Drugs, Health Technologies, Health Systems
Reimbursement Review
Venetoclax (Venclexta)
Sponsor: AbbVie Corporation
Therapeutic area: Mantle cell lymphoma (MCL)
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Clinical Review
Abbreviations
AE
adverse event
ASCT
autologous stem cell transplant
BTKi
Bruton’s tyrosine kinase inhibitor
CAR
chimeric antigen receptor
CI
confidence interval
CIT
chemoimmunotherapy
CNS
central nervous system
CR
complete response
ECOG PS
Eastern Cooperative Oncology Group performance status
FACT-Lym
Functional Assessment of Cancer Therapy — Lymphoma
GRADE
Grading of Recommendations Assessment, Development and Evaluation
Hem DAC
Hematology Cancer Drug Advisory Committee
HR
hazard ratio
HRQoL
health-related quality of life
IHC
immunohistochemistry
IRC
independent review committee
ITT
intention-to-treat
KM
Kaplan-Meier
MCL
mantle cell lymphoma
MID
minimal important difference
MRD
measurable residual disease
NE
not estimable
NHL
non-Hodgkin lymphoma
OH-CCO
Ontario Health Cancer Care Ontario
ORR
overall response rate
OS
overall survival
PFS
progression-free survival
PR
partial response
RCT
randomized controlled trial
TEAE
treatment-emergent adverse event
TESAE
treatment-emergent serious adverse event
TLS
tumour lysis syndrome
TTNT
time to next treatment
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Table 1: Background Information of Application Submitted for Review
Item | Description |
|---|---|
Drug product | Venetoclax (Venclexta), 10 mg, 50 mg, and 100 mg oral tablets |
Sponsor | AbbVie Corporation |
Indication | In combination with ibrutinib, for the treatment of adult patients with relapsed or refractory MCL. |
Reimbursement request | As per indication |
Health Canada approval status | NOC |
Health Canada review pathway | Standard |
NOC date | July 31, 2025 |
Recommended dose | On day 1, start venetoclax according to the 5-week ramp-up dosing schedule, in combination with ibrutinib 560 mg once daily. After completing the ramp-up phase (venetoclax daily dose — week 1: 20 mg [2 × 10 mg]; week 2: 50 mg [1 × 50 mg]; week 3: 100 mg [1 × 100 mg]; week 4: 200 mg [2 × 100 mg]; week 5: 400 mg [4 × 100 mg]), continue venetoclax at a dose of 400 mg once daily in combination with ibrutinib 560 mg once daily for an additional 23 months (a total duration of combination treatment for 24 months, including the ramp-up phase). Then, continue ibrutinib monotherapy 560 mg once daily until disease progression or unacceptable toxicity. |
MCL = mantle cell lymphoma; NOC = Notice of Compliance.
Source: Draft product monograph for venetoclax.1 Details included in the table are from the sponsor’s Summary of Clinical Evidence.2
Introduction
Mantle cell lymphoma (MCL) is a frequently aggressive subtype of B-cell non-Hodgkin lymphoma (NHL), accounting for approximately 5% to 7% of NHL cases.3,4 In Canada, NHL is estimated to account for 11,700 new cases in 2024,5 with a 5-year prevalence of 32,915 cases in 2018.6 MCL, although representing a small subset of NHL cases, remains a significant clinical challenge due to its aggressive nature. Nearly all patients with MCL require systemic therapy, and the vast majority eventually experience relapsed or refractory disease.7,8 MCL primarily affects older adults, with an average age of diagnosis between 60 and 70 years, and occurs 4 times more frequently in men.3,9 The disease follows a progressive course, often involving the lymph nodes, bone marrow, spleen, and gastrointestinal tract.10 Patients typically present with symptoms such as painless lymphadenopathy, fatigue, night sweats, fever, or weight loss, which can significantly impact their health-related quality of life (HRQoL). MCL has an unfavourable prognosis, with a varying median overall survival of 2 to 10 years.2,10-15 Diagnosis of MCL requires a comprehensive clinical evaluation, including a detailed patient history, physical examination, and specialized diagnostic testing. Diagnostic tests for MCL, including immunohistochemistry (IHC), molecular assays, and genetic testing, are widely available in Canada and are routinely used in clinical practice.2
According to the clinical experts consulted by the CDA-AMC review team, MCL is noncurable with most therapies, and the goal of first-line treatment is to achieve remission, delay progression, and improve survival. The choice of first-line chemoimmunotherapy (CIT) is determined based on patient age, fitness, comorbidities, and institutional preferences. Younger patients (aged up to approximately 65) who are medically fit and have not received prior treatment for MCL are typically treated with intensive rituximab-based CIT (e.g., rituximab, cyclophosphamide, doxorubicin hydrochloride [hydroxydaunomycin], vincristine sulfate [oncovin], and prednisone [R-CHOP] and rituximab, dexamethasone, cytarabine, and cisplatin [R-DHAP]; bendamustine-rituximab and cytarabine-rituximab; bendamustine-rituximab) followed by autologous stem cell transplant (ASCT) and rituximab maintenance therapy for responding patients.16 Older or medically unfit patients with treatment-naive MCL are typically treated with lower-intensity CIT (e.g., bendamustine-rituximab), followed by rituximab maintenance therapy.17 Most patients with MCL are not cured by first-line treatments and eventually experience disease progression and require second-line treatments.18 For these patients with relapsed or refractory MCL, ibrutinib, a first-generation covalent Bruton’s tyrosine kinase inhibitor (BTKi), is a standard second-line treatment in Canada.8 Zanubrutinib and acalabrutinib, second-generation BTKis, have been approved by Health Canada for relapsed or refractory MCL;19,20 however, neither of them are currently publicly funded in Canada. Furthermore, most patients with MCL are not cured by second-line treatment with ibrutinib and are treated with third-line treatment, according to the clinical experts consulted by the CDA-AMC review team. Chimeric antigen receptor (CAR) T-cell therapy with brexucabtagene autoleucel is the third-line standard of care in Canada for patients with relapsed or refractory MCL who have been treated with 2 or more lines of prior systemic therapy, including a BTKi.21
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of venetoclax, 10 mg, 50 mg, and 100 mg tablets, taken orally, in the treatment of adult patients with relapsed or refractory MCL.
Perspectives of Patients, Clinicians, and Drug Programs
The information in this section is a summary of input provided by the patient and clinician groups who responded to our call for input and from clinical expert(s) consulted by for the purpose of this review.
Patient Input
CDA-AMC received 1 patient group input for this review from Lymphoma Canada. Lymphoma Canada collected patient input through an online anonymous survey between January and March 2025, gathering 82 responses from patients with MCL, with 5 patients who had received venetoclax plus ibrutinib (3 from Canada). Most of all survey respondents were living in Canada (74%), aged between 65 to 74 years (36%), with diagnoses 3 to 5 years ago (27%), or 9 to 10 years ago or more (24%).
The survey respondents reported significant impacts of MCL on their quality of life, with 28% reporting fatigue and 15% experiencing neutropenia. Patients also reported psychological challenges (with 72% experiencing stress, 70% anxiety, and 64% fear of progression) as well as mental health challenges (with 74% reporting fear of relapse and 38% having difficulty sleeping). Aspects of daily life were impacted, such as the ability to travel (38%), work (28%), and engage in social activities (20%), with many patients highlighting the challenges of managing a compromised immune system, isolation, and physical limitations due to treatment side effects.
Regarding current treatments for MCL, most respondents received 1 (56%) line of treatment. In second line or beyond, 29% of the respondents received stem cell transplants and 15% received BTKis. While 78% were satisfied with first-line treatments, satisfaction dropped for second-line (27%) and third-line (13%) options, indicating a need for more alternatives. Side effects such as fatigue, nausea, and joint pain were common and severely impacted patients’ quality of life. Patients expressed their desire to have more treatment options, especially for second- and third-line therapies.
Patients with MCL surveyed by Lymphoma Canada highlighted key outcomes of new treatments, including longer disease remission and survival, and better quality of life and symptom control. A majority (91%) were willing to tolerate mild, short-term side effects for better options, and 76% valued having treatment choices based on side effects and outcomes.
Five patients in the survey received a combination of venetoclax and ibrutinib in the second-line setting, with 1 patient newly in remission, 3 patients in remission for 1 to 2 years, and 1 patient experiencing a relapse after treatment. Reported side effects included diarrhea (3 patients), neutropenia (2 patients), fatigue (2 patients), joint pain (1 patient), and constipation (1 patient). Psychological impacts included anxiety (3 patients) and fear of progression (2 patients).
Clinician Input
Input From Clinical Experts Consulted for This Review
The clinical experts consulted by the CDA-AMC review team noted that the goal of first-line treatment for MCL is to achieve remission, delay progression, and improve survival. Treatments for patients with relapsed or refractory MCL are usually not curative, and most patients eventually experience disease progression. The clinical experts noted that ibrutinib was a standard second-line treatment for patients with MCL that has relapsed or is refractory to first-line treatments, but most patients with a response to ibrutinib eventually experience progression. Therefore, there is an unmet need for treatments with long-lasting benefits that are well tolerated for patients with relapsed or refractory MCL in the second-line treatment setting.
All clinical experts agreed that venetoclax plus ibrutinib should become a standard second-line treatment for patients with relapsed or refractory MCL and also noted that ibrutinib and venetoclax may change the current treatment paradigm, replacing ibrutinib monotherapy as the standard second-line treatment for most patients with relapsed or refractory MCL. The clinical experts consulted by the CDA-AMC review team noted that ibrutinib monotherapy could remain an alternative second-line treatment option for some patients.
The clinical experts noted that patients who are best suited for venetoclax plus ibrutinib are those with relapsed or refractory MCL who have received at least 1 prior line of therapy. The clinical experts indicated that venetoclax plus ibrutinib may not be suitable for patients whose disease is refractory to BTKis or BCL2 inhibitors. Other patients unsuited for this therapy include those who are unable or unwilling to perform bloodwork for TLS monitoring; those with serious active infections, severe liver dysfunction, or inability to swallow or absorb oral medications; those who require ongoing treatment with moderate or strong CYP3A inhibitors or inducers; and those with relative contraindications to ibrutinib (e.g., uncontrolled cardiovascular disease).
Assessing response to venetoclax plus ibrutinib generally includes a radiographic assessment after 2 to 3 months of treatment, but assessment may vary between physicians and institutions. Patients with circulating lymphoma cells and/or bone marrow involvement may have a complete blood count with or without bone marrow sampling as part of response assessment. For patients who demonstrate a response to venetoclax plus ibrutinib, treatment is continued for up to 2 years followed by ibrutinib monotherapy until disease progression or unacceptable intolerance. Subsequent imaging depends on the depth of initial response and the discretion of the treating physician.
According to the clinical experts, venetoclax should be given for a fixed-duration course of up to 2 years, while ibrutinib should be continued indefinitely. Either drug may be discontinued earlier for patients who experience disease progression or develop refractory disease or for those who experience unacceptable toxicities. The clinical experts noted that, although drugs are normally discontinued due to disease progression, in real-world practice, they may be continued while planning for the next line of therapy. The clinical experts noted that, when 1 drug is discontinued due to intolerance, it does not necessarily mean the other drug should also be discontinued at the same time, given that ibrutinib and venetoclax have different side effect profiles. The decision to discontinue either or both drugs should be made by the treating physician.
According to the clinical experts consulted by the CDA-AMC review team, venetoclax plus ibrutinib should be prescribed by a hematologist or oncologist who is familiar with the management of MCL and has knowledge regarding the safety, efficacy, and monitoring requirements of each drug, particularly regarding risk of tumour lysis syndrome (TLS) with venetoclax and cardiovascular toxicities of ibrutinib. Venetoclax plus ibrutinib (including the ramp-up phase of venetoclax) can be administered in the outpatient setting at tertiary care and community hospitals in urban and rural locations.
Clinician Group Input
CDA-AMC received input from 2 clinician groups, the Ontario Health Cancer Care Ontario (OH-CCO) Hematology Cancer Drug Advisory Committee (Hem DAC) and Lymphoma Canada Physician Group. OH-CCO Hem DAC provided input via a teleconference involving 7 clinicians. Lymphoma Canada Physician Group reviewed clinical trials, provincial guidelines, and a review on relapsed or refractory MCL by 5 experts.
According to the clinician groups, the goal of therapy for patients with MCL is long-term progression-free survival (PFS) and overall survival (OS), resolution of lymphoma-related symptoms, and improvement in quality of life. The clinician groups noted that treatment for patients with relapsed or refractory MCL includes BTKis (ibrutinib, acalabrutinib, zanubrutinib, and pirtobrutinib), CIT, and bortezomib-based options. The groups highlighted that, while BTKis are standard second-line therapy, their effectiveness declines, and relapse after BTKi remains a major unmet need. Both clinician groups highlighted significant treatment gaps for relapsed or refractory MCL, as no curative therapies exist. Current treatments offer limited survival benefits, with poor outcomes after BTKi failure (average survival is under 6 months). The Lymphoma Canada Physician Group noted that, while CAR T-cell therapy is now funded in Canada, access remains restricted to specialized centres and selected patients. Most patients with MCL that relapses do not qualify, leaving palliative options as the only alternative. There is a critical need for novel, well-tolerated treatment combinations to improve survival, delay disease progression, and enhance quality of life for the majority of patients.
The clinician groups noted that venetoclax plus ibrutinib is suitable as a second-line treatment option for relapsed or refractory MCL. According to the clinician groups, suitable candidates include patients eligible for BTKi treatment, particularly those who do not have BTKi-refractory disease. They further noted that, as a fully oral therapy, the combination of venetoclax and ibrutinib is suited for outpatient care and accessible in both community and academic settings. It should be prescribed by a hematologist managing MCL.
Drug Program Input
Input was obtained from the drug programs that participate in the reimbursement review process. The following were identified as key factors that could affect the implementation of a recommendation for venetoclax.
Relevant comparators
Consideration for prescribing of therapy
Generalizability
Funding algorithm
Care provision issues
System and economic issues.
Clinical Evidence
Systematic Review
Description of Studies
One study (SYMPATICO) was identified from the sponsor-submitted systematic literature review. The SYMPATICO trial consisted of an open-label safety run-in phase, a double-blind randomized phase, and an open-label treatment-naive cohort. The primary focus for this review is the randomized phase of SYMPATICO, which was a phase III, multicentre, double-blind randomized controlled trial (RCT) investigating the efficacy and safety of venetoclax plus ibrutinib in patients with MCL who have received at least 1, but no more than 5, prior treatment regimens for MCL, including at least 1 prior rituximab- or anti-CD20–containing regimen. A total of 267 patients (including ██ patients in Canada) were randomized to the venetoclax plus ibrutinib group (n = 134) or the placebo plus ibrutinib group (n = 133). The primary objective of the randomized phase of SYMPATICO was to assess the efficacy of venetoclax plus ibrutinib relative to placebo plus ibrutinib, as measured by PFS per investigator assessment. Secondary end points included OS and harms. HRQoL outcomes such as Functional Assessment of Cancer Therapy — Lymphoma (FACT-Lym) total score and the lymphoma-specific subscale of FACT-Lym were also reported.
Patients in the intention-to-treat (ITT) population of the randomized phase of SYMPATICO had a median age of 68 years (range, ██ ██ ██). There were more male patients than female patients (79.0% versus 21.0%). Most patients were white (86.5%), followed by Asian (1.9%), and Black or African American (0.7%). Approximately 59.6%, 23.6%, and 16.9% of the ITT population had received 1, 2, or 3 or more lines of therapies before receiving venetoclax plus ibrutinib, respectively.
Efficacy Results
The data cut-off date was May 22, 2023 (database lock date: July 5, 2023). The median time on study was █████ ██████ (range, ███ to ████) for the venetoclax plus ibrutinib group and █████ months (range, ███ to ████) for the placebo plus ibrutinib group.
Overall Survival
In the interim analysis of OS, the proportion of the ITT population who had OS events was 51.5% in the venetoclax plus ibrutinib group versus 56.4% in the placebo plus ibrutinib group. The median OS was 44.9 months (95% confidence interval [CI], 31.9 months to not estimable [NE]) in the venetoclax plus ibrutinib group versus 38.6 months (95% CI, 25.2 to 53.4 months) in the placebo plus ibrutinib group. The hazard ratio (HR) for death was 0.854 (95% CI, 0.615 to 1.186). At 12 months, the probability of being alive was ████% (95% CI, ████ to ████) for the venetoclax plus ibrutinib group and ████% (95% CI, ████ to ████) for the placebo plus ibrutinib group (between-group difference = ████%; 95% CI, █████ ██ ███). At 24 months, the probability of being alive was 65.9% (95% CI, 57.2% to 73.3%) for the venetoclax plus ibrutinib group and 61.4% (95% CI, 52.5% to 69.1%) for the placebo plus ibrutinib group (between-group difference = 4.5%; 95% CI, −7.0% to 16.2%). At 36 months, the probability of being alive was ████% (95% CI, ████ to ████) for the venetoclax plus ibrutinib group and ████% (95% CI, ████ to ████) for the placebo plus ibrutinib group (between-group difference = ███%; 95% CI, ████ to ████). At 48 months, the probability of being alive was ████% (95% CI, ████ to ████) for the venetoclax plus ibrutinib group and ████% (95% CI, ████ to ████) for the placebo plus ibrutinib group (between-group difference = ███%; 95% CI, –███ to ████). At 60 months, the probability of being alive was ████% (95% CI, ████ to ████) for the venetoclax plus ibrutinib group and ████% (95% CI, ████ to ████) for the placebo plus ibrutinib group (between-group difference = ███%; 95% CI, █████ to ████).
PFS Per Investigator Assessment
The proportion of the ITT population who had PFS events was 54.5% in the venetoclax plus ibrutinib group and 70.7% in the placebo plus ibrutinib group. The median PFS per investigator assessment was 31.9 months (95% CI, 22.8 to 47.0 months) in the venetoclax plus ibrutinib group versus 22.1 months (95% CI, 16.5 to 29.5 months) in the placebo plus ibrutinib group. The HR for PFS per investigator assessment was 0.645 (95% CI, 0.474 to 0.878). At 12 months, the probability of being progression-free was ████% (95% CI, ████ to ████) for the venetoclax plus ibrutinib group and ████% (95% CI, ████ to ████) for the placebo plus ibrutinib group (between-group difference = ████%; 95% CI, ████ to ████). At 24 months, the probability of being progression-free was 56.8% (95% CI, 47.7% to 64.9%) for the venetoclax plus ibrutinib group and 45.4% (95% CI, 36.5% to 53.8%) for the placebo plus ibrutinib group (between-group difference = 11.4%; 95% CI, −0.8% to 23.7%). At 36 months, the probability of being progression-free was ████% (95% CI, ████ to ████) for the venetoclax plus ibrutinib group and ████% (95% CI, ████ to ████) for the placebo plus ibrutinib group (between-group difference = ████; 95% CI, ███ to ████). At 48 months, the probability of being progression-free was ████% (95% CI, ████ to ████) for the venetoclax plus ibrutinib group and ████% (95% CI, ████ to ████) for the placebo plus ibrutinib group (between-group difference = ████%; 95% CI, ███ to ████). At 60 months, the probability of being progression-free was ████% (95% CI, ████ to ████) for the venetoclax plus ibrutinib group and ████% (95% CI, ████ to ████) for the placebo plus ibrutinib group (between-group difference = ████%; 95% CI, ███ to ████).
The overall concordance for the PFS events was ████% for the venetoclax plus ibrutinib group and ████% for the placebo plus ibrutinib group.
FACT-Lym Total Score
The FACT-Lym total score ranges between 0 and 168, with a higher score indicating a better HRQoL.
The difference in change from baseline FACT-Lym total score between the venetoclax plus ibrutinib group and the placebo plus ibrutinib group was ████ points (95% CI, █████ to ███) at ██ ██████ and ███ ██████ (95% CI, █████ to ████) at ██ ██████.
Lymphoma-Specific Subscale of FACT-Lym
The lymphoma-specific subscale of FACT-Lym ranges between 0 and 60, with a higher score indicating a better HRQoL.
The difference in change from baseline for the lymphoma-specific subscale of FACT-Lym score between the venetoclax plus ibrutinib group and the placebo plus ibrutinib group was ████ ██████ (95% CI, ████ to ███) at ██ ██████ and ████ points (95% CI, ████ to ███) at ██ ██████.
Harms Results
The proportion of patients who had treatment-emergent adverse events (TEAEs) of grade 3 or higher was 83.6% in the venetoclax plus ibrutinib group versus 75.8% in the placebo plus ibrutinib group. The most common TEAEs of grade 3 or higher included neutropenia (31.3% in the venetoclax plus ibrutinib group versus 10.6% in the placebo plus ibrutinib group), pneumonia (12.7% in the venetoclax plus ibrutinib group versus 10.6% in the placebo plus ibrutinib group), thrombocytopenia (12.7% in the venetoclax plus ibrutinib group versus 7.6% in the placebo plus ibrutinib group), and worsening of MCL (6.7% in the venetoclax plus ibrutinib group versus 12.1% in the placebo plus ibrutinib group).
The proportion of patients who had treatment-emergent serious adverse events (TESAEs) was 60.4% in the venetoclax plus ibrutinib group versus 59.8% in the placebo plus ibrutinib group. The most common TESAE was pneumonia (12.7% in the venetoclax plus ibrutinib group versus 10.6% in the placebo plus ibrutinib group), followed by worsening of MCL (6.7% in the venetoclax plus ibrutinib group versus 12.9% in the placebo plus ibrutinib group).
Venetoclax or placebo were discontinued due to TEAEs in 22.4% of the patients in the venetoclax plus ibrutinib group versus 28.8% in the placebo plus ibrutinib group. Ibrutinib was discontinued due to TEAEs in 29.1% of the patients in the venetoclax plus ibrutinib group versus 31.1% in the placebo plus ibrutinib group. The proportion of patients with any adverse event (AE) with outcome of death was 16.4% in the venetoclax plus ibrutinib group versus 13.6% in the placebo plus ibrutinib group. The most common reason was worsening of MCL (3.0% in the venetoclax plus ibrutinib group versus 7.6% in the placebo plus ibrutinib group).
Treatment-emergent major hemorrhage, which included serious or grade 3 or higher hemorrhage and central nervous system (CNS) hemorrhage of any grade, occurred in ████ of the patients in the venetoclax plus ibrutinib group versus ████ in the placebo plus ibrutinib group. Atrial fibrillation of any grade occurred in 10.4% of the patients in the venetoclax plus ibrutinib group versus 10.6% in the placebo plus ibrutinib group. The percentage of patients who had cardiac arrhythmias (excluding atrial fibrillation) of any grade was █████ in the venetoclax plus ibrutinib group versus █████ in the placebo plus ibrutinib group. The percentage of patients who had TLS of any grade was 5.2% in the venetoclax plus ibrutinib group versus 2.3% in the placebo plus ibrutinib group. There were 4 deaths possibly due to cardiac-related causes in the venetoclax plus ibrutinib group and 2 deaths in the placebo plus ibrutinib group.
Critical Appraisal
Internal Validity
In the randomized phase of SYMPATICO, only results from the interim OS analysis were available for this review, which was considered immature, as the upper bound of the 95% CI of the median OS in the venetoclax plus ibrutinib group was NE. As a result, uncertainty remains in the interim OS evidence, which may be addressed by the final OS analysis. ██ █████ ██ ███ ██████████████ ████████ ██ ███████ ██ ████████████ ███ ███████ █████████ ████ █████ ██ ██ ████ ██ ██████ ██████████ ██ █████ █████ ████ ███ ███████ ██ █████ ███ ███ ██████ ██ ███████████ Two sets of censoring rules were used in estimating PFS: the global censoring rules for the primary analysis and the FDA censoring rules for 1 of the sensitivity analyses. In the global censoring rules, patients without progression or death were censored, while, in the FDA censoring rules, 2 additional censoring scenarios were added to the global censoring rules, i.e., patients without progressive disease or death, with subsequent anticancer therapy, or with 2 or more missed visits before the PFS event were censored. There was a large difference in median PFS in the venetoclax plus ibrutinib group (approximately a 10-month increase) but not in the placebo plus ibrutinib group (no change) between the primary PFS analysis (i.e., per the global censoring rules) and the PFS sensitivity analysis per the FDA censoring rules, as noted by the review team and other.23 This indicated that the patients in the venetoclax plus ibrutinib group who were censored by the additional 2 scenarios of the FDA rules were not equally likely to experience disease progression, compared to those who were not censored. Specifically, the additionally censored patients in the venetoclax plus ibrutinib group were at a higher risk, which would have violated the noninformative censoring assumption of the Kaplan-Meier (KM) method, skewed the KM curve, and resulted in an overestimation of median PFS in the analysis with the FDA censoring rules.23,24 Moreover, as Lesan et al. pointed out,23 the possibility of overestimation in the PFS primary analysis using the global censoring rules could not be ruled out because, for example, in the primary PFS analysis, patients who missed visits were not censored. Given that these patients could be at a higher risk of disease progression (as suggested by the sensitivity analysis using the FDA censoring rules), not counting these patients as having a PFS event may have overestimated median PFS. There was a risk of unblinding in patients or investigators due to a higher occurrence of digestive AEs in the venetoclax plus ibrutinib group compared to the placebo plus ibrutinib group and a higher percentage of patients in the venetoclax plus ibrutinib group who were treated for these digestive AEs. If patients became unblinded, there was a risk of bias in the assessment of HRQoL outcomes. There was also a risk of missing outcome data for HRQoL outcomes. For instance, around half of the ITT population was missing when assessing the FACT-Lym total score and the lymphoma-specific subscale of FACT-Lym at 24 months. There was no description of how the missing data were handled for the HRQoL outcomes. Therefore, it is uncertain how the missing HRQoL data impacted the results observed.
External Validity
The eligibility criteria of the randomized phase of SYMPATICO were in general aligned with the selection criteria in the Canadian setting when identifying eligible patients with MCL in the relapsed and refractory setting, according to the clinical experts consulted by the review team. However, the clinical experts noted that some patients who might benefit from venetoclax plus ibrutinib were not included in the randomized phase of SYMPATICO, including selected patients with an Eastern Cooperative Oncology Group performance status (ECOG PS) greater than 2; patients who have previously been exposed, but whose disease is not refractory, to venetoclax or ibrutinib; patients without at least 1 site of disease of 2.0 cm (e.g., leukemic MCL), and patients with CNS lymphoma, which is rare. Nonetheless, results from the randomized phase of SYMPATICO were still likely to be generalizable to these patients.
GRADE Summary of Findings and Certainty of the Evidence
For pivotal studies and RCTs identified in the sponsor’s systematic review, Grading of Recommendations Assessment, Development and Evaluation (GRADE) was used to assess the certainty of the evidence for outcomes considered most relevant to inform expert committee deliberations, and a final certainty rating was determined as outlined by the GRADE Working Group.25,26
Following the GRADE approach, evidence from RCTs started as high-certainty evidence and could be rated down for concerns related to study limitations (which refers to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias.
When possible, certainty was rated in the context of the presence of an important (nontrivial) treatment effect. If this was not possible, certainty was rated in the context of the presence of any treatment effect (i.e., the clinical importance is unclear). In all cases, the target of the certainty of evidence assessment was based on the point estimate and where it was located relative to the threshold for a clinically important effect (when a threshold was available) or to the null.
The reference points for the certainty of evidence assessment for OS and PFS per investigator assessment were set according to the presence of an important effect based on thresholds agreed upon by clinical experts consulted by the review team for this review. The reference points for the certainty of evidence assessment for the FACT-Lym total score, the lymphoma-specific subscale of FACT-Lym, and harms events were set according to the presence of any non-null effect.
The selection of outcomes for GRADE assessment was based on the sponsor’s Summary of Clinical Evidence, consultation with clinical experts, and input received from patient and clinician groups and public drug plans. The following list of outcomes was finalized in consultation with expert committee members:
Survival outcomes (OS, PFS per investigator assessment)
HRQoL outcomes (FACT-Lym total score, lymphoma-specific subscale of FACT-Lym)
Harms (TESAEs).
Results of GRADE Assessments
Table 2 presents the GRADE summary of findings for venetoclax plus ibrutinib versus placebo plus ibrutinib for patients with MCL who have received at least 1, but no more than 5, prior treatment regimens.
