Drugs, Health Technologies, Health Systems
Reimbursement Review
Lazertinib and Amivantamab (Lazcluze and Rybrevant)
Sponsor: Janssen Inc.
Therapeutic area: Locally advanced or metastatic non–small cell lung cancer
This multi-part report includes:
Clinical Review
Pharmacoeconomic Report
Clinical Review
Abbreviations
AE
adverse event
AESI
adverse event of special interest
BICR
blinded independent central review
CCSN
Canadian Cancer Survivor Network
CDA-AMC
Canada’s Drug Agency
CI
confidence interval
CNS
central nervous system
CR
complete response
DOR
duration of response
ECOG
Eastern Cooperative Oncology Group
EORTC QLQ-C30
European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30
GRADE
Grading of Recommendations, Assessment, Development and Evaluations
HR
hazard ratio
HRQoL
health-related quality of life
IRR
infusion-related reaction
LS
least squares
MID
minimal important difference
MMRM
mixed model for repeated measures
NGS
next-generation sequencing
NMA
network meta-analysis
NSCLC
non–small cell lung cancer
NSCLC-SAQ
Non–Small Cell Lung Cancer Symptom Assessment Questionnaire
OR
odds ratio
ORR
objective response rate
OS
overall survival
PFS
progression-free survival
PR
partial response
RCT
randomized controlled trial
RECIST
Response Evaluation Criteria in Solid Tumours
SAE
serious adverse event
SC
subcutaneous
SD
standard deviation
SLR
systematic literature review
TKI
tyrosine kinase inhibitor
VTE
venous thromboembolism
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Table 1: Background Information of Application Submitted for Review
Item | Description |
|---|---|
Drug product | Lazertinib 80 mg and 240 mg tablets Amivantamab 350 mg/7 mL (50 mg/mL) single-use vial for IV infusion |
Sponsor | Janssen Inc. |
Indication | Lazertinib in combination with amivantamab is indicated for the first-line treatment of adult patients with locally advanced (not amenable to curative therapy) or metastatic NSCLC with EGFR exon 19 deletions or exon 21 L858R substitution mutations |
Reimbursement request | As per indication |
Health Canada approval status | NOC |
Health Canada review pathway | Standard (Project Orbis) |
NOC date | March 6, 2025 |
Recommended dose | Lazertinib: The recommended dosage is 240 mg once daily, taken orally, in combination with amivantamab until disease progression or no longer tolerated by the patient. It is recommended to administer lazertinib any time before amivantamab when given on the same day. Amivantamab IV infusion: Lazertinib is to be used in combination with amivantamab. The recommended dosage of amivantamab is 1,050 mg (if body weight < 80 kg) or 1,400 mg (if body weight ≥ 80 kg) administered by IV infusion in 28-day cycles, once weekly for the first 4 weeks (with a split dose on days 1 and 2) and then once every 2 weeks at week 5 onwards. |
NOC = Notice of Compliance; NSCLC = non–small cell lung cancer.
Introduction
Lung cancer is the most diagnosed cancer and leading cause of cancer-related deaths in Canada.1 It is estimated that 1 in 14 Canadians will develop lung cancer, accounting for 1 in 4 cancer-related deaths.1 In 2024, 32,100 new cases of lung and bronchus cancer are projected, with 98% occurring in individuals aged 50 years or older.2 Non–small cell lung cancer (NSCLC) comprises 88% of cases and has a poor prognosis, with a 5-year survival rate of only 3% for advanced (stage IV) disease.1 Treatment aims to delay progression, prolong survival, manage symptoms, and improve quality of life.3
NSCLC often presents asymptomatically in early stages, and symptoms such as cough, chest pain, hemoptysis, and weight loss are often nonspecific.4 A key mechanism involves driver mutations that activate progrowth signalling pathways, most commonly in the EGFR gene.5 These driver mutations are found more frequently in patients with adenocarcinomas, nonsmokers, patients of Asian ethnicity, and in females.6 Diagnosis typically occurs at late stages and requires a biopsy for histologic confirmation.1 NSCLC is classified into adenocarcinoma, squamous cell carcinoma, and large cell carcinoma,7 with EGFR mutation testing recommended to guide treatment decisions.8 According to the clinical experts consulted by the review team, testing for EGFR mutations, including exon 19 deletions and exon 21 L858R substitution mutations, is currently performed as part of the standard of care for locally advanced or metastatic nonsquamous NSCLC in Canada.
According to the experts consulted for this review, osimertinib is the current standard treatment for NSCLC with EGFR exon 19 deletions or exon 21 L858R mutations, based on the FLAURA trial, which demonstrated superior progression-free survival (PFS) and overall survival (OS) compared to erlotinib and gefitinib.9 It is taken daily until disease progression or intolerance and has a favourable safety profile, making it suitable for the vast majority of patients, including older patients. Osimertinib plus platinum-based chemotherapy is also recommended for reimbursement as a first-line treatment of adult patients with locally advanced or metastatic NSCLC whose tumours have EGFR exon 19 deletions or exon 21 L858R mutations.10 It is currently undergoing price negotiations and therefore is not widely available.
Perspectives of Patient, Clinicians, and Drug Programs
The information in this section is a summary of input provided by the patient and clinician groups who responded to our call for input and from clinical experts consulted by for the purpose of this review.
Patient Input
For this review, patient input was jointly submitted by 3 organizations: Lung Cancer Canada, Canadian Cancer Survivor Network (CCSN), and the Lung Health Foundation. Information was gathered from 4 patients in Canada diagnosed with stage IV NSCLC with treatment experience with amivantamab (n = 3), or lazertinib plus amivantamab combination therapy (n = 1). Data were collected through virtual interviews and from previous patient input submissions to Canada’s Drug Agency (CDA-AMC).
The patient group input described the initial shock patients experience with their diagnosis, as they noted minimal initial symptoms consisting of back pain, a persistent cough, or shortness of breath. Three of the patients reported experience with currently available EGFR-targeted therapies including osimertinib, gefitinib, and afatinib, with limited side effects (e.g., significantly dry skin, thinning of hair, and diarrhea) before their disease progressed. As such, progression and treatment resistance remain a critical concern for patients. The input noted that patients desire a treatment that improves the management of their disease symptoms, delays further progression, shrinks their tumours, improves their quality of life, prolongs survival with independence and functionality, and has manageable side effects.
Three of the patients included in the input each had a different mutation (exon 20, exon 19, or exon 21 L858R) and reported successful tumour shrinkage and stable metastases after receiving amivantamab as a first-line, third-line, or later-line treatment. One patient developed additional metastases approximately 3 years after initiating third-line amivantamab and has since passed away. The patient who received lazertinib and amivantamab combination therapy as a second-line treatment for over 2.5 years to date had initial shrinking in their primary tumour and is currently experiencing stable metastases. Two patients reported significant side effects at treatment onset, including severe dry scalp and bleeding due to dryness, paronychia, and painful acne, as well as rashes on their scalp, back, and chest. The patient input noted that these side effects reduced in severity over time, were controlled with prescription medications, were not as severe as those experienced with chemotherapy, and were deemed worthwhile if the treatment was working. Two patients reported that they were able to return to a good quality of life by pursuing hobbies, travel, and spending time with family. The input also noted that patients preferred the ease and convenience of oral targeted therapies that can be taken at home versus long infusion times in the hospital with amivantamab.
Clinician Input
Input From Clinical Experts Consulted for This Review
The clinical experts noted that ultimately, all patients with NSCLC will experience disease progression; thus, there is a need for treatments that delay progression, extend survival, and have manageable side effects. The clinical experts noted that there is a risk of relapse with current therapies, particularly in the case of central nervous system (CNS) disease because EGFR-mutated NSCLC tends to present with brain metastases or has a high risk of their development. The current standard of care (osimertinib monotherapy) is generally well-tolerated, relieves disease-related symptoms quickly, can be administered to older patients, and as an oral medication, can be more convenient for patients. The clinical experts noted that there is a risk of added toxicity and potential inconvenience of IV chemotherapy administered every 3 weeks for the recently recommended osimertinib plus chemotherapy combination. Additionally, EGFR inhibitors are generally associated with serious toxicities (e.g., pneumonitis) which can impact quality of life.
The experts indicated that amivantamab plus lazertinib, osimertinib monotherapy, or osimertinib plus chemotherapy could all be considered first-line options for patients with the EGFR mutations in question. Amivantamab plus lazertinib and osimertinib plus chemotherapy would offer the opportunity for greater efficacy over osimertinib alone, although with trade-offs such as the risk of greater toxicity and more clinic visits. Amivantamab plus lazertinib could be an alternate option to osimertinib plus chemotherapy for a proportion of patients, particularly those who are younger, more fit, and with some poorer prognostic features including CNS metastases. The experts emphasized, however, that similar to other treatments, amivantamab plus lazertinib would not be curative.
The clinical experts noted that EGFR detection is routine across Canada and therefore misdiagnosis is unlikely. Patients with newly diagnosed locally advanced or metastatic NSCLC with EGFR exon 19 deletions or exon 21 L858R substitution, who were young, fit, or felt to be at high risk of poorer outcomes (for example, with liver metastases, brain metastases, or p53 mutations) would be most likely to be considered for this therapy. The experts noted that not all patients would be suitable for amivantamab plus lazertinib, potentially due to underlying comorbidities, frailty, lack of desire for IV treatment, or increased toxicities including thromboembolism. They stated that patient preference would be important to consider, and that the choice of treatment would routinely involve a discussion with patients regarding their treatment options. The experts noted that patients with prior EGFR tyrosine kinase inhibitor (TKI) experience were excluded from the pivotal trial; however, there is a possibility that osimertinib may be used as an adjuvant therapy after tumour resection. These patients (estimated by the experts to be approximately 10% to 15% of patients) would not have been included in the pivotal trial and therefore it is unclear whether they would be considered candidates for amivantamab plus lazertinib. They also noted that older patients (i.e., aged > 75 years) were not highly represented in the trial and may also be less tolerant of a more aggressive regimen.
The experts noted that patients are typically seen every 3 weeks to 4 weeks and imaging is conducted every 8 weeks to 12 weeks, depending on their treatment regimen. Objective response criteria (e.g., radiological assessment every 2 months to 3 months to determine disease progression) can be used to ensure disease response or control, along with clinical assessments of disease-related symptoms (e.g., cough, shortness of breath) and health-related quality of life (HRQoL) which the experts noted is not routinely assessed in clinical practice using standardized tools. The clinical experts stated that the discontinuation criteria for amivantamab plus lazertinib should be the same as other anticancer therapies where disease progression, intolerable toxicity or toxicity associated with deteriorating quality of life, and patient choice would all be grounds to discontinue. The experts noted that amivantamab plus lazertinib should only be prescribed under the care of oncology specialists in a cancer centre.
Clinician Group Input
Two clinician groups, including the Ontario Health-Cancer Care Ontario Lung and Thoracic Cancer Drug Advisory Committee and the Lung Cancer Canada Medical Advisory Committee, provided input. They emphasized the primary treatment goals for patients with stage IV NSCLC include prolonging survival, improving symptoms, and delaying disease progression. Osimertinib remains the standard first-line treatment for EGFR-mutated NSCLC, but resistance inevitably develops, and no publicly funded targeted therapies exist for patients who progress on osimertinib in Canada. The input noted that to address resistance, intensified first-line regimens, such as osimertinib plus chemotherapy have been explored. However, according to the clinician groups, not all patients respond to these therapies, highlighting the need for additional, intensified treatments in the first-line setting that improve survival, symptom control, and brain protection while maintaining manageable toxicity and convenience. The Ontario Health-Cancer Care Ontario Lung and Thoracic Cancer Drug Advisory Committee noted that amivantamab and lazertinib do not fully meet these criteria of convenience or low toxicity.
Both clinician groups agreed that the combination of amivantamab and lazertinib would be used as a first-line treatment in the population under review. Single-drug osimertinib will still be considered as a first-line option (as there will be patients who do not want to receive IV systemic therapy or prefer the logistics involved with an oral drug alone). In the event there is access to the combination of osimertinib plus chemotherapy in the future, this regimen would add an additional front-line therapeutic option. Following these regimens, chemotherapy would remain a viable second-line option. Patients best suited for this therapy are those with advanced EGFR-mutated NSCLC who can tolerate intensified treatment and increased monitoring. The input noted that it is not yet possible to identify specific patients who are more likely to respond to this therapy or which patients should receive osimertinib plus chemotherapy versus amivantamab plus lazertinib. The input stated that treatment response is assessed through side effect profiles, clinical outcomes, and imaging at regular intervals. Patients will require close monitoring, particularly for dermatologic side effects, with evaluations typically occurring every 2 months to 4 months. Lazertinib is taken at home, while amivantamab is administered in outpatient oncology units or hospitals by experienced personnel.
Drug Program Input
Input was obtained from the drug programs that participate in the CDA-AMC reimbursement review process. The following were identified as key factors that could potentially impact the implementation of a recommendation for amivantamab plus lazertinib:
relevant comparators
considerations for initiation of therapy
considerations for prescribing of therapy
generalizability
funding algorithm
care provision issues.
The clinical experts provided advice on the potential implementation issues raised by the drug program. Refer to Table 5 for more details.
Clinical Evidence
Systematic Review
Description of Studies
The MARIPOSA study is an ongoing randomized, multicentre, phase III trial comparing the efficacy and safety of first-line amivantamab plus lazertinib to osimertinib monotherapy in adult patients with EGFR-mutated NSCLC. The data contained in the submission were from a data cut-off date of August 11, 2023, which represented the cut-off for the primary analysis of PFS and interim analysis of OS. An updated clinical efficacy analysis of major secondary end points (i.e., OS) and exploratory end points with longer-term follow-up was conducted using a data cut-off of May 13, 2024. The MARIPOSA study enrolled adult (aged ≥ 18 years) patients with newly diagnosed, histologically or cytologically confirmed, locally advanced or metastatic NSCLC which was treatment-naive and not amenable to any curative therapy including surgical resection or chemotherapy. Patients also had to meet specific organ function thresholds and had to have an Eastern Cooperative Oncology Group (ECOG) status of 0 or 1. The tumour also had to have evidence of either the EGFR 19 deletion mutation or the EGFR exon 21 L858R substitution, as well as at least 1 lesion measurable by Response Evaluation Criteria in Solid Tumours (RECIST) 1.1 which had not been previously irradiated. Notable exclusion criteria included prior treatment for any locally advanced (stage III) or metastatic (stage IV) cancer, symptomatic brain metastases, and any prior EGFR TKI therapy.
A total of 1,074 patients were randomized 2:2:1 to either open-label amivantamab plus lazertinib (arm A; n = 429), double-blinded osimertinib (arm B; n = 429), or double-blinded lazertinib (arm C; n = 216), respectively. Randomization was stratified on mutation type (exon 19 deletion versus exon 21 L858R), race (Asian versus non-Asian), and history of brain metastases (present versus absent). Arm A received amivantamab 1,050 mg (1,400 mg if body weight ≥ 80 kg) by IV infusion in 28-day cycles, once weekly for the first 4 weeks (with a split dose on day 1 and day 2 in week 1) and then once every 2 weeks, and three 80 mg lazertinib tablets once daily. Arm B received osimertinib 80 mg plus 3 lazertinib placebo tablets once daily. Arm C received 1 osimertinib placebo capsule plus three 80 mg lazertinib tablets (240 mg total) once daily. The primary end point of the MARIPOSA study was PFS by blinded independent central review (BICR), with secondary end points including OS, objective response rate (ORR), duration of response (DOR), and HRQoL measures.
Efficacy Results
Results of the prespecified primary analysis of PFS and interim analysis of OS (August 11, 2023, data cut-off; median duration of follow-up = 22.01 months), as well as results from OS, ORR, and DOR from the additional May 13, 2024, reanalysis (median follow-up approximately 31 months) were reported.
PFS by BICR
As of the August 11, 2023, data cut-off, there were a total of 192 (44.8%) PFS events in the amivantamab plus lazertinib arm, and 252 (58.7%) PFS events in the osimertinib arm. Of these, 148 (77.1%) and 228 (90.5%) were due to progressive disease, and 44 (22.9%) and 24 (9.5%) were due to death without progressive disease in the amivantamab plus lazertinib and osimertinib arms, respectively. The median PFS in the amivantamab plus lazertinib arm was 23.72 months (95% confidence interval [CI], 19.12 months to 27.66 months), and in the osimertinib arm was 16.59 months (95% CI, 14.78 months to 18.46 months), in favour of amivantamab plus lazertinib (hazard ratio [HR] = 0.70; 95% CI, 0.58 to 0.85; P = 0.0002). The difference in the probability of being progression-free between amivantamab plus lazertinib and osimertinib at 6 months, 12 months, 18 months, and 24 months was ████ ████ ███ █████ ██ ██████ ████ ████ ███ ████ ██ ███████ █████ ████ ███ ████ ██ ███████ ███ █████ █████ ██ ██████, respectively.
PFS was not re-analyzed with data from the May 13, 2024, data cut-off as the primary end point was met in the primary analysis of PFS (August 11, 2023, data cut-off).
Overall Survival
As of the August 11, 2023, data cut-off, with 214 deaths observed from the amivantamab plus lazertinib and osimertinib arms combined at the data cut-off, the interim analysis of OS was evaluated at a 2-sided significance level of 0.0050. There was a total of 97 (22.6%) deaths in the amivantamab plus lazertinib arm, and 117 (27.3%) deaths in the osimertinib arm. The median OS was not reached in either study arm as of the data cut-off (HR = 0.80; 95% CI, 0.61 to 1.05; P = 0.1099). The OS event-free probability between study arms for the proportion of patients who were alive at 6 months, 12 months, 18 months, and 24 months was █████ ████ ███ █████ ██ ██████ ████ ████ ███ █████ ██ ██████ ████ ████ ███ █████ ██ ██████ ███ ████ ████ ███ █████ ██ ███████ respectively.
As of the May 13, 2024, data cut-off, there were 142 deaths (33.1%) in the amivantamab plus lazertinib arm and 177 deaths (41.3%) in the osimertinib arm. The median OS was not reached in the amivantamab plus lazertinib arm. The median OS was 37.32 months (95% CI, 32.53 months to not estimable) in the osimertinib arm, in favour of amivantamab plus lazertinib (HR = 0.77; 95% CI, 0.61 to 0.96; P = 0.0185). The OS event-free probability between study arms for the proportion of patients who were alive at 12 months, 24 months, and 36 months was ████ ████ ███ █████ ██ ██████ ████ ████ ███ █████ ██ ███████ ███ ████ ████ ███ ████ ██ ██████, respectively.
Objective Response Rate
As of the August 11, 2023, data cut-off, a total of 336 patients (79.8%; 95% CI, 75.7% to 83.5%) in the amivantamab plus lazertinib arm and 314 patients (75.8%; 95% CI, 71.4% to 79.9%) in the osimertinib arm had an objective response ██████████ ██ ██ ████ ███ █████ ███ █████████ ██ ██ █████ ███ ██████ ████████████). The odds ratio (OR) for response when compared to osimertinib arm was 1.27 (95% CI, 0.91 to 1.77).
As of the May 13, 2024, data cut-off, a total of ███ ████████ ██████ ████ ███ █████ ██ ███████ in the amivantamab plus lazertinib arm and ███ ████████ ██████ ████ ███ █████ ██ ███████ in the osimertinib arm had an objective response. The OR for response was ████ ████ ███ ████ ██ █████.
Duration of Response
As of the August 11, 2023, data cut-off, there were 336 confirmed responders in the amivantamab plus lazertinib arm and 314 in the osimertinib arm. The median DOR in the amivantamab plus lazertinib arm was 25.76 months (95% CI, 20.14 months to not estimable), and in the osimertinib arm the median DOR was 16.76 months (95% CI, 14.75 months to 18.53 months). The difference between study arms in the proportion of responders with DOR of 6 months, 12 months, 18 months, and 24 months was ████ ████ ███ █████ ██ ██████ █████ ████ ███ ████ ██ ███████ ████ ████ ███ █████ ██ ███████ ███ ████ ████ ███ █████ ██ █████, respectively.
As of the May 13, 2024, data cut-off, there were ███ confirmed responders in the amivantamab plus lazertinib arm and ███ in the osimertinib arm. The median DOR in the amivantamab plus lazertinib arm was 25.76 months (95% CI, 20.34 months to 33.87 months), and in the osimertinib arm the median DOR was 18.14 months (95% CI, 14.78 months to 201.4 months). The difference between study arms in the proportion of responders with DOR of 12 months, 24 months, and 30 months was █████ ████ ███ ████ ██ ███████ █████ ████ ███ ████ ██ ███████ ███ ████ ████ ███ █████ ██ █████, respectively.
European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30
The European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 (EORTC QLQ-C30) functional scales range from 0 to 100, with higher scores indicating better functioning. As of the August 11, 2023, data cut-off, the mean baseline EORTC QLQ-C30 Global Health Status score was █████ ██████ █████████ █████████ ████ █ ██████ in the amivantamab plus lazertinib arm, and █████ ██████ ███ █ ██████ in the osimertinib arm. At cycle 13, day 1, the least squares (LS) mean change from baseline was ███ ██████ ████ ███ ███ ██ ████ | | ████ in the amivantamab plus lazertinib arm and ████ ██████ ████ ███ ████ ██ █████ | | ████ in the osimertinib arm, representing a LS mean difference of ███ ██████ ████ ███ ████ ██ ████ | | ███████. At cycle 21, day 1, the LS mean change from baseline was ███ ██████ ████ ███ ███ ██ ████ | | ████ in the amivantamab plus lazertinib arm and ███ ██████ ████ ███ ███ ██ ████ | | ███) in the osimertinib arm, representing a LS mean difference of ████ ██████ ████ ███ ████ ██ ████ | | ████████ At cycle 27, day 1, the LS mean change from baseline was ███ ██████ ████ ███ ████ ██ ████ | | ███ in the amivantamab plus lazertinib arm and ███ ██████ ████ ███ ███ ██ ████ | | ███ in the osimertinib arm, representing a LS mean difference of ████ ██████ ████ ███ ████ ██ ████ | | ████████. .
███████ ███ █████ ███████ ██████ ██████ ██████ ████ ███ ████████ ██ ███ ███ ███ ████ ████ ███████.
Non–Small Cell Lung Cancer Symptom Assessment Questionnaire Total Score
The Non–Small Cell Lung Cancer Symptom Assessment Questionnaire (NSCLC-SAQ) contains 5 domains and the total score ranges from 0 to 20, with higher scores indicating more severe symptoms. As of the August 11, 2023, data cut-off, the mean baseline NSCLC-SAQ total score was ████ ██████ ███ █ █████ in the amivantamab plus lazertinib arm, and ████ ██████ ███ █ █████ in the osimertinib arm. At cycle 13, day 1, the LS mean change from baseline was ████ ██████ ████ ███ ████ ██ █████ | | ████ in the amivantamab plus lazertinib arm and ████ ██████ ████ ███ ████ ██ █████ | | ████ in the osimertinib arm, representing a LS mean difference of ███ ██████ ████ ███ ████ ██ ████ | | ███████. At cycle 21, day 1, the LS mean change from baseline was ████ ██████ ████ ███ ████ ██ █████ | | ████ in the amivantamab plus lazertinib arm and ████ ██████ ████ ███ ████ ██ █████ | | ████ in the osimertinib arm, representing a LS mean difference of ████ ████ ███ ████ ██ ████ | | ████████ At cycle 27, day 1, the LS mean change from baseline was ████ ██████ ████ ███ ████ ██ █████ | | ███ in the amivantamab plus lazertinib arm and ████ ██████ ████ ███ ████ ██ █████ | | ███ in the osimertinib arm, representing a LS mean difference of ████ ████ ███ ████ ██ ████ | | ████████.
███████ ███ █████████ █████ █████ ████ ███ ████████ ██ ███ ███ ███ ████ ████ ███████.
Harms Results
Harms from the lazertinib monotherapy arm were also reported to provide additional context into the harms associated with amivantamab.
Adverse Events
As of the August 11, 2023, data cut-off, all patients in the amivantamab plus lazertinib arm and lazertinib monotherapy arm, and 99.3% of patients in the osimertinib arm experienced an adverse event (AE). In addition, 75.1% of patients in the amivantamab plus lazertinib arm, 42.8% in the osimertinib arm, and 45.5% in the lazertinib arm experienced an AE of grade 3 or higher. The most commonly reported AEs were paronychia (68.4% in the amivantamab plus lazertinib arm, 28.3% in the osimertinib arm, and █████ in the lazertinib arm); infusion reactions (62.9% in the amivantamab plus lazertinib arm, 0% in the osimertinib arm, and ██ in the lazertinib arm); rash (61.8% in the amivantamab plus lazertinib arm, 30.6% in the osimertinib arm, and █████ in the lazertinib arm); hypoalbuminemia (48.5% in the amivantamab plus lazertinib arm, 6.1% in the osimertinib arm, and ████ in the lazertinib arm); increased alanine aminotransferase (36.1% in the amivantamab plus lazertinib arm, 13.3% in the osimertinib arm, and █████ in the lazertinib arm); and peripheral edema (35.6% in the amivantamab plus lazertinib arm, 5.6% in the osimertinib arm, and █████ in the lazertinib arm). These also represented numeric differences between the amivantamab plus lazertinib arm relative to the other 2 study arms.
Additional AEs which were reported in a numerically higher proportion of patients in the osimertinib arm relative to the other 2 study arms were diarrhea (44.4% in the osimertinib arm, 29.2% in the amivantamab plus lazertinib arm, and █████ in the lazertinib arm); leukopenia (15.4% in the osimertinib arm, 6.2% in the amivantamab plus lazertinib arm, and ████ in the lazertinib arm); and neutropenia (█████ in the osimertinib arm, ████ in the amivantamab plus lazertinib arm, and ████ in the lazertinib arm).
Serious Adverse Events
As of the August 11, 2023, data cut-off, a total of 48.7% of patients in the amivantamab plus lazertinib arm, 33.4% of patients in the osimertinib arm, and 35.2% of patients in the lazertinib arm reported serious AEs (SAEs). The most common SAEs (occurring in more than 1.5% of patients) which were also reported in numerically higher proportions in the amivantamab plus lazertinib arm relative to the osimertinib arm were pulmonary embolism (26 [6.2%] in the amivantamab plus lazertinib arm, 10 [2.3%] in the osimertinib arm, and ██████ in the lazertinib arm); deep vein thrombosis (12 [2.9%] in the amivantamab plus lazertinib arm, 2 [0.5%] in the osimertinib arm, and ██████ in the lazertinib arm); infusion-related reactions (IRRs) (9 [2.1%] in the amivantamab plus lazertinib arm and 0 in the osimertinib ███ ██████████ ████); respiratory failure (6 [1.4%] in the amivantamab plus lazertinib arm, 2 [0.5%] in the osimertinib arm, and | ██████ in the lazertinib arm); and rash (7 [1.7%] in the amivantamab plus lazertinib arm and ██ in the osimertinib and lazertinib arms).
Withdrawals Due to AEs
As of the August 11, 2023, data cut-off, a total of 34.9% of patients in the amivantamab plus lazertinib arm, 13.6% in the osimertinib arm, and █████ in the lazertinib arm had discontinued any study treatment due to AEs. The most common reason for study treatment discontinuation in the amivantamab plus lazertinib arm ███ ██████████ ███ ████████████ █████ ██ ██████████ in the osimertinib arm the most common reason for discontinuation was ████████████ ████████ ███ ███████████ █████████ █████ ██ ██████████.
Mortality
The proportion of patients who died was numerically similar across study arms (96 [22.8%] patients in the amivantamab plus lazertinib arm, 116 [27.1%] patients in the osimertinib arm, and ██ ███████ patients in the lazertinib arm). The most common reason for death was disease progression (11.6% of patients in the amivantamab plus lazertinib arm, 18.9% of patients in the osimertinib arm, and █████ of patients in the lazertinib arm), followed by AEs (9.3% of patients in the amivantamab plus lazertinib arm, 6.8% of patients in the osimertinib arm, and ████ of patients in the lazertinib arm).
Notable Harms
The AEs of special interest (AESIs) of rash, IRR, and pneumonitis or interstitial lung disease were prospectively identified based on the safety profile of amivantamab, and venous thromboembolism (VTE) was added as an AESI during the conduct of the study. A numerically higher proportion of patients in the amivantamab plus lazertinib arm reported rash (88.6% versus 49.1% in the osimertinib arm and █████ in the lazertinib arm), IRR (62.9% versus ██ in the osimertinib ███ ██████████ ████), and VTE (37.3% versus 9.1% in the osimertinib arm and █████ in the lazertinib arm). A total of 3.1% of patients in the amivantamab plus lazertinib arm, 3.0% of patients in the osimertinib arm, and ████ of patients in the lazertinib arm reported pneumonitis or interstitial lung disease.
Critical Appraisal
The amivantamab plus lazertinib arm was open label, which would impact the assessment of HRQoL outcomes due to participants knowing that they were receiving treatment with amivantamab plus lazertinib. It is also possible that patients randomized to the osimertinib or lazertinib monotherapy arms, while double-blinded, would also be aware that they were not receiving amivantamab plus lazertinib because amivantamab is an IV infusion and there was no matching placebo IV. In addition, the study protocol was amended several times after patient enrolment started, including the addition of AESIs and updating the inclusion and exclusion criteria, and there is an unknown risk of bias due to these changes, which impacts an unknown number of patients. The OS results of the study were based on an interim analysis; thus, there is a risk of overestimating the true treatment effect.11 The median OS and DOR were not estimable at the time of the prespecified data cut-off. While data with longer-term follow-up were provided for OS, ORR, and DOR, this did not represent a prespecified data cut-off and should be considered exploratory. The median OS was not reached in either the August or May data cut-offs. As of the August 11, 2023, data cut-off, (median follow-up of 22.01 months) a total of 25% of OS events had occurred across both study arms but as of the May 13, 2024, data cut-off, a total of ███ of OS events had occurred, suggesting that the data are largely immature for OS. The 75th percentile for the DOR result was likewise not estimable at the May 2024 data cut-off, suggesting the data are immature for this outcome as well. The long-term results associated with amivantamab plus lazertinib are therefore unclear for OS and DOR. In addition to this, ORR and DOR were not controlled for multiple comparisons and are only considered supportive of the overall effect of amivantamab and lazertinib. In general, the stratification factors used in randomization and other potential prognostic factors identified by the experts such as age, smoking status, ECOG status, and sex were balanced between study arms. The HRQoL end points were secondary in the MARIPOSA study and results were not adjusted for multiple comparisons; therefore, there is an increased risk of type I error, and these end points can only be considered supportive. HRQoL estimates had a substantial amount of missing data and were modelled using a mixed model for repeated measures (MMRM), which assumes the data are missing at random. However, the nature of the disease means that, because patients are censored at disease progression or death, among other reasons, it is likely that patients who remained on study are systematically different from patients who did not provide data, and there is a likelihood of bias in the results. While the NSCLC-SAQ analysis required that all 5 domains be complete to compute a total score, EORTC QLQ-C30 did not report any methods to account for missing responses, which also may impart a bias of unknown direction and degree.
There are also limitations impacting the external validity of the study. Per the clinical experts consulted for this review, the study inclusion and exclusion criteria and baseline characteristics were broadly representative of the patients in Canadian clinical practice settings, apart from the fact that the racial breakdown in the MARIPOSA study was slightly different than the typical patient population in a Canadian clinical setting. However, they noted that the MARIPOSA study limited enrolment to ECOG status 0 or 1, and patients with ECOG status of 2 or greater may be considered for this therapy. In addition, patients with a history of adjuvant therapy were enrolled if therapy was more than 12 months prior; the experts noted that if the treatment received in the adjuvant or neoadjuvant setting was a non-EGFR inhibitor (e.g., cytotoxic chemotherapy), then a period of 6 months could be considered. They also noted that patients who had any prior experience with EGFR TKIs were excluded, which might preclude patients from receiving amivantamab plus lazertinib who had received osimertinib in the adjuvant setting given its use for earlier-stage NSCLC in Canada. The clinical experts estimated this might affect approximately 10% or 15% of patients. Results of the trial would therefore not be generalizable to these patients. In addition, the median follow-up at the time of the May 13, 2024, data cut-off was approximately 31 months; however, the trial is still ongoing and longer-term results on efficacy and harms are not available and it is uncertain whether the results are generalizable to a longer treatment duration.
GRADE Summary of Findings and Certainty of the Evidence
The selection of outcomes for the Grading of Recommendations, Assessment, Development and Evaluations (GRADE) assessment was based on the sponsor’s summary of clinical evidence, consultation with clinical experts, and input received from patient and clinician groups and public drug plans. The following list of outcomes was finalized in consultation with expert committee members.
Clinical outcomes:
PFS at 24 months
OS at 24, 30, and 36 months.
HRQoL outcomes:
change from baseline to cycle 13, day 1, in EORTC QLQ-C30 Global Health Status and NSCLC-SAQ total score
change from baseline to cycle 27, day 1, in EORTC QLQ-C30 Global Health Status and NSCLC-SAQ total score.
Harms:
rash
VTE
IRRs
pneumonitis or interstitial lung disease.
Table 2: Summary of Findings for Amivantamab Plus Lazertinib vs. Osimertinib for Patients With Locally Advanced or Metastatic Non–Small Cell Lung Cancer
Outcome and follow-up | Patients, N (studies) | Absolute effects (95% CI) | Certainty | What happens | ||
|---|---|---|---|---|---|---|
Amivantamab plus lazertinib | Osimertinib | Difference | ||||
Survival outcomes | ||||||
Progression-free survival by BICR: August 11, 2023, data cut-off | ||||||
Proportion of patients who are progression-free at 24 months Median follow-up: 23.72 months versus 16.59 monthsa | 858 (1 RCT) | ███ ███ ████ █████ ██ ███ ███ █████ | ███ ███ ████ █████ ██ ███ ███ █████ | ███ ███ ████ ████ ██ ███ ███ █████ | Moderateb | Amivantamab plus lazertinib likely results in an increase in the proportion of patients progression-free at 24 months when compared with osimertinib. |
Overall survival: May 13, 2024, data cut-offc | ||||||
Proportion of patients who are alive at 24 months Median follow-up: ██ ███ █████ ██████ | 858 (1 RCT) | ███ ███ ████ █████ ██ ███ ███ █████ | ███ ███ ████ █████ ██ ███ ███ █████ | ██ ███ ████ ████ ██ ███ ███ █████ | Lowd,e | Amivantamab plus lazertinib may result in an increase in the proportion of patients alive at 24 months when compared with osimertinib. |
Proportion of patients who are alive at 30 months Median follow-up: ██ ███ █████ ██████ | 858 (1 RCT) | ███ ███ ████ █████ ██ ███ ███ █████ | ███ ███ ████ █████ ██ ███ ███ █████ | ██ ███ ████ ████ ██ ███ ███ █████ | Lowd,e | Amivantamab plus lazertinib may result in an increase in the proportion of patients alive at 30 months when compared with osimertinib. |
Proportion of patients who are alive at 36 months Median follow-up: ██ ███ █████ ██████ | 858 (1 RCT) | ███ ███ ████ █████ ██ ███ ███ █████ | ███ ███ ████ █████ ██ ███ ███ █████ | ██ ███ ████ ███ ██ ███ ███ █████ | Lowd,e | Amivantamab plus lazertinib may result in an increase in the proportion of patients alive at 36 months when compared with osimertinib. |
Health-related quality of life outcomes: August 11, 2023, data cut-offf | ||||||
EORTC QLQ-C30 Global Health Status Score (100 [best] to 0 [worst]) | ||||||
LS mean change from baseline to cycle 13, day 1 Median follow-up: 22.01 months | 858 (1 RCT) | ███ ████ ██ ████ | ███ ████ ██ ████ | ████ █████ ██ █████ | Very lowg,h | The evidence is very uncertain about the effect of amivantamab plus lazertinib on the change from baseline to cycle 13, day 1, in EORTC QLQ-C30 Global Health Status when compared with osimertinib. |
LS mean change from baseline to cycle 27, day 1 Median follow-up: 22.01 months | 858 (1 RCT) | ███ █████ ██ ████ | ███ ████ ██ ████ | ████ █████ ██ ████ | Very lowg,h | The evidence is very uncertain about the effect of amivantamab plus lazertinib on the change from baseline to cycle 27, day 1, in EORTC QLQ-C30 Global Health Status when compared with osimertinib. |
NSCLC-SAQ total score (0 [best] to 20 [worst]) | ||||||
LS mean change from baseline to cycle 13, day 1 Median follow-up: 22.01 months | 858 (1 RCT) | ████ █████ ██ █████ | ████ █████ ██ █████ | ███ █████ ██ ████ | Very lowg,i | The evidence is very uncertain about the effect of amivantamab plus lazertinib on the change from baseline to cycle 13, day 1, in NSCLC-SAQ total score when compared with osimertinib. |
LS mean change from baseline to cycle 27, day 1 Median follow-up: 22.01 months | 858 (1 RCT) | ████ █████ ██ █████ | ████ █████ ██ █████ | ████ █████ ██ ████ | Very lowg,i | The evidence is very uncertain about the effect of amivantamab plus lazertinib on the change from baseline to cycle 27, day 1, in NSCLC-SAQ total score when compared with osimertinib. |
Harms: August 11, 2023, data cut-off | ||||||
Proportion of patients with rash Median follow-up: 22.01 months | 858 (1 RCT) | ███ ███ ████ ████ ██ ███ | ███ ███ ████ ████ ██ ███ | ██ | Lowj | Amivantamab plus lazertinib may result in an increase in the proportion of patients with rash when compared with osimertinib. |
Proportion of patients with VTE Median follow-up: 22.01 months | 858 (1 RCT) | ███ ███ ████ ████ ██ ███ | | ███ ████████ ██ ███ | ██ | Lowj | Amivantamab plus lazertinib may result in an increase in the proportion of patients with VTE when compared with osimertinib. |
Proportion of patients with infusion reactions Median follow-up: 22.01 months: | 858 (1 RCT) | ███ ███ ████ ████ ██ ███ | ██ ███ ████ ████ ██ ███ | ██ | Lowj | Amivantamab plus lazertinib may result in an increase in the proportion of patients with infusion reactions when compared with osimertinib. |
Proportion of patients with pneumonitis or interstitial lung disease Median follow-up: 22.01 months | 858 (1 RCT) | ██ ███ ████ ████ ██ ███ | ██ ███ ████ ████ ██ ███ | ██ | Lowj | Amivantamab plus lazertinib may result in an increase in the proportion of patients with pneumonitis or interstitial lung disease when compared with osimertinib. |
BICR = blinded independent central review; CI = confidence interval; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; LS = least squares; MID = minimal important difference; NR = not reported; NSCLC-SAQ = Non–Small Cell Lung Cancer Symptom Assessment Questionnaire; RCT = randomized controlled trial; vs. = versus; VTE = venous thromboembolism.
