Drugs, Health Technologies, Health Systems
Reimbursement Review
Pembrolizumab (Keytruda)
Sponsor: Merck
Therapeutic area: Unresectable or metastatic microsatellite instability-high or mismatch repair deficient solid tumours
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Ethics Review
Clinical Review
Abbreviations
AE
adverse event
AEOSI
adverse event of special interest
APaT
all participants as treated
CCRAN
Colorectal Cancer Resource & Action Network
CDA-AMC
Canada’s Drug Agency
CI
confidence interval
CNS
central nervous system
CR
complete response
CRC
colorectal cancer
dMMR
mismatch repair deficient
DOR
duration of response
ECOG PS
Eastern Cooperative Oncology Group Performance Status
EGFR
epidermal growth factor receptor
EORTC QLQ-C30
European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30
ESS
effective sample size
FOLFIRI
leucovorin calcium (folinic acid) + fluorouracil + irinotecan hydrochloride
GHS
global health status
GRADE
Grading of Recommendations Assessment, Development and Evaluation
HR
hazard ratio
HRQoL
health-related quality of life
IHC
immunohistochemistry
IPD
individual patient data
IRRDC
International Replication Repair Deficiency Consortium
ITC
indirect treatment comparison
KM
Kaplan-Meier
LS
least squares
MAIC
matching-adjusted indirect comparison
MID
minimal important difference
MMR
mismatch repair
MSI
microsatellite instability
MSI-H
microsatellite instability-high
nab
nanoparticle albumin-bound
NGS
next-generation sequencing
ORR
objective response rate
OS
overall survival
PFS
progression-free survival
PR
partial response
QoL
quality of life
RCT
randomized controlled trial
RECIST 1.1
Response Evaluation Criteria in Solid Tumours Version 1.1
SAE
serious adverse event
SD
standard deviation
SLR
systematic literature review
SOC
standard of care
TAS-102
trifluridine and tipiracil hydrochloride
TPC
treatment of physician’s choice
VEGF
vascular endothelial growth factor
WES
whole-exome sequencing
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Table 1: Background Information of Application Submitted for Review
Item | Description |
|---|---|
Drug product | Pembrolizumab (Keytruda), 100 mg/4 mL vial, solution for infusion |
Sponsor | Merck Canada Inc. |
Indication | As monotherapy for the treatment of adult and pediatric patients with unresectable or metastatic microsatellite instability-high (MSI-H) or mismatch repair deficient (dMMR) solid tumours, as determined by a validated test, that have progressed following prior treatment and who have no satisfactory alternative treatment options. |
Reimbursement request | As per indication |
Health Canada approval status | Approved |
Health Canada review pathway | Standard |
NOC date | August 29, 2024 |
dMMR = mismatch repair deficient; MSI-H = microsatellite instability-high; NOC = Notice of Compliance.
Introduction
Mismatch repair (MMR) deficiency results in an inactivation of the DNA repair system and can be caused by mutations in genes encoding proteins that are responsible for detecting and correcting errors in mismatched base pairs.1-3 Microsatellites are repetitive stretches of 1 to 6 base pairs that can result from a defective MMR system or inactivation of the MMR system.2,3 MMR deficiency can be observed by comparing the variation in length of the microsatellite in the tumour tissue versus the same patient’s healthy tissue.4 This is often termed microsatellite instability (MSI) and large variation in microsatellite length is referred to as microsatellite instability-high (MSI-H).2,4 Cancers that are MSI-H or MMR deficient (dMMR) tend to have a high tumour mutational load and are more responsive to PD-1–based immunotherapy.4 Immune checkpoint inhibitors, such as pembrolizumab, prevent tumour cells from evading the immune system; the cancer cells are then recognized by T cells and can trigger an antitumour immune response.4
MSI-H or dMMR mutations have been detected in more than 30 cancers.5-8 It was reported in a meta-analysis from 2022 that there is an estimated pooled prevalence of 2.7% for MSI-H status and 2.9% for dMMR status across different solid tumour types in adults.6 Endometrial, colorectal, small intestine, and gastric cancers showed a higher prevalence of MSI-H (8.5% to 21.9%) compared with cervical, esophageal, bladder or urothelial, lung, and skin cancers, which showed a lower prevalence of MSI-H (less than 5%).6 According to the clinical experts consulted for this review, patients with metastatic solid tumours that have confirmed MSI-H or dMMR status have inferior outcomes when treated with conventional therapies and tend to show improved outcomes with immune checkpoint inhibitors. As a group, these patients have a worse prognosis compared with those whose tumours are not MSI-H or dMMR, although prognosis varies based on tumour type.9
There is high variability in first-line treatments and the standard of care (SOC) in solid tumours expressing MSI-H or dMMR mutations. In some instances, immunotherapy has become the SOC. In patients with MSI-H or dMMR unresectable or metastatic colorectal cancer (CRC), pembrolizumab received a recommendation to reimburse as a first-line therapy and is the currently funded SOC.10 Also, pembrolizumab received a recommendation to reimburse as a second-line or later therapy in adult patients with MSI-H or dMMR unresectable or metastatic endometrial cancer whose tumours have progressed following prior therapy and who have no satisfactory alternative treatment options, and it is currently funded in most jurisdictions.11 Regardless of tumour type, patients with unresectable or metastatic MSI-H or dMMR cancers that have progressed after prior standard systemic therapy have a very poor prognosis, and the SOC for these patients is typically chemotherapy-based regimens, which provide limited clinical benefit and are associated with significant cumulative toxicity.
Pembrolizumab is a high-affinity antibody against PD-1 that reactivates tumour-specific cytotoxic T lymphocytes in the tumour microenvironment.12 Pembrolizumab is available as a solution for infusion (100 mg per 4 mL vial) that is administered as an IV infusion over 30 minutes.12,13 The recommended dosage in adult patients is either 200 mg every 3 weeks or 400 mg every 6 weeks until unacceptable toxicity or disease progression, or up to 24 months or 35 doses of 200 mg or 18 doses of 400 mg, whichever is longer, in patients without disease progression.12,13 The recommended dosage in pediatric patients is 2 mg/kg (up to a maximum of 200 mg) every 3 weeks until disease progression or unacceptable toxicity, or up to 24 months or 35 doses, whichever is longer, in patients without disease progression.12,13 In Canada, pembrolizumab has been issued market authorization to treat numerous types of cancers and the drug has been reviewed by Canada’s Drug Agency (CDA-AMC) for several other indications.
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of pembrolizumab, 100 mg per 4 mL vial solution for infusion, in the treatment of adult and pediatric patients with unresectable or metastatic MSI-H or dMMR solid tumours, as determined by a validated test, that have progressed following prior treatment and who have no satisfactory alternative treatment options.
Testing Procedure Considerations
MSI-H and dMMR status can be assessed by next-generation sequencing (NGS) and immunohistochemistry (IHC). According to the clinical experts, testing for MSI-H and dMMR status is currently part of the SOC for the most common unresectable or metastatic solid tumour types in adult patients and is not part of the SOC for any pediatric patients. Potential increases in testing requirements to determine eligibility for pembrolizumab are not anticipated to substantially impact health care resources or pose an additional burden to patients and caregivers in either adult or pediatric populations.
Perspectives of Patients, Clinicians, and Drug Programs
The information in this section is a summary of input provided by the patient and clinician groups that responded to the CDA-AMC call for input and by the clinical experts consulted for the purpose of this review.
Patient Input
Patient group input for this review was submitted by Colorectal Cancer Canada and the Colorectal Cancer Resource & Action Network (CCRAN) (the latter working in collaboration with Canadian Cancer Survivor Network, Craig’s Cause Pancreatic Cancer Society, Canadian Breast Cancer Network, and Ovarian Cancer Canada). The 2 patient groups collected information through patient and caregiver interviews and online surveys. All contributions were from adult patients and/or their caregivers and do not include the perspectives of pediatric patients.
According to the respondents, symptoms of the disease as well as the side effects of the SOC treatments they received had the greatest impact on their physical, mental, and social health. The impact of diagnosis, disease recurrence, and treatment was felt by patients’ families, friends, and communities.
The most important outcomes noted by patients and caregivers included preventing disease progression and disease recurrence, prolonging survival, having a durable response, and improving health-related quality of life (HRQoL) and symptoms.
Patients who received pembrolizumab noted many benefits, including symptom relief, quick response to treatment, minimal adverse effects, being easier to receive than conventional treatments, providing better HRQoL, and avoiding long-term toxicities associated with conventional chemotherapies.
The groups emphasized the importance of wide and equitable access to biomarker testing, treatments for those with appropriate biomarker status (i.e., MSI-H or dMMR) that go beyond tumour type, and drugs to treat rare and pediatric cancers.
Clinician Input
Input From the Clinical Experts Consulted by CDA-AMC
The clinical experts highlighted the heterogeneity and aggressive phenotype of MSI-H and dMMR solid tumours. For adult patients with MSI-H and/or dMMR metastatic cancer, there is a need for effective therapeutic options if SOC or salvage chemotherapy fails. Meanwhile, for pediatric patients, there is a general need for new treatments because the current treatment options in both the front-line and relapsed setting are limited for this population.
The clinical experts highlighted that pembrolizumab is already indicated for use as SOC in non–MSI-H and non-dMMR tumours (e.g., kidney, urothelial, gastric, lung, or biliary tract) as well as in some cancers with MSI-H and/or dMMR mutations (e.g., CRC or endometrial); thus, pembrolizumab may not be considered in later lines of therapy, depending on prior response. For the pediatric population, 1 clinical expert highlighted that, in general, pembrolizumab and immune checkpoint inhibitors are used less frequently and, thus, experience with these is limited. In adult and pediatric patients, the clinical experts highlighted that, for the indication under review, pembrolizumab is intended for use after first-line therapy specific to the solid tumour site, although the ideal sequencing of treatments is unknown. The clinical experts noted that pembrolizumab would not be used in combination with existing treatments for any indication in this setting, based on currently available data.
The experts considered the patients most likely to benefit from treatment with pembrolizumab to be those with confirmed MSI-H and/or dMMR positivity as, at this time, there are no other validated biomarkers or clinical factors that can better predict treatment benefit for these patients than MSI-H and/or dMMR status. The clinical experts highlighted that underdiagnosis due to lack of testing is a risk, particularly in rarer cancers that are not reflexively tested using NGS or IHC and in pediatric patients, among whom testing is even more limited. One expert highlighted that up to 50% of patients will not benefit from treatment despite biomarker positivity. Additionally, the experts highlighted that, particularly for rarer cancers, treatment with SOC does not result in long-term benefits. The clinical experts also noted that the patients least suitable for pembrolizumab are those who are negative for the MSI-H and/or dMMR biomarker, those who have previously received and/or whose cancer did not respond to an immune checkpoint inhibitor during a previous line of therapy, and those with severe active autoimmune disease. In the pediatric setting, 1 clinical expert highlighted that the population of patients with high-grade gliomas, for which MSI and MMR mutations are known and the testing for which is more routine, would benefit from pembrolizumab. Conversely, the prevalence of MSI-H and/or dMMR mutations appears much lower in pediatric patients; thus, testing for MSI-H and/or dMMR mutations is uncommon (except for high-grade gliomas) in pediatric patients because clinicians do not often see pediatric patients with some of the more common adult cancers that harbour MSI-H or dMMR mutations (e.g., CRC, endometrial, or pancreatic).
In both the adult and pediatric populations, the primary aim of treatment is disease control and prolongation of life, with low toxicity. The clinical experts noted that complete responses are uncommon for these patients; thus, durability and stability are also important. Per the clinical experts, treatment tolerance is generally evaluated at each appointment, with radiologic response assessments typically occurring every 2 to 3 treatment cycles or approximately every 9 to 12 weeks, depending on local protocols.
There is extensive experience with pembrolizumab in oncology. The clinical experts highlighted that treatment with pembrolizumab is generally discontinued in the event of intolerable adverse events (AEs) and clear evidence of disease progression. One concern highlighted by the clinical experts is the potential risk of premature discontinuation due to pseudoprogression; therefore, treating physicians must carefully weigh the need to identify true disease progression against the risk of prematurely halting a therapy that may still offer significant clinical benefit to patients.
As noted, immune checkpoint inhibitors have become the SOC in the treatment of many adult cancers, and there is growing experience in their use across various health care settings, including academic and community settings; however, in the pediatric setting, this is likely limited to specialist tertiary hospitals. Specialists, such as medical oncologists (as well as pediatric oncologists in the case of pediatric patients), are needed to select appropriate patients for treatment and oversee the management of therapy.
Clinician Group Input
Five clinician groups submitted input for this CDA-AMC review: the Society of Gynecologic Oncology of Canada and 4 Ontario Health (Cancer Care Ontario) Drug Advisory Committees (for genitourinary cancer, breast cancer, gynecology cancer, and central nervous system [CNS] cancer).
The input from the clinician groups aligned with that of the clinical experts consulted for this review with regard to treatment goals, the unmet needs of this patient population, assessing treatment response, the drug’s place in therapy, deciding when to discontinue treatment, the types of specialists who should manage these patients, and when patients should be treated with pembrolizumab. The clinician groups noted that access to biomarker testing varies based on tumour type and jurisdiction.
Drug Program Input
The drug programs identified implementation issues relating to relevant comparators, considerations for the initiation of therapy, considerations for the prescribing of therapy, generalizability, the funding algorithm, care provision issues, and system and economic issues. Refer to Table 5 for more details.
Clinical Evidence
Systematic Review
Description of Studies
Three studies were included in this review: KEYNOTE-158, KEYNOTE-164, and KEYNOTE-051. All were single-arm trials that evaluated pembrolizumab in different solid tumours. The KEYNOTE-158 trial enrolled adult patients with advanced MSI-H or dMMR solid tumours (non-CRC) who had disease progression following prior therapy. The KEYNOTE-164 trial enrolled adult patients with advanced MSI-H or dMMR CRC that progressed following prior therapy into 2 cohorts. Cohort A included patients who had previously been treated with 2 or more lines of SOC therapies, which had to have included fluoropyrimidine, oxaliplatin, and irinotecan. Cohort B included patients previously treated with at least 1 line of prior systemic SOC therapy. The KEYNOTE-051 trial enrolled pediatric patients with MSI-H or dMMR cancers whose disease had progressed following prior therapy. Patients who had previously received anti–PD-1, anti–PD-L1, or anti–PD-L2 drugs were excluded from all trials. The primary end point for the KEYNOTE-158 and KEYNOTE-164 trials was objective response rate (ORR), and the secondary end points were duration of response (DOR), progression-free survival (PFS), overall survival (OS), safety, and tolerability. For the KEYNOTE-051 trial, the primary end points were safety, tolerability, and ORR, and the secondary end points were DOR, PFS, and OS.
The KEYNOTE-158 trial enrolled 373 patients with a variety of MSI-H and/or dMMR solid tumours, primarily endometrial (25%), gastric (14%), and small intestine and ovarian (7% each), among other rarer cancers (26%), who had disease progression after prior treatments. The mean age was 59.2 years (standard deviation [SD] = 13.1 years), and most patients (56%) had 2 or more prior lines of therapy. The KEYNOTE-164 trial enrolled 124 patients (61 in cohort A and 63 in cohort B) with MSI-H or dMMR CRC who had received 1 or more prior lines of therapy, while the majority had received 2 or more lines (76%). The mean age of included patients was 56.1 years (SD = 14.9 years), and there were slightly more males (56%) than females (44%). The KEYNOTE-051 trial included 7 pediatric patients with a mean age of 11 years (SD = 4.3 years), mostly with brain tumours (n = 6; 86%). In total, 57% of patients had received 1 prior therapy, while 29% had received 2 or more lines of therapy.
Efficacy Results
Response Rate
Adult: In the KEYNOTE-158 trial, the median duration of follow-up was 17 months (range, 0.2 to 71.4 months). The ORR per the Response Evaluation Criteria in Solid Tumours Version 1.1 (RECIST 1.1) was 33.8% (95% confidence interval [CI], 29.0% to 38.8%). The best objective response included a complete response (CR) in 40 patients (10.7%) and a partial response (PR) in 86 patients (23.1%). The tumour-specific ORR in the KEYNOTE-158 trial showed varied response rates, ranging from 4.8% (brain) to 59.3% (small intestine) across different cancer types. Tumours with higher ORRs compared with the pooled result included endometrial, gastric, small intestine, cholangiocarcinoma, urothelial, and salivary cancers. Tumours with lower ORRs included ovarian, pancreatic, brain, sarcoma, breast, cervical neuroendocrine, prostate, adrenocortical, mesothelioma, thyroid, small cell lung, and renal cancers.
For the KEYNOTE-164 trial, the median duration of follow-up was 31.4 months (range, 0.2 to 65.2 months) for cohort A and 52.7 months (range, 0.1 to 56.6 months) for cohort B. The pooled ORR (cohorts A and B) was 33.9% (95% CI, 25.6% to 42.9%); 9.7% had a CR and 24.2% had a PR. The ORR in cohort A was 32.8% (95% CI, 21.3% to 46.0%). The objective response included a CR in 3 patients (4.9%) and a PR in 17 patients (27.9%). The ORR in cohort B was 34.9% (95% CI, 23.3% to 48.0%). The objective response included a CR in 9 patients (14.3%) and a PR in 13 patients (20.6%).
Pediatric: In the KEYNOTE-051 trial, the median duration of follow-up was 5.2 months (range, 0.3 to 28.2 months), and the ORR was 0% (95% CI, 0.0% to 41.0%). No patients experienced a CR or PR, 1 patient (14.3%) had stable disease, and 5 patients (71.4%) experienced progressive disease. Tumour-specific ORR results were not analyzed in the KEYNOTE-051 trial because all but 1 patient had brain cancer.
Duration of Response
Adult: Among the 126 patients in the KEYNOTE-158 trial with a response, the median DOR was 63.2 months (range, 1.9 to 63.9 months). Both ends of the range represent patients who were ongoing in the study without the event at the time of the data cut-off. The tumour-specific median DORs were as follows (for tumours represented by at least 10 patients): endometrial cancer (63.2 months), gastric cancer (not reached), and small intestine cancer (not reached). The DOR event-free probability at 6, 12, and 24 months was 95.2%, 88.5%, and 72.3%, respectively.
In the KEYNOTE-164 trial, among the 42 patients with a response in the overall population, the median DOR was not reached (range, 4.4 to 58.5 months among patients with a response who were ongoing in the study). The DOR event-free probability at 6, 12, and 24 months was 97.6%, 95.1%, and 92.2%, respectively. Similarly, the median DOR in cohort A (n = 20) was not reached (range, 6.2 to 58.5 months among patients with a response who were ongoing), and not reached in cohort B (n = 22) (range, 4.4 to 52.4 months among patients with a response who were ongoing).
Pediatric: DOR was not measured in the KEYNOTE-051 trial because there were no patients with a response.
Overall Survival
Adult: A total of 230 of 373 patients (61.7%) in the KEYNOTE-158 trial died, with a median OS of 19.8 months (95% CI, 14.5 to 25.8 months). The OS event-free probability at 6, 12, and 24 months was 72.1%, 58.6%, and 46.5%, respectively.
In the KEYNOTE-164 trial, 63 of 124 patients (50.8%) died, with a median OS of 36.1 months (95% CI, 24.0 months to not reached). The OS event-free probability at 12 and 24 months was 74.2% and 59.1%, respectively. In cohort A, 38 of 61 patients died (62.3%), with a median OS of 31.4 months (95% CI, 21.4 to 58.0 months). In cohort B, 31 of 63 patients died (49.2%), with a median OS of 47.0 months (95% CI, 19.2 months to not reached).
Pediatric: In the KEYNOTE-051 trial, 5 of 7 patients (71.4%) died, representing a median OS of 7.7 months (95% CI, 1.9 months to not reached). The OS event-free probability at 6, 12, and 18 months was 50.0%, 33.3%, and 33.3%, respectively.
Progression-Free Survival
Adult: A total of 275 of 373 patients (73.7%) in the KEYNOTE-158 trial experienced a PFS event, with a median PFS of 4.0 months (95% CI, 2.4 to 4.3 months). The PFS event-free probability at 6, 12, and 24 months was 43.2%, 35.1%, and 28.8%, respectively.
In the KEYNOTE-164 trial, 83 of 124 patients (66.9%) experienced a PFS event, with a median PFS of 4.0 months (95% CI, 2.1 to 7.4 months). The PFS event-free probability at 6, 12, and 24 months was 45.8%, 37.5%, and 33.8%, respectively. In cohort A, 44 of 61 patients (72.1%) had a PFS event, with a median PFS of 2.3 months (95% CI, 2.1 to 8.1 months). In cohort B, 40 of 63 patients (63.5%) had a PFS event, with a median PFS of 4.1 months (95% CI, 2.1 to 18.9 months).
Pediatric: In the KEYNOTE-051 trial, 6 of 7 patients (85.7%) experienced a PFS event, with a median PFS of 1.7 months (95% CI, 0.4 months to not reached). The PFS event-free probability at 6 months was 16.7% and at 12 months it was not estimable.
Health-Related Quality of Life
Adult: In the KEYNOTE-158 trial, the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 (EORTC QLQ-C30) global health status (GHS) and quality of life (QoL) score (ranging from 0 for worst to 100 for best) had a baseline mean of 64.40 points (SD = 20.12 points) across 364 patients. By week 9, the mean GHS and QoL score was 67.48 points (SD = 22.48 points) in 265 patients, and the least squares (LS) mean change from baseline was 3.08 points (95% CI, 0.32 to 5.84 points). A total of 57 patients (21.5%) experienced a deterioration in HRQoL at week 9. Deterioration was defined as a negative change of 10 points or more for each EORTC QLQ-C30 scale or subscale.
HRQoL was not assessed in the KEYNOTE-164 trial.
Pediatric: HRQoL was not assessed in the KEYNOTE-051 trial.
Harms Results
Adult
In the KEYNOTE-158 trial, 96% of patients experienced at least 1 AE, with the most common being diarrhea (25%), fatigue (24%), nausea (21%), asthenia (20%), vomiting (19%), and pruritus (19%). At least 1 serious adverse event (SAE) was reported in 133 out of 373 patients (36%). The SAEs reported in at least 2% of patients included sepsis (2%) and pneumonia (2%). A total of 49 of 373 patients (13%) discontinued pembrolizumab in the KEYNOTE-158 trial, and 20 patients (5.4%) died due to AEs.
In the KEYNOTE-164 trial, 100% of patients experienced AEs, with the most frequent being fatigue (34%), diarrhea (32%), nausea (31%), abdominal pain (27%), and vomiting (26%). At least 1 SAE was reported in 56 of 124 patients (45%). SAEs reported in at least 2% of patients included dyspnea (4%), sepsis (4%), abdominal pain (3%), a small intestine obstruction (3%), urinary tract infection (3%), and ileus (2%). In total, 10 of 124 patients (8%) discontinued treatment due to AEs, and 4 of 124 patients (3%) had an AE that resulted in death.
Pediatric
In the KEYNOTE-051 trial, all patients experienced at least 1 AE, with the most common being anemia (71.4%), headache (71.4%), vomiting (57.1%), decreased lymphocyte count (42.9%), pyrexia (42.9%), and rash (42.9%). At least 1 SAE was reported in 6 of 7 patients (85.7%). The most common SAE was vomiting (28.6%). A total of 2 of 7 patients (28.6%) discontinued treatment due to AEs. There were no deaths due to AEs.
Critical Appraisal
KEYNOTE-158, KEYNOTE-164, and KEYNOTE-051 are all single-arm trials, which raised several important considerations due to the lack of any relevant comparison group. Single-arm trials are inherently limited in their ability to provide causal inferences, making it difficult to distinguish between treatment effects and natural disease progression. Only ORR and DOR can be definitively attributed to the antitumour activity of pembrolizumab because a response is unlikely to occur spontaneously. This absence of a direct comparator creates challenges in interpreting time-to-event end points (PFS, OS) and HRQoL. The open-label design may also introduce a risk of performance bias, although there is no clear evidence that this was a concern in the trials. There is a risk of bias in the measurement of the outcomes, particularly HRQoL and subjective AEs, because knowledge of the intervention can impact patient expectations and perceptions about the benefits and harms of treatment. This risk of bias in the outcome assessment was mitigated for the response outcomes (PFS, ORR, DOR) which, in the KEYNOTE-158 and KEYNOTE-164 trials, were assessed by an independent review committee. OS is an objective outcome unlikely to be affected by such bias. The assessment of HRQoL in the KEYNOTE-158 trial was at high risk of bias due to missing outcome data. Despite high adherence among available patients, close to 30% of outcome data were missing at week 9. The results of the KEYNOTE-158 trial, which included adult patients with varying tumour types, showed considerable heterogeneity in response across tumour types. Many tumour types were represented by the very small number of patients (< 20). The interpretation of the potential differences in response across small samples of different cancer types is therefore challenging because these may represent either actual differences in treatment effects or natural statistical variation. The Health Canada reviewers’ report also acknowledged the variation in therapeutic benefit across tumour types, citing small sample sizes and that the numbers of patients recruited for each histology reflects the natural prevalence of the MSI-H and/or dMMR biomarker, and that enrolling a larger number of patients may not have been feasible, given the broad indication. The Health Canada reviewers’ report also noted that the use of a pooled ORR and DOR in the KEYNOTE-158 trial is reasonable for pursuing a tissue-agnostic indication.14 There was a small degree of heterogeneity across cohorts A and B in the KEYNOTE-164 trial. In the KEYNOTE-051 trial, only 7 patients were included, which limits the reliability of assessing the efficacy and safety of pembrolizumab.
In the KEYNOTE-158, KEYNOTE-164, and KEYNOTE-051 trials, patients who had previously received anti–PD-1, anti–PD-L1, or anti–PD-L2 drugs were excluded. The clinical experts consulted by CDA-AMC indicated that only a small proportion of patients in Canada would meet this eligibility criterion because most MSI-H and/or dMMR solid tumours are treated with anti–PD-1 or anti–PD-L1 drugs as SOC in earlier lines of therapy. This limits the generalizability of the trial results to the smaller population of patients with MSI-H or dMMR cancers in Canada who would not have received anti–PD-1 or anti–PD-L1 drugs in an earlier line. For cancers such as colorectal, endometrial, and non–small cell lung cancer, pembrolizumab is already used in earlier treatment stages. Additionally, other immune checkpoint inhibitors are widely used in solid tumours like gastric, mesothelioma, breast, small cell lung, and biliary tract cancers, regardless of MSI-H or dMMR status. The KEYNOTE-051 trial included only 7 patients, primarily with brain cancers, which also limits the generalizability of the findings. This small cohort is unlikely to adequately represent the broader patient population in terms of age, sex, performance status, disease stage, and other factors. Furthermore, HRQoL was not assessed in 2 trials (KEYNOTE-164 and KEYNOTE-051); thus, the generalizability of any HRQoL results to other indications or populations remains uncertain.
GRADE Summary of Findings and Certainty of the Evidence
For the pivotal studies identified in the sponsor’s systematic review, Grading of Recommendations, Assessment, Development and Evaluation (GRADE) was used to assess the certainty of the evidence for the outcomes considered most relevant to inform CDA-AMC expert committee deliberations, and a final certainty rating was determined as outlined by the GRADE Working Group.15,16 Although GRADE guidance is not available for noncomparative studies, the review team assessed pivotal single-arm trials for study limitations (which refer to internal validity or risk of bias), inconsistency across studies (or populations), indirectness, and publication bias to present these important considerations. Because the lack of a comparator arm does not allow for a conclusion to be drawn on the effect of the intervention versus any comparator, the certainty of evidence for single-arm trials starts at very low certainty with no opportunity for rating up.
Table 2 presents a GRADE summary of the findings for pembrolizumab that were assessed in the KEYNOTE-158, KEYNOTE-164, and KEYNOTE-051 trials. The selection of outcomes for GRADE assessment was based on the sponsor’s summary of clinical evidence, consultation with clinical experts, and the input received from patient and clinician groups and public drug plans. The following list of outcomes was finalized in consultation with expert committee members:
response (ORR [CR and PR], and DOR)
survival (OS and PFS)
HRQoL (EORTC QLQ-C30)
notable harms (adverse events of special interest [AEOSIs]), i.e., immune-mediated AEs and infusion-related reactions.
Table 2: GRADE Summary of Findings for Pembrolizumab for Patients With Unresectable or Metastatic MSI-H and/or dMMR Solid Tumours
Outcome and | Patients (studies), N | Effect | Certaintya | What happens |
|---|---|---|---|---|
Response (RECIST 1.1) | ||||
ORR (CR or PR) Median follow-up: 17 (range, 0.2 to 71.4) | 373 adults with mixed solid tumours (1 single-arm trial) | 33.8 per 100 (95% CI, 29.0 to 38.8 per 100) | Very lowb,c | The evidence is very uncertain about the effects of pembrolizumab on ORR vs. any comparator. |
ORR (CR or PR) Median follow-up: cohort A, 31.4 (range, 0.2 to 65.2); cohort B, 52.7 (range, 0.1 to 56.6) | 124 adults with CRC (1 single-arm trial) | 33.9 per 100 (95% CI, 25.6 to 42.9 per 100) | Very low | The evidence is very uncertain about the effects of pembrolizumab on ORR vs. any comparator. |
ORR (CR plus PR) Median follow-up: 5.2 (range, 0.3 to 28.2) | 7 children with mixed solid tumours (1 single-arm trial) | 0 per 100 (95% CI, 0 to 41.0 per 100) | Very low | The evidence is very uncertain about the effects of pembrolizumab on ORR vs. any comparator. |
CR Median follow-up: 17 (range, 0.2 to 71.4) | 373 adults with mixed solid tumours (1 single-arm trial) | 10.7 per 100 (95% CI, 7.8 to 14.3 per 100) | Very lowb,c | The evidence is very uncertain about the effects of pembrolizumab on CR vs. any comparator. |
CR Median follow-up: cohort A, 31.4 (range, 0.2 to 65.2); cohort B, 52.7 (range, 0.1 to 56.6) | 124 adults with CRC (1 single-arm trial) | 8.9 per 100 (95% CI, NR) | Very low | The evidence is very uncertain about the effects of pembrolizumab on CR vs. any comparator. |
CR Median follow-up: 5.2 (range, 0.3 to 28.2) | 7 children with mixed solid tumours (1 single-arm trial) | 0 per 100 (95% CI, 0 to 41 per 100) | Very low | The evidence is very uncertain about the effects of pembrolizumab on CR vs. any comparator. |
Duration of response among responders | ||||
DOR Median follow-up: 17 (range, 0.2 to 71.4) | 126 adults with mixed solid tumours (1 single-arm trial) | Median: 63.2 months (range, 1.9+ to 63.9+ months) Event-free probability:
| Very lowb,c | The evidence is very uncertain about the effects of pembrolizumab on DOR vs. any comparator. |
DOR Median follow-up: cohort A, 31.4 (range, 0.2 to 65.2); cohort B, 52.7 (range, 0.1 to 56.6) | 42 adults with CRC (1 single-arm trial) | Median: not reached (range, 4.4 to 58.5+ months) Event-free probability:
| Very low | The evidence is very uncertain about the effects of pembrolizumab on DOR vs. any comparator. |
DOR Median follow-up: 5.2 (range, 0.3 to 28.2) | 0 children with mixed solid tumours (1 single-arm trial) | NA | NA | There is no evidence about the effects of pembrolizumab on DOR; no patient had a response. |
OS and PFS | ||||
OS Median follow-up: 17 (range, 0.2 to 71.4) | 373 adults with mixed solid tumours (1 single-arm trial) | Median: 19.8 months (95% CI, 14.5 to 25.8 months) Event-free probability:
| Very lowb,c | The evidence is very uncertain about the effects of pembrolizumab on OS vs. any comparator. |
OS Median follow-up: cohort A, 31.4 (range, 0.2 to 65.2); cohort B, 52.7 (range, 0.1 to 56.6) | 124 adults with CRC (1 single-arm trial) | Median: 36.1 months (95% CI, 24.0 months to not estimable) Event-free probability:
| Very low | The evidence is very uncertain about the effects of pembrolizumab on OS vs. any comparator. |
OS Follow-up: not reported Median follow-up: 5.2 (range, 0.3 to 28.2) | 7 children with mixed solid tumours (1 single-arm trial) | Median: 7.7 months (95% CI, 1.9 months to not estimable) Event-free probability:
| Very low | The evidence is very uncertain about the effects of pembrolizumab on OS vs. any comparator. |
PFS Median follow-up: 17 (range, 0.2 to 71.4) | 373 adults with mixed solid tumours (1 single-arm trial) | Median: 4.0 months (95% CI, 2.4 to 4.3 months) Event-free probability:
| Very lowb,c | The evidence is very uncertain about the effects of pembrolizumab on PFS vs. any comparator. |
PFS Median follow-up: cohort A, 31.4 (range, 0.2 to 65.2); cohort B, 52.7 (range, 0.1 to 56.6) | 124 adults with CRC (1 single-arm trial) | Median: 4.0 months (95% CI, 2.1 to 7.4 months) Event-free probability:
| Very low | The evidence is very uncertain about the effects of pembrolizumab on PFS vs. any comparator. |
PFS Median follow-up: 5.2 (range, 0.3 to 28.2) | 7 children with mixed solid tumours (1 single-arm trial) | Median: 1.7 months (95% CI, 0.4 months to not estimable) Event-free probability
| Very lowb | The evidence is very uncertain about the effects of pembrolizumab on PFS vs. any comparator. |
Health-related quality of lifeb | ||||
EORTC QLQ-C30 (global QoL score), LS mean change from baseline, points (0 [worst] to 100 [best]) Follow-up: To week 9 | 364 adults with mixed solid tumours (1 single-arm trial) | 3.08 (95% CI, 0.32 to 8.84) | Very lowd | The evidence is very uncertain about the effects of pembrolizumab on EORTC QLQ-C30 (global QoL score) vs. any comparator. |
Harms | ||||
Patients with ≥ 1 AEOSI Median follow-up: 17 (range, 0.2 to 71.4) | 373 adults with mixed solid tumours (1 single-arm trial) | 22 per 100 | Very lowc | The evidence is very uncertain about the effects of pembrolizumab on AEOSIs vs. any comparator. |
Patients with ≥ 1 AEOSI Median follow-up: cohort A, 31.4 (range, 0.2 to 65.2); cohort B, 52.7 (range, 0.1 to 56.6) | 124 adults with CRC (1 single-arm trial) | 30 per 100 | Very low | The evidence is very uncertain about the effects of pembrolizumab on AEOSIs vs. any comparator. |
Patients with ≥ 1 AEOSI Median follow-up: 5.2 (range, 0.3 to 28.2) | 7 children with mixed solid tumours (1 single-arm trial) | 28.6 per 100 | Very low | The evidence is very uncertain about the effects of pembrolizumab on AEOSIs vs. any comparator. |
Patients with ≥ 1 SAE Median follow-up: 17 (range, 0.2 to 71.4) | 373 adults with mixed solid tumours (1 single-arm trial) | 36 per 100 | Very lowc | The evidence is very uncertain about the effects of pembrolizumab on SAEs vs. any comparator. |
Patients with ≥ 1 SAE Median follow-up: cohort A, 31.4 (range, 0.2 to 65.2); cohort B, 52.7 (range, 0.1 to 56.6) | 124 adults with CRC (1 single-arm trial) | 45 per 100 | Very low | The evidence is very uncertain about the effects of pembrolizumab on SAEs vs. any comparator. |
Patients with ≥ 1 SAE Median follow-up: 5.2 (range, 0.3 to 28.2) | 7 children with mixed solid tumours (1 single-arm trial) | 85.7 per 100 | Very low | The evidence is very uncertain about the effects of pembrolizumab on SAEs vs. any comparator. |
AEOSI = adverse event of special interest (immune-mediated event or infusion-related reaction); CI = confidence interval; CR = complete response; CRC = colorectal cancer; dMMR = mismatch repair deficient; DOR = duration of response; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; GRADE = Grading of Recommendations Assessment, Development and Evaluation; MSI-H = microsatellite instability-high; NA = no assessment; NR = not reported; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; PR = partial response; QoL = quality of life; RECIST 1.1 = Response Evaluation Criteria in Solid Tumours Version 1.1; SAE = serious adverse event; vs. = versus.
Note: In column 3 (effect), “+” indicates the patient was ongoing in the study without the event at the time of analysis.
aIn the absence of a comparator group, conclusions about efficacy relative to any comparator cannot be drawn and the certainty of evidence is started at “very low” and cannot be rated up.
bRated down 1 level for serious study limitations because results are based on an interim analysis. There is a risk of overestimating treatment effects.
cRated down 1 level due to inconsistency for ORR, CR, and DOR. The KEYNOTE-158 trial included a mixed solid tumour population. There was heterogeneity in the effects across different solid tumours for these outcomes; there was no subgroup information for OS, PFS, or harms available to assess these outcomes.
dHRQoL data were not reported for the KEYNOTE-164 trial (adults with CRC) and the KEYNOTE-051 trial (children with mixed solid tumours). Rated down 2 levels for study limitations due to the risk of bias in the assessment of the outcome (open-label trial with subjective assessment) and due to missing outcome data.
Source: KEYNOTE-158,17 KEYNOTE-164,18 and KEYNOTE-05119 Clinical Study Reports.
Long-Term Extension Studies
No long-term extension studies were provided by the sponsor.
Indirect Comparisons
To support the economic evaluation for tumour-agnostic submissions, the sponsor submitted several indirect treatment comparisons (ITCs), each focusing on comparing pembrolizumab with other relevant treatments in 4 different solid tumour types: colorectal, endometrial, small intestine, and gastric cancers. In the CRC ITC, pembrolizumab was compared with pooled chemotherapy and anti–vascular endothelial growth factor (VEGF) plus chemotherapy using a naive indirect comparison, and trifluridine and tipiracil hydrochloride (TAS-102) through an unanchored matching-adjusted indirect comparison (MAIC). In the endometrial cancer ITC, an unanchored MAIC was conducted to compare pembrolizumab with the treatment of physician’s choice (TPC) (doxorubicin or paclitaxel). For the small intestine cancer ITC, a naive indirect comparison was used to compare pembrolizumab with nanoparticle albumin-bound (nab)-paclitaxel. The gastric cancer ITC included a naive indirect comparison to compare pembrolizumab with leucovorin calcium (folinic acid) + fluorouracil + irinotecan hydrochloride (FOLFIRI); ramucirumab plus paclitaxel; ramucirumab monotherapy; paclitaxel; and irinotecan.
Efficacy Results
Colorectal Cancer
The colorectal ITC included 2 naive ITCs comparing pembrolizumab with chemotherapy and chemotherapy plus anti-VEGF, and 1 MAIC comparing pembrolizumab with TAS-102. Only PFS and OS results were reported. In both of the naive ITCs, the pembrolizumab group had a lower median age and fewer patients with an Eastern Cooperative Oncology Group Performance Status (ECOG PS) of 0 compared with the comparator group. In the unanchored MAIC, matching factors included age, sex, and ECOG PS.
The naive ITC for OS estimated a hazard ratio (HR) of 0.30 (95% CI, 0.24 to 0.39) when compared with chemotherapy alone, and 0.37 (95% CI, 0.29 to 0.48) when compared with chemotherapy in combination with an anti-VEGF, favouring pembrolizumab. The naive ITC for PFS estimated an HR of 0.43 (95% CI, 0.34 to 0.54) when compared with chemotherapy alone, and 0.53 (95% CI, 0.42 to 0.67) when compared with chemotherapy in combination with an anti-VEGF, favouring pembrolizumab.
In the unanchored MAIC comparing pembrolizumab with TAS-102, the estimated HR for OS was 0.21 (95% CI, 0.15 to 0.30) and, for PFS, was 0.32 (95% CI, 0.23 to 0.45), both favouring pembrolizumab.
Endometrial Cancer
For the endometrial cancer ITC, an unanchored MAIC was conducted to compare pembrolizumab with TPC (doxorubicin or paclitaxel). ORR, PFS, and OS results were reported. Matching factors included age, race, ECOG PS, number of prior lines of therapy, and histology status.
In the unanchored MAIC, the estimated response ratio was 4.27 (95% CI, 2.11 to 8.64) for ORR, favouring pembrolizumab. The estimated HR was 0.31 (95% CI, 0.19 to 0.53) for PFS and 0.24 (95% CI, 0.13 to 0.45) for OS, both favouring pembrolizumab compared with TPC. In each case, sensitivity analyses yielded results that aligned with the main analysis in both the direction and magnitude of effect.
Small Intestine Cancer
For the small intestine cancer ITC, a naive ITC was conducted to compare pembrolizumab with nab-paclitaxel. Only PFS and OS results were presented. The pembrolizumab group had a similar median age and a greater number of patients with an ECOG PS of 0 compared with the comparator group.
The naive ITC estimated an HR of 0.18 (95% CI, 0.07 to 0.45) for OS and 0.22 (95% CI, 0.09 to 0.52) for PFS, both favouring pembrolizumab.
Gastric Cancer
For the gastric cancer ITC, a naive ITC was conducted to compare pembrolizumab with FOLFIRI, ramucirumab plus paclitaxel, ramucirumab monotherapy, paclitaxel, and irinotecan. Only OS and PFS results were presented. The pembrolizumab group had a higher median age and a greater number of patients with an ECOG PS of 0 compared with all comparator groups.
For OS, the naive ITC estimated an HR of 0.43 (95% CI, 0.26 to 0.69) versus FOLFIRI, 0.35 (95% CI, 0.22 to 0.53) versus ramucirumab, 0.44 (95% CI, 0.29 to 0.66) versus ramucirumab plus paclitaxel, and 0.38 (95% CI, 0.26 to 0.56) versus irinotecan, all favouring pembrolizumab. The evidence was insufficient to demonstrate a difference between pembrolizumab and paclitaxel.
For PFS, the naive ITC estimated an HR of 0.43 (95% CI, 0.28 to 0.67) versus FOLFIRI, 0.37 (95% CI, 0.24 to 0.58) versus ramucirumab, 0.45 (95% CI, 0.31 to 0.65) versus ramucirumab plus paclitaxel, and 0.33 (95% CI, 0.23 to 0.47) versus irinotecan, all favouring pembrolizumab. The evidence was insufficient to demonstrate a difference between pembrolizumab and paclitaxel.
Harms Results
No harms were evaluated in the submitted ITCs.
Critical Appraisal
The sponsor conducted systematic literature reviews (SLRs) to identify studies for inclusion in the 4 ITCs. Although the SLRs appeared comprehensive, an a priori protocol was not provided, which prevented the evaluation of the risk of selective reporting based on the magnitude, direction, or statistical significance of the effects. The included comparator studies were deemed to be primarily at a low or unclear risk of bias. Additionally, the literature searches for colorectal, endometrial, and small intestine cancer studies were conducted between July and August 2023; it is not clear whether any new relevant studies have become available since then. Violations of the proportional hazards assumption in most comparisons further undermine the validity of the estimated HRs.
The majority of the ITCs, except for the endometrial cancer ITC, included comparator studies that did not evaluate MSI-H or dMMR status because this was infeasible. According to the clinical experts consulted by the review team, patients with dMMR or MSI-H status typically have a worse prognosis compared with those whose tumours are not MSI-H or dMMR, although prognosis varies based on tumour type. Without the dMMR or MSI-H status of patients in the comparator arms, the impact cannot be quantified. Naive indirect comparisons were used due to substantial reductions in effective sample size (ESS) when attempting to match baseline characteristics; however, such methods are highly susceptible to confounding bias from differences in patient characteristics and study methodologies. Unanchored MAICs were employed in other cases. These matched on a small number of factors. Although these factors were relevant according to the clinical experts consulted by the review team, it is unlikely that they represent all known and unknown prognostic and effect-modifying variables. As a result, there is a high risk of residual confounding. Small ESSs after matching and differences in patient characteristics, such as ECOG PS scores, reduce the reliability of the results.
The colorectal, endometrial, and gastric cancer comparisons may no longer be highly relevant due to changes in the current SOC because patients are likely to have already received immunotherapy in the first-line setting. This shift means that comparisons may not accurately reflect current patient populations or outcomes. Additionally, the analyses did not assess harms or HRQoL outcomes.
Studies Addressing Gaps in the Evidence From the Systematic Review
Description of Studies
The International Replication Repair Deficiency Consortium (IRRDC) data came from an observational, registry-based study of pediatric patients (N = 18, including 1 patient who was aged 24 years with a total of 20 tumours) with confirmed or suspected DNA replication repair deficiency.20 A patient’s cancer type was categorized as either CNS tumours or non-CNS tumours. Patients were treated with pembrolizumab between May 2015 and March 2019. Objective tumour response was the outcome of interest. The data cut-off date was March 2022.
The whole-exome sequencing (WES) data were obtained from across the clinical development program and data were evaluated from 7 trials of pembrolizumab monotherapy.20 The patients (N = 21) consisted of adults (median age was 65 years) with advanced solid tumours (gastric or gastroesophageal junction cancer, prostate cancer, cholangiocarcinoma, head and neck squamous cell carcinoma, triple-negative breast cancer) who had previously received at least 1 systemic treatment. End points of interest included ORR, DOR, PFS, and OS.
Efficacy Results
From the IRRDC dataset (pediatric patients), 17 tumours had measurable disease at baseline (3 tumours were not measurable). Based on the 17 tumours, 4 patients (23.5%) experienced objective treatment response, and 9 patients (52.9%) experienced stable disease. Four tumours (23.5%) continued to progress. Furthermore, 11 of 20 tumours (55.0%) had not progressed by 6 months and 15 of 18 patients (83.3%) were alive at 12 months.
In the WES dataset (adults), the ORR was 52.4% (95% CI, 29.8% to 74.3%). Median PFS was 17.8 months (95% CI, lower limit of 4.3 months and upper limit not reached) while the PFS rates were 56.7% and 45.9% at 12 and 36 months (there were no CIs), respectively. Median DOR and median OS were not achieved. The OS rates were 66.7% and 61.5% at 12 and 24 months (there were no CIs), respectively.
Harms Results
The collection of safety data was not a specific intent of the IRRDC study (pediatric patients); therefore, harms data are limited.21 According to the summary of clinical safety, no new safety signals were identified, and pancreatitis was the only harm that occurred in more than 1 patient (N = 2). The following harms were reported in 1 patient each: diarrhea, pneumonia, gastritis, dry skin, transient hypothyroidism, tolerable intermittent elevations in liver enzymes, skin rash, severe headaches, and seizure.
Safety data were not reported for the WES dataset (adults).
Critical Appraisal
Although the datasets provide more efficacy information on pediatric and adult populations with MSI-H cancers, they are small, noncomparative, and do not address the lack of direct or indirect evidence for pembrolizumab in this setting. Moreover, no protocols were available for review and the methods were not well described; thus, there is a risk of selective reporting. It was noted that for the IRRDC study, the treatment of patients was at the discretion of the clinical team and changes to dosages may not have been standardized across patients, making it challenging to interpret the results. Outcome measures were reviewed centrally by a blinded, independent committee, which can lower the risk of bias in the outcome measurement. The tumour types in these datasets generally cover the same types as those found in the pivotal trials (i.e., the datasets provide limited information additional to what is already available). Based on the available information, more than half of the patients had an ECOG PS of 1, which may not be representative of patients in poorer health who could receive pembrolizumab for MSI-H or dMMR tumours in clinical practice in Canada. There were few data on pediatric patients contributing to the pivotal trial evidence, and the IRRDC dataset modestly increases the amount of information available for younger patients. There was limited reporting of harms (reported only for the IRRDC dataset); assessments of HRQoL were not reported. Despite the use of real-world registry data, which can improve the generalizability of the results, the internal and external validity issues minimize the utility and applicability of the findings to clinical practice.
Conclusions
Patients and clinicians emphasized a high unmet need for new, effective treatments for patients with unresectable or metastatic MSI-H and/or dMMR solid tumours if SOC or salvage chemotherapy fails. Evidence for this review consisted of 3 pivotal trials (KEYNOTE-158, KEYNOTE-164, and KEYNOTE-051), multiple ITCs, and 2 noncomparative datasets in pediatric and adult patients with MSI-H cancer (IRRDC and WES datasets). The evidence about the efficacy of pembrolizumab in adults from 2 pivotal trials, KEYNOTE-158 and KEYNOTE-164, was very uncertain due to the single-arm design. The clinical experts consulted by the review team indicated that the response to treatment (ORR) was clinically meaningful and durable (DOR) compared with what is typically observed with SOC treatments. However, responses were heterogeneous across specific cancer types, many of which were represented by a small number of patients. Despite an inability to draw causal conclusions regarding time-to-event end points (OS and PFS), the clinical experts stated that the results were promising based on the natural history of the disease and experience in clinical practice. The results for HRQoL were inconclusive due to the open-label design and missing data. Results for the WES dataset were supportive of the pivotal trials but were affected by similar limitations.
In the pediatric population, due to the small number of patients (N = 7) enrolled in the KEYNOTE-051 trial and the single-arm design, it is difficult to ascertain the benefit of pembrolizumab in this group of patients. No patients in the KEYNOTE-051 trial had a PR or CR. Supportive evidence from the single-arm IRRDC registry study provides preliminary evidence from a small sample of patients to suggest that some pediatric patients with MSI-H or dMMR malignancies may respond to pembrolizumab. No new safety signals were identified in any of the pembrolizumab trials.
The indirect comparative evidence from the ITCs (naive indirect comparisons and unanchored MAICs) was limited to 4 cancer types in adults: colorectal, endometrial, small intestine, and gastric. The results of the ITCs suggested that PFS and OS were improved compared with SOC, which aligned with the expectations of the clinical experts consulted by the review team. However, the ITCs had significant limitations that impacted the internal validity of the findings and precluded definitive conclusions about the comparative efficacy of pembrolizumab versus SOC treatments. Additionally, immune checkpoint inhibitors are now used in the first line for colorectal, endometrial, and gastric cancers, reducing the relevance of these comparisons. No comparative safety data were provided; thus, the relative safety of pembrolizumab compared with other treatments is unknown. However, the clinical experts consulted for this review emphasized the breadth of experience with using pembrolizumab to treat other cancers, highlighting that pembrolizumab is better tolerated and has fewer and less severe side effects than conventional chemotherapy.
Introduction
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of pembrolizumab, 100 mg per 4 mL vial solution for infusion, in the treatment of adult and pediatric patients with unresectable or metastatic MSI-H or dMMR solid tumours, as determined by a validated test, whose disease has progressed following prior treatment and who have no satisfactory alternative treatment options.
Disease Background
Contents within this section have been informed by materials submitted by the sponsor and by clinical expert input. The following has been summarized and validated by the CDA-AMC review team.
Error repair of mismatched base pairs during DNA replication is an essential function for the maintenance of genomic integrity.3 The MMR deficiency results in an inactivation of the DNA repair system and can be caused by sporadic or inherited mutations in the gene (e.g., MLH1, MSH2, MSH6, and PMS2) encoding proteins that are responsible for detecting and correcting errors in mismatched base pairs or by methylation of the MLH1 promoter.1-3
Microsatellites are repetitive stretches of 1 to 6 base pairs that can result from a defective MMR system or inactivation of the MMR system.2,3 The dMMR status can be observed by comparing the variation in length of the microsatellite in a patient’s tumour tissue versus their healthy tissue.4 This is often termed MSI, and a large variation in microsatellite length is referred to as MSI-H.2,4
Mutations in the DNA result in abnormal proteins that can be neoantigens (as opposed to self-antigens).4 Cancers that are MSI-H or dMMR tend to have a high tumour mutational load and are more responsive to PD-1–based immunotherapy.4 Immune checkpoint inhibitors, such as pembrolizumab, prevent tumour cells from evading the immune system so they can be recognized by T cells and can trigger an antitumour immune response.4
MSI-H or dMMR mutations have been detected in more than 30 cancers.5-8 It was reported in a meta-analysis from 2022 that there is an estimated pooled prevalence rate of 2.7% for MSI-H status and 2.9% for dMMR status across different solid tumour types in adults.6 Endometrial, colorectal, small intestine, and gastric cancers showed a higher prevalence of MSI-H (8.5% to 21.9%), compared with cervical, esophageal, bladder or urothelial, lung, and skin cancers, which showed a lower prevalence of MSI-H (less than 5%).6 The same meta-analysis noted that, when data were available by disease stage, dMMR and MSI statuses were identified more often in early-stage disease.6 The meta-analysis did not report on solid tumours in pediatric patients due to the limited evidence available.