Table 2: Summary of Findings for Venetoclax Plus Ibrutinib Versus Placebo Plus Ibrutinib for Patients With MCL Who Have Received at Least 1, But No More Than 5, Prior Treatment Regimens
Outcome and follow-up | Patients (studies), N | Relative effect (95% CI) | Absolute effects (95% CI) | Certainty | What happens | ||
|---|---|---|---|---|---|---|---|
Placebo plus ibrutinib | Venetoclax plus ibrutinib | Difference | |||||
OS (interim analysis, data cut-off date: May 22, 2023) | |||||||
Probability of being alive at 48 months Median follow-up duration (months):
| 267 (1 RCT) | ██ | ███ per 1,000 | ███ per 1,000 (███ to ███ per 1,000) | ██ ████ per 1,000 (██ █████ to ███ ████ per 1,000) | Lowa | Venetoclax plus ibrutinib may result in little or no difference in the probability of being alive at 48 months, compared to placebo plus ibrutinib. |
Probability of being alive at 60 months Median follow-up duration (months):
| 267 (1 RCT) | ██ | ███ per 1,000 | ███ per 1,000 (███ to ███ per 1,000) | ██ ████ per 1,000 (███ █████ to ███ ████ per 1,000) | Lowa | Venetoclax plus ibrutinib may result in little or no difference in the probability of being alive at 60 months, compared to placebo plus ibrutinib. |
PFS per investigator assessment (data cut-off date: May 22, 2023) | |||||||
Probability of being progression-free at 36 months Median follow-up duration (months):
| 267 (1 RCT) | ██ | ███ per 1,000 | ███ per 1,000 (███ to ███ per 1,000) | ███ ███ per 1,000 (██ ████ to ███ ████ per 1,000) | Moderateb | Venetoclax plus ibrutinib likely results in a clinically important difference in the probability of being progression-free at 36 months, compared to placebo plus ibrutinib. |
Probability of being progression-free at 60 months Median follow-up duration (months):
| 267 (1 RCT) | ██ | ███ per 1,000 | ███ per 1,000 (███ to ███ per 1,000) | ███ ████ per 1,000 (██ ████ to ███ ████ per 1,000) | Highc | Venetoclax plus ibrutinib results in a clinically important difference in the probability of being progression-free at 60 months, compared to placebo plus ibrutinib. |
FACT-Lym total score (data cut-off date: May 22, 2023) | |||||||
Mean change from baseline in the FACT-Lym total score (0 [worst] to 168 [best]) Follow-up: 24 months | ███ (██ RCT) | ██ | █████ ███ █ ██████ | █████ ███ █ ██████ | ████ ██████ ██ ████ | Very lowd | The evidence is uncertain about the effect of venetoclax plus ibrutinib on the FACT-Lym total score at 24 months, compared to placebo plus ibrutinib. |
Mean change from baseline in the FACT-Lym total score (0 [worst] to 168 [best]) Follow-up: 60 months | ██ (██ RCT) | ██ | █████ ███ █ ██████ | █████ ███ █ ██████ | ███ ██████ ██ █████ | Very lowd | The evidence is uncertain about the effect of venetoclax plus ibrutinib on the FACT-Lym total score at 60 months, compared to placebo plus ibrutinib. |
Lymphoma-specific subscale of FACT-Lym (data cut-off date: May 22, 2023) | |||||||
Mean change from baseline in the lymphoma-specific subscale of FACT-Lym (0 [worst] to 60 [best]) Follow-up: 24 months | ███ (██ RCT) | ██ | ████ ███ █ █████ | ████ ███ █ █████ | ████ █████ ██ ████ | Very lowd | The evidence is uncertain about the effect of venetoclax plus ibrutinib on the lymphoma-specific subscale of FACT-Lym at 24 months, compared to placebo plus ibrutinib. |
Mean change from baseline in the lymphoma-specific subscale of FACT-Lym (0 [worst] to 60 [best]) Follow-up: 60 months | ██ (██ RCT) | ██ | ████ ███ █ █████ | ████ ███ █ █████ | ████ █████ ██ ████ | Very lowd | The evidence is uncertain about the effect of venetoclax plus ibrutinib on the lymphoma-specific subscale of FACT-Lym at 60 months, compared to placebo plus ibrutinib. |
Harms (data cut-off date: May 22, 2023) | |||||||
TESAEs Follow-up: 60 months| | ███ (██ RCT) | ██ | ███ per 1,000 | ███ per 1,000 (███ to ███ per 1,000) | ████ per 1,000 (███ █████ to ███ ████ per 1,000) | Lowe | Venetoclax plus ibrutinib may result in little or no difference in TESAEs, compared to placebo plus ibrutinib. |
CI = confidence interval; FACT-Lym = Functional Assessment of Cancer Therapy — Lymphoma; MCL = mantle cell lymphoma; OS = overall survival; PFS = progression-free survival; RCT = randomized controlled trial; TESAE = treatment-emergent serious adverse event.
Note: Study limitations (which refer to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias were considered when assessing the certainty of the evidence. All serious concerns in these domains that led to the rating down of the level of certainty are documented in the table footnotes.
aRated down 2 levels for very serious imprecision. According to the clinical experts consulted by the CDA-AMC review team, a 5% difference (50 per 1,000) between the venetoclax plus ibrutinib group and the placebo plus ibrutinib group in the probability of being alive could be considered clinically important (i.e., minimal important difference [MID]). The point estimate suggested little to no difference, while the upper and lower bounds of the 95% CI crossed the MID and the null (i.e., 0), respectively.
bRated down 1 level for serious imprecision. According to the clinical experts consulted by the CDA-AMC review team, a 7% (70 per 1,000) difference between the venetoclax plus ibrutinib group and the placebo plus ibrutinib group in the probability of being progression-free could be considered clinically important (i.e., MID). The point estimate suggested benefits, while the upper bound of the 95% CI crossed the MID.
cCertainty of evidence was not rated down as there were no serious concerns in risk of bias, indirectness, inconsistency, and imprecision.
dRated down 2 levels for serious risk of bias. Although the randomized phase of SYMPATICO adopted a double-blind study design, there was a risk of unblinding due to the high between-group imbalance in the occurrence of some adverse events such as diarrhea (64.9% versus 34.1%) and nausea (31.3% versus 16.7%). Moreover, there was a risk of bias due to data missing from a high percentage of patients. Rated down 2 levels for very serious imprecision given that the 95% CIs of the mean difference crossed the null threshold of 0.
eRated down 2 levels for imprecision. The 95% CI crossed the null, suggesting both benefit and harm.
Source: SYMPATICO Clinical Study Report27 and sponsor response to CDA-AMC request for additional information.22,28
Long-Term Extension Studies
No long-term extension studies were identified for this review.
Indirect Comparisons
No indirect evidence was identified for this review.
Studies Addressing Gaps in the Evidence from the Systematic Review
No studies addressing gaps in the pivotal and RCT evidence were identified for this review.
Conclusions
The randomized phase of the SYMPATICO trial, a phase III, double-blind RCT, assessed the efficacy and safety of venetoclax plus ibrutinib relative to placebo plus ibrutinib in patients with MCL who have received at least 1, but no more than 5, prior treatment regimens for MCL. The interim analysis of OS, based on OS data that were immature at the time of analysis, indicated that venetoclax plus ibrutinib may result in little to no difference in the probability of being alive at 48 or 60 months, compared to placebo plus ibrutinib. The certainty of the interim OS evidence was low, which may be addressed in the final OS analysis. Added clinical benefit was observed with venetoclax plus ibrutinib in the trial’s designated primary efficacy outcome — PFS per investigator assessment. Venetoclax plus ibrutinib, compared to placebo plus ibrutinib, likely results in a clinically meaningful improvement in the probability of being progression-free at 36 and 60 months, based on moderate- to high-certainty evidence. However, the possibility of overestimation in the PFS benefits could not be ruled out due to the informative censoring observed in the PFS sensitivity analysis, whereby patients censored might have been at a higher risk of having disease progression. Venetoclax plus ibrutinib appears to be overall safe, and the safety profile of venetoclax plus ibrutinib is consistent with the known harms for the individual components of the regimen.
Introduction
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of venetoclax, 10 mg, 50 mg, and 100 mg tablets, taken orally, in the treatment of adult patients with relapsed or refractory MCL.
Disease Background
Contents within this section have been informed by materials submitted by the sponsor and clinical expert input. The following have been summarized and validated by the review team.
MCL is a frequently aggressive subtype of B-cell NHL, accounting for approximately 5% to 7% of NHL cases.3,4 It primarily affects older adults, with an average age of diagnosis between 60 and 70 years, and occurs 4 times more frequently in men.3,9 The disease follows a progressive course, often involving the lymph nodes, bone marrow, spleen, and gastrointestinal tract.10 Patients typically present with symptoms such as painless lymphadenopathy, fatigue, night sweats, fever, or weight loss, which can significantly impact their HRQoL. MCL has an unfavourable prognosis, with a varying median OS of 2 to 10 years.2,10-15,29-31
In Canada, NHL is estimated to account for 11,700 new cases in 2024,5 with a 5-year prevalence of 32,915 cases in 2018.6 MCL represents a small subset of these cases, yet it remains a significant clinical challenge due to its frequently aggressive nature. Nearly all patients with MCL require systemic therapy, and the majority eventually experience relapsed or refractory disease.7,8
Diagnosis of MCL requires a comprehensive clinical evaluation, including a detailed patient history, physical examination, and specialized diagnostic testing. A biopsy of an affected lymph node or bone marrow sample is essential for confirming the presence of MCL.32 Histopathological examination typically reveals a monomorphic proliferation of small to medium lymphoid cells with irregular nuclear contours.33 The disease is definitively diagnosed through IHC, detecting cyclin D1 overexpression in 98% of cases, or by identifying the t(11;14)(q13;32) translocation through molecular or cytogenetic methods.33
Accurate classification of MCL is crucial for treatment planning. The 2022 International Consensus Classification and WHO classifications divide MCL into indolent and aggressive forms.34,35 Classical MCL is the more common, aggressive subtype, whereas leukemic non-nodal MCL follows a more indolent course. Prognostic risk stratification includes assessment of the following: blastoid or pleomorphic morphology, increased Ki-67 nuclear protein (e.g., > 30% to 50%), and the Mantle Cell Lymphoma International Prognostic Index-combined.36 Additionally, genetic testing, including fluorescence in situ hybridization (FISH) or next-generation sequencing, may be conducted to assess high-risk mutations such as TP53 deletions or mutations, which are present in approximately 11% of patients with MCL and are associated with poor outcomes.17,37-40 Diagnostic tests for MCL, including IHC and FISH, are widely available in Canada and are routinely used in clinical practice.2 Molecular testing is not widely available in the standard-of-care setting.
Standards of Therapy
Contents in this section have been informed by materials submitted by the sponsor and clinical expert input. The following have been summarized and validated by the review team.
According to the clinical experts consulted by the CDA-AMC review team, MCL is not curable with most therapies, and the goal of first-line treatment is to achieve remission, delay progression, and improve survival. The choice of first-line CIT is based on patient age, fitness, comorbidities, and institutional preferences. Younger patients (aged up to approximately 65) and medically fit patients with treatment-naive MCL are typically treated with intensive rituximab-based CIT (e.g., R-CHOP and R-DHAP, bendamustine-rituximab and cytarabine-rituximab, bendamustine-rituximab), followed by ASCT and maintenance therapy with rituximab for responding patients.16 Older or medically unfit patients with treatment-naive MCL are typically treated with lower-intensity CIT (e.g., bendamustine-rituximab) followed by rituximab maintenance.17
Most patients with MCL are not cured by first-line treatments, eventually experience disease progression, and require second-line treatments.18 For these patients with relapsed or refractory MCL, ibrutinib, a first-generation covalent BTKi, is a standard second-line treatment in Canada.8 Zanubrutinib and acalabrutinib, second-generation BTKis, have been approved by Health Canada for relapsed or refractory MCL.19,20 However, neither of them are currently publicly funded in Canada. According to the clinical experts consulted by the CDA-AMC review team, zanubrutinib and acalabrutinib may be available through special access programs in Canada. A small number of patients with relapsed or refractory MCL who are ineligible for BTKi due to existing cardiovascular risk may receive CIT or other nonfunded therapies.8
Furthermore, most patients with MCL are not cured by second-line treatment with ibrutinib and will receive third-line treatment, according to the clinical experts consulted by the CDA-AMC review team. CAR T-cell therapy with brexucabtagene autoleucel is the third-line standard of care in Canada for medically fit patients with relapsed or refractory MCL and who have been treated with 2 or more lines of prior systemic therapy, including a BTKi.21 According to the clinical experts consulted by the CDA-AMC review team, for patients unsuitable for CAR T-cell therapy (e.g., older or patients with comorbidities), alternative options include noncovalent BTKis such as pirtobrutinib, which is not yet funded in Canada but may be available through compassionate access programs; bortezomib- or lenalidomide-based therapies, which are not universally funded in Canada; CIT; venetoclax, which may be available through compassionate access programs; investigational treatments through clinical trials; or palliative or best supportive care. Allogeneic hematopoietic cell transplant is also an option for younger, medically fit patients.
Drug Under Review
Key characteristics of venetoclax are summarized in Table 3 with other treatments available for MCL in adult patients. Venetoclax has not been previously reviewed by CDA-AMC for MCL.
Venetoclax exerts its antitumour effects by selectively inhibiting BCL2, a protein that prevents apoptosis in malignant cells.1 BCL2 overexpression is a key driver of chemotherapy resistance in many hematologic cancers, including MCL, making it a critical therapeutic target. By binding to BCL2 and disrupting its interaction with proapoptotic proteins, venetoclax restores apoptotic signalling, leading to cell death.1
Venetoclax was approved by Health Canada on July 31, 2025, for use in combination with ibrutinib for adult patients with relapsed or refractory MCL. Venetoclax is an oral BCL2 inhibitor available in 10 mg, 50 mg, and 100 mg film-coated tablets.1 The dosing regimen begins with a starting dose of 20 mg once daily for 7 days, followed by a weekly ramp-up schedule over 5 weeks to a recommended daily dose of 400 mg, i.e., 20 mg (2 × 10 mg) in week 1, 50 mg (1 × 50 mg) in week 2, 100 mg (1 × 100 mg) in week 3, 200 mg (2 × 100 mg) in week 4, and 400 mg (4 × 100 mg) in week 5.1 This gradual dose escalation helps reduce tumour burden and mitigate the risk of TLS.1 When used for MCL, venetoclax is initiated on day 1 alongside ibrutinib 560 mg once daily.1 After the 5-week ramp-up phase, venetoclax is continued at 400 mg daily with ibrutinib for an additional 23 months, followed by ibrutinib monotherapy until disease progression or unacceptable toxicity.1
Sensitivity to venetoclax is enhanced when combined with agents targeting complementary survival pathways, such as BTKis.41-45 BTKi, given as a single drug, is the current standard option for patients with relapsed or refractory MCL.2 Ibrutinib, the only BTKi currently reimbursed for relapsed or refractory MCL across CDA-AMC-participating drug plans, is used as the primary comparator in the pharmacoeconomic analysis.2
Table 3: Key Characteristics of Venetoclax Plus Ibrutinib and Ibrutinib Alone
Characteristic | Venetoclax plus ibrutinib | Ibrutinib alone |
|---|---|---|
Mechanism of action | Venetoclax is a selective and orally bioavailable small-molecule inhibitor of BCL2, a protein that inhibits cells from programmed cell death (apoptosis). Overexpression of BCL2 in various hematologic malignancies contributes to cancer cell survival. The dual-acting combination of ibrutinib and venetoclax works synergistically through distinct and complementary modes of action, targeting distinct cell compartments. | A small-molecule targeted BTKi. BTK is a signalling molecule of the B-cell antigen receptor pathway, which is implicated in the pathogenesis of several B-cell malignancies. Ibrutinib forms a covalent bond with a cysteine residue (Cys-481) in the BTK active site, leading to inhibition of BTK. |
Indication | In combination with ibrutinib, venetoclax is indicated for the treatment of adult patients with relapsed or refractory MCL. | For the treatment of adult patients with relapsed or refractory MCLa |
Route of administration | Oral for both venetoclax and ibrutinib | Oral |
Recommended dose | Venetoclax Week 1: 20 mg once daily Week 2: 50 mg once daily Week 3: 100 mg once daily Week 4: 200 mg once daily Week 5 onward: 400 mg once daily Maximum duration: 24 months Ibrutinib 560 mg once daily administered in combination with venetoclax for a maximum duration of 24 months and then continued until disease progression or until it is no longer tolerated by the patient. | The recommended dosage of ibrutinib for MCL is 560 mg once daily until disease progression or it is no longer tolerated by the patient. |
Serious adverse effects or safety issues | Venetoclax
Ibrutinib Second primary malignancies, cardiac toxicity, cerebrovascular accidents, TLS, cytopenia, lymphocytosis, leukostasis, hemorrhage, hepatic impairment, infections, teratogenic risk. |
|
Other | Notice of Compliance issued on July 31, 2025 | NA |
BTK = Bruton’s tyrosine kinase; BTKi = Bruton’s tyrosine kinase inhibitor; MCL = mantle cell lymphoma; NA = not applicable; TLS = tumour lysis syndrome.
aHealth Canada–approved indication.
Source: Product monograph for Imbruvica46 and draft product monograph for Venclexta.1
Perspectives of Patients, Clinicians, and Drug Programs
The full patient and clinician group submissions received are available in the consolidated patient and clinician group input document for this review on the project website.
Patient Group Input
This section was prepared by the review team based on the input provided by patient groups.
CDA-AMC received 1 patient group input for this review from Lymphoma Canada, a national charity dedicated to empowering patients and the lymphoma community through education, support, advocacy, and research, while collaborating with stakeholders to improve early detection, treatments, and outcomes for patients with lymphoma. Lymphoma Canada collected patient input through an anonymous online survey between January and March 2025, gathering 82 responses from patients with MCL, with 5 patients who had received combination therapy of venetoclax and ibrutinib. Three of these patients were from Canada. The majority of all survey respondents lived in Canada (74%), were aged between 65 to 74 years (36%), and had received diagnoses 3 to 5 years ago (27%), or 9 to 10 years ago or more (24%).
The survey respondents reported significant impacts of MCL on their quality of life, with common symptoms at diagnosis including fatigue (33%), enlarged lymph nodes (27%), and abdominal issues (22%). Psychosocial challenges were prevalent, with 72% experiencing stress, 70% anxiety, and 64% fear of progression. Approximately 28% of respondents reported fatigue, and 15% reported neutropenia as major concerns. Mental health challenges such as fear of relapse (74%) and difficulty sleeping (38%) were also significant. Aspects of daily life were impacted, such as the ability to travel (38%), work (28%), and engage in social activities (20%), with many patients highlighting the challenges of managing a compromised immune system, isolation, and physical limitations due to treatment side effects.
Regarding current treatments for MCL, 64% of patients required immediate treatment upon diagnosis, while 36% were placed on “watch and wait.” Most patients received 1 (56%) or more than 3 (22%) lines of treatment, with common first-line therapies including:
bendamustine-rituximab (35%)
R-CHOP (25%)
R-DHAP or a combination of carmustine or lomustine, etoposide, cytarabine, and melphalan (BEAM) (12%).
In second-line therapy or beyond, 29% received stem cell transplants and 15% received BTKis. While 78% were satisfied with first-line treatments, satisfaction dropped for second-line (27%) and third-line (13%) options, indicating a need for more alternatives. Side effects such as fatigue, nausea, and joint pain were common and severely impacted patients’ quality of life. Difficulties accessing treatments were reported by 10% of patients, with reasons including financial burdens such as travel and drug costs. These difficulties led to patient frustration over treatment availability and the financial implications of their care. Patients expressed a desire for more treatment options, especially for second- and third-line therapies.
Patients with MCL surveyed by Lymphoma Canada highlighted key outcomes of new treatments, including longer disease remission, survival, quality of life, and symptom control. A majority (91%) were willing to tolerate mild, short-term side effects for better options, and 76% valued having treatment choices based on side effects and outcomes. More than half considered the mode of administration (e.g., oral versus IV) important for their treatment. Most patients (87%) believed more therapy options were needed, emphasizing the importance of targeted therapies and improved treatment experiences.
Five patients responding to the survey had received the combination of venetoclax and ibrutinib in the second-line setting, with 1 newly in remission, 3 in remission for 1 to 2 years, and 1 experiencing relapse after treatment. Reported side effects included diarrhea (3 patients), neutropenia (2 patients), fatigue (2 patients), joint pain (1 patient), and constipation (1 patient). Psychological impacts included anxiety (3 patients) and fear of progression (2 patients). Three patients rated the therapy as very good, while 2 rated it satisfactory, but all 5 would recommend it to other patients with MCL. One patient emphasized the benefits of receiving oral treatment, avoiding hospitalization, and experiencing fewer side effects compared to traditional chemotherapy.
Clinician Input
Input From Clinical Experts Consulted for This Review
All CDA-AMC review teams include at least 1 clinical specialist with expertise regarding the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). The following input was provided by 3 clinical specialists with expertise in the diagnosis and management of MCL.
Unmet Needs
The clinical experts noted that the goal of first-line treatment for MCL is to achieve remission, delay progression, and improve survival. Treatments for patients with relapsed or refractory MCL are rarely curative, and most patients eventually experience disease progression.
The clinical experts noted that ibrutinib is a standard second-line treatment for patients with MCL that has relapsed or is refractory to first-line treatments. It is also the most commonly used, publicly funded second-line treatment for patients with MCL in Canada. The clinical experts indicated that, in most patients who are responding to ibrutinib, MCL will progress eventually, and there are few effective and well-tolerated third-line treatments available in Canada. Also, ibrutinib, although well tolerated by many patients, has potential cardiovascular and other toxicities that make it unsuitable for some patients or that can result in premature treatment discontinuation. Therefore, there is an unmet need for treatments that are more effective, have long-lasting benefits, and are well tolerated for patients with relapsed or refractory MCL in the second-line treatment setting.
Place in Therapy
All clinical experts agreed that venetoclax plus ibrutinib should become a standard second-line treatment for patients with relapsed or refractory MCL and that ibrutinib and venetoclax may change the current treatment paradigm, replacing ibrutinib monotherapy as the standard second-line treatment for most patients with relapsed or refractory MCL. The clinical experts indicated that ibrutinib monotherapy could remain an alternative treatment option in the second-line treatment setting for some patients, e.g., those who have significant renal dysfunction, those who have difficulty coming to hospital for the ramp-up dosing schedule of venetoclax, or those who choose not to receive venetoclax plus ibrutinib combination therapy.
Patient Population
The clinical experts noted that patients who are best suited for venetoclax plus ibrutinib are those who have relapsed or refractory MCL and have received at least 1 prior line of therapy. These patients would be identified by their treating hematologist or oncologist, and no diagnostic test is required. They noted that patients with CNS lymphoma, which is rare, might benefit from venetoclax plus ibrutinib in the real-world setting, given the ability of these drugs to penetrate the blood-brain barrier.
The clinical experts noted that patients with disease refractory to BTKis or BCL2 inhibitors may not be suitable for venetoclax plus ibrutinib. They also noted that there is an increase in the use of BTKis in the first-line treatment setting via compassionate access programs in Canada, although they are not currently funded as first-line therapy in Canada. According to the clinical experts, patients previously exposed to a BTKi or BCL2 inhibitor were excluded from the enrolment in the pivotal SYMPATICO trial. However, in real-world practice, it would be reasonable to re-treat a patient with venetoclax plus ibrutinib if they have achieved a reasonably durable remission (e.g., lasting > 6 to 12 months off treatment) and did not experience disease progression while on therapy.
The clinical experts noted that patients may not be suitable candidates for venetoclax plus ibrutinib in some rare occasions, such as patients who are unable or unwilling to perform bloodwork for TLS monitoring; patients with serious active infections, severe liver dysfunction, or inability to swallow or absorb oral medications; patients require ongoing treatment with moderate or strong CYP3A inhibitors or inducers; and patients with relative contraindications to ibrutinib (e.g., uncontrolled cardiovascular disease).
Assessing the Response Treatment
The clinical experts stated that assessing response to venetoclax plus ibrutinib, which may vary between physicians and institutions, generally includes a radiographic assessment (e.g., PET or CT) after 2 to 3 months of treatment. They noted that patients with circulating lymphoma cells and/or bone marrow involvement may have a complete blood count with or without bone marrow sampling as part of response assessment. Patients who demonstrate a response to venetoclax plus ibrutinib would continue for up to 2 years of treatment with venetoclax plus ibrutinib, followed by ibrutinib monotherapy until disease progression or unacceptable intolerance. Subsequent imaging would depend on the depth of initial response and the discretion of the treating physician.
Discontinuing Treatment
The clinical experts indicated that venetoclax should be given for a fixed-duration course of up to 2 years, while ibrutinib should be continued indefinitely. Either drug may be discontinued earlier for patients who experience disease progression or develop refractory disease while on treatment or for those who experience unacceptable toxicities. The clinical experts consulted by the CDA-AMC review team noted that, although drugs are normally discontinued due to disease progression, in real-world practice, they may be continued while planning for the next line of therapy. They further stated that, when 1 drug is discontinued due to intolerance, it does not necessarily mean the other drug should also be discontinued at the same time, because ibrutinib and venetoclax have different side effect profiles. The decision to discontinue either or both drugs should be made by the treating physician.
Prescribing Considerations
According to the clinical experts, venetoclax plus ibrutinib should be prescribed by a hematologist or oncologist who is familiar with the management of MCL and has knowledge regarding the safety, efficacy, and monitoring requirements of each drug, particularly regarding the TLS risk of venetoclax and cardiovascular toxicities of ibrutinib. They noted that TLS monitoring required during the venetoclax ramp-up may briefly require hospitalization, but most hematologists in Canada are well equipped at managing this. The clinical experts indicated that venetoclax plus ibrutinib (including the ramp-up phase of venetoclax) can be administered in the outpatient setting at tertiary care and community hospitals in urban and rural locations.
Clinician Group Input
This section was prepared by the review team based on the input provided by clinician groups.
CDA-AMC received input from 2 clinician groups, OH-CCO Hem DAC and Lymphoma Canada Physician Group. OH-CCO’s Drug Advisory Committees support the Provincial Drug Reimbursement Programs and the Systemic Treatment Program through timely, evidence-based recommendations on drug-related issues. Lymphoma Canada Physician Group is a national organization dedicated to research, education, and raising awareness. OH-CCO Hem DAC provided input via teleconference among 7 clinicians. Lymphoma Canada Physician Group reviewed clinical trials, provincial guidelines, and a review on relapsed or refractory MCL by 5 experts.
According to the clinician groups, the goal of therapy for patients with MCL is long-term PFS and OS, resolution of lymphoma-related symptoms, and improvement in quality of life. The clinician groups noted that treatment for patients relapsed or refractory MCL includes BTKis (ibrutinib, acalabrutinib, zanubrutinib, and pirtobrutinib), CIT, and bortezomib-based options. Brexucabtagene autoleucel is available as a third-line therapy. First-line treatment depends on patient characteristics and typically involves CIT, often followed by high-dose therapy and ASCT. The groups highlighted that, while BTKis are standard second-line therapy, their effectiveness declines, and relapse after BTKi remains a major unmet need.
Both groups highlighted significant treatment gaps for relapsed or refractory MCL, as no curative therapies exist. Current treatments offer limited survival benefits, with poor outcomes after BTKi failure (average survival is under 6 months). The Lymphoma Canada Physician Group noted that, while CAR T-cell therapy is now funded in Canada, access remains restricted to specialized centres and selected patients. Most patients with MCL that relapses do not qualify for CAR T-cell therapy, leaving palliative options as the only alternative. There is a critical need for novel, well-tolerated treatment combinations to improve survival, delay disease progression, and enhance quality of life for the majority of patients.
The clinician groups noted that the combination of venetoclax and ibrutinib is suitable as a second-line treatment option for relapsed or refractory MCL, as the pivotal trial results showed its benefit in improving PFS and delaying the need for third-line CAR T-cell therapy. According to the clinician groups, suitable candidates include patients eligible for BTKi treatment, particularly those who do not have BTKi-refractory disease. Regular assessments, including imaging and clinical evaluations, are required to monitor response. Discontinuation is recommended in cases of disease progression or severe toxicity, after dose reductions or substitution of ibrutinib with zanubrutinib are tried.
The clinician groups noted that, as a fully oral therapy, the combination of venetoclax and ibrutinib is suited for outpatient care and accessible in both community and academic settings. It should be prescribed by a hematologist managing MCL. The groups highlighted that additional laboratory monitoring for venetoclax-related risk of TLS is necessary. Also, cardiac evaluation may be needed due to ibrutinib’s risks.
Drug Program Input
The drug programs provide input on each drug being reviewed through the reimbursement review processes by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by for this review are summarized in Table 4.
Table 4: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Relevant comparators | |
For patients with relapsed or refractory MCL, treatment with a BTKi is the current Canadian standard. Ibrutinib is the only BTKi publicly reimbursed in Canada for patients with MCL who have received at least 1 prior therapy. Although acalabrutinib and zanubrutinib are both approved by Health Canada for relapsed or refractory MCL,19,20 acalabrutinib has not been reviewed by CDA-AMC and zanubrutinib received a negative recommendation due to the uncertainty associated with the 2 phase II single-arm trials assessed.47 The public reimbursement of ibrutinib for relapsed or refractory MCL was supported by the results of the phase III randomized controlled trial MCL-3001.48 The SYMPATICO trial compared venetoclax plus ibrutinib with ibrutinib in patients with MCL after 1 to 5 prior lines of therapy, including 1 prior rituximab- or anti-CD20–containing regimen. Bendamustine plus rituximab in relapsed or refractory MCL is also a funded option in some jurisdictions. | This is a comment from the drug plans to inform pERC deliberations. |
Considerations for prescribing of therapy | |
Venetoclax 5-week ramp-up beginning on day 1, which includes 20 mg, 50 mg, 100 mg, 200 mg, and 400 mg once daily for weeks 1 to 5, respectively. After completing the ramp-up, venetoclax 400 mg once daily is continued until disease progression or unacceptable toxicity for a total treatment duration of 24 months. Ibrutinib 560 mg once daily was taken in combination with venetoclax for the 24-month period, with ibrutinib alone 560 mg once daily continued beyond 24 months until disease progression or unacceptable toxicity. | This is a comment from the drug plans to inform pERC deliberations. |
Inpatient administration may be required during the first few ramp-up doses for patients at high risk for TLS. | This is a comment from the drug plans to inform pERC deliberations. |
If 1 study drug had to be discontinued, the participant was allowed to continue in the trial provided they are still on the other study drug. Question: If a patient experiences intolerance to ibrutinib, can treatments with venetoclax monotherapy be continued? | The clinical experts indicated that, when 1 drug is discontinued due to intolerance, it does not necessarily mean the other drug should also be discontinued at the same time, because ibrutinib and venetoclax have different toxicity profiles. The clinical experts noted that the decision to discontinue either or both drugs should be made at the clinician’s discretion. |
Generalizability | |
Patients with ECOG PS of 0 to 2 were included in the trial. Question: Can patients with ECOG PS of 3 be considered eligible? | Two clinical experts consulted noted that selected patients with ECOG PS 3 can be considered eligible for venetoclax plus ibrutinib, while the third clinical expert indicated that patients with ECOG PS 3 may benefit more from therapies with a palliative intent rather than venetoclax plus ibrutinib. The 2 clinical experts who supported the use of venetoclax plus ibrutinib in selected patients with ECOG PS 3 noted that worse performance status does not necessarily mean the patient is ineligible for venetoclax plus ibrutinib, and the decision on eligibility should be made on a case-by-case basis. For example, some patients have poor ECOG PS due to disease-related symptoms, which may improve with treatment. |
Question: On a time-limited basis, should patients currently on ibrutinib or other alternative treatments be eligible to switch to venetoclax plus ibrutinib? | The clinical experts indicated that, if a patient is currently stable and responding well on a treatment (e.g., ibrutinib or other alternative treatments), they would not switch to venetoclax plus ibrutinib. If a patient has disease progression while on treatment with ibrutinib, the clinical experts noted that they would not switch patients to venetoclax plus ibrutinib or any other covalent BTKi-containing regimen in the next line of therapy. In this case, the patient’s disease has already been refractory to ibrutinib, and no benefits would be expected from re-treatment with ibrutinib or similar covalent BTKis (e.g., acalabrutinib, zanubrutinib). The clinical experts indicated that they might switch patients who had just started ibrutinib or alternative treatments. |
Funding algorithm | |
There are upcoming reviews for MCL, so an algorithm will be helpful:
| This is a comment from the drug plans to inform pERC deliberations. |
Care provision issues | |
Venetoclax is available as 10 mg, 50 mg, and 100 mg tablets. The product monograph indicates it can be stored between 2°C and 30°C. | This is a comment from the drug plans to inform pERC deliberations. |
Venetoclax has the potential for drug-drug, drug-food, and drug-herb interactions. | This is a comment from the drug plans to inform pERC deliberations. |
System and economic issues | |
The budget impact is uncertain, given the upcoming reviews for BTKi-based regimens in first-line therapy, which may lessen the uptake for venetoclax plus ibrutinib. However, this is offset by the combination use of venetoclax plus ibrutinib (up to 2 years) followed by the use of ibrutinib alone until disease progression or unacceptable toxicity. | This is a comment from the drug plans to inform pERC deliberations. |
BTKi = Bruton’s tyrosine kinase inhibitor; CDA-AMC = Canada’s Drug Agency; ECOG PS = Eastern Cooperative Oncology Group performance status; MCL = mantle cell lymphoma; pERC = pan-Canadian Oncology Drug Review Expert Review Committee; TLS = tumour lysis syndrome.