Notes: Study limitations (which refer to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias were considered when assessing the certainty of the evidence. All serious concerns in these domains that led to the rating down of the level of certainty are documented in the table footnotes.
aFollow-up presented as amivantamab plus lazertinib versus osimertinib.
bRated down 1 level for serious imprecision. Based on an MID of 20% (200 per 1,000) difference between study arms provided by clinical experts consulted for this review, the point estimate and lower bound of the CI are below the threshold for clinically meaningful benefit.
cThe May 13, 2024, efficacy update was done at the request of the European Medicines Agency and does not represent a preplanned analysis.
dRated down 1 level for serious limitations. Median overall survival was not reached at the time of the progression-free survival–triggered interim analysis (August 11, 2023) ███ ███ ████ ███ ███████ ██ ███ ███ ███ ████ ████████ ██████. This implies that the overall survival data are immature and there is high uncertainty in the trends observed to date; therefore, the confidence with which the results predict the outcome in the long term is not clear.
eRated down 1 level for serious imprecision. Based on an MID of 10% (100 per 1,000) difference between study arms provided by clinical experts consulted for this review, the point estimate and lower bound of the CI are below the threshold for clinically meaningful benefit.
fResults for this outcome were not controlled for multiple comparisons and are considered supportive evidence.
gRated down 2 levels for serious study limitations. A considerable number of patient data were missing at the time points, and based on the study design, it is likely that the missingness is informative. The open-label design of the amivantamab plus lazertinib arm also imparts bias to these subjective study measures, as patients would be aware that they are randomized to the treatment arm, and patients randomized to the osimertinib arm may also be aware of their treatment assignment due to the lack of placebo IV administered in the study.
hRated down 1 level for serious imprecision. Based on an MID of 10 points provided by the sponsor, the point estimate and lower bound of the CI are below the MID.
iRated down 1 level for serious imprecision. Based on an MID of 2 points increase (worsening) or 3 points decrease (improvement) in total score provided by the sponsor, the point estimate and lower bound of the CI are below the MID.
jRated down 2 levels for serious limitations due to a lack of CI estimates, and lack of absolute differences between study arms.
Sources: Details included in the table are from the sponsor’s summary of clinical evidence, the MARIPOSA Clinical Study Report (August 11, 2023, data cut-off),12 MARIPOSA efficacy update (May 13, 2024, data cut-off),13 and additional information provided by the sponsor.14
Long-Term Extension Studies
The submission did not include any long-term extension studies.
Indirect Comparisons
The MARIPOSA study compared amivantamab plus lazertinib with osimertinib monotherapy; however, there was no other head-to-head trial that assessed the relative effectiveness and safety of amivantamab plus lazertinib compared to other potentially relevant first-line treatment options. In addition, results from the indirect evidence were incorporated into the pharmacoeconomic model, meriting a review of the indirect evidence. The body of indirect evidence consisted of 5 network meta-analyses (NMAs) informed by a systematic literature review (SLR).
Description of Studies
An SLR was conducted in May 2020 and updated in July 2022 searching for therapeutic or palliative options for patients with metastatic or surgically unresectable common EGFR-mutated NSCLC; the common EGFR mutations included exon 21 L858R substitutions and exon 19 deletions, T790M in exon 20, and C797S in exon 20.
On completion of the SLR, the feasibility of conducting NMAs to compare amivantamab plus lazertinib with key comparators was assessed. The feasibility assessment appraised studies on the following factors:
their alignment with the prespecified scope
similarity of patient characteristics
similarity of study characteristics
reported outcome measures
data availability and network connectivity.
All interventions were considered either as monotherapy or in combination with others, unless the combination was deemed not of interest. Exclusions on the basis of interventions were initially made considering network connectivity. Interventions which had come onto the market, but which were discontinued or deemed unlikely to come to market were excluded. The submission therefore included first-generation TKIs (erlotinib, gefitinib, icotinib), second-generation TKIs (afatinib, dacomitinib), third-generation TKIs (osimertinib, lazertinib, aumolertinib, furmonertinib), chemotherapy, and monoclonal antibodies (bevacizumab, ramucirumab, cetuximab, and amivantamab). The clinical experts consulted for this review highlighted osimertinib and osimertinib plus chemotherapy as relevant comparators in Canada, and a deviation request to exclude first-generation and second-generation EGFR TKIs (afatanib, erlotinib, gefitinib) and platinum-based chemotherapy was accepted by CDA-AMC. Results from the comparison to osimertinib monotherapy and osimertinib plus chemotherapy were therefore included in the review. Though other treatments were included in the NMA network, they were not considered appropriate or relevant comparators; thus, their results were not reported.
Treatment effect modifiers were identified by the sponsor during the feasibility assessment based on the available baseline characteristics (supplemented by searching ClinicalTrials.gov), through reference to published literature or treatment appraisals, and discussion with experts.
Efficacy and Harms Results
The results of the NMAs show there was insufficient evidence to detect a difference between amivantamab plus lazertinib and osimertinib for OS, ORR, all AEs, and all SAEs. Amivantamab plus lazertinib was favoured over osimertinib for PFS ███ █████ ███ ██ ████ ██ ██████ and osimertinib was favoured over amivantamab plus lazertinib for all SAEs ███ █████ ███ ██ ████ ██ ██████ There was insufficient evidence to detect a difference between amivantamab plus lazertinib and osimertinib plus chemotherapy for OS, PFS, all AEs, and all SAEs; amivantamab plus lazertinib was favoured for ORR ███ ████ ███ ██ ████ ██ ██████.
Critical Appraisal
The indirect evidence consisted of 5 NMAs informed by an SLR. The SLR was conducted in 2022 and therefore it is not known whether the most recent publications on other relevant comparators (or OS updates to publications) would have been captured in the search. In addition to this, while the study exclusion list and reasons for exclusion were provided, ██ studies were excluded on the basis of not having interventions of interest or useful connection. These terms were not defined in the report and it is not known whether the criteria for a “useful connection” might bias the NMA network. Furthermore, while the steps for the quality assessment were provided, the results of the quality assessment were not; therefore, the specific risks of bias in the individual studies are not known. Because the ██ studies included in the NMA had different designs (open label, mixed open label and double blind, and double blind), this could represent a source of bias and adds uncertainty to the results of the NMA.
The NMA methods themselves are also subject to minor limitations: the use of fixed effect models over random effect models increases the uncertainty as it does not account fully for potential heterogeneity between studies. In addition, the nature of the network meant that it was not possible to evaluate pairwise contrasts, and consistency was not evaluated in the submission. Although the impact of these is likely minor given all 3 trials were phase III randomized controlled trials (RCTs), these limitations also contribute to increasing the general uncertainty in the results.
The submission provided the criteria by which treatment effect modifiers were identified in the studies forming the NMA network, and ██████████ ████ ███████████ ███████ ██████ ██████████ ████████ ██ █████ ███████████ ████ ██ ██████████ ███ ██████ ████ ████████ as treatment effect modifiers. According to clinical experts consulted for this review, the list of effect modifiers was generally representative of important indicators in the disease, and the list of additional prognostic factors █████ ████ ███████ ██████) also included factors which would interact with effect modifiers or represented prognostic factors on their own. Treatment effect modifiers were generally balanced across the ██ studies included in the appraisal, with the exception of brain metastases, where the FLAURA study reported lower proportions of patients with CNS metastases. In addition, smoking status and cancer stage at screening were not reported in either the FLAURA or FLAURA2 studies. These represent potential prognostic indicators which could interact with treatment effect modifiers. Overall, the heterogeneities in these 3 areas increased the uncertainty in the results.
There were additional differences noted with regards to study design and inclusion criteria which were highlighted in the submission. The duration of follow-up in the studies was ███████ for the FLAURA study (at the time that the SLR was conducted) than for the MARIPOSA and FLAURA2 studies. With a ███████ ██████ ██ ████ over which events can accrue, this could bias the results in favour of the comparators in the FLAURA study (osimertinib). A more recent publication of OS results for the FLAURA study has been published, but was not included in the network. In addition, there were numeric differences noted in the frequency of assessments between the 3 studies: assessments were done at baseline, every 6 weeks (± 1 week) for 18 months, then every 12 weeks in the FLAURA study; every 8 weeks (± 1 week) for the first 30 months followed by every 12 weeks (± 1 week) thereafter in the MARIPOSA study; and baseline, week 6, week 12, then every 12 weeks in the FLAURA2 study. While there is potential for overestimating treatment effects when disease assessments occur less frequently,15 the nature of this bias is that the interval within which an event occurred is known, but the exact time of the event is not known. For survival outcomes, this bias is more likely to impact the median estimates, as the median considers the number of events in individual arms of the study at a particular time and may be sensitive to the timing of the assessment. The direction of bias of the HR estimates are less likely to be materially impacted by the frequency of assessment, and while there is increased uncertainty in the estimates and CIs, the extent and direction of this bias in the NMA network is unclear. Additional design differences included the ascertainment of results by BICR versus investigator: the FLAURA2 and MARIPOSA studies reported sensitivity analyses for PFS by BICR and PFS by investigator, respectively, and the results were consistent with the primary analyses16; therefore, this bias was also not considered to impact the results. The FLAURA2 study also required a minimum life expectancy for enrolment, but clinical experts consulted for this review noted that this was unlikely to have an impact on the results or comparability of the studies because patients with a life expectancy of less than 12 weeks would be considered too frail for treatment with interventions such as chemotherapy or amivantamab, due to toxicity concerns. Lastly, while the sponsor noted that there were also ███████████ ██ ███ █████████ ██ ██████ █████ ███████ ███ ███ ████████ ███ ██████████ ██████ █████ ███████, CNS outcomes were not appraised in the report. Overall, the differences in study design have the potential for bias but the degree of bias is unknown; therefore, this increases the uncertainty in the results but was not deemed likely to change the conclusions from the NMA.
Studies Addressing Gaps in the Evidence From the Systematic Review
The sponsor submitted 2 studies (SKIPPirr and PALOMA-3) that did not meet the eligibility criteria for inclusion in the systematic review.17,18
The sponsor noted that systemic IRRs, including severe reactions, which occur with the introduction of a new protein therapeutic infusion are frequently observed. The SKIPPirr study evaluated the potential of prophylactic strategies in reducing amivantamab-associated IRRs.
Following observed increases in VTE events with the combination of amivantamab plus lazertinib in the MARIPOSA study, a mitigation strategy involving prophylactic anticoagulation therapy per local guidelines during the first 4 months of therapy with enhanced monitoring was implemented in 2022 and integrated into the PALOMA-3 study protocol.
SKIPPirr Study: IRRs
The SKIPPirr study is an ongoing phase II study evaluating prophylactic strategies to reduce IRRs associated with amivantamab in patients with EGFR-mutated (exon 19 deletion or exon 21 L858R substitution) advanced or metastatic NSCLC. The SKIPPirr study included patients with disease progression on or after sequential osimertinib and platinum-based chemotherapy. The study uses Simon’s 2-stage design with 4 cohorts receiving different prophylactic treatments. Cohorts are as follows: oral dexamethasone on varying schedules (cohort A and cohort A2), oral montelukast (cohort B), or subcutaneous (SC) methotrexate (cohort C). Only the dexamethasone 8 mg cohort met both stage 1 and stage 2 criteria, reducing IRR incidence to 22.5% (versus 67.4% with standard management). The regimen was well-tolerated, with no grade 3 or higher IRRs or new safety signals. The most common symptoms were nausea, dyspnea, and hypotension.
PALOMA-3 Study: VTE Prevention
The PALOMA-3 study is a phase III study comparing SC and IV amivantamab plus lazertinib in patients with EGFR-mutated locally advanced or metastatic NSCLC who progressed after osimertinib and platinum-based chemotherapy. As such, all patients had at least 1 prior therapy, with a majority (89%) having at least 2 lines of prior therapy. Following increased VTE events in the MARIPOSA study, prophylactic anticoagulation was integrated into the PALOMA-3 study and recommended for the first 4 months of treatment per local guidelines. The overall VTE incidence was 11.8%, mostly grade 1 or grade 2. Prophylactic anticoagulation use was similar between the SC and IV groups (approximately 80%), but VTE rates were lower with SC administration (9.2% versus 14.3% for IV). Among patients who were anticoagulated, VTEs occurred in 7.3% (SC) and 11.7% (IV), while patients who were not anticoagulated had higher rates (16.7% SC and 25.6% IV). Bleeding events were more frequent with anticoagulation. Overall, SC amivantamab plus lazertinib showed a lower VTE incidence than IV, regardless of anticoagulation use.
Critical Appraisal
The SKIPPirr and PALOMA-3 studies provided data on prophylactic treatments for preventing IRRs and VTE events, respectively, in patients with EGFR-mutated advanced or metastatic NSCLC. However, both studies had limitations that impact the generalizability and interpretability of their findings. The SKIPPirr study was an open-label, nonrandomized study with a small sample size, increasing the risk of bias, particularly in comparison to the rigour of standardized RCTs. Patients were aware of their treatment, which may have contributed to detection and performance bias, and the open-label design may influence the reporting of AEs. Similarly, the PALOMA-3 study, while randomized and stratified based on key clinical factors, also had an open-label design, introducing similar biases. In both studies, patients had progressed on or after prior treatment with osimertinib and platinum-based chemotherapy, which does not align with the Health Canada–approved indication as a first-line treatment. Additionally, included patients had an ECOG Performance Status of 0 or 1, meaning they were relatively healthy, which may not fully represent the broader population that would receive prophylactic treatment in real-world clinical practice in Canada.
Conclusions
One phase III, ongoing, multicentre, active-controlled RCT (MARIPOSA) provided evidence for the efficacy and safety of amivantamab plus lazertinib as first-line treatment for 858 adult patients with locally advanced or metastatic NSCLC with exon 19 deletions or exon 21 L858R substitution mutations.
Patient and clinician groups highlighted improving symptoms, PFS, OS, quality of life, and manageable side effects as important outcomes of interest in a new treatment. The clinical experts consulted for the review noted that patient preference, desire for additional efficacy, and fitness to tolerate the side effects were also factors they would consider when identifying potential candidates for this treatment. The results of the interim analysis of the MARIPOSA study suggested that treatment with amivantamab plus lazertinib improved median PFS. The results of the GRADE assessment also suggested that amivantamab plus lazertinib likely results in an increase in the proportion of patients who were progression-free at 24 months and may result in an increase in the proportion of patients alive at 24 months, 30 months, and 36 months. However, the results are subject to imprecision and the point estimates for PFS and OS did not attain the minimal important differences (MIDs) provided by the clinical experts. The data for OS, ORR, and DOR are also limited by data immaturity, with median OS not reached in either arm as of the prespecified interim analysis and imprecisely estimated in the amivantamab plus lazertinib arm using additional study data (upper bound of the CI could not be estimated). HRQoL results suggested that score changes did not attain the MIDs for improvement and suggested no clinically meaningful change in HRQoL While the reporting of harms in the MARIPOSA study was also immature, harms results demonstrated a notable side effect burden attributable to amivantamab plus lazertinib including a greater proportion of patients reporting ██████████, rash, IRRs, and VTE were also reported more commonly in the amivantamab plus lazertinib arm. Deaths were generally balanced across treatment arms, with a slightly greater proportion of deaths in the osimertinib (and lazertinib monotherapy) groups; however, deaths due to AEs were greater in the amivantamab plus lazertinib arm (██ ██████ ███ ██ ████████).
There is no direct comparative evidence for amivantamab plus lazertinib compared to osimertinib plus chemotherapy. The sponsor submitted an NMA evaluating these treatments; however, there was insufficient evidence to detect a difference between amivantamab plus lazertinib and osimertinib or osimertinib plus chemotherapy for nearly all efficacy and safety-related outcomes, and the results are limited by uncertainty due to multiple sources of heterogeneity in the studies.
Introduction
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of amivantamab 50 mg/mL IV infusion plus lazertinib 80 mg and 240 mg oral tablets in the treatment of locally advanced (not amenable to curative therapy) or metastatic NSCLC with EGFR exon 19 deletions or exon 21 L858R substitution mutations in adults.
Disease Background
Contents within this section have been informed by materials submitted by the sponsor and clinical expert input. The following have been summarized and validated by the review team.
Lung cancer is the most commonly diagnosed cancer type in Canada, as well as the leading cause of cancer-related death in the country.1 It is estimated that 1 in 14 Canadians will be diagnosed with lung cancer in their lifetime and 1 in 4 cancer-related deaths in Canada will be attributed to the disease.1 Approximately 98% of lung cancer cases in Canada are expected to occur in people aged 50 years or older, with a slightly higher incidence in females than males.1 For 2024, the projected incidence of lung and bronchus cancer in Canada was 32,100 new cases.2 In Canada, excluding Quebec, approximately 88% of lung cancer cases with an identified histologic subtype are classified as NSCLC, a serious terminal illness that is associated with a poor prognosis and a 5-year net survival rate of only 3% for patients with advanced (stage IV) NSCLC. Goals of treatment for advanced NSCLC include delaying progression, prolonging survival, palliation of symptoms, and improving quality of life.3 Early-stage NSCLC is often asymptomatic and if patients do present with symptoms, they are often unspecific and difficult to directly attribute to a lung cancer diagnosis.4 The most common symptoms include unspecific cough, chest and shoulder pain, hemoptysis, weight loss, dyspnea, hoarseness, bone pain, and fever.4
Diagnosis of NSCLC often occurs at late-stage disease and requires a biopsy in which sufficient tissue is obtained for histologic confirmation.1 Following the biopsy, a diagnosis of 1 of the 3 distinct histological types of NSCLC (i.e., adenocarcinoma, squamous cell carcinoma, and large cell carcinoma) is made, and the tumour is staged.7 Assessment of EGFR mutation status is recommended as part of a sequential or parallel approach to facilitate treatment decision-making.8
A key mechanism of NSCLC involves driver mutations, which activate progrowth signalling pathways.5 The most common driver mutation in NSCLC leads to the activation of EGFR, which is found more frequently in patients with adenocarcinomas, nonsmokers, patients of Asian ethnicity, and in females.6 A 2013 meta-analysis of 94 studies found that individuals who identified as Asian from China, Hong Kong, Japan, Korea, Singapore, or Taiwan exhibited a higher prevalence of EGFR mutations in lung adenocarcinoma (47.9%) compared to individuals from Europe, North America, or Australia (19.2%).19 According to clinical experts consulted for this review, approximately 10% to 15% of all patients with NSCLC in Canada will have an EGFR mutation. The clinical experts noted that EGFR mutations occur more commonly in people who have never smoked, and in those of East Asian descent. The most frequently observed EGFR mutations, including the exon 19 deletion and exon 21 L858R substitution, account for 85% to 90% of cases with activating EGFR mutations in NSCLC. Less common EGFR mutations (e.g., exon 20 insertion) make up the remaining 10% to 15%.5
Standards of Therapy
Contents within this section have been informed by materials submitted by the sponsor and clinical expert input. The following have been summarized and validated by the review team.
For advanced or metastatic NSCLC, National Comprehensive Cancer Network guidelines recommend that histologic subtype be determined before therapy so that an appropriate treatment can be selected. EGFR mutation testing is recommended for patients with nonsquamous NSCLC or NSCLC not otherwise specified.20
The clinical experts noted that locally advanced or metastatic EGFR-mutated NSCLC is incurable, and treatment is considered palliative. The goals of therapy include relieving disease-related symptoms with minimal toxicity from treatment, maximizing quality of life, preventing further disease-related complications, and prolonging life.
The first-generation and second-generation TKIs erlotinib, afatinib, and dacomitinib are recommended for reimbursement by CDA-AMC for first-line use in advanced or metastatic NSCLC with activating EGFR mutations; however, the third-generation TKI osimertinib is most commonly used for exon 19 deletions or exon 21 L858R substitution mutations based on the results of the FLAURA trial showing improved PFS and OS relative to erlotinib and gefitinib.21,22 The clinical experts noted that osimertinib monotherapy is taken daily until disease progression or intolerance, and has a favourable safety profile making it suitable for the vast majority of patients, including older patients. Osimertinib plus platinum-based chemotherapy is also recommended for reimbursement as a first-line treatment of adult patients with locally advanced or metastatic NSCLC whose tumours have EGFR exon 19 deletions or exon 21 L858R mutations.10 It is currently undergoing price negotiations and therefore is not widely available.
Drug Under Review
Key characteristics of lazertinib in combination with amivantamab are summarized in Table 3 with other treatments available for locally advanced or metastatic NSCLC with EGFR exon 19 deletions or exon 21 L858R substitution mutations.
Lazertinib is a highly selective CNS-penetrating, oral, third-generation EGFR TKI.23,24 It selectively inhibits both primary activating EGFR mutations (exon 19 deletions and exon 21 L858R substitution mutations) and the EGFR T790M resistance mutation, while sparing wild-type EGFR. The recommended dosage of lazertinib is 240 mg once daily, taken orally, in combination with amivantamab.25 It is recommended to administer lazertinib any time before amivantamab when given on the same day. Amivantamab is a bispecific antibody that binds to the extracellular domains of the EGFR and MET receptors, disrupting EGFR and MET signalling functions through blocking ligand binding and enhancing degradation of these receptors.26
Amivantamab has previously been reviewed by CDA-AMC and received a recommendation to reimburse with conditions for the treatment of adult patients with locally advanced or metastatic NSCLC with activating EGFR exon 20 insertion mutations whose disease has progressed on or after platinum-based chemotherapy; as well as in combination with carboplatin and pemetrexed for the first-line treatment of adult patients with locally advanced (not amenable to curative therapy) or metastatic NSCLC with activating EGFR exon 20 insertion mutations. CDA-AMC is currently reviewing amivantamab in combination with carboplatin and pemetrexed for the treatment of patients with locally advanced or metastatic NSCLC with EGFR exon 19 deletions or exon 21 L858R substitution mutations, whose disease has progressed on or after treatment with osimertinib.27 Lazertinib has not been previously reviewed by CDA-AMC.
The indication for this review is lazertinib in combination with amivantamab for the first-line treatment of adult patients with locally advanced or metastatic NSCLC with EGFR exon 19 deletions or exon 21 L858R substitution mutations.25 The sponsor’s reimbursement request is consistent with the indication. The recommended administration for amivantamab is a once weekly IV infusion, at a dose of 1,050 mg (1,400 mg if body weight ≥ 80 kg) for 4 weeks (first dose is split, and given on day 1 and day 2), then every 2 weeks thereafter.26
Table 3: Key Characteristics of Lazertinib Plus Amivantamab and Relevant Comparators
Characteristic | Lazertinib plus amivantamab | Osimertinib alone or plus platinum-based chemotherapy plus pemetrexeda |
|---|---|---|
Mechanism of action | Lazertinib: Third-generation EGFR TKI that selectively inhibits both primary activating EGFR mutations (exon 19 deletions and exon 21 L858R substitution mutations) while having less activity against wild-type EGFR. Amivantamab: Bispecific antibody that binds to the extracellular domains of the EGFR and MET receptors, disrupting EGFR and MET signalling functions through blocking ligand binding and enhancing degradation of these receptors. The presence of EGFR and MET on the surface of tumour cells also allows for targeting of these cells for destruction by immune effector cells, such as natural killer cells and macrophages, through antibody-dependent cellular cytotoxicity and trogocytosis mechanisms, respectively. | Osimertinib: Selective irreversible EGFR inhibitor targeting sensitizing and T790M mutations, with limited wild-type activity. Platinum-based chemotherapy: Damages DNA, leading to cell death. Pemetrexed: An antifolate that inhibits DNA synthesis. |
Indication | 1L treatment of adult patients with locally advanced or metastatic NSCLC with EGFR exon 19 deletions or exon 21 L858R mutations. | 1L treatment of patients with locally advanced or metastatic NSCLC with EGFR exon 19 deletions or exon 21 L858R mutations. In combination with pemetrexed and platinum-based chemotherapy for the 1L treatment of patients with locally advanced or metastatic NSCLC with EGFR exon 19 deletions or exon 21 L858R mutations.a |
Route of administration | IV | Oral |
Recommended dose | Amivantamab: IV infusion of 1,050 mg (1,400 mg if body weight ≥ 80 kg), once weekly for 4 weeks, with first dose split on day 1 and day 2; administered every 2 weeks on day 1 thereafter. Lazertinib: 240 mg administered orally once daily. | Osimertinib: 80 mg administered orally once daily. Pemetrexed: IV infusion, 500 mg/m2 (with vitamin supplementation) on first day of each 21-day cycle until disease progression or unacceptable toxicity. Carboplatin:b IV infusion, AUC on first day of each 21-day cycle; total of 6 cycles. Cisplatin:b IV infusion, 75 mg/m2 on day 1 of each 21-day cycle; total of 6 cycles. |
Serious adverse effects or safety issues | Lazertinib: Interstitial lung disease, hepatotoxicity, VTE events, skin reactions, ocular disorders. Amivantamab: Infusion reactions, skin reactions, ocular disorders. | Osimertinib: Interstitial lung disease, QT prolongation; left ventricular dysfunction and cardiomyopathy. Platinum compounds: Serious infections, anaphylactic-like reactions, hypersensitivity, bone marrow suppression, veno-occlusive disease, hemolytic anemia, hemolytic-uremic syndrome. Pemetrexed: Serious hepatobiliary toxicity, rare fatal hepatic failure, gastrointestinal toxicity, bone marrow suppression, hypersensitivity, serious renal events, interstitial pneumonitis, rare bullous epidermolysis. |
1L = first line; AUC = area under the curve; CDA-AMC = Canada's Drug Agency; NSCLC = non–small cell lung cancer; TKI = tyrosine kinase inhibitor; VTE = venous thromboembolism.
aRecommended by CDA-AMC for reimbursement with conditions on October 3, 2024.10
bReimbursement condition: osimertinib should only be prescribed in combination with pemetrexed and platinum-based (i.e., cisplatin or carboplatin) chemotherapy.
Sources: Products monographs for Lazcluze,25 Tagrisso,28 Rybrevant,26 carboplatin,29 cisplatin,30 and pemetrexed.31
Testing Procedure Considerations
The treatment landscape of NSCLC is constantly evolving, as targeted therapies are being developed.32,33 For advanced or metastatic NSCLC in Canada, genomic profiling for the most likely actionable oncogenic driver mutations is the standard of care to match targeted therapies to the appropriate patients.32,34 According to the clinical experts consulted for this review, while there may be some variations in the tests performed between jurisdictions and cancer centres, most patients in this population will receive, at a minimum, testing for mutations in the ALK and EGFR genes as part of routine care.32 Consensus guidelines from Canada recommend testing all patients with advanced nonsquamous NSCLC for the most common EGFR alterations, including exon 19 deletions and exon 21 point mutations.32,34 Likewise, it is recommended that patients with advanced squamous NSCLC should be tested for EGFR mutations if there is no smoking history.32 Although the process may differ across provinces and territories, reflex testing for EGFR mutations (i.e., initiated by the pathologist during the diagnostic work-up) is the recommended standard of care in Canada.32-35
Testing for EGFR mutations is typically conducted on tissue samples collected through biopsy as part of routine diagnostic work-up. EGFR mutations can be identified by either polymerase chain reaction or next-generation sequencing (NGS) testing methods.35 NGS is the preferred method because targeted polymerase chain reaction may not detect certain types of alterations in EGFR.33-35 Consensus guidelines from Canada also recommend comprehensive genomic profiling using NGS over single-gene techniques due to overall efficiencies in turnaround times, costs, and tissue use.33,34 Approximately 10% of people with NSCLC may have insufficient biopsy tissue available to test for EGFR mutations.8 In these instances, NGS testing of cell-free circulating tumour DNA drawn using a noninvasive blood sample could be a comparable alternative.8,33,34,36 However, the clinical experts pointed out that patients may have to pay out of pocket for circulating tumour DNA testing.8 A positive circulating tumour DNA EGFR mutation result is usually actionable; however, a negative result would need to be verified with a repeat tissue biopsy.8,34
CDA-AMC considered the potential impacts of testing for EGFR exon 19 deletions or exon 21 L858R substitution mutations to ascertain eligibility for lazertinib in combination with amivantamab for the first-line treatment of adult patients with locally advanced (not amenable to curative therapy) or metastatic NSCLC, including impacts to health systems, patients (including families and caregivers), and costs. No new impacts are anticipated because EGFR testing is currently performed as the standard of care for patients with locally advanced or metastatic NSCLC across jurisdictions in Canada. Key considerations and relevant information available from materials submitted by the sponsor, input from the clinical experts consulted by the review team, and sources from the literature were validated by the review team when possible and are summarized in Table 4.
Table 4: Considerations for EGFR Exon 19 Deletion or Exon 21 L858R Substitution Mutation Testing to Establish Treatment Eligibility for Lazertinib in Combination With Amivantamab for the First-Line Treatment of Adult Patients With Locally Advanced or Metastatic NSCLC
Consideration | Criterion | Available information |
|---|---|---|
Health system related | Number of individuals in Canada expected to require the test (e.g., per year) | Based on the materials provided by the sponsor, in 2025, the estimated number of patients in Canada, excluding Quebec, expected to undergo testing for EGFR mutations to determine eligibility for lazertinib in combination with amivantamab is approximately 8,500 individuals, or 82% of individuals with advanced, nonsquamous NSCLC.37 The clinical experts mentioned that the testing proportion would be closer to 100% in cancer centres. Because testing for EGFR mutations is already part of the standard of care for locally advanced or metastatic NSCLC, there is no additional impact to health systems anticipated as part of establishing treatment eligibility for lazertinib in combination with amivantamab. |
Availability and reimbursement status of the testing procedure in jurisdictions across Canada | According to the clinical experts, testing for EGFR mutations, including exon 19 deletions and exon 21 L858R substitutions, using PCR or NGS is broadly available as part of the current standard of care for locally advanced or metastatic NSCLC. | |
Testing procedure as part of routine care | According to the clinical experts, testing for EGFR mutations, including exon 19 deletions and exon 21 L858R substitutions, is currently performed during the diagnostic work-up as part of the standard of care for locally advanced or metastatic NSCLC. | |
Repeat testing requirements | The clinical experts confirmed that testing for EGFR exon 19 deletions and exon 21 L858R substitution mutations does not need to be repeated. | |
Impacts on human and other health care resources by provision of the testing procedure | Because testing for EGFR mutations is currently part of the standard of care for locally advanced or metastatic NSCLC and publicly funded across jurisdictions, use of the test result to establish treatment eligibility is not anticipated to substantially impact human and other health care resources. | |
Patient related | Accessibility of the testing procedure in jurisdictions across Canada | The clinical experts mentioned that almost all patients with nonsquamous NSCLC being treated by a thoracic oncologist would receive EGFR mutation testing. This testing proportion may be lower in rural or remote areas with limited access to a tertiary cancer centre.38,39 However, because EGFR mutation testing is part of the current standard of care for locally advanced or metastatic NSCLC in Canada, there is no additional impact on access anticipated from the testing as part of establishing treatment eligibility for lazertinib in combination with amivantamab. |
Expected turnaround times for the testing procedure | Consensus guidelines from Canada recommend that EGFR mutation testing turnaround time does not exceed 21 calendar days.34 The clinical experts estimated that the turnaround time for EGFR mutation testing is approximately 1 to 2 weeks. This may be delayed up to several weeks in certain cases (e.g., if a repeat biopsy is needed due to insufficient tissue). However, the experts confirmed that, in general, test results are available by the time the oncologist needs to make a treatment decision. Therefore, there is no additional impact on turnaround times anticipated as part of establishing treatment eligibility for lazertinib in combination with amivantamab. | |
Burden associated with the testing procedure for patients, families, and/or caregivers | Because testing for EGFR mutations is currently part of the standard of care for locally advanced or metastatic NSCLC, there is no additional burden to patients, families, and/or caregivers anticipated from the testing as part of establishing treatment eligibility for lazertinib in combination with amivantamab. | |
Clinical | Clinical utility and validity of the testing procedure | There is evidence that demonstrates the diagnostic accuracy and clinical utility of PCR and NGS testing for EGFR mutations.a,35,40,41 |
Risks of harm associated with the testing procedure | Because testing for EGFR mutations is currently part of the standard of care for locally advanced or metastatic NSCLC, there is no additional risk of harm associated with the testing as part of establishing treatment eligibility for lazertinib in combination with amivantamab. | |
Cost | Projected cost of the testing procedure | A comprehensive genomic profile by NGS using biopsy tissue costs around $1,400 per sample.8 Because testing for EGFR mutations is currently part of the standard of care for locally advanced or metastatic NSCLC, there is no additional cost anticipated from the testing as part of establishing treatment eligibility for lazertinib in combination with amivantamab. |
CDA-AMC = Canada's Drug Agency; NGS = next-generation sequencing; NSCLC = non–small cell lung cancer; PCR = polymerase chain reaction.
aCDA-AMC has not evaluated or critically appraised this evidence to determine its validity or reliability.
Perspectives of Patients, Clinicians, and Drug Programs
The full patient and clinician group submissions received are available in the consolidated patient and clinician group input document for this review on the project website.
Patient Group Input
This section was prepared by the review team based on the input provided by patient groups.
For this review, patient input was jointly submitted by 3 organizations: Lung Cancer Canada, the CCSN, and the Lung Health Foundation. Information was gathered from 4 patients in Canada diagnosed with stage IV NSCLC with treatment experience with amivantamab (n = 3), or lazertinib plus amivantamab combination therapy (n = 1). Data were collected through virtual interviews and from previous patient input submissions to CDA-AMC.
The patient group input described the initial shock patients experienced with their diagnosis, as they noted minimal initial symptoms consisting of back pain, a persistent cough, or shortness of breath. Three of the patients reported experience with currently available EGFR-targeted therapies including osimertinib, gefitinib, and afatinib, with limited side effects (e.g., significantly dry skin, thinning of hair, and diarrhea) before their disease progressed. As such, progression and treatment resistance remain a critical concern for patients. The input noted that patients desire a treatment that improves the management of their disease symptoms, delays further progression, shrinks their tumours, improves their quality of life, prolongs survival with independence and functionality, and has manageable side effects.
Three of the patients included in the input each had a different mutation (exon 20, exon 19, or exon 21 L858R) and reported successful tumour shrinkage and stable metastases after receiving amivantamab as a first-line, third-line, or later-line treatment. One patient developed additional metastases approximately 3 years after initiating third-line amivantamab and has since passed away. The patient who received lazertinib and amivantamab combination therapy as a second-line treatment for over 2.5 years to date had initial shrinking in their primary tumour and is currently experiencing stable metastases. Two patients reported significant side effects at treatment onset, including severe dry scalp and bleeding due to dryness, paronychia, painful acne, as well as rashes on their scalp, back, and chest. The patient input noted that these side effects reduced in severity over time, were controlled with prescription medications, were not as severe as those experienced with chemotherapy, and were deemed worthwhile if the treatment was working. Two patients reported that they were able to return to a good quality of life by pursuing hobbies, travel, and spending time with family. The input also noted that patients preferred the ease and convenience of oral targeted therapies that can be taken at home versus long infusion times in the hospital with amivantamab.
Clinician Input
Input From Clinical Experts Consulted for This Review
All CDA-AMC review teams include at least 1 clinical specialist with expertise regarding the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). The following input was provided by 2 clinical specialists with expertise in the diagnosis and management of locally advanced or metastatic NSCLC with EGFR exon 19 deletions or exon 21 L858R substitution mutations.
Unmet Needs
The clinical experts noted that ultimately, all patients with NSCLC will experience disease progression; thus, there is a need for treatments that delay progression, extend survival, and have manageable side effects. The clinical experts noted that there is a risk of relapse with current therapies, particularly in the case of CNS disease because EGFR-mutated NSCLC tends to present with brain metastases or have a high risk of their development. Per the clinical experts, the current standard of care (osimertinib monotherapy) is generally well-tolerated, relieves disease-related symptoms quickly, can be administered to older patients, and as an oral medication, can be more convenient for patients. The clinical experts noted that there is a risk of added toxicity and potential inconvenience of IV chemotherapy administered every 3 weeks for the recently recommended osimertinib plus chemotherapy combination. Additionally, EGFR inhibitors are generally associated with serious toxicities (e.g., pneumonitis) which can impact quality of life.
Place in Therapy
The experts indicated that amivantamab plus lazertinib, osimertinib monotherapy, or osimertinib plus chemotherapy could all be considered first-line options for patients with the EGFR mutations in question. Amivantamab plus lazertinib and osimertinib plus chemotherapy would offer the opportunity for more efficacy over osimertinib alone, although with trade-offs such as the risk of greater toxicity and more clinic visits. Amivantamab plus lazertinib could be an alternate option to osimertinib plus chemotherapy for a proportion of patients, particularly those who are younger, more fit, and with some poorer prognostic features including CNS metastases. They emphasized, however, that similar to other treatments, amivantamab plus lazertinib would not be curative.
Patient Population
The clinical experts noted that EGFR detection is routine across Canada and therefore misdiagnosis is unlikely. Patients with newly diagnosed locally advanced or metastatic NSCLC with EGFR exon 19 deletion or exon 21 L858R substitution, who were young, fit, or felt to be at high risk of poorer outcomes (for example, with liver metastases, brain metastases, or p53 mutations) would be most likely to be considered for this therapy. The experts noted that not all patients would be suitable for amivantamab plus lazertinib, potentially due to underlying comorbidities, frailty, lack of desire for IV treatment, or increased toxicities including thromboembolism. They stated that patient preference would be important to consider, and that the choice of treatment would routinely involve a discussion with patients regarding their treatment options.
The experts noted that patients with prior TKI experience were excluded from the pivotal trial; however, osimertinib is recommended for reimbursement as adjuvant therapy after tumour resection in patients with stage IB to stage IIIA NSCLC, whose tumours have EGFR exon 19 deletions or exon 21 L858R substitution mutations.10 Therefore, there is the possibility that patients may use TKIs as an adjuvant therapy after tumour resection. These patients (estimated by the experts to be approximately 10% to 15% of patients) would not have been included in the pivotal trial and therefore it is unclear whether they would be considered candidates for amivantamab plus lazertinib. They also noted that older patients (i.e., aged > 75 years) were not highly represented in the trial and may also be less tolerant of a more aggressive regimen.
