Drugs, Health Technologies, Health Systems
Reimbursement Review
Nivolumab and Ipilimumab (Opdivo and Yervoy)
Sponsor: Bristol-Myers Squibb Canada Co.
Therapeutic area: Unresectable or metastatic MSI-H or dMMR colorectal cancer
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Clinical Review
Abbreviations
AE
adverse event
AESI
adverse event of special interest
BICR
blinded independent central review
CCC
Colorectal Cancer Canada
CCRAN
Colorectal Cancer Resource and Action Network
CDA-AMC
Canada’s Drug Agency
CGOEN
Canadian Gastrointestinal Oncology Evidence Network
CI
confidence interval
CRC
colorectal cancer
dMMR
deficient mismatch repair
ECOG PS
Eastern Cooperative Oncology Group Performance Status
EORTC QLQ-30
European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30
FOLFIRI
leucovorin calcium (folinic acid), fluorouracil, irinotecan hydrochloride
FOLFOX
leucovorin calcium (folinic acid), fluorouracil, oxaliplatin
GRADE
Grading of Recommendations Assessment, Development and Evaluation
GHS
global health status
HR
hazard ratio
HRQoL
health-related quality of life
IHC
immunohistochemistry
IMAE
immune-mediated adverse event
IRT
interactive response technology
ITC
indirect treatment comparison
ITT
intention to treat
KM
Kaplan-Meier
MAIC
matching-adjusted indirect comparison
mCRC
metastatic colorectal cancer
mFOLFOX
modified leucovorin calcium (folinic acid), fluorouracil, oxaliplatin
MID
minimal important difference
MMR
mismatch repair
MSI
microsatellite instability
MSI-H
microsatellite instability-high
NGS
next generation sequencing
NMA
network meta-analysis
OESI
other event of special interest
OH (CCO)
Ontario Health (Cancer Care Ontario)
OR
odds ratio
ORR
objective response rate
OS
overall survival
PCR
polymerase chain reaction
PFS
progression-free survival
PHA
proportional hazard assumption
RCT
randomized controlled trial
RECIST 1.1
Response Evaluation Criteria in Solid Tumours Version 1.1
SAE
serious adverse event
SLR
systematic literature review
SOC
standard of care
TEM
treatment-effect modifier
UI
utility index
VAS
visual analogue scale
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Table 1: Background Information of Application Submitted for Review
Item | Description |
|---|---|
Drug product | Nivolumab (Opdivo) and ipilimumab (Yervoy) Strength:
|
Sponsor | Bristol-Myers Squibb Canada Co. |
Indication | Opdivo (nivolumab), in combination with ipilimumab is indicated for the first-line treatment of adult patients with unresectable or metastatic microsatellite instability-high (MSI-H) or mismatch repair deficient (dMMR) colorectal cancer |
Reimbursement request | As per the indication: The reimbursement request is for the first-line treatment of adult patients with unresectable or metastatic MSI-H or dMMR colorectal cancer |
Health Canada approval status | NOC |
Health Canada review pathway | Standard |
NOC date | July 16, 2025 |
Recommended dose | Nivolumab at a dose of 240 mg nivolumab given in combination with ipilimumab at 1 mg/kg every 3 weeks for a total of 4 doses, then 480 mg nivolumab every 4 weeks until disease progression or unacceptable toxicity, or up to 2 years Route of administration: IV infusion |
dMMR = deficient mismatch repair; MSI-H = metastatic microsatellite instability-high; NOC = Notice Of Compliance.
Introduction
In Canada, colorectal cancer (CRC) was the third most prevalent cancer overall in 2024. CRC is also the fourth most commonly diagnosed cancer, as well as the second leading cause of cancer-related death (11% of all cancer deaths) among people living in Canada.1 In 2024, the incidence was 11,000 and 14,100 cases among males and females, respectively.2 Presenting symptoms can be nonspecific (diarrhea, constipation, abdominal pain, rectal bleeding or pain, unexplained weight loss, unexplained iron deficiency anemia, nausea, vomiting), contributing to delays in diagnosis.3,4 Around 20% to 25% of patients with CRC present with metastasis at diagnosis, and almost 50% of patients with nonmetastatic CRC will eventually develop metastases. Metastatic CRC (mCRC) is largely incurable, with a 5-year overall survival (OS) of less than 15%.5,6 The metastatic microsatellite instability-high (MSI-H) or deficient mismatch repair (dMMR) subtype of CRC arises from germline or sporadic impairments of the mismatch repair (MMR) system, the protein complex responsible for correcting errors during DNA replication.7 Overall, MSI-H and/or dMMR tumours account for 15% of CRC cases. However, the prevalence of microsatellite instability (MSI) differs across disease stages. It can range from 10% in stage II and 20% in stage III to approximately 5% to 7% in stage IV.8,9 According to the clinical experts consulted by the review team, testing for MMR and MSI status is currently part of the standard of care (SOC) for unresectable or mCRC, and testing is not anticipated to be a barrier to implementation.
Currently, pembrolizumab is the recommended first-line therapy in Canada indicated for patients with MSI- H or dMMR mCRC.10 Multiagent chemotherapy, along with targeted therapies against VEGFR and EGFR are the principle first-line therapies in patients with metastatic proficient MMR or microsatellite stable CRC. These agents may be used as the first-line treatment in a limited number of patients with dMMR or MSI-H mCRC in whom there is a severe contraindication to immunotherapy.
Nivolumab in combination with ipilimumab has been previously reviewed by Canada’s Drug Agency (CDA-AMC) in the population with melanoma,11,12 malignant pleural mesothelioma,13 non–small cell lung cancer,14,15 advanced or metastatic renal cell carcinoma,16 and metastatic melanoma.17 The combination is also currently under review for another indication in people with unresectable or advanced hepatocellular carcinoma.18
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of nivolumab plus ipilimumab (nivolumab: 40 mg/4 mL [10 mg/mL] and 100 mg/10 mL [10 mg/mL]; ipilimumab: 50 mg/10 mL [5 mg/mL] and 200 mg/40 mL [5 mg/mL], IV) in the first-line treatment of adult patients with unresectable or metastatic MSI-H or dMMR CRC.
Perspectives of Patients, Clinicians, and Drug Programs
The information in this section is a summary of input provided by the patient and clinician groups who responded to the call for input and from clinical experts consulted by CDA-AMC for the purpose of this review.
Patient Input
Two patient groups, Colorectal Cancer Resource and Action Network (CCRAN) and Colorectal Cancer Canada (CCC), provided input for this submission. CCRAN is a national, not-for-profit, patient advocacy group championing the health and well-being of people living in Canada by providing support, education, and advocacy to help improve patient outcomes, longevity, and quality of life. CCRAN used a multifaceted approach to contact medical oncologists based in Canada, Europe, and the US between July 24, 2024, to February 19, 2025, to gather lived patient experience. None of the clinicians in Canada had treated patients with MSI-H CRC. In collaboration with the Canadian Cancer Survivor Network, a social media campaign was conducted from July 16, 2024, to March 15, 2025. Patients from France (n = 2), Italy (n = 2), and the US (n = 2) shared their experience with nivolumab plus ipilimumab through either telephone interviews or written inputs. One patient from Canada with MSI-H mCRC without access to nivolumab plus ipilimumab provided input. Further, responses from a previous CRC survey distributed from March 17, 2024, to April 17, 2024, comprising 77 patients with CRC or their respective caregivers, were submitted.
CCC is a not-for-profit organization for patients with CRC dedicated to raising awareness, education, supporting patients and their caregivers, and advocating on their behalf. Patient and caregiver perspectives regarding nivolumab plus ipilimumab were gathered through an online survey and semistructured interviews from August 2024 to April 2025. Of the 11 patients and 1 caregiver who responded to the online survey, 1 patient lived in Australia, 3 patients lived in Canada, 1 caregiver lived in England, and 7 patients lived in the US. Among the 4 patients interviewed, 3 lived in Canada, and 1 lived in the US.
Those who responded to both patient group surveys highlighted how the inability to work, exercise, and participate in social activities and/or family obligations significantly impacted quality of life. They also highlighted that the inability to plan about the future, fear of recurrence, constant worry, and fatigue resulted in significant psychological impacts. Caregivers reported challenges caring for patients with CRC, including the inability to work outside, difficulty managing treatment-induced side effects, loss of income, and/or financial strain, time spent on medical appointments, and medication administration. Those who responded to the CCC survey indicated that symptoms such as abdominal cramps, gas, feeling bloated, abdominal pain, fatigue, and diarrhea were important to control.
Those who responded to both patient group surveys indicated the following side effects from available systemic treatments: fatigue, brain fog, diarrhea, loss of appetite, hair loss, peripheral neuropathy, nausea, and low white blood cell count. In addition, those who responded to the CCC survey highlighted that diarrhea, hand-foot syndrome, and fatigue are the most difficult side effects to tolerate. Those who responded to the CCRAN survey noted the burden of out-of-pocket expenses for additional mediations required to manage treatment-induced side effects. In addition, patients who were interviewed reported that ineffective chemotherapeutics to control cancer caused poor quality of life and negatively impacted mental health. The CCC survey results noted that 30% of those who responded to the survey believed that their needs were not met by currently available treatments. Five percent of patients indicated “no” and 45% indicated “somewhat” when asked whether available drug therapies were effective in controlling disease progression.
Both patient groups noted tumour shrinkage, tumour stability, reduced pain, improved breathing, and quality of life (e.g., improved mobility, improved sense of wellness, relief from side effects) as important outcomes with new treatments. Caregivers who responded to the CCRAN survey indicated that preventing death (i.e., survival) and stopping the spread of the illness were important treatment outcomes. Those who responded to the CCC survey (53%) indicated a willingness to accept a treatment with significant yet tolerable side effects (i.e., nausea, anemia, neutropenia) if it offered an OS of at least 3 or 4 months.
Four patients interviewed by CCRAN who received the combination therapy achieved a durable and complete response and maintained no evidence of disease for more than 5 years. Patients also noted that side effects were manageable, treatment administration was easily managed, and they were able to maintain a high quality of life. Those who responded to the CCC survey (11 of 12) indicated that nivolumab plus ipilimumab controlled their cancer and its spread to other organs. Sixty-four percent indicated that they were able to continue their daily activities while undergoing treatment. Most patients were able to complete treatment without interruptions, whereas 25% stopped treatment earlier or skipped doses due to side effects and/or complications. Anxiety and/or worry, fatigue, and management of side effects were noted as the most difficult adverse events (AEs) of receiving nivolumab plus ipilimumab. The top 5 side effects included skin itchiness, skin rash, joint stiffness, vomiting, and diarrhea. Several patients considered side effects with nivolumab plus ipilimumab as more manageable than those associated with chemotherapy. All patients interviewed experienced tumour shrinkage and/or stabilization during treatment with nivolumab plus ipilimumab and were able to return to daily activities. Patients noted that although there were considerable side effects, they resolved over time.
Clinician Input
Input From Clinical Experts Consulted for This Review
The clinical experts highlighted that the 3 most important goals of all therapies for metastatic MSI-H or dMMR CRC are to improve OS, to improve quality of life, and to reduce AEs and toxicity.
The clinical experts indicated that for patients with unresectable or metastatic MSI-H or dMMR CRC, pembrolizumab is the current funded standard first-line treatment. According to the clinical expert, a concern with the pembrolizumab monotherapy is that only approximately 40% of patients will respond to treatment, and patients with liver metastases may derive significantly less benefit. The clinical experts emphasized that nivolumab plus ipilimumab will likely replace pembrolizumab, particularly in the population of patients with liver metastases, given that the CheckMate-8HW trial showed consistent treatment benefit in this population of patients. However, the enhanced efficacy of using nivolumab plus ipilimumab comes at the expense of a higher risk of side effects and/or toxicity. Therefore, single-drug pembrolizumab will remain an important therapeutic alternative for patients experiencing frailty and who have comorbidities. The clinical experts noted that following disease progression on first-line therapy, the SOC second-line systemic treatment in Canada is chemotherapy (leucovorin calcium [folinic acid], fluorouracil, irinotecan hydrochloride [FOLFIRI] or leucovorin calcium [folinic acid], fluorouracil, oxaliplatin [FOLFOX]) in combination with bevacizumab. Following disease progression on 2 lines of therapy, the third-line treatment options become very limited in number and efficacy.
The clinical experts stated that patients with treatment-naive unresectable or metastatic MSI-H or dMMR CRC, with no contraindications to immunotherapy, reasonable performance status, and no concerns about the immunotherapy-related side effects, would be the ideal candidates for treatment with nivolumab plus ipilimumab. The clinical experts highlighted that while OS is the most important treatment outcome in this disease, progression-free survival (PFS) is considered an accepted surrogate outcome for OS in this setting. They noted that based on the statistically significant and clinical meaningful improvement in PFS reported in the CheckMate-8HW trial, OS improvement is very much expected. The clinical experts noted that patients should be assessed by a clinician after every 2 to 3 cycles of treatment, and more frequently if bothersome symptoms or side effects are occurring. Radiological assessment (e.g., CT scans) should be completed every 2 to 3 months. Tumour markers should be completed at least once every 4 weeks.
The clinical experts indicated that disease progression and/or unacceptable toxicities are the 2 main reasons to discontinue treatment with nivolumab plus ipilimumab.
The clinical experts noted that treatment with nivolumab plus ipilimumab could be safely administered in a hospital and should only be prescribed by or under the supervision of a specialist in medical oncology with expertise in managing immunotherapy-related side effects. One clinical expert further indicated that in some jurisdictions in Canada, private-pay immunotherapy is allowed to be administered in outpatient private infusion centres.
Clinician Group Input
Two clinician groups, Ontario Health (Cancer Care Ontario) (OH [CCO]) Gastrointestinal Cancer Drug Advisory Committee, and Canadian Gastrointestinal Oncology Evidence Network (CGOEN), in collaboration with the CCC Medical Advisory Board, provided their input for this submission. The OH (CCO) provides evidence-based clinical and health system guidance on drug-related issues in support of CCO’s mandate, including the Provincial Drug Reimbursement Programs and the Systemic Treatment Program. The group gathered information via emails, and 5 clinicians provided their input. The CGOEN is a network of gastrointestinal oncology clinicians in Canada who contribute to the knowledge of gastrointestinal cancer and its treatments by participating in clinical trials, conducting observational research, and engaging in local, provincial, and national clinical guideline development and health technology assessment. The Medical Advisory Board of CCC works alongside the patient group to ensure its activities and health information are relevant and useful for patients and caregivers. For this submission, 11 clinicians provided input based on relevant information from the CheckMate-8DW trial and evidence-based expert opinions.
Clinician groups agreed that improving survival and quality of life were important treatment goals. The OH (CCO) further noted the following treatment goals: prolong PFS, delay disease progression, potentially convert some patients to surgery, reduce the severity of symptoms, and minimize AEs. The CGOEN clinician group noted that about 30% to 40% of patients do not respond to pembrolizumab and progress within the first 2 to 3 months of treatment.
Clinician groups agreed that treatment with nivolumab plus ipilimumab would be the new standard first-line for patients with dMMR or MSI-H tumours. The CGOEN further mentioned that the treatment may be administered in any centre and by any specialist experienced in treating patients with mCRC using systemic therapy.
The CGOEN noted that the treatment should be limited to patients not amenable for surgical resection or with metastatic disease. They highlighted that patients would require regular clinical evaluations to assess clinical response and toxicity. They also noted routine imaging would be required at timed intervals for objective assessment and suggested that patient preference, tolerability of treatment, and quality of life be considered when assessing meaningful response to treatment. The CGOEN noted that disease progression (radiological or clinical), toxicity, clinician discretion, or patient request should be considered reasons for treatment discontinuation.
Drug Program Input
The drug programs provide input on each drug under review through the reimbursement review process by identifying issues that may affect their ability to implement a recommendation. The drug programs’ input, along with the corresponding responses from the clinical experts consulted by CDA-AMC, is summarized in Table 5.
Clinical Evidence
Systematic Review
Description of Studies
One pivotal trial (CheckMate-8HW) is included in this review. CheckMate-8HW is an ongoing multinational, phase III, open-label, active-controlled randomized controlled trial (RCT) to evaluate the efficacy and safety of nivolumab plus ipilimumab (N = 202) compared with chemotherapy (N = 101) in adult patients with unresectable or MSI-H or dMMR CRC. Key inclusion criteria included histologically confirmed recurrent or mCRC with no prior treatment history with chemotherapy and/or targeted drugs for metastatic disease and not amenable to surgery; locally confirmed MSI-H or dMMR status, and Eastern Cooperative Oncology Group Performance Status (ECOG PS) score of 1 or less. A total of 303 patients in 22 countries, including 204 patients (67.3%) from Canada, Europe, and the US, were randomized to receive treatment with nivolumab plus ipilimumab or chemotherapy (2:1 randomization). Randomization was conducted using an interactive response technology system and stratified by primary tumour location (sidedness: left versus right). The baseline demographic and disease characteristics were largely balanced between treatment groups. The median age of all patients was 63.0 years, ranging from 21 to 87 years. Most of the patients were white (86.1%), followed by Asian (10.6%), other (2.0%), and Black or African American (1.3%). Females represented 53.8% of all participants and males were 46.2%. An ECOG PS score of 0 was reported in 53.8% of patients, and an ECOG PS score of 1 was reported in 46.2% of patients. The primary efficacy outcome was PFS, assessed per a blinded independent central review (BICR) based on centrally confirmed MSI-H or dMMR mCRC. The secondary efficacy outcome was PFS, assessed per a BICR based on locally confirmed MSI-H or dMMR mCRC. The exploratory outcome included the health-related quality of life (HRQoL) (e.g., European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 [EORTC QLQ-C30]). The harm outcomes included AEs, serious adverse events (SAEs), discontinuation from the treatment due to AEs, immune-mediated adverse events (IMAEs), and other events of special interest (OESIs). The results of PFS presented in this report are based on the data cut-off on August 28, 2024 (with a median follow-up time of 42.05 months). Results of HRQoL were based on the data cut-off on October 12, 2023 (median follow-up of 31.57 months). Safety outcomes results were based on the safety population at the data cut-off on both October 12, 2023, and August 28, 2024.
Efficacy Results
Progression-Free Survival
After a median follow-up of 42.05 months, a total of 53 (31.0%) PFS events were observed in the nivolumab plus ipilimumab arm and 54 (64.3%) in the chemotherapy arm. The median PFS was 54.08 months (95% CI, 54.08 months to not available) in the nivolumab plus ipilimumab arm and 5.85 months (95% CI, 4.37 months to 7.79 months) in the chemotherapy arm (hazard ratio [HR] = 0.21, 95% CI, 0.14 to 0.31). In the landmark time points, compared with the chemotherapy, nivolumab plus ipilimumab showed a clinical meaningful higher PFS probability starting from 6 months and sustained to 36 months. Based on the Grading of Recommendations Assessment, Development and Evaluation (GRADE) assessment, nivolumab plus ipilimumab results in a clinically important increase in the probability of being progression-free at 12 months compared to chemotherapy. The PFS results for patients with MSI-H or dMMR mCRC were consistent whether the patients were centrally confirmed (primary outcome) or locally confirmed (a key secondary outcome).
The results of the predefined subgroup analysis showed a statistically significant improvement in PFS probability with nivolumab plus ipilimumab compared with chemotherapy in patients with liver metastasis (HR = 0.11; 95% CI, 0.05 to 0.25) and patients without liver metastasis (HR = 0.28; 95% CI, 0.17 to 0.46). Sensitivity analyses of PFS were consistent with the primary analysis.
HRQoL Assessed With EORTC QLQ-C30
Compared with chemotherapy, treatment with nivolumab plus ipilimumab demonstrated a statistically significant improvement from week 13 to week 37. The GRADE assessment suggested nivolumab plus ipilimumab may result in a clinically important improvement in EORTC QLQ-C30 global health status (GHS) score compared with chemotherapies at week 37.
Harms Results
After a median follow-up of 42.05 months, the overall proportion of patients with AEs were similar in both nivolumab plus ipilimumab compared with chemotherapy arm (nivolumab plus ipilimumab versus chemotherapy: 99.0% versus 98.9%). Compared to those in the nivolumab plus ipilimumab arm, more patients receiving chemotherapy reported all-cause grade 3 or 4 AEs (nivolumab plus ipilimumab versus chemotherapy: 50.5% versus 67.0%), all-causality SAEs (nivolumab plus ipilimumab versus chemotherapy: 35.5% versus 42.0%), and death (nivolumab plus ipilimumab versus chemotherapy: 25.5% versus 47.7%). The proportion of patients who discontinued treatment because of AEs was similar (nivolumab plus ipilimumab versus chemotherapy: 15.0% versus 15.9%). However, it should be noted that the AEs of special interest (AESIs) such as all-causality grade 3 to 4 IMAEs were much higher in the nivolumab plus ipilimumab arm than in the chemotherapy arm (nivolumab plus ipilimumab versus chemotherapy: 17.0% versus 1.1%). The between-group difference was 15.9% (95% CI, not reported). The GRADE assessment suggested that nivolumab plus ipilimumab likely result in clinically important increases in grade 3 or 4 IMAEs, compared with chemotherapies. The clinical experts consulted for this review indicated that the safety profile of nivolumab plus ipilimumab has been well established. The harms profile of nivolumab plus ipilimumab observed in the CheckMate-8HW trial was generally consistent with that of previously known AEs associated with nivolumab plus ipilimumab. No new safety signals were identified. Overall, most AEs were predictable and clinically manageable in most patients.
Critical Appraisal
The CheckMate-8HW study was a phase III, open-label RCT. Appropriate methods for randomization were reported. The outcomes assessed are clinically relevant, and statistical analyses were done using standard methods. Overall, the risk of selection bias and detection bias is considered very low for the key outcome (i.e., PFS per BICR). However, the open-label design introduces a potential bias in the subjective outcomes of HRQoL (e.g., EORTC QLQ-C30) and AEs (such as fatigue and nausea). However, the extent and direction of bias due to treatment knowledge is uncertain. In addition, the EORTC QLQ-C30 assessment may be further biased due to high attrition, particularly at a longer follow-up (e.g., at week 37).
The clinical experts highlighted that the inclusion and exclusion criteria of the CheckMate-8HW trial are standard for clinical trials, but stricter than what pertains in clinical practice. For example, they noted that patients with an ECOG PS score of more than 1 were not eligible for the trial, whereas patients with an ECOG PS score of 2 would be considered potential candidates for nivolumab plus ipilimumab in the clinical experience. However, the clinical experts considered that overall, the inclusion and exclusion criteria of the CheckMate-8HW trial are consistent with the clinical practice setting in Canada, and its findings present no major concerns regarding generalizability in terms of clinical practice in Canada.
GRADE Summary of Findings and Certainty of the Evidence
For pivotal studies and RCTs identified in the sponsor’s systematic review, GRADE was used to assess the certainty of the evidence for outcomes considered most relevant to inform expert committee deliberations, and a final certainty rating was determined as outlined by the GRADE Working Group.19,20 Following the GRADE approach, evidence from RCTs started as high-certainty evidence and could be rated down for concerns related to study limitations (which refers to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias.
When possible, certainty was rated in the context of the presence of an important (nontrivial) treatment effect. The target of the certainty of evidence assessment was based on the point estimate and where it was located relative to the threshold (minimal important difference [MID]) for a clinically important effect. In this review, the threshold (MID) assessment of between-group difference for PFS was based on published information21,22 in combination with the MID suggested by clinical experts consulted for this review. The threshold (MID) for HRQoL (i.e., EORTC QLQ-C30 GHS) assessment of between-group difference was based on the published information,23 which was aligned with the suggestion by the clinical experts consulted for this review. The threshold (MID) for assessment of between-group difference for harms (i.e., IMAEs) was suggested by clinical experts consulted for this review.
The selection of outcomes for GRADE assessment was based on the sponsor’s Summary of Clinical Evidence, consultation with clinical experts, and input received from patient and clinician groups and public drug plans. The following list of outcomes was finalized in consultation with expert committee members:
PFS
HRQoL
safety.
Table 2 presents the GRADE summary of findings for nivolumab plus ipilimumab versus chemotherapy for the first-line treatment of adult patients with unresectable or metastatic MSI-H or dMMR CRC.
Table 2: Summary of Findings of Nivolumab Plus Ipilimumab Combination Therapy vs. Chemotherapies for Patients With Unresectable or Metastatic MSI-H or dMMR CRC Receiving First-Line Treatment With Unresectable or Metastatic MSI-H or dMMR Colorectal Cancer
Outcome and follow-up | Patients (studies), N | Relative effect (95% CI) | Absolute effects (95% CI) | Certainty | What happens | ||
|---|---|---|---|---|---|---|---|
Chemotherapy | Nivolumab plus ipilimumab | Difference | |||||
PFS at data cut-off on August 28, 2024 (median follow-up of 42.05 months, 95% CI, NR) | |||||||
PFS probability at 12 months, centrally confirmed | 255 (1 RCT) | NR | 216 per 1,000 | 790 per 1,000 | 575 more per 1,000 (454 to 695 per 1,000) | High | Nivolumab plus ipilimumab results in a clinically important increase in the probability of being progression-free at 12 months, compared to chemotherapy. |
PFS probability at 12 months, locally confirmed | 303 (1 RCT) | NR | 240 per 1,000 | 710 per 1,000 | 470 more per 1,000 (366 to 575 more per 1,000) | High | Nivolumab plus ipilimumab results in a clinically important increase in the probability of being progression-free at 12 months, compared to chemotherapy. |
Health-related quality of life (EORTC QLQ-C30 GHS) at data cut-off on October 12, 2023 | |||||||
EORTC QLQ-C30 GHS total score, locally confirmed | 303 (1 RCT) | NR | ████ | ████ ██████ █████ | ████ █████ █████ | Lowa | Nivolumab plus ipilimumab may result in clinically important improvement in EORTC QLQ-C30 GHS, compared with chemotherapies at week 37. |
Notable harms (i.e., AESIs) at data cut-off on August 28, 2024 (median follow-up of 42.05 months, 95% CI, NR) | |||||||
All-causality grade 3 to 4 IMAEs within 100 days of last dose | |||||||
Total number of patients with grade 3 or 4 IMAEs (safety population), n (%) | 288 (1 RCT) | NR | ██ ███ █████ | ███ ███ ████ ██████ | ███ ████ ███ █████████ | Moderateb,c,d | Nivolumab plus ipilimumab likely results in a clinically important increase in grade 3 or 4 IMAEs, compared with chemotherapies over an overall median follow-up of 42.05 months. |
AE = adverse event; AESI = adverse event of special interest; CI = confidence interval; CRC = colorectal cancer; dMMR = deficient mismatch repair; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; GHS = global health status; IMAE = immune-mediated adverse event; MID = minimal important difference; MSI-H = microsatellite instability-high; NR = not reported; PFS = progression-free survival; RCT = randomized controlled trial; vs. = versus.
Notes: Study limitations (which refer to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias were considered when assessing the certainty of the evidence. All serious concerns in these domains that led to the rating down of the level of certainty are documented in the table footnotes.
The between-group MID for PFS at 12 months was based on the publications (≥ 10%),21,22 in combination with the MID suggested by the clinical experts consulted for this review. (i.e., 10% to 20% for PFS probabilities at 12 months).
Musoro et al. reported that the between-group MID for EORTC QLQ-C30 GHS total score was 6 points.23 The clinical experts consulted for this review suggested between-group difference MIDs for EORTC QLQ-C30 GHS total score at 37 weeks is 5 to 7 points.
There is no established between-group MID for the proportion of patients with grade 3 or 4 IMAEs after an overall median follow-up of 42.05 months. The clinical experts consulted for this review suggested a MID of 5% for the odds experiencing grade 3 or 4 IMAEs after an overall median follow-up of 42.05 months.
aRated down 2 levels for very serious study limitations for this outcome: There is risk of bias in measurement of the outcome due to open-label study design and risk of bias due to a substantial attrition rate; that is, only 119 patients (59%) in the nivolumab plus ipilimumab arm and 15 patients (15%) in the chemotherapy arm were included for the analysis at week 37.
bRated down 2 levels for very serious study limitations for this outcome: Because no 95% CI for between-group difference was reported, it was rated down 2 levels for imprecision.
cRated up 1 level for very large between-group difference.
dDespite it being an open-label study design, the evidence certainty is not rated down for the grade 3 or 4 IMAEs because the grade 3 or 4 IMAEs reported in the review are all objective), which were unlikely biased due to the open-label design.
Long-Term Extension Studies
No long-term extension studies were submitted by the sponsor.
Indirect Comparisons
Description of Studies
The sponsor conducted an indirect treatment comparison (ITC) using a matching-adjusted indirect comparison (MAIC) to estimate the relative efficacy (i.e., PFS) and network meta-analysis (NMA) for safety outcomes comparing nivolumab plus ipilimumab with pembrolizumab for the first-line treatment of MSI-H or dMMR mCRC.
Efficacy Results
Anchored MAIC: The point estimate of the time-varying HR of PFS is lower than 1 over the estimated 10-year period (HR < 1 indicates in favour of nivolumab plus ipilimumab compared with pembrolizumab). ███ ██ ██████ ███████ ████ ██ ██ ██████ ███ ████ ██ ██ ███████ The 95% CIs do not cross the null value (i.e., 1) at 12 months and 24 months, which indicates that PFS for nivolumab plus ipilimumab is favourable compared with pembrolizumab. However, starting from 36 months until 120 months, the 95% CI of HR includes the null value (i.e., 1), indicating the estimation of the HR is uncertain.
Constant HR-based scenario NMA: ███ ███ ██ ██ ████ ████ ████ ████ ██ ██████ ███ ██████ ████ ███ █████ ██ ███████ █████████ █ ██████████ ██ ███████ █████████ ████ ██████████████ ███ ██████ ██ ██████████ ████ ███ ████████████ ████████ ██ ██ ██████ ███ ██ ███████
Unanchored MAIC: ███ █████ ████████ ██ ███ ████████████ ██ ███ ███ ██ █████ ████ █ ████ ███ █████████ ███████ ███████ ███ ██ ██████ ████ ████ ██ ██ ██████ ██ ████ ██ ██ ███████ ███ ███ ███ ██ ██ ██ ███ █████ ███ ████ █████ ████ ██ ██████ ██ ██ ██ ███████ █████ █████████ ████ ███ ███ █████████ █ ██████████ ██ ██████████ ████████ ████ ██████████████ ████████ ██████ ██ ███████ ███ ██████ ██ ██ ███████ ███ ████ ██████ ██████████ ███ ██████████ ██ ███ ██ ███ ███ ██ ██████████
Constant HR-based scenario NMA analysis: ███ ███ ██ ██ ████ ███████ ████ ██ ██████ ███ ██████ ████ ███ █████ ██ ███████ █████████ █ ██████████ ██ ████████ ████ █████████ ██ ██████████████ ███ ██████ ██ ██████████ ████ ███ ████████████ ████████ ████ ██ ██████ ██ ██ ███████
In summary, all results of the ITC analysis (i.e., anchored MAIC using a time-varying HR approach, unanchored MAIC using a time-varying HR approach, and the scenario NMAs using constant HR approach) suggested a favourable PFS improvement in patients with nivolumab plus ipilimumab treatment compared with pembrolizumab, despite certain key limitations (e.g., not able to adjust all treatment effect modifiers [TEMs] and prognostic modifiers).
Harms Results
The evidence of the NMA was not sufficient to demonstrate the difference of grade 3 or higher AEs (█████ ███████ ███████████ █████████ ███ █████████) between the 2 treatments. It should be noted that no ITC was done for the overall AEs, overall SAEs, and discontinuation due to AEs, especially for the proportion of patients with total IMAEs.
Critical Appraisal
The key limitation for the MAICs was their inability to balance all (known or unknown) TEMs due to the unavailability of published summary statistics in the KEYNOTE-177 trial. Another key limitation for the NMA was that the heterogeneity in terms of TEMs between the 2 studies were not adjusted, which may threaten the transitivity assumption for the NMA analysis.
Studies Addressing Gaps in the Evidence From the Systematic Review
The sponsor-submitted evidence from the CheckMate-8HW trial comparing nivolumab plus ipilimumab to nivolumab monotherapy in patients with MSI-H or dMMR mCRC receiving treatment across all lines of therapy to inform questions on the contribution of ipilimumab in addition to nivolumab. Per the CDA-AMC Procedures for Reimbursement Reviews, nivolumab monotherapy does not meet the CDA-AMC definition of relevant comparator because it is neither approved by Health Canada nor reimbursed by participating drug plans in Canada for the first-line treatment of MSI-H or dMMR mCRC. Therefore, the evidence was considered out of scope for this review.
Conclusions
Evidence from the CheckMate-8HW trial showed that nivolumab plus ipilimumab results in a clinically important increase in the probability of being progression-free at 12 months, compared to chemotherapy in the first-line treatment of patients with unresectable or metastatic MSI-H or dMMR CRC. Based on the EORTC QLQ-C30 GHS, nivolumab plus ipilimumab may result in a clinically important improvement in patients’ HRQoL compared with chemotherapy, which was expected in this population. The evidence indicates that nivolumab plus ipilimumab likely results in a clinically important increase in grade 3 to 4 IMAEs, compared with chemotherapies. The harms profile of nivolumab plus ipilimumab reported in the CheckMate-8HW trial was generally consistent with that of previously known AEs associated with nivolumab plus ipilimumab. No new safety signal was identified. Overall, most AEs were predictable, and clinically manageable in most patients.
The results of the ITC suggested a more favourable PFS improvement with nivolumab plus ipilimumab treatment compared with pembrolizumab, despite certain limitations associated with the ITC methods. Due to the limitations associated with the NMA, a definitive conclusion could not be drawn on the comparative safety of nivolumab plus ipilimumab versus pembrolizumab in patients with MSI-H or dMMR mCRC. However, according to the clinical experts consulted on this review, nivolumab plus ipilimumab, being a double-drug immunotherapy, is expected to have an increased risk of side effects compared with the single-drug immunotherapy, and likely unsuitable for patients experiencing frailty or who have comorbidities.
Introduction
Disease Background
Contents within this section have been informed by materials submitted by the sponsor and clinical expert input. The following have been summarized and validated by the review team.
In Canada, CRC was the third most prevalent cancer overall in 2024. CRC is also the fourth most commonly diagnosed cancer, as well as the second leading cause of cancer-related death (11% of all cancer deaths) among residents of Canada.1 In 2024, the incidence was 11,000 and 14,100 cases among males and females, respectively.2 Presenting symptoms can be nonspecific (diarrhea, constipation, abdominal pain, rectal bleeding or pain, unexplained weight loss, unexplained iron deficiency anemia, nausea, vomiting), contributing to delays in diagnosis.3,4
Around 20% to 25% of patients with CRC present with metastasis at diagnosis, and almost 50% of patients with non-mCRC will eventually develop metastases. Based on the extent of metastasis, CRC can be either regional with metastasis limited to specific nodes, or distant with metastasis to distant organs.7 mCRC is largely incurable, with a 5-year OS of less than 15%.5,6 The MSI-H and/or dMMR subtype of CRC arises from germline or sporadic impairments of the MMR system, the protein complex responsible for correcting errors during DNA replication.7 Overall, MSI-H and/or dMMR accounts for 15% of CRC cases. However, the prevalence of MSI differs across disease stages. It can range from 10% in stage II and 20% in stage III to approximately 5% to 7% in stage IV.8,9
Diagnosis of CRC begins with a histologic examination of the colon, usually obtained from a biopsy,24 followed by a colonoscopy if CRC is suspected. Once a diagnosis of CRC is established, the local and distant extent of disease needs to be determined.24,25 The stage at diagnosis is the most important prognostic factor. The American Joint Committee on Cancer has defined 1 of the most common staging systems for CRC based on tumour, node, and metastases criteria. In Ontario, approximately 23% of patients present with stage IV CRC at diagnosis.26
MSI can be detected in fresh or fixed tumour specimens by amplification of specific microsatellite markers using polymerase chain reaction (PCR) or next generation sequencing (NGS).27 Immunohistochemistry (IHC) is a useful alternative strategy for identifying tumours with dMMR activity by searching for loss of expression of 1 of the proteins of the MMR system (generally MSH2, MLH1, MSH6, or PMS2).27 In Canada, between 95% to 100% of patients with CRC undergo MMR or MSI testing.28 The availability of MMR or MSI testing is not expected to be limited by access.
Standards of Therapy
Contents within this section have been informed by materials submitted by the sponsor and clinical expert input. The following have been summarized and validated by the review team.
Currently, pembrolizumab is the recommended first-line therapy in Canada that is indicated for patients with unresectable or metastatic MSI-H or dMMR CRC regardless of any other biomarker status.10 Multiagent chemotherapy, along with targeted therapies against VEGFR and EGFR are the principle first-line therapies in patients with metastatic proficient MMR and microsatellite stable CRC. These agents may be used as the first-line treatment in a limited number of patients with deficient MMR or MSI-H mCRC in whom there is a severe contraindication to immunotherapy.10
Per the CDA-AMC and the Institut national d’excellence en santé et en service sociaux (INESSS) treatment algorithms, a patient with mCRC with both MSI-H or dMMR and BRAF V600E mutations should receive pembrolizumab as first-line therapy. The use of encorafenib in combination with cetuximab or panitumumab29 should be reserved for use as a second-line regimen.10
Drug Under Review
Key characteristics of nivolumab plus ipilimumab are summarized in Table 3 with other treatments available for CRC.
According to the product monograph,30 240 mg nivolumab and 1 mg/kg ipilimumab are to be administered every 3 weeks for a maximum of 4 dosing cycles. The combination is administered intravenously over 30 minutes. Following the combination phase, nivolumab is administered as a single drug at a dose of 480 mg every 4 weeks or 240 mg every 2 weeks up to 2 years (unless disease progression or unacceptable toxicity occurs).
Nivolumab is a human immunoglobulin G4 monoclonal antibody that binds to the PD-1 receptor and blocks its interaction with PD-L1 and PD-L2, releasing PD-1 pathway-mediated inhibition of the immune response.30 Ipilimumab is a fully human monoclonal antibody to the CTLA-4 antigen.31 Combined nivolumab (anti–PD-1) and ipilimumab (anti–CTLA-4) mediated inhibition results in enhanced T-cell function and results in improved antitumour responses.
The Health Canada indication is “nivolumab in combination with ipilimumab for the first-line treatment of adult patients with unresectable or metastatic microsatellite instability-high (MSI-H) or mismatch repair deficient (dMMR) colorectal cancer.”30 The sponsor’s reimbursement request aligns with the Health Canada indication.
Nivolumab plus ipilimumab for the first-line treatment of unresectable or mCRC was approved by the European Medicines Agency in December 2024.32 The FDA approved nivolumab plus ipilimumab in patients aged 12 years and older with unresectable or metastatic MSI-H or dMMR CRC in April 2025.33 On May 8, 2025, the National Institute of Health and Care Excellence in England approved the use of nivolumab plus ipilimumab in adults with untreated unresectable or mCRC with MSI-H or dMMR.34 In May 2025, nivolumab plus ipilimumab was approved by regulatory agencies in Australia for the treatment of unresectable or mCRC, that is MSI-H or dMMR as determined by a validated test.35 The combination is under review by health technology agencies in Australia (Pharmaceutical Benefits Advisory Committee), and France (Haute Autorité de Santé).
