Drugs, Health Technologies, Health Systems
Reimbursement Review
Amivantamab (Rybrevant)
Sponsor: Janssen Inc.
Therapeutic area: Locally advanced or metastatic non–small cell lung cancer with EGFR exon 19 deletions or exon 21 L858R substitution mutations
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Clinical Review
Abbreviations
ACP
amivantamab plus carboplatin and pemetrexed
ACP-L
amivantamab plus carboplatin and pemetrexed plus lazertinib
AE
adverse event
AESI
adverse event of special interest
AUC 5
area under the concentration-time curve 5 mg/mL per minute
BICR
blinded independent central review
CCO
clinical cut-off
CCSN
Canadian Cancer Survivor Network
CDA-AMC
Canada’s Drug Agency
CI
confidence interval
CP
carboplatin and pemetrexed
CR
complete response
DAEI
dermatologic adverse event of interest
DCO
data cut-off
DOR
duration of response
ECOG
Eastern Cooperative Oncology Group
EORTC QLQ-C30
European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30
GRADE
Grading of Recommendations Assessment, Development and Evaluation
HR
hazard ratio
HRQoL
health-related quality of life
IA1
interim analysis 1
IA2
interim analysis 2
IRR
infusion-related reaction
LACP
lazertinib plus amivantamab plus carboplatin and pemetrexed
LCC
Lung Cancer Canada
LCC MAC
Lung Cancer Canada Medical Advisory Committee
LHF
Lung Health Foundation
MedDRA
Medical Dictionary for Regulatory Activities
MET
mesenchymal epithelial transition
MID
minimal important difference
NE
not estimable
NGS
next-generation sequencing
NOC
Notice of Compliance
NSCLC
non–small cell lung cancer
NSCLC-SAQ
Non–Small Cell Lung Cancer Symptom Assessment Questionnaire
OH (CCO)
Ontario Health (Cancer Care Ontario)
OR
odds ratio
ORR
objective response rate
OS
overall survival
PBC
platinum-based chemotherapy
PFS
progression-free survival
PR
partial response
PRO
patient-reported outcome
RCT
randomized controlled trial
RECIST
Response Evaluation Criteria in Solid Tumours
SAE
serious adverse event
SOC
standard of care
TEAE
treatment-related adverse event
TKI
tyrosine kinase inhibitor
TTSP
time to symptomatic progression
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Table 1: Background Information of Application Submitted for Review
Item | Description |
|---|---|
Drug product | Amivantamab (Rybrevant), 350 mg/7 mL (50 mg/mL) single-use vial for IV infusion |
Sponsor | Janssen Inc. |
Indication | In combination with carboplatin and pemetrexed for the treatment of patients with locally advanced (not amenable to curative therapy) or metastatic NSCLC with EGFR exon 19 deletions or exon 21 L858R substitution mutations, whose disease has progressed on or after treatment with osimertinib |
Reimbursement request | As per proposed indication |
Health Canada approval status | Approved |
Health Canada review pathway | Standard |
NOC date | January 13, 2025 |
Recommended dose |
|
AUC 5 = area under the concentration-time curve 5 mg/mL per minute; NOC = notice of compliance; NSCLC = non–small cell lung cancer.
Introduction
Lung cancer is the most commonly diagnosed cancer and leading cause of cancer death in Canada. An estimated 32,100 new cases of lung cancer were expected in Canada in 2024 and 20,700 deaths from lung cancer were expected in Canada in the same year. The overall 5-year survival rate for lung cancer in Canada is 22%; 5-year survival rates for lung cancer are 16% for those diagnosed at stage III and 3% for those diagnosed at stage IV.
The 2 main types of lung cancer are small cell lung cancer and non–small cell lung cancer (NSCLC). NSCLC accounts for approximately 88% of new lung cancer cases in Canada. A key mechanism of NSCLC involves driver mutations, which activate progrowth signalling pathways. The most common driver mutations in NSCLC lead to the activation of EGFR, and are found more frequently in patients with adenocarcinomas, nonsmokers, patients of Asian ethnicity, and females. EGFR mutations are present in approximately 15% of NSCLC cases, primarily of the nonsquamous histology per clinical expert input. A study characterizing EGFR mutations in patients with metastatic NSCLC in Canada found that among the 15% of patients with EGFR-mutated disease, exon 19 deletions and exon 21 L858R mutations accounted for 49% and 35%, respectively, of these cases.
Diagnosis of NSCLC involves imaging tests such as CT, PET-CT, and MRI to detect the presence of a tumour and its spread. Biopsy is performed to confirm the diagnosis and determine the specific type of cancer. For patients with newly diagnosed nonsquamous NSCLC, comprehensive tissue-based biomarker testing using next-generation sequencing (NGS) is standard of care (SOC) in Canada to identify actionable driver mutations that have a prognostic and predictive impact.
Patients with NSCLC, especially those with late-stage or progressive disease or receiving later lines of treatment, have reduced health-related quality of life (HRQoL) marked by impairments in emotional functioning (e.g., anxiety, depression) and physical functioning. Symptoms may include cough, fatigue, shortness of breath, difficulty remembering or focusing, chest pain, and pain in areas other than the chest.
Canada’s Drug Agency (CDA-AMC) has previously reviewed amivantamab for the following indications: for the treatment of adult patients with locally advanced or metastatic NSCLC with activating EGFR exon 20 insertion mutations whose disease has progressed on or after platinum-based chemotherapy (PBC), and in combination with carboplatin and pemetrexed (CP) for the first-line treatment of adult patients with locally advanced (not amenable to curative therapy) or metastatic NSCLC with activating EGFR exon 20 insertion mutations. Both were issued a recommendation by the pan-Canadian Oncology Drug Review Expert Review Committee (pERC) to reimburse with clinical criteria and/or conditions. Combination therapy with lazertinib and amivantamab is currently under review by CDA-AMC for the first-line treatment of adult patients with locally advanced (not amenable to curative therapy) or metastatic NSCLC with EGFR exon 19 deletions or exon 21 L858R substitution mutations.
Perspectives of Patients, Clinicians, and Drug Programs
The information in this section is a summary of input provided by the patient and clinician groups who responded to the call from CDA-AMC for input and from clinical expert(s) consulted by CDA-AMC for the purpose of this review.
Patient Input
A joint patient group submission was received from Lung Cancer Canada (LCC), the Canadian Cancer Survivor Network (CCSN), and the Lung Health Foundation (LHF). Information provided in this submission consisted of thoughts and experiences of patients with NSCLC and their caregivers, collected through virtual interviews, or was taken by the patient groups from previous submissions to CDA-AMC. Contributions from 5 patients located in Canada diagnosed with stage III or IV NSCLC were included in the patient group submission, including input from 2 patients with direct experience in the MARIPOSA-2 trial and 3 other patients with experience in other trials involving amivantamab or who received amivantamab via the sponsor’s compassionate access program.
Input from 2 patients described symptoms preceding diagnosis of NSCLC, including back pain, shortness of breath, and cough. Respondents’ experiences with osimertinib before receiving amivantamab varied, ranging from no side effects and good quality of life to side effects that limited day-to-day life. Upon disease progression with this osimertinib, symptoms reported by respondents included significant pain and respiratory and mobility symptoms.
The patient group submission identified an unmet need for additional treatment options for patients who have progressed on osimertinib that successfully treat their disease and delay further progression, and allow for good quality of life and for patients to make future plans for working, enjoying retirement, and spending time with loved ones. Outcomes of importance of treatment identified by patients included improved management of NSCLC-related symptoms, delaying disease progression and potentially shrinking tumours, maintaining full and worthwhile quality of life, prolonging life, allowing patients to maintain independence and ability to function to minimize caregiver burden, and having manageable side effects.
Regarding their experience with amivantamab, respondents described it as being successful in treating their disease while being durable. Input from 3 of the patients reported significant side effects upon starting treatment with amivantamab but noted that these ultimately improved with dose reductions and prescription medications. Side effects described by patients included mouth ulcers, loss of taste, constipation, skin issues, paronychia, ingrown toenails and infections around toenails, blood clots, tingling or numbness in fingers and toes, edema, tinnitus, dizziness, and weakness. Patients who were enrolled in the MARIPOSA-2 trial commented that, while on amivantamab treatment, they were able to return to having good quality of life, enjoying their hobbies, being active, and spending time with loved ones. Another patient reported terminating treatment with amivantamab due to the impact on energy levels and quality of life. Most respondents agreed that they would strongly prefer their experience on amivantamab over previous therapies. Some patients noted that injectable treatments requiring long infusion times in the hospital were less convenient than oral targeted therapies that can be taken at home.
Clinician Input
Input From Clinical Experts Consulted for This Review
Clinical experts consulted for this review noted that there is currently no well-established, evidence-based, second-line SOC for patients with EGFR-mutated NSCLC who experience disease progression on osimertinib. In practice, treatment decisions are often guided by extrapolation from first-line data, expert consensus, or access to PBC (typically CP). In certain cases of oligoprogression, local therapies, such as stereotactic radiotherapy, may allow continuation of osimertinib; however, these approaches are not always feasible, particularly for patients in rural settings or those lacking access to specialized testing or care.
The experts emphasized a high unmet need for therapies that can address known resistance mechanisms (e.g., mesenchymal epithelial transition [MET] amplification, small cell transformation), extend survival, and maintain quality of life. They noted that many patients are clinically stable at the time of progression, underscoring the importance of effective but tolerable treatment options in this setting.
The experts identified the combination of amivantamab plus carboplatin and pemetrexed (ACP) as an appropriate second-line treatment for patients with EGFR-mutated NSCLC following progression on osimertinib. This regimen is expected to become the new SOC for patients eligible for systemic chemotherapy, based on its demonstrated efficacy and targeted mechanism of action.
According to the clinical experts, the most appropriate candidates for amivantamab plus chemotherapy are adult patients with EGFR exon 19 deletions or exon 21 L858R substitution mutations whose disease has progressed on or after osimertinib and who are fit to receive systemic chemotherapy. Important factors to consider include Eastern Cooperative Oncology Group (ECOG) Performance Status score and the ability to tolerate corticosteroid-based premedications used to manage infusion-related reactions (IRRs). In cases of suspected histological transformation (e.g., to small cell histology), repeat biopsy was recommended. Patients unable to tolerate premedications or chemotherapy-related toxicities may be less suitable for this regimen. EGFR mutation testing is standardized in Canada, and no additional companion diagnostic was deemed necessary.
Response to treatment is typically assessed through symptom improvement (e.g., dyspnea, fatigue, cough), radiographic imaging, and functional status. The experts considered tumour shrinkage or disease stability on imaging, alongside clinical benefit, as indicative of a meaningful response. Imaging every 3 months was noted to be common practice, and meaningful response may vary by patient but generally includes symptom control and preserved quality of life.
Treatment discontinuation should occur upon confirmed clinical or radiographic disease progression. However, the experts advised that imaging alone may not always justify discontinuation, particularly if patients are experiencing ongoing clinical benefit (e.g., symptom improvement, functional stability). Continuation of treatment in such cases may be considered until progression is confirmed or functional decline occurs. Discontinuation should also be considered in the case of nonreversible grade 3 or higher toxicities. If a patient cannot tolerate 1 component of the regimen but continues to receive benefit, the remaining components may be continued at the discretion of the treating physician.
The clinical experts noted that the regimen is typically administered in an outpatient setting by clinicians experienced in systemic therapy and managing systemic therapies and infusion reactions. Initial concerns about IRRs have been largely addressed with appropriate premedication and monitoring protocols. Experts also noted the potential for a future subcutaneous (SC) formulation of amivantamab to reduce infusion-related complications and enhance convenience. A medical oncologist is required to prescribe this treatment.
Clinician Group Input
Two clinician groups consisting of 19 clinicians from the LCC Medical Advisory Committee (LCC MAC) and 5 clinicians from the Ontario Health (Cancer Care Ontario) (OH [CCO]) Lung Cancer Drug Advisory Committee provided input for this review.
Clinician groups identified that patients with advanced EGFR-mutated NSCLC following disease progression on osimertinib would currently primarily receive platinum (usually cisplatin or carboplatin) plus pemetrexed chemotherapy (followed by pemetrexed maintenance chemotherapy). The LCC MAC expressed that the most important goals for these patients are to maximize quality of life and prolong life and that secondary goals are to minimize toxicity and prolong control of disease. Clinician groups commented that response to chemotherapy treatment postprogression on osimertinib is low and identified an unmet need for more effective therapies with longer duration of benefit that target mechanisms of resistance that develop during osimertinib treatment.
Clinician groups agreed that, in patients with EGFR-mutated NSCLC, the amivantamab plus chemotherapy regimen investigated in the MARIPOSA-2 trial would be expected to replace platinum-doublet chemotherapy following progression on osimertinib (i.e., it would be used as second-line treatment following progression on osimertinib). Both clinician groups agreed that patients best suited for treatment with ACP would be those with advanced or incurable EGFR-mutated (exon 19 deletion or exon 21 L858R mutation) NSCLC who have experienced progression on osimertinib, noting other considerations, such as ECOG Performance Status score.
Clinically meaningful responses to treatment were stated by clinician groups as being improvement in overall survival (OS), delay in progression, and improvement in symptoms or quality of life. Clinician groups expressed that treatment with amivantamab and chemotherapy should be discontinued upon (symptomatic) disease progression, unacceptable toxicity, or patient choice.
Clinician groups stated that the appropriate setting for amivantamab and chemotherapy treatment is an outpatient unit (e.g., cancer centre or hospital setting) under the supervision of a medical oncologist and with personnel experienced in administering these drugs, with the LCC MAC noting that the risk of IRRs with the current mode of administration is high but manageable.
The unmet needs, treatment goals, place in therapy, patients best suited for treatment, assessment of treatment response, and discontinuation and prescribing criteria identified by the clinician groups were generally aligned with those described by clinical experts consulted by CDA-AMC for this review.
Drug Program Input
Input was obtained from the drug programs that participate in the CDA-AMC reimbursement review process. The following were identified as key factors that could potentially impact the implementation of a CDA-AMC recommendation for ACP:
consideration for initiation of therapy
consideration for discontinuation of therapy
considerations for prescribing of therapy
generalizability
funding algorithm and sequencing
care provision issues.
The clinical experts consulted by CDA-AMC provided advice on the potential implementation issues raised by the drug programs (refer to Table 4).
Clinical Evidence
Systematic Review
Description of Studies
One ongoing, phase III, randomized, open-label, multicentre trial (the MARIPOSA-2 trial; N = 657) assessed the efficacy and safety of ACP compared with CP alone in adult patients with locally advanced or metastatic nonsquamous EGFR-mutated NSCLC (exon 19 deletions or exon 21 L858R substitutions) whose disease had progressed on or after osimertinib. Patients were randomized in a 2:1:2 ratio to CP, ACP, or a third investigational arm (ACP plus lazertinib), which is not included in this review report. Results from 2 prespecified interim analyses (interim analysis 1 [IA1]: July 10, 2023; interim analysis 2 [IA2]: April 26, 2024) are included. The primary end point was progression-free survival (PFS) by blinded independent central review (BICR). Key secondary end points included OS, objective response rate (ORR), duration of response (DOR), time to symptomatic progression (TTSP), and patient-reported outcomes (PROs) (European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 [EORTC QLQ-C30], Non–Small Cell Lung Cancer Symptom Assessment Questionnaire [NSCLC-SAQ]).
Patients were required to have measurable disease by Response Evaluation Criteria in Solid Tumours (RECIST) 1.1, ECOG Performance Status score of 0 or 1, and documented progression on osimertinib as the most recent line of therapy. Randomization was stratified by line of prior osimertinib (first-line versus second-line), history of brain metastases, and race (Asian versus non-Asian). Patients received 21-day treatment cycles until progression or unacceptable toxicity. The ACP regimen included weight-based IV dosing of amivantamab (split in cycle 1), carboplatin area under the concentration-time curve 5 mg/mL per minute (AUC 5) for 4 cycles, and pemetrexed 500 mg/m2 with vitamin supplementation.
Baseline characteristics were generally well balanced between the ACP (n = 131) and CP (n = 263) arms. The mean age was ██ years; approximately ███ of patients were female. Most patients were Asian (███) or white (███); other racial groups included Black or African American (██) and other or unknown (██). An ECOG Performance Status score of 0 was reported in 42% of patients receiving ACP and 38% of patients receiving CP. A history of brain metastases was present in 44% and 46%, respectively. EGFR mutation types were exon 19 deletions (68% to 70%) and exon 21 L858R substitutions (30% to 32%). All patients had previously received osimertinib (first or second-line), and most had received only 1 prior line of systemic therapy in the advanced or metastatic setting.
Efficacy Results
At IA1 (data cut-off [DCO]: July 10, 2023), the median PFS by BICR was 6.28 months (95% confidence interval [CI], 5.55 to 8.41) in the ACP arm and 4.17 months (95% CI, 4.04 to 4.44) in the CP arm. At this data cut-off point, ██ PFS events (█████) occurred in the ACP arm and ███ events (█████) in the CP arm. The hazard ratio (HR) for PFS was 0.63 (95% CI, 0.47 to 0.84). The PFS rates at 6 and 12 months were █████ and █████, in the ACP arm, and █████ and █████ respectively, in the CP arm.
At IA1, the median OS was █████ months (███ ███ ██████ ██) in the ACP arm and █████ months (███ ███ ██████ ██) in the CP arm. At IA2 (DCO: April 26, 2024), median OS was 17.74 months (95% CI, 15.97 to 22.37) for ACP and 15.34 months (95% CI, 13.73 to 16.76) for CP. OS event rates at IA2 were █████ (ACP) and █████ (CP). The HR for OS at IA2 was 0.73 (95% CI, 0.54 to 0.99). Estimated OS rates at 6, 12, and 24 months were ███████████ and █████ for ACP and █████, ██████ and █████ for CP, respectively.
ORR by BICR at IA1 was 63.8% (95% CI, 55.0% to 72.1%) in the ACP arm and 36.2% (95% CI, 30.3% to 42.3%) in the CP arm. Complete responses were reported in 2 patients (1.5%) in ACP and 1 patient (0.4%) in CP.
DOR was 6.90 months (95% CI, 5.52 to not estimable [NE]) for ACP and 5.55 months (95% CI, 4.17 to 9.56) for CP. DOR greater than or equal to 6 months was observed in █████ of patients receiving ACP and █████ of patients receiving CP; duration greater than or equal to 12 months was observed in ███████ ██ ████ ██████ █████████ ██████ ██ ██████ ██ ██████ ██ ██████ ████.
At IA1, ██ TTSP events (█████) occurred in the ACP arm and ██ ███████ in the CP arm. Median TTSP was 14.88 months (95% CI, 11.30 to NE) for ACP and 13.01 months (95% CI, 9.20 to NE) for CP. At IA2, median TTSP was █████ months ████ ███ █████ ██ ██████ for ACP and █████ ██████ ████ ███ ████ ██ ██████ for CP. Kaplan-Meier TTSP rates at 12, 18, and 24 months were ██████, and ███ in ACP, and ███, ███, and ███ in CP, respectively.
At IA1, median intracranial PFS was 12.45 months in the ACP arm and 8.31 months in the CP arm (HR = 0.55; 95% CI, 0.38 to 0.79). At IA2, median intracranial PFS was █████ months in ACP and ████ months in CP ███ █ █████ ███ ███ ████ ██ ██████.
Intracranial ORR at IA1 was █████ in ACP and █████ in CP. At IA2, intracranial ORR was █████ in ACP and █████ in CP.
Median intracranial DOR was ████ months in CP and ███ █████████ in ACP at IA1. At IA2, median intracranial DOR was ████ months in CP and █████ months in ACP. Median time to intracranial disease progression was █████ months in CP and ███ █████████ in ACP at IA1, and █████ months in CP and █████ months in ACP at IA2 (██ █ █████ ███ ███ ████ ██ ████).
Harms Results
At IA1, treatment-emergent adverse events (TEAEs) were reported in 99.2% of patients in the ACP arm and 86.4% in the CP arm. Grade 3 or higher TEAEs occurred in 72.3% of patients in the ACP arm and 48.1% in the CP arm. Serious adverse events (SAEs) were reported in █████ and █████ of patients in the ACP and CP arms, respectively.
Discontinuation of any study treatment due to adverse events (AEs) occurred in 18.5% of patients receiving ACP and 3.7% of patients receiving CP. Fatal AEs were reported in 2.3% of patients in the ACP arm and 1.2% in the CP arm.
Premedication, including corticosteroids, antihistamines, and antipyretics, were used to mitigate IRRs. Discontinuation due to IRRs occurred in ████ of patients in the ACP arm. █████ ██ ███████████ ██████████ █████████████████ ██████ ██ ███ ███ █████ ██ ████ ██████ ██████ ██ ███ ███ ████ ██ ████ ███ ████████████████ █████ ██ ███ ███ ████ ██ ████ █████ ██ ███████ ███ ████████ ██ ████ ██ ████████ ██ ███ ███ ███ ███ ████ ██ ███ ██ ███.
The safety profile of amivantamab plus chemotherapy was consistent with the known adverse effects of the individual agents.
Patient-Reported Outcomes
At IA1, median time to sustained deterioration in NSCLC-SAQ total symptom score was 11.6 months (95% CI, 10.2 to 14.9) in the ACP arm and 8.5 months (95% CI, 7.2 to 10.1) in the CP arm (HR = 0.62; 95% CI, 0.43 to 0.88; P = 0.0057). At IA2, median time to deterioration in EORTC QLQ-C30 Global Health Status score was ████ ██████ ████ ███ ████ ██ █████ in the ACP arm and ████ ██████ ████ ███ ████ ██ █████ in the CP arm ███ █ █████ ███ ██████████.Twelve-month event-free rates for Global Health Status were ███ and ████ respectively.
Critical Appraisal
Randomization and stratification were appropriately implemented in the MARIPOSA-2 trial to reduce selection bias, and key efficacy end points, such as PFS, were assessed by BICR, minimizing the risk of bias in assessing end points. However, the open-label design introduces potential performance and detection bias, particularly for subjective end points, such as PROs and AE assessments. The primary end point (PFS) and the key secondary end point (OS) were included in a hierarchical testing strategy with appropriate control for multiplicity; however, multiplicity adjustments were not applied to other secondary end points, such as DOR and TTSP. Missing data were minimal for PFS and OS, but PRO data decreased over time, and missingness was not formally quantified or modelled, limiting interpretability of results from later cycles. Although censoring rates were generally balanced, the trial did not report sensitivity analyses to explore the impact of informative censoring on PROs. This may limit the interpretation of OS data. Postprogression treatment strategies were not explicitly defined. However, timelines for subsequent therapy suggest that patients generally received standard clinical management following disease progression, which may have introduced contamination bias and potentially underestimated the treatment effect on OS, thereby limiting the interpretability of the observed survival difference. The trial population was considered generally representative of patients anticipated by the clinical experts to receive ACP in a practice setting in Canada. However, generalizability may be limited for patients with poorer performance status (ECOG Performance Status score > 1) or comorbidities. According to the clinical experts, the inclusion of patients with treated or stable brain metastases improved external validity. The trial enrolled a globally diverse population, but representation of Indigenous, Black, and other racialized individuals living in Canada was limited. The clinical experts noted that the average participant age was slightly younger than the typical patient population with EGFR-mutated NSCLC in Canada. Overall, the clinical experts considered the ACP regimen to be implementable in Canada, if funded, although early administration may require access to specialized centres due to infusion-related precautions. Supportive medications for managing IRRs and dermatologic AEs may not be uniformly covered across jurisdictions.
GRADE Summary of Findings and Certainty of the Evidence
For the MARIPOSA-2 trial, which served as the pivotal trial for this review, the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach was used to assess the certainty of the evidence for outcomes considered most relevant to inform CDA-AMC expert committee deliberations. Certainty was rated following the GRADE Working Group.
Following the GRADE approach, evidence from the randomized controlled trial (RCT) started as high-certainty evidence and could be rated down for concerns related to study limitations (which refers to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias.
When possible, certainty was rated in the context of the presence of an important (nontrivial) treatment effect; if this was not possible, certainty was rated in the context of the presence of any treatment effect (i.e., the clinical importance is unclear). In all cases, the target of the certainty of evidence assessment was based on the point estimate and where it was located relative to the threshold for a clinically important effect (when a threshold was available) or to the null.
The reference points for the certainty assessments for OS, PFS, and SAEs were based on the presence or absence of an important effect, as informed by clinical experts consulted for this review. For the HRQoL outcomes (i.e., EORTC QLQ-C30 Global Health Status scores), the threshold for an important effect was informed by literature cited by the sponsor.
The selection of outcomes for GRADE assessment was based on the sponsor’s Summary of Clinical Evidence, consultation with clinical experts, and input received from patient and clinician groups and public drug plans. The following list of outcomes was finalized in consultation with expert committee members:
survival outcomes: PFS and OS (reported at multiple time points)
tumour response: ORR (complete response [CR] plus partial response [PR])
HRQoL: EORTC QLQ-C30 Global Health Status scores at 6 and 12 months
notable harms: SAEs.
Results of GRADE Assessments
Table 2 presents the GRADE summary of findings for ACP versus CP.
Table 2: Summary of Findings for ACP vs. CP for Patients With NSCLC Following Progression on Osimertinib (MARIPOSA-2 Trial)
Outcome and follow-up | Patients (studies), N | Relative effect (95% CI) | Absolute effects (95% CI) | Certainty | What happens | ||
|---|---|---|---|---|---|---|---|
CP | ACP | Difference | |||||
PFS – Full analysis set, IA1 | |||||||
Probability of PFS at 6 months Median follow-up: ████ months (ACP) and ████ months (CP) | 394 (1 RCT) | ██ | ███ | ███ | ███ | Higha | ACP results in a clinically important increase in the probability of PFS at 6 months when compared with CP. |
Probability of PFS at 12 months Median follow-up: ████ months (ACP) and ████ months (CP) | 394 (1 RCT) | ██ | ███ | ███ | ███ | Moderateb | ACP likely results in a clinically important improvement in PFS at 12 months compared to CP. |
OS – Full analysis set, IA2 | |||||||
Probability of OS at 12 months Median follow-up: ████ months (ACP) and ████ months (CP) | 394 (1 RCT) | ██ | ███ | ███ | ███ | Moderateb | ACP likely results in a clinically important improvement in OS at 12 months compared to CP. |
Probability of OS at 24 months (IA2) Median follow-up: ████ months (ACP) and ████ months (CP) | 394 (1 RCT) | ██ | ███ | ███ | ███ | Moderateb | ACP likely results in a clinically important improvement in OS at 24 months compared to CP. |
ORR – Full analysis set, IA1 | |||||||
ORR (CR + PR) Median follow-up: ████ months (ACP) and ████ months (CP) | 394 (1 RCT) | ██ | ███ | ███ | ███ | Highc | ACP improves ORR compared to CP. |
HRQoL – Full analysis set, IA2 | |||||||
EORTC QLQ-C30 Global Health Score/QoL at 6 months (IA2) Median follow-up: ████ months (ACP) and ████ months (CP) | 394 (1 RCT) | ██ | ███ | ███ | ███ | Lowd | ACP may result in a clinically important improvement in HRQoL at 6 months compared to CP. |
EORTC QLQ-C30 Global Health Score/QoL at 12 months (IA2) Median follow-up: ████ months (ACP) and ████ months (CP) | 394 (1 RCT) | ██ | ███ | ███ | ███ | Lowd | ACP may result in a clinically important improvement in HRQoL at 12 months compared to CP. |
Harms – Safety analysis set | |||||||
SAEs Median follow-up: ████ months (ACP) and ████ months (CP) and ████ | 394 (1 RCT) | ██ | ███ | ███ | ███ | Moderatee | ACP likely results in more serious adverse events when compared with CP. |
ACP = amivantamab plus carboplatin and pemetrexed; CI = confidence interval; CP = carboplatin and pemetrexed; CR = complete response; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; IA1 = interim analysis 1; IA2 = interim analysis 2; MID = minimal important difference; NA = not applicable; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; PR = partial response; PRO = patient-reported outcome; RCT = randomized controlled trial; SAE = serious adverse event; SD = standard deviation; vs. = versus.
Note: Study limitations (which refer to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias were considered when assessing the certainty of the evidence. All serious concerns in these domains that led to the rating down of the level of certainty are documented in the table footnotes.
aA between-group absolute risk difference of ███ ████ ████ ███ █████) at 6 months was clinically important according to the clinical experts (MID > 10%). The point estimate and entire CI exceeded the threshold.
bRated down 1 level for imprecision. Wide CI crossed the null and the clinical importance threshold according to the clinical experts (MID > 10%).
cA between-group absolute risk difference of █████ ████ ████ ██████ ███ █████ █████████ was clinically important according to the clinical experts (MID > 10%). The point estimate and entire CI exceeded the threshold.
dRated down 2 levels, 1 for serious imprecision due to the 95% CIs for the between-group differences ██ ██████ ██ █ ███████ █ ██████ ██ ██ ███████, including the possibility of no effect and not meeting the threshold for clinical importance. The MIDs were based on a 10-point change from baseline on the EORTC QLQ-C30 Global Health Status scale, as identified in the literature and suggested by the sponsor. Rated down 1 level for risk of bias due to missing outcome data and declining completion rates for PROs over time.
eCertainty of the evidence was rated down by 1 level for serious imprecision. Although the total safety population met the conservative information size, the 95% CI for the absolute risk difference ████ ████ ███ ██████ ███ ███ ██ █████ ██ ███ █████ crossed both the null effect and the threshold for a clinically important difference (10%). The wide CI reflects uncertainty regarding the presence and magnitude of a clinically important increase in SAEs.
Sources: Details included in the table are from the MARIPOSA-2 Clinical Study Report1 and additional information provided by the sponsor.
Long-Term Extension Studies
No long-term extension studies were submitted by the sponsor.
Indirect Comparisons
No indirect treatment comparisons were submitted by the sponsor.
Studies Addressing Gaps in the Evidence From the Systematic Review
The sponsor identified gaps in the systematic review evidence for which 2 studies were submitted as supportive evidence. The first evidence gap was regarding the impact of prophylactic strategies to reduce the risk of IRRs associated with amivantamab, for which results from the SKIPPirr study were submitted. The second identified evidence gap was regarding the impact of enhanced versus standard dermatologic management in patients with locally advanced or metastatic NSCLC with EGFR exon 19 deletions or exon 21 L858R substitution mutations treated with amivantamab, for which interim analysis results from the COCOON study (in patients treated with first-line amivantamab plus lazertinib) were submitted.
SKIPPirr Study
Description of Study
The SKIPPirr study (N = 68) is an ongoing, phase II, open-label, multicentre study evaluating oral dexamethasone, oral montelukast, or SC methotrexate for the prevention of IRRs associated with amivantamab in adult patients with advanced or metastatic NSCLC with EGFR exon 19 deletions or exon 21 L858R substitution mutations who have experienced disease progression on or after osimertinib treatment and on or after PBC and who may benefit from combination therapy with amivantamab and oral lazertinib. All study participants received standard prophylaxis with an antihistamine, antipyretic, and glucocorticoid (IV dexamethasone). The study used a Simon 2-stage design with an expansion stage where participants were eligible to move into subsequent stages if they met an IRR incidence criterion. The primary end point was the rate of IRRs occurring on cycle 1 day 1 following administration of lazertinib and amivantamab combination therapy. In the overall study population, the median age was 63.5 years; 65% of patients were female and 35% were male; 62% of patients were Asian, 26% were white, and 1% were Black or African American (race was not reported for 10% of patients); 75% of patients had an ECOG Performance Status score of 1; 44% had brain metastases; and 66% had an exon 19 deletion EGFR mutation type. In the dexamethasone 8 mg cohort, the median age was 62.0 years; 63% of patients were female and 37% were male; 59% of patients were Asian, 24% were white, and 2% were Black or African American (race was not reported for 15% of patients); 78% of patients had an ECOG Performance Status score of 1; 37% had brain metastases; and 71% had an exon 19 deletion EGFR mutation type.
Efficacy Results
Only the dexamethasone 8 mg cohort passed both stage I and stage II and proceeded to the expansion stage. In this cohort, the intervention was oral dexamethasone 8 mg twice daily on day −2 and day −1 (cycle 1) and 8 mg approximately 1 hour before the start of the infusion of amivantamab IV on cycle 1 day 1. Among the 40 patients in the dexamethasone 8 mg cohort, 9 (22.5%; ███ ███ ████ ██ ████) patients reported IRRs on cycle 1 day 1; 1 patient had an IRR on cycle 2 day 1. ███ ████ ██ ██ ███ ███ ██ █████ █ ████ █████ █ ██ ██ ██████ ███ ███ █████ █ ███ ██ █████ █ ███ ██.
Critical Appraisal
Patients and investigators were aware of the treatment intervention in the open-label SKIPPirr study. As such, there is the potential for bias in favour of the intervention; however, many signs of IRRs are objective (e.g., hypotension, fever, tachycardia) and are not as likely as subjective symptoms to be biased. Patients in the SKIPPirr study had previously received osimertinib and PBC and received amivantamab and lazertinib as background anticancer treatment, whereas anticancer treatment for the patient population of interest for this review is ACP. Although there are differences in the anticancer treatment regimens, clinical experts consulted by CDA-AMC commented that the SKIPPirr study is relevant in addressing the issue of IRR prevention in the population of interest for this review. Clinical experts also commented that the IRR rate on cycle 1 day 1 that was observed in the dexamethasone 8 mg cohort of the SKIPPirr study was clinically meaningfully less than what is expected in clinical practice with IV administration of amivantamab.
COCOON Study
Description of Study
The COCOON study (N = 138 at interim analysis) is an ongoing, phase II, randomized, open-label, multicentre study evaluating enhanced (n = 70) versus standard (n = 68) dermatologic management of locally advanced or metastatic NSCLC with EGFR exon 19 deletions or exon 21 L858R substitution mutations in adult patients who are treatment-naive for advanced disease; patients received anticancer treatment with amivantamab plus lazertinib. Enhanced dermatologic management consisted of doxycycline or minocycline 100 mg twice daily for 12 weeks, clindamycin 1% topical lotion on the scalp for 9 months starting in week 13, noncomedogenic moisturizer (La Roche Posay Lipikar AP+M) for 12 months, chlorhexidine 4% hand and foot wash for 12 months, and general skin prophylaxis recommendations. SOC dermatologic management consisted of general skin prophylaxis recommendations per local practice and reactive treatment, such as topical corticosteroids and systemic antibiotics. The primary end point was the incidence of grade 2 or higher dermatologic adverse events of interest (DAEIs) in the first 12 weeks after initiation of amivantamab plus lazertinib treatment. Only interim analysis results were available. In the overall study population, the median age was ████ years; █████ of patients were female; █████ and █████ of patients were Asian and white, respectively; █████ of patients had an ECOG Performance Status score of 1; █████ ███ █████ ███████████ ███ █████ ███ █████████ ████ ████████ █████.
Efficacy Results
The results of the interim analysis show that, by week 12, the incidence of grade 2 or higher DAEIs was ██ ██ ██ patients (38.6%; ███ ███ ████ ██ ████) in the enhanced dermatologic management arm and ██ ██ ██ patients (76.5%; ███ ██ ████ ██ ████) in the SOC dermatologic management arm (odds ratio [OR] = 0.19; 95% CI, 0.09, to 0.40; P < 0.0001).
Critical Appraisal
Patients and investigators were aware of the treatment intervention in the open-label COCOON study. As such, there is the potential for bias in favour of enhanced dermatologic management; however, many signs of DAEIs are objective and at a lower risk of bias. In addition, the findings should be interpreted with consideration that, although the primary end point was met at the interim analysis, certain data (e.g., treatment adherence, concomitant medications) were not available for appraisal. Patients in the COCOON study received amivantamab and lazertinib as background anticancer treatment as first-line treatment for advanced disease, whereas anticancer treatment for the patient population of interest for this review is ACP received following disease progression with osimertinib. Although there are differences in the anticancer treatment regimens, the clinical experts consulted by CDA-AMC commented that the COCOON study is relevant in addressing the issue of management of dermatologic AEs in the population of interest for this review. The clinical experts highlighted that chlorhexidine 4% availability may be limited and that the skin moisturizers used in the COCOON study are expensive and can be financially preclusive for patients. Clinical experts stated that the difference in the incidence of grade 2 or higher DAEIs between the 2 arms of the COCOON study (interim analysis results) is clinically meaningful.
Conclusions
Evidence from the MARIPOSA-2 trial suggests that, in adult patients with locally advanced or metastatic EGFR-mutated NSCLC who experience disease progressed on or after treatment with osimertinib, ACP results in clinically important improvement in PFS compared with CP. Improvements were also observed for ORR and DOR. These outcomes were supported by high to moderate certainty of evidence. Preliminary results on OS likely favour ACP; however, formal statistical testing for OS was not planned at this interim analysis, and the comparison is considered descriptive only. PROs suggested a potential benefit with ACP in delaying deterioration in HRQoL, though interpretation was limited by missing data over time. Treatment with ACP was associated with a higher frequency of AEs compared with CP, including increased risk of IRRs and dermatologic toxicities, which were generally manageable with supportive care and preinfusion prophylactic medications, such as corticosteroids, antihistamines, and antipyretics.
Introduction
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of amivantamab 50 mg/mL IV in combination with carboplatin (AUC 5) and pemetrexed (500 mg/m2) for the treatment locally advanced (not amenable to curative therapies) or metastatic NSCLC with EGFR exon 19 deletions or exon 21 L858R substitution mutations in patients whose disease has progressed on or after treatment with osimertinib.
Disease Background
Contents within this section have been informed by materials submitted by the sponsor and clinical expert input. The following has been summarized and validated by the review team.