According to the clinical experts consulted for this review, patients with metastatic solid tumours that have confirmed MSI-H or dMMR status have inferior outcomes (e.g., ORR, PFS, and DOR) when treated with conventional therapies, and tend to show improved outcomes with immune checkpoint inhibitors. They also noted that metastatic MSI-H or dMMR tumours can be characterized by faster disease progression during or after chemotherapy treatment, resulting in shorter survival times compared with patients with the same cancer stage and intact MMR. As a group, the former patients have a worse prognosis compared with those whose tumours are not MSI-H or dMMR, although prognosis varies based on tumour type.9
Standards of Therapy
Contents within this section have been informed by materials submitted by the sponsor and clinical expert input. The following has been summarized and validated by the CDA-AMC review team.
There is high variability in first-line treatments and in the SOC in solid tumours expressing MSI-H or dMMR mutations. In some instances, immunotherapy has become the SOC, with the clinical experts consulted for this review highlighting that pembrolizumab or other immune checkpoint inhibitors are available in earlier lines of therapy for most tumour types, regardless of MSI-H or dMMR status. In patients with MSI-H or dMMR unresectable or metastatic CRC, pembrolizumab received a recommendation to reimburse as a first-line therapy and is the currently funded SOC.10 Also, pembrolizumab received a recommendation to reimburse as a second-line or later therapy in adult patients with MSI-H or dMMR unresectable or metastatic endometrial cancer whose tumours have progressed following prior therapy and who have no satisfactory alternative treatment options, and it is currently funded in most jurisdictions.11 Regardless of tumour type, patients with unresectable or metastatic MSI-H or dMMR cancers that have progressed after prior standard systemic therapy and who have no satisfactory options have a very poor prognosis, and the SOC for these patients is typically chemotherapy-based regimens, which provide limited clinical benefit and are associated with significant cumulative toxicity.
The proposed place in therapy for pembrolizumab in this submission is in accordance with the Health Canada–approved indication, i.e., as monotherapy for the treatment of adult and pediatric patients with unresectable or metastatic MSI-H or dMMR solid tumours, as determined by a validated test, that have progressed following prior treatment and who have no satisfactory alternative treatment options.22 The clinical experts consulted for this review noted that when pembrolizumab or other immune checkpoint inhibitors are available as SOC, it is unlikely that patients would receive pembrolizumab in later lines of therapy.
Drug Under Review
Pembrolizumab is a high-affinity antibody against PD-1 that exerts a dual-ligand blockade of the PD-1 pathway, including PD-L1 and PD-L2, on antigen-presenting and tumour cells.12 By inhibiting the PD-1 receptor from binding to its ligands, pembrolizumab reactivates tumour-specific cytotoxic T lymphocytes in the tumour microenvironment.12
Pembrolizumab is available as a solution for infusion (100 mg per 4 mL vial) that is administered as an IV infusion over 30 minutes.12,13 The recommended dosage in adult patients is either 200 mg every 3 weeks or 400 mg every 6 weeks until unacceptable toxicity or disease progression, or up to 24 months or 35 doses of 200 mg or 18 doses of 400 mg, whichever is longer, in patients without disease progression.12,13 The recommended dosage in pediatric patients is 2 mg/kg (up to a maximum of 200 mg) every 3 weeks until disease progression or unacceptable toxicity, or up to 24 months or 35 doses, whichever is longer, in patients without disease progression.12,13
In Canada, pembrolizumab has been issued market authorization to treat numerous types of cancers and has been reviewed by CDA-AMC for several indications. The Health Canada–approved indication and reimbursement request for this review is as monotherapy for the treatment of adult and pediatric patients with unresectable or metastatic MSI-H or dMMR solid tumours, as determined by a validated test, that have progressed following prior treatment and who have no satisfactory alternative treatment options.12 Pembrolizumab received a Notice of Compliance on August 29, 2024.
Key characteristics of pembrolizumab and other treatments available for unresectable or metastatic MSI-H or dMMR solid tumours are summarized in Table 3.
Table 3: Key Characteristics of Pembrolizumab and Other Treatments for MSI-H or dMMR Tumours
Characteristic | Mechanism of action | Indicationa | Route of administration | Recommended dosage | Serious adverse effects or safety issues |
|---|---|---|---|---|---|
Pembrolizumab | Anti-PD-1 antibody that exerts dual-ligand blocking of PD-L1 and PD-L2. | Adult and pediatric patients with unresectable or metastatic MSI-H or dMMR solid tumours, as determined by a validated test, that have progressed following prior treatment and who have no satisfactory alternative treatment options. | IV | 200 mg q.3.w. | Risk of immune-mediated adverse reactions and infusion-related reactions. |
Trifluridine and tipiracil hydrochloride | Antineoplastic thymidine-based nucleoside analogue (trifluridine) and thymidine phosphorylase inhibitor (tipiracil) that interfere with DNA function to prevent cell proliferation. | Adult patients with metastatic CRC who have been previously treated with, or are not candidates for, available therapies, including fluoropyrimidine-, oxaliplatin-, and irinotecan-based chemotherapies, anti-VEGF biological drugs and, if RAS wild-type, anti-EGFR drugs. | Oral | 35 mg/m2 b.i.d. on days 1 to 5 and days 8 to 12 of each 28-day cycle. | Risk of myelosuppression and gastrointestinal toxicity. |
Paclitaxel | Antimicrotubule drug that stabilizes microtubules inhibiting the normal reorganization of microtubules that is essential for mitotic cellular functions. | Off-label for metastatic endometrial or gastric cancer in patients whose disease has progressed after ≥ 1 prior therapy. | IV | Endometrial: 80 mg/m2 on days 1, 8, 15, and 22 of each 28-day cycle. | Risk of bone marrow suppression, sepsis, pneumonitis, and greater toxicity (in patients aged ≥ 75 years in combination with gemcitabine). |
Nab-paclitaxel | Refer to paclitaxel. Modified nab delivery system suggested to offer better PK and PD characteristics than paclitaxel.23 | Off-label for metastatic small intestine cancer in patients whose disease has progressed after prior therapy. | IV | 260 mg/m2 q.3.w. | Refer to paclitaxel. |
Doxorubicin | Thought to be related to binding DNA and inhibiting nucleic acid synthesis. | Either as monotherapy or with other approved cancer chemotherapeutic agents for neoplastic conditions such as acute lymphoblastic leukemia, acute myeloblastic leukemia, Wilms tumour, neuroblastomas, soft tissue sarcomas, bone sarcomas, breast carcinomas, gynecologic carcinomas, testicular carcinomas, bronchogenic carcinomas, Hodgkin disease, non-Hodgkin lymphoma, thyroid carcinomas, bladder carcinomas, squamous cell carcinomas of the head and neck, and gastric carcinomas. | IV | 60 mg/m2 q.3.w. | Risk of cardiotoxicity, acute infusion reactions, myelosuppression, and secondary oral neoplasms. |
Ramucirumab | Antibody that mediates VEGF-induced angiogenesis, inhibiting the proliferation and migration of human endothelial cells. | For patients with advanced or metastatic gastric cancer or gastroesophageal junction adenocarcinoma, with disease progression on or after prior platinum and fluoropyrimidine chemotherapy. | IV | 8 mg/kg q.2.w. | Risk of hemorrhage, gastrointestinal perforations, and impaired wound healing. |
Ramucirumab and paclitaxel | Ramucirumab: Refer to ramucirumab. Paclitaxel: Refer to paclitaxel. | For patients with advanced or metastatic gastric cancer or gastroesophageal junction adenocarcinoma with disease progression on or after prior platinum and fluoropyrimidine chemotherapy. | IV | Ramucirumab 8 mg/kg on days 1 and 15 and paclitaxel 80 mg/m2 on days 1, 8, and 15 of each 28-day cycle. | Refer to ramucirumab and paclitaxel. |
Irinotecan | Antineoplastic drug that binds to the topoisomerase I DNA complex and prevents relegation of single-strand breaks. | Off-label for metastatic gastric cancer in patients whose disease has progressed after prior therapy. | IV | 150 mg/m2 q.2.w. | Risk of severe diarrhea, typhlitis, ulcerative and ischemic colitis, ileus and intestinal perforation, severe myelosuppression with grade 3 or 4 neutropenia, and serious infections. |
FOLFOX | Fluorouracil: Antineoplastic activity that interferes with the processing and functions of RNA. Leucovorin: Enhances the cytotoxicity of fluoropyrimidines (fluorouracil). Oxaliplatin: Platinum-type alkylating agent inhibiting DNA replication and transcription. | Treatment of metastatic CRC. | IV | Fluorouracil 2,800 mg/m2 q.2.w. Leucovorin 400 mg/m2 q.2.w. Oxaliplatin 85 mg/m2 q.2.w. | Fluorouracil: Contraindicated in people who are pregnant or have a poor nutritional state, severely depressed bone marrow function, potentially serious infections, known hypersensitivity to 5-fluorouracil, or a known complete absence of dihydropyrimidine dehydrogenase activity. Leucovorin: Risk of diarrhea and/or stomatitis or mucositis, gastrointestinal toxicity, myelosuppression, SJS, and TEN, and may reduce the effects of antiepileptic drugs. Oxaliplatin: Risk of anaphylactic reaction; cardiovascular, gastrointestinal, hepatotoxic, musculoskeletal, and respiratory complications; myelosuppression; sepsis; and neuropathy. |
FOLFIRI | Fluorouracil and leucovorin: Refer to FOLFOX. Irinotecan: Refer to irinotecan. | Off-label for metastatic CRC or gastric cancer in patients whose disease has progressed after prior therapy. | IV | Fluorouracil 2,800 mg/m2 q.2.w. Leucovorin 400 mg/m2 q.2.w. Irinotecan 180 mg/m2 q.2.w. | Fluorouracil and leucovorin: Refer to FOLFOX. Irinotecan: Refer to irinotecan. |
Bevacizumab and chemotherapy | Bevacizumab: Antibody that selectively binds to and neutralizes the biologic activity of human VEGF, reducing the vascularization of tumours. Chemotherapy: Refer to FOLFOX. | Bevacizumab with fluoropyrimidine-based chemotherapy is indicated for first-line treatment of patients with metastatic carcinoma of the colon or rectum. Used off-label in patients with CRC whose disease has progressed after prior therapy. | IV | Bevacizumab 10 mg/kg q.2.w. Fluorouracil 1,000 mg/m2 q.2.w. Leucovorin 400 mg/m2 q.2.w. Oxaliplatin 85 mg/m2 q.2.w. | Bevacizumab: Risk of gastrointestinal perforation, impaired wound healing, and hemorrhage. |
b.i.d. = twice daily; CRC = colorectal cancer; dMMR = mismatch repair deficient; EGFR = epidermal growth factor receptor; FOLFIRI = leucovorin calcium (folinic acid) + fluorouracil + irinotecan hydrochloride; FOLFOX = leucovorin calcium (folinic acid) + fluorouracil + oxaliplatin; MSI-H = microsatellite instability-high; nab = nanoparticle albumin-bound; PD = pharmacodynamics; PK = pharmacokinetics; q.2.w. = every 2 weeks; q.3.w. = every 3 weeks; RNA = ribonucleic acid; SJS = Stevens-Johnson syndrome; TEN = toxic epidermal necrolysis; VEGF = vascular endothelial growth factor.
aHealth Canada–approved indication.
Source: Product monographs and Cancer Care Ontario.4,12,24-34
Testing Procedure Considerations
Different testing methods are available to detect MSI-H and/or dMMR status. The expression of the 4 MMR proteins is assessed by IHC,35 whereas MSI-H status can be detected by NGS36 or polymerase chain reaction. NGS can also help define tumour mutational burden, which can function as a surrogate marker for MSI-H or dMMR status.37,38 According to the clinical experts consulted for this review, both IHC and NGS should be used concurrently to determine MSI-H and/or dMMR status. Molecular profiling using NGS and/or IHC has become part of SOC for many tumour types because targeted drugs tailored to be effective in the presence of certain alterations have likewise entered the SOC.39
Both IHC and NGS testing can be conducted using archival tumour tissue collected during diagnostic biopsy or surgical resection. If archival tumour tissue is not available, NGS testing can be conducted in certain tumour types using circulating tumour DNA obtained through a peripheral blood sample.40 A clinical expert noted that, in clinical practice, around 20% to 30% of patients do not have enough archival tissue available and may require testing of circulating tumour DNA; sometimes, a fresh biopsy is required.
The review team considered the potential impacts of MSI-H and/or dMMR testing conducted to ascertain eligibility for pembrolizumab as monotherapy for the treatment of adult and pediatric patients with unresectable or metastatic MSI-H or dMMR solid tumours that have progressed following prior treatment and who have no satisfactory alternative treatment options. Considerations included impacts to health systems, patients (including families and caregivers), and costs, and the team determined that these impacts are not anticipated to be substantial compared with the current SOC. Ethical considerations related to the increase in testing requirements are detailed in the Ethics Review report. Key considerations and relevant information were sourced from materials submitted by the sponsor, input from the clinical experts (including the clinical expert panel consulted by the review team), and sources from the literature. These were validated by the review team when possible and are summarized in Table 4.
Table 4: Considerations for MSI and MMR Testing for Establishing Treatment Eligibility With Pembrolizumab in Unresectable or Metastatic MSI-H or dMMR Solid Tumours
Consideration | Criterion | Available information |
|---|---|---|
Health system–related | Number of individuals in Canada expected to require the test (e.g., per year). | Based on materials provided by the sponsor,a around 31,000 new patients with persistent, recurrent, or metastatic solid tumours would have been diagnosed in 2024.41,42 The clinical experts confirmed that most of these patients would be tested for MSI-H and/or dMMR status as part of SOC. There would be a small number of additional patients who would be anticipated to undergo testing as part of establishing treatment eligibility with pembrolizumab; however, according to the clinical experts, the increase in the testing population would not be significant. |
Availability of the testing procedure in jurisdictions across Canada. | According to the clinical experts, IHC testing for MMR and NGS testing for MSI are broadly available as the SOC for providing access to targeted immunotherapy drugs to patients across Canada, including adult and pediatric populations. | |
Testing procedure as part of routine care. | According to the clinical experts, IHC testing for MMR and NGS testing for MSI are currently performed routinely for adult patients with any solid tumour type for which immunotherapy or another targeted treatment is already the SOC for metastatic disease (e.g., ICI therapy in endometrial and colorectal cancer; PARP-inhibitor therapy in breast, ovarian, prostate, and pancreatic cancer). Genomic testing is not part of routine care in other cancers for which targeted therapy is not an option (e.g., adrenal gland, salivary gland, and thyroid cancers). If pembrolizumab is approved for these tumours, there would be an additional need for testing in these populations. Furthermore, tumours in pediatric patients do not currently undergo testing for MSI-H or dMMR status as part of routine care, and there would likewise be an increased need for testing in that population. However, these potential increases in testing requirements are not anticipated to be substantial, considering the rarity of solid tumours that have progressed following treatment options among patients in both adult and pediatric populations who are still fit for systemic therapy and who have no satisfactory alternative treatment options. | |
Repeat testing requirements. | According to the clinical experts, testing for MSI or MMR is done once before starting treatment and would not need to be repeated in most cases. | |
Impact on human health care resources due to the provision of the testing procedure. | Testing for MSI-H and/or dMMR status is currently part of the SOC for the most common unresectable or metastatic solid tumour types and is publicly funded across jurisdictions. Patients with tumours that are not subjected to reflex testing (e.g., renal cell, urothelial, gastric, and biliary tract cancer, for which ICI therapy is already given as first-line treatment) would not be required to undergo testing. According to the clinical experts, MSI and/or MMR testing to establish treatment eligibility for pembrolizumab for adult patients with unresectable or metastatic solid tumours that are less common is not anticipated to substantially impact human health care and other resources. The panel also agreed that testing pediatric patients with solid tumours is unlikely to significantly impact health care resources. | |
Patient-related | Accessibility of the testing procedure in jurisdictions across Canada. | Because testing for MSI-H and/or dMMR status is already part of the SOC for the most common unresectable or metastatic solid tumour types in Canada, no additional testing-related access implications would be anticipated as part of establishing treatment eligibility for pembrolizumab in adult and pediatric populations. |
Expected wait times for the testing procedure. | According to the clinical experts, the current turnaround time for IHC results is 1 to 2 weeks and 3 to 4 weeks for NGS results. Because testing would be conducted in most cases as part of standard care when a patient is diagnosed, they anticipate no or minimal additional impact for patients or caregivers due to wait times. | |
Burden associated with the testing procedure for patients, families, and/or caregivers. | The clinical expert panel highlighted several patient-related considerations, such as the need for an informed consent model (especially for pediatric patients), a need for genetic counselling, or a need to test family members for possible hereditary tumour syndromes. However, these are existing concerns, and any additional burden to patients, families, and/or caregivers from broadening the testing as part of establishing treatment eligibility for pembrolizumab for rare MSI-H or dMMR solid tumour types is not anticipated to be substantial. | |
Clinical | Clinical utility and validity of the testing procedure. | There is evidence to demonstrate the clinical utility and validity of IHC testing for MMR and NGS testing for MSI in patients with solid tumours.b,2,36,43-45 |
Risks of harm associated with the testing procedure. | Testing for MSI-H and/or dMMR status is currently part of the SOC for the most common unresectable or metastatic solid tumour types in adult patients. MSI and/or MMR testing is most often conducted on archival tumour tissue obtained as part of a diagnostic biopsy or surgical resection. Any additional risk of harm from broadening the testing as part of establishing treatment eligibility for pembrolizumab for rare MSI-H or dMMR solid tumour types, or eligibility in pediatric patients, is not anticipated to be substantial. | |
Cost | Projected cost of the testing procedure. | Based on materials provided by the sponsor, IHC testing for MMR is estimated to cost $150 per test.46 NGS testing is estimated to be around $1,000 for a comprehensive panel.47 Testing for MSI-H and/or dMMR status is currently part of the SOC for the most common unresectable or metastatic MSI-H or dMMR solid tumour types in adult patients. There will be additional costs associated with broadening the testing requirement in adult and pediatric populations to include tumour sites where testing is currently not done routinely, and first-line treatment with an ICI is not funded. The extent of additional testing costs would depend on how common testing is currently performed and whether IHC, NGS, or both have been used to identify an eligible patient. |
CDA-AMC = Canada’s Drug Agency; dMMR = mismatch repair deficient; ICI = immune checkpoint inhibitor; IHC = immunohistochemistry; MMR = mismatch repair; MSI = microsatellite instability; MSI-H = microsatellite instability-high; NGS = next-generation sequencing; PARP = poly(adenosine diphosphate ribose) polymerase; SOC = standard of care.
aBudget impact analysis submitted by the sponsor.
bCDA-AMC has not evaluated or critically appraised this evidence to determine its validity or reliability.
Perspectives of Patients, Clinicians, and Drug Programs
The full patient and clinician group submissions received by CDA-AMC are available in the consolidated patient and clinician group input document for this review on the project website.
Patient Group Input
This section was prepared by the CDA-AMC review team based on the input provided by 2 patient groups.
There were 2 patient group input submissions for this review, which were provided by Colorectal Cancer Canada and CCRAN (the latter working in collaboration with Canadian Cancer Survivor Network, Craig’s Cause Pancreatic Cancer Society, Canadian Breast Cancer Network, and Ovarian Cancer Canada). Colorectal Cancer Canada gathered information from an interview with 1 patient with CRC in Canada in 2024 for the current review, and through an online survey conducted in 2023 for a previous review that included responses from 15 patients with CRC and 1 caregiver. The CCRAN submission collected information from 6 patient and caregiver interviews across 4 pathologies. All contributions were from adult patients and/or their caregivers and do not include the perspectives of pediatric patients.
Patients described specific symptoms related to their cancer before beginning any treatment (e.g., weight changes, pain, fatigue, itching, difficulty sleeping and/or eating, vomiting, bloating, and jaundice). Patients stated that cancer symptoms had the greatest impact on their ability to work, exercise, and participate in social activities. After diagnosis, most patients received SOC chemotherapy for their specific type of cancer (e.g., FOLFOX [leucovorin calcium (folinic acid) + fluorouracil + oxaliplatin], FOLFIRI, capecitabine) and experienced disease progression. The most common intolerable side effects included neuropathy, nausea, and fatigue. Other side effects that impacted their HRQoL including insomnia, brain fog, digestive concerns, and hair loss. The negative effects that treatments had on their physical health resulted in detriments to their mental, social, and emotional health and prevented patients from participating in normal activities, volunteering, and working. This was further compounded for patients who lived in rural communities because travel and time away from their homes and loved ones for treatment was burdensome. The patient groups highlighted that the impact of diagnosis, disease, recurrence, and treatment went beyond the patient and was felt by their families and caregivers, friends, and communities.
The patients with experience with pembrolizumab gained access to the drug through various channels, including clinical trials, private payment, special access or compassionate access programs, or provincial funding. Treatment duration ranged from 9 to 50 cycles. The patients interviewed for the CCRAN submission had a terminal diagnosis when they started pembrolizumab and, at the time of the interview, most had no evidence of disease. While on pembrolizumab, patients indicated experiencing symptom relief and a quick and measurable response to treatment based on imaging and laboratory results. They also noted minimal side effects (fatigue, joint pain, inflammation, hypothyroidism, skin rash and dryness, and asymptomatic elevated lipase or liver enzymes), which patients considered to be an acceptable trade-off. Of those contributing to the CCRAN input, 2 of 6 patients had to withhold therapy due to elevated enzyme levels but remained asymptomatic. Patients reported various benefits of pembrolizumab, including that it was easier to receive than the prior treatments, required fewer concomitant medications (e.g., antiemetics, steroids), had a shorter infusion time, provided a better HRQoL, and left them feeling that they had avoided the long-term toxicities associated with conventional chemotherapies and the risks associated with invasive procedures.
Input from both patient groups emphasized the need for new, safe, and effective treatment options that are accessible to treat refractory, metastatic disease. According to the respondents, there were general concerns around a notable delay in diagnosis, variable access to tumour biomarker testing, and the need for patients to relocate for treatment and be away from their families and friends for extended periods of time. Furthermore, patients advocated for wide and equitable access to biomarker testing, treatments for tumours with appropriate biomarker status (i.e., MSI-H or dMMR) that go beyond tumour type and, especially, for the availability of drugs to treat rare and pediatric cancers. The most important outcomes noted by patients and caregivers included preventing disease progression and disease recurrence, prolonging survival, having a durable response, and improving HRQoL and symptoms such as pain.
Clinician Input
Input From Clinical Experts Consulted by CDA-AMC
All CDA-AMC review teams include at least 1 clinical specialist with expertise in the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). As part of the review of pembrolizumab, a panel of 3 clinical experts from across Canada was convened to characterize unmet therapeutic needs, assist in identifying and communicating situations when there are gaps in the evidence that could be addressed through the collection of additional data, promote the early identification of potential implementation challenges, gain further insight into the clinical management of patients living with a condition, and explore the potential place in therapy of the drug (e.g., potential reimbursement conditions). A summary of this panel discussion follows.
Unmet Needs
MSI-H and dMMR solid tumours are a diverse and heterogenous group of cancers that typically have a more aggressive phenotype and a reduced sensitivity to SOC chemotherapeutic agents. For adult patients with MSI-H and/or dMMR metastatic cancer, there is a need for effective therapeutic options if SOC or salvage chemotherapy fails. Meanwhile, for pediatric patients, there is a general need for new treatments because the current treatment options in both the front-line and relapsed setting are limited for this population (for example, pediatric high-grade glioma). The clinical experts highlighted that pembrolizumab has the potential to address this unmet need by providing an efficacious treatment option for this niche population.
Place in Therapy
The clinical experts highlighted the variability in treatment options and sequencing, depending on tumour site and diagnosis. In adult and pediatric patients, the clinical experts highlighted that, for the indication under review, pembrolizumab is intended for use after first-line therapy specific to the solid tumour site, although the ideal sequencing of treatments is unknown. The clinical experts highlighted that pembrolizumab is already indicated for use as SOC in non–MSI-H and/or non-dMMR tumours (e.g., kidney, urothelial, gastric, lung, biliary tract) and in some cancers with MSI-H and/or dMMR mutations (e.g., CRC, endometrial); thus, pembrolizumab may not be considered in later lines of therapy, depending on prior response.
For the pediatric population, 1 clinical expert highlighted that, in general, pembrolizumab and immune checkpoint inhibitors are used less frequently and, thus, experience with these is limited (except in specific subpopulations such as Hodgkin lymphoma). However, it was noted that therapies that are proven safe and effective in the pediatric population would be used as indicated, and access to such therapies is important, given the lack of available treatments, particularly in the relapsed setting.
The clinical experts noted that pembrolizumab would not be used in combination with existing treatments for any indication in this setting based on currently available data.
Patient Population
MSI-H and/or dMMR mutations are present across a broad range of cancer types, occurring in both common and rarer cancers. As previously noted, hypermutated tumours are generally more aggressive and do not often respond to SOC treatments. Per the clinical experts, this represents a population of patients currently in need of new treatments because the options are limited and of limited effectiveness. The clinical experts highlighted that underdiagnosis due to lack of testing is a risk, particularly in rarer cancers that are not reflexively tested using NGS or IHC, or in pediatric patients, among whom testing is even more limited.
The experts considered that the patients most likely to benefit from treatment with pembrolizumab would be those with confirmed MSI-H and/or dMMR positivity because, at this time, there are no other validated biomarkers or clinical factors that can better predict treatment benefit for these patients than MSI-H and/or dMMR status. One expert highlighted that up to 50% of patients will not benefit from treatment despite biomarker positivity. Additionally, the experts highlighted that, particularly for rarer cancers, treatment with SOC does not result in long-term benefits.
The clinical experts also highlighted that the patients least suitable for pembrolizumab are those who are negative for the MSI-H and/or dMMR biomarker, those who have previously received and/or did not respond to an immune checkpoint inhibitor during a previous line of therapy, and those with severe active autoimmune disease. However, the experts noted that in the case of certain, well-controlled autoimmune diseases, pembrolizumab may be used, but this would be decided in discussion with patients (and caregivers).
In the pediatric setting, 1 clinical expert highlighted that the population of patients with high-grade gliomas would benefit from pembrolizumab because such cancers are known to potentially have MSI and MMR mutations and, thus, testing for these biomarkers is more routine. Conversely, the prevalence of MSI-H and dMMR mutations appears much lower in pediatric patients; thus, testing for these mutations is uncommon (except for high-grade gliomas) because clinicians do not often see pediatric patients with some of the more common adult cancers that harbour MSI-H and/or dMMR mutations (e.g., CRC, endometrial, pancreatic). It was also noted that classic MSI testing based on a limited number of loci may not always identify patients, such as those with constitutional dMMR mutations, who nevertheless have significant MSI (albeit at other loci).
Assessing the Response to Treatment
Pembrolizumab has been available as a treatment in multiple cancers for many years, and the clinical experts noted that it is generally well tolerated. The primary aim of treatment in the spectrum of MSI-H and/or dMMR cancers may vary but, generally, disease control and prolongation of life with reduced toxicity are the most important goals of treatment in both the adult and pediatric populations.
The clinical experts noted that current clinical trials aim to address important outcomes that are assessed in clinical practice. These outcomes generally include objective response, disease stability, DOR, and HRQoL. The clinical experts noted that CRs are uncommon for these patients; thus, durability and stability are also important. Standard imaging tests (CT, MRI, PET, and so forth) are generally used to measure treatment response. Per the clinical experts, treatment tolerance is usually evaluated at each appointment, with radiologic response assessments typically occurring every 2 to 3 treatment cycles or approximately every 9 to 12 weeks, depending on local protocols.
Discontinuing Treatment
The clinical experts referred to several situations in which treatment with pembrolizumab may be discontinued, including intolerable AEs and clear evidence of disease progression (e.g., clinical [worsening of symptoms] or radiographic evidence). As previously noted, there is extensive experience with pembrolizumab in oncology. The clinical experts highlighted that immune-related AEs with pembrolizumab are generally mild and manageable with treatment interruption, symptomatic measures, or medical therapy (e.g., topical or oral steroids). However, in the case of severe immune-related AEs, pembrolizumab should be discontinued. One expert highlighted that in cases of oligometastatic progression, when progression is limited to 1 or 2 lesions, local therapies such as stereotactic body radiation therapy may be employed to treat the progressing lesions while continuing immune checkpoint therapy. Ultimately, the decision to discontinue treatment must carefully weigh the need to identify true disease progression against the risk of prematurely halting a therapy that may still offer significant clinical benefit to patients.
One additional concern highlighted by the clinical experts is the potential risk of premature discontinuation due to pseudoprogression. Pseudoprogression has been shown to occur with the use of immune checkpoint inhibitors due to immune infiltration that presents as disease progression on imaging. However, patients may continue to improve clinically or demonstrate a late response; thus, premature discontinuation is a risk that must be considered.
Prescribing Considerations
As noted, immune checkpoint inhibitors have become the SOC in the treatment of many adult cancers, and there is growing experience in their use across various health care settings, including academic and community settings; however, in the pediatric setting, this is likely limited to specialist tertiary hospitals.
Specialists, such as medical oncologists (as well as pediatric oncologists in the case of pediatric patients), are needed to select appropriate patients for treatment and oversee the management of therapy. This includes monitoring side effects, managing toxicities, and determining when to continue or discontinue treatment. The clinical experts noted that while specialists play a key role in these decisions, the actual delivery and routine monitoring of the treatment is currently handled by other health care professionals, such as general practitioners, especially in community hospitals and rural facilities, with proper guidance.
Clinician Group Input
This section was prepared by the CDA-AMC review team based on the input provided by 5 clinician groups.
Five clinician groups submitted input for this CDA-AMC review: the Society of Gynecologic Oncology of Canada and 4 Ontario Health (Cancer Care Ontario) Drug Advisory Committees (for genitourinary cancer, breast cancer, gynecology cancer, and CNS cancer). The Society of Gynecologic Oncology of Canada consists of health care professionals involved in the treatment and prevention of gynecologic cancer. Information for the Society of Gynecologic Oncology of Canada’s submission was based on completed and published clinical trials as well as the expert opinion of the physician members of the organization’s board of directors. The 4 Ontario Health Drug Advisory Committees, which provide timely evidence-based clinical and health system guidance on drug-related issues, gathered information for the submissions via email, videoconference, and published literature.
According to the 5 clinician groups, the most important goals of treatment include prolonging life, delaying disease progression, reducing the severity of cancer-related symptoms, improving HRQoL, and minimizing treatment-related toxicities and adverse effects. For patients with recurrent cancer, there is a lack of safe and effective treatment options and therapy is often palliative in nature. Although treatments for recurrent disease are available, prognoses remain poor because many treatments have not been shown to improve OS or disease-related symptoms and they are often toxic.
According to the clinician groups, patients whose disease has progressed on prior therapy and who have confirmed MSI-H or dMMR tumours could receive pembrolizumab monotherapy if they have not previously received the drug in the metastatic or unresectable setting. Based on input from the Society of Gynecologic Oncology of Canada, patients can be identified by IHC assessment of primary tissue for dMMR status, highlighting that testing is well validated in this setting and can be requested on an as-needed basis for patients with advanced or recurrent disease, and that misdiagnosis is rare. However, the breast cancer Drug Advisory Committee stated that MSI-H or dMMR testing is not standard for breast cancer in Ontario. The clinician groups highlighted that the patients who would not receive pembrolizumab are those with poor performance status, at risk of significant toxicity, or who have contraindications to immunotherapy.
Treatment response is assessed based on the patient’s symptoms, a clinical examination, a tumour assessment by diagnostic imaging (CT or MRI), or tumour markers as determined by the treating physician. Symptoms and a clinical examination are completed before each treatment cycle, while diagnostic imaging is typically performed every 2 to 3 cycles (every 6 to 9 weeks). According to some clinician groups, a clinically meaningful response includes prolonged survival, maintaining radiographic disease control (i.e., tumour response or stabilization) with good treatment tolerance, and stable or improving symptoms (e.g., symptoms related to pain, vomiting, or functional status).
In line with the clinical experts consulted for this review, the CNS Cancer Drug Advisory Committee cautioned against premature discontinuation based on pseudoprogression. Patients with clinically stable disease would continue treatment; however, repeat imaging that confirms ongoing disease progression would warrant treatment discontinuation. For immune-related toxicities, treatment should be withheld and managed as per standard guidelines and, if the event has resolved, treatment could be reinitiated at the physician’s discretion; however, grade 4 toxicity would require discontinuation. Contraindication to immunotherapy, significant drug intolerance, and patient choice are other reasons for stopping the drug.
The clinician groups and the clinical experts consulted for this review agreed that patients should be managed at cancer care centres (e.g., hospital outpatient settings, tertiary cancer care centres, community satellite clinics) by oncologists with expertise in treating advanced disease, using systemic therapies, and managing immune-related AEs.
Drug Program Input
The drug programs provide input on each drug being reviewed through CDA-AMC reimbursement review processes by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CDA-AMC are summarized in Table 5.
Table 5: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Relevant comparators | |
The included studies (KEYNOTE-164, KEYNOTE-158, KEYNOTE-151) did not have active comparator treatments and included only cohorts that received pembrolizumab monotherapy. The KEYNOTE-164 study included patients with CRC. Later-line treatment options for this population can include:
The KEYNOTE-158 study included several tumour-type cohorts that have a broad range of available treatment options (e.g., endometrial cancer, small intestinal cancer, gastric cancer). In endometrial cancer, later-line treatment options include:
In small intestinal cancer, later-line treatment options include:
In gastric cancer, later-line treatment options include:
The KEYNOTE-051 study is an ongoing trial designed to establish pediatric dosing and tolerability for pembrolizumab. All 7 patients enrolled (all of whom have dMMR and/or MSI-H mutations) received pembrolizumab monotherapy. How does pembrolizumab monotherapy compare with existing later-line therapies in other indications? Would all solid tumour types with MSI-H or dMMR mutation be eligible for treatment for this indication? | The clinical experts indicated that yes, all tumour types with MSI-H and/or dMMR mutation should be eligible for treatment with pembrolizumab. The clinical experts highlighted that although there was no formal comparator in the available evidence, the results from the sponsor-submitted studies as well as other studies have demonstrated that pembrolizumab is associated with a good response rate and a good duration of response versus historical treatments. However, the clinical experts acknowledged the limitations in combining very different diseases and further highlighted that, in general, the results with SOC or conventional chemotherapy are underwhelming. |
Considerations for initiation of therapy | |
In KEYNOTE-164, patients in cohort A received 2 or more prior lines of therapy and patients in cohort B received 1 or more prior lines of therapy. In KEYNOTE-158, patients had to have received at least 1 prior line of therapy, except patients in cohort K (patients with CRC) who had to have received 2 prior lines of therapy. In KEYNOTE-051, pediatric patients could have had any number of prior therapies. How many lines of prior therapy should patients receive before pembrolizumab monotherapy? | The clinical experts noted that in line with the Health Canada indication, reimbursement request, and trial populations, at least 1 line of prior therapy would be required before initiating pembrolizumab monotherapy. |
Should patients who complete 2 years of treatment and experience disease progression and/or recurrence after pembrolizumab treatment be eligible for up to 1 year (17 cycles) of pembrolizumab re-treatment? | The clinical experts stated that rechallenging with a therapy proven to be previously highly effective is routine in oncology and should be considered standard in this setting as well. They also highlighted that most trials and health jurisdictions are now routinely permitting rechallenge at progression. Conversely, the clinical experts noted that in cancers for which pembrolizumab is already first-line or second-line SOC, if a patient’s disease did not respond to treatment with pembrolizumab, it should not be rechallenged later. |
Would patients with CNS metastases be eligible for pembrolizumab monotherapy? | The clinical experts stated that patients with CNS metastases could be eligible for pembrolizumab if or once their CNS metastases were considered clinically stable or managed. |
Pembrolizumab monotherapy was previously reviewed by CDA-AMC in patients with unresectable or metastatic MSI-H or dMMR endometrial cancer whose tumours have progressed following prior therapy and who have no satisfactory alternative treatment options. | Comment from drug plans for pERC consideration. |
Considerations for prescribing of therapy | |
For consistency, jurisdictions would plan on implementing pembrolizumab as weight-based dosing up to a cap, e.g., 2 mg/kg every 3 weeks to a maximum dose of 200 mg (in adult and pediatric patients) or 4 mg/kg every 6 weeks to a maximum of 400 mg (in adult patients only), similar to other indications. | Comment from drug plans for pERC consideration. |
Generalizability | |
Should patients with an ECOG PS of 2 or greater be eligible? | According to the clinical experts, patients with an ECOG PS of 0 to 2 would be considered eligible for treatment with pembrolizumab provided they were able to tolerate therapy. The experts noted that, situationally, patients with an ECOG PS of 3 might be considered eligible. For example, if they were young without comorbidities and/or they were experiencing cancer-related symptoms that might be alleviated with other treatments or local management, pembrolizumab might be considered. However, the clinical experts noted that ECOG PS is not used in the pediatric population, which would be assessed with another adequate performance score. |
Should patients with ampullary cancer, sarcomas, or mesenchymal tumours be eligible? | Despite the exclusion of these patients from the trials, the clinical experts highlighted that if the MSI-H and/or dMMR biomarker is present in these patients, then they should be eligible for treatment with pembrolizumab. The clinical experts also noted that sarcomas represent a larger proportion of pediatric solid tumours. |
Should patients actively on alternative later-line therapies be eligible to switch to pembrolizumab monotherapy? | The clinical experts suggested that patients who are doing well on current treatment should not be switched. |
Funding algorithm | |
Pembrolizumab monotherapy is currently funded by most jurisdictions as first-line therapy in dMMR and/or MSI-H CRC. Patients in the KEYNOTE-164 trial were excluded if they had received prior anti–PD-1, anti–PD-L1, or anti–PD-L2 therapy. Should patients who have previously received prior anti–PD-1, anti–PD-L1, or anti–PD-L2 therapy be eligible for pembrolizumab? | If a patient’s disease progressed following treatment with immune checkpoint inhibitor therapy, they would not be eligible for re-treatment with pembrolizumab. |
Care provision issues | |
Currently testing for MSI-H and/or dMMR mutations is in place for unresectable or metastatic CRC and endometrial cancers. In the KEYNOTE-158 study, cohorts A through J completed PCR-based central testing evaluating the 5 mononucleotide loci (BAT25, BAT26, NR21, NR24, Mono27) to retrospectively identify patients enrolled with MSI-H and/or dMMR tumours while testing of cohort K (patients with CRC) was performed locally. In clinical practice, how should MSI-H and dMMR testing be conducted for all patient populations when determining eligibility? | MSI-H and/or dMMR testing would be conducted using locally funded and standardized testing as available, which generally includes NGS, PCR, or IHC. While these tests are adequate for identifying this biomarker, IHC tends to be more readily accessible across regions (i.e., in community and hospital settings). However, the clinical experts also noted that the standard adult MSI panel is known to be inaccurate in pediatric populations; thus, they felt there should be flexibility in the type of tests conducted to determine biomarker status. |
System and economic issues | |
Confidential prices exist for pembrolizumab, bevacizumab, encorafenib, panitumumab, ramucirumab, and trifluridine plus tipiracil hydrochloride. | Comment from drug plans for pERC consideration. |
CDA-AMC = Canada’s Drug Agency; CNS = central nervous system; CRC = colorectal cancer; dMMR = mismatch repair deficient; ECOG PS = Eastern Cooperative Oncology Group Performance Status; EGFRi = epidermal growth factor receptor inhibitor; IHC = immunohistochemistry; MSI = microsatellite instability; MSI-H = microsatellite instability-high; NGS = next-generation sequencing; PCR = polymerase chain reaction; pERC = pan-Canadian Oncology Drug Review Expert Review Committee; SOC = standard of care; VEGF = vascular endothelial growth factor.
Clinical Evidence
The objective of this Clinical Review report is to review and critically appraise the clinical evidence submitted by the sponsor on the beneficial and harmful effects of pembrolizumab 200 mg IV or pembrolizumab 2 mg/kg IV in the treatment of patients with unresectable or metastatic MSI-H or dMMR solid tumours, as determined by a validated test, that have progressed following prior treatment and who have no satisfactory alternative treatment options. The focus will be placed on comparing pembrolizumab with relevant comparators and identifying gaps in the current evidence.
A summary of the clinical evidence included by the sponsor in the review of pembrolizumab is presented in 4 sections, with a critical appraisal of the evidence included at the end of each section. The first section, the systematic review, includes pivotal studies and randomized controlled trials (RCTs) that were selected according to the sponsor’s systematic review protocol. The CDA-AMC assessment of the certainty of the evidence in this first section using the GRADE approach follows the critical appraisal of the evidence. The second section would include sponsor-submitted long-term extension studies; however, none were submitted. The third section includes indirect evidence from the sponsor. The fourth section includes additional studies that were considered by the sponsor to address important gaps in the systematic review evidence.
Included Studies
Clinical evidence from the following is included in the CDA-AMC review and appraised in this document:
3 pivotal studies identified in the systematic review
ITCs for 4 tumour types (CRC, endometrial cancer, small intestine cancer, and gastric cancer)
2 additional studies addressing gaps in the evidence.
Systematic Review
Contents within this section have been informed by materials submitted by the sponsor. The following has been summarized and validated by the CDA-AMC review team.
Description of Studies
Three clinical trials with evidence relevant to the targeted reimbursement request were included in this review: KEYNOTE-158,48 KEYNOTE-164,49 and KEYNOTE-051.19
KEYNOTE-158 Trial
KEYNOTE-158 is an ongoing, single-arm, open-label, phase II basket trial that evaluated pembrolizumab monotherapy in adult patients with advanced (unresectable and/or metastatic) MSI-H solid tumours that have progressed on SOC therapy. Patients received pembrolizumab 200 mg intravenously every 3 weeks until progressive disease, unacceptable toxicity, or an intercurrent illness that prevents further administration of treatment. The primary end point was ORR and the secondary end points were DOR, PFS, OS, safety, and tolerability. Patients were enrolled across 60 centres in 18 countries (included 16 patients from 2 sites in Quebec and Ontario, Canada). A total of 373 patients with MSI-H and/or dMMR cancers were assessed in the KEYNOTE-158 trial.48 The database cut-off for the data presented herein was January 12, 2022.
KEYNOTE-164 Trial
KEYNOTE-164 is a single-arm, open-label, phase II trial that evaluated pembrolizumab in adult patients with locally advanced unresectable or metastatic (stage IV) dMMR or MSI-H CRC whose tumours have progressed on SOC therapy. The KEYNOTE-164 trial included patients in 2 cohorts, cohort A and cohort B, all of whom had received prior standard treatments. For cohort A, patients had to have been treated with at least 2 lines of SOC therapies that must have included fluoropyrimidine, oxaliplatin, and irinotecan. For cohort B, patients were required to have had at least 1 line of systemic SOC, including fluoropyrimidine plus oxaliplatin or fluoropyrimidine plus irinotecan, with or without an anti-VEGF or anti-epidermal growth factor receptor (EGFR) monoclonal antibody. All patients received pembrolizumab 200 mg intravenously every 3 weeks until progressive disease, unacceptable toxicity, or an intercurrent illness that prevents further administration of treatment. The primary end point was ORR and the secondary end points were DOR, PFS, OS, safety, and tolerability. Patients were enrolled across 34 centres in 10 countries (included 5 patients from 1 site in Quebec, Canada). A total of 124 patients were assessed in the KEYNOTE-164 trial.49 The database cut-off for the data presented herein was February 19, 2021.
KEYNOTE-051 Trial
The KEYNOTE-051 trial is an ongoing, single-arm, open-label, phase I and II basket trial that evaluated pembrolizumab in pediatric patients with MSI-H or dMMR cancers that has progressed on SOC therapy.50 Patients received pembrolizumab 2 mg/kg intravenously every 3 weeks for 35 cycles (approximately 24 months). The primary end points were safety, tolerability, and ORR, and the secondary end points were DOR, PFS, and OS. A total of 7 patients were included in the MSI-H cancer cohort in the KEYNOTE-051 trial.19 Patients were enrolled from 58 centres across 12 countries, including 2 sites in Canada. However, it is unclear from which sites the 7 patients were evaluated. The database cut-off for the data presented herein was January 18, 2022.
Table 6: Details of Sponsor Studies Included in the Systematic Review
Detail | KEYNOTE-158 trial | KEYNOTE-164 trial | KEYNOTE-051 trial |
|---|---|---|---|
Designs and populations | |||
Study design | Phase II single-arm basket trial. | Phase II single-arm 2-cohort trial. | Phase I and II single-arm basket trial |
Locations | The study was conducted at 60 centres in 18 countries (Australia, Brazil, Canada, Colombia, Denmark, France, Germany, Israel, Italy, Japan, Mexico, Netherlands, Norway, Republic of Korea, Russian Federation, South Africa, Spain, and US). | The study was conducted at 34 centres in 10 countries (locations not reported). | The study was conducted at 58 centres in 12 countries (Australia, Brazil, Canada, France, Germany, Israel, Italy, New Zealand, South Korea, Sweden, UK, and US). |
Patient enrolment dates | Start date: December 23, 2015 End date: study is ongoing Database cut-off date: January 12, 2022 | Start date: September 14, 2015 End date: February 19, 2021 Database cut-off date: February 19, 2021 | Start date: March 23, 2015 End date: study is ongoing Database cut-off date: January 18, 2022 |
Enrolled (N) | A total of 373 patients were enrolled in cohorts A to J (not included in this review), which were tumour-specific cohorts (anal, biliary, neuroendocrine, endometrial, cervical, vulvar, small cell lung, mesothelioma, thyroid, and salivary gland). Only patients with MSI-H cancers from these cohorts are included in the sponsor’s submission, plus patients in cohort K (patients with MSI-H and/or dMMR solid tumours). | 124 (cohort A + B). | 7 (MSI-H cancer cohort). |
Inclusion criteria |
|
|
|
Exclusion criteria |
|
|
|
Drugs | |||
Intervention | Pembrolizumab 200 mg IV q.3.w. | Pembrolizumab 200 mg IV q.3.w. | Pembrolizumab 2 mg/kg (up to a maximum of 200 mg) q.3.w. for 35 cycles (dose of 2 mg/kg for phase II established in phase I). |
Comparator | No comparator. | No comparator. | No comparator. |
Study duration | |||
Screening phase | Approximately 28 days before the first doses of study treatment. | Approximately 28 days before the first doses of study treatment. | Approximately 28 days before the first doses of study treatment. |
Treatment phase | Up to 35 cycles (approximately 24 months) or until disease progression, unacceptable toxicity, investigator decision, withdrawal of consent, or other reasons. | Up to 35 cycles (approximately 24 months) or until disease progression, unacceptable toxicity, investigator decision, withdrawal of consent, or other reasons. | Up to 35 cycles (approximately 24 months) or until disease progression, unacceptable toxicity, investigator decision, withdrawal of consent, or an intercurrent illness that prevents further administration of treatment, or other reasons. |
Follow-up phase | Follow-up: Every 9 weeks by radiologic imaging to monitor disease status until start of new anticancer therapy, disease progression, death, withdrawal of consent, pregnancy, end of study or, if the participant begins re-treatment with pembrolizumab, follow-up for the first year and then every 12 weeks. Survival follow-up: Every 12 weeks to assess for survival status until death, explicit withdrawal of consent for survival follow-up, or the end of the study, whichever occurs first. Safety follow-up: Approximately 30 days after the last dose of the study intervention. HRQoL follow-up: Questionnaires were administered at cycles 1, 2, 3, 4, 7, 10, 14, and every fourth cycle thereafter until disease progression or treatment discontinuation, and approximately 30 days after treatment discontinuation. | Follow-up: Every 9 weeks by radiologic imaging to monitor disease status until start of new anticancer therapy, disease progression, death, withdrawal of consent, pregnancy, end of study or, if the participant begins re-treatment with pembrolizumab, follow-up for the first year and then every 12 weeks. Survival follow-up: Every 8 weeks to assess for survival status until death, explicit withdrawal of consent for survival follow-up, or the end of the study, whichever occurs first. Safety follow-up: Approximately 30 days after the last dose of study intervention. | Follow-up: Every 8 weeks (56 days ± 7 days) by radiologic imaging to monitor disease status until start of new anticancer therapy, disease progression, death, withdrawal of consent, pregnancy, end of study, or if the participant begins re-treatment with pembrolizumab. Survival follow-up: Every 12 weeks to assess for survival status until death, explicit withdrawal of consent for survival follow-up, or the end of the study, whichever occurs first. Safety follow-up: Approximately 30 days after the last dose of study intervention. |
Outcomes | |||
Primary end point | ORR per RECIST 1.1 by IRC. | ORR per RECIST 1.1 by IRC. | Phase I: Dose finding. Phase II: Safety, tolerability, and ORR per RECIST 1.1 or INRC by investigator. |
Secondary and exploratory end points | Secondary: DOR, PFS, OS, safety, and tolerability. Exploratory: HRQoL (EORTC QLQ-C30). | Secondary: DOR, PFS, OS, safety, and tolerability. Exploratory: None relevant. | Secondary: DOR, PFS, and OS. Exploratory: None relevant. |
Publication status | |||
Publications | Marabelle et al. (2020),48 Maio et al. (2022).51-53 NCT02628067.33 | Le et al. (2020),49 Le et al. (2021),54 Le et al. (2023).55 NCT02460198.33 | No publication on the MSI-H/dMMR cohort. Geoerger et al. (2020).56 NCT02332668.33 |
AE = adverse event; CNS = central nervous system; CRC = colorectal cancer; dMMR = mismatch repair deficient; DOR = duration of response; ECOG PS = Eastern Cooperative Oncology Group Performance Status; EGFR = epidermal growth factor receptor; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; HRQoL = health-related quality of life; INRC = International Neuroblastoma Response Criteria; IRC = independent review committee; mAb = monoclonal antibody; MSI = microsatellite instability; MSI-H = microsatellite instability-high; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; q.3.w. = every 3 weeks; RECIST 1.1 = Response Evaluation Criteria in Solid Tumours Version 1.1; SOC = standard of care; VEGF = vascular endothelial growth factor.
Sources: Marabelle et al. (2020),48 Maio et al. (2022),51-53 Le et al. (2020),49 Le et al. (2021),54 Le et al. (2023),55 Geoerger et al. (2020),56 sponsor’s clinical summary for Keytruda for MSI-H,13 clinicaltrials.gov,33 and Clinical Study Reports for the KEYNOTE-158,17 KEYNOTE-051,19 and KEYNOTE-16418 trials.
Populations
Inclusion and Exclusion Criteria
The eligibility criteria for the 3 KEYNOTE trials included in this review are summarized in Table 6.