Clinical Evidence
The objective of this clinical review report is to review and critically appraise the clinical evidence submitted by the sponsor on the beneficial and harmful effects of venetoclax, 10 mg, 50 mg, and 100 mg tablets, taken orally, in the treatment of adult patients with relapsed or refractory MCL. The focus will be placed on comparing venetoclax to relevant comparators and identifying gaps in the current evidence.
A summary of the clinical evidence included by the sponsor in the review of venetoclax is presented in 1 section with our critical appraisal of the evidence at the end of each section. The first section, the systematic review, includes pivotal studies and RCTs that were selected according to the sponsor’s systematic review protocol. Our assessment of the certainty of the evidence in this first section using the GRADE approach follows the critical appraisal of the evidence. The sponsor did not submit any long-term extension studies, indirect evidence from the sponsor, or additional studies to address important gaps in the systematic review evidence.
Included Studies
Clinical evidence from the following is included in the review and appraised in this document:
One phase III, RCT (SYMPATICO) identified in the systematic review.
Systematic Review
Contents within this section have been informed by materials submitted by the sponsor. The following have been summarized and validated by the review team.
Description of Studies
One study (SYMPATICO) was identified from the sponsor-submitted systematic literature review. The SYMPATICO trial consisted of an open-label safety run-in phase, a double-blind randomized phase, and an open-label treatment-naive cohort. Of note, according to the sponsor, the primary focus for this review is the randomized phase of SYMPATICO. All information presented in the review is therefore for the double-blind randomized phase, unless otherwise stated.
The characteristics of the randomized phase of SYMPATICO are summarized in Table 5. The randomized phase of SYMPATICO is a phase III, multicentre, double-blind RCT, investigating the efficacy and safety of venetoclax plus ibrutinib in patients with MCL who have received at least 1, but no more than 5, prior treatment regimens for MCL, including at least 1 prior rituximab- or anti-CD20–containing regimen. A total of 267 patients (including ██ patients in Canada) were randomized, using an interactive response technology system, to the venetoclax plus ibrutinib group (n = 134) and the placebo plus ibrutinib group (n = 133). The randomization was stratified by the number of prior lines of therapy, ECOG PS, and TLS risk category. Patients, investigators, and the sponsor’s study team members remained blinded to the treatment assignment. The primary objective of the randomized phase of SYMPATICO was to assess the efficacy of venetoclax plus ibrutinib, compared to placebo plus ibrutinib, in patients with relapsed or refractory MCL, as measured by PFS. Secondary end points included OS, complete response (CR) rate, overall response rate (ORR), measurable residual disease (MRD)–negative remission rate, and harms.
Table 5: Details of Studies Included in the Systematic Review
Detail | SYMPATICO |
|---|---|
Designs and populations | |
Study design | Phase III, multinational, randomized, double-blind study that consists of:
Different patients participated in each cohort (i.e., patients in the safety run-in were not the same patients as in the randomized phase). According to the sponsor, the primary focus is the double-blind randomized phase. Unless otherwise stated, all details provided in this table are for this phase. |
Locations | The trial was performed at 94 sites in Poland, Italy, Czech Republic, France, Spain, UK, Hungary, Ukraine, Netherlands, Belgium, Germany, Turkey, Greece, US, Canada, Australia, and South Korea. There were ██ patients living in Canada, randomized across 6 sites. |
Patient enrolment dates | Between April 26, 2018, and August 28, 2019, patients were enrolled and randomized. |
Randomized (N) | Among 267 randomized:
|
Key inclusion criteria |
|
Key exclusion criteria |
|
Drugs | |
Intervention | Venetoclax plus ibrutinib
|
Comparator(s) | Placebo plus ibrutinib
|
Study duration (randomization phase) | |
Screening phase | Screening procedures were performed within 28 days of the first dose of ibrutinib and venetoclax or placebo. |
Treatment phase | From the first dose of ibrutinib and venetoclax or placebo until the end-of-treatment visit (due to disease progression or treatment discontinuation, whichever occurs first). Treatment discontinuation did not include discontinuation of placebo or venetoclax following a full 24-month course. |
Response follow-up | Patients who discontinued treatment for reasons other than disease progression entered response follow-up. Following disease progression, these patients entered long-term follow-up. |
Long-term follow-up | Patients who progressed (and had not withdrawn consent) entered long-term follow-up until death, patient withdrawal, or study termination by the sponsor, whichever occurred first. |
Outcomes | |
Primary end point | PFS |
Secondary and exploratory end points | Secondary:
Exploratory:
|
Publication status | |
Publications | Publication for the safety run-in Wang et al. (2021)49 Publication for the randomized phase (identified in systematic review) Wang et al. (2025)50 Key abstracts/presentations Wang et al. (2023)51 Wang et al. (2024)52 Clinicaltrials.gov identifier NCT03112174 |
AE = adverse event; BTKi = Bruton’s tyrosine kinase inhibitor; CNS = central nervous system; CR = complete response; DOR = duration of response; ECOG PS = Eastern Cooperative Oncology Group performance status; FACT-Lym = Functional Assessment of Cancer Therapy — Lymphoma; MCL = mantle cell lymphoma; MRD = measurable residual disease; ORR = overall response rate; OS = overall survival; PFS = progression-free survival; PR = partial response; TTNT = time to next treatment.
Source: SYMPATICO Clinical Study Report27 and SYMPATICO Clinical Study Protocol Amendment 4.53 Details included in the table are from the sponsor’s Summary of Clinical Evidence.2
Populations
Inclusion and Exclusion Criteria
The randomized phase of SYMPATICO included adult patients (≥ 18 years) with pathologically confirmed MCL who had received 1 to 5 prior therapies for MCL (including at least 1 prior rituximab- anti-CD20–containing regimen), failed to achieve at least partial response (PR), with or documented disease progression after the most recent treatment regimen, and had an ECOG PS of 0 to 2. Patients with a history or current evidence of CNS lymphoma or who had received anticancer therapy, including chemotherapy, radiotherapy, small-molecule, and investigational agents 21 days before the start of intervention were excluded.
Interventions
Venetoclax Plus Ibrutinib
Venetoclax was taken orally according to the 5-week ramp-up dosing schedule (i.e., week 1: 20 mg once daily; week 2: 50 mg once daily; week 3: 100 mg once daily; week 4: 200 mg once daily; week 5: 400 mg once daily). After completing the ramp-up phase, patients continued on venetoclax at a dosage of 400 mg once daily for an additional 23 months (a total duration of combination treatment for 24 months).
Ibrutinib was given at a dosage of 560 mg once daily, starting from day 1 until disease progression or unacceptable toxicity.
Placebo Plus Ibrutinib
Patients received placebo once daily for 24 months, matched to the dosing schedule (including the 5-week ramp-up) for venetoclax in the venetoclax plus ibrutinib group.
Ibrutinib 560 mg once daily was taken in combination with placebo for the 24-month period, with ibrutinib 560 mg once daily given as a single drug continued beyond 24 months until disease progression or unacceptable toxicity.
Outcomes
A list of efficacy end points assessed in this clinical review report is provided in Table 6, followed by descriptions of the outcome measures. Summarized end points are based on outcomes included in the sponsor’s Summary of Clinical Evidence as well as any outcomes identified as important to this review according to the clinical expert(s) consulted for this review and input from patient and clinician groups and public drug plans. Using the same considerations, we selected end points that were considered to be most relevant to inform expert committee deliberations and finalized this list of end points in consultation with members of the expert committee. All summarized efficacy end points were assessed using GRADE. Selected harms outcomes considered important for informing expert committee deliberations were also assessed using GRADE.
Table 6: Outcomes Summarized From the Randomized Phase of SYMPATICO
Outcome measure | Time point | SYMPATICO |
|---|---|---|
OSa | Months 12, 24, 36, 48, 60 | Secondaryb |
PFS per investigator assessment | Months 12, 24, 36, 48, 60 | Primaryb |
FACT-Lym total score | Months 24, 60 | Secondary |
Lymphoma-specific subscale of FACT-Lym | Months 24, 60 | Secondary |
FACT-Lym = Functional Assessment of Cancer Therapy — Lymphoma; OS = overall survival; PFS = progression-free survival.
aOnly the interim analysis of OS was available and assessed by the CDA-AMC review team.
bStatistical testing was adjusted for multiple comparisons (e.g., hierarchical testing).
Source: SYMPATICO Statistical Analysis Plan version 2,54 SYMPATICO Clinical Study Protocol Amendment 4,53 and sponsor response to CDA-AMC request for additional information.22
Descriptions of efficacy and safety outcomes presented in the randomized phase of SYMPATICO and appraised in the clinical review are as follows:53,54
Efficacy Outcomes
Overall Survival
OS was defined as the time from the date of randomization until death due to any cause. Patients without an OS event were censored at the date last known alive.
PFS Per Investigator Assessment
PFS was defined as time from the date of randomization to the date of the first documentation of progressive disease or the date of death due to any cause, whichever occurred first, regardless of study drug discontinuation or use of subsequent anticancer treatment. Of note, posttreatment stem cell transplant, CAR T-cell therapy, and other cellular therapies were not considered subsequent anticancer treatment for patients responding to treatment (CR or PR). Lugano Classification Criteria were used to determine disease progression.55 If patients did not have a baseline disease assessment or any adequate postbaseline disease assessment, they were censored at the date of randomization.
Health-Related Quality of Life
The summary of measurement properties of FACT-Lym is shown in Table 7.
Table 7: Summary of Outcome Measures and Their Measurement Properties
Outcome measure | Type | Conclusions about measurement properties | MID |
|---|---|---|---|
FACT-Lym | The total FACT-Lym consists of the Functional Assessment of Cancer Therapy — General (FACT-G) and a lymphoma-specific additional concerns subscale (Lym), with a 7-day recall period. Responses to all items are rated on a 5-point Likert scale ranging from 0 (“not at all”) to 4 (“very much.”)56 The lymphoma-specific subscale includes 15 items, with scores ranging from 0 to 60. Higher scores indicate better HRQoL.56 | The FACT-Lym was originally developed to assess functional status and well-being of patients with NHL.57,58 Reliability and validity have been assessed in a population of 84 patients with NHL.56 Validity: In the patients with NHL, the FACT-Lym subscale demonstrated concurrent validity, with significant correlations to SF-36 physical (r = 0.62) and mental (r = 0.48) summary scores.56 Reliability: In the patients with NHL, the FACT-Lym subscale exhibited good internal consistency across 3 time points (Cronbach alpha = 0.79, 0.85, 0.84 at baseline, 3 to 7 days, and 8 to 12 weeks) and strong test-retest reliability (r = 0.84).56 Responsiveness: In the patients with NHL, responsiveness exceeded established FACT subscale scores in detecting changes based on ECOG PS and treatment status. The subscale distinguished effectively between patients’ retrospective ratings of change (better, unchanged, worse; P < 0.001).56 The construct validity of the lymphoma subscale was tested in a single-arm, open-label study enrolling 60 patients with relapsed or refractory MCL. The mean lymphoma subscale score showed a significant decline from baseline to the 30-day assessment (−4.8 points, P < 0.05). Additionally, changes in scores from baseline to discontinuation significantly differed between patients with improved or stable ECOG PS (n = 20) and those with worsened ECOG PS (n = 16), with the latter experiencing significantly greater declines in scores.59 | Carter et al. reported a minimal important change score for the Lym subscale in a population with relapsed or refractory MCL ranging from approximately 2.9 to 5.4 points, based on within-group changes, using both distribution- and anchor-based methods.59 For the current review, the sponsor selected a 5-point change in the Lym subscale as an estimate of clinically meaningful deterioration in lymphoma symptoms.2,27 |
ECOG PS = Eastern Cooperative Oncology Group performance status; FACT-G = Functional Assessment of Cancer Therapy — General; FACT-Lym = Functional Assessment of Cancer Therapy — Lymphoma; HRQoL = health-related quality of life; MCL = mantle cell lymphoma; MID = minimal important difference; NHL = non-Hodgkin lymphoma; SF-36 = Short Form (36) Health Survey.
Harms Outcomes
The harms outcomes assessed in the review report included AEs, TESAEs, withdrawals due to AEs, mortality, and notable harms. Harms events were coded in accordance with the Medical Dictionary for Regulatory Activities 24.1. Severity of harms events were rated by the investigator according to the National Cancer Institute’s Common Terminology Criteria for Adverse Events version 4.03. The treatment-emergent period was defined as the period from the date of the first dose of study treatment up to 30 days after the date of the last dose of study treatment or the day before initiation of subsequent anticancer treatment, whichever came first. TEAEs were events that occurred or worsened during the treatment-emergent period or that were related to the study treatment.
Statistical Analysis
Sample Size and Power Calculation
In the randomization phase of SYMPATICO, sample size was powered based on the primary end point of PFS. Approximately 260 patients were planned to be randomized at a 1:1 ratio to the venetoclax plus ibrutinib group and the placebo plus ibrutinib group. The calculations were based on the following assumptions:
The target HR was 0.61, which corresponds to an improvement of 9 months in median PFS from 14 months to 23 months for the venetoclax plus ibrutinib group, compared to the placebo plus ibrutinib group.
A total of 134 PFS events would provide approximately 80% power at a 1-sided significance level of 0.025 for the study. No interim analysis was planned for PFS.
Assuming an enrolment rate of approximately 10 to 11 patients per month, enrolment was projected to be completed approximately 21 months after the enrolment of the first patient. The actual length of the study and the time to the primary analysis were dependent on the actual enrolment rate and the number of events.
Sample size and power calculation for the interim and final OS analyses were as follows:
The target HR was 0.65, which corresponds to an improvement of about 16 months in median OS from 30 months to 46.2 months for the venetoclax plus ibrutinib group, compared to the placebo plus ibrutinib group.
A total of 155 OS events would provide about 76% power at a 1-sided significance level of 0.025, adjusting for 1 interim analysis based on group sequential design with Lan-DeMets spending function with O’Brien-Fleming boundary.
It was anticipated that 112 and 155 OS events would be observed at the interim analysis (at about 40 months, corresponding to the timing of the primary PFS analysis) and at the final analysis (at about 57 months), respectively.
The calculation for OS was based on a log-rank test.
To address the impact of COVID-19 on the effect size (HR), the researchers planned to conduct the primary analysis after 150 PFS events occurred during the randomization phase. At the time of the database lock date (July 5, 2023), the actual number of investigator-assessed PFS events was ███.
At the time of the primary PFS analysis, an interim analysis for OS was performed, with a prespecified 2-sided alpha of 0.001. To maintain a 2-sided overall significance level of 0.05 for OS, the significance level of the OS final analysis has been adjusted for the OS interim analysis based on Haybittle-Peto boundary (i.e., 2-sided alpha of 0.001). The final OS analysis is planned after the last patient has been followed for at least 5 years or approximately 170 OS events are observed, whichever occurs first. ██ ███ ██████████████ ████████ ██ ███████ ██ █████ ███ ███████ ███ ███████ █████████ ████ █████ ██ ██ ████ ██ ██████ ██████████ ██ █████ █████ ████ ███ ███████ ██ █████ ███ ███ ██████ ██ ███████████
Statistical Testing
Details of the statistical analysis of efficacy end points in the randomization phase of SYMPATICO are presented in Table 8.
In the primary analysis of the primary end point (i.e., PFS per investigator assessment), hierarchical testing and censoring rules for PFS followed the global rules (i.e., patients were censored at the last nonprogressive disease assessment [i.e., CR, PR, and stable disease]). The 1-sided type I family-wise error rate was controlled at 0.025 by a closed testing procedure for testing PFS and some secondary end points, including CR rate per investigator assessment, time to next treatment (TTNT), OS, and ORR per investigator assessment. These secondary end points were tested when PFS reached statistical significance (1-sided 0.025) and were ranked and tested at a 1-sided statistical significance of 0.025 sequentially in the following hierarchical order: CR rate per investigator assessment, TTNT, OS, and ORR per investigator assessment. To maintain a 2-sided overall significance level of 0.05 for OS, the significance boundary of the OS interim analysis was 2-sided alpha of 0.001 based on the Haybittle-Peto boundary.
Of note, in 1 of the sensitivity analyses of PFS, the FDA rules were followed for hierarchical testing and censoring. Based on the FDA rules, the hierarchical order for secondary end points was CR rate per investigator assessment, OS, TTNT, and ORR per investigator assessment. In addition to the global censoring rule, 2 additional censoring rules were adopted for the FDA censoring rules, in which patients were censored when subsequent anticancer therapy was used before or without a PFS event or when 2 or more consecutive response assessments were missing before a PFS event.
For FACT-Lym total score and the lymphoma-specific subscale of FACT-Lym score, summary statistics were provided, and no statistical model or adjustment factors were considered.28
Table 8: Statistical Analysis of Efficacy End Points in the Randomized Phase of SYMPATICO
End point | Statistical model | Adjustment factors | Handling of missing data | Sensitivity analyses |
|---|---|---|---|---|
OS |
|
| Patients without an OS event were censored at the date last known alive. |
|
PFS per investigator assessment |
|
| If patients did not have a baseline disease assessment or any adequate postbaseline disease assessment, they were censored at the date of randomization. |
|
CI = confidence interval; HR = hazard ratio; IRC = independent review committee; KM = Kaplan-Meier; OS = overall survival; PFS = progression-free survival; TLS = tumour lysis syndrome
Source: SYMPATICO Statistical Analysis Plan version 254 and SYMPATICO Clinical Study Protocol Amendment 4.53 Details included in the table are from the sponsor’s Summary of Clinical Evidence.2
Analysis Populations
The analysis populations in the randomized phase of SYMPATICO are summarized in Table 9.
Table 9: Analysis Populations of the Randomized Phase of SYMPATICO
Population | Definition | Application |
|---|---|---|
ITT population | All patients randomized into the study | All efficacy analyses |
Safety population | All patients who received at least 1 dose of study treatment (ibrutinib and venetoclax or placebo) | Safety data |
ITT = intention-to-treat.
Source: SYMPATICO Clinical Study Report,27 SYMPATICO Clinical Study Protocol Amendment 4.53 Details included in the table are from the sponsor’s Summary of Clinical Evidence.2
Protocol Amendments and Deviations
In total, there were 7 versions of the study protocols for the randomized phase of SYMPATICO, including the initial protocol (protocol date: December 16, 2016) and 6 amendments, including Amendment 0.1, Amendment 1, Amendment 2, Amendment 2.1, Amendment 3, and Amendment 4. In Amendment 1 (November 17, 2017), trial inclusion criteria were modified, adding that a prior rituximab- or anti-CD20–containing regimen was required and that patients with ECOG PS of 2 were eligible. An interim analysis for OS at the time of the primary analysis for PFS at 134 events was added in Amendment 3 (March 25, 2021).
In the randomized phase of SYMPATICO, protocol deviations included inclusion or exclusion criteria violations, receipt of wrong treatment or incorrect dose of study drug, development of withdrawal criteria without being withdrawn, and use of prohibited concomitant medications. In total, ██ protocol deviations occurred during the randomized phase of SYMPATICO, of which the most common reason was ███ █████████ ████ ███████ ███ ██████████ ██ ███████ (██ ██████), followed by ███████████ ████████ █████████ █████████ ██████ ██ ████████ ██ ███████.
Results
Patient Disposition
The disposition of patients in the randomized phase of SYMPATICO is summarized in Table 10. In the venetoclax plus ibrutinib group, venetoclax was discontinued due to AEs in 12.7% of the patients, and ibrutinib was discontinued due to AEs in 14.9% of the patients. In the placebo plus ibrutinib group, placebo was discontinued due to AEs in 15.0% of the patients, and ibrutinib was discontinued due to AEs in 13.5% of the patients.
Table 10: Summary of Patient Disposition in the Randomized Phase of SYMPATICO (ITT Population)
Patient disposition | SYMPATICO | |||
|---|---|---|---|---|
Venetoclax plus ibrutinib (n = 134) | Placebo plus ibrutinib (n = 133) | |||
Ibrutinib, n (%) | Venetoclax, n (%) | Ibrutinib, n (%) | Placebo, n (%) | |
Screened, N | 325 | |||
Reason for screening failure, N (%) | 58 (17.8) | |||
Ineligible | 42 (12.9) | |||
Declined to participate | 16 (4.9) | |||
Randomized, N | 134 | 133 | ||
Treatment status, n (%) | ||||
Did not receive study treatment | 0 | 0 | 1 (0.8) | 1 (0.8) |
Ongoing | 40 (29.9) | 0 | 26 (19.5) | 0 |
Completed 2 years of venetoclax | NA | 60 (44.8) | NA | 46 (34.6) |
Study drug discontinuation | 94 (70.1) | 74 (55.2) | 106 (79.7) | 86 (64.7) |
Primary reason for study drug discontinuation, N (%) | ||||
Progressive disease determined by protocol criteria | ██ ██████ | ██ ██████ | ██ ██████ | ██ ██████ |
Clinical progression | █████ | █████ | █████ | █████ |
Adverse event not related to progressive disease | 20 (14.9) | 17 (12.7) | 18 (13.5) | 20 (15.0) |
Death | 15 (11.2) | 9 (6.7) | 7 (5.3) | 4 (3.0) |
Withdrawal of consent for treatment by patient | 7 (5.2) | 5 (3.7) | 4 (3.0) | 1 (0.8) |
Investigator decision | 11 (8.2) | 8 (6.0) | 9 (6.8) | 8 (6.0) |
Clinical deterioration | █████ | ██ | █████ | █████ |
Other | ██ █████ | █████ | █████ | █████ |
Lost to follow-up | 0 | 0 | 2 (1.5) | 2 (1.5) |
Patient status, N (%) | ||||
On study treatment | 40 (29.9) | 26 (19.5) | ||
Off treatment on study follow-up | ██ ██████ | ██ ██████ | ||
Off study | ██ ██████ | ██| ██████ | ||
Primary reason for study termination | ||||
Withdrawal of consent for follow-up observation | ██ █████ | | █████ | ||
Lost to follow-up | | █████ | | █████ | ||
Death | ██ ██████ | ██ ██████ | ||
Other | ██ | | █████ | ||
ITT = intention-to-treat; NA = not applicable.
| ███ ███████ ███ ███ ███████ █████ ██████████
Source: SYMPATICO Clinical Study Report.27 Details included in the table are from the sponsor’s Summary of Clinical Evidence.2
Baseline Characteristics
The baseline characteristics outlined in Table 11 are limited to those that are most relevant to this review or were believed to affect the outcomes or interpretation of the study results. Patients in the ITT population of the randomized phase of SYMPATICO had a median age of 68 years (range, ██ ██ ██). There were more male patients than female patients (79.0% versus 21.0%). Most of patients were white (86.5%), followed by Asian (1.9%), and Black or African American (0.7%). Approximately ████% of the ITT population had Ann Arbor stage IV disease, and 28.8% had a TP53 mutation. Approximately 59.6%, 23.6%, and 16.9% of the ITT population had received 1, 2, or 3 or more lines of therapies before receiving venetoclax plus ibrutinib, respectively.
Some differences in baseline characteristics were identified between the venetoclax plus ibrutinib group and the placebo plus ibrutinib group, including proportion of patients with high-risk simplified MCL International Prognostic Index scores (38.1% versus 30.8%), patients with bulky disease greater than or equal to 5 cm (46.3% versus 39.8%), lymphoma involvement in bone marrow biopsy (46% versus 41%), and patients with splenomegaly (31.3% versus 24.8%).
Table 11: Summary of Baseline Characteristics in the Randomized Phase of SYMPATICO (ITT Population)
Characteristic | SYMPATICO | |
|---|---|---|
Venetoclax plus ibrutinib (n = 134) | Placebo plus ibrutinib (n = 133) | |
Age (years) | ||
Mean (SD) | ████ ██████ | ████ ██████ |
Median | 69.0 | 67.0 |
Minimum, maximum | ███ ██ | ███ ██ |
Age groups, n (%) | ||
< 65 years | 41 (30.6) | 47 (35.3) |
≥ 65 years | 93 (69.4) | 86 (64.7) |
Gender, n (%) | ||
Male | 103 (76.9) | 108 (81.2) |
Female | 31 (23.1) | 25 (18.8) |
Race,a n (%) | ||
American Indian or Alaska Native | ██ | ██ |
Asian | 2 (1.5) | 3 (2.3) |
Black or African American | 1 (0.7) | 1 (0.8) |
Native Hawaiian or Pacific Islander | ██ | ██ |
White | 116 (86.6) | 115 (86.5) |
Not reported | 15 (11.2) | 14 (10.5) |
Ethnicity,a n (%) | ||
Hispanic or Latino | 8 (6.0) | 7 (5.3) |
Not Hispanic or Latino | 112 (83.6) | 110 (82.7) |
Not reported | 14 (10.4) | 16 (12.0) |
ECOG PS, n (%) | ||
0 | 74 (55.2) | 74 (55.6) |
1 to 2 | 60 (44.8) | 59 (44.4) |
Prior lines of treatment, n (%) | ||
1 | 80 (59.7) | 79 (59.4) |
2 | 32 (23.9) | 31 (23.3) |
≥ 3 | 22 (16.4) | 23 (17.3) |
Extranodal disease, n (%) | 64 (47.8) | 61 (45.9) |
Bone marrow involvement, n (%) | 62 (46.3) | 54 (40.6) |
Splenomegaly, n (%) | 42 (31.3) | 33 (24.8) |
Time from initial diagnosis to randomization in months | ||
Mean (SD) | ████ ██████ | ████ ██████ |
Median | ████ | ████ |
Minimum, maximum | ██ ███ | ██ ███ |
MCL histology, n (%) | ||
Typical | 88 (65.7) | 95 (71.4) |
Blastoid | 19 (14.2) | 17 (12.8) |
Pleomorphic | 8 (6.0) | 6 (4.5) |
Round cell (CLL-like) | 1 (0.7) | 0 |
Other | 18 (13.4) | 15 (11.3) |
Disease status at completion of treatment regimen preceding entry into the study, n (%) | ||
Relapsed from complete response | ██ ██████ | ██ ██████ |
Relapsed from partial response | ██ ██████ | ██ ██████ |
Refractory (stable disease or progressive disease) | ██ ██████ | ██ ██████ |
Ann Arbor stage, n (%) | ||
I | | █████ | | █████ |
IE | ██ | | █████ |
II | | █████ | | █████ |
IIE | | █████ | | █████ |
III | ██ █████ | ██ █████ |
IIIE | | █████ | | █████ |
IIIE, S | | █████ | ██ |
IV | ███ ██████ | ██ ██████ |
Bulky disease,b n (%) | ||
≥ 10 cm | 13 (9.7) | 10 (7.5) |
≥ 5 cm | 62 (46.3) | 53 (39.8) |
Simplified MIPI score, n (%) | ||
Low risk | 18 (13.4) | 23 (17.3) |
Intermediate risk | 63 (47.0) | 68 (51.1) |
High risk | 51 (38.1) | 41 (30.8) |
Missing | | █████ | █████ |
TP53,c n (%) | ||
Mutated | 40 (29.9) | 37 (27.8) |
Not mutated | 66 (49.3) | 57 (42.9) |
Not performed or missing | 28 (20.9) | 39 (29.3) |
CLL = chronic lymphocytic leukemia; ECOG PS = Eastern Cooperative Oncology Group performance status; ITT = intention-to-treat; MCL = mantle cell lymphoma; MIPI = Mantle Cell Lymphoma International Prognostic Index; SD = standard deviation.
aWording used in original study.
bPatients with bulky disease are patients with any lesion (nodal or extranodal) with any axis (short or long) ≥ 5 cm at screening or baseline.
cCentral laboratory testing was used as the primary source of data; a local laboratory was used only when central laboratory data were not available.