Lung cancer is the most commonly diagnosed cancer and leading cause of cancer death in Canada. An estimated 32,100 new cases of lung cancer were expected in Canada in 2024 and 20,700 deaths from lung cancer were expected in Canada in the same year.2
The 2 main types of lung cancer are small cell lung cancer and NSCLC. NSCLC accounts for approximately 88% of new lung cancer cases in Canada.4 A key mechanism of NSCLC involves driver mutations, which activate progrowth signalling pathways.5,6 The most common driver mutations in NSCLC lead to EGFR activation, and are found more frequently in patients with adenocarcinomas, nonsmokers, patients of Asian ethnicity, and females.7 EGFR mutations are present in approximately 15% of NSCLC cases,5,6 primarily with nonsquamous histology, per clinical expert input. A study characterizing EGFR mutations in patients with metastatic NSCLC in Canada found that, among the 15% of patients with EGFR-mutated disease, exon 19 deletions and exon 21 L858R substitution mutations accounted for 49% and 35% of these cases, respectively.6
The overall 5-year survival rate for lung cancer in Canada is 22%; 5-year survival rates for lung cancer are 16% for those diagnosed at stage III and 3% for those diagnosed at stage IV.3,8
Diagnosis of NSCLC involves imaging tests such as CT, PET-CT, and MRI to detect the presence of a tumour and its spread. Biopsy is performed to confirm the diagnosis and determine the specific type of cancer.9,10 For patients with newly diagnosed nonsquamous NSCLC, comprehensive tissue-based biomarker testing using NGS is accessible in Canada to identify actionable driver mutations that have a prognostic and predictive impact.9 According to a clinical expert consulted by CDA-AMC for this review, some centres will send for NGS by reflex, while others require it to be requested by an oncologist. The clinical experts consulted by CDA-AMC stated that EGFR mutations persist; therefore, patients previously identified as having NSCLC with EGFR exon 19 deletions or exon 21 L858R substitution mutations who experience treatment failure with first-line osimertinib would not require rebiopsy to confirm the presence of these EGFR mutations.
Patients with NSCLC, especially those with late-stage or progressive disease or receiving later lines of treatment, have reduced HRQoL marked by impairments in emotional functioning (e.g., anxiety, depression) and physical functioning.11 A qualitative interview study of patients with advanced or metastatic NSCLC with exon 19 deletions or exon 21 L858R substitution mutations reported that 77% and 82% of patients experienced negative impacts on daily living activities and emotional functioning, respectively. Furthermore, 35% reported physical impacts and 40% reported social impacts. The study also noted the most common symptoms reported by patients as pain in areas other than the chest, cough, fatigue, shortness of breath, difficulty remembering or focusing, and chest pain.12
Standards of Therapy
Contents within this section have been informed by materials submitted by the sponsor and clinical expert input. The following has been summarized and validated by the review team.
The SOC in Canada for patients with locally advanced or metastatic EGFR-mutated NSCLC who have experienced disease progression on osimertinib includes PBC, typically CP, which remains the predominant second-line treatment due to its established efficacy and tolerability. This regimen is widely used and recommended by Canadian guidelines, including the 2023 CADTH Provisional Funding Algorithm and the 2020 Canadian Consensus Statement, as well as the European Society for Medical Oncology and American Society of Medical Oncology 2023 guidelines.13-17 In clinical practice, osimertinib remains the preferred first-line therapy for patients with EGFR exon 19 deletions or exon 21 L858R substitution mutations, offering superior progression-free survival (PFS) and central nervous system penetration compared with earlier-generation EGFR tyrosine kinase inhibitors (TKIs).18-20 Some patients with oligoprogression may receive stereotactic body radiotherapy to delay the need for systemic therapy, while those with widespread progression often undergo a repeat biopsy to assess resistance mechanisms, such as MET amplification or small cell transformation, which may influence treatment decisions.20 In addition to systemic therapies, palliative radiation, nutritional and respiratory support, and psychosocial support programs help manage disease-related symptoms and maintain quality of life.21
Despite initial disease control with first-line osimertinib, nearly all patients eventually develop resistance, leading to disease progression.18-20 Resistance patterns are highly heterogeneous, and the incidence of EGFR-dependent resistance varies based on whether osimertinib was used in the first-line or second-line setting.22 Real-world data from Canada (N = 379) show that 37.9% of patients who received first-line osimertinib and 50.2% of those who received second-line osimertinib do not proceed to further treatment, primarily due to disease progression and death.23 The median OS from the initiation of available second-line therapy (e.g., PBC, afatinib, gefitinib, or immune-oncology therapies) after first-line or second-line osimertinib is 8.6 months (95% confidence interval [CI], 6.9 to 11.8) in clinical practice in Canada.23 In the US real-world setting, median PFS is reported to be 3.4 months and median OS is 9.2 months following osimertinib treatment, further highlighting the poor outcomes associated with current second-line therapies.24,25 Given the high attrition rates in later lines of therapy, the clinical experts consulted for this review emphasized that an optimal second-line treatment should prolong survival, improve symptom control, minimize toxicities, and enhance quality of life.
The proposed place in therapy for ACP is in the second-line setting for adult patients with locally advanced or metastatic EGFR-mutated NSCLC after disease progression on osimertinib.26 This aligns with international guidelines, which now recommend amivantamab plus PBC as the preferred treatment for patients with symptomatic progression and multiple lesions following osimertinib therapy.27-29 Currently, PBC alone is the SOC for postosimertinib treatment in Canada.16,17 The introduction of amivantamab plus PBC for this patient population would provide an alternative second-line option without altering treatment sequencing, or replacing or eliminating any existing therapies.16,17 Clinical experts consulted for this review expected that amivantamab plus PBC would become the preferred second-line treatment for patients with EGFR exon 19 deletions or exon 21 L858R substitution mutations who experience disease progression after osimertinib.
Drug Under Review
Key characteristics of amivantamab are summarized in Table 3 with other treatments available for EGFR-mutated NSCLC after osimertinib failure.
Amivantamab has been approved by Health Canada in combination with CP for the treatment of locally advanced (not amenable to curative therapy) or metastatic NSCLC with EGFR exon 19 deletions or exon 21 L858R substitution mutations in patients whose disease has progressed on or after treatment with osimertinib. A validated test is required to identify EGFR exon 19 deletion or exon 21 L858R substitution mutation positive status before treatment.30 The reimbursement request is per the Health Canada–approved indication. Amivantamab is a bispecific antibody that binds the extracellular domains of EGFR and MET receptors and blocks ligand binding and enhances degradation of these receptors, thereby disrupting EGFR and MET signalling functions. The presence of EGFR and MET on tumour cell surfaces allows for targeted destruction of these cells by immune effector cells, such as natural killer cells and macrophages via antibody-dependent cellular cytotoxicity and trogocytosis mechanisms, respectively.30
Amivantamab is available as a liquid concentrate for IV infusion after dilution, supplied in single-use vials each containing 350 mg of amivantamab per 7 mL (50 mg/mL). According to the product monograph, the recommended dose of amivantamab, when given in combination with CP, is based on baseline body weight (dose adjustments for subsequent body weight changes are not required). For patients weighing less than 80 kg, the recommended dose is 1,400 mg weekly at week 1 (split infusion on day 1 [350 mg] and day 2 [1,050 mg]) and weeks 2 to 4 (infusion on day 1), with no dose at weeks 5 and 6; this is followed by 1,750 mg every 3 weeks starting at week 7 and onward. For patients weighing 80 kg or more, the recommended dose is 1,750 mg weekly at week 1 (split infusion on day 1 [350 mg] and day 2 [1,400 mg]) and weeks 2 to 4 (infusion on day 1), with no dose at weeks 5 and 6; this is followed by 2,100 mg every 3 weeks .starting from week 7 onward. The indicated regimen in combination with amivantamab is pemetrexed 500 mg/m2 IV every 3 weeks until disease progression or unacceptable toxicity and carboplatin AUC 5 IV every 3 weeks, for up to 12 weeks. The order of administration should be pemetrexed first, carboplatin second, and amivantamab last, with preinfusion medications given before amivantamab administration to reduce the risk of IRRs. Recommended amivantamab dose reductions for adverse reactions are outlined in the product monograph. Amivantamab should be administered by health care professionals with appropriate medical support to manage IRRs. The product monograph recommends that amivantamab be administered until disease progression or unacceptable toxicity.30
On July 25, 2024, the European Medicines Agency Committee for Medicinal Products for Human Use adopted a positive opinion recommending a change to the terms of marketing authorization for amivantamab, with the following new indication: in combination with carboplatin and pemetrexed for the treatment of adult patients with advanced NSCLC with EGFR exon 19 deletions or exon 21 L858R substitution mutations after failure of prior therapy including an EGFR TKI.31 Similarly, on September 19, 2024, the FDA approved ACP for adult patients with locally advanced or metastatic NSCLC with EGFR exon 19 deletions or exon 21 L858R substitution mutations whose disease has progressed on or after treatment with an EGFR TKI.32
In addition to the indication under review, amivantamab has been approved by Health Canada as monotherapy for the treatment of adult patients with locally advanced or metastatic NSCLC with activating EGFR exon 20 insertion mutations, whose disease has progressed on or after PBC.30 Amivantamab has also been approved by Health Canada, in combination with CP, for the first-line treatment of adult patients with locally advanced (not amenable to curative therapy) or metastatic NSCLC with activating EGFR exon 20 insertion mutations.30 CDA-AMC has previously reviewed amivantamab for both of these indications, and both were issued a recommendation by pERC to reimburse with clinical criteria and/or conditions.33,34 Combination therapy with lazertinib and amivantamab is currently under review by CDA-AMC for the first-line treatment of adult patients with locally advanced (not amenable to curative therapy) or metastatic NSCLC with EGFR exon 19 deletions or exon 21 L858R substitution mutations.35
Table 3: Key Characteristics of Amivantamab and Platinum-Based Chemotherapy
Characteristic | Amivantamab | Platinum-based chemotherapy | |
|---|---|---|---|
Carboplatin + pemetrexed | Cisplatin + pemetrexed | ||
Mechanism of action | Amivantamab is a bispecific antibody that binds the extracellular domains of EGFR and MET receptors, blocks ligand binding, and enhances degradation of these receptors, thereby disrupting EGFR and MET signalling functions. Amivantamab also targets tumour cells for destruction by immune effector cells, such as natural killer cells and macrophages, via ADCC and trogocytosis mechanisms, respectively. | Carboplatin is a synthetic analogue of cisplatin that interferes with DNA intrastrand and interstrand crosslinks in cells. Pemetrexed is an antifolate antineoplastic drug that disrupts folate-dependent metabolic processes that are essential for cell replication. | The main mechanism of the cytotoxic action of cisplatin involves the binding of the drug to DNA in the cell nucleus to form intrastrand and interstrand cross-links, which interferes with normal transcription and/or DNA replication mechanisms, triggering processes that lead to cell death. Pemetrexed is an antifolate antineoplastic drug that disrupts folate-dependent metabolic processes that are essential for cell replication. |
Indicationa | In combination with carboplatin and pemetrexed for the treatment of patients with locally advanced (not amenable to curative therapy) or metastatic NSCLC with EGFR exon 19 deletions or exon 21 L858R substitution mutations, whose disease has progressed on or after treatment with osimertinib. | This combination is not officially indicated by Health Canada for the treatment of NSCLC. | This combination is not officially indicated by Health Canada for the treatment of locally advanced or metastatic NSCLC with EGFR exon 19 deletions or exon 21 L858R substitution mutations following disease progression on or after treatment with osimertinib. |
Route of administration | IV | IV | IV |
Recommended dose | Amivantamab (in combination with carboplatin and pemetrexed) Patients weighing < 80 kg at baselineb:
Patients weighing ≥ 80 kg at baselineb:
Treatment with amivantamab is recommended until disease progression or unacceptable toxicity. Carboplatin and pemetrexed (in combination with amivantamab) Pemetrexed 500 mg/m2 IV q.3.w. until disease progression or unacceptable toxicity Carboplatin AUC 5 IV q.3.w. for up to 12 weeks Order of treatment administration: pemetrexed first, carboplatin second, amivantamab last | Carboplatin AUC 5 on day 1 of each 21-day cycle for a usual total of 4 to 6 cycles, unless disease progression or unacceptable toxicity occurs Pemetrexed 500 mg/m2 on day 1 of each 21-day cycle for a usual total of 4 to 6 cycles, unless disease progression or unacceptable toxicity occurs | Cisplatin 75 mg/m2 on day 1 of each 21-day cycle for a usual total of 4 to 6 cycles, unless disease progression or unacceptable toxicity occurs Pemetrexed 500 mg/m2 on day 1 of each 21-day cycle for a usual total of 4 to 6 cycles, unless disease progression or unacceptable toxicity occurs |
Serious adverse effects or safety issues |
| Carboplatin:
Pemetrexed:
| Cisplatin:
Pemetrexed:
|
Other | Amivantamab should be administered in a setting with appropriate medical support necessary to treat IRRs. | Carboplatin should only be administered under the supervision of a physician experienced in the use of chemotherapeutic drugs; facilities should be available for appropriate management of therapy and possible complications. Pemetrexed should only be administered by, or under the supervision of, a physician experienced in cancer chemotherapy and in the management of related toxicities. | Cisplatin should be administered under the supervision of a physician experienced with the use of chemotherapeutic drugs; facilities should be available for appropriate management of therapy and complications. Pemetrexed should only be administered by, or under the supervision of, a physician experienced in cancer chemotherapy and in the management of related toxicities. |
ADCC = antibody-dependent cellular cytotoxicity; AML = acute myeloid leukemia; APL = acute promyelocytic leukemia; AUC 5 = area under the concentration-time curve 5 mg/mL per minute; HUS = hemolytic uremic syndrome; ILD = interstitial lung disease; IRR = infusion-related reaction; MDS = myelodysplastic syndrome; NSCLC = non–small cell lung cancer; q.3.w. = every 3 weeks; TLS = tumour lysis syndrome.
aHealth Canada–approved indication.
bDose adjustments not required for subsequent body weight changes.
Sources: Rybrevant (amivantamab) product monograph,30 carboplatin product monograph,36 cisplatin product monograph,37 pemetrexed product monograph,38 Cancer Care Ontario CRPPEME regimen,39 and Cancer Care Ontario CISPPEME regimen.40
Perspectives of Patients, Clinicians, and Drug Programs
The full patient and clinician group submissions received are available in the consolidated patient and clinician group input document for this review on the project website.
Patient Group Input
This section was prepared by the review team based on the input provided by patient groups.
A joint patient group submission was received from LCC, the CCSN, and the LHF. LCC is a registered national charitable organization that serves as Canada’s leading resource for lung cancer education, patient support, research, and advocacy. The CCSN is a national network of patients, families, survivors, friends, community partners, funders, and sponsors taking action to promote the very best SOC, including early diagnosis, timely treatment and follow-up care, support for patients with cancer, and issues related to survivorship or quality of end-of-life care. The LHF (previously Ontario Lung Association) is a registered charity that is a recognized leader, voice, and primary resource in the prevention and control of respiratory illness, as well as tobacco cessation and prevention and its effects on lung health. The LHF provides programs and services to patients and health care providers, invests in lung research, and advocates for improved policies in lung health.
Information provided by the LCC, CCSN, and LHF in this submission consisted of thoughts and experiences of patients with NSCLC and their caregivers, collected through virtual interviews with patients or caregivers (conducted in October and November 2024), or was taken by the patient groups from previous submissions to CDA-AMC. Contributions from 5 patients located in British Columbia, Alberta, and Ontario diagnosed with stage III or IV NSCLC were included in the patient group submission, including input from 2 patients with direct experience in the MARIPOSA-2 trial and 3 other patients with experience in other trials involving amivantamab or who had received amivantamab via the sponsor’s compassionate access program.
Input from 3 patients described their diagnoses with NSCLC as being unexpected and “a shock”; preceding symptoms for 2 of the patients included back pain, shortness of breath, and cough, with lung cancer being discovered incidentally for the third patient as they were completely asymptomatic. All 5 respondents (including those who participated in the MARIPOSA-2 trial) had experience with osimertinib before receiving amivantamab. One patient described experiencing many side effects of osimertinib that limited day-to-day life and contributed to an inability to maintain mental health and a healthy lifestyle, particularly nausea, diarrhea, dizziness, and muscle weakness. Another patient recalled osimertinib treatment being convenient but causing side effects of dry skin and thinning hair. Osimertinib treatment was effective for 3 months and 2 months, respectively, for these patients before disease progression occurred, which included significant respiratory and mobility symptoms for 1 patient. Both patients subsequently participated in the MARIPOSA-2 clinical trial. Another patient initially received gefitinib and experienced diarrhea with this treatment but described this as being tolerable. Upon progression about 1 year later, this patient received osimertinib and described having “incredible” quality of life and no side effects with this treatment. Osimertinib was successful at keeping the tumours stable for 4.5 years; upon progression, this patient received treatment with amivantamab in a clinical trial. Similarly, another patient experienced no side effects and generally normal day-to-day life while taking osimertinib but experienced disease progression with significant pain after 1 year of this treatment. Subsequent treatment with chemotherapy and radiation resulted in side effects (e.g., low energy level, hair loss, nausea) and was not very helpful, so this patient then received amivantamab in a clinical trial. The fifth respondent had previously received EGFR-targeted therapies, including afatinib and osimertinib, and, upon progression, had participated in clinical trials involving amivantamab but had not received the intervention (only SOC chemotherapy) and experienced further spread of cancer. This patient was later approved to receive amivantamab on a compassionate basis by the sponsor.
The patient group submission identified an unmet need for additional treatment options for patients who have experienced disease progression with osimertinib that successfully treat their disease and delay further progression, and allow for good quality of life and for patients to make future plans for working, enjoying retirement, and spending time with loved ones. Treatment outcomes of importance identified by patients included improved management of NSCLC-related symptoms, delaying disease progression, potentially shrinking tumours, maintaining full and worthwhile quality of life, prolonging life, maintaining independence and ability to function to minimize caregiver burden, and having manageable side effects.
The 5 patients who provided input for this submission started treatment with amivantamab between January 2021 and September 2023; 3 of the patients were still receiving this treatment as of September or December 2024, 1 patient discontinued treatment in October 2024 due to its impact on energy levels and quality of life, and 1 patient died. Patients described amivantamab as being successful in treating their disease (e.g., reducing lesion size, scans showing stable disease, preventing further disease spread) while providing durable therapeutic effects. Three of the patients reported significant side effects upon starting treatment with amivantamab but noted that these ultimately improved with dose reductions and prescription medications. Side effects described by patients included mouth ulcers, loss of taste, constipation, skin issues (e.g., rash, acne, dry and bleeding scalp with subsequent infections, growth of facial hair), paronychia, ingrown toenails and infections around toenails, blood clots, tingling or numbness in fingers and toes, edema, tinnitus, dizziness, and weakness. Patients who were enrolled in the MARIPOSA-2 trial noted that, while on amivantamab treatment, they were able to return to a good quality of life, enjoying their hobbies, being active, and spending time with loved ones. Another patient reported terminating treatment with amivantamab due to its impact on energy levels and quality of life. Most of the respondents agreed that they would strongly prefer their experience on amivantamab over previous therapies. One patient noted that, if osimertinib pills had been effective, this treatment would have been preferred due to the ease of taking it at home rather than needing to visit the hospital for long infusions; however, this patient expressed that, as long as treatment with amivantamab plus lazertinib is working, it is worth taking despite initial significant side effects. Another patient commented that, in terms of side effects, amivantamab was preferred as side effects had been more manageable than with previous therapies. From a quality-of-life perspective, this patient also noted a preference for the ease and convenience of oral targeted therapies over long infusions of amivantamab in a hospital every 3 weeks. One patient who stopped amivantamab due to side effects noted that amivantamab was preferred over previous treatments because it controlled their disease but expressed that, if other options were available, they would be preferred to amivantamab. Another patient commented that amivantamab was a lifesaver for patients who have no other option left.
Clinician Input
Input From Clinical Experts Consulted for This Review
All CDA-AMC review teams include at least 1 clinical specialist with expertise regarding the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). The following input was provided by 2 clinical specialists with expertise in the diagnosis and management of NSCLC.
Unmet Needs
The experts indicated that there is currently no well-established, evidence-based, second-line SOC for patients with EGFR-mutated NSCLC who experience disease progression with osimertinib. In clinical practice, treatment decisions are often based on extrapolation from first-line settings, expert consensus, or access to platinum-doublet chemotherapy (typically CP). In select cases of oligoprogression (i.e., limited progression at a few sites while most disease remains controlled), local therapies (e.g., stereotactic radiotherapy) may be used to enable continuation of osimertinib. However, these options are not always feasible, particularly for patients in rural areas or those unable to access specialized testing or care.
There is a high unmet need for therapies that can address common resistance mechanisms (e.g., MET amplification, small cell transformation), extend survival, and maintain quality of life. Both experts emphasized that patients are often clinically stable at the time of progression, highlighting the need for effective but tolerable regimens in this setting.
Place in Therapy
The clinical experts agreed that ACP is expected to become the new SOC for patients with EGFR-mutated NSCLC who progress on or after osimertinib and are eligible to receive systemic chemotherapy. They highlighted the regimen’s superior efficacy over chemotherapy alone and its targeted mechanism of action against common escape pathways. Neither expert indicated that patients must first try therapies other than osimertinib before initiating amivantamab; rather, this combination is considered an appropriate second-line treatment based on trial eligibility.
Patient Population
According to the clinical experts, appropriate candidates for treatment with ACP include adult patients with EGFR exon 19 deletions or exon 21 L858R substitution whose disease has progressed on or after osimertinib. Patients should be fit enough to receive systemic chemotherapy, with an adequate Performance Status score and ability to tolerate corticosteroid-based premedications (e.g., high-dose steroids, antihistamines, antipyretics) to mitigate IRRs. In cases where small cell transformation is suspected, repeat biopsy should be considered. Patients who cannot tolerate the required premedications or have contraindications to chemotherapy may not be suitable for this regimen.
Assessing Response to Treatment
Treatment response is typically assessed through a combination of symptom improvement (e.g., dyspnea, fatigue, cough), radiographic imaging, and functional status. The experts noted that a meaningful response includes tumour shrinkage or disease stability on imaging alongside clinical benefit. Routine imaging every 3 months is common practice and would be reflected by symptom control, preserved function, and improved or maintained quality of life.
Discontinuing Treatment
Treatment with amivantamab plus chemotherapy should be discontinued when there is clear and confirmed evidence of disease progression, either clinically (e.g., worsening symptoms or functional decline) or radiographically (e.g., new or growing lesions on imaging). However, both clinical experts advised that radiographic progression alone may not always warrant immediate discontinuation — particularly in patients who continue to show clinical improvement, such as reduced symptom burden, stable or improved performance status, and maintained daily functioning.
In such cases, treatment may be continued until progression is confirmed on subsequent imaging or the patient experiences clinical deterioration. Discontinuation should also be considered in the event of nonreversible, grade 3 or higher AEs attributable to 1 or more components of the regimen. If a patient develops intolerable toxicity to 1 drug but continues to benefit from the overall treatment, it may be appropriate to continue the tolerable components, based on clinical judgment.
Prescribing Considerations
The regimen can be delivered in an outpatient setting by clinics experienced in systemic therapy delivery and managing infusion reactions. Early concerns regarding IRRs have largely been addressed through premedication protocols. Experts noted that the anticipated SC formulation of amivantamab may further reduce infusion-related complications and improve treatment convenience. A medical oncologist is required to prescribe this regimen.
Clinician Group Input
This section was prepared by the review team based on the input provided by clinician groups.
Two clinician groups consisting of 19 clinicians from the LCC MAC and 5 clinicians from the OH (CCO) Lung Cancer Drug Advisory Committee provided input for this review. LCC is a national charity providing support and education to lung cancer patients, supporting research, and advocating for access to best care for patients with lung cancer. The LCC MAC is a group of clinicians and key opinion leaders who have provided input for submissions of new lung cancer drugs to the health technology assessment process for many years. OH (CCO) Drug Advisory Committees provide timely evidence-based clinical and health system guidance on drug-related issues in support of OH (CCO)’s mandate.
Regarding current treatments, the OH (CCO) Lung Cancer Drug Advisory Committee stated that patients with advanced NSCLC with common EGFR mutations (exon 19 deletion and exon 21 L858R substitution) following progression on osimertinib would receive platinum-pemetrexed chemotherapy followed by pemetrexed maintenance chemotherapy for those without contraindications. The LCC MAC also noted that patients with EGFR-mutated NSCLC whose cancer progresses more substantially than oligoprogression on osimertinib would primarily receive a platinum-doublet chemotherapy regimen, usually cisplatin and pemetrexed or CP. The LCC MAC expressed that the most important goals for patients with EGFR-mutated NSCLC who experience progression on osimertinib are to maximize quality of life and prolong life, and that secondary goals are to minimize toxicity and prolong control of disease. Clinician groups commented that response to chemotherapy treatment postprogression on osimertinib is low and identified an unmet need for more effective therapies with longer duration of benefit in this setting that target mechanisms of resistance that develop during osimertinib treatment.
The LCC MAC expressed that, in patients with EGFR-mutated NSCLC, the amivantamab plus chemotherapy regimen investigated in the MARIPOSA-2 trial would be expected to replace chemotherapy with platinum-doublet following progression on osimertinib. The OH (CCO) Lung Cancer Drug Advisory Committee anticipated that amivantamab in combination with chemotherapy would be used as second-line treatment following progression on osimertinib, noting that amivantamab has shown activity against a wide range of activating and resistance mutations in EGFR-mutated NSCLC and in patients with MET alterations. Both clinician groups agreed that patients best suited for treatment with ACP would be those with advanced or incurable EGFR-mutated (exon 19 deletion or exon 21 L858R mutation) NSCLC who have experienced progression on osimertinib. The OH (CCO) Lung Cancer Drug Advisory Committee added that patients best suited for this treatment would have an ECOG Performance Status score of 0 to 2 and no contraindications to chemotherapy, and would include patients with treated or untreated brain metastases. The LCC MAC acknowledged that patients would need to be fit, due to the risk of toxicity with this treatment, that the MARIPOSA-2 trial was limited to patients with ECOG Performance Status scores of 0 or 1, and that there are no other patient or disease characteristics that would limit provision of this treatment. The LCC MAC also noted that patients eligible for ACP would be identified through previous testing for EGFR mutation, previous treatment with osimertinib, and evidence of progression on osimertinib (typically shown through growth of disease identified via serial CT scans); no test or characteristic exists to identify patients who would be most likely to benefit from the addition of amivantamab therapy.
The OH (CCO) Lung Cancer Drug Advisory Committee noted that clinically meaningful response to treatment includes improvement in OS, delay in progression, and improvement in symptoms or quality of life. The LCC MAC noted that the outcomes used in clinical practice are aligned with the outcomes usually used in clinical trials, including clinical response, treatment response, and side effects, and commented that stable or improved radiological response is considered clinically meaningful and is usually reflected by clinical response (i.e., symptom improvement). Clinician groups identified that, in clinical practice, response to treatment is evaluated using clinical and radiological assessments, noting that clinical response, blood work, and tolerability are assessed before each treatment cycle, and radiographic assessment via CT with or without MRI or bone scan (depending on the location of metastatic disease) is performed every 2 to 4 months. The LCC MAC noted that, upon starting treatment with amivantamab and chemotherapy, patients would require more frequent assessment for side effects and tolerance, with less frequent in-person evaluation required once therapy is stable and side effects have been managed.
The clinician groups expressed that treatment with amivantamab and chemotherapy should be discontinued upon (symptomatic) disease progression, unacceptable toxicity, or patient choice.
The clinician groups stated that the appropriate setting for amivantamab and chemotherapy treatment is an outpatient unit (cancer centre or hospital setting, both academic and community) under the supervision of a medical oncologist and by personnel experienced in administering these drugs, with the LCC MAC noting that risk of IRRs with the current mode of administration is high but manageable.
The unmet needs, treatment goals, place in therapy, patients best suited for treatment, assessment of treatment response, and discontinuation and prescribing criteria identified by the clinician groups were generally aligned with those described by clinical experts consulted by CDA-AMC for this review.
Drug Program Input
The drug programs provide input on each drug being reviewed through the reimbursement review process by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by for this review are summarized in Table 4.
Table 4: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Relevant comparators | |
1. Issues with the choice of comparator in the submitted trial(s) The MARIPOSA-2 trial compared ACP followed by amivantamab-pemetrexed maintenance vs. carboplatin-pemetrexed followed by pemetrexed maintenance in locally advanced or metastatic EGFR-mutated (exon 19 deletion or exon 21 L858R substitution) NSCLC in patients whose disease had progressed on or after osimertinib monotherapy. At the time of this input, 1L osimertinib monotherapy is the funded standard of care, while 1L osimertinib-pemetrexed plus platinum chemotherapy is under consideration for funding. If the patient received 1L osimertinib, then the platinum chemotherapy (mainly platinum-pemetrexed followed by pemetrexed maintenance) would be the appropriate comparator. If 1L osimertinib-pemetrexed plus platinum chemotherapy (followed by osimertinib ± pemetrexed maintenance) is used, then an appropriate comparator would be docetaxel. | Comment from the drug plans to inform pERC deliberations. The clinical experts agreed that docetaxel would be an appropriate comparator following 1L osimertinib plus platinum chemotherapy plus pemetrexed, particularly when pemetrexed maintenance has been stopped. They also agreed that the timing of the last platinum-based chemotherapy would be a deciding factor in the choice of comparator. |
Considerations for initiation of therapy | |
1. Prior therapies required for eligibility Should patients who were previously treated with 1L osimertinib-pemetrexed plus platinum chemotherapy with or without osimertinib-pemetrexed maintenance be considered for ACP? If yes, what is the minimum disease-free interval required between the last dose of osimertinib plus chemotherapy and the first dose of amivantamab plus chemotherapy? | The clinical experts agreed that patients previously treated with 1L osimertinib-pemetrexed plus platinum chemotherapy with or without osimertinib-pemetrexed maintenance may be considered for treatment with ACP. A minimum interval of 6 months from the last platinum dose and 3 months from the last pemetrexed dose is generally required. Patients must also have documented disease progression with osimertinib and be clinically fit for systemic therapy (e.g., ECOG Performance Status score of 0 to 2, adequate renal function). Osimertinib must be discontinued upon initiation of amivantamab-based therapy. Disease stability or response should be confirmed at restaging before starting ACP. |
Considerations for discontinuation of therapy | |
1. Definition of loss of response, absence of clinical benefit, or disease progression What discontinuation criteria should be used for ACP? | The clinical experts stated that the trial criteria for discontinuation of treatment with ACP would apply in clinical practice and include radiographic disease progression, clinically evident worsening, unacceptable toxicity, or absence of clinical benefit as determined by the treating physician. |
Considerations for prescribing of therapy | |
1. Dosing, schedule or frequency, dose intensity Two types of dosing are available for amivantamab depending on the patient’s weight (1,400 mg weekly × 4 doses then 1,750 mg every 3 weeks if < 80 kg, vs. 1,750 mg weekly × 4 then 2,100 mg every 3 weeks if ≥ 80 kg). | Comment from the drug plans to inform pERC deliberations. The clinical experts confirmed that the patient’s weight is considered in determining the amivantamab dose: patients weighing < 80 kg receive 1,400 mg, and those weighing ≥ 80 kg receive 1,750 mg. The first dose is split: 350 mg on cycle 1 day 1 followed by 1,050 mg (or 1,400 mg) the same day. If tolerated, patients continue with 1,400 mg (or 1,750 mg) on cycle 1 days 8 and 15, and cycle 2 day 1. Starting on cycle 3 day 1, the dose is 1,750 mg or 2,100 mg every 3 weeks. |
2. Drug administration Premedications are recommended before each infusion to reduce the risk of infusion-related reactions. The initial dose of amivantamab is administered as a split infusion on days 1 and 2 of cycle 1, week 1. | Comment from the drug plans to inform pERC deliberations. |
3. Concerns related to combination usage: 3.1. If chemotherapy has to be discontinued, should amivantamab be continued as a single agent? 3.2. Can amivantamab be used with cisplatin-pemetrexed followed by pemetrexed maintenance? | 3. Concerns related to combination usage: 3.1. Yes, if there is documented disease control. This approach aligns with clinical trial protocol and is considered acceptable in practice. 3.2. Yes, this should be allowed, particularly at the discretion of the treating physician. |
Generalizability | |
1. Populations of interest matching the indication but with insufficient data Should ACP be used in the following scenarios?
| The trial included only patients with an ECOG Performance Status score of 0 to 1. Clinical experts advise that patients with an ECOG Performance Status score of 2 may be considered eligible at the discretion of the treating physician, if the patients are fit for systemic chemotherapy. |
2. Patients receiving active treatment with a time-limited opportunity to switch to the drug(s) under review On a time-limited basis, should eligible patients on existing treatments be switched to amivantamab-pemetrexed plus platinum chemotherapy followed by amivantamab-pemetrexed? | The clinical experts agreed that eligible patients receiving existing active treatment should be permitted to switch to amivantamab-pemetrexed plus platinum chemotherapy followed by amivantamab-pemetrexed on a time-limited basis if the treatment under review is funded. This may represent their only opportunity to access amivantamab. The clinical experts noted that the main consideration will be whether patients who have already started second-line platinum chemotherapy plus pemetrexed and are now receiving maintenance pemetrexed should be permitted to add amivantamab. They suggested the following criteria:
|
Funding algorithm | |
Request an initiation of a rapid provisional funding algorithm. Note that if the final reimbursement recommendation for this drug under review is “Do not reimburse,” the project will be suspended indefinitely. Drug may change place in therapy of drugs reimbursed in subsequent lines. | Comment from the drug plans to inform pERC deliberations. |
Other aspects: In the trial, participants who received prior neoadjuvant and/or adjuvant treatment were eligible if the disease progressed ≥ 12 months after the last dose and the patient’s disease progressed on or after osimertinib in the locally advanced or metastatic setting. Should amivantamab plus platinum chemotherapy plus pemetrexed be funded for patients who have received neoadjuvant and/or adjuvant therapy but whose disease progresses to the advanced stage within less than 12 months of the last dose of treatment? If so, what is the minimum disease-free interval? | The clinical experts noted that they would consider a patient eligible if disease progression occurred at least 6 months after completion of platinum-based adjuvant chemotherapy, while the patient was still receiving adjuvant osimertinib. If a patient progressed after completing adjuvant osimertinib, eligibility for amivantamab should depend on whether the patient meets criteria to retry osimertinib. If the patient is eligible for osimertinib reinitiation, they should not receive amivantamab. This eligibility scenario may become less relevant as clinical decisions and funding policies evolve in response to the broader evidence generated by the MARIPOSA-2 trial. Use of amivantamab plus chemotherapy in patients who experience disease progression within 6 months of platinum chemotherapy or 3 months of pemetrexed, in the presence of a new documented MET amplification or alteration, may be considered on a case-by-case basis at the discretion of the treating clinician. However, this falls outside the currently approved indication for this therapy. |
In the trial, participants must also have experienced disease progression on or after osimertinib monotherapy (wherein osimertinib must have been given as either first-line or second-line therapy). Should patients who have received adjuvant osimertinib and whose disease progresses while receiving osimertinib or within 6 months of the last dose of osimertinib be eligible for amivantamab plus platinum chemotherapy plus pemetrexed? | The clinical experts agreed that patients whose disease progresses during adjuvant osimertinib should be eligible for amivantamab plus chemotherapy, provided that at least 6 months have passed since their last osimertinib exposure. |
At the time of this input, there is an ongoing review for osimertinib for unresectable stage III NSCLC with EGFR exon 19 deletions or exon 21 L858R substitution mutations for patients whose disease has not progressed during or following platinum-based chemoradiation. Should these patients be considered for downstream amivantamab plus chemotherapy if the disease progresses while receiving osimertinib or within 6 months of the last dose of osimertinib? What minimum interval would be required from completion of platinum-based chemoradiation? | The clinical experts agreed that patients who progress while on or shortly after discontinuing osimertinib following chemoradiation or adjuvant chemotherapy may be eligible for amivantamab plus chemotherapy, provided that at least 6 months have passed since the last platinum exposure. Eligibility should be based on the same clinical criteria used for patients progressing on or after osimertinib in the metastatic setting, including a minimum of 6 months since the last platinum exposure. The clinical experts stated that, in the absence of supporting evidence, they would not recommend amivantamab for use in patients who have not received prior osimertinib. |
Care provision issues | |
1. Companion diagnostics (e.g., access issues, timing of testing) Confirmation of EGFR exon 19 deletion or exon 21 L858R substitution is required before starting treatment. EGFR mutation testing is part of routine clinical practice. | Comment from the drug plans to inform pERC deliberations. |
1L = first-line; ACP = amivantamab plus carboplatin and pemetrexed; ECOG = Eastern Cooperative Oncology Group; NSCLC = non–small cell lung cancer; pERC = pan-Canadian Oncology Drug Review Expert Review Committee.
Clinical Evidence
The objective of this Clinical Review report is to review and critically appraise the clinical evidence submitted by the sponsor on the beneficial and harmful effects of ACP in the treatment of locally advanced (not amenable to curative therapy) or metastatic NSCLC with EGFR exon 19 deletions or exon 21 L858R substitution mutations in adult patients whose disease has progressed on or after treatment with osimertinib.
A summary of the clinical evidence included by the sponsor is presented in 4 sections, with the CDA-AMC critical appraisal of the evidence included at the end of each section. The first section, the Systematic Review, includes a pivotal study and RCTs that were selected according to the sponsor’s systematic review protocol. The CDA-AMC assessment of the certainty of the evidence in this first section, using the GRADE approach, follows the critical appraisal of the evidence. The second section includes indirect evidence from the sponsor. The third section includes additional studies that were considered by the sponsor to address important gaps in the systematic review evidence.
Included Studies
Clinical evidence from the following are included in the review and appraised in this document:
1 pivotal study: the phase III MARIPOSA-2 RCT, evaluating amivantamab plus PBC versus PBC alone in following osimertinib in EGFR-mutated NSCLC
additional evidence: 2 studies addressing gaps in evidence, including real-world treatment patterns and survival outcomes.
Systematic Review
Contents within this section have been informed by materials submitted by the sponsor. The following has been summarized and validated by the review team.
Description of Studies
The MARIPOSA-2 trial (NCT04988295) is an ongoing, phase III, randomized, open-label, multicentre study designed to evaluate the efficacy and safety of ACP compared with CP alone in patients with locally advanced or metastatic NSCLC with EGFR exon 19 deletions or exon 21 L858R substitution mutations who have experienced disease progression on or after osimertinib (Figure 1). The trial was conducted across 235 sites in 29 countries, including Canada, and enrolled a total of 657 patients. Patients were randomized in a 2:1:2 ratio to receive 1 of the following:
CP (control arm)
ACP
lazertinib plus amivantamab plus carboplatin and pemetrexed (LACP) (data from this arm are not included in this review, as the combination does not align with the Health Canada product monograph).
The DCO dates for the results presented were July 10, 2023, for IA1 and April 26, 2024, for IA2. The study database lock occurred on the same respective dates for each analysis. Additional characteristics of the trial are summarized in Table 5.
