Drugs, Health Technologies, Health Systems
Reimbursement Review
Abemaciclib (Verzenio)
Sponsor: Eli Lilly Canada Inc.
Therapeutic area: HR-positive, HER2-negative advanced or metastatic breast cancer
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Clinical Review
Abbreviations
ABE
abemaciclib
AE
adverse event
AESI
adverse event of special interest
BCC
Breast Cancer Canada
CBCN
Canadian Breast Cancer Network
CDA-AMC
Canada’s Drug Agency
CDK
cyclin-dependent kinase
CI
confidence interval
CrI
credible interval
DAC
Drug Advisory Committee
DIC
deviance information criterion
ECOG PS
Eastern Cooperative Oncology Group Performance Status
ET
endocrine therapy
FP
fractional polynomial
FUL
fulvestrant
FUL 500
fulvestrant 500 mg
GRADE
Grading of Recommendations Assessment, Development and Evaluation
HRQoL
health-related quality of life
ITC
indirect treatment comparison
NMA
network meta-analysis
OH (CCO)
Ontario Health (Cancer Care Ontario)
ORR
objective response rate
OS
overall survival
pERC
pan-Canadian Oncology Drug Review Expert Review Committee
PFS
progression-free survival
RCT
randomized controlled trial
REAL
Research Excellence Active Leadership
RECIST 1.1
Response Evaluation Criteria in Solid Tumours Version 1.1
RWE
real-world evidence
SAE
serious adverse event
SLR
systematic literature review
TTF
time to treatment failure
VTE
venous thrombotic event
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Table 1: Background Information of Application Submitted for Review
Item | Description |
|---|---|
Drug product | Abemaciclib (Verzenio) Strength: 50 mg, 100 mg, 150 mg Dose form: tablet Route of administration: oral |
Sponsor | Eli Lilly Canada Inc. |
Indication |
|
Reimbursement request | This reassessment request for reimbursement is with respect to the treatment of HR-positive, HER2-negative advanced or metastatic breast cancer:
|
Health Canada approval status | NOC |
Health Canada review pathway | Standard review |
NOC date | April 5, 2019 |
Recommended dose | 150 mg twice daily, oral; when used as single agent, the recommended dose is 200 mg, oral, twice daily. |
GnRH = gonadotropin-releasing hormone; NOC = Notice of Compliance.
Introduction
Breast cancer is the most commonly diagnosed cancer and the second leading cause of cancer-related deaths among the female population of Canada. Approximately 75% of breast cancers are HR-positive and 66% to 75% are HER2-negative. In 2024, an estimated 30,500 new cases and 5,500 deaths were expected. Although early-stage disease is often curable, metastatic breast cancer remains incurable, with a 5-year survival rate of 23%. Treatment for HR-positive or HER2-negative advanced or metastatic breast cancer aims to prolong survival, maintain quality of life, and delay progression, with inhibitors of cyclin-dependent kinases (CDKs) 4 and 6 combined with endocrine therapy (ET) being the current standard of care.
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of abemaciclib in combination with fulvestrant for the treatment of females with HR-positive, HER2-negative advanced or metastatic breast cancer after progression on ET. Abemaciclib was previously reviewed by Canada’s Drug Agency (CDA-AMC) in 2019 and conditionally recommended for reimbursement based on demonstration of a significant benefit in progression-free survival (PFS) in the MONARCH 2 trial, although the data for overall survival (OS) were not conclusive.1,2 In this resubmission, the sponsor provided updated evidence from the MONARCH 2 trial, including an interim OS analysis (data cut-off: June 20, 2019) and a final OS analysis (data cut-off: March 18, 2022), reflecting more than 5 years of follow-up. This updated submission also includes revised network meta-analyses (NMAs) and updated economic models incorporating the new OS data.
Perspectives of Patient, Clinicians, and Drug Programs
The information in this section is a summary of input provided by the patient and clinician groups that responded to our call for input and from clinical experts consulted for the purpose of this review.
Patient Input
Three patient groups — Breast Cancer Canada (BCC), the Canadian Breast Cancer Network (CBCN), and Rethink Breast Cancer — provided input based on surveys, interviews, and patient networks. Patients emphasized the profound impact of HR-positive, HER2-negative advanced or metastatic breast cancer on their daily lives, describing significant emotional, physical, financial, and social burdens. The disease often disrupts employment, relationships, and overall quality of life, not only for patients but also for their families and caregivers.
Key outcomes identified as important by patients included extending OS, delaying disease progression, maintaining daily functioning and health-related quality of life (HRQoL), and having access to oral treatment options that postpone the need for IV chemotherapy. Patients emphasized a willingness to tolerate manageable side effects if the treatment provided meaningful clinical benefits. These perspectives align closely with the outcomes evaluated in the MONARCH 2 trial, reinforcing the relevance of improvements in PFS and OS observed with abemaciclib plus fulvestrant to patient priorities in the Canadian health care landscape.
Clinician Input
Input From Clinical Experts Consulted for This Review
The clinical experts consulted for this review emphasized that an unmet need remains for effective therapies that prolong survival and delay disease progression in patients with HR-positive, HER2-negative advanced or metastatic breast cancer after the failure of ET. They described abemaciclib plus fulvestrant as an important treatment option that offers continuous CDK4 and CDK6 inhibition with a manageable safety profile. The experts noted that abemaciclib provides flexibility for patients who may not tolerate other CDK4 and CDK6 inhibitors, such as those who experience hematologic toxicity on palbociclib or ribociclib. They also referred to the potential benefit of abemaciclib in patients with visceral disease, a subgroup often associated with poorer prognosis, and in those who have previously demonstrated endocrine resistance.
According to the experts, patients most likely to benefit from abemaciclib plus fulvestrant are those with a good performance status, visceral involvement, or evidence of aggressive disease biology. Patients least likely to benefit include those with rapidly progressing disease unsuitable for endocrine-based therapy, a poor performance status, or severe gastrointestinal comorbidities that could worsen treatment tolerability. Treatment initiation is recommended at the time of progression on ET, with monitoring based on imaging, clinical assessment, and biomarkers when applicable. Discontinuation should occur on evidence of disease progression or if toxicity becomes unmanageable despite dose modifications.
Additional considerations noted by the experts include the importance of dose-management strategies, patient education regarding early management of diarrhea, and the availability of oral administration as a patient-centred advantage compared with infusion-based therapies.
Clinician Group Input
Input was received from the Research Excellence Active Leadership (REAL) Canadian Breast Cancer Alliance (n = 16 participants) and the Ontario Health (Cancer Care Ontario) (OH [CCO]) Drug Advisory Committee (DAC) (n = 5 participants). Both groups emphasized that extending survival while maintaining quality of life is a key goal and identified a need for additional CDK4 and CDK6 inhibitor options, particularly for patients who experience toxicity with existing drugs.
The clinician groups anticipated that abemaciclib may have a role in delaying the need for chemotherapy and agreed that it fits within current treatment approaches. Their input was consistent with that of the clinical experts consulted for this review, with no major disagreements identified and general agreement that abemaciclib addresses an important unmet need.
Drug Program Input
The drug programs inquired whether abemaciclib had been directly compared with ribociclib, palbociclib, or capivasertib in combination with fulvestrant, noting that these are now relevant comparators in Canadian clinical practice. The clinical experts consulted for this review indicated that no head-to-head trials are available, and that comparisons would rely on cross-trial analyses or NMAs, which should be interpreted cautiously because of differences in study designs and populations. The experts emphasized that all CDK4 and CDK6 inhibitors approved for use in Canada demonstrate efficacy, but have differences in safety profiles and dosing schedules, and that subgroup outcomes guide treatment choice in practice. Regarding prescribing, the clinical experts agreed that guidance for abemaciclib should align with established protocols for ribociclib and palbociclib, including selection criteria, monitoring, and dose-adjustment strategies.
The drug programs also asked whether switching from ribociclib or palbociclib to abemaciclib would be reasonable. The clinical experts considered switching appropriate in certain cases, particularly when patients are intolerant to or have contraindications to other CDK4 and CDK6 inhibitors, although direct evidence supporting the efficacy of switching is lacking. The experts supported the idea that individualized clinical judgment and pharmacologic differences among drugs could justify switching in practice and recommended updating existing funding algorithms for CDK4 and CDK6 inhibitors to reflect the evolving body of evidence.
Clinical Evidence
Systematic Review
Description of Studies
The pivotal MONARCH 2 trial (N = 669) was a phase III, multicentre, double-blind, placebo-controlled study that compared abemaciclib plus fulvestrant to placebo plus fulvestrant in females with HR-positive, HER2-negative advanced or metastatic breast cancer who had experienced disease progression following ET. The primary outcomes were PFS and OS. At the time of the original review, only interim PFS data and OS results were available. The current submission provides updated data, including those from an interim OS analysis (data cut-off: June 20, 2019) and a final OS analysis (data cut-off: March 18, 2022), offering an assessment of long-term outcomes based on more than 5 years of follow-up.
Baseline characteristics were well balanced across treatment arms. The median age of enrolled patients was 60 years, with the majority being in the postmenopausal stage. Most patients had visceral metastases at baseline, and a high proportion demonstrated previous resistance to ET, reflecting a population with advanced disease and a poor prognosis.
Efficacy Results
At the interim analysis (data cut-off on June 20, 2019; median follow-up of 47.7 months), after 338 deaths had occurred, abemaciclib plus fulvestrant significantly improved OS compared to placebo plus fulvestrant, with a hazard ratio of 0.757 (95% confidence interval [CI], 0.606 to 0.945; P = 0.0137). The median OS was 46.72 months versus 37.25 months for placebo, representing a median survival gain of 9.47 months (95% CI not reported).
At the final OS analysis (data cut-off on March 18, 2022), after a median follow-up of approximately 80 months for both arms and 440 deaths, the survival benefit was maintained. The hazard ratio was 0.784 (95% CI, 0.644 to 0.955; nominal P = 0.0157). The median OS times were 45.80 months for the abemaciclib plus fulvestrant arm and 37.25 months for the placebo arm, corresponding to an improvement in median OS of 8.55 months (95% CI not reported).
At the time of the primary PFS analysis (data cut-off on February 14, 2017; median follow-up of 19.5 months), abemaciclib plus fulvestrant significantly improved PFS compared to placebo plus fulvestrant, with a hazard ratio of 0.553 (95% CI, 0.449 to 0.681; P < 0.001). The median PFS was 16.4 months versus 9.3 months for placebo, corresponding to a gain of 7.2 months (95% CI not reported). An updated PFS analysis at the interim OS data cut-off (June 20, 2019) produced consistent results, with a hazard ratio of 0.536 (95% CI, 0.445 to 0.645; P < 0.001). The median PFS was 16.87 months in the abemaciclib arm versus 9.27 months in the placebo arm, maintaining an advantage of 7.59 months (95% CI not reported). At the final analysis (data cut-off on March 18, 2022; median follow-up of 79.7 months), the PFS benefit remained sustained, with a hazard ratio of 0.539 (95% CI, 0.449 to 0.647). The median PFS times were again 16.87 months for the abemaciclib arm and 9.27 months for the placebo arm. Kaplan-Meier curves showed early separation at approximately 3 months, which was maintained over long-term follow-up, supporting the durability of the PFS benefit with abemaciclib plus fulvestrant.
Harms Results
In the MONARCH 2 trial, adverse events (AEs) were more frequently reported in the abemaciclib plus fulvestrant arm compared to placebo plus fulvestrant. The most common AEs included diarrhea (384 patients [87.1%] versus 62 patients [27.8%], respectively), neutropenia (220 patients [49.9%] versus 9 patients [4.0%], respectively), and infections (213 patients [48.3%] versus 59 patients [26.5%], respectively). Most were low-grade events and manageable with dose adjustments and supportive care. Treatment discontinuations because of AEs were infrequent, and the safety profile remained consistent with the known effects of CDK4 and CDK6 inhibition. Serious adverse events (SAEs) were reported more frequently in the abemaciclib arm (███ patients █████%]) compared to the placebo arm (██ patients █████%]), and were primarily related to infections and thromboembolic complications. Although the incidence of SAEs was higher with abemaciclib, most events were managed effectively with supportive interventions.
Adverse events of special interest (AESIs) occurred more frequently with abemaciclib than with placebo and included neutropenia, which was reported in ███ patients (████%) receiving abemaciclib plus fulvestrant compared to ██ patients (███%) receiving placebo. Diarrhea was reported in ███ patients (████%) treated with abemaciclib and ██ patients (████%) on placebo; venous thromboembolic events (VTEs) were reported in ██ patients in the abemaciclib group (████) versus ██ patients in the placebo group (███%); infections occurred in ███ patients (████%) in the abemaciclib group and ██ patients (████%) in the placebo group; and interstitial lung disease/pneumonitis occurred ██ patients receiving abemaciclib(███%) versus ██ patient in the placebo arm (███%). Most events were of a low grade and manageable.
Critical Appraisal
The MONARCH 2 study demonstrated strong internal validity, with appropriate randomization (2:1 ratio, stratified), maintained allocation concealment, and double-blinding. Although a higher incidence of diarrhea in the abemaciclib arm raised the potential for unblinding, this was unlikely to have affected objectively measured outcomes such as PFS and OS. Baseline characteristics were well balanced, adherence was high (████%), and relatively few data were missing. The study used hierarchical testing with appropriate control of type I error and prespecified subgroup and sensitivity analyses, supporting the robustness of the findings. While the final OS analysis was performed post hoc following a significant interim analysis, consistency between interim and final results reduces concerns about bias.
Overall, the findings of the MONARCH 2 trial were generalizable to the population of patients in Canada with HR-positive, HER2-negative advanced breast cancer progressing after ET. The study population, dosing regimens, and outcomes align closely with Canadian clinical practice. However, it is unknown if the generalizability of the findings would extend to patients with central nervous system metastases or visceral crisis, as they were excluded from the study. The use of supportive medications was largely balanced across treatment arms, with higher loperamide use in the abemaciclib arm reflecting expected management of diarrhea. No major concerns regarding cointerventions or external applicability were identified by the clinical experts consulted for this review.
Long-Term Extension Studies
No other long-term studies were submitted.
Indirect Comparisons
Description of Studies
The sponsor submitted the M2 indirect treatment comparison (ITC) using a Bayesian NMA to assess the relative efficacy of abemaciclib plus fulvestrant compared to other treatments for HR-positive, HER2-negative advanced or metastatic breast cancer. The network included 10 randomized controlled trials (RCTs) evaluating treatments, including fulvestrant monotherapy (500 mg and 250 mg), exemestane, capecitabine, everolimus plus exemestane, palbociclib plus fulvestrant, ribociclib plus fulvestrant, and dalpiciclib plus fulvestrant. The analysis incorporated both fixed- and random-effects models, with model selection based on the deviance information criterion (DIC). The report was divided into sections according to the methods or models used, the Cox proportional hazards models, and the fractional polynomial (FP) models that were applied as sensitivity analysis because violations of proportional hazards assumptions were detected. Consistency across the network was assumed rather than formally tested because of network sparsity.
Efficacy Results
The M2 ITC supports the results of the MONARCH 2 trial, specifically that abemaciclib plus fulvestrant had favourable PFS and OS compared with fulvestrant monotherapy. However, when comparing abemaciclib plus fulvestrant to other CDK4 and CDK6 inhibitors relevant to Canada’s clinical practice, such as palbociclib or ribociclib combined with fulvestrant, the results were less certain.
Hazard ratios for OS from the Cox proportional hazards model suggested numerically favourable outcomes for abemaciclib plus fulvestrant when compared to fulvestrant monotherapy (both 500 mg and 250 mg) and exemestane monotherapy. When compared to all other interventions the credible intervals (CrIs) were wide, reflecting imprecision. The same results were observed when assessing PFS, with the addition of numerically favourable effects when compared to everolimus.
Overall, the results produced by the FP models aligned with those of the Cox proportional hazards models. The effect estimates, presented as the mean difference between treatments in expected OS, showed that the effects of abemaciclib were numerically favourable when compared to those of exemestane and fulvestrant 250 mg. When compared to all other interventions, the CrIs were wide, reflecting imprecision. Similar results were observed when assessing PFS (also presented as the mean difference between treatments in expected PFS), with favourable effects of abemaciclib plus fulvestrant evident when compared to those of fulvestrant monotherapy (250 mg and 500 mg), exemestane, and everolimus.
Harms Results
No harms data were provided with either the hazard ratio or the FP approach.
Critical Appraisal
The systematic literature review (SLR) that informed the M2 ITC was generally well conducted, with appropriate prespecification of eligibility criteria, comprehensive database searches, duplicate review processes, and quality assessment using the Cochrane risk of bias tool. Four of the trials in the network were assessed as involving a high risk of bias, and several others had an unclear risk of bias. No trials that enrolled the same population as the MONARCH 2 trial were identified. Eligibility criteria were therefore broadened, which increased the heterogeneity across trials in the network and may have resulted in violation of the exchangeability assumption required to produce valid results. These included variations in patient characteristics, such as differences in visceral metastases, previous treatments, and follow-up durations. Because of network sparsity, consistency was assumed based on clinical judgment without performing formal checks; whether consistency was upheld is therefore unknown. Minor variations in patient characteristics, such as differences in visceral metastases, previous treatments, and follow-up durations, may have introduced potential effect modifiers, although the study designs and populations were deemed acceptable overall.
The selection of clinical outcomes relevant to the patient population, namely PFS and OS, was appropriate, but harms outcomes were not included, limiting the ability to assess comparative safety. While sensitivity analyses supported the robustness of findings, the small sample sizes for some treatments and wide CrIs indicated imprecision, particularly when comparing targeted therapy combinations to chemotherapy-based regimens.
The limitation related to violation of the proportional hazards assumption was addressed through a sensitivity analysis using FP models that do not require this assumption. The final models were selected from 88 options. None of the best-fitting models (by the DIC) could be selected because of clinically implausible survival plateaus, particularly for OS. A limited number of models with poorer fits to the observed data were therefore considered. The poorer fits of the chosen models and limited transparency in the selection process may have resulted in biased estimates of comparative effects. The CrIs produced do not account for the model-selection procedures and may be overly optimistic. The clinical experts consulted by the review team suspected that the comparative-effectiveness results produced by these extrapolations might not all be plausible. Limitations included misalignment of the comparative effect of fulvestrant on PFS versus OS, and lower-than-expected long-term projections at 5 and 10 years.
The included studies are largely reflective of the Canadian clinical context, although differences in disease severity and geographic variability may affect generalizability. Overall, the M2 ITC provides useful comparative evidence for efficacy outcomes but should be interpreted cautiously, given residual heterogeneity, untested consistency, and imprecision around some treatment-effect estimates.
Studies Addressing Gaps in the Evidence From the Systematic Review
Description of Studies
To address gaps related to real-world harms and tolerability, the sponsor submitted 4 real-world evidence (RWE) studies evaluating the use of abemaciclib in broader clinical practice settings. These included 1 expanded access program (I3Y-MC-JPBK) and 3 observational cohort studies. Across these studies, patient populations were more heterogeneous than in the MONARCH 2 trial, often including individuals with a wider range of disease burdens, comorbidities, and previous treatments. These studies provided complementary information on the harms profile of abemaciclib outside of the controlled environment of randomized trials.
Efficacy Results
The primary focus of the RWE studies was on harms, with limited information on treatment outcomes. Nonetheless, PFS times in these studies were generally consistent with the results observed in the MONARCH 2 trial. However, the absence of standardized follow-up protocols, variability in outcome definitions, and lack of adjustment limit the ability to interpret the findings causally.
Harms Results
Across the RWE studies, the safety profile of abemaciclib was consistent with that observed in the MONARCH 2 trial. Diarrhea, neutropenia, and infections were the most frequently reported AEs, with diarrhea remaining the most common. Most AEs were manageable with dose reductions, delays, or supportive-care measures, such as antidiarrheal medication. No new or unexpected harm signals were identified. The RWE studies suggested that AEs were manageable in clinical practice, although the rates of dose adjustments and treatment interruptions varied depending on patient characteristics and treatment settings.
Critical Appraisal
While the RWE studies provide useful supportive information on the safety and tolerability of abemaciclib, they are limited by their observational nature, small sample sizes, lack of standardized outcomes, and potential for selection bias. Studies were single-arm or lacked adjustment, limiting the ability to interpret the findings causally. Differences in clinical practice patterns and follow-up intensity across studies also limit generalizability. Nevertheless, the findings broadly support the profile established in RCTs and provide information on the management strategies for AEs used in the MONARCH 2 trial that are applicable to routine clinical care.
Conclusions
The totality of evidence reviewed supports a finding that abemaciclib plus fulvestrant provides a clinically meaningful improvement in both PFS and OS for patients with HR-positive, HER2-negative advanced breast cancer who have progressed on ET compared to those treated with fulvestrant alone. The updated MONARCH 2 trial results, including final OS data, confirm a survival benefit that was not demonstrated at the time of the initial submission, addressing a key evidence gap. The observed benefit aligns with patient priorities of delaying disease progression and prolonging survival. The safety profile of abemaciclib remains consistent with that of other CDK4 and CDK6 inhibitors, with diarrhea, neutropenia, and infections the most reported AEs. These events are considered by the clinical experts consulted for this review to be generally manageable with supportive care and dose modifications, as shown in both the MONARCH 2 trial and RWE studies.
Comparisons of abemaciclib with other CDK4 and CDK6 inhibitors relevant to Canadian practice, such as palbociclib and ribociclib, are limited by imprecise estimates, differences in patient populations, and the absence of direct head-to-head trials, which precluded making definitive conclusions about comparative effects. Important gaps, including limited evidence in specific subgroups, such as patients with central nervous system metastases or more aggressive disease, remain.
Introduction
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of abemaciclib 50 mg, 100 mg, 150 mg, oral tablets, in the treatment of HR-positive, HER2-negative advanced or metastatic breast cancer, specifically in combination with fulvestrant in female patients with disease progression following ET.
Disease Background
Contents within this section have been informed by materials submitted by the sponsor and clinical expert input. The following has been summarized and validated by the review team.
Breast cancer is the most diagnosed cancer and the second leading cause of cancer-related deaths among females in Canada, accounting for approximately 13.5% of cancer mortality. In 2024, an estimated 30,500 new cases and 5,500 deaths were expected among females in Canada because of breast cancer.3
Breast cancer is a biologically heterogeneous disease that is classified based on molecular and immunohistochemical characteristics. These classifications reflect specific oncogenic pathways and inform prognosis and treatment decisions. The most clinically relevant subtypes are defined by the presence or absence of hormone receptors (the estrogen receptor and/or progesterone receptor, collectively referred to as HR) and HER2. Approximately 75% of breast cancers are HR-positive, while 10% to 30% overexpress HER2, a feature associated with more aggressive disease and poorer outcomes.4 The HR-positive or HER2-negative subtype is the most prevalent, representing 66% to 75% of all cases of breast cancer in North America and Europe.5-7
Breast cancer typically progresses in a stepwise manner from noninvasive to invasive to metastatic disease. Noninvasive forms are confined to the breast ducts or lobules. Invasive disease involves the surrounding breast tissue, while locally advanced cases extend into adjacent structures, such as the skin or chest wall, without distant spread. Metastatic breast cancer is classified as stage IV and is defined by the presence of distant metastases. In HR-positive or HER2-negative breast cancer, the bone is the most frequent site of metastasis, followed by visceral organs (e.g., the liver and lungs), the brain, and lymph nodes.4,5
Although many individuals with early-stage breast cancer are cured with appropriate therapy, metastatic disease remains incurable. Approximately 5% of patients present with metastatic disease at initial diagnosis.8 Among those diagnosed with early or localized invasive disease, up to 30% may eventually experience distant recurrence.9,10 The 5-year survival rate for patients with metastatic breast cancer is approximately 23%.11 In addition to significantly reduced survival, patients with metastatic disease often experience debilitating symptoms, including pain, fatigue, cognitive impairment, and insomnia, which reduce the quality of life and functional independence, while also imposing substantial financial and emotional burdens.12
A diagnosis of HR-positive, HER2-negative locally advanced or metastatic breast cancer is confirmed through tissue biopsy using validated immunohistochemistry and/or in situ hybridization assays and pathological review.8,13 Biomarker testing for HR and HER2 status should be performed on all newly diagnosed primary or metastatic breast cancer cases to guide treatment decisions.8
In addition to histopathological confirmation, the diagnostic workup for metastatic breast cancer typically includes bloodwork (e.g., a complete blood count, metabolic panel, and liver function tests), imaging studies (e.g., bilateral diagnostic mammogram, bone scan, chest X-ray, PET and/or CT scan, or ultrasound), and, where appropriate, germline genetic testing.8
Molecular tests required to confirm HER2 and HR status, as well as other diagnostic testing requirements for breast cancer are widely available across Canada.
Standards of Therapy
Contents within this section have been informed by materials submitted by the sponsor and clinical expert input. The following has been summarized and validated by the review team.
In Canada, treatment for HR-positive, HER2-negative locally advanced metastatic breast cancer is primarily aimed at maintaining or improving quality of life, delaying disease progression, and prolonging survival, while minimizing treatment-related toxicity. This approach reflects the chronic and generally incurable nature of the disease. Therapeutic strategies, both pharmacological and nonpharmacological, are tailored to the patient’s treatment history, clinical characteristics, and tumour biology.
Treatment decisions are guided by comprehensive clinical practice guidelines, including those from the National Comprehensive Cancer Network,14 American Society of Clinical Oncology,15 European Society of Medical Oncology,16 and the Sixth and Seventh International Consensus Guidelines for Advanced Breast Cancer.8
In the first-line metastatic setting, the standard of care for patients who are not in visceral crisis is ET in combination with a CDK4 and CDK6 inhibitor. This recommendation is strongly supported across all major guidelines. In Canada, the most commonly used CDK4 and CDK6 inhibitors include ribociclib, palbociclib, and abemaciclib. Aromatase inhibitors (e.g., letrozole or anastrozole) or fulvestrant are typically used as the endocrine partner. ET alone, while no longer the preferred first-line option, may be used selectively in patients with significant comorbidities, poor performance status, or contraindications to CDK4 and CDK6 inhibitors. In patients in the premenopausal or perimenopausal stage, ET must be combined with ovarian suppression or ablation.
In the second line of treatment, upon disease progression, treatment selection is influenced by prior therapies (including whether a CDK4 and CDK6 inhibitor was used), disease biology, the pace of progression, and patient preferences. Guideline-recommended options in the second line and beyond include ET plus a CDK4 and CDK6 inhibitor (if not previously administered); everolimus plus ET, most commonly with exemestane (which is widely reimbursed in Canada), but also with fulvestrant or tamoxifen; ET monotherapy, including nonsteroidal aromatase inhibitors; steroidal agents such as exemestane; selective estrogen receptor degraders and selective estrogen receptor modulators; and targeted therapies for actionable mutations, such as alpelisib (a PI3K-alpha inhibitor) for patients with PIK3CA mutations and capivasertib (an AKT inhibitor) for tumours with AKT1, PIK3CA, or PTEN mutations (available in Canada via special access programs).
Chemotherapy is used for patients with endocrine-resistant disease, visceral crisis, or rapidly progressing disease, in which single-drug chemotherapy becomes the standard of care. Available drugs in Canada include anthracyclines (doxorubicin, liposomal doxorubicin), taxanes (paclitaxel and docetaxel), antimetabolites (capecitabine and gemcitabine), microtubule inhibitors (eribulin and vinorelbine), and platinum-based therapies (cisplatin and carboplatin). Combination chemotherapy is generally reserved for highly symptomatic patients or those with rapidly progressive, life-threatening disease because of higher toxicity.
The clinical experts consulted by CDA-AMC emphasized that CDK4 and CDK6 inhibitors with ET represent the current standard of care in the first-line setting and are widely used in Canada. For patients progressing on these regimens, mutational profiling (e.g., for PIK3CA, AKT1, and PTEN) is increasingly used to inform targeted treatment strategies. Subsequent therapies are personalized based on prior response, patient comorbidities, and goals of care
Drug Under Review
Abemaciclib (Verzenio) oral tablets (50 mg, 100 mg, and 150 mg), is indicated in both early breast cancer and advanced or metastatic breast cancer. In the advanced or metastatic breast cancer setting, the following indications were issued an NOC by Health Canada on April 5, 2019.
Key characteristics of abemaciclib are summarized in Table 2 with other treatments available for the treatment of HR-positive, HER2-negative, advanced or metastatic breast cancer.
Table 2: Key Characteristics of Abemaciclib, Ribociclib, Palbociclib, and Fulvestrant
Drug | Indication | Route of administration and dose | Serious adverse effects or safety issues |
|---|---|---|---|
Abemaciclib | For the treatment of HR-positive, HER2-negative advanced or metastatic breast cancer:
| When used in combination with endocrine therapy, the recommended dose is 150 mg taken orally twice daily When used as a single drug, the recommended dose is 200 mg taken orally twice daily For advanced or metastatic breast cancer, continue treatment until disease progression or unacceptable toxicity | Venous thromboembolism |
Ribociclib | In combination with:
In pre/perimenopausal women or men, the endocrine therapy should be combined with a luteinising hormone releasing hormone agonist (LHRH). | 600 mg (3 × 200 mg film-coated tablets) taken orally, once daily for 21 consecutive days followed by 7 days off treatment, resulting in a complete cycle of 28 days | QT interval prolongation, hepatotoxicity, neutropenia |
Palbociclib | For the treatment of HR-positive, HER2-negative locally advanced or metastatic breast cancer in combination with:
| 125 mg capsule taken orally once daily for 21 consecutive days followed by 7 days off treatment for a complete cycle of 28 days | Neutropenia |
Fulvestrant | For the:
| The recommended dose regimen is 500 mg administered intramuscularly as two 5 mL (250 mg/5 mL) injections, 1 in each buttock (gluteal area) The recommended dosing schedule is as follows: 500 mg dose to be administered on days 0, 14, 28 and then every 28 days thereafter | Hepatotoxicity |
GnRH = gonadotropin-releasing hormone; LHRH = luteinizing hormone releasing hormone agonist.
Note: Sex and gender were not differentiated in the original indications.
aHealth Canada–approved indication.
Source: Product monographs for abemaciclib,17 ribociclib,18 palbociclib,19 and fulvestrant.16
Reassessment by CDA-AMC and Reimbursement Request
Abemaciclib (Verzenio) was previously reviewed by CDA-AMC in 2019 for the treatment of HR-positive, HER2-negative advanced or metastatic breast cancer. Two separate final recommendations were issued.
The first recommendation pertained to the use of abemaciclib in combination with an aromatase inhibitor as initial endocrine-based therapy.1 This recommendation was based on interim (data cut-off on January 31, 2017) and final (data cut-off on November 7, 2017) PFS analyses from the MONARCH 3 trial, which was a randomized, double-blind, placebo-controlled phase III study evaluating abemaciclib plus anastrozole or letrozole versus placebo plus anastrozole or letrozole. The pan-Canadian Oncology Drug Review Expert Review Committee (pERC) conditionally recommended reimbursement for abemaciclib in combination with an aromatase inhibitor in patients with HR-positive, HER2-negative advanced or metastatic breast cancer as initial ET. The recommendation applied to male patients and female patients in the postmenopausal stage with a good performance status who were either intolerant to, or had contraindications for, other CDK4 and CDK6 inhibitors. The recommendation was based on a statistically significant and clinically meaningful improvement in PFS. However, the relatively narrow recommendation reflected concerns over the manageable but notable toxicity profile and a lack of conclusive evidence for an OS benefit at the time.
The second recommendation — and the focus of this reassessment — concerned abemaciclib in combination with fulvestrant for patients who had experienced disease progression following previous ET.1 This recommendation was supported by the primary PFS analysis (data cut-off on February 14, 2017) from the MONARCH 2 trial, a randomized, double-blind, placebo-controlled phase III study comparing abemaciclib plus fulvestrant versus placebo plus fulvestrant in female patients with disease progression and who had previously received ET. A conditional recommendation for the reimbursement of abemaciclib in this setting was made by pERC, again citing a significant PFS benefit.
The current CDA-AMC report addresses a reassessment and reimbursement request submitted by the sponsor for the use of abemaciclib in combination with fulvestrant in females with HR-positive, HER2-negative advanced or metastatic breast cancer whose disease has progressed following ET. In females in the premenopausal or perimenopausal stage, treatment must also include a gonadotropin-releasing hormone agonist.
New Clinical Evidence
Following the 2019 conditional recommendation, the sponsor submitted a reassessment request to CDA-AMC, accompanied by new clinical evidence from extended follow-up analyses of the phase III MONARCH 2 trial (for inclusion in this submission) and MONARCH 3 trial (in parallel with another submission to CDA-AMC running concurrently). For this report, the pertinent information stems from the MONARCH 2 trial, from which the sponsor has provided additional data from an interim OS analysis (data cut-off on June 20, 2019) and the final OS analysis (data cut-off on March 18, 2022).
These updated datasets reflect 5 years and 1 month of updated data for the MONARCH 2 trial. According to the sponsor, these data were submitted in response to pERC’s previously identified concerns in the 2019 recommendation regarding the immaturity of OS outcomes. The sponsor also submitted revised NMAs and updated economic models that incorporate the new OS data.
In addition, the sponsor requested that the language used in the 2019 recommendation be reviewed to ensure alignment with the current data and with the Health Canada–approved indication.
The sponsor also requested a deviation from the pharmacoeconomic requirement that the base case include all relevant comparators — that is, treatments currently reimbursed by at least 1 participating drug plan for the indication under review, treatments reimbursed but used off-label in Canadian clinical practice, or treatments previously recommended for reimbursement by CDA-AMC for the same indication. The rationale provided in the request to exclude capivasertib as a comparator for abemaciclib is that capivasertib is indicated for a biomarker-defined subpopulation and is typically used in patients with previous exposure to CDK4 and CDK6 inhibitors. CDA-AMC accepted this request to exclude these comparators from the base-case analysis.