Assessing the Response to Treatment
The experts noted that patients are typically seen every 3 weeks to 4 weeks and imaging is conducted every 8 weeks to 12 weeks, depending on their treatment regimen. Objective response criteria (e.g., radiological assessment every 2 months to 3 months to determine disease progression) can be used to ensure disease response or control, along with clinical assessments of disease-related symptoms and HRQoL, which the experts noted are not routinely assessed in clinical practice using standardized tools.
Discontinuing Treatment
The clinical experts stated that the discontinuation criteria for amivantamab plus lazertinib should be the same as other anticancer therapies, where disease progression, intolerable toxicity or toxicity associated with deteriorating quality of life, and patient choice would all be grounds to discontinue treatment.
Prescribing Considerations
The experts noted that amivantamab plus lazertinib should only be prescribed under the care of oncology specialists in a cancer centre.
Clinician Group Input
This section was prepared by the review team based on the input provided by clinician groups.
Two clinician groups — the Ontario Health-Cancer Care Ontario Lung and Thoracic Cancer Drug Advisory Committee and the Lung Cancer Canada Medical Advisory Committee — comprising a total of 31 clinicians provided input for this review. Both submissions noted that the main treatment goals for patients with stage IV NSCLC include prolonging life, improving symptoms, and delaying cancer progression. The input noted that in NSCLC with common EGFR mutations, the standard first-line treatment is osimertinib, an oral TKI which is widely funded and available throughout Canada. To overcome the inevitable resistance to osimertinib, intensified regimens have been tested in the first-line setting including adding chemotherapy to osimertinib, which has been approved by Health Canada and received a recommendation for reimbursement with conditions by the CDA-AMC in May 2024. The clinician groups noted that despite a high initial response rate, not all patients respond to osimertinib or osimertinib plus chemotherapy. The clinicians agreed that intensified regimens beyond osimertinib alone are needed. The clinician groups noted that there is a need for additional treatments that improve OS, symptoms, PFS, are more convenient, have manageable toxicity, and protect the brain from cancer growth to a greater degree than the current standard of care. However, the Ontario Health-Cancer Care Ontario Lung and Thoracic Cancer Drug Advisory Committee input stated that the amivantamab and lazertinib regimen does not fulfill the need for a treatment with greater convenience or manageable toxicity.
Both clinician groups agreed that the combination of amivantamab and lazertinib would be used as a first-line treatment in the population under review. Single-drug osimertinib will still be considered as a first-line option, as there will be patients who do not want to receive IV systemic therapy or prefer the logistics involved with an oral drug alone. In the event there is access to the combination of osimertinib plus chemotherapy in the future, this regimen would add an additional front-line therapeutic option. The input stated that following first-line treatment with amivantamab and lazertinib, chemotherapy would remain a viable second-line option as amivantamab and lazertinib are not expected to induce resistance to chemotherapy.
According to the input, patients best suited for the treatment under review are those with advanced EGFR-mutated NSCLC. Patients who are interested in intensified therapy, able to withstand side effects, and able to manage the increased visit schedule would also be good candidates for this therapy. The input noted that at this time, it is not yet possible to identify those specific patients who are more likely to respond to this therapy or which patients should receive osimertinib plus chemotherapy versus amivantamab plus lazertinib.
The input stated that outcomes used to assess response to treatment include side effect profiles, treatment response, and clinical response which are evaluated at regular intervals. The input suggested that patients will need to be seen more frequently initially when starting the treatment under review for AEs and tolerance assessments, especially for potential dermatologic AEs. In general, patients in clinical practice are often evaluated every 2 months to 4 months for evidence of response status with radiographic studies including CTs and MRIs depending on the sites of metastatic disease. Lazertinib as an oral medication is administered at home. The appropriate setting for amivantamab treatment includes systemic therapy outpatient units at cancer centres or in a hospital setting, by personnel experienced in administering these agents.
Drug Program Input
The drug programs provide input on each drug being reviewed through the reimbursement review process by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by for this review are summarized in Table 5.
Table 5: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Relevant comparators | |
The comparator in the MARIPOSA trial is osimertinib monotherapy, but osimertinib plus chemotherapy has also been recommended for reimbursement by CDA-AMC and both are potential comparators. | This is a comment from the drug plans and is intended to inform pERC deliberations. |
Considerations for initiation of therapy | |
The MARIPOSA trial included patients with ECOG status of 0 or 1. Would it be appropriate to allow patients with other ECOG statuses (e.g., 2) to be treated with amivantamab and lazertinib? | Selected patients with ECOG Performance Status of 2 could be considered for treatment especially if the performance status is at least in part related to disease-related factors. This would be based on clinical judgment. |
The MARIPOSA trial eligibility included previous adjuvant or neoadjuvant therapy for stage I and stage II disease, if treatment was completed at least 12 months ago. Could treatment with amivantamab and lazertinib be considered in patients with an interval of < 12 months? | If the treatment received in the adjuvant or neoadjuvant setting was a non-EGFR inhibitor (e.g., cytotoxic chemotherapy), then a period of 6 months could be considered. The experts also noted that osimertinib in the adjuvant setting is standard of care and that this would only apply to a rare subset of patients. There are no data on prior EGFR inhibitors in the adjuvant setting as patients with prior TKI use were excluded from MAIRPOSA. |
Alignment of the initiation criteria with osimertinib plus chemotherapy should be considered. | This is a comment from the drug plans and is intended to inform pERC deliberations. |
Considerations for prescribing of therapy | |
The combination contains an oral and IV drug and depending on jurisdiction, these may be funded differently. | This is a comment from the drug plans and is intended to inform pERC deliberations. |
Generalizability | |
When initially funded, would it be appropriate to switch patients from osimertinib plus chemotherapy to lazertinib plus amivantamab, assuming no progression? | Generally, patients would not switch unless there was a lack of efficacy, the patient was unable to tolerate osimertinib plus chemotherapy and a more intensive approach is indicated, or the patient was not considered to be a suitable candidate for osimertinib plus chemotherapy. |
If there is toxicity, would it be appropriate to switch patients from osimertinib plus chemotherapy to lazertinib plus amivantamab or vice versa? | Yes, if the toxicity is not considered related to the EGFR inhibitor, as the side effects of EGFR inhibitors will not be improved by switching to lazertinib plus amivantamab in this case. |
Funding algorithm | |
The initiation of a rapid provisional funding algorithm has been requested | This is a comment from the drug plans and is intended to inform pERC deliberations. |
Care provision issues | |
Venous thromboembolism has a higher incidence in the amivantamab plus lazertinib arm. Prophylaxis for the first 4 months is recommended, although funding of anticoagulants may be variable across jurisdictions and may include patient self-pay. | This is a comment from the drug plans and is intended to inform pERC deliberations. The experts commented that venous thromboembolism can be associated with considerable morbidity. |
System and economic issues | |
Confidential pricing exists for osimertinib. | This is a comment from the drug plans and is intended to inform pERC deliberations. |
CDA-AMC = Canada’s Drug Agency; ECOG = Eastern Cooperative Oncology Group; pERC = pan-Canadian Oncology Drug Review Expert Review Committee; TKI = tyrosine kinase inhibitor.
Clinical Evidence
The objective of this clinical review report is to review and critically appraise the clinical evidence submitted by the sponsor on the beneficial and harmful effects of amivantamab 350 mg/mL IV plus lazertinib 80 mg and 240 mg oral tablets in the treatment of locally advanced (not amenable to curative therapy) or metastatic NSCLC with EGFR exon 19 deletions or exon 21 L858R substitution mutations in adults. The focus will be placed on comparing amivantamab plus lazertinib to relevant comparators and identifying gaps in the current evidence.
A summary of the clinical evidence included by the sponsor in the review of amivantamab plus lazertinib is presented in 3 sections with the CDA-AMC critical appraisal of the evidence included at the end of each section. The first section, the systematic review, includes pivotal studies and RCTs that were selected according to the sponsor’s systematic review protocol. Our assessment of the certainty of the evidence in this first section using the GRADE approach follows the critical appraisal of the evidence. The second section includes indirect evidence from the sponsor. The third section includes additional studies that were considered by the sponsor to address important gaps in the systematic review evidence.
Included Studies
Clinical evidence from the following is included in the review and appraised in this document:
1 pivotal study or RCT identified in systematic review
indirect evidence consisting of 5 NMAs
2 additional studies addressing gaps in evidence.
Systematic Review
Contents within this section have been informed by materials submitted by the sponsor. The following have been summarized and validated by the review team.
Description of Studies
One pivotal trial, the MARIPOSA study, was included in the review. Characteristics of the MARIPOSA study are summarized in Table 6.
Table 6: Details of Studies Included in the Systematic Review
Detail | MARIPOSA |
|---|---|
Designs and populations | |
Study design | Ongoing phase III, randomized, multicentre RCT |
Locations | Conducted at 262 centres, of which 219 centres enrolled participants in Argentina, Australia, Belgium, Brazil, Canada, China, France, Germany, Hungary, India, Israel, Italy, Japan, Malaysia, Mexico, the Netherlands, Poland, Portugal, Russian Federation, South Korea, Spain, Taiwan, Thailand, Turkey, Ukraine, UK, and the US (including Puerto Rico) |
Patient enrolment dates | Start date: October 16, 2020 End date: Ongoing |
Randomized (N) | N = 1,074
|
Inclusion criteria |
|
Exclusion criteria |
|
Drugs | |
Intervention | Arm A (open label):
|
Comparator(s) |
|
Study duration | |
Screening phase | Screening for eligible participants was performed within 28 days before randomization. If a fresh tumour biopsy was required to meet eligibility, the biopsy could be obtained at any time before randomization, provided informed consent was given. |
Treatment phase | The treatment phase for a participant began on cycle 1, day 1, and continued as 28-day cycles until the end-of-treatment visit, which occurred approximately 30 days after discontinuation of study treatment. |
Follow-up phase | Participants who discontinued study treatment for any reason were followed for survival and symptomatic progression in the follow-up phase. Survival, subsequent anticancer treatment, and disease status were assessed at least every 12 weeks (± 14 days) after the last dose of study treatment or disease progression (whichever occurred first), until the end of study, death, loss to follow-up, or withdrawal of consent, whichever came first. |
Outcomes | |
Primary end point | PFS by BICR |
Secondary and exploratory end points | Secondary:
Exploratory:
|
Publication status | |
Publications | |
ANC = absolute neutrophil count; ALT = alanine aminotransferase; ART = antiretroviral therapy; AST = aspartate aminotransferase; BICR = blinded independent central review; CLIA = Clinical Laboratory Improvement Amendments; CYP = cytochrome P450; DOR = duration of response; ECOG = Eastern Cooperative Oncology Group; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; G-CSF = granulocyte colony-stimulating factor; ILD = interstitial lung disease; LLN = lower limit of normal; LVEF = left ventricular ejection fraction; NSCLC = non–small cell lung cancer; NSCLC-SAQ = Non–Small Cell Lung Cancer Symptom Assessment Questionnaire; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; PFS2 = progression-free survival after first subsequent therapy; RCT = randomized controlled trial; RECIST = Response Evaluation Criteria in Solid Tumours; TKI = tyrosine kinase inhibitor; TTD = time to treatment discontinuation; TTSP = time to subsequent therapy; TTST = time to subsequent therapy; ULN = upper limit of normal; VTE = venous thromboembolism.
Source: Details included in the table are from the sponsor’s summary of clinical evidence.44
The MARIPOSA study is an ongoing randomized, multicentre, phase III study comparing the efficacy and safety of first-line amivantamab plus lazertinib to osimertinib monotherapy in adult patients with EGFR-mutated NSCLC. Details of the study design are included in Figure 1. The data contained in the submission were from a data cut-off date of August 11, 2023, which represented the cut-off for the primary analysis of PFS and interim analysis of OS. An updated clinical efficacy analysis of major secondary end points (i.e., OS) and exploratory end points with longer-term follow-up was conducted using a data cut-off of May 13, 2024.
The study included 3 sites in Canada. A total of 1,074 patients were randomized using an interactive web response system in a 2:2:1 ratio to either open-label amivantamab plus lazertinib (arm A; n = 429), double-blinded osimertinib (arm B; n = 429), or double-blinded lazertinib (arm C; n = 216), respectively. Randomization was stratified based on mutation type (exon 19 deletion versus exon 21 L858R), race (Asian versus non-Asian), and history of brain metastases (present versus absent). Study treatment continued until documented disease progression using RECIST 1.1 confirmed by BICR, or until another reason for discontinuation was met. Of note, the lazertinib monotherapy arm functioned as a comparison to assess the action of amivantamab; however, no hypothesis testing was undertaken using the lazertinib monotherapy arm and it was not included in the statistical analysis.
Figure 1: Study Design of MARIPOSA
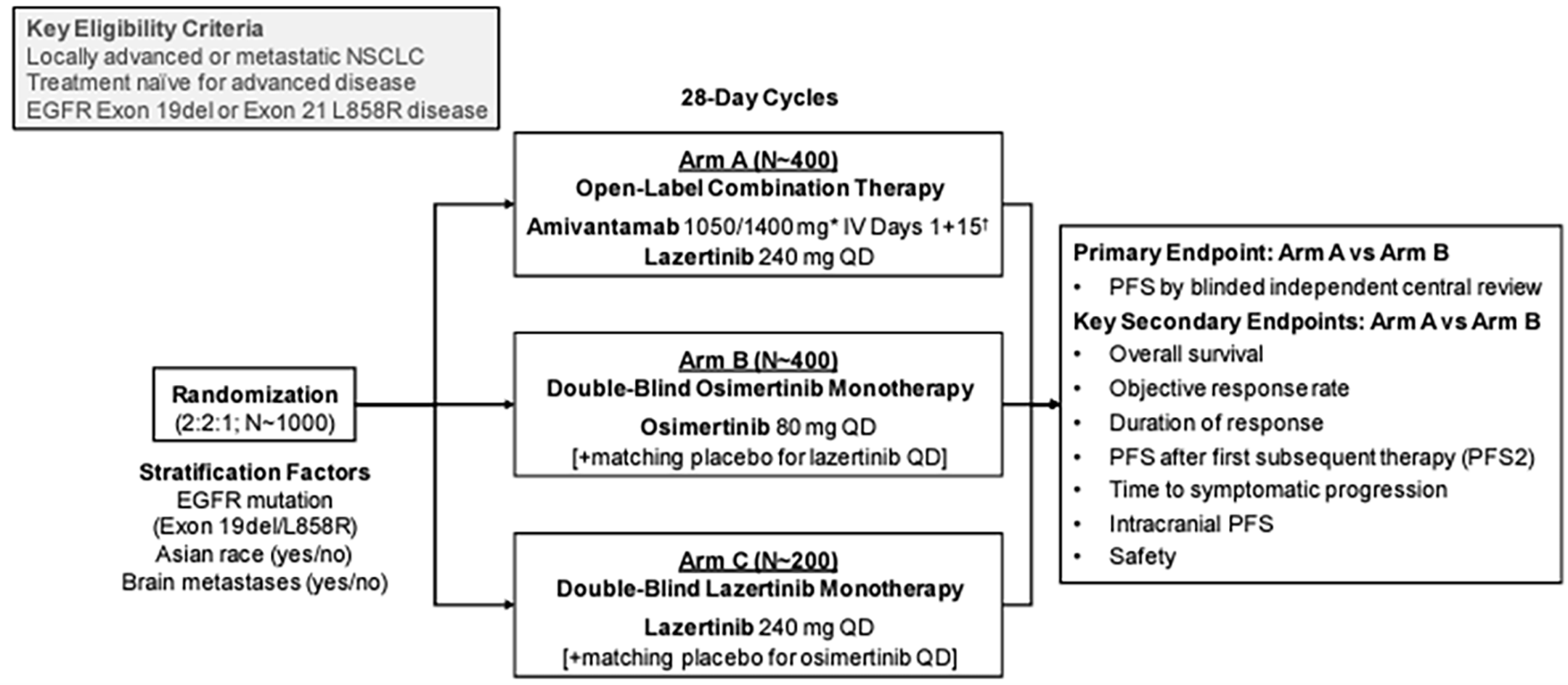
NSCLC = non–small cell lung cancer; PFS = progression-free survival; QD = every day.
* Weight-based dosing: < 80 kg/ ≥ 80 kg
† Cycle 1: days 1 to 2 (split dose), 8, 15, 22; Cycles 2 and beyond: days 1, 15
Source: Details included in the figure are from the MARIPOSA Clinical Study Report (August 11, 2023, data cut-off).12
Populations
Inclusion and Exclusion Criteria
The MARIPOSA study enrolled adult (aged ≥ 18 years) patients with newly diagnosed, histologically or cytologically confirmed, locally advanced or metastatic NSCLC which was treatment-naive and not amenable to any curative therapy including surgical resection or chemotherapy. Patients also had to meet specific organ function thresholds (e.g., hemoglobin, platelet liver enzyme) and had to have an ECOG status of 0 or 1. The tumour also had to have evidence of either the EGFR 19 deletion mutation or the EGFR exon 21 L858R substitution, as well as at least 1 lesion measurable by RECIST 1.1 which had not been previously irradiated. Notable exclusion criteria included prior treatment for any locally advanced (stage III) or metastatic (stage IV) cancer. Prior adjuvant treatment for stage I or stage II disease was permitted so long as it was administered more than 12 months before the development of the locally advanced or metastatic disease. The presence of symptomatic brain metastases was also an exclusion criterion, although the study protocol noted that patients with asymptomatic or previously treated and stable brain metastases and patients who received definitive radiation or surgical treatment for symptomatic or unstable brain metastases but who were clinically stable and asymptomatic for at least 2 weeks before randomization (either off corticosteroid treatment or receiving low-dose corticosteroid treatment [≤ 10 mg/day prednisone or equivalent] for at least 2 weeks before randomization) were eligible. Additional exclusion criteria of note included prior treatment with an EGFR TKI, and certain medications including potent cytochrome P450 3A4 and cytochrome P450 3A5 inducers which could not be stopped for an appropriate washout period. Detailed inclusion and exclusion criteria are described in Table 6.
Interventions
Treatment phases for a patient began on cycle 1, day 1, and continued as 28-day cycles until the end-of-treatment visit, which occurred approximately 30 days after discontinuation of study treatment. Patients were randomized to receive the following interventions, by treatment arm.
Arm A, amivantamab plus lazertinib: open-label combination therapy as amivantamab 1,050 mg (1,400 mg if body weight ≥ 80 kg) by IV infusion in 28-day cycles, once weekly for the first 4 weeks (with a split dose on day 1 and day 2 in week 1) and then once every 2 weeks, and three 80 mg lazertinib tablets once daily
Arm B, osimertinib: double-blind administration of 1 osimertinib 80 mg capsule and 3 placebo tablets once daily
Arm C, lazertinib: double-blind administration of 1 placebo capsule and three 80 mg lazertinib tablets (240 mg total) once daily
Amivantamab was supplied centrally by the sponsor in a glass vial containing 350 mg per vial with concentration 50 mg/mL in a 7 mL vial. Lazertinib was supplied as an 80 mg yellow film-coated tablet. The matching placebo tablet (for the osimertinib arm) was a yellow film-coated tablet, matched in appearance to the lazertinib 80 mg tablet. Osimertinib was supplied as over-encapsulated 80 mg tablets in red capsules to maintain the blinding, and as over-encapsulated 40 mg tablets in red capsules (as needed for dose reduction). Placebo capsules (for the lazertinib arm) were matched in appearance to the over-encapsulated osimertinib tablets.
After 12 cycles of amivantamab (approximately 1 year), patients receiving the full dosage of amivantamab were able to skip up to 3 doses in a year and patients on a reduced dose of amivantamab were able to skip up to 2 doses in a year, as needed, for life events. The skipped doses had to be at least 3 months apart and were to be avoided when feasible. Patients taking lazertinib and/or osimertinib had to take it at approximately the same time each day; if a dose was missed, they were permitted to take the missed dose within a 12-hour window.
Postrandomization disease assessments were conducted every 8 weeks (± 1 week) for the first 120 weeks and then every 12 weeks (± 1 week) until disease progression confirmed by BICR, even if a participant discontinued treatment before progression or received another systemic anticancer therapy. Serial brain MRIs (or CT scans if MRI was contraindicated) were conducted every 8 weeks (± 1 week) for the first 120 weeks and then every 12 weeks (± 1 week) until disease progression in participants with a history of brain metastasis at baseline. For patients without a history of brain metastasis at baseline, serial MRIs (or CT scans if MRI was contraindicated) were conducted every 12 weeks (± 1 week) until disease progression.
Patients’ study treatment would be discontinued if any of the following occurred.
The participant withdrew consent to receive study treatment.
The investigator believed that for safety reasons or tolerability reasons (e.g., AE) it was in the best interest of the patient to discontinue study treatment.
The participant became pregnant.
Nonadherence with study treatment or procedure requirements as judged by the investigator.
Radiographic disease progression (per RECIST 1.1) with 1 exception being in accordance with local practice, after consultation with the medical monitor, if the investigator believes the participant is deriving clinical benefit.
Disease progression that, at the discretion of the treating investigator, required the initiation of a new systemic anticancer treatment.
The submission did not provide a list of permitted or disallowed concomitant medications.
Outcomes
A list of efficacy end points assessed in this clinical review report is provided in Table 7, followed by descriptions of the outcome measures. Summarized end points are based on outcomes included in the sponsor’s summary of clinical evidence as well as any outcomes identified as important to this review according to the clinical experts consulted for this review and input from patient and clinician groups and public drug plans. Using the same considerations, the review team selected end points that were considered to be most relevant to inform expert committee deliberations and finalized this list of end points in consultation with members of the expert committee.
The included time-to-end-point outcomes (PFS and OS) were summarized in the clinical report and assessed at 24 months (PFS and OS), 30 months (OS only), and 36 months (OS only) using GRADE; these measures and time points were chosen because they are standard measures of response to treatment in oncology and provide the longest follow-up available from the MARIPOSA study, including the data update from May 13, 2024, requested by the European Medicines Agency. To provide additional context for efficacy, ORR and DOR were summarized in the clinical report but not evaluated using GRADE. The EORTC QLQ-C30 score and NSCLC-SAQ were summarized in the clinical report and included in GRADE; these measures were chosen as they measured quality of life in patients with cancer and quality of life in patients with NSCLC, respectively. Fewer numbers of patients provided data at later time points. To balance this, time points of cycle 13, day 1, and cycle 27, day 1, were chosen. Select notable harms outcomes considered important for informing expert committee deliberations were also assessed using GRADE. These included VTEs, IRRs, and dermatological AEs.
Table 7: Outcomes Summarized From MARIPOSA
Outcome measure | Definition | Time point | August 2023 data cut-off | May 2024 data cut-off |
|---|---|---|---|---|
PFS by BICR | The time from randomization until the date of objective disease progression (based on BICR using RECIST 1.1) or death, whichever came first. | Up to 32.8 months | Primarya | Not included |
OS | The time from the date of randomization until the date of death due to any cause. | Up to 60 months | Secondarya | Included |
ORR by BICR | Defined as participants achieving either CR or PR, as assessed by BICR per RECIST 1.1 criteria, among participants with measurable disease at baseline and responders. | Up to 42 months | Secondary | Included |
DOR by BICR | Defined as the time from the date of first documented response (PR or CR) until the data of documented progression of death, whichever comes first, for participants who have PR or CR. | Up to 42 months | Secondary | Included |
EORTC QLQ-C30 | Measured as change from baseline in Global Health Status score. | Up to 42 months | Secondary | Not included |
NSCLC-SAQ | Measured as change from baseline in total score. | Up to 42 months | Secondary | Not included |
BICR = blinded independent central review; CR = complete response; DOR = duration of response; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; NSCLC-SAQ = Non–Small Cell Lung Cancer Symptom Assessment Questionnaire; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; PR = partial response; RECIST = Response Evaluation Criteria in Solid Tumours.
aStatistical testing for these outcomes was controlled for multiple comparisons.
Source: Details included in the table are from the sponsor’s summary of clinical evidence.44
Survival Outcomes
Postbaseline disease assessments were conducted every 8 weeks (± 1 week) for the first 30 months followed by every 12 weeks (± 1 week) thereafter. Serial postbaseline brain MRI was required for all patients in the study. Participants with a history of brain metastasis at screening underwent postbaseline brain MRI every 8 weeks (± 1 week) for the first 30 months followed by every 12 weeks, while participants with no history of brain metastasis at screening underwent postbaseline brain MRI every 24 weeks (± 1 week).
Progression-Free Survival
PFS was the primary end point of the MARIPOISA study and was defined as the time from randomization until the date of objective disease progression (based on BICR using RECIST 1.1) or death, whichever came first. Patients who had not progressed or died at the time of analysis were censored at the time of the latest date of their last evaluable RECIST 1.1 assessment. If the patient progressed or died after 2 or more missed disease assessments, they were censored at the time of the last evaluable RECIST 1.1 assessment. PFS was analyzed using the data cut-off of August 11, 2023, as the primary analysis. PFS was not re-analyzed with data from the May 13, 2024, data cut-off because the primary end point was met in the primary analysis.
Prespecified subgroup analyses of interest to this review included patients with or without a history of brain metastases.
Overall Survival
OS was a secondary end point of the MARIPOSA study and was defined as the time from the date of randomization until the date of death due to any cause. Any patient not known to have died at the time of analysis was censored based on the last recorded date on which they were known to be alive. An interim analysis of OS was undertaken using the data cut-off on August 11, 2023, and updated using the second data cut-off from May 13, 2024.
Objective Response Rate
ORR was defined as patients achieving either complete response (CR) or partial response (PR), as assessed by BICR per RECIST 1.1 criteria, among patients with measurable disease at baseline. ORR was assessed using the data cut-off on August 11, 2023, and updated using the second data cut-off from May 13, 2024.
Duration of Response
DOR was defined as the time from the date of first documented response (PR or CR) until the date of documented progression of death, whichever comes first, for patients who have PR or CR. DOR was assessed using the data cut-off on August 11, 2023, and updated using the second data cut-off from May 13, 2024.
HRQoL Outcomes
A summary of the HRQoL outcomes and their measurement properties is presented in Table 8.
European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30
The EORTC QLQ-C30 is a 30-item, cancer-specific, patient-reported HRQoL questionnaire designed to assess the physical, psychological, and social functioning of patients with cancer. The functional scales range from 0 to 100, with higher scores indicating better functioning. The sponsor suggested an MID of 10 points as identified in studies of patients with breast and small cell lung cancer.45-47 Based on a study in patients with NSCLC, MID estimates for individual scales or items ranged from 5 points to 16 points for improvement when using the ECOG Performance Status as an anchor.48
Non–Small Cell Lung Cancer Symptom Assessment Questionnaire
The NSCLC-SAQ is a patient-reported tool designed to assess NSCLC symptoms. The tool contains 5 domains and the total score ranges from 0 to 20, with higher scores indicating more severe symptoms. A decrease of 3 points to 5 points in scores was used as MID for improvement in symptoms, and an increase of 2 points to 3 points in scores was used as MID for worsening of symptoms.49
Table 8: Summary of Outcome Measures and Their Measurement Properties
Outcome measure | Type | Conclusions about measurement properties | MID |
|---|---|---|---|
NSCLC-SAQ | A self-reported, symptom-based patient-reported outcome tool designed to assess 5 NSCLC symptoms: cough, pain, dyspnea, fatigue, and appetite. Respondents rate each of the 7 items using a 5-point scale for intensity (3 items) and frequency (4 items), with higher scores indicating more severe symptoms. The total score is the sum of the 5 domain scores (0 to 20).50 | Validity: Strong correlation (r > 0.5) between NSCLC-SAQ and FLSI-17.50 Moderate correlations (r = 0.3 to 0.5 or r > 0.5) with EORTC QLQ-C30, EORTC QLQ-LC13, EQ-5D-5L, and PGIS-LC.49 Reliability: Acceptable internal consistency; Cronbach alpha = 0.78 for 7 items and 0.72 for 5 domains.51 Responsiveness: total score Supported by longitudinal differences from baseline to week 18 among PGIS-LC improvement groups (P < 0.001).49 | Improvement: indicated by a decrease in total score of 3 points to 5 points.49 Worsening: indicated by an increase of 2 points to 3 points.52 |
EORTC QLQ-C30 | A cancer-specific, multidimensional HRQoL questionnaire with 30 items across 4 scales: functional scales, symptom scales, single-item symptoms, and Global Health Status/QoL. Most items use a 4-point scale (1 = “not at all” to 4 = “very much”), and global QoL uses a 7-point scale (1 = “very poor” to 7 = “excellent”).53 | In studies with patients with lung cancer: Validity: Moderate to strong correlations between the FACT-G and EORTC QLQ-C30 scales (r = 0.64 to 0.76);54 HADS anxiety scales with all EORTC QLQ-C30 functioning scales (r = 0.28 to 0.75); and BPI scales with all EORTC QLQ-C30 scales except for nausea/vomiting (r = 0.20 to 0.72),55 supporting convergent validity. Known-groups approach: Able to differentiate across different measures of cancer severity — cancer stages (d = 0.49), ECOG PS (d = 0.65), and self-reported health status (d = 1.36).54 Reliability: Cronbach alpha ranging from 0.56 to 0.93 with 7 scales having acceptable internal consistency (alpha > 0.70).56 Responsiveness: Group differences (improved versus deteriorated based on ECOG PS) over 28 days between pretreatment and on-treatment periods showed a statistically significant difference in global quality of life (P < 0.01) scale. No such difference was identified in patients whose ECOG PS remained unchanged.57 | In a study with patients with NSCLC: MID estimates for individual scales/items using the ECOG PS as an anchor: improvement = 5 to 16 points, deterioration = 4 to 7 points. When using weight change as an anchor: improvement = 4 to 7 points, deterioration = 4 to 11 points.48 The sponsor’s submission indicated a clinically relevant change as a ≥ 10-point change from baseline for scales or items.45-47 |
BPI = Brief Pain Inventory; ECOG PS = Eastern Cooperative Oncology Group Performance Status; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; EORTC QLQ-LC13 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Lung Cancer Module; FACT-G = Functional Assessment of Cancer Therapy–General; HADS = Hospital Anxiety and Depression Scale; HRQoL = health-related quality of life; MID = minimal important difference; NFLSI-17 = National Comprehensive Cancer Network/Functional Assessment of Cancer Therapy Lung Cancer Symptom Index–17-Item Version; NSCLC = non–small cell lung cancer; NSCLC-SAQ = Non–Small Cell Lung Cancer Symptom Assessment Questionnaire; PGIS-LC = Patient Global Impression of Severity–Lung Cancer symptoms; QoL = quality of life.
Statistical Analysis
The MARIPOSA study was an ongoing study with an event-driven trial design. Approximately 390 death events in arms A and B combined would trigger a final analysis of OS. At the time of the submission to CDA-AMC, this end point had not yet been triggered.
Sample Size and Power Calculations
The primary outcome of the MARIPOSA study was PFS by BICR, and the sample size calculation was based on the assumption that amivantamab plus lazertinib would result in a 27% reduction in the risk of either progression or death over the single-drug osimertinib therapy (HR = 0.73, prolonging the median PFS from 19 months to 26 months). A total of 450 PFS events in arm A and arm B would provide approximately 90% power to achieve a statistically significant difference between the 2 treatment arms with the stratified log-rank test (2-sided alpha = 0.05).
One interim analysis was planned for PFS when approximately 280 PFS events by BICR from the amivantamab plus lazertinib and osimertinib arms combined had occurred (approximately 62% of total planned 450 PFS events). When the interim PFS analysis was triggered, there were 321 PFS events by BICR observed from the amivantamab plus lazertinib and osimertinib arms combined and the efficacy stopping criteria had been met for PFS with a median duration of follow-up of 15.1 months. The sponsor committee decided to continue the study and maintain the blinding until the next protocol-specified PFS analysis; the sponsor study team and investigators remained blinded to treatment allocation. The PFS analysis was therefore tested using the nominal 2-sided 0.05 without an alpha penalty for the interim data analysis.
One interim analysis for OS was planned to be conducted at the final analysis of PFS; OS was to be tested only if statistical significance was reported for PFS. If statistical significance was not achieved, then final analysis of OS was to be conducted around 60 months after the first participant was enrolled, when approximately 390 deaths from the amivantamab plus lazertinib arm and osimertinib arm combined were anticipated.
Based on the power calculations, approximately 1,000 patients were to be randomized in a 2:2:1 ratio to the 3 arms (arm A:arm B:arm C). Assuming a 25-month recruitment period and an annual dropout rate of approximately 5%, 560 PFS events (approximately 450 events in arm A and arm B combined) were expected to occur approximately 42 months after the first patient was enrolled.
Statistical and Analytical Plans
Statistical Tests and Models
The baseline measurement was defined as the closest nonmissing measurement taken on or before the first administration of study drug (including time, if time was available). If the first administration date was missing or the administration was not done, then the baseline measurement was the closest nonmissing measurement taken on or before the corresponding visit date and if the visit date was not available, then randomization date was used. Continuous variables were summarized using the number of participants (n), mean, standard deviation (SD), median, minimum, and maximum. Discrete variables were summarized with number and percent. The hypothesis testing for PFS and OS was performed for the comparison between arm A and arm B; the comparison of the arm A with arm C (lazertinib monotherapy) was also performed using summary statistics for PFS and OS along with nominal P values; there was no preplanned hypothesis testing for this comparison and the results were not included in the review.
Time-to-Event and Response Outcome Analysis
Details of the statistical analysis for the included outcomes are summarized in Table 9. Briefly, the primary end point (PFS by BICR) was analyzed using a stratified Cox regression model with treatment as the sole explanatory variable to estimate the HR and associated 95% CIs. The Kaplan-Meier method was used to estimate the median and landmark PFS (at 6 months, 12 months, 18 months, and 24 months) with 95% CI.
The secondary end point of OS was analyzed using a log-rank test at the overall 2-tailed significance level of 0.05. One interim analysis of OS was conducted at the August 11, 2023, data cut-off for the final PFS analysis. The comparison of OS was conducted only if the results for PFS were statistically significant. Patients were then followed up for a final analysis of OS when 390 deaths from the amivantamab plus lazertinib and osimertinib arms combined occurred. A stratified Cox regression model with treatment as the sole explanatory variable was used to estimate the HR and associated 95% CI. The Kaplan-Meier method was used to estimate the median and landmark OS (at 6 months, 12 months, 18 months, and 24 months) with 95% CI.
ORR was analyzed using a logistic regression model adjusted by mutation type (exon 19 deletion or exon 21 L858R), race (Asian or non-Asian), and history of brain metastasis (present or absent), at the overall 2-tailed significance level of 0.05. Results were presented as an OR with 95% CI.
DOR was analyzed using a Kaplan-Meier plot with 95% CI and presented by treatment group.
HRQoL and Descriptive Statistics
Descriptive statistics were used for all variables, as appropriate, and presented by treatment group. Continuous variables were summarized using number of patients (n), mean, SD, median, minimum, and maximum. Discrete variables were summarized with number and percent.
Results for the change from baseline in EORTC QLQ-C30 Global Health Status were summarized descriptively, and change from baseline to day 1 of cycles 13, 21, and 27 in EORTC QLQ-C30 Global Health Status were modelled using a MMRM.
Results for the change from baseline in total NSCLC-SAQ score were summarized descriptively, and the change from baseline to day 1 of cycles 13, 21, and 27 were modelled using MMRM.
Table 9: Statistical Analysis of Efficacy End Points in MARIPOSA
End point | Statistical model | Adjustment factors | Handling of missing data | Sensitivity analyses |
|---|---|---|---|---|
PFS (by BICR) |
|
| Sensitivity analysis |
|
OS |
|
| NR | Unstratified log-rank test |
ORR (by BICR) |
|
| NR | NR |
DOR (by BICR) |
| NR | NR | NR |
EORTC QLQ-30 |
| NR | NR | NR |
NSCLC-SAQ |
| NR | All 5 domains must be nonmissing to compute a total score | NR |
BICR = blinded independent central review; DOR = duration of response; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; MMRM = mixed model for repeated measures; NR = not reported; NSCLC-SAQ = Non–Small Cell Lung Cancer Symptom Assessment Questionnaire; ORR = objective response rate; OS = overall survival; PFS = progression-free survival.
Source: Details included in the table are from the sponsor’s summary of clinical evidence.44
Subgroup and Sensitivity Analyses
The submission included several sensitivity and subgroup analyses. For PFS, sensitivity analyses were conducted using a nonstratified log-rank test and using investigator-assessed progression. For OS, a sensitivity test using unstratified log-rank tests was conducted. Sensitivity analyses were not specified for the other outcomes included in the review.
The following prespecified subgroup analyses were included in the MARIPOSA study:
age group (< 65 years, ≥ 65 years; < 75 years, ≥ 75 years)
sex (male, female)
race (Asian, Non-Asian)
weight (< 80 kg, ≥ 80 kg)
mutation type (exon 19 deletion, exon 21 L858R)
history of brain metastasis (yes, no)
ECOG Performance Status score (0, 1)
history of smoking (yes, no).
An exploratory subgroup analysis in study participants with additional high-risk disease features (i.e., history of liver metastasis [yes, no], TP53 co-mutation status [mutated, wild type], and circulating tumour DNA status at baseline [yes, no], as well as clearance at cycle 3, day 1 [yes, no]) was also performed.
The results from the PFS age subgroup analysis, the results of the sensitivity analysis using investigator assessment, and the results from the PFS analysis by history of brain metastases were included in Appendix 1.
Multiple Testing Procedure
To control the type I error rate at 0.05 for the study, a hierarchical testing approach for PFS and OS was used. The comparison between arm A and arm B for OS was to be conducted with a total 2-sided alpha of 0.05 only if the testing on PFS showed statistical significance.
Analysis Populations
Details of the analysis populations for the MARIPOSA study are presented in Table 10. All primary and secondary end points were analyzed using the full analysis set. The submission did not explicitly state whether a per-protocol or intent-to-treat analysis was undertaken.