The KEYNOTE-158 trial enrolled adult patients with advanced MSI-H or dMMR non-CRC cancers who had disease progression following prior standard first-line therapy. Patients were enrolled into cohorts A through J, depending on their cancer type (anal, biliary, neuroendocrine, endometrial, cervical, vulvar, small cell lung, mesothelioma, thyroid, or salivary gland); MSI-H status was retrospectively tested in these patients. Cohort K prospectively included patients with any solid tumour (except CRC) that was MSI-H. Only patients with MSI-H, non-CRC solid tumours (cohorts A through K) were of interest to this review. Patients had to have adequate organ function and an ECOG PS score of 0 or 1, and had to provide an archival or newly obtained tissue sample from a tumour lesion that had not been previously irradiated. Patients who had previously received anti–PD-1, anti–PD-L1, or anti–PD-L2 drugs were excluded.
The KEYNOTE-164 trial enrolled adult patients with advanced MSI-H or dMMR CRC into either cohort A, if they had been previously treated with at least 2 lines of SOC therapies that must have included fluoropyrimidine, oxaliplatin, and irinotecan, or cohort B, if they had been previously treated with at least 1 line of systemic SOC therapy (fluoropyrimidine and oxaliplatin or fluoropyrimidine plus irinotecan, with or without anti-VEGF or anti-EGFR monoclonal antibody). Patients had to have adequate organ function and an ECOG PS score of 0 or 1, and had to provide an evaluable tissue sample for biomarker analysis taken from a tumour lesion that had not been previously irradiated. Patients who had previously received anti–PD-1, anti–PD-L1, or anti–PD-L2 drugs were excluded.
The KEYNOTE-051 trial enrolled pediatric patients aged 6 months to 18 years with MSI-H or dMMR cancers who had disease progression following prior therapy. Patients had to have adequate organ function and an ECOG PS score of 0 or 1, and had to provide an archival or newly obtained tissue sample of a tumour lesion that had not been previously irradiated. Patients who had previously received anti–PD-1, anti–PD-L1, or anti–PD-L2 drugs were excluded.
Interventions
For the KEYNOTE-158 and KEYNOTE-164 trials, patients received pembrolizumab 200 mg intravenously every 3 weeks until progressive disease, unacceptable toxicity, or an intercurrent illness that prevents further administration of treatment. For the KEYNOTE-051 trial, patients received pembrolizumab 2 mg/kg intravenously every 3 weeks for 35 cycles (approximately 24 months).52,55,56 Patients in the KEYNOTE-158, KEYNOTE-164, and KEYNOTE-051 trials were prohibited from receiving certain therapies during the screening and treatment phase, including any re-treatment following relapse. The restricted therapies included antineoplastic systemic chemotherapy or biological therapy, any immunotherapy or chemotherapy not specified in the protocol, investigational drugs apart from pembrolizumab, and radiation therapy. Additionally, live vaccines were not allowed within 30 days before the first dose of trial treatment or during the trial. Systemic glucocorticoids were allowed only in specific circumstances, such as managing AEs for symptoms of immunologic etiology, with the sponsor’s approval.52,55,56
At the discretion of the investigator, patients with stable disease or better who discontinued pembrolizumab treatment after 24 months for reasons other than disease progression or intolerability, or participants who experienced a CR and stopped pembrolizumab treatment after 8 cycles and who had received at least 2 cycles administered after the date of the initial CR, could be eligible for up to 1 year of pembrolizumab re-treatment (second course) upon experiencing disease progression.52,55,56
Outcomes
A list of efficacy end points assessed in this Clinical Review report is provided in Table 7, followed by descriptions of the outcome measures. Summarized end points are based on outcomes included in the sponsor’s summary of clinical evidence as well as any outcomes identified as important to this review according to the clinical experts consulted by CDA-AMC and the input from the patient and clinician groups and public drug plans. Using the same considerations, the CDA-AMC review team selected end points that were considered to be most relevant to inform the deliberations of the CDA-AMC expert committee, and finalized this list of end points in consultation with members of the committee. All summarized efficacy end points were assessed using GRADE. Select notable harms outcomes that were considered important for informing the deliberations of the expert committee were also assessed using GRADE. The patient and clinician groups, as well as the clinical experts consulted, indicated that durable response, prevention of progression, prolongation of life, and improved HRQoL with a low number of harms were important goals of treatment. This was reflected in the included end points: ORR, DOR, PFS, OS, HRQoL, SAEs, and AEOSIs (immune-mediated and infusion-related reactions).
Table 7: Outcomes Summarized From the Included Studies
Outcome measure | Time points | KEYNOTE-158 trial | KEYNOTE-164 trial | KEYNOTE-051 trial |
|---|---|---|---|---|
ORR per RECIST 1.1 | Any time during the trial | Primary | Primary | Primary |
OS | Median, 12 months, 24 months | Secondary | Secondary | Secondary |
PFS | Median, 12 months, 24 months | Secondary | Secondary | Secondary |
DOR | Median, 12 months, 24 months | Secondary | Secondary | Secondary |
SAE | To the data cut-off | Secondary | Secondary | Primary |
AEOSI | To the data cut-off | Secondary | Secondary | Primary |
EORTC QLQ-C30 | 9 weeks | Tertiary | NR | NR |
AEOSI = adverse event of special interest (immune-mediated event or infusion-related reaction); DOR = duration of response; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; NR = not reported; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; RECIST 1.1 = Response Evaluation Criteria in Solid Tumours Version 1.1; SAE = serious adverse event.
Sources: Marabelle et al. (2020),48 Maio et al. (2022),51-53 sponsor’s clinical summary for Keytruda for MSI-H,13 clinicaltrials.gov,33 and Clinical Study Reports for the KEYNOTE-158,17 KEYNOTE-051,19 and KEYNOTE-16418 trials.
Efficacy Outcomes
Overall Survival
OS was defined as the time from either treatment allocation (KEYNOTE-158 trial) or treatment initiation (KEYNOTE-164 and KEYNOTE-051 trials) to death from any cause. In cases where a patient did not die but started a new anticancer therapy, the patient was censored at the time of the new treatment initiation. Missing OS observations were censored at the last recorded assessment. Patients without efficacy evaluation data or without survival data were censored at day 1 in the OS analyses.
Progression-Free Survival
PFS was defined as the time from day 1 of study treatment to the first documented disease progression per RECIST 1.1 or death due to any cause, whichever occurred first. In cases where a patient did not die or experience disease progression but started a new anticancer therapy, the patient’s data were censored at the time of treatment initiation. Missing PFS observations were censored at the last recorded assessment. Patients without efficacy evaluation data or survival data were censored at day 1 in the PFS analyses. The PFS end point was assessed by independent central radiological review (KEYNOTE-164 and KEYNOTE-158 trials) or by the investigator (KEYNOTE-051 trial).
Objective Response Rate
ORR was defined as the proportion of patients who have a confirmed CR or PR per RECIST 1.1 assessed by an independent central radiological review (KEYNOTE-158 and KEYNOTE-164 trials) or by the investigator (KEYNOTE-051 trial). Patients with no assessment (unknown or missing) were considered to have not experienced a response and were included in the denominator.
Duration of Response
DOR was assessed among patients with a CR or PR and defined as the time from first documented response to subsequent disease progression (per RECIST 1.1) or death from any cause, whichever occurred first. In the KEYNOTE-158 and KEYNOTE-164 trials, patients who were ongoing in the study, had started a subsequent treatment, or had missed at least 2 disease assessments were censored at the last adequate disease assessment. Patients who died or progressed after 1 missed assessment were considered to have had an event. Patients who were alive, had not progressed, had not initiated new anticancer treatment, and were not lost to follow-up were considered ongoing responders at the time of analysis.
Health-Related Quality of Life
HRQoL was only assessed in the KEYNOTE-158 trial using the EORTC QLQ-C30. The EORTC QLQ-C30 contains 30 items and measures, 5 functional dimensions (physical, role, emotional, cognitive, and social), 3 symptom items (fatigue, nausea or vomiting, and pain), 6 single items (dyspnea, sleep disturbance, appetite loss, constipation, diarrhea, and financial impact), and a global health and QoL scale. A summary of the questionnaire, its measurement properties, and estimated minimal important difference (MID) is in Table 8. Prespecified exploratory HRQoL end points included changes from baseline to week 9 in the EORTC QLQ-C30 GHS and QoL.13
A mean difference of 10 points or more has been estimated as a MID when interpreting data collected with the EORTC QLQ-C30 questionnaire.57 However, a more recent review has estimated an MID for within-group improvement in GHS ranging from 4 points (brain cancer) to 13 points (ovarian cancer), and for deterioration ranging from −5 points (head or neck, lung cancers) to −8 points (breast cancer).58,59
Harms Outcomes
AE reporting was identical across the KEYNOTE-158, KEYNOTE-164, and KEYNOTE-051 studies. AEs, irrespective of causality, were reported from the time of treatment initiation through 30 days after the last dose of study treatment or before the initiation of a new anticancer treatment, whichever occurred first (intensity was assessed by the investigator according to the National Cancer Institute Common Terminology Criteria for Adverse Events Version 4.03).
SAEs reported from the time of treatment initiation until 90 days after the last dose of study treatment or 30 days after discontinuation of study treatment if the patient initiated a new anticancer treatment, whichever occurred first (intensity was assessed by the investigator according to the National Cancer Institute Common Terminology Criteria for Adverse Events Version 4.03). SAEs included AEs that result in death or are life-threatening, require inpatient hospitalization or prolong existing hospitalization, or result in persistent or significant disability and/or incapacity. SAEs also included congenital anomalies and/or births, deaths, or other important medical events.
Notable harms of interest to this review included immune-mediated events and infusion-related reactions associated with pembrolizumab. A predefined list of preferred terms was developed by the sponsor to consistently characterize the nature and frequency of each AEOSI regardless of causality and as reported by investigators. These preferred terms are considered medically equivalent to immune-mediated events and infusion-related reactions.
Table 8: Summary of Outcome Measures and Their Measurement Properties
Outcome measure | Type | Conclusions about measurement properties | MID |
|---|---|---|---|
EORTC QLQ-C30 | A self-reported, 30-item, cancer-specific instrument that is used to assess 5 functional scales (physical, role, emotional, cognitive, and social), 3 symptom scales (fatigue, nausea or vomiting, and pain), 6 single items (dyspnea, sleep disturbance, appetite loss, constipation, diarrhea, and financial difficulties), and a global health status or quality of life scale.13,57,60 Scores are linearly transformed to range from 0 to 100, where a higher score represents better function (for functioning and global health scales) or increased symptom severity (for symptom scales).13,57,60 | The validity and reliability of the core questionnaire (and some of its translations) have been demonstrated in a variety of cancer types in adults, though information specifically for MSI-H or dMMR status was not identified from the literature.61-64 The groups of patients included those with breast cancer, ovarian cancer, and lung cancer, and a heterogenous group with different cancers. In general, convergent validity and reliability were demonstrated: item–scale correlations were between −0.65 and 0.95, while most scales had a Cronbach alpha > 0.70 (all scales had an alpha > 0.50). Changes in scores indicate that the instrument is responsive to different levels of disease severity, the effects of chemotherapy, and different ECOG PS levels.61 In other studies of patients with nonhematological cancers, the instrument generally demonstrated convergent and construct validity (correlation coefficient ≥ 0.40) and reliability among most scales (Cronbach alpha ≥ 0.70).62-64 | A 10-point within-patient change in score for all dimensions, except role function, is suggested as being clinically meaningful for advanced cancer, based on the literature.57 This estimate was based on data from a variety of cancer types. In a study of 9 cancer types (brain, colorectal, advanced breast, head and neck, lung, mesothelioma, melanoma, ovarian, and prostate cancers), anchor and distribution methods were used to estimate group-level MIDs.65 It was noted that the questionnaire scale, anchor used to estimate the MID, direction of change (improvement versus deterioration), and type of cancer impact the MID. Most MIDs (by individual scale and cancer type) were between 5 and 10 points for within-group changes (range, 4 to 19). Additionally, the magnitude of an MID for improvement was not always the same as that for deterioration. |
dMMR = mismatch repair deficient; ECOG PS = Eastern Cooperative Oncology Group Performance Status; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; MID = minimal important difference; MSI-H = microsatellite instability-high.
Statistical Analysis
Sample Size and Power Calculation
Sample size considerations were included for all KEYNOTE trials. For KEYNOTE-158, the trial planned to enrol a minimum of 200 patients and up to approximately 1,350 patients over a period of around 90 months. Because both the sample size and the underlying response rate were unknown, no power calculations were included in this study.
In the KEYNOTE-164 trial, approximately 60 patients were planned for each of cohorts A and B. For cohort A, with 60 patients, the study had 93% power to reject the null hypothesis of an ORR of 15%, with a 1-sided type I error rate of 2.5%, assuming a true ORR of 35%. Historically, the response rate had been less than 5%. For cohort B, with a historical response rate of about 20% and a sample size of 60 patients, if at least 19 responders were observed, the lower bound of the 95% CI for ORR would have exceeded 20%.
In the KEYNOTE-051 trial, power calculations were for the “all participants as treated” (APaT) population and had 25 patients per indication planned for enrolment. With up to 25 patients per indication, the study had 84% power to show that the ORR induced by pembrolizumab exceeded 10% at a 1-sided alpha level of 8%, assuming a true ORR of 35%. The null hypothesis of 10% assumed that the population consisted of patients with incurable solid tumours that had not responded to multiple lines of standard therapy.
Multiplicity
The KEYNOTE-158 trial allowed for multiple interim analyses to allow for hypothesis generation. Analyses were performed without multiplicity control.
In the KEYNOTE-164 trial, for cohort A, the overall type I error rate for ORR analyses was controlled at 2.5% (1-sided) using a group sequential approach for the interim analysis and final analysis. For cohort B, no multiplicity adjustment was applied.
In the KEYNOTE-051 trial, interim analyses were performed to monitor the ORR of the enrolled patients in the APaT set. Within a tumour type, after at least 10 patients had had at least 1 postbaseline response assessment, a sequential monitoring procedure was used to evaluate for efficacy and futility simultaneously, based on the number of patients with a confirmed or unconfirmed response. The design assumed a 1-sided type I error rate of 8%.
Statistical and Analytical Plans
The efficacy analyses included in this submission were based on the APaT populations (or relevant subsets of those populations) and included all participants with MSI-H and/or dMMR tumours in cohorts A through K who received at least 1 dose of pembrolizumab in the KEYNOTE-158 trial (N = 373), all participants in cohorts A and B who received at least 1 dose of pembrolizumab in the KEYNOTE-164 trial (N = 124), and all participants with MSI-H and/or dMMR tumours who received at least 1 dose of pembrolizumab in the KEYNOTE-051 trial (N = 7).
The data cut-off dates for the analyses were January 12, 2022, for the KEYNOTE-158 trial (interim analysis); February 19, 2021, for the KEYNOTE-164 trial (final analysis); and January 18, 2022, for the KEYNOTE-051 trial (interim analysis). The analysis methods were similar across all trials. The point estimate and 95% CI for the ORR, based on RECIST 1.1, were provided using an exact binomial distribution (Clopper and Pearson) method. Participants without response data (i.e., data were nonevaluable, missing, or unknown) were counted as nonresponders but included in the denominator. In the KEYNOTE-164 trial, a P value was to be provided for testing that showed the ORR was greater than 15% (cohort A); results for cohort B were descriptive. For the KEYNOTE-158 and KEYNOTE-051 trials, the results were provided descriptively. Time-to-event outcomes were presented as median values with 95% CIs. DOR, PFS, and OS were summarized by Kaplan-Meier (KM) methods.
In the KEYNOTE-158 trial, ORR and DOR were provided for the overall population as well as by tumour type. Results for the KEYNOTE-164 trial were provided for cohorts A and B and pooled within the sponsor’s submission. Results by tumour type were not provided for the KEYNOTE-051 trial because all but 1 patient in that trial had brain cancer. Sensitivity analyses were not described.
In the KEYNOTE-158 trial, an adherence summary was provided, defined as the proportion of patients who completed at least 1 item out of all eligible patients who were expected to complete questionnaires at a given time point. This calculation excluded patients missing due to the study design, such as death or study discontinuation. LS mean (95% CI) changes from baseline to week 9 in the EORTC QLQ-C30 GHS and QoL scores were presented using a repeated measures model, with missing data assumed to be missing at random. The proportion of participants showing improvement, deterioration, or stability in EORTC QLQ-C30 scores from baseline to week 9 was summarized with no imputation for missing data. Postbaseline scores were classified as “improved,” “stable,” or “deteriorated” according to a change of 10 points or more for each EORTC QLQ-C30 scale or subscale.
Analysis Populations
Analysis sets included in the KEYNOTE-158, KEYNOTE-164, KEYNOTE-051 trials are summarized in Table 9.
Table 9: Analysis Populations for the KEYNOTE-158, KEYNOTE-164, and KEYNOTE-051 Trials
Study | Population | Definition | Application |
|---|---|---|---|
KEYNOTE-158 | APaT (MSI-H participants) | All participants with MSI-H and/or dMMR cancers in cohorts A through K who received at least 1 dose of pembrolizumab | All efficacy and safety analyses |
FAS | All participants in the primary efficacy population (i.e., the APaT population) with at least 1 HRQoL assessment available | HRQoL analyses | |
KEYNOTE-164 | APaT | All participants in cohorts A and B, who received at least 1 dose of pembrolizumab | All efficacy and safety analyses |
KEYNOTE-051 | APaT (MSI-H cohort) | All participants with MSI-H and/or dMMR cancers who received at least 1 dose of pembrolizumab | All efficacy and safety analyses |
APaT = all participants as treated; dMMR = mismatch repair deficient; FAS = full analysis set; HRQoL = health-related quality of life; MSI-H = microsatellite instability-high.
Sources: KEYNOTE-158,17 KEYNOTE-051,19 and KEYNOTE-16418 Clinical Study Reports.
Results
Patient Disposition
In all 3 trials, all allocated patients received treatment: 373 (100%) in the KEYNOTE-158 trial, 124 (100%) in the KEYNOTE-164 trial, and 7 (100%) in the KEYNOTE-051 trial (Table 10). Data reported in the sponsor’s summary of clinical evidence for the KEYNOTE-164 trial pooled cohorts A and B. The proportion of patients with unsuccessful screening were not reported for the KEYNOTE-158 or KEYNOTE-051 trial. For the KEYNOTE-164 trial, 148 patients were screened, with 24 (16.2%) being screened out due to eligibility criteria not being met.
Study discontinuation rates were 62.5% in the KEYNOTE-158 trial, 55.6% in the KEYNOTE-164 trial, and 71.4% in the KEYNOTE-051 trial. The primary reason for discontinuation was death, occurring in 59.0% of patients in the KEYNOTE-158 trial, 46.0% in the KEYNOTE-164 trial, and 71.4% in the KEYNOTE-051 trial. Other reasons included withdrawal by the patient and AEs, with AEs causing discontinuation in 3.2% of patients in the KEYNOTE-164 trial, but no patients withdrew due to AEs in the KEYNOTE-158 or KEYNOTE-051 trials.
Table 10: Summary of Patient Disposition in the Systematic Review for Sponsor Studies
Patient disposition | KEYNOTE-158 trial | KEYNOTE-164 trial | KEYNOTE-051 trial |
|---|---|---|---|
Screened, N | NR | 148 | NR |
Reason for unsuccessful screening, n (%) | |||
Unsuccessful screening (eligibility criteria not met) | NR | 24 (16.2) | NR |
Allocated, N (%) | 373 (100) | 124 (100) | 7 (100) |
Treated, N (%) | 373 (100) | 124 (100) | 7 (100) |
Discontinuations, n (%) | |||
Discontinued from study, n (%) | 233 (62.5) | 69 (55.6) | 5 (71.4) |
Death | 220 (59.0) | 57 (46.0) | 5 (71.4) |
Lost to follow-up | 1 (0.3) | 2 (1.6) | 0 |
Withdrawal by patient | 12 (3.2) | 6 (4.8) | 0 |
Adverse event | 0 (0) | 4 (3.2) | 0 |
APaT, N | 373 | 124 | 7 |
Safety, N | 373 | 124 | 7 |
FAS, N | 364 | NA | NA |
APaT = all patients as treated; FAS = full analysis set; MSI-H = microsatellite instability-high; NA = not applicable; NR = not reported.
Sources: KEYNOTE-158,17 KEYNOTE-051,19 KEYNOTE-16418 Clinical Study Reports.
Baseline Characteristics
The summary of baseline characteristics in the 3 included trials is presented in Table 11. The baseline characteristics outlined are limited to those that are most relevant to this review or were felt to affect the outcomes or interpretation of the study results.
The KEYNOTE-158 trial enrolled 373 adult patients with MSI-H and/or dMMR tumours. The majority of the patients were female (61%), with a mean age of 59.2 (SD = 13.1) years, and 36% of the patients were aged 65 years or older. The most common cancer types in this cohort were colorectal (25%), endometrial (14%), and gastric (14%); there was a smaller representation (4% to 7%) of other cancers, including small intestine, ovarian, biliary, pancreatic, brain, sarcomas, and other rare cancers. Regarding metastatic status, 91% of the patients were classified as having M1 disease, indicating the presence of metastases. Regarding ECOG PS, 46% of the patients had an ECOG PS of 0, and 54% had an ECOG PS of 1. Most patients had undergone prior therapy, with 42% receiving 1 prior line of treatment and 56% receiving 2 or more lines.
The KEYNOTE-164 trial included 124 patients with MSI-H and/or dMMR CRC. The sex distribution for patients was 56% male and 44% female. The mean age was 56.1 years (SD = 14.9 years), and 33% were aged 65 years or older. Regarding ECOG PS, 41% of the patients had a status of 0 and 59% had a status of 1. In terms of metastatic status, 97% of patients were classified as M1, indicating metastatic disease. The majority of the patients (76%) had received 2 or more prior lines of treatment.
The KEYNOTE-051 trial included a cohort of 7 pediatric patients with MSI-H and/or dMMR tumours. The majority of the patients (71%) were female, and the age of patients ranged from 3 to 16 years, with a mean age of 11 years (SD = 4.3 years). This cohort mainly consisted of patients with brain tumours (86%), with 1 patient having another type of cancer (14%). Most patients (71%) were classified as having M1 disease, indicating their cancer was metastatic, and 57% of the patients had undergone 2 or more prior lines of therapy.
Table 11: Summary of Baseline Characteristics — Participants With MSI-H and/or dMMR Cancers in the KEYNOTE-158, KEYNOTE-164, and KEYNOTE-051 Trials (APaT)
Characteristic | KEYNOTE-158 trial | KEYNOTE-164 trial | KEYNOTE-051 trial |
|---|---|---|---|
Sex, n (%) | |||
Male | 147 (39) | 69 (56) | 2 (29) |
Female | 226 (61) | 55 (44) | 5 (71) |
Age | |||
≥ 65 years, n (%) | 135 (36) | 41 (33) | 0 (0) |
Mean, years (SD) | 59.2 (13.1) | 56.1 (14.9) | 11 (4.3) |
Median, years (range) | 60 (20 to 89) | 56 (21 to 84) | 11 (3 to 16) |
Race, n (%) | |||
Asian | 36 (10) | 33 (27) | 1 (14) |
Black | 9 (2) | 7 (6) | 0 (0) |
White | 301 (81) | 84 (68) | 6 (86) |
Other or missing | 27 (7) | 0 (0) | 0 (0) |
ECOG PS, n (%) | |||
0 | 172 (46) | 51 (41) | NR |
1 | 201 (54) | 73 (59) | NR |
Karnofsky score, n (%) | |||
100 | NR | NR | 4 (57) |
Cancer type, n (%) | |||
Colorectal | 0 (0) | 124 (100) | 0 (0) |
Endometrial | 94 (25) | 0 (0) | 0 (0) |
Gastric | 51 (14) | 0 (0) | 0 (0) |
Small intestine | 27 (7) | 0 (0) | 0 (0) |
Ovarian | 25 (7) | 0 (0) | 0 (0) |
Biliary | 22 (6) | 0 (0) | 0 (0) |
Pancreatic | 22 (6) | 0 (0) | 0 (0) |
Brain | 21 (6) | 0 (0) | 6 (86) |
Sarcoma | 14 (4) | 0 (0) | 0 (0) |
Other | 97 (26) | 0 (0) | 1 (14) |
Metastasis stage, n (%) | |||
MX | 21 (6) | 0 (0) | 0 |
M0 | 14 (4) | 4 (3) | 1 (14) |
M1 | 338 (91) | 120 (97) | 5 (71) |
Number of prior lines of therapy, n (%) | |||
0 | 8 (2) | 0 (0) | 1 (14) |
Adjuvant or neoadjuvant or definitive | 2 (1) | 0 (0) | 0 (0) |
1 | 155 (42) | 30 (24) | 4 (57) |
≥ 2 | 208 (56) | 94 (76) | 2 (29) |
APaT = all participants as treated; dMMR = mismatch repair deficient; ECOG PS = Eastern Cooperative Oncology Group Performance Status; MSI-H = microsatellite instability-high; M0 = cancer has not spread to other parts of the body; M1 = cancer has spread to other parts of the body; MX = metastasis cannot be measured; NR = not reported; SD = standard deviation.
Note: The data cut-off dates were January 12, 2022, for the KEYNOTE-158 trial (interim analysis), February 19, 2021, for the KEYNOTE-164 trial (final analysis), and January 18, 2022, for the KEYNOTE-051 trial (interim analysis).
Sources: Clinical Study Report for KEYNOTE-15817 and sponsor’s clinical summary.13
Exposure to Study Treatments
Patient exposure for the included studies is presented in Table 12.
In the KEYNOTE-158 trial, the median duration of treatment with pembrolizumab was 6.18 months (range, 0.03 to 29.67 months) and the mean duration of treatment was 10.19 months (SD = 9.42 months). Patients received a median treatment of 9 cycles (range, 1 to 35 cycles), with a mean of 15.06 cycles (SD = 13.14 cycles). Among all patients, 85.3% were treated for at least 1 month, 65.4% for 3 months or more, 50.4% for 6 months or more, and 37.0% for 12 months or more. Additionally, 28.2% of patients were treated for 18 months or more, and 25.7% were treated for 21 months or more.
In the KEYNOTE-164 trial, the median duration of treatment with pembrolizumab was 273 days (approximately 9.0 months) in cohort A (range, 1 to 1,405 days) and 226 days (approximately 7.4 months) in cohort B (range, 1 to 1,157 days). The mean duration of treatment was 427.41 days (SD = 403.01 days) for cohort A and 382.62 days (SD = 350.65 days) for cohort B. Patients received a median treatment of 14 cycles in cohort A (range, 1 to 52 cycles) and 11 cycles in cohort B (range, 1 to 48 cycles), with a mean of 18.90 cycles (SD = 15.10 cycles) in cohort A and 17.52 cycles (SD = 14.75 cycles) in cohort B. All patients (100%) were treated for more than 0 months, with 89.5% treated for at least 1 month, 73.4% for 3 months or more, 54.0% for 6 months or more, and 43.5% for 12 months or more. Additionally, 16.9% of patients were treated for 21 months or more, and 7.3% were treated for 24 months or more.
In the KEYNOTE-051 trial, which included 7 patients with MSI-H tumours, the median duration of treatment with pembrolizumab was 43 days (approximately 1.4 months; range, 1 to 453 days). The mean duration of treatment was 114.9 days (SD = 165.4 days). Patients received a median treatment of 3 cycles (range, 1 to 21 cycles), with a mean of 6.1 cycles (SD = 7.4 cycles). All patients (100%) were treated for more than 0 months, with 71.4% treated for at least 1 month. However, only 28.6% of patients were treated for 3 months or more, and the same proportion (28.6%) was treated for 6 months or more. One patient (14.3%) was treated for 12 months or more.
Table 12: Summary of Patient Exposure in the Systematic Review for Sponsor Studies
Exposure to pembrolizumab | KEYNOTE-158 trial | KEYNOTE-164 trial | KEYNOTE-051 trial |
|---|---|---|---|
Duration, mean (SD) | 10.19 months (9.42) | Cohort A (N = 61): 427.41 days (403.01) Cohort B (N = 63): 382.62 days (350.65) | 114.9 days (165.4) |
Duration, median (range) | 6.18 months (0.03 to 29.67) | Cohort A (N = 61): 273.00 days (1.00 to 1,405.00) Cohort B (N = 63): 226.00 days (1.00 to 1,157.00) | 43 days (1 to 453) |
Number of cycles, mean (SD) | 15.06 (13.14) | Cohort A: 18.90 (15.10) Cohort B: 17.52 (14.75) | 6.1 (7.4) |
Number of cycles, median (range) | 9.0 (1.00 to 35.00) | Cohort A: 14.00 (1.00 to 52.00) Cohort B: 11.00 (1.00 to 48.00) | 3 (1 to 21) |
Duration of follow-up, median (range) | 17.0 months (0.2 to 71.4) | Cohort A: 31.4 months (range, 0.2 to 65.2) Cohort B: 52.7 months (0.1 to 56.6) | 5.2 months (0.3 to 28.2) |
Patients exposed to treatment by duration, n (%) | |||
> 0 month | 373 (100.0) | 124 (100.0) | 7 (100.0) |
≥ 1 month | 318 (85.3) | 111 (89.5) | 5 (71.4) |
≥ 3 months | 244 (65.4) | 91 (73.4) | 2 (28.6) |
≥ 6 months | 188 (50.4) | 67 (54.0) | 2 (28.6) |
≥ 12 months | 138 (37.0) | 54 (43.5) | 1 (14.3) |
≥ 18 months | 105 (28.2) | NR | NR |
≥ 21 months | 96 (25.7) | NR | NR |
≥ 24 months | NR | 21 (16.9) | NR |
≥ 36 months | NR | 9 (7.3) | NR |
MSI-H = microsatellite instability-high; NR = not reported; SD = standard deviation.
Sources: KEYNOTE-158,17 KEYNOTE-051,19 and KEYNOTE-164 Clinical Study Reports.18 Details included in the table are from the sponsor’s summary of clinical evidence.
Concomitant Treatments
In the KEYNOTE-158 trial, a total of 5 patients (1.3%) received concomitant antineoplastic agents, 8 patients (2.1%) were receiving endocrine treatment, 3 patients (0.8%) were receiving immunostimulants, and 6 patients (1.6%) were receiving immunosuppressants.
In cohort A in the KEYNOTE-164 trial, a total of 25 patients (41.0%) received concomitant antineoplastic agents and 3 patients (4.9%) received endocrine therapy. In cohort B, a total of 24 patients (38.1%) received concomitant antineoplastic agents and 1 patient (1.6%) received an immunostimulant.
In the KEYNOTE-051 trial, all patients received concomitant treatments. The most frequently reported concomitant medications were acetaminophen and levetiracetam, in 4 participants each.
Efficacy
The summary of the efficacy outcomes for the sponsor’s studies is presented in Table 13 and Table 14. In the KEYNOTE-158 trial, the median duration of follow-up was 17 months (range, 0.2 to 71.4 months). For the KEYNOTE-164 trial, the median duration of follow-up was 31.4 months (range, 0.2 to 65.2 months) for cohort A and 52.7 months (range, 0.1 to 56.6 months) for cohort B. In the KEYNOTE-051 trial, the median length of follow-up was 5.2 months (range, 0.3 to 28.2 months).
Objective Response Rate
Adult
The ORR per RECIST 1.1 in the KEYNOTE-158 trial (varied tumours) was 33.8% (95% CI, 29.0% to 38.8%). The best objective response included 40 patients (10.7%) with a CR and 86 patients (23.1%) with a PR. The tumour-specific ORR in the KEYNOTE-158 trial showed varied response rates, ranging from 4.8% (brain) to 59.3% (small intestine) across different cancer types (Table 43). Tumours with higher ORRs compared with the pooled result included endometrial, gastric, small intestine, cholangiocarcinoma, urothelial, and salivary cancers. Tumours with lower ORRs included ovarian, pancreatic, brain, sarcoma, breast, cervical neuroendocrine, prostate, adrenocortical, mesothelioma, thyroid, small cell lung, and renal cancers.
The ORR in cohort A was 32.8% (95% CI, 21.3% to 46.0%). The objective response included a CR in 3 patients (4.9%) and a PR in 17 patients (27.9%), with 11 patients (18.0%) experiencing stable disease and 28 patients (45.9%) experiencing progressive disease. The ORR in cohort B was 34.9% (95% CI, 23.3% to 48.0%). The objective response included a CR in 9 patients (14.3%) and a PR in 13 patients (20.6%), with 13 patients (20.6%) experiencing stable disease and 25 patients (39.7%) experiencing progressive disease.
Pediatric
In the KEYNOTE-051 trial, the ORR was 0% (95% CI, 0.0% to 41.0%). No patients experienced a CR or PR; 1 patient (14.3%) had stable disease. Tumour-specific ORR results were not reported in the KEYNOTE-051 trial.
Table 13: Key Efficacy Outcomes in the KEYNOTE-158, KEYNOTE-164, and KEYNOTE-051 Trials, APaT Populations
Parameter | KEYNOTE-158 trial adult patients with MSI-H or dMMR tumours (N = 373) | KEYNOTE-164 trial adult patients with MSI-H or dMMR CRC (cohorts A + B) (N = 124) | KEYNOTE-051 trial pediatric patients with MSI-H or dMMR tumours (N = 7) |
|---|---|---|---|
ORR per RECIST 1.1 | |||
Number of patients contributing to the analysis | 373 | 124 | 7 |
ORR (CR + PR), n (%) | 126 (33.8) | 42 (33.9) | 0 (0.0) |
95% CI | 29.0 to 38.8 | 25.6 to 42.9 | 0.0 to 41.0 |
Tumour-specifica ORR, % (95% CI) | |||
Colorectal (n = 124) | NA | 33.9 (25.6 to 42.9) | NA |
Endometrial (n = 94) | 50.0 (39.5 to 60.5) | NA | |
Gastric (n = 51) | 39.2 (25.8 to 53.9) | NA | |
Small intestine (n = 27) | 59.3 (38.8 to 77.6) | NA | |
Ovarian (n = 25) | 32.0 (14.9 to 53.5) | NA | |
Biliary (n = 22) | 40.9 (20.7 to 63.6) | NA | |
Pancreatic (n = 22) | 18.2 (5.2 to 40.3) | NA | |
Brain (n = 21) | 4.8 (0.1 to 23.8) | NA | |
Best objective response per RECIST 1.1, n (%) [95% CI] | |||
CR | 40 (10.7) [7.8 to 14.3] | 11 (8.9) [NR] | 0 (0.0) [NR] |
PR | 86 (23.1) [18.9 to 27.7] | 31 (25.0) [NR] | 0 (0.0) [NR] |
Stable disease | 66 (17.7) [14.0 to 22.0] | 25 (21.2) [NR] | 1 (14.3) [NR] |
Progressive disease | 148 (39.7) [34.7 to 44.8] | 53 (42.7) [NR] | 5 (71.4) [NR] |
NE | 4 (1.1) [0.3 to 2.7] | 4 (3.2) [NR] | 0 (0.0) [NR] |
NAb | 29 (7.8) [5.3 to 11.0] | 0 (0.0) [NR] | 1 (14.3) [NR] |
DOR | |||
Number of patients contributing to the analysis | 126 | 42 | 0 |
Median in months (range) | 63.2 (1.9+ to 63.9+) | Not reached (4.4 to 58.5+) | NA |
Number of censored patients, n (%) | 91 (72.2) | NR | NA |
Participants who missed 2 or more consecutive disease assessments, n (%) | 5 (4.0) | NR | NA |
Participants who started new anticancer treatment, n (%) | 8 (6.3) | NR | NA |
Participants who were lost to follow-up, n | 0 | NR | NA |
Participants whose last adequate assessment was ≥ 5 months before data cut-off date, n (%) | 17 (13.5) | NR | NA |
Ongoing response, n (%) | 61 (48.4) | NR | NA |
Tumour-specific median DOR, months (range) | |||
Colorectal | NA | Not reached (4.4 to 58.5+) (n = 42) | NA |
Endometrial | 63.2 (2.9 to 63.2) n = 47 | NA | |
Gastric | Not reached (1.9+ to 63.0+) n = 20 | NA | |
Small intestine | Not reached (3.7+ to 57.3+) n = 16 | NA | |
Ovarian | Not reached (4.2 to 56.6+) n = 8 | NA | |
Biliary | 30.6 (6.2 to 49.0+) n = 9 | NA | |
Pancreatic | Not reached (8.1 to 24.3+) n = 4 | NA | |
Brain | 18.9 (18.9 to 18.9) n = 1 | NA | |
Probability of remaining in response, %b | |||
6 months | 95.2 | 97.6 | NA |
12 months | 88.5 | 95.1 | |
18 months | NR | 92.2 | |
24 months | 72.3 | 92.2 | |
36 months | 69.4 | 92.2 | |
48 months | 66.0 | Not reached | |
60 months | 66.0 | Not reached | |
PFS | |||
n | 373 | 124 | 7 |
Number (%) of PFS eventsa | 275 (73.7) | 83 (66.9) | 6 (85.7) |
Median PFS, in months (95% CI) | 4.0 (2.4 to 4.3) | 4.0 (2.1 to 7.4) | 1.7 (0.4 to not reached) |
PFS event-free probability, %c | |||
6 months | 43.2 | 45.8 | 16.7 |
12 months | 35.1 | 37.5 | Not reached |
18 months | NR | NR | NR |
24 months | 28.8 | 33.8 | NR |
36 months | 25.0 | 31.5 | NR |
48 months | 24.0 | NR | NR |
60 months | 22.0 | NR | NR |
72 months | Not reached | NR | NR |
OS | |||
n | 373 | 124 | 7 |
Number (%) of deaths | 230 (61.7) | 63 (50.8) | 5 (71.4) |
Median OS, months (95% CI) | 19.8 (14.5 to 25.8) | 36.1 (24.0 to not reached) | 7.7 (1.9 to not reached) |
OS event-free probability, %c | |||
At 6 months | 72.1 | NR | 50.0 |
At 12 months | 58.6 | 74.2 | 33.3 |
At 18 months | NR | NR | 33.3 |
At 24 months | 46.5 | 59.1 | NR |
At 36 months | 39.2 | 50.5 | NR |
At 48 months | 37.1 | 44.3 | NR |
At 60 months | 34.8 | NR | NR |
At 72 months | Not reached | NR | NR |
APaT = all participants as treated; CI = confidence interval; CR = complete response; CRC = colorectal cancer; dMMR = mismatch repair deficient; DOR = duration of response; MSI-H = microsatellite instability-high; NA = not applicable; NE = not evaluable; NR = not reported; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; PR = partial response; RECIST 1.1 = Response Evaluation Criteria in Solid Tumours Version 1.1; TTR = time to response.
Note: “+” indicates the TTR event (e.g., response, progression, survival) was ongoing at the time of the analysis.
aOnly tumours affecting ≥ 20 participants are reported.
bFrom product-limit (Kaplan-Meier) method for censored data.
cPatients with no postbaseline assessment at data cut-off, including missing, discontinued, or death before the first postbaseline scan. One of the 7 patients in the MSI-H cohort of the KEYNOTE-051 trial received the first dose of pembrolizumab just 9 days before the data cut-off date and therefore, no postbaseline imaging scans were available for efficacy analyses.
Sources: Sponsor’s clinical summary.13
Duration of Response
Adult
In the KEYNOTE-158 trial (varied tumours), among 126 patients with a response, the median DOR was 63.2 months (range, 1.9 to 63.9 months). Both ends of the range represent patients who were ongoing in the study without the event at the time of the data cut-off. Tumour-specific median DOR was as follows: endometrial cancer (63.2 months), gastric cancer (not reached), small intestine cancer (not reached), ovarian cancer (not reached), biliary tract cancer (30.6 months), pancreatic cancer (not reached), and brain cancer (18.9 months). Among patients who experienced a response, the event-free probabilities at 6, 12, 24, 36, 48, and 60 months after the first response were 95.2%, 88.5%, 72.3%, 69.4%, 66.0%, and 66.0%, respectively.
In the KEYNOTE-164 trial (all patients with CRC), among 42 patients with a response, the median DOR was not reached (range, 4.4 to 58.5 months for patients ongoing with response). Among patients who experienced a response, the event-free probabilities at 6, 12, 18, 24, and 36 months after the first response were 97.6%, 95.1%, 92.2%, 92.2%, and 92.2% respectively. The median DORs in cohorts A (n = 20) and B (n = 22) were not reached (range, 6.2 to 58.5 months for patients ongoing with response) and not reached (range, 4.4 to 52.4 months for patients ongoing with response), respectively.
Pediatric
DOR was not assessed in the KEYNOTE-051 trial because no patients had a response.
Overall Survival
Adult
At the data cut-off date, 230 out of 373 patients (61.7%) in the KEYNOTE-158 trial (varied tumours) had died. The median OS was 19.8 months (95% CI, 14.5 to 25.8 months). The OS event-free probabilities at 6, 12, 24, 36, 48, and 60 months were 72.1%, 58.6%, 46.5%, 39.2%, 37.1%, 34.8%, and not reached, respectively. The OS for individual tumour types was not reported.
In KEYNOTE-164 (all patients had CRC), 63 of 124 patients (50.8%) had died, with a median OS of 36.1 months (95% CI, 24.0 months to not estimable). The OS event-free probabilities at 12, 24, 36, and 48 months were 74.2%, 59.1%, 50.5%, 44.3%, respectively. In cohort A, 38 of 61 patients died (62.3%), with a median OS of 31.4 months (95% CI, 21.4 to 58.0 months). In cohort B, 31 of 63 patients died (49.2%), with a median OS of 47.0 months (95% CI, 19.2 months to not reached).
Pediatric
In the KEYNOTE-051 trial, 5 of 7 patients (71.4%) had died, with a median OS of 7.7 months (95% CI, 1.9 months to not estimable). The OS event-free probabilities at 6, 12, and 18 months were 50.0%, 33.3%, 33.3%, respectively. OS for individual tumour types was not reported.
Progression-Free Survival
Adult
At the cut-off date, 275 of 373 patients (73.7%) in the KEYNOTE-158 trial (varied tumours) had experienced a PFS event, with a median PFS of 4.0 months (95% CI, 2.4 to 4.3 months). The PFS event-free probabilities at 6, 12, 24, 36, 48, 60, and 72 months were 43.2%, 35.1%, 28.8%, 25.0%, 24.0%, 22.0%, and not reached, respectively. PFS for individual tumour types was not reported.
In KEYNOTE-164 (all patients had CRC), 83 of 124 patients (66.9%) had experienced a PFS event, with a median PFS of 4.0 months (95% CI, 2.1 to 7.4 months). The PFS event-free probabilities at 6, 12, 24, and 36 months were 45.8%, 37.5%, 33.8%, and 31.5%, respectively. In cohort A, 44 of 61 patients (72.1%) had a PFS event, with a median PFS of 2.3 months (95% CI, 2.1 to 8.1 months). In cohort B, 40 of 63 patients (63.5%) had a PFS event, with a median PFS of 4.1 months (95% CI, 2.1 to 18.9 months).
Pediatric
In the KEYNOTE-051 trial, 6 of 7 patients (85.7%) experienced a PFS event, with a median PFS of 1.7 months (95% CI, 0.4 months to not reached). The PFS event-free probability at 6 months was 16.7% and for 12 months it was not reached. PFS for individual tumour types was not reported.
Health-Related Quality of Life
Adult
In the KEYNOTE-158 trial (varied tumours) at baseline, adherence rates were 93.4% for the EORTC QLQ-C30. By week 9, adherence rates were 90%. After baseline, adherence rates ranged from 71.5% to 90.0% for the EORTC QLQ-C30 through week 111. Completion rates declined over time due to participant discontinuation as a result of disease progression, AEs, death, or physician decision.
The mean baseline EORTC QLQ-C30 GHS and QoL score was 64.40 points (SD = 20.12 points) across 364 patients. By week 9, the mean score was 67.48 points (SD = 22.48 points) in 265 patients, with an LS mean change from baseline of 3.08 points (95% CI, 0.32 to 5.84 points). A total of 57 patients (21.5%) experienced a deterioration in HRQoL at week 9, according to the sponsor’s 10-point threshold for any subscale. Based on the observed cases (n = 265), 32.8% of patients reported an improvement (≥ 10-point increase), 45.7% reported stability (< 10-point change), and 21.5% reported deterioration (≥ 10-point decrease) in GHS and QoL at week 9.
HRQoL was not assessed in the KEYNOTE-164 trial.
Pediatric
HRQoL was not assessed in the KEYNOTE-051 trial.
Table 14: Key HRQoL Outcomes (KEYNOTE-158 Trial, APaT Population)
Outcome measure | APaT population |
|---|---|
EORTC QLQ-C30 GHS and QoL | |
Number of patients at baseline | 364 |
Baseline score, mean (SD) | 64.40 (20.12) |
Number of patients at week 9 | 265 |
Score at week 9, mean (SD) | 67.48 (22.48) |
Change from baseline to week 9, LS mean (95% CI) | 3.08 (0.32 to 5.84) |
APaT = all participants as treated; CI = confidence interval; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; GHS = global health status; HRQoL = health-related quality of life; LS = least squares; QoL = quality of life; SD = standard deviation.
Note: Data cut-off date of January 12, 2022.
Source: KEYNOTE-158 Clinical Study Report.17
Harms
The summary of the harms outcomes for the included studies is presented in Table 15.
Adverse Events
Adult
At the January 12, 2022, cut-off date, 358 of 373 patients (96%) had experienced at least 1 AE in the KEYNOTE-158 trial. The most common AEs included diarrhea (25%), fatigue (24%), nausea (21%), vomiting (19%), and abdominal pain (14%). Of 373 patients, 197 (53%) had experienced at least 1 grade 3 to 5 AE. The grade 3 to 5 AEs that were reported in at least 5% of patients included anemia (6%) and abdominal pain (1%).
At the September 9, 2019, cut-off date, all 124 patients (100%) had experienced at least 1 AE. The most common AEs included fatigue (34%), diarrhea (32%), nausea (31%), abdominal pain (27%), and vomiting (26%). Of 124 patients, 68 (55%) had experienced at least 1 grade 3 to 5 AE. The grade 3 to 5 AEs that were reported in at least 5% of patients in the KEYNOTE-164 trial were anemia (7%) and abdominal pain (6%).
Pediatric
At the January 18, 2022, cut-off date, 7 of 7 patients (100%) had experienced at least 1 AE in the KEYNOTE-051 trial. The most common AEs included headache (71.4%), anemia (71.4%), vomiting (57.1%), pyrexia (42.9%), and rash (42.9%). A total of 5 of 7 patients (71.4%) had experienced at least 1 grade 3 to 5 AE. The grade 3 to 5 AEs that were reported in at least 5% of patients in the KEYNOTE-051 trial included anemia (14.3%) and abdominal pain (28.6%).
Serious Adverse Events
Adult
At the January 12, 2022, cut-off date, 133 of 373 patients (36%) had reported at least 1 SAE. The SAEs that were reported in at least 2% of patients in the KEYNOTE-158 trial included sepsis (2%) and pneumonia (2%).
At the September 9, 2019, cut-off date, 56 of 124 patients (45%) had reported at least 1 SAE. The SAEs that were reported in at least 2% of patients in the KEYNOTE-164 trial included dyspnea (4%), sepsis (4%), abdominal pain (3%), a small intestine obstruction (3%), urinary tract infection (3%), and ileus (2%).
Pediatric
At the January 18, 2022, cut-off date, 6 of 7 patients (85.7%) had reported at least 1 SAE. The SAE that was reported in at least 10% of patients in the KEYNOTE-051 trial was vomiting (28.6%).
Withdrawals Due to Adverse Events
Adult
At the January 12, 2022, cut-off date, 49 patients (13%) had discontinued pembrolizumab due to AEs in the KEYNOTE-158 trial.
At the September 9, 2019, cut-off date, 10 patients (8%) had discontinued treatment due to AEs in the KEYNOTE-164 trial.
Pediatric
At the January 18, 2022, cut-off date, 2 patients (28.6%) in the KEYNOTE-051 trial had discontinued pembrolizumab due to AEs.
Mortality
Adult
At the January 12, 2022, cut-off date, 220 patients had died in the KEYNOTE-158 trial; 20 of these patients died due to AEs.
At the September 9, 2019, cut-off date, 32 out of 61 patients (52.5%) had died in cohort A in the KEYNOTE-164 trial. In cohort B, 25 out of 63 patients (39.7%) had died. A total of 2 patients died in each cohort due to AEs.
Pediatric
At the January 18, 2022, cut-off date, 5 patients had died in the KEYNOTE-051 trial; none of these deaths were due to AEs.
Notable Harms
Notable harms of interest to this review were immune-mediated events and infusion-related reactions. The incidence of notable harms in the included trials is summarized in Table 15.
Adult
At the January 12, 2022, cut-off date, 83 out of 373 patients (22%) in the KEYNOTE-158 trial had experienced at least 1 AEOSI (immune-mediated event or infusion-related reaction associated with pembrolizumab). The most common AEOSIs were hypothyroidism (10%), hyperthyroidism (4%), pneumonitis (3%), and colitis (3%).
At the September 9, 2019, cut-off date, 37 out of 124 patients (30%) in the KEYNOTE-164 trial had experienced at least 1 AEOSI. The most common AEOSIs (immune-mediated events and infusion-related reactions associated with pembrolizumab) were hypothyroidism (15%), hyperthyroidism (8%), pneumonitis (2%), and colitis (2%).
Pediatric
At the January 18, 2022, cut-off date, 2 patients (28.6%) in the KEYNOTE-051 trial had experienced at least 1 AEOSI (immune-mediated event or infusion-related reaction associated with pembrolizumab). The AEOSIs reported were hypothyroidism (14.3%) and drug hypersensitivity (14.3%).