Nivolumab plus ipilimumab has been previously reviewed by CDA-AMC in the population with melanoma,11,12 malignant pleural mesothelioma,13 non–small cell lung cancer,14,15 advanced or metastatic renal cell carcinoma,16 and metastatic melanoma.17 The combination is also currently under review for another indication in people with unresectable or advanced hepatocellular carcinoma.18
Table 3: Key Characteristics of Nivolumab, Ipilimumab, Pembrolizumab, mFOLFOX6, FOLFIRI, Bevacizumab, Panitumumab, and Cetuximab
Drug name | Mechanism of action | Indicationa | Route of administration | Recommended dose | Serious adverse events or safety issues |
|---|---|---|---|---|---|
Nivolumab plus ipilimumab | Binds PD-1 ligands, PD-L1 and PD-L2, to the PD-1 receptor on T cells, inhibiting T-cell proliferation and cytokine production Combined nivolumab (anti–PD-1) and ipilimumab (anti–CTLA-4) mediated inhibition results in enhanced T-cell function and improved tumour responses | For the first line treatment of adult patients with unresectable or metastatic MSI-H or dMMR colorectal cancer, when used in combination with ipilimumab | IV | Combination phase: Nivolumab 240 mg every 3 weeks (30-minute IV infusion) with ipilimumab 1 mg/kg intravenously (30-minute IV infusion) Single drug phase administered 3 weeks after the last dose of the combination phase: 240 mg every 2 weeks or 480 mg every 4 weeks (30-minute IV infusion) |
|
Pembrolizumab | Activates antitumour immune response | Treatment, as monotherapy, of adult patients with metastatic MSI-H or dMMR colorectal cancer as determined by a validated test | IV | 200 mg every 3 weeks or 400 mg every 6 weeks, until disease progression, unacceptable toxicity, or up to 24 months or 35 doses for 200 mg or 18 doses for 400 mg, whichever is longer, in patients without disease progression (IV infusion over 30 minutes) |
|
mFOLFOX6 | Interferes with DNA synthesis and cellular replication | Treatment of patients with metastatic colorectal cancer | Oxaliplatin: IV Leucovorin: IV 5-Fluorouracil: bolus and/or infusion | Administered every 2 weeks for 12 cycles or until disease progression or unacceptable toxicity. Day 1:
| Oxaliplatin:
Leucovorin:
5-fluorouracil:
|
FOLFIRI | Interferes with DNA synthesis and cellular replication | First-line treatment for patients with metastatic carcinoma of the colon or rectum | Irinotecan: IV Leucovorin: IV 5-Fluorouracil: IV bolus and/or IV infusion | Irinotecan: 180 mg/m2 IV over 90 minutes once every 2 weeks (days 1, 15, 29), then 1 week rest Leucovorin: 200 mg/m2 IV over 2 hours on days 1 and 2 every 2 weeks (days 1, 2, 15, 16, 29, and 30), then 1 week rest 5-fluorouracil bolus and infusion: 400 mg/m2 IV bolus immediately followed by a 5-fluorouracil infusion of 2,400 mg/m2 IV over 46 hours on day 1, and every 2 weeks on days 1, 2, 15, 16, 29, and 30, then 1 week rest | Irinotecan:
Leucovorin and 5-fluorouracil: Refer to serious adverse events or safety issues listed for leucovorin and 5-fluorouracil in the mFOLFOX6 section. |
Bevacizumab (plus FOLFIRI or mFOLFOX6) | Inhibits microvascular growth and slows tissue growth | In combination with fluoropyrimidine-based chemotherapy for the first-line treatment of patients with metastatic carcinoma of the colon or rectum | Bevacizumab: IV infusion FOLFIRI or mFOLFOX6: Refer to previous sections on FOLFIRI and mFOLFOX6 on route of administration. | Bevacizumab: 5 mg/kg every 2 weeks FOLFIRI or mFOLFOX6: Refer to previous sections on FOLFIRI and mFOLFOX6 for recommended doses. | Bevacizumab:
FOLFIRI or mFOLFOX6: refer to previous sections on FOLFIRI and mFOLFOX6 for serious adverse events and safety issues. |
Panitumumab (plus FOLFIRI or mFOLFOX6) | Inhibits cell growth, survival, and proliferation | Treatment of wild-type RAS metastatic colorectal cancer | Panitumumab: IV FOLFIRI or mFOLFOX6: Refer to previous sections on FOLFIRI and mFOLFOX6. | Panitumumab: 6 mg/kg IV on day 1 every 2 weeks until disease progression or unacceptable toxicity FOLFIRI or mFOLFOX6: Refer to previous sections on FOLFIRI and mFOLFOX6. | Panitumumab:
FOLFIRI or mFOLFOX6: Refer to previous sections on FOLFIRI and mFOLFOX6. |
Cetuximab (plus FOLFIRI or mFOLFOX6) | Recombinant, chimeric monoclonal antibody that binds to the extracellular domain of human EGFR with high affinity | Treatment of EGFR-expressing Kras wild-type metastatic colorectal cancer
| Cetuximab: IV FOLFIRI or mFOLFOX6: Refer to previous sections on FOLFIRI and mFOLFOX6. | Cetuximab: 500 mg/m2 infusion on day 1 every 2 weeks until disease progression or unacceptable toxicity FOLFIRI or mFOLFOX6: Refer to previous sections on FOLFIRI and mFOLFOX6. | Cetuximab:
FOLFIRI or mFOLFOX6: Refer to previous sections on FOLFIRI and mFOLFOX6. |
dMMR = deficient mismatch repair; FOLFORI = leucovorin calcium (folinic acid), fluorouracil, irinotecan hydrochloride; FOLFOX = leucovorin calcium (folinic acid), fluorouracil, oxaliplatin; ; mCRC = metastatic colorectal cancer; mFOLFOX6 = modified leucovorin calcium (folinic acid), fluorouracil, oxaliplatin; MSI-H = microsatellite instability-high.
Note: Clinical experts noted that for patients with MSI-H or dMMR colorectal cancer, single-drug pembrolizumab was the standard of care first-line treatment in Canada. Following disease progression while receiving first-line therapy, the standard of care for patients with MSI-H or dMMR colorectal cancer requiring second-line treatment in Canada is chemotherapy (FOLFIRI or FOLFOX) in combination with bevacizumab. Following disease progression on 2 lines of therapy, treatment options are limited.
aHealth Canada–approved indication.
Sources: Product monographs of nivolumab (draft),30 ipilimumab,31 pembrolizumab,36 mFOLFOX6,37-39 FOLFIRI,38-40 bevacizumab,41 panitumumab,42 and cetuximab.43
Testing Procedure Considerations
MMR and MSI mutation status is an important prognostic factor in patients with CRC and can be used in clinical decision-making to determine eligibility for targeted treatments (e.g., immunotherapies).44-46 Current guidelines in Canada recommend testing all patients with CRC for MMR or MSI status, or both MMR and MSI status.44-46 The clinical experts consulted for this review indicated that reflexive MMR testing using IHC is currently done in jurisdictions across Canada as the SOC to identify dMMR or MSI-H tumours upon diagnosis with CRC. IHC is recommended for MMR testing instead of other methods, such as NGS or PCR testing of the MSI status, due to factors such as lower costs, shorter turnaround times, and being less resource intensive.47,48 However, the clinical experts noted that MSI testing is readily available and funded, but funding of NGS versus PCR testing may vary between jurisdictions.
Potential impacts were considered for MMR and MSI testing to ascertain eligibility for nivolumab plus ipilimumab for the first-line treatment of adult patients with unresectable or metastatic MSI-H or dMMR CRC, including those to health systems, patients (including families and caregivers), and costs. Because testing for MMR and MSI status is currently performed as the SOC for adult patients with CRC across jurisdictions in Canada, no new impacts are anticipated. Key considerations and relevant information available from materials submitted by the sponsor, input from the clinical experts consulted by the review team, and sources from the literature were validated by the review team when possible and are summarized in Table 4.
Table 4: Considerations for MMR and MSI Testing for Establishing Treatment Eligibility With Nivolumab Plus Ipilimumab in mCRC
Consideration | Criterion | Available information |
|---|---|---|
Health system related | Number of individuals in Canada expected to require the test (e.g., per year) | According to the sponsor-submitted BIA, based on a Canada-wide perspective (excluding Quebec), there will be approximately 16,000 incident cases of CRC per year over the next 3 years, and between 95% to 100% of patients diagnosed with CRC in Canada would undergo MMR or MSI testing.28 The clinical experts agreed with these estimates. |
Availability and reimbursement status of the testing procedure in jurisdictions across Canada | According to the clinical experts, MMR testing by IHC is broadly available and funded across all jurisdictions in Canada. | |
Testing procedure as part of routine care | MMR and MSI testing are a part of the minimum standard of care for CRC biomarker testing in Canada.44-46 The clinical experts confirmed that MMR testing by IHC is currently performed as part of the standard of care for patients with mCRC. Complementary MSI testing is only performed in select cases with high clinical suspicion of MSI-H CRC. Sequencing for MSI status may also be required in the absence of adequate tissue or cellularity to determine MMR status using IHC. | |
Repeat testing requirements | MMR testing usually only needs to be performed once and does not need to be repeated. However, according to the clinical experts, some patients who were proficient in MMR may be retested for MSI status using NGS or PCR if there is a high clinical suspicion of MSI-H disease (e.g., young patients with right-sided, poorly differentiated tumours). MSI status testing is rare, with less than 1% of patients being tested for both MMR and MSI status. | |
Impacts on human and other health care resources by provision of the testing procedure | Because testing for MMR and MSI status is currently part of the standard of care for CRC and publicly funded across jurisdictions in Canada, use of the test result to establish treatment eligibility for nivolumab plus ipilimumab is not anticipated to substantially impact human and other health care resources. | |
Patient related | Accessibility of the testing procedure in jurisdictions across Canada | The clinical experts noted that most, if not all, patients with CRC in Canada are tested for MMR status. Therefore, there is no additional accessibility concerns anticipated from the testing of MMR and MSI status as part of establishing treatment eligibility for nivolumab plus ipilimumab. |
Expected turnaround times for the testing procedure | According to the clinical experts, the expected turnaround time for MMR testing by IHC is 3 to 5 business days, but results may be available in as little as 24 hours. Because testing would be conducted in most cases as part of routine care, they anticipate minimal impact on patients or caregivers due to wait times. | |
Burden associated with the testing procedure for patients, families, and/or caregivers | Because testing for MMR and MSI status is currently part of the standard of care for CRC, there is no additional burden to patients, families, and/or caregivers anticipated from the testing as part of establishing treatment eligibility for nivolumab plus ipilimumab. | |
Clinical | Clinical utility and validity of the testing procedure | There is evidence from Canada to demonstrate the diagnostic accuracy and clinical utility of IHC testing for MMR mutation status.44-47,a According to the sponsor, MMR testing by IHC is highly sensitive (92.3%) and specific (100%) in detecting MSI-H tumours, and highly concordant with MSI testing (92%).47 These estimates were confirmed by the clinical experts. |
Risks of harm associated with the testing procedure | According to the clinical experts, MMR and MSI status is typically tested using the diagnostic biopsy sample. No additional risk of harm associated with the testing as part of establishing treatment eligibility for nivolumab plus ipilimumab were identified. | |
Cost | Projected cost of the testing procedure | According to the BIA submitted by the sponsor, the cost of diagnostic testing is approximately $77.13 for a 4 MMR protein IHC panel. Because testing for MMR and MSI status is currently part of the standard of care for unresectable CRC or mCRC, there is no additional cost associated impact from the testing as part of establishing treatment eligibility for nivolumab plus ipilimumab. |
BIA = budget impact analysis; CRC = colorectal cancer; IHC = immunohistochemistry; mCRC = metastatic colorectal cancer; MMR = mismatch repair; MSI = microsatellite instability; MSI-H = microsatellite instability-high; NGS = next generation sequencing; PCR = polymerase chain reaction.
aCDA-AMC has not evaluated or critically appraised this evidence to determine its validity or reliability.
Perspectives of Patients, Clinicians, and Drug Programs
The full patient and clinician group submissions received are available in the consolidated patient and clinician group input document for this review on the project website.
Patient Group Input
This section was prepared by the review team based on the input provided by patient groups.
Two patient groups, CCRAN and CCC, provided input for this submission. CCRAN is a national, not-for-profit, patient advocacy group championing the health and well-being of people living in Canada by providing support, education, and advocacy to help improve patient outcomes, longevity, and quality of life. CCRAN used a multifaceted approach to contact medical oncologists based in Canada, Europe, and the US between July 24, 2024, and February 19, 2025, to gather lived patient experience. None of the clinicians practising in Canada had treated any patients with MSI-H CRC. In collaboration with the Canadian Cancer Survivor Network, a social media campaign was conducted from July 16, 2024, to March 15, 2025. Patients from France (n = 2), Italy (n = 2), and the US (n = 2) shared their experience with nivolumab plus ipilimumab through either telephone interviews or written inputs. One patient from Canada with MSI-H mCRC without access to nivolumab and ipilimumab provided input. Further, responses from a previous CRC survey distributed from March 17, 2024, to April 17, 2024, comprising 77 patients with CRC or their respective caregivers, were submitted. CCC is a not-for-profit organization for patients with CRC dedicated to raising awareness, education, supporting patients and their caregivers, and advocating on their behalf. Patient and caregiver perspectives regarding nivolumab and ipilimumab were gathered through an online survey and semistructured interviews from August 2024 to April 2025. Of the 11 patients and 1 caregiver who responded to the online survey, 1 patient lived in Australia, 3 patients lived in Canada, 1 caregiver lived in England, and 7 patients lived in the US. Among the 4 patients interviewed, 3 lived in Canada, and 1 lived in the US.
Both patient group survey respondents highlighted how the inability to work, exercise, and participate in social activities and/or family obligations significantly impacted quality of life. They also highlighted that the inability to plan about the future, fear of recurrence, constant worry, and fatigue resulted in significant psychological impacts. Caregivers reported challenges caring for patients with CRC, including the inability to work outside, difficulty managing treatment-induced side effects, loss of income, and/or financial strain, time spent on medical appointments, and medication administration. Those who responded to the CCC survey indicated that symptoms such as abdominal cramps, gas, feeling bloated, abdominal pain, fatigue, and diarrhea were important to control.
Patients who responded to both patient group surveys indicated the following side effects from available systemic treatments: fatigue, brain fog, diarrhea, loss of appetite, hair loss, peripheral neuropathy, nausea, and low white blood cell count. In addition, those who responded to the CCC survey highlighted that diarrhea, hand-foot syndrome, and fatigue are the most difficult side effects to tolerate. Patients who responded to the CCRAN survey noted the burden of out-of-pocket expenses for additional mediations required to manage treatment-induced side effects. In addition, patients who were interviewed reported that ineffective chemotherapeutics to control cancer caused poor quality of life and negatively impacted mental health. The CCC survey results noted that 30% of patients who responded believed that their needs were not met by currently available treatments. Five percent of patients indicated “no” and 45% indicated “somewhat” when asked whether available drug therapies were effective in controlling disease progression.
Both patient groups noted tumour shrinkage, tumour stability, reduced pain, improved breathing, and quality of life (e.g., improved mobility, improved sense of wellness, relief from side effects) as important outcomes with new treatments. Caregivers who responded to the CCRAN survey indicated that preventing death (i.e., survival) and stopping the spread of the illness were important treatment outcomes. Those who responded to the CCC survey (53%) indicated a willingness to accept a treatment with significant yet tolerable side effects (i.e., nausea, anemia, neutropenia) if it offered an OS of at least 3 or 4 months.
Four patients interviewed by CCRAN who received the combination therapy achieved a durable and complete response and maintained no evidence of disease for more than 5 years. Patients also noted that side effects were manageable, treatment administration was easily managed, and they were able to maintain a high quality of life. Patients (11 of 12) who responded to the CCC survey indicated that nivolumab plus ipilimumab controlled their cancer and its spread to other organs. Sixty-four percent of patients indicated that they were able to continue their daily activities while undergoing treatment. Most were able to complete treatment without interruptions, whereas 25% stopped treatment earlier or skipped doses due to side effects and/or complications. Anxiety and/or worry, fatigue, and management of side effects were noted as the most difficult AEs of receiving nivolumab plus ipilimumab. The top 5 side effects included skin itchiness, skin rash, joint stiffness, vomiting, and diarrhea. Several patients considered side effects with nivolumab plus ipilimumab as more manageable than those associated with chemotherapy. All patients interviewed experienced tumour shrinkage and/or stabilization during treatment with nivolumab plus ipilimumab and were able to return to daily activities. Patients noted that although there were considerable side effects, they resolved over time.
Clinician Input
Input From Clinical Experts Consulted for This Review
All CDA-AMC review teams include at least 1 clinical specialist with expertise regarding the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). The following input was provided by 2 clinical specialists with expertise in the diagnosis and management of adult patients with unresectable or metastatic MSI-H or dMMR CRC.
Unmet Needs
The clinical experts highlighted that the 3 most important goals of all therapies for metastatic MSI-H or dMMR CRC are to improve OS, to improve quality of life, and to reduce AEs and toxicity. The clinical experts indicated that for patients with unresectable or metastatic MSI-H or dMMR CRC, pembrolizumab is the current funded standard first-line treatment. According to the clinical experts, a concern with pembrolizumab monotherapy is that only approximately 40% of patients will respond to treatment, and patients with liver metastases may derive significantly less benefit. The clinical experts emphasized that nivolumab plus ipilimumab will likely replace pembrolizumab, particularly in the population of patients with liver metastases, as the CheckMate-8HW trial showed consistent treatment benefit in this population of patients.
Place in Therapy
The clinical experts indicated that, in eligible patients without a contraindication to immunotherapy, the current first-line treatment with pembrolizumab is the funded SOC in these cases. This recommendation is based on the results of the KEYNOTE-177 phase III RCT.49
The clinical experts noted that following disease progression on first-line therapy, the SOC second-line systemic treatment in Canada is chemotherapy (FOLFIRI or FOLFOX) with or without bevacizumab. There is no high-quality evidence to support this recommendation. Following disease progression on first-line therapy, for patients with BRAF V600E mutations (whether they have comutations in MMR or MSI or not), the SOC second-line systemic treatment in Canada is encorafenib plus cetuximab based on the results of the BEACON phase III RCT. Following disease progression on first-line therapy for patients without a BRAF V600E mutation, the SOC treatment in Canada is to switch the chemotherapy regimen backbone. This recommendation is based on a GERCOR phase III RCT.50 In Canada, in the second-line setting, additional therapies on top of the chemotherapy backbone are not routinely used. It may vary across the jurisdictions.
The clinical experts indicated that following disease progression on 2 lines of therapy, treatment options become very limited in number and efficacy. The present SOC for most patients is TAS-102 plus bevacizumab based on the SUNLIGHT clinical trial.51 For patients with extended RAS wild-type tumours who have not previously been treated with EGFR inhibition, options could include single-drug panitumumab52 or irinotecan in combination with cetuximab.53 For other patients, treatment with either regorafenib monotherapy or TAS-102 (trifluridine-tipiracil) monotherapy are the treatment options in Canada based on the results of the phase III CORRECT RCT and the phase III RECOURSE RCT respectively, but these are very infrequently used due to their limited effectiveness and substantial toxicity.
Fruquintinib is another treatment option for patients with treatment-refractory mCRC based on the results of the phase III FRESCO-2 trial.54 However, access to this medication is very limited in Canada. Best supportive care without anticancer systemic therapy is a treatment option in all lines of treatment depending on patients’ performance status, values, and preferences. However, best supportive care is often given higher consideration after progression on second-line therapies due to the limited anticancer efficacy of these treatments in this setting.
The clinical experts stated that combining CTLA-4 inhibition (ipilimumab) to PD-1 inhibition (nivolumab) seems to be associated with a better response rate and PFS compared to PD-1 inhibition alone, as per the most recent update of the landmark phase III CheckMate-8HW trial. Very importantly, the findings in the CheckMate-8HW trial demonstrated that patients with liver metastases derived excellent benefit from the dual immunotherapy treatment. According to the clinical experts, this is not the first drug to address this disease process, but the hope is that it will represent a far more effective way to address this disease process, used as a first-line treatment. They considered the reported improvement in outcomes remarkable and expected that some patients can have a very durable response with stabilization of their cancer (i.e., delaying the need for a second-line treatment). The clinical experts further noted that if nivolumab plus ipilimumab is available, it would be appropriate to give eligible patients that treatment option.
The clinical experts further indicated that while nivolumab plus ipilimumab will likely become the preferred first-line therapy, the enhanced efficacy of using the double-drug immunotherapy comes at the expense of an increased risk of side effects or toxicity and may not be suitable for patients experiencing frailty and who have comorbidities. However, single-drug pembrolizumab will remain an important therapeutic alternative for such patients.
Patient Population
The clinical experts stated that patients with treatment-naive unresectable and/or metastatic MSI-H or dMMR CRC, with no contraindications to immuno-oncology, reasonable performance status, and no concerns about the immuno-oncology–related side effects would be the ideal candidates for this treatment option. These patients should be identified based on clinician assessment in addition to diagnostic testing.
Assessing the Response Treatment
Both clinical experts highlighted that 3 important outcomes measurements for this setting are HRQoL (e.g., EORTC QLC-30), safety, and PFS. They also noted that while OS is the most important treatment outcome in this disease, PFS is considered an accepted surrogate outcome for OS in this setting. The clinical experts noted that no mature OS data are yet available from the CheckMate-8HW trial. The magnitude of improvement in PFS from this study is remarkable. With such an improvement in PFS, OS improvement is expected. A delay in the need for a second-line treatment in patients with MSI-H mCRC would be expected. This is a substantial development. One expert noted that although OS and quality of life are most important outcomes, response rate is an important end point that should be considered in the mCRC setting. The clinical experts noted that patients should be assessed by a clinician after every 2 to 3 cycles of treatment, or more frequently if bothersome symptoms or side effects are occurring. Radiological assessment (e.g., CT scans) should be completed every 2 to 3 months. Tumour markers should be completed at least once every 4 weeks.
The clinical experts mentioned that there are 3 factors used to determine the response to treatment: patient-reported symptoms or side effects, cross-sectional imaging (e.g., CT scan or MRI), and tumour markers (e.g., CEA and Ca 19 to 9). In general, those factors are listed in descending hierarchical importance. The only truly clinically meaningful end points in all of oncology are OS and quality of life. PFS should be considered a surrogate outcome. However, it is of little relevance if PFS does not predict better OS or quality of life. Nevertheless, the early and dramatic separation of the PFS curves (in both the nivolumab plus ipilimumab versus chemotherapy) makes an OS benefit highly likely, especially due to the fact that there are no other dramatically effective therapies available for this population of patients.
Discontinuing Treatment
The clinical experts indicated that disease progression and/or unacceptable toxicities are the 2 main reasons to discontinue treatment with nivolumab plus ipilimumab. Principally, patient-reported symptoms, side effects, and well-being would be the major determinants for discontinuing therapy. Additionally, the results of the cross-sectional imaging and serum tumour markers would be used to provide context of how well the treatment was working to fully inform treatment decision-making. However, progression on imaging alone would be insufficient reason to discontinue therapy with immunotherapy due to concerns about “pseudo-progression.” The results of the imaging must be interpreted in the context of the patient’s general status, their symptoms or side effect, and the timing of imaging in relation to treatment.
Prescribing Considerations
The clinical experts noted that treatment with nivolumab plus ipilimumab could be safely administered in a hospital and should only be prescribed by or under the supervision of a specialist in medical oncology with expertise in managing immunotherapy-related side effects. One clinical expert further indicated that in some jurisdictions in Canada, private-pay immunotherapy is allowed to be administered in outpatient private infusion centres.
Clinician Group Input
This section was prepared by the review team based on the input provided by clinician groups.
Two clinician groups, OH (CCO) Gastrointestinal Cancer Drug Advisory Committee and CGOEN, in collaboration with the CCC Medical Advisory Board, provided their input for this submission. The OH (CCO) provides evidence-based clinical and health system guidance on drug-related issues in support of CCO’s mandate, including the Provincial Drug Reimbursement Programs and the Systemic Treatment Program. The group gathered information via emails, and 5 clinicians provided their input. The CGOEN is a network of gastrointestinal oncology clinicians in Canada who contribute to the knowledge of gastrointestinal cancer and its treatments by participating in clinical trials, conducting observational research, and engaging in local, provincial, and national clinical guideline development and health technology assessment. The Medical Advisory Board of CCC works alongside the patient group to ensure its activities and health information are relevant and useful for patients and caregivers. For this submission, 11 clinicians provided input based on relevant information from the CheckMate 8HW trial and evidence-based expert opinions.
Clinician groups agreed that improving survival and quality of life were important treatment goals. The OH (CCO) further noted the following treatment goals: prolong PFS, delay disease progression, potentially convert some patients to surgery, reduce the severity of symptoms, and minimize AEs. The CGOEN clinician group noted that about 30% to 40% of patients do not respond to pembrolizumab and progress within the first 2 to 3 months of treatment.
Clinician groups agreed that treatment with nivolumab plus ipilimumab would be the new standard first-line for patients with dMMR or MSI-H tumours. The CGOEN further mentioned that the treatment may be administered in any centre and by any specialist experienced in treating patients with mCRC using systemic therapy.
The CGOEN noted that the treatment should be limited to patients not amenable for surgical resection or with metastatic disease. They highlighted that patients would require regular clinical evaluations to assess clinical response and toxicity. They also noted routine imaging would be required at timed intervals for objective assessment and suggested that patient preference, tolerability of treatment, and quality of life be considered when assessing meaningful response to treatment. The CGOEN noted that disease progression (radiological or clinical), toxicity, clinician discretion, or patient request should be considered reasons for treatment discontinuation.
Drug Program Input
The drug programs provide input on each drug under review through the reimbursement review process by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted for this review are summarized in Table 5.
Table 5: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Relevant comparators | |
Issues with the choice of comparator in the submitted trial Patients in the CheckMate-8HW trial were randomized to receive either nivolumab plus ipilimumab combination therapy, nivolumab monotherapy, or the investigator’s choice of chemotherapy (including FOLFOX, FOLFIRI, with or without bevacizumab or cetuximab). Pembrolizumab monotherapy is funded in most jurisdictions for this indication and would be considered the current standard of care. Other treatment options can include combination chemotherapy with or without bevacizumab, panitumumab, as well as cetuximab in some jurisdictions. | This is a comment from the drug plans to inform pERC deliberations. One of the clinical experts noted that the chosen comparators in the clinical trial were appropriate at the time of the trial design. The most appropriate modern day comparator would be single-drug PD1 inhibition (e.g., pembrolizumab). |
Considerations for initiation of therapy | |
Eligibility to re-treatment Should patients who complete 2 years of treatment and experience disease progression or recurrence from nivolumab plus ipilimumab treatment be eligible for up to 1 year (17 cycles) of re-treatment? If yes, would this be nivolumab monotherapy or nivolumab plus ipilimumab combination therapy? | The clinical experts indicated that, consistent with all prior immunotherapy approvals, patients who completed 2 years of treatment of nivolumab plus ipilimumab treatment with ongoing response at time of discontinuation of therapy should be eligible for re-treatment for another 1 year if they have progression while on surveillance. The choice of re-treatment with either nivolumab monotherapy or a combination of nivolumab plus ipilimumab should be at the discretion of the treating clinician based on prior response or toxicity. |
Consistency with initiation criteria associated with other drugs reviewed by CDA-AMC in the same therapeutic space Consider alignment with existing pembrolizumab indication criteria. | This is a comment from the drug plans to inform pERC deliberations. |
Considerations for continuation or renewal of therapy | |
Consistency with renewal criteria associated with other drugs reviewed by CDA-AMC in the same therapeutic space Consider alignment with existing pembrolizumab indication criteria. | This is a comment from the drug plans to inform pERC deliberations. |
Considerations for discontinuation of therapy | |
Consistency with discontinuation criteria associated with other drugs reviewed by CDA-AMC in the same therapeutic space Consider alignment with existing pembrolizumab indication criteria. | This is a comment from the drug plans to inform pERC deliberations. |
Considerations for prescribing of therapy | |
Dosing, schedule and/or frequency, and dose intensity If therapy is funded and/or implemented, most jurisdictions are likely to implement a weight-based nivolumab dosing, as used for other funded indications (i.e., nivolumab 3 mg/kg IV every 3 weeks up to a maximum of 240 mg per dose for the first 4 cycles, and then 3 mg/kg IV every 2 weeks up to a maximum of 240 mg per dose or 6 mg/kg IV every 4 weeks up to a maximum of 480 mg per dose thereafter). Ipilimumab was weight-based in the CheckMate-8HW trial as 1 mg/kg IV every 3 weeks for the first 4 cycles. | This is a comment from the drug plans to inform pERC deliberations. |
Concerns related to combination usage In the trial, if ipilimumab had to be discontinued early due to toxicity, then nivolumab can still be continued. However, if nivolumab had to be discontinued, then ipilimumab was discontinued as well. Could pERC clarify whether patients can continue monotherapy of ipilimumab if nivolumab is discontinued due to toxicity? If yes, what would be the duration for ipilimumab monotherapy treatment? | The clinical experts did not support continuing with ipilimumab as monotherapy if a patient discontinued therapy with nivolumab due to toxicity. They endorsed sticking to the approach outlined in the trial protocol (i.e., if nivolumab has to be discontinued, then ipilimumab has to be discontinued as well). |
Consistency with prescribing criteria associated with other drugs reviewed by CDA-AMC in the same therapeutic space Consider alignment with existing pembrolizumab indication criteria. | This is a comment from the drug plans to inform pERC deliberations. |
Generalizability | |
Populations of interest matching the indication but with insufficient data Should patients with an ECOG PS score of 2 or greater be eligible? | The clinical experts indicated that they agree with expanding the eligibility to include patients with an ECOG PS score of 2 (but not more than 2). |
Funding algorithm | |
Request initiation of a rapid provisional funding algorithm. Note that if the final reimbursement recommendation for this drug under review is “Do not Reimburse,” the project will be suspended indefinitely. | This was a comment from the drug programs to inform pERC deliberations. |
Drug may change place in therapy of comparator drugs | This was a comment from the drug programs to inform pERC deliberations. |
Complex therapeutic space with multiple lines of therapy, subpopulations, or competing products | This was a comment from the drug programs to inform pERC deliberations. |
Other aspects: Under what clinical circumstances would nivolumab plus ipilimumab be preferred over pembrolizumab in this setting? | The clinical experts indicated that they would rather phrase it in the algorithm such that nivolumab plus ipilimumab is the preferred standard of care among patients with MSI-H mCRC. Pembrolizumab should be considered only if the treating physician has concerns about tolerability to nivolumab plus ipilimumab because the patient is experiencing frailty or comorbidities. |
Care provision issues | |
Drug preparation, storage, administration, or dispensing Preparation of both nivolumab plus ipilimumab is familiar to many jurisdictions due to their use in other indications. | This was a comment from the drug programs to inform pERC deliberations. |
Companion diagnostics (e.g., access issues, timing of testing) This indication requires MMR and MSI testing; however, this testing is established in this patient population in most jurisdictions. | This was a comment from the drug programs to inform pERC deliberations. |
System and economic issues | |
Presence of confidential negotiated prices for comparators Pembrolizumab has confidential pricing in place. | This was a comment from the drug programs to inform pERC deliberations. |
CDA-AMC = Canada’s Drug Agency; ECOG PS = Eastern Cooperative Oncology Group Performance Status; FOLFIRI = leucovorin calcium (folinic acid), fluorouracil, irinotecan hydrochloride; FOLFOX = leucovorin calcium (folinic acid), fluorouracil, oxaliplatin; mCRC = metastatic colorectal cancer; MMR = mismatch repair; MSI = microsatellite instability; MSI-H = microsatellite instability-high; pERC = pan-Canadian Oncology Drug Review Expert Review Committee.
Clinical Evidence
The objective of this Clinical Review report is to review and critically appraise the clinical evidence submitted by the sponsor on the beneficial and harmful effects of nivolumab plus ipilimumab, IV infusion for the first-line treatment of adult patients with unresectable or MSI-H or dMMR CRC. The focus will be placed on comparing nivolumab plus ipilimumab to relevant comparators and identifying gaps in the current evidence.
A summary of the clinical evidence included by the sponsor in the review of nivolumab plus ipilimumab is presented in 2 sections with a critical appraisal of the evidence included at the end of each section. The first section, the systematic review, includes pivotal studies and RCTs that were selected according to the sponsor’s systematic review protocol. The assessment of the certainty of the evidence in this first section using the GRADE approach follows the critical appraisal of the evidence. The second section includes indirect evidence from the sponsor.
Included Studies
Clinical evidence from the following studies is included in the review and appraised in this document:
1 pivotal study (i.e., RCT) identified in the systematic review
1 ITC.
Systematic Review
Contents within this section have been informed by materials submitted by the sponsor. The following studies have been summarized and validated by the review team.
Description of Studies
Characteristics of the included studies are summarized in Table 6. A schematic of the CheckMate-8HW study design is shown in Figure 1.
Table 6: Details of Studies Included in the Systematic Review
Designs and populations | CheckMate-8HW trial |
|---|---|
Study design | Phase III, randomized, 3-arm open-label study of nivolumab monotherapy (arm A),a nivolumab plus ipilimumab combination therapy (arm B), or investigator’s choice chemotherapy (arm C) for the treatment of MSI-H or dMMR mCRC The study enrolment includes 2 sequential parts. In part 1, enrolment was open to patients across all lines of therapy,a and in part 2 enrolment was open only to patients who had not received prior therapy for metastatic disease (patients receiving 1L therapy). Enrolment in part 2 started immediately after completion of the part 1 enrolment.a |
Locations | This study was conducted at 88 sites in 22 countries (Argentina, Australia, Austria, Belgium, Brazil, Canada, Chile, China, Czechia, Denmark, France, Germany, Greece, Ireland, Italy, Japan, Netherlands, Romania, Spain, Türkiye, the UK, and the US). |
Patient enrolment dates | Start date: August 5, 2019 End date: Enrolment ended April 10, 2023; study is ongoing |
Randomized (N) |
|
Inclusion criteria |
|
Exclusion criteria |
|
Intervention | Nivolumab plus ipilimumab combination therapy (arm B): Nivolumab 240 mg + ipilimumab 1 mg/kg IV q.3.w. for 4 doses, then nivolumab monotherapy 480 mg IV q.4.w. for up to 2 years |
Comparator(s) | Nivolumab monotherapy (arm A)a: Nivolumab 240 mg IV q.2.w. for 6 doses then nivolumab 480 mg IV q.4.w. for up to 2 years Chemotherapy (arm C): Investigator’s choice chemotherapy q.2.w. (patients in arm were allowed to crossover to receive nivolumab plus ipilimumab if their disease progressed) |
Study duration | |
Screening phase | Time required to confirm patients’ MSI-H or dMMR status per local standard of practice testing, followed by central confirmation of MSI-H or dMMR status based on tissue samples submitted to a central lab |
Treatment phase | Up to 2 years |
Follow-up phase | Up to 5 years |
Outcomes | |
Primary end point | 1L therapy only
All lines of therapya
|
Key secondary end points | 1L therapy only
Crossover cohortd
|
Exploratory end points |
|
Safety | Deaths, AEs, SAEs, select AEs, IMAEs, OESIs, and lab abnormalities |
Publications | Andre et al. (2024)55 Andre et al. (2025)56 |
1L = first line; AE = adverse event; BICR = blinded independent central review; CDA-AMC = Canada’s Drug Agency; CRC = colorectal cancer; dMMR = deficient mismatch repair; ECOG PS = Eastern Cooperative Oncology Group Performance Status; IMAE = immune-mediated adverse event; mCRC = metastatic colorectal cancer; MSI-H = microsatellite instability-high; OESI = other event of special interest; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; q.2.w. = every 2 weeks; q.3.w. = every 3 weeks; q.4.w. = every 4 weeks; RECIST 1.1 = Response Evaluation Criteria in Solid Tumours Version 1.1; SAE = serious adverse event; vs. = versus.
Notes: For all patients receiving first-line therapy in this study (data cut-off: October 12, 2023), prior surgery related to the current cancer and prior radiotherapy was allowed.57 Prior treatment with chemotherapy and/or targeted agents for metastatic disease was not allowed; however, patients treated with neoadjuvant and/or adjuvant chemotherapy were eligible if disease progression occurred 6 months or later following completion of chemotherapy.57
For key secondary outcomes and exploratory outcomes, only information and/or outcomes relevant to and reported in this review (i.e., the first-line treatment for patients who are treatment-naive; nivolumab plus ipilimumab vs. chemotherapy) are presented in this table.
aPer CDA-AMC Procedures for Reimbursement Reviews, the definition of relevant comparators, the nivolumab monotherapy arm, and all lines population are not relevant to this review.
bOS data were not provided for this review because OS data were not mature.
CORR data were not yet available for the nivolumab plus ipilimumab vs. chemotherapy comparison due to the hierarchical testing approach.
dThe crossover cohort included patients in the chemotherapy arm who experienced documented progression of disease (per RECIST 1.1) by BICR and crossed over to receive nivolumab plus ipilimumab therapy (nivolumab 240 mg q.2.w. + ipilimumab 1 mg/kg every 6 weeks for 2 cycles followed by nivolumab 480 mg q.4.w. + ipilimumab 1 mg/kg every 6 weeks). Patients must have completed at least 1 follow-up visit and met all other crossover criteria outlined in the protocol.
Source: Details included in the table are from the sponsor’s Summary of Clinical Evidence.58
Figure 1: Study Design of CheckMate-8HW
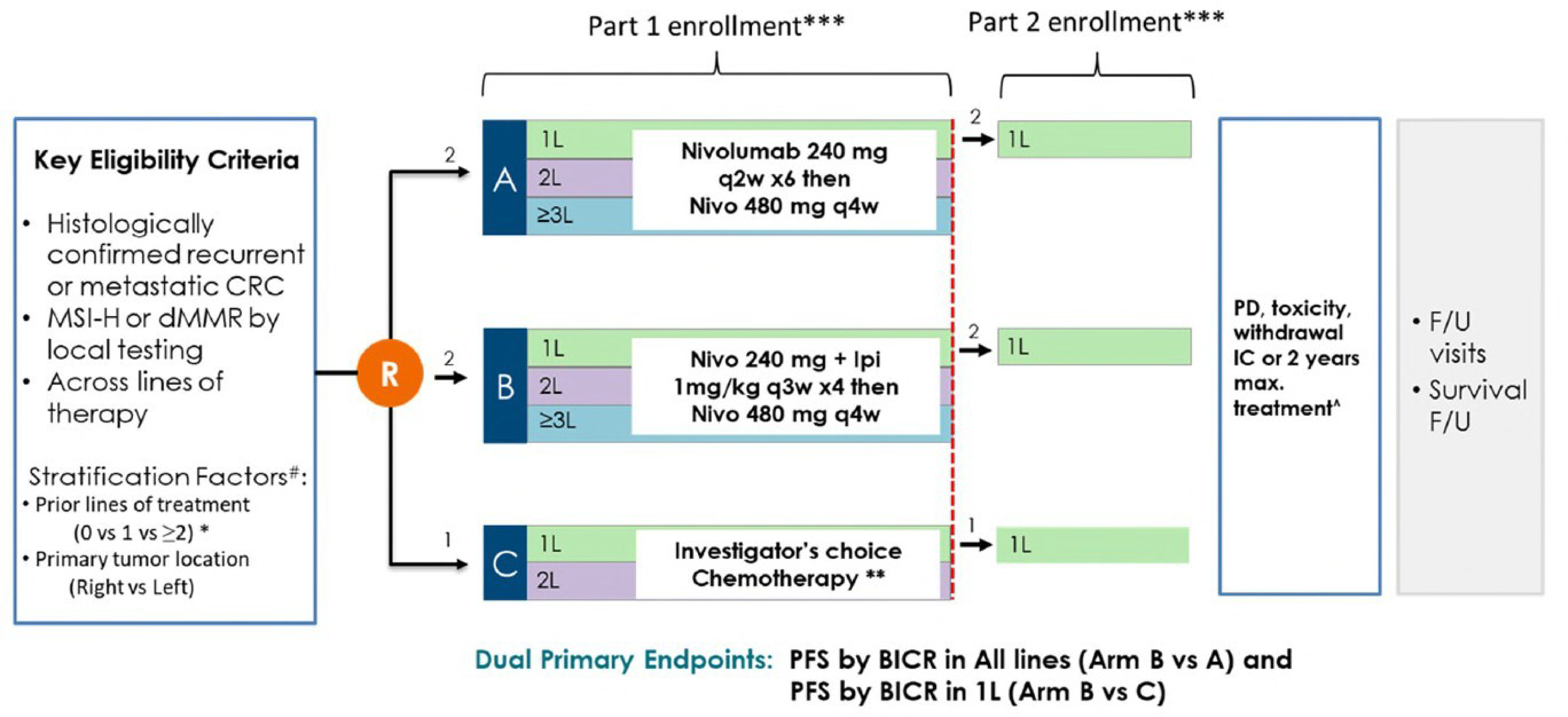
1L = first-line; 2L = second line; 3L = third line; BICR = blinded independent central review; CRC = colorectal cancer; CSR = Clinical Study Report; dMMR = deficient mismatch repair; FOLFORI = leucovorin calcium (folinic acid), fluorouracil, irinotecan hydrochloride; F/U = follow-up; IC = informed consent; Ipi = ipilimumab; mCRC = metastatic CRC; mFOLFOX6 = modified leucovorin calcium (folinic acid), fluorouracil, oxaliplatin; MSI-H = microsatellite instability-high; Nivo = nivolumab; PD = pharmacodynamics; PFS = progression-free survival; q.2.w. = every 2 weeks; q.3.w. = every 3 weeks; q.4.w. = every 4 weeks; vs. = versus.
