Drugs, Health Technologies, Health Systems
Reimbursement Review
Trastuzumab Deruxtecan (Enhertu)
Sponsor: AstraZeneca Canada Inc.
Therapeutic area: HER2-low or HER2-ultralow breast cancer
Summary
What Is Metastatic Breast Cancer With HER2-Low or HER2-Ultralow Expression?
Metastatic breast cancer (mBC) is a life-threatening disease in which breast cancer spreads beyond the breast and nearby lymph nodes to distant organs, such as the liver, brain, lungs, or bones. HER2-low and HER2-ultralow breast cancers contain low levels of HER2 protein, which is found on the surface of breast cancer cells and causes the cancer to grow and spread.
In 2024, there were an estimated 30,800 new cases of breast cancer diagnosed in Canada. Among these, 30,500 cases were in females and 290 were in males. Around 80% of breast cancers are currently classified as HER2-negative, a category that includes tumours with HER2 expression below the threshold for HER2 positivity. Among these, approximately 60% show low HER2 expression (i.e., immunohistochemistry [IHC] 1+ or IHC 2+ and negative for in situ hybridization), while in another 28.1% to 36.7%, the HER2 expression level is IHC 0. Some of the latter cases may exhibit ultralow levels of HER2 (i.e., IHC 0 with membrane staining).
Across Canada, HER2 status is routinely assessed using IHC during mBC diagnosis as part of standard of care. However, for HER2-negative mBC, HER2-low and HER2-ultralow status are not yet routinely reported across all sites in Canada.
What Are the Treatment Goals and Current Treatment Options for mBC With HER2-Low or HER2-Ultralow Expression?
Treatment goals for patients with HER2-low or HER2-ultralow mBC include prolonging overall survival (OS), delaying disease progression, preserving or improving health-related quality of life (HRQoL), and minimizing treatment-related toxicity.
Outcomes identified as important in the input from patient and clinician groups included improvements in progression-free survival (PFS), OS, and HRQoL; minimal side effects; and the ability to continue normal activities.
Current treatment options for HER2-low and HER2-ultralow mBC include chemotherapy regimens, such as capecitabine, nab-paclitaxel, and paclitaxel. The inputs received by clinician groups emphasized the importance of delaying the use of conventional generic chemotherapy, which is associated with poor outcomes in patients who have received at least 1 endocrine therapy (ET) and are not considered suitable for ET as the next line of therapy. No HER2-targeted therapies were previously approved for the target patient population before Enhertu.
What Is Enhertu, and Why Did Canada’s Drug Agency Conduct This Review?
Enhertu is a HER2-directed antibody-drug conjugate administered through IV infusion.
Canada’s Drug Agency (CDA-AMC) reviewed Enhertu to inform a recommendation to the participating public drug programs on whether Enhertu should be reimbursed for the treatment of adult patients with unresectable or metastatic HER2-low (IHC 1+ or IHC 2+/in situ hybridization–negative) or HER2-ultralow (IHC 0 with membrane staining) breast cancer who have received at least 1 ET in the metastatic setting and who are not considered suitable for ET as the next line of therapy. The Health Canada indication changed during the review to include the language “and who are not considered suitable for endocrine therapy as the next line of therapy,” which was aligned with the sponsor’s reimbursement request. Due to the timing of the revision, the report was not updated to remove references to differences between the proposed indicated population and the reimbursement request population.
How Did CDA-AMC Evaluate Enhertu?
CDA-AMC reviewed the clinical evidence on the beneficial and harmful effects, as well as the economic evidence, of Enhertu versus other treatments used in Canada for the treatment of adult patients with unresectable or metastatic HER2-low or HER2-ultralow breast cancer who have received at least 1 ET in the metastatic setting and are not considered suitable for ET as the next line of therapy.
Capecitabine, paclitaxel, and nab-paclitaxel were considered relevant comparators when reviewing the clinical evidence.
CDA-AMC considered the potential impacts of determining HER2-low or HER2-ultralow disease status using IHC to ascertain eligibility for Enhertu in patients with mBC, including those affecting health systems and patients (including their families and caregivers).
CDA-AMC identified equity and ethical considerations relevant to Enhertu and the treatment of unresectable or metastatic HER2-low or HER2-ultralow breast cancer.
The review was informed by materials submitted by the sponsor, which included clinical and economic evidence.
The review also considered input from 3 patient groups (Breast Cancer Canada and the McPeak-Sirois Group for Clinical Research in Breast Cancer; the Canadian Breast Cancer Network; and Rethink Breast Cancer), 2 clinician groups (the Ontario Health [Cancer Care Ontario] Breast Cancer Drug Advisory Committee and the REAL Alliance), and 1 industry group in response to the CDA-AMC call for input. Input from participating public drug programs was also reviewed regarding issues that could affect their ability to implement a recommendation.
Two clinical experts with expertise in the diagnosis and management of HER2-low or HER2-ultralow mBC contributed to the review.
What Were the Findings?
Clinical Evidence
CDA-AMC reviewed the following clinical evidence:
1 randomized, controlled, open-label, phase III trial (the DESTINY-Breast06 trial) comparing Enhertu with the investigators’ choice of chemotherapy (capecitabine, nab-paclitaxel, or paclitaxel) in 866 patients with unresectable or metastatic hormone receptor–positive, HER2-low or HER2-ultralow breast cancer; these patients had disease progression after receiving at least 2 lines of ET in the metastatic setting or 1 line of ET in the metastatic setting and demonstrated disease progression within 24 months of the start of adjuvant ET or within 6 months of starting first-line ET in combination with a CDK4/6 inhibitor in the metastatic setting.
For the comparison of Enhertu versus chemotherapy, based on the overall trial population of the DESTINY-Breast06 trial:
Compared with chemotherapy, treatment with Enhertu results in a clinically important improvement in PFS at 6 months and likely results in a clinically important improvement at 18 months. The certainty of the evidence was high at 6 months and moderate at 18 months due to imprecision.
Treatment with Enhertu likely results in a clinically important improvement in OS at 12 ███ ██ months compared with chemotherapy. The certainty of the evidence was moderate due to imprecision.
Compared with chemotherapy, treatment with Enhertu may result in little to no clinically important difference in HRQoL over 31 weeks (measured using the Global Health Status domain of the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30). The certainty of the evidence was low due to risk of bias.
Compared with chemotherapy, treatment with Enhertu may result in little to no clinically important difference in the occurrence of serious adverse events. The certainty of this evidence was moderate due to imprecision.
Compared with chemotherapy, treatment with Enhertu results in a clinically important increase in the occurrence of interstitial lung disease. The certainty of this evidence was high.
Economic Evidence
Trastuzumab deruxtecan is available as powder for IV infusion (100 mg). At the submitted price of $2,440.00 per vial, the cost of trastuzumab deruxtecan per 21-day cycle is expected to be $9,760 per patient (28-day cost = $13,013), based on the Health Canada–recommended dosage.
Clinical efficacy in the economic analysis (PFS, OS, and time to treatment discontinuation) was derived from the DESTINY-Breast06 trial, which compared trastuzumab deruxtecan with physician’s choice of single-drug chemotherapy (capecitabine, paclitaxel, or nab-paclitaxel). Evidence submitted by the sponsor indicates that trastuzumab deruxtecan is likely to improve PFS at 6 months and 18 months and OS at 12 ███ ██ months compared with chemotherapy among adult patients with unresectable or metastatic HER2-low or HER2-ultralow breast cancer who have received at least 1 ET in the metastatic setting and are not considered suitable for ET as the next line of therapy. The estimates for OS at 12 ███ ██ months are affected by serious imprecision; 95% confidence intervals include the possibility of a small difference between groups that is not considered clinically important. The interim nature of the OS analysis (with █████ ███ of the expected events) results in ████████ ████████ ████████████ ████████ ██ █████ ██ ███████ ███ ███ ████████ █████████ ██ ████ █████ ██ ██████. Therefore, longer follow-up is needed to draw definitive conclusions about longer-term OS.
The results of the CDA-AMC base case suggest that:
Trastuzumab deruxtecan is predicted to be associated with higher costs to the health care system than chemotherapy (incremental cost = $138,930). This higher cost is driven primarily by costs associated with drug acquisition.
Trastuzumab deruxtecan is predicted to be associated with a gain of 0.35 life-years compared to chemotherapy and may result in a gain of 0.31 quality-adjusted life-years (QALYs) compared to chemotherapy.
The incremental cost-effectiveness ratio of trastuzumab deruxtecan compared to chemotherapy was $453,869 per QALY gained in the CDA-AMC base case. Approximately 87% of the incremental QALYs were estimated based on extrapolations outside the trial period. No long-term data were submitted by the sponsor.
The magnitude of difference in OS between trastuzumab deruxtecan and chemotherapy may be lower in clinical practice in Canada than observed in the DESTINY-Breast06 trial because of greater use of trastuzumab deruxtecan in later lines of therapy (i.e., after disease progression on chemotherapy). If the incremental QALYs with trastuzumab deruxtecan are lower than predicted in the CDA-AMC base case, then further price reductions than those presented in this report may be required.
CDA-AMC estimates that the budget impact of reimbursing trastuzumab deruxtecan for the requested reimbursement population will be approximately $70 million over the first 3 years of reimbursement compared to the amount currently spent on chemotherapy, with an estimated expenditure of $155 million on trastuzumab deruxtecan over this period. The actual budget impact will depend on the number of eligible people, the uptake of trastuzumab deruxtecan, and the cost of subsequent treatment.
Abbreviations
AE
adverse event
BICR
blinded independent central review
CBCN
Canadian Breast Cancer Network
CDA-AMC
Canada’s Drug Agency
CI
confidence interval
DOR
duration of response
EORTC QLQ-BR45
European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire–Breast Cancer Module
EORTC QLQ-C30
European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30
ET
endocrine therapy
GRADE
Grading of Recommendations Assessment, Development and Evaluation
HR
hormone receptor
HRQoL
health-related quality of life
IA1
first interim analysis
IA2
second interim analysis
IHC
immunohistochemistry
ILD
interstitial lung disease
IQR
interquartile range
ISH
in situ hybridization
ITT
intention to treat
LVEF
left ventricular ejection fraction
mBC
metastatic breast cancer
MID
minimal important difference
OH (CCO) HCDAC
Ontario Health (Cancer Care Ontario) Breast Cancer Drug Advisory Committee
OR
odds ratio
ORR
objective response rate
OS
overall survival
PFS
progression-free survival
PRO
patient-reported outcome
QALY
quality-adjusted life-year
RCT
randomized controlled trial
RECIST
Response Evaluation Criteria in Solid Tumours
Background
Introduction
This report has 2 objectives:
One objective is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of trastuzumab deruxtecan at a dose of 5.4 mg/kg given as an IV infusion for the treatment of unresectable or metastatic HER2-low (immunohistochemistry [IHC] 1+ or IHC 2+/ in situ hybridization [ISH] negative) or HER2-ultralow (IHC 0 with membrane staining) breast cancer in adult patients who have received at least 1 endocrine therapy (ET) in the metastatic setting and are not considered suitable for further ET. The focus is on comparing trastuzumab deruxtecan to comparators considered relevant in clinical practice in Canada and identifying gaps in the current evidence. This focus is outlined in Table 1.
The additional objective is to review and critically appraise the economic information submitted by the sponsor, including a cost-effectiveness analysis and a budget impact analysis. The focus of the economic review is aligned with the scope of the clinical review unless otherwise stated. For most reviews, a base case is developed by Canada’s Drug Agency (CDA-AMC). The base case is informed by clinical expert input, available clinical evidence, and the best interpretation of the economic evidence using the information provided by the sponsor.
This application was submitted by the sponsor before the Notice of Compliance from Health Canada was available. This report reflects the anticipated indication and recommended dosage for trastuzumab deruxtecan during the initial CDA-AMC review period. The Health Canada indication changed during the review to include the language “and who are not considered suitable for endocrine therapy as the next line of therapy,” which was aligned with the sponsor’s reimbursement request. Due to the timing of the revision, the report was not updated to remove references to differences between the proposed indicated population and the reimbursement request population.
Table 1: Information on the Application Submitted for Review and on the CDA-AMC Review
Item | Description |
|---|---|
Information on the application submitted for review | |
Drug | Trastuzumab deruxtecan (Enhertu), powder for concentrate for solution for IV infusion (infusion/100 mg/vial) |
Sponsor | AstraZeneca Canada Inc. |
Health Canada indication | Proposed: For treatment of adult patients with unresectable or metastatic HER2-low (IHC 1+ or IHC 2+/ISH-) or HER2-ultralow (IHC 0 with membrane staining) breast cancer who have received at least 1 endocrine therapy in the metastatic setting. |
Health Canada approval status | Under review (pre-NOC) |
Health Canada review pathway | Standard review |
NOC date | October 27, 2025 |
Mechanism of action | Targets HER2-positive cells and releases topoisomerase I inhibitor to induce DNA damage and cell death |
Recommended dosage | 5.4 mg/kg administered as an IV infusion once every 3 weeks until disease progression or unacceptable toxicity |
Submission type | Initial |
Sponsor’s reimbursement request | For the treatment of adult patients with unresectable or metastatic HER2-low (IHC 1+ or IHC 2+/ISH-) or HER2-ultralow (IHC 0 with membrane staining) breast cancer who have received at least 1 endocrine therapy in the metastatic setting and are not considered suitable for endocrine therapy as the next line of therapy |
Submitted price | $2,440.00 per 100 mg vial |
Information on the CDA-AMC review | |
Review type | Standard |
Clinical review focusa | Population: As defined in the reimbursement request Subgroups: None Intervention: Trastuzumab deruxtecan, 5.4 mg/kg every 3 weeks through IV infusion Comparators: Capecitabine, paclitaxel, and nab-paclitaxel Outcomes: OS, PFS, HRQoL (EORTC QLQ-C30), EORTC QLQ-BR45, AEs, and interstitial lung disease, including pneumonitis |
AE = adverse event; CDA-AMC = Canada’s Drug Agency; EORTC QLQ-BR45 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire–Breast Cancer Module; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; HRQoL = health-related quality of life; IHC = immunohistochemistry; ISH = in situ hybridization; NOC = Notice of Compliance; OS = overall survival; PFS = progression-free survival.
aThe economic review aligns with the scope of the clinical review unless otherwise stated.
Submission History for the Drug Under Review
CDA-AMC previously reviewed trastuzumab deruxtecan through the reimbursement review process for the following indications and issued a recommendation to reimburse with conditions:
as monotherapy for the treatment of adult patients with unresectable or metastatic HER2-low (IHC 1+ or IHC 2+ and ISH-negative) breast cancer who have received at least 1 prior line of chemotherapy in the metastatic setting or developed disease recurrence during or within 6 months of completing adjuvant chemotherapy (patients with hormone receptor [HR]–positive breast cancer should have received at least 1 and be considered ineligible for ET)
for the treatment of adult patients with unresectable or metastatic HER2-positive breast cancer who have received prior treatment with an anti–HER2-based regimen in the metastatic setting or developed disease recurrence during or within 6 months of completing neoadjuvant or adjuvant therapy
as monotherapy for the treatment of adult patients with unresectable locally advanced or metastatic HER2-positive gastric or gastroesophageal junction adenocarcinoma who have received a prior trastuzumab-based regimen.
Sources of Information
The contents of this Reimbursement Review are informed by materials submitted by the sponsor, input received from interested parties (i.e., patient groups, clinician groups, and drug programs), and input from clinical experts consulted for this review.