The study included a screening phase conducted 1 to 28 days before randomization, during which patients with histologically or cytologically confirmed NSCLC were assessed for eligibility. Eligible patients had documented disease progression while receiving osimertinib, an ECOG Performance Status score of 0 or 1, and had received prior platinum-based therapy. Patients with untreated symptomatic brain metastases were excluded. Treatment randomization was stratified by:
line of prior osimertinib therapy (first-line versus second-line)
history of brain metastases (yes versus no)
race (Asian versus non-Asian).
The treatment phase involved the administration of study drugs in 21-day cycles until disease progression, intolerable toxicity, or patient withdrawal. The dosing regimen included:
amivantamab:
for patients weighing less than 80 kg: 1,400 mg IV on cycle 1, days 1 and 2 (split dose), then on day 1 of weeks 2 to 4, then 1,750 mg on day 1 of each subsequent 21-day cycle (starting cycle 3)
For patients weighing 80 kg or more: 1,750 mg IV on cycle 1, days 1 and 2 (split dose), then on day 1 of weeks 2 to 4, then 2,100 mg on day 1 of each subsequent 21-day cycle (starting cycle 3)
carboplatin: AUC 5 IV on day 1 of each 21-day cycle for up to 4 cycles.
pemetrexed: 500 mg/m2 IV on day 1 of each 21-day cycle for up to 4 cycles, followed by maintenance therapy with pemetrexed until disease progression.
The trial also included a follow-up phase to monitor safety and survival outcomes. Safety assessments were conducted up to 90 days after the last dose of the study drug, and survival was monitored at predefined intervals.
Although the trial included a treatment group for amivantamab plus lazertinib plus PBC, the sponsor is not seeking approval from Health Canada for this combination. Details regarding this group are summarized in Table 5 and associated texts for completeness.
Table 5: Details of Studies Included in the Systematic Review
Detail | MARIPOSA-2 study |
|---|---|
Designs and populations | |
Study design | Ongoing phase III, randomized, multicentre RCT |
Locations | 235 centres across 29 countries or territories |
Patient enrolment dates | Start date: November 17, 2021 End date: Study is ongoing IA1: July 10, 2023 (primary analysis) IA2: April 26, 2024 |
Randomized (N) | N = 657 LACP or ACP-L arm: N = 263 ACP arm: N = 131 CP arm: N = 263 |
Inclusion criteria |
|
Exclusion criteria |
|
Drugs | |
Intervention | ACP:
LACP (from start of study until November 6, 2022)a:
ACP-L (from November 7, 2022, onward)a:
|
Comparator(s) | CP:
|
Study duration | |
Screening phase | Up to 28 days before randomization |
Treatment phase | Started cycle 1 day 1 and continued in 21-day cycles until approximately 30 days after discontinuation of study treatment, due to either documented radiographic (RECIST 1.1) disease progression (confirmed by BICR), or if another criterion for discontinuation of study treatment was met |
Follow-up phase | Began 30 days after the discontinuation of treatment and continued until the end of study, death, lost to follow-up, or withdrawal of consent from participation in the study, whichever came first |
Outcomes | |
Primary end point | PFS by BICR |
Secondary and exploratory end points | Secondary:
Exploratory:
|
Publication status | |
Publications | Passaro et al. (2023)41 NCT04988295 |
ACP = amivantamab plus carboplatin and pemetrexed; ACP-L = amivantamab plus carboplatin and pemetrexed plus lazertinib; AUC 5 = area under the concentration-time curve 5 mg/mL per minute; BICR = blinded independent central review; CCO = clinical cut-off; CP = carboplatin and pemetrexed; CTCAE = Common Terminology Criteria for Adverse Events; DOR = duration of response; ECOG = Eastern Cooperative Oncology Group; EORTC QLQ-C30 = European Organisation for the Research and Treatment of Cancer Quality of Life Questionnaire Core 30; IA1 = interim analysis 1; IA2 = interim analysis 2; LACP = lazertinib plus amivantamab plus carboplatin and pemetrexed; NSCLC = non–small cell lung cancer; NSCLC-SAQ = Non–Small Cell Lung Cancer Symptom Assessment Questionnaire; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; PFS2 = progression-free survival after first subsequent therapy; PROMIS-PF = Patient-Reported Outcomes Measurement Information System – Physical Function; RCT = randomized controlled trial; RECIST = Response Evaluation Criteria in Solid Tumours; TKI = tyrosine kinase inhibitor; TTD = time to discontinuation; TTSP = time to symptomatic progression; TTST = time to subsequent therapy.
aBoth LACP and ACP-L regimens consisted of lazertinib plus amivantamab plus carboplatin and pemetrexed. For patients who received LACP, lazertinib was administered from cycle 1 day 1, and for patients who received ACP-L, lazertinib was started on cycle 5 day 1. While the efficacy of the LACP or ACP-L arm was reported in the MARIPOSA-2 trial, regulatory approval was not sought for this drug combination. As such, the remainder of this report will focus only on assessing the ACP arm compared with the CP arm in the postosimertinib common EGFR setting.
Sources: MARIPOSA-2 Clinical Study Report.1 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Figure 1: Study Design of MARIPOSA-2 Study
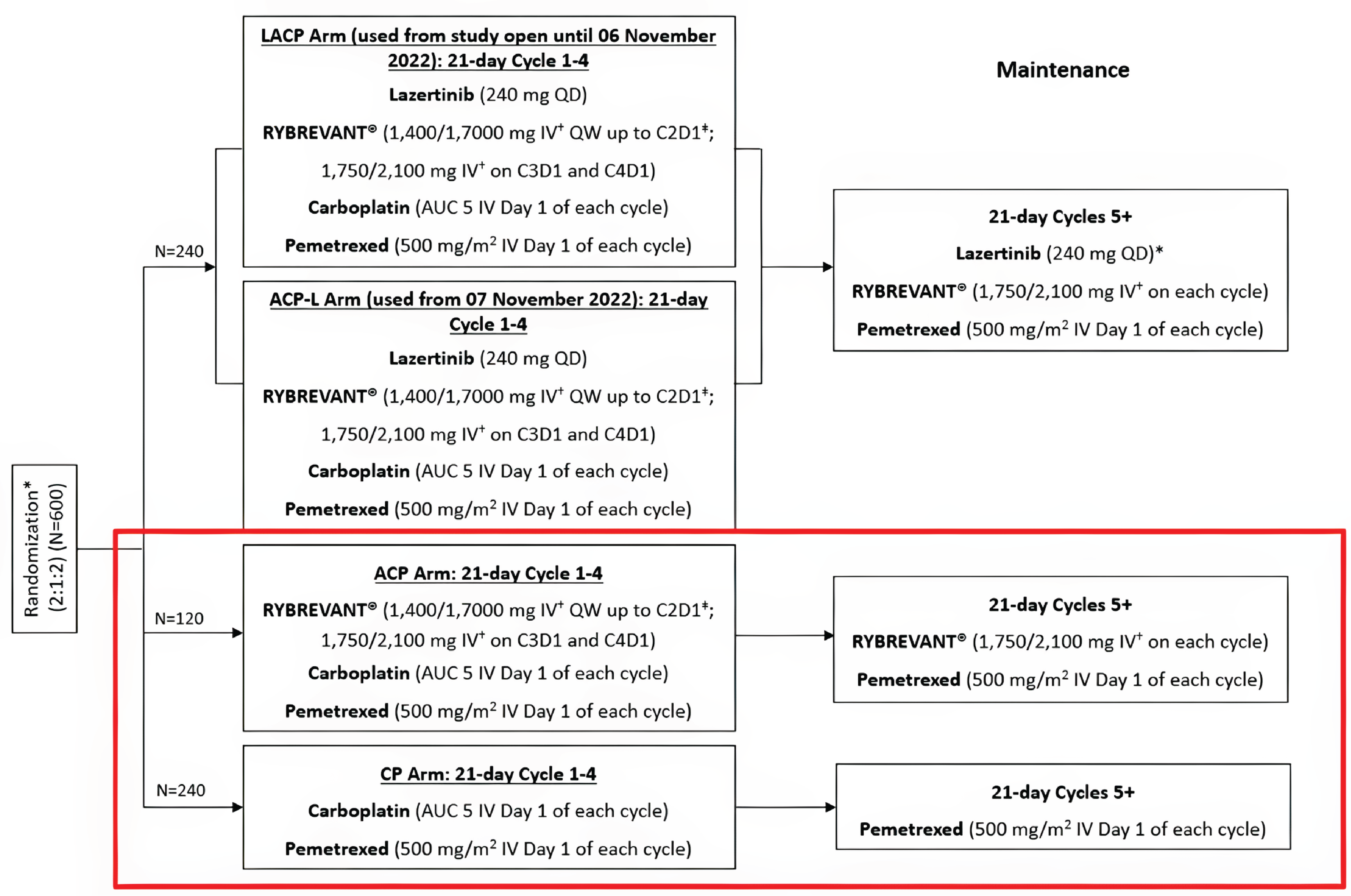
ACP = amivantamab plus carboplatin and pemetrexed; ACP-L = amivantamab plus carboplatin and pemetrexed plus lazertinib; AUC 5 = area under the concentration-time curve 5 mg/mL per minute; C2D1 = cycle 2 day 1; C3D1 = cycle 3 day 1; C4D1= cycle 4 day 1; LACP = lazertinib plus amivantamab plus carboplatin and pemetrexed; QD = once daily; QW = once weekly.
*Stratification factors: osimertinib line of therapy (first-line vs. second-line), history of brain metastases (yes vs. no), Asian race (yes vs. no).
†Doses shown by body weight (< 80 kg or ≥ 80 kg).
‡Cycle 1: Days 1 and 2 (split dose), 8, and 15; cycle 2: day 1.
Notes: Lazertinib for participants receiving dosing schedule 2 (ACP-L) may start sooner if carboplatin is discontinued earlier than cycle 4.
The red box highlights the study arms described in this report.
Source: MARIPOSA-2 Clinical Study Report.1
Populations
Inclusion and Exclusion Criteria
The MARIPOSA-2 trial included adult patients (aged ≥ 18 years) with histologically or cytologically confirmed, locally advanced or metastatic, nonsquamous NSCLC harbouring EGFR exon 19 deletions or exon 21 L858R substitution mutations. Eligible patients had measurable disease per RECIST 1.1, an ECOG Performance Status score of 0 or 1, and adequate organ and bone marrow function. All participants had disease progression on or after osimertinib monotherapy, either as a first-line treatment for locally advanced or metastatic disease or in the second-line setting following prior treatment with first-generation or second-generation EGFR TKIs. Patients with brain metastases were eligible if all lesions had been treated as clinically indicated and there was no need for further definitive local therapy.
Key exclusion criteria included prior systemic chemotherapy for locally advanced or metastatic disease, receipt of neoadjuvant or adjuvant therapy with progression to advanced disease within 12 months of the last dose, uncontrolled intercurrent illnesses, active cardiovascular disease, symptomatic brain metastases, and prior treatment with anti–PD-1 or anti–PD-L1 antibodies within 6 weeks of the first study dose.
Interventions
The MARIPOSA-2 trial assessed the efficacy and safety of ACP versus CP. Amivantamab was administered intravenously with a split dose in cycle 1 (1,400 mg for patients weighing < 80 kg or 1,750 mg for patients weighing ≥ 80 kg on days 1 and 2), then 1,750 mg (for those weighing < 80 kg) or 2,100 mg (for those weighing ≥ 80 kg) every 21 days starting in cycle 3 and until disease progression. Carboplatin (AUC 5) and pemetrexed (500 mg/m2) were given intravenously on day 1 of each 21-day cycle for up to 4 cycles, followed by pemetrexed maintenance until disease progression. Patients in both arms received preinfusion medications, including corticosteroids, antihistamines, and analgesics, to mitigate IRRs. Concomitant medications, such as folic acid, vitamin B12, and corticosteroids, were required for pemetrexed therapy. Rescue medications for infusion reactions included dexamethasone, diphenhydramine, and acetaminophen. The trial did not include a placebo due to differences in drug administration, making blinding unfeasible. Treatment continued until disease progression or unacceptable toxicity.
Outcomes
A list of efficacy end points assessed in this Clinical Review report is provided in Table 6, followed by descriptions of the outcome measures. Summarized end points are based on outcomes included in the sponsor’s Summary of Clinical Evidence as well as any outcomes identified as important to this review according to the clinical experts consulted for this review and input from patient and clinician groups and public drug plans. Using the same considerations, CDA-AMC selected end points that were considered to be the most relevant to inform expert committee deliberations and finalized this list of end points in consultation with members of the expert committee. All summarized efficacy end points were assessed using the GRADE approach. Select notable harms outcomes considered important for informing expert committee deliberations were also assessed using GRADE.
Table 6: Outcomes Summarized From the MARIPOSA-2 Study
Outcome measure | Time point | Primary analysis CCO July 10, 2023 (IA1) | Supportive analysis CCO April 26, 2024 (IA2) |
|---|---|---|---|
PFS by BICRa | Up to 28 Months | Primary | Not included |
OSa | Up to 48 months | Secondary | Included |
ORR by BICR | Up to 28 Months | Secondary | Included |
DOR by BICR | Up to 28 Months | Secondary | Included |
TTSP | Up to 28 Months | Secondary | Included |
EORTC QLQ-C30 | Up to 28 Months | Secondary | Included |
NSCLC-SAQ | Up to 28 months | Secondary | Not included |
BICR = blinded independent central review; CCO = clinical cut-off; DOR = duration of response; EORTC QLQ-C30 = European Organization of Research and Treatment of Cancer Quality of Life Questionnaire Core 30; IA1 = interim analysis 1; IA2 = interim analysis 2; NSCLC-SAQ: non–Small cell lung cancer symptom assessment questionnaire; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; TTSP = time to symptomatic progression.
aStatistical testing for these end points was adjusted for multiple comparisons (e.g., hierarchal testing).
Sources: MARIPOSA-2 Clinical Study Report.1 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Primary Outcome
PFS: PFS was the primary end point of the MARIPOSA-2 trial and was defined as the time from randomization to the first occurrence of objective disease progression or death from any cause, whichever occurred first. Disease progression was assessed by BICR using RECIST 1.1 criteria. Imaging assessments were conducted at screening, then at week 6, week 12, and every 12 weeks thereafter, with more frequent assessments (every 6 weeks) through to week 48. Participants who discontinued treatment before progression continued to undergo scheduled imaging assessments. Censoring rules were prespecified: participants who had not experienced disease progression or who had not died at the time of analysis were censored at the date of their last evaluable RECIST 1.1 assessment. If a participant had experienced disease progression or died after 2 or more consecutive missed assessments, censoring occurred at the time of the last evaluable RECIST 1.1 assessment. PFS was centrally adjudicated and analyzed as a time-to-event end point using standard survival analysis methods. No references were provided in the sponsor’s submission for a minimal important difference (MID) for PFS specifically in the patient population with locally advanced or metastatic NSCLC who had EGFR exon 19 deletions or exon 21 L858R substitution mutations.
Key Secondary Outcome
OS: OS was defined as the time from randomization to death from any cause. For participants not known to have died at the time of analysis, OS time was censored at the last recorded date the participant was known to be alive. Unlike PFS, OS was assessed through survival follow-up contacts, such as phone calls or medical record reviews, and was not dependent on imaging schedules. OS is widely considered the most clinically meaningful end point in oncology and was analyzed using standard time-to-event methods. No references were provided in the sponsor's submission for a MID for OS specifically in the patient population with locally advanced or metastatic NSCL who have EGFR exon 19 deletions or exon 21 L858R substitution mutations.
Other Secondary Outcomes
ORR: ORR by BICR was defined as the percentage of patients with a best overall response of CR or PR, as assessed by BICR using RECIST 1.1 criteria. Tumour responses must be confirmed by a follow-up scan at least 4 weeks after the initial documentation of response. Patients without a postbaseline tumour assessment or who did not achieve CR or PR were categorized as nonresponders. No references were provided in the sponsor’s submission for a MID for ORR.
DOR: DOR was defined as the time from the date of first documented response (CR or PR by BICR) until the date of documented disease progression (assessed by BICR) or death, whichever occurred first. No references were provided in the sponsor’s submission for a MID for DOR.
TTSP: TTSP was defined as the time from randomization to the onset of new or worsening lung cancer symptoms that required a change in anticancer therapy, clinical intervention, or resulted in death, whichever occurred first. This end point was investigator-assessed based on clinical judgment and was documented in the electronic case report form. It was not based on standardized symptom scales or imaging criteria, and was intended to capture the real-world impact of disease burden. References to support the validity or measurement properties of this outcome were not submitted by the sponsor. No references were provided in the sponsor’s submission for a MID for TTSP.
Intracranial PFS: Intracranial PFS was defined as the time from randomization to intracranial disease progression or death, whichever occurred first. No references were provided in the sponsor’s submission for a MID for intracranial PFS.
Intracranial ORR: Intracranial ORR was defined as the percentage of patients achieving a best overall intracranial response of CR or PR, confirmed by follow-up imaging at least 4 weeks later. No references were provided in the sponsor’s submission for a MID for intracranial ORR.
Intracranial DOR: Intracranial DOR was defined as the time from first documented intracranial response to intracranial progression or death. No references were provided in the sponsor’s submission for a MID for intracranial DOR.
Time to intracranial progression: Time to intracranial progression by BICR was defined as the time from randomization to the date of objective intracranial disease progression. This outcome was analyzed as a time-to-event end point using standard survival analysis methods. No references were provided in the sponsor’s submission for a MID for time to intracranial progression.
Patient-Reported Outcomes
EORTC QLQ-C30: The EORTC QLQ-C30 is a 30-item, cancer-specific, PRO instrument used to evaluate global health status, physical functioning, and symptom burden in cancer patients. It includes multiple functional and symptom subscales, with a 1-week recall period.42 Scores for each scale or item are linearly transformed to a 0 to 100 range, with higher scores indicating better functioning or worse symptoms, depending on the subscale. In the MARIPOSA-2 trial, the EORTC QLQ-C30 was used to assess change from baseline and time to deterioration for specific domains, including global health status and physical functioning. A MID of 10 points has been widely referenced in oncology, based on prior validation studies in breast cancer, small cell lung cancer, and later supported in broader cancer populations, including NSCLC.43,44
NSCLC-SAQ, symptom burden: The NSCLC-SAQ is a 7-item, disease-specific PRO instrument designed to assess symptom burden in advanced NSCLC. It includes 5 symptom domains — cough, dyspnea, fatigue, pain, and appetite loss — each measured using a 5-point Likert-type scale (0 to 4), with higher scores indicating greater symptom severity. The total score, ranging from 0 to 20, is calculated only if responses for all 5 domains are not missing. The instrument uses a 7-day recall period and was administered from cycle 1, day 1 through end of treatment and follow-up visits. Summary statistics were derived at predefined time points, and the outcome was centrally analyzed. A MID of 0.3 times the standard deviation of the baseline score has been cited in metastatic NSCLC literature.45
Harms Outcomes
SAEs: SAEs were defined as any AEs resulting in death, life-threatening condition, inpatient hospitalization or prolongation of hospitalization, persistent or significant disability or incapacity, or congenital anomaly or birth defect. SAEs were collected from the time of informed consent through at least 30 days after the last dose of study treatment. Events were reported and coded using the Medical Dictionary for Regulatory Activities (MedDRA) and graded per National Cancer Institute Common Terminology Criteria for Adverse Events Version 5.0.
TEAEs: TEAEs were coded using MedDRA version 25.0, based on verbatim terms used in the case report form by investigators and graded according to the National Cancer Institute Common Terminology Criteria for Adverse Events Version 5.0. TEAEs were defined as any AEs occurring at or after the initial administration of study treatment through the day of last dose plus 30 days, or until the start of subsequent anticancer therapy (if earlier).
Table 7: Summary of NSCLC-SAQ and EORTC QLQ-C30 Outcome Measures From the MARIPOSA-2 Trial and Their Measurement Properties
Outcome measure | Type | Conclusions about measurement properties | MID |
|---|---|---|---|
NSCLC-SAQ | A PRO measure containing 7 items intended for use in advanced NSCLC clinical trials. The items assess symptoms of NSCLC (i.e., cough, pain, dyspnea, fatigue, and poor appetite) over a 7‑day recall period and have a 5-point response scale ranging from 0 to 4.46-48 The total score ranges between 0 and 20, with higher scores indicating greater severe symptomatology.49 | Validity: A cross-sectional study of patients with advanced NSCLC (N = 152) showed a strong correlation between NSCLC-SAQ total score and NCCN/FLSI-17 (r = 0.83), and NSCLC-SAQ was able to differentiate between self-reported symptom severity levels, self-reported health status, and clinician-reported performance status (P < 0.001 for all).48 A study in patients with stage IV metastatic NSCLC (N = 560) reported Spearman correlations between NSCLC-SAQ total score and other PRO measures, as follows: EORTC QLQ‑C30 Global Health Status/QoL, r = −0.58; EQ‑5D‑5L VAS, r = −0.54; PGIS‑LC Version 2, r = 0.62.49 A study of patients with EGFR‑mutated locally advanced or metastatic NSCLC (N = 615) stated that the NSCLC‑SAQ presented adequate internal validity for clinical trial use. Over the study period, correlations for the NSCLC‑SAQ total score with the EORTC QLQ‑C30 Global ranged from −0.48 to −0.65.50 Reliability: The cross-sectional study (N = 152) reported internal consistency for the 7 items (Cronbach alpha = 0.78) and 5 domains (Cronbach alpha = 0.72). The test-retest reliability was examined in 148 patients who completed a retest (ICC = 0.87).48 In the study in stage IV metastatic NSCLC (N = 560), test-retest reliability was calculated between baseline and week 3 for patients with stable overall symptoms (N = 210), with ICC = 0.79.49 The study in EGFR‑mutated locally advanced or metastatic NSCLC (N = 615) stated that test-retest reliability for the NSCLC‑SAQ total score was rated “fair to good” (ICC = 0.69, from 268 stable participants).50 Responsiveness: The study in stage IV metastatic NSCLC (N = 560) reported that the NSCLC‑SAQ total score was able to detect improvement over time based on mean differences in change from baseline to week 18 among PGIS‑LC change score groups (P < 0.001).49 | In patients with metastatic NSCLC, the reported within-person MID for improvement was a decrease of 3 to 5 points.49 In patients with EGFR‑mutated locally advanced or metastatic NSCLC, the within-person MID for worsening was an increase of 2 to 3 points.50 |
EORTC QLQ-C30 | A 30-item PRO measure used to assess general aspects of HRQoL in patients with cancer. Dimensions include functional scales, symptom scales, a Global Health Status/QoL scale, and items addressing common cancer symptoms and financial impact.43 Responses are linearly transformed to be in the 0 to 100 range; a higher score represents a “better” level of functioning or “worse” level of symptoms.51 | Validity: In a study of EORTC QLQ‑C30 in patients with nonresectable lung cancer (N = 305), correlations (Pearson r) between the global QoL scale and the other scales of the EORTC QLQ‑C30 ranged from 0.26 to 0.62 before treatment and 0.31 to 0.61 after treatment. Most symptom and functional measures discriminated between patients with differing clinical status based on ECOG Performance Status score, weight loss, and treatment toxicity.52 Reliability: In the study in nonresectable lung cancer (N = 305), reliability coefficients (Cronbach alpha) for the multiitem scales ranged from 0.54 to 0.86 before treatment and from 0.52 to 0.89 during treatment. For functioning scales, coefficients ranged from 0.54 to 0.86 before treatment and from 0.52 to 0.89 during treatment. For symptom scales and/or items, coefficients ranged from 0.65 to 0.82 before treatment and from 0.73 to 0.85 during treatment.52 Responsiveness: In the study in nonresectable lung cancer (N = 305), over an average of 28 days, differences were reported for physical functioning (P < 0.001), role functioning (P < 0.001), fatigue (P < 0.01), nausea and vomiting (P < 0.05), and global QoL (P < 0.01) between patients whose condition improved or worsened based on ECOG Performance Status score during pretreatment and on-treatment periods. No changes were noted in EORTC QLQ‑C30 scores among patients whose Performance Status score did not change.52 | The MID estimates in patients with small cell lung cancer and breast cancer who reported “a little” change in a subjective significance questionnaire had corresponding changes in the EORTC QLQ‑C30 of 5 to 10 points, those who reported a “moderate” change had corresponding changes of about 10 to 20 points, and those who reported “very much” change had corresponding changes of more than 20 points.44 A within-patient MID of 10 points was reported in a study evaluating both the EORTC QLQ‑C30 and EORTC QLQ‑LC13 in NSCLC.43 Between-group MIDs for improvement (5 points) and deterioration (−5 points) for Global Health Status were identified for patients with lung cancer.53 |
ECOG = Eastern Cooperative Oncology Group; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; EORTC QLQ-LC13 = European Organisation for Research and Treatment of Cancer questionnaire for assessing quality of life in lung cancer; EQ VAS = EQ visual analogue scale; FLSI-17 = Functional Assessment of Cancer Therapy Lung Symptom Index-17; HRQoL = health-related quality of life; ICC = intraclass correlation coefficient; MID = minimal important difference; NCCN = National Comprehensive Cancer Network; NSCLC = non–small cell lung cancer; NSCLC-SAQ = non–small cell lung cancer symptom assessment questionnaire; PGIS-LC = Patient Global Impression of Severity Lung Cancer Symptom Assessment; PRO = patient-reported outcome; QoL = quality of life.
Statistical Analysis
The MARIPOSA-2 trial is an ongoing, randomized, phase III, open-label, multicentre study with an event-driven design aimed at assessing the efficacy and safety of ACP compared with CP in patients with EGFR-mutated NSCLC following progression on osimertinib. Data from this trial have been analyzed at multiple prespecified time points, with the primary analysis based on a clinical cut-off (CCO) date of July 10, 2023 (IA1), and a subsequent supportive analysis at a CCO of April 26, 2024 (IA2). Final OS analysis is planned after the occurrence of approximately 390 OS events.
Sample Size and Power Calculations
The MARIPOSA-2 trial is an event-driven trial that targets dual primary hypotheses comparing PFS for LACP or ACP-L versus CP and ACP versus CP.
A total of 394 participants were planned to be randomized at a 2:1 ratio to CP:ACP in the MARIPOSA-2 trial. The sample size was calculated based on the assumption that ACP reduces the risk of disease progression or death by 35% compared with CP, with an HR of 0.65. The trial aims to accrue 350 PFS events to ensure 93% power for the ACP-L versus CP comparison and 83% power for the ACP versus CP comparison.
Interim and final OS analyses are planned based on event counts. An interim OS analysis is to be conducted when 75% of total planned OS events (approximately 300 deaths) have been observed, and a final OS analysis is scheduled when 400 deaths occur across all arms.
Statistical and Analytical Plans
Statistical Tests and Models
Details of the statistical analysis for the included outcomes are summarized in Table 8. Time-to-event end points were analyzed using Kaplan-Meier methods to estimate survival functions and medians, with stratified log-rank tests for comparisons between treatment groups. Cox proportional hazards models were used to estimate HRs and 95% CIs. Stratification factors included EGFR mutation type (exon 19 deletion versus exon 21 L858R substitution), race (Asian versus non-Asian), and brain metastasis status (yes versus no).
PFS was analyzed using a stratified Cox proportional hazards model and stratified log-rank test. Time-to-event analyses were conducted in the full analysis set, with patients analyzed according to their randomized treatment assignment. Landmark PFS estimates were reported at 6, 12, 18, and 24 months. The interim and final analyses for PFS were planned, using a group sequential design based on an O’Brien-Fleming–-type alpha-spending function to control the overall type I error rate at a 2-sided 5% level. Prespecified nominal alpha boundaries were defined for interim analyses to determine statistical significance without inflating type I error.
OS was analyzed using similar time-to-event methods. Interim and final OS analyses were also governed by the O’Brien-Fleming approach, ensuring appropriate control of the family-wise error rate across end points.
ORR was analyzed using a stratified logistic regression model adjusting for randomization stratification factors, with results reported as ORs and 95% CIs.
DOR was estimated using the Kaplan-Meier method with 95% CIs.
TTSP was analyzed using a stratified Cox regression model.
Sensitivity analyses for all time-to-event end points were prespecified to account for intercurrent events, such as subsequent anticancer therapies or missed disease assessments.
Multiple Testing Procedures
To control the family-wise type I error rate at a 2-sided alpha of 0.05, a graphical approach was implemented using a group sequential design. Six hypotheses (i.e., PFS, ORR, and OS for each comparison) were grouped into 2 families: 1 for LACP versus CP and 1 for ACP versus CP. Within each family, end points were tested hierarchically, starting with PFS, followed by ORR, and then OS. The local alpha values were dynamically reallocated after each rejection according to a predefined weighting structure. This ensured appropriate control of multiplicity across interim and final analyses.
Data Imputation Methods
Time-to-event data (e.g., PFS, OS, DOR, TTSP) were censored at the last evaluable assessment if events were not observed. For PRO measures (e.g., NSCLC-SAQ), missing data were handled using a mixed model for repeated measures approach. No imputation was applied to ORR, which relied on confirmed response assessments using RECIST 1.1.
Subgroup Analyses
Prespecified subgroup analyses were conducted to explore potential treatment-effect heterogeneity based on EGFR mutation type, race, brain metastasis status, line of prior osimertinib therapy, age group (i.e., < 65 years or ≥ 65 years), sex, weight (i.e., < 80 kg or ≥ 80 kg), ECOG Performance Status score (0 versus 1), and smoking history. Subgroup effects were evaluated for PFS, OS, and ORR using interaction terms in the appropriate models.
Table 8: Statistical Analysis of Efficacy End Points
End point | Statistical model | Adjustment factors | Handling of missing data | Sensitivity analyses |
|---|---|---|---|---|
PFS (by BICR) | Stratified log-rank test; stratified Cox model; Kaplan-Meier | Line of osimertinib (1L vs. 2L), brain metastases (yes versus no), Asian race (yes versus no) | Missing data not imputed. Censoring handled using standard time-to-event methodology (e.g., last known alive or assessment date). | Unstratified log-rank; investigator-assessed PFS; proportional hazards assumption |
OS | Stratified log-rank test; stratified Cox model; Kaplan-Meier | Line of osimertinib (1L vs. 2L), brain metastases (yes vs. no), Asian race (yes vs. no) | Missing data not imputed. Censoring handled using standard time-to-event methodology (e.g., last known alive or assessment date). | Unstratified log-rank; OS interim analyses with alpha-spending function |
ORR by BICR | Stratified logistic regression model | Line of osimertinib (1L vs. 2L), brain metastases (yes vs. no), Asian race (yes vs. no) | Missing data analyzed as observed; no imputation conducted. Missingness mechanism not specified. | Investigator-assessed ORR |
DOR by BICR | Kaplan-Meier method | Not applicable | Missing data analyzed as observed; no imputation conducted. Missingness mechanism not specified. | Not reported |
TTSP | Stratified log-rank test; stratified Cox model; Kaplan-Meier | Line of osimertinib (1L vs. 2L), brain metastases (yes vs. no), Asian race (yes vs. no) | Missing data analyzed as observed; no imputation conducted. Missingness mechanism not specified | Not reported |
EORTC QLQ-C30 | Mixed effect model for repeated measures; | Line of osimertinib (1L vs. 2L), brain metastases (yes vs. no), Asian race (yes vs. no) | Missing data analyzed as observed; no imputation conducted. Missingness mechanism not specified. | Not reported |
NSCLC-SAQ | Mixed effect model for repeated measures; Kaplan-Meier | Line of osimertinib (1L vs. 2L), brain metastases (yes vs. no), Asian race (yes vs. no) | Missing data analyzed as observed; no imputation conducted. Missingness mechanism not specified. | Not reported |
1L = first line; 2L = second line; BICR = blinded independent central review; DOR = duration of response; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; NSCLC-SAQ = Non–Small Cell Lung Cancer Symptom Assessment Questionnaire; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; TTSP = time to symptomatic progression.
Sources: MARIPOSA-2 Clinical Study Report.1 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Analysis Populations
The analysis population and number of participants included in the CP and ACP arms of the MARIPOSA-2 trial, as well as their respective descriptions, are provided in Table 9.
Table 9: Analysis Populations of MARIPOSA-2 Trial
Population | Participants | Definition | Application |
|---|---|---|---|
Full analysis set | CP arm: N = 263 ACP arm: N = 131 | All randomized patients, classified according to their assigned treatment arm regardless of the actual treatment received | Used to summarize the population characteristics and efficacy data. |
Safety analysis set | CP arm: N = 243 (92.4%) ACP arm: N = 130 (99.2%) | Randomized patients who receive at least 1 dose of a study treatment and have at least 1 evaluable postbaseline concentration measurement. | Used to summarize the safety data. |
ACP = amivantamab plus carboplatin and pemetrexed; CP = carboplatin and pemetrexed.
Sources: MARIPOSA-2 Clinical Study Report.1 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Results
Patient Disposition
Full details of the patient’s disposition are presented in Table 10. Briefly, in the MARIPOSA-2 trial, 970 patients were screened. Of these, 394 patients (40.6%) were randomized to either ACP (n = 131) or CP (n = 263). Screening failure occurred in 302 patients (31.1%), with the primary reason being failure to meet eligibility criteria (n = 265; 27.3%). Among randomized patients, 130 of 131 (99.2%) in the ACP arm and 243 of 263 (92.4%) in the CP arm received at least 1 dose of study treatment.
At IA1 (CCO July 10, 2023), ██ of 131 patients (█████) in the ACP arm and ███ of 263 patients (█████) in the CP arm remained on study treatment. Study completion was reported for ██ patients (█████) in the ACP arm and ██ patients ██████) in the CP arm. Discontinuation of all study drugs occurred in 63 of 130 patients (48.5%) in the ACP arm and 188 of 243 patients (77.4%) in the CP arm. The most common reason for treatment discontinuation was disease progression, reported in 41 patients (31.5%) in the ACP arm and 152 patients (62.6%) in the CP arm. Discontinuation due to AEs occurred in 14 patients (10.8%) and 10 patients (4.1%) in the ACP and CP arms, respectively. Refusal of further treatment was documented for █ patients █████ in the ACP arm and ██ patients ██████ in the CP arm. Study discontinuation due to patient withdrawal was reported in █ patients (████) in the ACP group and ██ patients ██████) in the CP group.
At IA2 (CCO April 26, 2024), ██ of 131 patients ██████ in the ACP arm and ██ of 263 patients ███████ in the CP arm were still participating in the study. The number of patients who completed the study was ██ ███████ in the ACP arm and ███ ███████ in the CP arm. Discontinuation occurred in █ patients ██████ in the ACP arm and ██ patients ██████ in the CP arm. At this time point, the most common reason for discontinuation was ████ ██ █████████.
Table 10: Summary of Patient Disposition in MARIPOSA-2 Trial
Patient disposition | ACP (N = 131) | CP (N = 263) |
|---|---|---|
Screened, N | 970 | |
Screening failure, n (%) | 302 ████ | |
Reason for discontinuation during screening, n (%) | ||
Failure to meet eligibility criteria | 265 ████ | |
Patient withdrawal | 15 █████ | |
Other | 9 █████ | |
Missing | 8 █████ | |
Progressive disease | 3 █████ | |
Lost to follow-up | 1 █████ | |
Study terminated by sponsor | 1 █████ | |
Full analysis set at IA1 | ||
Randomized, N (%) | 394 ██████ | |
Randomized into each study arm, n (%) | 131 (100.0) | 263 (100.0) |
Randomized but not treated, n (%) | █████ | █████ |
Treated, n (%) | 130 █████ | 243 █████ |
Patients ongoing, n (%) | █████ | █████ |
Completed study participationa | █████ | █████ |
Discontinued from study, n (%) | █████ | █████ |
Reason for discontinuation, n (%) | ||
Withdrawal by patient | █████ | █████ |
Lost to follow-up | █████ | █████ |
Safety analysis set at IA1 | ||
Randomized, n (%) | 131 (100) | 263 (100) |
Patients ongoing, n (%) | 67 (51.5) | 55 (22.6) |
Discontinued all study drugs,b n (%) | 63 (48.5) | 188 (77.4) |
Reason for discontinuation of lastc study drug, n (%) | ||
Progressive disease | 41 (31.5) | 152 (62.6) |
Adverse event | 14 (10.8) | 10 (4.1) |
Adverse event – COVID-19 related | █████ | █████ |
Patient refused further study treatment | 3 (2.3) | 21 (8.6) |
Physician decisiond | 5 (3.8) | 5 (2.1) |
FAS, n (%) | 131 (100.0) | 263 (100.0) |
Safety, n (%) | 130 (99.2) | 243 (92.4) |
Full analysis set – IA2 | ||
Randomized, n (%) | 131 (100) | 263 (100) |
Randomized but not treated, n (%) | █████ | █████ |
Patients treated, n (%) | █████ | █████ |
Patients still on the study | █████ | █████ |
Completed study participationb | █████ | █████ |
Discontinued from study, n (%) | █████ | █████ |
Reason for discontinuation, n (%) | ||
Withdrawal by patient | █████ | █████ |
Lost to follow-up | █████ | █████ |
ACP = amivantamab plus carboplatin and pemetrexed; CP = carboplatin and pemetrexed; FAS = full analysis set; IA1 = interim analysis 1; IA2 = interim analysis 2.
aCompleted: if a patient had died before the end of study.
bIncludes patients who completed 4 cycles of carboplatin or discontinued carboplatin prematurely before cycle 4.
cRepresents the discontinuation of all study treatments.
dThe category of physician decision in the table included participants who discontinued treatment due to clinical progressive disease in the absence of radiographic progressive disease.
Sources: MARIPOSA-2 Clinical Study Report.1 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Baseline Characteristics
Baseline demographic and clinical characteristics were reported for patients in the MARIPOSA-2 trial (full analysis set), which included 131 patients in the ACP arm and 263 patients in the CP arm. The mean age was ██ years in both arms. In the ACP arm, ██ patients ██████ were aged 75 years or older, compared with ██ patients ██████ in the CP arm.
There were 81 females (61.8%) and 50 males (38.2%) in the ACP arm, and 157 females (59.7%) and 106 males (40.3%) in the CP arm. Race categories in the ACP arm included Asian (48.1%) and white (45.8%). In the CP arm, race categories included Asian (48.3%) and white (46.8%).
In the ACP arm, 55 patients (42.0%) had a baseline ECOG Performance Status score of 0, and 76 (58.0%) had a score of 1. In the CP arm, 101 patients (38.4%) had a score of 0 and 162 (61.6%) had a score of 1.
A history of smoking was reported in 41 patients (31.3%) in the ACP arm and 95 patients (36.1%) in the CP arm.