Table 10: Analysis Populations of MARIPOSA
Population | Number analyzed | Definition | Application |
|---|---|---|---|
Full analysis set | Arm A: n = 429 Arm B: n = 429 Arm C: n = 216 Total: N = 1,074 | All randomized participants, classified according to their assigned treatment arm regardless of the actual treatment received. | Used to summarize patient demographic and baseline disease characteristics as well as the efficacy data. |
Safety analysis set | Arm A: n = 421 Arm B: n = 428 Arm C: n = 213 Total: N = 1,062 | Randomized patients who receive at least 1 dose of study treatment. | Used to summarize the safety data. |
Source: Details included in the table are from the sponsor’s summary of clinical evidence.44
Protocol Amendments and Deviations
The latest version of the study protocol was implemented after the data cut-offs in the submission. Notable changes to the study protocol which were in place before the data cut-offs included adding VTE as an AESI plus dosing guidance, management, and detection (August 2022); adding guidance on dose reduction or withholding in case of AEs and managing dermatological AEs (August 2022); modifying the exclusion criteria to specify the exact stages of NSCLC permitted (September 2021); adding dose reduction clarifications for lazertinib (September 2021); adding guidance for IRRs (September 2021); adding information on suspected pulmonary toxicity (September 2021); and revising the inclusion and exclusion criteria to their current forms (April 2021).
Results
Patient Disposition
Full details of the patient and treatment disposition are presented in Table 11. Briefly, 1,375 patients were screened and 301 failed screening. The most common reason for screening failure was not meeting eligibility criteria (243 [17.7%] of screened patients); the submission did not specify which criteria were most commonly failed. At the time of the August 11, 2023, data cut-off, 45.4% of patients in the amivantamab plus lazertinib arm and 50.2% of patients in the osimertinib arm had discontinued all study drugs. In the safety analysis set, the most common reason for discontinuation in all study arms was disease progression (20.4% amivantamab plus lazertinib and 36.0% osimertinib). A numerically higher proportion of patients in the amivantamab plus lazertinib arm discontinued due to AEs (20.4% for amivantamab plus lazertinib and 11.7% for osimertinib). In addition, 21.9% of patients in the amivantamab plus lazertinib arm and 26.3% of patients in the osimertinib arm were reported to have died before the end of the study. The median duration of follow-up was 22.01 months (amivantamab plus lazertinib arm = 22.21 months; osimertinib arm = 21.98 months; lazertinib arm = 21.88 months).
Table 11: Summary of Patient and Treatment Disposition From MARIPOSA — August 11, 2023, Data Cut-Off
Category | Amivantamab lazertinib n = 429 | Osimertinib n = 429 | Lazertinib n = 216 |
|---|---|---|---|
Patient disposition (FAS) | |||
Screened, N | 1,375 | ||
Screening failure, n (%) | 301 (21.9) | ||
Failure to meet eligibility criteria | 243 (17.7) | ||
Participant withdrawal | ██ █████ | ||
AEs | | █████ | ||
Progressive disease | | █████ | ||
Death | | █████ | ||
Lost to follow-up | | █████ | ||
Other | | █████ | ||
Randomized, N (%) | 1,074 (78.1) | ||
Randomized into each study arm, n (%) | 429 (100.0) | 429 (100.0) | 216 (100.0) |
Randomized but not treated | 8 (1.9) | 1 (0.2) | 3 (1.4) |
Treated | 421 (98.1) | 428 (99.8) | 213 (98.6) |
On study at data cut-off (August 11, 2023) | 313 (73.0) | 297 (69.2) | 149 (69.0) |
Died before end of study | 94 (21.9) | 113 (26.3) | 54 (25.0) |
Discontinued the study, n (%) | 22 (5.1) | 19 (4.4) | 13 (6.0) |
Reason for discontinuation, n (%) | |||
Withdrawal by participant | 19 (4.4) | 18 (4.2) | 13 (6.0) |
Lost to follow-up | 3 (0.7) | 1 (0.2) | 0 (0.0) |
Patients still receiving any study treatment, n (%) | 230 (54.6) | 213 (49.8) | 106 (49.8) |
Treatment disposition (SAS) | |||
Discontinued from all study drugs, n (%) | 191 (45.4) | 215 (50.2) | 107 (50.2) |
Progressive disease | 86 (20.4) | 154 (36.0) | 72 (33.8) |
AEs | 86 (20.4) | 50 (11.7) | 29 (13.6) |
Patient refused further study treatment | 14 (3.3) | 10 (2.3) | 4 (1.9) |
Physician decision | 2 (0.5) | 1 (0.2) | 0 (0.0) |
Nonadherence to study drug | 1 (0.2) | 0 (0.0) | 1 (0.5) |
Lost to follow-up | 1 (0.2) | 0 (0.0) | 0 (0.0) |
Other | 1 (0.2) | 0 (0.0) | 1 (0.5) |
Analysis populations | |||
FAS, N (%) | 429 (100.0) | 429 (100.0) | 216 (100.0) |
SAS, N (%) | 421 (98.1) | 428 (99.8) | 213 (98.6) |
AE = adverse event; FAS = full analysis set; SAS = safety analysis set.
Source: Details included in the table are from the sponsor’s summary of clinical evidence44 and the MARIPOSA Clinical Study Report (August 11, 2023, data cut-off).12
Baseline Characteristics
The baseline characteristics outlined in Table 12 are limited to those that are most relevant to this review or were felt to affect the outcomes or interpretation of the study results. Briefly, the baseline characteristics were generally balanced across all 3 study arms, apart from a numerically lower proportion of patients in the lazertinib monotherapy arm reporting any prior therapy for lung cancer (19% of patients) relative to the amivantamab plus lazertinib arm (26.1%) and the osimertinib arm (24.2%). The mean age of patients was approximately 62 years and patients were mostly female (58.5% to 64.1% of patients were female across the 3 study arms; 35.9% to 41.5% were male) and of Asian descent (58.3% to 59.3% across study arms). The percentage of patients who identified as white was 36.6% to 38.5% across study arms, and less than 2% in each study arm identified as either American Indian or Alaska Native, Black or African American, Native Hawaiian or other Pacific Islander, other races, or multiple races. Most patients across study arms reported never smoking (66.2% to 69.7% of patients across study arms) and were ECOG status 1 (64.8% to 67.1%). Of the patients who had received any prior therapy for lung cancer, radiotherapy (13.9% to 17.0% of patients) was the most common prior therapy.
Table 12: Summary of Baseline Characteristics From MARIPOSA (FAS)
Characteristic | Amivantamab plus lazertinib n = 429 | Osimertinib n = 429 | Lazertinib n = 216 |
|---|---|---|---|
Demographic characteristics | |||
Age (years), mean (SD) | 62.7 (10.63) | 61.9 (11.52) | 61.3 (10.69) |
Sex, n (%) | |||
Female | 275 (64.1) | 251 (58.5) | 136 (63.0) |
Male | 154 (35.9) | 178 (41.5) | 80 (37.0) |
Race, n (%) | |||
American Indian or Alaska Native | 7 (1.6) | 7 (1.6) | 4 (1.9) |
Asian | 250 (58.3) | 251 (58.5) | 128 (59.3) |
Black or African American | 4 (0.9) | 3 (0.7) | 4 (1.9) |
Multiple | 1 (0.2) | 1 (0.2) | 0 (0.0) |
Native Hawaiian or other Pacific Islander | 1 (0.2) | 1 (0.2) | 0 (0.0) |
Unknown | 2 (0.5) | 1 (0.2) | 1 (0.5) |
White | 164 (38.2) | 165 (38.5) | 79 (36.6) |
Weight (kg), mean (SD) | 64.4 (13.43) | 63.8 (13.44) | 63.1 (13.22) |
Height (cm), mean (SD) | 161.3 (8.73) | 162.1 (8.98) | 163.1 (9.48) |
BMI (kg/m2), mean (SD) | 24.65 (4.265) | 24.15 (4.047) | 23.67 (3.982) |
Medical characteristics | |||
History of smoking, n (%) | |||
Yes | 130 (30.3) | 134 (31.2) | 73 (33.8) |
███████ | ██ █████ | ██ █████ | | █████ |
██████ | ███ ██████ | ███ ██████ | ██ ██████ |
No | 299 (69.7) | 295 (68.8) | 143 (66.2) |
Baseline ECOG score, n (%) | |||
0 | 141 (32.9) | 149 (34.7) | 76 (35.2) |
1 | 288 (67.1) | 280 (65.3) | 140 (64.8) |
History of brain metastasis, n (%) | |||
Present | 178 (41.5) | 172 (40.1) | 86 (39.8) |
Absent | 251 (58.5) | 257 (59.9) | 130 (60.2) |
Mutation type, n (%) | |||
Exon 19 deletion | 258 (60.1) | 257 (59.9) | 131 (60.6) |
Exon 21 L858R | 172 (40.1) | 172 (40.1) | 85 (39.4) |
Initial diagnosis NSCLC subtype, n (%) | |||
Adenocarcinoma | 417 (97.2) | 415 (96.7) | 212 (98.1) |
Large cell carcinoma | 3 (0.7) | 0 (0.0) | 0 (0.0) |
Squamous cell carcinoma | 6 (1.4) | 5 (1.2) | 2 (0.9) |
Other | 2 (0.5) | 9 (2.1) | 2 (0.9) |
Not reported | 1 (0.2) | 0 (0.0) | 0 (0.0) |
Histology grade at initial diagnosis, n (%) | |||
Poorly differentiated | 61 (14.2) | 61 (14.2) | 32 (14.8) |
Moderately differentiated | 90 (21.0) | 108 (25.2) | 42 (19.4) |
Well differentiated | 46 (10.7) | 50 (11.7) | 19 (8.8) |
Other | 14 (3.3) | 11 (2.6) | 11 (5.1) |
Not reported | 218 (50.8) | 199 (46.4) | 112 (51.9) |
Cancer stage at initial diagnosis, n (%) | |||
IA | 10 (2.3) | 9 (2.1) | 5 (2.3) |
IB | 12 (2.8) | 8 (1.9) | 2 (0.9) |
IIA | 2 (0.5) | 2 (0.5) | 2 (0.9) |
IIB | 5 (1.2) | 3 (0.7) | 0 (0.0) |
IIIA | 3 (0.7) | 6 (1.4) | 0 (0.0) |
IIIB | 14 (3.3) | 10 (2.3) | 3 (1.4) |
IIIC | 4 (0.9) | 5 (1.2) | 2 (0.9) |
IVA | 146 (34.0) | 150 (35.0) | 81 (37.5) |
IVB | 233 (54.3) | 236 (55.0) | 121 (56.0) |
Location of metastasis at screening, n (%) | |||
Bone | 206 (48.9) | 180 (42.5) | 90 (41.7) |
Liver | 64 (15.2) | 72 (17.0) | 32 (14.8) |
Brain | 178 (42.3) | 172 (40.6) | 86 (39.8) |
Lymph node | 282 (67.0) | 289 (68.2) | 144 (66.7) |
Adrenal gland | 41 (9.7) | 45 (10.6) | 19 (8.8) |
Lung | 257 (61.0) | 280 (66.0) | 135 (62.5) |
Other | 14 (3.3) | 16 (3.8) | 8 (3.7) |
Histology grade at screening, n (%) | |||
Poorly differentiated | 59 (13.8) | 66 (15.4) | 36 (16.7) |
Moderately differentiated | 86 (20.0) | 111 (25.9) | 40 (18.5) |
Well differentiated | 46 (10.7) | 49 (11.4) | 19 (8.8) |
Other | 18 (4.2) | 11 (2.6) | 13 (6.0) |
Not reported | 220 (51.3) | 192 (44.8) | 108 (50.0) |
Cancer stage at screening, n (%) | |||
IIIA | 1 (0.2) | 3 (0.7) | 0 (0.0) |
IIIB | 11 (2.6) | 5 (1.2) | 2 (0.9) |
IIIC | 3 (0.7) | 3 (0.7) | 2 (0.9) |
IVA | 131 (30.5) | 119 (27.7) | 66 (30.6) |
IVB | 283 (66.0) | 299 (69.7) | 146 (67.6) |
Time since initial lung cancer diagnosis (months), mean (SD) | 4.785 (14.8980) | 4.614 (15.2386) | 5.024 (22.1585) |
Time since initial metastatic disease diagnosis (months), mean (SD) | 1.669 (1.8189) | 1.491 (1.1084) | 1.443 (1.1156) |
Received any prior therapy for lung cancer, n (%) | 112 (26.1) | 104 (24.2) | 41 (19.0) |
Prior systemic therapy | 8 (1.9) | 10 (2.3) | 3 (1.4) |
Prior radiotherapy | 73 (17.0) | 65 (15.2) | 30 (13.9) |
Prior cancer-related surgery | 53 (12.4) | 49 (11.4) | 16 (7.4) |
Number of prior lines of systemic therapy, n (%) | |||
0 | 421 (98.1) | 419 (97.7) | 213 (98.6) |
1 | 8 (1.9) | 10 (2.3) | 3 (1.4) |
BMI = body mass index; ECOG = Eastern Cooperative Oncology Group; FAS = full analysis set; NSCLC = non–small cell lung cancer; SD = standard deviation.
Source: Details included in the table are from the sponsor’s summary of clinical evidence.44
Exposure to Study Treatments
Details of exposure to study treatments are presented in Table 13. As of the August 11, 2023, data cut-off, for patients in the amivantamab plus lazertinib arm, the median duration of treatment with amivantamab was numerically shorter (15.24 months) than the median duration of lazertinib (18.50 months); this was also reflected in the mean duration (12.13 months amivantamab exposure versus 16.97 months lazertinib exposure). Patients in the amivantamab plus lazertinib arm received a mean number of ████ ██████ ███ █ █████ of amivantamab. Of note, 59.1% of patients in the amivantamab plus lazertinib arm, 5.4% patients in the osimertinib arm, and █████ of patients in the lazertinib arm required a dose reduction of any study treatment. A total of 83.1% of patients in the amivantamab plus lazertinib arm, 38.6% in the osimertinib arm, and █████ in the lazertinib arm had interrupted any study drug treatment due to AEs, as of the data cut-off. In the amivantamab plus lazertinib arm, in most cases the drug which was either discontinued, reduced, or interrupted was amivantamab.
Table 13: Summary of Patient Exposure From MARIPOSA (SAS) — August 11, 2023, Data Cut-Off
Exposure | Amivantamab plus lazertinib | Osimertinib n = 428 | Lazertinib n = 213 | ||
|---|---|---|---|---|---|
Total N = 421 | Amivantamab n = 421 | Lazertinib n = 421 | |||
Total patient-years | █████ | █████ | █████ | █████ | █████ |
Duration (months), mean (SD) | █████ ███████ | █████ ███████ | █████ ███████ | █████ ███████ | █████ ███████ |
Duration (months), median (range) | 18.50 (0.2 to 31.4) | 15.24 (0.0 to 31.3) | 18.50 (0.2 to 31.4) | 18.00 (0.2 to 32.7) | 17.05 (0.4 to 32.1) |
Total number amivantamab cycles, mean (SD) | ████ ██████ | NA | NA | NA | NA |
NA = not applicable; SAS = safety analysis set; SD = standard deviation.
Source: Details included in the table are from the sponsor’s summary of clinical evidence.44
A list of permitted prior and concomitant medications in the MARIPOSA study was not provided; however, the most common concomitant medications received by patients in the MARIPOSA study are summarized in Table 14. Briefly, there were numerically higher proportions of patients in the amivantamab plus lazertinib arm receiving certain concomitant medications, relative to the osimertinib arm. The largest differences were in antibacterials for systemic use ██████ ███ █████ ██ ███ ███████████ █████ systemic corticosteroids ██████ ███ █████ ██ ███ ███████████ █████ antihistamines ██████ ███ █████ ██ ███ ███████████ █████ antithrombotic agents ██████ ███ █████ ██ ███ ███████████ █████ opthamologicals ██████ ███ █████ ██ ███ ███████████ █████ antibiotics and chemotherapeutics for dermatological use ██████ ███ █████ ██ ███ ███████████ █████ and emollients and protectives ██████ ███ █████ ██ ███ ███████████ █████.
Table 14: Summary of Most Common (≥ 20% of Patients) Concomitant Treatments in MARIPOSA (SAS)
Exposure | Amivantamab plus lazertinib n = 421 | Osimertinib n = 428 | Lazertinib n = 213 |
|---|---|---|---|
████████ ███ ███████████ ████████████ █ ███ | ███ █████ | ███ █████ | ███ █████ |
██████████████ ███ ████████ ███ | ███ █████ | ███ █████ | ███ █████ |
██████████ | ███ █████ | ███ █████ | ███ █████ |
███████████████ ███ ████████ ███ | ███ █████ | ███ █████ | ██ ██████ |
█████ ███ ████ ███████ █████████ | ███ █████ | ███ █████ | ██ ██████ |
██████████████ ███ ████████ ███ | ███ █████ | ███ █████ | ██ ██████ |
████████████████ ██████████████ ████████████ | ███ █████ | ███ █████ | ██ ██████ |
████████████████ ███ █████████████ ████████ | ███ █████ | ███ █████ | ██ ██████ |
██████████████ ██████ | ███ █████ | ███ █████ | ██ ██████ |
█████████████████ | ███ █████ | ███ █████ | ██ ██████ |
█████ ███ ████ ████████████ | ███ █████ | ███ █████ | ██ ██████ |
███████████ ██████ ███ ███████████ ████████ | ███ █████ | ███ █████ | ██ ██████ |
███████████████ ██████████ ██████████████████████████████ ██████ | ███ █████ | ███ █████ | ██ ██████ |
████████ | ███ █████ | ██ ██████ | ██ ██████ |
███████████ ███ █████████████████ ███ ██████████████ ███ | ███ █████ | ██ ██████ | ██ ██████ |
██████ ██████ ██ ███ █████████████████ ██████ | ███ █████ | ███ █████ | ██ ██████ |
█████ ███████████ ███ █████████ █████████ | ███ █████ | ██ ██████ | ██ ██████ |
██████████ ███ ███████████ | ███ █████ | ██ ██████ | ██ ██████ |
███████ ███████████ | ███ █████ | ██ ██████ | ██ ██████ |
████████ | ███ █████ | ███ █████ | ██ ██████ |
█████████████ | ███ █████ | ███ █████ | ██ ██████ |
█████ ███ ██████████ ████████████████ █████████ | ███ █████ | ██ ██████ | ██ ██████ |
█████ ███ ████████████ | ███ █████ | ██ ██████ | ██ ██████ |
█████ █████████ ██████ | ███ █████ | ██ ██████ | ██ ██████ |
█████████ | ███ █████ | ██ ██████ | ██ ██████ |
███████ ███████ ████████ | ██ █████ | ██ ██████ | ██ ██████ |
██████ ████████████ | ███ ████ | ██ ██████ | ██ ██████ |
██████████ ████████████ | ██ ██████ | ██ ██████ | ██ ██████ |
SAS = safety analysis set.
Source: Details included in the table are from the sponsor’s summary of clinical evidence.44
Details of the first subsequent therapy received by patients after discontinuing study treatment are summarized in Table 15. At the time of the May 13, 2024, data cut-off, █████ of patients in the amivantamab plus lazertinib arm and █████ of patients in the osimertinib arm were receiving their first subsequent line of therapy. The most common subsequent line in the amivantamab plus lazertinib arm was ██ ████████ ██ █████████ ███████ ████████ while in the osimertinib arm the most common regimen was a ████████████ ██ ███████████████████ ████████ ██████ ██ ██████████ The submission did not specify whether patients received lines of therapy after the first subsequent line.
Table 15: Summary of First Subsequent Systemic Therapies in MARIPOSA (FAS) — May 13, 2024, Data Cut-Off
Exposure | Amivantamab plus lazertinib n = 429 | Osimertinib n = 429 |
|---|---|---|
████████ █████████ █████ ██████████ ████████ █ ███ | ███ ██████ | ███ ██████ |
████████ █████ ████████ █ ███ | ██ ██████ | ███ ██████ |
█████ █████ | ██ ██████ | ██ ██████ |
█████ █ █████ █ ██ | | █████ | ██ █████ |
█████ █ █████ | | █████ | ██ █████ |
█████ █ ██ | | █████ | | █████ |
█████ | | █████ | | █████ |
███ ██████ ██ ███ █████ ███████ █ ███ | ██ ██████ | ██ ██████ |
███ | ██ ██████ | ██ ██████ |
███ █████ ███████ | ██ █████ | ██ █████ |
██████ ███ ███████ █████ ██████ █ ███ | | █████ | | █████ |
████ | | █████ | | █████ |
███████ █ ███ | | █████ | | █████ |
███ ███ ███ ████████ █████████ █ ███ | | █████ | | █████ |
██████ █ ███ | | █████ | | █████ |
IO = immunotherapy; MoA = monoclonal antibody; TKI = tyrosine kinase inhibitor.
Source: Details included in the table are from the sponsor’s MARIPOSA efficacy update of the Clinical Study Report (May 13, 2024, data cut-off).13
Efficacy
Survival Outcomes
Results of the prespecified primary analysis of PFS and interim analysis of OS (August 11, 2023, data cut-off) are reported in Table 16; the median duration of follow-up was 22.01 months. Results from OS, ORR, and DOR from the additional May 13, 2024, reanalysis are included in the text; the updated median follow-up was approximately 31 months.
PFS by BICR
As of the August 11, 2023, data cut-off, there were a total of 192 (44.8%) PFS events in the amivantamab plus lazertinib arm, and 252 (58.7%) PFS events in the osimertinib arm. Of these, ███ ███████ and 228 (90.5%) were due to progressive disease, and ██ ███████ ███ ██ ██████ were due to death without progressive disease in the amivantamab plus lazertinib and osimertinib arms, respectively. The median PFS in the amivantamab plus lazertinib arm was 23.72 months (95% CI, 19.12 months to 27.66 months), and in the osimertinib arm was 16.59 months (95% CI, 14.78 months to 18.46 months), in favour of amivantamab plus lazertinib (HR = 0.70; 95% CI, 0.58 to 0.85; P = 0.0002). The difference in the probability of being progression-free between amivantamab plus lazertinib and osimertinib at 6 months, 12 months, 18 months, and 24 months was ████ ████ ███ █████ ██ ██████ ████ ████ ███ ████ ██ ███████ █████ ████ ███ ████ ██ ███████ ███ █████ █████ ██ ███████ respectively.
Results for the prespecified subgroup of patients with a history of brain metastases at baseline and patients without a history of brain metastases at baseline are summarized in Figure 2. The magnitude of benefit in terms of median PFS was lower for patients with a history of brain metastases, and higher in patients without a history of brain metastases. In patients with a history of brain metastases, the median PFS was 18.3 months ████ ███ ████ ██ █████ for amivantamab plus lazertinib and ████ ██████ ████ ███ ████ ██ █████ ███ ███████████, in favour of amivantamab plus lazertinib ████ ████ ████ ███ ████ ██ ███████ In patients with no history of brain metastases, the median PFS was 27.5 months ████ ███ ████ ██ ███ ██████████ for amivantamab plus lazertinib and ████ ██████ ████ ███ ████ ██ █████ ███ ███████████, in favour of amivantamab plus lazertinib ████ ████ ████ ███ ████ ██ ███████.
PFS was not re-analyzed with data from the May 13, 2024, data cut-off, as the primary end point was met in the primary analysis of PFS (August 11, 2023, data cut-off).
Overall Survival
As of the August 11, 2023, data cut-off, with 214 deaths observed from the amivantamab plus lazertinib and osimertinib arms combined at the data cut-off, the interim analysis of OS was evaluated at a 2-sided significance level of 0.0050. There was a total of 97 (22.6%) deaths in the amivantamab plus lazertinib arm, and 117 (27.3%) deaths in the osimertinib arm. The median OS was not reached in either study arm as of the data cut-off (HR = 0.80; 95% CI, 0.61 to 1.05; P = 0.1099). The OS event-free probability between study arms for the proportion of patients who were alive at 6 months, 12 months, 18 months, and 24 months was █████ ████ ███ █████ ██ ██████ ████ ████ ███ █████ ██ ██████ ████ ████ ███ █████ ██ ██████ ███ ████ ████ ███ █████ ██ ███████ █████████████.
As of the May 13, 2024, data cut-off, there was ███ ██████ ███████ in the amivantamab plus lazertinib arm and ███ ██████ ███████ in the osimertinib arm. The median OS was not reached in the amivantamab plus lazertinib arm. The median OS was 37.32 months (95% CI, 32.53 months to not estimable) in the osimertinib arm, in favour of amivantamab plus lazertinib (HR = 0.77; 95% CI, 0.61 to 0.96; P = 0.0185). The OS event-free probability between study arms for the proportion of patients who were alive at 12 months, 24 months, and 36 months was ████ ████ ███ █████ ██ ██████ ████ ████ ███ █████ ██ ███████ ███ ████ ████ ███ ████ ██ ████████████████████.
Objective Response Rate
As of the August 11, 2023, data cut-off, a total of 336 patients (79.8%; 95% CI, 75.7% to 83.5%) in the amivantamab plus lazertinib arm and 314 patients (75.8%; 95% CI, 71.4% to 79.9%) in the osimertinib arm had an objective response (confirmed CR in 5.5% and 3.4% and confirmed PR in 74.3% and 72.5%, respectively). The OR for response when compared to the osimertinib arm was 1.27 (95% CI, 0.91 to 1.77).
As of the May 13, 2024, data cut-off, a total of ███ ████████ ██████ ████ ███ █████ ██ ███████ in the amivantamab plus lazertinib arm and ███ ████████ ██████ ████ ███ █████ ██ ███████ in the osimertinib arm had an objective response. The OR for response was ████ ████ ███ ████ ██ ██████.
Duration of Response
As of the August 11, 2023, data cut-off, there were 336 confirmed responders in the amivantamab plus lazertinib arm and 314 in the osimertinib arm. The median DOR in the amivantamab plus lazertinib arm was 25.76 months (95% CI, 20.14 months to not estimable), and in the osimertinib arm, the median DOR was 16.76 months (95% CI, 14.75 months to 18.53 months). The difference between study arms in the proportion of responders with DOR of 6 months, 12 months, 18 months, and 24 months was ████ ████ ███ █████ ██ ██████ █████ ████ ███ ████ ██ ███████ ████ ████ ███ █████ ██ ███████ ███ ████ ████ ███ █████ ██ ██████ █████████████.
As of the May 13, 2024, data cut-off, there were ███ confirmed responders in the amivantamab plus lazertinib arm and ███ in the osimertinib arm. The median DOR in the amivantamab plus lazertinib arm was 25.76 months (95% CI, 20.34 months to 33.87 months), and in the osimertinib arm, the median DOR was 18.14 months (95% CI, 14.78 months to 201.4 months). The difference between study arms in the proportion of responders with DOR of 12 months, 24 months, and 30 months was █████ ████ ███ ████ ██ ███████ █████ ████ ███ ████ ██ ███████ ███ ████ ████ ███ █████ ██ ██████ █████████████.
Table 16: Summary of Survival-Related Outcome Results From MARIPOSA (FAS) — August 11, 2023, Data Cut-Off
Variable | Amivantamab plus lazertinib n = 429 | Osimertinib n = 429 |
|---|---|---|
PFS by BICR: primary outcome | ||
Total events, n (%) | 192 (44.8) | 252 (58.7) |
Progressive disease | 148 (34.5) | 228 (53.1) |
Death without progressive disease | 44 (10.3) | 24 (5.6) |
Censored patients, n (%) | 237 (55.2) | 177 (41.3) |
Study cut-off | 210 (49.0) | 161 (37.5) |
Withdrawal of consent | 15 (3.5) | 8 (1.9) |
No progressive disease or death before ≥ 2 consecutively missing or unevaluable assessments | 11 (2.6) | 8 (1.9) |
Lost to follow-up | 1 (0.2) | 0 |
PFS (months), median (95% CI) | 23.72 (19.12 to 27.66) | 16.59 (14.78 to 18.46) |
HR (95% CI) versus osimertiniba | 0.70 (0.58 to 0.85) | |
P valueb | 0.0002 | |
Proportion (95% CI) of patients who were progression-free | ||
At 6 months | ███ █████ ████ | ███ █████ ████ |
Difference (95% CI) versus osimertinib | ███ ██████ ████ | |
At 12 months | ███ █████ ████ | ███ █████ ████ |
Difference (95% CI) versus osimertinib | ███ █████ █████ | |
At 18 months | ███ █████ ████ | ███ █████ ████ |
Survival difference (95% CI) versus osimertinib | ████ █████ █████ | |
At 24 months | ███ █████ ████ | ███ █████ ████ |
Survival difference (95% CI) versus osimertinib | ████ █████ █████ | |
OS: secondary outcome | ||
Deaths, n (%) | 97 (22.6) | 117 (27.3) |
Censored patients, n (%) | 332 (77.4) | 312 (72.7) |
OS (months), median (95% CI) | NE (NE to NE) | NE (NE to NE) |
HR (95% CI) versus osimertinib | 0.80 (0.61 to 1.05) | |
P value (2-sided significance level = 0.0050)b | 0.1099 | |
Proportion (95% CI) of patients who were alive | ||
At 6 months | ███ █████ ████ | ███ █████ ████ |
Survival difference (95% CI) versus osimertinib | ████ ██████ ████ | |
At 12 months | ███ █████ ████ | ███ █████ ████ |
Survival difference (95% CI) versus osimertinib | ███ ██████ ████ | |
At 18 months | ███ █████ ████ | ███ █████ ████ |
Survival difference (95% CI) versus osimertinib | ███ ██████ ████ | |
At 24 months | ███ █████ ████ | ███ █████ ████ |
Survival difference (95% CI) versus osimertinib | ███ ██████ █████ | |
ORR: secondary outcome | ||
Number of patients with measurable disease at baseline | 421 | 414 |
ORR (CR plus PR), n (%) | 336 (79.8) | 314 (75.8) |
95% CI for proportion | (75.7 to 83.5) | (71.4 to 79.9) |
Difference in proportion (95% CI) | 4.0 (–1.7 to 9.6) | |
OR (95% CI)c | 1.27 (0.91 to 1.77) | |
Best overall response, n (%) | ||
████████ ████████ | ██ █████ | ██ █████ |
███████ ████████ | ███ ██████ | ███ ██████ |
██████ ███████ | ██ ██████ | ██ ██████ |
███████████ ███████ | | █████ | ██ █████ |
███ █████████ | ██ █████ | ██ █████ |
DOR: secondary outcome | ||
Confirmed responders (CR plus confirmed PR) | 336 | 314 |
Median DOR | 25.76 (20.14 to NE) | 16.76 (14.75 to 18.53) |
≥ 6 months | 290 (86.3) | 267 (85.0) |
Difference in proportion (95% CI) | ███ ██████ ████ | |
≥ 12 months | 228 (67.9) | 181 (57.6) |
Difference in proportion (95% CI) | ████ █████ █████ | |
≥ 18 months | 115 (34.2) | 86 (27.4) |
Difference in proportion (95% CI) | ███ ██████ █████ | |
≥ 24 months | 34 (10.1) | 21 (6.7) |
Difference in proportion (95% CI) | ███ ██████ ███) | |
BICR = blinded independent central review; CI = confidence interval; CR = complete response; DOR = duration of response; FAS = full analysis set HR = hazard ratio; NE = not estimable; PR = partial response; OR = odds ratio; ORR = objective response rate; OS = overall survival; PFS = progression-free survival.
aHR is from a stratified proportional hazards model; HR < 1 favours amivantamab plus lazertinib.
bStatistical methods for this outcome were controlled for multiple comparisons.
cOR is from a stratified logistic regression model; OR > 1 favours amivantamab plus lazertinib.
Source: Details included in the table are from the sponsor’s summary of clinical evidence,44 the MARIPOSA Clinical Study Report (August 11, 2023, data cut-off),12 and additional information provided by the sponsor.14
HRQoL Outcomes
Details of the HRQoL outcomes as of the August 11, 2023, data cut-off are summarized in Table 17.
EORTC QLQ-C30 Global Health Status
██ ██ ███ ██████ ███ ████ ████ ███████ ███ ████ ████████ █████ ███████ ██████ ██████ ██████ █████ ███ █████ ██████ ███ █ ██████ ██ ███ ███████████ ████ ██████████ ████ ███ █████ ██████ ███ █ ██████ ██ ███ ███████████ ████ ██ █████ ███ ███ ██ ███ ██ ████ ██████ ████ ████████ ███ ███ ██████ ████ ███ ███ ██ ████ | | ████ ██ ███ ███████████ ████ ██████████ ███ ███ ████ ██████ ████ ███ ████ ██ █████ | | ████ ██ ███ ███████████ ████ ████████████ █ ██ ████ ██████████ ██ ███ ██████ ████ ███ ████ ██ ████ | | ████████ ██ █████ ███ ███ ██ ███ ██ ████ ██████ ████ ████████ ███ ███ ██████ ████ ███ ███ ██ ████ | | ████ ██ ███ ███████████ ████ ██████████ ███ ███ ███ ██████ ████ ███ ███ ██ ████ | | ████ ██ ███ ███████████ ████ ████████████ █ ██ ████ ██████████ ██ ████ ██████ ████ ███ ████ ██ ████ | | ████████ ██ █████ ███ ███ ██ ███ ██ ████ ██████ ████ ████████ ███ ███ ██████ ████ ███ ████ ██ ████ | | ███ ██ ███ ███████████ ████ ██████████ ███ ███ ███ ██████ ████ ███ ███ ██ ████ | | ███ ██ ███ ███████████ ████ ████████████ █ ██ ████ ██████████ ██ ████ ██████ ████ ███ ████ ██ ████ | | ████████
███████ ███ █████ ███████ ██████ ██████ ██████ ████ ███ ████████ ██ ███ ███ ███ ████ ████ ███████
NSCLC-SAQ Total Score
██ ██ ███ ██████ ███ ████ ████ ███████ ███ ████ ████████ █████████ █████ █████ ███ ████ ██████ ███ █ █████ ██ ███ ███████████ ████ ██████████ ████ ███ ████ ██████ ███ █ █████ ██ ███ ███████████ ████ ██ █████ ███ ███ ██ ███ ██ ████ ██████ ████ ████████ ███ ████ ██████ ████ ███ ████ ██ █████ | | ████ ██ ███ ███████████ ████ ██████████ ███ ███ ████ ██████ ████ ███ ████ ██ █████ | | ████ ██ ███ ███████████ ████ ████████████ █ ██ ████ ██████████ ██ ███ ██████ ████ ███ ████ ██ ████ | | ████████ ██ █████ ███ ███ ██ ███ ██ ████ ██████ ████ ████████ ███ ████ ██████ ████ ███ ████ ██ █████ | | ████ ██ ███ ███████████ ████ ██████████ ███ ███ ████ ██████ ████ ███ ████ ██ █████ | | ████ ██ ███ ███████████ ████ ████████████ █ ██ ████ ██████████ ██ ████ ████ ███ ████ ██ ████ | | ████████ ██ █████ ███ ███ ██ ███ ██ ████ ██████ ████ ████████ ███ ████ ██████ ████ ███ ████ ██ █████ | | ███ ██ ███ ███████████ ████ ██████████ ███ ███ ████ ██████ ████ ███ ████ ██ █████ | | ███ ██ ███ ███████████ ████ ████████████ █ ██ ████ ██████████ ██ ████ ████ ███ ████ ██ ████ | | ████████
███████ ███ █████████ █████ █████ ████ ███ ████████ ██ ███ ███ ███ ████ ████ ███████
Table 17: Summary of HRQoL Outcomes in MARIPOSA (FAS) — August 11, 2023, Data Cut-Off
Outcome | Amivantamab plus lazertinib n = 429 | Osimertinib n = 429 | |
|---|---|---|---|
EORTC QLQ-C30 Global Health Status | |||
Baseline score, mean (SD) | █████ ███████ | █████ ███████ | |
Change from baseline to cycle 13, day 1 | |||
Patients, n | ███ | ███ | |
LS mean (95% CI) | ███ █████ ████ | ███ █████ ████ | |
LS mean difference (95% CI) vs. osimertinib | ████ ██████ █████ | ||
P value vs. osimertinib | ██████ | ||
Change from baseline to cycle 21, day 1 | |||
Patients, n | ███ | ███ | |
LS mean (95% CI) | ███ █████ ████ | ███ █████ ████ | |
LS mean difference (95% CI) vs. osimertinib | ████ ██████ ████ | ||
P value vs. osimertinib | ██████ | ||
Change from baseline to cycle 27, day 1 | |||
Patients, n | ██ | ██ | |
Mean (95% CI) | ███ ██████ ████ | ███ █████ ████ | |
LS mean difference (95% CI) vs. osimertinib | ████ ██████ ████ | ||
P value vs. osimertinib | ██████ | ||
NSCLC-SAQ total score | |||
Baseline score, mean (SD) | ████ ██████ | ████ ██████ | |
Change from baseline to cycle 13, day 1 | |||
Patients, n | ███ | ███ | |
LS mean (95% CI) | ████ ██████ █████ | ████ ██████ █████ | |
LS mean difference (95% CI) vs. osimertinib | ███ ██████ ████ | ||
P value vs. osimertinib | ██████ | ||
Change from baseline to cycle 21, day 1 | |||
Patients, n | ███ | ███ | |
LS mean (95% CI) | ████ ██████ █████ | ████ ██████ █████ | |
LS mean difference (95% CI) vs. osimertinib | ████ ██████ ████ | ||
P value vs. osimertinib | ██████ | ||
Change from baseline to cycle 27, day 1 | |||
Patients, n | ██ | ██ | |
Mean (95% CI) | ████ ██████ █████ | ████ ██████ █████ | |
LS mean difference (95% CI) vs. osimertinib | ████ ██████ ████ | ||
P value vs. osimertinib | ██████ | ||
CI = confidence interval; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; FAS = full analysis set; HRQoL = health-related quality of life; LS = least squares; NSCLC-SAQ = Non–Small Cell Lung Cancer Symptom Assessment Questionnaire; SD = standard deviation; vs. = versus.
Source: Details included in the table are from the sponsor’s summary of clinical evidence44 and the MARIPOSA Clinical Study Report (August 11, 2023, data cut-off).12
Other Efficacy Outcomes
At the request of the sponsor, results for the secondary outcome of intracranial PFS, and exploratory outcomes of intracranial ORR, intracranial DOR, and time to intracranial progression were included (Table 25) to contextualize the specific needs of patients with CNS metastases owing to the associated morbidity and importance of CNS disease control.