Calls for patient and clinician group input are issued for each reimbursement review. For the current review, 3 patient group submissions were received. These were from Breast Cancer Canada and the McPeak-Sirois Group for Clinical Research (McPeak-Sirois Group), the Canadian Breast Cancer Network (CBCN), and Rethink Breast Cancer. Clinician group submissions were received from the Ontario Health (Cancer Care Ontario) Breast Cancer Drug Advisory Committee (OH [CCO] HCDAC) and the REAL Alliance.
In May 2025, the McPeak-Sirois Group distributed an electronic survey to patients living with a first recurrence (i.e., a first-line chemotherapy phase) of HR-positive, HER2-negative metastatic breast cancer (mBC) following resistance to ET. There were 12 respondents. In addition, an electronic survey was distributed in July 2023 to patients living with recurrent HR-positive, HER2-negative mBC and their caregivers. This survey had 171 respondents. There were no patients with experience of trastuzumab deruxtecan among the respondents of either survey.
CBCN noted that the information for this submission was collected from multiple sources, including an excerpt from project number PC0285-000 (2022) (which included 7 patients with HER2-positive mBC who had experience receiving trastuzumab deruxtecan and 1 patient with HR-negative, HER2-low mBC who had experience receiving trastuzumab deruxtecan); a literature review; and CBCN’s 2022 Triple Negative Breast Cancer Patient Survey. The CBCN survey was distributed to patients living with breast cancer. There were 981 respondents. CBCN shared the responses from 30 patients with HR-positive, HER2-negative mBC.
Rethink Breast Cancer gathered information through meetings with patients with breast cancer, an online survey conducted between September 2019 and April 2019 that gathered responses from 78 patients with mBC, and interviews conducted between February 2025 and May 2025 with 5 patients with mBC who had experience receiving trastuzumab deruxtecan.
The clinician group inputs were gathered through virtual meetings, email exchanges, and a literature review. In total, 22 clinicians contributed to the input: 17 clinicians from the REAL Alliance and 5 clinicians from OH (CCO) HCDAC.
The full submissions received are available on the project landing page in the consolidated input document. The drug programs provide input on each drug being reviewed through the reimbursement review process by identifying issues that may affect their ability to implement a recommendation.
Input from patient and clinician groups is considered throughout the review process, including in the selection of outcomes to include in the Clinical Review and in the interpretation of the clinical and economic evidence. Relevant patient and clinician group input is summarized in the Disease Background, Current Management, and Unmet Needs and Existing Challenges sections.
Each review team includes at least 1 clinical expert with expertise regarding the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process. Two medical oncologists with expertise in the diagnosis and management of unresectable or metastatic HER2-low or HER2-ultralow breast cancer participated as part of the review team, with representation from British Columbia and Manitoba. In addition, 1 expert pathologist from Ontario with expertise in testing procedures participated.
Disease Background
Breast cancer may not cause any signs or symptoms in its early stages. Signs and symptoms often appear when the tumour grows large enough to be felt as a lump in the breast or when the cancer spreads to surrounding tissues and organs.1 The most common symptoms in the metastatic setting are related to the site of metastasis; these can occur together with general symptoms, such as fatigue, depression, insomnia, and pain.2 In Canada, breast cancer is the second most commonly diagnosed cancer among all adults and the most commonly diagnosed cancer among women.3 In 2024, an estimated 30,800 new cases of breast cancer were diagnosed in Canada. Of these, 30,500 cases were in females and 290 were in males.3 Metastasis is present in 4% to 6% of breast cancer patients at diagnosis; 30% to 40% of patients diagnosed with early-stage or localized invasive disease will develop metastatic disease later.4 While the overall 5-year survival rate for breast cancer is 89%, for those with metastatic disease, the survival rate decreases to 23%.5 For HER2-low disease, the 5-year overall survival (OS) rate in early-stage disease is 97%, while in advanced disease, it may be only 36%.6 Around 80% of breast cancers are currently classified as HER2‑negative (including about 70% that are HR-positive and 11% that are HR-negative).7 Among HR‑positive, HER2-negative breast cancers, approximately 60% show low HER2 expression despite being traditionally considered negative.8,9 Additionally, studies indicate that 28.1% to 36.7% of HER2-negative cases have an HER2 expression level of IHC 0, some of which may exhibit ultralow levels of HER2.10-13 For more details on the estimated proportions of patients with HER2-negative disease with HER2-ultralow status, refer to Table 2.
Patient Group Input
According to the 3 patient group submissions (from the McPeak-Sirois Group, CBCN, and Rethink Breast Cancer), the challenges and uncertainties related to living with mBC affect both patients and the loved ones who support and help care for them. mBC has negative physical, social, mental, emotional, and financial impacts on patients’ and caregivers’ lives. More details on these impacts are provided in the Unmet Needs and Existing Challenges section.
Current Management
Treatment Goals
Patient group input: The treatment goals and key outcomes for mBC, including HER2-negative and HER2-low breast cancer, as reported across the 3 patient group submissions from the McPeak-Sirois Group, CBCN, and Rethink Breast Cancer, included effective cancer control, prolonged survival, delayed disease progression, relief from cancer-related symptoms, extended recurrence-free survival, minimal side effects, and improved quality of life. According to the McPeak-Sirois Group patient input, most patient respondents with metastatic HER2-negative disease are willing to accept significant compromises in daily functioning and personal time, as well as IV versus oral administration, if it means achieving key treatment goals, such as extended survival or recurrence-free periods.
Clinician group input: Across the 2 clinician group inputs from OH (CCO) HCDAC and REAL Alliance, the treatment goals and important outcomes for patients with HER2-low and HER2-ultralow mBC include prolonged progression-free survival (PFS) and OS, improved quality of life, reduction of treatment-related toxicities, and delayed use of conventional generic chemotherapy associated with poor outcomes.
Clinician input: Clinical experts consulted by CDA-AMC emphasized that treatment goals for patients with metastatic HER2-low or HER2-ultralow breast cancer include delaying disease progression, prolonging PFS and OS, and maintaining quality of life. They highlighted the importance of achieving disease control while minimizing treatment-related toxicity and avoiding adverse effects that may compromise quality of life or functional independence. Goals also included enabling patients to continue with day-to-day activities and minimizing the need for aggressive chemotherapy. For some patients, the potential for a meaningful clinical benefit, even if modest, is considered worthwhile if the treatment is better tolerated than standard options.
Current Treatment Options
Given that mBC is an incurable disease, the goal of treatment is palliative. The focus is on prolonging survival by delaying disease progression, reducing symptom burden, and improving quality of life.
Until recently, HER2-low tumours were not differentiated from tumours historically defined as HER2‑negative.10 Patients with HER2-low tumours were generally treated according to the standard of care for HER2-negative breast cancer. However, HER2-low status is now recognized as a distinct subtype of HER2‑negative disease,14 and treatment with anti–HER2-targeted therapies in patients with this subtype has been incorporated into treatment guidelines.15-17
There are currently no Canada-specific guidelines for the treatment of HR-positive, HER2-negative mBC. Oncologists in Canada typically follow international guidelines, including those from the National Comprehensive Cancer Network, the European Society for Medical Oncology, and the American Society of Clinical Oncology.15-19 These agencies have updated their recommendations to recognize HER2-low and, more recently, HER2-ultralow as distinct subtypes of HER2-negative mBC.15-17
For patients with HR-positive, HER2-negative mBC (which includes HER2-low and HER2-ultralow mBC), the standard initial treatment is ET plus a CDK4/6 inhibitor. Subsequent lines of treatment may include additional ET with or without targeted therapies (e.g., AKT, mTOR or PI3K inhibitors) or chemotherapy. The selection of therapy is influenced by factors such as prior treatment, disease aggressiveness, the toxicity profile of available therapies, and the patient’s biomarker or molecular profile.15-20
Once a tumour is no longer suitable for ET, international treatment guidelines recommend the use of sequential single-drug chemotherapy.15-20 For patients with HER2-low disease (defined as IHC 1+ or IHC 2+ and ISH-negative) who have received prior chemotherapy in the metastatic setting or who developed disease recurrence during or within 6 months of completing adjuvant chemotherapy, trastuzumab deruxtecan is a funded treatment option.21 In addition, to qualify for currently available treatment with trastuzumab deruxtecan, patients with HR-positive with HER2-low disease must have been treated with at least 1 prior line of ET and no longer be considered candidates for ET.21
In the TROPiCS-02 trial, for patients with HR-positive, HER2-negative (i.e., IHC 0, 1+, or 2+ and ISH‑negative) mBC who have received prior ET and at least 2 additional systemic chemotherapies in the metastatic setting, sacituzumab govitecan has also received a positive funding recommendation.22
Per the CDA-AMC provisional funding algorithm, trastuzumab deruxtecan and sacituzumab govitecan are not to be used sequentially (i.e., patients whose disease progresses while receiving 1 are not eligible to receive the other).23
The key characteristics of trastuzumab deruxtecan and relevant comparators are summarized in Appendix 1 of the Supplemental Material.
Unmet Needs and Existing Challenges
Patient Group Input
According to the 3 patient group inputs received by the McPeak-Sirois Group, CBCN, and Rethink Breast Cancer, there is a significant unmet need for first-line targeted chemotherapy in people with HR-positive, HER2-low or HER2-ultralow mBC whose disease is resistant to ET. Currently available chemotherapy options provide limited efficacy with considerable toxicity. The patient groups advocate for the adoption of newly available testing kits that have higher sensitivity to provide more consistent HER2-level results.
According to CBCN, many patients experience significant barriers and challenges around the availability of health care services and quality child care in their communities. Additionally, patients have expressed the need for access to the treatment that works best for them and the need for personal choice and autonomy. CBCN added that, in the 2017 survey, patients indicated that the time required to travel for treatment had a significant impact (26%) or some impact (40%) on their quality of life. Costs related to travelling for treatment had a significant impact of the quality of life of 12% of patients and some impact for 42%. The cost of prescription medications was indicated as having a significant impact on quality of life by 14% of respondents and some impact by 44%. The costs of other treatments (such as massage or physiotherapy) had a significant impact on quality of life for 26% and some impact for 34% of respondents. Costs related to devices had a significant impact on quality of life for 4% of patients and some impact for 24% of respondents.
Additionally, CBCN noted that in response to the 2012 survey questions about the availability of supports such as child care, transportation, and alternative treatments in their community:
Among patients with children or other dependents, 53% indicated that there is minimal or no access to appropriate care for these loved ones when they experience debilitating cancer-related symptoms, and 40% identified barriers to accessing quality care during cancer treatment.
Among survey respondents who had children at the time of their diagnosis, 24% reported that appropriate care for their children or other dependents when experiencing side effects of cancer treatments was not accessible, while 46% indicated that it was somewhat accessible. Appropriate care for children or other dependents during cancer treatment was not accessible for 29%, while 44% found it somewhat accessible.
CBCN added that among all patients with HER2-negative mBC from the 2017 survey, 14% indicated that transportation to appointments was not accessible, while 20% indicated that it was somewhat accessible. Mental health supports were somewhat accessible for 52% of respondents, while 10% indicated that it was not accessible. Cancer treatment in or near respondents’ communities was somewhat accessible for 38% and not accessible for 4%. Symptom management options in or near their communities was not accessible for 16% of respondents and somewhat accessible for 42%.
Based on the patient group inputs, most patients with mBC are without private third-party insurance or do not qualify for insurance at work. Financial insecurity and compounded years of reduced income are a particular concern for these patients.
Across the patient group inputs, some of the physical impacts of mBC that were reported to have significant or debilitating impacts on patients’ quality of life included pain, nausea, insomnia, fatigue, depression, lack of concentration, memory loss, and diarrhea. Additionally, some of the social impacts included restrictions on an patients’ employment and career, ability to care for children and dependents, ability to exercise, ability to socialize and participate meaningfully in their communities, and ability to spend time with loved ones. Specifically, when young people get breast cancer, it may be more aggressive, which can lead to tougher treatments. Those diagnosed in their twenties, thirties, and forties face age-specific issues, such as fertility or family planning challenges; diagnosis during pregnancy; impacts on child care; impacts on relationships, body image, dating, and sexuality; feelings of isolation from peers who do not have cancer; the need to take career hiatuses; and financial insecurity.
CBCN explained that other experiences identified by patients included guilt, the feeling of being a burden on caregivers, fear of death, poor body image, not knowing what functionality will be lost, fear of the impact of cancer and loss of a parent on children, not knowing what will happen to children, the loss of support of loved ones, and marital stress or the loss of fidelity and affection from a partner.
Clinician Input
According to the clinical experts consulted by CDA-AMC, there remains an unmet need for effective, well-tolerated therapies for patients with HR-positive, HER2-low or HER2-ultralow mBC whose disease has progressed on prior ET and CDK4/6 inhibitors. Treatment-related toxicities and limited duration of benefit with chemotherapy continue to be a challenge. There is a need for therapies that offer improved PFS and OS with a manageable toxicity profile.
The clinical experts consulted by CDA-AMC emphasized that some patients — particularly those who are older, have poor performance status, or reside in rural or remote locations — may experience barriers in accessing timely care or supportive services, including transportation and social support.
The clinical experts consulted by CDA-AMC noted that patients with HER2-low or HER2-ultralow disease have not historically been eligible for HER2-targeted therapy; currently available systemic treatment options are limited. The experts emphasized the need for treatments that are better tolerated and delay the need for more toxic chemotherapy. Disease-related symptoms, such as pain, fatigue, and functional decline, were highlighted as areas of unmet need that affect patients' health-related quality of life (HRQoL) and daily activities. The disease and treatment, especially in younger patients with dependent children, were also noted as concerns.
Considerations for Using the Drug Under Review
The contents of this section have been informed by input from the clinical experts consulted for the purpose of this review and by input from clinician groups. The implementation questions and corresponding responses from the clinical experts consulted for this review are summarized in the Supplemental Material document and in the Summary of Drug Program Input and Clinical Expert Responses table in Appendix 1. The following information has been summarized by the review team.
Place in Therapy
According to the clinical experts consulted by CDA-AMC, trastuzumab deruxtecan would be used as a second- or later-line treatment for patients with HR-positive, HER2-low or HER2-ultralow mBC whose disease has progressed on ET and CDK4/6 inhibitors. It would serve as a systemic option following failure of endocrine-based therapy, consistent with the proposed Health Canada indication.
Clinical experts consulted by CDA-AMC emphasized that trastuzumab deruxtecan is not intended to replace first-line ET, which remains the standard of care. Instead, it would be used after disease progression while receiving ET and CDK4/6 inhibitors. Its use in earlier lines of therapy or before exhausting endocrine options was not recommended.
Trastuzumab deruxtecan is expected to be used as monotherapy and could offer an alternative to conventional chemotherapy in the first line after ET. Clinical experts consulted by CDA-AMC noted that it may address an unmet need by providing a more effective, targeted option for patients with HR-positive, HER2-low or HER2-ultralow disease — a population for whom HER2-directed therapy was previously unavailable (for the HER2-ultralow subgroup) or not available in this line (for the HER2-low subgroup), but available after progression on 1 line of chemotherapy. The experts added that its availability may shift the treatment paradigm by enabling a HER2-targeted approach in a subgroup that was previously treated with nontargeted therapies.
Input received by 2 clinician groups indicated that there is a need for more effective treatment options in patients with HR-positive, HER2- low or HER2-ultralow mBC whose disease has progressed while receiving prior ET and CDK4/6 inhibitors. The REAL Alliance suggested that trastuzumab deruxtecan availability be expanded as a treatment option immediately after ET resistance in the transition to the first chemotherapy treatment for patients with advanced or metastatic HR-positive, HER2-low or HER2-ultralow breast cancer. The OH (CCO) HCDAC indicated that trastuzumab deruxtecan will be a new option for many patients with HER2-ultralow mBC and that these patients may have had multiple lines of chemotherapy.