A history of brain metastases was reported in 58 patients (44.3%) in the ACP arm and 120 patients (45.6%) in the CP arm.
EGFR mutation types in the ACP arm were exon 19 deletions in 67.9% and exon 21 L858R substitutions in 32.1%. In the CP arm, exon 19 deletions were reported in 69.8% and exon 21 L858R substitutions in 30.2%.
At initial diagnosis, adenocarcinoma was reported in 130 patients (99.2%) in the ACP arm and 260 patients (98.9%) in the CP arm. Other histological subtypes, including large cell carcinoma, squamous cell carcinoma, and unspecified types, were also recorded.
At screening, stage IVB disease was documented in ███ patients ██████ in the ACP arm and ███ patients ██████ in the CP arm. Locations of metastasis included █████ ██████ ██████ █████ ██████ ███████ ██████ █████ ███ █████ █████.
The mean time since initial lung cancer diagnosis was ████ months ██ ████ in the ACP arm and ████ months ███ ████ in the CP arm. The mean time since metastatic disease diagnosis was ████ months (██ ████) in the ACP arm and ████ months (██ ████) in the CP arm.
All patients had received prior systemic therapy for lung cancer. Prior radiotherapy was reported in ██ patients ██████ in the ACP arm and ███ patients ██████ in the CP arm. Prior cancer-related surgery was reported in ██ patients ██████ in the ACP arm and ██ patients ██████ in the CP arm.
Regarding prior lines of systemic therapy in the locally advanced or metastatic setting, 97 patients (74.0%) in the ACP arm and 181 patients (68.8%) in the CP arm had received 1 line of therapy. Osimertinib had been received as first-line therapy by 97 patients (74.0%) in the ACP arm and 181 patients (68.8%) in the CP arm. Prior systemic therapy settings included adjuvant therapy in ██████ patients █████ in the ACP arm and ██████ patients █████ in the CP arm. All patients enrolled in the MARIPOSA-2 trial had received osimertinib as first-line or second-line therapy in the advanced or metastatic setting; no patients had previously received osimertinib in the adjuvant setting.
The baseline characteristics outlined in Table 11 are limited to those that are most relevant to this review or were felt to affect the outcomes or interpretation of the study results.
Table 11: Summary of Baseline Characteristics From the MARIPOSA-2 Trial (FAS)
Characteristic | CP N = 263 | ACP N = 131 |
|---|---|---|
Age, years | ||
Mean (SD) | ██ █████ | ██ █████ |
Median | 62.0 | 62.0 |
Range | 31 to 85 | 36 to 84 |
< 65 years, n (%) | 166 (63.1) | 79 (60.3) |
≥ 65 years, n (%) | 97 (36.9) | 52 (39.7) |
███ | ██ █████ | ██ █████ |
███ | ██ █████ | ██ █████ |
Sex, n (%) | ||
Female | 157 (59.7) | 81 (61.8) |
Male | 106 (40.3) | 50 (38.2) |
Race, n (%) | ||
████████ ██████ ██ ██████ ██████ | ██ █████ | ██ █████ |
Asian | 127 (48.3) | 63 (48.1) |
█████ ██ ███████ ████████ | ██ █████ | ██ █████ |
White | 123 (46.8) | 60 (45.8) |
████████ | ██ █████ | ██ █████ |
███ ████████ | ██ █████ | ██ █████ |
███████ | ██ █████ | ██ █████ |
Weight, kg | ||
Mean (SD) | ██ █████ | ██ █████ |
Median | 63.0 | 63.0 |
Range | 37.2 to 118.0 | 38.5 to 111.9 |
< 80 kg, n (%) | 226 (85.9) | 113 (86.3) |
≥ 80 kg, n (%) | 37 (14.1) | 18 (13.7) |
Height, cm | ||
████ ████ | ██ █████ | ██ █████ |
██████ | ██ █████ | ██ █████ |
█████ | ██ █████ | ██ █████ |
Body mass index, kg/m2 | ||
████ ████ | ██ █████ | ██ █████ |
██████ | ██ █████ | ██ █████ |
█████ | ██ █████ | ██ █████ |
Baseline ECOG Performance Status score, n (%) | ||
0 | 101 (38.4) | 55 (42.0) |
1 | 162 (61.6) | 76 (58.0) |
History of smoking, n (%) | ||
Yes | 95 (36.1) | 41 (31.3) |
███████ | ██ █████ | ██ █████ |
██████ | ██ █████ | ██ █████ |
No | 168 (63.9) | 90 (68.7) |
History of brain metastasis, n (%) | ||
Yes | 120 (45.6) | 58 (44.3) |
No | 143 (54.4) | 73 (55.7) |
Mutation type, n (%) | ||
Exon 19 deletion | 183 (69.8) | 89 (67.9) |
Exon 21 L858R substitution | 79 (30.2) | 42 (32.1) |
NSCLC subtype at initial diagnosis, n (%) | ||
Adenocarcinoma | 260 (98.9) | 130 (99.2) |
█████ ████ █████████ | ██ █████ | ██ █████ |
████████ ████ █████████ | ██ █████ | ██ █████ |
█████ | ██ █████ | ██ █████ |
Histology grade at initial diagnosis, n (%) | ||
██████████ ██████████████ | ██ █████ | ██ █████ |
██████ ██████████████ | ██ █████ | ██ █████ |
████ ██████████████ | ██ █████ | ██ █████ |
Other | 166 (63.1) | 71 (54.2) |
Cancer stage at initial diagnosis, n (%) | ||
█████ | ██ █████ | ██ █████ |
█████ | ██ █████ | ██ █████ |
█████ | ██ █████ | ██ █████ |
█████ | ██ █████ | ██ █████ |
█████ | ██ █████ | ██ █████ |
█████ | ██ █████ | ██ █████ |
█████ | ██ █████ | ██ █████ |
█████ | ██ █████ | ██ █████ |
█████ | ██ █████ | ██ █████ |
█████ | ██ █████ | ██ █████ |
Histology grade at screening, n (%) | ||
█████ | ██ █████ | ██ █████ |
█████ | ██ █████ | ██ █████ |
█████ | ██ █████ | ██ █████ |
█████ | ██ █████ | ██ █████ |
Cancer stage at screening, n (%) | ||
████ | ██ █████ | ██ █████ |
████ | ██ █████ | ██ █████ |
████ | ██ █████ | ██ █████ |
███ | ██ █████ | ██ █████ |
███ | ██ █████ | ██ █████ |
Location of metastasis at screening, n (%)a,b | ||
████ | ██ █████ | ██ █████ |
█████ | ██ █████ | ██ █████ |
█████ | ██ █████ | ██ █████ |
█████ ████ | ██ █████ | ██ █████ |
███████ █████ | ██ █████ | ██ █████ |
████ | ██ █████ | ██ █████ |
█████ | ██ █████ | ██ █████ |
Time since initial lung cancer diagnosis (months), n (%) | ||
████ ████ | ██ █████ | ██ █████ |
██████ | ██ █████ | ██ █████ |
█████ | ██ █████ | ██ █████ |
Time since metastatic disease diagnosis (months), n (%) | ||
████ ████ | ██ █████ | ██ █████ |
██████ | ██ █████ | ██ █████ |
█████ | ██ █████ | ██ █████ |
Total number of patients with any prior therapies for lung cancer, n (%) | ||
█████ ████████ ███████ | ██ █████ | ██ █████ |
█████ ████████████ | ██ █████ | ██ █████ |
█████ ██████████████ ███████ | ██ █████ | ██ █████ |
Number of prior lines of systemic therapy in the locally advanced or metastatic setting, n (%) | ||
█████ | ██ █████ | ██ █████ |
█████ | ██ █████ | ██ █████ |
█████ | ██ █████ | ██ █████ |
Prior line of osimertinib line of therapy, n (%) | ||
1L | 181 (68.8) | 97 (74.0) |
2L | 82 (31.2) | 34 (26.0) |
███ | ██ █████ | ██ █████ |
Prior systemic therapy setting, n (%) | ||
████████ | ██ █████ | ██ █████ |
████████████ | ██ █████ | ██ █████ |
███████████████████████ █ | ██ █████ | ██ █████ |
██████████ ██████████████ | ██ █████ | ██ █████ |
1L = first line; 2L = second line; ACP = amivantamab plus carboplatin and pemetrexed; CP = carboplatin and pemetrexed; ECOG = Eastern Cooperative Oncology Group; FAS = full analysis set; NSCLC = non–small cell lung cancer.
Note: The n values for each parameter reflect nonmissing values. Percentages calculated with the number of subjects in each treatment group as the denominator.
aPatients could be counted in more than 1 category.
bRefers to a history of metastases in these organs.
Sources: MARIPOSA-2 Clinical Study Report.1 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Exposure to Study Treatments
Details of exposure to study treatments are presented in Table 12. In the MARIPOSA-2 trial (safety analysis set), 130 patients received ACP and 243 patients received CP. The total patient-years of exposure was █████ in the ACP arm and █████ in the CP arm. The mean duration of study treatment was ███ months (██ ███) in the ACP arm and ███ months ██ ███ in the CP arm. Median durations were ███ and ███ months, respectively.
In the ACP arm █████ ██ ████████ ████████ █ ██ █ █████████ ███████ █████ ████████ █ ██ ██ ███████ █████ ████████ ██ ██ ██ ███████ █████ ████████ ██ ██ ██ ███████ ███ ████ ████████ ██ ██ ██ ███████. In the CP arm, █████ ████████ █ ██ █ ███████ █████ █████.
Mean relative dose intensity was █████ ███ █████ ███ ████████████ ██████ ███ ████ ███████████████ ███ ███████ ███ ████ ███ ██████████ ██ ███ ███ ████ ██ ███ ██ ████ ████████ █████████████ ███ ██████ ███ ████ ███ ███████████ ███ ██████ ███ ████ ███ ███████████.
Table 12: Summary of Patient Exposure From the MARIPOSA-2 Trial (Safety Analysis Set)
Exposure | CP (N = 243) | ACP (N = 130) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
Total | Carboplatin | Pemetrexed | Total | Amivantamab | Carboplatin | Pemetrexed | ||||||
Duration of study treatment (months) | ||||||||||||
Mean (SD) | ██ █████ | ██ █████ | ||||||||||
Median | ██ █████ | ██ █████ | ||||||||||
Range | ██ █████ | ██ █████ | ||||||||||
Total duration of treatment, months (%) | ||||||||||||
< 3 | ██ █████ | ██ █████ | ||||||||||
3 to < 6 | ██ █████ | ██ █████ | ||||||||||
6 to < 9 | ██ █████ | ██ █████ | ||||||||||
9 to < 12 | ██ █████ | ██ █████ | ||||||||||
12 to < 15 | ██ █████ | ██ █████ | ||||||||||
15 to < 18 | ██ █████ | ██ █████ | ||||||||||
≥ 18 | ██ █████ | ██ █████ | ||||||||||
Treatment cycles, n (%) | ||||||||||||
Mean (SD) | ██ | ██ | ██ | ██ | ████ | ██ | ██ | |||||
Median | ██ | ██ | ██ | ██ | ████ | ██ | ██ | |||||
Range | ██ | ██ | ██ | ██ | ████ | ██ | ██ | |||||
1 to 5 | ██ | ██ | ██ | ██ | ████ | ██ | ██ | |||||
6 to 10 | ██ | ██ | ██ | ██ | ████ | ██ | ██ | |||||
11 to 15 | ██ | ██ | ██ | ██ | ████ | ██ | ██ | |||||
16 to 20 | ██ | ██ | ██ | ██ | ████ | ██ | ██ | |||||
21 to 25 | ██ | ██ | ██ | ██ | ████ | ██ | ██ | |||||
ACP = amivantamab plus carboplatin and pemetrexed; CP = carboplatin and pemetrexed.
Note: The total number of cycles represent the combination of individual therapies.
Sources: MARIPOSA-2 Clinical Study Report.1 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Subsequent Treatment
A summary of subsequent systemic therapies received by patients in the MARIPOSA-2 trial is provided in Table 13. At the time of the interim DCO (July 10, 2023), a lower proportion of patients in the ACP arm received subsequent systemic therapy compared with the CP arm (22.1% versus 43.3%, respectively). Most subsequent treatments in both arms were classified as antineoplastic drugs. Use of investigational therapies and other medication classes was limited across groups.
Table 13: Summary of Subsequent Treatment From the MARIPOSA-2 Trial (Full Analysis Set) [Redacted]
███████████████ | ██████████ | |
|---|---|---|
██████ | ██████ | |
███████████████ | ██████ | ██████ |
███████████████ | ██████ | ██████ |
███████████████ | ██████ | ██████ |
███████████████ | ██████ | ██████ |
███████████████ | ██████ | ██████ |
███ █ ████████████ ██████████████████████ █████████████ ██ █ ███████████████████████.
Source: MARIPOSA-2 Clinical Study Report.1
Concomitant Medications and Cointerventions
Details of the most common concomitant medications received by patients in MARIPOSA-2 are summarized in Table 14. ████████ ███ ████████████ ██ ████ █████████ ████ ████████ ██ █████ ███ ████████████ ██████████ ███ █████████████ ██ ███ ███ ████ ████████████████ ███████████████ ███ ██████████ ████ ████ █████ ██ ███████████ ████████ ██ ██████ █████ ████ ████ ████████ ████████████████ █████ █████ ███ ███████ ███ ████ ███████████ ██ ████ ██ █████ ██████████ ███████████ ████ ██ ████████████.
█████████████ ███████████ ████ ████████████ █████ ██ ████████ █████████ ██ ███ ███ ████ █████ ██ ████████████ ████████ █████████████ ████████████ ██ ███ ██ ████ █████ ████████ ███ ████ ████████████ ████████ ████████████ █████████████ █████████████████ ███████████████ ███ ███████████████████ ███ ██████ ████ ██ ████████ ██ ███ ███ ███ ███ █████ ██ ███ ██ ███ ████████ ██ █████ ███ ███████████ ███████████ ██████████ ███████ ████████ ████ ████████ ███████████ █████ ███ ████████████ ██████████ ██████████████ ███ ████████ ████ ███████████████ ███ ████████ ████ ██████████████ ███████ ███ ██████.
Table 14: Summary of Most Common (> 10% Patients) Concomitant Treatments in (SAS) [Redacted]
████████ ██ ███████████ ███ | ██████████ | |
|---|---|---|
██████████ | ██████████ | |
█████████████████████ | ██████████ | ██████████ |
██████████ | ██ ██████ | ██ ██████ |
█████ ███ ████ ███████ ████ | ██ ██████ | ██ ██████ |
██████████████ ███ ███████ | ██ ██████ | ██ ██████ |
███████████████ ███ ███████ | ██ ██████ | ██ ██████ |
██████████████ ██████ | ██ ██████ | ██ ██████ |
█████ ███ ██████████ ██████ | ██ ██████ | ██ ██████ |
█████ ███ ████████████ | ██ ██████ | ██ ██████ |
████████████████ | ██ ██████ | ██ ██████ |
█████ ███████████ ███ █ | ██ ██████ | ██ ██████ |
██████████████ ███ ███████ | ██ ██████ | ██ ██████ |
█████████████ | ██ ██████ | ██ ██████ |
████████████████ ████████ | ██ ██████ | ██ ██████ |
███████ ███████████ | ██ ██████ | ██ ██████ |
███████████ ███ █████████████ | ██ ██████ | ██ ██████ |
███████████ ████████████ | ██ ██████ | ██ ██████ |
█████████████████ ███ ██████ | ██ ██████ | ██ ██████ |
████████████████ | ██ ██████ | ██ ██████ |
████████ | ██ ██████ | ██ ██████ |
███████████ ██████ ███ ████ | ██ ██████ | ██ ██████ |
██████ ██████ ██ ███ ██████ | ██ ██████ | ██ ██████ |
███████████████ ██████████ | ██ ██████ | ██ ██████ |
███████████ ███ ██████████ | ██ ██████ | ██ ██████ |
█████ ███ ████ ███████████ | ██ ██████ | ██ ██████ |
█████ ███ █████████ ██ ████ | ██ ██████ | ██ ██████ |
█████████ | ██ ██████ | ██ ██████ |
██████████ ███ ███████████ | ██ ██████ | ██ ██████ |
█████ █████████ ██████ | ██ ██████ | ██ ██████ |
███████ ███████ ███████ | ██ ██████ | ██ ██████ |
████ ████████ ██████ | ██ ██████ | ██ ██████ |
████████████████ | ██ ██████ | ██ ██████ |
██████ ████████████ | ██ ██████ | ██ ██████ |
█████ ███ ███████████ ███ | ██ ██████ | ██ ██████ |
████████████████ | ██ ██████ | ██ ██████ |
███ █████ ███████████ ███ | ██ ██████ | ██ ██████ |
█████ ████ ██ ████████ | ██ ██████ | ██ ██████ |
██████████████ | ██ ██████ | ██ ██████ |
███ ████████ ███ ██████████ | ██ ██████ | ██ ██████ |
███████████ ███ ██████████ | ██ ██████ | ██ ██████ |
███ █ ████████████ ██████████████████████ █████████.
Source: MARIPOSA-2 Clinical Study Report.1
Efficacy
A summary of key efficacy outcomes (PFS, OS, ORR, DOR, and TTSP) from the MARIPOSA-2 trial’s primary analysis (IA1; July 10, 2023), as well as the supportive OS results from the updated longer-term follow-up (IA2; April 26, 2024) is presented in Table 15.
Table 15: Summary of Key Efficacy Results From the MARIPOSA-2 Trial (Full Analysis Set)
Key efficacy results | Primary analysis CCO: July 10, 2023 (IA1) | Updated analysis CCO: April 26, 2024 (IA2) | ||
|---|---|---|---|---|
ACP (N = 131) | CP (N = 263) | ACP (N = 131) | CP (N = 263) | |
Primary end point | ||||
PFS (by BICR) | ||||
Events, n (%) | ██ ████ | ███ ███ | ██ | |
Median time to event, months (95% CI) | 6.28 (5.55 to 8.41) | 4.17 (4.04 to 4.44) | ||
HR (95% CI)a; P valueb | 0.48 (0.36 to 0.64); < 0.0001 | |||
Event-free rate (95% CI) 6-month 9-month 12-month 18-month 24-month | ████ ███ ████ ███ ████ ███ ████ ███ ████ ███ | ████ ███ ████ ███ ████ ███ ████ ███ ████ ███ | ||
Key secondary end point | ||||
OS (full analysis set) | ||||
Events, n (%) | ████ ███ | ████ ███ | ████ ███ | ████ ███ |
Median time to event, months (95% CI) | ████ ███ | ████ ███ | ████ ███ | ████ ███ |
HR (95% CI)a; P valueb | 0.77 (0.49 to 1.21); 0.2531 | 0.73 (0.54 to 0.99); 0.0386 | ||
Event-free rate (95% CI) 6-month 9-month 12-month 18-month 24-month | ████ ███ ████ ███ ████ ███ ████ ███ ████ ███ | ████ ███ ████ ███ ████ ███ ████ ███ ████ ███ | ████ ███ ████ ███ ████ ███ ████ ███ ████ ███ | ████ ███ ████ ███ ████ ███ ████ ███ ████ ███ |
ORR (by BICR) | ||||
Number of subjects with measurable disease at baseline | ████ | ████ | ███ ████ ███ | |
ORR (CR + PR), n (%) | ████ (63.8%) | ████ (36.2%) | ||
95% CI | 55.0% to 72.1% | 30.3% to 42.3% | ||
Odds ratio (95% CI)c; P valued | 3.10 (2.00 to 4.80); < 0.0001 | |||
Best overall response, n (%) CR PR Stable disease Progressive disease Not evaluable | 2 (1.5) 81 (62.3) 30 (23.1) 10 (7.7) 7 (5.4) | 1 (0.4) 93 (35.8) 82 (31.5) 52 (20.0) 32 (12.3) | ||
DOR (by BICR)e | ||||
Number of patients with measurable disease at baseline, n | ████ | ████ | ████ █████ | |
Responder (confirmed CR + confirmed PR) | ████ | ████ | ||
Events, n (%) | ████ | ████ | ||
Median (95% CI)f time to event (months) | 6.90 (5.52 to NE) | 5.55 (4.17 to 9.56) | ||
DOR (%) ≥ 6 months ≥ 12 months ≥ 18 months | ████ ███ ████ ███ ████ ███ | ████ ███ ████ ███ ████ ███ | ||
TTSP | ||||
Events, n (%) | ████ | ████ | ████ | ████ |
Symptomatic PD | ████ | ████ | ████ | ████ |
Death without symptomatic PD | ████ | ████ | ████ | ████ |
Median time to event, months (95% CI) | 14.88 (11.30 to NE) | 13.01 (9.20 to NE) | ████ | ████ |
HR (95% CI)a; P valueb,g | 0.74 (0.51 to 1.07); 0.1026 | ████ | ||
Event-free rate (95% CI) 6-month 9-month 12-month 18-month 24-month | ████ ███ ████ ███ ████ ███ ████ ███ ████ ███ | ████ ███ ████ ███ ████ ███ ████ ███ ████ ███ | ████ ███ ████ ███ ████ ███ ████ ███ ████ ███ | ████ ███ ████ ███ ████ ███ ████ ███ ████ ███ |
Intracranial PFS (by BICR) | ||||
Events, n (%) | ████ ███ | ████ ███ | ████ ███ | ████ ███ |
Median months (95% CI) | 8.31 (7.29 to 11.27) | 12.45 (10.84 to NE) | ████ ███ | ████ ███ |
HR (95% CI)a; P valueb | 0.55 (0.38 to 0.79); 0.0011 | ████ ██ | ||
Event-free rate (95% CI) 6-month 9-month 12-month 18-month 24-month | ████ ███ ████ ███ ████ ███ ████ ███ ████ ███ | ████ ███ ████ ███ ████ ███ ████ ███ ████ ███ | ████ ███ ████ ███ ████ ███ ████ ███ ████ ███ | ████ ███ ████ ███ ████ ███ ████ ███ ████ ███ |
Intracranial ORR (by BICR)h | ||||
Number of subjects with intracranial disease at baseline, n | ████ ███ | ████ ███ | ████ ███ | ████ ███ |
ORRi | ████ ███ | ████ ███ | ████ ███ | ████ ███ |
95% CI | ████ ███ | ████ ███ | ████ ███ | ████ ███ |
Odds ratio (95% CI)c; P valuej | ████ ███ | ████ ███ | ||
Best overall response | ||||
CR | ████ ███ | ████ ███ | ████ ███ | ████ ███ |
PR | ████ ███ | ████ ███ | ████ ███ | ████ ███ |
Stable diseaseg | ████ ███ | ████ ███ | ████ ███ | ████ ███ |
Progressive disease | ████ ███ | ████ ███ | ████ ███ | ████ ███ |
Not evaluable | ████ ███ | ████ ███ | ████ ███ | ████ ███ |
Intracranial DOR (by BICR)k | ||||
Respondersi | ████ ███ | ████ ███ | ████ ███ | ████ ███ |
Events, n (%) | ████ ███ | ████ ███ | ████ ███ | ████ ███ |
Median (95% CI)f (months) | ████ ███ | ████ ███ | ████ ███ | ████ ███ |
DOR ≥ 6 months ≥ 9 months ≥ 12 months ≥ 18 months | ████ ███ ████ ███ ████ ███ ████ ███ | ████ ███ ████ ███ ████ ███ ████ ███ | ████ ███ ████ ███ ████ ███ ████ ███ | ████ ███ ████ ███ ████ ███ ████ ███ |
Time to intracranial disease progression (by BICR) | ||||
Events, n (%) | ████ ███ | ████ ███ | ████ ███ | ████ ███ |
Median (95% CI), months | ████ ███ | ████ ███ | ████ ███ | ████ ███ |
HR (95% CI)a; P valueb | ████ ███ | ████ ███ | ||
Event-free rate (95% CI) 6-month 9-month 12-month 18-month 24-month | ████ ███ ████ ███ ████ ███ ████ ███ ████ ███ | ████ ███ ████ ███ ████ ███ ████ ███ ████ ███ | ████ ███ ████ ███ ████ ███ ████ ███ ████ ███ | ████ ███ ████ ███ ████ ███ ████ ███ ████ ███ |
ACP = amivantamab plus carboplatin and pemetrexed; BICR = blinded independent central review; CCO = clinical cut-off; CI = confidence interval; CP = carboplatin and pemetrexed; CR = complete response; DOR = duration of response; HR = hazard ratio; IA1 = interim analysis 1; IA2 = interim analysis 2; NE = not estimable; ORR = objective response rate; OS = overall survival; PD = progressive disease; PFS = progression-free survival; PR = partial response; TTSP = time to symptomatic progression; vs. = versus.
aHR is from stratified proportional hazards model. HR less than 1 favours experimental treatment.
bP value is from a log-rank test stratified by osimertinib line of therapy (first-line vs. second-line), history of brain metastases (yes vs. no), and Asian race (yes vs. no).
cOdds ratio greater than 1 favours experimental treatment.
dP value is from a logistic regression stratified by osimertinib line of therapy (first-line vs. second-line), history of brain metastases (yes vs. no), and Asian race (yes vs. no).
ePercentages are based on the number of subjects who achieved CR or PR.
fQuartiles and 95% CIs are estimated with Kaplan-Meier method.
gNominal P value. TTSP was not included in the prespecified hierarchical testing strategy, and this analysis was not adjusted for multiplicity. The result should be interpreted as supportive evidence.
hFor IA1, CR does not have to be confirmed. For IA2, CR and PR do not have to be confirmed. Percent of responders is based on the number of patients with intracranial disease at baseline.
iFor IA1, only intracranial CRs are considered in this analysis because, as per the charter, brain lesions could not be selected as target lesions by BICR. For IA2, ORR includes CR or PR.
jP value is from a logistic regression (unstratified).
kFor IA1, CR does not have to be confirmed. Percentages are based on the number of patients who achieved CR. For IA2, CR and PR do not have to be confirmed. Percentages are based on the number of patients who achieved CR or PR.
Sources: MARIPOSA-2 Clinical Study Rreport;1 Tomasini et al., 2024;54 Janssen data on file.55 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Progression-Free Survival
The primary end point of PFS was met at the primary analysis, with ███ PFS events observed across both study arms combined. At the July 10, 2023, cut-off, a total of ██ PFS events (█████) had occurred in the ACP arm and ███ PFS events (█████) in the CP arm.
The median PFS was 6.28 months (95% CI, 5.55 to 8.41) in the ACP arm and 4.17 months (95% CI, 4.04 to 4.44) in the CP arm. The HR for disease progression or death was 0.48 (95% CI, 0.36 to 0.64; P < 0.0001). The number of patients censored at IA1 was ██ ███████ in the ACP arm and ██ ███████ in the CP arm. Prespecified subgroup analyses for PFS were consistent with the results of the intention-to-treat analysis.
The estimated proportion of patients who were progression-free at 6 months was █████ ████ ███ ████ ██ █████ in the ACP arm and █████ ████ ███ ████ ██ ███ in the CP arm. At 12 months, the estimated PFS rate was █████ ████ ███ ████ ██ █████ for ACP and █████ ████ ███ ███ ██ ████ for CP. Kaplan-Meier curves for IA1 PFS are presented in Figure 4 in Appendix 1.
At IA1, median intracranial PFS, assessed by BICR, was 12.45 months (95% CI, 10.84 to NE) in the ACP arm and 8.31 months (95% CI, 7.29 to 11.27) in the CP arm (HR = 0.55; 95% CI, 0.38 to 0.79; P = 0.0011). ██ ████ ██████ ████████████ ███ ███ █████ ██████ ████ ███ ██████ ██████ ██ ███ ███ ████ ██████ ████ ███ █████ ██████ ██ ██ ███ █ █████ ███ ███ ████ ██ █████████████. Estimated 12-month intracranial PFS event-free rates were ███ ████ ███ █████ ████ in the ACP group and ███ ████ ███ █████ ████ in the CP group at IA1, and ███ ████ ███ █████ ████ versus ███ ████ ███ █████ █████ at IA2.
Overall Survival
At IA1, a total of ██ deaths ██████ had occurred in the ACP arm and ██ deaths ██████ in the CP arm. The median OS was █████ ██████ ████ ███ ██████ ██) for ACP and █████ ██████ ████ ███ ██████ █ for CP. The HR for death was 0.77 (95% CI, 0.49 to 1.21); P = 0.2531.
At IA2, ██ deaths ██████ were reported in the ACP arm and ███ deaths ██████ in the CP arm. Median OS was 17.74 months (95% CI, 15.97 to 22.37) for ACP and 15.34 months (95% CI, 13.73 to 16.76) for CP. The HR for death was 0.73 (95% CI, 0.54 to 0.99; P = 0.0386).
Kaplan-Meier–estimated survival rates at 6 months were █████ ████ ███ ████ ██ ████ for ACP and █████ ████ ███ ████ ██ █████ for CP. At 12 months, the estimated OS rate was █████ ████ ███ ████ ██ ████ in the ACP arm and █████ ████ ███ ████ ██ ████ in the CP arm. At 24 months, estimated survival rates were █████ ████ ███ ████ ██ ████ and █████ ████ ███ ████ ██ ████ in the ACP and CP arms, respectively. Kaplan-Meier survival curves and the number of patients at risk by time point are presented in Figure 5 and Figure 6 in Appendix 1.
Objective Response Rate
At IA1, in the ACP arm, ██ ██ ███ patients (63.8%; 95% CI, 55.0% to 72.1%), and ██ ██ ███ patients (36.2%; 95% CI, 30.3% to 42.3%) in the CP arm achieved a confirmed response. The OR for response was 3.10 (95% CI, 2.00 to 4.80; P < 0.0001). CR was reported in 2 patients (1.5%) in the ACP arm and 1 patient (0.4%) in the CP arm.
At IA1, intracranial ORR by BICR was █████ ██ ██ ██ patients with intracranial disease at baseline; ███ ███ ████ ██ ████ in the ACP arm and █████ ██ ██ ██ patients; ███ ███ ███ ██ ████ in the CP arm (OR = █████ ███ ███ ████ ██ ███████████.
At IA2, intracranial ORR was █████ ██ ██ ██ patients; ███ ███ ██ in the ACP arm and █████ ███ ██ ██ patients; ███ ███ ███ ██ █████ in the CP arm (OR = █████ ███ ███ ████ ██.
Duration of Response
At IA1, the median DOR was 6.90 months (95% CI, 5.52 to NE) for the ACP arm and 5.55 months (95% CI, 4.17 to 9.56) for the CP arm. Events (progression or death) were reported in ██ patients (█████) in the ACP arm and ██ patients ██████ in the CP arm. Duration equal to or longer than 6 months was observed in ██ patients ██████ in the ACP arm and ██ patients ██████ in the CP arm. Duration of 12 months or longer was observed in ███████ ██ ████ ███ █████ ███ ████ ████ ███ ████ ██ ████████ ██ ██████ ███ ██████████ ████████ ███ ██ ██████ ██ ███████.
At IA1, median intracranial DOR by BICR was ████ months (███ ███ █████ ██) in the CP arm (██ responders) and ███ █████████ ████ ███ █████ ███ in the ACP arm (██ responders). Intracranial response duration equal to or longer than 6 months was observed in ██ patients ██████ in the CP arm and ██ patients (██████ in the ACP arm. ██ ████████ ██ ██████ ███ ███ ████████████ █████████ ███████ ███ ████ ██ ███ ██████. At IA2, median intracranial DOR was ████ months (███ ███ █████ ██) in the CP arm (██ responders) and █████ months (███ ███ █████ ██) in the ACP arm (██ responders). Duration equal to or longer than 6 months was observed in ██ ██ patients ██████ in the CP arm and ██ patients ██████ in the ACP arm. Duration equal to or longer than 12 months was observed in ██ patients (██████ in the ACP arm; ██ ████████ ██ ██████ █████ ███ ████████ ███ ██████.
Time to Symptomatic Progression
At IA1, ██ TTSP events (█████) occurred in the ACP arm and ██ events ██████) in the CP arm. Median TTSP was 14.88 months (95% CI, 11.30to NE) in the ACP group and 13.01 months (95% CI, 9.20 to NE) in the CP group. The HR was 0.74 (95% CI, 0.51 to 1.07; nominal P = 0.1026). At IA2, ██ TTSP events ██████ were observed in the ACP arm and ███ events ██████ in the CP arm. Median TTSP was █████ months ████ ███ █████ ██ █████) with ACP and █████ months (███ ███ ████ ██ █████) with CP. The HR was ████ ████ ███ ████ ██ █████ ███████████████ █████████ ACP. Kaplan-Meier event-free rates at 12 months were ███ ████ ███ ████ ██ █████ in the ACP arm and ███ ████ ███ ████ ██ ████ in the CP arm. By 18 months, rates declined to ███ (ACP) and ███ (CP), and at 24 months were ███ and ███, respectively.
At IA1, ██ intracranial progression events ██████ occurred in the ACP arm and ██ events ██████ in the CP arm. Median time to intracranial disease progression, assessed by BICR, was ███ █████████ ████ ███ █████ ██ ███ in the ACP arm and █████ months ████ ███ █████ ██ ██ in the CP arm. The HR was ████ ████ ███ ████ ██ █████ ████████████. At IA2, ██ intracranial progression events ██████ occurred in the ACP arm and ██ events ██████ in the CP arm. Median time to intracranial progression was █████ ██████ ████ ███ █████ ██ █████ with ACP and █████ ██████ ████ ███ █████ ██ ██████ with CP. The HR was ████ ████ ███ ████ ██ █████ ██████████████. Kaplan-Meier event-free rates at 12 months were ███ ████ ███ ████ ██ █████ in the ACP arm and ███ ████ ███ ████ ██ █████ in the CP arm. By 18 months, rates ████████ ██ ███ (ACP) and ███ (CP), and at 24 months were ███ █████████ (ACP) and ███ (CP).
HRQoL Outcomes
NSCLC-SAQ Total Score
For EORTC QLQ-C30 Global Health Status score (IA2), the median time to deterioration was ████ ██████ ████ ███ ████ ██ ████ in the ACP arm and ████ ██████ █ in the CP arm. The HR was ████ ████ ███ ████ ██ ████, with a P value of ██████. Twelve-month event-free rates were ███ in the ACP arm and ███ in the CP arm.
For the NSCLC-SAQ total symptom score (IA1), the median time to sustained deterioration was 11.6 months (95% CI, 10.2 to 14.9) in the ACP arm and 8.5 months (95% CI, 7.2 to 10.1) in the CP arm. The HR was 0.62 (95% CI, 0.43 to 0.88), with a P value of 0.0057.
Details are presented in Table 16 and Figure 7 in Appendix 1.
Table 16: Summary of EORTC QLQ-C30 and NSCLC-SAQ Outcomes in the MARIPOSA-2 Trial – FAS
Outcome | ACP (N = 131) | CP (N = 263) |
|---|---|---|
EORTC QLQ-C30; Time to deterioration in Global Health Status score (IA2) | ||
Events, n (%) | ███ ███ | ███ ███ |
Median time to event, months (95% CI) | ███ ███ | ███ ███ |
HR (95% CI);a P valueb | ███ ███ | |
Event-free rate (95% CI) | ||
6-month | ███ ███ | ███ ███ |
9-month | ███ ███ | ███ ███ |
12-month | ███ ███ | ███ ███ |
18-month | ███ ███ | ███ ███ |
24-month | ███ ███ | ███ ███ |
NSCLC-SAQ time to sustained deterioration in total symptom score over time (IA1) | ||
Time to event, months | ||
Median (95% CI) | 11.6 (10.2 to 14.9) | 8.5 (7.2 to 10.1) |
HR (95% CI);a P valueb | 0.62 (0.43 to 0.88); 0.0057 | |
ACP = amivantamab plus carboplatin and pemetrexed; CI = confidence interval; CP = carboplatin and pemetrexed; HR = hazard ratio; IA1 = interim analysis 1; EORTC QLQ-C30 = European Organization of Research and Treatment of Cancer Quality of Life Questionnaire Core 30; NSCLC-SAQ = non–small cell lung cancer symptom assessment questionnaire.
aHR is from a stratified proportional hazards model. HR less than 1 favours experimental treatment.
bP value is from a log-rank test stratified by osimertinib line of therapy (first-line vs. second-line), history of brain metastases (yes vs. no), and Asian race (yes vs. no).
Sources: MARIPOSA-2 Clinical Study Report;1 Tomasini et al., 2024;54 Janssen data on file.56 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Harms
Refer to Table 17 and Table 18 for harms data.
Adverse Events
TEAEs were reported in all patients in the ACP arm and in 93.4% of patients in the CP arm. Grade 3 or higher TEAEs occurred in 72.3% of patients receiving ACP and 48.1% receiving CP, indicating a higher frequency of severe events in both arms. AEs leading to death were reported in 3 patients (2.3%) in the ACP group and 3 patients (1.2%) in the CP group.
Gastrointestinal AEs, including nausea (44.6% in the ACP arm versus 37.0% in the CP arm), constipation (38.5% in the ACP arm versus 29.6% in the CP arm), and vomiting (24.6% in the ACP arm versus 17.3% in the CP arm), were commonly observed in both arms. Fatigue-related events, such as asthenia (26.2% in the ACP arm versus 16.5% in the CP arm), were also frequently reported.
Serious Adverse Events
SAEs were reported in 32.3% of patients in the ACP arm and 20.2% of those in the CP arm. The most frequently reported SAEs (≥ 2%) in the ACP arm included dyspnea (3.1%), thrombocytopenia (3.1%), pulmonary embolism (2.3%), and sepsis (2.3%). In the CP arm, SAEs occurring in at least 2% of patients included neutropenia (2.5%), pneumonia (2.1%), thrombocytopenia (2.1%), and febrile neutropenia (2.1%).
System organ classes with the highest incidence of SAEs in the ACP arm were infections and infestations (████), respiratory disorders (8.5%), and blood and lymphatic system disorders (████). In the CP arm, the most common SAE categories were blood and lymphatic disorders (████) and infections and infestations (████).
Discontinuation Due to AEs
Permanent discontinuation of any study drug due to TEAEs was more common in the ACP arm (18.5%) than the CP arm (3.7%). Dose reductions due to TEAEs occurred in 40.8% of patients receiving ACP and 15.2% receiving CP. Treatment interruptions were also more frequent in the ACP arm (64.6%) versus the CP arm (33.3%).
Mortality
During the study, 20.8% of patients in the ACP arm and 26.7% of patients in the CP arm died. The most common cause of death was disease progression, reported in 13.1% of patients in the ACP arm and 23.0% of patients in the CP arm. Deaths attributed to AEs occurred in 3.1% of patients in the ACP arm and 1.2% of patients in the CP arm.