Harms
Refer to Table 18 for harms data for amivantamab plus lazertinib and osimertinib. Harms were presented as of the August 11, 2023, data cut-off. Updated harms data were not available for the May 13, 2024, data cut-off. Harms from the lazertinib monotherapy arm were also reported to provide additional context into the harms associated with amivantamab.
Adverse Events
As of the August 11, 2023, data cut-off, all patients in the amivantamab plus lazertinib arm and lazertinib monotherapy arm, and 99.3% of patients in the osimertinib arm experienced an AE. In addition, 75.1% of patients in the amivantamab plus lazertinib arm, 42.8% in the osimertinib arm, and 45.5% in the lazertinib arm experienced an AE of grade 3 or higher. The most commonly reported AEs were ██████████ (68.4% in the amivantamab plus lazertinib arm, 28.3% in the osimertinib arm, and █████ in the lazertinib arm); infusion reactions (62.9% in the amivantamab plus lazertinib arm, 0% in the osimertinib arm, and ██ in the lazertinib arm); rash (61.8% in the amivantamab plus lazertinib arm, 30.6% in the osimertinib arm, and █████ in the lazertinib arm); hypoalbuminemia (48.5% in the amivantamab plus lazertinib arm, 6.1% in the osimertinib arm, and ████ in the lazertinib arm); increased alanine aminotransferase (36.1% in the amivantamab plus lazertinib arm, 13.3% in the osimertinib arm, and █████ in the lazertinib arm); and peripheral edema (35.6% in the amivantamab plus lazertinib arm, 5.6% in the osimertinib arm, and █████ in the lazertinib arm). These also represented numeric differences between the amivantamab plus lazertinib arm relative to the other 2 study arms.
Additional AEs which were reported in a numerically higher proportion of patients in the osimertinib arm relative to the other 2 study arms were diarrhea (44.4% in the osimertinib arm, 29.2% in the amivantamab plus lazertinib arm, and █████ in the lazertinib arm); leukopenia (15.4% in the osimertinib arm, 6.2% in the amivantamab plus lazertinib arm, and ████ in the lazertinib arm); and neutropenia (█████ in the osimertinib arm, ████ in the amivantamab plus lazertinib arm, and ████ in the lazertinib arm).
Serious Adverse Events
As of the August 11, 2023, data cut-off, a total of 48.7% of patients in the amivantamab plus lazertinib arm, 33.4% of patients in the osimertinib arm, and 35.2% of patients in the lazertinib arm reported SAEs. The most common SAEs (occurring in more than 1.5% of patients) which were also reported in numerically higher proportions in the amivantamab plus lazertinib arm relative to the osimertinib arm were pulmonary embolism (26 [6.2%] in the amivantamab plus lazertinib arm, 10 [2.3%] in the osimertinib arm, and | ██████ in the lazertinib arm); deep vein thrombosis (12 [2.9%] in the amivantamab plus lazertinib arm, 2 [0.5%] in the osimertinib arm, and ██████ in the lazertinib arm); IRRs (9 [2.1%] in the amivantamab plus lazertinib arm, and 0 in the osimertinib ███ ██████████ ████); respiratory failure (6 [1.4%] in the amivantamab plus lazertinib arm, 2 [0.5%] in the osimertinib arm, and ██████ in the lazertinib arm); and rash (7 [1.7%] in the amivantamab plus lazertinib arm, and 0 in the osimertinib ███ ██████████ ████).
Withdrawals Due to AEs
As of the August 11, 2023, data cut-off, a total of 34.9% of patients in the amivantamab plus lazertinib arm, 13.6% in the osimertinib arm, and █████ in the lazertinib arm had discontinued any study treatment due to AEs. The most common reason for study treatment discontinuation in the amivantamab plus lazertinib arm was ██████████ ███ ████████████ █████ ██ █████████; in the osimertinib arm the most common reason for discontinuation was ████████████ ████████ ███ ███████████ █████████ █████ ██ █████████.
Mortality
The proportion of patients who died was numerically similar across study arms (96 [22.8%] patients in the amivantamab plus lazertinib arm, 116 [27.1%] patients in the osimertinib arm, and ██ ███████ patients in the lazertinib arm). The most common reason for death was disease progression (11.6% of patients in the amivantamab plus lazertinib arm, 18.9% of patients in the osimertinib arm, and █████ of patients in the lazertinib arm), followed by AEs (9.3% of patients in the amivantamab plus lazertinib arm, 6.8% of patients in the osimertinib arm, and ████ of patients in the lazertinib arm).
Notable Harms
The AESIs of rash, IRR, and pneumonitis or interstitial lung disease were prospectively identified based on the safety profile of amivantamab, and VTE was added as an AESI during the conduct of the study. A numerically higher proportion of patients in the amivantamab plus lazertinib arm reported rash (88.6% versus 49.1% in the osimertinib arm and █████ in the lazertinib arm), IRR (62.9% versus 0 in the osimertinib ███ ██████████ ████), and VTE (37.3% versus 9.1% in the osimertinib arm and █████ in the lazertinib arm). A total of 3.1% of patients in the amivantamab plus lazertinib arm, 3.0% of patients in the osimertinib arm, and ████ of patients in the lazertinib arm reported pneumonitis or interstitial lung disease.
Table 18: Summary of Harms Results From MARIPOSA (SAS) — August 11, 2023, Data Cut-Off
AEs | Amivantamab plus lazertinib n = 421 | Osimertinib n = 428 | Lazertinib n = 213 |
|---|---|---|---|
Most common AEs (incidence ≥ 10% in any treatment group), n (%) | |||
≥ 1 AE | 421 (100.0) | 425 (99.3) | ███ ███████ |
≥ 1 grade 3 or higher AE | 316 (75.1) | 183 (42.8) | ██ ██████ |
Skin and subcutaneous tissue disorders | ███ ██████ | ███ ██████ | ███ ██████ |
Rash | 260 (61.8) | 131 (30.6) | ██ ██████ |
Dermatitis acneiform | 122 (29.0) | 55 (12.9) | ██ ██████ |
Pruritus | 99 (23.5) | 73 (17.1) | ██ ██████ |
Dry skin | 67 (15.9) | 60 (14.0) | ██ ██████ |
Alopecia | ██ █████ | ██ █████ | ██ ██████ |
Infections and infestations | ███ ██████ | ███ ██████ | ███ ██████ |
Paronychia | 288 (68.4) | 121 (28.3) | ██ ██████ |
COVID-19 | 111 (26.4) | 103 (24.1) | ██ ██████ |
Conjunctivitis | 46 (10.9) | 7 (1.6) | | █████ |
Upper respiratory tract infection | ██ █████ | ██ ██████ | ██ █████ |
Gastrointestinal disorders | ███ ██████ | ███ ██████ | ███ ██████ |
Constipation | 123 (29.2) | 55 (12.9) | ██ ██████ |
Diarrhea | 123 (29.2) | 190 (44.4) | ██ ██████ |
Stomatitis | 122 (29.0) | 90 (21.0) | ██ ██████ |
Nausea | 90 (21.4) | 58 (13.6) | ██ ██████ |
Vomiting | 52 (12.4) | 23 (5.4) | ██ ██████ |
General disorders and administration site conditions | ███ ██████ | ███ ██████ | ███ ██████ |
Edema peripheral | ███ ██████ | ██ █████ | ██ ██████ |
Asthenia | 78 (18.5) | 46 (10.7) | ██ ██████ |
Fatigue | 70 (16.6) | 42 (9.8) | ██ ██████ |
Pyrexia | 51 (12.1) | 37 (8.6) | ██ █████ |
Mucosal inflammation | ██ ██████ | ██ █████ | | █████ |
Metabolism and nutrition disorders | ███ ██████ | ███ ██████ | ██ ██████ |
Hypoalbuminemia | 204 (48.5) | 26 (6.1) | ██ █████ |
Decreased appetite | 103 (24.5) | 76 (17.8) | ██ ██████ |
Hypercalcemia | 88 (20.9) | 35 (8.2) | ██ █████ |
Hypokalemia | ██ ██████ | ██ █████ | ██ █████ |
Hyponatremia | ██ █████ | ██ █████ | ██ ██████ |
Injury, poisoning, and procedural complications | ███ ██████ | ██ █████ | ██ ██████ |
Infusion-related reaction | 265 (62.9) | 0 (0) | | ███ |
Investigations | ███ ██████ | ███ ██████ | ███ ██████ |
Alanine aminotransferase increased | 152 (36.1) | 57 (13.3) | ██ ██████ |
Aspartate aminotransferase increased | 121 (28.7) | 58 (13.6) | ██ ██████ |
Gamma-glutamyl transferase increased | 61 (14.5) | 31 (7.2) | ██ █████ |
Blood alkaline phosphatase increased | 52 (12.4) | 22 (5.1) | ██ █████ |
Blood lactate dehydrogenase increased | ██ ██████ | ██ █████ | ██ █████ |
Blood creatinine increased | ██ █████ | ██ ██████ | ██ ██████ |
Respiratory, thoracic, and mediastinal disorders | ███ ██████ | ███ ██████ | ███ ██████ |
Pulmonary embolism | 73 (17.3) | 20 (4.7) | ██ █████ |
Cough | 65 (15.4) | 88 (20.6) | ██ ██████ |
Dyspnea | 51 (12.1) | 68 (15.9) | ██ ██████ |
Nervous system disorders | ███ ██████ | ███ ██████ | ███ ██████ |
Paresthesia | ██ ██████ | ██ █████ | ██ ██████ |
Headache | ██ ██████ | ██ ██████ | ██ ██████ |
Dizziness | ██ ██████ | ██ █████ | ██ █████ |
Peripheral neuropathy | ██ █████ | | █████ | ██ ██████ |
Musculoskeletal and connective tissue disorders | ███ ██████ | ███ ██████ | ███ ██████ |
Muscle spasms | 70 (16.6) | 32 (7.5) | ██ ██████ |
Pain in extremity | 64 (15.2) | 22 (5.1) | ██ █████ |
Myalgia | 53 (12.6) | 19 (4.4) | ██ █████ |
Back pain | ██ ██████ | ██ ██████ | ██ ██████ |
Arthralgia | ██ █████ | ██ ██████ | ██ ██████ |
Blood and lymphatic system disorders | ███ ██████ | ███ ██████ | ██ ██████ |
Anemia | 96 (22.8) | 91 (21.3) | ██ ██████ |
Thrombocytopenia | 66 (15.7) | 84 (19.6) | ██ █████ |
Leukopenia | 26 (6.2) | 66 (15.4) | ██ █████ |
Neutropenia | ██ █████ | ██ ██████ | | █████ |
Vascular disorders | ███ ██████ | ██ ██████ | ██ ██████ |
Deep vein thrombosis | 61 (14.5) | 11 (2.6) | | █████ |
Psychiatric disorders | ██ ██████ | ██ ██████ | ██ ██████ |
Insomnia | 41 (9.7) | 48 (11.2) | ██ █████ |
SAEs, n (%) | |||
Patients with ≥ 1 SAE | 205 (48.7) | 143 (33.4) | ██ ██████ |
Respiratory, thoracic, and mediastinal disorders | ██ ██████ | ██ ██████ | ██ █████ |
Pulmonary embolism | 26 (6.2) | 10 (2.3) | | █████ |
Pleural effusion | 9 (2.1) | 17 (4.0) | | █████ |
Pneumonitis | 7 (1.7) | 8 (1.9) | | █████ |
Respiratory failure | 6 (1.4) | 2 (0.5) | | █████ |
Interstitial lung disease | 5 (1.2) | 5 (1.2) | | █████ |
Dyspnea | 4 (1.0) | 11 (2.6) | | █████ |
Infections and infestations | ██ ██████ | ██ █████ | ██ █████ |
Pneumonia | 17 (4.0) | 21 (4.9) | | █████ |
COVID-19 | 10 (2.4) | 10 (2.3) | | █████ |
Injury, poisoning, and procedural complications | ██ █████ | | █████ | | █████ |
Infusion-related reaction | 9 (2.1) | 0 (0.0) | | ███ |
Vascular disorders | ██ █████ | | █████ | | █████ |
Deep vein thrombosis | 12 (2.9) | 2 (0.5) | | █████ |
Venous thrombosis limb | | █████ | | █████ | | █████ |
Metabolism and nutrition disorders | ██ █████ | | █████ | | █████ |
Hypoalbuminemia | 5 (1.2) | 0 (0.0) | | ███ |
Hyponatremia | 5 (1.2) | 4 (0.9) | | ███ |
Cardiac disorders | ██ █████ | ██ █████ | | █████ |
Pericardial effusion | 4 (1.0) | 5 (1.2) | | █████ |
Cardiac failure | 1 (0.2) | 5 (1.2) | | █████ |
Investigations | ██ █████ | | █████ | | █████ |
Alanine aminotransferase increased | 8 (1.9) | 6 (1.4) | | █████ |
Aspartate aminotransferase increased | | █████ | | █████ | | █████ |
Skin and subcutaneous tissue disorders | ██ █████ | | █████ | | ███ |
Rash | 7 (1.7) | 0 (0.0) | | ███ |
Patients who stopped treatment due to AEs, n (%) | |||
Dose interruption of any study treatment | 350 (83.1) | 165 (38.6) | ██ ██████ |
Interruption of amivantamab | 328 (77.9) | NA | ██ |
Dose reduction of any study treatment | 249 (59.1) | 23 (5.4) | ██ ██████ |
Reduction of amivantamab | 193 (45.8) | NA | ██ |
Discontinuation of any study treatment | 147 (34.9) | 58 (13.6) | ██ ██████ |
Discontinuation of amivantamab | 145 (34.4) | NA | ██ |
Discontinuation of all study treatments | 86 (20.4) | 50 (11.7) | ██ ██████ |
Reasons for discontinuation, n (%) | |||
Infections and infestations | ██ █████ | ██ █████ | | █████ |
Paronychia | 14 (3.3) | 0 (0.0) | | █████ |
Pneumonia | 8 (1.9) | 3 (0.7) | | █████ |
Respiratory, thoracic, and mediastinal disorders | ██ █████ | ██ █████ | ██ █████ |
Pulmonary embolism | 8 (1.9) | 2 (0.5) | | █████ |
Pneumonitis | 7 (1.7) | 7 (1.6) | | █████ |
Interstitial lung disease | 5 (1.2) | 4 (0.9) | | █████ |
Skin and subcutaneous tissue disorders | ██ █████ | | █████ | | █████ |
Rash | 11 (2.6) | 0 (0.0) | | █████ |
Dermatitis acneiform | 6 (1.4) | 0 (0.0) | | █████ |
General disorders and administration site conditions | ██ █████ | | █████ | | █████ |
Asthenia | 5 (1.2) | 1 (0.2) | | ███ |
Edema peripheral | | █████ | | █████ | | ███ |
Injury, poisoning, and procedural complications | 21 (5.0) | 1 (0.2) | | ███ |
Infusion-related reaction | 19 (4.5) | 0 (0.0) | | ███ |
Metabolism and nutrition disorders | 9 (2.1) | 3 (0.7) | | ███ |
Hypoalbuminemia | 6 (1.4) | 0 (0.0) | | ███ |
Deaths, n (%) | |||
Patients who died during study | ██ ██████ | ███ ██████ | ██ ██████ |
Progressive disease | ██ ██████ | ██ ██████ | ██ ██████ |
AE | ██ █████ | ██ █████ | ██ █████ |
Other | | █████ | | █████ | | █████ |
AESIs, n (%)a | |||
Rash | 373 (88.6) | 210 (49.1) | ███ ██████ |
Infusion-related reaction | 265 (62.9) | 0 (0.0) | | ███ |
VTE | 157 (37.3) | 39 (9.1) | ██ ██████ |
Pneumonitis and/or interstitial lung disease | 13 (3.1) | 13 (3.0) | | █████ |
AE = adverse event; AESI = adverse event of special interest; SAE = serious adverse event; NA = not applicable; SAS = safety analysis set; VTE = venous thromboembolism.
aAESIs of rash, infusion-related reaction, and pneumonitis and/or interstitial lung disease were prospectively identified based on the safety profile of amivantamab. VTE was added as an AESI during the conduct of the study.
Source: Details included in the table are from the sponsor’s summary of clinical evidence44 and the MARIPOSA Clinical Study Report (August 11, 2023, data cut-off).12
Critical Appraisal
Internal Validity
The design of the MARIPOSA study is subject to some limitations. The amivantamab plus lazertinib arm was open label, which would impact the assessment of HRQoL outcomes due to participants knowing that they were receiving treatment with amivantamab plus lazertinib. It is also possible that patients randomized to the osimertinib or lazertinib monotherapy arms, while double-blinded, would also be aware that they were not receiving amivantamab plus lazertinib because amivantamab is an IV infusion and there was no matching placebo IV. In addition, the study protocol was amended several times after patient enrolment started, including the addition of AESIs and updating the inclusion and exclusion criteria, and therefore there is an unknown risk of bias due to these changes, and it is unknown how many patients were impacted. Randomization methods were likely at low risk of bias due to being centrally conducted, and ascertainment of the PFS, OS, ORR, and DOR outcomes was also likely at low risk of bias due to being assessed by BICR. Results of sensitivity analyses for PFS assessed by the investigator showed broadly similar results to the BICR analysis; thus, the conclusions of the analyses based on HR were the same. Allocation concealment to either the osimertinib or lazertinib arm was also adequate and at low risk of bias. In addition, according to the clinical experts consulted for the review, the frequency of clinical assessments was similar to the frequency of assessments in clinical practice.
The statistical methods of the MARIPOSA study were also subject to some limitations. In general, the stratification factors used during randomization and other potential prognostic factors identified by the experts such as age, smoking status, ECOG status, and sex were balanced between study arms. However, the OS results of the study were based on an interim analysis, thus there is a risk of overestimating the true treatment effect. The median OS and DOR were not estimable at the time of the prespecified data cut-off. While data with longer-term follow-up were provided for OS, ORR, and DOR, this did not represent a prespecified data cut-off and should be considered exploratory. The median OS was not reached in either the August or May data cut-offs. As of the August 11, 2023, data cut-off, (median follow-up of 22.01 months) a total of 25% of OS events had occurred across both study arms but as of the May 13, 2024, data cut-off, a total of ███ of OS events had occurred, suggesting that the data are largely immature for OS. The 75th percentile for the DOR result was likewise not estimable at the May 2024 data cut-off, suggesting the data are immature for this outcome as well. The long-term results associated with amivantamab plus lazertinib are therefore unclear for OS and DOR. In addition to this, ORR and DOR were not controlled for multiple comparisons and are only considered supportive of the overall effect of amivantamab and lazertinib.
The HRQoL end points were secondary in the MARIPOSA study and results were not adjusted for multiple comparisons; therefore, there is an increased risk of type I error, and these end points can only be considered supportive. HRQoL estimates had a substantial amount of missing data (| | ███ █████ in the amivantamab plus lazertinib arm and | | ███ █████ in the osimertinib arm at cycle 13, day 1; | | ███ █████ in the amivantamab plus lazertinib arm and | ████ █████ in the osimertinib arm at cycle 21, day 1; | | ██ █████ in the amivantamab plus lazertinib arm and | | ██ █████ in the osimertinib arm at cycle 27, days 1). Both measures were modelled using a MMRM model, which assumes the data are missing at random. However, the nature of the disease means that, because patients are censored at disease progression or death, among other reasons, it is likely that patients who remained on study are systematically different from patients who did not provide data, and there is a likelihood of bias in the results. While the NSCLC-SAQ analysis required that all 5 domains be complete to compute a total score, EORTC QLQ-C30 did not report any methods to account for missing responses, which also may impart a bias of unknown direction and degree.
External Validity
Per the clinical experts consulted for this review, the study inclusion and exclusion criteria and baseline characteristics were broadly representative of the patients in Canadian clinical practice settings, apart from the fact that the clinical experts noted the racial breakdown in the MARIPOSA study had a greater proportion of patients of Asian descent than may be seen in Canadian clinical practice. However, they noted that the MARIPOSA study limited enrolment to ECOG status 0 or 1, and patients with ECOG status of 2 or greater may be considered for this therapy. In addition, patients with a history of adjuvant therapy were enrolled if therapy was more than 12 months prior; the experts noted that if the treatment received in the adjuvant or neoadjuvant setting was a non-EGFR inhibitor (e.g., cytotoxic chemotherapy), then a period of 6 months could be considered. They also noted that patients who had any prior experience with TKIs were excluded, which might preclude patients from receiving amivantamab plus lazertinib who had received osimertinib in the adjuvant setting given its use for earlier-stage NSCLC in Canada. The clinical experts estimated this might affect approximately 10% or 15% of patients. Results of the trial would therefore not be generalizable to these patients. In addition, the median follow-up at the time of the May 13, 2024, data cut-off was approximately 31 months; however, the trial is still ongoing and longer-term results on efficacy and harms are not available and it is uncertain whether the results are generalizable to a longer treatment duration.
GRADE Summary of Findings and Certainty of the Evidence
Methods for Assessing the Certainty of the Evidence
For pivotal studies and RCTs identified in the sponsor’s systematic review, GRADE was used to assess the certainty of the evidence for outcomes considered most relevant to inform expert committee deliberations, and a final certainty rating was determined as outlined by the GRADE Working Group:58,59
High certainty: We are very confident that the true effect lies close to that of the estimate of the effect.
Moderate certainty: We are moderately confident in the effect estimate — the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. We use the word “likely” for evidence of moderate certainty (e.g., “X intervention likely results in Y outcome”).
Low certainty: Our confidence in the effect estimate is limited — the true effect may be substantially different from the estimate of the effect. We use the word “may” for evidence of low certainty (e.g., “X intervention may result in Y outcome”).
Very low certainty: We have very little confidence in the effect estimate — the true effect is likely to be substantially different from the estimate of effect. We describe evidence of very low certainty as “very uncertain.”
Following the GRADE approach, evidence from RCTs started as high-certainty evidence and could be rated down for concerns related to study limitations (which refers to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias.
When possible, certainty was rated in the context of the presence of an important (nontrivial) treatment effect; if this was not possible, certainty was rated in the context of the presence of any treatment effect (i.e., the clinical importance is unclear). In all cases, the target of the certainty of evidence assessment was based on the point estimate and where it was located relative to the threshold for a clinically important effect (when a threshold was available) or to the null. For PFS and OS, the target of the assessment was the presence or absence of an important effect based on thresholds provided by the clinical expert. For HRQoL outcomes, the target of the assessment was the presence or absence of an important effect based on thresholds provided by the sponsor.
Results of GRADE Assessments
Table 2 presents the GRADE summary of findings for amivantamab plus lazertinib versus osimertinib.
Long-Term Extension Studies
No long-term extension studies were included in the submission.
Indirect Evidence
Contents within this section have been informed by materials submitted by the sponsor. The following have been summarized and validated by the review team.
Objectives for the Summary of Indirect Evidence
The MARIPOSA study compared amivantamab plus lazertinib with osimertinib monotherapy; however, there was no other head-to-head trial that assessed the relative effectiveness and safety of amivantamab plus lazertinib compared to other potentially relevant first-line treatment options. In addition, results from the indirect evidence were incorporated into the pharmacoeconomic model, meriting a review of the indirect evidence.
Description of Indirect Comparisons
The body of indirect evidence consisted of 5 NMAs informed by a SLR.
NMA Design
Objectives
The objective of the indirect evidence provided in the submission was to determine the comparative effectiveness and safety of amivantamab plus lazertinib versus other potentially relevant first-line treatments in advanced or metastatic NSCLC with common EGFR mutations.
Study Selection Methods
Details of the study selection criteria are in Table 19. In summary, a SLR was conducted in May 2020 and updated in July 2022 searching for therapeutic or palliative options for patients with metastatic or surgically unresectable common EGFR-mutated NSCLC; the common EGFR mutations included exon 21 L858R substitutions and exon 19 deletions, T790M in exon 20, and C797S in exon 20.
Table 19: Study Selection Criteria and Methods for the NMAs
Characteristics | Indirect comparison |
|---|---|
Population | Adult (aged ≥ 18 years) patients with metastatic or surgically unresectable common EGFR-mutated NSCLC, specifically:
Patients aged < 18 years, with lung cancer not otherwise specified, without metastatic or unresectable NSCLC or studies where the outcome was not presented for the population of interest, or studies including only stage IIIA or stage IIII without including stage IV were excluded. |
Intervention | Any therapeutic or palliative intervention administered within the health care system, first-line or later than first-line treatment settinga |
Comparator |
|
Outcome |
|
Study designs | RCTs |
Publication characteristics |
|
Exclusion criteria |
|
Databases searched | Electronic databases, conference proceedings, clinical trial registries, and bibliographies of published SLRs and meta-analyses |
Selection process | Studies were screened by 2 independent reviewers at both the title and abstract and full text review stages. Discrepancies resolved through discussion or adjudication by a third reviewer |
Data extraction process | Data extraction was conducted by 1 reviewer and checked by a second independent reviewer, with discrepancies resolved through discussion or adjudication by a third reviewer |
Quality assessment | Study quality assessment, using the York Centre for Reviews and Dissemination tool, was conducted by 1 reviewer and checked by a second independent reviewer, with discrepancies resolved through discussion or adjudication by a third reviewer |
AE = adverse event; AESI = adverse event of special interest; CBR = clinical benefit rate; DFS = disease-free survival; DOR = duration of response; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; HRQoL = health-related quality of life; NMA = network meta-analysis; NSCLC = non–small cell lung cancer; NSCLS-SAQ = Non–Small Cell Lung Cancer Symptom Assessment Questionnaire; OECD = Organisation for Economic Co-operation and Development; ORR = overall response rate; OS = overall survival; PFS = progression-free survival; PFS2 = time to second progression; PGIC = Patient Global Impression of Change scale; PGIS = Patient Global Impression of Severity; PRO = patient-reported outcome; PROMIS-PF = Patient-Reported Outcomes Measurement Information System–Physical Function; RCT = randomized controlled or clinical trial; RFS = relapse or recurrence-free survival; SAE = serious adverse event; SF-36 = Short Form (36) Health Survey; SLR = systematic literature review; SOC = standard of care; TKI = tyrosine kinase inhibitor; TTNT = time to next treatment; WDAE = withdrawal due to adverse event.
aThe “first-line or later” setting was defined as studies where it could be confirmed that at least some patients were treatment-naive at study entry, but that other patients may have previously received treatment.
Source: Details included in the table are from the sponsor’s summary of clinical evidence44 and the NMA Technical Report.60
NMA Analysis Methods
On completion of the SLR, the feasibility of conducting NMAs to compare amivantamab plus lazertinib with key comparators was assessed. The feasibility assessment appraised studies on the following factors:
their alignment with the prespecified scope (as described in the SLR in Table 19)
similarity of patient characteristics
similarity of study characteristics
reported outcome measures
data availability and network connectivity.
All interventions were considered either as monotherapy or in combination with others, unless the combination was deemed not of interest. Exclusions on the basis of interventions were initially made considering network connectivity. Interventions that had come onto the market but were discontinued or interventions deemed unlikely to come to market were excluded. The submission therefore included first-generation TKIs (erlotinib, gefitinib, icotinib), second-generation TKIs (afatinib, dacomitinib), third-generation TKIs (osimertinib, lazertinib, aumolertinib, furmonertinib), chemotherapy, and monoclonal antibodies (bevacizumab, ramucirumab, cetuximab, and amivantamab). The clinical experts consulted for this review highlighted osimertinib and osimertinib plus chemotherapy as relevant comparators in Canada, and a deviation request to exclude first-generation and second-generation EGFR TKIs (afatanib, erlotinib, gefitinib) and platinum-based chemotherapy was accepted by CDA-AMC. Results from the comparison to osimertinib monotherapy and osimertinib plus chemotherapy were therefore included in the review. Though other treatments were included in the network, they were not considered appropriate or relevant comparators, thus, results for them were not reported.
Treatment effect modifiers were identified by the sponsor during the feasibility assessment based on the available baseline characteristics (supplemented by searching ClinicalTrials.gov), through reference to published literature or treatment appraisals, and discussion with experts. The feasibility assessment identified the following factors as treatment effect modifiers:
ECOG Performance Status, specifically the proportion of patients with ECOG Performance Status of 2
cancer histology
presence of brain metastases
race/ethnicity
specific common EGFR mutations.
Age, sex, and smoking status were also identified as potentially important prognostic indicators.
During construction of the network, erlotinib and gefitinib were combined into a single node and considered to be equivalent based on the FLAURA trial, which included osimertinib as a comparator but whose control group included patients tested with either erolotinib or gefitinib at the investigator’s discretion. All studies which investigated only erlotinib or gefitinib were excluded based on this decision to combine and also due to clinical evidence suggesting similar treatment effects.61
Full details of the NMA analysis methods are presented in Table 20.
Table 20: NMA Analysis Methods
Methods | Description |
|---|---|
Analysis methods | NMAs using Bayesian Markov Chain Monte-Carlo simulations, where the first 50,000 simulations (run-in or burn-in samples) were discarded, and the succeeding 50,000 simulations (posterior samples) were used for parameter estimation. The primary analyses included all eligible studies that were balanced for treatment effect modifiers. |
Priors | Noninformative priors were used for the baseline effects and treatment effects. In RE models, a uniform (0,1) distribution was used for the between-study standard deviation. |
Assessment of model fit |
|
Assessment of consistency | Network diagrams were investigated for presence of loops of evidence |
Assessment of convergence |
|
Outcomes | OS, PFS, ORR, AEs, and SAEs |
Follow-up time points | Comparator data reported at the first available data cut-off were prioritized to align with the follow-up time of 22 months from the MARIPOSA study |
Construction of nodes | The network connectivity of all included RCTs was checked and illustrated using a network plot, where each node represented a treatment regimen included in the network and lines represented direct comparisons between nodes. A plot was produced for each outcome assessed. |
Sensitivity analyses |
|
Subgroup analysis | None reported |
Methods for pairwise meta-analysis | Not reported |
AE = adverse event; BGR = Brooks-Gelman-Rubin; DIC = deviance information criterion; NMA = network meta-analysis; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; RCT = randomized controlled trial; RE = random effects; SAE = serious adverse event.
Source: Details included in the table are from the sponsor’s summary of clinical evidence.44
Results of NMA
Summary of Included Studies
███ ███ ██████████ ██ ███████ █████ ████████ ██ ████████ ██ █ ██████████ ██ ███████████████ ███████ ███ █████ ████████ ████ ██ ███ ██████ ████ █████████ ███ ██ █████ █████████ █ ██████ ████ ██████████ ██ ███ ██ █████ ████████ █ ██████ ████ █████████ ████ █████ █████ ███ ██████████ ██ ████████ ██████ ███ ███ ██████████████ ██ █████ █████ ████ ████████ ████████ █████ ██ ████ █████ ████ ████████ ██ ███ ███████████ ███████████ ███ ███ ████ ██████ ███████ ███ █████████ ██████ ███ ███████████ ██████████ ████ ███ █████████ ██ ████████████ ██ ████████ ██████ ███ ███ ███████ █████████ ███████ ███ ████████ ██ ███ ████████ ████████ ████████ ██ ███ ███████ █ ██████ ███████ ██████████ ██ █ ██ █████████ ███ ████ ██████ █ ████████ ██ ████████ ████ ██████ ████ ████████ ███ ███ █████████████ ███ ███ ██████████ ██ ████ ██████ ██ █ ██ █████████ █ █████ ██ ██ ███████ ████ ████████ ██████ ███ ███████████ ███████████ ███████ ██ ███████ ██ ███ ██████████ ███████ ███ █ █████ ██ ███ ███████████████ ███████ ██ ██ ████████ ██ ███ █████
A summary of key characteristics of the included studies is presented in Table 21, and a summary of the homogeneity assessment for the NMA is presented in Table 22.
Table 21: Summary of Relevant Studies From the NMA
Characteristic | MARIPOSA (amivantamab plus lazertinib) | FLAURA (osimertinib monotherapy) | FLAURA2a (osimertinib plus chemotherapy) |
|---|---|---|---|
Study characteristics |
|
|
|
Population key inclusion criteria |
|
|
|
Intervention |
|
|
|
Comparator |
|
|
|
Outcomes of interest |
|
|
|
Frequency of outcome assessment |
|
|
|
Duration of follow-up |
|
|
|
Key baseline characteristics (treatment arm) |
|
|
|
AE = adverse event; AUC5 = area under the curve 5 mg/mL; BICR = blinded independent central review; CNS = central nervous system; DOR = duration of response; ECOG = Eastern Cooperative Oncology Group; NMA = network meta-analysis; NR = not reported; NSCLC = non–small cell lung cancer; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; PS = performance status; q.3.w. = every 3 weeks; q.6.w. = every 6 weeks; q.8.w. = every 8 weeks; q.12.w. = every 12 weeks; RCT = randomized controlled trial; RECIST = Response Evaluation Criteria in Solid Tumours; SAE = serious adverse event; SD = standard deviation; SLR = systematic literature review; TKI = tyrosine kinase inhibitor; vs. = versus.
aThe sponsor’s NMA Technical Report included the conference abstract for the FLAURA2 study for the homogeneity assessment, and updated data from the first data cut-off in the NMA. Baseline characteristics and other study characteristics were obtained from the full publication (the Planchard et al. study).
Source: Details included in the table are from the sponsor’s summary of clinical evidence,44 the FLAURA trial (interim analysis publication cited in the NMA Technical Report),62 and the FLAURA2 trial.16
A summary of the homogeneity assessment for the 3 studies in the NMA is presented in Table 22. Briefly, some heterogeneity was noted in the 3 studies for the frequency of disease assessments, duration of follow-up, study design, potential prognostic indicators such as brain or CNS metastases, and unknown heterogeneity due to certain information not being reported such as proportion of smokers and the time since lung cancer diagnosis.
Table 22: Assessment of Homogeneity for the NMAs
Characteristics | Description and handling of potential effect modifiers |
|---|---|
Disease severity |
|
Treatment history | Treatment history requirements were generally similar. All 3 studies reported in the first-line setting and required patients be treatment-naive (with some exceptions for adjuvant chemotherapy > 12 months previously). |
Trial eligibility criteria | Trial eligibility criteria were generally similar. All 3 trials enrolled adult patients with newly diagnosed, locally advanced or metastatic NSCLC with exon 19 deletions or exon 21 L858R mutations. The FLAURA and FLAURA2 studies permitted this to be co-occurring with other EGFR mutations. The MARIPOSA study did not specify. |
Dosing of comparators | Osimertinib was dosed similarly across the 3 studies. |
Placebo response | Not reported. |
Definitions of end points | Standardized end points were used (PFS, OS, AEs). The submission noted that the definition of an SAE varied moderately between studies, but was still able to be compared in a single network. The proportional hazards assumption for PFS and OS were assessed using a preliminary visual assessment of Kaplan-Meier plots. |
Timing of end point evaluation | Some heterogeneity was noted in the frequency of disease assessments between studies. The disease assessments in the FLAURA study occurred at baseline, q.6.w. (± 1 week) for 18 months, then q.12.w. (± 1 week) until disease progression. Disease assessments in the MARIPOSA study occurred at q.8.w. (± 1 week) for the first 30 months followed by q.12.w. (± 1 week) thereafter. Disease assessments in the FLAURA2 study occurred at baseline, week 6, week 12, then q.12.w. until disease progression. Some heterogeneity was noted in the duration of follow-up in the studies at the time of the SLR and time of NMA analysis. The FLAURA study’s median duration of follow-up was 16.2 months (range, 0.1 months to 27.4 months) for patients receiving osimertinib and 11.5 months (range, 0 months to 26.2 months) for patients receiving erlotinib or gefitinib. The MARIPOSA study’s median duration of follow-up was 22.01 months (amivantamab plus lazertinib arm = 22.21 months; osimertinib arm = 21.98 months; and lazertinib arm = 21.88 months). The FLAURA2 study’s median duration of follow-up was 22.3 months in the osimertinib plus chemotherapy group and 19.3 months in the osimertinib group. |
Withdrawal frequency | Not reported |
Clinical trial setting | Not reported |
Study design | Heterogeneity was noted between the 3 relevant studies. The FLAURA study was double-blinded in both treatment arms, the MARIPOSA study had 1 open-label arm plus 2 double-blind arms, and the FLAURA2 study was open label in both treatment arms. |
AE = adverse event; CNS = central nervous system; NMA = network meta-analysis; NSCLC = non–small cell lung cancer; OS = overall survival; PFS = progression-free survival; q.6.w. = every 6 weeks; q.8.w. = every 8 weeks; q.12.w. = every 12 weeks; SAE = serious adverse event; SLR = systematic literature review.
Source: Details included in the table are from the sponsor’s summary of clinical evidence,44 the sponsor’s NMA Technical Report.60, the FLAURA trial (interim analysis publication cited in the NMA Technical Report),62 and the FLAURA2 trial.16
Results
The results of the comparators included in the appraisal are presented in Table 23. Briefly, the results of the NMAs show there was insufficient evidence to detect a difference between amivantamab plus lazertinib and osimertinib for OS, ORR, all AEs, and all SAEs. Amivantamab plus lazertinib was favoured over osimertinib for PFS, and osimertinib was favoured over amivantamab plus lazertinib for all SAEs. There was insufficient evidence to detect a difference between amivantamab plus lazertinib and osimertinib plus chemotherapy for OS, PFS, all AEs, and all SAEs; amivantamab plus lazertinib was favoured for ORR.
Table 23: NMA Results — Primary Base-Case Analysis
Detail | OS HR (95% CrI) | PFS HR (95% CrI) | ORR OR (95% CrI) | All AEs OR (95% CrI) | All SAEs OR (95% CrI) |
|---|---|---|---|---|---|
Number of studies (patients), N | ███████ ████ | ███████ ████ | ██████ ████ | ██████ ████ | ██████ ████ |
Model | █████ ██████ | █████ ██████ | ████ █████ | ████ █████ | ████ █████ |
Amivantamab plus lazertinib versus comparator | |||||
██████████ | ████ ██████ █████ | ████ ██████ █████ | █████████ | ███ █████ ██████ | ███ █████████ |
████████ █ ██████████ | ████ ██████ █████ | ████ ██████ █████ | █████████ | ███ █████ █████ | ███ █████ ████ |
AE = adverse event; CrI = credible interval; HR = hazard ratio; NMA = network meta-analysis; NR = not reported; OR = odds ratio; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; SAE = serious adverse event.
