Drugs, Health Technologies, Health Systems
Reimbursement Review
Pembrolizumab (Keytruda)
Sponsor: Merck Canada Inc.
Therapeutic area: Advanced or metastatic malignant pleural mesothelioma (MPM)
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Clinical Review
Abbreviations
AE
adverse event
BICR
blinded independent central review
CDA-AMC
Canada’s Drug Agency
CI
confidence interval
DIC
deviance information criterion
ECOG
Eastern Cooperative Oncology Group
ECOG PS
Eastern Cooperative Oncology Group Performance Status
EORTC QLQ-C30
European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30
EORTC QLQ-LC13
European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire 13-item lung cancer-specific questionnaire module
EU
European Union
GRADE
Grading of Recommendations Assessment, Development and Evaluation
HR
hazard ratio
HRQoL
health-related quality of life
ITC
indirect treatment comparison
ITT
intention to treat
MID
minimal important difference
MPM
malignant pleural mesothelioma
mRECIST
modified Response Evaluation Criteria in Solid Tumours
NMA
network meta-analysis
NPH-NMA
nonproportional hazards network meta-analysis
ORR
objective response rate
OS
overall survival
PH-NMA
proportional hazards network meta-analysis
PFS
progression-free survival
RCT
randomized controlled trial
RECIST
Response Evaluation Criteria in Solid Tumours
RMST
restricted mean survival time
SAE
serious adverse event
VAS
Visual Analogue Scale
WDAE
withdrawal due to adverse event
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Table 1: Background Information of Application Submitted for Review
Item | Description |
|---|---|
Drug product | Pembrolizumab (Keytruda), 100 mg/4 mL vial, solution for infusion, IV infusion |
Sponsor | Merck Canada Inc. |
Indication | In combination with pemetrexed and platinum chemotherapy, for the first-line treatment of adult patients with unresectable advanced or metastatic malignant pleural mesothelioma. |
Reimbursement request | As per indication |
Health Canada approval status | Approved |
Health Canada review pathway | Standard, Project Orbis |
NOC date | April 11, 2025 |
Recommended dose | Supplied as 100 mg/4 mL vial, solution for IV infusion. In adult patients 18 years and older:
|
NOC = Notice of Compliance.
Introduction
Malignant mesothelioma is a rare neoplasm arising from the mesothelial cells lining the pleura, peritoneum, pericardium, or testes. Malignant pleural mesothelioma (MPM) develops in the pleural cavity, which is the most common site of disease.1,2 The epithelioid histology subtype is the most common (60% to 70%) and is generally associated with a better prognosis compared with sarcomatoid or mixed histologies.3,4
MPM is primarily linked to occupational inhalational exposure to asbestos, with a latency period of 10 to 50 years.5,6 Symptoms include chest-wall pain, pleuritic pain, cough, pneumothorax, difficulty breathing, and unexplained weight loss, which can affect daily functioning and health-related quality of life (HRQoL).3,7 Diagnosis may consist of laboratory blood tests, imaging with chest X-ray or CT scan of the chest and upper abdomen, PET scan, and thoracentesis.8,9 The overall prognosis of mesothelioma is poor and cure with treatment is rare. The median overall survival (OS) for patients with MPM has been estimated to be less than 1 year.5,10
The primary goals of treatment are to improve symptoms, enhance HRQoL, and extend survival. Due to its long latency period and nonspecific symptoms, MPM is often diagnosed at an advanced stage, making it difficult to treat. Systemic therapy is the main treatment modality for MPM. First-line systemic therapies for unresectable advanced MPM include chemotherapy with pemetrexed plus cisplatin (or carboplatin) or combination immunotherapy with nivolumab-ipilimumab.
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of pembrolizumab (IV; 200 mg every 3 weeks or 400 mg every 6 weeks) for the treatment of adult patients with unresectable advanced or metastatic MPM.
Perspectives of Patient, Clinicians, and Drug Programs
The information in this section is a summary of input provided by the patient and clinician groups that responded to our call for input and from the clinical experts consulted for the purpose of this review.
Patient Input
This review received a joint submission by 3 patient groups: the Lung Health Foundation, Lung Cancer Canada, and the Canadian Cancer Survivor Network. Patients reported significant challenges in obtaining an accurate and timely diagnosis. Symptoms such as fatigue, shortness of breath, cough, nausea, and pain affected daily life, limiting work, physical activity, and hobbies while contributing to emotional distress and concerns about caregiver burden. While prior treatments provided symptom relief and prolonged survival, many patients struggled with lingering adverse effects like fatigue, neuropathy, and nausea, as well as financial barriers to accessing further treatment. Key concerns included better management of symptoms and adverse effects, along with treatment effectiveness in slowing or stopping disease progression with minimal toxicity.
Patients with MPM with experience using pembrolizumab reported experiencing tumour reduction and symptom relief, with 1 seeing rapid improvement after starting pembrolizumab in a clinical trial. However, disease progression eventually led to treatment switches, highlighting the need for sustained efficacy in advanced disease.
Clinician Input
Input From Clinical Experts Consulted for This Review
Two clinical experts with experience in the diagnosis and medical management of MPM were consulted by Canada’s Drug Agency (CDA-AMC).
Current treatments for MPM include chemotherapy and combination immunotherapy, but both have limitations, particularly for patients who cannot tolerate immunotherapy’s adverse effects. Pembrolizumab plus chemotherapy offers a first-line alternative that combines immunotherapy with chemotherapy in a more tolerable manner. The clinical experts emphasized its potential benefit for patients who may not tolerate nivolumab-ipilimumab, which is associated with a much higher rate of immune-related adverse events (AEs). While nivolumab-ipilimumab remains preferred for nonepithelioid histology MPM, pembrolizumab plus chemotherapy could serve as an alternative in this subgroup.
MPM remains incurable, with treatment primarily aimed at prolonging survival, maintaining HRQoL, and preventing disease progression. Oncologists monitor patients at each treatment cycle, assessing side effects, functional status, and tumour response with imaging every 2 to 4 cycles. Treatment discontinuation is recommended for disease progression, severe toxicity, or after 2 years, per the product monograph. Experts agreed that prescribing should be limited to experienced clinicians to ensure appropriate use and toxicity management.
Clinician Group Input
Input was received from 1 clinician group, the Ontario Health (Cancer Care Ontario) Lung Cancer Drug Advisory Committee, with contributions from 10 clinicians.
The clinician group identified nivolumab-ipilimumab as the standard first-line treatment for MPM, with platinum plus pemetrexed chemotherapy preferred for patients contraindicated to immunotherapy. Despite available treatments, OS remains poor, and patients experience a high symptom burden, highlighting the need for more effective and tolerable options. Pembrolizumab plus chemotherapy is expected to serve as a first-line alternative for patients with advanced unresectable MPM, with treatment decisions guided by patient and physician choice in the absence of direct comparative data. Regular clinical and radiological assessments are recommended to monitor treatment response, with tumour stability or shrinkage seen as meaningful outcomes for improving symptoms and HRQoL. Treatment should be administered under medical oncologist supervision and discontinued upon serious toxicity, disease progression, or completion of therapy.
Drug Program Input
Input was obtained from the drug programs that participate in the CDA-AMC reimbursement review process. The following were identified as key factors that could potentially impact the implementation of a recommendation by CDA-AMC for pembrolizumab plus chemotherapy:
considerations for initiation and discontinuation of therapy
considerations for prescribing therapy
generalizability
funding algorithm.
The clinical experts consulted by CDA-AMC provided advice on the potential implementation issues raised by the drug programs (refer to Table 4).
Clinical Evidence
Systematic Review
Description of Studies
One randomized controlled trial (RCT), KEYNOTE-483, was included in the sponsor’s systematic review.11 This open-label, multicentre, phase II/III study randomly assigned patients 1:1 to either pembrolizumab plus pemetrexed and cisplatin (or carboplatin) (N = 222) or pemetrexed plus platinum chemotherapy alone (N = 218), stratified by tumour histology. Patients in the KEYNOTE-483 trial were enrolled across 54 centres in 3 countries, including 13 study sites in Canada.
Patients had to be 18 years or older with histologically confirmed unresectable advanced and/or metastatic MPM and Eastern Cooperative Oncology Group (ECOG) Performance Status (ECOG PS) score of 0 or 1. Among all patients enrolled, 74% identified as male and 26% as female. Regarding race, participants self-identified as American Indian or Alaska Native (0.2%), Asian (0.2%), white (79%), other (3.6%), or did not report race (17%). The median age was 70 years.
The primary objective of the study was to evaluate whether pembrolizumab improves OS when added to standard chemotherapy in MPM.
Efficacy Results
At the data cut-off on September 16, 2022, with a median follow-up of 17.4 months (range, 0.8 months to 60.3 months), 175 patients (80.3%) in the chemotherapy-alone group and 167 patients (75.2%) in the pembrolizumab plus chemotherapy group had died. The Kaplan-Meier estimated differences in OS probabilities between groups favoured pembrolizumab plus chemotherapy by 6.2% (95% confidence interval [CI], –2.8% to 15.2%) at 24 months and 8.1% (95% CI, –0.2% to 16.4%) at 36 months.
Progression-free survival (PFS) based on modified Response Evaluation Criteria in Solid Tumours (mRECIST) by blinded independent central review (BICR) was achieved in 190 patients (85.6%) in the pembrolizumab plus chemotherapy group and 166 patients (76.1%) in the chemotherapy-alone group. The Kaplan-Meier estimated difference in PFS probability at 12 months was 9.1% (95% CI, 0.8% to 17.4%) in favour of pembrolizumab plus chemotherapy.
A higher percentage of patients treated with pembrolizumab plus chemotherapy achieved an objective response (mRECIST by BICR) compared with those receiving chemotherapy alone, with a between-group difference of 23.5% (95% CI, 14.6% to 32.0%) at the data cut-off.
Subgroup analyses suggested that patients with nonepithelioid histology MPM experienced greater treatment benefits with pembrolizumab plus chemotherapy versus chemotherapy alone for OS, PFS, and objective response rate (ORR) compared with those with epithelioid histology MPM. However, the trial was not designed to support causal inferences on subgroups.
HRQoL was assessed using several subscales of the European Organisation for Research and Treatment of Cancer Core Quality of Life Questionnaire Core 30 (EORTC QLQ-C30) and the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire 13-item lung cancer-specific questionnaire module (EORTC QLQ-LC13). No significant between-group differences were observed on any subscale.
Harms Results
A higher percentage of patients randomized to pembrolizumab plus chemotherapy had AEs compared with those who received chemotherapy alone (96.3% versus 91.4%). More patients treated with pembrolizumab plus chemotherapy experienced grade 3 and higher AEs of any cause. Serious adverse events (SAEs) were reported more frequently in patients treated with pembrolizumab plus chemotherapy (40.2%) compared with chemotherapy alone (19.0%). More patients treated with pembrolizumab plus chemotherapy (34.4%) discontinued treatment for any AE (withdrawal due to adverse event [WDAE]) compared with the chemotherapy-alone group (17.2%). A higher percentage of patients treated with pembrolizumab plus chemotherapy experienced death coded as an AE (7.1%) compared with those in the chemotherapy-alone group (2.2%). The most common cause of death was sepsis, occurring in 4 patients (1.7%) in the pembrolizumab plus chemotherapy group and 2 patients (0.9%) in the chemotherapy-alone group. Nearly 27% of patients in the pembrolizumab plus chemotherapy group and 7% in the chemotherapy-alone group experienced notable harms. The most frequently reported notable harms in the pembrolizumab group were immune-mediated (e.g., hypothyroidism).
Critical Appraisal
Internal Validity
The KEYNOTE-483 trial employed a web-based randomization system with stratification by histology, ensuring balance for this key prognostic factor. However, baseline imbalances in smoking history and prior therapies could introduce residual confounding, although the clinical experts deemed these differences to be unlikely to impact results significantly. The open-label design introduced risks of performance, detection, and reporting bias, particularly for subjective end points like HRQoL and AEs, although OS, the primary end point, is less prone to bias. A key concern is the higher posttrial use of nivolumab in the chemotherapy-alone group, which may have diluted the treatment effect of pembrolizumab plus chemotherapy, yet no sensitivity analysis assessed this potential impact. Delayed separation of Kaplan-Meier curves for OS and PFS suggests possible violations of the proportional hazards assumption, complicating interpretation of the hazard ratios (HRs). Additionally, the study’s original power calculations overestimated the expected treatment benefit, raising questions about whether the trial was sufficiently powered to detect smaller, yet clinically meaningful, effects. Subgroup analyses suggested differential efficacy by histology and by geographic region (European Union [EU] versus Canada) on OS and PFS, raising questions about potential variability in treatment effects. However, these analyses were exploratory, lacked formal interaction testing, and did not include confounder analyses, increasing the risk of spurious or misleading findings due to multiple comparisons. The validity of conclusions drawn from the subgroup analyses remains uncertain.
External Validity
The trial population was generally representative of patients in clinical practice in Canada receiving first-line treatment for advanced MPM, but the exclusion of patients with an ECOG PS score of 2 or greater limits generalizability to those with a poorer performance status. The comparator, pemetrexed plus platinum chemotherapy, aligned with standard clinical practice, with an appropriate distribution of carboplatin and cisplatin use. While the trial measured key outcomes relevant to patients, the short duration of HRQoL assessments (15 weeks) limits conclusions about long-term impacts on patient-reported outcomes.
GRADE Summary of Findings and Certainty of the Evidence
For the pivotal studies and RCTs identified in the sponsor’s systematic review, Grading of Recommendations Assessment, Development and Evaluation (GRADE) was used to assess the certainty of the evidence for outcomes considered most relevant to inform expert committee deliberations, and a final certainty rating was determined as outlined by the GRADE Working Group.12,13
Following the GRADE approach, evidence from RCTs started as high-certainty evidence and could be rated down for concerns related to study limitations (which refer to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias.
When possible, certainty was rated in the context of the presence of an important (nontrivial) treatment effect; if this was not possible, certainty was rated in the context of the presence of any treatment effect (i.e., the clinical importance is unclear). In all cases, the target of the certainty-of-evidence assessment was based on the point estimate and where it was located relative to the threshold for a clinically important effect (when a threshold was available) or to the null.
The reference points for the certainty-of-evidence assessment for OS, PFS, ORR, SAEs, WDAEs, and fatal AEs were set according to the presence or absence of an important effect based on thresholds informed by the clinical experts consulted for this review (Table 2). The reference point for the certainty-of-evidence assessment for EORTC QLQ-C30 global health status scale and quality of life scale score was set according to the presence or absence of an important effect based on a threshold that was informed by the literature.
Table 2: Summary of Findings for First-Line Pembrolizumab Plus Chemotherapy vs. Chemotherapy Alone for Adult Patients With Unresectable Advanced or Metastatic Malignant Pleural Mesothelioma
Outcome and follow-up | Patients (studies), N | Relative effect (95% CI) | Absolute effects (95% CI) | Certaintya | What happens | ||
|---|---|---|---|---|---|---|---|
Chemotherapy | Pembrolizumab + chemotherapy | Difference | |||||
OS | |||||||
Probability of OS at 24 months Median (range) follow-up: Pembrolizumab + chemotherapy, 17.4 months (0.8 months to 60.3 months) Chemotherapy alone, 16.8 months (0.8 months to 59.3 months) | 440 (1 RCT) | NR | 328 per 1,000 | 389 per 1,000 (325 to 453 per 1,000) | ██ ███ █████ ███ █████ ██ ███ ████ ███ ██████ | Moderateb | Compared with chemotherapy alone, pembrolizumab + chemotherapy likely results in an increase in OS at 24 months |
Probability of OS at 36 months Median (range) follow-up: Pembrolizumab + chemotherapy, 17.4 months (0.8 months to 60.3 months) Chemotherapy alone, 16.8 months (0.8 months to 59.3 months) | 440 (1 RCT) | NR | 173 per 1,000 | 253 per 1,000 (193 to 318 per 1,000) | ██ ███ █████ ██ █████ ██ ███ ████ ███ ██████ | Moderateb | Pembrolizumab + chemotherapy likely results in an increase in OS compared with chemotherapy alone at 36 months |
PFS per mRECIST by BICR | |||||||
Probability of PFS at 12 months Median (range) follow-up: Pembrolizumab + chemotherapy, 17.4 months (0.8 months to 60.3 months) Chemotherapy alone, 16.8 months (0.8 months to 59.3 months) | 440 (1 RCT) | NR | 171 per 1,000 | 263 per 1,000 (204 to 324 per 1,000) | ██ ███ █████ ██ ████ ██ ███ ████ ███ ██████ | Moderatec | Pembrolizumab + chemotherapy likely results in an increase in PFS compared with chemotherapy alone at 12 months |
Objective response rate per mRECIST by BICR | |||||||
ORR (mRECIST by BICR) Median (range) follow-up: Pembrolizumab + chemotherapy, 17.4 months (0.8 months to 60.3 months) Chemotherapy alone, 16.8 months (0.8 months to 59.3 months) | 440 (1 RCT) | ██ ████ █████ ██ █████ | 294 per 1,000 | 527 per 1,000 (459 more to 594 more per 1,000) | ███ ███ █████ ████ ████ ██ ███ ████ ███ ██████ | Highd | Pembrolizumab + chemotherapy results in a higher percentage of patients achieving an objective response compared with chemotherapy alone |
HRQoL | |||||||
Mean change from baseline in EORTC QLQ-C30 global health status scale and quality of life scale Time point: 15 weeks | 440 (1 RCT) | NR | –3.86 points (–6.80 to –0.92) | –2.87 points (–5.68 to –0.07) | LS mean difference 0.99 points (−2.88 to 4.86) | Lowe,f | Pembrolizumab + chemotherapy may result in little to no difference in HRQoL compared with chemotherapy alone |
Harms | |||||||
SAEs Follow-up: NR Time point: End of trial | 473 (1 RCT) | NR | 190 per 1,000 | 402 per 1,000 | ███ ███ █████ ████ ████ ██ ███ █████ | Highd | Pembrolizumab + chemotherapy results in an increase in SAEs compared with chemotherapy alone |
WDAEs Follow-up: NR Time point: End of trial | 473 (1 RCT) | NR | 172 per 1,000 | 344 per 1,000 | ███ ███ █████ ███ ████ ██ ███ ████ ███ ██████ | Moderateg | Pembrolizumab + chemotherapy likely results in an increase in WDAEs compared with chemotherapy alone |
Deaths as AEs Follow-up: NR Time point: End of trial | 473 (1 RCT) | NR | 22 per 1,000 | 71 per 1,000 | █████ █████ █ ██ ████ ██ ██████ | Lowh | Pembrolizumab + chemotherapy may result in an increase in deaths as AEs compared with chemotherapy alone |
AE = adverse event; BICR = blinded independent central review; CI = confidence interval; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; HRQoL = health-related quality of life; LS = least squares; MID = minimally important difference; mRECIST = modified Response Evaluation Criteria in Solid Tumours; NR = not reported; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; RCT = randomized controlled trial; SAE = serious adverse event; vs. = versus; WDAE = withdrawal due to adverse event.
aStudy limitations (which refer to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias were considered when assessing the certainty of the evidence. All serious concerns in these domains that led to the rating down of the level of certainty are documented in the table footnotes.
bRated down 1 level for imprecision. In the absence of a validated MID, the threshold was informed by the clinical experts consulted for this review. A between-group absolute risk difference of 5% (at least 50 fewer events per 1,000 patients) at 24 and 36 months was considered clinically significant by the clinical experts. While the point estimate and upper CI exceeded this threshold, the lower CI crossed zero, indicating uncertainty. The risk difference includes both meaningful benefit and the possibility of no effect. Certainty was not downgraded further for imprecision despite variations in the magnitude and statistical significance of OS estimates across different metrics — including median OS, Cox proportional HRs, and the difference in restricted mean survival time (RMST) at 24 months and by histology — because the direction of the treatment effect remained consistent.
cRated down 1 level for imprecision. In the absence of a validated MID, the threshold was informed by the clinical experts consulted for this review. A between-group absolute risk difference of 5% (at least 50 fewer events per 1,000 patients) at 12 months was considered clinically significant by the clinical experts. While the point estimate and upper CI exceeded this threshold, the lower CI did not, indicating uncertainty. The risk difference includes both meaningful benefit and the possibility of no effect.
dIn the absence of a validated MID, the threshold was informed by the clinical experts consulted for this review. A between-group absolute risk difference of 10% (at least 100 fewer events per 1,000 patients) was considered clinically significant by the clinical experts. The point estimate and entire CI exceeded the threshold.
eRated down 1 level for imprecision due to the wide CI, which includes both no effect and the published MID of 4 points. This uncertainty limits confidence in whether the observed effect is clinically meaningful.
fRated down 1 level for indirectness because the final analysis was conducted at 15 weeks, while the median follow-up duration for all participants was nearly 18 months. This discrepancy raises concerns about whether the reported results accurately reflect the longer-term impact on HRQoL.
gRated down 1 level for imprecision. In the absence of a validated MID, the threshold was informed by the clinical experts consulted for this review. A between-group absolute risk difference of 10% (at least 100 fewer events per 1,000 patients) was considered clinically significant by the clinical experts. Although the point estimate and upper CI exceed the clinician-defined threshold for clinical significance, the lower CI is slightly below this threshold, introducing uncertainty.
hRated down 2 levels for imprecision. In the absence of a validated MID, the threshold was informed by the clinical experts consulted for this review. A between-group absolute risk difference of 3% (at least 30 fewer events per 1,000 patients) was considered clinically significant by the clinical experts. Although the point estimate and upper CI exceed the clinician-defined threshold for clinical significance, the lower CI is slightly below this threshold, introducing uncertainty. Additionally, the number of deaths was low, making the effect estimate unstable and susceptible to meaningful changes with small variations in event counts.
Source: Clinical Study Report for KEYNOTE-483.11 Details included in the table are from the sponsor’s summary of clinical evidence.
Indirect Comparisons
One sponsor-provided indirect treatment comparison (ITC) was included to evaluate the comparative effectiveness and harms of pembrolizumab plus chemotherapy versus nivolumab-ipilimumab in the first-line treatment of unresectable advanced or metastatic MPM.14
Description of Studies
A systematic literature search was conducted that identified 3 reports from 2 RCTs that met the inclusion criteria for the ITC: the KEYNOTE-483 trial and the phase II IND.227 study for pembrolizumab plus chemotherapy, and the CheckMate 743 trial for nivolumab-ipilimumab.
Two analyses were reported:
The main analyses (base case) using the Bucher ITC method were used involving only 2 studies (KEYNOTE-483 and CheckMate 743) reporting OS, PFS, and ORR.
Sensitivity analyses performed through a Bayesian network meta-analysis (NMA) involving 3 studies (KEYNOTE-483, CheckMate 743, and IND.227) reporting OS, PFS, and ORR.
HRQoL and AE end points were not included in the ITC analyses.
Models were analyzed under both proportional hazards and nonproportional hazards assumptions for OS and PFS.
Efficacy Results
The base-case Bucher ITC analysis indicated that the HR for OS favoured nivolumab-ipilimumab over pembrolizumab plus chemotherapy (████████████████████████. However, the difference was not statistically significant because the 95% CIs crossed unity (upper CI was > 1).
The Bucher ITC analysis indicated that the HR for PFS favoured pembrolizumab plus chemotherapy over nivolumab-ipilimumab ██████████████████████████. However, the difference was not statistically significant because the 95% CI crossed unity (lower CI < 1).
The Bucher ITC analysis indicated that the odds ratio for ORR favoured pembrolizumab plus chemotherapy over nivolumab-ipilimumab █████████████████████████.
Harms Results
Not estimated.
Critical Appraisal
The systematic literature review and ITC of pembrolizumab versus nivolumab-ipilimumab, using chemotherapy as the common comparator, aligned with Reimbursement Review requirements. The ITC aimed to estimate the relative treatment effects for OS, PFS, and ORR, rather than formally test for superiority, equivalence, or inferiority. Key ITC assumptions — similarity and transitivity — were assessed and generally met, but no adjustments were made for baseline imbalances, and no subgroup analyses were conducted on important effect modifiers such as histology, reducing interpretability. The sponsor employed fixed-effects models for all analyses due to the small number of trials, which was deemed acceptable but may not fully capture treatment-effect heterogeneity. Long-term extrapolations (up to 15 years) introduced uncertainty because survival in advanced MPM is much shorter, and comparisons at this time point may not be generalizable. No comparisons for HRQoL or AEs were conducted, limiting insights into patient-centred outcomes and potential differences in tolerability between regimens. Overall, while the ITC followed standard methodology, concerns about long-term extrapolations, lack of HRQoL and AE assessments, and potential baseline imbalances impact the robustness of its conclusions.
Studies Addressing Gaps in the Evidence From the Systematic Review
No studies were submitted.
Conclusions
The KEYNOTE-483 trial provided moderately certain evidence that pembrolizumab plus chemotherapy offers a clinically significant improvement in OS and PFS for some patients with unresectable advanced or metastatic MPM compared with chemotherapy alone. ITC evidence did not establish a clear difference in OS or PFS between pembrolizumab plus chemotherapy versus nivolumab-ipilimumab. Estimates for OS generally favoured nivolumab-ipilimumab and estimates for PFS favoured pembrolizumab plus chemotherapy, but the uncertainty around the results (e.g., wide CIs) precludes firm conclusions. While pembrolizumab plus chemotherapy demonstrated a higher ORR than chemotherapy alone and nivolumab-ipilimumab, this did not translate into evidence of improved HRQoL and symptoms compared with chemotherapy alone. The relative impact on HRQoL and symptoms compared with nivolumab-ipilimumab remains unknown due to a lack of comparative data. Pembrolizumab plus chemotherapy was associated with increased rates of SAEs, WDAEs, and possibly fatal AEs compared with chemotherapy alone. The comparative harms for pembrolizumab plus chemotherapy versus nivolumab-ipilimumab have not been formally evaluated, making it unclear whether pembrolizumab plus chemotherapy offers a meaningful safety advantage. Despite these uncertainties, pembrolizumab plus chemotherapy represents an additional first-line systemic therapy option for adult patients with unresectable advanced or metastatic MPM.
Introduction
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of pembrolizumab (IV; 200 mg every 3 weeks or 400 mg every 6 weeks) for the treatment of adult patients with unresectable advanced or metastatic MPM.
Disease Background
Contents within this section have been informed by materials submitted by the sponsor and clinical expert input. The following has been summarized and validated by the review team.
Malignant mesothelioma is a rare neoplasm arising from the mesothelial cells lining the pleura, peritoneum, pericardium, or testes. The most common site of disease — accounting for at least 80% of reported mesotheliomas — is in the pleural cavity, followed by 15% to 20% of cases in the peritoneum, and less than 1% in the pericardium or testes.1,2 Malignant mesothelioma is broadly classified as epithelioid, sarcomatoid, or biphasic (mixed histology). The epithelioid histology subtype is the most common (60% to 70%) and is generally associated with a better prognosis compared with sarcomatoid or mixed histologies.3,4
Occupational, environmental, or domestic asbestos exposure has been implicated in up to 85% of MPM cases, although other contributing etiologic factors such as genetic susceptibility have been suggested.5,6 Inhalational exposure to asbestos has been widely recognized as a risk factor, and the latency period between exposure and development of MPM is estimated to range between 10 and 50 years, depending on the severity and duration of exposure.15,16 In response, Canada banned asbestos and asbestos-containing products in 2018.17 The risk of developing this cancer increases with age, with a median age of diagnosis of around 70 years.18,19 MPM is generally more common in males than in females, which is thought to be due to males being historically more likely to work in industries with asbestos exposure. While mesothelioma incidence rates appear to have plateaued after 2010, due to decreases in incidence among males, incidence rates among females appear to be increasing.5,20
Symptoms of MPM include unilateral or bilateral chest-wall pain, pleuritic pain, cough, pneumothorax, difficulty breathing, and unexplained weight loss. These symptoms can affect daily functioning and HRQoL.3,7 Because these signs and symptoms are nonspecific to MPM and the latency of this disease is long, diagnosis is often difficult. MPM is considered an aggressive cancer, and patients often have advanced disease by the time symptoms develop.3 A standard diagnostic workup for mesothelioma consists of laboratory blood tests and imaging with chest X-ray and CT scan of the chest and upper abdomen and, more recently, PET scans.9,21 Imaging can reveal pleural thickening and masses, as well as pleural effusion (fluid in the pleural cavity between the chest wall and the lungs), and is useful for disease staging.9 Thoracentesis can also be employed in patients with pleural effusion, for cytological examination of fluid in the pleural cavity.8 However, the diagnostic guidelines recommend a thoracoscopic biopsy for patients with planned antineoplastic treatment for confirming diagnosis and aid in clinical staging before initiating treatments.8,9
Incidence rates of MPM vary considerably between countries.3 In 2019, 460 people in Canada (excluding Quebec) were diagnosed with mesothelioma, 355 (77%) of whom were males and 105 (23%) of whom were females, corresponding to an incidence rate of 1.6 per 100,000 population.22,23 The overall prognosis of mesothelioma is poor and cure with treatment is rare. Using data from the Ontario Cancer Registry gathered between 1993 and 2017 and the Canadian Cancer Registry, the Occupational Cancer Research Centre in Ontario estimated that, between 2013 and 2017, the 5-year survival rate for mesothelioma was 6.3%.24 A similar study performed in British Columbia demonstrated a poorer prognosis, with a 5-year survival rate of 3.7% between 2012 and 2016.25 The median OS for patients with MPM has been estimated to be less than 1 year.5,10
Standards of Therapy
Contents within this section have been informed by materials submitted by the sponsor and clinical expert input. The following was summarized and validated by the review team.
MPM is an incurable disease, and the primary goals of treatment are to improve symptoms, enhance HRQoL, and prolong survival. Treatment options for patients who are newly diagnosed with MPM include surgery, radiation therapy, and/or systemic therapy.4,26 However, due to its long latency period and nonspecific symptoms, MPM is often diagnosed at an advanced stage, making it difficult to treat.