Source: SYMPATICO Clinical Study Report.27 Details included in the table are from the sponsor’s Summary of Clinical Evidence.2
Exposure to Study Treatments
A summary of patient disposition in the randomized phase of SYMPATICO is presented in Table 12. The median overall treatment duration was 22.2 months (range, ███ to ████) in the venetoclax plus ibrutinib group and 17.7 months (range, ███ to ████) in the placebo plus ibrutinib group. SYMPATICO measured treatment compliance as relative dose intensity, which was similar between the venetoclax plus ibrutinib group and the placebo plus ibrutinib group. The proportion of patients with dose reduction due to an AE for ibrutinib was 25.4% in the venetoclax plus ibrutinib group and 16.7% in the placebo plus ibrutinib group. The proportion of patients with dose reduction due to an AE was 23.1% for venetoclax in the venetoclax plus ibrutinib group and 11.4% for placebo in the placebo plus ibrutinib group.
Table 12: Summary of Patient Exposure in the Randomized Phase of SYMPATICO (Safety Population)
Exposure | SYMPATICO | |||
|---|---|---|---|---|
Venetoclax plus ibrutinib (n = 134) | Placebo plus ibrutinib (n = 132) | |||
Ibrutinib | Venetoclax | Placebo | Venetoclax | |
Treatment duration in monthsa | ||||
N | 134 | 134 | 132 | 132 |
Mean (SD) | ████ █████ | ████ ████ | ████ █████ | ████ ████ |
Median | ████ | ████ | ████ | ████ |
Minimum, maximum | ████ ████ | ████ ████ | ████ ████ | ████ ████ |
< 3 months | ██ ██████ | ██ ██████ | ██ ██████ | ██ ██████ |
3 to < 6 months | ██ ██████ | ██ ██████ | ██ ██████ | ██ ██████ |
6 to < 12 months | ██ ██████ | ██ ██████ | ██ ██████ | ██ ██████ |
12 to < 24 months | ██ ██████ | ██ ██████ | ██ ██████ | ██ ██████ |
24 to < 36 months | ██ ██████ | ██ ██████ | ██ ██████ | ██ █████ |
≥ 36 months | ██ ██████ | ██ | ██ ██████ | ██ |
Relative dose intensity (%)b | ||||
N | ███ | ███ | ███ | ███ |
Mean (SD) | ██████████ | ████ █████ | ████ █████ | ████ █████ |
Median | ████ | ████ | ████ | ████ |
Minimum, maximum | ███ ███ | ██ ███ | ███ ███ | ██ ███ |
Patients with dose reduction due to an AE | 34 (25.4) | 31 (23.1) | 22 (16.7) | 15 (11.4) |
AE = adverse event; SD = standard deviation.
aTreatment duration in months was calculated as (last dose date of study drug − first dose date of study drug + 1) / 30.4375.
bRelative dose intensity was calculated as (actual dose intensity / planned dose intensity) × 100. Planned dose intensity was ███ ██████ for ibrutinib and █████ mg per day for venetoclax or placebo.
Source: SYMPATICO Clinical Study Report.27 Details included in the table are from the sponsor’s Summary of Clinical Evidence.2
Prior Anticancer Therapy
Details about prior anticancer therapy in the randomized phase of SYMPATICO are shown in Table 13.
Concomitant Medications
Details about concomitant medications in the randomized phase of SYMPATICO, which consisted of any medication taken on or after first dose date and up to last dose date of study drug, are shown in Table 14.
Table 13: Prior Anticancer Therapies in the Randomized Phase of SYMPATICO (ITT Population)
Prior anticancer therapy | SYMPATICO | |
|---|---|---|
Venetoclax plus ibrutinib (n = 134) | Placebo plus ibrutinib (n = 133) | |
Number of prior lines of therapies, n | ||
Mean (SD) | ███ ██████ | ███ ██████ |
Median | ███ | ███ |
Range | ██ | ██ |
Group by prior lines of treatment, n (%) | ||
1 | ██ ██████ | ██ ██████ |
2 | ██ ██████ | ██ ██████ |
≥ 3 | ██ ██████ | ██ ██████ |
Any treatment related to transplant, n (%) | ||
Yes | ██ ██████ | ██ ██████ |
No | ██ ██████ | ██ ██████ |
Type of transplant, n (%) | ||
Autologous | ██ ██████ | ██ ██████ |
Allogeneic | █████ | ██ |
Radiation therapy, n (%) | ||
Yes | ██ █████ | ██ █████ |
No | ███ ██████ | ███ ██████ |
Surgery/procedures performed with therapeutic intent, n (%) | ||
Yes | ██ █████ | ██ █████ |
No | ██ ██████ | ██ ██████ |
Missing | ███ ██████ | ███ ██████ |
Prior high intensity, n (%) | ||
Hyper CVAD | ██ ██████ | ██ ██████ |
Stem cell transplant | 39 (29.1) | 50 (37.6) |
Received prior anticancer agents, n (%) | ||
Anti-CD20 monoclonal antibody | ███ ██████ | ███ ██████ |
Alkylator | ███ ██████ | ███ ██████ |
Vinca alkaloid | ███ ██████ | ███ ██████ |
Anthracycline | ██ ██████ | ███ ██████ |
Antimetabolite | ██ ██████ | ██ ██████ |
Plant alkaloid | ██ ██████ | ██ ██████ |
Platinum-containing | ██ ██████ | ██ ██████ |
Folic acid analogue | █████ | ██ ██████ |
Lenalidomide | █████ | █████ |
Bortezomib | █████ | █████ |
Antineoplastic drug | █████ | █████ |
Antineoplastic and immunomodulating drug | █████ | █████ |
HDAC-inhibitor | █████ | ██ |
Temsirolimus | █████ | █████ |
PI3-kinase inhibitor | █████ | ██ |
HDAC = histone deacetylases; hyper CVAD = chemotherapy regimen including cyclophosphamide, vincristine, doxorubicin, dexamethasone, methotrexate, and cytarabine; ITT = intention to treat; SD = standard deviation.
Source: SYMPATICO Clinical Study Report.27
Table 14: Concomitant Medications (≥ 30% of Patients in Either Arm) During Study Treatment in the Randomized Phase of SYMPATICO (Safety Population)
Therapeutic class | SYMPATICO | |
|---|---|---|
Venetoclax plus ibrutinib (n = 134) | Placebo plus ibrutinib (n = 132) | |
Number of patients who received any concomitant medication, n (%) | ███ █████ | ███ █████ |
Antigout preparations | ███ ██████ | ███ ██████ |
Antibacterials for systemic use | ███ ██████ | ███ ██████ |
Drugs for acid-related disorders | ██ ██████ | ██ ██████ |
Antivirals for systemic use | ██ ██████ | ██ ██████ |
Analgesics | ██ ██████ | ██ ██████ |
Antidiarrheals, intestinal anti-inflammatory or anti-infective agents | ██ ██████ | ██ ██████ |
Blood substitutes and perfusion solution | ██ ██████ | ██ ██████ |
Antithrombotic agents | ██ ██████ | ██ ██████ |
Mineral supplements | ██ ██████ | ██ ██████ |
Agents acting on the renin-angiotensin system | ██ ██████ | ██ ██████ |
Beta-blocking drugs | ██ ██████ | ██ ██████ |
Vaccines | ██ ██████ | ██ ██████ |
Psycholeptics | ██ ██████ | ██ ██████ |
Diuretics | ██ ██████ | ██ ██████ |
Source: SYMPATICO Clinical Study Report.27 Details included in the table are from the sponsor’s Summary of Clinical Evidence.2
Subsequent Anticancer Therapies
The summary of subsequent anticancer therapies in the randomized phase of SYMPATICO is shown in Table 15. Thirty-nine patients (29.1%) in the venetoclax plus ibrutinib group and 54 patients (40.9%) in the placebo plus ibrutinib group received subsequent antineoplastic agents. The most common antineoplastic agents (> 5 patients) in the venetoclax plus ibrutinib group were rituximab (20.9%), bendamustine (11.9%), cytarabine (9.0%), cyclophosphamide (6.0%), bortezomib (5.2), doxorubicin (5.2%), and ibrutinib (5.2%). The most common antineoplastic agents (> 5 patients) in the placebo plus ibrutinib group were rituximab (29.5%), bendamustine (22.0%), cytarabine (14.4%), venetoclax (11.4%), ibrutinib (9.1%), and cyclophosphamide (6.1%).
Table 15: Summary of Subsequent Anticancer Therapies in the Randomized Phase of SYMPATICO (Safety Population)
Treatment | SYMPATICO | |
|---|---|---|
Venetoclax plus ibrutinib (n = 134) | Placebo plus ibrutinib (n = 132) | |
Antiemetics and antinauseants, n (%) | ██ | █████ |
Granisetron | ██ | █████ |
Subsequent antineoplastic agents, n (%) | 39 (29.1) | 54 (40.9) |
Rituximab | 28 (20.9) | 39 (29.5) |
Bendamustine | 16 (11.9) | 29 (22.0) |
Cytarabine | 12 (9.0) | 19 (14.4) |
Cyclophosphamide | 8 (6.0) | 8 (6.1) |
Bortezomib | 7 (5.2) | 3 (2.3) |
Doxorubicin | 7 (5.2) | 4 (3.0) |
Ibrutinib | 7 (5.2) | 12 (9.1) |
Vincristine | 5 (3.7) | 4 (3.0) |
Methotrexate | 4 (3.0) | 5 (3.8) |
Venetoclax | 3 (2.2) | 15 (11.4) |
Carboplatin | 2 (1.5) | 0 |
Cisplatin | 2 (1.5) | 3 (2.3) |
Etoposide | 2 (1.5) | 3 (2.3) |
Investigational antineoplastic drugs | 2 (1.5) | 3 (2.3) |
Ocaliplatin | 2 (1.5) | 0 |
Brexucabtagene autoleucel | 1 (0.7) | 1 (0.8) |
Bruton’s tyrosine kinase inhibitors | 1 (0.7) | 0 |
CAR T-cells not otherwise specified | 1 (0.7) | 1 (0.8) |
Chlorambucil | 1 (0.7) | 0 |
Fludarabine | 1 (0.7) | 2 (1.5) |
Gemcitabine | 1 (0.7) | 1 (0.8) |
Ifosfamide | 1 (0.7) | 0 |
Loncastuximab tesirine | 1 (0.7) | 0 |
Obinutuzumab | 1 (0.7) | 3 (2.3) |
Protein kinase inhibitors | 1 (0.7) | 0 |
Umbralisib | 1 (0.7) | 0 |
Valemetostat | 1 (0.7) | 0 |
AZD 5991 | 0 | 1 (0.8) |
Daunorubicin | 0 | 1 (0.8) |
Decitabine | 0 | 1 (0.8) |
Glofitamab | 0 | 2 (1.5) |
Lenalidomide | 0 | 1 (0.8) |
Melphalan | 0 | 1 (0.8) |
Mosunetuzumab | 0 | 3 (2.3) |
Odronextamab | 0 | 1 (0.8) |
Parsaclisib | 0 | 2 (1.5) |
Phosphatidylinositol-3-kinase inhibitors | 0 | 2 (1.5) |
Pirtobrutinib | 0 | 1 (0.8) |
Polutuzumab vedotin | 0 | 3 (2.3) |
Rituximab; vorhyaluronidase alfa | 0 | 1 (0.8) |
Tafasitamab | 0 | 1 (0.8) |
Thiotepa | 0 | 1 (0.8) |
Antivirals for systemic use, n (%) | ██ | █████ |
█████████ | ██ | █████ |
████████ ██████████ | ██ | █████ |
Corticosteroids for systemic use, n (%) | 13 (9.7) | 11 (8.3) |
Dexamethasone | 6 (4.5) | 5 (3.8) |
Prednisone | 4 (3.0) | 4 (3.0) |
Methylprednisolone | 3 (2.2) | 4 (3.0) |
Prednisolone | 2 (1.5) | 0 |
Hydrocortisone | 1 (0.7) | 0 |
Drugs for functional gastrointestinal disorders, n (%) | ██ | █████ |
████████ | ██ | █████ |
Immunosuppressants, n (%) | 11 (8.2) | 6 (4.5) |
Lenalidomide | 10 (7.5) | 6 (4.5) |
Ublituximab | 1 (0.7) | 0 |
Investigational drugs, n (%) | 3 (2.2) | 1 (0.8) |
Nemtabrutinib | 1 (0.7) | 0 |
Subasumstat | 1 (0.7) | 0 |
Other | 1 (0.7) | 1 (0.8) |
Source: SYMPATICO Clinical Study Report.27 Details included in the table are from the sponsor’s Summary of Clinical Evidence.2
Efficacy
Key efficacy results from the randomized phase of SYMPATICO are presented in Table 16. The data cut-off date was May 22, 2023 (database lock date: July 5, 2023). The median time on study was █████ ██████ (range, ███ to ████) for the venetoclax plus ibrutinib group and █████ months (range, ███ to ████) for the placebo plus ibrutinib group.
Table 16: Summary of Key Efficacy Results in the Randomized Phase of SYMPATICO (ITT Population)
Efficacy end points | SYMPATICO | |
|---|---|---|
Venetoclax plus ibrutinib (n = 134) | Placebo plus ibrutinib (n = 133) | |
OS | ||
Deaths, n (%) | 69 (51.5) | 75 (56.4) |
Censored, n (%) | ██ ██████ | ██ ██████ |
Median (months) (95% CI)a | 44.9 (31.9 to NE) | 38.6 (25.2 to 53.4) |
Minimum, maximum | ████ █████ | ████ █████ |
HR (95% CI)b | 0.854 (0.615 to 1.186) | |
P valuec, d | 0.3465 | |
Probability of being alive at 12 months, % (95% CI)a | ████ █████ ██ █████ | ████ █████ ██ █████ |
Difference in OS probability, % (95% CI) | ████ ██████ ██ ████ | |
Probability of being alive at 24 months, % (95% CI)a | 65.9 (57.2 to 73.3) | 61.4 (52.5 to 69.1) |
Difference in OS probability, % (95% CI) | 4.5 (████ ██ █████ | |
Probability of being alive at 36 months, % (95% CI)a | ████ █████ ██ █████ | ████ █████ ██ █████ |
Difference in OS probability, % (95% CI) | ███ █████ ██ █████ | |
Probability of being alive at 48 months, % (95% CI)a | ████ █████ ██ █████ | ████ █████ ██ █████ |
Difference in OS probability, % (95% CI) | ███ █████ ██ █████ | |
Probability of being alive at 60 months, % (95% CI)a | ████ █████ ██ █████ | ████ █████ ██ █████ |
Difference in OS probability, % (95% CI) | ███ ██████ ██ █████ | |
PFS per investigator assessment (primary analysis) | ||
Number (%) of PFS events | 73 (54.5) | 94 (70.7) |
Disease progression, n | ██ | ██ |
Death, n | ██ | ██ |
Censored, n (%) | 61 (45.5) | 39 (29.3) |
Active without disease progression or death | 51 (38) | 30 (23) |
No postbaseline assessments | 2 (1) | 1 (1) |
Lost to follow-up | 1 (1) | 1 (1) |
Patient withdrawal | 7 (5) | 7 (5) |
Median (months) (95% CI)a | 31.9 (22.8 to 47.0) | 22.1 (16.5 to 29.5) |
Minimum, maximum | ██████ █████ | ██████ █████ |
HR (95% CI)b | 0.645 (0.474 to 0.878) | |
P valuec, d | 0.0052 | |
Probability of being progression-free at 12 months, % (95% CI)a | ████ █████ ██ █████ | ████ █████ ██ █████ |
Difference in PFS probability, % (95% CI) | ████ █████ ██ █████ | |
Probability of being progression-free at 24 months, % (95% CI)a | 56.8 (47.7 to 64.9) | 45.4 (36.5 to 53.8) |
Difference in PFS probability, % (95% CI) | 11.4 █████ ██ █████ | |
Probability of being progression-free at 36 months, % (95% CI)a | ████ █████ ██ █████ | ████ █████ ██ █████ |
Difference in PFS probability, % (95% CI) | ████ ████ ██ █████ | |
Probability of being progression-free at 48 months, % (95% CI)a | ████ █████ ██ █████ | ████ █████ ██ █████ |
Difference in PFS probability, % (95% CI) | ████ ████ ██ █████ | |
Probability of being progression-free at 60 months, % (95% CI)a | ████ █████ ██ █████ | ████ █████ ██ █████ |
Difference in PFS probability, % (95% CI) | ████ ████ ██ █████ | |
PFS per IRC assessment (sensitivity analysis) | ||
Number (%) of PFS events | ██ ██████ | ██ ██████ |
Disease progression, n | ██ | ██ |
Death, n | ██ | ██ |
Censored, n (%) | ██ ██████ | ██ ██████ |
Median (months) (95% CI)a | ████ █████ ██ █████ | ████ █████ ██ █████ |
Minimum, maximum | ██████ █████ | ██████ █████ |
HR (95% CI)b | █████ ██████ ██ ██████ | |
P valuec | ██████ | |
Probability of being progression-free at 12 months, % (95% CI)a | ████ █████ ██ █████ | ████ █████ ██ █████ |
Difference in PFS probability, % (95% CI) | ███ █████ ██ █████ | |
Probability of being progression-free at 24 months, % (95% CI)a | ████ █████ ██ █████ | ████ █████ ██ █████ |
Difference in PFS probability, % (95% CI) | ████ ████ ██ █████ | |
Probability of being progression-free at 36 months, % (95% CI)a | ████ █████ ██ █████ | ████ █████ ██ █████ |
Difference in PFS probability, % (95% CI) | ████ ████ ██ █████ | |
Probability of being progression-free at 48 months, % (95% CI)a | ████ █████ ██ █████ | ████ █████ ██ █████ |
Difference in PFS probability, % (95% CI) | ████ ████ ██ █████ | |
Probability of being progression-free at 60 months, % (95% CI)a | ██ ███ ██ ███ | ████ █████ ██ █████ |
Difference in PFS probability, % (95% CI) | ██ ███ ██ ███ | |
PFS per investigator assessment using the FDA censoring rules (sensitivity analysis)e | ||
Number (%) of PFS events | ██ ██████ | ██ ██████ |
Disease progression, n | ██ | ██ |
Death, n | ██ | ██ |
Censored, n (%) | ██ ██████ | ██ ██████ |
Median (months) (95% CI)a | 42.6 (27.3 to NE) | 22.1 (16.5 to 29.5) |
Minimum, maximum | ██████ █████ | ██████ █████ |
HR (95% CI)b | 0.603 (0.436 to 0.833) | |
P valuec | 0.0021 | |
Probability of being progression-free at 12 months, % (95% CI)a | ████ █████ ██ █████ | ████ █████ ██ █████ |
Difference in PFS probability, % (95% CI) | ██ | |
Probability of being progression-free at 24 months, % (95% CI)a | ████ █████ ██ █████ | ████ █████ ██ █████ |
Difference in PFS probability, % (95% CI) | ██ | |
Probability of being progression-free at 36 months, % (95% CI)a | ████ ██████ █████ | ████ █████ ██ █████ |
Difference in PFS probability, % (95% CI) | ██ | |
Probability of being progression-free at 48 months, % (95% CI)a | ████ █████ ██ █████ | ████ █████ ██ █████ |
Difference in PFS probability, % (95% CI) | ██ | |
Probability of being progression-free at 60 months, % (95% CI)a | ████ █████ ██ █████ | ████ █████ ██ █████ |
Difference in PFS probability, % (95% CI) | ██ | |
FACT-Lym total score | ||
Baseline | ||
N | ███ | ███ |
Mean (SD) | █████ ███████ | █████ ███████ |
Median | █████ | █████ |
Minimum, maximum | ███ ███ | ███ ███ |
Difference (95% CI) | ████ █████ ██ ████ | |
Month 24 | ||
N | ██ | ██ |
Mean (SD) | █████ ███████ | █████ ███████ |
Median | █████ | █████ |
Minimum, maximum | ███ ███ | ███ ███ |
Difference (95% CI) | ████ ██████ ██ ████ | |
Month 60 | ||
N | ██ | ██ |
Mean (SD) | █████ ███████ | █████ ███████ |
Median | █████ | █████ |
Minimum, maximum | ███ ███ | ████ ███ |
Difference (95% CI) | ███ ██████ ██ █████ | |
Lymphoma-specific subscale of FACT-Lym | ||
Baseline | ||
N | ███ | ███ |
Mean (SD) | ████ ██████ | ████ ██████ |
Median | ████ | ████ |
Minimum, maximum | ███ ██ | ███ ██ |
Difference (95% CI) | ████ █████ ██ ████ | |
Month 24 | ||
N | ██ | ██ |
Mean (SD) | ████ ██████ | ████ ██████ |
Median | ████ | ████ |
Minimum, maximum | ███ ██ | ███ ██ |
Difference (95% CI) | ████ █████ ██ ████ | |
Month 60 | ||
N | ██ | ██ |
Mean (SD) | ████ ██████ | ████ ██████ |
Median | ████ | ████ |
Minimum, maximum | ███ ██ | ███ ██ |
Difference (95% CI) | ████ █████ ██ ████ | |
CI = confidence interval; FACT-Lym = Functional Assessment of Cancer Therapy — Lymphoma; HR = hazard ratio; IRC = independent review committee; ITT = intention-to-treat; NE = not estimable; NR = not reported; OS = overall survival; PFS = progression-free survival; SD = standard deviation.
+Indicates censored observation.
aEstimated by KM method.
bHR is estimated using stratified Cox regression model with treatment as the only covariate.
cP value was from a stratified log-rank test.
dP value has been adjusted for multiple testing.
eIn the primary analysis of PFS, the global censoring rules (i.e., patients without progression or death were censored at last visit) were applied. In the sensitivity analyses, the FDA censoring rules were adopted for PFS per investigator assessment. On top of the global censoring rule, 2 additional censoring rules were included in the FDA censoring rules: patients were censored when subsequent anticancer therapy was used before or without a PFS event or when 2 or more consecutive response assessments were missing before a PFS event.
Source: SYMPATICO Clinical Study Report.27 Sponsor response to CDA-AMC request for additional information.22,28
Overall Survival
In the interim analysis of OS, the proportion of patients in the ITT population who had OS events was 51.5% in the venetoclax plus ibrutinib group versus 56.4% in the placebo plus ibrutinib group. The median OS was 44.9 months (95% CI, 31.9 months to NE) in the venetoclax plus ibrutinib group versus 38.6 months (95% CI, 25.2 to 53.4 months) in the placebo plus ibrutinib group. The HR for death was 0.854 (95% CI, 0.615 to 1.186). At 12 months, the probability of being alive was ████% (95% CI, ████ ██ ████) for the venetoclax plus ibrutinib group and ████% (95% CI, ████ ██ ████) for the placebo plus ibrutinib group (between-group difference = ████%; 95% CI, █████ ██ ███). At 24 months, the probability of being alive was 65.9% (95% CI, 57.2% to 73.3%) for the venetoclax plus ibrutinib group and 61.4% (95% CI, 52.5% to 69.1%) for the placebo plus ibrutinib group (between-group difference = 4.5%; 95% CI, ████ ██ ████). At 36 months, the probability of being alive was ████% (95% CI, ████ ██ ████) for the venetoclax plus ibrutinib group and ████% (95% CI, ████ ██ ████) for the placebo plus ibrutinib group (between-group difference = ███%; 95% CI, ████ ██ ████). At 48 months, the probability of being alive was ████% (95% CI, ████ ██ ████) for the venetoclax plus ibrutinib group and ████% (95% CI, ████ ██ ████) for the placebo plus ibrutinib group (between-group difference = ███%; 95% CI, ████ ██ ████). At 60 months, the probability of being alive was ████% (95% CI, ████ ██ ████) for the venetoclax plus ibrutinib group and ████% (95% CI, ████ ██ ████) for the placebo plus ibrutinib group (between-group difference = ███%; 95% CI, █████ ██ ████). The KM plot for OS at the interim analysis is presented in Figure 1.
Figure 1: KM Curves for OS in the Randomized Phase of SYMPATICO (ITT Population, Interim Analysis)
![The vertical axis plots the survival probability, and the horizontal axis plots time by months. The median OS was 44.9 months (95% CI, 31.9 months to NE) in the venetoclax plus ibrutinib group versus 38.6 months (95% CI, 25.2 to 53.4 months) in the placebo plus ibrutinib group. The HR for OS was 0.854 (95% CI, 0.615 to 1.186). The difference in the probability of being alive between the venetoclax plus ibrutinib group and the placebo plus ibrutinib group was [redacted] (95% CI, [redacted]) at 48 months and [redacted] (95% CI, [redacted]) at 60 months.](https://canjhealthtechnol.ca/index.php/cjht/article/download/PC0402r/version/1378/3172/12204/PC0402-Clinical_Review-fig01.png)
CI = confidence interval; HR = hazard ratio; ITT = intention-to-treat; KM = Kaplan-Meier; OS = overall survival.
+ Indicates censored observation.
* Stratified test or model was based on 2 randomization stratification factors: number of prior lines of therapy (1 to 2 versus ≥ 3) and TLS category (low-risk versus increased risk) at randomization.
Source: SYMPATICO Clinical Study Report.27
PFS per Investigator Assessment
In the primary analysis of PFS, the proportion of patients in the ITT population who had PFS events was 54.5% in the venetoclax plus ibrutinib group versus 70.7% in the placebo plus ibrutinib group. The median PFS per investigator assessment was 31.9 months (95% CI, 22.8 to 47.0 months) in the venetoclax plus ibrutinib group versus 22.1 months (95% CI, 16.5 to 29.5 months) in the placebo plus ibrutinib group. The HR for progression per investigator assessment was 0.645 (95% CI, 0.474 to 0.878). At ██ ██████, the probability of being progression-free was ████% (95% CI, ████ ██ ████) for the venetoclax plus ibrutinib group and ████% (95% CI, ████ ██ ████) for the placebo plus ibrutinib group (between-group difference = ████%; 95% CI, ████ ██ ████). At 24 months, the probability of being progression-free was 56.8% (95% CI, 47.7 to 64.9) for the venetoclax plus ibrutinib group and 45.4% (95% CI, 36.5% to 53.8%) for the placebo plus ibrutinib group (between-group difference = 11.4%; 95% CI, −0.8% to 23.7%). At ██ ██████, the probability of being progression-free was ████% (95% CI, ████ ██ ████) for the venetoclax plus ibrutinib group and ████% (95% CI, ████ ██ ████) for the placebo plus ibrutinib group (between-group difference = ████; 95% CI, ███ ██ ████). At ██ ██████, the probability of being progression-free was ████% (95% CI, ████ ██ ████) for the venetoclax plus ibrutinib group and ████% (95% CI, ████ ██ ████) for the placebo plus ibrutinib group (between-group difference = ████%; 95% CI, ███ ██ ████). At ██ ██████, the probability of being progression-free was ████% (95% CI, ████ ██ ████) for the venetoclax plus ibrutinib group and ████% (95% CI, ████ ██ ████) for the placebo plus ibrutinib group (between-group difference = ████%; 95% CI, ███ ██ ████). The KM plot for PFS per investigator assessment is shown in Figure 2.
Figure 2: KM Curves for PFS per Investigator Assessment in the Randomized Phase of SYMPATICO (ITT Population)
![The figure presents the KM curves for PFS per investigator assessment in the ITT population of the randomized phase of SYMPATICO. The vertical axis plots the survival probability, and the horizontal axis plots time by months. The median PFS per investigator assessment was 31.9 months (95% CI, 22.8 to 47.0 months) in the venetoclax plus ibrutinib group versus 22.1 months (95% CI, 16.5 to 29.5 months) in the placebo plus ibrutinib group. The HR for PFS per investigator assessment was 0.645 (95% CI, 0.474 to 0.878). The difference in the probability of being progression-free between the venetoclax plus ibrutinib group and the placebo plus ibrutinib group was [redacted]% (95% CI, [redacted]) at 36 months and [redacted]% (95% CI, [redacted]) at 60 months.](https://canjhealthtechnol.ca/index.php/cjht/article/download/PC0402r/version/1378/3172/12205/PC0402-Clinical_Review-fig02.png)
CI = confidence interval; HR = hazard ratio; ITT = intention-to-treat; KM = Kaplan-Meier; PFS = progression-free survival.
+ Indicates censored observation.
* Stratified test or model was based on 2 randomization stratification factors: number of prior lines of therapy (1 to 2 versus ≥ 3) and TLS category (low-risk versus increased risk) at randomization.
Source: SYMPATICO Clinical Study Report.27
One of the sensitivity analyses examined PFS per independent review committee (IRC) assessment in the ITT population using the same censoring rule (i.e., global censoring rules) as the primary analysis did. In this sensitivity analysis, the proportion of patients in the ITT population who had PFS events was ████% in the venetoclax plus ibrutinib group versus ████% in the placebo plus ibrutinib group. The median PFS per IRC assessment was 31.8 months (95% CI, 20.9 to 47.0 months) in the venetoclax plus ibrutinib group versus 20.9 months (95% CI, 16.3 to 25.2 months) in the placebo plus ibrutinib group. The HR for PFS per IRC assessment was 0.669 (95% CI, 0.492 to 0.911). The difference in the probability of being progression-free between the venetoclax plus ibrutinib group and the placebo plus ibrutinib group was ███% (95% CI, ████ ██ ████) at 12 months, ████% (95% CI, ███ ██ ████) at 24 months, ████% (95% CI, ███ ██ ████) at 36 months, ████% (95% CI, ███ ██ ████) at 48 months, and ██ (95% CI, ██ ██ ██) at 60 months. Information on the concordance in progressive disease between the primary PFS analysis (i.e., PFS per investigator assessment using global censoring rules) versus the sensitivity analysis (i.e., PFS per IRC assessment using global censoring rules) is shown in Table 17. The overall concordance for the PFS events was ████% for the venetoclax plus ibrutinib group and ████% for the placebo plus ibrutinib group.