Table 15: Key Harms Data (APaT Population) for Sponsor Studies
AEs | KEYNOTE-158 trial (N = 373) | KEYNOTE-164 trial (N = 124) | KEYNOTE-051 trial (N = 7) |
|---|---|---|---|
Most common AEs, n (%) | |||
Patients with ≥ 1 AE | 358 (96) | 124 (100) | 7 (100) |
AEs reported in ≥ 10% of patients in either trial, n (%) | |||
Fatigue | 89 (24) | 42 (34) | 2 (28.6) |
Diarrhea | 93 (25) | 40 (32) | 1 (14.3) |
Nausea | 77 (21) | 39 (31) | 1 (14.3) |
Abdominal pain | 51 (14) | 34 (27) | 1 (14.3) |
Vomiting | 72 (19) | 32 (26) | 4 (57.1) |
Arthralgia | 69 (18) | 25 (20) | 1 (14.3) |
Pyrexia | 48 (13) | 26 (21) | 3 (42.9) |
Constipation | 53 (14) | 25 (20) | 1 (14.3) |
Cough | 40 (11) | 23 (19) | 1 (14.3) |
Anemia | 64 (17) | 23 (19) | 5 (71.4) |
Decreased appetite | 53 (14) | 23 (19) | 0 (0) |
Dyspnea | 41 (11) | 19 (15) | 1 (14.3) |
Back pain | 43 (12) | 22 (18) | 0 (0) |
Edema peripheral | 27 (7.2) | 20 (16) | 2 (28.6) |
Pruritus | 72 (19) | 18 (15) | 2 (28.6) |
Rash | 41 (11) | 17 (14) | 3 (42.9) |
Headache | 40 (11) | 16 (13) | 5 (71.4) |
Upper respiratory tract infection | 22 (5.9) | 16 (13) | 0 (0) |
Alanine aminotransferase increased | 44 (12) | 15 (12) | 2 (28.6) |
Asthenia | 73 (20) | 14 (11) | 0 (0) |
Urinary tract infection | 49 (13) | 8 (6) | 0 (0) |
Aspartate aminotransferase increased | 40 (11) | 8 (6) | 2 (28.6) |
Hypothyroidism | 38 (10) | 19 (15) | 1 (14.3) |
SAEs, n (%) | |||
Patients with ≥ 1 SAEs | 133 (36) | 56 (45) | 6 (85.7) |
SAEs reported in ≥ 2% of patients, n (%) | |||
Dyspnea | 0 (0) | 5 (4) | 0 (0) |
Sepsis | 8 (2) | 5 (4) | 0 (0) |
Abdominal pain | 3 (0.8) | 4 (3) | 0 (0) |
Small intestinal obstruction | 3 (0.8) | 4 (3) | 0 (0) |
Urinary tract infection | 4 (1.1) | 4 (3) | 0 (0) |
Ileus | 1 (0.3) | 3 (2) | 0 (0) |
Pneumonia | 8 (2) | 1 (1) | 0 (0) |
Vomiting | 1 (0.3) | 1 (1.6) | 2 (28.6) |
Patients who stopped treatment due to AEs, n (%) | |||
Patients who stopped pembrolizumab | 49 (13) | 10 (8) | 2 (28.6) |
Deaths, n (%) | |||
Patients who died due to an AE | 20 (5) | 4 (3) | 0 (0) |
Notable harms, n (%) | |||
Patients with ≥ 1 AEOSIs | 83 (22) | 37 (30) | 2 (28.6) |
Colitis | 11 (3) | 2 (2) | 0 (0) |
Drug hypersensitivity | 0 (0) | 1 (0.8) | 1 (14.3) |
Guillain-Barre syndrome | 2 (0.5) | 0 (0) | 0 (0) |
Hepatitis | 6 (2) | 1 (0.8) | 0 (0) |
Hyperthyroidism | 16 (4) | 10 (8) | 0 (0) |
Hypothyroidism | 38 (10) | 19 (15) | 1 (14.3) |
Infusion reactions | 4 (1) | 1 (0.8) | 0 (0) |
Myocarditis | 1 (0.3) | 0 (0) | 0 (0) |
Nephritis | 2 (0.5) | 0 (0) | 0 (0) |
Pancreatitis | 2 (0.5) | 1 (0.8) | 0 (0) |
Pneumonitis | 12 (3) | 3 (2) | 0 (0) |
Rhabdomyolysis | 0 (0) | 1 (0.8) | 0 (0) |
Severe skin reactions | 6 (2) | 1 (0.8) | 0 (0) |
Sarcoidosis | 0 (0) | 1 (0.8) | 0 (0) |
Type 1 diabetes mellitus | 3 (0.8) | 0 (0) | 0 (0) |
Uveitis | 1 (0.3) | 0 (0) | 0 (0) |
APaT = all participants as treated; AE = adverse event; AEOSI = adverse event of special interest (immune-mediated event or infusion-related reaction associated with pembrolizumab); SAE = serious adverse event.
Note: The data cut-off dates were January 12, 2022, for the KEYNOTE-158 trial and February 19, 2021, for the KEYNOTE-164 trial.
Sources: KEYNOTE-158,17 KEYNOTE-164,18 and KEYNOTE-05119 Clinical Study Reports.
Critical Appraisal
Internal Validity
KEYNOTE-158, KEYNOTE-164, and KEYNOTE-051 are all single-arm trials, which raised several important considerations due to the lack of any comparison group. A single-arm study design is usually used to provide preliminary evidence of the efficacy of a treatment and to collect safety data and not intended to be confirmatory for efficacy.66 Formal statistical hypothesis tests were not presented. According to the FDA, ORR is a direct measure of antitumour activity that may be attributed to the study drug and is evaluable with a single-arm design.67 However, single-arm trials are inherently limited in their ability to unambiguously support causal conclusions versus any comparator because it is not possible to distinguish between treatment effects, placebo effects, and natural history. Although the inclusion and exclusion criteria for the trials were stated, the selection procedures were not described; therefore, the potential for selection bias cannot be excluded.
An open-label design can introduce a risk of performance bias (i.e., the care or concomitant treatments received may differ based on knowledge of the intervention), but there was no evidence that this occurred. Similarly, the open-label design could introduce a risk of bias in the measurement of the outcomes, particularly HRQoL and subjective AEs. A relevant tool (EORTC QLQ-C30) with evidence of validity, reliability, and responsiveness was used in the assessment of HRQoL. However, the assessment of subjective end points can be biased because knowledge of the intervention can impact patient expectations and perceptions about the benefits and harms of treatment (i.e., there is a possibility for both to be overestimated). This risk of bias in the outcome assessment was mitigated for the response outcomes (PFS, ORR) in the KEYNOTE-158 and KEYNOTE-164 trials because these were outcomes assessed by an independent review committee. The measurement of these outcomes was done by the investigator in the KEYNOTE-051 trial, which might introduce some bias; however, this likely did not occur for the ORR because no patients responded. OS is an objective outcome that is not likely to be affected by such bias. However, it should be noted that OS results would be reflective of the influence of both pembrolizumab and subsequent treatments.
The risk of bias due to missing outcome data was considered to be low across all trials for the response and time-to-event outcomes because the rate of withdrawal from the studies was relatively low. In the assessment of ORR, patients with missing data were considered to be nonresponders, which would be a conservative assumption in a single-arm design. The assessment of HRQoL in the KEYNOTE-158 trial was at high risk of bias because, despite high adherence among available patients, close to 30% of the outcome data were missing at week 9. The analysis of the change from baseline employed a mixed model for repeated measures in which missing data are implicitly imputed under the assumption that they are missing at random. However, the reasons for the missing data suggest that this assumption is not valid, and no sensitivity analyses were provided to judge the robustness of the results.
The results of the KEYNOTE-158 and KEYNOTE-164 trials, which included adult patients with varying tumour types, show considerable heterogeneity in response across tumour types. Several tumour types were represented by a very small number of enrolled patients, which reduces the reliability of the results (i.e., the effects may be unstable and not reproducible in a larger sample). The interpretation of the potential differences in response across small samples of different cancer types is challenging because these may represent either actual differences in treatment effects or natural statistical variation. However, in its review, Health Canada acknowledged that the numbers of patients recruited for each histology reflects the natural prevalence of the MSI-H and/or dMMR biomarker, and that enrolling a larger number of patients may not have been feasible, given the broad indication.14 In the KEYNOTE-051 trial, only 7 pediatric patients were included (below the target of 25), which limits the reliability of assessing the efficacy and safety of pembrolizumab in this population. Additionally, rare or delayed AEs may not be adequately captured, leading to gaps in the harms profile, although there is extensive experience with pembrolizumab in many cancer indications. Quantification of the extent of uncertainty was challenged by a lack of CIs presented across several outcomes in this trial.
External Validity
In the KEYNOTE-158, KEYNOTE-164, and KEYNOTE-051 trials, patients who had previously received anti–PD-1, anti–PD-L1, or anti–PD-L2 drugs were excluded. The clinical experts consulted by CDA-AMC indicated that only a small proportion of the patient population in Canada would meet this eligibility criterion because most MSI-H and/or dMMR solid tumours are now treated with anti–PD-1 or anti–PD-L1 drugs that are the SOC in earlier lines of therapy. For cancers such as colorectal, endometrial, non–small cell lung cancer, kidney cancer, and urothelial carcinoma, pembrolizumab is already used in earlier treatment stages. Additionally, other immune checkpoint inhibitors are widely used in solid tumours like those found in gastric, mesothelioma, breast, small cell lung, and biliary tract cancers. Therefore, most of the available evidence in adults (KEYNOTE-158 and KEYNOTE-164 trials) is for tumours that are now treated with immune checkpoint inhibitors in earlier lines of therapy. The KEYNOTE-051 trial included only 7 pediatric patients, primarily with brain cancers, which also limits the generalizability of the findings. This small cohort may not adequately represent the broader patient population in terms of age, sex, performance status, disease stage, and other factors. As a result, it becomes difficult to confidently apply the outcomes of this trial to a broader population. Furthermore, HRQoL was not assessed in 2 trials (KEYNOTE-164 and KEYNOTE-051); thus, the generalizability of any HRQoL results to the CRC cohort and pediatric patients remains uncertain.
GRADE Summary of Findings and Certainty of the Evidence
Methods for Assessing the Certainty of the Evidence
For the pivotal studies identified in the sponsor’s systematic review, GRADE was used to assess the certainty of the evidence for outcomes considered most relevant to inform the deliberations of the CDA-AMC expert committee, and a final certainty rating was determined as outlined by the GRADE Working Group:15,16
High certainty: We are very confident that the true effect lies close to that of the estimate of the effect.
Moderate certainty: We are moderately confident in the effect estimate. The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. We use the word “likely” for evidence of moderate certainty (e.g., “X intervention likely results in Y outcome”).
Low certainty: Our confidence in the effect estimate is limited. The true effect may be substantially different from the estimate of the effect. We use the word “may” for evidence of low certainty (e.g., “X intervention may result in Y outcome”).
Very low certainty: We have very little confidence in the effect estimate. The true effect is likely to be substantially different from the estimate of effect. We describe evidence of very low certainty as “very uncertain.”
Although GRADE guidance is not available for noncomparative studies, to present these important considerations, the CDA-AMC review team assessed pivotal single-arm trials for study limitations (which refer to internal validity or risk of bias), inconsistency across studies (or populations), indirectness, and publication bias. Because the lack of a comparator arm does not allow for a conclusion to be drawn on the effect of the intervention versus any comparator, the certainty of evidence for single-arm trials started at very low certainty with no opportunity for rating up.
Although pooled evidence is available for the KEYNOTE-158 and KEYNOTE-164 trials, there are clinical characteristics that differ between these trials, such as cancer type, which may have an impact on important clinical outcomes. Therefore, GRADE was assessed separately in 3 patient groups based on these differences, as follows: adults with mixed solid tumours, adults with CRC, and children with mixed solid tumours.
Results of the GRADE Assessments
Table 2 presents the GRADE summary of findings for pembrolizumab for the treatment of unresectable or metastatic MSI-H or dMMR solid tumours assessed in adult and pediatric patients from the KEYNOTE-158, KEYNOTE-164, and KEYNOTE-051 trials.
Long-Term Extension Studies
No long-term evidence was submitted by the sponsor for this review.
Indirect Evidence
Contents within this section have been informed by materials submitted by the sponsor. The following has been summarized and validated by the CDA-AMC review team.
Objectives for the Summary of Indirect Evidence
No comparative evidence was available in the pivotal trials for patients with unresectable or metastatic MSI-H or dMMR solid tumours that progressed following prior treatment. This section provides a summary and appraisal of the indirect evidence submitted by the sponsor to address these knowledge gaps. These data were used to inform the pharmacoeconomic model.
Description of Indirect Comparisons
A total of 4 ITC reports were submitted, each focusing on a different solid tumour type: colorectal, endometrial, small intestine, and gastric cancers. ITCs were conducted only in tumour types for which there was a sufficient number of pembrolizumab-treated patients to conduct the analysis. All of the submitted ITCs were for the adult population only.
In the CRC ITC, pembrolizumab was compared with pooled chemotherapy, anti-VEGF plus chemotherapy, and TAS-102, representing the SOC interventions. Naive indirect comparisons were used for comparisons between pembrolizumab and pooled chemotherapy or anti-VEGF plus chemotherapy, while an unanchored MAIC was used to compare pembrolizumab with TAS-102. In the endometrial cancer ITC, an unanchored MAIC was conducted to compare pembrolizumab with TPC (doxorubicin or paclitaxel). For the small intestine cancer ITC, a naive indirect comparison was used to compare pembrolizumab with nab-paclitaxel. The gastric cancer ITC included a naive indirect comparison to compare pembrolizumab with FOLFIRI, ramucirumab plus paclitaxel, ramucirumab monotherapy, paclitaxel, and irinotecan.
Study Selection Methods
A systematic review was conducted to identify clinical trials evaluating treatments in adult patients with advanced or metastatic colorectal carcinoma who have received at least 1 prior line of therapy, irrespective of MSI-H or dMMR status. CDA-AMC did not receive any protocols outlining the systematic review and ITC for the different tumour types. The dates of the searches for the SLRs were in August 2023 (CRC ITC), May 2023 (small intestine cancer ITC), and June 2023 (gastric cancer ITC). Details of the study selection criteria can be found in Table 16. Two reviewers, working independently, reviewed all abstracts and proceedings identified by the search according to the selection criteria, with the exception of outcome criteria, which were only applied during the screening of full-text publications. The full texts of the studies identified as eligible during abstract screening were then screened by the same 2 reviewers. The studies selected at this stage were then included for data extraction. A third reviewer was included to reach consensus for any discrepancies.
For the endometrial cancer ITC, the KEYNOTE-775 trial was identified and selected based on a previous reimbursement submission reviewed by CDA-AMC.11 KEYNOTE-775 was a phase III RCT that evaluated the combination of pembrolizumab and lenvatinib versus TPC chemotherapy (doxorubicin or paclitaxel) for patients with advanced endometrial carcinoma following at least 1 prior platinum-based regimen in any setting. The study included subgroup analyses of ORR, PFS, and OS by MMR status (i.e., proficient MMR versus dMMR). For consistency, the ITC presented in this section and the comparator study selection methods are similar to those methods found in the material recently reviewed by CDA-AMC for the reimbursement recommendation for pembrolizumab monotherapy for the treatment of adult patients with unresectable or metastatic MSI-H or dMMR endometrial cancer whose tumours have progressed following prior therapy and who have no satisfactory alternative treatment options.11 This indication is already reimbursed by a majority of jurisdictions in Canada. The comparator in the previous submission was deemed to be still clinically relevant and no updated ITC was conducted. The ITC methods and results are summarized in Table 16.
ITC Design: CRC
Objectives
To compare the treatment efficacy of pembrolizumab as part of the KEYNOTE-164 trial versus SOC interventions in patients with MSI-H colorectal carcinomas and at least 1 prior line of therapy.
ITC Analysis Methods
A dataset with the individual patient data (IPD) from the KEYNOTE-164 trial and the pseudo-IPD from the comparator studies was used. The comparator studies were chosen based on SLRs of treatments commonly used for patients with MSI-H colorectal carcinoma and at least 1 prior line of therapy. The comparator group was pooled from multiple studies, although the pooling method was not specified. These individual comparators included pooled chemotherapy, anti-VEGF plus chemotherapy, and TAS-102, representing SOC interventions. To allow a treatment effect estimation on OS and PFS within the context of time-to-event analyses, a software tool was used to replicate the data from the published KM curves.71 Pseudo-IPD were derived for comparator interventions by using the number of participants at risk over time alongside the digitized KM curves, per the methods developed by Guyot et al.75
The baseline characteristics of the KEYNOTE-164 participants were reweighted to align with those of participants from the selected comparator studies to assess the potential reduction in ESS. For chemotherapy and anti-VEGF comparisons, where most studies included participants with only 1 prior line of therapy, KEYNOTE-164 participants with more than 1 prior line of therapy were excluded from the analyses, reducing the sample size from 124 to 30. Further reweighting for age, sex, and ECOG PS resulted in a significant reduction in ESS and, as a result, only unadjusted ITCs could be conducted for these comparators.
Table 16: Study Selection Criteria and Methods for Indirect Comparisons
Characteristic | Colorectal cancer | Endometrial cancer | Small intestine cancer | Gastric cancer | ||
|---|---|---|---|---|---|---|
Population | Patients with advanced or metastatic colorectal carcinoma, irrespective of MSI-H or dMMR status, who have received ≥ 1 prior line of therapy and:
| Adult patients with unresectable or MSI-H (dMMR) endometrial cancer whose tumours have progressed following prior therapy and who have no satisfactory alternative treatment options. Subgroups:
| Patients with advanced unresectable or metastatic small intestine or small bowel adenocarcinoma, irrespective of MSI-H or dMMR status, who have received ≥ 1 prior line of therapy and:
| Patients with histologically or cytologically confirmed recurrent or metastatic gastric or gastroesophageal junction adenocarcinoma, irrespective of MSI-H or dMMR status, who have received ≥ 1 prior line of therapy and:
| ||
Intervention |
|
|
|
| ||
Comparator | Unrestricted | Single-agent chemotherapy:
Hormonal therapy:
| Unrestricted | |||
Outcome | ≥ 1 of the following outcomes:
| Efficacy outcomes:
Harms:
| ≥ 1 of the following outcomes:
| |||
Time | From 2000 onward | No limits | From 2000 onward | |||
Study designs |
|
|
| |||
Language | English | No limits | English | |||
Exclusion criteria | ECOG PS ≥ 2, population with stage I or II disease, studies in patients with CNS metastasis, no intervention of interest, studies in patients previously treated with anti–PD-1 or anti–PD-L1 drugs, no outcome of interest, observational studies (prospective or retrospective noninterventional studies), case reports, case series. | Not reported. | Patients not previously treated, ECOG PS ≥ 2, no intervention of interest, no outcome of interest, populations with stage I or II disease, studies in patients with CNS metastases, studies in patients previously treated with an anti–PD-1 or anti–PD-L1 drug, ampulla of Vater cancers, radiation without chemotherapy, surgical intervention with or without systemic treatment, observational studies (prospective or retrospective noninterventional studies), case reports, case series. | ECOG PS ≥ 2, population with stage I or II disease, studies in patients with CNS metastasis, no intervention of interest, radiation without chemotherapy, surgical intervention with or without systemic treatment, studies in patients previously treated with anti–PD-1 or anti–PD-L1 drugs, no outcome of interest, observational studies (prospective or retrospective noninterventional studies), case reports, case series. | ||
Databases searched | Relevant studies were identified by searching the following databases through the Ovid platform:
The searches were executed on August 24, 2023 (CRC), May 18, 2023 (small intestine cancer), and May 31, 2024 (gastric cancer). Hand searches for relevant materials from the following scientific conferences were conducted on July 25, 2023 (CRC), June 2, 2023 (small intestine cancer), and June 6, 2023 (gastric cancer); the following conference abstracts were not searched for endometrial cancer:
Manual searches of the US National Institutes of Health Clinical Trial Registry (clinicaltrials.gov) were conducted to identify trials with posted results that have not yet been released in an abstract or full-text form. Additional manual searches conducted for endometrial cancer included only WHO’s International Clinical Trials Registry Platform search portal, Health Canada’s Clinical Trials Database, and the European Union Clinical Trials Register. | |||||
Selection process | Study selection followed a 2-stage screening process. First, a review of titles and/or abstracts against the PICOS selection criteria was conducted. Second, a full-text review of publications identified in the first step against the PICOS selection criteria was conducted. During both stages of study selection (i.e., title and/or abstract and full-text article) each publication was assessed by 2 independent investigators. Any disagreements were resolved by discussion between investigators, including a third researcher, if needed. A third investigator was not included in the endometrial cancer study selection process. | |||||
Data extraction process | Data from the included studies were extracted into a standardized table template developed in Microsoft Excel. Data were captured independently by 2 reviewers and reconciled. Any discrepancies were resolved by discussion between investigators, including a third researcher, if needed. A third investigator was not included in the endometrial cancer data extraction process. | |||||
Quality assessment | Two independent reviewers assessed study quality. Following reconciliation between the 2 investigators, a third investigator was included to reach consensus for any remaining discrepancies. Version 2 of the Cochrane risk-of-bias tool was used to assess the risk of bias in the included clinical trials.68 The Newcastle-Ottawa Scale was used to assess the study quality of the non-RCTs, including single-arm interventional trials.69 | Not reported. | Two independent reviewers assessed study quality. Following reconciliation between the 2 investigators, a third investigator was included to reach consensus for any remaining discrepancies. Version 2 of the Cochrane Collaboration’s risk-of-bias tool was used to assess the risk of bias in the included clinical trials.68 The Newcastle-Ottawa Scale was used to assess the study quality of the non-RCTs, including single-arm interventional trials.69 | |||
5-FU = 5-fluorouracil; AE = adverse event; ASCO = American Society of Clinical Oncology; CAPOX = capecitabine and oxaliplatin; CENTRAL = Cochrane Central Register of Controlled Trials; CNS = central nervous system; CRC = colorectal cancer; dMMR = mismatch repair deficient; DOR = duration of response; ECOG PS = Eastern Cooperative Oncology Group Performance Status; ESMO = European Society for Medical Oncology; FIGO = International Federation of Gynecology and Obstetrics; FOLFIRI = leucovorin calcium (folinic acid) + fluorouracil + irinotecan hydrochloride; FOLFOX = leucovorin calcium (folinic acid) + fluorouracil + oxaliplatin; FOLFOXIRI = folinic acid, 5-fluorouracil, oxaliplatin, and irinotecan; HRQoL = health-related quality of life; ICU = intensive care unit; ITC = indirect treatment comparison; MSI-H = microsatellite instability-high; nab = nanoparticle albumin-bound; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; PICOS = population, intervention, comparator, outcomes, and study design; RCT = randomized controlled trial; SAE = serious adverse event; SLR = systematic literature review; TAS-102 = trifluridine and tipiracil hydrochloride; WDAE = withdrawal due to adverse event.
Sources: Colorectal cancer SLR report,70 Merck Canada colorectal cancer ITC report,71 small intestine adenocarcinoma SLR report,72 Merck Canada small intestine cancer ITC report,73 gastric cancer SLR report,74 Merck Canada gastric cancer ITC report.73
Unadjusted ITCs, without adjustment for confounders or effect modifiers, were performed using Cox proportional hazard models, applying both pseudo-IPD from comparator arms and the KEYNOTE-164 data. The model included treatment as the sole covariate. The results summarized for each time-to-event end point included HRs with 95% CIs, P values, median survival times with corresponding CIs, and the number and percentage of events per treatment arm (pembrolizumab versus pooled comparators). In cases with 0 events in 1 treatment group, the 2-sided Wald test was replaced by a 2-sided score test. Log-cumulative hazard plots and Schoenfeld residual plots were generated for diagnostic purposes. When multiple suitable comparator arms were identified, pseudo-IPD data were merged, and baseline characteristics were summarized using weighted averages.
An unanchored MAIC approach was used for the comparison of pembrolizumab to TAS-102 (Table 17). To account for differences in baseline characteristics between participants in KEYNOTE-164 and the aggregated data from comparator studies (Table 44), IPD from the KEYNOTE-164 trial were reweighted to align with the mean baseline characteristics reported in the external studies, following the methods described by Signorovitch et al. (2012)76 and Signorovitch et al. (2010).77 Before reweighting, any participants in the KEYNOTE-164 trial who did not meet the eligibility criteria of the comparator trials were excluded. Potential effect modifiers and prognostic factors identified as relevant matching variables, based on input from the clinical experts, included age, sex, and ECOG PS.
For all comparisons in CRC, the proportional hazards assumption did not hold for both OS and PFS outcomes. Time-varying HR analyses were not conducted due to the limited sample size of the colorectal carcinoma subpopulation in the KEYNOTE-164 trial, which could have caused parametrization issues. Diagnostic plots were provided to aid in interpreting this assumption.71
Table 17: ITC Analysis Methods — Colorectal Cancer
Methods | Description |
|---|---|
Analysis methods | Naive indirect comparison using a Cox proportional hazard model for chemotherapy with or without anti-VEGF comparators; unanchored MAIC for TAS-102 comparators |
Outcomes |
|
Follow-up time points | Based on follow-up available from the digitized KM curves; length of follow-up not reported |
Sensitivity analyses | Removing 1 matching variable (ECOG PS) in the MAIC |
ECOG PS = Eastern Cooperative Oncology Group Performance Status; ITC = indirect treatment comparison; KM = Kaplan-Meier; MAIC = matching-adjusted indirect comparison; OS = overall survival; PFS = progression-free survival; TAS-102 = trifluridine and tipiracil hydrochloride; VEGF = vascular endothelial growth factor.
Source: Merck Canada colorectal cancer ITC report.71
Results of ITC: CRC
Summary of Included Studies
Baseline characteristics for selected comparator studies are provided in Table 18, Table 19, and Table 20. Table 18 and Table 19 provide a summary of the key patient characteristics in the pembrolizumab arm (KEYNOTE-164 study) and the pooled chemotherapy arm of the ITC and the anti-VEGF plus chemotherapy arm used in the naive indirect comparisons. For these 2 comparators, patients had received at least 1 prior line of systemic therapy. For the chemotherapy with or without anti-VEGF comparators, because the majority of comparator studies included only participants with 1 prior line of therapy, patients in the KEYNOTE-164 trial with more than 1 prior line of therapy were excluded from the naive indirect comparison. The results of the risk-of-bias assessment or quality of the included studies was not provided.
The characteristics of the patients in the pembrolizumab arm versus the TAS-102 arm after reweighting in the unanchored MAIC are described in Table 20; these patients had all received at least 2 prior lines of systemic treatment. For the TAS-102 comparison, there was a limitation in comparing the baseline characteristics of the comparator studies. It was assumed, for matching purposes within the MAIC framework, that all participants had received at least 2 prior lines of therapy. However, there may have been a small proportion of participants in the comparator studies who had fewer than 2 prior lines of therapy, which could impact the accuracy of the comparison.
The homogeneity assessment of included studies is provided in Table 21; few characteristics were available for comparison.
Table 18: Key Baseline Characteristics for Participants With MSI-H CRC and at Least 1 Line of Prior Therapy — Pembrolizumab Versus Pooled Chemotherapy (APaT Population)
Characteristic | Pembrolizumab (Na = 124) | Pooled chemotherapy (Nb = 2,890) |
|---|---|---|
Sex, n (%) | ||
Male | 69 (55.6) | 1,727 (59.8) |
Female | 55 (44.4) | 1,163 (40.2) |
Age (years), n (%) | ||
≤ 65 | 83 (66.9) | NR (NR) |
> 65 | 41 (33.1) | NR (NR) |
Mean (SD) | 56.1 (14.9) | NR (NR) |
Median (Q1; Q3) | 55.5 (45.0; 67.5) | 61.0 (NR; NR) |
Range | 21.0 to 84.0 | NR |
ECOG PS at screening, n (%) | ||
0 | 51 (41.1) | 1,548 (53.6) |
1 | 73 (58.9) | NR (NR) |
MSI-H, n (%) | 123 (99.2) | NR (NR) |
APaT = all participants as treated; CRC = colorectal cancer; ECOG PS = Eastern Cooperative Oncology Group Performance Status; MSI-H = microsatellite instability-high; NR = not reported; Q1 = quartile 1; Q3 = quartile 3; SD = standard deviation.
aNumber of participants: Included the APaT population of patients with MSI-H CRC and at least 1 line of prior therapy. Database cut-off date: February 19, 2021.
bNumber of participants was based on Aparicio et al. (2022), Giantonio et al. (2007), Graeven et al. (2007), Li et al. (2018), Masi et al. (2015), Moore et al. (2016), Passardi et al. (2017), Peeters et al. (2013), Pietrantonio et al. (2020), Randolph Hecht et al. (2017), Rothenberg et al. (2008), Tabernero et al. (2015), Van Cutsem et al. (2012), Van Cutsem et al. (2011), and Yasui et al. (2015); modified APaT population.
Source: Merck Canada CRC indirect treatment comparison report.71
Table 19: Key Baseline Characteristics for Participants With MSI-H CRC and at Least 1 Line of Prior Therapy — Pembrolizumab Versus Anti-VEGF and Chemotherapy (APaT Population)
Characteristic | Pembrolizumab | Anti-VEGF and chemotherapy |
|---|---|---|
Sex, n (%) | ||
Male | 69 (55.6) | 1,139 (59.0) |
Female | 55 (44.4) | 791 (41.0) |
Age (years), n (%) | ||
≤ 65 | 83 (66.9) | NR (NR) |
> 65 | 41 (33.1) | NR (NR) |
Mean (SD) | 56.1 (14.9) | NR (NR) |
Median (Q1; Q3) | 55.5 (45.0; 67.5) | 61.0 (NR; NR) |
Range | 21.0; 84.0 | NR; NR |
ECOG PS at screening, n (%) | ||
0 | 51 (41.1) | 1,194 (61.9) |
1 | 73 (58.9) | NR (NR) |
MSI-H, n (%) | 123 (99.2) | NR (NR) |
APaT = all participants as treated; CRC = colorectal cancer; ECOG PS = Eastern Cooperative Oncology Group Performance Status; MSI-H = microsatellite instability-high; NR = not reported; Q1 = quartile 1; Q3 = quartile 3; SD = standard deviation; VEGF = vascular endothelial growth factor.
aNumber of participants: Included the APaT population of patients with MSI-H CRC and at least 1 line of prior therapy. Database cut-off date: February 19, 2021.
bNumber of participants: Based on Bendell et al. (2013), Bendell et al. (2013), Cunningham et al. (2013), Giantonio et al. (2007), Iwamoto et al. (2015), Iwamoto et al. (2015), Li et al. (2018), Li et al. (2021), Masi et al. (2015), O’Neil et al. (2014), Passardi et al. (2017), Shi et al. (2017), Van Cutsem et al. (2012), modified APaT population.
Source: Merck Canada CRC indirect treatment comparison report.71
Table 20: Key Baseline Characteristics Before and After Weighting for Participants With MSI-H CRC and at Least 2 Lines of Prior Therapy — Pembrolizumab Versus TAS-102 (APaT Population)
Characteristic | Pembrolizumab | TAS-102 (Nb = 1,210) | |
|---|---|---|---|
Before weighting (Na = 94) | After weighting (N = 90.48) | ||
Sex, n (%) | |||
Male | 54 (57.4) | NR | 724 (59.8) |
Female | 40 (42.6) | NR (40.2) | 486 (40.2) |
Age (years), n (%) | |||
≤ 65 | 61 (64.9) | NR | NR (NR) |
> 65 | 33 (35.1) | NR | NR (NR) |
Mean (SD) | 57.1 (14.8) | NR | NR (NR) |
Median (Q1; Q3) | 59.0 (45.0; 69.0) | 63.0 (NR) | 63.0 (NR; NR) |
Range | 21.0 to 84.0 | NR | 24.0 to 90.0 |
ECOG PS at screening, n (%) | |||
0 | 43 (45.7) | NR (46.1) | 558 (46.1) |
1 | 51 (54.3) | NR | 648 (53.6) |
MSI-H, n (%) | 93 (98.9) | NR | NR (NR) |
Race | NR | NR | NR |
APaT = all participants as treated; CRC = colorectal cancer; ECOG PS = Eastern Cooperative Oncology Group Performance Status; MSI-H = microsatellite instability-high; NR = not reported; Q1 = quartile 1; Q3 = quartile 3; SD = standard deviation; TAS-102 = trifluridine and tipiracil hydrochloride.
aNumber of participants: Included the APaT population of patients with MSI-H CRC and at least 2 lines of prior therapy. Database cut-off date: February 19, 2021.
bNumber of participants: Based on Mayer et al. (2015), Pfeiffer et al. (2023), Prager et al. (2023), Xu et al. (2018), and Yoshino et al. (2012); modified APaT population.
Source: Merck Canada CRC indirect treatment comparison report.71
Table 21: Assessment of Homogeneity — Colorectal Cancer
Characteristic | Description and handling of potential effect modifiers |
|---|---|
ECOG PS |
|
Patient characteristics | The pooled comparator trials did not assess MSI-H and/or dMMR status. Several characteristics were unavailable for comparison.
|
Definitions of end points |
|
Timing of end point evaluation | OS and PFS were estimated based on Kaplan-Meier curves with varied follow-up periods. |
dMMR = mismatch repair deficient; ECOG PS = Eastern Cooperative Oncology Group Performance Status; MSI-H = microsatellite instability-high; OS = overall survival; PFS = progression-free survival; TAS-102 = trifluridine and tipiracil hydrochloride; VEGF = vascular endothelial growth factor.
Source: Merck Canada colorectal cancer indirect treatment comparison report.71
Results
In the naive indirect comparisons, pembrolizumab was favoured for OS versus chemotherapy alone or in combination with an anti-VEGF drug. The unadjusted OS analysis estimated an HR of 0.30 (95% CI, 0.24 to 0.39) when compared with chemotherapy alone, and an HR of 0.37 (95% CI, 0.29 to 0.48) when compared with chemotherapy in combination with an anti-VEGF drug. The unadjusted PFS analysis estimated an HR of 0.43 (95% CI, 0.34 to 0.54) when compared with chemotherapy alone, and an HR of 0.53 (95% CI, 0.42 to 0.67) when compared with chemotherapy in combination with an anti-VEGF drug, favouring pembrolizumab.
In the unanchored MAIC comparing pembrolizumab with TAS-102, pembrolizumab was favoured for OS and PFS. The unanchored OS and PFS analysis after matching estimated HRs of 0.21 (95% CI, 0.15 to 0.30) and 0.32 (95% CI, 0.23 to 0.45), respectively (Table 22, Table 23, Table 24, Table 25).
Table 22: Unadjusted Indirect OS Comparison of Pembrolizumab Versus Selected Comparators for Participants With MSI-H CRC and at Least 1 Prior Therapy (APaT Population)
Characteristic | Pembrolizumab | Pooled chemotherapy | Anti-VEGF and chemotherapy |
|---|---|---|---|
N | 124 | 3,283 | 1,642 |
Events, n (%) | 69 (55.6) | 2,654 (80.8) | 1,233 (75.1) |
Median OS,a months (95% CI) | 36.1 (24.0 to not reported) | 12.0 (11.7 to 12.4) | 14.3 (13.6 to 14.9) |
HRb (95% CI) | NA | 0.30 (0.24 to 0.39) | 0.37 (0.29 to 0.48) |
P valuec | NA | < 0.001 | < 0.001 |
APaT = all participants as treated; CI = confidence interval; CRC = colorectal cancer; HR = hazard ratio; MSI-H = microsatellite instability-high; NA = not applicable; OS = overall survival; VEGF = vascular endothelial growth factor.
aFrom product-limit (Kaplan-Meier) method.
bBased on Cox regression model with treatment as a covariate.
cTwo-sided P value using Wald test (score test in case of 0 events in 1 treatment group).
Source: Merck Canada CRC indirect treatment comparison report.71
Table 23: Unanchored OS MAIC of Pembrolizumab Versus TAS-102 for Participants With MSI-H CRC and at Least 2 Prior Therapies (APaT Population)
Characteristic | Pembrolizumaba,b | TAS-102c | ||
|---|---|---|---|---|
Before weighting | After weighting | Before weighting | After weighting | |
N | 94 | 92.2 | 1,210 | 1,210 |
Events, n (%) | 55 (58.5) | 34.4 (21.6 to 58.0) | 867 (71.7) | 867 (71.7) |
Median OS,d months (95% CI) | 55 (59.7) | 31.4 (21.4 to 58.0) | 7.5 (7.2 to 8.0) | 7.5 (7.2 to 8.0) |
HRe (95% CI) | NA | NA | 0.21 (0.14 to 0.30) | 0.21 (0.15 to 0.30) |
P valuef | NA | NA | < 0.001 | < 0.001 |
APaT = all participants as treated; CI = confidence interval; CRC = colorectal cancer; HR = hazard ratio; MAIC = matching-adjusted indirect comparison; MSI-H = microsatellite instability-high; NA = not applicable; OS = overall survival; TAS-102 = trifluridine and tipiracil hydrochloride.
Note: Matching covariates included age (median), sex, and Eastern Cooperative Oncology Group Performance Status.
aDatabase cut-off date: February 19, 2021.
bNumber of participants: APaT population with MSI-H CRC and at least 2 lines of prior therapy.
cNumber of participants: APaT population based on Mayer et al. (2015), Pfeiffer et al. (2023), Prager et al. (2023), Xu et al. (2018), Yoshino et al. (2012).
dFrom product-limit (Kaplan-Meier) method.
eBased on Cox regression model with treatment as a covariate.
fTwo-sided P value using Wald test (score test in case of 0 events in 1 treatment group).
Source: Merck Canada CRC indirect treatment comparison report.71
Table 24: Unadjusted Indirect PFS Comparison of Pembrolizumab Versus Selected Comparators for Participants With MSI-H CRC and at Least 1 Prior Therapy (APaT Population)
Characteristic | Pembrolizumab | Pooled chemotherapy | Anti-VEGF and chemotherapy |
|---|---|---|---|
N | 124 | 3,332 | 2,010 |
Events, n (%) | 84 (67.7) | 2,940 (88.2) | 1,593 (79.2) |
Median PFS,a months (95% CI) | 4.0 (2.1 to 7.4) | 4.8 (4.5 to 5.0) | 7.0 (6.7 to 7.3) |
HRb (95% CI) | NA | 0.43 (0.34 to 0.54) | 0.53 (0.42 to 0.67) |
P valuec | NA | < 0.001 | < 0.001 |
APaT = all participants as treated; CI = confidence interval; CRC = colorectal cancer; HR = hazard ratio; MSI-H = microsatellite instability-high; NA = not applicable; PFS = progression-free survival; VEGF = vascular endothelial growth factor.
aFrom product-limit (Kaplan-Meier) method.
bBased on Cox regression model with treatment as a covariate.
cTwo-sided P value using Wald test (score test in case of 0 events in 1 treatment group).
Source: Merck Canada CRC indirect treatment comparison report.71
Table 25: Unanchored PFS MAIC of Pembrolizumab Versus TAS-102 for Participants With MSI-H CRC and at Least 2 Prior Therapies (APaT Population)
Characteristic | Pembrolizumaba,b | TAS-102c | ||
|---|---|---|---|---|
Before weighting | After weighting | Before weighting | After weighting | |
N | 94 | 92.2 | 1,210 | 1,210 |
Events, n (%) | 63 (67.0) | 63 (68.3) | 1,066 (88.1) | 1,066 (88.1) |
Median PFS,d months (95% CI) | 4.0 (2.1 to 10.3) | 3.9 (2.1 to 10.2) | 2.1 (2.0 to 2.2) | 2.1 (2.0 to 2.2) |
HRe (95% CI) | NA | NA | 0.32 (0.23 to 0.44) | 0.32 (0.23 to 0.45) |
P valuef | NA | NA | < 0.001 | < 0.001 |
APaT = all participants as treated; CI = confidence interval; CRC = colorectal cancer; HR = hazard ratio; MAIC = matching-adjusted indirect comparison; MSI-H = microsatellite instability-high; NA = not applicable; PFS = progression-free survival; TAS-102 = trifluridine and tipiracil hydrochloride.
Note: Matching covariates included age (median), sex, and Eastern Cooperative Oncology Group Performance Status.
aDatabase cut-off date: February 19, 2021.
bNumber of participants: APaT population of patients with MSI-H CRC and at least 2 lines of prior therapy.
cNumber of participants: Based on Mayer et al. (2015), Pfeiffer et al. (2023), Prager et al. (2023), Xu et al. (2018), Yoshino et al. (2012), modified APaT population.
dFrom product-limit (Kaplan-Meier) method.
eBased on Cox regression model with treatment as a covariate.
fTwo-sided P value using Wald test (score test in case of 0 events in 1 treatment group).
Source: Merck Canada CRC indirect treatment comparison report.71
ITC Design: Endometrial Cancer
Objectives
The objective was to compare pembrolizumab in participants with MSI-H endometrial carcinoma that were part of the KEYNOTE-158 study (particularly in cohort K and some in cohort D; data cut-off date of January 12, 2022) against the comparator arm (doxorubicin or paclitaxel, denoted as TPC) in the dMMR subpopulation of the KEYNOTE-775 trial using information from Makker et al. (2021).78
ITC Analysis Methods
The endometrial cancer ITC used unanchored MAICs to assess the relative efficacy of pembrolizumab monotherapy in participants with previously treated MSI-H or dMMR advanced or metastatic endometrial carcinoma, compared with SOC (Table 26). The following baseline characteristics, identified as potential effect modifiers or key prognostic factors based on clinical expertise, were selected as matching variables:
age (median)
race (Asian, Black, white, other)
ECOG PS (0 versus 1)
number of prior lines of therapy (1 versus ≥ 2)
histology status (endometrioid carcinoma, others).
For time-to-event end points (such as OS and PFS), an unstratified Cox proportional hazards model was applied, with treatment as the only covariate and using the Efron method for handling ties. This model used a universal weight of 1 for the comparator arm (pseudo-IPD for TPC from the KEYNOTE-775 trial) and weights derived from the MAIC matching step for the pembrolizumab arm (IPD from the KEYNOTE-158 trial). HRs for pembrolizumab versus TPC and the corresponding 95% CIs were estimated both before and after weighting, using the sandwich (empirical) covariance matrix. A 2-sided Wald test was applied (all treatment groups had ≥ 1 event).
For the end point (i.e., ORR), a weighted response ratio with no stratification factor was used to estimate the treatment difference between pembrolizumab and TPC, with a universal weight 1 for the comparator arm (pseudo-IPD for TPC from the KEYNOTE-775 trial) and the weights from the MAIC matching step for the pembrolizumab arm (IPD from the KEYNOTE-158 trial).
Table 26: ITC Analysis Methods — Endometrial Cancer
Methods | Description |
|---|---|
Analysis methods | Unanchored MAIC |
Outcomes |
|
Follow-up time points | Based on follow-up available from the digitized KM curves; length of follow-up not reported |
Sensitivity analyses | Sensitivity analyses were performed to investigate the MAIC OS, PFS, and ORR results according to different matching variables (age, ECOG PS, race, prior lines of therapy, prior adjuvant or neoadjuvant therapy)79 |
ECOG PS = Eastern Cooperative Oncology Group Performance Status; ITC = indirect treatment comparison; KM = Kaplan-Meier; MAIC = matching-adjusted indirect comparison; ORR = objective response rate; OS = overall survival; PFS = progression-free survival.
Source: Merck Canada endometrial cancer ITC report.80
Results of ITC: Endometrial Cancer
Table 27 provides a summary of the key patient characteristics in the pembrolizumab arm (KEYNOTE-158 study) and the TPC arm of the ITC. The baseline homogeneity assessment of included studies is provided in Table 28.
Summary of Included Studies
Table 27: MAIC of Pembrolizumab Versus Selected Comparators for Participants With MSI-H Endometrial Carcinoma and at Least 1 Line of Prior Therapy
Characteristic | TPC (Na = 65) | KEYNOTE-158 trialb | |
|---|---|---|---|
Before weighting (Nc = 94) | After weighting (Nd = 46.11) | ||
Age (years) | |||
Median | 63.0 | 64.0 | 62.0 |
ECOG PS (%) | |||
0 | 52.3 | 44.7 | 52.3 |
1 | 47.7 | 55.3 | 47.7 |
Race (%) | |||
Asian | 18.5 | 7.4 | 18.5 |
Black | 7.7 | 3.2 | 7.7 |
White | 53.8 | 84.0 | 53.8 |
Other | 20.0 | 5.3 | 20.0 |
Prior lines of therapy (%) | |||
1 | 78.5 | 52.1 | 78.5 |
≥ 2 | 21.5 | 47.9 | 21.5 |
Prior adjuvant or neoadjuvant therapy (%) | |||
Yes | 49.2 | 26.6 | 49.2 |
APaT = all participants as treated; ECOG PS = Eastern Cooperative Oncology Group Performance Status; ESS = effective sample size; MAIC = matching-adjusted indirect comparison; MSI-H = microsatellite instability-high; TPC = treatment of physician’s choice (doxorubicin or paclitaxel).
aNumber of participants and comparators based on Makker et al. (2021).
bDatabase cut-off date: January 12, 2022.
cNumber of participants: Included the APaT population of patients in the KEYNOTE-158 trial with MSI-H endometrial carcinoma (cohorts D and K) and at least 1 line of prior therapy.
dESS computed as the square of the summed weights divided by the sum of the squared weights. Weighted according to matched baseline characteristics of selected comparators.
Source: Merck Canada endometrial cancer indirect treatment comparison report.80
Table 28: Assessment of Homogeneity — Endometrial Cancer
Characteristic | Description and handling of potential effect modifiers |
|---|---|
Disease severity | Disease stage was similar in the KEYNOTE-158 and KEYNOTE-775 (patients with advanced endometrial cancer that did not respond to 1 previous line of therapy) trials. |
Patient characteristics | There were some notable differences in the distribution of ECOG PS (0 versus 1), race (Asian, Black, white, other), the number of prior lines of therapy (1 versus 2 or more) and histology status (endometrioid carcinoma, others) between patients in the pembrolizumab arm and the TPC arm of the ITC. Median age was relatively similar in the 2 arms (63 versus 64 years). |
Definitions of end points | KEYNOTE-158 and KEYNOTE-775 trials:
|
Timing of end point evaluation | OS and PFS were estimated based on mature KM curves. |
ECOG PS = Eastern Cooperative Oncology Group Performance Status; ITC = indirect treatment comparison; KM = Kaplan-Meier; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; TPC = treatment of physician’s choice (doxorubicin or paclitaxel).
Source: Merck Canada endometrial cancer ITC report.80
Table 29: Unanchored MAIC Analysis of OS (Pembrolizumab Versus TPC) for Patients With MSI-H Endometrial Carcinoma and at Least 1 Line of Prior Therapy
Characteristic | Pembrolizumaba | TPC | ||
|---|---|---|---|---|
Before weighting | After weightingb | Before weighting | After weightingb | |
Nc | 94 | 58.2d | 65 | 65 |
Events, n (%) | 41 (43.6) | 19 (32.6) | 42 (64.6) | 42 (64.6) |
Median OS,e months (95% CI) | 65.4 (29.5; not reached) | Not reached (0.5 to 1.5) | 8.6 (5.5 to 12.9) | 8.6 (5.5 to 12.9) |
HRf (95% CI) | NA | NA | 0.34 (0.21 to 0.54) | 0.24 (0.13 to 0.45) |
P valuef,g | NA | NA | < 0.001 | < 0.001 |
CI = confidence interval; ECOG PS = Eastern Cooperative Oncology Group Performance Status; HR = hazard ratio; MAIC = matching-adjusted indirect comparison; MSI-H = microsatellite instability-high; NA = not applicable; OS = overall survival; TPC = treatment of physician’s choice (doxorubicin or paclitaxel).
aDatabase cut-off date: January 12, 2022.
bMatching was done on the following covariates: age (median), ECOG PS, race, prior lines of therapy, and histology status.
cNumber of participants: For pembrolizumab, this included all participants with MSI-H endometrial carcinoma (cohorts D and K) and at least 1 line of prior therapy in the as-treated population of the KEYNOTE-158 trial. For TPC, the data were based on Makker et al. (2021).
dSample size after matching computed as the sum of the weights.
eFrom product-limit (Kaplan-Meier) method for censored data.
fBased on Cox regression model with treatment as a covariate.
gTwo-sided P value using Wald test (score test in case of 0 events in 1 treatment group).
Source: Merck Canada endometrial cancer indirect treatment comparison report.80
Results
OS results for the unanchored MAIC between pembrolizumab from the KEYNOTE-158 trial and the TPC data from the KEYNOTE-775 trial are presented in Table 29. After weighting, the HR was 0.24 (95% CI, 0.13 to 0.45) favouring pembrolizumab compared with TPC. The sensitivity analysis for OS yielded results that aligned with the main analysis in both the direction and magnitude of effect.
Table 30: Unanchored MAIC Analysis of PFS (Pembrolizumab Versus TPC) for Patients With MSI-H Endometrial Carcinoma and at Least 1 Line of Prior Therapy
Characteristic | Pembrolizumaba | TPC | ||
|---|---|---|---|---|
Before weighting | After weightingb | Before weighting | After weightingb | |
Nc | 94 | 58.2d | 65 | 65 |
Events, n (%) | 58 (61.7) | 35 (60.1) | 48 (73.8) | 48 (73.8) |
Median PFS,e months (95% CI) | 13.1 (4.3 to 25.7) | 14.2 (not reported) | 3.7 (3.1 to 4.4) | 3.7 (3.1 to 4.4) |
HRf (95% CI) | NA | NA | 0.42 (0.28 to 0.64) | 0.31 (0.19 to 0.53) |
P valuef,g | NA | NA | < 0.001 | < 0.001 |
CI = confidence interval; ECOG PS = Eastern Cooperative Oncology Group Performance Status; HR = hazard ratio; MAIC = matching-adjusted indirect comparison; MSI-H = microsatellite instability-high; NA = not applicable; PFS = progression-free survival; TPC = treatment of physician’s choice (doxorubicin or paclitaxel).
aDatabase cut-off date: January 12, 2022.
bMatching was done on the following covariates: age (median), ECOG PS, race, prior lines of therapy, and histology status.
cNumber of participants: For pembrolizumab, this included all participants in the as-treated population in the KEYNOTE-158 trial with MSI-H endometrial carcinoma (cohorts D and K) and at least 1 line of prior therapy. For TPC, the number of participants was based on Makker et al. (2021).
dThe sample size after matching was computed as the sum of the weights.
eFrom product-limit (Kaplan-Meier) method for censored data.
fBased on Cox regression model with treatment as a covariate.
gTwo-sided P value using Wald test (score test in case of 0 events in 1 treatment group).
Source: Merck Canada endometrial cancer indirect treatment comparison report.80
Table 31: Unanchored MAIC Analysis of ORR (Pembrolizumab Versus TPC) for Patients With MSI-H Endometrial Carcinoma and at Least 1 Line of Prior Therapy
Characteristic | Pembrolizumaba | TPCb | ||
|---|---|---|---|---|
Before weighting | After weightingc | Before weighting | After weightingc | |
N | 94 | 58.2d | 65 | 65 |
Patients with ORR (%) | 47 (50.00) | 32.2 (55.36) | 8 (12.31) | 8 (12.31) |
Response ratioe (95% CI) | NA | NA | 4.06 (2.06 to 8.02) | 4.50 (2.22 to 9.10) |
P valuef | NA | NA | < 0.001 | < 0.001 |
CI = confidence interval; ECOG PS = Eastern Cooperative Oncology Group Performance Status; ESS = effective sample size; MAIC = matching-adjusted indirect comparison; MSI-H = microsatellite instability-high; NA = not applicable; ORR = objective response rate; TPC = treatment of physician’s choice (doxorubicin or paclitaxel).
aNumber of participants: This included all participants in the as-treated population of the KEYNOTE-158 trial with MSI-H endometrial carcinoma (cohorts D and K) and at least 1 line of prior therapy. Database cut-off date: January 12, 2022.
bNumber of participants: Based on Makker et al. (2021).
cMatching was done on the following covariates: age (median), ECOG PS, race, prior lines of therapy, and prior adjuvant or neoadjuvant therapy.
dESS after matching computed as the sum of the weights.
eBased on a robust sandwich estimator using PROC GENMOD in the safety analysis set.
fTwo-sided P value based on Wald test.
Source: Merck Canada endometrial cancer indirect treatment comparison report.80
For PFS, the results are detailed in Table 30. Following weighting, the HR was 0.31 (95% CI, 0.19 to 0.53), favouring pembrolizumab compared with TPC. The sensitivity analysis for PFS yielded results that aligned with the main analysis in both the direction and magnitude of effect.
The ORR results are outlined in Table 31. After weighting, the response ratio was 4.27 (95% CI, 2.11 to 8.64), favouring pembrolizumab compared with TPC. The sensitivity analysis for ORR yielded results that aligned with the main analysis in both the direction and magnitude of effect.
ITC Design: Small Intestine Cancer
Objectives
To compare pembrolizumab in participants with MSI-H small intestine cancer who were part of the KEYNOTE-158 trial versus selected interventions.
ITC Analysis Methods
A naive indirect comparison was performed based on Cox proportional hazard models using pseudo-IPD for the nab-paclitaxel arm and IPD from the KEYNOTE-158 trial for the pembrolizumab arm (Table 32). The model included treatment as a single covariate. The following results were summarized for each time-to-event end point analyzed: HRs with corresponding 95% CIs and P values, median survival time with corresponding 95% CIs, and number and percentage of events by treatment arm (pembrolizumab versus nab-paclitaxel). Log-cumulative hazard plots as well as Schoenfeld residual plots were produced for diagnostic purposes. KM curves for OS and PFS from Overman et al.81 were used to derive pseudo-IPD for the nab-paclitaxel arm of the ITC. Digital software was used to replicate the data from the published KM curves. Pseudo-IPD were derived using the number of participants at risk over time alongside the digitized KM curves, per the methods developed by Guyot et al.75 Due to the reduction in the ESS after matching, the baseline characteristics of participants with MSI-H small intestine cancer in the KEYNOTE-158 trial versus the aggregated baseline characteristics of the selected comparator study, the impact on ESS was deemed too substantial to perform an MAIC. As a result, only naive unadjusted ITCs were conducted.