Perspectives of Patients, Clinicians, and Drug Programs
The full patient and clinician group submissions received are available in the consolidated patient and clinician group input document for this review on the project website.
Patient Group Input
This section was prepared by the review team based on the input provided by patient groups.
Three patient groups, BCC, CBCN, and Rethink Breast Cancer, provided input for this submission. BCC is a national organization in Canada that encourages precision oncology research and collaboration among physicians and researchers. Information for this submission was gathered by an electronic survey distributed from July 6 to 21, 2023, to 171 patients living with recurrent HR-positive or HER2-negative metastatic breast cancer (i.e., those undergoing second-line treatment and beyond) and their caregivers. The survey responses included 108 patients identified as the target group for this submission. Approximately 76% of respondents were receiving second-line treatment, approximately 11% were currently receiving third-line treatment, and 13% were receiving treatment in the fourth line or more.
CBCN is a leading, patient-directed, national health charity committed to ensuring the best quality of care for all Canadians affected by breast cancer through the promotion of information, education, and advocacy activities. Information for this submission was gathered via excerpts and key interviews from past submissions to CDA-AMC. This included results from a 2012 survey of 71 patients with metastatic breast cancer and 16 caregivers, and a 2017 survey of 180 patients in Canada living with metastatic breast cancer. In addition, information from a review of current studies and grey literature to highlight issues and experiences commonly shared among individuals living with breast cancer, and relevant disease experience findings from a 2022 survey of 30 patients in Canada who had HR-positive, HER2-negative metastatic breast cancer was submitted.
Rethink Breast Cancer is a Canadian charity known for making positive change by educating, empowering, and advocating for system changes to improve the experience and outcomes of those with breast cancer. Information for this submission was gathered through observations and insights drawn through programs and meetings with 24 key breast cancer patient advisors, as well as an online survey of 78 patients and caregivers documenting the lived experience with metastatic breast cancer conducted from September 2018 to April 2019. In addition, 4 people living with HR-positive, HER2-negative metastatic breast cancer who had experience with abemaciclib were interviewed from January to February 2025.
Analysis of the 2012 CBCN survey found that fatigue, insomnia, and pain resulted in significant or debilitating impacts on patient quality of life. Respondents also described moderate to significant restrictions in their ability to exercise, pursue hobbies and personal interests, participate in social events and activities, and spend time with loved ones. Patient groups noted that the disease also affected caregivers and loved ones, undermined mental health, imposed a physical and emotional toll during diagnosis, and caused fear of recurrence and financial toxicity.
Patient groups indicated the following barriers faced by respondents with existing treatments: AEs (e.g., fatigue, nausea, depression, problems with concentration, memory loss, diarrhea, and insomnia), financial impacts (e.g., not qualifying for insurance, an inability to change employers because of loss of insurance, and prohibitive costs of new treatment options), minimal or no access to appropriate care when experiencing debilitating symptoms, and challenges accessing quality care during cancer treatment. Patients emphasized the importance of and need for a choice of treatment options to determine a therapy that suited them. The CBCN patient group noted that efficacy, followed by quality of life, work, and costs were ranked as the most to least important when considering a treatment. The BCC input noted that patients who received second-line treatment reported a definitive improvement in HRQoL whereas those on third-, fourth- or later-line therapy were less certain of an HRQoL improvement.
All patient groups that provided input for this submission noted that extended cancer control and improved survival, combined with delayed progression, a delay in IV chemotherapy, and improved quality of life were the most important desired outcomes of treatment. CBCN also emphasized the importance of manageable AEs and noted that the respondents sought improvement to extend their life beyond what was expected and be able to choose an oncologist and therapy that suited them. BCC also noted that patients were in favour of receiving at-home, oral therapy that preserves quality of life. Rethink Breast Cancer suggested that patients valued long-term health outcomes over immediate concerns, such as reducing symptoms or managing side effects.
The BCC patient group characterized delaying IV chemotherapy treatment at each recurrence of metastatic breast cancer as a primary treatment goal and noted that more effective oral options were required in frontline and second-or-later lines of therapy. They also pointed out that abemaciclib was only funded in the province of Quebec for first and second-or-later lines of therapy, resulting in inequitable access. The BCC survey emphasized the financial strain caused by metastatic breast cancer, either from living on a single income, reduced retirement funds, and/or medical costs after their loved one has died. Many respondents reported that their out-of-pocket medical expenses were higher than expected.
Of the 4 patients who were interviewed, 2 were on abemaciclib and letrozole, 1 was on abemaciclib and Faslodex (fulvestrant), and another was on abemaciclib as an 11th line of treatment. Patients described their condition as well managed, with no signs of progression and tolerable side effects that could be managed with dose reductions or other medications, and that they were able to travel. One patient expressed comfort with frequent monitoring (scans every 6 months), a preference for oral treatment, and valued having multiple treatment options. The patient who received abemaciclib as an 11th line of treatment noted that, even after being heavily pretreated, the treatment worked for a year.
Rethink Breast Cancer indicated that testing required for this treatment is already accessible and covered in jurisdictions across Canada, but the clinical experts consulted by CDA-AMC noted that this is only the case for early-stage breast cancer, and it is not relevant to the advanced or metastatic treatment setting. BCC also indicated that no companion diagnostic testing was required for abemaciclib plus ET in the first and second-or-later lines for advanced or metastatic breast cancer.
The Rethink Breast Cancer and BCC patient groups agreed that expanding access to CDK4 and CDK6 inhibitors to include abemaciclib, without limiting its use to only patients unsuitable or intolerant to other options, promotes a more equitable treatment approach across provinces. They emphasized that this would help reduce drug-related out-of-pocket costs for a financially vulnerable population. Rethink Breast Cancer added that patient and physician choice is an important part of treatment, and health care professionals should be able to tailor treatment plans to individual patient needs.
Clinician Input
Input From Clinical Experts Consulted for This Review
All CDA-AMC review teams include at least 1 clinical specialist with expertise in the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). The following input was provided by 2 clinical specialists with expertise in the diagnosis and management of metastatic breast cancer.
Unmet Needs
The clinical experts noted that, while currently available CDK4 and CDK6 inhibitors are associated with demonstrated improvements in PFS and OS for patients with HR-positive, HER2-negative metastatic breast cancer, important treatment gaps remain. Not all patients respond to existing therapies, and resistance — either primary or acquired — limits long-term disease control. Side effects, such as neutropenia, abnormal heart rhythms known as QT prolongation, gastrointestinal issues, and fatigue, also affect HRQoL and treatment adherence. Moreover, limited biomarker-driven personalization and regional inequities in access persist. The experts noted a continued need for well-tolerated, accessible therapies that offer durable disease control, maintain quality of life, and provide options for patients who cannot tolerate or have contraindications to other CDK4 and CDK6 inhibitors.
Place in Therapy
The clinical experts described abemaciclib as an additional option within the class of CDK4 and CDK6 inhibitors rather than a disruptor of the current treatment paradigm. While not expected to replace other drugs, it may provide a preferable choice based on the toxicity profiles or previous intolerance. The experts emphasized that, unlike ribociclib and palbociclib, abemaciclib does not require a treatment break and may offer continuous inhibition of the cell cycle. They added that abemaciclib has demonstrated an ability to act in high-risk subgroups, including patients with visceral disease, central nervous system involvement, and primary endocrine resistance. Abemaciclib is used both in first-line settings (with aromatase inhibitors) and second-line settings (with fulvestrant), offering flexibility in treatment sequencing. The experts did not suggest a requirement for other CDK4 and CDK6 inhibitors to fail before patients initiate abemaciclib, particularly in cases in which toxicity or comorbidities may influence drug selection.
Patient Population
The clinical experts indicated that the target population (patients with HR-positive, HER2-negative metastatic breast cancer) is not small. According to the experts, the patients best suited for abemaciclib include those with visceral metastases, a high disease burden, primary endocrine resistance, or intolerance to other CDK4 and CDK6 inhibitors. Patients enrolled in the MONARCH 2 trial were broadly representative of the real-world population, although those with severe gastrointestinal disorders or who relapsed early after treatment with adjuvant abemaciclib may be less suitable. Clinical identification of candidates is based on HR and HER2 testing, disease extent, and treatment history. No companion diagnostic is required. Laboratory tests such as a complete blood count and liver function panels, alongside imaging and clinical evaluation, are used to guide treatment decisions.
Assessing the Response Treatment
The clinical experts recommended that treatment response be assessed using a combination of clinical evaluation (symptoms and physical findings), laboratory testing (including tumour markers), and imaging (typically CT scans of the chest, abdomen, and pelvis). Response is typically evaluated every 1 to 3 months, with flexibility for longer intervals in stable patients. Clinically meaningful responses include symptom improvement, tumour stabilization or shrinkage, and delay in the need for chemotherapy. The experts agreed that treatment should be continued only if the patient experiences a clinical benefit and is tolerating therapy.
Discontinuing Treatment
The clinical experts noted that abemaciclib should be discontinued in the event of disease progression (as determined by radiographic or clinical analysis) or if AEs, particularly severe diarrhea, liver toxicity, or interstitial lung disease, persist despite dose adjustments. Patient preference and HRQoL were also described as important factors. The experts emphasized that discontinuation should be based on objective evidence of a lack of benefit or intolerance, and should align with the thresholds used in both clinical trials and routine practice.
Prescribing Considerations
The clinical experts stated that abemaciclib should be initiated by a medical oncologist, although ongoing management can involve other professionals trained in oncology, including nurse practitioners and oncology pharmacists. Appropriate settings include both academic and community oncology clinics. While continuous dosing requires patient adherence and monitoring, no specific restrictions on combination therapy or dosage were proposed beyond those already reflected in product monographs. No major issues with regional variation were noted, although collaboration among care providers is essential to support optimal use.
Additional Considerations
The experts indicated that abemaciclib likely has a role to play in delaying the initiation of chemotherapy, which is considered a clinically meaningful outcome for patients. They also emphasized the importance of real-world data in understanding long-term tolerability and adherence. The potential role of abemaciclib in future combination regimens (e.g., with oral selective estrogen-receptor degraders or HER2-targeted drugs) and in other disease settings (e.g., central nervous system involvement or HER2-positive subtypes) was noted as an evolving area of interest. Emerging trial data and biomarker-driven strategies may further refine the use of abemaciclib in clinical practice.
Clinician Group Input
This section was prepared by the review team based on the input provided by 2 clinician groups: the REAL Canadian Breast Cancer Alliance (n = 16) and the OH (CCO) DAC, (n = 5). The REAL Alliance is a multidisciplinary national group that develops clinical consensus recommendations, while the OH (CCO) DAC provides evidence-based guidance to support Ontario’s cancer drug funding programs. Input was gathered through literature reviews, clinical trial data, and expert discussion, including a teleconference with members of the OH (CCO) DAC.
Both groups emphasized the importance of extending PFS and OS while preserving quality of life and delaying chemotherapy. They noted the need for additional CDK4 and CDK6 inhibitor options to improve treatment flexibility. Limited access to abemaciclib across provinces and concerns with limitations of existing options, such as QTc prolongation with ribociclib and lack of OS benefit with palbociclib identified as key gaps. The OH (CCO) DAC emphasized the potential OS benefit of abemaciclib, particularly in patients with visceral disease.
REAL Alliance clinicians reported that side effects (e.g., diarrhea and nausea) from abemaciclib are typically low-grade and manageable with supportive care. They noted that compared to other CDK4 and CDK6 inhibitors, abemaciclib causes less neutropenia and allows for continuous dosing. Its use would not alter treatment sequencing or add cost or complexity. The efficacy of abemaciclib was described as consistent regardless of alterations to the ESR1 or PI3K pathway, potentially reducing the need for biomarker testing.
The patient population best suited for abemaciclib plus fulvestrant aligns with the MONARCH-2 study criteria: those progressing on first-line ET. It is considered less suitable for patients with previous ribociclib use, contraindications, or rapid disease progression following treatment with palbociclib.
Response to treatment is assessed through clinical evaluations, restaging scans every 3 months, and standard blood work, with closer monitoring during the first 4 months. Both clinician groups agreed that treatment should be discontinued at disease progression or if toxicity is persistent or unacceptable.
The OH (CCO) DAC noted that fulvestrant administration requires monthly clinic visits, while abemaciclib is an oral take-home therapy. The REAL group emphasized that treatment and monitoring can be integrated into existing workflows with support from pharmacists and nurses, without additional burden.
Drug Program Input
Drug programs provide input on each drug being reviewed through the Reimbursement Review processes by identifying issues that may affect their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by for this review are summarized in Table 3.
Table 3: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert responses |
|---|---|
Relevant comparators | |
The comparator in the MONARCH 2 study of fulvestrant is placebo. However, the standard of care now is ribociclib or palbociclib. Is there any evidence comparing abemaciclib to either ribociclib or palbociclib (with fulvestrant)? In the second-line setting, capivasertib or fulvestrant may also be a comparator. Is there any evidence comparing capivasertib to abemaciclib? | In both settings, because of lack of head-to-head clinical trials directly comparing abemaciclib with ribociclib or palbociclib in combination with fulvestrant, the comparative-effectiveness across these CDK4 and CDK6 inhibitors must be inferred indirectly through cross-trial comparisons or network meta-analyses and be interpreted accordingly with caution because the studies may have different designs and patient populations. While the efficacy of all 3 in combination with endocrine therapy has been demonstrated, they differ in safety profiles, dosing schedules, and some subgroup outcomes, which may guide individual treatment decisions in clinical practice. |
Considerations for prescribing of therapy | |
This is an oral therapy: 150 mg p.o. twice daily when used in combination with endocrine therapy; 200 mg p.o. twice daily when used as a single drug with or without food. Consistency with recommendations for ribociclib and palbociclib would be helpful. | Prescribing guidance should align with existing protocols for ribociclib and palbociclib, including clear criteria for patient selection, monitoring, and dose adjustments based on tolerability. |
Generalizability | |
In this specific indication, would it be reasonable to switch patients from ribociclib or palbociclib to abemaciclib? | While there is no direct clinical trial evidence evaluating the consequences of switching from ribociclib or palbociclib to abemaciclib, switching is reasonable in certain scenarios, particularly when patients are intolerant to 1 drug or have contraindications to others. Clinical experience and pharmacologic differences among CDK4 and CDK6 inhibitors support individualized switching, although efficacy following progression on a previous CDK4 and CDK6 inhibitor remains an area of active investigation. |
Funding algorithm (oncology only) | |
It would be helpful to update the existing funding algorithm. | An update to the existing funding algorithm for CDK4 and CDK6 inhibitors would be beneficial. |
CDK = cyclin-dependent kinase; p.o. = orally.
Clinical Evidence
The objective of this clinical review report is to review and critically appraise the clinical evidence submitted by the sponsor on the beneficial and harmful effects of abemaciclib oral tablets (50 mg, 100 mg, 150 mg), in the treatment of HR-positive, HER2-negative, advanced or metastatic breast cancer. The focus is on comparing abemaciclib to relevant comparators and identifying gaps in the current evidence.
A summary of the clinical evidence on abemaciclib submitted by the sponsor is presented in 3 sections, with a critical appraisal of the evidence included at the end of each section. The first section, the systematic review, includes pivotal studies and RCTs that were selected according to the sponsor’s systematic review protocol. The second section includes indirect evidence from the sponsor. The third section includes additional studies that were considered by the sponsor to address important evidence gaps in the systematic review.
Included Studies
Clinical evidence from the following is included in the review and appraised in this document:
1 pivotal study identified in the systematic review (the MONARCH 2 study), which includes 2 versions of updated data from the original submission (an interim OS analysis with a data cut-off of June 20, 2019, and a final OS analysis with a data cut-off of March 18, 2022)
1 ITC using an NMA (2 reports within using 2 different models)
4 additional studies addressing gaps in evidence.
Systematic Review
Contents within this section have been informed by materials submitted by the sponsor. The following has been summarized and validated by the review team.
Description of Study
Characteristics of the included pivotal study (the MONARCH 2 study) are summarized in Table 4.
Table 4: Details of Study Included in the Systematic Review (MONARCH 2 Study)
Detail | Designs and populations |
|---|---|
Study design | Multicentre, randomized, double-blind, placebo-controlled, phase III study |
Locations | 146 sites in 20 countries, including the US, Australia, Canada, Belgium, Denmark, Finland, France, Germany, Greece, Italy, Japan, Korea, Mexico, Poland, Puerto Rico, Romania, Russia, Spain, Switzerland, and Taiwan |
Patient enrolment dates | Start date: August 7, 2014 Data cut-off date:
End date: December 2025 |
Randomized (N) | Total randomized (N) = 669
|
Inclusion criteria |
|
Exclusion criteria |
|
Drugs | |
Intervention | Abemaciclib 150 mg orally twice daily on days 1 to 28 of 28-day cycles plus fulvestrant 500 mg by intramuscular injection on days 1 and 15 of the first 28-day cycle, and on day 1 of subsequent cycles |
Comparator | Placebo capsules orally twice daily on days 1 to 28 of 28-day cycles plus fulvestrant 500 mg by intramuscular injection on days 1 and 15 of the first 28-day cycle, and on day 1 of subsequent cycles |
Study duration | |
Screening phase | 28 days |
Treatment phase | Until progressive disease as defined by RECIST 1.1, death, enrolment in any other clinical trial involving an investigational drug or enrolment in any other type of medical research judged not to be scientifically or medically compatible with this study, investigator decision, patient decision, or sponsor decision |
Follow-up phase |
|
Outcomes | |
Primary end point | PFS |
Secondary and exploratory end points | Secondary
Exploratory
|
Publication status | |
Publications | Sledge et al. (2020)20 Sledge et al. (2017)21 Kaufman et al. (2020).22 Tokunaga et al. (2024)23 Toi et al. (2023)24 Inoue et al. (2021)25 Neven et al. (2021)26 |
CBR = clinical benefit rate; CDK = cyclin-dependant kinase; DCR = disease control rate; DOR = duration of response; ECOG PS = Eastern Cooperative Oncology Group Performance Status; EORTC QLQ-BR23 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Breast Cancer; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; GnRH = gonadotropin-releasing hormone; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; RANK-L = receptor activator of nuclear factor kappa beta; RECIST 1.1 = Response Evaluation Criteria in Solid Tumours Version 1.1.
aPatients may not have received more than 1 line of endocrine therapy or any previous chemotherapy for metastatic disease.
Source: Details included in the table are from the sponsor’s Summary of Clinical Evidence.
The objective of the MONARCH 2 study was to evaluate the efficacy and safety of abemaciclib in combination with fulvestrant compared to placebo plus fulvestrant in patients with HR-positive, HER2-negative advanced breast cancer who had disease progression during or shortly after ET. Primary and key secondary end points included PFS, OS, and HRQoL. The study was a global, randomized, double-blind, placebo-controlled, phase III trial. A total of 669 patients were randomized 2:1 to the 2 treatment groups, which are described in more detail in Table 4. Randomization was stratified by the site of metastasis (visceral, bone-only, or other) and ET resistance (primary or secondary). A permuted block randomization method was used within stratification factors.
Populations
Inclusion and Exclusion Criteria
Eligible participants were adult (older than 18 years) females (premenopausal, perimenopausal with ovarian suppression, or postmenopausal) with HR-positive, HER2-negative advanced breast cancer (Table 4). Disease progression must have occurred during neoadjuvant or adjuvant ET, within 12 months of completing adjuvant ET, or during first-line ET for advanced disease. ET in the neoadjuvant or adjuvant setting was permitted if the patient had a disease-free interval greater than 12 months from the completion of ET. Patients with previous exposure to fulvestrant, CDK4 and CDK6 inhibitor therapy, chemotherapy for advanced disease, or central nervous system metastasis were excluded.
Interventions
At study initiation, patients in the abemaciclib arm initially received 200 mg orally twice daily on days 1 to 28 of 28-day cycles. After a review of safety data and dose reduction rates, the protocol was amended to reduce the starting dose to 150 mg for new patients, and all patients who were receiving 200 mg underwent a mandatory dose reduction to 150 mg. Patients also received 500 mg of fulvestrant by intramuscular injection on days 1 and 15 of the first 28-day cycle, and on day 1 of subsequent cycles. Patients randomized to the placebo arm received placebo capsules taken orally twice daily on days 1 to 28 of 28-day cycles plus 500 mg of fulvestrant by intramuscular injection on days 1 and 15 of the first 28-day cycle, and on day 1 of subsequent cycles.
For both arms, fulvestrant 500 mg was to be administered intramuscularly, slowly (1 to 2 minutes per injection), as two 250 mg injections, 1 in each buttock; however, for patients with moderate (Child-Pugh Class B) hepatic impairment, including any patient who develops moderate hepatic impairment during study treatment, fulvestrant250 mg was to be administered intramuscularly into the buttock slowly (1 to 2 minutes) as a single 250 mg injection.
Outcomes
A list of efficacy end points assessed in this Clinical Review Report is provided in Table 5, followed by descriptions of the outcome measures. Summarized end points are based on outcomes included in the sponsor’s Summary of Clinical Evidence as well as any outcomes identified as important to this review by the clinical experts consulted by CDA-AMC and input from patient and clinician groups and public drug plans. Using the same considerations, we selected end points that were most relevant to inform expert committee deliberations and finalized this list of end points in consultation with members of the expert committee.
This resubmission is based on updated survival data available from the MONARCH 2 trial. Only OS, PFS, and harms outcomes are presented in detail in the main report. A summary of the other key secondary outcomes, as reported in the 2019 clinical review report, are presented in Appendix 1 without update.
Table 5: Outcomes Summarized From the Study Included in the Systematic Review
Outcome measure | Time point | MONARCH 2 study |
|---|---|---|
Progression-free survivala | From the date of randomization to the date of objective progression or the date of death because of any cause, whichever is earlier | Primary end point |
Overall survivala | The time from the date of study randomization to the date of death from any cause | Secondary end point |
Harms | All patients treated with the intervention drug, from randomization to last follow-up | Secondary end point |
aStatistical testing for these end points was adjusted for multiple comparisons (e.g., hierarchal testing).
Source: Details included in the table are from the sponsor’s Summary of Clinical Evidence.
For those patients with nonmeasurable, bone-only disease, objective progression was established if at least 1 of the following criteria was met:
the appearance of 1 or more new lesions (in bone or outside of bone)
unequivocal progression of existing bone lesions.
According to Response Evaluation Criteria in Solid Tumours Version 1.1 (RECIST 1.1), a finding of a new lesion should be unequivocal and not attributable to something other than a tumour (e.g., “new” bone lesions that may have been simply healing or a flare of preexisting lesions). Pathologic fractures, new compression fractures, or complications of bone metastases were not considered to be evidence of disease progression, unless at least 1 of these 2 criteria was met.
For those patients with locoregionally recurrent disease for whom surgery was performed with no postoperative evidence of residual disease, objective progression was established if at least 1 of the following criteria was met:
local and/or regional recurrence
new development of metastatic disease.
For patients with locoregionally recurrent disease for whom surgery was performed while on study with postoperative evidence of residual disease, new baseline measurements should have been taken and RECIST 1.1 applied. If a patient was not known to have progressed or died at the time of analysis, PFS time was censored at the last known progression-free assessment. Additionally, patients with documented progression or death after 2 or more consecutive postbaseline assessments were censored at the date of randomization or last assessment, whichever was later.
Overall survival, defined as the time from randomization to death from any cause, was a key secondary end point in the MONARCH 2 study. Patients who had not died at the time of the analysis were censored at the date of last contact.
In the current report, OS is the primary outcome evaluated, as it provides updated information based on data provided by the study sponsor.
Harms outcomes included AEs, SAEs, withdrawals because of AEs, AESIs, and death (Table 17). AESIs were defined as neutropenia, infections, diarrhea, hepatic events, VTEs, and interstitial lung disease and/or pneumonitis.
Statistical Analysis
A summary of statistical analyses for the trial end points that are assessed in this submission is presented in Table 6.
Table 6: Statistical Analysis of Efficacy End Points, MONARCH 2 Study
End point | Statistical model | Adjustment factors | Handling of missing data | End point |
|---|---|---|---|---|
PFS | Kaplan-Meier method to estimate the PFS in each treatment arm followed by stratified Cox proportional hazard model to estimate the hazard ratio between the 2 treatment arms and the corresponding CI and Wald P value from a stratified log-rank test | Stratified by nature of disease and previous (neo)adjuvant endocrine therapy | — |
|
OS | Kaplan-Meier method to estimate the OS curve for each treatment arm, followed by stratified Cox proportional hazard model to estimate the hazard ratio between the 2 treatment arms and the corresponding CI and Wald P value from a stratified log-rank test. | Stratified by nature of disease and prior (neo)adjuvant endocrine therapy | — |
|
CI = confidence interval; OS = overall survival; PFS = progression-free survival.
Sources: MONARCH 2 Statistical Analysis Plan. Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Following the initial study protocol, the MONARCH 2 trial planned to enrol 450 endocrine-pretreated patients. A protocol amendment (Amendment A) reduced the starting dose of the blinded study drug from 200 mg every 12 hours to 150 mg every 12 hours, consistent with the Health Canada–approved dosage. Patients already receiving 200 mg every 12 hours were dose-reduced to 150 mg every 12 hours. To enable robust safety analyses at the approved dose, enrolment continued until 450 patients had been switched to the 150 mg starting dose, resulting in a final sample size of approximately 630 patients.
A 2-look group-sequential design was used for the primary end point of investigator-assessed PFS, with 1 planned interim analysis (at approximately 265 events) and 1 final analysis (at 378 events). Three interim analyses and 1 final analysis were planned for OS, which was tested hierarchically following PFS significance, with overall control of the 1-sided type I error at 0.025. PFS and OS analyses were conducted using Kaplan-Meier methods, stratified Cox proportional hazards models, and restricted mean survival time analyses. A Lan-DeMets alpha-spending function was used to preserve the cumulative type I error rate across interim and final analyses.
This report presents results from the latest interim OS analysis (data cut-off on June 20, 2019) and the final OS analysis (data cut-off on March 18, 2022). The primary PFS analysis (data cut-off on February 14, 2017) had been previously submitted to CDA-AMC in the 2018 review of abemaciclib for the treatment of HR-positive, HER2-negative advanced or metastatic breast cancer. At the time of the initial submission, the evidence was insufficient to draw conclusions for OS.
Prespecified subgroup analyses of PFS and OS were performed for each of the following potential prognostic subgroup variables:
all baseline stratification factors
starting dose (200 mg versus 150 mg)
measurable disease at baseline (yes versus no)
number of organs involved (1 versus 2 versus 3 or more)
age (younger than 65 years versus 65 years or older)
region (North America, Europe, and Asia)
race (White, Asian, and other)
progesterone receptor status (positive versus negative)
baseline ECOG PS (0 versus 1).
If a level of a factor consisted of less than 5% of randomized patients, analysis within that level was omitted.
Analyses were conducted within subgroups and, separately, across subgroups with a test of interactions of subgroups with treatment performed. Estimated hazard ratios and CIs within subgroup analyses were presented as a forest plot along with P values for tests of interactions between subgroup variables and treatment. Other subgroup analyses were permitted as appropriate. If any safety analyses identified important imbalances between arms, subgroup analyses of these end points were permitted.
Analysis Populations
Three different populations for analysis from the MONARCH 2 study are presented in this report and described in Table 7.
Table 7: Populations of the MONARCH 2 Study
Population | Definition | Application |
|---|---|---|
Entered population | All patients who signed the ICF | All disposition analyses |
Enrolled or ITT | All randomized patients within the EP strata (either primary endocrine resistance or secondary endocrine resistance), per IWRS | All patient characteristic and efficacy analyses |
Safety or RT | All randomized EP patients who received at least 1 dose of abemaciclib, placebo, or fulvestrant | All safety and exposure analyses |
EP = endocrine therapy pretreated; ICF = informed consent form; ITT = intention to treat; IWRS = interactive web response system; RT = randomized and treated.
Source: MONARCH 2 Clinical Study Report.27
Results
Patient Disposition
A total of 669 patients were randomized in the MONARCH 2 trial (446 to abemaciclib plus fulvestrant and 223 to placebo plus fulvestrant). Overall, 99.3% of randomized patients received study treatment, and 91.3% of patients discontinued treatment by the data cut-off (March 18, 2022). The most common reason for treatment discontinuation was disease progression, which was reported in 71% of patients (Table 8).
There were no major concerns identified regarding patient disposition.
Table 8: Summary of Patient Disposition in the MONARCH 2 Study
Population | Definition | Application |
|---|---|---|
Entered population | All patients who signed the ICF | All disposition analyses |
Enrolled or ITT | All randomized patients within the EP strata (either primary endocrine resistance or secondary endocrine resistance), per interactive web response system | All patient characteristic and efficacy analyses |
Safety or RT | All randomized patients who received at least 1 dose of abemaciclib, placebo, or fulvestrant | All safety and exposure analyses |
EP = eligibility period; ICF = informed consent form; ITT = intention to treat; RT = randomized treatment.
aAt the time of data cut-off on March 18, 2022.
bIncludes patients who were off treatment, as well as patients who were randomized but never treated.
Sources: MONARCH 2 Clinical Study Report (data cut-off date: March 18, 2022).27 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Baseline Characteristics
Baseline characteristics of patients enrolled in the MONARCH 2 trial are presented in Table 9. Overall, characteristics were well balanced between arms. All 669 enrolled patients were female, and the majority were white or Asian. The median age was 60.0 years, and 424 patients (63.4%) were younger than 65 years. Most patients (551 [82.4%]) at study entry were in the postmenopausal stage. The median duration of disease (from initial diagnosis of disease to randomization) was ████ months. Most patients (96.9%) entered the study with metastatic disease. The baseline characteristics outlined in Table 9 are limited to those that are most relevant to this review or were assumed to affect the outcomes or interpretation of the study results.
Table 9: Summary of Baseline Characteristics in the MONARCH 2 Study
Characteristic | Abemaciclib + fulvestrant (N = 446) | Placebo + fulvestrant (N = 223) | ||
|---|---|---|---|---|
Female, n (%) | 446 (100.0) | 223 (100.0) | ||
Age, mean (SD) | 59.3 (11.2) | 61.1 (11.7) | ||
Race, n (%) | ||||
Asian | 149 (33.4) | 65 (29.1) | ||
American Indian or Alaska Native [wording from original source] | ██ █████ | | █████ | ||
Black or African American | | █████ | | █████ | ||
White | 237 (53.1) | 136 (61.0) | ||
Missing | ██ █████ | | █████ | ||
Region, n (%) | ||||
Asia | ███ ██████ | ██ ██████ | ||
Europe | ███ ██████ | ███ ██████ | ||
North America | ███ ██████ | ██ ██████ | ||
Menopausal status, n (%) | ||||
Postmenopausal | 371 (83.2) | 180 (80.7) | ||
Premenopausal or perimenopausal | 72 (16.1) | 42 (18.8) | ||
Missing | | █████ | | █████ | ||
Duration of disease (months)a | 433 | 221 | ||
Mean | ████ ██████ | ████ ██████ | ||
Median (first to third quartile) | ████ ████ ████ | ████ ████ ████ | ||
Minimum to maximum | ████ █████ | ████ █████ | ||
ECOG Performance Status score, n (%) | ||||
0 | 264 (59.2) | 136 (61.0) | ||
1 | 176 (39.5) | 87 (39.0) | ||
2 | | █████ | ██ | ||
Missing | | █████ | ██ | ||
Disease stage at study entry, n (%) | ||||
Locally advanced | ██ █████ | | █████ | ||
Metastatic | ███ ██████ | ███ ██████ | ||
Unknown | | █████ | ██ | ||
Endocrine therapy sensitivity, n (%) | ||||
No prior endocrineb | | █████ | | █████ | ||
Primary resistance | ███ ██████ | ██ ██████ | ||
Secondary resistance | ███ ██████ | ███ ██████ | ||
Missing | | █████ | ██ | ||
Nature of disease, n (%) | ||||
Visceral | 245 (54.9) | 128 (57.4) | ||
Bone only | 123 (27.6) | 57 (25.6) | ||
Other | 75 (16.8) | 38 (17.0) | ||
Disease-free interval among patients with adjuvant therapy, n | 338 | 176 | ||
n with available information (%)c | ███ ██████ | ███ ██████ | ||
Median (minimum to maximum), months | ███ ███ ████ | ███ ███ ████ | ||
≤ 24 months, n (%)c | ██ ██████ | ██ ██████ | ||
> 24 months n (%)c | ███ ██████ | ███ ██████ | ||
ECOG = Eastern Cooperative Oncology Group; IWRS = interactive web response system; SD = standard deviation.
aDuration of disease is the time from the date of initial diagnosis to the date of randomization.
bThese 8 patients were stratified as primary endocrine resistance or secondary endocrine resistance in the IWRS and are included in the ITT population.
cThe denominator was based on the number of patients with adjuvant therapy.
Sources: MONARCH 2 Clinical Study Report.27 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Exposure to Study Treatments
Patient exposure was longer in the abemaciclib plus fulvestrant arm, with a median treatment duration of 52 weeks compared to 34 weeks in the placebo plus fulvestrant arm. The median number of treatment cycles was higher in the abemaciclib group (13 versus 9 cycles for the placebo arm), and no major discrepancies in treatment exposure were observed (Table 10).
Use of concomitant medications was common and balanced between groups (████% versus ████%). However, loperamide use was notably greater in the abemaciclib arm (██% versus ██% for the placebo arm), which can be explained by the higher risk of diarrhea in the abemaciclib group. No other major imbalances in concomitant medication use were noted (Table 11).
Following discontinuation of study treatment, a larger proportion of patients in the placebo arm received systemic therapies compared with the abemaciclib plus fulvestrant arm (████% versus ████%, respectively), particularly chemotherapy (████% versus ████%, respectively). No major issues with adherence to study treatments were reported (Table 12).