In the primary analysis of PFS, the global censoring rules were applied. In the sensitivity analysis where the FDA censoring rules were adopted, the proportion of patients in the ITT population who had PFS events was ████% in the venetoclax plus ibrutinib group versus ████% in the placebo plus ibrutinib group. The median PFS per investigator assessment was 42.6 months (95% CI, 27.3 months to NE) in the venetoclax plus ibrutinib group versus 22.1 months (95% CI, 16.5 to 29.5 months) in the placebo plus ibrutinib group. The HR for PFS per investigator assessment was 0.603 (95% CI, 0.436 to 0.833).
FACT-Lym Total Score
The FACT-Lym total score ranges between 0 and 168, with a higher score indicating a better HRQoL.
The difference in change from baseline FACT-Lym total score between the venetoclax plus ibrutinib group and the placebo plus ibrutinib group was ████ ██████ (95% CI, █████ ██ ███) at ██ ██████ and ███ ██████ (95% CI, █████ ██ ████) at ██ ██████.
Table 17: Concordance in Progressive Disease per Investigator Assessment Versus per IRC Assessment (ITT Population)
Items | SYMPATICO | |
|---|---|---|
Venetoclax plus ibrutinib (n = 134) | Placebo plus ibrutinib (n = 133) | |
Overall concordance,a n (%) | ███ ██████ | ███ ██████ |
Progressive disease by investigator, n | ██ | ██ |
Progressive disease by IRC, n (%) | ██ ██████ | ██ ██████ |
Complete concordance in date of first progressive disease | ██ ██████ | ██ ██████ |
Concordance with later date of first progressive disease by IRC | ██ | | █████ |
Concordance with earlier date of first progressive disease by IRC | | ██████ | ██ ██████ |
Nonprogressive disease by IRC, n (%) | ██████ | ██ ██████ |
Nonprogressive disease by investigator, n | ██ | ██ |
Progressive disease by IRC, n (%) | █████ | █████ |
Nonprogressive disease by IRC, n (%) | ██ ██████ | ██ ██████ |
CR = complete response; IRC = independent review committee; ITT = intention-to-treat; PR = partial response.
Notes: The percentage for overall concordance was based on the number of patients in the ITT population as the denominator. Other percentages were based the number of patients with progressive disease by investigator and number of patients with nonprogressive disease by investigator as the denominators.
aIncluding patients who had progressive disease by both investigator and IRC and patients who had nonprogressive disease by both investigator and IRC.
Source: SYMPATICO Clinical Study Report.27
Lymphoma-Specific Subscale of FACT-Lym
The lymphoma-specific subscale of FACT-Lym ranges between 0 and 60, with a higher score indicating a better HRQoL.
The difference in change from baseline lymphoma-specific subscale of FACT-Lym score between the venetoclax plus ibrutinib group and the placebo plus ibrutinib group was ████ ██████ (95% CI, ████ ██ ███) at ██ ██████ and ████ ██████ (95% CI, ████ ██ ███) at ██ ██████.
Harms
Harms data from the randomized phase of SYMPATICO are presented in Table 18.
TEAEs
All patients in the venetoclax plus ibrutinib group and 98.5% of the patients in the placebo plus ibrutinib group had at least 1 TEAE of any grade. The most common TEAEs included diarrhea (64.9% in the venetoclax plus ibrutinib group versus 34.1% in the placebo plus ibrutinib group), neutropenia (34.3% in the venetoclax plus ibrutinib group versus 14.4% in the placebo plus ibrutinib group), nausea (31.3% in the venetoclax plus ibrutinib group versus 16.7% in the placebo plus ibrutinib group), fatigue (29.1% in the venetoclax plus ibrutinib group versus 27.1% in the placebo plus ibrutinib group), anemia (22.4% in the venetoclax plus ibrutinib group versus 12.1% in the placebo plus ibrutinib group), pyrexia (20.9% in the venetoclax plus ibrutinib group versus 19.7% in the placebo plus ibrutinib group), and cough (20.1% in the venetoclax plus ibrutinib group versus 27.3% in the placebo plus ibrutinib group).
The proportion of patients who had TEAEs of grade 3 or higher was 83.6% in the venetoclax plus ibrutinib group versus 75.8% in the placebo plus ibrutinib group. The most common TEAEs of grade 3 or higher included neutropenia (31.3% in the venetoclax plus ibrutinib group versus 10.6% in the placebo plus ibrutinib group), pneumonia (12.7% in the venetoclax plus ibrutinib group versus 10.6% in the placebo plus ibrutinib group), thrombocytopenia (12.7% in the venetoclax plus ibrutinib group versus 7.6% in the placebo plus ibrutinib group), and worsening of MCL (6.7% in the venetoclax plus ibrutinib group versus 12.1% in the placebo plus ibrutinib group).
TESAEs
The proportion of patients who had TESAEs was 60.4% in the venetoclax plus ibrutinib group versus 59.8% in the placebo plus ibrutinib group. The most common TESAE was pneumonia (12.7% in the venetoclax plus ibrutinib group versus 10.6% in the placebo plus ibrutinib group), followed by worsening of MCL (6.7% in the venetoclax plus ibrutinib group versus 12.9% in the placebo plus ibrutinib group).
Treatment Discontinuation Due to TEAEs
Discontinuation of venetoclax or placebo due to TEAEs occurred in 22.4% of the patients in the venetoclax plus ibrutinib group versus 28.8% in the placebo plus ibrutinib group.
Discontinuation of ibrutinib due to TEAEs occurred in 29.1% of the patients in the venetoclax plus ibrutinib group versus 31.1% in the placebo plus ibrutinib group.
Mortality
The proportion of patients with any AE with outcome of death was 16.4% in the venetoclax plus ibrutinib group versus 13.6% in the placebo plus ibrutinib group. The most common reason was worsening of MCL (3.0% in the venetoclax plus ibrutinib group versus 13.6% in the placebo plus ibrutinib group).
Notable Harms
Treatment-emergent major hemorrhage, which included serious or grade ≥ 3 hemorrhage and CNS hemorrhage of any grade, occurred in ███% of the patients in the venetoclax plus ibrutinib group versus ███% in the placebo plus ibrutinib group. Atrial fibrillation of any grade occurred in 10.4% of the patients in the venetoclax plus ibrutinib group versus 10.6% in the placebo plus ibrutinib group. The percentage of patients who had cardiac arrhythmias (excluding atrial fibrillation) of any grade was ████% in the venetoclax plus ibrutinib group versus ████% in the placebo plus ibrutinib group. The percentage of patients who had TLS of any grade was 5.2% in the venetoclax plus ibrutinib group versus 2.3% in the placebo plus ibrutinib group. There were 4 deaths possibly due to cardiac-related causes in the venetoclax plus ibrutinib group and 2 deaths in the placebo plus ibrutinib group.
Table 18: Summary of Harms Results in the Randomized Phase of SYMPATICO (Safety Population)
Harms | Venetoclax plus ibrutinib (n = 134) | Placebo plus ibrutinib (n = 132) |
|---|---|---|
Most common TEAEs, n (%) | ||
≥ 1 TEAE of any grade (reported in ≥ 10% of patients in either treatment group) | 134 (100.0) | 130 (98.5) |
Diarrhea | 87 (64.9) | 45 (34.1) |
Neutropenia | 46 (34.3) | 19 (14.4) |
Nausea | 42 (31.3) | 22 (16.7) |
Fatigue | 39 (29.1) | 36 (27.3) |
Anemia | 30 (22.4) | 16 (12.1) |
Pyrexia | 28 (20.9) | 26 (19.7) |
Cough | 27 (20.1) | 36 (27.3) |
Asthenia | 26 (19.4) | 18 (13.6) |
Thrombocytopenia | 26 (19.4) | 21 (15.9) |
Vomiting | 25 (18.7) | 15 (11.4) |
Pneumonia | 24 (17.9) | 20 (15.2) |
Vision blurred | 24 (17.9) | 23 (17.4) |
Upper respiratory tract infection | 23 (17.2) | 16 (12.1) |
Decreased appetite | 22 (16.4) | 15 (11.4) |
Arthralgia | 21 (15.7) | 23 (17.4) |
Hypokalemia | 21 (15.7) | 8 (6.1) |
COVID-19 | 20 (14.9) | 15 (11.4) |
Constipation | 19 (14.2) | 22 (16.7) |
Dyspepsia | 19 (14.2) | 10 (7.6) |
Visual acuity reduced | 19 (14.2) | 15 (11.4) |
Dry eye | 18 (13.4) | 19 (14.4) |
Hypertension | 18 (13.4) | 21 (15.9) |
Rash maculo-papular | 18 (13.4) | 14 (10.6) |
Dyspnea | 17 (12.7) | 18 (13.6) |
Lacrimation increased | 17 (12.7) | 16 (12.1) |
Abdominal pain | 15 (11.2) | 10 (7.6) |
Edema peripheral | 15 (11.2) | 21 (15.9) |
Atrial fibrillation | 14 (10.4) | 14 (10.6) |
Dizziness | 14 (10.4) | 20 (15.2) |
Headache | 14 (10.4) | 20 (16.7) |
Hypomagnesemia | 14 (10.4) | 4 (3.0) |
Oropharyngeal pain | 14 (10.4) | 15 (11.4) |
Pruritus | 14 (10.4) | 15 (11.4) |
Urinary tract infection | 14 (10.4) | 11 (8.3) |
Weight decreased | 14 (10.4) | 7 (5.3) |
Eye irritation | 13 (9.7) | 20 (15.2) |
Myalgia | 13 (9.7) | 17 (12.9) |
Muscle spasms | 11 (8.2) | 32 (24.2) |
(Worsening of) MCLa | 9 (6.7) | 19 (14.4) |
Back pain | 9 (6.7) | 16 (12.1) |
Epistaxis | 10 (7.5) | 14 (10.6) |
Paresthesia | 5 (3.7) | 14 (10.6) |
≥ 1 TEAE of grade 3 or higher (reported in ≥ 5% of patients in either treatment group) | 112 (83.6) | 100 (75.8) |
Neutropenia | 42 (31.3) | 14 (10.6) |
Pneumonia | 17 (12.7) | 14 (10.6) |
Thrombocytopenia | 17 (12.7) | 10 (7.6) |
Anemia | 13 (9.7) | 4 (3.0) |
Diarrhea | 11 (8.2) | 3 (2.3) |
Leukopenia | 10 (7.5) | 0 (0) |
(Worsening of) MCL | 9 (6.7) | 16 (12.1) |
Atrial fibrillation | 7 (5.2) | 7 (5.3) |
COVID-19 | 7 (5.2) | 1 (0.8) |
Hypertension | 6 (4.5) | 12 (9.1) |
TESAEs, n (%) (reported in ≥ 2% of patients in either treatment) | ||
Patients with ≥ 1 TESAE | 81 (60.4) | 79 (59.8) |
Anemia | 5 (3.7) | 2 (1.5) |
Thrombocytopenia | 3 (2.2) | 2 (1.5) |
Febrile neutropenia | 1 (0.7) | 3 (2.3) |
Atrial fibrillation | 6 (4.5) | 3 (2.3) |
Atrial flutter | 5 (3.7) | 0 |
Cardiac failure congestive | 0 | 3 (2.3) |
Gastrointestinal hemorrhage | 3 (2.2) | 1 (0.8) |
Pneumonia | 17 (12.7) | 14 (10.6) |
COVID-19 | 6 (4.5) | 1 (0.8) |
COVID-19 pneumonia | 5 (3.7) | 2 (1.5) |
Sepsis | 0 | 3 (2.3) |
Upper respiratory tract infection | 0 | 3 (2.3) |
Accidental overdose | 7 (5.2) | 2 (1.5) |
Tumour lysis syndrome | 4 (3.0) | 1 (0.8) |
(Worsening of) MCL | 9 (6.7) | 17 (12.9) |
Acute kidney injury | 3 (2.2) | 2 (1.5) |
Respiratory failure | 2 (1.5) | 4 (3.0) |
Dyspnea | 1 (0.7) | 4 (3.0) |
Pleural effusion | 1 (0.7) | 4 (3.0) |
Hypotension | 1 (0.7) | 3 (2.3) |
Patients who stopped treatment with venetoclax or placebo due to AEs, n (%) (reported in ≥ 1% of patients in either treatment arm) | ||
Patients with any AE leading to discontinuation | 30 (22.4) | 38 (28.8) |
(Worsening of) MCL | 5 (3.7) | 13 (9.8) |
Diarrhea | 4 (3.0) | 0 |
Atrial fibrillation | 2 (1.5) | 0 |
COVID-19 | 2 (1.5) | 0 |
Patients who stopped treatment with ibrutinib due to AEs, n (%) (reported in ≥ 1% of patients in either treatment arm) | ||
Patients with any AE leading to discontinuation | 39 (29.1) | 41 (31.1) |
(Worsening of) MCL | 5 (3.7) | 15 (11.4) |
Atrial fibrillation | 3 (2.2) | 0 |
COVID-19 | 3 (2.2) | 0 |
Diarrhea | 3 (2.2) | 1 (0.8) |
COVID-19 pneumonia | 2 (1.5) | 2 (1.5) |
Subdural hematoma | 2 (1.5) | 0 |
Deaths, n (%) | ||
Patients with any AE with outcome of death | 22 (16.4) | 18 (13.6) |
(Worsening of) MCL | 4 (3.0) | 10 (7.6) |
COVID-19 | 2 (1.5) | 0 |
COVID-19 pneumonia | 2 (1.5) | 2 (1.5) |
Cardiac arrest | 2 (1.5) | 0 |
Respiratory failure | 2 (1.5) | 2 (1.5) |
Cardiac death | 1 (0.7) | 0 |
Cerebrovascular accident | 1 (0.7) | 0 |
Clostridium colitis | 1 (0.7) | 0 |
Death | 1 (0.7) | 0 |
Gastric ulcer perforation | 1 (0.7) | 0 |
Hemorrhage intracranial | 1 (0.7) | 0 |
Lymphoma | 1 (0.7) | 0 |
Pneumonia | 1 (0.7) | 0 |
Subarachnoid hemorrhage | 1 (0.7) | 0 |
Sudden death | 1 (0.7) | 0 |
Cardiac failure | 0 | 1 (0.8) |
Intestinal ischemia | 0 | 1 (0.8) |
Metabolic acidosis | 0 | 1 (0.8) |
Necrotizing fasciitis | 0 | 1 (0.8) |
Notable harms, n (%) | ||
Treatment-emergent major hemorrhage of any grade | 13 (9.7) | 8 (6.1) |
Grade 3 or 4 | 8 (6.0) | 7 (5.3) |
Grade 5 | 2 (1.5) | 0 (0) |
Atrial fibrillation of any grade | 14 (10.4) | 14 (10.6) |
Grade 3 or 4 | 7 (5.2) | 7 (5.3) |
Grade 5 | 0 (0) | 0 (0) |
Cardiac arrhythmias (excluding atrial fibrillation) of any grade | 30 (22.4) | 18 (13.6) |
Grade 3 or 4 | 7 (5.2) | 6 (4.5) |
Grade 5 | 4 (3.0) | 0 (0) |
Fatal events possibly due to cardiac-related causes | ||
Cardiac arrest | 2 (1.5) | 0 (0) |
Cardiac failure | 0 | 1 (0.8) |
Cardiac death | 1 (0.7) | 0 (0) |
Death | 0 (0) | 1 (0.8) |
Sudden death | 1 (0.7) | 0 (0) |
Tumour lysis syndrome of any grade | 7 (5.2) | 3 (2.3) |
Grade 3 or 4 | 6 (4.5) | 3 (2.3) |
Grade 5 | 0 (0) | 0 (0) |
AE = adverse event; MCL = mantle cell lymphoma; TEAE = treatment-emergent adverse event; TESAE = treatment-emergent serious adverse event.
aMCL was recorded as an AE if it was worsening of MCL that did not meet Cheson criteria for progressive disease.
Source: SYMPATICO Clinical Study Report.27 Details included in the table are from the sponsor’s Summary of Clinical Evidence.2
Critical Appraisal
Internal Validity
The randomized phase of the SYMPATICO study was a phase III, double-blind RCT. An interactive response technology system, which was used to generate the randomization list and code, assigned patients to the venetoclax plus ibrutinib group or the placebo plus ibrutinib group. A stratified randomization procedure based on the number of prior lines of therapy (1 to 2 versus 3), ECOG PS (0 versus 1 to 2), and TLS risk category (low versus increased risk) were also carried out. While the distribution of most baseline characteristics was similar between the venetoclax plus ibrutinib group and the placebo plus ibrutinib group, some between-group imbalances were observed, such as the proportion of patients with high-risk simplified MCL International Prognostic Index scores (38.1% versus 30.8%), patients with bulky disease 5 cm or greater (46.3% versus 39.8%), lymphoma involvement in bone marrow biopsy (46% versus 41%), patients with splenomegaly (31.3% versus 24.8%), and history of prior autologous transplant (28.4% versus 37.6%). The clinical experts consulted by the CDA-AMC review team noted no major concerns about these imbalances in terms of biasing the treatment effect estimates. The CDA-AMC review team determined that the risk of selection bias associated with inadequate randomization was overall low.
It was noted that the trial inclusion criteria were modified in Study Protocol Amendment 1, which added that a prior rituximab- or anti-CD20–containing regimen was required and that patients with ECOG PS of 2 were eligible. The amendment was made in 2017 which was before patients were enrolled and randomized in 2018, leading to no major concern. The clinical experts consulted by the CDA-AMC review team noted that many of the concomitant medications reported in the randomized phase of SYMPATICO were used to manage side effects caused by venetoclax or ibrutinib and these concomitant medications were unlikely to impact the assessment of survival outcomes (i.e., OS, PFS). A higher proportion of patients in the placebo plus ibrutinib group, compared to the venetoclax plus ibrutinib group, received subsequent anticancer therapy (40.9% versus 29.1%). The clinical experts consulted by the CDA-AMC review team determined that this imbalance in subsequent anticancer therapy was unlikely to cause biased results.
PFS and OS were reported in SYMPATICO as survival outcomes. The clinical experts consulted by the CDA-AMC review team acknowledged OS as the most clinically important outcome for patients with MCL. Yet only results from the interim OS analysis were available for this review. The 1-sided type I family-wise error rate was controlled at 0.025 by a closed testing procedure for testing PFS and some secondary end points, including OS. To maintain a 2-sided overall significance level of 0.05 for OS, the significance boundary of the OS interim analysis was 2-sided alpha of 0.001, based on the Haybittle-Peto boundary, which was considered by the review team as appropriate. Nonetheless, the interim OS data were immature, and the upper bound of the 95% CI of the median OS in the venetoclax plus ibrutinib group was NE. As a result, uncertainty remains in the interim OS evidence, which may be addressed by the final OS analysis. ██ █████ ██ ███ ██████████████ ████████ ██ ███████ ██ █████ ███ ███████ ███ ███████ █████████ ████ █████ ██ ██ ████ ██ ██████ ██████████ ██ █████ █████ ████ ███ ███████ ██ █████ ███ ███ ██████ ██ ███████████
PFS per investigator assessment was the primary efficacy end point in the randomized phase of SYMPATICO. The clinical experts consulted by the CDA-AMC review team noted that the selection of PFS as primary efficacy end point was necessary and informative. MCL is noncurable, especially in the relapsed or refractory setting, and PFS could provide information on the relative treatment effects on disease control and stabilization. Two sets of censoring rules were used in estimating PFS: the global censoring rules for the primary analysis and the FDA censoring rules for 1 of the sensitivity analyses. In the global censoring rules, patients without progression or death were censored, while, in the FDA censoring rules, 2 additional censoring scenarios were added to the global censoring rules, i.e., patients with subsequent anticancer therapy, or with 2 or more missed visits before the PFS event, were censored. The CDA-AMC review team noticed that, compared to the median PFS in the venetoclax plus ibrutinib group from the primary analysis, there was a marked increase in the median PFS from the sensitivity analysis using FDA censoring rules (approximately a 10-month increase from 31.9 months to 42.6 months). However, no change was observed in the median PFS in the placebo plus ibrutinib group between the analyses (with the same median PFS of 22.1 months). The large difference in median PFS in the venetoclax plus ibrutinib group but not in the placebo plus ibrutinib group between these 2 analyses, as noted by the review team and others,23 indicated that the patients in the venetoclax plus ibrutinib group who were censored by the additional 2 scenarios of the FDA rules were not equally likely to experience disease progression, compared to those who were not censored. Specifically, the additionally censored patients in the venetoclax plus ibrutinib group were at a higher risk, which would have violated the noninformative censoring assumption of the KM method, skewed the KM curve, and resulted in an overestimation of median PFS in the analysis with the FDA censoring rules.23,24 Moreover, as Lesan et al. pointed out,23 the possibility of overestimation in the PFS primary analysis using the global censoring rules could not be ruled out because, for example, in the primary PFS analysis, patients who missed visits were not censored. Given that these patients were possibly at a higher risk of disease progression (as suggested by the sensitivity analysis using the FDA censoring rules), not counting these patients as having a PFS event may have overestimated median PFS.
Patients, trial investigators, and representatives of the study sponsor were blinded to treatment assignment in the randomized phase of SYMPATICO, which overall minimized the risk of bias associated with patient performance or outcome assessment. However, there was a risk of unblinding in patients or investigators because there was a higher occurrence of digestive AEs in the venetoclax plus ibrutinib group compared to that in the placebo plus ibrutinib group (i.e., diarrhea [64.9% versus 34.1%], nausea [31.3% versus 16.7%], and vomiting [18.7% versus 11.4%]) and because a higher percentage of patients in the venetoclax plus ibrutinib group were treated for these AEs (e.g., ████% of the patients in the venetoclax plus ibrutinib group versus ███% of the patients in the placebo plus ibrutinib group were treated with ██████████ ███ ████████). The CDA-AMC review team determined that the risk of bias due to unblinding affecting survival outcomes (e.g., PFS, OS) was minimal. First, disease progression was evaluated using the Lugano Classification Criteria55 by both the investigator and the IRC. Second, the overall concordance for the PFS events was ████% for the venetoclax plus ibrutinib group and ████% for the placebo plus ibrutinib group, suggesting good agreement between the ways of assessing the primary outcome.
The potential bias due to the risk of unblinding in reporting or assessing HRQoL outcomes could not be ruled out. In addition to the unblinding risk, there was also a risk of missing data for HRQoL outcomes. For instance, only ██ ███ ██ ███ ████████ in the venetoclax plus ibrutinib group and ██ ██ ███ ████████ in the placebo plus ibrutinib group contributed to the FACT-Lym total score and the lymphoma-specific subscale of FACT-Lym at 24 months; ██████ ████ of the ITT population was missing. There was no description of how the missing data for the HRQoL outcomes were handled, and therefore the direction and magnitude of the bias due to missing outcome data remained unknown.
External Validity
The eligibility criteria of the randomized phase of SYMPATICO were in general aligned with the criteria in the Canadian setting for selecting eligible patients with MCL in the relapsed and refractory setting, according to the clinical experts consulted by the review team. However, the clinical experts noted that some patients who might benefit from venetoclax plus ibrutinib were not included in the randomized phase of SYMPATICO, including selected patients with an ECOG PC greater than 2; patients who have previously been exposed, but whose disease is not refractory, to venetoclax or ibrutinib; patients without at least 1 site of disease 2.0 cm (e.g., leukemic MCL), and patients with CNS lymphoma, which is rare. Nonetheless, results from the randomized phase of SYMPATICO were still likely to be generalizable to these patients.
Concerning the prior therapies received, the randomized phase of SYMPATICO required eligible patients to have at least 1 rituximab- or anti-CD20–containing regimen, while the Health Canada indication and the reimbursement request proposed by the sponsor do not. The clinical experts noted that all first-line therapies that are currently funded for patients with MCL in Canada contain an anti-CD20 drug. Almost all patients would receive a rituximab- or anti-CD20–containing regimen in the first-line setting, unless they have a reason not to (e.g., a patient is intolerant to rituximab). As a result, the clinical experts noted no concerns generalizing the results from the randomized phase of SYMPATICO to the indicated population.
GRADE Summary of Findings and Certainty of the Evidence
Methods for Assessing the Certainty of the Evidence
For pivotal studies and RCTs identified in the sponsor’s systematic review, GRADE was used to assess the certainty of the evidence for outcomes considered most relevant to inform expert committee deliberations, and a final certainty rating was determined as outlined by the GRADE Working Group:25,26
High certainty: We are very confident that the true effect lies close to that of the estimate of the effect.
Moderate certainty: We are moderately confident in the effect estimate — that is, the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. We use the word “likely” for evidence of moderate certainty (e.g., “X intervention likely results in Y outcome”).
Low certainty: Our confidence in the effect estimate is limited — that is, the true effect may be substantially different from the estimate of the effect. We use the word “may” for evidence of low certainty (e.g., “X intervention may result in Y outcome”).
Very low certainty: We have very little confidence in the effect estimate — that is, the true effect is likely to be substantially different from the estimate of effect. We describe evidence of very low certainty as “very uncertain.”
Following the GRADE approach, evidence from RCTs started as high-certainty evidence and could be rated down for concerns related to study limitations (which refers to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias.
When possible, certainty was rated in the context of the presence of an important (nontrivial) treatment effect. If this was not possible, certainty was rated in the context of the presence of any treatment effect (i.e., the clinical importance is unclear). In all cases, the target of the certainty of evidence assessment was based on the point estimate and where it was located relative to the threshold for a clinically important effect (when a threshold was available) or to the null.
The reference points for the certainty of evidence assessment for OS and PFS per investigator assessment were set according to the presence of an important effect based on thresholds agreed upon by clinical experts consulted by the review team for this review. The reference points for the certainty of evidence assessment for the FACT-Lym total score, the lymphoma-specific subscale of FACT-Lym, and harms events were set according to the presence of any non-null effect.
Results of GRADE Assessments
Table 2 presents the GRADE summary of findings for venetoclax plus ibrutinib versus placebo plus ibrutinib for patients with MCL who have received at least 1, but no more than 5, prior treatment regimens.
Long-Term Extension Studies
No long-term extension studies were identified for this review.
Indirect Evidence
No indirect evidence was identified for this review.
Studies Addressing Gaps in the Systematic Review Evidence
No studies addressing gaps in the pivotal and RCT evidence were identified for this review.
Discussion
Summary of Available Evidence
The randomized phase of the SYMPATICO study was submitted by the sponsor in the systematic review of this clinical report. The randomized phase of SYMPATICO is a phase III, multicentre, double-blind RCT, investigating the efficacy and safety of venetoclax plus ibrutinib in patients with MCL who have received at least 1, but no more than 5, prior treatment regimens for MCL including at least 1 prior rituximab- or anti-CD20–containing regimen. A total of 267 patients (including ██ patients in Canada) were randomized to the venetoclax plus ibrutinib group (n = 134) and the placebo plus ibrutinib group (n = 133). The primary objective of the randomized phase of SYMPATICO was to assess the efficacy of venetoclax plus ibrutinib relative to placebo plus ibrutinib as measured by PFS per investigator assessment. Secondary end points included OS and harms. HRQoL outcomes, such as FACT-Lym total score and lymphoma-specific subscale of FACT-Lym, were also reported. Patients in the ITT population of the randomized phase of SYMPATICO had a median age of 68 years (range, ██ ██ ██). There were more male patients than female patients (79.0% versus 21.0%). Most of patients were white (86.5%), followed by Asian (1.9%) and Black or African American (0.7%). Approximately 59.6%, 23.6%, and 16.9% of the ITT population had received 1, 2, or 3 or more lines of therapies before receiving venetoclax plus ibrutinib, respectively.
Interpretation of Results
Efficacy
Survival (i.e., OS, PFS) and HRQoL outcomes (i.e., FACT-Lym, lymphoma-specific subscale of FACT-Lym) were reported in the randomized phase of the SYMPATICO study. These efficacy end points were selected based on the input from patients and clinician groups as well as the input from the clinical experts consulted by the CDA-AMC review team. These efficacy outcomes aligned with patients’ expectation of important outcomes which included prolonging life, achieving longer disease remission, controlling disease symptoms, and improving quality of life.
The evidence regarding OS reviewed in the clinical report was based on the interim analysis, and data were immature at the time of this analysis. Overall, there remains a gap in the evidence regarding OS, which may be addressed by the final analysis. The interim OS analysis showed a between-group difference of ███% (95% CI, ████ ██ ████) in the probability of being alive at ██ ██████ and ███% (95% CI, █████ ██ ████) in the probability of being alive at ██ ██████. Based on the assessment of certainty of evidence using the GRADE approach, venetoclax plus ibrutinib may result in little to no difference in the probability of being alive at 48 or 60 months, compared to venetoclax plus ibrutinib, based on low-certainty evidence. The main reason for the low certainty in OS results was the imprecision identified in the point estimates and the 95% CIs of the between-group difference in the probability of being alive. A 5% difference (50 per 1,000) between the venetoclax plus ibrutinib group and the placebo plus ibrutinib group was considered clinically important (i.e., MID) by the clinical experts consulted by the review team. The point estimate of the between-group difference in the probability of being alive at ██ ██████ (i.e., ███%) and ██ ██████ (i.e., ███%) did not reach the MID of 5%, suggesting little to no clinically meaningful difference. Moreover, the upper and lower bounds of the 95% CIs of the probability of being alive at ██ ██████ (i.e., ████% to ████%) and ██ ██████ (i.e., █████% to ████%) crossed both the null (i.e., between-group difference = 0) and the MID (i.e., 5%), respectively, indicating a high level of uncertainty around the point estimates.