Overall, 5.4% of the deaths in the ACP arm and 2.9% of the deaths in the CP arm occurred within 30 days of the last dose. Among these, 2.3% of the deaths in the ACP arm and 1.2% of the deaths in the CP arm were attributed to AEs. Deaths due to disease progression occurred in 3.1% of patients in the ACP group and 1.6% of patients in the CP group.
Notable Harms
SAEs occurred more frequently in the ACP arm, particularly those known to be associated with amivantamab. These included IRRs (58.5% in the ACP arm versus 0.4% in the CP arm), rash (43.1% versus 4.9%), paronychia (36.9% versus 0.4%), and stomatitis (31.5% versus 8.6%). Hematologic toxicities, such as neutropenia (56.9% versus 41.6%), thrombocytopenia (43.8% versus 29.6%), and anemia (39.2% versus 33.9%), were also commonly reported in both groups.
Venous thromboembolism, including pulmonary embolism and deep vein thrombosis, was observed more frequently in the ACP arm (pulmonary embolism: 2.3% versus 0.4%; deep vein thrombosis: < 2% in both arms), aligning with the known safety profile of amivantamab.
Table 17: Summary of Treatment-Emergent Safety Outcomes From the MARIPOSA-2 Trial; April 26, 2024, Data Cut-Off (Safety Analysis Set)
Outcome | ACP (N = 130) | CP (N = 243) |
|---|---|---|
AEs, n (%) | 130 (100.0) | 227 (93.4) |
Grade 3 or greater AEs, n (%) | 94 (72.3) | 117 (48.1) |
Serious AEs, n (%) | 42 (32.3) | 49 (20.2) |
AEs leading to death,a n (%) | 3 (2.3) | 3 (1.2) |
Any AEs leading to the following: | ||
Dose reduction of any study drug, n (%) | 53 (40.8) | 37 (15.2) |
Drug interruption of any study drug, n (%)b | 84 (64.6) | 81 (33.3) |
Discontinuation of any study drug, n (%) | 24 (18.5) | 9 (3.7) |
ACP = amivantamab plus carboplatin and pemetrexed; AE = adverse event; CP = carboplatin and pemetrexed.
aAEs leading to death are based on the “Fatal” AE outcome.
bExcludes infusion-related reactions.
Sources: MARIPOSA-2 Clinical Study Report.1 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
No new safety signals were identified. However, IRRs, rash, and venous thromboembolism were notable harms that may require active monitoring and management in clinical practice.
Table 18: Summary of Harms Results From the MARIPOSA-2 Trial; July 10, 2023, Data Cut-Off (Safety Analysis Set)
AEs | ACP (N = 130) | CP (N = 243) |
|---|---|---|
Patients with 1 or more TEAEs, n (%) | 130 (100.0) | 227 (93.4) |
Patients with 1 or more grade ≥ 3 TEAEs, n (%) | 94 (72.3) | 117 (48.1) |
Maximum toxicity grade, n (%) | ||
Grade 1 | ███ ███ | ███ ███ |
Grade 2 | ███ ███ | ███ ███ |
Grade 3 | ███ ███ | ███ ███ |
Grade 4 | ███ ███ | ███ ███ |
Grade 5 | ███ ███ | ███ ███ |
TEAEs with incidence ≥ 10% subjects in either treatment group, n (%) | ||
System organ class or preferred term | ||
Blood and lymphatic system disorders | ███ ███ | ███ ███ |
Neutropenia | 74 (56.9) | 101 (41.6) |
Anemia | 51 (39.2) | 97 (39.9) |
Thrombocytopenia | 57 (43.8) | 72 (29.6) |
Leukopenia | 37 (28.5) | 68 (28.0) |
Lymphopenia | ███ ███ | ███ ███ |
Gastrointestinal disorders | ███ ███ | ███ ███ |
Nausea | 58 (44.6) | 90 (37.0) |
Constipation | 50 (38.5) | 72 (29.6) |
Vomiting | 32 (24.6) | 42 (17.3) |
Stomatitis | 41 (31.5) | 21 (8.6) |
Diarrhea | 18 (13.8) | 16 (6.6) |
General disorders and administration site conditions | ███ ███ | ███ ███ |
Fatigue | 36 (27.7) | 47 (19.3) |
Asthenia | 34 (26.2) | 40 (16.5) |
Pyrexia | ███ ███ | ███ ███ |
Edema peripheral | ███ ███ | ███ ███ |
Investigations | ███ ███ | ███ ███ |
Alanine aminotransferase increased | 26 (20.0) | 67 (27.6) |
Aspartate aminotransferase increased | 19 (14.6) | 57 (23.5) |
Gamma-glutamyltransferase increased | ███ ███ | ███ ███ |
Weight decreased | ███ ███ | ███ ███ |
Blood creatinine increased | ███ ███ | ███ ███ |
Metabolism and nutrition disorders | ███ ███ | ███ ███ |
Decreased appetite | 40 (30.8) | 51 (21.0) |
Hypoalbuminemia | 29 (22.3) | 21 (8.6) |
Hyponatremia | 13 (10.0) | 16 (6.6) |
Hypokalemia | 24 (18.5) | 15 (6.2) |
Hyperglycemia | ███ ███ | ███ ███ |
Hypocalcemia | 16 (12.3) | 9 (3.7) |
Hypomagnesemia | ███ ███ | ███ ███ |
Infections and infestations | ███ ███ | ███ ███ |
COVID-19 | 27 (20.8) | 25 (10.3) |
Paronychia | 48 (36.9) | 1 (0.4) |
Respiratory, thoracic, and mediastinal disorders | ███ ███ | ███ ███ |
Cough | ███ ███ | ███ ███ |
Dyspnea | ███ ███ | ███ ███ |
Epistaxis | ███ ███ | ███ ███ |
Pulmonary embolism | ███ ███ | ███ ███ |
Nervous system disorders | ███ ███ | ███ ███ |
Headache | ███ ███ | ███ ███ |
Dizziness | ███ ███ | ███ ███ |
Skin and subcutaneous tissue disorders | ███ ███ | ███ ███ |
Pruritus | 20 (15.4) | 17 (7.0) |
Rash | 56 (43.1) | 12 (4.9) |
Dermatitis acneiform | 26 (20.0) | 7 (2.9) |
Dry skin | ███ ███ | ███ ███ |
Musculoskeletal and connective tissue disorders | ███ ███ | ███ ███ |
Back pain | ███ ███ | ███ ███ |
Injury, poisoning, and procedural complications | ███ ███ | ███ ███ |
IRR | 76 (58.5) | 1 (0.4) |
SAEs, n (%) | ||
Subjects with 1 or more SAEs | 42 (32.3) | 49 (20.2) |
System organ class or preferred term | ||
Blood and lymphatic disorders | ███ ███ | ███ ███ |
Neutropenia | 2 (1.5) | 6 (2.5) |
Thrombocytopenia | 4 (3.1) | 5 (2.1) |
Febrile neutropenia | 2 (1.5) | 5 (2.1) |
Anemia | 2 (1.5) | 2 (0.8) |
Myelosuppression | 2 (1.5) | 0 |
Infections and infestations | ███ ███ | ███ ███ |
Pneumonia | 0 (0.0) | 5 (2.1) |
Sepsis | 3 (2.3) | 1 (0.4) |
COVID-19 | 2 (1.5) | 0 (0.0) |
Skin infection | 2 (1.5) | 0 (0.0) |
General disorders and administration site conditions | ███ ███ | ███ ███ |
Pyrexia | 2 (1.5) | 3 (1.2) |
Respiratory, thoracic, and mediastinal disorders | ███ ███ | ███ ███ |
Pulmonary embolism | 3 (2.3) | 3 (1.2) |
Pleural effusion | 1 (0.8) | 3 (1.2) |
Dyspnea | 4 (3.1) | 2 (0.8) |
Nervous system disorders | ███ ███ | ███ ███ |
Metabolism and nutritional disorders | ███ ███ | ███ ███ |
Hepatobiliary disorders | ███ ███ | ███ ███ |
Gastrointestinal disorders | ███ ███ | ███ ███ |
Injury, poisoning, and procedural complications | ███ ███ | ███ ███ |
IRR | 2 (1.5) | 0 (0.0) |
Vascular disorders | ███ ███ | ███ ███ |
Deep vein thrombosis | 2 (1.5) | 1 (0.4) |
Cardiac disorders | ███ ███ | ███ ███ |
Supraventricular tachycardia | 2 (1.5) | 0 |
AEs of special interest, n (%) | ||
Subjects with 1 or more AEs of special interest | ███ ███ | ███ ███ |
Skin reaction | ███ ███ | ███ ███ |
Rash | 56 (43.1) | 12 (4.9) |
Dermatitis acneiform | 26 (20.0) | 7 (2.9) |
Rash maculopapular | ███ ███ | ███ ███ |
Acne | ███ ███ | ███ ███ |
Rash erythematous | ███ ███ | ███ ███ |
Folliculitis | ███ ███ | ███ ███ |
Dermatitis | ███ ███ | ███ ███ |
Rash pustular | ███ ███ | ███ ███ |
VTE | 13 (10.0) | 11 (4.5) |
Pulmonary embolism | ███ ███ | ███ ███ |
Deep vein thrombosis | ███ ███ | ███ ███ |
IRRs | 76 (58.5) | 1 (0.4) |
Pneumonitis or interstitial lung disease | ███ ███ | ███ ███ |
Deaths, n (%) | ||
Deaths during study | 27 (20.8) | 65 (26.7) |
Progressive disease | 17 (13.1) | 56 (23.0) |
AEs | 4 (3.1) | 3 (1.2) |
Other | 5 (3.8) | 6 (2.5) |
COVID-19 | 1 (0.8) | 0 (0.0) |
Deaths within 30 days of last dosea | 7 (5.4) | 7 (2.9) |
AEs | 3 (2.3) | 3 (1.2) |
Progressive disease | 4 (3.1) | 4 (1.6) |
Other | 0 (0.0) | 0 (0.0) |
ACP = amivantamab plus carboplatin and pemetrexed; AE = adverse event, CP = carboplatin and pemetrexed; IRR = infusion-related reaction; SAE = serious adverse event; TEAE = treatment-emergent adverse event; VTE = venous thromboembolism.
Note: Patients were counted only once for any given event, regardless of the number of times they experienced the event. AEs are coded using the Medical Dictionary for Regulatory Activities Version 25.0.
aPatients who died within 30 days were counted in both categories.
Sources: MARIPOSA-2 Clinical Study Report.63 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Critical Appraisal
Internal Validity
In the MARIPOSA-2 trial, randomization and stratification were appropriately implemented to reduce selection bias and ensure balance across treatment groups. Patients were randomized in a 2:1:2 ratio to CP or ACP, and LACP (not included in this report) and stratification was performed by line of prior osimertinib therapy (first-line versus second-line), presence of brain metastases, and Asian race. These were appropriate given their prognostic relevance in EGFR-mutated NSCLC.
However, the trial was open-label, and no blinding was used for treatment assignment. This design introduces the potential for performance and detection bias, particularly in the assessment of subjective end points, such as HRQoL and AEs. Primary and select secondary efficacy end points, including PFS, were assessed using RECIST 1.1 criteria by BICR, which mitigates the risk of assessment bias. The hierarchical testing strategy controlled for multiplicity across the primary end point (PFS) and the key secondary end point (OS), both of which were adequately powered. No multiplicity adjustments were applied to secondary end points, such as DOR and TTSP. The MARIPOSA-2 trial employed a sequential interim analysis design, which further structured the timing and control of statistical testing.
Patient characteristics were generally well balanced. No major imbalances were observed in age, sex, ECOG status, EGFR mutation subtype, brain metastases, or prior chemotherapy exposure. Chemotherapy before enrolment was reported in █████ of the CP arm and █████ of the ACP arm. Brain metastases were present in █████ of the CP arm and █████ of the ACP arm. Concomitant medications were significantly higher in the ACP arm than the CP arm, whereas subsequent therapies were lower in the ACP arm than the CP arm. For example, corticosteroids for systemic use ███ ██ ███ in ACP versus CP, respectively) along with many other concomitant drugs uses, such as antihistamines (███ ██ ███), antibacterials (███ ██ ███), may have been needed to control the more frequent AEs in the ACP arm compared with the CP arm. Subsequent antineoplastic agents were ██████ ██████ with CP (███) compared with ACP (███). The imbalance of these drug uses between treatment arms might have biased the HRQoL results in favour of ACP, and might have biased the OS assessment against ACP.
Crossover to amivantamab was not permitted per-protocol in the MARIPOSA-2 trial. A prespecified sensitivity analysis using inverse probability of censoring weighting was planned to adjust for potential confounding due to postprogression use of amivantamab-containing regimens in the CP arm. The proportion of patients who received amivantamab after progression was not reported, and postprogression treatment strategies were not defined in the protocol; therefore, interpretation of OS results may have been confounded by subsequent therapies that were not systematically documented or controlled.
Only ████ of patients in each of the CP and ACP arms were censored due to missing or unevaluable tumour assessments. The patterns appeared balanced between groups, suggesting minimal bias for time-to-event outcomes. In contrast, PROs (EORTC QLQ-C30 and NSCLC-SAQ scores) decreased in completeness of data reporting due to dropouts in later treatment cycles. Given the likely association between dropout and clinical deterioration, this incomplete data reporting might have limited the interpretability of later-cycle PRO results.
For PFS, censoring occurred at the last valid tumour assessment before a nonprogression event or DCO, and progression was confirmed by BICR. For OS, censoring occurred at the last known date the patient was alive. Due to the disproportionate rate in discontinuation of study, the potential for informative censoring, particularly in the ACP arm where AEs were more frequent, cannot be entirely ruled out. The trial did not report sensitivity analyses to explore the impact of censoring assumptions, which limits the ability to assess potential bias in the primary PFS analysis.
A total of █████ of patients in the ACP arm and █████ in the CP arm discontinued study treatment. The most common reason was disease progression (█████ ███ █████), while AEs accounted for █████ and ████, respectively. All patients who discontinued were followed for survival, and those without RECIST-defined progression continued undergoing scheduled assessments, which reduced attrition bias.
PFS was considered a robust and objective primary outcome, minimally influenced by lack of blinding. Regulatory agencies recognize PFS as meaningful when supported by consistent sensitivity analyses. In the MARIPOSA-2 trial, PFS benefits were consistent across prespecified subgroups. However, its ability to predict OS benefit in postosimertinib NSCLC would still remain uncertain as the overall treatment effect on the improvement in OS is modest compared with that of PFS.
External Validity
Based on clinical expert opinion, the MARIPOSA-2 trial population and interventions are generally applicable to practice in Canada. Eligible patients had EGFR-mutated advanced NSCLC that progressed on osimertinib (first-line or second-line) and an ECOG Performance Status score of 0 or 1, representing a relatively fit population that would be potentially less generalizable to patients with poor performance status or significant comorbidities. Inclusion of patients with treated or stable brain metastases enhances external validity. In the MARIPOSA-2 trial, █████ and █████ of patients in the ACP arm and CP arm, respectively, had a history of brain metastasis at baseline. The MARIPOSA-2 trial population may not be generalizable to patients who received osimertinib in the adjuvant setting or in combination with chemotherapy in the first-line setting, as these scenarios were excluded from trial eligibility.
The trial enrolled a globally diverse population; however, representation of Indigenous, Black, and other racialized groups living in Canada was limited. The mean participant age was 61 years, with more than one-third aged 65 years or older — somewhat younger than the typical population with EGFR-mutated NSCLC in Canada. Female predominance and high rates of having never smoked or being a former smoker were consistent with the epidemiology of this disease in Canada.
The ACP regimen is considered feasible in Canada but may require initial administration in specialized centres due to the need for prolonged observation and premedication during early cycles of amivantamab. Transition to outpatient care may be feasible once patients tolerate initial infusions.
Clinical experts confirmed that pemetrexed and carboplatin are standard in oncology practice in Canada and accessible through provincial formularies. Amivantamab is not yet publicly funded. IRRs, rash, and paronychia may require dermatology referral and supportive medications (e.g., steroid creams, antibiotics, antihistamines), which may not be universally covered.
The PBC comparator reflects Canadian SOC and validates the relevance of the control arm. While short-term survival results were clinically meaningful, longer-term follow-up is needed to assess the durability of benefit and late toxicities, particularly given the open-label design and median follow-up of 12.2 months at IA2. Real-world evidence will be important to confirm the applicability and implementation of findings in broader populations in Canada.
GRADE Summary of Findings and Certainty of the Evidence
Methods for Assessing the Certainty of the Evidence
For pivotal studies and RCTs identified in the sponsor’s systematic review, GRADE was used to assess the certainty of the evidence for outcomes considered most relevant to inform expert committee deliberations, and a final certainty rating was determined as outlined by the GRADE Working Group.57,58
High certainty: CDA-AMC is very confident that the true effect lies close to that of the estimate of the effect.
Moderate certainty: CDA-AMC is moderately confident in the effect estimate. The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. CDA-AMC uses the word “likely” for evidence of moderate certainty (e.g., “X intervention likely results in Y outcome”).
Low certainty: CDA-AMC has limited confidence in the effect estimate. The true effect may be substantially different from the estimate of the effect. CDA-AMC uses the word “may” for evidence of low certainty (e.g., “X intervention may result in Y outcome”).
Very low certainty: CDA-AMC has very little confidence in the effect estimate. The true effect is likely to be substantially different from the estimate of effect. CDA-AMC describes evidence of very low certainty as “very uncertain.”
Following the GRADE approach, evidence from RCTs started as high-certainty evidence and could be rated down for concerns related to study limitations (which refer to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias.
When possible, certainty was rated in the context of the presence of an important (nontrivial) treatment effect. If this was not possible, certainty was rated in the context of the presence of any treatment effect (i.e., the clinical importance is unclear). In all cases, the target of the certainty of evidence assessment was based on the point estimate and where it was located relative to the threshold for a clinically important effect (when a threshold was available) or to the null.
The selection of outcomes for GRADE assessment was based on the sponsor’s Summary of Clinical Evidence, consultation with clinical experts, and input received from patient and clinician groups and public drug plans. The following list of outcomes was finalized in consultation with expert committee members:
PFS
OS
ORR
HRQoL (EORTC QLQ-C30)
SAEs.
The reference points for the certainty of evidence assessment for PFS, OS, and ORR were set according to the presence or absence of an important effect based on thresholds informed by clinical experts consulted for this review. The reference points for the certainty of evidence assessment for the EORTC QLQ-C30 Global Health Status scores were determined based on a threshold suggested by the sponsor and informed by the literature, which identified a 10-point change from baseline as clinically meaningful. The reference points for the certainty of evidence assessment for SAEs and pneumonitis were set according to the presence or absence of a clinically important increase in the frequency of these harms, as informed by clinical expert input.
Results of GRADE Assessments
Table 2 presents the GRADE summary of findings for ACP versus CP for Patients with NSCLC following progression on osimertinib in theMARIPOSA-2 trial.
Long-Term Extension Studies
No long-term extension studies were submitted by the sponsor.
Indirect Evidence
No indirect treatment comparisons were submitted by the sponsor.
Studies Addressing Gaps in the Systematic Review Evidence
Contents within this section have been informed by materials submitted by the sponsor. The following has been summarized and validated by the review team.
The sponsor identified gaps in the systematic review evidence for which 2 phase II studies were submitted as supportive evidence (Table 19). A summary of the studies addressing gaps in the systematic review evidence is presented in Table 20.47
Table 19: Summary of Gaps in the Systematic Review Evidence
Evidence gap | Study description | Summary of key results |
|---|---|---|
Impact of prophylactic strategies to reduce the risk of IRRs with amivantamab | The SKIPPirr study is an ongoing, phase II, open-label, multicentre study evaluating oral dexamethasone, oral montelukast, or SC methotrexate for the prevention of IRRs associated with amivantamab in patients with advanced EGFR exon 19 deletion or exon 21 L858R substitution mutated NSCLC who have experienced disease progression on or after osimertinib treatment and on or after PBC. The study used a Simon 2-stage design with an expansion stage where cohorts were eligible to move into subsequent stages if they met an IRR incidence criterion. | Only the dexamethasone 8 mg cohort passed both stage I and stage II and proceeded to the expansion stage. Among the 40 patients in the dexamethasone 8 mg cohort, 9 patients (22.5%) reported IRRs on cycle 1 day 1; 1 patient had an IRR on cycle 2 day 1. All IRRs up to the end of cycle 3 were grade 1 to 2, except for 1 grade 3 IRR on cycle 2 day 1. |
Impact of enhanced dermatologic management to reduce the risk of dermatologic AEs | The COCOON study is an ongoing, phase II, randomized, open-label, multicentre study evaluating enhanced vs. standard dermatologic management in patients with advanced or metastatic EGFR-mutated NSCLC receiving amivantamab plus lazertinib. | At the interim analysis, by week 12, the incidence of grade ≥ 2 DAEIs was 27 of 70 patients (38.6%; 95% CI, 27.2% to 51.0%) in the enhanced dermatologic management arm and 52 of 68 patients (76.5%; 95% CI, 64.6% to 85.9%) in the SOC dermatologic management arm (OR = 0.19; 95% CI, 0.09 to 0.40; P < 0.0001). |
AE = adverse event; CI = confidence interval; DAEI = dermatologic adverse event of interest; IRR = infusion-related reaction; NSCLC = non–small cell lung cancer; OR = odds ratio; PBC = platinum-based chemotherapy; SC = subcutaneous; SOC = standard of care; vs. = versus.
Sources: Sponsor’s Summary of Clinical Evidence;47 SKIPPirr Clinical Study Protocol;59 SKIPPirr Study Summary;60 Spira et al., 2025;61 and COCOON Clinical Summary.62
Table 20: Details of Studies Addressing Gaps in the Systematic Review Evidence
Detail | SKIPPirr study | COCOON study |
|---|---|---|
Designs and populations | ||
Study design | Ongoing, phase II, open-label, multicentre study | Ongoing, phase II, randomized, open-label, multicentre study |
Enrolled, N | 68 (all cohorts) | 200 (planned enrolment) |
Key inclusion criteria |
|
|
Key exclusion criteria |
|
|
Drugs | ||
Intervention | Cohort A: Oral dexamethasone 4 mg twice daily (8 mg total daily dose) on day −1 (cycle 1) before the first dose of oral lazertinib and amivantamab IV combination therapy Cohort A2: Oral dexamethasone 8 mg twice daily (16 mg total daily dose) on day −2 and −1 (cycle 1) and 8 mg approximately 1 hour before the start of the infusion of amivantamab IV on cycle 1 day 1 Cohort B: Oral montelukast 10 mg in the morning on days −4, −3, −2, −1, and cycle 1 day 1 (5 doses total) before the first dose of oral lazertinib and amivantamab IV combination therapy Cohort C: Single dose of SC methotrexate 25 mg between day −7 and day −3 (cycle 1) before the first dose of oral lazertinib and amivantamab IV combination therapy Sequential enrolment was applied throughout the study, beginning with stage I in the following order: cohort A, cohort B, cohort C, cohort A2 All patients received background anticancer therapy with IV amivantamab 1,050 mg (for participants < 80 kg) or 1,400 mg (for participants ≥ 80 kg) once weekly for 4 weeks then every 2 weeks thereafter and oral lazertinib 240 mg once daily. All participants received standard prophylaxis with an antihistamine (diphenhydramine or equivalent), antipyretic (acetaminophen or equivalent), and glucocorticoid (IV dexamethasone). | Arm A: Amivantamab plus lazertinib plus enhanced dermatologic management; IV amivantamab 1,050 mg (1,400 mg if ≥ 80 kg) once weekly for 4 weeks and every 2 weeks thereafter; oral lazertinib 240 mg once daily; enhanced dermatologic management
Management also included general skin prophylaxis recommendations. |
Comparator(s) | NA All patients received background anticancer therapy with IV amivantamab 1,050 mg (for participants < 80 kg) or 1,400 mg (for participants ≥ 80 kg) once weekly for 4 weeks then every 2 weeks thereafter and oral lazertinib 240 mg once daily All participants also received standard prophylaxis with an antihistamine (diphenhydramine or equivalent), antipyretic (acetaminophen or equivalent), and glucocorticoid (IV dexamethasone). | Arm B: Amivantamab plus lazertinib plus standard dermatologic management; IV amivantamab 1,050 mg (1,400 mg if ≥ 80 kg) once weekly for 4 weeks and every 2 weeks thereafter; oral lazertinib 240 mg once daily; standard dermatologic management
|
Outcomes | ||
Primary end point | Rate of IRRs occurring on cycle 1 day 1 following administration of lazertinib and amivantamab combination therapy | Incidence of grade ≥ 2 DAEIsa in the first 12 weeks after initiation of amivantamab plus lazertinib treatment in arm A vs. arm B |
Select secondary end points |
|
|
Notes | ||
Publications | Spira et al., 202561 (NCT05663866) | None (NCT06120140) |
DAEI = dermatologic adverse event of interest; DOR = duration of response; ECOG = Eastern Cooperative Oncology Group; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; ILD = interstitial lung disease; INV = investigator; IRR = infusion-related reaction; NA = not applicable; NCI-CTCAE = National Cancer Institute Common Terminology Criteria for Adverse Events; NSCLC = non–small cell lung cancer; ORR = objective response rate; PBC = platinum-based chemotherapy; SC = subcutaneous; TKI = tyrosine kinase inhibitor; vs. = versus.
aDAEIs comprise rash, dermatitis, paronychia, skin fissures, acne, erythema, skin exfoliation, skin lesion, skin irritation, eczema, scalp rash, and more.
Sources: Sponsor’s Summary of Clinical Evidence;47 SKIPPirr Clinical Study Protocol;59 SKIPPirr Clinical Study Report;63 Cho et al., 2024;64 COCOON Clinical Study Protocol (Amendment 3/CHN-1);65 Kam et al., 2025.65,66
SKIPPirr Study
Description of Study
The SKIPPirr study is an ongoing, phase II, open-label, multicentre study evaluating oral dexamethasone, oral montelukast, or SC methotrexate for the prevention of IRRs associated with amivantamab in adult patients with advanced or metastatic EGFR exon 19 deletion or exon 21 L858R substitution mutated NSCLC who have experienced disease progression on or after osimertinib treatment and on or after PBC and who may benefit from combination therapy with amivantamab and oral lazertinib. Key inclusion and exclusion criteria and details of the study regimens are described in Table 20. All study participants received standard prophylaxis with an antihistamine, antipyretic, and glucocorticoid (IV dexamethasone). The SKIPPirr study used a Simon 2-stage design with an expansion stage where cohorts were eligible to move into subsequent stages if they met an IRR incidence criterion.47,59,60 The SKIPPirr study design is summarized in Figure 2.
Outcomes
The primary and select secondary end points of the SKIPPirr study are listed in Table 20. The end point of interest to this review (identified by clinical experts as clinically relevant) was the primary end point of IRRs occurring on cycle 1 day 1 following administration of lazertinib and amivantamab. This was defined as IRR events with onset time within 24 hours of the start of the first amivantamab infusion and before the start of amivantamab infusion on cycle 1 day 2 if there was an infusion on day 2, otherwise it was within 24 hours of the start of the first amivantamab infusion.47,59,68 The sponsor was not aware of a reported MID specific to the population with an EGFR exon 19 deletion or exon 21 L858R substitution mutation.47
Results
In the overall study population, the median age was 63.5 years; 65% of patients were female and 35% were male; 62% and 26% of patients were Asian and white, respectively; 75% of patients had an ECOG Performance Status score of 1; 44% had brain metastases; and 66% had an exon 19 deletion EGFR mutation type. In the dexamethasone 8 mg cohort, the median age was 62.0 years; 63% of patients were female and 37% were male; 59% and 24% of patients were Asian and white, respectively; 78% of patients had an ECOG Performance Status score of 1; 37% had brain metastases; and 71% had an exon 19 deletion EGFR mutation type.47,60,69
Figure 2: SKIPPirr Study Design
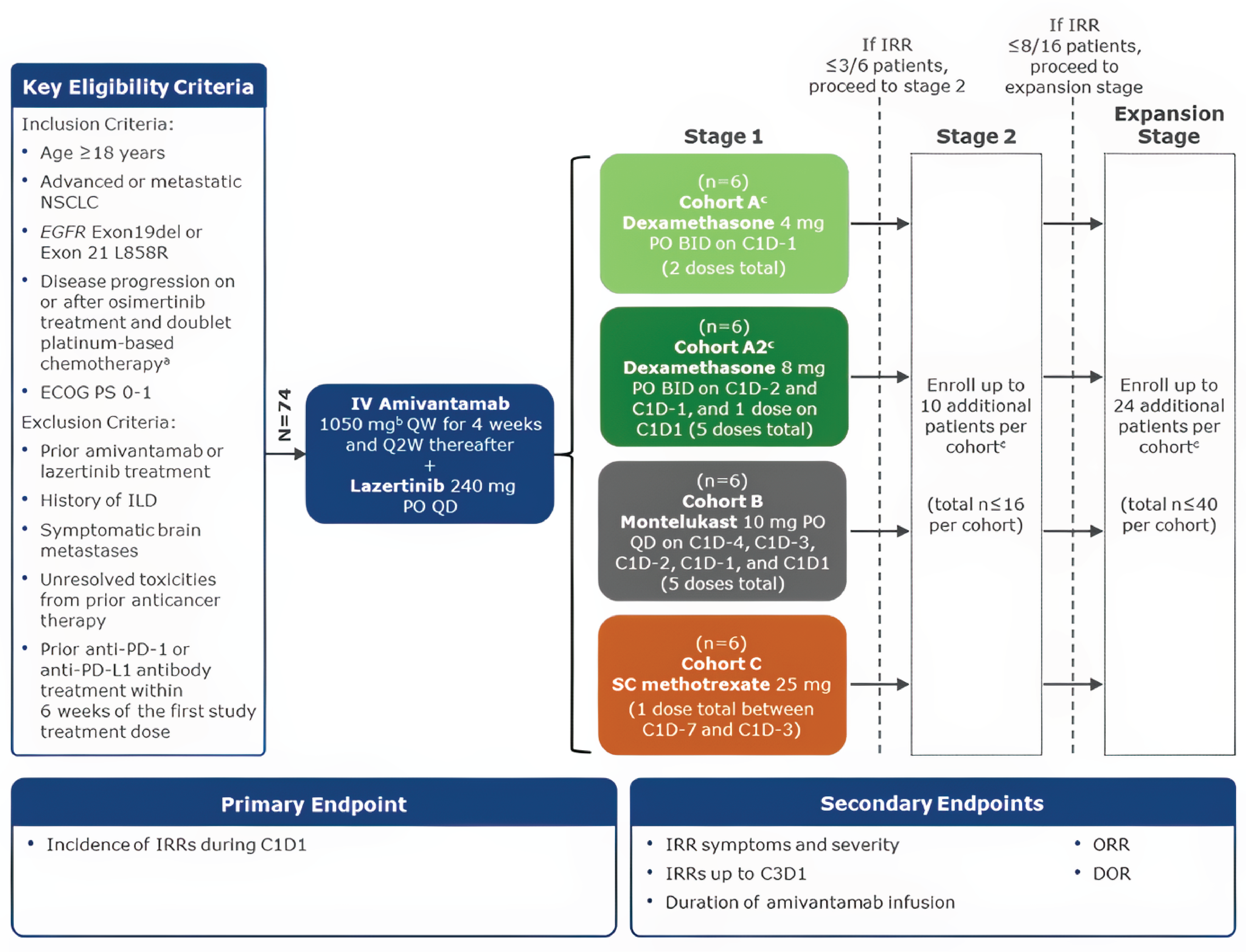
BID = twice daily; C = cycle; D = day; DOR = duration of response; ECOG = Eastern Cooperative Oncology Group; ILD = interstitial lung disease; IRR = infusion-related reaction; NSCLC = non–small cell lung cancer; ORR = objective response rate; PO = orally; QD = daily; Q2W = every 2 weeks; SC = subcutaneous.
Note: The data cut-off date was February 7, 2024.
aPrior use of a first-generation or second-generation EGFR tyrosine kinase inhibitor is allowed if administered before osimertinib.
bThe dose is 1,400 mg if body weight ≥ 80 kg.
cIf both cohorts A and A2 have positive results, only 1 will move on to stage II as determined by the study evaluation team.
Source: SKIPPirr Study Summary.67
Results for the primary end point (IRR rate on cycle 1 day 1) were available for the dexamethasone 8 mg cohort (A2), as it was the only cohort that passed both stage 1 and 2 and proceeded to the expansion stage.47,60,61 During stages 1 and 2, IRRs were reported in ███ ██ ██ ███████ ███ ███ ████ ██ █████ patients in this cohort.63 At the February 7, 2024, DCO, an additional █████ patients were enrolled in the expansion stage. Among the ████ patients with available efficacy data, IRRs on cycle 1 day 1 were reported for ███ patients. At the April 1, 2024, DCO, an additional ████ patients were enrolled in the expansion stage.47,60,70 At the June 24, 2024, DCO, an additional ████ patients were enrolled in the expansion stage.47,60,69 ███ ███████████ did not receive amivantamab on cycle 1 day 1 per-protocol and was not included in the analysis of the primary end point.61 Among the 40 patients in the dexamethasone 8 mg cohort, 9 (22.5%; ███ ███ ████ ██ ████) patients reported IRRs on cycle 1 day 1; 1 patient had an IRR on cycle 2 day 1.47,61,63 All IRRs up to the end of cycle 3 were grades 1 to 2, except for 1 grade 3 IRR on cycle 2 day 1.47,61 Authors compared the 22.5% IRR rate on cycle 1 day 1 in the dexamethasone 8 mg cohort to historical data in which participants who had received standard IRR management of antihistamines, antipyretics, and glucocorticoids experienced an IRR rate of 67.4% over the entire study period in the CHRYSALIS study.61
Critical Appraisal
Because patients and investigators were aware of the treatment intervention, there is the potential for bias in favour of the intervention; however, many signs of IRRs are objective (e.g., hypotension, fever, tachycardia) and are not as likely as subjective symptoms to be biased. Patients in the SKIPPirr study had previously received osimertinib and PBC and received amivantamab and lazertinib as background anticancer treatment, whereas the anticancer treatment for the patient population of interest for this review is ACP. The authors of the SKIPPirr study compared the IRR rate on cycle 1 day 1 in the dexamethasone 8 mg cohort (22.5%) to a historical IRR rate from the entire study period of the CHRYSALIS study (67.4%), which is higher than the IRR incidence reported throughout the MARIPOSA-2 trial in the ACP treatment arm (58.5%). Although there are differences in the anticancer treatment regimens, clinical experts consulted by CDA-AMC commented that the SKIPPirr study is relevant in addressing the issue of IRR prevention in the population of interest for this review because IRRs would be attributable to the amivantamab component of the regimen. They noted that historical control IRR rate cited is a reasonable reflection of what would be expected in clinical practice. Clinical experts also commented that the IRR rate on cycle 1 day 1 that was observed in the dexamethasone 8 mg cohort of the SKIPPirr study is less clinically meaningfully than what is expected in clinical practice with IV administration of amivantamab.
COCOON Study
Description of Study
The COCOON study is an ongoing, phase II, randomized, open-label, multicentre study evaluating enhanced versus standard dermatologic management in adult patients with locally advanced or metastatic (not amenable to curative therapy) EGFR exon 19 deletion or exon 21 L858R substitution mutated NSCLC receiving amivantamab plus lazertinib.47 Key inclusion and exclusion criteria and details of the study regimens are described in Table 20. Participants in the COCOON study were randomized 1:1 to receive either enhanced dermatologic management or SOC dermatologic management. The COCOON study design is summarized in Figure 3. The results presented are based on the planned interim analysis (DCO: November 13, 2024).71
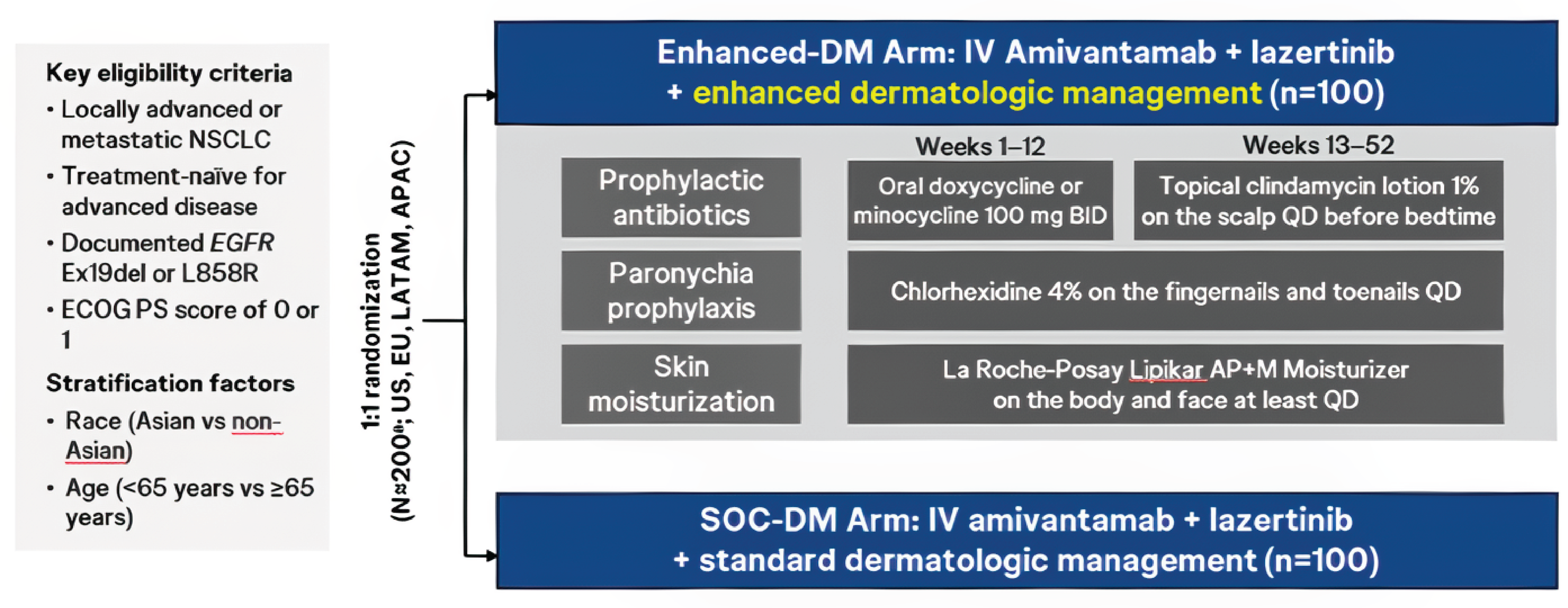
APAC = Asia-Pacific; BID = twice daily; DM = dermatologic management; ECOG = Eastern Cooperative Oncology Group; EU = Europe; LATAM = Latin America; NSCLC = non–small cell lung cancer; PS = Performance Status; QD = daily; SOC = standard of care.
