Drugs, Health Technologies, Health Systems
Reimbursement Review
Amivantamab (Rybrevant)
Sponsor: Janssen Inc.
Therapeutic area: Locally advanced or metastatic non-small cell lung cancer
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Clinical Review
Abbreviations
20ins
20 insertion
AE
adverse event
ATO
average treatment effect in the overlap
ATT
average treatment effect in the treated
AUC
area under the curve
BICR
blinded independent central review
CCSN
Canadian Cancer Survivor Network
CDA-AMC
Canada’s Drug Agency
CI
confidence interval
CSR
Clinical Study Report
ctDNA
circulating tumour DNA
ECOG
Eastern Cooperative Oncology Group
ECOG PS
Eastern Cooperative Oncology Group Performance Status
EMR
electronic medical record
EORTC QLQ-C30
European Organization of Research and Treatment of Cancer Quality of Life Questionnaire Core 30
ESS
effective sample size
GRADE
Grading of Recommendations Assessment, Development and Evaluation
GHS
Global Health Status
HR
hazard ratio
HRQoL
health-related quality of life
IO
immunotherapy
IPCW
inverse probability of censoring weighting
ITC
indirect treatment comparison
LCC
Lung Cancer Canada
LHF
Lung Health Foundation
MedDRA
Medical Dictionary for Regulatory Activities
MET
mesenchymal-epithelial transition
MID
minimal important difference
NE
not estimable
NGS
next-generation sequencing
NSCLC
non–small cell lung cancer
OR
odds ratio
ORR
objective response rate
OS
overall survival
PFS
progression-free survival
PFS2
progression-free survival after first subsequent therapy
PROMIS PF
Patient-Reported Outcomes Measurement Information System – Physical Function
RCT
randomized controlled trial
RECIST
Response Evaluation Criteria in Solid Tumours
RPSFT
rank-preserving structural failure time
RW-PFS
real-world progression-free survival
SAE
serious adverse event
SMD
standardized mean difference
TEAE
treatment-emergent adverse event
TKI
tyrosine kinase inhibitor
TSE
two-stage estimation
TTNT
time to next treatment
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Table 1: Background Information of Application Submitted for Review
Item | Description |
|---|---|
Drug product | Amivantamab (Rybrevant) 350 mg/7 mL (50 mg/mL) single-use vial |
Sponsor | Janssen Inc. |
Indication | In combination with carboplatin and pemetrexed for the first-line treatment of adult patients with locally advanced (not amenable to curative therapy) or metastatic non–small cell lung cancer with activating epidermal growth factor receptor exon 20 insertion mutations. |
Reimbursement request | As per indication |
Health Canada approval status | NOC |
Health Canada review pathway | Standard |
NOC date | June 28, 2024 |
Recommended dose | Amivantamab (Rybrevant) 1,400 mg (1,750 mg if body weight is ≥ 80 kg) by IV infusion once weekly for 4 weeks (first dose split on days 1 and 2), then 1,750 mg (2,100 mg if body weight is ≥ 80 kg) on day 1 of each 21-day cycle, starting with cycle 3. |
NOC = Notice of Compliance.
Introduction
Lung cancer is the most commonly diagnosed cancer type in Canada, as well as the leading cause of cancer-related death in the country.1 Canadian Cancer Statistics (2023) estimate that 1 in 14 Canadians will be diagnosed with lung cancer in their lifetime and that 1 in 4 cancer-related deaths in Canada will be attributed to the disease.1 The overwhelming majority of newly diagnosed lung cancer cases in Canada are attributed to non–small cell lung cancer (NSCLC) (88%), and the 5-year net survival rates for patients in Canada with advanced (stage IV) NSCLC is only 3%.1 Goals of treatment for advanced NSCLC include delaying progression, prolonging survival, palliation of symptoms, and improving quality of life.2 EGFR exon 20 insertion (20ins) is a rare mutation that is associated with aggressive, highly symptomatic disease and significant clinical burden. Multiple studies have found that patients with EGFR exon 20ins-positive NSCLC are typically female, nonsmokers, and diagnosed with metastatic disease at approximately 60 years of age.3-6 In Canada, it has been estimated that EGFR exon 20ins account for approximately 5% of EGFR mutations and between 0.4% to 1.2% of all NSCLC cases, with provincial variation likely being driven by differences in population demographics (exon 20ins mutations are more prevalent in those with East Asian ethnicity).7-20 According to the clinical experts consulted by the review team, testing for EGFR exon 20ins mutations is currently performed as part of the standard of care for locally advanced or metastatic NSCLC in Canada.
Currently, there are no approved targeted therapies for patients with EGFR exon 20ins in the first-line setting. The current recommended standard of care remains chemotherapy (cisplatin or carboplatin, generally in combination with pemetrexed, followed by pemetrexed maintenance therapy).21,22 Treatment with chemotherapy alone does not provide a durable treatment benefit for patients with EGFR exon 20ins and is associated with poor survival outcomes (median progression-free survival [PFS] ranging from 4.2 to 6.9 months and median overall survival [OS] from 16.1 to 22.4 months).8,23-28
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of amivantamab 1,400 mg IV infusion for the first-line treatment of adult patients with locally advanced (not amenable to curative therapy) or metastatic NSCLC with activating EGFR exon 20ins mutations.
Perspectives of Patients, Clinicians, and Drug Programs
The information in this section is a summary of input provided by the patient and clinician groups who responded to the Canada’s Drug Agency (CDA-AMC) call for input and from clinical expert(s) consulted by CDA-AMC for the purpose of this review.
Patient Input
This section was prepared by the CDA-AMC review team based on the input provided by patient groups. The full patient and clinician group submissions received by CDA-AMC are available in the consolidated patient and clinician group input document for this review on the project website.
The patient input was submitted jointly by Lung Cancer Canada (LCC), the Canadian Cancer Survivor Network (CCSN), and the Lung Health Foundation (LHF). Nine patients with NSCLC provided input through virtual interviews by LCC and the CCSN. Among them, 7 patients were from Canada, 1 from the US, and 1 from the UK. All data were collected between May and July in 2024. Based on the input, patients with exon 20ins mutations face a unique challenge, as the mutation is insensitive to conventional tyrosine kinase inhibitors (TKIs). Thus, patients face a poorer prognosis, necessitating different treatment options. Patient groups indicated that there is an urgent unmet need for novel treatment options for patients with EGFR-positive exon 20ins NSCLC. According to the patient group input, improved management of disease symptoms, quality of life, and survival, as well as delayed disease progression and manageable side effects, are considered important outcomes by patients with NSCLC. All participants (n = 9) had experience with amivantamab. Generally, patients indicated that amivantamab was effective in stabilizing disease and maintaining quality of life with manageable side effects. The most common side effects reported included facial and scalp rashes, cuts on fingers and toes, paronychia, eye dryness, sensitivity to the sun, fatigue, skin sensitivity, and nausea.
Clinician Input
Input From Clinical Experts Consulted by CDA-AMC
The clinical experts consulted by CDA-AMC on this review noted the toxicities associated with cytotoxic chemotherapy, its limited efficacy, and the need for targeted therapies with better efficacy.
The clinical experts noted that amivantamab would be added to current standard doublet therapy in the first-line setting. The clinical experts believed that the patients most likely to respond to amivantamab are those with the EGFR exon 20ins mutation.
The clinical experts noted that response would be determined by serial physical and symptom assessments and radiography, typically with CT scans every 8 to 12 weeks during therapy or if there were new symptoms suggesting progression. The clinical experts believed that treatment should be discontinued when patients experience unacceptable toxicity or significant progression or choose to stop treatment.
Clinician Group Input
Two clinician groups submitted input — the LCC Medical Advisory Committee (MAC) and the Ontario Health — Cancer Care Ontario (OH-CCO) Lung Cancer Drug Advisory Committee. In total, 32 clinicians from the LCC MAC and 7 clinicians from OH-CCO Lung Cancer Drug Advisory Committee provided input to the submissions.
The clinician groups agreed with the clinical experts consulted by CDA-AMC that, because of poor outcomes with current available treatments, there is a significant unmet need for novel targeted therapies with better efficacy. The clinician groups agreed with the clinical experts consulted by CDA-AMC that amivantamab plus carboplatin-pemetrexed should be used in the first-line setting, and clinicians from the OH-CCO Lung Cancer Drug Advisory Committee indicated that amivantamab plus carboplatin-pemetrexed can replace pembrolizumab or ipilimumab and/or nivolumab. All clinicians agreed that patients with EGFR exon 20ins mutations are best suited for treatment with amivantamab plus carboplatin-pemetrexed. Clinicians from the LCC MAC suggested radiological response assessments every 6 to 9 weeks, and clinicians from the OH-CCO Lung Cancer Drug Advisory Committee suggested response assessments every 9 to 12 weeks. All clinicians agreed that disease progression and unacceptable toxicities should be considered when deciding to discontinue treatment. All clinicians agreed that specialists with experience in using systemic therapy in cancer care are required for the treatment with amivantamab; outpatient cancer centres, satellite facilities, or hospitals would be appropriate settings.
Drug Program Input
Input was obtained from the drug programs that participate in the CDA-AMC reimbursement review process. The clinical experts consulted by CDA-AMC provided advice on the potential implementation issues raised by the drug programs (Table 5).
Clinical Evidence
Systematic Review
Description of Study
The PAPILLON study is an ongoing, phase III, multicentre, open-label trial conducted in 131 centres across 25 countries, including 3 study sites in Canada. Patients were ≥ 18 years of age with treatment-naive EGFR exon 20ins mutated locally advanced or metastatic NSCLC. The primary objective of the study was to assess the efficacy of amivantamab plus carboplatin-pemetrexed compared with carboplatin-pemetrexed in the first-line treatment of patients with EGFR exon 20ins mutated NSCLC. A total of 308 patients were randomized 1:1 to either the amivantamab plus carboplatin-pemetrexed or carboplatin-pemetrexed arm from December 2020 to November 2022. The clinical cut-off date for data inclusion was May 2023. The treatment phase for each participant started at cycle 1 day 1 and continued in 21-day cycles until the end of treatment visit (approximately 30 days after discontinuation of study treatment), and patients continued treatment until documented radiographic disease progression. Eligible patients in the carboplatin-pemetrexed arm who experienced disease progression were given the option to enter the crossover phase and receive amivantamab monotherapy in 21-day cycles. The primary outcome was PFS, assessed by blinded independent committee review (BICR), and secondary outcomes included OS and objective response rate (ORR).
Patients in the PAPILLON trial were 60 years of age, on average, and the majority were female and had no smoking history (58% each). Of total patients, 65% had an Eastern Cooperative Oncology Group Performance Status (ECOG PS) of 1 and the remainder had an ECOG score of 0, and the majority of patients (77%) had no history of brain metastases. Almost all patients had adenocarcinoma and had not used prior EGFR inhibitors (99% each). Almost all patients had either stage IVA (45%) or IVB (54%) NSCLC at screening. All patients had prior surgery for lung cancer, and 35% had prior radiotherapy. Although there were some differences in specific baseline characteristics between the amivantamab plus carboplatin-pemetrexed and carboplatin-pemetrexed groups, the clinical experts consulted by CDA-AMC on this review did not believe them to be clinically relevant.
Efficacy Results
As of the data cut-off in May 2023, there was a median follow-up of 14.92 months.
Progression-Free Survival
Analyses were performed after 216 events had been observed (amivantamab plus carboplatin-pemetrexed arm: 84, carboplatin-pemetrexed arm: 132). A treatment effect favouring amivantamab plus carboplatin-pemetrexed was observed, with an HR of 0.395 (95% confidence interval [CI], 0.296 to 0.528; P < 0.0001). The median PFS by BICR in the amivantamab plus carboplatin-pemetrexed arm was 11.37 months (95% CI, 9.79 to 13.70) compared with the carboplatin-pemetrexed arm (6.70 months; 95% CI, 5.59 to 7.33). Preplanned sensitivity analyses evaluating PFS, as assessed by the treating investigator, as well as a nonstratified analysis were consistent with the primary analysis. At the 6-month time point, the absolute difference in event-free probability between amivantamab plus carboplatin-pemetrexed and carboplatin-pemetrexed groups was █████ ████ ███ ████ ██ ███████ and at 12 months was █████ ████ ███ ████ ██ ██████ and at 18 months was █████ ████ ███ ████ ██ ███████. Note that by 18 months there were only 17 patients (15 in the amivantamab plus carboplatin-pemetrexed group and 2 in the carboplatin-pemetrexed group) remaining at risk.
Overall Survival
As of the data cut-off in May 2023, there were a total of 70 deaths reported across both groups (amivantamab plus carboplatin-pemetrexed arm: 28 deaths, carboplatin-pemetrexed arm: 42 deaths). At this point, 65 patients from the carboplatin-pemetrexed group had crossed over to amivantamab monotherapy, and the HR was 0.675 (95% CI, 0.418 to 1.090; P = 0.106). Median OS in the amivantamab plus carboplatin-pemetrexed arm was not estimable (NE), and the median OS in the carboplatin-pemetrexed arm was 24.38 (95% CI, 22.08 to NE) months. The final planned OS analysis will be conducted on more mature OS data, approximately 48 months after the first participant was randomized, when approximately 210 deaths overall are anticipated. Results of the stratified sensitivity analysis were consistent with unstratified analysis. At the 12-month time point, the absolute difference in event-free probability between amivantamab plus carboplatin-pemetrexed and carboplatin-pemetrexed groups was ████ ████ ███ ████ ██ ███████ and at 18 months was ████ ████ ███ ████ ██ ██████ and at 24 months was █████ ████ ███ ████ ██ ███████. Note that by 18 months there were only 11 patients (5 in the amivantamab plus carboplatin-pemetrexed group and 6 in the carboplatin-pemetrexed group) who remained at risk. The sponsor also conducted sensitivity analyses to adjust for patients who crossed over to amivantamab monotherapy from carboplatin-pemetrexed: inverse probability of censoring weighting (IPCW) (adjusted HR of ████ ████ ███ █████ ████), two-stage estimation (TSE) (adjusted HR of ████ ████ ███ █████ ████) and rank-preserving structural failure time (RPSFT) (adjusted HR of ███ ████ ███ █████ ████) analyses.
Objective Response Rates
Based on BICR assessment in patients with measurable disease at baseline (n = 304), there was a higher percentage of responders in the amivantamab plus carboplatin-pemetrexed arm (111 patients [72.5%]), compared with the carboplatin-pemetrexed arm (72 patients [46.4%]) at the data cut-off for an odds ratio (OR) of █████ ████ ███ ██████ ██████ ████████), favouring amivantamab plus carboplatin-pemetrexed. The absolute difference between groups ███ ███ ████ ███ ███ ██ ███). The percentage of patients with progressive disease as the best response in the amivantamab plus carboplatin-pemetrexed arm was ████ compared with █████ in the carboplatin-pemetrexed arm. Results of the sensitivity analysis evaluating ORR, as assessed by the treating investigator, were consistent with the assessment by BICR.
Health-Related Quality of Life
For the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 (EORTC QLQ-C30) Global Health Status (GHS) (range, 0 [worst] to 100 [best] points), the mean change from baseline to 12 months was ███ ████ ███ █████ ███) in the amivantamab plus carboplatin-pemetrexed group and ████ ████ ███ █████ ███) in the carboplatin-pemetrexed group. The mean difference between amivantamab plus carboplatin-pemetrexed and carboplatin-pemetrexed groups for change from baseline to 12 months was ███ ████ ███ █████ ███).
Progression-Free Survival After First Subsequent Therapy
At the data cut-off, there were ██ of 153 patients ███████ in the amivantamab plus carboplatin-pemetrexed group and ██ of 155 patients in the carboplatin-pemetrexed group (██████ who had PFS after first subsequent therapy (PFS2) event. The HR was 0.493 (95% CI, 0.32 to 0.759; P = 0.001). This analysis was not adjusted for multiplicity. The median PFS2 was NE (95% CI, 22.77 to NE) in the amivantamab plus carboplatin-pemetrexed arm and 17.25 months (95% CI, 13.96 to 21.52) in the carboplatin-pemetrexed arm.
Harms Results
Adverse Events
Overall, all 151 patients (100%) in the amivantamab plus carboplatin-pemetrexed group and 152 patients (98.1%) in the carboplatin-pemetrexed group experienced at least 1 adverse event (AE). The most common AE was rash, which occurred in 81 patients (53.6%) in the amivantamab plus carboplatin-pemetrexed group and 12 patients (7.7%) in the carboplatin-pemetrexed group. Other common AEs with large differences between groups included dermatitis acneiform, in 47 patients (31.1%) in the amivantamab plus carboplatin-pemetrexed group and 5 patients (3.2%) in the carboplatin-pemetrexed group; hypoalbuminemia, in 62 (41.1%) patients in the amivantamab plus carboplatin-pemetrexed group and 15 (9.7%) patients in the carboplatin-pemetrexed group; peripheral edema, in 45 (29.8%) of patients in the amivantamab plus carboplatin-pemetrexed group and 16 (10.3%) patients in the carboplatin-pemetrexed group; and infusion-related reaction, in 63 (41.7%) patients in the amivantamab plus carboplatin-pemetrexed group and 2 (1.3%) patients in the carboplatin-pemetrexed group.
Serious Adverse Events
Treatment-emergent serious AEs (SAEs) were reported in 56 patients (37.1%) in the amivantamab plus carboplatin-pemetrexed group and 48 patients (31.0%) in the carboplatin-pemetrexed group. The most common SAEs in the amivantamab plus carboplatin-pemetrexed group were pneumonia (6 patients [4.0%] versus 4 patients [2.6%] in the carboplatin-pemetrexed group), pneumonitis (4 patients [2.6%] and no patients in carboplatin-pemetrexed), and pulmonary embolism (4 patients [2.6%] in each group). All other SAEs in the amivantamab plus carboplatin-pemetrexed group had an incidence of less than 2%. The most common SAE in the carboplatin-pemetrexed arm was anemia (6 patients [3.9%] and 1 patient [0.7%] in the amivantamab plus carboplatin-pemetrexed group).
Withdrawals Due to Adverse Events
Overall, from study initiation through the data cut-off, 36 patients (23.8%) in the amivantamab plus carboplatin-pemetrexed arm and 16 patients (10.3%) in the carboplatin-pemetrexed arm had treatment-emergent AEs (TEAEs) leading to discontinuation of at least 1 study treatment. Of the 36 patients in the amivantamab plus carboplatin-pemetrexed arm who discontinued any study treatment, 17 discontinued amivantamab. Pneumonitis was the most common cause of discontinuation of amivantamab (4 patients [2.6%]), followed by dermatitis acneiform (████████ ████████ Thrombocytopenia (3 patients [1.9%]) and neutropenia (2 patients [1.3%]) were the most common reasons for treatment discontinuation of either carboplatin or pemetrexed in the carboplatin-pemetrexed arm. Most of the TEAEs leading to study treatment discontinuation occurred at a frequency of less than 2% in both treatment arms.
Mortality
There were 4 patients (2.6%) in the amivantamab plus carboplatin-pemetrexed group and 9 patients (5.8%) in the carboplatin-pemetrexed group who died due to an AE during the study, and 3 patients (2.0%) in the amivantamab plus carboplatin-pemetrexed group and 4 patients (2.6%) in the carboplatin-pemetrexed group who died due to an AE within 30 days of the last dose.
Notable Harms
The notable harms identified for this review were rash and infusion reactions. As noted previously, rash was the most common AE, occurring in 81 (53.6%) patients in the amivantamab plus carboplatin-pemetrexed group and 12 (7.7%) patients in the carboplatin-pemetrexed group. Under the grouping skin and subcutaneous disorders, there were ███ ████████ ███████ ████████ in the amivantamab plus carboplatin-pemetrexed group and ██ ███████ patients in the carboplatin-pemetrexed group with such an event. Infusion-related reactions were reported in 63 (41.7%) patients in the amivantamab plus carboplatin-pemetrexed group and 2 (1.3%) patients in the carboplatin-pemetrexed group.
Critical Appraisal
The lack of blinding in the PAPILLON trial introduces significant potential for bias in the assessment of patient-reported outcomes such as health-related quality of life (HRQoL). There was a large number of patients (42%) who crossed over from the carboplatin-pemetrexed group to the amivantamab monotherapy after disease progression, which is a major confounder when assessing OS. Another limitation of assessment of OS is that the data are not yet mature.
With respect to external validity, the clinical experts consulted on this review believed the population enrolled in the PAPILLON trial to be generalizable to the patients they expect to be treated with amivantamab in Canada, although they would likely consider expanding the population to an ECOG PS of 2, rather than limiting it to ECOG PS of 0 or 1, as was seen in the trial.
GRADE Summary of Findings and Certainty of the Evidence
The selection of outcomes for Grading of Recommendations Assessment, Development and Evaluation (GRADE) assessment was based on the sponsor’s Summary of Clinical Evidence, consultation with clinical experts, and input received from patient and clinician groups and public drug plans. The following list of outcomes was finalized in consultation with expert committee members:
PFS
OS
ORR
HRQoL (EORTC QLQ-C30 GHS)
Notable harms: rash, infusion-related reactions.
The target of the certainty-of-evidence assessment was the presence or absence of a clinically important effect based on thresholds informed by the clinical experts consulted for this review for PFS and OS. The literature-based minimal important difference (MID) of 10 points was used for the EORTC QLQ-C30 GHS.29,30 This MID has been estimated for within-group changes and was applied in the absence of an estimate of the MID for a between-group difference. The target of the certainty of evidence was the presence or absence of any (non-null) effect for the ORR because a threshold for a clinically important between-group difference could not be estimated.
