Drugs, Health Technologies, Health Systems
Reimbursement Review
Pembrolizumab (Keytruda)
Sponsor: Merck Canada Inc.
Therapeutic area: Cervical Cancer
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Clinical Review
Abbreviations
AE
adverse event
AESI
adverse event of special interest
BICR
blinded independent central review
CCRAN
Colorectal Cancer Resource & Action Network
CDA-AMC
Canada's Drug Agency
CI
confidence interval
CPS
combined positive score
CRT
chemoradiotherapy
EBRT
external beam radiotherapy
ECOG PS
Eastern Cooperative Oncology Group Performance Status
EORTC QLQ-C30
European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30
EORTC QLQ-C30 GHS/QoL
European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 Global Health Status/Quality of Life subscale
FIGO
Fédération internationale de gynécologie et d’obstétrique
GOC
Society of Gynecologic Oncology of Canada
GRADE
Grading of Recommendations Assessment, Development and Evaluation
HR
hazard ratio
HRQoL
health-related quality of life
LACC
locally advanced cervical cancer
LSM
least squares mean
OH (CCO)
Ontario Health (Cancer Care Ontario)
OS
overall survival
PFS
progression-free survival
RCT
randomized controlled trial
RECIST 1.1
Response Evaluation Criteria in Solid Tumours, version 1.1
SAE
serious adverse event
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Table 1: Background Information of Application Submitted for Review
Item | Description |
|---|---|
Drug product | Pembrolizumab (Keytruda), 100 mg/4 mL vial, solution for infusion |
Sponsor | Merck Canada Inc. |
Indication | Treatment of adult patients with FIGO 2014 Stage III-IVA cervical cancer, in combination with chemoradiotherapy. |
Reimbursement request | Treatment of adult patients with FIGO 2014 stage III to IVA cervical cancer, in combination with chemoradiotherapy. |
Health Canada approval status | NOC |
Health Canada review pathway | Standard |
NOC date | July 14, 2025 |
Recommended dose | For the treatment of FIGO 2014 stage III to IVA cervical cancer, patients should receive pembrolizumab 200 mg every 3 weeks or 400 mg every 6 weeks until disease progression or unacceptable toxicity or up to 24 months. Pembrolizumab should be administered before chemoradiotherapy when given on the same day. |
FIGO = Fédération internationale de gynécologie et d’obstétrique; NOC = Notice of Compliance.
Introduction
Cervical cancer is the fourth most common cancer in women globally, with incidence varying considerably by region.1-3 Most cervical cancers are HPV infection–related, which makes them highly immunogenic diseases,1,4,5 and only 5% are HPV independent.5 PD-1 and its ligand 1 (PD-L1) play a crucial role in the disease pathogenesis by inhibiting T-cell response to HPV infection.6 PD-L1 expression is a potential biomarker that is overexpressed in cervical cancers and surrounding inflammatory cells.7 High PD-L1 expression also correlates with poorer overall survival (OS) in patients with cervical cancer, establishing it as a potential prognostic indicator.8 Other risk factors commonly associated with cervical cancer include smoking, parity, oral contraceptive use, early sexual debut, multiple sexual partners, sexually transmitted infections, autoimmune diseases, and chronic immunosuppression.5
At the time of diagnosis, patients undergo imaging, biopsy, clinical evaluation for histologic confirmation of squamous cell carcinoma, adenocarcinoma, or adenosquamous carcinoma of the cervix, and staging according to the Fédération internationale de gynécologie et d’obstétrique (FIGO) staging criteria. Before 2018, FIGO 2014 staging criteria were used for cervical cancer screening, including FIGO stages IA to IVB. As per the FIGO 2014 staging criteria, stage I (IA to IC3) referred to a tumour confined to the cervix, stage II (IIA and IIB) included cancer that has spread beyond the cervix but not to the pelvic wall or lower third of the vagina, stage III (IIIA to IIIC) referred to cancer that has spread to the pelvic wall and/or involves the lower third of the vagina and/or causes hydronephrosis or nonfunctioning kidney, and stage IV (IVA and IVB) included cancer that has spread beyond the true pelvis or involves the bladder or rectal mucosa.9 The 2018 FIGO staging classification expanded the 2014 system and added stages IIIC1 and IIIC2, which specifically account for pelvic and para-aortic nodal disease, respectively.10-13 Patients with FIGO 2014 or 2018 stage III to IVA have particularly poor prognosis and constitute the target population for this reimbursement submission.
Current treatment guidelines align with input from the clinical experts consulted during the review. Standard protocols recommend cisplatin 40 mg/m2 IV weekly for 5 to 6 cycles plus external beam radiotherapy (EBRT) followed by brachytherapy for patients with locally advanced (per FIGO 2014 stage IB2 to IVA or FIGO 2018 stage IB3 to IVA) cervical cancer.14,15 For patients who cannot tolerate or who are ineligible for cisplatin, the National Comprehensive Cancer Network5 and Cancer Care Alberta guidelines15 recommend carboplatin (area under the curve 2 IV weekly)16 as an alternative to cisplatin. Although the current standard of care with chemoradiotherapy (CRT) is reportedly effective in ensuring disease-free survival and OS, these benefits have remained suboptimal over time, particularly in patients with advanced FIGO stage disease or nodal involvement.17-22 Hence the need for new treatments that improve OS or cure rates for patients.
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of pembrolizumab (200 mg every 3 weeks or 400 mg every 6 weeks, solution for infusion) in combination with CRT for the treatment of FIGO 2014 stage III to IVA cervical cancer in adult patients.
Perspectives of Patients, Clinicians, and Drug Programs
The information in this section is a summary of input provided by the patient and clinician groups who responded to the Canada’s Drug Agency (CDA-AMC) call for input and from clinical expert(s) consulted for the purpose of this review.
Patient Input
Input from 1 patient group was submitted for this review by the Colorectal Cancer Resource & Action Network (CCRAN) in collaboration with the Canadian Cancer Survivor Network and HPV Global Action. CCRAN is a national, not-for-profit patient advocacy group that provides support and education to patients with colorectal cancer to improve longevity and quality of life; CCRAN has expanded its mandate to serve patients aside from those with colorectal cancer through collaboration with patient advocacy groups associated with other tumour types. CCRAN also participates in patients’ evidence submissions for health technology assessments, educational events, and advocacy initiatives for patients with cancers other than colorectal cancer. To gather input for this submission, CCRAN conducted telephone interviews with 5 patients (3 from Canada, specifically, Quebec, Ontario, and Alberta, and 2 from the US). Additional information on patients’ experiences with the disease and previously available treatments was gathered through a survey from April to May 2022, with 8 responses (5 from Canada — specifically, Nova Scotia, Quebec, Ontario, Manitoba, Alberta, and British Columbia — and 3 from the US).
CCRAN noted that cervical cancer affects only individuals assigned female sex at birth. Cervical cancer research and treatments tend to be underfunded. In addition, cervical cancer disproportionately impacts equity-denied communities in Canada, who often experience barriers such as low health literacy, poor health care access, and lack of culturally appropriate care. The patients interviewed by CCRAN described health care providers initially dismissing their symptoms and delays in diagnosis, particularly due to limited access to primary care during the COVID-19 pandemic. The survey respondents identified fatigue (57%), uncertainty about the future (43%), loss of appetite (29%), and anxiety, panic attacks, or depression (29%) as the most pressing symptoms to manage. Many of the patients said that receiving their diagnosis felt overwhelming and final, and that it made it difficult to plan for the future or maintain a sense of stability in their personal relationships. Patients need to undergo frequent and intrusive pelvic examinations, including colposcopies. Because cervical cancer is linked to HPV, a sexually transmitted infection, patients often experience stigma, guilt, and shame, despite that HPV is a common infection that many people acquire at some point in their lives.
The survey respondents reported that prior treatments included cisplatin (29%), carboplatin/paclitaxel/bevacizumab (14%), palliative care (14%), alternative treatments (14%), and pembrolizumab (14%), with most rating these as “somewhat effective.” The interviewees reported receiving chemotherapy, radiation, brachytherapy, laser therapy, loop electrosurgical excision procedures, hysterectomy, and total pelvic exenteration. Most of the interviewees indicated that adverse events (AEs) associated with treatments options available to patients significantly impacted their quality of life during treatment. Radiation therapy was also associated with severe toxicity, including fatigue, appetite loss, and rapid weight loss. The patients also highlighted the long-term effects of treatments they received such as impaired sexual and vaginal function as a result of pelvic radiation and loss of fertility following hysterectomy.
Controlling cancer spread was the top priority for most interviewees. Survey respondents also valued improved quality of life, delayed symptom onset, and better treatment tolerability. Across the interviews and survey, most of the patients noted that access to pembrolizumab plus chemoradiation is a key priority. All the interviewed patients believed that pembrolizumab offered the improvements they sought, particularly better response rates, short infusion times, and minimal side effects.
Of the 5 interviewees, 4 had direct experience with pembrolizumab, as did 3 of the 8 survey respondents. The survey respondents reported that while receiving pembrolizumab, they experienced better symptom control, had fewer AEs, and found pembrolizumab administration to be easier. The most common AEs were nausea, fatigue, diarrhea, rash, joint pain, fever, and interstitial nephritis. The 4 interviewees had received pembrolizumab plus carboplatin and either paclitaxel (Taxol) or radiation for 4 to 6 cycles, followed by pembrolizumab monotherapy for 2 to 35 cycles. Most reported durable responses: 2 had no evidence of disease, 1 with aggressive recurrence had no progression, and 1 had a 1-year response before developing possible lymph node involvement, requiring treatment with bevacizumab. The interviewees reported pain relief, reduced mental burden, and a return to normal activities while receiving pembrolizumab. On a scale of 1 to 10, interviewees rated their quality of life while receiving pembrolizumab at an average of 8.9.
Clinician Input
Input From Clinical Experts Consulted for This Review
Two clinical experts with experience in the diagnosis and clinical management of cervical cancer were consulted by CDA-AMC.
Current standard of care includes chemoradiation (cisplatin 40 mg/m2 IV weekly for 5 to 6 cycles plus EBRT followed by brachytherapy administered with curative intent). The experts said that carboplatin and paclitaxel in addition to cisplatin (based on evidence from the INTERLACE trial)23 were other chemotherapy treatments, although these are not widely adopted across jurisdictions due to challenges with administering radiation. The experts noted that pembrolizumab will cause a shift in the current treatment paradigm, fitting as a first-line therapy in combination with CRT. The experts noted that treatment with pembrolizumab addresses the underlying disease process as the HPV infection pathway will be addressed through immunotherapy.
According to the experts, patients best suited for treatment with concurrent pembrolizumab plus CRT will include those with FIGO 2014 stage III to IVA disease. Given the small number of patients with stage III to IVA disease with PD-L1–positive tumour combined positive scores (CPSs) less than 1 enrolled in the KEYNOTE-A18 trial, it was unclear to the experts whether they would benefit from treatment.
The most important treatment goals for patients with stage III to IVA cervical cancer highlighted by the experts consulted include improving survival or cure, delaying disease progression, reducing symptoms, and improving health-related quality of life (HRQoL). Although current treatments (chemotherapy and radiation) prolong life and improve cure rates, they do not modify the underlying disease mechanism. There is therefore a need for treatments with reduced toxicity profiles that ensure a long-term cure over shorter treatment periods. Both clinical experts agreed that they would consider discontinuing treatment if immune-related toxicity is significant during treatment, which typically occurs if the liver, gastrointestinal tract, or lungs are affected.
Clinician Group Input
Input from 2 clinician groups were submitted for this review, the Society of Gynecologic Oncology of Canada (GOC) and the Ontario Health (Cancer Care Ontario) (OH [CCO]) Gynecologic Cancer Drug Advisory Committee. The GOC is a nonprofit multidisciplinary organization comprising physicians, nurses, pharmacists, and scientists involved in the treatment and prevention of gynecologic cancer. OH (CCO) provides timely evidence-based clinical and health system guidance on drug-related issues, including the Provincial Drug Reimbursement Programs and the Systemic Treatment Program. Information was gathered for this submission through a review of published trials and direct clinical experience treating locally advanced cervical cancer (LACC).
The clinician groups indicated that for patients with LACC (stage II, III, and IVA), key treatment goals are to prolong OS and progression-free survival (PFS) while improving quality of life. The current standard of care for these patients, provided with curative intent, is concurrent cisplatin and pelvic EBRT, followed by brachytherapy. The clinician groups agreed that this protocol, which has not been updated since its establishment in 1999, demonstrates only modest OS and PFS benefits; OH (CCO) noted that the OS rate of patients with stage III to IVA cervical cancer is between 32% to 35% in Canada. The clinician groups highlighted a need for new treatments with improved OS and PFS for patients with stage III to IVA cervical cancer.
The clinician groups agreed that pembrolizumab would be used first-line for patients with FIGO 2014 stage III or IVA cervical cancer who are undergoing curative-intent therapy, regardless of nodal status, as a complement to chemoradiation. The clinician groups anticipated that approval of pembrolizumab would shift the current treatment paradigm, such that any eligible patient initiating chemoradiation would also receive pembrolizumab. The groups noted that with pembrolizumab as a first-line curative-intent therapy, it would not be appropriate to try other treatments before initiating pembrolizumab with chemoradiation. The groups agreed that patients with newly diagnosed FIGO 2014 stage III (irrespective of nodal status) or stage IVA histologically confirmed squamous cell carcinoma, adenocarcinoma, or adenosquamous carcinoma of the cervix, with no previous treatment targeting the cancer, are most likely to respond to treatment. Patients for whom this treatment is least suited are those who are unable to tolerate radiation, chemotherapy, or immunotherapy.
According to the GOC, a clinically meaningful response to treatment would be defined as clinical and radiographic resolution of disease with tolerable toxicity. The clinician groups suggested using tumour imaging (per Response Evaluation Criteria in Solid Tumours, version 1.1 [RECIST 1.1]) to determine treatment response. However, the groups had slightly different suggestions on the schedule for follow-up. OH (CCO) suggested aligning the imaging follow-up schedule with the KEYNOTE-A18 trial, every 12 weeks for years 1 and 2, every 24 weeks in year 3, and once yearly thereafter. The GOC suggested initial imaging with a pelvic MRI, CT scan, or PET-CT scan, followed by tumour imaging 3 months after chemoradiation completion, and ongoing response assessments by clinical assessment and imaging every 3 to 6 months thereafter. Discontinuation should be considered in the event of disease progression, unacceptable toxicity (especially grade 4 immune-related events), or patient choice. Treatment would be administered as outpatient therapy in a comprehensive cancer setting by specialist physicians with experience in treating gynecologic cancer, including medical oncologists, radiation oncologists, or gynecologic oncologists.
Drug Program Input
Input was obtained from the drug programs that participate in the CDA-AMC reimbursement review process. The following were identified as key factors that could potentially impact the implementation of a CDA-AMC recommendation for pembrolizumab plus CRT:
Considerations for initiation and discontinuation of therapy
Considerations for prescribing therapy
Generalizability
Funding algorithm
Relevant comparators
Care provision issues
System and economic issues
The clinical experts consulted by CDA-AMC provided advice on the potential implementation issues raised by the drug programs (refer to Table 4).
Clinical Evidence
Systematic Review
Description of Studies
One randomized controlled trial (RCT), the KEYNOTE-A18 trial, was included in the sponsor’s systematic review. The KEYNOTE-A18 trial is an ongoing, randomized, double-masked, placebo-controlled, phase III trial with a sequential study design that is evaluating the efficacy and safety of concurrent use of pembrolizumab with and after CRT compared with placebo and CRT alone in patients with newly diagnosed high-risk (FIGO 2014 stage IB2 to IIB node-positive disease or stage III to IVA regardless of node status) LACC. The coprimary outcomes assessed in the study were PFS as assessed by an investigator per RECIST 1.1 and OS. Other outcomes included HRQoL (using the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 Global Health Status/Quality of Life [EORTC QLQ-C30 GHS/QoL] subscale) and safety. Overall, patients enrolled in the KEYNOTE-A18 trial were randomized by stratification factors in a 1:1 ratio to the pembrolizumab plus CRT and placebo plus CRT treatment arms.
The Health Canada indication is limited to FIGO 2014 stage III to IVA disease. The sponsor’s reimbursement request is in line with the Health Canada indication. Therefore, this report focuses on the post hoc analyses of the subgroup of patients enrolled in the KEYNOTE-A18 trial who are living with FIGO 2014 stage III to IVA disease regardless of node status at interim analysis 2 data cut-off.24
At the interim analysis 2 data cut-off (January 8, 2024), 296 patients were included in the pembrolizumab plus CRT arm and 305 in the placebo plus CRT arm of the PFS analysis. Baseline demographics and disease characteristics in both treatment arms in the FIGO 2014 stage III to IVA disease subgroup were generally similar. The percentage of patients with PD-L1–positive tumour CPS greater than or equal to 1 was high in both treatment arms (93.9% in the pembrolizumab plus CRT arm and 92.1% in the placebo plus CRT arm).24 The majority of patients were aged 65 years or younger (85.8% in the pembrolizumab plus CRT arm and 81.3% in the placebo plus CRT arm) and had disease with positive pelvic and or para-aortic lymph node involvement (72.0% in the pembrolizumab plus CRT arm and 69.5% in the placebo plus CRT arm).
Efficacy Results
Progression-Free Survival
The hazard ratio (HR) for investigator-assessed PFS was 0.57 (95% confidence interval [CI], 0.43 to 0.76) in the FIGO 2014 stage III to IVA disease population. The median PFS was not reached in the pembrolizumab plus CRT arm and not reached (95% CI, 26.3 to not reached) in the placebo plus CRT arm. The Kaplan-Meier estimated between-group differences in PFS probabilities at 18, 24, and 30 months were 14.8% (95% CI, 7.3% to 22.2%), 16.0% (95% CI, 7.9% to 24.0%), and 17.9% (95% CI, 9.4% to 26.5%), respectively, in favour of pembrolizumab plus CRT. These findings were consistent with PFS per blinded independent central review (BICR) analysis and the primary analysis in the overall population (FIGO 2014 stage IB2 to IIB node-positive disease or stage III to IVA disease regardless of node status).
Overall Survival
The HR for OS was 0.57 (95% CI, 0.39 to 0.83; nominal P = 0.0016) in the FIGO 2014 stage III to IVA disease subpopulation. The median OS was not reached in both treatment arms. The Kaplan-Meier estimated between-group differences in OS probabilities at 24, 30, and 36 months were 8.9% (95% CI, 2.5% to 15.3%), 11.9% (95% CI, 4.7% to 19.2%), and 11.5% (95% CI, 3.5% to 19.5%), respectively, in favour of pembrolizumab plus CRT. These findings were consistent with the primary analysis of the overall population.
Health-Related Quality of Life
At interim analysis 2, 261 patients in the pembrolizumab plus CRT arm and 270 patients in the placebo plus CRT arm contributed to the analysis at baseline, and 200 and 198 patients, respectively, were included in the analysis at week 36. The mean change from baseline showed improvements in the EORTC QLQ-C30 GHS/QoL subscale score at week 36 in both the pembrolizumab plus CRT arm (least squares mean [LSM] = 10.67 points; 95% CI, 7.73 points to 13.62 points) and the placebo plus CRT arm (LSM = 11.32 points; 95% CI, 8.39 points to 14.26 points). The between-group difference was –0.65 points (95% CI, –4.19 points to 2.89 points), with no added benefit observed for pembrolizumab plus CRT compared to placebo plus CRT. These findings were consistent with the primary analysis of the overall population.
Harms
The proportion of overall AEs were comparable in the 2 treatment arms (100% in the pembrolizumab plus CRT arm versus 99.3% in the placebo plus CRT arm). The most frequently reported AEs (incidence ≥ 25%) were anemia, nausea, diarrhea, and decreased white blood cell counts. Overall, serious adverse events (SAEs) were high in proportion with no major differences between the 2 treatment arms (33.9% in the pembrolizumab plus CRT arm versus 32.6% in the placebo plus CRT arm). The most frequent SAEs included anemia (4.4%), urinary tract infection (3.1%), and pyrexia (2.0%) in the pembrolizumab plus CRT arm, and urinary tract infection (4.3%) and acute kidney injury (2.0%) in the placebo plus CRT arm.
Rates of treatment discontinuation due to AEs were generally higher (21.0% versus 15.1%) in the pembrolizumab plus CRT arm than in the placebo plus CRT arm, and included events in the system organ class such as blood and lymphatic system disorders (5.1% versus 3.3%, respectively), gastrointestinal disorders (1.7% versus 2.0%, respectively) and investigations (6.1% versus 7.2%, respectively). Deaths due to grade 5 AEs were reported among 4 patients (1.4%) in the pembrolizumab plus CRT arm and 6 patients (2.0%) in the placebo plus CRT arm. The most frequently reported notable harm (adverse events of special interest) in the pembrolizumab plus CRT arm was immune-mediated reactions, reported by 40.7% of patients compared to 17.8% of patients in the placebo plus CRT arm.
Critical Appraisal
Internal Validity
The KEYNOTE-A18 trial is a randomized, double-masked, placebo-controlled, phase III trial designed to evaluate the efficacy and safety of pembrolizumab and CRT in patients with high-risk FIGO 2014 stage IB2 to IIB (with node-positive disease) or stage III to IVA (either node-positive or node-negative disease) LACC. Although the enrolled patients were stratified by FIGO 2014 stage III to IVA disease at randomization, the subgroup analysis of interest was not prespecified and, as such, the evidence informing this submission is based on a post hoc analysis. There is a risk that the statistically significant results may have been due to chance, due to multiple testing, though the risk is likely low given that the subgroup results were consistent with those of the primary analysis of the overall population. The trial is ongoing at the time of this review, and the available data were based on an interim analysis that could be considered exploratory. There were also concerns about imprecision as evidenced by the wide CIs associated with PFS and OS at various time points; these included the clinical threshold of important difference suggested by the clinical experts consulted during the review.
Baseline demographic and disease characteristics were generally similar in the FIGO 2014 stage III to IVA subgroup treatment arms, thus ensuring that confounding effect from these factors at baseline is an unlikely explanation for any differences in treatment outcomes between the 2 groups.
The double-masked design minimized the risk of detection bias and reporting bias, particularly for subjective end points like PFS. Results from BICR for PFS were consistent with the investigator’s assessment. This would indicate that the between-group differences in PFS are unlikely to be due to subjective bias in the investigator’s assessment.
The proportion of patients who discontinued from study treatment was high in both treatment arms (39.7% in the pembrolizumab plus CRT arm versus 46.7% in the placebo plus CRT arm). Differential treatment discontinuation was primarily due to radiographic progression (19.3% versus 30.9%) and AEs (11.2% versus 4.9%) for the pembrolizumab plus CRT arm and the placebo plus CRT arm, respectively. Although overall treatment exposure appeared to be similar in the treatment arms for the completion of CRT, the shorter duration of exposure to treatment in the placebo plus CRT arm versus the pembrolizumab plus CRT arm (20 versus 16 months in median duration and 17 versus 15 in median number of treatment cycles) may have biased the efficacy results in favour of pembrolizumab plus CRT.
The use of subsequent anticancer therapy may increase the risk of bias in OS against pembrolizumab plus CRT (e.g., antineoplastic agents 15.9% versus 27.6%). Therefore, the benefit of pembrolizumab on OS may have been underestimated.
External Validity
The KEYNOTE-A18 trial is a multicentre study with 3 sites in Canada. The inclusion and exclusion criteria were considered appropriate for the clinical trial setting, and the baseline characteristics of patients enrolled in the overall trial and the subgroup did not suggest any notable issues with generalizability to patients in clinical practice in Canada. One exception is the low proportion of patients with CPS less than 1 (< 7%), which resulted in uncertainty regarding whether these patients would benefit from this treatment.
The use of CRT was considered appropriate and the number of cycles and dosing reflected clinical practice. Although carboplatin was not specified as an alternative to cisplatin in the trial and it is not frequently prescribed by physicians in clinical practice in Canada, the clinical experts consulted for this review noted that some patients who may not be eligible for cisplatin could receive carboplatin or paclitaxel instead.
Concomitant and subsequent medications also generally reflected current clinical practice, with no discrepancies identified.
Key outcomes important for clinical decision-making by the clinicians and patient groups consulted by CDA-AMC were investigated in the KEYNOTE-A18 trial; these included PFS, OS, and HRQoL. Time points for assessment considered in the trial were appropriate, and the clinical experts agreed that 18, 24, and 30 months were clinically meaningful for PFS as were 24, 30, and 36 months for OS. PFS assessments by the investigator using the RECIST 1.1 criteria reflected current practice settings. Patient groups also indicated that improvements in HRQoL were important. HRQoL (measured using the EORTC QLQ-C30 GHS/QoL subscale) was considered clinically relevant and a better indicator of changes in quality of life during treatment.
GRADE Summary of Findings and Certainty of the Evidence
For pivotal studies and RCTs identified in the sponsor’s systematic review, Grading of Recommendations Assessment, Development and Evaluation (GRADE) was used to assess the certainty of the evidence for outcomes considered most relevant to informing expert committee deliberations, and a final certainty rating was determined as outlined by the GRADE Working Group.25,26
Following the GRADE approach, evidence from RCTs started as high-certainty evidence and could be rated down for concerns related to study limitations (which refers to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias.
Whenever possible, certainty was rated in the context of the presence of an important (nontrivial) treatment effect; if this was not possible, certainty was rated in the context of the presence of any treatment effect (i.e., the clinical importance is unclear). In all cases, the target of the certainty-of-evidence assessment was based on the point estimate and where it was located relative to the threshold for a clinically important effect (when a threshold was available) or to the null.
The selection of outcomes for GRADE assessment was based on the sponsor’s Summary of Clinical Evidence, consultation with clinical experts, and input received from patient and clinician groups and public drug plans. The following list of outcomes was finalized in consultation with expert committee members: OS, PFS, and HRQoL (measured using the EORTC QLQ-C30 GHS/QoL subscale), and safety outcomes (SAEs, discontinuation due to AEs, and immune-related AEs). The EORTC QLQ-C30 GHS/QoL subscale was determined to be the most appropriate single measures of HRQoL for the CDA-AMC assessment of evidence using the GRADE guidelines because this subscale provides a comprehensive, patient-centred measure of overall well-being, integrating physical, emotional, and social aspects of health that the clinical experts considered most relevant to patients.
The reference points for the certainty-of-evidence assessment for OS, PFS, and safety outcomes (SAEs and immune-related AEs leading to discontinuation) were set according to the presence or absence of an important effect based on thresholds informed by the clinical experts consulted for this review. The reference point for the certainty-of-evidence assessment for the EORTC QLQ-C30 GHS/QoL subscale score was set according to the presence or absence of an important effect based on a threshold informed by the literature.
Results of GRADE Assessments
Table 2 shows the GRADE summary of findings for pembrolizumab plus CRT versus placebo plus CRT for the treatment of FIGO 2014 stage III to IVA cervical cancer in adult patients.
Table 2: Summary of Findings for Pembrolizumab Plus CRT Versus Placebo Plus CRT for Patients With FIGO 2014 Stage III to IVA Cervical Cancer
Outcome and follow-up | Patients (studies), N | Relative effect (95% CI) | Absolute effects (95% CI) | Certainty | What happens | ||
|---|---|---|---|---|---|---|---|
Pembrolizumab plus CRT | Placebo plus CRT | Difference | |||||
Overall survival | |||||||
OS rate Follow-up: 24 months | 601 (1 RCT) | HR = 0.57 (0.39 to 0.83) | ████ ██ | 780 per 1,000 | ████ ██ | Moderatea | Compared with placebo plus CRT, pembrolizumab plus CRT likely results in a clinically important increase in OS at 24 months. |
OS rate Follow-up: 30 months | ████ ██ | 724 per 1,000 | ████ ██ | Moderatea | Compared with placebo plus CRT, pembrolizumab plus CRT likely results in a clinically important increase in OS at 30 months. | ||
OS rate Follow-up: 36 months | ████ ██ | 707 per 1,000 | ████ ██ | Moderatea | Compared with placebo plus CRT, pembrolizumab plus CRT likely results in a clinically important increase in OS at 36 months. | ||
PFS assessed by investigator | |||||||
PFS rate Follow-up: 18 months | 601 (1 RCT) | HR = 0.57 (0.43 to 0.76) | ████ ██ | 628 per 1,000 | ████ ██ | Moderateb | Compared with placebo plus CRT, pembrolizumab plus CRT likely results in a clinically important increase in PFS at 18 months. |
PFS rate Follow-up: 24 months | ████ ██ | 569 per 1,000 | ████ ██ | Moderateb | Compared with placebo plus CRT, pembrolizumab plus CRT likely results in a clinically important increase in PFS at 24 months. | ||
PFS rate Follow-up: 30 months | ████ ██ | 537 per 1,000 | ████ ██ | Moderateb | Compared with placebo plus CRT, pembrolizumab plus CRT likely results in a clinically important increase in PFS at 30 months. | ||
Health-related quality of life | |||||||
EORTC QLQ-C30 GHS/QoL LSM change from baseline Follow-up: week 36 | 531 (1 RCT) | NR | ████ ██ | 11.32 points (8.39 points to 14.26 points) | ████ ██ | Lowc | Compared with placebo plus CRT, pembrolizumab plus CRT may result in little-to-no clinically important difference in HRQoL. |
Harms | |||||||
SAEs Follow-up: 36 months | 599 (1 RCT) | NR | ████ ██ | 326 per 1,000 | ████ ██ | Moderated | Compared with placebo plus CRT, pembrolizumab plus CRT likely leads to little-to-no clinically important difference in SAEs. |
Withdrawal due to immune-related AEs Follow-up: 36 months | 599 (1 RCT) | NR | ████ ██ | 7 per 1,000 | ████ ██ | Highe | Compared with placebo plus CRT, pembrolizumab plus CRT does not result in a clinically important difference in withdrawals due to immune-related AEs. |
AE = adverse event; CI = confidence interval; CRT = chemoradiotherapy; EORTC QLQ-C30 GHS/QoL = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 Global Health Status/Quality of Life; FIGO = Fédération internationale de gynécologie et d’obstétrique; HR = hazard ratio; HRQoL = health-related quality of life; LSM = least squares mean; MID = minimal important difference; NR = not reported; OS = overall survival; PFS = progression-free survival; RCT = randomized controlled trial; SAE = serious adverse event.
Note: Study limitations (which refer to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias were considered when assessing the certainty of the evidence. All serious concerns in these domains that led to the rating down of the level of certainty are documented in the Table 2 footnotes.
aRated down 1 level for imprecision. In the absence of a validated MID, the threshold was informed by clinical experts consulted for this review. The clinical experts considered a between-group absolute risk difference of 5% (50 or more OS events per 1,000 patients) at 24, 30, and 36 months to be clinically significant. The 95% CIs included values that were considered unimportant, indicating uncertainty.
bRated down 1 level for imprecision. In the absence of a validated MID, the threshold was informed by clinical experts consulted for this review. The clinical experts considered a between-group absolute risk difference of 10% (100 or more PFS events per 1,000 patients) at 18, 24, and 30 months to be clinically significant. The 95% CI included values that may be considered unimportant, indicating uncertainty.
cRated down 1 level for imprecision. The 95% CI crossed the MID, suggesting the possibility of harm or no clinically meaningful benefit. Rated down 1 level for risk of bias due to missing data.
dIn the absence of a validated MID, the null was used. Rated down 1 level for imprecision due to the wide 95% CIs, which crossed the null, suggesting the possibility of a benefit and no benefit.
eIn the absence of a validated MID, the threshold was informed by clinical experts consulted for this review. The clinical experts considered a between-group absolute risk difference of 10% (100 or more AEs per 1,000 patients) clinically significant. The point estimate and entire CI did not reach or exclude the threshold.