While acknowledging OS as the most clinically relevant efficacy end point for patients with MCL, the clinical experts consulted by the CDA-AMC review team also considered PFS as a necessary and informative efficacy end point due to the noncurable nature of MCL, especially in the relapsed or refractory setting. The difference in the probability of being progression-free between the venetoclax plus ibrutinib group and the placebo plus ibrutinib group was ████% (95% CI, ███ ██ ████) at ██ ████ and ████% (95% CI, ███ ██ ████) at ██ ██████. Both point estimates at ██ ███ ██ ██████ exceeded the MID (i.e., 7%) suggested by the clinical experts consulted by the CDA-AMC review team, while the lower bound of the 95% CI of the probability of being progression-free at ██ ██████ excluded the MID. Based on the GRADE approach, venetoclax plus ibrutinib likely results in a clinically meaningful benefit in PFS at ██ ███ ██ ██████, compared to placebo plus ibrutinib, based on moderate- to high-certainty evidence. However, it should be noted that there was a risk of overestimation of median PFS due to the possibility of informative censoring, as discussed previously in the Internal Validity section.23
No between-group difference in HRQoL outcomes, including FACT-Lym and the lymphoma-specific subscale of FACT-Lym, was observed at 24 and 60 months. Both the CDA-AMC review team and the clinical experts consulted by the review team agreed that the HRQoL findings were difficult to interpret, mainly due to missing data. ██████ ████ of the ITT population were missing data for these outcomes at 24 months, and ████ ██ ███ ████████ ██ ███) were missing data at 60 months. It remains unclear how the missing data would affect the HRQoL assessment.
Harms
In the randomized phase of the SYMPATICO study, the proportion of patients who had TEAEs of grade 3 or higher was greater in the venetoclax plus ibrutinib group than in the placebo plus ibrutinib group (83.6% versus 75.8%). In addition, 22.4% of the patients in the venetoclax plus ibrutinib group and 28.8% in the placebo plus ibrutinib group discontinued venetoclax or placebo due to TEAEs, and 29.1% in the venetoclax plus ibrutinib group and 31.1% in the placebo plus ibrutinib group discontinued ibrutinib due to TEAEs. AEs led to death in 16.4% of the patients in the venetoclax plus ibrutinib group and 13.6% in the placebo plus ibrutinib group.
TLS, cardiac deaths, and sudden deaths were noted by the clinical experts consulted by the CDA-AMC review team as important notable harms. Although a higher percentage of patients in the venetoclax plus ibrutinib group had TLS compared with the placebo plus ibrutinib group (5.2% versus 2.3%), the clinical experts consulted were not concerned and considered the mainly laboratory TLS events manageable. Only 1 patient in the venetoclax plus ibrutinib group had a cardiac death and 1 had a sudden death, while no patients died due to these reasons in the placebo plus ibrutinib group. According to the clinical experts, it was uncertain whether venetoclax plus ibrutinib would cause more cardiac deaths or sudden deaths than placebo plus ibrutinib due to the small number of events and the fact that such events are more likely attributable to ibrutinib than to venetoclax.
The CDA-AMC review team noted that worsening of MCL (those cases that did not meet Cheson criteria for progressive disease) was recorded as an AE. When excluding the patients who had worsening of MCL, the proportion of patients who had harms events became generally higher in the venetoclax plus ibrutinib group than that in the placebo plus ibrutinib group: 76.9% versus 63.7% for TEAEs of grade 3 or higher, 18.5% versus 19% for discontinuation of venetoclax or placebo due to TEAEs, 25.4% versus 19.7% for discontinuation of ibrutinib due to TEAEs, and 13.4% versus 6% for deaths. According to the clinical experts consulted by the CDA-AMC review team, compared to placebo plus ibrutinib, adding venetoclax to ibrutinib is expected to increase the risk of AEs. Regardless of whether worsening of MCL was included, the clinical experts consulted by the CDA-AMC review team determined that the safety profile of venetoclax plus ibrutinib is overall manageable and consistent with the known toxicities of the individual components of the regimen. The clinical experts consulted by the CDA-AMC review team noted that many hematologists in Canada are experienced at managing the adverse effects of both drugs, and that this regimen is better tolerated than other therapies used in relapsed MCL, such as CAR T-cell therapy or allogeneic stem cell transplant.
Conclusion
The randomized phase of the SYMPATICO trial, a phase III, double-blind RCT, assessed the efficacy and safety of venetoclax plus ibrutinib relative to placebo plus ibrutinib in patients with MCL who have received at least 1, but no more than 5, prior treatment regimens for MCL. The interim analysis of OS, based on OS data that were immature at the time of analysis, indicated that venetoclax plus ibrutinib may result in little to no difference in the probability of being alive at 48 or 60 months, compared to placebo plus ibrutinib. The certainty of the interim OS evidence was low, and this low certainty may be addressed in the final OS analysis. Added clinical benefit was observed with venetoclax plus ibrutinib in the trial’s designated primary efficacy outcome — PFS per investigator assessment. Venetoclax plus ibrutinib, compared to placebo plus ibrutinib, likely results in a clinically meaningful improvement in the probability of being progression-free at 36 and 60 months based on moderate- to high-certainty evidence. However, the possibility of overestimation in the PFS benefits could not be ruled out due to the informative censoring observed in the PFS sensitivity analysis. Patients censored might have been at a higher risk of having disease progression. Venetoclax plus ibrutinib appears to be overall safe, and the safety profile of venetoclax plus ibrutinib is consistent with the known harms for the individual components of the regimen.
References
1.AbbVie Corporation. Venclexta (venetoclax): 10 mg, 50 mg, and 100 mg, oral tablets [product monograph]. July 31, 2025.
2.AbbVie Corporation. Sponsor's summary of clinical evidence [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Venclexta (venetoclax), 10 mg, 50 mg, and 100 mg, oral tablets February 20, 2025.
3.Dreyling M, Campo E, Hermine O, et al. Newly diagnosed and relapsed mantle cell lymphoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2017;28(suppl_4):iv62-iv71. doi:10.1093/annonc/mdx223 PubMed
4.Leukemia and Lymphoma Society. Mantle cell lymphoma facts. 2014. Accessed by sponsor, no date provided. https://www.lls.org/sites/default/files/file_assets/mantlecelllymphoma.pdf
5.Brenner DR, Gillis J, Demers AA, et al. Projected estimates of cancer in Canada in 2024. Can Med Assoc J. 2024;196(18):E615-E623. doi:10.1503/cmaj.240095 PubMed
6.Canadian Cancer Statistics Advisory Committee, Canadian Cancer Society, Statistics Canada, et al. Canadian Cancer Statistics: A 2022 special report on cancer prevalence. Canadian Cancer Society; November 2022. Accessed by sponsor, no date provided. https://cancer.ca/Canadian-Cancer-Statistics-2022-EN
7.Narkhede M, Goyal G, Shea L, et al. Evaluating real-world treatment patterns and outcomes of mantle cell lymphoma. Blood Adv. 2022;6(14):4122-4131. doi:10.1182/bloodadvances.2022007247 PubMed
8.Villa D, Kansara R, Lemieux C, et al. Updates in the treatment of mantle cell lymphoma: A Canadian expert framework. Canadian Hematology Today. 2022:2–11-2–11. doi:10.58931/cht.2022.1S1227
9.Alnassfan T, Cox-Pridmore MJ, Taktak A, et al. Mantle cell lymphoma treatment options for elderly/unfit patients: A systematic review. EJHaem. 2022;3(1):276-290. doi:10.1002/jha2.311 PubMed
10.Silkenstedt E, Linton K, Dreyling M. Mantle cell lymphoma – advances in molecular biology, prognostication and treatment approaches. Br J Haematol. 2021;195(2):162-173. doi:10.1111/bjh.17419 PubMed
11.Le Gouill S, Długosz-Danecka M, Rule S, et al. Final results and overall survival data from a phase II study of acalabrutinib monotherapy in patients with relapsed/refractory mantle cell lymphoma, including those with poor prognostic factors. Haematologica. 2024;109(1):343-350. doi:10.3324/haematol.2022.282469 PubMed
12.Wang M, Munoz J, Goy A, et al. Three-Year follow-up of KTE-X19 in patients with relapsed/refractory mantle cell lymphoma, including high-risk subgroups, in the ZUMA-2 study. J Clin Oncol. 2023;41(3):555-567. doi:10.1200/jco.21.02370 PubMed
13.Wang M, Munoz J, Goy A, et al. KTE-X19 CAR T-cell therapy in relapsed or refractory mantle-cell lymphoma. N Engl J Med. 2020;382(14):1331-1342. doi:10.1056/NEJMoa1914347 PubMed
14.Wang M, Rule S, Zinzani PL, et al. Acalabrutinib in relapsed or refractory mantle cell lymphoma (ACE-LY-004): a single-arm, multicentre, phase 2 trial. Lancet. 2018;391(10121):659-667. doi:10.1016/s0140-6736(17)33108-2 PubMed
15.Wang ML, Jurczak W, Jerkeman M, et al. Ibrutinib plus bendamustine and rituximab in untreated mantle-cell lymphoma. N Engl J Med. 2022;386(26):2482-2494. doi:10.1056/NEJMoa2201817 PubMed
16.Gong IY, Kuruvilla J, Crump M. Mantle cell lymphoma: Evolving frontline treatment strategies. Canadian Hematology Today. 2024;3(2):5–21. doi:10.58931/cht.2024.3251
17.Eskelund CW, Dahl C, Hansen JW, et al. TP53 mutations identify younger mantle cell lymphoma patients who do not benefit from intensive chemoimmunotherapy. Blood. 2017;130(17):1903-1910. doi:10.1182/blood-2017-04-779736 PubMed
18.Jain P, Wang ML. Mantle cell lymphoma in 2022-A comprehensive update on molecular pathogenesis, risk stratification, clinical approach, and current and novel treatments. Am J Hematol. 2022;97(5):638-656. doi:10.1002/ajh.26523 PubMed
19.AstraZeneca Canada Inc. Calquence (acalabrutinib tablets): 100 mg acalabrutinib (as acalabrutinib maleate) for oral use [product monograph]. June 24, 2025. Accessed by sponsor, no date provided. https://www.astrazeneca.ca/content/dam/az-ca/downloads/productinformation/calquence-product-monograph-en.pdf
20.BeiGene Switzerland Gmb H. Brukinsa (zanubrutinib capsules): capsules, 80 mg, oral, Bruton’s Tyrosine Kinase (BTK) Inhibitor[product monograph] January 31, 2024. Accessed by sponsor, no date provided. https://pdf.hres.ca/dpd_pm/00074465.PDF
21.Gilead Sciences Canada I. Tecartus (brexucabtagene autoleucel) [product monograph]. 2022. Accessed by sponsor, no date provided. https://www.gilead.ca/-/media/gilead-canada/pdfs/medicines/tecartus_english_pm_e230191-gs-001.pdf
22.AbbVie Corporation. AbbVie Corporation response to Canada's Drug Agency request for additional information regarding Venclexta (venetoclax) review on March 21, 2025 [internal additional sponsor's information]. Mar 31, 2025.
23.Lesan V, Olivier T, Prasad V. Progression-free survival estimates are shaped by specific censoring rules: Implications for PFS as an endpoint in cancer randomized trials. Eur J Cancer. 2024;202doi:10.1016/j.ejca.2024.114022
24.Campigotto F, Weller E. Impact of informative censoring on the Kaplan-Meier estimate of progression-free survival in phase II clinical trials. J Clin Oncol. 2014;32(27):3068-74. doi:10.1200/jco.2014.55.6340 PubMed
25.Balshem H, Helfand M, Schünemann HJ, et al. GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol. 2011;64(4):401-6. doi:10.1016/j.jclinepi.2010.07.015 PubMed
26.Santesso N, Glenton C, Dahm P, et al. GRADE guidelines 26: informative statements to communicate the findings of systematic reviews of interventions. J Clin Epidemiol. 2020;119:126-135. doi:10.1016/j.jclinepi.2019.10.014 PubMed
27.AbbVie Corporation. Clinical Study Report: R&D/21/0809. Phase 3 Study of ibrutinib in combination with venetoclax in subjects with mantle cell lymphoma [internal sponsor's report]. February 22, 2024.
28.AbbVie Corporation. AbbVie Corporation response to Canada's Drug Agency request for additional information regarding Venclexta (venetoclax) review on April 11, 2025 [internal additional sponsor's information]. Apr 22, 2025.
29.Sarkozy C, Thieblemont C, Oberic L, et al. Long-term follow-up of rituximab maintenance in young patients with mantle-cell lymphoma included in the LYMA Trial: A LYSA study. J Clin Oncol. 2024;42(7):769-773. doi:10.1200/jco.23.01586 PubMed
30.Cencini E, Calomino N, Franceschini M, et al. Survival outcomes of patients with mantle cell lymphoma: A retrospective, 15-year, real-life study. Hematol Rep. 2024;16(1):50-62. doi:10.3390/hematolrep16010006 PubMed
31.Lynch DT, Koya S, Dogga S, et al. Mantle cell lymphoma. In: StatPearls [Internet] StatPearls Publishing; 2023. Accessed May 14, 2025. https://www.ncbi.nlm.nih.gov/books/NBK536985/#:~:text=Treatment%20/%20Management,standard%20treatment%20established%20for%20MCL.
32.National Organization for Rare Disorders. Mantle Cell Lymphoma. 2021. Accessed November 18, 2022. https://rarediseases.org/rare-diseases/mantle-cell-lymphoma/
33.Vose JM. Mantle cell lymphoma: 2017 update on diagnosis, risk-stratification, and clinical management. Am J Hematol. 2017;92(8):806-813. doi:10.1002/ajh.24797 PubMed
34.Alaggio R, Amador C, Anagnostopoulos I, et al. The 5th edition of the World Health Organization classification of haematolymphoid tumours: Lymphoid neoplasms. Leukemia. 2022;36(7):1720-1748. doi:10.1038/s41375-022-01620-2
35.Campo E, Jaffe ES, Cook JR, et al. The international consensus classification of mature lymphoid neoplasms: a report from the Clinical Advisory Committee. Blood. 2022;140(11):1229-1253. doi:10.1182/blood.2022015851 PubMed
36.Hoster E, Dreyling M, Klapper W, et al. A new prognostic index (MIPI) for patients with advanced-stage mantle cell lymphoma. Blood. 2008;111(2):558-65. doi:10.1182/blood-2007-06-095331 PubMed
37.Jain P, Wang M. Mantle cell lymphoma: 2019 update on the diagnosis, pathogenesis, prognostication, and management. Am J Hematol. 2019;94(6):710-725. doi:10.1002/ajh.25487 PubMed
38.Jares P, Colomer D, Campo E. Molecular pathogenesis of mantle cell lymphoma. J Clin Invest. 2012;122(10):3416-23. doi:10.1172/jci61272 PubMed
39.Navarro A, Beà S, Jares P, et al. Molecular pathogenesis of mantle cell lymphoma. Hematol Oncol Clin North Am. 2020;34(5):795-807. doi:10.1016/j.hoc.2020.05.002 PubMed
40.Veloza L, Ribera-Cortada I, Campo E. Mantle cell lymphoma pathology update in the 2016 WHO classification. Annals of Lymphoma. 2019;3doi:10.21037/aol.2019.03.01
41.Zhao X, Bodo J, Sun D, et al. Combination of ibrutinib with ABT-199: synergistic effects on proliferation inhibition and apoptosis in mantle cell lymphoma cells through perturbation of BTK, AKT and BCL2 pathways. Br J Haematol. 2015;168(5):765-8. doi:10.1111/bjh.13149 PubMed
42.Portell CA, Axelrod M, Brett LK, et al. Synergistic cytotoxicity of ibrutinib and the BCL2 antagonist, ABT-199(GDC-0199) in mantle cell lymphoma (MCL) and chronic lymphocytic leukemia (CLL): Molecular analysis reveals mechanisms of target interactions. Blood. 2014;124(21):509. doi:10.1182/blood.V124.21.509.509
43.Axelrod M, Ou Z, Brett LK, et al. Combinatorial drug screening identifies synergistic co-targeting of Bruton’s tyrosine kinase and the proteasome in mantle cell lymphoma. Leukemia. 2014;28(2):407-410. doi:10.1038/leu.2013.249 PubMed
44.Li Y, Bouchlaka MN, Wolff J, et al. FBXO10 deficiency and BTK activation upregulate BCL2 expression in mantle cell lymphoma. Oncogene. 2016;35(48):6223-6234. doi:10.1038/onc.2016.155 PubMed
45.Wang ML, Rule S, Martin P, et al. Targeting BTK with ibrutinib in relapsed or refractory mantle-cell lymphoma. N Engl J Med. 2013;369(6):507-16. doi:10.1056/NEJMoa1306220 PubMed
46.Janssen Inc. Imbruvica (ibrutinib): tablets, 140 mg, 280 mg, 420 mg, 560 mg, oral; ibrutinib capsules; capsules, 140 mg, oral; ibrutinib oral suspension; suspension, 70 mg/ml, oral [product monograph]. 2023. Accessed by sponsor, no date provided. https://pdf.hres.ca/dpd_pm/00071920.PDF#page=2.09
47.Canada’s Drug Agency. CADTH reimbursement recommendation: Zanubrutinib (Brukinsa) 2022. Accessed by sponsor, no date provided. https://www.cda-amc.ca/zanubrutinib-0
48.Canada’s Drug Agency. pCODR Expert Review Committee (pERC) final recommendation. Ibrutinib (Imbruvica) Accessed by sponsor, no date provided. https://www.cda-amc.ca/imbruvica-mantle-cell-lymphoma-relapsedrefractory
49.Wang M, Ramchandren R, Chen R, et al. Concurrent ibrutinib plus venetoclax in relapsed/refractory mantle cell lymphoma: the safety run-in of the phase 3 SYMPATICO study. J Hematol Oncol. 2021;14(1):179. doi:10.1186/s13045-021-01188-x PubMed
50.Wang M, Jurczak W, Trneny M, et al. Ibrutinib plus venetoclax in relapsed or refractory mantle cell lymphoma (SYMPATICO): a multicentre, randomised, double-blind, placebo-controlled, phase 3 study. Lancet Oncol. 2025;26(2):200-213. doi:10.1016/S1470-2045(24)00682-X PubMed
51.Wang M, Jurczak W, Trněný M, et al. Ibrutinib combined with venetoclax in patients with relapsed/refractory mantle cell lymphoma: Primary analysis results from the randomized phase 3 Sympatico Study. Blood. 2023;142(Supplement 2):LBA-2-LBA-2. doi:10.1182/blood-2023-191921
52.Wang M, Jurczak W, Trneny M, et al. Efficacy and safety of ibrutinib plus venetoclax in patients with mantle cell lymphoma (MCL) and <i>TP53</i> mutations in the SYMPATICO study. J Clin Oncol. 2024;42(16_suppl):7007-7007. doi:10.1200/JCO.2024.42.16_suppl.7007
53.AbbVie Corporation. Clinical Study Protocol amendment 4: PCYC-1143-CA. Phase 3 study of ibrutinib in combination with venetoclax in subjects with mantle cell lymphoma [internal sponsor's report]. September 16, 2022.
54.AbbVie Corporation. Statistical Analysis Plan version 2: PCYC-1143-CA. Phase 3 study of ibrutinib in combination with venetoclax in subjects with mantle cell lymphoma [internal sponsor's report]. June 22, 2023.
55.Cheson BD, Fisher RI, Barrington SF, et al. Recommendations for initial evaluation, staging, and response assessment of Hodgkin and non-Hodgkin lymphoma: the Lugano classification. J Clin Oncol. 2014;32(27):3059-68. doi:10.1200/jco.2013.54.8800 PubMed
56.Hlubocky FJ, Webster K, Beaumont J, et al. A preliminary study of a health related quality of life assessment of priority symptoms in advanced lymphoma: the National Comprehensive Cancer Network-Functional Assessment of Cancer Therapy - Lymphoma Symptom Index. Leuk Lymphoma. 2013;54(9):1942-6. doi:10.3109/10428194.2012.762977 PubMed
57.Cella D, Webster K, Cashy J, et al. Development of a measure of health-related quality of life for non-hodgkin’s lymphoma clinical research: The Functional Assessment of Cancer Therapy-Lymphoma (FACT-Lym). Blood. 2005;106(11):750. doi:10.1182/blood.V106.11.750.750
58.Webster K, Cashy J, Cella D, et al. P-218/1650/ Measuring quality of life (QOL) in patients with non-Hodgkin's lymphoma (NHL): The Functional Assessment of Cancer Therapy-Lymphoma (FACT-Lym). Qual Life Res. 2005;14(9):2103-2103.
59.Carter GC, Liepa AM, Zimmermann AH, et al. Validation of the functional assessment of cancer therapy–lymphoma (FACT-LYM) in patients with relapsed/refractory mantle cell lymphoma. Blood. 2008;112(11):2376. doi:10.1182/blood.V112.11.2376.2376
Pharmacoeconomic Review
Abbreviations
AE
adverse event
BIA
budget impact analysis
CDA-AMC
Canada’s Drug Agency
CUA
cost-utility analysis
ICER
incremental cost-effectiveness ratio
LY
life-year
MCL
mantle cell lymphoma
OS
overall survival
PFS
progression-free survival
QALY
quality-adjusted life-year
RDI
relative dose intensity
Economic Review
The objective of the economic review is to review and critically appraise the pharmacoeconomic evidence submitted by the sponsor on the cost-effectiveness and budget impact of venetoclax in combination with ibrutinib compared to ibrutinib alone for the treatment of adult patients with mantle cell lymphoma (MCL) who have received at least 1 prior therapy.
Item | Description |
|---|---|
Drug product | Venetoclax (Venclexta), 10 mg, 50 mg, and 100 mg oral tablets |
Indication | In combination with ibrutinib, for the treatment of adult patients with relapsed or refractory MCL. |
Submitted price | Venetoclax
|
Health Canada approval status | NOC |
Health Canada review pathway | Standard |
NOC date | July 31, 2025 |
Reimbursement request | As per indication |
Sponsor | AbbVie Corporation |
Submission history | Previously reviewed: Yes Indication: In combination with obinutuzumab for previously untreated CLL Recommendation date: November 28, 2024 Recommendation: Recommended with clinical criteria and/or conditions Indication: In combination with low-dose cytarabine for newly diagnosed AML in patients who are 75 years or older, or who have comorbidities that preclude use of intensive induction chemotherapy Recommendation date: August 23, 2021 Recommendation: Do not reimburse Indication: In combination with azacitidine for newly diagnosed AML in patients who are 75 years or older, or who have comorbidities that preclude use of intensive induction chemotherapy Recommendation date: August 20, 2021 Recommendation: Recommended with clinical criteria and/or conditions Indication: In combination with obinutuzumab for previously untreated CLL who are fludarabine ineligible Recommendation date: November 17, 2020 Recommendation: Recommended with clinical criteria and/or conditions Indication: In combination with rituximab for CLL in adults who have received at least 1 prior therapy Recommendation date: May 31, 2019 Recommendation: Recommended with clinical criteria and/or conditions Indication: For the treatment of CLL in patients who have received at least 1 prior therapy and who have failed a B-cell receptor inhibitor Recommendation date: March 2, 2018 Recommendation: Recommended with clinical criteria and/or conditions |
AML = acute myeloid leukemia; CLL = chronic lymphocytic leukemia; MCL = mantle cell lymphoma; NOC = Notice of Compliance.
Key Messages
Venetoclax is supplied as 10 mg, 50 mg, and 100 mg tablets. At the submitted unit price (refer to Table 1), the cost of venetoclax is $1,834 per patient in the first 28-day cycle (subsequent cycles: $7,930), based on the Health Canada–recommended dosage. When used in combination with ibrutinib, the total cost is $13,016 per patient in the first 28-day cycle and $19,111 in subsequent cycles. The total recommended duration of venetoclax is 24 months.
Clinical efficacy data used in the economic analysis were derived from the randomized phase of the SYMPATICO trial, which compared venetoclax plus ibrutinib to placebo plus ibrutinib.1,2 Evidence from the SYMPATICO trial suggests that venetoclax plus ibrutinib likely results in a clinically meaningful improvement in the probability of being progression-free at 60 months compared to ibrutinib alone, with little to no difference in survival at 60 months.
The results of the Canada’s Drug Agency (CDA-AMC) base case suggest:
Venetoclax plus ibrutinib is predicted to be associated with higher costs to the health care system than ibrutinib alone (incremental costs = $172,576), primarily driven by increased acquisition costs associated with venetoclax.
Venetoclax plus ibrutinib is predicted to be associated with an incremental gain of 0.51 life-years (LYs) compared to ibrutinib alone and may result in a gain of 0.48 quality-adjusted life-years (QALYs) compared to ibrutinib alone.
The incremental cost-effectiveness ratio (ICER) of venetoclax plus ibrutinib versus ibrutinib alone was $360,148 per QALY gained in the CDA-AMC base case. The estimated ICER was highly sensitive to the predicted overall survival (OS) benefit, and more than 85% of the incremental benefit was gained in the extrapolated period (i.e., after 60 months). In the absence of long-term data, these projected benefits are highly uncertain and may be overestimated. Additional price reductions may therefore be required.
CDA-AMC estimates that the budget impact of reimbursing venetoclax for use in combination with ibrutinib for relapsed or refractory MCL will be approximately $43 million over the first 3 years of reimbursement compared to the amount currently spent on ibrutinib alone. The expenditure on venetoclax over this period is predicted to be approximately $40 million. The actual budget impact of reimbursing venetoclax will depend on the number of eligible patients, market uptake, and the use of other treatments.
Summary of the Submitted Economic Evaluation
The sponsor submitted a cost-utility analysis (CUA) to assess the cost-effectiveness of venetoclax in combination with ibrutinib from the perspective of a public health care payer in Canada, using a lifetime time horizon (33 years). The modelled population included adult patients with MCL who had received at least 1 prior therapy.3 This population aligns with the Health Canada indication and reimbursement request, as well as the patient population enrolled in the SYMPATICO trial.1,2
In the sponsor’s base-case analysis, costs considered included drug acquisition (based on the submitted price for venetoclax and public list prices for comparators), health-state resource use, management of tumour lysis syndrome, subsequent treatment, and adverse events (AEs). Compared with ibrutinib alone, venetoclax plus ibrutinib was associated with an incremental cost of $173,713 and a gain of 0.90 QALYs, resulting in an ICER of $192,741 per QALY gained. Of the incremental benefit, 87% of the incremental LYs and 85% of the incremental QALYs were predicted to be accrued after the duration of the SYMPATICO trial. Further details on the sponsor’s submission are provided in Appendix 3.
CDA-AMC identified several key issues with the sponsor’s analysis (refer to Table 2; full details are provided in Appendix 4).
Table 2: Key Issues With the Sponsor’s Economic Submission
Issue | What evidence is there to inform this issue? | How was this issue addressed by CDA-AMC? | Did CDA-AMC explore uncertainty in a scenario analysis? |
|---|---|---|---|
The long-term benefits of venetoclax plus ibrutinib are uncertain. | The sponsor’s model predicts a gain of 0.99 LYs and 0.90 QALYs for venetoclax plus ibrutinib compared to ibrutinib alone, with 87% of the incremental LYs and 85% of the incremental QALYs accrued through extrapolation. Interim OS data from the SYMPATICO trial are immature and suggest little to no difference in OS at 60 months of follow-up. Clinical expert input received by CDA-AMC indicated that the predicted survival rates were overly optimistic. | In the CDA-AMC base case, data from the SYMPATICO trial were adopted for the trial period and an alternative distribution (exponential) was adopted for extrapolation of OS for both venetoclax plus ibrutinib and ibrutinib alone, based on clinical expert input. | CDA-AMC explored alternative OS extrapolations in scenario analyses. |
Relevant comparators were excluded from the sponsor’s economic evaluation. | The sponsor’s economic evaluation compared venetoclax plus ibrutinib to ibrutinib alone. Clinical expert input received by CDA-AMC noted that some patients receive other treatment regimens, including bortezomib- and rituximab-based chemoimmunotherapy.a | CDA-AMC could not address this issue owing to a lack of comparative efficacy data for venetoclax plus ibrutinib vs. treatments other than ibrutinib alone. | No scenario analysis was conducted. |
Health-state utility values lack face validity. | The utility values used by the sponsor were derived from SYMPATICO trial data but were considered overly optimistic by clinical experts for patients with relapsed or refractory MCL (preprogression: ████; postprogression: ████). The CDA-AMC Clinical Review noted concerns about potential bias in self-reported HRQoL owing to the open-label design of the trial and missing data. | CDA-AMC adopted utility values from the literature (preprogression: 0.78; postprogression: 0.68).4 Clinical experts indicated that these values had better face validity than those derived from SYMPATICO trial data. | No scenario analysis was conducted. |
CDA-AMC = Canada’s Drug Agency; HRQoL = health-related quality of life; LY = life-year; MCL = mantle cell lymphoma; OS = overall survival; QALY = quality-adjusted life-year; vs. = versus.
Note: Full details of the issues identified by CDA-AMC are provided in Appendix 3.
aIn addition, acalabrutinib and zanubrutinib may be received by some patients as second-line treatment (e.g., via compassionate access programs). Acalabrutinib is approved by Health Canada for treatment of patients with MCL who have received at least 1 prior therapy; however, it has not been submitted to CDA-AMC for this indication. Zanubrutinib received a recommendation of do not reimburse for the treatment of MCL in patients who have received at least 1 prior therapy from CDA-AMC in 2022.
CDA-AMC Assessment of Cost-Effectiveness
The CDA-AMC base case was derived by making changes to model parameter values and assumptions (refer to Table 6), in consultation with clinical experts. Detailed information about the base case is provided in Appendix 4.
Impact on Health Care Costs
Venetoclax plus ibrutinib is expected to be associated with additional health care costs compared to ibrutinib alone (incremental costs = $172,576). This increase in health care spending results from drug acquisition costs associated with venetoclax (refer to Figure 1).