Table 2: Summary of Findings for Amivantamab Plus Carboplatin-Pemetrexed Versus Carboplatin-Pemetrexed for Patients With NSCLC With Exon 20ins
Outcome and follow-up | Patients (studies), N | Relative effect (95% CI) | Absolute effects (95% CI) | Certainty | What happens | ||
|---|---|---|---|---|---|---|---|
CP | Amivantamab + CP | Difference | |||||
PFS (median follow-up of 14.9 months [range, 0.3 to 27.0]) | |||||||
Probability of being progression-free at 6 months | 308 (1 RCT) | NA | ██ ███ ███ | | ██ ███ ███ ███ ██ ██ ███ █████ | ████ ████ ███ ███ █████ ██ ████ ████ ███ ████ | Higha | Amivantamab + CP results in a clinically important improvement in the probability of being progression-free compared to CP alone. |
Probability of being progression-free at 12 months | 308 (1 RCT) | NA | ██ ███ ███ | ██ ███ ███ ███ ██ ██ ███ ████ | ████ ████ ███ ███ █████ ██ ████ ██ ████ ███ ████ | Higha | Amivantamab + CP results in a clinically important improvement in the probability of being progression-free compared to CP alone. |
Probability of being progression-free at 18 months | 308 (1 RCT) | NA | | ███ ███ | ██ ███ ███ ███ ██ ██ ███ ████ | ████ ████ ███ ███ █████ ██ ████ ████ ███ ████ | Higha | Amivantamab + CP likely results in a clinically important improvement in the probability of being progression-free compared to CP alone. |
OS (median follow-up of 14.9 months [range, 0.3 to 27.0]) | |||||||
Probability of being alive at 12 months | 308 (1 RCT) | NA | ██ ███ ███ | ██ ███ ███ ███ ██ ██ ███ ████ | ███ ████ ███ ███ ████ █████ ██ ████ ████ ███ ████ | Lowb | Amivantamab + CP may result in a clinically important improvement in the probability of being alive compared to CP alone. |
Probability of being alive at 18 months | 308 (1 RCT) | NA | ██ ███ ███ | ██ ███ ███ ███ ██ ██ ███ ████ | ███ ████ ███ ███ ████ █████ ██ ████ ████ ███ ████ | Lowb | Amivantamab + CP may result in a clinically important improvement in the probability of being alive compared to CP alone. |
Probability of being alive at 24 months | 308 (1 RCT) | NA | ██ ███ ███ | ██ ███ ███ ███ ██ ██ ███ ████ | ████ ████ ███ ███ ████ █████ ██ ████ ████ ███ ████ | Lowb | Amivantamab + CP may result in a clinically important improvement in the probability of being alive compared to CP alone. |
ORR (median follow-up of 14.9 months [range, 0.3 to 27.0]) | |||||||
ORR by BICR Follow-up: Data cut-off | 304 (1 RCT) | ██ █ ████ █████ ██ █████ | ██ ███ ███ | | ██ ███ ███ ███ ██ ██ ███ ████ | ██ ████ ███ ███ ███ ██ ██ ████ ███ ████ | Moderatec | Amivantamab + CP likely results in an improvement in ORR compared to CP alone. The clinical importance is uncertain. |
HRQoL: EORTC QLQ-C30 Global Health Status | |||||||
EORTC QLQ-C30 Global Health Status, mean change from baseline (0 [worst] to 100 [best]), points Follow-up: 12 months | 308 (1 RCT) | NA | ████ █████ ██ ████ | ███ █████ ██ █████ | ███ █████ ██ ████ | Lowd | Amivantamab + CP may result in little to no difference in HRQoL compared to CP alone. |
Notable harms | |||||||
Rashe Follow-up: to data cut-off | 308 (1 RCT) | NR | | ███ ███ | ██ ███ ███ █████ | ██ ████ ███ ███ ███ ██ ██ ████ ███ ████ | Moderatef | Amivantamab + CP likely results in an increase in rash compared to CP alone. The clinical significance of the rash is unknown. |
Infusion-related reaction Follow-up: to data cut-off | 308 (1 RCT) | NR | | ███ ████ | ██ ███ ███ ████ | ██ ████ ███ ███ ███ ██ ██ ████ ███ ████ | Moderatef | Amivantamab + CP likely results in an increase in infusion-related reactions compared to CP alone. The clinical significance of the infusion-related reactions is unknown. |
BICR = blinded independent central review; CI = confidence interval; CP = carboplatin-pemetrexed; EORTC QLQ-C30 = European Organization for the Research and Treatment of Cancer Quality of Life Questionnaire Core 30; HRQoL = health-related quality of life; NA = not applicable; NR = not reported; NSCLC = non–small cell lung cancer; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; RCT = randomized controlled trial.
Notes: Study limitations (which refer to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias were considered when assessing the certainty of the evidence. All serious concerns in these domains that led to the rating down of the level of certainty are documented in the table footnotes.
Cycle 17 day 1 and cycle 25 day 1 were selected to correspond 12- and 18-month time points, respectively. For EORTC QLQ-C30 GHS, means and 95% CIs are derived based on the mixed-effects model with repeated measures, in which the dependent variable is change from baseline in score, and independent variables are baseline, visit, treatment, and visit by treatment interaction as fixed effects and individual patient as random effect.
The between-group differences for PFS, OS, HRQoL, and notable harms were not part of the sponsor’s statistical analysis plan and were requested by the review team to facilitate interpretation.
aThe clinical experts consulted by the review team considered that both the point estimate and lower bound of the CI constituted clinically meaningful benefit.
bRated down 1 level for study limitations; results are from an interim analysis and there is a risk of bias due to confounding as a result of crossover of patients from the carboplatin-pemetrexed group to amivantamab monotherapy postprogression. Rated down 1 level for imprecision; the point estimate suggests benefit and CI includes little to no difference and in some cases, potential harm (threshold of 5% suggested by clinical experts).
cNo threshold of clinical importance could be established; effects were appraised using the null. Rated down 1 level for indirectness; this is a surrogate end point without strong evidence that it predicts the treatment effect on OS.
dRated down 2 levels for study limitations; there is risk of bias due to (a) lack of blinding and a subjective outcome, (b) substantial missing outcome data. Based on a MID of 10 points, the point estimate and both bounds of the CI suggest little to no difference. The 10-point MID has been estimated for within-group changes, and was applied in the absence of an estimate of a between-group MID. However, both within- and between- group differences were smaller than the MID.
eLower-level rash was used instead of higher-level rash because it was thought to capture rash events more specifically.
fRated down 1 level for study limitations; there is a risk of bias due to lack of blinding and potential subjectivity in the outcomes.
Sources: Details included in the table are from the sponsor’s Summary of Clinical Evidence.31 Data request of the sponsor, and the Clinical Study Report (CSR) for the PAPILLON trial.
Long-Term Extension Studies
No long-term extension studies were submitted.
Indirect Comparisons
The sponsor submitted an indirect treatment comparison (ITC) report that included analyses that used individual patient data from the PAPILLON trial and real-world databases and inverse probability of treatment weighting (IPTW) methods to reduce the risk of bias due to confounding. This was considered by the review team as a nonrandomized study and is reported in the following section.
Studies Addressing Gaps in the Evidence From the Systematic Review
This section includes the contents of the ITC report submitted by the sponsor, which were considered by the review team to be a nonrandomized study, as it utilized individual patient data for each arm in the comparison.
Description of the Nonrandomized Study
The sponsor performed a nonrandomized study using IPTW. These analyses used individual patient data from the PAPILLON trial for amivantamab plus carboplatin-pemetrexed and from real-world databases COTA and ConcertAI for EGFR TKI monotherapy and platinum chemotherapy plus immunotherapy (IO). The analyses examined the outcomes of OS, PFS, real-world PFS, and time to next treatment (TTNT).
Covariates were identified by the sponsor that were considered treatment effect modifiers or prognostic factors. The base-case results were adjusted for ECOG at index date, history of brain metastases, history of liver metastases, and age at index date. The full model adjusted for all the variables in the base case, plus Asian race, history of smoking, sex, and history of other metastases.
For the PAPILLON trial versus EGFR TKI comparison, before weighting, moderate differences (absolute standardized mean difference [SMD] ████ ███ ████) were observed for ECOG at index date and history of smoking, and substantial differences (absolute SMD ████) were seen for history of liver metastases, age, Asian race, sex, and history of other metastases. In the primary analysis, base-case average treatment effect in the treated (ATT) weighting balanced (SMD ████) all 4 covariates between cohorts. In the full model, however, all 8 of the included factors had absolute SMDs ████, indicating lack of balance, with moderate differences observed for 6 factors (ECOG at index date, history of liver metastases, age, history of smoking, sex, history of other metastases), and substantial differences observed for the remaining 2 factors (history of brain metastases, Asian race). The resulting effective sample size (ESS) in the EGFR TKI cohort was ████ ███ ████ for the base case and full model, respectively, compared to the original ██ observations.
For the PAPILLON trial versus platinum plus IO comparison, before weighting, substantial (absolute SMD ████) differences were observed for ECOG at index date, history of liver metastases, history of brain metastases, age, Asian race, and history of other metastases. In the primary analysis, ATT weighting reduced the proportion of categories with absolute SMDs ████ from ████ ██████ ██ ███ ██████, with only moderate differences observed for the 2 remaining factors (ECOG at index date, age). The balance between populations in the full model, on the other hand, remained the same (6 of 8 factors balanced) following weighting, although moderate differences were observed for 3 factors (ECOG at index date, history of brain metastases, history of smoking) and substantial differences were observed for the remaining 3 factors (history of liver metastases, Asian race, history of other metastases). The resulting ESS in the platinum plus IO cohort was █████ ███ ████ for the base case and full model, respectively, compared to the original ██ observations.
Efficacy Results
The unadjusted comparison of OS for the PAPILLON trial versus EGFR TKI produced an HR of ████ ████ ███ █████ █████ ███████) in favour of amivantamab plus carboplatin-pemetrexed. The primary analysis, using base-case ATT weighting, produced results in favour of amivantamab plus carboplatin-pemetrexed, with an HR of ████ ████ ███ █████ █████ ███████). The unadjusted comparison of OS for the PAPILLON trial versus platinum plus IO, produced an HR of ████ ████ ███ █████ █████ ███████) in favour of amivantamab plus carboplatin-pemetrexed. The primary analysis, using base-case ATT weighting, produced a point estimate favouring amivantamab plus carboplatin-pemetrexed, but the 95% CI crossed the null, with an HR of ████ ████ ███ █████ █████ ███████).
The unadjusted comparison of PFS for the PAPILLON trial versus EGFR TKI produced an HR of ████ ████ ███ █████ █████ ███████); the point estimate favoured amivantamab plus carboplatin-pemetrexed, but the 95% CI crossed the null. Similarly, the primary analysis, using base-case ATT weighting, produced an HR of ████ ████ ███ █████ █████ ███████). The unadjusted comparison of PFS for the PAPILLON trial versus platinum plus IO produced an HR of ████ ████ ███ █████ █████ ███████), favouring amivantamab plus carboplatin-pemetrexed. The primary analysis, using base-case ATT weighting, produced results in favour of amivantamab plus carboplatin-pemetrexed, with an HR of ████ ████ ███ █████ █████ ███████).
The unadjusted comparison of real-world PFS (RW-PFS) for the PAPILLON trial versus EGFR TKI produced an HR of ████ ████ ███ █████ █████ ████████, favouring amivantamab plus carboplatin-pemetrexed. The primary analysis, using base-case ATT weighting, produced results in favour of amivantamab plus carboplatin-pemetrexed, with an HR of ████ ████ ███ █████ █████ ███████). The unadjusted comparison of RW-PFS for the PAPILLON trial versus platinum plus IO produced an HR of ████ ████ ███ █████ █████ ███████), favouring amivantamab plus carboplatin-pemetrexed. The primary analysis, using base-case ATT weighting, produced results in favour of amivantamab plus carboplatin-pemetrexed, with an HR of ████ ████ ███ █████ █████ ███████).
The unadjusted comparison of TTNT for the PAPILLON trial versus EGFR TKI produced an HR of ████ ████ ███ █████ █████ ███████) favouring amivantamab plus carboplatin-pemetrexed. The primary analysis, using base-case ATT weighting, produced results in favour of amivantamab plus carboplatin-pemetrexed, with an HR of ████ ████ ███ █████ █████ ███████). The unadjusted comparison of TTNT for the PAPILLON trial versus platinum plus IO produced an HR of ████ ████ ███ █████ █████ ███████), favouring amivantamab plus carboplatin-pemetrexed. The primary analysis, using base-case ATT weighting, produced results in favour of amivantamab plus carboplatin-pemetrexed, with an HR of ████ ████ ███ █████ █████ ███████).
Results of the other sensitivity analyses (not shown) were mostly in the direction of favouring amivantamab plus carboplatin-pemetrexed, but in some cases the results were imprecise, with CIs that crossed the null.
Harms Results
Harms were not assessed in the nonrandomized studies.
Critical Appraisal
There was no predefined protocol available, and the search and selection criteria, data extraction, and methods to appraise the risk of bias were not described. There was minimal information related to the real-world data source regarding data quality and completeness, suitability, and validity of any algorithms used to identify patients and classify outcomes. Additionally, due to the lack of protocol, there is an increased risk of bias in the selection of the reported results.
Propensity score–based methods aim to reduce the risk of bias due to confounding. However, it is important to note that no comparisons using data from randomized cohorts were used in the sponsor’s analysis. Lack of randomization within the datasets introduces the possibility of imbalance of patient characteristics, which could lead to comparing groups of patients who do not possess similar prognostic risk. While the methods used by the sponsor serve to reduce confounding, the results indicate that a high risk of residual confounding is present in the analyses, even after the adjustments that were made on prognostic and effect-modifying covariates. While a sensitivity analysis of the full model including all 8 factors was conducted, the primary analysis of the base case only adjusted for 4 factors; it is unlikely that this represents all relevant prognostic and effect-modifying variables. In many cases, the full model was associated with high SMDs, indicating evidence of differences in baseline characteristics between the groups being compared. The base-case model, which used 4 factors, also had notable imbalances.
The use of real-world data has several limitations. Participants in the PAPILLON trial were monitored more strictly than were the patients included in the ITC from the real-world databases. Monitoring of patients in the real-world databases was likely to be less rigorous. OS measurements may include errors or missing deaths, or censoring may differ between the clinical and real-word data sources. The sponsor suggested that missing deaths in real-world data may result in an overestimation of OS. The handling of missing data in the databases and in the analyses was not clearly described in the sponsor’s report.
The effective sample sizes were very small in the base case and in several of the full model analyses. For example, the ESS was ██ in the IPTW-ATT full model for the EGFR TKI group. In the full model, the majority of the 8 included factors remained unbalanced (SMDs ████) following ATT weighting for both the the PAPILLON trail versus EGFR TKI (all 8 factors imbalanced) and platinum plus IO comparisons (6 of 8 factors were imbalanced). Therefore, the reliability of the results from the full model is expected to be low due to risk of bias and the small sample size. The results of the base-case model are based on populations that have greater similarity to one another (in comparison to the full model). However, imbalances remained, and the base-case model did not control for all the important baseline prognostic covariates.
The selection of comparators in the analyses lack clinical relevance in the context of Canada. The relevance is also limited by the lack of analyses, including patient-reported outcomes such as HRQoL.
Conclusions
There is evidence from 1 pivotal, phase III, open-label, randomized controlled trial (RCT) (PAPILLON, n = 308) that amivantamab plus carboplatin-pemetrexed results in a clinically important improvement in PFS compared to carboplatin-pemetrexed alone in patients with locally advanced NSCLC with an exon 20ins mutation. Evidence from the trial suggested that amivantamab plus carboplatin-pemetrexed may improve OS over carboplatin-pemetrexed alone. However, conclusions regarding OS are limited because the OS data are not yet mature, a large number of crossovers occurred in this trial, and the estimates were imprecise (i.e., 95% CIs included effects that may not be clinically important and crossed the null). The combination of amivantamab plus carboplatin-pemetrexed likely improves ORR compared to carboplatin-pemetrexed alone, although the clinical significance of this improvement is less clear, given that ORR is a surrogate outcome without strong evidence of a potential to predict the treatment effect on OS. Amivantamab plus carboplatin-pemetrexed may result in little to no difference in HRQoL; the results of this assessment were likely biased by the open-label design of the trial and patient attrition. Rash and infusion-related reactions are more likely to occur when amivantamab is added to carboplatin-pemetrexed. The most common notable harm associated with amivantamab was rash. However, this only rarely resulted in serious harm or prompted the patient to stop therapy.
A nonrandomized study using individual patient data from the PAPILLON trail and real-world databases, as well as IPTW methods to reduce the risk of bias due to confounding, aimed at determining the comparative efficacy of amivantamab plus carboplatin-pemetrexed versus EGFR TKI and chemotherapy plus IO for several efficacy outcomes (OS, PFS, RW-PFS, TTNT). Despite the analyses suggesting superiority of amivantamab plus carboplatin-pemetrexed for most outcomes, the evidence was insufficient to draw definitive conclusions on the relative efficacy of amivantamab plus carboplatin-pemetrexed or the precise magnitude of any potential difference. The clinical experts consulted by the review team suggested that superiority of amivantamab plus chemotherapy over EGFR TKI monotherapy or chemotherapy plus IO is plausible, given that the 2 comparators are not known to be efficacious in patients with NSCLC with EGFR exon 20ins mutations. The nonrandomized study provided no information on HRQoL, an outcome of importance to patients, or on harms.
Introduction
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of amivantamab 1,400 mg IV infusion for the first-line treatment of adult patients with locally advanced (not amenable to curative therapy) or metastatic NSCLC with activating EGFR exon 20ins mutations.
Disease Background
Contents within this section have been informed by materials submitted by the sponsor and clinical expert input. The following have been summarized and validated by the CDA-AMC review team.
Lung cancer is the most commonly diagnosed cancer type in Canada, as well as the leading cause of cancer-related death in the country.1 Canadian Cancer Statistics (2023) estimate that 1 in 14 Canadians will be diagnosed with lung cancer in their lifetime and that 1 in 4 cancer-related deaths in Canada will be attributed to the disease.1 It is estimated that in 2024 there were 32,100 Canadians diagnosed with lung and bronchus cancer.32 The overwhelming majority of newly diagnosed lung cancer cases in Canada are attributed to NSCLC (88%), which is a serious terminal illness that is associated with a poor prognosis, as the 5-year net survival rate for patients in Canada with advanced (stage IV) NSCLC is only 3%.1 Goals of treatment for advanced NSCLC include delaying progression, prolonging survival, palliation of symptoms, and improving quality of life.2
Scientific advances over the past decade have allowed for a better understanding of advanced NSCLC and its mechanisms of action.19,33 One key mechanism are “driver” mutations, which activate progrowth signalling pathways. The most prevalent driver mutation in NSCLC results in the activation of EGFR, which has been identified in 15% of Western populations34 and 40% to 50% of Asian populations.35 EGFR mutations can be classified into 2 distinct groups: common EGFR mutations, which comprise 85% to 90% of all EGFR mutations and include exon 19 deletions and exon 21 L858R point mutations, and uncommon EGFR mutations, which constitute the remaining 10% to 15% and include exon 20ins mutations.8,19, 36-38 EGFR exon 20ins is a rare mutation that is associated with aggressive, highly symptomatic disease and significant clinical burden. EGFR exon 20ins mutations are heterogenous at the molecular level, with more than 70 types of mutations described to date.3,19,36,39 Multiple studies have found that patients with EGFR exon 20ins-positive NSCLC are typically female, nonsmokers, and diagnosed with metastatic disease at approximately 60 years of age.3-6 In Canada, it has been estimated that EGFR exon 20ins account for approximately 5% of EGFR mutations and between 0.4% to 1.2% of all NSCLC cases, with provincial variation likely being driven by differences in population demographics (exon 20ins mutations are more prevalent in those with East Asian ethnicity).7-10,12-20 Patients with EGFR exon 20ins experience a poor HRQoL due to frequent disease-related symptoms, such as fatigue, pain, shortness of breath and cough, and negative impacts on daily activities, including self-care, social activities, and family life.40-43
Diagnosis of NSCLC often occurs at late-stage disease and requires a biopsy in which sufficient tissue is obtained for histologic confirmation.1 Following the biopsy, a diagnosis of 1 of the 3 distinct histological types of NSCLC (i.e., adenocarcinoma, squamous cell carcinoma, and large cell carcinoma) is made, and the tumour is staged.44 Assessment of EGFR mutation status is recommended as part of a sequential or parallel approach to facilitate treatment decision-making.45
Standards of Therapy
Contents within this section have been informed by materials submitted by the sponsor and clinical expert input. The following have been summarized and validated by the CDA-AMC review team.