Source: Details in the table are from the sponsor’s Summary of Clinical Evidence.24
Conclusions
A post hoc subgroup analysis conducted in the KEYNOTE-A18 trial provided evidence of safety and efficacy for the use of pembrolizumab plus CRT versus placebo plus CRT for the treatment of FIGO 2014 stage III to IVA LACC. The evidence suggested that, compared to placebo plus CRT, pembrolizumab plus CRT likely results in clinically important improvement in OS and delays disease progression. Although the findings on OS and PFS reported across time points were consistent and considered clinically meaningful, there is uncertainty due to imprecision. While the FIGO 2014 stage III to IVA disease subgroup analysis showed little-to-no clinically meaningful difference in change in HRQoL between the 2 treatment arms, the short duration of HRQoL assessments and the potential risk of bias mean that no conclusion can be reached on the effectiveness of pembrolizumab in improving or maintaining better quality of life when pembrolizumab is added to standard-of-care CRT.
Overall, the frequencies of AEs and SAEs were similar in the 2 treatment arms, and treatment with pembrolizumab plus CRT did not result in a clinically important difference in withdrawals due to immune-related AEs compared to placebo plus CRT. The long-term impact of pembrolizumab plus CRT is uncertain due to the lack of long-term safety and efficacy data for the indication under review; however, this was not a major concern given the prevalence of the use of pembrolizumab for the treatment of other cancers in Canada.
Introduction
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of pembrolizumab (200 mg every 3 weeks or 400 mg every 6 weeks, solution for infusion), in combination with CRT, for the treatment of adult patients with FIGO 2014 stage III to IVA cervical cancer.
Disease Background
The contents in this section have been informed by materials submitted by the sponsor and clinical expert input. The following have been summarized and validated by the review team.
Cervical cancer is the fourth most common cancer in women globally, with incidence varying considerably by region.1-3 In Canada, comprehensive screening and vaccination programs have reduced its impact, ranking it 15th in cancer incidence rates among females.27-29 The primary histologic types of cervical cancer are squamous cell carcinoma (70% to 80% of cervical cancers) and adenocarcinoma (10% to 25%).2,30,31 Less common variants include adenosquamous carcinoma, small cell carcinoma, and neuroendocrine tumours, collectively representing less than 5% of cases.2,31 PD-1 and its ligand, PD-L1, play a crucial role in the pathogenesis of cervical cancer by inhibiting T-cell response to HPV infection.6 PD-L1 expression is a potential biomarker as it is overexpressed in cervical cancers and surrounding inflammatory cells.7 High PD-L1 expression also correlates with poorer OS in patients with cervical cancer, which establishes it as a potential prognostic indicator.8 Most cervical cancers are HPV infection–related, which makes them highly immunogenic diseases,1,4,5 and only 5% are HPV independent.5 Other risk factors include smoking, high parity, oral contraceptive use, early sexual debut, multiple sexual partners, sexually transmitted infections, autoimmune diseases, and chronic immunosuppression.32 Cervical cancer and its treatment can generate psychological and physical challenges, including anxiety, mood changes, uncertainty about the future, physical debilitation, and sleep disruption, which can affect employment and result in financial and relationship challenges.33 Compared with healthy individuals or patients who undergo surgery, those who receive definitive concurrent CRT experience greater social, physical, and psychological challenges, which results in diminished quality of life.34
At the time of diagnosis, patients undergo imaging, biopsy, clinical evaluation for histologic confirmation of squamous cell carcinoma, adenocarcinoma, or adenosquamous carcinoma of the cervix and staging according to the FIGO criteria. Before 2018, FIGO 2014 criteria were used in cervical cancer screening. FIGO 2014 stage I (IA to IC3) referred to a tumour confined to the cervix, stage II (IIA and IIB) included cancer that has spread beyond the cervix but not to the pelvic wall or lower third of the vagina, stage III (IIIA to IIIC) referred to cancer that has spread to the pelvic wall and/or involves the lower third of the vagina and/or causes hydronephrosis or nonfunctioning kidney, and stage IV (IVA and IVB) included cancer that had spread beyond the true pelvis or involved the bladder or rectal mucosa.9 The 2018 FIGO staging classification expanded the 2014 system and added stages IIIC1 and IIIC2, which specifically account for pelvic and para-aortic nodal disease, respectively.10-13 Patients with FIGO 2014 stage III to IVA have particularly poor prognosis and constitute the target population for this reimbursement submission.
Cancer stage at diagnosis is a critical determinant of treatment options and prognosis, and individuals with locally advanced (FIGO 2014 stage IB2 to IVA) cervical cancer have been shown to have a higher rate of recurrence and poorer survival than those with early-stage disease.1,32,35 Approximately 54% of cervical cancers are diagnosed at stage I in Canada, resulting in favourable outcomes and contributing to a 5-year survival probability of 74% across all stages combined.32,36 Those with locally advanced disease (an estimated 37% of cases globally1) have a 5-year survival probability of approximately 60%, despite standard curative-intent CRT.32,36 For patients with locally advanced cancers, prognosis worsens with more advanced disease (based on FIGO stage) or nodal involvement.17,19,20,22,37,38
Standards of Therapy
The contents in this section have been informed by materials submitted by the sponsor and clinical expert input. The following have been summarized and validated by the review team.
The current standard of care in Canada for LACC aligns with input from the clinical experts consulted during the review. Standard CRT protocols recommend cisplatin 40 mg/m2 IV weekly for 5 to 6 cycles plus EBRT followed by brachytherapy.14,15 For patients who are unable to tolerate or who are ineligible for cisplatin, the National Comprehensive Cancer Network5 and the Cancer Care Alberta guidelines15 recommend carboplatin (area under the curve 2 IV weekly)16 as an alternative to cisplatin.15 For locally advanced squamous cell carcinoma, adenocarcinoma, or adenosquamous carcinoma of the cervix, the primary treatment per international and regional guidelines consists of EBRT with concurrent platinum-containing chemotherapy, followed by brachytherapy. While surgery followed by risk-adapted adjuvant radiotherapy or CRT remains an alternative for treating patients with stage IB2 to IIA2 (per FIGO 2014) or IB3 to IIA2 (per FIGO 2018), concurrent CRT is preferrable, based on supporting evidence.15,39-41
Although current standard of care (since 1999) has demonstrated superior benefits in achieving disease-free survival and OS compared to EBRT alone, these benefits have remained suboptimal over time, particularly for patients with advanced disease (based on FIGO stage) or nodal involvement;17-22 hence the need for new treatments that improve OS or cure rates. The clinical experts also referred to the use of short-course induction chemotherapy (carboplatin administered once weekly) followed by standard cisplatin-based CRT as another treatment option, as per the protocol used in the INTERLACE trial;23 however, few centres in Canada have adopted this protocol.
Drug Under Review
PD-1 is an immune-checkpoint receptor that limits the activity of T lymphocytes in peripheral tissues. Pembrolizumab is a high-affinity antibody against PD-1. It exerts a dual-ligand blockade of the PD-1 pathway, including PD-L1 and PD-L2, on antigen-presenting or tumour cells. By inhibiting the PD-1 receptor from binding to its ligands, tumour-specific cytotoxic T lymphocytes in the tumour microenvironment are reactivated.
Key characteristics of pembrolizumab and other treatments available for FIGO 2014 stage III to IVA cervical cancer are summarized in Table 3.
Pembrolizumab is currently under review by Health Canada for the treatment of adult patients with FIGO 2014 stage III to IVA cervical cancer, in combination with CRT. The sponsor’s reimbursement request aligns with the indication.
Pembrolizumab is administered as an IV infusion over 30 minutes. The recommended dose is 200 mg every 3 weeks or 400 mg every 6 weeks until disease progression, unacceptable toxicity, or up to 24 months. Pembrolizumab should be administered before CRT when given on the same day.
Table 3: Key Characteristics of Pembrolizumab and Cisplatin
Characteristic | Pembrolizumab | Cisplatin |
|---|---|---|
Mechanism of action | High-affinity antibody that exerts a dual-ligand blockade of the PD-1 pathway, an immune-checkpoint inhibitor, resulting in reactivation of tumour-specific cytotoxic T lymphocytes in the tumour microenvironment | A bifunctional alkylating agent, binding to genomic DNA in the cell nucleus to form cross-links and interfere with normal transcription and replication, resulting in cell death |
Indicationa | For the treatment of adult patients with FIGO 2014 stage III to IVA cervical cancer, in combination with CRT | Indicated as palliative therapy, to be employed in addition to other modalities, or in established combination therapy with other chemotherapeutic agents in the treatment of:
|
Route of administration | IV infusion | IV infusion |
Recommended dose | 200 mg q.3.w. or 400 mg q.6.w. until disease progression, unacceptable toxicity, or up to 24 months To be administered before CRT when given on the same day | 40 mg/m2 IV weekly (maximum 5 to 6 cycles) plus EBRT followed by brachytherapy14,15 |
Serious adverse events or safety issues |
|
|
CRT = chemoradiotherapy; EBRT = external beam radiotherapy; FIGO = Fédération internationale de gynécologie et d’obstétrique; q.3.w. = every 3 weeks; q.6.w. = every 6 weeks.
aHealth Canada–approved indication.
Sources: Pembrolizumab Draft Product Monograph;42 Cisplatin Product Monograph;43 BC Cancer Protocol Summary GOCXCRT;14 Cancer Care Alberta Clinical Practice Guidelines.15
Perspectives of Patients, Clinicians, and Drug Programs
The full patient and clinician group submissions received are available in the consolidated patient and clinician group input document for this review on the project website.
Patient Group Input
This section was prepared by the review team based on the input provided by patient groups.
Input from 1 patient group was submitted for this review by CCRAN in collaboration with the Canadian Cancer Survivor Network and HPV Global Action. CCRAN is a national, not-for-profit patient advocacy group that provides support and education to patients with colorectal cancer to improve longevity and quality of life; CCRAN has expanded its mandate to serve patients aside from those with colorectal cancer through collaboration with patient advocacy groups associated with other tumour types. CCRAN also participates in patients’ evidence submissions for health technology assessments, educational events, and advocacy initiatives for patients with cancers other than colorectal space. To gather input for this submission, CCRAN conducted telephone interviews with 5 patients (3 from Canada, 2 from the US; representation from Quebec, Ontario, and Alberta). Additional information on patients’ experiences with the disease and previously available treatments was gathered through a survey from April to May 2022, with 8 responses (5 from Canada — specifically, Nova Scotia, Quebec, Ontario, Manitoba, Alberta, and British Columbia — and 3 from the US
CCRAN noted that cervical cancer affects only individuals assigned female sex at birth. Cervical cancer research and treatments tend to be chronically underfunding. CCRAN also emphasized that cervical cancer disproportionately affects equity-denied communities in Canada, where individuals often encounter barriers such as low health literacy, difficulties navigating the health care system, and a lack of culturally appropriate care. The patients interviewed by CCRAN described health care providers initially dismissing their symptoms and delays in diagnosis, particularly due to limited access to primary care during the COVID-19 pandemic. The survey respondents identified fatigue (57%), uncertainty about the future (43%), loss of appetite (29%), and anxiety, panic attacks, or depression (29%) as the most pressing symptoms to manage. Many of the patients said that receiving their diagnosis felt overwhelming and final, and made it difficult to plan for the future or maintain a sense of stability in their personal relationships. Patients need to undergo frequent and intrusive pelvic examinations, including colposcopies. Because cervical cancer is linked to HPV, a sexually transmitted infection, patients often experience stigma, guilt, and shame, despite that HPV is a common infection that many people acquire at some point in their lives.
The survey respondents reported that prior treatments included cisplatin (29%), carboplatin/paclitaxel/bevacizumab (14%), palliative care (14%), alternative treatments (14%), and pembrolizumab (14%), with most rating these as “somewhat effective.” The interviewees also reported receiving chemotherapy, radiation, brachytherapy, laser therapy, loop electrosurgical excision procedures, hysterectomy, and total pelvic exenteration. Most of the interviewees indicated that the AEs associated with the treatments available to them significantly impacted their quality of life during treatment. One patient stated, “I did nothing. I had no quality of life. Went nowhere, did nothing, very depressed. Alone, just pretty useless, I guess.” Radiation therapy was also associated with severe toxicity, including fatigue, appetite loss, and rapid weight loss. The patients also highlighted the long-term effects of treatments they received such as impaired sexual and vaginal function from pelvic radiation and loss of fertility following hysterectomy.
Controlling cancer spread was the top priority for most interviewees. Survey respondents also valued improved quality of life, delayed symptom onset, and better treatment tolerability. Across the interviews and the survey, most of the patients noted that access to pembrolizumab plus chemoradiation is a key priority. All the interviewed patients believed that pembrolizumab offered the improvements they sought, in particular, better response rates, short infusion times, and minimal side effects.
Of the 5 interviewees, 4 had direct experience with pembrolizumab, as did 3 of the 8 survey respondents. The survey respondents reported that they experienced better symptom control, had fewer adverse events, and found pembrolizumab administration to be easier. The most common AEs were nausea, fatigue, diarrhea, rash, joint pain, fever, and interstitial nephritis. The 4 interviewees had received pembrolizumab plus carboplatin treatment and either paclitaxel or radiation for 4 to 6 cycles, followed by pembrolizumab monotherapy for 2 to 35 cycles. Most reported durable responses: 2 had no evidence of disease, 1 with aggressive recurrence had no progression, and 1 had a 1-year response before developing possible lymph node involvement, requiring treatment with bevacizumab. The interviewees reported pain relief, reduced mental burden, and a return to normal activities while receiving pembrolizumab. On a scale of 1 to 10, interviewees rated their quality of life while receiving pembrolizumab at an average of 8.9.
Clinician Input
Input From Clinical Experts Consulted for This Review
All CDA-AMC review teams include at least 1 clinical specialist with expertise in the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). The following input was provided by 2 clinical specialists with expertise in the diagnosis and management of cervical cancer.
Unmet Needs
The consulted experts noted that the most important treatment goals for patients with stage III to IVA cervical cancer include improved survival or cure, delayed disease progression, reduced symptoms, and improved HRQoL.
Current standard of care includes chemoradiation (cisplatin 40 mg/m2 IV weekly for 5 to 6 cycles plus EBRT followed by brachytherapy, administered with curative intent). Carboplatin and paclitaxel in addition to cisplatin (based on evidence from the INTERLACE trial23) were other chemotherapy treatments considered potential alternatives to cisplatin, although they are not widely adopted by jurisdictions due to the challenges with administering radiation.
The experts noted that although current treatments (chemotherapy and radiation) prolong life and improve cure rates, they do not modify the underlying disease mechanism. Therefore, there is a need for new treatments that ensure long-term cure, reduce toxicity, and have shorter treatment periods. In addition, treatments that optimize initial response are needed for those who do not experience response with CRT alone, including those with bulky nodal disease, particularly in the para-aortic area.
Place in Therapy
According to the clinical experts, pembrolizumab will cause a shift in the current treatment paradigm as it will fit as first-line treatment in combination with CRT. The addition of pembrolizumab will impact the underlying disease process as the HPV infection pathway will be addressed through immunotherapy. According to the experts, all eligible patients, including new patients, would receive the combination therapy, as they expect that it would give patients the best chance of a cure, decrease the rate of recurrence, and improve survival. The experts considered that it would not be appropriate to allow patients to try other treatments, which could be less effective and may result in chemoradiation resistance. According to the experts, once patients do not experience a response following treatment, salvage is difficult, and cure rates are low.
Patient Population
According to the clinical experts consulted, patients best suited for treatment with concurrent pembrolizumab plus CRT will include those with FIGO 2014 stage III to IVA disease. Given that most of the patients with stage III to IVA disease enrolled in the KEYNOTE-A18 trial had PD-L1 CPS greater than or equal to 1, it was unclear to the experts whether those with PD-L1 CPS less than 1 would benefit from treatment due to the small number enrolled in the trial. Given that LACCs include stage IB2 to IVA disease, according to FIGO 2014 classification, it was unclear to the clinical experts why patients with FIGO stage IB to IIB disease, who typically have better OS due to early disease stage, did not experience similar benefits to patients with FIGO 2014 stage III to IVA disease in the overall KEYNOTE-A18 trial. According to 1 expert, although benefits for patients with FIGO 2014 stage IB to IIB disease were smaller, benefit may improve with longer follow-up.
According to clinical experts, the diagnosis and staging of cervical cancer is performed clinically and radiologically (CT scan or MRI or PET-CTscan) with no companion testing required for staging. However, the experts indicated that a central path review often occurs during diagnosis to avoid misclassification of some endometrial cancers. The clinical experts indicated that given the switch from the FIGO 2014 to 2018 staging guidelines, the new recommendations for staging may impact patient populations in clinical practice because nodal disease detected radiologically or pathologically will recategorize cases from stage IB (according to FIGO 2014 criteria) to IIIC (according to FIGO 2018 criteria). According to the clinical experts, clinicians will likely offer this treatment to all patients with node-positive disease in clinical practice.
Assessing the Response to Treatment
The experts considered the outcomes assessed in the KEYNOTE-A18 trial to reflect clinical practice. The experts mentioned that it is challenging to assess patient response to treatment in practice, especially for those with bulky disease. The experts noted that radiology assessments are frequently used to assess tumours, although it can take several weeks to months for clinicians to observe meaningful changes, and sometimes these changes may be confused with tumour necrosis. In practice, patient symptoms are commonly assessed as surrogate markers for response to treatment while waiting for changes in the tumour.
According to the clinical experts, a clinically meaningful response to treatment would translate to a reduction in tumour mass or eradication of the tumour, the absence of recurrence, and symptom alleviation. Although the ranges are not universally established, the experts generally agreed that an improvement of 10% to 15% in PFS would be clinically important and an improvement of 5% to 10% in OS would be considered clinically meaningful.
According to the clinical experts, a response to treatment would typically be assessed in practice every 3 to 4 months in the first 2 years of treatment.
Discontinuing Treatment
Both clinical experts agreed that they would consider discontinuing treatment if immune-related toxicity is significant during treatment, which typically occurs if the liver, gastrointestinal tract, or lungs are affected. Toxicity can affect almost any organ in the body, although mild toxicity can be managed with dose adjustments (reduced dosing), while severe toxicity can be managed by permanent discontinuation.
Prescribing Considerations
Both experts agreed that a specialist familiar with cervical cancer and chemoradiation is required to diagnose, treat, and monitor patients. A gynecologic oncologist would be required to diagnose and treat, while a radiology oncologist could prescribe radiation. A gynecologist, an oncologist, or a medical oncologist will be needed to access pembrolizumab.
Both experts noted that cancer centres and hospitals that specialize in managing cancer would be appropriate for administering pembrolizumab and CRT. According to 1 expert, initial therapy may be in a cancer centre, and subsequent maintenance could be at a satellite clinic that is closer to where patients live.
Clinician Group Input
This section was prepared by the review team based on the input provided by clinician groups.
Input from 2 clinician groups, the GOC and the OH (CCO) Gynecologic Cancer Drug Advisory Committee, were submitted for this review. The GOC is a nonprofit multidisciplinary organization comprising physicians, nurses, pharmacists, and scientists involved in the treatment and prevention of gynecologic cancer. OH (CCO) provides timely evidence-based clinical and health system guidance on drug-related issues, including the Provincial Drug Reimbursement Programs and the Systemic Treatment Program. Information was gathered for this submission through a review of published trials and direct clinical experience treating LACC.
The clinician groups indicated that for patients with LACC (stage II, III, and IVA), key treatment goals are to prolong OS and PFS while improving quality of life. The current standard of care for these patients, provided with curative intent, is concurrent cisplatin and pelvic EBRT followed by brachytherapy. Clinician groups agreed that this protocol, which has not been updated since its establishment in 1999, demonstrates only modest benefits in OS and PFS; OH (CCO) noted that the OS rate of patients with stage III to IVA cervical cancer is between 32% to 35% in Canada. Thus, the clinician groups highlighted a need for new treatments with improved OS and PFS for patients with stage III to IVA cervical cancer.
The clinician groups agreed that pembrolizumab would be used first-line for patients with FIGO 2014 stage III or IVA cervical cancer who are undergoing curative-intent therapy, regardless of nodal status, as a complement to chemoradiation. The clinician groups anticipated that approval of pembrolizumab would shift the current treatment paradigm, such that any eligible patient initiating chemoradiation would also receive pembrolizumab. The groups noted that with pembrolizumab as a first-line curative-intent therapy, it would not be appropriate to first try other treatments before initiating pembrolizumab with chemoradiation. The groups agreed that patients with newly diagnosed FIGO stage III (irrespective of nodal status) or stage IVA histologically confirmed squamous cell carcinoma, adenocarcinoma, or adenosquamous carcinoma of the cervix with no previous cancer-directed treatment are most likely to respond to treatment. The treatment is least suitable for those patients who are unable to tolerate radiation, chemotherapy, or immunotherapy.
According to the GOC, a clinically meaningful response to treatment would be defined as clinical and radiographic resolution of disease with tolerable toxicity. Clinician groups suggested using tumour imaging (per RECIST 1.1) to determine treatment response. However, the groups had slightly different suggestions on the schedule for follow-up. OH (CCO) suggested aligning the imaging follow-up schedule with the KEYNOTE-A18 trial, every 12 weeks for years 1 and 2, every 24 weeks in year 3, and once yearly thereafter. The GOC suggested initial imaging with a pelvic MRI or a CT or PET-CT scan, followed by tumour imaging 3 months after chemoradiation completion, and ongoing response assessments by clinical assessment and imaging every 3 to 6 months thereafter. Discontinuation should be considered in the event of disease progression, unacceptable toxicity (especially grade 4 immune-related events), or patient choice. Treatment would be administered as outpatient therapy in a comprehensive cancer setting by specialist physicians with experience in treating gynecologic cancer, including medical oncologists, radiation oncologists, or gynecologic oncologists.
Drug Program Input
The drug programs provide input on each drug being reviewed through the reimbursement review processes by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted for this review are summarized in Table 4.
Table 4: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical experts’ responses |
|---|---|
Relevant comparators | |
In the KEYNOTE-A18 trial, patients received 5 cycles every 3 weeks of concurrent platinum-based CRT plus pembrolizumab (or placebo) with an optional sixth dose at the investigator’s discretion, followed by 15 cycles of pembrolizumab monotherapy every 6 weeks. Could pERC confirm the recommended number of cycles for concurrent CRT plus pembrolizumab? | According to the clinical experts consulted, dosing and number of cycles for chemotherapy and radiation treatment outlined in the trial protocol aligns with clinical practice in Canada. Additional cycles for chemotherapy (up to 6 cycles) would be at the discretion of the practising physician. According to the experts, pembrolizumab administration in practice will align with the trial’s procedures. |
Considerations for initiation of therapy | |
The submitted indication uses the FIGO 2014 staging system to establish the stage III to IVA patient population. Does this align with the FIGO 2018 stage III to IVA patient population? Which FIGO edition is recommended by pERC for staging this patient population? | According to the clinical experts, the FIGO 2018 guidelines are currently in use in clinical practice in Canada. Patients with disease staged as IB2 according to the FIGO 2014 guidelines would now be considered stage IIIC per the FIGO 2018 guidelines. |
Are patients who receive pembrolizumab plus CRT in this setting eligible for downstream immunotherapy in the metastatic setting? What would be an appropriate disease-free interval? | The clinical experts noted that due to the lack of evidence on the use of this combination in the metastatic setting, they could not confirm whether downstream use of pembrolizumab would benefit patients or what the appropriate disease-free interval would be. |
Considerations for discontinuation of therapy | |
If progression occurs during a drug holiday, can treatment be resumed? | The experts indicated that treatment can be resumed if progression occurs during a drug holiday. They also indicated that radiotherapy is administered immediately after treatment with cisplatin. If chemotherapy is interrupted due to AEs or lack of tolerability, radiotherapy will be put on hold and administered once treatment resumes. |
If a patient cannot tolerate the chemotherapy combination, are they able to continue with pembrolizumab plus radiotherapy alone? | The experts indicated that pembrolizumab plus radiotherapy would be an option for patients who cannot tolerate the chemotherapy combination. |
Is there a minimum number of CRT cycles that must be given concurrently with pembrolizumab? | The experts did not consider that there is a minimum number of CRT cycles that must be given with pembrolizumab as the CRT cycles administered in practice will likely follow guidelines for standard of care, and pembrolizumab will be used in addition to CRT following the KEYNOTE-A18 trial’s procedures. |
Considerations for prescribing therapy | |
Pembrolizumab should be implemented using weight-based dosing up to a cap (e.g., 2 mg/kg every 3 weeks to a maximum dose of 200 mg or 4 mg/kg every 6 weeks to a maximum of 400 mg), similar to other indications. | This is a comment from the drug plans to inform pERC deliberations. |
Generalizability | |
Should patients with ECOG PS of 2 or greater be eligible? | The experts indicated that they would administer pembrolizumab plus CRT to patients with ECOG PS of 2 or greater. |
Should patients who are unable to tolerate platinum-based chemotherapy be eligible for pembrolizumab plus CRT using an alternative chemotherapy? | The experts considered that if patients are unable to tolerate cisplatin, they could receive another chemotherapy such as carboplatin or paclitaxel in combination with radiotherapy and pembrolizumab or pembrolizumab plus radiotherapy. |
Should pembrolizumab be added to the treatment patients are currently receiving or administered to those who have just completed receiving concurrent CRT? | The experts indicated that there is no evidence to support the addition of pembrolizumab for patients who have already initiated CRT because the patients participating in the KEYNOTE-A18 trial were naive to treatment before receiving the drug combination of interest. However, the experts noted that they would consider adding pembrolizumab to the ongoing treatment based on when patients in current practice began receiving CRT. |
Funding algorithm | |
Pembrolizumab in combination with bevacizumab and chemotherapy is indicated in the metastatic setting for cervical cancer. | This is a comment from the drug plans to inform pERC deliberations. |
Care provision issues | |
Preparation of pembrolizumab is familiar to many jurisdictions due to its use in other indications. | This is a comment from the drug plans to inform pERC deliberations. |
System and economic issues | |
Feasibility of adoption (budget impact), as this will become the new standard of care. | This is a comment from the drug plans to inform pERC deliberations. |
AE = adverse event; CRT = chemoradiotherapy; ECOG PS = Eastern Cooperative Oncology Group Performance Status; FIGO = Fédération internationale de gynécologie et d’obstétrique; pERC = pan-Canadian Oncology Drug Review Expert Review Committee.
Clinical Evidence
The objective of this Clinical Review Report is to review and critically appraise the clinical evidence submitted by the sponsor on the beneficial and harmful effects of pembrolizumab (200 mg every 3 weeks or 400 mg every 6 weeks, solution for infusion) in combination with CRT for the treatment of adult patients with FIGO 2014 stage III to IVA cervical cancer. The focus is on comparing pembrolizumab to relevant comparators and identifying gaps in the current evidence.
A summary of the clinical evidence included by the sponsor in the review of pembrolizumab is presented in this section, with the CDA-AMC critical appraisal of the evidence is in the Critical Appraisal subsection. The systematic review includes a pivotal study selected according to the sponsor’s systematic review protocol. The CDA-AMC assessment of the certainty of the evidence using the GRADE approach follows the critical appraisal of the evidence, in the GRADE Summary of Findings and Certainty of the Evidence subsection.
Included Studies
Clinical evidence from 1 RCT identified in the systematic review is appraised in this Clinical Review Report.
Systematic Review
The contents in this section have been informed by materials submitted by the sponsor. The following have been summarized and validated by the review team.
Description of Studies
Characteristics of the included studies are summarized in Table 5.
Table 5: Details of Study Included in the Systematic Review
Characteristic | KEYNOTE-A18 |
|---|---|
Designs and populations | |
Study design | Randomized, phase III, double-masked study |
Locations | 176 centres in 30 countries: Australia, Austria, Belgium, Brazil, Canada, Chile, China, Colombia, Czechia, France, Germany, Greece, Guatemala, Hungary, Ireland, Israel, Italy, Japan, South Korea, Norway, Peru, Russia, Spain, Sweden, Taiwan, Thailand, Türkiye, Ukraine, UK, and US |
Patient enrolment dates | Start date: May 12, 2020 End date: January 08, 2024 |
Randomized (N) | Primary analysis: A total of 1,060 eligible patients randomized, 529 to pembrolizumab plus CRT and 531 to placebo plus CRT FIGO stage III to IVA disease subgroup analysis: 601 randomized, 296 to pembrolizumab plus CRT and 305 to placebo plus CRT |
Inclusion criteria |
|
Exclusion criteria |
|
Intervention |
|
Comparator(s) |
|
Study duration | |
Screening phase | 42 days |
Treatment phase |
|
Follow-up phase | 4 or more (first interim analysis occurred at 28 months) |
Outcomes | |
Primary end point |
|
Secondary and exploratory end points | Secondary:
|
Publication status | |
Publications and presentations | Lorusso (2024_2),45 KEYNOTE-A18 CSRv02,46 KEYNOTE-A18 Health Technology Assessment Report,47 Duska (2024),48 Lorusso (2024_3),49 Lorusso (2023),44 Randall (2024),50 and Xiang (2024)51 |
BICR = blinded independent central review; CTLA-4 = cytotoxic T-lymphocyte–associated antigen 4; CRR = complete response rate; CRT = chemoradiotherapy; EBRT = external beam radiotherapy; ECOG PS = Eastern Cooperative Oncology Group Performance Status; EORTC QLQ-C30 GHS/QoL = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 Global Health Status/Quality of Life; EORTC QLQ-CX24 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Cervical Cancer Module; FIGO = Fédération internationale de gynécologie et d’obstétrique; LACC = locally advanced cervical cancer; ORR = objective response rate; OS = overall survival; OX40 = tumour necrosis factor receptor superfamily, member 4; PFS = progression-free survival; PFS2 = progression-free survival for subsequent anticancer therapy; q.3.w. = every 3 weeks; q.6.w. = every 6 weeks; RECIST 1.1 = Response Evaluation Criteria in Solid Tumours, version 1.1; VAS = visual analogue scale.
Data cut-off date: January 8, 2024.
Source: KEYNOTE-A18 Clinical Study Report v02.46 Details included in the table are from the sponsor’s Summary of Clinical Evidence.24
The KEYNOTE-A18 study is an ongoing randomized, double-masked, placebo-controlled, phase III trial and a sequential design with 2 interim analyses evaluating the efficacy and safety of concurrent pembrolizumab with and after CRT against placebo plus CRT in patients with newly diagnosed high-risk (FIGO 2014 stage IB2 to IIB node-positive disease or stage III to IVA disease regardless of node status) LACC.24 The coprimary outcomes assessed in the overall trial were PFS assessed by investigator or by histopathologic confirmation of suspected disease progression, per RECIST 1.1, and OS. Key secondary outcomes of interest for this review included HRQoL (using the EORTC QLQ-C30 GHS/QoL subscale) and safety.