Source: COCOON Clinical Summary.62
Outcomes
The primary and select secondary end points of the COCOON study are listed in Table 20. The end point of interest to this review (identified by clinical experts as clinically relevant) was the primary end point of the incidence of grade 2 or higher DAEIs in the first 12 weeks after initiation of amivantamab plus lazertinib treatment in patients who received enhanced dermatologic management versus patients who received SOC dermatologic management. DAEIs included rash, dermatitis, paronychia, skin fissures, acne, erythema, skin exfoliation, skin lesion, skin irritation, eczema, and more.64,65
Results
In the overall study population (N = 138 at interim analysis), the median age was ████ years; █████ of patients were female; █████ and █████ of patients were Asian and white, respectively; █████ of patients had an ECOG Performance Status score of 1; █████ had brain metastases; and █████ had an exon 19 deletion EGFR mutation type.62
Results for the primary end point (incidence of grade ≥ 2 DAEIs by Week 12) were available from the interim analysis. The results of the interim analysis show that, by week 12, the incidence of grade 2 or higher DAEIs was 27 of 70 patients (38.6%; ███ ███ ████ ██ ████) in the enhanced dermatologic management arm and 52 of 68 patients (76.5%; ███ ██ ████ ██ ████) in the SOC dermatologic management arm (OR = 0.19; 95% CI, 0.09 to 0.40; P < 0.0001). The most common grade 2 or higher DAEIs in the first 12 weeks (≥ 10% of participants in either arm) in the enhanced dermatologic management and SOC dermatologic management arms were ██████████ ██████ ███ ██████ respectively), ████ ██████ ███ █████, and ██████████ █████████ █████ ███ █████.
Critical Appraisal
Because patients and investigators were aware of the treatment intervention, there is the potential for bias in favour of enhanced dermatologic management; however, many signs of DAEIs are objective and at less risk of bias. In addition, the findings should be interpreted with consideration that although the primary end point was met at the interim analysis, certain data (e.g., treatment adherence, concomitant medications) were not available for appraisal. Patients in the COCOON study received amivantamab and lazertinib as background anticancer treatment as first-line treatment for advanced disease, whereas anticancer treatment for the patient population of interest for this review is ACP, received following disease progression with osimertinib. Although there were differences in the anticancer treatment regimens, the clinical experts consulted by CDA-AMC commented that the COCOON study is relevant in addressing the issue of management of dermatologic AEs in the population of interest for this review. The clinical experts stated that, where possible, the enhanced dermatologic management treatments used in the COCOON study are currently implemented in clinical practice, but they highlighted that chlorhexidine 4% availability may be limited and the skin moisturizers used in the COCOON study are expensive and can be financially preclusive for patients. The clinical experts stated that the difference in the incidence of grade 2 or higher DAEIs between the 2 arms of the COCOON study (interim analysis results) is clinically meaningful.
Discussion
Summary of Available Evidence
The clinical evidence for the effects of ACP in patients with EGFR exon 19 deletion or exon 21 L858R substitution-mutated NSCLC who experience disease progression on or after osimertinib is primarily derived from the MARIPOSA-2 trial. This was a phase III, randomized, open-label, multicentre trial that enrolled 657 patients with locally advanced or metastatic nonsquamous NSCLC. Patients were randomized in a 2:1:2 ratio to receive CP, ACP, or an investigational regimen (LACP or ACP-L) that was not assessed in this review. The primary end point was PFS assessed by BICR, with key secondary end points including OS, ORR, DOR, TTSP, and HRQoL. Results from 2 prespecified interim analyses, conducted on July 10, 2023 (IA1), and April 26, 2024 (IA2), were included in the clinical review.
Baseline characteristics of the MARIPOSA-2 trial population were generally well balanced between treatment arms and considered by the clinical experts to be applicable to the Canadian setting. The mean age was ███ ████ ███ years in both groups, and most patients were female (61.8% in the ACP arm and 59.7% in the CP arm) and of Asian or white descent. All enrolled patients had an ECOG Performance Status score of 0 or 1. Brain metastases were reported in 44% of patients in the ACP arm and 46% in the CP arm. Most patients had received osimertinib as their only prior line of systemic therapy (74% in the ACP arm and 69% in the CP arm). The distribution of EGFR mutations was consistent across arms, with exon 19 deletions present in 68% to 70% of patients and exon 21 L858R substitutions in 30% to 32%.
Two studies addressing gaps in the systematic review evidence were submitted. The SKIPPirr study, an ongoing, phase II open-label trial, evaluated strategies to reduce the incidence of IRRs in patients receiving amivantamab-based therapy. The COCOON study, a phase II, randomized, open-label trial, assessed enhanced versus standard dermatologic management in patients receiving first-line amivantamab plus lazertinib. Enhanced management significantly reduced the incidence of grade 2 or higher dermatologic AEs in the first 12 weeks (38.6% versus 76.5%) compared with SOC. Although the study population differed from the MARIPOSA-2 trial population, the clinical experts concluded that the COCOON study results were relevant for managing dermatologic toxicities in patients receiving amivantamab in other combinations, including ACP.
Interpretation of Results
Efficacy
In the MARIPOSA-2 trial, ACP demonstrated clinically meaningful improvements in efficacy outcomes compared with chemotherapy alone in patients with EGFR-mutated NSCLC following progression on osimertinib.
PFS, the primary end point, showed a statistically significant and clinically important improvement with ACP, with a median PFS of 6.28 months (95% CI, 5.55 to 8.41) versus 4.17 months (95% CI, 4.04 to 4.44) in the CP arm at IA1. The absolute difference in 6-month PFS probability (███ ████ ███ █████) exceeded the prespecified MID threshold of 10%, supporting the robustness of this finding. Improvements in PFS were supported by high-certainty evidence in the GRADE assessment.
OS, a key secondary end point, also favoured ACP across both interim analyses. Hypothesis testing for OS was not performed at IA1. At IA2, median OS was 17.74 months (95% CI, 15.97 to 22.37) in the ACP arm versus 15.34 months (95% CI, 13.73 to 16.76) in the CP arm and results reached statistical significance (HR = 0.73; 95% CI, 0.54 to 0.99). The absolute difference in 12-month OS probability (█████ ███ █████) exceeded the 10% MID threshold and was supported by moderate-certainty evidence. OS probabilities at 24 months were similar between groups (█████ ███ ███ █████ ██). These findings suggest that ACP likely extends survival in a patient population with limited treatment options. However, interpretation of OS is limited by potential risk of bias due to imbalances in the frequency of subsequent therapies between arms (█████ ██ ██ ███ █████ ██ ███), which may have influenced OS estimates.
The combination also showed improved tumour response, with a higher ORR in the ACP arm (███ ███ █████) compared with CP (███ ███ █████). The absolute improvement of ███ ████ responders per 1,000 patients exceeded the MID and was supported by high-certainty evidence. DOR was longer in the ACP arm (6.9 months) compared with the CP arm (5.55 months), ████████ the proportion of patients with responses lasting at least 12 months was ███ ██ ████ ██████ ██████████████ ██ ████.
PRO analyses suggested a trend toward improved HRQoL with ACP, particularly in Global Health Status scores measured by the EORTC QLQ-C30 at 6 months and 12 months. The median time to deterioration was slightly longer with ACP (████ ██████ ███ ████ ███████ ██ █████ ███ ███ ████ █ ███████████). However, these findings were associated with moderate-certainty evidence due to limitations, such as missing data and risk of bias, and the observed differences did not consistently exceed the predefined MID of 10 points. In addition, interpretation of PRO results may be limited by declining completion rates over time and potential influence from concomitant treatments, which may have affected symptom perception and response.
These findings align with the unmet need identified by patients and clinicians for therapies that delay disease progression, prolong life, and maintain quality of life. According to patient input, these outcomes were key priorities. Although ACP may address these priorities, it remains uncertain whether the observed improvements in PROs translate into meaningful advantages across all patients, given the variability in HRQoL outcomes and limitations in the available data.
While the MARIPOSA-2 trial is the only direct comparative evidence available for this setting, its open-label design introduces potential risk of bias in subjective outcomes such as HRQoL and symptom progression, although objective end points (i.e., PFS and ORR) were evaluated by BICR, strengthening the internal validity of these results.
Finally, evidence from studies addressing gaps in the systematic review supports the feasibility of managing amivantamab-related toxicities. Although the anticancer treatment in the studies included amivantamab and lazertinib, both provided evidence that IRRs and dermatologic AEs can be mitigated in clinical practice using appropriate adverse effects management strategies.
Harms
The addition of amivantamab to chemotherapy in the MARIPOSA-2 trial was associated with a higher frequency of AEs compared with chemotherapy alone. Grade 3 or higher TEAEs occurred in 72.3% of patients in the ACP arm versus 48.1% in the CP arm. SAEs were also more common in the ACP arm (32.3% versus 20.2%). While no new safety signals were identified, the incidence of several clinically important toxicities — including IRRs (58.5%); hematologic AEs, such as neutropenia and thrombocytopenia; and dermatologic toxicities, including rash and paronychia — was notably higher in the ACP arm.
IRRs occurred in 58.5% of patients receiving ACP, consistent with the known risk profile of amivantamab. Although most IRRs were grade 1 or 2 and occurred during the first infusion, grade 3 or higher IRRs were reported in ████ of the patients, and ████ discontinued treatment due to IRRs. These findings underscore the importance of appropriate premedication and monitoring strategies during initial infusions.
The SKIPPirr study addressed this safety concern by evaluating prophylactic interventions to reduce IRRs. Among patients who received oral dexamethasone 8 mg twice a day (administered on days −2 and −1, and 1 dose preinfusion on cycle 1 day 1), the IRR rate on cycle 1 day 1 was 22.5%, representing a clinically meaningful reduction compared with historical rates of approximately 67.4% with standard prophylaxis. No grade 3 or higher IRRs were reported with this regimen. Although the SKIPPirr study involved a different treatment base (i.e., amivantamab plus lazertinib), clinical experts confirmed the findings were relevant to the current review, given that IRRs were primarily attributed to the amivantamab component.
Dermatologic AEs were more common with ACP, including higher incidences of rash and paronychia. The COCOON study provided supportive evidence on mitigation strategies for dermatologic toxicities. Enhanced dermatologic management significantly reduced the incidence of grade 2 or higher DAEIs (38.6% versus 76.5%) during the first 12 weeks of treatment compared with SOC. Although the COCOON study was conducted in the first-line setting with amivantamab plus lazertinib, the study population differed from the MARIPOSA-2 trial. Nonetheless, clinical experts concluded that the findings were relevant for managing dermatologic toxicities in patients receiving amivantamab in other combinations, including ACP. Patient input noted that, while some respondents experienced significant toxicity with amivantamab — including skin and nail changes, fatigue, and infections — these side effects were manageable in most cases with dose adjustments and supportive care. However, 1 patient reported stopping treatment due to side effects affecting energy and quality of life. From a clinician perspective, tolerability of the ACP regimen was considered acceptable for patients who were fit for systemic chemotherapy, and the safety profile was not expected to limit use in appropriately selected individuals.
The harms observed in the MARIPOSA-2 trial were consistent with the known safety profiles of amivantamab, carboplatin, and pemetrexed. The frequency of SAEs was higher in the ACP group. The absolute increase in incidence exceeded the MID threshold of 10% and was deemed clinically important. The certainty of evidence for harms was rated as moderate due to the absence of statistical comparisons and limited event counts for specific SAEs. Overall, the potential for increased toxicity with ACP must be weighed against the observed clinical benefits in efficacy and PROs.
Other Considerations
Several additional factors are relevant to the interpretation of the clinical evidence for ACP. Although no indirect treatment comparisons were submitted, clinician and patient input consistently emphasized the lack of effective second-line options for patients with EGFR-mutated NSCLC who experience disease progression while taking osimertinib. In current Canadian practice, treatment decisions are largely guided by expert consensus and extrapolation from earlier-line data, underscoring the value of direct comparative evidence, such as that from the MARIPOSA-2 trial.
There are no long-term extension studies currently available; thus, the durability of response and long-term safety of amivantamab remain uncertain. This represents an evidence gap, particularly given the limited availability of effective third-line options and the need to optimize outcomes during second-line therapy. Ongoing follow-up from the MARIPOSA-2 trial may help address this uncertainty.
Patient group input highlighted several implementation considerations, including the need for convenient and tolerable treatment options. While many respondents reported positive experiences with amivantamab, the requirement for IV administration and premedication to mitigate IRRs was perceived as burdensome by some, particularly compared to oral EGFR-targeted therapies. Additionally, dermatologic side effects were noted to impact quality of life and body image, especially early in treatment. Evidence from the COCOON and SKIPPirr studies suggests that these concerns may be addressed through enhanced prophylactic and supportive care strategies, which could improve treatment satisfaction and may potentially enhance clinical benefits by promoting patient adherence and forestalling treatment discontinuation or interruption due to adverse effects.
From a clinical perspective, the clinical experts consulted for this review expect ACP to become the new SOC in the second-line setting for patients with EGFR-mutated NSCLC who have experienced disease progression while taking osimertinib and are eligible for systemic chemotherapy. This includes patients with an ECOG Performance Status score of 0 or 1. However, access to infusion services, supportive medications, and specialized oncology care may vary across Canadian jurisdictions, which could impact the consistency of implementation.
Conclusion
When considering the totality of evidence, ACP demonstrated clinically meaningful improvements in PFS, ORR, and DOR compared with chemotherapy alone in patients with EGFR exon 19 deletion or exon 21 L858R substitution-mutated NSCLC who experienced disease progression on or after osimertinib. These outcomes were supported by moderate to high certainty of evidence. Preliminary OS results likely favour ACP; however, formal statistical testing was not planned at the interim analysis, and the comparison should be considered descriptive. PROs suggested a potential benefit with ACP in delaying deterioration in HRQoL, although interpretation was limited by missing data over time. The evidence for PFS and ORR was supported by high certainty, while the certainty for OS and HRQoL was moderate due to imprecision and limitations in PRO data completeness.
The harms profile of ACP was consistent with the known safety of its individual components, although the incidence of SAEs, IRRs, and dermatologic AEs was higher than with chemotherapy alone. Supporting evidence from the SKIPPirr and COCOON studies suggested that IRRs and dermatologic toxicities may be manageable with appropriate prophylactic measures, which could improve patient tolerability in clinical practice.
The findings are relevant to Canadian clinical practice and reflect outcomes that matter to patients, including disease control, prolonged survival, and maintenance of quality of life. However, key gaps remain. Real-world data may be needed to assess the generalizability of trial results to broader patient populations, including those with poorer performance status or limited access to supportive care services.
Overall, the evidence suggests that ACP provides added clinical benefit compared with chemotherapy alone in the second-line setting for EGFR-mutated NSCLC following treatment with osimertinib. These conclusions are supported by moderate- to high-certainty evidence for key outcomes.
References
1.A Phase 3, Open-Label, Randomized Study of Amivantamab and Lazertinib in Combination with Platinum-Based Chemotherapy Compared with Platinum-Based Chemotherapy in Patients with EGFR-Mutated Locally Advanced or Metastatic Non-Small Cell Lung Cancer After Osimertinib Failure (Preliminary Analysis), Pub. L. No. 61186372NSC3002, (2024).
2.Brenner DR, Gillis J, Demers AA, et al. Projected estimates of cancer in Canada in 2024. CMAJ. May 12 2024;196(18):E615-E623. doi:10.1503/cmaj.240095 PubMed
3.Committee CCSA. Canadian Cancer Statistics 2023. Accessed March 21, 2025, https://cdn.cancer.ca/-/media/files/research/cancer-statistics/2023-statistics/2023_pdf_en.pdf?rev=7e0c86ef787d425081008ed22377754d&hash=DBD6818195657364D831AF0641C4B45C
4.Canadian Cancer Society SC, the Public Health Agency of Canada. Canadian Cancer Statistics A 2020 special report on lung cancer. Accessed March 21, 2025, https://cdn.cancer.ca/-/media/files/cancer-information/resources/publications/2020-canadian-cancer-statistics-special-report/2020-canadian-cancer-statistics-special-report-en.pdf?rev=15c66a0b05f5479e935b48035c70dca3&hash=3D51B0D0FB5C3F7E659F896D66495CE8&_ga=2.1870065.1988674510.1635847835-1688650972.1629385192
5.O'Sullivan DE, Jarada TN, Yusuf A, et al. Prevalence, Treatment Patterns, and Outcomes of Individuals with EGFR Positive Metastatic Non-Small Cell Lung Cancer in a Canadian Real-World Setting: A Comparison of Exon 19 Deletion, L858R, and Exon 20 Insertion EGFR Mutation Carriers. Curr Oncol. Sep 30 2022;29(10):7198-7208. doi:10.3390/curroncol29100567 PubMed
6.Boyne DJ, Jarada TN, Yusuf A, et al. 51P Testing Patterns and Outcomes of Different EGFR-positive Metastatic Non-Small Cell Lung Cancer Patients in a Canadian Real-world Setting. Ann Oncol. 2022;33(2)(Supplement):S56.
7.Janne PA, Johnson BE. Effect of epidermal growth factor receptor tyrosine kinase domain mutations on the outcome of patients with non-small cell lung cancer treated with epidermal growth factor receptor tyrosine kinase inhibitors. Clin Cancer Res. Jul 15 2006;12(14 Pt 2):4416s-4420s. doi:10.1158/1078-0432.CCR-06-0555 PubMed
8.Society CC. Survival statistics for non–small cell lung cancer. Accessed May 8, 2025, https://cancer.ca/en/cancer-information/cancer-types/lung/prognosis-and-survival/non-small-cell-lung-cancer-survival-statistics
9.Ontario H. Plasma-based comprehensive genomic profiling DNA assays for non–small cell lung cancer: a health technology assessment. Ont Health Technol Assess Series. 2024;24(8):1-306; Available at: https://www.hqontario.ca/Portals/0/Documents/evidence/reports/hta-plasma-based-comprehensive-genomic-profiling-DNA-assays-for-non%E2%80%93small-cell-lung-cancer.pdf. PubMed
10.Society CC. Diagnosis of lung cancer. Accessed March 21, 2025, https://cancer.ca/en/cancer-information/cancer-types/lung/diagnosis
11.Enstone A, Panter C, Manley Daumont M, Miles R. PRM47: Societal burden and impact on health related quality of life (HRQOL) of non-small cell lung cancer (NSCLC) in Europe. Value Health. 2015;18:A335-A766.
12.Horn MK, Mathias SD, Colwell HH, et al. Qualitative Research to Evaluate Perceptions around Biomarker Testing and Patient-Reported Outcomes (PROs) for Use in Studies of Non-Small Cell Lung Cancer (NSCLC). presented at: European Lung Cancer Congress (ELCC); 29 March to 1 April 2023 2023; Copenhagen, Denmark.
13.Hendriks LE, Kerr KM, Menis J, et al. Oncogene addicted metastatic non-small-cell lung cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up(†). Ann Oncol. Jan 3 2023;doi:10.1016/j.annonc.2022.12.013 PubMed
14.Singh N, Jaiyesimi IA, Ismaila N, et al. Therapy for Stage IV Non–Small-Cell Lung Cancer With Driver Alterations: ASCO Living Guideline, Version 2023.1. J Clin Oncol. 2023/05/20 2023;41(15):e42-e50. doi:10.1200/JCO.23.00281
15.Singh N, Jaiyesimi IA, Ismaila N, et al. Therapy for Stage IV Non–Small-Cell Lung Cancer Without Driver Alterations: ASCO Living Guideline, Version 2023.1. J Clin Oncol. 2023/05/20 2023;41(15):e51-e62. doi:10.1200/JCO.23.00282
16.Melosky B, Banerji S, Blais N, et al. Canadian consensus: a new systemic treatment algorithm for advanced EGFR-mutated non-small-cell lung cancer. Curr Oncol. Apr 2020;27(2):e146-e155. doi:10.3747/co.27.6007 PubMed
17.CADTH. Provisional Funding Algorithm: Advanced or metastatic non-small cell lung cancer with activating epidermal growth factor receptor mutations. 2023. January, 2024. https://www.cadth.ca/sites/default/files/DRR/2023/PH0028-NSCLC-EGFR.pdf
18.Fu K, Xie F, Wang F, Fu L. Therapeutic strategies for EGFR-mutated non-small cell lung cancer patients with osimertinib resistance. J Hematol Oncol. Dec 8 2022;15(1):173. doi:10.1186/s13045-022-01391-4 PubMed
19.Koulouris A, Tsagkaris C, Corriero AC, Metro G, Mountzios G. Resistance to TKIs in EGFR-Mutated Non-Small Cell Lung Cancer: From Mechanisms to New Therapeutic Strategies. Cancers (Basel). Jul 8 2022;14(14)doi:10.3390/cancers14143337 PubMed
20.Lin YT, Tsai TH, Wu SG, Liu YN, Yu CJ, Shih JY. Complex EGFR mutations with secondary T790M mutation confer shorter osimertinib progression-free survival and overall survival in advanced non-small cell lung cancer. Lung Cancer. Jul 2020;145:1-9. doi:10.1016/j.lungcan.2020.04.022 PubMed
21.Sari S, Andayani T, Endarti D, Widayati K. Health-Related Quality of Life in Non-Small Cell Lung Cancer (NSCLC) Patients with Mutation of Epidermal Growth Factor Receptor (EGFR) in Indonesia Research Journal of Pharmacy and Technology. 2020;
22.Passaro A, Janne PA, Mok T, Peters S. Overcoming therapy resistance in EGFR-mutant lung cancer. Nat Cancer. Apr 2021;2(4):377-391. doi:10.1038/s43018-021-00195-8 PubMed
23.Cheung WY, Carbonell C, Navani V, et al. Real-World Treatment Patterns, Health Outcomes, and Healthcare Resource Use in Advanced Common EGFR-Positive Non-Small Cell Lung Cancer Patients Treated with Osimertinib in Alberta. Curr Oncol. Jul 31 2024;31(8):4382-4396. doi:10.3390/curroncol31080327 PubMed
24.Sabari J, Pisano S, Gemmler K, et al. Treatment Patterns and Outcomes Among Patients With EGFR-mutant Advanced NSCLC in the Frontline and Post-osimertinib Settings. presented at: World Conference on Lung Cancer (WCLC); 2022; Vienna, Austria.
25.Girard N, Besse B, Caro RB, et al. Treatment Patterns, Outcomes, Healthcare Utilization, and Costs in EGFR-mutant Frontline and Post-osimertinib Advanced NSCLC. presented at: World Conference on Lung Cancer (WCLC); 2022; Vienna, Austria.
26.Janssen Inc. RYBREVANT (amivantamab). 2024.
27.NCCN Clinical Practice Guidelines in Oncology. NCCN Guidelines Version 2.2024 Non-Small Cell Lung Cancer. February 9 2024;
28.ESMO. ESMO Oncogene-Addicted Metastatic Non-Small-Cell Lung Cancer Living Guideline Version 1.2. 2025. https://www.esmo.org/living-guidelines/esmo-oncogene-addicted-metastatic-non-small-cell-lung-cancer-living-guideline
29.Bazhenova L, Ismaila N, Rous FA, et al. Therapy for Stage IV Non–Small Cell Lung Cancer With Driver Alterations: ASCO Living Guideline, Version 2024.2. Journal of Clinical Oncology. 2024;0(0):JCO-24-02133. doi:10.1200/jco-24-02133 PubMed
30.Inc. J. RYBREVANT amivantamab for injection Concentrate for Solution for Intravenous Infusion 350 mg / 7 mL (50 mg/mL) single-use vial [product monograph]. Mar 30, 2022. Updated January 13, 2025 Accessed March 21, 2025.
31.Agency EM. EMA/CHMP/335044/2024 Committee for Medicinal Products for Human Use (CHMP) Summary of opinion (post authorisation) Rybrevantamivantamab. March 18, 2025, https://www.ema.europa.eu/en/documents/smop/chmp-post-authorisation-summary-positive-opinion-rybrevant-ii-11_en.pdf
32.Administration USFD. FDA approves amivantamab-vmjw with carboplatin and pemetrexed for non-small cell lung cancer with EGFR exon 19 deletions or L858R mutations. March 18, 2025, https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-amivantamab-vmjw-carboplatin-and-pemetrexed-non-small-cell-lung-cancer-egfr-exon-19
33.Agency CsD. PC0289-000 amivantamab. March 18, 2025, https://www.cda-amc.ca/amivantamab
34.Agency CsD. PC0376-000 amivantamab. March 18, 2025, https://www.cda-amc.ca/amivantamab-0
35.Agency CsD. PC0392-000 lazertinib and amivantamab. March 21, 2025, https://www.cda-amc.ca/lazertinib-and-amivantamab
36.ULC PC. CARBOPLATIN INJECTION (Carboplatin Injection) Sterile solution 10 mg / mL (50 mg, 150 mg, 450 mg, 600 mg of carboplatin per vial) [product monograph]. January 3, 1986 Updated August 23, 2023. Accessed March 19, 2025.
37.ULC PC. CISPLATIN INJECTION BP (Cisplatin injection) Sterile solution 1 mg / mL (50 mg and 100 mg cisplatin per vial) [product monograph]. August 18, 1986. Updated October 24, 2023. Accessed March 19, 2025.
38.Inc. AP. Pemetrexed Disodium for Injection Sterile Powder for Solution 100 mg, 500 mg or 1000 mg pemetrexed per vial Pemetrexed (as pemetrexed disodium hemipentahydrate) [product monograph]. June 29, 2021. Updated June 29, 2021. Accessed March 19, 2025.
39.Ontario CC. CRBPPEME Regimen CARBOplatin-Pemetrexed. Accessed March 19, 2025, https://www.cancercareontario.ca/sites/ccocancercare/files/CRBPPEME_LU_NSC_AP.pdf
40.Ontario CC. CISPPEME Regimen CISplatin-Pemetrexed. Accessed March 19, 2025, https://www.cancercareontario.ca/sites/ccocancercare/files/CISPPEME_LU_NSCADV.pdf
41.Passaro A, Wang J, Wang Y, et al. Amivantamab plus chemotherapy with and without lazertinib in EGFR-mutant advanced NSCLC after disease progression on osimertinib: primary results from the phase III MARIPOSA-2 study. Ann Oncol. 2024;35(1):77-90. doi:10.1016/j.annonc.2023.10.117 PubMed
42.Montazeri A, Gillis CR, McEwen J. Quality of life in patients with lung cancer: a review of literature from 1970 to 1995. Chest. Feb 1998;113(2):467-81. doi:10.1378/chest.113.2.467 PubMed
43.Coon CD, Schlichting M, Zhang X. Interpreting Within-Patient Changes on the EORTC QLQ-C30 and EORTC QLQ-LC13. Patient. Nov 2022;15(6):691-702. doi:10.1007/s40271-022-00584-w PubMed
44.Osoba D, Rodrigues G, Myles J, Zee B, Pater J. Interpreting the significance of changes in health-related quality-of-life scores. J Clin Oncol. Jan 1998;16(1):139-44. doi:10.1200/JCO.1998.16.1.139 PubMed
45.Reinmuth N, Paz-Ares L, Chiara Garassino M, et al. Patient-Reported Outcomes (PROs) from the Phase 3 EVOKE-01 Trial of Sacituzumab Govitecan (SG) vs Docetaxel (Doc) in Metastatic Non-Small Cell Lung Cancer (mNSCLC). 2024.
46.McCarrier KP, Atkinson TM, DeBusk KP, Liepa AM, Scanlon M, Coons SJ. Qualitative Development and Content Validity of the Non-small Cell Lung Cancer Symptom Assessment Questionnaire (NSCLC-SAQ), A Patient-reported Outcome Instrument. Clin Ther. Apr 2016;38(4):794-810. doi:10.1016/j.clinthera.2016.03.012 PubMed
47.Inc. J. Sponsor's Summary of Clinical Evidence RYBREVANT® in Combination with Carboplatin and Pemetrexed in the Treatment of EGFRm NSCLC After Osimertinib Failure [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: RYBREVANT® (amivantamab); 350 mg/7mL (50 mg/mL) single-use vial for intravenous infusion February 19, 2025.
48.Bushnell DM, Atkinson TM, McCarrier KP, Liepa AM, DeBusk KP, Coons SJ. Non-Small Cell Lung Cancer Symptom Assessment Questionnaire: Psychometric Performance and Regulatory Qualification of a Novel Patient-Reported Symptom Measure. Curr Ther Res Clin Exp. 2021;95:100642. doi:10.1016/j.curtheres.2021.100642 PubMed
49.Williams P, Burke T, Norquist JM, et al. Non-Small Cell Lung Cancer Symptom Assessment Questionnaire (NSCLC-SAQ): Measurement Properties and Estimated Clinically Meaningful Thresholds From a Phase 3 Study. JTO Clin Res Rep. Apr 2022;3(4):100298. doi:10.1016/j.jtocrr.2022.100298 PubMed
50.Houts CR, Savord A, Gardner MJ, et al. Patient-reported outcomes in non-small cell lung cancer: psychometric evaluation of the PROMIS PF-SF 8c and NSCLC-SAQ in two phase 3 clinical trials. Qual Life Res. Mar 2025;34(3):751-762. doi:10.1007/s11136-024-03846-2 PubMed
51.Janssen R, Development. (Data on File). MARIPOSA-2 Statistical Analysis Plan. A Phase 3, Open-Label, Randomized Study of Amivantamab and Lazertinib in Combination with Platinum-Based Chemotherapy Compared with Platinum-Based Chemotherapy in Patients with EGFR-Mutated Locally Advanced or Metastatic Non Small Cell Lung Cancer After Osimertinib Failure. 2022.
52.Aaronson NK, Ahmedzai S, Bergman B, et al. The European Organization for Research and Treatment of Cancer QLQ-C30: a quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst. Mar 3 1993;85(5):365-76. doi:10.1093/jnci/85.5.365 PubMed
53.Musoro JZ, Coens C, Sprangers MAG, et al. Minimally important differences for interpreting EORTC QLQ-C30 change scores over time: A synthesis across 21 clinical trials involving nine different cancer types. Eur J Cancer. Jul 2023;188:171-182. doi:10.1016/j.ejca.2023.04.027 PubMed
54.Tomasini P, Blasco Cordellat A, Dooms C, et al. 8P Amivantamab plus chemotherapy vs chemotherapy in EGFR-mutant advanced NSCLC after progression on osimertinib: Secondary analyses of patient-relevant endpoints from MARIPOSA-2. ESMO Open. 2024;9(Supplement 3):102587. European Lung Cancer Congress (ELCC) 2024. Prague Czechia. doi:10.1016/j.esmoop.2024.102587
55.Janssen Inc. (Data on File) Overview of Efficacy Results from Interim Analysis 2. 2024;
56.Janssen. MARIPOSA-2 Patient-Reported Outcomes Report: Interim Analysis 2. 2024.
57.Balshem H, Helfand M, Schünemann HJ, et al. GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol. Apr 2011;64(4):401-6. doi:10.1016/j.jclinepi.2010.07.015 PubMed
58.Santesso N, Glenton C, Dahm P, et al. GRADE guidelines 26: informative statements to communicate the findings of systematic reviews of interventions. J Clin Epidemiol. Mar 2020;119:126-135. doi:10.1016/j.jclinepi.2019.10.014 PubMed
59.LLC JRD. Clinical Study Protocol: 61186372NSC2005. Subcutaneous Methotrexate, Oral Dexamethasone or Oral Montelukast for the Prevention of Infusion Related Reaction Associated with Amivantamab, an EGFR-MET bispecific antibody, Among Post-osimertinib Treated EGFRm NSCLC; SKIPPirr, a Phase 2 Study [internal sponsor's report]. August 21, 2023.
60.Janssen R, Development. (Data on File). SKIPPirr: Study Summary. Approved Effective Date: 3 October 2024. 2024;
61.Spira AI, Paz-Ares L, Han JY, et al. Preventing Infusion-Related Reactions With Intravenous Amivantamab-Results From SKIPPirr, a Phase 2 Study: A Brief Report. J Thorac Oncol. Jan 24 2025;doi:10.1016/j.jtho.2025.01.018 PubMed
62.Janssen. Clinical Summary (Based on Interim Analysis): COCOON Study 61186372NSC2007 [internal sponsor's report]. 2025. Updated January 10, 2025.
63.Development JR. Clinical Study Report: 61186372NSC2005. Subcutaneous Methotrexate, Oral Dexamethasone or Oral Montelukast for the Prevention of Infusion Related Reaction Associated with Amivantamab, an EGFR-MET bispecific antibody, Among Post-osimertinib Treated EGFRm NSCLC; SKIPPirr, a Phase 2 Study [internal sponsor's report]. February 5, 2025.
64.Cho BC, Girard N, Sauder MB, et al. Enhanced vs Standard Dermatologic Management with Amivantamab-Lazertinib in Advanced NSCLC: Phase 2 COCOON Study. Presented at WCLC 2024; San Diego, CA. WCLC 2024 Full Conference Abstract Book. 2024;https://wclc2024.iaslc.org/wp-content/uploads/2024/09/WCLC-2024-Full-Conference-Abstract-Book.pdf.
65.Development JR. Clinical Protocol: 61186372NSC2007. A Phase 2, open-label, randomizedtrial evaluating the impact of enhanced versus standard dermatologic management on selected dermatologic adverse events among patients with locally advanced or metastatic EGFR-mutated NSCLC treated first-line with amivantamab + lazertinib [internal sponsor's report]. January 17, 2025.
66.Kam J, Simoes J. J&J Data at European Lung Cancer Congress 2025. 2025;
67.Janssen. Amivantamab SKIPPirr Study [internal sponsor's report]. 10/3/2024.
68.LLC JRD. Statistical Analysis Plan: 61186372NSC2005. Subcutaneous Methotrexate, Oral Dexamethasone or Oral Montelukast for the Prevention of Infusion Related Reaction Associated with Amivantamab, an EGFR-MET bispecific antibody, Among Post-osimertinib Treated EGFRm NSCLC; SKIPPirr, a Phase 2 Study [internal sponsor's report]. June 14, 2024.
69.Paz-Ares LG, Spira AI, Han JY, et al. 1269P-Preventing infusion-related reactions with intravenous amivantamab: Updated results from SKIPPirr, a phase II study. Ann Oncol. 2024;35(S2)
70.Lopes G, Spira AI, Shih JY, et al. MA12.08-Preventing Infusion-Related Reactions with Intravenous Amivantamab: Primary Results from SKIPPirr, a Phase 2 Study. J Thorac Oncol. 2024;19(10):S104-S105.
71.Janssen. Topline Results (Based on Interim Analysis): COCOON Study 61186372NSC2007 [internal sponsor's report]. 2025. Updated January 10, 2025.
Appendix 1: Detailed Outcome Data
Please note that this appendix has not been copy-edited.
Figure 4: Primary End Point: PFS by BICR for ACP vs. CP (IA1); Full Analysis Set
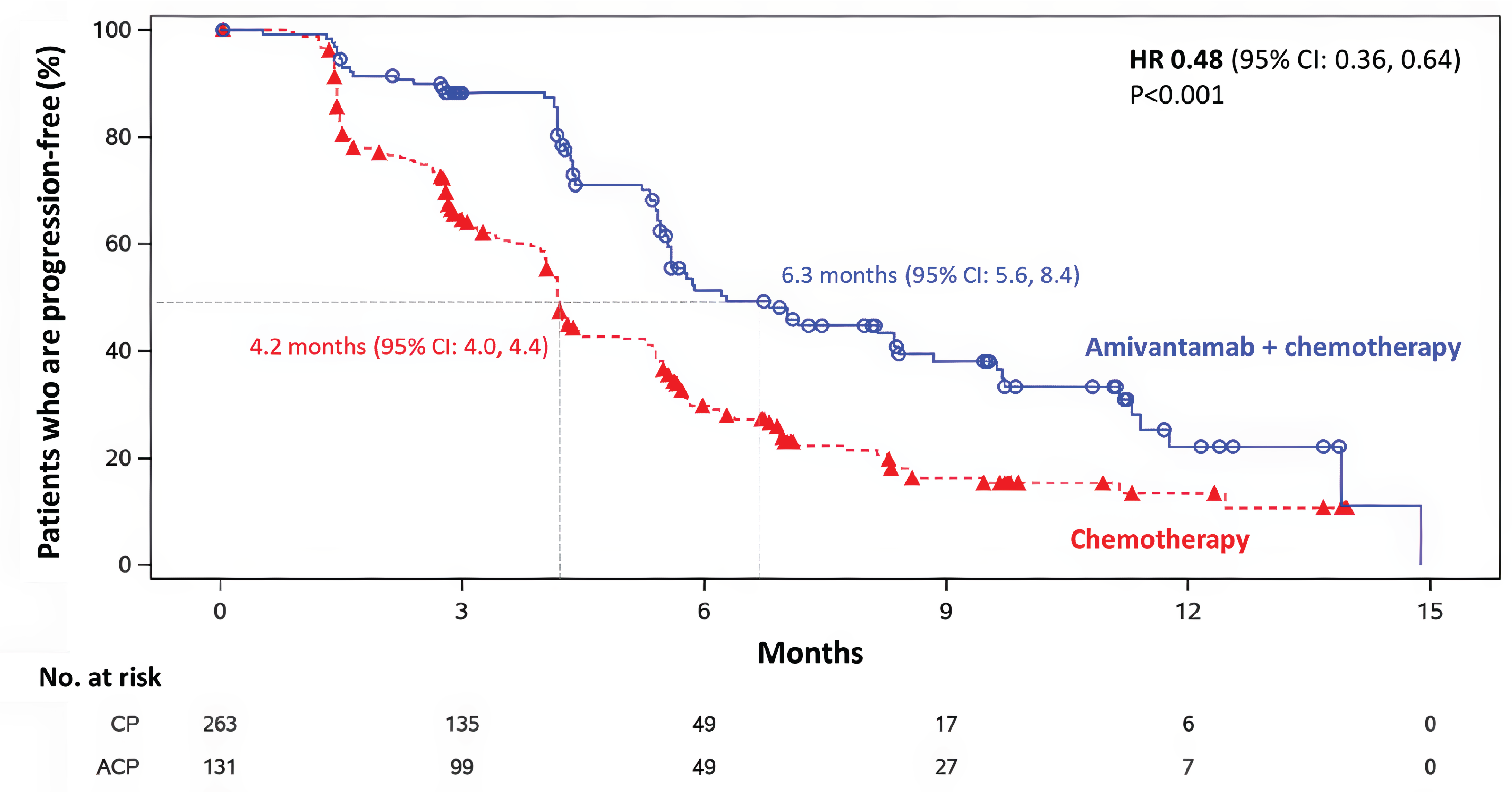
ACP = amivantamab plus carboplatin and pemetrexed; CP = carboplatin and pemetrexed; IA1 = interim analysis 1; vs. = versus.