Notes: First line is defined as 0 prior lines of systemic therapy); second line is defined as 1 prior line of systemic therapy; third line or later is defined as 2 or more prior lines of systemic therapy. Line of therapy was not a stratification factor during part 2 enrolment. The populations for the dual primary end points were patients receiving first-line treatment and randomized (arm B vs. arm C) with centrally confirmed MSI-H or dMMR mCRC or patients who were randomized (arm B vs. arm A) with centrally confirmed MSI-H/dMMR mCRC. Investigator’s choice chemotherapy included mFOLFOX6 or FOLFIRI with or without bevacizumab or cetuximab. Maximum treatment duration was not applicable for patients in arm C.
*Patients who had received 2 or more prior lines of therapy were randomized only to arm A or arm B during part 1; only patients with 0 prior lines of therapy were randomized during part 2.
**Optional crossover for arm C with 6 doses of nivolumab 240 mg every 2 weeks, then nivolumab 480 mg every 4 weeks plus ipilimumab 1 mg/kg every 6 weeks.
***Part 1 enrolment allowed randomization of approximately 560 patients across lines of therapy with locally confirmed MSI-H or dMMR mCRC. Part 2 enrolment allowed randomization of approximately 271 additional patients with locally confirmed MSI-H or dMMR who had not received prior therapy for metastatic disease (first line).
Source: Details included in the table are from the sponsor’s Summary of Clinical Evidence and interim CSR.57
Populations
Inclusion and Exclusion Criteria
Eligibility Criteria
Patients included in the CheckMate-8HW trial were aged 18 years or older. Among the first-line treatment population (i.e., the Health Canada population of indication), patients had histologically confirmed recurrent or metastatic CRC with no prior treatment history with chemotherapy and/or targeted drugs for metastatic disease and not amenable to surgery. Patients were also required to have known dMMR or MSI-H status per local standard of practice testing and an ECOG PS score of 1 or lower. Patients were excluded from the trial if they had an active, known, or suspected autoimmune disease, history of interstitial lung disease or pneumonitis, or a known history of a positive test for HIV or known AIDS.
Interventions
Eligible patients receiving first-line treatment were randomized (2:1 ratio) to receive nivolumab plus ipilimumab or chemotherapy, respectively. Patients in the chemotherapy arm who experienced documented progression of disease per the Response Evaluation Criteria in Solid Tumours Version 1.1 (RECIST 1.1) by BICR had an option to crossover to receive nivolumab plus ipilimumab therapy if they had completed at least 1 follow-up visit and met all other crossover criteria; crossover started when the patients started nivolumab plus ipilimumab treatment.
Interventions were as follows:
Nivolumabplus plus ipilimumab arm: Nivolumab (240 mg) plus ipilimumab (1 mg/kg) were both administered as IV infusion every 3 weeks for up to 4 doses, followed by 480 mg of nivolumab administered as IV infusion every 4 weeks until disease progression, unacceptable toxicity, withdrawal of consent, or until reaching the maximum treatment duration of 2 years.
Chemotherapy arm: Patients received 1 of 6 investigator’s choice chemotherapy regimens (modified leucovorin calcium [folinic acid], fluorouracil, oxaliplatin [mFOLFOX6], mFOLFOX6 plus bevacizumab, mFOLFOX6 plus cetuximab, FOLFIRI, FOLFIRI plus bevacizumab, or FOLFIRI plus cetuximab) administered every 2 weeks until disease progression, unacceptable toxicity, or withdrawal of consent.
Crossover cohort (nivolumab plus ipilimumab): Patients received 240 mg of nivolumab every 2 weeks for up to 6 doses plus ipilimumab 1 mg/kg every 6 weeks for 2 doses, both administered as IV infusion, followed by 480 mg of nivolumab every 4 weeks plus ipilimumab 1 mg/kg every 6 weeks, both administered as IV infusion.
Dose reductions or escalations of nivolumab were not permitted. However, dose adjustments of ipilimumab (1 mg/kg) were permitted if the participant’s weight on the day of dosing differed by greater than 10% from the weight used to calculate the initial dose; in such cases, the dose was recalculated. Dose reductions were permitted for chemotherapy. Doses could be delayed or interrupted and/or the IV infusion rate reduced.
Outcomes
Table 7 summarizes the outcome measures assessed in patients receiving first-line treatment in the CheckMate-8HW trial available at the time of the data cut-off date of October 12, 2023, and August 28, 2024. Of note, per the hierarchical testing strategy, not all outcomes planned for analysis have yet been evaluated for statistical significance at this time. For example, because statistically significant PFS results of nivolumab plus ipilimumab versus nivolumab monotherapy were not available (refer to Figure 2, although nivolumab monotherapy is not the relevant comparator to this review), the results for the objective response rate (ORR) are not yet available for the nivolumab plus ipilimumab arm compared with the chemotherapy arm.
Table 7: Summary of Outcomes Relevant to the Systematic Review
Outcome measure | Patients receiving first-line treatment (data cut-off: October 12, 2023, or August 28, 2024) | |
|---|---|---|
Population | Time point | |
Primary efficacy outcome | ||
PFS per BICR | Patients receiving first-line treatment and who were randomized with centrally confirmed MSI-H or dMMR mCRC | Supplemental analysis conducted using August 28, 2024, data cut-off (median follow-up of 42.05 months) |
Secondary efficacy outcome | ||
PFS per BICR | Patients receiving first-line treatment and who were randomized with locally confirmed MSI-H or dMMR mCRC | Supplemental analysis conducted using August 28, 2024, data cut-off (median follow-up of 42.05 months) |
Exploratory outcomes | ||
EORTC QLQ-C30 | Patients receiving first-line treatment and who were randomized with central and local testing for MSI-H or dMMR mCRC | First interim analysis conducted using October 12, 2023, data cut-off (median follow-up of 31.51 months) |
EQ-5D-3L VAS and UI | Patients receiving first-line treatment and who were randomized with central and local testing for MSI-H or dMMR mCRC | First interim analysis conducted using October 12, 2023, data cut-off (median follow-up of 31.51 months) |
Safety outcomes | ||
Safety and tolerability | Patients receiving first-line treatment with central and local testing for MSI-H or dMMR mCRC | First interim analysis conducted using October 12, 2023, data cut-off (median follow-up of 31.51 months) Supplemental analysis conducted using August 28, 2024, data cut-off (median follow-up of 42.05 months) |
BICR = blinded independent central review; CSR = Clinical Study Report; dMMR = deficient mismatch repair; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; mCRC = metastatic colorectal cancer; MSI-H = microsatellite instability-high; PFS = progression-free survival; UI = utility index; VAS = visual analogue scale.
Note: Only relevant outcomes reported in the section of results in this review were presented in this table.
Sources: Details included in the table are from the sponsor’s Summary of Clinical Evidence, Bristol-Myers Squibb, 2024 (Interim CSR);57 Bristol-Myers Squibb, 2025 (Supplemental Analysis).59
Progression-Free Survival
The primary outcome was BICR-assessed PFS based on the centrally confirmed MSI-H or dMMR mCRC, defined as the time from randomization to the date of the first documented disease progression per RECIST 1.1 or death due to any cause, whichever occurred first. Patients who did not progress and remained alive were censored on the date of their last tumour assessment. Patients who did not have any on-study tumour assessments and remained alive were censored on their randomization date. Patients who started any subsequent anticancer therapy or switched to crossover without a prior reported progression or before death were censored at the last tumour assessment conducted on or before initiation of the subsequent anticancer therapy or crossover.60
The sponsor submitted 3 publications61-63 as evidence to support the use of PFS as a surrogate end point for OS in the population with mCRC. Roodhart et al. (2025),61 examined previously untreated patients with mCRC and reported a correlation between PFS and OS. In the Cicero et al. (2018)62 study, results aggregated from multiple mCRC trials supported the use of PFS as a surrogate, particularly in first-line and second-line settings. A study by Sidhu et al. (2013),63 with pooled data (n = 20,438) from 24 randomized mCRC trials evaluated chemotherapy and targeted drugs (panitumumab, cetuximab, bevacizumab, and aflibercept), and the results indicated that PFS efficacy reasonably predicted a benefit in OS in the mCRC setting.63
The sponsor noted that the CheckMate-8HW trial measured PFS using a predefined criterion of progression, such as RECIST 1.1 criteria, and the use of central reviewers blinded to study treatments to ascertain lack of assessment bias, as per FDA recommendations.64
BICR-assessed PFS based on locally confirmed MSI-H or dMMR mCRC was a key secondary outcome of interest. It was defined the same way as the primary outcome, and conditions (e.g., patients who were censored) applied in a similar manner.
Exploratory Outcomes
The exploratory outcomes in the CheckMate-8HW trial included the following:
EORTC QLQ-C30 (cancer-specific) includes GHS, 5 functional scales, 3 multi-item symptom scales, and 6 symptom single items. The sponsor did not submit any information regarding the psychometric properties (validity, reliability, and responsiveness) of the EORTC QLQ-C30 in the population with metastatic colorectal disease (Table 8).
EQ-5D-3L (visual analogue scale [VAS] and utility index [UI]) descriptive systems have 5 dimensions with 3 levels: “no problems” (level 1), “some problems” (level 2), and “extreme problems” (level 3).” Responses to the descriptive system were converted to a single UI score. Respondents used VAS to rate their current health on a 101-point scale: 0 = “worst” to 100 = “best imaginable health.” The sponsor did not submit any information regarding the psychometric properties of EQ-5D-3L in the population of mCRC (Table 8).
A description of the EORTC QLQ-C30 and EQ-5D-3L outcome measures is presented in Table 8.
Table 8: Summary of the EORTC QLQ-C30 and EQ-5D-3L Outcome Measures and Their Measurement Properties
Outcome measure | Type | Conclusions about measurement properties | MID |
|---|---|---|---|
EORTC QLQ-C30 | A cancer-specific questionnaire, comprising of 30 items measuring:
Patients complete the questionnaire based on a 1 week recall period by rating most items on a 4-point Likert-type scale (1 = not at all; 2 = a little; 3 = quite a bit; 4 = very much). For the 2 items in the GHS scale, the response format is a 7-point Likert-type scale (1 = very poor; 7 = excellent).65 Scores are then converted to a 0 to 100 scale.66,67 | The sponsor did not submit any information regarding the psychometric properties (validity, reliability, and responsiveness) of the EORTC QLQ-C30 in the population with metastatic colorectal disease. | The sponsor indicated that ≥ 10 points improvement or deterioration was considered as clinically meaningful.68 |
EQ-5D-3L | A generic patient-reported outcome measure of HRQoL that consists of both a VAS and a descriptive system that can be used to yield utility index scores.7 There are 5 dimensions with 3 levels:
Responses to the descriptive system are converted to a single UI score. Respondents use VAS to rate their current health on a 101-point scale: 0 = “worst” to 100 = “best imaginable health.” | The sponsor did not submit any information regarding the psychometric properties of EQ-5D-3L in the population of mCRC. | The sponsor indicated that the MID was determined as a change from baseline of 0.08 in health UI scores and a change of 7 for the EQ-5D-3L VAS.69 |
EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; GHS = global health status; HRQoL = health-related quality of life; mCRC = metastatic colorectal cancer; MID = minimal important difference; QoL = quality of life; UI = utility index; VAS = visual analogue scale.
Source: Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Safety End Points
The assessment of safety was based on the incidence of AEs, SAEs, AEs leading to discontinuation, AEs leading to dose modification, select AEs, IMAEs, OESIs, and deaths.
Statistical Analysis
A summary of statistical analyses used in the CheckMate-8HW trial is provided in Table 9.
Table 9: Statistical Analysis of Efficacy and Safety End Points
End point | Statistical model | Adjustment factors | Handling of missing data | Sensitivity analyses |
|---|---|---|---|---|
Primary end point | ||||
PFS per BICR (centrally confirmed population) |
|
|
|
|
Secondary and exploratory end points | ||||
PFS per BICR (locally confirmed population) | As the primary end point | As the primary end point | As the primary end point | As the primary end point |
EORTC QLQ-C30 |
| NA |
| NA |
EQ-5D-3L VAS and UI |
| NA |
| NA |
Safety |
| NA | NR | NA |
BICR = blinded independent central review; CI = confidence interval; CTCAE = Common Terminology Criteria for Adverse Events; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; GHS = global health status; HR = hazard ratio; KM = Kaplan-Meier; MID = minimally important difference; MMRM = mixed models for repeated measures; NA = not applicable; NCI = National Cancer Institute; NR = not reported; PFS = progression-free survival; QoL = quality of life; SD = standard deviation; UI = utility index; VAS = visual analogue scale; vs. = versus.
Note: Only relevant outcomes reported in the Results section in this review were presented.
Source: Details included in the table are from the sponsor’s Summary of Clinical Evidence - Bristol-Myers Squibb, 2023 [Statistical Analysis Plan].70
Sample Size and Power Calculation
The study characteristics, design, and statistical testing strategy of the CheckMate-8HW trial are described in Table 6, Figure 1, and Figure 2, respectively. The following description focuses on content from the study considered relevant to this Reimbursement Review report.
To control the overall type I error of 0.05, alpha was split among various hypotheses. An alpha of 0.044 was used for PFS (nivolumab plus ipilimumab versus chemotherapy) in first-line treatment and the remaining 0.006 was used for all lines. Sample size determination for PFS was calculated assuming a piecewise exponential distribution in the nivolumab plus ipilimumab arm and exponential distribution in the chemotherapy arm. Based on simulations, approximately 125 PFS events in first-line treatment would provide about 99% power to reject an alternative hypothesis of a model-averaged HR of 0.55 with an overall type I error of 0.044 (2-sided). Under the assumption of a staggered enrolment and the assumed event distribution, it would require randomizing approximately 230 patients receiving first-line treatment with nivolumab plus ipilimumab compared with chemotherapy at a 2:1 ratio. An interim analysis was planned to be conducted when 85% of the total number of events were observed (approximately 106 events) and after the last participant was randomized.
Statistical Testing
Statistical analysis of efficacy outcomes in the CheckMate-8HW trial was controlled for overall type I error by using a hierarchical testing strategy. The testing strategy in Figure 2 controlled the family wise error rate at an alpha level of 5% for the primary and key secondary end points. The testing procedure only allowed testing of secondary outcomes if all the precedent outcomes completed their tests. Testing was only performed in the forwarding path (no retrospective testing).
Figure 2: Testing Strategy for the Primary and Secondary Outcomes
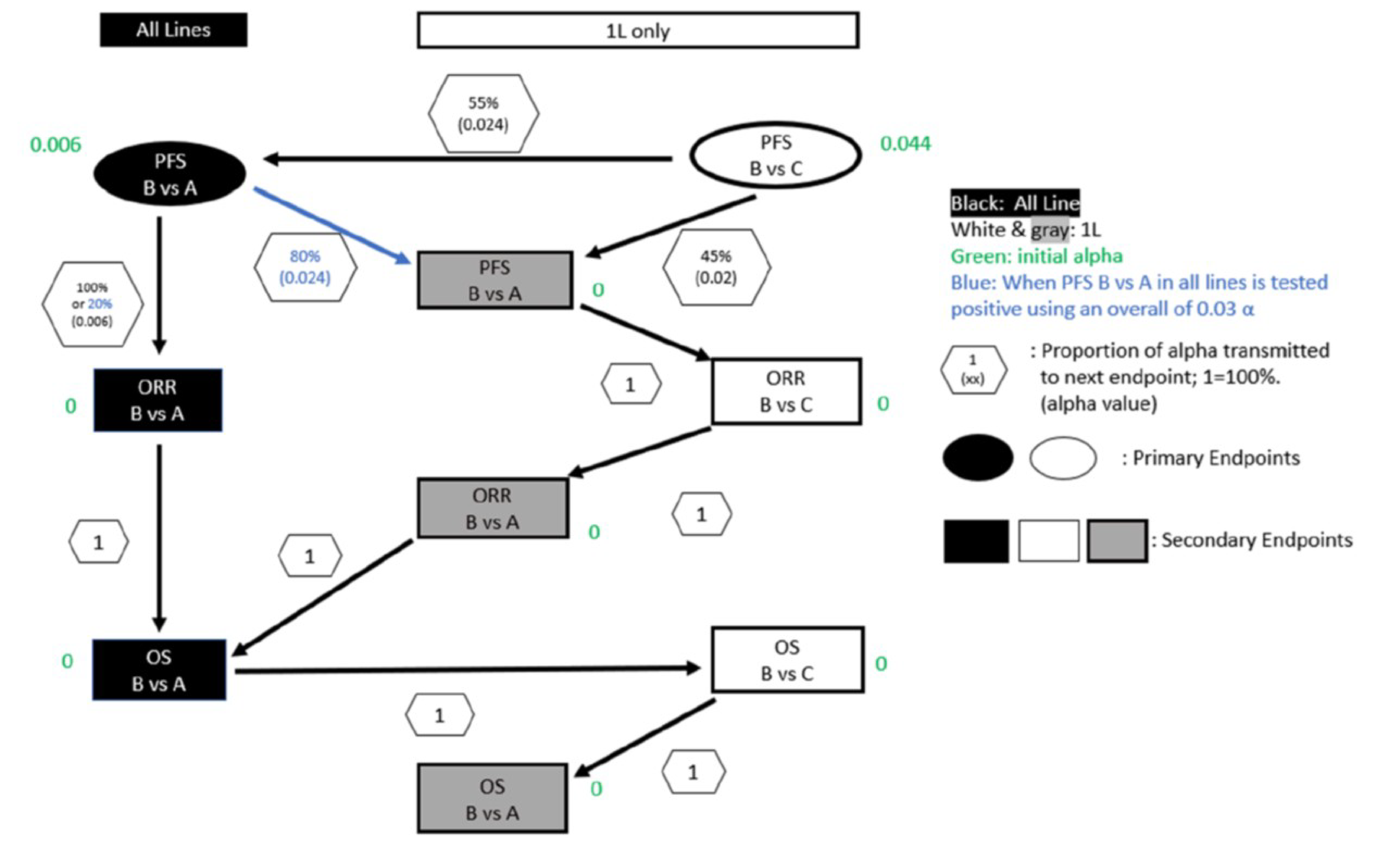
1L = first line; dMMR = deficient mismatch repair; MSI-H = microsatellite instability-high; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; vs. = versus.
Sources: Bristol-Myers Squibb, 2023 (Statistical Analysis Plan).70 Details included in the figure are from the sponsor’s Summary of Clinical Evidence.
PFS by BICR
Primary Analyses
The primary outcome PFS analysis based on centrally confirmed MSI-H or dMMR mCRC was conducted using a log-rank test stratified on tumour sidedness (left versus right). The HR across treatment groups along with its corresponding CI were estimated using a stratified Cox model. Ties were handled using the exact method. The PFS survival curve within each treatment arm was estimated using the Kaplan-Meier (KM) estimator. A 2-sided 95% confidence interval (CI) for median PFS in each treatment arm was computed via a log-log transformation. PFS probability at fixed time points (e.g., 6 and 12 months) were presented along with their corresponding 95% CIs calculated using Greenwood’s formula.71
PFS based on locally confirmed MSI-H or dMMR mCRC (a key secondary outcome) was assessed using the same method as the primary outcome analysis.
Subgroup Analyses
Prespecified subgroup analyses for PFS by BICR was conducted based on important baseline and demographic characteristics including age, sex, race, region, ECOG PS, disease stage at initial diagnosis, tumour sidedness, time from initial disease diagnosis to randomization, liver metastasis per BICR, and BRAF, KRAS, NRAS mutation status, and so forth. For each comparison, the median PFS based on the KM product-limit method along with 2-sided 95% CIs were produced. Forest plots of the unstratified PFS HRs (along with the 95% CIs) were produced. Median and HRs were not reported if the number of patients in the subgroup category per treatment arm was less than 10.
Sensitivity Analysis
Sensitivity analyses were conducted, including analysis of PFS per BICR including imbalanced baseline characteristics as covariates; analysis of PFS per BICR using unstratified Cox model; analysis of PFS per BICR using stratification factors as covariates; and analysis of PFS per BICR accounting for missing tumour assessment before PFS event (Table 9).
EORTC QLQ-C30 (Exploratory Outcomes)
For EORTC QLQ-C30, all scales and single items were scored on categorical scales and linearly transformed to 0 to 100 scales with higher scores for functional scales or items (and EORTC QLQ-C30 GHS) representing higher levels of functioning or quality of life and higher scores for symptom scales or items representing a higher level of symptoms. For EORTC QLQ-30, a meaningful difference in the change from baseline was defined as a change of 10 or more points.68,72
For EORTC QLQ-C30, the following descriptive analyses were conducted:
The EORTC QLQ-C30 questionnaire completion rate was analyzed, defined as the proportion of questionnaires received out of the expected number (i.e., number of patients receiving treatment or in follow-up), and summaries for each assessment time point by treatment group, based on all patients who were randomized and all patients with locally confirmed MSI-H or dMMR status who were randomized.
The mean score and mean change from baseline in EORTC QLQ-C30 GHS, functional scales, and symptom scales were summarized using descriptive statistics (N, mean with standard deviation, and 95% CI) for all scales at each assessment time point).
A mixed model repeated measures model was used to generate the results.
EQ-5D-3L (Exploratory End Point)
For EQ-5D-3L VAS, patients rated their general health using a scale ranging from 0 to 100 with 0 being the worst imaginable health state and 100 being the best imaginable health state. The MID from baseline was 7 points for EQ-5D-3L VAS scores.73
For the EQ-5D-3L UI, patients rated their health state for each of the 5 dimensions in the descriptive system (mobility, self-care, usual activities, pain or discomfort, anxiety or depression). Responses to the descriptive system then define 1 of 243 possible health states. A single UI score was calculated by applying a value or weight to each of the levels in each dimension. The UK time trade-off value set was used to calculate UI scores, which range from −0.594 to 1.000, where 1 reflects full health, 0 reflects death, and negative scores reflect a health state perceived to be worse than death.74 The MID was 0.08 for EQ-5D-3L UI scores.73
Safety Analyses
All safety analyses were based on the safety analysis set. Safety assessments included the frequency of deaths, AEs, SAEs, AEs leading to discontinuation of study treatment or dose modification, IMAEs, and OESIs. Descriptive statistics of safety were presented by treatment arm for all patients who were treated. Analyses were conducted using the 30 day and/or 100-day safety window from the day of the last dose received (data cut-off date: October 12, 2023, and data cut-off date: August 28, 2024).
Analysis Populations
The analysis populations for patients receiving first-line treatment randomized to nivolumab plus ipilimumab and chemotherapy are defined in Table 10.
Table 10: Analysis Populations
Population | Definition | Application |
|---|---|---|
Patients with centrally confirmed MSI-H or dMMR | All patients who were randomized with centrally confirmed MSI-H or dMMR status by either central test (IHC or PCR) | Primary outcome |
Patients with locally confirmed MSI-H or dMMR | All patients who were randomized with locally confirmed MSI-H or dMMR status (i.e., ITT population) | Secondary outcome |
dMMR = deficient mismatch repair; IHC = immunohistochemistry; ITT = intention to treat; MSI-H = microsatellite instability-high; PCR = polymerase chain reaction.
Sources: Bristol-Myers Squibb, 2023 [Statistical Analysis Plan].70 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Results
Patient Disposition
The patient disposition for the CheckMate-8HW trial is presented in Table 11. At the data cut-off date on October 12, 2023, the median follow-up for patients who were randomized and receiving first-line treatment was 31.57 months (range, 6.1 months to 48.4 months).57 A total of 303 patients were randomized to the nivolumab plus ipilimumab arm (n = 202) or to chemotherapy arm (N = 101). Of these patients, 288 patients (95.0%) were treated: 200 with nivolumab plus ipilimumab and 88 with chemotherapy. The most common reason for discontinuation of treatment was disease progression in both treatment arms (19% in the nivolumab plus ipilimumab arm and 69% in the chemotherapy arm). Of the 303 patients who were randomized and receiving first-line treatment, 255 had centrally confirmed MSI-H or dMMR status: 171 in the nivolumab plus ipilimumab arm and 84 in the chemotherapy arm. The overall patient disposition was consistent between all patients randomized to receive first-line treatment (i.e., locally confirmed MSI-H or dMMR, intention-to-treat [ITT] population) and patients who were randomized and receiving first-line treatment with centrally confirmed MSI-H or dMMR.
Table 11: Patient Disposition — Patients Randomized to Receive First-Line Treatment in the Nivolumab Plus Ipilimumab and Chemotherapy Arms (ITT)
Patient disposition | DCO: October 12, 2023 | |
|---|---|---|
Nivolumab plus ipilimumab (n = 202) | Chemotherapy (n = 101) | |
Screened, N | ||||| | |
Unsuccessful screening | ||| |||||||| | |
Reason for unsuccessful screening, n (%) | ||
Adverse event | 2 (0.3) | |
Patient withdrew consent | 19 (3.2) | |
Death | 6 (1.0) | |
Poor or noncompliance | 3 (0.5) | |
Patient no longer met study criteria | 236 (39.5) | |
Other | 28 (4.7) | |
Not reported | 1 (0.2) | |
Randomized, N (%) | 202 | 101 |
Treated, n (%) | 200 (99.0) | 88 (87.1) |
Not treated | 2 (1.0) | 13 (12.9) |
Reason for not treated | ||
Patient withdrew consent | 0 | 6 (5.9) |
Patient no longer met study criteria | 1 (0.5) | 2 (2.0) |
Othera | 1 (0.5) | 5 (5.0) |
Ongoing treatment, n (%) | 42 (21.0) | 6 (6.8) |
Completed treatment, n (%) | 62 (31.0) | 0 |
Discontinued treatment, n (%) | 96 (48.0) | 82 (93.2) |
Reason for treatment discontinuation, n (%) | ||
Withdrew consent | 0 | 1 (1.1) |
Death | 2 (1.0) | 0 |
Pregnancy | 1 (0.5) | 0 |
No longer met study criteria | 1 (0.5) | 0 |
Disease progression | 38 (19.0) | 61 (69.3) |
Study drug toxicity | 36 (18.0) | 4 (4.5) |
AE unrelated to study drug | 12 (6.0) | 5 (5.7) |
Maximum clinical benefit | 0 | 8 (9.1) |
Discontinued treatment due to COVID-19 | 2 (1.0) | 0 |
Other | 6 (3.0) | 3 (3.4) |
Protocol deviation | 10 (5.0) | 6 (5.9) |
Next expected study phase, n (%) | ||
Follow-up | 138 (69.0) | 73 (83.0) |
Survival follow-up | 5 (2.5) | 2 (2.3) |
Ongoing study,b n (%) | 152 (76.0) | 50 (56.8) |
Discontinued study,b n (%) | 48 (24.0) | 38 (43.2) |
Reason for discontinuation of study, n (%) | ||
Death | 44 (22.0) | 32 (36.4) |
Lost to follow-up | 1 (0.5) | 0 |
Withdrew consent | 2 (1.0) | 3 (3.4) |
Other | 1 (0.5) | 3 (3.4) |
ITT, Nc (%) | 202 (100) | 101 |
PP, N (%) | 192 (95) | 95 (94.1) |
Safety, Nd (%) | 200 (99.1) | 88 (87.1) |
AE = adverse event; CDA-AMC = Canada’s Drug Agency; CSR = Clinical Study Report; DCO = data cut-off; ITT = intent to treat; PP = per protocol.
██ █████████ ██ ███ ████████ ███ █████████ ███████ ████ ███ ██ █████████ ██ █████████ ██████████ █████ ███ ███████████ ███████ ████████ ████ ███████ ██████ ███████ ██████████ ██ █████████ ██████████ ███ ███ ██████████ ████████████ ██ ███ ████ ███████ ██ ████████ ███ ███ ██████████ █████████████ ██ ████ ██ ████████████ ██████████ ██ ███ █ ███ █ ██ ███ ██████
aThe reasons include randomized in error for the participant in the nivolumab plus ipilimumab arm and the following in the chemotherapy arm: participant refused chemotherapy (3 patients); participant changed their mind (1 participant); and participant requested to discontinue (1 participant).
bIncludes data from crossover period or cohort. The crossover cohort included patients in the chemotherapy arm who experienced documented progression of disease and crossed over to receive nivolumab plus ipilimumab therapy. Percentages are based on patients entering the period. End of treatment status was evaluated at the end of the main period treatment for patients who continued to crossover.
cThe ITT population corresponds to the population who were randomized.
dThe safety population included all patients who were treated (i.e., the population who were treated).
Sources: Bristol-Myers Squibb, 2024 (Interim CSR).57 Details included in the table are from the sponsor’s Summary of Clinical Evidence, as well as additional information provided by the sponsor at the request of CDA-AMC.
Baseline Characteristics
Baseline characteristics of all patients randomized to receive first-line treatment in the CheckMate-8HW trial for the ITT population (i.e., locally confirmed MSI-H or dMMR) are presented in Table 12. The baseline characteristics outlined in Table 12 are limited to those that are most relevant to this review or were felt to affect the outcomes or interpretation of the study results. Baseline characteristics for patients randomized to receive first-line treatment with centrally confirmed MSI-H or dMMR were consistent with those for all patients randomized to receive first-line treatment. The 2 treatment arms had generally similar demographic, clinical, and disease characteristics. No major imbalances were noted. Among all patients, the median age was 63 years (range, 21 to 87 years). More patients were aged 65 years or older in the chemotherapy arm than in the nivolumab plus ipilimumab arm (54.5% versus 42.1%). Slightly more patients were female (53.8%), and a majority were white (86.1%). Patients were distributed across Asia (9.9%); Canada, Europe, or the US (67.3%); and the rest of the world (22.8%). The number of patients who were enrolled from Canada was not reported. A total of 53.8% patients had an ECOG PS score of 0, and 46.2% had an ECOG PS score of 1. Overall, 44.2% of patients had stage IV disease at initial diagnosis. Overall tumour sidedness was 32% in the left side and 68% in the right side. The proportion of patients who had liver metastasis, lung metastasis, and peritoneal metastasis at baseline were 38.9%, 22.8% and 41.9% respectively.
Table 12: Baseline Characteristics of Patients Randomized to Receive First-Line Treatment in the Nivolumab Plus Ipilimumab and Chemotherapy Arms (ITT)
Characteristic | Data cut-off date: October 12, 2023 | ||
|---|---|---|---|
Nivolumab plus ipilimumab (n = 202) | Chemotherapy (n = 101) | Total (N = 303) | |
Age, years, median (range) | 62.0 (21 to 86) | 65.0 (26 to 87) | 63.0 (21 to 87) |
Age group, years, n (%) | |||
< 65 | 117 (57.9) | 46 (45.5) | 163 (53.8) |
≥ 65 | 85 (42.1) | 55 (54.5) | 140 (46.2) |
Sex, n (%) | |||
Female | 107 (53.0) | 56 (55.4) | 163 (53.8) |
Male | 95 (47.0) | 45 (44.6) | 140 (46.2) |
Race, n (%) | |||
Asian | 19 (9.4) | 13 (12.9) | 32 (10.6) |
Black or African American | 2 (1.0) | 2 (2.0) | 4 (1.3) |
White | 176 (87.1) | 85 (84.2) | 261 (86.1) |
Other | 5 (2.5) | 1 (1.0) | 6 (2.0) |
Geographic region, n (%) | |||
Asia | 19 (9.4) | 11 (10.9) | 30 (9.9) |
Canada, Europe, or the US | 133 (65.8) | 71 (70.3) | 204 (67.3) |
Rest of the world | 50 (24.8) | 19 (18.8) | 69 (22.8) |
ECOG PS, n (%) | |||
0 | 111 (55.0) | 52 (51.5) | 163 (53.8) |
1 | 91 (45.0) | 49 (48.5) | 140 (46.2) |
Weight (kg), median (range) | 67.45 (37.0 to 178.0) | 71.00 (39.3 to 128.0) | 68.00 (37.0 to 178.0) |
Disease stage at initial diagnosis, n (%) | |||
Stage II | 43 (21.3) | 17 (16.8) | 60 (19.8) |
Stage III | 73 (36.1) | 35 (34.7) | 108 (35.6) |
Stage IV | 85 (42.1) | 49 (48.5) | 134 (44.2) |
Not reported | 1 (0.5) | 0 | 1 (0.3) |
Disease stage at study entry, n (%) | |||
Stage IVA | 80 (39.6) | 43 (42.6) | 123 (40.6) |
Stage IVB | 60 (29.7) | 27 (26.7) | 87 (28.7) |
Stage IVC | 62 (30.7) | 31 (30.7) | 93 (30.7) |
Not reported | 0 | 0 | 0 |
Tumour sidedness (CRF), n (%) | |||
Left | 64 (31.7) | 33 (32.7) | 97 (32.0) |
Right | 138 (68.3) | 68 (67.3) | 206 (68.0) |
Metastasis site per BICR, n (%) | |||
Liver | 76 (37.6) | 42 (41.6) | 118 (38.9) |
Lung | 44 (21.8) | 25 (24.8) | 69 (22.8) |
Peritoneal | 84 (41.6) | 43 (42.6) | 127 (41.9) |
PD-L1 status, n (%) | |||
≥ 1% | 43 (21.3) | 12 (11.9) | 55 (18.2) |
< 1% | 145 (71.8) | 80 (79.2) | 225 (74.3) |
NE or indeterminate | 3 (1.5) | 0 | 3 (1.0) |
NA | 11 (5.4) | 9 (8.9) | 20 (6.6) |
BRAF, KRAS, and NRAS mutation status, n (%) | |||
BRAF, KRAS, and NRAS all wild-type | 47 (23.3) | 23 (22.8) | 70 (23.1) |
BRAF mutant | 52 (25.7) | 24 (23.8) | 76 (25.1) |
KRAS or NRAS mutant | 43 (21.3) | 21 (20.8) | 64 (21.1) |
BRAF, and KRAS, or NRAS mutant | 5 (2.5) | 2 (2.0) | 7 (2.3) |
Unknown | 55 (27.2) | 31 (30.7) | 86 (28.4) |
Lynch syndrome,a n (%) | |||
Yes | 22 (10.9) | 17 (16.8) | 39 (12.9) |
No | 135 (66.8) | 49 (48.5) | 184 (60.7) |
Unknown | 44 (21.8) | 30 (29.7) | 74 (24.4) |
Not reported | 1 (0.5) | 5 (5.0) | 6 (2.0) |
BICR = blinded independent central review; CSR = Clinical Study Report; dMMR = deficient mismatch repair; ECOG PS = Eastern Cooperative Oncology Group Performance Status; ITT = intention to treat; MMR = mismatch repair; MSI = microsatellite instability; NA = not applicable; NE = not evaluable; NGS = next generation sequencing; PCR = polymerase chain reaction; pMMR = proficient mismatch repair.
Notes: For local and central MSI or MMR assessment, “not available” includes both not evaluable and not tested. MSI test per local assessment includes both PCR and NGS test.
Racial categories used in the table are as reported in the source and may not align with Canada's Drug Agency inclusive language guidelines.
aInformation on Lynch syndrome was collected based on the participant’s medical history.
Sources: Bristol-Myers Squibb, 2024 (Interim CSR);57 Andre et al. (2024).55 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Exposure to Study Treatments
Study Treatments
Patient exposure data for first-line treatment only supplemental analysis with a data cut-off date of August 28, 2024, is provided in Table 13. At the data cut-off, the median duration of therapy was 19.04 months in the nivolumab plus ipilimumab arm (nivolumab: 19.04 months; ipilimumab: 2.10 months) and 3.96 months in the chemotherapy arm.59 Detailed patient exposure information for the first-line treatment only interim analysis with a data cut-off on October 12, 2023, is provided in Table 31 in Appendix 1.
Table 13: Duration of Study Therapy in Patients Receiving First-Line Treatment in the Nivolumab Plus Ipilimumab and Chemotherapy Arms (ITT)
Duration of therapy (months) | Data cut-off date: August 28, 2024 | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
Nivolumab plus ipilimumab (n = 200) | Chemotherapy (n = 88) | ||||||||||
Nivolumab (n = 200) | Ipilimumab (n = 200) | Overall (n = 200) | Oxaliplatin (n = 51) | Leucovorin (n = 87) | Fluorouracil bolus (n = 86) | Fluorouracil IV (n = 88) | Bevacizumab (n = 56) | Cetuximab (n = 10) | Irinotecan (n = 37) | Overall (n = 88) | |
Mean (range) | 14.90 (0 to 35.9) | 1.96 (0 to 3.7) | 14.90 (0 to 32.3) | 2.67 (0 to 32.7) | 5.43 (0 to 27.4) | 5.18 (0 to 32.7) | 5.71 (0 to 32.8) | 5.821 (0 to 26.7) | 3.19 (0 to 8.8) | 4.87 (0 to 20.8) | 5.74 (0.1 to 32.8) |
Median | 19.04 | 2.10 | 19.04 | 2.83 | 3.89 | 3.56 | 3.96 | 3.83 | 2.66 | 3.45 | 3.96 |
ITT = intention to treat.
Source: Bristol-Myers Squibb, 2025 (Supplemental Analyses).59 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Prior Treatment
For all patients receiving first-line treatment in this study, prior surgery related to the current cancer and prior radiotherapy was allowed.57 Prior treatment with chemotherapy and/or targeted drugs for metastatic disease was not allowed; however, patients treated with neoadjuvant and/or adjuvant chemotherapy were eligible if disease progression occurred 6 months or later after completion of chemotherapy. Most patients (96.7%) randomized to first-line treatment received prior cancer therapy.57
Concomitant Medications and Cointerventions
████ ██ ██████████ ████████ ███████ ████████ ███████████ ██████████████ ████ ██████████ ███ █████ █████ ██ ██████████ ████████ ████ █████████ █████████ ████ ███████ ███████████ ███████████ ████ ██ ████ ██ ███ █████ ██████████ ███ ██████████ ██ █████ ███ █████████████████ ███████████ ███████████ ███████ █████████ ████████████████ █████████████████ ███████ █████████████████ ███████ ███ ████████████████ ████ ████████████ ██ █████ ███████ ███ ██ █████ ██ ████████ ██ ███ █████████ █ ██████████ ███ ███ █████ ██ ████████ ██ ███ ████████████ ██████ ████ ████████ ██ ███ ██████████ ██████████ ████ ██████████████ █████████ ███████████████████ ██████████ ███ ████████████ ████ ██ ████████████ ████ ████████ █████ ████████ ██ ███ ██████████ ██████████ ████ █████████████ ████ ██ ███ ████████████ ████
Table 14: Concomitant Medications Used in 10% or More of Patients Randomized to Receive First-Line Treatment in the Nivolumab Plus Ipilimumab and Chemotherapy Arms (ITT)
Concomitant medication, n (%) | Data cut-off: October 12, 2023 | ||
|---|---|---|---|
Nivolumab plus ipilimumab (n = 202) | Chemotherapy (n = 101) | Total (N = 303) | |
||||||||||| | || |||||| | || |||||| | ||| |||||| |
||||||||||| | || |||||| | || |||||| | || |||||| |
|||||||||||||| | || |||||| | | ||||| | || |||||| |
|||||||||| | || |||||| | || |||||| | || |||||| |
||||||||||||| |||||| | || |||||| | || | || ||||| |
||||||||| | || |||||| | | ||||| | || |||||| |
|||||||||||| | || |||||| | || |||||| | || |||||| |
|||||||||||||||||| | || |||||| | | ||||| | || |||||| |
|||||||||| | || |||||| | | ||||| | || |||||| |
|||||||||||| |||||||||| |||| | || |||||| | | ||||| | || |||||| |
|||||||||| ||||||||||||| | || |||||| | || |||||| | || |||||| |
|||||||||||||| | || |||||| | || |||||| | || |||||| |
||||||||||||||| |||| | || |||||| | | ||||| | || ||||| |
|||||||||| |||||| | || |||||| | | ||||| | || ||||| |
|||||||||| | || |||||| | || |||||| | || |||||| |
|||||||||||| | || |||||| | | ||||| | || ||||| |
|||||||||||| |||||| ||||||||||||| | || |||||| | | ||||| | || ||||| |
||||||||||| | || ||||| | || |||||| | || |||||| |
||||||||||||| | || ||||| | || |||||| | || |||||| |
|||||||||||||| ||||||||||||| | || ||||| | || |||||| | || ||||| |
|||||||||||| ||||||| |||||||||| |||||| | || ||||| | || |||||| | || ||||| |
|||||||| | || ||||| | || |||||| | || ||||| |
||||||||| |||||||| | || ||||| | || |||||| | || ||||| |
|||||||||||| | || ||||| | || |||||| | || ||||| |
|||||| |||||||| | || ||||| | || |||||| | || ||||| |
|||||||| | || | || |||||| | || ||||| |
CSR = Clinical Study Report; ITT = intention to treat.