Pretreatment evaluation is important for staging, assessing surgical eligibility (based on age, extent of disease, comorbidities, and other factors), and determining the histologic subtype of MPM.4,21 Among patients eligible for surgery, evidence suggests that the benefits are primarily seen in those with earlier-stage disease (stage I to IIIA) and with pure epithelioid histology MPM, as part of a multimodal treatment strategy that includes chemotherapy and radiation therapy. However, the role of surgical resection is limited and has become more controversial because the MARS2 randomized trial demonstrated that surgery (pleurectomy decortication) plus chemotherapy was associated with higher morbidity and poorer survival compared with chemotherapy alone in patients with resectable (early stage) disease.27 Due to the typically advanced stage of disease at diagnosis, most patients are ineligible for surgical resection anyway.
Similarly, radiation therapy is a treatment option for select patients within a multimodal treatment strategy, but it is not recommended as monotherapy because delivering it to the entire pleural surface without serious toxicity is challenging.4
Systemic therapy is the main treatment modality for MPM. It is recommended for patients with good performance status who are medically inoperable, refuse surgery, present with advanced MPM regardless of histology, or who have sarcomatoid or biphasic histology, regardless of clinical stage.4 First-line systemic therapies for unresectable MPM include chemotherapy with pemetrexed plus cisplatin or combination immunotherapy with nivolumab-ipilimumab. Both regimens are approved by Health Canada for the first-line treatment of unresectable MPM and both are publicly reimbursed. Cisplatin may be substituted for carboplatin, especially if there are concerns with tolerability.19
Treatment with nivolumab-ipilimumab may be preferred based on the results of the CheckMate 743 trial, which demonstrated prolonged OS compared with chemotherapy.28 This combination may be particularly effective in patients with nonepithelioid histology MPM, which is generally less responsive to chemotherapy. However, not all patients are eligible for immunotherapy (e.g., those with active autoimmune comorbidities or who may be unable to tolerate the adverse effects associated with combination immunotherapy).
Drug Under Review
Key characteristics of pembrolizumab and other treatments for MPM are summarized in Table 3. Pembrolizumab is a human immunoglobulin G4 monoclonal antibody that binds to the PD-1 receptor on T cells to block its interaction with PD-L1 and PD-L2. This binding prevents PD-1 pathway–mediated inhibition of the antitumour immune response.
The recommended dosage of pembrolizumab for the treatment of MPM in adults is either 200 mg every 3 weeks or 400 mg every 6 weeks. Pembrolizumab is administered as an IV infusion over 30 minutes. Treatment is continued until disease progression or unacceptable toxicity, or until maximum treatment duration is reached without disease progression. Maximum treatment duration is either 2 years, 35 doses at the 200 mg dosage, or 18 doses at 400 mg, whichever results in the longest duration of treatment.
Pembrolizumab was approved by Health Canada on April 11, 2025, for the following indication: in combination with pemetrexed and platinum chemotherapy for the first-line treatment of adult patients with unresectable advanced or metastatic MPM. The sponsor is requesting reimbursement as per the anticipated indication. Pembrolizumab was recently approved in the US, in combination with pemetrexed and platinum chemotherapy, as first-line treatment of adult patients with unresectable advanced or metastatic MPM.29 In the EU, pembrolizumab is currently under review, in combination with pemetrexed and platinum chemotherapy, for the first-line treatment of adults with unresectable nonepithelioid MPM.30
Table 3: Key Characteristics of Pembrolizumab and Nivolumab-Ipilimumab
Characteristic | Pembrolizumab | Nivolumab-ipilimumab |
|---|---|---|
Mechanism of action | Human IgG4 monoclonal antibody that binds to the PD-1 receptor on T cells to block its interaction with PD-L1 and PD-L2, preventing PD-1 pathway–mediated inhibition of the antitumour immune response. | Nivolumab: Human IgG4 monoclonal antibody that binds to the PD-1 receptor on T cells to block its interaction with PD-L1 and PD-L2, preventing PD-1 pathway–mediated inhibition of the antitumour immune response. Ipilimumab: Recombinant human monoclonal antibody that binds to CTLA-4, preventing inhibition of T cell–mediated antitumour immune response. |
Indicationa | In combination with pemetrexed and platinum chemotherapy for the first-line treatment of adult patients with unresectable advanced or metastatic MPM. | Nivolumab-ipilimumab is indicated for the treatment of adult patients with unresectable MPM who have not received prior systemic therapy for MPM. |
Route of administration | IV | IV |
Recommended dose | 200 mg q.3.w. or 400 mg q.6.w. | Nivolumab 3 mg/kg q.2.w. or 360 mg q.3.w. with ipilimumab 1 mg/kg q.6.w. |
Serious adverse effects or safety issues |
| |
Other | Maximum treatment duration: 2 years or 35 doses (200 mg) or 18 doses (400 mg), whichever is longer | Maximum treatment duration: 2 years |
IgG4 = immunoglobulin G4; MPM = malignant pleural mesothelioma; q.2.w. = every 2 weeks; q.3.w. = every 3 weeks; q.6.w. = every 6 weeks.
aHealth Canada–approved indication.
Sources: Product monographs for pembrolizumab (Keytruda),31 nivolumab (Opdivo),32 and ipilimumab (Yervoy).33
Perspectives of Patients, Clinicians, and Drug Programs
The full patient and clinician group submissions received are available on the project website in the consolidated patient and clinician group input document for this review.
Patient Group Input
This section was prepared by the review team based on the input provided by patient groups.
This review received a joint submission by 3 patient groups: the Lung Health Foundation, Lung Cancer Canada, and the Canadian Cancer Survivor Network. The Lung Health Foundation is a registered charity that assists and empowers individuals living with or caring for others with lung disease. Lung Cancer Canada is a registered national charitable organization serving as a resource for lung cancer education, patient support, research, and advocacy. The Canadian Cancer Survivor Network is a national network of patients, caregivers, community partners, and sponsors promoting standard of care improvements for individuals with cancer. The input was based on information collected by the Lung Health Foundation, gathering 70 responses to an online survey available between June 2023 to November 2024. There was representation from across Canada, with provincial breakdowns as follows: Ontario (68), Alberta (9), British Columbia (8), Manitoba (4), Quebec (4), New Brunswick (3), and Nova Scotia (2). Of all those who responded to the survey, 59 were patients with lung cancer (non–small cell and small cell) of various stages and 11 were caregivers for individuals with lung cancer; 6 patients with lung cancer had experience with pembrolizumab. In addition to this survey, the Lung Health Foundation gathered information through interviews for previous review submissions with 5 patients living in Canada who had direct experience with pembrolizumab, 2 of whom had pleural mesothelioma.
When asked about their disease experience, those who responded to the survey reported substantial challenges obtaining an accurate and timely diagnosis. Reported symptoms and challenges due to lung cancer included fatigue (67%), shortness of breath (67%), cough (23%), nausea (23%), and pain (20%). Survey respondents also noted chest tightness, wheezing, weight loss, diminished appetite, low mood or depressive periods, and challenges with physical and emotional intimacy. When asked how lung cancer negatively impacts their day-to-day life, survey respondents highlighted their inability to work (48%), participate in physical activities (33%), do housework (21%), use stairs (22%), or partake in hobbies (21%). Most survey respondents indicated that living with lung cancer negatively impacts their emotional well-being through feelings of isolation, challenges with symptom management, and perceived burden on caregivers and family.
Survey respondents reported some benefit from previous treatments, such as reduced cough and shortness of breath, increased participation in daily activities, ability to exercise, prolonged life, delayed disease progression, and a reduction in the severity of other disease-related symptoms. However, survey respondents also reported struggling with lingering side effects of surgery and medications, including deconditioning, chronic fatigue, extreme itching, brain fog, fatigue, nausea, vomiting, mood changes, diminished appetite, weight loss, hair loss, anemia, and neuropathy. The input noted that patients face difficulties accessing certain therapies due to high treatment costs; patients on targeted therapies expressed concerns about their ability to access the next line of treatment if their disease progresses.
Disease aspects that were most important to control included improved management of disease symptoms as well as management of the pain and side effects from therapy. Survey respondents indicated that key treatment outcomes to consider when evaluating new therapies include stopping or slowing disease progression with minimal side effects and effectiveness in advanced disease. Survey respondents also highlighted efficacy as an outcome of interest, with 1 noting they would be more receptive to side effects if there was robust evidence that the medication would stop or slow their disease progression.
The 2 patients with MPM reported substantial tumour shrinkage while receiving pembrolizumab. One patient diagnosed in 2020 experienced a 50% tumour reduction within 2 months of treatment with nivolumab-ipilimumab. The second patient, diagnosed in 2016 with inoperable MPM and metastasis to the diaphragm, liver, and heart, was given 3 months to live. After enrolling in a clinical trial for pembrolizumab, there was patient-reported symptom and appetite improvement within 10 hours of treatment initiation. The tumour began growing 2 years after the trial, prompting reinitiation of pembrolizumab, which was switched to nivolumab-ipilimumab due to a lack of response.
Clinician Input
Input From the Clinical Experts Consulted for This Review
All review teams with CDA-AMC include at least 1 clinical specialist with expertise regarding the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). The following input was provided by 2 clinical specialists with expertise in the diagnosis and management of mesothelioma.
Unmet Needs
The currently available treatments for MPM consist of either chemotherapy or combination immunotherapy regimens, each with limitations that leave important unmet needs for patients. The benefit of combination immunotherapy approaches is especially observed in patients with nonepithelioid histology MPM, but many cannot tolerate these regimens due to their adverse effects. Although both chemotherapy and immunotherapy have demonstrated efficacy in MPM, until now, patients have not had an opportunity to receive both in a combined approach. The natural course of MPM varies, with some patients maintaining prolonged disease control and being rechallenged with first-line therapy, but most experience disease progression with few viable second-line options. The clinical experts indicated that a pembrolizumab plus chemotherapy regimen may be an attractive alternative because it offers immunotherapy exposure in a more tolerable manner compared with combination immunotherapy while leveraging chemotherapy’s established role in treatment.
Place in Therapy
Pembrolizumab plus chemotherapy would be used as a first-line treatment for MPM and as an alternative treatment to chemotherapy alone and to combination immunotherapy (nivolumab-ipilimumab).
The clinical experts emphasized the importance of a treatment option among patients who could benefit from immunotherapy but have tolerability concerns (e.g., those with active autoimmune disease).
It was also noted by the clinical experts that chemotherapy alone is less effective in nonepithelioid versus epithelioid MPM than immunotherapy-based regimens; nivolumab-ipilimumab is currently preferred in this subpopulation of patients with MPM. Therefore, the experts anticipate that pembrolizumab plus chemotherapy — with an immunotherapy component — would be an alternative to nivolumab-ipilimumab in patients with MPM and nonepithelioid histology.
Patient Population
The clinical experts stated that the target population in practice for pembrolizumab plus chemotherapy aligns with the indication and with the current use of chemotherapy and nivolumab-ipilimumab in the first-line setting for unresectable MPM. They noted that no additional tests or assessments are needed beyond those already used for diagnosis, clinical characterization of MPM, and treatment planning.
Assessing the Response to Treatment
The clinical experts stated that MPM is incurable, but the primary goal of treatment remains prolonged survival. Maintaining good HRQoL and tumour response (preventing progression and reducing tumour burden) are also key patient priorities.
Medical oncologists typically conduct medical assessments of patients with MPM at every treatment cycle, monitoring AEs, tolerability, functional status, symptoms, and HRQoL. Radiologic assessments to evaluate treatment effectiveness are conducted every 2 to 4 cycles.
Discontinuing Treatment
There was agreement among the clinical experts that treatment with pembrolizumab plus chemotherapy should stop for disease progression or uncontrollable or serious immunotherapy associated toxicity. Also, the maximum duration of treatment should be 2 years, in accordance with the product monograph.
Prescribing Considerations
The prescribing of pembrolizumab plus chemotherapy should be restricted to clinicians and centres with experience in immuno-oncology and treating MPM. The clinical experts agreed that this approach helps to ensure the appropriate patients receive treatment with pembrolizumab plus chemotherapy and to optimize toxicity management. This approach is consistent with current prescribing and monitoring of treatment of MPM using chemotherapy alone and with nivolumab-ipilimumab.
Clinician Group Input
This section was prepared by the review team based on the input provided by clinician groups.
Input for this review was provided by 1 clinician group, the Ontario Health (Cancer Care Ontario) Lung Cancer Drug Advisory Committee, with contributions from 10 clinicians.
The clinician group indicated that the standard first-line treatment of MPM is combination immunotherapy with nivolumab-ipilimumab, following the results of the CheckMate 743 trial. For patients who are contraindicated to this immunotherapy doublet, such as those with autoimmune disease or those who are on long-term immunosuppressive therapy, the clinician group noted that platinum plus pemetrexed chemotherapy is the preferred treatment option. According to the clinician group, current treatment goals include improving the patient’s OS, PFS, and response rates to alleviate their symptoms and improve HRQoL. However, the clinician group highlighted that median OS remains poor in patients with unresectable advanced MPM despite these available treatment options, and patients continue to experience high symptom burden and morbidity. The clinician group emphasized the need for treatments with improved efficacy and tolerability.
The clinician group anticipates that pembrolizumab plus chemotherapy will be used as a first-line alternative to nivolumab-ipilimumab in patients with advanced unresectable MPM. Due to a lack of head-to-head comparative data, treatment decisions will rely on patient and physician choice. In the absence of demonstrated superiority, the clinician group emphasized the importance of keeping platinum-based chemotherapy available as a second-line option.
Pembrolizumab plus chemotherapy is best suited for adults with MPM who are unsuitable for surgery, have not received prior systemic therapy for advanced unresectable disease, and do not have untreated central nervous system metastases or significant pneumonitis. Patients least suited to the treatment are those with poor performance status, uncontrolled autoimmune disease, or significant contraindications to platinum or pemetrexed chemotherapy. Companion diagnostic biomarkers (e.g., PD-L1 status) have not been shown to be predictive of treatment effects with immunotherapies for MPM and are unlikely to identify patients who may preferentially benefit from treatment.
To assess treatment benefit, the clinician group suggested clinical and radiological evaluation. Clinical assessments should occur before each treatment cycle to monitor symptom burden and tolerability of treatment. Radiological assessments, including CT scans and/or chest X-rays, should occur every 3 months while on treatment. In this group’s opinion, a clinically meaningful outcome of treatment is tumour response or stability, which may alleviate symptoms, delay disease progression, improve HRQoL, and improve OS.
Pembrolizumab plus chemotherapy should be administered as an outpatient procedure under supervision by a medical oncologist. Treatment should be discontinued in the event of serious and/or life-threatening AEs, disease progression, or completion of therapy.
Drug Program Input
The drug programs provide input on each drug being reviewed through the reimbursement review processes by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted for this review are summarized in Table 4.
Table 4: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Relevant comparators | |
When is pembrolizumab plus chemotherapy preferable to nivolumab-ipilimumab? | Combination immunotherapy with nivolumab-ipilimumab immunotherapy may be too toxic for certain patients. Pembrolizumab plus platinum-based chemotherapy offers an alternative to all-immunotherapy or all-chemotherapy approaches, leveraging the known effectiveness of both types of regimens in MPM while providing a different adverse-effect profile. Pembrolizumab plus chemotherapy is a well-tolerated regimen in patients with NSCLC, where there is substantial experience with the regimen. The clinical experts noted that although no head-to-head comparisons exist for pembrolizumab plus chemotherapy, clinicians may prefer combination immunotherapy (nivolumab-ipilimumab) over a chemotherapy-containing regimen for patients with nonepithelioid histology MPM. Nonepithelioid tumours are associated with a higher symptom burden, poorer prognosis, and weaker response to chemotherapy than to immunotherapy. |
Are the trial results generalizable to allow patients to switch from nivolumab-ipilimumab to pembrolizumab plus chemotherapy if there are adverse effects without disease progression? | There is currently no evidence to support switching treatments, including from the KEYNOTE-483 trial. However, the clinical experts noted that switching may be considered in practice, particularly if adverse effects from nivolumab-ipilimumab are serious or difficult to manage. They emphasized that the different adverse-effect profile of pembrolizumab plus chemotherapy, combined with its expected benefit, could justify switching in such cases. |
Considerations for initiation of therapy | |
For disease diagnosis and scoring or staging for eligibility, is PD-L1 status required or applicable? | Oncologists who treat MPM do not routinely test for PD-L1 because it is not considered a key factor in treatment decision-making. This is based on findings from the CheckMate 743 trial, which showed no clear association between PD-L1 expression and outcomes with nivolumab-ipilimumab in MPM. Similarly, the KEYNOTE-483 trial did not indicate a subgroup effect based on PD-L1 status. The clinical experts stated that reimbursement for pembrolizumab plus chemotherapy should not be linked to a patient’s PD-L1 status. They noted that this would be consistent with the reimbursement criteria for nivolumab-ipilimumab in the same patient population. |
The KEYNOTE-483 trial eligibility included the following criteria:
Would these criteria be appropriate to apply for identifying patients who are eligible for reimbursement of pembrolizumab plus chemotherapy? | The eligibility criteria for the KEYNOTE-483 trial are generally appropriate for identifying the target population for pembrolizumab treatment. However, the clinical experts noted that patients with an ECOG PS score of 2 or higher would be considered for pembrolizumab plus chemotherapy because performance status could be influenced by tumour-related symptoms that may improve with treatment. This approach is also applied when considering treatment with nivolumab-ipilimumab. The clinical experts agreed that the reimbursement-initiation conditions specified in the pERC recommendation for nivolumab-ipilimumab could similarly be applied to pembrolizumab plus chemotherapy if recommended for public reimbursement. |
Would patients who had partial tumour resection be eligible for pembrolizumab and chemotherapy regimen? | The clinical experts noted that the KEYNOTE-483 trial did not include patients who had undergone an initial resection; however, it was also noted that a partial resection, by definition, is not curable. The experts indicated that it would be reasonable to offer treatment with pembrolizumab plus chemotherapy to patients with a tumour that has undergone partial resection upon disease progression post resection, or symptomatic progression after resection. |
The KEYNOTE-483 trial excluded patients with the following:
Would patients with these trial-exclusion criteria be eligible for treatment with pembrolizumab with chemotherapy? | Interstitial lung disease and noninfectious pneumonitis are not absolute contraindications to pembrolizumab, but they are considered risk factors that require careful consideration and monitoring, including treatment modifications, as per the product monograph. The clinical experts noted that CNS metastases are very rare in MPM and that patients with stable and asymptomatic brain metastases would be eligible for pembrolizumab plus chemotherapy. |
If pembrolizumab is discontinued for reasons other than disease progression or toxicity, would patients with advanced MPM be considered eligible for an additional 12 months of treatment at the time of disease recurrence? Should re-treatment consist of pembrolizumab monotherapy or pembrolizumab plus chemotherapy? | The clinical experts indicated that re-treatment with pembrolizumab plus chemotherapy may be considered in this scenario, especially if a patient had stopped taking pembrolizumab for at least 6 months without disease progression, indicating an initial strong, objective, and durable response to treatment. However, they were not aware of evidence to inform the use of pembrolizumab re-treatment in patients with advanced MPM. In clinical practice, decisions would be informed by experience with pembrolizumab re-treatment in NSCLC. Yet, the clinical experts noted that very few patients with advanced MPM would meet these criteria, making this scenario rare. It was the opinion of the clinical experts that, in this scenario, rechallenge with the combination of pembrolizumab plus chemotherapy would be preferred to pembrolizumab monotherapy. There is evidence for and considerable clinical experience that some patients can achieve repeated responses to platinum-based chemotherapy with pemetrexed, suggesting no strong rationale for withholding this treatment upon disease recurrence. While the role of immunotherapy in the rechallenge setting remains uncertain due to limited direct evidence, chemotherapy is expected to provide clinical benefit in this context. However, for patients who previously achieved a durable response to pembrolizumab and did not experience disease progression while receiving it, rechallenge with both pembrolizumab and chemotherapy would be a clinically justifiable option. |
Consider alignment with reimbursement conditions for nivolumab-ipilimumab for MPM. | This is a comment from the drug plans to inform pERC deliberations. |
Considerations for discontinuation of therapy | |
If there is disease progression during a treatment break, can pembrolizumab and chemotherapy be resumed? If a patient cannot tolerate 1 of the components of the treatment, would treatment continue with the remaining components? Is there a minimum number of chemotherapy cycles that must be given concurrently with pembrolizumab? | The clinical experts stated that if disease progression occurred during a treatment break, then they would resume pembrolizumab plus chemotherapy treatment. The clinical experts indicated that continuing treatment with pembrolizumab alone would be clinically appropriate if the patient experiences an adverse event from chemotherapy, in the absence of disease progression. This approach was permitted in the KEYNOTE-483 trial and would align with current treatment practices. Monotherapy with the remaining drug should stop if the patient experiences serious adverse effects, has disease progression, or after completion of 2 years of therapy. The clinical experts noted that at least 1 cycle of chemotherapy should be administered concurrently with pembrolizumab. In cases where an infusion reaction to platinum-based chemotherapy occurred in the first cycle, then switching to nivolumab-ipilimumab may be considered; however, the experts noted that is typically a rare scenario. |
Consider alignment with reimbursement conditions for nivolumab-ipilimumab for MPM. | This is a comment from the drug plans to inform pERC deliberations. |
Considerations for prescribing of therapy | |
Jurisdictions would plan on implementing pembrolizumab as weight-based dosing up to a cap (e.g., 2 mg/kg every 3 weeks to a maximum dose of 200 mg) if reimbursed for MPM, similar to other indications. | This is a comment from the drug plans to inform pERC deliberations. |
Consider alignment with reimbursement conditions for nivolumab-ipilimumab for MPM. | This is a comment from the drug plans to inform pERC deliberations. |
Generalizability | |
Can pembrolizumab and chemotherapy also be given to patients with advanced peritoneal mesothelioma? | Malignant peritoneal mesothelioma is not currently an approved indication for pembrolizumab. Patients with malignant peritoneal mesothelioma and other nonpleural mesotheliomas were not included in the KEYNOTE-483 trial. The clinical experts indicated that malignant peritoneal mesothelioma is a distinct disease from MPM. No high-level studies (i.e., RCTs) have evaluated pembrolizumab with or without chemotherapy in patients with unresectable malignant peritoneal mesothelioma. Currently, evidence on the effects of pembrolizumab in this population is limited to retrospective data.34 However, accumulating clinical evidence and guideline recommendations suggest a potential role for this regimen in peritoneal mesothelioma. The clinical experts noted UK practitioners have extrapolated data from the CheckMate 743 trial (evaluating ipilimumab-nivolumab) to peritoneal mesothelioma. Increasing clinical experience with this regimen is helping to shift perspectives on the role of these treatments in peritoneal mesothelioma. Additionally, the NCCN guidelines4 list both nivolumab-ipilimumab and pembrolizumab plus chemotherapy as treatment options for peritoneal mesothelioma. The study by Marmarelis et al.,34 while small and retrospective, reported objective response rates that are clinically important, in the experts’ opinions. It was noted that peritoneal mesothelioma is more commonly epithelioid in nature, making chemotherapy a key component of treatment. The clinical experts also noted that given the rarity of peritoneal mesothelioma, randomized studies are less likely to be conducted. However, the accumulation of smaller studies, clinical experience, and evolving guidelines increasingly support a clinical rationale for using pembrolizumab plus chemotherapy in this setting. |
Could patients actively receiving alternative first-line systemic treatment for MPM who have not experienced disease progression and who otherwise meet eligibility criteria be switched to pembrolizumab plus chemotherapy? | The clinical experts noted there is no evidence to inform switching from chemotherapy or nivolumab-ipilimumab to pembrolizumab plus chemotherapy. However, it was their opinion that patients who had received fewer than 4 cycles of chemotherapy without disease progression or toxicity could be switched to pembrolizumab plus chemotherapy to potentially improve the likelihood of an objective response and delay progression. Switching from nivolumab-ipilimumab before completing the regimen would primarily be considered for patients who experienced serious adverse effects or toxicity from dual immunotherapy. |
Funding algorithm | |
Drug may change place in therapy of comparator drugs. | This is a comment from the drug plans to inform pERC deliberations. |
CNS = central nervous system; ECOG PS = Eastern Cooperative Oncology Group Performance Status; MPM = malignant pleural mesothelioma; NCCN = National Comprehensive Cancer Network; NSCLC = non–small cell lung cancer; pERC = pan-Canadian Oncology Drug Review Expert Review Committee; RCT = randomized controlled trial.
Clinical Evidence
The objective of this Clinical Review report is to review and critically appraise the clinical evidence submitted by the sponsor on the beneficial and harmful effects of pembrolizumab 100 mg/4 mL solution for IV infusion, in combination with pemetrexed and platinum chemotherapy, for the first-line treatment of adult patients with unresectable advanced or metastatic MPM. The focus will be placed on comparing pembrolizumab with relevant comparators and identifying gaps in the current evidence.
A summary of the clinical evidence included by the sponsor in the review of pembrolizumab is presented in 4 sections, with the critical appraisal by CDA-AMC of the evidence included at the end of each section. The first section, the systematic review, includes pivotal studies and RCTs that were selected according to the sponsor’s systematic review protocol. The assessment by CDA-AMC of the certainty of the evidence in this first section using the GRADE approach follows the critical appraisal of the evidence. The third section includes a sponsor-submitted ITC of pembrolizumab compared with nivolumab-ipilimumab. There were no long-term extension studies (section 2), nor any additional studies to address important gaps in the systematic review evidence (section 4) submitted by the sponsor.
Included Studies
Clinical evidence from the following is included in the review and appraised in this document:
1 pivotal RCT identified in systematic review (KEYNOTE-483 trial)
1 sponsor-provided ITC.
Systematic Review
Contents within this section have been informed by materials submitted by the sponsor. The following has been summarized and validated by the review team.
Description of Studies
Characteristics of the included study is summarized in Table 5.
Table 5: Details of Studies Included in the Systematic Review
Details | KEYNOTE-483 trial |
|---|---|
Designs and populations | |
Study design | Randomized, open-label, multicentre, phase II and III |
Locations | Study was conducted at 54 centres in 3 countries: Canada, France, and Italy. |
Patient enrolment dates |
|
Randomized (N) | Phase III: Efficacy (N = 440)
Phase II and III: Safety (N = 473)
|
Inclusion criteria |
|
Exclusion criteria |
|
Drugs | |
Intervention | IV infusions of pembrolizumab (200 mg q.3.w.) in combination with platinum (cisplatin 75 mg/m2 or carboplatin [AUC 5 mg/mL per min to 6 mg/mL per min] could be substituted) and pemetrexed (500 mg/m2 q.3.w.) |
Comparator | IV infusions of platinum (cisplatin 75 mg/m2 or carboplatin [AUC 5 mg/mL per min to 6 mg/mL per min] could be substituted) plus pemetrexed (500 mg/m2 q.3.w.) |
Study duration | |
Screening phase | NR |
Treatment phase |
|
Follow-up phase |
|
Outcomes | |
Primary end point | OS |
Secondary and exploratory end points | Secondary end points
Exploratory end points
|
Publication status | |
Publications | Unpublished records:
Published records: |
AE = adverse event; AUC = area under the concentration-time curve; CFB = change from baseline; CNS = central nervous system; ECOG PS = Eastern Cooperative Oncology Group Performance Status; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; EORTC QLQ-LC13 = European Organisation for Research and Treatment of Cancer 13-item lung cancer-specific questionnaire module; MPM = malignant pleural mesothelioma; mRECIST = modified Response Evaluation Criteria in Solid Tumours; NR = not reported; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; q.3.w. = every 3 weeks; TTD = time to deterioration; VAS = visual analogue scale.
Source: Clinical Study Report for KEYNOTE-483.11 Details included in the table are from the sponsor’s summary of clinical evidence.
One RCT, KEYNOTE-483 (NCT02784171), was included in the sponsor’s systematic review. This open-label, multicentre, phase II and III study, initiated as the IND.227 trial by the Canadian Cancer Trials Group in collaboration with the National Cancer Institute Naples, compared pembrolizumab with or without chemotherapy versus chemotherapy alone in untreated advanced MPM. Participants were randomized 1:1:1 to arm A (chemotherapy), arm B (pembrolizumab plus chemotherapy), or arm C (pembrolizumab). After an interim analysis showed arm B had higher response rates and improved OS compared with arm A, arm C was discontinued due to lower disease control. The study was subsequently adjusted to phase III, with Canadian Cancer Trials Group sponsorship and support from Merck (e.g., pembrolizumab supply and statistical analyses).
The phase III study design is presented in Figure 1. The objective of the KEYNOTE-483 trial was to examine the effects of the addition of pembrolizumab to chemotherapy (pemetrexed plus cisplatin or carboplatin) compared with chemotherapy alone in participants with MPM receiving first-line treatment for unresectable advanced or metastatic disease.
All eligible participants were randomly assigned 1:1 to study treatments, stratified by histology. Randomization was done through a web-based electronic data capture system. Patients in the KEYNOTE-483 trial were enrolled across 54 centres in 3 countries, including 13 study sites in Canada. Patients were recruited between January 2017 and September 2020. The final database lock date for the KEYNOTE-483 trial was December 16, 2022.