Source: MARIPOSA-2 Clinical Study Report.1
Figure 5: Interim OS Analysis for ACP vs. CP Chemotherapy (IA1); Full Analysis Set
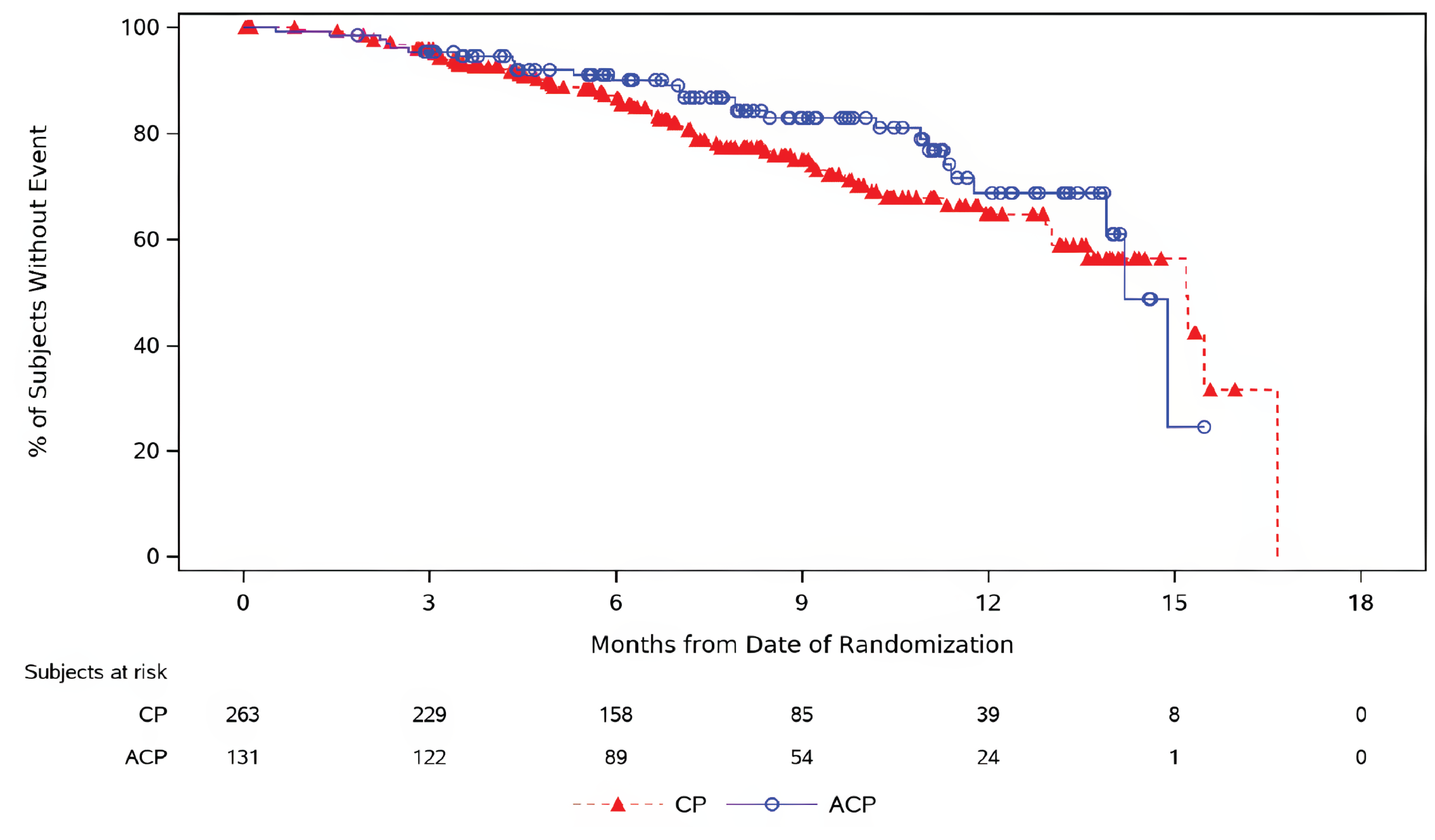
ACP = amivantamab plus carboplatin and pemetrexed; CCO = clinical cut-off; CP = carboplatin and pemetrexed; IA1 = interim analysis 1; OS = overall survival; vs. = versus.
Source: MARIPOSA-2 Clinical Study Report.1
Figure 6: Interim OS Analysis for ACP vs. CP (IA2); Full Analysis Set [Redacted]

██████████████████████ █████████████ ██ █ ██████████ █████████ ██ █ ██████ ██████ ███ █ ███████ ████████ █ █████ ██ █████ ██████ ██ █ ███████ ██ █ ███████ ████████.
ACP = amivantamab plus carboplatin and pemetrexed; CP = carboplatin and pemetrexed; IA1 = interim analysis 1; vs. = versus.
Source: Janssen data on file.55
Figure 7: Time to Sustained Deterioration in Total Symptom Score Over Time by NSCLC-SAQ
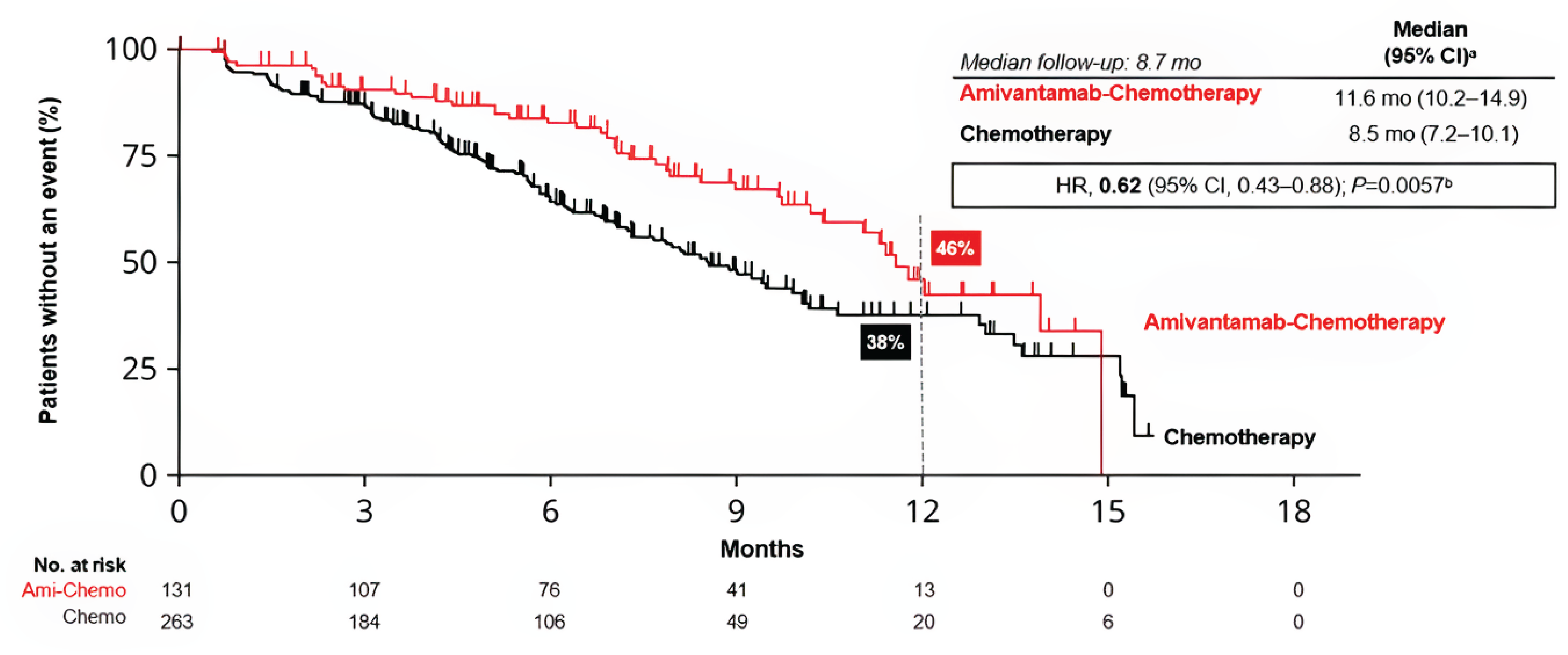
Ami-chemo = amivantamab plus carboplatin and pemetrexed chemotherapy; chemo = carboplatin and pemetrexed chemotherapy; CI = confidence interval; HR = hazard ratio; mo = months; NSCLC-SAQ: Non–Small Cell Lung Cancer Symptom Assessment Questionnaire.
aTime to sustained deterioration was defined as the time from randomization until the date of the first clinically meaningful deterioration (i.e., decrease of ≥ 2.5 points relative to baseline) or death that was not subsequently followed by a score that is more than the meaningful deterioration threshold at any later visits.
bKaplan-Meier analyses of PROs are influenced by disease progressions, which are not part of the “deterioration” definition, and patients postprogression have fewer PRO data than those before progression.
Source: Tomasini et al., 2024.54
Pharmacoeconomic Review
Abbreviations
ACP
amivantamab plus carboplatin and pemetrexed
AE
adverse event
BIA
budget impact analysis
CEAC
cost-effectiveness acceptability curve
CDA-AMC
Canada’s Drug Agency
CP
carboplatin and pemetrexed
CUA
cost-utility analysis
ICER
incremental cost-effectiveness ratio
ITC
indirect treatment comparison
LY
life-year
NOC
Notice of Compliance
NSCLC
non–small cell lung cancer
OS
overall survival
PBC
platinum-based chemotherapy
PFS
progression-free survival
PSM
partitioned survival model
QALY
quality-adjusted life-year
QoL
quality of life
Economic Review
The objective of the economic review is to review and critically appraise the pharmacoeconomic evidence submitted by the sponsor on the cost-effectiveness and budget impact of amivantamab plus carboplatin and pemetrexed (ACP) compared with carboplatin and pemetrexed (CP) alone for the treatment of locally advanced (not amenable to curative therapy) or metastatic non–small cell lung cancer (NSCLC) with EGFR exon 19 deletion mutations or exon 21 L858R substitution mutations in patients whose disease has progressed on or after treatment with osimertinib.
Item | Description |
|---|---|
Drug product | Amivantamab (Rybrevant), 350 mg/7 mL (50 mg/mL) solution (single-use vial) |
Indication | In combination with carboplatin and pemetrexed for the treatment of patients with locally advanced (not amenable to curative therapy) or metastatic NSCLC with EGFR exon 19 deletions or exon 21 L858R substitution mutations, whose disease has progressed on or after treatment with osimertinib |
Submitted price | Amivantamab: $1,676.00 per 7 mL vial |
Health Canada approval status | NOC |
Health Canada review pathway | Standard |
NOC date | January 13, 2025 |
Reimbursement request | Per indication |
Sponsor | Janssen Inc. |
Submission history | Previously reviewed: Yes Indication: The first-line treatment of adult patients with locally advanced (not amenable to curative therapy) or metastatic NSCLC with activating EGFR exon 20 insertion mutations Recommendation date: January 10, 2025 Recommendation: Reimburse with clinical criteria and/or conditions Indication: Treatment of adult patients with locally advanced or metastatic NSCLC with activating EGFR exon 20 insertion mutations whose disease has progressed on, or after platinum-based chemotherapy Recommendation date: March 1, 2023 Recommendation: Reimburse with clinical criteria and/or conditions |
NOC = Notice of Compliance; NCSLC = non–small cell lung cancer.
Summary
Amivantamab is available as a solution for infusion (50 mg/mL). At the submitted price of $1,676.00 per vial, the estimated per-cycle cost of amivantamab is as follows: $6,342 for the first cycle, $2,436 for the second cycle, $2,781 for the third and fourth cycles, and $2,424 for each subsequent cycle, based on the Health Canada–recommended dosage.
Clinical efficacy in the economic analysis was derived from the MARIPOSA-2 trial,1 which compared ACP to CP alone. Evidence submitted by the sponsor indicates that ACP is likely to improve progression-free survival (PFS) and overall survival (OS) compared with CP alone.
The results of the Canada’s Drug Agency (CDA-AMC) base case suggest that ACP will be associated with higher costs to the health care system than CP alone (incremental costs = $128,544), primarily driven by increased drug acquisition costs associated with amivantamab.
The results of the CDA-AMC base case suggest that ACP will result in a potential gain of 0.74 life-years (LYs) compared with CP alone. When the impact on health-related quality of life (HRQoL) is also considered, ACP may result in a gain of approximately 0.44 quality-adjusted life-years (QALYs) compared to CP alone.
The incremental cost-effectiveness ratio (ICER) of ACP compared with CP alone was $292,610 per QALY gained in the CDA-AMC base case. The estimated ICER was highly sensitive to the choice of model used for long-term OS extrapolation and to assumptions regarding dose skipping.
CDA-AMC estimates that the budget impact of reimbursing ACP for the indicated population will be approximately $46.7 million over the first 3 years of reimbursement, compared with the amount currently spent on CP alone, with an estimated expenditure of $48 million on ACP over this period. The actual budget impact of reimbursing ACP will depend on the number of people eligible for treatment.
Although the CDA-AMC base case estimated increased QALYs with ACP compared with CP alone (incremental QALYs = 0.44), approximately 86% of the incremental benefit was gained in the extrapolated period. In the absence of comparative evidence beyond the trial period and uncertainty in the comparative clinical evidence, the incremental QALYs for ACP predicted in the CDA‑AMC base case are highly uncertain and may be overestimated. Additional price reductions may therefore be required. Clinical experts consulted by CDA-AMC noted that amivantamab requires prolonged chair time and incurs significant administration costs, which may pose barriers to implementation in clinical practice.
Summary of the Submitted Economic Evaluation
The sponsor submitted a cost-utility analysis (CUA) to estimate the cost-effectiveness of ACP from the perspective of a public drug plan payer in Canada over a 15-year horizon. The modelled population comprised adult patients with locally advanced (not amenable to curative therapy) or metastatic NSCLC with activating EGFR exon 19 deletions or exon 21 L858R substitution mutations, whose disease had progressed on or after treatment with osimertinib, which is aligned with the Health Canada indication and reimbursement request and was based on the participants in the MARIPOSA-2 trial. The sponsor’s base-case analysis included costs related to drug acquisition, premedication, drug administration, monitoring, disease management, adverse event (AE) management, subsequent treatments, central nervous system progression, and end-of-life care.
In the sponsor’s base case, ACP was associated with incremental costs of $127,839 and 0.67 incremental QALYs relative to CP. This resulted in an ICER of $189,622 per QALY gained. Additional information about the sponsor’s submission is summarized in Appendix 3.
CDA-AMC identified several key issues with the sponsor’s analysis (refer to Table 2; full details are provided in Appendix 4). A revised base case was therefore developed.
Table 2: Key Issues With the Sponsor’s Economic Submission
Issue | What evidence is there to inform this issue? | How was this issue addressed by CDA-AMC? | Did CDA-AMC explore Uncertainty in a scenario analysis? |
|---|---|---|---|
The sponsor used a unit cost for 50 mg of carboplatin, which was higher than what is typically paid in Canadian clinical settings. As a result, the total treatment costs for both the ACP and the CP groups were underestimated in the economic model. | The sponsor assumed a cost of $106.12 for each 50 mg vial of carboplatin based on a McKesson price list from August 2024. However, this price is higher than the publicly available prices typically paid for carboplatin in Canada. | CDA-AMC used a public list price of $70.00 for each 50 mg vial of carboplatin in the sponsor-corrected base case. | No scenario analysis was conducted because CDA‑AMC used the best available evidence. |
The overall survival benefit predicted for ACP relative to CP is likely overestimated in the sponsor’s base case. | The sponsor estimated that about 12% of patients would be alive at 5 years, based on their survival projection. However, clinical experts consulted by CDA‑AMC found this overly optimistic. | CDA-AMC adopted an alternative extrapolation for OS as a base-case change. This extrapolation better reflects clinical expectation. | Because there is limited long-term data, the effect of ACP on OS is uncertain. CDA-AMC tested different ways to estimate long-term survival and explored other methods to predict PFS because those data were only available for 12 months. |
The sponsor’s estimates of patients receiving subsequent therapy were based on trial conditions and do not reflect real-world clinical practice in Canada. | This assumption is not aligned with how ACP is expected to be used in clinical practice, as noted by the clinical experts. | CDA-AMC assumed that a smaller proportion of patients would receive subsequent treatment after disease progression, and that fewer patients would be treated with immunotherapy. | No scenario analysis was conducted as changes in the distribution of subsequent treatments are expected to have minimal impact on the overall cost-effectiveness results. |
The sponsor’s analysis likely overestimated the quality of life associated with different health states, which may overestimate the overall benefits of ACP. | The sponsor’s health utility estimates for health states in the base case were likely overestimated due to optimistic assumptions, unadjusted averaging across treatment arms, and unaddressed missing data in the MARIPOSA-2 trial. CDA‑AMC was also concerned about the validity and reliability of the quality-of-life inputs used in the model. | CDA-AMC adopted utility values from the 2 real-world studies, which were considered a more appropriate source of utility values and better reflect patient preferences.2,3 | No scenario analysis was conducted because CDA‑AMC used the best available evidence. |
ACP = amivantamab plus carboplatin and pemetrexed; CDA-AMC = Canada’s Drug Agency; OS = overall survival; CP = carboplatin and pemetrexed; PFS = progression-free survival.
Note: Full details of the CDA-AMC identified issues are provided in Appendix 3.
CDA-AMC Assessment of Cost-Effectiveness
The CDA-AMC base case was derived by making changes to model parameter values and assumptions (refer to Table 7), in consultation with clinical experts. Detailed information about the base case is provided in Appendix 4.
Impact on Health Care Costs
ACP is expected to be associated with additional health care costs, compared with CP alone (incremental costs = $128,544). This increase in health care spending was a result of drug acquisition costs associated with amivantamab (refer to Figure 1).
Figure 1: Impact of Amivantamab Plus CP vs. CP on Health Care Costs
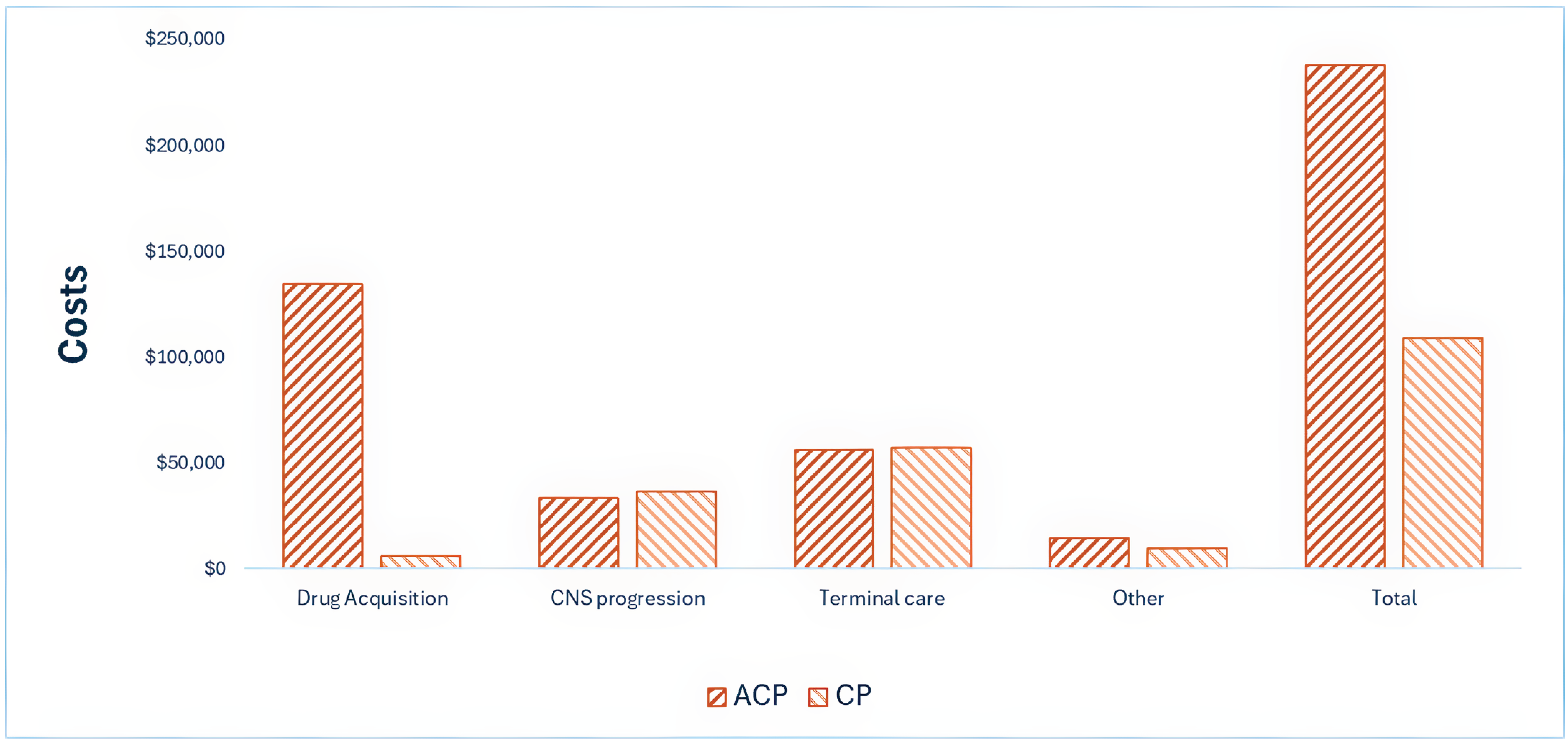
ACP = amivantamab plus carboplatin and pemetrexed; CNS = central nervous system; CP = carboplatin and pemetrexed; vs. = versus.
Note: “Other” includes drug administration, premedication, adverse events, subsequent treatments, and monitoring or follow-up costs.
Impact on Health
Relative to CP alone, ACP is expected to increase the amount of time a patient remains in the progression-free state by approximately 0.24 years and to extend OS by 0.74 years (refer to Figure 2). Considering the impact on both quality and length of life, ACP is expected to result in an additional 0.44 QALYs per patient compared to CP alone.
Figure 2: Impact of ACP vs. CP on Patient Health
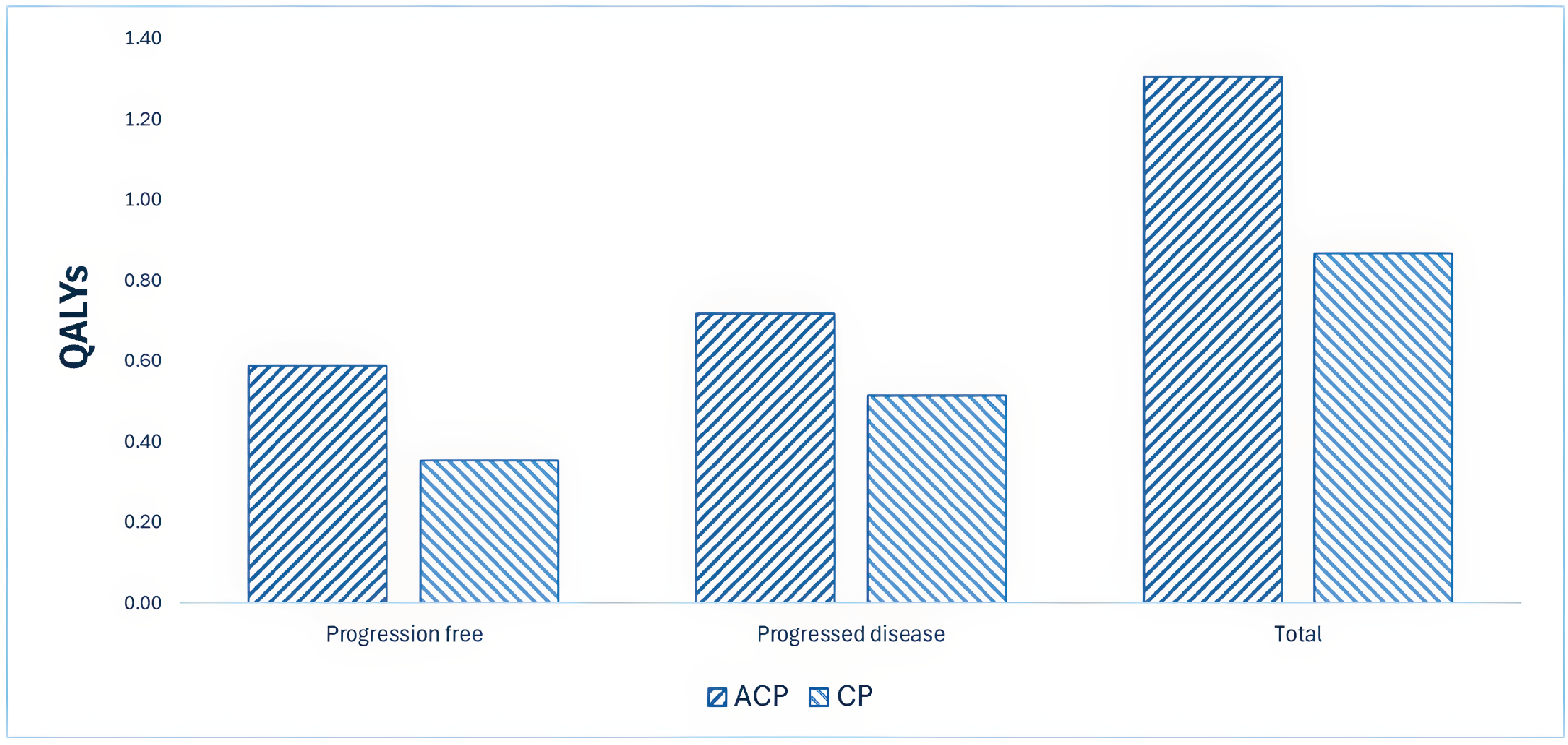
ACP = amivantamab plus carboplatin and pemetrexed; QALY = quality-adjusted life-year; CP = carboplatin and pemetrexed; vs. = versus.
Overall Results
The results of the CDA-AMC base case suggest an ICER of $292,610 per QALY gained for ACP compared with CP alone (refer to Table 3). Additional details on the CDA-AMC base case are available in Appendix 4.
Table 3: Summary of CDA-AMC Economic Evaluation Results
Drug | Total costs ($) | Total QALYs | ICER vs. CP ($/QALY) |
|---|---|---|---|
CP | 109,151 | 0.87 | Reference |
ACP | 237,695 | 1.31 | 292,610 |
ACP = amivantamab plus carboplatin and pemetrexed; ICER = incremental cost-effectiveness ratio; CP = carboplatin and pemetrexed; QALY = quality-adjusted life-year; vs. = versus.
Note: Publicly available list prices were used for all comparators.
Uncertainty and Sensitivity
Due to the lack of long-term evidence, extrapolation of OS and PFS was uncertain. The impact of uncertainty on long-term OS and PFS for patients receiving ACP was explored in scenario analyses (refer to Table 2). Based on the results of these analyses, the ICER for ACP may range from $241,592 to $336,878 per QALY gained, compared with CP alone (refer to Table 11, Appendix 4).
Summary of the Budget Impact
The sponsor submitted a budget impact analysis to estimate the 3-year (2026 to 2028) budget impact of reimbursing ACP for the treatment of locally advanced (not amenable to curative therapy) or metastatic NSCLC with EGFR exon 19 deletions or exon 21 L858R substitution mutations in patients whose disease has progressed on or after treatment with osimertinib. The sponsor assumed that the payer would be CDA-AMC–participating public drug plans and derived the size of the eligible population using an epidemiologic approach. The price of ACP was aligned with the price included in the sponsor’s economic evaluation, while the prices of comparators were based on the publicly available list prices. Additional information pertaining to the sponsor’s submission is provided in Appendix 5.
CDA-AMC identified a number of issues with the sponsor’s estimated budget impact and made changes to model parameters and assumptions in consultation with clinical experts to derive the CDA-AMC base case (Appendix 5). CDA-AMC estimated that 820 patients would be eligible for treatment with ACP over a 3-year period (year 1 = 267; year 2 = 273; year 3 = 280), of whom 370 are expected to receive ACP (year 1 = 107; year 2 = 123; year 3 = 140). The estimated incremental budget impact of reimbursing ACP is expected to be approximately $46.7 million over the first 3 years, with an expected expenditure of $48 million on ACP. The actual budget impact of reimbursing ACP will depend on the number of people eligible for treatment.
Conclusion
Based on the CDA-AMC base case, amivantamab for use in combination with CP would be considered cost-effective at the submitted price if the public health care system was willing to pay at least $292,610 for each additional QALY gained. If the public health care system is not willing to pay that amount, a price reduction should be considered (refer to Figure 3; full details of the impact of price reductions on cost-effectiveness are presented in Table 10).
The budget impact of reimbursing ACP to the public drug plans in the first 3 years is estimated to be approximately $46.7 million. The 3-year expenditure on ACP (i.e., not accounting for current expenditure on comparators) is estimated to be $48 million.
Figure 3: Summary of the CDA-AMC Economic Analysis and Price Reduction
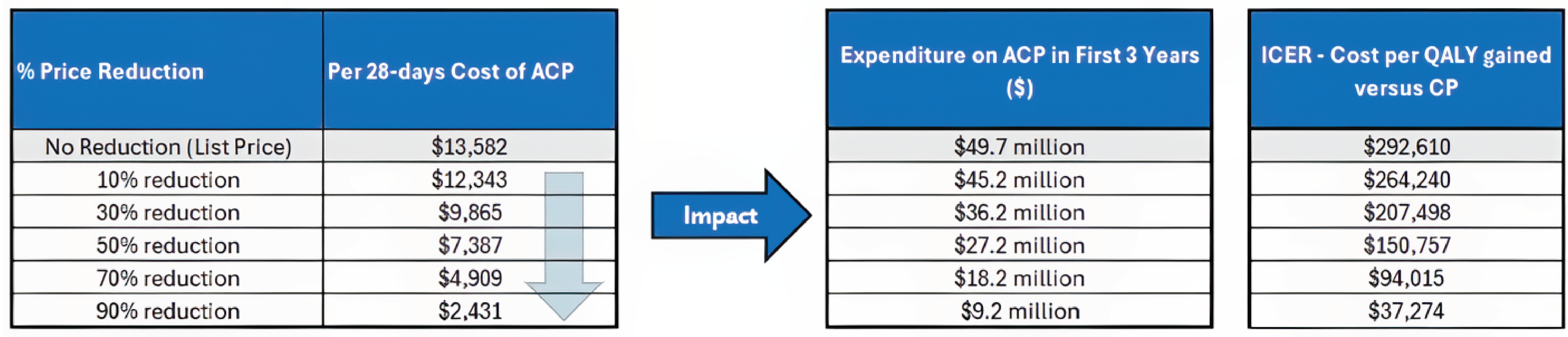
ACP = amivantamab plus carboplatin and pemetrexed; CDA-AMC = Canada’s Drug Agency; ICER = incremental cost-effectiveness ratio; CP = carboplatin and pemetrexed; QALY = quality-adjusted life-year.
Note: “Expenditure” includes only the drug cost of amivantamab. If the term “dominant” is used in the figure, add the following: The term dominant indicates that a drug costs less and provides more QALYs than the comparator.
References
1.Janssen. MARIPOSA-2 Clinical study report [sponsor supplied reference]. 2023.
2.Naik H, Howell D, Su S, et al. EQ-5D Health Utility Scores: Data from a Comprehensive Canadian Cancer Centre. Patient. 2017;10(1):105-115. doi:10.1007/s40271-016-0190-z PubMed
3.O'Kane GM, Su J, Tse BC, et al. The Impact of Brain Metastases and Associated Neurocognitive Aspects on Health Utility Scores in EGFR Mutated and ALK Rearranged NSCLC: A Real World Evidence Analysis. Oncologist. 2019;24(7):e501-e509. doi:10.1634/theoncologist.2018-0544 PubMed
4.Iqvia. DeltaPA [sponsor supplied reference]. 2023. https://www.iqvia.com/
5.Janssen Inc. Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Rybrevant (amivantamab for injection): concentrate for solution for intravenous infusion, 350 mg / 7 mL (50 mg/mL) single-use vial. February 20, 2025.
6.Passaro A, Wang J, Wang Y, et al. Amivantamab plus chemotherapy with and without lazertinib in EGFR-mutant advanced NSCLC after disease progression on osimertinib: primary results from the phase III MARIPOSA-2 study. Ann Oncol. 2024;35(1):77-90. doi:10.1016/j.annonc.2023.10.117 PubMed
7.Roughley A, Damonte E, Taylor-Stokes G, Rider A, Munk VC. Impact of Brain Metastases on Quality of Life and Estimated Life Expectancy in Patients with Advanced Non-Small Cell Lung Cancer. Value Health. 2014;17(7):A650. doi:10.1016/j.jval.2014.08.2364 PubMed
8.Chouaid C, Agulnik J, Goker E, et al. Health-related quality of life and utility in patients with advanced non-small-cell lung cancer: a prospective cross-sectional patient survey in a real-world setting. J Thorac Oncol. 2013;8(8):997-1003. doi:10.1097/JTO.0b013e318299243b PubMed
9.Brenner DR, Gillis J, Demers AA, et al. Projected estimates of cancer in Canada in 2024. CMAJ. 2024;196(18):E615-E623. doi:10.1503/cmaj.240095 PubMed
10.Felip E, Shu CA, Aguilar A, et al. 2MO Amivantamab plus chemotherapy vs chemotherapy as first-line treatment in EGFR exon 20 insertion-mutated advanced NSCLC: Analysis of post-progression endpoints from PAPILLON. ESMO Open. 2024;9(Supplement 3):102581. doi:10.1016/j.esmoop.2024.102581
11.Mack PC, Miao J, Redman MW, et al. Circulating Tumor DNA Kinetics Predict Progression-Free and Overall Survival in EGFR TKI-Treated Patients with EGFR-Mutant NSCLC (SWOG S1403). Clin Cancer Res. 2022;28(17):3752-3760. doi:10.1158/1078-0432.CCR-22-0741 PubMed
12.Song Y, Hu C, Xie Z, et al. Circulating tumor DNA clearance predicts prognosis across treatment regimen in a large real-world longitudinally monitored advanced non-small cell lung cancer cohort. Transl Lung Cancer Res. 2020;9(2):269-279. doi:10.21037/tlcr.2020.03.17 PubMed
13.Jiang T, Cheng R, Zhang G, et al. Characterization of Liver Metastasis and Its Effect on Targeted Therapy in EGFR-mutant NSCLC: A Multicenter Study. Clin Lung Cancer. 2017;18(6):631-639 e2. doi:10.1016/j.cllc.2017.04.015 PubMed
14.Li J, Niu C, Guo Z, et al. TY-4028: a novel, targeted therapy for non small-cell lung cancer with EGFR exon 20 or HER2 exon 20 insertion mutations. Cancer Res. 2023;83(7 Supplement):4488. doi:10.1158/1538-7445.Am2023-4488
15.Choi D, Jung HA, Park S, et al. A study of the efficacy and safety of amivantamab in EGFR exon 20 insertion (E20I) mutations in NSCLC. Ann Oncol. 2023;34(Supplement 4):S1696. doi:10.1016/j.annonc.2023.10.655
16.Stock-Martineau S, Laurie K, McKinnon M, Zhang T, Wheatley-Price P. Evolution of Systemic Treatment Uptake and Survival in Advanced Non-Small Cell Lung Cancer. Curr Oncol. 2020;28(1):60-68. doi:10.3390/curroncol28010008 PubMed
17.Melosky B, Banerji S, Blais N, et al. Canadian consensus: a new systemic treatment algorithm for advanced EGFR-mutated non-small-cell lung cancer. Curr Oncol. 2020;27(2):e146-e155. doi:10.3747/co.27.6007 PubMed
18.Stockhammer P, Grant M, Wurtz A, et al. Co-Occurring Alterations in Multiple Tumor Suppressor Genes Are Associated With Worse Outcomes in Patients With EGFR-Mutant Lung Cancer. J Thorac Oncol. 2024;19(2):240-251. doi:10.1016/j.jtho.2023.10.001 PubMed
Appendix 1: Cost Comparison Table
Please note that this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical experts and CDA-AMC–participating public drug plans. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans
Table 4: Cost Comparison for Non–Small Cell Lung Cancer
Treatment | Strength and/or concentration | Form | Price | Recommended dosage | Daily cost ($) | 28-day cost ($) |
|---|---|---|---|---|---|---|
Amivantamab (Rybrevant) | 50 mg/mL | 7 mL (350 mg) Solution for IV infusion | 1,676.0000 | Body weight < 80 kg: 1,400 mg weekly for 4 weeks, then 1,750 every 3 weeks starting at week 7 Body weight ≥ 80 kg: 1,750 mg weekly for 4 weeks, then 2,100 mg every 3 weeks starting at week 7 | First 28 days: 957.71 to 1,197.14 Thereafter: 399.05 to 478.86 | First 28 days: 26,816 to 33,520 Thereafter: 11,173 to 13,408 |
CISPPME plus amivantamab | — | — | — | — | First 28 days: 998.43 to 1,237.86 Thereafter: 439.76 to 519.57 | First 28 days: 27,956 to 34,660 Thereafter: 12,313 to 14,548 |
CRBPPME plus amivantamab | — | — | — | — | First 28 days: 1,026.05 to 1,265.48 Thereafter: 467.38 to 547.19 | First 28 days: 28,729 to 35,433 Thereafter: 13,087 to 15,321 |
Platinum-based chemotherapy | ||||||
Carboplatin (Generic) | 50 mg/5 mL 150 mg/15 mL 450 mg/45 mL 600 mg/60 mL | Vial for IV infusion | 70.0000 210.0000 599.9985 775.0020 | Target AUC 5 on day 1 Q3W, 750 mg/mL for a total of 4 cycles | 46.9 | 1,313 |
Cisplatin (Generic) | 50 mg/50 mL 100 mg/100 mL | Vial for IV infusion | 135.0000 270.0000 | 75 mg/m2 Q3W, for a total of 4 cycles | 19.29 | 540 |
Pemetrexed (Generic) | 100 mg 500 mg 1,000 mg | Powder for solution for infusion | 50.0000 250.0000 4,290.0000 | 500 mg/m2 Q3W | 21.43 | 600 |
CISPPME | — | — | — | — | 40.71 | 1,140 |
CRBPPME | — | — | — | — | 68.33 | 1,913 |
CDA-AMC = Canada’s Drug Agency; CISPPME = cisplatin and pemetrexed regimen; CRBPPME = carboplatin and pemetrexed regimen; Q3W = every 3 weeks.