Figure 1: Impact of Venetoclax Plus Ibrutinib vs. Ibrutinib Alone on Health Care Costs
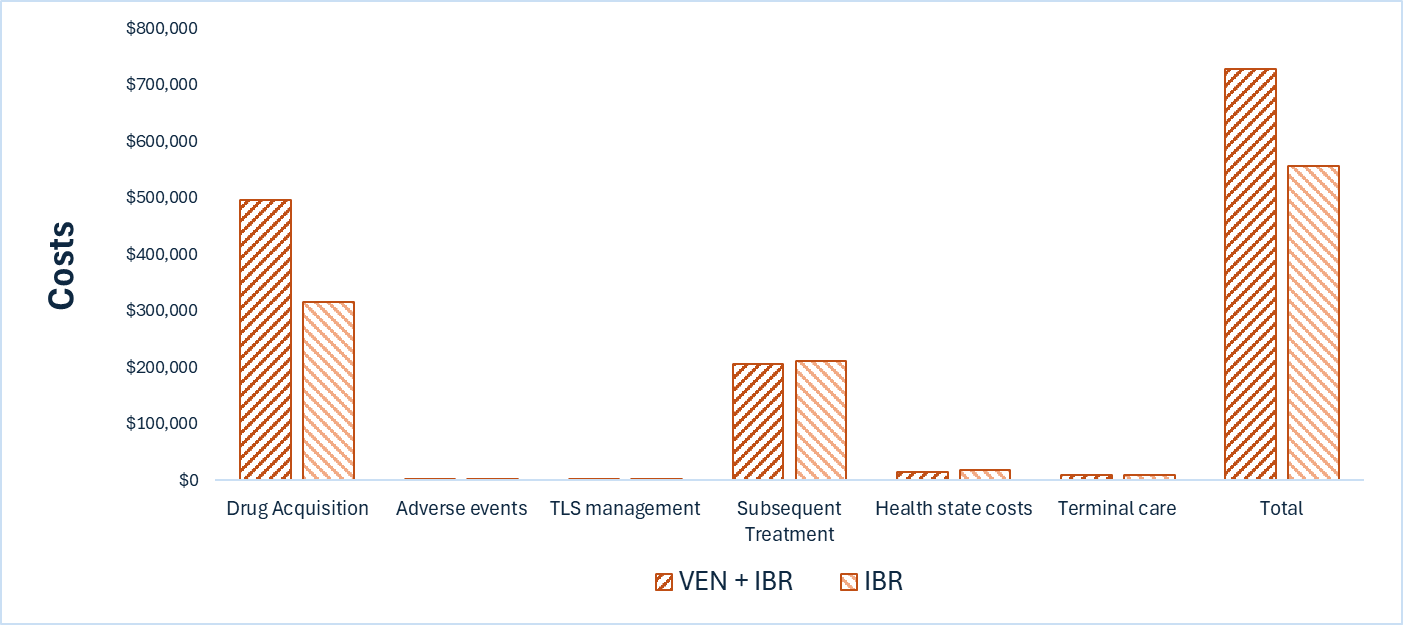
IBR = ibrutinib; TLS = tumour lysis syndrome; VEN = venetoclax; vs. = versus.
Impact on Health
Relative to ibrutinib alone, venetoclax plus ibrutinib is predicted to increase the amount of time a patient remains progression-free by approximately 1.38 years, with an incremental gain of 0.51 LYs, compared to ibrutinib alone. Considering the impact of treatment on both quality and length of life, venetoclax plus ibrutinib is predicted to result in 0.48 QALYs per patient compared to ibrutinib alone (refer to Figure 2 and Table 7). Approximately 85% of the predicted incremental QALYs were accrued on the basis of extrapolation.
Figure 2: Impact of Venetoclax Plus Ibrutinib vs. Ibrutinib Alone on Patient Health
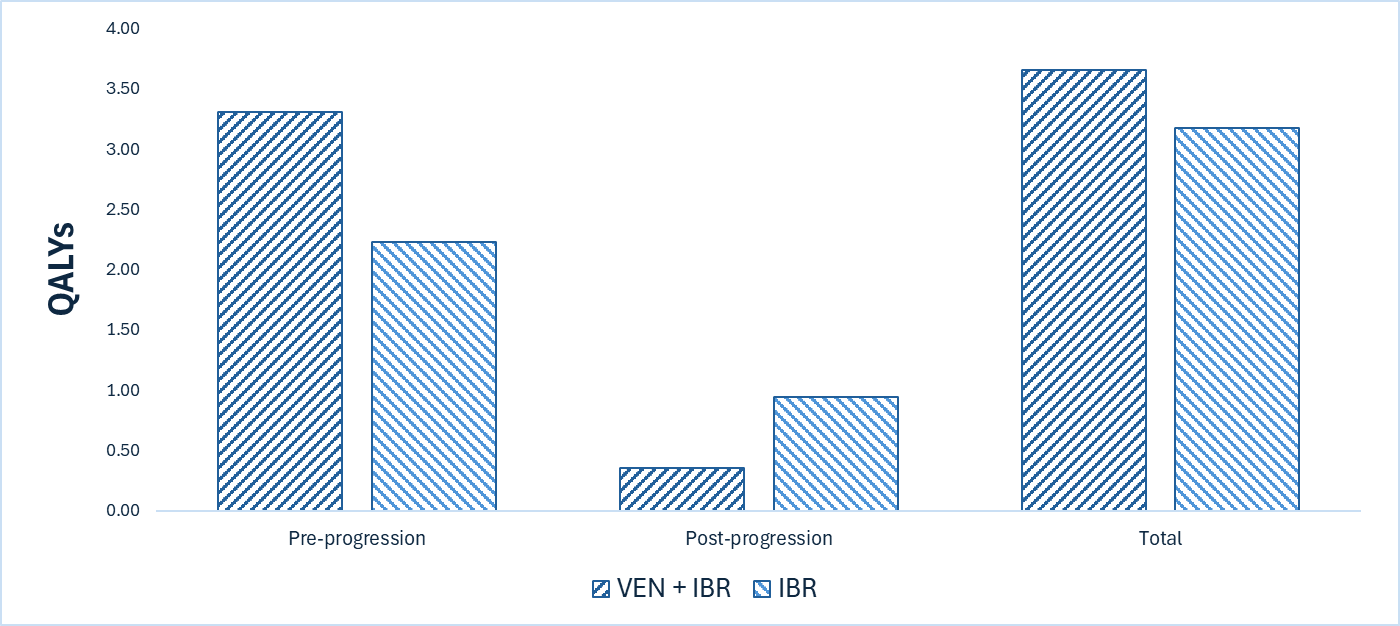
IBR = ibrutinib; QALY = quality-adjusted life-year; VEN = venetoclax; vs. = versus.
Overall Results
The results of the CDA-AMC base case suggest an ICER of $360,148 per QALY gained for venetoclax plus ibrutinib compared to ibrutinib alone (refer to Table 3). Additional details on the CDA-AMC base case are available in Appendix 4.
Table 3: Summary of CDA-AMC Economic Evaluation Results
Drug | Total costs ($) | Total LYs | Total QALYs | ICER vs. ibrutinib ($/QALY) |
|---|---|---|---|---|
Ibrutinib | 556,277 | 4.25 | 3.17 | Reference |
Venetoclax + ibrutinib | 728,854 | 4.76 | 3.65 | 360,148 |
CDA-AMC = Canada’s Drug Agency; ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year; vs. = versus.
Note: Publicly available list prices were used for comparators.
Uncertainty and Sensitivity
Uncertainty was explored in the scenario analyses outlined in Table 2, which included adopting an alternative extrapolation model for OS and assuming 100% relative dose intensity (RDI) (refer to Table 10, Appendix 4). Based on the results of these analyses, the ICER for venetoclax plus ibrutinib may range from $228,921 to $409,769 per QALY gained compared with ibrutinib alone.
Summary of the Budget Impact
The sponsor submitted a budget impact analysis (BIA) to estimate the 3-year (2026 to 2029) budget impact of reimbursing venetoclax for use in combination with ibrutinib in adult patients with MCL that have received at least 1 prior therapy.3 The sponsor assumed that the payers would be CDA-AMC–participating public drug plans and derived the size of the eligible population using an epidemiologic approach.5 The price of venetoclax was aligned with the price included in the sponsor’s economic evaluation, while the prices of comparators were based on the publicly available list prices.1,6-8 Additional information pertaining to the sponsor’s submission is provided in Appendix 5.
CDA-AMC identified a number of issues with the sponsor’s estimated budget impact and made changes to model parameters and assumptions in consultation with clinical experts to derive the CDA-AMC base case (Table 13). CDA-AMC estimated that 1,216 patients would be eligible for treatment with venetoclax plus ibrutinib over a 3-year period (year 1 = 396; year 2 = 405; year 3 = 415), of whom 449 are expected to receive venetoclax plus ibrutinib (year 1 = 79; year 2 = 162; year 3 = 207). The estimated incremental budget impact of reimbursing venetoclax plus ibrutinib is expected to be approximately $43 million over the first 3 years, with an expected expenditure of $40 million on venetoclax (refer to Table 14). The actual budget impact will depend on the number of eligible patients, the uptake of venetoclax plus ibrutinib, and confidentially negotiated prices of venetoclax and ibrutinib.
Conclusion
Based on the CDA-AMC base case, venetoclax in combination with ibrutinib would be considered cost-effective at the submitted price if the public health care system was willing to pay at least $360,148 for each additional QALY gained. If the public health care system is not willing to pay that amount, a price reduction should be considered (refer to Figure 3; full details of the impact of price reductions on cost-effectiveness are presented in Table 9). In the absence of long-term data, these projected benefits are highly uncertain and may be overestimated. Additional price reductions may therefore be required.
The budget impact of reimbursing venetoclax for use in combination with ibrutinib to the public drug plans in the first 3 years is estimated to be approximately $43 million. The 3-year expenditure on venetoclax (i.e., not accounting for current expenditure on comparators) is estimated to be $40 million. The estimated budget impact will depend on the number of eligible patients, the uptake of venetoclax plus ibrutinib, and confidentially negotiated prices of venetoclax and ibrutinib.
Figure 3: Summary of the CDA-AMC Economic Analysis and Price Reduction

CDA-AMC = Canada’s Drug Agency; IBR = ibrutinib; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; VEN = venetoclax.
Note: Expenditure includes only the drug cost of venetoclax. The term dominant indicates that a drug costs less and provides more QALYs than the comparator.
References
1.AbbVie Corporation. Drug Reimbursement Review sponsor submission: Venclexta (venetoclax), 10 mg, 50 mg, and 100 mg, oral tablets [internal sponsor's package]. February 20, 2025.
2.Wang M, Jurczak W, Trneny M, et al. Ibrutinib plus venetoclax in relapsed or refractory mantle cell lymphoma (SYMPATICO): a multicentre, randomised, double-blind, placebo-controlled, phase 3 study. Lancet Oncol. 2025;26(2):200-213. doi:10.1016/S1470-2045(24)00682-X PubMed
3.AbbVie Corporation. Venclexta (venetoclax): 10 mg, 50 mg, and 100 mg, oral tablets [product monograph]. September 27, 2016. Updated August 2024.
4.NICE. Ibrutinib for treating relapsed or refractory mantle cell lymphoma: Technology appraisal guidance (TA502) [sponsor supplied reference]. https://www.nice.org.uk/guidance/ta502
5.AbbVie Corporation. Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Venclexta (venetoclax), 10 mg, 50 mg, and 100 mg, oral tablets. February 20, 2025.
6.IQVIA. DeltaPA. 2025. Accessed May, 2025. https://www.iqvia.com/
7.Government of Ontario. Exceptional Access Program product prices [sponsor provided reference]. Accessed May 2025, https://www.ontario.ca/page/exceptional-access-program-product-prices
8.Ontario Go. Ontario Drug Benefit Formulary/Comparative Drug Index [sponsor supplied reference]. May 2025. https://www.formulary.health.gov.on.ca/formulary/
9.Friedberg JW, Vose JM, Kelly JL, et al. The combination of bendamustine, bortezomib, and rituximab for patients with relapsed/refractory indolent and mantle cell non-Hodgkin lymphoma. Blood. 2011;117(10):2807-12. doi:10.1182/blood-2010-11-314708 PubMed
10.Latimer NR. NICE Decision Support Unit Technical Support Documents. Survival Analysis For Economic Evaluations Alongside Clinical Trials-Extrapolation with Patient Level Data. National Institute for Health and Care Excellence (NICE); 2013.
11.Villa D, Kansara R, Lemieux C, Kuruvilla J. Updates in the treatment of mantle cell lymphoma: A Canadian expert framework. Canadian Hematology Today. 2022:2–11-2–11.
12.Cancer Care Alberta. Clinical Practice Guideline LYHE-002 V20: Lymphoma [sponsor provided reference]. https://www.albertahealthservices.ca/assets/info/hp/cancer/if-hp-cancer-guide-lyhe002-lymphoma.pdf
13.PeriPharm Inc. Burden of Illness and Health Care Resource Utilization in the Management of Patients with Relapse/Refractory Mantle Cell Lymphoma in Canada [sponsor supplied reference]. 2024.
14.Yan J, Xie S, Johnson JA, et al. Canada population norms for the EQ-5D-5L. Eur J Health Econ. 2024;25(1):147-155. doi:10.1007/s10198-023-01570-1 PubMed
15.NICE. Ibrutinib with venetoclax for untreated chronic lymphocytic leukaemia (Technology appraisal guidance TA891) [sponsor supplied reference]. https://www.nice.org.uk/guidance/ta891
16.AbbVie Corporation. Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Venclexta (venetoclax), 10 mg, 50 mg, and 100 mg, oral tablets. February 20, 2025.
17.Statistics Canada. Table 17-10-0005-01 Population estimates on July 1st, by age and sex. DOI: https://doi.org/10.25318/1710000501-eng [sponsor provided reference].
18.Non-Insured Health Benefits Program. First Nations and Inuit Health Branch: Annual report 2022 to 2023. Accessed at: https://www.sac-isc.gc.ca/eng/1713194236054/1713194280612 [sponsor supplied reference].
19.Canadian Cancer Statistics Advisory Committee, Canadian Cancer Society, Statistics Canada, Public Health Agency of Canada. Canadian Cancer Statistics: a 2024 special report on the economic impact of cancer in Canada. Canadian Cancer Society; 2024. Accessed May 15, 2025. https://cdn.cancer.ca/-/media/files/research/cancer-statistics/2024-statistics/2024-special-report/2024_pdf_en.pdf
20.Leukemia and Lymphoma Society. 2014. Mantle Cell Lymphoma Facts. Accessed at: https://www.lls.org/sites/default/files/file_assets/mantlecelllymphoma.pdf [sponsor supplied reference].
21.Narkhede M, Goyal G, Shea L, Mehta A, Giri S. Evaluating real-world treatment patterns and outcomes of mantle cell lymphoma. Blood Adv. 2022;6(14):4122-4131. doi:10.1182/bloodadvances.2022007247 PubMed
22.Sutherland G, Dihn T. Understanding the gap: a pan-Canadian analysis of prescription drug insurance coverage. The Conference Board of Canada; 2017. Accessed May 15, 2025. https://www.conferenceboard.ca/e-library/abstract.aspx?did=9326
23.Ibrutinib/PCI-32765 PCYC-1143-CA (SYMPATICO). Primary Analysis Clinical Study Report. Data cut-off: July 5, 2023 [sponsor supplied reference].
24.Bock AM, Gile JJ, Larson MC, et al. Evolving treatment patterns and improved outcomes in relapsed/refractory mantle cell lymphoma: a prospective cohort study. Blood Cancer J. 2023;13(1):169. doi:10.1038/s41408-023-00942-3 PubMed
25.Hess G, Dreyling M, Oberic L, et al. Real-world experience among patients with relapsed/refractory mantle cell lymphoma after Bruton tyrosine kinase inhibitor failure in Europe: The SCHOLAR-2 retrospective chart review study. Br J Haematol. 2023;202(4):749-759. doi:10.1111/bjh.18519. PubMed
Appendix 1: Cost Comparison Table
Please note that this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical experts and CDA-AMC–participating public drug plans. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table, and, as a result, the table may not represent the actual costs to public drug plans
Table 4: Cost Comparison for Relapsed or Refractory MCL
Treatment | Strength and/or concentration | Form | Price ($) | Recommended dosage | Daily cost ($) | 28-day cost ($) |
|---|---|---|---|---|---|---|
Venetoclax + ibrutinib | ||||||
Venetoclax | 10 mg 50 mg 100 mg | Tablet | 7.0800a 35.4000a 70.8000a | Cycle 1: 20 mg daily for the first week; 50 mg daily for the second week; 100 mg daily for the third week; and 200 mg daily during the fourth week Cycle 2+: 400 mg daily for up to 24 months total | Cycle 1: 65.49 Cycle 2+: 283.20 | Cycle 1: 1,834 Cycle 2+: 7,930 |
Ibrutinib | 140 mg | Capsule | 99.8350b | 560 mg daily in combination with venetoclax until disease toxicity | 399.34 | 11,182 |
Venetoclax + ibrutinib | — | — | — | — | Cycle 1: 464.83 Cycle 2+: 682.54 | Cycle 1: 13,016 Cycle 2+: 19,111 |
BTK inhibitors | ||||||
Acalabrutinibc | 100 mg | Tablet | 142.7700b | 100 mg twice daily | 285.55 | 7,995 |
Ibrutinib | 140 mg | Capsule | 99.8350b | 560 mg daily | 399.34 | 11,182 |
Zanubrutinibc | 80 mg | Capsule | 67.9800b | 160 mg twice daily | 271.93 | 7,614 |
Chemotherapy and chemoimmunotherapy | ||||||
Bortezomib monotherapy | ||||||
Bortezomib | 3.5 mg | Powder in vial | 654.3100d | 1.3 mg/m2 on days 1, 4, 8, and 11 for 8, 21-day cycles | 124.63 | 3,490 |
Bendamustine + rituximab | ||||||
Bendamustine | 25 mg 100 mg | 5 mg/mL vial for IV infusion | 250.0000d 1,000.0000d | 90 mg/m2 on days 1 and 2 for 6 28-day cycles | 125.00 | 3,500 |
Rituximab | 100 mg 500 mg 1,400 mg 1,600 mg | 10 mg/mL vial for IV infusion Solution for subcutaneous injection | 297.0000d 1,485.0000d 2,880.2807d 3,832.1893d | 375 mg/m2 on day 1 of each 28-day cycle Cycle 2+: either 375 mg/m2 or 1,400 mg subcutaneously every 28 daysf | Cycle 1: 74.25 Cycle 2+: 74.25 or 102.87 | Cycle 1: 2,079 Cycle 2+: 2,079 or 2,880 |
Bendamustine + rituximab | — | — | — | — | 199.25 or 227.87 | 5,579 or 6,380 |
Bortezomib + rituximab | ||||||
Bortezomib | 3.5 mg | Powder in vial | 654.3100d | 1.6 mg/m2 on days 1, 8, 15, and 22 every 35 dayse | 74.78 | 2,094 |
Rituximab | 100 mg 500 mg | 10 mg/mL vial for IV infusion | 297.0000d 1,485.0000d | 375 mg/m2 on days 1, 8, 15, and 22 every 35 dayse | 237.60 | 6,653 |
Bortezomib + rituximab | — | — | — | — | 312.38 | 8,747 |
Bendamustine + rituximab + bortezomib | ||||||
Bendamustine | 25 mg 100 mg | 5 mg/mL vial for IV infusion | 250.0000d 1,000.0000d | 90 mg/m2 on days 1 and 4 every 28 dayse | 125.00 | 3,500 |
Rituximab | 100 mg 500 mg | 10 mg/mL vial for IV infusion | 297.0000d 1,485.0000d | 375 mg/m2 on day 1 every 28 dayse | 74.25 | 2,079 |
Bortezomib | 3.5 mg | Powder in vial | 654.3100d | 1.3 mg/m2 on days 1, 4, 8, and 11 every 28 dayse | 93.47 | 2,617 |
Bendamustine + rituximab + bortezomib | — | — | — | — | 292.72 | 8,196 |
Bendamustine + cytarabine + rituximab | ||||||
Bendamustine | 25 mg 100 mg | 5 mg/mL vial for IV infusion | 250.0000d 1,000.0000d | 70 mg/m2 on days 2 and 3 every 28 days | 104.14 | 3,000 |
Rituximab | 100 mg 500 mg 1,400 mg 1,600 mg | 10 mg/mL vial for IV infusion Solution for subcutaneous injection | 297.0000d 1,485.0000d 2,880.2807d 3,832.1893d | Cycle 1: 375 mg/m2 on day 1 every 28 days Cycle 2+: 375 mg/m2 or 1,400 mg subcutaneously every 28 daysf | Cycle 1: 74.25 Cycle 2+: 74.25 or 102.87 | Cycle 1: 2,079 Cycle 2+: 2,079 or 2,880 |
Cytarabine | 500 mg 2000 mg | 100 mg/mL vial for IV infusion | 76.85d 306.5000d | 500 to 800 mg/m2 on days 2 to 4 every 28 days | 16.47 to 24.70 | 461.10 to 691.65 |
Bendamustine + cytarabine + rituximab | — | — | — | — | 197.86 to 206.09 or 226.48 to 234.71 | 5,540 to 5,771 or 6,341 to 6,572 |
Lenalidomide + rituximab | ||||||
Lenalidomide | 2.5 mg 5 mg 10 mg 15 mg 20 mg 25 mg | Capsule | 82.3752g 85.0000g 90.2500g 95.5000g 100.7500g 106.0000g | Cycle 1, 2 to 5, and 6 to 12: 20 mg daily from day 1 to 21 of a 28-day cycle | Cycle 1, 2 to 5, and 6 to 12: 75.56 | Cycle 1, 2 to 5, and 6 to 12: 2,116 |
Rituximab | 100 mg 500 mg | 10 mg/mL vial for IV infusion | 297.0000d 1,485.0000d | Cycle 1: 375 mg/m2 on days 1, 8, 15, and 22 of a 28-day cycle Cycle 2 to 5: 375 mg/m2 on day 1 for each 28-day cycle | Cycle 1: 297.00 Cycle 2 to 5: 74.25 | Cycle 1: 2,116 Cycle 2 to 5: 2,079 |
Lenalidomide + rituximab | — | — | — | — | Cycle 1: 372.56 Cycle 2 to 5: 149.81 Cycle 6 to 12: 75.56 | Cycle 1: 10,432 Cycle 2 to 5: 4,195 Cycle 6 to 12: 2,116 |
Cyclophosphamide + doxorubicin + vincristine + prednisone + rituximab (CHOP + R) | ||||||
Rituximab | 100 mg 500 mg | 10 mg/mL vial for IV infusion | 297.0000d 1,485.0000d | Cycle 1: 375 mg/m2 on day 1 every 21 days Cycle 2+: 375 mg/m2 or 1,400 mg subcutaneously every 21 daysf | 99.00 or 137.16 | 2,772 or 3,840 |
Vincristine | 1 mg 2 mg 5 mg | 1 mg/mL vial for IV infusion | 30.6000d 62.0000d 153.0000d | 1.4 mg/m2 on day 1 every 21 days | 2.95 | 83.00 |
Doxorubicin | 10 mg 50 mg 200 mg | 2 mg/mL vial for IV infusion | 50.0000d 252.2500d 770.0000d | 50 mg/m2 on day 1 every 21 days | 21.54 | 603.00 |
Cyclophosphamide | 500 mg 1,000 mg 2,000 mg | 20 mg/mL vial for IV infusion | 101.7100d 184.3600d 339.2000d | 750 mg/m2 on day 1 every 21 days | 13.62 | 381.43 |
Oral prednisone | 50 mg | Tablet | 0.1735g | 100 mg daily from day 1 to 5 of a 21-day cycle | 0.08 | 2.00 |
CHOP + R | — | — | — | — | 137.19 or 175.35 | 3,841 or 4,910 |
BSA = body surface area; BTK = Bruton’s tyrosine kinase; MCL = mantle cell lymphoma.
Note: Patient weight and BSA were assumed 75 kg and 1.8 m2, respectively. All off-label treatment recommended dosages were obtained from Cancer Care Ontario and verified by clinical experts consulted by CDA-AMC. Dispensing fees are not included. All drug cost calculations assume 100% relative drug intensity.
aSponsor’s submitted price.1
bOntario Exceptional Access Program (accessed May 2025).7
cAcalabrutinib and zanubrutinib are funded through compassionate care programs.
dIQVIA Delta PA database (accessed May 2025).6
eRecommended dosage obtained from published literature and verified by clinical experts consulted for this review by CDA-AMC.9
fSubcutaneous rituximab may only be initiated starting at cycle 2 for regimens that include subcutaneous administration.
gOntario Drug Benefit Formulary (accessed May 2025).8
Appendix 2: Input Relevant to the Economic Review
Please note that this appendix has not been copy-edited.
This section is a summary of the input received from the patient groups, clinician groups, and drug plans that participated in the CDA-AMC review process.
Patient input was received from Lymphoma Canada, collected through a survey of 82 people with MCL (74% from Canada; 5 with experience with venetoclax plus ibrutinib). Patients described physical symptoms associated with MCL that included persistent fatigue, enlarged lymph nodes, abdominal discomfort (e.g., bloating, indigestion), night sweats, weight loss, and leukocytosis. Patients also noted psychosocial impacts, such as fear of disease progression or relapse, restrictions on travel, limitations in employment and volunteer activities, and anxiety related to having a weakened immune system. Respondents reported having received various lines of therapy, with many having undergone 1 or more than 3 lines of treatment. Challenging side effects with treatment included fatigue, nausea, insomnia, appetite and weight loss, hair loss, constipation, joint pain, bodily aches and pain, neuropathy, mouth sores, muscle weakness, and diarrhea. More than half of respondents emphasized the need for additional treatment options in the second and third-line settings. Patients identified prolonged survival, longer remission, improved quality of life, and fewer side effects as important areas of unmet need. Among the 5 patients who had experience with venetoclax plus ibrutinib, the most frequently reported side effects were diarrhea, neutropenia, and fatigue, while some patients reported muscle pain and constipation; however, overall, feedback from respondents was positive.
Clinician group input was received from the Ontario Health Cancer Care Ontario Hematology Cancer Drug Advisory Committee and Lymphoma Canada Physician Group. Clinician group input noted that current treatment options for patients with relapsed or refractory MCL include ibrutinib monotherapy alone, rituximab-based chemoimmunotherapy or chemotherapy alone (for patients refractory to rituximab), bortezomib-containing regimens, and brexucabtagene autoleucel (third-line only), as well as drugs accessed through compassionate access programs (i.e., acalabrutinib, zanubrutinib, pirtobrutinib). Input from the clinician groups noted that unmet needs for MCL include improved survival, delayed disease progression, resolution of symptoms, and preserved health-related quality of life; as such, these are key goals of treatment. Clinicians noted that venetoclax plus ibrutinib is anticipated to be most beneficial for BTK inhibitor–naive patients, although it may also be appropriate for use in patients who are not refractory to BTK inhibitors, due to the limited number of available treatment options in this setting. Clinicians emphasized the notable improvement in progression-free survival (PFS) associated with venetoclax plus ibrutinib across all risk groups, suggesting that disease characteristics such as stage or cytogenetics would not prevent its use. Given that venetoclax plus ibrutinib is orally administered, highlight a key advantage for its use, as this increases its accessibility to patients without the need for specialized care apart from the routine bloodwork monitoring necessary.
Input from CDA-AMC–participating drug plans noted that, in addition to ibrutinib, other comparators (e.g., rituximab-bendamustine) are funded in some jurisdictions for this indication. Drug plans noted that the current standard of care involves BTK inhibitor therapy, with ibrutinib being the only funded option. Plans noted that other BTK inhibitors, such as zanubrutinib and acalabrutinib, were not included as comparators in the submission for venetoclax plus ibrutinib. Plans noted that inpatient administration may be required during the first few ramp-up doses for patients at high risk for tumour lysis syndrome. Plans noted that the SYMPATICO trial included patients with Eastern Cooperative Oncology Group performance status of 0 to 2 and questioned whether the results can be generalized to patients with a status of 3. Plans asked whether patients receiving ibrutinib or other treatments could be eligible to switch to venetoclax plus ibrutinib. Lastly, drug plans were interested in how the evolving treatment landscape of MCL might impact access to treatments for patients with relapsed or recurrent disease.
Several of these concerns were addressed in the sponsor’s model:
The submitted model incorporated the impact of venetoclax plus ibrutinib on survival, disease progression, and health-related quality of life.
The model accounted for additional laboratory monitoring and supportive care measures required to mitigate the risk of tumour lysis syndrome. The model also considered additional clinic visits and ongoing monitoring requirements.
Key AEs associated with the combination therapy, including diarrhea and fatigue, were incorporated into the model.
The submitted economic model accounted for CDA-AMC addressed some of these concerns as follows:
The base-case analysis incorporated an alternative assumption for OS beyond the trial period and health-related quality of life, to reflect clinicians’ and patients’ concerns regarding the unmet needs in MCL.
CDA-AMC was unable to address the following concerns:
Ibrutinib alone was selected as the comparator. However, the submission did not include rituximab-bendamustine and other BTK inhibitors, such as zanubrutinib or acalabrutinib, as comparators. CDA-AMC could not address this limitation due to the absence of comparative efficacy data for these BTK inhibitors in the relevant patient population.
Appendix 3: Summary of the Sponsor’s Submission
Please note that this appendix has not been copy-edited.
Summary of the Sponsor’s Economic Evaluation
For the pharmaceutical reviews program, clinical and economic information is submitted to CDA-AMC by the sponsor. The CDA-AMC health economics team reviews the submitted economic information and appraises the information in collaboration with clinical experts and the clinical review team to evaluate key assumptions, influential parameters, and the overall rigour of the economic submission. Based on what the team learns through this process, adjustments may be made to the sponsor’s model to produce the CDA-AMC base case. The CDA-AMC base case represents the team’s current understanding of the clinical condition, clinical evidence currently available, and best interpretation of the economic evidence based on the information provided.