Table 32: ITC Analysis Methods — Small Intestine Cancer
Methods | Description |
|---|---|
Analysis methods | Naive indirect comparison using Cox proportional hazard model |
Outcomes |
|
Follow-up time points | At least 6 months of follow-up was required for all patients considered in the KEYNOTE-158 trial IPD and, for the comparator study, data were used as derived from the digitization process. |
IPD = individual patient data; ITC = indirect treatment comparison; OS = overall survival; PFS = progression-free survival.
Source: Merck Canada small intestine cancer ITC report.82
Results of ITC: Small Intestine Cancer
Table 33 provides a summary of the key patient characteristics in the pembrolizumab arm (KEYNOTE-158 study) and the nab-paclitaxel arm of the ITC. In these 2 treatment arms, all patients had received at least 1 prior line of systemic therapy; the median number of lines of prior therapy was 1 in the pembrolizumab arm versus 2 in the nab-paclitaxel arm. The homogeneity assessment of included studies is provided in Table 34.
Table 33: Key Baseline Characteristics for Participants With MSI-H Small Intestine Carcinoma and at Least 1 Line of Prior Therapy
Characteristic | Pembrolizumab | Nab-paclitaxel |
|---|---|---|
Sex, n (%) | ||
Male | 17 (63.0) | 6 (46.2) |
Female | 10 (37.0) | 7 (54.8) |
Age (years), n (%) | ||
< 65 | 18 (66.7) | NR (NR) |
≥ 65 | 9 (33.3) | NR (NR) |
Mean (SD) | 57.6 (13.1) | NR (NR) |
Median (Q1; Q3) | 58.0 (53.0; 67.0) | 58.0 (NR; NR) |
Range | 21.0 to 77.0 | 40.0 to 76.0 |
Race, n (%) | ||
American Indian or Alaska Native | 2 (7.4) | NR (NR) |
Asian | 3 (11.1) | 2 (15.0) |
Black or African American | 0 (0.0) | 4 (31.0) |
White | 22 (81.5) | 7 (54.0) |
ECOG PS, n (%) | ||
0 | 15 (55.6) | 6 (46.0) |
1 | 12 (44.4) | 7 (54.0) |
Number of prior lines of therapy | ||
Participants with data | 27 | 13 |
Mean (SD) | 1.5 (0.9) | NR (NR) |
Median (Q1; Q3) | 1.0 (1.0; 2.0) | 2.0 (NR; NR) |
Range | 0.0 to 4.0 | 1.0 to 7.0 |
ECOG PS = Eastern Cooperative Oncology Group Performance Status; MSI-H = microsatellite instability-high; nab = nanoparticle albumin-bound; NR = not reported; Q1 = first quartile; Q3 = third quartile; SD = standard deviation.
aNumber of participants: For the pembrolizumab efficacy analysis, this included all participants with MSI-H small intestine carcinoma and at least 1 line of prior therapy in the as-treated population in the KEYNOTE-158 trial. Database cut-off date: January 12, 2022.
bNumber of participants: mAPaT population based on Overman (2018).
Source: Merck Canada small intestine cancer indirect treatment comparison report.82
Results
The naive indirect comparisons resulted in an HR of 0.18 (95% CI, 0.07 to 0.45) for OS (Table 35) and an HR of 0.22 (95% CI, 0.09 to 0.52) for PFS (Table 36), both favouring pembrolizumab.
Table 34: Assessment of Homogeneity — Small Intestine Cancer
Characteristic | Description and handling of potential effect modifiers |
|---|---|
Disease severity |
|
Patient characteristics |
|
Definitions of end points | Cannot assess homogeneity because OS and PFS definitions are not stated in Overman et al.81 |
Timing of end point evaluation | OS and PFS were estimated based on KM curves with a range of follow-up periods; the length of follow-up was not reported. |
dMMR = mismatch repair deficient; ECOG PS = Eastern Cooperative Oncology Group Performance Status; KM = Kaplan-Meier; MSI-H = microsatellite instability-high; nab = nanoparticle albumin-bound; OS = overall survival; PFS = progression-free survival.
Source: Merck Canada small intestine cancer indirect treatment comparison report.82
Table 35: Unadjusted OS Analysis — Unadjusted ITC of Pembrolizumab Versus Nab-Paclitaxel for Patients With MSI-H Small Intestine Carcinoma and at Least 1 Line of Prior Therapy
Characteristic | Pembrolizumab | TPC |
|---|---|---|
Na | 27 | 10 |
Events, n (%) | 10 (37.0) | 10 (100.0) |
Median OS,b months (95% CI) | Not reached (16.2 to not reached) | 10.9 (3.9 to 15.3) |
HRc (95% CI) | NA | 0.18 (0.07 to 0.45) |
P valuec,d | NA | < 0.001 |
APaT = all participants as treated; CI = confidence interval; HR = hazard ratio; ITC = indirect treatment comparison; KM = Kaplan-Meier; MSI-H = microsatellite instability-high; nab = nanoparticle albumin-bound; NA = not applicable; OS = overall survival; TPC = treatment of physician’s choice (doxorubicin or paclitaxel).
aNumber of participants: For the pembrolizumab efficacy analysis, this included all participants with MSI-H small intestine carcinoma and at least 1 line of prior therapy in the as-treated population in the KEYNOTE-158 trial; database cut-off date: January 12, 2022. For TPC, the data were based on the Overman (2018) modified APaT population.
bFrom product-limit (Kaplan-Meier) method.
cBased on Cox regression model with treatment as a covariate.
dTwo-sided P value using Wald test (score test in case of 0 events in 1 treatment group).
Source: Merck Canada small intestine cancer ITC report.82
Table 36: Unadjusted PFS Analysis — Unadjusted ITC of Pembrolizumab Versus Nab-Paclitaxel for Patients With MSI-H Small Intestine Carcinoma and at Least 1 Line of Prior Therapy
Characteristic | Pembrolizumab | TPC |
|---|---|---|
Na | 27 | 10 |
Events, n (%) | 14 (51.9) | 10 (100.0) |
Median PFS,b months (95% CI) | 29.2 (4.3 to not reached) | 3.2 (2.0 to 6.5) |
HRc (95% CI) | NA | 0.22 (0.09 to 0.52) |
P valuec,d | NA | < 0.001 |
APaT = all participants as treated; CI = confidence interval; HR = hazard ratio; ITC = indirect treatment comparison; KM = Kaplan-Meier; MSI-H = microsatellite instability-high; NA = not applicable; nab = nanoparticle albumin-bound; PFS = progression-free survival; TPC = treatment of physician’s choice (doxorubicin or paclitaxel).
aNumber of participants: For the pembrolizumab efficacy analysis, this included all patients with MSI-H small intestine carcinoma and at least 1 line of prior therapy in the as-treated population of the KEYNOTE-158 trial; database cut-off date: January 12, 2022. For TPC, the data were based on the Overman (2018) modified APaT population.
bFrom product-limit (Kaplan-Meier) method.
cBased on Cox regression model with treatment as a covariate.
dTwo-sided P value using Wald test (score test in case of 0 events in 1 treatment group).
Source: Merck Canada small Iintestine cancer ITC report.82
ITC Design: Gastric Cancer
Objectives
To compare the efficacy in patients with MSI-H gastric carcinomas in the KEYNOTE-158 trial who received pembrolizumab versus selected interventions.
ITC Analysis Methods
Naive indirect comparisons were performed based on Cox proportional hazard models using pseudo-IPD for the comparator arms and IPD from the KEYNOTE-158 trial for the pembrolizumab arm (Table 37). In some cases, the comparator arm included pooled data across multiple studies, but it was not clear how this pooling was undertaken. The model included treatment as a single covariate. The following results were summarized for each time-to-event end point analyzed: HRs with corresponding 95% CIs and P values, median survival time with the corresponding 95% CI, and number and percentage of events by treatment arm (pembrolizumab versus selected comparators). If there were no events in 1 of the treatment groups, the 2-sided Wald test was replaced with a 2-sided score test. Log-cumulative hazard plots as well as Schoenfeld residual plots were produced for diagnostic purposes. A software tool was used to replicate the data from the published KM curves. Pseudo-IPD were derived using the number of participants at risk over time alongside the digitized KM curves, per the methods developed by Guyot et al.75 Due to the reduction in the ESS after matching the baseline characteristics of participants with MSI-H gastric cancer in the KEYNOTE-158 trial to the aggregated baseline characteristics of the selected comparator studies, the impact on ESS was deemed too substantial to perform an MAIC. As a result, only unadjusted ITCs were conducted.
Table 37: ITC Analysis Methods — Gastric Cancer
Method | Description |
|---|---|
Analysis methods | Naive indirect comparison using Cox proportional hazard model |
Outcomes |
|
Follow-up time points | Based on follow-up available from the digitized KM curves with a range of follow-up periods; length of follow-up not reported |
ITC = indirect treatment comparison; KM = Kaplan-Meier; OS = overall survival; PFS = progression-free survival.
Source: Merck Canada gastric cancer ITC report.73
Results of ITC: Gastric Cancer
Summary of Included Studies
The selected comparator studies are listed in Table 45 of Appendix 1. The baseline characteristics of the patients in each treatment group of interest in each study is reported in Table 38. The comparators trials did not assess MSI-H or dMMR status. The comparator interventions include FOLFIRI, ramucirumab plus paclitaxel, ramucirumab, paclitaxel, and irinotecan. The homogeneity assessment of the included studies is provided in Table 39.
Table 38: Baseline Characteristics of the ITC Treatment Arms
Characteristic | Pembrolizumab (Na = 51) | FOLFIRI (Nb = 75) | Ramucirumab (Nb = 278) | Paclitaxel (Nb = 12) | Ramucirumab and paclitaxel (Nb = 506) | Irinotecan (Nb = 600) |
|---|---|---|---|---|---|---|
Sex, n (%) | ||||||
Male | 33 (64.7) | 44 (58.7) | 198 (71.2) | 8 (66.7) | 346 (68.4) | 459 (76.5) |
Female | 18 (35.3) | 31 (41.3) | 80 (28.8) | 4 (33.3) | 160 (31.6) | 141 (23.5) |
Age (years), n (%) | ||||||
Median (Q1; Q3) | 67.0 (59.0; 76.0) | 57.0 (NR; NR) | 60.0 (NR; NR) | 63.0 (NR; NR) | 61.0 (NR; NR) | 65.0 (NR; NR) |
Range | 41.0 to 89.0 | 28.0 to 84.0 | NR | 43.0 to 75.0 | NR | 35.0 to 78.0 |
ECOG PS, n (%) | ||||||
0 | 23 (45.1) | NR (NR) | 80 (28.8) | 4 (33.3) | 191 (37.7) | NR (NR) |
1 | 28 (54.9) | NR (NR) | 197 (70.9) | 8 (66.7) | 314 (62.1) | NR (NR) |
Number of prior lines of therapy | ||||||
Mean (SD) | 1.8 (1.0) | NR (NR) | NR (NR) | NR (NR) | NR (NR) | NR (NR) |
Median (Q1; Q3) | 1.0 (1.0; 2.0) | NR (NR; NR) | NR (NR; NR) | NR (NR; NR) | NR (NR; NR) | NR (NR; NR) |
Range | 1.0 to 5.0 | NR | NR | NR | NR | NR |
Race | NR | NR | NR | NR | NR | NR |
ECOG PS = Eastern Cooperative Oncology Group Performance Status; FOLFIRI = leucovorin calcium (folinic acid) + fluorouracil + irinotecan hydrochloride; ITC = indirect treatment comparison; mAPaT = modified all participants as treated; MSI-H = microsatellite instability-high; NR = not reported; Q1 = quartile 1; Q3 = quartile 3; SD = standard deviation.
aNumber of participants: The efficacy analysis included all participants with MSI-H gastric carcinoma and at least 1 line of prior therapy in the KEYNOTE-158 trial in the as-treated population; database cut-off date: January 12, 2022.
bNumber of participants: Based on comparator-specific pooled data for the mAPaT population from the sources reported in Table 45.
Source: Merck Canada gastric cancer ITC report.73
Table 39: Assessment of Homogeneity — Gastric Cancer
Characteristic | Description and handling of potential effect modifiers |
|---|---|
Disease severity |
|
Patient characteristics | Pooled comparators trials did not assess MSI-H or dMMR status. Comparison with:
|
Definitions of end points | The definitions of the 2 end points, OS and PFS, were similar to the definitions in the KEYNOTE-158 trial and the selected comparative trials. |
Timing of end point evaluation | OS and PFS were estimated based on KM curves with a range of follow-up periods (not specified). |
dMMR = mismatch repair deficient; ECOG PS = Eastern Cooperative Oncology Group Performance Status; FOLFIRI = leucovorin calcium (folinic acid) + fluorouracil + irinotecan hydrochloride; KM = Kaplan-Meier; MAIC = matching-adjusted indirect comparison; MSI-H = microsatellite instability-high; OS = overall survival; PFS = progression-free survival.
Source: Merck Canada gastric cancer indirect treatment comparison report.73
Results
The naive indirect comparisons demonstrated that pembrolizumab was favoured for OS (Table 40) and PFS (Table 41) compared with FOLFIRI, ramucirumab, ramucirumab and paclitaxel, and irinotecan in patients with gastric cancer. The evidence was insufficient to demonstrate a difference between pembrolizumab and paclitaxel.
Table 40: Unadjusted OS Analysis — ITC of Pembrolizumab Versus Comparators for Patients With MSI-H Gastric Carcinoma and at Least 1 Line of Prior Therapy
Detail | Pembrolizumab | FOLFIRI | Ramucirumab | Paclitaxel | Ramucirumab and paclitaxel | Irinotecan |
|---|---|---|---|---|---|---|
Na | 51 | 75 | 278 | 12 | 506 | 600 |
Median OS,b months (95% CI) | 19.9 (6.6; not reached) | 7.5 (4.5 to 9.7) | 5.3 (4.5 to 5.8) | 8.1 (2.0 to 16.6) | 8.9 (8.0 to 9.8) | 8.4 (7.8 to 9.3) |
HRc (95% CI) | NA | 0.43 (0.26 to 0.69) | 0.35 (0.22 to 0.53) | 0.53 (0.25 to 1.10) | 0.44 (0.29 to 0.66) | 0.38 (0.26 to 0.56) |
P valuec,d | NA | < 0.001 | < 0.001 | 0.089 | < 0.001 | < 0.001 |
CI = confidence interval; FOLFIRI = leucovorin calcium (folinic acid) + fluorouracil + irinotecan hydrochloride; HR = hazard ratio; ITC = indirect treatment comparison; MSI-H = microsatellite instability-high; mAPaT = modified all participants as treated; NA = not applicable; OS = overall survival.
aNumber of participants: For the pembrolizumab efficacy analysis, this included all participants with MSI-H gastric carcinoma and at least 1 line of prior therapy in the as-treated population in the KEYNOTE-158 trial; database cut-off date: January 12, 2022. For comparators, the analysis was based on comparator-specific pooled data for the mAPaT population from the sources reported in Table 45.
bFrom product-limit (Kaplan-Meier) method.
cBased on Cox regression model with treatment as covariate.
dTwo-sided P value using Wald test (score test in case of 0 events in 1 treatment group).
Source: Merck Canada gastric cancer ITC report.73
Table 41: Unadjusted PFS Analysis — ITC of Pembrolizumab Versus Comparators for Patients With MSI-H Gastric Carcinoma and at Least 1 Line of Prior Therapy
Characteristic | Pembrolizumab | FOLFIRI | Ramucirumab | Paclitaxel | Ramucirumab and paclitaxel | Irinotecan |
|---|---|---|---|---|---|---|
Na | 51 | 75 | 278 | 12 | 506 | 600 |
Median PFS,b months (95% CI) | 4.1 (2.1 to 24.6) | 3.1 (2.3 to 5.3) | 1.8 (1.5 to 2.6) | 2.9 (1.7 to 13.8) | 4.5 (4.2 to 5.2) | 3.0 (2.6 to 3.3) |
HRc (95% CI) | NA | 0.43 (0.28 to 0.67) | 0.37 (0.24 to 0.58) | 0.73 (0.35 to 1.50) | 0.45 (0.31 to 0.65) | 0.33 (0.23 to 0.47) |
P valuec,d | NA | < 0.001 | < 0.001 | 0.387 | < 0.001 | < 0.001 |
APaT = all participants as treated; CI = confidence interval; FOLFIRI = leucovorin calcium (folinic acid) + fluorouracil + irinotecan hydrochloride; ITC = indirect treatment comparison; MSI-H = microsatellite instability-high; NA = not applicable; PFS = progression-free survival.
aNumber of participants: For the pembrolizumab efficacy analysis, this included all patients with MSI-H gastric carcinoma and at least 1 line of prior therapy in the as-treated population in the KEYNOTE-158 trial; database cut-off date: January 12, 2022. For comparators, the analysis was based on comparator-specific pooled data for the modified APaT population from the sources reported in Table 45.
bFrom product-limit (Kaplan-Meier) method.
cBased on Cox regression model with treatment as covariate.
dTwo-sided P value using Wald test (score test in case of 0 events in 1 treatment group).
Source: Merck Canada gastric cancer ITC report.73
Critical Appraisal of ITCs
The sponsor-submitted SLRs that were used to identify studies for inclusion in all of the submitted ITCs, except the ITC for endometrial cancer, appeared comprehensive. However, an a priori protocol and subsequent analyses were not provided, which prevented any evaluation of the risk of selective-results reporting (i.e., based on the magnitude, direction, or statistical significance of the effects). The included comparator studies were deemed to be primarily at a low or unclear risk of bias. Additionally, the SLR search for colorectal and small intestine cancer was conducted in July and August 2023; it is not clear whether new relevant studies have become available since then. In some cases, data were pooled across a number of studies to produce comparator arms for the analyses. The rationale and methods for pooling were not provided; thus, it should be considered that the pooling may have introduced bias and/or obscured heterogeneity in the results across the comparator studies. The sponsor noted that the proportional hazards assumption may have been violated in most comparisons (excluding the small intestine cancer ITC and the gastric cancer ITC with irinotecan and paclitaxel as comparators), which would undermine the validity of the estimated HRs.
All ITCs, except for the endometrial cancer ITC, included comparator studies that did not evaluate MSI-H or dMMR status. According to the clinical experts consulted by the review team, patients with dMMR or MSI-H tumours typically have a worse prognosis compared with those with cancer that is not MSI-H or dMMR, although prognosis varies based on tumour type. Without data on the dMMR or MSI-H status of patients in the comparator arms, the impact is not clear. Most of the ITCs conducted were unadjusted (naive), except for the endometrial cancer ITC and the pembrolizumab versus TAS-102 comparison for the CRC ITC. Unadjusted indirect comparisons were undertaken due to substantial reductions in ESS when attempting to match baseline characteristics across study arms. However, naive indirect comparisons are not considered a valid method to produce comparative effect estimates for decision-making because they are at high risk of bias due to confounding (which may be substantial). Such confounding may be due to both differences in patient characteristics and the methodologies across studies (e.g., different length of follow-up). As a result, it is not possible to discern whether the effects produced by these analyses are the result of the treatments or the differences in known or unknown prognostic and/or effect-modifying variables.
The other indirect comparisons used unanchored MAIC methodology, in which a small number of potential effect-modifying or prognostic variables were selected for matching by the sponsor based on clinical expert input. In the CRC MAIC between pembrolizumab and TAS-102, age, sex, and ECOG PS were identified as matching factors. For the endometrial cancer MAIC, adjusting factors included age, race, ECOG PS, number of prior lines of therapy, and histology. The clinical experts consulted by the review team considered these factors to be relevant. While the baseline characteristics included in the matching and reweighting are important, a key requirement for the validity of an unanchored MAIC is that all prognostic factors and effect modifiers have been identified and included in the weighting process. As this is a strong assumption that is likely not possible to meet, it has been proposed by the National Institute for Health and Care Excellence (NICE) that the extent of residual confounding be assessed statistically.83 In the absence of such analyses for the MAICs presented, the magnitude of residual bias in the relative treatment effect estimates produced by the unanchored MAICs is unknown and could be substantial.83 Additionally, the MAIC approach cannot adjust for methodological differences that may exist across the treatment arms (e.g., length of follow-up). In the endometrial cancer MAIC, there was a notable reduction in ESS following matching, which suggests that the results may be driven by a small subset of the original KEYNOTE-158 population. Some comparisons included a small sample size (e.g., the small intestine ITC), which would reduce the reliability of the effect estimates.
Several external validity considerations were identified. The colorectal, endometrial, and gastric cancer comparisons may no longer be highly relevant due to changes in the current SOC because patients would have already received immune checkpoint inhibitors in the first-line setting. This shift means that the comparisons may not accurately reflect current patient populations or outcomes. Furthermore, no harms or HRQoL outcomes were assessed in the analyses; therefore, it is not possible to inform on the comparative effects of these outcomes, despite them being important to patients. Another limitation is that the matching in an MAIC produces a population that is more similar to the comparator trials, which could differ from the population considered for the indication, potentially affecting the generalizability of the results.
Studies Addressing Gaps in the Systematic Review Evidence
Contents within this section have been informed by materials submitted by the sponsor. The following has been summarized and validated by the CDA-AMC review team.
The sponsor submitted 2 studies, Le et al. (2015) and Bellone et al. (2021), that did not meet the eligibility criteria for inclusion in the systematic review:50,84
The study by Le et al. (2015)84 did not evaluate the Health Canada–approved dosage for pembrolizumab and was therefore not eligible for inclusion in this review.
The study by Bellone et al. (2021)50 assessed pembrolizumab in patients with dMMR and/or MSI-H endometrial cancer that progressed after standard therapy. Because there was pivotal evidence for these patients from the KEYNOTE-158 trial (summarized in the systematic review), CDA-AMC did not consider the study to provide additional insight. The clinical experts consulted for this review highlighted a gap in the evidence of pembrolizumab rechallenging in patients who previously received pembrolizumab and whose disease responded to immune checkpoint inhibitors and then progressed later. However, because patients with prior exposure to immune checkpoint inhibitors were excluded from the study, the potential gap for patients who were previously treated with these drugs and subsequently received pembrolizumab remains unaddressed; therefore, the study by Bellone et al. (2021) was not included.
A summary of the evidence gaps and studies that may address these gaps is included in Table 42.
Table 42: Summary of Gaps in the Systematic Review Evidence
Evidence gap | Studies that address gaps | |
|---|---|---|
Study description | Summary of key results | |
Clinical trials from the systematic review lacked comparators. As a result, the FDA requested additional efficacy data be submitted. | Note that the following datasets contribute noncomparative efficacy data.
|
|
IRRDC = International Replication Repair Deficiency Consortium; MSI-H = microsatellite instability-high; ORR = objective response rate; WES = whole-exome sequencing.
Source: Details included in the table are from the sponsor’s summary of clinical evidence.13
Description of Studies
The IRRDC data came from an observational, registry-based study of pediatric patients (including 1 patient who was aged 24 years) with confirmed or suspected DNA replication repair deficiency.20 Data were collected for the treatment administered and from medical records (demographics, cancer diagnosis, date of initiation and completion of anti–PD-1 therapy, choice of anti–PD-1 therapy, and survival outcomes), ongoing radiological monitoring, response assessment, and management of adverse effects. Patients were treated with pembrolizumab between May 2015 and March 2019. Pathology, radiology, molecular, and biomarker analyses were centrally assessed. Imaging data were collected to assess objective tumour response and the radiologist was blinded to the clinically determined response. Tumour measurements were documented according to the Response Assessment in Neuro-Oncology criteria or by RECIST 1.1. The data cut-off date was March 2022.
The WES data were obtained from across the drug’s clinical development program and data were evaluated from 7 trials of pembrolizumab monotherapy.20 Patients included adults who had advanced solid tumours and previously received systemic treatment. End points included ORR, DOR, and PFS based on a blinded independent central review (RECIST 1.1) and OS.
Populations
The IRRDC dataset consisted of 18 patients who had 20 tumours. The median age was 14 years (range, 4 to 24 years) and the proportion of females and males was split evenly. The type of cancer was categorized as either CNS tumours (10 patients with glioblastoma, 2 patients with astrocytoma, and 1 patient with high-grade glioma) or non-CNS tumours (7 patients with colorectal adenocarcinoma). The 2 patients with 2 types of cancer had both glioblastoma and colorectal adenocarcinoma. All patients received pembrolizumab 2 mg/kg (up to 200 mg) IV every 3 weeks. Discontinuations and follow-up duration were not reported for the IRRDC dataset.
The WES dataset consisted of 21 patients with MSI-H tumours from the KEYNOTE-028, KEYNOTE-012, KEYNOTE-059, KEYNOTE-061, KEYNOTE-055, KEYNOTE-199, and KEYNOTE-086 trials. The median age was 65 years (range, 51 to 89 years) and 57.1% were female, while 42.9% were male. Overall, 11 patients (52.4%) had an ECOG PS score of 1 and scores were not reported for other patients. Cancer types included gastric or gastroesophageal junction cancer (76.2%), prostate cancer (9.5%), cholangiocarcinoma (4.8%), head and neck squamous cell carcinoma (4.8%), and triple-negative breast cancer (4.8%). All patients had previously received at least 1 prior systemic therapy and 95.2% had metastatic disease. All patients received pembrolizumab. Of the 21 patients, 6 (28.1%) completed the study and 12 (57.1%) discontinued pembrolizumab. The main reason for treatment discontinuation was progressive disease, while the main reason for study discontinuation was death. The median follow-up was 18.2 months (range, 1.0 to 55.4 months).
Efficacy
From the IRRDC dataset (pediatric patients), 17 tumours were measurable at baseline (3 tumours were not measurable). Based on the 17 tumours, 4 patients (23.5%) experienced an objective treatment response and 9 patients (52.9%) experienced stable disease. Four tumours (23.5%) continued to progress. Furthermore, 11 of 20 tumours (55.0%) had not progressed by 6 months and 15 of 18 patients (83.3%) were alive at 12 months.
In the WES dataset (adults), the ORR was 52.4% (95% CI, 29.8% to 74.3%). Median PFS was 17.8 months (95% CI, 4.3 months to upper limit not reached) while the PFS rates were 56.7% and 45.9% at 12 and 36 months (there were no CIs), respectively. Median DOR and median OS were not achieved. The OS rates were 66.7% and 61.5% at 12 and 24 months (there were no CIs), respectively.
Harms
The collection of safety data was not a specific intent of the IRRDC study (pediatric patients); therefore, harms data are limited.21 According to the summary of clinical safety, no new safety signals were identified, and pancreatitis was the only harm that occurred in more than 1 patient (n = 2). The following harms were reported in 1 patient each: diarrhea, pneumonia, gastritis, dry skin, transient hypothyroidism, tolerable intermittent elevations in liver enzymes, skin rash, severe headaches, and seizure.
Safety data were not reported for the WES dataset (adults).
Critical Appraisal
Internal Validity
Although the datasets provide more efficacy data in pediatric and adult populations with MSI-H cancers, they are small, noncomparative, and do not address the lack of direct or indirect evidence for pembrolizumab in this setting. Moreover, no protocols were available for review and the methods were not well described; thus, there is a risk of selective reporting. It was noted that, for the IRRDC study, the treatment of patients was at the discretion of the clinical team and changes to dosages may not have been standardized across patients, making it challenging to interpret the results. Outcome measures were reviewed centrally by a blinded, independent committee, which can lower the risk of bias in the outcome measurement. While registries allow for access to additional data that clinical trials may not have, concerns with the use of this type of data include the lack of randomization, uncertain data quality (e.g., accuracy and consistency of collecting and maintaining the data), and missing or incomplete data that can bias results, particularly when compared with the rigour of standardized RCT follow-up.85,86
External Validity
Tumour types in these datasets generally covered the same types as those in the pivotal trials (i.e., the datasets provide limited information additional to what is already available). Based on what has been reported for the WES dataset, more than half of the patients had an ECOG PS of 1 indicating that these patients were relatively healthy, which may not be representative of patients in poorer health who may receive pembrolizumab for MSI-H or dMMR tumours in clinical practice in Canada. The IRRDC dataset only modestly increases the amount of information available for younger patients with MSI-H cancers treated with pembrolizumab because there were few pediatric patients contributing to the pivotal trial evidence. There was limited reporting of harms and only for the IRRDC dataset; assessments of HRQoL were not reported. Despite the use of real-world registry data, which could improve the generalizability of the results, the internal and external validity issues minimize the utility and applicability of the findings to clinical practice.
Discussion
Summary of Available Evidence
The systematic review included 3 clinical trials: KEYNOTE-158, KEYNOTE-164, and KEYNOTE-051. Both KEYNOTE-158 and KEYNOTE-164 were phase II trials, while KEYNOTE-051 was a combined phase I and II trial. All were single-arm trials that evaluated pembrolizumab in different solid tumour cancers. The KEYNOTE-158 trial enrolled 373 adult patients with advanced MSI-H or dMMR non-CRC who experienced disease progression after prior treatments. The KEYNOTE-164 trial enrolled 124 adult patients with advanced MSI-H or dMMR CRC that had progressed following 1 or 2 prior lines of therapy (i.e., after treatment with fluoropyrimidine and either oxaliplatin or irinotecan, with or without an anti-VEGF or anti-EGFR-based therapy). The KEYNOTE-051 trial is an ongoing, open-label, multicentre study aimed at establishing the pediatric dosing regimen for pembrolizumab and evaluating the tolerability of pembrolizumab in 7 pediatric patients with MSI-H or dMMR cancers.
In the KEYNOTE-158 trial, the mean age was 59.2 years (SD = 13.1 years), and 36% of the patients were aged 65 years or older. The majority of the participants were female (61%). The majority of tumours were endometrial (25%), followed by gastric (14%). Other rarer cancers represented 26% of the cancer types. Regarding ECOG PS, 46% of the patients had a status of 0, and 54% had a status of 1. The majority of patients (56%) had received 2 or more prior lines of therapy. In the KEYNOTE-164 trial, the mean age of patients was 56.1 years (SD = 14.9 years), and 33% were aged 65 years or older. There were slightly more males (56%) than females (44%). In total, 41% of patients had an ECOG PS of 0, and 59% had an ECOG PS of 1. Most patients (76%) had received 2 or more prior lines of therapy. In the KEYNOTE-051 trial, the mean age of the 7 pediatric patients was 11 years (SD = 4.3 years) and ranged from 3 to 16 years. ECOG PS was not reported for this cohort, but 57% of the patients had a Karnofsky score of 100. In total 57% of patients had received only 1 prior therapy, while 29% had received 2 or more lines of therapy.
The sponsor submitted several ITCs, each focusing on comparing pembrolizumab with other relevant treatments in different solid tumour types: colorectal, endometrial, small intestine, and gastric cancers. The CRC ITCs compared pembrolizumab with pooled chemotherapy, anti-VEGF plus chemotherapy, and TAS-102. Naive indirect comparisons were used for comparisons between pembrolizumab and pooled chemotherapy or anti-VEGF plus chemotherapy, while an unanchored MAIC was used to compare pembrolizumab with TAS-102. For endometrial cancer, an unanchored MAIC was conducted to compare pembrolizumab with TPC (doxorubicin or paclitaxel). For small intestine cancer, a naive indirect comparison was used to compare pembrolizumab with nab-paclitaxel. For gastric cancer, naive indirect comparisons were used to compare pembrolizumab with multiple comparators, which included FOLFIRI, ramucirumab plus paclitaxel, ramucirumab monotherapy, paclitaxel, and irinotecan.
The sponsor submitted evidence from 4 studies to address gaps in the pivotal evidence; however, 2 were excluded for not providing sufficient additional insight to support using pembrolizumab for the treatment of unresectable or metastatic MSI-H or dMMR solid tumours. Two datasets were included, the IRRDC (N = 18) dataset and the WES pooled dataset (N = 21) that included pediatric and adult patients, respectively, with MSI-H status tumours who received pembrolizumab.
Interpretation of Results
Efficacy
The 3 pivotal sponsor trials (KEYNOTE-158, KEYNOTE-164, and KEYNOTE-051) included different patient populations. The KEYNOTE-158 trial included adult patients with multiple solid tumour types, including endometrial, gastric, small intestine, ovarian, biliary, pancreatic, brain, sarcomas, and other rare cancers; KEYNOTE-164 included adult patients with CRC; and KEYNOTE-051 included pediatric patients with solid tumours that consisted mainly of brain tumours. All sponsor-provided studies were single-arm trials; therefore, the findings need to be interpreted in consideration of the single-arm design, which typically cannot support causal conclusions about the effect of a drug versus any comparator. However, ORR is a surrogate end point that can be evaluated as a direct measure of antitumour activity in a single-arm design by considering the magnitude of the effect and the proportion of CRs.67 It is not possible to robustly evaluate evidence for time-to-event end points (i.e., PFS, OS) in a single-arm design; therefore, the interpretation of the findings for these end points from the single-arm trials is informed primarily by expert opinion.
There are limited treatment options available for patients with solid tumours when SOC options were unsuccessful, particularly for adults with rare cancers and pediatric patients. The clinical experts consulted by CDA-AMC stated that the efficacy observed in the adult trials represents a notable improvement compared with SOC, based on their clinical experience. The experts noted that they would not expect SOC treatments to result in a CR or PR, rather, the goal at an advanced disease stage is stabilization and is typically what is observed in terms of response. However, the clinical experts indicated that only a small proportion of the patient population in Canada would meet the eligibility criteria to receive pembrolizumab for the submitted indication because most solid tumours are now treated with anti–PD-1 or anti–PD-L1 drugs in earlier lines of therapy (e.g., pembrolizumab is funded as SOC in the first line for MSI-H and dMMR CRC, and in the second line in MSI-H and dMMR endometrial cancer among other cancers for which immune checkpoint inhibitors are available as first-line or second-line therapy). This limits the number of patients in Canada who will be eligible to receive pembrolizumab in later lines of therapy and limits the generalizability of the studies because the majority of the patients in the included studies are not representative of the eligible population in Canada. Furthermore, there are no data to support pembrolizumab after the failure of immune checkpoint inhibitors because patients with prior exposure were excluded from the studies.
Because the KEYNOTE trials that were conducted in adults enrolled a small number of patients with tumours relevant to this indication, the generalizability of the trial results to the broader population in Canada is limited. It is important to note that the KEYNOTE-158 trial encompassed multiple solid tumour types, with variability in ORR and DOR observed across these different tumours. Despite this variability and the limited evidence for several tumour types, the tumour-agnostic indication was based on the biological rationale that MSI-H and dMMR alterations drive similar mechanisms of immune invasion, regardless of tumour type.14
In the pediatric study (KEYNOTE-051), no patients experienced an objective response (CR or PR). The small sample size of the KEYNOTE-051 trial, which included only 7 patients, also limits the generalizability of its findings and restricts the ability to draw robust conclusions about pembrolizumab’s efficacy and safety across the broader pediatric population with MSI-H or dMMR tumours that have progressed on prior therapy. The IRRDC study included a small sample of children and provided preliminary evidence to suggest that some MSI-H and dMMR tumours are responsive to pembrolizumab in this population. The clinical experts noted that the prevalence of MSI-H or dMMR in the pediatric population appears much lower because clinicians do not often see patients with some of the more common adult cancers that harbour MSI-H or dMMR mutations (e.g., CRC, endometrial, pancreatic). Given the limited evidence regarding MSI-H malignancies in children, the biological plausibility of pembrolizumab's efficacy in this population is mainly theoretical.14
Several ITCs were conducted to compare pembrolizumab with various comparators across different cancer types. Due to limitations in the available data, suboptimal methods were employed, including naive comparisons and unanchored MAICs that matched on few variables. Naive comparisons are generally not considered valid for deriving comparative effect estimates because they do not adjust for potential confounders. Unanchored MAICs require assumptions that are difficult or impossible to fully satisfy, such as the absence of unmeasured confounding. The analyses typically suggested that pembrolizumab may be favoured over the comparators in terms of OS, PFS, and ORR. The clinical experts believed it was plausible that pembrolizumab would outperform the comparators based on the single-arm trial results. However, these findings must be interpreted with caution due to significant methodological limitations. These concerns included the absence of a predefined protocol, violation of the proportional hazards assumption, lack of quality appraisals, a high risk of bias due to confounding, and small sample sizes for some comparisons. As a result, robust conclusions could not be drawn from the indirect comparisons.
Harms
Generally, no new safety signals were identified in the sponsor-provided KEYNOTE trials. The open-label design of the trials may introduce bias in reporting subjective harms, potentially affecting the reliability of the safety data. Additionally, there is limited safety information available for pediatric patients, which restricts the understanding of pembrolizumab's safety profile in this population. Because the sponsor did not provide ITCs for safety outcomes, the relative safety of pembrolizumab compared with other treatments remains unknown.
Conclusion
Patients and clinicians emphasized a high unmet need for new, effective treatments for patients with unresectable or metastatic MSI-H and/or dMMR solid tumours if SOC or salvage chemotherapy fails. Evidence for this review consisted of 3 pivotal trials (KEYNOTE-158, KEYNOTE-164, and KEYNOTE-051), multiple ITCs, and 2 noncomparative datasets in pediatric and adult patients with MSI-H cancer (IRRDC and WES). The evidence on the efficacy of pembrolizumab in adults from 2 pivotal trials, KEYNOTE-158 and KEYNOTE-164, was very uncertain due to the single-arm design. The clinical experts consulted by the review team indicated that the response to treatment (ORR) was clinically meaningful and durable (DOR) compared with what is typically observed with SOC treatments. However, responses were heterogeneous across specific cancer types, many of which were represented by a small number of patients. Despite an inability to draw causal conclusions regarding time-to-event end points (OS and PFS), the clinical experts stated that the results were promising based on the natural history of the disease and experience in clinical practice. The results for HRQoL were inconclusive due to the open-label design and missing data. The results from the WES dataset were supportive of the pivotal trials but were affected by similar limitations.
In the pediatric population, due to the small number of patients (N = 7) enrolled in the KEYNOTE-051 trial and the single-arm design, it is difficult to ascertain the benefit of pembrolizumab in this group of patients. No patients in the KEYNOTE-051 trial had a PR or CR. Supportive evidence from the single-arm IRRDC registry study provides preliminary evidence from a small sample of patients to suggest that some pediatric patients with MSI-H or dMMR malignancies may respond to pembrolizumab. No new safety signals were identified in any of the pembrolizumab trials.
The indirect comparative evidence from the ITCs (naive indirect comparisons and unanchored MAICs) was limited to 4 cancer types in adults: colorectal, endometrial, small intestine, and gastric. Results of the ITCs suggested improved PFS and OS compared with SOC, which aligned with the expectations of the clinical experts consulted by the review team. However, the ITCs had significant limitations that impacted the internal validity of the findings and precluded drawing definitive conclusions about the comparative efficacy of pembrolizumab versus SOC treatments. Additionally, immune checkpoint inhibitors are now used in the first line for colorectal, endometrial, and gastric cancers, reducing the relevance of these comparisons. No comparative safety data were provided; thus, the relative safety of pembrolizumab compared with other treatments is unknown. However, the clinical experts consulted for this review emphasized the breadth of experience with using pembrolizumab in other cancers, highlighting that pembrolizumab is better tolerated and has fewer and less severe side effects than conventional chemotherapy.
References
1.Marcus L, Lemery SJ, Keegan P, Pazdur R. FDA Approval Summary: Pembrolizumab for the Treatment of Microsatellite Instability-High Solid Tumors. Clin Cancer Res. 2019;25(13):3753-3758. PubMed
2.Mishima S, Naito Y, Akagi K, et al. Japanese Society of Medical Oncology/Japan Society of Clinical Oncology/Japanese Society of Pediatric Hematology/Oncology-led clinical recommendations on the diagnosis and use of immunotherapy in patients with DNA mismatch repair deficient (dMMR) tumors, third edition. Int J Clin Oncol. 2023;28(10):1237-1258.
3.Olave MC, Graham RP. Mismatch repair deficiency: The what, how and why it is important. Genes Chromosomes Cancer. 2022;61(6):314-321. PubMed
4.Overman MJ, Morse M. Tissue-agnostic cancer therapy: DNA mismatch repair deficiency, tumor mutational burden, and response to immune checkpoint blockade in solid tumors. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2024: https://www.uptodate.com. Accessed 2024 Jul 17.
5.Akagi K, Oki E, Taniguchi H, et al. Real-world data on microsatellite instability status in various unresectable or metastatic solid tumors. Cancer Sci. 2021;112(3):1105-1113. PubMed
6.Kang YJ, O'Haire S, Franchini F, et al. A scoping review and meta-analysis on the prevalence of pan-tumour biomarkers (dMMR, MSI, high TMB) in different solid tumours. Sci Rep. 2022;12(1):20495. PubMed
7.Lorenzi M, Amonkar M, Zhang J, Mehta S, Liaw K-L. Epidemiology of Microsatellite Instability High (MSI-H) and Deficient Mismatch Repair (dMMR) in Solid Tumors: A Structured Literature Review. J Oncol. 2020;2020:1-17.
8.Programme de gestion thérapeutique des médicaments. Inhibiteurs du point de contrôle immunitaire (IPCI) pour le traitement des tumeurs avec instabilité microsatellitaire élevée/déficience du système de réparation des erreurs d’apariements (MSI-H / dMMR). Rapport d’évaluation [sponsor supplied reference]. 2021.
9.Li K, Luo H, Huang L, Luo H, Zhu X. Microsatellite instability: a review of what the oncologist should know. Cancer Cell Int. 2020;20(1):16. PubMed
10.CADTH Reimbursement Recommendation: Pembrolizumab (Keytruda). Can J Health Technol. 2021;1(7). https://www.cadth.ca/sites/default/files/attachments/2021-07/PC0235%20Keytruda%20-%20CADTH%20Final%20Rec%20revised_1.pdf. Accessed 2023 Nov 24.
11.CADTH Reimbursement Recommendation: Pembrolizumab (Keytruda). Can J Health Technol. 2023;3(2). https://www.cadth.ca/sites/default/files/DRR/2023/PC0280%20Keytruda%20-%20Final%20CADTH%20Recommendation.pdf. Accessed 2023 Nov 24.
12.Keytruda (pembrolizumab): solution for infusion 100 mg/4 mL vial [product monograph DRAFT]. Kirkland (QC): Merck Canada Inc.; 2023 Aug 18.
13.Keytruda Clinical Evidence [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Keytruda (pembrolizumab), solution for infusion 100 mg/4 mL vial Kirkland (QC): Merck Canada Inc.; 2024.
14.Health Canada reviewer's report: Keytruda (pembrolizumab) [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: pembrolizumab, 200 mg Q3W IV solution for infusion. Merck Canada Inc.
15.Balshem H, Helfand M, Schunemann HJ, et al. GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol. 2011;64(4):401-406. PubMed
16.Santesso N, Glenton C, Dahm P, et al. GRADE guidelines 26: informative statements to communicate the findings of systematic reviews of interventions. J Clin Epidemiol. 2020;119:126-135. PubMed
17.Merck Sharp & Dohme. Data on file. Pembrolizumab (MK-3475) - MSI-H Cancer (KEYNOTE-158). Clinical Study Report P158V11MK3475. 2022.
18.Merck Sharp & Dohme. Data on file. Pembrolizumab (MK-3475) - KEYNOTE-164. Clinical Study Report P164V04MK3475 (end of study synoptic report). 2022.
19.Merck Sharp & Dohme. Data on file. Pembrolizumab (MK-3475) - Pediatric Advanced Solid Tumors or Lymphomas (KEYNOTE-051). Clinical Study Report P051V03MK3475. 2022.
20.Common Technical Document section 2.7.3: summary of clinical efficacy [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Keytruda (pembrolizumab), solution for infusion 100 mg/4 mL vial. Kirkland (QC): Merck Canada Inc.; 2023.
21.Common Technical Document section 2.7.4: summary of clinical safety [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Keytruda (pembrolizumab), solution for infusion 100 mg/4 mL vial. Kirkland (QC): Merck Canada Inc.; 2023.
22.KEYTRUDA (pembrolizumab) draft version [product monograph]. Merck Canada, Inc.; 2023 Oct 11.
23.Tian Z, Yao W. Albumin-Bound Paclitaxel: Worthy of Further Study in Sarcomas. Front Oncol. 2022;12:815900. PubMed
24.Lonsurf (trifluridine and tipiracil): tablet, 15 mg trifluridine/6.14 mg tipiracil (as tipiracil hydrochloride), 20 mg trifluridine/8.19 mg tipiracil (as tipiracil hydrochloride) [product monograph]. Oakville (ON): Taiho Pharma Canada, Inc.; 2020 Oct 29: https://pdf.hres.ca/dpd_pm/00058926.PDF. Accessed 2024 Aug 15.
25.PACLitaxel powder for injectable suspension nanoparticle, albumin-bound paclitaxel: 100 mg paclitaxel/vial, lyophilized powder [product monograph]. Toronto (ON): Apotex Inc.; 2021 Nov 16: https://pdf.hres.ca/dpd_pm/00071231.PDF. Accessed 2024 Aug 15.
26.Cyramza (ramucirumab): intravenous injection 10 mg ramucirumab/mL [product monograph]. Toronto (ON): Eli Lilly Canada Inc.; 2022 Jun 9: https://pdf.hres.ca/dpd_pm/00067328.PDF. Accessed 2024 Aug 15.
27.Leucovorin calcium injection: solution, 10 mg/mL, intravenous and intramuscular [product monograph]. Toronto (ON): Teva Canada Limited 2023 Nov 30: https://pdf.hres.ca/dpd_pm/00073616.PDF. Accessed 2024 Aug 15.
28.Irinotecan hydrochloride injection: solution, 20 mg/mL, intravenous [product monograph]. Toronto (ON): Teva Canada Limited 2023 Mar 28: https://pdf.hres.ca/dpd_pm/00070343.PDF. Accessed 2024 Aug 15.
29.Fluorouracil solution: 50 mg / mL, intravenous [product monograph]. Boucherville (QC): Sandoz Canada Inc.; 2024 May 31: https://pdf.hres.ca/dpd_pm/00075846.PDF. Accessed 2024 Aug 15.
30.Oxaliplatin injection: 5 mg/mL, sterile concentrate 50 mg / 10 mL, 100 mg / 20 mL, 200 mg / 40 mL for intravenous infusion [product monograph]. Boucherville (QC): Sandoz Canada Inc.; 2024 Jul 30: https://pdf.hres.ca/dpd_pm/00076515.PDF. Accessed 2024 Aug 15.
31.Abraxane (paclitaxel) powder for injectable suspension, nanoparticle, albumin-bound (nab®) paclitaxel: 100 mg paclitaxel/vial, intravenous [product monograph]. Saint-Laurent (QC): Bristol-Myers Squibb Canada; 2024 Mar 8: https://pdf.hres.ca/dpd_pm/00074884.PDF. Accessed 2024 Aug 15.
32.Caelyx (pegylated liposomal doxorubicin hydrochloride) for injection: suspension, 2 mg/mL, for intravenous administration [product monograph]. Mississauga (ON): Baxter Corporation; 2024 Apr 2: https://pdf.hres.ca/dpd_pm/00075111.PDF. Accessed 2024 Aug 15.
33.ClinicalTrials.gov [accessed by sponsor]. Bethesda (MD): U.S. National Library of Medicine: https://clinicaltrials.gov/. Accessed 2024 May 22.
34.Cancer Care Ontario. Drug Formulary. 2024; https://www.cancercareontario.ca/en/cancer-treatments/chemotherapy/drug-formulary. Accessed 2024 May 28.
35.Al-Mansor E, Mahoney M, Chenard-Poirier M, et al. Eastern Canadian Gastrointestinal Cancer Consensus Conference 2023. Curr Oncol. 2023;30(9):8172-8185. PubMed
36.Shimozaki K, Hayashi H, Tanishima S, et al. Concordance analysis of microsatellite instability status between polymerase chain reaction based testing and next generation sequencing for solid tumors. Sci Rep. 2021;11(1):20003. PubMed
37.Rizzo A, Ricci AD, Gadaleta-Caldarola G. MSI-H/dMMR and cancer immunotherapy: current state and future implications. Expert Review of Precision Medicine and Drug Development. 2021;6(6):345-347.
38.Trabucco SE, Gowen K, Maund SL, et al. A Novel Next-Generation Sequencing Approach to Detecting Microsatellite Instability and Pan-Tumor Characterization of 1000 Microsatellite Instability-High Cases in 67,000 Patient Samples. J Mol Diagn. 2019;21(6):1053-1066. PubMed
39.Yip S, Christofides A, Banerji S, et al. A Canadian guideline on the use of next-generation sequencing in oncology. Curr Oncol. 2019;26(2):e241-e254. PubMed
40.Gilson P, Merlin JL, Harle A. Detection of Microsatellite Instability: State of the Art and Future Applications in Circulating Tumour DNA (ctDNA). Cancers (Basel). 2021;13(7). PubMed
41.Canadian Cancer Statistics Advisory Committee. Canadian Cancer Statistics: A 2020 special report on lung cancer. Toronto (ON): Canadian Cancer Society; 2020: https://cancer.ca/Canadian-Cancer-Statistics-2020-EN. Accessed 2024 Jul 11.
42.Canadian Centre for Cancer Information. Cancer incidence. 2023; https://cancer-data.canada.ca/stats/incidence-eng.htm. Accessed 2024 Jul 11.
43.Fanale D, Corsini LR, Scalia R, et al. Can the tumor-agnostic evaluation of MSI/MMR status be the common denominator for the immunotherapy treatment of patients with several solid tumors? Crit Rev Oncol Hematol. 2022;170:103597. PubMed
44.Cicek MS, Lindor NM, Gallinger S, et al. Quality assessment and correlation of microsatellite instability and immunohistochemical markers among population- and clinic-based colorectal tumors results from the Colon Cancer Family Registry. J Mol Diagn. 2011;13(3):271-281. PubMed
45.Le DT, Durham JN, Smith KN, et al. Mismatch repair deficiency predicts response of solid tumors to PD-1 blockade. Science. 2017;357(6349):409-413. PubMed
46.Peterse EFP, Naber SK, Daly C, et al. Cost-effectiveness of Active Identification and Subsequent Colonoscopy Surveillance of Lynch Syndrome Cases. Clin Gastroenterol Hepatol. 2020;18(12):2760-2767 e2712. PubMed
47.Makarem M, Ezeife DA, Smith AC, et al. Reflex ROS1 IHC Screening with FISH Confirmation for Advanced Non-Small Cell Lung Cancer-A Cost-Efficient Strategy in a Public Healthcare System. Curr Oncol. 2021;28(5):3268-3279. PubMed
48.Marabelle A, Le DT, Ascierto PA, et al. Efficacy of Pembrolizumab in Patients With Noncolorectal High Microsatellite Instability/Mismatch Repair-Deficient Cancer: Results From the Phase II KEYNOTE-158 Study. J Clin Oncol. 2020;38(1):1-10. PubMed
49.Le DT, Kim TW, Van Cutsem E, et al. Phase II Open-Label Study of Pembrolizumab in Treatment-Refractory, Microsatellite Instability-High/Mismatch Repair-Deficient Metastatic Colorectal Cancer: KEYNOTE-164. J Clin Oncol. 2020;38(1):11-19. PubMed
50.Bellone S, Roque DM, Siegel ER, et al. A phase II evaluation of pembrolizumab in recurrent microsatellite instability-high (MSI-H) endometrial cancer patients with Lynch-like versus MLH-1 methylated characteristics (NCT02899793). Ann Oncol. 2021;32(8):1045-1046. PubMed
51.Maio M, Amonkar MM, Norquist JM, et al. Health-related quality of life in patients treated with pembrolizumab for microsatellite instability-high/mismatch repair-deficient advanced solid tumours: Results from the KEYNOTE-158 study. Eur J Cancer. 2022;169:188-197. PubMed
52.Maio M, Ascierto PA, Manzyuk L, et al. Pembrolizumab in microsatellite instability high or mismatch repair deficient cancers: updated analysis from the phase II KEYNOTE-158 study. Ann Oncol. 2022;33(9):929-938. PubMed
53.Maio M, Ascierto PA, Motola-Kuba D, et al. Pembrolizumab in microsatellite instability-high/mismatch repair deficient advanced solid tumors: An update of the phase 2 KEYNOTE-158 trial [accessed by sponsor]. European Society for Medical Oncology Congress 2022; September 9-13, 2022, 2022; Paris, France.