Treatment of EGFR-mutated NSCLC is not a “one size fits all” approach, as key differences exist in the mechanisms of action between common and uncommon mutations.19 While common EGFR mutations respond well to EGFR TKIs, they are largely ineffective against EGFR exon 20ins mutations.46,47 Given the paucity of effective treatment options and lack of approved first-line targeted therapies, survival outcomes are worse in patients diagnosed with EGFR exon 20ins mutations versus common EGFR mutations.8 A population-based study of patients with EGFR-positive NSCLC in Alberta, Canada, found real-world median OS in patients with EGFR exon 20ins was significantly worse than in patients with EGFR exon 19 deletions or exon 21 L858R mutations.7
As per the clinical experts consulted by the review team, current treatment goals for patients with advanced NSCLC include prolonging PFS and OS and maintaining or improving HRQoL. In 2023, the American Society of Clinical Oncology and the European Society for Medical Oncology published treatment guidelines recommending chemotherapy for patients with EGFR exon 20ins-positive NSCLC in the first-line setting.48,49 According to the clinical experts consulted by the review team, platinum-doublet chemotherapy in first-line treatment, and then other cytotoxic chemotherapies (e.g., docetaxel), would be offered to the present patient target population. Patients with EGFR exon 20ins mutations do not respond to standard EGFR targeting TKIs, such as osimertinib, that have led to much better outcomes in patients with sensitizing EGFR mutations, i.e., exon 19 deletion and exon 21 L858R substitution, compared to platinum-doublet chemotherapy. Further, the patient target population does not have meaningful responses to IO checkpoint inhibitors. Current therapy with cytotoxic chemotherapy provides a modest survival benefit over best supportive care. However, benefits are typically short-lived, and chemotherapies can have significant toxicities, according to the clinical experts consulted by the review team. Treatment with chemotherapy in patients with EGFR exon 20ins has been associated with poor survival outcomes (median PFS ranging from 4.2 to 6.9 months and median OS from 16.1 to 22.4 months).8,23-28
Currently, there are no approved targeted therapies for patients with exon 20ins in the first-line setting. The current recommended standard of care remains chemotherapy (cisplatin or carboplatin, generally in combination with pemetrexed, followed by pemetrexed maintenance).21,22
Drug Under Review
Key characteristics of amivantamab are summarized in Table 3 with other treatments available for locally advanced (not amenable to curative therapy) or metastatic NSCLC with activating EGFR exon 20ins mutations.
The recommended dosage for amivantamab is a once weekly IV infusion, at a dose of 1,400 mg (1,750 mg if body weight is 80 kg or greater) for 4 weeks (first dose split on days 1 and 2), then 1,750 mg (2,100 mg if body weight is ≥ 80 kg) on day 1 of each 21-day cycle, starting with cycle 3. Amivantamab has received Health Canada approval for the first-line treatment of adult patients with locally advanced (not amenable to curative therapy) or metastatic NSCLC with activating EGFR exon 20ins mutations. The sponsor’s reimbursement request is consistent with the indication. Amivantamab is a bispecific antibody that binds to both the EGFR and mesenchymal-epithelial transition (MET) receptor. It is thought that the EGFR and MET pathways compensate for each other in situations where 1 pathway is inhibited, leading to the so-called “kinase switch” drug resistance (seen with EGFR TKIs).50 Thus, simultaneous inhibition of both EGFR and MET may improve overall treatment efficacy by limiting the compensatory pathway activation.50
Table 3: Key Characteristics of Amivantamab Plus Carboplatin-Pemetrexed, Platinum-Based Chemotherapy, EGFR TKI, and IO
Characteristic | Amivantamab + pemetrexed + carboplatin | Immunotherapy + chemotherapya56 | ||
|---|---|---|---|---|
Mechanism of action | EGFR and MET inhibitor. Both pathways are drivers of cell division, and when 1 is blocked, the other compensates. | Platinum-based chemotherapy damages DNA. Pemetrexed is an antifolate that inhibits DNA synthesis. | Blocks EGFR, a driver of cell division. | Blocks PD-1, an immune checkpoint, thereby activating cytotoxic T lymphocytes. |
Indication | Anticipated: first-line treatment of treatment-naive adult patients with EGFR exon 20ins-mutated locally advanced NSCLC. | Indicated for the first-line treatment of patients with locally advanced or metastatic nonsquamous NSCLC. | Afatinib: Indicated as monotherapy for the treatment of TKI-naive patients with locally advanced or metastatic NSCLC after progressing on platinum-based chemotherapy. Erlotinib: Indicated as monotherapy for the treatment of patients with locally advanced or metastatic NSCLC after failure of at least 1 prior chemotherapy regimen, and whose EGFR expression status is positive or unknown. Gefitinib: Indicated for the first-line treatment of patients with locally advanced or metastatic NSCLC who have activating mutations of the EGFR tyrosine kinase. | Pembrolizumab + carboplatin + pemetrexed: Indicated for the treatment of adult patients with metastatic nonsquamous NSCLC with no EGFR or ALK genetic tumour aberrations, and no prior systemic chemotherapy treatment for metastatic NSCLC. Pembrolizumab + cisplatin + pemetrexed: Indicated for the treatment of adult patients with metastatic nonsquamous NSCLC with no EGFR or ALK genetic tumour aberrations and no prior systemic chemotherapy treatment for metastatic NSCLC. |
Route of administration | IV | IV | Oral | IV |
Recommended dose | Amivantamab: Dose of 1,400 mg (1,750 if body weight ≥ 80 kg) by IV infusion once weekly for 4 weeks (first dose split on days 1 and 2), then 1,750 mg (2,100 mg if body weight is ≥ 80 kg) on day 1 of each 21-day cycle, starting with cycle 3. Pemetrexed: 500 mg/m2 (with vitamin supplementation) on day 1 of each 21-day cycle, in combination with carboplatin for up to 4 cycles, and then as maintenance monotherapy until disease progression. Carboplatin: AUC 5 on day 1 of each 21-day cycle, for up to 4 cycles. | Carboplatin: AUC on day 1 of each 21-day cycle. Pemetrexed: 500 mg/m2 (with vitamin supplementation) on day 1 of each 21-day cycle. Treatment continues for a total of six 21-day cycles unless disease progression or unacceptable toxicity occurs. Cisplatin: 75 mg/m2 infused over 2 hours beginning approximately 30 minutes after completion of the administration of pemetrexed. Pemetrexed: 500 mg/m2 administered as IV infusion over 10 minutes on day 1 of each 21-day cycle. | Afatinib: 40 mg administered orally once daily. Erlotinib: 150 mg administered orally once daily. Gefitinib: 250 mg administered orally once daily. | Pembrolizumab + carboplatin + pemetrexed: Either 200 mg every 3 weeks, or 400 mg every 6 weeks until disease progression, unacceptable toxicity, or up to 24 months or 35 doses for 200 mg or 18 doses for 400 mg, whichever is longer, in patients without disease progression. Pembrolizumab + cisplatin + pemetrexed: 200 mg every 3 weeks, or 400 mg every 6 weeks until disease progression, unacceptable toxicity, or up to 24 months or 35 doses for 200 mg or 18 doses for 400 mg, whichever is longer, in patients without disease progression. |
Serious adverse effects or safety issues | Infusion reactions | Platinum compounds:
| Interstitial lung disease Gastrointestinal perforation Hepatotoxicity | Immune-mediated reactions |
AUC = area under the curve; CP = carboplatin-pemetrexed; exon 20ins = exon 20 insertion; IO = immunotherapy; NSCLC = non–small cell lung cancer; PD-1 = programmed cell death protein 1; TKI = tyrosine kinase inhibitor.
aAlthough IO plus chemotherapy is not currently indicated for the first-line treatment of patients with EGFR exon 20ins NSCLC, it is commonly prescribed to patients while waiting to receive next-generation sequencing (NGS) testing results for EGFR tumour aberrations. Refer to page 17 for more information on this treatment regimen.
Source: Product monographs for amivantamab, carboplatin, pemetrexed, afatinib, gefitinib, erlotinib, and pembrolizumab.53-59
Testing Procedure Considerations
The clinical experts consulted for this review confirmed that testing for EGFR exon 20ins mutations is currently done as routine care in patients with advanced nonsquamous NSCLC. Although the process varies across different provinces and territories, reflex testing for EGFR mutations, including exon 20ins, is the recommended standard of care in Canada.60,61 According to the clinical experts, depending on the jurisdiction, EGFR testing can be ordered directly by the pathologist (reflex testing), referred directly by the lab or pathologist to an external testing site (reflex referral), or ordered by a health care provider such as oncologist or surgeon.
Testing for EGFR exon 20ins mutations is conducted on tissue samples collected through biopsy as part of the routine diagnostic work-up. EGFR exon 20ins mutations can be identified by either polymerase chain reaction or next-generation sequencing (NGS) testing methods.60 NGS is the preferred method, since targeted polymerase chain reaction (PCR) may under-detect EGFR exon 20ins mutations.60,61 In instances where there is inadequate biopsy tissue available to test, NGS testing of cell-free circulating tumour DNA (ctDNA) drawn using a noninvasive blood sample could be a comparable alternative.61,62 However, the clinical experts consulted for this review pointed out that patients may have to pay out of pocket for ctDNA testing. According to the clinical experts, about 10% of nonsquamous NSCLC patients in Canada are tested for EGFR exon 20ins mutations by ctDNA analysis.
We considered the potential impacts of EGFR exon 20ins mutation testing to ascertain eligibility for the first-line treatment with amivantamab plus PC for locally advanced or metastatic NSCLC, including impacts to health systems, patients (including families and caregivers), and costs; these impacts are not anticipated to be substantial. Key considerations and relevant information available from materials submitted by the sponsor, input from the clinical experts consulted by the review team, and sources from the literature were validated by the review team and are summarized in Table 4.
Table 4: Considerations for EGFR Exon 20ins Mutation Testing for Establishing Treatment Eligibility for Amivantamab in Locally Advanced or Metastatic NSCLC
Consideration | Criterion | Available information |
|---|---|---|
Health system | Availability of the testing procedure in jurisdictions across Canada | According to the clinical experts, testing for EGFR exon 20ins mutations is broadly available as part of the current standard of care for locally advanced or metastatic NSCLC. In locations where genetic testing is not available, samples are shipped to larger centres for testing. |
Number of individuals in Canada expected to require the test (e.g., per year) | The clinical experts estimated that around 15,000 patients with locally advanced or metastatic nonsquamous NSCLC will be tested for EGFR mutations in Canada per year. Based on the materials provided by the sponsor, excluding Quebec, the number of patients undergoing testing is estimated to be around 10,300 annually.63, a However, because testing is already part of the standard of care for locally advanced or metastatic NSCLC, there is no additional impact to health systems anticipated as part of establishing treatment eligibility. | |
Testing procedure as part of routine care | According to the clinical experts, EGFR exon 20ins mutation testing is currently performed as part of the standard of care for locally advanced or metastatic NSCLC, almost always using NGS. | |
Repeat testing requirements | According to the clinical experts, testing for EGFR exon 20ins mutations does not need to be repeated. | |
Impact on health care human resources by provision of the testing procedure | Because testing for EGFR exon 20ins mutations is currently part of the standard of care for locally advanced or metastatic NSCLC and publicly funded across jurisdictions, use of the test result to establish treatment eligibility is not anticipated to substantially impact health care human resources. | |
Patient-oriented | Accessibility of the testing procedure in jurisdictions across Canada | Since EGFR exon 20ins mutation testing is part of the current standard of care for locally advanced or metastatic NSCLC in Canada, there is no additional impact of access anticipated from the testing as part of establishing treatment eligibility. |
Expected wait times for the testing procedure | According to the clinical experts, the wait time for EGFR exon 20ins mutation testing can be extremely variable, depending on the region of Canada, especially if the tissue has to be referred out for testing. There could be many delays from the time of biopsy to the receipt of mutational information by the oncologist, such as those related to the shipment of tissue and integration of results to the electronic medical records. However, there is no additional impact of wait times to patients anticipated as part of establishing treatment eligibility for amivantamab. | |
Burden associated with the testing procedure for patients, families, and/or caregivers | Because testing for EGFR exon 20ins mutations is currently part of the standard of care for locally advanced or metastatic NSCLC, there is no additional burden to patients, families, and/or caregivers anticipated from the testing as part of establishing treatment eligibility. | |
Clinical | Clinical utility of the testing procedure | There is evidence that demonstrates the diagnostic accuracy and clinical utility of NGS testing for EGFR exon 20ins mutations.60,64 |
Risks of harm associated with the testing procedure | Because testing for EGFR exon 20ins mutations is currently part of the standard of care for locally advanced or metastatic NSCLC, there is no additional risk of harm associated with the testing as part of establishing treatment eligibility. | |
Cost | Projected cost of the testing procedure | Because testing for EGFR exon 20ins mutations is currently part of the standard of care for locally advanced or metastatic NSCLC, there is no additional cost anticipated from the testing as part of establishing treatment eligibility. |
exon 20ins = exon 20 insertion; NGS = next-generation sequencing; NSCLC = non–small cell lung cancer.
aCDA-AMC have not evaluated or critically appraised this evidence to determine its validity or reliability.
Source: Sponsor’s Summary of Clinical Evidence.31
Perspectives of Patients, Clinicians, and Drug Programs
Patient Group Input
This section was prepared by the CDA-AMC review team based on the input provided by patient groups. The full patient and clinician group submissions received by CDA-AMC are available in the consolidated patient and clinician group input document for this review on the project website.
Patient Input
The patient input submission was jointly submitted by LCC, the CCSN, and the LHF. LCC serves as a leading resource for lung cancer education, patient support, research, and advocacy in Canada. The CCSN is a national network of patients, families, survivors, friends, community partners, funders, and sponsors who have come together to take action to promote the very best standard of care. The LHF (previously named the Ontario Lung Association) assists and empowers people living with or caring for others with lung disease. Nine patients with NSCLC provided inputs through virtual interviews by LCC and the CCSN. Among them, 7 patients were from Canada, 1 from the US, and 1 from the UK. All participants (n = 9) had experience with amivantamab. All data were collected between May and July in 2024.
Most (6 of 9) patients had stage 4 NSCLC, with metastases to bone, liver, lymph nodes, and/or brain when first diagnosed with NSCLC. Patient groups highlighted that the most common subsets of EGFR mutations include exon 19 deletion and exon 21 L858R mutations, while EGFR exon 20 mutations are much less common, with a frequency of roughly 0.1% to 4% in NSCLC. Patients with exon 20 mutations face a unique challenge as the mutation is insensitive to conventional TKIs and, thus, face a poorer prognosis, necessitating different treatment options. Platinum-doublet chemotherapy followed by single-drug docetaxel is the current standard of care for patients with EGFR-positive exon 20ins NSCLC. However, chemotherapy is limited as a viable long-term treatment option due to its nature as a systemic treatment with harsh and toxic side effects, which often creates additional burden on patients, leading to decreased function, poorer quality of life, and increased dependence on caregivers for daily activities. Immunotherapies, such as EGFR-specific TKIs, are available treatment options for patients with EGFR-positive exon 20ins NSCLC but have limited benefit, as patients may experience insensitivity. Additionally, radiotherapy, such as whole-brain radiation therapy, is effective in stabilizing brain metastases but may cause memory loss. Therefore, patient groups indicated that there is an urgent unmet need for novel treatment options for patients with EGFR-positive exon 20ins NSCLC. According to the patient group input, improved management of disease symptoms, quality of life, and survival, as well as delayed disease progression and manageable side effects, are considered important outcomes by patients with NSCLC. Generally, patients indicated that amivantamab was effective in stabilizing disease and maintaining quality of life with manageable side effects. The most common side effects reported were facial and scalp rashes, cuts on fingers and toes, paronychia, eye dryness, sensitivity to the sun, fatigue, skin sensitivity, and nausea. Other less common side effects noted by patients included low appetite, mild peripheral neuropathy, muscle aches, tinnitus, and gastrointestinal issues (constipation or diarrhea).
Clinician Input
Input From Clinical Experts Consulted by CDA-AMC
All CDA-AMC review teams include at least 1 clinical specialist with expertise regarding the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). The following input was provided by 2 clinical specialists with expertise in the diagnosis and management of NSCLC.
Unmet Needs
The clinical experts consulted by CDA-AMC on this review noted that chemotherapy is not well-tolerated and the benefit is modest and short-lived; not all patients respond to chemotherapy and most who do respond quickly become refractory. Targeted therapies with better efficacy are needed, as they directly target the underlying mechanisms of malignant proliferation. According to the clinical experts consulted for this review, the goals of therapy would be to prolong survival, delay time to progression of disease, and maintain maximum quality of life.
Place in Therapy
According to the clinical experts, amivantamab would be added to current standard doublet chemotherapy in the first-line setting, per the evidence from the PAPILLON trail.65 If a patient did not tolerate the cytotoxic chemotherapy component, that could be dropped, and the patient could continue on amivantamab monotherapy, as the mechanism is independent from that of chemotherapy. According to the clinical experts, this would preclude patients who do not tolerate chemotherapy from having to move on to a distinct second line of chemotherapy due to intolerance to first-line chemotherapy.
Patient Population
The clinical experts believed that the patients most suited to receive amivantamab would be those with an identified exon 20ins mutation, noting that testing for this mutation is widely available in Canada, although the wait time for EGFR exon 20ins mutation testing can be variable, depending on the region of Canada. One clinical expert noted that some jurisdictions are still struggling with timely testing results, meaning that mutation testing results are not available when a patient needs to start therapy. This clinical expert also noted that, if an exon 20ins mutation was identified after a patient had already started platinum-doublet chemotherapy, the patient should be allowed to add amivantamab at that point in time. The clinical experts noted that underdiagnosis may occur in settings with inadequate tissue for NGS testing; ctDNA testing may play a role to fill that gap.
Assessing the Response to Treatment
The clinical experts noted that tumour response is determined in clinical practice with serial physical and symptom assessments and serial radiography, typically with serial CT scans every 8 to 12 weeks during therapy or in the setting of new symptoms concerning disease progression during therapy. The clinical experts added that a meaningful response to treatment would involve a patient whose cancer is shrinking or has stopped growing, or even a rate of growth that has slowed significantly in the setting of a clinical benefit.
Discontinuing Treatment
The clinical experts believed that treatment should be discontinued when patients experience unacceptable toxicity despite appropriate supportive care and dose reductions, or significant progression of disease, or when patients choose to stop treatment.
Prescribing Considerations
With respect to setting, the clinical experts believed that amivantamab should be administered in systemic therapy units with experience in managing acute infusion reactions, under the supervision of a medical oncologist.
Clinician Group Input
This section was prepared by the CDA-AMC review team based on the input provided by clinician groups. The full patient and clinician group submissions received by CDA-AMC are available in the consolidated patient and clinician group input document for this review on the project website.
Two clinician groups submitted inputs, the LCC MAC and the OH-CCO Lung Cancer Drug Advisory Committee. In total, 32 clinicians from the LCC MAC and 7 clinicians from OH-CCO Lung Cancer Drug Advisory Committee provided input to the submissions.
The clinician groups agreed with the clinical experts consulted by CDA-AMC that, because of poor outcomes with current available treatments, there is a significant unmet need for novel targeted therapies with better efficacy. The clinician groups agreed with the clinical experts consulted by CDA-AMC that amivantamab plus carboplatin-pemetrexed should be used in the first-line setting, and clinicians from the OH-CCO Lung Cancer Drug Advisory Committee indicated that amivantamab plus carboplatin-pemetrexed can replace pembrolizumab or ipilimumab and/or nivolumab. All clinicians agreed that patients with EGFR exon 20ins mutations are best suited for treatment with amivantamab plus carboplatin-pemetrexed. Clinicians from the LCC MAC suggested radiological response assessments every 6 to 9 weeks, and clinicians from the OH-CCO Lung Cancer Drug Advisory Committee suggested response assessments every 9 to 12 weeks. All clinicians agreed that disease progression and unacceptable toxicities should be considered when deciding to discontinue treatment. All clinicians agreed that specialists with experience in using systemic therapy in cancer care are required for the treatment with amivantamab; outpatient cancer centres, satellite facilities, or hospitals would be appropriate settings.
Drug Program Input
The drug programs provide input on each drug being reviewed through the CDA-AMC reimbursement review processes by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CDA-AMC are summarized in Table 5.