Figure 1: Schematic of the KEYNOTE-483 Clinical Trial Design
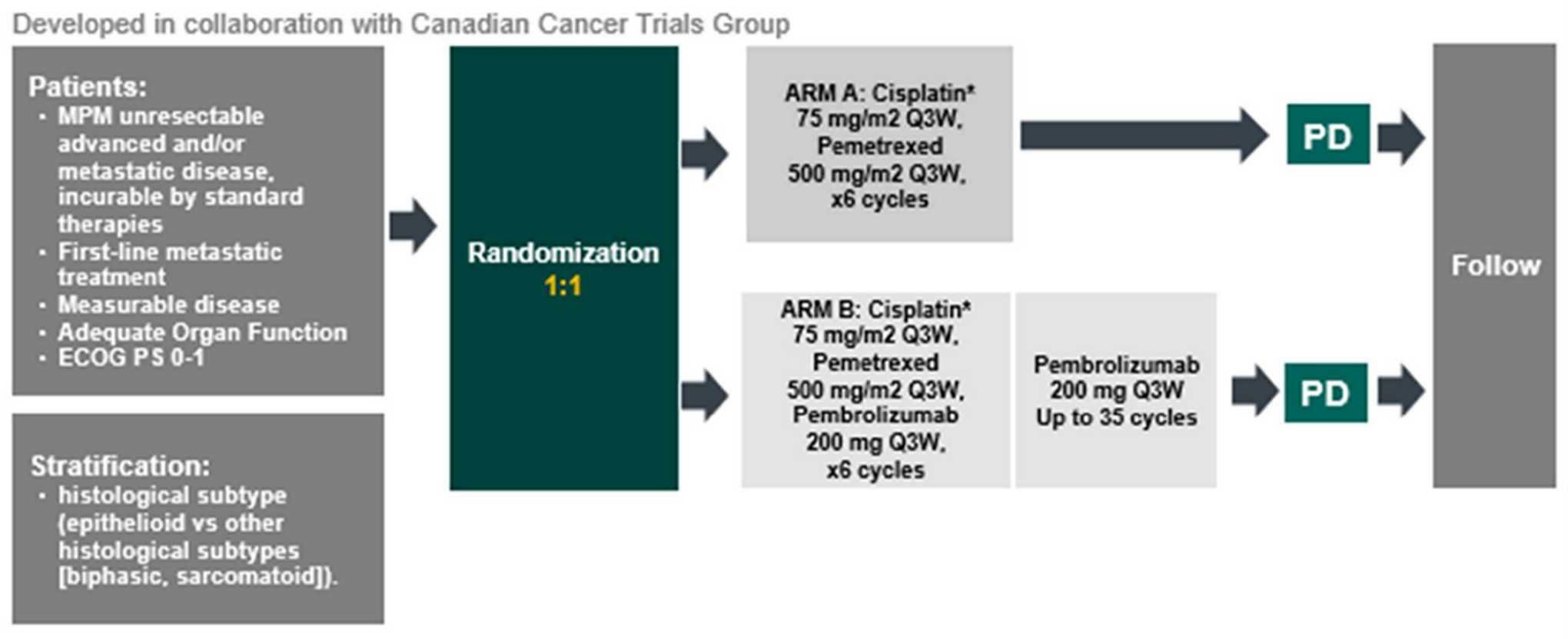
ECOG PS = Eastern Cooperative Oncology Group Performance Status; MPM = malignant pleural mesothelioma; PD = progressive disease; Q3W = every 3 weeks; vs = versus.
*Carboplatin was allowed instead of cisplatin with Canadian Cancer Trials Group approval.
Source: Clinical Study Report for KEYNOTE-483.11
Populations
Inclusion and Exclusion Criteria
Key eligibility criteria required patients to be aged 18 years or older with histologically confirmed unresectable advanced and/or metastatic MPM. At least 1 site of the disease was measurable according to mRECIST. Patients had no previous systemic therapy; however, neoadjuvant chemotherapy was permitted if it was stopped more than 1 year before the start of this trial. Patients had an ECOG PS score of 0 or 1. Patients were excluded if they had other malignancies, untreated central nervous system metastases or pneumonitis, or immunodeficiency or autoimmune disease that required systemic treatment.
Interventions
Patients were randomized to receive either chemotherapy alone or pembrolizumab plus chemotherapy.
All patients received IV cisplatin 75 mg/m2 (or carboplatin area under the curve 5 mg/mL to 6 mg/mL per minute) every 3 weeks and pemetrexed 500 mg/m2 every 3 weeks for up to 6 cycles. Patients also received standard premedication for chemotherapy, including antiemetics, hydration (for cisplatin), vitamin supplementation, and corticosteroid prophylaxis (the latter 2 for pemetrexed). Patients randomly assigned to the pembrolizumab group also received IV pembrolizumab 200 mg every 3 weeks for up to 35 cycles (2 years).
Pembrolizumab and chemotherapy were continued until disease progression, unacceptable toxic effects occurred, the investigator decided to stop, the patient withdrew consent, planned treatment was complete, or other reasons, whichever occurred first. Participants who discontinued pembrolizumab for toxicity could not restart pembrolizumab after they completed chemotherapy. Patients were permitted to continue pembrolizumab alone if they stopped treatment with chemotherapy for adverse effects.
In the event pembrolizumab interruption or discontinuation was warranted, the process was conducted in accordance with the recommended dose modifications procedures outlined in the product monograph.
Concomitant Medications and Cointerventions
All treatments that the investigator considered necessary for a patient’s welfare could be administered at the discretion of the investigator in keeping with the community standards of medical care, except for antineoplastic systemic chemotherapy or biological therapy, radiation therapy, live vaccines, or systemic glucocorticoids. Patients who, in the assessment of the investigator, required the use of any of these treatments for clinical management could be removed from trial therapy.
Subsequent Treatment
The choice of subsequent treatments was at the discretion of the investigator. No crossover was planned.
Outcomes
A list of efficacy end points assessed in this Clinical Review report is provided in Table 6, followed by descriptions of the outcome measures. The summarized end points are based on outcomes included in the sponsor’s summary of clinical evidence as well as any outcomes identified as important to this review according to the clinical experts consulted for this review and input from patient and clinician groups and public drug plans. Using the same considerations, the CDA-AMC reviewers selected end points that were most relevant to inform expert committee deliberations and finalized this list of end points in consultation with members of the expert committee. All summarized efficacy and harms end points assessed using GRADE are identified.
Table 6: Outcomes Summarized From the Studies Included in the Systematic Review
Outcome measure | Time point | Type |
|---|---|---|
OSa | At months 24 and 36: KM estimate At the time of data cut-off: HR and median | Primary |
PFS per mRECIST by BICRa | At month 12: KM estimate At the time of data cut-off: HR and median | Secondaryb |
ORR per mRECIST by BICRa | At the time of data cut-off | Secondaryb |
Harms outcomes: AEs, SAEs,a WDAEs,a fatal AEs,a notable harms | At the time of data cut-off | Secondary |
HRQoL, change from baseline in EORTC QLQ-C30:
| At week 15 | Exploratory |
HRQoL, change from baseline in EORTC QLQ-LC13:
| At week 15 | Exploratory |
HRQoL, EQ-5D-5L VAS | At week 15 | Exploratory |
AE = adverse event; BICR = blinded independent central review; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; EORTC QLQ-LC13 = European Organisation for Research and Treatment of Cancer 13-item lung cancer-specific questionnaire module; GRADE = Grading of Recommendations Assessment, Development and Evaluation; HR = hazard ratio; HRQoL = health-related quality of life; KM = Kaplan-Meier; mRECIST = modified Response Evaluation Criteria in Solid Tumours; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; SAE = serious adverse event; VAS = visual analogue scale; WDAE = withdrawal due to adverse event.
aIncluded in the GRADE summary of findings in Table 2 for being the most relevant to inform expert committee deliberations.
bStatistical testing for these end points was adjusted for multiple comparisons (e.g., hierarchal testing).
Source: Clinical Study Report for KEYNOTE-483.11
Efficacy Outcomes
OS was the primary end point of the KEYNOTE-483 trial. OS was defined as the time from randomization to death from any cause. Patients alive at data cut-off were censored at the last day known alive. Kaplan-Meier estimates of the probability of OS were estimated at several time points. Discussion with the clinical experts consulted for this review identified estimates at 24 and 36 months to be clinically relevant for this review; these time points were used in the GRADE assessment of OS.
PFS was a secondary outcome in the KEYNOTE-483 trial and was defined as the time from day of random assignment until the first observation of progression per mRECIST38 or death due to any cause. Patients who were alive without progression were censored at their last date of disease assessment unless definitive therapy had been initiated, or 2 or more consecutive assessments were missed. Like OS, Kaplan-Meier probabilities of PFS were estimated at several time points. The estimate at 12 months was identified — with help from the clinical experts consulted — as a clinically important time point for the GRADE assessment of PFS.
ORR was also a secondary outcome in the KEYNOTE-483 trial and was defined as the percentage of participants who achieve a complete or partial response, per mRECIST. Complete response was defined as the disappearance of target and nontarget lesions and the normalization of tumour markers. Partial response was defined as at least a 30% decrease in the sum of measures (longest diameter for tumour lesions and short axis measure for nodes) of target lesions, taking as reference the baseline sum of diameters. The clinical experts consulted by CDA-AMC indicated that reducing tumour size and burden is a patient-important outcome. Advanced MPM tumours spread diffusely along the pleura, often encasing the lung and extending to the chest wall, diaphragm, and mediastinum. Tumour burden directly contributes to key symptoms that impact patients’ lives, including chest pain, breathlessness, and reduced physical functioning. Therefore, objective response, reflecting tumour shrinkage, may alleviate these symptoms and improve functioning and HRQoL in patients with advanced MPM.
For assessing both PFS and ORR, CT scans were the preferred mode of tumour imaging to assess disease response and were conducted every 6 weeks for 3 assessments, then every 12 weeks during treatment. They were also conducted 4 weeks after the completion of treatment and, if applicable, every 12 weeks until confirmed disease progression post treatment and then every 24 weeks until death.
HRQoL and other patient-reported outcomes were measured using the EORTC QLQ-C30 (global health status scale and quality of life scale, and physical functioning and dyspnea subscales), EORTC QLQ-LC13 (cough and chest pain subscales), and EQ-5D-5L Visual Analogue Scale (VAS). The EORTC QLQ-C30 subscales were evaluated as time to deterioration (secondary end points) and change from baseline to week 15 (exploratory end points). The EQ-5D-5L VAS was evaluated as an exploratory end point as change from baseline to week 15.
The EORTC QLQ-C30 is a self-administered cancer-specific questionnaire that consists of multi-item scales and single-item measures, including 5 functioning domains, a global HRQoL domain, 3 symptom domains, and 6 single items.39 The QLQ-LC13 module includes questions assessing lung cancer–associated symptoms and pain medication.40 The QLQ-LC13 module is used in conjunction with the QLQ-C30 and includes 13 questions that share the 4-level ordinal response with the QLQ-C30. More details about these instruments, including minimal important differences (MIDs) are presented in Table 7.
The EQ-5D-5L is a standardized instrument for use as a measure of health outcomes that is typically used to develop health utilities for use in health economic analyses.41 It includes a graded vertical VAS that ranges from 0 (worst imaginable health) to 100 (best imaginable health) on which the participant rates their general state of health at the time of the assessment.
The EORTC QLQ-C30 global health status scale and quality of life scale was included in the GRADE assessment because it provides a comprehensive, patient-centred measure of overall well-being, integrating physical, emotional, and social aspects of health that are most relevant to patients. While the other subscales provide valuable clinical insights, their inclusion in GRADE could lead to an overemphasis on specific symptoms without adequately capturing the full patient experience. Given that GRADE prioritizes outcomes that are most meaningful to patients and that best inform decision-making, the global health status scale and quality of life scale was determined to be the most appropriate single measure to represent HRQoL in this context. Additionally, the review prioritizes change from baseline for each of HRQoL end point to capture improvement, deterioration, or stability in the treatment effects, rather than focusing on time to deterioration.
Harms Outcomes
Harms were assessed continuously throughout the trial. Events relevant for the CDA-AMC review are SAEs, discontinuation or WDAEs, any AEs, AEs of grade 3 or higher, and fatal AEs. Immune-mediated AEs are included as notable harms. SAEs, WDAEs, and fatal AEs were assessed in GRADE because these outcomes likely have more impact on patients, clinical decision-making, and health care resource implications.
Table 7: Summary of Outcome Measures and Their Measurement Properties
Outcome measure | Type | Conclusions about measurement properties | MID |
|---|---|---|---|
EORTC QLQ-C30 | A self-reported, 30-item, cancer-specific instrument that is used to assess 5 functional scales (physical, role, emotional, cognitive, and social), 3 symptom scales (fatigue, nausea or vomiting, and pain), 6 single items (dyspnea, sleep disturbance, appetite loss, constipation, diarrhea, and financial difficulties), and a global health status scale and quality of life scale.42 Scores are linearly transformed to range from 0 to 100, where a higher score represents better functioning and global health scales, or increased symptom severity for symptom scales.42 | Psychometric properties have been evaluated in patients with MPM. Validity Construct validity:43
Criterion validity: Subscales correlate with clinical measures such as tumour stage, performance status, and lung function tests.43 Reliability Cronbach alpha ranging from 0.57 to 0.87 with 6 of the 8 subscales with estimates having an internal consistency alpha > 0.80.43 Responsiveness Sensitivity to change: The EORTC QLQ-C30 is responsive to changes in clinical status. For instance, improvements in dyspnea, pain, insomnia, and cough were observed with chemotherapy in mesothelioma patients.7 Predictive validity: Functional domains and symptom scales from the EORTC QLQ-C30 have demonstrated predictive validity for survival, with certain scales showing strong correlations with survival outcomes.7 | Anchor-based and distribution-based MID estimates of patients with MPM and lung cancer who were pooled.44,45 Between-group MIDs for improvement:
Between-group MIDs for deterioration:
|
EORTC QLQ- LC13 | The EORTC QLQ-LC13 is a tumour-specific questionnaire used to supplement the EORTC QLQ-C30. It contains 13 items related to lung cancer symptoms and treatment side effects, including a 3-item scale assessing dyspnea and 9 single items: pain in chest, pain in arm or shoulder, pain in other parts, coughing, hemoptysis, sore mouth or tongue, dysphagia, peripheral neuropathy, and alopecia.39 All the scales range in score from 0 to 100. Higher scores on the symptom scales indicate worse symptoms.39 | Psychometric properties have been evaluated in patients with MPM and lung cancer. Validity Construct validity has been established between pain score and disease type (P < 0.001). Also, based on ECOG PS, construct validity was confirmed in dyspnea, coughing, and pain (P < 0.001) scores.40 Correlation between spirometry result and dyspnea score was found to be weak (r = 0.24). BPI intensity score and EORTC QLQ-LC13 pain score were found to be modestly correlated (r > 0.4).43 Reliability Good internal consistency reliability for the dyspnea multi-item scale (alpha = 0.81).47 However, internal consistency was found to be unacceptable for pain scores (alpha = 0.53 to 0.54) when EORTC QLQ-LC13 was used alone without EORTC QLQ-C30 questionnaire pain items.47 The reliability estimate for dyspnea scale was confirmed to be acceptable, i.e., alpha = 0.76, in another study.43 Responsiveness Dyspnea, coughing, and pain scores improved significantly over time between the pretreatment and on-treatment period (P < 0.001 for all except for extra thoracic pain, which showed P < 0.05). Responsiveness of chest pain (P < 0.01), dyspnea (P < 0.001), and coughing (P < 0.001) to change in ECOG PS was also noted.40 | An MID was not identified for patients with MPM. However, in other lung cancers, generally, a 10 points or greater worsening from baseline represents a clinically relevant deterioration.46 |
6MWD = 6-minute walk distance; BPI = Brief Pain Inventory; ECOG PS = Eastern Cooperative Oncology Group Performance Status; EORTC QLQ-C30 = European Organization for the Research and Treatment of Cancer Quality of Life Questionnaire Core 30; EORTC QLQ-LC13 = European Organization for the Research and Treatment of Cancer 13-item lung cancer-specific questionnaire module ; HADS = Hospital Anxiety and Depression Scale; MID = minimal important difference; MPM = malignant pleural mesothelioma.
Statistical Analysis
A summary of statistical analyses for the efficacy end points in the KEYNOTE-483 trial is presented in Table 8.
Sample-Size and Power Calculation
The sample-size and power calculations for OS and PFS were estimated based on prior trials in unresectable MPM, including the CheckMate 743 and LUME-Meso trials.28,47 In the KEYNOTE-483 trial, the median OS for the chemotherapy-alone group was estimated as 16 months. To detect an increase in median OS to 22.9 months (HR = 0.70) in the pembrolizumab plus chemotherapy group, with 90% power at a 2-sided 0.05 significance level, a minimum of 334 events were required across both treatment arms. It was estimated that the required number of events would be observed by accruing a total of up to 430 patients over a 34-month accrual period with a 31-month follow-up. Assuming 10 patients would drop out earlier, the final sample size of patients who were randomized was estimated at 440 (220 per arm).
The median PFS for the chemotherapy-alone group was estimated as 7 months. To detect an increase in median PFS to 10 months (HR = 0.70) by the pembrolizumab plus chemotherapy group, with 90.6% power at a 2-sided 0.035 level, a minimum of 376 events were required across both treatment arms with a total of 440 patients randomized, assuming a 13% annual dropout rate. With this sample size, ORR testing at a 2-sided level would have approximately 87.5% power to detect a 17% difference, assuming an ORR of 43% in the chemotherapy-alone group and 60% in the pembrolizumab plus chemotherapy group.
A total of 520 patients were planned for enrolment, including 440 in the phase III component. In the phase II component, 40 patients were enrolled in each treatment group and included in the interim disease control rate analysis. These patients were also part of the overall safety analysis. An additional 40 patients were enrolled in the pembrolizumab monotherapy arm before its closure to accrual.
Statistical Testing
An interim efficacy analysis was conducted on OS and PFS during the phase III component, approximately 11 months after the last participant was randomized (data cut-off: July 30, 2021). The OS and PFS results presented in this review are from the final analysis (data cut-off: September 16, 2022).
To control for multiplicity in multiple hypotheses and interim analyses, the trial used the graphical method of Maurer and Bretz. Figure 2 illustrates the initial 2-sided alpha allocation for each hypothesis. The initial 2-sided alpha of 0.05 was assigned to OS. PFS was tested at a 2-sided 0.035 significance level only if the OS hypothesis test was significant or 0 at the interim analysis. The stratified log-rank test was used to compare PFS between treatment arms, with statistical significance determined using the Lan-DeMets methodology with O’Brien-Fleming–type boundaries.
The ORR hypothesis was tested at the interim analysis at a 2-sided 0.015 alpha level if the OS hypothesis was rejected. If the PFS hypothesis was rejected, its alpha could be transferred to ORR, allowing testing at the full 2-sided 0.05 level. Conversely, if the ORR hypothesis was rejected, its alpha could be transferred to PFS for testing at the full 2-sided 0.05 level.
Figure 2: Multiplicity Schema for Type I Error Control in the KEYNOTE-483 Trial
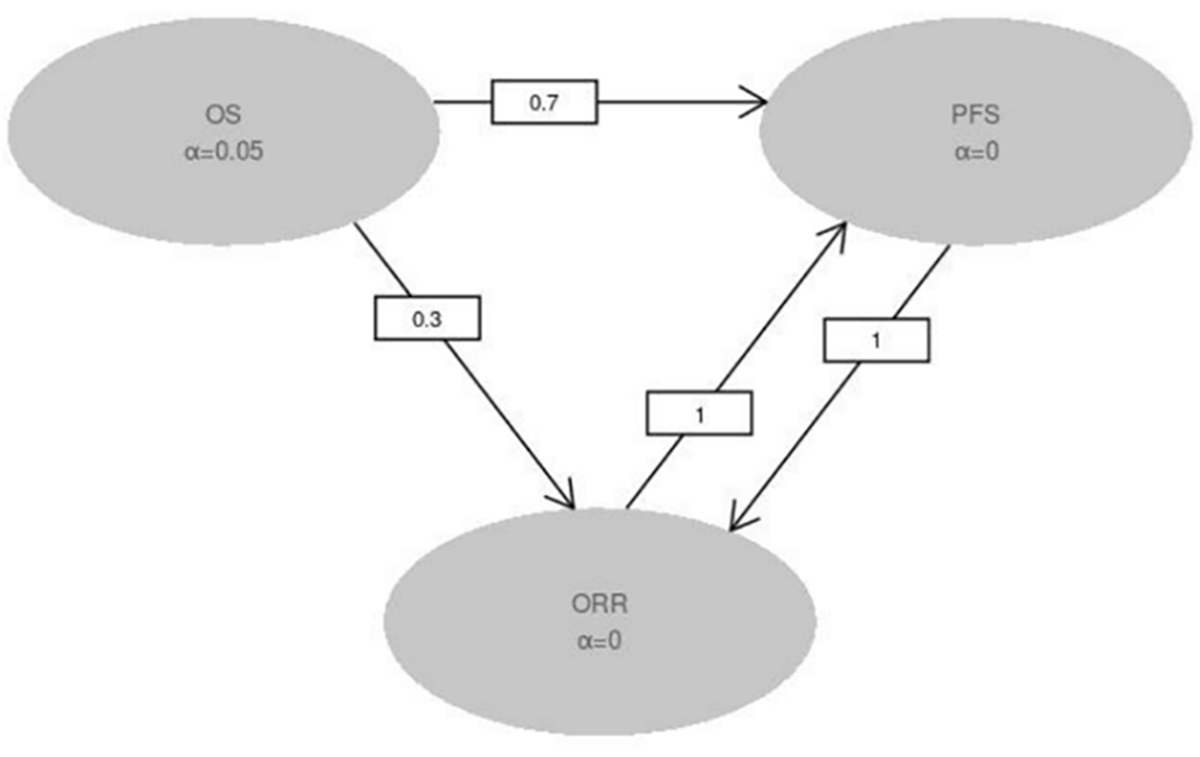
ORR = objective response rate; OS = overall survival; PFS = progression-free survival.
Source: Clinical Study Report for KEYNOTE-483.11
The nonparametric Kaplan-Meier method was used to estimate the survival curves for the OS and PFS end points. The HR and its 95% CIs were reported for OS and PFS, using the statistical methods described in Table 8. For the PFS end point, because disease progression was assessed periodically, progressive disease could occur at any point between the last assessment where progressive disease was not documented and the subsequent assessment where progression was documented. The true date of disease progression was approximated by the earlier of the date of the first assessment at which progressive disease was objectively documented per mRECIST and the date of death. If a participant met multiple criteria for censoring, the earliest applicable censoring criterion was applied.
The treatment difference in terms of the change from baseline in the least squares mean was estimated from the constrained longitudinal data-analysis model together with the 95% CI for the HRQoL end point measures. Model-based least square means with 95% CIs were provided by treatment group for each instrument at week 15.
Data Imputation Methods
The methods for handling missing data are described in Table 8.
Subgroup Analyses
Subgroup analyses were planned to determine whether the treatment effect was consistent across various subgroups. The between-group treatment effect for OS and PFS were estimated by the treatment group within each category of the following subgroup variables:
geographic region (EU versus non-EU)
ECOG PS (0 versus 1)
initial choice of platinum chemotherapy (cisplatin versus carboplatin)
PD-L1 combined positive score (positive versus negative)
age category (< 65 years versus ≥ 65 years) (< 65 years, or 65 to 74 years, or 75 to 84 years, or ≥ 85 years)
sex (female versus male)
race (white versus all other races)
smoking history (never versus current or former)
histological subtype (epithelioid versus other subtypes).
The subgroup analyses for PFS and OS were conducted using an unstratified Cox model.
Histological subtype was selected as the subgroups most relevant to this Reimbursement Review based on input from the clinical experts consulted by CDA-AMC, previous reviews for the same indication, and information from the available literature regarding clinically important prognostic factors and effect modifiers.
Sensitivity and Supportive Analyses
The sensitivity analyses reported in the sponsor’s clinical summary of evidence are described in Table 8.
The statistical analysis plan for the KEYNOTE-483 trial noted that a re-randomization sensitivity analysis might be conducted; however, no results of this sensitivity analysis were reported in the sponsor’s summary of clinical evidence for the Clinical Study Report for the trial, suggesting it was not performed. A supplemental analysis of OS was conducted using RMST, but it was not reported in the statistical analysis plan.
Supplemental analyses were conducted for PFS (using the intention-to-treat [ITT] population) in addition to the sensitivity analyses reported in Table 8. These analyses included:
PFS based on investigator assessment per mRECIST (primary censoring rule)
PFS based on investigator assessment per mRECIST (sensitivity censoring rule 1)
PFS based on BICR per Response Evaluation Criteria in Solid Tumours (RECIST) (primary censoring rule)
PFS based on RMST.
As with OS, the supplementary analyses for PFS were not found in the statistical analysis plan, except for PFS based on investigator assessment per mRECIST (primary censoring rule).
Table 8: Statistical Analysis of Efficacy End Points From the KEYNOTE-483 Trial
End points | Statistical model | Adjustment factors | Handling of missing data | Sensitivity analyses |
|---|---|---|---|---|
OS | Testing: Stratified log-rank test Estimation: Stratified Cox model with Efron tie-handling method | Adjusting for histology (epithelioid vs. other). | Censored at the date participant was last known to be alive. | Re-randomization test using the log-rank statistics stratified by histological subtype, assuming 1:1 randomization starting from the first participant randomized in the phase III ITT population. |
PFS | Testing: Stratified log-rank test Estimation: Stratified Cox model with Efron tie-handling method | Adjusting for histology (epithelioid vs. other). |
|
|
CFB in EORTC QLQ-C30, EORTC QLQ-LC13 scores, and EQ-5D-5L VAS | Constrained longitudinal data-analysis model | Adjusting for histology (epithelioid vs. other). | Model-based: Constrained longitudinal data-analysis model implicitly treats missing data as missing at random. | NA |
CFB = change from baseline; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Core Quality of Life Questionnaire Core 30; EORTC QLQ-LC13 = European Organisation for Research and Treatment of Cancer 13-item lung cancer-specific questionnaire module; NA = not applicable; OS = overall survival; PD = progressive disease; PFS = progression-free survival; VAS = visual analogue scale; vs. = versus.
Source: Clinical Study Report for the KEYNOTE-483 trial.11
Analysis Populations
As presented in Table 9, the efficacy results presented in the KEYNOTE-483 Clinical Study Report and the sponsor’s summary of clinical evidence are from patients enrolled in the phase III trial (ITT population); no results were presented from the phase II IND.277 study portion because the end points were assessed differently. Additionally, the harms results were combined from both the phase II and III portions of the trial (the population comprising all participants as treated) for transparency and to align with recommendations from regulatory agencies.
Table 9: Analysis Populations of the KEYNOTE-483 Trial
Study | Population | Definition | Application |
|---|---|---|---|
KEYNOTE-483 | Phase III ITT population | All participants randomized | Efficacy end points |
APaT population | All participants who received treatment | Safety end points | |
PRO FAS population | All participants in the phase III ITT population who had at least 1 PRO assessment available for the specific end point and received at least 1 dose of the study intervention | HRQoL end points |
APaT = all participants as treated; FAS = full analysis set; HRQoL = health-related quality of life; ITT = intention to treat; PRO = patient-reported outcome.
Source: Clinical Study Report for KEYNOTE-483.11
Results
Patient Disposition
The patient disposition as of the final analysis data cut-off date (September 16, 2022) is reported in Table 10. A total of 440 patients were randomized, with 222 assigned to the pembrolizumab plus chemotherapy arm and 218 to the chemotherapy-alone arm. All patients in the pembrolizumab plus chemotherapy group and 96.8% of those in the chemotherapy-alone group received treatment. At the data cut-off date, a lower percentage of participants in the pembrolizumab plus chemotherapy group completed the study intervention compared with the chemotherapy-alone group (10.4% versus 72.5%), due to differences in the maximum allowed number of cycles in each arm (up to 35 cycles of pembrolizumab and up to 6 cycles of chemotherapy).
Table 10: Summary of Patient Disposition From the KEYNOTE-483 Trial, Phase III
Patient disposition | Pembrolizumab + platinum + pemetrexed (N = 222) | Platinum + pemetrexed (N = 218) |
|---|---|---|
Screened, N | NR | |
Reason for unsuccessful screening, N (%) | NR | |
Randomized, N (%) | 222 (100) | 218 (100) |
Treated, N (%) | 222 (100) | 211 (96.8) |
Completed, N (%) | 23 (10.4) | 153 (72.5) |
Discontinued from study, N (%) | 168 (75.7) | 185 (84.9) |
Death | 167 (75.2) | 175 (80.3) |
Lost to follow-up | 0 | 1 (0.5) |
Withdrawal by patient | 1 (0.5) | 9 (4.1) |
Discontinued treatment, N (%) | 199 (89.6) | 58 (27.5) |
AEs related to protocol therapy | 39 (17.6) | 17 (8.1) |
Death | 4 (1.8) | 1 (0.5) |
Intercurrent illness: AEs unrelated to protocol treatment | 5 (2.3) | 4 (1.9) |
Other reason | 3 (1.4) | 1 (0.5) |
Patient refusal (not related to AE) | 3 (1.4) | 8 (3.8) |
Progressive disease (objective) | 137 (61.7) | 23 (10.9) |
Symptomatic progression | 8 (3.6) | 4 (1.9) |
Participants, ongoing, N (%) | 54 (24.3) | 33 (15.1) |
Safety, N (APaT population) | 241 | 232 |
ITT, N (%) | 222 (100) | 218 (100) |
PRO FAS, N (%) | 220 (99.1) | 209 (95.9) |
AE = adverse event; APaT = all participants as treated; FAS = full analysis set; ITT = intention to treat; NR = not reported; PRO = patient-reported outcome.
Source: Clinical Study Report for KEYNOTE-483.11
Baseline Characteristics
The baseline characteristics outlined in Table 11 have been limited to those that are most relevant to this review or considered to have impacted the study outcomes or their interpretation. Demographic and disease characteristics were generally similar between treatment groups, with 2 exceptions: there was a higher percentage of current or former patients who smoked in the pembrolizumab plus chemotherapy group and a higher percentage of patients in the chemotherapy arm who had received prior treatments (surgery, radiation, and neoadjuvant or adjuvant chemotherapy).