Source: Details included in the figure are from the sponsor’s NMA Technical Report.60
Critical Appraisal of NMAs
The indirect evidence consisted of 5 NMAs informed by an SLR. Generally speaking, the SLR covered a relevant study population including the EGFR mutations of interest to the review, along with outcomes of interest to the review. While the SLR had a protocol and used generally accepted methods for searching, screening, quality assessment, and data extraction, the SLR was conducted in 2022 and therefore it is not known whether the most recent publications on other relevant comparators (or OS updates to publications) would have been captured in the search. For example, the NMA Technical Report did not include the most recent publications of some studies, such as the final OS follow-up from the FLAURA study. In addition to this, while the study exclusion list and reasons for exclusion were provided, ██ studies were excluded on the basis of not having an intervention of interest or useful connection; these terms were not defined in the report and it is not known whether the criteria for a “useful connection” might bias the NMA network. Furthermore, while the steps for the quality assessment were provided, the results of the quality assessment were not; therefore, the specific risks of bias in the individual studies are not known. Because the ██ studies included in the NMA had different designs (open label, mixed open label and double blind, and double blind), this could represent a source of bias and adds uncertainty to the results of the NMA.
The NMA methods themselves are also subject to minor limitations: the use of fixed effect models over random effect models increases the uncertainty as it does not account fully for potential heterogeneity between studies. In addition, the nature of the network meant that it was not possible to evaluate pairwise contrasts, and consistency was not evaluated in the submission. Although the impact of these is likely minor given all 3 trials were phase III RCTs, these limitations also contribute to increasing the general uncertainty in the results.
The submission provided the criteria by which treatment effect modifiers were identified in the studies forming the NMA network, and identified ████ ███████████ ███████ ██████ ██████████ ████████ ██ █████ ███████████ ████ ██ ██████████ ███ ██████ ████ ████████ as treatment effect modifiers. According to clinical experts consulted for this review, the list of effect modifiers was generally representative of important indicators in the disease, and the list of additional prognostic factors (████ ████ ███████ ██████) also included factors which would interact with effect modifiers or represented prognostic factors on their own. Treatment effect modifiers were generally balanced across the ██ studies included in the appraisal with the exception of brain metastases where the FLAURA study reported lower proportions of patients with CNS metastases. In addition, smoking status and cancer stage at screening were not reported in either the FLAURA or FLAURA2 studies. These represent potential prognostic indicators which could interact with treatment effect modifiers. Overall, the heterogeneities in these 3 areas increased the uncertainty in the results.
There were additional differences noted with regards to study design and inclusion criteria which were highlighted in the submission. The duration of follow-up in the studies was ███████ for the FLAURA study (at the time that the SLR was conducted) than for the MARIPOSA and FLAURA2 studies; with a ███████ ██████ ██ ████ over which events can accrue, this could bias the results in favour of the comparators in the FLAURA study (osimertinib). A more recent publication of OS results for the FLAURA study has been published but was not included in the network. In addition, there were numeric differences noted in the frequency of assessments between the 3 studies: assessments were done at baseline, every 6 weeks (± 1 week) for 18 months, then every 12 weeks in the FLAURA study; every 8 weeks (± 1 week) for the first 30 months followed by every 12 weeks (± 1 week) thereafter in the MARIPOSA study; and baseline, week 6, week 12, and then every 12 weeks for the FLAURA2 study. While there is potential for overestimating treatment effects when disease assessments occur less frequently, the nature of this bias is that the interval within which an event occurred is known, but the exact time of the event is not known.
For survival outcomes, this bias is more likely to impact the median estimates, as the median considers the number of events in individual arms of the study at a particular time and may be sensitive to the timing of the assessment. The direction of bias of the HR estimates are less likely to be materially impacted by the frequency of assessment, and while there is increased uncertainty in the estimates and CIs, the extent and direction of this bias in the NMA network is unclear. Additional design differences included the ascertainment of results by BICR versus investigator. The FLAURA2 and MARIPOSA studies reported sensitivity analyses for PFS by BICR and PFS by investigator, respectively, and the results were consistent with the primary analyses; therefore, this bias was also not considered to impact the results. The FLAURA2 study also required a minimum life expectancy for enrolment, but clinical experts consulted for this review noted that this was unlikely to have an impact on the results or comparability of the studies because patients with a life expectancy of less than 12 weeks would be considered too frail for treatment with interventions such as chemotherapy or amivantamab, due to toxicity concerns. Lastly, while the sponsor noted that there were also ███████████ ██ ███ █████████ ██ ██████ █████ ███████ ███ ███ ████████ ███ ██████████ ██████ █████ ███████, CNS outcomes were not appraised in the report, and it remains unclear what impact this may have on the results. Overall, the differences in study design have the potential for bias but the degree of bias is unknown; therefore, this increases the uncertainty in the results but was not deemed likely to change the conclusions from the NMA.
Studies Addressing Gaps in the Systematic Review Evidence
Contents within this section have been informed by materials submitted by the sponsor. The following have been summarized and validated by the review team.
The sponsor submitted 2 studies (SKIPPirr and PALOMA-3) that did not meet the eligibility criteria for inclusion in the systematic review.17,18
The sponsor noted that systemic IRRs, including severe reactions, which occur with the introduction of a new protein therapeutic infusion are frequently observed. The SKIPPirr study evaluated the potential of prophylactic strategies in reducing amivantamab-associated IRRs.
Following observed increases in VTE events with the combination of amivantamab plus lazertinib in the MARIPOSA study, a mitigation strategy involving prophylactic anticoagulation therapy per local guidelines during the first 4 months of therapy with enhanced monitoring was implemented in 2022 and integrated into the PALOMA-3 study protocol.
Evidence Gap: Preventing IRRs With Amivantamab
The SKIPPirr study (NCT05663866) is an ongoing phase II, open-label, multicentre study evaluating strategies to manage IRRs associated with amivantamab in patients with EGFR-mutated (exon 19 deletion or exon 21 L858R substitution) advanced or metastatic NSCLC. The SKIPPirr study included patients with disease progression on or after sequential osimertinib and platinum-based chemotherapy. Using Simon’s 2-stage design with an expansion phase, the study evaluated 4 cohorts (n = 6 patients each) receiving prophylactic treatment before the first infusion of amivantamab with oral lazertinib. Cohorts were as follows: oral dexamethasone on varying schedules (cohort A and cohort A2), oral montelukast (cohort B), or SC methotrexate (cohort C). Cohorts passed stage 1 if 3 or fewer patients experienced an IRR. In stage 2, up to 10 additional patients could be enrolled per cohort. Cohorts passed stage 2 if 8 or fewer patients experienced an IRR. The primary end point was the rate of IRRs within 24 hours of the first amivantamab infusion. Safety end points included AEs and SAEs.
To date, among all cohorts (N = 68), the median age was 63.5 years, 65% were female, and 62% Asian, with a median of 3 (range = 2 to 9) prior lines of treatment. Only the dexamethasone 8 mg cohort passed both stage 1 (2 of 6 patients with IRRs) and stage 2 (6 of 16 patients with IRRs), advancing to the expansion stage. Prophylactic treatment with dexamethasone 8 mg oral was twice a day for 2 days before amivantamab administration, followed by 1 dose an hour before the amivantamab infusion (5 doses total). As of the data cut-off of June 24, 2024, among the 41 patients in the dexamethasone 8 mg cohort, 10 (24%) patients reported IRRs, 1 of which was greater than or equal to grade 3 in severity. Other common treatment-emergent AEs were nausea, epistaxis, dyspnea, and hypotension. No new safety signals were observed.
Evidence Gap: Preventing VTE Events With Amivantamab Plus Lazertinib
The PALOMA-3 study is a phase III, randomized, open-label, multicentre study evaluating the pharmacokinetic noninferiority of SC amivantamab plus lazertinib compared to IV amivantamab plus lazertinib in patients with EGFR-mutated locally advanced or metastatic NSCLC who progressed after osimertinib and platinum-based chemotherapy. As such, all patients had at least 1 prior therapy, with a majority (89%) having at least 2 lines of prior therapy. A subgroup analysis of patients treated with IV amivantamab in the PALOMA-3 study was conducted to provide supportive information on the safety and efficacy of prophylactic anticoagulation in patients receiving the combination of amivantamab and lazertinib.
Eligible patients were randomized 1:1 to receive SC or IV amivantamab plus lazertinib in 28-day cycles. Amivantamab SC was administered by manual injection, while IV administration included split doses during cycle 1. Lazertinib was given orally at 240 mg daily. Randomization was stratified by baseline brain metastases, EGFR mutation type, race, and prior therapy. Prophylactic anticoagulation was recommended for the first 4 months of treatment per local guidelines. A total of 416 patients (206 patients in the amivantamab SC plus lazertinib group and 210 patients in the amivantamab IV plus lazertinib group) received at least 1 dose of study treatment.
The overall incidence of VTEs was 11.8%, occurring in 9.2% of patients in the SC group and 14.3% of patients in the IV group, with most classified as grade 1 or grade 2 events. Prophylactic anticoagulation use was similar between the SC and IV treatment groups (79.6% versus 81.4%, respectively). Among patients receiving anticoagulation, VTEs occurred in 7.3% of the SC group and 11.7% of the IV group, whereas in patients who were not anticoagulated, the incidence was higher (16.7% for the SC group versus 25.6% for the IV group). Bleeding events were more frequent in patients on prophylactic anticoagulation (26.8% for the SC group versus 28.1% for the IV group) than in patients who were not anticoagulated (11.9% for the SC group and 12.8% for the IV group). Overall, SC amivantamab plus lazertinib was associated with a lower VTE incidence than IV administration, regardless of anticoagulation use.
Critical Appraisal
The SKIPPirr and PALOMA-3 studies provided data on prophylactic treatments for preventing IRRs and VTE events, respectively, in patients with EGFR-mutated advanced or metastatic NSCLC. However, both studies had limitations that impact the generalizability and interpretability of their findings. The SKIPPirr study was an open-label, nonrandomized study with a small sample size, increasing the risk of bias, particularly in comparison to the rigour of standardized RCTs. Patients were aware of their treatment, which may have contributed to detection and performance bias, and the open-label design may influence the reporting of AEs. Similarly, the PALOMA-3 study, while randomized and stratified based on key clinical factors, also had an open-label design, introducing similar biases. In both studies, patients had progressed on or after prior treatment with osimertinib and platinum-based chemotherapy, which does not align with the Health Canada–approved indication as a first-line treatment. Additionally, included patients had an ECOG Performance Status of 0 or 1, meaning they were relatively healthy, which may not fully represent the broader population that would receive prophylactic treatment in real-world clinical practice in Canada.
Discussion
Summary of Available Evidence
This report summarizes the evidence for amivantamab plus lazertinib compared to osimertinib monotherapy for the treatment of locally advanced or metastatic NSCLC with exon 19 deletions or exon L858R substitution mutations in adult patients who are candidates for systemic therapy. The evidence appraisal was based on results from the first interim analysis of an ongoing phase III multisite RCT (MARIPOSA; N = 1,074), where patients were randomized to 1 of 3 treatment arms consisting of either open-label amivantamab plus lazertinib (n = 429), double-blind osimertinib (n = 429), or double-blind lazertinib (n = 216). Results for the lazertinib monotherapy arm were included for contextualization of harms but were otherwise not reported. The primary end point of the MARIPOSA study was PFS by BICR, and secondary end points included OS, ORR, DOR, and HRQoL. The submission also included a body of indirect evidence consisting of 5 NMAs, and results comparing amivantamab plus lazertinib to osimertinib monotherapy and osimertinib plus chemotherapy were appraised. No long-term extension studies were included, but 2 studies addressing gaps in the evidence were appraised. The SKIPPirr study (N = 68) is an ongoing phase II, open-label, multicentre trial designed to evaluate prophylactic treatments for IRRs (oral dexamethasone, oral montelukast, or SC methotrexate) before amivantamab infusion with oral lazertinib in patients with advanced EGFR-mutated NSCLC who have progressed after osimertinib and platinum chemotherapy. The primary outcome was the rate of IRRs within 24 hours of the first infusion. The PALOMA-3 study (N = 416) is a phase III, randomized, open-label, multicentre trial assessing the pharmacokinetic noninferiority of SC amivantamab plus lazertinib compared to IV administration in patients with EGFR-mutated locally advanced or metastatic NSCLC who have progressed after osimertinib plus platinum-based chemotherapy, for the purpose of managing VTEs associated with amivantamab plus lazertinib.
The baseline characteristics of the patients in the MARIPOSA study were generally balanced between study arms. Included patients mainly had metastatic disease, ECOG status of 1, had never smoked, and were naive to prior systemic therapy. The mean age was approximately 62 years. The clinical experts noted that the study inclusion and exclusion criteria, as well as the baseline characteristics, broadly characterized patients in the Canadian clinical setting who would be candidates for amivantamab plus lazertinib, with some caveats. They noted that there was a greater proportion of patients of Asian descent than they might see in clinical practice in Canada, and they also noted that few patients aged older than 75 years were included which would impact their decision to use this treatment in older patients. Patients with ECOG status of 2 were not enrolled but it was noted such patients would be unlikely to use this treatment given the safety profile of amivantamab plus lazertinib, except in very select cases. Additionally, the MARIPOSA study excluded patients with any prior TKI exposure, and because osimertinib is also approved for use in the adjuvant setting for patients with exon 19 deletions and exon L858R mutations, the results of the trial might not apply to this patient population. The experts estimated this might impact 10% to 15% of patients eligible for treatment with EGFR inhibitor-based treatment.
Interpretation of Results
Efficacy
Patient and clinician groups highlighted improved symptoms, delayed progression, prolonged life, improved quality of life, and manageable side effects were the most important outcomes of new treatments. Clinician groups pointed out a specific unmet need for the exon 19 deletions and exon L858R substitution mutations in the indication under review because patients eventually progress on treatment with osimertinib, and because osimertinib plus chemotherapy may be an option in some, but not all patients. The outcomes in the MARIPOSA study included survival outcomes and cancer-specific HRQoL measures and therefore evaluated several outcomes of importance to patients and clinicians.
As noted, PFS was the primary end point of the MARIPOSA study and the results were from a prespecified interim analysis. The median PFS was reached in the study for both treatment arms and the results were statistically significant (median PFS in amivantamab plus lazertinib arm = 23.72 months; 95% CI, 19.12 months to 27.66 months and HR = 0.70; 95% CI, 0.58 to 0.85), suggesting a small benefit relative to osimertinib monotherapy. At the time of the August 11, 2023, data cut-off, the median follow-up was 22.01 months (amivantamab plus lazertinib arm = 22.21 months; osimertinib arm = 21.98 months; lazertinib arm = 21.88 months). When it came to the clinical meaningfulness of the results, clinical experts consulted for this review considered 12 months of follow-up to be too early to determine clinical benefit between study arms, and noted 24 months would be more reasonable to assess benefit. They also felt that, given the additional toxicity associated with amivantamab and the existing results observed with osimertinib, an absolute benefit of at least 20% between study arms for the proportion of patients who were progression-free at 24 months was clinically meaningful. Based on this assessment, the results are impacted by imprecision because the point estimate and lower bound of the CI did not reach this threshold at 24 months, and therefore PFS likely results in an increase in the proportion of patients progression-free at 24 months, but the CI contains the possibility of benefit that may or may not be clinically meaningful.
At the request of the European Medicines Agency, an additional analysis was conducted on OS, ORR, and DOR using data up to May 13, 2024; these data were included in the GRADE assessment although the analysis was not prespecified in the statistical analysis plan, and is considered supportive evidence. The results for OS are largely limited by imprecision and data immaturity; median OS was not reached in either study arm at the August 2023 data cut-off (22.6% of deaths had occurred in the amivantamab plus lazertinib arm and 27.3% of deaths had occurred in the osimertinib arm). At the May 2024 efficacy update, the median OS in the amivantamab plus lazertinib arm was still not fully reached in either arm (█████ of deaths had occurred in the amivantamab plus lazertinib arm and █████ of deaths had occurred in the osimertinib arm with a median follow-up of approximately 31 months). The clinical experts agreed that an event-free benefit in OS of at least 10% between study arms for the proportion of patients alive at 24 months onwards would be clinically meaningful. Results for OS at 24, 30, and 36 months were not considered clinically meaningful as the point estimates and lower bound of the 95% CI did not attain this 10% threshold. Two important considerations for the survival data are that the efficacy update provides results from nearly 3 years of follow-up and the active comparator, osimertinib, is associated with a generally favourable response according to clinical experts. However, the immaturity of the data suggests that the comparative efficacy of amivantamab plus lazertinib with osimertinib remain uncertain for OS, and the confidence with which long-term survival trends can be predicted from these results is unknown.
In the recent CDA-AMC Canadian Drug Expert Committee recommendation for osimertinib plus chemotherapy published in October 2024, the pan-Canadian Oncology Drug Review Expert Review Committee noted that prevention of CNS metastasis and CNS disease control are important treatment goals in patients with NSCLC. As such, the sponsor requested that CNS efficacy outcomes in the MARIPOSA trial be included in the report. Results for subgroup analyses of PFS in patients with history of brain metastases were generally consistent with the primary analysis, favouring amivantamab plus lazertinib over osimertinib; however, the median PFS in patients without brain metastases was numerically greater than the primary analysis population in both treatment groups. Conversely, in patients with brain metastases, the median PFS was numerically lower in both treatment groups compared to the primary analysis population. Subgroup analyses were not controlled for multiplicity and were only considered supportive of the overall effect of amivantamab plus lazertinib. For intracranial time-to-event outcomes (intracranial PFS, intracranial DOR, and time to intracranial progression) and response-related outcomes (intracranial ORR), the results generally suggested no difference between amivantamab plus lazertinib and osimertinib.
HRQoL was assessed in the MARIPOSA study using 2 cancer-specific measures: EORTC QLQ-C30, which assesses quality of life, and NSCLC-SAQ, which assesses symptom burden and is specific to NSCLC. The submission also contained NSCLC-specific MIDs for the NSCLC-SAQ; therefore, results for this outcome were able to be interpreted directly in the context of the disease. Changes from baseline in EORTC QLQ-C30 scores were ███████████ ███████ for the osimertinib arm than for the amivantamab plus lazertinib arm at all time points, suggesting ██████ █████ ████ ███████████. ████ ██ ████████ ███████ were reported for the NSCLC-SAQ. Overall, none of the reported score changes attained the MIDs for clinically meaningful change, likely suggesting no improvement or no detriment to HRQoL with amivantamab plus lazertinib compared to osimertinib. The results for HRQoL were impacted by high levels of attrition. For both measures, approximately ███ of patients in the amivantamab plus lazertinib arm and ███ of patients in the osimertinib arm contributed data at cycle 13; ███ ███ ███ in each arm at cycle 21; and ███ ███ ███ in each arm at cycle 27. While the NSCLC-SAQ required all domains be complete to count as a whole score, no measures were reported for missing data in the EORTC QLQ-C30. In addition, stratified models were used for the analyses and LS mean change from baseline was modelled using an MMRM analysis, which assumes the data are missing at random. However, the high attrition and small sample sizes at later time points raise a concern of poor model fit and also whether the missing-at-random assumption is valid. The nature of the disease is such that patients who are missing are likely missing for reasons related to their disease; therefore, it is likely that this missingness is not random. Overall, the evidence was unclear on the impact of amivantamab plus lazertinib on HRQoL outcomes when compared to osimertinib monotherapy.
The main comparators identified by clinical experts for this review were osimertinib monotherapy and osimertinib plus chemotherapy. Clinical experts noted that if all 3 treatments were available, they would consider each of these for a newly diagnosed patient and decide which is appropriate based on the individual patient. There were 5 NMAs assessing efficacy (PFS, OS, ORR) and safety (all AEs, all SAEs) of amivantamab plus lazertinib (the MARIPOSA study), osimertinib (the FLAURA study), and osimertinib plus chemotherapy (the FLAURA2 study) appraised in the review. Overall, amivantamab plus lazertinib was favoured over osimertinib for PFS and there was insufficient evidence to detect a difference for OS and ORR. For the comparison to osimertinib plus chemotherapy, amivantamab plus lazertinib was favoured for ORR but there was insufficient evidence to detect a difference for OS and PFS. The interpretation of the NMA results is limited by heterogeneity in the studies and the fact that some comparators or recent evidence may have been excluded, as the SLR was completed in 2022. The 3 studies included in the review had a mix of study designs. The FLAURA study was double blind, the FLAURA2 study was open label, and the MARIPOSA study had a mix of double-blind comparator arms and an open-label intervention arm. In addition, there was heterogeneity in 1 known treatment effect modifier — ███ ████████ ██ █████ ██████████ — and unknown information on 2 potential prognostic factors, which increase the uncertainty of the results. Lastly, differences in study design such as follow-up duration and frequency of disease assessments may also bias the results to an unknown extent and direction. Overall, the NMA contained multiple limitations which together contributed to increasing the uncertainty of the results, but do not impact the overall conclusions.
Harms
Given the known adverse reactions associated with amivantamab (IRRs, interstitial lung disease or pneumonitis, and skin and nail reactions), harms were highlighted by the clinical experts and clinician group input as an important consideration for amivantamab plus lazertinib. The clinical experts noted that nail, skin, mucosal toxicity, and VTEs are often associated with considerable patient morbidity and infusion reactions are inconvenient. They also noted that the IV administration and additional potential for toxicity would impact the patients they might consider for this therapy, and 1 of the clinician groups noted that amivantamab did not quite meet their criteria for manageable convenience or low toxicity. The MARIPOSA study is ongoing, and therefore the harms reporting is not yet complete, and some additional harms may not have been captured in this data. In addition, the lack of a long-term extension study means that long-term harms data are not available. Lazertinib is a new drug not previously approved by Health Canada; however, amivantamab was approved by Health Canada in 2022 for NSCLC with EGFR exon 20 insertion mutations and therefore the safety profile and management are becoming more familiar.
Though the overall frequency of AEs was similar between the 2 study arms and the lazertinib monotherapy arm, the overall frequency of individual events between study arms suggested a higher burden of harms in the amivantamab plus lazertinib arm as there was a considerably greater proportion of patients reporting AEs including ██████████, IRRs, rash, hypoalbuminemia, increased alanine aminotransferase, and peripheral edema. For the AESIs specified in the study, rash and VTE could occur across all study arms (as opposed to infusion reactions, because no IV was administered in the osimertinib and lazertinib monotherapy arms) and overall, these were reported more commonly in the amivantamab plus lazertinib arm than the other 2 study arms. Amivantamab plus lazertinib was also associated with more severe AEs with 75.1% of patients in the amivantamab plus lazertinib arm experiencing an AE of grade 3 or higher compared to 42.8% in the osimertinib arm and 45.5% in the lazertinib arm, and 48.7% of patients in the amivantamab plus lazertinib arm experiencing SAEs compared to 33.4% of patients in the osimertinib arm, and 35.2% of patients in the lazertinib arm.
Results from the sponsor-submitted indirect treatment comparison suggested that there is insufficient evidence to conclude any difference in AEs or SAEs between amivantamab plus lazertinib when compared to osimertinib plus chemotherapy or osimertinib monotherapy. The use of AEs and SAEs as an outcome without further specificity on the type of toxicity (i.e., preferred term) is a limitation in the indirect evidence, as certain harms can have greater morbidity than others per the clinical experts consulted for this review.
The proportion of patients who died was numerically similar between study arms (█████ ██ █████ across all 3 study arms), caused primarily by disease progression, and while high proportions of patients in the amivantamab plus lazertinib arm reported dose interruption ███████ and dose reduction ████████ these proportions were numerically higher than the proportion of patients who discontinued due to AEs ███████ — of note, these proportions were all higher than those reported in the osimertinib arm ██████ ████████ ████ ██████████████ ████ ████████ ████ ███████████ ███ █████ ████████ ██████████████████ Input from clinical experts consulted for this review suggested that they would consider younger, fitter patients for this treatment given the potential toxicities. They also highlighted that the withdrawals due to AEs were high and, in their view, require a clear OS benefit to justify the additional toxicity. The results of harms to date also reinforce the importance of discussing with patients the trade-offs of efficacy and side effect burden when it comes to treatment options for advanced or metastatic NSCLC.
The product monograph for amivantamab contains information on premedication for IRRs, dose reduction guidance for AEs, and guidance for specific AEs such as interstitial lung disease, IRRs, and skin and nail reactions. The product monograph for lazertinib also contains a warning about interstitial lung disease. The sponsor submitted additional information pertaining to the safety data for amivantamab which evaluated the impact of preventive measures to reduce the risk of IRRs, VTE events, and dermatologic AEs to further inform the toxicity profile of amivantamab plus lazertinib. Results from the SKIPPirr study suggested that pretreatment with dexamethasone reduces the incidence of IRRs in patients receiving IV amivantamab plus lazertinib, potentially improving its tolerability. In the PALOMA-3 trial, the overall incidence of VTE events was lower in patients receiving SC amivantamab compared to those receiving IV amivantamab, regardless of anticoagulation use. The safety profile of SC administration was comparable to IV administration, with similar rates of treatment-emergent AEs. Bleeding events were more frequent in patients with anticoagulants than those without. In general, the additional evidence provides potential avenues for mitigating certain safety concerns with amivantamab. However, it is also limited by factors such as small sample size, open-label design, and patient populations that differ from the population in the indication (the studies were conducted in a patient population who had progressed on osimertinib plus chemotherapy). The additional evidence also does not address all AESIs (e.g., rash).
Conclusion
One phase III, ongoing, multicentre, active-controlled RCT (MARIPOSA) provided evidence for the efficacy and safety of amivantamab plus lazertinib as first-line treatment for 858 adult patients with locally advanced or metastatic NSCLC with exon 19 deletions or exon 21 L858R substitution mutations.
Patient and clinician groups highlighted improving symptoms, PFS, OS, quality of life, and manageable side effects as important outcomes of interest in a new treatment. The clinical experts consulted for the review noted that patient preference, desire for additional efficacy, and fitness to tolerate the side effects were also factors they would consider when identifying potential candidates for this treatment. The results of the interim analysis of the MARIPOSA study suggested that treatment with amivantamab plus lazertinib improved median PFS. The results of the GRADE assessment also suggested that amivantamab plus lazertinib likely results in an increase in the proportion of patients who are progression-free at 24 months and may result in an increase in the proportion of patients alive at 24 months, 30 months, and 36 months. However, the results are subject to imprecision and the point estimates for PFS and OS did not attain the MIDs provided by the clinical experts. The data for OS, ORR, and DOR are also limited by data immaturity, with median OS not reached in either arm as of the prespecified interim analysis and imprecisely estimated in the amivantamab plus lazertinib arm using additional study data (upper bound of the CI could not be estimated). HRQoL results suggested that score changes did not attain the MIDs for improvement and suggested no clinically meaningful change in HRQoL. While the reporting of harms in the MARIPOSA study was also immature, the results demonstrated a notable side effect burden attributable to amivantamab plus lazertinib including a greater proportion of patients reporting ██████████, rash, IRRs, and VTE were also reported more commonly in the amivantamab plus lazertinib arm. Deaths were generally balanced across treatment arms, with a slightly greater proportion of deaths in the osimertinib monotherapy and lazertinib monotherapy groups; ████████ ██████ ███ ██ ███ ████ ███████ ██ ███ ███████████ ████ ██████████ ███ ███ ██████ ███ ██ ████████.
There is no direct comparative evidence for amivantamab plus lazertinib compared to osimertinib plus chemotherapy. The sponsor submitted an NMA evaluating these treatments; however, there was ████████████ ████████ ██ ██████ █ ██████████ ███████ ███████████ ████ ██████████ ███ ███████████ ██ ███████████ ████ ████████████ ███ ██████ ███ ████████ ███ ██████████████ █████████ and the results are limited by uncertainty due to multiple sources of heterogeneity in the studies.
References
1.Canadian Cancer Statistics Advisory Committee, Canadian Cancer Society, Statistics Canada, Public Health Agency of Canada. Canadian Cancer Statistics 2023. Canadian Cancer Society; 2023. Accessed May 7, 2024. https://cancer.ca/Canadian-Cancer-Statistics-2023-EN
2.Canadian Cancer Society. Lung and bronchus cancer statistics. 2024. Accessed June 23, 2025. https://cancer.ca/en/cancer-information/cancer-types/lung/statistics
3.Plunkett TA, Chrystal KF, Harper PG. Quality of life and the treatment of advanced lung cancer. Clin Lung Cancer. 2003;5(1):28-32. doi: 10.3816/CLC.2003.n.018 PubMed
4.Birring SS, Peake MD. Symptoms and the early diagnosis of lung cancer. Thorax. 2005;60(4):268-9. doi: 10.1136/thx.2004.032698 PubMed
5.Vyse S, Huang PH. Targeting EGFR exon 20 insertion mutations in non-small cell lung cancer. Signal Transduct Target Ther. 2019;4:5. doi: 10.1038/s41392-019-0038-9 PubMed
6.Janne PA, Johnson BE. Effect of epidermal growth factor receptor tyrosine kinase domain mutations on the outcome of patients with non-small cell lung cancer treated with epidermal growth factor receptor tyrosine kinase inhibitors. Clin Cancer Res. 2006;12(14 Pt 2):4416s-4420s. doi: 10.1158/1078-0432.CCR-06-0555 PubMed
7.Lababede O, Meziane MA. The Eighth Edition of TNM Staging of Lung Cancer: Reference Chart and Diagrams. Oncologist. 2018;23(7):844-848. doi: 10.1634/theoncologist.2017-0659
8.Ontario Health. Plasma-based comprehensive genomic profiling DNA assays for non–small cell lung cancer: a health technology assessment. Ont Health Technol Assess Series. 2024;24(8):1-306. Accessed June 23, 2025. https://www.hqontario.ca/Portals/0/Documents/evidence/reports/hta-plasma-based-comprehensive-genomic-profiling-DNA-assays-for-non%E2%80%93small-cell-lung-cancer.pdf PubMed
9.Ramalingam SS, Vansteenkiste J, Planchard D, et al. Overall Survival with Osimertinib in Untreated, EGFR-Mutated Advanced NSCLC. N Engl J Med. 2020;382(1):41-50. doi: 10.1056/NEJMoa1913662 PubMed
10.Canada's Drug Agency. Reimbursement recommendation: osimertinib (Tagrisso). Can J Health Technol. 2024;4(10). doi: 10.51731/cjht.2024.100
11.Soon YY, Marschner IC, Schou M, et al. Challenges of estimating treatment effects after a positive interim analysis. Eur J Cancer. 2024;209:114230. doi: 10.1016/j.ejca.2024.114230 PubMed
12.Janssen Research & Development, LLC. Clinical Study Report: 73841937NSC3003, MARIPOSA, Primary Endpoint Analysis. A Phase 3, Randomized Study of Amivantamab and Lazertinib Combination Therapy Versus Osimertinib Versus Lazertinib as First-Line Treatment in Patients with EGFR-Mutated Locally Advanced or Metastatic Non-Small Cell Lung Cancer [internal sponsor's report]. November 28, 2023.
13.Janssen Research & Development, LLC. Clinical Study Report: 73841937NSC3003, MARIPOSA, overview of updated efficacy. A Phase 3, Randomized Study of Amivantamab and Lazertinib Combination Therapy Versus Osimertinib Versus Lazertinib as First-Line Treatment in Patients with EGFR-Mutated Locally Advanced or Metastatic Non-Small Cell Lung Cancer [internal sponsor's report]. August 5, 2024.
14.Janssen Inc. Janssen Inc. response to Canada's Drug Agency request for additional information regarding amivantamab plus lazertinib on February 6, 2025 [internal additional sponsor's information]. February 13, 2025.
15.Zhong Z, Yang M, Ni S, et al. The heterogeneity effect of surveillance intervals on progression free survival. J Appl Stat. 2024;51(4):646-663. doi: 10.1080/02664763.2022.2145272 PubMed
16.Planchard D, Janne PA, Cheng Y, et al. Osimertinib with or without Chemotherapy in EGFR-Mutated Advanced NSCLC. N Engl J Med. 2023;389(21):1935-1948. doi: 10.1056/NEJMoa2306434 PubMed
17.Paz-Ares LG, Spira AI, Han JY, et al. 1269P Preventing infusion-related reactions with intravenous amivantamab: Updated results from SKIPPirr, a phase II study. Ann Oncol. 2024;35(S2). doi: 10.1016/j.annonc.2024.08.1326
18.Leighl NB, Akamatsu H, Lim SM, et al. Subcutaneous Versus Intravenous Amivantamab, Both in Combination With Lazertinib, in Refractory Epidermal Growth Factor Receptor-Mutated Non-Small Cell Lung Cancer: Primary Results From the Phase III PALOMA-3 Study. J Clin Oncol. 2024;42(30):3593-3605. doi: 10.1200/JCO.24.01001 PubMed
19.Dearden S, Stevens J, Wu YL, Blowers D. Mutation incidence and coincidence in non small-cell lung cancer: meta-analyses by ethnicity and histology (mutMap). Ann Oncol. 2013;24(9):2371-6. doi: 10.1093/annonc/mdt205 PubMed
20.Riely GJ, Wood DE, Ettinger DS, et al. Non-Small Cell Lung Cancer, Version 4.2024, Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw. 2024;22(4):249-274. doi: 10.6004/jnccn.2204.0023 PubMed
21.Melosky B, Banerji S, Blais N, et al. Canadian consensus: a new systemic treatment algorithm for advanced EGFR-mutated non-small-cell lung cancer. Curr Oncol. 2020;27(2):e146-e155. doi: 10.3747/co.27.6007 PubMed
22.Canada's Drug Agency. Reimbursement Review: Provisional Funding Algorithm for advanced or metastatic non-small cell lung cancer with activating epidermal growth factor receptor mutations. December 2024. Accessed by sponsor, no date provided. https://www.cda-amc.ca/sites/default/files/DRR/2024/PH0054-FINAL_NSCLC_EGFR.pdf
23.Cho BC, Han JY, Kim SW, et al. A Phase 1/2 Study of Lazertinib 240 mg in Patients With Advanced EGFR T790M-Positive NSCLC After Previous EGFR Tyrosine Kinase Inhibitors. J Thorac Oncol. 2022;17(4):558-567. doi: 10.1016/j.jtho.2021.11.025 PubMed
24.Ahn MJ, Han JY, Lee KH, et al. Lazertinib in patients with EGFR mutation-positive advanced non-small-cell lung cancer: results from the dose escalation and dose expansion parts of a first-in-human, open-label, multicentre, phase 1-2 study. Lancet Oncol. 2019;20(12):1681-1690. doi: 10.1016/S1470-2045(19)30504-2 PubMed
25.Janssen Inc. Lazcluze (lazertinib): 80 mg and 240 mg oral tablets [product monograph]. July 19, 2024.
26.Janssen Inc. Rybrevant (amivantamab for injection): 50 mg/mL concentrate for solution for intravenous infusion, in single use vial [product monograph]. March 30, 2022. Updated June 28, 2024.
27.Canada's Drug Agency. Reimbursement Review: amivantamab (Rybrevant) in combination with carboplatin and pemetrexed. Updated June 4, 2025. Accessed January 21, 2025. https://www.cda-amc.ca/amivantamab-1
28.AstraZeneca Canada Inc. Tagrisso (osimertinib): 40 mg and 80 mg, oral tablets [product monograph]. 2024. [sponsor supplied reference].
29.Pfizer Canada ULC. Carboplatin Injection BP: 10 mg / mL sterile solution (50 mg, 150 mg, 450 mg, 600 mg of carboplatin per vial), for injection [product monograph]. December 16, 2019. https://pdf.hres.ca/dpd_pm/00054389.PDF
30.Pfizer Canada ULC. Cisplatin Injection BP: 1 mg / mL sterile solution (50 mg and 100 mg cisplatin per vial), for injection [product monograph]. December 7, 2018. Accessed June 24, 2025. https://pdf.hres.ca/dpd_pm/00048673.PDF
31.Apotex Inc. Pemetrexed (pemetrexed disodium): 100 mg or 500 mg pemetrexed per vial, lyophilized powder, for intravenous injection [product monograph]. June 01, 2016. Accessed June 24, 2025. https://pdf.hres.ca/dpd_pm/00035165.PDF
32.Melosky B, Blais N, Cheema P, et al. Standardizing biomarker testing for Canadian patients with advanced lung cancer. Curr Oncol. 2018;25(1):73-82. doi: 10.3747/co.25.3867 PubMed
33.Ionescu DN, Stockley TL, Banerji S, et al. Consensus Recommendations to Optimize Testing for New Targetable Alterations in Non-Small Cell Lung Cancer. Curr Oncol. 2022;29(7):4981-4997. doi: 10.3390/curroncol29070396 PubMed
34.Cheema PK, Gomes M, Banerji S, et al. Consensus recommendations for optimizing biomarker testing to identify and treat advanced EGFR-mutated non-small-cell lung cancer. Curr Oncol. 2020;27(6):321-329. doi: 10.3747/co.27.7297 PubMed
35.NCCN Guidelines. Non-small lung cancer, version 3.2025. National Comprehensive Cancer Network; 2025. Accessed February 12, 2025. https://www.nccn.org/professionals/physician_gls/pdf/nscl.pdf
36.Sebastião MM, Ho RS, de Carvalho JPV, Nussbaum M. Diagnostic Accuracy of Next Generation Sequencing Panel using Circulating Tumor DNA in Patients with Advanced Non-Small Cell Lung Cancer: A Systematic Review and Meta-Analysis. J Health Econ Outcomes Res. 2020;7(2):158-163. doi: 10.36469/jheor.2020.17088 PubMed
37.Janssen Inc. Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Lazcluze (lazertinib), 80 mg and 240 mg oral tablets, and Rybrevant (amivantamab), 50 mg/mL concentrate for solution for intravenous infusion. Decemeber 18, 2024.
