Drugs, Health Technologies, Health Systems
Reimbursement Review
Abemaciclib (Verzenio)
Sponsor: Eli Lilly Canada Inc.
Therapeutic area: HR-positive, HER2-negative advanced or metastatic breast cancer
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Clinical Review
Abbreviations
AE
adverse event
AI
aromatase inhibitor
BCC
Breast Cancer Canada
CBCN
Canadian Breast Cancer Network
CBR
clinical benefit rate
CDA-AMC
Canada’s Drug Agency
CI
confidence interval
CR
complete response
CrI
credible interval
CTCAE
Common Terminology Criteria for Adverse Events
DAC
Drug Advisory Committee
DIC
deviance information criterion
ECOG PS
Eastern Cooperative Oncology Group Performance Status
EHR
electronic health record
EORTC QLQ-C30
European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30
FP
fractional polynomial
HR
hormone receptor
HRQoL
health-related quality of life
ITC
indirect treatment comparison
ITT
intention to treat
KM
Kaplan-Meier
NMA
network meta-analysis
NSAI
nonsteroidal aromatase inhibitor
OH (COO)
Ontario Health (Cancer Care Ontario)
ORR
overall response rate
OS
overall survival
PD
progressive disease
pERC
pan-Canadian Oncology Drug Review Expert Review Committee
PFS
progression-free survival
PH
proportional hazard
REAL
Research Excellence, Active Leadership
RCT
randomized controlled trial
RECIST
Response Evaluation Criteria in Solid Tumours
RWE
real-world evidence
SAE
serious adverse event
SD
standard deviation
SLR
systematic literature review
TEAE
treatment-emergent adverse event
TTSD
time to sustained deterioration
VIS
visceral disease population
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Table 1: Background Information of Application Submitted for Review
Item | Description |
|---|---|
Drug product | Drug product: Abemaciclib (VERZENIO) Strength: 50 mg, 100 mg, 150 mg Dosage form: Tablet Route of administration: Oral |
Sponsor | Eli Lilly Canada Inc. |
Indication | VERZENIO is indicated in both early breast cancer and advanced breast cancer or metastatic breast cancer. In the advanced breast cancer or metastatic breast cancer setting the following indications were issued NOC by Health Canada on April 5, 2019: VERZENIO (abemaciclib) is indicated for the treatment of HR-positive, HER2-negative advanced or metastatic breast cancer as follows:
|
Reimbursement request | For the treatment of HR-positive, HER2-negative advanced or metastatic breast cancer in combination with an aromatase inhibitor in females who are postmenopausal as initial endocrine-based therapy.a |
Health Canada approval status | NOC |
Health Canada review pathway | Standard review |
NOC date | April 5, 2019 |
Recommended dose | When used in combination with endocrine therapy, the recommended dose of Verzenio is 150 mg taken orally, twice daily. When used as a single drug, the recommended dose of Verzenio is 200 mg taken orally, twice daily. For advanced or metastatic breast cancer, treatment is continued until disease progression or unacceptable toxicity. |
HR = hormone receptor; NOC = notice of compliance.
aA separate, concurrent review was conducted in parallel for the treatment of HR-positive, HER2-negative advanced breast cancer or metastatic breast cancer in combination with fulvestrant in females with disease progression following endocrine therapy. Females who are premenopausal or perimenopausal must also be treated with a gonadotropin-releasing hormone agonist.
Basis of Reassessment
Abemaciclib (Verzenio) was previously reviewed by Canada’s Drug Agency (CDA-AMC) for the treatment of advanced or metastatic breast cancer in adults with hormone receptor (HR)-positive, HER2-negative disease.1 Within this indication, there are 2 subpopulations of interest:
Patients who are postmenopausal as initial endocrine-based therapy, given in combination with an aromatase inhibitor (AI), sometimes also referred to as a nonsteroidal aromatase inhibitor (NSAI). This population is also referred to as “endocrine-naive,” “endocrine-sensitive,” or “first-line systemic therapy” (first-line for advanced or metastatic disease, specifically).
Patients with disease progression following endocrine therapy, in combination with fulvestrant. Patients who are premenopausal or perimenopausal must be treated with a gonadotropin-releasing hormone agonist. This population is also referred to as “endocrine-resistant.”
The evidence provided for the original review of abemaciclib included the pivotal trials, MONARCH 2 (endocrine resistant, in combination with fulvestrant, N = 669) and MONARCH 3 (endocrine sensitive, in combination with AI [letrozole or anastrozole per investigator’s choice], N = 493), which were both phase III, multicentre, randomized, double-blind controlled studies in patients with advanced breast cancer or metastatic breast cancer. This report focuses on the population who are endocrine sensitive as studied in the MONARCH 3 study; a concurrent reimbursement review is under way for the population who are endocrine resistant as studied in the MONARCH 2 study, which will not be discussed in detail in this review.
In the initial submission in 2019, for the population who were endocrine sensitive, the sponsor noted that the pan-Canadian Oncology Drug Review Expert Review Committee (pERC) recommended that abemaciclib should be reimbursed only in patients who are unable to tolerate or have a contraindication to other available CDK4/6 inhibitors as a result of the immature and uncertain overall survival (OS) results and the side effect profile; this represents a narrower population than the reimbursement request and the Health Canada indication, which did not stipulate limiting abemaciclib to patients who could not receive other CDK4/6 inhibitors. As such, the sponsor has filed a reassessment of abemaciclib to lift the restriction for patients who are unable to tolerate or have a contraindication to other available CDK4/6 inhibitors, as mature OS data, representing an additional 5 years and 10 months of follow-up data since the first evaluation of the preplanned final OS analysis (data cut-off: September 29, 2023) has become available from the MONARCH 3 trial. The focus of this reassessment is the new clinical evidence pertaining to OS, and any updated progression-free survival (PFS) results as available (although it is worth noting that the final preplanned analysis of PFS was already assessed in the 2019 review), as well as updated harms and adverse event (AE) results. Results for other key outcomes such as overall response rate (ORR), clinical benefit rate (CBR), and health-related quality of life (HRQoL) end points are presented in Appendix 1 for reference, but these outcomes were already assessed by pERC in 2019 and are not updated from how they were presented at the time of the original review. Chemotherapy-free survival, an exploratory outcome in the MONARCH 3 study that was not assessed by pERC in 2019, was also updated as of the latest data cut-off and these results are presented briefly in Appendix 1.
As such, the objective of this report is to evaluate the newly available evidence for OS and whether the totality of evidence supports lifting the restriction on the reimbursement recommendation regarding intolerance or contraindication to other CDK4/6 inhibitors, in combination with AI as an initial endocrine-based therapy in adult patients who are postmenopausal with HR-positive, HER2-negative advanced or metastatic breast cancer.
Introduction
Breast cancer was the second leading cause of death in females living in Canada in 2024 and accounted for 13% of cancer-related mortality. It was estimated that 30,500 new cases in females and 5,500 deaths would occur as a result of breast cancer in Canada in 2024.2 Major molecular subtypes of breast cancer have been defined based on the expression of cell surface receptors HR and HER2.3 HR-positive and HER2-negative breast cancer is the most common molecular subtype, accounting for at least 66% to 75% of all breast cancer cases in North America and Europe.4-7 Metastatic cancer occurs when cancer spreads beyond the primary tumour site to other parts of the body, forming secondary metastatic tumours.8 Currently, first-line standard of care in patients with advanced or metastatic breast cancer is the combination of an AI (in patients who were endocrine sensitive) or fulvestrant (in patients who were endocrine resistant) with a CDK4/6 inhibitor. Upon disease progression, patients may switch to an alternative endocrine drug alone or in combination with another targeted therapy, or to chemotherapy, or antibody-drug conjugates. Abemaciclib is a CDK4/6 inhibitor approved by Health Canada for the treatment of HR-positive, HER2-negative advanced or metastatic breast cancer, in combination with an AI in patients who are postmenopausal as initial endocrine-based therapy (i.e., endocrine-sensitive disease), or in combination with fulvestrant in females with recurrent disease while receiving adjuvant endocrine therapy, or after disease progression following endocrine therapy (i.e., endocrine-resistant disease). Other CDK4/6 inhibitors used in Canada in this patient population include palbociclib and ribociclib.
Abemaciclib (Verzenio) has previously been reviewed for this indication as well as other indications by CDA-AMC. The objective of this report is to review and critically appraise the updated evidence provided by the sponsor on the beneficial and harmful effects of abemaciclib plus an NSAI in the treatment of HR-positive, HER2-negative advanced or metastatic breast cancer in adult patients who are postmenopausal as a first-line endocrine-based therapy.
Perspectives of Patients, Clinicians, and Drug Programs
The information in this section is a summary of input provided by the patient and clinician groups who responded to our call for input and from clinical experts consulted by for the purpose of this review.
Patient Input
Three patient groups, Breast Cancer Canada (BCC), Canadian Breast Cancer Network (CBCN), and Rethink Breast Cancer, provided their input for this submission. BCC is a national organization in Canada which encourages precision oncology research and awareness collaboration among physicians and researchers. Information for this submission was gathered via an electronic survey, distributed to 169 patients living with a first recurrence (i.e., first line) of HR-positive, HER2-negative metastatic breast cancer from February 15 to 23, 2025. The survey responses included 54 patients identified as the target group for this input submission; 2% in both Nova Scotia and New Brunswick, 3% in Quebec, 64% in Ontario,18% in Alberta, and 11% in British Columbia. The CBCN is a leading, patient-directed, national health charity committed to ensuring the best quality of care for all people living in Canada affected by breast cancer through the promotion of information, education, and advocacy activities. Information for this submission was gathered via excerpts and key interviews from past submissions to CDA-AMC, including results from a 2012 survey in 71 patients with metastatic breast cancer and 16 caregivers, and a 2017 survey in 180 patients in Canada living with metastatic breast cancer. Additionally, information from a review of current studies and grey literature to highlight issues and experiences commonly shared among females living with breast cancer, and relevant disease experience and treatment considerations from a 2022 survey in 30 patients in Canada who had HR-positive, HER2-negative metastatic breast cancer was submitted. ReThink Breast Cancer is a charity in Canada known for making positive change by educating, empowering, and advocating for system changes to improve the experience and outcomes of those with breast cancer. Information for this submission was gathered through observations and insights drawn through programs and meetings with 24 key patient advisors with a history of breast cancer, as well as an online survey documenting the lived experience with metastatic breast cancer from 78 patients and caregivers, conducted from September 2018 to April 2019. In addition, 4 people living with HR-positive, HER2-negative metastatic breast cancer who had experience with abemaciclib were interviewed from January to February 2025.
Results from the 2012 CBCN survey highlighted that fatigue, insomnia, and pain resulted in significant or debilitating impact on quality of life. Respondents also stated moderate to significant restrictions in their ability to exercise, pursue hobbies and personal interests, participate in social events and activities, and in their ability to spend time with loved ones. Patient groups noted that the disease further impacted mental health, with a physical and emotional toll associated with diagnosis, fear of recurrence, affecting caregivers and loved ones, and financial toxicity.
Patient groups highlighted the following barriers faced by respondents with existing treatments: AEs (e.g., fatigue, nausea, depression, problems with concentration, memory loss, diarrhea, and insomnia), financial impact (e.g., not qualifying for insurance, inability to change employers due to loss of insurance, prohibitive cost of new treatment options), minimal or no access to appropriate care when experiencing debilitating symptoms, and challenges accessing quality care during cancer treatment. Patients emphasized the importance of having a choice of treatment options to determine a therapy that suited them. The CBCN patient group specifically noted that efficacy, followed by quality of life, work, and cost were ranked as the most important to least important when considering treatment options.
All patient groups that provided input for this submission noted that extending cancer control and improved survival, combined with delayed progression (at least 6 to 9 months more than front line treatments), a delay in IV chemotherapy, and improved quality of life were the most important outcomes of treatment. The CBCN also highlighted manageable AEs, although in the BCC survey, respondents noted that they were willing to accept higher rates of diarrhea as a trade-off for better recurrence-free survival outcomes. BCC also noted that patients were in favour of providing at-home, oral therapy that preserves quality of life. Rethink Breast Cancer suggested that patients valued long-term health outcomes over immediate concerns like reducing symptoms or managing side effects.
Of the 4 patients who were interviewed, 2 patients were receiving abemaciclib and letrozole, 1 receiving abemaciclib and fulvestrant, and another receiving abemaciclib as their 11th line of treatment. Patients mentioned their condition was well managed, with no signs of progression, and tolerable side effects that could be managed with dose reductions or other medications, and that they had the ability to travel. One patient expressed comfort with frequent monitoring (scans every 6 months), a preference for oral treatment, and valued having multiple treatment options. The patient who received abemaciclib as their 11th line of treatment mentioned that, even after being heavily pretreated, the treatment worked for a year.
Patient groups indicated that testing required for this treatment is already accessible and covered in jurisdictions across Canada but noted that this is only the case in early-stage breast cancer and it is not relevant to the advanced or metastatic treatment setting. ReThink Breast Cancer and BCC agreed that expanding the range of available CDK4/6 inhibitor therapies with abemaciclib, without restriction to only unsuitable or intolerance to other CDK4/6 inhibitors, would ensure a more equitable approach to treatment across all provinces for patients while minimizing drug-related out-of-pocket costs in this population experiencing financial insecurity. ReThink Breast Cancer further added that because patient and physician choice was an important part of treatment, health care professionals should be able to tailor treatment plans to meet patient needs.
Clinician Input
Input From Clinical Experts Consulted for This Review
The clinical experts consulted for this review noted that treatment goals include prolonging life, delaying disease progression, and improving HRQoL. They also noted that not all patients respond to current treatments, and primary resistance to endocrine therapy in HR-positive disease remains a major challenge. Even among those who initially respond, resistance to CDK4/6 inhibitors often leads to disease progression, necessitating a transition to less effective and/or more toxic therapies. The clinical experts noted that there are currently 3 (including abemaciclib) CDK4/6 inhibitors that have demonstrated benefit in the first-line advanced or metastatic setting, and that clinicians generally perceive them to be approximately equivalent for the outcome of PFS. The experts agreed that choice of CDK4/6 inhibitor varies by patient and by clinician, and that a key decision-making factor was not just the prevalence of AEs, but also the particular type(s) of AE associated with each CDK4/6 inhibitor, as different side-effect profiles will be more or less tolerable to different patients depending on their background health status and comorbid conditions. For instance, the clinical experts noted that ribociclib may not be the drug of choice if long-QT is an issue, and palbociclib may be avoided if neutropenia is an issue, while abemaciclib is generally associated with more diarrhea.
According to both clinical experts consulted by CDA-AMC, abemaciclib would not be the first drug in its class considered for this indication. However, it remains a valuable treatment option not only for patients with contraindications or intolerance to other CDK4/6 inhibitors, but also for other patients based on their individual health status, previous exposure to therapies in the adjuvant setting, duration between adjuvant therapy and diagnosis of metastatic disease, rate of disease progression, location and involvement of tumour sites, clinical status and comorbidities of the patients, and individual preferences. The clinicians noted that the best suited patients for treatment with abemaciclib are those with HR-positive HER2-negative advanced or metastatic breast cancer. One expert noted that more significant benefit from the addition of abemaciclib may be observed in patients with high-risk features, such as visceral disease, progesterone receptor–negative tumours, prior AI therapy, and high metastatic burden.
The clinicians noted that monitoring for treatment response involves a combination of clinical findings, bloodwork (including tumour markers), and imaging, and assessments should be performed at every visit, typically ranging from once monthly (before each cycle) to once every 3 months. In some patients whose disease remained stable and who are receiving treatment for several years, clinicians may extend the interval between assessments to longer than 3 months. Clinically meaningful outcomes, according to the experts, included improved survival, reduction in disease-related symptom frequency and severity, improved ability to perform daily activities, improvements in quality of life, and delaying the receipt of chemotherapy. The clinicians stated that abemaciclib should be discontinued upon evidence of disease progression, whether clinically or radiographically (e.g., Response Evaluation Criteria in Solid Tumours [RECIST] criteria), or in the event of intolerable side effects that cannot be managed supportively (e.g., dosage modification) and that significantly impact the patient’s quality of life. Patient preference is also considered. The experts noted that only a medical oncologist is qualified to initiate treatment with abemaciclib. Monitoring and continuing patients after initiation can be performed by other members of the health care team, including family physicians in oncology, nurse practitioners, and oncology pharmacists.
Clinician Group Input
Two clinician groups, the Research Excellence, Active Leadership (REAL) Canadian Breast Cancer Alliance and Ontario Health (Cancer Care Ontario) (OH [CCO]) Breast Cancer Drug Advisory Committee (DAC) provided their input for this submission. REAL Canadian Breast Cancer Alliance is a standing committee of multidisciplinary clinical-academic oncologists across Canada and publishes national clinical consensus recommendations. Recommendations published by REAL Canadian Breast Cancer Alliance are routinely updated for timely health policy, funding, and consistent clinical adoption to ensure optimal outcomes for patients with breast cancer across all provinces and territories in Canada. A total of 16 clinicians provided their input, along with a literature review, clinical trial data, and recent data releases from international congresses, as well as collective clinical expertise of the members. The OH (CCO) Breast Cancer DAC provides evidence-based clinical and health system guidance on drug-related issues including the Provincial Drug Reimbursement Programs and the Systemic Treatment Program. Input from 5 clinicians was gathered via teleconference.
Both clinician groups indicated that CDK4/6 inhibitors plus endocrine therapy was the gold or current standard for the first-line treatment of HR-positive, HER2-negative advanced or metastatic breast cancer. The REAL Canadian Breast Cancer Alliance clinician group indicated that CDK4/6 inhibitors, when combined with endocrine therapy, were associated with significantly improved PFS in the first-line metastatic setting compared to endocrine therapy alone.
In line with the clinical experts consulted for this review, the REAL Canadian Breast Cancer Alliance clinician group noted that the goals of treatment were to extend life, maintain quality of life, delay the need for chemotherapy, and minimize treatment-related AEs. They highlighted that among current publicly funded CDK4/6 inhibitors, ribociclib was the preferred first-line treatment option for HR-positive, HER2-negative advanced or metastatic breast cancer, given its proven OS benefit. They noted that the choice of therapy (i.e., ribociclib, palbociclib, and abemaciclib) was dependent not only on efficacy but also on the tolerability of side effects by patients and that expanding the range of available CDK4/6 inhibitor therapies would allow a more personalized approach to treatment, which aligned with the opinion of clinical experts consulted by CDA-AMC.
The REAL Canadian Breast Cancer Alliance clinician group noted that the population receiving CDK4/6 inhibitors would not be expected to expand; rather abemaciclib would be included as 1 of the treatment options for patients for whom CDK4/6 inhibitors are already considered standard of care. The REAL Canadian Breast Cancer Alliance clinician group noted that monitoring would mostly be required in the first 4 months of abemaciclib initiation and include bloodwork, assessing toxicities, and assessing treatment adherence, and AEs ware manageable with early interventions, including dose reduction and standard supportive care. Both clinician groups agreed that treatment discontinuation should be considered at the first sign of disease progression or due to persistent toxicity, as per the product monograph. The prescribing considerations noted by the group aligned with the opinion of clinical experts consulted by CDA-AMC. The REAL Canadian Breast Cancer Alliance clinician group noted that treatment initiation would be done by oncologists with experience in treating patients with breast cancer. The OH (CCO) Breast Cancer DAC noted that because abemaciclib and AI are oral therapies, an outpatient setting would be appropriate.
Drug Program Input
The following were identified as key factors that could potentially impact the implementation of an updated recommendation for abemaciclib:
considerations for initiation of therapy
considerations for prescribing of therapy
system and economic issues.
The clinical experts provided advice on the potential implementation issues raised by the drug programs. Refer to Table 3 for more details.
Clinical Evidence
Systematic Review
Description of Studies
MONARCH 3 was a phase III, multicentre, randomized, double-blind, placebo-controlled study of abemaciclib or placebo plus an NSAI in patients who were postmenopausal with HR-positive, HER2-negative advanced or metastatic breast cancer who had not received any previous systemic therapy in the advanced or metastatic setting. The study was conducted in 158 centres in 22 countries.
The baseline demographic and disease characteristics were well balanced between the study arms. All patients who were enrolled were female and postmenopausal, with a mean age of 63 years (standard deviation [SD] = 9.92 years). The majority of patients were white (56.7%, and 61.8% in the abemaciclib and placebo arms, respectively) or of Asian ethnicity (31.4%, and 27.3% in the abemaciclib and placebo arms, respectively), and had a measurable disease (81.4%, and 78.8% in the abemaciclib and placebo arms, respectively). Prior treatments were also well-balanced between the 2 study arms. Approximately 40% of the patients in each arm had received a prior adjuvant or neoadjuvant chemotherapy. At the baseline, 25.9% of patients in the abemaciclib plus AI arm and 30.3% of those in the placebo plus AI arm had received a prior AI.
Efficacy Results
Due to the nature of the reassessment, only OS and PFS are discussed here as these outcomes have been updated since the prior review. Results are presented for both the November 3, 2017, data cut-off (i.e., the time of the final planned PFS analysis) and the September 29, 2023, data cut-off (i.e., the time of the final planned OS analysis). Results from the November 3, 2017, data cut-off are only provided for context as these results have previously been appraised by CDA-AMC and considered by pERC in 2019.
Overall Survival
The data for OS were immature at the time of the original review. At the January 3, 2017, data cut-off date, there were a total of 49 deaths (32 deaths [9.8%] in the abemaciclib plus AI arm and 16 deaths [9.9%] in the placebo plus AI arm). The median OS was not reached in either arm.
As of the final OS analysis (data cut-off: September 29, 2023), 314 OS events (deaths) were observed in the intention-to-treat (ITT) population; 198 patients (60.4%) experienced OS events, and ███ ████████ ███████ were censored in the abemaciclib plus NSAI arm, and 116 patients (70.3%) experienced OS events, and ██ ████████ ███████ were censored in the placebo plus NSAI arm. The hazard ratio for OS in the ITT population was 0.804 (95% confidence interval [CI], 0.637 to 1.015; 2-sided stratified log-rank P value = 0.0664). Based on the O’Brien-Fleming boundary, the 2-sided P value boundary for OS was 0.034 for the ITT population. Median OS was 66.81 months (95% CI, 59.21 months to 74.83 months) in the abemaciclib arm and 53.72 months (95% CI, 44.75 months to 59.34 months) in the placebo arm, that is, an absolute difference of 13.09 months in the ITT population (95% CI of absolute difference was not reported). In the Kaplan-Meier (KM) plot of OS, sustained separation favouring the abemaciclib plus NSAI arm became apparent at approximately 35 months. The OS rate at 5 years and 6 years was 54.5% (95% CI, █████ ████) and 45.7% (95% CI, █████ ████) in the abemaciclib plus NSAI arm, and 42.1% (95% CI, █████ ████) and 35.2% (95% CI, █████ ████) in the placebo plus NSAI arms, respectively.
Progression-Free Survival
In the final PFS analysis (November 3, 2017, data cut-off), after a median follow-up duration of 26.73 months, 246 investigator-assessed PFS events had occurred (138 events [42.1%] the abemaciclib plus AI arm and 108 events [65.5%] in the placebo plus AI arm). The median PFS was 28.18 months in the abemaciclib plus AI arm compared to 14.76 months in the placebo plus AI arm (hazard ratio = 0.540; 95% CI, 0.418 to 0.698); P = 0.000002). The PFS benefit was maintained across the predefined patient subgroup analyses.
Updated PFS data were provided based on the September 29, 2023, data cut-off, which was the time of the final planned OS analysis. At this data cut-off, 350 patients experienced PFS events (i.e., progressive disease [PD] or death), including 213 (64.9%) in the abemaciclib plus NSAI group and 137 (83.0%) in the placebo plus NSAI group. Median PFS was 29.03 months (95% CI, █████ ██ █████) in the abemaciclib plus NSAI arm and 14.76 months (95% CI, █████ ██ █████) in the placebo plus NSAI arm (hazard ratio = 0.535; 95% CI, 0.429 to 0.668]). These results corresponded to a 14.27-month increase in the median PFS (95% CI of difference not reported) for patients treated with abemaciclib plus an NSAI. In the KM plot of PFS, early and sustained separation by treatment arm was apparent beginning at approximately 2 months and continued to separate.
Harms Results
Data in this section were from the most recent data cut-off (i.e., September 29, 2023).
Adverse Events
Compared to placebo, a higher percentage of patients receiving abemaciclib experienced any treatment-emergent adverse event (TEAE) (98.8% versus 94.4%), or grade 3 or higher TEAEs (69.4% versus 28.6%). The most frequently reported TEAE was diarrhea (83.5% versus 34.2%). Other AEs with a between-group difference of 20% included neutropenia (46.8% versus 1.9%), anemia (35.2% versus 9.9%), increased blood creatinine (25.1% versus 4.3%), and leukopenia (24.5% versus 3.1%). The most common grade 3 or higher TEAEs were neutropenia (27.5% versus 1.2%) and leukopenia (10.7% versus 0.6%).
Serious Adverse Events
The incidence of serious adverse events (SAEs) was higher in the abemaciclib plus NSAI arm compared with the placebo plus NSAI arm ██████ ███ ███████. The most common causes of SAEs in the abemaciclib plus NSAI arm by system organ class were infections and infestations (█████), followed by ████████████████ █████████ ██████. The most common SAEs (at least 2%) regardless of causality in the abemaciclib plus NSAI arm by preferred term were █████████ ██████ ███ ████████ ███████. In the placebo plus NSAI arm, no SAEs occurred in more than 2% of patients. The most common SAEs were ███████ ████████████████ █████████ █████████ █████ ████████████ ███ █████ ████████ ████████ █████ ██████.
Withdrawals Due to AEs
In the abemaciclib plus NSAI arm versus the placebo plus NSAI arm, ██ ███████ ███ █ ██████ patients discontinued all study treatments due to AEs, respectively. The most common reason for stopping treatment due to AEs in the abemaciclib plus NSAI group was increased ███████ ████████████████ █████ ███ ██████ All other withdrawals due to AEs were at a frequency of less than 2%.
Mortality
In total, 198 patients (60.4%) in the abemaciclib plus NSAI arm and 116 patients (70.3%) in the placebo plus NSAI arm died in the study. Deaths due to AEs on study therapy or within 30 days of treatment discontinuation were reported in ██ ████████ ██████ ██ ███ ███████████ ████ ████ ███ ███ █ ████████ ██████ in the placebo plus NSAI arm. A total of ███ patients died after 30 days of treatment discontinuation. AEs were the cause of death in ████████ ██████ in the abemaciclib plus NSAI arm.
Notable Harms
Prespecified AEs of special interest included neutropenia (46.8% in the abemaciclib group and 1.9% in the placebo group), ██████████ ██████ ███ ██████, diarrhea (83.5% and 34.2%), alanine transaminase increase (22.0% and 8.1%), venous thromboembolisms (7.6% and 1.2%), and interstitial lung disease or pneumonitis (7.0% and 0.6%). The incidence of each of these events was higher in the abemaciclib plus NSAI group compared to the placebo plus NSAI group.
Critical Appraisal
The MONARCH 3 trial has previously been reviewed and appraised by CDA-AMC, and many of the critical appraisal points still apply. Briefly, critical appraisal points at the time of the initial review were the MONARCH 3 study was a phase III, double blind, placebo-controlled randomized controlled trial (RCT) that evaluated abemaciclib plus an NSAI versus placebo plus an NSAI as a first-line therapy in adult patients who were postmenopausal with HR-positive, HER2-negative advanced or metastatic breast cancer. Choice of an NSAI therapy (letrozole or anastrozole) was determined by the treating physician in each case. Randomization, allocation, allocation concealment and blinding methods were conducted to reduce the risk of systematic bias in the selection and assignment of patients, and in the interpretation of observed treatment effects (benefits and harms). Patients were stratified by the nature of disease (visceral metastases versus bone-only metastases versus other), and prior (neo)adjuvant endocrine therapy (AI therapy versus other versus no prior endocrine therapy). Blinded independent central review was used for assessment of radiological scans to reduce detection bias. At baseline, demographic, disease characteristics, and prior treatments in the ITT population were balanced across study arms.
As of the updated efficacy analysis (data cut-off: September 29, 2023), the median duration of follow-up was just over 8 years in either treatment arm (█████ ██████ ███ █████ ██████). Discontinuation of treatment was higher in the placebo group and was most commonly due to PD in both treatment groups (█████ ██████ █████), but there was a higher incidence of discontinuation due to AEs in the group receiving abemaciclib (█████ ██████ ████), which is aligned with the generally higher rate of overall AEs and SAEs observed compared to the placebo group.
Although the hazard ratio at the final OS analysis (hazard ratio = 0.804; 95% CI, 0.637 to 1.015) was improved compared to the primary analysis (hazard ratio = 1.057; 95% CI, 0.683 to 1.633), and the estimated benefit in OS was an absolute difference in median OS of 13.09 months (95% CI of absolute difference not reported), the results were not statistically significant. However, in consultation with clinical experts, the reported difference in median OS was considered clinically important despite not being statistically significant.
The treatment setting, demographics, disease characteristics, and treatment history of recruited patients were considered to reasonably reflect real-world clinical practice in Canada with regards to this indication. Patients enrolled in MONARCH 3 were required to have an Eastern Cooperative Oncology Group Performance Status (ECOG PS) score of 0 to 1, and therefore there is no evidence on the efficacy and safety of abemaciclib in patients of ECOG PS score of 2 or greater; however, most patients in clinical practice will have a performance status of 0 to 1, and so this was not considered to represent a concern for external validity. The clinical experts consulted by CDA-AMC noted that the results of this study of abemaciclib were as expected for CDK4/6 inhibitors and were relatively similar to their experiences in clinical practice with abemaciclib as well as other CDK4/6 inhibitors, although each drug has its own unique safety profile. Overall, there were no major generalizability concerns related to the MONARCH 3 study.
Long-Term Extension Studies
No long-term extension studies were identified for this review.
Indirect Comparisons
Description of Studies
As the MONARCH 3 study was a placebo-controlled trial, there is a lack of direct evidence comparing abemaciclib to key comparators. The sponsor submitted Bayesian network meta-analyses (NMAs) to compare abemaciclib (from the MONARCH 3 study) with other CDK4/6 inhibitors and other treatments commonly used in HR-positive, HER2-negative advanced breast cancer or metastatic breast cancer in the treatment of patients who were postmenopausal without prior systemic treatment for advanced disease. The sponsor conducted a systematic literature review (SLR) to identify studies aligning with the indication.
For the purpose of this reassessment, only PFS, OS, and grade 3 and 4 AEs were assessed in depth. Other outcomes submitted by the sponsor (CBR, complete response [CR], and ORR) can be found in Appendix 2.
Efficacy Results
Overall Survival
Results of the NMA analysis for OS did not demonstrate a difference in hazard ratios between abemaciclib plus an NSAI, an NSAI alone, ribociclib plus letrozole, ribociclib plus fulvestrant, palbociclib plus letrozole, fulvestrant 200 mg or 500 mg, tamoxifen, or exemestane, as all credible intervals (CrIs) were wide and overlapped null.
Progression-Free Survival
Results of the NMA analysis for PFS favoured abemaciclib plus an NSAI compared to fulvestrant 500 mg, fulvestrant 250 mg, and tamoxifen monotherapies. However, the comparisons of abemaciclib plus an NSAI against ribociclib plus letrozole, ribociclib plus fulvestrant, palbociclib plus letrozole, palbociclib plus fulvestrant, and dalpiciclib plus anastrozole-letrozole, did not demonstrate a difference and the hazard ratios were comparable.
Harms Results
For the NMA of grade 3 or 4 AEs abemaciclib plus an NSAI was favoured compared to palbociclib plus letrozole, palbociclib plus fulvestrant, and dalpiciclib plus anastrozole or letrozole. Conversely, anastrozole or letrozole, fulvestrant 500 mg, and exemestane were favoured over abemaciclib plus AI. There was no difference detected against ribociclib plus letrozole.
Critical Appraisal
The sponsor conducted an appropriate SLR to identify studies of interest for indirect treatment comparisons (ITCs) and assessed the study design, eligibility criteria, baseline characteristics, outcome definitions, and outcome assessment for homogeneity. Studies included in the SLR were appraised for risk of bias by the sponsor using the Cochrane tool; there was some elevated or unknown risk of bias, particularly for open-label studies, which naturally, had elevated risk of bias for domains related to allocation concealment and blinding. Bayesian NMAs were conducted for several outcomes of interest. The proportional hazard (PH) assumption was evaluated and found to be violated in several cases, including in the MONARCH 3 study (for the outcome of OS); NMAs using the fractional polynomial (FP) method were conducted as sensitivity analyses for PFS and OS as this approach does not rely on the PH assumption. There were important differences in the trial design, eligibility criteria, and patient baseline characteristics across several domains that could impact comparability with the MONARCH 3 study, for example, HR status, country that the study was conducted in, open-label trials, disease severity, and location of disease. The results of the NMA analyses generally suggested that there was no difference between abemaciclib plus an NSAI and other available combination CDK4/6 inhibitors for OS, PFS, and grade 3 and grade 4 AEs. The clinical experts noted that it is important to consider specific, individual AEs (e.g., diarrhea or neutropenia), rather than aggregate AEs as this is an important consideration in treatment selection. Regardless, the limitations previously outlined, in combination with the wide 95% CrIs, reduce the precision of the results, and preclude definitive conclusions on the comparative effectiveness of abemaciclib and other CDK4/6 inhibitors.
Studies Addressing Gaps in the Evidence From the Systematic Review
Description and Appraisal of Studies
The sponsor submitted 4 observational studies to address the safety issues identified in the pivotal evidence; however, only 2 were summarized and appraised as they were deemed to contain potentially relevant information of interest to this review. The other 2 studies were not considered relevant as they mostly evaluated a population that received abemaciclib plus fulvestrant as the endocrine partner, which was not the indication under review.
US Database Study
The US database study by Price et al. (2022)9 was provided by the sponsor to address the gap in the pivotal study concerning safety issues of abemaciclib relative to other CDK4/6 inhibitors. This was a retrospective study examining the management of AEs among female patients with HR-positive, HER2-negative metastatic breast cancer receiving CDK4/6 inhibitors. Data for 396 patients from the US Oncology Network iKnowMed electronic health record (EHR) database were analyzed, of which 163 patients received palbociclib, 142 patients received abemaciclib, and 91 patients received ribociclib. The mean age was 64.3 years (SD = 11.9 years) and included patients with varying stages of disease (stage I = 10.1%, stage II = 35.6%, stage IIIA = 18.2%, and stage IV = 31.1%). More than one-half of the patients received CDK4/6 inhibitors as first-line therapy (84.6% for ribociclib, 65.5% for abemaciclib, and 63.8% for palbociclib). For patients receiving palbociclib and ribociclib, letrozole was the most prescribed combination therapy in first line, while for the abemaciclib cohort, fulvestrant was the most prescribed combination therapy in first line (N = 45 of 93; 31.7%). Across all lines of therapy, one-half of the patients in the abemaciclib cohort received fulvestrant as combination therapy, and one-half received either anastrozole or letrozole.
The most common AEs reported included neutropenia (palbociclib: 44.8%, abemaciclib: 10.6%, and ribociclib: 36.3%), diarrhea (palbociclib: 8.0%, abemaciclib: 43.0%, and ribociclib: 8.8%), and fatigue (palbociclib: 12.9%, abemaciclib: 17.6%, and ribociclib: 16.5%). Treatment holds due to neutropenia were reported in 47 patients and were more frequently reported in the palbociclib cohort (N = 33 [45.2%]) and ribociclib cohort (N = 13 [39.4%]) than the abemaciclib cohort (N = 1 [6.7%]). Dose reductions due to neutropenia were reported in 25 patients (34.2%) who received palbociclib, 8 patients (53.3%) who received abemaciclib, and 11 patients (33.3%) who received ribociclib. Treatment discontinuations due to neutropenia were reported in 10 patients in the palbociclib cohort and 2 patients in the ribociclib cohort. Treatment holds due to diarrhea were reported in 24 patients: 5 in the palbociclib cohort, 18 in the abemaciclib cohort, and 1 in the ribociclib cohort. Dose reductions due to diarrhea were reported in 22 patients, most frequently in the abemaciclib cohort (N = 18), followed by 3 patients who received palbociclib and 1 patient who received ribociclib. In total, 17 patients discontinued treatment due to diarrhea, most frequently in the abemaciclib cohort (N = 11), followed by the palbociclib cohort (N = 4), and the ribociclib cohort (N = 2). Eleven patients discontinued treatment due to fatigue, of which 9 patients received abemaciclib and 1 patient received palbociclib and ribociclib. Hospitalizations due to AEs occurred for 13 patients (3.3%) overall (4.3%, 3.5%, and 1.1% for patients in the palbociclib, abemaciclib, and ribociclib cohorts, respectively). The study noted lower frequencies of AEs but higher dose reductions when compared to data from clinical trials.
The study had some notable limitations. Data were collected from an EHR system, and any AE-related data managed outside of the network and not documented may lead to underreporting. An unadjusted observational analysis limits the reported estimates to be interpreted causally. Furthermore, documentation of the validity and accuracy of data were not provided. The analysis did not adjust for baseline demographics, disease characteristics, or comorbidities, and included patients of varying disease stages which could impact response to treatment and tolerability of treatment. It is unclear how many patients included in the analysis aligned with the indication under review given the different lines of therapy, and differing endocrine partners received with abemaciclib (i.e., one-half of all patients received combination fulvestrant, which is not part of the reimbursement request for this review). The National Cancer Institute – Common Terminology Criteria for Adverse Events (CTCAE) grading was not collected during clinical practice and not available for this study. The study was only conducted in the US. As such, the generalizability of the results of this retrospective chart study to the population under review is unclear.
Real-World Evidence Study From Slovenia
The sponsor-provided real-world evidence (RWE) study from Slovenia by Matos et al. (2024)10 provides additional safety and efficacy data of abemaciclib in the real-world setting, as well as insight into relevant subgroups such as older patients (age groups analyzed were < 70 years and ≥ 70 years). This study was an institutional retrospective study evaluating the real-world efficacy and safety of abemaciclib in patients with HR-positive, HER2-negative metastatic breast cancer. Data of 134 patients (133 female, 1 male) who were prescribed abemaciclib with AI or fulvestrant in the first, second, or subsequent line of treatment were retrospectively collected from institutional medical records. Real-world PD was determined by the treating physician based on radiological, laboratory, or clinical assessment. Median follow-up was 42 months (95% CI, 28.28 months to 45.71 months). The median age at treatment initiation was 62 years, and most patients had recurrent metastatic disease at presentation (100 [74.6%]). A total of 69 patients (51.5%) received abemaciclib in combination with endocrine therapy in first line, of which 47 patients (68.1%) received AI and 22 patients (31.9%) received fulvestrant as the endocrine partner. Thirty-two patients and 33 patients received abemaciclib in the second and third or later lines, respectively.
The median real-world PFS for the entire cohort was 15 months (95% CI, 9.52 months to 20.48 months), and was 21 months in first line (95% CI, 15.12 months to 26.88 months), 20 months in the second line (95% CI, 6.38 months to 33.60 months), and 7 months in the third line (95% CI, 4.19 months to 9.81 months), respectively. For the entire cohort, the median OS was 29 months (95% CI, 24.15 months to 33.84 months). Median OS was not reached in the first line setting but was 29 months for second line (95% CI, 26.09 months to 39.90 months) and 19 months for third or later lines (95% CI, 7.59 months to 30.49 months), respectively.
The most common AEs (any grade) were diarrhea (68.7%), anemia (64.9%), and increased serum creatinine (63.4%). Grade 3 or 4 diarrhea was reported in 7 patients, and grade 2 diarrhea in 27 patients. Grade 2 neutropenia was reported in 39 patients and grades 3 or 4 neutropenia were reported in 17 patients, respectively. Grade 2 anemia was reported in 21 patients. Dose reductions occurred in 41 patients (30.6%), primarily due to diarrhea (19 [32.2%]). Dose reductions were more frequent in patients aged 70 years or older (40%) compared to patients aged younger than 70 years (28%). Eighty-seven patients discontinued abemaciclib either due to disease progression (n = 64) or AEs (n = 23). Grade 3 or 4 neutropenia were more common in patients aged younger than 70 years (16%) versus 70 years or older (5%). Grade 3 or 4 diarrhea was more frequently reported in patients 70 years or older (7.5%) versus patients aged younger than 70 years (4.3%).
Several limitations were noted for this study. Data were collected from an EHR system, and any inconsistent AE incident collection may lead to underreporting. An unadjusted observational analysis limits the reported estimates to be interpreted causally. There was heterogeneity in the patient population analyzed with respect to age, line of treatment, and endocrine therapy used, though it was primarily AI. This study also had a small sample size, and many patients (n = 87) discontinued abemaciclib at study cut-off due to disease progression or AEs. It is worth noting that the results for median PFS and OS were numerically lower in this study compared to the pivotal trial, though the reason for this naive difference is unknown, which further undermines the generalizability of the results.
Conclusions
Abemaciclib plus an NSAI has been previously reviewed by CDA-AMC for the treatment of adult patients with endocrine-sensitive, HR-positive, HER2-negative advanced or metastatic breast cancer as a first-line endocrine-based therapy. In the initial review, it was concluded that evidence from the phase III double-blind RCT, MONARCH 3, demonstrated a clinically significant improvement in PFS when compared to placebo plus an NSAI in this population. Additionally, the safety profile of abemaciclib was not insignificant but was considered to be manageable in the treatment of this population. At the time of the initial review, OS data were immature, and conclusions could not be drawn. The recommendation by CDA-AMC was to conditionally reimburse abemaciclib in the treatment of this patient population but with stipulation that patients must be intolerant to or have a contraindication to other CDK4/6 inhibitors, which is narrower than the indication approved by Health Canada.
The current reassessment is based on updated data from the MONARCH 3 study, including updated PFS results, the final preplanned OS analysis, and updated safety results, given an additional 5 years and 10 months of follow-up time. Additionally, an updated sponsor-submitted ITC provided indirect comparison against other CDK4/6 inhibitors, and 2 real-world observational studies were appraised to assist in the assessment of AEs, particularly diarrhea.
The updated PFS results were aligned with the conclusions drawn from the final preplanned PFS analysis, in that abemaciclib plus an NSAI was associated with prolonged PFS relative to placebo plus an NSAI in this patient population. Although the results of the final OS analysis of the MONARCH 3 study suggest an improvement in OS for abemaciclib plus an NSAI compared to placebo, the results were not statistically significant, and there is uncertainty in the magnitude of benefit because of the wide 95% CI. However, the clinical experts consulted for this review considered the approximately 13-month difference in median OS between abemaciclib and placebo to be clinically meaningful in the context of metastatic breast cancer. In the absence of head-to-head data comparing with other CDK4/6 inhibitors, indirect comparisons in the form of NMAs demonstrated no evidence of difference between abemaciclib plus an NSAI and other CDK4/6 inhibitors plus an NSAI for the outcomes of OS or PFS, and there was considerable uncertainty due to between-trial heterogeneity and wide CrIs that crossed null.