Table 10: Summary of Patient Exposure in the MONARCH 2 Study
Exposure detail | Abemaciclib + fulvestrant (N = 441) | Placebo + fulvestrant (N = 223) |
|---|---|---|
Patients who received abemaciclib or placebo, n (%)a | 441 (100.0) | 223 (100.0) |
Cycles received per patientb | ||
Median | █████ | ████ |
First to third quartile | ████ █ █████ | ████ █ █████ |
Minimum to maximum | ████ █ █████ | ████ █ █████ |
Mean (SD) | █████ ███████ | █████ ███████ |
Duration of therapy (weeks) | ||
Median | █████ | █████ |
First to third quartile | █████ █ ██████ | █████ █ █████ |
Minimum to maximum | ████ █ ██████ | ████ █ ██████ |
Mean (SD) | █████ ████████ | █████ ███████ |
SD = standard deviation.
aNumber of patients who received at least 1 dose of abemaciclib or placebo, either partial or complete.
bPatients were considered to have received a treatment cycle after receiving at least 1 dose of abemaciclib or placebo, either partial or complete.
Sources: MONARCH 2 Clinical Study Report.27 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Table 11: Summary of Concomitant Medications in the MONARCH 2 Study
Preferred term | Abemaciclib + fulvestrant (N = 441) n (%) | Placebo + fulvestrant (N = 223) n (%) |
|---|---|---|
Patients with ≥ 1 medication | ███ ██████ | ███ ██████ |
Loperamide | ███ ██████ | ██ ██████ |
Paracetamol | ███ ██████ | ██ ██████ |
Denosumab | ███ ██████ | ██ ██████ |
Metoclopramide | ██ ██████ | ██ █████ |
Zoledronic acid | ██ ██████ | ██ ██████ |
Ondansetron | ██ ██████ | ██ █████ |
Ibuprofen | ██ ██████ | ██ █████ |
Acetylsalicylic acid | ██ ██████ | ██ █████ |
Goserelin | ██ ██████ | ██ ██████ |
Potassium | ██ ██████ | ██ █████ |
Omeprazole | ██ ██████ | ██ ██████ |
Levofloxacin | ██ ██████ | ██ █████ |
Oxycodone | ██ ██████ | ██ █████ |
Calcium carbonate-cholecalciferol | ██ ██████ | ██ █████ |
Levothyroxine | ██ ██████ | ██ ██████ |
Pantoprazole | ██ ██████ | ██ █████ |
Amoxicillin-clavulanic acid | ██ ██████ | ██ █████ |
Tramadol | ██ ██████ | ██ █████ |
Dexamethasone | ██ █████ | ██ █████ |
Furosemide | ██ █████ | ██ █████ |
Loxoprofen | ██ █████ | ██ █████ |
Source: MONARCH 2 Clinical Study Report.27
Table 12: Summary of Postdiscontinuation Treatment in the MONARCH 2 Study
Treatment | Abemaciclib + fulvestrant (N = 446) n (%) | Placebo + fulvestrant (N = 223) n (%) |
|---|---|---|
Surgical procedure | ██ █████ | | █████ |
Radiotherapy | ██ ██████ | ██ ██████ |
Systemic therapy | ||
Overall | ███ ██████ | ███ ██████ |
Chemotherapy | ███ ██████ | ███ ██████ |
Endocrine | ███ ██████ | ███ ██████ |
Other | ██ ██████ | ██ ██████ |
Targeted therapy | ███ ██████ | ███ ██████ |
Sources: MONARCH 2 Clinical Study Report27 and the sponsor’s Summary of Clinical Evidence.
Efficacy
Since the 2019 recommendation, the preplanned interim OS analysis (data cut-off: June 20, 2019) and final OS analysis (data cut-off: March 18, 2022) have become available, representing an additional 5 years and 1 month of data. The results of the interim and final OS analyses (outlined in detail in this section) address pERC’s initial concerns from the 2019 recommendation that the OS information was insufficient to make strong conclusions.
Overall Survival (Interim Analysis, June 20, 2019)
The interim OS analysis was performed after 338 deaths (211 [49.8%] in the abemaciclib arm and 127 [57.0%] in the placebo arm) had occurred (data cut-off: June 20, 2019; median follow-up of 47.7 months). The 2-sided P-value boundary for significance was 0.0208. The median OS times were 46.72 months in the abemaciclib plus fulvestrant arm and 37.25 months in the placebo plus fulvestrant arm (Table 13). These results corresponded to an increase of 9.47 months (95% CI not reported) in the median OS for patients treated with abemaciclib plus fulvestrant. The addition of abemaciclib to fulvestrant resulted in a hazard ratio of 0.757 (95% CI, 0.606 to 0.945; P = 0.0137), favouring abemaciclib plus fulvestrant. Figure 1 displays a Kaplan-Meier plot of OS at this cut-off point.
Table 13: Summary of Interim Overall Survival Analysis (ITT Population, Cut-Off Date: June 20, 2019) in the MONARCH 2 Study
Variable | Abemaciclib + fulvestrant (N = 446) n (%) | Placebo + fulvestrant (N = 223) n (%) | Treatment effect/ difference/P valuea |
|---|---|---|---|
Deaths, n (%) | 211 (47.3) | 127 (57.0) | — |
Patients censored, n (%) | ███ ██████ | ██ ██████ | ██ |
Alive | ███ ██████ | ██ ██████ | ██ |
Lost to follow-up | ██ █████ | ██ █████ | ██ |
Withdrawal by patient | ██ █████ | ██ █████ | ██ |
Median (95% CI) months | ███ █████ ████ | █████ ███████ ██████ | ███ |
P value (2-sided) log-rank stratifiedb | ██ | ██ | ██████ |
Hazard ratio (95% CI) stratifiedb | ██ | ██ | █████ ███████ ██████ |
OS rate, % (95% CI)c | |||
12 months | ████ █████ █████ | ████ ████ █████ | ███ █████ ████ |
24 months | ████ █████ █████ | ████ ████ █████ | ███ █████ ████ |
36 months | ████ █████ █████ | ████ ████ █████ | ███ ████ █████ |
48 months | ████ █████ █████ | ████ ████ █████ | ████ ███ █████ |
CI = confidence interval; ITT = intention to treat; IWRS = interactive web response system; OS = overall survival.
aTreatment effect, difference, and P values are computed based on comparator placebo.
bStratified by IWRS sensitivity to endocrine therapy and IWRS nature of disease.
cThe 95% CIs and 2-sided P values for the difference between rates were calculated based on normal approximation.
Note: Quartiles and OS rates were estimated using the Kaplan-Meier method. Corresponding 95% CIs were estimated using the methods of Brookmeyer and Crowley (1982), and Greenwood (1926), respectively.
Sources: MONARCH 2 Clinical Study Report (data cut-off date: June 20, 2019).27 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Figure 1: Kaplan-Meier Plot of OS (ITT Population, Data Cut-Off Date: June 20, 2019), MONARCH 2
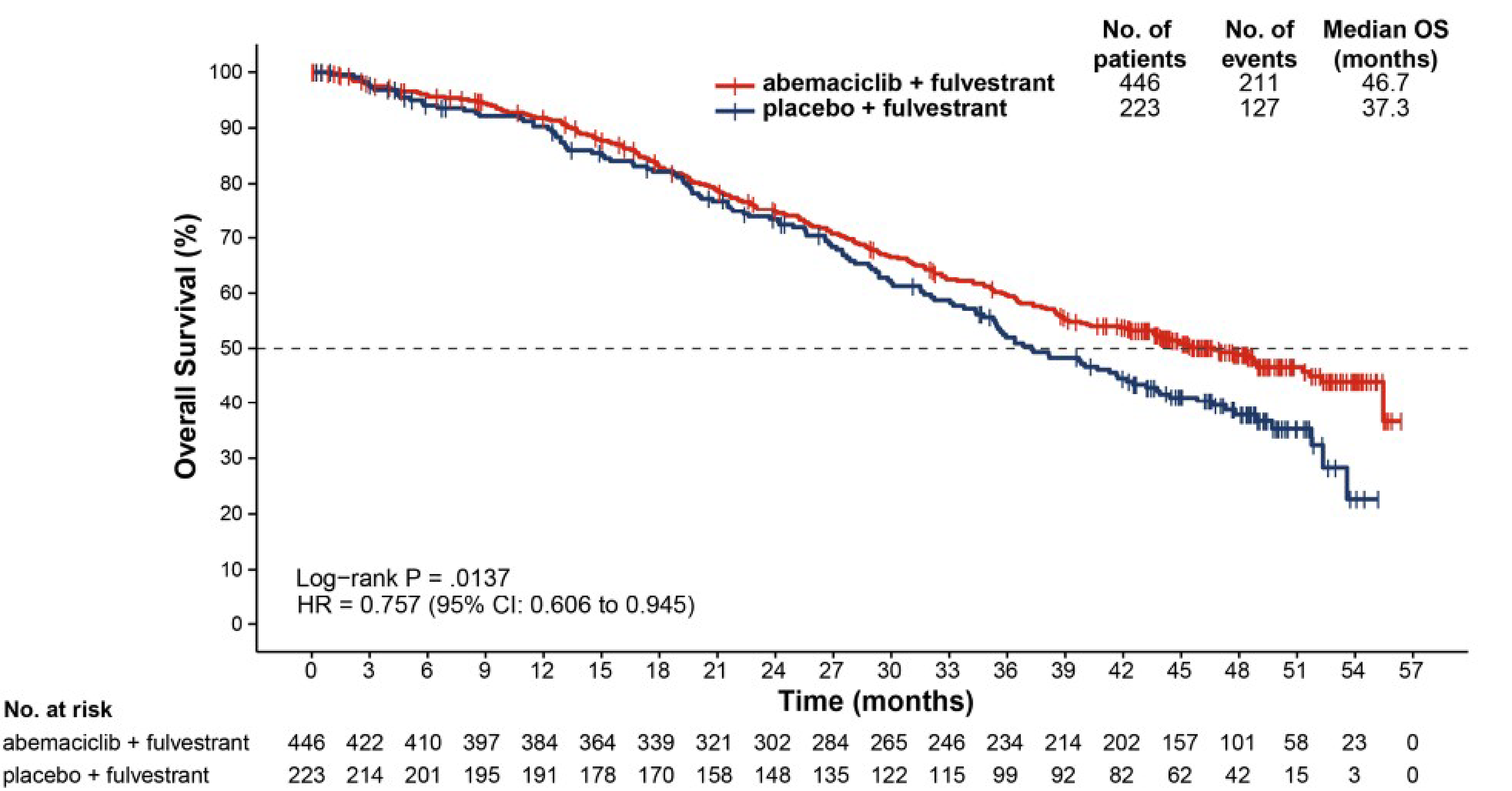
CI = confidence interval; HR = hazard ratio; ITT = intention to treat; OS = overall survival.
Source: MONARCH 2 Clinical Study Report27 (data cut-off date: June 20, 2019).
Subgroup Analysis
Prespecified subgroup analyses of OS were performed. No statistically significant interactions were observed, except for the interaction between the starting doses before and after Amendment A and treatment (P = 0.015). Improvement in OS was also consistent across the additional subgroups. Numerically stronger effects were observed in patients with premenopausal status or poor prognostic factors, such as absence of bone-only metastases, a high tumour grade, and a younger age (< 65 years). Smaller effects were observed in patients with bone metastases, a low or intermediate tumour grade, and an older age (65 to 84 years).
Further analyses illustrated the interaction between the starting doses before and after Amendment A and treatment was no longer statistically significant after adjustment for multiplicity and confounding factors of prespecified subgroup analyses.
Sensitivity Analysis
In the prespecified OS sensitivity analysis, OS time was censored at the date of death for patients who had died because of reasons not related to disease. The statistical significance and magnitude of treatment effect of the main OS analysis were supported by the prespecified analysis, as demonstrated by a hazard ratio of █████ (95% CI, █████ to █████), with a 2-sided P value of ██████.
OS (Final Analysis, March 18, 2022)
The prespecified final OS analysis was performed after approximately 441 OS events had been observed in the intention-to-treat population (data cut-off: March 18, 2022). The median follow-up times were similar for the abemaciclib plus fulvestrant and placebo plus fulvestrant arms (79.79 months versus 79.73 months, respectively). Because statistical significance was reached at the interim OS analysis, this prespecified, final OS analysis was considered post hoc by the sponsor.
A total of 440 patients died, including 283 patients (63.5%) in the abemaciclib plus fulvestrant arm and 157 patients (70.4%) in the placebo plus fulvestrant arm. The improvement in OS previously observed at the interim OS analysis (June 20, 2019 data cut-off) was maintained in the abemaciclib plus fulvestrant arm compared to the placebo plus fulvestrant arm, with a hazard ratio of █████ (95% CI, █████, █████, nominal P = ██████). Median OS values were 45.80 months in the abemaciclib plus fulvestrant arm and 37.25 months in the placebo plus fulvestrant arm (Table 14). These results corresponded to an 8.55-month (95% CI not reported) increase in median OS for patients treated with abemaciclib plus fulvestrant. Figure 2 displays a Kaplan-Meier plot of OS with additional follow-up since the June 20, 2019, dataset.
Sensitivity Analysis
In the prespecified OS sensitivity analysis, OS time was censored at the date of death for patients who had died because of reasons not related to disease. The statistical significance and magnitude of treatment effect of the main OS analysis were supported by the prespecified analysis, as demonstrated by a hazard ratio of █████ (95% CI, █████ to █████).
Table 14: Summary of Final Overall Survival (ITT Population, Data Cut-Off Date: March 18, 2022), MONARCH 2 Study
Variable | Abemaciclib + fulvestrant (N = 446) n (%) | Placebo + fulvestrant (N = 223) n (%) | Treatment effect/ difference/P valuea |
|---|---|---|---|
Deaths, n (%) | 283 (63.5) | 157 (70.4) | — |
Patients censored, n (%) | ███ ██████ | ██ ██████ | ██ |
Alive | ███ ██████ | ██ ██████ | ██ |
Lost to follow-up | ██ █████ | | █████ | ██ |
Withdrawal by patient | ██ █████ | ██ █████ | ██ |
Median (95% CI) months | ███ █████ ████ | █████ ███████ ██████ | ████ |
P value (2-sided) log-rank stratifiedb | ██ | ██ | ██████ |
Hazard ratio (95% CI) stratifiedb | ██ | ██ | ████ █████ ██████ |
OS rate, % (95% CI)c | |||
12 months | ████ █████ ████ | ████ ████ ████ | ███ ████ ████ |
24 months | ████ █████ ████ | ████ ████ ████ | ███ ████ ████ |
36 months | ████ █████ ████ | ████ ████ ████ | ███ ████ ████ |
48 months | ████ █████ ████ | ████ ████ ████ | ████ ███ ████ |
60 months | ████ █████ ████ | ████ ████ ████ | ████ ███ ████ |
72 months | ████ █████ ████ | ████ ████ ████ | ████ ███ ████ |
CI = confidence interval; ITT = intention to treat; IWRS = interactive web response system; OS = overall survival.
aTreatment effect/difference/P values are computed based on comparator (placebo).
bStratified by IWRS sensitivity to endocrine therapy and IWRS nature of disease.
c95% CIs and 2-sided P values for the difference between rates were calculated based on normal approximation.
Note: Quartiles and OS rates were estimated using the Kaplan-Meier method. Corresponding 95% CIs were estimated using the methods of Brookmeyer and Crowley (1982), and Greenwood (1926), respectively.
Source: MONARCH 2 Clinical Study Report27 (data cut-off date: March 18, 2022).
Figure 2: Kaplan-Meier Plot of OS (ITT Population, Cut-Off Date: March 18, 2022), MONARCH 2 Study
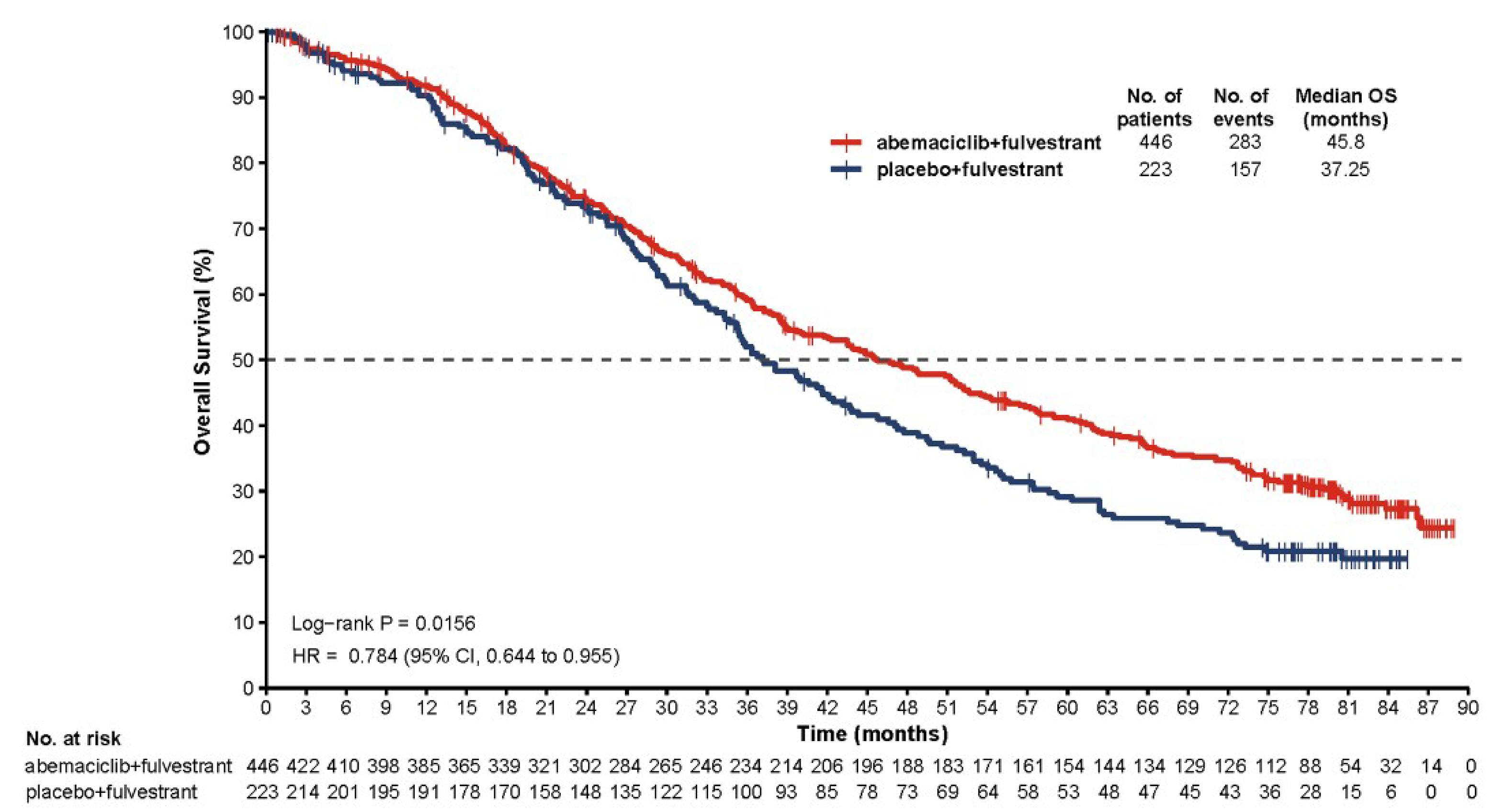
CI = confidence interval; HR = hazard ratio; ITT = intention to treat; OS = overall survival.
Source: MONARCH 2 Clinical Study Report27 (data cut-off date: March 18, 2022).
Subgroup Analysis
Results from the prespecified subgroup analyses were aligned with the subgroup analysis results from the interim OS analysis. The treatment effect of abemaciclib plus fulvestrant in terms of OS benefit was consistent across most analyzed subgroups (Figure 3).
Figure 3: Forest Plot of Summary of OS by Prespecified Subgroups (ITT Population, Cut-Off Date: March 18, 2022), MONARCH 2 Study
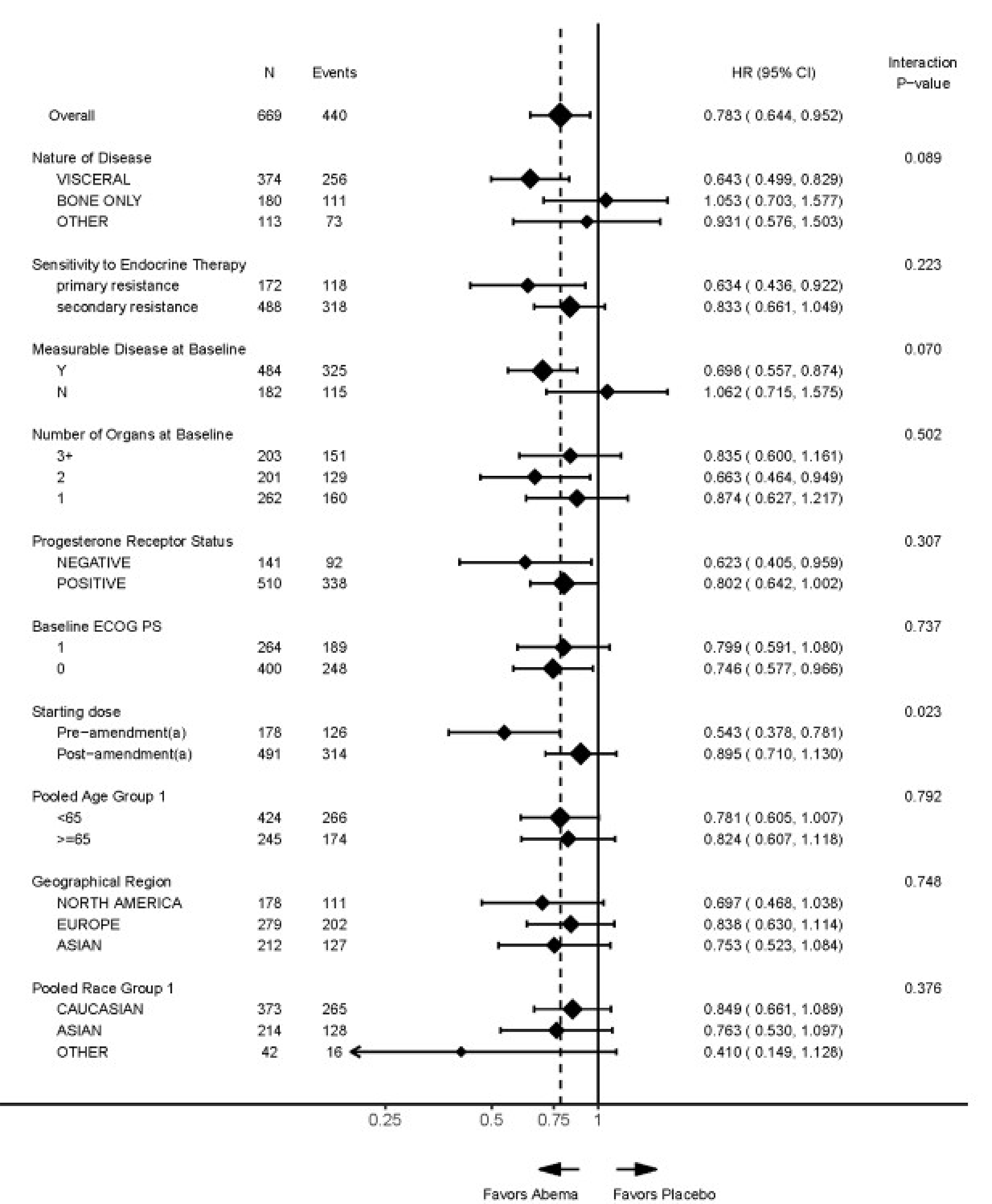
CI = confidence interval; ECOG PS = Eastern Cooperative Oncology Group Performance Status; HR = hazard ratio; ITT = intention to treat; OS = overall survival.
Note: OS hazard ratios and 95% CIs are indicated by diamonds and the crossing of horizontal lines, respectively. HRs for overall and within subgroups are unstratified; subgroup HRs are estimated with the adjustment of arm*subgroup interaction. Factor levels that consisted of less than 5% of randomized patients were omitted from the analysis.
Source: MONARCH 2 Clinical Study Report27 (data cut-off date: March 18, 2022).
No statistically significant interactions were observed, except for the interaction between the starting doses before and after Amendment A and treatment (P = █████). The interaction between starting doses before and after Amendment A and treatment was no longer statistically significant after adjustment for multiplicity and confounding factors of prespecified subgroup analyses.
Results from the prespecified subgroup analyses aligned with the subgroup analysis results from the interim OS analysis. The treatment effect of abemaciclib plus fulvestrant in terms of OS benefit was consistent across analyzed subgroups. The following were found to be prognostic factors of OS: endocrine resistance, number of organs at baseline, age, race, region, and baseline Eastern Cooperative Oncology Group Performance Status (ECOG PS). Accordingly, the subgroup analyses for each of the 10 prespecified variables were rerun using a multivariate Cox model with the selected prognostic main effects and the subgroup by treatment interaction term included. After accounting for these prognostic main effects, the interaction P value for the subgroups for starting doses before and after Amendment A was no longer significant (P = █████). Improvement in OS was also consistent across additional subgroups evaluated. Numerically stronger effects were observed in patients with a premenopausal status or poor prognostic factors, such as absence of bone-only metastases, presence of baseline liver metastases, and a high tumour grade.
PFS (Updated at the Time of Interim OS Analysis, June 20, 2019)
The efficacy results at the time of the primary analysis of the PFS end point (data cut-off on February 14, 2017) occurred when 379 investigator-assessed PFS events had been observed (222 [49.8%] in the abemaciclib arm and 157 [70.4%] in the placebo arm). The hazard ratio was 0.553 (95% CI, 0.449 to 0.681; 2-sided P < 0.000001), favouring abemaciclib plus fulvestrant. The abemaciclib arm achieved a median PFS of 16.4 months compared with 9.3 months in the placebo arm. These results corresponded to an increase of 7.2 months (95% CI not reported) in median PFS for patients treated with abemaciclib plus fulvestrant. At this time, 5 sensitivity analyses showed magnitudes of benefit similar to those of the primary analysis: PFS by investigator assessment; censoring for receiving subsequent systemic anticancer therapy; considering nonobjective progression as a PFS event; forward-dating progressions at unscheduled assessments; and adjusting for selected prognostic factors. There was a relatively consistent magnitude of effect across all subgroups.
At the June 20, 2019, data cut-off, an updated PFS analysis was performed (median follow-up of 47.7 months). A total of 490 patients experienced PFS events, including 297 patients (66.6%) in the abemaciclib plus fulvestrant arm and 193 patients (86.5%) in the placebo plus fulvestrant arm. Consistent with the primary PFS analysis, the hazard ratio was 0.536 (95% CI, 0.445 to 0.645; 2-sided P < 0.001) favouring abemaciclib plus fulvestrant (Table 15). The median PFS times were 16.87 months in the abemaciclib plus fulvestrant arm and 9.27 months in the placebo plus fulvestrant arm. These results corresponded to an increase of 7.59 months (95% CI not reported) in median PFS for patients treated with abemaciclib plus fulvestrant.
Table 15: Summary of PFS (ITT Population, Data Cut-Off Date: June 20, 2019), MONARCH 2 Study
Variable | Abemaciclib + fulvestrant (N = 446) n (%) | Placebo + fulvestrant (N = 223) n (%) | Treatment effect/difference/P valuea |
|---|---|---|---|
Deaths, n (%) | 297 (66.6) | 193 (86.5) | — |
Death without PD | ██ █████ | | █████ | — |
PD | ███ ██████ | ███ ██████ | — |
Number of patients censored, n (%) | ███ ██████ | ██ ██████ | ██ |
Death or PD after ≥ 2 missed tumour assessments | ██ █████ | | █████ | ██ |
No baseline tumour assessment | | █████ | ██ | ██ |
No postbaseline tumour assessment | | █████ | | █████ | ██ |
No documented PD with regular assessment | ███ ██████ | ██ █████ | ██ |
Median (95% CI) months | ████ █████ ████ | ███ ████ ████ | ███ |
P value (2-sided) log-rank stratifiedb | ██ | ██ | █████████ |
Hazard ratio (95% CI) stratifiedb | ██ | ██ | ███ ████ █████ |
PFS survival rate, % (95% CI)c | |||
12 months | ███ ████ █████ | ████ ███ █████ | ████ ███ █████ |
24 months | ████ ████ ████ | ████ ███ █████ | ████ ███ █████ |
36 months | ████ ████ █████ | ████ ███ █████ | ████ ███ █████ |
CI = confidence interval; ITT = intention to treat; IWRS = interactive web response system; PD = progressive disease; PFS = progression-free survival.
aTreatment effect, difference, and P values are computed based on comparator placebo.
bRounded numbers.
cStratified by IWRS sensitivity to endocrine therapy, IWRS nature of disease.
d95% CIs and 2-sided P values for the difference between rates were calculated based on normal approximation.
Note: Quartiles and PFS rates were estimated using the Kaplan-Meier method. Corresponding 95% CIs were estimated using the methods of Brookmeyer and Crowley (1982), and Greenwood (1926), respectively.
Source: MONARCH 2 Clinical Study Report27 (data cut-off date: June 20, 2019).
A Kaplan-Meier plot of updated PFS is displayed in Figure 4. Early and sustained separation by treatment arm, which was apparent beginning at approximately 3 months, showed clinically meaningful improvement in PFS. The 3-year PFS rate was 29.9% (95% CI, ████ to ████) in the abemaciclib plus fulvestrant versus 10.1% (95% CI, ███ to ████) in the placebo plus fulvestrant arm.
Figure 4: Kaplan-Meier Plot of Progression-Free Survival (ITT Population, Data Cut-Off Date: June 20, 2019), MONARCH 2 Study
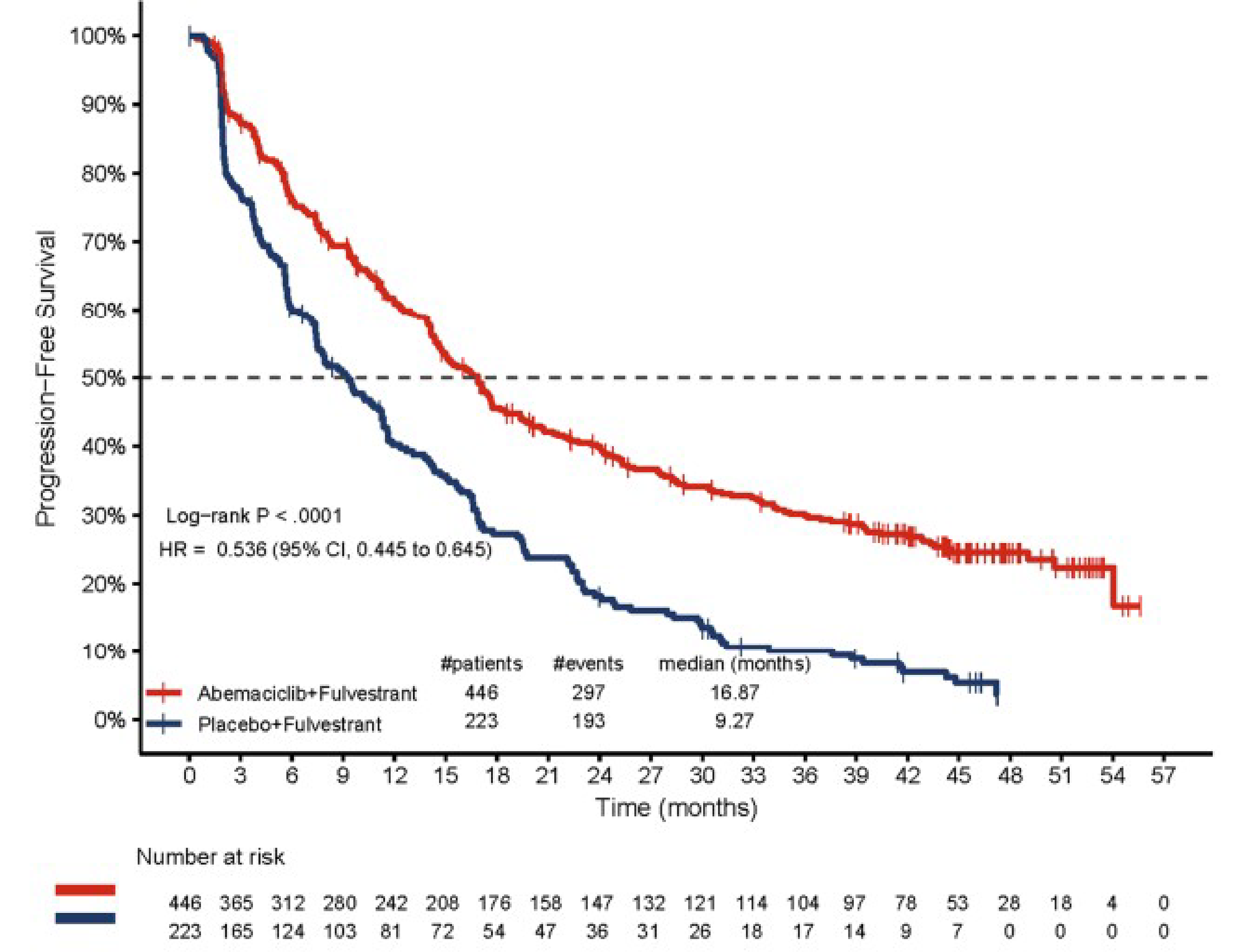
CI = confidence interval; HR = hazard ratio; ITT = intention to treat.
Source: MONARCH 2 Clinical Study Report27 (data cut-off date: June 20, 2019).