Table 11: Summary of Baseline Characteristics From the KEYNOTE-483 Trial (ITT Population)
Characteristics | Pembrolizumab + platinum + pemetrexed (N = 222) | Platinum + pemetrexed (N = 218) |
|---|---|---|
Sex, n (%) | ||
Male | 165 (74.3) | 168 (77.1) |
Female | 57 (25.7) | 50 (22.9) |
Age (years) | ||
Median (range) | 70.0 (33 to 86) | 70.0 (28 to 87) |
Mean (SD) | 69.3 (NR) | 68.5 (NR) |
Region, n (%) | ||
North America | 70 (31.5) | 67 (30.7) |
European Union | 152 (68.5) | 151 (69.3) |
Race,a n (%) | ||
American Indian or Alaska Native | 0 | 1 (0.5) |
Asian | 1 (0.5) | 0 |
White | 175 (78.8) | 172 (78.9) |
Not reported | 37 (16.7) | 38 (17.4) |
Unknown | 9 (4.1) | 7 (3.2) |
Baseline ECOG PS | ||
0 | 101 (45.5) | 105 (48.2) |
1 | 121 (54.5) | 113 (51.8) |
Histological subtypes, n (%) | ||
Epithelioid | 176 (79.3) | 169 (77.5) |
Mixed or biphasic | 31 (14.0) | 30 (13.8) |
Sarcomatoid | 12 (5.4) | 18 (8.3) |
Other | 3 (1.4) | 1 (0.5) |
EORTC prognostic score, n (%) | ||
≤ 1.27b | 77 (35.0) | 76 (35.0) |
> 1.27 | 145 (65.0) | 141 (65.0) |
Unknown | 0 | 0 |
PD-L1 CPS status, n (%) | ||
CPS ≥ 1 | 131 (59.0) | 132 (60.6) |
CPS < 1 | 70 (31.5) | 6 3 (28.9) |
Unknown | 7 (3.2) | 6 (2.8) |
Not done | 14 (6.3) | 17 (7.8) |
Smoking status, n (%) | ||
Current or former | 129 (58.1) | 116 (53.2) |
Never | 91 (41.0) | 102 (46.8) |
Unknown | 2 (0.9) | 0 |
Prior therapy, n (%) | ||
Previous major surgeryc | 17 (7.7) | 24 (11.0) |
Previous radiation | 9 (4.1) | 16 (7.3) |
Previous neoadjuvant or adjuvant chemotherapy | 3 (1.4) | 9 (4.1) |
CPS = combined positive score; ECOG PS = Eastern Cooperative Oncology Group Performance Status; EORTC = European Organisation for Research and Treatment of Cancer; ITT = intention to treat; NR = not reported; SD = standard deviation.
aCategories are as reported in study.
bgood prognosis is defined as a score of 1.27 or less.
cPrior major surgeries included decortication, pleurectomy, pneumonectomy, and wedge resection.
Source: Clinical Study Report for KEYNOTE-483.11
Exposure to Study Treatments
The median duration of exposure (Table 12) was longer in the pembrolizumab plus chemotherapy group than in the chemotherapy-alone group (211 days versus 107 days, respectively), reflecting the longer treatment duration in the pembrolizumab plus chemotherapy group. The median number of treatment cycles was 10 in the pembrolizumab plus chemotherapy group compared with 6 in the chemotherapy-alone group.
Platinum chemotherapy use in the KEYNOTE-483 trial is summarized in Table 13.
Table 12: Summary of Patient Exposure From the KEYNOTE-483 Trial (APaT Population)
Exposure | Pembrolizumab + platinum + pemetrexed (N = 241) | Platinum + pemetrexed (N = 232) |
|---|---|---|
Number of cycles, mean (SD) | 13.2 (9.5) | 5.1 (1.6) |
Number of cycles, median (range) | 10.0 (1.0 to 36.0) | 6.0 (1.0 to 8.0) |
Duration in days, mean (SD) | 278.8 (212.3) | 95.6 (38.3) |
Duration in days, median (range) | 211.0 (1.0 to 767.0) | 107.0 (1.0 to 192.0) |
APaT = all participants as treated; SD = standard deviation.
Source: Clinical Study Report for KEYNOTE-483.11
Table 13: Platinum Chemotherapy Use in the KEYNOTE-483 Trial (ITT Population)
Platinum chemotherapy used | Pembrolizumab + platinum + pemetrexed (N = 222) | Platinum + pemetrexed (N = 218) |
|---|---|---|
Cisplatin only, n (%) | 94 (42.3) | 100 (45.9) |
Carboplatin only, n (%) | 96 (43.2) | 84 (38.5) |
Switching from cisplatin to carboplatin, n (%) | 32 (14.4) | 27 (12.4) |
Not treated | 0 | 7 (3.2) |
ITT = intention to treat.
Source: Clinical Study Report for KEYNOTE-483.11
Concomitant Medications and Cointerventions
All treatments that the investigator considered necessary for a patient’s welfare could be administered at the investigator’s discretion, in accordance with the community standards of medical care, except for antineoplastic systemic chemotherapy or biological therapy, radiation therapy, live vaccines, or systemic glucocorticoids not specified in the protocol. All patients in both treatment groups received concomitant medications, with similar percentages between groups. The types of concomitant medications were primarily supportive and typical for patients undergoing antineoplastic treatment (i.e., antianemic preparations and antiemetics).
Subsequent Treatment
Greater than one-half of the patients in both treatment groups received subsequent oncologic treatment after disease progression at the investigator’s discretion (Table 14). The most common subsequent oncologic therapies (≥ 5% of participants in either treatment group) were bevacizumab, carboplatin, gemcitabine, ipilimumab, nivolumab, pemetrexed, and vinorelbine. Pembrolizumab was used as a subsequent therapy in 3 patients (1.2%) in the pembrolizumab plus chemotherapy group and 11 patients (4.7%) in the chemotherapy-alone group.
Table 14: Summary of Subsequent Treatment in the KEYNOTE-483 Trial (APaT Population)
Subsequent treatmenta | Pembrolizumab + platinum + pemetrexed (N = 241) | Platinum + pemetrexed (N = 232) |
|---|---|---|
Patients with ≥ 1 subsequent anticancer treatments, n (%) | 133 (55.2) | 135 (58.2) |
Antineoplastic drugs, n (%) | 132 (54.8) | 135 (58.2) |
Most commonb | ||
Bevacizumab | 9 (3.7) | 15 (6.5) |
Carboplatin | 57 (23.7) | 61 (26.3) |
Gemcitabine | 65 (27.0) | 68 (29.3) |
Ipilimumab | 7 (2.9) | 15 (6.5) |
Nivolumab | 12 (5.0) | 47 (20.3) |
Pemetrexed | 68 (28.2) | 64 (27.6) |
Vinorelbine | 41 (17.0) | 35 (15.1) |
All other therapeutic products, n (%) | 1 (0.4) | 0 |
APaT = all participants as treated.
aEvery participant is counted a single time for each specific subsequent oncologic. A participant with multiple subsequent anticancer treatments within an oncologic category is counted a single time for that category.
bSpecific medications represent those with a frequency of ≥ 5% of participants in either treatment group.
Source: Clinical Study Report for KEYNOTE-483.11
Efficacy
Overall Survival
At the data cut-off on September 16, 2022, with a median follow-up of 17.4 months (range, 0.8 months to 60.3 months), 342 patients had died, including 175 (80.3%) in the chemotherapy-alone group and 167 (75.2%) in the pembrolizumab plus chemotherapy group (Table 15). The following Kaplan-Meier plot (Figure 3) shows the OS curves for each treatment group. The Kaplan-Meier estimated differences in OS probabilities between groups were 6.2% (95% CI, –2.8% to 15.2%) at 24 months and 8.1% (95% CI, –0.2% to 16.4%) at 36 months in favour of pembrolizumab plus chemotherapy.
OS by histology was consistent with the overall ITT study population, favouring pembrolizumab plus chemotherapy (HRs < 1); however, only the CIs for the subgroup with nonepithelioid histology MPM were entirely below unity.
Supplemental OS analyses indicated a RMST difference of 0.95 months (95% CI, –0.52 months to 2.41 months) at a 24-month follow-up, favouring pembrolizumab plus chemotherapy (Appendix 1, Table 23). Analyses with a 36-month RMST follow-up were not reported in the KEYNOTE-483 Clinical Study Report.
Figure 3: Kaplan-Meier Plot of Overall Survival From the KEYNOTE-483 Trial (ITT Population)
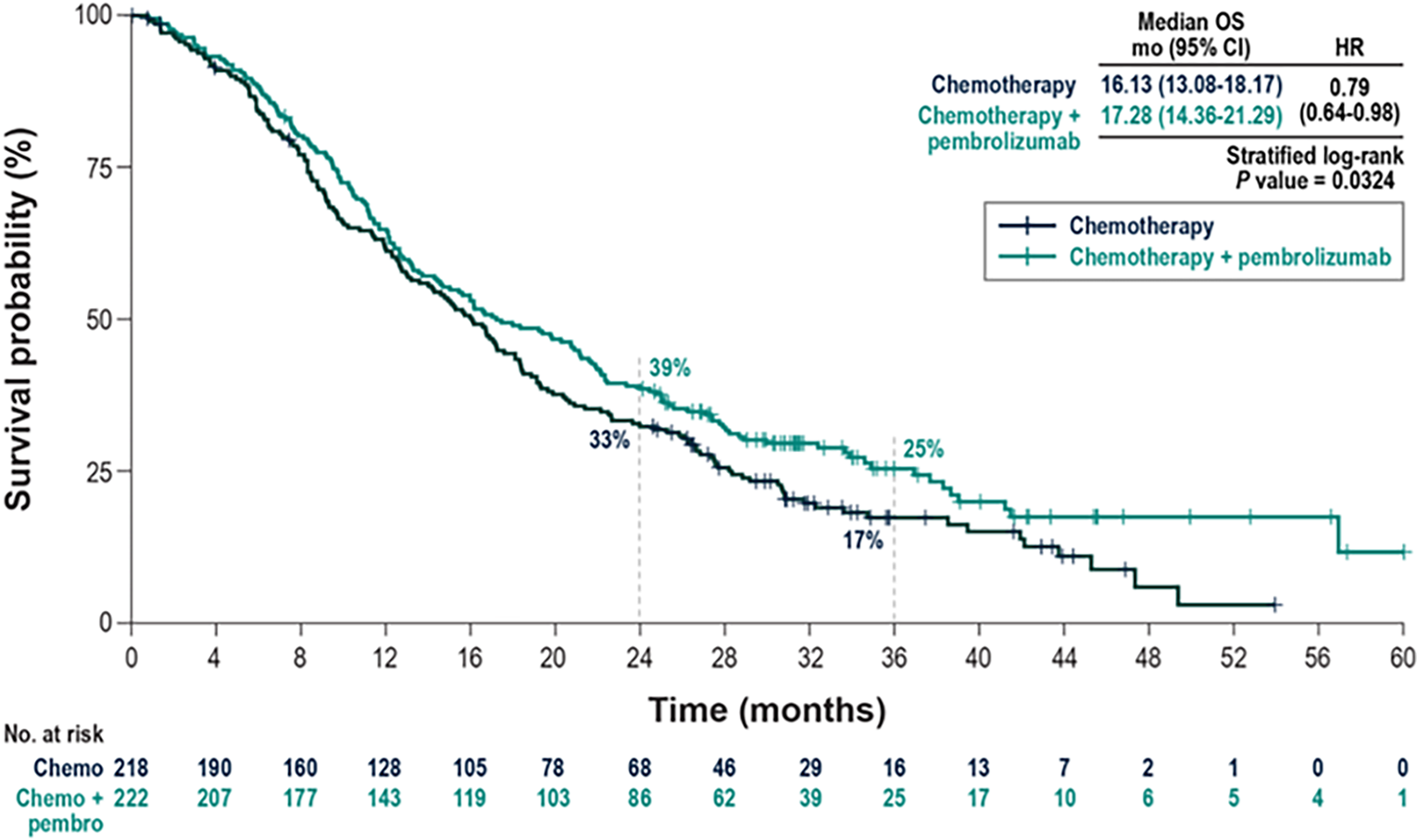
chemo = chemotherapy; CI = confidence interval; HR = hazard ratio; ITT = intention to treat; mo = months; OS = overall survival; pembro = pembrolizumab.
Source: Sponsor’s clinical summary.48
Table 15: Summary of Survival Results From the KEYNOTE-483 Trial (ITT Population)
Outcomes | Pembrolizumab + platinum + pemetrexed (N = 222) | Platinum + pemetrexed (N = 218) |
|---|---|---|
OS (database cut-off date: September 16, 2022) | ||
Number of patients contributing to the analysis | 222 | 218 |
Number of patients with events, n (%) | 167 (75.2) | 175 (80.3) |
OS probability at 24 months, % (95% CI)a | 38.9 (32.5 to 45.3) | 32.8 (26.5 to 39.2) |
Difference (95% CI) | 6.2 (–2.8 to 15.2) | |
OS probability at 36 months, % (95% CI)a | 25.3 (19.3 to 31.8) | 17.3 (12.1 to 23.2) |
Difference (95% CI) | 8.1 (–0.2 to 16.4) | |
Median, months (95% CI)a | 17.3 (14.36 to 21.29) | 16.1 (13.08 to 18.17) |
HR (95% CI)b | 0.79 (0.64 to 0.98) | |
P valuec,d | 0.0162 | |
Subgroups | ||
Epithelioid histology, events/N | 130/176 | 131/169 |
HR (95% CI)e | 0.89 (0.70 to 1.13) | |
Nonepithelioid histology, events/N | 37/46 | 44/49 |
HR (95% CI)e | 0.57 (0.36 to 0.89) | |
PFS: mRECIST by BICR (database cut-off date: September 16, 2022) | ||
Number of patients contributing to the analysis | 222 | 218 |
Number of patients with progression-free disease, n (%) | 190 (85.6) | 166 (76.1) |
Death | 19 (8.6) | 20 (9.2) |
Documented progression | 171 (77.0) | 146 (67.0) |
PFS probability at 12 months, % (95% CI)a | 26.3 (20.4 to 32.4) | 17.1 (11.8 to 23.3) |
Difference (95% CI) | 9.1 (8.0 to 17.4) | |
Median, months (95% CI)a | 7.1 (6.9 to 8.1) | 7.1 (6.8 to 7.7) |
HR (95% CI)b | 0.80 (0.65 to 0.99) | |
P valuec,f | 0.0194 | |
Subgroups | ||
Epithelioid histology, events/N | 154/176 | 128/169 |
HR (95% CI)e | 0.92 (0.73 to 1.17) | |
Nonepithelioid histology, events/N | 36/46 | 38/49 |
HR (95% CI)e | 0.47 (0.29 to 0.77) | |
ORR: mRECIST by BICR (database cut-off date: September 16, 2022) | ||
Number of patients achieving an objective response | 117 | 64 |
Percentage (%) (95% CI) | 52.7 (45.9 to 59.4) | 29.4 (23.4 to 35.9) |
Difference (95% CI)g | 23.5 (14.6 to 32.0) | |
Subgroups | ||
Epithelioid histology, responders/N (%) | 98/176 (55.7) | 61/169 (36.1) |
Difference, % (95% CI) | 19.6 (9.1 to 29.6) | |
Nonepithelioid histology, responders/N (%) | 19/46 (41.3) | 3/49 (6.1) |
Difference, % (95% CI) | 35.2 (19.2 to 50.7) | |
BICR = blinded independent central review; CI = confidence interval; HR = hazard ratio; ITT = intention to treat; mRECIST = modified Response Evaluation Criteria in Solid Tumours; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; vs. = versus.
aBased on Kaplan-Meier estimates.
bBased on Cox regression model with the Efron method of tie handling, with treatment as a covariate stratified by histological subtype at randomization (epithelioid vs. other subtypes).
cOne-sided P value based on log-rank test stratified by histological subtype at randomization (epithelioid vs. other subtypes).
dOne-sided P value boundary = 0.0204.
eBased on unstratified Cox regression model with treatment as a covariate.
fP value tested within a hierarchical testing strategy to control for multiple comparisons. One-sided P value boundary = 0.0227, with all alpha reallocated to the PFS hypothesis after both OS and ORR were statistically significant.
gBased on Miettinen and Nurminen method stratified by histological subtype (epithelioid vs. nonepithelioid).
Source: Clinical Study Report for KEYNOTE-483.11
Progression-Free Survival
More patients experienced progression-free disease (mRECIST by BICR) in the pembrolizumab group than in the chemotherapy group at the data cut-off on September 16, 2022: 190 patients (85.6%) versus 166 patients (76.1%), respectively (Table 15). The number of PFS events recorded as deaths was similar between groups (8.6% in the pembrolizumab group versus 9.2% in the chemotherapy group), but a higher percentage of patients in the pembrolizumab plus chemotherapy group experienced disease-progression events (77.0%) compared with the chemotherapy-alone group (67.0%). The following Kaplan-Meier plot (Figure 4) shows the PFS curves for each treatment group. The Kaplan-Meier estimated difference in PFS probability at 12 months was 9.1% (95% CI, 0.8% to 17.4%) in favour of pembrolizumab plus chemotherapy.
PFS by histology was consistent with the overall ITT study population, favouring pembrolizumab plus chemotherapy (HRs < 1); however, only the CIs for the subgroup with nonepithelioid histology MPM were completely below unity.
Sensitivity analyses generally supported the main PFS results (Appendix 1, Table 24), although the statistical significance of the treatment effects (HRs) with pembrolizumab plus chemotherapy varied, depending on the censoring rule used.
Supplemental PFS analyses indicated an RMST difference of 0.42 months (95% CI, –0.23 months to 1.08 months) at a 12-month follow-up, favouring pembrolizumab plus chemotherapy (Appendix 1, Table 23).
Objective Response Rate
As shown in Table 15, a higher percentage of patients treated with pembrolizumab plus chemotherapy achieved an objective response (mRECIST by BICR) compared with those receiving chemotherapy alone at the data cut-off on September 16, 2022, with a between-group difference of 23.5% (95% CI, 14.6% to 32.0%). Consistent with the OS and PFS results, the difference in ORR between groups was greater for patients with nonepithelioid histology MPM than for those with epithelioid histology, although the CIs for both ORR estimates were above unity.
Figure 4: Kaplan-Meier Plot of Progression-Free Survival From the KEYNOTE-483 Trial (Phase III ITT Population)
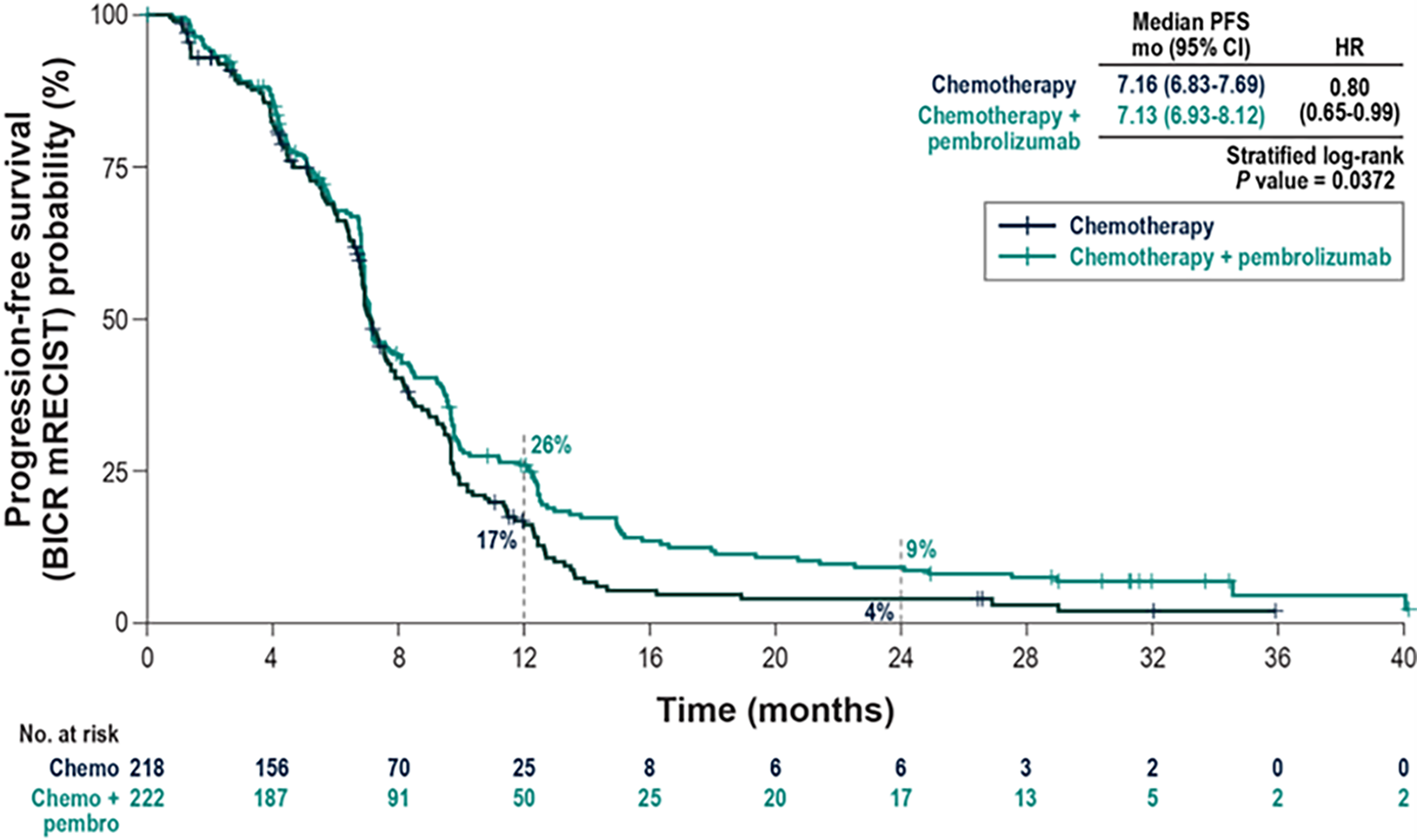
BICR = blinded independent central review; chemo = chemotherapy; CI = confidence interval; HR = hazard ratio; mo = months; mRECIST = modified Response Evaluation Criteria in Solid Tumours; ITT = intention to treat; PFS = progression-free survival.
Source: Sponsor’s clinical summary.48
Health-Related Quality of Life
Table 16 presents the results for the HRQoL end points from the KEYNOTE-483 trial. Mean changes from baseline showed similar improvements across all 3 instruments for both treatment groups, with no statistically significant differences between the groups at week 15.
Table 16: Summary of Health-Related Quality of Life Results From the KEYNOTE-483 Trial (PRO FAS Population)
Outcomesa | Pembrolizumab + platinum + pemetrexed (N = 222) | Platinum + pemetrexed (N = 218) |
|---|---|---|
EORTC QLQ-C30 global health status scale and quality of life scale | ||
Baseline, N | 217 | 208 |
Mean (SD) score | 62.90 (21.15) | 62.90 (20.36) |
Week 15, N | 154 | 139 |
Mean (SD) score | 61.47 (20.53) | 61.69 (21.23) |
CFB to week 15, N | 220 | 209 |
LS mean (95% CI) | –2.87 (–5.68 to –0.07) | –3.86 (–6.80 to –0.92) |
Difference in LS means (95% CI)b | 0.99 (–2.88 to 4.86) | |
P value | 0.6164 | |
EORTC QLQ-C30 physical functioning | ||
Baseline, N | 218 | 208 |
Mean (SD) score | 79.51 (18.36) | 80.87 (19.97) |
Week 15, N | 154 | 139 |
Mean (SD) score | 76.02 (21.40) | 79.93 (20.15) |
CFB to week 15, N | 220 | 209 |
LS mean (95% CI) | –5.91 (–8.38 to –3.45) | –4.30 (–6.89 to –1.70) |
Difference in LS means (95% CI)b | –1.62 (–5.15 to 1.91) | |
P value | 0.3679 | |
EORTC QLQ-C30 dyspnea | ||
Baseline, N | 218 | 207 |
Mean (SD) score | 34.10 (30.60) | 28.34 (29.23) |
Week 15, N | 154 | 139 |
Mean (SD) score | 29.44 (28.51) | 25.42 (27.97) |
CFB to week 15, N | 220 | 209 |
LS mean (95% CI) | –1.76 (–5.69 to 2.17) | –1.59 (–5.71 to 2.52) |
Difference in LS means (95% CI)b | –0.17 (–5.51 to 5.18) | |
P value | 0.9508 | |
EORTC QLQ-LC13 chest pain | ||
Baseline, N | 218 | 206 |
Mean (SD) score | 17.13 (24.00) | 16.67 (24.14) |
Week 15, N | 153 | 139 |
Mean (SD) score | 12.42 (23.22) | 12.95 (22.88) |
CFB to week 15, N | 220 | 209 |
LS mean (95% CI) | –4.08 (–7.33 to –0.82) | –1.02 (–4.42 to 2.39) |
Difference in LS means (95% CI)b | –3.06 (–7.53 to 1.41) | |
P value | 0.1791 | |
EORTC QLQ-LC13 cough | ||
Baseline, N | 218 | 208 |
Mean (SD) score | 24.16 (24.53) | 22.12 (24.13) |
Week 15, N | 154 | 139 |
Mean (SD) score | 17.10 (22.62) | 16.31 (22.47) |
CFB to week 15, N | 220 | 209 |
LS mean (95% CI) | –5.82 (–9.38 to –2.26) | –5.79 (–9.50 to –2.08) |
Difference in LS means (95% CI)b | –0.03 (–4.69 to 4.63) | |
P value | 0.9892 | |
EQ-5D-5L VAS | ||
Baseline, N | 183 | 176 |
Mean (SD) score | 69.22 (18.06) | 70.27 (19.51) |
Week 15, N | 129 | 118 |
Mean (SD) | 67.93 (19.19) | 69.82 (17.91) |
CFB to week 15, N | 190 | 183 |
LS mean (95% CI) | –2.22 (–4.73 to 0.28) | –2.68 (–5.30 to –0.07) |
Differences in LS means (95% CI)b | 0.46 (–3.02 to 3.94) | |
P value | 0.7964 | |
CFB = change from baseline; CI = confidence interval; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; EORTC QLQ-LC13 = European Organisation for Research and Treatment of Cancer 13-item lung cancer-specific questionnaire module; FAS = full analysis set; LS = least squares; PRO = patient-reported outcome; SD = standard deviation; VAS = visual analogue scale.
aDatabase cut-off date was September 16, 2022.
bBased on a constrained longitudinal data-analysis model with the PRO scores as the response variable, with covariates for treatment by study visit interaction and stratified by histological subtype at randomization (epithelioid versus other subtypes).
Source: Clinical Study Report for KEYNOTE-483.11
Harms
Refer to Table 17 for harms data.
Adverse Events
A higher percentage of patients randomized to pembrolizumab plus chemotherapy had AEs compared with those who received chemotherapy alone (96.3% versus 91.4%). More patients treated with pembrolizumab plus chemotherapy experienced grade 3 and higher AEs of any cause.
Serious Adverse Events
SAEs were reported more frequently in patients treated with pembrolizumab plus chemotherapy (40.2% of patients) compared with chemotherapy alone (19.0% of patients). The most frequently reported SAE was febrile neutropenia, reported by 5.0% of patients treated with pembrolizumab plus chemotherapy compared with 1.3% of patients treated with chemotherapy alone.
Discontinuation Due to Adverse Events
More patients treated with pembrolizumab plus chemotherapy discontinued treatment for any AE (34.4% versus 17.2%) and for SAEs (20.7% versus 4.3%) compared with the chemotherapy-alone group.
Mortality
A higher percentage of patients treated with pembrolizumab plus chemotherapy died (death was coded as an AE) compared with those in the chemotherapy-alone group (7.1% versus 2.2%). The most common cause of death was sepsis, occurring in 4 patients (1.7%) in the pembrolizumab plus chemotherapy group and 2 patients (0.9%) in the chemotherapy-alone group.
Notable Harms
There were 64 patients (26.6%) in the pembrolizumab plus chemotherapy group and 16 patients (6.9%) in the chemotherapy-alone group who experienced notable harms. The most frequently reported notable harms (≥ 4% of participants in either group) in the pembrolizumab plus chemotherapy group were hypothyroidism (9.1%), infusion reactions (5.8%), and pneumonitis (5.0%). A total of 6.6% of participants experienced grade 3 AEs, and no grade 4 or grade 5 notable AEs were reported. No notable harms with death as an outcome occurred during the reporting period (up to 90 days after last dose). In total, 40.6% of patients in the pembrolizumab plus chemotherapy group and 18.8% of those in the chemotherapy-alone group had unresolved notable harms at the end of follow-up.
Table 17: Summary of Harms Results From the KEYNOTE-483 Trial (APaT Population)
AEs | Pembrolizumab + platinum + pemetrexed (N = 241) | Platinum + pemetrexed (N = 232) |
|---|---|---|
AEs, n (%) | ||
Patients with ≥ 1 AE | 232 (96.3) | 212 (91.4) |
Most common AEs (≥ 10% in either treatment group) | ||
Fatigue | 148 (61.4) | 141 (60.8) |
Nausea | 128 (53.1) | 109 (47.0) |
Constipation | 77 (32.0) | 51 (22.0) |
Diarrhea | 74 (30.7) | 34 (14.7) |
Dyspnea | 69 (28.6) | 51 (22.0) |
Vomiting | 63 (26.1) | 37 (15.9) |
Pyrexia | 54 (22.4) | 23 (9.9) |
Stomatitis | 54 (22.4) | 42 (18.1) |
Decreased appetite | 52 (21.6) | 48 (20.7) |
Cough | 42 (17.4) | 27 (11.6) |
Rash | 42 (17.4) | 20 (8.6) |
Pruritus | 40 (16.6) | 11 (4.7) |
Noncardiac chest pain | 34 (14.1) | 22 (9.5) |
Abdominal pain | 32 (13.3) | 11 (4.7) |
Peripheral sensory neuropathy | 32 (13.3) | 21 (9.1) |
Lacrimation increased | 31 (12.9) | 18 (7.8) |
Back pain | 28 (11.6) | 14 (6.0) |
Dysgeusia | 28 (11.6) | 32 (13.8) |
Embolism | 28 (11.6) | 21 (9.1) |
Insomnia | 28 (11.6) | 12 (5.2) |
Edema peripheral | 28 (11.6) | 16 (6.9) |
Arthralgia | 27 (11.2) | 2 (0.9) |
Dizziness | 24 (10.0) | 16 (6.9) |
Grade ≥ 3 AEs | 106 (44.0) | 70 (30.2) |
SAEs, n (%) | ||
Patients with ≥ 1 SAE | 97 (40.2) | 44 (19.0) |
Most common SAEs (> 2% in either treatment group) | ||
Febrile neutropenia | 12 (5.0) | 3 (1.3) |
Pneumonia | 10 (4.1) | 5 (2.2) |
Diarrhea | 8 (3.3) | 3 (1.3) |
Pneumonitis | 8 (3.3) | 0 |
Anemia | 7 (2.9) | 0 |
Sepsis | 7 (2.9) | 2 (0.9) |
Platelet count decreased | 6 (2.5) | 1 (0.4) |
Abdominal pain | 5 (2.1) | 2 (0.9) |
Embolism | 5 (2.1) | 6 (2.6) |
Nausea | 5 (2.1) | 1 (0.4) |
Pyrexia | 5 (2.1) | 2 (0.9) |
Vomiting | 5 (2.1) | 0 |
Patients who stopped treatment due to an AE, n (%) | ||
Discontinued any drug due to an AE | 83 (34.4) | 40 (17.2) |
Discontinued any drug due to an SAE | 50 (20.7) | 10 (4.3) |
Deaths, n (%) | ||
Patients who died | 17 (7.1) | 5 (2.2) |
Sepsis | 4 (1.7) | 2 (0.9) |
Assisted suicide | 2 (0.8) | 0 |
Cardiac arrest | 2 (0.8) | 0 |
Ill-defined disorder | 2 (0.8) | 0 |
Death | 1 (0.4) | 0 |
Dyspnea | 1 (0.4) | 0 |
Febrile neutropenia | 1 (0.4) | 0 |
Mesothelioma | 1 (0.4) | 0 |
Myocardial infarction | 1 (0.4) | 1 (0.4) |
Neutrophil count decreased | 1 (0.4) | 0 |
Pleural effusion | 1 (0.4) | 0 |
Sudden death | 1 (0.4) | 0 |
Hemorrhage intracranial | 0 | 1 (0.4) |
Neoplasm malignant | 0 | 1 (0.4) |
Notable AEs, n (%) | ||
Patients with ≥ 1 notable AE | 64 (26.6) | 16 (6.9) |
Hypothyroidism | 22 (9.1) | 4 (1.7) |
Infusion reactions | 14 (5.8) | 4 (1.7) |
Pneumonitis | 12 (5.0) | 0 |
Severe skin reactions | 7 (2.9) | 3 (1.3) |
Colitis | 6 (2.5) | 0 |
Hyperthyroidism | 4 (1.7) | 2 (0.9) |
Adrenal insufficiency | 2 (0.8) | 1 (0.4) |
Gastritis | 2 (0.8) | 2 (0.9) |
Nephritis | 2 (0.8) | 0 |
Pancreatitis | 2 (0.8) | 0 |
Uveitis | 2 (0.8) | 1 (0.4) |
Vasculitis | 2 (0.8) | 0 |
Hypophysitis | 1 (0.4) | 0 |
Myelitis | 1 (0.4) | 0 |
Myositis | 1 (0.4) | 0 |
AE = adverse event; APaT = all participants as treated; SAE = serious adverse event.