For the review of venetoclax in combination with ibrutinib, the sponsor provided a CUA and a BIA. The sponsor’s economic submission is summarized in Table 5.
Table 5: Key Components of the Sponsor’s Economic Evaluation
Component | Description |
|---|---|
Treatment information | |
Drug under review | Venetoclax (Venclexta), 10, 50, and 100 mg oral tablets |
Submitted price of drug under review | Venetoclax
|
Regimen | Venetoclax: 5-week ramp-up to 400 mg once daily (1 week each of 20 mg daily, 50 mg daily, 100 mg daily, 200 mg daily, and 400 mg daily); 400 mg once daily thereafter for a total of 24 28-day cycles. Ibrutinib: 560 mg once daily until disease progression or the occurrence of unacceptable toxicity (24 months in combination with venetoclax, then as monotherapy). |
28-day cycle cost | The estimated cost of venetoclax during the first 28 days is $1,834 (a total regimen cost of $11,897 when used in combination with ibrutinib). For subsequent cycles, the average 28-day cost of venetoclax is $7,930 (a combined regimen cost of $17,993 per cycle) |
Model information | |
Type of economic evaluation | Cost-utility analysis PSM |
Treatment | Venetoclax in combination with ibrutinib |
Included comparator | Ibrutinib alone |
Perspective | Publicly funded health care payer perspective |
Time horizon | Lifetime (33 years) |
Cycle length | 7 days |
Modelled population | Adult patients with MCL who have received at least 1 prior therapy |
Characteristics of modelled population | Derived from the SYMPATICO trial (mean age: ████ years, 79% male, BSA ████ m2, weight ████ kg) |
Model health states |
|
Data sources | |
Comparative efficacy | PFS and OS data for venetoclax plus ibrutinib and ibrutinib alone were derived from the SYMPATICO trial. |
Natural history and/or clinical pathway |
|
Health-related utilities and disutilities |
|
Costs included in the model |
|
Summary of the submitted results | |
Base-case results | ICER = $192,741 per QALY gained vs. ibrutinib alone (incremental costs = $173,713; incremental QALYs = 0.90) |
Scenario analysis resultsb |
|
AE = adverse event; BSA = body surface area; ICER = incremental cost-effectiveness ratio; MCL = mantle cell lymphoma; OS = overall survival; PFS = progression-free survival; PSM = partitioned survival model; QALY = quality-adjusted life-years; vs. = versus.
Appendix 4: Additional Details of CDA-AMC Reanalyses
Please note that this appendix has not been copy-edited.
Clinical Data in the Economic Model
The key clinical efficacy data in the model (OS, PFS, HRQoL) were derived from the randomized portion of the SYMPATICO trial (data cut-off May 22, 2023) for venetoclax plus ibrutinib and ibrutinib alone (placebo plus ibrutinib).1,2 Evidence from this trial suggests that venetoclax plus ibrutinib likely results in a clinically meaningful improvement in PFS at 36 and 60 months compared to ibrutinib alone, with little to no difference in OS at 48 or 60 months (refer to the Clinical Review report). The OS data remain immature at the time of interim analysis and the effects of venetoclax plus ibrutinib on OS beyond 60 months is uncertain.
In the economic model submitted by the sponsor, PFS and OS for venetoclax plus ibrutinib and ibrutinib were extrapolated beyond the SYMPATICO trial period, over the 33-year lifetime time horizon. Notably, 87% and 85% of the incremental gains in survival and QALYs, respectively, with venetoclax plus ibrutinib in the sponsor’s model were accrued beyond the observed trial follow-up of 60 months, contributing to additional uncertainty in the projected LYs and QALYs gained. Additionally, the Clinical Review report noted the possibility of overestimation of the PFS effect of venetoclax plus ibrutinib in the SYMPATICO trial due to informative censoring, as well as the potential for bias in HRQoL estimates (e.g., due to unblinding and missing data). Although the direction of benefit favours venetoclax plus ibrutinib compared with ibrutinib alone, the magnitude of the effect, particularly for PFS, and HRQoL, remains uncertain. As such, the estimated incremental gain in LYs and QALYs predicted by the sponsor’s model for venetoclax plus ibrutinib alone, as well as in the CDA-AMC base case, are highly uncertain.
Key Issues of the Submitted Economic Evaluation
CDA-AMC identified the following key issues with the sponsor’s analysis:
The long-term benefits of venetoclax plus ibrutinib are uncertain: The sponsor submitted a partitioned survival model (PSM), in which treatment efficacy is represented by PFS and OS curves informed by observations from the SYMPATICO trial (maximum follow-up of 62 months) and extrapolated over the model’s horizon (33 years).The parametric distributions chosen by the sponsor for extrapolation resulted in an incremental gain of 0.99 LYs and 0.90 QALYs for venetoclax plus ibrutinib compared to ibrutinib alone. Of these, 87% of the incremental LYs and 85% of the incremental QALYs were accrued during the extrapolated portion of the model. As noted in the CDA-AMC Clinical Review, while venetoclax plus ibrutinib is likely to result in a clinically meaningful improvement in the probability of being progression-free at 60 months, the PFS benefit of venetoclax plus ibrutinib may be overestimated.
Additionally, the sponsor’s selected parametric distribution for OS predicted a median survival of 46 months. The sponsor’s model predicted that approximately 39% of patients who receive venetoclax plus ibrutinib and 34% of those who receive ibrutinib alone would be alive at 5 years. Clinical expert input received by CDA-AMC suggested that these estimates are overly optimistic, with approximately 20% of patients with relapsed/refractory MCL expected to survive at 5 years. Moreover, CDA-AMC noted a slight increase in modelled OS at the tail of the curve (in both treatment arms). This is a known artifact of the parametric survival distribution used in the sponsor’s base case for OS extrapolation (log-normal) and can produce nonmonotonic extrapolations beyond the observed data.10 This behaviour is not clinically plausible and may further contribute to the overestimation of long-term survival.
CDA-AMC was unable to fully assess the concerns identified within this limitation. In the base case, CDA-AMC adopted the Kaplan-Meier estimates of OS from the SYMPATICO trial and adopted an exponential distribution for long-term extrapolation of OS for both venetoclax plus ibrutinib and ibrutinib alone. This approach may still overestimate survival; however, the predicted survival is better aligned clinical experts’ expectations and has improved plausibility of the long-term projections.
Relevant comparators were excluded from the sponsor’s economic evaluation: The sponsor’s economic evaluation compared venetoclax plus ibrutinib to ibrutinib alone. CDA-AMC notes that the sponsor requested a deviation from the CDA-AMC pharmacoeconomic requirements to exclude treatments other than ibrutinib from the economic model, based on clinical expert opinion obtained by the sponsor, prior CDA-AMC reviews, and practice guidelines.11,12 Although this request was approved by CDA-AMC, the sponsor was advised that if it was subsequently determined that there are other relevant comparators for the indication under review, the exclusion of those comparators may be identified as an important limitation of the application which may impact the recommendation.
CDA-AMC acknowledges that ibrutinib is a standard second-line treatment in Canada for relapsed or refractory MCL. However, the sources cited by the sponsor, as well as input received by CDA-AMC for this review, indicates that chemoimmunotherapy regimens may be used for some patients with relapsed or refractory MCL, including R-BAC (rituximab plus bendamustine plus cytarabine), which may potentially “achieve rapid disease control in the short term and open a window for consolidative strategies, such as CAR T-cell or allogeneic stem cell transplant.”11 A study commissioned by the sponsor suggests that ███ of patients with relapsed or refractory MCL receive ibrutinib monotherapy as a second-line treatment, while approximately ███ of patients receive a rituximab-based chemotherapy.13 Additionally, clinician input received by CDA-AMC indicated that other rituximab-based chemotherapy regimens, bortezomib-based chemoimmunotherapy regimens, and chemotherapy alone (e.g., for patients with rituximab-refractory disease) may also be considered for patients with relapsed or refractory MCL.
CDA-AMC was unable to address this limitation.
The health-state utility values lack face validity: The sponsor derived health-state utility values from EQ-5D-5L observations from the SYMPATICO trial. Clinical experts consulted by CDA-AMC considered these values to be overly optimistic for patients with relapsed or refractory MCL for both the preprogression health state (████) and the postprogression health state (████). Notably, the utility value for the progression-free state is equivalent to the estimated utility value for individuals in a similar age group in Canada,14 raising concerns about the face validity of the estimates.
Further, the Clinical Review noted concerns about the internal validity of the trial-based HRQoL data. Although the SYMPATICO trial was double-blind, there was a risk of unblinding, which may have introduced bias in self-reported HRQoL. Additionally, there was a risk of missing data for HRQoL measures, which may have further biased the utility estimates if data were not missing at random. These limitations introduce uncertainty into the model’s health utility inputs and may overstate the quality-adjusted survival benefits associated with treatment.
In the base case, CDA-AMC adopted health-state utility values from a UK National Institute of Health and Care Excellence (NICE) evaluation of ibrutinib for the treatment of relapsed or refractory MCL.15
Use of RDI may underestimate actual drug costs. In their base case, the sponsor adjusted drug costs based on the RDI observed in the SYMPATICO trial for venetoclax and ibrutinib, which results in reduced drug costs. In the model, RDI is applied for the duration of treatment (i.e., trial period plus extrapolated time on treatment). Based on the draft product monograph, any dose adjustments of venetoclax are expected to be temporary and over time a patient will return to the full recommended dose. Therefore, RDI is likely lowest during the trial period, as patients may receive a reduced dose because of an AE. Over time, patients who cannot tolerate AEs are more likely to discontinue treatment, and those who remain on treatment are likely to achieve a stable dose. In the SYMPATICO trial, approximately 23% of patients had a venetoclax dose reduction due to an AE, ███ had a dose held due to an AE, and 22% discontinued venetoclax due to an AE. Thus, applying trial-based RDI over a lifetime horizon may underestimate total drug costs.
RDI as observed in the SYMPATICO trial was maintained in the CDA-AMC base case. In scenario analysis, CDA-AMC adopted an RDI of 100%.
Additional issues were identified but were not considered to be key issues:
The sponsor assumed that patients would remain on ibrutinib for a maximum of 10 years, whereas clinical experts consulted by CDA-AMC indicated that ibrutinib is typically continued until disease progression or intolerance. However, given that the observed maximum time on treatment in the SYMPATICO trial for patients who received placebo plus ibrutinib was 58.9 months (approximately 5 years), this assumption is expected to have minimal impact on the overall cost-effectiveness results.
Administration costs were not included for venetoclax. This may underestimate total treatment costs, given that clinical experts and CDA-AMC–participating drug plans noted that ramp-up dosing schedule for venetoclax requires frequent clinic visits, particularly during the first 5 weeks of treatment. Given the short time period and that costs related to tumour lysis syndrome prevention and management were included separately, the exclusion of administration costs is unlikely to have an important impact on the cost-effectiveness results.
CDA-AMC Reanalysis of the Economic Evaluation
The CDA-AMC base case was derived by making changes in model parameter values and assumptions, in consultation with clinical experts (refer to Table 6). The impact of these changes, individually and collectively, is presented in Table 7.
Table 6: Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CDA-AMC value or assumption |
|---|---|---|
1. Overall survival | VEN + IBR: Log-normal IBR: Generalized gamma | Trial period:
Beyond the trial period:
|
2. Health-state utility values | Preprogression: ████ Postprogression: ████ | Preprogression: 0.78 Postprogression: 0.68 |
CDA-AMC base case | ― | 1 + 2 |
CDA-AMC = Canada’s Drug Agency; IBR = ibrutinib; KM = Kaplan-Meier; VEN = venetoclax.
Table 7: Summary of the Stepped Analysis
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALY) |
|---|---|---|---|---|
Sponsor’s base case | IBR | 578,124 | 4.88 | Reference |
VEN + IBR | 744,944 | 5.90 | 163,897 | |
Sponsor’s base case (probabilistic) | IBR | 570,402 | 4.95 | Reference |
VEN + IBR | 744,114 | 5.85 | 192,741 | |
CDA-AMC reanalysis 1 | IBR | 566,033 | 3.62 | Reference |
VEN + IBR | 730,602 | 4.13 | 319,800 | |
CDA-AMC reanalysis 2 | IBR | 578,124 | 4.23 | Reference |
VEN + IBR | 744,944 | 5.17 | 176,370 | |
CDA-AMC base case: (Reanalysis 1 + 2) | IBR | 566,033 | 3.17 | Reference |
VEN + IBR | 730,602 | 3.69 | 319,218 | |
CDA-AMC base case (Reanalysis 1 + 2) (probabilistic) | IBR | 556,277 | 3.19 | Reference |
VEN + IBR | 728,854 | 3.65 | 360,148 |
CDA-AMC = Canada’s Drug Agency; IBR = ibrutinib; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; VEN = venetoclax.
Note: The CDA-AMC reanalysis is based on the publicly available prices of the comparator treatments. Deterministic results are presented, unless otherwise indicated.
Table 8: Disaggregated Results of the CDA-AMC Base Case
Parameter | VEN + IBR | IBR |
|---|---|---|
Discounted LYs | ||
Total | 4.76 | 4.25 |
By health state | ||
Preprogression | 4.24 | 2.86 |
Postprogression | 0.51 | 1.39 |
Discounted QALYs | ||
Total | 3.65 | 3.17 |
By health state | ||
Preprogression | 3.31 | 2.23 |
Postprogression | 0.35 | 0.94 |
AE disutilities | –0.01 | 0.00 |
Discounted costs ($) | ||
Total | 728,854 | 556,277 |
Drug acquisition | 495,911 | 315,078 |
Administration | 0 | 0 |
AE | 2,200 | 1,543 |
Management of tumour lysis syndrome | 641 | 644 |
Subsequent treatment | 205,955 | 211,347 |
Health-state costs | 14,906 | 18,348 |
Terminal care costs | 9,240 | 9,318 |
AE = adverse event; CDA-AMC = Canada’s Drug Agency; IBR = ibrutinib; LY = life-year; QALY = quality-adjusted life-year; VEN = venetoclax.
Price Reduction Analysis
CDA-AMC conducted price reduction analyses using the sponsor’s base case and the CDA-AMC base case (refer to Table 9).
Table 9: Results of the Price Reduction Analysis
Price reduction | Unit drug cost ($) | Cost per 28 daysa ($) | ICERs for VEN + IBR vs. IBR ($/QALY) | |
|---|---|---|---|---|
Sponsor base case | CDA-AMC base case | |||
No price reduction | 7.08b | 7,695 | 192,741 | 360,148 |
10% | 6.37 | 6,926 | 178,546 | 336,296 |
20% | 5.66 | 6,156 | 164,351 | 312,444 |
30% | 4.96 | 5,387 | 150,157 | 288,592 |
40% | 4.25 | 4,617 | 135,962 | 264,740 |
50% | 3.54 | 3,848 | 121,767 | 240,888 |
60% | 2.83 | 3,078 | 107,573 | 217,036 |
70% | 2.12 | 2,309 | 93,378 | 193,184 |
80% | 1.42 | 1,539 | 79,183 | 169,332 |
90% | 0.71 | 770 | 64,988 | 145,480 |
CDA-AMC = Canada’s Drug Agency; IBR = ibrutinib; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; VEN = venetoclax; vs. = versus.
aBased on the average cost of the ramp-up and maintenance schedules.
bSponsor’s submitted price for venetoclax.16
Assessment of Uncertainty
CDA-AMC conducted scenario analyses to address uncertainty within the economic evaluation, using the CDA-AMC base case. Results are provided in Table 10.
Assuming an RDI of 100% for venetoclax and ibrutinib.
Adopting OS data from the Kaplan-Meier estimates from the SYMPATICO trial for the in-trial period, and the sponsor-chosen parametric models (log-normal for venetoclax plus ibrutinib and generalized gamma for ibrutinib alone) for long-term extrapolation of OS.
Table 10: Results of CDA-AMC Scenario Analyses
Analysisa | Drug | Total costs ($) | Total QALYs | ICER ($/QALYs) |
|---|---|---|---|---|
CDA-AMC base case | IBR | 495,051 | 3.17 | Reference |
VEN + IBR | 728,854 | 3.65 | 360,148 | |
CDA-AMC scenario 1: Assuming 100% RDI | IBR | 583,419 | 3.16 | Reference |
VEN + IBR | 783,639 | 3.65 | 409,769 | |
CDA-AMC scenario 2: Adopting alternative OS in-trial and extrapolation curves | IBR | 567,074 | 4.02 | Reference |
VEN + IBR | 740,001 | 4.77 | 228,921 |
CDA-AMC = Canada’s Drug Agency; IBR = ibrutinib; ICER = incremental cost-effectiveness ratio; KM = Kaplan-Meier; OS = overall survival; QALY = quality-adjusted life-year; RDI = relative dose intensity; VEN = venetoclax.
aProbabilistic analyses.
Issues for Consideration
Venetoclax and ibrutinib have successfully completed negotiations with the pan-Canadian Pharmaceutical Alliance for non-MCL indications. It is therefore likely that both treatments are reimbursed by jurisdictional drug plans at confidential prices that are lower than publicly listed prices. Thus, the actual price paid by the drug plans may be lower than those used in the sponsor’s model, which was based on the submitted price and public list prices, respectively.
Acalabrutinib has been approved by Health Canada for use in patients with relapsed or refractory MCL but has not been reviewed by CDA-AMC for this indication. Zanubrutinib received a negative recommendation from CDA-AMC for relapsed or refractory MCL. Both drugs are reimbursed by some CDA-AMC–participating drug plans for other indications. Clinical input indicates that acalabrutinib and zanubrutinib are accessible to patients relapsed or refractory MCL through manufacturer-sponsored compassionate access programs. The cost-effectiveness of venetoclax plus ibrutinib compared to these treatments is unknown.
Appendix 5: Budget Impact Analysis
Please note that this appendix has not been copy-edited.
Summary of the Submitted BIA
The sponsor submitted a BIA that estimated the expected incremental budgetary impact of reimbursing venetoclax plus ibrutinib for the treatment of adult patients with MCL that have received at least 1 prior therapy.
The BIA was conducted from the perspective of public drug plan payers over a 3-year time horizon (2026 to 2029), with 2025 as the base year. The sponsor’s estimate reflects the aggregated results from the jurisdictional provincial budgets (excluding Quebec) as well as the Non-Insured Health Benefits Program. The sponsor estimated the eligible population using an epidemiologic approach. The sponsor’s base case included drug acquisition costs. The market uptake for venetoclax plus ibrutinib was estimated using internal market share estimates.5 The key inputs to the BIA are documented in Table 11.
The sponsor estimated that the 3-year incremental budget impact associated with reimbursing venetoclax plus ibrutinib for the treatment of adult patients with MCL that have received at least 1 prior therapy would be $41,997,557 (year 1 = $3,616,375; year 2 = $13,889,558; year 3 = $24,491,624).
Table 11: Key Model Parameters
Parameter | Sponsor’s estimate (reported as year 1 / year 2 / year 3 if appropriate) |
|---|---|
Target population | |
Starting number of people (base year) | 26,908,36517 |
Population growth rate | |
Incidence of non-Hodgkin lymphoma (2024) | 0.033%19 |
Percentage of patients with MCL | 6.0%20 |
Percentage of patients who receive first-line therapy | 93.1%21 |
Percentage of patients who experience relapse and receive treatment | 90.0%11 |
Percentage of patients with public drug plan coveragea | Jurisdiction specific (86.6% average)22 |
Percentage of patients ineligible for BTKi-based therapy in the second line | 0% / 0% / 10%5 |
Number of patients eligible for drug under review | 396 / 405 / 373 |
Market shares (reference scenario) | |
Venetoclax plus ibrutinib | 0% / 0% / 0% |
Ibrutinib | 100% / 100% / 100% |
Market shares (new drug scenario) | |
Venetoclax plus ibrutinib | ███ █ ███ █ ███ |
Ibrutinib | ███ █ ███ █ ███ |
Cost of treatment (per patient per 28 days) | |
Venetoclax plus ibrutinibb | Cycle 1: $13,016; Subsequent cycles: $19,111 |
Ibrutinibb | $11,182 |
BTKi = Bruton’s tyrosine kinase inhibitor; MCL = mantle cell lymphoma.
aWeighted average across all jurisdictions, taking into account the proportion of patients estimated to be younger or older than 65 years (obtained from the SYMPATICO trial).
bTreatment duration was derived from the SYMPATICO trial. Mean treatment duration for venetoclax plus ibrutinib was ████ ██████ ███████ █████ for venetoclax and ████ ██████ ███████ █████ for ibrutinib. For ibrutinib monotherapy, the mean treatment duration was ████ ██████ ███████ █████.
Key Issues of the Submitted BIA
CDA-AMC identified several key issues to the sponsor’s analysis that have notable implications on the results of the BIA:
The number of patients eligible for venetoclax plus ibrutinib is uncertain. The sponsor used an epidemiologic approach to estimate the number of eligible patients, starting with the incidence of non-Hodgkin lymphoma (derived from estimates provided by Statistics Canada and the Non-Insured Health Benefits Program).17,18 The sponsor then used estimates from the US Leukemia and Lymphoma Society, an analysis of claims data from the US, and a narrative review of first-line treatments to determine the proportion of patients with MCL, the proportion who receive first-line therapy, and the proportion who relapse following first-line therapy and receive second-line therapy, respectively.11,20,21 There are several sources of uncertainty associated with these estimates, particularly whether data from the US are generalizable to patients in Canada, for example, because access to health care in the US is dependent, at least in part, on insurance payers’ and patients’ ability to pay a co-payment.
Further, the sponsor assumed that, by year 3 of the BIA, 10% of patients will have received acalabrutinib plus bendamustine and rituximab in the first-line setting and thus be ineligible for re-treatment with a BTKi-based treatment in subsequent lines.5 Acalabrutinib for use in combination with bendamustine and rituximab is currently undergoing review by Health Canada and CDA-ACM for previously untreated MCL. At this time, it is highly uncertain whether this regimen will become publicly reimbursed and, if so, what proportion of patients will receive it in the first line.
Finally, the sponsor assumed that all patients will be eligible for public drug coverage in several CDA-AMC–participating jurisdictions (British Columbia, Alberta, Saskatchewan, Manitoba, Non-Insured Health Benefits). For the remaining jurisdictions, the sponsor estimated public drug plan coverage using the age distribution in the SYMPATICO trial (33% < 65 years; 67%3 65 years), with all patients aged 65 and older assumed to be eligible for public coverage.23 Clinical expert input received by CDA-AMC, as well as several studies from the literature, suggests that the SYMPATICO trial population may be younger than patients seen in clinical practice.24,25 If patients in clinical practice in Canada are older than those in the SYMPATICO trial, a higher proportion will qualify for public drug plan coverage.
In the CDA-AMC base case, first-line use of acalabrutinib plus bendamustine and rituximab was excluded. CDA-AMC was unable to address other sources of uncertainty in the number of eligible patients.
The market uptake of venetoclax plus ibrutinib may be underestimated: In the base case, the sponsor estimated that ███ of eligible patients will receive venetoclax plus ibrutinib in year 1, with ███ and ███ receiving venetoclax plus ibrutinib in year 2 and 3, respectively, based on an unpublished study undertaken by the sponsor.5 Clinical expert input received by CDA-AMC indicates that uptake of venetoclax plus ibrutinib is likely to be higher than projected by the sponsor, potentially reaching 40% in year 1, 45% in year 2, and 60% in year 3. If the uptake is higher than estimated by the sponsor, the corresponding expenditure and budget impact will be higher than is predicted.
CDA-AMC explored the impact of uncertainty in the uptake of venetoclax plus ibrutinib in scenario analysis.
Costs associated with subsequent therapy were excluded from the BIA: The sponsor did not include costs associated with subsequent therapy in the estimated budget impact, which is inconsistent with the approach taken in the CUA (refer to Appendix 3). In the CUA, the sponsor assumed that all living patients whose disease progressed would receive subsequent therapy (equates to █████ of patients in the SYMPATICO trial, after adjustment for those who died).23 Clinical expert input received by CDA-AMC indicated that, at present, the majority of patients with MCL who receive second-line treatment will eventually experience disease progression and receive subsequent treatment.
CDA-AMC was unable to address this limitation owing to the structure of the sponsor’s model.
Relevant comparators were excluded from the sponsor’s economic evaluation: The sponsor’s BIA included only ibrutinib as a comparator. As noted in the Key Issues of the Submitted Economic Evaluation, while ibrutinib is currently standard second-line treatment in Canada, other treatment options exist. CDA-AMC notes that these treatments (refer to Table 4) have a lower 28-day cycle cost; however, the impact of excluding these treatments on the estimated cost of reimbursing venetoclax plus ibrutinib will depend on market share and displacement.
CDA-AMC was unable to address this limitation.
The prices paid by public drug plans is uncertain: Venetoclax and ibrutinib have successfully completed negotiations with the pan-Canadian Pharmaceutical Alliance for non-MCL indications. It is therefore likely that both treatments are reimbursed by jurisdictional drug plans at confidential prices that are less than publicly available list prices, as any potential confidential rebates are not reflected in list prices.
CDA-AMC was unable to address this limitation.
CDA-AMC Reanalyses of the BIA
CDA-AMC revised the sponsor’s submitted analyses by making changes in model parameter values and assumptions, in consultation with clinical experts, as outlined in Table 12.
Table 12: Revisions to the Submitted BIA
Stepped analysis | Sponsor’s value or assumption | CDA-AMC value or assumption |
|---|---|---|
1. Acalabrutinib plus bendamustine and rituximab as a first-line treatment for MCL | Included. The sponsor assumed that 10% of potentially eligible patients in year 3 would have received this regimen in the first line and thus be ineligible for re-treatment with a BTKi inhibitor (i.e., venetoclax) in the second line | Excluded |
CDA-AMC base case | ― | Reanalysis 1 |
BIA = budget impact analysis; BTKi = Bruton’s tyrosine kinase inhibitor; CDA-AMC = Canada’s Drug Agency; MCL = mantle cell lymphoma.
The results of the CDA-AMC reanalysis are presented in summary format in Table 13 and a more detailed breakdown is presented in Table 14. In the CDA-AMC base case, the 3-year budget impact of reimbursing venetoclax for use in combination with ibrutinib for the indication under review was $42,943,592 (year 1 = $3,616,375; year 2 = $13,889,558; year 3 = $25,437,592).
Table 13: Summary of the Stepped Analysis of the CDA-AMC Base Case
Stepped analysis | Three-year total ($) |
|---|---|
Submitted base case | 41,997,557 |
CDA-AMC reanalysis 1 | 42,943,592 |
CDA-AMC base case | 42,943,592 |
CDA-AMC = Canada’s Drug Agency.
Note: The CDA-AMC reanalysis is based on publicly available prices of comparators.
CDA-AMC used the CDA-AMC base case to conduct scenario analyses to explore uncertainty in the estimated budget impact of reimbursing venetoclax plus ibrutinib. The results are provided in Table 14.
Adopting a higher market share for venetoclax plus ibrutinib (year 1: 30%; year 2: 45%; year 3: 60%).
Table 14: Disaggregated Summary of the BIA
Stepped analysis | Scenario | Year 0 (current situation) ($) | Year 1 ($) | Year 2 ($) | Year 3 ($) | Three-year total ($) |
|---|---|---|---|---|---|---|
Submitted base case | Reference total | 28,256,427 | 85,416,835 | 109,037,891 | 108,513,418 | 302,968,144 |
VEN + IBR | 0 | 0 | 0 | 0 | 0 | |
IBR | 28,256,427 | 85,416,835 | 109,037,891 | 108,513,418 | 302,968,144 | |
New drug total | 28,256,427 | 89,033,210 | 122,927,449 | 133,005,042 | 344,965,701 | |
VEN + IBRa | 0 | 9,397,171 | 37,277,818 | 66,187,084 | 112,862,073 | |
IBR | 28,256,427 | 79,636,039 | 85,649,631 | 66,817,958 | 232,103,629 | |
Budget Impact | 0 | 3,616,375 | 13,889,558 | 24,491,624 | 41,997,557 | |
CDA-AMC base case | Reference total | 28,256,427 | 85,416,835 | 109,037,891 | 111,537,903 | 305,992,629 |
VEN + IBR | 0 | 0 | 0 | 0 | 0 | |
IBR | 28,256,427 | 85,416,835 | 109,037,891 | 111,537,903 | 305,992,629 | |
New drug total | 28,256,427 | 89,033,210 | 122,927,449 | 136,975,562 | 348,936,221 | |
VEN + IBRb | 0 | 9,397,171 | 37,277,818 | 68,645,361 | 115,320,350 | |
IBR | 28,256,427 | 79,636,039 | 85,649,631 | 68,330,201 | 233,615,871 | |
Budget Impact | 0 | 3,616,375 | 13,889,558 | 25,437,659 | 42,943,592 | |
CDA-AMC scenario analyses | ||||||
Scenario 1: Increased venetoclax plus ibrutinib market share | Reference total | 28,256,427 | 85,416,835 | 109,037,891 | 111,537,903 | 305,992,629 |
New drug total | 28,256,427 | 90,841,397 | 127,097,762 | 141,876,435 | 359,815,594 | |
Budget Impact | 0 | 5,424,562 | 18,059,872 | 30,338,532 | 53,882,966 | |
BIA = budget impact analysis; CDA-AMC = Canada’s Drug Agency; IBR = ibrutinib; VEN = venetoclax.
Note: The CDA-AMC reanalysis is based on the publicly available prices of comparators.
aThe expenditure on VEN alone in the sponsor’s base case (New Drug Scenario) is predicted to be $3,616,375 in year 1, $13,889,558 in year 2; and $21,793,919 in year 3.
bThe expenditure on VEN alone in the CDA-AMC base case (New Drug Scenario) is predicted to be $3,616,375 in year 1, $13,889,558 in year 2; and $22,739,954 in year 3.
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.