Patient Population
The clinical experts consulted by CDA-AMC noted that trastuzumab deruxtecan is best suited for patients with unresectable or metastatic HR-positive, HER2-low or HER2-ultralow breast cancer whose disease progressed while receiving prior ET and a CDK4/6 inhibitor, who are no longer candidates for ET, and who may or may not have received prior chemotherapy in the metastatic setting. The patients most likely to benefit are those with early disease progression on ET or those considered to have endocrine-resistant disease.
Some patients may prefer an oral chemotherapy option, such as capecitabine, immediately following progression on ET; in this scenario, patients with HER2-low disease would be eligible for trastuzumab deruxtecan after 1 line of chemotherapy.
The clinical experts consulted by CDA-AMC noted that trastuzumab deruxtecan would not be appropriate for patients who have a recent diagnosis or limited metastatic burden or who remain candidates for ET. A history of interstitial lung disease (ILD) was identified as a contraindication due to the known risk of ILD with trastuzumab deruxtecan. While brain metastases would not preclude treatment, the patient’s ability to tolerate therapy is an important consideration.
The clinical experts consulted by CDA-AMC specified that HER2-low status should be confirmed using IHC, with IHC 1+ or IHC 2+ and ISH-negative criteria. They acknowledged variability and challenges in HER2 scoring for HER2-ultralow disease. There was no indication that misdiagnosis was a major concern; however, the clinical experts consulted by CDA-AMC did acknowledge some inconsistency in HER2 scoring across institutions.
The clinical experts consulted by CDA-AMC did not propose prespecified initiation conditions beyond HER2-low or HER2-ultralow status and disease progression with prior ET with or without a CDK4/6 inhibitor.
According to the OH (CCO) HCDAC, patients with HR-positive and HER2-low or HER2-ultralow disease whose disease has progressed on a prior line of therapy, including an ET and/or a CDK4/6 inhibitor — and are fit enough for further systemic treatment — are the most suitable patients for treatment with trastuzumab deruxtecan. The least suitable patients would be those who are newly diagnosed and those at significant risk for neutropenia and/or ILD.
The REAL Alliance noted that the best-suited patients are those with advanced or metastatic HR‑positive, HER2-low or HER2-ultralow breast cancer who have exhausted ET and had at least 1 prior ET-based treatment in the advanced setting. The alliance stated that this population has been clearly shown to derive PFS and objective response rate (ORR) benefits and that treatment is recommended for this target population when progression of disease occurs within 24 months while receiving adjuvant ET.
Based on the REAL Alliance input, the least suitable patient populations would include those who were ineligible for the DESTINY Breast06 study and those who have a contraindication to trastuzumab deruxtecan.
Testing Procedure Considerations
In breast malignancies, HER2 status is determined through IHC and ISH tests that are performed on tissue biopsy samples. These tests are routinely conducted in several tertiary clinical centres across Canada at first diagnosis, recurrence, and metastatic diagnosis as part of standard of care.20 There is recognition now that HER2-negative status represents a spectrum of HER2 expression that includes HER2-low, HER2-ultralow, and HER2-null, and that these can be considered as additional clinical designations.24 Table 2 outlines the previous and updated classifications of HER2 status in mBC.
Clinical and pathology experts consulted by CDA-AMC for this review stated that IHC staining levels (IHC 0, 1, and 2) are reported for all HER2-negative mBC; however, HER2-low and HER2-ultralow statuses are not routinely reported in Canada.25,26 They noted that there is increasing awareness among clinicians of the need to adopt the updated classification for newly diagnosed patients and expected that this will become standard practice in the near future. However, to inform the eligibility of existing patients for the drug under review, patients with HER2-negative mBC who have an IHC staining level of 0 (approximately 40% of patients currently classified as HER2-negative) may need to have their disease reclassified as HER2-ultralow or HER2-null.27 The pathology expert anticipated that this reclassification may require additional resources, primarily in terms of pathologists’ time. According to the clinical experts, for the vast majority of patients in active care (around 90%), their existing IHC stains would be of sufficient quality to be reassessed and reclassified. In rare instances, new IHC assays using existing tissue samples may be required; in even rarer instances, new samples might be warranted. CDA-AMC estimates that reclassification will be required for up to approximately 960 patients (upper estimate) in the first year.27 The clinical and pathology experts agreed with this estimate and noted that reclassification would be conducted only at the request of the oncologist. The number of patients who may require reclassification in subsequent years would likely decrease as laboratories adopt the updated classification guidelines.
CDA-AMC considered the potential impacts of determining HER2-low or HER2-ultralow status to ascertain eligibility for trastuzumab deruxtecan in patients with mBC, including those to health systems, patients (including their families and caregivers), and costs. Because existing patients with HER2-negative, IHC 0 status may need to be reclassified, there will be some impact on health systems, especially pathologists’ time and resources. Pathology experts expected that, overall, this impact will be minimal; minimal implementation challenges related to testing and reclassification are expected as part of determining treatment eligibility for trastuzumab deruxtecan. The key considerations and relevant available information were validated by the review team when possible and are summarized in Table 4 of Appendix 1 in the Supplemental Material.
Table 2: Summary of Previous and Updated Classification Guidelines for HER2 Status in mBC
Previous classification28 | Updated classification25 | Implications for reclassification | |||
|---|---|---|---|---|---|
HER2 status | IHC and ISH results | HER2 status | IHC and ISH results | Estimated proportion of patients with HER2-negative disease | |
HER2-negative | IHC 0 IHC 1+ IHC 2+ and ISH-negative | HER2-nulla | IHC 0 without membrane staining and ISH-negative | 10% to 20%27 | Existing IHC stains may require reassessment and then reclassification. |
HER2-ultralowa | IHC 0 with membrane staining and ISH-negative | 20% to 30%27 | Existing IHC stains may require reassessment and then reclassification. | ||
HER2-lowa | IHC 1+ IHC 2+ and ISH-negative | 60%27 | Updated classification can be inferred.29 | ||
HER2-positive | IHC 2+ and ISH-positive IHC 3+ | HER2-positive | IHC 2+ and ISH-positive IHC 3+ | NA | No reassessment or reclassification is required. |
IHC = immunohistochemistry; ISH = in situ hybridization; mBC = metastatic breast cancer; NA = not applicable.
aHER2-null is the terminology proposed in the DESTINY-Breast06 trial protocol and corroborated by the European Society for Medical Oncology to describe cases scored as IHC 0 with no membrane staining.30 According to the experts, the terms HER2-null, HER2-ultralow, and HER2-low are used primarily by clinicians, but may not be consistently used by pathologists or in the literature.
Assessing the Response to Treatment
According to clinical experts consulted by CDA-AMC, the main approaches used in clinical practice to evaluate whether patients are benefiting from treatment with trastuzumab deruxtecan include radiologic imaging (to assess tumour response) and clinical assessments of changes in symptoms. Tumour response is typically assessed using Response Evaluation Criteria in Solid Tumours Version 1.1 (RECIST 1.1), with scans performed every 2 to 3 months. Clinical experts consulted by CDA-AMC also considered symptom improvement (e.g., in fatigue and pain) as indicators of treatment response.
Clinical experts consulted by CDA-AMC indicated that continuation of therapy is generally based on radiographic evidence of disease control (i.e., stable disease or response) and the patient’s ability to tolerate the treatment. If patients are deriving clinical benefit without unacceptable toxicity, treatment would typically be continued. The clinical experts consulted by CDA-AMC did not identify a strict minimum response threshold, but they emphasized the importance of overall clinical benefit.
The clinical experts consulted by CDA-AMC agreed that the use of standard clinical assessments for monitoring treatment response and toxicity would be appropriate and feasible to implement in clinical practice in Canada.
According to input from the 2 clinician groups, in practice, monitoring for recurrence would occur when clinically indicated, as per the current standard of care for the post-ET setting. The REAL Alliance added that CT imaging would be performed every 3 to 6 months and echocardiograms every 3 months. Pulmonary function tests would be conducted as needed to diagnose ILD.
Discontinuing Treatment
According to the clinical experts consulted by CDA-AMC, treatment with trastuzumab deruxtecan should be discontinued in patients who experience disease progression or develop unacceptable treatment-related toxicities.
The clinical experts consulted by CDA-AMC indicated that discontinuation is typically considered in the event of radiographic progression based on RECIST 1.1 criteria, symptomatic deterioration, or adverse events (AEs), such as ILD or other significant toxicities.
The clinical experts consulted by CDA-AMC emphasized that if a patient is no longer deriving clinical benefit or is unable to tolerate the treatment despite supportive care interventions, therapy should be stopped.
The clinician groups noted that treatment should be discontinued upon disease progression or treatment-related toxicities.
Prescribing Considerations
According to the clinical experts consulted by CDA-AMC, trastuzumab deruxtecan should be prescribed by oncologists experienced in managing advanced breast cancer. Due to the risk of ILD, prescribing and monitoring should take place in settings with expertise in ILD management. The clinical experts consulted by CDA-AMC also emphasized the importance of pathology expertise for the accurate identification of patients with HER2-low and HER2-ultralow disease using IHC or ISH.
Trastuzumab deruxtecan is expected to be used as monotherapy. Clinical experts consulted by CDA-AMC did not recommend combining it with other systemic therapies.
Across the clinician group, it was noted that oncologists with experience in treating breast cancer patients are required for recommending and monitoring treatment. In addition, pathology expertise is required for the correct identification of patients with HER2-low and HER2 ultralow disease. Access to ILD monitoring and to experts for ILD management is also required.
Clinical Review
Methods
The review team considered pivotal studies and randomized controlled trials (RCTs) from the sponsor’s systematic review in the evidence for inclusion. The sponsor did not submit long-term extension studies, indirect treatment comparisons, or studies addressing gaps in the evidence for inclusion. Eligible studies for the systematic review included published and unpublished pivotal studies and phase III and IV RCTs. Relevant patients and interventions were defined by the reimbursement request and the recommended dosage in the product monograph. Although HER2-low and HER2-ultralow were prespecified subgroups in the trial — and outcomes were reported separately for these subgroups — the clinical experts consulted by CDA-AMC did not identify any subgroup findings as potentially important for informing the reimbursement recommendation. The intervention under review was trastuzumab deruxtecan 5.4 mg/kg administered intravenously every 3 weeks. Comparators in the trial included physician’s choice of single-drug chemotherapy, namely capecitabine, paclitaxel, or nab-paclitaxel.
CDA-AMC selected outcomes and follow-up times for review, considering the sponsor’s Summary of Clinical Evidence, clinical expert input, and patient and clinician group input. The included outcomes are those considered relevant to the expert committee deliberations and were selected in consultation with committee members. Evidence from the systematic review for the most important outcomes was assessed using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach. The following outcomes were assessed using GRADE because these are efficacy or safety measures that address at least 1 of the main treatment goals for mBC and were considered important to patients, according to patient and clinician group inputs: PFS (6 and 12 months), OS (12 ███ ██ months), European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 (EORTC QLQ-C30) scores, ILD, and serious AEs (SAEs). As noted by the clinical experts consulted for this review, PFS may be viewed as a meaningful short-term efficacy outcome. As per the FDA guidance, PFS reflects tumour growth and can be assessed before the determination of a survival benefit. Its determination is not confounded by subsequent therapy.31 The following outcomes are included in the review to provide context, but were not part of the GRADE assessment because these were not considered most critical to inform the reimbursement recommendation: ORR, duration of response (DOR), and EORTC Quality of Life Questionnaire–Breast Cancer Module (QLQ-BR45) scores.
The methods used for data extraction, risk of bias appraisal, and certainty of evidence assessment are in the Supplemental Material document in Appendix 2.
Clinical Evidence
In this report, the following source of evidence submitted by the sponsor is reviewed and appraised:
1 pivotal RCT, the DESTINY-Breast06 trial, was included in the systematic review.
Systematic Review
Description of Studies
Study Characteristics
Characteristics of the included study are summarized in Table 3. Details pertaining to the comparators and relevant outcome measures are in the Supplemental Material document in Appendix 3.
The DESTINY-Breast06 trial is an ongoing, phase III, global, open-label RCT evaluating the efficacy and safety of trastuzumab deruxtecan compared with physician’s choice of chemotherapy (i.e., capecitabine, paclitaxel, or nab-paclitaxel) in adult patients with unresectable or metastatic HR-positive, HER2-low (i.e., IHC 1+ or IHC 2+ and ISH-negative) or HER2-ultralow (i.e., IHC 0 with membrane staining) breast cancer whose disease has progressed after at least 2 lines of ET in the metastatic setting, or after 1 line of ET in the metastatic setting with progression within 24 months of the start of adjuvant ET or within 6 months of starting first-line ET in combination with a CDK 4/6 inhibitor in the metastatic setting. Patients had not received previous chemotherapy for metastatic breast cancer.
A total of 866 patients were randomized 1:1 to receive trastuzumab deruxtecan (5.4 mg/kg every 3 weeks; n = 436) or physician’s choice of chemotherapy (n = 430). Randomization was stratified by HER2 expression (IHC 2+ and ISH-negative vs. IHC 1+ vs. IHC > 0 to < 1+); prior use of CDK4/6 inhibitors (yes or no); and prior taxane use in the nonmetastatic setting (yes or no).
Eligible patients were chemotherapy-naive in the metastatic setting and had received greater than or equal to 2 prior lines of ET or 1 prior line with early progression (≤ 6 months) or recurrence (≤ 24 months) after adjuvant ET. Treatment continued until disease progression per RECIST 1.1, unacceptable toxicity, or withdrawal.
The study included HER2-low and HER2-ultralow subgroups. While the primary objective was to compare PFS by blinded independent central review (BICR) in the population of patients with HER2-low cancer, key secondary objectives included PFS in the intention-to-treat (ITT) population and OS in the HER2-low and ITT populations. Other secondary outcomes relevant to this review included ORR, DOR, patient-reported outcomes (PROs), and safety and tolerability. Exploratory objectives included efficacy and safety outcomes in the prespecified subgroup of patients with HER2-ultralow disease.
Assessments of efficacy were conducted through tumour imaging every 6 weeks for the first 12 months and every 9 weeks thereafter. Safety assessments were conducted at each treatment visit throughout the study.
The trial was conducted at 273 study sites across 28 countries, including 10 sites in Canada that enrolled 35 patients. The first patient was randomized on July 24, 2020, and the last patient was randomized on April 13, 2023. The primary data cut-off date for efficacy and safety analyses was March 18, 2024. A second interim data cut-off date was March 24, 2025, with final database lock pending. The trial is sponsored by AstraZeneca.