Note: All prices are from IQVIA Delta PA (accessed January 2025),4 unless otherwise indicated, and do not include dispensing fees. Dosing is based on Cancer Care Ontario product monographs. For treatments using weight-based, CDA-AMC assumed 64.5 kg, and 1.70m2 based on the MARIPOSA-2 trial.1
Appendix 2: Input Relevant to the Economic Review
Please note that this appendix has not been copy-edited.
This section is a summary of the input received from the patient groups, clinician groups, and drug plans that participated in the CDA-AMC review process. Input was collected in Canada through virtual interviews conducted directly with the patients.
Patient input was received from 3 organizations: Lung Cancer Canada (LCC), the Canadian Cancer Survivor Network, and the Lung Health Foundation. Five patients from British Columbia, Alberta, and Ontario with Stage III or IV NSCLC contributed to the submission, including 2 with direct experience in the MARIPOSA 2 trial and others who had used amivantamab through clinical trials or compassionate access. Several patients described their diagnoses as unexpected, with symptoms including back pain, shortness of breath, and cough, while 1 was asymptomatic. All of the patients had previously been treated with osimertinib, with varying responses; some experienced significant side effects, while others had a high QoL until disease progression. The patient group highlighted the need for additional treatment options beyond osimertinib to maintain QoL, delay progression, and support independence. Patients described amivantamab as effective in treating their disease, with some experiencing side effects that improved over time with dose adjustments. While some preferred the convenience of oral therapies, most agreed that amivantamab was a valuable option, with 1 patient calling it a “lifesaver” for those without alternatives.
Clinician group input was received from 19 clinicians from Lung Cancer Canada’s (LCC) Medical Advisory Committee and 5 from Ontario Health (Cancer Care Ontario)’s Lung Cancer Drug Advisory Committee contributed to this review. Current treatment for advanced NSCLC with EGFR mutations following progression on osimertinib typically involves platinum-based chemotherapy (PBC), but clinicians noted low response rates and an unmet need for more effective therapies. Both clinician groups anticipated that amivantamab combined with chemotherapy could replace PBC as second-line treatment following osimertinib progression, given its activity against various EGFR resistance mutations and MET alterations. Patients best suited for this treatment would have advanced, EGFR-mutated NSCLC, good functional status (ECOG 0 to 2), and no contraindications to chemotherapy, with fit patients being preferred due to potential toxicity risks. Treatment response would be evaluated through clinical and radiological assessments, focusing on symptom improvement, disease stability, and overall survival. Clinicians recommended discontinuing amivantamab upon disease progression, unacceptable toxicity, or patient preference. The treatment would be administered in outpatient cancer centres or hospitals under the supervision of experienced oncology teams, with careful management of infusion-related reactions.
Input from CDA-AMC–participating drug plans noted that the implementation of ACP raises several considerations. Amivantamab requires weight-based dosing with an initial split infusion and premedications to manage infusion-related reactions, adding complexity to administration. Diagnostic confirmation of EGFR exon 19 deletions or exon 21 L858R substitution mutations is essential and, although part of standard practice, may introduce timing and access considerations. Plans also noted uncertainty about the criteria for initiation in patients previously treated with osimertinib plus PBC and emphasized the need for clear discontinuation criteria, especially in the context of loss of response or disease progression. Additionally, questions were raised about the continuation of amivantamab as monotherapy if chemotherapy must be discontinued.
Several of these concerns were addressed in the sponsor’s model:
The sponsor’s economic model accounted for the extended progression-free survival, improved overall survival, enhanced QoL, and higher risk of side effects associated with ACP.
The sponsor assumed ACP would replace PBC as a second-line treatment following progression with osimertinib.
CDA-AMC addressed some of these concerns as follows:
A scenario analysis was conducted to assess the impact of amivantamab combined with PBC on long-term PFS and OS.
CDA-AMC did not identify any unaddressed concerns.
Appendix 3: Summary of the Sponsor’s Submission
Please note that this appendix has not been copy-edited.
Summary of the Sponsor’s Economic Evaluation
For the pharmaceutical reviews program, clinical and economic information is submitted to CDA-AMC by the sponsor. The CDA-AMC health economics team reviews the submitted economic information and appraises the information in collaboration with clinical experts and the clinical review team to evaluate key assumptions, influential parameters, and the overall rigour of the economic submission. Based on what the team learns through this process, adjustments may be made to the sponsor’s model to produce the CDA-AMC base case. The CDA-AMC base case represents the team’s current understanding of the clinical condition, clinical evidence currently available, and best interpretation of the economic evidence based on the information provided.
For the review of ACP, the sponsor provided a CUA and a budget impact analysis. The sponsor’s economic submission is summarized in Table 5.
Table 5: Key Components of the Sponsor’s Economic Evaluation
Component | Description |
|---|---|
Treatment information | |
Drug under review | Amivantamab (Rybrevant), 350 mg/7mL (50 mg/mL) single-use vial for IV infusion |
Submitted price of drug under review | Amivantamab: $1,676.0000 per 7 mL vial |
Regimen | Amivantamab Body weight at baseline < 80 kg:
Body weight at baseline ≥ 80 kg:
Pemetrexed: 500 mg/m2 on Day 1 of each 21-day cycle, in combination with carboplatin for up to 4 cycles, and then as maintenance until disease progression. Carboplatin: AUC 5 mg/mL per minute IV once every 3 weeks for up to 12 weeks |
Per-cycle cost of drug under review | Amivantamab: $5,850 per patient for Cycle 1, $1,950 per patient for Cycle 2, $2,295 per patienta for Cycle 3 and subsequent cycles |
Model information | |
Type of economic evaluation | Cost-utility analysis PSM |
Treatment | Amivantamab plus platinum-based chemotherapy (pemetrexed and carboplatin) |
Included comparator | Platinum-based chemotherapy (pemetrexed and carboplatin or cisplatin) |
Perspective | Publicly funded health care payer perspective |
Time horizon | Lifetime (15 years) |
Cycle length | One week |
Modelled population | Adult patients with locally advanced (not amenable to curative therapy) or metastatic non–small cell lung cancer with EGFR exon 19 deletions or exon 21 L858R substitution mutations, whose disease has progressed on or after treatment with osimertinib |
Characteristics of modelled population | Derived from the MARIPOSA-2 trial (mean age 60.6 years, % female 61.8%, mean weight 64.7 kg, mean BSA 1.71 m2) |
Model health states |
For additional information, refer to Model Structure |
Data sources | |
Comparative efficacy |
|
Natural history and/or clinical pathway |
|
Health-related utilities and disutilities | Health-state utility values were derived from EQ-5D data collected in the MARIPOSA-2 trial. Adverse event disutilities were obtained from the literature. |
Costs included in the model |
|
Summary of the submitted results | |
Base case results | Amivantamab plus platinum-based chemotherapy were associated with an ICER of $189,622 per QALY gained (incremental costs = $127,839; incremental QALYs = 0.67) |
Scenario analysis resultsb |
|
AE = adverse event; AUC = area under the curve; BSA = body surface area; CIHI = Canadian Institute for Health Information; CNS = central nervous system; ICER = incremental cost-effectiveness ratio; PFS = progression-free survival; PSM = partitioned survival model; OS = overall survival; QALY = quality-adjusted life-year; TTD = time to discontinuation.
aAmivantamab plus platinum-based chemotherapy = $6,329 per patient for cycle 1, $2,429 per patient for cycle 2, $2,773 per patient for cycle 3, and $2,416 per patient for cycle 4.
bResults of scenario analyses that had a meaningful impact on the estimated ICER compared to the sponsor’s base case. Additional scenarios were submitted that had no meaningful impact on the estimated ICER included using INV PFS assessment and applying vial sharing assumption.
cSubmitted scenarios included changing a time horizon, adopting different discount rates, alternative PFS and OS curves, alternative PFS assessment (BICR vs. INV), alternative clinical data cut-off, vial sharing, and dose sharing assumptions.
Model Structure
The cost-utility model uses a partitioned survival model (PSM) to estimate the proportion of patients in 3 health states over time: progression-free, progressed disease, and dead. All patients start in the progression-free state and can transition to postprogression or death but not back to progression-free. The PSM estimates health-state occupancy using the area under the curve of PFS and OS curves. Specifically, the proportion dead is calculated as 1 minus OS; progression-free as the PFS projection; and postprogression as the difference between OS and PFS.
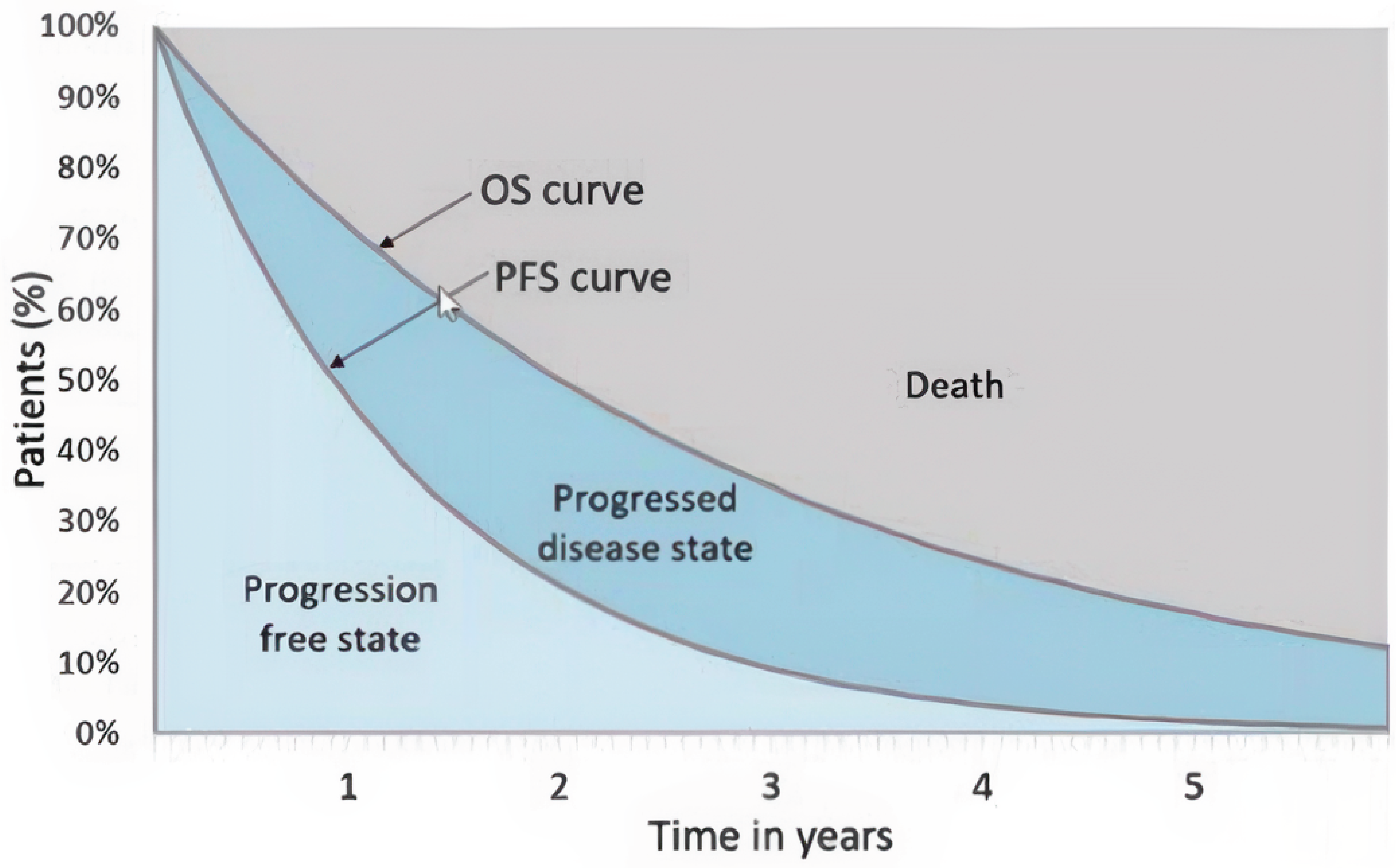
OS = overall survival; PFS = progression-free survival.
Source: Sponsor’s pharmacoeconomic submission.5
Table 6: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER vs. ($/QALY) |
|---|---|---|---|---|---|
CP | $113,638 | Reference | 1.11 | Reference | Reference |
ACP | $241,477 | $127,839 | 1.79 | 0.67 | $189,622 |
ACP = amivantamab plus carboplatin and pemetrexed; ICER = incremental cost-effectiveness ratio; CP = carboplatin and pemetrexed; QALY = quality-adjusted life-year.
Appendix 4: Additional Details of CDA-AMC Reanalyses
Please note that this appendix has not been copy-edited.
Clinical Data in the Economic Model
The CDA-AMC Clinical Review found that, in patients with locally advanced or metastatic EGFR-mutated NSCLC who experienced disease progression on or after osimertinib, ACP improved PFS, objective response rate, and duration of response compared with CP alone. These outcomes were supported by high to moderate certainty of evidence. While preliminary OS data suggested a possible benefit with ACP, the data were immature and insufficient to allow for statistical inference. Patient-reported outcomes indicated a potential delay in HRQoL deterioration with ACP, but interpretation was limited due to high levels of missing data. Treatment with ACP was associated with more AEs than CP, notably infusion-related reactions and dermatologic toxicities, although these were considered manageable with supportive care.
Key clinical inputs for the economic evaluation — PFS and OS — were derived from the pivotal trial. OS was extrapolated based on interim data using parametric survival models. The CDA-AMC review noted that, due to the lack of long-term OS data, survival projections are highly uncertain. Health utility and AE data were incorporated into the model but were affected by data limitations. Consequently, the model’s estimates of incremental QALYs and cost-effectiveness may overstate the long-term benefits of ACP.
Key Issues of the Submitted Economic Evaluation
CDA-AMC identified the following key issues with the sponsor’s analysis:
Uncertainty in OS extrapolation and limitations of the PSM approach: The sponsor extrapolated OS for amivantamab using parametric survival models based on data from the MARIPOSA-2 trial,6 which had a median follow-up of 22 months. This extrapolation extended out to a 15-year model horizon. At the second interim analysis (IA2), median OS was 17.74 months for ACP versus 15.34 months for CP, with a hazard ratio of 0.73 (95% CI, 0.54 to 0.99). The absolute difference in 12-month OS (70.0% versus 63.0%) exceeded the minimum important difference threshold of 10% and was supported by moderate-certainty evidence. However, the 24-month OS probabilities were nearly identical between groups (31.0% for ACP versus 32.0% for CP), raising concerns about the durability of benefit and the plausibility of long-term extrapolations.
Further uncertainty arises from methodological limitations. Postprogression treatment strategies were not clearly defined. This omission further reduce confidence in the validity of the observed OS effect.
The sponsor’s extrapolated OS curve predicted a 5-year survival of 11.9%, with 85% of LYs and 81% of QALYs gained occurring beyond the observed trial period. Clinical experts consulted by CDA-AMC advised that this estimate is likely overly optimistic, suggesting that 9% was a more realistic 5-year survival for this patient population.
Additionally, the use of a PSM compounds the risk of overestimation. In a PSM, postprogression survival is derived as the difference between OS and PFS. When the extrapolated OS is overestimated, especially in the absence of corresponding long-term PFS data, the model may substantially inflate the time patients are assumed to spend in the postprogression state, leading to an overstatement of both LYs and QALYs. This structural feature of the PSM amplifies uncertainty in survival projections and may distort cost-effectiveness outcomes.
CDA-AMC used a log-logistic model, which was deemed reasonable by clinical experts, to extrapolate the long-term OS in the CDA-AMC base case.
Inappropriate estimation of subsequent therapy distributions: The sponsor’s approach to estimating the proportion of patients receiving subsequent therapy does not align with clinical practice in Canada. Using longer-term data from the MARIPOSA-2 trial (IA2; data cut-off April 26, 2024), the sponsor calculated these proportions based on the number of patients who received third-line treatment — 56 in the ACP arm and 158 in the CP arm — divided by those who discontinued treatment before death (96 in the ACP arm and 225 in the CP arm). This resulted in estimated proportions of 58.3% for the ACP arm and 70.2% for the CP arm. These estimates raise several concerns. First, they reflect outcomes under controlled trial conditions, which often involve younger and fitter patients, and may not generalize to the broader real-world population, particularly those who are older, frailer, or experience rapid clinical deterioration. Second, the estimates do not account for key access barriers within the health care systems in Canada, including funding limitations, regional variability, and patient eligibility criteria. Additionally, the sponsor assumed that 30% of patients receiving third-line therapy would be treated with immunotherapies, which clinical experts considered to be an overestimate.
Based on input from clinical experts consulted by CDA-AMC, more conservative assumptions were applied: 35% of patients in the ACP arm and 45% in the PBC arm were assumed to receive third-line therapy, and the proportion receiving immunotherapies was reduced to 20%. These adjustments are considered more reflective of treatment patterns and access in Canadian clinical practice.
Validity of health-state utility: The health utility values used in the sponsor’s base case raise concerns regarding their face validity and the methodological approach applied. Utility estimates for the progression-free and progressed disease health states were derived using the arithmetic mean of EQ-5D scores pooled across all treatment arms in the MARIPOSA-2 trial. The sponsor assumed utilities of 0.82 (0.01) for progression-free disease, 0.79 (0.01) for progressed disease without CNS progression, and 0.59 (0.06) for progressed disease with CNS progression. To account for CNS progression, the sponsor applied a utility multiplier of 0.75 based on a citation from Roughley et al. (2014),7 under the assumption that the MARIPOSA-2 data did not fully capture the impact of CNS involvement. However, the utility multiplier was derived from a cross-sectional comparison of patients with brain metastases versus those with contralateral lung metastases, which is not the most appropriate source for modelling CNS progression. The sponsor compared 2 distinct static patient groups, and this does not reflect how utility changes for a patient transitioning from non-CNS progression to CNS progression. While it is appropriate to apply a decrement for CNS progression, the overall utility values appear optimistic given the clinical context. For example, a study conducted at a centre in Canada reported a mean utility of 0.77 (0.03) for patients with metastatic lung cancer, suggesting that the progression-free utility in the sponsor’s model may overestimate real-world patient QoL.2
From a methodological standpoint, the sponsor's reliance on unadjusted arithmetic means does not account for variability in baseline characteristics or changes over time. More rigorous methods, such as mixed-effects models, are typically preferred to control for these factors and provide more reliable utility estimates. Additionally, as noted in the CDA-AMC Clinical Review, the MARIPOSA-2 trial had declining completion rates for patient-reported outcomes over time, and missing data were not formally addressed or modelled. This may introduce bias if patients in poorer health, who are likely to report lower utility, were underrepresented in later cycles.
To address these limitations, CDA-AMC adopted alternative health-state utility values from a large, multinational prospective study involving patients with advanced NSCLC across 25 centres in Europe, Canada, Australia, and Turkey.8 EQ-5D data from this study were used, and a similar approach was followed to apply a decrement for CNS progression. Specifically, a utility value of 0.74 (0.15) was applied for patients with newly diagnosed brain metastases based on data from Princess Margaret Cancer Centre. CDA-AMC considered these values to be more reflective of the real-world patient experience.3
CDA-AMC Reanalysis of the Economic Evaluation
The CDA-AMC base case was derived by making changes in model parameter values and assumptions, in consultation with clinical experts (refer to Table 7). The impact of these changes, individually and collectively, is presented in Table 8.
Table 7: Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CDA-AMC value or assumption |
|---|---|---|
Correction | Carboplatin 50 mg price/vial: $106.12 | Carboplatin 50 mg price/vial: $70.00 |
1. Overestimation of OS extrapolation | ACP: Log-normal CP: Gamma | ACP: Log-logistic CP: Gamma |
2. Unrealistic distribution of subsequent therapies | Proportion of patients receiving subsequent 3-line treatments:
Distribution of subsequent treatments:
| Proportion of patients receiving subsequent 3-line treatments:
Distribution of subsequent treatments:
|
3. Lack of face validity of health-state utility values |
|
|
CDA-AMC base case (health care payer perspective) | ― | Reanalysis 1 + 2 + 3 |
ACP = amivantamab plus carboplatin and pemetrexed; CDA-AMC = Canada’s Drug Agency; CNS = central nervous system; OS = overall survival; CP = carboplatin and pemetrexed.
Table 8: Summary of the Stepped Analysis
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALY) |
|---|---|---|---|---|
Sponsor’s base case | CP | 114,000 | 1.11 | Reference |
ACP | 241,348 | 1.77 | 192,079 | |
Sponsor’s corrected base case | CP | 112,907 | 1.11 | Reference |
ACP | 239,971 | 1.77 | 191,652 | |
CDA-AMC reanalysis 1 | CP | 112,907 | 1.11 | Reference |
ACP | 239,705 | 1.65 | 233,568 | |
CDA-AMC reanalysis 2 | CP | 109,409 | 1.11 | Reference |
ACP | 237,504 | 1.77 | 193,205 | |
CDA-AMC reanalysis 3 | CP | 112,907 | 0.87 | Reference |
ACP | 239,971 | 1.37 | 244,147 | |
CDA-AMC base case: Reanalysis 1 + 2 + 3 (deterministic) | CP | 109,409 | 0.87 | Reference |
ACP | 237,237 | 1.30 | 295,705 | |
CDA-AMC base case Reanalysis 1 + 2 + 3 (probabilistic) | CP | 109,151 | 0.87 | Reference |
ACP | 237,695 | 1.31 | 292,610 |
ACP = amivantamab plus carboplatin and pemetrexed; CDA-AMC = Canada’s Drug Agency; ICER = incremental cost-effectiveness ratio; CP = carboplatin and pemetrexed; QALY = quality-adjusted life-year.
Note: The CDA-AMC reanalysis is based on the publicly available prices of the comparator treatments. Deterministic results are presented, unless otherwise indicated.
Table 9: Disaggregated Results of the CDA-AMC Base Case
Parameter | ACP | CP |
|---|---|---|
Discounted LYs | ||
Total | 2.25 | 1.51 |
By health state | ||
Progression-free | 0.85 | 0.51 |
Progressed disease | 1.40 | 1.01 |
Discounted QALYs | ||
Total | 1.31 | 0.87 |
By health state | ||
Progression-free | 0.59 | 0.35 |
Progressed disease | 0.72 | 0.51 |
Adverse events | –0.00 | –0.00 |
Discounted costs ($) | ||
Total | 237,695 | 109,151 |
Drug acquisition | 134,124 | 5,763 |
Administration | 2,265 | 596 |
Premedications | 121 | 49 |
Monitoring and routine follow-up | 5,612 | 3,722 |
Subsequent treatments | 2,230 | $3,641 |
CNS progression | 33,212 | 36,500 |
Adverse events management | 4,217 | 1,741 |
End-of-life | 55,909 | 57,138 |
ACP = amivantamab plus carboplatin and pemetrexed; CDA-AMC = Canada’s Drug Agency; CNS = central nervous system; LY = life-year; CP = carboplatin and pemetrexed; QALY = quality-adjusted life-year.
Price Reduction Analysis
CDA-AMC conducted price reduction analyses using the sponsor’s base case and the CDA-AMC base case (refer to Table 10).
Table 10: Results of the Price Reduction Analysis
Price reduction | Unit drug cost ($) | Cost per 28 days ($) | ICERs for ACP vs. CP ($/QALY) | |
|---|---|---|---|---|
Sponsor-corrected base case | CDA-AMC base case | |||
No price reduction | 1,676a | 13,582 | 189,210 | 292,610 |
10% | 1,508 | 12,343 | 170,724 | 264,240 |
20% | 1,341 | 11,104 | 152,237 | 235,869 |
30% | 1,173 | 9,865 | 133,751 | 207,498 |
40% | 1,006 | 8,626 | 115,264 | 179,127 |
50% | 838 | 7,387 | 96,778 | 150,757 |
60% | 670 | 6,148 | 78,291 | 122,386 |
70% | 503 | 4,909 | 59,805 | 94,015 |
80% | 335 | 3,670 | 41,318 | 65,644 |
90% | 168 | 2,431 | 22,832 | 37,274 |
ACP = amivantamab plus carboplatin and pemetrexed; CDA-AMC = Canada’s Drug Agency; ICER = incremental cost-effectiveness ratio; CP = carboplatin and pemetrexed; vs. = versus.
aSponsor’s submitted price for amivantamab.5
Assessment of Uncertainty
CDA-AMC used the CDA-AMC base case to conduct scenario analyses to address uncertainty within the economic evaluation. The results are provided in Table 11.
Scenario 1: Alternative parametric distribution for overall survival extrapolation. To explore uncertainty in the long-term survival benefit of amivantamab plus chemotherapy, a log-normal distribution was used in place of a log-logistic distribution for extrapolating overall survival.
Scenario 2: Alternative parametric distribution for progression-free survival extrapolation. Given the limited follow-up period in the MARIPOSA-2 trial, a spline (1-knot normal) model was used instead of the log-logistic distribution to assess the impact of model choice on long-term progression-free survival estimates for amivantamab plus chemotherapy.
Scenario 3: Removing dose skipping assumptions for second-line therapies. This scenario assumed patients did not skip doses of second-line therapies, using a sponsor-provided option to remove dose-skipping behaviour. However, percentage dose reductions — as reported in the MARIPOSA-2 trial — were still applied.
Table 11: Results of CDA-AMC Scenario Analyses
Analysisa | Drug | Total costs ($) | Total QALYs | ICER ($/QALYs) |
|---|---|---|---|---|
CDA-AMC base case | CP | $109,151 | 0.87 | Reference |
ACP | $237,695 | 1.31 | $292,610 | |
CDA-AMC scenario 1: Adopting alternative (log-normal) distribution for OS extrapolation | CP | $109,570 | 0.87 | Reference |
ACP | $238,838 | 1.41 | $241,592 | |
CDA-AMC scenario 2: Adopting alternative (spline, normal, 1 knot) distribution for PFS extrapolation | CP | $109,339 | 0.87 | Reference |
ACP | $238,121 | 1.30 | $298,473 | |
CDA-AMC scenario 3: Removing dose skipping | CP | $110,041 | 0.87 | Reference |
ACP | $260,094 | 1.31 | $336,878 |
ACP = amivantamab plus carboplatin and pemetrexed; CDA-AMC = Canada’s Drug Agency; ICER = incremental cost-effectiveness ratio; OS = overall survival; CP = carboplatin and pemetrexed; PFS = progression-free survival; QALY = quality-adjusted life-year.
aProbabilistic analyses.
Issues for Consideration
Amivantamab has received Health Canada approval for the treatment of adult patients with locally advanced or metastatic NSCLC with activating EGFR exon 20 insertion mutations whose disease has progressed on or after PBC. It was also approved in combination with carboplatin and pemetrexed for the first-line treatment of the same patient population. In parallel, a separate submission for the combination of amivantamab plus lazertinib is currently under review by CDA-AMC for the first-line treatment of EGFR-mutated NSCLC (exon 19 deletions or exon 21 L858R substitutions). The cost of amivantamab applied in the current submission may not reflect the confidential net price that jurisdictions pay in practice. This has implications for the durability of the cost-effectiveness estimates presented in this report.
Furthermore, there are implications for future changes to the treatment landscape, including the potential approval of amivantamab for a broader EGFR-mutated population (e.g., exon 19 or exon 21 mutations), as well as anticipated competition from pipeline EGFR-targeted therapies. These developments may affect the comparative clinical positioning and the economic value proposition of amivantamab in this and other indications.
Given the administration requirements of amivantamab (IV infusion with extended initial dosing), access may be limited to patients receiving care at larger cancer centres with the infrastructure to manage complex infusion protocols, including those related to infusion-related reactions. This could disproportionately impact patients in rural or underserved regions, raising concerns about equitable access.
Drug plan input indicated that first-line osimertinib monotherapy is the current funded standard of care, while the combination of first-line osimertinib with pemetrexed and platinum is under consideration for funding. If this combination (followed by osimertinib with or without pemetrexed maintenance) becomes standard practice, docetaxel would be a more appropriate comparator in the postprogression setting. However, CDA-AMC was unable to address this concern due to the lack of comparative efficacy data between ACP and docetaxel.
Appendix 5: Budget Impact Analysis
Please note that this appendix has not been copy-edited.
Summary of the Submitted BIA
The sponsor submitted a BIA that estimated the expected incremental budgetary impact of reimbursing ACP for the treatment of patients with locally advanced (not amenable to curative therapy) or metastatic NSCLC with EGFR exon 19 deletions or exon 21 L858R substitution mutations, whose disease has progressed on or after treatment with osimertinib.
The BIA was conducted from the perspective of public drug plan payers over a 3-year time horizon (2026 to 2028), with 2025 as the base year. The sponsor’s estimate reflects the aggregated results from the jurisdictional provincial budgets (excluding Quebec) as well as the Non-Insured Health Benefits Program. The sponsor estimated the eligible population using an epidemiological approach. The sponsor’s base case included drug acquisition costs only and no mark-ups or dispensing fees were included in the cost calculations. Median PFS from the MARIPOSA-2 trial were applied to each cycle to determine the duration on treatment. The market uptake for ACP was estimated using sponsor obtained clinician input. The key inputs to the BIA are documented in Table 12.
The sponsor estimated the 3-year incremental budget impact associated with reimbursing ACP for the treatment of patients with locally advanced (not amenable to curative therapy) or metastatic NSCLC with EGFR exon 19 deletions or exon 21 L858R substitution mutations, whose disease has progressed on or after treatment with osimertinib would be $36,670,793 (year 1 = $10,592,993; year 2 = $12,200,143; year 3 = $13,877,657).
Table 12: Key Model Parameters
Parameter | Sponsor’s estimate (reported as year 1 / year 2 / year 3 if appropriate) |
|---|---|
Target population | |
Incident lung cancer cases | 23,267 / 23,820 / 24,3859 |
% NSCLC | 88%10 |
% advanced NSCLC | |
% nonsquamous NSCLC | 83.1%15 |
% tested for EGFR mutations | 81.6%16 |
% positive for EGFR mutations | 14.3%16 |
% positive for EGFR exon 19 deletion or exon 21 L858R substitution | 84.3%17 |
% initiated first-line treatment | 83.1%18 |
Number of patients eligible for drug under review | 267 / 273 / 280 |
Market shares (reference scenario) | |
Amivantamab + CP | 0% / 0% / 0% |
CP | 100% / 100% / 100% |
Market shares (new drug scenario) | |
Amivantamab + CP | ███ / ███ / ███ |
CP | ███ / ███ / ███ |
Cost of treatment (per patient per 21-days) | |
Amivantamab + CP | $8,604 |
CP | $425 |
NSCLC = non–small lung cancer; CP = carboplatin and pemetrexed.
Key Issues of the Submitted BIA
CDA-AMC identified several key issues to the sponsor’s analysis that have notable implications on the results of the BIA:
Median PFS values as a proxy for the duration of treatment. To estimate the maximum budgetary impact in the target population, the sponsor included median PFS values for each regimen to be used as a proxy for the duration of treatment. The median PFS values were derived from the MARIPOSA-2 trial, with values of 8.18 and 4.21 months for ACP and CP, respectively. However, the MARIPOSA-2 trial captured TTD, which was used to represent duration of treatment in the CUA. In the CUA submission, TTD was defined as the time from the date of randomization to discontinuation of treatment for any reason, including disease progression, treatment toxicity, and death. Median TTD in the MARIPOSA-2 trial was 10.4 and 4.5 months for ACP and CP, respectively.1
To address this limitation, CDA-AMC performed a reanalysis to align duration of treatment with the median TTD from the MARIPOSA-2 trial.
The total number of eligible patients is uncertain. The sponsor derived, through an epidemiologic approach, that approximately 261 patients would be eligible for treatment with ACP at baseline, with an increase in total eligible patients to 280 over 3 years. Clinical expert feedback obtained by CDA-AMC noted that since amivantamab has been approved for first-line treatment of metastatic NSCLC, the number of patients receiving amivantamab assumed by the sponsor as a second-line treatment may be overestimated.
To address the uncertainty in the target population assumed by the sponsor, CDA-AMC undertook a scenario analysis to estimate the impact of decreasing the total number of eligible patients by 50%.
Percentage of patients tested for EGFR mutation is uncertain. In the sponsor submitted model, Albertan population-based data were used to estimate the percentage of patients tested for EGFR mutations (81.6%). When inquired, clinical expert feedback obtained by CDA-AMC suggested that this value may be underestimated. While the clinical experts noted that it may differ by jurisdiction, the percentage of patients tested for EGFR mutations are likely closer to 100%. By assuming a lower percentage, the total number of eligible patients is underestimated and in turn, underestimates the total budget impact.
In the absence of evidence to support the total percentage of patients tested for EGFR mutations, CDA-AMC undertook a scenario analysis to estimate the impact of 100% of patients receiving testing.
Additional issues were identified but were not considered to be key issues. These issues include incorrect list price of carboplatin and exclusion of wastage in the intervention cost calculations.
CDA-AMC Reanalyses of the BIA
CDA-AMC revised the sponsor’s submitted analyses by making changes in model parameter values and assumptions, in consultation with clinical experts, as outlined in Table 12.
Table 13: Revisions to the Submitted BIA
Stepped analysis | Sponsor’s value or assumption | CDA-AMC value or assumption |
|---|---|---|
1. Pricing for carboplatin | 50 mg/5 mL: $106.12 | 50 mg/5 mL: $70 |
2. Wastage | Not included | Included |
3. Duration of treatment | Median PFS | Median TTD |
CDA-AMC base case | ― | Reanalysis 1 + 2 + 3 |
BIA = budget impact analysis; CDA-AMC = Canada’s Drug Agency; PFS = progression-free survival; TTD = time to treatment discontinuation.
Note: The results of the CDA-AMC stepwise reanalysis are presented in summary format in Table 14, and a more detailed breakdown is presented in Table 15. In the CDA-AMC base case, the 3-year budget impact of reimbursing ACP for the treatment of patients with locally advanced (not amenable to curative therapy) or metastatic NSCLC with EGFR exon 19 deletions or exon 21 L858R substitution mutations, whose disease has progressed on or after treatment with osimertinib was $46,738,071 (year 1 = $13,501,101; year 2 = $15,549,464; year 3 = $17,687,507).
Table 14: Summary of the Stepped Analysis of the CDA-AMC Base Case
Stepped analysis | Three-year total ($) |
|---|---|
Submitted base case | 36,670,793 |
CDA-AMC reanalysis 1 | 36,510,425 |
CDA-AMC reanalysis 2 | 36,721,180 |
CDA-AMC reanalysis 3 | 46,901,518 |
CDA-AMC base case (reanalysis 1 + 2 + 3) | 46,738,071 |
CDA-AMC = Canada’s Drug Agency.
Note: The CDA-AMC reanalysis is based on publicly available prices of the comparator treatments.
Pagebreak
CDA-AMC used the CDA-AMC base case to conduct scenario analyses to explore uncertainty in the estimated budget impact of reimbursing ACP. The results are provided in Table 15.
Decrease in number of eligible patients by 50% to account for reimbursement of amivantamab as a first-line treatment.
Increase in percent of patients tested for EGFR mutations to 100%.
Table 15: Disaggregated Summary of the BIA
Stepped analysis | Scenario | Year 0 (current situation) ($) | Year 1 ($) | Year 2 ($) | Year 3 ($) | Three-year total ($) |
|---|---|---|---|---|---|---|
Submitted | Reference total | 970,133 | 993,173 | 1,016,760 | 1,040,908 | 3,050,841 |
ACP | 0 | 0 | 0 | 0 | 0 | |
All other comparators | 970,133 | 993,173 | 1,016,760 | 1,040,908 | 3,050,841 | |
New drug total | 970,133 | 11,586,166 | 13,216,904 | 14,918,564 | 39,721,634 | |
ACP | 0 | 10,990,262 | 12,657,685 | 14,398,111 | 38,046,058 | |
All other comparators | 970,133 | 595,904 | 559,218 | 520,454 | 2,645,709 | |
Budget Impact | 0 | 10,592,993 | 12,200,143 | 13,877,657 | 36,670,793 | |
CDA-AMC base case | Reference total | 949,020 | 971,559 | 994,633 | 1,018,255 | 2,984,446 |
ACP | 0 | 0 | 0 | 0 | 0 | |
All other comparators | 949,020 | 971,559 | 994,633 | 1,018,255 | 2,984,446 | |
New drug total | 949,020 | 14,472,659 | 16,544,096 | 18,705,762 | 49,722,517 | |
ACP | 0 | 13,889,724 | 15,997,048 | 18,196,634 | 48,083,407 | |
All other comparators | 949,020 | 582,935 | 547,048 | 509,127 | 2,588,130 | |
Budget Impact | 0 | 13,501,101 | 15,549,464 | 17,687,507 | 46,738,071 | |
CDA-AMC scenario analyses | ||||||
Scenario 1: 50% decrease in total eligible patients | Reference total | 474,510 | 485,779 | 497,316 | 509,127 | 1,492,223 |
New drug total | 474,510 | 7,236,330 | 8,272,048 | 9,352,881 | 24,861,259 | |
Budget Impact | 0 | 6,750,550 | 7,774,732 | 8,843,753 | 23,369,036 | |
Scenario 2: 100% of patients tested for EGFR mutations | Reference total | 1,163,015 | 1,190,636 | 1,218,913 | 1,247,861 | 3,657,409 |
New drug total | 1,163,015 | 17,736,102 | 20,274,628 | 22,923,727 | 60,934,458 | |
Budget Impact | 0 | 16,545,467 | 19,055,715 | 21,675,866 | 57,277,048 | |
BIA = budget impact analysis; CDA-AMC = Canada’s Drug Agency.
Note: The CDA-AMC reanalysis is based on the publicly available prices of the comparator treatments.
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@cda-amc.ca.