Updated PFS (at the Time of Final OS Analysis, Data Cut-Off Date: March 18, 2022)
At the March 18, 2022, data cut-off (median follow-up of ████ months), another updated PFS analysis was performed. A total of ███ patients experienced PFS events, including ███ patients (████%) in the abemaciclib plus fulvestrant arm and ███ patients (████%) in the placebo plus fulvestrant arm.
The increase in PFS was maintained from the previous interim OS analysis (June 20, 2019, data cut-off) in the abemaciclib plus fulvestrant arm compared to the placebo plus fulvestrant arm, with a hazard ratio of █████ (95% CI, █████ to █████). The median PFS times were █████ months in the abemaciclib plus fulvestrant arm and ████ months in the placebo plus fulvestrant arm (Table 16). These results corresponded to an increase of ████ months in the median PFS for patients treated with abemaciclib plus fulvestrant.
A Kaplan-Meier plot of updated PFS is displayed in Figure 5. Early and sustained separation by treatment arm was apparent beginning at approximately 3 months and continued to separate with an additional follow-up.
Table 16: Summary of PFS (ITT, Data Cut-Off Date: March 18, 2022), MONARCH 2 Study
Variable | Abemaciclib + fulvestrant (N = 446) n (%) | Placebo + fulvestrant (N = 223) n (%) | Treatment effect/ difference/P valuea |
|---|---|---|---|
Deaths, n (%) | ███ ██████ | ███ ██████ | ██ |
Death without PD | ██ █████ | █████ | ██ |
PD | ███ ██████ | ███ ██████ | ██ |
Patients censored, n (%) | ███ ██████ | ██ ██████ | ██ |
Death or PD after ≥ 2 missed tumour assessments | ██ █████ | ██ █████ | ██ |
No baseline tumour assessment | | █████ | ██ | ██ |
No postbaseline tumour assessment | | █████ | | █████ | ██ |
No documented PD with regular assessment | ██ ██████ | ██ █████ | ██ |
Median (95% CI) months | █████ ███████ ██████ | ████ ████ ████ | ████ |
P value (2-sided) log-rank stratifiedb | ██ | ██ | ████████ |
Hazard ratio (95% CI) stratifiedb | ██ | ██ | █████ ███████ ██████ |
PFS survival rate, % (95% CI)c | |||
12 months | ████ ████ █████ | ████ ████ ████ | ████ ███ ████ |
24 months | ████ ████ █████ | ████ ████ ████ | ████ ███ ████ |
36 months | ████ ████ █████ | ███ █████ ████ | ████ ███ ████ |
48 months | ████ ████ █████ | ███ █████ ████ | ████ ███ ████ |
60 months | ████ ████ █████ | ███ █████ ████ | ████ ███ ████ |
72 months | ████ ████ █████ | ███ █████ ████ | ████ ███ ████ |
CI = confidence interval; ITT = intention to treat; IWRS = interactive web response system; PD = progressive disease; PFS = progression-free survival.
aTreatment effect/difference/P values are computed based on comparator placebo.
bStratified by IWRS sensitivity to endocrine therapy, IWRS nature of disease.
c95% CIs and 2-sided P values for the difference between rates were calculated based on normal approximation.
Note: Quartiles and PFS rates were estimated using the Kaplan-Meier method. Corresponding 95% CIs were estimated using the methods of Brookmeyer and Crowley (1982), and Greenwood (1926), respectively.
Source: MONARCH 2 Clinical Study Report27 (data cut-off date: March 18, 2022).
Figure 5: Kaplan-Meier Plot of PFS (ITT Population, March 18, 2022), MONARCH 2 Study
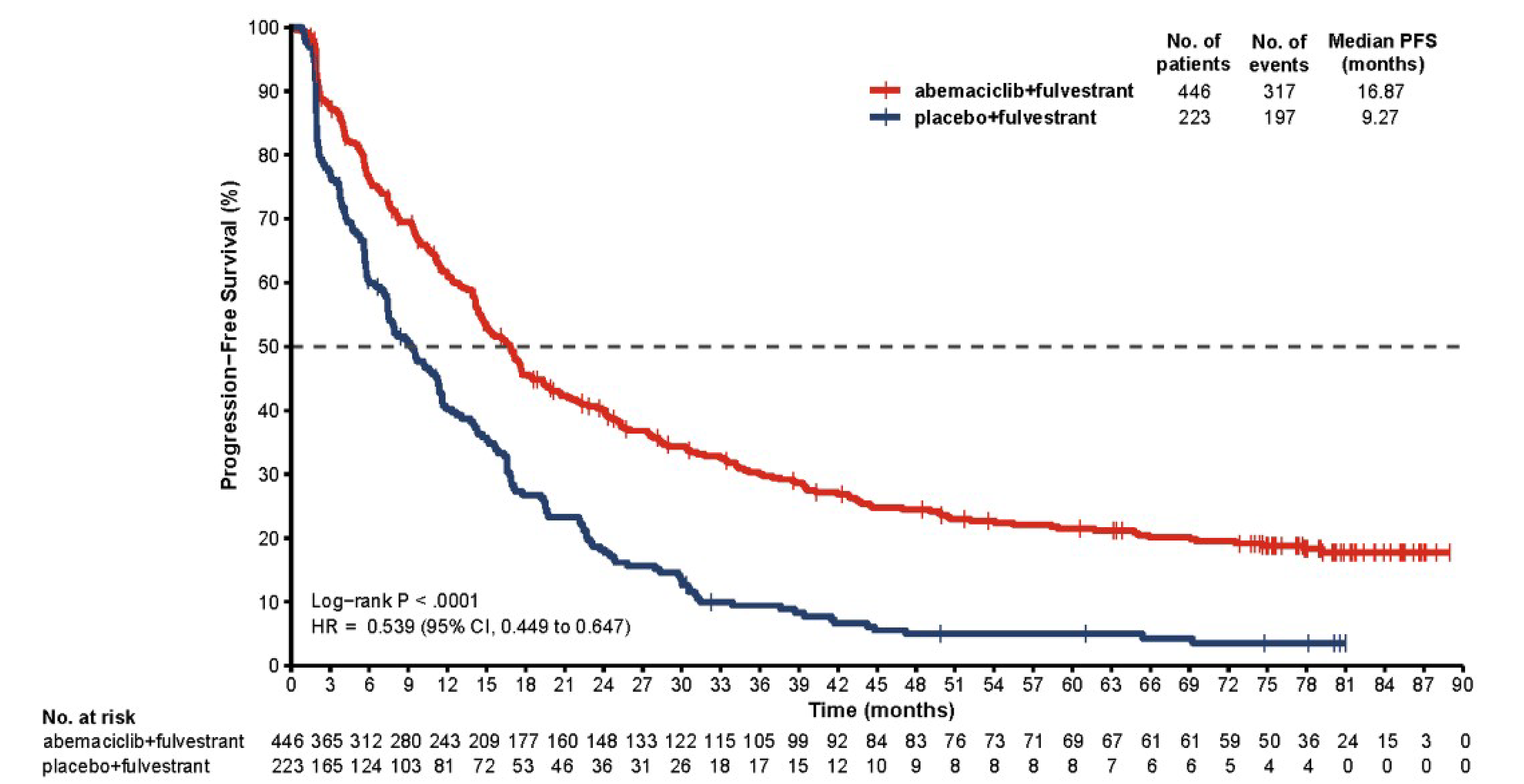
CI = confidence interval; HR = hazard ratio; ITT = intention to treat; PFS = progression-free survival.
Source: MONARCH 2 Clinical Study Report27 (data cut-off date: March 18, 2022).
Harms
Overview of Safety
A summary of AEs, SAEs, withdrawals due to AEs, AESIs, and deaths due to AEs is provided in Table 17.
Table 17: Key Harms Data for the MONARCH 2 Study
Variable | Abemaciclib + fulvestrant (N = 441), n (%) | Placebo + fulvestrant (N = 223), n (%) |
|---|---|---|
Adverse events, n (%) | ||
Patients with ≥ 1 adverse event | ███ ██████ | ███ ██████ |
Diarrhea | ███ ██████ | ██ ██████ |
Neutropenia | ███ ██████ | | █████ |
Nausea | ███ ██████ | ██ ██████ |
Fatigue | ███ ██████ | ██ ██████ |
Abdominal pain | ███ ██████ | ██ ██████ |
Anemia | ███ ██████ | ██ █████ |
Leukopenia | ███ ██████ | | █████ |
Vomiting | ███ ██████ | ██ ██████ |
Decreased appetite | ███ ██████ | ██ ██████ |
Headache | ███ ██████ | ██ ██████ |
Upper respiratory tract infection | ██ ██████ | ██ █████ |
Dysgeusia | ██ ██████ | | █████ |
Stomatitis | ██ ██████ | ██ ██████ |
Increased AST | ██ ██████ | ██ █████ |
Increased ALT | ██ ██████ | ██ █████ |
Thrombocytopenia | ██ ██████ | | █████ |
Arthralgia | ██ ██████ | ██ ██████ |
Cough | ██ ██████ | ██ ██████ |
Alopecia | ██ ██████ | | █████ |
Constipation | ██ ██████ | ██ ██████ |
Dizziness | ██ ██████ | ██ █████ |
Serious adverse events, n (%) | ||
Patients with ≥ 1 serious adverse event | ███ ██████ | ██ ██████ |
Pneumonia | ██ █████ | | █████ |
Sepsis | | █████ | | █████ |
Skin infection | | █████ | | █████ |
Diarrhea | | █████ | | █████ |
Embolism | | █████ | | █████ |
Patients who stopped treatment due to adverse events, n (%) | ||
Patients discontinued any study treatment due to adverse eventsa | ██ ██████ | ██ █████ |
Neutropenia | ██ █████ | | ███ |
Diarrhea | ██ █████ | | ███ |
Patients only discontinued abemaciclib or placebo due to adverse eventsb | ██ ██████ | | █████ |
Neutropenia | ██ █████ | | ███ |
Diarrhea | | █████ | | ███ |
Deaths, n (%) | ||
All deaths | ███ ██████ | ███ ██████ |
Deaths on therapy or within 30 days of treatment discontinuation | ██ █████ | ██ █████ |
Reasons for death | ||
Adverse events | ██ █████ | | █████ |
Sepsis | | █████ | | ███ |
Study disease | ██ █████ | | █████ |
Adverse events of special interest (any grade), n (%) | ||
Neutropenia | ███ ██████ | | █████ |
Infections | ███ ██████ | ██ ██████ |
Diarrhea | ███ ██████ | ██ ██████ |
Increased AST | ██ ██████ | ██ █████ |
Increased ALT | ██ ██████ | ██ █████ |
Interstitial lung disease or pneumonitis | ██ █████ | | █████ |
aPatients may be counted in more than 1 category.
bIncludes events that were considered related to study treatment as judged by the investigator.
cNew event reported since June 20, 2019, data cut-off.
dCryptogenic organizing pneumonia coded as pneumonia as determined by Common Terminology Criteria for Adverse Events.
Note: Results for greater than 15% of adverse events, 2% for serious adverse events and adverse events of special interest.
Source: MONARCH 2 Clinical Study Report27 (data cut-off date: March 18, 2022).
Adverse Events
AEs were reported in ███ (████%) patients in the abemaciclib plus fulvestrant arm and ███ patients (████%) in the placebo plus fulvestrant arm. The most common AEs (occurring at a frequency of 20% or more) in either treatment arm (abemaciclib plus fulvestrant versus placebo plus fulvestrant) were diarrhea (████% versus ████%, respectively), neutropenia (████% versus ███%), nausea (████% versus ████%), fatigue (████% versus ████%), abdominal pain (████% versus ████%), anemia (████ versus ███%), leukopenia (████% versus ███%), vomiting (████% versus ████%), decreased appetite (████% versus ████%), headache (████% versus ████%), and upper respiratory tract infection (████% versus ███%).
Serious AEs
A total of ███ patients (████%) in the abemaciclib plus fulvestrant arm, and ██ patients (████%) in the placebo plus fulvestrant arm experienced at least 1 SAE. In the abemaciclib plus fulvestrant arm, the most frequently reported SAEs were pneumonia (███%), diarrhea (███%), and embolism (███%). In the placebo plus fulvestrant arm, SAEs were more frequently reported within the system organ class of respiratory, thoracic, and mediastinal disorders (███%). Pleural effusion was the most frequently reported SAE in the placebo plus fulvestrant arm (███%).
Withdrawals Due to AEs
The number of AEs leading to treatment discontinuation in the abemaciclib plus fulvestrant arm was ██ patients (████%) at the time of the final OS analysis (Table 18).
Table 18: Adverse Events Reported as Reason for Any Study Drug Discontinuation Experienced by 2 or More Patients in Either Arm, Preferred Term by Decreasing Frequency Safety Population
Adverse events | Abemaciclib + fulvestrant (N = 441), n (%) | Placebo + fulvestrant (N = 223), n (%) |
|---|---|---|
Patients discontinued any study treatment due to adverse eventsa | ██ ██████ | ██ █████ |
Neutropenia | ██ █████ | | ███ |
Diarrhea | ██ █████ | | ███ |
Sepsis | | █████ | | ███ |
Embolism | | █████ | | ███ |
Anemia | | █████ | | ███ |
Leukopenia | | █████ | | ███ |
Increased ALT | | █████ | | █████ |
Increased AST | | █████ | | █████ |
Muscular weakness | | █████ | | ███ |
Pneumonia | | █████ | | ███ |
Pneumonitis | | █████ | | ███ |
Cerebrovascular accident | | █████ | | ███ |
Nausea | | █████ | | ███ |
Decreased weight | | █████ | | ███ |
Drug-induced liver injury | | █████ | | ███ |
Rash | | █████ | | ███ |
Patients only discontinued abemaciclib or placebo due to adverse eventsb | ██ ██████ | | █████ |
Neutropenia | ██ █████ | | ███ |
Diarrhea | | █████ | | ███ |
Leukopenia | | █████ | | ███ |
Increased ALT | | █████ | | ███ |
Embolism | | █████ | | ███ |
Rash | | █████ | | ███ |
aSubject may have been counted in more than 1 category.
bIf the date of the patient’s last dose of abemaciclib was on or before the discontinuation date of fulvestrant or abemaciclib or placebo only, then the patient was considered as to have discontinued abemaciclib alone.
Source: MONARCH 2 Clinical Study Report27 (data cut-off date: March 18, 2022).
AEs of Special Interest
Neutropenia was reported in ███ patients (████%) receiving abemaciclib plus fulvestrant compared to ██ patients (███%) with placebo. Dose reductions and omissions because of neutropenia occurred in ██ (████%) and ██ (████%) patients, respectively, in the abemaciclib group.
Infections, mostly low-grade, occurred in ███ patients (████%) in the abemaciclib group and ██ patients (████%) in the placebo group. Grade 3 or higher infections were reported in ██ patients (███%) receiving abemaciclib and ██ patients (███%) receiving placebo.
Diarrhea was reported in 384 patients (87.1%) treated with abemaciclib and 62 patients (27.8%) with placebo. Grade 3 or higher diarrhea occurred in 64 patients (14.5%) in the abemaciclib arm. Dose reductions because of diarrhea were required in ██ patients (████%), and ██ patients (███%) discontinued any study drug for this reason.
Hepatic events requiring dose modification (elevated ALT or AST) occurred in ██ patients (███%) in the abemaciclib group and ██ patients (███%) in the placebo group. No new hepatic safety signals were observed.
VTEs were reported in ██ patients (███%) in the abemaciclib group and ██ patients (███%) in the placebo group. Treatment discontinuations because of VTEs occurred in ██ patients (███%) receiving abemaciclib.
Cases of interstitial lung disease or pneumonitis were reported in ██ patients (███%) treated with abemaciclib and in ██ patient (███%) in the placebo group. Most cases were grade 1 or 2, with 3 patients (███%) experiencing grade 3 or higher events.
Critical Appraisal
Internal Validity
The MONARCH 2 study used an appropriate randomization process (2:1 ratio, stratified by site of metastasis and ET resistance) and maintained allocation concealment. Baseline demographics and disease characteristics were well balanced across treatment arms. No significant imbalances were observed that would threaten the validity of treatment comparisons. The study was double-blind; however, the higher incidence of diarrhea in the abemaciclib arm (87.1% versus 27.8% with placebo) could have led to unblinding. This potential unblinding risk may have influenced subjectively reported outcomes (e.g., patient-reported HRQoL, for which data are provided in Appendix 1), but is unlikely to have affected objectively measured end points such as PFS and OS.
Patients who were lost to follow-up were censored at the last adequate disease assessment for PFS and the date of last contact for OS. Loss to follow-up and censoring for this reason was relatively limited and similar across arms, and treatment adherence was high (████% treated). No evidence suggests that missing data meaningfully biased the results. Because patient-reported outcomes were not updated in the final OS dataset, no updated imputation assessment was needed. The study used prespecified hierarchical testing (PFS before OS) and controlled the overall type I error rate across end points and interim analyses at █████. Kaplan-Meier methods and stratified Cox proportional hazards models were appropriate for time-to-event end points. Subgroup analyses were prespecified and exploratory, and no statistically significant interactions remained after multiplicity adjustment for likely effect modification. Sensitivity analyses supported the robustness of the OS and PFS results, with consistent direction of results, although the magnitude of effects varied.
The study was event-driven, with the final OS analysis performed post hoc (after significance was achieved at the interim analysis), but the findings were consistent with the interim results, reducing concerns about bias from multiple analyses.
Overall, the study was rigorously designed with strong blinding, randomization, appropriate control of type I error, clinically relevant end points (PFS and OS), and relatively little missing data for OS and PFS. Sensitivity and subgroup analyses showing consistency in the direction of effects further support the internal validity.
External Validity
The study population included patients with HR-positive, HER2-negative advanced breast cancer with previous exposure to ET, aligning them with the clinical population in Canada for this resubmission. Patients with visceral crisis or central nervous system metastases were excluded, limiting generalizability to those populations. The abemaciclib dosing (150 mg twice daily) was consistent with the Health Canada–approved regimen, as was the use of fulvestrant, making the intervention and comparator reflective of Canadian clinical practice. Primary and secondary outcomes (PFS and OS) are clinically meaningful and align with those used in routine clinical decision-making. Follow-up at the latest analysis was adequate to warrant confidence in the treatment effects. HRQoL was assessed but not updated in the final OS dataset. Comparative evidence of benefit and harm versus relevant comparators (ribociclib plus fulvestrant, palbociclib plus fulvestrant) was not available in the MONARCH 2 trial.
Long-Term Extension Studies
No long-term extension studies were submitted by the sponsor.
Indirect Evidence
Contents within this section have been informed by materials submitted by the sponsor. The following has been summarized and validated by the review team.
Objectives for the Summary of Indirect Evidence
To evaluate the relative efficacy (PFS and OS) estimates for treatment regimens prescribed for the management of women with HR-positive, HER2-negative advanced breast cancer who had disease progression on or within 12 months of completing (neo)adjuvant endocrine therapy or who had disease progression on their first-line ET for advanced disease.
Description of Indirect Comparison
The sponsor submitted an ITC (M2, Table 19) using a Bayesian NMA to assess the relative efficacy of abemaciclib plus fulvestrant 500 mg (ABE + FUL 500) compared with other therapies for patients with HR-positive, HER2-negative advanced or metastatic breast cancer who progressed on or after ET. The analysis includes PFS and OS outcomes and considers both fixed- and random-effects models. FP models were used because violations of the proportional hazards’ assumption were identified. Two reports were submitted: 1 using the Cox proportional hazards models28 and 1 using the FP models.29 The evidence network included treatments such as fulvestrant monotherapy, exemestane, everolimus plus exemestane, capecitabine, palbociclib plus fulvestrant, ribociclib plus fulvestrant, and dalpiciclib plus fulvestrant.
Table 19: Study Selection Criteria and Methods for the M2 ITC
Characteristics | M2 ITC |
|---|---|
Population |
|
Intervention | For inclusion, studies must compare at least 1 listed treatment or placebo, monotherapy or in combination: abemaciclib, alpelisib, capecitabine, chidamide, dalpiciclib, docetaxel, doxorubicin, doxorubicin (liposomal), eribulin, everolimus, exemestane, fulvestrant, imlunestrant, amcenestrant, camizestrant, elacestrant, giredestrant, rintodestrant, gemcitabine, paclitaxel, paclitaxel (nanoparticle-bound), palbociclib, ribociclib, tamoxifen, vinorelbine |
Comparator | The listed interventions or placebo |
Outcome | Efficacy: OS, PFS, PD, PR, CR, SD, DFS, ORR, DCR, DOR, CBR Safety: overall discontinuations, discontinuations because of AEs, treatment-related deaths, overall incidence of grade 3 to 4 AEs, overall serious AEs Health-related quality of life: EORTC QLQ-C30, EQ-5D, Functional Assessment of Cancer Therapy–Breast |
Study designs |
|
Publication characteristics | No restrictions specified |
Exclusion criteria |
|
Databases searched | OVID database The following medical literature databases were searched to October 2022 using the OVID platform to identify relevant publications for inclusion in the SLR:
Conference search To complement the searches of electronic databases, a hand search of abstracts and posters at conference proceedings held since the last SLR update (February 2020):
|
Selection process | The records were screened by 2 reviewers in accordance with the eligibility criteria and any disagreements were resolved by a third reviewer through consensus |
Data extraction process | Data were extracted by a single reviewer; extractions were independently verified and validated by a second reviewer |
Quality assessment | The risk-of-bias assessment was restricted to RCTs described in peer-reviewed publications, using the Cochrane risk of bias tool (version 1);30 as important aspects of risk of bias were not normally reported in conference abstracts because of text restrictions, it was not possible to conduct a critical appraisal of these disclosures |
AE = adverse event; CBR = clinical benefit rate; CR = complete response; DCR = disease control rate; DFS = disease-free survival; DOR = duration of response; EORTC QLQ-C30 = European Organisation for the Research and Treatment of Cancer Quality of Life Questionnaire Core 30; ET = endocrine therapy; HR = hormone receptor; ORR = overall response rate; OS = overall survival; PD = progressive disease; PFS = progression-free survival; PR = partial response; RCT = randomized controlled trial; SD = stable disease; SLR = systematic literature review.
Sources: Indirect treatment comparison hazard ratio report28 and indirect treatment comparison fractional polynomial report.29
ITC Design
Study Selection Methods
The sponsor conducted an SLR to identify studies for inclusion in the M2 ITC. Studies were screened by 2 independent reviewers, with disagreements resolved by a third reviewer through consensus.
Databases searched via OVID included MEDLINE (All and In-Process), Embase, and the Cochrane Central Register of Controlled Trials (CENTRAL) up to October 2022, as well as hand searches of key conference proceedings (e.g., American Society of Clinical Oncology, European Society of Medical Oncology, and San Antonio Breast Cancer Symposium) from February 2020 to March 2023 and searches of ClinicalTrials.gov and the WHO International Clinical Trials Registry Platform for ongoing studies. To assess the feasibility of the analysis, the authors assessed the trials that formed a connected network of evidence for the end points of interest; this required assessing the treatment arms to ensure that dosing and dosing schedules for treatments included in more than 1 trial were comparable. Following development of the evidence network, an assessment of heterogeneity between the trials was conducted.
ITC Analysis Methods
Data were extracted by a single reviewer and independently verified by a second reviewer against clean copies of publications or abstracts. Any discrepancies were resolved through discussion. Risk of bias was assessed for RCTs using the Cochrane risk of bias tool (version 1).30 RCTs reported only in abstracts were not formally appraised because of limited information.
Efficacy outcomes included PFS, defined as the time from randomization to disease progression or death, as determined by investigator assessment using RECIST 1.1 where available. OS was defined as the time from randomization to death from any cause. Harms outcomes were not analyzed in the M2 ITC.
A Bayesian NMA approach was used to synthesize relative treatment effects, exploring both fixed-effects and random-effects models, with model selection based on the DIC in the Cox proportional hazards NMA. Vague priors were applied, and convergence was assessed through Brooks-Gelman-Rubin plots, trace plots, R-hat statistics, and adjustments for autocorrelation when needed. Proportional hazards assumptions were evaluated using Grambsch-Therneau tests, log-cumulative hazard plots, and Schoenfeld residuals. Homogeneity and similarity were qualitatively assessed across studies, and sensitivity analyses explored exclusions based on HER2 status and predominant Asian populations. Given the sparse network, consistency was assumed rather than formally tested. Treatments were grouped by drug and backbone ET without pooling across doses or administration routes. Differences in follow-up times were accepted. When multiple end-point assessments were available, investigator-assessed PFS was prioritized to align with the MONARCH 2 trial. More details are shown in Table 20.
To address violations of the proportional hazards assumption, an FP NMA, which does not require this assumption, was performed as a sensitivity analysis. The FP model specifies a collection of parametric forms for the log hazard of each treatment arm. The power of the linear predictor’s P1 and P2 were chosen from a set of predefined values with different choices corresponding to hazard functions in a range of shapes. A total of 8 first-order and 36 second-order fixed-effects and random-effects models were considered for each end point, for a total of 88 models. Model selection was informed by the DIC, visual inspection of fit to the observed data, and the plausibility of the long-term extrapolations. Assessment of convergence was performed according to the Cox proportional NMA. Consistency was not assessed.
Table 20: Indirect Comparison Analysis Methods
Methods | M2 ITC |
|---|---|
Analysis methods | NMAs using a Bayesian approach; fixed- and random-effects models were considered |
Priors | Vague (flat or uninformative) priors were used for all models, and informative priors were only considered for heterogeneity parameters |
Assessment of model fit | Alternative model specifications were compared using the deviance information criterion |
Assessment of consistency | Consistency was not tested |
Assessment of convergence | Convergence within and between chains was assessed using Brooks-Gelman-Rubin plots and by examining trace plots; convergence was assumed to be adequate if the parameter estimate range was consistent, and if there was little deviation in the estimates as the number of simulations increased; the R-hat statistic was investigated for all parameters estimated in the models Where autocorrelation was high, the number of simulations was increased or chains thinned in an attempt to reduce the autocorrelation |
Outcomes | PFS and OS |
Follow-up time points | Duration of follow-ups ranged from 18 months to 56.3 months for PFS and 28.2 to 56.3 for OS |
Construction of nodes | Treatments were grouped by drug and backbone endocrine therapy without pooling across doses or administration routes |
Sensitivity analyses | Based on the PH assumption assessment results performed for the survival outcomes in the trials included in the networks, there were some violations of the PH; the FP NMA was completed as a sensitivity analysis for OS and PFS |
Subgroup analysis | Scenario analyses were conducted to restrict to or exclude studies enrolling predominantly Asian patients, investigate potential differences in the assessment of PFS (i.e., investigator assessment and independent review committee), and investigate potential differences because of the enrolment of HER2-negative–specific populations A scenario analysis was conducted where, as feasible, HER2-negative data were used to more closely align with the inclusion/exclusion criteria of the MONARCH 2 trial; for the base analysis, the population aligned with the inclusion criteria for the SLR, and for the SoFEA trial, HER2 data were reported and used within scenario analysis; where HER2-specific data were not available, ITT population data were used |
FP = fractional polynomial; HER2 = human epidermal growth factor receptor 2; ITC = indirect treatment comparison; ITT = intention to treat; NMA = network meta-analysis; OS = overall survival; PFS = progression-free survival; PH = proportional hazards; SLR = systematic literature review.
Sources: Indirect treatment comparison: hazard ratio report28 and indirect treatment comparison: fractional polynomial report.29
Results of the NMA
Summary of Included Studies
The M2 ITC included 10 RCTs encompassing various treatments for patients with HR-positive, HER2-negative advanced or metastatic breast cancer who progressed on or after ET. Across the studies, the total number of patients contributing to the networks varied depending on the end point analyzed (PFS or OS), with all trials contributing to PFS analyses and 9 trials included in the OS network.
The included trials evaluated a range of interventions: ABE + FUL 500, palbociclib plus fulvestrant, ribociclib plus fulvestrant, everolimus plus exemestane, dalpiciclib plus fulvestrant, capecitabine, and fulvestrant monotherapy at 500 mg or 250 mg doses, and exemestane monotherapy. Treatments were administered in accordance with Health Canada–approved or standard international dosing regimens. Notable differences across trials included variations in fulvestrant dosing schedules (500 mg loading dose schedules versus older 250 mg schedules) and variations in previous lines of therapy allowed, with some trials permitting previous chemotherapy for advanced disease (unlike the MONARCH 2 trial, which excluded it). Capecitabine and everolimus plus exemestane introduced chemotherapeutic and targeted-therapy backbones not used in all studies, potentially introducing heterogeneity.
No trials identified in the SLR included the same population used in the MONARCH 2 trial. Some baseline patient characteristics were similar across studies, although heterogeneity was apparent for several characteristics. Most patients had an ECOG PS of 0 or 1, but some studies enrolled small proportions of patients with an ECOG PS of 2. The proportion of patients with visceral metastases, liver involvement, and previous exposure to ETs varied across studies. The number of previous therapies and/or the ET received in the advanced setting differed across trials, as did the requirement for HR-positive, HER2-negative status.
Quality assessments of the included RCTs were performed using the Cochrane risk of bias tool (Version 1). Most studies were peer-reviewed full publications with a low to unclear risk of bias across key domains, such as randomization, blinding, and outcome assessment. Four studies (the BOLERO-6, MANTA, PEARL, and SoFEA studies) were at high risk of bias for allocation concealment and/or blinding of outcome assessment and/or incomplete outcome data. Studies reported only in abstract form were not formally appraised because of insufficient information. No studies were excluded based solely on risk of bias.
A review of study characteristics confirmed that most included trials met the prespecified eligibility criteria outlined in the M2 ITC protocol. An assessment of heterogeneity across trials is displayed in Table 21.
Table 21: Assessment of Homogeneity
Characteristics | Description and handling of potential effect modifiers |
|---|---|
Disease severity | Not reported |
Treatment history | The MONARCH 2 study included patients who received ≤ 1 previous ET and no previous chemotherapy in the advanced setting. Except for the MONALEESA-3 study, all comparator studies allowed for previous chemotherapy in the advanced setting. Several studies permitted the use of > 1 previous ET in the advanced setting. |
Baseline characteristics | The mean and median age reported by arm ranged from 53.1 years to 66 years (mean) and 50.7 to 66.5 years (median) across the included studies. > 80% of patients in the study arms of the included studies had an ECOG PS of 0 or 1. All studies included patients in the postmenopausal stage within their population. Some studies, such as the DAWNA-1 study, included patients who were in the premenopausal stage and patients who were in the postmenopausal stage. The proportion of patients with visceral involvement ranged from 13.5% to 100% of patients in each study arm of the included studies, where reported. This characteristic was often not reported, and when reported the definitions were not consistent. Adjustments for differences were not considered feasible. The MONARCH 2 eligibility criteria included patients with an HR-positive, HER2-negative status. This varied across the other included studies, with several studies not reporting these criteria. The authors looked to assess whether subgroup data for an HR-positive, HER2-negative population were available from the included studies. Except for the PALOMA 3 study, this was not identified in any other study. As the full population of the PALOMA 3 included HR-positive, HER2-negative patients, there were no alternative data to include in the analysis. Given the lack of reporting on this status, no adjustment for these differences was considered feasible. |
Dosing of comparators | Focusing on the treatments included in multiple studies (e.g., fulvestrant 500 mg, fulvestrant 250 mg, exemestane, capecitabine, and capecitabine plus fulvestrant), there we no major concerns about the dose, treatment schedule, or treatment discontinuation rules. |
Placebo response | Not reported |
Definitions of end points | Two assessments of disease progression were conducted in the MONARCH 2 trial: IA (primary end point) and IRC. The IA PFS data for the MONARCH 2 trial were used in the NMA as it was the primary end point in the MONARCH 2 trial. Most of the comparator publications also reported IA PFS data. Given that most publications reported IA PFS, this was preferred over IRC in cases where both were available. This sensitivity of results to this decision was also tested in scenario analyses for the PFS end point. The end points for PFS and time to progression are sometimes reported interchangeably in the literature. To ensure that the study data included in the analysis were based on a true definition for PFS (time to progression death) the reported definitions were reviewed for all studies and only data corresponding to a true PFS definition were included. |
Timing of end point evaluation | The duration of follow-up ranged from 18 months to 56.3 months for PFS and 28.2 to 56.3 for OS. The sponsor deemed the duration of follow-up to be suitable to capture treatment efficacy for both end points in all studies where the duration of follow-up was reported. |
Withdrawal frequency | No major concerns about the treatment discontinuation rules were reported. |
Clinical trial setting | The trials included a range of locations, with most studies being multicentre international studies, with notable exceptions: MONARCH plus study (using Cohort B of the study) and the DAWNA-1 study enrolled predominantly Asian patients. |
Study design | No major key differences between trials were reported, with the exception of the PEARL study, in which patients were permitted to crossover to CDK4 and CDK6 inhibitor treatment upon disease progression, if they had not received capecitabine plus fulvestrant 500 mg at randomization. The PEARL study reports that 55.1% of patients receiving capecitabine had a CDK4 and CDK6 inhibitor as a subsequent line of therapy, most patients received the CDK4 and CDK6 inhibitor as their first subsequent line of therapy. The high use of CDK4 and CDK6 inhibitor (fulvestrant 500 mg) following disease progression was not expected to affect PFS but could affect OS. Other studies permitted treatment crossover (e.g., MONALEESA-3 and CONFIRM). This was considered unlikely to bias results as the crossover was allowed after final study results. |
Trial phase and timing | All studies were phase III trials, with the exception of the phase II BOLERO-6 study. |
CDK = cyclin-dependent kinase; ECOG PS = Eastern Cooperative Oncology Group Performance Status; ET = endocrine therapy; HER2 = human epidermal growth factor receptor 2; HR = hormone receptor; IA = investigator assessment; IRC = independent review committee; NMA = network meta-analysis; OS = overall survival; PFS = progression-free survival.