Source: Clinical Study Report for KEYNOTE-483.11
Critical Appraisal
Internal Validity
The randomization sequence in the KEYNOTE-483 trial was adequately generated using a web-based system. Although it was not explicitly stated in the protocol, allocation was likely concealed, given the method of randomization. Randomization was stratified by histology, which is a clinically relevant prognostic factor. Baseline characteristics were generally similar between treatment groups, except for a higher percentage of current and former smokers in the pembrolizumab plus chemotherapy group, and more patients in the chemotherapy-alone group who had received prior therapies. The clinical experts consulted by CDA-AMC did not expect these differences to have a clinically significant confounding effect on the results.
Seven patients were randomized to receive chemotherapy alone but did not receive any treatment. The KEYNOTE-483 Clinical Study Report did not explain why these patients did not initiate treatment, nor did it explicitly describe how they were handled in the efficacy analyses. The sponsor subsequently clarified that these patients were included in the final sample in accordance with the ITT principle, and that standard end point definitions, censoring, and event rules were applied (e.g., patients without postrandomization assessments were censored at randomization). While this approach technically adheres to the ITT principle, the lack of reporting on the reasons for the noninitiation of treatment and the censoring of patients at baseline introduces potential risk of bias. If the decision or inability to initiate treatment was related to underlying prognosis, then these early censored observations may have differed systematically from those who received treatment. This raises concerns about potential bias due to deviations from intended intervention or missing outcome data. Without clear justification or transparency in the trial documentation, it is not possible to fully assess the potential impact on internal validity. Nevertheless, it is anticipated that the magnitude of the bias, if present, would be small, given only 7 patients were involved.
The study design was open-label and therefore susceptible to reporting, performance, and detection biases because both patients and investigators were aware of treatment assignments after randomization. OS was the primary end point of the trial and is an objective measure that is less likely to be biased by the open-label study design. However, the influence of subsequent anticancer therapies may impact the OS estimates, especially because the choice of subsequent therapies was at the discretion of the investigator, who would have been aware of the study treatment assignment. A similar percentage of patients in both treatment groups received subsequent systemic therapy (54.8% in the pembrolizumab plus chemotherapy group versus 58.2% in the chemotherapy-alone group; Table 14). Subsequent immunotherapy — namely nivolumab — was administered to more patients in the chemotherapy-alone group (> 20%) compared with the pembrolizumab plus chemotherapy group (< 10%). The input from the clinical experts in the treatment of MPM indicated that emerging evidence suggests that nivolumab monotherapy in the second-line setting may improve OS. Given this, the greater use of nivolumab in the chemotherapy-alone group may have diluted the treatment-effect estimate for pembrolizumab plus chemotherapy. If nivolumab meaningfully prolonged OS, the difference between treatment groups may have been underestimated, potentially biasing the results toward the null. The lack of sensitivity analyses to assess the impact of subsequent anticancer therapies on OS further limits the ability to determine the true effect of pembrolizumab plus chemotherapy.
PFS is more susceptible to detection bias in an open-label trial design; however, the main analysis for PFS was done by a BICR committee to mitigate the potential for bias. The open-label design is also a concern for the HRQoL and harms end points because patient and/or investigator knowledge of treatment assignment could have influenced the assessment and reporting of these outcomes. However, no clear differences in HRQoL were observed between groups (albeit with only 15 weeks of follow-up), and the reported AEs were consistent with the known and documented profiles (per the product monographs). Therefore, there is no evidence that the results for PFS, HRQoL end points, and harms were biased by the open-label design.
The study protocol for the KEYNOTE-483 trial was amended 6 times. Key amendments included the switch from a phase II to a phase III confirmatory design, with OS as the primary outcome instead of PFS; the revision of antitumour activity assessment from RECIST to a mesothelioma-specific modification; and the implementation of alpha spending rules to account for multiplicity, including interim analyses. Following this change in the primary end point, the alpha level and the required number of events for OS analyses (interim and final) were adjusted. The number of patients already enrolled in the trial at the time of these amendments was not reported in the KEYNOTE-483 Clinical Study Report. Additionally, the changes to the end points and statistical assumptions were informed by external trial data (phase II IND.227 results and results from the KEYNOTE-604 trial). However, these modifications were made before the efficacy data from the KEYNOTE-483 trial became available, reducing the likelihood that the changes were driven by emerging trial results. Overall, these amendments likely improved the internal validity and generalizability of the trial, particularly the switch from PFS to OS as the primary outcome, given the objective nature and clinical relevance of OS.
The study provided several definitions of PFS based on different censoring rules. One of these rules censored patients who received new anticancer therapy. This may lead to biased results (inflated estimates of PFS) through informative censoring — i.e., the likelihood of receiving new therapy is related to a patient's prognosis or disease trajectory. As mentioned, the study conducted several sensitivity and supplemental analyses (Appendix 1, Table 24) to test various censoring assumptions. Overall, the treatment effects were similar (consistent median PFS and HRs) to those from the main PFS analysis, although the lack of consistent statistical significance across some sensitivity analyses (e.g., BICR with censoring rules 1 and 2) suggests that the treatment effect on PFS may not be uniformly reliable under all scenarios.
The analysis of OS and PFS treatment-effect estimates was based on a stratified Cox proportional hazards model, which assumes that the HR between treatments remains constant over time. At the final analysis, the results for OS indicated superiority of pembrolizumab plus chemotherapy over chemotherapy alone. However, the Kaplan-Meier OS curves (Figure 3) initially overlapped, showed some separation at approximately 6 months, but did not clearly diverge until after 18 months. Similarly, the Kaplan-Meier curves for PFS (Figure 4) crisscrossed and/or touched up to approximately 8 months and did not distinctly separate until after 10 months. These visual patterns suggest potential time-varying effects, which could violate the proportional hazards assumption. The statistical analysis plan and Clinical Study Report did not indicate whether visual examination or statistical tests were conducted to assess the proportional hazards assumption for OS and PFS. The sponsor-provided ITC technical report included a proportional hazards assessment for OS and PFS (refer to the ITC section of this review for details). The sponsor also provided statistical tests of the proportional hazards test with comments on a draft of this review report. They included the time-dependent covariate test (P = 0.81), supremum test (P = 0.85), and Grambsch-Therneau test (P = 0.68), all of which indicated no violation of the assumption for OS and PFS. These results were similar to the evaluation done for the ITC analysis using the Grambsch-Therneau test. These are established tests and provide evidence supporting proportionality. However, while global statistical tests for proportional hazards are commonly recommended, their reliability depends on sample size. In smaller samples, these tests may lack power to detect violations, increasing the risk of false negatives.49 Moreover, these tests may not adequately account for time-varying effects, potentially leading to incorrect conclusions about the validity of the proportional hazards assumptions. Reliance on statistical tests of the proportional hazards assumption, therefore, can lead to P value misinterpretation.50,51
Supplemental analyses using RMST, which does not rely on the proportional hazards assumption, were performed for both end points. While the RMST differences between groups were consistent in direction with the HRs, they were not statistically significant, possibly due to limited statistical power. The non–statistically significant RMST results and wide CIs suggest potential deviations from the proportional hazards assumption, further complicating the interpretation of the HRs. If the proportional hazards assumption does not hold, the HR may not provide a stable, long-term estimate of the treatment effect. This concern is reinforced by the delayed separation of the Kaplan-Meier curves, which suggests that treatment effects may not be constant over the study period.
The sample-size calculations for the KEYNOTE-483 trial assumed that pembrolizumab plus chemotherapy would provide a clinically meaningful improvement in both OS and PFS compared with chemotherapy alone. Specifically, the assumed median OS benefit was a 7-month improvement (23 versus 16 months), and the assumed median PFS benefit was a 3-month improvement (10 versus 7 months). However, the actual results showed only a 1.2-month improvement in median OS (17.3 versus 16.1 months) and no difference in median PFS (both groups had a median PFS of 7.1 months). These findings indicate that the assumptions used in the power calculations overestimated the treatment effect of pembrolizumab plus chemotherapy. The smaller-than-expected differences suggest that pembrolizumab may not provide the level of benefit anticipated, particularly for PFS, where no improvement in the median was observed. This discrepancy raises questions as to whether the trial was sufficiently powered to detect a more modest benefit and whether the treatment effect is durable and robust.
The treatment benefit for OS, PFS, and ORR appears to differ by histology. The upper 95% CIs for OS and PFS in the epithelioid histology MPM subgroup crossed unity, indicating the benefit is statistically nonsignificant and uncertain. Conversely, the 95% CIs for OS and PFS in the nonepithelioid histology MPM subgroup were entirely below unity (HR < 1.0), suggesting a statistically significant difference between groups favouring pembrolizumab plus chemotherapy. Additionally, the percentage of patients with an objective response in the nonepithelioid histology MPM subgroup was nearly double that of the epithelioid histology MPM subgroup, although the CIs were less than 1.0 for both subgroups. The subgroup results are difficult to interpret because the study was not designed to support causal inferences from subgroup analyses, and no test for interaction between treatment and histology status was conducted. This raises concerns about potential confounding or effect modification because differences in baseline characteristics between histologic subgroups could contribute to the observed differences in treatment benefit. Additionally, the lack of a prespecified statistical plan for subgroup analyses increases the risk of spurious findings due to multiple comparisons.
Geographic region — EU or non-EU — was not initially a subgroup of priority for this review. However, because the non-EU subgroup is entirely represented by patients in Canada, the differences in the results for OS and PFS in this subgroup were notable. The HR for patients in the Canada subgroup for OS was 0.97 (95% CI, 0.67 to 1.40), and for PFS, the HR was 0.93 (95% CI, 0.65 to 1.33). In comparison, the HR for the OS estimate for patients in the EU group was 0.74 (95% CI, 0.57 to 0.96); for PFS, the HR was 0.76 (95% CI, 0.59 to 0.99). The same limitations for histology also apply here for the subgroup analyses, including the lack of a prespecified hypothesis, the potential for spurious findings due to multiple comparisons, and the absence of statistical tests for interaction. The observed differences by geographic region may be due to variations in baseline patient characteristics, access to subsequent therapies, or differences in clinical practice patterns rather than a true differential treatment effect. No analyses exploring these potential confounders were reported in the Clinical Study Report for the trial; the validity of any conclusions drawn from the regional subgroup analyses remains uncertain.
External Validity
The KEYNOTE-483 trial was designed and conducted by the Canadian Cancer Trials Group. As a result, nearly one-third of the patients enrolled were from Canada, with the remaining participants from France and Italy. The clinical experts consulted by CDA-AMC noted that the trial population was consistent with the population expected to receive treatment for advanced MPM in Canada. However, the study eligibility criteria were restricted to patients with an ECOG PS score of 0 to 1, whereas, in clinical practice, patients with an ECOG PS score of 2 — and, in select cases, those with a worse performance status — may still be considered for systemic treatment.
Pemetrexed plus platinum chemotherapy was considered an appropriate comparator for first-line systemic treatment of MPM. The clinical experts noted that carboplatin is frequently used in place of cisplatin in this regimen, and the distribution of use in the KEYNOTE-483 trial aligned with standard clinical practice.
The trial measured clinically meaningful outcomes relevant to patients with MPM. However, a key limitation was the incomplete measurement of HRQoL because assessments were only conducted up to 15 weeks of treatment. Given that HRQoL was identified as a key outcome in the patient and clinician input, the lack of long-term data is a notable shortcoming.
GRADE Summary of Findings and Certainty of the Evidence
Methods for Assessing the Certainty of the Evidence
For pivotal studies and RCTs identified in the sponsor’s systematic review, GRADE was used to assess the certainty of the evidence for outcomes considered most relevant to inform expert committee deliberations, and a final certainty rating was determined as outlined by the GRADE Working Group:12,13
High certainty: We are very confident that the true effect lies close to that of the estimate of the effect.
Moderate certainty: We are moderately confident in the effect estimate. The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. We use the word “likely” for evidence of moderate certainty (e.g., “X intervention likely results in Y outcome”).
Low certainty: Our confidence in the effect estimate is limited. The true effect may be substantially different from the estimate of the effect. We use the word “may” for evidence of low certainty (e.g., “X intervention may result in Y outcome”).
Very low certainty: We have very little confidence in the effect estimate. The true effect is likely to be substantially different from the estimate of effect. We describe evidence of very low certainty as “very uncertain.”
Following the GRADE approach, evidence from the RCTs started as high-certainty evidence and could be rated down for concerns related to study limitations (which refer to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias.
When possible, certainty was rated in the context of the presence of an important (nontrivial) treatment effect; if this was not possible, certainty was rated in the context of the presence of any treatment effect (i.e., the clinical importance is unclear). In all cases, the target of the certainty-of-evidence assessment was based on the point estimate and where it was located relative to the threshold for a clinically important effect (when a threshold was available) or to the null.
The reference points for the certainty-of-evidence assessment for OS, PFS, ORR, SAEs, WDAEs, and fatal AEs were set according to the presence or absence of an important effect based on thresholds informed by the clinical experts consulted for this review. The reference point for the certainty-of-evidence assessment for EORTC QLQ-C30 global health status scale and quality of life scale score was set according to the presence or absence of an important effect based on a threshold that was informed by the literature.
Results of GRADE Assessments
Table 2 presents the GRADE summary of findings for pembrolizumab plus chemotherapy versus chemotherapy alone for the first-line treatment of adult patients with unresectable advanced or metastatic MPM.
Long-Term Extension Studies
No long-term extension studies were submitted.
Indirect Evidence
Contents within this section have been informed by materials submitted by the sponsor. The following has been summarized and validated by the review team.
Objectives for the Summary of Indirect Treatment Evidence
The KEYNOTE-483 trial provided comparative evidence for pembrolizumab plus chemotherapy in the treatment of MPM, using 1 of the 2 relevant comparator treatments, i.e., chemotherapy alone. No head-to-head RCTs compared pembrolizumab plus chemotherapy with the other relevant comparator, nivolumab-ipilimumab. As a result, indirect treatment evidence was used to inform the comparative effectiveness and harms of these 2 regimens in the first-line treatment of patients with advanced MPM.
Description of Indirect Treatment Comparison
To evaluate the comparative effectiveness and harms of pembrolizumab plus chemotherapy versus nivolumab-ipilimumab in the first-line treatment of unresectable advanced or metastatic MPM, the sponsor provided a systematic literature review and an ITC.14
Table 18: Study Selection Criteria and Methods for Indirect Treatment Comparisons Submitted by the Sponsor
Characteristics | Criteria and methods |
|---|---|
Population | Patients aged ≥ 12 years with unresectable advanced or metastatic MPM |
Intervention | Pembrolizumab 200 mg IV infusion + pemetrexed 500 mg/m2 + platinum (cisplatin 75 mg/m2 or carboplatin AUC 5 mg/mL per min to 6 mg/mL per min) |
Comparator | Nivolumab 3 mg/kg + ipilimumab 1 mg/kg |
Outcome |
|
Study designs | Published and unpublished RCTs |
Publication characteristics | Full-text publications available in English |
Databases searched | Databases:
|
Selection process | All citations were screened by 2 independent reviewers; a third reviewer reconciled any discrepancies. The first screening stage included a review of citations based on their titles and abstracts. Citations that did not match the eligibility criteria were excluded at the first-pass stage. Duplicates of citations (due to the overlap in the coverage of databases) were excluded at the first-pass stage. Full-text copies of all references that potentially met the eligibility criteria were obtained. After the completion of the first-stage screening, the full texts of the relevant studies were examined in more detail to determine a final list of included studies. |
Data extraction process | Two independent reviewers extracted data from the studies, and a third independent reviewer reconciled any discrepancies. |
Quality assessment | A critical appraisal of the included studies was conducted using the Cochrane RoB tool version 2.0. All studies were assessed by 2 independent reviewers, with a third reviewer performing a quality check. The overall RoB assessment indicated “some concerns” for all 3 publications (2 RCTs). None of the studies were judged to have a high RoB in any domain. Given that all studies demonstrated a low risk of bias, no further sensitivity analysis based on the quality assessment results was deemed necessary. |
AUC = area under the curve; EU = European Union; ITC = indirect treatment comparison; MPM = malignant pleural mesothelioma; RCT = randomized controlled trial; RoB = risk of bias.
Source: ITC technical report.14
Indirect Treatment Comparison Methods
Feasibility Assessment
A literature search was conducted based on the details in Table 18. Two RCTs reported in 3 publications met the inclusion criteria with the relevant comparator, nivolumab-ipilimumab:
the KEYNOTE-483 and IND.227 trials for pembrolizumab plus chemotherapy
the CheckMate 743 trial for nivolumab-ipilimumab.
The feasibility assessment examined the comparability of these trials:
Trial characteristics: KEYNOTE-483 and CheckMate 743 were phase III studies, while IND.227 was the phase II portion of the KEYNOTE-483 trial. All 3 studies included pemetrexed plus platinum as the common comparator, with similar administration schedules.
Efficacy outcomes: OS and PFS were consistently reported across the KEYNOTE-483 and CheckMate 743 trials. The definitions of these end points were aligned in these trials but not explicitly defined in the IND.227 study. Tumour response evaluations in the KEYNOTE-483 and IND.227 trials followed mRECIST criteria, while CheckMate 743 used adapted mRECIST for pleural lesions and RECIST for nonpleural lesions.
Harms outcomes: While pembrolizumab and nivolumab are both immune checkpoint inhibitors, their combination regimens differ. KEYNOTE-483 assessed immunotherapy with chemotherapy, whereas CheckMate 743 studied dual immunotherapy. These distinct regimens have different AE profiles due to their mechanisms of action.
The feasibility assessment determined that the KEYNOTE-483 and CheckMate 743 trials were suitable for an ITC, while the IND.227 study was included only in sensitivity analyses. Noted limitations included differences in efficacy outcome definitions, response assessment methods, and patient populations, although these were considered manageable within the ITC framework. However, differences in AE reporting and small patient counts for certain AEs limited the feasibility of meaningful comparisons, so no ITC for harms end points was performed.
Similarity Assessment
Due to a limited number of studies, a sensitivity analysis for potential heterogeneity was not feasible. However, clinical heterogeneity was assessed through comparison of the trial design, study characteristics, patient characteristics, and outcome assessments (Table 19).
Table 19: Sponsor’s Assessment of Similarity Between the Trials Included in the ITC
Characteristics | Description and handling of potential effect modifiers |
|---|---|
Study design | Of the 3 included trials (CheckMate 743, KEYNOTE-483, and IND.227), 2 were in phase III and 1 was in phase II. In terms of the blinding status, all 3 studies were open-label, and the study setting indicates a multicentre approach across all 3 studies. Both the KEYNOTE-483 and CheckMate 743 trials had a large sample size, randomizing > 400 patients. The IND.227 trial included a smaller sample size, with < 50 patients randomized. Partly because of this, the IND.227 study was not included in the main analysis. |
Disease severity | Across all studies, every patient had an ECOG PS score of 0 or 1. Comparison of the KEYNOTE-483 and CheckMate 743 trials concerning ECOG PS showed that the KEYNOTE-483 trial had more patients with an ECOG PS score of 0. A total of 47% of patients in the KEYNOTE-483 trial had an ECOG PS score of 0 (46% in the pembrolizumab plus chemotherapy arm and 48% in the chemotherapy-alone arm), and 40% (38% in the nivolumab-ipilimumab arm and 42% in the chemotherapy-alone arm) in the CheckMate 743 trial had an ECOG PS score of 0. A total of 35.2% of patients in the IND.227 study had an ECOG PS score of 0. Of the 2 studies, CheckMate 743 was the only trial that reported data on disease staging for patients with unresectable MPM; thus, further comparison based on disease staging was not possible. |
Treatment history | In the CheckMate 743 study, 10% of patients had received prior radiation therapy in the nivolumab-ipilimumab arm and 9% in the chemotherapy-alone arm, whereas, in the KEYNOTE-483 trial, 4% of patients had received prior radiation therapy in the pembrolizumab plus chemotherapy arm and 7% in the chemotherapy-alone arm. |
Smoking history | In the CheckMate 743 study, 57% of patients were current smokers, while, in the KEYNOTE-483 trial, 55.6% were former or current smokers. The IND.227 study did not report baseline smoking status data. |
PD-L1 status | Distribution of patients in terms of PD-L1 status (PD-L1 ≥ 1% vs. PD-L1 < 1%) varied between the KEYNOTE-483 and CheckMate 743 trials. A total of 66% of patients in the KEYNOTE-483 trial had PD-L1 ≥ 1% (65% in the pembrolizumab plus chemotherapy arm and 68% in the chemotherapy-alone arm) and 77% (80% in the nivolumab-ipilimumab arm and 74% in the chemotherapy-alone arm) in the CheckMate 743 trial had PD-L1 ≥ 1%. In the IND.227 study, 60% of patients had PD-L1 ≥ 1%. |
Patient characteristics | Patients were predominantly male (> 75%) in all 3 studies: 87.5% in the IND.227 study, 77% in the CheckMate 743 trial, and 75.5% in the KEYNOTE-483 trial. Both the KEYNOTE-483 and IND.227 trials reported a median age of 69 years, and the CheckMate 743 study reported a median age of 71 years. |
Trial population | In all studies, efficacy analyses were conducted on the ITT population. |
Follow-up time | The median follow-up period ranged from 14.6 months to 43.1 months across studies. The median follow-up for the KEYNOTE-483 trial with a December 15, 2022, database cut-off was 16.2 months, while the median follow-up for the CheckMate 743 trial with a May 7, 2021, database cut-off was 43.1 months. The median follow-up for the IND.227 study, as per the January 2022 database cut-off, was 14.6 months. |
Dosing of comparators | The dosing of the comparator arm was very similar across trials. In the KEYNOTE-483 and IND.227 trials, the comparator arm was pemetrexed 500 mg/m2 IV on day 1 every 21 days for 6 cycles plus cisplatin 75 mg/m2 IV (or carboplatin AUC 5 mg/mL/min to 6 mg/mL/min) on day 1 and every 21 days for 6 cycles. For the CheckMate 743 trial, the comparator was pemetrexed 500 mg/m2 plus cisplatin 75 mg/m2 (or carboplatin AUC 5 mg/mL/min) every 21 days for a maximum of 6 cycles. |
Comparator response | The median OS for the comparator arm (chemotherapy alone) in the IND.227 study was 9 months, which was shorter than in the comparator arms of the KEYNOTE-483 (median OS of 16 months) and CheckMate 743 (median OS of 14.1 months) trials. Partly because of this, the IND.227 trial was not included in the main analysis. |
Definitions of end points | No variability was observed in the KEYNOTE-483 and CheckMate 743 trials for the definition of OS and PFS because it was commonly defined as the time from randomization to death from any cause (OS) and time from randomization to disease progression or death (PFS). All 3 publications provided data on the median OS. Both the KEYNOTE-483 and CheckMate 743 trials provided data on the median PFS based on BICR. However, the IND.227 study did not report the specific definition of OS and PFS. OS was the primary outcome of both the CheckMate 743 and KEYNOTE-483 trials, while PFS was the primary outcome of the IND.227 study. The CheckMate 743 trial evaluated response using adapted mRECIST for pleural lesions and/or RECIST for nonpleural lesions based on a BICR assessment. In the KEYNOTE-483 trial, response was assessed by BICR, whereas in the IND.227 study, it was assessed by the investigator. |
Clinical trial setting | Both the IND.227 and KEYNOTE-483 trials were conducted in 3 countries, Canada, Italy, and France, while CheckMate 743 was a global study with no Canadian sites. |
AUC = area under the curve; BICR = blinded independent central review; ECOG PS = Eastern Cooperative Oncology Group Performance Status; ITC = indirect treatment comparison; ITT = intention to treat; MPM = malignant pleural mesothelioma; mRECIST = modified Response Evaluation Criteria in Solid Tumours; OS = overall survival; PFS = progression-free survival; RECIST = Response Evaluation Criteria in Solid Tumours; vs. = versus.
Source: ITC technical report.14
Consistency Assessment
An assessment of inconsistency to compare direct and indirect evidence was not possible due to the absence of direct comparison between pembrolizumab plus chemotherapy versus nivolumab-ipilimumab.
Proportional Hazards Assumption
Tests for the proportional hazards assumption were conducted after regenerating individual patient data from published Kaplan-Meier curves, following the Guyot et al. (2012) method.52 The probabilities were extracted by digitizing the published Kaplan-Meier plots for OS and PFS.
To assess proportionality:
Log-log plots were used for visual inspection (nonparallel log[–log] curves or crossing survival curves indicate potential violations). However, visual assessment can be subjective and may lack sensitivity in detecting nonproportionality.
Statistical tests, including the Harrell test and the Grambsch-Therneau global test for the proportional hazards assumption,53,54 were used to formally evaluate whether the proportional hazards assumption was met.
The evaluation found that the proportional hazards assumption was not met for PFS in the CheckMate 743 trial, as indicated by the P value from the global test (Grambsch-Therneau test) (Table 20).
Table 20: Proportional Hazards Assumption Testing for Studies Reporting OS and PFS Curves
Publication (year) (trial name) | Outcome | Grambsch-Therneau test values | Proportional hazards assumption true (yes or no) by log-log plota |
|---|---|---|---|
Peters et al. (2022) (CheckMate 743) | OS | 0.0047; P = 0.93 | No |
Chu et al. (2023)35 (KEYNOTE-483) | OS | 0.47; P = 0.5 | No |
Piccirillo et al. (2023)36 (IND.227) | OS | 2.34; P = 0.31 | No |
Peters et al. (2022) (CheckMate 743) | PFS | 57.7; P < 0.05b | No |
Chu et al. (2023)35 (KEYNOTE-483) | PFS | 1.7; P = 0.19 | No |
Piccirillo et al. (2023)36 (IND.227) | PFS | 0.841; P = 0.66 | No |
OS = overall survival; PFS = progression-free survival.
aThe proportional hazards assumption was determined by visual inspection of the log-log plots for each outcome.
bA Grambsch-Therneau test with a P value of < 0.05 indicates the proportional hazards assumption was violated. This was used for definitively concluding whether the proportional hazards assumption was met.
Source: Indirect treatment comparison technical report.14
Statistical Model
Two types of analyses were reported:
the main (base-case) analyses, which used the Bucher ITC method55 and involved only 2 studies (KEYNOTE-483 and CheckMate 743), reporting OS, PFS, and ORR
sensitivity analyses, which were performed via a Bayesian NMA involving 3 studies (KEYNOTE-483, CheckMate 743, and IND.227), reporting OS, PFS, and ORR.
The proportional hazards network meta-analysis (PH-NMA) was performed using summary data from the included trials, synthesizing HRs for OS and PFS. A Bayesian NMA was implemented with linear models assuming a normal likelihood distribution for time-to-event outcomes (log HR and standard error). The analysis was conducted in WinBUGS (version 1.4.3, MRC Biostatistics Unit, Cambridge, UK) using coding from Dias et al. (2013)56
Key details included:
Iterations: 200,000 (3 chains)
Burn-in: 50,000 iterations
Convergence assessment: Visual inspection of trace plots and Gelman plots
Accuracy check: Monte Carlo error was assessed, ensuring it remained less than 1% of the posterior standard deviation or less than 0.05 when divided by posterior standard deviations.
The results were presented as point estimates (median of the posterior) with the 95% credible intervals.
Nonproportional Hazards Network Meta-Analysis
Given the proportional hazards assumption was violated for PFS in the CheckMate 743 trial, a nonproportional hazards network meta-analysis (NPH-NMA) was performed. This analysis used pseudo–patient level data from the CheckMate 743 and KEYNOTE-483 trials (main analysis), with the IND.227 study included in the sensitivity analysis.
The NPH-NMA included:
simulated analysis of mean OS and PFS
simulated landmark survival probabilities and survival curves, extrapolated over 15 years.
To handle nonproportional hazards, both nonparametric and parametric methods were used:
RMST analysis
fractional polynomial models fitted to pseudo–patient level data
first- and second-order fractional polynomial models following Jansen.57
The analysis was conducted in R using the RJAGS package with coding from Dias et al. (2018).58
Key details:
Iterations: 250,000 (3 chains)
Burn-in: 50,000 iterations
Convergence assessment: Trace plots and the Gelman-Rubin statistic.