There is extensive experience with abemaciclib, having been available to patients in Canada since 2019. The updated safety results were consistent with the previously reported safety profile, which demonstrated that compared to placebo, abemaciclib is associated with an increase in AEs, serious AEs, and grade 3 and 4 AEs, most notably diarrhea. Real-world observational studies suggested that the risk of diarrhea is typically managed through dose reduction, proactive intervention plans, and concomitant medications. This safety profile is significant but was described by the clinical experts to be manageable in the treatment of this patient population. Overall, the NMAs evaluating harms were limited by the reporting of aggregate AE results, as individual AEs by preferred term were considered more clinically relevant when comparing CDK4/6 inhibitors. As such, whether there is a clinically meaningful difference in overall safety profile between the CDK4/6 inhibitors available in this population remains uncertain.
Introduction
The objective of this reassessment is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of abemaciclib (Verzenio) in the treatment of HR-positive HER2-negative advanced breast cancer or metastatic breast cancer in combination with an AI in patients who were postmenopausal and endocrine sensitive considering the longer follow-up data from the pivotal trial, MONARCH 3.
Disease Background
Contents within this section have been informed by materials submitted by the sponsor and clinical expert input. The following have been summarized and validated by the review team.
Breast cancer is the most commonly diagnosed cancer in females and was the second leading cause of death among females in Canada in 2024, accounting for 13% of cancer-related mortality.2 It was estimated that 30,500 new female cases and 5,500 deaths would occur as a result of breast cancer in Canada in 2024.2 While many females diagnosed with early stage breast cancer will be cured with treatment, there remains no cure for metastatic breast cancer.11 A small percentage of patients with breast cancer (approximately 5%) present with metastatic disease at diagnosis. Of those who are diagnosed with early-stage or localized invasive disease, approximately 30% will relapse with metastatic disease,12,13 where the 5-year survival rate is 23%.14
Breast cancer is heterogenous, composed of several biologic subtypes that have distinct behaviours and responses to therapy.15 Major molecular subtypes of breast cancer have been defined based on the expression of the cell surface receptors HR and HER2.3 Roughly 70% to 80% of all breast cancers are HR-positive.16 Overexpression of the HER2 receptor (i.e., HER2 positive), occurs in approximately 10% to 30% of invasive breast cancers, and is associated with an aggressive form of the disease and a worse prognosis compared to an absence of expression of this receptor (i.e., HER2 negative).17 HR-positive and HER2-negative breast cancer is the most common molecular subtype, accounting for at least 66% to 75% of all breast cancer cases in North America and Europe.4-7
Metastatic cancer, classified as stage IV disease, occurs when cancer spreads beyond the primary tumour site to other parts of the body, forming secondary, metastatic tumours.8 Bone is the most common and often the primary metastatic site in HR-positive, HER2-negative breast cancer, while other common metastatic sites include visceral organs (liver and lung), the brain, and lymph nodes.5,17 Symptoms of metastatic breast cancer, include pain, fatigue, cognitive difficulties, and insomnia, and the disease imposes significant financial burdens as well as limitations on the activities of daily living of patients.18
Diagnosis of breast cancer is defined by the presence of invasive cancer cells on biopsy.19 Other diagnostic workup for metastatic breast cancer includes blood tests (complete blood count, metabolic profile, and liver function tests), imaging tests (mammographic screening, bone scan, X-ray, PET or CT scan, and ultrasound), and genetic testing.11 According to the American Society of Clinical Oncology or College of American Pathologists guidelines, biomarker assessment of HR and HER2 status is performed using validated immunohistochemistry testing or in situ hybridization assays to determine the molecular subtype and guide treatment decision-making.11,20,21 Molecular tests required to confirm HER2 and HR status as well as other diagnostic testing requirements for breast cancer are widely available across Canada.
Standards of Therapy
Contents within this section have been informed by materials submitted by the sponsor and clinical expert input. The following have been summarized and validated by the review team.
HR-positive, HER2-negative advanced or metastatic breast cancer is considered to be incurable according to the clinical experts consulted by CDA-AMC. For patients with this disease, therapies are therefore chosen to prolong life, delay progression, and improve HRQoL. Treatments are often selected considering a variety of factors, including previous exposure to therapies in the adjuvant setting, duration between adjuvant therapy and diagnosis of metastatic disease, rate of disease progression, location and involvement of tumour sites, clinical status and comorbidities of the patients, individual preferences, and provincial treatment funding.
Endocrine therapy (e.g., AIs) is the cornerstone of initial treatment for most patients with HR-positive advanced or metastatic breast cancer, with a key objective in delaying the need to initiate chemotherapy, as this can preserve the patient’s quality of life. However, the development of resistance to estrogen-based therapies poses a significant challenge to long-term disease-control according to the clinical experts consulted.
The experts noted that over the past decade, several novel targeted drugs have been introduced as add-ons to endocrine therapy, including CDK4/6 inhibitors such as ribociclib, palbociclib, and abemaciclib. Currently, first-line standard of care in this population is the combination of an AI or fulvestrant with a CDK4/6 inhibitor for patients with HR-positive advanced or metastatic breast cancer. Upon disease progression, patients may switch to an alternative endocrine drug in combination with another targeted therapy, or to chemotherapy, or antibody-drug conjugates.
Drug Under Review
Abemaciclib is an inhibitor of CDK4/6 and was most active against cyclin D1/CDK4 in enzymatic assays. Abemaciclib prevents retinoblastoma protein phosphorylation, blocking progression from G1 into S phase of the cell cycle, leading to suppression of tumour growth in preclinical models following short duration target inhibition. In estrogen receptor–positive breast cancer cell lines, sustained target inhibition by abemaciclib prevents rebound of retinoblastoma phosphorylation and cell cycle re-entry, resulting in senescence and apoptosis.22
The recommended dose of abemaciclib is 150 mg taken orally, twice daily. Females who are premenopausal or perimenopausal treated with abemaciclib in combination with an AI should be treated with a gonadotropin-releasing hormone agonist according to local clinical practice. Doses may need to be modified, or treatment may need to be suspended for management of AEs (e.g., diarrhea, hepatotoxicity).
In the advanced or metastatic setting, abemaciclib is approved by Health Canada “for the treatment of HR-positive, HER2-negative advanced or metastatic breast cancer:
in combination with an aromatase inhibitor in post-menopausal women as initial endocrine-based therapy.
in combination with fulvestrant in women with disease progression following endocrine therapy. Pre- or perimenopausal women must also be treated with a gonadotropin-releasing hormone agonist.
as a single agent in women with disease progression following endocrine therapy and at least 2 prior chemotherapy regimens. At least 1 chemotherapy regimen should have been administered in the metastatic setting, and at least 1 should have contained a taxane.”
Abemaciclib has been previously reviewed by CDA-AMC for both early and metastatic breast cancer indications:
In July 2019, a conditional positive reimbursement recommendation was issued for abemaciclib for the treatment of HR-positive, HER2-negative, advanced or metastatic breast cancer in combination with an AI in females who are postmenopausal as initial endocrine-based therapy.23
In July 2019, a conditional positive reimbursement recommendation was issued for abemaciclib for the treatment of HR-positive, HER2-negative, advanced or metastatic breast cancer in combination with fulvestrant in females with disease progression following endocrine therapy. Females who are premenopausal or perimenopausal must also be treated with a gonadotropin-releasing hormone agonist.23
In September 2022, a conditional positive reimbursement recommendation was issued for abemaciclib in combination with endocrine therapy for the adjuvant treatment of adult patients with HR-positive, HER2-negative, node-positive, early breast cancer at high risk of disease recurrence based on clinicopathological features and a Ki-67 score of at least 20%.24
In October 2024, a conditional positive reimbursement was issued for abemaciclib in combination with endocrine therapy for the adjuvant treatment of adult patients with HR-positive, HER2-negative, node-positive, early breast cancer at high risk of disease recurrence based on clinicopathological features.25
Key characteristics of abemaciclib are summarized in Table 2 with other treatments available for HR-positive, HER2-negative, advanced or metastatic breast cancer in combination with an AI in patients who are endocrine sensitive and postmenopausal.
Table 2: Key Characteristics of Abemaciclib, Palbociclib, Ribociclib, Fulvestrant, Letrozole, Anastrozole, Everolimus, and Exemestane for Advanced or Metastatic Breast Cancer
Drug | Indicationa | Mechanism of action | Route of administration | Recommended dose | Serious adverse events or safety issues |
|---|---|---|---|---|---|
Abemaciclib | For the treatment of HR-positive, HER2-negative advanced or metastatic breast cancer:
| Abemaciclib is a CDK4/6 inhibitor and blocks retinoblastoma protein phosphorylation, suppressing tumour growth, inducing senescence and apoptosis in ER-positive breast cancer, and reducing tumour size in xenograft models alone or with antiestrogens. | Oral | In combination with endocrine therapy: 150 mg, twice daily As a single drug: 200 mg, twice daily |
For advanced or metastatic breast cancer, continue treatment until disease progression or unacceptable toxicity. |
Palbociclib | For the treatment of HR-positive, HER2-negative locally advanced or metastatic breast cancer in combination with:
Pre- or perimenopausal women must also be treated with a luteinizing hormone-releasing hormone agonist. | Palbociclib is a selective, reversible, small molecule inhibitor of CDK4/6. Cyclin D and CDK4/6 are downstream of multiple signalling pathways that lead to cellular proliferation. Through inhibition of cyclin D-CDK4/6 complex activity, palbociclib inhibits the phosphorylation of retinoblastoma protein, blocking cell cycle progression from G1 into S phase. | Oral | 125 mg capsule once daily for 21 consecutive days followed by 7 days off treatment to comprise a complete cycle of 28 days |
|
Ribociclib | In combination with:
In pre/perimenopausal women or males, the endocrine therapy should be combined with a luteinizing hormone-releasing hormone agonist. | Ribociclib is a CDK4/6 inhibitor that reduces cell cycle progression and proliferation by decreasing retinoblastoma protein phosphorylation, leading to tumour regression and a senescent phenotype in breast cancer models. | Oral | 600 mg (3 × 200 mg film-coated tablets), once daily for 21 consecutive days followed by 7 days off treatment resulting in a complete cycle of 28 days |
Ribociclib should be administered by health professionals experienced with anticancer drugs. |
Fulvestrant | Indicated for the treatment of females who are postmenopausal with:
| Fulvestrant is a nonagonist ER antagonist that blocks the trophic actions of estrogens without itself having any partial agonist (estrogen-like) activity. | Intramuscular injection | 500 mg administered intramuscularly as 2 × 5 mL injections (250 mg per 5 mL) on days 0, 14, 28, and then every 28 days after |
|
Everolimus with exemestane | Everolimus in combination with exemestane is indicated for the treatment of females who are post-menopausal with HER2-negative, advanced breast cancer after recurrence or progression following treatment with a nonsteroidal aromatase inhibitor (letrozole or anastrozole). Exemestane is indicated for the treatment of females with advanced breast cancer with naturally or artificially induced postmenopausal status whose disease has progressed from antiestrogen therapy. | Everolimus reduces cell proliferation by inhibiting mTORC1, glycolysis, and angiogenesis in solid tumours in vivo, both through direct antitumour cell activity and inhibition of the tumour stromal compartment. Exemestane is a potent competitive human placental aromatase inhibitor that lowers circulating estrogen concentrations in females who are postmenopausal. | Oral | Everolimus is administered in 2.5 mg, 5 mg, or 10 mg tablets once daily. Exemestane is administered in 25 mg tablets once daily. | Everolimus:
Exemestane:
|
Letrozole |
| Letrozole is an AI that inhibits the aromatase enzyme by competitively binding to the heme of the cytochrome P450 subunit of the enzyme, resulting in a reduction of estrogen biosynthesis in all tissues. | Oral | 2.5 mg tablet once daily |
|
Anastrozole | For hormonal treatment of advanced breast cancer in females who are postmenopausal | Anastrozole is a selective nonsteroidal aromatase inhibitor that lowers serum estradiol concentrations, helping to reduce estrogen levels and thereby decreasing tumour mass or slowing tumour progression in many breast cancers, which often grow due to estrogen stimulation. | Oral | 1 mg, once a day |
|
ER = estrogen receptor; HR = hormone receptor.
aHealth Canada–approved indication.
Source: Product monographs of abemaciclib (Verzenio),22 palbociclib (Ibrance),26 ribociclib (Kisqali),27 fulvestrant (Faslodex),28 everolimus,29 exemestane (Aromasin),30 anastrozole (Arimidex),31 letrozole.32
Submission History
Basis of Reassessment
Abemaciclib (Verzenio) was previously reviewed by CDA-AMC for the treatment of advanced or metastatic breast cancer in adults with HR-positive, HER2-negative disease.1 Within this indication, there were 2 subpopulations of interest:
Patients who are postmenopausal as initial endocrine-based therapy, given in combination with an AI, sometimes also referred to as an NSAI. This population is also referred to as “endocrine-naive,” “endocrine-sensitive,” or “first-line systemic therapy” (first-line for advanced or metastatic disease, specifically).
Patients with disease progression following endocrine therapy, in combination with fulvestrant. Patients who are premenopausal or perimenopausal must be treated with a gonadotropin-releasing hormone agonist. This population is also referred to as “endocrine-resistant.”
The evidence provided for the original review of abemaciclib included the pivotal trials, MONARCH 2 (endocrine resistant, in combination with fulvestrant, N = 669) and MONARCH 3 (endocrine sensitive, in combination with AI [letrozole or anastrozole per investigator’s choice], N = 493), which were both phase III, multicentre, randomized, double-blind controlled studies in patients with advanced or metastatic breast cancer. This report focuses on the population who are endocrine sensitive as studied in the MONARCH 3 study; a concurrent reimbursement review is under way for the population who are endocrine resistant as studied in the MONARCH 2 study, which will not be discussed in detail here.
In the initial submission in 2019, for the population who were endocrine sensitive, the sponsor noted that the pERC recommended that abemaciclib should be reimbursed only in patients who are unable to tolerate or have a contraindication to other available CDK4/6 inhibitors as a result of the immature and uncertain OS results and the side effect profile; this represents a narrower population than the reimbursement request and the Health Canada indication, which did not stipulate limiting abemaciclib to patients who could not receive other CDK4/6 inhibitors. As such, the sponsor has filed a reassessment of abemaciclib to lift the restriction for patients who are unable to tolerate or have a contraindication to other available CDK4/6 inhibitors, as mature OS data, representing an additional 5 years and 10 months of follow-up data since the first evaluation of the preplanned final OS analysis (data cut-off: September 29, 2023) has become available from the MONARCH 3 trial. The focus of this reassessment is the new clinical evidence pertaining to OS, and any updated PFS results as available (although it is worth noting that the final preplanned analysis of PFS was already assessed in the 2019 review), as well as updated harms and AE results. Results for other key outcomes such as ORR, CBR, and HRQoL end points will be presented in the appendices for reference, but these outcomes were already assessed by pERC in 2019 and are not updated from how they were presented at the time of the original review.
As such, the objective of this report is to evaluate the newly available evidence for OS and whether the totality of evidence supports lifting the restriction on the reimbursement recommendation regarding intolerance or contraindication to other CDK4/6 inhibitors, in combination with AI as an initial endocrine-based therapy in adult patients who are postmenopausal with HR-positive, HER2-negative advanced or metastatic breast cancer.
Perspectives of Patients, Clinicians, and Drug Programs
The full patient and clinician group submissions received are available in the consolidated patient and clinician group input document for this review on the CDA-AMC abemaciclib project website.
Patient Group Input
This section was prepared by the review team based on the input provided by patient groups.
Three patient groups, BCC, CBCN, and Rethink Breast Cancer, provided their input for this submission. BCC is a national organization in Canada which encourages precision oncology research and awareness collaboration among physicians and researchers. The CBCN is a leading, patient-directed, national health charity committed to ensuring the best quality of care for all people living in Canada affected by breast cancer through the promotion of information, education, and advocacy activities. ReThink Breast Cancer is a charity in Canada known for making positive change by educating, empowering, and advocating for system changes to improve the experience and outcomes of those with breast cancer.
Information for this submission from BCC was gathered via an electronic survey, distributed to 169 patients living with a first recurrence (i.e., first line) of HR-positive, HER2-negative metastatic breast cancer from February 15 to 23, 2025. The survey responses included 54 patients identified as the target group for this input submission; 2% in both Nova Scotia and New Brunswick, 3% in Quebec, 64% in Ontario,18% in Alberta, and 11% in British Columbia. From the input provided by the CBCN, information for this submission was gathered via excerpts and key interviews from past submissions to CDA-AMC, including results from a 2012 survey in 71 patients with metastatic breast cancer and 16 caregivers, and a 2017 survey in 180 patients in Canada living with metastatic breast cancer. Additionally, information from a review of current studies and grey literature to highlight issues and experiences commonly shared among females living with breast cancer, and relevant disease experience and treatment considerations from a 2022 survey in 30 patients in Canada who had HR-positive, HER2-negative metastatic breast cancer was submitted. Information for this submission from ReThink Breast Cancer was gathered through observations and insights drawn through programs and meetings with 24 key patient advisors with a history of breast cancer, as well as an online survey documenting the lived experience with metastatic breast cancer from 78 patients and caregivers, conducted from September 2018 to April 2019. In addition, 4 people living with HR-positive, HER2-negative metastatic breast cancer who had experience with abemaciclib were interviewed from January to February 2025.
Results from the 2012 CBCN survey highlighted that fatigue, insomnia, and pain resulted in significant or debilitating impact on quality of life. Respondents also stated moderate to significant restrictions in their ability to exercise, pursue hobbies and personal interests, participation in social events and activities, and ability to spend time with loved ones. Patient groups noted that the disease further impacted mental health, with a physical and emotional toll associated with diagnosis, fear of recurrence, affecting caregivers and loved ones, and financial toxicity.
Patient groups highlighted the following barriers faced by respondents with existing treatments: AEs (e.g., fatigue, nausea, depression, problems with concentration, memory loss, diarrhea, and insomnia), and financial impact (e.g., not qualifying for insurance, inability to change employers due to loss of insurance, and prohibitive cost of new treatment options), minimal or no access to appropriate care when experiencing debilitating symptoms, and challenges accessing quality care during cancer treatment. Patients emphasized the importance of having a choice of treatment options to determine a therapy that suited them. The CBCN patient group specifically noted that efficacy, followed by quality of life, work, and cost were ranked as the most important to least important when considering treatment options.
All patient groups that provided input for this submission noted that extending cancer control and improved survival, combined with delayed progression (at least 6 to 9 months more than front-line treatments), a delay in IV chemotherapy, and improved quality of life were the most important outcomes of treatment. The CBCN also highlighted manageable AEs, although in the BCC survey, respondents noted that they were willing to accept higher rates of diarrhea as a trade-off for better recurrence-free survival outcomes. BCC also noted that patients were in favour of providing at-home, oral therapy that preserves quality of life. Rethink Breast Cancer suggested that patients valued long-term health outcomes over immediate concerns like reducing symptoms or managing side effects.
Of the 4 patients who were interviewed, 2 patients were receiving abemaciclib and letrozole, 1 was receiving abemaciclib and fulvestrant, and another was receiving abemaciclib as their 11th line of treatment. Patients mentioned their condition was well managed, with no signs of progression, and tolerable side effects that could be managed with dose reductions or other medications, and that they had the ability to travel. One patient expressed comfort with frequent monitoring (scans every 6 months), a preference for oral treatment, and valued having multiple treatment options. The patient who received abemaciclib as their 11th line mentioned that even after being heavily pretreated, the treatment worked for a year.
Patient groups indicated that testing required for this treatment is already accessible and covered in jurisdictions across Canada but noted that this is only the case in early-stage breast cancer, and it is not relevant to the advanced or metastatic treatment setting. ReThink Breast Cancer and BCC agreed that expanding the range of available CDK4/6 inhibitor therapies with abemaciclib, without restriction to only unsuitable or intolerance to other CDK4/6 inhibitors, would ensure a more equitable approach to treatment across all provinces for patients while minimizing drug-related out-of-pocket costs for people experiencing financial insecurity. ReThink Breast Cancer further added that because patient and physician choice was an important part of treatment, health care professionals should be able to tailor treatment plans to meet patient needs.
Clinician Input
Input From Clinical Experts Consulted for This Review
All CDA-AMC review teams include at least 1 clinical specialist with expertise regarding the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). The following input was provided by 2 clinical specialists with expertise in the diagnosis and management of advanced and metastatic breast cancer.
Unmet Needs
The clinical experts consulted for this review noted that HR-positive, HER2-negative advanced or metastatic breast cancer is generally considered to be incurable, and as a result, treatment is chosen with goals to prolong life, delay disease progression, and improve HRQoL. Not all patients respond to current treatments, and primary resistance to endocrine therapy in HR-positive disease remains a major challenge. The experts noted that even among those who initially respond, acquired resistance to drugs such as CDK4/6 inhibitors often leads to disease progression, necessitating a transition to less effective and/or more toxic therapies.
Place in Therapy
The clinical experts noted that there are currently 3 (including abemaciclib) CDK4/6 inhibitors that have demonstrated benefit in the first-line advanced or metastatic setting, and that clinicians generally perceive them to be approximately equivalent in terms of efficacy. The experts agreed that choice of CDK4/6 inhibitor varies by patient and by clinician, and that a key decision-making factor was not just the prevalence of AEs, but also the particular type(s) of AE associated with each CDK4/6 inhibitor, as different side-effect profiles will be more or less tolerable to different patients depending on their background health status and comorbid conditions. For instance, ribociclib may not be the drug of choice if long-QT is an issue, and palbociclib may be avoided if neutropenia is an issue, while abemaciclib is generally associated with more diarrhea.
Patient Population
The clinicians noted that the patients who are best suited for treatment with abemaciclib are those with HR-positive, HER2-negative advanced or metastatic breast cancer. The experts noted that there is no way to determine which patients are more likely to exhibit a response to abemaciclib compared to other CDK4/6 inhibitor; however, 1 expert noted that more significant benefit from the addition of abemaciclib may be observed in patients with high-risk features, such as visceral disease, PR-negative tumours, prior AI therapy, and high metastatic burden. According to both clinical experts consulted by CDA-AMC, abemaciclib remains a valuable treatment option not only for patients with contraindications or intolerance to other CDK4/6 inhibitors, but also for other patients based on their individual health status, previous exposure to therapies in the adjuvant setting, duration between adjuvant therapy and diagnosis of metastatic disease, rate of disease progression, location and involvement of tumour sites, clinical status and comorbidities of the patients, and individual preferences. Conversely, abemaciclib would be a less preferable option for patients who have previously received adjuvant abemaciclib for early-stage breast cancer.
Assessing the Response Treatment
The clinicians described that monitoring for treatment response involves a combination of clinical findings, bloodwork including tumour markers, and imaging. Treatment response should be assessed at every visit which typically occurs between once monthly (before each cycle) to once every 3 months. In select patients whose condition has not changed while receiving treatment for several years, clinicians may extend the assessments longer than 3 months apart. Clinically important outcomes according to the experts included improved survival, reduction in disease-related symptom frequency and severity, improved ability to perform daily activities, improvements in quality of life, and delaying the receipt of chemotherapy.
Discontinuing Treatment
The clinicians stated that abemaciclib should be discontinued upon evidence of disease progression, whether clinically or radiographically (e.g., RECIST criteria), or in the event of intolerable side effects that cannot be managed supportively (e.g., dosage modification) and significantly impact the patient’s quality of life. Patient preference is also considered.
Prescribing Considerations
The experts noted that only a medical oncologist is qualified to initiate treatment with abemaciclib. Monitoring patients and continuing treatment with abemaciclib after initiation can be performed by other members of the health care team, including family physicians in oncology, nurse practitioners, and oncology pharmacists.
Clinician Group Input
This section was prepared by the review team based on the input provided by clinician groups.
Two clinician groups, the REAL Canadian Breast Cancer Alliance, and OH (CCO) Breast Cancer DAC provided their input for this submission. The REAL Canadian Breast Cancer Alliance is a standing committee of multidisciplinary clinical-academic oncologists across Canada that publishes national clinical consensus recommendations. Recommendations published by the REAL Canadian Breast Cancer Alliance are routinely updated for timely health policy, funding, and consistent clinical adoption to ensure optimal outcomes for patients with breast cancer across all provinces and territories in Canada. A total of 16 clinicians provided their input, along with a literature review, clinical trial data, and recent data releases from international congresses, as well as collective clinical expertise of the members. The OH (CCO) Breast Cancer DAC provides evidence-based clinical and health system guidance on drug-related issues including the Provincial Drug Reimbursement Programs and the Systemic Treatment Program. Input from 5 clinicians was gathered via teleconference.
Both clinician groups indicated that CDK4/6 inhibitors plus endocrine therapy was the gold or current standard for the first-line treatment of HR-positive, HER2-negative advanced or metastatic breast cancer. The REAL Canadian Breast Cancer Alliance clinician group indicated that CDK4/6 inhibitors, when combined with endocrine therapy, were associated with significantly improved PFS in the first line metastatic setting compared to endocrine therapy alone.
In line with the clinical experts consulted for this review, the REAL Canadian Breast Cancer Alliance clinician group noted that the goals of treatment were to extend life, maintain quality of life, delay the need for chemotherapy, and minimize treatment-related AEs. They highlighted that among currently publicly funded CDK4/6 inhibitors, ribociclib was the preferred first-line treatment option for HR-positive, HER2-negative advanced or metastatic breast cancer, given its proven OS benefit. They noted that the choice of therapy (i.e., ribociclib, palbociclib, and abemaciclib) was dependent not only on efficacy but also on the tolerability of side effects by patients and that expanding the range of available CDK4/6 inhibitor therapies would allow a more personalized approach to treatment, which aligned with the opinion of clinical experts consulted by CDA-AMC.
The REAL Canadian Breast Cancer Alliance clinician group noted that the population receiving CDK4/6 inhibitors would not be expected to expand; rather abemaciclib would be included as 1 of the treatment options for patients for whom CDK4/6 inhibitors are already considered standard of care.
The REAL Canadian Breast Cancer Alliance clinician group noted that monitoring would mostly be required in the first 4 months of abemaciclib initiation and include bloodwork, assessing toxicities, assessing treatment adherence, and whether AEs were manageable with early interventions, including dose reduction and standard supportive care. Both clinician groups agreed that treatment discontinuation should be considered at the first sign of disease progression or due to persistent toxicity, as per the product monograph. The prescribing considerations noted by the group aligned with the opinion of clinical experts consulted by CDA-AMC. The REAL Canadian Breast Cancer Alliance clinician group noted that treatment initiation would be done by oncologists with experience in treating patients with breast cancer. OH (CCO) Breast Cancer DAC noted that because abemaciclib and AI are oral therapies, an outpatient setting would be appropriate.
Drug Program Input
The drug programs provide input on each drug being reviewed through the reimbursement review processes by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted for this review are summarized in Table 3.
Table 3: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Considerations for initiation of therapy | |
Should initiation criteria be consistent with CDA-AMC recommendations for ribociclib and palbociclib + AI in the same therapeutic space (e.g., have not received prior endocrine therapy for metastatic disease but may have received up to 1 line of chemotherapy for metastatic disease; are not resistant to [neo]adjuvant NSAI therapy; and do not have active or uncontrolled CNS metastases)? | Yes. The clinical experts consulted by CDA-AMC indicated that initiation criteria should be similar across CDK4/6 inhibitors in the treatment of this patient population, as they are considered broadly similar in efficacy and safety, albeit with differences in specific elements of the safety profiles that factors into clinician and patient decision-making. |
Do the criteria from the previous CDA-AMC recommendation for abemaciclib + AI still apply? Specifically:
| Yes. The clinical experts consulted by CDA-AMC did not indicate any need to change these criteria. |
Would it be reasonable to switch patients from ribociclib or palbociclib to abemaciclib (when there is toxicity to CDK4/6 inhibitor without progression)? | The clinical experts indicated that this scenario would be uncommon but would be an option for some patients having side effects from other CDK4/6 inhibitors but would only be done in the absence of disease progression. The experts noted that different CDK4/6 inhibitors may be tolerated differently in a given patient due to differences in side-effect profile. |
Considerations for prescribing of therapy | |
Note that the recommended dosing is twice daily dosing for abemaciclib vs. once daily for the other CDK4/6 inhibitors. | This is a comment from the drug programs to inform pERC deliberations. |
System and economic issues | |
Ribociclib and palbociclib have successfully gone through price negotiations for the same indication. | This is a comment from the drug programs to inform pERC deliberations. |
Request an initiation of a rapid provisional funding algorithm. An update to the algorithm to incorporate the recommendation if positive. | This is a comment from the drug programs to inform pERC deliberations. |
CDA-AMC = Canada’s Drug Agency; CNS = central nervous system; NSAI = nonsteroidal aromatase inhibitor; pERC = pan-Canadian Oncology Drug Review Expert Review Committee; vs. = versus.
Clinical Evidence
The objective of this Clinical Review report is to review and critically appraise the clinical evidence submitted by the sponsor on the beneficial and harmful effects of abemaciclib (Verzenio), an orally administered tablet (available in 50 mg, 100 mg, and 150 mg tablets), in the treatment of HR-positive, HER2-negative advanced or metastatic breast cancer in combination with an AI in patients who are endocrine sensitive and postmenopausal. The focus will be placed on comparing abemaciclib to relevant comparators and identifying gaps in the current evidence.
A summary of the clinical evidence included by the sponsor in the review of abemaciclib is presented in 4 sections with our critical appraisal of the evidence included at the end of each section. The first section, the systematic review, includes pivotal studies and RCTs that were selected according to the sponsor’s systematic review protocol. The second section includes sponsor-submitted long-term extension studies, although none were submitted for this review. The third section includes indirect evidence from the sponsor. The fourth section includes additional studies that were submitted by the sponsor to address important gaps in the systematic review evidence.
Included Studies
Clinical evidence from the following studies is included in the review and appraised in this document:
1 phase III, multicentre, placebo-controlled pivotal RCT identified in the systematic review (MONARCH 3)
1 indirect treatment comparison
2 additional studies addressing gaps in evidence.
Systematic Review
Contents within this section have been informed by materials submitted by the sponsor. The following have been summarized and validated by the review team.
Description of Studies
Characteristics of the included studies are summarized in Table 4. The MONARCH 2 and MONARCH 3 studies were identified in the sponsor’s systematic review, which comprised 2 indications in the advanced or metastatic breast cancer setting. The MONARCH 2 study (which investigated abemaciclib plus fulvestrant) is relevant to patients who are endocrine resistant, while the MONARCH 3 study (which investigated abemaciclib plus AI) is relevant to patients who are endocrine sensitive. This report pertains to the latter indication only.
The MONARCH 3 trial has previously been summarized and appraised in the previous review of abemaciclib.1 MONARCH 3 was a phase III, multicentre, randomized, double-blind, placebo-controlled study of abemaciclib or placebo plus NSAI in females who were postmenopausal with HR-positive, HER2-negative advanced or metastatic breast cancer who had not received any previous systemic therapy in the advanced or metastatic setting. The study was conducted in 158 centres in 22 countries, including 8 centres enrolling 25 patients in Canada.
Table 4: Details of Studies Included in the Systematic Review
Detail | MONARCH 3 |
|---|---|
Designs and populations | |
Study design | Multicentre, randomized, double-blind, placebo-controlled, phase III study |
Locations | 155 sites in 22 countries including the US, Australia, Canada, Belgium, Japan, Korea, Austria, France, Germany, Greece, Isreal, Italy, Mexico, the Netherlands, New Zealand, Russia, Slovakia, Spain, Sweden, Taiwan, Türkiye, and the UK |
Patient enrolment dates | Start date: November 18, 2014 Data cut-off date: September 29, 2023 (final analysis of overall survival) End date: December 2025 |
Randomized (N) | Total randomized: N = 493
|
Inclusion criteria |
|
Exclusion criteria |
|
Drugs | |
Intervention | Abemaciclib 150 mg orally twice daily on days 1 to 28 of 28-day cycles plus either anastrozole 1 mg or letrozole 2.5 mg (as determined by the investigator) orally once daily on days 1 to 28 of 28-day cycles |
Comparator(s) | Placebo capsules orally twice daily on days 1 to 28 of 28-day cycles plus either anastrozole 1 mg or letrozole 2.5 mg (as determined by the investigator) orally once daily on days 1 to 28 of 28-day cycles |
Study duration | |
Screening phase | 28 days |
Treatment phase | Until progressive disease as defined by RECIST v1.1, death, enrolment in any other clinical trial involving an investigational drug or enrolment in any other type of medical research judged not to be scientifically or medically compatible with this study, investigator decision, patient decision or sponsor decision |
Follow-up phase | 30 day short-term follow up Continued access period (optional; patients continue to receive study treatment until 1 of the criteria for discontinuation is met) |
Outcomes | |
Primary end point | Progression-free survival |
Secondary and exploratory end points | Secondary:
Exploratory: Change in tumour size |
Publication status | |
Publications | Goetz et al. (2024) 33; Johnston et al. (2019) 34; Goetz et al. (2017) 35; Goetz et al. (2020) 36; Takahashi et al. (2022)37 |
Clinical trial record number | NCT02246621 |
ECOG PS = Eastern Cooperative Oncology Group Performance Status; EORTC QLQ-BR23 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Breast Cancer 23; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; HR = hormone receptor; NSAI = nonsteroidal aromatase inhibitor; RECIST = Response Evaluation Criteria in Solid Tumours Version 1.1.
Source: Details included in the table are from the sponsor’s Summary of Clinical Evidence.38
Randomization was performed using a centralized interactive web-based randomization system. Patients were randomized into abemaciclib plus AI or placebo plus AI arms in a 2:1 ratio. Randomization was stratified based on 2 factors:
nature of disease (visceral, bone only, or other)
prior (neo)adjuvant therapy (AI, no endocrine therapy, or other).
The study was double-blinded. Blinding of study participants and investigators was performed through the use of placebo capsules that were similar to abemaciclib capsules. A limited number of Eli Lilly Canada Inc. personnel had access to the randomization table and study assignments before study completion. Patients remained blinded until the final OS analysis. Blinding codes could be broken if necessary for patient safety or after a patient discontinued treatment due to disease progression, if deemed essential for the selection of the patient’s next treatment regimen. The Eli Lilly Canada Inc. clinical research physician had to be consulted before unblinding. If the investigator or patient became unblinded, the patient was transitioned to postdiscontinuation follow-up.
After completing study screening, follow-up visits occurred on day 1 of each 28-day cycle. Tumour assessment (breast MRI, CT scan, or MRI of the chest, abdomen, and pelvis) was conducted on days 21 to 28 of cycle 2, every second cycle thereafter through cycle 18, and on days 21 to 28 of every third cycle beyond cycle 18. If there was any evidence of clinical progression, imaging was performed within 14 days of the event. Bone scintigraphy was conducted on days 21 to 28 of every sixth cycle starting with cycle 6. For patients with bone lesions identified at baseline, X-ray, CT scan with bone windows, or MRI were performed on days 21 to 28 of every second cycle starting with cycle 2 through cycle 18, and every third cycle thereafter. For patients with new lesions identified by postbaseline scintigraphy, targeted assessment with X-ray, CT scan with bone windows, or MRI was required to confirm findings. Upon RECIST-defined disease progression, the study drug was discontinued.
Populations
Eligible patients in the MONARCH 3 study were females aged 18 years or older who were postmenopausal and who had not received prior systemic therapy for advanced disease. Endocrine therapy in the neoadjuvant or adjuvant setting was permitted if the patient had a disease-free interval greater than 12 months from the completion of endocrine therapy.
Interventions
Study Therapies
Patients who were randomized to the intervention arm received abemaciclib 150 mg orally twice daily on days 1 to 28 of 28-day cycles plus either letrozole 2.5 mg or anastrozole 1 mg taken orally once daily on days 1 to 28 of 28-day cycles.
Patients who were randomized to the placebo arm received placebo capsules taken orally twice daily on days 1 to 28 of 28-day cycles plus either anastrozole 1 mg or letrozole 2.5 mg taken orally once daily on days 1 to 28 of 28-day cycles.
The specific NSAI (letrozole or anastrozole) administered to patients was determined by the investigator. Abemaciclib or placebo (blinded study drug) was supplied as capsules for oral administration.
Dose Modifications
For patients who reported significant treatment-related toxicities, dose modifications (interruptions or reductions) were permitted for abemaciclib or placebo according to prespecified dose-adjustment procedures. There were 2 recommended dose adjustment schedules (150 mg to 100 mg and 100 mg to 50 mg, all administered twice daily). Based on the US Prescribing Information, single dose strengths are approved for letrozole and anastrozole. In special circumstances, in the absence of evidence of progression, and in consultation with an Eli Lilly Canada Inc. clinical research physician, a change in the NSAI drug could be made. When treatment interruption was deemed necessary for 1 of the study drugs in the combination, treatment with the other drug could be continued.
For patients requiring dose reductions, re-escalation to a previous dose was permitted only after consultation with an Eli Lilly Canada Inc. clinical research physician.
Concomitant and Subsequent Interventions
The use of megestrol acetate as an appetite stimulant was prohibited in the MONARCH 3 trial. To prevent drug interactions, the use of the following drugs was required to be avoided or substituted: carbamazepine, dexamethasone, phenobarbital, phenytoin, rifampin, rifabutin, St. John’s Wort, HIV protease inhibitors, clarithromycin, itraconazole, ketoconazole, and nefazodone. Dexamethasone was permitted as a supportive care therapy where indicated, preferably for a treatment course of 7 days or less.
Patients with bone metastases present at the time of baseline imaging must have received bisphosphonates or RANK ligand targeted drugs (e.g., denosumab) per respective approved labels. Initiation of treatment with bone-modifying drugs must have begun at least 7 days before randomization. Patients receiving bisphosphonates or RANK ligand targeted drugs should not have switched treatments (e.g., replaced a bisphosphonate with denosumab) while on study treatment.
Outcomes
Selection of Outcomes
A list of efficacy end points assessed in this Clinical Review report is provided in Table 5, followed by descriptions of the outcome measures. Summarized end points are based on outcomes included in the sponsor’s Summary of Clinical Evidence as well as any outcomes identified as important to this review according to the clinical experts consulted for this review and input from patient and clinician groups and public drug plans. Selected end points that were considered to be most relevant to inform expert committee deliberations were assessed using GRADE.
Updated survival data available from the MONARCH 3 study are presented in detail in this reassessment report. A summary of the other key secondary outcomes, as reported in the 2019 Clinical Review report, are presented in Appendix 1 without update, and analysis of these end points is not described within this report.
Since the receipt of the 2019 final recommendation (data cut-offs of January 2017 and November 2017), later data cut-offs have become available and are reported in this submission:
MONARCH 3 interim OS analysis 1 (data cut-off: February 3, 2020)
MONARCH 3 interim OS analysis 2 (data cut-off: July 2, 2021)
MONARCH 3 final OS analysis (data cut-off: September 29, 2023).
These later data cuts-offs represent an additional 5 years and 10 months of follow-up data for the MONARCH 3 study. The OS analyses are based on the final data cut-off. The data cut-offs submitted in 2019 (i.e., the planned final PFS analysis and OS analyses) are presented alongside for comparison given the context of the reassessment but are not the focus of this report.
Table 5: Outcomes Summarized From the MONARCH 3 Study
Outcome measure | 2019 submission | 2025 reassessment | MONARCH 3 |
|---|---|---|---|
PFS |
| Data cut from September 29, 2023 (updated from final) | Primarya |
OS | Data cut from January 31, 2017 (immature; median OS had not been reached) | Data cut from September 29, 2023 (final)b | Key secondary a |
Safety and tolerability | Data cut from February 14, 2017 | Data cut from September 29, 2023 | Safety |
OS = overall survival; PFS = progression-free survival.
aStatistical testing for these end points was adjusted for multiple comparisons (e.g., hierarchal testing).
bInterim data cut-offs of OS from February 3, 2020, and July 2, 2021, are also available but are not the focus of this review.
Source: Details included in the table are from the sponsor’s Summary of Clinical Evidence38 and the MONARCH 3 Clinical Study Report.39
Outcome Definitions
The primary end point of the study was investigator-assessed PFS, defined as the time from randomization to disease progression (according to RECIST Version 1.1) or death for any reason.
For those patients with locoregionally recurrent disease for whom surgery was performed with no evidence of residual disease postoperatively, objective progression was established if at least 1 of the following criteria was met:
local and/or regional recurrence
new development of metastatic disease.
OS, a key secondary outcome, was defined as the time from randomization to death from any cause.
Statistical Analysis
Sample Size and Power Calculations
The study planned to enrol approximately 450 patients in a 2:1 randomization. A 2-look group-sequential design of the primary end point of investigator-assessed PFS was used to accommodate an event-driven plan for the interim and final PFS analyses. There was 1 planned interim analysis, and 1 planned final analysis for PFS in this study. The interim analysis was planned to take place after approximately 189 investigator-assessed PFS events had occurred. The final PFS analysis was planned to be performed after 240 PFS events had occurred. The cumulative 1-sided type I error rate of 0.025 was maintained using methods described in the subsections that follow. Assuming a hazard ratio of 0.67, this sample size yielded more than 80% statistical power to detect superiority of the abemaciclib plus NSAI arm over the placebo plus NSAI arm with the use of a 1-sided log-rank test and a type I error of 0.025. If the true median PFS for the placebo plus NSAI arm was 10 months, then the hazard ratio of 0.67 amounted to an approximately 5-month (50%) improvement in median PFS for the abemaciclib plus NSAI arm under an additional assumption of exponential survival distribution.
Efficacy Outcomes
A summary of the statistical analysis of PFS and OS in the MONARCH 3 study is described in Table 6. Other outcomes not relevant to the purpose of the reassessment have been omitted from this report.
Table 6: Statistical Analysis of Updated PFS and OS End Points in the MONARCH 3 Study for the Reassessment
End point | Statistical model | Adjustment factors | Handling of missing data | Sensitivity analyses |
|---|---|---|---|---|
MONARCH 3 study | ||||
PFSa,b | The Kaplan-Meier method was used to estimate PFS in each treatment arm. Treatment efficacy was estimated using a stratified Cox proportional hazard model. | Stratified by nature of disease and prior (neo)adjuvant endocrine therapy | NA |
|
OSa,c | The Kaplan-Meier method was used to estimate the OS curve for each treatment arm. Treatment efficacy was estimated using a stratified Cox proportional hazard model. | Stratified by nature of disease and prior (neo)adjuvant endocrine therapy | NA | Based on overall survival time from date of study enrolment to date of death due to study disease |
NA = not applicable; OS = overall survival; PFS = progression-free survival.
aStatistical testing for these end points was adjusted for multiple comparisons (e.g., hierarchal testing). New data cut-offs for these outcomes have been provided by the sponsor for this submission.
bPrimary end point.
cKey secondary end point.