Table 5: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Relevant comparators | |
The trial compared amivantamab + carboplatin-pemetrexed and with carboplatin-pemetrexed. The currently funded first-line treatments for patients with EGFR exon 20 insertion mutations are platinum-doublet chemotherapy (usually cisplatin or carboplatin-pemetrexed, followed by pemetrexed maintenance therapy). Is there evidence to inform the use of amivantamab in combination with alternative platinum-doublet chemotherapy options? | The clinical experts did not note any evidence for use of amivantamab with other platinum-doublet options. However, the clinical experts suggested that some clinicians might prefer to use cisplatin over carboplatin, which was felt to be reasonable, given that cisplatin has a similar side effect profile and efficacy as carboplatin. |
Considerations for initiation of therapy | |
The trial protocol specified nonsquamous NSCLC, and 99% of patients had adenocarcinoma. Please confirm the histological types of NSCLC that would be eligible for first-line combination with amivantamab. | The clinical experts believed that patients with nonsquamous histology should be eligible for first-line combination with amivantamab. In the absence of evidence for amivantamab + carboplatin-pemetrexed in patients with other histological types of NSCLC, generalizability of the PAPILLION study results to these patients remains uncertain. |
The trial protocol allowed neoadjuvant or adjuvant treatments only if given 12 months prior. If prior adjuvant or neoadjuvant treatment was given, what is the minimum disease-free interval to be eligible for first-line combination with amivantamab? | The clinical experts believed that 6 months would be the minimum disease-free interval to be eligible for first-line combination with amivantamab. |
The trial only included patients with ECOG PS 0 or 1. Patients with treated brain metastases were eligible if they were “asymptomatic, if their condition was clinically stable, and if they had received no glucocorticoid treatment for at least 2 weeks before randomization.” Should patients with ECOG PS greater than 1 be considered for first-line combination with amivantamab? Should patients with CNS disease be eligible for first-line combination with amivantamab, as outlined in inclusion criteria for the PAPILLON trail? | The clinical experts felt that patients with ECOG PS 2 would be eligible for amivantamab + carboplatin-pemetrexed, noting that in clinical trials the patient populations selected tend to be healthier than those seen in clinical practice. The clinical experts noted that they typically offer platinum-doublet therapy to patients with ECOG PS 2, and that the evidence does not suggest a noteworthy increase in harms when adding amivantamab to platinum-doublet therapy. Patients with untreated brain metastases were excluded from the PAPILLION trial. A total of 23.1% of participants had a history of brain metastasis. According to the clinical experts, patients with stable or treated metastases should be eligible for amivantamab. Further, the experts agreed that patients with unstable or new clinically relevant CNS metastasis should not be eligible to receive amivantamab before receiving treatment for the CNS metastases. However, the clinical experts cautioned to leave it up to the discretion of the treating clinician to apply some flexibility in identifying “clinically relevant” metastases. For instance, a patient may experience significant disease progression and at the same time have a new but small brain metastases which may not qualify for radiation. It would be reasonable to leave it up to the discretion of the treating clinician to initiate amivantamab in such a patient, according to the clinical experts. |
Considerations for discontinuation of therapy | |
In the trial, treatment beyond confirmed disease progression was allowed if the investigator deemed that the participant was deriving continued clinical benefit. What discontinuation criteria should be used for first-line combination therapy with amivantamab in clinical practice? | The clinical experts believed that patients who experience unacceptable toxicity despite appropriate supportive care and dose reductions, or significant progression, or those who choose to stop, should discontinue therapy. |
Considerations for prescribing of therapy | |
Amivantamab adds multiple treatment visits and pharmacy preparations to each treatment cycle versus comparators. Greater than or equal to 80 kg: 1,750 mg weekly for 4 weeks, then 2,100 mg once every 3 weeks starting at week 7, and continued until disease progression or unacceptable toxicity (week 1 dose given as split infusion on day 1 and day 2) Less than 80 kg: 1,400 mg weekly for 4 weeks, then 1,750 mg once every 3 weeks starting at week 7, and continued until disease progression or unacceptable toxicity (week 1 dose given as split infusion on day 1 and day 2) | This was a comment from the drug programs to inform pERC deliberations. |
Administration rates for amivantamab follow an escalation schedule for the first few doses (rates vary for 1,400 mg and 1,750 mg doses). These escalating infusion rate schedules will require additional monitoring by nursing staff. Target doses are administered over 2 hours at a fixed rate. The administration of the first dose is split over 2 days. This represents a notable increase in resources versus comparator therapies and has impacts on patients, the chemotherapy treatment room, and pharmacy. | This was a comment from the drug programs to inform pERC deliberations. |
The PAPILLON trial used chemotherapy for up to 4 cycles in combination with amivantamab. Should there be intolerance to chemotherapy before completion of 4 cycles, can amivantamab be continued as monotherapy? | The clinical experts believed that, if there is intolerance to chemotherapy before completion of 4 cycles, amivantamab can be continued as monotherapy, noting that the mechanism of amivantamab is distinct from that of cytotoxic chemotherapy, and that there is evidence for its use as monotherapy from second-line trials. |
Generalizability | |
On a time-limited basis, for patients who are currently receiving first-line therapy or who have recently completed first-line therapy, should amivantamab in combination with platinum-doublet chemotherapy be funded for patients, provided that disease progression has not occurred to alternative first-line therapy? | The clinical experts believed that yes, amivantamab + carboplatin-pemetrexed should be funded for patients who have not progressed on their previous first-line therapy on a time-limited basis. |
Funding algorithm | |
Are patients eligible for amivantamab if they received EGFR TKI therapy for a duration of less than 8 weeks with a documented lack of response? What are the subsequent treatment options after patients progress on amivantamab? | The clinical experts believed that patients should be eligible for amivantamab + carboplatin-pemetrexed if they previously had a documented lack of response to an EGFR TKI, because these drugs work by a different mechanism. If any resistance had developed, this should not impact the efficacy of amivantamab. The clinical experts believed that most patients would receive chemotherapy (single-drug docetaxel) as subsequent treatment. |
Care provision issues | |
Available as 350 mg vials. Recommended doses and dose adjustments correspond to available vial size and should minimize wastage. The product monograph indicates a need to withdraw a volume from the infusion bag equal to the volume of drug being added, and the volume in the infusion bag should be 250 mL. It is extra work to ensure a final volume of exactly 250 mL. | This was a comment from the drug programs to inform pERC deliberations. |
Additional therapies may be required for the management of skin toxicities (e.g., emollient creams, topical corticosteroids, oral or IV antibiotics, oral steroids). | This was a comment from the drug programs to inform pERC deliberations. |
Companion diagnostics (e.g., access issues, timing of testing). Timely confirmation of EGFR exon 20 insertion mutation is needed to confirm eligibility. What method of testing should be used for detection of EGFR exon 20 insertion mutations? In the event the patient has already started alternative systemic therapy before the exon 20 insertion mutation results are available, can the patient be switched to amivantamab + carboplatin-pemetrexed? | The clinical experts noted that NGS testing is the current standard. However, there are emerging technologies, such as rapid tests, that are being used in some jurisdictions. The clinical experts believed that it would be reasonable to allow patients who have had already started alternative systemic therapy to switch to amivantamab + carboplatin-pemetrexed once their status is confirmed. |
System and economic issues | |
There are confidential prices for comparators (chemotherapy). | This was a comment from the drug programs to inform pERC deliberations. |
CNS = central nervous system; ECOG PS = Eastern Cooperative Oncology Group Performance Status; NGS = next-generation sequencing; NSCLC = non–small cell lung cancer; pERC = pan-Canadian Oncology Review Expert Review Committee; TKI = tyrosine kinase inhibitor.
Clinical Evidence
The objective of the CDA-AMC Clinical Review report is to review and critically appraise the clinical evidence submitted by the sponsor on the beneficial and harmful effects of amivantamab in the first-line treatment of adult patients with locally advanced (not amenable to curative therapy) or metastatic NSCLC in patients with activating EGFR exon 20ins mutation. The focus will be placed on assessment of comparative effectiveness and safety comparing amivantamab to relevant comparators, including identifying gaps in the current evidence.
A summary of the clinical evidence included by the sponsor in the review of amivantamab is presented in 4 sections, with the CDA-AMC critical appraisal of the evidence included at the end of each section. The first section, the systematic review, includes pivotal studies and RCTs that were selected according to the sponsor’s systematic review protocol. The CDA-AMC assessment of the certainty of the evidence in this first section using the GRADE approach follows the critical appraisal of the evidence. The second section included indirect evidence from the sponsor; the sponsor submitted an ITC report that used individual patient data for both arms. This was considered as a nonrandomized study by the review team and presented in the Studies Addressing Gaps section. No long-term extension studies were submitted.
Included Studies
Clinical evidence from the following are included in the CDA-AMC review and appraised in this document:
1 pivotal RCT identified in systematic review
1 study addressing gaps in the systematic review evidence (submitted by the sponsor as an ITC report).
Systematic Review
Contents in this section have been informed by materials submitted by the sponsor. The following have been summarized and validated by the CDA-AMC review team.
Description of Studies
Characteristics of the included studies are summarized in Table 6.
The PAPILLON trial is an ongoing, phase III, multicentre, open-label trial conducted in 131 centres across 25 countries, including 3 sites in Canada. Patients were 18 years of age or older, with treatment-naive EGFR exon 20ins mutated locally advanced or metastatic NSCLC. The primary objective of the study was to assess the efficacy of amivantamab plus carboplatin-pemetrexed compared with carboplatin-pemetrexed in the first-line treatment of patients with EGFR exon 20ins mutated NSCLC. A total of 308 patients were randomized 1:1 to either the amivantamab plus carboplatin-pemetrexed or carboplatin-pemetrexed arm using an interactive web response system, from December 2020 to November 2022. The clinical cut-off date for data inclusion was May 2023. A screening period 28 days before randomization was used to ensure study eligibility, which was assessed through a baseline radiographic assessment of disease sites and a review of test results and/or tumour biopsy to confirm EGFR exon 20ins mutation status. The treatment phase for each patient started at cycle 1 day 1 and continued in 21-day cycles until the end of treatment visit (approximately 30 days after discontinuation of study treatment).
Eligible patients in the carboplatin-pemetrexed arm who experienced disease progression were given the option to enter the crossover phase and receive amivantamab monotherapy in 21-day cycles (described in additional detail in Appendix 3). Patients discontinued study treatment for documented radiographic disease progression (confirmed by BICR, according to Response Evaluation Criteria in Solid Tumours [RECIST] v1.1) or if they met another criterion for discontinuation of study treatment. Patients who discontinued assigned study treatment were followed for subsequent therapy, disease status, survival, and symptomatic progression in the follow-up phase. This phase started after the end of treatment visit and continued until the end of the study, death, loss to follow-up, or withdrawal of consent from participation in the study, whichever came first (refer to Figure 1 for a schematic overview of the study design).
Figure 1: Schematic Overview of the PAPILLON Study Design
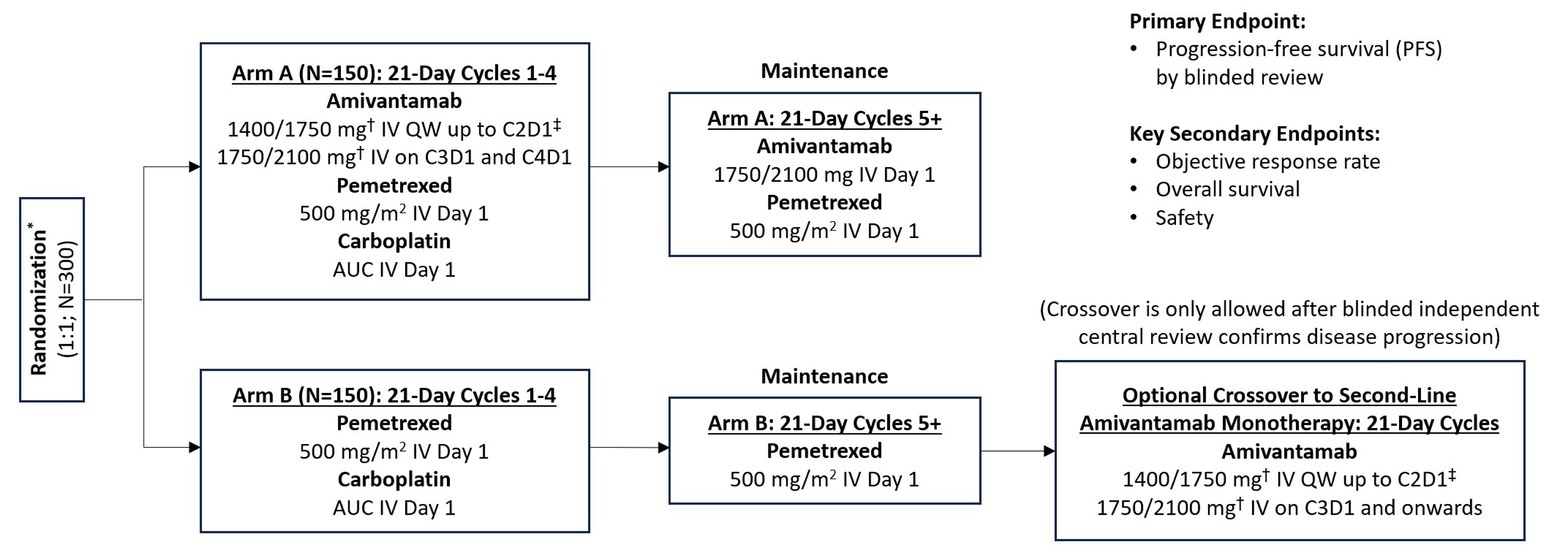
AUC = area under the curve; C2D1 = cycle 2 day 1; C3D1 = cycle 3 day 1; C4D1 = cycle 4 day 1; QW = once weekly.
* Stratification factors: Brain metastases (yes or no); ECOG PS (0 or 1); prior EGFR TKI use (yes or no).
† Doses shown by body weight (< 80 kg/≥ 80 kg).
‡ Cycle 1: first dose split between days 1 and 2, then doses on days 8 and 15; cycle 2: day 1.
Table 6: Details of Studies Included in the Systematic Review
Detail | PAPILLON |
|---|---|
Designs and populations | |
Study design | Phase III, open-label RCT |
Locations | 131 centres across 25 countries: Australia, Belgium, Brazil, Canada, China, France, Germany, Hungary, India, Israel, Italy, Japan, Malaysia, Mexico, Poland, Portugal, Russian Federation, South Korea, Spain, Taiwan, Thailand, Türkiye, Ukraine, UK, US. Canada had 3 study sites. |
Patient enrolment dates | Start date: December 2020 End date: Study is ongoing. CCO: May 2023 |
Randomized (N) | N = 308 ACP: N = 153 CP: N = 155 |
Inclusion criteria |
|
Exclusion criteria |
|
Drugs | |
Intervention |
|
Comparator(s) |
|
Study duration | |
Screening phase | Up to 28 days before randomization. |
Treatment phase | Started cycle 1 day 1 and continued in 21-day cycles until approximately 30 days after discontinuation of study treatment, due to either documented radiographic (RECIST v1.1) disease progression (confirmed by the blinded independent central review [BICR]), or if another criterion for discontinuation of study treatment was met. |
Follow-up phase | Began 30 days after the discontinuation of treatment and continued until the end of study, death, loss to follow-up, or withdrawal of consent from participation in the study, whichever came first. |
Outcomes | |
Primary end point | The primary end point was PFS by BICR, defined as the time from randomization until the date of objective disease progression based on RECIST v1.1 or death (by any cause), whichever comes first. This was evaluated using the full analysis set. |
Secondary and exploratory end points | Key secondary:
Secondary outcomes:
Key exploratory:
|
Publication status | |
Publications | Zhou et al. (2023)66 NCT04538664 |
ACP = amivantamab + carboplatin-pemetrexed; AUC = area under the curve; BICR = blinded independent central review; CCO = clinical cut-off date; CP = carboplatin-pemetrexed; DOR = duration of response; ECOG = Eastern Cooperative Oncology Group; EORTC QLQ-C30 = European Organization for the Research and Treatment of Cancer Quality of Life Questionnaire Core 30; exon 20ins = exon 20 insertion; ILD = interstitial lung disease; NSCLC = non–small cell lung cancer; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; PFS2 = progression-free survival after first subsequent therapy; PRO = patient-reported outcomes; PROMIS PF = Patient-Reported Outcomes Measurement Information System — Physical Function; RECIST = Response Evaluation Criteria in Solid Tumours; RCT = randomized controlled trial; TTD = time to discontinuation; TTSP = time to symptomatic progression; TTST = time to subsequent therapy.
Note: 2 additional reports were included (CSR for PAPILLON, sponsor submission to CDA-AMC).
Source: Details included in the table are from the sponsor’s Summary of Clinical Evidence.31
Populations
Inclusion and Exclusion Criteria
Key inclusion criteria include patients 18 years of age or older, with histologically or cytologically confirmed, locally advanced or metastatic, nonsquamous NSCLC with documented primary EGFR exon 20ins mutations, measurable disease according to RECIST v1.1, ECOG PS 0 or 1, and adequate organ and bone marrow function. Key exclusion criteria include having received any prior systemic treatment for locally advanced or metastatic disease, with evidence of synchronous NSCLC disease, or with untreated brain metastases.
Interventions
Patients in the amivantamab plus carboplatin-pemetrexed arm received the following study treatment:
amivantamab 1,400 mg (1,750 mg if body weight is ≥ 80 kg) by IV infusion once weekly through cycle 1 (day 1 on weeks 1, 2, and 3) and on cycle 2 day 1 (day 1 week 4); then 1,750 mg (2,100 mg if body weight is ≥ 80 kg) on day 1 of each 21-day cycle, starting at week 7 (cycle 3 day 1)
pemetrexed 500 mg/m2 (with vitamin supplementation) on day 1 of each 21-day cycle, in combination with carboplatin for up to 4 cycles, and then as maintenance monotherapy until disease progression
carboplatin area under the curve (AUC) 5 on day 1 of each 21-day cycle, for up to 4 cycles.
The entire regimen was infused in an outpatient chemotherapy suite and took between 2 and 6 hours depending on cycle, day, and dose. Patients in the carboplatin-pemetrexed arm received the following study treatment:
pemetrexed 500 mg/m2 (with vitamin supplementation) on day 1 of each 21-day cycle, in combination with carboplatin for up to 4 cycles, and then as maintenance monotherapy until disease progression
carboplatin AUC 5 of day 1 of each 21-day cycle, for up for 4 cycles.
Assigned study treatment was continued until documented radiographic (RECIST v1.1) disease progression, confirmed by BICR or another criterion for discontinuation, was met. Continuation of study treatment after confirmed disease progression was allowed after approval from the medical monitor, if the investigator believed the participant was deriving clinical benefit.
Patients in the carboplatin-pemetrexed group were allowed to switch to amivantamab monotherapy once they had progressed, referred to as the crossover phase. All participants in the crossover phase received amivantamab in 21-day cycles at a dose of 1,400 mg (1,750 mg if body weight ≥ 80 kg) by IV infusion once weekly up to cycle 2 day 1, then 1,750 mg (2,100 mg if body weight ≥ 80 kg) on day 1 of each 21-day cycle, starting with cycle 3.
Participants who discontinued assigned study treatment for any reason were followed for subsequent therapy, disease status, survival, and symptomatic progression in the follow-up phase. For the secondary end points related to subsequent therapy, a crossover from carboplatin-pemetrexed to amivantamab monotherapy was also considered as initiation of a subsequent systemic therapy.
Throughout the study, investigators were allowed to prescribe any concomitant medications or treatments deemed necessary to provide adequate supportive care, except for those listed as prohibited therapies. Prohibited therapies included any chemotherapy, anticancer therapy, experimental therapies, radiotherapy to tumour lesions being assessed for response, phenytoin or phosphenytoin (with carboplatin), and live or attenuated vaccines. Medications that were permitted (with caution) included concurrent use of a nonsteroidal anti-inflammatory with pemetrexed in patients with creatinine clearance less than 80 mL/min, ibuprofen specifically, within 2 days (before or after) of administration of pemetrexed, and any drug that may decrease serum magnesium, due to the hypomagnesemia that can occur with EGFR inhibitors.
There were both required and optional concomitant medications given specifically with amivantamab to prevent infusion-related reactions. The required medications were IV glucocorticoids (cycle 1 day 2), IV or oral antihistamines (before amivantamab infusion), and IV or oral antipyretics (before amivantamab infusion). Optional medications included IV or oral glucocorticoids (cycle 1 day 8 and onwards), IV histamine H2-receptor antagonists (any cycle), and antiemetics (ondansetron oral or IV, any cycle). The pre- and postinfusion medications given for chemotherapy included corticosteroids, folic acid, and vitamin B12, given concomitantly with pemetrexed.
Outcomes
A list of efficacy end points assessed in this Clinical Review Report is provided in Table 7, followed by descriptions of the outcome measures. Summarized end points are based on outcomes included in the sponsor’s Summary of Clinical Evidence as well as any outcomes identified as important to this review, according to the clinical expert(s) consulted by CDA-AMC and patient, clinician, and drug program input. Using the same considerations, the CDA-AMC review team selected end points that were considered to be most relevant to inform the CDA-AMC expert committee deliberations and finalized this list of end points in consultation with members of the expert committee. All summarized efficacy end points were assessed using GRADE. Select notable harms outcomes considered important for informing the CDA-AMC expert committee deliberations were also assessed using GRADE. Based on the input received, PFS, OS, ORR, and HRQoL were identified as important outcomes. The clinical experts consulted for this review selected these end points based on their relevance to patients and their use in making treatment decisions. For HRQoL, the EORTC QLQ-C30 GHS was chosen as the outcome to assess with GRADE as the clinical experts believed it to be a key HRQoL measure with relevance to patients. Patient-Reported Outcomes Measurement Information System — Physical Function (PROMIS PF) total score was included in the Appendix 1 of this Clinical Review Report in support of patients’ HRQoL. The time points chosen to perform GRADE analyses were chosen to balance the need to obtain as late a follow-up as possible (particularly for outcomes like OS and PFS) with the reality that, at these later time points, very few patients remain at risk, therefore limiting any conclusions that can be drawn from these data. The clinical experts believed that rash and infusion-related reactions were key notable harms.
Progression-Free Survival
The primary end point was PFS, defined as the time from randomization until the date of objective disease progression (based on BICR using RECIST v1.1) or death (by any cause), whichever comes first. Participants who had not progressed or died at the time of analysis were censored at the time of the latest date of their last evaluable RECIST v1.1 assessment. If the participant progressed or died after 2 or more consecutive missed disease assessments, the participant was censored at the time of the last evaluable RECIST v1.1 assessment. If the participant had no evaluable visits or did not have any baseline data, they were censored at day 1, unless they died within 2 visits of baseline. Radiographic disease progression was assessed during imaging at regular 6-week intervals. The sponsor is not aware of a reported MID specific to the EGFR exon 20ins population.
PFS After First Subsequent Therapy 2
PFS2 by investigator was defined as the time from randomization until the date of second objective disease progression, after initiation of subsequent anticancer therapy, based on investigator assessment (after that used for PFS) or death, whichever came first. The sponsor is not aware of a reported MID specific to the EGFR exon 20ins population.