38.O'Sullivan DE, Jarada TN, Yusuf A, et al. Prevalence, Treatment Patterns, and Outcomes of Individuals with EGFR Positive Metastatic Non-Small Cell Lung Cancer in a Canadian Real-World Setting: A Comparison of Exon 19 Deletion, L858R, and Exon 20 Insertion EGFR Mutation Carriers. Curr Oncol. 2022;29(10):7198-7208. doi: 10.3390/curroncol29100567 PubMed
39.Snow S, Brezden-Masley C, Carter MD, et al. Barriers and Unequal Access to Timely Molecular Testing Results: Addressing the Inequities in Cancer Care Delays across Canada. Curr Oncol. 2024;31(3):1359-1375. doi: 10.3390/curroncol31030103 PubMed
40.Zou D, Ye W, Hess LM, et al. Diagnostic Value and Cost-Effectiveness of Next-Generation Sequencing-Based Testing for Treatment of Patients with Advanced/Metastatic Non-Squamous Non-Small-Cell Lung Cancer in the United States. J Mol Diagn. 2022;24(8):901-914. doi: 10.1016/j.jmoldx.2022.04.010 PubMed
41.Brenner DR, O'Sullivan DE, Jarada TN, et al. The impact of population-based EGFR testing in non-squamous metastatic non-small cell lung cancer in Alberta, Canada. Lung Cancer. 2023;175:60-67. doi: 10.1016/j.lungcan.2022.11.017 PubMed
42.Cho BC, Lu S, Felip E, et al. Amivantamab plus Lazertinib in Previously Untreated EGFR-Mutated Advanced NSCLC. N Engl J Med. 2024;391(16):1486-1498. doi: 10.1056/NEJMoa2403614 PubMed
43.Felip E, Cho BC, Gutierrez V, et al. Amivantamab plus lazertinib versus osimertinib in first-line EGFR-mutant advanced non-small-cell lung cancer with biomarkers of high-risk disease: a secondary analysis from MARIPOSA. Ann Oncol. 2024;35(9):805-816. doi: 10.1016/j.annonc.2024.05.541 PubMed
44.Lazcluze + Rybrevant: First-line (1L) Treatment of Locally Advanced (not amenable to curative therapy) or Metastatic Non-Small Cell Lung Cancer (NSCLC) with EGFR exon 19 deletions or exon 21 L858R substitution mutations [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Lazcluze (lazertinib), 80 mg and 240 mg oral tablets, and Rybrevant (amivantamab), 50 mg/mL concentrate for solution for intravenous infusion Janssen, Inc.; 2024.
45.Janssen Inc. Drug Reimbursement Review sponsor submission: Lazcluze (lazertinib), 80 mg and 240 mg oral tablets, and Rybrevant (amivantamab), 50 mg/mL concentrate for solution for intravenous infusion [internal sponsor's package]. December 18, 2024.
46.Osoba D, Rodrigues G, Myles J, Zee B, Pater J. Interpreting the significance of changes in health-related quality-of-life scores. J Clin Oncol. 1998;16(1):139-44. doi: 10.1200/JCO.1998.16.1.139 PubMed
47.Coon CD, Schlichting M, Zhang X. Interpreting Within-Patient Changes on the EORTC QLQ-C30 and EORTC QLQ-LC13. Patient. 2022;15(6):691-702. doi: 10.1007/s40271-022-00584-w PubMed
48.Maringwa JT, Quinten C, King M, et al. Minimal important differences for interpreting health-related quality of life scores from the EORTC QLQ-C30 in lung cancer patients participating in randomized controlled trials. Support Care Cancer. 2011;19(11):1753-60. doi: 10.1007/s00520-010-1016-5 PubMed
49.Williams P, Burke T, Norquist JM, et al. Non-Small Cell Lung Cancer Symptom Assessment Questionnaire (NSCLC-SAQ): Measurement Properties and Estimated Clinically Meaningful Thresholds From a Phase 3 Study. JTO Clin Res Rep. 2022;3(4):100298. doi: 10.1016/j.jtocrr.2022.100298 PubMed
50.Bushnell DM, Atkinson TM, McCarrier KP, et al. Non-Small Cell Lung Cancer Symptom Assessment Questionnaire: Psychometric Performance and Regulatory Qualification of a Novel Patient-Reported Symptom Measure. Curr Ther Res Clin Exp. 2021;95:100642. doi: 10.1016/j.curtheres.2021.100642 PubMed
51.Reeve BB, Wyrwich KW, Wu AW, et al. ISOQOL recommends minimum standards for patient-reported outcome measures used in patient-centered outcomes and comparative effectiveness research. Qual Life Res. 2013;22(8):1889-905. doi: 10.1007/s11136-012-0344-y PubMed
52.Houts CR, Savord A, Gardner MJ, et al. Patient-reported outcomes in non-small cell lung cancer: psychometric evaluation of the PROMIS PF-SF 8c and NSCLC-SAQ in two phase 3 clinical trials. Qual Life Res. 2025;34(3):751-762. doi: 10.1007/s11136-024-03846-2 PubMed
53.Fayers PM, Aaronson NK, Bjordal K, et al. EORTC QLQ-C30 Scoring Manual. 3rd ed. European Organisation for Research and Treatment of Cancer; 2001. Accessed January 21, 2025. https://www.eortc.org/app/uploads/sites/2/2018/02/SCmanual.pdf
54.Teckle P, Peacock S, McTaggart-Cowan H, et al. The ability of cancer-specific and generic preference-based instruments to discriminate across clinical and self-reported measures of cancer severities. Health Qual Life Outcomes. 2011;9:106. doi: 10.1186/1477-7525-9-106 PubMed
55.Nicklasson M, Bergman B. Validity, reliability and clinical relevance of EORTC QLQ-C30 and LC13 in patients with chest malignancies in a palliative setting. Qual Life Res. 2007;16(6):1019-28. doi: 10.1007/s11136-007-9210-8 PubMed
56.Ozturk A, Sarihan S, Ercan I, Karadag M. Evaluating quality of life and pulmonary function of long-term survivors of non-small cell lung cancer treated with radical or postoperative radiotherapy. Am J Clin Oncol. 2009;32(1):65-72. doi: 10.1097/COC.0b013e31817e6ec2 PubMed
57.Aaronson NK, Ahmedzai S, Bergman B, et al. The European Organization for Research and Treatment of Cancer QLQ-C30: a quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst. 1993;85(5):365-76. doi: 10.1093/jnci/85.5.365 PubMed
58.Balshem H, Helfand M, Schünemann HJ, et al. GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol. 2011;64(4):401-6. doi: 10.1016/j.jclinepi.2010.07.015 PubMed
59.Santesso N, Glenton C, Dahm P, et al. GRADE guidelines 26: informative statements to communicate the findings of systematic reviews of interventions. J Clin Epidemiol. 2020;119:126-135. doi: 10.1016/j.jclinepi.2019.10.014 PubMed
60.Janssen Inc. Network meta-analysis report: first-line treatments for patients with advanced cEGFR-mutated NSCLC [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Lazcluze (lazertinib), 80 mg and 240 mg oral tablets, and Rybrevant (amivantamab), 50 mg/mL concentrate for solution for intravenous infusion. February 27, 2024.
61.Qi Y, Xia X, Shao L, et al. An updated network meta-analysis of EGFR-TKIs and combination therapy in the first-line treatment of advanced EGFR mutation positive non-small cell lung cancer. Front Oncol. 2022;12:616546. doi: 10.3389/fonc.2022.616546 PubMed
62.Soria JC, Ohe Y, Vansteenkiste J, et al. Osimertinib in Untreated EGFR-Mutated Advanced Non-Small-Cell Lung Cancer. N Engl J Med. 2018;378(2):113-125. doi: 10.1056/NEJMoa1713137 PubMed
Appendix 1: Detailed Outcome Data
Please note that this appendix has not been copy-edited
Figure 2: Subgroup Analyses of PFS From MARIPOSA by Age Category and History of Brain Metastases (August 11, 2023, Data Cut-Off)
![Forest plot of the results of the PFS subgroup analysis by the following age categories: under 65 years (HR 0.50, 95% CI, 0.39 to 0.65), 65 years of age and older (HR 1.06, 95% CI, 0.80 to 1.41), under 75 years (HR 0.70, 95% CI, 0.57 to 0.85), 75 years of age and older (HR 0.77, 95% CI, 0.46, 1.30); and the PFS analysis by the history of brain metastases; No (HR, 0.69 [95% CI, 0.53 to 0.89]), or Yes (HR, 0.69 [95% CI, 0.53 to 0.92]).](https://canjhealthtechnol.ca/index.php/cjht/article/download/PC0392r/version/1309/2923/11297/PC0392-Clinical_Review-fig02.png)
A + L = amivantamab plus lazertinib; CI = confidence interval; eCRF = electronic case report form; HR = hazard ratio; NE = not estimable; Osi = osimertinib.
Note: HR from the subgroup analysis is from an unstratified proportional hazards model.
a Based on investigator-reported data recorded on the eCRF page.
Source: details included in the figure are from the MARIPOSA Clinical Study Report (August 11, 2023, data cut-off).12
Table 24: Summary of PFS as Assessed by Investigator — August 11, 2023, Data Cut-Off
Variable | MARIPOSA | |
|---|---|---|
Amivantamab plus Lazertinib N = 429 | Osimertinib N = 429 | |
PFS | ||
Total events, n (%) | 189 (44.1) | 230 (53.6) |
Censored patients, n (%) | 240 (55.9) | 199 (46.4) |
PFS (months), median (95% CI) | 23.92 (20.30, 29.54) | 19.94 (17.08, 21.98) |
HR (95% CI) vs Osimertiniba | 0.79 (0.65, 0.95) | |
P valueb | 0.0139 | |
Proportion (95% CI) of patients who were progression-free | ||
At 6 months | ███ █████ ████ | ███ █████ ████ |
Difference (95% CI) vs. Osimertinib | ██ | |
At 12 months | ███ █████ ████ | ███ █████ ████ |
Difference (95% CI) vs. Osimertinib | ██ | |
At 18 months | ███ █████ ████ | ███ █████ ████ |
Survival difference (95% CI) vs. Osimertinib | ██ | |
At 24 months | ███ █████ ████ | ███ █████ ████ |
Survival difference (95% CI) vs. Osimertinib | ██ | |
CI = confidence interval; HR = hazard ratio; NR = not reported; PFS = progression-free survival.
Source: details included in the figure are from the MARIPOSA CSR (August 11, 2023, data cut-off).12
Table 25: Summary of CNS Efficacy Outcomes in MARIPOSA (FAS)
PFS outcome | Primary analysis (August 11, 2023 DCO) | Updated efficacy analysis (May 13, 2024, DCO) | ||
|---|---|---|---|---|
Amivantamab plus lazertinib N = 429 | Osimertinib N = 429 | Amivantamab plus lazertinib N = 429 | Osimertinib N = 429 | |
Intracranial PFS by BICR (secondary end point) | ||||
Median icPFS, months | NE (18.43, NE) | 21.09 (18.40, NE) | █████ ███████ ██████ | █████ ███████ ██████ |
HR (95% CI)a; P valueb | 0.96 (0.70, 1.33); 0.8168 | ████ █████ █████ █████ | ||
6-month event-free rate (%) | 0.87 (0.81, 0.91) | 0.88 (0.82, 0.92) | ███ █████ ████ | ███ █████ ████ |
12-month event-free rate (%) | 0.71 (0.64, 0.77) | 0.75, 0.68, 0.81) | ███ █████ ████ | ███ █████ ████ |
18-month event-free rate (%) | 0.59 (0.51, 0.66) | 0.58 (0.50, 0.66) | ███ █████ ████ | ███ █████ ████ |
24-month event-free rate (%) | 0.51 (0.42, 0.59) | 0.46 (0.36, 0.55) | ███ █████ ████ | ███ █████ ████ |
30-month event-free rate (%) | NR | NR | ███ █████ ████ | ███ █████ ████ |
36-month event-free rate (%) | NR | NR | ███ █████ ████ | ███ █████ ████ |
Intracranial objective response rate (exploratory end point) | ||||
Intracranial disease at baseline, N | 180 | 187 | ███ | ███ |
icORR CR plus PR, (95% CI) | 76.7% (69.8, 82.6) | 76.5% (69.7, 82.4) | ████ █████ ████ | ███ ███ ████ |
OR (95% CI); p-valuec | 1.00 (0.61. 1.63); 0.9964 | ███ █████ ████ ██████ | ||
Complete response | 112 (62.2%) | 108 (57.8%) | ██ ██████ | ██ ██████ |
Partial response | 26 (14.4%) | 35 (18.7%) | █ ██████ | █ ██████ |
Stable diseased | 35 (19.4%) | 39 (20.9%) | █ ██████ | █ ██████ |
Progressive disease | 3 (1.7%) | 2 (1.1%) | | ██████ | | ██████ |
Not evaluable | 4 (2.2%) | 3 (1.6%) | | ██████ | | ██████ |
Intracranial duration of response (exploratory end point) | ||||
Median icDOR (95% CI) | NE (20.24, NE) | NE (NE, NE) | ██ ███ ███ | ███ ██████ |
≥ 6 months | 107 (77.5%) | 111 (77.6%) | ███ ██████ | ███ ██████ |
≥ 12 months | 80 (58.0%) | 77 (53.8%) | ██ ███████ | ██ ███████ |
≥ 18 months | 43 (31.2%) | 30 (21.0%) | ██ ███████ | ██ ███████ |
≥ 24 months | 14 (10.1%) | 6 (4.2%) | ██ ███████ | ██ ███████ |
≥ 30 months | NR | NR | ██ ███████ | ██ ██████ |
≥ 36 months | NR | NR | | ██████ | | ██████ |
Time to intracranial disease progression (exploratory end point) | ||||
██████ ████ ███ | ██ ████ ███ | ██ ████ ███ | ███ | ███ |
██ ████ ███ ███████ | ████ █████ █████ █████ | ███ | ||
███████ ███████████ ███ | ███ █████ ████ | ███ █████ ████ | ███ | ███ |
██████ ████████ ███ ███ | ███ █████ ████ | ███ █████ ████ | ███ | ███ |
███████ ██████ ███ ███ | ███ █████ ████ | ███ █████ ████ | ███ | ███ |
██████ ████████ █████ | ███ █████ ████ | ███ █████ ████ | ███ | ███ |
BICR = blinded independent central review; CI = confidence interval; CR = complete response; DCO = data cut-off; HR = hazard ratio; icDOR = intracranial duration of response; icORR = intracranial objective response rate; icPFS = intracranial PFS; NE = not estimable; OR = odds ratio; PFS = progression-free survival.
aHR is from a stratified proportional hazards model. HR < 1 favours amivantamab plus lazertinib.
bP value is from a log-rank test stratified by mutation type (Exon 19del or Exon 21 L858R), race (Asian or Non-Asian), and history of brain metastasis (present or absent).
cP value and OR are from logistic regression model stratified by mutation type (exon 19dle or exon 21 L858R) and race (Asian or non-Asian). OR > 1 favours amivantamab plus lazertinib.
dIncludes non-CR/non-PD in subjects with only nontarget lesions at baseline. e Quartiles and 95% CIs are estimated with Kaplan-Meier method.
Source: Details included in the table are from the sponsor’s summary of clinical evidence,44 the MARIPOSA CSR (August 11, 2023 data cut)12 and MARIPOSA Efficacy Update CSR (May 13, 2024 data cut-off).13
Figure 3: Complete NMA Network for OS, PFS, and ORR [Redacted]

████ █████████ ████ ████████████ ████ ████████████ ████ ██████████ ████ ██████████ ███ ████████████████████ ██ █████████████████████ ████████████ █████████ ████ ██████████ ████ ██████████ ████ ███████████ ████ ███████████ ████ ████████████████████ ███████ ████████ ██ ███ ██████ ███ ████ ███ █████████ ███ █████████ ███████
Figure 4: Complete NMA Network for AEs and SAEs [Redacted]

████ █████████ ████ ████████████ ████ ████████████ ███ ████████████████████ ██ ███████████ ██████████ ████████████ █████████ ████ ██████████ ████ ██████████ ████ ███████████ ████ ████████████████████ ███████ ████████ ██ ███ ██████ ███ ████ ███ █████████ ███ █████████ ███████
Pharmacoeconomic Report
Abbreviations
AE
adverse event
BIA
budget impact analysis
CDA-AMC
Canada's Drug Agency
ICER
incremental cost-effectiveness ratio
LY
life-year
NMA
network meta-analysis
NSCLC
non–small cell lung cancer
OS
overall survival
PBC
platinum-based chemotherapy
PFS
progression-free survival
QALY
quality-adjusted life-year
SAE
serious adverse event
TTD
time to treatment discontinuation
WTP
willingness to pay
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Amivantamab (Rybrevant), liquid concentrate for IV fusion, 50 mg/mL Lazertinib (Lazcluze), 80 mg and 240 mg tablets |
Indication | For the first-line treatment of adult patients with locally advanced (not amenable to curative therapy) or metastatic NSCLC with EGFR exon 19 deletions or exon 21 L858R substitution mutations |
Health Canada approval status | NOC |
Health Canada review pathway | Standard review (Project Orbis) |
NOC date | March 6, 2025 |
Reimbursement request | As per indication |
Sponsor | Janssen Inc. |
Submission history | Previously reviewed: No |
NOC = Notice of Compliance; NSCLC = non–small cell lung cancer.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis PSM |
Target population | Adult patients with locally advanced (not amenable to curative therapy) or metastatic NSCLC with EGFR exon 19 deletions or exon 21 L858R substitution mutations in the first-line setting |
Treatments | Amivantamab plus lazertinib |
Dose regimen | Amivantamab:
Lazertinib:
|
Submitted price | Amivantamab liquid concentrate for IV fusion, 50 mg/mL: $1,676.00 Lazertinib tablets, 80 mg: $103.60 and 240 mg: $310.82 |
Submitted treatment cost | $12,135 per 28-day cycle |
Comparators |
|
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs, LYs |
Time horizon | Lifetime (15 years) |
Key data sources | MARIPOSA trial: amivantamab plus lazertinib compared with osimertinib monotherapy NMA: amivantamab plus lazertinib compared with osimertinib plus PBC |
Submitted results |
|
Key limitations |
|
CDA-AMC reanalysis results |
|
AE = adverse event; CDA-AMC = Canada's Drug Agency; ICER = incremental cost-effectiveness ratio; LY = life-year; NMA = network meta-analysis; NSCLC = non–small cell lung cancer; OS = overall survival; PBC = platinum-based chemotherapy; PFS = progression-free survival; PSM = partitioned survival model; QALY = quality-adjusted life-year; SAE = serious adverse event; vs. = versus; WTP = willingness to pay.
Conclusions
The sponsor submitted evidence from 1 pivotal randomized, open-label trial (MARIPOSA) which demonstrated that amivantamab plus lazertinib was associated with a benefit compared with osimertinib monotherapy in terms of progression-free survival (PFS) for the treatment of adult patients with locally advanced (not amenable to curative therapy) or metastatic non–small cell lung cancer (NSCLC) with EGFR exon 19 deletions or exon 21 L858R substitution mutations in the first-line setting. However, the most relevant comparator for amivantamab plus lazertinib in practice in Canada was determined by clinical experts to be osimertinib plus platinum-based chemotherapy (PBC). In the absence of head-to-head evidence for amivantamab plus lazertinib compared with osimertinib plus PBC, the sponsor submitted a network meta-analysis (NMA) to inform the comparative PFS and overall survival (OS) parameters used within the economic evaluation. The clinical review by Canada’s Drug Agency (CDA-AMC) noted inconsistent timing of disease assessments between the MARIPOSA and FLAURA2 trials, along with factors such as heterogeneity in the presence of █████ ██████████ and unknown information on 2 potential prognostic factors. As a result, the CDA-AMC Clinical Review reported that there was insufficient evidence to detect any difference between amivantamab plus lazertinib compared to osimertinib plus PBC for OS, PFS, adverse events (AEs) and serious AEs (SAEs).
CDA-AMC identified several limitations with the sponsor’s pharmacoeconomic analysis, which mostly resulted from limitations with the submitted comparative evidence. The incremental quality-adjusted life-years (QALYs) gained for amivantamab plus lazertinib compared with osimertinib is largely derived from long-term parametric extrapolations of OS from the MARIPOSA trial. The incremental QALYs gained for amivantamab plus lazertinib compared with osimertinib plus PBC are largely derived based on the hazard ratio estimated from the NMA. Incremental cost for both comparators is largely driven by differences in drug acquisition costs (93% for osimertinib plus PBC and 97% for osimertinib monotherapy). The CDA-AMC base case addresses the clinical uncertainty by assuming equivalent clinical efficacy between amivantamab plus lazertinib compared to osimertinib plus PBC, and using the Gompertz extrapolation function to estimate long-term OS for amivantamab plus lazertinib compared to osimertinib monotherapy.
The CDA-AMC base-case results align with the sponsor’s, indicating that amivantamab plus lazertinib is not cost-effective at a willingness-to-pay (WTP) threshold of $50,000 per QALY gained, relative to osimertinib monotherapy. Results from the CDA-AMC base case suggest that osimertinib plus PBC was associated with fewer costs and equal benefit compared to amivantamab plus lazertinib (incremental costs = $81,302), and amivantamab plus lazertinib was associated with an incremental cost-effectiveness ratio (ICER) of $305,328 per QALY gained compared to osimertinib monotherapy. At the submitted price for amivantamab and lazertinib, the regimen would require a price reduction of 87% for amivantamab plus lazertinib to be considered cost-effective at a WTP threshold of $50,000 per QALY, compared to osimertinib monotherapy. There was insufficient clinical evidence to justify a price premium for amivantamab plus lazertinib over the cost of osimertinib plus PBC.
Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, clinician groups, and drug plans that participated in the CDA-AMC review process.
Patient input was received from 3 organizations: Lung Cancer Canada, Canadian Cancer Survivor Network, and Lung Health Foundation. Input was collected in Canada through virtual interviews conducted directly with the patients. Three of the patients reported experience with currently available EGFR-targeted therapies including osimertinib, gefitinib, and afatinib with limited side effects (significantly dry skin, thinning of hair, or diarrhea) before their disease progressed. As such, progression and treatment resistance remain a critical concern for these patients. The input noted that patients desire a treatment that improves the management of their disease symptoms, delays further progression, shrinks their tumours, improves their quality of life, prolongs survival with independence and functionality, and has manageable side effects. The input noted that 3 patients, each with a different mutation (exon 20, exon 19, or exon 21 L858R), reported successful tumour shrinkage and stable metastases after receiving amivantamab as a first-line, third-line, or later treatment, respectively. One of these patients developed additional metastases approximately 3 years after initiating third-line amivantamab and has since passed away. The input also noted that 1 patient has been receiving lazertinib and amivantamab combination therapy as a second-line treatment for more than 2.5 years to date with initial shrinking in their primary tumour and is currently experiencing stable metastases. Two patients reported significant side effects at treatment onset, including severe dry scalp and bleeding due to dryness, paronychia, painful acne, as well as rashes on their scalp, back, and chest. The input also noted that patients preferred the ease and convenience of oral targeted therapies that can be taken at home versus long infusion times in the hospital with amivantamab.
Clinician input was received from 2 groups: the Ontario Health (Cancer Care Ontario) Lung and Thoracic Cancer Drug Advisory Committee and the Lung Cancer Canada Medical Advisory Committee. The input noted that in NSCLC with EGFR mutations, the standard first-line treatment for the common mutations is osimertinib, an oral tyrosine kinase inhibitor which is widely funded and available throughout Canada. To overcome the inevitable resistance to osimertinib, intensified regimens have been tested in the first-line setting including adding pemetrexed and platinum chemotherapy to osimertinib; this has been approved by Health Canada (recommended for reimbursement with conditions by CDA-AMC in May 2024). The clinicians agreed that all patients on osimertinib eventually develop treatment resistance and there are currently no publicly funded targeted therapies available for patients progressing on osimertinib in Canada. As such, the clinician groups noted that there is a need for additional treatments that improve OS, symptoms, and PFS, and are more convenient, have manageable toxicity, and protect the brain from cancer growth to a greater degree than the current standard of care. Both clinician groups agreed that the combination of amivantamab and lazertinib would be used as a first-line treatment in patients with advanced EGFR-mutated NSCLC. According to the input, patients best suited for the treatment under review are those with advanced EGFR-mutated NSCLC.
Drug plan input received for this review noted that as the regimen under review contains an oral and IV drug, and depending on the jurisdiction, the treatments may be funded differently. The plans questioned if it would be appropriate to switch patients from osimertinib plus PBC to amivantamab plus lazertinib, if this treatment was funded. Drug plan input noted that venous thromboembolism has a higher incidence in the amivantamab plus lazertinib treatment arm, and that prophylaxis for the first 4 months of treatment is recommended. The plans noted the presence of confidential prices for osimertinib.
Several of these concerns were addressed in the sponsor’s model.
The sponsor included AEs, including venous thromboembolism.
In addition, CDA-AMC addressed some of these concerns as follows.
CDA-AMC noted the limitation of confidential pricing for comparators in the both the cost-utility analysis and budget impact analysis (BIA).
CDA-AMC was unable to address the following concerns raised from the received input.
Cost-effectiveness of amivantamab plus lazertinib was not compared to osimertinib plus PBC due to limitations surrounding the NMA evidence.
Economic Review
The current review is for amivantamab (Rybrevant) plus lazertinib (Lazcluze) for adult patients with locally advanced (not amenable to curative therapy) or metastatic NSCLC with EGFR exon 19 deletions or exon 21 L858R substitution mutations in the first-line setting.
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted a cost-utility analysis of amivantamab plus lazertinib for the first-line treatment of adult patients with locally advanced (not amenable to curative therapy) or metastatic NSCLC with EGFR exon 19 deletions or exon 21 L858R substitution mutations.1 The model population is consistent with the Health Canada–approved indication and the reimbursement request, and these populations are aligned with the sponsor’s MARIPOSA trial population.
Amivantamab is available as a 50 mg/mL liquid concentrate for IV fusion. The recommended dose is 1,050 mg (1,400 mg if the body weight is ≥ 80 kg) by IV infusion once weekly for the first 4 weeks, then once every 2 weeks starting at week 5.2 The first infusion is split in 2 and given on day 1 and day 2 in week 1. Lazertinib is available as an 80 mg or 240 mg tablet.3 The recommended dose is 240 mg orally once daily or until disease progression or unacceptable toxicity.3 At the sponsor’s submitted price of $1,676 (350 mg/7 mL) for amivantamab and $103.6 per 80 mg tablet or $310.82 per 240 mg tablet for lazertinib, the 28-day cost of amivantamab plus lazertinib was $12,135. First-line comparator treatments considered in the cost-utility analysis included osimertinib monotherapy, and osimertinib plus PBC. PBC was defined as 2 combination regimens of either cisplatin plus pemetrexed or carboplatin plus pemetrexed. The sponsor submitted a deviation request to exclude first-generation and second-generation EGFR tyrosine kinase inhibitors (erlotinib, gefitinib, and afatinib), based on osimertinib’s efficacy profile when compared to erlotinib or gefitinib in the FLAURA trial.4,5
The clinical outcomes modelled were PFS and OS. The economic outcomes of interest were QALYs and life-years (LYs). The patient age at model entry was 62.1 years and the economic analysis was undertaken over a lifetime time horizon (assumed to be 15 years) from the perspective of the Canadian publicly funded health care system. Costs and QALYs were discounted at a rate of 1.5% per annum.
Model Structure
The sponsor submitted a partitioned survival model with 3 health states: progression-free, post-progression, and death. The proportion of patients in each health state was estimated over time based on the OS and PFS curves for each intervention. All patients entered the model in the progression-free health state, where they received 1 of the treatment options, with state occupancy defined by PFS and OS. The cycle length selected for the model was 1 week to account for different treatment schedules. A half-cycle correction was applied in the model.
Model Inputs
The modelled population generally reflected the baseline characteristics of the enrolled population in the MARIPOSA trial, a phase III, randomized, open-label, multicentre clinical trial that was designed to evaluate the efficacy of amivantamab plus lazertinib compared with osimertinib for the first-line treatment of patients with locally advanced (not amenable to curative therapy) or metastatic NSCLC with EGFR exon 19 deletions or exon 21 L858R substitution mutations. The sponsor’s model used a mean age of 62.1 years, a mean weight of 63.9 kg, and a mean body surface area of 1.68 m2.6-8
Key efficacy inputs (OS and PFS) for amivantamab plus lazertinib and osimertinib were derived from an August 2023 cut-off of MARIPOSA trial data. Efficacy inputs for osimertinib plus PBC were estimated based on results from an NMA that assessed the relative efficacy and safety of amivantamab plus lazertinib compared with other potentially relevant first-line treatment options, including osimertinib plus PBC.9
The sponsor extrapolated OS, PFS, and time to treatment discontinuation (TTD) from the MARIPOSA trial Kaplan-Meier for amivantamab plus lazertinib versus osimertinib and plotted curves alongside the Kaplan-Meier data. Survival distributions were selected based on clinical plausibility of long-term projections, visual inspection of fit, and the Akaike information criterion and Bayesian information criterion. The Weibull curve was selected for the base case, as it was determined to be the most clinically plausible for amivantamab plus lazertinib and osimertinib for PFS and TTD. Spline, hazard, 1 knot curve was selected for the base case, as it was determined to be the most clinically plausible for amivantamab plus lazertinib and osimertinib for OS. For osimertinib plus PBC, PFS and OS were modelled using the hazard ratios reported from the primary analysis for the NMA of PFS in the submitted indirect treatment comparison technical report. The hazard ratios for duration of treatment were assumed to be the same as the PFS hazard ratios.
AEs included in the model were limited to grade 3 or greater events that occurred in at least 5% of the patients in any treatment arm, as well as grade 1 to grade 2 infusion-related reactions and venous thromboembolisms. The grade 3 or greater AEs included in the model were alanine aminotransferase increased, anemia, dermatitis acneiform, hypoalbuminemia, infusion-related reactions, neutropenia, paronychia, pulmonary embolism, rashes, and thrombocytopenia.
Health state utility values were sourced from EQ-5D-5L data collected in the MARIPOSA trial and published estimates. The EQ-5D-5L data collected in the MARIPOSA trial were used to derive utility values for the progression-free (0.85) and progressed disease (0.81) health states. EQ-5D-5L scores were converted to a utility value using the Canadian value set for the EQ-5D-5L questionnaire.10 Disutilities for AEs were either sourced from the literature or based on assumptions and incorporated as a single disutility as an exception in the first cycle.
The model incorporated treatment acquisition costs for amivantamab plus lazertinib, comparators, and subsequent therapies. Dosing details were sourced from Health Canada product monographs, with lazertinib acquisition costs derived from the sponsor's submitted price1 and IQVIA Delta Price for other treatments.11 The dosage of treatments, including chemotherapy regimens, were estimated from the average body surface area estimates (1.68 m2) from the MARIPOSA trial's patient population.8 In the base-case analysis, the total number of administrations per week for amivantamab plus lazertinib and osimertinib monotherapy were adjusted to account for dose skipping and dose reductions, based on the MARIPOSA trial. Skipped doses were determined by first calculating the expected number of doses for each patient based on their treatment duration and planned dosing schedule; the proportion of doses that were skipped were then calculated as 1 minus the total number of doses administered in the trial divided by the expected total number of doses.12 Dose reductions were calculated as 1 minus the total cumulative dose recorded in the trial divided by the expected total cumulative dose. Treatment wastage was not applied to treatments where dose skipping and dose reductions were applied. Other costs included drug administration, premedication and comedication, monitoring, management of AEs, and subsequent treatment costs. Administration costs were sourced from the Ontario Schedule of Benefits for Physician Services,13 monitoring costs were obtained from the Ontario Schedule of Benefits for Laboratory Services,14 and costs of managing AEs were sourced from Ontario Case Costing Initiative 2015 and 2017 and the Canadian Institute for Health Information Patient Cost Estimator.15,16 End-of-life (terminal care) costs were included as a 1-time cost, applied at the time of death, sourced from the study by De Oliveria and colleagues.17
Summary of Sponsor’s Economic Evaluation Results
The base-case analysis was run probabilistically (1,000 iterations for the base case). The deterministic and probabilistic results were similar. The probabilistic findings are presented in the following.
Base-Case Results
The submitted analyses were based on publicly available prices of the comparator treatments. Results from the base case of the submitted economic evaluation are presented in Table 3. Additional results from the sponsor’s submitted economic evaluation base case are presented in Appendix 3.
In the sponsor’s base-case analysis, over a 15-year time horizon, the expected total costs and QALYs for amivantamab plus lazertinib were $580,321 and 4.17, respectively. Amivantamab plus lazertinib was associated with a gain of 1.43 QALYs at an additional cost of $241,626, resulting in an ICER of $169,413 compared to osimertinib monotherapy. Based on the sequential analysis, compared to osimertinib plus PBC, amivantamab plus lazertinib was associated with a gain of 0.27 QALYs at an additional cost of $81,830, resulting in an ICER of $304,970. Amivantamab plus lazertinib was cost-effective at a WTP threshold of $50,000 per QALY in approximately 1.5% of the iterations. Drug acquisition costs were responsible for 93% ($81,860) and 97% ($233,727) of the incremental cost between amivantamab plus lazertinib versus osimertinib plus PBC and osimertinib monotherapy, respectively. Fifty-seven percent of the QALYs in the sponsor-submitted model were calculated through extrapolation beyond the observation period of the MARIPOSA trial (31 months).
Table 3: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total costs ($) | Total QALYs | Sequential ICER ($/QALY) |
|---|---|---|---|
Osimertinib | 338,695 | 2.75 | Reference |
Osimertinib plus PBC | 498,491 | 3.91 | 138,001 vs. osimertinib |
Amivantamab plus lazertinib | 580,321 | 4.17 | 304,970 vs. osimertinib plus PBC |
ICER = incremental cost-effectiveness ratio; PBC = platinum-based chemotherapy; QALY = quality-adjusted life-year; vs. = versus.
Source: Sponsor’s pharmacoeconomic submission.1
Sensitivity and Scenario Analysis Results
The sponsor performed scenario analyses to assess the impact of the model’s structural and methodological assumptions, including discount rates; time horizon; and choice of extrapolated curves for OS, PFS, and TTD, including prophylactic anticoagulation and vial sharing. Dose skipping and dose reduction were excluded. Scenarios that produced the most favourable ICERs included those that considered a lower discount rate (i.e., 0%), a longer time horizon (i.e., 20 years), or alternative curve distributions for PFS, OS, and TTD (for amivantamab plus lazertinib and osimertinib monotherapy).The model was most sensitive to assumptions around dose skipping and dose reductions, which resulted in the highest ICERs of all scenarios tested as a result of the total increased costs. No scenario analysis was conducted using a perspective other than the health care payer.
CDA-AMC Appraisal of the Sponsor’s Economic Evaluation
CDA-AMC identified several key limitations to the sponsor’s analysis that have notable implications on the economic analysis.
Inconsistent definition of PFS between the FLAURA2 and MARIPOSA studies resulted in uncertainty surrounding clinical efficacy of osimertinib plus PBC. As noted in the sponsor’s submission, while the MARIPOSA clinical trial (which evaluated the efficacy of amivantamab plus lazertinib versus osimertinib) and the FLAURA2 clinical trial (which evaluated the efficacy of osimertinib plus PBC versus osimertinib), were conducted in the same target patient population, the absolute and relative level of benefits observed in the MARIPOSA and FLAURA2 studies have substantial methodological heterogeneity that limits the comparisons. Disease assessments were conducted more frequently in the MARIPOSA study than in the FLAURA2 study. In the MARIPOSA clinical trial, disease assessments were conducted at baseline, then every 8 weeks for the first 30 months, then every 12 weeks relative to randomization until disease progression. In the FLAURA2 clinical trial, disease assessments were conducted at baseline, week 6, week 12, and then every 12 weeks relative to first dose until disease progression. When questioned on the impact of the difference in disease assessment, clinical expert feedback highlighted that the comparison would be flawed. This ultimately introduces face validity concerns in the extrapolation of clinical benefit due to lack of comparability between the disease assessment timeline in the MARIPOSA and FLAURA2 studies. Therefore, this introduced uncertainty surrounding the comparison of clinical benefit between osimertinib plus PBC and amivantamab plus lazertinib. The CDA-AMC Clinical Review also noted that while the clinical evidence suggested that amivantamab plus lazertinib was superior to osimertinib monotherapy in terms of PFS, there was insufficient evidence to detect any difference between amivantamab plus lazertinib and osimertinib plus PBC for OS, PFS, all AEs, and all SAEs due to heterogeneity in the presence of █████ ██████████, unknown information on 2 potential prognostic factors, and the aforementioned differences in the study design. Additionally, clinical expert feedback obtained by CDA-AMC highlighted that because amivantamab is associated with notable adverse effects and requires more visits for infusion, and because of the absence of clear differences between osimertinib plus PBC and amivantamab plus lazertinib, physicians would likely prefer to prescribe osimertinib plus PBC for patients in the indicated population.
In the absence of direct evidence comparing amivantamab plus lazertinib to osimertinib plus PBC and owing to the limitations of the sponsor’s NMA, the extent to which amivantamab plus lazertinib offers a net benefit over osimertinib plus PBC remains uncertain. To address this limitation, CDA-AMC performed a reanalysis assuming equivalent clinical efficacy between amivantamab plus lazertinib and osimertinib plus PBC.
Impact of amivantamab plus lazertinib on long-term OS is highly uncertain. The sponsor submitted a partitioned survival model with survival parameters based on the population enrolled in the amivantamab plus lazertinib treatment arm of the MARIPOSA trial. OS for amivantamab plus lazertinib was extrapolated from MARIPOSA trial data, which had a median follow-up of 31 months. The sponsor estimated that 44% of patients receiving amivantamab plus lazertinib would be alive at 5 years. At 10 years, the sponsor projected that 16% of patients would still be alive. Clinical experts consulted by CDA-AMC suggested that the extrapolated estimates of OS at 5 years and 10 years did not match their expectations and were likely overestimated. The sponsor’s base case therefore likely estimated a larger benefit in the amivantamab plus lazertinib treatment arm than would be realized in clinical practice. Additionally, the estimated incremental QALYs for osimertinib plus PBC compared to osimertinib monotherapy estimated in the sponsor’s base case (1.16 QALYs) was much larger than the increment estimated in a previous CDA-AMC Reimbursement Review18 that evaluated osimertinib plus PBC compared to osimertinib monotherapy using the same FLAURA2 trial data (0.25 QALYs). Distinct methods were used to estimate relative efficacy in this previous review, and direct comparisons between the 2 estimates of incremental efficacy should be viewed as highly uncertain. However, the magnitude of this finding suggests that the sponsor’s extrapolation assumptions likely overestimate the incremental effectiveness of osimertinib plus PBC, and potentially that of amivantamab plus lazertinib.
According to the CDA-AMC Clinical Review, as of the data cut-off on August 11, 2023, the median OS had not been reached. Additionally, the analysis was conducted using a Cox proportional hazards model which only stratified on treatment assignment, while randomization was stratified on known treatment effect modifiers. The randomization factors were not included in the model, which may increase the uncertainty in the PFS and OS outcomes. Given the lack of robust long-term data, the projected OS benefit for patients receiving amivantamab plus lazertinib in the post-trial period of the model is highly uncertain.