Patients enrolled in the KEYNOTE-A18 study were randomized in a 1:1 ratio to pembrolizumab plus CRT followed by pembrolizumab and to placebo plus CRT followed by placebo.24 Randomization was stratified by planned type of external beam radiotherapy (intensity-modulated radiotherapy or volumetric-modulated arc therapy versus non–intensity-modulated radiotherapy and non–volumetric-modulated arc therapy), cervical cancer stage at screening (FIGO 2014 stage IB2 to IIB node-positive disease versus FIGO 2014 stage III to IVA disease regardless of node status, and planned total radiotherapy (EBRT plus brachytherapy) dose (< 70 Gy versus ≥ 70 Gy). The KEYNOTE-A18 study was conducted at 176 centres in 30 countries across Asia, Australia, Europe, North America (3 centres in Canada), and South America.24
The KEYNOTE-A18 study was designed with efficacy end points for the intention-to-treat primary population, which included patients with FIGO 2014 stage IB2 to IIB node-positive disease or stage III to IVA regardless of node status. The Health Canada indication is restricted to the FIGO 2014 stage III to IVA subgroup, which diverged from the trial design. The focus of the sponsor’s reimbursement request is patients with FIGO 2014 stage III to IVA disease, and this report presents efficacy findings of the FIGO 2014 stage III to IVA subgroup at interim analysis 2.24
Populations
Inclusion and Exclusion Criteria
The inclusion and exclusion criteria for the subgroup analysis were identical to the criteria used for the overall population, with the exception of limiting the population to patients with FIGO 2014 stage III to IVA cervical cancer (regardless of node status). Eligible patients were aged 18 years or older, and had newly diagnosed, high-risk (FIGO 2014 stage III to IVA, regardless of node status), locally advanced and histologically confirmed squamous cell carcinoma, adenocarcinoma, or adenosquamous carcinoma of the cervix. Eligible patients had not previously received any definitive surgical, radiation, or systemic therapy for cervical cancer, including investigational agents, and were immunotherapy naive. Previous surgical procedure for localized cervical tumour was allowed. Eligible patients had an Eastern Cooperative Oncology Group Performance Status (ECOG PS) score of 0 or 1, evaluable disease per RECIST 1.1, and adequate organ function.24
Patients were excluded if they had FIGO 2014 stage IVB disease; had a known additional malignancy that was progressing or had required active treatment within the past 3 years; had a diagnosis of immunodeficiency, received chronic systemic steroid therapy (in dosing exceeding 10 mg daily of prednisone equivalent), or any other form of immunosuppressive therapy within 7 days before the first dose of study medication; had received prior therapy with a PD-1, PD-L1, or anti–PD-L2 agent or with an agent directed to another stimulatory or coinhibitory T-cell receptor; and had received prior systemic anticancer therapy, including investigational agents, within 4 weeks before randomization.
Interventions
Patients in the pembrolizumab plus CRT arm received 5 cycles of pembrolizumab 200 mg every 3 weeks plus CRT, followed by 15 cycles of pembrolizumab 400 mg every 6 weeks. Patients in the placebo plus CRT arm received 5 cycles of placebo every 3 weeks plus CRT, followed by 15 cycles of placebo every 6 weeks. Pembrolizumab, placebo, and chemotherapy were administered intravenously.47
The interval between cycle 5 and cycle 6 was 3 weeks (± 3 days). Dosing every 6 weeks started from cycle 6. Chemotherapy, EBRT, and brachytherapy were administered during the every-3-week dosing regimen. Pembrolizumab or placebo infusions were continued during cisplatin or radiotherapy delay. On treatment days when both pembrolizumab or placebo and cisplatin were administered, it was preferable to administer pembrolizumab or placebo before cisplatin. If pembrolizumab-related AEs occurred, the dose could be withheld or discontinued, but not reduced.47
The CRT regimen included 5 cycles (with an optional sixth dose at the investigator’s discretion, per local protocol) of cisplatin 40 mg/m2 once weekly with concurrent pelvic EBRT, followed by brachytherapy to obtain maximal tumour regression. Cisplatin dose interruptions due to treatment-related toxicity were allowed as per local standard. Dose reductions to 30 mg/m2 were also allowed. The overall CRT treatment (including both EBRT and brachytherapy) had to be administered within 50 days of initiation (with an extension to a maximum of 56 days for unforeseen delays).47
Treatment was continued for the planned number of cycles for each treatment component or until radiographic progression, disease recurrence, unacceptable toxicity, confirmed positive pregnancy test, investigator decision, or participant withdrawal of consent.
Outcomes
A list of efficacy end points assessed in this Clinical Review Report is provided in Table 6. Summaries of the outcome measures are listed in Table 7. Summarized end points are based on outcomes included in the sponsor’s Summary of Clinical Evidence as well as any outcomes identified as important to this review by the consulted clinical expert(s) and according to input from patient and clinician groups and public drug plans. CDA-AMC selected those end points considered the most relevant to informing expert committee deliberations and finalized this list of end points in consultation with members of the expert committee. All summarized efficacy end points were assessed using the GRADE approach. Select notable harms outcomes considered important for informing expert committee deliberations were also assessed using the GRADE approach.
Table 6: Outcomes Summarized From the Study Included in the Systematic Review
Outcome measure | Time point | End point |
|---|---|---|
Survival outcomes | ||
PFS (investigator assessed) | 18, 24, and 30 months | Primary |
OS | 24, 30, and 36 months | Primary |
Health-related quality of life | ||
EORTC QLQ-C30 GHS/QoL | Week 36 | Secondary |
Safety | ||
Serious adverse events | Interim analysis | Secondary |
Discontinuation due to immune-related adverse events | Interim analysis | Secondary |
EORTC QLQ-C30 GHS/QoL= European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 Global Health Status/Quality of Life; OS = overall survival; PFS = progression-free survival.
Data cut-off date: January 8, 2024.
Sources: KEYNOTE-A18 Clinical Study Report v0246 and KEYNOTE-A18 Health Technology Assessment Report.47 Details included in the table are from the sponsor’s Summary of Clinical Evidence.24
Efficacy Outcomes
Progression-Free Survival and Overall Survival
PFS, assessed per RECIST 1.1 by investigator review or by histopathologic confirmation of suspected progression, was the primary end point. PFS was defined as the time from randomization to the first documented disease progression or death due to any cause, whichever occurred first. Images were submitted to a contracted imaging research organization and underwent BICR to minimize bias in response assessments. In addition, the final determination of radiologic progression was based on the central assessment of progression, rather than a local site investigator or radiology assessment.52
OS was defined as the time from randomization to death due to any cause.
European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30
The EORTC QLQ-C30 is widely used to assess the quality of life of patients living with cancer. The EORTC QLQ-C30 contains 30 items and measures 5 functional dimensions (physical, role, emotional, cognitive, and social), 3 symptom items (fatigue, nausea/vomiting, and pain), and 6 single items (dyspnea, sleep disturbance, appetite loss, constipation, diarrhea, and financial impact) and has a global health status and quality of life subscale. The EORTC QLQ-C30 is a psychometrically and clinically validated instrument appropriate for assessing quality of life in oncology studies.52 The EORTC QLQ-C30 uses a 1-week recall period to assess functional status and symptoms. All scales and single-item measures are scored from 0 to 100. Most questions have 4 response options (“not at all,” “a little,” “quite a bit,” or “very much”), with scores on these items ranging from 1 to 4. For the 2 items that form the global HRQoL scale, the response format is a 7-point Likert-type scale with anchors at 1 (equivalent to “very poor”) and 7 (equivalent to “excellent”). Raw scores for each scale are computed as the average of the items that contribute to a particular scale. Scale sum scores are transformed such that a high score on the functional scales represents a high or healthy level of functioning, a high score on the symptom scales represents a high level of symptomatology, and a high score on the global health status and quality of life subscale represents a high HRQoL. According to the EORTC QLQ-C30 scoring algorithm, if items on a scale are missing (i.e., the participant did not provide a response), the score for the scale can still be computed if there are responses for at least half of the items. The values for missing items are interpolated with the average of the respondent-completed items (Table 7).53
Harms Outcomes
Safety outcomes of interest were AEs, SAEs, death due to AEs, adverse events of special interest (AESIs), and study treatment discontinuations due to AEs. AEs and laboratory abnormalities were graded according to the National Cancer Institute Common Terminology Criteria for Adverse Events, version 5.0. The AEs and SAEs included were reported from time of randomization to treatment through 90 days after the last study treatment dose or 30 days after discontinuation of study treatment if the patient initiated a new anticancer treatment, whichever occurred first. Deaths due to AEs were considered grade 5 AEs. Discontinuations due to AEs included permanent discontinuations of any study treatment due to any toxicity specified as a reason for the permanent discontinuation, as defined in the Common Terminology Criteria for Adverse Events, version 5.0 guidelines for dose modification due to AEs. AESIs were immune-mediated events and infusion-related reactions associated with pembrolizumab reported from the time of randomization through 90 days after the last dose of study treatment or 30 days after discontinuation of study treatment if the patient initiated a new anticancer treatment, whichever occurred first.52
Table 7: Summary of the Outcome Measures and Their Measurement Properties in the Study Included in the Systematic Review
Outcome measure | Type | Conclusions about measurement properties | MID |
|---|---|---|---|
EORTC QLQ-C30 | The EORTC QLQ-C30 is a widely used cancer-specific HRQoL instrument that contains 30 items and measures 5 functional dimensions (physical, role, emotional, cognitive, and social), 3 symptom items (fatigue, nausea/vomiting, and pain), and 6 single items (dyspnea, sleep disturbance, appetite loss, constipation, diarrhea, and financial impact) and includes a Global Health Status/Quality of Life subscale. | The validity, reliability, and responsiveness of the EORTC QLQ-C30 for use among patients with cancer is well-documented. In a 2021 study of Kenyan patients with cervical cancer, the EORTC QLQ-C30 demonstrated reliability (Cronbach alpha coefficient 0.72 to 0.95) and clinical validity (interscale correlations statistically significant).54 While fewer studies have assessed the psychometric performance of the EORTC QLQ-C30 in populations with cervical cancer populations, they have shown some evidence of its validity, reliability, and responsiveness across diverse settings (China, Kenya, and multinational studies). Construct validity: The tool has shown success in distinguishing between early and advanced disease stages.54,55 Reliability: The tool has been shown to have high internal consistency across domains, with alpha ≥ 0.70 for functional and symptom scales.54 Responsiveness: There is limited longitudinal evidence of responsiveness to change with the QLQ-C30, but it has shown some sensitivity to clinical changes during treatment in oncological settings, particularly in the global health, nausea/vomiting, and fatigue scales.56 | In a study of 21 published EORTC phase III trials of 9 cancer types (brain, colorectal, advanced breast, head/neck, lung, mesothelioma, melanoma, ovarian, and prostate), anchor-based MIDs generally ranged between 5 and 10 points.57 Distribution-based MIDs ranged between 4 and 11 points per cancer type.57 |
EORTC QLQ-CX24 | The EORTC QLQ-CX24 is a disease-specific module of the EORTC QLQ that is used to measure quality of life of patients with cervical cancer. The EORTC QLQ-CX24 consists of 24 items classified into 3 multi-item scales, 11 items with symptom experience domain, 3 items with body image domain, and 4 items with sexual/vaginal functioning domain. The other domains of the questionnaire are single-item scales, including lymphedema, peripheral neuropathy, menopausal symptoms, sexual worry, sexual activity, and sexual enjoyment. | Multiple studies with patients with cervical cancer have demonstrated the validity, reliability, and responsiveness of the EORTC QLQ-CX24.55,56,58-60 Validity: Some scale scores (e.g., menopausal symptoms) have been shown to correlate appropriately with disease stage.55,56 Reliability: The tool has shown high internal consistency (alpha ≥ 0.70) across many multi-item scales.54,56 Responsiveness: There is limited longitudinal evidence for the EORTC QLQ-CX24; however, some studies have reported its ability to detect meaningful changes in domains over time, with sensitivity to long-term treatment effects.56 | No MID was identified. |
EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; EORTC QLQ-CX24 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Cervical Cancer Module; HRQoL = health-related quality of life; MID = minimal important difference.
Source: KEYNOTE-A18 Clinical Study Report v02.46 Details included in the table are from the sponsor’s Summary of Clinical Evidence.24
Statistical Analysis
Subgroup FIGO 2014 Stage III to IVA Disease
The statistical analysis plan of the KEYNOTE-A18 study was designed to assess the superiority of pembrolizumab plus CRT compared to placebo plus CRT in patients with high-risk LACC. Given that the subgroup analyses by disease stage in the primary analysis of the KEYNOTE-A18 study suggested favourable PFS and OS at interim analysis 2 for the subgroup with FIGO stage III to IVA cervical cancer regardless of node status, regulatory review at Health Canada is limited to this subpopulation. To align with regulatory approval requirements, post hoc analyses were conducted and presented to supplement the current reimbursement request for this population.
Sample Size and Power Calculation
There were no predefined sample size and power calculations for OS and PFS for the subgroup with FIGO stage III to IVA cervical cancer.52
Statistical Testing
No formal hypothesis tests and alpha allocations were predefined for the subgroup with FIGO stage III to IVA cervical cancer.
Time-to-event end points in the subgroup were estimated using nonparametric Kaplan-Meier methodology, with Cox proportional hazards models using Efron's method for tie handling and treatment as a covariate to assess differences between arms (HR and 95% CI). One-sided P values were calculated using log-rank tests for OS and PFS (Table 8).
In the primary analysis for overall population, the overall type I error rate over the multiple analyses of end points in the primary analysis was controlled at 2.5% (1-sided) with initially 1.25% allocated to test PFS superiority and 1.25% allocated to test OS superiority. No multiplicity adjustments were conducted for the subgroup.
For PFS, the true date of disease progression was approximated by the date of the first assessment at which progressive disease was objectively documented per RECIST 1.1 (based on BICR for primary analysis). Death was considered a confirmed progressive disease event. Participants who did not experience a PFS event were censored at the last disease assessment. A similar analysis was performed for comparisons of PFS based on investigator assessment.
For OS, patients without a documented death at the time of analysis were censored at the date of last known contact. A restricted mean survival time method was performed for OS to account for possible nonproportional hazards effect.52
In alignment with the primary analysis, HRQoL assessments were also conducted in the FIGO 2014 stage III to IVA disease subgroup. A constrained longitudinal data analysis model was used, with the patient-reported outcome score as the response variable and the treatment-by-time interaction and stratification factors as covariates. LSM changes from baseline were summarized. Group-wise comparisons were performed, and the model-based LSM score was provided by treatment arm and study visit.52
Data Imputation Methods
There were no reports on how missing data were handled in the subgroup analysis.
Sensitivity Analysis
No sensitivity analyses assessing the robustness of PFS results in the subgroup analysis were reported. However, the robustness of PFS results was assessed in the primary overall patient population through sensitivity analyses. Sensitivity analysis 1 considered progressive disease or deaths as events regardless of missed study visits or initiation of new anticancer therapy, and sensitivity analysis 2 considered discontinuation of treatment or initiation of an anticancer treatment subsequent to discontinuation of study-specified treatments, whichever occurred later, as a progressive disease event for patients without documented progressive disease or death.52
Table 8: Statistical Analysis of Efficacy End Points in the FIGO Stage III to IVA Disease Subgroup in the KEYNOTE-A18 Study
End point | Statistical model | Adjustment factors | Handling of missing data | Sensitivity analyses |
|---|---|---|---|---|
PFS | Survival curve estimated using the Kaplan-Meier product-limit method. Magnitude of difference between treatment arms estimated using Cox proportional hazards model with Efron’s method of tie handling. One-sided P values based on log-rank test. | Treatment used as covariate in Cox model. | Not reported | Not reported |
OS | Survival curve estimated using the Kaplan-Meier product-limit method. Magnitude of difference between treatment arms estimated using Cox proportional hazards model with Efron’s method of tie handling. One-sided P values based on log-rank test. | Treatment used as covariate in Cox model. | Not reported | Not reported |
HRQoL | HRQoL assessed using a constrained longitudinal data analysis, with the patient-reported outcome score as the response variable and the treatment-by-time interaction and stratification factors as covariates. Stratified log-rank test and HR estimation using stratified Cox model with Efron’s method of tie handling. | Not reported | Not reported | Not reported |
FIGO = Fédération internationale de gynécologie et d’obstétrique; HR = hazard ratio; HRQoL = health-related quality of life; OS = overall survival; PFS = progression-free survival.
Data cut-off date: January 8, 2024.
Source: Sponsor’s Summary of Clinical Evidence.24
Analysis Populations
A summary of the analysis populations for the FIGO 2014 stage III to IVA disease subgroup population of the KEYNOTE-A18 study is available in Table 9.
Table 9: Analysis Populations of the FIGO 2014 Stage III to IVA Disease Subgroup in the KEYNOTE-A18 Study
Population | Definition | Application |
|---|---|---|
ITT population | All randomized participants were included in this population. Participants were analyzed in the treatment arm to which they were randomized. | Efficacy end points |
APaT population | The APaT population consisted of all randomized and allocated participants who received at least 1 dose of study treatment. | Safety end points |
PRO population | Included all participants who have at least 1 PRO assessment available and have received at least 1 dose of study medication. | HRQoL end points |
APaT = all participants as treated; FIGO = Fédération internationale de gynécologie et d’obstétrique; HRQoL = health-related quality of life; ITT = intention to treat; PRO = patient-reported outcome.
Source: Sponsor’s Summary of Clinical Evidence.24
Results
Patient Disposition
At the interim analysis 2 data cut-off (January 8, 2024), of the 1,060 patients randomized in the KEYNOTE-A18 study, 601 (56.7%) were included in FIGO 2014 stage III to IVA intention-to-treat subgroup. Table 10 presents patient disposition in the FIGO stage III to IVA disease subgroup. In total, 296 patients were included in the pembrolizumab plus CRT arm and 305 patients in the placebo plus CRT arm. In total, 17.9% of patients in the pembrolizumab plus CRT arm and 25.9% of patients in the placebo plus CRT arm stopped participating in the KEYNOTE-A18 study. A higher proportion of participants in the placebo plus CRT group (46.7%) than in the pembrolizumab plus CRT group (39.7%) discontinued the study intervention. The most frequent reasons for discontinuing all study interventions in both treatment arms were radiographic progression and AEs. Completion rates were 43.4% in the pembrolizumab plus CRT arm versus 35.9% in the placebo plus CRT arm. Patient disposition in the overall population of the KEYNOTE-A18 study is presented in Table 17, Appendix 1.
Table 10: Patient Disposition in the FIGO 2014 Stage III to IVA Disease Subgroup in the KEYNOTE-A18 Study (ITT Population)
Disposition | Pembrolizumab plus CRT (N = 296) | Placebo plus CRT (N = 305) |
|---|---|---|
Discontinued trial, n(%) | 53 (17.9) | 79 (25.9) |
Death | 41 (13.9) | 73 (23.9) |
Lost to follow-up | 2 (0.7) | 1 (0.3) |
Patients who withdrew from trial | 10 (3.4) | 5 (1.6) |
Completed study treatment, n (%) | 128 (43.4) | 109 (35.9) |
Discontinued treatment, n (%) | 117 (39.7) | 142 (46.7) |
AE | 33 (11.2) | 15 (4.9) |
Clinical progression | 3 (1.0) | 7 (2.3) |
Excluded medication | 1 (0.3) | 0 (0.0) |
Lost to follow-up | 1 (0.3) | 0 (0.0) |
Noncompliance with study drug | 3 (1.0) | 1 (0.3) |
Non–study anticancer therapy | 1 (0.3) | 0 (0.0) |
Physician decision | 6 (2.0) | 4 (1.3) |
Progressive disease | 0 | 4 (1.3) |
Protocol violation | NR | NR |
Radiographic progression | 57 (19.3) | 94 (30.9) |
Withdrawal of patient | 12 (4.1) | 17 (5.6) |
Patients still ongoing | 243 (82.1) | 226 (74.1) |
ITT, N (%) | 601 | |
Safety, N (APaT) | 599 | |
AE = adverse event; APaT = all participants as treated; CRT = chemoradiotherapy; FIGO = Fédération internationale de gynécologie et d’obstétrique; ITT = intention to treat; NR = not reported.
Data cut-off date: January 8, 2024.
Source: Sponsor’s Summary of Clinical Evidence.24
Baseline Characteristics
Demographic and baseline disease characteristics of participants in the FIGO 2014 stage III to IVA disease subgroup are presented in Table 11. Baseline characteristics and demographics were generally similar in the treatment arms. Of the patients with known CPS tumour status, 93.9% in the pembrolizumab plus CRT arm and 92.1% in the placebo plus CRT arm had CPS greater than or equal to 1.24 All the participants were assigned female sex at birth. The majority were younger than 65 years (85.8% versus 81.3% ); were Asian (35.1% versus 32.5%, respectively) or white (35.1% versus 37.0%); had a baseline ECOG PS of 0 (65.5% versus 69.5%); had squamous histology subtype (82.4% versus 84.6%); and had positive pelvic and/or para-aortic lymph node involvement (72.0% versus 69.5%) in the pembrolizumab plus CRT and placebo plus CRT arms, respectively.
These demographic and baseline disease characteristics were in line with those of the overall primary population in the KEYNOTE-A18 study (refer to Table 18, Appendix 1).
Table 11: Summary of Baseline Disease Characteristics of FIGO 2014 Stage III to IVA Disease Subgroup in the KEYNOTE-A18 Study (ITT Population)
Characteristic | Pembrolizumab plus CRT (N = 296) | Placebo plus CRT (N = 305) |
|---|---|---|
Sex, n (%) | ||
Female | 296 (100.0) | 305 (100.0) |
Age (years), n (%) | ||
< 65 | 254 (85.8) | 248 (81.3) |
≥ 65 | 42 (14.2) | 57 (18.7) |
Race, n (%) | ||
American Indian or Alaska Native | 21 (7.1) | 20 (6.6) |
Asian | 104 (35.1) | 99 (32.5) |
Black or African American | 6 (2.0) | 3 (1.0) |
Multiple | 60 (20.3) | 69 (22.6) |
Native Hawaiian or Other Pacific Islander | 1 (0.3) | 1 (0.3) |
White | 104 (35.1) | 113 (37.0) |
Geographic region, n (%) | ||
Asia Pacific | 103 (34.8) | 99 (32.5) |
EMEA | 70 (23.6) | 78 (25.6) |
Latin America | 109 (36.8) | 111 (36.4) |
North America | 14 (4.7) | 17 (5.6) |
Baseline ECOG PS, n (%) | ||
0 | 194 (65.5) | 212 (69.5) |
1 | 102 (34.5) | 93 (30.5) |
Presence of lymph node, n (%) | ||
Positive pelvic and/or para-aortic | 213 (72.0) | 212 (69.5) |
No positive pelvic nor para-aortic | 83 (28.0) | 93 (30.5) |
Histology subtype, n (%) | ||
Nonsquamous | 52 (17.6) | 47 (15.4) |
Squamous | 244 (82.4) | 258 (84.6) |
Planned type of EBRT, n (%) | ||
IMRT or VMAT | 255 (86.1) | 264 (86.6) |
non-IMRT and non-VMAT | 41 (13.9) | 41 (13.4) |
Planned total radiation therapy dose per EQD2, n (%) | ||
< 70 Gy | 32 (10.8) | 29 (9.5) |
≥ 70 Gy | 264 (89.2) | 276 (90.5) |
PD-L1 status, n (%) | ||
CPS < 1 | 14 (4.7) | 20 (6.6) |
CPS ≥ 1 | 278 (93.9) | 281 (92.1) |
Missing | 4 (1.4) | 4 (1.3) |
CPS = combined positive score; CRT = chemoradiotherapy; EBRT = external beam radiotherapy; ECOG PS = Eastern Cooperative Oncology Group Performance Status; EMEA = Europe, the Middle East, and Africa; EQD2 = equivalent dose in 2-Gy fractions; FIGO = Fédération internationale de gynécologie et d’obstétrique; IMRT = intensity-modulated radiotherapy; ITT = intention to treat; VMAT = volumetric-modulated arc therapy.
Data cut-off date: January 8, 2024.
Source: Sponsor’s Summary of Clinical Evidence.24
Exposure to Study Treatments
At interim analysis 2, the median duration of therapy in the FIGO 2014 stage III to IVA subpopulation was 20.04 months (range, 0.39 months to 31.74 months) in the pembrolizumab plus CRT arm and 15.97 months (range, 0.13 months to 31.87 months) in the placebo plus CRT arm (Table 12). Patients in the pembrolizumab plus CRT arm received a higher median number of treatment cycles (17.0 versus 15.0 for the placebo plus CRT arm). Treatment adherence was comparable in both arms, with mean rates of 99.4% and 99.9%, respectively.24 Patient exposure to treatments in the overall population in the KEYNOTE-A18 study is presented in Table 19, Appendix 1.
Table 12: Treatment Exposure in the FIGO 2014 Stage III to IVA Disease Subgroup in the KEYNOTE-A18 Study (ITT Population)
Exposure | Pembrolizumab plus CRT | Placebo plus CRT |
|---|---|---|
na | 295 | 304 |
Duration of all therapy (months)b | ||
Mean (SD) | 16.48 (8.27) | 15.04 (8.32) |
Median (range) | 20.04 (0.39 to 31.74) | 15.97 (0.13 to 31.87) |
Number of cycles of pembrolizumab or placebo | ||
Mean (SD) | 14.67 (6.05) | 13.70 (6.08) |
Median (range) | 17.00 (1.00 to 20.00) | 15.00 (1.00 to 20.00) |
Adherence (% of actual vs. expected doses administered), mean (SD)c | 99.4 (2.53) | 99.9 (1.16) |
Number of cisplatin administrations | ||
Mean (SD) | 4.98 (0.82) | 4.94 (0.92) |
Median (range) | 5 (1.0 to 7.0) | 5 (1.0 to 7.0) |
Duration of exposure by EBRT (days) | ||
Mean (SD) | 39.41 (7.66) | 39.47 (11.29) |
Median (range) | 37 (12 to 102) | 37 (4 to 143) |
Duration of exposure on brachytherapy (days) | ||
na | 286 | 285 |
Mean (SD) | 13.36 (6.50) | 13.29 (5.54) |
Median (range) | 12 (1.0 to 74.0) | 13 (2.0 to 57.0) |
Exposure to treatment by duration (months), n (%) | ||
> 0 | 295 (100.0) | 304 (100.0) |
≥ 1 | 294 (99.7) | 299 (98.4) |
≥ 3 | 273 (92.5) | 281 (92.4) |
≥ 6 | 242 (82.0) | 246 (80.9) |
≥ 12 | 207 (70.2) | 188 (61.8) |
≥ 18 | 158 (53.6) | 140 (46.1) |
≥ 24 | 37 (12.5) | 22 (7.2) |
CRT = chemoradiotherapy; EBRT = external beam radiotherapy; FIGO = Fédération international de gynécologie et d’obstétrique; ITT = intention to treat; SD = standard deviation; vs. = versus.
aNumber of patients with available information.
bDuration of exposure is the time from the date of the first dose to the date of the last dose.
cDefined as the actual number of doses received divided by the expected number of doses and then multiplied by 100. Pembrolizumab was administered every 3 weeks for 5 infusions (5 cycles) and then every 6 weeks for 15 infusions (15 cycles). The expected number of doses that participants would have received up to the data cut-off date was based on the protocol-specified interval for administering each treatment component, given that the participant continues to receive treatment. The expected number of doses was limited to the maximum number of doses that a participant could receive as per study protocol. The expected number of dose administrations per participant for all cycles was calculated as a sum of expected number of dose administrations in cycles 1 to 5 and cycles 6+.
Data cut-off date: January 8, 2024.
Source: Sponsor’s Summary of Clinical Evidence.24
Concomitant Medications and Cointerventions
Concomitant medication and intervention use was generally similar in the 2 treatment arms, except for the following medication categories, where incidence was 5 or more percentage points higher in the pembrolizumab plus CRT arm compared to the placebo plus CRT arm: antidiarrheals, intestinal anti-inflammatory or anti-infective agents (67.5% versus 55.6%); sex hormones and modulators of the genital system (16.9% versus 11.5%); antihistamines for systemic use (50.8% versus 43.1%), thyroid therapy (28.8% versus 12.5%); all other nontherapeutic products (51.9% versus 45.1%); and homeopathic preparations (70.2% versus 59.5%) (Table 13).24
In the overall population in the KEYNOTE-A18 study, concomitant medication use was generally well-balanced in the pembrolizumab plus CRT and the placebo plus CRT arms (Appendix 1).
Subsequent Treatment
In the FIGO 2014 stage III to IVA subgroup, a smaller proportion of patients in the pembrolizumab plus CRT arm required subsequent antineoplastic therapy compared to the placebo plus CRT arm (15.9% versus 27.6%) (Table 14). The most commonly used (≥ 5% in any treatment arm) subsequent therapies were paclitaxel (13.9% versus 24.3%), carboplatin (11.2% versus 20.1%), bevacizumab (7.1% versus 10.5%), cisplatin (3.7% versus 6.3%), and pembrolizumab (1.4% versus 6.3%) in the pembrolizumab plus CRT arm versus the placebo plus CRT arm, respectively.24 Subsequent oncology treatments reported in the overall population of the KEYNOTE-A18 study were consistent with the subgroup population (Table 20, Appendix 1).