Source: MONARCH 3 Clinical Study Report.39
The primary analysis of investigator-assessed PFS was performed on the ITT population, which included all patients who were randomized. A sensitivity analysis was additionally conducted to assess PFS by a full, blinded independent central review. PFS was analyzed using a log-rank test stratified by metastatic site and prior neoadjuvant or adjuvant endocrine therapy. Unless otherwise stated, all hypothesis tests were performed at the 2-sided 0.05 statistical significance level, and all CIs were estimated at a 95% confidence level. Exploratory subgroup analyses were conducted within prespecified protocol subgroups as well as relevant subgroups identified in the literature.
Statistical Testing Structure
For the outcomes of PFS and OS, the difference between abemaciclib plus an NSAI and placebo plus an NSAI was evaluated using a 1-sided log-rank test and stratified by metastatic site and prior neoadjuvant or adjuvant endocrine therapy. Estimates of the hazard ratio were constructed using a stratified Cox model, stratified by metastatic site and prior neoadjuvant or adjuvant endocrine therapy.
The overall type I error rate was controlled with a gate-keeping strategy between the primary (PFS) and secondary (OS) end points; OS was tested for significance only if PFS was statistically significant. All hypothesis tests were performed at the 1-sided 0.025 level and CIs used a 95% confidence level.
A 4-look approach was planned for the analysis of OS data. There was a 2% alpha allocation for OS in the ITT population and 0.5% allocation for alpha in the visceral disease population. Type I error was to be shared between the 2 OS end points. The cumulative 1-sided type I error rate within each population was maintained using the Lan-Demets method. The planned analysis time points were as follows:
the interim PFS analysis (189 PFS events)
the final PFS analysis (240 PFS events)
approximately 189 OS events in the ITT population, regardless of the number of events in the visceral disease population (VIS)
approximately 252 OS events in the ITT population, regardless of the number of events in the VIS
final OS analysis: At least 315 OS events in the ITT population and at least 189 events in the VIS.
The first interim analysis was planned to take place after approximately 189 investigator-assessed PFS events have occurred. If statistical significance was not declared at the interim PFS analysis, the final PFS analysis was to be performed after 240 PFS events have been observed based on investigator assessment. Following a positive PFS result, a 1-sided alpha of 0.025 was allocated to test for OS within the VIS and ITT populations, with an initial allocation of 0.005 for the VIS population and 0.020 for the ITT population.
Progression-Free Survival
A KM model was used to estimate the PFS curve for each treatment arm. Point estimates and CIs for the first quartile, median, and third quartile for the PFS curve of each arm were estimated. The difference in survival probability of PFS for each arm — along with their Wald type CIs — was compared at 4-month intervals up to 24 months.
The difference in restricted means of PFS was estimated over various intervals indexed by T. The restriction time T was chosen as the largest time point at which the standard error of the survival estimate within each treatment group was no more than 0.075.
Overall Survival
A KM model was used to estimate the OS curve for each treatment arm. Point estimates and CIs for the first quartile, median, and third quartile for the OS curve of each arm were estimated. The difference in survival probability of OS at 1, 2, and 3 years for each arm were estimated along with their corresponding Wald type CIs.
The difference in restricted means of OS was estimated over various intervals indexed by T. The restriction time T was chosen as the largest time point at which the SE of the survival estimate within each treatment group was no more than 0.075.
Safety Outcomes
Safety was assessed in all patients who received at least 1 dose of study drug (i.e., the safety population). Safety and tolerability of abemaciclib was graded using the CTCAE (version 4.03), and the results were reported descriptively.
Treatment emergent AEs were defined as any AE that began between the day of the first dose and 30 days after the last dose of any study drug (or any time, if they were serious and related to study treatment), or any pre-existing condition that increased in CTCAE grade between the day of the first dose and 30 days after the last dose of the study drug. A serious AE was any AE during the study that resulted in death, initial or prolonged hospitalization, a life-threatening experience, persistent or significant disability, congenital anomaly or birth defect, or was otherwise considered significant.
At randomization, patients received instructions on the management of diarrhea. In the event of diarrhea, supportive measures were initiated as early as possible. These included the following:
At the first sign of loose stools, the patient should initiate antidiarrheal therapy (e.g., loperamide) and notify the investigator for further instructions and appropriate follow-up.
Patients were encouraged to drink fluids (e.g., 8 to 10 glasses of clear liquids per day).
Site personnel should assess response within 24 hours.
If diarrhea did not resolve with antidiarrheal therapy within 24 hours to at least grade 1, blinded study drug should be suspended until diarrhea resolved to at least grade 1.
When blinded study drug recommenced, dosing should be adjusted: dose adjustment level 0 would constitute an oral dose of 150, while dose adjustment level 2 would be a dose of 100 mg, and level 2 would be a dose of 50 mg. In all cases, dose frequency is every 12 hours.
In severe cases of diarrhea, the measuring of neutrophil counts and body temperature and proactive management of diarrhea with antidiarrheal drugs should be considered. If diarrhea was severe (requiring IV rehydration) and/or associated with fever or severe neutropenia, broad-spectrum antibiotics such as fluoroquinolones were prescribed.
Subgroup Analyses
Prespecified subgroup analyses of PFS and OS were performed for each of the following potential prognostic subgroup variables:
all baseline stratification factors
NSAI received at cycle 1 (letrozole versus anastrozole)
disease setting (de novo metastatic versus recurrent metastatic versus locoregionally recurrent)
measurable disease at baseline (yes versus no)
number of organs involved (1 versus 2 versus 3 or more)
age (< 65 years versus ≥ 65 years)
region (North America, Europe, Asia, and other)
race (Asian, white, and other)
progesterone receptor status (positive versus negative)
baseline ECOG PS (0 versus 1).
If a level of a factor consists of fewer than 10% of patients who were randomized, analysis within that level was omitted.
Analyses were conducted within subgroups and, separately, across subgroups using a test of interactions between subgroups and treatment. Estimated hazard ratios and CIs for the within-subgroup analyses were presented as a forest plot along with P values for tests of interactions between subgroup variables and treatment.
Other subgroup analyses were performed as deemed appropriate. If any safety analyses identified important imbalances between arms, subgroup analyses of these end points were permitted.
Analysis Populations
The analysis populations of the MONARCH 3 study are presented in Table 7.
Table 7: Analysis Populations of the MONARCH 3 Study
Population | Definition | Application |
|---|---|---|
Entered population | All patients who signed the informed consent form | All disposition analyses |
Enrolled or ITT | All patients who were randomized | All patient characteristic and efficacy analyses |
VIS population | All patients who were randomized with visceral disease at baseline as per the CRF | Alpha-controlled OS analysis |
Randomized and treated | All patients who were randomized who received at least 1 dose of abemaciclib, placebo, or NSAI | All safety and exposure analyses |
CRF = case report form; ITT = intention to treat; NSAI = nonsteroidal aromatase inhibitor; OS = overall survival; VIS = visceral disease population.
Source: MONARCH 3 Clinical Study Report.39
Results
Patient Disposition
In the MONARCH 3 study, 493 patients were randomized into the ITT population; among them, 328 patients were randomized into the abemaciclib plus NSAI group, and 165 patients were randomized into the placebo plus NSAI group.
At the January 31, 2017, data cut-off date, ███ ████████ were still on study treatment in the abemaciclib plus AI arm, as compared with ██ ████████ in the placebo plus AI arm. A total of ███ ████████ ███████ in the abemaciclib plus AI arm and ██ ████████ ███████ in the placebo plus AI arm had discontinued the study treatment. At the time of final PFS analysis (November 3, 2017, data cut-off), ███ ████████ in the abemaciclib plus AI and ██ ████████ the placebo plus AI arm were still on study treatment. A total of ███ ████████ ███████ in the abemaciclib plus AI arm and ███ ████████ ███████ in the placebo plus AI arm had discontinued the study treatment.
At the time of the final OS analysis (September 29, 2023), 23 patients (7%) who received abemaciclib plus an NSAI and 5 patients (3%) who received placebo plus an NSAI remained on the study-assigned treatment. The majority of patients discontinued due to disease progression. A summary of the patient disposition of the MONARCH 3 study at the time of the final OS analysis is reported in Table 8.
Table 8: Summary of Patient Disposition in the MONARCH 3 Study
Value | Abemaciclib + NSAI (N = 328) n (%) | Placebo + NSAI (N = 165) n (%) | Total (N = 493) n (%) |
|---|---|---|---|
Entered, N | 579 | ||
Not randomized, N | 86 | ||
Screening unsuccessful | 55 | ||
Withdrawal by patient | 18 | ||
Physician decision | ████ ██ | ||
Progressive disease | ████ ██ | ||
Enrolled or randomized, N | 493 | ||
Randomized, but never treated | 2 (0.6) | 3 (1.8) | 5 (1.0) |
Treated | 326 (99.4) | 162 (98.2) | 488 (99.0) |
On treatmenta | 23 (7.0) | 5 (3.0) | 28 (5.7) |
Off treatmenta | 303 (92.4) | 157 (95.2) | 460 (93.3) |
Reason for discontinuation of treatment | |||
Progressive disease | ████ ██ | ████ ██ | ████ ██ |
Adverse event | ████ ██ | ████ ██ | ████ ██ |
Withdrawal by patient | ████ ██ | ████ ██ | ████ ██ |
Death | ████ ██ | ████ ██ | ████ ██ |
Physician decision | ████ ██ | ████ ██ | ████ ██ |
Noncompliance with study drug | ████ ██ | ████ ██ | ████ ██ |
Protocol violation | ████ ██ | ████ ██ | ████ ██ |
Posttreatment discontinuation follow-upa,b | |||
No | 21 (6.4) | 6 (3.6) | 27 (5.5) |
Yes | 284 (86.6) | 154 (93.3) | 438 (88.8) |
On posttreatment discontinuation follow-upa,b | ████ ██ | ████ ██ | ████ ██ |
Continue with protocol procedures | ████ ██ | ████ ██ | ████ ██ |
Continue only for survival status | ████ ██ | ████ ██ | ████ ██ |
Off posttreatment discontinuation follow-upa,b | ████ ██ | ████ ██ | ████ ██ |
Reasons for end of postdiscontinuation follow-up | |||
Death | ████ ██ | ████ ██ | ████ ██ |
Lost to follow-up | ████ ██ | ████ ██ | ████ ██ |
Withdrawal by patient | ████ ██ | ████ ██ | ████ ██ |
ITT, N | 328 | 165 | 493 |
VIS, N | 173 | 90 | 263 |
Safety, N | 327 | 161 | 488 |
ITT = intention-to-treat; NSAI = nonsteroidal aromatase inhibitor; VIS = visceral disease population.
aAt the time of data cut-off on September 29, 2023.
bIncludes patients who were off treatment as well as patients who were randomized but never treated.
Source: MONARCH 3 Clinical Study Report.39 Data cut-off date: September 29, 2023.
Baseline Characteristics
The baseline characteristics outlined in Table 9 are limited to those most relevant to patient and clinician values or were considered plausible prognostic factors for the reported outcomes and may affect the interpretation of the study results. All 493 patients who were enrolled in the MONARCH 3 trial were female, and the majority were white (58.4%) or of Asian ethnicity (30.0%). The median age was 63 years, and ███ ████████ ███████ were aged less than 65 years. Overall, the median duration of disease from initial diagnosis of disease to randomization was ████ ██████. Most patients ███████ entered the study with metastatic disease.
In the MONARCH 3 study, a total of 135 patients (27.4%) had received prior endocrine therapy with AI, 95 patients (19.3%) had received other prior endocrine therapy, and 263 patients (53.3%) had received no prior endocrine therapy (Table 10). Endocrine therapy was received by ███ ████████ ████████ including | ████████ ██████ in the neoadjuvant setting and ███ ████████ ███████ in the adjuvant setting. Per protocol, a patient may have received 2 or fewer weeks of NSAI in the locally advanced or metastatic disease setting preceding screening if they agreed to discontinue the NSAI until study treatment initiation. ████████████ ████████ met this criterion.
Table 9: Summary of Baseline Characteristics in the MONARCH 3 Study
Characteristic | Abemaciclib + NSAI (N = 328) | Placebo + NSAI (N = 165) | Total (N = 493) |
|---|---|---|---|
Female, n (%) | 328 (100.0) | 165 (100.0) | 493 (100.0) |
Age, mean (SD) | 63.13 (9.92) | 62.92 (9.96) | 63.05 (9.92) |
Race,a n (%) | |||
American Indian or Alaska Native | ████ ██ | ████ ██ | ████ ██ |
Asian | 103 (31.4) | 45 (27.3) | 148 (30.0) |
Black or African American | ████ ██ | ████ ██ | ████ ██ |
Native Hawaiian or Pacific Islander | ████ ██ | ████ ██ | ████ ██ |
White | 186 (56.7) | 102 (61.8) | 288 (58.4) |
Multiple | ████ ██ | ████ ██ | ████ ██ |
Region, n (%) | |||
Europe | ████ ██ | ████ ██ | ████ ██ |
Asia | ████ ██ | ████ ██ | ████ ██ |
North America | ████ ██ | ████ ██ | ████ ██ |
ECOG PS, n (%) | |||
0 | 192 (58.5) | 104 (63.0) | 296 (60.0) |
1 | 136 (41.5) | 61 (37.0) | 197 (40.0) |
Duration of disease in monthsb | |||
Mean (SD) | ████ ██ | ████ ██ | ████ ██ |
Median (range) | ████ ██ | ████ ██ | ████ ██ |
Disease stage at study entry, n (%) | |||
Recurrent locally advanced | ████ ██ | ████ ██ | ████ ██ |
Metastatic | ████ ██ | ████ ██ | ████ ██ |
Unknown | ████ ██ | ████ ██ | ████ ██ |
Prior endocrine therapy ([neo]adjuvant), n (%) | |||
Prior AI therapy | 85 (25.9) | 50 (30.3) | 135 (27.4) |
Other prior endocrine therapy | 65 (19.8) | 30 (18.2) | 95 (19.3) |
No prior endocrine therapy | 178 (54.3) | 85 (51.5) | 263 (53.3) |
ECOG PS = Eastern Cooperative Oncology Group Performance Status; NSAI = nonsteroidal aromatase inhibitor; SD = standard deviation.
aFrom original source.
bDuration of disease is the time in months from the date of initial diagnosis to the date of randomization.
Source: MONARCH 3 Clinical Study Report39 Data cut-off Date: January 31, 2017.
Table 10: Summary of Reported Prior Therapy in the MONARCH 3 Study (ITT Population)
Therapy | Abemaciclib + NSAI (N = 328) | Placebo + NSAI (N = 165) | Total (N = 493) |
|---|---|---|---|
Prior anticancer therapy, n (%) | |||
Surgical procedure | ████ ██ | ████ ██ | ████ ██ |
Systemic therapy | ████ ██ | ████ ██ | ████ ██ |
Radiotherapy | ████ ██ | ████ ██ | ████ ██ |
Systemic therapy: reason and type, n (%) | |||
Neoadjuvant and/or adjuvanta | ████ ██ | ████ ██ | ████ ██ |
Chemotherapy | 125 (38.1) | 66 (40.0) | 191 (38.7) |
Endocrine | ████ ██ | ████ ██ | ████ ██ |
Other | ████ ██ | ████ ██ | ████ ██ |
Targeted | ████ ██ | ████ ██ | ████ ██ |
Neoadjuvant | ████ ██ | ████ ██ | ████ ██ |
Chemotherapy | ████ ██ | ████ ██ | ████ ██ |
Endocrine | ████ ██ | ████ ██ | ████ ██ |
Other | ████ ██ | ████ ██ | ████ ██ |
Targeted | ████ ██ | ████ ██ | ████ ██ |
Adjuvant | ████ ██ | ████ ██ | ████ ██ |
Chemotherapy | ████ ██ | ████ ██ | ████ ██ |
Endocrine | ████ ██ | ████ ██ | ████ ██ |
Other | ████ ██ | ████ ██ | ████ ██ |
Targeted | ████ ██ | ████ ██ | ████ ██ |
ITT = intention to treat; NSAI = nonsteroidal aromatase inhibitor.
aPatients may have received treatment in more than 1 setting.
Source: MONARCH 3 Clinical Study Report39 Data cut-off date: January 31, 2017.
Exposure to Study Treatments
As of the data cut-off date of September 29, 2023, the median treatment duration was longer in the abemaciclib plus NSAI group compared to the placebo plus NSAI group (66.57 months versus 60.29 months). The median number of cycles received per patient in the abemaciclib plus NSAI group was also higher than that of the placebo plus NSAI group.
Table 11: Summary of Patient Exposure in the MONARCH 3 Study (Data Cut-Off: September 29, 2023)
Exposure | Abemaciclib + NSAI (N = 327) | Placebo + NSAI (N = 161) |
|---|---|---|
Number of patients who received abemaciclib or placebo, n (%)a | ████ ██ | ████ ██ |
Cycles received per patientb | ||
Median (range) | ████ ██ | ████ ██ |
Mean (SD) | ████ ██ | ████ ██ |
Duration of therapy (weeks) | ||
Median (range) | ████ ██ | ████ ██ |
Mean (SD) | ████ ██ | ████ ██ |
NSAI = nonsteroidal aromatase inhibitor; SD = standard deviation.
aNumber of patients who received at least 1 dose of the study drug abemaciclib or placebo either partially or completely.
bPatient is considered to have received a treatment cycle after receiving at least 1 dose of the study drug.
Source: MONARCH 3 Clinical Study Report39 Data cut-off date: September 29, 2023.
As of the final OS analysis | ███ ███████ patients receiving abemaciclib in the abemaciclib plus NSAI group had at least 1 dose adjustment (██ ██████ and ███ ███████ in patients receiving anastrozole or letrozole, respectively) compared to ██ ███████ in the patients receiving placebo (| ██████ and ██ ███████ in patients receiving anastrozole or letrozole, respectively). The most common reason for dose reductions were AEs (███ ███████ versus ██ ██████), mostly due to ███████████ ███ ████████.
Concomitant Medications
A total of 323 patients (98.8%) in the abemaciclib plus NSAI group and 152 patients (94.4%) in the abemaciclib plus placebo arm received at least 1 concomitant medication (Table 12). Concomitant medications that were reported for more than ███ of patients in either arm included:
loperamide (█████ in the abemaciclib plus NSAI group and █████ in the placebo plus NSAI group)
paracetamol (█████ in the abemaciclib plus NSAI group and █████ in the placebo plus NSAI group)
denosumab (█████ in the abemaciclib plus NSAI group and █████ in the placebo plus NSAI group).
The use of bone-modifying drugs was balanced between the arms, with the most common bone-modifying drugs being denosumab and zoledronic acid.
Table 12: Summary of Concomitant Medication in the MONARCH 3 Study (Data Cut-Off: September 29, 2023)
Preferred term | Abemaciclib + NSAI (N = 327) n (%) | Placebo + NSAI (N = 161) n (%) | Total (N = 488) n (%) |
|---|---|---|---|
Patients with ≥ 1 medication | ████ ██ | ████ ██ | ████ ██ |
Loperamide | ████ ██ | ████ ██ | ████ ██ |
Paracetamol | ████ ██ | ████ ██ | ████ ██ |
Denosumab | ████ ██ | ████ ██ | ████ ██ |
Zoledronic acid | ████ ██ | ████ ██ | ████ ██ |
Metoclopramide | ████ ██ | ████ ██ | ████ ██ |
Amoxicillin | ████ ██ | ████ ██ | ████ ██ |
Amoxicillin-clavulanic acid | ████ ██ | ████ ██ | ████ ██ |
Acetylsalicylic acid | ████ ██ | ████ ██ | ████ ██ |
Calcium carbonate-colecalciferol | ████ ██ | ████ ██ | ████ ██ |
Pantoprazole | ████ ██ | ████ ██ | ████ ██ |
Amlodipine | ████ ██ | ████ ██ | ████ ██ |
Omeprazole | ████ ██ | ████ ██ | ████ ██ |
Ibuprofen | ████ ██ | ████ ██ | ████ ██ |
Levothyroxine | ████ ██ | ████ ██ | ████ ██ |
Tramadol | ████ ██ | ████ ██ | ████ ██ |
Dexamethasone | ████ ██ | ████ ██ | ████ ██ |
Ondansetron | ████ ██ | ████ ██ | ████ ██ |
Sodium chloride | ████ ██ | ████ ██ | ████ ██ |
Levofloxacin | ████ ██ | ████ ██ | ████ ██ |
Atorvastatin | ████ ██ | ████ ██ | ████ ██ |
Oxycodone | ████ ██ | ████ ██ | ████ ██ |
NSAI = nonsteroidal aromatase inhibitor.
Source: MONARCH 3 Clinical Study Report39 Data cut-off date: September 29, 2023.
Subsequent Treatment
After study treatment discontinuation in the MONARCH 3 study, patients were allowed to start new anticancer treatment. A total of 234 patients in the abemaciclib plus NSAI group and 142 patients in the placebo plus NSAI group received a new systemic anticancer treatment after discontinuing study treatment. A summary of postdiscontinuation therapies as of September 29, 2023, is provided in Table 13.
Table 13: Postdiscontinuation Therapy in the MONARCH 3 Study (Data Cut-Off: September 29, 2023)
Therapy | Abemaciclib + NSAI (N = 328) n (%) | Placebo + NSAI (N = 165) n (%) |
|---|---|---|
Surgical procedure | ████ ██ | ████ ██ |
Radiotherapy | ████ ██ | ████ ██ |
Systemic therapy | ||
Overall (any subsequent line) | 234 (71.3) | 142 (86.1) |
Endocrine | 196 (59.8) | 121 (73.3) |
Chemotherapy | 136 (41.5) | 102 (61.8) |
Targeted therapy | 94 (28.7) | 80 (48.5) |
CDK4/6 inhibitora | 38 (11.6) | 52 (31.5) |
Everolimus | ████ ██ | ████ ██ |
Other | ████ ██ | ████ ██ |
Investigational drug | ████ ██ | ████ ██ |
NSAI = nonsteroidal aromatase inhibitor.
aPostdiscontinuation CDK4/6 inhibitor therapy includes abemaciclib, ribociclib, or palbociclib.
Source: MONARCH 3 Clinical Study Report39 Data cut-off date: September 29, 2023.
Efficacy
Results for PFS and OS at both the November 3, 2017, data cut-off (i.e., the time of the final planned PFS analysis) and the September 29, 2023, data cut-off (i.e., the time of the final planned OS analysis) are presented in Table 14 and subsequently summarized. Additional interim data cut-offs for PFS and OS are not included.
Additional outcomes including ORR, CBR, and HRQoL are summarized in Appendix 1. These outcomes remain unchanged since the 2019 review of abemaciclib (Verzenio).
Overall Survival
At the time of the November 3, 2017, data cut-off, a total of ██ ██████ (███████ █████) had occurred in the abemaciclib plus NSAI arm, and ██ ██████ (███████ █████) had occurred in the placebo plus NSAI arm; median OS had not been reached in either treatment group. The hazard ratio was 1.057 (95% CI, 0.683 to 1.633), and the 2-sided stratified log-rank test P value was 0.8017.
As of the final OS analysis (data cut-off: September 29, 2023), the median duration of follow-up was █████ and █████ months in the abemaciclib plus NSAI arm and the placebo plus NSAI arm, respectively. More than 80% of patients were followed up for at least 90 months, and 314 OS events (deaths) were observed in the ITT population. In the abemaciclib plus NSAI arm, 198 patients (60.4%) experienced OS events and ███ ████████ (█████) were censored, whereas in the placebo plus NSAI arm, 116 patients (70.3%) experienced OS events and ██ ████████ (█████) were censored. The hazard ratio for OS was 0.804 (95% CI, 0.637 to 1.015; 2-sided stratified log-rank P value = 0.0664). Based on the O’Brien-Fleming boundary, the 2-sided P value boundary for OS was 0.034. Median OS was 66.81 months (95% CI, █████ ██ █████) in the abemaciclib arm and 53.72 months (95% CI, █████ ██ █████) in the placebo arm, representing an absolute difference of 13.09 months (95% CI not reported). In the KM plot of OS, sustained separation favouring the abemaciclib plus NSAI group became apparent at approximately 35 months (Figure 1). The OS probabilities at 5 years and 6 years was 54.5% (95% CI, ████ ██ ████) and 45.7% (95% CI, ████ ██ ████), respectively, in the abemaciclib plus NSAI arm, and 42.1% (95% CI, ████ ██ ████) and 35.2% (95% CI, ████ ██ ████), respectively, in the placebo plus NSAI arm.
Results in the subgroup of patients with visceral disease were similar for OS, with a hazard ratio of 0.758 (95% CI, 0.558 to 1.030; 2-sided unstratified log-rank P value = 0.0757).
Figure 1: Kaplan-Meier Plot of Overall Survival in the MONARCH 3 Study (ITT) (Data Cut-Off: September 29, 2023)
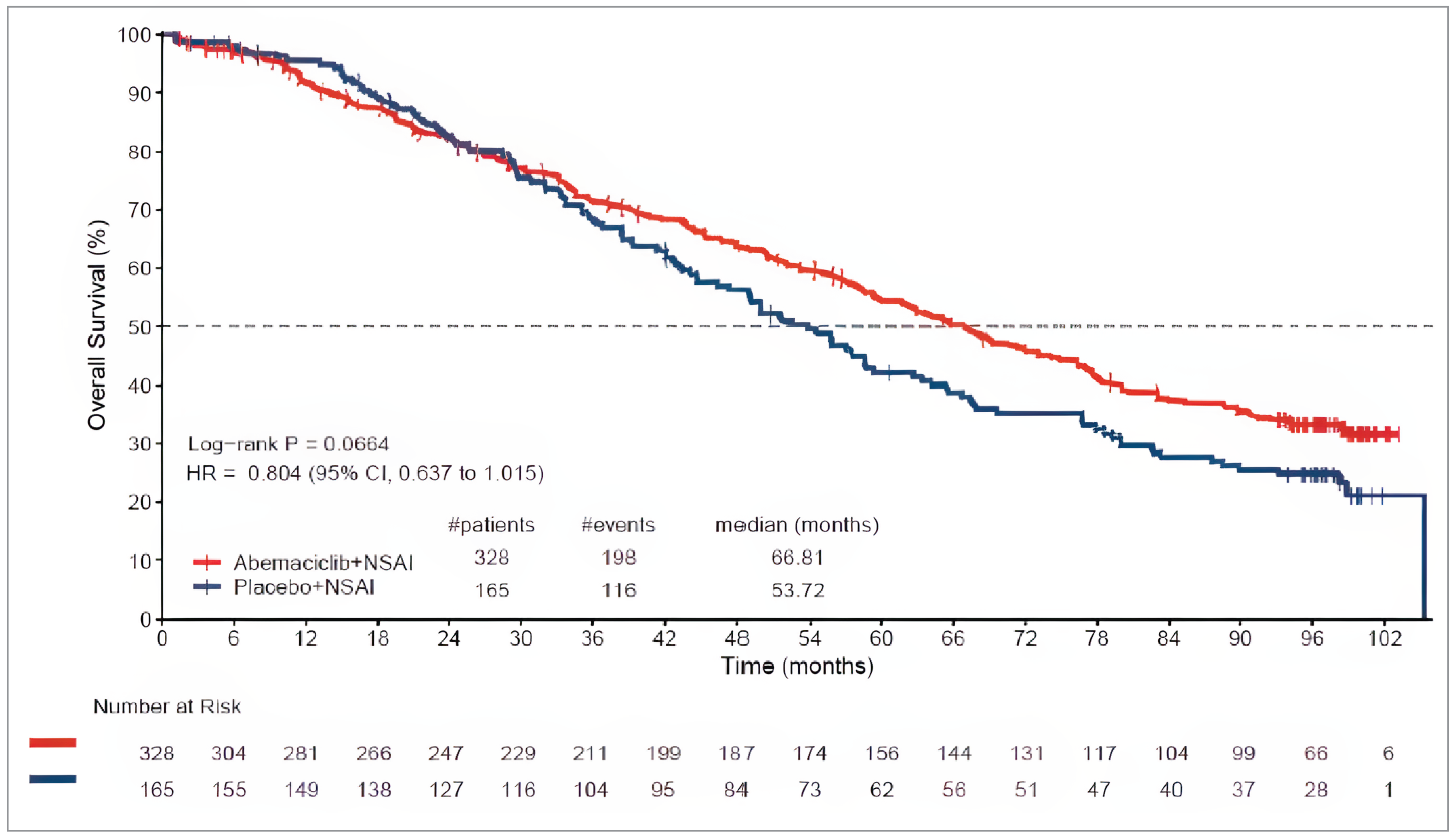
CI = confidence interval; HR = hazard ratio; ITT = intention to treat; NSAI = nonsteroidal aromatase inhibitor.
Source: MONARCH 3 Clinical Study Report39 (data cut-off date: September 3, 2023).
Progression-Free Survival
At the time of the final PFS analysis (November 3, 2017, data cut-off), a total of 246 patients experienced PFS events (i.e., PD or death), including 138 patients (42.1%) in the abemaciclib plus NSAI group and 108 patients (65.5%) in the placebo plus NSAI group. Median PFS was 28.18 months (95% CI, 23.51 months to not reached) in the abemaciclib plus NSAI group and 14.76 months (95% CI, 11.24 months to 19.20 months) in the placebo plus NSAI group, with a hazard ratio of 0.540 (95% CI, 0.418 to 0.698; 2-sided P = 0.000002).
Updated PFS data were provided for the September 29, 2023, data cut-off, which marked the time of the final planned OS analysis. At this data cut-off, 350 patients had experienced PFS events (i.e., PD or death), including 213 (64.9%) in the abemaciclib plus NSAI group and 137 (83.0%) in the placebo plus NSAI group. Median PFS was 29.03 months (95% CI, █████ ██ █████) in the abemaciclib plus NSAI arm and 14.76 months (95% CI, 11.24 months to 19.20 months) in the placebo plus NSAI arm (hazard ratio = 0.535; 95% CI, 0.429 to 0.668). These results indicated a 14.27-month increase in the median PFS (95% CI not reported) for patients treated with abemaciclib plus an NSAI. In the KM plot of PFS, early and sustained separation by treatment arm was apparent beginning at approximately 2 months (Figure 2).
Figure 2: Kaplan-Meier Plot of Progression-Free Survival in MONARCH 3 (ITT) (Data Cut-Off: September 29, 2023)
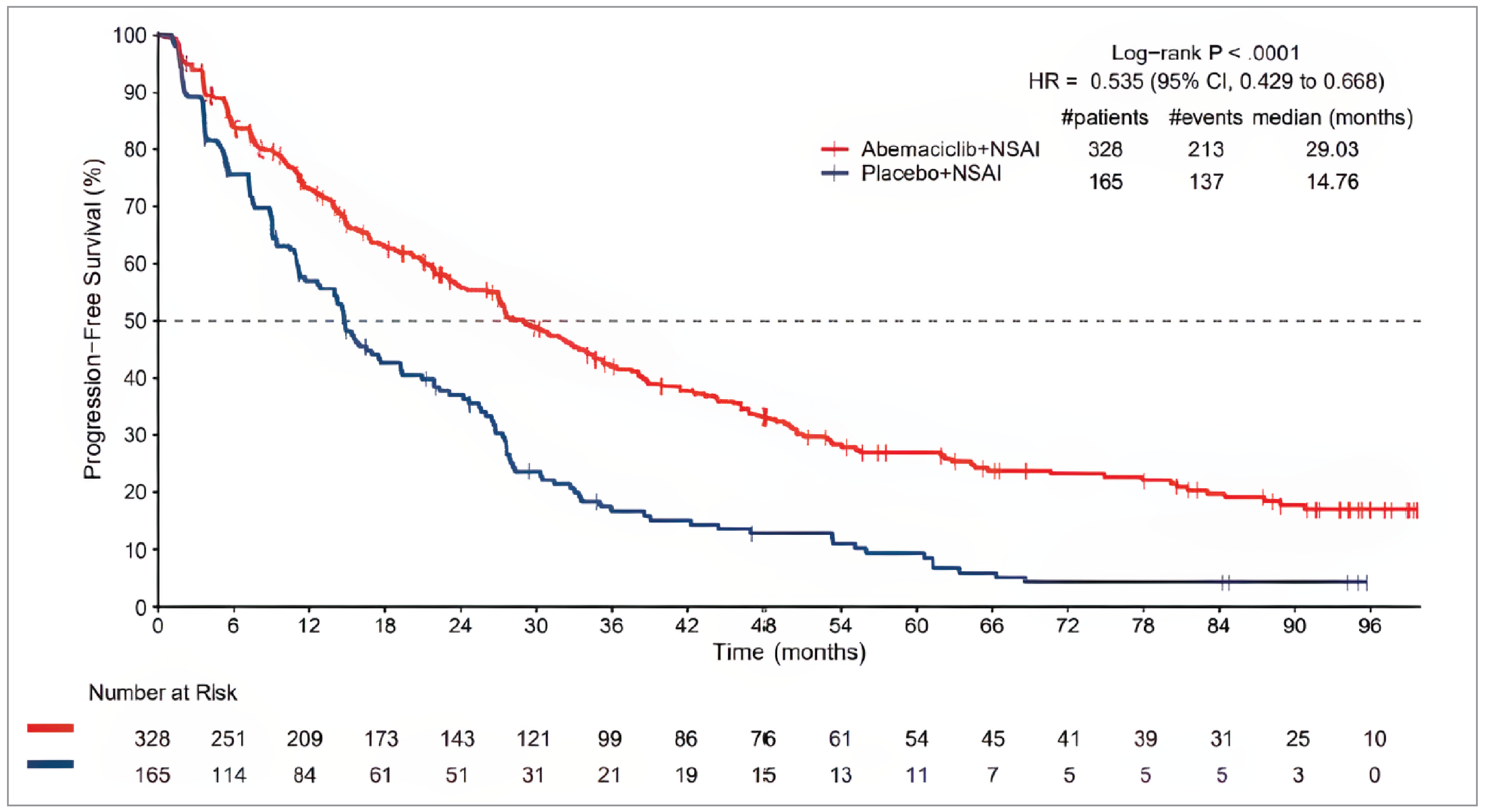
CI = confidence interval; HR = hazard ratio; ITT = intention to treat; NSAI = nonsteroidal aromatase inhibitor.
Source: MONARCH 3 Clinical Study Report39 (data cut-off date: September 29, 2023).
Table 14: Summary of Outcomes for PFS and OS in the MONARCH 3 Study (ITT)
Results | Planned final PFS analysis (Cut-off date: November 3, 2017) | Final planned final OS analysis (Cut-off date: September 29, 2023) | ||
|---|---|---|---|---|
Abemaciclib + NSAI (N = 328) | Placebo + NSAI (N = 165) | Abemaciclib + NSAI (N = 328) | Placebo + NSAI (N = 165) | |
PFS | ||||
Number of events, n (%) | 138 (42.1) | 108 (65.5) | 213 (64.9) | 137 (83.0) |
Death without PD, n (%) | ████ ██ | ████ ██ | ████ ██ | ████ ██ |
PD, n (%) | ████ ██ | ████ ██ | ████ ██ | ████ ██ |
Number of patients censored, n (%) | ████ ██ | ████ ██ | ████ ██ | ████ ██ |
Death or PD after ≥ 2 missed tumour assessments, n (%) | ████ ██ | ████ ██ | ████ ██ | ████ ██ |
No baseline tumour assessment, n (%)b | ████ ██ | ████ ██ | ████ ██ | ████ ██ |
No postbaseline tumour assessment, n (%) | ████ ██ | ████ ██ | ████ ██ | ████ ██ |
No documented PD with regular assessment, n (%) | ████ ██ | ████ ██ | ████ ██ | ████ ██ |
Median PFS (95% CI), months | 28.18 (23.51 to not reached) | 14.76 (11.24 to 19.20) | 29.03 (23.97 to 34.06) | 14.76 (11.24 to 19.20) |
Difference in median PFS, months | NR | 14.27 | ||
Hazard ratio (95% CI) stratifieda | 0.540 (0.418 to 0.698)c | 0.535 (0.429 to 0.668) | ||
P value (2-sided) log-rank stratifieda | 0.000002c | < 0.0001 | ||
OS | ||||
Number of deaths, n (%) | 63 (19.2) | 30 (18.2) | 198 (60.4) | 116 (70.3) |
Number of patients censored, n (%) | ████ ██ | ████ ██ | ████ ██ | ████ ██ |
Alive, n (%) | ████ ██ | ████ ██ | ████ ██ | ████ ██ |
Lost to follow-up, n (%) | ████ ██ | ████ ██ | ████ ██ | ████ ██ |
Withdrawal by patient, n (%) | ████ ██ | ████ ██ | ████ ██ | ████ ██ |
Median OS (95% CI) months | Not reached | Not reached | 66.81 (59.21 to 74.83) | 53.72 (44.75 to 59.34) |
Difference in Median OS, months | NR | NR | 13.09 | |
Hazard ratio (95% CI) stratifieda | 1.057 (0.683 to 1.633) | 0.804 (0.637 to 1.015) | ||
P value (2-sided) log-rank stratifieda | 0.8017 | 0.0664 | ||
Proportion of patients who were alive, % (95% CI)d | ||||
At 12 months | ████ ██ | ████ ██ | ████ ██ | ████ ██ |
Difference at 12 months | ████ ██ | ████ ██ | ||
At 24 months | ████ ██ | ████ ██ | ████ ██ | ████ ██ |
Difference at 24 months | ████ ██ | ████ ██ | ||
At 36 months | ████ ██ | ████ ██ | ████ ██ | ████ ██ |
Difference at 36 months | ████ ██ | ████ ██ | ||
At 48 months | ████ ██ | ████ ██ | ████ ██ | ████ ██ |
Difference at 48 months | ████ ██ | ████ ██ | ||
At 60 months | ████ ██ | ████ ██ | ████ ██ | ████ ██ |
Difference at 60 months | ████ ██ | ████ ██ | ||
At 72 months | ████ ██ | ████ ██ | ████ ██ | ████ ██ |
Difference at 72 months | ████ ██ | ████ ██ | ||
CI = confidence interval; ITT = intention to treat; IWRS = interactive web recognition system; NR = not reported; NSAI = nonsteroidal aromatase inhibitor; OS = overall survival; PD = progressive disease; PFS = progression-free survival.
aStratified by IWRS endocrine therapy and IWRS nature of disease.
bBetween January 31, 2017, and November 3, 2017, the baseline assessment date for 1 patient was updated; therefore, the number of patients in the abemaciclib plus NSAI group with no baseline tumour assessment decreased from 2 patients (as presented in earlier data cut-offs of the MONARCH 3 Clinical Study Report) to 1 patient (in the updated September 29, 2023, data cut-off).
cThe 95% CIs and 2-sided P values for the difference between rates were calculated based on normal approximation.
dThe 95% CIs and 2-sided P values for the difference between rates were calculated based on normal approximation.
Source: MONARCH 3 Clinical Study Report39 (data cut-off dates: November 3, 2017, and September 29, 2023).
Harms
Refer to Table 15 for harms data. Data in this section were from the most recent data cut-off (i.e., September 29, 2023).
Adverse Events
Compared to placebo, a higher percentage of patients receiving abemaciclib experienced any TEAE (98.8% versus 94.4%), or grade 3 or higher TEAEs (69.4% versus 28.6%). The most frequently reported TEAE was diarrhea (83.5% versus 34.2%). Other AEs with a between-group difference of 20% included neutropenia (46.8% versus 1.9%), anemia (35.2% versus 9.9%), increased blood creatinine (25.1% versus 4.3%), and leukopenia (24.5% versus 3.1%). The most common grade 3 or higher TEAEs were neutropenia (27.5% versus 1.2%) and leukopenia (10.7% versus 0.6%).
Serious Adverse Events
The incidence of SAEs was higher in the abemaciclib plus NSAI arm compared with the placebo plus NSAI arm (█████ ███ █████). The most common causes of SAEs in the abemaciclib plus NSAI arm by system organ class were infections and infestations (█████), followed by ████████████████ █████████ ███████ The most common SAEs (at least 2%) regardless of causality in the abemaciclib plus NSAI arm by preferred term were █████████ ██████ ███ ████████ ██████. In the placebo plus NSAI arm, no SAEs occurred in more than 2% of patients. The most common SAEs were ███████ ████████████████ █████████ █████████ █████ ████████████ ███ █████ ████████ ████████ █████ █████.
Withdrawals Due to AEs
In the abemaciclib plus NSAI arm versus placebo plus NSAI arm, ██ ███████ ███ █ ██████ patients discontinued all study treatments due to AEs, respectively. The most common reason for stopping treatment due to AEs in the abemaciclib plus NSAI group was increased ███████ ████████████████ █████ ███ ██████. All other withdrawals due to AEs were at a frequency less than 2%.
Mortality
In total, 198 patients (60.4%) died in the abemaciclib plus NSAI arm, and 116 patients (70.3%) died in the placebo plus NSAI arm. Deaths due to AEs on study therapy or within 30 days of treatment discontinuation were reported in ██ ████████ ██████ ██ ███ ███████████ ████ ████ ███ ███ █ ████████ ██████ in the placebo plus NSAI arm. A total of ███ patients died after 30 days of treatment discontinuation. AEs were the cause of death in ████████ ██████ in the abemaciclib plus NSAI arm.