Objective Response Rate
ORR was defined as the proportion of participants who achieved either a complete response or partial response, as defined by BICR using RECIST v1.1. Data obtained up until progression or last evaluable disease assessment in the absence of progression was included in the assessment of ORR. However, any complete response or partial response that occurred after a further anticancer therapy was received was not included in the numerator for the ORR calculation. Participants who did not have a tumour response assessment for any reason were considered nonresponders and were included in the denominator when calculating the response rate. The sponsor is not aware of a reported MID specific to the EGFR exon 20ins population.
Overall Survival
OS was defined as the time from the date of randomization until the date of death due to any cause. Any participant not known to have died at the time of analysis was censored based on the last recorded date on which the participant was known to be alive. The sponsor is not aware of a reported MID specific to the EGFR exon 20ins population. The clinical experts consulted by the review team considered a 5% between-group difference as the smallest clinically important difference.
European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30
EORTC QLQ-C30 is used to measure self-reported functioning for all cancer types in patients with cancer. It includes 30 items resulting in 5 functional scales (physical functioning, role functioning, emotional functioning, cognitive functioning, and social functioning), 1 GHS and quality of life scale, 3 symptom scales (fatigue, nausea and vomiting, and pain), and 6 single items (dyspnea, insomnia, appetite loss, constipation, diarrhea, and financial difficulties). The instrument contains 28 items using a verbal rating scale with 4 response options: “Not at All,” “A Little,” “Quite a Bit,” and “Very Much” (scored 1 to 4). Two additional items use response options (1 to 7): 1 = Very Poor to 7 = Excellent. All scale and item scores were linearly transformed to be in the range from 0 to 100 according to the algorithm in EORTC QLQ-C30 scoring manual, version 3.0.67 A higher score represents a higher (“better”) level of functioning, or a higher (“worse”) level of symptoms. This was measured as change from baseline and time to deterioration for symptom, GHS, and physical functioning scores. The meaningful worsening threshold for time to deterioration in the PAPILLON trail was specified by the sponsor as an increase of 10 points or more for symptom scales and a decrease of 10 points or more for health status and functioning scales.
PROMIS PF Short Form V2.0
Another measure of patient-reported outcomes supportive of HRQoL outcomes in the target patient population was the PROMIS PF short form. In the presence of survival and EORTC QLQ-C30 data, this instrument was not considered to be most critical to guide treatment selection in clinical practice. Results are included in Appendix 1 and not assessed with GRADE. For a description of the measure and its meaningful worsening threshold identified in the literature, please refer to Table 8.
Safety Evaluation Plan
The verbatim terms used in the case report form by investigators to identify AEs were coded using the Medical Dictionary for Regulatory Activities (MedDRA) Version 25.0. Any AE occurring at or after the initial administration of study treatment through the day of last dose plus 30 days or until the start of subsequent anticancer therapy (if earlier) was considered to be treatment-emergent. Treatment-related AEs were those judged by the investigator to be at least possibly related to the study medication. Patients with multiple occurrences of events were only counted once at the maximum severity to study medication for each preferred team, system organ class, and overall. Deaths that occurred within 30 days after the last dose of study medication were defined as on-study deaths.
Data for PFS2 were also summarized in the main section of the report because the clinical experts believed this outcome to be of some relevance in the population. However, a GRADE assessment was not performed because this was not considered an outcome of critical importance for decision-making.
Table 7: Outcomes Summarized From the Studies Included in the Systematic Review
Outcome measure | Time point | PAPILLON |
|---|---|---|
PFSa | 6 months | Primary |
12 months | ||
18 months | ||
OSa | 12 months | Key secondary |
18 months | ||
24 months | ||
ORRa | Data cut-off | Key secondary |
HRQOL — EORTC QLQ-C30 | 12 months | Secondary |
PFS2 | Data cut-off | Secondary |
Notable harms — rash | End of treatment | Safety |
Notable harms — infusion reactions | End of treatment | Safety |
EORTC QLQ-C30 = European Organization for the Research and Treatment of Cancer Quality of Life Questionnaire Core 30; HRQoL = health-related quality of life; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; PFS2 = progression-free survival after first subsequent therapy.
aStatistical testing for these end points was adjusted for multiple comparisons (e.g., hierarchal testing).
Source: Details included in the table are from the sponsor’s Summary of Clinical Evidence.31
Table 8: Summary of Outcome Measures and Their Measurement Properties
Outcome measure | Type | Conclusions about measurement properties | MID |
|---|---|---|---|
EORTC QLQ-C30 | Self-reported HRQoL questionnaire that includes 30 items used to assess functioning domains and common cancer symptoms with recall in the past week.68 All scale and item scores are linearly transformed to be in the range from 0 to 100 in accordance with the scoring manual version 3.0.67 A higher score represents a higher (better) level of functioning on the functioning scales or a higher (worse) level of symptoms on the symptom scales. | Validity Results support the EORTC QLQ-C30 as a valid measure of the quality of life of a typical cancer patient.69 All interscale correlations were moderate, indicating that the scales were assessing distinct components of the quality of life construct. Most of the functional and symptom measures discriminated clearly between patients differing in clinical status, as defined by the Eastern Cooperative Oncology Group Performance Status scale, weight loss, and treatment toxicity. Reliability Scales of the QLQC30 have good test–retest reliability.69 Internal consistency is supported by Cronbach alphas > 0.8.70 Responsiveness The QLQ-C30 is responsive to the effects of cancer treatment. Studies show strong correlations between changes in performance status and changes in QLQ-C30 domains in the expected directions.70,71 | The MID threshold of 10 points was originally established with patients with breast cancer or small cell lung cancer and was subsequently supported in studies with patients with other types of cancer, including non–small cell lung cancer.29,30 |
PROMIS PF short form v2.0 (8c 7-day version) | The Patient-Reported Outcomes Measurement Information System — Physical Function (PROMIS PF) short form v2.0 (8c [8 item] 7-day version) is used to assess level of physical ability and conduct of activities of daily living.72 The form includes 8 items relevant to cancer patients. It is scored using the sum score to scale score conversion table in the PROMIS physical function scoring manual.73 All 8 items must be nonmissing to compute the score. The scale for PROMIS PF 8c ranges from 15 (lowest functioning) to 61.3 (highest functioning). | Validity PROMIS PF short forms showed convergent validity (Fatigue, Pain Interference, FACT Physical Well-Being all r ≥ 0.68) and discriminant validity (unrelated domains all r ≤ 0.3) across survey short forms, age, and race-ethnicity.74 Known group differences by demographic, clinical, and functional characteristics performed as hypothesized. Reliability PROMIS PF short forms showed high internal consistency (Cronbach alpha = 0.92 to 0.96).74 Responsiveness: Clinical trial data showed that the PROMIS PF 8c is responsive to change. Change correlations between PROMIS PF 8c scores and other PRO measure variables all conformed to expectations.75 The strongest correlations were found with the EORTC QLQ-C30 Physical Function variable, as expected.76 | The meaningful worsening threshold was estimated to be a decrease of 6 to 7 points, using data from patients with advanced non–small cell lung cancer.75 |
EORTC QLQ-C30 = European Organization for the Research and Treatment of Cancer Quality of Life Questionnaire Core 30; HRQoL = health-related quality of life; MID = minimal important difference; PF = physical function; PRO = patient-reported outcomes.
Statistical Analysis
Sample Size and Power Calculation
The total sample size needed for the PAPILLON trail was approximately 300 participants (150 per group). This was calculated given that a total of 200 PFS events would provide approximately 90% power to detect a hazard ratio (HR) of 0.625 at a 2-sided alpha level of 0.05. This estimation corresponded to an extension of at least 3 months in the median PFS, which was estimated at 8 months in the amivantamab plus carboplatin-pemetrexed group and 5 months in the carboplatin-pemetrexed group. The basis for these estimates was not reported. The sample size calculation took into consideration an annual dropout rate of 5%.
Statistical Test or Model
In the PAPILLON trail, all primary and secondary efficacy end points were analyzed using the full analysis set.
The primary end point (PFS by BICR) was analyzed using a log-rank test at the overall 2-tailed significance level of 0.05. The log-rank test was stratified by ECOG PS (0 or 1) and history of brain metastases (yes or no) using the Breslow approach for handling ties. The Kaplan-Meier product limit was used to estimate the median PFS, and a stratified Cox model using the same stratification factors as the log-rank test was used to estimate the HR, along with the associated 95% CIs. The proportional hazards assumption was examined by plotting log(-log[estimated survival distribution function]) against log(survival time). In addition, a treatment by logarithm-transformed time interaction term was added into the primary Cox model and tested. A P value greater than 0.05 for the interaction term was interpreted as no statistical evidence against the proportional hazards assumption.
Multiple Testing Procedure
A hierarchical fixed-sequence testing strategy was used to control the overall type I error rate for hypotheses testing of primary and key secondary end points ORR and OS at 5%. If the testing for the primary end point of PFS was statistically significant, key secondary end points, including ORR and OS, were sequentially tested, with an overall 2-sided alpha of 0.05. The test for ORR was to be conducted before the test for OS.
Based on the O’Brien Fleming alpha spending approach, a 2-sided alpha of 0.0008 was allocated to the interim analysis, approximately 48 months after the first participant was randomized, when approximately 210 deaths overall are anticipated. The final analysis will be conducted at a 2-sided alpha of 0.0498.
Data Imputation Methods
No imputation method was used for handling missing or incomplete data.
Subgroup Analyses
Prespecified subgroup analyses were performed for the efficacy and/or safety end points. Only the subgroup data reported for the primary outcome was of interest for this report. The following subgroups were used:
age group (< 65 years, ≥ 65 years; < 75 years, ≥ 75 years)
sex (male, female)
race (Asian, non-Asian)
weight (< 80 kg, ≥ 80 kg)
history of brain metastasis (yes, no)
ECOG PS (0, 1)
history of smoking (yes, no).
HRs with 95% CI were reported for each of the individual subgroups. However, no P values were reported and no tests for interactions appeared to have been performed.
Sensitivity Analyses
The sensitivity analyses performed for the primary outcome included an unstratified log-rank test and an assessment of the proportional hazards assumption by plotting log (-log[estimated survival distribution function]) against log (survival time). Additionally, a treatment by logarithm-transformed time interaction term was added into the primary Cox model and tested. A P value greater than 0.05 for the interaction term was interpreted as no statistical evidence against the proportional hazards assumption. An additional sensitivity analysis, which used investigator assessments for radiographic progression, does not appear to have been prespecified.
Secondary Outcomes
The secondary end point of ORR was analyzed using a logistic regression model at the overall 2-tailed significance level of 0.05 and stratified by ECOG PS (0 or 1) and history of brain metastases (yes or no). Results were presented as an OR with its associated 95% CIs.
The secondary end point of OS was tested sequentially following significance of PFS and ORR end points. OS was tested with a nonstratified log-rank test as the primary analysis and a sensitivity analysis using a stratified log-rank test (using the same methodology and model as for the analysis of PFS). The analysis of OS was a priori planned to be conducted at 2 time points: (1) at the time of the primary analysis of PFS, when approximately 85 deaths overall were anticipated, and (2) approximately 48 months after the first patient was randomized, when about 210 deaths overall are anticipated. To try to account for the large number of crossovers, the sponsor performed 3 different sensitivity analyses specifically for OS: IPCW, TSE methods, and RPSFT models. IPCW artificially censors patients whose NSCLC had progressed when they switched from carboplatin-pemetrexed to amivantamab, and the remaining observations from patients whose NSCLC had not yet progressed when they switched to amivantamab are upweighted to represent the censored patients. This weighting process aims to account for the similarities in baseline and time-varying factors between the patients whose NSCLC had progressed who were censored and those who were not, thereby mitigating the selection bias caused by censoring. In the TSE method, the impact of crossover is estimated by comparing those patients who crossed over to those who did not after a disease-related secondary baseline. The TSE method uses a parametric survival regression model to estimate the effect of crossover by accounting for confounders (baseline and at secondary baseline) as covariates and is therefore reliant upon the “no unmeasured confounding” assumption. RPSFT uses a counterfactual framework to estimate the causal effect of the intervention. It uses the g-estimation method and assumes that the treatment effect in those who crossed over is the same as those who were originally assigned to the intervention. The estimated treatment effect (in terms of time shrinkage) is later applied to adjust for the benefit that those who crossed over obtained from receiving the active treatment, to remove the impact of crossover on the observed results.
The remaining secondary end points, including PFS2, were analyzed using the same methodology and model as for the analysis of PFS. For end points related to subsequent therapy, a crossover from the carboplatin-pemetrexed arm to amivantamab monotherapy was also considered as an initiation of a subsequent systemic therapy.
For EORTC QLQ-C30 domain scores and the PROMIS Physical Function Tscore, descriptive statistics were reported at baseline and at each visit for absolute value and for change from baseline. Statistical tests were not adjusted for multiplicity. All P values were nominal. Instrument level compliance for patient-reported outcomes was summarized for patients expected to complete patient-reported outcome assessments at each time point. The change of scores from baseline over time was assessed using a mixed-effects model for repeated measures analysis based on restricted maximum likelihood. The model included participants as a random effect and baseline value, treatment group, time in week, treatment-by-time interaction, and stratification factors as fixed effects. The treatment comparison was based on the least squares means, and the 2-sided 95% CI was estimated. Randomized participants who received at least 1 dose of study treatment and had at least 1 evaluable postbaseline measurement were included in the analysis.
With respect to harms, all reported TEAEs were included in the analysis. For each AE, the number and percentage of patients who experienced at least 1 occurrence of the given event were summarized by treatment arm. For each treatment group, AE incidence rates were summarized with frequency and percentage by system organ class and preferred term, with all patients treated in that treatment group as the denominator, unless otherwise specified. In addition, AE incidence rates were summarized by severity and relationship to study medication.
Analysis Populations
Refer to Table 9 for analysis populations in the PAPILLON trail.
Table 9: Analysis Populations of PAPILLON
Population | Analysis | Number analyzed | Definition | Application |
|---|---|---|---|---|
Full analysis set | Study population Efficacy | ACP arm: n = 153 CP arm: n = 155 | All randomized participants, classified according to their assigned treatment arm, regardless of the actual treatment received | Used to summarize the population characteristics as well as the efficacy data |
Safety analysis set | Safety | ACP arm: n = 151 CP arm: n = 155 | Randomized participants who received at least 1 dose of study treatment | Used to summarize the safety data |
ACP = amivantamab + carboplatin-pemetrexed; CP = carboplatin-pemetrexed.
Source: PAPILLON Clinical Study Report.33
Results
Patient Disposition
There were more patients in the carboplatin-pemetrexed group who discontinued treatment compared to amivantamab plus carboplatin-pemetrexed (84.5% versus 52.9%), with the most common reason being disease progression (69.0% versus 33.1%) (Table 10). A total of █████ of patients in the carboplatin-pemetrexed group crossed over to amivantamab monotherapy, as was allowed in the protocol. An additional 6 patients in the carboplatin-pemetrexed group crossed over to amivantamab monotherapy off protocol. All patients who crossed over were treated in the crossover phase.
Baseline Characteristics
The baseline characteristics outlined in Table 11 are limited to those that are most relevant to this review or were felt to affect the outcomes or interpretation of the study results.
Patients in the PAPILLON trail were 60 years of age, on average, and the majority were female (57.8%) and had no smoking history (58%). There were 65% of patients with an ECOG PS of 1 (the remainder had an ECOG PS of 0), and the majority of patients (77%) had no history of brain metastases. Almost all patients had adenocarcinoma (98.7%) and had not used prior EGFR inhibitors (99% each). Almost all patients were either stage IVA (███) or IVB (███) at screening. ███ patients had prior surgery for lung cancer and ███ had prior radiotherapy. Although there were some differences in specific baseline characteristics between amivantamab plus carboplatin-pemetrexed and carboplatin-pemetrexed groups (location of metastasis at screening, time since diagnosis, histology, and prior radiotherapy), the clinical experts consulted by CDA-AMC on this review did not believe them to be clinically relevant.
Table 10: Summary of Patient Disposition From PAPILLON
Patient disposition | ACP (N = 153) | CP (N = 155) |
|---|---|---|
Screened, N | 542 | |
Screening failure, N (%) | 234 (43.2) | |
Reason for screening failure | ||
Met exclusion criteria | 130 (24.0) | |
Did not meet inclusion criteria | 104 (19.2) | |
Other | 4 (0.7) | |
Adverse event | 1 (0.2) | |
Lost to follow-up | 1 (0.2) | |
Randomized, N (%) | 153 (100.0) | 155 (100.0) |
Randomized but not treated, N (%) | 2 (1.3) | 0 (0.0) |
Patients treated, N (%) | 151 (98.7) | 155 (100.0) |
Discontinued all study treatment, N (%) | 81 (52.9) | 131 (84.5) |
Reason for discontinuation,a,b N (%) | ||
Progressive disease | 50 (33.1) | 107 (69.0) |
Adverse event | 14 (9.3) | 14 (9.0) |
Adverse event — COVID-19-related | 2 (1.3) | 0 (0.0) |
Patient refused further study treatment | 12 (7.9) | 5 (3.2) |
Noncompliance with study drug | 1 (0.7) | 2 (1.3) |
Death | 1 (0.7) | 1 (0.6) |
Physician decision | 1 (0.7) | 0 (0.0) |
Other | 2 (1.3) | 2 (1.3) |
Discontinued study, n (%) | ██ ██████ | | ██████ |
Reason for discontinuation | ||
Withdrawal by patient | | ██████ | | ██████ |
Lost to follow-up | | ██████ | | ██████ |
Patients ongoing,b N (%) | ██ ██████ | 24 (15.5) |
FAS, N (%) | ███ ███████ | 155 (100.0) |
PP, N (%) | ███ ███████ | 155 (100.0) |
Crossover to amivantamab monotherapy, N (%) (65 patients on protocol and 6 patients off protocol crossed over) | NA | 71 (████) |
Safety, N (%) | 151 (98.7) | 155 (100.0) |
ACP = amivantamab + carboplatin-pemetrexed; CP = carboplatin-pemetrexed; FAS = full analysis set; NA = not applicable; PP = per protocol.
aThe reason for discontinuation for all study treatment is the reason for discontinuation for the last study treatment received.
bNumbers and percentages represent analysis conducted on safety analysis set.
Source: Details included in the table are from the sponsor’s Summary of Clinical Evidence.31
Table 11: Summary of Baseline Characteristics From PAPILLON, FAS
Characteristic | ACP (N = 153) | CP (N = 155) |
|---|---|---|
Age, years | N = 153 | N = 155 |
Mean (SD) | ████ ███████ | ████ ███████ |
Median | 61.0 | 62.0 |
Range | 27 to 86 | 30 to 92 |
Age category, n (%) | ||
18 to 25 | ██ | ██ |
26 to 50 | ██ ██████ | ██ ██████ |
51 to 64 | ██ ██████ | ██ ██████ |
65 to 74 | ██ ██████ | ██ ██████ |
≥ 75 | ██ █████ | ██ █████ |
Sex, n (%) | N = 153 | N = 155 |
Female | 85 (55.6) | 93 (60.0) |
Male | 68 (44.4) | 62 (40.0) |
Race, n (%)a | N = 151 | N = 152 |
American Indian or Alaska Native | 1 (0.7) | 2 (1.3) |
Asian | 97 (64.2) | 89 (58.6) |
Black or African American | 2 (1.3) | 0 (0.0) |
White | 49 (32.5) | 60 (39.5) |
Multipleb | 1 (0.7) | 0 (0.0) |
Unknown | 1 (0.7) | 1 (0.7) |
Ethnicity, n (%) | N = 153 | N = 155 |
Hispanic or Latino | ██ █████ | | █████ |
Not Hispanic or Latino | ███ ██████ | ███ ██████ |
Not reported | | █████ | | █████ |
Unknown | | █████ | | █████ |
Weight, kg | N = 153 | N = 155 |
Mean (SD) | ████ ███████ | ████ ███████ |
Median | 61.8 | 66.5 |
Range | 39; 127 | 37; 112 |
< 80 kg, n (%) | 132 (86.3) | 128 (82.6) |
≥ 80 kg, n (%) | 21 (13.7) | 27 (17.4) |
Height, cm | N = 153 | N = 155 |
Mean (SD) | █████ █████ | █████ █████ |
Median | █████ | █████ |
Range | ████ ███ | ████ ███ |
Body mass index, kg/m2 | N = 153 | N = 155 |
Mean (SD) | ████ █████ | ████ █████ |
Median | ████ | ████ |
Range | ███ ██ | ███ ██ |
Baseline ECOG PS, n (%) | N = 153 | N = 155 |
0 | 54 (35.3) | 55 (35.5) |
1 | 99 (64.7) | 100 (64.5) |
History of smoking, n (%) | N = 153 | N = 155 |
Yes | 65 (42.5) | 64 (41.3) |
No | 88 (57.5) | 91 (58.7) |
History of brain metastasis, n (%) | N = 153 | N = 155 |
No | 118 (77.1) | 119 (76.8) |
Yes | 35 (22.9) | 36 (23.2) |
Prior EGFR TKI use,c n (%) | N = 153 | N = 155 |
No | ███ ██████ | ███ ██████ |
Yes | | █████ | | █████ |
Initial diagnosis NSCLC subtype, n (%) | N = 153 | N = 155 |
Adenocarcinoma | 151 (98.7) | 153 (98.7) |
Large cell carcinoma | 0 (0.0) | 1 (0.6) |
Squamous cell carcinoma | 0 (0.0) | 0 (0.0) |
Other | 2 (1.3) | 1 (0.6) |
Histology grade at initial diagnosis,d n (%) | N = 146 | N = 142 |
Poorly differentiated | ██ ██████ | ██ ██████ |
Moderately differentiated | ██ ██████ | ██ ██████ |
Well differentiated | ██ █████ | | █████ |
Other | ██ ██████ | ██ ██████ |
Cancer stage at initial diagnosis, n (%) | N = 153 | N = 149 |
IA | | █████ | | █████ |
IB | | █████ | | █████ |
IIA | | █████ | | █████ |
IIB | | █████ | | █████ |
IIIA | | █████ | | █████ |
IIIB | | █████ | | █████ |
IIIC | | █████ | | █████ |
IVA | ██ ██████ | ██ ██████ |
IVB | ██ ██████ | ██ ██████ |
Location of metastasis at screening,e n (%) | N = 151 | N = 153 |
Bone | ██ ██████ | ██ ██████ |
Liver | ██ ██████ | ██ ██████ |
Brain | ██ ██████ | ██ ██████ |
Lymph node | ███ ██████ | ███ ██████ |
Adrenal gland | ██ █████ | ██ ██████ |
Lung | ███ ██████ | ███ ██████ |
Other | ██ ██████ | ██ ██████ |
Histology grade at screening,d n (%) | N = 145 | N = 143 |
Poorly differentiated | ██ ██████ | ██ ██████ |
Moderately differentiated | ██ ██████ | ██ ██████ |
Well differentiated | ██ █████ | ██ █████ |
Other | ██ ██████ | ██ ██████ |
Cancer stage at screening, n (%) | N = 153 | N = 155 |
IIIB | | █████ | | █████ |
IIIC | | █████ | | █████ |
IVA | ██ ██████ | ██ ██████ |
IVB | ██ ██████ | ██ ██████ |
Time since initial lung cancer diagnosis (months) | N = 153 | N = 155 |
Mean | ████ ████████ | ████ ████████ |
Median | ████ | ████ |
Range | ████ ████ | ████ ████ |
Time since metastatic disease diagnosis (months) | N = 151 | N = 154 |
Mean | ████ ███████ | ████ ███████ |
Median | ████ | ████ |
Range | ████ ████ | ████ ████ |
Total number of patients with any prior therapies for lung cancer (%)f | N = 151 | N = 155 |
Prior systemic therapy | | █████ | ██ █████ |
Prior radiotherapy | ██ ██████ | ██ ██████ |
Prior cancer-related surgeryg | ███ █████ | ███ █████ |
Prior systemic therapy, n (%)f | N = 151 | N = 155 |
Adjuvant/neoadjuvant | ||
Adjuvant | | █████ | ██ █████ |
Neoadjuvant | | █████ | | █████ |
Palliative | ||
Palliativeh,i | | █████ | | █████ |
ACP = amivantamab + carboplatin-pemetrexed; CP = carboplatin-pemetrexed; ECOG = Eastern Cooperative Oncology Group; NSCLC = non–small cell lung cancer; SD = standard deviation; TKI = tyrosine kinase inhibitor.