Prior Distribution
Noninformative priors were used to model between study heterogeneity for OS and PFS as recommended by the National Institute for Health and Care Excellence (NICE).59 To model the excess heterogeneity arising due to low study count, the prior selection technique by Turner et al. was used.60
Model Fit
Model fit was assessed using the deviance information criterion (DIC) and posterior residual deviance (median estimate).
If fixed-effects and random-effects models had a DIC difference of fewer than 5 points, the fixed-effects model was preferred for parsimony and interpretability.
With only 3 studies, the random-effects model was considered unreliable and was not recommended.
For the NPH-NMA, model selection followed these criteria:
DIC values and convergence diagnostics (trace plots, R-hat statistics).
Top 5 fractional polynomial models were evaluated based on RMST analysis and clinical plausibility.
Clinical plausibility was assessed by ensuring the predicted OS and PFS curves converged toward a low survival probability. Models showing plateauing at high survival probabilities were excluded as best-fit choices.
Final model selection also considered how well the predicted OS and PFS curves aligned with the observed Kaplan-Meier curves during the trial period. The RMST time point was based on the minimum common follow-up across trials:
52 months for OS (CheckMate 743 trial)
40 months for PFS (KEYNOTE-483 trial).
Results of ITC
The network of interlinked studies for the Bucher ITC (base case) and PH-NMA (sensitivity analysis) for all outcomes is presented in Figure 5.
Figure 5: Global Evidence Network Diagram
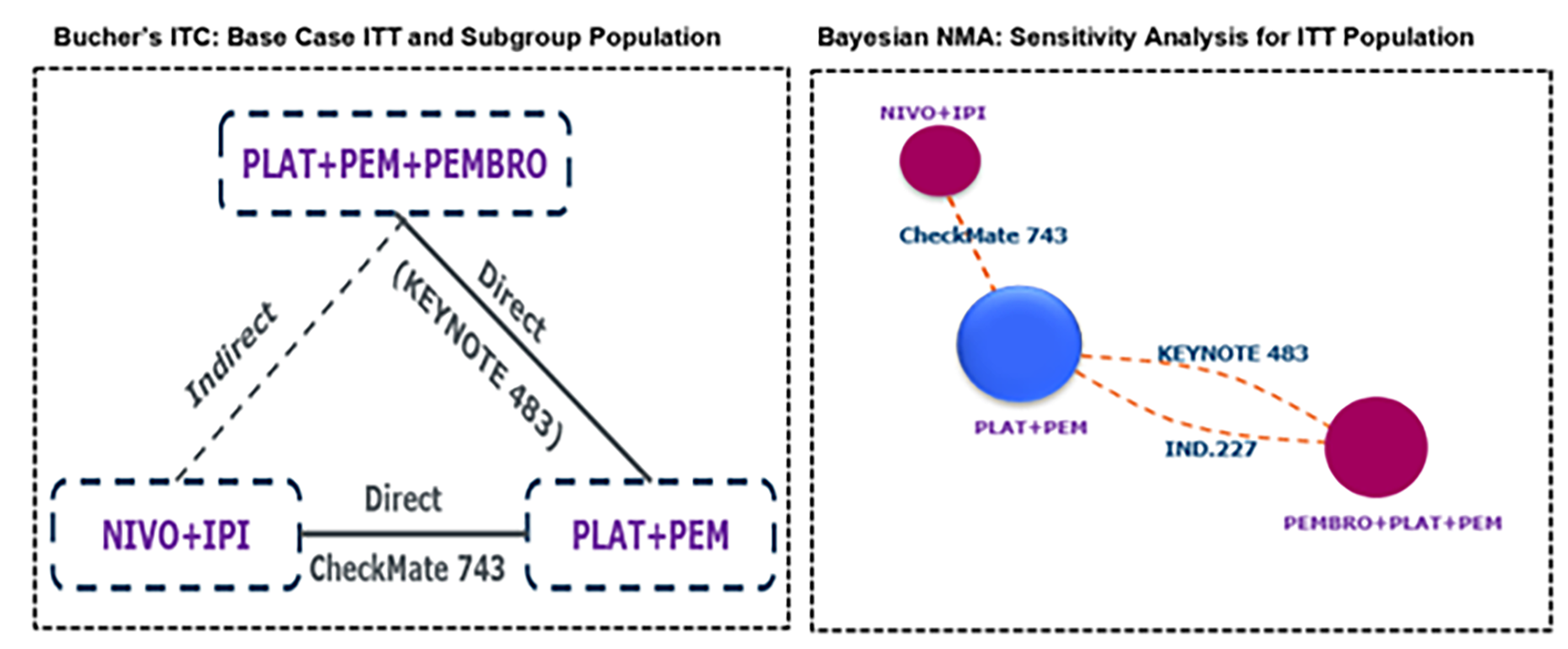
IPI = ipilimumab; ITC = indirect treatment comparison; ITT = intention to treat; NIVO = nivolumab; NMA = network meta-analysis; PEMBRO = pembrolizumab; PLAT = platinum; PEM = pemetrexed; RCT = randomized controlled trial.
Note: The network included 2 RCTs based on 3 publications.
Source: ITC technical report.14
Efficacy
Overall Survival, Base Case
The Bucher ITC analysis indicated that the HR for OS favoured nivolumab-ipilimumab over pembrolizumab plus chemotherapy. However, the difference was not statistically significant because the 95% CIs crossed unity (upper CI was > 1) (Table 21).
The NPH-NMA first-order fractional polynomial model (using P1 = –1) predicted that at 15 years, the restricted mean survival would be 2.32 months longer with nivolumab-ipilimumab versus pembrolizumab plus chemotherapy. The 60-month OS probability was 6.5% with pembrolizumab plus chemotherapy and 9.3% with nivolumab-ipilimumab.
Overall Survival, Sensitivity Analyses
Results from the PH-NMA sensitivity analysis, which included the IND.227 study, were consistent with the base-case analysis (Table 21).
However, the NPH-NMA sensitivity analysis predicted greater survival benefits for pembrolizumab plus chemotherapy in restricted mean OS at 15 years using a fractional polynomial model (P1 = –0.5, P2 = 0):
This model estimated an additional 3.1 months of OS with pembrolizumab plus chemotherapy compared with nivolumab-ipilimumab.
The 60-month OS probabilities were 10.7% for pembrolizumab plus chemotherapy and 6.65% for nivolumab-ipilimumab.
Table 21: Summary of ITC OS Results
OS model (trials) | Nivolumab-ipilimumab vs. pembrolizumab + platinum + pemetrexed |
|---|---|
Base case (KEYNOTE-483, CheckMate-743) | Bucher ITC ██████████████████████████ NPH-NMA FE (P1 = –1)b RMST: + 2.32 months at 15 years in favour of nivolumab-ipilimumab 60 months OS probability: 6.5% in pembrolizumab + platinum + pemetrexed vs. 9.3% in nivolumab-ipilimumab |
Sensitivity analysis (KEYNOTE-483, IND.227, CheckMate-743) | PH-NMA FE ███████████████████████████ NPH-NMA FE (P1 = –0.5, P2 = 0)c RMST: + 3.1 months at 15 years in favour of pembrolizumab + platinum + pemetrexed 60 months OS probability: 10.7% in pembrolizumab + platinum + pemetrexed vs. 6.65% in nivolumab-ipilimumab |
CI = confidence interval; CrI = credible interval; DIC = deviance information criterion; FE = fixed effects; HR = hazard ratio; ITC = indirect treatment comparison; NPH-NMA = nonproportional hazards network meta-analysis; OS = overall survival; PH-NMA = proportional hazards network meta-analysis; RMST = restricted mean survival time; vs. = versus.
aContent linked to this footnote has been redacted at the sponsor’s request.
bFive fractional polynomial models were considered. Based on the lowest DIC goodness of fit, the P1 = –1 model (DIC = 784.6) was chosen as best fit because the other top 4 second-order models showed plateauing of survival at high probability.
cFive fractional polynomial models were considered. Based on the lowest DIC goodness of fit, the P1 = –0.5 and P2 = 0 model (DIC = 904.2) was chosen as best fit because the other top 4 second-order models showed plateauing of survival at high probability.
Source: ITC technical report.14
Progression-Free Survival, Base Case
The Bucher ITC analysis indicated that the HR for PFS favoured pembrolizumab plus chemotherapy over nivolumab-ipilimumab. However, the difference was not statistically significant because the 95% CI crossed unity (lower CI < 1) (Table 22).
The NPH-NMA fractional polynomial model (P1 = 0; P2 = 0.5) simulated that at 15 years, the restricted mean PFS would be 1.04 months longer with nivolumab-ipilimumab compared with pembrolizumab plus chemotherapy.
The 60-month PFS probability was 3.7% with pembrolizumab plus chemotherapy and 4.9% with nivolumab-ipilimumab.
Progression-Free Survival, Sensitivity Analyses
Results from the PH-NMA sensitivity analysis, which included IND.227, were consistent with the base case (Table 22).
The NPH-NMA sensitivity analysis predicted a slight additional benefit for nivolumab-ipilimumab, estimating 0.15 additional months of PFS compared with pembrolizumab plus chemotherapy at 15 years, using a fractional polynomial model (P1 = 0, P2 = 0).
The 60-month PFS probabilities were 2.95% for pembrolizumab plus chemotherapy and 3.95% for nivolumab-ipilimumab.
Table 22: Summary of ITC Progression-Free Survival Results
PFS model (trials) | Nivolumab-ipilimumab vs. pembrolizumab + platinum + pemetrexed |
|---|---|
Base case (KEYNOTE-483 and CheckMate-743 trials) | Bucher ITC ██████████████████████████ NPH-NMA FE (P1 = 0 and P2 = 0.5)b RMST: + 1.04 months at 15 years in favour of nivolumab-ipilimumab 60 months PFS probability: 3.71% in pembrolizumab + platinum + pemetrexed vs. 4.94% in nivolumab-ipilimumab |
Sensitivity analysis (KEYNOTE-483, IND.227, and CheckMate-743 trials) | PH-NMA FE ██████████████████████████ NPH-NMA FE (P1 = 0, P2 = 0)c RMST: + 0.15 months at 15 years in favour of nivolumab-ipilimumab 60 months PFS probability: 2.95% in pembrolizumab + platinum + pemetrexed vs. 3.95% in nivolumab-ipilimumab |
CI = confidence interval; CrI = credible interval; DIC = deviance information criterion; FE = fixed effects; HR = hazard ratio; ITC = indirect treatment comparison; NPH-NMA = nonproportional hazards network meta-analysis; PFS = progression-free survival; PH-NMA = proportional hazards network meta-analysis; RMST = restricted mean survival time; vs. = versus.
aContent linked to this footnote has been redacted at the sponsor’s request.
bFive fractional polynomial models were considered. Based on the lowest DIC goodness of fit, the P1 = 0 and P2 = 0.5 model (DIC = 724.4) was chosen as best fit because the other top 4 second-order models showed plateauing of survival at high probability.
cFive fractional polynomial models were considered. Based on the lowest DIC goodness of fit, the P1 = 0 and P2 = 0 model (DIC = 846.6) was chosen as best fit because the other top 4 second-order models showed plateauing of survival at high probability.
Source: ITC technical report.14
Objective Response Rate, Base Case
The Bucher ITC analysis indicated that the odds ratio for ORR favoured pembrolizumab plus chemotherapy over nivolumab-ipilimumab (█████████████████████████.
Objective Response Rate, Sensitivity Analysis
The estimated ORR remained similar to the base case after the IND.227 study was added to the ████████████████████ ███████████████.
Critical Appraisal of ITC
The PICOS (population, intervention, comparison, outcomes, and study) criteria specified for the systematic literature search were transparently reported and generally aligned with the Reimbursement Review’s scope, except that disease control rate and duration of response were not end points of importance for the Reimbursement Review. The identification of nivolumab-ipilimumab and pemetrexed plus cisplatin or carboplatin as relevant comparators was appropriate, given current clinical practice and the objectives of the systematic review and ITC. Study identification and selection followed standard systematic review methods, although restriction to English language reports may result in publication bias. Nonetheless, the included reports from 2 unique RCTs aligned with both the evidence base for this review and the Reimbursement Review of nivolumab-ipilimumab for MPM.
A risk-of-bias assessment based on the Cochrane risk-of-bias tool version 2.0 for RCTs was performed. A low risk of bias across most domains was reported, except for uncertainty related to the lack of blinding, given the open-label design of the studies. The risk-of-bias assessment was consistent with that done by CDA-AMC for each study.
The ITC analysis estimated relative treatment effects for OS, PFS, and ORR comparing pembrolizumab plus chemotherapy with nivolumab-ipilimumab using chemotherapy alone as a common comparator. However, the base-case analysis using the Bucher ITC method has inherent limitations due to its reliance on similarity (clinical and methodological homogeneity) and transitivity (exchangeability of comparators), which were assessed but not fully validated.
Differences in patient populations, trial designs, and chemotherapy regimens used as the common comparator could invalidate the key assumptions and introduce bias. Similarity between studies was assessed using patent characteristics and design features of the included trial (refer to Table 19). Characteristics of the trial populations and designs were generally similar between the KEYNOTE-483 and CheckMate 743 trials; however, some factors, such as baseline MPM stage, could not be assessed for lack of reporting. The design and differences in patients’ characteristics in the phase II IND.227 study led to its appropriate exclusion from the base-case analysis. The Bucher approach cannot account for effect modifiers,55 and no additional analyses (either via the NMA or other ITC methods) were performed to adjust for baseline imbalances between trials. Given the known heterogeneity in MPM prognosis by histology subtype (epithelioid versus nonepithelioid) and the observed differences in treatment effects by histology in the trials, subgroup analyses could have provided clinically relevant insights.
While superiority or inferiority could be inferred from statistically significant results, conclusions of similarity were difficult without prespecified equivalence margins, particularly given the sensitivity of ITC results to model assumptions.
The Grambsch-Therneau test indicated a potential proportional hazards violation for PFS in the CheckMate 743 trial. An NPH-NMA was conducted, yielding results consistent with the proportional hazards-based models. While this mitigates concerns, residual uncertainty remains. Additionally, as noted in the critical appraisal of the KEYNOTE-483 trial, concerns persist regarding whether the proportional hazards assumption was met for OS and PFS. Therefore, analyses based on the nonproportional hazards assumption are likely more appropriate for comparing the treatment regimens.
The ITC used fixed-effects models, citing limited trials and a model fit comparable to random-effects models. However, fixed-effects models assume homogeneity across studies and may underestimate variability in oncology ITCs, where treatment-effect heterogeneity is expected.
The NPH-NMA involved long-term (i.e., 15 year) extrapolation of OS and PFS data. However, the sponsor did not report the results of follow-up for the included trials or the methods used to handle differences in the trial follow-ups within the NMA. Long-term extrapolations of this nature may be subject to bias because trials typically do not report data over such extended periods. The results of the NPH-NMA showed inconsistent findings for long-term OS and PFS, with some models favouring pembrolizumab plus chemotherapy and others favouring nivolumab-ipilimumab. Additionally, no formal comparisons were conducted for the 60-month OS and PFS probability simulations, preventing any firm conclusions from being drawn. Furthermore, estimates of long-term efficacy may be over- or underestimated due to differences in trial duration, follow-up, and censoring for outcomes, as well as general concerns regarding extrapolating estimated treatment effects beyond the duration of the included studies. Additionally, the clinical experts consulted by CDA-AMC indicated that such extrapolations are unrealistic, given that survival in advanced MPM, even with treatment, is much less than 15 years. Therefore, comparative outcomes at that time point are not generalizable to practice.
Despite the importance of HRQoL and AE data for reimbursement decisions, no formal comparisons were conducted. The ITC technical report cited challenges due to differences in AE profiles (chemotherapy-related toxicities versus immune-related AEs), reporting standards, and treatment-exposure differences. While it is accurate that the regimens present distinct AE profiles due to differing mechanisms of action — immunotherapy (anti–PD-1) plus chemotherapy versus dual immunotherapy (anti–PD-1 and anti–CTLA-4) — and that specific AE patterns are expected to differ (e.g., chemotherapy-related hematologic toxicity versus immune-related AEs). As well, differences in treatment exposure, including dose modifications, or AE management protocols between trials and follow-up duration, could influence AE reporting and the comparability of events. However, aggregate harm end points, such as SAEs, treatment discontinuations due to AEs, and fatal AEs, often have standardized definitions and reporting conventions (e.g., Common Terminology Criteria for Adverse Events [CTCAE] Version 4.0 was used in both trials), which could allow for meaningful comparisons between treatments, provided that sufficient data were available. It is unclear from the technical report whether the feasibility of such comparisons was evaluated.
Regarding HRQoL, the technical report did not explicitly state the comparability of the trials. Given the differing treatment regimens and toxicity profiles, HRQoL could be a critical determinant in assessing the relative benefits of each therapy. Failure to evaluate HRQoL comparisons limits the ability to assess patient-centred outcomes, particularly given the potential for different tolerability profiles and long-term quality-of-life implications associated with chemotherapy plus immunotherapy versus dual immunotherapy regimens. Without this information, the comparative patient-reported burden of treatment remains uncertain.
Studies Addressing Gaps in the Systematic Review Evidence
No studies were provided in the submission.
Discussion
Summary of Available Evidence
KEYNOTE-483 was an open-label, multicentre, phase II and III trial that randomized adult patients with untreated and unresectable advanced or metastatic MPM to treatment with pembrolizumab plus chemotherapy (N = 222) or chemotherapy alone (N = 218). The trial was initiated in Canada and included study sites in France and Italy. The primary efficacy outcome was OS and the key secondary end points were PFS and ORR.
Most patients enrolled were male (77%) and white (79%), with a median age of 70 years. Nearly one-third of participants were from centres in Canada. At the data cut-off on September 16, 2022, patients had a median follow-up of 17.4 months (range, 0.8 months to 60.3 months).
A sponsor-submitted ITC estimated the comparative effectiveness of pembrolizumab plus chemotherapy versus nivolumab-ipilimumab for the indication under review.
Interpretation of Results
Efficacy
Patients with mesothelioma identified significant challenges in obtaining timely diagnoses and managing symptoms related to MPM, such as fatigue, shortness of breath, and chest pain, which impacted their daily lives and led to feelings of isolation. While treatments provided symptom relief and extended survival, patients reported struggling with adverse effects and high treatment costs. The key treatment outcomes valued by patients included effective disease control with minimal adverse effects and improved HRQoL. Similarly, clinician input (from the clinician group and experts consulted by CDA-AMC) emphasized the need for treatments with improved efficacy and tolerability, noting that current options are associated with a high symptom burden and relatively poor OS. Evidence from the KEYNOTE-483 trial suggests that pembrolizumab plus chemotherapy may meet some of the needs of patients and clinicians.
There is moderate-certainty evidence that OS was improved with pembrolizumab plus chemotherapy compared with chemotherapy alone. The clinical experts consulted for this review suggested a 5% absolute difference in OS probability as the threshold for clinical significance. The observed differences at both 24 and 36 months exceed this threshold, suggesting a clinically meaningful effect. However, the lower bounds of the CIs crossed zero, indicating uncertainty, because the estimates include the possibility of no survival benefit or even potential harm. Additional uncertainty arises from variability in the magnitude and statistical significance of OS measures. The trial’s sample-size calculations were based on an expected median OS difference of approximately 7 months between treatment arms, yet the observed difference was only 1.2 months. The HR for OS (0.79; 95% CI, 0.64 to 0.98) suggests a reduced risk of death with pembrolizumab plus chemotherapy, but the upper confidence limit being just below unity highlights the potential fragility of the effect estimate. Further uncertainty stems from whether the proportional hazards assumption was met; formal evaluation of proportionality was not planned for the trial, and a supplemental RMST analysis at 24 months estimated a between-group difference of 0.95 months (95% CI, –0.52 months to 2.41 months), indicating no clear survival benefit over this period. Other sources of uncertainty include the effects of subsequent anticancer therapies (which may have biased the results toward the null, although the actual direction is hard to predict or determine without more data) and differential survival benefits by histology, with greater magnitude and precision observed in patients with nonepithelioid histology MPM compared with those with epithelioid histology MPM. However, despite imprecision in the estimates, all measures of OS favoured pembrolizumab plus chemotherapy over chemotherapy alone, suggesting a real treatment benefit.
The ITC of pembrolizumab plus chemotherapy versus nivolumab-ipilimumab also showed variability in OS estimates. As with the direct trial results versus chemotherapy, modelling choices regarding the proportional hazards assumption affected the OS estimates but, overall, the ITC did not indicate that either regimen was superior.
For PFS, there is moderate-certainty evidence that pembrolizumab plus chemotherapy provides a benefit over chemotherapy alone. The observed difference in PFS probability at 12 months was ████████████████████████ surpassing the 5% threshold for clinical significance set by the clinical experts consulted. However, the lack of improvement in median PFS (7.1 months in both treatment groups) suggests that any potential benefit is not reflected in this central measure of time to progression. The HR for PFS (0.80; 95% CI, 0.65 to 0.99) indicates a reduction in the rate of progression or death, but the CI includes 0.99, reflecting imprecision. Similarly, the ITC analysis comparing pembrolizumab plus chemotherapy with nivolumab-ipilimumab showed imprecise HR estimates for PFS, and neither treatment was superior to the other.
ORR was highlighted by the clinical experts as an important outcome for patients with advanced MPM because tumour size reduction and tumour distribution directly impact symptoms and functional status. There is high-certainty evidence that pembrolizumab plus chemotherapy leads to a clinically significant improvement in ORR compared with chemotherapy alone. Moreover, the ITC analysis suggested that pembrolizumab plus chemotherapy achieved a higher ORR than nivolumab-ipilimumab, although the implications of this difference for long-term outcomes remain uncertain.
Despite the observed benefit in ORR, there was no difference in HRQoL between pembrolizumab plus chemotherapy versus chemotherapy alone, as measured by the EORTC QLQ-C30 global health status scale and quality of life scale. The EORTC QLQ-C30 global scale captures a broad perspective of HRQoL, which may not be specific enough to detect symptom improvements associated with tumour burden reduction, such as relief from chest pain. Similarly, no differences were observed on other EORTC QLQ-C30 and EORTC QLQ-LC13 subscales. However, the EORTC QLQ-LC13 chest pain item showed a between-group difference of –3.06 points (95% CI, –7.53 points to 1.41 points) favouring pembrolizumab plus chemotherapy over chemotherapy alone, although the result was not statistically significant and of unknown clinical significance. HRQoL was not assessed in the ITC comparison with nivolumab-ipilimumab, representing a gap in the comparative evidence for pembrolizumab plus chemotherapy.
The clinical experts consulted for this review emphasized that all 3 available first-line systemic treatment options — pembrolizumab plus chemotherapy, nivolumab-ipilimumab, and chemotherapy alone — have a similar role in treating patients with unresectable advanced MPM. Treatment selection is largely individualized based on patient eligibility for immunotherapy and personal preferences. The primary distinction between regimens is tumour histology because immunotherapy is more effective in nonepithelioid histology MPM than in epithelioid histology MPM. Additionally, tolerability considerations (discussed in the next section) play a crucial role in decision-making because AE profiles differ between regimens. Pembrolizumab plus chemotherapy appears to provide another option with seemingly similar efficacy to nivolumab-ipilimumab for OS and PFS, and no clear difference from chemotherapy alone in patients with epithelioid histology MPM.
Harms
The AEs observed in the KEYNOTE-483 trial were consistent with the established harms profiles for pembrolizumab and pemetrexed plus platinum-based chemotherapy. As expected, the combination of immunotherapy plus chemotherapy resulted in a higher frequency of AEs compared with chemotherapy alone, including a greater frequency of SAEs, WDAEs, and potentially more fatal AEs. The sponsor’s summary of evidence attributed the higher percentage of fatal AEs in the pembrolizumab plus chemotherapy group to differences in treatment exposure. When adjusted for exposure, the rate of deaths due to AEs was reportedly similar between the 2 groups. Notably, many of the reported fatal AEs in the pembrolizumab plus chemotherapy group were related to the underlying disease. The most common cause of death was sepsis, occurring in 4 participants in the pembrolizumab plus chemotherapy group and 2 in the chemotherapy-alone group.
As noted by the clinical experts, pembrolizumab plus chemotherapy may fill an important gap in therapy for patients eligible for immunotherapy who are either unlikely to tolerate or have not tolerated nivolumab-ipilimumab. However, the ITC did not evaluate the comparative harms between these regimens. Although there is a sound rationale for pembrolizumab plus chemotherapy as an alternative treatment option, the absence of direct comparative harms data makes it unclear whether any potential reduction in toxicity relative to nivolumab-ipilimumab is clinically meaningful.
Conclusion
The KEYNOTE-483 trial provided moderately certain evidence that pembrolizumab plus chemotherapy offers a clinically significant improvement in OS and PFS for some patients with unresectable advanced or metastatic MPM compared with chemotherapy alone. The ITC evidence did not establish a clear difference in OS or PFS between pembrolizumab plus chemotherapy versus nivolumab-ipilimumab. Estimates for OS generally favoured nivolumab-ipilimumab and estimates for PFS favoured pembrolizumab plus chemotherapy, but the uncertainty around the results (e.g., wide CIs) precludes firm conclusions. While pembrolizumab plus chemotherapy demonstrated a higher ORR than chemotherapy alone and nivolumab-ipilimumab, this did not translate into evidence of improved HRQoL and symptoms compared with chemotherapy alone. The relative impact on HRQoL and symptoms compared with nivolumab-ipilimumab remains unknown due to a lack of comparative data. Pembrolizumab plus chemotherapy was associated with increased rates of SAEs, WDAEs, and possibly fatal AEs compared with chemotherapy alone. The comparative harms for pembrolizumab plus chemotherapy versus nivolumab-ipilimumab have not been formally evaluated, making it unclear whether pembrolizumab plus chemotherapy offers a meaningful safety advantage. Despite these uncertainties, pembrolizumab plus chemotherapy represents an additional first-line systemic therapy option for adult patients with unresectable advanced or metastatic MPM.
References
1.Ontario Health (Cancer Care Ontario). Types of Cancer: Mesothelioma. Accessed February 18, 2025. https://www.cancercareontario.ca/en/types-of-cancer/mesothelioma
2.Mezei G, Chang ET, Mowat FS, Moolgavkar SH. Epidemiology of mesothelioma of the pericardium and tunica vaginalis testis. Ann Epidemiol. 2017;27(5):348-359.e11. doi: 10.1016/j.annepidem.2017.04.001 PubMed
3.Fels Elliott DR, Jones KD. Diagnosis of Mesothelioma. Surg Pathol Clin. 2020;13(1):73-89. doi: 10.1016/j.path.2019.10.001 PubMed
4.NCCN Guidelines. Mesothelioma: Pleural. 2024 [sponsor supplied reference].
5.Ontario Health (Cancer Care Ontario). Trends in mesothelioma incidence rates are changing for men and women in Ontario. 2021. Accessed February 18, 2025. https://www.cancercareontario.ca/en/cancer-facts/trends-mesothelioma-incidence-rates-are-changing-men-and-women-ontario
6.Cancer Care Ontario, Occupational Cancer Research Centre. Burden of occupational cancer in Ontario: Major workplace carcinogens and prevention of exposure. Queen's Printer for Ontario; 2017. Accessed February 18, 2025. https://www.cancercareontario.ca/sites/ccocancercare/files/assets/OCRCBurdenofOccupationalCancerReport.pdf
7.Nowak AK, Stockler MR, Byrne MJ. Assessing quality of life during chemotherapy for pleural mesothelioma: feasibility, validity, and results of using the European Organization for Research and Treatment of Cancer Core Quality of Life Questionnaire and Lung Cancer Module. J Clin Oncol. 2004;22(15):3172-80. doi: 10.1200/JCO.2004.09.147 PubMed
8.de Perrot M, Vella ET, Bradbury P, et al. Endorsement of the 2018 American Society of Clinical Oncology Treatment of Malignant Pleural Mesothelioma Guideline. 2018 [sponsor supplied reference].
9.Alberta Health Services. Clinical practice guideline: Malignant pleural mesothelioma, version 2. 2012. Accessed by sponsor, no date provided. https://www.albertahealthservices.ca/assets/info/hp/cancer/if-hp-cancer-guide-lu009-mesothelioma.pdf
10.Ellison LF. Progress in net cancer survival in Canada over 20 years. Health Rep. 2018;29(9):10-18. Accessed June 27, 2025. https://www150.statcan.gc.ca/n1/en/pub/82-003-x/2018009/article/00002-eng.pdf PubMed
11.Merck Sharp & Dohme LLC. Clinical Study Report: P483V01MK3475. A phase 2/3 randomized study of pembrolizumab in patients with advanced malignant pleural mesothelioma [internal sponsor's report]. March 21, 2024.
12.Balshem H, Helfand M, Schünemann HJ, et al. GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol. 2011;64(4):401-6. doi: 10.1016/j.jclinepi.2010.07.015 PubMed
13.Santesso N, Glenton C, Dahm P, et al. GRADE guidelines 26: informative statements to communicate the findings of systematic reviews of interventions. J Clin Epidemiol. 2020;119:126-135. doi: 10.1016/j.jclinepi.2019.10.014 PubMed
14.Merck Canada Inc. A systematic literature review and indirect treatment comparison for pembrolizumab in combination with pemetrexed and platinum chemotherapy for the first-line treatment of unresectable advanced or metastatic malignant pleural mesothelioma [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Keytruda (pembrolizumab), solution for infusion 100 mg/4 mL vial. November 2024.