Table 3: Characteristics of Studies Included in the Systematic Review
Study name, design, and sample size | Key inclusion criteria | Key exclusion criteria | Intervention and comparators | Relevant end points |
|---|---|---|---|---|
DESTINY-Breast06 trial Multicentre, open-label, phase III RCT Total N = 866 |
|
| Intervention: Trastuzumab deruxtecan 5.4 mg/kg, administered through IV once every 3 weeks until disease progression or unacceptable toxicity Dose interruptions or reductions of trastuzumab deruxtecan were allowed. The starting dose was 5.4 mg/kg every 3 weeks, with reductions to 4.4 mg/kg or 3.2 mg/kg permitted for clinically significant or unacceptable toxicity. Comparators: Capecitabine: 1,000 mg/m2 or 1,250 mg/m2 orally b.i.d. on days 1 to 14 of a 21‑day cycle until disease progression or unacceptable toxicity Paclitaxel: 80 mg/m2 through IV once weekly for 3 weeks of a 4-week cycle until disease progression or unacceptable toxicity Nab-paclitaxel: 100 mg/m2 through IV once weekly for 3 weeks of a 4-week cycle until disease progression or unacceptable toxicity Chemotherapy could be delayed up to 28 days; longer delays required discussion with the sponsor. |
|
ADC = antibody-drug conjugate; BICR = blinded independent central review; b.i.d. = twice daily; DOR = duration of response; EORTC QLQ-BR45 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire–Breast Cancer Module; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; ER = estrogen receptor; ET = endocrine therapy; IHC = immunohistochemistry; ILD = interstitial lung disease; ISH = in situ hybridization; ITT = intent to treat; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; PR = progesterone receptor; RCT = randomized controlled trial; SAE = serious adverse event.
aPatients with prior (neo)adjuvant chemotherapy were eligible if the interval between the completion of chemotherapy and the diagnosis of metastatic disease was greater than 12 months.
Source: Details included in the table are from the sponsor’s Summary of Clinical Evidence and the DESTINY-Breast06 trial Clinical Study Report.32
Statistical Testing and Analysis Populations
The DESTINY-Breast06 study intended to randomize about 850 patients (700 with HER2-low disease status and 150 with HER2-ultralow disease status). A total of 456 PFS events were required to achieve at least 95% power to detect a hazard ratio of 0.55 (corresponding to an increase in median PFS from 5.5 months to 10 months) in the population with HER2-low disease at a 2-sided significance level of 5%. A total of 521 OS events were required to achieve 80% power to detect a hazard ratio of 0.77 (i.e., increase in median OS from 20.5 months to 26.6 months) in the population of patients with HER2-low disease.
The type I error rate across PFS and OS in the population with HER2-low disease and the ITT populations was controlled at 5% (2-sided) using a fixed sequence testing procedure. PFS was first tested in the population of patients with HER2-low disease, after which the alpha was distributed across PFS in the ITT population (1.5%) and OS in the population of patients with HER2-low disease (3.5%), with alpha recycling if either were significant. If both were significant, then OS was to be tested in the ITT population. If PFS in the ITT population was significant, the adjusted significance levels at each analysis time point for OS in the HER2-low and ITT populations were updated per the group sequential Holm variable procedure.
An interim futility analysis for the population with HER2-ultralow disease was planned for after the first 70 patients were randomized and had at least 24 weeks of follow-up. PFS in the population with HER2-low disease and in the ITT populations was to be tested once when about 65% maturity (456 events) was reached in the population of patients with HER2-low disease. Two event-driven interim analyses (IAs) and a final analysis for OS were planned, with the 3.5% initial alpha being distributed across the analyses using the Lan DeMets spending function. In the DESTINY-Breast06 trial, the difference in OS in the population of patients with HER2-low disease was not statistically significant; therefore, the ITT population was not formally tested. Other end points and populations (e.g., those with HER2-ultralow disease) were unadjusted for multiplicity.
Efficacy analyses were conducted in 3 prespecified analysis populations:
The population of patients with HER2-low disease (n = 713) included those whose disease had centrally confirmed HER2 IHC 1+ or IHC 2+ and ISH-negative expression. This was the primary population for the efficacy analyses.
The population of patients with HER2-ultralow disease (n = 152) included those whose disease was HER2-ultralow and IHC 0 with membrane staining per central lab results.
The ITT population (n = 866) included all randomized patients. The safety population included all randomized patients who received at least 1 dose of the study drug; it was analyzed according to the actual treatment received.
The results within this report represent the final analysis of PFS at the first IA (IA1) and second IA (IA2) of OS. The date of the data cut-off for IA1 was March 18, 2024; the date of the data cut-off for IA2 was March 24, 2025. The results for the final OS analysis were not available when this report was prepared. The final analysis is expected to occur approximately 57 months after the first patient is randomized.
Patient Disposition
Results in the following section are summarized for the March 24, 2025, data cut-off date. Results for both the March 18, 2024, and March 24, 2025, data cut-off dates are summarized in Appendix 4 of the Supplemental Material.
In the DESTINY-Breast06 trial, 2,311 patients were enrolled and 866 patients were randomized: 436 to trastuzumab deruxtecan and 430 to chemotherapy. Of those randomized, 434 patients (99.5%) in the trastuzumab deruxtecan arm and 417 patients (97.0%) in the chemotherapy arm received at least 1 dose of treatment. At the time of the data cut-off, ███ patients in the trastuzumab deruxtecan arm (█████) and ███ patients in the chemotherapy arm (█████) had discontinued study treatment.
The most common reason for treatment discontinuation was disease progression, reported for ███ patients in the trastuzumab deruxtecan arm (█████) and ███ patients in the chemotherapy arm (██████. Discontinuation due to AE was reported in ██ patients in the trastuzumab deruxtecan arm (█████) and ██ patients in the chemotherapy arm (████). Other reported reasons for discontinuation included patient decision (██ ██████ vs. ██ ██████ patients) and other (██ ██████ vs. ██ ██████ patients) in the trastuzumab deruxtecan and chemotherapy arm, respectively.
At the time of data cut-off, ███ patients in the trastuzumab deruxtecan arm (█████) and ███ patients in the chemotherapy arm (█████) remained in the study. The main reason for study termination was █████ ██████ in the trastuzumab deruxtecan arm vs. █████ in the chemotherapy arm). Withdrawals by patients were higher in the chemotherapy arm (████) compared to the trastuzumab deruxtecan arm (████).
No notable protocol deviations were identified.
Baseline Characteristics
Baseline demographic and disease characteristics for patients enrolled in the DESTINY-Breast06 trial are summarized in Table 4. These characteristics were generally similar between treatment arms. In the trastuzumab deruxtecan arm, the mean age was 58.2 years (standard deviation = 11.46); in the chemotherapy arm, the mean age was 58.2 years (standard deviation = 10.92). All enrolled patients were female except for 1 male in the chemotherapy arm. Most patients had HER2-low disease (359 patients [82.3%] in the trastuzumab deruxtecan arm and 354 patients [82.3%] in the chemotherapy arm), while a smaller proportion had HER2-ultralow disease (76 patients [17.4%] in each arm). ET with CDK4/6 inhibitors had been used previously in 89.0% of patients in the trastuzumab deruxtecan arm and in 89.5% of patients in the chemotherapy arm. The median number of prior lines of ET for metastatic disease was 2 in both arms.
Table 4: Summary of Baseline Characteristics in the DESTINY-Breast06 Trial (ITT Population)
Characteristic | Trastuzumab deruxtecan (N = 436) | Chemotherapy (N = 430) |
|---|---|---|
Age (years)a | ||
Mean (SD) | 58.2 (11.46) | 58.2 (10.92) |
Median (minimum to maximum) | 58.0 (28 to 87) | 57.0 (32 to 83) |
Age group (years), n (%) | ||
< 65 | 302 (69.3) | 297 (69.1) |
≥ 65 | 134 (30.7) | 133 (30.9) |
Sex, n (%) | ||
Female | 436 (100) | 429 (99.8) |
Male | 0 (0) | 1 (0.2) |
Race, n (%) | ||
American Indian or Alaska Native | 1 (0.2) | 0 (0) |
Asian | 154 (35.3) | 151 (35.1) |
Black or African-American | 4 (0.9) | 3 (0.7) |
White | 231 (53.0) | 230 (53.5) |
Other | 7 (1.6) | 12 (2.8) |
Not reported | 39 (8.9) | 34 (7.9) |
Ethnic group, n (%) | ||
Hispanic or Latino | 28 (6.4) | 32 (7.4) |
Not Hispanic or Latino | 397 (91.1) | 387 (90.0) |
Missing | 11 (2.5) | 11 (2.6) |
ECOG Performance Status score, n (%)b | ||
0 | 252 (57.8) | 257 (59.8) |
1 | 178 (40.8) | 163 (37.9) |
2 | 1 (0.2) | 1 (0.2) |
Missing | 5 (1.1) | 9 (2.1) |
AJCC stage at diagnosis of breast cancer, n (%) | ||
Stage 0 | ██ ██████ | ██ ██████ |
Stage I | ██ ██████ | ██ ██████ |
Stage II | ██ ██████ | ██ ██████ |
Stage III | ██ ██████ | ██ ██████ |
Stage IV | 133 (30.5) | 132 (30.7) |
Missing | ██ ██████ | ██ ██████ |
ER and PR status, n (%)c,d | ||
ER-negative, PR-negative | 1 (0.2) | 0 |
ER-positive, PR-negative | 167 (38.3) | 181 (42.1) |
ER-negative, PR-positive | 3 (0.7) | 2 (0.5) |
ER-positive, PR-positive | 253 (58.0) | 237 (55.1) |
ER-positive, PR missing | 12 (2.8) | 10 (2.3) |
HER2 status, n (%)e | ||
IHC 0 | 1 (0.2) | 1 (0.2) |
IHC > 0 < 1+ (i.e., HER2-ultralow) | 76 (17.4) | 76 (17.7) |
IHC 1+ (i.e., HER2-low) | 239 (54.8) | 234 (54.4) |
IHC 2+ and ISH-negative (i.e., HER2-low) | 117 (26.8) | 118 (27.4) |
IHC 2+ | 3 (0.7) | 1 (0.2) |
Endocrine resistance at baseline, n (%)f | ||
Primary | 128 (29.4) | 140 (32.6) |
Secondary | 308 (70.6) | 288 (67.0) |
ET for metastatic disease, n (%)g | ||
Median number of lines (range) | 2 (1 to 4) | 2 (1 to 5) |
1 line | 65 (14.9) | 82 (19.2) |
First-line ET with CDK4/6 inhibitor for ≤ 6 months | 37 (8.5) | 40 (9.3) |
2 lines | 295 (67.8) | 288 (67.3) |
≥ 3 lines | 75 (17.2) | 58 (13.6) |
Previous therapies for metastatic disease, n (%) | ||
Endocrine monotherapy | 230 (52.8) | 223 (51.9) |
Any ETh | 435 (99.8) | 428 (99.5) |
ET with CDK4/6 inhibitor | 388 (89.0) | 385 (89.5) |
ET with targeted therapy other than CDK4/6 inhibitori | 143 (32.8) | 127 (29.5) |
AJCC = American Joint Committee on Cancer; ECOG = Eastern Cooperative Oncology Group; ER = estrogen receptor; ET = endocrine therapy; IHC = immunohistochemistry; IPD = important protocol deviation; ISH = in situ hybridization; ITT = intention to treat; mBC = metastatic breast cancer; PD = progressed disease; PR = progesterone receptor; SD = standard deviation.
Racial categories used in the table are as reported in the source and may not align with Canada's Drug Agency inclusive language guidelines.
aAge calculated at randomization.
bECOG Performance Status scores are assessed on a 5-point scale, with higher scores indicating greater disability. A total of 14 patients in the ITT population (5 patients in the trastuzumab deruxtecan arm and 9 patients in the chemotherapy arm) had missing ECOG Performance Status scores at baseline but had a score of 0 or 1 recorded within 6 days after randomization.
cThe most recent results available at study entry are summarized.
dER-positive and PR-positive correspond to the results 1% to 10%, > 10%, and positive. ER-negative and PR-negative correspond to the results < 1% and negative.
eIn 4 patients with HER2 IHC 2+, ISH was not evaluable per central laboratory. In 2 patients, the final baseline HER2 IHC score per central laboratory was 0; IPDs were reported for all 6 patients.
fPrimary endocrine resistance was defined as either relapse during the first 2 years of adjuvant ET, or PD within the first 6 months of first-line ET for mBC while receiving ET. Secondary (acquired) endocrine resistance was defined as relapse while receiving adjuvant ET, but after the first 2 years, or relapse within 12 months of completing adjuvant ET, or PD greater than 6 months after initiating ET for mBC while on ET.
gThe number of patients in the trastuzumab deruxtecan arm was 435; the number of patients in the chemotherapy arm was 428.
hAny ET included both monotherapy and combination therapy.
iOther targeted therapies in the trastuzumab deruxtecan arm and chemotherapy arms in the ITT population included mammalian target of rapamycin inhibitors (in 23.9% of the patients in the trastuzumab deruxtecan arm and in 23.7% of those in the chemotherapy arm), PI3K inhibitors (in 5.5% and 2.8%, respectively), or poly(adenosine diphosphate–ribose) polymerase inhibitors (in 0.7% and 1.2%, respectively).
Sources: Details included in the table are from the sponsor’s Summary of Clinical Evidence and the DESTINY-Breast06 Clinical Study Report.32
Treatment Exposure and Concomitant Medications
Refer to Appendix 4 for full details related to treatment exposure, concomitant medications, and subsequent treatments.
At the March 24, 2025, data cut-off date, the median durations of treatment in the ITT population were ████ months (range, ███ to ████) in the trastuzumab deruxtecan treatment arm and ███ months (range, ███ to ████) in the chemotherapy treatment arm.
The use of concomitant mediations was reported for the March 18, 2024, data cut-off date; there was no significant update in concomitant medications received by the March 25, 2025, data cut-off date. Concomitant medication use was reported for ███ patients ███████ in the trastuzumab deruxtecan treatment arm and ███ patients ██████) in the chemotherapy treatment arm. The most commonly used concomitant medications (i.e., those administered to ≥ 20% of patients in either treatment arm) included █████████ ██████ ███████████ ████ patients ███████ trastuzumab deruxtecan, ███ patients ███████ chemotherapy), ███████████████ ████ ████████ ███ █████████ ██████ ████ ██████████ ████ ████████ ███ █████████ ████████ ████ ████████ ███ █████████ ███ ███████████ ███ █████████████ ████ ████████ ██ █████████ Additional commonly used agents included ███████ █ ███ █████████ ███ ████████ ██ █████████ █████████ ████ ███████████ ███ ████████ ██ ████████, and ██████████████ ███████████ ████ ████████ ██ █████████ Concomitant ██████████ ████████████ was administered to ████████ ██████ in the trastuzumab deruxtecan arm and ████████ ██████ in the chemotherapy arm. ███ ████████ used disallowed concomitant medications.
At the March 24, 2025, data cut-off date, following treatment discontinuation, █████ of patients in the trastuzumab deruxtecan arm and █████ in the chemotherapy arm received at least 1 subsequent anticancer therapy. The most common subsequent treatments were ████████████ (trastuzumab deruxtecan vs. chemotherapy: █████ vs. █████) and ████████ ████████ ██████ █████ (████ vs. ████) or ██ ███████████ ████ ████████ ███████ (████ vs. ████) or ██████ ██████████ (████ vs. ████). Subsequent treatment with ███████ ████████ ████ █████████ █████ was reported in ████ of patients in the trastuzumab deruxtecan arm and █████ in the chemotherapy arm.
Critical Appraisal
Internal Validity
There is low risk of bias in the randomization process. A computer software program was used to generate the randomization sequence, which was stratified by HER2 status (low vs. ultralow), prior treatment with CDK4/6 inhibitors (yes vs. no), and prior taxane use in the nonmetastatic setting (yes vs. no). The stratification ensured that randomization was maintained in the groups with HER2-low and HER2-ultralow disease. The use of interactive response technology was adequate to conceal the allocation. Baseline characteristics were generally balanced between treatment arms across stratification factors and relevant prognostic variables. All patients had received prior ET; the median number of prior lines of therapy in the metastatic setting was 2 (range, 0 to 8), which is consistent with the intended treatment setting. DOR was measured among patients with a disease response. Randomization is not guaranteed to be maintained in this group; the result can be considered at risk of bias.