Source: Indirect treatment comparison: hazard ratio report,28 and indirect treatment comparison: fractional polynomial report.29
Results
Results are presented for both the hazard ratio and FP approaches. A view of the geometry of the complete base-case evidence networks are presented in Figure 6 and Figure 7.
Figure 6: Base-Case Complete Evidence Network — Overall Survival
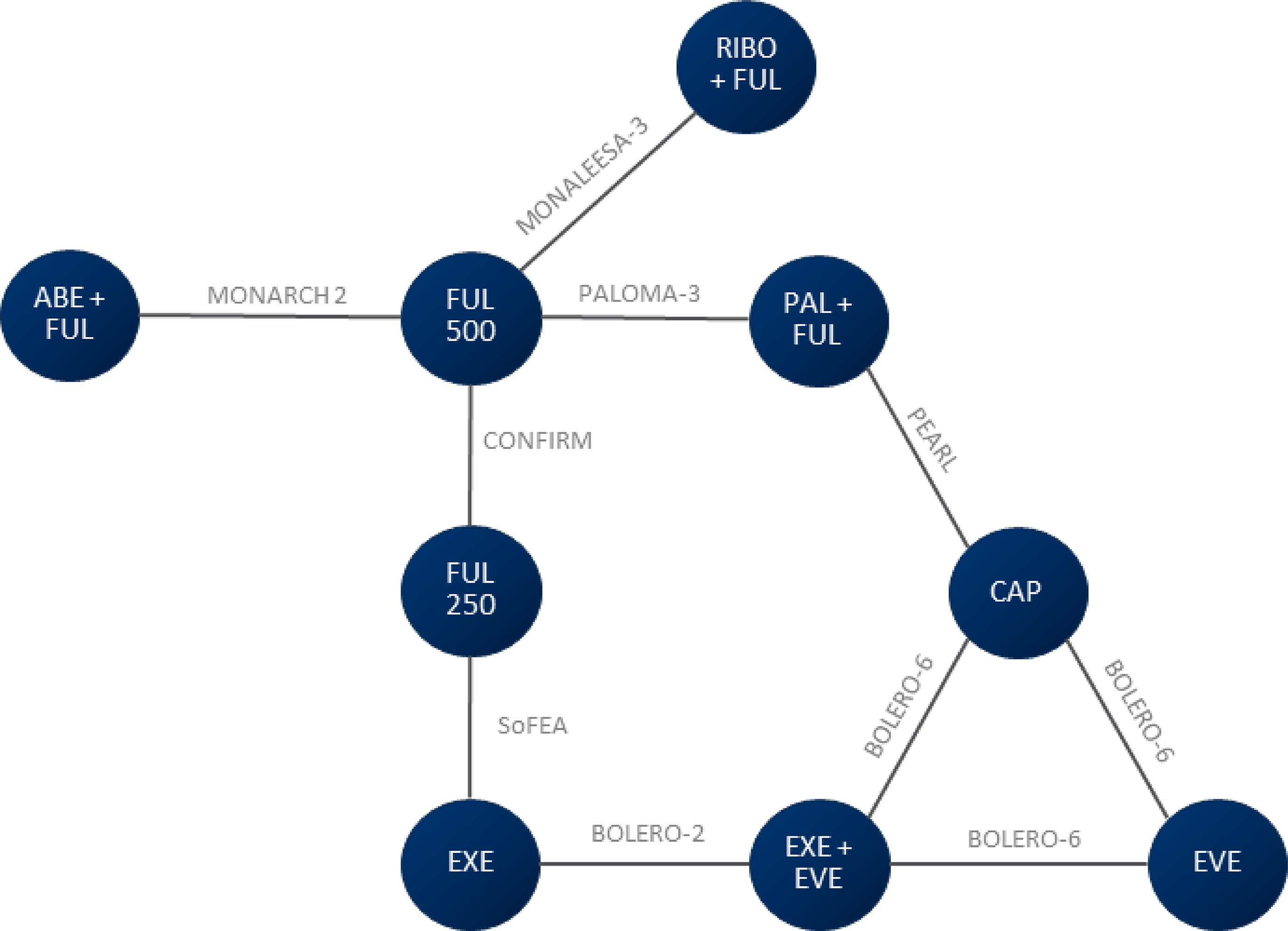
ABE = abemaciclib; CAP = capecitabine; EVE = everolimus; EXE = exemestane; FUL 250 = fulvestrant 250 mg; FUL 500 = fulvestrant 500 mg; PAL = palbociclib; RIBO = ribociclib.
Note: RIBO-FUL 500 data were from a subgroup population of the MONALEESA-3 trial.
Source: Indirect treatment comparison: hazard ratio report28 and indirect treatment comparison: fractional polynomial report.29
Figure 7: Base-Case Complete Evidence Network — Progression-Free Survival
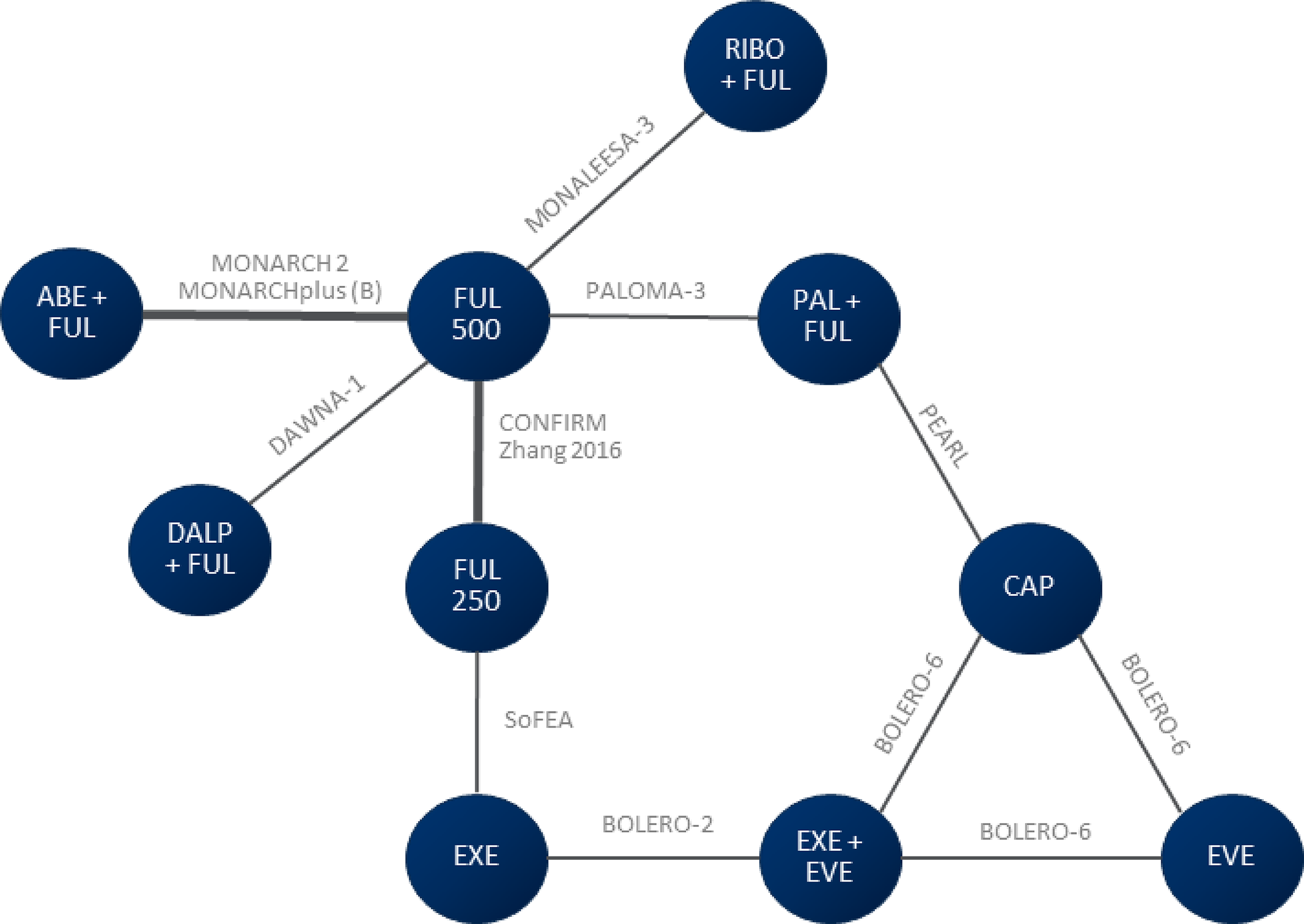
ABE = abemaciclib; CAP = capecitabine; EVE = everolimus; EXE = exemestane; FUL 250 = fulvestrant 250 mg; FUL 500 = fulvestrant 500 mg; PAL = palbociclib; RIBO = ribociclib.
Note: RIBO-FUL 500 data were from a subgroup population of the MONALEESA-3 trial.
Source: Indirect treatment comparison: hazard ratio report28 and indirect treatment comparison: fractional polynomial report.29
Efficacy Results, Cox Proportional Hazards Approach
Overall Survival
The OS treatment effects of different comparisons are shown in Table 22.
The combination therapy of ABE + FUL 500 had greater OS benefit compared to fulvestrant 500 mg (hazard ratio = ████; 95% CrI ████, ████). ABE + FUL 500 also was statistically superior compared to fulvestrant 250 mg (hazard ratio = ████; 95% CrI ████ to ████) and exemestane (hazard ratio = ████; 95% CrI, ████ to ████). For the rest of the comparisons, ABE + FUL 500 showed effects with wide CrIs. Sensitivity analysis including studies that enrolled HER2-negative populations showed similar results to the OS base-case analysis (results not shown here).
Progression-Free Survival
Results on PFS are presented in Table 23 and Figure 8. The combination therapy of ABE + FUL 500 had a greater PFS benefit compared to fulvestrant 500 mg (hazard ratio = ████; 95% CrI, ████ to ████). ABE + FUL 500 also had a statistically greater PFS compared to fulvestrant 250 mg (hazard ratio = ████; 95% CrI, ████ to ████), everolimus (hazard ratio = ████; 95% CrI, ████ to ████), and exemestane (hazard ratio = ████; 95% CrI, ████ to ████). For the rest of the comparisons, ABE + FUL 500 showed effects with wide CrIs.
Sensitivity analyses performed by restricting studies enrolling predominantly Asian patients and based on an independent review committee assessment of PFS showed no meaningful differences to the base-case analysis in the direction of effects (data not shown).
Table 22: League Table of Treatment Effects for OS Using an FE Model — Base Case (Hazard Ratio and 95% CrI), Cox Proportional Hazards Approach
Treatment | FUL 500 | ABE + FUL 500 | CAP | EVE | EXE | EXE-EVE | FUL 250 | PAL + FUL 500 |
|---|---|---|---|---|---|---|---|---|
FUL 500 | ██ | █████ ███████ ██████ | █████ ███████ ██████ | █████ ███████ ██████ | ████ ███████ ██████ | █████ ███████ ██████ | ████ ███████ ██████ | █████ ███████ ██████ |
ABE + FUL 500 | █████ ███████ ██████ | ██ | █████ ███████ ██████ | █████ ███████ ██████ | █████ ███████ ██████ | █████ ███████ ██████ | █████ ███████ ██████ | █████ ███████ ██████ |
CAP | ██████ ███████ ██████ | ██████ ███████ ██████ | ██ | █████ ███████ ██████ | █████ ███████ ██████ | █████ ███████ ██████ | █████ ███████ ██████ | █████ ███████ ██████ |
EVE | ██████ ███████ ██████ | █████ ███████ ██████ | █████ ███████ ██████ | ██ | █████ ███████ ██████ | █████ ███████ ██████ | █████ ███████ ██████ | █████ ███████ ██████ |
EXE | █████ ███████ █████ | █████ ███████ ██████ | █████ ███████ ██████ | █████ ███████ ██████ | ██ | █████ ███████ ██████ | █████ ███████ ██████ | ████ ███████ ██████ |
EXE-EVE | █████ ███████ ██████ | █████ ███████ ██████ | █████ ███████ ██████ | █████ ███████ ██████ | ██████ ███████ ██████ | ██ | █████ ███████ ██████ | █████ ███████ ██████ |
FUL 250 mg | █████ ███████ ██████ | █████ ███████ ██████ | █████ ███████ █████ | █████ ███████ ██████ | █████ ███████ ██████ | █████ ███████ ██████ | ██ | █████ ███████ ██████ |
PAL + FUL 500 mg | ██████ ███████ ██████ | ████ ███████ ██████ | ███ ███████ ██████ | ████ ███████ ██████ | █████ ███████ ██████ | ██████ ███████ ██████ | ██████ ███████ ██████ | ██ |
RIBO + FUL 500 mg | ██████ ███████ ██████ | ██████ ███████ ██████ | ██████ ███████ ██████ | ██████ ███████ ██████ | ██████ ██████ ██████ | ██████ ███████ █████ | ██████ ███████ ██████ | ██████ ███████ ██████ |
ABE = abemaciclib; CAP = capecitabine; CrI = credible interval; EVE = everolimus; EXE = exemestane; FE = fixed-effects; FUL 500 = fulvestrant 500 mg; OS = overall survival; PAL = palbociclib; RIBO = ribociclib.
Note: Bold numbers are results with statistical significance (excluding the null effect) of the ABE + FUL 500 mg comparisons.
Source: Indirect treatment comparison: hazard ratio report28 and indirect treatment comparison: fractional polynomial report.29
Table 23: League Table of Treatment Effects for PFS Using FE model; Base Case (Hazard Ratio and 95% CrI), Cox Proportional Hazards Approach
Treatment | FUL 500 | ABE + FUL 500 | CAP | DALP + FUL 500 | EVE | EXE | EXE-EVE | FUL 250 | PAL + FUL 500 | RIBO + FUL 500 |
|---|---|---|---|---|---|---|---|---|---|---|
FUL 500 | ██ | ████ █████ █████ | █████ ██████ ██████ | █████ ██████ ██████ | █████ ██████ ██████ | ████ ██████ ██████ | █████ ██████ ██████ | ████ ██████ ██████ | | ██████ ██████ | █████ ██████ ██████ |
ABE + FUL 500 | █████ ██████ ██████ | ██ | █████ ██████ ██████ | █████ ██████ ██████ | █████ ██████ ██████ | █████ ██████ ██████ | ████ ██████ ██████ | █████ ██████ ██████ | █████ ██████ █████ | █████ ██████ ██████ |
CAP | █████ ██████ ██████ | █████ ██████ ██████ | ██ | ████ ██████ ██████ | ████ ██████ █████ | ████ ██████ ██████ | ████ ██████ ██████ | ████ ██████ ██████ | ████ ██████ ██████ | ████ ██████ ██████ |
DALP + FUL 500 | █████ ██████ ██████ | █████ ██████ ██████ | ████ ██████ █████ | ██ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | █████ ██████ █████ |
EVE | █████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ██ | ████ ██████ █████ | ████ ██████ █████ | ███ ██████ █████ | █████ ██████ ██ | ████ ██████ █████ |
EXE | ████ ██████ █████ | ████ ██████ █████ | █████ ██████ ██████ | ████ ██████ █████ | ████ ██████ █████ | ██ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ |
EXE-EVE | █████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | ██ | ████ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ |
FUL 250 | ████ ██████ █████ | ████ ██████ █████ | ███ ██████ █████ | ████ ██████ █████ | ████ ██████ █████ | █████ ██████ █████ | ████ ██████ █████ | ██ | ████ ██████ █████ | ████ ██████ ████ |
PAL-FUL 500 | ███ ██████ ████ | █████ ██████ █████ | █████ ██████ ██████ | ███ ██████ █████ | ██ █████ █████ | █████ ██████ █████ | █████ ██████ █████ | ████ ██████ █████ | ██ | ████ ██████ █████ |
RIBO- FUL 500 | ████ ██████ █████ | █████ ██████ ██████ | ███ ██████ █████ | ████ ██████ █████ | █████ ██████ █████ | █████ ██████ ████ | █████ ██████ █████ | █████ ██████ █████ | ████ ██████ █████ | ██ |
ABE = abemaciclib; CAP = capecitabine; CrI = credible interval; DALP = dalpiciclib; EVE = everolimus; EXE = exemestane; FE = fixed effect; FUL 500 = fulvestrant 500 mg; PAL = palbociclib; PFS = progression-free survival; RIBO = ribociclib.
Note: Bold numbers are results with statistical significance (excluding the null effect) of the ABE + FUL 500 comparisons.
Source: Indirect treatment comparison: hazard ratio report28 and indirect treatment comparison: fractional polynomial report.29
Figure 8: Forest Plot of Treatment Effects and 95% CrI Relative to FUL 500 for PFS Using FE Model; Base Case, HR [Redacted]

Efficacy Results, FP Approach
Overall Survival
Table 24 presents the differences in median survival between ABE + FUL 500 and other comparator treatments and difference in survival across multiple time points. The results indicate that ABE + FUL 500 treatments results in an increase in survival compared to fulvestrant 500 mg at ██ months (median difference:███ months; 95% CrI, █████ to █████) and ███ months (difference of █████ months; 95% CrI █████ to █████). These benefits in survival at ██ and ███ months remain modest but are those that are excluding a null effect in favour of ABE + FUL 500. However, for the rest of comparison, the wide CrIs suggest uncertainty in the effect estimates.
All of the best-fitting models based on the DIC had long-term extrapolations that included clinically implausible survival plateaus. A broader range of DIC statistics (beyond 5 points from the best-fitting model) was considered to identify a more clinically plausible model. The chosen model was the random-effects second-order model (P1 = −1, P2 = −1). Differences (restricted means, ██ to ██ months) between treatments in expected OS (with 95% CrIs) — base case, FP approach — are presented in Appendix 2.
Table 24: Differences (95% CrI) in Median Time to Event for Abemaciclib Plus Fulvestrant vs. Comparators, Overall Survival
Variable and comparison | ABE + FUL 500 vs. FUL 500 | ABE + FUL 500 vs. RIBO-FUL 500 | ABE + FUL 500 vs. PAL-FUL 500 | ABE + FUL 500 vs. EXE-EVE |
|---|---|---|---|---|
Difference in median survival (months) | █████ ██████ ███████ | ████ ██████ ███████ | █████ ███████ ███████ | ████ █████ ██████ |
Difference in survival at 12 months | █████ ████ ███████ | ████ ████ ██████ | ████ ██████ ███████ | ████ ██████ ███████ |
Difference in survival at 60 months | █████ █████ ██████ | ████ █████ ███████ | ████ ██████ ███████ | ████ ██████ ███████ |
Difference in survival at 120 months | █████ █████ ██████ | ████ ██████ ███████ | ████ ███████ ██████ | ████ ██████ ███████ |
ABE = abemaciclib; CAP = capecitabine; CrI = credible interval; EVE = everolimus; EXE = exemestane; FUL 500 = fulvestrant 500 mg; PAL = palbociclib; RIBO = ribociclib; vs. = versus.
Note: Bold results imply a statistically significant estimate (with CrI excluding the null).
Sources: Indirect treatment comparison: hazard ratio report,28 indirect treatment comparison: fractional polynomial report,29 and information updated from sponsor.
Progression-Free Survival
Table 25 presents the differences in median survival and PFS at ███ ███ ███ ███ months between ABE + FUL 500 and other comparator treatments. The findings indicate that ABE + FUL 500 shows a survival benefit compared to FUL 500 alone, with a median survival difference of █████ months, but the 95% CrI (█████ to █████) still shows imprecision as it includes the null effect. The effect is less precise when compared to ribociclib plus FUL 500 and palbociclib plus FUL 500. Similarly, the progression-free survival benefits at ██, ██, and ███ months are present against FUL 500, with the largest positive effect observed in the ██-months. In the rest of comparisons, the confidence intervals include 0, suggesting uncertainty and lack of statistical significance for several outcomes, and indicating that the treatment effect may not be consistent across comparators.
All of the best-fitting models based on the DIC had long-term extrapolations that included clinically implausible survival plateaus. A broader range of DIC statistics (beyond 5 points from the best-fitting model) was considered to identify a more clinically plausible model. The chosen model was the random-effects first-order model (P1 = −0.5). Differences (restricted means, ██ to ██ months) between treatments in expected PFS (with 95% CrI) — base case, FP approach — are presented in Appendix 2.
Table 25: Differences (95% CrI) in Median Time to Event for Abemaciclib Plus Fulvestrant vs. Comparators, Progression-Free Survival
Variable and comparison | ABE + FUL 500 vs. FUL 500 | ABE + FUL 500 vs. RIBO + FUL 500 | ABE + FUL 500 vs. PAL + FUL 500 | ABE + FUL 500 vs. EXE-EVE |
|---|---|---|---|---|
Difference in median survival (months) | ████ ██████ ██████ | ███ ███████ ██████ | █████ █████ ██████ | █████ █████ ██████ |
Difference in progression-free at 12 months | ████ ██████ █████ | ████ ██████ ██████ | █████ ████ ██████ | █████ ████ ██████ |
Difference in progression-free at 60 months | ████ ██████ █████ | ████ ██████ ███████ | █████ █████ ██████ | ████ █████ ██████ |
Difference in progression-free at 120 months | ████ █████ ██████ | ████ █████ ██████ | ████ █████ ██████ | █████ █████ ██████ |
ABE = abemaciclib; CAP = capecitabine; CrI = credible interval; EVE = everolimus; EXE = exemestane; FUL = fulvestrant 500 mg; PAL = palbociclib; RIBO = ribociclib; vs. = versus.
Note: Bold results imply a statistically significant estimate (with a CrI excluding the null).
Sources: Indirect treatment comparison: hazard ratio report,28 indirect treatment comparison: fractional polynomial report,29 and information updated from sponsor.
Harms
No harms data were provided with either the Cox proportional hazards or the FP approach.
Critical Appraisal of ITC
The M2 ITC SLR used appropriate prespecification of eligibility criteria through patient, intervention, comparison, and outcome (PICO) elements, comprehensive database searches, and the use of duplicate reviewers for study selection. The last database search was carried out in October 2022; there may be newer relevant studies that were not captured. Data extraction was verified by a second reviewer, and risk-of-bias assessments were conducted using the Cochrane risk of bias tool for full publications. Risk-of-bias assessments were conducted at the study level, which ignores that a risk of bias may differ by effect estimate.31 Four of the trials in the network were assessed as having a high risk of bias; the risk for several others was unclear.
A Bayesian NMA approach was used, exploring both fixed- and random-effects models with model selection based on DIC values. The fixed-effects model was chosen in the Cox proportional hazards NMA. Violation of the proportional hazards assumption was identified for some studies in analyses of PFS and OS, which could have biased the comparative-effect estimates. However, the direction of the results using the FP model generally aligned with those of the Cox proportional hazards NMA.
No trials identified in the SLR enrolled the same population as used in the MONARCH 2 trial. Eligibility criteria were therefore broadened, which increased the heterogeneity across trials in the network and may have resulted in violation of the exchangeability assumption required to produce valid results. These sources of heterogeneity may have acted as potential effect modifiers. There were important differences in the proportion of patients with visceral metastases, liver involvement, and previous exposure to endocrine therapies across trials. Trials involving chemotherapy-based comparators (e.g., capecitabine) likely enrolled patients with more aggressive disease compared to endocrine-only regimens, which could bias indirect comparisons. Minor differences in fulvestrant dosing (500 mg versus 250 mg) may have introduced some additional heterogeneity. Variations in follow-up duration was a source of uncertainty in the analysis, as the sponsor described the OS data in some of the trials as “immature.” Overall, the clinical experts consulted by the review team agreed that the enrolled populations across trials are expected to be heterogeneous, and that this limitation needs to be considered when interpretating the findings. Consistency in the NMA was assumed rather than tested because of the sparsity of the network; it is therefore not known whether this was upheld.
Clinical outcomes relevant to the patient population (i.e., PFS and OS) were appropriately selected and defined. Harm outcomes were not included in the M2 ITC, which limits the ability to fully assess the profile of the treatments compared. No data reconstruction, rescaling, or major imputation methods were reported, and investigator-assessed PFS was prioritized to maintain consistency with the primary end point of the MONARCH 2 trial. Sensitivity analyses addressing potential heterogeneity (e.g., exclusion of studies enrolling predominantly Asian patients) were conducted and resulted in similar findings. However, small sample sizes for some treatments and the wide CrIs observed in many comparisons indicate a degree of imprecision, particularly when comparing targeted therapy combinations to chemotherapy-based regimens. Use of vague priors in the Bayesian model was appropriate, and no concerning sensitivity to priors was reported.
The limitation related to violation of the proportional hazards assumption was addressed through sensitivity analysis using FP models that do not require this assumption. The final models were selected from a choice of 88 possible models. None of the best-fitting models (by the DIC) could be selected because of clinically implausible survival plateaus, particularly for OS. A limited number of models with a poorer fit to the observed data were therefore considered, with selection based on plausibility of the long-term extrapolations; these contributed to the economic evaluation. The poorer fit of the chosen models and limited transparency in the selection process may result in biased comparative-effect estimates. The CrIs produced do not account for the model selection procedures and may be overly optimistic. The clinical experts consulted by the review team noted that the comparative-effectiveness results produced by these extrapolations may not all be plausible. Limitations included misalignment of the comparative effect of fulvestrant on the PFS versus OS, and lower-than-expected long-term projections at 5 and 10 years.
The included studies largely reflect the target population in Canada with HR-positive, HER2-negative advanced breast cancer progressing after ET, although differences in disease severity, previous treatment history, and geographic variability (e.g., enrolment of predominantly Asian populations) may affect generalizability. Some trials permitted previous chemotherapy for advanced disease, unlike the MONARCH 2 trial. While interventions and comparators were aligned with the standard of care in Canada, the exclusion of harm outcomes limits the assessment of comparative tolerability.
Overall, the M2 ITC provides comparative evidence for PFS and OS but should be interpreted with consideration of the limitations previously mentioned. Overall, the ITC methodology was appropriate, and the primary limitations relate to the risk of bias in the included studies, residual clinical heterogeneity, untested consistency assumptions, and imprecision around treatment-effect estimates. These limitations should be considered when interpreting the results.
Studies Addressing Gaps in the Systematic Review Evidence
Contents within this section have been informed by materials submitted by the sponsor. The following has been summarized and validated by the review team.
Description of Studies
The sponsor submitted 4 observational studies (3 retrospective analyses32-34 and 1 prospective analysis35) to address the gaps in safety information identified in the pivotal evidence. The studies are briefly summarized in text.
US Database Study by Price et al. (2022)
The US Database Study by Price et al. (2022)32 addresses the gap in the pivotal study concerning safety issues as it evaluates the safety outcomes of abemaciclib compared to other CDK4 and CDK6 inhibitors (i.e., ribociclib and palbociclib) and AE outcomes (i.e., neutropenia, fatigue, and diarrhea) including health care resource utilization. This was a retrospective study examining the management of AEs among female patients with HR-positive, HER2-negative metastatic breast cancer receiving CDK4 and CDK6 inhibitors. Data of 396 patients from the US Oncology Network iKnowMed electronic health records database were analyzed, with 163, 142, and 91 patients in the palbociclib, abemaciclib and ribociclib cohorts, respectively. Most patients received total daily doses of 125 mg for palbociclib, 300 mg for abemaciclib, and 600 mg for ribociclib, which aligned with the respective product labels. The most common AEs were neutropenia (palbociclib: 44.8%; abemaciclib: 10.6%; ribociclib: 36.3%), diarrhea (palbociclib: 8.0%; abemaciclib: 43.0%; ribociclib: 8.8%), and fatigue (palbociclib: 12.9%; abemaciclib: 17.6%; ribociclib: 16.5%). Treatment holds because of neutropenia were reported in 47 patients and were more frequent in the palbociclib (n = 33 [45.2%]) and ribociclib cohorts (n = 13 [39.4%]) than in the abemaciclib cohort (n = 1 [6.7%]). Dose reductions because of neutropenia were reported in 44 patients, of which 25 (34.2%) patients, 8 (53.3%) patients and 11 (33.3%) patients received palbociclib, abemaciclib, and ribociclib, respectively. Treatment discontinuations because of neutropenia were reported in 10 patients in the palbociclib cohort and 2 patients in the ribociclib cohort. Treatment holds because of diarrhea were reported in 24 patients, of whom 5, 18, and 1 patient were in the palbociclib, abemaciclib, and ribociclib cohorts, respectively. Dose reductions because of diarrhea were reported in 22 patients, of whom 18 received abemaciclib, 3 received palbociclib, and 1 received ribociclib. Of the 17 patients who reported discontinuing treatment because of diarrhea, discontinuations were more frequently reported in the abemaciclib cohort (n = 11) than in the palbociclib (n = 4) and ribociclib cohorts (n = 2). Eleven patients permanently discontinued treatment because of fatigue, 9 of whom received abemaciclib, and 1 each received palbociclib and ribociclib. Hospitalizations because of AEs occurred for 13 patients (3.3%) overall (4.3%, 3.5%, and 1.1% for patients in the palbociclib, abemaciclib, and ribociclib cohorts, respectively). The study noted lower frequencies of AEs but higher dose reductions when compared to data from clinical trials. The study has some notable limitations. The analysis did not adjust for baseline demographic, disease characteristics, or comorbidities. An unadjusted observational analysis limits the reported estimates to be interpreted causally. Data were collected from an electronic health records system, and any AE-related data managed outside of the network and not documented may lead to under-reporting. Documentation of the validity and accuracy of data was not provided. National Cancer Institute Common Terminology Criteria for Adverse Events grading was not collected during clinical practice and not available for this study. The study was only conducted in the US. No statistical comparisons were conducted on AE occurrence and management.
RWE Study by Takada et al. (2023)
The Japanese RWE Study by Takada et al. (2023)33 provides additional safety and tolerability data of abemaciclib in a real-world setting. This was a retrospective study examining real-world data of Japanese patients with advanced breast cancer to identify factors that may help patients stay on abemaciclib treatment for longer and achieve a time to treatment failure (TTF) of greater than 1 year. The incidence of AEs and time of occurrence, reasons for treatment discontinuation and dose reduction, and time of treatment discontinuation were collected from medical records. Data from 120 patients who received abemaciclib therapy from December 2018 to March 2021 at a single cancer centre in Japan were analyzed. The evaluation of AEs covered a 4-week period to record AEs and determine the need for dose reductions and whether to continue treatment. Patients were classified into 3 groups based on dose reduction (100 mg, 200 mg, and 300 mg). Patients on a 300 mg dose had a median TTF of 7.4 months, whereas patients on a 100 mg dose or a 200 mg dose had a median TTF of 17.9 months or 17.3 months, respectively. Dose reduction was identified as the only effective factor that can be modified to achieve TTF at 365 days (OR = 3.95, 95% CI, 1.68 to 9.36, P = 0.002). Frequently reported AEs (any grade) included anemia (90%), increased blood creatinine levels (83%), diarrhea (82%), and neutropenia (75%). Common reasons for treatment discontinuation were disease progression (n = 35), interstitial pneumonia (n = 10), patient convenience (n = 6), liver dysfunction (n = 4), anorexia (n = 3), neutropenia (n = 2), skin rash (n = 2), and other (n = 9). Eighty-four patients (70%) had a 1-level dose reduction because of neutropenia (29%), fatigue (17%) or diarrhea (14%). Twenty-four patients (20%) had a 2-level dose reduction because of neutropenia (33%), fatigue (21%), or diarrhea (21%). The study has several limitations. An unadjusted observational analysis limits the reported estimates to causal interpretation. The number of patients included were limited and from a single-country, single-site study. The patient population may not be representative of the broader population. Institutional practices, dosing regimens, and management and monitoring of AEs limit the generalizability of the findings.
RWE Study by Matos et al. (2024)
The Slovenian RWE Study by Matos et al. (2024)34 provides additional safety and efficacy data of abemaciclib in the real-world setting, as well as insight into relevant subgroups, such as older patients (age groups analyzed < 70 years and ≥ 70 years). The study was an institutional retrospective study evaluating the real-world efficacy and safety of abemaciclib in patients with HR-positive, HER2-negative metastatic breast cancer. Data from 134 patients (133 female, 1 male) who were prescribed abemaciclib with an aromatase inhibitor or fulvestrant in the first, second, or subsequent line of treatment were collected retrospectively from institutional medical records. Real-world progressive disease was determined by the treating physician based on radiological, laboratory or clinical assessments. The median follow-up was 42 months (95% CI, 28.28 to 45.71 months). A total of 69 patients (51.5%) received abemaciclib in combination with ET in the first line, of whom 47 received an aromatase inhibitor and 22 patients received fulvestrant as the ET. Thirty-two patients and 33 patients received abemaciclib in the second and third-or-later lines, respectively. The median PFS times were 21 months (95% CI, 15.12 to 26.88), 20 months (95% CI, 6.38 to 33.60), and 7 months (95% CI, 4.19 to 9.81) in first, second, and third line, respectively. The median OS times were 29 months (95% CI, 26.09 to 39.90) and 19 months (7.59 to 30.49) for the second line and third-or-later lines, respectively. The median OS was not reached in the first-line setting. The median real-world PFS and median OS were 15 months and 25 months, respectively, in patients aged 70 years and older. No significant difference was observed for the median real-world PFS and OS in the group of patients aged 70 years and older compared with younger patients (aged < 70 years). The most common AEs (any grade) were diarrhea (68.7%), anemia (64.9%) and increased serum creatinine (63.4%). Grade 3 or 4 diarrhea was reported in 7 patients and grade 2 diarrhea in 27 patients. Grade 2 and grade 3 or 4 neutropenia were reported in 39 patients and 17 patients, respectively. Grade 2 anemia was reported in 21 patients. Eighty-seven patients discontinued abemaciclib either because of disease progression (n = 64) or AEs (n = 23). Grade 3 or 4 neutropenia was more common in patients aged less than 70 years (16%) versus 70 years and older (5%). Grade 3 or 4 diarrhea was more frequently reported in patients aged 70 years and older (7.5%) versus patients aged less than 70 years (4.3%). Dose reductions were frequent in patients aged 70 years or older (40%) compared to patients aged less than 70 years (28%). Several limitations were noted for this study. An unadjusted observational analysis limits the number of reported estimates that can be interpreted causally. Data were collected from an electronic health records system, and any inconsistent AE incident collection may lead to under-reporting. There was heterogeneity in the patient population analyzed (age, line of treatment, and ET used) as well as a small sample size, with a sizeable number of patients (n = 87) discontinuing abemaciclib at study cut-off due to disease progression or AEs.