54.Le DT, Diaz LA, Jr., Kim TW, et al. Pembrolizumab for previously treated, microsatellite instability-high/mismatch repair-deficient advanced colorectal cancer: Final analysis of KEYNOTE-164 [accessed by sponsor]. European Society for Medical Oncology Virtual Congress 2021; September 16-21, 2021, 2021.
55.Le DT, Diaz LA, Jr., Kim TW, et al. Pembrolizumab for previously treated, microsatellite instability-high/mismatch repair-deficient advanced colorectal cancer: final analysis of KEYNOTE-164. Eur J Cancer. 2023;186:185-195. PubMed
56.Geoerger B, Kang HJ, Yalon-Oren M, et al. Pembrolizumab in paediatric patients with advanced melanoma or a PD-L1-positive, advanced, relapsed, or refractory solid tumour or lymphoma (KEYNOTE-051): interim analysis of an open-label, single-arm, phase 1-2 trial. Lancet Oncol. 2020;21(1):121-133. PubMed
57.King MT. The interpretation of scores from the EORTC quality of life questionnaire QLQ-C30. Qual Life Res. 1996;5(6):555-567. PubMed
58.Cocks K, King MT, Velikova G, et al. Evidence-based guidelines for interpreting change scores for the European Organisation for the Research and Treatment of Cancer Quality of Life Questionnaire Core 30. Eur J Cancer. 2012;48(11):1713-1721. PubMed
59.Cocks K, King MT, Velikova G, Martyn St-James M, Fayers PM, Brown JM. Evidence-based guidelines for determination of sample size and interpretation of the European Organisation for the Research and Treatment of Cancer Quality of Life Questionnaire Core 30. J Clin Oncol. 2011;29(1):89-96. PubMed
60.Clinical Study Report: P158V11MK3475. A Clinical Trial of Pembrolizumab (MK-3475) Evaluating Predictive Biomarkers in Subjects with Advanced Solid Tumors (KEYNOTE-158) [internal sponsor's report]. Kirkland (QC): Merck Canada, Inc.; 2022.
61.Osoba D, Zee B, Pater J, Warr D, Kaizer L, Latreille J. Psychometric properties and responsiveness of the EORTC quality of Life Questionnaire (QLQ-C30) in patients with breast, ovarian and lung cancer. Qual Life Res. 1994;3(5):353-364. PubMed
62.Davda J, Kibet H, Achieng E, Atundo L, Komen T. Assessing the acceptability, reliability, and validity of the EORTC Quality of Life Questionnaire (QLQ-C30) in Kenyan cancer patients: a cross-sectional study. J Patient Rep Outcomes. 2021;5(1):4. PubMed
63.Jayasekara H, Rajapaksa LC, Aaronson NK. Quality of life in cancer patients in South Asia: psychometric properties of the Sinhala version of the EORTC QLQ-C30 in cancer patients with heterogeneous diagnoses. Qual Life Res. 2008;17(5):783-791. PubMed
64.Silpakit C, Sirilerttrakul S, Jirajarus M, Sirisinha T, Sirachainan E, Ratanatharathorn V. The European Organization for Research and Treatment of Cancer Quality of Life Questionnaire (EORTC QLQ-C30): validation study of the Thai version. Qual Life Res. 2006;15(1):167-172. PubMed
65.Musoro JZ, Coens C, Sprangers MAG, et al. Minimally important differences for interpreting EORTC QLQ-C30 change scores over time: A synthesis across 21 clinical trials involving nine different cancer types. Eur J Cancer. 2023;188:171-182. PubMed
66.Evans SR. Clinical trial structures. J Exp Stroke Transl Med. 2010;3(1):8-18. PubMed
67.Clinical Trial Endpoints for the Approval of Cancer Drugs and Biologics: Guidance for Industry. Silver Spring (MD): U.S. Food and Drug Administration (FDA); 2018: https://www.fda.gov/media/71195/download. Accessed 2024 Oct 4.
68.Higgins JPT, Thomas J, Chandler J, et al. Cochrane handbook for systematic reviews of interventions [accessed by sponsor]. John Wiley & Sons; 2019.
69.Wells GA, Wells G, Shea B, et al. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses [accessed by sponsor]. 2014.
70.Precision Heor. Systematic literature review of studies on interventions for advanced colorectal cancer that has progressed after prior treatment. Technical Report [sponsor supplied reference]. Version 3 ed2024.
71.Keytruda (MK-3475) KN164 MSI-H Colorectal Carcinoma. ITCs of pembrolizumab and SoC interventions. Database Cutoff Date 19-Feb-2021. Version 4 [sponsor supplied reference]. Bards Hta Statistics for Merck Canada; 2024.
72.Precision Heor. Systematic literature review of studies on interventions for advanced small intestine adenocarcinoma that has progressed after prior treatment. Technical Report [sponsor supplied reference]. Version 4 ed2024.
73.Keytruda (MK-3475), KN158 MSI-H Gastric Carcinoma. ITCs of pembrolizumab vs. SoC interventions. Data cutoff date of January 12, 2022. Version 1.0 [sponsor supplied reference]. Bards Hta Statistics for Merck Canada; 2023.
74.Precision Heor. Systematic literature review of studies on interventions relevant to health technology assessment submission in Canada for advanced gastric cancer progressing after prior treatment. Technical Report [sponsor supplied reference]. Version 2 ed2024.
75.Guyot P, Ades AE, Ouwens MJNM, Welton NJ. Enhanced secondary analysis of survival data: reconstructing the data from published Kaplan-Meier survival curves. BMC Med Res Methodol. 2012;12(1):9. PubMed
76.Signorovitch JE, Sikirica V, Erder MH, et al. Matching-adjusted indirect comparisons: a new tool for timely comparative effectiveness research. Value Health. 2012;15(6):940-947. PubMed
77.Signorovitch JE, Wu EQ, Yu AP, et al. Comparative effectiveness without head-to-head trials: a method for matching-adjusted indirect comparisons applied to psoriasis treatment with adalimumab or etanercept. Pharmacoeconomics. 2010;28(10):935-945. PubMed
78.Makker V, Colombo N, Herráez AC, et al. O002/#43 Randomized phase 3 study of lenvatinib plus pembrolizumab for advanced endometrial cancer (aec): subgroup analysis of patients with DNA mismatch repair deficient (DMMR) tumors. International Journal of Gynecologic Cancer. 2021;31(Suppl 4):A1.
79.KEYTRUDA. Cancer colorectal métastatique. Avis au ministre en mai 2021 [accessed by sponsor]. Quebec (QC): INESSS: https://www.inesss.qc.ca/fileadmin/doc/INESSS/Inscription_medicaments/Avis_au_ministre/Juin_2021/Keytruda_2021_05.pdf.
80.Keytruda (MK-3475), MSI-H Endometrial Carcinoma. ITCs KN158 vs. KN775. Version 2.0 [sponsor provided reference]. Bards Hta Statistics for Merck Canada; 2024.
81.Overman MJ, Adam L, Raghav K, et al. Phase II study of nab-paclitaxel in refractory small bowel adenocarcinoma and CpG island methylator phenotype (CIMP)-high colorectal cancer. Ann Oncol. 2018;29(1):139-144. PubMed
82.Keytruda (MK-3475), KN158 MSI-H Small Intestine Carcinoma. ITCs of pembrolizumab vs. SoC interventions. Data cutoff date of January 12, 2022. Version 1.0 [sponsor supplied reference]. Bards Hta Statistics for Merck Canada; 2023.
83.Phillippo D, Ades T, Dias S, Palmer S, Abrams KR, Welton N. NICE DSU Technical Support Document 18: Methods for population-adjusted indirect comparisons in submissions to NICE. 2016: https://research-information.bris.ac.uk/ws/portalfiles/portal/94868463/Population_adjustment_TSD_FINAL.pdf. Accessed 2024 Oct 2.
84.Le DT, Uram JN, Wang H, et al. PD-1 Blockade in Tumors with Mismatch-Repair Deficiency. N Engl J Med. 2015;372(26):2509-2520. PubMed
85.Rubinger L, Ekhtiari S, Gazendam A, Bhandari M. Registries: Big data, bigger problems? Injury. 2023;54 Suppl 3:S39-S42. PubMed
86.Pop B, Fetica B, Blaga ML, et al. The role of medical registries, potential applications and limitations. Med Pharm Rep. 2019;92(1):7-14. PubMed
Appendix 1: Detailed Outcome Data
Please note that this appendix has not been copy-edited.
Table 43: Response Outcomes for the KEYNOTE-158 Trial by Tumour Types
Tumour type | N | ORR (CR + PR), n (%) [95% CI] | CR, n (%) [95% CI] | PR, n (%) [95% CI] |
|---|---|---|---|---|
Endometrial | 94 | 47 (50.0) [39.5 to 60.5] | 15 (16.0) [9.2 to 25.0] | 32 (34.0) [24.6 to 44.5] |
Gastric | 51 | 20 (39.2) [25.8 to 53.9] | 8 (15.7) [7.0 to 28.6] | 12 (23.5) [12.8 to 37.5] |
Small intestine | 27 | 16 (59.3) [38.8 to 77.6] | 4 (14.8) [4.2 to 33.7] | 12 (44.4) [25.5 to 64.7] |
Ovarian | 25 | 8 (32.0) [14.9 to 53.5] | 4 (16.0) [4.5 to 36.1] | 4 (16.0) [4.5 to 36.1] |
Cholangiocarcinoma | 22 | 9 (40.9) [20.7 to 63.6] | 3 (13.6) [2.9 to 34.9] | 6 (27.3) [10.7 to 50.2] |
Pancreatic | 22 | 4 (18.2) [5.2 to 40.3] | 1 (4.5) [0.1 to 22.8] | 3 (13.6) [2.9 to 34.9] |
Brain | 21 | 1 (4.8) [0.1 to 22.8] | 0 (0.0) [0.0 to 16.1] | 1 (4.8) [0.1 to 22.8] |
Sarcoma | 14 | 3 (21.4) [4.7 to 50.5] | 1 (7.1) [0.2 to 33.5] | 2 (14.3) [1.8 to 43.8] |
Breast | 13 | 1 (7.7) [0.2 to 36.0] | 0 (0.0) [0.0 to 24.7] | 1 (7.7) [0.2 to 36.0] |
Other (pooled) | 12 | 4 (33.3) [9.9 to 65.1] | 1 (8.3) [0.2 to 38.5] | 3 (25.0) [5.5 to 57.2] |
Cervical | 11 | 1 (9.1) [0.2 to 41.3] | 0 (0.0) [0.0 to 28.5] | 1 (9.1) [0.2 to 41.3] |
Neuroendocrine | 11 | 1 (9.1) [0.2 to 41.3] | 0 (0.0) [0.0 to 28.5] | 1 (9.1) [0.2 to 41.3] |
Prostate | 8 | 1 (12.5) [0.3 to 52.7] | 0 (0.0) [0.0 to 36.9] | 1 (12.5) [0.3 to 52.7] |
Adrenocortical | 7 | 1 (14.3) [0.4 to 57.9] | 0 (0.0) [0.0 to 41.0] | 1 (14.3) [0.4 to 57.9] |
Mesothelioma | 7 | 0 (0.0) [0.0 to 41.0] | 0 (0.0) [0.0 to 41.0] | 0 (0.0) [0.0 to 41.0] |
Thyroid | 7 | 1 (14.3) [0.4 to 57.9] | 1 (14.3) [0.4 to 57.9] | 1 (14.3) [0.4 to 57.9] |
Small cell lung cancer | 6 | 2 (33.3) [4.3 to 77.7] | 1 (16.7) [0.4 to 64.1] | 1 (16.7) [0.4 to 66.7] |
Urothelial | 5 | 3 (50.0) [11.8 to 88.2] | 0 (0.0) [0.0 to 45.9] | 3 (50.0) [11.8 to 88.2] |
Salivary | 5 | 2 (40.0) [5.3 to 85.3] | 1 (20.0) [0.5 to 71.6] | 1 (20.0) [0.5 to 71.6] |
Renal | 4 | 1 (25.0) [0.6 to 80.6] | 0 (0.0) [0.0 to 60.2] | 1 (25.0) [0.6 to 80.6] |
CI = confidence interval; CR = complete response; ORR = objective response rate; PR = partial response.
Source: KEYNOTE-158 trial.17
Table 44: Colorectal Carcinoma SLR — Summary of Participant Characteristics
Source | Registry number | Treatment | Trial arm | N mAPaT | Median age, years (range) | Sex, female | Race: Asian (%), Black (%), white (%), other (%) | ECOG PS | Number of prior lines of therapy |
|---|---|---|---|---|---|---|---|---|---|
Kemeny (2004) | NR | FOLFOX4 | Arm 2 | 110 | 63 (NR to NR) | 51 (46) | NR, NR, NR, NR | NR, NR, NR | NR, NR, NR |
Giantonio (2007) | NR | Bevacizumab + FOLFOX4 | Arm 1 | 286 | 62 (21 to 85) | 113 (40) | NR, NR, NR, NR | 49, 47, 4 | NR, NR, NR |
Giantonio (2007) | NR | FOLFOX4 | Arm 2 | 291 | 61 (25 to 84) | 114 (39) | NR, NR, NR, NR | 51, 43, 6 | NR, NR, NR |
Graeven (2007) | NR | Irinotecan + 5-fluorouracil + folinic acid | Arm 1 | 28 | 66 (44 to 77) | 12 (43) | NR, NR, NR, NR | 18, 75, 7 | NR, NR, NR |
Rothenberg (2008) | NCT00069108 | FOLFOX4 | Arm 1 | 314 | 60 (26 to 83) | 123 (39) | NR, NR, NR, NR | 46, 47, 7 | NR, NR, NR |
Galal (2009) | NR | Chemotherapy (FOLFOX6/FOLFIRI) | Arm 2 | 17 | 62 (NR to NR) | 9 (53) | NR, NR, NR, NR | NR, NR, 53 | NR, NR, NR |
Galal (2009) | NR | Chemotherapy (FOLFOX6/FOLFIRI) + bevacizumab | Arm 3 | 16 | 57 (NR to NR) | 7 (44) | NR, NR, NR, NR | NR, NR, 44 | NR, NR, NR |
Van Cutsem (2011) | NCT00056446 | Placebo + FOLFOX4 | Arm 2 | 429 | NR (18 to 81) | 161 (38) | 11, 4, 83, 2 | 52, 42, 5 | NR, NR, NR |
Van Cutsem (2012) | NCT00561470 | FOLFIRI + placebo | Arm 1 | 614 | 61 (19 to 86) | 261 (43) | 8, 4, 85, 2 | 57, 41, 2 | 0, 100, NR |
Van Cutsem (2012) | NCT00561470 | FOLFIRI + aflibercept | Arm 2 | 612 | 61 (21 to 82) | 247 (40) | 6, 3, 90, 2 | 57, 41, 2 | 0, 100, NR |
Yoshino (2012) | JapicCTI-090880 | TAS-102 | Arm 1 | 112 | 63 (28 to 80) | 48 (43) | NR, NR, NR, NR | 64, 33, 3 | 0, NR, NR |
Bendell (2013) | NCT00615056 | Bevacizumab + FOLFIRI | Arm 2 | 51 | 58 (34 to 80) | 24 (47) | 16, 4, 80, 0 | 71, 29, NR | NR, NR, NR |
Bendell (2013) | NCT00615056 | Bevacizumab + FOLFOX | Arm 4 | 35 | 60 (41 to 77) | 11 (31) | 20, 0, 77, 3 | 71, 29, NR | NR, NR, NR |
Cunningham (2013) | NCT00278889 | Bevacizumab (10 mg/kg) + mFOLFOX6 | Arm 3 | 66 | NR (NR to NR) | 27 (41) | 0, 3, 96, 2 | 73, 24, 3 | 0, 100, NR |
Peeters (2013) | NCT00752570 | Placebo + FOLFIRI | Arm 2 | 49 | 55 (29 to 79) | 25 (51) | 24, 0, 76, NR | 45, 55, NR | NR, NR, NR |
O'Neil (2014) | NCT00707889 | Bevacizumab + mFOLFOX6 | Arm 1 | 49 | 57 (22 to 71) | 20 (41) | 37, 2, 61, NR | 43, 55, 2 | 0, NR, NR |
Xie (2014) | NR | FOLFIRI | Arm 1 | 155 | 58 (21 to 86) | 57 (37) | NR, NR, NR, NR | NR, NR, 21 | 0, 100, NR |
Yasui (2015) | NCT00284258 | FOLFIRI | Arm 1 | 213 | 63 (32 to 75) | 90 (42) | NR, NR, NR, NR | 75, 25, NR | NR, NR, NR |
Cao (2015) | NR | FOLFIRI | Arm 1 | 77 | NR (24 to 81) | 29 (38) | NR, NR, NR, NR | NR, NR, 31 | NR, NR, NR |
Cao (2015) | NR | Bevacizumab + FOLFIRI | Arm 2 | 65 | NR (30 to 79) | 25 (39) | NR, NR, NR, NR | NR, NR, 32 | NR, NR, NR |
Masi (2015) | NCT00720512 | FOLFOX/FOLFIRI | Arm 1 | 92 | 67 (38 to 75) | 23 (25) | NR, NR, NR, NR | 82, 17, 1 | NR, NR, NR |
Masi (2015) | NCT00720512 | BEV + FOLFOX/FOLFIRI | Arm 2 | 92 | 62 (38 to 75) | 40 (43) | NR, NR, NR, NR | 82, 16, 2 | NR, NR, NR |
Iwamoto (2015) | UMIN000002557 | Bevacizumab (5 mg/kg) + FOLFIRI | Arm 1 | 181 | 66 (36 to 84) | 79 (44) | NR, NR, NR, NR | 86, 14, NR | NR, 100, NR |
Iwamoto (2015) | UMIN000002557 | Bevacizumab (10 mg/kg) + FOLFIRI | Arm 2 | 188 | 65 (31 to 88) | 81 (43) | NR, NR, NR, NR | 87, 13, NR | NR, 100, NR |
Mayer (2015) | NCT01607957 | TAS-102 | Arm 1 | 534 | 63 (27 to 82) | 208 (39) | 34, NR, 57, NR | 56, 44, NR | NR, NR, 40 |
Tabernero (2015) | NCT01183780 | FOLFIRI + placebo | Arm 2 | 536 | 62 (33 to 87) | 210 (39) | 19, 3, 77, NR | 48, 51, NR | 0, 100, NR |
Moore (2016) | NCT01111604 | mFOLFOX-6 | Arm 1 | 49 | NR (NR to NR) | 21 (43) | NR, NR, NR, NR | 43, 55, 2 | NR, NR, NR |
Randolph Hecht (2017) | NCT01479465 | FOLFIRI + placebo | Arm 3 | 80 | 61 (32 to 85) | 41 (51) | 1, 10, 84, 1 | 54, 45, 1 | NR, NR, NR |
Passardi (2017) | NCT01878422 | Bevacizumab + FOLFOX4/FOLFIRI | Arm 1 | 31 | 64 (45 to 81) | 11 (36) | NR, NR, NR, NR | 83, NR, NR | NR, NR, NR |
Passardi (2017) | NCT01878422 | FOLFOX4/FOLFIRI | Arm 1 | 25 | 63 (44 to 82) | 9 (36) | NR, NR, NR, NR | 80, NR, NR | NR, NR, NR |
Shi (2017) | NR | Bevacizumab + FOLFOX4 | Arm 2 | 65 | NR (38 to 72) | 23 (35) | NR, NR, NR, NR | 54, 34, 12 | 0, 100, NR |
Li (2018) | NCT01661270 | Aflibercept + FOLFIRI | Arm 1 | 223 | 56 (26 to 77) | 95 (43) | NR, NR, NR, NR | 40, 60, NR | NR, 100, NR |
Li (2018) | NCT01661270 | FOLFIRI | Arm 2 | 109 | 55 (27 to 80) | 46 (42) | NR, NR, NR, NR | 39, 61, NR | NR, 100, NR |
Xu (2018) | NCT01955837 | TAS-102 | Arm 1 | 271 | 58 (26 to 81) | 101 (37) | 100, 0, 0, NR | 24, 76, NR | NR, NR, 50 |
Pietrantonio (2020) | NCT02414009 | FOLFIRI | Arm 2 | 43 | 67 (61 to 73) | 19 (44) | NR, NR, NR, NR | 51, 49, NR | NR, NR, NR |
Li (2021) | NCT04718038 | Bevacizumab + FOLFOX/FOLFIRI | Arm 2 | 51 | 59 (24 to 74) | 20 (39) | NR, NR, NR, NR | 65, 35, NR | NR, 100, NR |
Aparicio (2022) | NCT03751176 | FOLFIRI + Panitumumab | Arm 1 | 18 | 59 (31 to 78) | 8 (44) | NR, NR, NR, NR | 56, 44, NR | NR, 100, NR |
Zhang et al. (2022) | NCT02935764 | FOLFIRI | Arm 1 | 88 | 59 (50 to 66) | 36 (41) | NR, NR, NR, NR | NR, NR, 2 | NR, NR, NR |
Pfeiffer et al. (2023) | EudraCT 2016 to 005241 to 23 | TAS-102 | Arm 1 | 47 | 67 (58 to 72) | 17 (36) | NR, NR, NR, NR | 32, 68, NR | NR, NR, 45 |
Prager et al. (2023) | NCT04737187 | TAS-102 | Arm 2 | 246 | 64 (24 to 90) | 112 (46) | 0, 1, 89, 2 | 43, 57, 0 | NR, 6, 94 |
ECOG PS = Eastern Cooperative Oncology Group Performance Status; EudraCT = European Union Drug Regulating Authorities Clinical Trials Database; FOLFIRI = leucovorin calcium (folinic acid) + fluorouracil + irinotecan hydrochloride; FOLFOX = leucovorin calcium (folinic acid) + fluorouracil + oxaliplatin; mAPaT = modified all participants as treated; mFOLFOX6 = modified fluorouracil, leucovorin, and oxaliplatin; NR = not reported; SLR = systematic literature review; TAS-102 = trifluridine and tipiracil hydrochloride.
Note: Selection of baseline characteristics based on frequency of reported characteristics across selected studies.
The mAPaT population was defined as the analysis populations used to report comparator study results.
Source: Merck Canada colorectal cancer indirect treatment comparison report.71
Table 45: Summary of Studies Included in the ITCs
Target population | Internal data source | External (comparator) | Outcomes |
|---|---|---|---|
MSI-H gastric carcinoma with at least 1 prior line of therapy | Pembrolizumab: IPD from the KEYNOTE-158 trial Data cut-off: January 12, 2022 | FOLFIRI from SUN-CASE and Sym et al. studies (2013):
Ramucirumab + paclitaxel from RAMIRIS, MORPHEUS-GC, JVCZ, and RAINBOW studies:
Ramucirumab from REGARD and JVDB studies:
Irinotecan from AIO, JACCRO GC-05, TRICS/UMIN, KCSG ST10 to 01, WJOG 4007, TCOG GI-, Sym et al. (2013), Satoh et al. (2015), Roy et al. (2013), and Kang et al. (2012) studies:
Paclitaxel from the KEYNOTE-061 study:
|
|
FOLFIRI = leucovorin calcium (folinic acid) + fluorouracil + irinotecan hydrochloride; IPD = individual patient data; ITC = indirect treatment comparison; MSI-H = microsatellite instability-high; OS = overall survival; PFS = progression-free survival.
Source: Merck Canada gastric cancer ITC report.73
Pharmacoeconomic Review
Abbreviations
AE
adverse event
BIA
budget impact analysis
CDA-AMC
Canada’s Drug Agency
CRC
colorectal cancer
dMMR
mismatch repair deficient
DOR
duration of response
FOLFIRI
leucovorin calcium (folinic acid) + fluorouracil + irinotecan hydrochloride
FOLFOX
leucovorin calcium (folinic acid) + fluorouracil + oxaliplatin
HR
hazard ratio
ICER
incremental cost-effectiveness ratio
ITC
indirect treatment comparison
KM
Kaplan-Meier
MSI-H
microsatellite instability-high
NSCLC
non–small cell lung cancer
ORR
objective response rate
OS
overall survival
PFS
progression-free survival
QALY
quality-adjusted life-year
RDI
relative dose intensity
SCLC
small cell lung cancer
SOC
standard of care
TTD
time to treatment discontinuation
VEGF
vascular endothelial growth factor
WTP
willingness to pay
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Pembrolizumab (Keytruda), $4,400.00 per 100 mg/4 mL vial |
Indication | As monotherapy for the treatment of adult and pediatric patients with unresectable or metastatic microsatellite instability-high (MSI-H) or mismatch repair deficient (dMMR) solid tumours, as determined by a validated test, that have progressed following prior treatment and who have no satisfactory alternative treatment options. |
Health Canada approval status | NOC |
Health Canada review pathway | Standard review |
NOC date | August 29, 2024 |
Reimbursement request | As per indication |
Sponsor | Merck Canada Inc. |
Submission history | Previously reviewed: Yes Pembrolizumab (Keytruda) has been reviewed for numerous indications by CDA-AMC. |
CDA-AMC = Canada’s Drug Agency; dMMR = mismatch repair deficient; MSI-H = microsatellite instability-high; NOC = Notice of Compliance.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation |
|
Target population | Adult and pediatric patients with unresectable or metastatic MSI-H or dMMR solid tumours, as determined by a validated test, that have progressed following prior treatment and who have no satisfactory alternative treatment options |
Treatment | Pembrolizumab |
Dose regimen | 200 mg every 3 weeks for up to 35 cycles or until progression. |
Submitted price | Pembrolizumab: $4,400 per 100 mg/4 mL vial |
Submitted treatment cost | $8,800 per cycle ($308,000 for 35 cycles) |
Comparators | SOC defined by tumour site:
|
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs, LYs |
Time horizon | Lifetime (40 years) |
Key data sources |
|
Submitted results | Weighted ICER for pembrolizumab versus SOC across all tumour sites = $35,618 per QALY gained (incremental costs: $117,657; incremental QALYs: 3.30) |
Key limitations |
|
CDA-AMC reanalysis results |
|
CDA-AMC = Canada’s Drug Agency; CRC = colorectal; dMMR = mismatch repair deficient; FOLFIRI = leucovorin calcium (folinic acid) + fluorouracil + irinotecan hydrochloride; FOLFOX = leucovorin calcium (folinic acid) + fluorouracil + oxaliplatin; ICER = incremental cost-effectiveness ratio; ITC = indirect treatment comparison; KM = Kaplan-Meier; LY = life-year; MSI-H = microsatellite instability-high; nab = nanoparticle albumin–bound; NSCLC = non–small cell lung cancer; OS = overall survival; PFS = progression-free survival; PSM = partitioned survival model; QALY = quality-adjusted life-year; SCLC = small cell lung cancer; SOC = standard of care; TTD = time to treatment discontinuation; VEGF = vascular endothelial growth factor.
Conclusions
Evidence from the single-arm trials, KEYNOTE-158 and KEYNOTE-164, assessed the efficacy of pembrolizumab in adult patients with metastatic or unresectable microsatellite instability-high (MSI-H) or mismatch repair deficient (dMMR) solid tumours. The clinical experts consulted by Canada’s Drug Agency (CDA-AMC) found that the response to treatment (objective response rate [ORR]) was clinically meaningful and durable (duration of response [DOR]) compared with what is typically observed with standard of care (SOC) treatments. There was considerable variability in response rates across different tumour types, but interpretation of this heterogeneity was challenged by small sample sizes. In the pediatric population, it is difficult to ascertain the benefit of pembrolizumab in this group of patients due to the small number or patients enrolled in the KEYNOTE-051 trial. A key limitation of the sponsor-submitted studies is that they were all single-arm trials, limiting the ability to directly compare pembrolizumab's efficacy and safety with SOC treatment options. The absence of randomized data makes it difficult to draw definitive conclusions regarding pembrolizumab's impact on overall survival (OS), progression-free survival (PFS), or quality of life relative to existing therapies. The comparative evidence from the indirect treatment comparisons (ITCs) was limited to 4 cancer types in adults (colorectal, endometrial, small intestine, and gastric) and suggested improved PFS and OS with pembrolizumab compared with SOC, which aligned with the expectations of the clinical experts consulted by CDA-AMC. However, the ITCs that were submitted had significant limitations that impacted the internal validity of the findings.
In the absence of randomized evidence or robust indirect comparisons, it is uncertain to what degree differences in the OS benefit for pembrolizumab versus different SOCs are driven by confounding rather than treatment effect. Conclusions from the economic analysis are contingent on the submitted indirect evidence that is associated with methodological limitations, as noted by the Clinical Review. Likewise, the survival analysis conducted on the trial evidence is limited by small sample sizes and a heterogenous population. The economic analysis may therefore not accurately reflect the true incremental difference between pembrolizumab versus current SOC.
The CDA-AMC base-case results align with those of the sponsor’s submitted analysis, indicating that pembrolizumab is cost-effective at a willingness-to-pay (WTP) threshold of $50,000 per quality-adjusted life-year (QALY) gained, relative to SOC. In the CDA-AMC base case, pembrolizumab is associated with a weighted incremental cost-effectiveness ratio (ICER) of $32,001 per QALY gained compared with SOC, which was driven by the OS benefit associated with pembrolizumab, which was estimated to be 3.35 life-years compared with those treated with SOC. Across different modelled tumour sites, the ICER ranged from $23,213 (small intestine) to $36,880 (gastric) per QALY gained. The tumour sites modelled (small intestine, endometrial, gastric, and colorectal) represented 80% of patients with MSI-H or dMMR solid tumours. For unmodelled tumours, the sponsor assumed a full incremental cost for pembrolizumab versus SOC and no additional benefit (0 QALYs). The results assume no additional testing costs associated with the funding of pembrolizumab in this indication. Based on the sponsor’s budget impact analysis (BIA), there may be additional testing costs in tumour sites where testing is not currently routine. Inclusion of these costs may add an additional $1,109 to $7,394 per patient in health care costs to the analysis. However, because pembrolizumab is currently approved for some tumour sites where MSI-H and dMMR prevalence is low (e.g., breast cancer), it is unclear if funding of pembrolizumab will drastically change testing uptake in all tumour sites where it is not currently routine.
The clinical experts consulted by CDA-AMC noted that rechallenging with pembrolizumab or another immune checkpoint inhibitor after disease progression in an earlier line of treatment is not expected to happen in clinical practice. Pembrolizumab and other immune checkpoint inhibitors are already funded for treating various cancers, including colorectal cancer (CRC), endometrial, gastric, renal, urothelial, mesothelioma, breast, non–small cell lung cancer (NSCLC), small cell lung cancer (SCLC), and biliary tract tumour sites. Therefore, it is anticipated that pembrolizumab will be used predominately in tumour sites for which there is very little evidence for this drug.
Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, clinician groups, and drug plans that participated in the CDA-AMC review process.
Two patient groups provided input for this review: Colorectal Cancer Canada and the Colorectal Cancer Resource & Action Network, the latter working in collaboration with the Canadian Cancer Survivor Network, Craig’s Cause Pancreatic Cancer Society, Canadian Breast Cancer Network, and Ovarian Cancer Canada. Information was collected from international and Canadian respondents through a survey and interviews and included 7 patients and caregivers. Overall, patients’ disease experiences were influenced by the physical symptoms associated with cancer (e.g., fatigue, pain, weakness), the psychosocial effect associated with fear of death and a poor disease prognosis (e.g., anxiety, distress, depression), and the adverse side effects of treatment with chemotherapy and radiation (e.g., nausea, vomiting, neuropathy). The most important outcomes for patients included delaying disease progression and achieving long-term remission, with the ultimate objective of improving survival, experiencing minimal side effects from treatments, preserving independence to minimize the burden on caregivers, and maintaining an optimal quality of life. The current standard of treatment for patients is a chemotherapy regimen, specifically, leucovorin calcium (folinic acid) + fluorouracil + oxaliplatin (FOLFOX); leucovorin calcium (folinic acid) + fluorouracil + irinotecan hydrochloride (FOLFIRI); capecitabine; and panitumumab were noted to be used for CRC. Survey respondents treated with pembrolizumab reported going from a terminal diagnosis to no evidence of disease, while diminishing the need for traditional systemic therapies that have limited efficacy and severe side effects.
Registered clinician input was received from 5 groups: 4 Ontario Health (Cancer Care Ontario) Drug Advisory Committees (breast genitourinary, gynecology, and central nervous system cancer), and the Gynecologic Oncologic Society of Canada. According to the clinician input, the current pathway of care comprises various chemotherapy regimens and varies by tumour site, although patients would be treated with palliative intent. There is an unmet need due to pembrolizumab’s restriction to specific solid tumour locations with eligible MSI-H or dMMR alterations, when it is expected that patients with the same class of alterations will benefit from pembrolizumab, agnostic of primary tumour location. The clinician input noted that patients with any eligible alteration regardless of primary tumour location would be eligible for pembrolizumab, and that treatment has been shown to offer considerable response and disease control and, in some patients, durable long-term benefit.
The drug plan input received by CDA-AMC noted the single-arm evidence for pembrolizumab and expressed interest in knowing how pembrolizumab compared with existing later line therapies and which solid tumour types should be included for this indication given the available clinical evidence. Feedback noted that pembrolizumab monotherapy is currently funded by most jurisdictions as first-line therapy in MSI-H and dMMR malignancies in the CRC tumour site. The drug plans questioned the number of prior therapies required for eligibility and whether re-treatment would be allowed in clinical practice. The drug plans also noted that patients will be required to have mismatch repair and microsatellite instability testing in some disease settings where it is not regularly conducted (e.g., testing is currently in place for unresectable or metastatic CRC and endometrial patients). The drug plans stated they intended to adopt weight-based dosing for pembrolizumab (e.g., 2 mg/kg every 3 weeks to a maximum dose of 200 mg in adult and pediatric patients, or 4 mg/kg every 6 weeks to a maximum of 400 mg in adult patients only), similar to other indications. The drug plans noted the presence of confidential listing prices for pembrolizumab, bevacizumab, encorafenib, panitumumab, ramucirumab, and trifluridine and tipiracil hydrochloride.
Several of these concerns were addressed in the sponsor’s model:
PFS and OS were included in the model.
Costs and utility decrements related to adverse events (AEs) were included in the model.
In addition, CDA-AMC addressed some of these concerns as follows:
Weight-based dosing for pembrolizumab (2 mg/kg every 3 weeks) was incorporated in a reanalysis.
CDA-AMC was unable to address the following concerns raised from the input received:
Uncertainty in the comparative efficacy of pembrolizumab, given the single-arm trial evidence.
Confidential listing prices for pembrolizumab and select comparators.
Economic Review
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted a cost-utility analysis of pembrolizumab compared with SOC.1 The model population comprised adult and pediatric patients with unresectable or metastatic MSI-H or dMMR solid tumours, as determined by a validated test, that have progressed following prior treatment and who have no satisfactory alternative treatment options. The modelled cohort is aligned with the Health Canada–indicated population and the sponsor’s reimbursement request.
Pembrolizumab is available as a 100 mg/4 mL vial for IV infusion at a submitted price of $4,400.00 per vial and the recommended dosage is 200 mg every 3 weeks up to 35 cycles or until disease progression.2 At the submitted price of $4,400 per 4 mL vial, the cost of pembrolizumab per 3-week cycle was estimated by the sponsor to be $8,624 (assuming 98% relative dose intensity [RDI] averaged across modelled tumour sites) up to 104 weeks for modelled tumour sites.1 In unmodelled tumour sites, the sponsor assumed a total cost of $73,111 per patient for pembrolizumab based on the per 3-week cycle treatment cost multiplied by the weighted average SOC time on treatment (0.49 years).1 The comparator for this analysis was SOC defined based on tumour site and comprised pooled FOLFOX-FOLFIRI, anti-vascular endothelial growth factor (VEGF) + chemotherapy, and trifluridine-tipiracil hydrochloride for CRC tumour sites; paclitaxel and doxorubicin for endometrial tumour sites, paclitaxel, irinotecan, ramucirumab + paclitaxel, FOLFORI, and ramucirumab for gastric tumour sites; and nanoparticle albumin-bound (nab)-paclitaxel, anti-VEGF + chemotherapy, and taxane-based treatment for small intestine tumour sites. The drug acquisition cost per administration of SOC ranged from $240 to $3,590 for CRC tumour sites, $416 to $1,440 for endometrial tumour sites, $103 to $2,684 for gastric tumour sites, and $1,440 to $4,544 for small intestine tumour sites.1
The outcomes of interest included QALYs and life-years. The economic evaluation was conducted over a lifetime horizon of 40 years from the perspective of the Canadian public health care payer. Discounting (1.5% per annum) was applied for both costs and outcomes and a cycle length of 1 week was used.
Model Structure
The sponsor submitted a partitioned survival model with 3 health states: “progression-free,” “progressed disease,” and “death” (Figure 1).1 The proportions of patients who were progression-free, experienced progressed disease, or were dead at any time over the model horizon were derived from nonmutually exclusive survival curves. All patients entered the model in the progression-free state and could either remain progression-free, experience disease progression, or die. Patients could discontinue treatment before or after disease progression based on the estimated time to treatment discontinuation (TTD), after which the cost of first-line treatment would no longer be incurred. Patients could also remain on treatment while in the progressed disease state. Disease progression was determined by investigator assessment according to Response Evaluation Criteria in Solid Tumours Version 1.1 (RECIST 1.1) criteria. Patients who transitioned to the progressed disease state incurred costs associated with subsequent treatment. Patients can transition to the death state from any health state.
Model Inputs
The modelled population reflected the baseline characteristics of participants from the phase II nonrandomized, single-arm KEYNOTE-1583 and KEYNOTE-1644 trials, which enrolled patients with a wide variety of tumour sites; however the economic model only included data from relevant patients with MSI-H or dMMR solid tumours (N = 296; mean age = 56 to 66 years across tumour sites; proportion male = 0% to 64.7% across tumour sites; mean weight = 62 kg to 72 kg across tumour sites).
The sponsor’s analysis was stratified per tumour tissue location based on the availability of data on CRC, endometrial, gastric, and small intestine tumour sites from the KEYNOTE-158 and KEYNOTE-164 trials.5 All other tumour sites were defined as “unmodelled,” with no additional clinical benefit attributed to pembrolizumab while incurring the costs of treatment. These unmodelled tumour sites included ovarian, pancreatic, cholangiocarcinoma, brain, sarcoma, breast, cervical, neuroendocrine, prostate, adrenocortical, mesothelioma, thyroid, SCLC, urothelial, salivary, renal, and other tumour sites.
Key clinical efficacy inputs (PFS, OS, TTD) for pembrolizumab were derived from the KEYNOTE-158 and KEYNOTE-164 trials (data cut-off date: January 12, 2022, and February 19, 2021, respectively)5 to inform data for CRC, endometrial, gastric, and small intestine tumour sites.1 The sponsor used parametric survival modelling to estimate survival outcomes for pembrolizumab after the trial follow-up period using survival data from the KEYNOTE-158 and KEYNOTE-164 trials to extrapolate health state transition probabilities for the entire lifetime horizon of the model (40 years). The selection of parametric survival models used in the base case was based on clinical plausibility of long-term survival projections, visual inspection of model fit, as well as Akaike and Bayesian information criterion of statistical fit.1 For SOC treatments, approaches to modelling survival outcomes varied based on availability of data for each, including standard parametric survival modelling fit to pseudo–individual patient-level data derived from ITC Kaplan-Meier (KM) data and hazard ratios (HRs) derived using matching-adjusted indirect comparisons where feasible.1,6 TTD for pembrolizumab was modelled directly using KM data from the pivotal trials and TTD for comparators was modelled by applying a constant HR of 1 to PFS derived from the ITCs. The proportion of patients receiving subsequent treatments after discontinuation for each tumour site were based on data from the KEYNOTE-158 and KEYNOTE-164 trials.5 The model accounted for grade 3 or higher treatment-related AEs that were reported in at least 1% of patients treated with pembrolizumab and at least 3% of patients treated with SOC based on data from the KEYNOTE-158 and KEYNOTE-164 trials or published literature.1,6
Health state utility values were derived using EQ-5D-3L data collected in the KEYNOTE-158 trial and applying a Canadian value set.1 A linear mixed-effects regression method was used to estimate health-state and tumour site–specific values. Disutility due to AEs was calculated in each treatment arm as a function of the mean duration of AEs, the estimated disutility associated with grade 3+ AEs, and the proportion of AEs sourced from National Institute for Health and Care Excellence (NICE) technology appraisals or based on assumption.1
The model included costs related to drug acquisition and administration, health care resource use, AEs, and end-of-life costs. Drug acquisition costs were calculated by the sponsor as a function of unit drug costs, dosing schedules, RDI, and the proportion of patients on treatment. Acquisition costs were based on the sponsor’s submitted price for pembrolizumab and were sourced from IQVIA DeltaPA for SOC treatments.1,7 Administration costs were included for IV treatments only. Health care resource use differed by health state and tumour site. Resource use costs included those for medical consultation follow-ups, CT scans, liver function tests, and MRIs for CRC tumour sites; medical consultation follow-ups, electrolytes, CT scans, blood counts, and liver function tests for endometrial tumour sites; medical consultations, electrolytes, echocardiograms, gastroscopy, blood counts, and liver function tests for gastric tumour sites; and CT scans, liver function tests, MRI scans, and renal function tests for small intestine tumour sites. Costs associated with AE management were sourced from the Ontario Case Costing Initiative and Canadian Institute for Health Information Patient Cost Estimator.8,9 The sponsor assumed that polymerase chain reaction and immunohistochemistry were used for MSI-H and dMMR testing, and that 100% of patients across all modelled tumour sites would have already received MSI-H or dMMR testing in clinical practice and therefore pembrolizumab testing costs are $0.1 End-of-life costs were sourced from published literature.10
Summary of Sponsor’s Economic Evaluation Results
All analyses were run probabilistically (1,000 iterations for the base-case and scenario analyses). The deterministic and probabilistic results were similar. The probabilistic findings are presented subsequently.
Base-Case Results
In the sponsor’s base case, pembrolizumab was associated with an incremental cost of $117,657 and an incremental QALY gain of 3.30 compared with SOC, resulting in a weighted ICER of $35,618 per QALY gained across all tumour sites. The weighted ICER was estimated by calculating ICERs across each individual tumour site and weighting them based on tumour site prevalence (using Canadian epidemiology data from the Canadia Cancer Society).11 Across modelled tumour sites (i.e., CRC, gastric, endometrial, and small intestine), the ICER for pembrolizumab compared with SOC was between $27,341 per QALY (endometrial) and $47,539 per QALY (gastric). For all nonmodelled tumour sites (which made up 20% of the population), the sponsor assumed no incremental benefit (0 QALYs) while assuming the full cost of pembrolizumab would be incurred (incremental costs = $46,571).
The sponsor’s analysis predicted that pembrolizumab was associated with a longer duration of life than SOC (incremental life-years = 4.71). Given the duration of the KEYNOTE-158 and KEYNOTE-164 trials (maximum follow-up ranging from 277 to 306 weeks across tumour sites) in contrast to the model’s lifetime horizon (40 years), the majority (e.g., approximately 57% in CRC) of incremental QALYs realized by patients receiving pembrolizumab relative to SOC were derived during the period beyond which there are observed trial data (i.e., extrapolated period).
The probability that pembrolizumab was cost-effective at a $50,000 per QALY gained threshold was 100%.
Table 3: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER versus SOC ($/QALY) |
|---|---|---|---|---|---|
SOC | 105,413 | Reference | 0.83 | Reference | Reference |
Pembrolizumab | 223,070 | 117,657 | 4.13 | 3.30 | 35,618 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; SOC = standard of care.
Note: The submitted analysis is based on publicly available prices of comparator treatments. The weighted ICER was estimated by calculating ICERs across each individual tumour site and weighting them based on tumour site prevalence (using Canadian epidemiology data from the Canadian Cancer Society).11
Source: Sponsor’s pharmacoeconomic submission.1
Additional results from the sponsor’s submitted economic evaluation base case are presented in Appendix 3.
Sensitivity and Scenario Analysis Results
The sponsor conducted several deterministic scenario analyses that included adopting alternative modelling assumptions (i.e., alternate discount rates and time horizons) as well as alternate assumptions related to removing the pembrolizumab limit of 35 cycles of therapy, excluding end-of-life costs, applying a RDI for pembrolizumab of 100%, excluding subsequent therapy costs, and excluding AE disutilities. The sponsor’s scenario analyses were conducted on the modelled population only (i.e., CRC, gastric, endometrial, and small intestine). The ICERs for pembrolizumab versus SOC ranged from $29,894 to $48,968 per QALY; the scenario that adopted a 10-year time horizon had the largest ICER.
The sponsor conducted a scenario analysis from a societal perspective that included additional costs associated with labour productivity lost. In this analysis, relative to SOC, the ICER was $32,320 per QALY gained in modelled tumour sites. This was similar to the sponsor’s base-case analysis for modelled tumour sites using a health care payer perspective.
CDA-AMC Appraisal of the Sponsor’s Economic Evaluation
CDA-AMC identified several key limitations to the sponsor’s analysis that have notable implications on the economic analysis:
Uncertainty in the comparative efficacy of pembrolizumab versus SOC across tumour sites: The sponsor modelled 4 tumour sites (CRC, endometrial, gastric, small intestine) due to the lack of data available for the remaining unmodelled tumour sites (ovarian, pancreatic, cholangiocarcinoma, brain, sarcoma, breast, cervical, neuroendocrine, prostate, adrenocortical, mesothelioma, thyroid, SCLC, urothelial, salivary, renal, and others). Due to this lack of data, the sponsor assumed no clinical benefit attributed to pembrolizumab while incurring costs of treatment for unmodelled tumour sites, which is aligned with the CDA-AMC guidelines for tumour-agnostic products.12 Although the clinical experts consulted by CDA-AMC suggested that pembrolizumab is expected to be efficacious across all tumour sites, the cost-effectiveness of pembrolizumab versus SOC in unmodelled tumour types is highly uncertain due to the lack of available clinical data. Notably, data from the KEYNOTE-158 trial suggested that the ORRs for ovarian and biliary tumour sites were relatively comparable to the ORRs observed in the 4 modelled tumour sites, suggesting that the sponsor’s modelling approach may be conservative by assuming there is no benefit in unmodelled tumour sites.
The modelling of SOC survival outcomes was based on standard parametric survival modelling fit to pseudo–individual patient-level data derived from ITCs in the base-case analysis. Across all sources of published data included in the ITCs, however, the majority of sources used did not represent data specific to patients with MSI-H or dMMR solid tumours. There remains a lack of head-to-head clinical trial evidence comparing pembrolizumab to comparator treatments in this patient population and it is therefore uncertain whether survival data from the ITC appropriately represents PFS and OS for patients receiving SOC. It is not known whether patients with MSI-H or dMMR solid tumours would experience similar outcomes to those without these biomarkers in response to SOC treatments. The CDA-AMC Clinical Review concluded that the submitted ITCs were subject to considerable limitations that impacted the internal validity of the findings, including lack of adjustment for potential confounders and small sample size. Naive indirect comparisons are not considered a valid method to produce comparative effect estimates for decision-making because they are at high risk of bias due to confounding, which may be substantial. It is therefore not possible to discern whether the effects produced by these analyses are the result of the treatments or differences in known or unknown prognostic and/or effect-modifying variables.
Furthermore, the sponsor’s model was parameterized using data from the KEYNOTE-158 and KEYNOTE-164 trials that enrolled adult patients aged 18 and older with MSI-H or dMMR solid tumours across various tumour sites. However, the proposed Health Canada indication for pembrolizumab is for the treatment of adult and pediatric patients. Given that the clinical data used to parameterize the economic model did not include patients younger than 18 years old, the modelled population represents an older cohort of patients compared with those who might receive pembrolizumab in clinical practice in Canada. The clinical experts consulted by noted there were very few patients (N = 7) included in the KEYNOTE-051 trial that assessed the efficacy of pembrolizumab in pediatric patients. However, immune checkpoint inhibitors have been used in pediatric patients historically and, therefore, pediatric patients are not expected to be excluded from treatment eligibility due to age. The clinical experts consulted also noted that there is safety data available from larger studies to infer safety in the pediatric population. CDA-AMC notes that any conclusions surrounding the cost-effectiveness of pembrolizumab in pediatric patients can only be extrapolated from results in an adult population.
Feedback from the clinical experts noted that pembrolizumab is available and used in an earlier line of treatment in CRC, endometrial, and NSCLC tumour sites, and that an alternative immune checkpoint inhibitor (i.e., nivolumab) is available and used in an earlier line of treatment in the gastric, renal, urothelial, mesothelioma, breast, NSCLC, SCLC, and biliary tract tumour sites. If an alternative immune checkpoint inhibitor such as nivolumab is used in a previous line of therapy and patients experience disease progression, this substantially reduces the likelihood of rechallenge with another immune checkpoint inhibitor, such as pembrolizumab. Therefore, the most relevant remaining tumour sites in which pembrolizumab would be newly available under the current reimbursement request and therefore impacted in clinical practice would be small intestine, ovarian, pancreatic, brain, sarcoma, cervical, neuroendocrine, prostate, adrenocortical, thyroid, salivary, and others. Notably, the only modelled tumour site included in the relevant remaining sites in which pembrolizumab would be newly available is small intestine. The cost-effectiveness of pembrolizumab in the relevant remaining tumour sites is unknown, given the lack of evidence for the majority of these sites.
CDA-AMC could not address this limitation in reanalysis. The evidence informing the economic analysis is only valid if the difference between SOC and pembrolizumab is driven entirely by the pembrolizumab treatment effect with no confounding.
Uncertainty in the long-term survival benefit associated with pembrolizumab: The sponsor used parametric modelling to extrapolate OS beyond the observable time points in the KEYNOTE-158 and KEYNOTE-164 trials (maximum follow-up time ranging from 277 to 306 weeks across modelled tumour sites) to a lifetime horizon of 40 years. The parametric distribution chosen by the sponsor resulted in an incremental gain of 5.89 life-years and 4.13 QALYs among patients treated with pembrolizumab. Notably, the majority of the total incremental QALYs are accrued by patients from the period beyond which there are no observed clinical data (e.g., 57% for CRC). The extrapolation assumptions are influenced by the end-of-trial cut-off, which has a small sample size and high censoring, further compounding this uncertainty. Additionally, the following limitations were noted with the sponsor’s chosen extrapolation.