Table 13: Concomitant Medication Use (Incidence > 0% in 1 or Both Treatment Arms) in the FIGO 2014 III to IVA Disease Subgroup in the KEYNOTE-A18 Study (APaT Population)
Characteristic | Pembrolizumab plus CRT (N = 295) | Placebo plus CRT (N = 304) |
|---|---|---|
Patients in the population, n (%) | ||
With 1 or more concomitant medications | 295 (100.0) | 302 (99.3) |
With no concomitant medication | 0 | 2 (0.7) |
Antidiarrheal, intestinal anti-inflammatory, and anti-infective agents | 199 (67.5) | 169 (55.6) |
Antiemetics and antinauseants | 285 (96.6) | 289 (95.1) |
Drugs for acid-related disorders | 214 (72.5) | 221 (72.7) |
Drugs for constipation | 221 (74.9) | 219 (72.0) |
Drugs for functional gastrointestinal disorders | 166 (56.3) | 165 (54.3) |
Drugs used in diabetes | 34 (11.5) | 41 (13.5) |
Mineral supplements | 222 (75.3) | 229 (75.3) |
Other alimentary tract and metabolism products | 50 (16.9) | 76 (25.0) |
Stomatologic preparations | 279 (94.6) | 275 (90.5) |
Vitamins | 81 (27.5) | 79 (26.0) |
Antibacterials for systemic use | 193 (65.4) | 189 (62.2) |
Antimycotics for systemic use | 15 (5.1) | 16 (5.3) |
Antivirals for systemic use | 21 (7.1) | 22 (7.2) |
Vaccines | 62 (21.0) | 61 (20.1) |
Antineoplastic agents | 31 (10.5) | 35 (11.5) |
Bevacizumab | 1 (0.3) | 2 (0.7) |
Carboplatin | 2 (0.7) | 2 (0.7) |
Celecoxib | 24 (8.1) | 28 (9.2) |
Fluorouracil | 1 (0.3) | 0 (0.0) |
Methotrexate | 1 (0.3) | 0 (0.0) |
Methotrexate sodium | 1 (0.3) | 0 (0.0) |
Paclitaxel | 1 (0.3) | 3 (1.0) |
Pembrolizumab | 0 (0.0) | 1 (0.3) |
Propranolol | 2 (0.7) | 1 (0.3) |
Trastuzumab | 1 (0.3) | 1 (0.3) |
Tretinoin | 1 (0.3) | 0 (0.0) |
Endocrine therapy | 34 (11.5) | 24 (7.9) |
Anastrozole | 1 (0.3) | 0 (0.0) |
Estradiol | 6 (2.0) | 5 (1.6) |
Estradiol cypionate | 1 (0.3) | 1 (0.3) |
Estrogens | 1 (0.3) | 1 (0.3) |
Estrogens conjugated | 2 (0.7) | 1 (0.3) |
Medroxyprogesterone acetate | 5 (1.7) | 3 (1.0) |
Megestrol acetate | 20 (6.8) | 13 (4.3) |
Relugolix | 0 (0.0) | 1 (0.3) |
Immunostimulants | 114 (38.6) | 114 (37.5) |
Filgrastim | 59 (20.0) | 62 (20.4) |
Glutathione | 14 (4.7) | 14 (4.6) |
Granulocyte colony–stimulating factor | 47 (15.9) | 43 (14.1) |
Granulocyte-macrophage colony–stimulating factor | 2 (0.7) | 2 (0.7) |
Inosine | 4 (1.4) | 9 (3.0) |
Lenograstim | 4 (1.4) | 2 (0.7) |
Leucogen | 9 (3.1) | 10 (3.3) |
Methyluracil | 4 (1.4) | 9 (3.0) |
Antianemic preparations | 130 (44.1) | 116 (38.2) |
Antihemorrhagics | 88 (29.8) | 76 (25.0) |
Antithrombotic agents | 75 (25.4) | 72 (23.7) |
Blood substitutes and perfusion solutions | 246 (83.4) | 240 (78.9) |
Antihypertensives | 121 (41.0) | 121 (39.8) |
Beta-blocking agents | 36 (12.2) | 21 (6.9) |
Calcium channel blockers | 39 (13.2) | 33 (10.9) |
Cardiac therapy | 89 (30.2) | 85 (28.0) |
Diuretics | 101 (34.2) | 87 (28.6) |
Vasoprotective drugs | 257 (87.1) | 264 (86.8) |
Antibiotics and chemotherapeutics for dermatologic use | 136 (46.1) | 128 (42.1) |
APaT = all participants as treated; CRT = chemoradiotherapy; FIGO = Fédération internationale de gynécologie et d’obstétrique.
Data cut-off date: January 8, 2024.
Source: Sponsor’s Summary of Clinical Evidence.24
Table 14: Subsequent Oncologic Therapies Administered in the FIGO 2014 Stage III to IVA Disease Subgroup in the KEYNOTE-A18 Study (ITT Population)
Drug | Pembrolizumab plus CRT (N = 295) | Placebo plus CRT (N = 304) |
|---|---|---|
Antineoplastic agents, n (%) | 47 (15.9) | 84 (27.6) |
Bevacizumab | 21 (7.1) | 32 (10.5) |
Cadonilimab | 2 (0.7) | 1 (0.3) |
Capecitabine | 1 (0.3) | 0 (0.0) |
Carboplatin | 33 (11.2) | 61 (20.1) |
Catequentinib | 2 (0.7) | 0 (0.0) |
Cemiplimab | 1 (0.3) | 2 (0.7) |
Cisplatin | 11 (3.7) | 19 (6.3) |
Cyclophosphamide | 0 (0.0) | 1 (0.3) |
Docetaxel | 1 (0.3) | 1 (0.3) |
Doxorubicin | 1 (0.3) | 1 (0.3) |
Doxorubicin hydrochloride | 1 (0.3) | 0 (0.0) |
Gemcitabine | 1 (0.3) | 9 (3.0) |
Gemcitabine hydrochloride | 1 (0.3) | 1 (0.3) |
Irinotecan | 0 (0.0) | 1 (0.3) |
Marsdenia tenacissima stem | 0 (0.0) | 1 (0.3) |
Paclitaxel | 41 (13.9) | 74 (24.3) |
Paclitaxel nanoparticle albumin-bound | 2 (0.7) | 9 (3.0) |
Pembrolizumab | 4 (1.4) | 19 (6.3) |
Pemetrexed disodium | 1 (0.3) | 0 (0.0) |
Sintilimab | 1 (0.3) | 0 (0.0) |
Tisotumab vedotin | 1 (0.3) | 0 (0.0) |
Topotecan | 3 (1.0) | 2 (0.7) |
Topotecan hydrochloride | 0 (0.0) | 1 (0.3) |
Vincristine | 0 (0.0) | 1 (0.3) |
Vinorelbine tartrate | 0 (0.0) | 1 (0.3) |
Zimberelimab | 0 (0.0) | 1 (0.3) |
Endocrine therapy, n (%) | ||
Anastrozole | 1 (0.3) | 0 (0.0) |
CRT = chemoradiotherapy; FIGO = Fédération internationale de gynécologie et d’obstétrique; ITT = intention to treat.
Data cut-off date: January 8, 2024.
Source: Sponsor’s Summary of Clinical Evidence.24
Efficacy
Progression-Free Survival
At interim analysis 2, the HR for PFS based on investigator assessment was 0.57 (95% CI, 0.43 to 0.76, P < 0.0001) in the FIGO 2014 stage III to IVA disease subgroup. The median PFS was not reached in the pembrolizumab plus CRT arm and not reached (95% CI, 26.3 to not reached) in the placebo plus CRT group. The Kaplan-Meier estimated between-group differences in PFS probabilities at 18, 24, and 30 months were 14.8% (95% CI, 7.3% to 22.2%), 16.0% (95% CI, 7.9% to 24.0%), and 17.9% (95% CI, 9.4% to 26.5%), respectively, in favour of pembrolizumab plus CRT (Table 15). These findings were confirmed by the BICR assessment (HR = 0.60; 95% CI, 0.44 to 0.82) and were also consistent with the primary analysis of the overall population (Table 21, Appendix 1).24
Figure 1: Kaplan-Meier Estimates of PFS (Primary Censoring Rule) per Investigator Assessment in the FIGO 2014 Stage III to IVA Disease Subgroup in the KEYNOTE-A18 Study (ITT Population)
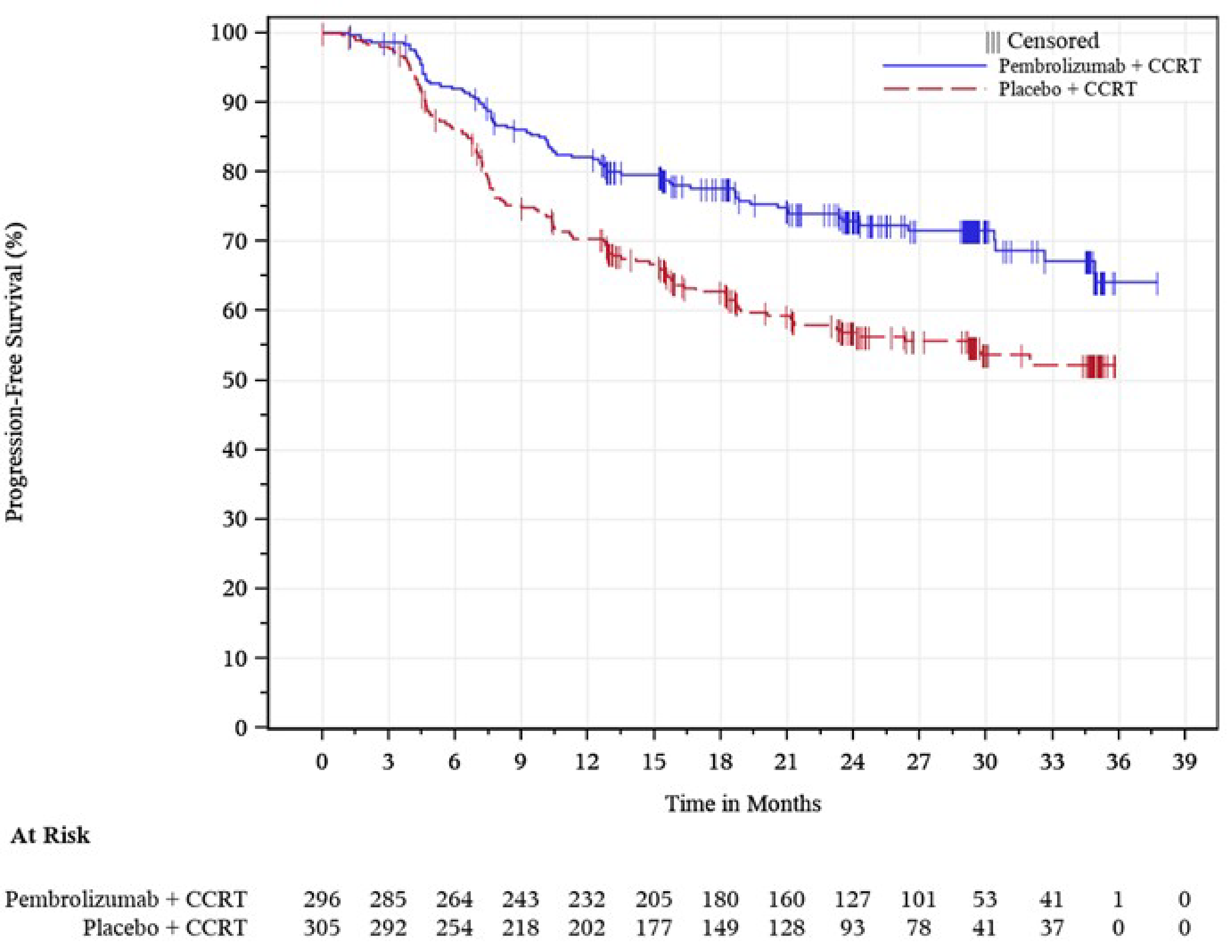
CCRT = cisplatin chemoradiotherapy; CRT = chemoradiotherapy; FIGO = Fédération internationale de gynécologie et d’obstétrique; ITT = intention to treat; PFS = progression-free survival.
Data cut-off date: January 08, 2024.
Source: Sponsor’s Summary of Clinical Evidence.24
Overall Survival
At interim analysis 2, the HR for OS was 0.57 (95% CI, 0.39 to 0.83; nominal P = 0.0016) in the FIGO 2014 stage III to IVA disease subpopulation. The Kaplan-Meier estimated between-group differences in OS probabilities at 24, 30, and 36 months were 8.9% (95% CI, 2.5% to 15.3%), 11.9% (95% CI, 4.7% to 19.2%), and 11.5% (95% CI, 3.5% to 19.5%), respectively, in favour of pembrolizumab plus CRT (Table 15).24 These findings were consistent with the primary analysis of the overall population (Table 21, Appendix 1).
Figure 2: Kaplan-Meier Estimates of OS in the FIGO 2014 Stage III to IVA Disease Subgroup in the KEYNOTE-A18 Study (ITT Population)
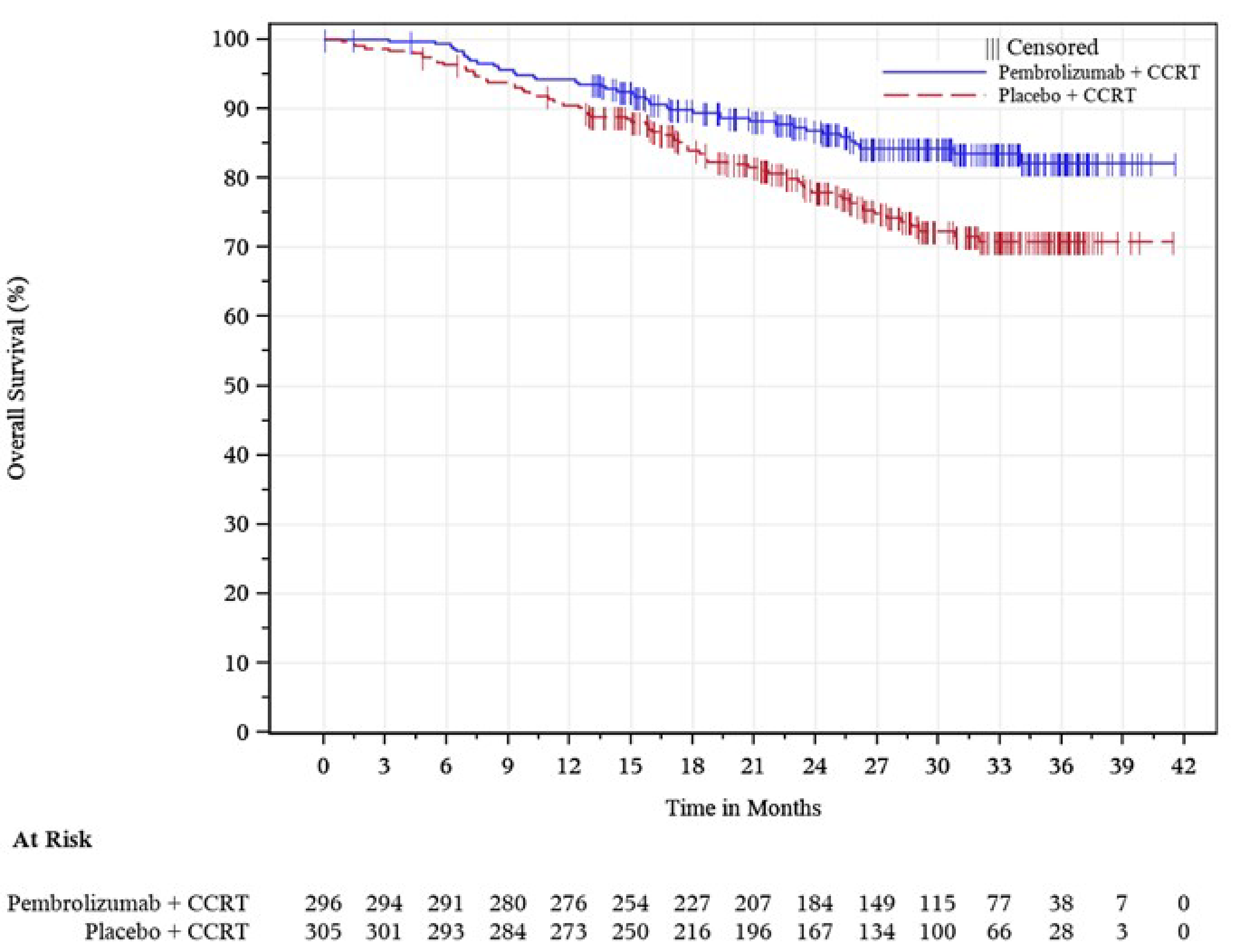
CCRT = cisplatin chemoradiotherapy; CRT = chemoradiotherapy; FIGO = Fédération internationale de gynécologie et d’obstétrique; ITT = intention to treat; OS = overall survival.
Data cut-off date: January 8, 2024.
Source: Sponsor’s Summary of Clinical Evidence.24
Health-Related Quality of Life
Mean change from baseline showed improvements in the EORTC QLQ-C30 GHS/QoL scale at week 36 in both the pembrolizumab plus CRT arm (LSM = 10.67 points; 95% CI, 7.73 points to 13.62 points) and the placebo plus CRT arm (LSM = 11.32 points; 95% CI, 8.39 points to 14.26 points). The between-group difference was –0.65 points (95% CI, –4.19 points to 2.89 points) (Table 15).24 These findings were consistent with the primary analysis of the overall population (Table 21, Appendix 1).
Table 15: Key Efficacy Outcomes of Patients With FIGO 2014 Stage III to IVA Disease in the KEYNOTE-A18 Study (ITT Population)
Outcome | Pembrolizumab plus CRT | Placebo plus CRT |
|---|---|---|
PFS (investigator assessed) | ||
N | 296 | 305 |
Number (%) of events | 79 (26.7) | 125 (41.0) |
PFS (months), median (95% CI) | Not reached (not reached to not reached) | Not reached (26.3 to not reached) |
HR (95% CI) | 0.57 (0.43 to 0.76) | |
Nominal P valuea | < 0.0001 | |
PFS rate at 18 months, % (95% CI) | 77.6 (72.2 to 82.0) | 62.8 (56.9 to 68.2) |
Difference in PFS rates at 18 months, % (95% CI)b | 14.8 (7.3 to 22.2) | |
PFS rate at 24 months, % (95% CI) | 72.9 (67.1 to 77.9) | 56.9 (50.7 to 62.6) |
Difference in PFS rates at 24 months, % (95% CI)b | 16.0 (7.9 to 24.0) | |
PFS rate at 30 months, % (95% CI) | 71.6 (65.6 to 76.8) | 53.7 (47.0 to 59.9) |
Difference in PFS rates at 30 months, % (95% CI)b | 17.9 (9.4 to 26.5) | |
OS | ||
N | 296 | 305 |
Number (%) of events | 43 (14.5) | 73 (23.9) |
OS (months), median (95% CI) | Not reached (not reached to not reached) | Not reached (not reached to not reached) |
HR (95% CI) | 0.57 (0.39 to 0.83) | |
Nominal P valuea | 0.0016 | |
OS rate at month 24 (%), (95% CI) | 86.8 (82.2 to 90.4) | 78.0 (72.5 to 82.5) |
Difference in OS rates at 24 months, % (95% CI)b | 8.9 (2.5 to 15.3) | |
OS rate at month 30 (%), (95% CI) | 84.3 (79.2 to 88.2) | 72.4 (66.2 to 77.6) |
Difference in OS rates at 30 months, % (95% CI)b | 11.9 (4.7 to 19.2) | |
OS rate at month 36 (%), (95% CI) | 82.2 (76.2 to 86.8) | 70.7 (64.3 to 76.3) |
Difference in OS rates at 36 months, % (95% CI)b | 11.5 (3.5 to 19.5) | |
EORTC QLQ-C30 GHS/QoL | ||
Number of patients contributing to the analysis at baselinea | 261 | 270 |
Baseline score, mean (SD) | 64.46 (23.68) | 64.14 (21.93) |
Number of patients at week 36c | 200 | 198 |
Score at week 36, mean (SD) | 76.75 (18.67) | 77.61 (18.57) |
Change from baseline to week 36, LSM (95% CI)d | 10.67 (7.73 to 13.62) | 11.32 (8.39 to 14.26) |
Treatment arm difference at week 36, LSM (95% CI)d | –0.65 (–4.19 to 2.89) | |
Nominal P valued | 0.7195 | |
CI = confidence interval; CRT = chemoradiotherapy; EORTC QLQ-C30 GHS/QoL = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 Global Health Status/Quality of Life; FIGO = Fédération internationale de gynécologie et d’obstétrique; HR = hazard ratio; ITT = intention to treat; LSM = least squares mean; OS = overall survival; PFS = progression-free survival; SD = standard deviation.
aAll P values were nominal due to the lack of formal hypothesis testing for the subgroup.
bFor the subgroups, analysis is based on unstratified Cox regression model with treatment as a covariate.
cNumber of participants in each treatment arm with nonmissing assessments at the specific time point.
dBased on a constrained longitudinal data analysis model with the patient-reported outcome scores as the response variable with covariates for treatment by study visit interaction. P values are nominal.
Data cut-off date: January 8, 2024.
Source: Sponsor’s Summary of Clinical Evidence.24
Harms
All treatment-emergent AEs, SAEs, deaths due to AEs, AESIs, and discontinuations due to AEs were reported. Safety data presented in this section represents data for the FIGO 2014 stage III to IVA disease safety population (all participants as treated population, N = 599) at interim analysis 2 (Table 16).24 Harms reported in the overall population are presented in Table 22 in Appendix 1.
Adverse Events
Overall, the proportions of patients reporting any AE were similar in the 2 arms (100% for the pembrolizumab plus CRT arm versus 99.3% for the placebo plus CRT arm). The most frequently reported AEs (incidence ≥ 25%) were anemia (68.8% versus 66.1%), nausea (56.6% versus 62.5%), diarrhea (50.5% versus 50.7%), white blood cell counts decreased (38.0% versus 41.8%), neutrophil count decreased (35.6% versus 32.9%), vomiting (33.9% versus 35.2%), and urinary tract infection (29.5% versus 31.3%) in the pembrolizumab plus CRT arm and the placebo plus CRT arm, respectively.24
Serious Adverse Events
The proportion of patients with SAEs was similar in the 2 arms (33.9% in the pembrolizumab plus CRT arm versus 32.6% in the placebo plus CRT arm). Most frequent SAEs included anemia (4.4%), urinary tract infection (3.1%), and pyrexia (2.0%) in the pembrolizumab plus CRT arm, and urinary tract infection (4.3%) and acute kidney injury (2.0%) in the placebo plus CRT arm. Anemia and pyrexia are well-established events associated with CRT; urinary tract infections are commonly associated with pelvic radiotherapy as well as with cervical cancer.24
Mortality
Deaths due to AEs were reported among 4 patients (1.4%) in the pembrolizumab plus CRT arm and 6 patients (2.0%) in the placebo plus CRT arm.24
Discontinuation Due to Adverse Events
Rates of treatment discontinuation due to AEs were 21.0% versus 15.1% in the pembrolizumab plus CRT arm and the placebo plus CRT arm, respectively, and included events in the system organ class such as blood and lymphatic system disorders (5.1% versus 3.3%, respectively), gastrointestinal disorders (1.7% versus 2.0%, respectively), and investigations (6.1% versus 7.2%, respectively).24
Notable Harms
AESIs occurred more frequently in the pembrolizumab plus CRT arm (40.7%) than in the placebo plus CRT arm (17.8%).24 Incidence of hypothyroidism (23.1% versus 8.2%), hyperthyroidism (12.9% versus 3.3%), and thyroiditis (2.7% versus 0.3%) were higher in the pembrolizumab plus CRT arm than the placebo plus CRT arm.
Table 16: Key Harms Data for the FIGO 2014 Stage III to IVA Disease Subgroup in the KEYNOTE-A18 Study (APaT Population)
Characteristic | Pembrolizumab plus CRT (N = 295) | Placebo plus CRT (N = 304) |
|---|---|---|
Patients with ≥ 1 AEs | 295 (100.0) | 302 (99.3) |
Most common (≥ 10% incidence in any treatment arm) AEs, n (%) | ||
Anemia | 203 (68.8) | 201 (66.1) |
Nausea | 167 (56.6) | 190 (62.5) |
Diarrhea | 149 (50.5) | 154 (50.7) |
White blood cell counts decreased | 112 (38.0) | 127 (41.8) |
Neutrophil count decreased | 105 (35.6) | 100 (32.9) |
Vomiting | 100 (33.9) | 107 (35.2) |
Urinary tract infection | 87 (29.5) | 95 (31.3) |
Platelet count decreased | 72 (24.4) | 70 (23.0) |
Hypomagnesemia | 71 (24.1) | 67 (22.0) |
Hypokalemia | 68 (23.1) | 51 (16.8) |
Hypothyroidism | 67 (22.7) | 25 (8.2) |
Alanine aminotransferase increased | 58 (19.7) | 41 (13.5) |
Constipation | 58 (19.7) | 60 (19.7) |
Aspartate aminotransferase increased | 56 (19.0) | 40 (13.2) |
Neutropenia | 56 (19.0) | 48 (15.8) |
Weight decreased | 56 (19.0) | 58 (19.1) |
Patients with ≥ 1 SAEs, n (%) | 100 (33.9) | 99 (32.6) |
SAE with incidence ≥ 0.5% in 1 or both treatment arms | ||
Anemia | 13 (4.4) | 3 (1.0) |
Urinary tract infection | 9 (3.1) | 13 (4.3) |
Pyrexia | 6 (2.0) | 3 (1.0) |
Diarrhea | 5 (1.7) | 2 (0.7) |
Hydronephrosis | 5 (1.7) | 3 (1.0) |
Acute kidney injury | 4 (1.4) | 6 (2.0) |
Hypokalemia | 4 (1.4) | 2 (0.7) |
Urosepsis | 4 (1.4) | 1 (0.3) |
Gastroenteritis radiation | 3 (1.0) | 0 (0.0) |
Platelet count decreased | 3 (1.0) | 0 (0.0) |
Patients who discontinued any treatment due to AEs, n (%) | 62 (21.0) | 46 (15.1) |
Blood and lymphatic system disorders | 15 (5.1) | 10 (3.3) |
Anemia | 7 (2.4) | 3 (1.0) |
Thrombocytopenia | 3 (1.0) | 1 (0.3) |
Gastrointestinal disorders | 5 (1.7) | 6 (2.0) |
Diarrhea | 3 (1.0) | 1 (0.3) |
Hepatobiliary disorders | 1 (0.3) | 1 (0.3) |
Liver disorder | 1 (0.3) | 0 (0.0) |
Immune system disorders | 2 (0.7) | 0 (0.0) |
Hypersensitivity | 1 (0.3) | 0 (0.0) |
Infections and infestations | 5 (1.7) | 0 (0.0) |
Urinary tract infection | 1 (0.3) | 0 (0.0) |
Investigations | 18 (6.1) | 22 (7.2) |
Neutrophil count decreased | 5 (1.7) | 2 (0.7) |
Nervous system disorders | 5 (1.7) | 1 (0.3) |
Guillain-Barre syndrome | 1 (0.3) | 0 (0.0) |
Deaths, n (%) | 4 (1.4) | 6 (2.0) |
Patients with ≥ 1 AESI, n (%) | 120 (40.7) | 54 (17.8) |
Colitis | 8 (2.7) | 3 (1.0) |
Gastritis | 9 (3.1) | 10 (3.3) |
Hyperthyroidism | 38 (12.9) | 10 (3.3) |
Hypothyroidism | 68 (23.1) | 25 (8.2) |
Infusion reactions | 6 (2.0) | 6 (2.0) |
Pneumonitis | 5 (1.7) | 3 (1.0) |
Thyroiditis | 8 (2.7) | 1 (0.3) |
Type 1 diabetes | 1 (0.3) | 0 (0.0) |
Uveitis | 1 (0.3) | 0 (0.0) |
Vasculitis | 1 (0.3) | 0 (0.0) |
AE = adverse event; AESI = adverse event of special interest; APaT = all participants as treated; CRT = chemoradiotherapy; FIGO = Fédération internationale de gynécologie et d’obstétrique; SAE = serious adverse event.
Data cut-off date: January 8, 2024.
Source: Sponsor’s Summary of Clinical Evidence.24
Critical Appraisal
Internal Validity
The KEYNOTE-A18 study is an ongoing, randomized, double-masked, placebo-controlled, phase III designed to evaluate the efficacy and safety of pembrolizumab and CRT in patients with high-risk LACC. Included were patients with FIGO 2014 stage IB2 to IIB (with node-positive disease) or stage III to IVA (either node-positive or node-negative disease). The indication under review is limited to patients with stage III to IVA (either node-positive or node-negative) disease, and therefore the focus of this review is this subgroup. Appropriate methods (interactive web response system) were implemented to ensure random assignment and allocation concealment. Randomization was stratified using relevant prognostic factors (e.g., type of EBRT, cervical cancer stages IB2 to IIB and III to IVA), which would have likely ensured the balance in patient baseline and disease characteristics in the 2 arms of the subgroup of interest. Baseline demographic and disease characteristics were generally similar in the treatment arms for the FIGO 2014 stage III to IVA subgroup. This would have ensured that a confounding effect from these factors at baseline is an unlikely explanation for any differences in efficacy outcomes in the treatment arms.
Although patients enrolled in the KEYNOTE-A18 study were stratified by the subgroup of interest at randomization, the subgroup analysis of patients with FIGO 2014 stage III to IVA disease was not prespecified and, as such, the evidence informing this submission is based on a post hoc analysis. There is a potential risk that the statistically significant results may have been due to chance, due to multiple testing, even though the risk is likely low given that the subgroup results were consistent with the results of the primary analysis of the overall population.
The double-masked design minimized the risk of detection bias and reporting bias, particularly for subjective end points like PFS. BICR assessments of PFS were consistent with those of the investigator. This indicates that it is unlikely that any between-group differences in investigator-assessed PFS are due to subjective bias.
Treatment discontinuations were high overall (40% in the pembrolizumab plus CRT arm versus 47% in the placebo plus CRT arm). Differential treatment discontinuation was observed between treatment arms primarily due to radiographic progression (19.3% versus 30.9%) and AEs (11.2% versus 4.9%) for pembrolizumab plus CRT and placebo plus CRT, respectively. The proportion of treatment completion was also higher in the pembrolizumab plus CRT arm than in the placebo plus CRT arm (43.4% versus 35.9%, respectively). Although overall treatment exposure appeared to be similar between the treatment arms for the completion of CRT, the shorter duration of exposure to treatment in the placebo arm compared to pembrolizumab (20 months versus 16 months in median duration and 17 versus 15 in median treatment cycles) may potentially bias the efficacy results in favour of pembrolizumab plus CRT.
The use of subsequent anticancer therapy may increase the risk of bias in OS against pembrolizumab plus CRT (e.g., antineoplastic agents 15.9% versus 27.6%). Therefore, the benefit of pembrolizumab on OS may have been underestimated.
The KEYNOTE-A18 study was ongoing at the time of this review and the findings were based on interim analysis that could be considered exploratory. There were also concerns about imprecision as evidenced by the wide CIs at various time points for PFS and OS, which included the clinical threshold of important difference suggested by the clinical experts consulted during the review.
External Validity
The KEYNOTE-A18 study is a multicentre study with 3 sites in Canada. The inclusion and exclusion criteria were considered appropriate and inclusive for the clinical trial setting by the clinical experts consulted for this review. Although the proportion of enrolled patients with PD-L1 CPS greater than or equal to 1, ECOG PS of 0, squamous cancer cell histology type, planned type of EBRT, and positive pelvic and/or para-aortic lymph node presence was higher in the overall trial and subgroup, the impact of these factors on the generalizability of the results in both populations was considered minimal. However, there was uncertainty about whether patients with PD-L1 CPS less than 1 would benefit from this treatment given that the proportion of these patients was lower in the overall study.
The use of CRT was considered appropriate and the number of cycles and dosing reflected clinical practice in Canada. Although carboplatin was not specified as an alternative to cisplatin in the trial and it is not frequently prescribed by physicians, the clinical experts consulted for this review noted that some patients who are not be eligible for cisplatin may receive carboplatin or paclitaxel instead.23
Concomitant medications were permitted in the KEYNOTE-A18 study. No discrepancies were identified in the medications used in the trial relative to those administered in current practice. Subsequent chemotherapy was also permitted according to local site standard-of-care requirements. While this may impact the internal validity of certain end points, this is consistent with treatment patterns in real-world practice.