Table 15: Summary of Harms Results From the MONARCH 3 Study
AEs | Abemaciclib + NSAI N = 327 | Placebo + NSAI N = 161 | ||
|---|---|---|---|---|
Any grade n (%) | Grade ≥ 3 n (%) | Any grade n (%) | Grade ≥ 3 n (%) | |
Most common AEs (≥ 20% of population in either group), n (%) | ||||
Patients with ≥ 1 TEAE | ███ | ███ | ███ | ███ |
Diarrhea | 273 (83.5) | 32 (9.8) | 55 (34.2) | 2 (1.2) |
Neutropenia | ███ | 90 (27.5) | ███ | ███ |
Fatigue | ███ | ███ | ███ | ███ |
Nausea | ███ | ███ | ███ | ███ |
Anemia | ███ | 31 (9.5) | ███ | ███ |
Abdominal pain | ███ | ███ | ███ | ███ |
Vomiting | ███ | ███ | ███ | ███ |
Decreased appetite | ███ | ███ | ███ | ███ |
Alopecia | ███ | ███ | ███ | ███ |
Blood creatinine increased | ███ | ███ | ███ | ███ |
Leukopenia | ███ | 35 (10.7) | ███ | ███ |
Arthralgia | ███ | ███ | ███ | ███ |
Headache | ███ | ███ | ███ | ███ |
Hepatic events | ███ | ███ | ███ | ███ |
ALT increased | ███ | ███ | ███ | ███ |
AST increased | ███ | ███ | ███ | ███ |
Constipation | ███ | ███ | ███ | ███ |
Infections and infestations | ███ | ███ | ███ | ███ |
SAEs, n (%) | ||||
Patients with ≥ 1 SAE | ███ | ███ | ||
Pneumonia | ███ | ███ | ||
Urinary tract infection | ███ | ███ | ||
Sepsis | ███ | ███ | ||
Gastroenteritis | ███ | ███ | ||
Diarrhea | ███ | ███ | ||
Vomiting | ███ | ███ | ||
Abdominal pain | ███ | ███ | ||
Pneumonitis | ███ | ███ | ||
Embolism | ███ | ███ | ||
Osteonecrosis of jaw | ███ | ███ | ||
Dehydration | ███ | ███ | ||
Acute coronary syndrome | ███ | ███ | ||
Anemia | ███ | ███ | ||
Cerebrovascular accident | ███ | ███ | ||
Acute kidney injury | ███ | ███ | ||
Patients who stopped treatment due to AEs, n (%) | ||||
Patients who stopped all study drugs due to an AE | ███ | ███ | ||
Alanine aminotransferase increased | ███ | ███ | ||
Pneumonia | ███ | ███ | ||
Neutropenia | ███ | ███ | ||
Diarrhea | ███ | ███ | ||
Embolism | ███ | ███ | ||
Deaths, n (%) | ||||
All deaths | ███ | ███ | ||
Patients who died on therapy or within 30 days of treatment discontinuation | ███ | ███ | ||
Due to study disease | ███ | ███ | ||
Due to an AE | ███ | ███ | ||
Pneumonia | ███ | ███ | ||
Cerebral ischemia | ███ | ███ | ||
Embolism | ███ | ███ | ||
Respiratory failure | ███ | ███ | ||
Pneumonitis | ███ | ███ | ||
Cerebrovascular accident | ███ | ███ | ||
General physical health deterioration | ███ | ███ | ||
Sudden death | ███ | ███ | ||
Deaths after 30 days of treatment discontinuation | ███ | ███ | ||
Due to study disease | ███ | ███ | ||
Due to AE | ███ | ███ | ||
Aspiration | ███ | ███ | ||
Embolism | ███ | ███ | ||
Intracranial aneurysm | ███ | ███ | ||
Sudden death | ███ | ███ | ||
Unknown AEa | ███ | ███ | ||
Deathb | ███ | ███ | ||
AE = adverse event; ALT = alanine aminotransferase; AST = aspartate aminotransferase; NSAI = nonsteroidal aromatase inhibitor; SAE = serious adverse event; TEAE = treatment-emergent adverse event.
aOne patient in each treatment arm discontinued from the study due to an AE; however, the AE was not entered into the database and is reported as unknown.
bThis entry is reproduced as reported in the Clinical Study Report. The meaning and why this is separate from other death-related data are unclear.
Source: Details included in the table are from the sponsor’s Summary of Clinical Evidence38 and the MONARCH 3 Clinical Study Report39 (data cut-off date: September 29, 2023).
Notable Harms
Prespecified AEs of special interest included neutropenia (46.8% in the abemaciclib group and 1.9% in the placebo group), ██████████ ██████ ███ ███████ diarrhea (83.5% and 34.2%), alanine transaminase increase (22.0% and 8.1%), venous thromboembolisms (7.6% and 1.2%), and interstitial lung disease or pneumonitis (7.0% and 0.6%). The incidence of each of these events was higher in the abemaciclib plus NSAI group compared to the placebo plus NSAI group.
Critical Appraisal
Internal Validity
The MONARCH 3 trial has previously been reviewed and appraised by CDA-AMC, and many of the critical appraisal points still apply. This reassessment focuses on the outcomes of PFS, OS, and AEs, which include updated results as part of the most recent data cut-off (September 29, 2023), representing an additional 5 years and 10 months of follow-up. Outcomes including ORR, duration of response, disease control rate, CBR, and HRQoL were not updated, and therefore not included in this report.
Briefly, critical appraisal points at the time of the initial review were the MONARCH 3 study was a phase III, double blind, placebo-controlled RCT that evaluated abemaciclib plus an NSAI versus placebo plus an NSAI as a first-line therapy in adult patients who were postmenopausal with HR-positive, HER2-negative advanced or metastatic breast cancer. Choice of an NSAI therapy (letrozole or anastrozole) was determined by the treating physician in each case. Outcomes evaluated in the MONARCH 3 study were considered to be standard and appropriate in the evaluation of treatments for this disease population.
Randomization, allocation, allocation concealment, and blinding methods were conducted to reduce the risk of systematic bias in the selection and assignment of patients, and in the interpretation of observed treatment effects (benefits and harms). Patients were stratified by the nature of disease (visceral metastases versus bone-only metastases versus other), and prior (neo)adjuvant endocrine therapy (AI therapy versus other versus no prior endocrine therapy). Blinded independent central review was used for assessment of radiological scans to reduce detection bias. The study adjusted for multiplicity for the analysis of the key secondary outcome of OS but lacked a testing procedure for other secondary end points. A sensitivity analysis was performed to support the estimates of PFS efficacy using a full, blinded independent central review, and there were no reported inconsistencies with the primary analysis. The conduct of the trial and choice of stratification factors were considered appropriate based on clinical expert input. At baseline, demographic, disease characteristics, and prior treatments in the ITT population were balanced across study arms.
In the updated efficacy analysis (data cut-off: September 29, 2023), the median duration of follow-up was just over 8 years in either treatment arm (█████ ██████ ███ █████ ██████). A slightly greater proportion of patients assigned to abemaciclib plus NSAI ████ remained on-study compared to patients in the placebo plus NSAI arm ████. Discontinuation of treatment was most commonly due to PD in both treatment groups (█████ versus █████), but there was a higher incidence of discontinuation due to AEs in the group receiving abemaciclib (█████ versus ████). There was generally a higher rate of overall AEs and SAEs observed in the abemaciclib group compared to the placebo group, notably the case with diarrhea (83.5% versus █████) and neutropenia (█████ versus ████), which are AEs of special interest for abemaciclib. Risk of unblinding may have been elevated in the abemaciclib group due to the unbalanced nature and prevalence of AEs across study groups.
Although the hazard ratio at the final OS analysis (hazard ratio = 0.804; 95% CI, 0.637 to 1.015) was improved compared to the primary analysis (hazard ratio = 1.057; 95% CI, 0.683 to 1.633), and the estimated benefit in OS was an absolute difference in median OS of 13.09 months (95% CI of absolute difference not reported), the results were not statistically significant as the 95% CI of the hazard ratio crossed null, which contributes to uncertainty in the true presence or magnitude of benefit associated with abemaciclib. In the KM curve for OS, survival was marginally higher in the placebo group at first, but the survival curves crossed and progressively separated at approximately 29 to 30 months, whereafter the curve showed a benefit of abemaciclib on survival compared to placebo. The median OS at final analysis was 63.72 months in the abemaciclib group and 48.82 months in the placebo group. In consultation with clinical experts, the reported difference in median OS was considered clinically important despite not being statistically significant.
The updated results for PFS from the September 29, 2023, data cut-off (hazard ratio = 0.535; 95% CI, 0.429 to 0.668) were consistent with the results of the previously reported final preplanned analysis of PFS from the November 3, 2017, data cut-off (hazard ratio = 0.540; 95% CI, 0.418 to 0.698), and these results were considered by the experts to be clinically meaningful. Similarly, the updated safety data such as AEs were consistent with those previously reported and assessed in the initial review of abemaciclib by CDA-AMC. While the AEs associated with abemaciclib are not insignificant, they are considered by the clinical experts to be manageable in the context of treating patients with advanced or metastatic breast cancer.
External Validity
According to clinical experts consulted for this review, the treatment setting, demographics, disease characteristics, and treatment history of patients who were recruited were considered reflective of clinical practice in Canada. Patients enrolled in the MONARCH 3 study were required to have an ECOG PS score of 0 to 1, and therefore there is no evidence on the comparative effectiveness and potential harms of abemaciclib in patients with an ECOG PS score of 2 or greater. However, the clinical experts noted that there is a potential for patients with ECOG PS scores of 2 to receive treatment at the discretion of treating clinicians, which is consistent with clinical practice. There were no major generalizability concerns interpreting the efficacy results of the MONARCH 3 study to the setting in Canada.
Long-Term Extension Studies
No long-term extension studies were included.
Indirect Evidence
Contents within this section have been informed by materials submitted by the sponsor. The following have been summarized and validated by the review team.
Objectives for the Summary of Indirect Evidence
To address a gap in the comparative effectiveness of abemaciclib plus AI compared to available therapies used in clinical practice, an indirect comparison was conducted. In this reassessment, updated NMAs were provided, focusing on the updated results for OS and PFS from the MONARCH 3 trial. Additionally, a new NMA was provided pertaining to safety outcomes (specifically, grade 3 or 4 AEs). For the purpose of this reassessment, the NMA results for OS, PFS, and AEs are presented herein. Data from the MONARCH 3 study in these networks are from the updated data cut-off (September 29, 2023) as well as updated comparator data from an updated SLR conducted by the sponsor to facilitate this reassessment. Other outcomes presented in the updated report (ORR, CBR, and CR) can be found in Appendix 2; these same outcomes were assessed in the initial review of abemaciclib, but the results presented in Appendix 2 reflect the updated NMAs that incorporate (if applicable) new comparator data from the updated SLR. To our knowledge, the MONARCH 3 study data for these other outcomes were not updated as the final analyses were already conducted at the time of the initial review.
Description of Indirect Comparison
The sponsor submitted NMAs to compare abemaciclib with other CDK4/6 inhibitors and other treatments commonly used in the treatment of females who are postmenopausal without prior systemic treatment for advanced disease with HR-positive, HER2-negative advanced or metastatic breast cancer.
Table 16: Study Selection Criteria and Methods for NMA
Characteristics | Indirect comparison |
|---|---|
Population |
Limited previous treatment for locoregionally recurrent or metastatic disease. Exclude studies where:
Greater than 10% of the whole study population are currently receiving or have previously received chemotherapy for locoregionally recurrent or MBC. (Note: Patients may be enrolled if they received prior (neo)adjuvant chemotherapy for localized disease). |
Intervention | For inclusion, studies must compare to at least 1 listed treatment or PBO:
|
Comparator | As per the list previously mentioned in the Intervention section or PBO |
Outcome | Efficacy:
Safety:
HRQoL:
|
Study designs |
|
Publication characteristics | Publication was required |
Exclusion criteria | Exclude the following:
|
Databases searched | OVID database:
Conference search: From February 2020 to current (March 2023) Clinicaltrials.gov and the WHO International Clinical Trials Registry were searched to identify relevant ongoing trials. |
Selection process | The records were screened by 2 independent reviewers in accordance with the eligibility criteria and any disagreements were resolved by a third reviewer. |
Data extraction process | Not reported |
Quality assessment | A quality assessment of included studies was conducted as part of the SLR. The assessment was restricted to RCTs described in peer-reviewed publications. RCTs reported only in conference abstracts were not assessed due to limited reporting. Studies were assessed using the Cochrane ROB tool, version 1 (ROB 1.0). |
ABE = abemaciclib; AE = adverse event; ANAS = anastrozole; CBR = clinical benefit rate; CR = complete response; DALP = dalpiciclib; DCR = disease control rate; DFS = disease-free survival; DOR = duration of response; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; FACT-B = Functional Assessment of Cancer Therapy-Breast; FUL = fulvestrant; HR = hormone receptor; LTZ = letrozole; MBC = metastatic breast cancer; NMA = network meta-analysis; ORR = overall response rate; OS = overall survival; PAL = palbociclib; PBO = placebo; PD = progressive disease; PFS = progression-free survival; RCT = randomized controlled trial; RIBO = ribociclib; ROB = risk of bias; SD = stable disease; SLR = systematic literature review; TMX = Tamoxifen.
aMenopause may be due to any of (but not limited to) natural age-related menopause, surgical menopause, or ovarian suppression methods.
Source: Sponsor-submitted updated indirect treatment comparison report.40
Indirect Treatment Comparison Design
Objectives
The objective of the ITC was to compare abemaciclib with other CDK4/6 inhibitors and other treatments commonly used in the treatment of females who are postmenopausal without prior systemic treatment for advanced disease with HR-positive, HER2-negative advanced or metastatic breast cancer.
Study Selection Methods
The sponsor conducted an SLR and assessed the feasibility of an ITC to produce a connected network, then assessed the heterogeneity in study designs, inclusion and exclusion criteria, patient and disease characteristics, as well as definitions, measurement, and availability of outcomes. Outcomes of interest were defined by the sponsor as: PFS, OS, ORR, CBR, CR, time to chemotherapy, grade 3 and 4 AEs, and mean change from baseline in the index score of the EQ-5D, although, as previously noted, only outcomes of OS, PFS, and harms were included in this report.
ITC Analysis Methods
According to the sponsor summary of methods, the relative efficacy and safety of abemaciclib plus anastrozole or letrozole versus existing treatments was estimated in the overall population using a Bayesian NMA.
For time-to-event outcomes (OS and PFS), hazard ratios were estimated using a Cox model. The PH assumption was evaluated using the Grambsch-Therneau statistical test, visual inspection of the log-cumulative hazard curves, and visual inspection of the Schoenfeld residuals. If there was an indication that the PH assumption was violated for the PFS and OS outcomes, a sensitivity analyses using an FP NMA in the ITT population was conducted.
Table 17: ITC Analysis Methods
Methods | Description |
|---|---|
Analysis methods | Bayesian NMA |
Priors | Vague (flat or uninformative) priors were used for all models, and informative priors were only considered for heterogeneity parameters. |
Assessment of model fit | Alternative model specifications were compared using the DIC. |
Assessment of consistency | Not reported |
Assessment of convergence | The model parameters were estimated using a Markov Chain Monte Carlo method and the Gelman-Rubin statistic was applied to check the convergence. |
Outcomes | PFS, OS, ORR, CBR, CR, and grade 3 and 4 AEsa |
Follow-up time points | Median study follow-up was not reported in 7 studies. In the remaining 22 studies, median follow-up ranged from 7.36 months to 90.1 months. Median OS follow-up was reported in 25 studies and ranged from 12.9 months to 90.1 months. In the MONARCH 3 trial, it was 8.1 years. |
Construction of nodes | All comparators could be integrated into a network with the exception of DALP plus ANAS or LTZ and for PAL plus FUL for OS. No data were available for RIBO plus FUL for ORR, CR, and CBR. Also, MONALEESA-2 and PALOMA-2 used PBO plus LTZ as control treatment, whereas the MONARCH 3 trial used PBO plus ANAS or LTZ. |
Sensitivity analyses | Sensitivity analyses were based on the PH assumption assessment results performed for the survival outcomes in the trials included in the networks. Because there were violations of the PH assumptions, a FP NMA was completed as a sensitivity analysis for OS and PFS. |
Subgroup analysis | For the PFS and the OS outcomes, a subgroup analysis was conducted that included only studies with patients who were HR-positive, and another analysis included only patients with a performance status of 0 or 1. |
AE = adverse event; ANAS = anastrozole; CBR = clinical benefit rate; CR = complete response; DALP = dalpiciclib; DIC = deviance information criterion; FP = fractional polynomial; FUL = fulvestrant; HR: hormone receptor; ITC = indirect treatment comparison; LTZ = letrozole; NMA = network meta-analysis; ORR = overall response rate; OS = overall survival; PAL = palbociclib; PBO = placebo; PFS = progression-free survival; PH = proportional hazards; RIBO = ribociclib; SLR = systematic literature review.
aFor the purpose of this reassessment, only PFS, OS, and grade 3 and 4 AEs are described in detail in this report. Additional information about ORR, CBR, and CR can be found in the appendices. For PFS, OS, and AEs, data from the MONARCH 3 study reflects the updated data cut-off of September 29, 2023. For all outcomes, the comparator data are from an updated SLR conducted by the sponsor to facilitate this reassessment, so the comparator data may differ from that in the initial submission.
Source: Sponsor-submitted updated indirect treatment comparison report.40
Results
Summary of Included Studies
Study Design and Patient Eligibility Criteria
For the analysis of each specific outcome, a different network was used due to differences in outcome reporting across studies. A summary of the studies included in the networks for OS, PFS, and/or grade 3 and 4 AEs is presented in Table 18, and outcome-specific network diagrams for each NMA are presented in Appendix 2. Comparator arms in the studies that included letrozole, anastrozole, or allowed physician choice between letrozole and anastrozole (with or without placebo) were considered equivalent for the sake of the NMAs and were pooled into 1 anastrozole or letrozole or NSAI node to function as the central anchoring node for the networks.
Across the included studies, there were differences in the study design and eligibility criteria. Specifically, differences in ECOG PS (e.g., less than or equal to 1 versus 0 to 2), different requirements for the breast cancer stage, differences in HR or HER2 status reporting, and different requirements for the number of prior lines of chemotherapy and/or endocrine therapy. The studies were also heterogenous in the reporting for the presence of central nervous system metastases, and the presence of visceral crisis, lymphangitic spread, or leptomeningeal carcinomatosis (only the MONARCH 3 study explicitly excluded all 3). The study locations varied and some studies such as PALOMA-4 only included patients of Asian ethnicity.
Table 18: Summary of Studies Included in the Networks for OS, PFS, and/or Grade 3 and 4 AEs
Trial name | Study design | Brief summary of eligibility criteria | Treatment groupsa | Included in networks |
|---|---|---|---|---|
DAWNA-241 | RCT 2:1, phase III, double blind, multicentre, N = 458 | Females aged 18 to 75 years, any menopausal status, HR-positive HER2-negative, locally recurrent advanced breast cancer or metastatic breast cancer, ECOG PS score ≤ 1, no prior systemic therapy in advanced setting, no prior treatment with CDK4/6 | Dalpiciclib + letrozole or anastrozole Placebo + letrozole or anastrozole | PFS Grade 3 and 4 AEs |
FALCON42 | RCT 1:1, phase III, double blind, multicentre, N = 462 | Adult females who are postmenopausal, HR-positive locally advanced breast cancer or metastatic breast cancer, ET-naive, WHO performance status 0 to 2, at least 1 measurable or unmeasurable lesion, no hormonal therapy | Fulvestrant Anastrozole | PFS Grade 3 and 4 AEs |
FIRST43 | RCT 1:1, phase III, open label, multicentre, N = 205 | Females who are postmenopausal, HR-positive locally advanced breast cancer or metastatic breast cancer not amenable to curative therapy, WHO performance status 0 to 2, measurable disease per modified RECIST criteria or at least 1 bone lesion with a lytic component, no prior ET in advanced setting | Fulvestrant Anastrozole | OS |
FLIPPER44 | RCT 1:1, phase II, double blind, multicentre, N = 189 | Adult females who are postmenopausal, HR-positive HER2-negative locoregional or distant metastatic breast cancer not amenable to curative therapy, at least 5 years of ET in the adjuvant setting and remained disease-free for > 12 months or de novo metastatic disease, at least 1 measurable and/or unmeasurable lesion, no prior systemic therapy in metastatic setting, no prior treatment with fulvestrant | Palbociclib + fulvestrant Placebo + fulvestrant | PFS |
Howell et al.45 | RCT 1:1, phase NR, double blind, multicentre, N = 587 | Females who are postmenopausal, at least 1 measurable lesion, or 1 unmeasurable lesion evaluable by UICC criteria, WHO performance status ≤ 2, no prior treatment with ET for breast cancer or prior fulvestrant | Fulvestrant Tamoxifen | PFS OS |
Iwata et al.46 | RCT 1:1, phase III, double blind, multicentre, N = 298 | Adult females who are postmenopausal, HR-positive progressive or locally recurrent advanced breast cancer or metastatic breast cancer, inoperable (prior ET in the adjuvant setting was permitted), ECOG PS score 0 to 1 | Exemestane Anastrozole | OS Grade 3 and 4 AEs |
Milla-Santos et al.47 | RCT 1:1, phase III, blinding NR, single-centre, N = 238 | Adult females who are postmenopausal, HR-positive advanced breast cancer (prior chemotherapy in the adjuvant setting was permitted), bidimensional measurable lesions or evaluable lytic bone metastases, ECOG PS score 0 to 2, no CNS metastases | Toremifene Tamoxifen | OS |
MONALEESA-2 et al.48 | RCT 1:1, phase III, double blind, multicentre, N = 668 | Females who are postmenopausal, HR-positive, HER2-negative locoregionally recurrent advanced breast cancer or metastatic breast cancer not amenable to curative therapy, no prior systemic therapy in the advanced setting (patients who received adjuvant or neoadjuvant therapy were eligible), no prior CDK4/6, measurable disease as per RECIST criteria, or unmeasurable disease with at least 1 lytic bone lesion, ECOG PS score ≤ 1 | Ribociclib + letrozole Letrozole | PFS OS Grade 3 and 4 AEs |
RCT 2:1, phase III, double blind, multicentre, N = 493 | Adult females who are postmenopausal, HR-positive, HER2-negative locoregionally recurrent advanced breast cancer or metastatic breast cancer, measurable disease or unmeasurable bone-only disease (blastic, lytic, or mixed) as per RECIST v1.119, no prior systemic therapy for advanced disease (ET in the neoadjuvant or adjuvant setting was permitted if the patient had a DFS > 12 months from the completion of ET), ECOG-PS ≤ 1 | Abemaciclib + anastrozole or letrozole Placebo + anastrozole or letrozole | PFS Grade 3 and 4 AEs | |
MONARCHplus49 | RCT 2:1, phase III, double blind, multicentre, N = 372 | Adult females who are postmenopausal, HR-positive, HER2-negative locally advanced breast cancer or metastatic breast cancer not amenable to curative therapy (patients who received adjuvant or neoadjuvant ET or chemotherapy were eligible), measurable disease as per RECIST 1.1 criteria, or unmeasurable bone-only disease, ECOG PS score ≤ 1, no prior CDK4/6 or prior chemotherapy or ET in advanced setting, no CNS metastases | Abemaciclib + anastrozole or letrozole Placebo + anastrozole or letrozole | PFS Grade 3 and 4 AEs |
Nordic Study50 | RCT 1:1, phase III, double blind, multicentre, N = 415 | Adult females who are postmenopausal, ER-positive or unknown, inoperable primary advanced breast cancer or metastatic breast cancer (patients who received adjuvant or neoadjuvant ET or chemotherapy were eligible), at least 1 measurable or evaluable bone lesion, Karnofsky performance status ≥ 50% | Toremifene Tamoxifen | PFS OS |
PALOMA-251 | RCT 2:1, phase III, double blind, multicentre, N = 666 | Adult females who are postmenopausal, ER-positive locoregionally recurrent advanced breast cancer or metastatic breast cancer not amenable to curative therapy, no prior systemic anticancer therapy for advanced ER-positive disease, measurable disease as per RECIST criteria or bone-only disease, ECOG PS score 0 to 2 | Palbociclib + letrozole Letrozole | PFS OS Grade 3 and 4 AEs |
PALOMA-452 | RCT 1:1, phase III, double blind, multicentre, N = 340 | Adult females of Asian ethnicity who are postmenopausal, ER-positive locoregionally recurrent advanced breast cancer or metastatic breast cancer not amenable to curative therapy, no prior systemic anticancer therapy for advanced ER-positive disease, no evidence of HER2-positive disease | Palbociclib + letrozole Placebo + letrozole | PFS |
PALOMA-1/TRIO-1853 | RCT 2:1, phase II, open label, multicentre, N = 165 | Females who are postmenopausal, inoperable ER-positive HER2-negative advanced breast cancer or metastatic breast cancer, no prior or concomitant treatment for advanced breast cancer | Letrozole + palbociclib Letrozole | PFS OS Grade 3 and 4 AEs |
PARSIFAL54 | RCT 1:1, phase II, open label, multicentre, N = 486 | Adult female postmenopausal, HR-positive, HER2-negative local advanced breast cancer or metastatic breast cancer not amenable to curative therapy, no prior chemotherapy in the metastatic setting, measurable disease as per RECIST version 1.1 criteria, or unmeasurable disease, ECOG PS score 0 to 1, no active CNS metastases | Palbociclib + fulvestrant Palbociclib + letrozole | PFS |
TARGET and North American55 | RCT 1:1, phase NR, double blind, multicentre, N = 1,021 | Adult females who are postmenopausal, locally advanced breast cancer or metastatic breast cancer suitable for ET (prior adjuvant or neoadjuvant ET or chemotherapy was allowed), no prior treatment in metastatic setting | Anastrozole Tamoxifen | PFS OS |
AE = adverse event; CNS = central nervous system; DFS = disease-free survival; ECOG PS = Eastern Cooperative Oncology Group Performance Status; ER = estrogen receptor; ET = endocrine therapy; HR = hormone receptor; NR = not reported; OS: overall survival; PFS = progression-free survival; RCT = randomized controlled trial; RECIST = Response Evaluation Criteria in Solid Tumours; UICC = Union for International Cancer Control.
aAll arms of letrozole, anastrozole, placebo plus letrozole, placebo plus anastrozole, or combinations thereof were pooled as 1 NSAI node for the sake of creating connected networks.
Source: Sponsor-submitted updated indirect treatment comparison report.40
Characteristics of Patients at Baseline
The ages of patients in most included studies were similar, except the MONARCH plus and PALOMA-4 studies, which included younger patients (median age was 43 to 54 years). Most studies recruited patients with HR-positive disease, but in some cases HR-positive disease was not specified as a criterion or the proportion was not reported (DAWNA-2, Nordic Study, and TARGET and North American Study). Some studies did not specify a requirement of HER2-negative disease or did not report the proportion with HER2-negative or HER2-positive disease. In the FIRST study, roughly 48% of patients had confirmed HER2-negative disease. Some studies allowed recruitment of patients with unknown receptor status with regards to HR and HER2.
In the PALOMA-1/TRIO-18, PARSIFAL, and DAWNA-2 studies, 95% to 100% of patients had an ECOG PS score of greater than 1, indicating greater disease severity than in the MONARCH 3 study. In the MONARCH 3 study, 38.1% to 40.0% of patients had received (neo)adjuvant chemotherapy; this was similar in the MONALEESA-2 and PALOMA-2 studies but was substantially lower (5.0% to 28.0%) in several studies: FALCON, FIRST, FLIPPER, MONALEESA-3, MONARCH plus, PARSIFAL, TARGET and North American Study, PALOMA-4, and in the study by Howell et al.45
In the MONARCH plus and FALCON studies, some patients received chemotherapy for advanced disease (< 1% to 18%), in contrast to the MONARCH 3 study — and most other included studies — that excluded these patients. Most studies had a comparable proportion of patients with prior endocrine therapy in the (neo)adjuvant setting versus the MONARCH 3 study, but some studies reported a lower proportion (1% in the FALCON study, and between 13.0% to 27.0% in the FIRST study, the TARGET and North American Study, and the Howell et al.45 study).
Studies also differed in the proportion of patients who had visceral metastases, bone metastases, 3 or more organ sites, or measurable disease. Many studies did not report this information, and there was a substantial amount of between-study heterogeneity across those that did.
Efficacy Outcomes
For the purpose of this reassessment, only OS, PFS, and grade 3 and 4 AEs will be assessed in depth. Other outcomes submitted by the sponsor (CBR, CR, and ORR) can be found in Appendix 2.
Overall Survival
An evidence network for OS is reported in Figure 9 of Appendix 2, and 2 approaches to the NMA are subsequently described (the Cox approach and the FP approach). The network included 12 studies evaluating 9 treatments.
Cox PHs NMA: Results of the NMA analysis did not demonstrate a difference in hazard ratios, as all CrIs were wide and overlapped null. While both fixed and random effects models were fitted, the random effects model was deemed the model of choice based on the deviance information criterion (DIC) values.
Figure 3: Forest Plot for OS in the ITT Population – RE Model [Redacted]

ITT = intention to treat; OS = overall survival; RE = random effects.
Table 19: Fractional Polynomial ITC – OS
Treatment | Median OSa, months (95% CrI) | Median difference in OS of ABE + NSAI, months (95% CrI)a,b | OS probability (95% CrI)c | ||
|---|---|---|---|---|---|
12 months | 60 months | 120 months | |||
ABE + NSAI | ███ | ███ | ███ | ███ | ███ |
NSAI | ███ | ███ | ███ | ███ | ███ |
PAL + NSAI | ███ | ███ | ███ | ███ | ███ |
RIBO + NSAI | ███ | ███ | ███ | ███ | ███ |
ABE = abemaciclib; CrI = credible interval; ITC = indirect treatment comparison; OS = overall survival; PAL = palbociclib; RIBO = ribociclib; NSAI = nonsteroidal aromatase inhibitor (referring to anastrozole or letrozole).
aProbabilistic average; average of medians of posterior distributions.
bNumbers greater than 0 favour ABE plus NSAI.
cBayesian fixed-effects first order fractional polynomial model; power = −0.5.
Sources: Sponsor response to request for additional information.56
Figure 4: Fitted OS Curve Based on the FP Model,a Time in Months [Redacted]

FP = fractional polynomial; OS = overall survival.
Progression-Free Survival
For the outcome of PFS, 2 approaches to the NMA are subsequently described (the Cox approach and the FP approach). The network included 13 studies evaluating 10 treatments (e.g., refer to Figure 8 in Appendix 2).
Cox PHs NMA: Based on DIC selection criteria, a fixed-effects NMA was selected over a random effects NMA.
Estimated hazard ratios comparing abemaciclib plus an NSAI to fulvestrant 500 mg, fulvestrant 250 mg, and tamoxifen monotherapies favoured abemaciclib plus an NSAI.
The comparisons of abemaciclib plus an NSAI against ribociclib plus letrozole, ribociclib plus fulvestrant, palbociclib plus letrozole, palbociclib plus fulvestrant, and dalpiciclib plus anastrozole or letrozole, did not demonstrate a difference and the hazard ratios were comparable.
Figure 5: Forest Plot for Progression-Free Survival in ITT Population – FE Model [Redacted]

FE = fixed-effects model; ITT = intention to treat.
FP Model: The FP model specifies a collection of parametric forms for the log hazard of each treatment arm. Each parametric model was indexed by P, which took values from the set (−2, −1.5, −1, −0.5, 0, 0.5, 1, 1.5, and 2) in a first-order FP model. Second-order FP models had 2 indices from the same set. The NMA included 7 studies and the 6 corresponding treatment arms from the ITT population. Both random and fixed effects models were considered. The Gelman-Rubin diagnostic suggested good convergence of the model parameters (all values were smaller than 1.1) and low autocorrelation between samples was indicated. In total, 18 first-order models were considered — up to 52 second-order models were considered but did not converge — and based on DIC criteria the (P = −2) FE model was chosen.
Table 20: Fractional Polynomial ITC – PFS
Treatment | Median PFSa, months (95% CrI) | Median difference in PFS of ABE + NSAI, months (95% CrI)a,b | Progression-free survival probability (95% CrI)c | ||
|---|---|---|---|---|---|
12 months | 60 months | 120 months | |||
ABE + NSAI | ███ | ███ | ███ | ███ | ███ |
NSAI | ███ | ███ | ███ | ███ | ███ |
PAL + NSAI | ███ | ███ | ███ | ███ | ███ |
RIBO + NSAI | ███ | ███ | ███ | ███ | ███ |
ABE = abemaciclib; CrI = credible interval; ITC = indirect treatment comparison; PAL = palbociclib; PFS = progression-free survival; RIBO = ribociclib; NSAI = nonsteroidal aromatase inhibitor (referring to anastrozole or letrozole).
aProbabilistic average; average of medians of posterior distributions.
bNumbers greater than 0 favour ABE plus NSAI.
cBayesian fixed-effects first order fractional polynomial model; power = −2.
Sources: Sponsor response to request for additional information.56
Figure 6: Fitted PFS Curve Based on the FP Model,a Time in Months [Redacted]

FP = fractional polynomial; PFS = progression-free survival.
Safety Outcomes
Grade 3 and 4 AEs
Nine studies reported grade 3 and 4 AEs and were included in the network (e.g., refer to Figure 10 of Appendix 2). It was not possible to construct a connected network for studies with SAEs because only 2 studies reported this outcome. Both fixed and random effects models were fitted, and the fixed effects model was selected as the model of choice by the sponsor based on the inspection of DIC values.
The results are presented in Figure 7. Abemaciclib plus an NSAI was favoured compared to palbociclib plus letrozole, palbociclib plus fulvestrant, and dalpiciclib plus anastrozole or letrozole. Conversely, anastrozole or letrozole, fulvestrant 500 mg, and exemestane were favoured over abemaciclib plus AI. There was no difference detected against ribociclib plus letrozole.
Figure 7: Forest Plot for Grade 3 and 4 AEs in the ITT Population – FE Model [Redacted]

AE = adverse event; FE = fixed effects; ITT = intention to treat.
Critical Appraisal of ITC
The sponsor-conducted SLR identified an appropriate catalogue of studies for an ITC. The sponsor appraised the studies included in the SLR for risk of bias using the Cochrane tool,57 which evaluates selection, performance, detection, attrition, and reporting biases. Of the 18 studies included across all NMAs (including those relevant only for other outcomes in Appendix 2), 7 had a low risk of bias related to randomization, 5 in allocation concealment, 17 in group comparability at the outset, 13 in the blinding of care providers, participants, and outcome assessors, 8 in terms of balanced dropout between arms, 12 in reporting, and 6 in using an ITT analysis. In most cases that were not considered low risk of bias, the risk was unknown, except for open-label studies, which had a higher risk of bias in allocation concealment and blinding. The clinical experts consulted for this review provided additional input on the heterogeneity of the included studies based on study design, eligibility criteria, baseline characteristics, and outcome definitions, and noted that there were several between-study differences that contributed to heterogeneity when compared to the MONARCH 3 study, such as differences in baseline HR status, study location, disease severity, and disease location. The NMA was adequately conducted; however, the results could be biased to an unknown degree for these reasons and challenge any interpretation of comparative effectiveness among people living in Canada. Subgroup and sensitivity analyses included analyses of patients who were HR-positive only, patients with baseline ECOG PS score of 0 to 1, patients with visceral metastases, patients with de novo metastatic breast cancer, and patients with recurrent metastatic breast cancer, and the results were generally consistent with the base case analyses.
The sponsor provided methodology summaries on testing for inconsistency but did not specify if these methods were employed and did not present the results of any analysis of inconsistency. It is therefore unknown whether inconsistency was appropriately tested and ultimately whether there was inconsistency detected in the networks.
Random effects and fixed effects models were compared for each end point, and the model of best fit was selected using DIC. The primary analysis used a Cox PH model; however, diagnostic inspection showed a violation of the PH assumption. A FP model was used to estimate median and restricted mean PFS and OS as a sensitivity analysis. However, the model selection of a first-order FP model with P equal to −0.5 (PFS) was conducted using DIC, and this approach may be biased and overly optimistic due to its failure to account for the model selection step in the final inference.58 Because the final model was selected from up to 78 choices of models, the best fitting model based on DIC may be overfit, resulting in a larger difference between treatments than if one had corrected for the additional variability introduced by the selection step. This overfitting is a compounded problem for the economic evaluation, which must also extrapolate beyond the observed data into the future. While the estimated effects of the treatments were comparable, the magnitude of the CrIs are likely overestimated and should be interpreted with caution.
The results of the NMA analyses suggested that there was no difference between abemaciclib plus an NSAI to other available combination CDK4/6 inhibitors for PFS and OS. There is also uncertainty around these comparisons due to large CrIs, heterogeneity across the included studies, and underreporting of the variability due to the model selection process. It is possible for abemaciclib to have better or worse effectiveness with regards to the outcomes of PFS and OS when compared to the other CDK4/6 inhibitors, ribociclib or palbociclib, in the setting in Canada.
The results for grade 3 and 4 AEs showed that monotherapies were associated with fewer events, which is as expected because the combination therapies are known to be more aggressive, and CDK4/6 inhibitors are associated with a side-effect profile that is weighed against potentially increased efficacy. The clinical experts consulted for this review noted that while the findings of this NMA (in the comparisons to other combination therapies that include CDK4/6 inhibitors) may appear to differ from clinical expectations, it is important to consider not just the relative proportion of all AEs or grade 3 and 4 AEs, but also the nature and type of AEs associated with each therapy. These factors must be carefully weighed against the patient's health status and preferences.
Studies Addressing Gaps in the Systematic Review Evidence
Contents within this section have been informed by materials submitted by the sponsor. The following have been summarized and validated by the review team.
The sponsor submitted 4 observational studies to address the safety issues identified in the pivotal evidence; however, only 2 were summarized and appraised as they were deemed to contain potentially relevant information of interest to this review. The other 2 studies were not considered relevant as they mostly evaluated a population that received abemaciclib plus fulvestrant as the endocrine partner, which was not the indication under review.
US Database Study
The US Database Study by Price et al. (2022)9 was provided by the sponsor to address the gap in the pivotal study concerning safety issues of abemaciclib relative to other CDK4/6 inhibitors. This was a retrospective study examining the management of AEs among female patients with HR-positive, HER2-negative metastatic breast cancer receiving CDK4/6 inhibitors. Data of 396 patients from the US Oncology Network iKnowMed EHR database was analyzed, of which 163 patients received palbociclib, 142 patients received abemaciclib, and 91 patients received ribociclib. The mean age was 64.3 years (SD = 11.9 years) and included patients with varying stages of disease (stage I = 10.1%; stage II = 35.6%; stage IIIA = 18.2%; and stage IV = 31.1%). More than one-half of patients received CDK4/6 inhibitors as first-line therapy (84.6% for ribociclib, 65.5% for abemaciclib, and 63.8% for palbociclib). For patients receiving palbociclib and ribociclib, letrozole was the most prescribed combination therapy in first line, while for the abemaciclib cohort, fulvestrant was the most prescribed combination therapy in first line (N = 45 of 93; 31.7%). Across all lines of therapy, one-half of patients in the abemaciclib cohort received fulvestrant as combination therapy, and one-half received either anastrozole or letrozole.
The most common AEs reported included neutropenia (palbociclib: 44.8%, abemaciclib: 10.6%, ribociclib: 36.3%), diarrhea (palbociclib: 8.0%, abemaciclib: 43.0%, ribociclib: 8.8%), and fatigue (palbociclib: 12.9%, abemaciclib: 17.6%, ribociclib: 16.5%). Treatment holds due to neutropenia were reported in 47 patients and were more frequently reported in the palbociclib (N = 33; 45.2%) and ribociclib cohorts (N = 13; 39.4%) than the abemaciclib cohort (N = 1; 6.7%). Dose reductions due to neutropenia were reported in 25 patients (34.2%) who received palbociclib, 8 patients (53.3%) who received abemaciclib, and 11 patients (33.3%) who received ribociclib. Treatment discontinuations due to neutropenia were reported in 10 patients in the palbociclib cohort and 2 patients in the ribociclib cohort. Treatment holds due to diarrhea were reported in 24 patients, 5 in the palbociclib cohort, 18 in the abemaciclib cohort, and 1 in the ribociclib cohorts. Dose reductions due to diarrhea were reported in 22 patients, most frequently in the abemaciclib cohort (N = 18), followed by 3 patients who received palbociclib and 1 patient who received ribociclib. In total, 17 patients discontinued treatment due to diarrhea, most frequently in the abemaciclib cohort (N = 11), followed by the palbociclib (N = 4) and ribociclib cohorts (N = 2). Eleven patients discontinued treatment due to fatigue, of which 9 patients received abemaciclib and 1 patient each received palbociclib and ribociclib. Hospitalizations due to AEs occurred for 13 patients (3.3%) overall (4.3%, 3.5%, and 1.1% for patients in the palbociclib, abemaciclib, and ribociclib cohorts, respectively). The study noted lower frequencies of AEs but higher dose reductions when compared to data from clinical trials.
The study had some notable limitations. Data were collected from an EHR system, and any AE-related data managed outside of the network and not documented may lead to underreporting. An unadjusted observational analysis limits the reported estimates to be interpreted causally. Furthermore, documentation of the validity and accuracy of data were not provided. The analysis did not adjust for baseline demographic, disease characteristics, or comorbidities, and included patients of varying disease stages which could impact response to treatment and tolerability of treatment. It is unclear how many patients included in the analysis aligned with the indication under review given the different lines of therapy, and differing endocrine partners received with abemaciclib (i.e., one-half of all patients received combination fulvestrant, which is not part of the reimbursement request for this review), The National Cancer Institute-CTCAE grading was not collected during clinical practice and not available for this study. The study was only conducted in the US. As such, the generalizability of the results of this retrospective chart study to the population under review is unclear.
RWE Study From Slovenia
The sponsor-provided RWE study from Slovenia by Matos et al. (2024),10 provides additional safety and efficacy data of abemaciclib in the real-world setting, as well as insight into relevant subgroups such as older patients (age groups analyzed < 70 years and ≥ 70 years). This study was an institutional retrospective study evaluating the real-world efficacy and safety of abemaciclib in patients with HR-positive, HER2-negative metastatic breast cancer. Data of 134 patients (133 female, 1 male) who were prescribed abemaciclib with AI or fulvestrant in the first, second, or subsequent line of treatment were retrospectively collected from institutional medical records. Real-world PD was determined by the treating physician based on radiological, laboratory, or clinical assessment. Median follow-up was 42 months (95% CI, 28.28 months to 45.71 months). The median age at treatment initiation was 62 years, and most patients had recurrent metastatic disease at presentation (100 [74.6%]). A total of 69 patients (51.5%) received abemaciclib in combination with endocrine therapy in first line, of which 47 patients (68.1%) received AI and 22 patients (31.9%) received fulvestrant as the endocrine partner. Thirty-two and 33 patients received abemaciclib in the second and third or later lines, respectively.
The median real-world PFS for the entire cohort was 15 months (95% CI, 9.52 months to 20.48 months), and was 21 months (95% CI, 15.12 months to 26.88 months), 20 months (95% CI, 6.38 months to 33.60 months), and 7 months (95% CI, 4.19 months to 9.81 months) in first, second, and third line, respectively. For the entire cohort, the median OS was 29 months (95% CI, 24.15 months to 33.84 months). Median OS was not reached in the first line setting, but was 29 months (95% CI, 26.09 months to 39.90 months) and 19 months (95% CI, 7.59 months to 30.49 months) for second and third or later lines, respectively.