Note: Percentages calculated with the number of patients in each treatment group as denominator.
aIn some regions, reporting of race is not required.
b“Multiple” includes 1 patient who selected Black or African American and white.
cProtocol allowed for prior TKI therapy if certain criteria were met per exclusion criterion 1.
d“Other” includes unknown histology grade.
ePatients can be counted in more than 1 category.
fAnalyses completed on safety set instead of full analysis set.
gPrior cancer-related surgery includes tumour biopsies performed for diagnosis.
hPalliative was captured on the electronic case report form as Curative/Palliative/Any other intent.
iOne patient received both adjuvant and palliative therapy.
Source: Details included in the table are from the sponsor’s Summary of Clinical Evidence.31
Exposure to Study Treatments
Overall, there was a difference in exposure to regimen between amivantamab plus carboplatin-pemetrexed and carboplatin-pemetrexed, █████ patient-years versus ████ patient-years. While exposure to carboplatin was similar between groups, exposure to pemetrexed was █████ patient-years in amivantamab plus carboplatin-pemetrexed and ████ patient-years in carboplatin-pemetrexed.
With respect to concomitant medications, there was a relatively large numerical difference in frequency of use between amivantamab plus carboplatin-pemetrexed and carboplatin-pemetrexed groups for antibacterials for systemic use (88.1% and 35.5%, respectively), corticosteroids for systemic use (74.2% and 27.1%, respectively), corticosteroids and dermatological preparations (59.6% and 11.6%, respectively), ophthalmologicals (46.4% and 18.7%, respectively), and emollients and protectives (33.8% and 5.2%, respectively).
Table 12: Summary of Patient Exposure From PAPILLON
Exposure | ACP | CP | |||||
|---|---|---|---|---|---|---|---|
Amivantamab (N = 151) | Carboplatin (N = 151) | Pemetrexed (N = 151) | Total (N = 151) | Carboplatin (N = 155) | Pemetrexed (N = 155) | Total (N = 155) | |
Total patient-yearsa | █████ | ████ | █████ | █████ | ████ | ████ | ████ |
Duration of study treatment (months) | |||||||
Mean (SD) | 10.19 (6.085) | 2.12 (0.594) | 9.58 (6.009) | ██████ | 2.17 (0.463) | 7.32 (4.140) | ██████ |
Median | 9.26 | 2.14 | 8.34 | ████ | 2.14 | 6.74 | ████ |
Range | (0.0 to 26.9) | (0.0 to 3.8) | (0.0 to 24.9) | ██████ | (0.0 to 3.9) | (0.0 to 25.3) | ██████ |
Total number of treatment cycles | |||||||
Mean (SD) | 13.99 (7.873) | 3.77 (0.668) | 13.50 (7.857) | ██████ | 3.88 (0.514) | 10.77 (5.768) | ██████ |
Median | 14.00 | 4.00 | 13.00 | █████ | 4.00 | 10.00 | █████ |
Range | (1.0 to 39.0) | (1.0 to 4.0) | (1.0 to 34.0) | ██████ | (1.0 to 5.0) | (1.0 to 37.0) | ██████ |
Relative dose intensityb | |||||||
Mean (SD) | ██████ | ██████ | ██████ | ██ | ██████ | ██████ | ██ |
Median | ██████ | ██████ | ██████ | ██ | ██████ | ██████ | ██ |
Range | ██████ | ██████ | ██████ | ██ | ██████ | ██████ | ██ |
ACP = amivantamab + carboplatin-pemetrexed; CP = carboplatin-pemetrexed; SD = standard deviation.
Notes: Analyses conducted on the safety analysis set. Percentages are calculated with the number of patients in each treatment group as the denominator. Amivantamab is administered once weekly (with the first dose split over days 1 and 2) up to cycle 2 day 1, and then administered once every 3 weeks.
aTotal exposure is the sum of treatment duration for each patient.
bRelative dose intensity (%) is calculated as the ratio of total received dose versus total prepared dose.
Source: Details included in the table are from the sponsor’s Summary of Clinical Evidence.31
Table 13: Patient Exposure to Concomitant Medications in PAPILLON (Safety Analysis Set)
Exposure to concomitant medication classes taken by > 10% of patients | ACP (N = 151) | CP (N = 155) |
|---|---|---|
Patients taking any concomitant medications, n (%) | 151 (100.0) | 155 (100.0) |
Analgesics | ███ ██████ | ██ ██████ |
Drugs for acid-related disorders | ███ ██████ | ██ ██████ |
Antibacterials for systemic use | ███ ██████ | ██ ██████ |
Corticosteroids for systemic use | ███ ██████ | ██ ██████ |
Drugs for constipation | ██ ██████ | ██ ██████ |
Anti-inflammatory and antirheumatic products | ██ ██████ | ██ ██████ |
Antiemetics and antinauseants | ██ ██████ | ██ ██████ |
Psycholeptics | ██ ██████ | ██ ██████ |
Corticosteroids, dermatological preparations | ██ ██████ | ██ ██████ |
Drugs for functional gastrointestinal disorders | ██ ██████ | ██ ██████ |
Antithrombotic drugs | ██ ██████ | ██ ██████ |
Immunostimulants | ██ ██████ | ██ ██████ |
Ophthalmologicals | ██ ██████ | ██ ██████ |
Antihistamines for systemic use | ██ ██████ | ██ ██████ |
Unspecified herbal and traditional medicine | ██ ██████ | ██ ██████ |
Mineral supplements | ██ ██████ | ██ ██████ |
Antianemic preparations | ██ ██████ | ██ ██████ |
Blood substitutes and perfusion solutions | ██ ██████ | ██ ██████ |
Cough and cold preparations | ██ ██████ | ██ ██████ |
Vitamins | ██ ██████ | ██ ██████ |
Lipid-modifying drugs | ██ ██████ | ██ ██████ |
Diuretics | ██ ██████ | ██ ██████ |
Drugs for treatment of bone diseases | ██ ██████ | ██ ██████ |
Vaccines | ██ ██████ | ██ ██████ |
Drugs for obstructive airway diseases | ██ ██████ | ██ ██████ |
Emollients and protectives | ██ ██████ | | █████ |
Agents acting on the renin-angiotensin system | ██ ██████ | ██ ██████ |
Bile and liver therapy | ██ ██████ | ██ ██████ |
Antibiotics and chemotherapeutics for dermatological use | ██ ██████ | | █████ |
Calcium channel blockers | ██ ██████ | ██ ██████ |
Antidiarrheals, intestinal anti-inflammatory and anti-infective drugs | ██ ██████ | ██ ██████ |
All other therapeutic products | ██ ██████ | ██ ██████ |
Drugs used in diabetes | ██ ██████ | ██ ██████ |
Throat preparations | ██ ██████ | ██ █████ |
Antivirals for systemic use | ██ ██████ | ██ █████ |
Psychoanaleptics | ██ ██████ | ██ ██████ |
Beta-blocking drugs | ██ ██████ | ██ ██████ |
Antiseptics and disinfectants | ██ ██████ | | █████ |
Sex hormones and modulators of the genital system | ██ ██████ | ██ ██████ |
Antiepileptics | ██ ██████ | ██ █████ |
Antifungals for dermatological use | ██ ██████ | | █████ |
Vasoprotectives | ██ ██████ | | █████ |
General nutrients | ██ ██████ | ██ █████ |
Gynecological anti-infective and antiseptics | ██ ██████ | | █████ |
Antihemorrhagics | ██ ██████ | ██ █████ |
Cardiac therapy | ██ ██████ | | █████ |
Anesthetics | ██ ██████ | | █████ |
Antimycotics for systemic use | ██ ██████ | | █████ |
Antiacne preparations | ██ ██████ | | █████ |
ACP = amivantamab + carboplatin-pemetrexed; CP = carboplatin-pemetrexed.
Source: PAPILLON Clinical Study Report.77
Subsequent therapies received by patients in the PAPILLON trail are summarized in Table 14. There were fewer patients in the amivantamab plus carboplatin-pemetrexed than in the carboplatin-pemetrexed group that had received subsequent therapy, 28% versus 61%, respectively, and the most common subsequent therapy was a drug that targeted the EGFR or a TKI-based regimen (8% versus 53%, respectively).
Table 14: Summary of Subsequent Treatment From PAPILLON
Exposure | ACP (N = 153) | CP (N = 155) |
|---|---|---|
Patients receiving first subsequent therapy, N (%) | 43 (28.1) | 94 (60.6) |
EGFR monoclonal antibody/TKI or TKI-based regimen, N (%) | 12 (7.8) | 82 (52.9) |
EGFR monoclonal antibody | 1 (0.7) | 71 (45.8) |
TKI | 9 (5.9) | 7 (4.5) |
TKI-based regimena | 2 (1.3) | 4 (2.6) |
Chemotherapy- and/or IO-based regimen, N (%) | 23 (15.0) | 11 (7.1) |
Chemotherapy alone | 13 (8.5) | 2 (1.3) |
Chemotherapy + VEGFi | 6 (3.9) | 1 (0.6) |
Chemotherapy + VEGFi + IO | 1 (0.7) | 5 (3.2) |
Chemotherapy + IO | 2 (1.3) | 1 (0.6) |
IO alone | 1 (0.7) | 2 (1.3) |
Other, N (%) | 8 (5.2) | 1 (0.6) |
Patients crossing over from CP to amivantamab monotherapy | NA | 65 (41.9) |
ACP = amivantamab + carboplatin-pemetrexed; CP = carboplatin-pemetrexed; IO = immunotherapy; TKI = tyrosine kinase inhibitor; VEGFi = vascular endothelial growth factor inhibitor.
aTKI in combination with chemotherapy, IO, or vascular endothelial growth factor inhibitor therapies are only counted in the TKI-based regimen category.
Source: Details included in the table are from the sponsor’s Summary of Clinical Evidence.31
Efficacy
As of the data cut-off in May 2023, there was a median follow-up of 14.92 (range, 0.3 to 27.0) months.
Progression-Free Survival
Analyses were performed after 216 events had been observed (amivantamab plus carboplatin-pemetrexed arm: 84, carboplatin-pemetrexed arm: 132). The HR for amivantamab plus carboplatin-pemetrexed versus carboplatin-pemetrexed was 0.395 (95% CI, 0.296 to 0.528; P < 0.0001), favouring amivantamab plus carboplatin-pemetrexed (Table 15). The median PFS by BICR in the amivantamab plus carboplatin-pemetrexed arm was 11.37 months (95% CI, 9.79 to 13.70) compared with 6.70 months (95% CI, 5.59 to 7.33) in the carboplatin-pemetrexed arm. The Kaplan-Meier plot of PFS by BICR is in Figure 2.
At the 6-month time point, the absolute difference in PFS rate between amivantamab plus carboplatin-pemetrexed and carboplatin-pemetrexed groups was █████ ████ ███ ████ ██ █████), at 12 months it was █████ ████ ███ ████ ██ █████), and at 18 months the PFS rate was █████ ████ ███ ████ ██ ███████ Note that by 18 months there were only 17 patients (15 in the amivantamab plus carboplatin-pemetrexed group and 2 in the carboplatin-pemetrexed group) remaining at risk. A preplanned sensitivity analysis evaluating PFS, as assessed by the treating investigator, was consistent with the primary analysis. The test for proportional hazards and the residual plots showed that the assumption was satisfied.
Figure 2: Primary End Point: PFS by BICR for Amivantamab Plus Carboplatin and Pemetrexed Versus Carboplatin and Pemetrexed
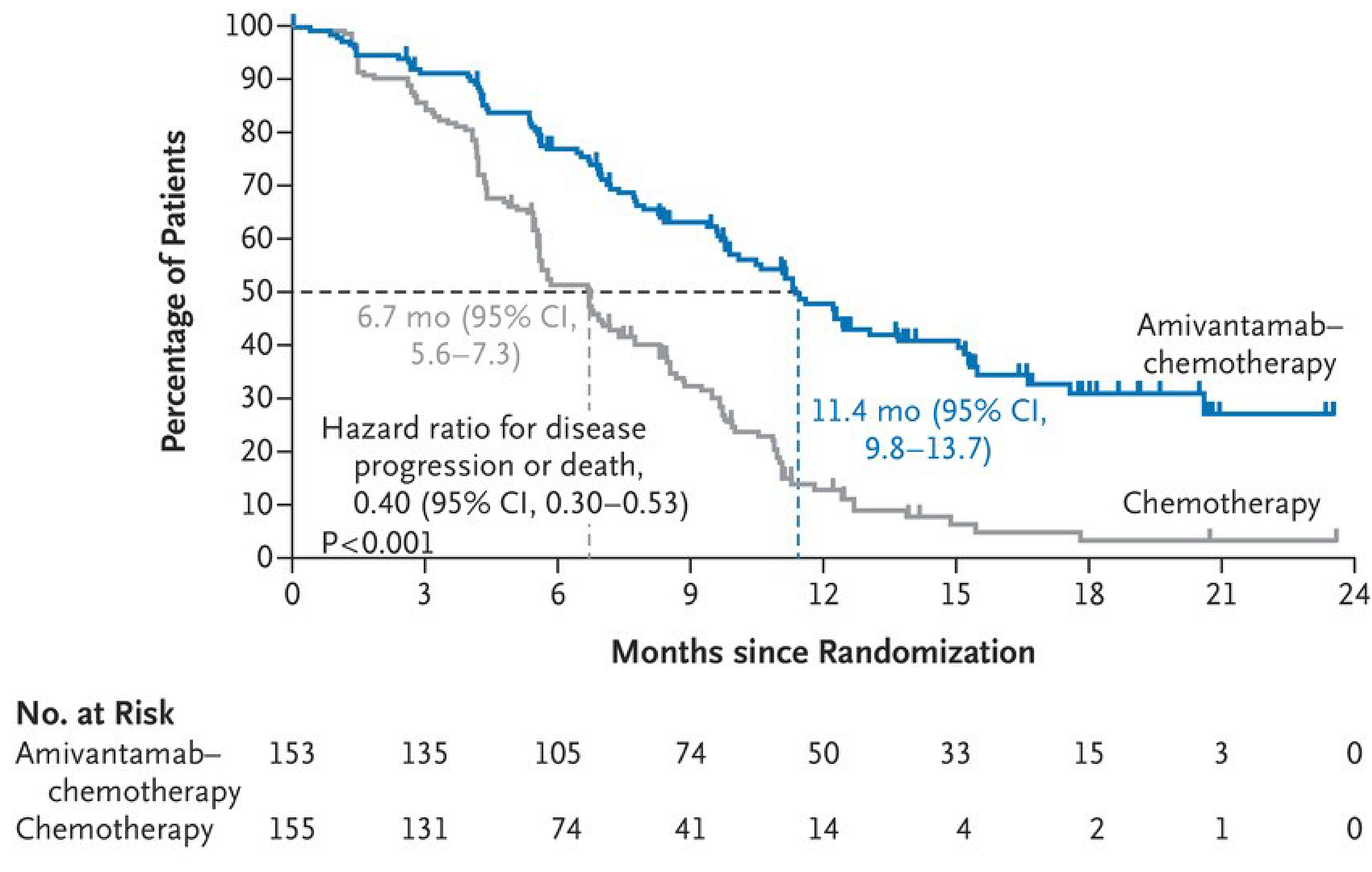
BICR = blinded independent central review; CI = confidence interval; mo = months; PFS = progression-free survival.
Note: Censoring of data is indicated by tick marks, and median PFS is indicated by dashed lines.
Source: PAPILLON Clinical Summary.65
Subgroup analyses, based on the primary outcome of PFS by BICR, are reported in Table 33, Appendix 1. The reported HR with CIs suggest that the treatment effect is consistent across various subgroups based on sex, race (Asian versus non-Asian), weight (< 80 kg versus ≥ 80 kg), ECOG PS (0 or 1), and history of smoking. However, there was some indication that the magnitude of effects of amivantamab plus carboplatin-pemetrexed versus carboplatin-pemetrexed may differ depending on history of brain metastasis (HR of 0.63; 95% CI, 0.38 to 1.06) or no history of brain metastasis (HR of 0.33; 95% CI, 0.23 to 0.46) and possibly the age of patients, i.e., 75 years of age or older (HR of ████ ████ ███ █████ ████), and age younger than 75 (HR of ████ ████ ███ █████ ███████, although it should be noted that the 75 or older age group had a relatively small sample of only ██ patients across groups, compared to ███ patients in those aged younger than 75. The sample for the subgroup of patients with brain metastases was also relatively small (N = ██) across both groups. The purpose of the subgroup analyses was not to test for subgroup differences.
Key Secondary End Points
Objective Response Rates
Based on BICR assessment in patients with measurable disease at baseline (n = 304), there was a higher percentage of responders in the amivantamab plus carboplatin-pemetrexed arm (111 patients [72.5%]), compared with the carboplatin-pemetrexed arm (72 patients [46.4%]) at the data cut-off, for an OR of █████ ████ ███ ██████ ██████ █████████ favouring amivantamab plus carboplatin-pemetrexed (Table 15). The percentage of patients with progressive disease as the best response in the amivantamab plus carboplatin-pemetrexed arm was ████, compared with █████ in the carboplatin-pemetrexed arm. Results of the sensitivity analysis evaluating ORR, as assessed by the treating investigator, were consistent with the assessment by BICR.
Overall Survival
As of the data cut-off in May 2023, after a median follow-up time of 14.92 months, a total of 70 deaths were reported across both groups (amivantamab plus carboplatin-pemetrexed arm: 28 deaths, carboplatin-pemetrexed arm: 42 deaths). At this point, 65 patients from the carboplatin-pemetrexed group had crossed over to amivantamab monotherapy and the HR was 0.675 (95% CI, 0.418 to 1.090; P = 0.106) (Table 15). Median OS in the amivantamab plus carboplatin-pemetrexed arm was NE, and the median OS in the carboplatin-pemetrexed arm was 24.38 (95% CI, 22.08 to NE) months. At the 12-month time point, the absolute difference in OS rate between amivantamab plus carboplatin-pemetrexed and carboplatin-pemetrexed groups was ████ ████ ███ ████ ██ ███████; at 18 months, it was ████ ████ ███ ████ ██ ██████; and at 24 months, it was █████ ████ ███ ████ ██ ███████ Note that by 24 months there were only 11 patients (5 in the amivantamab plus carboplatin-pemetrexed group and 6 in the carboplatin-pemetrexed group) who contributed to the analysis.