Note: Concomitant medications are listed in order of most used in the nivolumab plus ipilimumab arm.
Source: Bristol-Myers Squibb, 2024 (Interim CSR).57
Subsequent Treatment
Subsequent cancer therapy was defined as any systemic therapy, surgery, or radiotherapy for the treatment of tumours occurring after discontinuation of the study treatment. Among all patients randomized to first-line treatment (data cut-off date was on October 12, 2023), a lower proportion of patients received subsequent cancer therapy (systemic therapy in majority) in the nivolumab plus ipilimumab arm than in the chemotherapy arm (22.3% versus 68.3%). Crossover treatment (nivolumab plus ipilimumab) was received by 45 patients (44.6%) in the chemotherapy arm who experienced BICR-documented disease progression; this crossover treatment was included under subsequent systemic therapy. An additional 20.8% of patients received subsequent immuno-oncology therapy outside of the crossover cohort. Taken together, 65.4% of patients in the chemotherapy arm received subsequent immuno-oncology therapy. A summary of subsequent cancer therapy for all patients randomized to first-line treatment is provided in Table 15.
Table 15: Subsequent Cancer Treatment — Patients Randomized to Receive First-Line Treatment in the Nivolumab Plus Ipilimumab and Chemotherapy Arms (ITT)
Exposure | Data cut-off: October 12, 2023 | |
|---|---|---|
Nivolumab plus ipilimumab (n = 202) | Chemotherapy (n = 101) | |
Patients with any subsequent therapy, n (%)a | 45 (22.3) | 69 (68.3) |
Patients who received subsequent radiotherapy, n (%) | 1 (0.5) | 1 (1.0) |
Patients who received subsequent surgery, n (%) | 5 (2.5) | 5 (5.0) |
Patients who received subsequent systemic therapy, n (%)b | 39 (19.3) | 68 (67.3) |
Crossover treatment, n (%) | 0 | 45 (44.6) |
Nonstudy systemic therapy, n (%) | 39 (19.3) | 23 (22.8) |
Anti-CTL4A | 0 | 2 (2.0) |
Ipilimumab | 0 | 2 (2.0) |
Anti-PD1 or anti-PDL1 | 8 (4.0) | 21 (20.8) |
Pembrolizumab | 6 (3.0) | 15 (14.9) |
Nivolumab | 2 (1.0) | 4 (4.0) |
EGFR inhibitors | 11 (5.4) | 2 (2.0) |
Cetuximab | 9 (4.5) | 1 (1.0) |
Panitumumab | 3 (1.5) | 1 (1.0) |
Platinum compounds | 20 (9.9) | 5 (5.0) |
Oxaliplatin | 20 (9.9) | 5 (5.0) |
VEGFR-targeted therapy | 15 (7.4) | 7 (6.9) |
Bevacizumab | 15 (7.4) | 7 (6.9) |
Aflibercept | 3 (1.5) | 0 |
Other systemic anticancer therapy | 30 (14.9) | 9 (8.9) |
Fluorouracil | 25 (12.4) | 5 (5.0) |
Irinotecan | 18 (8.9) | 5 (5.0) |
Capecitabine | 4 (2.0) | 3 (3.0) |
Irinotecan hydrochloride | 1 (0.5) | 0 |
Raltitrexed | 1 (0.5) | 0 |
Tipiracil hydrochloride; trifluridine | 1 (0.5) | 0 |
Tipiracil; trifluridine | 1 (0.5) | 0 |
MEK, NRAS, and BRAF inhibitors | 3 (1.5) | 1 (1.0) |
Encorafenib | 3 (1.5) | 1 (1.0) |
CSR = Clinical Study Report; ITT = intention to treat.
aParticipant may have received more than 1 type of subsequent therapy. Subsequent therapy was defined as therapy started on or after first dosing date (randomization date if the participant was never treated).
bPatients who received crossover treatment in chemotherapy are included.
Source: Bristol-Myers Squibb, 2024 (Interim CSR).57 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Efficacy
The primary outcome was defined as PFS per BICR based on centrally confirmed MSI-H or dMMR mCRC, with a data cut-off of August 28, 2024.
The median PFS was 54.08 months (95% CI, 54.08 months to not available) in the nivolumab plus ipilimumab arm and 5.85 months (95% CI, 4.37 months to 7.79 months) in the chemotherapy arm. The HR was 0.21 (95% CI, 0.14 to 0.31) (Table 16). The between-group difference in PFS at 12 months for nivolumab plus ipilimumab versus chemotherapy was 57.45% (95%CI, 45.41% to 69.49%). PFS results are presented in Figure 3, Table 16, and Table 17.
Figure 3: PFS per BICR for Nivolumab Plus Ipilimumab Versus Chemotherapy in Patients With Centrally Confirmed MSI-H or dMMR mCRC Randomized to Receive First-Line Treatment (DCO: August 28, 2024)
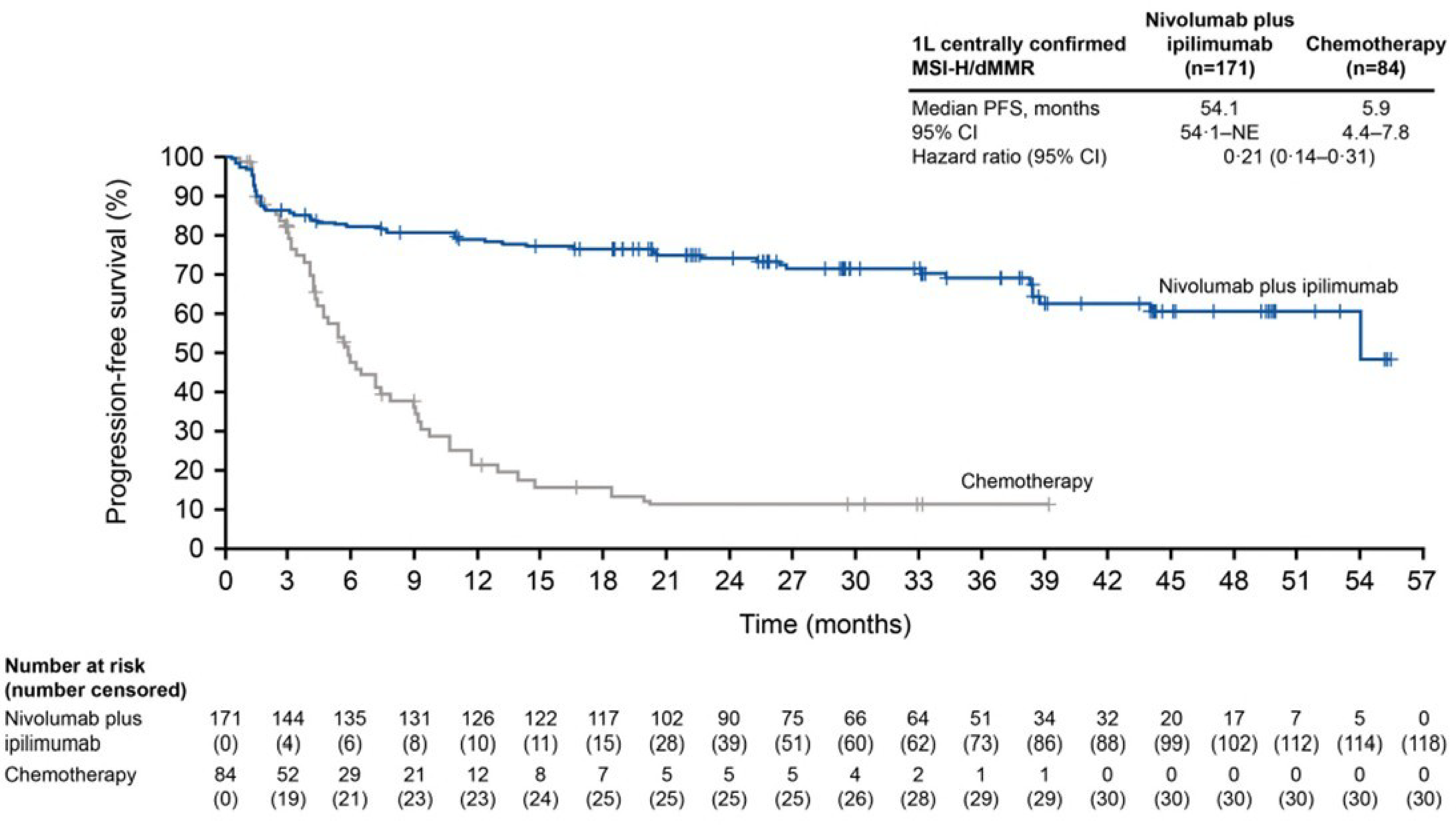
1L = first line; BICR = blinded independent central review; CI = confidence interval; DCO = data cut-off date; dMMR = deficient mismatch repair; HR = hazard ratio; IRT = interactive response technology; KM = Kaplan-Meier; mCRC = metastatic colorectal cancer; MSI-H = microsatellite instability-high; NE = not estimable; PFS = progression-free survival.
Notes: Statistical model for HR and P value: stratified Cox proportional hazard model and stratified log-rank test by tumour sidedness (left versus right) as per IRT. Symbols represent censored observations. Excludes data collected on or after first crossover dose date. KM plot was generated only if there were at least 10 patients in each treatment arm in population or subgroup.
Source: Andre et al., Lancet 2025 – supplement.56 Bristol-Myers Squibb, 2025 [Supplemental Analyses.].59 Reprinted from The Lancet, 405(10476), Andre T, Elez E, Lenz H-J, et al. Nivolumab plus ipilimumab versus nivolumab in microsatellite instability-high metastatic colorectal cancer (CheckMate 8HW): a randomized, open-label, phase 3 trial., Pages No.383 to 395, Copyright (2025), with permission from Elsevier. doi: https://doi.org/10.1016/S0140-6736(24)02848-4. Details included in the figure are from the sponsor’s Summary of Clinical Evidence.
Table 16: Results of PFS per BICR, Patients Randomized to First-Line Treatment With Centrally Confirmed MSI-H or dMMR mCRC
PFS per BICR | Data cut-off: August 28, 2024 | |
|---|---|---|
Nivolumab plus ipilimumab (n = 171) | Chemotherapy (n = 84) | |
Events, n (%) | 53 (31.0) | 54 (64.3) |
Median PFS, months (95% CI) | 54.08 (54.08 to NA) | 5.85 (4.37 to 7.79) |
HR (95% CI)a | 0.21 (0.14 to 0.31) | |
P value | NRb | |
PFS rate, % (95% CI) | ||
6-month | 82.08 (75.37 to 87.11) | 47.64 (35.03 to 59.21) |
Between-group mean difference, % (95% CI) | 34.44 (21.00 to 47.87) | |
12-month | 79.00 (71.99 to 84.45) | 21.55 (12.13 to 32.74) |
Between-group mean difference, % (95% CI) | 57.45 (45.41 to 69.49) | |
18-month | 76.49 (69.26 to 82.24) | 15.67 (7.63 to 26.32) |
Between-group mean difference, % (95% CI) | 60.82 (49.44 to 72.19) | |
24-month | 74.21 (66.70 to 80.27) | 11.20 (4.47 to 21.39) |
Between-group mean difference, % (95% CI) | 63.01 (52.16 to 73.86) | |
36-month | 69.00 (60.55 to 76.00) | 11.20 (4.47 to 21.39) |
Between-group mean difference, % (95% CI) | 57.80 (46.34 to 69.49) | |
BICR = blinded independent central review; CI = confidence interval; dMMR = deficient mismatch repair; HR = hazard ratio; mCRC = metastatic colorectal cancer; MSI-H = microsatellite instability-high; NR = not retested; PFS = progression-free survival.
aBased on Kaplan-Meier estimates.
bNot retested because P < 0.0001 was reported based on the data cut off date of October 12, 2023.
Source: Bristol-Myers Squibb, 2025 (Supplemental Analyses).59 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Table 17: Reason for Censoring, PFS per BICR for Nivolumab Plus Ipilimumab vs. Chemotherapy in Patients With Centrally Confirmed MSI-H or dMMR mCRC Randomized to Receive First-Line Treatment (Data Cut-off Date: August 28, 2024)
Item | Nivolumab plus ipilimumab (n = 171) | Chemotherapy (n = 84) |
|---|---|---|
||||||| | ||| | || |||||| | || |||||| |
|||||||||||| | || |||||| | || |||||| |
||||| | | ||||| | | ||||| |
|||||| || |||||||| ||||||||| | ||| | ||| |||||| | || |||||| |
|||||||| || |||| || ||||||||||||| | | ||||| | | ||||| |
|| |||||||| |||||| ||||||||||| | | ||||| | | ||||| |
||||| ||||||| | | ||||| | || |
||||| | | ||||| | | ||||| |
|| |||||||| |||||| |||||||||| ||| || |||||| | || | | ||||| |
||||| ||||||| | || | | ||||| |
||||| | || | || |
|||||||| || |||| || |||| |||||| |||||||||| |||||||| || || |||| || |||||||||||||| | ||| |||||| | || |||||| |
|||||||| |||||||||| ||||||||||| |||||||| | || ||||| | || |||||| |
|||||||| |||||||||| |||||||| ||||||| | | ||||| | || |||||| |
|||||||| |||||||||| |||||||||||| | || | | ||||| |
|||||||| |||||||||| ||||||| | | ||||| | | ||||| |
||||| |||||||||||| | || |||||| | || |
|| ||||||||| | || |||||| | | ||||| |
||| ||||| | | ||||| | | ||||| |
|||| || ||||||||| | || | || |
|||||||| ||||||| | || | | ||||| |
||||| | | ||||| | || |
BICR = blinded independent central review; dMMR = deficient mismatch repair; mCRC = metastatic colorectal cancer; MSI-H = microsatellite instability-high; PFS = progression-free survival; RECIST 1.1 = Response Evaluation Criteria in Solid Tumours Version 1.1; vs. = versus.
Note: Excludes data collected on or after first crossover dose date.
aRECIST 1.1 criteria.
bTumour assessments and death if any, occurring after the start of subsequent anticancer therapy were not considered.
cPatients who received subsequent anticancer therapy before first on-study scan were censored on randomization date.
dIncludes patients, regardless of treatment status, who received subsequent anticancer therapy without a prior reported PFS event. Those patients were censored at the last evaluable tumour assessment before or on the start date of subsequent anticancer therapy.
Sources: Bristol-Myers Squibb, 2025 [Supplemental Analyses].59 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Subgroup Analyses
Most subgroup analyses of PFS per BICR for patients with centrally confirmed MSI-H or dMMR mCRC were consistent with the primary analysis. Specifically, HRs were less than 1 in favour of nivolumab plus ipilimumab, and the corresponding 95% CIs did not include 1 (Figure 4). Of note, statistically significant improvements in PFS were observed in both patients with liver metastases (HR = 0.11; 95% CI, 0.05 to 0.25) and those without liver metastases (HR = 0.28; 95% CI, 0.17 to 0.46).
Figure 4: PFS per BICR in Predefined Subgroups for Nivolumab Plus Ipilimumab Versus Chemotherapy in Patients With Centrally Confirmed MSI-H or dMMR mCRC Randomized to Receive First-Line Treatment [Redacted]

BICR = blinded independent central review; dMMR = deficient mismatch repair; mCRC = metastatic colorectal cancer; MSI-H = microsatellite instability-high; PFS = progression-free survival.
Sensitivity Analyses
Sensitivity analyses for PFS per BICR based on centrally confirmed MSI-H or dMMR mCRC were consistent with primary analysis (Table 18).
Table 18: Sensitivity Analysis for PFS per BICR for Nivolumab Plus Ipilimumab vs. Chemotherapy in Patients With Centrally Confirmed MSI-H or dMMR mCRC Randomized to Receive First-Line Treatment
Sensitivity analysis | Nivolumab plus ipilimumab vs. chemotherapy | |
|---|---|---|
HR (97.91% CI) | P value | |
Analysis of PFS per BICR including imbalanced baseline characteristics as covariatesa,b | 0.22 (0.13 to 0.36) | < 0.0001 |
Analysis of PFS per BICR using unstratified Cox model | 0.21 (0.13 to 0.34) | < 0.0001 |
Analysis of PFS per BICR using stratification factors as covariates | 0.21 (0.13 to 0.34) | < 0.0001 |
Analysis of PFS per BICR accounting for missing tumour assessment before the PFS eventa | |||| |||||| ||||| | < 0.0001 |
BICR = blinded independent central review; CI = confidence interval; dMMR = deficient mismatch repair; HR = hazard ratio; IRT = interactive response technology; mCRC = metastatic colorectal cancer; MSI-H = microsatellite instability-high; PFS = progression-free survival; PD-L1 = programmed death-ligand 1 vs. = versus.
Note: Excludes data collected on or after first crossover dose date.
aCox proportional hazard model stratified by time-dependent Cox model by tumour sidedness (left versus right) per IRT.
bThe following imbalanced baseline characteristics are included in the model: PD-L1.
Sources: Bristol-Myers Squibb, data on file. Data cut-off date: October 12, 2023.57 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
The secondary outcome was PFS per BICR results based on locally confirmed dMMR or MSI-H mCRC in the ITT population (data cut-off date: August 28, 2024).
The median PFS was 54.08 months (95% CI, 38.44 months to not achieved) in the nivolumab plus ipilimumab arm and 5.95 months (95% CI, 4.86 months to 9.03 months) in the chemotherapy arm. The HR was 0.30 (95% CI, 0.21 to 0.43) (Table 19). The between-group difference in PFS at 12 months for nivolumab plus ipilimumab versus chemotherapy was 47.01% (95% CI, 36.57% to 57.45%). PFS results are presented in Figure 5 and Table 19.
Figure 5: PFS per BICR for Nivolumab Plus Ipilimumab Versus Chemotherapy in Patients With Locally Confirmed MSI-H or dMMR mCRC Randomized to Receive First-Line Treatment (ITT) (DCO: August 28, 2024) [Redacted]

BICR = blinded independent central review; DCO = data cut-off; dMMR = deficient mismatch repair; ITT = intention to treat; mCRC = metastatic colorectal cancer; MSI-H = microsatellite instability-high; PFS = progression-free survival.
Table 19: PFS per BICR for Nivolumab Plus Ipilimumab vs. Chemotherapy in Patients With Locally Confirmed MSI-H or dMMR mCRC Randomized to Receive First-Line Treatment (ITT)
Parameters and time points | Data cut-off date: August 28, 2024 | |
|---|---|---|
Nivolumab plus ipilimumab (n = 202) | Chemotherapy (n = 101) | |
|||||| |||||||||| |||||| | ||||| | |
|||||| || |||||| ||| | || |||||| | || |||||| |
|||||| ||| |||| |||| || |||||| | ||||| ||||||| ||| | |||| |||||| ||||| |
|| |||| |||| | |||| |||||| ||||| | |
||||||| | | | |||||| | |
||| ||||||||||| | ||
|| | ||||||| | ||||||| | ||||| ||||||| |||||| | ||||| ||||||| |||||| |
||||||| ||||| |||| ||||||||||| | ||||||| | ||||| ||||||| |||||| | |
|| || ||||||| | ||||||| | ||||| ||||||| |||||| | ||||| ||||||| |||||| |
||||||| ||||| |||| ||||||||||| | ||||||| | ||||| ||||||| |||||| | |
|| || ||||||| | ||||||| | ||||| ||||||| |||||| | ||||| |||||| |||||| |
||||||| ||||| |||| ||||||||||| | ||||||| | ||||| ||||||| |||||| | |
|| || ||||||| | ||||||| | ||||| ||||||| |||||| | ||||| |||||| |||||| |
||||||| ||||| |||| ||||||||||| | ||||||| | ||||| ||||||| |||||| | |
███ █████ █████ ████ █ ███████ ███████████ ███████ ███████ ██ █ ██████████ █████████ ███ █ ████ ████████ ████ █ █████████ ████████ ███████ ████ █ ██████████ ██████████ ███████ █████ █ ██████████████ ███████████ █████ ██ █ ███ ███████████ ████ █ ███ █ █████████ █ ██████████████ ██████████ ██ ████████ ████ ██████ ████████████████ ██ ████████ ██████████ █████ ██ ████████████ ███████████ █████ ████ █████████ ██ ██ █████ █████ █████████ ████ ████ ███ █████████ ████████ █████████████ ███████ ████ ██████████████ ████████████ ███ ████ ███ ██████████ ███████████ ████████ ██ ███ ███████ ██ ███ ███████ ██ ████████
BICR = blinded independent central review; dMMR = deficient mismatch repair; ITT = intention to treat; mCRC = metastatic colorectal cancer; MSI-H = microsatellite instability-high; PFS = progression-free survival; vs. = versus.
The results observed in the August 28, 2024, data cut-off date (median follow-up: 42.05 months) were consistent with the PFS results from the primary analysis, sensitivity analysis, and subgroup analysis based on the October 12, 2023, data cut-off date (median follow-up: 31.57 months).
Health-Related Quality of Life
European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30
At the data cut-off for the first-line treatment interim analysis (data cut-off: October 12, 2023), the completion rates for the EORTC QLQ-C30 at baseline were 95.3% for patients in the nivolumab plus ipilimumab arm and 86.9% in the chemotherapy arm.57
Mean baseline EORTC QLQ-C30 scores were generally similar in the 2 treatment arms (Figure 6 and Table 20). The results for EORTC QLQ-C30 GHS in the nivolumab plus ipilimumab arm showed a trend for improvement from baseline during the treatment period (Figure 6). In contrast, EORTC QLQ-C30 GHS results for the chemotherapy arm were either stable or showed a trend for worsening from baseline during the treatment period (Figure 6). At week 37, the between-group mean differences of change from baseline was 14.0 (95% CI, 5.9 to 22.1).
No subgroup or sensitivity analyses were conducted for EORTC QLQ-C30.
Figure 6: Mean Change From Baseline for EORTC QLQ-C30 GHS Scores by Time Points in Patients With Locally Confirmed MSI-H or dMMR mCRC Randomized to Receive First-Line Treatment in the Nivolumab Plus Ipilimumab and Chemotherapy Arms (ITT) (Data Cut-Off Date: October 12, 2023) [Redacted]

dMMR = deficient mismatch repair; EORTC QLQ-C30 = European Organization for Research and Treatment of Cancer Quality of Life Core 30; GHS = global health status; ITT = intention to treat; mCRC = metastatic colorectal cancer; MSI-H = microsatellite instability-high.
Table 20: EORTC QLQ-C30 GHS, EQ-5D-3L VAS, and EQ-5D-3L UI Scores — Longitudinal Analysis (MMRM) Change From Baseline Results by Time Points (Patients With Locally Confirmed MSI-H or dMMR mCRC Randomized to Receive First-Line Treatment) (ITT)
Outcomes and time points | Data cut-off date: October 12, 2023 | |
|---|---|---|
Nivolumab plus ipilimumab N = 202 | Chemotherapy N = 101 | |
||||||||||||| | ||| | ||
|| || ||||| | ||
|||||| || |||||||| |||||||||||| || ||| ||||||||| | ||| | ||| | || |
|||||| |||| ||||||||| |||| |||| ||| | |||| |||||| ||||| | |||| |||||| ||||| |
|||| ||||||||||| |||| ||| | ||| ||||| ||||| | |
|| || ||||| | ||
|||||| || |||||||| |||||||||||| || ||| ||||||||| | ||| | ||| | || |
|||||| |||| ||||||||| |||| |||| ||| | |||| |||||| ||||| | |||| |||||| ||||| |
|||| ||||||||||| |||| ||| | |||| ||||| ||||| | |
|| || ||||| | ||
|||||| || |||||||| |||||||||||| || ||| ||||||||| | ||| | ||| | || |
|||||| |||| ||||||||| |||| |||| ||| | |||| |||||| ||||| | |||| |||||| ||||| |
|||| ||||||||||| |||| ||| | |||| ||||| ||||| | |
|||||||| ||| | ||
|| || ||||| | ||
|||||| || |||||||| |||||||||||| || ||| ||||||||| | ||| | ||| | || |
|||||| |||| ||||||||| |||| |||| ||| | |||| |||||| ||||| | |||| |||||| ||||| |
|||| ||||||||||| |||| ||| | ||| |||||| |||| | |
|| || ||||| | ||
|||||| || |||||||| |||||||||||| || ||| ||||||||| | ||| | ||| | || |
|||||| |||| ||||||||| |||| |||| ||| | |||| |||||| ||||| | |||| |||||| ||||| |
|||| ||||||||||| |||| ||| | |||| ||||| ||||| | |
|||||||| ||||||| ||||| |||| | ||
|| || ||||| | ||
|||||| || |||||||| |||||||||||| || ||| ||||||||| | ||| | ||| | || |
|||||| |||| ||||||||| |||| |||| ||| | ||||| ||||||| |||||| | ||||| ||||||| |||||| |
|||| ||||||||||| |||| ||| | ||||| ||||||| |||||| | |
|| || ||||| | ||
|||||| || |||||||| |||||||||||| || ||| ||||||||| | ||| | ||| | || |
|||||| |||| ||||||||| |||| |||| ||| | ||||| ||||||| |||||| | ||||| ||||||| |||||| |
|||| ||||||||||| |||| ||| | ||||| ||||||| |||||| | |
CDA-AMC = Canada’s Drug Agency; CI = confidence interval; dMMR = deficient mismatch repair; EORTC QLQ-C30 = European Organization for Research and Treatment of Care Quality of Life Questionnaire Core 30; GHS = global health status; ITT = intention to treat; mCRC = metastatic colorectal cancer; MMRM = mixed model repeated measure; MSI-H = microsatellite instability-high; VAS = visual analogue scale; UI = utility index.
Note: A mixed model repeated measures model was used to generate the results in this table.
Source: Additional information was provided by the sponsor at the request of CDA-AMC.
The results of EORTC QLQ-C30 GHS based on the centrally confirmed patient population was consistent with the locally confirmed patient population.
EQ-5D-3L Questionnaire
████████ ███ ████ ████████ ███ ███ ██ ██████ ███ ███ ██ ██████████ ████████████ ████ ███████ █████████ ██████████ ████ ████████ ███████████ ████ ████ ██████ █████████ ██ ████ █████ ███ ██ █ ███████ ██████ ██ ███ █████████ ████ ██████████ ███ ████████ ████ ███ ████████████ ██████████ ███
Harms
At the October 12, 2023, data cut-off for the first-line treatment interim analysis, patients had a median treatment duration of 13.52 months for the nivolumab plus ipilimumab arm (nivolumab: 13.52 months; ipilimumab: 2.10 months) and 3.96 months for the chemotherapy arm.57 At the August 28, 2024, data cut-off, patients had a median treatment duration of 19.04 months for the nivolumab plus ipilimumab arm (nivolumab: 19.04 months; ipilimumab: 2.10 months) and 3.96 months for the chemotherapy arm.57 The median follow-up time was 31.57 months and 42.05 months as of the October 12, 2023, and the August 28, 2024, data cut-offs, respectively. The narrative that follows will focus on the updated data from the August 28, 2024, data cut-off, except where that information was not provided. The harms outcomes are summarized in Table 21.
Table 21: Safety Results for Patients Receiving First-Line Treatment (Safety Population)
Safety parameters | Data cut-off date: October 12, 2023 | Data cut-off date: August 28, 2024 | ||||||
|---|---|---|---|---|---|---|---|---|
Nivolumab plus ipilimumab (n = 200) | Chemotherapy (n = 88) | Nivolumab plus ipilimumab (n = 200) | Chemotherapy (n = 88) | |||||
Any grade AE | Grade 3 to 4 AE | Any grade AE | Grade 3 to 4 AE | Any grade AE | Grade 3 to 4 AE | Any grade AE | Grade 3 to 4 AE | |
Most common AEs, n (%) | ||||||||
Patients with ≥ 1 all-causality AEs, n (%) | 197 (98.5) | 96 (48.0) | 86 (97.7) | 59 (67.0) | ||| |||||| | ||| |||||| | || |||||| | || |||||| |
Patients with all-causality AEs reported in ≥ 6% patients with grade 3 to 4 AEs in either group, n (%) | ||||||||
Neutrophil count decreased | 3 (1.5) | 1 (0.5) | 14 (15.9) | 6 (6.8) | || | || | || | || |
Neutropenia | 6 (3.0) | 2 (1.0) | 23 (26.1) | 9 (10.2) | || | || | || | || |
Hypertension | 14 (7.0) | 3 (1.5) | 12 (13.6) | 6 (6.8) | || | || | || | || |
SAEs, n (%) | ||||||||
Patients with ≥ 1 all-causality SAEs | || |||||| | || |||||| | || |||||| | || |||||| | || |||||| | || |||||| | || |||||| | || |||||| |
Patients with all-causality SAEs reported in ≥ 3% patients with grade 3 to 4 SAEs in either group, n (%) | ||||||||
Abdominal pain | | ||||| | | ||||| | | ||||| | | ||||| | || | || | || | || |
Pneumonia | | ||||| | 3 (1.5) | | ||||| | 3 (3.4) | || | || | || | || |
Adrenal insufficiency | | ||||| | 6 (3.0) | || | 0 | || | || | || | || |
Patients who stopped treatment due to AEs, n (%) | ||||||||
All-causality AEs leading to discontinuationa | || |||||| | || |||||| | || |||||| | || |||||| | || |||||| | || |||||| | || |||||| | || |||||| |
AEs of special interest, n (%) | ||||||||
All-causality IMAEs within 100 days of last dose: Patients with grade 3 to 4 IMAEs, n (%) | || | || |||||| | || | | ||||| | || | || |||||| | || | | ||||| |
Treatment group absolute difference (nivolumab plus ipilimumab vs. chemotherapy), % (95% CI) | |||| | |||| | |||| | |||| | ||||||
Diarrhea or colitis | 13 (6.5) | 9 (4.5) | 1 (1.1) | 0 | || ||||| | | ||||| | | ||||| | || |
Hepatitis | 11 (5.5) | 6 (3.0) | 0 | 0 | || ||||| | | ||||| | || | || |
Pneumonitis | 4 (2.0) | 3 (1.5) | 0 | 0 | | ||||| | | ||||| | || | || |
Nephritis or renal dysfunction | 2 (1.0) | 1 (0.5) | 0 | 0 | | ||||| | | ||||| | || | || |
Adrenal insufficiency | 21 (10.5) | 7 (3.5) | 0 | 0 | || |||||| | | ||||| | || | || |
Hypophysitis | 10 (5.0) | 5 (2.5) | 0 | 0 | || ||||| | | ||||| | || | || |
All-causality OESIs within 100 days of last doseb Patients with grade 3 to 4 OESIs, n (%) | || | | |||||| | || | | ||||| | || | | ||||| | || | || |
Pancreatitis | | ||||| | || | || | || | | ||||| | || | | ||||| | || |
Encephalitis | | ||||| | | ||||| | || | || | | ||||| | | ||||| | || | || |
Myositis or rhabdomyolysis | | ||||| | | ||||| | || | || | | ||||| | | ||||| | || | || |
Myocarditis | | ||||| | | ||||| | || | || | | ||||| | | ||||| | || | || |
Death | || |||||| | || |||||| | || |||||| | || |||||| | ||||
AEs = adverse event; CI = confidence interval; CSR = Clinical Study Report; DCO = data cut-off; IMAE = immune-mediated adverse event; OESI = other event of special interest; SAE = serious adverse event; vs. = versus.
Notes: AE included events reported between first dose and 30 days after last dose of study therapy, unless otherwise indicated. Excluded data collected on or after first crossover dose date, except for the summary of deaths.
aDiscontinuation of any drug in the regimen.
bNo OESIs were reported in the following categories: demyelination, Guillain-Barre syndrome, graft vs. host disease, autoimmune eye disorder, and immune-mediated arthritis. All-causality OESIs within 100 days of last dose with or without immune modulating medication by category.
cOne patient with grade 5 OESIs was observed in the nivolumab plus ipilimumab arm on top of the grade 3 to 4 OESIs events.
Sources: Bristol-Myers Squibb, 2024 (Interim CSR);57 Bristol-Myers Squibb, 2025 (Supplemental analyses).59
Adverse Events
The overall frequency of grade 3 to 4 all-causality AEs were reported in █████ ███ █████ in the nivolumab plus ipilimumab arm and in the chemotherapy arm, respectively (data cut-off: August 28, 2024) (Table 21). The most frequently reported all-causality grade 3 to 4 AEs (occurred in 6% or more of patients in either arm) were neutropenia (nivolumab plus ipilimumab versus chemotherapy: 1.0% versus 10.2%), decreased neutrophil count (0.5% versus 6.8%), and hypertension (1.5% versus 6.8%) (data cut-off: October 12, 2023) (Table 21).
Serious Adverse Events
The overall frequency of grade 3 to 4 SAEs was █████ ███ █████ in the nivolumab plus ipilimumab arm and in the chemotherapy arm, respectively (data cut-off: August 28, 2024) (Table 21). The most frequently reported all-causality grade 3 to 4 SAEs (occurred in more than 3% of patients in either arm) were adrenal insufficiency (nivolumab plus ipilimumab versus chemotherapy: 3% versus 0%) and pneumonia (1.5% versus 3.4%) (data cut-off: October 12, 2023) (Table 21).
Withdrawals Due to AEs
The overall frequency of all-causality AEs leading to discontinuation of treatment was █████ in the nivolumab plus ipilimumab arm and █████ in the chemotherapy arm, respectively (data cut-off: August 28, 2024) (Table 21). Grade 3 to 4 AEs leading to discontinuation of study drug were reported in a similar proportion of patients (nivolumab plus ipilimumab versus chemotherapy: █████ ███ █████) in both arms (data cut-off: August 28, 2024) (Table 21). ███ ████ ██████████ ████████ ███ ███████ ██ █████████ ███████████████ ██ ███ █████████ █ ██████████ ███ ████ █████████ ████ ████ ███████ █████████████ ██████ ███ ███████████████ █████████████ █████████ ██ ███ ████████████ ████ ███ ████ ██████████ ████████ ███ ███████ ██ █████████ ███████████████ ████ ██████████ ██████████ ███ █████████████ █████ ██████ ███ ██████████ ███████ ██████████ ███████ ███ █████████ ███ ███████ ██ █ ████ █████ ██ █████████ ████ ████████ ██ ██ ███████ ████████ ██ ███ █████████ █ ██████████ ███ ███ ██ ███████ ████████ ██ ███ ████████████ ██████ ███ ████ ██████████ ████████ ███ ███████ ██ █ ████ █████ ██ █████████ ████ ████████ ███████ ████████ ███████ ███ █████████ ███ ███ █████████ ███ █████ █████ ██ ███ █████████ █ ██████████ ███ ███ ███████████ ████████ ████████ ████████ ████████ ████████ ███ █████████ ██████████ █████ ███████ ██ ███ ████████████ ██████
Notable Harms (AESIs)
The AESIs of special interest reported in this report include IMAEs and OESIs.
Immune-Mediated AEs
A total of ███ patients in the nivolumab plus ipilimumab arm and ████ patients in the chemotherapy arm experienced grade 3 to 4 IMAEs. The difference between groups (nivolumab plus ipilimumab versus chemotherapy) was ████ | (95% CI, not reported). The most frequently reported grade 3 to 4 IMAEs (occurred in 3% or more of patients in either arm) were ████████████████ ███████████ ██████████ ███ █████████████ ████ ███ ████ █████████ █████ ███ ████ ███ ███████ █████████████ █████ ███ ███
These results were consistent with those reported in the data cut-off on October 12, 2023 (Table 21).
Other Events of Special Interest
A total of 2% patients in the nivolumab plus ipilimumab arm and 0% of patients in the chemotherapy arm experienced grade 3 to 4 OESIs. ███ ████ ██████████ ████████ █████ ███ ████ █████████ ██ | | | ████████ ██ ██████ ████ ████ ████████████ ███████████ ██████████ ███ █████████████ ████ ███ ████ ███ ███████████ █████ ███ ████
Mortality
All-cause mortality was █████ in the nivolumab plus ipilimumab arm and █████ in the chemotherapy arm (Table 21).
Critical Appraisal
Internal Validity
The CheckMate-8HW study was a phase III, open-label RCT. Stratified randomization via interactive response technology ensured concealment of the randomized groups until allocation. Baseline characteristics were balanced across the treatment groups, suggesting that the randomization was reasonably successful. The clinical experts consulted for this review indicated that the concomitant treatments used in both arms are reflective of practice in Canada, and it is unlikely to have introduced bias in efficacy for PFS. The open-label design introduces a potential bias in the assessment of PFS; however, this bias was mitigated by using BICR for disease assessment. Knowledge of the assigned treatment could have led to bias in the reporting and measurement of subjective outcomes, including patient-reported outcomes (e.g., EORTC QLQ-C30) and subjective AEs (such as fatigue and nausea). Two patients (1%) randomized in the nivolumab plus ipilimumab arm and 13 patients (12.9%) in the chemotherapy arm did not receive the treatment. Protocol deviations were low and balanced in both arms (nivolumab plus ipilimumab versus chemotherapy: 4.95% versus 5.94%). Overall, the risk of selection bias and detection bias are considered low.
The clinical experts CDA-AMC consulted for this review indicated that OS is the most important end point in this disease setting. The primary efficacy end point of PFS was considered appropriate for the disease setting and was considered a valid surrogate for OS in this indication in the patient population with mCRC.61-63 A longer-term follow-up is needed to inform the true effect of nivolumab plus ipilimumab compared with chemotherapy on OS. Most subgroup results for PFS were consistent with the primary analysis, favouring nivolumab plus ipilimumab, although some of these analyses were limited by small sample sizes. However, there was no multiplicity control for the subgroup analyses.
█████ ███ █ ███████████ █████████ ████ ███ █████ █████ ██████ ███████ █████ █████ ███ ████████ ████ ██ ███ █████████ █████ ███████ ██████ ████ ███████ █████ ███ ███████ ███ ███ █████ ██ █████ ██ █████ ████ ███ █████ ███ ██████████ █████████ ████ █████████ ████████ ██ ███ █████ ███ █████████ █████████ █████ ██ ████ ███ ███ ███ ██ ██████████████ ██ ███ ███████ ███████ ███████████ ██ ██████ ███████████ █████ ██ █████ █████ ███ ██████ ██ ██████████ ██████████ ████████ ████ ████████████ ██ █████ ███ ██ █ ████ ████ ██ █████████ █████ ████████████ ██ ██████ █████████ ██████ ██ ████ ████
External Validity
The clinical experts highlighted that the inclusion and exclusion criteria of the CheckMate-8HW trial are standard for clinical trials, but stricter than what pertains in clinical practice. For example, they noted that patients with an ECOG PS score of greater than 1 were not eligible for the trial, whereas patients with an ECOG PS score of 2 would be considered potential candidates for nivolumab plus ipilimumab in the clinical experience. However, the clinical experts considered that overall, the inclusion and exclusion criteria of the CheckMate-8HW trial are consistent with the clinical practice setting in Canada and present no major generalizability concern of its findings in clinical practice in Canada.
The clinical experts indicated that the enrolment of the patients based on the locally confirmed MSI-H or dMMR mCRC is aligned with the clinical practice. In addition, according to the clinical experts consulted, the demographic and disease characteristics of the CheckMate-8HW trial population were reflective of patients living in Canada with mCRC. The drugs and dose regimens used in the chemotherapy arm were also consistent with that used in practice in Canada. Therefore, the results are considered to be generalizable to clinical practice in Canada.
GRADE Assessment Summary of Findings and Certainty of the Evidence
Methods for Assessing the Certainty of the Evidence
For pivotal studies and RCTs identified in the sponsor’s systematic review, GRADE assessment was used to assess the certainty of the evidence for outcomes considered most relevant to inform expert committee deliberations, and a final certainty rating was determined as outlined by the GRADE Working Group:19,20
High certainty: We are very confident that the true effect lies close to that of the estimate of the effect.
Moderate certainty: We are moderately confident in the effect estimate — the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. We use the word “likely” for evidence of moderate certainty (e.g., “X intervention likely results in Y outcome”).
Low certainty: Our confidence in the effect estimate is limited — the true effect may be substantially different from the estimate of the effect. We use the word “may” for evidence of low certainty (e.g., “X intervention may result in Y outcome”).