The most common AEs (any grade) were diarrhea (68.7%), anemia (64.9%) and increased serum creatinine (63.4%). Grade 3 or 4 diarrhea was reported in 7 patients, grade 2 diarrhea in 27 patients. Grade 2 and grade 3 or 4 neutropenia was reported in 39 patients and 17 patients, respectively. Grade 2 anemia was reported in 21 patients. Dose reductions occurred in 41 patients (30.6%), primarily due to diarrhea (19 [32.2%]). Dose reductions were more frequent in patients aged 70 years or older (40%) compared to patients aged younger than 70 years (28%). Eighty-seven patients discontinued abemaciclib either due to disease progression (n = 64) or AEs (n = 23). Grade 3 or 4 neutropenia was more common in patients aged younger than 70 years (16%) versus 70 years or older (5%). Grade 3 or 4 diarrhea was more frequently reported in patients aged 70 years or older (7.5%) versus patients aged younger than 70 years (4.3%).
Several limitations were noted for this study. Data were collected from an EHR system, and any inconsistent AE incident collection may lead to underreporting. An unadjusted observational analysis limits the reported estimates to be interpreted causally. There was heterogeneity in the patient population analyzed with respect to age, line of treatment, and endocrine therapy used, though it was primarily AI. This study also had a small sample size, and many patients (n = 87) discontinued abemaciclib at study cut-off due to disease progression or AEs. It is worth noting that the results for median PFS and OS were numerically lower in this study compared to the pivotal trial, though the reason for this naive difference is unknown, which further undermines the generalizability of the results.
Discussion
Summary of Available Evidence
Abemaciclib was previously reviewed by CDA-AMC in 2019 for the treatment of HR-positive, HER2-negative advanced or metastatic breast cancer in combination with an AI in females who are postmenopausal as initial endocrine-based therapy and received a positive recommendation from pERC based on evidence of PFS benefit and a manageable, although not insignificant safety profile. At the time of the initial review, the OS results were insufficient to draw definitive conclusions on the survival benefit of abemaciclib. The sponsor noted that the toxicity profile and lack of clinical evidence demonstrating a clinically meaningful and statistically significant improvement in OS resulted in pERCs restriction of the reimbursement recommendation solely to patients who are unable to tolerate or who have a contraindication to other available CDK4/6 inhibitors. To address pERCs concerns, the sponsor has filed a reassessment based on updated efficacy results for survival outcomes and harms from the MONARCH 3 trial.
The evidence included in this reassessment consisted of an updated analysis of PFS, OS, and harms from the MONARCH 3 trial, providing an additional 5 years and 10 months of follow-up data (more than 8 years median follow-up), an indirect treatment comparison in the form of an NMA using the updated data, and 4 observational studies addressing gaps in the evidence related to AEs.
The MONARCH 3 trial was a phase III, multicentre, randomized, double-blind, placebo-controlled study of abemaciclib or placebo plus an NSAI in females who are postmenopausal with HR-positive, HER2-negative advanced or metastatic breast cancer who had not received any previous systemic therapy in the advanced or metastatic setting. The study was conducted in 158 centres in 22 countries. Baseline demographic and disease characteristics of patients were well-balanced between the treatment groups. Of the 493 patients enrolled, all were female, and the majority were white (58.4%) or of Asian ethnicity (30.0%). The median age was 63 years, and ███ ████████ ███████ were aged younger than 65 years. The median duration of disease before randomization was ████ ██████. Most patients (█████) had metastatic disease at study entry. Prior endocrine therapy included AI in 27.4%, other endocrine drugs in 19.3%, and no prior endocrine therapy in 53.3%. A total of █████ had received endocrine therapy in the (neo)adjuvant setting, including ████ in the neoadjuvant and █████ in the adjuvant setting. Per protocol, a patient could have received 2 weeks or less of an NSAI in the locally advanced or metastatic disease setting preceding screening if discontinued before study treatment; 27 patients met this criterion.
In the absence of direct comparative evidence between abemaciclib and relevant comparators, the sponsor submitted an updated NMA to estimate the relative efficacy and safety of abemaciclib plus an NSAI compared with ribociclib plus an NSAI, palbociclib plus an NSAI, and various endocrine therapies in the treatment of females who are postmenopausal without prior systemic treatment for advanced disease with HR-positive, HER2-negative advanced or metastatic breast cancer. Outcomes of interest for the reassessment included OS, PFS, and grade 3 and 4 AEs.
Four observational real-world studies identified by the sponsor were reviewed to address a gap in the comparative safety and tolerability of abemaciclib compared to other available treatment options; however, only 2 were summarized and appraised.
Interpretation of Results
Efficacy
As previously noted, this reassessment focused on OS, PFS, and AEs, which were included as part of the updated results of the MONARCH 3 trial. In the initial submission, it was concluded that there was evidence of a clinically meaningful benefit associated with abemaciclib compared to placebo for the outcome of PFS, but data pertaining to OS was immature and inconclusive at the time of the review. Based on updated evidence from the MONARCH 3 phase III pivotal study (September 29, 2023 data cut-off), treatment with abemaciclib is likely associated with a clinically significant improvement in PFS compared to placebo in patients who are endocrine sensitive and have HR-positive, HER2-negative advanced or metastatic breast cancer (absolute difference in median PFS = 14.27 months; 95% CI not reported; hazard ratio = 0.535; 95% CI, 0.429 to 0.668), which was consistent with the findings of the initial review of abemaciclib. Treatment with abemaciclib, compared to placebo, may also be associated with an improvement in OS (absolute difference in median OS: 13.09 months; 95% CI not reported; hazard ratio = 0.804; 95% CI, 0.637 to 1.015) but there is uncertainty in the presence and magnitude of benefit because the CI associated with the hazard ratio for OS was not statistically significant, and no 95% CI was reported for the absolute difference in medians. The clinical experts consulted by CDA-AMC considered the absolute difference in median OS observed in the MONARCH 3 study to be clinically meaningful, although acknowledged the aforementioned uncertainty.
Results from the updated NMAs suggested no difference between abemaciclib for the outcomes of OS and PFS when compared to other CDK4/6 inhibitors, in combination with NSAIs. However, there was considerable uncertainty in the magnitude of difference due to trial heterogeneity and statistical considerations.
When asked about their preference in CDK4/6 inhibitors in patients with advanced breast cancer or metastatic breast cancer in the first-line setting, the clinical experts expressed that physician and patient choice depend both on the efficacy and safety profile of available therapies. The experts noted that ribociclib is more commonly the first choice due to its stronger OS data, but it is also considered the least tolerable of the 3 available CDK4/6 inhibitors based on clinician experience (refer also to Harms section). Each patient’s individual health status and preference as well as clinician opinion will factor into the decision-making for the most appropriate CDK4/6 inhibitor to treat within this setting. The experts stated that there would sometimes be cases where the first choice of CDK4/6 inhibitor for a specific patient may be abemaciclib, even in absence of contraindication or evidence of intolerability to other CDK4/6 inhibitors, but that this would be a minority of patients. Therefore, the clinical experts noted that the current requirement of intolerability or contraindication to other CDK4/6 inhibitors may limit clinician and patient choice in treating patients with advanced breast cancer or metastatic breast cancer.
Harms
As of the updated analysis, the abemaciclib treatment group experienced a higher incidence of AEs across all categories compared to the placebo group. Nearly all patients experienced at least 1 AE (98.8% versus 94.4%), and █████ and █████ of patients in the abemaciclib and placebo groups experienced at least 1 SAE, respectively. Prespecified AEs of special interest included neutropenia, infections, diarrhea, hepatic events, venous thromboembolism, and interstitial lung disease or pneumonitis, all of which occurred more frequently in the abemaciclib plus NSAI group than in the placebo plus NSAI group. As noted in the original review, abemaciclib is associated with a side-effect profile that, while not insignificant, is considered manageable.
The safety profile of abemaciclib differs from those of other CDK4/6 inhibitors. The clinical experts consulted by CDA-AMC highlighted that abemaciclib is associated with a higher incidence of diarrhea, whereas palbociclib is more strongly associated with neutropenia. Ribociclib, in contrast, has been linked to an increased risk of QT interval prolongation — especially when used with other QT-prolonging drugs — and impaired liver function. It is also associated with a higher risk of neutropenia. Overall, the clinical experts considered the updated safety profile of abemaciclib to be consistent with expectations for a CDK4/6 inhibitor used in the treatment of advanced or metastatic breast cancer, although differences between the safety profile of each drug may inform treatment decisions for each patient.
In the NMA analysis of grade 3 and 4 AEs, it was reported that abemaciclib may be associated with fewer grade 3 and 4 AEs than palbociclib plus letrozole, palbociclib plus fulvestrant, and dalpiciclib plus anastrozole-letrozole, but more grade 3 and 4 AEs than anastrozole or letrozole alone, fulvestrant 500 mg, and exemestane. Additionally, there was no evidence of difference when compared to ribociclib plus letrozole due to the 95% CrI overlapping null. The clinical experts noted that some findings, such as a lower incidence of AEs compared to palbociclib-based therapies, do not reflect their experiences with real-world tolerability. The NMA evaluated an aggregate measure of harms (i.e., the proportion of patients with any grade 3 or 4 AEs), but the clinical experts consulted for this review noted that real-world decision-making and experience of tolerability of these therapies depends more on differences in specific, individual types of AEs and how that interacts with each patient’s health status and preferences. This discrepancy may therefore stem from differences in the type and nature of AEs experienced, which are not fully captured by aggregate measures of AE or severity grades evaluated in the NMA.
Additionally, to address the concerns related to harms, 2 observational studies evaluating the safety and tolerability of abemaciclib were summarized and appraised. Overall, results from these RWE studies demonstrated that AEs due to abemaciclib treatment, in particular diarrhea, may be adequately managed through dose reductions, proactive intervention plans, and comedications. However, interpretations from these studies are limited by their study design, data sources, and small sample sizes. In addition, generalizability to the setting in Canada was limited by the heterogeneity in patient populations, dosing regimens, monitoring, and management of AEs.
Conclusion
Abemaciclib plus an NSAI has been previously reviewed by CDA-AMC for the treatment of adult patients with endocrine-sensitive, HR-positive, HER2-negative advanced or metastatic breast cancer as a first-line endocrine-based therapy. In the initial review, it was concluded that evidence from the phase III, double-blind RCT, MONARCH 3, demonstrated a clinically significant improvement in PFS when compared to placebo plus an NSAI in this population. Additionally, the safety profile of abemaciclib was not insignificant but was considered to be manageable in the treatment of this population. At the time of the initial review, OS data were immature and conclusions could not be drawn. The recommendation by CDA-AMC was to conditionally reimburse abemaciclib in the treatment of this patient population, but with stipulation that patients must be intolerant to or have a contraindication to other CDK4/6 inhibitors, which is narrower than the indication approved by Health Canada.
This reassessment is based on updated data from the MONARCH 3 study, including updated PFS results, the final preplanned OS analysis, and updated safety results, given an additional 5 years and 10 months of follow-up time. Additionally, an updated sponsor-submitted ITC provided indirect comparison against other CDK4/6 inhibitors, and 2 real-world observational studies were appraised to assist in the assessment of AEs, particularly diarrhea.
The updated PFS results were aligned with the conclusions drawn from the final preplanned PFS analysis, in that abemaciclib plus an NSAI was associated with prolonged PFS relative to placebo plus an NSAI in this patient population. Although the results of the final OS analysis of the MONARCH 3 study suggest an improvement in OS for abemaciclib plus an NSAI compared to placebo, the results were not statistically significant, and there is uncertainty in the magnitude of benefit because of the wide 95% CI. However, the clinical experts consulted for this review considered the approximately 13-month difference in median OS between abemaciclib and placebo to be clinically meaningful in the context of metastatic breast cancer. In the absence of head-to-head data comparing to other CDK4/6 inhibitors, indirect comparisons in the form of NMAs demonstrated no evidence of difference between abemaciclib plus an NSAI and other CDK4/6 inhibitors plus an NSAI for the outcomes of OS or PFS, and there was considerable uncertainty due to between-trial heterogeneity and wide CrIs that crossed null.
There is extensive experience with abemaciclib, having been available to patients in Canada since 2019. The updated safety results were consistent with the previously reported safety profile, which demonstrated that compared to placebo, abemaciclib is associated with an increase in AEs, serious AEs, and grade 3 and 4 AEs, most notably diarrhea. The real-world observational studies suggested that the risk of diarrhea is typically managed through dose reduction, proactive intervention plans, and concomitant medications. This safety profile is significant but was described by the clinical experts to be manageable in the treatment of this patient population. Overall, the NMAs evaluating harms were limited by the reporting of aggregate AE results, as individual AEs by preferred term were considered more clinically relevant when comparing CDK4/6 inhibitors. As such, whether there is a clinically meaningful difference in overall safety profile between the CDK4/6 inhibitors available in this population remains uncertain.
References
1.CADTH. Drug Reimbursement review clinical guidance report: abemaciclib (Verzenio) for metastatic breast cancer July 5, 2019. Accessed April 23, 2025. https://www.cda-amc.ca/sites/default/files/pcodr/Reviews2019/10161AbemaciclibMBC_fnCGR_NOREDACT_Post_05Jul2019_final.pdf
2.Canadian Cancer Society. Cancer statistics at a glance. Accessed September 2024. https://cancer.ca/en/research/cancer-statistics/cancer-statistics-at-a-glance
3.Turashvili G, Brogi E. Tumor Heterogeneity in Breast Cancer. Front Med (Lausanne). 2017;4:227. doi: 10.3389/fmed.2017.00227 PubMed
4.National Cancer Institute. Cancer Stat Facts: Female Breast Cancer Subtypes. 2023. Accessed by sponsor, no date provided. https://seer.cancer.gov/statfacts/html/breast-subtypes.html
5.Lobbezoo DJ, van Kampen RJ, Voogd AC, et al. Prognosis of metastatic breast cancer subtypes: the hormone receptor/HER2-positive subtype is associated with the most favorable outcome. Breast Cancer Res Treat. 2013;141(3):507-14. doi: 10.1007/s10549-013-2711-y PubMed
6.Khan NAJ, Abdallah M, Tirona MT. Hormone Receptor Positive/HER2 Negative Breast Cancer With Isolated Bladder Metastasis: A Rare Case. J Investig Med High Impact Case Rep. 2021;9:23247096211022186. doi: 10.1177/23247096211022186 PubMed
7.Huppert LA, Gumusay O, Idossa D, Rugo HS. Systemic therapy for hormone receptor-positive/human epidermal growth factor receptor 2-negative early stage and metastatic breast cancer. CA Cancer J Clin. 2023;73(5):480-515. doi: 10.3322/caac.21777 PubMed
8.American Cancer Society. Types of breast cancer [sponsor supplied reference]. 2017. Accessed October 2024. https://www.cancer.org/cancer/types/breast-cancer/understanding-a-breast-cancer-diagnosis.html
9.Price GL, Sudharshan L, Ryan P, et al. Real world incidence and management of adverse events in patients with HR+, HER2- metastatic breast cancer receiving CDK4 and 6 inhibitors in a United States community setting. Curr Med Res Opin. 2022;38(8):1319-1331. doi: 10.1080/03007995.2022.2073122 PubMed
10.Matos E, Cankar K, Rezun N, Dejanovic K, Ovcaricek T. Abemaciclib for the Treatment of HR+HER2- Metastatic Breast Cancer: An Institutional Experience. Cancers (Basel). 2024;16(10):1828. doi: 10.3390/cancers16101828 PubMed
11.Cardoso F, Paluch-Shimon S, Schumacher-Wulf E, et al. 6th and 7th International consensus guidelines for the management of advanced breast cancer (ABC guidelines 6 and 7). Breast. 2024;76:103756. doi: 10.1016/j.breast.2024.103756 PubMed
12.Early Breast Cancer Trialists' Collaborative Group (EBCTCG). Effects of chemotherapy and hormonal therapy for early breast cancer on recurrence and 15-year survival: an overview of the randomised trials. Lancet. 2005;365(9472):1687-717. doi: 10.1016/S0140-6736(05)66544-0 PubMed
13.National Cancer Institute. SEER*Explorer: An interactive website for SEER cancer statistics. Surveillance Research Program [sponsor supplied reference]. April 2024. Accessed October 2024. https://seer.cancer.gov/statistics-network/explorer
14.Canadian Cancer Society. Survival statistics for breast cancer. August 2023. Accessed November 2024. https://cancer.ca/en/cancer-information/cancer-types/breast/prognosis-and-survival/survival-statistics
15.Burstein HJ. Selection and administration of adjuvant chemotherapy for HER2-negative breast cancer. UpToDate; 2024. Accessed February 19, 2025. http://www.uptodate.com
16.Dixon JM. Neoadjuvant management of newly diagnosed hormone receptor-positive, HER2-negative breast cancer. UpToDate; 2024. Accessed February 19, 2025. http://www.uptodate.com
17.DeKoven M, Bonthapally V, Jiao X, et al. Treatment pattern by hormone receptors and HER2 status in patients with metastatic breast cancer in the UK, Germany, France, Spain and Italy (EU-5): results from a physician survey. J Comp Eff Res. 2012;1(5):453-63. doi: 10.2217/cer.12.43 PubMed
18.Irvin W, Jr., Muss HB, Mayer DK. Symptom management in metastatic breast cancer. Oncologist. 2011;16(9):1203-14. doi: 10.1634/theoncologist.2011-0159 PubMed
19.Joe BN. Clinical features, diagnosis, and staging of newly diagnosed breast cancer. UpToDate; 2024. Accessed February 19, 2025. http://www.uptodate.com
20.NCCN Guidelines. Breast Cancer, version 1.2025. National Comprehensive Cancer Network. Accessed by sponsor, no date provided. https://www.nccn.org/
21.Wolff AC, Hammond MEH, Allison KH, et al. Human Epidermal Growth Factor Receptor 2 Testing in Breast Cancer: American Society of Clinical Oncology/College of American Pathologists Clinical Practice Guideline Focused Update. J Clin Oncol. 2018;36(20):2105-2122. doi: 10.1200/JCO.2018.77.8738 PubMed
22.Eli Lilly Canada Inc. Verzenio (abemaciclib): 50 mg, 100 mg, 150 mg, or 200 mg, oral tablet [product monograph]. April 4, 2019. Updated December 1, 2023.
23.CADTH. Drug Reimbursement Expert Review Committee final recommendation: Abemaciclib (Verzenio - Eli Lilly Canada Inc.). July 5, 2019. Accessed April 14, 2025. https://www.cda-amc.ca/sites/default/files/pcodr/Reviews2019/10161AbemaciclibMBC_fnRec_ApprovedbyChair_v01_2019-07-04_Post_05Jul2019_final.pdf
24.CADTH. Reimbursement recommendation: abemaciclib (Verzenio). Can J Health Technol. 2022;2(10). doi: 10.51731/cjht.2022.475
25.Canada’s Drug Agency. Reimbursement recommendation: abemaciclib (Verzenio). Can J Health Technol. 2024;4(10). doi: 10.51731/cjht.2024.1007
26.Pfizer Canada Inc. Ibrance (palbociclib): 75 mg, 100 mg and 125 mg, oral capsules [product monograph; sponsor supplied reference]. 2018.
27.Novartis Pharmaceuticals Canada Inc. Kisqali (ribociclib as ribociclib succinate): 200 mg oral tablets [product monograph; sponsor supplied reference]. 2018.
28.AstraZeneca Canada Inc. Faslodex (fulvestrant): 50 mg/mL in pre-filled syringe, for injection [product monograph; sponsor supplied reference]. June 2020.
29.Natco Pharma (Canada) Inc. NAT-Everolimus (everolimus): 2.5mg, 5mg, 7.5 mg, and 10 mg, oral tablets [product monograph; sponsor supllied reference]. 2023.
30.Pfizer Canada ULC. Aromasin (exemestane tablets): 25 mg, oral tablets [product monograph; sponsor supplied reference]. 2022.
31.AstraZeneca Canada Inc. Arimidex (anastrozole): 1 mg, oral use tablet [product monograph; sponsor supplied reference]. November 2022.
32.Teva Canada Limited. Letrozole (letrozole): 2.5 mg, oral tablets [product monograph; sponsor supplied reference]. February 2010.
33.Goetz MP, Toi M, Huober J, et al. Abemaciclib plus a nonsteroidal aromatase inhibitor as initial therapy for HR+, HER2- advanced breast cancer: final overall survival results of MONARCH 3. Ann Oncol. 2024;35(8):718-727. doi: 10.1016/j.annonc.2024.04.013 PubMed
34.Johnston S, Martin M, Di Leo A, et al. MONARCH 3 final PFS: a randomized study of abemaciclib as initial therapy for advanced breast cancer. NPJ Breast Cancer. 2019;5:5. doi: 10.1038/s41523-018-0097-z PubMed
35.Goetz MP, Toi M, Campone M, et al. MONARCH 3: Abemaciclib As Initial Therapy for Advanced Breast Cancer. J Clin Oncol. 2017;35(32):3638-3646. doi: 10.1200/JCO.2017.75.6155 PubMed
36.Goetz MP, Martin M, Tokunaga E, et al. Health-Related Quality of Life in MONARCH 3: Abemaciclib plus an Aromatase Inhibitor as Initial Therapy in HR+, HER2- Advanced Breast Cancer. Oncologist. 2020;25(9):e1346-e1354. doi: 10.1634/theoncologist. 2020-0084 PubMed
37.Takahashi M, Tokunaga E, Mori J, et al. Japanese subgroup analysis of the phase 3 MONARCH 3 study of abemaciclib as initial therapy for patients with hormone receptor-positive, human epidermal growth factor receptor 2-negative advanced breast cancer. Breast Cancer. 2022;29(1):174-184. doi: 10.1007/s12282-021-01295-0 PubMed
38.Eli Lilly Canada Inc. Sponsor Summary of Clinical Evidence: Verzenio (abemaciclib) [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Verzenio (abemaciclib), 50 mg, 100 mg, or 150 mg, oral tablet, with an aromatase inhibitor. February 14, 2025.
39.Eli Lilly and Company. Clinical Study Report: I3Y-MC-JPBM, final overall survival analysis. MONARCH 3: A Randomized, Double-Blind, Placebo-Controlled, Phase 3 Study of Nonsteroidal Aromatase Inhibitors (Anastrozole or Letrozole) plus LY2835219, a CDK4/6 Inhibitor, or Placebo in Postmenopausal Women with Hormone Receptor-Positive, HER2-Negative Locoregionally Recurrent or Metastatic Breast Cancer with No Prior Systemic Therapy in This Disease Setting [internal sponsor's report].
40.Eli Lilly Canada Inc. Abemaciclib in combination with aromatase inhibitors for the first-line treatment of postmenopausal women with HR+, HER2− advanced/metastatic breast cancer: Indirect Treatment Comparisons Report, version 1.0 [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Verzenio (abemaciclib), 50 mg, 100 mg, or 150 mg, oral tablet, with an aromatase inhibitor. December 5th, 2024.
41.Zhang P, Zhang Q, Tong Z, et al. Dalpiciclib plus letrozole or anastrozole versus placebo plus letrozole or anastrozole as first-line treatment in patients with hormone receptor-positive, HER2-negative advanced breast cancer (DAWNA-2): a multicentre, randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2023;24(6):646-657. doi: 10.1016/S1470-2045(23)00172-9 PubMed
42.Robertson JFR, Bondarenko IM, Trishkina E, et al. Fulvestrant 500 mg versus anastrozole 1 mg for hormone receptor-positive advanced breast cancer (FALCON): an international, randomised, double-blind, phase 3 trial. Lancet. 2016;388(10063):2997-3005. doi: 10.1016/S0140-6736(16)32389-3 PubMed
43.Robertson JF, Llombart-Cussac A, Rolski J, et al. Activity of fulvestrant 500 mg versus anastrozole 1 mg as first-line treatment for advanced breast cancer: results from the FIRST study. J Clin Oncol. 2009;27(27):4530-5. doi: 10.1200/JCO.2008.21.1136 PubMed
44.Albanell J, Martinez MT, Ramos M, et al. Randomized phase II study of fulvestrant plus palbociclib or placebo in endocrine-sensitive, hormone receptor-positive/HER2-advanced breast cancer: GEICAM/2014-12 (FLIPPER). Eur J Cancer. 2022;161:26-37. doi: 10.1016/j.ejca.2021.11.010 PubMed
45.Howell A, Robertson JF, Abram P, et al. Comparison of fulvestrant versus tamoxifen for the treatment of advanced breast cancer in postmenopausal women previously untreated with endocrine therapy: a multinational, double-blind, randomized trial. J Clin Oncol. 2004;22(9):1605-13. doi: 10.1200/JCO.2004.02.112 PubMed
46.Iwata H, Masuda N, Ohno S, et al. A randomized, double-blind, controlled study of exemestane versus anastrozole for the first-line treatment of postmenopausal Japanese women with hormone-receptor-positive advanced breast cancer. Breast Cancer Res Treat. 2013;139(2):441-51. doi: 10.1007/s10549-013-2573-3 PubMed
47.Milla-Santos A, Milla L, Portella J, et al. Anastrozole versus tamoxifen as first-line therapy in postmenopausal patients with hormone-dependent advanced breast cancer: a prospective, randomized, phase III study. Am J Clin Oncol. 2003;26(3):317-22. doi: 10.1097/01.COC.0000047126.10522.F9 PubMed
48.O'Shaughnessy J, Petrakova K, Sonke GS, et al. Ribociclib plus letrozole versus letrozole alone in patients with de novo HR+, HER2- advanced breast cancer in the randomized MONALEESA-2 trial. Breast Cancer Res Treat. 2018;168(1):127-134. doi: 10.1007/s10549-017-4518-8 PubMed
49.Zhang QY, Sun T, Yin YM, et al. MONARCH plus: abemaciclib plus endocrine therapy in women with HR+/HER2- advanced breast cancer: the multinational randomized phase III study. Ther Adv Med Oncol. 2020;12:1758835920963925. doi: 10.1177/1758835920963925 PubMed
50.Pyrhonen S, Valavaara R, Modig H, et al. Comparison of toremifene and tamoxifen in post-menopausal patients with advanced breast cancer: a randomized double-blind, the 'nordic' phase III study. Br J Cancer. 1997;76(2):270-7. doi: 10.1038/bjc.1997.375 PubMed
51.Finn RS, Martin M, Rugo HS, et al. Palbociclib and Letrozole in Advanced Breast Cancer. N Engl J Med. 2016;375(20):1925-1936. doi: 10.1056/NEJMoa1607303 PubMed
52.Xu B, Hu X, Li W, et al. Palbociclib plus letrozole versus placebo plus letrozole in Asian postmenopausal women with oestrogen receptor-positive/human epidermal growth factor receptor 2-negative advanced breast cancer: Primary results from PALOMA-4. Eur J Cancer. 2022;175:236-245. doi: 10.1016/j.ejca.2022.08.012 PubMed
53.Finn RS, Crown JP, Lang I, et al. The cyclin-dependent kinase 4/6 inhibitor palbociclib in combination with letrozole versus letrozole alone as first-line treatment of oestrogen receptor-positive, HER2-negative, advanced breast cancer (PALOMA-1/TRIO-18): a randomised phase 2 study. Lancet Oncol. 2015;16(1):25-35. doi: 10.1016/S1470-2045(14)71159-3 PubMed
54.Llombart-Cussac A, Perez-Garcia JM, Bellet M, et al. Fulvestrant-Palbociclib vs Letrozole-Palbociclib as Initial Therapy for Endocrine-Sensitive, Hormone Receptor-Positive, ERBB2-Negative Advanced Breast Cancer: A Randomized Clinical Trial. JAMA Oncol. 2021;7(12):1791-1799. doi: 10.1001/jamaoncol.2021.4301 PubMed
55.Bonneterre J, Buzdar A, Nabholtz JM, et al. Anastrozole is superior to tamoxifen as first-line therapy in hormone receptor positive advanced breast carcinoma. Cancer. 2001;92(9):2247-58. doi: 10.1002/1097-0142(20011101)92:9<2247::aid-cncr1570>3.0.co;2-y PubMed
56.Eli Lilly Canada Inc. Eli Lilly Canada Inc. response to Canada's Drug Agency request for additional information regarding Verzenio review on April 15, 2025 [internal additional sponsor's information]. April 24, 2025.
57.Higgins JP, Altman DG, Gotzsche PC, et al. The Cochrane Collaboration's tool for assessing risk of bias in randomised trials. BMJ. 2011;343:d5928. doi: 10.1136/bmj.d5928 PubMed
58.Leeb H, Pötscher BM. Model selection and inference: Facts and fiction. Econometric Theory. 2005;21(1):21-59.
Appendix 1: Additional Data From the MONARCH 3 Study
Please note that this appendix has not been copy-edited.
Outcomes From the Initial Review of Abemaciclib Based on Earlier Data Cut-Offs of the MONARCH 3 Study
The interpretation of the results presented in this section are reflective of those reported by CDA-AMC during the reimbursement review conducted in 2019.
Efficacy
The primary efficacy end point was investigator-assessed PFS (according to RECIST Version 1.1). Key secondary end points included ORR, duration of response, OS, and CBR.
Progression-Free Survival
In the final PFS analysis (November 7, 2017, data cut-off), after a median follow-up duration of 26.73 months, 246 investigator-assessed PFS events had occurred (138 [42.1%] events the abemaciclib plus AI arm and 108 [65.5%] events in the placebo plus AI arm). The median PFS was 28.18 months in the abemaciclib plus AI arm compared to 14.76 months in the placebo plus AI arm (hazard ratio = 0.540; 95% CI, 0.418, 0.698); P = 0.000002). The PFS benefit was maintained across the predefined patient subgroup analyses.
Overall Survival
The data for OS were immature at the time of the original review. At the January 3, 2017, data cut-off date, there were a total of 49 deaths (32 deaths [9.8%] in the abemaciclib plus AI arm and 16 deaths [9.9%] in the placebo plus AI arm). The median OS was not reached in either of the arms.
Overall Response Rate
ORR was a secondary end point in the MONARCH 3 trial. As of January 31, 2017, data cut-off date, after a median follow-up duration of 17.8 months, ORR was reported to be 48.2% (95% CI, 42.8% to 53.6%) in the abemaciclib plus AI arm and 34.5% (95% CI, 27.3% to 41.8%) in the placebo plus AI arm (P = 0.002). Of these responders, 135 patients (101 [63.9%] in the abemaciclib plus AI arm and 34 [59.6%] in the placebo plus AI arm) were continuing with treatment at the time of the analysis. For patients with measurable disease, ORR was 59.2% (95% CI, 53.3% to 65.1%) in the abemaciclib plus AI arm and 43.8% (95% CI, 35.3% to 52.4%) in the placebo plus AI arm (P = 0.004).
At the November 7, 2017, data cut-off date, the ORR was 49.7% (95% CI, 44.3% to 55.1%) in the abemaciclib plus AI arm and 37.0% (95% CI, 29.6% to 44.3%) in the placebo plus AI arm (P = 0.005). For the subset of 399 patients (80.9%) with measurable disease, the ORR was 61.0% (95% CI, 55.2% to 66.9%) in the abemaciclib plus AI arm and 45.5% (95% CI, 37.0% to 53.9%) in the placebo arm (P = 0.003).
Clinical Benefit Rate
CBR, a secondary end point in the MONARCH 3 trial, was defined as complete or partial response or stable disease of at least 24 weeks duration. At the January 31, 2017, data cut-off date, CBR was achieved by 78.0% of patients (95% CI, 73.6% to 82.5%) in the abemaciclib plus AI arm and 71.5% of patients (95% CI, 64.6% of 78.4%) in the placebo arm.
Quality of Life
No peer-reviewed publications reporting on the HRQoL data from the MONARCH 3 trial were identified at the time of the review. The following data were extracted from a conference abstract and its related poster presentation that was provided by the submitter:
A clinically meaningful (≥ 10 points) and statistically significant worsening in diarrhea was reported in the abemaciclib plus AI arm. There was a statistically significant and clinically meaningful worsening in European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 (EORTC QLQ-C30) diarrhea symptom score in patients treated with abemaciclib (mean change = 18.68; 95% CI ██████ █████; P < 0.001). Changes from baseline in the following symptom scores were statistically different (but not clinically meaningful) between the 2 study arms, all favouring the placebo arm: nausea and vomiting (mean change = 2.77; 95% CI, █████ ████; P = 0.013), appetite loss (mean change = 4.03; 95% CI, █████ ████; P = 0.034), and fatigue (mean change = 4.96; 95% CI, 1.58 to 8.35; P = 0.004). In addition, a statistically significant worsening was observed with abemaciclib in global health status, role functioning, social functioning, body image, and the composite score for the systemic therapy symptoms.
Since the initial CDA-AMC review, quality of life data and post hoc analyses have been published in a peer-reviewed publication by Goetz et al. (2020) (based on data from final PFS analysis [data cut-off date: November 3, 2017]).36 The underlying data are the same as previously described, but additional details have become available compared to the poster that was assessed at the time of the 2019 review (albeit consistent with the original conclusions). The between-group differences in change from baseline for each item of the EORTC QLQ-C30 and EORTC QLQ Breast Cancer 23 by cycle were analyzed. Goetz et al. (2020) further evaluated the time to sustained deterioration (TTSD) in a post hoc analysis, defined as time from randomization to the time of a 10-point or more deterioration.
For both EORTC QLQ-C30 and EORTC QLQ Breast Cancer 23, there were no clinically meaningful difference (≥ 10 points) between treatment differences in change from baseline scores for any functioning scores and the majority of symptom scores. Similarly, with the TTSD analysis, there were no statistically significant or clinically meaningful differences between treatment arms for global HRQoL, most symptoms, or any functional items. The exception to these results was diarrhea, as patients in the abemaciclib arm experienced both a clinically meaningful and statistically significant worsening from baseline (18.68 ± 1.80; P < 0.001) and a shorter TTSD compared with patients in the placebo arm.
These results as extracted from the publication were consistent with previously disclosed safety data from MONARCH 3 and other abemaciclib trials showing diarrhea to be the most commonly reported AEs. Although there was an overall increase in diarrhea in patients taking abemaciclib, it was predominantly low grade (72.8% of all cases in the abemaciclib arm being grade 1 or 2) with no cases of grade 4 diarrhea. The median onset for diarrhea was 8 days in the abemaciclib arm, and the median duration was 10.5 days for grade 2, and 8 days for grade 3. Importantly diarrhea did not frequently result in abemaciclib discontinuation, with less than 2% of patients discontinuing due to diarrhea (1.8%). There is evidence that when abemaciclib-related diarrhea is treated at the first loose stool with over-the-counter antidiarrheal medication and/or dose modifications, it resolves over time with no impact on efficacy and returns to baseline levels after discontinuation.
Abbreviated Conclusions From the Original Submission
The PFS results observed in MONARCH 3 were concluded to be statistically significant and clinically meaningful. Although the most common side effects experienced with abemaciclib plus AI in this trial were not life threatening, they do require monitoring by an experienced health care team familiar with the toxicities associated with this combination, as a higher incidence of AEs may occur in an unselected nonclinical trial population. There was a statistically significant and clinically meaningful worsening in EORTC QLQ-C30 diarrhea symptom score in patients treated with abemaciclib (mean change = 18.68; 95% CI, ██████ █████; P < 0.001). Overall, CDA-AMC concluded that there is a net overall clinical benefit to the addition of abemaciclib as an initial therapy with a NSAI in patients who were postmenopausal with HR-positive HER2-negative advanced breast cancer or metastatic breast cancer who had no prior systemic therapy in the advanced setting. As previously mentioned in the Basis for the Reassessment section, there were concerns regarding uncertainty of benefit in OS (due to immature study data).
Additional Updated Outcomes From the Most Recent Data Cut-Off of the MONARCH 3 Study
Chemotherapy-Free Survival
Delay of chemotherapy is a goal of treatment in this population. It was not assessed in the original review of abemaciclib. This was an exploratory outcome in the MONARCH 3 study and updated data were provided for the data-cut that took place at the final OS analysis (i.e., September 29, 2023). The end point was measured from the date of randomization to initiation of first postdiscontinuation chemotherapy or death due to any cause, whichever was earlier. A total of 237 patients received postdiscontinuation chemotherapy, including ███ ███████ in the abemaciclib arm, and 102 (61.8%) in the placebo arm. At the September 29, 2023, data cut-off, the hazard ratio between the abemaciclib group and placebo group was 0.693 (95% CI, 0.557 to 0.863; 2-sided stratified log-rank P value = 0.0010). The median chemotherapy-free survival was 46.65 months (95% CI, █████ ██ █████ months) in the abemaciclib group and 30.58 months (95% CI, █████ ██ █████ months) in the placebo group. Additional data are reported in Table 21.
Table 21: Summary of Chemotherapy-Free Survival (ITT Population) in the MONARCH 3 Study (Data Cut-Off: September 29, 2023)
Value | Abemaciclib + NSAI (N = 328) n (%) | Placebo + NSAI (N = 165) n (%) | Treatment effect, difference, P value |
|---|---|---|---|
Number of deaths, n (%) | ███ █ | ███ █ | ███ █ |
Death without chemotherapy | ███ █ | ███ █ | ███ █ |
Received postdiscontinuation chemotherapy | ███ █ | ███ █ | ███ █ |
Number of patients censored, n (%) | ███ █ | ███ █ | ███ █ |
Off treatment, in follow-up without chemotherapy | ███ █ | ███ █ | ███ █ |
Off treatment, lost to follow-up without chemotherapy | ███ █ | ███ █ | ███ █ |
On treatment | ███ █ | ███ █ | ███ █ |
Median (95% CI) months | ███ █ | ███ █ | ███ █ |
P value (2-sided) log-rank stratifieda | ███ █ | ███ █ | ███ █ |
Hazard ratio (95% CI) stratifieda | ███ █ | ███ █ | ███ █ |
Chemotherapy-free survival rate, % (95% CI)b | |||
12 months | ███ █ | ███ █ | ███ █ |
24 months | ███ █ | ███ █ | ███ █ |
36 months | ███ █ | ███ █ | ███ █ |
48 months | ███ █ | ███ █ | ███ █ |
60 months | ███ █ | ███ █ | ███ █ |
72 months | ███ █ | ███ █ | ███ █ |
CFS = chemotherapy free survival; CI = confidence interval; IWRS = interactive web recognition system; ITT = intention to treat; N/A = not applicable; NSAI = nonsteroidal aromatase inhibitor.
Note: CFS rates were estimated using the Kaplan-Meier method. Corresponding 95% CIs were estimated using the methods of Brookmeyer and Crowley, and Greenwood, respectively.
aStratified by IWRS endocrine therapy, IWRS nature of disease.
b95% CIs and 2-sided P values for the difference between rates were calculated based on normal approximation.
Source: MONARCH 3 Clinical Study Report.39
Appendix 2: Additional Data from Sponsor-Submitted NMAs
Please note that this appendix has not been copy-edited.