Key outcomes important for clinical decision-making by the clinicians and patient groups consulted by CDA-AMC were investigated in the KEYNOTE-A18 study, including PFS, OS, and HRQoL. The time points considered in the trial were appropriate and the clinical experts consulted agreed on 18, 24, and 30 months as clinically meaningful for PFS and 24, 30, and 36 months for OS. PFS assessments by investigator using the RECIST 1.1 criteria reflect current practice settings. Patient groups also indicated that improvements in HRQoL were important. HRQoL (measured using the EORTC QLQ-C30 GHS/QoL subscale) was considered clinically relevant and a better indicator of changes in quality of life during treatment. However, a key limitation was the incomplete measurement of HRQoL, as assessments were only conducted up to 36 weeks of treatment. Even though no important differences between the 2 treatment arms were observed, the lack of long-term HRQoL data resulted in uncertainty regarding the generalizability of the efficacy and safety results.
GRADE Summary of Findings and Certainty of the Evidence
Methods for Assessing the Certainty of the Evidence
For pivotal studies and RCTs identified in the sponsor’s systematic review, GRADE was used to assess the certainty of the evidence for outcomes considered most relevant to inform expert committee deliberations, and a final certainty rating was determined as outlined by the GRADE Working Group:25,26
High certainty: We are very confident that the true effect lies close to that of the estimate of the effect.
Moderate certainty: We are moderately confident in the effect estimate — The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. We use the word “likely” for evidence of moderate certainty (e.g., “X intervention likely results in Y outcome”).
Low certainty: Our confidence in the effect estimate is limited — The true effect may be substantially different from the estimate of the effect. We use the word “may” for evidence of low certainty (e.g., “X intervention may result in Y outcome”).
Very low certainty: We have very little confidence in the effect estimate — The true effect is likely to be substantially different from the estimate of effect. We describe evidence of very low certainty as “very uncertain.”
Following the GRADE approach, evidence from RCTs started as high-certainty evidence and could be rated down for concerns related to study limitations (which refers to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias.
Whenever possible, certainty was rated in the context of the presence of an important (nontrivial) treatment effect; if this was not possible, certainty was rated in the context of the presence of any treatment effect (i.e., the clinical importance is unclear). In all cases, the target of the certainty-of-evidence assessment was based on the point estimate and where it was located relative to the threshold for a clinically important effect (when a threshold was available) or to the null.
The reference points for the certainty-of-evidence assessment for OS, PFS, and harms outcomes (SAEs, discontinuations, and immune-related AEs leading to discontinuation) were set according to the presence or absence of an important effect based on thresholds informed by the clinical experts consulted for this review. The reference point for the certainty-of-evidence assessment for the EORTC QLQ-C30 GHS/QoL score was set according to the presence or absence of an important effect based on a threshold informed by the literature.
Results of GRADE Assessments
Table 2 shows the GRADE summary of findings for pembrolizumab plus CRT versus placebo plus CRT for the treatment of adult patients with FIGO 2014 stage III to IVA cervical cancer.
Long-Term Extension Studies
No long-term extension studies were provided in the submission.
Indirect Evidence
No indirect treatment comparisons were provided in the submission.
Studies Addressing Gaps in the Systematic Review Evidence
No studies addressing gaps in the evidence were provided in the submission.
Discussion
Summary of Available Evidence
One RCT, the KEYNOTE-A18 study, was included in the sponsor’s systematic review. The KEYNOTE-A18 study is an ongoing randomized, double-masked, placebo-controlled, phase III trial evaluating the efficacy and safety of the concurrent use of pembrolizumab with CRT against placebo and CRT alone in patients with newly diagnosed high-risk (FIGO 2014 stage IB2 to IIB node-positive disease or stage III to IVA regardless of node status) LACC. The coprimary outcomes assessed in the subgroup were PFS according to investigator assessment per RECIST 1.1 and OS. Other outcomes included HRQoL (using the EORTC QLQ-C30 GHS/QoL subscale) and safety.
Subgroup analyses in the KEYNOTE-A18 study revealed that the benefits of pembrolizumab on PFS and OS at interim analysis 2 were primarily driven by improvements among patients with FIGO 2014 stage III to IVA disease. Benefits were limited among patients with FIGO 2014 stage IB2 to IIB cervical cancer. Consequently, the Health Canada indication is limited to FIGO 2014 stage III to IVA disease. The sponsor’s reimbursement request is in line with the Health Canada indication. This report focuses on results of the post hoc analyses of the subpopulation of patients with FIGO 2014 stage III to IVA disease at interim analysis 2.24
Baseline demographics and disease characteristics in the FIGO 2014 stage III to IVA subgroup were generally similar in both the pembrolizumab plus CRT arm and the placebo plus CRT arm. There were more patients with PD-L1–positive tumours with CPS greater than or equal to 1 in both treatment arms (93.9% and 92.1%, respectively).24 The majority of patients were aged 65 years or younger (85.8% versus 81.3%, respectively) and had disease with positive pelvic and or para-aortic lymph node involvement (72.0% versus 69.5%, respectively).24
Interpretation of Results
Efficacy
The clinical experts, patient groups, and clinician groups consulted during the review highlighted that the most important treatment goals for high-risk LACC is to improve survival, cure the disease, delay disease progression, reduce symptoms, and improve HRQoL. The clinical experts noted that although current standard of care (commonly, cisplatin and radiation) prolongs life and improves cure rates, these treatments do not address the underlying disease mechanism. In addition, patients may experience lack of response to CRT, leading to poorer outcomes with later lines of therapy. There is therefore a need for treatments with reduced toxicity profiles that lead to a long-term cure over shorter treatment periods. Evidence from the FIGO 2014 stage III to IVA subgroup in the KEYNOTE-A18 study suggests that pembrolizumab plus CRT may meet, in part, patient needs as identified by patients and clinicians.
Although the KEYNOTE-A18 study was designed to evaluate coprimary (PFS and OS) and secondary efficacy end points in the overall population, the reimbursement sought is narrowed to a subgroup population. Due to the methodological limitations of the subgroup analysis, that is, the lack of predefined hypothesis testing and uncontrolled alpha in in the multiple testing, these findings were considered at a potential increased risk of uncertainty, including imprecision. Therefore, the subgroup findings were considered exploratory.
PFS was considered relevant for decision-making by the clinicians consulted for this review and for deliberations by the committee panel members. Overall, the subgroup findings showed that the patients receiving pembrolizumab plus CRT likely experienced a reduction in risk of disease progression. PFS probability rates at 18, 24, and 36 months were better and clinically meaningful in the pembrolizumab plus CRT arm compared to the placebo plus CRT arm, based on a clinically meaningful threshold of 10% suggested by the clinical experts consulted during the review. The between-group differences consistently increased at 18, 24, and 36 months (14.8%, 16.0%, and 17.9%, respectively) in favour of pembrolizumab plus CRT. PFS assessments by BICR were consistent with investigator findings of PFS. Overall, PFS findings were considered clinically meaningful by the clinical experts consulted for this review. However, because of the methodological limitations of the subgroup analysis, these findings are at increased risk due to chance. There was also uncertainty arising from imprecision (where the lower CI bounds were less than 10%), potentially due to the small sample size.
OS findings in the subgroup also suggest that patients receiving pembrolizumab plus CRT likely experienced improved survival compared to those receiving placebo plus CRT, based on a 5% threshold of clinically meaningful significance suggested by clinical experts. At month 24, 30, and 36, the between-group differences increased and were consistent across time points (8.9%, 11.9%, and 11.5%, respectively). These findings were considered clinically meaningful by the clinical experts consulted for this review; however, in addition to a potentially increased risk of results due to chance, there was imprecision, as shown by the wide 95% CI, with the lower bound less than 5% (i.e., 2.5% at 24 months, 4.7% at 30 months, and 3.5% at 36 months). Other sources of uncertainty included the use of subsequent anticancer therapies, which could potentially bias OS estimates toward the null and which would likely have resulted in underestimating the benefit.
The patient groups and clinical experts consulted noted the importance of quality of life during treatment. The experts noted that patients usually experience worsening symptoms during treatment with CRT before improvement. The EORTC QLQ-C30 GHS/QoL subscale score was considered a clinically relevant patient-reported outcome because the subscale provides a comprehensive, patient-centred measure of overall well-being, integrating physical, emotional, and social aspects of health that are most relevant to patients receiving treatment. The between-group differences showed that pembrolizumab plus CRT may result in little-to-no clinically meaningful change in HRQoL, compared to placebo plus CRT, based on the published minimal important difference of 4 points.57 In addition to the highlighted methodological challenges, sources of uncertainty included the use of concomitant medications, which may have impacted quality of life, the lack of long-term data, and the lack of accounting for missing data. Failure to account for missing data may introduce bias when the missingness is not at random.
Tumour stage was considered a clinically meaningful prognostic variable, according to the experts consulted, as it impacts patient response to treatment and may have contributed to the plausible response observed in the subgroup of interest.1,32,35 Among patients with locally advanced cancers (which include FIGO 2014 stage III to IVA disease), prognosis worsens with more advanced disease or nodal involvement.17,19,20,22,37,38 Compared to patients with early-stage cervical cancer, patients with locally advanced disease experience significantly lower cure rates, with a 5-year disease-free survival rate of 68% and a 5-year OS rate of 73% to 74%;18,20,61 hence, the need for new treatments that improve OS or cure rates for patients.
Harms
The majority of patients receiving CRT with or without pembrolizumab in the subgroup experienced at least 1 AE, and these AEs were consistent with the known safety profiles of both pembrolizumab and CRT according to the clinical experts.
The median number of chemotherapy cycles and radiotherapy exposures aligned with clinical experts’ input, indicating that the reported AEs were not influenced by how long patients were exposed to treatment. Overall, frequencies of AEs were similar in the 2 treatment arms, and certainty was moderate that pembrolizumab plus CRT leads to little-to-no clinically meaningful changes in SAEs compared to placebo plus CRT. AESIs occurred more frequently among patients in the pembrolizumab plus CRT arm (40.7%) than among those in the placebo plus CRT arm (17.8%).
Colitis, hyperthyroidism, hypothyroidism, thyroiditis, and hepatotoxicity were a few of the immune-related AEs identified that could result in treatment discontinuation in clinical practice. Although the frequencies of their occurrence were generally higher in the pembrolizumab plus CRT arm, they were considered clinically manageable in real-world practice, by way of dose adjustments or treatment discontinuation if the events are severe. The certainty-of-evidence assessment showed that pembrolizumab plus CRT did not result in a clinically meaningful change in withdrawals due to immune-related AEs compared to placebo plus CRT because the CIs included values (0 fewer to 4.7 more per 100 patients) smaller than the threshold (10%) suggested by the clinical experts during the review.
Physicians are generally familiar with pembrolizumab based on their experience with its use in clinical practice. No new safety concerns were identified by the KEYNOTE-A18 study, and the safety profiles of both pembrolizumab and CRT were considered manageable in practice, according to the clinical experts.
Other Considerations
The 2014 FIGO staging system used to identify patients in the KEYNOTE-A18 study was identified as a potential implementation issue for this review because FIGO 2018 staging is currently used in diagnosis and cervical cancer management in Canada. As noted in the sponsor’s submission,24 benefits were limited among patients with FIGO 2014 stage IB2 to IIB. Given that patients with FIGO 2014 stage IB2 to IIB (node-positive) disease will now be considered as having stage IIIC disease per the FIGO 2018 staging system, translating the KEYNOTE-A18 study subgroup results to the 2018 staging system is challenging.
Another implementation concern was the exclusion of patients with vaginal cancers and patients with ECOG PS of 2 or greater. The clinical experts believed that these patients would potentially benefit from treatment in clinical practice due to the similarities of vaginal cancers to cervical cancers in terms of causation (both are HPV infection–related) and in terms of the treatment approaches. Patients with ECOG PS of 2 or greater were also excluded from the KEYNOTE-A18 study due to poor prognosis; however, the experts considered that these patients would potentially benefit from treatment given that the best chance of cure is during the initial therapy and once patients develop resistance to chemoradiation, cure rates are low.
Conclusion
A post hoc subgroup analysis conducted in the KEYNOTE-A18 study provided evidence of safety and efficacy for the use of pembrolizumab plus CRT versus placebo plus CRT in patients with FIGO 2014 stage III to IVA LACC. The evidence suggests that compared to placebo plus CRT, treatment with pembrolizumab plus CRT likely results in clinically important improvement in OS and likely delays disease progression. Although the findings on OS and PFS reported across time points were consistent and considered clinically meaningful, there is uncertainty due to imprecision. While the subgroup analysis showed little-to-no clinically meaningful change in HRQoL between the 2 treatment arms, the short duration of HRQoL assessments and the potential risk of bias mean that no conclusions can be reached on the effectiveness of pembrolizumab in improving or maintaining better quality of life when added to standard-of-care CRT.
Overall, the frequencies of AEs and SAEs were similar in the 2 treatment arms in the subgroup, and pembrolizumab did not result in a clinically important difference in withdrawals due to immune-related AEs compared to placebo plus CRT. There is uncertainty in the long-term impact of pembrolizumab plus CRT due to the lack of long-term safety and efficacy data for the indication under review; however, this was not a major concern given the prevalence of the use of pembrolizumab for the treatment of other cancers in Canada.
References
1.Monk BJ, Tan DSP, Hernandez Chagui JD, et al. Proportions and incidence of locally advanced cervical cancer: a global systematic literature review. Int J Gynecol Cancer. 2022;32(12):1531-1539. doi: 10.1136/ijgc-2022-003801 PubMed
2.Vora C, Gupta S. Targeted therapy in cervical cancer. ESMO Open. 2018;3(Suppl 1):e000462. doi: 10.1136/esmoopen-2018-000462 PubMed
3.World Health Organization. Fact Sheets: Cervical Cancer. 2024. Accessed January 7, 2025. https://www.who.int/news-room/fact-sheets/detail/cervical-cancer
4.Girda E, Randall LM, Chino F, Monk BJ, Farley JH, O'Cearbhaill RE. Cervical cancer treatment update: A Society of Gynecologic Oncology clinical practice statement. Gynecol Oncol. 2023;179:115-122. doi: 10.1016/j.ygyno.2023.10.017 PubMed
5.National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines: Cervical Cancer. Version 3.2025. Accessed March 4, 2025. https://www.nccn.org/professionals/physician_gls/pdf/cervical.pdf
6.Grau-Bejar JF, Garcia-Duran C, Garcia-Illescas D, Mirallas O, Oaknin A. Advances in immunotherapy for cervical cancer. Ther Adv Med Oncol. 2023;15:17588359231163836. doi: 10.1177/17588359231163836 PubMed
7.Grau JF, Farinas-Madrid L, Oaknin A. A randomized phase III trial of platinum chemotherapy plus paclitaxel with bevacizumab and atezolizumab versus platinum chemotherapy plus paclitaxel and bevacizumab in metastatic (stage IVB), persistent, or recurrent carcinoma of the cervix: the BEATcc study (ENGOT-Cx10/GEICO 68-C/JGOG1084/GOG-3030). Int J Gynecol Cancer. 2020;30(1):139-143. doi: 10.1136/ijgc-2019-000880 PubMed
8.Gu X, Dong M, Liu Z, et al. Elevated PD-L1 expression predicts poor survival outcomes in patients with cervical cancer. Cancer Cell Int. 2019;19(1):146. doi: 10.1186/s12935-019-0861-7 PubMed
9.World Health Organization. Comprehensive Cervical Cancer Control: A Guide to Essential Practice. 2nd ed. 2014. Accessed June 12, 2025. https://www.ncbi.nlm.nih.gov/books/NBK269617/
10.FIGO Committee on Gynecologic Oncology. FIGO staging for carcinoma of the vulva, cervix, and corpus uteri. Int J Gynaecol Obstet. 2014;125(2):97-8. doi: 10.1016/j.ijgo.2014.02.003 PubMed
11.Bhatla N, Aoki D, Sharma DN, Sankaranarayanan R. Cancer of the cervix uteri. Int J Gynaecol Obstet. 2018;143 Suppl 2(S2):22-36. doi: 10.1002/ijgo.12611
12.Bhatla N, Berek JS, Cuello Fredes M, et al. Revised FIGO staging for carcinoma of the cervix uteri. Int J Gynaecol Obstet. 2019;145(1):129-135. doi: 10.1002/ijgo.12749 PubMed
13.Salib MY, Russell JHB, Stewart VR, et al. 2018 FIGO Staging Classification for Cervical Cancer: Added Benefits of Imaging. Radiographics. 2020;40(6):1807-1822. doi: 10.1148/rg.2020200013 PubMed
14.B. C. Cancer. BC Cancer Protocol Summary GOCXCRT. Treatment of High Risk Squamous Carcinoma, Adenocarcinoma, or Adenosquamous Carcinoma of the Cervix with Concurrent CISplatin and Radiation. 1998. Accessed January 6, 2025. https://www.bccancer.bc.ca/chemotherapy-protocols-site/Documents/Gynecology/GOCXCRT_Protocol.pdf
15.Cancer Care Alberta. Clinical Practice Guidelines GYNE-004 Version 6. Cancer of the Uterine Cervix. 2021. Accessed January 6, 2025. https://www.albertahealthservices.ca/assets/info/hp/cancer/if-hp-cancer-guide-gyne004-cervical.pdf
16.Xue R, Cai X, Xu H, Wu S, Huang H. The efficacy of concurrent weekly carboplatin with radiotherapy in the treatment of cervical cancer: A meta-analysis. Gynecol Oncol. 2018;150(3):412-419. doi: 10.1016/j.ygyno.2018.07.005 PubMed
17.Cetina L, Rivera L, Hinojosa J, et al. Routine management of locally advanced cervical cancer with concurrent radiation and cisplatin. Five-year results. BMC Womens Health. 2006;6:3. doi: 10.1186/1472-6874-6-3 PubMed
18.Eifel PJ, Winter K, Morris M, et al. Pelvic irradiation with concurrent chemotherapy versus pelvic and para-aortic irradiation for high-risk cervical cancer: an update of radiation therapy oncology group trial (RTOG) 90-01. J Clin Oncol. 2004;22(5):872-80. doi: 10.1200/JCO.2004.07.197 PubMed
19.Macdonald OK, Chen J, Dodson M, Lee CM, Gaffney DK. Prognostic significance of histology and positive lymph node involvement following radical hysterectomy in carcinoma of the cervix. Am J Clin Oncol. 2009;32(4):411-6. doi: 10.1097/COC.0b013e31819142dc PubMed
20.Potter R, Tanderup K, Schmid MP, et al. MRI-guided adaptive brachytherapy in locally advanced cervical cancer (EMBRACE-I): a multicentre prospective cohort study. Lancet Oncol. 2021;22(4):538-547. doi: 10.1016/S1470-2045(20)30753-1 PubMed
21.Shrivastava S, Mahantshetty U, Engineer R, et al. Cisplatin Chemoradiotherapy vs Radiotherapy in FIGO Stage IIIB Squamous Cell Carcinoma of the Uterine Cervix: A Randomized Clinical Trial. JAMA Oncol. 2018;4(4):506-513. doi: 10.1001/jamaoncol.2017.5179 PubMed
22.Sturdza A, Potter R, Fokdal LU, et al. Image guided brachytherapy in locally advanced cervical cancer: Improved pelvic control and survival in RetroEMBRACE, a multicenter cohort study. Radiother Oncol. 2016;120(3):428-433. doi: 10.1016/j.radonc.2016.03.011 PubMed
23.McCormack M, Eminowicz G, Gallardo D, et al. Induction chemotherapy followed by standard chemoradiotherapy versus standard chemoradiotherapy alone in patients with locally advanced cervical cancer (GCIG INTERLACE): an international, multicentre, randomised phase 3 trial. Lancet. 2024;404(10462):1525-1535. doi: 10.1016/S0140-6736(24)01438-7 PubMed
24.Merck Canada Inc. Sponsor's clinical summary of clinical evidence [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Keytruda (pembrolizumab), 200 mg every 3 weeks or 400 mg every 6 weeks, solution for infusion. March 25, 2025.
25.Balshem H, Helfand M, Schunemann HJ, et al. GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol. 2011;64(4):401-6. doi: 10.1016/j.jclinepi.2010.07.015 PubMed
26.Santesso N, Glenton C, Dahm P, et al. GRADE guidelines 26: informative statements to communicate the findings of systematic reviews of interventions. J Clin Epidemiol. 2020;119:126-135. doi: 10.1016/j.jclinepi.2019.10.014 PubMed
27.Brenner DR, Gillis J, Demers AA, et al. Projected estimates of cancer in Canada in 2024. CMAJ. 2024;196(18):E615-E623. doi: 10.1503/cmaj.240095 PubMed
28.Canadian Cancer Statistics Advisory Committee in collaboration with the Canadian Cancer Society, Statistics Canada, and the Public Health Agency of Canada. Canadian Cancer Statistics 2024. Canadian Cancer Society; 2024. Accessed July 17, 2024. https://cdn.cancer.ca/-/media/files/research/cancer-statistics/2024-statistics/2024-cmaj/2024_cancer-specific-stats.pdf
29.CADTH Reimbursement Recommendation: Pembrolizumab (Keytruda). Can J Health Technol. 2022;2(12). doi:10.51731/cjht.2022.527
30.Mahmud A, Brydon B, Tonita J, Hanna TP, Schmidt M, Tai P. A population-based study of cervix cancer: incidence, management and outcome in the Canadian province of Saskatchewan. Clin Oncol (R Coll Radiol). 2011;23(10):691-5. doi: 10.1016/j.clon.2011.05.002 PubMed
31.Saleh M, Virarkar M, Javadi S, Elsherif SB, de Castro Faria S, Bhosale P. Cervical Cancer: 2018 Revised International Federation of Gynecology and Obstetrics Staging System and the Role of Imaging. AJR Am J Roentgenol. 2020;214(5):1182-1195. doi: 10.2214/AJR.19.21819 PubMed
32.National Cancer Institute. Surveillance, Epidemiology, and End Results Program. Cancer Stat Facts: Cervical Cancer. 2024. Accessed January 6, 2025. https://seer.cancer.gov/statfacts/html/cervix.html
33.pan-Canadian Oncology Drug Review Final Clinical Guidance Report for Bevacizumab (Avastin) for Cervical Cancer. 2015. Accessed January 7, 2025. https://www.cadth.ca/sites/default/files/pcodr/pcodr-avastin-cc-fn-cgr.pdf
34.Conway JL, Felder S, Tang J, et al. Long-term patient-reported distress in locally advanced cervical cancer patients treated with definitive chemoradiation. Clin Transl Radiat Oncol. 2020;23:1-8. doi: 10.1016/j.ctro.2020.04.005 PubMed
35.Canadian Cancer Society. Survival statistics for cervical cancer. Accessed January 6, 2025. https://cancer.ca/en/cancer-information/cancer-types/cervical/prognosis-and-survival/survival-statistics
36.Canadian Cancer Statistics Advisory Committee. Canadian Cancer Statistics. A 2018 special report of cancer incidence by stage (supplementary data). Canadian Cancer Society; 2018. Accessed June 12, 2024. https://cdn.cancer.ca/-/media/files/research/cancer-statistics/2018-statistics/canadian-cancer-statistics-2018-en.pdf
37.Cho O, Chun M. Management for locally advanced cervical cancer: new trends and controversial issues. Radiat Oncol J. 2018;36(4):254-264. doi: 10.3857/roj.2018.00500 PubMed
38.Kidd EA, Siegel BA, Dehdashti F, et al. Lymph node staging by positron emission tomography in cervical cancer: relationship to prognosis. J Clin Oncol. 2010;28(12):2108-13. doi: 10.1200/JCO.2009.25.4151 PubMed
39.Chuang LT, Temin S, Camacho R, et al. Management and Care of Women With Invasive Cervical Cancer: American Society of Clinical Oncology Resource-Stratified Clinical Practice Guideline. J Glob Oncol. 2016;2(5):311-340. doi: 10.1200/JGO.2016.003954 PubMed
40.Marth C, Landoni F, Mahner S, et al. Cervical cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2017;28(suppl_4):iv72-iv83. doi: 10.1093/annonc/mdx220 PubMed
41.Restaino S, Pellecchia G, Arcieri M, et al. Management for Cervical Cancer Patients: A Comparison of the Guidelines from the International Scientific Societies (ESGO-NCCN-ASCO-AIOM-FIGO-BGCS-SEOM-ESMO-JSGO). Cancers (Basel). 2024;16(14). doi: 10.3390/cancers16142541 PubMed
42.Merck Canada Inc. KEYTRUDA (pembrolizumab): solution for infusion 100 mg/4 mL vial [draft product monograph]. May 19, 2015. Updated August 15, 2024.
43.Teva Canada Limited. Cisplatin Injection: Solution, 1 mg / mL (10 mg, 50 mg and 100 mg cisplatin per vial), Intravenous [product monograph]. March 15, 2013. Updated June 25, 2024. Accessed June 11, 2025. https://pdf.hres.ca/dpd_pm/00076100.PDF
44.Lorusso D, Xiang Y, Hasegawa K, et al. LBA38 Pembrolizumab plus chemoradiotherapy for high-risk locally advanced cervical cancer: A randomized, double-blind, phase III ENGOT-cx11/GOG-3047/KEYNOTE-A18 study. Ann Oncol. 2023;34:S1279-S1280. doi: j.annonc.2023.10.032.
45.Lorusso D, Xiang Y, Hasegawa K, et al. Pembrolizumab or placebo with chemoradiotherapy followed by pembrolizumab or placebo for newly diagnosed, high-risk, locally advanced cervical cancer (ENGOT-cx11/GOG-3047/KEYNOTE-A18): overall survival results from a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet. 2024;404(10460):1321-1332. doi: 10.1016/S0140-6736(24)01808-7 PubMed
46.Merck, Sharp, and Dohme LLC. Clinical Study Report: PA18V02MK3475. A Randomized, Phase 3, Double-Blind Study of Chemoradiotherapy With or Without Pembrolizumab for the Treatment of High-risk, Locally Advanced Cervical Cancer (KEYNOTE-A18/ENGOT-cx11/GOG-3047). 08-JANV-2024 data cutoff date [internal sponsor's report]. January 8, 2024.
47.Bards HTA. Health Technology Assessment (HTA) Report of MK3475, Protocol A-18. A Randomized, Phase 3, Double-Blind Study of Chemoradiotherapy With or Without Pembrolizumab for the Treatment of High-risk, Locally Advanced Cervical Cancer. Participants with FIGO III to IVA. Database Cutoff 08-Jan-2024 (Interim Analysis #2). Rest or World (ROW) Report [sponsor supplied reference]. 2024.
48.Duska L, Xiang Y, Hasegawa K, et al. Pembrolizumab plus chemoradiotherapy for high-risk locally advanced cervical cancer: A randomized, double-blind, phase III ENGOT-cx11/GOG-3047/KEYNOTE-A18 study. Gynecol Oncol. 2024;190:S8-S9. doi: j.ygyno.2024.07.019.
49.Lorusso D, Xiang Y, Hasegawa K, et al. 709O Pembrolizumab plus chemoradiotherapy for high-risk locally advanced cervical cancer: Overall survival results from the randomized, double-blind, phase III ENGOT-cx11/GOG-3047/KEYNOTE-A18 study. Ann Oncol. 2024;35:S544. doi: j.annonc.2024.08.771.
50.Randall L, Sukhin V, Colombo N, et al. Patient-reported outcomes from the phase III, randomized, double-blind, placebo-controlled ENGOT-cx11/GOG-3047/KEYNOTE-A18 Study of pembrolizumab plus concurrent chemoradiotherapy among patients with high-risk, locally advanced cervical cancer. Gynecol Oncol. 2024;190:S9. doi: 10.1016/j.ygyno.2024.07.020
51.Xiang Y, Hasegawa K, Zhu H, et al. 23O A randomized, phase III, double-blind study of chemoradiotherapy with or without pembrolizumab in patients with high-risk, locally advanced, cervical cancer (KEYNOTE-A18/ENGOT-cx11/GOG-3047): Results for patients enrolled in Asia. ESMO Open. 2024;9. doi: j.esmoop.2024.103523.
52.Merck Canada Inc. Drug Reimbursement Review sponsor submission: Keytruda (pembrolizumab), 200 mg every 3 weeks or 400 mg every 6 weeks, solution for infusion [internal sponsor's package]. March 25, 2025.
53.Fayers P, Bottomley A, EORTC Quality of Life Group, Quality of Life Unit. Quality of life research within the EORTC-the EORTC QLQ-C30. European Organisation for Research and Treatment of Cancer. Eur J Cancer. 2002;38 Suppl 4:S125-33. doi: 10.1016/s0959-8049(01)00448-8 PubMed
54.Davda J, Kibet H, Achieng E, Atundo L, Komen T. Assessing the acceptability, reliability, and validity of the EORTC Quality of Life Questionnaire (QLQ-C30) in Kenyan cancer patients: a cross-sectional study. J Patient Rep Outcomes. 2021;5(1):4. doi: 10.1186/s41687-020-00275-w PubMed
55.Hua CH, Guo HM, Guan XL, et al. Validation of the European Organization for Research and Treatment of Cancer cervical cancer module for Chinese patients with cervical cancer. Patient Prefer Adherence. 2013;7:1061-6. doi: 10.2147/PPA.S52498 PubMed
56.Greimel ER, Kuljanic Vlasic K, Waldenstrom AC, et al. The European Organization for Research and Treatment of Cancer (EORTC) Quality-of-Life questionnaire cervical cancer module: EORTC QLQ-CX24. Cancer. 2006;107(8):1812-22. doi: 10.1002/cncr.22217 PubMed
57.Musoro JZ, Coens C, Sprangers MAG, et al. Minimally important differences for interpreting EORTC QLQ-C30 change scores over time: A synthesis across 21 clinical trials involving nine different cancer types. Eur J Cancer. 2023;188:171-182. doi: 10.1016/j.ejca.2023.04.027 PubMed
58.Singer S, Kuhnt S, Momenghalibaf A, et al. Patients' acceptance and psychometric properties of the EORTC QLQ-CX24 after surgery. Gynecol Oncol. 2010;116(1):82-7. doi: 10.1016/j.ygyno.2009.09.022 PubMed
59.Jayasekara H, Rajapaksa LC, Greimel ER. The EORTC QLQ-CX24 cervical cancer-specific quality of life questionnaire: psychometric properties in a South Asian sample of cervical cancer patients. Psychooncology. 2008;17(10):1053-7. doi: 10.1002/pon.1310 PubMed
60.Paradowska D, Tomaszewski KA, Balajewicz-Nowak M, et al. Validation of the Polish version of the EORTC QLQ-CX24 module for the assessment of health-related quality of life in women with cervical cancer. Eur J Cancer Care (Engl). 2014;23(2):214-20. doi: 10.1111/ecc.12103 PubMed
61.Massobrio R, Bianco L, Campigotto B, et al. New Frontiers in Locally Advanced Cervical Cancer Treatment. J Clin Med. 2024;13(15). doi: 10.3390/jcm13154458 PubMed
Appendix 1: Detailed Outcome Data
Please note that this appendix has not been copy-edited.