Very low certainty: We have very little confidence in the effect estimate — the true effect is likely to be substantially different from the estimate of effect. We describe evidence of very low certainty as “very uncertain.”
Following the GRADE approach, evidence from RCTs started as high-certainty evidence and could be rated down for concerns related to study limitations (which refers to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias.
When possible, certainty was rated in the context of the presence of an important (nontrivial) treatment effect. The target of the certainty of evidence assessment was based on the point estimate and where it was located relative to the threshold (MID) for a clinically important effect. In this review, the threshold (MID) assessment of between-group difference for PFS were based on published information21,22 in combination with the MID suggested by clinical experts consulted for this review. The threshold (MID) for HRQoL (i.e., EORTC QLQ-C30 GHS) assessment of between-group difference was based on the published information,23 which was aligned with the suggestion by the clinical experts consulted for this review. The threshold (MID) for assessment of between-group difference for harms (i.e., IMAEs) was suggested by clinical experts consulted for this review.
Results of GRADE Assessments
Table 2 presents the GRADE summary of findings for nivolumab plus ipilimumab combination therapy versus chemotherapies for the first-line treatment of patients with unresectable or MSI-H or dMMR CRC. The reference points for the certainty of evidence assessment for PFS, HRQoL, and harms were set according to the presence of an important effect based on thresholds identified from the literature and agreed or suggested by clinical experts consulted for this review.
Long-Term Extension Studies
No long-term extension studies were submitted by the sponsor.
Indirect Evidence
Contents within this section have been informed by materials submitted by the sponsor. The following have been summarized and validated by the review team.
Objectives for the Summary of Indirect Evidence
In the absence of evidence from a direct head-to-head comparison, the sponsor submitted an ITC using MAIC for PFS and NMA for safety outcomes to compare nivolumab plus ipilimumab versus other comparators. The scope of the sponsor’s search strategy and study selection criteria for the systematic literature review (SLR) that informed the ITC were broader than that of this review, which focuses on pembrolizumab considered the current relevant comparator in Canada. The objective of this section is to summarize and critically appraise the sponsor-submitted ITC in patients receiving first-line treatment for MSI-H or dMMR mCRC.
Description of Indirect Comparison
Objectives
The objective of this ITC was to compare the efficacy in terms of PFS and safety outcomes of nivolumab plus ipilimumab with that of pembrolizumab for patients with MSI-H or dMMR mCRC receiving first-line treatment.
ITC Design
Study Selection Methods
An SLR was conducted following the recommendations of the Preferred Reporting Items for Systematic review and Meta-Analysis Protocols checklist.76,77 A summary of the methods used to conduct the SLR is provided in Table 22.
Table 22: Study Selection Criteria and Methods for Indirect Comparisons
Characteristics | Indirect comparison |
|---|---|
Population | Adults aged ≥ 18 years with untreated MSI-H or dMMR mCRC status |
Intervention | Any 1L therapy administered in patients with MSI-H or dMMR mCRC, including off-licence administration |
Comparator | Any 1L treatment |
Outcome | Survival
Response
Safety
|
Study designs |
|
Other | Studies published in the English language |
Exclusion criteria | Population:
Study design:
Publications:
|
Databases searched | Relevant studies were identified by searching (search date: April 2, 2024) the following databases from inception through the Ovid platform:
Supplemental searches for relevant materials from the scientific conferences were conducted for the past 2 years (2022-2024):
Grey literature searches were also conducted to capture studies from sources that were not included in the main literature databases. Finally, bibliographies of relevant SLRs or meta-analyses captured in the electronic searches were screened for additional primary records that were not retrieved via electronic searches. |
Selection process | Dual screening of study abstracts and/or sources identified from the electronic database and the grey literature searches were conducted by 2 independent researchers blinded to each other’s decisions to determine eligibility according to the inclusion and exclusion criteria. Any disagreement on study or source eligibility was resolved via a consensus between the researchers. A senior researcher was consulted where a consensus could not be reached. This same process was also applied at the full-text screening stage once publications were retrieved. A PRISMA diagram was developed as a graphical representation of included and excluded articles at each screening level for each evidence type. |
Data extraction process | A data extraction form, developed in Microsoft Excel, was used to extract articles by a single reviewer and was then quality-checked by a second reviewer. The data extraction form included study information, treatment characteristics, patient characteristics, survival, response, and safety outcomes. Data were extracted from full-text publications and conference abstracts. All relevant full-text and non–full-text references were linked to the original primary source, where appropriate. |
Quality assessment | Randomized controlled trials and nonrandomized clinical trials were included in the review. Relevant risk of bias tools such as the Cochrane Collaboration’s tool for assessing risk of bias in randomized trial (version 2) were used to assess the internal validity of the studies. Risk of bias was assessed by a single reviewer, and then quality-checked by a second reviewer. This instrument was used to evaluate bias arising in 5 domains: randomization process, deviations from intended interventions, missing outcome data, measurement of the outcome, and selection of reported result. The risk of bias tool was used to assign summary assessments of within-study bias: low risk of bias (low risk of bias in all domains), some concerns (some concerns in at least 1 domain but not high risk of bias for any domain), or high-risk of bias (high-risk of bias in at least 1 domain or some concerns in multiple domains). |
1L = first line; AE = adverse event; ASCO = American Society of Clinical Oncology; ASCO GI = American Society of Clinical Oncology Gastrointestinal Cancers; CR = complete response; DFS = disease-free survival; dMMR = deficient mismatch repair; DOR = duration of response; ESCP = European Society of Coloproctology; ESMO GI = European Society for Medical Oncology Gastrointestinal Cancers; mCRC = metastatic colorectal cancer; MSI-H = microsatellite instability-high; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; PR = partial response; RFS = recurrence-free survival; SAE = serious adverse event; SD = stable disease; SLR = systematic literature review; TRM = treatment-related mortality; TTP = time to progression; TTTF = time to treatment failure.
aRelevant SLRs or meta-analyses were included for bibliographic checks for primary publications that were not retrieved via other search methods. Once reviewed at the full-text screening stage, SLRs or meta-analyses were excluded from this review.
Source: Bristol-Myers Squibb, 2022.78 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
SLR Results and ITC Feasibility Assessment
Based on the similarity of the studies (population, intervention, comparator, outcome, and study design), the phase III RCTs KEYNOTE-177 and CheckMate-8HW were included for the ITC. The feasibility assessment found the 2 trials to be comparable across study designs, inclusion and exclusion criteria, most baseline characteristics assessed (minor differences in patient-reported race), common comparator treatments, and outcome definitions. Therefore, an indirect comparison was deemed feasible.
Identification of TEMs
A multistep approach, incorporating a literature review and input or validation from clinical experts consulted by the ITC team (including input from a clinical expert in Canada), was used to identify important prognostic factors in MSI-H or dMMR mCRC. The subgroup forest plots used to inform TEM selection are presented in Figure 9 and Figure 10 in Appendix 1. Seven TEMs were finally identified for matching based on the forest plots and availability of published data from the KEYNOTE-177 trial, namely, age, ECOG PS, BRAF, KRAS, and NRAS mutation status, side of primary tumour (left or right), liver metastasis, liver or lung metastasis, and region.
Proportional Hazards Assumption Validation
The proportional hazards assumption (PHA) for PFS in the KEYNOTE-177 trial was tested using the pseudoindividual patient data generated from the published KM curves. The results of the test suggested that the PHA was violated, indicating that the use of a constant HR-based ITC method may be biased.
ITC Analysis Methods
A summary of the analytical approaches used to conduct the ITC is provided in Table 23. Both an anchored and unanchored MAIC were conducted for efficacy analyses.79
Table 23: Indirect Comparison Analysis Methods
Methods | Description |
|---|---|
Analysis methods | Analyses were performed in a Bayesian framework for the constant HR. Fixed effects models were employed due to the limited evidence network (i.e., only 2 studies and only 2 treatment arms). A parametric model was used to estimate the time-varying HR. All analyses were performed using the RStan package (the R interface to Stan) and the multinma package. |
Priors | Normal noninformative prior distributions (mean 0 and precision 0.0001) were used for the prior distribution of the treatment effect (log HR). |
NMA model selection | Time-varying HR MAIC: Parametric distributions tested included exponential, Weibull, Gompertz, log-logistic, log normal, gamma, and generalized gamma. Models were assessed for goodness of fit based on the AIC and BIC. Constant HR NMA: No model comparison was conducted. |
Assessment of model fit | Model selection based on statistical model fit was based on the AIC and BIC scores for the models. Models were also assessed based on the visual fit following the recommendations in the NICE DSU Technical Support Document 14.84 Additionally, a visual assessment of the smoothed hazard curves was performed. The smoothed hazard curve indicates whether observed hazards are likely to be constant, monotonic, or nonmonotonic. |
Assessment of consistency | NA; the ITC is not based on a closed loop network, and therefore no assessment of consistency was conducted. |
Assessment of convergence | Convergence of Bayesian models was assessed through the Gelman-Rubin statistic, size of the Monte Carlo error, autocorrelation, trace plots, and Kernel density plots. |
Outcomes | PFSa |
Follow-up time points | The CheckMate-8HW trial had a median follow-up of 42.05 months and 5-year follow-up data were available for KEYNOTE-177. In cases where no HR was reported but the trial reported KM curves, HRs were derived using the Guyot algorithm.75 Time-varying HR NMA: The time-specific HRs are presented for all times between 0 and 120 months in graphical format, as well as in tabular format at 12-month intervals. |
Sensitivity or scenario analyses | An unanchored unweighted analysis is presented in the ITC report. |
Subgroup analysis | None |
AIC = Akaike information criterion; BIC = Bayesian information criterion; DSU = Decision Support Unit; HR = hazard ratio; ITC = indirect treatment comparison; KM = Kaplan-Meier; MAIC = matching-adjusted indirect comparison; NA = not available; NICE = National Institute for Health and Care Excellence; NMA = network meta-analysis; PFS = progression-free survival.
aAnalyses involving overall survival could not be conducted at the time as this data from the CheckMate-8HW trial was still immature.
Source: Bristol-Myers Squibb, 2025 [ITC Report].79 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
The detailed information of the assessment of homogeneity for the ITC is presented in Table 24 and Table 25.
Table 24: Assessment of Homogeneity for ITC
Characteristics | Description and handling of potential effect modifiers |
|---|---|
Disease severity | Disease severity was similar in both the CheckMate-8HW and KEYNOTE-177 trials. |
Treatment history | Enrolled patients had not previously received systemic treatment for their metastatic disease in both trials. |
Trial eligibility criteria | Comparable inclusion criteria used in both the CheckMate-8HW and KEYNOTE-177 trials. |
Balance of the baseline characteristics (i.e., potential treatment effect and/or prognostic modifies) | Unable to fully address. The author noted that 3 recommended and 14 suggested prognostic variables are not adjusted because these data on distributions in the KEYNOTE-177 trial were unavailable. |
Dosing of comparators | Both trials had a similar comparator arm, consisting of the same choices of chemotherapy regimens. |
Definitions of end points | The definition of PFS in both trials was the same. |
Timing of end point evaluation | The CheckMate-8HW trial had a median follow-up of 42.05 months. The 5-year follow-up data were available for KEYNOTE-177. In cases where no HR was reported but the trial reported KM curves, HRs were derived using the Guyot algorithm.75 |
Withdrawal frequency | KEYNOTE-177: In the chemotherapy group, 11 patients (7%) did not begin their assigned trial treatment, while in the pembrolizumab group, all patients began assigned trial treatment. CheckMate-8HW trial: based on the locally confirmed population, in the chemotherapy group, 13 patients (13%) did not begin their assigned trial treatment and in the nivolumab plus ipilimumab group, 2 patients (1%) did not begin their assigned trial treatment. |
Clinical trial setting | In both trials, patients received their treatments and were followed in hospital cancer centres. |
Study design | Both trials were international, multicentric, phase III, open-label, randomized controlled trials with a similar comparator arm. In both trials, patients in the comparator arm were allowed to crossover to the intervention arm after disease progression. |
Follow-up time | The KEYNOTE-177 trial had a median follow-up of 73.3 months and the CheckMate-8HW trial had a median follow-up of 42.05 months (based on IPD from August 28, 2024 DCO, corresponding to the September 2024 database lock).56,59,80,81 |
DCO = data cut-off; HR = hazard ratio; IPD = individual patient data; ITC = indirect treatment comparison; KM = Kaplan-Meier; PFS = progression-free survival.
Source: The sponsor’s submission.58 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
The key baseline characteristics of the KEYNOTE-177 and CheckMate-8HW trials are presented in Table 25.
Baseline characteristics for first-line treatment trials in mCRC were classified according to 1 of 3 levels: most relevant (i.e., suggested stratification factors), recommended set, and suggested set.82 The distribution of these baseline characteristics were compared between the CheckMate-8HW and KN-177 trials, with a specific focus on the distribution of TEMs across trials to assess any potential imbalances (Table 25). The 2 trials were comparable across most of the baseline characteristics assessed with only minor differences noticed in the distribution of race of patients (i.e., with the CheckMate-8HW trial having a greater proportion of patients who were white and fewer patients who were Asian compared to the KEYNOTE-177 trial). Table 25 compares the patients’ baseline characteristics based on each trial’s population with locally confirmed MSI-H or dMMR mCRC status.
Table 25: Assessment of Heterogeneity in mCRC-Specific Baseline Characteristics
Baseline characteristics82 | KEYNOTE-177 trial | CheckMate-8HW trial | ||
|---|---|---|---|---|
Chemotherapy (N = 154) | Pembrolizumab (N = 153) | Chemotherapy (N = 101) | Nivolumab plus ipilimumab (N = 202) | |
Most relevant prognostic variables | ||||
ECOG PS score of 0a | 84 (55%) | 75 (49%) | 52 (51%) | 111 (55%) |
Primary tumour location (sidedness)a | ||||
Right side | 107 (69%) | 102 (67%) | 68 (67%) | 137 (68%) |
Left side | 42 (27%) | 46 (30%) | 33 (33%) | 65 (32%) |
Other site or site missing or both sides | 5 (3%) | 5 (3%) | 0 | 0 |
Liver-only disease | NRb | NRb | NRb | NRb |
Mutation status (RAS or BRAF)a | ||||
BRAF, KRAS, NRAS all wild-type | 35 (23%) | 34 (22%) | 23 (23%) | 47 (23%) |
KRAS or NRAS mutantc | 41 (27%) | 33 (22%) | 23 (23%) | 48 (24%) |
BRAF V600E mutantc | 43 (28%) | 34 (22%) | 26 (26%) | 57 (28%) |
Could not be evaluated | 38 (25%) | 52 (34%) | 31 (31%) | 55 (27%) |
Recommended prognostic variables | ||||
Median age (range)a | 62.5 (26 to 90) | 63.0 (24 to 93) | 65 (26 to 87) | 62 (21 to 86) |
Prior chemotherapy | ||||
Adjuvant | 37 (24%) | 33 (22%) | 31 (31%)d | 64 (32%)d |
Neoadjuvant with or without adjuvant systemic therapy | 8 (5%) | 5 (3%) | ||
None | 109 (71%) | 115 (75%) | 70 (69%) | 138 (68%) |
Liver involvementa | 54 (35%) | 71 (46%) | 42 (42%) | 76 (38%) |
Synchronous or metachronous metastases | ||||
Recurrent metachronous | 74 (48%) | 80 (52%) | NR | NR |
Newly diagnosed with metastatic disease | 80 (52%) | 73 (48%) | NR | NR |
MSI-H status | 153 (99%) | 153 (100%) | 101 (100%) | 200 (99%) |
Suggested prognostic variables | ||||
Sex: Male | 82 (53%) | 71 (46%) | 45 (45%) | 95 (47%) |
Stage at diagnosis: IV (vs. stage I to III) | NR | NR | 49 (49%) | 85 (42%) |
Race | ||||
Asian | 26 (17%) | 24 (16%) | 13 (13%) | 19 (9%) |
Black | 5 (3%) | 9 (6%) | 2 (2%) | 2 (1%) |
White | 116 (75%) | 113 (74%) | 85 (84%) | 176 (87%) |
Other | 0 | 0 | 1 (1%) | 5 (3%) |
Not reported or missing | 7 (5%) | 7 (5%) | 0 | 0 |
Ethnicity | ||||
Hispanic or Latino | 10 (7%) | 11 (7%) | 8 (8%) | 24 (12%) |
Not Hispanic or Latino | 131 (85%) | 128 (84%) | 55 (54%) | 96 (48%) |
Not reported or missing | 13 (8%) | 14 (9%) | 38 (38%) | 82 (41%) |
ECOG PS = Eastern Cooperative Oncology Group Performance Status; ITC = indirect treatment comparison; mCRC = metastatic colorectal cancer; MSI-H = microsatellite instability-high; NR = not reported; TEM = treatment-effect modifier; vs. = versus.
Note: Three recommended and 14 suggested prognostic variables are not listed in the table as data on distributions in the KEYNOTE-177 trial were unavailable.
Race and ethnicity categories used in the table are as reported in the source and may not align with Canada's Drug Agency inclusive language guidelines.
aPotential TEMs.
bNot reported, but liver involvement (under recommended prognostic variables) was reported.
cThree patients from the KEYNOTE-177 trial and 7 patients from the CheckMate-8HW trial who had both a BRAF mutation and a KRAS or NRAS mutation are included. Totals do not add up to 100%.
dThe CheckMate-8HW trial reported the number of patients who received prior systemic therapy in adjuvant or neoadjuvant setting.
Sources: Bristol-Myers Squibb, 2024 (ITC Report Appendix).79 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Treatments of the chemotherapy arm in the KEYNOTE-177 trial and the CheckMate-8HW trial consisted of the same 6 chemotherapy treatments with or without targeted therapies, with the same dosing regimens. The distribution of treatments in the SOC (i.e., chemotherapy) arm for the KEYNOTE-177 trial and the CheckMate-8HW trial are comparable (Table 32 in Appendix 1). In both the KEYNOTE-177 trial and the CheckMate-8HW trial, PFS was similarly defined. Both trials were phase III, randomized, open-label studies with blinded independent review for assessing PFS. Both trials allowed crossover after disease progression. The KEYNOTE-177 trial had a median follow-up of 73.3 months and the CheckMate-8HW trial had a median follow-up of 42.05 months (based on individual patient data from the data cut-off of August 28, 2024.56,59,80,81
Based on the feasibility assessment, 2 approaches were recommended for the ITC: an anchored MAIC that allows for adjustment of present heterogeneity in TEMs without requiring PHA to hold, and a proportional HR-based NMA that serves as a scenario analysis even though PHA is violated. The anchored MAIC is the methodologically preferred method, relying on fewer assumptions compared to the unanchored MAIC as randomization is preserved. Therefore, unanchored MAIC was performed as a sensitivity analysis. Unanchored MAIC matched the nivolumab plus ipilimumab trial arm to the pembrolizumab trial arm in terms of TEMs and prognostic variables.
Estimation of MAIC Weights
For the weighted analyses, inverse odds for trial inclusion were estimated for each patient in the CheckMate-8HW trial. These weights were estimated using a matching approach.
Anchored MAIC
Weighting
TEMs were matched in the MAIC methodology and the patient population in the CheckMate-8HW trial was reweighted such that the resulting population aligned with the KEYNOTE-177 population with regards to TEM distribution. Baseline characteristics used for matching and their distribution before and after matching of the CheckMate-8HW trial to the KEYNOTE-177 trial are provided in Table 26. Following matching, an effective sample size corresponding to █████ ███ of the original CheckMate-8HW trial sample size was observed.
Table 26: Patient Characteristics Included in the Anchored MAIC
Identified TEMs | Pembrolizumab KEYNOTE-177 trial (N = 307) | Nivolumab plus Ipilimumab CheckMate-8HW trial (N = 303) Unadjusted | |||||| || |||||||||||||||| ||||||||| |
|---|---|---|---|
Age (years), median (range) | 63 (24 to 93) | 63 (21 to 87) | || ||| | ||| |
ECOG PS score of 0 | 159 (52%) | 163 (54%) | ||||| ||||| |
BRAF, KRAS, NRAS mutation status | |||
BRAF, KRAS, NRAS all wild-type | 69 (22%) | 74 (24%) | |||| ||||| |
KRAS or NRAS mutant | 74 (24%) | 76 (25%) | |||| ||||| |
BRAF mutant | 77 (25%) | 87 (29%) | |||| ||||| |
Could not be evaluated | 90 (29%) | 75 (25%) | |||| ||||| |
Site of primary tumour (sidedness) | |||
Right | 219 (71%)a | 205 (68%) | ||||| ||||| |
Left | 88 (29%) | 98 (32%) | |||| ||||| |
Liver metastasis | 125 (41%) | 118 (39%) | |||| ||||| |
Liver or lung metastasis | 159 (52%) | 156 (51%) | ||||| ||||| |
Region | |||
Asia | 48 (16%) | 30 (10%) | |||| ||||| |
Western Europe or North Americab | 222 (72%) | 178 (59%) | ||||| ||||| |
Rest of the world | 37 (12%) | 95 (31%) | |||| ||||| |
ECOG PS = Eastern Cooperative Oncology Group Performance Status; ITC = indirect treatment comparison; MAIC = matching-adjusted indirect comparison; TEM = treatment-effect modifier.
aIncludes 10 patients who were classified as “both sided.”
bThe CheckMate-8HW trial reported patients classified as “Canada, Europe, or US” from Czech Republic and Romania were reclassified to the rest of the world.
Source: Bristol-Myers Squibb, 2025 (ITC Report).79 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Weighting did not change the survival estimates significantly (Figure 11 in Appendix 1).
Unanchored MAIC
The unanchored MAIC methodology is similar to the methodology described in the preceding section for the anchored analyses. However, in the unanchored MAIC, only the intervention arm populations of interest (e.g., nivolumab plus ipilimumab and pembrolizumab) were matched. The unanchored analysis adjusted for both the chosen TEMs and 2 prognostic variables (prior chemotherapy and synchronous or recurrent metachronous metastasis).79
Baseline characteristics before and after matching the CheckMate-8HW trial to the KEYNOTE-177 trial are provided in Table 27. Following matching, an effective sample size corresponding with about █████ of the original nivolumab plus ipilimumab arm sample size was observed.
Table 27: Patient Characteristics Included in the Unanchored MAIC
Identified TEMs | Pembrolizumab KEYNOTE-177 trial (N = 153) | Nivolumab plus ipilimumab CheckMate-8HW trial (N = 202) Unadjusted | |||| | ||||||||||| | | |||||||||||||||| ||||||||| |
|---|---|---|---|
Age (years), median (range) | 63 (24 to 93) | 62 (21 to 86) | || ||| | ||| |
ECOG PS score of 0 | 75 (49%) | 111 (55%) | |||| ||||| |
BRAF, KRAS, NRAS mutation status | |||
BRAF, KRAS, NRAS all wild-type | 34 (22%) | 49 (24%) | |||| ||||| |
KRAS or NRAS mutant | 33 (22%) | 50 (25%) | ||||||||| |
BRAF mutant | 34 (22%) | 60 (30%) | |||| ||||| |
Could not be evaluated | 52 (34%) | 50 (25%) | |||| ||||| |
Site of primary tumour (sidedness) | |||
Right | 107a (70%) | 137 (68%) | |||| ||||| |
Left | 46 (30%) | 65 (32%) | |||| ||||| |
Liver metastasis | 71 (46%) | 75 (37%) | |||| ||||| |
Liver or lung metastasis | 36 (24%) | 44 (22%) | |||| ||||| |
Region | |||
Asia | 22 (14%) | 19 (9%) | |||| ||||| |
Western Europe or North Americab | 109 (71%) | 115 (57%) | |||| ||||| |
Rest of the world | 22 (14%) | 68 (34%) | |||| ||||| |
ECOG PS = Eastern Cooperative Oncology Group Performance Status; ITC = indirect treatment comparison; MAIC = matching-adjusted indirect comparison; TEM = treatment effect modifier.
aIncludes 5 patients who were classified as “both sided.”
bThe CheckMate-8HW trial reported patients classified as “Canada, Europe, or US” from Czech Republic and Romania were reclassified to the rest of the world.
Source: Bristol-Myers Squibb, 2025 (ITC Report).79 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Weighting did not change the survival estimates significantly (Figure 12 in Appendix 1).
Adverse Events NMA
A Bayesian fixed effect NMA of AEs was conducted comparing the incidence of the following AEs in the CheckMate-8HW trial and the KEYNOTE-177 trial: any AEs of grade 3 or higher occurring in 5% or more of a treatment arm and immuno-oncology therapy related AEs recommended by clinical experts for inclusion in the analysis (diarrhea, hypophysitis, rash, adrenal insufficiency, hepatitis, hyperthyroidism, and pneumonia).83
Results of ITC
Summary of Included Studies
Two studies, KEYNOTE-177 and CheckMate-8HW, were included in the ITC.
Evidence Networks
CheckMate-8HW and KEYNOTE-177 were the 2 trials included in the evidence base for which chemotherapy (SOC) was the common comparator. The network diagram is presented in Figure 13 in Appendix 1.
Efficacy
Anchored MAIC
Seven parametric survival distributions were fitted. The PFS KM curves for weighted CheckMate-8HW and KEYNOTE-177 trials, as well as the long-term extrapolation based on the best-fitting generalized gamma distribution, are shown in Figure 14 in Appendix 1.
Base-Case Analysis: Time-Varying HR of Nivolumab Plus Ipilimumab Versus Pembrolizumab
███ █████████ ████████████ ██████ █████ ██ ███ ███ █████████ █ ██████████ ███ █████████████ ██ ██████████ ██ ██████ █ ███ █████ ███ ███ █████ ████████ ██ ███ ████████████ ██ ██ ███ ██ █████ ████ █ ████ ███ █████████ ███████ ███████ ████ ██ ███████ ███████ ████ ██ ██ ██████ ███ ████ ██ ██ ███████ █████ █████████ ████ ███ ███ █████████ █ ██████████ ██ ██████████ █████████ ████ ██████████████ ████████ ████████ ████ ██ ██████ █████ ██ ███████ ███ █████ ██ ██ ███████ ███ ████ █████ ██████ ███
Figure 7: Results of the Generalized Gamma Model Anchored MAIC — Time-Varying PFS HR of Nivolumab Plus Ipilimumab Versus Pembrolizumab [Redacted]

HR = hazard ratio; MAIC = matching-adjusted indirect comparison; PFS = progression-free survival.
Table 28: Results of Anchored MAIC (Time-Varying PFS HR) and NMA (Constant PFS HR)
ITC methods | Time (months) | Nivolumab plus ipilimumab vs. pembrolizumab PFS HR (95% CI) |
|---|---|---|
|||||||| |||||||||||||||||| ||| || |||||||||| || |||||||| | || | |||| |||||| ||||| |
|| | |||| |||||| ||||| | |
|| | |||| |||||| ||||| | |
|| | |||| |||||| ||||| | |
|| | |||| |||||| ||||| | |
|||| |||||||| ||| || ||||||||| | || |||| |||| | |||| |||||| ||||| | |
██ █ ██████████ █████████ ███ █ ████████ █████████ ██ █ ██████ █████ ███ █ ███████████ ████ █ ██████████ ███ █ ███████ ██████████████ ████ █ ██████████████ ███ █ ███████████████ ██████████| ████ ████ █████████ █████ ███████████ ████████| ████████ █████████ ████████ █████████ █████████ ██ ██ ███ ███ ███ █████ ██ █████ ██████ ████████ ███ █████████ ████████ ████████████ █████████████ ███████ ████ ████ ██████████ ████████ ████████ ██ ███ █████ ███ ████ ███ █████████ ███████ ██ ████████ █████████
CI = confidence interval; HR = hazard ratio; ITC = indirect treatment comparison; MAIC = matching-adjusted indirect comparison; PFS = progression-free survival; NMA = network meta-analysis; vs. = versus.
Scenario Analysis Using a Constant HR-Based NMA for Anchored MAIC
A constant HR-based NMA was performed as a scenario analysis. The estimated PFS HR is ████ ████ ████ ████ ██ ██████
Unanchored MAIC
The results of a generalized gamma model in the unanchored MAIC for PFS is presented in Figure 15 in Appendix 1. As a sensitivity analysis, an unanchored MAIC analysis of PFS using time-varying HRs was also estimated. The estimated time-varying PFS for nivolumab plus ipilimumab versus pembrolizumab is presented in Figure 8 and Table 29. The estimated HRs are ██ ██ ██████ ███ ████ ██ ██ ██████, which indicates that PFS for nivolumab plus ipilimumab is favourable comparing with pembrolizumab. However, ██████ ██ ███████ the HR efficacy of nivolumab plus ipilimumab compared to pembrolizumab is uncertain because the 95% CI for the HR include the null value (i.e., 1).
Figure 8: Results of the Generalized Gamma Model Unanchored MAIC — Time-Varying PFS HR of Nivolumab Plus Ipilimumab Versus Pembrolizumab [Redacted]

HR = hazard ratio; MAIC = matching-adjusted indirect comparison; PFS = progression-free survival.
Table 29: Results of Unanchored MAIC (Time-Varying PFS HRs) and NMA (Constant PFS HR)
ITC methods | Time (months) | Nivolumab plus ipilimumab vs. pembrolizumab HR (95% CI) |
|---|---|---|
Unanchored MAIC: Time-varying PFS HR approach,a HR (95% CI) | | | |||| |||||| ||||| |
|| | |||| |||||| ||||| | |
|| | |||| |||||| ||||| | |
|| | |||| |||||| ||||| | |
NMA: Constant PFS HR approach,b HR (95% CrI) | |||| |||||| ||||| | |
CDA-AMC = Canada’s Drug Agency; CI = confidence interval; Crl = credible interval; HR = hazard ratio; ITC = indirect treatment comparison; MAIC = matching-adjusted indirect comparison; NMA = network meta-analysis; PFS = progression-free survival; vs. = versus.
aBase-case analysis, using frequentist approach.
bScenario analysis: Estimates of HR and 95% CI based on Cox proportional hazards model (assuming constant HRs).
Source: Bristol-Myers Squibb, 2025 (ITC Report).79 Details included in the table are from the additional information provided by the sponsor at the request of CDA-AMC.
Scenario NMA Analysis Using Constant PFS HR Approach for Unanchored MAIC
A constant HR-based NMA was performed as a scenario analysis. The PFS HR is ████ ███████ ████ ██ ██████. The result was consistent with the time-varying analyses (Table 29).
Harms
Estimated ORs (95% CrI) are provided in Table 30.
The 95% CrIs of all ORs of all assessed individual AEs include 1, which indicates the uncertainty of the comparative safety findings when comparing nivolumab plus ipilimumab with pembrolizumab in all assessed individual AEs.
Table 30: Main Results of AEs in the NMA (Grade ≥ 3 AEs Occurring in ≥ 5% in Either of the Treatment Arms)
AE | Pembrolizumab vs. nivolumab plus ipilimumab OR (95% CrI) |
|---|---|
||||||| ||||||||||||| | |||| |||||||||||| |
||||||||| | |||| |||||| ||||||| |
||||||||||| | |||| |||||| |||||| |
|||||||||| | |||| |||||| |||||| |
██ █ ███████ ██████ ███ █ ████████ █████████ ███ █ ███████████ ████ ███████████ ██ █ ████ ██████ ████ █ ███████████████| ███ ████████ ███ ███ ███████ █ ████ ████████████████ ██ ████ █████████ ████ █████████████ ███ █ █████ ████ ██ ███████████ █████████████ ███████ ████ ████ ██████ ████████████████ ████████ ██ ███ █████ ███ ████ ███ █████████ ███████ ██ ████████ █████████
AE = adverse event; Crl = credible interval; MAIC = matching-adjusted indirect comparison; OR = odds ratio; NMA = network meta-analysis; vs. = versus.
Critical Appraisal of ITC
The search for eligible studies was comprehensive, and the methods used to select relevant studies, extract data, and assessment of the risk of bias of included studies were adequate. The use of an MAIC estimation procedure was conducted according to existing standards. In the ITC, the anchored MAIC was considered the preferred method because it relied on fewer methods assumptions compared with an unanchored MAIC. However, the sponsor indicated that the anchored analysis did not sufficiently match the chemotherapy comparator arms across studies, with the chemotherapy arm of CheckMate-8HW displaying a poorer PFS than the KEYNOTE-177 chemotherapy arm. In either case, at least 3 known potential TEMS were not included in the analysis, which could contribute to bias of the results. In the unanchored setting, 14 suggested prognostic variables were not adjusted because these data on distributions in KEYNOTE-177 were unavailable. Consequently, the bias of the effects in the unanchored MAIC can be substantial and the CI may be overly optimistic.
In addition to the anchored and unanchored MAIC time-varying HR models, 2 Bayesian NMAs using a constant HR model were conducted. The estimates from these models are considered to be biased and challenging to interpret except as supportive evidence of the time-varying model estimates. The differences across trials and imbalances in the distribution of TEMs and prognostic factors introduces substantial differences in the populations being compared. Furthermore, any long-term extrapolation beyond the support of observed follow-up is uncertain,79 and relies exclusively on the model fit rather than data.
Finally, for the harms outcome, a fixed effects Bayesian NMA of AEs was conducted comparing the incidence of any AEs of grade 3 or higher occurring in 5% or more of a treatment arm and immuno-oncology therapy related AEs reported in the CheckMate-8HW trial and KEYNOTE-177 trial, including diarrhea, hypophysitis, rash, adrenal insufficiency, hepatitis, hyperthyroidism, and pneumonia.83 As the sponsor pointed out, AEs were not consistently reported or measured across trials, and differences between these measurements may persist, potentially biasing the NMA. ███ ███████ ███ ████ ████████ ███ ██ ████ ████ ██████████ █████████ ███ █████████ ███ ███████ ███ ███ ███████████ ████████ ██ █████████ ██ ███ ███ ████ ███ ██████ █████ ███████████████ ███ ██ ███████ ███████ ████
Studies Addressing Gaps in the Systematic Review Evidence
The sponsor-submitted evidence from the CheckMate-8HW trial comparing nivolumab plus ipilimumab to nivolumab monotherapy in patients with MSI-H or dMMR mCRC receiving treatment across all lines of therapy to inform questions on the contribution of ipilimumab in addition to nivolumab. Per the CDA-AMC Procedures for Reimbursement Reviews, nivolumab monotherapy does not meet the CDA-AMC definition of relevant comparator because it is neither approved by Health Canada nor reimbursed by participating drug plans in Canada for the first-line treatment of MSI-H or dMMR mCRC. Therefore, the evidence was considered out of scope for this review.
Discussion
Summary of Available Evidence
The evidence included in this review consisted of 1 pivotal study (CheckMate-8HW) and 1 ITC. The CheckMate-8HW trial is an ongoing multinational, phase III, open-label, active-controlled RCT evaluating the efficacy and safety of nivolumab plus ipilimumab (N = 202) versus chemotherapy (N = 101) in adult patients with unresectable or metastatic MSI-H or dMMR CRC. A total of 303 patients across 22 countries, including 204 patients (67.3%) from Canada, Europe, and the US, were randomized (2:1 randomization) to receive treatment with nivolumab plus ipilimumab compared with chemotherapy. Key inclusion criteria included histologically confirmed recurrent or metastatic CRC with no prior treatment history with chemotherapy and/or targeted drugs for metastatic disease and not amenable to surgery; locally confirmed MSI-H or dMMR status, ECOG PS score of 1 or less. The median age of all patients was 63.0 years, ranging from 21 to 87 years. Most of the patients were white (86.1%), and 53.8% of all participants were female. Patients had an ECOG PS score of 0 (53.8%) or 1 (46.2%). The primary efficacy outcome was PFS per BICR based on centrally confirmed MSI-H or dMMR mCRC. The secondary efficacy outcome was PFS per BICR based on locally confirmed MSI-H or dMMR mCRC. The exploratory outcome includes HRQoL (e.g., EORTC QLQ-C30). The harms outcomes included AEs, SAEs, discontinuation from the treatment due to AEs, IMAEs, and OESI, and so forth.
In the absence of direct comparative evidence of nivolumab plus ipilimumab versus the relevant comparator, pembrolizumab (considered the current relevant comparator in Canada), the sponsor submitted an ITC using a MAIC to estimate the comparative efficacy (i.e., PFS) and NMA for safety of nivolumab plus ipilimumab versus pembrolizumab as the first-line treatment in adult patients with unresectable or metastatic MSI-H or dMMR CRC. The outcomes of interest in the ITC included PFS and safety outcomes.
Interpretation of Results
Efficacy
After a median follow-up of 42.05 months, the use of nivolumab plus ipilimumab results in a clinically important increase in the probability of being progression free at 12 months compared with chemotherapy, with a between-group difference of 57.45% (95% CI, 45.41% to 69.49%) in favour of nivolumab plus ipilimumab. The patients in the nivolumab plus ipilimumab arm demonstrated a clinically meaningful longer median PFS than that in chemotherapy arm (treatment group difference: 48.23 months). At landmark time points, compared with the chemotherapy, nivolumab plus ipilimumab showed a clinically important increase in the probability of being progression free starting from 6 months (between-group difference, 34.44% [95% CI, 21.00% to 47.87%]) and sustained to 36 months (between-group difference, 57.80% [95% CI, 46.34% to 69.49%]) in favour of nivolumab plus ipilimumab. Similarly, the results of the prespecified subgroup and sensitivity analyses were overall consistent with the results of primary analyses, indicating rigour in the finding and suggesting that the open-label trial design of the CheckMate-8HW study was unlikely to have biased the estimates.
The clinical experts CDA-AMC consulted for this review indicated that a particular concern of the current standard treatment (i.e., single-drug pembrolizumab) is that the patients with liver metastases may derive significantly less benefit. However, the predefined subgroup analysis in the CheckMate-8HW trial demonstrated that treatment with nivolumab plus ipilimumab resulted in a statistically significant improvement PFS probability in both patients with liver metastasis (HR = 0.11; 95% CI, 0.05 to 0.25) and patients without liver metastasis (HR = 0.28; 95% CI, 0.17 to 0.46).
One of the enrolment criteria in the CheckMate-8HW trial was MSI-H or dMMR status per local standard of practice. The clinical experts CDA-AMC consulted for this review noted that eligibility for the treatment based on the locally confirmed MSI-H or dMMR status reflects the current standard practice in Canada. However, they also expressed ongoing concerns about the accuracy of MMR testing. Notably, approximately 16% of patients were not centrally confirmed to have MSI-H or dMMR mCRC, and the potential false-positives could not be ruled out. Despite this, the PFS results for patients with MSI-H or dMMR mCRC were consistent whether the patients were centrally confirmed (primary outcome) or locally confirmed (a key secondary outcome), further supporting the robustness and reliability of the findings from the CheckMate-8HW trial.
Input from patient group, clinician group, and clinical experts CDA-AMC consulted for this review noted improvements in OS and quality of life as part of the most important treatment goals for unresectable or metastatic MSI-H or dMMR CRC. OS data from the CheckMate-8HW trial was immature at the cut-off dates for analyses, and a conclusive determination could not be made about the comparative OS benefit of nivolumab plus ipilimumab. However, evidence from the literature indicate that the PFS is an acceptable surrogate for OS in this setting.61-63 Furthermore, the clinical experts noted that the magnitude of improvement in PFS in nivolumab plus ipilimumab compared with chemotherapy reported in the CheckMate-8HW trial is remarkable and suggests that improvement in OS is expected.
The EORTC QLQ-C30 results from the CheckMate-8HW trial suggest that treatment with nivolumab plus ipilimumab may result in clinically important HRQoL improvement compared with chemotherapy from week 13 to week 37. However, EORTC QLQ-C30 is based on subjective patient-reported outcomes, and the open-label design of the CheckMate-8HW trial could have introduced performance bias, potentially favouring the nivolumab plus ipilimumab arm regarding these outcomes. Additionally, the nivolumab plus ipilimumab arm had significantly more patients than the chemotherapy arm (64% versus 13%, respectively), contributing data to the week 37 assessment. This discrepancy raises concerns about attrition bias, which could further skew results in favour of the treatment with nivolumab plus ipilimumab.
The clinical experts highlighted that the inclusion and exclusion criteria of the CheckMate-8HW trial are standard for clinical trials, but stricter than what pertains in clinical practice. For example, they noted that patients with an ECOG PS score of greater than 1 were not eligible for the trial, whereas patients with an ECOG PS score of 2 would be considered potential candidates for nivolumab plus ipilimumab in the clinical experience. However, the clinical experts considered that overall, the inclusion and exclusion criteria of the CheckMate-8HW trial are consistent with clinical practice in the setting in Canada and present no major generalizability concern of its findings in clinical practice in Canada.