The open-label design introduces a risk of bias for PROs (HRQoL) and reporting of subjective AEs. The measurement of OS is unaffected, and the use of BICR mitigates the risk of bias in assessing PFS. The timing of assessment could affect the PFS results if scans occurred outside the protocol-scheduled time points; however, this is not an important concern because a sensitivity analysis addressing the timing of assessments showed results that were consistent with those of the primary analysis. The lack of blinding can also result in bias due to deviations from the intended intervention; however, evidence from the trial does not suggest that this is an important concern. Treatment discontinuations were primarily due to progressive disease and AEs, as expected in practice. A slightly higher proportion of patients in the placebo group discontinued treatment due to patient decision (possibly due to the open-label design). Clinical experts consulted by the review team indicated that the use of concomitant treatments appeared consistent with clinical practice. There was minimal use of disallowed treatments. No major protocol deviations were expected to compromise the validity of the results.
Time-to-event outcomes were analyzed using stratified Cox proportional hazards models and Kaplan-Meier estimates. The proportional hazards assumption was assessed using log-log survival plots. By visual inspection, the CDA-AMC review team judged that the assumption held approximately for PFS and OS in the ITT population and population of patients with HER2‑low disease. In the population of patients with HER2-ultralow disease, separation of the Kaplan-Meier curves was delayed; the curves came together or crossed in later follow-up when few patients remained at risk. This implies that the hazard ratio is not constant over time; therefore, reliance on this statistic alone to inform the effects of trastuzumab deruxtecan versus chemotherapy among patients with HER2-ultralow disease may be misleading. The evaluation of specific time points on the Kaplan-Meier curves does not require the proportional hazards assumption; therefore, it provides a more appropriate interpretation of the difference between groups over time.
The statistical analysis plan prespecified the primary and secondary analyses with appropriate control for multiplicity. Due to earlier failure of the statistical hierarchy, the analysis of OS in the ITT population was not formally tested. The prespecified subgroup analyses in patients with HER2-ultralow status were exploratory; no formal statistical testing was performed in this population. IAs were conducted under the oversight of an independent data monitoring committee. Given that the results of PFS and OS are from an interim analysis, there is some potential that the treatment effect (hazard ratio) is overestimated.33
The information fraction (observed events vs. total expected events) in the ITT population for OS was ██████████ █████ ██████) at the time of IA2 due to the relatively short follow-up time frame. Kaplan-Meier estimates are affected by imprecision at 12 ███ ██ months, at which time the 95% confidence interval (CI) included small effects that were not considered clinically important or crossed the null value. An important amount of █████████ ████████ ██ █████ ██ ██████ limits the ability to draw definitive conclusions regarding potential long-term survival benefit. The final OS analysis, which is planned for at an information fraction of 70%, is needed to confirm the robustness of the positive trend observed in the DESTINY-Breast06 trial.
As is common in oncology trials, the results for OS reflect the effects of trastuzumab deruxtecan versus chemotherapy and any subsequent non–protocol-specified treatments. This is considered a relevant estimand when subsequent treatments are reflective of usual clinical practice.34 The clinical experts consulted by the review team noted that they would have expected a larger proportion of patients in the chemotherapy arm to receive subsequent trastuzumab deruxtecan treatment — specifically, at least 75% of the population of patients with HER2-low expression who progressed compared to the observed ████ who received trastuzumab deruxtecan immediately after chemotherapy and █████ who received it at any point during subsequent lines of therapy. This may have inflated the treatment effect on OS. However, the magnitude of the impact on the results is uncertain.
PFS may be used as a surrogate to predict longer-term OS. However, there remains some uncertainty regarding its validity. An analysis of 40 RCTs including patients with HR-positive, HER2-negative breast cancer showed a moderate correlation between hazard ratios for PFS and OS.35 The surrogate threshold effect (i.e., the minimum PFS benefit below which there is no predicted OS benefit) for predicting OS was 5 to 6 months of incremental PFS benefit. The validity of a surrogate is context specific; therefore, there is some uncertainty in the application of this information to treatment with trastuzumab deruxtecan versus chemotherapy in the population of interest.
Relatively few patients discontinued the trial for reasons other than death, and there is no indication of an important degree of informative censoring for the analyses of PFS and OS. Additionally, a sensitivity analysis that included events that occurred following 2 missed assessments supported the robustness of the primary PFS analysis result. PROs were assessed using validated instruments (i.e., the EORTC QLQ-C30 and EORTC QLQ-BR45). The timing and frequency of PRO data collection appeared appropriate for the mBC population. However, the number of patients with available assessments declined substantially over time. At week 25, ███ and ███ of patients were available to provide assessments in the trastuzumab deruxtecan and chemotherapy groups, respectively; by week 31, these percentages had decreased to ███ and ███. The PRO data were analyzed using a mixed model for repeated measures, which implicitly handles missing data under the missing-at-random assumption. Given the reasons for data being missing, this assumption may not be plausible, and no sensitivity analyses were conducted to assess the impacts of different reasonable assumptions about the missingness. Therefore, the results are considered at risk of bias.
The focus of this submission is the ITT population because it aligns with the population in the reimbursement request. The treatment effects observed in the ITT population were largely influenced by the population with HER2-low disease, who made up most of the sample. Results for OS and PFS in the populations of patients with HER2-low and HER2-ultralow disease were directionally consistent. However, analyses of the latter population were exploratory, and given the small sample size of this group, baseline imbalances in characteristics (e.g., American Joint Committee on Cancer stage and Eastern Cooperative Oncology Group status) were observed and are likely due to chance. The impact of these imbalances on interpretation is uncertain, and the results had wide CIs that substantially crossed the null for PFS. The Kaplan-Meier curves for this group come together or cross late in the follow-up for both PFS and OS; however, the implication is difficult to ascertain because of uncertainty in the findings attributable to a low number of patients remaining at risk at later time points, which may render the effects unstable.
External Validity
The DESTINY-Breast06 trial enrolled 866 patients from 273 sites across 28 countries. Ten sites were located in Canada. The inclusion and exclusion criteria were considered appropriate by clinical experts consulted by CDA-AMC and aligned with real-world clinical practice. All enrolled patients had HR-positive disease and HER2-low or HER2-ultralow expression confirmed by central pathology review.
The enrolled population was heavily pretreated, with a median of 2 prior lines of therapy in the metastatic setting; more than 90% had received prior CDK4/6 inhibitors. These characteristics generally reflect the population of patients eligible for trastuzumab deruxtecan in second-line or later settings.
The comparator arm included chemotherapy drugs commonly used in Canada (capecitabine, paclitaxel, or nab-paclitaxel), administered according to local practice. The treatment setting, administration procedures, and follow-up schedules are considered applicable to clinical practice in Canada. Outcomes assessed in the DESTINY-Breast06 trial included PFS, OS, ORR, DOR, PROs, and safety, all of which are relevant to clinicians and patients. The trial follow-up period was adequate to assess the primary outcome (median PFS), but longer follow-up is desirable to understand the long-term impact of trastuzumab deruxtecan on OS. As noted by the clinical experts consulted for this review, OS is an important outcome of interest in mBC, and PFS may be viewed as a meaningful short-term efficacy outcome if supported by consistent improvements in quality of life and safety. However, clinical experts noted that the proportion of patients receiving trastuzumab deruxtecan as subsequent therapy (i.e., after progression on chemotherapy) is substantially higher in clinical practice in Canada (approximately 75% among patients with HER2-low disease) than in the DESTINY-Breast06 trial (approximately █████). This difference may affect the OS estimates in the trial; however, the magnitude of this potential overestimation of the true effect in practice is uncertain.
Overall, the trial population, intervention, comparator, outcomes, and setting are broadly applicable to clinical practice in Canada. There is some uncertainty regarding the generalization of the ITT results to the group with HER2-ultralow disease, given the exploratory nature of this group, the reliance on a relatively smaller sample size, and the resulting wide CIs. However, point estimates of effect in the groups with HER2-low or HER2-ultralow disease were directionally consistent, and it was the opinion of clinical experts consulted by the review team that trastuzumab deruxtecan would be expected to have a similar benefit across groups with either HER2-low or HER2-ultralow disease. HRQoL results were not reported for patients with HER2-ultralow disease, specifically. Longer follow-up is needed to further characterize longer-term OS and confirm the robustness of the findings.
Results
The key efficacy and harms results and findings from the GRADE assessment are presented in this section. At the March 18, 2024, data cut-off date, the median duration of follow-up for all patients was 18.6 months. At the March 24, 2025, data cut-off date, the median duration of follow-up was ████ months. For PFS, at the March 24, 2025, data cut-off date, the median durations of follow-up in the ITT population were ████ months in the trastuzumab deruxtecan arm and ███ months in the chemotherapy arm. Detailed efficacy and harms results can be found in Appendix 4 in the Supplemental Material document.
Efficacy
PFS by BICR and investigator assessment: At the primary analysis (i.e., the March 18, 2024, data cut-off date), median PFS durations in the population of patients with HER2-low expression were 13.2 months (95% CI, 11.4 months to 15.2 months) in the trastuzumab deruxtecan treatment arm and 8.1 months (95% CI, 7.0 months to 9.0 months) in the chemotherapy arm. The hazard ratio was 0.62 (95% CI, 0.52 to 0.75; P < 0.0001), favouring trastuzumab deruxtecan. In the ITT population, the median PFS durations were 13.2 months (95% CI, 12.0 months to 15.2 months) for trastuzumab deruxtecan and 8.1 months (95% CI, 7.0 months to 9.0 months) for chemotherapy. The hazard ratio was 0.64 (95% CI, 0.54 to 0.76; P < 0.0001), favouring trastuzumab deruxtecan. The results of the investigator assessment were consistent with those of the BICR. In the population of patients with HER2-low expression, the median PFS durations were 13.2 months (95% CI, 9.8 months to 17.3 months) with trastuzumab deruxtecan and 8.3 months (95% CI, 5.8 months to 15.2 months) with chemotherapy. The hazard ratio was 0.78 (95% CI, 0.5 to 1.21).
Refer to Appendix 4 for PFS KM curves for the ITT, HER2-low, and HER2-ultralow populations.
OS: At the time of the March 24, 2025, data cut-off date (the IA2 for OS), a total of ███ OS events had accrued, corresponding to an information fraction of █████ in the ITT population. In the population of patients with HER2-low expression, median OS was ████ months (95% CI, ████ to ████) with trastuzumab deruxtecan and ████ months (95% CI, ████ to ████) with chemotherapy. The HR was ████ (95% CI, ████ to ████, P = ██████), although the █████ ███ ███ █████ ██ ███ ███████ ████████ ████████ ██ ███████ ██████████ ███ ███ ██████████ ███ ███ ████████ ██████. In the ITT population, median OS was ████ months (95% CI, ████ to ████) for trastuzumab deruxtecan and ████ months (95% CI, ████ to ████) for chemotherapy. The HR was ████ (95% CI, ████ to ████). In the population of patients with HER2-ultralow expression, median OS was ████ months (95% CI, ████ ██ ██) for trastuzumab deruxtecan and ████ months (95% CI, ████ ██ ████) for chemotherapy. The HR was ████ (95% CI████ ██ ████
Refer to Appendix 4 for the OS KM curves for the ITT, HER2-low, and HER2-ultralow populations.
ORR: At the time of the March 18, 2024, data cut-off, in the population of patients with HER2-low disease, ORR by BICR was confirmed in 203 patients (56.5%) receiving trastuzumab deruxtecan and in 114 patients (32.2%) receiving chemotherapy, corresponding to an odds ratio (OR) of 2.74 (95% CI, 2.02 to 3.73). In the ITT population, ORR was confirmed in 250 patients (57.3%) receiving trastuzumab deruxtecan and in 134 patients (31.2%) receiving chemotherapy, with an OR of 2.98 (95% CI, 2.26 to 3.94). In the population of patients with HER2-ultralow disease, ORR was confirmed in 47 patients (61.8%) receiving trastuzumab deruxtecan and in 20 patients (26.3%) receiving chemotherapy, with an OR of 4.54 (95% CI, 2.31 to 9.20). Between-group differences for the proportions of patients with confirmed ORR by BICR were not reported. Results from the investigator assessment were consistent with those of the BICR.
DOR: Based on the BICR assessment, the median confirmed DORs among patients with a confirmed disease response in the population of patients with HER2-low disease were 14.1 months (interquartile range [IQR], 6.9 months to 25.5 months) in the trastuzumab deruxtecan arm and 8.6 months (IQR, 4.2 months to 15.9 months) in the chemotherapy arm. In the ITT population, the median confirmed DORs were 14.3 months (IQR, 7.0 months to 25.5 months) with trastuzumab deruxtecan and 8.6 months (IQR, 4.4 months to 17.6 months) with chemotherapy. In the population of patients with HER2-ultralow expression, the median DOR was not reported for either arm. The absolute between-group differences in the percentages of patients with maintained disease response were not reported.
Patient-Reported Outcomes
EORTC QLQ-C30
In the population of patients with HER2-low disease, the adjusted mean changes from baseline over 31 weeks in EORTC QLQ-C30 Global Health Status were −1.7 (95% CI, −4.1 to 0.7) in the trastuzumab deruxtecan treatment arm and −2.7 (95% CI, −5.2 to 0.3) in the chemotherapy arm, with an adjusted mean between-group difference of 1.0 (95% CI, −1.6 to −3.6; P = 0.46).
In the ITT population, the adjusted mean changes from baseline over 31 weeks in EORTC QLQ-C30 Global Health Status were −0.9 (95% CI, −3.0 to 1.2) for trastuzumab deruxtecan and −2.0 (95% CI, −4.2 to 0.2) for chemotherapy, with an adjusted mean between-group difference of 1.1 (95% CI, −1.2 to 3.4; P = 0.35).
No patient-reported EORTC QLQ-C30 outcome data were reported for the population with HER2-ultralow disease.
EORTC QLQ-BR45
Overall, the adjusted mean change from baseline analysis over 31 weeks did not appear to show clinically meaningful differences between treatment arms in the EORTC QLQ-BR45 scales, based on the 10-point minimal important difference (MID) proposed in the submitted Clinical Study Report,32 except for the skin mucositis symptom scale. In the ITT population, the between-group difference in adjusted mean change from baseline on the skin mucositis symptoms scale met the clinically meaningful threshold of 10 points, with greater deterioration observed in the chemotherapy group compared to the trastuzumab deruxtecan group at weeks 10, 13, 16, 22, 25, 28, and 31. In the ITT population, the adjusted mean changes from baseline over 31 weeks in EORTC QLQ-BR45 skin mucosis symptoms were 2.0 (95% CI, 0.2 to 3.8) in the trastuzumab deruxtecan arm and 11.5 (95% CI, 9.7 to 13.4) in the chemotherapy arm. The adjusted between-group difference was −9.5 (95% CI, −11.5 to −7.5; P < 0.0001).
Results were similar in the population of patients with HER2-low expression. No patient-reported EORTC QLQ-BR45 outcome data were reported for the population of patients with HER2-ultralow expression. Refer to Appendix 4 for the summary of changes from baseline for the EORTC QLQ-C30 and EORTC QLQ-BR45 questionnaires for the HER2-low and ITT populations.
Harms
Key results for the overall safety analysis set at the March 24, 2025, data cut-off date are discussed in this section.
Treatment-emergent AEs were reported in ███ patients (█████) in the trastuzumab deruxtecan treatment arm and ███ patients (█████) in the chemotherapy arm. The most common AEs (≥ 10% of patients in either arm) were ██████ ██████ trastuzumab deruxtecan vs. █████ chemotherapy), ████████ ██████ ███ ██████, ██████ ██████ ███ ██████, ████████ ██████ ███ ██████, ████████ ██████ ███ ██████, and ████████████ ██████ ███ ██████.