15.Molinari L, Moncivais K. Mesothelioma Latency Period. Mesothelioma.com. 2024. Accessed February 18, 2025. https://www.mesothelioma.com/mesothelioma/latency-period/
16.Reid A, de Klerk NH, Magnani C, et al. Mesothelioma risk after 40 years since first exposure to asbestos: a pooled analysis. Thorax. 2014;69(9):843-50. doi: 10.1136/thoraxjnl-2013-204161 PubMed
17.Government of Canada. Prohibition of Asbestos and Products Containing Asbestos Regulations (SOR/2018-196). 2018. Accessed February 18, 2025. https://pollution-waste.canada.ca/environmental-protection-registry/regulations/view?Id=150
18.Asciak R, George V, Rahman NM. Update on biology and management of mesothelioma. Eur Respir Rev. 2021;30(159):200226. doi: 10.1183/16000617.0226-2020 PubMed
19.Kindler HL, Ismaila N, Armato SG, 3rd, et al. Treatment of Malignant Pleural Mesothelioma: American Society of Clinical Oncology Clinical Practice Guideline. J Clin Oncol. 2018;36(13):1343-1373. doi: 10.1200/JCO.2017.76.6394 PubMed
20.Huang J, Chan SC, Pang WS, et al. Global Incidence, Risk Factors, and Temporal Trends of Mesothelioma: A Population-Based Study. J Thorac Oncol. 2023;18(6):792-802. doi: 10.1016/j.jtho.2023.01.095 PubMed
21.Popat S, Baas P, Faivre-Finn C, et al. Malignant pleural mesothelioma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up☆. Ann Oncol. 2022;33(2):129-142. doi: 10.1016/j.annonc.2021.11.005 PubMed
22.Canadian Cancer Society. Mesothelioma statistics. 2024. Accessed February 18, 2025. https://cancer.ca/en/cancer-information/cancer-types/mesothelioma/statistics
23.Statistics Canada. Table 13-10-0111-01 Number and rates of new cases of primary cancer, by cancer type, age group and sex. Accessed by sponsor, no date provided. https://doi.org/10.25318/1310011101-eng
24.Occupational Cancer Research Centre. Mesothelioma Surveillance & Prognosis in Ontario: research brief. 2020. Accessed by sponsor, no date provided. https://www.occupationalcancer.ca/wp-content/uploads/2023/03/ON-Meso-Research-Brief.pdf
25.Partnership for Work, Health and Safety, UBC. Mesothelioma Surveillance and Prognosis in BC. 2021. Accessed by sponsor, no date provided. https://pwhr.sites.olt.ubc.ca/files/2021/05/BC-mesothelioma-research-brief-2021.pdf
26.Tsao AS, Wistuba I, Roth JA, Kindler HL. Malignant pleural mesothelioma. J Clin Oncol. 2009;27(12):2081-90. doi: 10.1200/JCO.2008.19.8523 PubMed
27.Lim E, Waller D, Lau K, et al. Extended pleurectomy decortication and chemotherapy versus chemotherapy alone for pleural mesothelioma (MARS 2): a phase 3 randomised controlled trial. Lancet Respir Med. 2024;12(6):457-466. doi: 10.1016/S2213-2600(24)00119-X PubMed
28.Baas P, Scherpereel A, Nowak AK, et al. First-line nivolumab plus ipilimumab in unresectable malignant pleural mesothelioma (CheckMate 743): a multicentre, randomised, open-label, phase 3 trial. Lancet. 2021;397(10272):375-386. doi: 10.1016/S0140-6736(20)32714-8 PubMed
29.Merck Sharp Dohme. Prescribing information: Keytruda (pembrolizumab) injection, for intravenous use. U.S. Food and Drug Administration; 2024. Accessed February 18, 2025. https://www.accessdata.fda.gov/drugsatfda_docs/label/2024/125514s161lbl.pdf
30.ESMO. EMA Recommends Extension of Indications for Pembrolizumab to Malignant Pleural Mesothelioma. 2024. Accessed February 18, 2025. https://www.esmo.org/oncology-news/ema-recommends-extension-of-indications-for-pembrolizumab-to-malignant-pleural-mesothelioma
31.Merck Canada Inc. Keytruda (pembrolizumab): solution for infusion 100 mg/4 mL vial [product monograph]. 2024.
32.Bristol-Myers Squibb Canada Co. Opdivo (nivolumab): intravenous Infusion, 10 mg/mL vials [product monograph]. 2021 [sponsor supplied reference].
33.Bristol-Myers Squibb Canada. Yervoy (ipilimumab for injection): intravenous Infusion, 5 mg/mL vials [product monograph]. February 1, 2012. Updated December 7, 2023. Accessed February 18, 2025. https://pdf.hres.ca/dpd_pm/00074279.PDF
34.Marmarelis ME, Wang X, Roshkovan L, et al. Clinical Outcomes Associated With Pembrolizumab Monotherapy Among Adults With Diffuse Malignant Peritoneal Mesothelioma. JAMA Netw Open. 2023;6(3):e232526. doi: 10.1001/jamanetworkopen.2023.2526 PubMed
35.Chu Q, Perrone F, Greillier L, et al. Pembrolizumab plus chemotherapy versus chemotherapy in untreated advanced pleural mesothelioma in Canada, Italy, and France: a phase 3, open-label, randomised controlled trial. Lancet. 2023;402(10419):2295-2306. doi: 10.1016/S0140-6736(23)01613-6 PubMed
36.Piccirillo MC, Chu Q, Bradbury P, et al. Brief Report: Canadian Cancer Trials Group IND. 227: A phase 2 randomized study of pembrolizumab in patients with advanced Malignant pleural mesothelioma (NCT02784171). J Thorac Oncol. 2023;18(6):813-819. doi: 10.1016/j.jtho.2023.02.003 PubMed
37.Chu QS, Piccirillo MC, Greillier L, et al. IND227 phase III (P3) study of cisplatin/pemetrexed (CP) with or without pembrolizumab (pembro) in patients (pts) with malignant pleural mesothelioma (PM): A CCTG, NCIN, and IFCT trial. J Clin Oncol. 2023;41(17_suppl):LBA8505-LBA8505. doi: 10.1200/JCO.2023.41.17_suppl.LBA8505
38.Armato SG, 3rd, Nowak AK. Revised Modified Response Evaluation Criteria in Solid Tumors for Assessment of Response in Malignant Pleural Mesothelioma (Version 1.1). J Thorac Oncol. 2018;13(7):1012-1021. doi: 10.1016/j.jtho.2018.04.034 PubMed
39.Aaronson NK, Ahmedzai S, Bergman B, et al. The European Organization for Research and Treatment of Cancer QLQ-C30: a quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst. 1993;85(5):365-76. doi: 10.1093/jnci/85.5.365 PubMed
40.Bergman B, Aaronson NK, Ahmedzai S, Kaasa S, Sullivan M. The EORTC QLQ-LC13: a modular supplement to the EORTC Core Quality of Life Questionnaire (QLQ-C30) for use in lung cancer clinical trials. EORTC Study Group on Quality of Life. Eur J Cancer. 1994;30A(5):635-42. doi: 10.1016/0959-8049(94)90535-5 PubMed
41.Rabin R, de Charro F. EQ-5D: a measure of health status from the EuroQol Group. Ann Med. 2001;33(5):337-43. doi: 10.3109/07853890109002087 PubMed
42.King MT. The interpretation of scores from the EORTC quality of life questionnaire QLQ-C30. Qual Life Res. 1996;5(6):555-67. doi: 10.1007/BF00439229 PubMed
43.Nicklasson M, Bergman B. Validity, reliability and clinical relevance of EORTC QLQ-C30 and LC13 in patients with chest malignancies in a palliative setting. Qual Life Res. 2007;16(6):1019-28. doi: 10.1007/s11136-007-9210-8 PubMed
44.Musoro JZ, Coens C, Sprangers MAG, et al. Minimally important differences for interpreting EORTC QLQ-C30 change scores over time: A synthesis across 21 clinical trials involving nine different cancer types. Eur J Cancer. 2023;188:171-182. doi: 10.1016/j.ejca.2023.04.027 PubMed
45.Koller M, Musoro JZ, Tomaszewski K, et al. Minimally important differences of EORTC QLQ-C30 scales in patients with lung cancer or malignant pleural mesothelioma - Interpretation guidance derived from two randomized EORTC trials. Lung Cancer. 2022;167:65-72. doi: 10.1016/j.lungcan.2022.03.018 PubMed
46.Coon CD, Schlichting M, Zhang X. Interpreting Within-Patient Changes on the EORTC QLQ-C30 and EORTC QLQ-LC13. Patient. 2022;15(6):691-702. doi: 10.1007/s40271-022-00584-w PubMed
47.Scagliotti GV, Gaafar R, Nowak AK, et al. Nintedanib in combination with pemetrexed and cisplatin for chemotherapy-naive patients with advanced malignant pleural mesothelioma (LUME-Meso): a double-blind, randomised, placebo-controlled phase 3 trial. Lancet Respir Med. 2019;7(7):569-580. doi: 10.1016/S2213-2600(19)30139-0 PubMed
48.Merck Canada Inc. Clinical summary [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Keytruda (pembrolizumab) solution for infusion 100 mg/4 mL vial. November 27, 2024.
49.Latimer N. NICE DSU Technical Support Document 14: Undertaking survival analysis for economic evaluations alongside clinical trials - extrapolation with patient-level data. Decision Support Unit, ScHARR, University of Sheffield; 2011. Updated March 2013. Accessed March 25, 2025. https://www.sheffield.ac.uk/media/34225/download?attachment
50.In J, Lee DK. Survival analysis: part II - applied clinical data analysis. Korean J Anesthesiol. 2019;72(5):441-457. doi: 10.4097/kja.19183 PubMed
51.Austin PC. Statistical power to detect violation of the proportional hazards assumption when using the Cox regression model. J Stat Comput Simul. 2018;88(3):533-552. doi: 10.1080/00949655.2017.1397151 PubMed
52.Guyot P, Ades AE, Ouwens MJ, Welton NJ. Enhanced secondary analysis of survival data: reconstructing the data from published Kaplan-Meier survival curves. BMC Med Res Methodol. 2012;12:9. doi: 10.1186/1471-2288-12-9 PubMed
53.Grambsch PM, Therneau TM. Proportional hazards tests and diagnostics based on weighted residuals. Biometrika. 1994;81(3):515-526. doi: 10.1093/biomet/81.3.515
54.Harrell FE, Jr., Lee KL, Mark DB. Multivariable prognostic models: issues in developing models, evaluating assumptions and adequacy, and measuring and reducing errors. Stat Med. 1996;15(4):361-87. doi: 10.1002/(SICI)1097-0258(19960229)15:4<361::AID-SIM168>3.0.CO;2-4 PubMed
55.Bucher HC, Guyatt GH, Griffith LE, Walter SD. The results of direct and indirect treatment comparisons in meta-analysis of randomized controlled trials. J Clin Epidemiol. 1997;50(6):683-91. doi: 10.1016/s0895-4356(97)00049-8 PubMed
56.Dias S, Sutton AJ, Ades AE, Welton NJ. Evidence synthesis for decision making 2: a generalized linear modeling framework for pairwise and network meta-analysis of randomized controlled trials. Med Decis Making. 2013;33(5):607-17. doi: 10.1177/0272989X12458724 PubMed
57.Jansen JP. Network meta-analysis of survival data with fractional polynomials. BMC Med Res Methodol. 2011;11:61. doi: 10.1186/1471-2288-11-61 PubMed
58.Dias S, Ades AE, Welton NJ, Jansen JP, Sutton AJ. Network Meta-Analysis of Survival Outcomes. In: Dias S, Ades AE, Welton NJ, Jansen JP, Sutton AJ, eds. Network Meta-Analysis for Decision Making. 2018. https://doi.org/10.1002/9781118951651.ch10
59.Dias S, Welton NJ, Sutton AJ, Ades AE. NICE DSU technical support document 2: a generalised linear modelling framework for pairwise and network meta-analysis of randomised controlled trials. 2011 [sponsor supplied reference].
60.Turner RM, Jackson D, Wei Y, Thompson SG, Higgins JP. Predictive distributions for between-study heterogeneity and simple methods for their application in Bayesian meta-analysis. Stat Med. 2015;34(6):984-98. doi: 10.1002/sim.6381 PubMed
Appendix 1: Detailed Outcome Data
Please note that this appendix has not been copy-edited.
Table 23: Analysis of Restricted Mean Survival Times of Overall Survival (ITT Population) in the KEYNOTE-483 Trial
RMST follow-up duration | Pembrolizumab + platinum + pemetrexed (N = 222) | Platinum + pemetrexed (N = 218) | RMST difference (95% CI) | ||
|---|---|---|---|---|---|
Number of events | RMST (months) | Number of events | RMST (months) | ||
Overall survival | |||||
24 months | 135 | 16.29 | 140 | 15.34 | 0.95 (–0.52 to 2.41) |
36 months | NR | NR | NR | NR | NR |
Progression-free survival (mRECIST by BICR) | |||||
12 months | 153 | 7.76 | 146 | 7.33 | 0.42 (–0.23 to 1.08) |
BICR = blinded independent central review; CI = confidence interval; ITT = intention to treat; mRECIST = modified Response Evaluation Criteria in Solid Tumours; NR = not reported; RMST = restricted mean survival time.
Note: The database cut-off date was September 16, 2022.
Source: Clinical Study Report for KEYNOTE-483.11
Table 24: Sensitivity Analyses and Supplemental Analyses of Progression-Free Survival (ITT Population) in the KEYNOTE-483 Trial
Analyses | Pembrolizumab + platinum + pemetrexed (N = 222) | Platinum + pemetrexed (N = 218) |
|---|---|---|
PFS — mRECIST by BICR: Sensitivity analysis censoring rule 1a | ||
Number of patients contributing to the analysis | 222 | 218 |
Number of patients with events, n (%) | 207 (93.2) | 200 (91.7) |
Death | 34 (15.3) | 52 (23.9) |
Documented progression | 173 (77.9) | 148 (67.9) |
Progression-free probability at 12 months, % (95% CI)b | 26.9 (21.2 to 32.9) | 22.8 (17.3 to 28.7) |
Median, months (95% CI)b | 7.2 (6.9 to 8.3) | 7.2 (6.9 to 7.9) |
HR (95% CI)c | 0.88 (0.72 to 1.07) | |
P valued | 0.0983 | |
PFS — mRECIST by BICR: Sensitivity analysis censoring rule 2e | ||
Number of patients contributing to the analysis | 222 | 218 |
Number of patients with events, n (%) | 213 (95.9) | 207 (95.0) |
Death | 34 (15.3) | 52 (23.9) |
Documented progression | 173 (77.9) | 148 (67.9) |
Progression-free probability at 12 months, % (95% CI)b | 26.6 (21.0 to 32.5) | 21.9 (16.6 to 27.7) |
Median, months (95% CI)b | 7.1 (6.9 to 8.1) | 7.2 (6.9 to 7.8) |
HR (95% CI)c | 0.88 (0.72 to 1.06) | |
P valued | 0.0895 | |
PFS — mRECIST by investigator: Sensitivity analysis primary censoring rulef | ||
Number of patients contributing to the analysis | 222 | 218 |
Number of patients with events, n (%) | 200 (90.1) | 185 (84.9) |
Death | 16 (7.2) | 17 (7.8) |
Documented progression | 184 (82.9) | 168 (77.1) |
Progression-free probability at 12 months, % (95% CI)b | 26.5 (20.8 to 32.6) | 14.2 (9.6 to 19.6) |
Median, months (95% CI)b | 7.1 (6.9 to 7.7) | 6.9 (6.7 to 7.2) |
HR (95% CI)c | 0.75 (0.61 to 0.93) | |
P valued | 0.0034 | |
PFS — mRECIST by investigator: Supplemental analysis censoring rule 1a | ||
Number of patients contributing to the analysis | 222 | 218 |
Number of patients with events, n (%) | 208 (93.7) | 203 (93.1) |
Death | 23 (10.4) | 34 (15.6) |
Documented progression | 185 (83.3) | 169 (77.5) |
Progression-free probability at 12 months, % (95% CI)b | 26.5 (20.8 to 32.4) | 17.8 (13.0 to 23.3) |
Median, months (95% CI)b | 7.1 (6.9 to 7.7) | 6.9 (6.7 to 7.2) |
HR (95% CI)c | 0.82 (0.67 to 1.00) | |
P valued | 0.0221 | |
PFS — RECIST 1.1 by BICR: Supplemental analysis primary censoring rulef | ||
Number of patients contributing to the analysis | 222 | 218 |
Number of patients with events, n (%) | 193 (86.9) | 171 (78.4) |
Death | 19 (8.6) | 21 (9.6) |
Documented progression | 174 (78.4) | 150 (68.8) |
Progression-free probability at 12 months, % (95% CI)b | 26.1 (20.3 to 32.2) | 14.9 (10.0 to 20.7) |
Median, months (95% CI)b | 7.1 (6.9 to 7.9) | 7.0 (6.8 to 7.4) |
HR (95% CI)c | 0.78 (0.63 to 0.96) | |
P valued | 0.0104 | |
BICR = blinded independent central review; CI = confidence interval; HR = hazard ratio; ITT = intention to treat; mRECIST = modified Response Evaluation Criteria in Solid Tumours; PFS = progression-free survival; RECIST = Response Evaluation Criteria in Solid Tumours Version.
Note: The database cut-off date was September 16, 2022.
aFollowed the ITT principle, i.e., progressive disease events and deaths were counted as events regardless of missed study visits or initiation of new anticancer therapy.
bBased on Kaplan-Meier estimates.
cBased on Cox regression model using the Efron method of tie handling, with treatment as a covariate stratified by histological subtype at randomization (epithelioid versus other subtypes).
dOne-sided P value based on log-rank test stratified by histological subtype at randomization (epithelioid versus other subtypes).
eConsidered initiation of new anticancer treatment or discontinuation of treatment due to reasons other than complete response, whichever occurred later, to be a progressive disease event for participants without documented progressive disease event or death.
fPrimary censoring rules described in Table 8.
Source: Clinical Study Report for KEYNOTE-483.11
Pharmacoeconomic Review
Abbreviations
BIA
budget impact analysis
CDA-AMC
Canada’s Drug Agency
CMA
cost-minimization analysis
HRQoL
health-related quality of life
ITC
indirect treatment comparison
MPM
malignant pleural mesothelioma
NMA
network meta-analysis
ORR
objective response rate
OS
overall survival
PFS
progression-free survival
RDI
relative dose intensity
ToT
time on treatment
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Pembrolizumab (Keytruda), solution for infusion, 100 mg/4 mL vial (25 mg/mL) |
Submitted price | Pembrolizumab, 25 mg/mL, solution for infusion, $4,400 per 100 mg vial |
Indication | Proposed: In combination with pemetrexed and platinum chemotherapy for the first-line treatment of adult patients with unresectable advanced or metastatic malignant pleural mesothelioma. |
Health Canada approval status | Approved |
Health Canada review pathway | Standard |
NOC date | April 11, 2025 |
Reimbursement request | As per indication |
Sponsor | Merck Canada Inc. |
Submission history | Previously reviewed: Yes Pembrolizumab (Keytruda) has been reviewed for multiple indications by CDA-AMC:
|
CDA-AMC = Canada’s Drug Agency; NOC = Notice of Compliance; NSCLC = non–small cell lung cancer; T2a = tumour stage IIa; TPS = tumour proportion score.
Table 2: Summary of Economic Information
Component | Description |
|---|---|
Type of economic evaluation | Cost-minimization analysis |
Target population | Proposed: In combination with pemetrexed and platinum chemotherapy, it is indicated for the first-line treatment of adult patients with unresectable advanced or metastatic malignant pleural mesothelioma. |
Treatment | Pembrolizumab plus chemotherapy (i.e., pemetrexed and cisplatin or carboplatin) |
Comparator | Nivolumab-ipilimumab |
Perspective | Canadian publicly funded health care payer |
Time horizon | Lifetime (31 years) |
Key data source | An ITC was conducted to evaluate the efficacy of pembrolizumab plus chemotherapy compared with nivolumab-ipilimumab. The ITC compared evidence from the CheckMate 743 trial and the KEYNOTE-483 trial. The KEYNOTE-483 trial was a phase II/III randomized controlled study that assessed the efficacy and safety of pembrolizumab plus chemotherapy versus pemetrexed plus cisplatin or carboplatin alone in patients with advanced or metastatic MPM. |
Costs considered | Drug acquisition and administration costs |
Submitted results | Incremental costs = $4,663 per patient over a lifetime time horizon |
Key limitations |
|
CDA-AMC reanalysis results | CDA-AMC did not perform reanalyses for the base case and accepted the sponsor’s submitted base case. Based on publicly available list prices, pembrolizumab plus chemotherapy is a cost saving compared with nivolumab-ipilimumab. The cost savings associated with pembrolizumab plus chemotherapy are contingent on confidentially negotiated prices. If the actual price paid for nivolumab-ipilimumab is lower than the publicly listed prices, reimbursing pembrolizumab at the price submitted by the sponsor could result in higher costs for the public health payer. Changes to the RDI assumptions resulted in cost savings for nivolumab-ipilimumab, with pembrolizumab plus chemotherapy being associated with higher costs. All other scenario analyses, including weight-based dosing and the proportion of patients receiving subsequent therapy, resulted in cost savings. |
CDA-AMC = Canada’s Drug Agency; ITC = indirect treatment comparison; MPM = malignant pleural mesothelioma; OS = overall survival; PFS = progression-free survival; RDI = relative dose intensity.
Conclusions
The Clinical Review by Canada’s Drug Agency (CDA-AMC) determined that the available evidence aimed to estimate relative treatment effects for overall survival (OS), progression-free survival (PFS), and objective response rate (ORR) rather than formally test for superiority, equivalence, or inferiority between pembrolizumab plus chemotherapy (i.e., pemetrexed and carboplatin or cisplatin) versus nivolumab-ipilimumab. The sponsor’s indirect treatment comparison (ITC) showed that OS results favoured nivolumab-ipilimumab over pembrolizumab plus chemotherapy, while PFS favoured pembrolizumab plus chemotherapy over nivolumab-ipilimumab; however, in both cases, the difference was not statistically significant. Other outcomes, such as ORR and health-related quality of life (HRQoL), were not included in the sponsor’s economic analysis of pembrolizumab plus chemotherapy. The CDA-AMC Clinical Review noted that the nonepithelioid subgroup appeared to derive more treatment benefit compared with the epithelioid subgroup; however, the sponsor did not conduct subgroup analyses to confirm these observed benefits. The CDA-AMC Clinical Review concluded there is insufficient evidence to establish nonsimilarity between pembrolizumab plus chemotherapy and nivolumab-ipilimumab. Additionally, comparative safety data between pembrolizumab plus chemotherapy and nivolumab-ipilimumab were not formally evaluated, leaving uncertainty regarding whether pembrolizumab plus chemotherapy offers similar safety to nivolumab-ipilimumab. No revisions were undertaken for the sponsor’s base case; at the sponsor’s submitted price for pembrolizumab and all other drugs in the economic analysis, pembrolizumab plus chemotherapy was a cost saving over a lifetime horizon. These cost savings are relatively small compared with the overall cost of treatment ($4,663 savings versus $123,525 treatment cost) and are highly uncertain.
CDA-AMC notes that the cost equivalence for pembrolizumab plus chemotherapy is contingent on the publicly listed drug prices for the comparators. If the actual drug prices paid by the plans for nivolumab-ipilimumab are lower by 3%, pembrolizumab plus chemotherapy is no longer a cost saving. CDA-AMC found that pembrolizumab plus chemotherapy and nivolumab-ipilimumab are cost-equivalent. Changes to relative dose intensity (RDI) resulted in pembrolizumab plus chemotherapy costing more than nivolumab-ipilimumab. Given the uncertainty in the clinical evidence and the sensitivity of relative treatment cost to several assumptions within the economic analysis, the evidence does not support a price premium for pembrolizumab plus chemotherapy over nivolumab-ipilimumab.
Economic Review
The current review is for pembrolizumab (Keytruda) for malignant pleural mesothelioma (MPM).
Economic Information
Summary of Sponsor’s Economic Information
The sponsor submitted a cost-minimization analysis (CMA) comparing pembrolizumab plus chemotherapy (i.e., pemetrexed and cisplatin or carboplatin) to nivolumab-ipilimumab for the first-line treatment of unresectable advanced or metastatic MPM.1 The evaluation was conducted from the public health payer perspective and used population data from the KEYNOTE-483 clinical trial, alongside inputs from other relevant sources.2
The eligible population for pembrolizumab plus chemotherapy includes adults with unresectable MPM.3 This was aligned with the anticipated Health Canada indication. Baseline patient characteristics were based on values from the KEYNOTE-483 trial.4 The mean age of the model cohort was 68.9 years.4 The analysis assumed that both regimens provided similar clinical benefits, supported by an ITC comparing evidence from the KEYNOTE-483 and CheckMate-743 trials.2 Maximum treatment durations were 104 weeks (35 cycles) for pembrolizumab and 18 weeks (6 cycles) for chemotherapy, consistent with their respective product monographs.5 Time-on-treatment (ToT) estimates for pembrolizumab were based on patient-level data.6 Among patients receiving nivolumab-ipilimumab, the ToT was derived using an exponential model informed by the CheckMate 743 trial with a treatment duration of 104 weeks, consistent with its product monograph.7
Drug acquisition costs were calculated based on defined dosing schedules, unit prices, and RDIs. Pembrolizumab was administered at 200 mg every 3 weeks for up to 2 years, pemetrexed at 500 mg/m2 every 3 weeks for 6 cycles, and cisplatin at 75 mg/m2 every 3 weeks for 6 cycles.5,8 In cases where cisplatin was contraindicated, carboplatin was substituted at an area under the curve (AUC) of 5 mg/mL per min to 6 mg/mL per min for 6 cycles.5 Dosing for nivolumab-ipilimumab was sourced from product monographs and included a fixed dose of nivolumab at 360 mg every 3 weeks and ipilimumab at 1 mg/kg every 6 weeks for up to 2 years.9,10 Drug administration costs for first-line treatments were calculated by multiplying the hourly administration cost of $131.77 by the infusion duration for each drug, with durations sourced from trial protocols and literature. Pembrolizumab required an infusion time of 0.5 hours per dose, as reported in the KEYNOTE-483 trial, resulting in an administration cost of $65.89 per infusion.11 Cisplatin, with a 2-hour infusion time based on BC Cancer protocols, incurred a cost of $263.54 per infusion.12,13 Carboplatin required 0.5 hours per infusion, costing $65.89.12,13 Pemetrexed, when paired with carboplatin, had an infusion duration of 0.17 hours, costing $21.96 per infusion.14 However, when coadministered with cisplatin, pemetrexed’s administration cost was assumed to be covered by cisplatin’s prehydration process and, thus, incurred no additional cost. For the nivolumab-ipilimumab regimen, both drugs had infusion durations of 0.5 hours each, as stated in their respective product monographs, resulting in administration costs of $65.89 per infusion for each drug.9,10 The CMA incorporated vial-sharing assumptions, reducing wastage to 5%.
Subsequent treatment assumptions were informed by data from the KEYNOTE-483 trial, with the sponsor assuming that patients in both treatment arms — pembrolizumab plus chemotherapy and nivolumab-ipilimumab — would receive the same subsequent therapies.1 The distribution of subsequent market shares was derived from treatment discontinuation data and applied equally across both arms. Costs were calculated as the weighted averages of the regimens used. The sponsor assumed that 46% of patients would not initiate subsequent therapy, while the remaining patients were distributed across carboplatin and pemetrexed (22%), gemcitabine (14%), pemetrexed (7%), and vinorelbine (7%), with all other subsequent therapies accounting for less than 4%.6 By assuming identical subsequent therapy distributions for both arms, the sponsor minimized potential cost differences between the treatment arms.
The sponsor conducted an ITC alongside a network meta-analysis (NMA) and a nonproportional hazard NMA to assess the comparative effectiveness of pembrolizumab plus chemotherapy and nivolumab-ipilimumab. Because the included studies shared a common comparator, a Bucher ITC was deemed an appropriate method for synthesizing the indirect evidence.2 Time-dependent outcomes, such as OS and PFS, were key end points, and the proportional hazards assumption was applied where applicable. The Bucher ITC combined data from 2 pivotal studies, KEYNOTE-483 and CheckMate 743, to compare OS, PFS, and ORR. For the NMA, 3 studies — KEYNOTE-483, CheckMate 743, and IND.227 — were included to evaluate the same outcomes.2 In cases where nonproportional hazards were observed, Kaplan-Meier curves were used to generate pseudo–patient level data, enabling the use of nonproportional hazard NMA. The ITC conducted by the sponsor found no significant differences in OS or PFS between pembrolizumab plus chemotherapy and nivolumab-ipilimumab, supporting the assumption of comparable clinical efficacy.2 However, pembrolizumab plus chemotherapy demonstrated a statistically superior ORR.2
A summary of the sponsor’s base case is presented in Table 3. In the sponsor’s base-case analysis, pembrolizumab plus chemotherapy was associated with cost savings over a 31-year lifetime horizon compared with nivolumab-ipilimumab. This cost difference was primarily driven by reduced drug acquisition costs and assumptions regarding RDI. The total lifetime cost for pembrolizumab plus chemotherapy was estimated at $123,525 compared with $128,188 for nivolumab-ipilimumab, resulting in a cost saving of $4,663. Disaggregated results of the sponsor’s analysis can be found in Table 5.
Table 3: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total drug costs ($) | Incremental drug costs ($) | Total costs ($) | Incremental costs ($) |
|---|---|---|---|---|
Pembrolizumab plus chemotherapy | 118,350 | Reference | 123,525 | Reference |
Nivolumab-ipilimumab | 124,241 | −5,891 | 128,188 | −4,663 |
Source: Sponsor’s economic submission.1
The sponsor conducted several scenario analyses. Although the model was sensitive to assumptions related to vial sharing, RDI, the absence of wastage with vial sharing, and the use of the median ToT across all treatments, pembrolizumab plus chemotherapy consistently demonstrated cost savings compared with nivolumab-ipilimumab in all scenarios except the scenario involving RDI. Given that the cost savings associated with pembrolizumab are less than 5% of the total cost, CDA-AMC assumed pembrolizumab to be cost-equivalent to nivolumab-ipilimumab.
CDA-AMC Appraisal of the Sponsor’s Economic Information
CDA-AMC identified several key limitations to the sponsor’s analysis that have notable implications for the economic analysis:
The sponsor’s assumption of similar equivalence between pembrolizumab plus chemotherapy and nivolumab-ipilimumab is uncertain: Key clinical outcomes, including OS, PFS, and ORR, were identified as critical factors for evaluation. The ITC evidence did not establish a clear difference in OS or PFS between pembrolizumab plus chemotherapy and nivolumab-ipilimumab. While estimates for OS generally favoured nivolumab-ipilimumab and estimates for PFS favoured pembrolizumab plus chemotherapy, the uncertainty around the results (e.g., wide confidence intervals) precludes firm conclusions. While pembrolizumab plus chemotherapy demonstrated a higher ORR than chemotherapy alone and nivolumab-ipilimumab, this did not translate into improved HRQoL, an outcome not assessed in the studies.