There was no direct evidence comparing nivolumab plus ipilimumab with pembrolizumab identified in a literature review. The sponsor submitted an ITC using a MAIC to estimate the relative efficacy comparing nivolumab plus ipilimumab with pembrolizumab on PFS and NMA for safety outcomes. Results of the ITC analyses suggested a favourable PFS improvement in patients with nivolumab plus ipilimumab treatment compared with that in pembrolizumab, despite certain key limitations such as inability to adjust for some relevant treatment effect and prognostic modifiers. The clinical experts consulted for this review indicated that the findings of the ITC are aligned with expected use in clinical practice in Canada.
Harms
The overall proportion of patients with AEs were similar in both the nivolumab plus ipilimumab compared with chemotherapy arms. More patients in the hemotherapy arm reported all-cause grade 3 to 4 AEs than in the nivolumab plus ipilimumab arm, all-causality SAEs, and deaths. The proportion of patients who discontinued treatment because of AEs was similar. However, AESIs — specifically, all-cause grade 3 to 4 IMAEs — were significantly more frequent in the nivolumab plus ipilimumab arm ███████ compared to chemotherapy ███████ with a between-group difference of ██████ The 95% CI for this difference was not reported, introducing uncertainty regarding the precision of this estimate. The GRADE assessment suggested that nivolumab plus ipilimumab likely result in a clinically important increase in grade 3 to 4 IMAEs, compared with chemotherapies. The clinical experts consulted for this review indicated that the safety profile of nivolumab plus ipilimumab has been well established. The harms profile of nivolumab plus ipilimumab reported in the CheckMate-8HW trial was generally consistent with that of previously known AEs associated with nivolumab plus ipilimumab, with no new safety signals identified. According to the clinical experts consulted for this review, most AEs were predictable, and clinically manageable in most patients.
Results from the NMA showed odds ratios (ORs) with wide CIs for the assessed grade 3 or higher AEs, indicating uncertainty. In addition, due to the limitations of the NMA methods (e.g., potential heterogeneity between the 2 trials), the evidence of the NMA was insufficient to demonstrate the difference of grade 3 or higher AEs (e.g., ███████ ███████████ █████████ ███ █████████) between nivolumab plus ipilimumab compared with pembrolizumab. A definitive conclusion could not be drawn on the comparative safety of the 2 therapies in patients with MSI-H or dMMR mCRC. The clinical experts noted that the use of double-drug immunotherapy (e.g., nivolumab plus ipilimumab) is expected to cause an increased risk of side effects or toxicity compared with the single-drug immunotherapy (e.g., pembrolizumab).
Conclusion
Evidence from the CheckMate-8HW trial showed that nivolumab plus ipilimumab results in a clinically important increase in the probability of being progression free at 12 months, compared to chemotherapy in the first-line treatment of patients with unresectable or metastatic MSI-H or dMMR CRC. Based on the EORTC QLQ-C30 GHS, nivolumab plus ipilimumab may result in clinically important improvement in patients’ HRQoL compared with chemotherapy, which was expected in this population. The evidence indicates that nivolumab plus ipilimumab likely result in a clinically important increase in grade 3 to 4 IMAEs, compared with chemotherapies. The harms profile of nivolumab plus ipilimumab reported in the CheckMate-8HW trial was generally consistent with that of previously known AEs associated with nivolumab plus ipilimumab. No new safety signal was identified. Overall, most AEs were predictable, and clinically manageable in most patients.
The results of the ITC suggested a more favourable PFS improvement with nivolumab plus ipilimumab treatment compared with pembrolizumab, despite certain limitations associated with the ITC methods. Due to the limitations associated with the NMA, a definitive conclusion could not be drawn on the comparative safety of nivolumab plus ipilimumab versus pembrolizumab in patients with MSI-H or dMMR mCRC. However, according to the clinical experts consulted on this review, nivolumab plus ipilimumab, being a double-drug immunotherapy, is expected to have an increased risk of side effects compared with the single-drug immunotherapy, and likely unsuitable for patients experiencing frailty or who have comorbidities.
References
1.Canadian Cancer Society. Canadian cancer statistics 2023. 2024. Accessed March 5, 2025. https://cdn.cancer.ca/-/media/files/research/cancer-statistics/2023-statistics/2023_pdf_en
2.Canadian Cancer Society. Colorectal cancer statistics. 2024. Accessed March 5, 2025. https://cancer.ca/en/cancer-information/cancer-types/colorectal/statistics
3.Fletcher RH. Colorectal cancer screening: for prevention or cure? J Epidemiol Community Health. 2009;63(7):505-6. doi:10.1136/jech.2008.083675 PubMed
4.Power E, Simon A, Juszczyk D, et al. Assessing awareness of colorectal cancer symptoms: measure development and results from a population survey in the UK. BMC Cancer. 2011;11:366. doi:10.1186/1471-2407-11-366 PubMed
5.Copija A, Waniczek D, Witkoś A, et al. Clinical significance and prognostic relevance of microsatellite instability in sporadic colorectal cancer patients. Int J Mol Sci. 2017;18(1)doi:10.3390/ijms18010107 PubMed
6.Statistics Canada. Five-year cancer survival by stage at diagnosis in Canada. 2023. Accessed March 5, 2025. https://www150.statcan.gc.ca/n1/pub/82-003-x/2023001/article/00001-eng.htm
7.Van Cutsem E, Cervantes A, Nordlinger B, et al. Metastatic colorectal cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2014;25 Suppl 3:iii1-9. doi:10.1093/annonc/mdu260 PubMed
8.Gelsomino F, Barbolini M, Spallanzani A, et al. The evolving role of microsatellite instability in colorectal cancer: A review. Cancer Treat Rev. 2016;51:19-26. doi:10.1016/j.ctrv.2016.10.005 PubMed
9.Gutierrez C, Ogino S, Meyerhardt JA, et al. The prevalence and prognosis of microsatellite instability-high/mismatch repair-deficient colorectal adenocarcinomas in the United States. JCO Precis Oncol. 2023;7:e2200179. doi:10.1200/po.22.00179 PubMed
10.Canada's Drug Agency. Provisional funding algorithm. Indication: metastatic colorectal cancer. PH0062. 2025. Accessed by sponsor, no date provided. https://www.cda-amc.ca/sites/default/files/DRR/2025/PH0062-mCRC_Rapid_Algorithm_Report.pdf
11.Canada's Drug Agency. Drug Reimbursement Review: nivolumab and ipilimumab (N/A) for first-line treatment of adult patients with advanced (unresectable or metastatic) melanoma when patients progress during or within 6 months of adjuvant PD-1 therapy. 2024. Accessed May 28, 2025. https://www.cda-amc.ca/nivolumab-and-ipilimumab
12.Canada's Drug Agency. Drug Reimbursement Review: nivolumab and ipilimumab (N/A) for neoadjuvant setting for resectable stage III melanoma. 2025. Accessed May 28, 2025. https://www.cda-amc.ca/nivolumab-ipilimumab-0
13.Canada's Drug Agency. Drug Reimbursement Review: nivolumab and ipilimumab (Opdivo & Yervoy) for treatment of adult patients with unresectable malignant pleural mesothelioma (MPM) who have not received prior systemic therapy for MPM. 2021. Accessed May 28, 2025. https://www.cda-amc.ca/nivolumab-ipilimumab
14.Canada's Drug Agency. Drug Reimbursement Review: nivolumab and ipilimumab (Opdivo & Yervoy) for non-small cell lung cancer. 2021. Accessed May 28, 2025. https://www.cda-amc.ca/nivolumab-ipilimumab-non-small-cell-lung-cancer-details
15.Canada's Drug Agency. Drug Reimbursement Review: nivolumab and ipilimumab (Opdivo-Yervoy) for the first-line treatment of patients with metastatic or recurrent NSCLC with no EGFR or ALK genomic tumor aberrations. 2020. Accessed May 28, 2025. https://www.cda-amc.ca/nivolumab-ipilimumab-1
16.Canada's Drug Agency. Drug Reimbursement Review: nivolumab and ipilimumab (Opdivo & Yervoy) for Intermediate/poor risk patients with previously untreated, advanced or metastatic renal cell carcinoma (RCC). 2018. Accessed May 28, 2025. https://www.cda-amc.ca/opdivo-combo-yervoy-renal-cell-carcinoma-details
17.Canada's Drug Agency. Drug Reimbursement Review: nivolumab and ipilimumab (Opdivo & Yervoy) for treatment-naïve adult patients with advanced (unresectable or metastatic) melanoma, regardless of BRAF status. 2017. Accessed May 28, 2025. https://www.cda-amc.ca/opdivo-combo-yervoy-metastatic-melanoma-details
18.Canada's Drug Agency. Drug Reimbursement Review: nivolumab and ipilimumab (Opdivo-Yervoy) for the first-line treatment of adult patients with unresectable or advanced hepatocellular carcinoma (HCC). 2025. Accessed May 28, 2025. https://www.cda-amc.ca/nivolumab-and-ipilimumab-1
19.Balshem H, Helfand M, Schünemann HJ, et al. GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol. 2011;64(4):401-6. doi:10.1016/j.jclinepi.2010.07.015 PubMed
20.Santesso N, Glenton C, Dahm P, et al. GRADE guidelines 26: informative statements to communicate the findings of systematic reviews of interventions. J Clin Epidemiol. 2020;119:126-135. doi:10.1016/j.jclinepi.2019.10.014 PubMed
21.Cherny NI, Dafni U, Bogaerts J, et al. ESMO-magnitude of clinical benefit scale version 1.1. Ann Oncol. 2017;28(10):2340-2366. doi:10.1093/annonc/mdx310 PubMed
22.Ko YJ, Abdelsalam M, Kavan P, et al. What is a clinically meaningful survival benefit in refractory metastatic colorectal cancer? Curr Oncol. 2019;26(2):e255-e259. PubMed
23.Musoro JZ, Coens C, Sprangers MAG, et al. Minimally important differences for interpreting EORTC QLQ-C30 change scores over time: A synthesis across 21 clinical trials involving nine different cancer types. Eur J Cancer. 2023;188:171-182. doi:10.1016/j.ejca.2023.04.027 PubMed
24.Macrae FA, Parikh AR, Riccardi R. Tanabe KK, ed. Clinical presentation, diagnosis, and staging of colorectal cancer. UpToDate; 2025. Accessed May 9, 2025. http://www.uptodate.com
25.Kolligs FT. Diagnostics and epidemiology of colorectal cancer. Visc Med. 2016;32(3):158-64. doi:10.1159/000446488 PubMed
26.Cancer Care Ontario. Ontario cancer statistics 2022: Chapter 4 - cancer incidence. 2022. Accessed March 5, 2025. https://www.cancercareontario.ca/en/data-research/view-data/statistical-reports/ontario-cancer-statistics-2022/ch-4-cancers-incidence-2022
27.Boland CR, Thibodeau SN, Hamilton SR, et al. A National Cancer Institute workshop on microsatellite instability for cancer detection and familial predisposition: development of international criteria for the determination of microsatellite instability in colorectal cancer. Cancer Res. 1998;58(22):5248-57. PubMed
28.Adelphi Real World. A comparative analysis of MSI-H/dMMR prevalence, testing patterns, and treatment uptake in first-line metastatic colorectal cancer in EU4 (France, Germany, Italy, Spain), the UK and Canada. April 2024. [BMS DOF] [sponsor supplied reference]. 2024.
29.Institut national d'excellence en santé et en services sociaux. Algorithmes d’investigation, de traitement et de suivi du cancer colorectal. 2024. Accessed by sponsor, no date provided. https://inesss.algorithmes-onco.info/fr/algorithmes-d-investigation-de-traitement-et-de-suivi-du-cancer-colorectal
30.Bristol-Myers Squibb Canada. Opdivo (nivolumab) [DRAFT product monograph; sponsor supplied reference]. 2024.
31.Bristol-Myers Squibb Canada. Yervoy (Ipilimumab) [product monograph; sponsor supplied reference]. 2023.
32.European Medicines Agency. Opdivo (nivolumab): European Commission decision. 2024. Accessed April 17, 2025. https://www.ema.europa.eu/en/medicines/human/EPAR/opdivo#product-info
33.U.S. Food and Drug Administration. FDA approves nivolumab with ipilimumab for unresectable or metastatic MSI-H or dMMR colorectal cancer. April 8, 2025. Accessed April 17, 2025. https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-nivolumab-ipilimumab-unresectable-or-metastatic-msi-h-or-dmmr-colorectal-cancer
34.National Institute of Health and Care Excellence. Nivolumab plus ipilimumab for untreated unresectable or metastatic colorectal cancer with high microsatellite instability or mismatch repair deficiency (Technology appraisal guidance). May 28, 2025. Accessed June 10, 2025. https://www.nice.org.uk/guidance/ta1065/resources/nivolumab-plus-ipilimumab-for-untreated-unresectable-or-metastatic-colorectal-cancer-with-high-microsatellite-instability-or-mismatch-repair-deficiency-pdf-2973528577772485
35.Therapeutic Goods Administration. OPDIVO in combination with ipilimumab is indicated for the treatment of adult patients with unresectable or metastatic colorectal cancer (CRC) that is MSI-H or dMMR as determined by a validated test. 2025. Accessed July 9, 2025. https://www.tga.gov.au/resources/prescription-medicines-registrations/opdivo-bristol myers-squibb-australia-pty-ltd-17
36.Merck Canada Inc. Keytruda (pembrolizumab) [product monograph; sponsor supplied reference]. 2023.
37.Pfizer Canada U. L. C. Oxaliplatin (oxaliplatin injection): 5 mg/mL oxaliplatin, 50 mg / 10 mL, 100 mg / 20 mL, 200 mg / 40 mL; sterile concentrate for intravenous infusion [product monograph]. July 3, 2020. Accessed by sponsor, no date provided. https://pdf.hres.ca/dpd_pm/00057007.PDF
38.General Medical Partners Inc. Leucovorin calcium injection (leucovorin): solution for injection, 10 mg/mL for intramuscular injection or intravenous use [product monograph]. August 13, 2018. Accessed by sponsor, no date provided. https://pdf.hres.ca/dpd_pm/00046946.PDF
39.Accord Healthcare Inc. Fluorouracil injection: 50 mg / mL (5 g / 100 mL) [product monograph]. October 30, 2019. Accessed by sponsor, no date provided. https://pdf.hres.ca/dpd_pm/00053796.PDF
40.Auro Pharma Inc. Irinotecan Hydrochloride Injection (irinotecan hydrochloride trihydrate): sterile solution 20 mg / mL; house standard (40 mg / 2 mL, 100 mg / 5 mL, 300 mg / 15 mL and 500 mg / 25 mL) [product monograph]. June 30, 2020. Accessed by sponsor, no date provided. https://pdf.hres.ca/dpd_pm/00056704.PDF
41.Hoffman-La Roche Limited. Avastin (bevacizumab for injection): 100 mg and 400 mg vials (25 mg/mL solution for injection) [product monograph]. August 4, 2023. Accessed by sponsor, no date provided. https://assets.roche.com/f/173850/x/5c3325cd99/avastin_pm_e.pdf
42.Amgen Canada Inc. Vectibix (panitumumab for injection): sterile solution 100 mg, 400 mg (20 mg / mL) [product monograph]. October 25, 2021. Accessed by sponsor, no date provided. https://www.amgen.ca/en-CA/-/media/Themes/CorporateAffairs/Redesign/Amgen-ca/Amgen-ca/pdf/products/en/vectibix_pm.pdf
43.Eli Lilly Canada Inc. Erbitux (cetuximab intravenous injection): intravenous Injection, 2 mg cetuximab / mL, 50 mL and 100 mL vials [product monograph]. January 10, 2018. Accessed by sponsor, no date provided. https://pdf.hres.ca/dpd_pm/00043071.PDF
44.Al-Mansor E, Mahoney M, Chenard-Poirier M, et al. Eastern Canadian Gastrointestinal Cancer Consensus Conference 2023. Curr Oncol. 2023;30(9):8172-8185. doi:10.3390/curroncol30090593 PubMed
45.Yu IS, Aubin F, Goodwin R, et al. Tumor biomarker testing for metastatic colorectal cancer: A Canadian consensus practice guideline. Ther Adv Med Oncol. 2022;14:17588359221111705. doi:10.1177/17588359221111705 PubMed
46.Gill S, Ahmed S, Anderson B, et al. Report from the 24th Annual Western Canadian Gastrointestinal Cancer Consensus Conference on Colorectal Cancer, Richmond, British Columbia, 28-29, October 2022. Curr Oncol. 2023;30(9):7964-7983. doi:10.3390/curroncol30090579 PubMed
47.Shia J. Immunohistochemistry versus microsatellite instability testing for screening colorectal cancer patients at risk for hereditary nonpolyposis colorectal cancer syndrome. Part I. The utility of immunohistochemistry. J Mol Diagn. 2008;10(4):293-300. doi:10.2353/jmoldx.2008.080031 PubMed
48.Bartley AN, Mills AM, Konnick E, et al. Mismatch repair and microsatellite instability testing for immune checkpoint inhibitor therapy: Guideline From the College of American Pathologists in Collaboration with the Association for Molecular Pathology and Fight Colorectal Cancer. Arch Pathol Lab Med. 2022;146(10):1194-1210. doi:10.5858/arpa.2021-0632-CP PubMed
49.André T, Shiu KK, Kim TW, et al. Pembrolizumab in microsatellite-instability-high advanced colorectal cancer. N Engl J Med. 2020;383(23):2207-2218. doi:10.1056/NEJMoa2017699 PubMed
50.Tournigand C, André T, Achille E, et al. FOLFIRI followed by FOLFOX6 or the reverse sequence in advanced colorectal cancer: a randomized GERCOR study. J Clin Oncol. 2004;22(2):229-37. doi:10.1200/jco.2004.05.113 PubMed
51.Prager GW, Taieb J, Fakih M, et al. Trifluridine-tipiracil and bevacizumab in refractory metastatic colorectal cancer. N Engl J Med. 2023;388(18):1657-1667. doi:10.1056/NEJMoa2214963 PubMed
52.Van Cutsem E, Peeters M, Siena S, et al. Open-label phase III trial of panitumumab plus best supportive care compared with best supportive care alone in patients with chemotherapy-refractory metastatic colorectal cancer. J Clin Oncol. 2007;25(13):1658-64. doi:10.1200/jco.2006.08.1620 PubMed
53.Cunningham D, Humblet Y, Siena S, et al. Cetuximab monotherapy and cetuximab plus irinotecan in irinotecan-refractory metastatic colorectal cancer. N Engl J Med. 2004;351(4):337-45. doi:10.1056/NEJMoa033025 PubMed
54.Dasari A, Lonardi S, Garcia-Carbonero R, et al. Fruquintinib versus placebo in patients with refractory metastatic colorectal cancer (FRESCO-2): an international, multicentre, randomised, double-blind, phase 3 study. Lancet. 2023;402(10395):41-53. doi:10.1016/s0140-6736(23)00772-9 PubMed
55.Andre T, Elez E, Cutsem EV, et al. Nivolumab plus ipilimumab in microsatellite-instability–high metastatic colorectal cancer. N Engl J Med. 2024;391(21):2014-2026. doi:doi:10.1056/NEJMoa2402141 PubMed
56.Andre T, Elez E, Lenz H-J, et al. Nivolumab plus ipilimumab versus nivolumab in microsatellite instability-high metastatic colorectal cancer (CheckMate 8HW): a randomised, open-label, phase 3 trial. Lancet. 2025;Feb 1(10476)(405):383-395. doi:10.1016/S0140-6736(24)02848-4
57.Bristol Myers Squibb. DOF - Interim Clinical Study Report for Study CA2098HW. A phase 3 randomized clinical trial of nivolumab alone, nivolumab in combination with ipilimumab, or investigator’s choice chemotherapy in participants with microsatellite instability high (MSI-H) or mismatch repair deficient (DMMR) metastatic colorectal cancer. DCO: 12-Oct-2023 [sponsor supplied reference]. 2024.
58.Bristol-Myers Squibb Canada. Drug Reimbursement Review sponsor submission: Opdivo plus Yervoy (nivolumab plus ipilimumab), 240 mg and 1 mg/kg intravenous infusions [internal sponsor's package]. March 24, 2025.
59.Bristol-Myers Squibb. DOF - CheckMate-8HW IA1b supplemental data. September 2024 database lock - arm B and arm C - first line. DCO: 28-Aug-2024 [sponsor supplied reference]. 2025.
60.Bristol Myers Squibb. DOF - Clinical Protocol CA2098HW. A phase 3 randomized clinical trial of nivolumab alone, nivolumab in combination with ipilimumab, or investigator’s choice chemotherapy in participants with microsatellite instability high (MSI-H) or mismatch repair deficient (DMMR) metastatic colorectal cancer. Revised Protocol 04 [sponsor supplied reference]. 2020.
61.Roodhart JML, Dave K, Dixon M, et al. Can overall survival benefit be predicted from improvements in progression-free survival (PFS) for previously metastatic colorectal cancer? [321]. presented at: Gastrointestinal Cancers Symposium (ASCO-GI); 23-25 January 2025; San Francisco, US.
62.Cicero G, De Luca R, Dieli F. Progression-free survival as a surrogate endpoint of overall survival in patients with metastatic colorectal cancer. Onco Targets Ther. 2018;11:3059-3063. doi:10.2147/ott.S151276 PubMed
63.Sidhu R, Rong A, Dahlberg S. Evaluation of progression-free survival as a surrogate endpoint for survival in chemotherapy and targeted agent metastatic colorectal cancer trials. Clin Cancer Res. 2013;19(5):969-76. doi:10.1158/1078-0432.Ccr-12-2502 PubMed
64.U.S. Food and Drug Administration. Clinical trial endpoints for the approval of cancer drugs and biologics: Guidance for industry. 2018.
65.Fayers P, Bottomley A. Quality of life research within the EORTC—the EORTC QLQ-C30. Eur J Cancer. 2002;38:125-133. doi:10.1016/S0959-8049(01)00448-8 PubMed
66.de Lima Lopes G, Nahas GR. Chimeric antigen receptor T cells, a savior with a high price. Chin Clin Oncol. 2018;7(2):21. doi:10.21037/cco.2018.04.02 PubMed
67.Brigand T, Prokupkova A, Muller G. CAR-T Cell Therapies: How much for survival? Association of European Cancer Leagues; 2018. Accessed Mar 20, 2025. https://www.cancer.eu/wp-content/uploads/2018/06/CAR-T-ECL-Article_Final_20062018.pdf
68.Nolte S, Liegl G, Petersen MA, et al. General population normative data for the EORTC QLQ-C30 health-related quality of life questionnaire based on 15,386 persons across 13 European countries, Canada and the Unites States. Eur J Cancer. 2019;107:153-163. doi:10.1016/j.ejca.2018.11.024 PubMed
69.Institut national d'excellence en santé et en services sociaux. Keytruda - Cancer colorectal métastatique. 2021. Accessed by sponsor, no date provided. https://www.inesss.qc.ca/fileadmin/doc/INESSS/Inscription_medicaments/Avis_au_ministre/Juin_2021/Keytruda_2021_05.pdf
70.Bristol Myers Squibb. Protocol CA209-8HW. DOF - Statistical Analysis Plan (SAP) for Clinical Study Report (CSR). A phase 3 randomized clinical trial of nivolumab alone, nivolumab in combination with ipilimumab, or investigator’s choice chemotherapy in participants with microsatellite instability high (MSI-H) or mismatch repair deficient (DMMR) metastatic colorectal cancer. Version 3.0 [sponsor supplied reference]. 2023.
71.Greenwood M. The errors of sampling of the survivorship tables [sponsor supplied reference]. Reports on Public Health and Statistical Participants. HMSO; 1926.
72.Osoba D, Rodrigues G, Myles J, et al. Interpreting the significance of changes in health-related quality-of-life scores. J Clin Oncol. 1998;16(1):139-44. doi:10.1200/jco.1998.16.1.139 PubMed
73.Pickard AS, Neary MP, Cella D. Estimation of minimally important differences in EQ-5D utility and VAS scores in cancer. Health Qual Life Outcomes. 2007;5:70. doi:10.1186/1477-7525-5-70 PubMed
74.Dolan P. Modeling valuations for EuroQol health states. Med Care. 1997;35(11):1095-108. doi:10.1097/00005650-199711000-00002 PubMed
75.Guyot P, Ades AE, Ouwens MJ, et al. Enhanced secondary analysis of survival data: reconstructing the data from published Kaplan-Meier survival curves. BMC Med Res Methodol. 2012;12:9. doi:10.1186/1471-2288-12-9
76.Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj.n71 PubMed
77.Shamseer L, Moher D, Clarke M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: elaboration and explanation. BMJ. 2015;350:g7647. doi:10.1136/bmj.g7647 PubMed
78.Adelphi Values. Comparative efficacy and safety of 1L therapies in patients with MSI-H/DMMR metastatic colorectal cancer: Systematic literature review. Report No: BS9950A. Version 3.0 - July 18, 2024 [sponsor supplied reference]. 2024.
79.Bristol Myers Squibb. DOF - Indirect treatment comparison for nivolumab + ipilimumab in microsatellite instability-high/mismatch-repair-deficient metastatic colorectal cancer. Version 1.0-September 2024 DBL updated; 2025 January 8 [sponsor supplied reference]. 2025.
80.André T, Shiu KK, Kim TW, et al. Pembrolizumab versus chemotherapy in microsatellite instability-high or mismatch repair-deficient metastatic colorectal cancer: 5-year follow-up from the randomized phase III KEYNOTE-177 study. Ann Oncol. 2024;doi:10.1016/j.annonc.2024.11.012 PubMed
81.Shiu KK, André T, Kim TW, et al. LBA32 Pembrolizumab versus chemotherapy in microsatellite instability-high (MSI-H)/mismatch repair-deficient (dMMR) metastatic colorectal cancer (mCRC): 5-year follow-up of the randomized phase III KEYNOTE-177 study. Ann Oncol. 2023;34:S1271-S1272.
82.Goey KKH, Sørbye H, Glimelius B, et al. Consensus statement on essential patient characteristics in systemic treatment trials for metastatic colorectal cancer: Supported by the ARCAD Group. Eur J Cancer. 2018;100:35-45. doi:10.1016/j.ejca.2018.05.010 PubMed
83.Open Health. Cost-effectiveness analysis of Nivo + Ipi for 1L MSI-H/dMMR mCRC - Model version 9.1 [sponsor supplied reference]. 2025.
84.Nice. NICE DSU Technical Support Document 14: Survival Analysis for Economic Evaluations Alongside Clinical Trials - Extrapolation with Patient-level Data [sponsor provided reference]. 2011. June 2011.
Appendix 1: Detailed Outcome Data
Table 31: Duration of Study Therapy, Cumulative Dose, and Relative Dose Intensity in Patients Receiving First-Line Treatment in the Nivolumab Plus Ipilimumab and Chemotherapy Arms (Data Cut-Off Date: October 12, 2023)
Parameters | Nivolumab plus ipilimumab (n=200) | Chemotherapy (n=88) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
Nivolumab (n=200) | Ipilimumab (n=200) | Overall (n=200) | Oxaliplatin (n=51) | Leucovorin (n=87) | Fluorouracil bolus (n=86) | Fluorouracil IV (n=88) | Bevacizumab (n=56) | Cetuximab (n=10) | Irinotecan (n=37) | Overall (n=88) | |
Duration of therapy (months) | |||||||||||
Mean (range) | ||||||||| ||||| | |||||||| |||| | |||||||| ||| | |||||||| ||||| | |||||||| ||||| | |||||||| ||||| | |||||||||| ||||| | |||||||| ||||| | |||||||| |||| | |||||||| ||||| | ||||||||||||| |
Median | 13.52 | 2.10 | 13.52 | 2.83 | 3.94 | 3.56 | 3.96 | 3.83 | 2.66 | 3.45 | 3.96 |
Number of doses received | |||||||||||
Mean (SD) | |||| |||||| | ||| |||||| | || | ||| |||||| | |||||||||| | |||| |||||| | |||| |||||| | |||| |||||| | ||| |||||| | ||| |||||| | || |
Median (range) | ||||| ||| ||| | ||| |||| || | || | |||| ||| ||| | |||| ||| ||| | |||| ||| ||| | ||| |||| ||| | ||| |||| ||| | ||| |||| ||| | |||| ||| ||| | || |
Relative dose intensity, n (%) | |||||||||||
≥110% | || | | ||||| | || | || | || | || | || | | ||||| | || | | ||||| | || |
90% to < 110% | ||| |||||| | ||| |||||| | || | || |||||| | || |||||| | || |||||| | || |||||| | || |||||| | | |||||| | || |||||| | || |
70% to <90% | || |||||| | || |||||| | || | || |||||| | || |||||| | || |||||| | || |||||| | || |||||| | | |||||| | || |||||| | || |
50% to <70% | | ||||| | | ||||| | || | || |||||| | || |||||| | || |||||| | || |||||| | | ||||| | | |||||| | | |||||| | || |
<50% | || | || | || | || | | ||||| | | ||||| | | ||||| | || | || | || | || |
CSR = Clinical Study Report; SD = standard deviation.
Note: This table has not been copy-edited.
Excludes data collected on or after the first crossover dose date. Dose unit: nivolumab in mg, ipilimumab in mg/kg; oxaliplatin, leucovorin, fluorouracil, cetuximab, irinotecan in mg/m2; and bevacizumab in mg/kg.
Source: Bristol-Myers Squibb, 2024 (Interim CSR).57 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Table 32: Treatment Regimen Distribution in the KEYNOTE-177 Trial and the CheckMate-8HW Trial
Treatment | SOC, % Chemotherapy arm in KEYNOTE-177 trial (N=143) | SOC, % Chemotherapy arm in CheckMate-8HW trial (N=88) |
|---|---|---|
mFOLFOX6 | 7.7 | 10.2 |
FOLFIRI | 11.2 | 13.6 |
mFOLFOX6 + cetuximab | 3.5 | 5.7 |
FOLFIRI + cetuximab | 7.7 | 6.8 |
mFOLFOX6 + bevacizumab | 44.8 | 42.0 |
FOLFIRI + bevacizumab | 25.2 | 21.6 |
FOLFIRI = leucovorin calcium (folinic acid), fluorouracil, irinotecan hydrochloride; ITC = indirect treatment comparison; mFOLFOX = modified leucovorin calcium (folinic acid), fluorouracil, oxaliplatin; SOC = standard of care.
Note: This table has not been copy-edited.
Source: Bristol-Myers Squibb, 2024 (ITC Report).79 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Figure 9: Subgroup Forest Plot Informing TEM Selection Based on the KEYNOTE-177 Trial
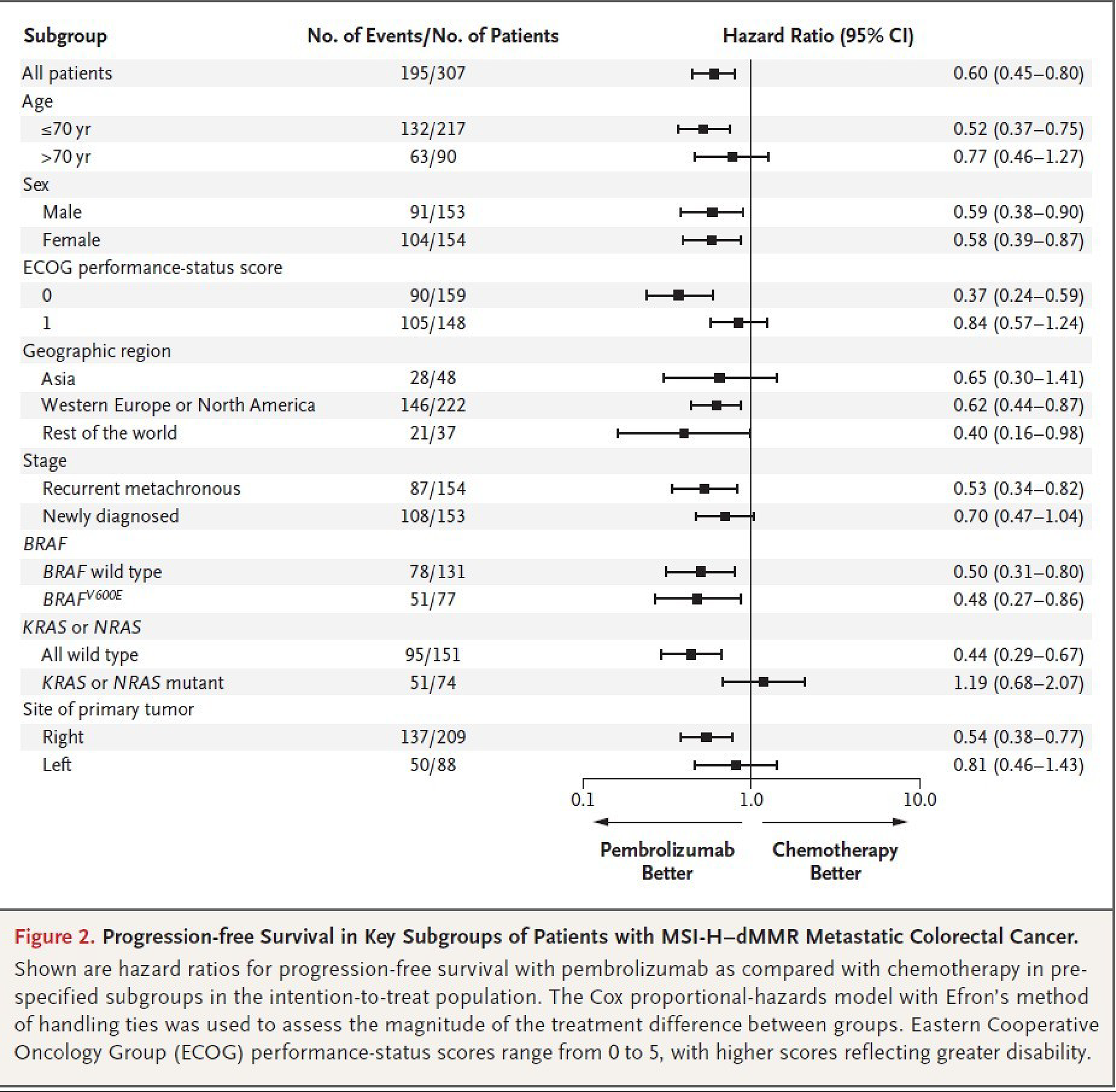
CI = confidence interval; dMMR = deficient mismatch repair; ECOG PS = Eastern Cooperative Oncology Group Performance Status; HR = hazard ratio; mCRC = metastatic colorectal cancer; MSI-H = microsatellite instability-high; no. = number; PFS = progression-free survival; TEM = treatment-effect modifier; yr = year.
Notes: Shown are hazard ratios for PFS with pembrolizumab compared with chemotherapy in prespecified subgroups in the intention-to-treat population. The Cox proportional hazards model with Efron method of handling ties was used to assess the magnitude of difference between groups.
Source: Andre et al., NEJM 2020.49 The New England Journal of Medicine, André T, Shiu KK, Kim TW, et al., Pembrolizumab in Microsatellite-Instability-High Advanced Colorectal Cancer., 383(23):2207 to 2218. Copyright (2020) Massachusetts Medical Society. Reprinted with permission from Massachusetts Medical Society. Details included in the figure are from the sponsor’s Summary of Clinical Evidence.
Figure 10: Subgroup Forest Plot Informing TEM Selection Based on the CheckMate-8HW Trial [Redacted]

TEM = treatment-effect modifier.
Figure 11: Anchored MAIC — KM Plot of Survival Estimates in the CheckMate-8HW Trial Before and After Matching [Redacted]

KM = Kaplan-Meier; MAIC = matching-adjusted indirect comparison.
Figure 12: Unanchored MAIC — KM Plot of Survival Estimates of Pembrolizumab (KEYNOTE-177 Trial) and Nivolumab Plus Ipilimumab (CheckMate-8HW Trial) Before and After Matching [Redacted]

KM = Kaplan-Meier; MAIC = matching-adjusted indirect comparison.
Figure 13: Network of Evidence for PFS — Nivolumab Plus Ipilimumab, Pembrolizumab, Nivolumab Monotherapy, and SOC Chemotherapy (CheckMate-8HW and KEYNOTE-177 Trials)
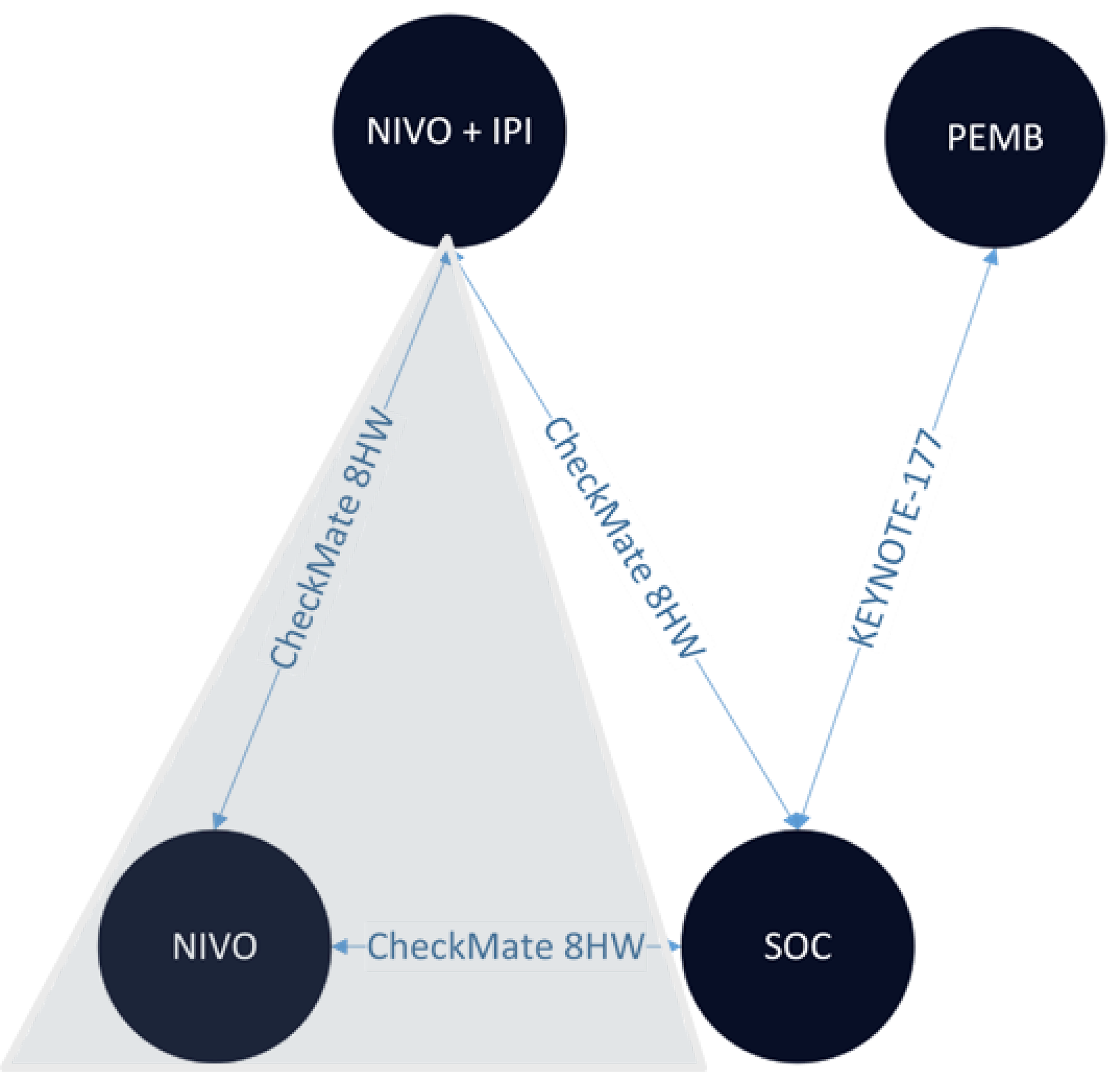
IPI = ipilimumab; Nivo = nivolumab; PEMB = pembrolizumab; PFS = progression-free survival; SOC = standard of care.
Note: Data for nivolumab monotherapy were not available in the September 2024 database lock of the CheckMate-8HW trial. Hence, the feasibility assessment includes only nivolumab plus ipilimumab and chemotherapy arms from the trial.
Source: Bristol-Myers Squibb, 2025 (ITC Report).79 Details included in the figure are from the sponsor’s Summary of Clinical Evidence.