Table 17: Patient Disposition in the Overall Population in the KEYNOTE-A18 Study (ITT Population)
Disposition | Pembrolizumab plus CRT (N = 529) | Placebo plus CRT (N = 531) |
|---|---|---|
Screened | 1,562 | |
Nonrandomized | 502 | |
Reason for screen failure | ||
Inclusion criteria not met | 498 | |
Other | 4 | |
Randomized | 1,060 | |
Randomized to stage III to IVA group | NA | |
Patients in the population, n (%) | ||
Patients who discontinued trial | 91 (17.2) | 119 (22.4) |
Death | 71 (13.4) | 109 (20.5) |
Lost to follow-up | 2 (0.4) | 3 (0.6) |
Patients who withdrew from trial | 18 (3.4) | 7 (1.3) |
Status for study medication in trial, n (%) | ||
Started study treatment, n (%) | 86 (16.3) | 85 (16.0) |
Completed study treatment, n (%) | 219 (41.5) | 209 (39.4) |
Discontinued study treatment, n (%) | 223 (42.2) | 236 (39.4) |
Reason for treatment discontinuation, n (%) | ||
AE | 64 (12.1) | 24 (4.5) |
Clinical progression | 4 (0.8) | 9 (1.7) |
Excluded medication | 1 (0.2) | 0 |
Lost to follow-up | 1 (0.2) | 1 (0.2) |
Noncompliance with study drug | 3 (0.6) | 1 (0.2) |
Nonstudy anticancer therapy | 1 (0.2) | 0 |
Physician decision | 8 (1.5) | 7 (1.3) |
Progressive disease | 2 (0.4) | 8 (1.5) |
Protocol violation | 1 (0.2) | 0 |
Radiographic progression | 108 (20.5) | 158 (29.8) |
Withdrawal of patient | 30 (5.7) | 28 (5.3) |
Patients ongoing | 438 (82.8) | 412 (77.6) |
Number randomized to treatment (ITT) | 529 | 531 |
Received allocated intervention (APaT) | 528 | 530 |
AE = adverse event; APaT = all participants as treated; CRT = chemoradiotherapy; FIGO = Fédération internationale de gynécologie et d’obstétrique; ITT = intention to treat; n = number of patients; NA = not applicable.
Data cut-off: January 8, 2024.
Source: KEYNOTE-A18 Clinical Study Report v02.46
Table 18: Baseline Characteristics in the Overall Population of the KEYNOTE-A18 Study (ITT Population)
Characteristics | Pembrolizumab plus CRT (N = 539) | Placebo plus CRT (N = 531) |
|---|---|---|
Sex, n (%) | ||
Female | 529 (100) | 531 (100) |
Age (years), n (%) | ||
< 65 | 473 (89.4) | 454 (85.5) |
≥ 65 | 56 (10.6) | 77 (14.5) |
Race, n (%) | ||
American Indian or Alaska Native | 24 (4.5) | 22 (4.1) |
Asian | 156 (29.5) | 148 (27.9) |
Black or African American | 14 (2.6) | 8 (1.5) |
Multiple | 78 (14.7) | 86 (16.2) |
Native Hawaiian or Other Pacific Islander | 2 (0.4) | 1 (0.2) |
White | 254 (48) | 264 (49.7) |
Missing | 1 (0.2) | 2 (0.4) |
Geographic region, n (%) | ||
Asia Pacific | 155 (29.3) | 150 (28.2) |
EMEA | 186 (35.2) | 183 (34.5) |
North America | 34 (6.4) | 45 (8.5) |
Latin America | 154 (29.1) | 153 (28.8) |
Baseline ECOG PS, n (%) | ||
0 | 380 (71.8) | 398 (75.0) |
1 | 149 (28.2) | 133 (25.0) |
Presence of lymph node, n (%) | ||
Positive pelvic and/or para-aortic | 445 (84.1) | 438 (82.5) |
No positive pelvic nor para-aortic | 84 (15.9) | 93 (17.5) |
Histology subtype, n (%) | ||
Nonsquamous | 95 (18.0) | 80 (15.1) |
Squamous | 434 (82.0) | 451 (84.9) |
Planned type of EBRT, n (%) | ||
IMRT or VMAT | 469 (88.7) | 470 (88.5) |
non-IMRT and non-VMAT | 60 (11.3) | 61 (11.5) |
Planned total radiation therapy dose per EQD2, n (%) | ||
< 70 Gy | 47 (8.9) | 46 (8.7) |
≥ 70 Gy | 482 (91.1) | 485 (91.3) |
PD-L1 status, n (%) | ||
CPS < 1 | 22 (4.2) | 28 (5.3) |
CPS ≥ 1 | 502 (94.9) | 498 (93.8) |
Missing | 5 (0.9) | 5 (0.9) |
CPS = combined positive score; CRT = chemoradiotherapy; EBRT = external beam radiotherapy; ECOG PS = Eastern Cooperative Oncology Group Performance Status; EMEA = Europe, the Middle East, and Africa; EQD2 = equivalent dose in 2-Gy fractions; IMRT = intensity-modulated radiotherapy; ITT = intention to treat; n = number of participants; VMAT = volumetric-modulated arc therapy.
Data cut-off: January 8, 2024.
Source: KEYNOTE-A18 Clinical Study Report v02.46
Concomitant Medications and Cointerventions in the Overall Population
In the overall population in the KEYNOTE-A18 study, concomitant medications were generally well-balanced between the pembrolizumab plus chemoradiotherapy versus placebo plus chemoradiotherapy groups except for antidiarrheal, intestinal anti-inflammatory, or anti-infective agents (69.3% versus 60.2%), antihistamines for systemic use (49.1% versus 42.6%), thyroid therapy (26.5% versus 10.9%), and homeopathic preparations (71.8% versus 62.1%) were higher (≥ 5 percentage point difference) in the pembrolizumab plus chemoradiotherapy group compared to placebo plus chemoradiotherapy, respectively.46
Exposure to Study Treatments
Table 19: Treatment Exposure in the Overall Population in the KEYNOTE-A18 Study (ITT Population)
Exposure | Pembrolizumab plus CRT | Placebo plus CRT |
|---|---|---|
n | 528 | 530 |
Duration in months | ||
Mean (SD) | 16.19 (8.14) | 15.81 (8.17) |
Median (range) | 18.96 (0.03 to 31.74) | 18.14 (0.07 to 31.87) |
Number of cycles | ||
Mean (SD) | 14.52 (6.00) | 14.29 (6.00) |
Median (range) | 17 (1.00 to 20.00) | 16 (1.00 to 20.00) |
Adherence (% of actual vs. expected doses administered), mean (SD)a | NR | NR |
Exposure by chemotherapy | ||
n | 527 | 530 |
Number of cisplatin administrations | ||
Mean (SD) | 4.96 (0.77) | 5.0 (0.82) |
Median (range) | 5.0 (1.0 to 7.0) | 5.0 (1.0 to 7.0) |
Duration of EBRT (days) | ||
Mean (SD) | 39.39 (8.26) | 39.18 (10.08) |
Median (range) | 37.0 (12.0 to 139.0) | 37.0 (2.0 to 143.0) |
Duration on brachytherapy (days) | ||
n | 513 | 504 |
Mean (SD) | 12.94 (6.05) | 13.03 (5.72) |
Median (range) | 12.0 (1.0 to 74.0) | 12.0 (1.0 to 59.0) |
Exposure to treatment by duration, n (%) | ||
> 0 m | 528 (100.0) | 530 (100) |
≥ 1 m | 526 (99.6) | 523 (98.7) |
≥ 3 m | 490 (92.8) | 494 (93.2) |
≥ 6 m | 440 (83.3) | 444 (83.8) |
≥ 12 m | 356 (67.4) | 345 (65.1) |
≥ 18 m | 276 (52.3) | 266 (50.2) |
≥ 24 m | 57 (10.8) | 44 (8.3) |
APaT = all participants as treated; CRT = chemoradiotherapy; EBRT = external beam radiotherapy; FIGO = Fédération international de gynécologie et d’obstétrique; ITT = intention to treat; m = month(s); n = number of patients who have the information available; NR = not reported; SD = standard deviation.
aDefined as the actual number of doses received divided by the expected number of doses and then multiplied by 100. Pembrolizumab was administered every 3 weeks (q.3.w.) for 5 infusions (5 cycles) followed by every 6 weeks (q.6.w.) for 15 infusions (15 cycles). The expected number of doses that participants would have received up to the database cut-off date based on the protocol-specified interval for administering each treatment component, given that the participant is remaining on treatment. It is limited to the maximum number of doses that a participant may receive as per study protocol. Expected number of dose administrations per participant for all cycles was calculated as a sum of expected number of dose administrations in cycles 1 to 5 and cycles 6+.
Data cut-off: January 8, 2024.
Source: KEYNOTE-A18 Clinical Study Report v02.46
Subsequent Treatment in the Overall Population of the KEYNOTE-A18 Study
In the overall population of patients enrolled in the KEYNOTE-A18 study, more patients in the placebo plus chemoradiotherapy group (27.4%) required subsequent oncology treatments compared to the pembrolizumab plus chemoradiotherapy group (18.4%). The most frequently reported subsequent oncological therapy (≥ 5% of participants in both groups) included bevacizumab, carboplatin, and paclitaxel. In the placebo plus chemoradiotherapy group, 41 (7.7%) patients used pembrolizumab, 1 (0.2%) patient used pembrolizumab plus vibostolimab, and 65 (12.3%) patients used bevacizumab as subsequent oncologic therapy.46
Table 20: Subsequent Oncologic Therapies Administered in the Overall Population of the KEYNOTE-A18 Study (ITT Population)
Drug | Pembrolizumab plus CRT | Placebo plus CRT |
|---|---|---|
Antineoplastic agents, n (%) | 96 (18.2) | 145 (27.4) |
Bevacizumab | 45 (8.5) | 65 (12.3) |
Cadonilimab | 2 (0.4) | 1 (0.2) |
Capecitabine | 2 (0.4) | 1 (0.2) |
Carboplatin | 69 (13.1) | 104 (19.6) |
Catequentinib | 2 (0.4) | 0 |
Cemiplimab | 1 (0.2) | 8 (1.5) |
Cisplatin | 26 (4.9) | 33 (6.2) |
Cyclophosphamide | 0 | 1 (0.2) |
Docetaxel | 1 (0.2) | 1 (0.2) |
Doxorubicin | 2 (0.4) | 1 (0.2) |
Doxorubicin hydrochloride | 1 (0.2) | 0 |
Gemcitabine | 6 (1.1) | 11 (2.1) |
Gemcitabine hydrochloride | 1 (0.2) | 1 (0.2) |
Irinotecan | 1 (0.2) | 3 (0.6) |
Marsdenia tenacissima stem | 0 | 1 (0.2) |
Paclitaxel | 85 (16.1) | 128 (24.2) |
Paclitaxel nanoparticle albumin-bound | 2 (0.4) | 9 (1.7) |
Pembrolizumab | 11 (2.1) | 41 (7.7) |
Pemetrexed disodium | 2 (0.4) | 0 |
Sintilimab | 1 (0.2) | 0 |
Tisotumab vedotin | 3 (0.6) | 1 (0.2) |
Topotecan | 6 (1.1) | 4 (0.8) |
Topotecan hydrochloride | 0 | 3 (0.6) |
Vincristine | 0 | 1 (0.2) |
Vinorelbine tartrate | 0 | 1 (0.2) |
Zimberelimab | 0 | 1 (0.2) |
Endocrine therapy, n (%) | ||
Anastrozole | 1 (0.2) | 0 |
CRT = chemoradiotherapy; ITT = intention to treat.
Data cut-off: January 8, 2024.
Source: KEYNOTE-A18 Clinical Study Report v02.46
Table 21: Key Efficacy Outcomes, Patients in the Overall Population of the KEYNOTE-A18 Study (ITT Population)
Outcome | Pembrolizumab plus CRT (N = 529) | Placebo plus CRT (N = 531) |
|---|---|---|
PFS (investigator assessed) | ||
Number (%) of events | 155 (29.3) | 210 (39.5) |
Death | 17 (3.2) | 17 (3.2) |
Documented progression | 138 (26.1) | 193 (36.3) |
PFS (months), median (95% CI) | Not reached (not reached to not reached) | Not reached (32.0 to not reached) |
HR (95% CI) | 0.68 (0.56 to 0.84) | |
P value | 0.0002 | |
PFS rate at 18 months, % (95% CI) | 75.0 (71.0 to 78.6) | 65.4 (61.1 to 69.4) |
Difference in PFS rates at 18 months, % (95% CI) | Not reached | Not reached |
PFS rate at 24 months, % (95% CI) | 70.6 (66.3 to 74.5) | 58.6 (54 to 62.9) |
Difference in PFS rates at 24 months, % (95% CI) | Not reported | Not reported |
PFS rate at 30 months, % (95% CI) | 67.6 (62.9 to 71.9) | 55.2 (50.3 to 59.9) |
Difference in PFS rates at 30 months, % (95% CI) | Not reached | Not reached |
OS | ||
Number (%) of events | 75 (14.2) | 109 (20.5) |
OS (months), median (95% CI) | Not reached (not reached to not reached) | Not reached (not reached to not reached) |
HR (95% CI) | 0.67 (0.50 to 0.90) | |
P value | 0.0040 | |
OS rate at month 24 (%) (95% CI) | 87.2 (83.9 to 89.9) | 82.2 (78.4 to 85.4) |
Difference in OS rates at 24 months, % (95% CI) | Not reached | Not reached |
OS rate at month 30 (%) (95% CI) | 83.8 (79.9 to 87.0) | 76.6 (72.2 to 80.4) |
Difference in OS rates at 30 months, % (95% CI) | Not reported | Not reported |
OS rate at month 36 (%) (95% CI) | 82.6 (78.4 to 86.1) | 74.8 (70.1 to 78.8) |
Difference in OS rates at 36 months, % (95% CI) | Not reached | Not reached |
EORTC QLQ-C30 GHS/QoL | ||
Number of patients contributing to the analysis at baselinea | 475 | 484 |
Baseline score, mean (SD) | 66.53 (22.77) | 65.69 (22.25) |
Number of patients at week 36a | 375 | 372 |
Score at week 36, mean (SD) | 75.47 (20.12) | 74.89 (19.91) |
Change from baseline to week 36, LSM (95% CI)b | 7.5 (5.30 to 9.73) | 7.44 (5.23 to 9.66) |
Treatment group difference at week 36, LSM (95% CI)b | 0.07 (–2.66 to 2.80) | |
P valueb | 0.9593 | |
CI = confidence interval; CRT = chemoradiotherapy; EORTC QLQ-C30 GHS/QoL = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 Global Health Status/Quality of Life; HR = hazard ratio; ITT = intention to treat; LSM = least squares mean; OS = overall survival; PFS = progression-free survival; SD = standard deviation.
Data cut-off date: January 8, 2024.
Source: KEYNOTE-A18 Clinical Study Report v02.46
Table 22: AEs Reported in the Overall Population of the KEYNOTE-A18 Study (APaT Population)
Characteristic | Pembrolizumab plus CRT (N = 528) | Placebo plus CRT (N = 530) |
|---|---|---|
Patients with ≥ 1 AEs, n (%) | 528 (100) | 526 (99.2) |
Most common (≥ 10% incidence in any treatment arm) AEs, n (%) | ||
Anemia | 358 (67.8) | 349 (65.8) |
Nausea | 320 (60.6) | 338 (63.8) |
Diarrhea | 301 (57.0) | 298 (56.2) |
White blood cell counts decreased | 175 (33.1) | 186 (35.1) |
Neutrophil count decreased | 164 (31.1) | 152 (28.7) |
Vomiting | 160 (30.3) | 152 (28.7) |
Urinary tract infection | 121 (22.9) | 146 (27.5) |
Platelet count decreased | 118 (22.3) | 113 (21.3) |
Hypomagnesemia | 130 (24.6) | 124 (23.4) |
Hypokalemia | 116 (22.0) | 92 (17.4) |
Hypothyroidism | 118 (22.3) | 36 (6. 8) |
Alanine aminotransferase increased | 115 (21.8) | 87 (16.4) |
Constipation | 118 (22.3) | 124 (23.4) |
Aspartate aminotransferase increased | 106 (20.1) | 71 (13.4) |
Neutropenia | 123 (23.3) | 109 (20.6) |
Weight decreased | 82 (15.5) | 81 (15.3) |
Patients with ≥ 1% serious adverse events, n (%) | ||
Anemia | 16 (3.0) | 13 (2.5) |
Urinary tract infection | 17 (3.2) | 14 (2.6) |
Pyrexia | 14 (2.7) | 10 (1.9) |
Diarrhea | 10 (1.9) | 6 (1.1) |
Hydronephrosis | 6 (1.1) | 3 (0.6) |
Acute kidney injury | 4 (0.8) | 6 (1.1) |
Sepsis | 6 (1.1) | 5 (0.9) |
Patients who discontinued any treatment due to AEs, n (%) | ||
Blood and lymphatic system disorders | 2 (0.4) | 1 (0.2) |
Gastrointestinal disorders | 12 (2.3) | 2 (0.4) |
Hepatobiliary disorders | 1 (0.2) | 2 (0.4) |
Immune system disorders | 1 (0.2) | 0 |
Infections and infestations | 5 (0.9) | 1 (0.2) |
Investigations | 7 (1.3) | 5 (0.9) |
Nervous system disorders | 4 (0.8) | 3 (0.6) |
Deaths, n (%) | 5 (0.9) | 7 (1.3) |
Patients with ≥ 0% adverse events of special interest, n (%) | ||
Colitis | 16 (3. 0) | 11 (2.1) |
Gastritis | 22 (4. 2) | 20 (3. 8) |
Hyperthyroidism | 64 (12.1) | 1 5 (2.8) |
Hypothyroidism | 119 (22.5) | 36 (6.8) |
Infusion reactions | 9 (1. 7) | 9 (1.7) |
Pneumonitis | 10 (1.9) | 5 (0.9) |
Thyroiditis | 12 (2.3) | 2 (0.4) |
Type 1 diabetes mellitus | 1 (0.2) | 0 |
Uveitis | 2 (0. 4) | 0 |
Vasculitis | 1 (0.2) | 1 (0.2) |
AE = adverse event; APaT = all participants as treated; CRT = chemoradiotherapy.
Data cut-off date: January 8, 2024.
Source: KEYNOTE-A18 Clinical Study Report v02.46
Pharmacoeconomic Review
Abbreviations
BIA
budget impact analysis
CDA-AMC
Canada’s Drug Agency
CRT
chemoradiotherapy
FIGO
Fédération internationale de gynécologie et d’obstétrique
HR
hazard ratio
ICER
incremental cost-effectiveness ratio
LACC
locally advanced cervical cancer
KM
Kaplan-Meier
OS
overall survival
PD
progressive disease
PFS
progression-free survival
QALY
quality-adjusted life-year
TTD
time to discontinuation
TTP
time to progression
Economic Review
The objective of the economic review undertaken by Canada’s Drug Agency (CDA-AMC) is to review and critically appraise the pharmacoeconomic evidence submitted by the sponsor on the cost-effectiveness and budget impact of pembrolizumab in combination with chemoradiotherapy (CRT) compared to CRT alone for the treatment of adult patients with Fédération internationale de gynécologie et d’obstétrique (FIGO) 2014 stage III to IVA cervical cancer.
Item | Description |
|---|---|
Drug product | Pembrolizumab (Keytruda), 100 mg/mL solution for infusion. |
Indication | Proposed: For the treatment of adult patients with FIGO 2014 Stage III-IVA cervical cancer, in combination with chemoradiotherapy (CRT). |
Submitted price | Pembrolizumab: $4,400.00 per 100 mg/4 mL vial |
Health Canada approval status | NOC |
Health Canada review pathway | Standard |
NOC date | July 14, 2025 |
Reimbursement request | Per indication |
Sponsor | Per application overview |
Submission history | Previously reviewed: Yes Indication: Persistent, recurrent, or metastatic cervical cancer Recommendation date: December 19, 2022 Recommendation: Reimburse with clinical criteria and/or conditions |
FIGO = Fédération internationale de gynécologie et d’obstétrique; NOC = Notice of Compliance.
Key Messages
Pembrolizumab is available as a solution for infusion (25 mg/mL).1 At the submitted price of $4,400 per 4 mL vial, the cost of pembrolizumab is expected to be $11,733 per patient per 28 days, based on a fixed-based dosage following the Health Canada–recommended dosing schedule.1,2 This decreases to $8,096 assuming a weight-based dose (2 mg/kg) and an average weight of 69 kg.
Clinical efficacy in the economic analysis was derived from a subgroup analysis of the KEYNOTE-A18 trial, which compared pembrolizumab plus CRT with CRT alone.2 Evidence submitted by the sponsor indicates that pembrolizumab plus CRT is likely to result in a clinically meaningful improvement for progression-free survival (PFS) and overall survival (OS) compared with CRT alone among patients with FIGO 2014 stage III to IVA cervical cancer. Although the findings on OS and PFS reported across time points were consistent and considered clinically meaningful, there is uncertainty due to imprecision.
The results of the CDA-AMC base case suggest the following:
Pembrolizumab plus CRT will be associated with higher costs to the health care system than CRT alone (incremental costs = $99,988), primarily driven by increased costs associated with drug acquisition.
Pembrolizumab plus CRT will be associated with a gain of 2.04 life-years compared to CRT alone. When the impact on health-related quality of life is also considered, pembrolizumab plus chemoradiotherapy CRT results in a gain of 1.76 quality-adjusted life-years (QALYs) compared to CRT.
The incremental cost-effectiveness ratio (ICER) of pembrolizumab plus CRT compared to CRT was $56,745 per QALY gained in the CDA-AMC base case.
Trial evidence is only approximately 2 years in length, and incremental benefit is contingent on long-term OS. Given that the evidence used to inform long-term OS was informed from another clinical trial (KEYNOTE-826) with different patient characteristics, the incremental QALYs for pembrolizumab plus CRT predicted in the CDA-AMC base case are uncertain and may be overestimated. Scenario analyses conducted indicate that if postprogression survival is improved such that patients who received CRT alone live longer, the ICER for pembrolizumab plus CRT compared to CRT alone increases to $74,284 per QALY gained.
CDA-AMC estimates that the budget impact of reimbursing pembrolizumab for use in combination with CRT for the indicated population will be approximately $73 million over the first 3 years of reimbursement, compared to the amount currently spent on CRT, with an estimated expenditure of $75 million on pembrolizumab plus CRT over this period. The actual budget impact of reimbursing pembrolizumab plus CRT will depend on the number of people eligible for treatment and the market uptake of pembrolizumab.
Summary of the Submitted Economic Evaluation
The sponsor submitted a cost-utility analysis to estimate the cost-effectiveness of pembrolizumab in combination with CRT from the perspective of a public drug plan payer in Canada over a lifetime horizon (50 years).3 The modelled population comprised adult patients with FIGO 2014 stage III to IVA cervical cancer, which is aligned with the Health Canada indication and was based on the participants in the subgroup population of the KEYNOTE-A18 trial.3 The sponsor’s base-case analysis included costs related to drug acquisition, administration, adverse event management, subsequent treatment, and terminal care.3
In the sponsor’s base case, pembrolizumab plus CRT was associated with incremental costs of $189,149 and 2.8 incremental QALYs relative to CRT alone. This resulted in an ICER of $67,007 per QALY gained.3 Approximately 99% of the incremental benefit (2.8 QALYs) was predicted to be accrued after the treatment duration of the FIGO 2014 stage III to IVA disease subgroup of the KEYNOTE-A18 trial (median treatment period = 20 months).3 Additional information about the sponsor’s submission is summarized in Appendix 3.
CDA-AMC identified several key issues with the sponsor’s analysis (refer to Table 2; full details are provided in Appendix 4). A revised base case was therefore developed.
Table 2: Key Issues With the Sponsor’s Economic Submission
Issue | What evidence is there to inform this issue? | How was this issue addressed by CDA-AMC? | Did CDA-AMC explore uncertainty in a scenario analysis? |
|---|---|---|---|
The selected parametric distribution for PFS and TTP did not reflect the natural history of cervical cancer. | Patients with locally advanced cervical cancer are treated with curative intent, which results in a reduction in progression events over time. The sponsor’s selected parametric distribution did not consider an achievable cure when treated with pembrolizumab plus CRT or CRT alone. | CDA-AMC revised the PFS and TTP parametric distribution to better reflect clinical expectation and the published literature. | Given the lack of long-term data on pembrolizumab plus CRT, CDA-AMC explored alternative extrapolations of PFS and TTP in scenario analyses. |
The generalizability of the KEYNOTE-826 trial outcomes for postprogression outcomes is associated with uncertainty. | Postprogression transition probabilities were informed by the KEYNOTE-826 trial. Given the differences in the characteristics of the patients who progressed in the KEYNOTE-A18 trial and those who entered the KEYNOTE-826 trial, there is uncertainty associated with applying survival curves based on KEYNOTE-826 trial data. | CDA-AMC was unable to address this issue in the base case due to the absence of robust data. | CDA-AMC conducted a scenario analysis to explore alternative extrapolations of postprogression survival outcomes. |
Cost savings associated with subsequent treatment use is uncertain because the negotiated price of pembrolizumab for patients with progressed disease is unknown. | Pembrolizumab is currently used as a subsequent therapy for patients who progress. Using pembrolizumab at an earlier stage would reduce its use in later lines. The cost savings associated with this will be influenced by any negotiated price arrangement currently in place. | CDA-AMC did not address this limitation in the base case because the negotiated price of pembrolizumab as subsequent treatment is unknown. | CDA-AMC conducted a scenario analysis that reduced the costs associated with subsequent therapies. |
The proportion of patients treated with pembrolizumab as subsequent treatment was overestimated. This overestimated the cost of pembrolizumab plus CRT. | Clinical expert feedback indicated that 20% of patients who previously received pembrolizumab plus CRT may receive pembrolizumab as a subsequent treatment. | CDA-AMC adjusted the proportion of patients who received pembrolizumab after pembrolizumab plus CRT to 20%, aligned with clinical expert feedback. | No scenario analysis was conducted. |
A fixed dose was assumed for pembrolizumab. This does not align with current administration. | In line with other indications, a weight-based dose will likely be implemented for pembrolizumab. | CDA-AMC selected the sponsor-provided weight-based dosing option. | No scenario analysis was conducted. |
The parametric fit for the TTD curve was not appropriate. This underestimated the cost of pembrolizumab plus CRT. | The sponsor’s parametric fit for TTD did not match the data from the KEYNOTE-A18 trial. | CDA-AMC adjusted the TTD curve to match the trial data. | No scenario analysis was conducted. |
Poor modelling practices were employed in relation to the probabilistic analysis. | To test the parametric uncertainty of the CDA-AMC base case, the sponsor’s PSA was used; however, it would occasionally result in indeterminant calculation. | CDA-AMC modified the sponsor’s model to allow for a functional PSA. | No scenario analysis was conducted. |
CDA-AMC = Canada’s Drug Agency; CRT = chemoradiotherapy; HR = hazard ratio; PFS = progression-free survival; PSA = probabilistic sensitivity analysis; TTD = time to discontinuation; TTP = time to progression.
Note: Details of the issues identified by CDA-AMC are provided in full in Appendix 3.
CDA-AMC Assessment of Cost-Effectiveness
The CDA-AMC base case was derived by making changes to model parameter values and assumptions (refer to Table 7), in consultation with clinical experts. Detailed information about the base case is provided in Appendix 4.
Impact on Health Care Costs
Pembrolizumab plus CRT is expected to be associated with additional health care costs compared to CRT alone (incremental costs = $99,988). Although treatment with pembrolizumab plus CRT results in an additional $146,769 in drug acquisition costs in the first-line setting, as fewer patients receive pembrolizumab upon progression there is a $50,182 reduction in subsequent treatment costs (refer to Figure 1). All other costs to the health system are similar in both treatments.
Figure 1: Impact of Pembrolizumab Plus CRT Versus CRT Alone on Health Care Costs
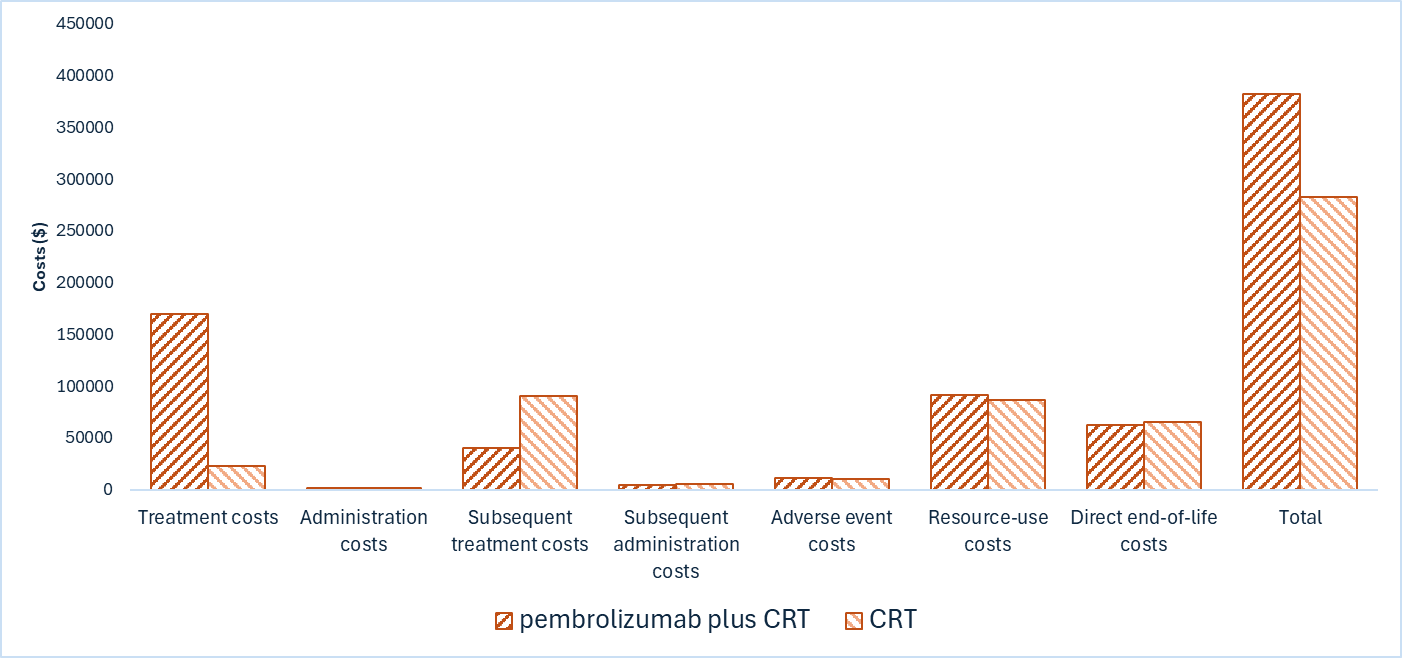
CRT = chemoradiotherapy.