Table 22: Sponsor-Submitted Assessment of Homogeneity for ITC
Characteristics | Description |
|---|---|
Disease severity | Breast cancer stage: In most studies, patients with ABC-MBC were eligible, including the MONARCH 3 trial. Two studies included patients with recurrent or progressing cancer without specifying eligibility of ABC or MBC (Paterson et al. [1990], Howell et al. [2004]). In the SONIA trial, patients with local ABC were not amenable to curative therapy were eligible. |
Treatment history | Prior systemic treatment for ABC-MBC: Similar to the MONARCH 3 trial, most included studies explicitly stated that only patients without prior systemic therapy for advanced disease were eligible for inclusion. One line of chemotherapy (but not ET) was permitted in the FALCON trial and in the LEONARDA-1 trial. In the LEONARDA-1 trial, chemotherapy at the ABC-MBC stage was indeed received by 28.5% to 29.0% of patients in the 2 arms at baseline. Whether prior use of chemotherapy, ET, or both was permitted in the advanced disease setting was unclear in 5 studies (Paterson et al. [1990], Muss et al. [1985], Gill et al. [1993], Milla-Santos et al. [2001], Milla-Santos et al. [2003]). Finally, the PADA-1 study enrolled patients who were already undergoing first-line ABC-MBC treatment with PAL plus AI, and who had newly presented or increased bESR1mut in circulating tumour DNA during treatment (i.e., an early indicator of potential treatment resistance). Patients were randomly assigned to continue with PAL plus AI or to switch to PAL plus FUL. This contrasts with the MONARCH 3 trial, where patients had not received prior ET for ABC-MBC. The LEONARDA-1 and PADA-1 studies were excluded from further heterogeneity assessment. Prior treatment with a CDK4/6 inhibitor or EVE: Twelve studies excluded patients previously treated with a CDK4/6 inhibitor, including the MONARCH 3 trial (LEONARDA-1, DAWNA-2, FLIPPER, PALOMA-2, PALOMA-4, PADA-1, MONARCH plus, SONIA, MONALEESA-2, MONALEESA-3, and MONALEESA-7 trials). The remaining studies did not mention relevant eligibility criteria. Only the MONARCH 3 trial excluded patients with prior EVE treatment. |
Trial eligibility criteria | The following key eligibility criteria were examined in the evidence base and compared with those of the MONARCH 3 trial: Sex and menopausal status: Twenty-one of 29 studies, including the MONARCH 3 trial, recruited adult females who were postmenopausal. Most studies reported similar criteria, although the LEONARDA-1, SONIA, and DAWNA-2 trials recruited females of any menopausal status and the MONALEESA-7 trial included females who were premenopausal and perimenopausal. Three studies (Milla-Santos et al. [2003], Mouridsen et al. [2001], and Yardley et al. [2009]) did not report sex or menopausal status among the eligibility criteria. HR (ER-PgR) status: Twenty-two of 29 studies, including the MONARCH 3 trial, recruited patients with HR-positive or ER+ disease. The remaining studies allowed the inclusion of patients with unknown HR status or made no mention of HR status in the eligibility criteria. HER2 status: Eleven of 29 studies, including the MONARCH 3 trial, recruited patients with HER2-negative disease, and 2 additional studies excluded patients with HER2+ or unknown HER2 status. No information relevant to HER2 status was reported in the remaining 16 studies. Disease severity: In 14 of 29 studies, disease severity was appraised using the ECOG PS, which measures patients’ ability to fulfill daily life activities. Most of these studies, including the MONARCH 3 trial, recruited patients with ECOG PS score ≤ 1, except for 3 RCTs, which recruited patients with ECOG PS score ≤ 2 (PALOMA-2, Yardley et al. [2009], and Mila-Santos et al. [2001]). Four studies used WHO criteria to appraise disease severity and included patients with WHO performance status ≤ 2 (SONIA, FALCON, FIRST, and Howell et al. [2004]). Finally, the Nordic trial included patients with Karnofsky performance status ≥ 50%. The remaining 10 studies did not report eligibility criteria regarding patient functionality. Presence of visceral crisis, lymphangitic spread, or leptomeningeal carcinomatosis: Only the MONARCH plus trial and the MONARCH 3 trial excluded patients with visceral crisis, lymphangitic spread, or leptomeningeal carcinomatosis. Seven studies excluded patients with visceral crisis (PALOMA-2, PALOMA-4, MONALEESA-3, LEONARDA-1, PADA-1, PARSIFAL, and TARGET and North American), 2 studies excluded patients with symptomatic pulmonary lymphangitic spread (FALCON trial, Howell et al. [2004]), and only the PADA-1 study excluded patients with leptomeningeal carcinomatosis. Presence of CNS metastasis: Seventeen patients with CNS metastasis were excluded. The remaining studies had no relevant eligibility criteria. Other key eligibility criteria: One study used inclusion or exclusion criteria relevant to ethnicity and included only females of Asian ethnicity (PALOMA-4 trial). The population from Asia was also specifically included in 2 more studies (DAWNA-2, Iwata 2013) even though this was not explicitly part of the inclusion criteria. Overall, the LEONARDA-1 study was excluded due to prior chemotherapy for ABC-MBC being permitted and received by approximately one-third of patients at baseline. The PADA-1 study was excluded due to participants being enrolled and randomized during receipt of systemic treatment for advanced disease. The MONALEESA-7 study was excluded because it included only females who were premenopausal and perimenopausal. Compared to the MONARCH 3 trial, both pivotal studies assessing CDK4/6 inhibitors plus NSAI (i.e., MONALEESA-2 and PALOMA-2 trials) had similar eligibility criteria. The exception is the PALOMA-2 trial that included patients with ECOG PS score of 0 to 2. |
Dosing of comparators | In the MONARCH 3 trial, patients were randomized 2:1 to receive ABE 150 mg twice a day plus an NSAI (investigator choice of either 1 mg ANAS or 2.5 mg LTZ), or PBO plus an NSAI (either 1 mg ANAS or 2.5 mg LTZ). All drugs were orally administered and taken daily during each 28-day cycle until disease progression or intolerable safety. ABE plus ET ABE plus ANAS-LTZ: The MONARCH 3 trial and the MONARCH plus trial assessed ABE twice a day (28-day cycle) plus investigator’s choice of either 1 mg ANAS or 2.5 mg LTZ every day. The 2 studies used the same treatment schedule. PAL plus ET PAL plus LTZ: Three studies assessed 125 mg PAL every day (21-day cycle) plus 2.5 mg LTZ every day. PAL plus FUL: Two studies assessed 125 mg PAL every day (21-day cycle) plus FUL (500 mg every day or 250 mg twice a day, thrice a month). RIBO plus ET RIBO plus LTZ: One study (MONALEESA-2) assessed 600 mg RIBO every day (21-day cycle) plus LTZ 2.5 mg every day. RIBO plus FUL: One study (MONALEESA-3) assessed 600 mg RIBO every day (21-day cycle) plus FUL 500 mg twice a day, thrice a month. DALP plus ET DALP plus ANAS-LTZ: Findings on the efficacy of DALP plus ANAS-LTZ is derived from 1 phase II RCT. The study was considered further for heterogeneity assessment because it may pose a comparator of interest for ABE in the future. DALP was administered at 150 mg every day (cycle duration not reported). ANAS and LTZ were given in the same schedule as in the MONARCH 3 trial (1 mg ANAS or 2.5 mg LTZ every day). CDK4/6 inhibitor (ABE, RIBO or PAL) plus ET The SONIA study assessed investigator’s choice of CDK4/6 inhibitor (ABE, RIBO, or PAL) plus NSAI in patients without previous systemic treatment for advanced disease (first line). Patients who progressed on the initial treatment in the experimental arm then received FUL as second-line treatment. Inclusion of the SONIA study in the ITC depends on the availability of outcome data for each CDK4/6 inhibitor subgroup. ET without a CDK4/6 inhibitor ANAS-LTZ: Four studies assessed ANAS, LTZ, or investigator’s choice of either ANAS or LTZ, without cointervention with a CDK4/6 inhibitor. ANAS was administered as 1 mg every day in 2 studies (schedule not reported by Milla-Santos et al. [2003]) and LTZ was administered as 2.5 mg every day in 1 study. FUL: Three studies assessed FUL. In all 3 RCTs, FUL was administered by intramuscular injection at 28-day cycles. In Howell et al. (2004), a 250 mg injection was administered once monthly, whereas in the FIRST and FALCON studies, patients received 500 mg (two 250 mg injections) thrice in the first month, followed by once monthly injections. Due to the difference in dosage and scheduling, the FUL arm in Howell et al. (2004), is handled separately from the FIRST and FALCON studies, denoted as FUL 250 and FUL 500, respectively, in the networks. TMX: Seven RCTs assessed TMX. TMX was the SOC for the indication of interest. Currently, TMX has been replaced by AIs as the SOC for previously untreated, hormone-sensitive ABC-MBC, and is recommended only for females for whom AIs are contraindicated or not well tolerated. Therefore, studies assessing TMX were considered comparatively less relevant than AI as comparators for ABE in the present ITC. |
Placebo response | Not applicable |
Definitions of end points | PFS: The primary outcome of the MONARCH 3 trial was PFS, defined as time from randomization to first disease progression or death. The same definition was used in 12 more studies. Five studies did not report PFS outcome data (SONIA, FIRST, Mouridsen et al. [2021], Milla-Santos et al. [2003], and Iwata et al. [2013]) OS: Four studies did not report OS outcome data (PALOMA-4, DAWNA-2, FLIPPER, and PARSIFAL). CR: The MONARCH 3 trial defined CR using IA and RECIST 1.1 criteria. Of the 14 studies that reported CR outcome data, 5 additional studies used RECIST 1.1 criteria to assess response, 1 study used RECIST 1.0 criteria and 3 studies used RECIST criteria without specifying the criteria version. Two studies used UICC criteria, and 1 study used International Union Against Cancer criteria. Finally, 1 study used WHO criteria for measurable disease and ECOG PS criteria for unmeasurable lesions. All studies reported using investigator-assessed response except for 5, in which the assessment approach was not reported (FIRST, Milla-Santos et al. [2003], Iwata et al. [2013], Howell et al. [2004], TARGET, and North American) and in Mouridsen et al. (2001) the investigator and a central radiologist independently reviewed outcome data and resolved disagreements. Five studies did not report CR data (PARSIFAL, FALCON, MONALEESA-3, SONIA, and DAWNA-2). ORR: The MONARCH 3 trial defined ORR as CR or partial response. Response was assessed using IA and RECIST 1.1 criteria. Of the 14 studies that reported ORR outcome data, 5 studies did not provide a definition, and the remaining studies provided a definition in alignment with the MONARCH 3 trial. Response was assessed using RECIST 1.1 criteria (n = 7), 1 study used RECIST 1.0 criteria (n = 1), RECIST criteria without reported version (n = 2), 2 studies used UICC criteria (n = 2), International Union Against Cancer criteria (n = 1), and WHO-ECOG PS criteria (n = 1). All studies where the assessor was reported using investigator-assessed response except for Mouridsen et al. (2001). Four studies did not report ORR data (SONIA, FALCON, FIRST, and MONALEESA-3). CBR: The MONARCH 3 trial defined CBR as the best response of CR, PR, or SD for ≥ 6 months. Thirteen additional studies reported CBR outcome data, of which 8 provided no outcome definition. In the remaining 5 (FLIPPER, Howell et al. [2004], MONALEESA-2, PALOMA-2, and PALOMA-4), CBR was defined in the same manner. Response was defined based on RECIST criteria in all studies except for Howell et al. (2004) (UICC criteria). Overall, no studies were excluded due to outcome definition. Regarding safety end points, the MONARCH 3 trial reported overall grade ≥ 3 TEAEs for patients with ≥ 1 CTCAE. A TEAE was defined as any AE that began between the day of first dose and 30 days after treatment discontinuation (or up to any time if the event was serious and related to the study treatment), or any pre-existing condition that increased in CTCAE grade between the day of first dose and 30 days after treatment discontinuation (or up to any time if it was serious and related to the study treatment). Severity was assessed according to the National Cancer Institute-CTCAE version 4.0. In the studies included in the feasibility assessment, the outcome definitions considered were either overall grade ≥ 3 AE or overall serious AE. Data for specific events (e.g., grade ≥ 3 neutropenia) were not assessed. The following categories of safety outcome definitions were identified: Nine studies reported grade 3 and 4 or grade ≥ 3 AEs, including the MONARCH 3 study: specifically, 3 reported grade ≥ 3 TEAE (MONARCH plus, MONARCH 3 studies) or AE (FALCON), and 6 reported grade 3 and 4 AE (DAWNA-2, FLIPPER, MONALEESA-2, PALOMA-1/TRIO-18, PALOMA-2, Iwata et al. [2013] studies). Information regarding assessing treatment relevance of these AE, which was used in the MONARCH 3 trial to measure TEAE, was not reported in these studies Two studies reported grade 3 or 4 AEs occurring in ≥ 10% of patients: PALOMA-4 and PARSIFAL. Two studies reported serious AE: FIRST and TARGET and North American (serious AE). SONIA reported the outcome only after first MBC progression Four studies did not report any safety data of interest: MONALEESA-3, Milla-Santos et al. (2003), Howell et al. (2004), and Mouridsen et al. (2001). Overall, 8 studies were excluded because they either did not report any safety outcomes (n = 4) or reported serious AEs (n = 2), or grade 3 or 4 AEs ≥ 10% of patients (n = 2), which was considered a different definition of safety compared to grade 3 and 4 AE. The SONIA study was also excluded, as the outcomes were reported only after first MBC progression. Grade 3 and 4 AEs reported from 9 studies. Compared to the MONARCH 3 trial, both pivotal studies assessing CDK4/6 inhibitors plus NSAI (i.e., MONALEESA-2, PALOMA-2 studies) had similar safety outcome definitions. |
Timing of end point evaluation | Follow-up duration: Median study follow-up was not reported in 7 studies. In the remaining 22 studies, median follow-up ranged from 7.36 months to 90.1 months. Follow-up in the MONARCH 3 trial was 26.7 months. Median OS follow-up: Median OS follow-up was reported in 25 studies and ranged from 12.9 months to 90.1 months. In the MONARCH 3 trial, it was 8.1 years. |
Withdrawal frequency | Not reported |
Clinical trial setting | Not reported |
Study design | Six of the 35 studies identified in the SLR were single-arm studies (Saeki [2004], RIBECCA, Takahashi [2019], INGE-B, COMPLEEMENT-1, and Danciu et al. [2021]). The remaining 29 studies were RCTs, including the MONARCH 3 trial. Seventeen studies were double-blinded, including the MONARCH 3 trial. Five studies were open-label, and blinding was not reported in the remaining 7 studies. Crossover was allowed in 9 studies, and it was not allowed in 6 studies, including the MONARCH 3 trial. Twelve studies did not report whether crossover was allowed or not. |
Trial phase | Twenty-one of 29 studies were phase III studies, including the MONARCH 3 trial. Five were phase II studies, and the phase was not reported in the remaining 3 studies. |
ABC = advanced breast cancer; ABE = abemaciclib; AE = adverse event; AI = aromatase inhibitor; ANAS = anastrozole; CBR = clinical benefit rate; CNS = central nervous system; CR = complete response; CTCAE = Common Terminology Criteria for Adverse Events; DALP = dalpiciclib; ECOG PS = Eastern Cooperative Oncology Group Performance Status; ER = endocrine receptor; ET = endocrine therapy; EVE = everolimus; FUL = fulvestrant; HR-positive = hormone receptor–positive; IA = investigator assessed; ITC = indirect treatment comparison; LTZ = letrozole; MBC = metastatic breast cancer; NSAI = non-steroidal aromatase inhibitor; ORR = overall response rate; OS = overall survival; PAL = palbociclib; PBO = placebo; PFS = progression-free survival; PgR = progesterone receptor; PR = partial response; RCT = randomized controlled trial; RECIST = Response Evaluation Criteria in Solid Tumours; RIBO = ribociclib; SOC = standard of care; SD = stable disease; SLR = systematic literature review; TEAE = treatment-emergent adverse event; TMX = tamoxifen; UICC = Union for International Cancer Control.
Source: Sponsor-submitted updated indirect treatment comparison report.40
Highlight of Results in the Studies of CDK4/6 Inhibitors
Other CDK4/6 inhibitors are key comparators for abemaciclib in this setting. Pivotal studies evaluating a CDK4/6 inhibitor, including the MONARCH 3 study, are described as provided by the sponsor in Table 23 for reference, including the basic population, treatment groups, and the median PFS and OS of each study. This table includes both first-line and second-line studies.
Table 23: Summary of Results in CDK4/6 Pivotal Studies
Trial name | Population | Treatment | Median PFS (months) | PFS HR (95% CI) | Median OS (months) | OS HR (95% CI) |
|---|---|---|---|---|---|---|
MONALEESA-2 | First-line patients who are postmenopausal with HR-positive, HER2-negative advanced breast cancer | Ribociclib + letrozole | 23.5 | 0.57 (0.46 to 0.70) | 63.9 | 0.76 (0.63 to 0.93) |
Letrozole | 16.0 | Reference | 51.4 | Reference | ||
MONALEESA-3 | First-line or second-line patients who are postmenopausal with HR-positive, HER2-negative advanced breast cancer | Ribociclib + fulvestrant | 20.5 | 0.59 (0.48 to 0.73) | 52.2 | 0.75 (0.62 to 0.92) |
Fulvestrant | 12.8 | Reference | 41.5 | Reference | ||
MONALEESA-7 | First-line patients who are premenopausal or perimenopausal with HR-positive, HER2-negative advanced breast cancer | Ribociclib + (tamoxifen- letrozole- anastrozole) + goserelin | 23.8 | 0.55 (0.44 to 0.69) | 58.7 | 0.76 (0.61 to 0.96) |
(Tamoxifen- letrozole- anastrozole) + goserelin | 13.0 | Reference | 48.0 | Reference | ||
MONARCH 2 | First-line or second-line patients who are perimenopausal or postmenopausal with HR-positive, HER2-negative advanced breast cancer | Abemaciclib + fulvestrant | 16.4 | 0.55 (0.45 to 0.68) | 45.8 | 0.78 (0.64 to 0.95) |
Fulvestrant | 9.3 | Reference | 37.2 | Reference | ||
MONARCH 3 | First-line patients who are postmenopausal with HR-positive HER2-negative advanced breast cancer | Abemaciclib + (anastrozole-letrozole) | 29.0 | 0.54 (0.43 to 0.67) | 66.8 | 0.804 (0.637 to 1.015) |
Anastrozole-letrozole | 14.8 | Reference | 53.7 | Reference | ||
PALOMA-2 | First-line patients who are postmenopausal with HR-positive, HER2-negative advanced breast cancer | Palbociclib + letrozole | 27.6 | 0.56 (0.46 to 0.69) | 53.9 | 0.96 (0.78 to 1.18) |
Letrozole | 14.5 | Reference | 51.2 | Reference | ||
PALOMA-3 | Second-line patients who are postmenopausal patients with HR-positive, HER2-negative advanced breast cancer | Palbociclib + fulvestrant | 9.5 | 0.46 (0.36 to 0.59) | 34.8 | 0.81 (0.65 to 0.99) |
Fulvestrant | 4.6 | Reference | 28.0 | Reference |
CI = confidence interval; HR = hazard ratio; HR-positive = hormone receptor–positive; OS = overall survival; PFS = progression-free survival.
Source: Sponsor-submitted updated indirect treatment comparison report.40
Network Diagrams for the NMAs of PFS, OS, and Safety
Figure 8: PFS Evidence Network (ITT)
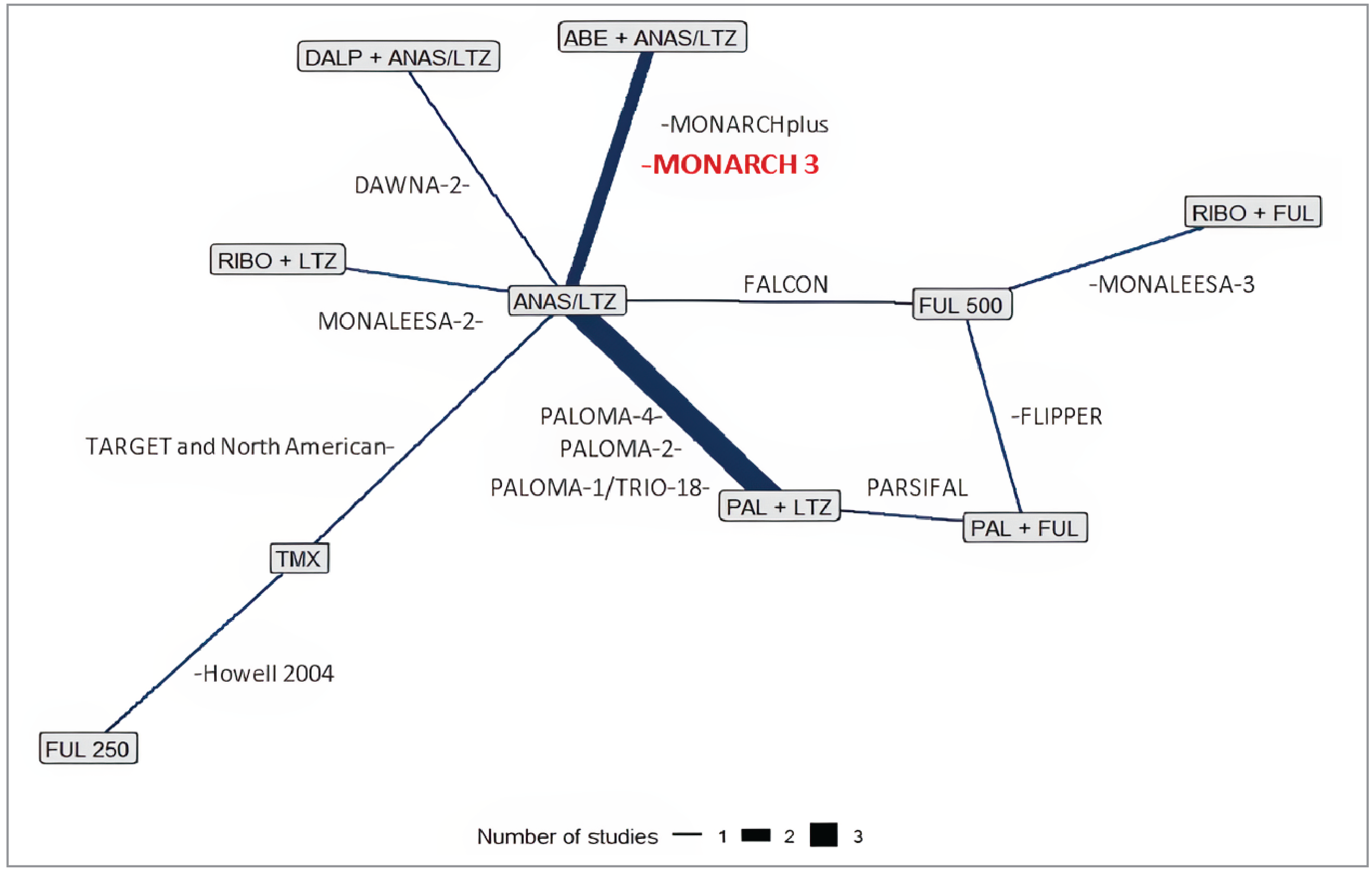
ABE = abemaciclib; ANAS = anastrozole; DALP = dalpiciclib; FUL = fulvestrant; ITT: intention to treat; LTZ = letrozole; PAL = palbociclib; PFS = progression-free survival; RIBO = ribociclib; TMX = tamoxifen.
Source: Sponsor-submitted updated indirect treatment comparison report.40
Figure 9: OS Evidence Network (ITT)
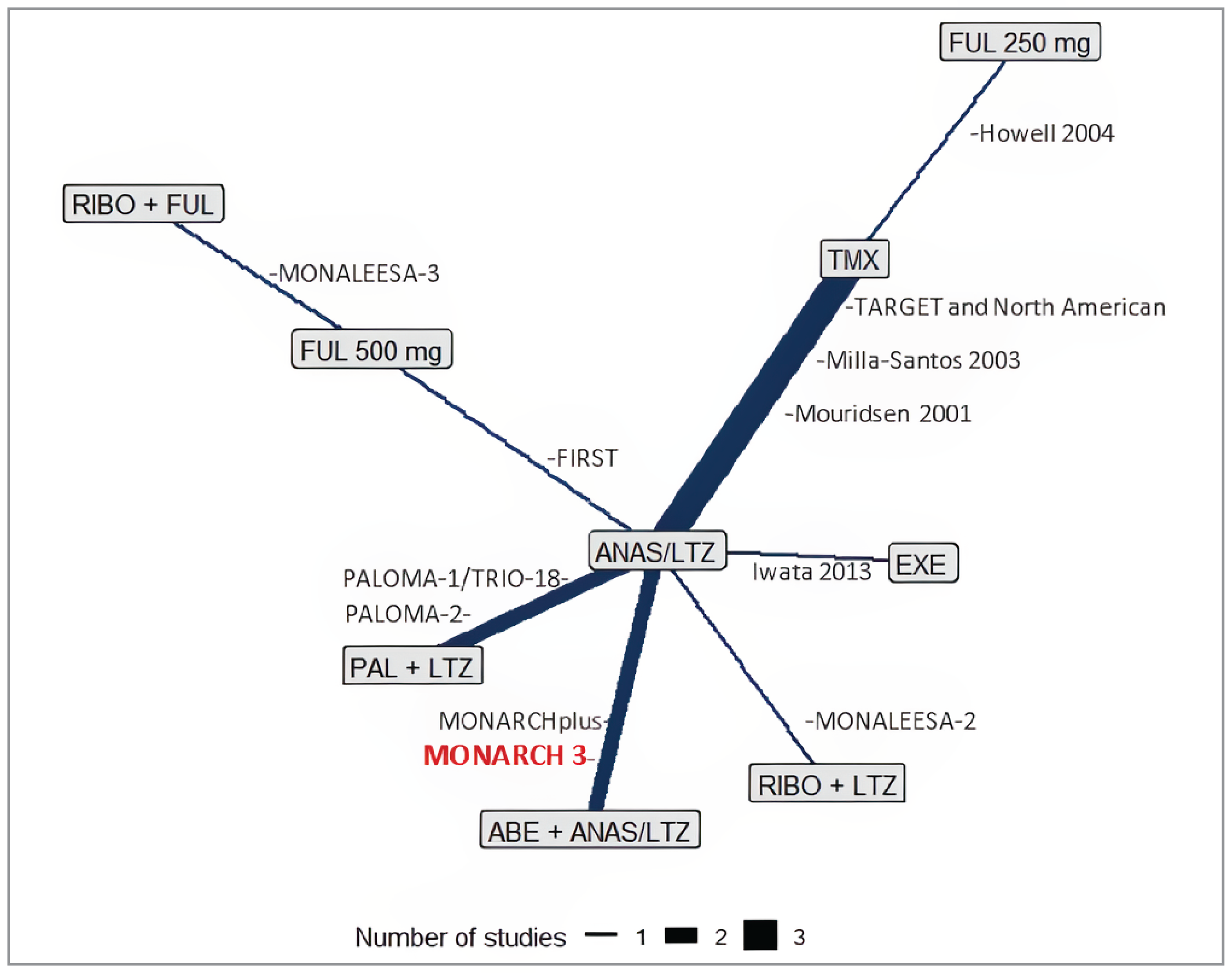
ABE = abemaciclib; ANAS = anastrozole; EXE = exemestane; FUL = fulvestrant; ITT = intention to treat; LTZ = letrozole; OS = overall survival; PAL = palbociclib; RIBO = ribociclib; TMX = tamoxifen.
Source: Sponsor-submitted updated indirect treatment comparison report.40
Figure 10: Safety Evidence Network (ITT)
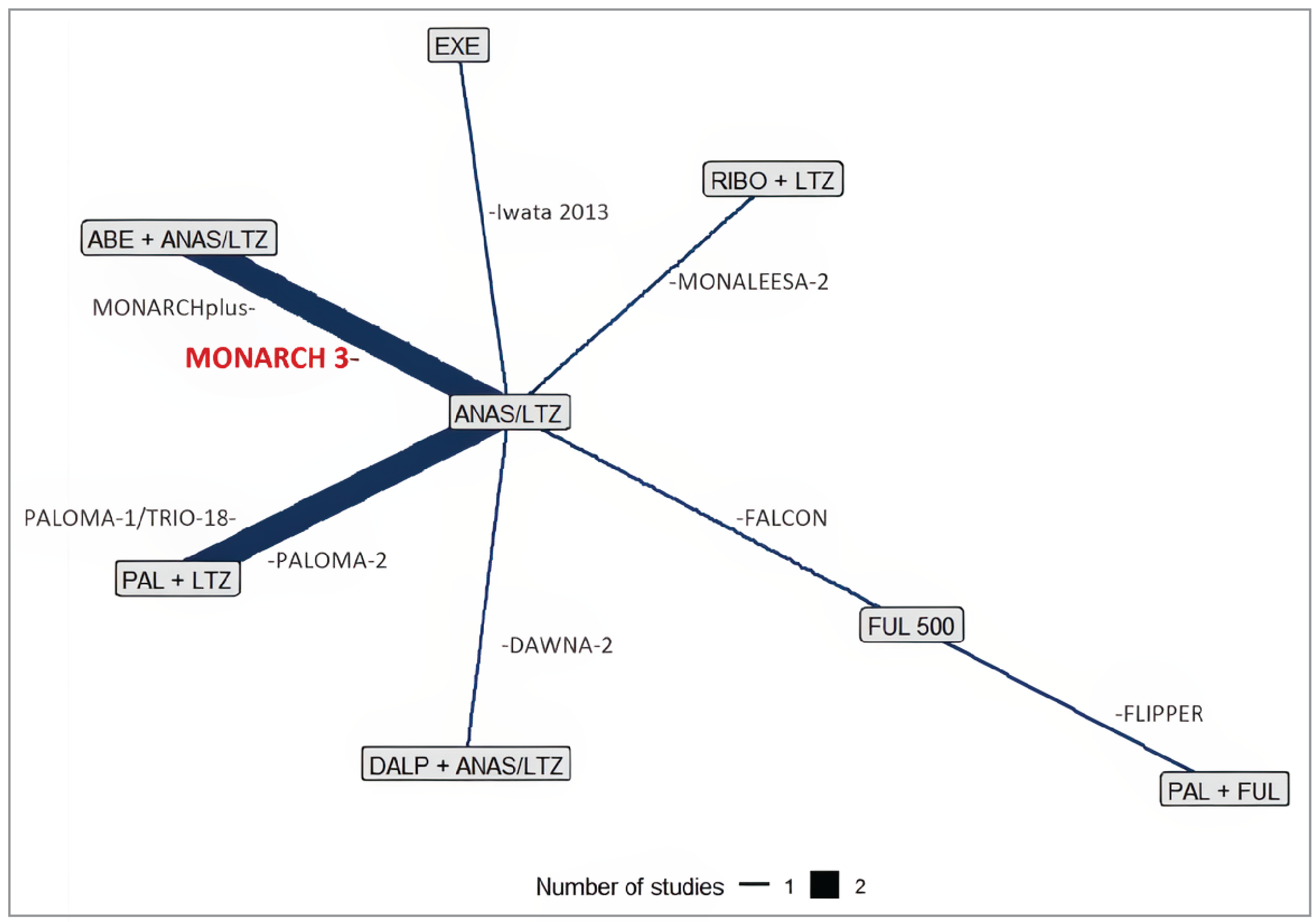
ABE = abemaciclib; ANAS = anastrozole; DALP = dalpiciclib; EXE = exemestane; FUL = fulvestrant; ITT = intention to treat; LTZ = letrozole; PAL = palbociclib; RIBO = ribociclib.
Note: Although it is likely that safety results were presented in safety analysis populations rather than ITT populations, the sponsor’s network diagram heading stated this network was in the ITT population, ergo it has been reproduced here as written.
Source: Sponsor-submitted updated indirect treatment comparison report.40
Additional Outcomes From the NMA
Objective Response Rate NMA
The network included 14 studies evaluating 10 treatments.
Values higher than 1 indicate that results are favourable for abemaciclib plus anastrozole-etrozole versus the comparators. Results showed that abemaciclib plus anastrozole-letrozole was statistically superior, in terms of ORR, to anastrozole-letrozole, palbociclib plus letrozole, palbociclib plus fulvestrant, fulvestrant 500 mg, fulvestrant 250 mg and tamoxifen. Comparisons with the other comparators (ribociclib plus letrozole, dalpiciclib plus anastrozole-letrozole and exemestane) did not achieve statistical significance.
Figure 11: Network Diagram for ORR (ITT)
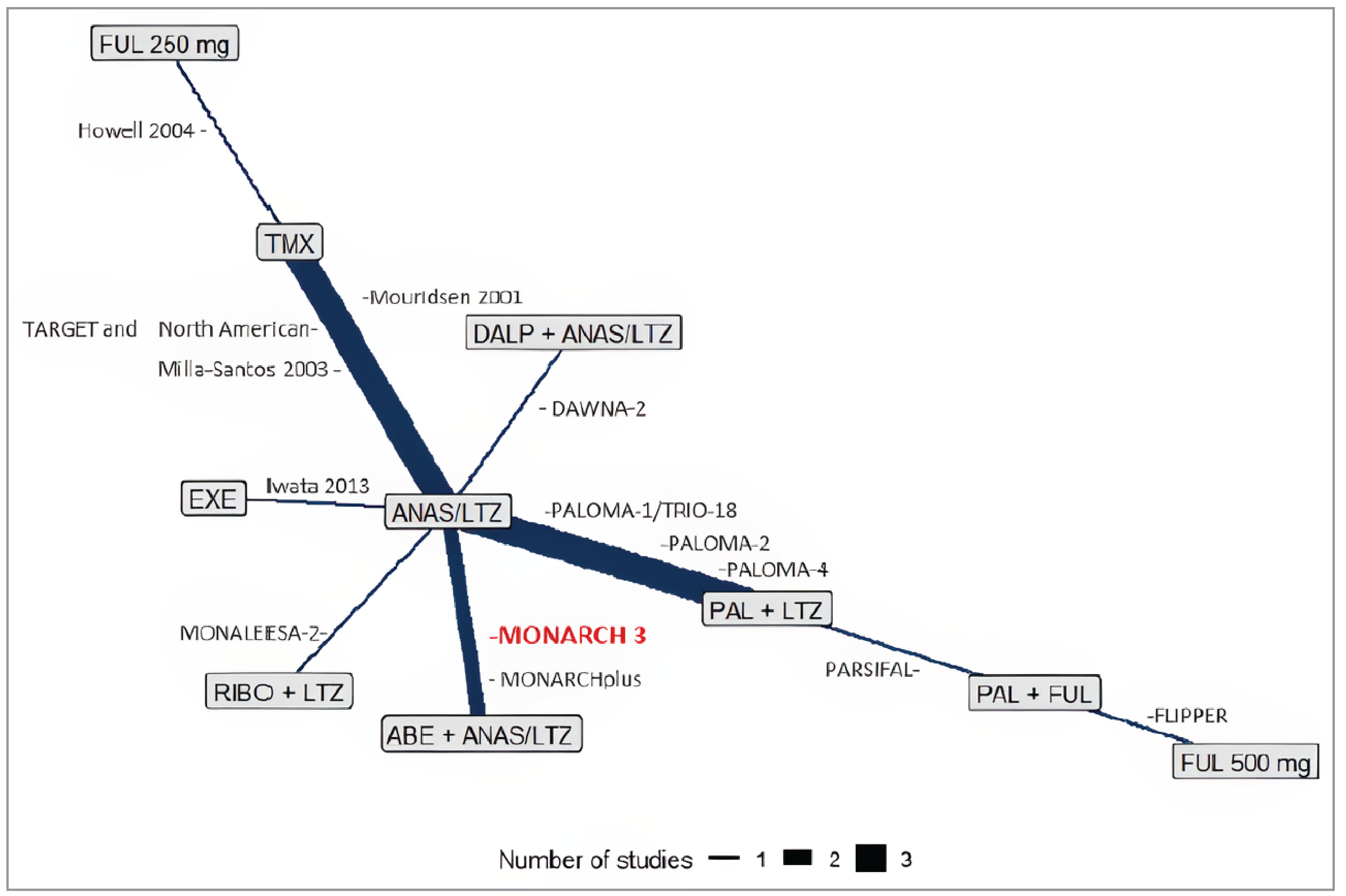
ABE = abemaciclib; ANAS = anastrozole; DALP = dalpiciclib; EXE = exemestane; FUL = fulvestrant; ITT = intention-to-treat; LTZ = letrozole; ORR = overall response rate; PAL = palbociclib; RIBO = ribociclib; TMX = tamoxifen.
Source: Sponsor-submitted updated indirect treatment comparison report.40
Figure 12: Forest Plot for ORR in the ITT Population – FE Model
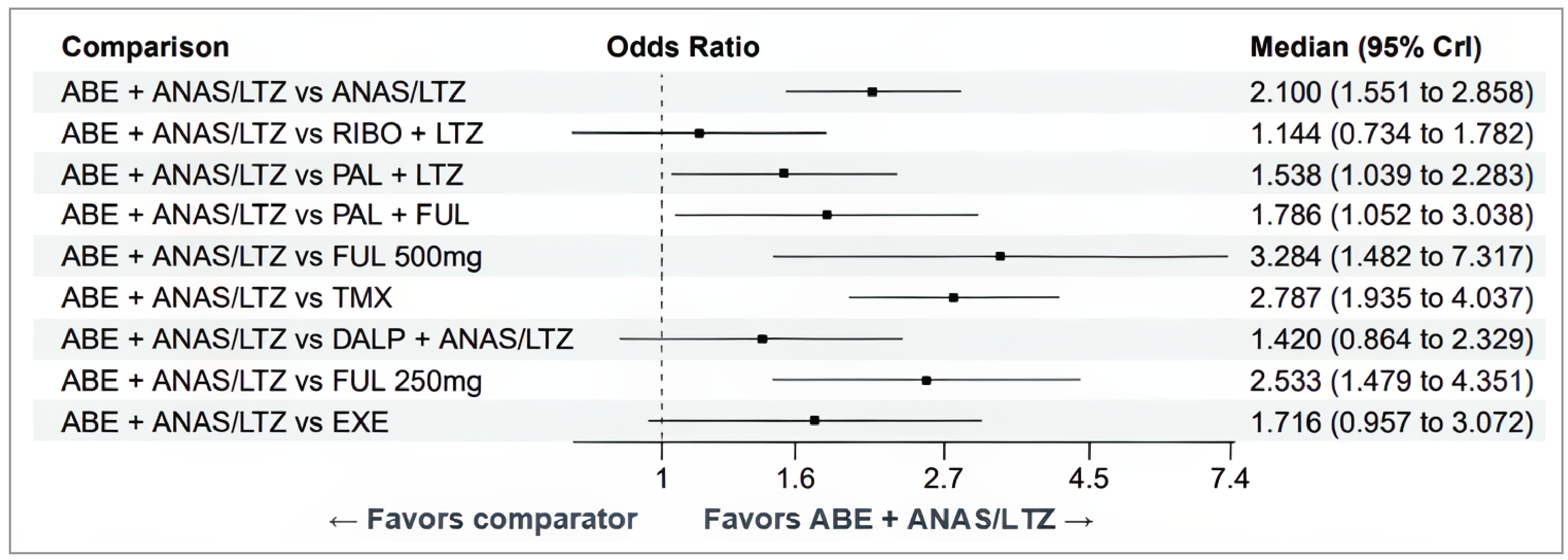
ABE = abemaciclib; anastrozole = anastrozole; CI = confidence interval; DALP = dalpiciclib; EXE = exemestane; FE = fixed effects; FUL = fulvestrant; ITT = intention to treat; LTZ = letrozole; ORR = overall response rate; PAL = palbociclib; RIBO = Ribociclib; TMX = tamoxifen.
Source: Sponsor-submitted updated indirect treatment comparison report.40
Clinical Benefit Rate NMA
The network included 14 trials evaluating 10 treatments.
The results showed no statistical significance for any comparisons, as all CrIs crossed the line of no difference.
Figure 13: Network Diagram for CBR (ITT)
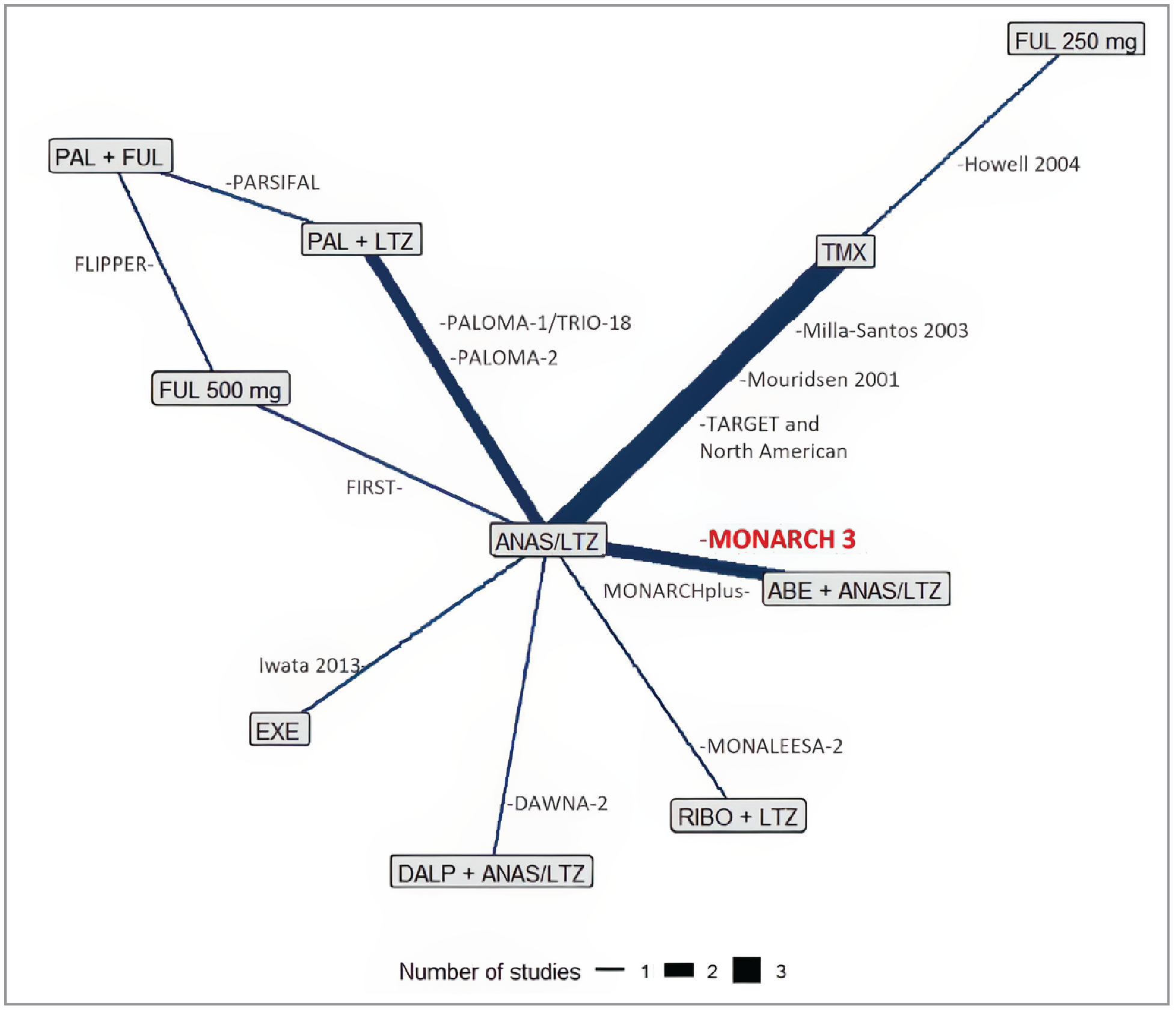
ABE = abemaciclib; ANAS = anastrozole; CBR = clinical benefit rate; DALP = dalpiciclib; EXE = exemestane; FUL = fulvestrant; ITT = intention to treat; LTZ = letrozole; PAL = palbociclib; RIBO = ribociclib; TMX = tamoxifen.
Source: Sponsor-submitted updated indirect treatment comparison report.40
Figure 14: Forest Plot for CBR in the ITT Population – RE Model
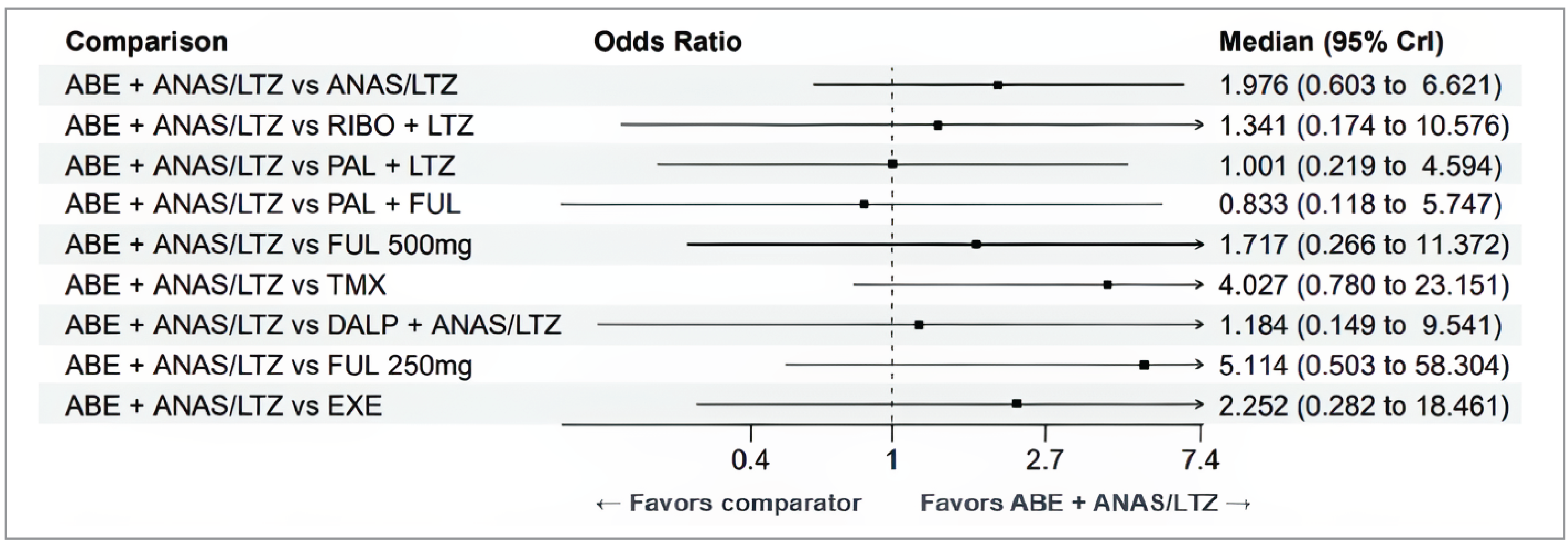
ABE = abemaciclib; ANAS = anastrozole; CBR = clinical benefit rate; CR = complete response; DALP = dalpiciclib; EXE = exemestane; FUL = fulvestrant; ITT = intention to treat; LTZ = letrozole; PAL = palbociclib; RE = random effects; RIBO = ribociclib; TMX = tamoxifen.