The small patient numbers lead to challenges in conducting a survival analysis. Curves that fit the available data lead to implausible outcomes, such as patients living indefinitely. Survival curves had to therefore be capped at general population survival, which indicates that the underlying parametric function is likely incorrectly specified. Given that some patients may respond well to pembrolizumab, and others may not, this heterogeneity may lead to a less accurate survival analysis, which assumes a homogenous population.
Based on the sponsor’s selection of curves, the hazard rate for mortality is assumed to continuously decrease over time for patients who receive pembrolizumab. By assuming that mortality hazard rates decrease over time, the proportion of patients alive at 15 years is predicted to be 22% for those receive pembrolizumab. At 30 years, 11% of patients who received pembrolizumab would be predicted to remain alive, and survival would be expected to be equivalent to that of the general population. This would suggest that, for some patients, pembrolizumab has alleviated the all-mortality risk associated with the cancer. Feedback obtained from the clinical experts for this review noted it is not expected that patients would have the same risk of mortality as those in the general population. If patients are essentially cured of disease and excess mortality because a metastatic cancer has been removed, these patients are still likely to have a higher mortality risk than the general population due to comorbidities. For example, patients with metastatic disease may have experienced the surgical removal of tumour site tissue and may have a higher risk of other cancer types due to Lynch syndrome, which is characteristic of MSI-H and dMMR solid tumours.13
Overall, the durability and magnitude of the predicted survival benefit associated with pembrolizumab is uncertain, given the limitations with the available data.
CDA-AMC addressed this limitation by using the gamma distribution for extrapolating OS for pembrolizumab in the CRC, endometrial, and gastric tumour sites, and using the exponential distribution for extrapolating OS for pembrolizumab in the small intestine tumour site. These functions were selected because they ensure that the number of patients who have better predicted survival than the general population risk of mortality is minimized.
A scenario analysis was conducted assuming a treatment waning effect from 5 to 7 years for all tumour sites. This assumes after 5 years there would be no additional benefit associated with pembrolizumab. The Gompertz function was selected to interpolate the data because it had the best fit. This analysis was conducted to explore the impact that extrapolation, as opposed to interpolation, has on the results. Figures 2, 3, 4 and 5 outline what long term overall survival looks like in this analysis for each tumour site. This was seen as more appropriate than an analysis that imposed a shorter time horizon.
Weight-based dosing for pembrolizumab is used in clinical practice: The modelled dose of pembrolizumab was a fixed dose of 200 mg intravenously every 3 weeks, aligned with the KEYNOTE-156 and KEYNOTE-164 trials. However, input from the participating public drug plans indicated that jurisdictions would most likely implement weight-based dosing for pembrolizumab of 2 mg/kg every 3 weeks to a maximum dose of 200 mg in adult and pediatric patients, like other indications for which pembrolizumab is reimbursed. Weight-based dosing will increase the cost savings associated with pembrolizumab, as weight-based dosing using the weighted mean weight of patients across the 4 modelled tumour sites (69.4 kg) resulted in patients requiring a dose of 138.7 mg every 3 weeks rather than 200 mg every 3 weeks when a fixed-dose approach is used.
CDA-AMC applied weight-based dosing for pembrolizumab of 2 mg/kg, resulting in a dose of 138.7 mg every 3 weeks per patient.
Approach taken to estimate time on treatment for pembrolizumab was inappropriate: The sponsor directly used TTD KM data from the pivotal trials to model time on treatment for pembrolizumab. Although this data depicts treatment discontinuation over the 24-month period for pembrolizumab, conducting a survival analysis to fit a curve to the TTD KM data would be preferable, given the small sample size, to derive a smoother function for estimating TTD. Reviewing the data, PFS and TTD appear to be similar. This is expected because patients would likely receive pembrolizumab until unacceptable toxicity or disease progression, meaning PFS and TTD are intrinsically linked. Furthermore, the sponsor’s method for modelling TTD differed between pembrolizumab versus SOC. For SOC, TTD was modelled by applying a constant HR of 1 versus PFS, essentially making the TTD for SOC equivalent to the PFS based on the ITC results. To reduce bias, it would be preferable to employ the same approach for all treatments in the model. The impact of uncertainty when assessed probabilistically is not adequately assessed when using KM TTD data, as it is sampled independently of PFS. This would create unlikely scenarios where TTD would vastly differ from PFS. Given the high correlation between the 2 parameters, it is more appropriate to link the 2 such that if PFS improves, then the TTD also improves and vice versa.
CDA-AMC modelled TTD by making it equal to PFS (modelled using a standard partitioned survival model) for pembrolizumab up to week 104, after which a stopping rule aligned with the product monograph was applied. This method is aligned with TTD modelling methods for SOC.
Testing costs are uncertain: Feedback from the drug plans indicates that patients will be required to have mismatch repair and microsatellite instability testing in some disease settings where it is not regularly conducted. Testing costs were not included in the sponsor’s base case because it was assumed that patients already receive MSI-H and dMMR testing in current clinical practice in the modelled tumour sites. The CDA-AMC testing procedures considerations state that testing for MSI-H and dMMR status is currently part of the SOC for the most common unresectable or metastatic solid tumour types and is publicly funded across jurisdictions. However, this does not apply to all tumour sites, as highlighted by the sponsor’s submitted BIA. In the BIA, the sponsor notes that testing uptake is currently at 50% for the following tumour sites: ovarian, pancreatic, cholangiocarcinoma, brain, sarcoma, breast, cervical, neuroendocrine, prostate, adrenocortical, mesothelioma, thyroid, SCLC, urothelial, salivary, renal, and other. If pembrolizumab were to receive a positive funding decision for this indication, then testing uptake would increase to 70%. If pembrolizumab is not funded for this indication, then testing uptake would be unchanged (remain at 50%). This implies that funding pembrolizumab would be associated with an increase in testing uptake.
Given the very low proportion of patients with dMMR or MSI-H malignancies in some tumour sites, testing costs to identify 1 patient can be high. For example, the sponsor notes that only 0.20% of patients with breast cancer have dMMR or MSI-H tumours. This would mean 500 patients would need to be tested to identify 1 patient eligible for this treatment. If immunohistochemistry testing were used, which costs $150 based on sponsor estimates, this would equate to $75,000 in testing costs to identify 1 patient. If a higher cost panel test was used ($1,000 per test), this cost rises to $500,000.
CDA-AMC used the sponsor’s BIA values to estimate potential testing costs. The results are outlined in Table 14.
Subsequent treatment costs are uncertain: The sponsor included a proportion of patients receiving 1 or more subsequent therapies as per data from the KEYNOTE-164 and KEYNOTE-158 trials. Subsequent therapies varied by tumour site and included anti-VEGF plus chemotherapy; capecitabine; FOLFOX; FOLFIRI; irinotecan, regorafenib, and trifluridine plus tipiracil hydrochloride for CRC tumour sites; anti-VEGF plus chemotherapy; carboplatin; carboplatin plus paclitaxel; cisplatin plus doxorubicin; doxorubicin monotherapy; gemcitabine, megestrol, paclitaxel monotherapy, and tamoxifen for endometrial tumour sites; capecitabine, FOLFIRI, irinotecan, paclitaxel, and ramucirumab plus paclitaxel for gastric tumour sites; and anti-VEGF plus chemotherapy, FOLFIRI, gemcitabine, and gemcitabine plus paclitaxel for small intestine tumour sites.
However, based on the Health Canada indication, no “satisfactory” treatment options are available to the modelled patient population. The clinical experts consulted by CDA-AMC noted that while these patients have generally received multiple lines of therapy and have no satisfactory alternative treatment options, it is still expected in clinical practice that a proportion of patients would receive subsequent therapy with SOC options or potentially continue treatment with pembrolizumab, depending on the extent of disease progression (e.g., some patients who progress with disease that is oligometastatic may continue treatment with pembrolizumab). This is aligned with data from the pivotal trials indicating that 19.61% to 45.97% of patients (depending on tumour site) received 1 or more subsequent therapies. It is uncertain whether patients who receive pembrolizumab versus SOC would be similarly likely to receive a subsequent line of therapy. In the absence of robust head-to-head Canadian data, the impact that pembrolizumab has on subsequent therapy usage is uncertain. In the sponsor’s base case, costs related to subsequent therapy were lower for patients receiving pembrolizumab because these patients remained progression-free for a longer period and, therefore, more patients died before progression.
CDA-AMC could not address this limitation in the reanalysis due to a lack of comparative clinical data. Any cost savings due to the delay or avoidance of subsequent therapy is highly uncertain. Given that subsequent therapy costs are small in the model, this limitation is unlikely to influence cost-effectiveness conclusions.
Drug acquisition costs for several comparator treatments were not aligned with most up-to-date sources: The sponsor modelled oxaliplatin costs as $36.27 per 10 mL vial, $72.54 per 20 mL vial, and $145.08 per 40 mL vial; however, a recent DeltaPA database search indicates that these costs should be $45.00, $90.00, and $180.00, respectively.14 Similarly, costs for ramucirumab were included as $627.22 per 10 mL vial and $3,131.58 per 50 mL vial, whereas data from the DeltaPA database indicates these costs should be $690.63 and $3,453.16, respectively.14 Pack sizes for ramucirumab were also incorrectly included as 30 units per pack instead of 1 unit per pack.
CDA-AMC corrected the drug acquisition costs for oxaliplatin and ramucirumab in the reanalysis.
The probabilistic analysis does not capture the full degree of uncertainty associated with the underlying data: When the model is run probabilistically, the model samples different OS curves for each comparator based on the trial data. However, based on the Clinical Review, due to the lack of control over confounding, the results are inherently uncertain. The analysis was conducted under the assumption that the underlying data for pembrolizumab and the comparator treatments represent the same patient population. However, if confounding has not been adequately controlled for, then the population may not be representative. This uncertainty is not captured in the probabilistic analysis. Likewise, OS and PFS curves are sampled independently from each other. This assumes no correlation between any of the parameters, which is unlikely because improved PFS likely correlates with better OS.
CDA-AMC could not address the limitation but notes the probabilistic analysis does not accurately reflect the full range of uncertainty associated with the decision problem and overestimates the certainty of certain outcomes.
Additionally, the following key assumptions were made by the sponsor and have been appraised by CDA-AMC (refer to Table 5).
Table 4: Key Assumptions of the Submitted Economic Evaluation (Not Noted as Limitations to the Submission)
Sponsor’s key assumption | CDA-AMC comment |
|---|---|
The patient demographics from the KEYNOTE-158 and KEYNOTE-164 trials were assumed to be generalizable to the patient population in Canada. | Reasonable. The clinical experts consulted during this review commented that the baseline and demographic characteristics for the KEYNOTE-158 and KEYNOTE-164 trials were a reasonable reflection of the target patient population in Canada. |
The sponsor applies RDI to estimate drug acquisition costs for pembrolizumab and comparators. | Likely reasonable. Under fixed dosing for pembrolizumab, it is expected that patients may experience dose reductions or skipping at a higher frequency than if weight-based dosing were employed. The sponsor’s trial-based RDI for pembrolizumab using fixed dosing was a weighted 98.47% across the modelled tumour sites, which was likely a reasonable reflection of dosing in practice. CDA-AMC notes that although the RDI associated with weight-based dosing for pembrolizumab is not available, the impact is expected to be minimal, given the proximity of the fixed-dosing RDI to 100%. |
CDA-AMC = Canada’s Drug Agency; RDI = relative dose intensity.
CDA-AMC Reanalyses of the Economic Evaluation
Base-Case Results
The CDA-AMC base case was derived by making changes in model parameter values and assumptions, in consultation with the clinical experts. CDA-AMC used a gamma distribution to extrapolate long-term OS data for pembrolizumab in CRC, endometrial, and gastric tumour sites, used an exponential distribution to extrapolate long-term OS data for pembrolizumab in small intestine tumour sites, applied weight-based dosing of 2 mg/kg for pembrolizumab, and set TTD to be equal to PFS up to 104 weeks, after which pembrolizumab was discontinued. CDA-AMC was unable to address uncertainty related to the comparative clinical data across tumour sites.
Table 5: CDA-AMC Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CDA-AMC value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
1. Drug acquisition costs |
|
|
Changes to derive the CDA-AMC base case | ||
1. OS extrapolation for pembrolizumab |
|
|
2. Pembrolizumab dosing | 200 mg q.3.w. (i.e., fixed dosing) | 2 mg/kg q.3.w. up to a maximum of 200 mg q.3.w. (weight-based dosing) |
3. Time on treatment for pembrolizumab |
|
|
CDA-AMC base case | — | Reanalysis 1 + 2 |
CDA-AMC = Canada’s Drug Agency; CRC = colorectal cancer; KM = Kaplan-Meier; OS = overall survival; PFS = progression-free survival; q.3.w. = every 3 weeks; SOC: standard of care; TTD = time to treatment discontinuation.
Results of the CDA-AMC base case suggest that pembrolizumab was associated with an incremental cost of $77,054 and an incremental QALY gain of 2.41 compared with SOC, resulting in a weighted ICER of $32,001 per QALY gained across all tumour sites. The CDA-AMC base case is based on publicly available prices of the comparator treatments. A detailed breakdown of the disaggregated results is available in Appendix 4.
The CDA-AMC base-case results align with those of the sponsor’s submitted analysis, indicating that pembrolizumab is cost-effective at a WTP threshold of $50,000 per QALY gained relative to SOC. In the CDA-AMC reanalysis, the majority of incremental QALYs realized by patients receiving pembrolizumab relative to SOC were derived in the first 5 years of receiving pembrolizumab (period for which trial data exists).
Table 6: Summary of the Stepped Analysis of the CDA-AMC Reanalysis Results
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALY) |
|---|---|---|---|---|
Sponsor’s base case | SOC | 104,180 | 0.81 | Reference |
Pembrolizumab | 222,493 | 4.16 | 35,302 | |
Sponsor’s base case (corrected) | SOC | 109,493 | 0.81 | Reference |
Pembrolizumab | 223,263 | 4.16 | 33,946 | |
CDA-AMC reanalysis 1 | SOC | 109,493 | 0.81 | Reference |
Pembrolizumab | 219,420 | 3.22 | 45,560 | |
CDA-AMC reanalysis 2 | SOC | 109,493 | 0.81 | Reference |
Pembrolizumab | 186,900 | 4.16 | 23,097 | |
CDA-AMC reanalysis 3 | SOC | 109,493 | 0.81 | Reference |
Pembrolizumab | 229,234 | 4.16 | 35,729 | |
CDA-AMC base case (reanalysis 1 + 2 + 3) | SOC | 109,493 | 0.81 | Reference |
Pembrolizumab | 187,186 | 3.22 | 32,202 | |
CDA-AMC base case (reanalysis 1 + 2 + 3) (probabilistic) | SOC | 110,826 | 0.83 | Reference |
Pembrolizumab | 187,880 | 3.23 | 32,001 |
CDA-AMC = Canada’s Drug Agency; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; SOC = standard of care.
Note: The CDA-AMC reanalysis is based on publicly available prices of the comparator treatments. The results of all steps are presented deterministically unless otherwise indicated, while the cumulative CDA-AMC base case is always presented both deterministically and probabilistically.
Scenario Analysis Results
CDA-AMC undertook price reduction analyses based on the sponsor’s submitted results and the CDA-AMC base-case reanalysis.
Table 7: CDA-AMC Price Reduction Analyses
Analysis price reduction | Unit drug cost ($) | ICERs for pembrolizumab versus SOC ($/QALY) | |
|---|---|---|---|
$ | Sponsor’s corrected base case | CDA-AMC reanalysis | |
No price reduction | 4,400 | 33,946 | 32,202 |
10% | 3,960 | 30,407 | 28,624 |
20% | 3,520 | 26,867 | 25,047 |
30% | 3,080 | 23,327 | 21,469 |
40% | 2,640 | 19,787 | 17,892 |
50% | 2,200 | 16,247 | 14,314 |
60% | 1,760 | 12,707 | 10,737 |
70% | 1,320 | 9,167 | 7,160 |
80% | 880 | 5,627 | 3,582 |
90% | 440 | 2,087 | 5 |
CDA-AMC = Canada’s Drug Agency ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; SOC = standard of care.
Note: Price reduction analyses were conducted on the deterministic results of the sponsor’s corrected base case and CDA-AMC base case.
CDA-AMC conducted a scenario analysis to determine the impact of the extrapolation of OS on the cost-effectiveness of pembrolizumab:
Assumed a treatment waning effect from 5 to 7 years indicating no further benefit beyond 7 years.
Results of the CDA-AMC scenario analyses are available in Table 17. The weighted ICER for pembrolizumab increased to $42,771 per QALY compared with SOC. Weighted QALYs across all tumour sites decreased from 2.41 to 1.77. This demonstrates that the QALY benefit is largely driven from the trial data and assumptions regarding extrapolation do not have a substantial impact on conclusions regarding cost-effectiveness. Therefore, given the conservative nature of this scenario analysis, although long-term evidence is uncertain, this does not drastically shift the ICER.
Issues for Consideration
Pembrolizumab has been previously reviewed by CDA-AMC for multiple indications, including patients with unresectable or metastatic MSI-H or dMMR endometrial cancer whose tumours have progressed following prior therapy and who have no satisfactory alternative treatment options, and patients with MSI-H or dMMR CRC as first-line therapy. The final recommendations (February 3, 2023, and July 27, 2021, respectively)15,16 state that pembrolizumab is recommended for reimbursement conditional on improved cost-effectiveness.
Overall Conclusions
Evidence from the single-arm trials, KEYNOTE-158 and KEYNOTE-164, assessed the efficacy of pembrolizumab in adult patients with metastatic or unresectable MSI-H or dMMR solid tumours. The clinical experts consulted by CDA-AMC found that the response to treatment (ORR) was clinically meaningful and durable (DOR) compared with what is typically observed with SOC treatments. There was considerable variability in response rates across different tumour types, but interpretation of this heterogeneity was challenged by small sample sizes. In the pediatric population, it is difficult to ascertain the benefit of pembrolizumab in this group of patients due to the small number of patients enrolled in the KEYNOTE-051 trial. A key limitation of the sponsor-submitted studies is that they were all single-arm trials, limiting the ability to directly compare pembrolizumab's efficacy and safety with SOC treatment options. The absence of randomized data makes it difficult to draw definitive conclusions regarding pembrolizumab’s impact on OS, PFS, or quality of life relative to existing therapies. The comparative evidence from the ITCs was limited to 4 cancer types in adults (colorectal, endometrial, small intestine, and gastric) and suggested improved PFS and OS with pembrolizumab compared with SOC, which was aligned with the expectations of the clinical experts consulted by CDA-AMC. However, the ITCs that were submitted had significant limitations that impacted the internal validity of the findings.
In the absence of randomized evidence or robust indirect comparisons, it is uncertain to what degree differences in the OS benefit for pembrolizumab versus different SOC therapies are driven by confounding rather than treatment effect. Conclusions from the economic analysis are contingent on the submitted indirect evidence, which is associated with methodological limitations, as noted in the Clinical Review. Likewise, survival analysis conducted on the trial evidence is limited by small sample sizes and a heterogenous population. The economic analysis may therefore not accurately reflect the true incremental difference between pembrolizumab versus current SOC. The CDA-AMC base-case results align with those of the sponsor’s submitted analysis, indicating that pembrolizumab is cost-effective at a WTP threshold of $50,000 per QALY gained, relative to SOC. In the CDA-AMC base case, pembrolizumab is associated with a weighted ICER of $32,001 per QALY gained compared with SOC, which was driven by the OS benefit associated with pembrolizumab, with an estimated OS benefit of 3.35 life-years compared with SOC treatment. Across different modelled tumour sites, the ICER ranged from $23,213 (small intestine) to $36,880 (gastric) per QALY gained. The tumour sites that were modelled (small intestine, endometrial, gastric, and colorectal) represented 80% of patients with MSI-H or dMMR solid tumours. For unmodelled tumours, the sponsor assumed a full incremental cost for pembrolizumab versus SOC and no additional benefit (0 QALYs).
Although long-term extrapolation is uncertain, it did not drastically influence the results. A scenario analysis was conducted that assumed pembrolizumab would provide no additional benefit beyond 5 years; this would assume substantial treatment waning and no long-term survivors. This was considered unlikely by the clinical experts consulted for this review. Even with this conservative assumption, pembrolizumab still generated an additional 1.77 QALYs, resulting in an ICER of $42,771 per QALY gained. This is because, in the period for which evidence is available, pembrolizumab has much better OS in comparison with the current SOC therapies across the modelled tumour sites. The main uncertainty is therefore not the modelling approach but rather the data that feed into it.
The clinical experts consulted by CDA-AMC noted that rechallenging with pembrolizumab or another immune checkpoint inhibitor after disease progression in an earlier line of treatment is not expected in clinical practice. Pembrolizumab or other immune checkpoint inhibitors are already funded in CRC, endometrial, gastric, renal, urothelial, mesothelioma, breast, NSCLC, SCLC, and biliary tract tumour sites. Therefore, it is anticipated that pembrolizumab will be used predominately in tumour sites for which there is no evidence.
The results assume no additional testing costs associated with the funding of pembrolizumab in this indication. However, based on the submitted BIA, testing is not routine in tumour sites with low MSI-H and dMMR prevalence. Because prevalence in these tumour sites is low, the cost to identify a single patient is high. Based on the assumption testing, the uptake is 50% in tumour sites where testing is not routinely conducted and would increase to 100% upon pembrolizumab funding; this additional testing cost equates to $1,109 to $7,394 per patient. This accounts for the fact that incremental testing costs associated with pembrolizumab funding are $0 for most identified cases. The cost is driven by substantially higher testing costs to identify 1 additional patient, for example, if more than 100 patients would need to be tested to identify 1 case. Because pembrolizumab is currently indicated in some tumour sites where MSI-H and dMMR prevalence is low (e.g., breast cancer), it is unclear if the funding of pembrolizumab will drastically change testing uptake in all tumour sites where such testing is not currently routine.
References
1.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Keytruda (pembrolizumab), 100 mg/4 mL vial, solution for infusion. Kirkland (QC): Merck Canada Inc.; 2024 Jul 16.
2.Keytruda (pembrolizumab): 100 mg/4 mL vial, solution for infusion [product monograph]. Merck Canada Inc.; 2023 Aug 18.
3.Clinical Study Report: P158V11MK3475. A Clinical Trial of Pembrolizumab (MK-3475) Evaluating Predictive Biomarkers in Subjects with Advanced Solid Tumors (KEYNOTE-158) [internal sponsor's report]. Merck Canada, Inc.; 2022.
4.Merck S, Dohme C. Data on file. Pembrolizumab (MK-3475) - KEYNOTE-164. Clinical Study Report P164V04MK3475 (end of study synoptic report). 2021;
5.Keytruda Clinical Evidence [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Keytruda (pembrolizumab), solution for infusion 100 mg/4 mL vial Merck Canada Inc.; 2024.
6.Sponsor's NMA report title [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Keytruda (pembrolizumab), 100 mg/4 mL vial, solution for infusion. Kirkland (QC): Merck Canada Inc.; 2024 Jul 16.
7.Iqvia. IQVIA DeltaPA. Ontario. 2024.
8.Ontario Case Costing Initiative (OCCI). Ontario Health and Long-Term Care; 2017. Accessed 1800 Jan 1. https://data.ontario.ca/dataset/ontario-case-costing-initiative-occi
9.Patient cost estimator. Canadian Institute for Health Information. Accessed 1800 Jan 1, https://www.cihi.ca/en/patient-cost-estimator
10.De Oliveira C, Pataky R, Bremner KE, et al. Estimating the Cost of Cancer Care in British Columbia and Ontario: A Canadian Inter-Provincial Comparison. Healthc Policy. Feb 2017;12(3):95-108. Estimation du cout des soins contre le cancer en Colombie-Britannique et en Ontario: une comparaison interprovinciale au Canada. PubMed
11.Canadian Cancer S. Canadian Cancer Statistics. Accessed 11 July 2024, https://cancer.ca/en/research/cancer-statistics/canadian-cancer-statistics
12.Cadth. Guidance for Economic Evaluations of Tumour-Agnostic Products. Accessed 11 July 2024, https://www.cadth.ca/sites/default/files/pdf/mh0016-cadth-economic-guidance-for-tumor-agnostic-products-rev-june22.pdf
13.Bucksch K, Zachariae S, Aretz S, et al. Cancer risks in Lynch syndrome, Lynch-like syndrome, and familial colorectal cancer type X: a prospective cohort study. BMC Cancer. May 24 2020;20(1):460. doi:10.1186/s12885-020-06926-x PubMed
14.DeltaPA. IQVIA; 2023. Accessed 2024 Sept. https://www.iqvia.com/
15.pan-Canadian Oncology Drug Review Committee (pERC) final recommendation: Pembrolizumab (Keytruda). CADTH; 2021. Accessed 2024 Oct 1. https://www.cda-amc.ca/sites/default/files/attachments/2021-07/PC0235%20Keytruda%20-%20CADTH%20Final%20Rec%20revised_1.pdf
16.pan-Canadian Oncology Drug Review Committee (pERC) final recommendation: Pembrolizumab (Keytruda). CADTH; 2023. Accessed 2024 Oct 1. https://www.cda-amc.ca/sites/default/files/DRR/2023/PC0280%20Keytruda%20-%20Final%20CADTH%20Recommendation.pdf
17.Cancer Care O. MFOLFOX6. Accessed 11 July 2024, https://www.cancercareontario.ca/en/drugformulary/regimens/71591
18.Cancer Care O. TRIFTIPI. Accessed 11 July 2024, https://www.cancercareontario.ca/en/drugformulary/regimens/monograph/52701
19.Cancer Care O. PACL(W) for endometrial cancer. Accessed 11 July 2024, https://www.cancercareontario.ca/en/drugformulary/regimens/monograph/50491
20.Cancer Care O. DOXO. Accessed 11 July 2024, https://www.cancercareontario.ca/en/drugformulary/regimens/monograph/45206
21.Cancer Care O. PACL(W) + RAMU. Accessed 11 July 2024, https://www.cancercareontario.ca/en/drugformulary/regimens/monograph/47456
22.Cancer Care O. Ramucirumab. Accessed 11 July 2024, https://www.cancercareontario.ca/en/drugformulary/drugs/ramucirumab
23.Cancer Care O. PACL(W) for gastrointestinal cancer. Accessed 11 July 2024, https://www.cancercareontario.ca/en/drugformulary/regimens/monograph/49036
24.Cancer Care O. IRIN. Accessed 11 July 2024, https://www.cancercareontario.ca/en/drugformulary/regimens/monograph/46116
25.Cancer Care O. FOLFIRI. Accessed 11 July 2024, https://www.cancercareontario.ca/en/drugformulary/regimens/monograph/49306
26.Giantonio BJ, Catalano PJ, Meropol NJ, et al. Bevacizumab in combination with oxaliplatin, fluorouracil, and leucovorin (FOLFOX4) for previously treated metastatic colorectal cancer: results from the Eastern Cooperative Oncology Group Study E3200. Clinical Trial, Phase III Multicenter Study Randomized Controlled Trial Research Support, N.I.H., Extramural. J Clin Oncol. Apr 20 2007;25(12):1539-44. PubMed
27.Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Keytruda (pembrolizumab), 100 mg/4 mL vial, solution for infusion. Kirkland (QC): Merck Canada Inc.; 2024 Jul 16.
Appendix 1: Cost Comparison Table
Table 8: CDA-AMC Cost Comparison Table for the Treatment of MSI-H or dMMR Solid Tumours
Treatment | Strength or concentration | Form | Price ($) | Recommended dosage | Daily cost ($) | Average 28-day cost ($) |
|---|---|---|---|---|---|---|
Pembrolizumab (Keytruda) | 100 mg vial | 100 mg/4 mL IV solution | 4,400a | 21-day cycles: 2 mg/kg up to 200 mg (weight-based dosing) | 291.24 | 8,155 |
21-day cycles: 200 mg q.3.w. (fixed dosing) | 419.05 | 11,733 | ||||
Colorectal | ||||||
Pooled FOLFOX and FOLFIRI | ||||||
Leucovorin (generics) | 50 mg vial 500 mg vial | 10 mg/mL IV solution | 68.9400 689.0000 | 400 mg/m2 every 14 days | 73.91 | 2,069 |
Oxaliplatin (generics) | 50 mg vial 100 mg vial 200 mg vial | 5 mg/mL IV solution | 45.0000 90.0000 180.0000 | 85 mg/m2 every 14 days | 12.86 | 360 |
Fluorouracil (generics) | 5,000 mg vial | 50 mg/mL IV solution | 160.9000 | 400 mg/m2 on day 1, then 2,400 mg/m2 continuous infusion over 46 hours starting day 1 every 14 days | 22.99 | 644 |
Pooled FOLFOX and FOLFIRI regimen cost (21-day cycle) | 109.75 | 3,073 | ||||
Anti-VEGF + chemotherapy | ||||||
Bevacizumab (generics) | 100 mg vial 400 mg vial | 25 mg/mL IV solution | 347.0000b | 10 mg/kg every 14 days | 173.50 | 4,858 |
Leucovorin (generics) | 50 mg vial 500 mg vial | 10 mg/mL IV solution | 68.9400 689.0000 | 400 mg/m2 every 14 days | 73.91 | 2,069 |
Oxaliplatin (generics) | 50 mg vial 100 mg vial 200 mg vial | 5 mg/mL IV solution | 45.0000 90.0000 180.0000 | 85 mg/m2 every 14 days | 12.86 | 360 |
Fluorouracil (generics) | 5,000 mg vial | 50 mg/mL IV solution | 160.9000 | 1,000 mg/m2 every 14 days | 11.49 | 322 |
Anti-VEGF + chemotherapy regimen cost (21-day cycle) | 271.76 | 7,609 | ||||
Trifluridine/ (Lonsurf) | 15 mg / 6.14 mg | Tablet | 76.2500 | 35 mg / m2 twice daily on days 1 to 5 and 8 to 12. Repeat 28-day cycle until disease progression or unacceptable toxicity | 176.71 | 4,948 |
Endometrial | ||||||
Paclitaxel (generics) | 30 mg vial 100.2 mg vial 150 mg vial 300 mg vial | 6 mg/mL IV solution | 300.00 1,002.00 1,500.00 3,000.00 | 80 mg/m2 every 7 days | 214.29 | 6,000 |
Doxorubicin (generics) | 10 mg vial 50 mg vial 100 mg vial | 2 mg/mL lyophilized powder | 50.0000 255.0000 1,304.2000 | 60 mg/m2 every 21 days | 64.49 | 1,806 |
Gastric | ||||||
Ramucirumab + paclitaxel | ||||||
Ramucirumab (Cyramza) | 100 mg vial 500 mg vial | 10 mg/mL IV solution | 690.6300 3,453.1600 | 8 mg/kg every 14 days | 295.99 | 8,288 |
Paclitaxel (generics) | 30 mg vial 100.2 mg vial 150 mg vial 300 mg vial | 6 mg/mL IV solution | 300.00 1,002.00 1,500.00 3,000.00 | 80 mg/m2 days 1, 8, 15 every 28 days | 160.71 | 4,500 |
Ramucirumab + paclitaxel regimen cost (21-day cycle) | 456.70 | 12,788 | ||||
Ramucirumab (Cyramza) | 100 mg vial 500 mg vial | 10 mg/mL IV solution | 690.6300 3,453.1600 | 8 mg/kg every 14 days | 295.99 | 8,288 |
Paclitaxel (generics) | 30 mg vial 100.2 mg vial 150 mg vial 300 mg vial | 6 mg/mL IV solution | 300.00 1,002.00 1,500.00 3,000.00 | 80 mg/m2 days 1, 8, and 15 every 28 days | 160.71 | 4,500 |
Irinotecan (generics) | 40 mg vial 100 mg vial 500 mg vial | 20 mg/mL IV solution | 208.3500 520.8500 2,675.0000 | 150 mg/m2 days 1 and 15 every 28 days | 104.17 | 2,917 |
FOLFIRI | ||||||
Leucovorin (generics) | 50 mg vial 500 mg vial | 10 mg/mL IV solution | 68.9400 689.0000 | 400 mg/m2 every 14 days | 73.91 | 2,069 |
Fluorouracil (generics) | 5,000 mg vial | 50 mg/mL IV solution | 160.9000 | 400 mg/m2 on day 1, then 2,400 mg/m2 continuous infusion over 46 hours starting day 1 every 14 days | 22.99 | 644 |
Irinotecan (generics) | 40 mg vial 100 mg vial 500 mg vial | 20 mg/mL IV solution | 208.3500 520.8500 2,675.0000 | 180 mg/m2 days 1 and 15 every 28 days | 126.49 | 3,542 |
FOLFIRI regimen cost | 223.39 | 6,255 | ||||
Small intestine | ||||||
Nab-paclitaxel (Abraxane) | 100 mg vial | 2 mg/mL lyophilized powder | 971.0000 | 260 mg/m2 every 21 days | 231.19 | 6,473 |
Anti-VEGF + chemotherapy | ||||||
Bevacizumab (generics) | 100 mg vial 400 mg vial | 25 mg/mL IV solution | 347.0000b | 10 mg/kg every 14 days | 173.50 | 4,858 |
Leucovorin (generics) | 50 mg vial 500 mg vial | 10 mg/mL IV solution | 68.9400 689.0000 | 400 mg/m2 every 14 days | 73.91 | 2,069 |
Oxaliplatin (generics) | 50 mg vial 100 mg vial 200 mg vial | 5 mg/mL IV solution | 45.0000 90.0000 180.0000 | 85 mg/m2 every 14 days | 12.86 | 360 |
Fluorouracil (generics) | 5,000 mg vial | 50 mg/mL IV solution | 160.9000 | 1,000 mg/m2 every 14 days | 11.49 | 322 |
Anti-VEGF + chemotherapy regimen cost (21-day cycle) | 271.76 | 7,609 | ||||
Paclitaxel (generics) | 30 mg vial 100.2 mg vial 150 mg vial 300 mg vial | 6 mg/mL IV solution | 300.00 1,002.00 1,500.00 3,000.00 | 80 mg/m2 on days 1, 8, and 15 every 28 days | 160.71 | 4,500 |
CDA-AMC = Canada’s Drug Agency; dMMR = mismatch repair deficient; FOLFIRI = leucovorin calcium (folinic acid) + fluorouracil + irinotecan hydrochloride; FOLFOX = leucovorin calcium (folinic acid) + fluorouracil + oxaliplatin; nab = nanoparticle albumin-bound; MSI-H = microsatellite instability-high; q.3.w. = every 3 weeks; VEGF = vascular endothelial growth factor.
Note: The comparators presented in Table 8 have been deemed to be appropriate based on feedback from clinical experts. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
All prices are IQVIA DeltaPA wholesale list prices (September 2024),14 unless otherwise indicated, and do not include dispensing fees or administration. Costs assume a body weight of approximately 70 kg or a body surface area of 1.8 m2 and include wastage of unused medication in vials.5 Total cost estimates per regimen are based on the cheapest combination of the component drugs. Costs have been prorated to a 28-day period. Regimen dosing is from the Cancer Care Ontario regimen database unless otherwise indicated.17-25
Note: This table has not been copy-edited.
aSponsor’s submitted price.1
bDosing schedule for bevacizumab followed the dose used in the BEYOND study (GEMCAD 17 to 01) for metastatic colorectal cancer after progression.26
Appendix 2: Submission Quality
Please note that this appendix has not been copy-edited.
Description | Yes or no | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | Yes | No comment. |
Model has been adequately programmed and has sufficient face validity | No | Refer to CDA-AMC appraisal section regarding uncertainty in the durability of long-term survival benefit associated with pembrolizumab. |
Model structure is adequate for decision problem | Yes | No comment. |
Data incorporation into the model has been done adequately | Yes | No comment. |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | No | Refer to the CDA-AMC appraisal section regarding the probabilistic analysis. |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | Yes | However, the submitted model was not clear in the options used in the base-case analysis (e.g., TTD approach) and it was not immediately clear whether this was aligned with the pharmacoeconomic report. |
CDA-AMC = Canada’s Drug Agency; TTD = time to treatment discontinuation.
Appendix 3: Additional Information on the Submitted Economic Evaluation
Please note that this appendix has not been copy-edited.
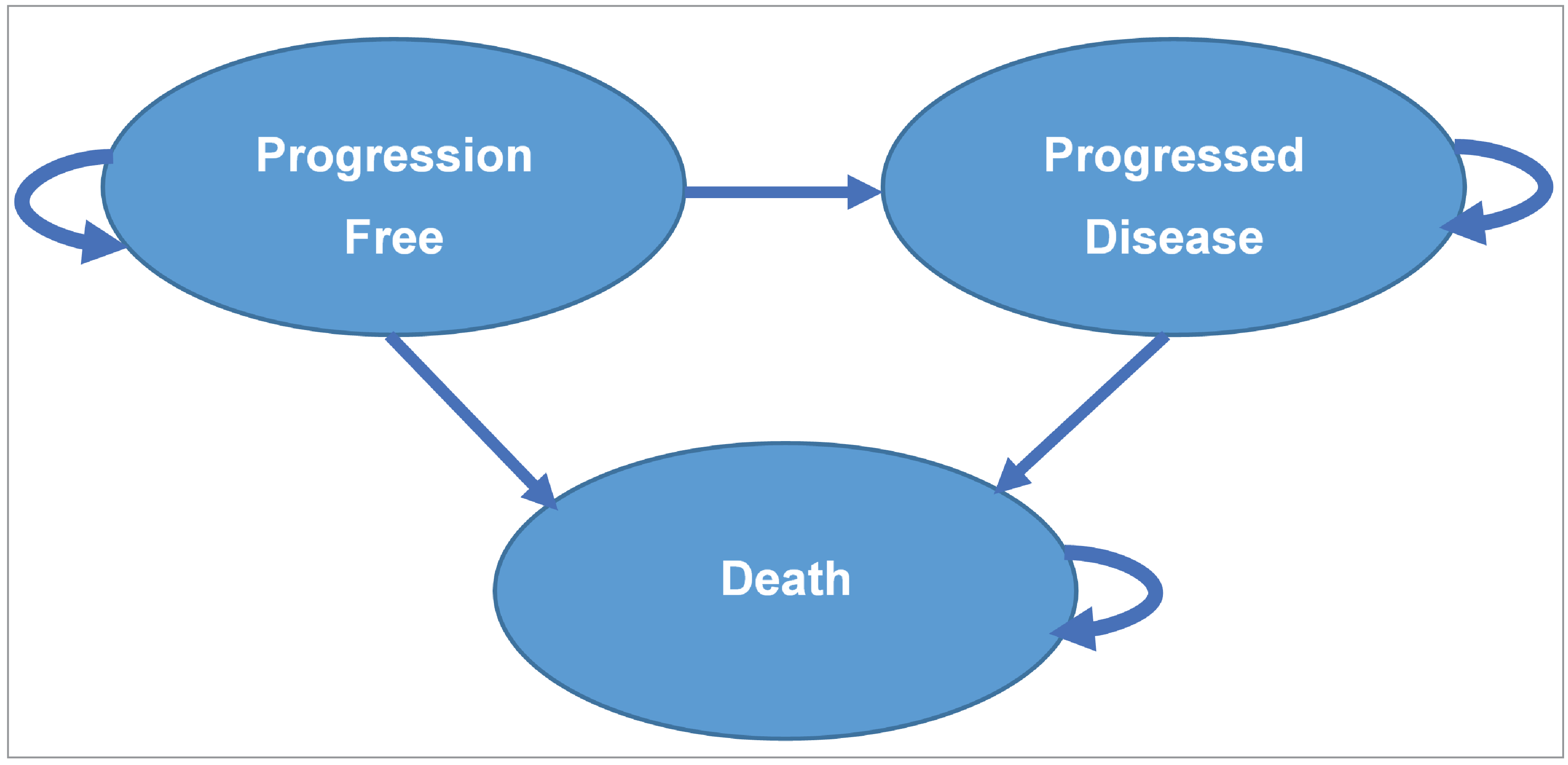
Detailed Results of the Sponsor’s Base Case
Table 10: Disaggregated Summary of the Sponsor’s Economic Evaluation Results Across Modelled Tumour Sites
Parameter | Pembrolizumab | SOC |
|---|---|---|
Discounted LYs | ||
Total | 5.93 | 1.22 |
Discounted QALYs | ||
Total | 4.96 | 0.83 |
Progression-free | 3.02 | 0.37 |
Disease progression | 1.94 | 0.46 |
Discounted costs ($) | ||
Total | 259,620 | 124,872 |
Acquisition | 148,289 | 27,475 |
Administration | 683 | 670 |
Subsequent treatment acquisition | 12,367 | 13,092 |
Subsequent treatment administration | 327 | 345 |
Testing costs | 0 | 0 |
Resource utilization | 27,556 | 5,493 |
End-of-life | 70,381 | 77,579 |
Adverse events | 16 | 218 |
dMMR = mismatch repair deficient; ICER = incremental cost-effectiveness ratio; LY = life-year; MSI-H = microsatellite instability–high; QALY = quality-adjusted life-year; SOC = standard of care.
Note: The weighted ICER was estimated by calculating ICERs across each individual tumour site and weighting them based on tumour site prevalence (Canadian epidemiology data from the Canadia Cancer Society).11 The tumour sites modelled (small intestine, endometrial, gastric, and colorectal) represented 80% of patients with MSI-H or dMMR solid tumours. The results in Table 10 do not reflect the full Health Canada indication that includes all other tumour sites.
Source: Sponsor’s pharmacoeconomic submission.1
Table 11: Sponsor’s Economic Evaluation Results (Tumour Site–Specific)
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALYs) |
|---|---|---|---|---|
Sponsor’s base case (probabilistic) all tumour sites | SOC | 105,413 | 0.83 | Ref. |
Pembrolizumab | 223,070 | 4.13 | 35,618 | |
CRC | SOC | 131,692 | 0.912 | Ref. |
Pembrolizumab | 253,424 | 5.02 | 29,646 | |
Endometrial | SOC | 102,897 | 0.92 | Ref. |
Pembrolizumab | 242,013 | 6.00 | 27,341 | |
Gastric | SOC | 130,393 | 0.67 | Ref. |
Pembrolizumab | 268,607 | 3.57 | 47,539 | |
Small intestine | SOC | 136,187 | 0.73 | Ref. |
Pembrolizumab | 333,550 | 7.79 | 27,955 |
CRC = colorectal; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; Ref. = reference; SOC = standard of care.
Source: Sponsor’s pharmacoeconomic submission.1
Appendix 4: Additional Details on the CDA-AMC Reanalyses and Sensitivity Analyses of the Economic Evaluation
Please note that this appendix has not been copy-edited.
Detailed Results of CDA-AMC Base Case
Figure 2: Extrapolation of Overall Survival for Patients With CRC Receiving Pembrolizumab
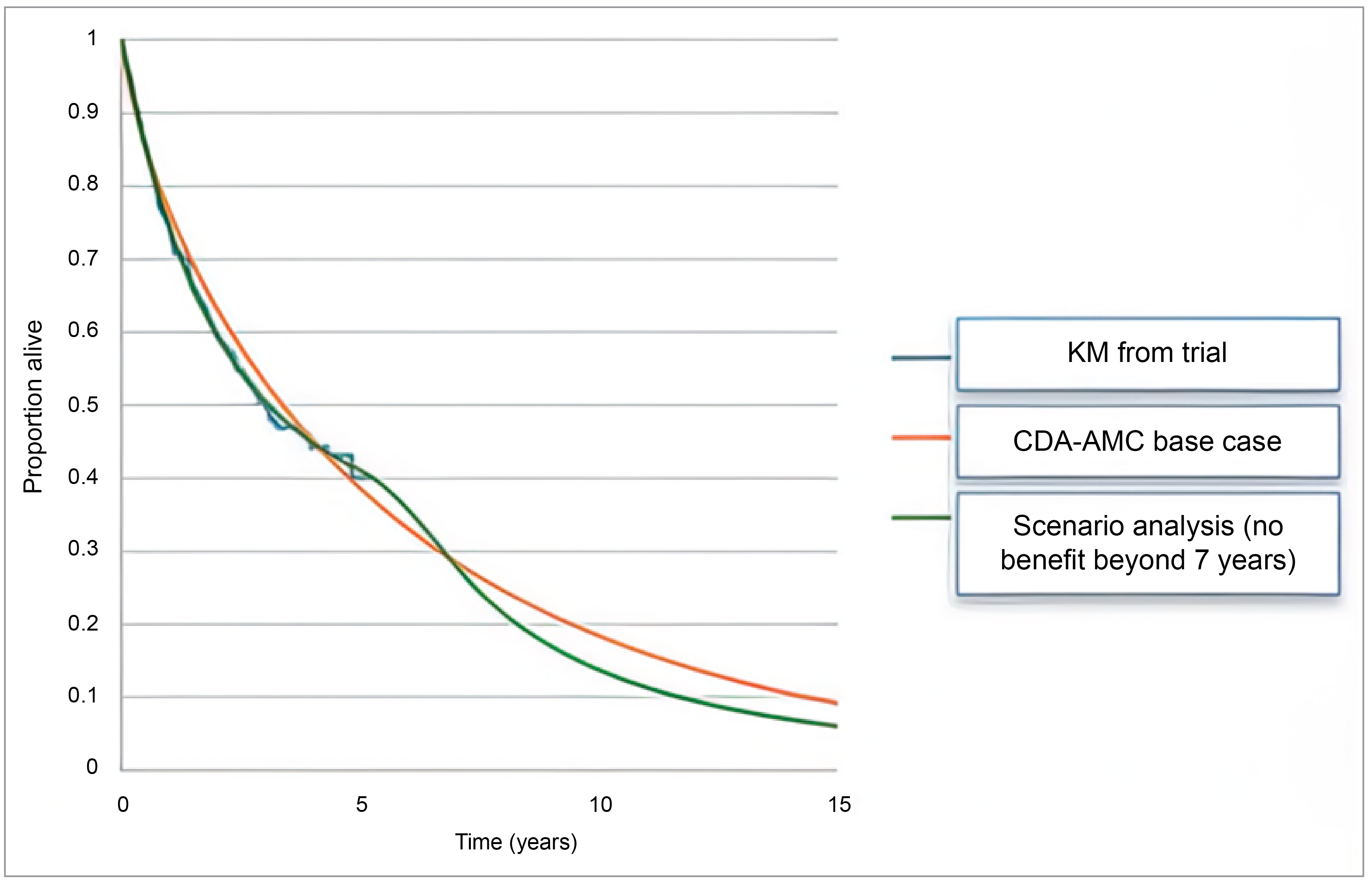
CDA-AMC = Canada’s Drug Agency; CRC = colorectal cancer; KM = Kaplam-Meier; OS = overall survival.
Figure 3: Extrapolation of Overall Survival for Patients With Endometrial Cancer Receiving Pembrolizumab
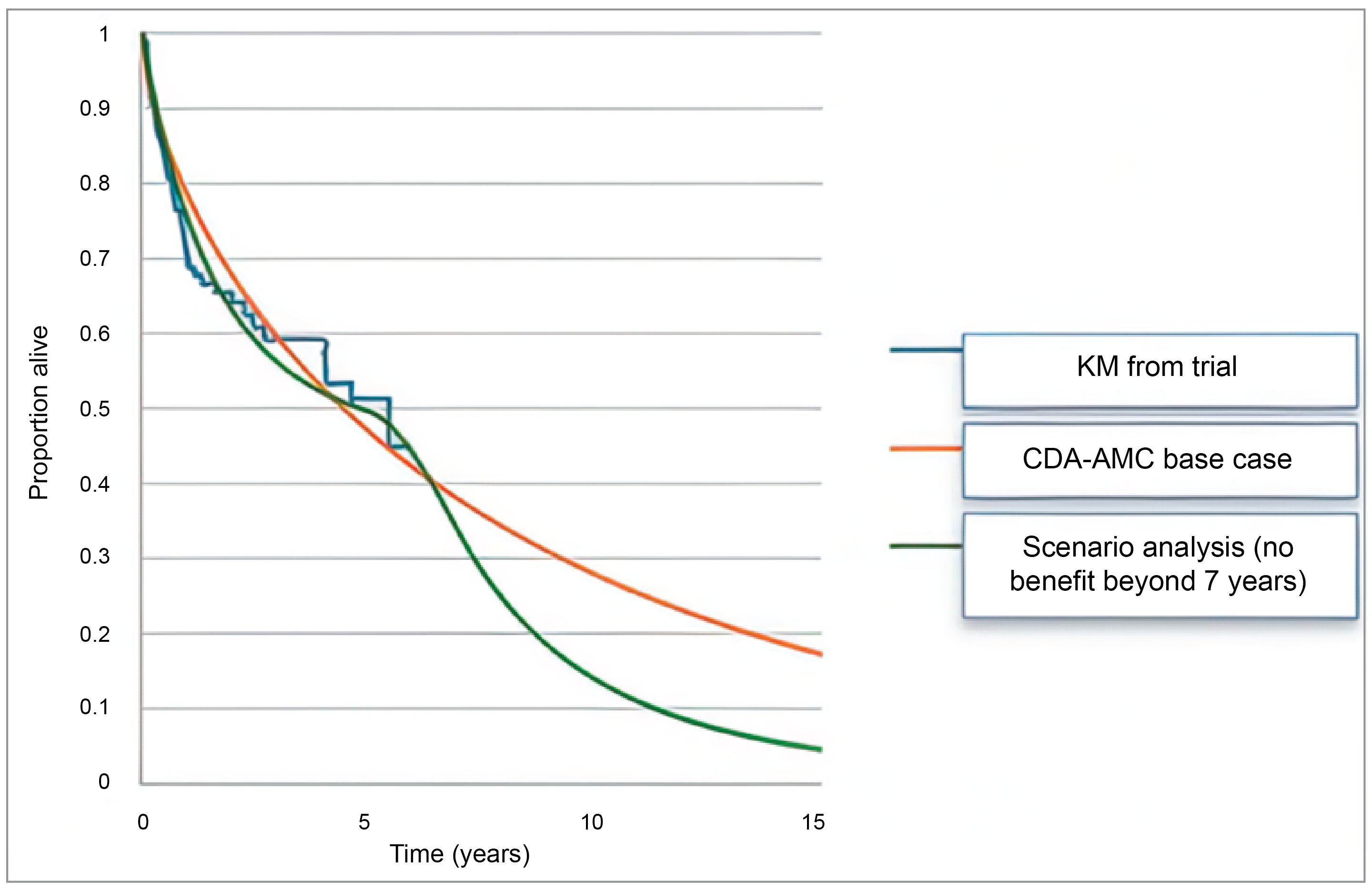
CDA-AMC = Canada’s Drug Agency; CRC = colorectal cancer; KM = Kaplam-Meier; OS = overall survival.