RWE Study by Gebbia et al. (2023)
The exploratory analysis of real-life data by Gebbia et al. (2023)35 provides insight into clinical factors potentially linked with diarrhea incidence and severity in patients with HR-positive, HER2-negative advanced breast cancer treated with abemaciclib plus an aromatase inhibitor or fulvestrant. This was a multicentre, prospective, observational study carried out in 6 oncology centres in Italy. All patients were treated with abemaciclib at 150 mg twice daily as starting dose, according to the Italian label indication for the drug. ET consisted of letrozole 2.5 mg or anastrozole 1 mg administered once daily continuously or and intramuscular injection of fulvestrant 500 mg every 2 weeks for the first cycle, a loading dose, and then monthly. Eighty women with advanced breast cancer were included in the study, of whom 91% had metastatic disease and 9% had locally advanced disease unsuitable for radical treatment. Most patients (86%) had visceral metastases and 11% had bone-only disease. Diarrhea was the most frequent toxicity, with 31 patients reporting grade 1 events, and 25 patients reporting grade 2 or 3 events. Diarrhea occurred mainly in the first treatment cycle, and in most cases was effectively managed by antidiarrheal medications and dose adjustments (maximum dose reduction to 100 mg daily for grade 2 or 3). The median duration of grade 2 or 3 diarrhea was 8 days (range, 4 to 10 days). Several risk factors including age (< 70 or ≥ 70 years), the number of concomitant medications, and the presence of concomitant or previous intestinal diseases correlated significantly with grade 2 or 3 diarrhea. Several study limitations were noted. An unadjusted observational analysis limits the reported estimates to be interpreted causally. There was a limited sample size, and all but 4 patients had an ECOG PS of no more than 1. No information was reported on the previous lines of treatment. Data were entered in an electronic database, and patients with incomplete information on toxicity or those lost to follow-up were excluded from analysis. Incomplete data or incorrect coding of data may therefore lead to under-reporting or mischaracterization of severity. No information on dose interruptions and limited demographic characteristics of patients were available.
Discussion
Summary of Available Evidence
The body of evidence for abemaciclib plus fulvestrant in the treatment of HR-positive, HER2-negative advanced breast cancer includes data from 1 pivotal randomized controlled trial (the MONARCH 2 trial), an ITC (M2), and 4 additional real-world observational studies addressing gaps in harms evidence.
The MONARCH 2 trial was a multicentre, double-blind, placebo-controlled phase III trial that enrolled 669 patients to compare abemaciclib plus fulvestrant with placebo plus fulvestrant, with PFS and OS as key outcomes. Updated PFS and OS data with longer follow-up were submitted by the sponsor to address the limitations of the original submission, which included only interim PFS results (data cut-off: February 14, 2017) and limited follow-up for OS data. The updated evidence includes both an interim OS analysis (data cut-off: June 20, 2019) and a final OS analysis (data cut-off: March 18, 2022), providing a more complete assessment of survival outcomes. Patients enrolled in the MONARCH 2 trial were primarily patients who were in the postmenopausal stage with advanced or metastatic HR-positive, HER2-negative breast cancer who had progressed on ET, with a median age of 60 years. Baseline characteristics were well balanced across treatment arms.
The M2 ITC synthesized evidence from 10 RCTs using a Bayesian NMA to compare abemaciclib plus fulvestrant with other standard treatments, focusing on PFS and OS.
In addition to the MONARCH 2 trial and the M2 ITC, 4 RWE studies were submitted to further characterize the safety and tolerability of abemaciclib in broader clinical practice. These included 1 database and 3 observational cohort studies. Across these studies, patients had baseline characteristics similar to those enrolled in the MONARCH 2 trial but often presented with greater heterogeneity in disease burden, previous treatments, and comorbidities, reflecting real-world practice. The findings from these studies were generally consistent with the clinical trial safety profile, with diarrhea, neutropenia, and infections identified as the most common AEs. No new safety signals were observed. However, differences in study design, follow-up duration, and reporting standards limit direct comparisons with randomized controlled trial data.
Interpretation of Results
Efficacy
The MONARCH 2 trial found that abemaciclib plus fulvestrant significantly improved PFS and OS compared to fulvestrant alone in patients with HR-positive, HER2-negative advanced breast cancer who had progressed on ET. The clinical experts consulted by the review team considered these improvements to be clinically meaningful. The primary PFS analysis (data cut-off on February 14, 2017; median follow-up of 19.5 months) established a statistically significant reduction in the risk of disease progression or death, supporting the initial clinical benefit of abemaciclib. However, OS data were immature and insufficient at the time of the initial submission to draw conclusions regarding any long-term survival benefit. The updated final OS analysis (data cut-off on March 18, 2022; median follow-up ████ months) confirmed a statistically significant improvement in OS, with a hazard ratio of ████ (95% CI, ████ to ████) and a median OS improvement of 8.6 months. The survival benefit was consistent in direction across key subgroups and supported by sensitivity analyses, strengthening the evidence supporting abemaciclib plus fulvestrant as an effective option when compared to placebo plus fulvestrant following progression on ET. No updated HRQoL outcomes were available in the final MONARCH 2 dataset, although patient input emphasized the importance of delaying disease progression and maintaining quality of life, outcomes that the observed improvements in PFS and OS are expected to support, according to clinical experts consulted by CDA-AMC.
Findings from the MONARCH 2 trial were supported by indirect evidence from the M2 ITC, in which abemaciclib plus fulvestrant demonstrated favourable PFS and OS outcomes compared with fulvestrant monotherapy. However, the M2 ITC comparisons of abemaciclib against other relevant treatments in Canadian clinical practice (i.e., ribociclib or palbociclib plus fulvestrant) were subject to considerable uncertainty because of imprecise estimates, differences in patient populations across trials (such as previous chemotherapy exposure, presence of visceral metastases, liver involvement, and previous exposure to endocrine therapies), and limited generalizability. In the M2 NMA, sensitivity analyses, including the use of FP models to address proportional hazards violations, generally came to similar overall conclusions as the main analysis from the Cox proportional hazards NMA. Nonetheless, wide CrIs, variations in patient characteristics, and the lack of formal consistency assessment introduced uncertainty.
The 4 RWE studies evaluating the safety of abemaciclib in broader clinical practice had findings consistent with the MONARCH 2 trial, with no new harm signals identified, and diarrhea, neutropenia, and infections cited as the most common AEs. Differences in study design and patient populations limit direct comparisons with randomized trial data.
Harms
Treatment with abemaciclib plus fulvestrant was associated with a higher incidence of AEs compared to placebo plus fulvestrant, particularly regarding diarrhea, neutropenia, and infections. Most AEs were manageable with dose adjustments and supportive care, as observed in the MONARCH 2 trial and further supported by findings from RWE studies, which reported similar patterns of tolerability. Diarrhea, although frequent, was generally low-grade, both in the clinical trial and in real-world settings.
The sponsor-submitted M2 ITC did not include safety outcomes, preventing a formal indirect comparison of harms with abemaciclib versus relevant treatments. Nevertheless, the available evidence suggests that the AE profile of abemaciclib is consistent with that of other CDK4 and CDK6 inhibitors. Real-world studies also did not identify any new harm signals beyond those reported in the MONARCH 2 trial. Patient input indicated that tolerable AEs were considered acceptable if balanced by meaningful improvements in disease control and survival outcomes.
Conclusion
The totality of evidence demonstrates that abemaciclib plus fulvestrant provides a clinically meaningful improvement in both PFS and OS for patients with HR-positive, HER2-negative advanced breast cancer who have progressed on ET when compared to fulvestrant alone. The updated MONARCH 2 results, including final OS data, confirm a survival benefit that was not demonstrated at the time of the initial submission, addressing a key evidence gap. The observed benefit aligns with patient priorities of delaying disease progression and prolonging survival. The safety profile of abemaciclib remains consistent with that of other CDK4 and CDK6 inhibitors, with diarrhea, neutropenia, and infections the most reported AEs. These events are considered by clinical experts to be generally manageable with supportive care and dose modifications, as shown in both the MONARCH 2 trial and RWE studies.
Comparisons of abemaciclib with other CDK4 and CDK6 inhibitors relevant to Canadian practice, such as palbociclib and ribociclib, are limited by imprecise estimates, differences in patient populations, and the absence of direct head-to-head trials, which precluded making definitive conclusions about comparative effects. Furthermore, important gaps exist, including limited evidence in specific subgroups, such as patients with central nervous system metastases or more aggressive disease.
References
1.CADTH. Drug Reimbursement review clinical guidance report: abemaciclib (Verzenio) for metastatic breast cancer. July 5, 2019. Accessed May 20, 2025. https://www.cda-amc.ca/sites/default/files/pcodr/Reviews2019/10161AbemaciclibMBC_fnCGR_NOREDACT_Post_05Jul2019_final.pdf
2.CADTH. Drug Reimbursement Expert Review Committee final recommendation: Abemaciclib (Verzenio - Eli Lilly Canada Inc.). July 5, 2019. Accessed May 20, 2025. https://www.cda-amc.ca/sites/default/files/pcodr/Reviews2019/10161AbemaciclibMBC_fnRec_ApprovedbyChair_v01_2019-07-04_Post_05Jul2019_final.pdf
3.Canadian Cancer Society. Cancer statistics at a glance. Accessed September 2024. https://cancer.ca/en/research/cancer-statistics/cancer-statistics-at-a-glance
4.DeKoven M, Bonthapally V, Jiao X, et al. Treatment pattern by hormone receptors and HER2 status in patients with metastatic breast cancer in the UK, Germany, France, Spain and Italy (EU-5): results from a physician survey. J Comp Eff Res. 2012;1(5):453-63. doi: 10.2217/cer.12.43 PubMed
5.Lobbezoo DJ, van Kampen RJ, Voogd AC, et al. Prognosis of metastatic breast cancer subtypes: the hormone receptor/HER2-positive subtype is associated with the most favorable outcome. Breast Cancer Res Treat. 2013;141(3):507-14. doi: 10.1007/s10549-013-2711-y PubMed
6.Khan NAJ, Abdallah M, Tirona MT. Hormone Receptor Positive/HER2 Negative Breast Cancer With Isolated Bladder Metastasis: A Rare Case. J Investig Med High Impact Case Rep. 2021;9:23247096211022186. doi: 10.1177/23247096211022186 PubMed
7.Huppert LA, Gumusay O, Idossa D, Rugo HS. Systemic therapy for hormone receptor-positive/human epidermal growth factor receptor 2-negative early stage and metastatic breast cancer. CA Cancer J Clin. 2023;73(5):480-515. doi: 10.3322/caac.21777 PubMed
8.Cardoso F, Paluch-Shimon S, Schumacher-Wulf E, et al. 6th and 7th International consensus guidelines for the management of advanced breast cancer (ABC guidelines 6 and 7). Breast. 2024;76:103756. doi: 10.1016/j.breast.2024.103756 PubMed
9.Early Breast Cancer Trialists' Collaborative Group (EBCTCG). Effects of chemotherapy and hormonal therapy for early breast cancer on recurrence and 15-year survival: an overview of the randomised trials. Lancet. 2005;365(9472):1687-717. doi: 10.1016/S0140-6736(05)66544-0 PubMed
10.Canadian Cancer Statistics Advisory, Canadian Cancer Society, Statistics Canada, Public Health Agency of Canada. Canadian Cancer Statistics: a 2022 special report on cancer prevalence. 2022. Accessed November 2024. https://cancer.ca/Canadian-Cancer-Statistics-2022-EN
11.Cardoso F, Paluch-Shimon S, Senkus E, et al. 5th ESO-ESMO international consensus guidelines for advanced breast cancer (ABC 5). Ann Oncol. 2020;31(12):1623-1649. doi: 10.1016/j.annonc.2020.09.010 PubMed
12.Irvin W, Jr., Muss HB, Mayer DK. Symptom management in metastatic breast cancer. Oncologist. 2011;16(9):1203-14. doi: 10.1634/theoncologist.2011-0159 PubMed
13.NCCN Guidelines. Breast Cancer, version 1.2025. National Comprehensive Cancer Network. Accessed by sponsor, no date provided. https://www.nccn.org/
14.Canada's Drug Agency. Provisional Funding Algorithm: breast cancer that is hormone receptor (HR) positive, human epidermal growth factor receptor 2 (HER2) negative, with inclusion of HER2 low. 2024. Accessed August 20, 2025. https://www.cda-amc.ca/sites/default/files/DRR/2024/PH0053-HRPositive-HER2-Breast-Cancer.pdf
15.Burstein HJ, Somerfield MR, Barton DL, et al. Endocrine Treatment and Targeted Therapy for Hormone Receptor-Positive, Human Epidermal Growth Factor Receptor 2-Negative Metastatic Breast Cancer: ASCO Guideline Update. J Clin Oncol. 2021;39(35):3959-3977. doi: 10.1200/JCO.21.01392 PubMed
16.AstraZeneca Canada Inc. Faslodex (fulvestrant): 50 mg/mL in pre-filled syringe, for injection [product monograph; sponsor supplied reference]. June 2020.
17.Eli Lilly Canada Inc. Verzenio (abemaciclib): 50 mg, 100 mg, 150 mg, or 200 mg, oral tablet [product monograph]. April 4, 2019. Updated December 1, 2023.
18.Novartis Pharmaceuticals Canada Inc. Kisqali (ribociclib as ribociclib succinate): 200 mg oral tablets [product monograph; sponsor supplied reference]. 2018.
19.Pfizer Canada Inc. Ibrance (palbociclib): 75 mg, 100 mg and 125 mg, oral capsules [product monograph; sponsor supplied reference]. 2018.
20.Sledge GW, Jr., Toi M, Neven P, et al. The Effect of Abemaciclib Plus Fulvestrant on Overall Survival in Hormone Receptor-Positive, ERBB2-Negative Breast Cancer That Progressed on Endocrine Therapy-MONARCH 2: A Randomized Clinical Trial. JAMA Oncol. 2020;6(1):116-124. doi: 10.1001/jamaoncol.2019.4782 PubMed
21.Sledge GW, Jr., Toi M, Neven P, et al. MONARCH 2: Abemaciclib in Combination With Fulvestrant in Women With HR+/HER2- Advanced Breast Cancer Who Had Progressed While Receiving Endocrine Therapy. J Clin Oncol. 2017;35(25):2875-2884. doi: 10.1200/JCO.2017.73.7585 PubMed
22.Kaufman PA, Toi M, Neven P, et al. Health-Related Quality of Life in MONARCH 2: Abemaciclib plus Fulvestrant in Hormone Receptor-Positive, HER2-Negative Advanced Breast Cancer After Endocrine Therapy. Oncologist. 2020;25(2):e243-e251. doi: 10.1634/theoncologist.2019-0551 PubMed
23.Tokunaga E, Miyoshi Y, Dozono K, Kawaguchi T, Toi M. Association of Neutrophil-to-Lymphocyte Ratio and Absolute Lymphocyte Count With Clinical Outcomes in Advanced Breast Cancer in the MONARCH 2 Trial. Oncologist. 2024;29(3):e319-e329. doi: 10.1093/oncolo/oyad301 PubMed
24.Toi M, Huang CS, Im YH, et al. Abemaciclib plus fulvestrant in East Asian women with HR+, HER2- advanced breast cancer: Overall survival from MONARCH 2. Cancer Sci. 2023;114(1):221-226. doi: 10.1111/cas.15600 PubMed
25.Inoue K, Masuda N, Iwata H, et al. Japanese subpopulation analysis of MONARCH 2: phase 3 study of abemaciclib plus fulvestrant for treatment of hormone receptor-positive, human epidermal growth factor receptor 2-negative breast cancer that progressed on endocrine therapy. Breast Cancer. 2021;28(5):1038-1050. doi: 10.1007/s12282-021-01239-8 PubMed
26.Neven P, Rugo HS, Tolaney SM, et al. Abemaciclib plus fulvestrant in hormone receptor-positive, human epidermal growth factor receptor 2-negative advanced breast cancer in premenopausal women: subgroup analysis from the MONARCH 2 trial. Breast Cancer Res. 2021;23(1):87. doi: 10.1186/s13058-021-01463-2 PubMed
27.Eli Lilly and Company. Clinical Study Report: I3Y-MC-JPBL, addendum final overall survival analysis. MONARCH 2: A Randomized, Double-Blind, Placebo-Controlled, Phase 3 Study of Fulvestrant with or without Abemaciclib, a CDK4/6 Inhibitor, for Women with Hormone Receptor Positive, HER2 Negative Locally Advanced or Metastatic Breast Cancer [internal sponsor's report]. June 15, 2022.
28.Eli Lilly Canada Inc. Update to network meta-analysis of systemic anti-cancer treatments for patients with HR+, HER2- advanced breast cancer: Hazard ratio NMA report [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Verzenio (abemaciclib), 50 mg, 100 mg, or 150 mg, oral tablet, with fulvestrant. September 16, 2024.
29.Eli Lilly Canada Inc. Update to network meta-analysis of systemic anti-cancer treatments for patients with HR+, HER2- advanced breast cancer: Fractional polynomial NMA report [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Verzenio (abemaciclib), 50 mg, 100 mg, or 150 mg, oral tablet, with fulvestrant. September 16, 2024.
30.Higgins JP, Altman DG, Gotzsche PC, et al. The Cochrane Collaboration's tool for assessing risk of bias in randomised trials. BMJ. 2011;343:d5928. doi: 10.1136/bmj.d5928 PubMed
31.Sterne JAC, Savovic J, Page MJ, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366:l4898. doi: 10.1136/bmj.l4898 PubMed
32.Price GL, Sudharshan L, Ryan P, et al. Real world incidence and management of adverse events in patients with HR+, HER2- metastatic breast cancer receiving CDK4 and 6 inhibitors in a United States community setting. Curr Med Res Opin. 2022;38(8):1319-1331. doi: 10.1080/03007995.2022.2073122 PubMed
33.Takada S, Maeda H, Umehara K, et al. Clinical Management of Potential Toxicity of Abemaciclib and Approaches to Ensure Treatment Continuation. Asian Pac J Cancer Prev. 2023;24(6):1955-1962. doi: 10.31557/APJCP.2023.24.6.1955 PubMed
34.Matos E, Cankar K, Rezun N, Dejanovic K, Ovcaricek T. Abemaciclib for the Treatment of HR+HER2- Metastatic Breast Cancer: An Institutional Experience. Cancers (Basel). 2024;16(10):1828. doi: 10.3390/cancers16101828 PubMed
35.Gebbia V, Martorana F, Sano MV, et al. Abemaciclib-associated Diarrhea: An Exploratory Analysis of Real-life Data. Anticancer Res. 2023;43(3):1291-1299. doi: 10.21873/anticanres.16276 PubMed
Appendix 1: Outcomes From the MONARCH 2 Trial Established in the Initial Submission
Please note that this appendix has not been copy-edited.
Objective Response Rate (Endocrine-Resistant)
Objective response rate (ORR) was a secondary end point in the MONARCH 2 trial. As of the February 14, 2017, data cut-off date, after a median follow-up duration of 19.5 months, ORR was reported to be 35.2% (95% CI 30.8, 39.6) in the abemaciclib + fulvestrant arm and 16.1% (95% CI 11.3, 21.0) in the placebo + fulvestrant arm (P < 0.001). Overall, 14 patients (3.1%) in the abemaciclib + fulvestrant arm and 1 patient (0.4%) in the placebo + fulvestrant arm achieved a CR.
For patients with measurable disease, ORR was 48.1% (95% CI 42.6, 53.6) in the abemaciclib + fulvestrant arm versus 21.3% (95% CI 15.1, 27.6) in the placebo + fulvestrant arm (P < 0.001).
Duration of Response (Endocrine-Resistant)
Duration of response was a secondary end point in the MONARCH 2 trial. At the data cut-off date, the median time to response was estimated to be 3.7 months (interquartile range [IQR] 1.7, 16.9) with abemaciclib + fulvestrant and 4.0 months (IQR 1.9, 14.7) with placebo + fulvestrant. The median duration of response for patients in the abemaciclib + fulvestrant arm was not reached (95% CI, 18.05 months, not estimable), and 90 responders (57.3%) were continuing to receive treatment at the time of the primary analysis.
Clinical Benefit Rate (Endocrine-Resistant)
The clinical benefit rate was a secondary end point in the MONARCH 2 trial and was defined as response (CR or PR) or prolonged stable disease (≥ 6 months) according to the RECIST version 1.1.9 At the February 14, 2017, data cut-off date, the clinical benefit rate was 72.2% (95% CI, 68.0% to 76.4%) in the abemaciclib + fulvestrant arm and 56.1% (95% CI, 49.5% to 62.6%) in the placebo + fulvestrant arm (P < 0.001). Best response of prolonged stable disease was lower in the abemaciclib + fulvestrant arm (9.0%) than that in the placebo + fulvestrant arm (20.2%).
HRQoL (Endocrine-Resistant)
The questionnaire completion rates for the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire Core 30, European Organization for Research and Treatment of Cancer Quality of Life Questionnaire Breast Cancer, EQ 5D‐5L, and mBPI‐sf were reported to be greater than 90% for most cycles.
The primary health reported outcome was time to progression of pain as measured by the mBPI-sf. Treatment with abemaciclib plus fulvestrant delayed the median time to worsening pain was by approximately 5 months (████ months in the abemaciclib arm versus ████ months in the placebo arm). However, this difference was not statistically significant (HR = █████; 95% CI █████, █████; P = ████).
Changes from baseline in the following 3 European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 scales were statistically different between the 2 study arms, all favouring the placebo arm: nausea and vomiting (mean change = ████; 95% CI ████, ████; P < █████), appetite loss (mean change = ████; 95% CI ████, ████; P < █████), and diarrhea (mean change = █████; 95% CI █████, █████; P < █████). There was also a clinically meaningful (≥ 10 points) difference between the 2 groups in terms of change from the baseline in diarrhea score.
No statistically significant or clinically meaningful differences were observed between the 2 groups in terms of European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Breast Cancer functional scales, except for systemic therapy side effects (dry mouth, eye symptoms, hair loss, and hot flashes) which were significantly worse in the abemaciclib plus fulvestrant arm (mean change = ████; 95% CI ████, ████; P < █████).
Appendix 2: Other Outcomes Evaluated in the NMAs
Please note that this appendix has not been copy-edited.
Table 26: Difference (Restricted Mean, 0 to 80 Months) Between Treatments in Expected OS (95% CrI) — Base Case, FP Approach
Treatment | FUL 500 | ABE + FUL 500 | CAP | EVE | EXE | EXE-EVE | FUL 250 | PAL-FUL 500 |
|---|---|---|---|---|---|---|---|---|
FUL 500 | — | — | — | — | — | — | — | — |
ABE + FUL 500 | −5.3 (0.5 to −10.38) | — | — | — | — | — | — | — |
CAP | −3.923 (8.03 to −10.87) | 1.372 (14.55 to −7.75) | — | — | — | — | — | — |
EVE | −4.107 (11.58 to −13.85) | 1.154 (17.85 to −10.23) | −0.22525 (10.49 to −10.7) | — | — | — | — | — |
EXE | 3.715 (9.77 to −2.6) | 8.96 (16.93 to 0.43) | 7.62 (14.89 to −4.6) | 7.818 (16.98 to −8.01) | — | — | — | — |
EXE-EVE | 1.988 (8.83 to −5.16) | 7.222 (15.81 to −1.95) | 5.894 (12.81 to −6.12) | 6.093 (14.5 to −9.2) | −1.73 (2.89 to −6.38) | — | — | — |
FUL 250 | 2.348 (6.15 to −1.48) | 7.616 (14.01 to 0.68) | 6.267 (13.42 to −5.98) | 6.462 (16.07 to −9.37) | −1.374 (4.02 to −6.51) | 0.3549 (7 to −6) | — | — |
PAL-FUL 500 | −0.801 (40.18 to −7.8) | 5.273 (47.59 to −4.91) | 3.457 (46.45 to −5.99) | 4.834 (48.82 to −9.86) | −3.677 (38.6 to −13.17) | −1.847 (40.93 to −11.73) | −2.786 (38.46 to −10.92) | — |
RIBO-FUL 500 | −4.712 (2.1 to −10.98) | 0.56825 (9.12 to −8.04) | −0.8109 (8.95 to −14.77) | −0.5896 (11.3 to −17.99) | −8.379 (0.82 to −17.11) | −6.642 (3.15 to −15.97) | −7.051 (0.74 to −14.38) | −5.045 (5.99 to −47.61) |
ABE = abemaciclib; CAP = capecitabine; CrI = credible interval; EVE = everolimus; EXE = exemestane; FP = fractional polynomial; FUL = fulvestrant; OS = overall survival; PAL = palbociclib; RIBO = ribociclib.
Sources: Indirect treatment comparison: HR report,28 and indirect treatment comparison: FP report.29
Table 27: Difference (Restricted Mean, 0 to 80 months) Between Treatments in Expected PFS (With 95% CrI) — Base Case, FP Approach
Treatment | FUL 500 | ABE + FUL 500 | CAP | DALP-FUL 500 | EVE | EXE | EXE-EVE | FUL 250 | PAL-FUL 500 |
|---|---|---|---|---|---|---|---|---|---|
FUL 500 | — | — | — | — | — | — | — | — | — |
ABE + FUL 500 | -11.4 (−7.73 to −14.83) | — | — | — | — | — | — | — | — |
CAP | −11.71 (−6.42--16.93) | −0.3311 (6.07--6.74) | — | — | — | — | — | — | — |
DALP-FUL 500 | −12.72 (−7.05--18.65) | −1.345 (5.26--8.25) | −1.019 (6.75--9.06) | — | — | — | — | — | — |
EVE | −4.025 (0.31--9.37) | 7.322 (12.89 to 0.92) | 7.584 (12.25 to 2.58) | 8.623 (16.1 to 0.91) | — | — | — | — | — |
EXE | 4.265 (7.96 to 0.44) | 15.67 (20.65 to 10.33) | 15.92 (21.76 to 10.36) | 16.99 (24.02 to 10.11) | 8.263 (14.09 to 3.58) | — | — | — | — |
EXE-EVE | −7.909 (−3.36--12.61) | 3.474 (9.23--2.53) | 3.763 (8.9--1.27) | 4.815 (12.3--2.59) | −3.841 (0.98--8.1) | −12.16 (−8.4--16.16) | — | — | — |
FUL 250 | 2.332 (4.77 to 0.07) | 13.76 (17.86 to 9.43) | 14.05 (19.35 to 8.8) | 15.07 (21.46 to 8.96) | 6.369 (11.72 to 2.14) | −1.896 (1.03--4.82) | 10.25 (14.58 to 6.22) | — | — |
PAL-FUL 500 | −9.603 (−6.22--13.17) | 1.774 (6.75--3.41) | 2.139 (6.6--2.79) | 3.1 (10.03--3.66) | −5.5165 (−0.26--10.39) | −13.88 (−9--18.79) | −1.673 (3.37--6.88) | −11.95 (−8.09--16.01) | — |
RIBO-FUL 500 | −7.489 (−2.05--12.51) | 3.887 (10.42--2.28) | 4.24 (11.82--3.12) | 5.263 (13.25--2.32) | −3.382 (4.21--10.16) | −11.74 (−5--18.04) | 0.443 (7.68--6.38) | −9.849 (−3.81--15.44) | 2.145 (8.69--4.03) |
ABE = abemaciclib; CAP = capecitabine; CrI = credible interval; DALP = dalpiciclib; EVE = everolimus; EXE = exemestane; FP = fractional polynomial; FUL = fulvestrant; PAL = palbociclib; PFS = progression-free survival; RIBO = ribociclib.
Sources: Indirect treatment comparison: HR report,28 and indirect treatment comparison: FP report.29
Pharmacoeconomic Review
Abbreviations
AE
adverse event
BIA
budget impact analysis
CDA-AMC
Canada’s Drug Agency
CDK
cyclin-dependent kinase
ET
endocrine therapy
FP
fractional polynomial
LY
life-year
NMA
network meta-analysis
OS
overall survival
PFS
progression-free survival
PH
proportional hazard
QALY
quality-adjusted life-year
TTD
time to treatment discontinuation
Economic Review
The objective of the economic review is to review and critically appraise the pharmacoeconomic evidence submitted by the sponsor, including an economic evaluation comparing the cost-effectiveness and budget impact analysis (BIA) of abemaciclib plus fulvestrant for the treatment of HR-positive, HER2-negative advanced or metastatic breast cancer in females with disease progression following endocrine therapy (ET). This is narrower than the Health Canada indication for this patient population, which also includes the use of abemaciclib in combination with an aromatase inhibitor as a first-line treatment, or its use as a single agent in females with disease progression following ET and at least 2 prior chemotherapy regimens. The use of abemaciclib in combination with an aromatase inhibitor is being assessed in a separate review,1 and Canada’s Drug Agency (CDA-AMC) approved a deviation request submitted by the sponsor to exclude abemaciclib as a single drug from this review. The focus of this review is on the use of abemaciclib in combination with fulvestrant in the second line to treat advanced or metastatic breast cancer.
Item | Description |
|---|---|
Drug product | Abemaciclib (Verzenio), 50 mg, 100 mg, and 150 mg, oral tables |
Indication | For the treatment of HR-positive, HER2-negative advanced or metastatic breast cancer in combination with fulvestrant in women with disease progression following endocrine therapy. Pre- or perimenopausal women must also be treated with a GnRH agonist. |
Submitted price | Abemaciclib 50 mg tablet: $116.97 100 mg tablet: $115.89 150 mg tablet: $116.22 |
Health Canada approval status | NOC |
Health Canada review pathway | Standard review |
NOC date | April 05, 2019 |
Reimbursement request | Per indication |
Sponsor | Eli Lilly Canada Inc. |
Submission history | Previously reviewed: Yes Indication: In combination with endocrine therapy for the adjuvant treatment of adult patients with HR-positive, HER2-negative, node-positive, early breast cancer at high risk of disease recurrence based on clinicopathological features and a Ki-67 score ≥ 20%. Recommendation date: September 29, 2022 Recommendation: Reimburse with clinical criteria and/or conditions Indication: For the treatment of HR-positive, HER2-negative, advanced, or metastatic breast cancer. In combination with an aromatase inhibitor in postmenopausal women as initial endocrine-based therapy. In combination with fulvestrant in women with disease progression following endocrine therapy. Recommendation date: July 5, 2019 Recommendation: Reimburse with clinical criteria and/or conditions Additionally, CDA-AMC is currently reviewing abemaciclib resubmission for patients with HR-positive, HER2-negative advanced or metastatic breast cancer who have not received prior systemic treatment in the advanced setting.1 |
CDA-AMC = Canada’s Drug Agency; GnHR = gonadotropin-releasing hormone; NOC = Notice of Compliance.
Key Messages
Abemaciclib is available as 50 mg, 100 mg, and 150 mg tablets. At the submitted price of $116.22 per 150 mg, the 28-day cycle of abemaciclib is predicted to be $6,508 per patient, based on the Health Canada–recommended dosage. The 28-day cost of abemaciclib plus fulvestrant is $7,324 per patient in the first cycle and $6,916 in subsequent cycles, for HR-positive, HER2-negative advanced or metastatic breast cancer. Treatment should be continued until disease progression or unacceptable toxicity.
Clinical efficacy in the economic analysis for abemaciclib plus fulvestrant in comparison to fulvestrant was derived from the MONARCH 2 trial. Evidence submitted by the sponsor indicates that abemaciclib plus fulvestrant is likely to improve PFS and OS compared with fulvestrant alone among patients with HR-positive, HER2-negative advanced or metastatic breast cancer. For abemaciclib plus fulvestrant compared to ribociclib plus fulvestrant, palbociclib plus fulvestrant, and exemestane plus everolimus, comparative clinical efficacy was informed by a sponsor-submitted network meta-analysis (NMA), which was subject to considerable uncertainty due to imprecise estimates and methodological limitations. This precluded CDA-AMC from drawing definitive conclusions about the comparative efficacy of abemaciclib plus fulvestrant compared to palbociclib plus fulvestrant, ribociclib plus fulvestrant, and exemestane plus everolimus. The safety profile of abemaciclib remains consistent with that of other inhibitors of cyclin-dependent kinases (CDKs) 4 and 6, with diarrhea, neutropenia, and infections the most reported adverse events (AEs), most of which are manageable with dose adjustments and supportive care. However, AEs were not assessed in the NMA, and long-term comparative safety data beyond the pivotal trial period and direct comparisons remain limited.
The results of the CDA-AMC base case suggest:
fulvestrant alone, palbociclib plus fulvestrant, and ribociclib plus fulvestrant are on the cost-effectiveness frontier
abemaciclib plus fulvestrant is less effective and more costly than ribociclib plus fulvestrant (i.e., dominated); these results are driven by increased drug acquisition costs, lower survival (−0.16 life-years [LYs]), and a reduction in quality-adjusted life-years (QALYs) (incremental QALYs: −0.05).
This finding is associated with uncertainty due to limitations with the comparative-effectiveness estimates obtained from the sponsor’s submitted NMA that are applicable regardless of the statistical methods (i.e., Cox proportional hazards [PH] models or fractional polynomial [FP] models). Although the PH assumption is violated, applying the FP model estimates into the economic evaluation produced implausible survival estimates that lacked face validity, according to clinical expert input sought by CDA-AMC. Applying estimates from the Cox PH models, while not preferable given the violation of PH assumptions within the trial period, produced overall survival (OS) and progression-free survival (PFS) curves in the economic model that were more clinically plausible.