SAEs were reported in ██ patients (█████) in the trastuzumab deruxtecan arm and ██ patients (█████) in the chemotherapy arm. The most common SAEs (≥ 1%) in the trastuzumab deruxtecan arm were ████████████ ████ ███████ ███████ ███████████ ███████ ████████ ███████ ███████ ███████████ ███████ ███ ███████████ ███████ In the chemotherapy arm, the most common SAEs (≥ 1%) were ██████████ ██████ ███ ███████ ████████ ███████
AEs leading to treatment discontinuation were reported in ██ patients ███████ in the trastuzumab deruxtecan arm and ██ patients ██████ in the chemotherapy arm. Common reasons for AEs in the trastuzumab deruxtecan arm were ███████████ ██████ ███ ████████████ ████ ███████ ███████
Deaths due to AEs occurred in ██ patients ██████ in the trastuzumab deruxtecan arm and in patients ██████ in the chemotherapy arm. In the trastuzumab deruxtecan group, the most common AEs with fatal outcomes were classified as ██████████ ███ ████████████, occurring in patients ██████. In the chemotherapy group, all AEs leading to death occurred in ████ █ ██ patients each.
ILD events, adjudicated as AEs of special interest, were reported in ██ ████████ ███████ treated with trastuzumab deruxtecan and ███████ ██████ treated with chemotherapy.
In the safety analysis set, grade 2 left ventricular ejection fraction (LVEF) events occurred in █████ of patients receiving trastuzumab deruxtecan and ████ of those receiving chemotherapy. Grade 3 events occurred in ████ of patients receiving trastuzumab deruxtecan and ████ of patients receiving chemotherapy. Among those with grade 2 LVEF decline who had a postgrade measurement, █████ of patients receiving trastuzumab deruxtecan and █████ of patients receiving chemotherapy recovered to 90% or more of their baseline LVEF. The mean changes in LVEF from baseline to end of treatment were █████ for trastuzumab deruxtecan and █████ for chemotherapy. No patients in either group experienced a drop in LVEF to less than 40% by end of treatment (the threshold requiring permanent discontinuation, according to the product monograph).
Summary of Findings and Certainty of the Evidence
Literature-based MID estimates were used as the thresholds for the EORTC QLQ-C30 Global Health Status domain. The anchor-based MIDs for between-group change over time ranged from –13 to –6 for deterioration and from 8 to 11 for improvement. Refer to the summary of outcome measures in Appendix 3 of the Supplemental Material document for additional information. In the absence of literature-based MID estimates, thresholds for a clinically important effect suggested by the clinical experts consulted were used for the following outcomes: PFS (threshold: 10%), OS (threshold: 5%), and SAEs (threshold: 5%). For ILD, clinical experts consulted considered any non-null effect to be clinically important. The certainty was rated accordingly.
Table 5: Summary of Findings for Trastuzumab Deruxtecan vs. Chemotherapy for Patients With HER2-Low and HER2‑Ultralow Breast Cancer
Outcome and follow-up | Patients (studies), N | Relative effects (95% CI) | Absolute effects (95% CI) | Certainty | What happens | ||
|---|---|---|---|---|---|---|---|
Chemotherapy | Trastuzumab deruxtecan | Difference | |||||
Efficacy outcome, PFS, ITT population, IA1 | |||||||
PFS at 6 months Median follow-up: T-DXd ████ months, chemotherapy ███ months | 866 (1 RCT) | NA | ███ ███ █████ | ███ ███ █████ ████ ██ ████ | ███ ████ ███ █████ ███ ████ ██ ███ | Higha | Trastuzumab deruxtecan results in a clinically important improvement in PFS at 6 months compared with chemotherapy. |
PFS at 18 months Median follow-up: T-DXd ████ months, chemotherapy ███ months | 866 (1 RCT) | NA | ███ ███ █████ | ███ ███ █████ ████ ██ ████ | ███ ████ ███ █████ ███ ████ ██ ███ █████ | Moderateb (serious imprecision) | Trastuzumab deruxtecan likely results in a clinically important improvement in PFS at 18 months compared with chemotherapy. |
Efficacy outcome, OS, ITT population, ███ | |||||||
OS at 12 months Median follow-up: T-DXd ████ months, chemotherapy ████ months | 866 (1 RCT) | NA | ███ ███ █████ | ███ ███ █████ ████ ██ ████ | ██ ████ ███ █████ ███ ████ ██ ███ █████ | Moderatec (serious imprecision) | Trastuzumab deruxtecan likely results in a clinically important improvement in OS at 12 months compared with chemotherapy. |
OS at ██ ██████ Median follow-up: T-DXd ████ months, chemotherapy ████ months | 866 (1 RCT) | NA | ███ ███ █████ | ███ ███ █████ ████ ██ ████ | ██ ████ ███ █████ ██ ████ ██ ███ █████ | Moderate (serious imprecision) | Trastuzumab deruxtecan likely results in a clinically important improvement in OS at ██ ██████ compared with chemotherapy. |
Patient-reported outcomes, ITT population, IA1 | |||||||
EORTC QLQ-C30 Global Health Status mean change from baseline (up to 7 months or PD) (0 to 100, where a higher score means better QoL) | 866 (1 RCT) | NA | ████ | ████ █████ ██ ████ | ███ █████ ██ ████ | Lowd (very serious risk of bias) | Trastuzumab deruxtecan may result in little to no clinically important difference in Global Health Status at 31 weeks when compared with chemotherapy. |
Harms, ███ | |||||||
SAEs Follow-up: date of AE onset > date of last dose of study treatment + 47 days | 851 (1 RCT) | ████ ██████ █████ | ███ ███ █████ | ███ ███ █████ ████ ██ ████ | ██ ████ ███ █████ ███ █████ ██ ███ █████ | Moderatee (serious imprecision) | Trastuzumab deruxtecan likely results in little to no clinically important difference in SAEs compared with chemotherapy. |
Adjudicated ILD events Follow-up: date of AE onset > date of last dose of study treatment + 47 days | 851 (1 RCT) | █████ ██████ ███████ | ███ ████ | ███ ███ █████ ████ ██ ████ | ███ ████ ███ █████ ███ ████ ██ ███ █████ | High | Trastuzumab deruxtecan results in a clinically important increase in ILD compared with chemotherapy. |
AE = adverse event; CI = confidence interval; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; IA1 = interim analysis 1; ILD = interstitial lung disease; ITT = intention to treat; NA = not available; OS = overall survival; PFS = progression-free survival; RCT = randomized controlled trial; SAE = serious adverse event; T-DXd = trastuzumab deruxtecan; vs. = versus.
Notes: Study limitations (which refer to internal validity or risk of bias), indirectness, imprecision of effects, and publication bias were considered when assessing the certainty of the evidence. All serious concerns in these domains that led to the rating down of the level of certainty are documented in the table footnotes.
The risk differences presented in this table are derived from the sponsor-submitted analyses and reflect estimates based on 2 × 2 contingency tables with associated 95% CIs. These values may differ slightly from crude differences (e.g., 207 to 161 or 136 to 2 per 1,000) due to rounding. Rounded percentage-based risk differences are from the safety dataset (e.g., 20.7% to 16.1% for SAEs and 13.6% to 0.2% for ILD).
aNot rated down for imprecision. The point estimate for the between-group difference suggested a clinically important difference between the 2 groups, and the CDA-AMC review team determined that the lower bound of the 95% CI did not appreciably cross the 10% threshold.
bRated down 1 level for serious imprecision; although the absolute risk difference exceeded the threshold of 10% suggested by clinical experts, the lower bound of the 95% CI included the potential for little to no clinically important difference. Certainty was not rated down for indirectness for PFS as a surrogate outcome for OS. While direct validation of PFS as a surrogate for OS in the setting of unresectable or metastatic HER2-low or HER2-ultralow disease treated with trastuzumab deruxtecan is lacking, the clinical experts considered PFS to be clinically relevant for patients with respect to delaying disease progression and administering more toxic treatment.
cRated down 1 level for serious imprecision; although the absolute risk difference exceeded the threshold of 5% suggested by clinical experts, the lower bound of the 95% CI included the potential for little to no clinically important difference.
dRated down 2 levels for very serious study limitations; there is high risk of bias due to the open-label study design, subjectivity in patient-reported outcomes, and substantial missing outcome data.
eRated down 1 level for serious imprecision; the 95% CI includes the potential for harm or little to no difference with trastuzumab deruxtecan.
Sources: Details included in the table are from the sponsor’s Summary of Clinical Evidence and the DESTINY-Breast06 Clinical Study Report.32
Long-Term Extension Studies
No long-term extension study was submitted.
Indirect Evidence
No indirect evidence was submitted.
Studies Addressing Gaps in the Systematic Review Evidence
No study addressing gaps in the systematic review was submitted.
Discussion
Efficacy
The DESTINY-Breast06 trial evaluated trastuzumab deruxtecan in patients with HER2-low or HER2-ultralow breast cancer who had received prior ET and no prior chemotherapy in the advanced setting. This is a population for whom treatment options are limited. No targeted therapy has previously been available for patients with HER2-low or HER2-ultralow disease in this setting.
The sponsor confirmed that the eligibility criteria of the DESTINY-Breast06 trial aligned with the target patient population in the sponsor’s reimbursement request. As per the sponsor, the mention of “not considered suitable for endocrine therapy” in the reimbursement request aligns with the population of patients in the DESTINY-Breast06 trial who have either developed disease resistance to ET or exhausted all available ET-based options; these patients would ordinarily progress to chemotherapy. The clinical experts consulted by CDA-AMC indicated that determining suitability for ET in patients whose disease has progressed while receiving at least 1 ET involves clinician judgment and is preferred over rigid definitions that may not capture all relevant clinical scenarios.
The DESTINY-Breast06 trial provides the primary evidence submitted to inform the evaluation of trastuzumab deruxtecan in the target patient population. The trial enrolled patients representative of those seen in clinical practice in Canada, including those with an Eastern Cooperative Oncology Group Performance Status of 0 or 1, and stratified patients’ disease prospectively by HER2 expression (low vs. ultralow). The comparator treatments (capecitabine, paclitaxel, or nab-paclitaxel) represent currently available therapies, supporting the generalizability of the findings.
Clinically meaningful improvements in PFS were observed in the ITT population, with high certainty of evidence at 6 months and moderate certainty of evidence at 18 months, due to imprecision. The findings were consistent in the group with HER2-low disease. PFS in the group with HER2-ultralow disease was analyzed in a prespecified subgroup analysis and was considered exploratory, with no formal statistical testing. The results showed point estimates that were directionally consistent with the ITT population; however, the smaller sample size resulted in imprecision. Based on the 10% threshold provided by the clinical experts consulted, the results suggested a trend toward clinically meaningful PFS benefit at 6 months and 12 months, and little to no difference at 18 months, in the population of patients with HER2‑ultralow disease. The estimates were limited by serious imprecision at 6 months and 12 months (with CIs encompassing small effects near the null) and by very serious imprecision at 18 months (with CIs including the possibility of both substantial harm and benefit). Clinical experts emphasized that patients with either HER2-low or HER2-ultralow disease are managed similarly in practice, and that despite the more limited evidence for HER2-ultralow disease, it remains their opinion that trastuzumab deruxtecan would have a similar benefit for patients with either HER2-low or HER2-ultralow disease.
Trastuzumab deruxtecan also showed benefits across secondary efficacy end points, including improved ORR and longer DOR (not reported for the group with HER2-ultralow disease), indicating better tumour control compared with chemotherapy.
OS was evaluated during IA1 and IA2. While no statistically significant difference was observed between treatment groups in the population of patients with HER2-low disease, the data indicated a favourable trend toward trastuzumab deruxtecan. In accordance with the hierarchical testing procedure, OS was not formally tested in the ITT population; however, a similar positive trend was observed in this group. A relatively short follow-up for OS resulted in █████ ████ of the expected events having accrued at the IA2, which limits the ability to draw conclusions regarding potential longer-term survival benefit. The final OS analysis, which is planned to take place when an information fraction of 70% is reached, is needed to confirm the robustness of the positive trend observed in the DESTINY-Breast06 trial. According to the GRADE assessment, the evidence showed likely clinically meaningful improvements in OS at 12 ███ ██ months in the ITT population. However, there was imprecision in the observed differences, such that the 95% CI was near or crossing the null, including effects that were considered not clinically important. Findings for the HER2-low subgroup were consistent, overall, with those for the ITT population; the clinical experts’ selected threshold of 5% for the between-group difference was ████████ ██ ██ ███ ██ █████ ███ █████ ██ █████ ███ ██ ████ ██. Experts noted that postprogression use of trastuzumab deruxtecan is more common in clinical practice in Canada (used by about 75% of patients with HER2-low disease) than in the DESTINY-Breast06 trial (about █████) — a difference that could possibly improve OS with chemotherapy in practice. This may have inflated the treatment effect of trastuzumab deruxtecan on OS; however, the magnitude of this potential overestimation of the true effect in practice is uncertain.
Exploratory results for OS in the HER2-ultralow population were directionally consistent with those in the ITT population, with numerically higher OS rates favouring trastuzumab deruxtecan across 12- ██ ██ -months landmark time points. By █████ ███ ███ ██████ ██ ████████ █████████ ██ ████ ███ ████ ███ and interpretation of long-term survival was more uncertain. The estimates were limited by very serious imprecision at 12 months (with CIs including the possibility of both substantial harm and benefit) and at ███████ ███████████ ██ ██ ███ ██ ██████ (with CIs ███████████ █████ ███████ ████ ███ ████.
Based on EORTC QLQ-C30 results over 31 weeks, trastuzumab deruxtecan may result in little to no clinically important difference in Global Health Status compared with chemotherapy. The findings are limited by risk of bias due to the open-label design and substantial missing data. Results for the EORTC QLQ-BR45 instrument were consistent overall with those of the EORTC QLQ-C30, with similar uncertainty in the estimates.
The clinical experts considered the improvements in PFS observed with trastuzumab deruxtecan to be clinically meaningful, especially given the lack of targeted therapies for patients with HER2-low or HER2‑ultralow mBC in the target population. Overall, trastuzumab deruxtecan demonstrated a likely added clinical benefit in delaying disease progression, achieving tumour response, and yielding short-term OS improvements in the studied population.
Harms
The safety profile of trastuzumab deruxtecan observed in the DESTINY-Breast06 trial, including the notable risk of ILD, is consistent with its established safety profile in the treatment of breast cancer. ILD remains a clinically significant concern due to its potential severity, including rare fatal outcomes. Product monograph warnings and precautions appropriately reflect this risk. According to clinical experts, proactive monitoring and early intervention can support the management of ILD and other known toxicities in routine practice.
Higher proportions of patients in the trastuzumab deruxtecan group had gastrointestinal toxicities, such as nausea, vomiting, diarrhea, and constipation, compared with the chemotherapy group. According to the sponsor’s submission, these AEs were generally manageable with supportive medication and dose modifications.32
Limitations in the safety evidence include the open-label study design, which may have introduced reporting bias for subjective AEs, and the exclusion of patients with baseline pulmonary disease, which reduces the generalizability of ILD findings to broader real-world populations. Additionally, while serious AEs were not substantially different between treatment arms overall, the increased incidence of ILD and treatment discontinuation due to AEs in the trastuzumab deruxtecan arm suggests a distinct safety profile that differs from that of conventional chemotherapy. The trial's follow-up duration also limits the ability to draw conclusions about long-term or cumulative harms.