The Kaplan-Meier plot of OS is depicted in Figure 4, Appendix 1 of this clinical report. After a slight imbalance in deaths during the first 3 months of the study (██ in the amivantamab plus carboplatin-pemetrexed group and ██ in the carboplatin-pemetrexed group; refer to Harms — Mortality section in this report), the Kaplan-Meier curves described a favourable trend in OS, starting from approximately 9 months, in patients treated with amivantamab plus carboplatin-pemetrexed. The curves are seen to come together approximately between 10 and 11 months before showing evidence of separating again.
The final planned OS analysis will be conducted on more mature OS data, approximately 48 months after the first participant was randomized, when approximately 210 deaths overall are anticipated. Results of the stratified sensitivity analysis were consistent with unstratified analysis.
The sponsor also conducted sensitivity analyses to adjust for patients who crossed over to amivantamab monotherapy from carboplatin-pemetrexed. The OS results were similar in the IPCW (adjusted HR of ████ ████ ███ █████ ██████ and TSE (adjusted HR of ████ ████ ███ █████ ████) analyses and differed slightly from those in the RPSFT (adjusted HR of ███ ████ ███ █████ ████).
PFS After First Subsequent Therapy
At the data cut-off, there were ██ of 153 patients (██████ in the amivantamab plus carboplatin-pemetrexed group and ██ of 155 patients in the carboplatin-pemetrexed group (██████ who had a PFS2 event, for an HR of 0.493 (95% CI, 0.32 to 0.759; P = 0.001) (Table 15). This end point was not controlled for multiplicity, and there is an increased risk of type I error (i.e., erroneously rejecting the null hypothesis). The median PFS2 was NE (95% CI, 22.77 to NE) in the amivantamab plus carboplatin-pemetrexed arm and was 17.25 months (95% CI, 13.96 to 21.52) in the carboplatin-pemetrexed arm.
Health-Related Quality of Life
A summary of the EORTC QLQ-C30 GHS score is presented in Table 15. Baseline compliance was ████ in both the amivantamab plus carboplatin-pemetrexed and carboplatin-pemetrexed treatment groups; compliance exceeded ███ through cycle 31 in both study arms. The number of patients available to complete the measure ██████████ with each cycle. After cycle 9, the number of patients available to complete assessments had ███████ ██ ████ ████ ███ after cycle 9 and after cycle 13 in the carboplatin-pemetrexed and the amivantamab plus carboplatin-pemetrexed groups, respectively. At the 12-month follow-up (cycle 17 day 1), the mean change from baseline on the EORTC QLQ-C30 was ███ ████ ███ █████ ████ in the amivantamab plus carboplatin-pemetrexed group ███ ████ ████ ███ █████ ████ in the carboplatin-pemetrexed group, with a mean difference of change between amivantamab plus carboplatin-pemetrexed and carboplatin-pemetrexed groups of ███ ████ ███ █████ ███) points. The point estimates for the between-group difference in this score did not meet the MID identified from the literature (a ≥ 10-point decrease for health status).
A summary of the PROMIS PF total score is presented in Table 33, Appendix 1. Baseline compliance was ████ in both the amivantamab plus carboplatin-pemetrexed and carboplatin-pemetrexed treatment groups; compliance exceeded ███ through cycle 31 in both study arms. The number of patients available to complete the measure ██████████ with each cycle. The number of patients available to complete assessments had ███████ ██ ████ ████ ███ after cycle 9 and after cycle 13 in the carboplatin-pemetrexed and the amivantamab plus carboplatin-pemetrexed groups, respectively. At the 12-month follow-up (cycle 17 day 1), the mean change from baseline on the PROMISE-PF total score was ████ ████ ███ █████ █████ in the amivantamab plus carboplatin-pemetrexed group and ████ ████ ███ ██████ ████ in the carboplatin-pemetrexed group, with a mean difference in change between amivantamab plus carboplatin-pemetrexed and carboplatin-pemetrexed groups of ████ ██████ ████ points.
Table 15: Summary of Key Efficacy Results From PAPILLON
Variable | ACP N = 153 | CP N = 155 |
|---|---|---|
PFS by BICR | ||
Number of patients analyzed, N (%) | 153 (100) | 155 (100) |
Events, n (%) | 84 (54.9) | 132 (85.2) |
Progressive disease | ██ ██████ | ███ ██████ |
Death without progressive disease | | █████ | | █████ |
Censored, n (%) | ██ ██████ | ██ ██████ |
Study cut-off | ██ ██████ | ██ ██████ |
No progressive disease or death before ≥ 2 consecutively missing or unevaluable assessments | | █████ | | █████ |
Lost to follow-up | | █████ | | █████ |
Withdrawal of consent | | █████ | ██ |
Time to event (months) | ||
25th percentile (95% CI) | ███ █████ ████ | ████ ██████ █████ |
Median (95% CI) | ████ █████ █████ | ████ ██████ █████ |
75th percentile (95% CI) | ██ ███████ ███ | ████ ██████ ██████ |
Range | ██████ ██████ | ██████ ██████ |
Event-free rate (95% CI) | ||
6 months | ███ █████ ████ | ███ █████ ████ |
12 months | ███ █████ ████ | ███ ████ ████ |
18 months | ███ █████ ████ | ██ ████ ███ |
HR (95% CI)a | █████ ███████ ██████ | |
P valueb | ███████ | |
OS | ||
Event, n (%) | ██ ██████ | ██ ██████ |
Censored, n (%) | ███ ██████ | ███ ██████ |
Time to event (months) | ||
25th percentile (95% CI) | █████ ███████ ███ | ███████████████ |
Median (95% CI) | ██ ████ ███ | █████ ███████ ███ |
75th percentile (95% CI) | ██ ████ ███ | █████ ███████ ███ |
Range | ██████ ██████ | █████ ██████ |
Event-free probability (95% CI) | ||
6 months | ███ █████ ████ | ███ ██████ ████ |
12 months | ███ █████ ████ | ███ █████ ████ |
18 months | ███ ██████ ████ | ███ █████ ████ |
24 months | ███ █████ ████ | ███ █████ ████ |
HR (95% CI)c | █████ ███████ ██████ | |
P valued | ██████ | |
ORR | ||
Patients with measurable disease at baseline, n (%) | 152 (99.3) | 152 (98.1) |
ORR, n (%) | 111 (72.5) | 72 (46.4) |
95% CI | (65.2% to 79.9%) | (39.2% to 55.6%) |
OR (95% CI) | █████ ███████ ██████ | |
P valuee | ███████ | |
Best overall response, n (%) | ||
Complete response | 6 (3.9) | 1 (0.7) |
Partial response | 105 (69.1) | 71 (46.7) |
Stable disease | 29 (19.1) | 62 (40.8) |
Progressive disease | 4 (2.6) | 16 (10.5) |
Not evaluable | 8 (5.3) | 2 (1.3) |
HRQoL: EORTC QLQ-C30 Global Health Status | ||
Mean (SD) baseline | █████ ██████████████ | █████ ██████████████ |
Mean change from baseline to 12 months (cycle 17 day 1) (95% CI)f | ██████ █████████ | ████ ██████ █████████ |
Mean change from baseline to 18 months (cycle 25 day 1) (95% CI)f | ███ ██████ █████████ | ███ ██████ █████████ |
PFS2 | ||
Event | ██ ██████ | ██ ██████ |
Censored | ███ ██████ | ██ ██████ |
Time to event (months) | ||
25th percentile (95% CI) | █████ ███████ ██████ | █████ ██████ ██████ |
Median (95% CI) | ██ ███████ ███ | █████ ███████ ██████ |
75th percentile (95% CI) | ██ ████ ███ | █████ ███████ ███ |
Range | ██████ ██████ | ██████ ███████ |
Event-free rate (95% CI) | ||
6 months | ███ █████ ████ | ███ █████ ████ |
12 months | ███ █████ ████ | ███ █████ ████ |
18 months | ███ █████ ████ | ███ █████ ████ |
24 months | ███ █████ ████ | ███ █████ ████ |
HR (95% CI)a | █████ ███████ ██████ | |
P valueb,g | ██████ | |
ACP = amivantamab + carboplatin-pemetrexed; BICR = blinded independent central review; CI = confidence interval; CP = carboplatin-pemetrexed; EORTC QLQ-C30 = European Organization for the Research and Treatment of Cancer Quality of Life Questionnaire Core 30; HR = hazard ratio; HRQoL = health-related quality of life; NE = not estimable; OR = odds ratio; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; PFS2 = progression-free survival after first subsequent therapy; SD = standard deviation.
Note: + = censored observation.
aHR is from stratified proportional hazards model. HR less than 1 favours ACP.
bP value is from a log-rank test stratified by ECOG PS (0 or 1) and history of brain metastases (yes or no).
cHR is from proportional hazards mode. HR less than 1 favours ACP.
dP value is from a log-rank test.
eP value is from a logistic regression model stratified by ECOG PS (0 or 1) and history of brain metastases (yes or no).
fMeans and 95% CIs are derived based on the mixed-effects model with repeated measures, in which the dependent variable is change from baseline in score, and independent variables are baseline, visit, treatment, and visit by treatment interaction as fixed effects, and individual patient as random effect.
gNot adjusted for multiple comparisons. There is an increased risk of type I error (i.e., erroneously rejecting the null hypothesis).
Source: Details included in the table are from the sponsor’s Summary of Clinical Evidence.31
Harms
Refer to Table 16 for harms data.
Adverse Events
Overall, all 151 patients (100%) in the amivantamab plus carboplatin-pemetrexed group and 152 patients (98.1%) in the carboplatin-pemetrexed group experienced at least 1 TEAE. The most common TEAE was rash, which occurred in 81 patients (53.6%) in the amivantamab plus carboplatin-pemetrexed group and 12 patients (7.7%) in the carboplatin-pemetrexed group. Other common TEAEs with large differences between groups included dermatitis acneiform, in 47 patients (31.1%) in the amivantamab plus carboplatin-pemetrexed group and 5 (3.2%) in the carboplatin-pemetrexed group; hypoalbuminemia, in 62 (41.1%) patients in amivantamab plus carboplatin-pemetrexed and 15 (9.7%) patients in carboplatin-pemetrexed; peripheral edema, in 45 (29.8%) patients in amivantamab plus carboplatin-pemetrexed and 16 (10.3%) patients in carboplatin-pemetrexed; and infusion-related reaction, in 63 (41.7%) patients in amivantamab plus carboplatin-pemetrexed and 2 (1.3%) patients in carboplatin-pemetrexed.
Grade 3 and Higher
Overall, there were 114 patients (75.5%) in the amivantamab plus carboplatin-pemetrexed group and 83 patients (53.5%) in the carboplatin-pemetrexed group who reported at least 1 TEAE that was grade 3 or higher. The most common grade 3 or higher TEAE was neutropenia, occurring in 50 patients (33.1%) in the amivantamab plus carboplatin-pemetrexed group and 35 patients (22.6%) of the carboplatin-pemetrexed group. Other common grade 3 or higher TEAEs where there was a notable (> 5%) difference in incidence between groups were paronychia, occurring in 10 patients (6.6%) in the amivantamab plus carboplatin-pemetrexed group and no patients in the carboplatin-pemetrexed group; rash, which occurred in 17 patients (11.3%) in the amivantamab plus carboplatin-pemetrexed group and no patients in the carboplatin-pemetrexed group; and hypokalemia, occurring in 13 patients (8.6%) in the amivantamab plus carboplatin-pemetrexed group and 2 patients (1.3%) in the carboplatin-pemetrexed group.
Serious Adverse Events
Treatment-emergent SAEs were reported in 56 patients (37.1%) in the amivantamab plus carboplatin-pemetrexed group and 48 patients (31.0%) in the carboplatin-pemetrexed group. The most common treatment-emergent SAEs in the amivantamab plus carboplatin-pemetrexed group were pneumonia (6 patients [4.0%] versus 4 patients [2.6%] in the carboplatin-pemetrexed group), pneumonitis (4 patients [2.6%] and no patients in the carboplatin-pemetrexed group), and pulmonary embolism (4 patients [2.6%] in each group). All other SAEs in the amivantamab plus carboplatin-pemetrexed group had an incidence of less than 2%. The most common SAE in the carboplatin-pemetrexed arm was anemia (6 patients [3.9%] and 1 patient [0.7%] in amivantamab plus carboplatin-pemetrexed group).
Withdrawals Due to Adverse Events
Overall, from study initiation through the data cut-off, 36 patients (23.8%) in the amivantamab plus carboplatin-pemetrexed arm and 16 patients (10.3%) in the carboplatin-pemetrexed arm had TEAEs leading to discontinuation of at least 1 study treatment. Of the 36 patients in the amivantamab plus carboplatin-pemetrexed arm who discontinued any study treatment, 17 discontinued amivantamab (discontinuations were considered to be drug-related in 10 patients). Pneumonitis was the most common cause of discontinuation of amivantamab (4 patients [2.6%]), followed by dermatitis acneiform (2 patients [1.3%]). Thrombocytopenia (3 patients [1.9%]) and neutropenia (████████ ███████ were the most common reasons for treatment discontinuation of either carboplatin or pemetrexed in the carboplatin-pemetrexed arm. Most of the TEAEs leading to study treatment discontinuation occurred at a frequency of less than 2% in both treatment arms.
Mortality
There were 4 patients (2.6%) in the amivantamab plus carboplatin-pemetrexed group and 9 patients (5.8%) in the carboplatin-pemetrexed group who died due to an AE during the study, and 3 patients (2.0%) in the amivantamab plus carboplatin-pemetrexed group and 4 patients (2.6%) in the carboplatin-pemetrexed group who died due to an AE within 30 days of the last dose. Excluding the crossover phase, there were 7 patients (4.6%) and 4 (2.6%) patients in the amivantamab plus carboplatin-pemetrexed and carboplatin-pemetrexed groups, respectively, who died due to an AE within 30 days of the last dose. Six out of the 7 AEs in the amivantamab plus carboplatin-pemetrexed group leading to death occurred within the first 90 days of cycle 1 day 1, compared with 1 death in the carboplatin-pemetrexed group. In the amivantamab plus carboplatin-pemetrexed group, these 6 deaths included 1 event each of cardiorespiratory arrest, sepsis, stroke, death, COVID-19, and COVID-19 pneumonia. Each of these deaths was reported to be a unique event in patients with comorbidities with no clear pattern of etiology identified.
Notable Harms
The notable harms identified for this review were rash and infusion reactions. As noted previously, rash was the most common AE, occurring in 81 (53.6%) patients in the amivantamab plus carboplatin-pemetrexed group and 12 (7.7%) patients in the carboplatin-pemetrexed group. Under the grouping skin and subcutaneous disorders, there were ███ ████████ ███████ in the amivantamab plus carboplatin-pemetrexed group and ██ ███████ patients in the carboplatin-pemetrexed group with such an event. Infusion-related reactions were reported in 63 (41.7%) patients in the amivantamab plus carboplatin-pemetrexed group and 2 (1.3%) patients in the carboplatin-pemetrexed group.
Table 16: Summary of Harms Results From PAPILLON
Harm | Amivantamab + CP N = 153 | CP N = 155 |
|---|---|---|
Most common adverse events, n (%) | ||
≥ 1 adverse event | 151 (100.0) | 152 (98.1) |
Skin and subcutaneous tissue disorders | ███ ██████ | ██ ██████ |
Rash | 81 (53.6) | 12 (7.7) |
Dermatitis acneiform | 47 (31.1) | 5 (3.2) |
Dry skin | ██ ██████ | | █████ |
Alopecia | ██ █████ | | █████ |
Pruritus | ██ █████ | ██ █████ |
Skin ulcer | ██ █████ | | █████ |
Erythema | | █████ | | █████ |
Gastrointestinal disorders | ███ ██████ | ███ ██████ |
Constipation | 60 (39.7) | 47 (30.3) |
Nausea | 55 (36.4) | 65 (41.9) |
Stomatitis | 38 (25.2) | 9 (5.8) |
Vomiting | 32 (21.2) | 29 (18.7) |
Diarrhea | 31 (20.5) | 20 (12.9) |
Hemorrhoids | ██ ██████ | | █████ |
Mouth ulceration | ██ █████ | | █████ |
Abdominal bleeding | ██ █████ | | █████ |
Gingival bleeding | | █████ | | █████ |
Abdominal distension | | █████ | ██ █████ |
Abdominal pain upper | | █████ | | █████ |
Infections and infestations | ███ ██████ | ██ ██████ |
Paronychia | 85 (56.3) | 0 (0.0) |
COVID-19 | 36 (23.8) | 21 (13.5) |
Pneumonia | ██ ██████ | ██ █████ |
Conjunctivitis | | █████ | | █████ |
Upper respiratory tract infection | | █████ | | █████ |
Urinary tract infection | | █████ | | █████ |
Metabolism and nutrition disorders | ███ ██████ | ██ ██████ |
Hypoalbuminemia | 62 (41.1) | 15 (9.7) |
Decreased appetite | 54 (35.8) | 43 (27.7) |
Hypokalemia | 32 (21.2) | 13 (8.4) |
Hypomagnesemia | ██ ██████ | ██ █████ |
Hypocalcemia | ██ ██████ | | █████ |
Hyponatremia | ██ ██████ | ██ █████ |
Hypophosphatasemia | ██ █████ | | █████ |
Hypoproteinemia | ██ █████ | | █████ |
Hyperglycemia | | █████ | ██ █████ |
Hyperkalemia | | █████ | | █████ |
Blood and lymphatic system disorders | ███ ██████ | ███ ██████ |
Neutropenia | 89 (58.9) | 70 (45.2) |
Anemia | 76 (50.3) | 85 (54.8) |
Leukopenia | 57 (37.7) | 50 (32.3) |
Thrombocytopenia | 55 (36.4) | 46 (29.7) |
Lymphopenia | | █████ | ██ █████ |
General disorders and administration site conditions | ███ ██████ | ██ ██████ |
Edema peripheral | ██ ██████ | ██ ██████ |
Asthenia | 30 (19.9) | 29 (18.7) |
Pyrexia | 24 (15.9) | 9 (5.8) |
Fatigue | 23 (15.2) | 32 (20.6) |
Malaise | ██ ██████ | ██ █████ |
Mucosal inflammation | ██ █████ | | █████ |
Edema | ██ █████ | | █████ |
Investigations | ██ ██████ | ██ ██████ |
Alanine aminotransferase increased | ██ ██████ | ██ ██████ |
Aspartate aminotransferase increased | ██ ██████ | ██ ██████ |
Gamma-glutamyltransferase increased | ██ ██████ | ██ ██████ |
Weight decreased | ██ ██████ | ██ █████ |
Blood alkaline phosphatase increased | ██ ██████ | ██ █████ |
Blood lactate dehydrogenase increased | ██ █████ | | █████ |
Blood creatinine increased | ██ █████ | ██ █████ |
Injury, poisoning, and procedural complications | ██ ██████ | ██ █████ |
Infusion-related reaction | 63 (41.7) | 2 (1.3) |
Respiratory, thoracic, and mediastinal disorders | ██ ██████ | ██ ██████ |
Cough | 21 (13.9) | 24 (15.5) |
Dyspnea | ██ ██████ | ██ ██████ |
Pulmonary embolism | ██ █████ | | █████ |
Productive cough | | █████ | | █████ |
Pleural effusion | | █████ | | █████ |
Nervous system disorders | ██ ██████ | ██ ██████ |
Dizziness | ██ █████ | ██ █████ |
Dysgeusia | | █████ | ██ █████ |
Headache | | █████ | ██ █████ |
Musculoskeletal and connective tissue disorders | ██ ██████ | ██ ██████ |
Back pain | ██ ██████ | ██ ██████ |
Arthralgia | ██ █████ | ██ █████ |
Myalgia | | █████ | | █████ |
Eye disorders | ██ ██████ | ██ ██████ |
Lacrimation increased | | █████ | | █████ |
Vascular disorders | ██ ██████ | ██ ██████ |
Deep vein thrombosis | ██ █████ | | █████ |
Hypertension | | █████ | ██ █████ |
Hepatobiliary disorders | ██ ██████ | ██ █████ |
Hyperbilirubinemia | ██ █████ | | █████ |
Psychiatric disorders | ██ ██████ | ██ ██████ |
Insomnia | ██ ██████ | ██ ██████ |
Most common treatment-emergent serious adverse events (≥ 1% patients in either treatment group), n (%) | ||
Patients with ≥ 1 SAE | 56 (37.1) | 48 (31.0) |
Infections and infestations | ██ ██████ | ██ █████ |
Pneumonia | 6 (4.0) | 4 (2.6) |
COVID-19 | 3 (2.0) | 1 (0.6) |
Cellulitis | 2 (1.3) | 1 (0.6) |
Pustular rash | 2 (1.3) | 0 (0.0) |
Skin infection | 2 (1.3) | 0 (0.0) |
Gastrointestinal disorders | ██ █████ | | █████ |
Vomiting | 3 (2.0) | 1 (0.6) |
Diarrhea | 2 (1.3) | 1 (0.6) |
Respiratory, thoracic, and mediastinal disorders | | █████ | ██ █████ |
Pneumonitis | 4 (2.6) | 0 (0.0) |
Pulmonary embolism | 4 (2.6) | 4 (2.6) |
Dyspnea | 1 (0.7) | 5 (3.2) |
Pleural effusion | 1 (0.7) | 5 (3.2) |
Metabolism and nutrition disorders | | █████ | | █████ |
Hypokalemia | 3 (2.0) | 1 (0.6) |
Blood and lymphatic system disorders | | █████ | ██ █████ |
Thrombocytopenia | 3 (2.0) | 5 (3.2) |
Neutropenia | 2 (1.3) | 0 (0.0) |
Anemia | 1 (0.7) | 6 (3.9) |
Febrile neutropenia | 1 (0.7) | 3 (1.9) |
Deaths, n (%) | ||
Deaths during studya | 28 (18.3) | 42 (27.1) |
Progressive disease | 20 (13.1) | 30 (19.4) |
Adverse event | 4 (2.6) | 9 (5.8) |
Other | 2 (1.3) | 3 (1.9) |
COVID-19 | 2 (1.3) | 0 (0.0) |
Deaths within 30 days of last dosea,b | 7 (4.6) | 7 (4.5) |
Adverse event | 3 (2.0) | 4 (2.6) |
Progressive disease | 1 (0.7) | 2 (1.3) |
COVID-19 | 2 (1.3) | 0 (0.0) |
Other | 1 (0.7) | 1 (0.6) |
Deaths within 30 days of last dose (main study)b,c | 7 (4.6) | 4 (2.6) |
Adverse event | 3 (2.0) | 2 (1.3) |
COVID-19 | 2 (1.3) | 0 (0.0) |
Other | 1 (0.7) | 1 (0.6) |
Progressive disease | 1 (0.7) | 1 (0.6) |
Adverse events of special interest, n (%) | ||
Patients with 1 or more AEs of special interest | 139 (92.1) | 30 (19.4) |
Rash | 135 (89.4) | 28 (18.1) |
Rash | 81 (53.6) | 12 (7.7) |
Dermatitis acneiform | 47 (31.1) | 5 (3.2) |
Dermatitis | | █████ | | █████ |
Pustular rash | | █████ | | █████ |
Acne | | █████ | | █████ |
Folliculitis | | █████ | | █████ |
Maculopapular rash | | █████ | | █████ |
Pustule | | █████ | | █████ |
Rash popular | | █████ | | █████ |
Pruritic rash | | █████ | | █████ |
Skin lesion | | █████ | | █████ |
Erythema | | █████ | | █████ |
Macular rash | | █████ | | █████ |
Infusion-related reaction | 63 (41.7) | 2 (1.3) |
Pneumonitis/ILD | | █████ | | █████ |
Pneumonitis | | █████ | | █████ |
AE = adverse event; CP = carboplatin-pemetrexed; ILD = interstitial lung disease; SAE = serious adverse event.