Pharmacoeconomic Review
Abbreviations
BIA
budget impact analysis
CDA-AMC
Canada’s Drug Agency
dMMR
deficient mismatch repair
HR
hazard ratio
HRQoL
health-related quality of life
ICER
incremental cost-effectiveness ratio
ITC
indirect treatment comparison
MAIC
matching-adjusted indirect comparison
mCRC
metastatic colorectal cancer
MSI-H
microsatellite instability-high
OS
overall survival
PFS
progression-free survival
QALY
quality-adjusted life-year
Economic Review
The objective of the economic review undertaken by Canada’s Drug Agency (CDA-AMC) is to review and critically appraise the pharmacoeconomic evidence submitted by the sponsor on the cost-effectiveness and budget impact of nivolumab (Opdivo) in combination with ipilimumab (Yervoy) compared to other relevant treatments for first-line treatment of adult patients with unresectable or metastatic microsatellite instability-high (MSI-H) or mismatch repair deficient (dMMR) colorectal cancer.
Item | Description |
|---|---|
Drug product | Nivolumab (Opdivo) at a dose of 240 mg given in combination with ipilimumab (Yervoy) at 1 mg/kg once every 3 weeks for a total of 4 doses followed by nivolumab at 480 mg every 4 weeks as maintenance therapy. |
Indication | First-line treatment of adult patients with unresectable or metastatic microsatellite instability-high (MSI-H) or mismatch repair deficient (dMMR) colorectal cancer |
Submitted price | Nivolumab $782.22 per 4 mL vial at 10 mg/mL Ipilimumab $5,800.00 per 10 mL vial at 5 mg/mL |
Health Canada approval status | NOC |
Health Canada review pathway | Standard |
NOC date | July 16, 2025 |
Reimbursement request | Per indication |
Sponsor | Bristol-Myers Squibb Canada Co. |
Submission history | Previously reviewed: No |
dMMR = mismatch repair deficient; MSI-H = microsatellite instability-high; NOC = Notice of Compliance.
Summary
Nivolumab is available as an IV solution at a strength of 10 mg/mL. At the submitted price of $782.22 per 4 mL, the per-cycle cost of nivolumab is expected to be $4,693 per patient for the first 4 doses and $9,387 for subsequent doses, based on the Health Canada–recommended dosage. Ipilimumab is available as an IV infusion at a strength of 5 mg/mL. At the submitted price of $5,800.00 per 10 mL, the per-cycle cost of ipilimumab is expected to be $11,600 per patient, based on the Health Canada–recommended dosage. For the first 4 doses, nivolumab is administered as a flat dose of 240 mg, and ipilimumab is assumed to be administered as a weight-based dose of 1 mg/kg IV every 3 weeks. After 4 doses, nivolumab is administered as a flat dose of 480 mg until disease progression, death, or other reasons for discontinuation up to a maximum of 2 years.
Clinical efficacy in the economic analysis for nivolumab plus ipilimumab versus chemotherapy was derived from the CheckMate-8HW trial. Evidence submitted by the sponsor indicates that nivolumab plus ipilimumab is likely to improve time to progression or death compared with chemotherapy among patients with unresectable or metastatic MSI-H or dMMR colorectal cancer. For nivolumab plus ipilimumab versus pembrolizumab, clinical efficacy was informed by sponsor-submitted indirect treatment comparison (ITC), which suggests that nivolumab plus ipilimumab may improve time to progression compared with pembrolizumab.
The results of the CDA-AMC base case suggest the following:
Nivolumab plus ipilimumab will be associated with higher costs to the health care system than chemotherapy (incremental costs = $118,050), primarily driven by increased costs associated with drug acquisition.
Nivolumab plus ipilimumab is associated with a gain of 4.81 life-years compared to chemotherapy. When the impact on health-related quality of life (HRQoL) is also considered, nivolumab plus ipilimumab may result in a gain of 3.98 quality-adjusted life-years (QALYs) compared to chemotherapy.
The incremental cost-effectiveness ratio (ICER) of nivolumab plus ipilimumab compared to chemotherapy was $30,522 per QALY gained in the CDA-AMC base case.
The incremental costs and QALYs compared to pembrolizumab are uncertain. Comparative progression-free survival (PFS) versus pembrolizumab was estimated using an unanchored matching-adjusted indirect comparison (MAIC), which could not control for potential treatment confounders. While the CDA-AMC base case estimated a gain in QALYs with nivolumab plus ipilimumab compared to pembrolizumab (incremental: 1.42), more than 89% of the incremental benefit was gained in the extrapolated period (i.e., after 42.05 months). In the absence of direct comparative evidence during the trial period and a high degree of uncertainty in the long-term extrapolation from the indirect evidence, the duration of time that patients spend in the progression-free state is uncertain. Given that time in this state is a primary driver of incremental costs and incremental QALYs, the estimated ICER in the CDA-AMC base case is highly uncertain and may be overestimated. In the CDA-AMC base case, nivolumab plus ipilimumab extendedly dominates pembrolizumab.
CDA-AMC estimates that the budget impact of reimbursing nivolumab plus ipilimumab for the first-line treatment of adult patients with unresectable or metastatic MSI-H or dMMR metastatic colorectal cancer (mCRC) will be a savings of approximately $235,000 for the first 3 years of reimbursement compared to the amount currently spent on pembrolizumab and chemotherapies, with an estimated expenditure of $114 million on nivolumab plus ipilimumab for this period. The actual budget impact of reimbursing nivolumab plus ipilimumab will depend on the proportion of eligible patients who receive nivolumab plus ipilimumab and if the treatments will be dosed by weight or a flat dose.
Summary of the Submitted Economic Evaluation
The sponsor submitted a cost-utility analysis to estimate the cost-effectiveness of nivolumab plus ipilimumab from the perspective of a public drug plan payer in Canada over a lifetime horizon (40 years). The modelled population comprised of adults (aged 18 years and older) with unresectable or metastatic MSI-H or dMMR colorectal cancer treated in the first-line setting, which is aligned with the Health Canada indication and was based on the participants in the CheckMate-8HW trial. The sponsor’s base-case analysis included costs related to drug acquisition, administration, monitoring, terminal care, and adverse reactions.
In the sponsor’s base case, nivolumab plus ipilimumab was associated with incremental costs of –$4,172 and 3.07 incremental QALYs relative to pembrolizumab. This resulted in nivolumab plus ipilimumab dominating pembrolizumab. Of the incremental benefit compared to pembrolizumab (3.14 incremental QALYs in the deterministic base case), approximately 93% of benefit was predicted to be accrued after the treatment duration of the CheckMate-8HW trial (median observation = 42.05 months). Additional information about the sponsor’s submission is summarized in Appendix 3.
CDA-AMC identified several key issues with the sponsor’s analysis (Table 2 with full details provided in Appendix 4). A revised base case was therefore developed.
Table 2: Key Issues With the Sponsor’s Economic Submission
Issue | What evidence is there to inform this issue? | How was this issue addressed by CDA-AMC? | Did CDA-AMC explore uncertainty in a scenario analysis? |
|---|---|---|---|
The PFS benefit predicted for nivolumab plus ipilimumab relative to pembrolizumab is likely overestimated in the sponsor’s base case. | The sponsor assumed that nivolumab plus ipilimumab provides a lifelong protective effect over pembrolizumab, beyond the maximum duration of treatment. This assumption is not supported by long-term evidence. The MAIC suggests the effect diminishes over time. Clinical experts agreed that the relative effect would wane over time. | CDA-AMC adopted an alternative relative effect of nivolumab plus ipilimumab compared to pembrolizumab. Using the results of the MAIC which suggest the relative effect equals 1 after 27 months (about 2.5 years). | No scenario analysis was conducted because the impact on cost-effectiveness was small. |
The PFS benefit predicted for nivolumab plus ipilimumab relative to pembrolizumab is likely overestimated in the sponsor’s base case. | The sponsor assumed that the relative hazard was an additive function and that background mortality can be subtracted to estimate progression. | CDA-AMC chose a less optimistic parametric function to describe PFS. | No scenario analysis was conducted. |
The PFS benefit predicted for nivolumab plus ipilimumab relative to pembrolizumab does not consider the uncertainty appropriately. | The use of parametric methods to extrapolate the relative effect underestimates the uncertainty in the relative effect. | CDA-AMC could not address this issue in the base case because insufficient data were provided. | No scenario analysis was conducted because insufficient data were provided. |
The background mortality is highly uncertain. | The sponsor assumed that the waning effect seen in the MAIC was due to background mortality, but in the model assumed that background mortality was the same. | CDA-AMC could not address this issue in the base case because insufficient data were provided. | No scenario analysis was conducted because insufficient data were provided. |
The background mortality is likely underestimated in the sponsor’s base case. | The sponsor assumed there would be no increased mortality of metastatic cancer compared to the general population of patients in the first 2 years of treatment. | CDA-AMC applied an increased background mortality to all patients regardless of treatment or time spent on treatment. | No scenario analysis was conducted. |
The terminal care costs of patients that die from the progression-free state are underestimated, decreasing the total cost of nivolumab plus ipilimumab. | The sponsor assumed that patients who die from the progression-free state would have the same costs of patients without cancer who die. Clinical experts stated that patients with cancer are likely to incur higher terminal care costs than patients without cancer. | In the CDA-AMC base case, the terminal care costs for those who died from the progression-free state were set equal to those who die from progressed disease. | No scenario analysis was conducted. |
There is substantial uncertainty around the choice of parametric distribution for the extrapolation of PFS. | The ICER ranged widely depending on the parametric distribution chosen. All predictions underestimated the 5-year mortality of patients treated with pembrolizumab. | In the base case, CDA-AMC chose the Weibull distribution for PFS parametric extrapolation. | No scenario analysis was conducted. |
The sponsor averaged the cost across chemotherapy regimens which can obscure important differences in the cost-effectiveness of individual treatments. | The cost of individual chemotherapy treatments was provided by the sponsor. | CDA-AMC conducted a sensitivity analysis comparing nivolumab plus ipilimumab to each of the most common chemotherapy regimens individually, using regimen-specific cost estimates. | The 4 most commonly prescribed chemotherapy regimens were tested. No meaningful difference was found in total cost or cost-effectiveness. |
Treatment costs were not reflective of current prices in Canada. | CDA-AMC found more up to date prices for some chemotherapy drugs. Additionally, the sponsor’s base case assumed flat dosing for immunotherapy and assumed that excess drugs in vials would be wasted. These assumptions were not supported by the clinical experts consulted by CDA-AMC for this review. | In reanalysis, the drug prices were updated to reflect current prices and dosage. Weight-based dosing was assumed. CDA-AMC assumed zero drug wastage. | No scenario analysis was conducted. |
CDA-AMC = Canada’s Drug Agency; ICER = incremental cost-effectiveness ratio; MAIC = match-adjusted indirect comparison; PFS = progression-free survival.
Note: Full details of the issues identified by CDA-AMC are provided in Appendix 3.
CDA-AMC Assessment of Cost-Effectiveness
The CDA-AMC base case was derived by making changes to model parameter values and assumptions (Table 7), in consultation with clinical experts. Detailed information about the base case is provided in Appendix 4.
Impact on Health Care Costs
Nivolumab plus ipilimumab is expected to be associated with additional health care costs compared with chemotherapy (incremental costs = $143,534). This increase in health care spending results from drug acquisition costs associated with nivolumab plus ipilimumab (Figure 1).
Compared to pembrolizumab, nivolumab plus ipilimumab is expected to be associated with higher health care costs (incremental costs = $70,140). This increase in health care spending is due to higher drug acquisition costs associated with nivolumab plus ipilimumab (Figure 1).
Figure 1: Impact of Nivolumab Plus Ipilimumab Versus Chemotherapy and Pembrolizumab on Health Care Costs
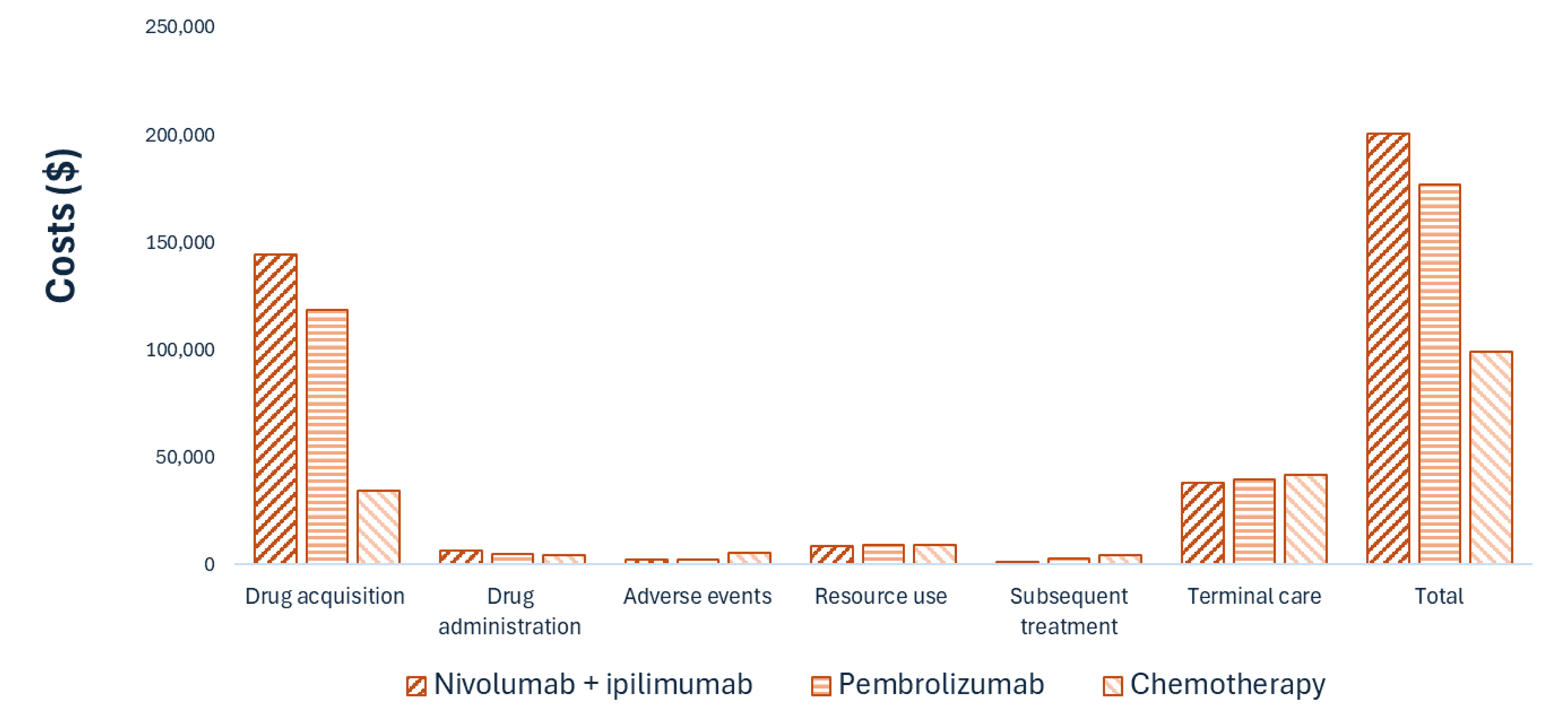
Note: Resource use refers to testing and oncologist visit costs.
Impact on Health
Relative to chemotherapy, nivolumab plus ipilimumab is expected to increase the amount of time a patient remains in the progression-free health state by approximately 5.76 years (Figure 2). Nivolumab plus ipilimumab is expected to increase the life-years to 10.07 compared to 5.41 for chemotherapy. Considering the impact of treatment on both quality and length of life, nivolumab plus ipilimumab is expected to result in 3.85 additional QALYs per patient compared to chemotherapy (Table 8).
Relative to pembrolizumab, nivolumab plus ipilimumab is expected to increase the amount of time a patient remains in the progression-free health state by approximately 2.07 years, and total life-years by 1.68 years (Figure 2). Considering the impact of treatment on both quality and length of life, nivolumab plus ipilimumab is expected to result in 1.39 additional QALYs per patient compared to pembrolizumab (Table 8).
Figure 2: Impact of Nivolumab Plus Ipilimumab Versus Chemotherapy and Pembrolizumab on Patient Health
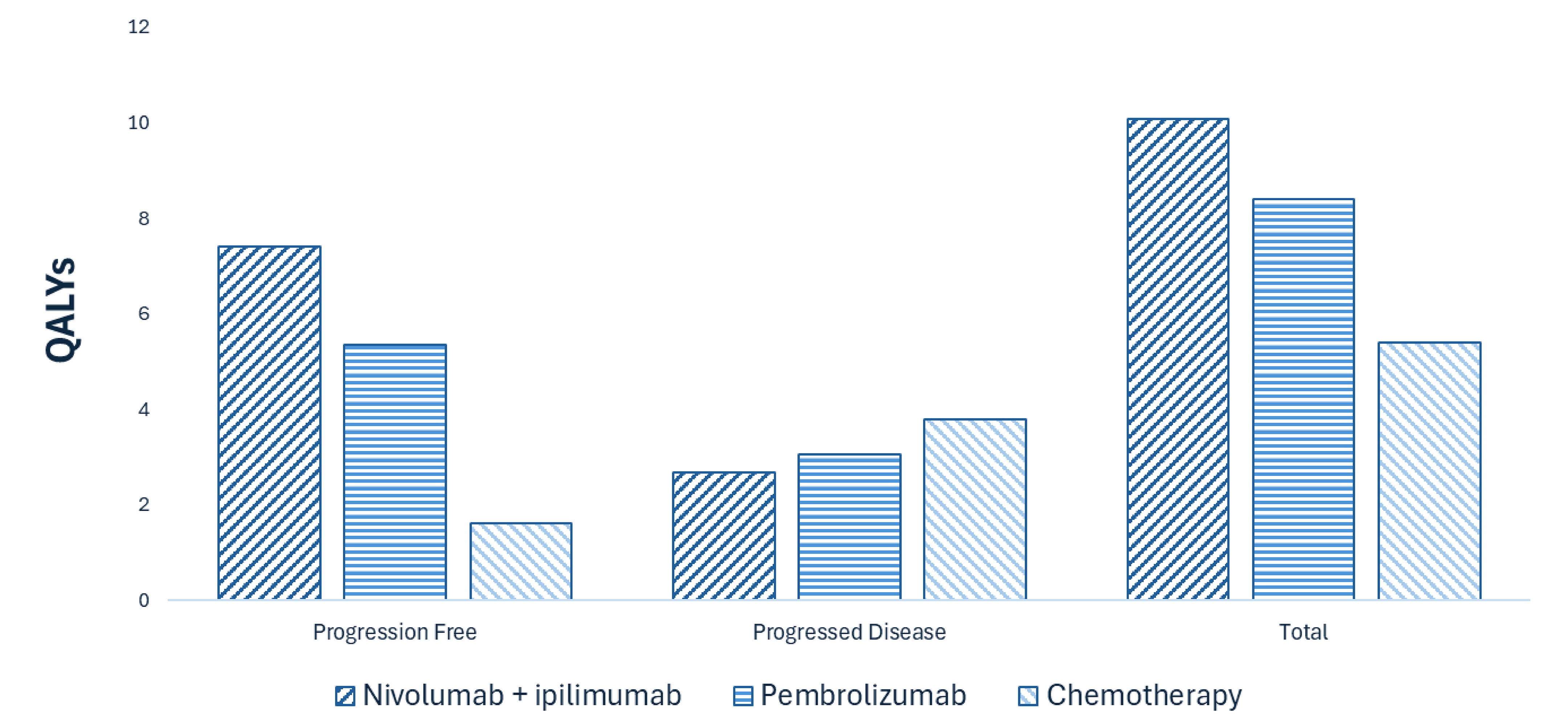
QALY = quality-adjusted life-year.
Overall Results
The results of the CDA-AMC base case suggest an ICER of $36,863 per QALY gained for nivolumab plus ipilimumab compared to chemotherapy (Table 3). Pembrolizumab is subject to extended dominance by nivolumab plus ipilimumab. Additional details on the CDA-AMC base case are available in Appendix 4.
Table 3: Summary of CDA-AMC Economic Evaluation Results
Drug | Total costs ($) | Total QALYs | Sequential ICER ($/QALY) |
|---|---|---|---|
Chemotherapy | 99,031 | 4.31 | Reference |
Pembrolizumab | 177,118 | 6.79 | Extendedly dominated |
Nivolumab plus ipilimumab | 217,081 | 8.18 | 30,522 |
CDA-AMC = Canada’s Drug Agency; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Note: Publicly available list prices were used for all comparators.
Uncertainty and Sensitivity
Uncertainty in the price of chemotherapy was performed. The model results were robust to these scenario analyses (nivolumab plus ipilimumab was more costly and more effective than chemotherapy).
Summary of the Budget Impact
The sponsor submitted a budget impact analysis (BIA) to estimate the 3-year (2026 to 2028) budget impact of reimbursing nivolumab plus ipilimumab for the first-line treatment of adult patients with unresectable or metastatic MSI-H or dMMR mCRC. The sponsor assumed that the payer would be CDA-AMC–participating public drug plans and derived the size of the eligible population using an epidemiologic approach. The price of nivolumab plus ipilimumab was aligned with the price included in the sponsor’s economic evaluation, while the prices of comparators were based on the publicly available list prices. Additional information pertaining to the sponsor’s submission is provided in Appendix 5. CDA-AMC identified a number of issues with the sponsor’s estimated budget impact and made changes to model parameters and assumptions in consultation with clinical experts to derive the CDA-AMC base case (Appendix 5). CDA-AMC estimated that 1,786 patients would be eligible for treatment with nivolumab plus ipilimumab over a 3-year period (year 1 = 381 patients; year 2 = 710 patients; year 3 = 695 patients), of whom 1,068 patients are expected to receive nivolumab plus ipilimumab (year 1 = 197 patients; year 2 = 407 patients; year 3 = 464 patients). The estimated budgetary savings associated with reimbursing nivolumab plus ipilimumab is expected to be approximately $235,000 for the first 3 years, with an expected expenditure of $114 million on nivolumab plus ipilimumab. The actual budget impact of reimbursing nivolumab plus ipilimumab will depend on the proportion of eligible patients who receive nivolumab plus ipilimumab and if the treatments will be dosed by weight or a flat dose.
Conclusion
Based on the CDA-AMC base case, nivolumab plus ipilimumab would be considered cost-effective at the submitted price if the public health care system was willing to pay at least $30,522 for each additional QALY gained. If the public health care system is not willing to pay that amount, a price reduction should be considered (Figure 3 with full details of the impact of price reductions on cost-effectiveness presented in Table 10). The estimated cost-effectiveness of nivolumab plus ipilimumab compared to pembrolizumab is uncertain due to a number of assumptions about the relative effect of nivolumab plus ipilimumab compared to pembrolizumab that could not be incorporated into the base case. In the CDA-AMC base case and all scenario analyses, nivolumab plus ipilimumab extendedly dominated pembrolizumab at the public list price.
The budgetary savings associated with reimbursing nivolumab plus ipilimumab to the public drug plans in the first 3 years is estimated to be approximately $235,000. The 3-year expenditure on nivolumab plus ipilimumab (i.e., not accounting for current expenditure on comparators) is estimated to be $114 million.
Figure 3: Summary of the CDA-AMC Economic Analysis and Price Reduction
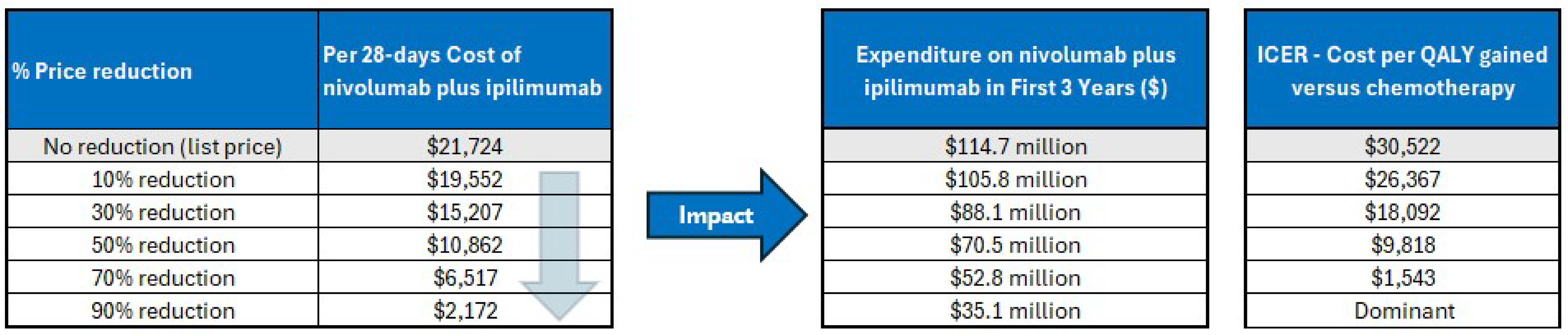
CDA-AMC = Canada’s Drug Agency; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Note: Expenditure includes only the drug cost of nivolumab plus ipilimumab. The term dominant indicates that a drug costs less and provides more QALYs than the comparator.
References
1.Iqvia. DeltaPA. 2023. Accessed January 1, 1800. https://www.iqvia.com/
2.Government of A. Interactive drug benefit list. Accessed January 1, 1800. https://idbl.ab.bluecross.ca/idbl/load.do
3.Canada's Drug Agency. CADTH Reimbursement Review - Pembrolizumab (Keytruda). 2023. https://www.cadth.ca/sites/default/files/DRR/2023/PC0280-Keytruda_combined.pdf
4.Cancer Care O. Funded evidence-informed regimens. Accessed January 1, 1800. https://www.cancercareontario.ca/en/drugformulary/regimens
5.Andre T, Elez E, Lenz H-J, et al. Nivolumab plus ipilimumab versus nivolumab in microsatellite instability-high metastatic colorectal cancer (CheckMate 8HW): a randomised, open-label, phase 3 trial. The Lancet. 2025;Feb 1(10476)(405):383-395. doi: 10.1016/S0140-6736(24)02848-4
6.Bristol-Myers S. Indirect Treatment Comparison for Nivolumab + Ipilimumab in Microsatellite Instability-High/Mismatch-Repair-Deficient Metastatic Colorectal Cancer Adverse Events, DBL Sept. 2024. 2025.
7.Global Cancer Observatory: Cancer T. GLOBOCAN 2022 – All Cancers. 2024. https://gco.iarc.who.int/media/globocan/factsheets/cancers/39-all-cancers-fact sheet.pdf
8.Ontario Ministry of H. Schedule of benefits for physician services under the Health Insurance Act: (June 29, 2023 (effective July 24, 2023)). 2023. Accessed January 1, 1800. https://www.health.gov.on.ca/en/pro/programs/ohip/sob/physserv/sob_master.pdf
9.Ontario Ministry of H. Schedule of benefits for laboratory services: (effective July 24, 2023). 2023. Accessed January 1, 1800. https://www.ontario.ca/files/2024-01/moh-ohip-schedule-of-benefits-laboratory-services-2024-01-24.pdf
10.Canadian Institute for Health I. Patient Cost Estimator. https://www.cihi.ca/en/patient-cost-estimator
11.Bristol-Myers Squibb Canada. Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Opdivo plus Yervoy (nivolumab plus ipilimumab), 240 mg and 1 mg/kg intravenous infusions. March 26, 2025.
12.van Oostrum I, Ouwens M, Remiro-Azócar A, et al. Comparison of parametric survival extrapolation approaches incorporating general population mortality for adequate health technology assessment of new oncology drugs. Value Health. 2021;24(9):1294-1301. PubMed
13.Dias S, Welton NJ, Sutton AJ, Ades AE. NICE DSU technical support document 2: a generalised linear modelling framework for pairwise and network meta-analysis of randomised controlled trials. 2011.
14.de Oliveira C, Pataky R, Bremner KE, et al. Phase-specific and lifetime costs of cancer care in Ontario, Canada. BMC Cancer. 2016;16:1-12. PubMed
15.Cadth. Guidelines for the economic evaluation of health technologies: Canada. 4th ed. 2017. Accessed January 1, 1800. https://www.cda-amc.ca/guidelines-economic-evaluation-health-technologies-canada-0
16.Brenner DR, Gillis J, Demers AA, et al. Projected estimates of cancer in Canada in 2024; Updated Version: 21 Aug 2024. CMAJ. 2024;196(18):E615-e623. doi: 10.1503/cmaj.240095 PubMed
17.Canadian Cancer S. Canadian Cancer Statistics 2023. 2024. Accessed March 5. https://cdn.cancer.ca/-/media/files/research/cancer-statistics/2023-statistics/2023_pdf_en
18.Cancer Care O. Ontario Cancer Statistics 2022: Chapter 4 - Cancer Incidence. 2022. Accessed March 5. https://www.cancercareontario.ca/en/data-research/view-data/statistical-reports/ontario-cancer-statistics-2022/ch-4-cancers-incidence-2022
19.Adelphi Real W. A Comparative Analysis of MSI-H/dMMR Prevalence, Testing Patterns, and Treatment Uptake in First-Line Metastatic Colorectal Cancer in EU4 (France, Germany, Italy, Spain), the UK and Canada. [internal study]. 2024.
20.Institut national d’excellence en santé et en services s. Keytruda - Cancer colorectal métastatique. 2021. https://www.inesss.qc.ca/fileadmin/doc/INESSS/Inscription_medicaments/Avis_au_ministre/Juin_2021/Keytruda_2021_05.pdf
Appendix 1: Cost Comparison Table
Please note that this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical experts and CDA-AMC–participating public drug plans. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 4: Cost Comparison for mCRC
Treatment | Strength or concentration | Form | Price ($) | Recommended dosage | Daily cost ($) | Average 28-day cost ($)a |
|---|---|---|---|---|---|---|
Nivolumab (Opdivo) | 40 mg vial 100 mg vial | 10 mg/mL IV solution | 782.2200 1,955.5600 | Flat dose Initiation: 240 mg every 3 weeks for a maximum of 4 doses Maintenance: 480 mg every 4 weeks until disease progression, unacceptable toxicity, or up to 2 years | Initiation: 223 Maintenance: 335 | Initiation: 6,258 Maintenance: 9,387 |
Nivolumab (Opdivo) | 40 mg vial 100 mg vial | 10 mg/mL IV solution | 782.2200 1,955.5600 | Weight-based dose Initiation: 3 mg/kg every 3 weeks for the first 4 doses Maintenance: 3 mg/kg every 2 weeks or 6 mg/kg every 4 weeks | Initiation: 223 Maintenance: 307 to 335 | Initiation: 6,258 Maintenance: 8,604 to 9,387 |
Ipilimumab (Yervoy) | 50 mg vial | 5 mg/mL IV solution | 5,800.0000 | 1 mg/kg every 3 weeks for a maximum of 4 doses | 552 | 15,467 |
Nivolumab + ipilimumab (Nivolumab flat dose) | — | — | — | — | Initiation: 776 Maintenance: 335 | Initiation: 21,724 Maintenance: 9,387 |
Nivolumab + ipilimumab (Nivolumab weight-based dose) | — | — | — | — | Initiation: 776 Maintenance: 307 to 335 | Initiation: 21,724 Maintenance: 8,604 to 9,387 |
Bevacizumab | ||||||
Bevacizumab (Mvasi) | 25 mg/mL | 4 mL vial 16 mL vial | 146.9300 587.7200 | 5 mg/kg every 2 weeks | 42 | 1,175 |
Cetuximab | ||||||
Cetuximab (Erbitux) | 2 mg/mL | 50 mL vial | 378.7500 | Initiation: 400 mg/m2; maintenance: 250 mg/m2 weekly | 260 to 293 | 7,280 to 8,190 |
FOLFOX | ||||||
Oxaliplatin (generic) | 5 mg/mL | 10 mL vial 20 mL vial 40 mL vial | 45.0000 90.0000 180.0000 | 85 mg/m2 every 2 weeks | 13 | 360 |
Folinic acid (Leucovorin) | 10 mg/mL | 5 mL vial 50 mL vial | 68.9430b 350.1900 | 400 mg/m2 every 2 weeks | 74 | 2,067 |
Fluorouracil bolus | 50 mg/mL | 100 mL vial | 160.9000 | 400 mg/m2 every 2 weeks | 2 | 47 |
Fluorouracil infusion | 50 mg/mL | 100 mL vial | 160.9000 | 2,400 mg/m2 every 2 weeks | 12 | 324 |
FOLFOX | — | — | — | — | 98 | 2,754 |
Bevacizumab + FOLFOX | — | — | — | — | 140 | 3,927 |
Cetuximab + FOLFOX | — | — | — | — | 358 to 391 | 10,032 to 10,942 |
FOLFIRI | ||||||
Irinotecan (generic) | 20 mg/mL | 2 mL vial 5 mL vial 25 mL vial | 208.3400 520.8500 2,604.2500 | 180 mg/m2 every 2 weeks | 126 | 3,542 |
Folinic acid (Leucovorin) | 10 mg/mL | 5 mL vial 50 mL vial | 68.9430b 350.1900 | 400 mg/m2 every 2 weeks | 74 | 2,067 |
Fluorouracil bolus | 50 mg/mL | 100 mL vial | 160.9000 | 400 mg/m2 every 2 weeks | 2 | 47 |
Fluorouracil infusion | 50 mg/mL | 100 mL vial | 160.9000 | 2,400 mg/m2 every 2 weeks | 12 | 324 |
FOLFIRI | — | — | — | — | 212 | 5,934 |
Bevacizumab + FOLFIRI | — | — | — | — | 254 | 7,109 |
Cetuximab + FOLFIRI | — | — | — | — | 472 to 504 | 13,214 to 14,124 |
Pembrolizumab | ||||||
Pembrolizumab (Keytruda) | 100 mg vial | 100 mg / 4 mL IV solution | 4,400.0000c | 2 mg/kg (max 200 mg) on Day 1 every 3 weeksd | 295 | 8,272 |
CDA-AMC = Canada’s Drug Agency; FOLFIRI = leucovorin calcium (folinic acid), fluorouracil, irinotecan hydrochloride; FOLFOX = leucovorin calcium (folinic acid), fluorouracil, oxaliplatin.
Note: All prices are from the Delta IQVIA database (accessed April 2025),1 unless otherwise indicated, and do not include dispensing fees. Recommended dosage is based on Cancer Care Ontario monographs, unless otherwise indicated. For dosing that depends on weight or body surface area, CDA-AMC assumed 70.5 kg or 1.8 m2 that was validated by clinical expert feedback. Total cost estimates per regimen are based on the least costly combination of the component drugs, with wastage considered for single-use vials.
aWhen initiation and maintenance dosages differ, cost is based on the maintenance dose, unless otherwise stated. Costs for 21-day treatment regimens have been prorated to a 28-day period.
bAlberta Health Care Insurance Plan.2
cCADTH review of pembrolizumab.3
dDespite a fixed-dosing in the product monograph, Cancer Care Ontario Drug Formulary references a weight-based dosing (confirmed by clinical experts and drug plans feedback as the current practice across jurisdictions) and does not include wastage.4
Appendix 2: Input Relevant to the Economic Review
Please note that this appendix has not been copy-edited.
This section is a summary of the input received from the patient groups, clinician groups, and drug plans that participated in the CDA-AMC review process.
Patient input was provided by the Colorectal Cancer Resource and Action Network in collaboration with the Canadian Cancer Survivor Network, with data gathered through interviews, surveys, and outreach to both people living in Canada and international patients with metastatic MSI-H or dMMR colorectal cancer. Among those who responded, several patients living in Canada were included, although access to nivolumab plus ipilimumab in Canada was limited, prompting reliance on clinical trials, special access programs, or out-of-country treatment. Patients reported significant challenges with current treatment options, primarily chemotherapy regimens such as leucovorin calcium (folinic acid), fluorouracil, oxaliplatin (FOLFOX) and leucovorin calcium (folinic acid), fluorouracil, irinotecan hydrochloride (FOLFIRI), which often failed to control disease progression and came with severe side effects that diminished quality of life. Patients identified a clear unmet need for more effective and better-tolerated therapies. Several patients with direct experience using nivolumab plus ipilimumab shared overwhelmingly positive outcomes, including durable complete responses, significant symptom relief, improved quality of life, and the ability to resume normal daily activities, often contrasting this experience favourably with chemotherapy. Some patients strongly advocated for public reimbursement to improve equitable access in Canada.
Clinician group input was received from the Canadian Gastrointestinal Oncology Evidence Network and the Medical Advisory Board of Colorectal Cancer Canada, as well as the Ontario Health (Cancer Care Ontario) Gastrointestinal Drug Advisory Committee. These clinician groups outlined that the current standard of care for dMMR or MSI-H mCRC in Canada is pembrolizumab monotherapy, which has shown significant improvements over chemotherapy in terms of survival and quality of life. However, they noted that up to 30% to 40% of patients do not respond adequately to pembrolizumab, leading to early disease progression. Clinicians identified this as a key treatment gap and expressed strong support for nivolumab plus ipilimumab as a new first-line option. They expect the combination therapy to improve PFS, reduce primary resistance to immunotherapy, and potentially convert some patients to surgical candidates. Importantly, they emphasized the regimen’s potential to become the new standard of care, particularly for patients with more aggressive disease features such as liver metastases, while still recognizing that monotherapy may be preferred in select cases. The introduction of this combination therapy is anticipated to enhance clinical outcomes and broaden treatment personalization within oncology practice.
Input from CDA-AMC–participating drug plans noted that nivolumab plus ipilimumab is familiar in terms of preparation and administration, as both drugs are used in other indications. Microsatellite instability or mismatch repair testing is already established across most jurisdictions, minimizing diagnostic access issues. Most provinces are expected to adopt weight-based dosing protocols similar to current nivolumab regimens. Drug plans raised questions about eligibility criteria — such as whether patients previously treated for metastatic disease or those with an Eastern Cooperative Oncology Group Performance Status score of 2 or higher would qualify — and requested alignment with pembrolizumab criteria for initiation, continuation, and discontinuation. Concerns were also noted around managing treatment if 1 component of the combination must be stopped due to toxicity. There were requests for guidance on re-treatment eligibility and sequencing, especially in relation to pembrolizumab. Given its potential to shift the treatment paradigm, plans support the development of a rapid funding algorithm and emphasize consideration of existing confidential pricing agreements for comparators.
Several of these concerns were addressed in the sponsor’s model:
The model reflected changes in PFS and HRQoL.
CDA-AMC addressed some of these concerns as follows:
CDA-AMC considered a scenario in which weight-based dosing was used for pembrolizumab and nivolumab.
CDA-AMC was unable to address the following concerns:
Issues related to the alignment of eligibility criteria and discontinuation due to toxicity could not be addressed in reanalysis due to the lack of clinical evidence.
Appendix 3: Summary of the Sponsor’s Submission
Please note that this appendix has not been copy-edited.
Summary of the Sponsor’s Economic Evaluation
For the pharmaceutical reviews program, clinical and economic information is submitted to CDA-AMC by the sponsor. The CDA-AMC health economics team reviews the submitted economic information and appraises the information in collaboration with clinical experts and the clinical review team to evaluate key assumptions, influential parameters, and the overall rigour of the economic submission. Based on what the team learns through this process, adjustments may be made to the sponsor’s model to produce the CDA-AMC base case. The CDA-AMC base case represents the team’s current understanding of the clinical condition, clinical evidence currently available, and best interpretation of the economic evidence based on the information provided.
For the review of nivolumab plus ipilimumab, the sponsor provided a cost-utility analysis and a BIA. The sponsor’s economic submission is summarized in Table 5.