Patient groups have acknowledged the risks of toxicities, particularly ILD, but considered these acceptable when weighed against the potential for prolonged disease control. This view was consistent with the expert input, which emphasized that, for appropriately selected patients, the benefits of trastuzumab deruxtecan are likely to outweigh the safety risks, if supported by appropriate clinical oversight.
Overall, while trastuzumab deruxtecan presents some notable safety concerns, particularly related to ILD, the risk profile appears manageable in clinical practice. Key uncertainties remain regarding the long-term safety of the drug, the impact of postmarketing surveillance, and the relevance of findings in underrepresented subgroups, such as patients with poor baseline pulmonary function.
Ethics and Equity Considerations
The DESTINY-Breast06 trial included patients with unresectable or metastatic HER2-low or HER2-ultralow, HR-positive breast cancer. Although the trial enrolled participants across 28 countries, including Canada, data regarding the representation of equity-deserving groups (e.g., racial or ethnic minorities, Indigenous populations, and gender-diverse individuals) were not reported, which limits the ability to assess the generalizability of findings to all populations in Canada.
Access-related considerations include the requirement for HER2 testing using IHC to determine HER2-low or HER2-ultralow expression, which may not be uniformly available across all practice settings in Canada. In addition, the use of trastuzumab deruxtecan requires IV administration every 3 weeks, typically in oncology infusion centres; this may pose barriers for patients in rural or remote regions or for those with mobility or transportation challenges.
Additionally, patients and their families may experience treatment-related burdens, including time away from work, travel costs, and caregiver responsibilities, particularly given the ongoing nature of treatment (i.e., until disease progression or unacceptable toxicity). While the cost of the drug is expected to be covered through public funding if recommended, ancillary costs (e.g., transportation, parking, or time off work) may pose financial strain for some patients.
Conclusion
The DESTINY-Breast06 trial met its primary end point and showed clinically meaningful improvement in PFS (as assessed by BICR) for patients with HER2-low disease; the evidence was rated as high and moderate certainty at 6 months and 18 months, respectively. PFS results in the ITT population were a key secondary outcome and demonstrated results that were consistent with those of the primary analyses. Response outcomes (ORR and DOR) were supportive of the PFS results.
Per the hierarchical testing procedure, OS in the ITT population was not formally tested, given that no statistically significant difference was observed in the group with HER2-low disease. However, the OS data in both the ITT population and for those with HER2-low disease indicated a favourable trend toward trastuzumab deruxtecan. According to the GRADE assessment, the evidence showed likely clinically meaningful improvements in OS at 12 ███ ██ months in the ITT population with moderate certainty of evidence. A relatively short OS follow-up at IA2 (with ████ █████ ███ of expected events) limits the ability to draw definitive conclusions about long-term survival benefit. In addition, the clinical experts consulted by CDA-AMC noted that trastuzumab deruxtecan would be used more often for postprogression in patients with HER2-low disease in clinical practice, possibly improving OS with chemotherapy in real-world settings. This may have inflated the drug’s observed OS benefit; however, the magnitude of this potential overestimation of the true effect in practice is uncertain.
Exploratory prespecified subgroup analyses for patients with HER2-ultralow disease were informed by a small number of patients, yielding wide CIs and uncertain findings; however, the point estimates for the PFS and OS results were directionally consistent overall with the ITT population.
Trastuzumab deruxtecan may result in little to no difference in terms of HRQoL (low certainty of evidence), as measured using the Global Health Status domain of the EORTC QLQ-C30 instrument. Results in the ITT population and in those with HER2-low disease were limited by risk of bias due to the open-label design and substantial missing outcome data. There was no information reported about HRQoL in the population of patients with HER2-ultralow disease.
The harms profile of trastuzumab deruxtecan, particularly the risk of ILD, reflects known toxicities associated with HER2-directed antibody-drug conjugates. Trastuzumab deruxtecan likely results in little to no difference in SAEs compared to chemotherapy. The risk of ILD was meaningfully higher with trastuzumab deruxtecan than with chemotherapy.
Economic Review
Methods
The review team appraised the pharmacoeconomic evidence submitted by the sponsor on the cost-effectiveness and budget impact of trastuzumab deruxtecan compared to chemotherapy for the treatment of unresectable or metastatic HER2-low (i.e., IHC 1+ or IHC 2+ and ISH-negative) or HER2-ultralow (i.e., IHC 0 with membrane staining) breast cancer in adults who have received at least 1 ET in the metastatic setting and are not considered suitable for ET as the next line of therapy. CDA-AMC approved a request by the sponsor to restrict the pharmacoeconomic evaluation and budget impact analysis to the requested reimbursement population (that is, patients not considered suitable for ET as the next line of therapy, which is not specified as part of the Health Canada indication.
Summary of the Submitted Economic Evaluation
The sponsor submitted a cost-utility analysis to estimate the cost-effectiveness of trastuzumab deruxtecan from the perspective of a public health care payer in Canada over a lifetime horizon (i.e., 11 years). The modelled population reflects that of the DESTINY-Breast06 trial population, which is aligned with the reimbursement request. The sponsor’s base-case analysis included costs related to drug acquisition, treatment administration, disease management, AE management, subsequent treatment, and end of life. No costs related to genetic testing were included.
In the sponsor’s base case, trastuzumab deruxtecan was associated with an incremental cost of $85,781 and 0.30 incremental quality-adjusted life-years (QALYs) relative to chemotherapy. This resulted in an incremental cost-effectiveness ratio of $287,326 per QALY gained. Of the incremental benefit compared to chemotherapy (0.30 incremental QALYs), approximately 87% was predicted to be accrued after the treatment duration of the DESTINY-Breast06 trial (median observation period = 19.3 months). Additional information about the sponsor’s submission is summarized in Supplemental Material, Appendix 10.
CDA-AMC identified several key issues with the sponsor’s analysis (refer to Table 6; full details are provided in Supplemental Material, Appendix 11).
Table 6: Key Issues With the Sponsor’s Economic Submission
Issue | What evidence is there to inform this issue? | How was this issue addressed by CDA-AMC? | Did CDA-AMC explore uncertainty in a scenario analysis? |
|---|---|---|---|
The long-term efficacy of trastuzumab deruxtecan is uncertain. | The sponsor’s analysis predicts an incremental gain in LYs for trastuzumab deruxtecan vs. chemotherapy. While a gain in LYs is supported by OS data from the DESTINY-Breast06 trial, the magnitude of the gain is highly uncertain.a Further, OS estimates from this trial for chemotherapy are lower than expected in clinical practice in Canada; as such, the incremental QALYs gained in clinical practice may be lower than predicted by the sponsor’s base case. | CDA-AMC could not address this issue. No long-term data were submitted by the sponsor to support a long-term difference in effectiveness between trastuzumab deruxtecan and chemotherapy, and the magnitude of incremental benefit that will be realized in clinical practice in Canada is highly uncertain. | CDA-AMC conducted a scenario analysis in which the incremental difference in OS between trastuzumab deruxtecan and chemotherapy is lower than in the base case. |
The acquisition cost of trastuzumab deruxtecan is likely underestimated. | The sponsor derived drug acquisition costs using TTD observations from the DESTINY-Breast06 trial. The independent modelling of TTD and PFS resulted in patients being off treatment for approximately 20% of the time spent in the progression-free health state. Clinical experts consulted by CDA‑AMC indicated that patients who are deriving clinical benefit without unacceptable toxicity would typically continue treatment until disease progression. | CDA-AMC could not address this issue. | CDA-AMC explored uncertainty in the time spent on treatment in a scenario analysis in which time on treatment was assumed to be equivalent to PFS. |
The costs and benefits with subsequent therapy are highly uncertain. | The sponsor assumed that 75% of patients who receive subsequent therapy after chemotherapy will receive trastuzumab deruxtecan. This proportion is notably higher than that observed in the DESTINY-Breast06 trial (approximately ███). This change increased the total treatment cost of chemotherapy without a corresponding impact on OS. | CDA-AMC aligned the percentage of patients who received trastuzumab deruxtecan as subsequent therapy with observations from the DESTINY-Breast06 trial. | No scenario analysis was conducted. |
CDA-AMC = Canada’s Drug Agency; LY = life-year; OS = overall survival; PFS = progression-free survival; QALY = quality-adjusted life-year; TTD = time to discontinuation; vs. = versus.
Note: Full details of the issues identified by CDA-AMC are provided in the Supplemental Material, Appendix 10.
aPoint estimates at 12 months and ██ months from the DESTINY-Breast06 trial suggest clinically important benefit but are affected by imprecision; the lower bound of the confidence intervals includes the potential for small differences near the null that are not considered clinically important. The interim nature of the analysis (with █████ ███ of the expected events) results in ████████ ████████ ████████████ ████████ ██ █████ ██ ███████ ███ ███ ████████ █████████ ██ ████ █████ ██ ██████. Longer follow-up is needed to draw definitive conclusions about potential longer-term OS benefits.
CDA-AMC Assessment of Cost-Effectiveness
The CDA-AMC base case was derived by making changes to model parameter values and assumptions (refer to Supplementary Material, Appendix 11, Table 16) in consultation with clinical experts. Detailed information about the CDA-AMC base case is provided in Appendix 11.
Impact on Health Care Costs
Trastuzumab deruxtecan is predicted to be associated with additional health care costs compared to chemotherapy (incremental cost = $138,930). Although treatment with trastuzumab deruxtecan results in an additional $176,411 in drug acquisition costs, it is expected that fewer patients will receive trastuzumab deruxtecan after disease progression on chemotherapy, resulting in a $38,681 reduction in subsequent therapy costs (refer to Figure 1). All other costs to the health system are similar between treatments.
Figure 1: Impact of Trastuzumab Deruxtecan vs. Chemotherapy on Health Care Costs
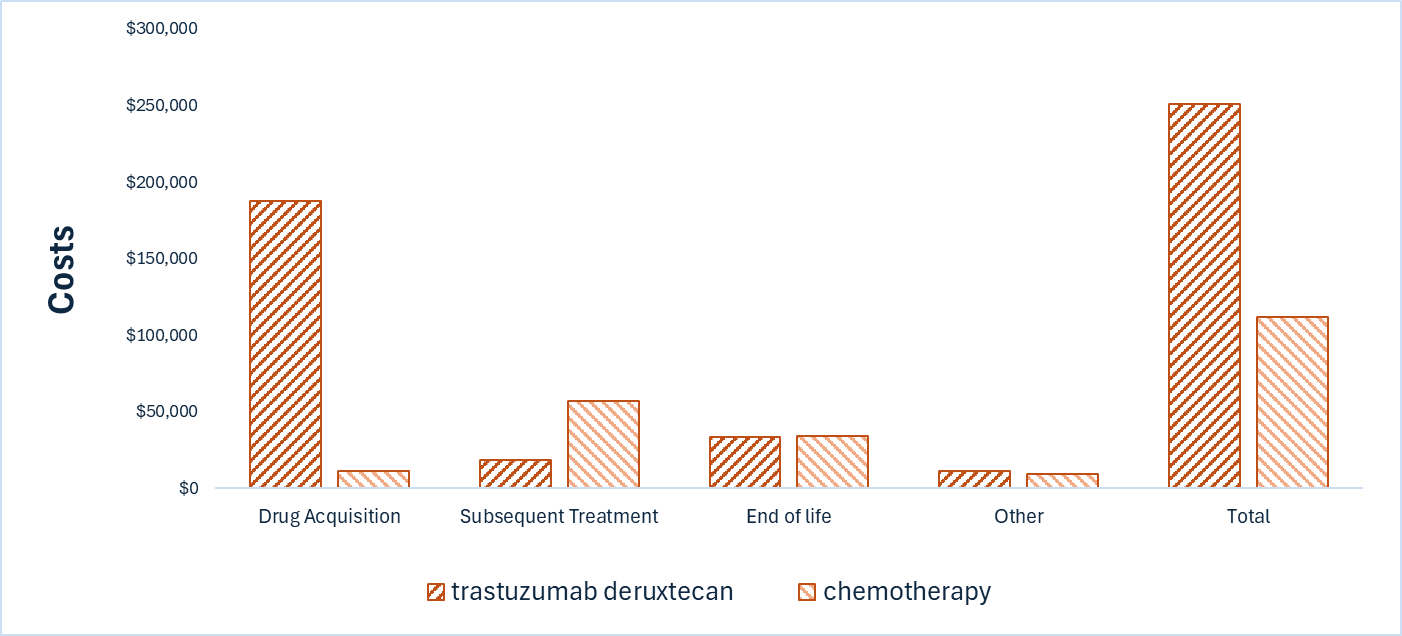
Vs. = versus.
Note: Other includes costs associated with drug administration, health care resource use, and management of adverse events.
Impact on Health
Relative to chemotherapy, trastuzumab deruxtecan is predicted to increase the amount of time a patient remains in the progression-free state by approximately 0.54 years and to extend OS by 0.35 years (refer to Figure 2). Considering the impact of treatment on both quality and length of life, trastuzumab deruxtecan is predicted to result in 0.31 additional QALYs per patient compared to chemotherapy over the 11-year time horizon. Approximately 86% of the predicted incremental QALY benefit was accrued on the basis of extrapolation.
Figure 2: Impact of Trastuzumab Deruxtecan vs. Chemotherapy on Patient Health
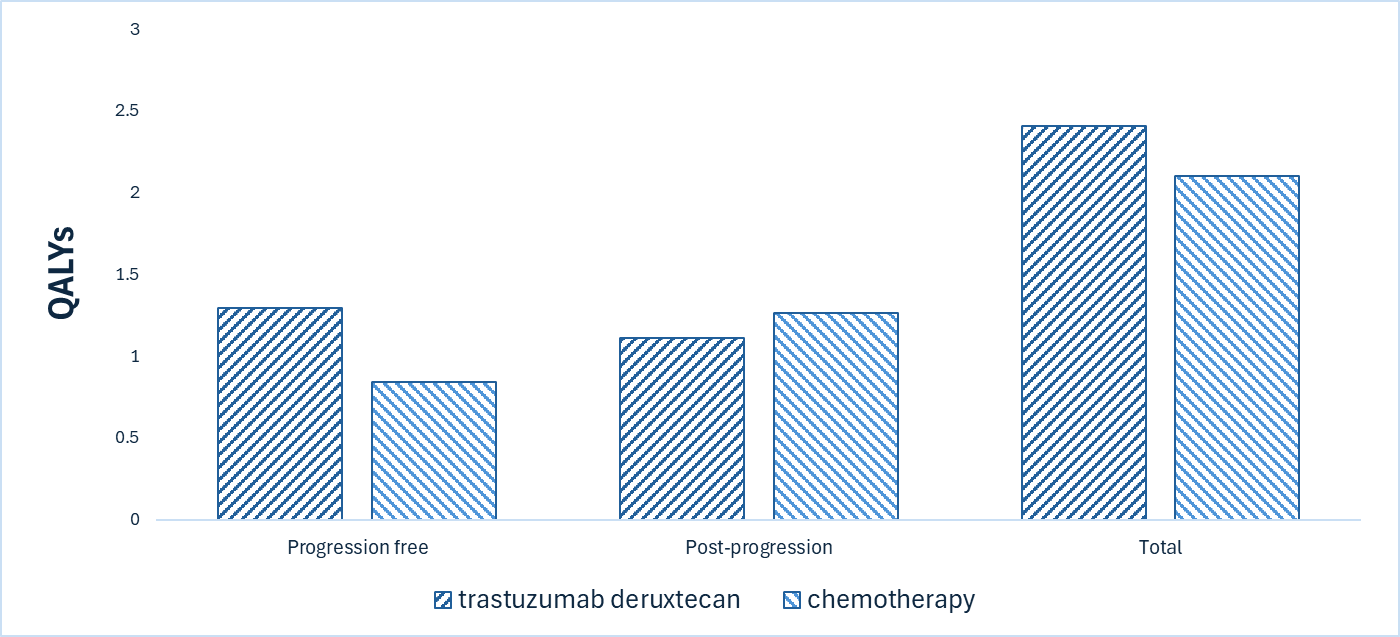
QALY = quality-adjusted life-year; vs. = versus.