Source: Sponsor-submitted updated indirect treatment comparison report.40
Complete Response NMA
The network included 13 studies evaluating 10 treatments.
Results showed that abemaciclib plus anastrozole-letrozole was statistically superior to tamoxifen, but the CrI was extremely wide. No other comparisons achieved statistical significance, and there were very wide CrIs for all comparisons.
Figure 15: Network Diagram for CR (ITT)
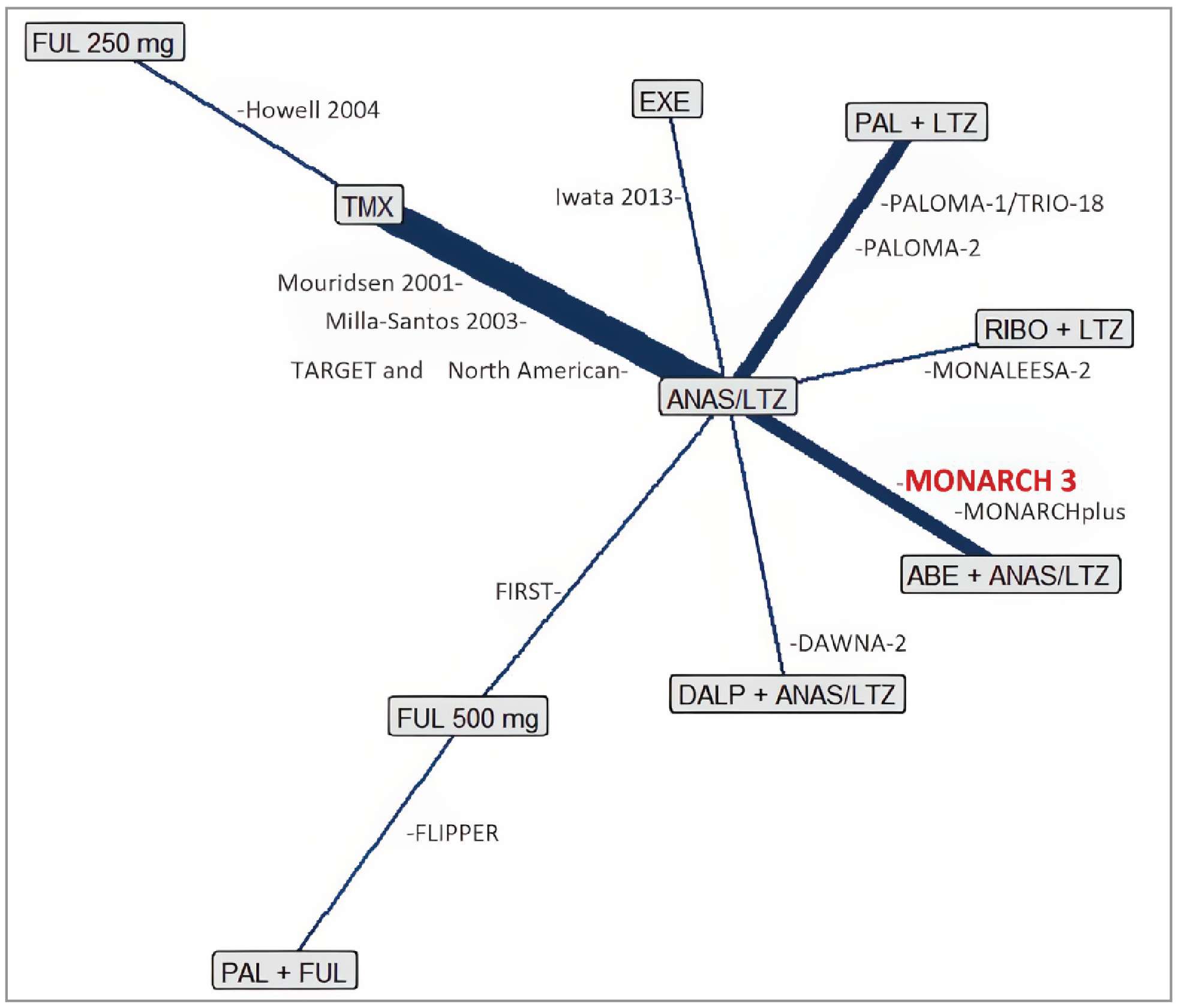
ABE = abemaciclib; ANAS = anastrozole; CR = complete response; DALP = dalpiciclib; EXE = exemestane; FUL = fulvestrant; ITT = intention to treat; LTZ = letrozole; PAL = palbociclib; RIBO = ribociclib; TMX = tamoxifen.
Source: Sponsor-submitted updated indirect treatment comparison report.40
Figure 16: Forest Plot for CR in the ITT population – FE model
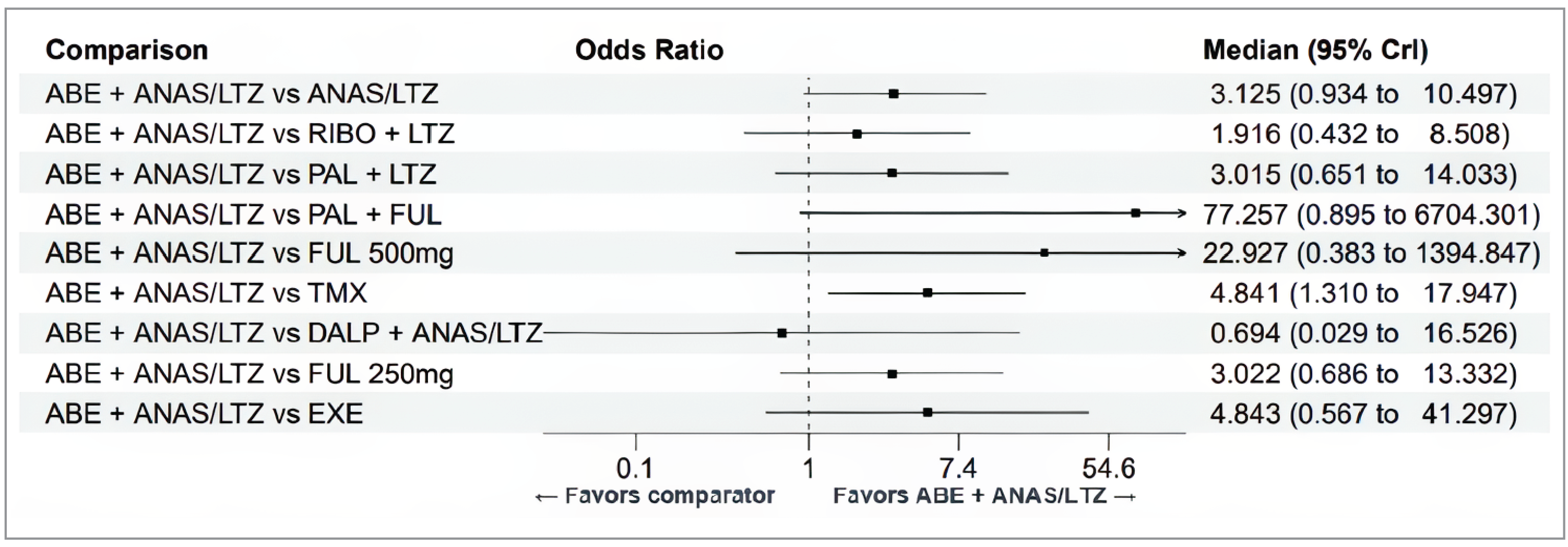
ABE = abemaciclib; ANAS = anastrozole; CR = complete response; DALP = dalpiciclib; EXE = exemestane; FE = Fixed effects; FUL = fulvestrant; ITT = intention to treat; LTZ = letrozole; PAL = palbociclib; RIBO = ribociclib; TMX = tamoxifen.
Source: Sponsor-submitted updated indirect treatment comparison report.40
Pharmacoeconomic Review
Abbreviations
AE
adverse event
BIA
budget impact analysis
CDA-AMC
Canada’s Drug Agency
FP
fractional polynomial
HR
hormone receptor
ICER
incremental cost-effectiveness ratio
NMA
network meta-analysis
NSAI
nonsteroidal aromatase inhibitor
OS
overall survival
PFS
progression-free survival
PH
proportional hazard
QALY
quality-adjusted life-year
TTD
time to treatment discontinuation
Economic Review
The objective of the economic review is to review and critically appraise the pharmacoeconomic evidence submitted by the sponsor on the cost-effectiveness and budget impact of abemaciclib plus a nonsteroidal aromatase inhibitor (NSAI) compared to an NSAI alone, ribociclib plus an NSAI, and palbociclib plus an NSAI “for the treatment of hormone receptor (HR)-positive, HER2-negative advanced or metastatic breast cancer in post-menopausal women as initial endocrine-based therapy.” This is narrower than the Health Canada indication for this patient population, which additionally includes the use of abemaciclib “in combination with fulvestrant as second-line treatment following endocrine therapy, or its use as a single agent in women with disease progression following endocrine therapy and at least 2 prior chemotherapy regimens.” The use of abemaciclib in combination with fulvestrant is being assessed in a separate review,1 and Canada’s Drug Agency (CDA-AMC) approved a deviation request submitted by the sponsor to exclude abemaciclib used as a single drug from this review. Thus, the focus of this review is on the use of abemaciclib in combination with an NSAI in the first-line advanced or metastatic breast cancer setting.
Item | Description |
|---|---|
Drug product | Abemaciclib (Verzenio), 50 mg, 100 mg, and 150 mg oral tablets |
Indication | VERZENIO is indicated in both early breast cancer and advanced breast cancer or metastatic breast cancer. In the advanced breast cancer or metastatic breast cancer setting the following indications were issued NOC by Health Canada on April 5, 2019: VERZENIO (abemaciclib) is indicated for the treatment of HR-positive, HER2-negative advanced or metastatic breast cancer as follows:
|
Submitted price | Abemaciclib: 50 mg tablet: $116.97 100 mg tablet: $115.89 150 mg tablet: $116.22 |
Health Canada approval status | NOC |
Health Canada review pathway | Standard review |
NOC date | April 5, 2019 |
Reimbursement request | Per 1 of the indications: For the treatment of hormone receptor HR-positive, HER2-negative advanced or metastatic breast cancer in combination with an aromatase inhibitor in post-menopausal women as initial endocrine-based therapy |
Sponsor | Eli Lilly Canada Inc. |
Submission history | Previously reviewed: Yes Indication: In combination with endocrine therapy for the adjuvant treatment of adult patients with HR-positive, HER2-negative, node-positive, early breast cancer at high risk of disease recurrence based on clinicopathological features and a Ki 67 score ≥ 20%. Recommendation date: September 29, 2022 Recommendation: Reimburse with clinical criteria and/or conditions. Indication: For the treatment of HR-positive, HER2-negative, advanced, or metastatic breast cancer. In combination with an aromatase inhibitor in postmenopausal women as initial endocrine-based therapy. In combination with fulvestrant in women with disease progression following endocrine therapy. Recommendation date: July 5, 2019 Recommendation: Reimburse with clinical criteria and/or conditions. Additionally, CDA-AMC is currently reviewing abemaciclib resubmission for patients with HR-positive, HER2-negative advanced breast cancer, who had disease progression on or within 12 months of completion of (neo)adjuvant ET or who had disease progression on their first-line ET for advanced disease.1 |
CDA-AMC = Canada’s Drug Agency; ET = endocrine therapy; HR = hormone receptor; NOC = Notice of Compliance.
Key Messages
Abemaciclib is available as 50 mg, 100 mg, and 150 mg tablets. At the submitted price of $116.22 per 150 mg, the 28-day cycle of abemaciclib is predicted to be $6,508 per patient, based on the Health Canada–recommended dosage. The 28-day per patient cost of abemaciclib plus a nonsteroidal aromatase inhibitor (NSAI) for advanced or metastatic breast cancer as initial endocrine-based therapy is predicted to be $6,535 if using anastrozole and $6,547 if using letrozole. Treatment should be continued until disease progression or unacceptable toxicity.
Clinical efficacy in the economic analysis for abemaciclib plus an NSAI versus an NSAI alone was derived from the MONARCH 3 trial. Evidence submitted by the sponsor indicates that abemaciclib plus an NSAI resulted in clinically significant improvement in progression-free survival (PFS). There is uncertainty regarding the benefit and magnitude of abemaciclib plus an NSAI in overall survival (OS), compared with an NSAI alone, in the first line among patients with advanced or metastatic breast cancer, as the results for OS were not statistically significant, although the clinical experts consulted for this review noted that they are clinically important. For abemaciclib plus an NSAI compared with ribociclib plus an NSAI and with palbociclib plus an NSAI, clinical efficacy was informed by a sponsor-submitted network metanalysis (NMA), which was subject to considerable uncertainty due to imprecise estimates and methodological limitations. It is possible for abemaciclib to have better or worse effectiveness with respect to the outcomes of PFS and OS when compared to the other CDK4/6 inhibitors, ribociclib or palbociclib, in the setting in Canada. Grade 3 and 4 adverse events (AEs) were assessed in the NMA. Although there is no strong evidence of substantial differences in the overall safety profile of abemaciclib compared with the other CDK4/6 inhibitors, based on clinical experience each drug is associated with an elevated risk of different types of AEs. Diarrhea, neutropenia, and infections were the most commonly reported AEs associated with abemaciclib in the MONARCH 3 trial, and most were manageable with dose adjustments and supportive care.
The results of the Canada’s Drug Agency (CDA-AMC) base case suggest:
Abemaciclib plus an NSAI is predicted to be associated with the highest costs to the health care system and the greater number of quality-adjusted life-years (QALYs) than all comparators (Table 3).
When considering the next most cost-effective treatment (ribociclib plus an NSAI), abemaciclib plus an NSAI is associated with greater costs (incremental costs = $64,375, primarily driven by increased drug acquisition costs associated with abemaciclib).
When considering the next most cost-effective treatment (ribociclib plus an NSAI), abemaciclib plus an NSAI is predicted to be associated with a gain of 0.02 life-years and may result in a gain of 0.06 QALYs.
The incremental cost-effectiveness ratio (ICER) of abemaciclib plus an NSAI compared with ribociclib plus an NSAI is $1,047,838 per QALY gained in the CDA-AMC base case. The estimated ICER was highly sensitive to assumptions about treatment duration and long-term efficacy. Approximately 14% of the incremental benefit was gained in the extrapolated period (i.e., after ███ months).
These findings are highly uncertain due to the limitations with the indirect comparative evidence and the lack of comparative evidence on time to treatment discontinuation (TTD) across combination therapies, both of which were key drivers to the submitted economic model. Therefore, there is no robust evidence to support a price premium for abemaciclib plus an NSAI over other relevant combination therapies to treat the same patient population. The incremental cost of abemaciclib plus an NSAI is driven primarily by the drug acquisition cost. Of note, there has been a recent availability of generic drugs for palbociclib, which has a similar mechanism of action (i.e., CDK4/6 inhibitor).
CDA-AMC estimates that the budget impact of reimbursing abemaciclib plus an NSAI for the treatment of HR-positive, HER2-negative advanced or metastatic breast cancer in females who are postmenopausal as initial endocrine-based therapy will be approximately $83 million over the first 3 years of reimbursement, compared with the amount currently spent on comparators. The expenditure on abemaciclib plus an NSAI is predicted to be $261 million over this period. The actual budget impact of reimbursing abemaciclib plus an NSAI will depend on the remaining number of people eligible for treatment with abemaciclib due to previous exposure, and the uptake of generic drugs for palbociclib. At the submitted price, the incremental budget impact of reimbursing abemaciclib plus an NSAI is predicted to be more than $40 million in year 3, and the economic feasibility of adoption must be addressed. Additionally, the magnitude of uncertainty in the budget impact must be addressed to ensure the feasibility of adoption, given the difference between the sponsor’s estimate and the CDA-AMC estimate.
Summary of the Submitted Economic Evaluation
The sponsor submitted a cost-utility analysis to estimate the cost-effectiveness of abemaciclib plus an NSAI from the perspective of a public health care payer in Canada over a 15-year horizon. The modelled population comprised patients with HR-positive, HER2-negative advanced or metastatic breast cancer who have not received prior systemic treatment in the advanced setting, based on the participants in the MONARCH 3 trial. This is narrower than the Health Canada population but reflects the reimbursement request for this submission. The sponsor’s base-case analysis included costs related to drug acquisition, administration, disease management, adverse events (AEs), subsequent therapies, and terminal care.
In the sponsor’s base case, only an NSAI alone and abemaciclib plus an NSAI remained on the cost-effectiveness frontier. Abemaciclib plus an NSAI was associated with incremental costs of $202,665 and 0.77 incremental quality-adjusted life-years (QALYs) relative to an NSAI alone. This resulted in an incremental cost-effectiveness ratio (ICER) of $261,782 per QALY gained. Of the incremental benefit compared to an NSAI alone, approximately 13% of benefit was predicted to be accrued after the duration of the MONARCH 3 trial (maximum follow-up = ███ months). Additional information about the sponsor’s submission is summarized in Appendix 3.
CDA-AMC identified several key issues with the sponsor’s analysis (refer to Table 2; full details in Appendix 4). A revised base case was therefore developed.
Table 2: Key Issues With the Sponsor’s Economic Submission
Issue | What evidence is there to inform this issue? | How was this issue addressed by CDA-AMC? | Did CDA-AMC explore uncertainty in a scenario analysis? |
|---|---|---|---|
The comparative efficacy between CDK4/6 inhibitors and extrapolations beyond the trial data are highly uncertain and lacks face validity. | There is a lack of direct head-to-head evidence comparing abemaciclib plus fulvestrant to other combination therapies. The CDA-AMC Clinical Review of the sponsor’s NMA found the results too uncertain. It is possible for abemaciclib plus an NSAI to have better or worse efficacy compared to ribociclib plus an NSAI or palbociclib plus an NSAI. | CDA-AMC could not address this issue in the base case as alternative models using the fractional polynomial model were not provided by the sponsor. | To explore uncertainty, CDA-AMC conducted a scenario analysis using the Cox proportional hazards models submitted by the sponsor to estimate PFS and OS, with an alternate distribution selected for an NSAI alone to result in more clinically plausible long-term estimates according to clinical expert input. |
The modelling approach to TTD results in a disproportionately larger gap between TTD and PFS curves for abemaciclib plus an NSAI compared to other CDK4/6 inhibitors. | TTD was not included as an outcome assessed within the submitted NMA. The sponsor used the unadjusted median TTDs vs. NSAI alone (naive comparison). Clinical input obtained by CDA-AMC does not expect TTD or time from discontinuation to progression across CDK4/6 inhibitors to be different (i.e., similar class effect). | CDA-AMC assumed that TTD was equivalent to PFS across all comparators to decrease the relative differences in time between TTD and progression across combination therapies. | No scenario analysis was conducted. |
The long-term efficacy of abemaciclib plus an NSAI is uncertain. | The sponsor assumed no treatment waning effect with abemaciclib plus an NSAI, indicating that the treatment effect persists indefinitely within the submitted model. Comparative efficacy across CDK4/6 inhibitors is sensitive to this assumption. | CDA-AMC could not address this issue in the base case due to the lack of long-term clinical data. | To explore uncertainty, CDA-AMC conducted scenario analysis assuming treatment waning for abemaciclib plus an NSAI. |
The quality of life associated with disease progression is uncertain and lacked face validity. | The utility value used by the sponsor (0.59) was based on an average from different published literature. While data were collected in the MONARCH 3, the evidence was deemed insufficient by the sponsor. Evidence from the MONARCH 2 trial suggests that the overall utility in a sicker patient population is higher (0.68). | CDA-AMC adopted utility values from the MONARCH 2 trial (0.68). Clinical expert input obtained by CDA-AMC considered this to be the lowest plausible utility value for disease progression. | No scenario analysis was conducted. |
The cost of palbociclib was overestimated. | The sponsor used a price of $253.91 per tablet although generic formulations are available at $126.96 per tablet. | CDA-AMC used the latest publicly available price for palbociclib in the base case. | No scenario analysis was conducted. |
CDA-AMC = Canada’s Drug Agency; NMA = network metanalysis; NSAI = nonsteroidal aromatase inhibitor; OS = overall survival; PFS = progression-free survival; TTD = time to treatment discontinuation; vs. = versus.
Note: Full details of the CDA-AMC identified issues are provided in Appendix 3.
CDA-AMC Assessment of Cost-Effectiveness
The CDA-AMC base case was derived by making changes to model parameter values and assumptions (refer to Table 7), in consultation with clinical expert input. Detailed information about the base case is provided in Appendix 4.
Impact on Health Care Costs
Abemaciclib plus an NSAI is predicted to be associated with the highest costs to the health care system. When considering the next most cost-effective treatment (ribociclib plus an NSAI), abemaciclib plus an NSAI is associated with greater costs (incremental costs = $64,375). This increase in health care spending results from drug acquisition costs associated with abemaciclib (refer to Figure 1 and to Table 3 for full results).
Figure 1: Impact of Abemaciclib Plus an NSAI Versus Comparators on Health Care Costs
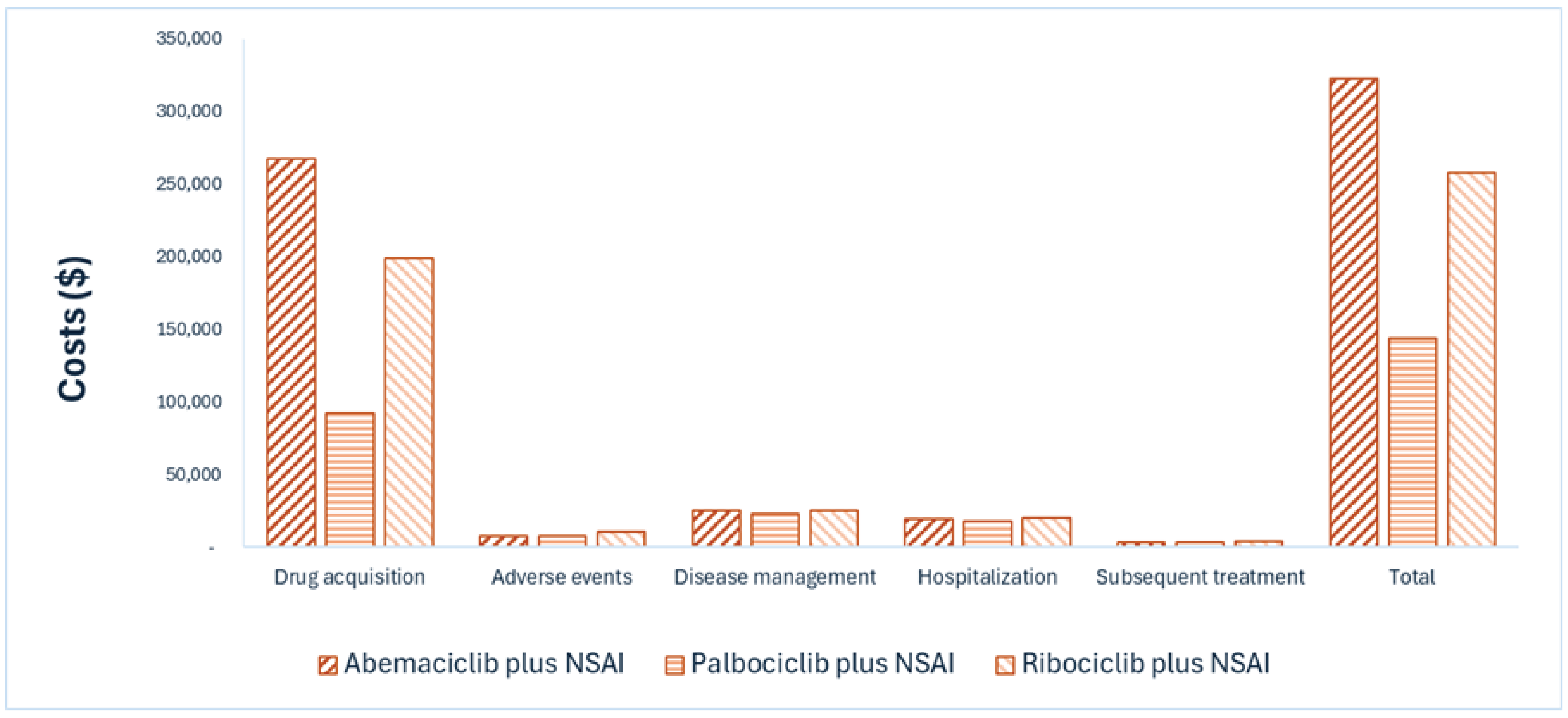
NSAI = nonsteroidal aromatase inhibitor.
Note: Results for NSAI alone are not presented in Figure 1. Refer to Appendix 4 for full results.
Impact on Health
Abemaciclib plus an NSAI is predicted to provide the greatest health benefits, as it extends the time a patient remains in the preprogressed disease state by approximately 5 months (refer to Figure 2 and to Table 3 for full results). When considering the next most cost-effective treatment (ribociclib plus an NSAI), considering the impact of treatment on both quality and length of life, abemaciclib plus an NSAI is predicted to result in 0.06 additional QALYs per patient. Approximately 14% of the predicted incremental benefit was accrued on the basis of extrapolation.
Overall Results
Based on the CDA-AMC analysis, abemaciclib plus an NSAI is associated with the greatest total costs to the health care system and the largest number of QALYs. Treatments appear on the cost-effectiveness frontier in the following order: an NSAI alone, palbociclib plus an NSAI, ribociclib plus an NSAI, and abemaciclib plus an NSAI. Compared with the next drug on the frontier (i.e., ribociclib plus an NSAI), the ICER for abemaciclib plus an NSAI is predicted at $1,047,838 per QALY gained (refer to Table 3). Additional details on the CDA-AMC base case are available in Appendix 4.
Figure 2: Impact of Abemaciclib Plus an NSAI Versus Comparators on Patient Health
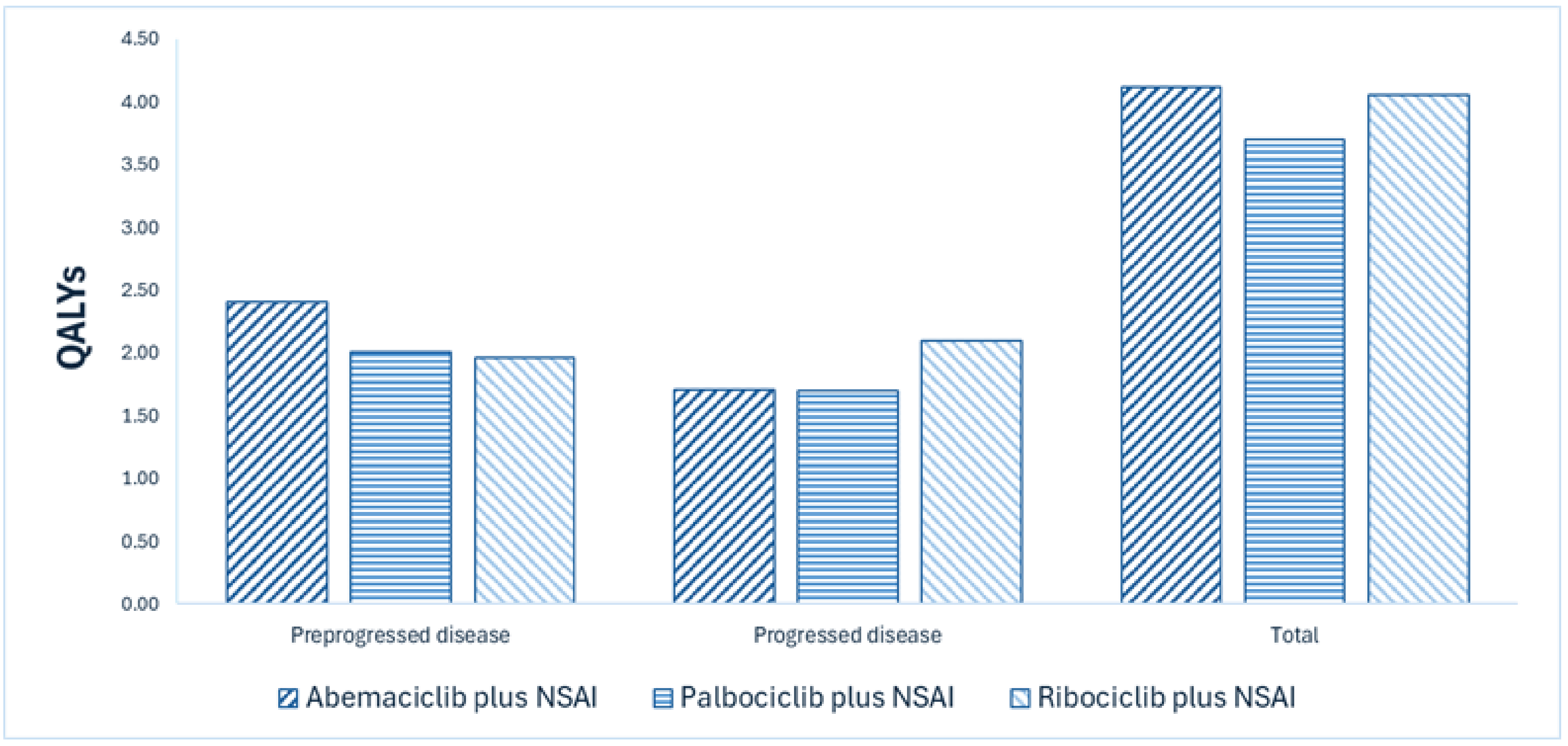
NSAI = nonsteroidal aromatase inhibitor; QALY = quality-adjusted life-year.
Note: Results for NSAI alone are not presented in Figure 2. Refer to Appendix 4 for full results.
Table 3: Summary of CDA-AMC Economic Evaluation Results
Drug | Total costs ($) | Total LYs | Total QALYs | Sequential ICER ($/QALY) |
|---|---|---|---|---|
NSAI alone | 71,014 | 4.79 | 3.40 | Reference |
Palbociclib plus NSAI | 162,384 | 5.12 | 3.70 | 297,961 vs. NSAI alone |
Ribociclib plus NSAI | 275,936 | 5.64 | 4.05 | 325,691 vs. palbociclib plus NSAI |
Abemaciclib plus NSAI | 340,311 | 5.66 | 4.11 | 1,047,838 vs. ribociclib plus NSAI |
CDA-AMC = Canada’s Drug Agency; ICER = incremental cost-effectiveness ratio; LY = life-year; NSAI = nonsteroidal aromatase inhibitor; QALY = quality-adjusted life-year; vs. = versus.
Note: Publicly available list prices were used for all comparators. Refer to Appendix 4 for full disaggregated costs and QALYs for all comparators.
Uncertainty and Sensitivity
Due to a lack of direct comparative evidence, particularly the absence of direct comparison with other combination therapies or comparative time to treatment discontinuation (TTD), these issues were addressed as thoroughly as possible in reanalyses; however, some uncertainty still remains surrounding the modelling approach to extrapolate PFS and OS and treatment waning (refer to Table 2).
Based on the results of the scenario analysis using Cox proportional hazards (PH) models to extrapolate progression-free survival (PFS) and overall survival (OS), abemaciclib plus an NSAI may be dominated (i.e., higher cost and lower benefit relative to ribociclib plus an NSAI).
When including treatment waning for OS, the ICER for abemaciclib plus an NSAI may be increased to $6,261,324 per QALY gained compared to ribociclib plus an NSAI due to the minimal difference in incremental QALYs.
Summary of the Budget Impact
The sponsor submitted a budget impact analysis (BIA) to estimate the 3-year (2026 to 2028) budget impact of reimbursing abemaciclib plus an NSAI for use in the treatment of HR-positive, HER2-negative advanced or metastatic breast cancer in females who are postmenopausal as initial endocrine-based therapy. The sponsor assumed that the payer would be CDA-AMC–participating public drug plans and derived the size of the eligible population using an epidemiologic approach. The price of abemaciclib plus an NSAI was aligned with the price included in the sponsor’s economic evaluation, while the prices of comparators were based on the publicly available list prices. Additional information pertaining to the sponsor’s submission is provided in Appendix 5.
CDA-AMC identified a number of issues with the sponsor’s estimated budget impact and made changes to model parameters and assumptions after clinical expert feedback to derive the CDA-AMC base case (Appendix 5). CDA-AMC estimated that 2,956 to 3,048 patients would be eligible for treatment with abemaciclib plus an NSAI over a 3-year period (year 1 = 2,956; year 2 = 3,002; year 3 = 3,048). The estimated incremental budget impact of reimbursing abemaciclib plus an NSAI is predicted to be approximately $83 million over the first 3 years, with a predicted expenditure of $261 million on abemaciclib plus an NSAI. The actual budget impact is uncertain and will depend on the remaining number of people eligible for treatment with abemaciclib due to previous exposure, and the uptake of generic drugs for palbociclib.
Conclusion
Based on the CDA-AMC base case, abemaciclib plus an NSAI would be considered cost-effective at the submitted price if the public health care system was willing to pay at least $1,047,838 for each additional QALY gained. If the public health care system is not willing to pay that amount, a price reduction should be considered (refer to Figure 3; refer to Table 10 for full details). The estimated cost-effectiveness of abemaciclib plus an NSAI compared with ribociclib plus an NSAI and palbociclib plus an NSAI is uncertain due to a lack of available head-to-head trial data to inform comparative efficacy to other combination therapies and methodological limitations with the network meta-analysis (NMA).
The budget impact of reimbursing abemaciclib plus an NSAI to the public drug plans in the first 3 years is estimated to be approximately $83 million. The 3-year expenditure on abemaciclib plus an NSAI (i.e., not accounting for current expenditure on comparators) is estimated to be $261 million. The estimated budget impact is uncertain due to uncertainty in uptake of treatment with abemaciclib due to previous exposure to abemaciclib in earlier lines of therapy, and the uptake of generic palbociclib.
Figure 3: Summary of the CDA-AMC Economic Analysis and Price Reduction

CDA-AMC = Canada’s Drug Agency; ICER = incremental cost-effectiveness ratio; NSAI = nonsteroidal aromatase inhibitor; QALY = quality-adjusted life-year; vs. = versus.
Note: Expenditure includes only the drug cost of abemaciclib plus an NSAI.
References
1.Canada's Drug Agency. Drug Reimbursement Review: abemaciclib (Verzenio), with fulvestrant, for HR-positive, HER2-negative advanced or metastatic breast cancer. 2025. Accessed May 6, 2025. https://www.cda-amc.ca/abemaciclib-2
2.Ontario Ministry of Health. Ontario drug benefit formulary/comparative drug index [Canada's Drug Agency reference]. Accessed March 10, 2025. https://www.formulary.health.gov.on.ca/formulary/
3.Eli Lilly Canada Inc. Drug Reimbursement Review sponsor submission: Verzenio (abemaciclib), 50 mg, 100 mg, or 150 mg, oral tablet, with an aromatase inhibitor [internal sponsor's package]. February 14, 2025.
4.Ontario Ministry of Health. Exceptional Access Program product prices [Canada's Drug Agency reference]. Accessed March 10, 2025. https://www.ontario.ca/page/exceptional-access-program-product-prices
5.Eli Lilly Canada Inc. Verzenio (abemaciclib): 50 mg, 100 mg, 150 mg, or 200 mg, oral tablet [product monograph]. April 4, 2019. Updated December 1, 2023.
6.Eli Lilly Canada Inc. Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Verzenio (abemaciclib), 50 mg, 100 mg, or 150 mg, oral tablet, with an aromatase inhibitor. February 14, 2025.
7.Eli Lilly and Company. Clinical Study Report: I3Y-MC-JPBM. MONARCH 3: A Randomized, Double-Blind, Placebo-Controlled, Phase 3 Study of Nonsteroidal Aromatase Inhibitors (Anastrozole or Letrozole) plus LY2835219, a CDK4/6 Inhibitor, or Placebo in Postmenopausal Women with Hormone Receptor-Positive, HER2-Negative Locoregionally Recurrent or Metastatic Breast Cancer with No Prior Systemic Therapy in This Disease Setting [internal sponsor's report].
8.Eli Lilly Canada Inc. Abemaciclib in combination with aromatase inhibitors for the first-line treatment of postmenopausal women with HR+, HER2− advanced/metastatic breast cancer: Indirect Treatment Comparisons Report, version 1.0 [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Verzenio (abemaciclib), 50 mg, 100 mg, or 150 mg, oral tablet, with an aromatase inhibitor. December 5, 2024.
9.Eli Lilly Canada Inc. Update to network meta-analysis of systemic anti-cancer treatments for patients with HR+, HER2- advanced breast cancer: Fractional polynomial NMA report [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Verzenio (abemaciclib), 50 mg, 100 mg, or 150 mg, oral tablet, with an aromatase inhibitor. September 16, 2024.
10.Bansback N, Tsuchiya A, Brazier J, Anis A. Canadian valuation of EQ-5D health states: preliminary value set and considerations for future valuation studies. PLoS One. 2012;7(2):e31115. doi: 10.1371/journal.pone.0031115 PubMed
11.Ontario Ministry of Health. Ontario drug benefit formulary/comparative drug index, effected from August 31, 2023 [sponsor supplied reference]. https://www.formulary.health.gov.on.ca/formulary
12.Ontario Ministry of Health. Exceptional Access Program product prices [sponsor supplied reference]. https://www.ontario.ca/page/exceptional-access-program-product-prices
13.Government of Ontario. Ontario Case Costing Initiative [sponsor supplied reference]. 2017.
14.Government of Ontario. Schedule of benefits [sponsor supplied reference]. 2024. https://www.ontario.ca/files/2024-08/moh-schedule-benefit-2024-08-30.pdf
15.Yu M, Guerriere DN, Coyte PC. Societal costs of home and hospital end-of-life care for palliative care patients in Ontario, Canada. Health Soc Care Community. 2015;23(6):605-18. doi: 10.1111/hsc.12170 PubMed
16.Jansen JP. Network meta-analysis of survival data with fractional polynomials. BMC Med Res Methodol. 2011;11:61. doi: 10.1186/1471-2288-11-61 PubMed
17.Hortobagyi GN, Stemmer SM, Burris HA, et al. Updated results from MONALEESA-2, a phase III trial of first-line ribociclib plus letrozole versus placebo plus letrozole in hormone receptor-positive, HER2-negative advanced breast cancer. Ann Oncol. 2018;29(7):1541-1547. doi: 10.1093/annonc/mdy155 PubMed
18.Coyle D, Haines A, Lee K. Extrapolating Clinical Evidence Within Economic Evaluations. Can J Health Technol. 2023;3(5). doi: 10.51731/cjht.2023.649 PubMed
19.Lloyd A, Nafees B, Narewska J, Dewilde S, Watkins J. Health state utilities for metastatic breast cancer. Br J Cancer. 2006;95(6):683-90. doi: 10.1038/sj.bjc.6603326 PubMed
20.National Institute for Health and Care Excellence. Ribociclib with an aromatase inhibitor for previously untreated, hormone receptor-positive, HER2-negative, locally advanced or metastatic breast cancer technology appraisal guidance. (Technology appraisal guidance TA496). 2017. Accessed by sponsor, no date provided. https://www.nice.org.uk/guidance/ta496
21.Sledge GW, Jr., Toi M, Neven P, et al. MONARCH 2: Abemaciclib in Combination With Fulvestrant in Women With HR+/HER2- Advanced Breast Cancer Who Had Progressed While Receiving Endocrine Therapy. J Clin Oncol. 2017;35(25):2875-2884. doi: 10.1200/JCO.2017.73.7585 PubMed
22.IQVIA. PharmaStat. 2023. Accessed March 10, 2025. https://www.iqvia.com/
23.CADTH. Drug Reimbursement Expert Review Committee final recommendation: abemaciclib (Verzenio - Eli Lilly Canada Inc.). July 5, 2019. Accessed by sponsor, no date provided. https://www.cda-amc.ca/sites/default/files/pcodr/Reviews2019/10161AbemaciclibMBC_fnRec_ApprovedbyChair_v01_2019-07-04_Post_05Jul2019_final.pdf
24.Canada's Drug Agency. Drug Reimbursement Review: abemaciclib (Verzenio), with an aromatase inhibitor, for HR-positive, HER2-negative advanced or metastatic breast cancer. 2025. Accessed May 6, 2025. https://www.cda-amc.ca/abemaciclib-1
25.Canada's Drug Agency. Reimbursement recommendation: abemaciclib (Verzenio). Can J Health Technol. 2024;4(10). doi: 10.51731/cjht.2024.1007
26.Eli Lilly Canada Inc. Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Verzenio (abemaciclib), 50 mg, 100 mg, or 150 mg, oral tablet, with an aromatase inhibitor. February 14, 2025.