Table 5: Key Components of the Sponsor’s Economic Evaluation
Component | Description |
|---|---|
Treatment information | |
Drug under review | Nivolumab (Opdivo) in combination with ipilimumab (Yervoy) |
Submitted price of drug under review | Nivolumab $782.22 per 4 mL vial at 10 mg/mL Ipilimumab $5,800.00 per 10 mL vial at 5 mg/mL |
Regimen | Nivolumab (Opdivo) at a dose of 240 mg given in combination with ipilimumab (Yervoy) at 1mg/kg once every 3 weeks for a total of 4 doses followed by nivolumab at 480 mg every 4 weeks as maintenance therapy |
Per-course cost of drug under review | The per-cycle cost of nivolumab is expected to be $4,693 per patient for the first 4 doses and $9,387 for subsequent doses, the per-cycle cost of ipilimumab is expected to be $11,600a per patient. |
Model information | |
Type of economic evaluation | Cost-utility analysis Markov model |
Treatment | Nivolumab plus ipilimumab |
Included comparator(s) |
|
Perspective | Publicly funded health care payer perspective |
Time horizon | Lifetime (40 years) |
Cycle length | 28 days |
Modelled population | First-line treatment of adult patients with unresectable or metastatic MSI-H or dMMR colorectal cancer |
Characteristics of modelled population | The model is based on the patient characteristics of the locally confirmed ITT population from the CheckMate-8HW trial. Female: 53.8% Age at start: 60.9 years Average weight: 70.5 kg Mean body surface area: 1.8 m2 |
Model health states | Progression-free Progressed disease Death |
Data sources | |
Comparative efficacy | Comparative efficacy is based on time to progression. Time to progression for nivolumab plus ipilimumab, nivolumab monotherapy, and chemotherapy were estimated from the CheckMate-8HW trial data from the September 2024 database lock (DCO: August 28, 2025). A matched adjusted indirect treatment comparison was performed comparing pembrolizumab with first-line nivolumab plus ipilimumab population using aggregate data from KN-177 and individual patient data from the CheckMate-8HW trial.5 |
Natural history and/or clinical pathway |
|
Health-related utilities and disutilities |
|
Costs |
|
Summary of the submitted results | |
Base-case results | Nivolumab plus ipilimumab was associated with an ICER of $16,431 per QALY gained compared to chemotherapy (incremental costs = $102,520; incremental QALYs = 6.24) and strictly dominates pembrolizumab. |
Scenario analysis resultsb | Time horizon 5 years ($120,625 per QALY gained compared to chemotherapy) Time horizon 10 years ($43,324 per QALY gained compared to chemotherapy) Societal perspective ($30,196 per QALY gained compared to chemotherapy) |
AE = adverse event; CDA-AMC = Canada’s Drug Agency; CIHI = Canadian Institute of Health Information; dMMR = deficient mismatch repair; DCO = data cut-off; FOLFIRI = leucovorin calcium (folinic acid), fluorouracil, irinotecan hydrochloride; ICER = incremental cost-effectiveness ratio; ITT = intention to treat; mFOLFOX = modified leucovorin calcium (folinic acid), fluorouracil, oxaliplatin; MSI-H = microsatellite instability-high; QALY = quality-adjusted life-years.
Note: Nivolumab plus ipilimumab = $16,293 per patient per cycle for the first 4 cycles.
aThe average patient weight of 70.5 kg was used to determine the use of 2 vials for costing ipilimumab.
bResults of scenario analyses that had a meaningful impact on the estimated ICER compared to the sponsor’s base case. Additional scenarios were submitted that had no meaningful impact on the estimated ICER included discount rate; unadjusted anchored and adjusted anchored indirect comparisons; constant hazard ratio; utilities; treatment duration; wastage; dosing strategy; and progression free to death transition.
Model Structure
The sponsor developed a semi-Markov cohort model with 3 states: progression-free, progressed disease, and death (Figure 4). Patients begin in the progression-free state and can transition to progressed disease, transition to death, or remain progression-free. Once a patient has progressed, they can transition to death or remain progressed. Death is the absorbing state. All transition probabilities in the model are time varying. For example, the transition probability from progressed disease to death and the probability of remaining in progressed disease depend on the time spent in the progressed disease state. Transitions from progression-free to progressed disease are treatment specific. For nivolumab plus ipilimumab and chemotherapy, these are based on the individual patient data from the CheckMate-8HW trial. For pembrolizumab, this transition is based on a matched ITC using data from the CheckMate-8HW trial and the KEYNOTE-177 trial. Time to progression was extrapolated beyond the observed period of CheckMate-8HW based on different parametric distributions (Figure 5). The chosen distribution is based on the fit of the distribution which relies on 42.05 months of median follow-up and is extrapolated to 39.1 years. The generalized gamma distribution was chosen based on the Akaike and Bayesian information criterion.
The other transitions in the model are not treatment specific. Transitions from progression-free to death are based on background mortality. Transitions from progressed disease to death are based on the CheckMate-142 trial. Adverse events were modelled separately for each treatment and were based on trial data.
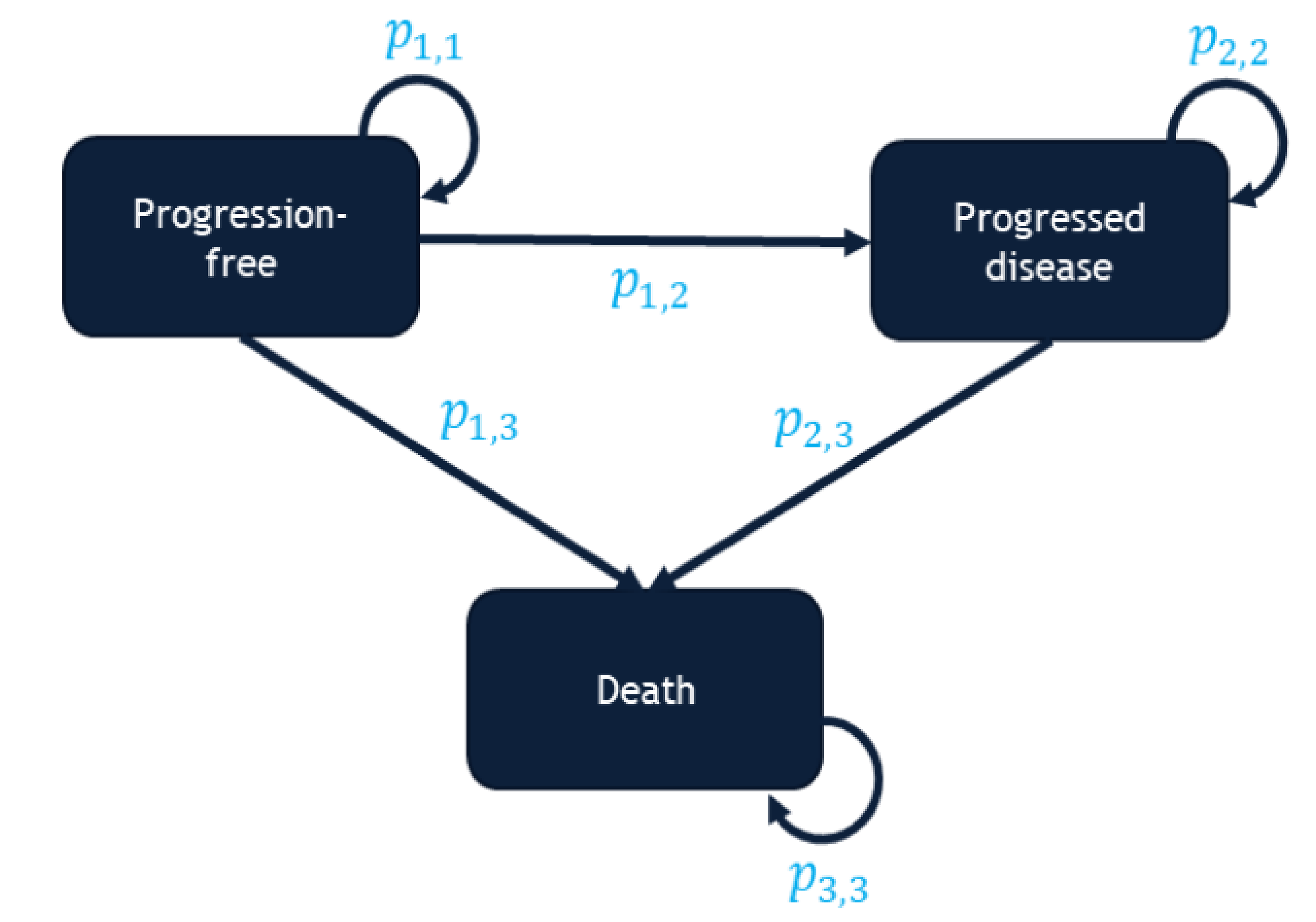
p1,1 = transition probability for remaining in progression-free; p1,2 = transition probability from progression-free to progressed disease; p1,3 = transition probability from progression-free to death; p2,2 = transition probability for remaining in progressed disease; p2,3 = transition probability from progressed disease to death; p3,3 = transition probability for remaining in death.
Source: Sponsor’s pharmacoeconomic submission.11
Figure 5: Parametric Extrapolation of Progression-Free Survival for Patients Treated With Nivolumab Plus Ipilimumab [Redacted]

Table 6: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total costs ($) | Total QALYs | Sequential ICER ($/ QALY) |
|---|---|---|---|
Chemotherapy | 119,132 | 4.37 | Reference |
Nivolumab plus ipilimumab | 221,652 | 10.61 | 16,431 |
Pembrolizumab | 225,824 | 7.54 | Dominated |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Appendix 4: Additional Details of CDA-AMC Reanalyses
Please note that this appendix has not been copy-edited.
Clinical Data in the Economic Model
The CDA-AMC Clinical Review found that, in patients with unresectable or metastatic MSI-H or dMMR colorectal cancer, nivolumab plus ipilimumab improves PFS and patient HRQoL compared with chemotherapy. No statistically significant improvement in overall survival (OS) was found in the CheckMate-8HW trial, but the Clinical Review noted that PFS is correlated with OS in this patient population. Clinical experts consulted by CDA-AMC for this review said they expected OS improvements given the magnitude of the PFS improvement observed in the trial.
For comparisons to pembrolizumab, the sponsor used data from an ITC, which took the form of an unanchored MAIC that estimated a time-varying hazard ratio (HR). The Clinical Review identified limitations with the analysis, including the unanchored nature of the MAIC and the inability to control for all treatment-effect modifiers. Despite these limitations the Clinical Review concluded that nivolumab plus ipilimumab likely improves PFS compared to pembrolizumab.
The economic model used PFS data derived from a different estimate of the effect of nivolumab plus ipilimumab versus pembrolizumab on PFS. In the economic analysis, the sponsor modified the HR used to calculate the transition probabilities from the progression-free to progressed disease states for pembrolizumab using a method described in the literature.12,13 As a result of this modification, the time-varying HR was assumed to be relatively constant and lower than 1.0 over the time horizon of the model, rather than approaching 1.0 over time as it does in the ITC appraised in the Clinical Review. The majority (93%) of incremental QALYs for nivolumab plus ipilimumab versus pembrolizumab were generated through extrapolation beyond the median follow-up of 42.05 months of the CheckMate-8HW trial. Postprogression survival was assumed to be equal for nivolumab plus ipilimumab and pembrolizumab. The probability of death from causes other than colorectal cancer for patients who have not experienced progression was derived from life tables for Canada, which were then mathematically adjusted to reflect the higher rate of background mortality expected among patients in this indicated population.
Key Issues of the Submitted Economic Evaluation
CDA-AMC identified the following key issues with the sponsor’s analysis:
Uncertainty in treatment effectiveness compared to pembrolizumab: In the absence of direct comparative evidence between nivolumab plus ipilimumab and pembrolizumab, the relative probability of experiencing progression in the sponsor’s model was informed by a time-varying HR that was derived from an unanchored MAIC conducted by the sponsor. Results from the anchored MAIC were explored through scenario analysis. In the economic model, the sponsor used a modified estimate of this time-varying HR that was adjusted in an attempt to control for background mortality. The HR in the economic model remains low (lower than 0.5, indicating a strong improvement in PFS) over the full model time horizon. While the 95% confidence interval around the HR remains lower than 1 (i.e., statistically significant relative improvement in PFS) in the economic analysis, it reaches 1.0 (i.e., no relative improvement in PFS) at 27 months in the ITC that was appraised in the CDA-AMC Clinical Review (i.e., the anchored MAIC). The sponsor justified this choice by noting that while the ITC showed the HR moving closer to 1.0 (i.e., no effect) over time, data from the CheckMate-8HW and KEYNOTE-177 trials suggested that this was due to background mortality events, not progression events. This approach taken by the sponsor raises several concerns.
First, this approach raises face validity concerns. The sponsor’s model is based on the implied assumption that nivolumab plus ipilimumab provides a strong and lifelong protective effect compared to pembrolizumab, beyond the maximum duration of treatment (2 years). This assumption is not supported by long-term evidence. It is the result of a statistical analysis that uses parametric survival functions to extrapolate beyond the available trial evidence. The available trial evidence does suggest a protective effect that diminishes over time. Clinical experts consulted by CDA-AMC for this review agreed that the relative effect versus pembrolizumab was not likely to persist indefinitely and would wane over time.
Second, the method chosen by the sponsor assumes that the relative hazard is an additive function, and that the estimated rate of progression can be estimated by statistically removing the effect of background mortality. It is reasonable to assume that progression and background mortality are multiplicative rather than additive functions, as having cancer is likely correlated with an increased risk of death from other causes. The sponsor themselves seems to support this conclusion, given that they use a multiplicative function (a mortality ratio) to reflect an increased risk of death from causes other than colorectal cancer.
Third, the sponsor’s method estimates an HR for PFS with a constant rate of statistical uncertainty over time. In the ITC that was appraised in the Clinical Review, the 95% confidence interval around this HR increased over time, reflecting an increase in the level of uncertainty as the number of observed events decreases. However, in the economic model the uncertainty is fixed over time. This effect is a property of the parametric methods used in the extrapolation. It also artificially restricts the model’s ability to accurately reflect decision uncertainty.
Fourth, the effect of background mortality is not reflected in an internally consistent way. The sponsor justified a fixed relative rate of progression rather than a waning one by suggesting that the apparent waning effect seen in the ITC was due to background mortality. This would suggest a differential rate of background mortality events between the treatment arms in the MAIC (i.e., different rates of noncancer mortality between nivolumab plus ipilimumab and pembrolizumab). However, the sponsor simultaneously assumed an identical rate of background mortality between the 2 treatments in calculating their transition probabilities for noncancer death in patients who had not experienced progression. This was compounded by the fact that the background mortality data used to adjust the HR to estimate progression was not adjusted by the same mortality ratio that was used to estimate background mortality in the model.
Fifth, the sponsor’s model adjusts background mortality in patients with mCRC by a multiplicative factor of 1.59. This increase in background mortality is only applied after the maximum duration of treatment, which is 2 years. The sponsor did not provide justification for not adjusting background mortality before the end of treatment.
The impact that these limitations have on the estimated cost-effectiveness of nivolumab plus ipilimumab compared to pembrolizumab is unknown. However, differential time spent in the progression-free state is the key driver of cost-effectiveness results in the sponsor’s model. The lack of treatment waning means that incremental QALYs are likely overestimated, while incremental costs are likely underestimated.
CDA-AMC introduced a treatment waning effect by setting relative treatment efficacy to be equal after 27 months.
The issues related to multiplicative risk, statistical uncertainty, and variations in the implementation of background mortality could not be addressed in reanalysis.
Terminal care costs: The sponsor includes terminal care costs in the model, recognizing that the final 3 months of life for patients with colorectal cancer often require palliative services not captured under routine care. In the model, patients who die with progressed disease are assigned a terminal care cost of $45,107.61, based on data from an Ontario cohort of patients with colorectal cancer who died from cancer. In contrast, patients who die in the progression-free state are assigned a lower terminal care cost of $9,769.75, based on a broader cohort that includes all deaths in Ontario, regardless of cause. This assumption reduces the overall cost of the nivolumab plus ipilimumab strategy because patients receiving this treatment are more likely to remain in the progression-free state longer and, consequently, more likely to die while still in that state.
A study by de Oliveira et al. estimated that the average end-of-life cost for patients with colorectal cancer was $32,408 in 2009 (equivalent to $46,260 in 2025).14 This estimate does not distinguish between cancer-related and noncancer-related deaths. Comparing this figure to the model’s cancer-specific terminal cost ($45,107.61) suggests that including noncancer deaths may not significantly reduce the average terminal care cost for patients with cancer. Furthermore, clinical experts consulted by CDA-AMC for this review noted that patients with cancer are likely to incur higher terminal care costs than patients without cancer, and that the much lower value used by the sponsor likely underestimates end-of-life costs for patients dying in the progression-free state.
In reanalysis, CDA-AMC assigned the same terminal care cost to patients regardless of whether they died with progressed disease or while progression-free.
Extrapolation uncertainty: The transition from the progression-free to the progressed health state for nivolumab plus ipilimumab was modelled using data from the CheckMate-8HW trial, which had a median follow-up of 42.05 months (approximately 3.5 years). Survival models were selected based on statistical goodness-of-fit criteria, including the Akaike and Bayesian information criterion, and were extrapolated over a 39.1-year time horizon. However, because long-term extrapolations rely heavily on the tail behaviour of the fitted curves — and the observed data only covers a small portion of that time horizon — there is substantial uncertainty around the choice of parametric distribution. The initial fit of the curve may not accurately capture long-term survival trends, leading to uncertainty in the model's long-term projections. Given the lack of long-term evidence and the fact that the majority (77%) of incremental QALYs were estimated through extrapolation, the choice of parametric function may overestimate incremental effectiveness, introducing a bias that favours nivolumab plus ipilimumab.
In reanalysis, CDA-AMC chose a less optimistic distribution (Weibull) for PFS parametric extrapolation. The sponsor’s base-case extrapolation (generalized gamma) was investigated through scenario analysis.
Inappropriate characterization of decision uncertainty: For the relative risk of progression between nivolumab plus ipilimumab versus pembrolizumab, the sponsor’s model assumed that the variation around the HR was plus or minus 20% of the log of the mean HR at all time points. This assumption means that the uncertainty around the transition to progressed disease is only a function of the mean HR and does not change over time even as survival is extrapolated years into the future. This means that the total decision uncertainty related to this key model driver is not only not supported by the observed evidence, but is artificially restricted, making the decision look more certain than may be warranted.
CDA-AMC could not address this issue through reanalysis.
Treatment costs: The sponsor reports monthly costs with wastage, of different treatment regimens in their submission. References to cost inputs, dosing regimens, and treatment durations were also provided. However, these costs differ from those reported in Table 4. The sponsor’s base case also assumed full drug wastage in their base case, which is likely not representative of treatment practice in larger cancer centres. Additionally, the sponsor’s base case assumed that immunotherapies would be provided as flat doses, rather than as weight-based dosing. Input from drug plans suggested that weight-based dosing is preferred.
In reanalysis, CDA-AMC used the cost estimates presented in Table 4, including the use of weight-based dosing and assuming no wastage.
Relative dose intensity: The sponsor’s report states “A dose intensity of 100% was assumed for all comparators”; however, the sponsor’s base case used treatment specific relative dose intensities.
In reanalysis, CDA-AMC changed all relative dose intensities to 100%.
Costs of chemotherapy: The cost of chemotherapy was estimated using a weighted average of multiple chemotherapy regimens. However, the Canadian Guidelines for Economic Evaluation of Health Technologies recommends that when more than 2 interventions are compared, expected costs and outcomes should be calculated separately and sequentially to enable proper incremental analysis.15 Averaging the cost across regimens can obscure important differences in the cost-effectiveness of individual treatments.
CDA-AMC conducted a sensitivity analysis comparing nivolumab plus ipilimumab to each of the most common chemotherapy regimens individually, using regimen-specific cost estimates.
CDA-AMC Base Case of the Economic Evaluation
The CDA-AMC base case was derived by making changes in model parameter values and assumptions, in consultation with clinical experts (refer to Table 7). The impact of these changes, individually and collectively, is presented in Table 8.
Table 7: Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CDA-AMC value or assumption |
|---|---|---|
1. Uncertainty in the time-varying hazard ratios | Time-varying hazard ratios between nivolumab plus ipilimumab and pembrolizumab | Hazard ratio between nivolumab plus ipilimumab and pembrolizumab equal to 1.00 after 27 months |
2. Increased mortality | Increased mortality was initiated after 2 years | Increased mortality from start |
3. Terminal care costs | Terminal care costs differ by whether patients were progressed or progression-free before death | Terminal care costs are the same |
4. Extrapolation uncertainty | Used the generalized gamma distribution | Used the Weibull distribution |
5. Mean relative dose intensity | Relative dose intensity specific to treatments | Relative dose intensity equal to 100% |
6. Treatment costs | Sources from older CDA-AMC reviews | Updated costs from most recent sources (Appendix 1) |
7. Weight-based dosing | Flat dosing for immunotherapy | Weight-based dosing for immunotherapy |
8. Drug wastage | Assume full wastage | Assume no wastage |
CDA-AMC base case (health care payer perspective) | — | Base case 1 + 2 + 3 + 4 + 5 + 6 |
CDA-AMC = Canada’s Drug Agency.
Table 8: Summary of the Stepped Analysis
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALY) |
|---|---|---|---|---|
Sponsor base case | Chemotherapy | 119,347 | 4.26 | Reference |
Pembrolizumab | 226,031 | 7.51 | Dominated | |
Nivolumab plus ipilimumab | 220,688 | 10.65 | 15,853 | |
Uncertainty in time-varying hazard ratios | Chemotherapy | 119,347 | 4.26 | Reference |
Pembrolizumab | 222,669 | 8.32 | Dominated | |
Nivolumab plus ipilimumab | 220,688 | 10.65 | 15,853 | |
Increased mortality | Chemotherapy | 119,080 | 4.20 | Reference |
Pembrolizumab | 225,666 | 6.96 | Dominated | |
Nivolumab plus ipilimumab | 220,459 | 9.57 | 18,882 | |
Terminal care costs | Chemotherapy | 119,976 | 4.26 | Reference |
Pembrolizumab | 232,278 | 7.51 | Extendedly dominated | |
Nivolumab plus ipilimumab | 233,103 | 10.65 | 17,697 | |
Extrapolation uncertainty (Weibull) | Chemotherapy | 119,347 | 4.26 | Reference |
Pembrolizumab | 232,531 | 5.94 | Dominated | |
Nivolumab plus ipilimumab | 229,593 | 8.78 | 24,382 | |
Mean relative dose intensity | Chemotherapy | 129,651 | 4.26 | Reference |
Pembrolizumab | 235,681 | 7.51 | Dominated | |
Nivolumab plus ipilimumab | 230,005 | 10.65 | 15,699 | |
Treatment costs | Chemotherapy | 97,421 | 4.26 | Reference |
Pembrolizumab | 224,621 | 7.51 | Dominated | |
Nivolumab plus ipilimumab | 220,021 | 10.65 | 19,179 | |
Weight-based dosing | Chemotherapy | 119,347 | 4.26 | Reference |
Pembrolizumab | 204,300 | 7.51 | Extendedly dominated | |
Nivolumab plus ipilimumab | 209,444 | 10.65 | 14,094 | |
Drug wastage | Chemotherapy | 113,842 | 4.26 | Reference |
Pembrolizumab | 211,789 | 7.51 | Dominated | |
Nivolumab plus ipilimumab | 211,162 | 10.65 | 15,224 | |
CDA-AMC base case 1 + 2 + 3 + 4 + 5 + 6 + 7 + 8 (deterministic) | Chemotherapy | 99,199 | 4.20 | Reference |
Pembrolizumab | 176,618 | 6.77 | Extendedly dominated | |
Nivolumab plus ipilimumab | 216,695 | 8.18 | 29,531 | |
CDA-AMC base case 1 + 2 + 3 + 4 + 5 + 6 (probabilistic) | Chemotherapy | 99,031 | 4.31 | Reference |
Pembrolizumab | 177,118 | 6.79 | Extendedly dominated | |
Nivolumab plus ipilimumab | 217,081 | 8.18 | 30,522 |
CDA-AMC = Canada’s Drug Agency; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-years.
Note: The CDA-AMC base case is based on the publicly available prices of the comparator treatments.
Table 9: Disaggregated Results of the CDA-AMC Base Case
Parameter | Nivolumab plus ipilimumab | Pembrolizumab | Chemotherapy |
|---|---|---|---|
Discounted LYs | |||
Total | 10.08 | 8.37 | 5.27 |
Progression free | 7.47 | 5.37 | 1.53 |
Progressed disease | 2.61 | 3.00 | 3.74 |
Discounted QALYs | |||
Total | 8.18 | 6.77 | 4.20 |
Progression free | 6.10 | 4.38 | 1.23 |
Progressed disease | 2.09 | 2.39 | 2.97 |
Discounted costs ($) | |||
Total | 200,683 | 176,613 | 99,199 |
Drug acquisition | 144,103 | 118,680 | 34,571 |
Administration | 6,331 | 4,711 | 4,218 |
Adverse events | 2,064 | 2,297 | 5,437 |
Resource use | 8,781 | 8,895 | 9,225 |
Subsequent treatment | 1,271 | 2,686 | 4,216 |
Terminal care | 38,133 | 39,342 | 41,532 |
CDA-AMC = Canada’s Drug Agency; LY = life-year; QALY = quality-adjusted life-year.
CDA-AMC conducted price reduction analyses using the sponsor’s base case and the CDA-AMC base case (Table 10).
Table 10: Price Reduction Analysis
Price reduction | Unit drug cost ($) | Cost per 28 days ($)a | ICERs for nivolumab plus ipilimumab vs. pembrolizumab and chemotherapy ($/QALY) | |
|---|---|---|---|---|
Sponsor base case | CDA-AMC base case | |||
No price reduction | Nivolumab: $782 per 4 mL vial at 10 mg/mL Ipilimumab: $5,800 per 10 mL vial at 5 mg/mLb | Nivolumab: $4,693 for the first 4 doses and $9,387 for subsequent doses Ipilimumab: $11,600 | 16,431 compared to chemotherapy | 30,522 compared to chemotherapy |
10% | Nivolumab: $704 per 4 mL vial at 10 mg/mL Ipilimumab: $5,220 per 10 mL vial at 5 mg/mL | Nivolumab: $4,224 for the first 4 doses and $8,448 for subsequent doses Ipilimumab: $10,440 | 13,047 compared to chemotherapy | 26,367 compared to chemotherapy |
20% | Nivolumab: $626 per 4 mL vial at 10 mg/mL Ipilimumab: $4,640 per 10 mL vial at 5 mg/mL | Nivolumab: $3,754 for the first 4 doses and $7,510 for subsequent doses Ipilimumab: $9,280 | 10,242 compared to chemotherapy | 22,229 compared to chemotherapy |
30% | Nivolumab: $548 per 4 mL vial at 10 mg/mL Ipilimumab: $4,060 per 10 mL vial at 5 mg/mL | Nivolumab: $3,285 for the first 4 doses and $6,571 for subsequent doses Ipilimumab: $8,120 | 7,436 compared to chemotherapy | 18,092 compared to chemotherapy |
40% | Nivolumab: $469 per 4 mL vial at 10 mg/mL Ipilimumab: $3,480 per 10 mL vial at 5 mg/mL | Nivolumab: $2,816 for the first 4 doses and $5,632 for subsequent doses Ipilimumab: $6,960 | 4,630 compared to chemotherapy | 13,955 compared to chemotherapy |
50% | Nivolumab: $391 per 4 mL vial at 10 mg/mL Ipilimumab: $2,900 per 10 mL vial at 5 mg/mL | Nivolumab: $2,347 for the first 4 doses and $4,694 for subsequent doses Ipilimumab: $5,800 | 1,824 compared to chemotherapy | 9,818 compared to chemotherapy |
60% | Nivolumab: $313 per 4 mL vial at 10 mg/mL Ipilimumab: $2,320 per 10 mL vial at 5 mg/mL | Nivolumab: $1,877 for the first 4 doses and $3,755 for subsequent doses Ipilimumab: $4,640 | Dominant | 5,681 compared to chemotherapy |
70% | Nivolumab: $235 per 4 mL vial at 10 mg/mL Ipilimumab: $1,740 per 10 mL vial at 5 mg/mL | Nivolumab: $1,408 for the first 4 doses and $2,816 for subsequent doses Ipilimumab: $3,480 | Dominant | 1,543 compared to chemotherapy |
80% | Nivolumab: $156 per 4 mL vial at 10 mg/mL Ipilimumab: $1,160 per 10 mL vial at 5 mg/mL | Nivolumab: $939 for the first 4 doses and $1,877 for subsequent doses Ipilimumab: $2,320 | Dominant | Dominant |
CDA-AMC = Canada’s Drug Agency; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; vs. = versus.
aThe cost of ipilimumab in this column assumes the use of 2 vials.
bSponsor’s submitted price for nivolumab plus ipilimumab.
Assessment of Uncertainty
CDA-AMC conducted scenario analyses to address uncertainty around the cost of chemotherapy within the economic evaluation, using the CDA-AMC base case. The model’s results were robust to all prices tested in these scenario analyses.
Appendix 5: Budget Impact Analysis
Please note that this appendix has not been copy-edited.
Summary of the Submitted BIA
The sponsor submitted a BIA that estimated the expected incremental budgetary impact of reimbursing nivolumab plus ipilimumab for the first-line treatment of adult patients with unresectable or metastatic MSI-H or dMMR colorectal cancer.
The BIA was conducted from the perspective of public drug plan payers over a 3-year time horizon (2026 to 2028), with 2025 as the base year. The sponsor’s estimate reflects the aggregated results from the jurisdictional provincial budgets (excluding Quebec as well as the Non-Insured Health Benefits Program). The sponsor estimated the eligible population using an epidemiological approach. The sponsor’s base case included drug acquisition and subsequent therapy costs. The market uptake for nivolumab plus ipilimumab was estimated using internal sponsor estimates. The sponsor assumed the reimbursement of nivolumab plus ipilimumab would only capture market shares from pembrolizumab. The key inputs to the BIA are documented in Table 11.
The sponsor estimated the 3-year incremental budget impact associated with reimbursing nivolumab plus ipilimumab for the first-line treatment of adult patients with unresectable or metastatic MSI-H or dMMR colorectal cancer would be $78,826 (year 1 = cost savings of $1,222,080; year 2 = $588,881; year 3 = $712,026).
Table 11: Key Model Parameters
Parameter | Sponsor’s estimate (reported as year 1 / year 2 / year 3 if appropriate) |
|---|---|
Target population | |
Incidence of colorectal cancer per 100,000 | 53.516 |
% change in incidence rate | −3.5%17 |
% stage I at diagnosis | 20.2%18 |
% stage II at diagnosis | 27.1%18 |
% stage III at diagnosis | 29.7%18 |
% stage IV at diagnosis | 23%18 |
% tested for MSI or dMMR | 100%19 |
% positive for MSI-H or dMMR with stage I | 20%20 |
% positive for MSI-H or dMMR with stage II | 20%20 |
% positive for MSI-H or dMMR with stage III | 10%20 |
% positive for MSI-H or dMMR with stage IV | 5%20 |
% of patients who progress to metastatic disease with stage I | 0%20 |
% of patients who progress to metastatic disease with stage II | 4%20 |
% of patients who progress to metastatic disease with stage III | 42%20 |
% receiving first-line treatment | 85%20 |
Number of patients eligible for drug under review | 381 / 372 / 363 |
Market shares (reference scenario) | |
Nivolumab + ipilimumab | 0% / 0% / 0% |
Pembrolizumab | 94% / 94% / 94% |
Chemotherapy | 6% / 6% / 6% |
Market shares (new drug scenario) | |
Nivolumab + ipilimumab | ███ █ ███ █ ███ |
Pembrolizumab | ███ █ ███ █ ███ |
Chemotherapy | 6% / 6% / 6% |
Cost of treatment (per patient per 28-day course) | |
Nivolumab + ipilimumab | $22,687a |
Pembrolizumab | $12,117 |
Chemotherapy | $9,240b |
dMMR = deficient DNA mismatch repair; FOLFIRI = leucovorin calcium (folinic acid), fluorouracil, irinotecan hydrochloride; mFOLFOX = modified leucovorin calcium (folinic acid), fluorouracil, oxaliplatin; MSI = microsatellite instability; MSI-H = microsatellite instability-high.
aInitiation costs. Maintenance cost is $9,694 per patient per 28-day course for up to 2 years.
bWeighted cost including mFOLFOX6, mFOLFOX6 + bevacizumab, mFOLFOX6 + cetuximab, FOLFIRI, FOLFIRI + bevacizumab, and FOLFIRI + cetuximab.
Key Issues of the Submitted BIA
CDA-AMC identified several key issues to the sponsor’s analysis that have notable implications on the results of the BIA:
The total number of eligible patients is uncertain. The sponsor derived, through an epidemiologic approach, that approximately 392 patients would be eligible for treatment with nivolumab plus ipilimumab at baseline, with a decrease in the total eligible patients to 363 over 3 years (in terms of incidence). Clinical expert feedback obtained by CDA-AMC noted that while the epidemiologic method was used to determine the incidence of patients eligible for treatment, the final value did not align with their expectations and may be underestimated. The clinical experts noted that this could be due to the underestimation of the percentage of patients that are treated with first-line therapy. When inquired, the clinical experts noted that the total number of patients eligible for treatment with nivolumab plus ipilimumab better aligns with clinical expectations when 100% of patients are assumed to receive first-line treatment (as opposed to 85%). By assuming a lower percentage, the total number of eligible patients is underestimated and in turn, underestimates the total budget impact.
In the absence of evidence to support the total percentage of patients eligible for first-line treatment, CDA-AMC undertook a scenario analysis to estimate the impact of 100% of patients receiving first-line treatment.
Use of relative drug intensity (RDI) to estimate actual drug costs is inappropriate. The sponsor’s base-case analysis incorporated relative dose intensities for nivolumab plus ipilimumab and the other comparators using data from the CheckMate-8HW trial. The consideration of RDI is problematic as this parameter can be influenced by several factors. The dose received by a patient may differ from the full planned dose of the drug due to dose delays, missed doses, dose reductions to manage toxicity, or subsequent dose re-escalation; each of these have differing impacts on drug costs.
In the CDA-AMC reanalysis, 100% RDI was adopted for nivolumab plus ipilimumab, pembrolizumab, and chemotherapies (weighted basket of modified leucovorin calcium [folinic acid], fluorouracil, oxaliplatin [mFOLFOX6], mFOLFOX6 plus bevacizumab, mFOLFOX6 plus cetuximab, leucovorin calcium [folinic acid], fluorouracil, irinotecan hydrochloride [FOLFIRI], FOLFIRI plus bevacizumab, and FOLFIRI plus cetuximab).
Weight-based dosing for nivolumab plus ipilimumab and pembrolizumab. In the sponsor’s base-case analysis, flat dosing was used to model the budgetary impact of reimbursing nivolumab plus ipilimumab. Participating public drug plan input received by CDA-AMC indicates that a weight-based dosage will likely be implemented for pembrolizumab (2 mg/kg [up to 200 mg] every 3 weeks or 4 mg/kg [up to 400 mg] every 6 weeks), nivolumab (3 mg/kg every 3 weeks [up to 240 mg] for first 4 cycles, then 3 mg/kg every 2 weeks [up to 240 mg] or 6 mg/kg every 4 weeks [up to 480 mg]), and ipilimumab (1 mg/kg every 3 weeks for the first 4 cycles).
In a scenario analysis, weight-based dosing for pembrolizumab, nivolumab, and ipilimumab was adopted.
The price of drugs paid by public drug plans is uncertain. Analyses by both the sponsor and CDA-AMC are based on publicly available list prices for all comparators. The actual costs paid by public drug plans are unknown.
CDA-AMC was unable to address this limitation.
Additional issues were identified but were not considered to be key issues. These issues include incorrect comparator pricing for bevacizumab and oxaliplatin.
CDA-AMC Reanalyses of the BIA
CDA-AMC revised the sponsor’s submitted analyses by making changes in model parameter values and assumptions, in consultation with clinical experts, as outlined in Table 11 and Table 12.
Table 12: Revisions to the Submitted BIA
Stepped analysis | Sponsor’s value or assumption | CDA-AMC value or assumption |
|---|---|---|
1. Comparator pricing | Bevacizumab 100 mg/mL: $347.00 Oxaliplatin 50mg/mL: $36.27 | Bevacizumab 100 mg/mL: $146.93 Oxaliplatin 50mg/mL: $45.00 |
2. RDI | < 100% (varied by drug) | 100% for all drugs |
CDA-AMC base case | — | Reanalysis 1 + 2 |
BIA = budget impact analysis; CDA-AMC = Canada’s Drug Agency; RDI = relative drug intensity.
The results of the CDA-AMC stepwise reanalysis are presented in summary format in Table 13 and a more detailed breakdown is presented in Table 14. In the CDA-AMC base case, the 3-year budgetary savings of reimbursing nivolumab plus ipilimumab for first-line treatment of adult patients with unresectable or metastatic MSI-H or dMMR mCRC was $235,994 (year 1 = $1,388,990 [incremental savings]; year 2 = $518,014 [incremental cost]; year 3 = $634,982 [incremental cost]).
Table 13: Summary of the Stepped Analysis of the CDA-AMC Base Case
Stepped analysis | Three-year total ($) |
|---|---|
Submitted base case | 78,826 |
CDA-AMC reanalysis 1 | 117,257 |
CDA-AMC reanalysis 2 | −277,664 |
CDA-AMC base case: reanalysis 1 + 2 | −235,994 |
CDA-AMC = Canada’s Drug Agency.
Note: The CDA-AMC reanalysis is based on publicly available prices of the comparator treatments
CDA-AMC used the CDA-AMC base case to conduct scenario analyses to explore uncertainty in the estimated budget impact of reimbursing nivolumab plus ipilimumab. The results are provided in Table 14.
100% of patients are eligible for first-line treatment.
Removal of subsequent therapy costs.
Weight-based dosing for pembrolizumab, and nivolumab plus ipilimumab.
Table 14: Disaggregated Summary of the BIA
Stepped analysis | Scenario | Year 0 (current situation) ($) | Year 1 ($) | Year 2 ($) | Year 3 ($) | Three-year total ($) |
|---|---|---|---|---|---|---|
Submitted base case | Reference total | 55,005,493 | 53,499,329 | 60,930,306 | 59,544,840 | 173,974,476 |
Nivolumab + ipilimumab | 0 | 0 | 0 | 0 | 0 | |
All other comparators | 55,005,493 | 53,499,329 | 60,930,306 | 59,544,840 | 173,974,476 | |
New drug total | 55,005,493 | 52,277,249 | 61,519,187 | 60,256,866 | 174,053,302 | |
Nivolumab + ipilimumab | 0 | 27,446,809 | 38,444,850 | 43,532,568 | 109,424,227 | |
All other comparators | 55,005,493 | 24,830,440 | 23,074,337 | 16,724,298 | 64,629,075 | |
Budget Impact | 0 | −1,222,080 | 588,881 | 712,026 | 78,826 | |
CDA-AMC base case | Reference total | 57,906,872 | 56,321,263 | 63,975,917 | 62,521,619 | 182,818,800 |
Nivolumab + ipilimumab | 0 | 0 | 0 | 0 | 0 | |
All other comparators | 57,906,872 | 56,321,263 | 63,975,917 | 62,521,619 | 182,818,800 | |
New drug total | 57,906,872 | 54,932,273 | 64,493,931 | 63,156,602 | 182,582,805 | |
Nivolumab + ipilimumab | 0 | 28,788,788 | 40,274,403 | 45,603,256 | 114,666,447 | |
All other comparators | 57,906,872 | 26,143,485 | 24,219,528 | 17,553,346 | 67,916,359 | |
Budget Impact | 0 | −1,388,990 | 518,014 | 634,982 | −235,994 | |
CDA-AMC scenario analyses | ||||||
Scenario 1: 100% patients eligible for first-line treatment | Reference total | 68,125,732 | 66,260,309 | 75,265,785 | 73,554,846 | 215,080,941 |
New drug total | 68,125,732 | 64,626,203 | 75,875,213 | 74,301,885 | 214,803,300 | |
Budget Impact | 0 | −1,634,106 | 609,428 | 747,038 | −277,640 | |
Scenario 2: Removal of subsequent therapy costs | Reference total | 57,741,083 | 56,160,013 | 59,876,690 | 58,525,392 | 174,562,095 |
New drug total | 57,741,083 | 54,771,023 | 60,779,362 | 59,603,497 | 175,153,883 | |
Budget Impact | 0 | −1,388,990 | 902,672 | 1,078,106 | 591,788 | |
Scenario 3: Weight-based dosing for pembrolizumab, and nivolumab + ipilimumab | Reference total | 50,855,197 | 49,462,677 | 56,648,673 | 55,359,776 | 161,471,125 |
New drug total | 50,855,197 | 50,296,746 | 59,636,722 | 58,779,021 | 168,712,488 | |
Budget Impact | 0 | 834,069 | 2,988,049 | 3,419,245 | 7,241,363 | |
BIA = budget impact analysis; CDA-AMC = Canada’s Drug Agency.
Note: The CDA-AMC reanalysis is based on the publicly available prices of the comparator treatments.
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.