Overall Results
The results of the CDA-AMC base-case analysis suggest an incremental cost-effectiveness ratio of $453,869 per QALY gained for trastuzumab deruxtecan compared to chemotherapy (refer to Table 7). Additional details on the CDA-AMC base case are available in Supplemental Material, Appendix 11.
Table 7: Summary of CDA-AMC Economic Evaluation Results
Drug | Total costs ($) | Total LYs | Total QALYs | ICER vs. chemotherapy ($/QALY) |
|---|---|---|---|---|
Chemotherapy | 112,081 | 2.54 | 2.10 | Reference |
Trastuzumab deruxtecan | 251,011 | 2.89 | 2.41 | 453,869 |
CDA-AMC = Canada’s Drug Agency; ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year; vs. = versus.
Note: Publicly available list prices were used for all comparators.
Summary of the Budget Impact
The sponsor submitted a budget impact analysis to estimate the 3-year (2026 to 2028) budget impact of reimbursing trastuzumab deruxtecan for use in the reimbursement requested population. The sponsor assumed that the payer would be CDA-AMC–participating public drug plans and derived the size of the eligible population using an epidemiologic approach. The price of trastuzumab deruxtecan was aligned with the price included in the sponsor’s economic evaluation, while the prices of comparators were based on publicly available list prices. Additional information pertaining to the sponsor’s submission is provided in Supplemental Material, Appendix 12. CDA-AMC identified a number of issues with the sponsor’s estimated budget impact and made changes to model parameters and assumptions in consultation with clinical experts to derive the CDA-AMC base case (refer to Supplemental Material, Appendix 12). CDA-AMC estimated that 3,453 patients would be eligible for treatment over a 3-year period based on the requested reimbursement population (year 1 = 1,125 patients; year 2 = 1,151 patients; year 3 = 1,177 patients), of whom █████ are expected to receive trastuzumab deruxtecan (year 1 = ███; year 2 = ███; year 3 = ███). The estimated incremental budget impact of reimbursing trastuzumab deruxtecan for the requested reimbursement population is predicted to be approximately $70 million over the first 3 years, with an expected expenditure of $155 million on trastuzumab deruxtecan. The actual budget impact will depend on the number of eligible patients, the uptake of trastuzumab deruxtecan, and the cost of subsequent treatment.
Conclusion
Based on the CDA-AMC base case, trastuzumab deruxtecan would be considered cost-effective at the submitted price if the public health care system were willing to pay at least $453,869 for each additional QALY gained. If the public health care system were not willing to pay that amount, a price reduction should be considered (refer to Figure 3; full details of the impact of price reductions on cost-effectiveness are presented in the Supplemental Material, Appendix 11, Table 19).
The estimated cost-effectiveness of trastuzumab deruxtecan compared to chemotherapy is highly uncertain due to uncertainty in both the long-term efficacy estimates and the costs and benefits of subsequent therapy. Based on clinical expert opinion, use of trastuzumab deruxtecan as part of subsequent therapy in current clinical practice in Canada is anticipated to be higher than observed in the DESTINY-Breast06 trial. As such, the CDA-AMC base case may overestimate the life-years gained relative to current practice, but also underestimate the costs associated with subsequent therapy. If the incremental QALYs with trastuzumab deruxtecan are lower than predicted in the CDA-AMC base case, further price reductions than those presented in this report may be required.
The budget impact of reimbursing trastuzumab deruxtecan to the public drug plans in the first 3 years is estimated to be approximately $70 million for the requested reimbursement population. The 3-year expenditure on trastuzumab deruxtecan (i.e., not accounting for current expenditure on comparators) is estimated to be $155 million. The actual budget impact will depend on the number of eligible patients, the uptake of trastuzumab deruxtecan, and the cost of subsequent treatment.
Figure 3: Summary of the CDA-AMC Economic Analysis and Price Reduction
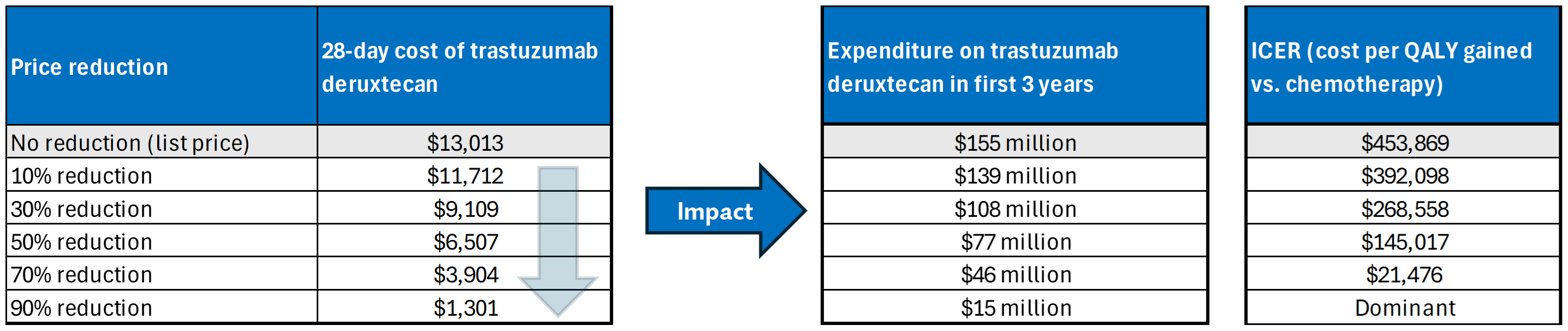
CDA-AMC = Canada’s Drug Agency; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; vs = versus.
Note: Expenditure includes only the drug cost of trastuzumab deruxtecan. The term dominant indicates that a drug costs less and provides more QALYs than the comparator.
References
1.Canadian Cancer Society. Symptoms of breast cancer. Updated N/A. Accessed June 2025. https://cancer.ca/en/cancer-information/cancer-types/breast/signs-and-symptoms
2.Irvin W, Jr., Muss HB, Mayer DK. Symptom management in metastatic breast cancer. Oncologist. 2011;16(9):1203-14. doi: 10.1634/theoncologist.2011-0159 PubMed
3.Brenner DR, Gillis J, Demers AA, et al. Projected estimates of cancer in Canada in 2024. CMAJ. 2024;196(18):E615-E623. doi: 10.1503/cmaj.240095 PubMed
4.Visovsky C. Treatment Considerations for the Management of Patients With Hormone Receptor-Positive Metastatic Breast Cancer. J Adv Pract Oncol. 2014;5(5):321-30. PubMed
5.Canadian Cancer Society. Survival statistics for breast cancer. Updated N/A. Accessed June 2025. https://cancer.ca/en/cancer-information/cancer-types/breast/prognosis-and-survival/survival-statistics
6.Rubio-Anguiano BL, Valencia-Cedillo R, Grajales R. Overall survival in patients with HER2-low breast cancer at a reference hospital in Mexico. J Clin Oncol. 2024;42(16_suppl):e12578-e12578. doi: 10.1200/JCO.2024.42.16_suppl.e12578
7.Institute NC. Cancer Stat Facts: Female Breast Cancer Subtypes. 2022. https://seer.cancer.gov/statfacts/html/breast-subtypes.html
8.Viale G, Basik M, Niikura N, et al. Retrospective study to estimate the prevalence and describe the clinicopathological characteristics, treatments received, and outcomes of HER2-low breast cancer. ESMO Open. 2023;8(4):101615. doi: 10.1016/j.esmoop.2023.101615 PubMed
9.Tommasi C, Airò G, Pratticò F, et al. Hormone Receptor-Positive/HER2-Positive Breast Cancer: Hormone Therapy and Anti-HER2 Treatment: An Update on Treatment Strategies. J Clin Med. 2024;13(7). doi: 10.3390/jcm13071873 PubMed
10.Schettini F, Chic N, Braso-Maristany F, et al. Clinical, pathological, and PAM50 gene expression features of HER2-low breast cancer. NPJ Breast Cancer. 2021;7(1):1. doi: 10.1038/s41523-020-00208-2 PubMed
11.Tarantino P, Hamilton E, Tolaney SM, et al. HER2-Low Breast Cancer: Pathological and Clinical Landscape. J Clin Oncol. 2020;38(17):1951-1962. doi: 10.1200/JCO.19.02488 PubMed
12.Viale G, Niikura N, Tokunaga E, et al. Retrospective study to estimate the prevalence of HER2-low breast cancer (BC) and describe its clinicopathological characteristics. J Clin Oncol. 2022;40(16_suppl):1087-1087. doi: 10.1200/JCO.2022.40.16_suppl.1087
13.Denkert C, Seither F, Schneeweiss A, et al. Clinical and molecular characteristics of HER2-low-positive breast cancer: pooled analysis of individual patient data from four prospective, neoadjuvant clinical trials. Lancet Oncol. 2021;22(8):1151-1161. doi: 10.1016/S1470-2045(21)00301-6 PubMed
14.Modi S, Jacot W, Yamashita T, et al. Trastuzumab Deruxtecan in Previously Treated HER2-Low Advanced Breast Cancer. N Engl J Med. 2022;387(1):9-20. doi: 10.1056/NEJMoa2203690 PubMed
15.European Society for Medical Oncology. ESMO Metastatic Breast Cancer Living Guidelines v1.2 April 2025. Available from: https://www.esmo.org/guidelines/living-guidelines/esmo-living-guideline-metastatic-breast-cancer.
16.National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) Breast Cancer. Version 4.2025 — April 17, 2025.
17.Moy B, Rumble RB, Carey LA, null n. Chemotherapy and Targeted Therapy for Human Epidermal Growth Factor Receptor 2–Negative Metastatic Breast Cancer That Is Either Endocrine-Pretreated or Hormone Receptor–Negative: ASCO Guideline Rapid Recommendation Update. Journal of Clinical Oncology. 2022;40(26):3088-3090. doi: 10.1200/JCO.22.01533 PubMed
18.Gennari A, Andre F, Barrios CH, et al. ESMO Clinical Practice Guideline for the diagnosis, staging and treatment of patients with metastatic breast cancer. Ann Oncol. 2021;32(12):1475-1495. doi: 10.1016/j.annonc.2021.09.019 PubMed
19.Moy B, Rumble RB, Carey LA, null n. Chemotherapy and Targeted Therapy for Endocrine-Pretreated or Hormone Receptor–Negative Metastatic Breast Cancer: ASCO Guideline Rapid Recommendation Update. Journal of Clinical Oncology. 2023;41(6):1318-1320. doi: 10.1200/JCO.22.02807 PubMed
20.Jerzak KJ, Bouganim N, Brezden-Masley C, et al. HR+/HER2- Advanced Breast Cancer Treatment in the First-Line Setting: Expert Review. Curr Oncol. 2023;30(6):5425-5447. doi: 10.3390/curroncol30060411 PubMed
21.CDA-AMC. CDA-AMC Reimbursement Recommendation. Enhertu (trastuzumab deruxtecan) [PC0305; DB-04]. Available from: https://www.cda-amc.ca/sites/default/files/DRR/2023/PC0305%20Enhertu%20-%20Final%20CADTH%20Recommendation%20(with%20redactions)%20June%2029%2C%202023%20-%20KH_KAS%20-%20KH-meta.pdf.
22.Rugo HS, Bardia A, Marme F, et al. Overall survival with sacituzumab govitecan in hormone receptor-positive and human epidermal growth factor receptor 2-negative metastatic breast cancer (TROPiCS-02): a randomised, open-label, multicentre, phase 3 trial. Lancet. 2023;402(10411):1423-1433. doi: 10.1016/S0140-6736(23)01245-X PubMed
23.Canada's Drug Agency. Provisional Funding Algorithm for HR-Positive HER2-Negative Breast Cancer, With Inclusion of HER2 Low (PH0053-000). December 2024. Available from: https://www.cda-amc.ca/hr-positive-her2-negative-breast-cancer-0.
24.Venetis K, Crimini E, Sajjadi E, et al. HER2 Low, Ultra-low, and Novel Complementary Biomarkers: Expanding the Spectrum of HER2 Positivity in Breast Cancer. Front Mol Biosci. 2022;9:834651. doi: 10.3389/fmolb.2022.834651 PubMed
25.Wolff AC, Somerfield MR, Dowsett M, et al. Human Epidermal Growth Factor Receptor 2 Testing in Breast Cancer: ASCO-College of American Pathologists Guideline Update. J Clin Oncol. 2023;41(22):3867-3872. doi: 10.1200/JCO.22.02864 PubMed
26.College of American Pathologists. Reporting Template for Reporting Results of Biomarker Testing of Specimens from Patients with Carcinoma of the Breast. 2025. Accessed July 01, 2025. https://documents.cap.org/documents/New-Cancer-Protocols-March-2025/Breast.Bmk_1.6.0.0.REL.CAPCP.pdf
27.AstraZeneca Canada Inc. Budget impact analysis report [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: ENHERTU (trastuzumab deruxtecan), 100 mg intravenous infusion. May 15, 2025.
28.Wolff AC, Hammond MEH, Allison KH, et al. Human Epidermal Growth Factor Receptor 2 Testing in Breast Cancer: American Society of Clinical Oncology/College of American Pathologists Clinical Practice Guideline Focused Update. J Clin Oncol. 2018;36(20):2105-2122. doi: 10.1200/JCO.2018.77.8738 PubMed
29.AstraZeneca Canada Inc. Clinical Study Protocol: A Phase 3, Randomized, Multi-center, Open-label Study of Trastuzumab Deruxtecan (T-DXd) Versus Investigator’s Choice Chemotherapy in HER2-low, Hormone Receptor Positive Breast Cancer Patients whose Disease has Progressed on Endocrine Therapy in the Metastatic Setting (DESTINY-Breast06). 2023. Accessed July 01, 2025. https://cdn.clinicaltrials.gov/large-docs/25/NCT04494425/Prot_002.pdf
30.Tarantino P, Viale G, Press MF, et al. ESMO expert consensus statements (ECS) on the definition, diagnosis, and management of HER2-low breast cancer. Ann Oncol. 2023;34(8):645-659. doi: 10.1016/j.annonc.2023.05.008 PubMed
31.Clinical trial endpoints for the approval of cancer drugs and biologics. (2018).
32.DESTINY-Breast06 Clinical Study Report. Data cut-off: March 18, 2024 [sponsor supplied reference].
33.Bassler D, Briel M, Montori VM, et al. Stopping randomized trials early for benefit and estimation of treatment effects: systematic review and meta-regression analysis. JAMA. 2010;303(12):1180-1187. PubMed
34.Manitz J, Kan‐Dobrosky N, Buchner H, et al. Estimands for overall survival in clinical trials with treatment switching in oncology. Pharm Stat. 2022;21(1):150-162. PubMed
35.Forsythe A, Chandiwana D, Barth J, Thabane M, Baeck J, Tremblay G. Progression-free survival/time to progression as a potential surrogate for overall survival in HR+, HER2− metastatic breast cancer. Breast Cancer (London). 2018:69-78.
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.