To address this limitation, CDA-AMC undertook a reanalysis using a Gompertz function to extrapolate long-term OS for amivantamab plus lazertinib in the base case. Clinical experts consulted by CDA-AMC for this review suggested that the 5-year and 10-year survival estimates produced with this function were more aligned with their expectations for survival in this population.
Additionally, the following key assumptions were made by the sponsor and have been appraised by CDA-AMC (refer to Table 4).
Table 4: Key Assumptions of the Submitted Economic Evaluation (Not Noted as Limitations to the Submission)
Sponsor’s key assumption | CDA-AMC comment |
|---|---|
Use of spline models for extrapolated OS outcomes | Uncertain. In the sponsor’s submitted model, spline hazard curves were selected for modelling amivantamab plus lazertinib vs. osimertinib monotherapy curves for OS in the base case. While spline models may be attractive in recognizing the nonstandard shape of both hazards and hazard ratios for the period covered by the trial duration, there is the potential that the modelling of long-term outcomes is based on extrapolation from the tail of the KM curve and thus derived from a lesser volume of data.19 |
CDA-AMC = Canada's Drug Agency; KM = Kaplan-Meier; OS = overall survival; vs. = versus.
CDA-AMC Reanalyses of the Economic Evaluation
Base-Case Results
The CDA-AMC base case was derived by making changes in the model parameter values and assumptions, in consultation with clinical experts. The review team undertook a stepped analysis, incorporating each change detailed in Table 5 into the sponsor’s model to highlight the impact of each change. The summary results of the CDA-AMC reanalysis are presented in Table 6 (sequentially) and the stepped results are in Appendix 4.
Table 5: CDA-AMC Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CDA-AMC value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
1. Cost of carboplatin | 50 mg/5 mL: $106.12 | 50 mg/5 mL: $70.00 |
Changes to derive the CDA-AMC base case | ||
1. Comparative clinical efficacy between amivantamab plus lazertinib vs. osimertinib plus PBC | Osimertinib plus PBC PFS HR = 0.88 OS HR = 1.12 | Osimertinib plus PBC PFS HR = 1.0 OS HR = 1.0 |
2. Parametric extrapolation of amivantamab plus lazertinib | Spline, hazard, 1 knot | Gompertz |
CDA-AMC base case | ― | Reanalysis 1 + 2 |
CDA-AMC = Canada's Drug Agency; HR = hazard ratio; OS = overall survival; PBC = platinum-based chemotherapy; PFS = progression-free survival; vs. = versus.
Results of the CDA-AMC reanalysis demonstrate that osimertinib plus PBC was associated with fewer costs and equal benefit compared to amivantamab plus lazertinib (incremental costs of $81,302). Selecting the Gompertz distribution resulted in amivantamab plus lazertinib being associated with $201,023 in incremental costs and an incremental gain of 0.66 QALYs compared to osimertinib monotherapy, resulting in an ICER of $305,328. The probability that amivantamab plus lazertinib is cost-effective at a WTP threshold of $50,000 per QALY is 1.5%. Approximately 88% of the incremental QALYs for amivantamab plus lazertinib, relative to osimertinib monotherapy, were gained in the extrapolated period of the model.
Table 6: Summary of the CDA-AMC Reanalysis Results (Sequential)
Drug | Total costs ($) | Total QALYs | Sequential ICER ($/QALY) |
|---|---|---|---|
Sponsor base case (probabilistic; corrected) | |||
Osimertinib | 338,695 | 2.75 | Reference |
Osimertinib plus PBC | 497,157 | 3.91 | 136,849 vs. osimertinib |
Amivantamab plus lazertinib | 580,321 | 4.17 | 309,942 vs. osimertinib plus PBC |
CDA-AMC base case (probabilistic) | |||
Osimertinib | 338,695 | 2.75 | Reference |
Osimertinib plus PBC | 458,416 | 3.41 | 181,325 |
Dominated treatments | |||
Amivantamab plus lazertinib | 539,718 | 3.41 | Dominated by osimertinib plus PBC |
CDA-AMC = Canada's Drug Agency; ICER = incremental cost-effectiveness ratio; PBC = platinum-based chemotherapy; QALY = quality-adjusted life-year; vs. = versus.
Source: Sponsor’s pharmacoeconomic submission.1
Scenario Analysis Results
CDA-AMC undertook price reduction analyses based on the sponsor’s results and the CDA-AMC base case. The CDA-AMC base case suggested that an 87% price reduction for amivantamab would be required for amivantamab plus lazertinib to achieve cost-effectiveness relative to osimertinib at a WTP threshold of $50,000 per QALY gained. In Appendix 4, the price reduction analyses based on the sponsor’s results and CDA-AMC base case for a WTP threshold of $100,000 per QALY gained were presented. The sponsor’s results highlighted that a 47% price reduction for amivantamab would be required to achieve cost-effectiveness at the $100,000 per QALY gained threshold. The CDA-AMC base case suggested that a 70% price reduction for amivantamab would be required to achieve cost-effectiveness at a WTP threshold of $100,000 per QALY gained.
Table 7: CDA-AMC Price Reduction Analyses
Analysis: price reduction | Unit drug cost: amivantamab ($) | Unit drug cost: lazertinib ($) | ICERs for amivantamab plus lazertinib vs. osimertinib ($/QALY) | |
|---|---|---|---|---|
Sponsor base case | CDA-AMC reanalysis | |||
No price reduction | 1,676 | 311 | 169,413 | 305,506 |
10% | 1,508 | 280 | 154,756 | 276,112 |
20% | 1,341 | 249 | 140,069 | 246,719 |
30% | 1,173 | 218 | 125,381 | 217,325 |
40% | 1,006 | 186 | 110,694 | 187,932 |
50% | 838 | 155 | 96,007 | 158,538 |
60% | 670 | 124 | 81,320 | 129,144 |
70% | 503 | 93 | 66,633 | 99,751 |
80% | 335 | 62 | 51,945 | 70,357 |
90% | 168 | 31 | Amivantamab plus lazertinib is dominant | Amivantamab plus lazertinib is dominant |
CDA-AMC = Canada's Drug Agency; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; vs. = versus.
Issue for Consideration
CDA-AMC reanalyses are based on the public list prices of amivantamab plus lazertinib and other comparator treatments, which may differ from any confidential prices paid by the CDA-AMC–participating drug plans and may influence the results of the cost-effectiveness and BIA.
Overall Conclusions
The sponsor submitted evidence from 1 pivotal randomized, open-label trial (MARIPOSA) which demonstrated that amivantamab plus lazertinib was associated with a benefit compared with osimertinib monotherapy in terms of PFS for the treatment of adult patients with locally advanced (not amenable to curative therapy) or metastatic NSCLC with EGFR exon 19 deletions or exon 21 L858R substitution mutations in the first-line setting. However, the most relevant comparator for amivantamab plus lazertinib in practice in Canada was determined by clinical experts to be osimertinib plus PBC. In the absence of head-to-head evidence for amivantamab plus lazertinib compared with osimertinib plus PBC, the sponsor submitted an NMA to inform the comparative PFS and OS parameters used within the economic evaluation. The CDA-AMC Clinical Review noted inconsistent timing of disease assessments between the MARIPOSA and FLAURA2 trials, along with factors such as heterogeneity in the presence of █████ ██████████ and unknown information on 2 potential prognostic factors. As a result, the CDA-AMC Clinical Review reported that there was insufficient evidence to detect any difference between amivantamab plus lazertinib compared to osimertinib plus PBC for OS, PFS, AEs, and SAEs.
CDA-AMC identified several limitations with the sponsor’s pharmacoeconomic analysis, which mostly resulted from limitations with the submitted comparative evidence. The incremental QALYs gained for amivantamab plus lazertinib compared with osimertinib monotherapy are largely derived from long-term parametric extrapolations of OS from the MARIPOSA trial. The incremental QALYs gained for amivantamab plus lazertinib compared with osimertinib plus PBC are largely based on the hazard ratio estimated from the NMA. Incremental cost for both comparators is largely driven by differences in drug acquisition costs (93% and 97% for osimertinib plus PBC and osimertinib monotherapy, respectively). The CDA-AMC base case addresses the uncertainty surrounding these limitations by assuming equivalent clinical efficacy between amivantamab plus lazertinib compared to osimertinib plus PBC and using the Gompertz extrapolation function to estimate long-term OS for amivantamab plus lazertinib compared to osimertinib monotherapy.
The CDA-AMC base-case results align with those of the sponsor’s submitted analysis, indicating that amivantamab plus lazertinib is not cost-effective at a WTP threshold of $50,000 per QALY gained, relative to osimertinib monotherapy. Results from the CDA-AMC base case suggest that osimertinib plus PBC was associated with fewer costs and equal benefit compared to amivantamab plus lazertinib (incremental costs = $81,302) and amivantamab plus lazertinib was associated with an ICER of $305,328 per QALY gained compared to osimertinib monotherapy. At the submitted price for amivantamab and lazertinib, the regimen would require a price reduction of 87% for amivantamab plus lazertinib to be considered cost-effective at a WTP threshold of $50,000 per QALY, compared to osimertinib monotherapy. There was insufficient evidence to justify a price premium for amivantamab plus lazertinib over the cost of osimertinib plus PBC.
References
1.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Lazcluze (lazertinib), 80 mg and 240 mg oral tablets, and Rybrevant (amivantamab), 50 mg/mL concentrate for solution for intravenous infusion. Toronto (ON): Janssen Inc.; 2024 Dec 18.
2.Janssen Inc. Rybrevant (amivantamab for injection): 50 mg/mL concentrate for solution for intravenous infusion, in single use vial [draft product monograph]. June 28, 2024.
3.Lazcluze (lazertinib): 80 mg and 240 mg oral tablets [product monograph]. Janssen Inc.; July 19, 2024.
4.Melosky B, Banerji S, Blais N, et al. Canadian consensus: a new systemic treatment algorithm for advanced EGFR-mutated non-small-cell lung cancer. Curr Oncol. 2020;27(2):e146-e155. doi: 10.3747/co.27.6007 PubMed
5.Canada's Drug Agency. Reimbursement Review Provisional Funding Algorithm: advanced or metastatic non–small cell lung cancer with activating epidermal growth factor receptor mutations. December 2024. Accessed December 16, 2024. https://www.cda-amc.ca/sites/default/files/DRR/2024/PH0054-FINAL_NSCLC_EGFR.pdf
6.Cho BC, Lu S, Felip E, et al. Amivantamab plus Lazertinib in Previously Untreated EGFR-Mutated Advanced NSCLC. N Engl J Med. 2024;391(16):1486-1498. doi: 10.1056/NEJMoa2403614 PubMed
7.Soria JC, Ohe Y, Vansteenkiste J, et al. Osimertinib in Untreated EGFR-Mutated Advanced Non-Small-Cell Lung Cancer. N Engl J Med. 2018;378(2):113-125. doi: 10.1056/NEJMoa1713137 PubMed
8.Janssen Research & Development, LLC. Clinical Study Report: 73841937NSC3003, MARIPOSA, Primary Endpoint Analysis. A Phase 3, Randomized Study of Amivantamab and Lazertinib Combination Therapy Versus Osimertinib Versus Lazertinib as First-Line Treatment in Patients with EGFR-Mutated Locally Advanced or Metastatic Non-Small Cell Lung Cancer [internal sponsor's report]. November 28, 2023.
9.Janssen Inc. Network meta-analysis report: first-line treatments for patients with advanced cEGFR-mutated NSCLC [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Lazcluze (lazertinib), 80 mg and 240 mg oral tablets, and Rybrevant (amivantamab), 50 mg/mL concentrate for solution for intravenous infusion. February 27, 2024.
10.Xie F, Pullenayegum E, Gaebel K, et al. A Time Trade-off-derived Value Set of the EQ-5D-5L for Canada. Med Care. 2016;54(1):98-105. doi: 10.1097/MLR.0000000000000447 PubMed
11.IQVIA. DeltaPA. 2023. Accessed January 15, 2025. https://www.iqvia.com/
12.Janssen. (Data on file). MARIPOSA dose skipping and dose reductions. 2024 [sponsor supplied reference].
13.Ontario Ministry of Health. Schedule of benefits for physician services under the Health Insurance Act: (February 20, 2024 (effective April 1, 2024)). 2024. Accessed April 18, 2024. https://www.ontario.ca/files/2024-04/moh-schedule-benefit-2024-02-20.pdf [sponsor supplied reference]
14.Ontario Ministry of Health. Schedule of benefits for laboratory services: (effective July 24, 2023). 2023. Accessed April 18, 2024. https://www.ontario.ca/files/2024-01/moh-ohip-schedule-of-benefits-laboratory-services-2024-01-24.pdf [sponsor supplied reference]
15.Ontario Ministry of Health. OCCI Tool (2017-2018). 2018 [sponsor supplied reference].
16.Canadian Institute for Health Information. Patient Cost Estimator (2021-2022). 2022. Accessed April 23, 2024. https://www.cihi.ca/en/patient-cost-estimator
17.De Oliveira C, Pataky R, Bremner KE, et al. Estimating the Cost of Cancer Care in British Columbia and Ontario: A Canadian Inter-Provincial Comparison. Healthc Policy. 2017;12(3):95-108. PubMed
18.Canada's Drug Agency. Reimbursement Recommendation: osimertinib (Tagrisso). Can J Health Technol. 2024;4(10). doi: 10.51731/cjht.2024.1006
19.Coyle D, Haines A, Lee K. Extrapolating clinical evidence within economic evaluations. Can J Health Technol. 2023;3(5). doi: 10.51731/cjht.2023.649 PubMed
20.National Kidney Foundation. Estimated Glomerular Filtration Rate (eGFR). Updated July 13, 2022. Accessed October 1, 2024. https://www.kidney.org/kidney-topics/estimated-glomerular-filtration-rate-egfr
21.Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Lazcluze (lazertinib), 80 mg and 240 mg oral tablets, and Rybrevant (amivantamab), 50 mg/mL concentrate for solution for intravenous infusion. Toronto (ON): Janssen Inc.; 2024 Dec 18.
22.Brenner DR, Gillis J, Demers AA, et al. Projected estimates of cancer in Canada in 2024. CMAJ. 2024;196(18):E615-E623. doi: 10.1503/cmaj.240095 PubMed
23.Canadian Cancer Statistics Advisory Committee. Canadian Cancer Statistics: A 2020 special report on lung cancer. Canadian Cancer Society; 2020. Accessed October 18, 2024. https://cancer.ca/Canadian-Cancer-Statistics-2020-EN
24.Vinod SK, Wai E, Alexander C, Tyldesley S, Murray N. Stage III non-small-cell lung cancer: population-based patterns of treatment in British Columbia, Canada. J Thorac Oncol. 2012;7(7):1155-63. doi: 10.1097/JTO.0b013e31824fea07 PubMed
25.Seung SJ, Hurry M, Walton RN, Evans WK. Retrospective cohort study of unresectable stage III non-small-cell lung cancer in Canada. Curr Oncol. 2020;27(4):e354-e360. doi: 10.3747/co.27.6047 PubMed
26.Agulnik J, Kasymjanova G, Pepe C, et al. Understanding clinical practice and survival outcomes in patients with unresectable stage III non-small-cell lung cancer in a single centre in Quebec. Curr Oncol. 2020;27(5):e459-e466. doi: 10.3747/co.27.6241 PubMed
27.Moore S, Leung B, Wu J, Ho C. Real-World Treatment of Stage III NSCLC: The Role of Trimodality Treatment in the Era of Immunotherapy. J Thorac Oncol. 2019;14(8):1430-1439. doi: 10.1016/j.jtho.2019.04.005 PubMed
28.Seung SJ, Hurry M, Walton RN, Evans WK. Real-world treatment patterns and survival in stage IV non-small-cell lung cancer in Canada. Curr Oncol. 2020;27(4):e361-e367. doi: 10.3747/co.27.6049 PubMed
29.Brenner DR, O'Sullivan DE, Jarada TN, et al. The impact of population-based EGFR testing in non-squamous metastatic non-small cell lung cancer in Alberta, Canada. Lung Cancer. 2023;175:60-67. doi: 10.1016/j.lungcan.2022.11.017 PubMed
Appendix 1: Cost Comparison Table
Please note that this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical experts and drug plan. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 8: CDA-AMC Cost Comparison Table for Non–Small Cell Lung Cancer
Treatment | Strength / concentration | Form | Price | Recommended dosage | Daily cost ($) | 28-day cost ($) |
|---|---|---|---|---|---|---|
Amivantamab (Rybrevant) | 50 mg/mL | 7 mL (350 mg) Solution for IV infusion | 1,676.0000 | Body weight < 80 kg: 1,050 mg weekly for 4 weeks, then every 2 weeks Body weight ≥ 80 kg: 1,400 mg weekly for 4 weeks, then every 2 weeks | First 28 days: 718.29 to 957.71 Thereafter: 359.14 to 478.86 | First 28 days: 20,112 to 26,816 Thereafter: 10,056 to 13,408 |
Lazertinib (Lazcluze) | 80 mg 240 mg | Tablet | 103.6400a 310.9200a | 240 mg once daily | 310.92 | 8,706 |
Amivantamab plus lazertinib | First 28 days: 1,029 to 1,269 Thereafter: 670.06 to 789.78 | First 28 days: 28,818 to 35,522 Thereafter: 18,762 to 22,114 | ||||
Osimertinib monotherapy | ||||||
Osimertinib (Tagrisso) | 40 mg 80 mg | Tablet | 322.1280 | 80 mg once daily until disease progression or unacceptable toxicity | 322.12 | 9,020 |
Osimertinib plus carboplatin and pemetrexed | ||||||
Osimertinib (Tagrisso) | 40 mg 80 mg | Tablet | 322.1280 | 80 mg once daily until disease progression or unacceptable toxicity | 322.12 | 9,020 |
Carboplatin (generic) | 50 mg/5 mL 150 mg/15 mL 450 mg/45 mL 600 mg/60 mL | Vial for IV infusion | 70.0000 210.0000 599.9985 775.0020 | Target AUC 5 on day 1 Q3W, 750 mg/mL for a total of 4 cycles | 35.24 | 987 |
Pemetrexed (generic) | 100 mg 500 mg 1,000 mg | Powder for solution for infusion | 50.0000 250.0000 4,290.0000 | 500 mg/m2 Q3W | 21.43 | 600 |
CRBPPME plus osimertinib | 378.79 | 10,606 | ||||
Osimertinib plus cisplatin and pemetrexed | ||||||
Osimertinib (Tagrisso) | 40 mg 80 mg | Tablet | 322.1280 | 80 mg once daily until disease progression or unacceptable toxicity | 322.12 | 9,020 |
Cisplatin (Generic) | 50 mg/50 mL 100 mg/100 mL | Vial for IV infusion | 135.0000 270.0000 | 75 mg/m2 Q3W, for a total of 4 cycles | 19.29 | 540 |
Pemetrexed (Generic) | 100 mg 500 mg 1,000 mg | Powder for solution for infusion | 50.0000 250.0000 4,290.0000 | 500 mg/m2 Q3W | 21.43 | 600 |
CISPPME plus osimertinib | 362.84 | 10,160 | ||||
CISPPME = cisplatin and pemetrexed regimen; CRBPPME = carboplatin and pemetrexed regimen; IV = IV; Q3W = every 3 weeks.
Notes: All prices are from IQVIA Delta PA (accessed January 2025),11 unless otherwise indicated, and do not include dispensing fees. Dosing is based on Cancer Care Ontario product monographs. For treatments using weight-based, CDA-AMC assumed 63.9 kg, and 1.68m2 based on the MARIPOSA trial.8 An eGFR of 85 mL/min was assumed.20
aThe sponsor’s application was filed on a pre-NOC basis and its pharmacoeconomic submission is reflected of the proposed treatment cost that was initially submitted to CDA-AMC. During the submission process, the sponsor provided updated pricing information for lazertinib, where the price for the 80 mg tablet changed from $103.6000 to $103.6400 and the price of the 240 mg tablet changed from $310.8163 to $310.9200. The updated price of the tablets is reflected in the cost table. However, when the impact of the pricing change was explored in the cost-utility analysis and BIA, the magnitude and direction of the results did not meaningfully change. The analyses in the report align with the sponsor-submitted pharmacoeconomic files.
Appendix 2: Submission Quality
Please note that this appendix has not been copy-edited.
Description | Yes or No | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | No | The OS data used in the model for amivantamab plus lazertinib was immature. |
Model has been adequately programmed and has sufficient face validity | Yes | No comment. |
Model structure is adequate for decision problem | Yes | No comment. |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | Yes | No comment. |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | No | Refer to key limitation “Inconsistent definition of PFS between FLAURA2 and MARIPOSA resulted in uncertainty surrounding clinical efficacy of osimertinib plus PBC.” |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | Yes | No comment. |
Appendix 3: Additional Information on the Submitted Economic Evaluation
Please note that this appendix has not been copy-edited.
Detailed Results of the Sponsor’s Base Case
Table 10: Disaggregated Summary of the Sponsor’s Economic Evaluation Results
Parameter | Amivantamab plus lazertinib | Osimertinib | Osimertinib plus PBC |
|---|---|---|---|
Discounted LYs | |||
Total | 5.15 | 3.34 | 4.80 |
PF | 2.35 | 1.73 | 2.60 |
PD | 2.80 | 1.62 | 2.20 |
Discounted QALYs | |||
Total | 4.17 | 2.75 | 3.91 |
PF | 1.98 | 1.46 | 2.19 |
PD | 2.20 | 1.29 | 1.72 |
Disutilities | −0.003 | −0.001 | −0.002 |
Discounted costs ($) | |||
Total | 580,321 | 338,695 | 498,461 |
Acquisition | 493,780 | 260,053 | 405,431 |
Administration | 5,020 | 0 | 6,248 |
Premedication/comedication | 118 | 0 | 319 |
Monitoring | 0 | 119 | 991 |
Subsequent treatment | 13,182 | 14,337 | 22,384 |
Disease management - PF | 5,956 | 4,378 | 6,595 |
Disease management - PD | 6,371 | 3,675 | 4,991 |
End-of-life care | 51,015 | 55,625 | 51,808 |
AE management | 4,880 | 508 | 1,925 |
AE = adverse event; LY = life-year; PBC = platinum-based chemotherapy; PD = progressed disease; PF = progression-free; QALY = quality-adjusted life-year
Source: Sponsor’s pharmacoeconomic submission.1
Appendix 4: Additional Details on the CDA-AMC Reanalyses and Sensitivity Analyses of the Economic Evaluation
Please note that this appendix has not been copy-edited.
Detailed Results of CDA-AMC Base Case
Table 11: Summary of the Stepped Analysis of the CDA-AMC Base-Case Results
Stepped analysis | Drug | Total costs ($) | Total QALYs | Sequential ICER ($/QALY) |
|---|---|---|---|---|
Sponsor base case | Osimertinib | 338,695 | 2.75 | Reference |
Osimertinib plus PBC | 498,491 | 3.91 | 138,001 | |
Amivantamab plus lazertinib | 580,321 | 4.17 | 304,970 | |
Corrected base case | Osimertinib | 341,501 | 2.72 | Reference |
Osimertinib plus PBC | 506,775 | 3.84 | 147,368 | |
Amivantamab plus lazertinib | 580,579 | 4.14 | 247,544 | |
1. CDA-AMC reanalysis 1: comparative clinical efficacy between amivantamab plus lazertinib vs. osimertinib plus PBC | Osimertinib | 341,501 | 2.72 | Reference |
Osimertinib plus PBC | 506,533 | 4.14 | 116,154 | |
Dominated treatments | ||||
Amivantamab plus lazertinib | 580,579 | 4.14 | Dominated by osimertinib plus PBC | |
2. CDA-AMC reanalysis 2: parametric extrapolation of amivantamab plus lazertinib | Osimertinib | 341,501 | 2.72 | Reference |
Osimertinib plus PBC | 457,305 | 3.03 | 370,606 | |
Amivantamab plus lazertinib | 544,823 | 3.21 | 490,470 | |
CDA-AMC base case (deterministic) (reanalysis 1 + 2) | Osimertinib | 341,501 | 2.72 | Reference |
Osimertinib plus PBC | 464,646 | 3.21 | 250,266 | |
Dominated treatments | ||||
Amivantamab plus lazertinib | 544,823 | 3.21 | Dominated by osimertinib plus PBC | |
CDA-AMC base case (probabilistic) (reanalysis 1 + 2) | Osimertinib | 338,695 | 2.75 | Reference |
Osimertinib plus PBC | 458,416 | 3.41 | 181,325 | |
Dominated treatments | ||||
Amivantamab plus lazertinib | 539,718 | 3.41 | Dominated by osimertinib plus PBC | |
ICER = incremental cost-effectiveness ratio; PBC = platinum-based chemotherapy; QALY = quality-adjusted life-years.
Notes: The CDA-AMC reanalysis is based on publicly available prices of the comparator treatments. The results of all steps are presented deterministically unless otherwise indicated, while the cumulative CDA-AMC base case is always presented both deterministically and probabilistically.
Table 12: Disaggregated Summary of the CDA-AMC Economic Evaluation Results
Parameter | Amivantamab plus lazertinib | Osimertinib | Osimertinib plus PBC |
|---|---|---|---|
Discounted LYs | |||
Total | 4.16 | 3.34 | 4.16 |
PF | 2.31 | 1.73 | 2.32 |
PD | 1.85 | 1.62 | 1.85 |
Discounted QALYs | |||
Total | 3.41 | 2.75 | 3.41 |
PF | 1.95 | 1.46 | 1.95 |
PD | 1.50 | 1.29 | 1.46 |
Disutilities | −0.003 | −0.001 | −0.002 |
Discounted costs ($) | |||
Total | 539,718 | 338,695 | 458,416 |
Acquisition | 452,971 | 260,053 | 365,138 |
Administration | 4,622 | 0 | 3,837 |
Premedication/comedication | 109 | 0 | 289 |
Monitoring | 0 | 119 | 895 |
Subsequent treatment | 13,312 | 14,337 | 22,707 |
Disease management - PF | 5,867 | 4,378 | 5,872 |
Disease management – PD | 4,194 | 3,695 | 4,192 |
End-of-life care | 53,765 | 55,625 | 53,762 |
AE management | 4,880 | 508 | 1,725 |
AE = adverse event; LY = life-year; PBC = platinum-based chemotherapy; PD = progressed disease; PF = progression-free; QALY = quality-adjusted life-year.
Scenario Analyses
Table 13: CDA-AMC Price Reduction Analyses (100,000 WTP)
Analysis: price reduction | Unit drug cost ($) | Unit drug cost ($): lazertinib | ICERs for amivantamab plus lazertinib vs. osimertinib ($/QALY) | |
|---|---|---|---|---|
Sponsor base case | CDA-AMC reanalysis | |||
No price reduction | 1,676 | 311 | 169,413 | $305,506 |
10% | 1,508 | 280 | 154,756 | $276,112 |
20% | 1,341 | 249 | 140,069 | $246,719 |
30% | 1,173 | 218 | 125,381 | $217,325 |
40% | 1,006 | 186 | 110,694 | $187,932 |
50% | 838 | 155 | Amivantamab plus lazertinib is dominant | $158,538 |
60% | 670 | 124 | Amivantamab plus lazertinib is dominant | $129,144 |
70% | 503 | 93 | Amivantamab plus lazertinib is dominant | Amivantamab plus lazertinib is dominant |
80% | 335 | 62 | Amivantamab plus lazertinib is dominant | Amivantamab plus lazertinib is dominant |
90% | 168 | 31 | Amivantamab plus lazertinib is dominant | Amivantamab plus lazertinib is dominant |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
During the submission process, the sponsor provided updated pricing information for lazertinib, where the price for the 80 mg tablet changed from $103.6000 to $103.6400 and the price of the 240 mg tablet changed from $310.8163 to $310.9200. The updated price of the tablets is reflected in Table 8. The CDA-AMC base case was re-run deterministically with the updated price. In this analysis, treatment with amivantamab plus lazertinib was associated with total treatment costs of $544,911. This represented a $168 difference from the deterministic cost calculated in the CDA-AMC base case.
Appendix 5: Submitted BIA and CDA-AMC Appraisal
Please note that this appendix has not been copy-edited.
Table 14: Summary of Key Take-Aways
Key take-aways of the budget impact analysis |
|---|
|
Summary of Sponsor’s BIA
The sponsor’s submitted BIA assessed the impact resulting from reimbursing amivantamab plus lazertinib for the first-line treatment of locally advanced (not amenable to curative therapy) or metastatic NSCLC with EGFR exon 19 deletions or exon 21 L858R substitution mutations.21 The BIA was conducted from the perspective of the Canadian public drug plans over a 3-year (2026 to 2028) time horizon with 2025 as the base year, using an epidemiologic approach. The sponsor’s pan-Canadian estimates reflect the aggregated results from provincial budgets (excluding Quebec) as well as the Non-Insured Health Benefits (NIHB) program. Adjustments were made to the provincial populations to remove NIHB patients to estimate the provincial public plan population. The sponsor’s base case included drug acquisition costs only and no mark-ups or dispensing fees were included in the cost calculations. TTD curves from the MARIPOSA trial were applied to each cycle to determine the proportion of patient who discontinued treatment. Patients who discontinued from treatments were eligible to receive subsequent treatment. Key inputs to the BIA are documented in Table 15.
The following key assumptions were made by the sponsor:
An average body surface area of 1.68 m2 and average weight of 63.9 kg were used in the drug acquisition calculations and were derived from the MARIPOSA trial.
Sponsor included dose skipping and dose reductions in drug costs.
Market share assumptions were informed by clinical expert opinion, as well as confidential market-access discussions.
Table 15: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as year 1 / year 2 / year 3 if appropriate) |
|---|---|
Target population | |
Incident lung cancer cases % NSCLC % advanced NSCLC % nonsquamous NSCLC % tested for EGFR mutations % positive for EGFR mutations | 23,267 / 23,820 / 24,38522 88%23 83.1%28 81.6%29 14.3%29 |
Number of patients eligible for drug under review | 884 / 905 / 926 |
Market uptake (3 years) | |
Uptake (reference scenario) Osimertinib Osimertinib plus PBC | ███ █ ██ █ ████ ███ █ ███ █ ███ |
Uptake (new drug scenario) Amivantamab plus lazertinib Osimertinib Osimertinib plus PBC | ██ █ ██ █ ████ ██ █ ███ █ ███ ██ █ ███ █ ███ |
Cost of treatment (per patient, per 28-days) | |
Amivantamab plus lazertinib Osimertinib Osimertinib plus PBC | $16,328 $8,877 $9,297 |
NSCLC = non–small cell lung cancer; PBC = platinum-based chemotherapy.
Summary of the Sponsor’s BIA Results
The sponsor’s base case reported that the reimbursement for amivantamab plus lazertinib for the treatment for first-line treatment of patients with locally advanced or metastatic NSCLC whose tumours have EGFR econ 19 deletions or exon 21 L858R substitution mutations would result in an incremental budget impact of $3,475,705 in year 1, $8,299,350 in year 2, $13,719,181 in year 3. The total 3-year incremental cost of reimbursing amivantamab plus lazertinib is $25,494,236.
CDA-AMC Appraisal of the Sponsor’s BIA
CDA-AMC identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
Percentage of patients tested for EGFR mutation is uncertain. In the sponsor-submitted model, Albertan population-based data were used to estimate the percentage of patients tested for EGFR mutations (81.6%). When inquired, clinical expert feedback obtained by CDA-AMC suggested that this value may be underestimated. While the clinical experts noted that it may differ by jurisdiction, the percentage of patients tested for EGFR mutations are likely closer to 100%. By assuming a lower percentage, the total number of eligible patients is underestimated and in turn, underestimates the total budget impact.
In the absence of evidence to support the total percentage of patients tested for EGFR mutations, CDA-AMC undertook a scenario analysis to estimate the impact of 100% of patients receiving testing.
Market shares in reference and new drug scenario for comparator treatments do not align with clinical expectations: In the sponsor-submitted model, the market shares estimated to be ████ ████ ███ ███ ███ ████ ███ ███ ███ for osimertinib and osimertinib plus PBC, respectively, over a 3-year time horizon. Clinical expert feedback obtained by CDA-AMC suggests that a 5% increase year over year for osimertinib plus PBC is underestimated and does not align with clinical expectations. The experts noted that, assuming pCPA negotiations are successful for osimertinib plus PBC, it is more reasonable to expect the opposite market capture of osimertinib and osimertinib plus PBC, where osimertinib plus PBC would capture 75%, 70%, and 65% of the market over 3 years and osimertinib would capture 25%, 30% and 35%. The clinical experts noted that as PBC is commonly used in clinical practice, the addition of the therapy to osimertinib would not require a ramp-up and that physicians would choose osimertinib plus PBC for incident cases. Similarly, in the new drug scenario, clinical experts expect a higher uptake of osimertinib plus PBC compared to osimertinib monotherapy.
To address this limitation, CDA-AMC conducted a reanalysis where in the reference scenario osimertinib plus PBC captures 75%, 70%, and 65% of the market in Years 1, 2, and 3, respectively. In turn, osimertinib captures the remaining market, decreasing to 25%, 30% and 35% in Year 1, 2, and 3, respectively. In the new drug scenario, osimertinib plus PBC captures 77%, 78% and 79%, and osimertinib monotherapy capture s18%, 13% and 7% of the market in Years 1, 2, and 3, respectively.
Additional limitations were identified, but were not considered to be key limitations. These limitations include incorrect list price of carboplatin.
CDA-AMC Reanalyses of the BIA
Table 16: CDA-AMC Revisions to the Submitted Budget Impact Analysis
Stepped analysis | Sponsor’s value or assumption | CDA-AMC value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
1. Wastage | Not included | Included |
2. Cost of carboplatin | 50mg/ 5mL $106.12 | 50mg/ 5mL $70.00 |
Changes to derive the CDA-AMC base case | ||
1. Reference scenario market shares for osimertinib and osimertinib plus PBC | Year: Base / 1 / 2 / 3 Osimertinib: ███ █ ███ █ ███ █ ███ Osimertinib plus PBC: ███ █ ███ █ ███ █ ███ | Year: Base / 1 / 2 / 3 Osimertinib: 20% / 25% / 30% / 35% Osimertinib plus PBC: 80% / 75% / 70% / 65% |
2. New drug scenario market shares for osimertinib and osimertinib plus PBC | Year: Base / 1 / 2 / 3 Osimertinib: ███ █ ███ █ ███ █ ███ Osimertinib plus PBC: ███ █ ███ █ ███ █ ███ | Year: Base / 1 / 2 / 3 Osimertinib: 20% / 18% / 13% / 7% Osimertinib plus PBC: 80% / 77% / 78% / 79% |
CDA-AMC base case | Reanalysis 1 + 2 | |
PBC = platinum-based chemotherapy
The results of the CDA-AMC step-wise reanalysis are presented in summary format in Table 17 and a more detailed breakdown is presented in Table 18. The analysis indicates that funding amivantamab plus lazertinib for the first-line treatment of locally advanced (not amenable to curative therapy) or metastatic NSCLC with EGFR exon 19 deletions or exon 21 L858R substitution mutations would result in an incremental budget impact of $3,881,198 in year 1, $10,459,802 in year 2, and $20,500,384 in year 3. This results in a 3-year budgetary impact of $34,841,383.
Table 17: Summary of the CDA-AMC Reanalyses of the Budget Impact Analysis
Stepped analysis | Three-year total ($) |
|---|---|
Submitted base case | 25,494,326 |
Corrected base case | 25,659,997 |
CDA-AMC reanalysis 1 | −67,507,014 |
CDA-AMC reanalysis 2 | 128,008,394 |
CDA-AMC base case (reanalysis 1 + 2) | 34,841,383 |
BIA = budget impact analysis
CDA-AMC conducted the following scenario analyses to address remaining uncertainty, using the CDA-AMC base case (results are provided in Table 18):
Assuming 100% of patients are tested for EGFR mutations.
Table 18: Detailed Breakdown of the CDA-AMC Reanalyses of the BIA
Stepped analysis | Scenario | Year 0 (current situation) ($) | Year 1 ($) | Year 2 ($) | Year 3 ($) | Three-year total ($) |
|---|---|---|---|---|---|---|
Submitted base case | Reference | 83,117,121 | 153,079,286 | 166,779,079 | 174,641,005 | 557,616,491 |
New drug | 83,117,121 | 156,554,991 | 175,078,430 | 188,360,186 | 603,110,727 | |
Budget impact | 0 | 3,475,705 | 8,299,350 | 13,719,181 | 25,494,236 | |
Corrected base case | Reference | 82,876,022 | 152,770,755 | 166,400,049 | 174,188,300 | 493,359,105 |
New drug | 82,876,022 | 156,271,142 | 174,749,937 | 187,998,023 | 519,019,102 | |
Budget impact | 0 | 3,500,387 | 8,349,888 | 13,809,722 | 25,659,997 | |
CDA-AMC base case | Reference | 88,455,668 | 171,308,913 | 207,067,884 | 208,149,319 | 586,526,116 |
New drug | 88,455,668 | 175,190,111 | 217,527,686 | 228,649,702 | 621,367,499 | |
Budget impact | 0 | 3,881,198 | 10,459,802 | 20,500,384 | 34,841,383 | |
CDA-AMC scenario analysis 1: Assuming 100% of patients tested for EGFR mutations | Reference | 108,401,553 | 209,937,394 | 253,759,662 | 255,084,949 | 718,782,005 |
New drug | 108,401,553 | 214,693,763 | 266,578,046 | 280,207,968 | 761,479,778 | |
Budget impact | 0 | 4,756,370 | 12,818,384 | 25,123,019 | 42,697,773 |
BIA = budget impact analysis; EGFR = epidermal growth factor receptor.
During the submission process, the sponsor provided updated pricing information for lazertinib, where the price for the 80 mg tablet changed from $103.6000 to $103.6400 and the price of the 240 mg tablet changed from $310.8163 to $310.9200. The updated price of the tablets is reflected in Table 8. The CDA-AMC BIA base case was re-run deterministically with the updated price. In this updated analysis, the 3-year budget impact associated with amivantamab plus lazertinib was $34,851,480. This represented a $10,097 difference from the CDA-AMC BIA base case calculated with the original lazertinib price.
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.