Impact on Health
Relative to CRT alone, pembrolizumab plus CRT is expected to extend mean OS by 2.04 years. This is achieved by preventing progression in some patients and those with progressed disease have a higher mortality risk than those who do not progress. Considering the impact of treatment on both quality and length of life, pembrolizumab plus CRT is expected to result in 1.76 additional QALYs per patient compared to CRT alone (refer to Figure 2).
Figure 2: Impact of Pembrolizumab Plus CRT Versus CRT Alone on Patient Health
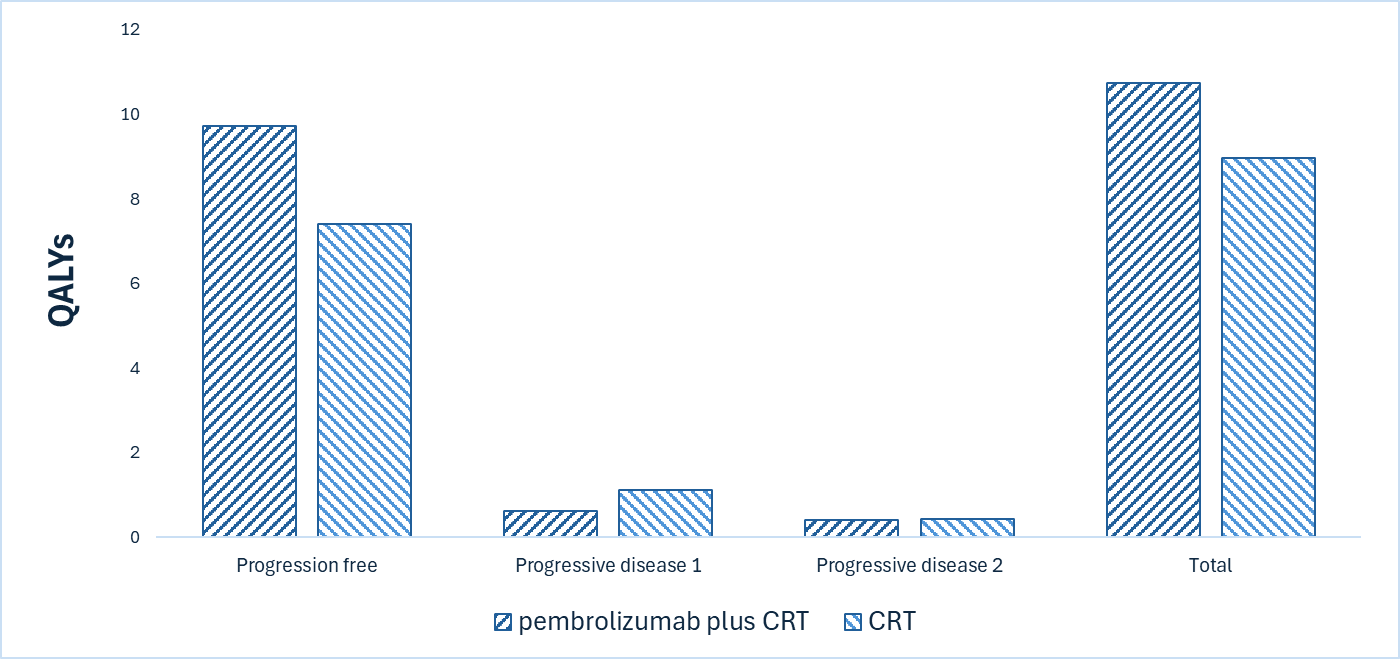
CRT = chemoradiotherapy; QALY = quality-adjusted life-year.
Overall Results
The results of the CDA-AMC base case suggest an ICER of $56,745 per QALY gained for pembrolizumab plus CRT compared to CRT alone (refer to Table 3). Additional details on the CDA-AMC base case are available in Appendix 4.
Table 3: Summary of the CDA-AMC Economic Evaluation Results
Drug | Total costs ($) | Total QALYs | ICER vs. CRT ($/QALY) |
|---|---|---|---|
CRT | 282,284 | 8.98 | Reference |
Pembrolizumab plus CRT | 382,272 | 10.74 | 56,745 |
CDA-AMC = Canada’s Drug Agency; CRT = chemoradiotherapy; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; vs. = versus.
Note: Publicly available list prices were used for all comparators.
Uncertainty and Sensitivity
Uncertainty was explored in the scenario analyses outlined in Table 2 (refer to Table 11, Appendix 4). If the base-case analysis underestimates postprogression survival for those who receive CRT alone then the ICER is underestimated. Scenario analysis shows that an alternative extrapolation of postprogression survival increases the ICER to $74,284 per QALY gained. Conversely, if pembrolizumab continues to reduce progression risk beyond 5 years, the ICER is reduced to $48,999 per QALY gained. Finally, if subsequent treatment costs are reduced by 50%, the ICER would increase to $70,892 per QALY gained.
Summary of the Budget Impact
The sponsor submitted a budget impact analysis (BIA) to estimate the 3-year (2026 to 2029) budget impact of reimbursing pembrolizumab in combination with CRT for use in adult patients with FIGO 2014 stage III to IVA cervical cancer.4 The sponsor assumed that the payer would be participating public drug plans and derived the size of the eligible population using an epidemiologic approach.4 The price of pembrolizumab was aligned with the price included in the sponsor’s economic evaluation, while the prices of comparators were based on the publicly available list prices.2,4 Additional information pertaining to the sponsor’s submission is provided in Appendix 5.
CDA-AMC identified several issues with the sponsor’s estimated BIA and made changes to model parameters and assumptions in consultation with clinical experts to derive the CDA-AMC base case (Appendix 5). CDA-AMC estimated that 868 patients would be eligible for treatment with pembrolizumab plus CRT over a 3-year period (year 1 = 278; year 2 = 289; year 3 = 300), of whom 762 would be expected to receive pembrolizumab plus CRT (year 1 = 202; year 2 = 275; year 3 = 285). The estimated incremental budget impact of reimbursing pembrolizumab plus CRT is expected to be approximately $73 million over the first 3 years, with an expected expenditure of $75 million on pembrolizumab plus CRT. The actual budget impact will depend on the number of people eligible for treatment and its uptake.
Conclusion
Based on the CDA-AMC base case, pembrolizumab plus CRT would be considered cost-effective at the submitted price if the public health care system was willing to pay at least $56,745 for each additional QALY gained. If the public health care system is not willing to pay that amount, a price reduction should be considered (refer to Figure 3; full details of the impact of price reductions on cost-effectiveness are presented in Appendix 4, Table 10). The estimated cost-effectiveness of pembrolizumab plus CRT compared to CRT alone is uncertain due to a lack of long-term evidence, uncertain generalizability of KEYNOTE-826 trial end points, and the presence of confidential list prices for subsequent therapies.
The budget impact of reimbursing pembrolizumab plus CRT to the public drug plans in the first 3 years is estimated to be approximately $73 million. The 3-year expenditure on pembrolizumab (i.e., not accounting for current expenditure on comparators or subsequent treatments) is estimated to be $75 million.
Figure 3: Summary of the CDA-AMC Economic Analysis and Price Reduction
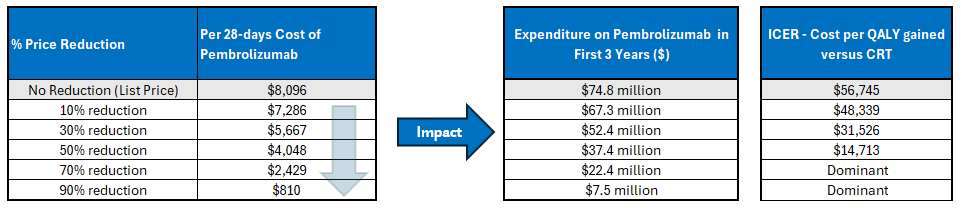
CDA-AMC = Canada’s Drug Agency; CRT = chemoradiotherapy; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Note: Expenditure includes only the drug cost of pembrolizumab in the first-line setting. The term “dominant” indicates that a drug costs less and provides more QALYs than the comparator. The 28-day cost of pembrolizumab assumes a weight-based dose, vial sharing, and an average body weight of 69 kg. The cost used in the model is slightly different as it is based on weight estimates gathered from trial data.
References
1.Merck Canada Inc. Keytruda (pembrolizumab): solution for infusion 100 mg/4 mL vial [product monograph]. May 19, 2015. Updated August 15, 2024.
2.Merck Canada Inc. Drug Reimbursement Review sponsor submission: Keytruda (pembrolizumab), solution for infusion 100 mg/4 mL vial [internal sponsor's package]. March 25, 2025.
3.Merck Canada Inc. Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Keytruda (pembrolizumab), solution for infusion 100 mg/4 mL vial. March 25, 2025.
4.Merck Canada Inc. Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Keytruda (pembrolizumab), solution for infusion 100 mg/4 mL vial. March 25, 2025.
5.Merck, Sharp, and Dohme. Clinical Study Report: KEYNOTE-A18/ENGOT-cx11/GOG-3047. A Randomized, Phase 3, Double-Blind Study of Chemoradiotherapy With or Without Pembrolizumab for the Treatment of High-risk, Locally Advanced Cervical Cancer. Data cutoff 09 Jan 2023 (interim analysis 1) [internal sponsor's report]. June 30, 2023.
6.Merck, Sharp, and Dohme. Statistical analyses of KN-A18 trial data. Data cutoff 08 Jan 2024 (interim analysis 2) [sponsor supplied reference]. 2024.
7.Monk BJ, Colombo N, Tewari KS, et al. KEYNOTE-826: Final overall survival results from a randomized, double-blind, phase 3 study of pembrolizumab + chemotherapy vs placebo + chemotherapy for first-line treatment of persistent, recurrent, or metastatic cervical cancer. J Clin Oncol. 2023;41(16_suppl):5500-5500. doi: 10.1200/JCO.2023.41.16_suppl.5500
8.Statistics Canada. Table: 13-10-0114-01. Life expectancy and other elements of the life table, Canada, all provinces except Prince Edward Island. Accessed April 26, 2025. https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310011401
9.Merck, Sharp, and Dohme. Keytruda (MK-3475) Cervical Cancer HECON Report - Patient Reported Outcomes (Overall) [sponsor supplied reference]. 2022. Accessed December 20.
10.Merck, Sharp, and Dohme. Health Technology Assessment (HTA) Report for Economic Modeling of MK3475, Protocol A-18, A Randomized, Phase 3, Double-Blind Study of Chemoradiotherapy With or Without Pembrolizumab for the Treatment of High-risk, Locally Advanced Cervical Cancer: HECON Report (Participants with III-IVA (node-negative or node-positive disease) FIGO 2014 Stage at Screening). Data cutoff 08 Jan 2024 (interim analysis 2). Version 4 [sponsor supplied reference]. 2024. Accessed July 12.
11.Ara R, Brazier JE. Populating an economic model with health state utility values: moving toward better practice. Value Health. 2010;13(5):509-18. doi: 10.1111/j.1524-4733.2010.00700.x PubMed
12.Mittmann N, Liu N, Cheng SY, et al. Health system costs for cancer medications and radiation treatment in Ontario for the 4 most common cancers: a retrospective cohort study. CMAJ open. 2020;8(1):E191-E198. doi: 10.9778/cmajo.20190114 PubMed
13.Canadian Institute for Health Information. Case mix group 507 [sponsor supplied reference]. 2019. https://www.cihi.ca/en/submit-data-and-view-standards/methodologies-and-decision-support-tools/case-mix
14.De Oliveira C, Pataky R, Bremner KE, et al. Estimating the Cost of Cancer Care in British Columbia and Ontario: A Canadian Inter-Provincial Comparison. Healthc Policy. 2017;12(3):95-108. PubMed
15.Pendrith C, Thind A, Zaric GS, Sarma S. Costs of cervical cancer treatment: population-based estimates from Ontario. Curr Oncol. 2016;23(2):e109-15. doi: 10.3747/co.23.2598 PubMed
16.CADTH Reimbursement Review: Pembrolizumab (Keytruda). Can J Health Technol. 2023;3(3). doi:10.51731/cjht.2022.596
17.Colombo N, Dubot C, Lorusso D, et al. Pembrolizumab for Persistent, Recurrent, or Metastatic Cervical Cancer. N Engl J Med. 2021;385(20):1856-1867. doi: 10.1056/NEJMoa2112435 PubMed
18.Monk BJ, Sill MW, McMeekin DS, et al. Phase III trial of four cisplatin-containing doublet combinations in stage IVB, recurrent, or persistent cervical carcinoma: a Gynecologic Oncology Group study. J Clin Oncol. 2009;27(28):4649-55. doi: 10.1200/JCO.2009.21.8909 PubMed
19.Canadian Institute for Health Information. Patient Cost Estimator 2021-22. 2022. Accessed February 24, 2025. https://www.cihi.ca/en/patient-cost-estimator
20.Wehler E, Zhao Z, Pinar Bilir S, Munakata J, Barber B. Economic burden of toxicities associated with treating metastatic melanoma in eight countries. Eur J Health Econ, 2017;18(1):49-58. doi: 10.1007/s10198-015-0757-y PubMed
21.CADTH Reimbursement Recommendation: Pembrolizumab (Keytruda). Can J Health Technol. 2022;2(12). doi:10.51731/cjht.2022.527
22.Coyle D, Haines A, Lee K. Extrapolating Clinical Evidence Within Economic Evaluations. Can J Health Technol. 2023;3(5). doi: 10.51731/cjht.2023.649 PubMed
23.Kim TE, Park BJ, Kwack HS, Kwon JY, Kim JH, Yoon SC. Outcomes and prognostic factors of cervical cancer after concurrent chemoradiation. J Obstet Gynaecol Res. 2012;38(11):1315-20. doi: 10.1111/j.1447-0756.2012.01871.x PubMed
24.Pan XB, Lu Y, Wei YS, Yao DS. Efficacy of treatment patterns based on concurrent chemoradiotherapy in patients with stage IIB cervical squamous cell carcinoma. BMC Cancer. 2024;24(1):106. doi: 10.1186/s12885-023-11372-6 PubMed
25.Shin W, Ham TY, Park YR, Lim MC, Won YJ. Comparing survival outcomes for cervical cancer based on the 2014 and 2018 International Federation of Gynecology and Obstetrics staging systems. Sci Rep. 2021;11(1):6988. doi: 10.1038/s41598-021-86283-2 PubMed
26.Lorusso D, Xiang Y, Hasegawa K, et al. Pembrolizumab or placebo with chemoradiotherapy followed by pembrolizumab or placebo for newly diagnosed, high-risk, locally advanced cervical cancer (ENGOT-cx11/GOG-3047/KEYNOTE-A18): a randomised, double-blind, phase 3 clinical trial. Lancet. 2024;403(10434):1341-1350. doi: 10.1016/S0140-6736(24)00317-9 PubMed
27.Monk BJ, Colombo N, Tewari KS, et al. First-Line Pembrolizumab + Chemotherapy Versus Placebo + Chemotherapy for Persistent, Recurrent, or Metastatic Cervical Cancer: Final Overall Survival Results of KEYNOTE-826. J Clin Oncol. 2023;41(36):5505-5511. doi: 10.1200/JCO.23.00914 PubMed
28.Canadian Cancer Statistics Advisory Committee in collaboration with the Canadian Cancer Society, Statistics Canada, and the Public Health Agency of Canada. Canadian Cancer Statistics 2024. Canadian Cancer Society; 2024. Accessed April 26, 2025. https://cancer.ca/Canadian-Cancer-Statistics-2024-EN
29.Mahmud A, Brydon B, Tonita J, Hanna TP, Schmidt M, Tai P. A population-based study of cervix cancer: incidence, management and outcome in the Canadian province of Saskatchewan. Clin Oncol (R Coll Radiol). 2011;23(10):691-5. doi: 10.1016/j.clon.2011.05.002 PubMed
30.Tian T, Gong X, Gao X, Li Y, Ju W, Ai Y. Comparison of survival outcomes of locally advanced cervical cancer by histopathological types in the surveillance, epidemiology, and end results (SEER) database: a propensity score matching study. Infect Agent Cancer. 2020;15:33. doi: 10.1186/s13027-020-00299-3 PubMed
31.Brenner DR, Poirier A, Woods RR, et al. Projected estimates of cancer in Canada in 2022. CMAJ. 2022;194(17):E601-E607. doi: 10.1503/cmaj.212097 PubMed
32.Grigsby PW, Massad LS, Mutch DG, et al. FIGO 2018 staging criteria for cervical cancer: Impact on stage migration and survival. Gynecol Oncol. 2020;157(3):639-643. doi: 10.1016/j.ygyno.2020.03.027 PubMed
Appendix 1: Cost Comparison Table
Please note that this appendix has not been copy-edited.
The comparators presented in Table 4 have been deemed to be appropriate based on feedback from clinical experts and CDA-AMC–participating public drug plans. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in Table 4 and, as such, Table 4 may not represent the actual costs to public drug plans.
Table 4: Cost Comparison for Cervical Cancer
Treatment | Strength and/or concentration | Form | Price ($) | Recommended dosage | Daily cost ($) | 28-day cost ($)a |
|---|---|---|---|---|---|---|
Pembrolizumab in combination with CRT | ||||||
Pembrolizumab | 100 mg/4 mL | Solution for infusion | $4,400.0000 | Fixed dosage: 200 mg once every 3 weeks, or 400 mg once every 6 weeks | 419 | 11,733 |
Weight-based dosage: 2 mg/kg (up to 200 mg) once every 3 weeks or 4 mg/kg (up to 400 mg) once every 6 weeksb | 289 | 8,096 | ||||
Cisplatin | 50 mg/mL 100 mg/mL | Solution for infusion | $135.0000 $270.0000 | BSA dose: 40 mg/m2 IV infusion every week for 6 weeks | 39 | 1,080 |
Pembrolizumab plus CRT | — | — | — | — | 328 to 458 | First 6 weeks: 9,176 to 12,813 Post 6 weeks: 8,096 to 11,733 |
CRT (cisplatin) | ||||||
Cisplatin | 50 mg/mL 100 mg/mL | Solution for infusion | $135.0000 $270.0000 | BSA dose: 40 mg/m2 IV infusion every week for 6 weeks | 39 | 1,080 |
CRT | — | — | — | — | 39 | 1,080 |
CRT (carboplatin) | ||||||
Carboplatin | 5 mL (10 mg/mL) 15 mL (10 mg/mL) 45 mL (10 mg/mL) 60 mL (10 mg/mL) | Solution for infusion | $70.0000 $210.0000 $600.0000 $775.0000 | 2 AUC infusions every week for 6 weeksc | 60 | 1,680 |
CRT | — | — | — | — | 60 | 1,680 |
AUC = area under the curve; BSA = body surface area; CRT = chemoradiotherapy.
Note: All prices are from the Ontario Drug Benefit Formulary (accessed May 2025), unless otherwise indicated, and do not include dispensing fees.
aThe maximum number of cycles for pembrolizumab and cisplatin treatment is 35 and 6, respectively.
bInput from clinical experts and participating drug plans indicated that weight-based dosage may be used for pembrolizumab. Weight-based dosage assumes a mean weight of 69 kg and vial sharing.
cAUC calculated based on a GFR = 125 mL/min.
Appendix 2: Input Relevant to the Economic Review
Please note that this appendix has not been copy-edited.
This section is a summary of the input received from the patient groups, clinician groups, and drug plans that participated in the CDA-AMC review process.
Joint patient input was received from 3 groups: Colorectal Cancer Resource and Action Network in collaboration with the Canadian Cancer Survivor Network and HPV global action. A total of 8 survey respondents (5 resided in Canada) and 5 interviewees (3 resided in Canada) highlighted the importance of controlling the spread of disease and the significant impacts to quality of life. Patients who were interviewed reported previous treatment with cisplatin, carboplatin, paclitaxel, bevacizumab, palliative care, and alternative methods. All patients who answered the survey were seeking to maintain quality of life and access a new treatment option. Patient input also indicated that some patients were seeking to reduce side effects from current treatments and delay onset of symptoms. 4 of the 5 patients interviewed had experience with pembrolizumab, and most reported having a positive experience including ease of use, control of symptoms, and positive clinical response with minimal side effects.
Clinician group input was received from 2 clinician groups: Ontario Health (Cancer Care Ontario) and Gynecologic Oncology of Canada. Clinician feedback highlighted that there are few therapy options for patients with FIGO 2014 stage III to IVA cervical cancer, namely: concurrent chemoradiation, or induction chemotherapy and subsequent chemoradiation. Clinician group input indicated that current treatment goals are to improve OS, PFS, and quality of life. Clinician group input stated that the most suitable for pembrolizumab in combination with chemoradiotherapy (CRT) treatment are FIGO stage III and IV patients who have not received prior treatment.
Input from CDA-AMC–participating drug plan input noted concerns about the generalizability of the FIGO 2014 to FIGO 2018 staging criteria. Drug plans additionally noted that the place in therapy would change from the metastatic to the locally advanced setting. Drug plans questioned eligibility if patients were unable to tolerate chemotherapy, if patients had Eastern Cooperative Oncology Group Performance Status scores of 2 or greater, or if patients recently completed CRT treatment. Drug plans indicated that, if a positive recommendation, a weight-based dosing schedule would be implemented.
Several of these concerns were addressed in the sponsor’s model:
PFS, quality of life, and adverse events were captured.
CDA-AMC addressed some of these concerns as follows:
A weight-based dose was captured in the CDA-AMC base case.
CDA-AMC was unable to address the following concerns:
Patients who could not tolerate chemotherapy, had recently receive CRT, or had an Eastern Cooperative Oncology Group Performance Status score greater than 2 were not captured due to a lack of available evidence.
Appendix 3: Summary of the Sponsor’s Submission
Please note that this appendix has not been copy-edited.
Summary of the Sponsor’s Economic Evaluation
For the pharmaceutical reviews program, clinical and economic information is submitted to CDA-AMC by the sponsor. The CDA-AMC health economics team reviews the submitted economic information and appraises the information in collaboration with clinical experts and the clinical review team to evaluate key assumptions, influential parameters, and the overall rigour of the economic submission. Based on what the team learns through this process, adjustments may be made to the sponsor’s model to produce the CDA-AMC base case. The CDA-AMC base case represents the team’s current understanding of the clinical condition, clinical evidence currently available, and best interpretation of the economic evidence based on the information provided.
For the review of pembrolizumab in combination with CRT, the sponsor provided a cost-utility analysis and a BIA. The sponsor’s economic submission is summarized in Table 5.
Table 5: Key Components of the Sponsor’s Economic Evaluation
Component | Description |
|---|---|
Treatment information | |
Drug under review | Pembrolizumab (Keytruda), IV (IV) solution (100 mg/4 mL) in combination with CRT |
Submitted price of drug under review | Pembrolizumab: $4,400.0000 per vial |
Regimen | 200 mg q.3.w. or 400 mg q.6.w. (fixed-based dose) |
28-day cost of drug under review | Pembrolizumab: $11,733 per patient |
Model information | |
Type of economic evaluation | Cost-utility analysis State-transition cohort model |
Treatment | Pembrolizumab in combination with CRT |
Included comparator | CRT: cisplatin, radiotherapy (external beam radiotherapy and brachytherapy) |
Perspective | Publicly funded health care payer perspective |
Time horizon | Lifetime (50 years) |
Cycle length | 1 week cycles |
Modelled population | Adult patients with FIGO 2014 stage III to IVA cervical cancer |
Characteristics of modelled population | Derived from subgroup of KEYNOTE-A18 trial (mean age: 49.8 years, body weight: 63.1 kg, BSA: 1.7 m2) |
Model health states |
For additional information, refer to Model Structure |
Data sources | |
Comparative efficacy | |
Natural history and/or clinical pathway |
|
Health-related utilities and disutilities | |
Costs |
|
Summary of the submitted results | |
Base case results | ICER = $67,007 per QALY gained (incremental costs = $189,149; incremental QALYs = 2.8) |
Scenario analysis resultsb | |
AE = adverse event; BSA = body surface area; CIHI = Canadian Institute for Health Information; CRT = chemoradiotherapy; FIGO = Fédération internationale de gynécologie et d’obstétrique; ICER = incremental cost-effectiveness ratio; PFS = progression-free survival; PPS = postprogression survival; q.3.w. = every 3 weeks; q.6.w. = every 6 weeks; QALY = quality-adjusted life-years; TTD = time to discontinuation; TTP = time to progression.
aPembrolizumab + CRT = $9,880 to $12,813 per patient per 28-day cycle based on a weight of 63.1 kg and BSA of 1.7 m2.
bResults of scenario analyses that had a meaningful impact on the estimated ICER compared to the sponsor’s base case. Additional scenarios submitted that had no meaningful impact on the estimated ICER included alternate discounting, using KEYNOTE-A18 trial findings to model TTP2 and PPS, exclusion of the age utility adjustment, calculating utilities based on multivariate regression, exclusion of AE disutility, exclusion of terminal care costs, including indirect costs, including a progressive disease 2 (PD2) disutilities, no half-cycle correction, and allowing vial sharing.
Model Structure
The sponsor submitted a state-transition cohort model with time-dependent probabilities with 1-week cycle lengths consisting of 4 health states (i.e., progression free, progressive disease 1 (PD1), PD2, and death [Figure 4]).3 All patients enter the model diagnosed with FIGO 2014 stage III to IVA cervical cancer and, upon beginning treatment, enter the model in the progression-free health state.3 State membership was estimated from an AUC approach from 3 independent survival curves (time to progression [TTP], PFS, and postprogression survival).3 A fourth survival curve, time-to-treatment discontinuation (TTD) was used to determine the proportion of patients in the progression-free state who were no longer on treatment.3
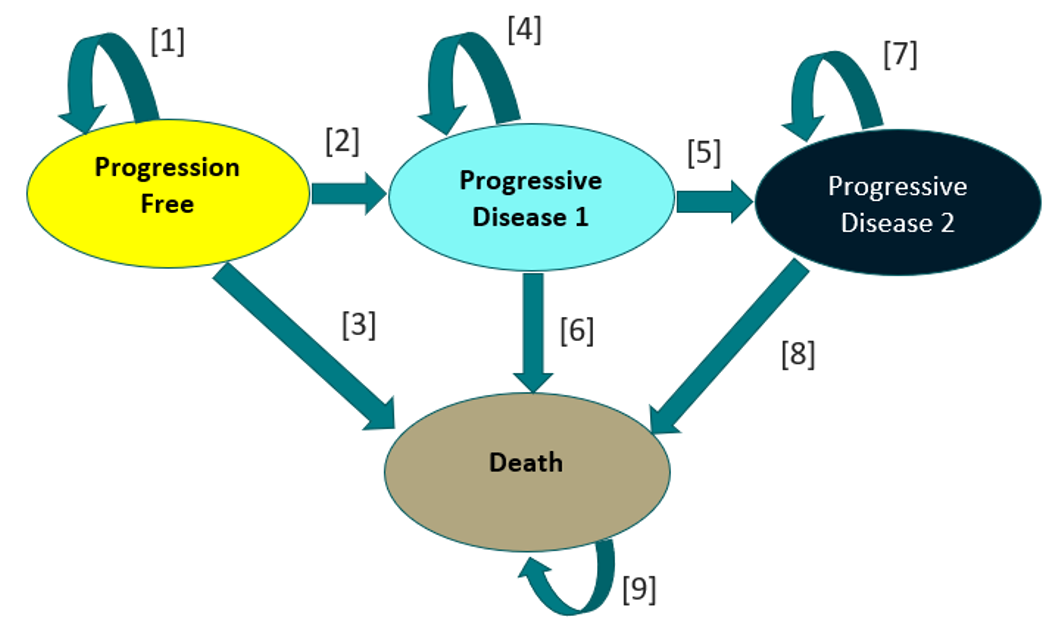
Table 6: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER vs. ($/QALY) |
|---|---|---|---|---|---|
CRTa | 348,144 | Reference | 6.4 | Reference | Reference |
Pembrolizumab in combination with CRT | 537,293 | 189,149 | 9.2 | 2.8 | 67,007 |
CRT = chemoradiotherapy; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; vs. = versus.
aCRT comprises cisplatin, external beam radiotherapy, brachytherapy.
Appendix 4: Additional Details of CDA-AMC Reanalyses
Please note that this appendix has not been copy-edited.
Clinical Data in the Economic Model
The CDA-AMC clinical review found that pembrolizumab plus CRT likely results in a clinically important increase in OS and PFS when compared to placebo plus CRT. The post hoc subgroup analysis conducted based on the KEYNOTE-A18 trial across time points (i.e., 18, 24, 30, and 36 months) were consistent and considered clinically meaningful. Additionally, adverse event frequency was similar for patients treated with chemotherapy with or without pembrolizumab, and the safety profile for pembrolizumab plus chemotherapy was considered manageable in practice. However, the sponsor’s post hoc subgroup analysis is associated with uncertainty due to the risk of type I error and imprecision of point estimates.
Estimates for the transition probabilities for the PD1 and PD2 health states were informed by the KEYNOTE-826 trial, which was not included in the sponsor’s clinical evidence for this review. However, KEYNOTE-826 was appraised in a previous CDA-AMC submission, where it was noted that pembrolizumab plus standard of care had a statistically significant benefit in PFS and OS when compared to placebo plus standard of care.21 While patients with persistent, recurrent, or metastatic cervical cancer can benefit from pembrolizumab treatment, it is uncertain if the clinical outcomes from KEYNOTE-826 are generalizable to a patient population who were previously treated with pembrolizumab (i.e., patients with locally advanced cervical cancer [LACC]).
Key Issues of the Submitted Economic Evaluation
CDA-AMC identified the following key issues with the sponsor’s analysis:
Modelled disease progression and patient outcomes do not reflect the natural history of disease. The sponsor’s submitted economic model chose a log-normal distribution for TTP and PFS. The log-normal distribution was chosen based on visual inspection, statistical fit parameters, and clinical expert opinion.3 While visual inspection and statistical fit parameters are appropriate selection methods for interpolation, additional rationale should be considered for extrapolation such as reviewing and validating survival estimates with published literature.22 The sponsor-selected log-normal TTP distribution predicted that approximately 40% and 18% of patients would remain progression free at 10 years for the pembrolizumab and CRT, and CRT arms, respectively.3 Clinical experts consulted for this review indicated that the current standard of care is provided with curative intent, and the likelihood of a progression event decreases rapidly after 3 years. After 5 years the probability of progression is expected to be small. Therefore, clinical experts noted that the sponsor’s base case likely underestimated OS and PFS for both the pembrolizumab plus CRT and CRT arms, as a cure is possible for a proportion of patients. This was corroborated by published literature as survival estimates for patients diagnosed with FIGO 2018 stage IIB to IIIC LACC demonstrate a plateau after 36 months, suggesting a reduction in mortality risk over time.23-25 As such, It is likely that the risk of long-term progression is smaller than that estimated by the sponsor.
Based on feedback from clinical experts and published literature the rate of progression is expected to substantially drop after 5 years. Therefore, CDA-AMC selected the sponsor-provided generalized gamma distribution for extrapolating TTP and PFS, which was considered plausible according to clinical expert feedback and projects a reduction in progression over time. Finally, the generalized gamma had the best Akaike information criterion and Bayesian information criterion rank meaning it has the best statistical fit to the trial data.