Figure 4: Extrapolation of Overall Survival for Patients with Gastric Cancer Receiving Pembrolizumab
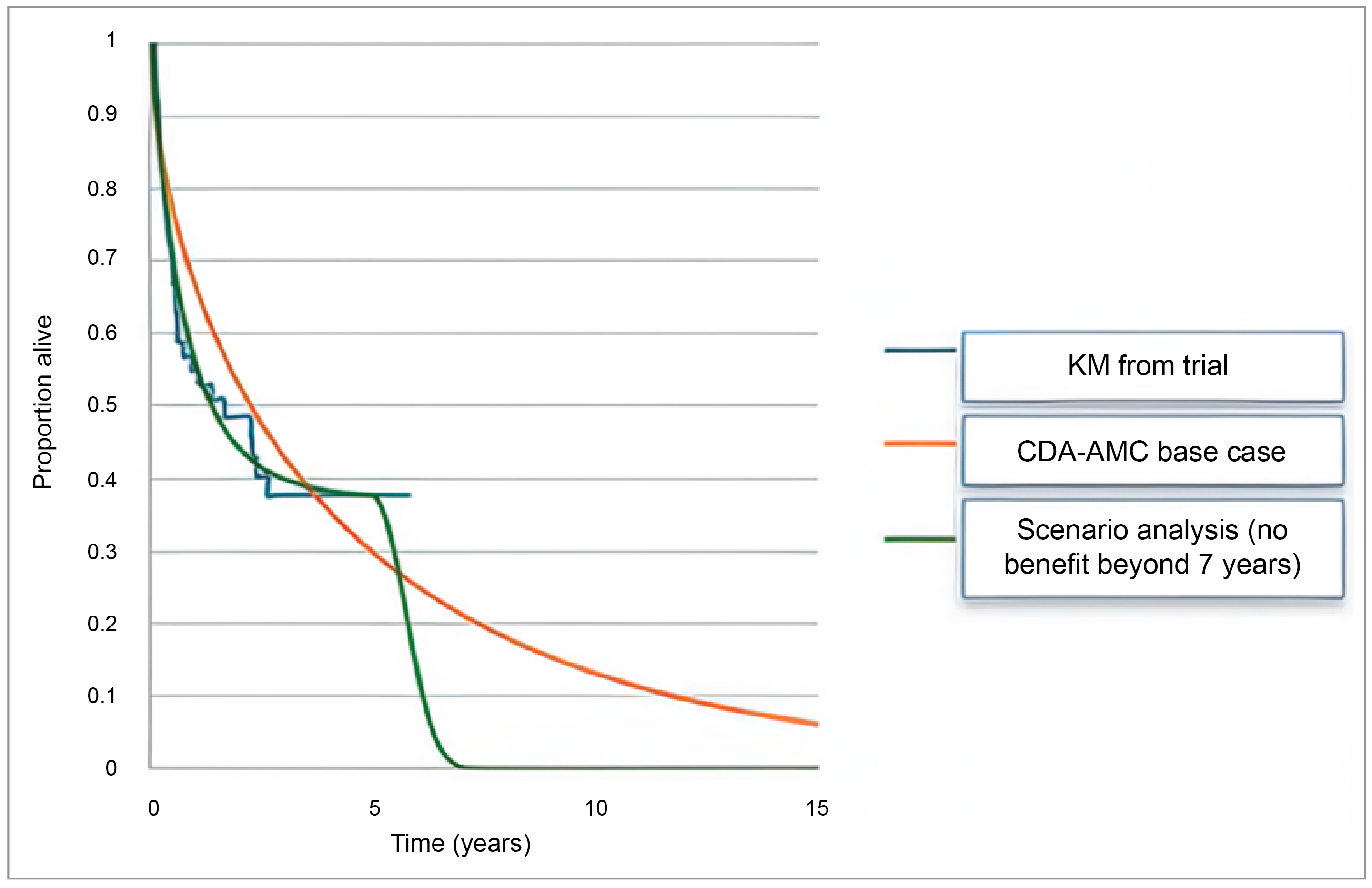
CDA-AMC = Canada’s Drug Agency; CRC = colorectal cancer; KM = Kaplam-Meier; OS = overall survival.
Figure 5: Extrapolation of Overall Survival for Patients With Small Intestine Cancer Receiving Pembrolizumab
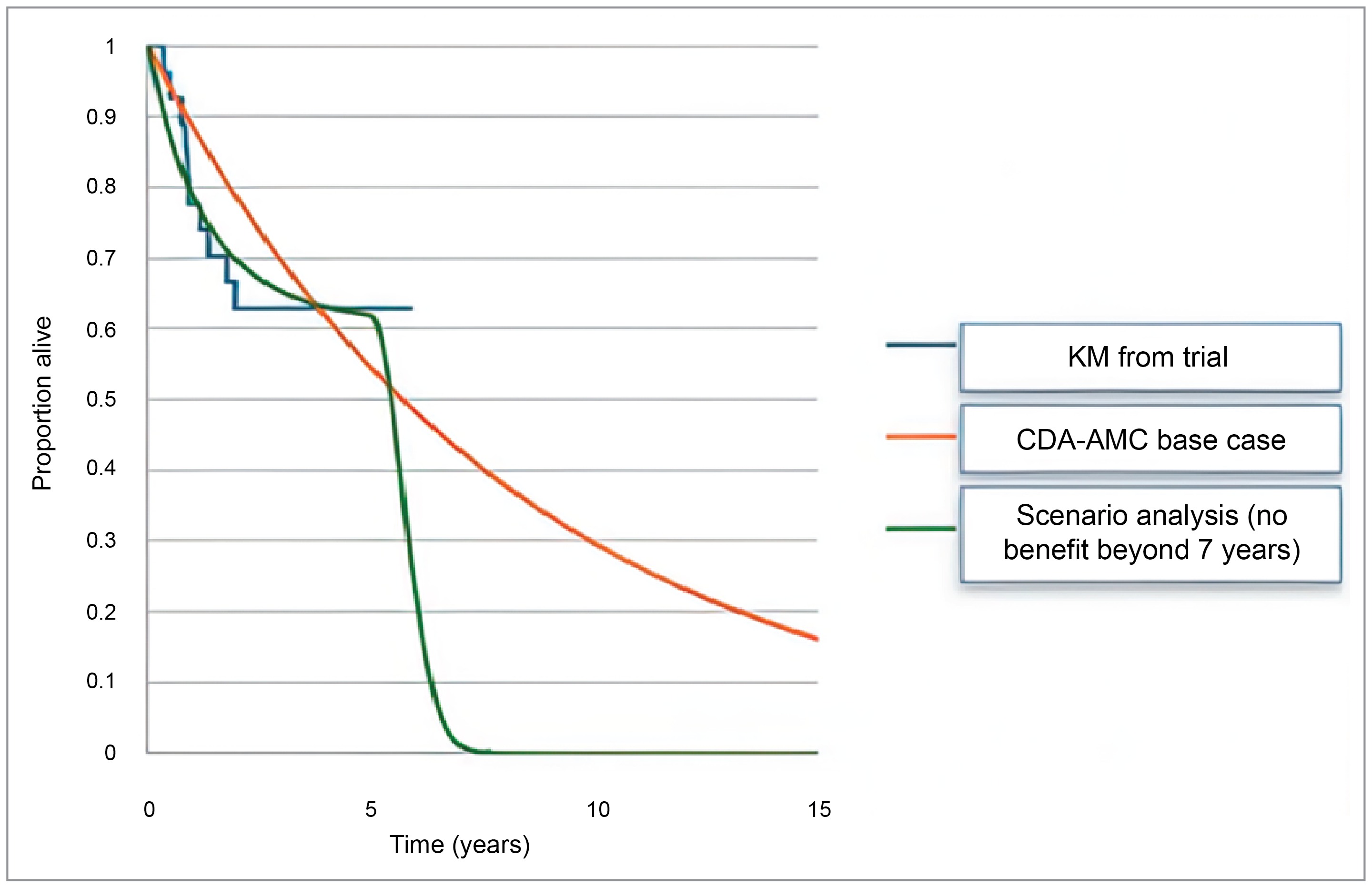
CDA-AMC = Canada’s Drug Agency; CRC = colorectal cancer; KM = Kaplam-Meier; OS = overall survival.
Tumour site | Number tested to identify 1 patienta | % identified through current testing strategies | Additional cost to identify each remaining eligible patient using IHC testing ($150 per test) | Additional cost to identify each remaining eligible patient using panel testing ($1,000 per test) | Proportion of patients that make up indication |
|---|---|---|---|---|---|
Colorectal | 24 | 100% | $0 | $0 | 33% |
Endometrial | 6 | 100% | $0 | $0 | 18% |
Gastric | 12 | 100% | $0 | $0 | 24% |
Small intestine | 7 | 85% | $157 | $1,049 | 4% |
Ovarian | 59 | 50% | $4,412 | $29,412 | 1% |
Pancreatic | 111 | 50% | $8,333 | $55,556 | 3% |
Cholangiocarcinoma | 71 | 50% | $5,357 | $35,714 | 0% |
Brain | 167 | 50% | $12,500 | $83,333 | 1% |
Sarcoma | 56 | 50% | $4,167 | $27,778 | 0% |
Breast | 500 | 50% | $37,500 | $250,000 | 0% |
Cervical | 67 | 50% | $5,000 | $33,333 | 0% |
Neuroendocrine | 71 | 50% | $5,357 | $35,714 | 0% |
Prostate | 15 | 50% | $1,136 | $7,576 | 5% |
Adrenocortical | 25 | 50% | $1,875 | $12,500 | 3% |
Mesothelioma | 25 | 50% | $1,875 | $12,500 | 1% |
Thyroid | 167 | 50% | $12,500 | $83,333 | 0% |
Small cell lung cancer | 250 | 50% | $18,750 | $125,000 | 0% |
Urothelial | 143 | 50% | $10,714 | $71,429 | 1% |
Salivary | 200 | 50% | $15,000 | $100,000 | 0% |
Renal | 59 | 50% | $4,412 | $29,412 | 2% |
Other (pooled) | 25 | 50% | $1,875 | $12,500 | 0% |
Weighted average cost per patient | $1,109 to $7,394 | ||||
IHC = immunohistochemistry.
aCalculated by dividing 1 by prevalence. Prevalence rates can be found in Table 15.
Source: Sponsors budget impact analysis based on values presented in Table 15.
Table 13: Disaggregated Summary of the CDA-AMC Economic Evaluation Results
Parameter | Pembrolizumab | SOC |
|---|---|---|
Discounted LYs | ||
Total | 5.39 | 1.21 |
Discounted QALYs | ||
Total | 3.83 | 0.82 |
Progression-free | 2.68 | 0.37 |
Disease progression | 1.15 | 0.45 |
Discounted costs ($) | ||
Total | 215,628 | 130,485 |
Acquisition | 106,774 | 31,924 |
Administration | 710 | 670 |
Subsequent treatment acquisition | 13,472 | 14,065 |
Subsequent treatment administration | 331 | 346 |
Resource utilization | 21,418 | 5,429 |
End of life | 72,904 | 77,833 |
Adverse events | 17 | 218 |
CDA-AMC = Canada’s Drug Agency; LY = life-year; QALY = quality-adjusted life-year; SOC = standard of care.
Note: The weighted ICER in Table 7 was estimated by calculating ICERs across each modelled tumour site and weighting them based on tumour site prevalence (Canadian epidemiology data from Canadia Cancer Society).11 The tumour sites modelled (small intestine, endometrial, gastric, and colorectal) represented 80% of patients with MSI-H or dMMR solid tumours. The results in this table do not reflect the full Health Canada indication that includes all other tumour sites.
Table 14: CDA-AMC Economic Evaluation Results (Tumour Site–Specific)
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALYs) |
|---|---|---|---|---|
CDA-AMC base case (probabilistic) average across all tumour sites | SOC | 110,826 | 0.83 | Ref. |
Pembrolizumab | 187,880 | 3.23 | 32,001 | |
CRC | SOC | 131,931 | 0.91 | Ref. |
Pembrolizumab | 206,457 | 3.56 | 28,163 | |
Endometrial | SOC | 102,274 | 0.91 | Ref. |
Pembrolizumab | 196,131 | 4.93 | 23,353 | |
Gastric | SOC | 148,993 | 0.66 | Ref. |
Pembrolizumab | 236,102 | 3.02 | 36,880 | |
Small intestine | SOC | 136,084 | 0.74 | Ref. |
Pembrolizumab | 255,090 | 5.86 | 23,213 |
CDA-AMC = Canada’s Drug Agency; CRC = colorectal cancer; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; Ref. = reference; SOC = standard of care.
Scenario Analyses
Table 15: Scenario Analyses Conducted on the CDA-AMC Base Case
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALYs) |
|---|---|---|---|---|
CDA-AMC base case (probabilistic) | SOC | 110,826 | 0.83 | Reference |
Pembrolizumab | 187,880 | 3.23 | 32,001 | |
CDA-AMC scenario 1: treatment waning | SOC | 110,820 | 0.83 | Reference |
Pembrolizumab | 186,378 | 2.60 | 42,771 |
CDA-AMC = Canada’s Drug Agency; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; SOC = standard of care.
Appendix 5: Submitted Budget Impact Analysis and CDA-AMC Appraisal
Please note that this appendix has not been copy-edited.
Table 16: Summary of Key Takeaways
Key takeaways of the budget impact analysis |
|---|
|
CDA-AMC = Canada’s Drug Agency; dMMR = mismatch repair deficient; MSI-H = microsatellite instability-high.
Summary of Sponsor’s Budget Impact Analysis
The sponsor submitted a BIA to estimate the incremental 3-year budget impact of reimbursing pembrolizumab for the treatment of adult and pediatric patients with unresectable or metastatic MSI-H or dMMR solid tumours, as determined by a validated test, that have progressed following prior treatment and who have no satisfactory alternative treatment options.27 The BIA was undertaken from the perspective of a Canadian public payer over a 3-year time horizon (2024 through 2027) using a tumour site–specific epidemiologic approach. The tumour sites considered in the BIA model are colorectal, endometrial, gastric, small intestine, ovarian, pancreatic, cholangiocarcinoma, brain, sarcoma, breast, cervical, neuroendocrine, prostate, adrenocortical, mesothelioma, thyroid, SCLC, urothelial, salivary, renal, and other. Data to inform the model were obtained from various sources, including the published literature, the sponsor’s internal data, and input from clinical experts consulted by the sponsor, and key inputs to the BIA are documented in Table 17.
The sponsor compared a reference scenario in which patients received current SOC defined by tumour site (pooled FOLFOX and FOLFIRI, anti-VEGF + chemotherapy, and trifluridine plus tipiracil hydrochloride for CRC tumour sites; paclitaxel and doxorubicin for endometrial tumour sites, paclitaxel, irinotecan, ramucirumab + paclitaxel, FOLFIRI, and ramucirumab for gastric tumour sites; and nanoparticle albumin-bound (nab)-paclitaxel, anti-VEGF + chemotherapy, and taxane-based treatment for small intestine tumour sites) to a new drug scenario in which pembrolizumab was reimbursed. The sponsor’s analysis included drug acquisition costs and dosing modelled for pembrolizumab reflected the product monograph. Key inputs to the BIA are documented in Table 16.
Figure 6: Sponsor’s Estimation of the Size of the Eligible Population
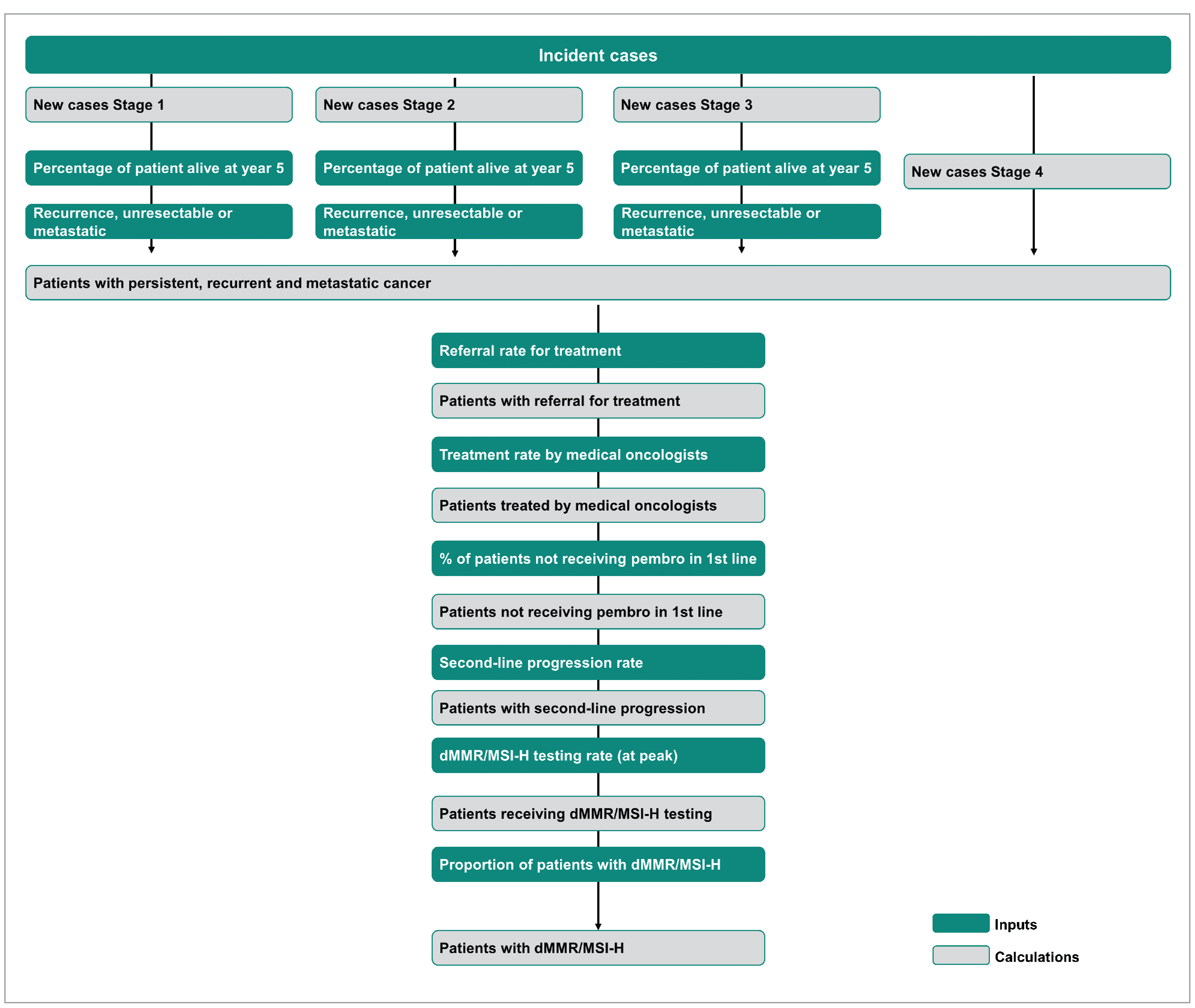
dMMR = mismatch repair deficient; MSI-H = microsatellite instability-high.
Source: Sponsor’s budget impact analysis submission.27
Table 17: Sponsor’s Estimation of the Size of the Eligible Population
Tumour | % of new cases | % of patients | % of cancer patients with stage IV | Referral rate for treatment (%) | Treatment rate by medical oncologists (%) | % of patients not receiving pembro in 1L | 2L progression rate (%) | dMMR/MSI-H testing rate | % of patients with DMMR/ MSI-H | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
stage I | stage II | stage III | With persistent stage I | With persistent stage II | With persistent stage III | without pembrolizumab | with pembrolizumab | |||||||
CRC | 24.40a | 24.50a | 30.30a | 9.10c | 26.60c | 26.60c | 20.70a | 100e | 100e | 100e | 67.50f | 100f | 100f | 4.10k |
Endometrial | 76.00a | 6.00a | 11.00a | 5.10c | 30.20c | 30.00c | 7.00a | 100e | 85e | 100e | 63g | 100e | 100e | 17.60k |
Gastric | 16.13a | 14.06a | 22.12a | 25.30c | 65.40c | 65.40c | 47.70a | 100e | 85e | 100e | 80.30h | 100e | 100e | 8.20k |
Small intestine | 32.20b | 34.00b | 25.50b | 15.30c | 21.60c | 21.60c | 8.30b | 100e | 85e | 100e | 67.50i | 85e | 100e | 14.30k |
Ovarian | 25.94a | 9.73a | 47.13a | 7.60c | 27.10c | 27.10c | 17.21a | 100e | 85e | 100e | 52m | 50e | 70e | 1.70k |
Pancreatic | 8.13a | 24.96a | 7.99a | 55.70c | 83.80c | 83.80c | 58.92a | 100e | 85e | 100e | 44m | 50e | 70e | 0.90k |
Cholangio-carcinoma | 40.70b | 25.30b | 18.40b | 33.50c | 71.70c | 71.70c | 15.60b | 100e | 85e | 100e | 33.33p | 50e | 70e | 1.40k |
Brain | 74.70b | 13.40b | 2.20b | 64.00c | 78.50c | 78.50c | 9.70b | 100e | 85e | 100e | 57n | 50e | 70e | 0.60k |
Sarcoma | 52.60b | 16.30b | 5.10b | 17.60c | 40.20c | 40.20c | 26.10b | 100e | 850e | 100e | 38m | 50e | 70e | 1.80k |
Breast | 43.30a | 32.77a | 11.60a | 0.70c | 13.70c | 13.70c | 4.61a | 100e | 85e | 100e | 64r | 50e | 70e | 0.20k |
Cervical | 56.59a | 13.93a | 17.17a | 8.80c | 40.20c | 40.20c | 12.31a | 100e | 85e | 100e | 48.75j | 50e | 70e | 1.50k |
Neuroendocrine | 0.00k | 0.00k | 100k | 0.00k | 0.00k | 0.00k | 100 | 100e | 85e | 100e | 49.82o | 50e | 70e | 1.40k |
Prostate | 23.27a | 53.61a | 14.23a | 0.00c | 0.20c | 0.20c | 8.89a | 100e | 85e | 100e | 27m | 50e | 70e | 6.60k |
Adrenocortical | 11.70l | 18.30l | 57.50l | 77.50l | 84.40l | 84.40l | 12.50l | 100e | 85e | 100e | 67l | 50e | 70e | 4.00k |
Mesothelioma | 11.70b | 18.30b | 57.50b | 77.50c | 84.40c | 84.40c | 12.50b | 100e | 85e | 100e | 67m | 50e | 70e | 4.00k |
Thyroid | 68.50a | 8.20a | 14.24a | 0.10c | 1.70c | 1.70c | 9.06a | 100e | 85e | 100e | 58m | 50e | 70e | 0.60k |
SCLC | 3.50a | 3.38a | 25.12a | 67.60c | 8.17c | 8.17c | 68.00a | 100e | 85e | 100e | 28p | 50e | 70e | 0.40k |
Urothelial | 23.16a | 8.12a | 4.47a | 29.10c | 60.80c | 60.80c | 9.23a | 100e | 85e | 100e | 46s | 50e | 70e | 0.70k |
Salivary | 46.00b | 29.80b | 16b | 5.40c | 31.50c | 31.50c | 8.20b | 100e | 85e | 100e | 38m | 50e | 70e | 0.50k |
Renal | 58.34a | 6.44a | 18.12a | 7.10c | 26.20c | 26.20c | 17.10a | 100e | 85e | 100e | 50q | 50e | 70e | 1.70k |
Other (pooled) | 0.00e | 0.00e | 0.00e | 0.00e | 0.00e | 0.00e | 100e | 100e | 85e | 100e | 0.00e | 50e | 70e | 4.00k |
1L = first line; CRC = colorectal cancer;; GI = gastrointestinal; pembro = pembrolizumab; SCLC = small cell lung cancer.
aCanadian Cancer Statistics staging report 2018.
bStage distributions of SEER (Surveillance, Epidemiology, and End Results Program) incidence cases, 2011 to 2020.
cNational Cancer Institute, 5-year survival probabilities by stage.
dCADTH recommendation for KEYNOTE-177. Maximum market share of 80% for pembro was assumed by CADTH.
eMerck assumption.
fCADTH recommendation for KEYNOTE-177 (65% to 70%).
gCADTH Reimbursement Review of KEYNOTE-775, 2021.
hMerck assumption, derived from KEYNOTE-811 in patients who did not receive pembrolizumab.
IMerck assumption. Assumed to match CRC based on the premise of similarity in lower GI.
jMerck assumption, Expert opinion from advisory board for KEYNOTE-826. Confidential.
kKang et al. (2022).
lAssumption. Matched to mesothelioma on premise of cancer rarity.
mEpicOncology survey.
nInstitut national d’excellence en santé et en services sociaux (INESSS) Imfinzi reimbursement review, 2023.
oMerck assumption, average of other sites as cancer is disseminated.
pCADTH Reimbursement Review, Lurbinectedin (Zepzela), 2022.
qCADTH Reimbursement Review, KEYNOTE-426, renal cell carcinoma.
rFrom KEYNOTE-355 subsequent treatment rates.
sONCO-CAPPS (Oncology Continuous Audit of Patients and Prescriptions Syndicated) MAT December 2015. Used in KEYNOTE-045. Pembrolizumab used in second line.
Source: Sponsor’s budget impact analysis submission.27
Table 18: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as year 1 / year 2 / year 3, if appropriate) |
|---|---|
Target population | |
Number of patients eligible for drug under review | 538 / 552 / 566 |
Market uptake (3 years) | |
Uptake (reference scenario) | |
CRC, gastric, cervical, urothelial, renal tumour sites Pembrolizumab SOC | 0% / 0% / 0% 100% / 100% / 100% |
Endometrial tumour site Pembrolizumab SOC | 20% / 30% / 40% 80% / 70% / 60% |
Breast tumour site Pembrolizumab SOC | 0% / 0% / 0% 100% / 100% / 100% |
Small intestine, ovarian, pancreatic, cholangiocarcinoma, brain, sarcoma, neuroendocrine, prostate, adrenocortical, mesothelioma, thyroid, SCLC, salivary, and other tumour sites Pembrolizumab SOC | 0% / 0% / 0% 100% /100% / 100% |
Uptake (new drug scenario) | |
CRC, endometrial, gastric, cervical, urothelial, renal tumour sites Pembrolizumab SOC | 20% / 30% / 40% 80% / 70% / 60% |
Endometrial tumour site Pembrolizumab SOC | 20% / 30% / 40% 80% / 70% / 60% |
Breast tumour site Pembrolizumab SOC | 51% / 64% / 80% 49% / 36% / 20% |
Small intestine, ovarian, pancreatic, cholangiocarcinoma, brain, sarcoma, neuroendocrine, prostate, adrenocortical, mesothelioma, thyroid, SCLC, salivary, and other tumour sites Pembrolizumab SOC | 58% / 72% / 90% 42% / 28% / 10% |
Cost of treatment (per patient) | |
Pembrolizumab SOC | $135,054 to $197,510 across modelled tumour sites $73,111 across unmodelled tumour sites $17,641 to $65,035 for CRC $3,550 to $36,885 for endometrial $815 to $33,248 for gastric $21,712 to $36,471 for small intestine $26,539 for unmodelled tumour sites |
CRC = colorectal; FOLFIRI = leucovorin calcium (folinic acid) + fluorouracil + irinotecan hydrochloride; FOLFOX = leucovorin calcium (folinic acid) + fluorouracil + oxaliplatin; nab = nanoparticle albumin-bound; SCLC = small cell lung cancer; SOC = standard of care; VEGF = vascular endothelial growth factor.
Note: SOC varied across modelled tumour sites; CRC included pooled FOLFOX and FOLFIRI, anti-VEGF + chemotherapy, and trifluridine plus tipiracil hydrochloride; endometrial included paclitaxel and doxorubicin; gastric included paclitaxel, irinotecan, ramucirumab + paclitaxel, FOLFIRI, and ramucirumab; and small intestine included nab-paclitaxel, anti-VEGF + chemotherapy, and taxane-based. For unmodelled tumour sites, pembrolizumab drug acquisition costs are assumed to be equal to pembrolizumab per cycle average treatment cost multiplied by the weighted average SOC time on treatment for modelled tumour sites. For the unmodelled tumour sites, comparator costs are assumed to be equal to the weighted average SOC treatment costs for modelled tumour sites. Costs of treatment were outputted from the submitted cost-utility analysis model and were aligned.
Summary of the Sponsor’s BIA Results
The sponsor estimated that the 3-year budget impact of reimbursing pembrolizumab for the treatment of adult and pediatric patients with unresectable or metastatic MSI-H or dMMR solid tumours, as determined by a validated test, that have progressed following prior treatment and who have no satisfactory alternative treatment options would be $7,693,858 in year 1, $15,164,965 in year 2, and $20,628,337 in year 3, for a 3-year cumulative total of $43,487,160 across all tumour sites.
CDA-AMC Appraisal of the Sponsor’s BIA
CDA-AMC identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
Uncertainty regarding market shares of pembrolizumab: The market uptake of pembrolizumab was assumed to differ across tumour sites based on availability of pembrolizumab as earlier-line treatment. The sponsor assumed that patients with prior exposure to immunotherapy would have lower uptake because of low expected re-treatment rates with the majority reaching 40% uptake by year 3 (e.g., CRC, gastric, endometrial, cervical, urothelial, breast, and renal sites). For other tumour sites, a gradual uptake is applied where pembrolizumab becomes the predominant treatment option for these patients reaching 90% uptake by year 3 (e.g., small intestine, ovarian, pancreatic, cholangiocarcinoma, brain, sarcoma, neuroendocrine, prostate, adrenocortical, mesothelioma, thyroid, SCLC, salivary, and others).
Clinical experts consulted by CDA-AMC noted that uptake of pembrolizumab was likely overestimated in the tumour sites with immune checkpoint inhibitors currently available as earlier-line treatment. Feedback from clinical experts noted that pembrolizumab is available and used in an earlier line of treatment in the CRC, endometrial, and NSCLC tumour sites, and that an alternative immune checkpoint inhibitor (i.e., nivolumab) is available and used in an earlier line of treatment in the gastric, renal, urothelial, mesothelioma, breast, NSCLC, SCLC, and biliary tract tumour sites. In addition to clinician expectations that re-treatment with pembrolizumab is generally unlikely, if an alternative immune checkpoint inhibitor such as nivolumab is used in a previous line of therapy and patients experience disease progression, this substantially reduces the likelihood of rechallenge with another immune checkpoint inhibitor such as pembrolizumab. The anticipated uptake of pembrolizumab upon reimbursement in the current indication is likely overestimated and clinical expert feedback indicated this is more likely to resemble 10% accounting for a small proportion of patients who did not receive pembrolizumab in a prior line despite being eligible or may be retreated in the identified tumour sites. Therefore, the tumour sites in which 90% of uptake will be reached are small intestine, ovarian, pancreatic, cholangiocarcinoma, brain, sarcoma, cervical, neuroendocrine, prostate, adrenocortical, thyroid, salivary, and “other.” The uptake of pembrolizumab was therefore likely overestimated in the sponsor’s base case, however the market uptake of pembrolizumab remains uncertain.
CDA-AMC adjusted tumour-specific market shares to reflect uptake of 90% by year 3 in the tumour sites where immune checkpoint inhibitors are not currently available in a previous line of treatment if not already assumed by the sponsor (e.g., cervical).
CDA-AMC adjusted tumour-specific market shares to reflect uptake of 10% across all 3 years in the tumour sites where immune checkpoint inhibitors are available in previous lines of treatment (e.g., CRC, endometrial, gastric, renal, urothelial, mesothelioma, breast, SCLC).
Drug acquisition costs were estimated inappropriately: Costs from the BIA model are directly pulled from the cost-utility analysis model. Therefore, as aligned with the critical appraisal section of the cost-utility model, the estimation of drug acquisition costs using weight-based dosing and the approach taken to estimate time on treatment for pembrolizumab was found to be inappropriate. Refer to the critical appraisal points of the cost-utility model, “weight-based dosing for pembrolizumab is used in clinical practice” and “approach taken to estimate time on treatment for pembrolizumab was inappropriate.”
CDA-AMC used the sponsor-provided option to update the BIA model costing inputs based on the cost-utility analysis results, which addressed issues regarding fixed dosing and modelling of TTD. Weight-based dosing was therefore applied in the BIA and TTD was modelled by setting it equal to PFS up to week 104.
Testing uptake is uncertain: The sponsor assumes testing uptake will be 100% in gastric, small intestine, endometrial, and CRC. However, for all other tumour sites, testing uptake will be 70%. Given pembrolizumab or another immune checkpoint inhibitor is not available in many of these other cancer sites testing uptake may be higher than 70%.
As a scenario analysis CDA-AMC explored the impact of 100% testing uptake.
CDA-AMC Reanalyses of the BIA
Table 19: CDA-AMC Revisions to the Submitted Budget Impact Analysis
Stepped analysis | Sponsor’s value or assumption | CDA-AMC value or assumption |
|---|---|---|
Changes to derive the CDA-AMC base case | ||
1. Market shares |
|
|
2. Drug acquisition costs for pembrolizumab (TTD and weight-based dosing) |
|
|
CDA-AMC base case | Reanalysis 1 + 2 | |
CDA-AMC = Canada’s Drug Agency; CRC = colorectal; KM = Kaplan-Meier; PFS = progression-free survival; q.3.w. = every 3 weeks; SCLC = small cell lung cancer; TTD = time to treatment discontinuation.
The results of the CDA-AMC stepwise reanalysis are presented in summary format in Table 18 and a more detailed breakdown is presented in Table 19.
The CDA-AMC base case estimated that 3-year budget impact of reimbursing pembrolizumab for the treatment of adult and pediatric patients with unresectable or metastatic MSI-H or dMMR solid tumours, as determined by a validated test, that have progressed following prior treatment and who have no satisfactory alternative treatment options would be $4,480,035 in year 1, $7,614,489 in year 2, and $8,777,897 in year 3, for a 3-year cumulative total of $20,872,421 across all tumour sites.
Table 20: Summary of the CDA-AMC Reanalyses of the Budget Impact Analysis
Stepped analysis | Three-year total ($) |
|---|---|
Submitted base case | 43,487,160 |
CDA-AMC reanalysis 1 | 29,222,551 |
CDA-AMC reanalysis 2 | 28,906,967 |
CDA-AMC base case | 20,872,421 |
CDA-AMC = Canada’s Drug Agency.
Note: The submitted analysis is based on the publicly available prices of pembrolizumab and comparator treatments.
CDA-AMC conducted the following scenario analysis to address remaining uncertainty, using the CDA-AMC base case (results are provided in Table 19):
Assuming 100% testing uptake across all tumour sites.
Table 21: Detailed Breakdown of the CDA-AMC Reanalyses of the BIA
Stepped analysis | Scenario | Year 0 (current situation) ($) | Year 1 ($) | Year 2 ($) | Year 3 ($) | Three-year total ($) |
|---|---|---|---|---|---|---|
Submitted base case | Reference | 18,853,552 | 22,041,882 | 23,618,812 | 25,663,142 | 90,177,387 |
New drug | 18,853,552 | 29,735,740 | 38,783,777 | 46,291,479 | 133,664,547 | |
Budget impact | 0 | 7,693,858 | 15,164,965 | 20,628,337 | 43,487,160 | |
CDA-AMC base case | Reference | 19,640,342 | 21,937,139 | 22,680,899 | 23,198,047 | 87,456,427 |
New drug | 19,640,342 | 26,417,174 | 30,295,388 | 31,975,943 | 108,328,848 | |
Budget impact | 0 | 4,480,035 | 7,614,489 | 8,777,897 | 20,872,421 | |
CDA-AMC scenario analysis 1: 100% testing uptake | Reference | 19,640,342 | 21,937,139 | 22,680,899 | 23,198,047 | 87,456,427 |
New drug | 19,640,342 | 28,158,954 | 32,287,598 | 34,289,513 | 114,376,407 | |
Budget impact | 0 | 6,221,815 | 9,606,699 | 11,091,466 | 26,919,980 |
BIA = budget impact analysis; CDA-AMC = Canada’s Drug Agency.
Table 22: Budget Impact by Tumour Site
Stepped analysis | Three-year budget impact ($) |
|---|---|
Colorectal | 2,777,210 |
Endometrial | 2,583,174 |
Gastric | 2,608,317 |
Small intestine | 4,511,454 |
Ovarian | 555,927 |
Pancreatic | 1,446,671 |
Cholangiocarcinoma | 112,290 |
Brain | 420,780 |
Sarcoma | 215,182 |
Breast | 81,591 |
Cervical | 213,426 |
Neuroendocrine | 0 |
Prostate | 2,703,413 |
Adrenocortical | 1,665,033 |
Mesothelioma | 202,104 |
Thyroid | 105,173 |
SCLC | 53,470 |
Urothelial | 185,396 |
Salivary | 28,053 |
Renal | 403,757 |
Other (pooled) | 0 |
Total budget impact across all tumour sites | 20,872,421 |
SCLC = small cell lung cancer.
Note: The submitted analysis is based on the publicly available prices of pembrolizumab and comparator treatments.
Ethics Review
Abbreviations
CDA-AMC
Canada’s Drug Agency
dMMR
mismatch repair deficient
HRQoL
health-related quality of life
ITC
indirect treatment comparison
MSI-H
microsatellite instability-high
ORR
objective response rate
OS
overall survival
PFS
progression-free survival
SOC
standard of care
Ethical Considerations
Mismatch repair deficiency can occur due to spontaneous or inherited mutations in the genes responsible for the stability of microsatellites (i.e., short segments of DNA with repeating sequences of nucleotides).1-3 High microsatellite instability (MSI-H) or mismatch repair deficient (dMMR) malignancies have been detected in more than 30 cancers with various prevalences and prognoses.4-7 Across different cancer types, there is an estimated pooled prevalence of 2.7% and 2.9% for MSI-H and dMMR status, respectively.5 MSI-H is higher in endometrial, colorectal, small intestine, and gastric cancers (8.5 to 21.9%) and lower in cervical, esophageal, bladder and urothelial, lung, and skin cancers (< 5%).5 People with hereditary conditions such as Lynch syndrome and constitutional mismatch repair deficiency syndrome are at a greater risk of MSI-H and dMMR cancers.
The clinical experts and clinician group input reported that cancers with MSI-H or dMMR solid tumours typically have worse prognoses than those without MSI-H or dMMR status. MSI-H and dMMR cancers are associated with high mutational burden and excessive expression of immune checkpoints such as PD-1.8 Pembrolizumab inhibits the activation of the PD-1 pathway, resulting in the reactivation of T cells that trigger antitumour responses.9 In Canada, pembrolizumab has been issued market authorization to treat various types of cancers, but funding for its use in treating MSI-H and dMMR cancers varies across jurisdictions. Funding is also limited to certain cancer types (i.e., endometrial, colorectal, and small intestine adenocarcinomas). Pembrolizumab has recently been granted tumour-agnostic authorization for treating MSI-H and dMMR solid tumours, as determined by a validated test, that have progressed following prior treatment and for which there are no satisfactory alternative treatment options in Canada.
This report is informed by the sponsor’s submission; patient group, clinician group, and drug plan input received by Canada’s Drug Agency (CDA-AMC) for this review; direct consultation with 3 clinical experts (2 adult medical oncologists and 1 pediatric medical oncologist) with experience treating patients with MSI-H or dMMR solid tumours; and engagement with CDA-AMC clinical, economic, and testing procedure–assessment reviewers. This report highlights ethical considerations regarding the use of pembrolizumab for the treatment of adult and pediatric patients with unresectable or metastatic MSI-H or dMMR solid tumours, as determined by a validated test, that have progressed following prior treatment and who have no satisfactory alternative treatment options. It outlines considerations relevant for decision-making regarding the public reimbursement and implementation of pembrolizumab for this tumour-agnostic indication in Canada. However, it does not present an exhaustive list of all ethical considerations associated with unresectable or metastatic MSI-H or dMMR solid tumours and their treatment.
Pagebreak
Diagnosis, Treatment, and Experiences of People Living With MSI-H or dMMR Solid Tumours
As reported in the Testing Procedure Considerations section of the Clinical Review report, testing for MSI-H and dMMR alterations is routinely performed across Canada for all adult patients with solid tumour types for which immunotherapy or other targeted treatment is already standard of care (SOC) for metastatic disease. However, testing is not routinely performed in the context of pediatric cancers or adult cancers where targeted therapies (including pembrolizumab) are currently not authorized or reimbursed. Should pembrolizumab be funded for the proposed tumour-agnostic indication, testing all people with unresectable or metastatic solid tumours that could have MSI-H or dMMR alterations would enable equitable access to targeted therapy. Testing for such alterations can also benefit patients and families by providing opportunities to pursue genetic testing and counselling for related hereditary tumour syndromes.
The clinician groups and clinical experts reported that people with unresectable or metastatic MSI-H or dMMR solid tumours that have progressed following prior treatment typically only have chemotherapy-based regimens, which are associated with limited clinical benefit and significant cumulative toxicity, as treatment options. Living with and undergoing treatment for unresectable or metastatic MSI-H or dMMR solid tumours causes substantial physical and psychosocial burdens that adversely impact patients’ and their caregivers’ health-related quality of life (HRQoL). Patient group input detailed how physical symptoms and side effects of treatments (especially chemotherapy) can be intolerable and limit functioning in daily activities. Psychosocial impacts of these cancers include experiencing anxiety, fear, sadness, and hopelessness about the future. Additional impacts include a reduced ability to engage in employment, exercise, and social activities.
Patients with MSI-H or dMMR tumour types for which pembrolizumab is currently not funded may experience emotional distress knowing that a targeted therapy such as pembrolizumab exists, but that it is only funded currently for selected MSI-H and dMMR tumour types. People with such cancers have a high unmet need and desire for effective treatments with manageable toxicity that can increase their overall survival (OS) and progression-free survival (PFS) and improve HRQoL.
Clinical Evidence Used in the Evaluation of Pembrolizumab
The safety and efficacy of pembrolizumab was evaluated in 3 single-arm, multicentre, nonrandomized, open-label, multicohort studies: KEYNOTE-158, KEYNOTE-164, and KEYNOTE-051. KEYNOTE-158 was a phase II, basket trial that enrolled 373 adult patients with various types of MSI-H and dMMR tumours. KEYNOTE-164 was a phase II trial that enrolled 124 adults with MSH-H or dMMR colorectal cancer. The phase I and II KEYNOTE-051 basket trial included 7 pediatric patients with MSI-H or dMMR tumours, 6 of whom had brain tumours. Indirect treatment comparisons (ITCs) for colorectal, endometrial, small intestine, and gastric cancers evaluated comparative efficacy versus SOC treatments among adult patients. These ITCs consisted of naive indirect comparisons and unanchored matching-adjusted indirect comparisons. The Clinical Review report provides further details on these 3 studies and the ITCs.
Durable response to treatment, improved OS and PFS, and improved HRQoL are important outcomes to patients and clinicians. The clinical experts believed that the KEYNOTE-158 and KEYNOTE-164 studies demonstrated clinically meaningful and durable improvements in objective response rate (ORR) compared with what is typically observed with SOC treatments. They also felt the evidence regarding OS and PFS was promising based on the natural history of disease and their clinical practice experience. However, the Clinical Review reports there is uncertainty regarding the efficacy of pembrolizumab relative to SOC across tumour sites due to the trials’ single-arm designs. The ITCs suggested that pembrolizumab improved OS and PFS compared with SOC. However, the Clinical Review reports that the ITCs had significant limitations that impacted the validity of the findings and precluded drawing definitive conclusions about comparative efficacy. Responses to pembrolizumab were heterogenous across specific cancer types, and patients with some cancer types had limited representation or small sample sizes in the trials, limiting the generalizability of the results.
None of the trials identified new safety signals. However, because the ITCs did not include comparative safety data, the safety of pembrolizumab compared with SOC treatments for MSI-H and dMMR solid tumours is unknown. Still, the clinical experts emphasized there is a breadth of experience in the use of pembrolizumab in other cancers and perceived that pembrolizumab is better tolerated and has fewer and less severe side effects than conventional chemotherapy. The median follow-up times at the data cut-off for ORR in the clinical trials ranged from 52.7 months (for the cohort of participants in the KEYNOTE-164 trial who had received at least 1 line of prior systemic SOC therapy for colorectal cancer) and 5.2 months (for participants in the KEYNOTE-051 trial). Follow-up times for ORR of individual participants across all trials ranged from 0.1 to 71.4 months. The clinical experts highlighted that further safety data may not be necessary to inform decision-making, given the body of pre-existing research on the use of pembrolizumab for various cancers. However, they acknowledged the potential benefit of the ongoing collection of efficacy data on its use for the proposed indication (e.g., through registries) to further support clinical and health systems decision-making.
The available evidence also raises ethical considerations related to limited representation or underrepresentation in clinical trials. It is difficult to ascertain the potential benefit or harms of pembrolizumab in pediatric patients, given the small number of participants in and single-arm design of the KEYNOTE-051 study. Clinical experts also acknowledged the underrepresentation of racialized persons (with 77% of pooled participants with MSI-H or dMMR tumours in the KEYNOTE-158 and KEYNOTE-164 trials and 86% in the KEYNOTE-105 trial reported as being white). Cancers where MSI-H is more common (i.e., colorectal, endometrial, and gastric) had the greatest representation in the data from the KEYNOTE-158 and KEYNOTE-164 trials, while the representation of other cancers in these data was lower. The clinical experts and patient group input reported that these groups of patients (with rare cancers) are frequently underrepresented or have limited representation in clinical trials and research on cancer therapies. Underrepresentation or limited representation of children, racialized persons, and people with rarer MSI-H and dMMR tumours may limit the generalizability of the findings to these groups.
Clinical Use of Pembrolizumab
The clinical experts reported they would use pembrolizumab for the treatment of adult and pediatric patients with metastatic, unresectable MSI-H or dMMR solid tumours whose disease has progressed following prior treatment and who have no effective and tolerable alternative treatment options. They supported this tumour-agnostic indication, emphasizing the substantial unmet need for effective and tolerable treatments for these patients, despite uncertain — though promising — evidence for outcomes important to patients and clinicians, such as a durable improvement in ORR and improved OS and PFS.
The clinical experts and patient group input provided insight into how pembrolizumab could lead to improvements in HRQoL for patients. Patients with MSI-H or dMMR solid tumours reported positive experiences with pembrolizumab, which they described as “life-changing” when reducing tumour burden and, in turn, alleviating cancer symptoms and prolonging survival. Those patients who received treatment with pembrolizumab reported experiencing reduced physical and psychosocial burdens related to cancer. They appreciated the ease of use of pembrolizumab compared with chemotherapy: fewer additional medications to manage adverse events, quicker infusion times, and no need for infusion pumps at home. The clinical experts and patients generally perceived the adverse effects associated with the use of pembrolizumab as manageable, especially when compared with chemotherapy.
The experts and patient group input noted that reimbursing pembrolizumab for the proposed tumour-agnostic indication could alleviate current inequities in access to treatment options for people with MSI-H or dMMR tumours where treatment with pembrolizumab is not currently reimbursed.
The clinical experts anticipated that most adult patients with MSI-H or dMMR solid tumours eligible for pembrolizumab in Canada would not have trouble accessing the treatment, were it reimbursed, given that the infrastructure required to prescribe, administer, and monitor the drug is already in place. However, because pembrolizumab is administered in hospitals or outpatient settings as a 30-minute IV infusion, people without access to transportation or living far from these settings may experience barriers to access. While these considerations are not novel in the context of cancer treatment, they emphasize the importance of providing patient supports to facilitate equitable access.
The clinical experts anticipated that children would experience disproportionate difficulty accessing pembrolizumab, as fewer pediatric providers would have experience with the treatment. These providers may also require educational supports to identify and treat eligible patients. Pediatric patients would likely receive their infusions at specialist centres, which may be especially challenging for those living far away to access.
To promote autonomous, informed decision-making, robust consent conversations should include disclosures about the uncertain benefits and risks of treatment with pembrolizumab. The clinical experts reported they would prescribe pembrolizumab for eligible patients from groups that were underrepresented or had limited representation in clinical trials (i.e., eligible racialized persons, children, and people with rare tumour types) due to unmet need. However, clinicians should disclose the limitations in the evidence available for these groups as well as their limited experience using pembrolizumab to treat children and people with cancers for which it formerly was not authorized or reimbursed. Consent conversations should also consider the vulnerabilities of patients with life-limiting conditions and uphold appropriate processes for obtaining consent and assent from pediatric patients. Disclosing that pembrolizumab is not a curative therapy may also be important to mitigate harms associated with unmet expectations. Finally, people without satisfactory alternative treatment options and who are ineligible for pembrolizumab may need appropriate psychosocial supports.
Health Systems Impact
The pharmacoeconomic report found that pembrolizumab may be cost-effective at a threshold of $50,000 per quality-adjusted life-year gained, relative to current SOC. However, due to the absence of both direct evidence and robust indirect evidence, there is uncertainty regarding the magnitude of benefit pembrolizumab provides versus SOC across all tumour sites. In some tumour sites, no evidence is available. This makes the estimation of cost-effectiveness highly uncertain and, in turn, may challenge understandings of opportunity costs and decision-making about the fair allocation of limited health system resources. Further collection of long-term data on efficacy and safety outcomes following pembrolizumab’s use for the proposed indication in the real world may better inform this decision-making.
As detailed in the Clinical Review, the clinical experts anticipated there would only be a “small” number of patients who would require testing for MSI-H and dMMR status who would not already receive it as standard care. For this reason, they did not anticipate that the additional testing required for implementing pembrolizumab for the proposed indication would substantially increase health system resource use. Still, the Pharmacoeconomic Review report details that, while testing costs associated with the tumour-agnostic indication are uncertain, costs would vary substantially by tumour type. Given the very low proportion of patients with MSI-H or dMMR status in some tumour sites, testing costs to identify 1 patient can be high. However, making MSI-H and dMMR testing standard for potentially eligible children and people with cancers for which targeted therapy is not already available would ensure these groups have equal opportunity to benefit from pembrolizumab.
The experts did not anticipate the administration of pembrolizumab for the proposed indication in Canada would require new health system structures or substantially greater use of health system resources. Providers already administer pembrolizumab and similar immunotherapies to adults with numerous solid tumour types in hospitals and clinics across Canada. Additionally, the clinical experts anticipated that many otherwise eligible patients with common tumour types may have already accessed pembrolizumab or other immune checkpoint inhibitors in earlier lines of therapy.
References
1.Olave MC, Graham RP. Mismatch repair deficiency: The what, how and why it is important. Genes Chromosomes Cancer. 2022;61(6):314-321. PubMed
2.Marcus L, Lemery SJ, Keegan P, Pazdur R. FDA approval summary: Pembrolizumab for the treatment of microsatellite instability-high solid tumors. Clin Cancer Res. 2019;25(13):3753-3758. PubMed
3.Mishima S, Naito Y, Akagi K, et al. Japanese Society of Medical Oncology/Japan Society of Clinical Oncology/Japanese Society of Pediatric Hematology/Oncology-led clinical recommendations on the diagnosis and use of immunotherapy in patients with DNA mismatch repair deficient (dMMR) tumors, third edition. Int J Clin Oncol. 2023;28(10):1237-1258.
4.Akagi K, Oki E, Taniguchi H, et al. Real-world data on microsatellite instability status in various unresectable or metastatic solid tumors. Cancer Sci. 2021;112(3):1105-1113. PubMed
5.Kang YJ, O'Haire S, Franchini F, et al. A scoping review and meta-analysis on the prevalence of pan-tumour biomarkers (dMMR, MSI, high TMB) in different solid tumours. Sci Rep. 2022;12(1):20495. PubMed
6.Lorenzi M, Amonkar M, Zhang J, Mehta S, Liaw K-L. Epidemiology of microsatellite instability high (MSI-H) and deficient mismatch repair (dMMR) in solid tumors: A structured literature review. J Oncol. 2020;2020:1-17.
7.Inhibiteurs du point de contrôle immunitaire (IPCI) pour le traitement des tumeurs avec instabilité microsatellitaire élevée/déficience du système de réparation des erreurs d’apariements (MSI-H / dMMR). Rapport d’évaluation [accessed by sponsor]. Programme de gestion thérapeutique des médicaments; 2021.
8.Overman MJ, Morse M. Tissue-agnostic cancer therapy: DNA mismatch repair deficiency, tumor mutational burden, and response to immune checkpoint blockade in solid tumors. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2024: https://www.uptodate.com. Accessed 2024 Jul 17.
9.KEYTRUDA (pembrolizumab): solution for infusion 100 mg/4 mL vial [product monograph]. Kirkland (QC): Merck Canada, Inc; 2023 Oct 11.
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.