As noted in the CDA-AMC Clinical Review, the usefulness of comparisons of abemaciclib with other CDK4 and CDK6 inhibitors relevant to Canadian practice is limited as no definitive conclusions could be reached about the comparative effect. There is therefore no robust evidence to support a price premium for abemaciclib plus fulvestrant over other relevant combination therapies to treat the same patient population. Of note, generics for palbociclib, which has a similar mechanism of action (i.e., CDK4 and CDK6 inhibition) have recently become available.
CDA-AMC estimates that the budget impact of reimbursing abemaciclib plus fulvestrant for the treatment of HR-positive, HER2-negative advanced or metastatic breast cancer will be approximately $29.3 million over the first 3 years of reimbursement compared to the amount currently spent on comparators. The expenditure on abemaciclib over this period is predicted to be $79.6 million (and $84.9 million for abemaciclib plus fulvestrant). The actual budget impact of reimbursing abemaciclib plus fulvestrant will depend on the remaining number of people eligible for treatment with abemaciclib in the second line due to previous exposure to abemaciclib, and the uptake of generics for palbociclib. At the submitted price, the magnitude of uncertainty in the budget impact must be addressed to ensure the feasibility of adoption given the difference between the sponsor’s estimate and the CDA-AMC estimate.
Summary of the Submitted Economic Evaluation
The sponsor submitted a cost-utility analysis to estimate the cost-effectiveness of abemaciclib plus fulvestrant from the perspective of a public payer in Canada over a lifetime horizon of 20 years. The modelled population aligned with the MONARCH 2 trial population and comprised the treatment of HR-positive, HER2-negative advanced or metastatic breast cancer in combination with fulvestrant in females with disease progression following ET. This is narrower than the Health Canada–indicated population but reflects the reimbursement request for this submission. The sponsor’s base-case analysis included costs related to drug acquisition, administration costs, AEs, health care resource use, subsequent therapies, and terminal care.
In the sponsor’s base case, abemaciclib plus fulvestrant was associated with incremental costs of $98,411 and 0.81 incremental QALYs relative to fulvestrant. This resulted in an incremental cost-effectiveness ratio of $122,203 per QALY gained. Of the incremental benefit compared to fulvestrant, approximately 42% was predicted to accrue after the duration of the MONARCH 2 trial (maximum follow-up = ██ months). Abemaciclib plus fulvestrant was estimated to dominate all other comparators. Additional information about the sponsor’s submission is summarized in Appendix 3.
CDA-AMC identified several key issues with the sponsor’s analysis (Table 2). Full details are provided in Appendix 4.
Table 2: Key Issues With the Sponsor’s Economic Submission
Issue | What evidence is there to inform this issue? | How was this issue addressed by CDA-AMC? | Did CDA-AMC explore uncertainty in a scenario analysis? |
|---|---|---|---|
The comparative efficacy between CDK4 and CDK6 inhibitors is highly uncertain and extrapolations beyond the trial data lack face validity. | There is a lack of direct head-to-head evidence comparing abemaciclib plus fulvestrant to other combination therapies. The results of the sponsor-submitted NMA are too uncertain to determine the comparative effects of abemaciclib plus fulvestrant over other combination therapies, regardless of the statistical methods employed (i.e., similar conclusions by Cox PH or FP models). The long-term predictions generated by the FP model (chosen for the sponsor) produced implausible results that are not substantiated by the evidence (e.g., they underestimated overall survival). This resulted in large differences in efficacy across CDK4 and CDK6 inhibitors in the extrapolated period (i.e., an additional 0.27 LYs for abemaciclib plus fulvestrant versus ribociclib), and estimated similar overall survival between monotherapy and some combination therapies (i.e., palbociclib plus fulvestrant and exemestane plus everolimus). | CDA-AMC used the Cox PH models in its base-case reanalysis to better reflect the available evidence and the clinical expert input sought by CDA-AMC. Although a Cox PH model is not the preferred method to make comparisons within the trials period given PH violation in some trials, in the economic model, it resulted in more plausible long-term survival extrapolations. | To explore uncertainty around the Cox PH models, CDA-AMC explored alternative parametric extrapolations of OS in scenario analyses. |
TTD curves lack face validity and underestimate the cost of abemaciclib plus fulvestrant relative to other CDK4 and CDK6 inhibitors. | The calibration method used to estimate TTD (i.e., ratio of median TTD and PFS from each primary trial) was inappropriate because it resulted in abemaciclib plus fulvestrant having a lower TTD relative to other CDK4 and CDK6 inhibitors. TTD was not included in the NMA, and there is therefore no evidence that the gap between TTD and PFS curves would differ across CDK4 and CDK6 inhibitors. Clinical expert input sought by CDA-AMC expected to see no difference in TTD is across CDK4 and CDK6 inhibitor treatments. | CDA-AMC could not address this issue in the base case because of a lack of comparative clinical data to inform how TTD may differ by CDK4 and CDK6 inhibitor treatments. | To explore uncertainty around this issue, CDA-AMC conducted a scenario analysis assuming TTD is equal to PFS for all comparators. |
The cost of some comparators were overestimated. | For everolimus, the sponsor considered only the use of two 5 mg tablets instead of the 10 mg tablet available in Canada (offered at flat prices). Palbociclib has generic formulations available. | CDA-AMC used the latest publicly available price for generic palbociclib and 10 mg everolimus in its base case. | No scenario analysis was conducted. |
CDA-AMC = Canada’s Drug Agency; CDK = cyclin-dependent kinase; FP = fractional polynomial; LY = life-year; OS = overall survival; PFS = progression-free survival; PH = proportional hazard; QALY = quality-adjusted life-year; TTD = time to treatment discontinuation.
Note: Full details of the issues identified by CDA-AMC are provided in Appendix 3.
CDA-AMC Assessment of Cost-Effectiveness
The CDA-AMC base case was derived by making changes to model parameter values and assumptions (Table 7), after clinical expert input. Detailed information about the base case is provided in Appendix 4. The following treatments were on the cost-effectiveness frontier, from lowest to highest expected costs: fulvestrant alone, palbociclib plus fulvestrant and ribociclib plus fulvestrant.
Impact on Health Care Costs
Abemaciclib plus fulvestrant is predicted to be associated with additional health care costs compared to ribociclib plus fulvestrant (incremental costs = $4,519). This increase in health care spending primarily results from drug acquisition costs associated with abemaciclib plus fulvestrant (Table 8 and Figure 1).
Figure 1: Impact of Abemaciclib Plus Fulvestrant vs. Comparators on Health Care Costs
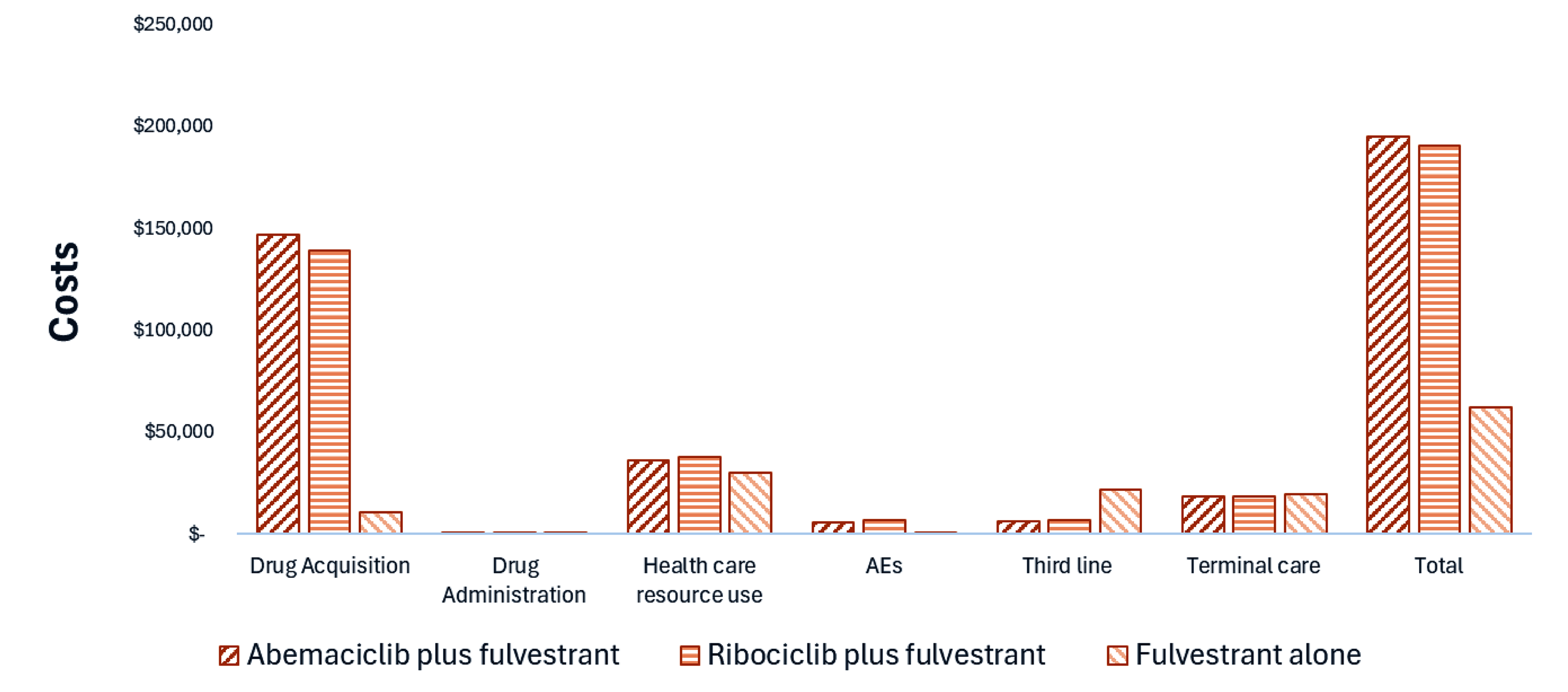
AE = adverse event; vs. = versus.
Note: Health care resource use includes follow-up care costs, hospitalization costs, and best standard of care costs. Results for palbociclib plus fulvestrant and exemestane plus everolimus are not presented. Appendix 4 provides full disaggregated costs and QALYs for all comparators.
Impact on Health
Abemaciclib plus fulvestrant is predicted to result in 0.16 fewer LYs and 0.05 fewer QALYs per patient, compared to ribociclib plus fulvestrant, over a patient lifetime horizon (Table 8 and Figure 2). This aligns with the NMA’s Cox hazard ratio indicating that, on average, ribociclib plus fulvestrant would result in slightly higher OS in comparison with abemaciclib plus fulvestrant (OS hazard ratio = 0.73 versus 0.76 for ribociclib versus abemaciclib, respectively). Most importantly, the use of Cox models reduced uncertainty in the extrapolated period by reducing the differences in efficacy across CDK4 and CDK6 inhibitors (e.g., incremental LYs versus ribociclib plus fulvestrant in the extrapolated period reduced from 0.27 LYs [FP model] to −0.03 [Cox PH model]).
Figure 2: Impact of Abemaciclib Plus Fulvestrant vs. Comparators on Patient Health
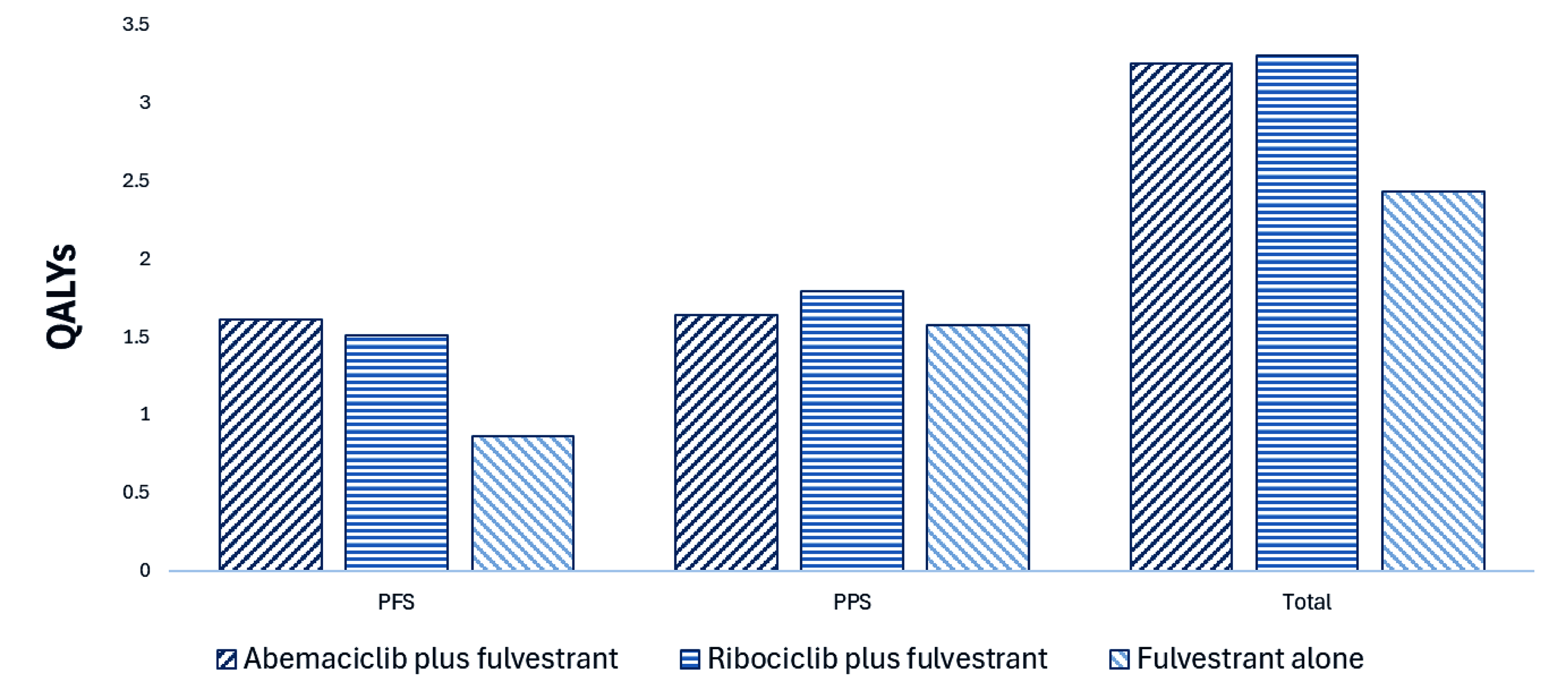
PFS = progression-free survival; PPS = postprogression survival; QALY = quality-adjusted life-year; vs. = versus.
Note: Results for palbociclib plus fulvestrant and exemestane plus everolimus are not presented. Appendix 4 provides full results.
Overall Results
Based on the CDA-AMC base case, the following treatments are on the cost-effectiveness frontier (that is, they are not dominated by other treatments): fulvestrant alone, palbociclib plus fulvestrant, and ribociclib plus fulvestrant. Abemaciclib plus fulvestrant is dominated by ribociclib plus fulvestrant (Table 3). Additional details on the CDA-AMC base case are available in Appendix 4.
Table 3: Summary of CDA-AMC Economic Evaluation Results
Drug | Total costs ($) | Total LYs | Total QALYs | Sequential ICER ($/QALY) |
|---|---|---|---|---|
Fulvestrant | 81,453 | 4.26 | 2.46 | Reference |
Palbociclib plus fulvestrant | 148,925 | 5.15 | 3.15 | 92,938 vs. fulvestrant |
Ribociclib plus fulvestrant | 208,596 | 5.56 | 3.30 | 416,809 vs. palbociclib plus fulvestrant |
Abemaciclib plus fulvestrant | 213,115 | 5.40 | 3.25 | Dominated by ribociclib plus fulvestrant |
CDA-AMC = Canada’s Drug Agency; ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year; vs. = versus.
Note: Publicly available list prices were used for all comparators. Appendix 4 provides the full disaggregated costs and QALYs for all comparators.
Uncertainty and Sensitivity
Due to uncertainty in the comparative clinical evidence, particularly the absence of direct comparisons with other combination therapies or comparative times to treatment discontinuation (TTD), these issues were addressed as thoroughly as possible in reanalyses; however, some uncertainty remains, as outlined in Table 2. Uncertainty around the comparative OS or TTD assumptions had the largest impact on cost-effectiveness, but abemaciclib plus fulvestrant remained dominated by ribociclib plus fulvestrant (Table 11, Appendix 4).
Summary of the Budget Impact
The sponsor submitted a BIA to estimate the 3-year (2026 to 2028) budget impact of reimbursing abemaciclib plus fulvestrant for use in the treatment of HR-positive, HER2-negative advanced or metastatic breast cancer in females with disease progression following ET. The sponsor assumed that the payer would be CDA-AMC–participating public drug plans and derived the size of the eligible population using an epidemiologic approach. The price of abemaciclib was aligned with the price included in the sponsor’s economic evaluation, while the prices of comparators were based on publicly available list prices. Additional information pertaining to the sponsor’s submission is provided in Appendix 5.
CDA-AMC identified a number of issues with the sponsor’s estimated budget impact and made changes to model parameters and assumptions after clinical expert input to derive the CDA-AMC base case (Appendix 5). CDA-AMC estimated that 1,019 to 1,051 patients would be eligible for treatment with abemaciclib plus fulvestrant over the 3-year period (1,019 in year 1 followed by 1,034 in year 2 and 1,051 in year 3). The estimated incremental budget impact of reimbursing abemaciclib plus fulvestrant is predicted to be approximately $29.3 million over the first 3 years, with a predicted expenditure of $84.9 million on abemaciclib plus fulvestrant. The estimated budget impact is uncertain due to uncertainty in the uptake of treatment with abemaciclib as a second-line treatment if patients have been previously exposed to abemaciclib in earlier lines of therapy, and the uptake of generic palbociclib.
Conclusion
Based on the CDA-AMC base case, abemaciclib plus fulvestrant would be considered dominated by ribociclib plus fulvestrant at the submitted price (i.e., it would be more costly and less effective). A price reduction for abemaciclib should be considered to put this treatment on the cost-effectiveness frontier (Figure 3; full details presented in Table 10). However, both the sponsor’s reanalysis and the CDA-AMC reanalysis are highly uncertain due to limitations of the sponsor’s submitted NMA, which informed the comparative efficacy within the economic model as these limitations could not be adequately addressed. As noted in the CDA-AMC Clinical Review, the NMA estimates were imprecise, with heterogeneity evident in patient populations across trials. Overall, the results had limited generalizability. Consequently, the added clinical value of abemaciclib plus fulvestrant relative to other combination therapies in clinical practice in Canada remains too uncertain to be determined.
The budget impact of reimbursing abemaciclib plus fulvestrant to the public drug plans in the first 3 years is estimated to be approximately $29.3 million. The 3-year expenditure on abemaciclib plus fulvestrant (i.e., not accounting for current expenditures on comparators) is estimated to be $84.9 million. The estimated budget impact is uncertain due to uncertainty in uptake of treatment with abemaciclib as a second-line treatment if patients have been previously exposed to abemaciclib in earlier lines of therapy, and the uptake of generic palbociclib.
Figure 3: Summary of the CDA-AMC Economic Analysis and Price Reduction

CDA-AMC = Canada’s Drug Agency; Ext. = extendedly; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; vs. = versus.
Note: Expenditure includes only the drug cost of abemaciclib plus fulvestrant. The term dominated indicates that a drug costs more and provides fewer QALYs than a comparator.
References
1.Canada's Drug Agency. Drug Reimbursement Review: abemaciclib (Verzenio), with an aromatase inhibitor, for HR-positive, HER2-negative advanced or metastatic breast cancer. 2025. Accessed May 6, 2025. https://www.cda-amc.ca/abemaciclib-1
2.Ontario Ministry of Health. Ontario drug benefit formulary/comparative drug index. Accessed March 2025. https://www.formulary.health.gov.on.ca/formulary
3.Ontario Ministry of Health. Exceptional Access Program product prices. Accessed March 2025. https://www.ontario.ca/page/exceptional-access-program-product-prices
4.Eli Lilly Canada Inc. Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Verzenio (abemaciclib), 50 mg, 100 mg, or 150 mg, oral tablet, with fulvestrant. February 14, 2025.
5.Eli Lilly Canada Inc. Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Verzenio (abemaciclib), 50 mg, 100 mg, or 150 mg, oral tablet, with fulvestrant. February 14, 2025.
6.National Institute for Health and Care Excellence. Fulvestrant for the treatment of locally advanced or metastatic breast cancer. (Technology appraisal guidance TA239). 2011. Accessed May 1, 2025. https://www.nice.org.uk/Guidance/TA239
7.Ontario Ministry of Health. Ontario Case Costing Initiative (OCCI). Accessed February 14, 2025. https://data.ontario.ca/dataset/ontario-case-costing-initiative-occi
8.Ontario Ministry of Health. Schedule of benefits for physician services under the Health Insurance Act: (February 20, 2024 (effective April 1, 2024)). 2023. Accessed February 14, 2025. https://www.ontario.ca/files/2024-08/moh-schedule-benefit-2024-08-30.pdf
9.IQVIA. DeltaPA. 2023. Accessed February 14, 2025. https://www.iqvia.com/
10.Yu M, Guerriere DN, Coyte PC. Societal costs of home and hospital end-of-life care for palliative care patients in Ontario, Canada. Health Soc Care Community. 2015;23(6):605-18. doi: 10.1111/hsc.12170 PubMed
11.Jansen JP. Network meta-analysis of survival data with fractional polynomials. BMC Med Res Methodol. 2011;11(1):61. doi: 10.1186/1471-2288-11-61 PubMed
12.Eli Lilly Canada Inc. Clinical Study Report: I3Y-MC-JPBL, addendum final overall survival analysis. MONARCH 2: A Randomized, Double-Blind, Placebo-Controlled, Phase 3 Study of Fulvestrant with or without Abemaciclib, a CDK4/6 Inhibitor, for Women with Hormone Receptor Positive, HER2 Negative Locally Advanced or Metastatic Breast Cancer [internal sponsor's report]. June 15, 2022.
13.Neven P, Fasching PA, Chia S, et al. Updated overall survival from the MONALEESA-3 trial in postmenopausal women with HR+/HER2- advanced breast cancer receiving first-line ribociclib plus fulvestrant. Breast Cancer Res. 2023;25(1):103. doi: 10.1186/s13058-023-01701-9 PubMed
14.IQVIA. PharmaStat. 2025. Accessed April 30, 2025. https://www.iqvia.com/
15.CADTH. Drug Reimbursement Expert Review Committee final recommendation: abemaciclib (Verzenio - Eli Lilly Canada Inc.). July 5, 2019. Accessed by sponsor, no date provided. https://www.cda-amc.ca/sites/default/files/pcodr/Reviews2019/10161AbemaciclibMBC_fnRec_ApprovedbyChair_v01_2019-07-04_Post_05Jul2019_final.pdf
16.Canada's Drug Agency. Drug Reimbursement Review: abemaciclib (Verzenio), with fulvestrant, for HR-positive, HER2-negative advanced or metastatic breast cancer. 2025. Accessed May 6, 2025. https://www.cda-amc.ca/abemaciclib-2
17.Canada's Drug Agency. Reimbursement recommendation: abemaciclib (Verzenio). Can J Health Technol. 2024;4(10). doi: 10.51731/cjht.2024.1007
18.CADTH. Reimbursement recommendation: capivasertib (Truqap). Can J Health Technol. 2024;4(9). doi: 10.51731/cjht.2024.977
Appendix 1: Cost Comparison Table
Please note that this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate after clinical expert input and feedback from CDA-AMC–participating public drug plans. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and, as such, the table may not represent the actual costs to public drug plans.
Table 4: Cost Comparison for HR-Positive, HER2-Negative Advanced or Metastatic Breast Cancer
Treatment | Strength and/or concentration | Form | Price | Recommended dosage | Daily cost ($) | 28-day cost ($) |
|---|---|---|---|---|---|---|
CDK4 and CDK6 plus fulvestrant | ||||||
Abemaciclib | 50 mg 100 mg 150 mg | Tablet | 116.9725a 115.8889 116.2173 | 150 mg, twice dailya | 232.43 | 6,508 |
Ribociclibb | 200 mg | Tablet | 94.1271 | 600 mg, once daily on days 1 to 21 of each 28-day cycle | 211.79 | 5,930 |
Palbociclib | 75 mg 100 mg 125 mg | Capsule | 126.9562 126.9562 126.9562 | 125 mg, once daily on days 1 to 21 of each 28-day cycle | 95.22 | 2,666 |
Abemaciclib plus fulvestrant | — | — | — | — | Cycle 1: 261.58 Cycle 2+: 247.01 | Cycle 1: 7,324 Cycle 2+: 6,916 |
Ribociclib plus fulvestrant | — | — | — | — | Cycle 1: 240.93 Cycle 2+: 226.36 | Cycle 1: 6,746 Cycle 2+: 6,338 |
Palbociclib plus fulvestrant | — | — | — | — | Cycle 1: 124.36 Cycle 2+: 109.79 | Cycle 1: 3,482 Cycle 2+:3,074 |
Fulvestrant alone | ||||||
Fulvestrant | 250 mg (50 mg/mL) | Prefilled syringe injection | 40.8027 per mL | 500 mg, intramuscular, on Day 1 and Day 15 of cycle 1, and then on Day 1 of each subsequent 28-day cycle | Cycle 1: 29.14 Cycle 2+: 14.57 | Cycle 1: 816 Cycle 2+: 408 |
Exemestane plus everolimus | ||||||
Exemestane | 25 mg | Tablet | 1.3263 | 25 mg, once daily | 1.33 | 37 |
Everolimus | 2.5 mg 5 mg 10 mg | Tablet | 172.2559 172.2559 172.2559 | 10 mg, once daily | 172.26 | 4,823 |
Exemestane plus everolimusc | — | — | — | — | 173.58 | 4,860 |
CDK = cyclin-dependent kinase.
aSponsor’s submitted price and recommended dosage.
bPrice from the Ontario Exceptional Access Program (accessed March 2025).3
cRecommended dosage based on Cancer Care Ontario.
Note: All prices, except for abemaciclib, are from the Ontario Drug Benefit Formulary (accessed March 2025), unless otherwise indicated, and do not include dispensing fees.2 Recommended dosages are based on product monographs, unless otherwise indicated.
Appendix 2: Input Relevant to the Economic Review
Please note that this appendix has not been copy-edited.
This section is a summary of the input received from the patient groups, clinician groups, and drug plans that participated in the CDA-AMC review process.
Patient input was received from Breast Cancer Canada, Rethink Breast Cancer, and Canadian Breast Cancer Network, collected via online surveys (171 respondents), and interviews (4 interviews) including patients with advanced breast cancer in Canada. The majority of patients reported to go on oral therapy after first-line progression, including single agent ET (e.g., anastrozole, letrozole, or tamoxifen), CDK4 and CDK6 inhibitors (ribociclib or palbociclib) plus ET and capecitabine. Patient input highlighted that patients place a high value on oral therapies that provide extended cancer control and meaningful quality of life, while delaying IV chemotherapy. Patient input noted that controlling disease and extending life expectancy are the most important treatment goals, while also avoiding chemotherapy. They also noted that the AE profile of available CDK4 and CDK6 inhibitors differ, as does the dosing schedule and the monitoring schedule and having more options would increase the ability to adhere to treatment. Patients considered relevant to highlight that abemaciclib is currently only funded in Quebec for second-line therapy. All 4 respondents with abemaciclib experience received it in combination with aromatase inhibitors (e.g., anastrozole, letrozole, exemestane) as first-line treatment for advanced breast cancer. Most patients reported manageable AEs, although all of them reported some degree of side effects, particularly diarrhea, which impaired quality of life when severe. AEs were mostly successfully managed by reducing abemaciclib dosage. No input from patients receiving abemaciclib plus fulvestrant as second-line treatment was received.
Clinician group input was received from Research Excellence, Active Leadership Canadian Breast Cancer Alliance. Current treatment options include, fulvestrant combined with a CDK4/6 inhibitor (ribociclib or palbociclib), for patients who did not have first-line treatment with CDK4 and CDK6 inhibitors, and everolimus combined with exemestane. The treatment goals include extending PFS and OS while minimizing AEs to preserve quality of life. Another treatment goal highlighted by the clinical input is delaying the need for subsequent chemotherapy. Abemaciclib plus fulvestrant is placed in the care pathway as another CDK4 and CDK6 inhibitor choice in the second-line setting.
Input from CDA-AMC–participating drug plans noted that ribociclib and palbociclib are the current standard of care in Canada for this indication. The drug plan inquired whether it would be reasonable to switch patients between ribociclib or palbociclib to abemaciclib.
Several of these concerns were addressed in the sponsor’s model:
Treatment goals of PFS and OS, as well as AEs, were modelled.
The model considers differences in the dose schedule of different treatment options.
CDA-AMC was unable to address the following concerns:
CDA-AMC was not able to estimate the impact of patients switching from other CDK4 and CDK6 inhibitors to abemaciclib plus fulvestrant if this regimen becomes available in Canada.
Appendix 3: Summary of the Sponsor’s Submission
Please note that this appendix has not been copy-edited.
Summary of the Sponsor’s Economic Evaluation
For the pharmaceutical reviews program, clinical and economic information is submitted to CDA-AMC by the sponsor. The CDA-AMC health economics team reviews the submitted economic information and appraises the information together with clinical expert input and the clinical review team to evaluate key assumptions, influential parameters, and the overall rigour of the economic submission. Based on what the team learns through this process, adjustments may be made to the sponsor’s model to produce the CDA-AMC base case. The CDA-AMC base case represents the team’s current understanding of the clinical condition, clinical evidence currently available, and best interpretation of the economic evidence based on the information provided.
For the review of abemaciclib plus fulvestrant, the sponsor provided a cost-utility analysis and a BIA.4,5 The sponsor’s economic submission is summarized in Table 5.
Table 5: Key Components of the Sponsor’s Economic Evaluation
Component | Description |
|---|---|
Treatment information | |
Drug under review | Abemaciclib (Verzenio), oral tablets (50, 100, and 150 mg) |
Submitted price of drug under review | Abemaciclib: 50 mg: $116.97 100 mg: $115.89 150 mg: $116.22 |
Regimen | Abemaciclib 150 mg orally twice daily until disease progression or unacceptable toxicity; administered in combination with fulvestrant 500 mg intramuscular on day 1 and day 15 of cycle 1, and then on day 1 of each subsequent 28-day cycle. |
Per 28-day cost of drug under review | Abemaciclib: $6,508 per patient Abemaciclib plus fulvestrant = $7,324 in cycle 1 and $6,916 in subsequent cycles |
Model information | |
Type of economic evaluation | Cost-utility analysis PSM |
Treatment | Abemaciclib plus fulvestrant |
Included comparators |
|
Perspective | Publicly funded health care payer perspective |
Time horizon | Lifetime (20 years) |
Cycle length | 7 days |
Modelled population | Patients with HR-positive, HER2-negative advanced breast cancer, who had disease progression on or within 12 months of completion of (neo)adjuvant ET or who had disease progression on their first-line ET for advanced disease |
Characteristics of modelled population | Derived from the MONARCH 2 trial (mean age: 59.3 years; BSA: 1.69 m2; weight: 66.7 kg) |
Model health states |
|
Data sources | |
Comparative efficacy |
|
Natural history and/or clinical pathway |
|
Health-related utilities and disutilities |
|
Costs included in the model |
|
Summary of the submitted results | |
Base case results |
|
Scenario analysis results |
|
AE = adverse event; BSA = body surface area; ET = endocrine therapy; GGT = gamma-glutamyl transferase; ICER = incremental cost-effectiveness ratio; NICE = National Institute for Health and Care Excellence; NMA = network meta-analysis; OS = overall survival; PFS = progression-free survival; PSM = partitioned survival model; PPS = postprogression survival; QALY = quality-adjusted life-year; RDI = relative dose reduction; TTD = time to treatment discontinuation.
Table 6: Summary of the Sponsor’s Economic Evaluation Results — Probabilistic
Drug | Total costs ($) | Total LYs | Total QALYs | Sequential ICER ($ per QALY) |
|---|---|---|---|---|
Fulvestrant | 68,903 | 3.39 | 1.90 | Reference |
Abemaciclib plus fulvestrant | 167,315 | 4.50 | 2.71 | 122,203 |
Palbociclib plus fulvestrant | 117,733 | 2.61 | 1.59 | Dominated by fulvestrant alone |
Ribociclib plus fulvestrant | 152,452 | 4.20 | 2.49 | Extendedly dominated through fulvestrant alone and abemaciclib plus fulvestrant |
Exemestane plus everolimus | 169,454 | 3.31 | 2.02 | Dominated by ribociclib plus fulvestrant and abemaciclib plus fulvestrant |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Appendix 4: Additional Details of CDA-AMC Reanalyses
Please note that this appendix has not been copy-edited.
Clinical Data in the Economic Model
The key clinical efficacy data (i.e., PFS and OS) used to inform the economic model were derived from the MONARCH 2 trial (data cut-off date: March 18, 2022, maximum follow-up ██ months) for abemaciclib plus fulvestrant and for fulvestrant alone, and from a sponsor-submitted NMA for all other comparators due to the lack of head-to-head trials against palbociclib plus fulvestrant, ribociclib plus fulvestrant, or exemestane plus everolimus.