27.Statistics Canada. Table: 17-10-0005-01. Population estimates on July 1st, by age and sex [sponsor supplied reference]. https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1710000501
28.Canadian Cancer Society. Canadian Cancer Statistics: Cancer Specific Statistics [sponsor supplied references]. 2024. Accessed November 2024. https://cancer.ca/en/research/cancer-statistics/canadian-cancer-statistics
29.Canadian Cancer Statistics Advisory, Canadian Cancer Society, Statistics Canada, Public Health Agency of Canada. A 2022 special report on cancer prevalence. 2022. Accessed November 2024. https://cancer.ca/Canadian-Cancer-Statistics-2022-EN
30.Brezden-Masley C, Fathers KE, Coombes ME, Pourmirza B, Xue C, Jerzak KJ. A population-based comparison of treatment patterns, resource utilization, and costs by cancer stage for Ontario patients with hormone receptor-positive/HER2-negative breast cancer. Breast Cancer Res Treat. 2021;185(2):507-515. doi: 10.1007/s10549-020-05960-4 PubMed
31.Sheffield KM, Peachey JR, Method M, et al. A real-world US study of recurrence risks using combined clinicopathological features in HR-positive, HER2-negative early breast cancer. Future Oncol. 2022;18(21):2667-2682. doi: 10.2217/fon-2022-0310 PubMed
32.Surveillance Research Program, National Cancer Institute. SEER*Explorer: An interactive website for SEER cancer statistics [sponsor supplied reference]. April 2024. Accessed October 2024. https://seer.cancer.gov/statistics-network/explorer
33.Heer E, Harper A, Escandor N, Sung H, McCormack V, Fidler-Benaoudia MM. Global burden and trends in premenopausal and postmenopausal breast cancer: a population-based study. Lancet Glob Health. 2020;8(8):e1027-e1037. doi: 10.1016/S2214-109X(20)30215-1 PubMed
34.Tolaney SM, Punie K, Carey LA, et al. Real-world treatment patterns and outcomes in patients with HR+/HER2- metastatic breast cancer treated with chemotherapy in the United States. ESMO Open. 2024;9(9):103691. doi: 10.1016/j.esmoop.2024.103691 PubMed
35.Sutherland G, Dihn T. Understanding the gap: a pan-Canadian analysis of prescription drug insurance coverage [sponsor supplied reference]. The Conference Board of Canada; 2017. https://www.conferenceboard.ca/product/understanding-the-gap-a-pan-canadian-analysis-of-prescription-drug-insurance-coverage/
Appendix 1: Cost Comparison Table
Please note that this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical expert feedback and CDA-AMC–participating public drug plans. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans
Table 4: Cost Comparison for HR-Positive, HER2-Negative Advanced or Metastatic Breast Cancer
Treatment | Strength and/or concentration | Form | Price | Recommended dosage | Daily cost ($) | 28-day cost ($)a |
|---|---|---|---|---|---|---|
Abemaciclib | 50 mg 100 mg 150 mg | Tablet | 116.9725 115.8889 116.2173 | 150 mg twice dailya | 232.43 | 6,508 |
Abemaciclib plus anastrozole | — | — | — | — | 233.39 | 6,535 |
Abemaciclib plus letrozole | — | — | — | — | 233.81 | 6,547 |
CDK inhibitor | ||||||
Ribociclib | 200 mg | Tablet | 94.1271b | 600 mg once daily for 21 consecutive days followed by 7 days off treatment | 211.79 | 5,930 |
Palbociclib | 75 mg 100 mg 125mg | Capsule | 126.9562 126.9562 126.9562 | 125 mg, once daily on days 1 to 21 of each 28-day | 95.22 | 2,666 |
Ribociclib plus anastrozole | — | — | — | — | 212.74 | 5,957 |
Ribociclib plus letrozole | — | — | — | — | 213.16 | 5,969 |
Palbociclib plus anastrozole | — | — | — | — | 96.18 | 2,693 |
Palbociclib plus letrozole | — | — | — | — | 96.61 | 2,705 |
Nonsteroidal aromatase inhibitor | ||||||
Anastrozoled (Arimidex) | 1 mg | Tablet | 0.9522 | 1 mg, once dailyc | 0.95 | 27 |
Letrozoled (Femara) | 2.5 mg | Tablet | 1.3780 | 2.5 mg, once dailyc | 1.38 | 39 |
HR = hormone receptor.
Notes All prices are from the Ontario Drug Benefit Formulary (accessed March 2025),2 unless otherwise indicated, and do not include dispensing fees. Recommended dosages are based on product monographs, unless otherwise indicated.
aSponsor’s submitted price and recommended dosage.3
bPrice from the Ontario Exceptional Access Program (accessed March 2025).4
cCancer Care Ontario Formulary.
dNot recommended for females who are premenopausal according to the Cancer Care Ontario Formulary.
Appendix 2: Input Relevant to the Economic Review
Please note that this appendix has not been copy-edited.
This section is a summary of the input received from the patient groups, clinician groups, and drug plans that participated in the CDA-AMC review process.
Patient input was received from Breast Cancer Canada, Rethink Breast Cancer, and Canadian Breast Cancer Network, collected via online surveys (685 total respondents across 5 independent surveys), and 4 interviews from patients living in Canada with advanced breast cancer. Frontline treatment experience for patients was reported to largely consist of CK4/6 inhibitor plus endocrine therapy (35% ribociclib, 26% palbociclib, 3% abemaciclib), although patients also receive endocrine therapy alone, or IV-based chemotherapy. Patient input highlighted that patients place a high value on oral therapies that provide extended cancer control and meaningful quality of life, while delaying IV chemotherapy. Patient input noted that controlling disease and extending life expectancy are the most important treatment goals, while also avoiding chemotherapy. They also noted that the AEs profile of available CDK4/6 inhibitors differ, as does the dosing schedule and the monitoring schedule and having more options would increase the ability to adhere to treatment. All 4 respondents with abemaciclib experience received it in combination with aromatase inhibitor as first-line treatment for advanced breast cancer. Most patients reported manageable AEs, although all of them reported some degree of side effects, particularly diarrhea, which impaired quality of life when severe. AEs were mostly successfully managed by reducing abemaciclib dosage.
Clinician group input was received from Ontario Health (Cancer Care Ontario) Breast Cancer Drug Advisory Committee and the Research Excellence, Active Leadership Canadian Breast Cancer Alliance. Current pathway of care for patients includes ribociclib or palbociclib plus aromatase inhibitor in the first-line setting. The treatment goals include extending PFS and OS while minimizing AEs to preserve quality of life, in addition to delaying the need for subsequent chemotherapy. Input indicated that treatment with abemaciclib plus aromatase inhibitor would be an additional option in the first-line setting where palbociclib or ribociclib plus aromatase inhibitor reside in the treatment algorithm.
Input from CDA-AMC–participating drug plans highlighted the lack of evidence comparing abemaciclib plus aromatase inhibitor versus ribociclib or palbociclib plus aromatase inhibitor, which are the current standard of care. Drug plans highlighted concerns with twice daily dosing versus once daily dosing versus the other CDK4/6 inhibitors and inquired whether it would be reasonable to switch patients from ribociclib or palbociclib to abemaciclib. Drug plans highlighted the presence of confidential negotiated prices for ribociclib and palbociclib for the same indication.
Several of these concerns were addressed in the sponsor’s model:
Treatment goals of PFS and OS were captured in the sponsor’s model.
AEs such as alanine aminotransferase increase, anemia, aspartate aminotransferase increase, diarrhea, leukopenia, lymphopenia, nausea, and neutropenia were modelled.
CDA-AMC addressed some of these concerns as follows:
CDA-AMC adopted alternative assumptions for quality of life postprogression and the most updated publicly available prices for comparators.
CDA-AMC was unable to address the following concerns:
Lack of head-to-head trial data for abemaciclib plus NSAI versus ribociclib plus NSAI and palbociclib plus NSAI.
CDA-AMC was not able to estimate the impact of patients switching from other CDK 4/6 inhibitors to abemaciclib plus aromatase inhibitor if this regimen becomes available in Canada.
Appendix 3: Summary of the Sponsor’s Submission
Please note that this appendix has not been copy-edited.
Summary of the Sponsor’s Economic Evaluation
For the pharmaceutical reviews program, clinical and economic information is submitted to CDA-AMC by the sponsor. The CDA-AMC health economics team reviews the submitted economic information and appraises the information in collaboration with clinical expert feedback and the clinical review team to evaluate key assumptions, influential parameters, and the overall rigour of the economic submission. Based on what the team learns through this process, adjustments may be made to the sponsor’s model to produce the CDA-AMC base case. The CDA-AMC base case represents the team’s current understanding of the clinical condition, clinical evidence currently available, and best interpretation of the economic evidence based on the information provided.
For the review of abemaciclib plus NSAI, the sponsor provided a cost-utility analysis and a budget impact analysis. The sponsor’s economic submission is summarized in Table 5.
Table 5: Key Components of the Sponsor’s Economic Evaluation
Component | Description |
|---|---|
Treatment information | |
Drug under review | Abemaciclib (Verzenio), oral tablets (50 mg, 100 mg, and 150 mg), Abemaciclib is administered in combination with an NSAI (e.g., anastrozole or letrozole). |
Submitted price of drug under review | Abemaciclib: 50 mg: $116.97 100 mg: $115.88 150 mg: $116.21 |
Regimen | 150 mg orally twice daily until disease progression or unacceptable toxicity; administered in combination with anastrozole (1 mg once daily) or letrozole (2.5 mg once daily)5 |
Per 28-day course cost of drug under review | Abemaciclib: $6,508 per patient6 Abemaciclib plus NSAI = $6,544 per patient. |
Model information | |
Type of economic evaluation | Cost-utility analysis PSM |
Treatment | Abemaciclib plus NSAI |
Included comparators |
|
Perspective | Publicly funded health care payer perspective |
Time horizon | 15 years |
Cycle length | 28 days |
Modelled population | Patients with HR-positive, HER2-negative advanced or metastatic breast cancer who have not received prior systemic treatment in the advanced setting. |
Characteristics of modelled population | Derived from the MONARCH 3 trial (mean age: 63 years; BSA: 1.70 m2; weight: 67.99 kg)6 |
Model health states |
|
Data sources | |
Comparative efficacy | |
Natural history and/or clinical pathway |
|
Health-related utilities and disutilities | |
Costs included in the model |
|
Summary of the submitted results | |
Base case results | Abemaciclib plus NSAI was associated with an ICER of $261,782 per QALY gained compared to NSAI alone (incremental costs = $202,666; incremental QALYs = 0.77) |
Scenario analysis results |
|
AE = adverse event; BSA = body surface area; FP = fractional polynomial; ICER = incremental cost-effectiveness ratio; HR = hormone receptor; NMA = network meta-analysis; NSAI = nonsteroidal aromatase inhibitor; OS = overall survival; PD = progressed disease; PFS = progression-free survival; PH = proportional hazard; PSM = partitioned survival model; QALY = quality-adjusted life-years; RDI = relative dose intensity; TTD = time to treatment discontinuation; vs. = versus.
Table 6: Summary of the Sponsor’s Economic Evaluation Results — Probabilistic
Drug | Total costs ($) | Total LYs | Total QALYs | Sequential ICER ($/ QALY) |
|---|---|---|---|---|
NSAI alone | 71,013 | 4.79 | 3.12 | Reference |
Abemaciclib plus NSAI | 273,679 | 5.65 | 3.89 | 261,782 vs. NSAI alone |
Palbociclib plus NSAI | 231,805 | 5.12 | 3.49 | Extendedly dominated |
Ribociclib plus NSAI | 259,352 | 5.64 | 3.78 | Extendedly dominated |
ICER = incremental cost-effectiveness ratio; LY = life-year; NSAI = nonsteroidal aromatase inhibitor; QALY = quality-adjusted life-year; vs. = versus.
Appendix 4: Additional Details of CDA-AMC Reanalyses
Please note that this appendix has not been copy-edited.
Clinical Data in the Economic Model
The key clinical efficacy data (i.e., PFS and OS) used to inform the economic model were derived from the MONARCH 3 trial (data cut-off date: September 29, 2023, maximum follow-up ███ months) for abemaciclib plus NSAI and for NSAI alone, and from a sponsor-submitted NMA for all other comparators due to the lack of head-to-head trials against palbociclib plus NSAI, and ribociclib plus NSAI.
The CDA-AMC Clinical Review of the MONARCH 3 trial found that abemaciclib plus NSAI resulted in clinically significant benefit in PFS in comparison to placebo plus NSAI. There is uncertainty regarding the benefit and magnitude of benefit of abemaciclib on OS due to the 95% CI crossing the null threshold. Nevertheless, the clinical expert feedback input sought by CDA-AMC deemed that the observed 13-month median difference in OS between placebo and abemaciclib noted in MONARCH 3 was clinically meaningful in the context of metastatic breast cancer. The CDA-AMC Clinical Review of the sponsor-submitted NMA considered the main analysis using fixed-effect Cox PH models with a sensitivity analysis using fractional polynomial models submitted to address violation of the PH assumptions in some included studies. However, there is uncertainty around these comparisons due to large credible intervals, heterogeneity across the included studies, and underreporting of the variability due to the model selection process. It is possible for abemaciclib to have better or worse effectiveness with regards to the outcomes of PFS and OS when compared to the other CDK4/6 inhibitors, ribociclib or palbociclib, in the setting in Canada. Aggregate grade 3 and 4 AEs were assessed in the NMA and there is no strong evidence of substantial differences in the overall safety profile of abemaciclib compared to the other CDK4/6 inhibitors. Based on clinical experience, each drug is associated with an elevated risk of different types of AEs. Diarrhea, neutropenia, and infections were the most commonly reported AEs associated with abemaciclib in the MONARCH 3 trial, and most were manageable with dose adjustments and supportive care.
In the sponsor’s economic model, PFS and OS were extrapolated beyond the MONARCH 3 trial period using a fractional polynomial (FP) model over a 15-year lifetime time horizon. Notably, of the total incremental QALYs gained over the model horizon, approximately 13% were accrued in the extrapolated period (i.e., after ███ months). The absence of comparative clinical data for relevant nontrial comparators limited the ability of CDA-AMC to validate the sponsor’s results. Several additional sources of uncertainty related to the clinical efficacy inputs in the economic model were noted (refer to Key Components of the Submitted Economic Evaluation). Consequently, the reanalysis by the sponsor and CDA-AMC remain highly uncertain.
Key Issues of the Submitted Economic Evaluation
CDA-AMC identified the following key issues with the sponsor’s analysis:
The comparative efficacy between CDK4/6 inhibitors and extrapolations beyond the trial data are highly uncertain and lack face validity: There are several sources of uncertainty related to the clinical data in the economic model. First, there is a lack of direct head-to-head evidence comparing abemaciclib plus NSAI to ribociclib plus NSAI and palbociclib plus NSAI. Indirect evidence was informed by a sponsor-submitted NMA. Given the violation of proportion hazard assumption observed in OS for the MONARCH 3 trial and in the NMA network, the sponsor used an FP model from the NMA to inform PFS and OS curves for all comparators in the economic model. The FP model uses a multidimensional relative treatment effect rather than a single parameter for treatment effect, which allows more flexible time-varying hazard ratio models.16 The sponsor’s choice of FP model in the NMA (out of 78 choices of FP models) was based on statistical criteria (i.e., the model with the lowest deviance information criterion) with no further details or justification on the choice of different powers used, beyond stating that some second order models were a poor fit to data and did not converge. Hence, the FP model may be over-fit, and the magnitude of the confidence intervals are likely overoptimistic. This may result in a larger difference between treatments than if 1 had corrected for the additional variability introduced by the selection step. However, for the cost-utility analysis, the sponsor submitted only 1 first order FP model and did not provide flexibility within the economic evaluation to incorporate alternative FP models. This substantially limited the ability of the CDA-AMC to validate the impact and appropriateness of different survival curves derived by using different FP model.
Clinical expert input sought by CDA-AMC also noted that the long-term predictions generated by the sponsor’s choice of FP model for the economic analysis underestimated PFS and OS compared to clinical trial data and overestimated differences in efficacy across combination therapies and lacks face validity. For instance, for patients receiving abemaciclib plus NSAI, the economic model predicted OS and PFS at 5 years as 50.0% and 21.6%, respectively, while data from the MONARCH-3 study showed an OS of 54.8% and PFS of 26.9% at 5 years, respectively. Further, given the NMA evidence available, it was not expected that abemaciclib plus NSAI would consistently result in higher PFS or OS estimates in comparison to other CDK4/6 combination therapies. However, abemaciclib was consistently predicted superior to other combination therapies for both outcomes. These differences across CDK4/6 combination therapies persisted and proportionally increased in the long-term. Importantly, the estimated PFS associated with palbociclib plus NSAI also did not meet face validity as it was consistently estimated to be superior to ribociclib plus NSAI, which was not expected according to clinical expert feedback input. Notably, CDK4/6 inhibitors (palbociclib, ribociclib, and abemaciclib) are expected to have relatively similar efficacy, with exception of ribociclib plus NSAI presenting with the only statistically significant OS trial result compared to NSAI alone.17 Thus, if any differences were expected across combination therapies, it was for ribociclib plus NSAI to have potentially higher OS over other combination therapies when they are all modelled against NSAI alone.
Finally, regardless of method used (FP or proportional HR), the CDA-AMC Clinical Review could not conclude that abemaciclib plus NSAI had superior efficacy in comparison to the other CDK4/6 inhibitors, namely palbociclib plus NSAI and ribociclib plus NSAI. Although the proportional HR approach would not be the preferred method to make comparisons within the trial periods due to the violation of PH assumptions for OS, it did result in more plausible long-term extrapolations estimates for OS, which is more aligned with the available evidence and clinical expert input sought by CDA-AMC.
CDA-AMC conducted a scenario analysis using the proportional HR method to estimate PFS and OS. The sponsor’s default parametric distributions were mostly maintained (generalized gamma), with exception for NSAI alone (changed to log-normal) to result in more clinically plausible long-term PFS and OS results according to clinical expert feedback obtained by CDA-AMC for this review.
TTD for patients receiving abemaciclib plus NSAI and comparators is uncertain: In the model, TTD was used to estimate drug acquisition costs. TTD for patients receiving abemaciclib plus NSAI and NSAI alone were informed by extrapolations derived from time-to-event analysis using individual patient data from the MONARCH 3 trial. For nontrial comparators TTD was modelled by applying hazard ratios to the NSAI alone TTD curve. These hazard ratios were estimated as the ratio of the median TTDs versus NSAI alone, across the individual trials. These data were not adjusted for patient characteristics or between-trial differences, as it was a naive estimation approach (i.e., not included in the NMA). The sponsor’s modelling approach disproportionately estimates a larger gap between TTD and PFS curves for abemaciclib plus NSAI versus palbociclib plus NSAI and ribociclib plus NSAI, which results in an underestimation of treatment duration and associated drug acquisition costs for abemaciclib plus NSAI and biases cost-effectiveness results in favour of abemaciclib plus NSAI. Furthermore, the model assumed no correlation between TTD and PFS for these trial arms, meaning patients were assumed to discontinue treatment while remaining progression-free. Clinical expert feedback obtained by CDA-AMC indicated that although it is plausible for patients to discontinue treatment and remain progression free, there is no biological mechanism or evidence that a benefit would be different among CDK4/6 inhibitors or sustained for more than a couple of months after discontinuation (i.e., expected similar class effect).
CDA-AMC set TTD equal to PFS for all comparators in the base case, as it is not expected that there would be differences in sustained PFS benefit after treatment discontinuation across CDK4/6 inhibitors. This change is likely to overestimate the costs of drug acquisition for all treatments; however, it decreases the relative difference in time between TTD and progression across combination therapies.
Uncertainty in the long-term efficacy of abemaciclib plus NSAI: The sponsor assumed no treatment waning effect with abemaciclib plus NSAI, meaning that the treatment effect of abemaciclib plus NSAI was experienced indefinitely in the model. This assumption implies that the treatment effect of abemaciclib plus NSAI will persist for approximately 7 years after treatment discontinuation. Clinical expert feedback consulted by CDA-AMC for this review indicated that they are unaware of evidence that may support this assumption and that it is plausible for treatment effect waning to occur. In the absence of evidence to support the long-term effectiveness of abemaciclib plus NSAI, CDA-AMC assumed that treatment waning would begin after the duration of the MONARCH 3 trial (i.e., ███ months) and would last an additional 77 months, which is aligned with the sponsor’s submitted scenario analysis that included treatment waning for OS. According to the CDA-AMC methods and guidelines for extrapolating clinical evidence within economic evaluations,18 including a treatment waning effect is appropriate in the context where uncertainty remains, and long-term clinical data are lacking.
CDA-AMC conducted a scenario analysis where treatment waning for OS with abemaciclib begins at ███ months and ends after 77 additional months.
Utility values for the progressed disease health state are uncertain: The sponsor included utility values for preprogressed disease (0.767) based on EQ-5D-3L data from the MONARCH 3 trial but opted to use published literature to inform the health state utility value for progressed disease (0.591). This was an average of values from Lloyd et al. (2006)19 and NICE TA496.20 The sponsor justifies that EQ-5D-3L data collected from the MONARCH 3 trial to inform the progressed disease health state utility value (0.744) was insufficient to provide a reliable estimate as it was collected only for 30 days following disease progression. However, the average from the published literature lacked face validity in comparison to other alternate utility values available to the sponsor and appeared to overestimate the decline in quality of life after disease progression. For example, the estimated overall utility from MONARCH 2 trial (0.679)21 is considerably higher than the average utility for progressed disease in the sponsor’s base case (0.591). Yet, patients from MONARCH-2 trial are likely a patients experiencing more severe illness than in MONARCH 3 trial. According to clinical expert feedback consulted by CDA-AMC, the decline in quality of life after disease progression in breast cancer is not as quick or severe compared to other metastatic cancers. Therefore, it was deemed more appropriate to assume the utility value for the disease progressed health state derived from MONARCH-2 trial as the lowest plausible utility value after progression. This may still be overestimating the decline in quality of life after disease progression, but to a lesser extent than the sponsor’s assumptions.
CDA-AMC assumed a utility value of 0.679 from the MONARCH 2 trial for the progressed disease health state in the base case.
The model overestimated the price of palbociclib. CDA-AMC noted that palbociclib has generic formulations available for more than 6 months, with flat prices reduced from $253.9123 to $126.9562 per tablet, for all strengths, based on the Ontario Drug Benefit Formulary.2,22 The outdated cost of palbociclib resulted in overestimation of the palbociclib plus the NSAI regimen total cost in the model.
CDA-AMC used the latest publicly available prices for palbociclib in the base case.
CDA-AMC Reanalysis of the Economic Evaluation
The CDA-AMC base case was derived by making changes in model parameter values and assumptions, after clinical expert feedback (refer to Table 7). The impact of these changes, individually and collectively, is presented in Table 8.
Table 7: Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CDA-AMC value or assumption |
|---|---|---|
1. Treatment discontinuation |
|
|
2. Utility value for postprogression health state | Postprogression utility value based on an average of 2 values from published literature (0.591) | Postprogression utility value based on MONARCH-2 trial data (0.679) |
3. Price of palbociclib | $253.9123 | $126.9562 |
CDA-AMC base case (health care payer perspective) | ― | Reanalysis 1 + 2 + 3 |
CDA-AMC = Canada’s Drug Agency; NSAI = nonsteroidal aromatase inhibitor; PFS = progression-free survival; TTD = time to treatment discontinuation; vs. = versus.
Note: CDA-AMC was unable to resolve the issues with the lack of direct comparative evidence for abemaciclib plus NSAI vs. palbociclib plus NSAI and ribociclib plus NSAI.
Table 8: Summary of the Stepped Analysis
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALY) |
|---|---|---|---|---|
Sponsor base case | NSAI alone | 79,867 | 3.12 | Reference |
Palbociclib plus NSAI | 232,977 | 3.50 | Extendedly dominated | |
Ribociclib plus NSAI | 263,069 | 3.84 | Extendedly dominated | |
Abemaciclib plus NSAI | 274,927 | 3.93 | 238,939 | |
CDA-AMC reanalysis 1: TTD equal to PFS | NSAI alone | 79,881 | 3.12 | Reference |
Palbociclib plus NSAI | 254,998 | 3.50 | Extendedly Dominated | |
Ribociclib plus NSAI | 279,743 | 3.84 | 278,564 | |
Abemaciclib plus NSAI | 343,285 | 3.93 | 642,530 | |
CDA-AMC reanalysis 2: postprogression utility | NSAI alone | 79,867 | 3.40 | Reference |
Palbociclib plus NSAI | 232,977 | 3.72 | Extendedly dominated | |
Ribociclib plus NSAI | 263,069 | 4.11 | Extendedly dominated | |
Abemaciclib plus NSAI | 274,927 | 4.16 | 255,417 | |
CDA-AMC reanalysis 3: palbociclib costs | NSAI alone | 79,867 | 3.12 | Reference |
Palbociclib plus NSAI | 152,666 | 3.50 | 190,804 | |
Ribociclib plus NSAI | 263,069 | 3.84 | Extendedly dominated | |
Abemaciclib plus NSAI | 274,927 | 3.93 | 281,175 | |
CDA-AMC base case Reanalysis 1 + 2 + 3) (deterministic) | NSAI alone | 79,881 | 3.40 | Reference |
Palbociclib plus NSAI | 163,756 | 3.72 | 258,514 | |
Ribociclib plus NSAI | 279,743 | 4.11 | 296,387 | |
Abemaciclib plus NSAI | 343,285 | 4.16 | 1,326,243 | |
CDA-AMC base case Reanalysis 1 + 2 + 3) (probabilistic) | NSAI alone | 71,014 | 3.40 | Reference |
Palbociclib plus NSAI | 162,384 | 3.70 | 297,961 | |
Ribociclib plus NSAI | 275,936 | 4.05 | 325,691 | |
Abemaciclib plus NSAI | 340,311 | 4.11 | 1,047,838 |
CDA-AMC = Canada’s Drug Agency; ICER = incremental cost-effectiveness ratio; NSAI = nonsteroidal aromatase inhibitor; PFS = progression-free survival; QALY = quality-adjusted life-years; TTD = time to treatment discontinuation.
Notes: The CDA-AMC reanalysis is based on the publicly available prices of the comparator treatments. All analyses are reported deterministically unless otherwise indicated, while the cumulative CDA-AMC base case is presented both deterministically and probabilistically.
Table 9: Disaggregated Results of the CDA-AMC Base Case
Parameter | Abemaciclib plus NSAI | NSAI alone | Palbociclib plus NSAI | Ribociclib plus NSAI |
|---|---|---|---|---|
Discounted LYs | ||||
Total | 5.66 | 4.79 | 5.12 | 5.64 |
Discounted QALYs | ||||
Total | 4.11 | 3.40 | 3.70 | 4.05 |
Preprogressed disease | 2.40 | 1.25 | 2.01 | 1.96 |
Progressed disease | 1.71 | 2.15 | 1.70 | 2.09 |
Disutility | −0.0009 | −0.0001 | −0.0005 | −0.0010 |
Discounted costs ($) | ||||
Total | 340,311 | 71,014 | 162,384 | 275,936 |
Drug acquisition | 267,502 | 762 | 92,292 | 198,808 |
Administration | 0 | 0 | 0 | 0 |
Adverse events | 7,266 | 986 | 7,591 | 10,401 |
Subsequent treatment | 2,874 | 11,262 | 3,213 | 3,663 |
Disease management (PPD) | 14,690 | 7,627 | 12,263 | 11,971 |
Disease management (PD) | 10,783 | 13,534 | 10,686 | 13,199 |
Terminal care | 17,996 | 19,208 | 18,681 | 17,990 |
Hospitalization (PPD) | 8,785 | 4,561 | 7,334 | 7,158 |
Hospitalization (PD) | 10,416 | 13,075 | 10,324 | 12,746 |
CDA-AMC = Canada’s Drug Agency; LY = life-year; NSAI = nonsteroidal aromatase inhibitor; QALY = quality-adjusted life-year; PD = progressed disease; PPD = preprogressed disease.
Price Reduction Analysis
CDA-AMC conducted price reduction analyses using the sponsor’s base case and the CDA-AMC base case (refer to Table 10).
Table 10: Results of the Price Reduction Analysis
Price reduction | Unit drug cost ($) | Cost per 28 days ($) | ICERs for abemaciclib plus NSAI vs. comparators ($/QALY) | |
|---|---|---|---|---|
Sponsor base case | CDA-AMC base case | |||
No price reduction | 117a | 6,508 | 261,782 | 1,047,838 vs. ribociclib plus NSAI |
10% | 105 | 5,857 | 236,004 vs. NSAI alone | 612,229 vs. ribociclib plus NSAI |
20% | 94 | 5,206 | 210,225 vs. NSAI alone | 303,359 vs. palbociclib plus NSAI |
30% | 82 | 4,556 | 184,447 vs. NSAI alone | 263,710 vs. NSAI alone |
40% | 70 | 3,905 | 158,669 vs. NSAI alone | 226,372 vs. NSAI alone |
50% | 58 | 3,254 | 132,890 vs. NSAI alone | 189,033 vs. NSAI alone |
60% | 47 | 2,603 | 107,112 vs. NSAI alone | 151,694 vs. NSAI alone |
70% | 35 | 1,952 | 81,333 vs. NSAI alone | 114,355 vs. NSAI alone |
80% | 23 | 1,302 | 55,555 vs. NSAI alone | 77,016 vs. NSAI alone |
90% | 12 | 651 | 29,777 vs. NSAI alone | 39,678 vs. NSAI alone |
CDA-AMC = Canada’s Drug Agency; ICER = incremental cost-effectiveness ratio; NSAI = nonsteroidal aromatase inhibitor; QALY = quality-adjusted life-year; vs. = versus.
aSponsor’s submitted price for abemaciclib for 150 mg tablet.6 Abemaciclib is also available in 50 mg and 100 mg tablets at the price of $116.9725 and $115.8889 per tablet, respectively.
Assessment of Uncertainty
CDA-AMC used the CDA-AMC base case to conduct scenario analyses to address uncertainty within the economic evaluation. The results are provided in Table 11.
Scenario 1: The sponsor-provided option to use parametric extrapolations from the MONARCH 3 trial (for abemaciclib plus NSAI and comparators) and Cox PH models (for other combination therapies) to estimate OS and PFS. In this scenario, a parametric distribution was selected for NSAI alone that resulted in more reasonable long-term extrapolations across all comparators based on clinical expert input.
Scenario 2: Treatment waning for OS was implemented for abemaciclib plus NSAI based on the sponsor-provided option. Treatment waning began at ███ months and persisted for 77 additional months.
Table 11: Results of CDA-AMC Scenario Analyses
Analysisa | Drug | Total costs ($) | Total QALYs | ICER ($/QALYs) |
|---|---|---|---|---|
CDA-AMC base case | NSAI alone | 71,014 | 3.40 | Reference |
Palbociclib plus NSAI | 162,384 | 3.70 | 297,961 | |
Ribociclib plus NSAI | 275,936 | 4.05 | 325,691 | |
Abemaciclib plus NSAI | 340,311 | 4.11 | 1,047,838 | |
CDA-AMC scenario 1: Constant hazard ratio approach | NSAI alone | 74,278 | 3.74 | Reference |
Palbociclib plus NSAI | 203,860 | 4.06 | Extendedly dominated | |
Ribociclib plus NSAI | 370,418 | 4.55 | 364,963 | |
Abemaciclib plus NSAI | 408,155 | 4.51 | Dominated | |
CDA-AMC scenario 2: OS treatment waning for abemaciclib plus NSAI | NSAI alone | 71,032 | 3.40 | Reference |
Palbociclib plus NSAI | 162,442 | 3.70 | 296,318 | |
Ribociclib plus NSAI | 276,115 | 4.06 | 322,477 | |
Abemaciclib plus NSAI | 340,117 | 4.07 | 6,261,324 |
CDA-AMC = Canada’s Drug Agency; ICER = incremental cost-effectiveness ratio; NSAI = nonsteroidal aromatase inhibitor; OS = overall survival; QALY = quality-adjusted life-year.
aProbabilistic analyses.
Issues for Consideration
CADTH had previously reviewed abemaciclib for the treatment of HR-positive, HER2-negative advanced or metastatic breast cancer in 2019.23 Abemaciclib was conditionally recommended for reimbursement based on a significant PFS benefit demonstrated in the MONARCH 2 trial, although OS data were not sufficient to draw conclusions. In this resubmission, the sponsor provided updated trial evidence from MONARCH 3 reflecting over 8 years of follow-up. This updated submission also includes revised NMAs and updated economic models incorporating the new OS data. Additionally, CDA-AMC is currently reviewing abemaciclib resubmission split into 2 distinct indications: PC0400 for patients with HR-positive, HER2-negative advanced or metastatic breast cancer who have not received prior systemic treatment in the advanced setting;24 and PC0409 for patients with HR-positive, HER2-negative advanced breast cancer, who had disease progression on or within 12 months of completion of (neo)adjuvant endocrine therapy or who had disease progression on their first-line endocrine therapy for advanced disease.1
CADTH also previously reviewed abemaciclib in combination with endocrine therapy for the adjuvant treatment of adult patients with HR-positive, HER2-negative, node-positive, early breast cancer at high risk of disease recurrence based on clinicopathological features. The pan-Canadian Oncology Drug Reviews’ Expert Committee (pERC) recommended that abemaciclib be reimbursed for this indication with clinical criteria and conditions on October 3, 2024.25
Appendix 5: Budget Impact Analysis
Please note that this appendix has not been copy-edited.
Summary of the Submitted BIA
The sponsor submitted a BIA that estimated the expected incremental budgetary impact of reimbursing abemaciclib plus NSAI for the treatment of HR-positive, HER2-negative advanced or metastatic breast cancer in females who were postmenopausal as initial endocrine-based therapy.26
The BIA was conducted from the perspective of public drug plan payers over a 3-year time horizon (2026 to 2028), with 2025 as the base year. The sponsor’s estimate reflects the aggregated results from the jurisdictional provincial budgets (excluding Quebec) as well as the Non-Insured Health Benefits Program. The sponsor estimated the eligible population using an epidemiological approach. Abemaciclib plus NSAI was assumed to displace ribociclib plus NSAI and palbociclib plus NSAI. The sponsor’s base case included drug acquisition costs. The market uptake for abemaciclib plus NSAI was estimated using internal estimates. The key inputs to the BIA are documented in Table 12.
The sponsor estimated the 3-year incremental budget impact associated with reimbursing abemaciclib plus NSAI would be $34,231,013 (year 1 = $3,968,213; year 2 = $11,692,371; year 3 = $18,570,429).
Table 12: Key Model Parameters
Parameter | Sponsor’s estimate (reported as year 1 / year 2 / year 3 if appropriate) |
|---|---|
Target population | |
Starting number of people27 | 26,987,736 |
Prevalence of disease28 | 0.37% |
Incidence of disease29 | 0.08% |
Proportion of patients with HR-positive, HER2-negative disease (among both incident and prevalent cases)30,a | 70.2% |
Annual recurrence rate (among prevalent cases)31 | 7.1% |
Proportion of patients > 12 months following adjuvant ET (among prevalent cases)a | 77.0% |
De novo MBC (of incident patients)32,a | 5.5% |
Total de novo and recurrent (> 12 months) patients (prevalent and incident cases combined) Proportion of postmenopausal (among both incident and prevalent cases)33 | 82.6% |
Receive first-line ET-based therapy (among both incident and prevalent cases)30,34 | 90% |
5% | |
Proportion of patients who attained adequate response after receiving first-line chemotherapy, and therefore are eligible for abemaciclib plus NSAIa | 100% |
Total population eligible for abemaciclib plus NSAI | 3,663 |
Percentage of patients covered by public drug plan35 | 79.9% |
Number of patients eligible for drug under review | 2,971 / 3,018 / 3,065 |
Market shares (reference scenario) | |
Abemaciclib plus NSAI | 0% / 0% / 0% |
Palbociclib plus NSAI | 43% / 43% / 43% |
Ribociclib plus NSAI | 51% / 51% / 51% |
NSAI alone | 6% / 6% / 6% |
Market shares (new drug scenario) | |
Abemaciclib plus NSAI | 12% / 23% / 29% |
Palbociclib plus NSAI | 38% / 33% / 30% |
Ribociclib plus NSAI | 44% / 38% / 35% |
NSAI alone | 6% / 6% / 6% |
Cost of treatment (per patient per total treatment course)b | |
Abemaciclib plus NSAI | $85,368 |
Palbociclib plus NSAI | $70,027 |
Ribociclib plus NSAI | $77,826 |
NSAI alone | $471 |
ET = endocrine therapy; HR = hormone receptor; MBC = metastatic breast cancer; NSAI = nonsteroidal aromatase inhibitors.
aSponsor’s assumption.
bTreatment durations were aligned with the mean number of cycles received in the MONARCH 3 trial for abemaciclib plus NSAI and for NSAI alone. This was estimated to be 29.2 cycles of 28 days for abemaciclib plus NSAI and 22.1 cycles of 28 days for NSAI alone. The sponsor assumed that palbociclib plus NSAI and ribociclib plus NSAI would be administered for the same duration as abemaciclib plus NSAI, assuming 29.2 cycles of 28 days for each.
Key Issues of the Submitted BIA
CDA-AMC identified several key issues to the sponsor’s analysis that have notable implications on the results of the BIA:
The proportion of patients with adequate response to chemotherapy following visceral crisis is overestimated. The sponsor assumed that the proportion of patients with adequate response to chemotherapy following visceral crisis was 100%. CDA-AMC obtained clinical expert feedback that suggested that although the rate of adequate response in clinical practice is high, it is unlikely that all patients will respond.
In the CDA-AMC reanalysis, the rate of adequate response to chemotherapy following visceral crisis was adjusted to 90% based on clinical expert feedback.
The market uptake of abemaciclib plus NSAI may be overestimated: The sponsor’s submitted budget impact analysis indicated that abemaciclib plus NSAI would result in a market uptake of 12% in year 1, 23% in year 2, and 29% in year 3 based on internal estimates. However, CDA-AMC obtained clinical expert feedback indicating that this market uptake may be overestimated as patients will increasingly have been exposed to abemaciclib in earlier lines of therapy and no longer be eligible for re-treatment with abemaciclib.
CDA-AMC undertook a scenario analysis revising the market shares for abemaciclib plus fulvestrant in the new drug scenario to 12% in year 1, 20% in year 2, and 20% in year 3.
The price of palbociclib used in the BIA model was outdated. CDA-AMC noted that palbociclib has generic formulations available, reducing its prices from $253.9123 to $126.9562 per tablet.2 This resulted in overestimation of the palbociclib plus NSAI regimen total cost in the model.
In the CDA-AMC base case, the updated price from Ontario Drug Benefit Formulary was used for palbociclib.
The price of drugs paid by public drug plans is uncertain: The analyses by both the sponsor and CDA-AMC are based on publicly available list prices for all comparators. Actual costs paid by public drug plans are unknown.
CDA-AMC was unable to address this limitation in reanalysis.
CDA-AMC Reanalyses of the BIA
CDA-AMC revised the sponsor’s submitted analyses by making changes in model parameter values and assumptions, after clinical expert feedback, as outlined in Table 12.
Table 13: Revisions to the Submitted BIA
Stepped analysis | Sponsor’s value or assumption | CDA-AMC value or assumption |
|---|---|---|
1. Proportion of patients with adequate response to chemotherapy following visceral crisis | 100% | 90% |
2. Cost of palbociclib | $253.9123 | $126.9562 |
CDA-AMC base case | ― | Reanalysis 1 + 2 |
BIA = budget impact analysis; CDA-AMC = Canada’s Drug Agency.
The results of the CDA-AMC step-wise reanalysis are presented in summary format in Table 14 and a more detailed breakdown is presented in Table 15.
In the CDA-AMC base case, the 3-year budget impact of reimbursing abemaciclib plus NSAI for HR-positive, HER2-negative advanced or metastatic breast cancer in females who were postmenopausal as initial endocrine-based therapy was $82,997,394 (year 1 = $9,621,431; year 2 = $28,349,624; year 3 = $45,026,339) (refer to Table 15).
CDA-AMC estimated that 2,956 to 3,048 patients would be eligible for treatment with abemaciclib plus NSAI over the 3-year period (year 1 = 2,956; year 2 = 3,002; year 3 = 3,048).
Table 14: Summary of the Stepped Analysis of the CDA-AMC Base Case
Stepped analysis | Three-year total ($) |
|---|---|
Submitted base case | 34,231,013 |
CDA-AMC reanalysis 1 | 34,050,849 |
CDA-AMC reanalysis 2 | 83,436,533 |
CDA-AMC base case: Reanalysis 1 + 2 | 82,997,394 |
CDA-AMC = Canada’s Drug Agency.
Note: The CDA-AMC reanalysis is based on publicly available prices of the comparator treatments.
CDA-AMC used the CDA-AMC base case to conduct scenario analyses to explore uncertainty in the estimated budget impact of reimbursing abemaciclib plus NSAI. The results are provided in Table 15.
Scenario 1: Lower market uptake for abemaciclib plus NSAI in years 2 and 3 (20%).
Table 15: Disaggregated Summary of the BIA
Stepped analysis | Scenario | Year 0 (current situation) ($) | Year 1 ($) | Year 2 ($) | Year 3 ($) | Three-year total ($) |
|---|---|---|---|---|---|---|
Submitted base case | Reference total | 204,253,461 | 411,660,273 | 467,225,686 | 474,501,256 | 1,353,387,215 |
Abemaciclib plus NSAI | 0 | 0 | 0 | 0 | 0 | |
All other comparators | 204,253,461 | 411,660,273 | 467,225,686 | 474,501,256 | 1,353,387,215 | |
New drug total | 204,253,461 | 415,628,486 | 478,918,057 | 493,071,685 | 1,387,618,228 | |
Abemaciclib plus NSAI | 0 | 30,438,198 | 89,686,397 | 142,444,575 | 262,569,170 | |
All other comparators | 204,253,461 | 385,190,288 | 389,231,660 | 350,627,109 | 1,125,049,057 | |
Budget Impact | 0 | 3,968,213 | 11,692,371 | 18,570,429 | 34,231,013 | |
CDA-AMC base case | Reference total | 159,412,409 | 321,280,463 | 364,642,901 | 370,321,067 | 1,056,244,432 |
Abemaciclib plus NSAI | 0 | 0 | 0 | 0 | 0 | |
All other comparators | 159,412,409 | 321,280,463 | 364,642,901 | 370,321,067 | 1,056,244,432 | |
New drug total | 159,412,409 | 330,901,894 | 392,992,525 | 415,347,406 | 1,139,241,825 | |
Abemaciclib plus NSAI | 0 | 30,277,997 | 89,214,363 | 141,694,867 | 261,187,227 | |
All other comparators | 159,412,409 | 300,623,897 | 303,778,162 | 273,652,539 | 878,054,598 | |
Budget Impact | 0 | 9,621,431 | 28,349,624 | 45,026,339 | 82,997,394 | |
CDA-AMC scenario analyses | ||||||
Scenario 1: Alternate market shares for abemaciclib plus NSAI | Reference total | 159,412,409 | 321,280,463 | 364,642,901 | 370,321,067 | 1,056,244,432 |
New drug total | 159,412,409 | 330,901,894 | 390,549,717 | 405,462,025 | 1,126,913,636 | |
Budget Impact | 0 | 9,621,431 | 25,906,816 | 35,140,957 | 70,669,204 | |
BIA = budget impact analysis; CDA-AMC = Canada’s Drug Agency; NSAI = nonsteroidal aromatase inhibitor.
Note: The CDA-AMC reanalysis is based on the publicly available prices of the comparator treatments.
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@cda-amc.ca.