CDA-AMC was unable to address this limitation. The economic base case retained the assumption that pembrolizumab plus chemotherapy is equally effective to nivolumab-ipilimumab.
Drug prices are based on publicly listed prices: The prices used in the CMA for pembrolizumab plus chemotherapy are based on publicly available list prices and do not account for potential confidential pricing agreements negotiated by public drug plans. Because the projected cost savings for pembrolizumab plus chemotherapy are based on public list prices for comparators, price reductions may be necessary for pembrolizumab plus chemotherapy to achieve cost parity if the actual prices of the comparators are lower than their listed prices.
CDA-AMC was unable to address this limitation through reanalysis.
Fixed dosing for pembrolizumab is not reflective of clinical practice: The sponsor assumed a fixed-dosing regimen of pembrolizumab at 200 mg intravenously every 3 weeks in the base-case model.15 However, CDA-AMC notes that, in line with other indications for pembrolizumab, jurisdictions would likely implement a weight-based dose of 2 mg/kg (up to a cap of 200 mg) every 3 weeks.
CDA-AMC conducted 1 scenario analysis in which pembrolizumab used weight-based dosing methods and another in which both pembrolizumab and nivolumab were both weight-based.
The RDI obtained for pembrolizumab may be inappropriate: The sponsor used trial data to estimate RDI values between 95.1% and 98.6% for pembrolizumab and chemotherapy, respectively.6 The sponsor assumed that patients receiving pembrolizumab plus chemotherapy received a lower proportion of the recommended dose compared with patients in the comparator arm, who were presumed to receive the full dose. This assumption reduced the cumulative cost attributed to pembrolizumab plus chemotherapy. The clinical experts consulted by CDA-AMC indicated that an RDI of 100% was expected for pembrolizumab and that the chemotherapy assumptions were appropriate. However, due to the toxicity profile of nivolumab-ipilimumab, the clinical experts anticipated a lower RDI, similar to the sponsor’s assumption for pembrolizumab. Because the actual price of treatments is uncertain, this approach introduces a bias in favour of the pembrolizumab plus chemotherapy and potentially overestimates its cost savings.
CDA-AMC conducted a scenario analysis in which the RDI was assumed to be 100% among patients receiving pembrolizumab, and 95% among patients receiving nivolumab-ipilimumab.
The distribution of subsequent therapy may be inappropriate: The sponsor assumed that subsequent therapies initiated by patients receiving pembrolizumab plus chemotherapy or nivolumab-ipilimumab would be the same. Based on observations from the KEYNOTE-483 trial, the sponsor assumed that patients in clinical practice would follow subsequent treatment patterns similar to those observed in the trial, despite the possibility that real-world subsequent therapies may differ from those used in the study.6 Approximately one-half of trial participants did not proceed with subsequent treatment, while most of the remainder were prescribed carboplatin plus pemetrexed or gemcitabine, with a smaller proportion receiving other therapies. Notably, 0.5% and 1% of patients continued treatment with nivolumab-ipilimumab and pembrolizumab monotherapy, respectively.6 Based on input from the clinical experts, the proportion of patients not receiving subsequent therapy was adjusted from 46% to 60%. Additionally, among patients receiving pembrolizumab plus chemotherapy, the clinical experts anticipated a lower likelihood of patients being rechallenged with immunotherapies.
CDA-AMC conducted a scenario analysis in which 60% of patients receiving pembrolizumab were assumed not to continue onto subsequent therapy, as well as 0% of patients in both treatment arms continuing to get rechallenged with other immunotherapies.
CDA-AMC Reanalyses of the Economic Information
CDA-AMC did not conduct a base-case reanalysis and accepted the sponsor’s submitted base case. CDA-AMC conducted scenario analyses to evaluate the impact of assuming weight-based dosing among patients receiving pembrolizumab and nivolumab in accordance with CDA-AMC guidelines on weight-based dosing for immunotherapies (Table 6). This scenario resulted in $33,133 in cost savings for pembrolizumab plus chemotherapy over the 31-year lifetime horizon. CDA-AMC also conducted scenario analyses on RDI, resulting in cost savings for nivolumab-ipilimumab over pembrolizumab plus chemotherapy. The remaining scenario analyses on weight-based dosing assumptions and the proportion of subsequent therapies resulted in cost savings for pembrolizumab plus chemotherapy over nivolumab-ipilimumab (Table 6).
Issues for Consideration
Subgroup analysis: Clinical evidence suggests that treatment response differs between epithelioid and nonepithelioid mesothelioma tumours. The Canadian Cancer Society identifies epithelioid mesothelioma as the most common subtype, and the clinical experts consulted for this review estimated that between 60% and 70% of mesothelioma tumours are epithelioid.16,17 These findings highlight the importance of considering histological differences when assessing treatment effectiveness.
Place in therapy: Although pembrolizumab is indicated for use in the first-line setting, the clinical experts noted it is unlikely that patients with advanced and/or metastatic MPM would not have received prior therapy.
Anticipated expiry of patents: The patents for nivolumab and ipilimumab are set to expire in 2026, and this is anticipated to influence the treatment landscape for MPM.18,19 If any nivolumab and ipilimumab generic drugs become available that are considered clinically equivalent to pembrolizumab for the treatment of MPM, the cost of pembrolizumab at the submitted price may be less attractive to drug plans.
Conclusions
The CDA-AMC Clinical Review determined that the available evidence did not establish whether pembrolizumab plus chemotherapy (i.e., pemetrexed and carboplatin or cisplatin) was superior, inferior, or equivalent to nivolumab-ipilimumab. The sponsor’s ITC showed that OS results favoured nivolumab-ipilimumab over pembrolizumab plus chemotherapy, while PFS favoured pembrolizumab plus chemotherapy over nivolumab-ipilimumab; however, in both cases, the difference was not statistically significant. Other outcomes, such as ORR and HRQoL, were not included in the sponsor’s economic analysis of pembrolizumab plus chemotherapy. The CDA-AMC Clinical Review noted that the nonepithelioid subgroup appeared to derive more treatment benefit compared with the epithelioid subgroup; however, the sponsor did not conduct subgroup analyses to confirm these observed benefits. The CDA-AMC Clinical Review concluded there is insufficient evidence to establish nonsimilarity between pembrolizumab plus chemotherapy and nivolumab-ipilimumab. Additionally, comparative safety data between pembrolizumab plus chemotherapy and nivolumab-ipilimumab were not formally evaluated, leaving uncertainty regarding whether pembrolizumab plus chemotherapy offers similar safety to nivolumab-ipilimumab.
No revisions were undertaken for the sponsor’s base case. At the sponsor’s submitted price for pembrolizumab and all other drugs in the economic analysis, pembrolizumab plus chemotherapy resulted in cost savings over a lifetime horizon. These cost savings are relatively small compared with the overall cost of treatment ($4,663 savings versus $123,525 treatment cost) and are highly uncertain.
CDA-AMC notes that the cost equivalence of pembrolizumab plus chemotherapy is contingent on the publicly listed drug prices for the comparators. If the actual drug prices paid by the plans for nivolumab-ipilimumab are lower by 3%, pembrolizumab plus chemotherapy is no longer a cost saving. CDA-AMC found that pembrolizumab plus chemotherapy and nivolumab-ipilimumab are cost-equivalent. Changes to the RDI resulted in pembrolizumab plus chemotherapy costing more than nivolumab-ipilimumab. Given the uncertainty in the clinical evidence and the sensitivity of relative treatment cost to several assumptions within the economic analysis, the evidence does not support a price premium for pembrolizumab and chemotherapy over nivolumab-ipilimumab.
References
1.Merck Canada Inc. Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Keytruda (pembrolizumab), solution for infusion 100 mg/4 mL vial. November 19, 2024.
2.Merck Canada Inc. A systematic literature review and indirect treatment comparison for pembrolizumab in combination with pemetrexed and platinum chemotherapy for the first-line treatment of unresectable advanced or metastatic malignant pleural mesothelioma [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Keytruda (pembrolizumab), solution for infusion 100 mg/4 mL vial. November 2024.
3.Merck Canada Inc. Keytruda (pembrolizumab): solution for infusion 100 mg/4 mL vial[product monograph]. April 11, 2025.
4.Canadian Cancer Trials Group. NCT02784171: pembrolizumab in patients with advanced malignant pleural mesothelioma. ClinicalTrials.gov. Accessed by sponsor, no date provided. https://www.clinicaltrials.gov/ct2/show/NCT02784171
5.Cancer Care Ontario: funded evidence-informed regimens. 2024. Accessed February 17, 2025. https://www.cancercareontario.ca/en/drugformulary/regimens
6.BARDS Health Technology Assessment Statistical Report. First-Line Advanced/Metastatic Malignant Pleural Mesothelioma. Protocol 483. Database cut off: 16SEP2022 (Final Analysis). 2022. Accessed September 16 [sponsor supplied reference].
7.Baas P, Scherpereel A, Nowak AK, et al. First-line nivolumab plus ipilimumab in unresectable malignant pleural mesothelioma (CheckMate 743): a multicentre, randomised, open-label, phase 3 trial. Lancet. 2021;397(10272):375-386. doi: 10.1016/S0140-6736(20)32714-8 PubMed
8.Merck Canada Inc. Keytruda (pembrolizumab): solution for infusion 100 mg/4 mL vial [product monograph]. Draft for proposed new indication [sponsor supplied reference].
9.Bristol-Myers Squibb Canada. Yervoy (ipilimumab for injection): intravenous Infusion, 5 mg/mL vials [product monograph]. February 1, 2012. Updated December 7, 2023. Accessed by sponsor, no date provided. https://pdf.hres.ca/dpd_pm/00074279.PDF
10.Bristol-Myers Squibb Canada Co. Opdivo (nivolumab): intravenous Infusion, 10 mg/mL vials [product monograph]. September 25, 2015. Updated June 28, 2024. Accessed by sponsor, no date provided. https://pdf.hres.ca/dpd_pm/00076152.PDF
11.Piccirillo MC, Chu Q, Bradbury P, et al. Brief Report: Canadian Cancer Trials Group IND.227: A Phase 2 Randomized Study of Pembrolizumab in Patients With Advanced Malignant Pleural Mesothelioma (NCT02784171). J Thorac Oncol. 2023;18(6):813-819. doi: 10.1016/j.jtho.2023.02.003 PubMed
12.BC Cancer. BC Cancer Protocol Summary for the Treatment of Malignant Mesothelioma using Ipilimumab and Nivolumab 3mg/kg. 2022. Accessed by sponsor, no date provided. http://www.bccancer.bc.ca/chemotherapy-protocols-site/Documents/Lung/LUMMIPNI_Protocol.pdf
13.BC Cancer. BC Cancer Protocol Summary for the Treatment of Malignant Mesothelioma using Ipilimumab and 3-Weekly Nivolumab 4.5mg/kg. 2022. Accessed by sponsor, no date provided. http://www.bccancer.bc.ca/chemotherapy-protocols-site/Documents/Lung/LUMMIPNI3_Protocol.pdf
14.Hazarika M, White RM, Johnson JR, Pazdur R. FDA drug approval summaries: pemetrexed (Alimta). Oncologist. 2004;9(5):482-8. doi: 10.1634/theoncologist.9-5-482 PubMed
15.Chu Q, Perrone F, Greillier L, et al. Pembrolizumab plus chemotherapy versus chemotherapy in untreated advanced pleural mesothelioma in Canada, Italy, and France: a phase 3, open-label, randomised controlled trial. Lancet. 2023;402(10419):2295-2306. doi: 10.1016/S0140-6736(23)01613-6 PubMed
16.Fels Elliott DR, Jones KD. Diagnosis of Mesothelioma. Surg Pathol Clin. 2020;13(1):73-89. doi: 10.1016/j.path.2019.10.001 PubMed
17.NCCN Guidelines. Malignant Pleural Mesothelioma, version 2.2020. National Comprehensive Cancer Network (NCCN); 2020. Accessed February 18, 2025. https://www.nccn.org/
18.Health Canada. Patent Register - Form IV summaries: Yervoy (ipilimumab). 2025. Accessed March 07, 2025. https://pr-rdb.hc-sc.gc.ca/pr-rdb/patent_result-resultat_brevet.do?action=search_recherche&formId=9948&din=02379384&drugId=2815&lang=fr&patentNumber_numeroBrevet=2607147
19.Health Canada. Patent Register - Form IV summaries: Opdivo (nivolumab). 2025. Accessed March 07, 2025. https://pr-rdb.hc-sc.gc.ca/pr-rdb/patent_result-resultat_brevet.do?action=search_recherche&formId=9945&din=02446626&drugId=4869&lang=fr&patentNumber_numeroBrevet=2607147
20.DeltaPA. IQVIA; 2023. Accessed January 13, 2025. https://www.iqvia.com/
21.CADTH. Reimbursement Review: nivolumab (Opdivo) in combination with ipilimumab (Yervoy). Can J Health Technol. 2021;1(9). doi: 10.51731/cjht.2021.168
22.Merck Canada Inc. Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Keytruda (pembrolizumab), solution for infusion 100 mg/4 mL vial. Merck Canada Inc; November 27, 2024.
23.Statistics Canada. Table 13-10-0111-01 Number and rates of new cases of primary cancer, by cancer type, age group and sex. 2024. Accessed by sponsor, no date provided. https://doi.org/10.25318/1310011101-eng
Appendix 1: Additional Economic Information
Please note that this appendix has not been copy-edited.
Cost Comparison Table
The comparators presented in the following table have been deemed to be appropriate based on feedback from the clinical expert consulted and the public drug plans. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and, as such, the table may not represent the actual costs to public drug plans.
Table 4: CDA-AMC Cost Comparison Table for Malignant Pleural Mesothelioma
Treatment | Strength and concentration | Form | Price | Recommended dosage | Daily cost | 21-day costa |
|---|---|---|---|---|---|---|
Pembrolizumab | 25 mg/mL | 4 mL vial | 4,400.0000 | 200 mg every 21 days for 2 years | 419.05 | 8,800 |
Pemetrexed | 100 mg 500 mg | Lyophilized powder for IV infusion | 50.0000 250.0000 | 500 mg/m2 on day 1 for six 21-day cycles | 21.43 | 450 |
Cisplatin | 1 mg/mL | 50 mL vial 100 mL vial | 135.0000 270.0000 | 75 mg/m2 on day 1 for six 21-day cycles | 19.29 | 405 |
Carboplatin | 10 mg/mL | 5 mL vial 15 mL vial 45 mL vial 60 mL vial | 70.0000 210.0000 600.0000 778.0000 | AUC 5 mg/mL per min on day 1 for six 21-day cycles | 46.90 | 985 |
Pembrolizumab plus pemetrexed and cisplatin | 459.76 | 9,655 | ||||
Pembrolizumab plus pemetrexed and carboplatin | 487.38 | 10,235 | ||||
Nivolumab-ipilimumab | ||||||
Nivolumab | 10 mg/mL | 4 mL vial 10 mL vial | 782.2200 1,955.5600 | 360 mg every 21 days for 2 years | 353.86 | 7,431 |
Ipilimumab | 5 mg/mL | 10 mL vial 40 mL vial | 5,800.0000 23,200.0000 | 1 mg/kg every 42 days for 2 years | 276.19 | 5,800 |
Nivolumab-ipilimumab | 630.05 | 13,231 | ||||
AUC = area under the curve; CDA-AMC = Canada’s Drug Agency.
Note: All prices are from IQVIA Delta PA (accessed January 2025), unless otherwise indicated, and do not include dispensing fees.20 The prices align with CDA-AMC wastage assumptions.
aPrices reflect IQVIA Delta PA wholesale list prices (accessed January 2025).20
Additional Details on the Sponsor’s Submission
Table 5: Disaggregated Summary of the Sponsor’s Economic Evaluation Results
Cost category | Pembrolizumab with platinum and pemetrexed ($) | Nivolumab-ipilimumab ($) | Incremental cost ($) |
|---|---|---|---|
Drug acquisition | 118,350 | 124,241 | −5,892 |
Drug administration | 2,310 | 1,080 | 1,230 |
Total first-line drug cost | 120,659 | 125,321 | −4,662 |
Subsequent drug acquisition | 2,686 | 2,687 | −1 |
Subsequent drug administration | 180 | 180 | 0 |
Total subsequent treatment cost | 2,866 | 2,867 | −1 |
Total costs | 123,525 | 128,188 | −4,663 |
Source: Sponsor’s economic submission.1
Additional Details on the CDA-AMC Reanalyses and Additional Analyses
Table 6: Scenario Analyses Conducted by CDA-AMC on the Sponsor’s Base Case
Scenario analysis | Drug | Drug cost ($) | Incremental drug cost ($) | Total cost ($) | Incremental cost ($) |
|---|---|---|---|---|---|
Sponsor’s base case | Pembrolizumab with platinum + pemetrexed | 121,036 | Reference | 123,525 | Reference |
Nivolumab-ipilimumab | 126,928 | 5,892 | 128,188 | 4,663 | |
CDA-AMC scenario 1: Weight-based dosing for pembrolizumab | Pembrolizumab with platinum + pemetrexed | 89,880 | Reference | 94,981 | Reference |
Nivolumab-ipilimumab | 124,241 | 34,362 | 128,113 | 33,133 | |
CDA-AMC scenario 2: Weight-based dosing for pembrolizumab and nivolumab-ipilimumab | Pembrolizumab with platinum + pemetrexed | 89,880 | Reference | 95,029 | Reference |
Nivolumab-ipilimumab | 115,461 | 25,582 | 119,382 | 24,353 | |
CDA-AMC scenario 3: Increased RDI for pembrolizumab and decreased RDI for nivolumab-ipilimumab | Pembrolizumab with platinum + pemetrexed | 124,168 | Reference | 129,348 | Reference |
Nivolumab-ipilimumab | 118,166 | −6,002 | 122,118 | −7,231 | |
CDA-AMC scenario 4: Distribution of subsequent therapies | Pembrolizumab with platinum + pemetrexed | 118,350 | Reference | 122,234 | Reference |
Nivolumab-ipilimumab | 124,241 | 5,892 | 126,896 | 4,662 |
CDA-AMC = Canada’s Drug Agency; RDI = relative dose intensity.
Source = Sponsor’s economic submission.1
Appendix 2: Submitted Budget Impact Analysis and CDA-AMC Appraisal
Please note that this appendix has not been copy-edited.
Table 7: Summary of Key Take-Aways
Key take-aways of the BIA |
|---|
State the key components revised in the CDA-AMC base case:
CDA-AMC did not conduct a base-case reanalysis. BIA results were sensitive to all scenarios undertaken by CDA-AMC (i.e., incremental budget impact when pembrolizumab’s market share was increased; increased cost savings when the weight-based dosing was applied to the pembrolizumab and increased budget expenditure when RDI assumptions were changed). |
BIA = budget impact analysis; CDA-AMC = Canada’s Drug Agency; RDI = relative dose intensity.
Summary of Sponsor’s BIA
The sponsor submitted a budget impact analysis (BIA) to estimate the 3-year budget impact of reimbursing pembrolizumab plus chemotherapy for the first-line treatment of patients with advanced or metastatic MPM.1 The BIA was conducted from the public drug plan perspective (excluding Quebec) over a 3-year time horizon (2026 to 2029).
The sponsor used an epidemiological approach to estimate the eligible market, based on data from the previous nivolumab-ipilimumab submission and clinical expert assumptions. Among patients with mesothelioma, 75% were identified as having MPM, with 95% of these cases identified to have unresectable MPM.21 The sponsor further assumed that 100% of patients with MPM received referrals to medical oncologists for treatment and that 75% of these patients were eligible for immuno-oncology therapy.21,22 In the reference scenario, the sponsor assumed that nivolumab-ipilimumab capture 95% of the market share annually over 3 years, with the remaining 5% attributed to patients enrolled in clinical trials.22 In the new-drug scenario, the sponsor projected that pembrolizumab plus chemotherapy would achieve a 17% market share in year 1, primarily by displacing nivolumab-ipilimumab.22 Over the following 2 years, pembrolizumab plus chemotherapy market share was projected to stabilize at 33% annually.22 Key inputs to the BIA are documented in Table 8.
State the key assumptions:
The sponsor assumed 95.1% to 98.6% RDI for pembrolizumab plus chemotherapy and 100% RDI for nivolumab-ipilimumab.6,7
Five percent of patients categorized as being in clinical trials were not assigned a treatment and represent a proportion of patients not receiving therapy.22
Table 8: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as year 1 / year 2 / year 3, if appropriate) |
|---|---|
Target population | |
Annual % growth rate | 0.58%23 |
Incidence rate of mesothelioma | 1.7 per 100,00022 |
Percentage of MPM cases | 75%21 |
Percentage of population with unresectable disease | 95%21 |
Percentage referred to for treatment | 100%21 |
Percentage of patients treated by medical oncologists | 100%22 |
Percentage of patients eligible for immuno-oncology | 75%21 |
Number of patients eligible for drug under review | 231/ 232 / 233 |
Market uptake (3 years) | |
Uptake (reference scenario) Nivolumab-ipilimumab Clinical trials | 95% / 95% / 95% 5% / 5% / 5% |
Uptake (new-drug scenario) Pembrolizumab + chemotherapy Nivolumab-ipilimumab Clinical trials | 17% / 33% / 33% 79% / 63% / 63% 4% / 3% / 3% |
Cost of treatment (per patient) | |
Cost of treatment per cycle Pembrolizumab Cisplatin Carboplatin Pemetrexed Nivolumab Ipilimumab | $8,800 $373.28 $697.41 $452.50 $7,040 $8,691 |
RDI | |
Pembrolizumab Cisplatin Carboplatin Pemetrexed Nivolumab Ipilimumab | 95.11% 98.64% 98.64% 98.64% 100.00% 100.00% |
Distribution of subsequent therapies | Pembrolizumab group and nivolumab-ipilimumab group |
No active treatment Carboplatin-pemetrexed Gemcitabine Gemcitabine-ramucirumab Nivolumab-ipilimumab Pembrolizumab Pemetrexed Vinorelbine | 46.40% 22.04% 14.33% 2.00% 0.50% 1.00% 7.11% 6.61% |
MPM = malignant pleural mesothelioma; RDI = relative dose intensity.
Summary of the Sponsor’s BIA Results
The cumulative net budget impact of funding pembrolizumab plus chemotherapy for patients with advanced or metastatic MPM, was –$180,818 in year 1, –$277,114 in year 2, and –$30,270 in year 3, resulting in a total budget impact of $488,202 in cost savings over 3 years.
The budget impact of excluding RDI from the base-case results in total incremental budget impact of $396,639 over the 3-year time horizon (year 1: –$91,873; year 2: $71,220; year 3: $417,288), excluding RDI results in a budget differential of $884,841 from the base case.
CDA-AMC Appraisal of the Sponsor’s BIA
CDA-AMC identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
Market share of pembrolizumab may be underestimated: The sponsor’s submitted BIA indicated that pembrolizumab plus chemotherapy would result in a market uptake of 16% in year 1, 33% in year 2, and 33% in year 3 based on the sponsor’s internal market share analysis.22 However, CDA-AMC obtained clinical expert consultation indicating that the market uptake of 33% in year 2 and 3 does not align with clinical expectations and indicated the sponsor likely underestimated pembrolizumab plus chemotherapy’s uptake. Clinical experts consulted by CDA-AMC expected a 40% market share in years 2 and 3 for pembrolizumab plus chemotherapy with the remainder being distributed to nivolumab-ipilimumab.
CDA-AMC conducted a scenario analysis in which the market share for pembrolizumab plus chemotherapy in the new-drug scenario was set to 40% in years 2 and 3, with the balance of the market share redistributed to nivolumab-ipilimumab.
Fixed dosing for pembrolizumab is not reflective of clinical practice: Consistent with the limitation in the CMA, the sponsor assumed a fixed-dosing regimen of pembrolizumab at 200 mg intravenously every 3 weeks in the base-case model.15 However, CDA-AMC notes that, in line with other indications for pembrolizumab, jurisdictions would likely implement a weight-based dose of 2 mg/kg (up to a cap of 200 mg) every 3 weeks. The only immunotherapy to which the sponsor applied weight-based dosing was for ipilimumab, dosed at 1 mg/kg. Using a fixed-dosing regimen may result in an overestimation of the sponsor’s budget impact.
CDA-AMC conducted a scenario analysis in which pembrolizumab and nivolumab were administered using a weight-based dosing regimen. This adjustment affected only pembrolizumab and nivolumab, as ipilimumab was already modelled using a weight-based approach.
RDI obtained for pembrolizumab may be inappropriate: The sponsor assumed that the RDI would reflect the values observed in the trial and applied these values in both the BIA and CMA. The reported RDI for pembrolizumab plus chemotherapy ranged from 95.1% to 98.6%, respectively, based on data from the trial.6 In contrast, patients receiving nivolumab-ipilimumab were assumed to receive 100% of the planned dosage.7 These RDI assumptions are subject to the same limitations outlined in the CMA analysis.
CDA-AMC conducted a scenario analysis in which RDI was assumed to be 100% among patients receiving pembrolizumab, and 95% among patients receiving nivolumab-ipilimumab.
Uncertainty in the price paid by the public drug plans: The sponsor used publicly available list prices for the treatments under evaluation, which do not account for the confidential pricing agreements negotiated by public drug plans. Consequently, the projected cost savings for pembrolizumab plus chemotherapy, which are based on the public list prices, may not be realized. Similar to the CMA discussed previously, this limitation is set to the same limitation as stated previously.
CDA-AMC was unable to address this limitation in the reanalysis.
The impact of subsequent therapy was excluded from the BIA: Inconsistent with the CMA, the sponsor did not include the impact of subsequent therapy on the budget impact model.22 The sponsor only included the cost of treatment and administration cost for the drug under review and the comparator in the first-line setting.
CDA-AMC was unable to address this limitation as the sponsor’s model did not have provisions to consider the impact of subsequent therapy in the BIA.
CDA-AMC Reanalyses of the BIA
In the absence of reliable estimates to inform the parameters of the BIA, the sponsor’s base-case assumptions were retained. CDA-AMC anticipates that the budget impact is uncertain with regard to variations in market share distribution, dosing assumptions, and RDI. This uncertainty was explored in the scenario analyses conducted by CDA-AMC, which demonstrated an increase in budget impact when market share and RDI assumptions were adjusted. Conversely, modifications to dosing assumptions resulted in greater cost savings. Further details are provided in Table 11.
Table 9: CDA-AMC Revisions to the Submitted BIA
Stepped analysis | Sponsor’s value or assumption | CDA-AMC value or assumption | ||
|---|---|---|---|---|
Pembrolizumab | Nivolumab | Pembrolizumab | Nivolumab | |
1. Pembrolizumab market share (year 1 / year 2 / year 3) | 17% / 33% / 33% | — | 17% / 40% / 40% | 83% / 60% / 60% |
2. Dosing assumptions | Fixed dosing | Fixed dosing | Weight-based dosing | Weight-based dosing |
3. RDI assumptions | 95.11% | 100% | 100% | 95% |
BIA = budget impact analysis; CDA-AMC = Canada’s Drug Agency; RDI = relative dose intensity.
The results of the CDA-AMC stepwise reanalysis are presented in summary format in Table 10, and a more detailed breakdown is presented in Table 11.
Increasing pembrolizumab plus chemotherapy's market share to 40% in years 2 and 3 led to a $2,395,163 increase in the sponsor’s budget impact, resulting in an incremental total budget impact of $1,906,961.
Implementing weight-based dosing in the BIA resulted in cost savings of $3,880,785.
Assuming an RDI of 100% for pembrolizumab and 95% for nivolumab-ipilimumab increased the total 3-year net budget impact to $1,283,564.
Table 10: Summary of the CDA-AMC Reanalyses of the BIA
Stepped analysis | Three-year total ($) |
|---|---|
Submitted base case | −488,202 |
CDA-AMC scenario 1: Increased pembrolizumab market share | 1,906,961 |
CDA-AMC scenario 2: Weight-based dosing regimen | −3,880,785 |
CDA-AMC scenario 3: RDI assumptions | 1,283,564 |
BIA = budget impact analysis; CDA-AMC = Canada’s Drug Agency; RDI = relative dose intensity.
Table 11: Detailed Breakdown of the CDA-AMC Reanalyses of the BIA
Stepped analysis | Scenario | Year 0 (current situation) ($) | Year 1 ($) | Year 2 ($) | Year 3 ($) | Three-year total ($) |
|---|---|---|---|---|---|---|
Submitted base case | Reference | 15,140,235 | 25,674,441 | 27,368,025 | 27,526,451 | 80,568,917 |
New drug | 15,140,235 | 25,493,623 | 27,090,911 | 27,496,181 | 80,080,715 | |
Budget impact | 0 | –180,818 | –277,114 | –30,270 | –488,202 | |
CDA-AMC scenario analysis: 40% pembrolizumab market share in years 2 and 3 | Reference | 15,140,235 | 25,674,441 | 27,368,025 | 27,526,451 | 80,568,917 |
New drug | 15,140,235 | 26,160,959 | 27,990,840 | 28,324,080 | 82,475,878 | |
Budget impact | 0 | 486,517 | 622,815 | 797,629 | 1,906,961 | |
CDA-AMC scenario analysis: Using weight-based dosing | Reference | 14,443,603 | 24,461,269 | 26,069,634 | 26,220,545 | 76,751,448 |
New drug | 14,443,603 | 23,948,408 | 24,462,217 | 24,460,038 | 72,870,663 | |
Budget impact | 0 | –512,861 | –1,607,418 | –1,760,506 | –3,880,785 | |
CDA-AMC scenario analysis: RDI assumption | Reference | 14,399,878 | 24,418,961 | 26,029,729 | 26,180,408 | 76,629,097 |
New drug | 14,399,878 | 24,424,004 | 26,454,693 | 27,033,964 | 77,912,661 | |
Budget impact | 0 | 5,043 | 424,965 | 853,556 | 1,283,564 |
BIA = budget impact analysis; CDA-AMC = Canada’s Drug Agency; RDI = relative dose intensity.
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.