The CDA-AMC Clinical Review of the MONARCH 2 trial concluded that abemaciclib plus fulvestrant, compared to fulvestrant alone, significantly increased patient PFS (median improvement: 7.6 months; hazard ratio = 0.539; 95% CI, 0.449 to 0.647), and OS (median improvement: 8.6 months; hazard ratio = 0.784; 95% CI, 0.644 to 0.955). The CDA-AMC Clinical Review of the sponsor-submitted NMA considered the main analysis using fixed-effect Cox PH models with a sensitivity analysis using FP models submitted to address violation of the PH assumptions in some included studies. Both models came to similar conclusions and are subject to many of the same methodological limitations. Comparisons against other relevant combination treatments available in clinical practice in Canada were subject to considerable uncertainty due to imprecise estimates, differences in patient populations across trials (such as prior chemotherapy exposure and geographic variability), and limited generalizability. This precluded CDA-AMC from drawing definitive conclusions about comparative effect of abemaciclib plus fulvestrant compared to palbociclib plus fulvestrant, ribociclib plus fulvestrant, and exemestane plus everolimus. The safety profile of abemaciclib remains consistent with that of other CDK4 and CDK6 inhibitors, with diarrhea, neutropenia, and infections as the most reported AEs, most manageable with dose adjustments and supportive care. However, AEs were not assessed in the NMA, and long-term comparative safety data beyond the pivotal trial period and direct comparisons remain limited.
In the sponsor’s economic model, PFS and OS were extrapolated beyond the MONARCH 2 trial period using a FP model over a 20-year lifetime time horizon. Notably, of the total incremental QALYs gained over the model horizon, approximately 42% were accrued in the extrapolated period (i.e., after ██ months), contributing to additional uncertainty in the projected LYs and QALYs gained. The sponsor indicated that none of the best-fitting models (by deviance information criterion [DIC]) could be selected because their extrapolations produced clinically implausible survival plateaus, particularly for OS. The range of the DIC to inform FP model selection was broadened, and the sponsor chose between a limited number of FP models suggested to have plausible extrapolations. However, the FP model selected by the sponsor’s for the economic evaluation generated unplausible long-term extrapolations based on clinical expert input sought by CDA-AMC. Several additional sources of uncertainty related to the clinical efficacy inputs in the economic model were noted (Refer to Key Issues of the Submitted Economic Evaluation). As such, the estimated incremental gain in LYs and QALYs predicted by the sponsor’s model for abemaciclib plus fulvestrant are highly uncertain.
Key Issues of the Submitted Economic Evaluation
CDA-AMC identified the following key issues with the sponsor’s analysis:
The comparative efficacy between CDK4 and CDK6 inhibitors is highly uncertain and extrapolations beyond the trial data lack face validity: There are several sources of uncertainty related to the clinical data in the economic model. First, due to lack of direct head-to-head evidence comparing abemaciclib plus fulvestrant to ribociclib plus fulvestrant, palbociclib plus fulvestrant, and exemestane plus everolimus, relative effectiveness was informed by the sponsor’s submitted NMA. Given the violation of proportion hazard assumption observed in OS for the MONARCH 2 and SoFEA trials, and in PFS for the BOLERO-2 trial, the sponsor used a FP model from the NMA to inform the PFS and OS curves for all comparators in the economic model. The FP model uses a multidimensional relative treatment effect rather than a single parameter for treatment effect, which allows more flexible time-varying hazard ratio models.11 FP models require careful model building and model selection strategies. The sponsor’s choice of FP models for the NMA considered DIC statistics, visual inspection of fit and clinical plausibility. The final models were selected from a choice of ██ possible models. None of the best-fitting models (by DIC) were selected because their extrapolations produced clinically implausible survival plateaus according to the sponsor’s own assessment, particularly for OS. The range of DIC to inform selection was then broadened (beyond 5 points), and the sponsor chose between a limited number of models suggested to have plausible extrapolations. However, for the cost-utility analysis, the sponsor included only 1 FP model and did not provide flexibility within the economic evaluation to incorporate alternative FP models. This substantially limited CDA-AMC ability to validate the impact and appropriateness of different survival curves derived by using different FP models.
Clinical expert input sought by CDA-AMC noted that the long-term predictions generated by the sponsor’s choice of FP model for the economic analysis underestimated survival compared to clinical trials data, and lacks face validity. For instance, the model predicted OS at year 5 for patients receiving abemaciclib plus fulvestrant and ribociclib plus fulvestrant to be 33% and 30%, respectively. However, the unadjusted 5-year survival from MONARCH 212 and MONALEESA-313 showed a survival of 41.2% and 39.7%, respectively. Further, treatment with fulvestrant alone was predicted to have lower PFS estimates in comparison to all combination therapies. Yet, the model’s OS extrapolations based on the FP model led to comparable or slightly better OS estimates for fulvestrant alone when compared to palbociclib plus fulvestrant and exemestane plus everolimus. Lastly, although the model predicted comparable OS efficacy in the first 3 years for CDK4 and CDK6 inhibitors (palbociclib, ribociclib and abemaciclib showed 48%, 50%, and 50% of patients alive, respectively), the long-term OS projections are higher for abemaciclib plus fulvestrant than ribociclib and palbociclib (3%, 1.4%, and 0.3% at year 20, respectively). This is not substantiated by the submitted clinical evidence as no long-term data exist to suggest that abemaciclib plus fulvestrant would be superior to other CDK4 and CDK6 inhibitors. In fact, the proportional hazard ratios are smaller for ribociclib plus fulvestrant compared with abemaciclib plus fulvestrant (0.73 versus 0.76 for ribociclib versus abemaciclib, respectively. This suggests that on average, ribociclib plus fulvestrant would result in slightly higher OS in comparison with abemaciclib plus fulvestrant.
Regardless of the statistical method used in the NMA (Cox PH or FP models), the CDA-AMC Clinical Review did not identify evidence demonstrating that abemaciclib plus fulvestrant offered superior efficacy in comparison to other CDK4 and CDK6 inhibitors, namely palbociclib and ribociclib. Clinical expert input sought by CDA-AMC noted that abemaciclib would be an additional option within the class of CDK4/6 inhibitors rather than a disruptor of the current treatment paradigm.
In the CDA-AMC base case, Cox PH models were used to extrapolate survival data beyond the clinical trial period using hazard ratios against fulvestrant alone. CDA-AMC specifically chose gamma and exponential distributions for PFS and OS of fulvestrant, respectively. Although the Cox PH models would not be the preferred method to make comparisons within the trial periods due to the violation of PH assumptions for PFS and OS, in the economic model, it resulted in more plausible long-term extrapolations estimates for OS at years 5 and 10 that are more aligned with the available evidence and clinical expert input. As a result of selecting the Cox PH model, the long-term comparative efficacy across CDK4 and CDK6 inhibitors reduced (e.g., incremental QALYs versus ribociclib plus fulvestrant in the extrapolated period reduced from 0.27 LYs [FP model] to −0.03 [Cox PH model]). During CDA-AMC reanalyses, it was noted that the submitted model contained some coding errors when calculating PFS for ribociclib plus fulvestrant when using the Cox PH model (e.g., assumed equal to abemaciclib plus fulvestrant’s PFS) and these coding errors were fixed as part of the reanalysis. Alternative parametric functions for fulvestrant PFS and OS were explored in scenario analysis based on model fit within the trial period.
TTD curves lack face validity: The sponsor estimated TTD for each treatment option using a calibration method justifying that the Kaplan-Meier data on TTD for ribociclib plus fulvestrant, palbociclib plus fulvestrant, and exemestane plus everolimus were not reported in their primary publications. In the calibration method, the sponsor used a ratio of medians to estimate a hazard ratio (i.e., based on the median TTD and median PFS reported in the individual trials). This ratio was then applied to the PFS curve of each treatment to attain their relative estimates of TTD. There is no evidence that the difference between TTD and PFS is proportional throughout the entire time horizon or different across CDK4 and CDK6 inhibitors. Finally, this approach resulted in abemaciclib plus fulvestrant having a lower TTD relative to other CDK4 and CDK6 inhibitors (reaching a difference of more than 2 months at some time points compared to palbociclib plus fulvestrant). This likely favours abemaciclib plus fulvestrant compared to the other CDK4/6 inhibitors by underestimating abemaciclib treatment costs. Clinical expert input sought by CDA-AMC for this review indicated that, although it is plausible for patients to discontinue treatment and remain progression-free, this is not expected to continue for more than a couple of months after discontinuation nor is it expected to be different across CDK4 and CDK6 inhibitors (i.e., expected similar class effect).
CDA-AMC undertook a scenario analysis by changing TTD to be equal to PFS for all treatments. This change is likely to overestimate the costs of drug acquisition; however, it maintains the relative difference in costs among treatment options.
The model overestimated the cost of some comparators. For everolimus, the sponsor estimated its cost considering the use of two 5 mg tablets in the model, to achieve the daily dosage of 10 mg (i.e., 2 tablets). Everolimus is available in Canada with flat prices for all strengths (2.5 mg, 5 mg or 10 mg),2 which results in lower cost per mg depending on what presentation is used to calculate the total cost of a daily dose (e.g., $34.45 and $17.25 per mg with the 5 mg and 10 mg strengths, respectively).2 In addition, CDA-AMC noted that palbociclib has generic formulations available for more than 6 months,14 with flat prices reduced from $253 to $126 for all strengths (75 mg, 100 mg and 125 mg) based on Ontario Drug Benefit Formulary.2 As such, total cost in the sponsor’s model for the exemestane plus everolimus and palbociclib plus fulvestrant regimens were overestimated.
CDA-AMC used the latest publicly available prices for palbociclib in the base case and costed everolimus based on one 10 mg tablet daily.
CDA-AMC Reanalysis of the Economic Evaluation
The CDA-AMC base case was derived by making changes in model parameter values and assumptions, after clinical expert input (refer to Table 7). The impact of these changes, individually and collectively, is presented in Table 8.
Table 7: Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CDA-AMC value or assumption |
|---|---|---|
1. Method for comparative effectiveness | Fractional polynomial model for PFS and OS | Proportional hazard ratio model FUL PFS: gamma distribution FUL OS: exponential distribution Recode ribociclib plus fulvestrant PFS curve to apply the HR against fulvestrant alone (instead of assuming equal to abemaciclib PFS) |
2. Comparators costs | Everolimus: Used two 5 mg tablets Palbociclib: $253.9123 per capsule | Everolimus: Used one 10 mg tablet Palbociclib: $126.9562 per capsule |
CDA-AMC base case (health care payer perspective) | ― | 1 + 2 |
CDA-AMC = Canada’s Drug Agency; FUL = fulvestrant alone; PFS = progression-free survival; OS = overall survival; TTD = time to treatment discontinuation.
Note: CDA-AMC was unable to resolve the issues with TTD lack of face validity for the comparators that were not part of MONARCH 2 trial.
Table 8: Summary of the Stepped Analysis
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALY) |
|---|---|---|---|---|
Sponsor base case | Fulvestrant (Fulv) | 68,992 | 1.89 | Reference |
Palbociclib plus fulvestrant (PF) | 151,408 | 2.21 | Ext. dominated by Fulv and AF | |
Ribociclib plus fulvestrant (RF) | 153,459 | 2.47 | Ext. dominated by Fulv and AF | |
Abemaciclib plus fulvestrant (AF) | 165,104 | 2.70 | 119,375 vs. Fulv | |
Exemestane plus everolimus (EE) | 168,348 | 1.97 | Dominated by PF, RF, and AF | |
CDA-AMC reanalysis 1 | Fulvestrant | 81,591 | 2.43 | Reference |
Ribociclib plus fulvestrant (RF) | 206,848 | 3.30 | 143,112 vs. Fulv | |
Abemaciclib plus fulvestrant (AF) | 211,866 | 3.24 | Dominated by RF | |
Palbociclib plus fulvestrant (PF) | 212,222 | 3.14 | Dominated by RF and AF | |
Exemestane plus everolimus (EE) | 225,914 | 2.55 | Dominated by PF, RF, and AF | |
CDA-AMC reanalysis 2 | Fulvestrant (Fulv) | 68,992 | 1.89 | Reference |
Exemestane plus everolimus (EE) | 107,980 | 1.97 | Ext. dominated by Fulv and AF | |
Palbociclib plus fulvestrant (PF) | 109,537 | 2.21 | Ext. dominated by Fulv and AF | |
Ribociclib plus fulvestrant (RF) | 153,459 | 2.47 | Ext. dominated by Fulv and AF | |
Abemaciclib plus fulvestrant (AF) | 165,104 | 2.70 | 119,375 vs. Fulv | |
CDA-AMC base case Reanalysis 1 + 2 (deterministic) | Fulvestrant (Fulv) | 81,591 | 2.43 | Reference |
Exemestane plus everolimus (EE) | 139,865 | 2.55 | Ext. dominated by Fulv and AF, and Fulv and RF | |
Palbociclib plus fulvestrant (PF) | 148,382 | 3.14 | 94,016 vs. Fulv | |
Ribociclib plus fulvestrant (RF) | 206,848 | 3.30 | 354,731 vs. PF | |
Abemaciclib plus fulvestrant (AF) | 211,866 | 3.24 | Dominated by RF | |
CDA-AMC base case Reanalysis 1 + 2 (probabilistic) | Fulvestrant (Fulv) | 81,453 | 2.46 | Reference |
Exemestane plus everolimus (EE) | 141,894 | 2.58 | Ext. dominated by Fulv and PF, and Fulv and RF | |
Palbociclib plus fulvestrant (PF) | 148,925 | 3.15 | 92,938 vs. Fulv | |
Ribociclib plus fulvestrant (RF) | 208,596 | 3.30 | 416,809 vs. PF | |
Abemaciclib plus fulvestrant (AF) | 213,115 | 3.25 | Dominated by RF |
AF = abemaciclib plus fulvestrant; CDA-AMC = Canada’s Drug Agency; EE = exemestane plus everolimus. Fulv = fulvestrant alone; ICER = incremental cost-effectiveness ratio; PF = palbociclib plus fulvestrant; QALY = quality-adjusted life-years; RF = ribociclib plus fulvestrant; vs. = versus.
Note All analyses are reported deterministically unless otherwise indicated, while the cumulative CDA-AMC base case is presented both deterministically and probabilistically. The CDA-AMC reanalysis is based on the publicly available prices of the comparator treatments.
Table 9: Disaggregated Results of the CDA-AMC Base Case
Parameter | Abemaciclib plus fulvestrant | Ribociclib plus fulvestrant | Palbociclib plus fulvestrant | Exemestane plus everolimus | Fulvestrant |
|---|---|---|---|---|---|
Discounted LYs | |||||
Total | 5.40 | 5.56 | 5.15 | 4.17 | 4.26 |
By health state | |||||
PFS | 2.15 | 2.01 | 2.29 | 1.97 | 1.14 |
PPS | 3.25 | 3.55 | 2.86 | 2.20 | 3.12 |
Discounted QALYs | |||||
Total | 3.25 | 3.30 | 3.15 | 2.58 | 2.43 |
By health state or data source | |||||
PFS | 1.61 | 1.51 | 1.71 | 1.47 | 0.86 |
PPS | 1.64 | 1.79 | 1.44 | 1.11 | 1.57 |
Discounted costs ($) | |||||
Total | 213,115 | 208,596 | 148,925 | 141,894 | 81,453 |
Drug acquisition | 146,467 | 138,971 | 84,055 | 88,688 | 10,500 |
Administration | 126 | 129 | 152 | 0 | 80 |
Follow-up (PFS) | 250 | 234 | 267 | 229 | 133 |
Follow-up (PPS) | 975 | 1,066 | 856 | 659 | 772 |
BSC | 23,663 | 24,393 | 22,571 | 18,271 | 18,684 |
AEs | 5,572 | 6,519 | 6,548 | 2,550 | 479 |
Hospitalization | 11,250 | 12,021 | 10,231 | 8,019 | 10,074 |
Third line treatment | 6,317 | 6,914 | 5,564 | 4,219 | 21,484 |
Terminal care | 18,495 | 18,350 | 18,681 | 19,260 | 19,246 |
AE = adverse event; BSC = best supportive care; CDA-AMC = Canada’s Drug Agency; LY = life-year; QALY = quality-adjusted life-year; PFS = progression-free survival; PPS = postprogression survival.
Price Reduction Analysis
CDA-AMC conducted price reduction analyses using the sponsor’s base case and the CDA-AMC base case (refer to Table 10).
Table 10: Results of the Price Reduction Analysis
Price reduction | Unit drug cost ($) | Cost per 28 days ($) | ICERs for abemaciclib plus fulvestrant vs. comparators ($/QALY) | |
|---|---|---|---|---|
Sponsor base case | CDA-AMC base case | |||
No price reduction | 117a | 6,508 | 98,412 vs. fulvestrant alone | Dominated by ribociclib plus fulvestrant |
10% | 105 | 5,857 | 89,118 vs. fulvestrant alone | Ext. dominated by fulvestrant alone and palbociclib plus fulvestrant; and fulvestrant alone and ribociclib plus fulvestrant |
20% | 94 | 5,207 | 79,824 vs. fulvestrant alone | 407.601 vs. palbociclib plus fulvestrant |
30% | 82 | 4,556 | 70,530 vs. fulvestrant alone | 271,364 vs. palbociclib plus fulvestrant |
40% | 70 | 3,905 | 61,236 vs. fulvestrant alone | 135,127 vs. palbociclib plus fulvestrant |
50% | 58 | 3,254 | 51,942 vs. fulvestrant alone | 82,117 vs. fulvestrant alone |
60% | 47 | 2,603 | 42,648 vs. fulvestrant alone | 66,443 vs. fulvestrant alone |
70% | 35 | 1,952 | 33,354 vs. fulvestrant alone | 50,768 vs. fulvestrant alone |
80% | 23 | 1,302 | 24,060 vs. fulvestrant alone | 35,093 vs. fulvestrant alone |
90% | 12 | 651 | 14,766 vs. fulvestrant alone | 19,419 vs. fulvestrant alone |
CDA-AMC = Canada’s Drug Agency; ICER = incremental cost-effectiveness ratio; vs. = versus.
aSponsor’s submitted price for abemaciclib for 150 mg tablet.5 Abemaciclib is also available in 50 mg and 100 mg tablets at the price of $116.9725 and $115.8889 per tablet, respectively.
Assessment of Uncertainty
CDA-AMC used the CDA-AMC base case to conduct scenario analyses to address uncertainty within the economic evaluation. The results are provided in Table 11.
Scenario 1: Changed the distribution for fulvestrant alone OS to log-normal. Based on the sponsor’s report, log-normal distribution provided the best fit within MONARCH 2 trial data for abemaciclib plus fulvestrant and fulvestrant alone.
Scenario 2: Changed TTD to be equal to PFS for all comparators.
Table 11: Results of CDA-AMC Scenario Analyses
Analysisa | Drug | Total costs ($) | Total QALYs | ICER ($/QALYs) |
|---|---|---|---|---|
CDA-AMC base case | Fulvestrant | 81,591 | 2.43 | Reference |
Exemestane plus everolimus | 139,865 | 2.55 | Ext. dominated by fulvestrant and palbociclib plus fulvestrant and fulvestrant and ribociclib plus fulvestrant | |
Palbociclib plus fulvestrant | 148,382 | 3.14 | 94,016 | |
Ribociclib plus fulvestrant | 206,848 | 3.30 | 354,731 | |
Abemaciclib plus fulvestrant | 211,866 | 3.24 | Dominated by ribociclib plus fulvestrant | |
CDA-AMC scenario 1: Use log-normal distribution for fulvestrant alone OS | Fulvestrant | 89,320 | 2.71 | Reference |
Exemestane plus everolimus | 144,406 | 2.82 | Ext. dominated by fulvestrant alone and palbociclib plus fulvestrant and fulvestrant alone and ribociclib plus fulvestrant | |
Palbociclib plus fulvestrant | 153,929 | 3.49 | 83,582 | |
Ribociclib plus fulvestrant | 212,767 | 3.68 | 304,038 | |
Abemaciclib plus fulvestrant | 217,646 | 3.61 | Dominated by ribociclib plus fulvestrant | |
CDA-AMC scenario 2: Assumed TTD equal to PFS | Fulvestrant | 83,530 | 2.43 | Reference |
Palbociclib plus fulvestrant | 169,069 | 3.14 | 120,406 | |
Exemestane plus everolimus | 176,167 | 2.55 | Dominated by palbociclib plus fulvestrant | |
Ribociclib plus fulvestrant | 247,424 | 3.30 | 475,404 | |
Abemaciclib plus fulvestrant | 271,691 | 3.24 | Dominated by ribociclib plus fulvestrant |
CDA-AMC = Canada’s Drug Agency; Ext. = extendedly; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; TTD = time to treatment discontinuation.
aDeterministic analyses.
Issues for Consideration
CADTH already reviewed abemaciclib for the treatment of HR-positive, HER2-negative advanced or metastatic breast cancer in 2019.15 Abemaciclib was conditionally recommended for reimbursement based on a significant PFS benefit demonstrated in the MONARCH 2 trial, although OS data were not sufficient to draw conclusions. In this resubmission, the sponsor provided updated evidence from the MONARCH 2 trial, including an interim OS analysis (data cut-off: 20 June 2019) and a final OS analysis (data cut-off: 18 March 2022), reflecting over 5 years of follow-up. This updated submission also includes revised NMAs and updated economic models incorporating the new OS data. Additionally, CDA-AMC is currently reviewing abemaciclib resubmission split into 2 distinct indications: (PC0400) for patients with HR-positive, HER2-negative advanced or metastatic breast cancer who have not received prior systemic treatment in the advanced setting;1 and (PC0409) for patients with HR-positive, HER2-negative advanced breast cancer, who had disease progression on or within 12 months of completion of (neo)adjuvant ET or who had disease progression on their first-line ET for advanced disease.16
CDA-AMC also has reviewed abemaciclib in combination with ET for the adjuvant treatment of adult patients with HR-positive, HER2-negative, node-positive, early breast cancer at high risk of disease recurrence based on clinicopathological features. The pan-Canadian Oncology Drug Reviews’ Expert Committee (pERC) recommended that abemaciclib be reimbursed for this indication with clinical criteria and conditions on October 3, 2024.17
With the increased use of abemaciclib in the adjuvant setting or earlier lines of therapy, there may be fewer patients who will be eligible for re-treatment with abemaciclib in the second line. However, for those who have no prior exposure to abemaciclib or other CDK4/6 inhibitors, based on clinical input obtained by CDA-AMC, abemaciclib was considered as an important treatment option that offers continuous CDK4/6 inhibition with a manageable safety profile. The experts noted that abemaciclib provides flexibility for patients who may not tolerate other CDK4/6 inhibitors, such as those with hematologic toxicity on palbociclib or ribociclib. They also highlighted the potential benefit of abemaciclib in patients with visceral disease, a subgroup often associated with poorer prognosis, and in those who have previously demonstrated endocrine resistance.
Appendix 5: Budget Impact Analysis
Please note that this appendix has not been copy-edited.
Summary of the Submitted BIA
The sponsor submitted a BIA that estimated the expected incremental budgetary impact of reimbursing abemaciclib plus fulvestrant for the treatment of HR-positive, HER2-negative advanced or metastatic breast cancer in females with disease progression following ET.4
The BIA was conducted from the perspective of public drug plan payers over a 3-year time horizon (2026 to 2028), with 2025 as the base year. The sponsor’s estimate reflects the aggregated results from the jurisdictional provincial budgets (excluding Quebec) as well as the Non-Insured Health Benefits Program. The sponsor estimated the eligible population using an epidemiological approach. The sponsor’s base case included drug acquisition costs. The market uptake for abemaciclib plus fulvestrant was estimated using sponsor’s internal estimates. Abemaciclib plus fulvestrant was assumed to displace ribociclib plus fulvestrant and palbociclib plus fulvestrant. The key inputs to the BIA are documented in Table 12.
The sponsor estimated the 3-year incremental budget impact associated with reimbursing abemaciclib plus fulvestrant would be $11,218,683 (year 1 = $1,462,355; year 2 = $3,954,624; year 3 = $5,801,884).
Table 12: Key Model Parameters
Parameter | Sponsor’s estimate (reported as year 1 / year 2 / year 3 if appropriate) |
|---|---|
Target population | |
Adult population in Canada | 26,987,736 |
Prevalence of breast cancer | 0.37% |
Proportion of patients HR-negative, HER2-positive | 70.2% |
Annual rate of recurrence | 7.1% |
Recurrence after 12 months following adjuvant therapy | 77% |
Recurrence within 12 months of adjuvant ET | 23% |
Recurrence within 12 months after receiving ET | 90% |
Recurrence within 12 months after receiving first-line chemotherapy due to visceral crisis | 5% |
Incidence of breast cancer | 0.08% |
Proportion of patients HR-negative, HER2-positive | 70.2% |
Annual rate of recurrence | 5.5% |
Receive first-line NSAI monotherapy for de novo or recurrence advanced or metastatic cancer (after 12 months following adjuvant ET) | 6% |
Progression on first-line NSAI | 80% |
Percentage of patients covered by public drug plan | Range 49.1% to 100% (weighted average 76.8%) |
Number of patients eligible for drug under review | 1,023 / 1,039 / 1,055 |
Market shares (reference scenario) | |
Abemaciclib plus fulvestrant | 0% / 0% / 0% |
Palbociclib plus fulvestrant | 46% / 46% / 46% |
Ribociclib plus fulvestrant | 54% / 54% / 54% |
Everolimus plus exemestane | 0% / 0% / 0% |
Fulvestrant | 0% / 0% / 0% |
Market shares (new drug scenario) | |
Abemaciclib plus fulvestrant | 12% / 23% / 29% |
Palbociclib plus fulvestrant | 40% / 35% / 33% |
Ribociclib plus fulvestrant | 48% / 42% / 38% |
Everolimus plus exemestane | 0% / 0% / 0% |
Fulvestrant | 0% / 0% / 0% |
Cost of treatment (per patient per 28-day cycle) | |
Abemaciclib plus fulvestranta | $6,916 |
Palbociclib plus fulvestranta | $5,740 |
Ribociclib plus fulvestranta | $6,338 |
Everolimus plus exemestane | $1,455 |
Fulvestranta | $408 |
ET = endocrine therapy; NSAI = nonsteroidal aromatase inhibitor.
aThe sponsor used the cost of subsequent cycles as they didn’t include the costs of 2 doses of fulvestrant incurring in cycle 1.
Key Issues of the Submitted BIA
CDA-AMC identified several key issues to the sponsor’s analysis that have notable implications on the results of the BIA:
The proportion of patients with adequate response to chemotherapy following visceral crisis is overestimated. The sponsor assumed that the proportion of patients with adequate response to chemotherapy following visceral crisis was 100%. Clinical expert input sought by CDA-AMC suggested that although the rate of adequate response in clinical practice is high, it is unlikely that all patients will respond.
In the CDA-AMC reanalysis, the rate of adequate response to chemotherapy following visceral crisis was adjusted to 90% based on clinical expert input.
The market share estimates for exemestane plus everolimus and fulvestrant alone do not align with clinical expectations. In the submitted BIA, the sponsor assumed that exemestane plus everolimus and fulvestrant alone had 0% of the current market shares. Clinical expert input sought by CDA-AMC indicated that some patients would continue to have contraindications to the use of CDKs 4/6 inhibitors. Therefore, both options could still be used by a small proportion of patients (i.e., just below 10% of patients) with a higher distribution to fulvestrant alone, as not all jurisdictions reimburse exemestane plus everolimus. Finally, they do not expect any displacement of these options by the availability of abemaciclib plus fulvestrant.
In the CDA-AMC reanalysis, the market shares of exemestane plus everolimus and fulvestrant alone in the reference scenario and new drug scenario were adjusted to 2% and 6%, respectively, to better align with expectations of clinical practice in Canada.
The market uptake of abemaciclib plus fulvestrant may be overestimated: The sponsor’s submitted BIA indicated that abemaciclib plus fulvestrant would result in a market uptake of 12% in Year 1, 23% in Year 2, and 29% in Year 3 based on internal estimates. However, clinical expert input sought by CDA-AMC indicated that this market uptake may be overestimated as patients will increasingly have been exposed to abemaciclib in earlier lines of therapy and no longer be eligible for retreatment with abemaciclib.
CDA-AMC undertook a scenario analysis revising the market uptake for abemaciclib plus fulvestrant in the new drug scenario to 12% in Year 1, 20% in Year 2, and 20% in Year 3.
The price of comparators used in the BIA model was outdated. The sponsor sourced the price for everolimus ($52 per 10 mg) from a previous CDA-AMC submission dated from 2024.18 However, the most updated public price of everolimus available from Ontario Drug Benefit Formulary is much higher ($172 per 10 mg). In addition, CDA-AMC noted that palbociclib has generic formulations available, reducing its prices from $253 to $126 per tablet. These limitations resulted in underestimation of exemestane plus everolimus total cost and overestimation of the palbociclib plus fulvestrant total costs.
In the CDA-AMC reanalysis, updated prices from Ontario Drug Benefit Formulary were used for everolimus and palbociclib.
The price of drugs paid by public drug plans is uncertain: Both the sponsor and CDA-AMC analyses are based on publicly available list prices for all comparators. The actual costs paid by public drug plans are unknown.
CDA-AMC was unable to address this limitation in reanalysis.
CDA-AMC Reanalyses of the BIA
CDA-AMC revised the sponsor’s submitted analyses by making changes in model parameter values and assumptions, after clinical expert input, as outlined in Table 12.
Table 13: Revisions to the Submitted BIA
Stepped analysis | Sponsor’s value or assumption | CDA-AMC value or assumption |
|---|---|---|
1. Proportion of patients with adequate response to chemotherapy following visceral crisis | 100% | 90% |
2. Market shares in the reference scenario for exemestane plus everolimus and fulvestrant alone | Exemestane plus everolimus: 0% Fulvestrant alone: 0% | Exemestane plus everolimus: 2% Fulvestrant alone: 6% |
3. Comparators price | Everolimus: $50.6636 Palbociclib: $253.9123 | Everolimus: $172.2559 Palbociclib: $126.9562 |
CDA-AMC base case | ― | Reanalysis 1 + 2 + 3 |
BIA = budget impact analysis; CDA-AMC = Canada’s Drug Agency.
The results of the CDA-AMC step-wise reanalysis are presented in summary format in Table 14 and a more detailed breakdown is presented in Table 15. In the CDA-AMC base case, the 3-year budget impact of reimbursing abemaciclib plus fulvestrant for HR-positive, HER2-negative advanced or metastatic breast cancer in females with disease progression following ET was $29,330,031 (year 1 = $3,823,104; year 2 = $10,338,768; year 3 = $15,168,159).
CDA-AMC estimated that 1,019 to 1,051 patients would be eligible for treatment with abemaciclib plus fulvestrant over the 3-year period (year 1 = 1,019; year 2 = 1,034; year 3 = 1,051).
Table 14: Summary of the Stepped Analysis of the CDA-AMC Base Case
Stepped analysis | Three-year total ($) |
|---|---|
Submitted base case | $11,218,863 |
CDA-AMC reanalysis 1 | $11,169,900 |
CDA-AMC reanalysis 2 | $11,198,061 |
CDA-AMC reanalysis 3 | $29,572,176 |
CDA-AMC base case: Reanalysis 1 + 2 + 3 | $29,330,031 |
CDA-AMC = Canada’s Drug Agency.
Note: The CDA-AMC reanalysis is based on publicly available prices of the comparator treatments.
CDA-AMC used the CDA-AMC base case to conduct scenario analyses to explore uncertainty in the estimated budget impact of reimbursing abemaciclib plus fulvestrant. The results are provided in Table 15.
Scenario 1: lower market uptake of abemaciclib plus fulvestrant in years 2 and 3 (20%).
Table 15: Disaggregated Summary of the BIA
Stepped analysis | Scenario | Year 0 (current situation) ($) | Year 1 ($) | Year 2 ($) | Year 3 ($) | Three-year total ($) |
|---|---|---|---|---|---|---|
Submitted base case | Reference total | $79,297,930 | $140,311,820 | $142,493,447 | $144,709,983 | $427,515,250 |
Abemaciclib plus fulvestrant | $0 | $0 | $0 | $0 | $0 | |
All other comparators | $79,297,930 | $140,311,820 | $142,493,447 | $144,709,983 | $427,515,250 | |
New drug total | $79,297,930 | $141,774,175 | $146,448,071 | $150,511,867 | $438,734,113 | |
Abemaciclib plus fulvestrant | $0 | $11,126,023 | $30,049,960 | $44,068,500 | $85,244,484 | |
All other comparators | $79,297,930 | $130,648,151 | $116,398,111 | $106,443,367 | $353,489,629 | |
Budget Impact | $0 | $1,462,355 | $3,954,624 | $5,801,884 | $11,218,863 | |
CDA-AMC base case | Reference total | $55,915,914 | $98,043,455 | $99,567,789 | $101,116,554 | $298,727,798 |
Abemaciclib plus fulvestrant | $0 | $0 | $0 | $0 | $0 | |
All other comparators | $55,915,914 | $98,043,455 | $99,567,789 | $101,116,554 | $298,727,798 | |
New drug total | $55,915,914 | $101,866,559 | $109,906,557 | $116,284,713 | $328,057,829 | |
Abemaciclib plus fulvestrant | $0 | $11,077,468 | $29,918,819 | $43,876,181 | $84,872,468 | |
All other comparators | $55,915,914 | $90,789,090 | $79,987,738 | $72,408,532 | $243,185,360 | |
Budget Impact | $0 | $3,823,104 | $10,338,768 | $15,168,159 | $29,330,031 | |
CDA-AMC scenario analyses | ||||||
Scenario 1: Lower market uptake for abemaciclib plus fulvestrant | Reference total | $55,915,914 | $98,043,455 | $99,567,789 | $101,116,554 | $298,727,798 |
New drug total | $55,915,914 | $101,866,559 | $108,935,916 | $112,591,921 | $323,394,395 | |
Budget Impact | $0 | $3,823,104 | $9,368,127 | $11,475,367 | $24,666,597 | |
BIA = budget impact analysis; CDA-AMC = Canada’s Drug Agency.
Note: The CDA-AMC reanalysis is based on the publicly available prices of the comparator treatments.
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.