At 5 years, progression rates are likely similar between those who received pembrolizumab and those who did not. To account for this treatment waning was applied using the sponsor prebuilt functionality such that progression rates were equal at 5 years.
To address the uncertainty from long-term outcomes, CDA-AMC conducted a scenario analysis where treatment waning was set to 7 years.
Generalizability of outcomes from the KEYNOTE-826 trial as a proxy for postprogression outcomes is associated with uncertainty. In the KEYNOTE-A18 trial very few patients received pembrolizumab as a subsequent therapy. Although 125 patients in the CRT arm experienced a progression event, only 15% (19/125) received pembrolizumab. Experts noted that up to 80% of patients would likely receive pembrolizumab meaning survival outcomes in the postprogression state were likely underestimated in the A18 trial. To account for this, the sponsor also provided an option to use survival curves from the KEYNOTE-826 trial which looks at pembrolizumab efficacy in the progressed setting. Transitions from the progressed health states were informed from KEYNOTE-826.3,17 The survival curves based on KEYNOTE-826 were subjected to a hazard ratio (HR) to estimate the benefit of patients who were treated with pembrolizumab plus platinum-based chemotherapy with or without bevacizumab in subsequent treatment compared to platinum-based chemotherapy with or without bevacizumab.3 However, 1 limitation with this approach is that there is uncertainty regarding the differences in the baseline characteristics of the patients in KEYNOTE-826 versus the characteristics of those who progress in KEYNOTE-A18.17,26 For example, 18.8% of patients did not receive previous therapy, and 44.6% of patients did not receive CRT with or without surgery in the pembrolizumab arm of KEYNOTE-826. The sponsor’s submitted model implicitly assumed that all patients in the progressed health state received prior therapy.17 As such, there is uncertainty associated with applying survival curves based on a patient population with differing baseline characteristics.
CDA-AMC was unable to address this limitation as KEYNOTE-A18 data postprogression was immature and the proportion of patients who received pembrolizumab as a subsequent treatment in KEYNOTE-A18 was lower than clinical expert expectations, which does not accurately reflect clinical practice in Canada.
Outcomes from the KEYNOTE-A18 trial postprogression may be accurate for those who received pembrolizumab as few patients are expected to be retreated with pembrolizumab in Canada. In a scenario analysis, an HR of 0.60 was applied to the rate of death postprogression for those who progressed on CRT only. This matches the HR for OS in the KEYNOTE-826 trial.27 This analysis likely overestimates postprogression survival for those receiving CRT pembrolizumab as it assumes everyone receives pembrolizumab and that prior exposure to pembrolizumab has no impact on postprogression outcomes. This can be seen as a potential upper limit of postprogression survival for those receiving CRT.
Subsequent treatment costs may be overestimated. To calculate subsequent therapy costs the sponsor applied a 1-time cost based on the mean duration of treatment informed by a point estimate in the KEYNOTE-826 trial3 (Pembrolizumab: 11.8 months; platinum-based chemotherapy: 4.1 months; Bevacizumab: 9.4 months). It would be more suitable for parametric distributions based on TTD from the KEYNOTE-826 trial to predict the duration of treatment. Additionally, using TTD curves would allow for the characterization of parameter uncertainty during the probabilistic sensitivity analysis. The current approach may misestimate subsequent treatment cost, especially in the probabilistic analysis where TTP will vary independently from time on treatment. If subsequent treatment costs were overestimated, the pembrolizumab plus CRT arm would be favoured as patients spend less time in the PD1 and PD2 health states compared to the CRT arm. Pembrolizumab also has a letter of intent from the pan-Canadian Pharmaceutical Alliance, meaning that there is a negotiated price. All cost savings associated with reducing subsequent therapy use are based on public list prices and are therefore overestimated.
CDA-AMC was unable to revise the method to calculate subsequent treatment costs due to the sponsor’s model structure.
To explore the uncertainty of subsequent treatment costs, CDA-AMC conducted a scenario analysis which reduced subsequent therapy costs associated by 50%.
The proportion of patients treated with pembrolizumab as subsequent treatment was overestimated. The sponsor assumed 80% of patients who previously received pembrolizumab plus CRT would receive pembrolizumab as a subsequent treatment after their first progression.3 Clinical expert feedback obtained by CDA-AMC indicated that only 20% of those patients would be expected to be treated with pembrolizumab after their first progression as pembrolizumab treatment had previously failed.
CDA-AMC revised the proportion of patients receiving pembrolizumab plus chemotherapy with or without bevacizumab as a subsequent treatment was 20%, in line with clinical expert feedback.
Weight-based dosing for pembrolizumab. The pembrolizumab dosage in KEYNOTE-A18 was a fixed dose of 200 mg every 21 days or 400 mg every 42 days. CDA-AMC notes that in line with other indications for pembrolizumab, jurisdictions would likely implement a weight-based dose for pembrolizumab of 2 mg/kg (up to a cap of 200 mg) every 3 weeks with the possibility of extended dosing intervals to every 6 weeks (4 mg/kg up to a 400 mg cap). The clinical experts agreed that this approach seemed reasonable given the clear interchangeable use in dosing for other cancer sites.
CDA-AMC selected the sponsor-provided weight-based dose option to determine the cost of pembrolizumab for initial and subsequent treatment. Vial sharing was also assumed.
Choice of parametric distribution for a TTD curve for pembrolizumab. The sponsor’s base-case analysis independently fitted parametric distribution based on the TTD Kaplan-Meier (KM) curve from KEYNOTE-A18.26 However, the trial implemented a stopping rule at 2 years meaning at 2 years the TTD KM quickly falls to 0%. Given this, there are no suitable parametric functions that can account for this enforced reduction to the curve. As such, the sponsor’s selected Gompertz distribution curve significantly deviated from the TTD KM curve. Figure 5 demonstrates the difference between the sponsors assumed TTD and the trial data. Finally, as discontinuation of treatment likely occurs when patients experience progression, TTD is highly correlated to PFS and should not be fitted independently.
Figure 5: Time-to-Treatment Discontinuation Comparison
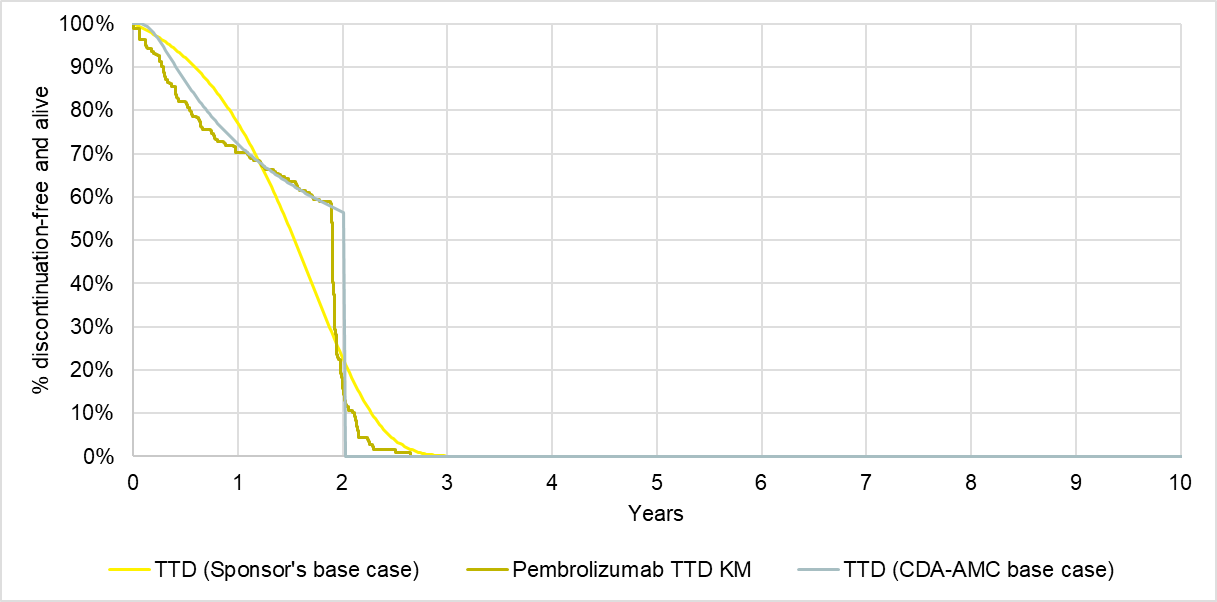
CDA-AMC = Canada’s Drug Agency; KM = Kaplan-Meier; TTD = time-to-treatment discontinuation.
In reanalysis, CDA-AMC selected to estimate TTD based on PFS with an HR of 1.8 and revised discontinuation of pembrolizumab after 2 years to 100%, in line with stopping rules according to the product monograph. Figure 5 outlines the assumed TTD in the CDA-AMC base case.
Poor modelling practices in relation to the probabilistic analysis. For the sponsor’s probabilistic sensitivity analysis, random draws allowed for the testing of parametric uncertainty; however, the sponsor’s method to adjust survival curves occasionally resulted in indeterminant calculations, resulting in a nonfunctioning probabilistic sensitivity analysis.
CDA-AMC conducted changes to allow for a functioning probabilistic sensitivity analysis.
CDA-AMC Reanalysis of the Economic Evaluation
The CDA-AMC base case was derived by making changes in model parameter values and assumptions, in consultation with clinical experts (refer to Table 7). The impact of these changes, individually and collectively, is presented in Table 8.
Table 7: Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CDA-AMC value or assumption |
|---|---|---|
1. Survival Curve distribution | KEYNOTE-A18 TTP: log-normal KEYNOTE-A18 PFS: log-normal No treatment waning | KEYNOTE-A18 TTP: gen gamma KEYNOTE-A18 PFS: gen gamma Treatment waning 2 to 5 years |
2. Subsequent treatment distribution for pembrolizumab plus CRT | Pembrolizumab: 80% | Pembrolizumab: 20% |
3. Weight-based dosing for pembrolizumab | Fixed to 200 mg q.3.w. or 400 mg q.6.w. | Weight-based: 2 mg/kg q.3.w. or 4 mg/kg q.6.w. Vial sharing assumed |
4. TTD parametric distribution for pembrolizumab plus CRT | Gompertz distribution | Based on PFS with an HR of 1.8 |
CDA-AMC base case (health care payer perspective) | ― | 1 + 2 + 3 + 4 |
CDA-AMC = Canada’s Drug Agency; CRT = chemoradiotherapy; HR = hazard ratio; PFS = progression-free survival; q.3.w. = every 3 weeks; q.6.w. = every 6 weeks; TTD = time to discontinuation, TTP = time to progression.
Note: CDA-AMC was unable to resolve the issues with poor modelling practices.
Table 8: Summary of the Stepped Analysis
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALY) |
|---|---|---|---|---|
Sponsor’s base case (probabilistic) | CRT | 348,144 | 6.41 | Reference |
Pembrolizumab plus CRT | 537,293 | 9.23 | 67,007 | |
Sponsor’s base case (deterministic) | CRT | 349,184 | 6.46 | Reference |
Pembrolizumab plus CRT | 538,857 | 9.31 | 66,507 | |
CDA-AMC reanalysis 1 | CRT | 314,826 | 9.06 | Reference |
Pembrolizumab plus CRT | 520,528 | 11.21 | 95,496 | |
CDA-AMC reanalysis 2 | CRT | 349,184 | 6.46 | Reference |
Pembrolizumab plus CRT | 467,044 | 8.94 | 47,511 | |
CDA-AMC reanalysis 3 | CRT | 305,876 | 6.46 | Reference |
Pembrolizumab plus CRT | 427,873 | 9.31 | 42,777 | |
CDA-AMC reanalysis 4 | CRT | 349,184 | 6.46 | Reference |
Pembrolizumab plus CRT | 551,103 | 9.31 | 70,801 | |
CDA-AMC base case: (1 + 2 + 3 + 4) (deterministic) | CRT | 282,448 | 9.06 | Reference |
Pembrolizumab plus CRT | 382,890 | 10.91 | 54,072 | |
CDA-AMC base case (1 + 2 + 3 + 4) (probabilistic) | CRT | 282,284 | 8.98 | Reference |
Pembrolizumab plus CRT | 382,272 | 10.74 | 56,745 |
CDA-AMC = Canada’s Drug Agency; CRT = chemoradiotherapy; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Note: The CDA-AMC reanalysis is based on the publicly available prices of the comparator treatments. Deterministic results are presented, unless otherwise indicated.
Table 9: Disaggregated Results of the CDA-AMC Base Case (Probabilistic)
Parameter | Pembrolizumab + CRT | CRT |
|---|---|---|
Discounted LYs | ||
Total | 13.02 | 10.97 |
Progression free | 11.67 | 8.90 |
Progressive disease 1 | 0.82 | 1.50 |
Progressive disease 2 | 0.53 | 0.58 |
Discounted QALYs | ||
Total | 10.74 | 8.98 |
Progression free | 9.72 | 7.42 |
Progressive disease 1 | 0.62 | 1.12 |
Progressive disease 2 | 0.40 | 0.44 |
Discounted costs ($) | ||
Total | 382,272 | 282,284 |
Treatment | 169,552 | 22,783 |
Administration | 1,730 | 1,264 |
Subsequent treatment | 40,387 | 90,569 |
Subsequent administration | 4,335 | 5,664 |
Adverse events | 11,677 | 10,404 |
Resource use | 91,850 | 86,399 |
Direct end-of-life | 62,741 | 65,201 |
CDA-AMC = Canada’s Drug Agency; LY = life-year; CRT = chemoradiotherapy; QALY = quality-adjusted life-year.
Price Reduction Analysis
CDA-AMC conducted price reduction analyses using the sponsor’s base case and the CDA-AMC base case (refer to Table 10).
Table 10: Results of the Price Reduction Analysis
Price reduction | Unit drug cost ($) | Cost per 28 days ($) | ICERs for pembrolizumab plus CRT vs. CRT ($/QALY) | |
|---|---|---|---|---|
Sponsor base case | CDA-AMC base case | |||
No price reduction | 4,400a | 8,096 | 67,007 | 56,745 |
10% | 3,960 | 7,286 | 56,121 | 48,339 |
20% | 3,520 | 6,477 | 45,234 | 39,932 |
30% | 3,080 | 5,667 | 34,347 | 31,526 |
40% | 2,640 | 4,858 | 23,460 | 23,119 |
50% | 2,200 | 4,048 | 12,573 | 14,713 |
60% | 1,760 | 3,238 | 1,687 | 6,306 |
70% | 1,320 | 2,429 | Dominant | Dominant |
80% | 880 | 1,619 | Dominant | Dominant |
90% | 440 | 810 | Dominant | Dominant |
CDA-AMC = Canada’s Drug Agency; CRT = chemoradiotherapy; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; vs. = versus.
aSponsor’s submitted price for pembrolizumab.2
Assessment of Uncertainty
CDA-AMC used the CDA-AMC base case to conduct scenario analyses to address uncertainty within the economic evaluation. The results are provided in Table 11.
Scenario 1: applying HRs for OS from KEYNOTE-826 to KEYNOTE-A18 data to inform postprogression survival for those receiving CRT only.
Scenario 2: treatment waning from 2 to 7 years.
Scenario 3: reduce subsequent therapy costs of pembrolizumab by 50%.
Table 11: Results of CDA-AMC Scenario Analyses
Analysisa | Drug | Total costs ($) | Total QALYs | ICER ($/QALYs) |
|---|---|---|---|---|
CDA-AMC base case | CRT | 282,448 | 9.06 | Reference |
Pembrolizumab plus CRT | 382,890 | 10.91 | 54,072 | |
CDA-AMC scenario 1: alternative PPS extrapolation | CRT | 289,725 | 9.80 | Reference |
Pembrolizumab plus CRT | 377,412 | 10.98 | 74,284 | |
CDA-AMC scenario 2: longer treatment waning | CRT | 282,448 | 9.06 | Reference |
Pembrolizumab plus CRT | 384,026 | 11.13 | 48,999 | |
CDA-AMC scenario 3: reduction in subsequent therapy costs | CRT | 253,191 | 8.99 | Reference |
Pembrolizumab plus CRT | 376,528 | 10.73 | 70,892 |
CDA-AMC = Canada’s Drug Agency; CRT = chemoradiotherapy; ICER = incremental cost-effectiveness ratio; PPS = postprogression survival; QALY = quality-adjusted life-year.
aProbabilistic analyses.
Figure 6: CDA-AMC Scenario Analysis 3 — Impact of Reducing the Price of Pembrolizumab in the Subsequent Treatment Line Only on the ICER (Deterministic)
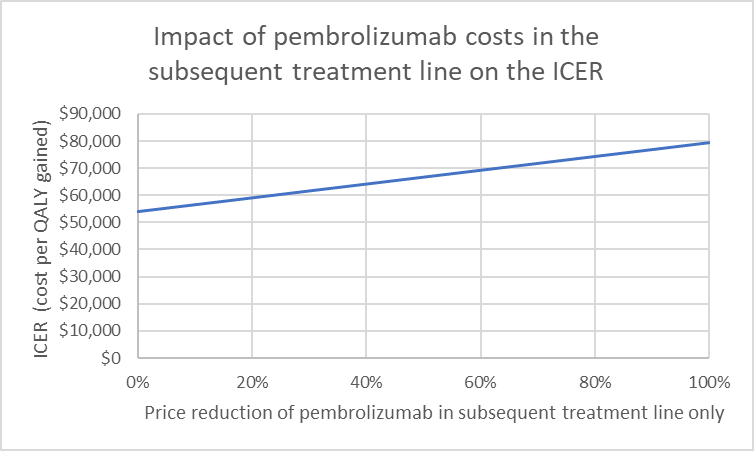
CDA-AMC = Canada’s Drug Agency; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Issues for Consideration
This review is indicated for patients with FIGO 2014 stage III to IVA LACC, clinician experts indicated that staging is currently performed using the FIGO 2018 criteria, which may include patients who were diagnosed with stage II or lower disease based on the FIGO 2014 criteria. It is uncertain if the results from the KEYNOTE-A18 subgroup analysis is generalizable to patients with stage II or lower FIGO 2014 LACC.
Pembrolizumab is currently under review for the treatment of adult patients with resectable locally advanced head and neck squamous cell carcinoma as neoadjuvant treatment, continued as adjuvant treatment in combination with radiotherapy with or without platinum-containing chemotherapy and then as monotherapy.
The pan-Canadian Pharmaceutical Alliance concluded negotiations with a letter of intent for pembrolizumab covering multiple indications. As such, pembrolizumab has a confidential negotiated price, and is currently funded by jurisdictional cancer formularies. The CDA-AMC reanalyses are based on the publicly available price of pembrolizumab, which may differ from the confidential price and may influence the results of the cost-effectiveness and BIAs.
Appendix 5: Budget Impact Analysis
Please note that this appendix has not been copy-edited.
Summary of the Submitted BIA
The sponsor submitted a BIA that estimated the expected incremental budgetary impact of reimbursing pembrolizumab in combination with CRT for the treatment of adult patients with FIGO 2014 stage III to IVA cervical cancer.4
The BIA was conducted from the perspective of public drug plan payers over a 3-year time horizon (July 2026 to July 2029), with 2025 to 2026 as the base year.4 The sponsor’s estimate reflects the aggregated results from the jurisdictional provincial budgets (excluding Quebec) as well as the Non-Insured Health Benefits Program.4 The sponsor estimated the eligible population using an epidemiological approach.4 The sponsor estimated drug acquisition and subsequent treatment cost by a function of an estimated weekly incidence, the proportion of patients on each treatment, and the parametric fit of the time-on-treatment KM curve.4 The sponsor’s base case included drug acquisition and subsequent treatment costs.4 The market uptake for pembrolizumab in combination with CRT was assumed to capture 80% market share in 52 weeks, estimated using logarithmic regression.4 The key inputs to the BIA are documented in Table 12.
The sponsor estimated the 3-year incremental budget impact associated with reimbursing pembrolizumab in combination with CRT for the treatment of adult patients with FIGO 2014 stage III to IVA cervical cancer would be $98,506,693 (year 1 = $10,889,281; year 2 = $36,103,257; year 3 = $51,514,155).4
Table 12: Key Model Parameters
Parameter | Sponsor’s estimate (reported as year 1 / year 2 / year 3 if appropriate) |
|---|---|
Target population | |
Number of new cases of cervical cancer | 1,25528 |
Proportion of new cases with local advanced designation | 38.0%29 |
Proportion of new localized advanced cervical cancer cases with FIGO stage III to IVA designation | Stage III: 52.4%30 Stage IVA: 3.4%30 |
Proportion of patients with high-risk locally advanced cervical cancer | 100%3 |
Proportion of patients referred for treatment | 100%3 |
Proportion of patients treated | 95.0%3 |
Yearly growth rate | |
Number of patients eligible for drug under review | 278 / 289 / 300 |
Market shares (reference scenario) | |
Pembrolizumab + CRT | 0% / 0% / 0% |
CRT | 100% / 100% / 100% |
Market shares (new drug scenario) | |
Pembrolizumab + CRT | 61% / 80% / 80% |
CRT | 39% / 20% / 20% |
Cost of treatment (per patient per 21-day cycle) | |
Pembrolizumab + CRT | $9,350.80 |
CRT | $550.18 |
CRT = chemoradiotherapy; FIGO = Fédération internationale de gynécologie et d’obstétrique.
Key Issues of the Submitted BIA
CDA-AMC identified several key issues to the sponsor’s analysis that have notable implications on the results of the BIA:
The market size is underestimated. The sponsor’s base case estimated the budget impact of reimbursing pembrolizumab plus CRT for the FIGO 2014 LACC population in line with the proposed Health Canada indication. However, clinical experts noted that currently diagnosis is assessed based on the updated FIGO 2018 version in clinical practice. Additionally, patients with FIGO 2018 stage IB3 and greater were noted to be suitable for pembrolizumab + CRT treatment. Based on published literature, this would increase the population size of patients eligible for pembrolizumab plus CRT treatment.32
CDA-AMC conducted a scenario analysis to reflect the proportion of patients with FIGO 2018 stage IB3 and greater LACC (75%).32
Market uptake of pembrolizumab may be underestimated. A log function was used to calculate the market uptake of pembrolizumab plus CRT with an assumed maximum value of 80%.4 In consultation with clinical experts, the market uptake of pembrolizumab is expected to be greater than 80% as health care providers for this indication are familiar with pembrolizumab as it is currently reimbursed for subsequent treatment.
CDA-AMC revised the maximum value of pembrolizumab plus CRT market uptake to 95% in line with clinical expert expectations.
Subsequent treatment costs for the pembrolizumab arm were overestimated. Similar to the economic evaluation, the sponsor assumed that 80% of patients who were previously treated with pembrolizumab plus CRT would receive pembrolizumab as a subsequent treatment.4 Clinical experts indicated that patients who progress after pembrolizumab plus CRT treatment are unlikely to be treated with pembrolizumab again.
In reanalysis, CDA-AMC revised the proportion of patients who received pembrolizumab as a subsequent treatment to 20% for the pembrolizumab plus CRT arm.
CDA-AMC conducted a scenario analysis on the duration of treatment for subsequent treatments are aligned with the median duration of treatment from KEYNOTE-826.
Assumptions about time on treatment for pembrolizumab in combination with CRT and for CRT may be inappropriate. The sponsor’s model estimated the volume of patients by determining the matrix product of the time-on-treatment data from KEYNOTE-A18 and the inverted weekly incident of patients.4 The time on treatment was estimated using the raw KM data from KEYNOTE-A18; these data neither capture the potential uncertainty related to treatment discontinuation nor provide a smooth function to estimate TTD.
CDA-AMC could not address this limitation due to the model structure.
The budget impact model does not fully capture costs of treatment: The sponsor assumed gradual weekly initiation of treatment, with a total of approximately 5 patients starting pembrolizumab plus CRT every week in year 1.4 This approach was further utilized to project market capture of pembrolizumab in years 2 and 3. In an incidence-based model, market shares represent the proportion of new patients on treatment at any point during the year, inherently accounting for changes in treatment over the course of the year. The sponsor’s assumption of a gradual treatment initiation may underestimate total treatment costs associated with the reimbursement of pembrolizumab. Over time the BIA will continue to increase as it will take longer for the budget impact to stabilize. This means the budget impact seen in year 3 will continue to increase for the next few years until stabilizing.
CDA-AMC could not address this limitation given how initiation of treatment was coded in the sponsor’s submitted BIA.
The fixed dosing of pembrolizumab does not reflect clinical practice: The sponsor’s model assumed fixed dosing for pembrolizumab. However, as noted in the appraisal of the economic evaluation, current clinical practice and public drug plan policies prefer a weight-based dose for pembrolizumab. As a result, the average administered dose and associated treatment costs of pembrolizumab in the sponsor’s model are likely overestimated.
The CDA-AMC base case was revised to incorporate weight-based dosing, aligning with the approach used in the cost-utility analysis.
The budget impact model has limited transparency and flexibility. The sponsor’s submitted BIA model is overly complex, using circular referencing and hard coding, which increases validity issues when making changes to the model and ensuring consistency throughout the budget impact model. Furthermore, the model lacks transparency and has limited flexibility to allow the reviewers to assess the impact of changing the sponsor’s base assumptions on estimated budgetary impact.
CDA-AMC could not address this limitation; therefore, the results presented should be treated with a degree of caution as the validity of the model calculations could not be thoroughly appraised.
CDA-AMC Reanalyses of the BIA
CDA-AMC revised the sponsor’s submitted analyses by making changes in model parameter values and assumptions, in consultation with clinical experts, as outlined in Table 13.
Table 13: Revisions to the Submitted BIA
Stepped analysis | Sponsor’s value or assumption | CDA-AMC value or assumption |
|---|---|---|
1. Market uptake of pembrolizumab | Maximum: 80% | Maximum: 95% |
2. Subsequent treatment for the pembrolizumab plus CRT arm | Pembrolizumab + platinum + paclitaxel = 48% Pembrolizumab + platinum + paclitaxel + bevacizumab = 32% platinum + paclitaxel = 12% platinum + paclitaxel + bevacizumab = 8% | Pembrolizumab + platinum + paclitaxel = 12% Pembrolizumab + platinum + paclitaxel + bevacizumab = 8% platinum + paclitaxel = 48% platinum + paclitaxel + bevacizumab = 32% |
3. Weight based | Fixed-based dose | Weight-based dose |
CDA-AMC base case | ― | (Reanalysis 1 + 2 + 3) |
BIA = budget impact analysis; CDA-AMC = Canada’s Drug Agency; CRT = chemoradiotherapy.
Note: CDA-AMC was unable to resolve the issues with the time-to-treatment assumptions, model approach, and model transparency.
The results of the CDA-AMC step-wise reanalysis are presented in summary format in Table 14 and a more detailed breakdown is presented in Table 15. In the CDA-AMC base case, the 3-year budget impact of reimbursing pembrolizumab plus CRT for the treatment of adult patients with FIGO 2014 stage III to IVA cervical cancer was $73,285,339 (year 1 = $8,118,346; year 2 = $26,869,349; year 3 = $38,297,644).
Table 14: Summary of the Stepped Analysis of the CDA-AMC Base Case
Stepped analysis | Three-year total ($) |
|---|---|
Submitted base case | 98,506,693 |
CDA-AMC reanalysis 1 | 116,976,698 |
CDA-AMC reanalysis 2 | 97,765,913 |
CDA-AMC reanalysis 3 | 62,098,588 |
CDA-AMC base case: (reanalysis 1 + 2 + 3) | 73,285,339 |
CDA-AMC = Canada’s Drug Agency.
Note: The CDA-AMC reanalysis is based on publicly available prices of the comparator treatments
CDA-AMC used the CDA-AMC base case to conduct scenario analyses to explore uncertainty in the estimated budget impact of reimbursing pembrolizumab plus CRT. The results are provided in Table 15.
Adjusting the population to include patients with FIGO 2018 stage IB3 and greater LACC.
Revising the duration of treatment for subsequent treatments.
Table 15: Disaggregated Summary of the BIA
Stepped analysis | Scenario | Year 0 (current situation) ($) | Year 1 ($) | Year 2 ($) | Year 3 ($) | Three-year total ($) |
|---|---|---|---|---|---|---|
Submitted base case | Reference total | 724,275 | 1,758,230 | 2,453,366 | 2,964,426 | 7,176,022 |
Pembrolizumab plus CRT | 0 | 0 | 0 | 0 | 0 | |
CRT only | 236,248 | 255,485 | 265,362 | 275,621 | 796,468 | |
Subsequent therapies | 488,026 | 1,502,745 | 2,188,004 | 2,688,805 | 6,379,554 | |
New drug total | 724,275 | 12,647,510 | 38,556,624 | 54,478,581 | 105,682,715 | |
Pembrolizumab plus CRT | 0 | 11,158,342 | 36,804,074 | 52,460,626 | 100,423,042 | |
CRT only | 236,248 | 107,600 | 53,119 | 55,124 | 215,843 | |
Subsequent therapies | 488,026 | 1,381,567 | 1,699,432 | 1,962,830 | 5,043,829 | |
Budget impact | 0 | 10,889,281 | 36,103,257 | 51,514,155 | 98,506,693 | |
CDA-AMC base case | Reference total | 578,789 | 1,307,957 | 1,797,123 | 2,157,710 | 5,262,789 |
Pembrolizumab plus CRT | 0 | 0 | 0 | 0 | 0 | |
CRT only | 236,248 | 255,485 | 265,362 | 275,621 | 796,468 | |
Subsequent therapies | 342,540 | 1,052,472 | 1,531,760 | 1,882,088 | 4,466,321 | |
New drug total | 578,789 | 9,426,302 | 28,666,472 | 40,455,354 | 78,548,128 | |
Pembrolizumab plus CRT | 0 | 8,425,887 | 27,670,755 | 39,406,022 | 75,502,664 | |
CRT only | 236,248 | 79,872 | 13,323 | 13,781 | 106,976 | |
Subsequent therapies | 342,540 | 920,543 | 982,394 | 1,035,550 | 2,938,488 | |
Budget impact | 0 | 8,118,346 | 26,869,349 | 38,297,644 | 73,285,339 | |
CDA-AMC scenario analyses | ||||||
Scenario 1: FIGO 2018 stage IB3 and greater | Reference total | 777,942 | 1,758,006 | 2,415,487 | 2,900,147 | 7,073,641 |
New drug total | 777,942 | 12,669,761 | 38,530,204 | 54,375,475 | 105,575,440 | |
Budget Impact | 0 | 10,911,755 | 36,114,717 | 51,475,328 | 98,501,800 | |
Scenario 2: Subsequent treatment duration | Reference total | 564,738 | 1,258,246 | 1,722,882 | 2,065,701 | 5,046,828 |
New drug total | 564,738 | 9,382,798 | 28,622,833 | 40,412,932 | 78,418,564 | |
Budget impact | $0 | 8,124,553 | 26,899,951 | 38,347,231 | 73,371,735 | |
BIA = budget impact analysis; CDA-AMC = Canada’s Drug Agency; CRT = chemoradiotherapy; FIGO = Fédération internationale de gynécologie et d’obstétrique.
Note: The CDA-AMC reanalysis is based on the publicly available prices of the comparator treatments.
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.