Note: Subjects are counted only once for any given event, regardless of the number of times they actually experienced the event. Adverse events are coded using MedDRA Version 25.0. Deaths due to COVID-19 are not included in the other causes of death (i.e., subjects are only counted in one row).
aSubjects who died during the Crossover phase are included.
bSubjects who died within 30 days will be counted in deaths during study as well.
cSubjects who died during the Crossover phase are excluded.
Source: Details included in the table are from the sponsor’s Summary of Clinical Evidence.31
Table 17: Summary of Discontinuations Due to AEs
Harm | Amivantamab | Carboplatin | Pemetrexed | Carboplatin | Pemetrexed |
|---|---|---|---|---|---|
AE leading to discontinuation of study drug (≥ 1% patients in either treatment group), n (%) | |||||
≥ 1 AE leading to discontinuation of any study treatment | ██ ████ | ██ █████ | ████████ | | █████ | ██ █████ |
Infections and infestations | | █████ | | █████ | | █████ | | █████ | | █████ |
Pneumonia | | █████ | | █████ | | █████ | | █████ | | █████ |
Skin infection | | █████ | | █████ | | █████ | | █████ | | █████ |
Blood and lymphatic system disorders | | █████ | | █████ | | █████ | | █████ | | █████ |
Anemia | | █████ | | █████ | | █████ | | █████ | | █████ |
Neutropenia | | █████ | | █████ | | █████ | | █████ | | █████ |
Thrombocytopenia | | █████ | | █████ | | █████ | | █████ | | █████ |
Skin and subcutaneous tissue disorders | | █████ | | █████ | | █████ | | █████ | | █████ |
Dermatitis acneiform | | █████ | | █████ | | █████ | | █████ | | █████ |
Rash | | █████ | | █████ | | █████ | | █████ | | █████ |
Skin ulcer | | █████ | | █████ | | █████ | | █████ | | █████ |
General disorders and administration site conditions | | █████ | | █████ | | █████ | | █████ | | █████ |
Asthenia | | █████ | | █████ | | █████ | | █████ | | █████ |
Fatigue | | █████ | | █████ | | █████ | | █████ | | █████ |
Respiratory, thoracic, and mediastinal disorders | | █████ | | █████ | | █████ | | █████ | | █████ |
Pneumonitis | | █████ | | █████ | | █████ | | █████ | | █████ |
Injury, poisoning, and procedural complications | | █████ | | █████ | | █████ | | █████ | | █████ |
Infusion-related reaction | | █████ | | █████ | | █████ | | █████ | | █████ |
Metabolism and nutrition disorders | | █████ | | █████ | | █████ | | █████ | | █████ |
Decreased appetite | | █████ | | █████ | | █████ | | █████ | | █████ |
AEs leading to drug interruption of any study drug | ██ ████ | ██ ████ | ██ ██████ | ██ ████ | ██ ████ |
AEs leading to dose reduction of any study drug | ██ ████ | ██ ████ | ██ ██████ | ██ ████ | ██ ████ |
AE = adverse event; CP = carboplatin-pemetrexed; ILD = interstitial lung disease; SAE = serious adverse event.
Source: Details included in the table are from the sponsor’s Summary of Clinical Evidence.31
Critical Appraisal
Internal Validity
The methods used in the PAPILLON trail to generate the randomization sequence and conceal the allocation until treatment assignment were adequate. Baseline characteristics were relatively well balanced between groups, which suggests that the randomization was successful. The few baseline imbalances that were identified (e.g., location of metastasis at screening, time since diagnosis, histology, and prior radiotherapy) were not believed to have an important impact on the efficacy and harm evaluation. There were some imbalances observed in the use of some concomitant medications. However, the clinical experts consulted on this review did not believe these differences would result in a differential impact on treatment effect.
Following randomization, the study was not blinded. Patients’ knowledge of their assigned treatment may bias the measurement of subjective outcomes, including patient-reported outcomes such as HRQoL. Assessments of disease progression and tumour response are based on subjective interpretation of radiographic images and clinical evaluation. However, both PFS and ORR were ascertained by BICR, which would mitigate the impact of bias in measurement of those outcomes. Patients’ knowledge of treatment assignment also has potential to bias assessment of harms; for example, diarrhea is a relatively common adverse effect of EGFR inhibitors and perhaps more subjective in its reporting.
A power calculation was performed; however, no rationale or source was provided for the underlaying assumptions of expected effect size. A hierarchical fixed-sequence testing strategy was used to control the overall type I error rate for hypotheses testing of primary outcome, PFS (by BICR), and key secondary end points, ORR and OS. Assessment of other important outcomes, such as PFS2, were not adjusted for multiple comparisons and therefore any analyses reported, and any P values, should be considered supportive in nature.
There was a considerable amount of missing data for the patient-reported outcomes, such as the EORTC QLQ-C30 and PROMIS PF. The number of patients available to complete the measure diminished with each cycle. After cycle 9, the number of patients available to complete assessments had ███████ ██ ████ ████ ███ after cycle 9 and after cycle 13 in the carboplatin-pemetrexed and the amivantamab plus carboplatin-pemetrexed groups, respectively. Only █████████ of the original randomized population (██ ██ ███ █████████ was available to provide assessments at the 12-month time point (cycle 17 day 1) in the amivantamab plus carboplatin-pemetrexed group and only slightly more than ███ ███ ██ ███ ████████) in the carboplatin-pemetrexed group. The sponsor employed mixed-effects model for repeated measures to estimate the change from baseline, an approach that assumes data to be missing at random. Although most of these missing data could be accounted for by patients leaving the study or crossing over to amivantamab monotherapy, it means that the remaining patients available to provide assessments were all responders, which may bias results in both groups, and does not suggest data were missing at random.
OS results are a reflection of both the study drug and subsequent treatments. Switching patients in the control group whose disease is not responding to their carboplatin-pemetrexed regimen to amivantamab monotherapy may have improved outcomes in these patients. Thus, there is a risk of bias toward the null. Given the large number of patients who switched from carboplatin-pemetrexed to amivantamab, the potential for underestimation of the treatment effect may be significant. For example, of the 155 patients in the carboplatin-pemetrexed group, ███ had a PFS event (death or progression), ███ of them had progressive disease, and 71 of 107 (66.4%) patients with disease progression switched to amivantamab monotherapy. On average, patients who switched were exposed to amivantamab for nearly as much time as they were exposed to carboplatin-pemetrexed, suggesting that switching may have had a significant impact on OS results, as well as influencing subsequent assessment of PFS2. In an effort to account for this potential bias, the sponsor performed several post hoc sensitivity analyses of OS results, including IPCW, TSE, and RPSFT. The OS results were similar in the IPCW (adjusted ██ ██ ████ ████ ███ █████ ████) and TSE (adjusted HR of ████ ████ ███ █████ ████) analyses and differed slightly from those in the RPSFT (adjusted HR ██ ███ ████ ███ █████ ████). CIs were wide in all cases (i.e., including small effects) and crossed the null for the RPSFT model. A key assumption of the IPCW and TSE approaches is that there is no unmeasured confounding, while a key assumption of the RPSFT model is that there is a common treatment effect. These assumptions cannot be objectively verified, and, if deemed implausible, would undermine the validity of the estimated effects. Several potential confounding variables were considered in the IPCW and TSE analyses. However, numerous subjective factors may influence which patients cross over (versus those who do not), which makes it difficult to fully justify the assumption that all potential confounding has been accounted for.78 Similarly, in relation to the RPSFT model, it might not be clinically reasonable to assume the treatment effect to be equivalent regardless of whether it is received at randomization or postprogression. Ultimately, all of these sensitivity analyses are considered to provide supportive information about the true treatment effect of amivantamab plus carboplatin-pemetrexed compared to carboplatin-pemetrexed but are limited due to their dependence on unverifiable assumptions.
External Validity
The clinical experts believed that the patients enrolled in the PAPILLON trail were generally representative of the patients who would receive this drug in Canada. The clinical experts consulted for this review noted that, although inclusion in the PAPILLON trail was restricted to patients with an ECOG performance status of 0 or 1, they would likely also offer amivantamab plus carboplatin-pemetrexed to patients with an ECOG of 2.
The clinical experts believed OS to be an important outcome in assessing response in these patients; however, these data are still immature. Specifically, there were a total of 70 (about 23%) patients who had died at the time of the data cut-off (median follow-up of 14.92 months), while the final analysis of OS is planned to be conducted 48 months after the first patient was randomized, with an anticipated 210 deaths. The clinical experts believed that PFS is an appropriate primary outcome, particularly since OS is difficult to assess in clinical trials in this setting, given the tendency to allow patients whose disease progressed on their control treatment, to cross over to the treatment group.
The background therapy, carboplatin-pemetrexed, is appropriate for these patients, according to the clinical experts consulted for this review. The clinical experts suggested that some clinicians might prefer to use cisplatin over carboplatin, which was felt to be reasonable, given cisplatin is anticipated to have a similar side effect profile and efficacy as carboplatin.
GRADE Summary of Findings and Certainty of the Evidence
Methods for Assessing the Certainty of the Evidence
For pivotal studies and RCTs identified in the sponsor’s systematic review, GRADE was used to assess the certainty of the evidence for outcomes considered most relevant to inform the CDA-AMC expert committee deliberations, and a final certainty rating was determined as outlined by the GRADE Working Group.79,80
High certainty: We are very confident that the true effect lies close to that of the estimate of the effect.
Moderate certainty: We are moderately confident in the effect estimate. The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. We use the word “likely” for evidence of moderate certainty (e.g., “X intervention likely results in Y outcome”).
Low certainty: Our confidence in the effect estimate is limited. The true effect may be substantially different from the estimate of the effect. We use the word “may” for evidence of low certainty (e.g., “X intervention may result in Y outcome”).
Very low certainty: We have very little confidence in the effect estimate. The true effect is likely to be substantially different from the estimate of effect. We describe evidence of very low certainty as “very uncertain.”
Following the GRADE approach, evidence from RCTs started as high-certainty evidence and could be rated down for concerns related to study limitations (which refers to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias.
When possible, certainty was rated in the context of the presence of an important (nontrivial) treatment effect; if this was not possible, certainty was rated in the context of the presence of any treatment effect (i.e., the clinical importance is unclear). In all cases, the target of the certainty-of-evidence assessment was based on the point estimate and where it was located relative to the threshold for a clinically important effect (when a threshold was available) or to the null. The target of the certainty-of-evidence assessment was the presence or absence of a clinically important effect based on thresholds informed by the clinical experts consulted for this review for PFS and OS. The literature-based MID of 10 points was used for the EORTC QLQ-C30 GHS.29,30 This MID has been estimated for within-group changes and was applied in the absence of an estimate of the MID for a between-group difference. The target of the certainty of evidence was the presence or absence of any (non-null) effect for the ORR because a threshold for a clinically important between-group difference could not be estimated.
Results of GRADE Assessments
Table 2 presents the GRADE summary of findings for amivantamab plus carboplatin-pemetrexed versus carboplatin-pemetrexed.
Long-Term Extension Studies
Contents in this section have been informed by materials submitted by the sponsor. The following have been summarized and validated by the CDA-AMC review team.
No long-term extension studies were available at the time of filing the application.
Indirect Evidence
The sponsor submitted an ITC report that included analyses that used individual patient data from the PAPILLON trail and real-world databases and IPTW methods to reduce the risk of bias due to confounding. This was considered by the review team as a nonrandomized study and is reported in the Studies Addressing Gaps section.
This section includes the contents of the ITC report submitted by the sponsor, which was considered by the review team to include a nonrandomized study, as it utilized individual patient data for each arm in the comparisons.
Objectives for the Nonrandomized Study
The objective of this section is to summarize and critically appraise the methods and findings of the nonrandomized study submitted by the sponsor. The sponsor submitted a nonrandomized study that assessed the relative effectiveness between amivantamab plus carboplatin-pemetrexed (assessed in the PAPILLON study), and other common treatment options used in real-world clinical practice (EGFR TKI monotherapy and platinum chemotherapy plus IO).
The sponsor stated that comparisons of amivantamab plus carboplatin-pemetrexed to EGFR TKIs, and IO, in head-to-head clinical studies of patients with EGFR exon 20ins mutated advanced NSCLC in the first-line setting, have not been conducted.
Description of the Nonrandomized Study
The sponsor’s analysis included a nonrandomized study using propensity score weighting to reduce the impact of bias due to confounding. The analyses used individual patient data from the PAPILLON trail for amivantamab plus carboplatin-pemetrexed and from real-world databases COTA and ConcertAI for EGFR TKI monotherapy and platinum chemotherapy plus IO.
Nonrandomized Study
Objectives
The sponsor submitted a nonrandomized study that assessed the relative effectiveness between amivantamab plus carboplatin-pemetrexed (assessed in the PAPILLON study) and other common treatment options used in real-world clinical practice (EGFR TKI monotherapy and platinum chemotherapy plus IO). The comparative clinical efficacy of chemotherapy alone versus EGFR TKIs or chemotherapy alone versus IO plus chemotherapy was not the purpose of assessment.
Study Selection Methods
The sponsor did not submit a predetermined protocol or undertake a systematic review to identify studies for inclusion in the analysis. There was no evidence that the sponsor employed a literature search or utilized a priori selection criteria to select the studies for the analysis. There was no description of data extraction methods or appraisal of risk of bias of the contributing data sources.
Data Sources
PAPILLON Study
Individual patient data for amivantamab plus carboplatin-pemetrexed consisted of data from 1 arm of the PAPILLON trial. the PAPILLON trail is an ongoing, phase III, open-label, parallel, multicentre RCT that enrolled 308 patients. Treatment was administered in cycles of 21 days (3 weeks) until patient discontinuation or disease progression. This study is described in detail in other sections of this report.
Real-World Database: COTA
COTA’s Real-World Evidence database comprises longitudinal, Health Insurance Portability and Accountability Act (HIPAA)-compliant data pertaining to the diagnosis, clinical management, and outcomes of patients with cancer in the US. Data are abstracted from the electronic health records of health care provider sites, representing diverse treatment settings, including academic, for-profit, community sites, and hospital systems. COTA leverages both human abstraction and technologic methods to transform structured and unstructured data into a standard data model. Abstractors receive in-depth training on oncology, data abstraction, and electronic medical record navigation and are required to achieve an acceptable accuracy rate on abstraction of test records against a gold standard before abstracting in COTA’s production database. The COTA deidentified retrospective dataset includes data on a cohort of patients with NSCLC and confirmed EGFR exon 20ins mutation from 5 unique sites of care; 79% of patients were treated at academic medical centres and 21% were treated in the community oncology setting. Patients are excluded from the dataset if they:
are younger than aged 18 years at the time of diagnosis
do not have the malignancy of interest
are not evaluated at the accessible provider site for the malignancy
have concurrent primary malignancies
have no date of diagnosis in the electronic health record
have no clinician note available in the electronic health record
are diagnosed with a malignancy after the diagnosis of the malignancy of interest before evaluation for the malignancy of interest at the accessible provider site
are initially misdiagnosed and treated for another malignancy but are later confirmed to have the malignancy of interest
are on therapy, active surveillance, or observation for a malignancy diagnosed before the diagnosis of the malignancy of interest at the time of diagnosis of the malignancy of interest
have metastatic malignancy, including leukemias and multiple myeloma, diagnosed before the malignancy of interest
were only seen once at the provider site for the malignancy of interest
had low-grade (inclusive of grades 1 and 2) neuroendocrine histology.
Real-World Database: ConcertAI
ConcertAI sources clinical data from multiple partnerships spanning a broad range of US locations, regardless of electronic medical record (EMR) provider. This includes data from various organizations aggregating data from oncology practices to create rapid learning systems for providers to improve patient care. ConcertAI’s data source partners receive copies of the practice’s complete EMR, including unstructured notes and scanned documents attached to the EMR. ConcertAI’s data partners are EMR agnostic and have customer-implementation teams assigned to each practice for procurement of structured and unstructured information. ConcertAI processes all available oncology data (patient documents, physician notes, structured EMR data) into an Observational Medical Outcomes Partnership (OMOP)-based Common Data Model designed for easier query and analyses. The split of organization type across the data product varies by indication (with an overall average of approximately 70% community and approximately 30% academic). The geographic split across the data product also varies by indication (with an overall average of approximately 15% northeast, approximately 25% midwest, approximately 40% south, and approximately 20% west). Patients were extracted from both the Patient360 and Genome360 data samples and pooled into a single “ConcertAI” cohort.
Patient360
ConcertAI screens patients for curation based on a structured International Classification of Diseases (ICD)-10 diagnosis for the indication of interest and, at a minimum, the diagnosis year. Once a screening list has been generated with these 2 criteria, ConcertAI randomly pulls in patients by first curating and confirming diagnosis and diagnosis date (based on pathology reports and other unstructured data). All patients must be older than 18 years of age at first diagnosis date. Patients are selected for inclusion in data products through the quality-control processes, identifying whether there are conflicts in the patient record, using structured or both structured and curated data, depending on the data product. Patients were not filtered by ConcertAI based on data completeness to avoid introduction of selection bias.
Genome360
Apart from the criteria used to select patients for Patient360 curation, as detailed previously, patients were further selected for Genome360 only if the patient record contained a somatic NGS report, which is determined through natural language processing algorithms and further confirmed by manual screening.
Table 18: Analysis Populations of the Included Studies in the Nonrandomized Study
Study | Patient characteristics |
|---|---|
PAPILLON cohort | The PAPILLON trial cohort consisted of patients who were randomized to amivantamab + CP, received or initiated treatment, and satisfied the key criteria:
The index date was determined as the date the first dose of amivantamab + CP therapy was received. |
Real-world comparator cohorts | Real-world cohorts consisted of patients with advanced NSCLC EGFR exon 20ins from the COTA and ConcertAI databases who received EGFR TKI monotherapy or platinum chemotherapy + IO. Eligible medications within each treatment class were:
These regimens were considered the most relevant first-line comparators for inclusion (separately) within the current analysis, due to the rarity of EGFR exon 20ins mutation, lack of standard of care, limited use of VEGFis in combination with other therapies in this patient population in the US (and Canada), and consistency with treatment patterns observed in previous US real-world evidence publications. Definitions used to identify the first-line advanced NSCLC EGFR exon 20ins population in the COTA and Concert AI databases were the following:
Included patients in the present analysis also met the following key inclusion criteria to align with the PAPILLON trial:
The study index date was determined as the date of the initiation of first-line treatment for advanced NSCLC disease with confirmed EGFR exon 20ins mutation. |
CP = carboplatin-pemetrexed; ECOG = Eastern Cooperative Oncology Group; exon 20ins = exon 20 insertion; IO = immunotherapy; NSCLS = non–small cell lung cancer; RECIST = Response Evaluation Criteria in Solid Tumours; TKI = tyrosine kinase inhibitor; ULN = upper limit of normal; VEGFi = vascular endothelial growth factor inhibitor.
Source: Sponsor’s ITC.81
Feasibility Assessment
The sponsor did not provide a feasibility assessment or a systematic review of the literature.
Analysis Methods
Outcomes Analyzed
Overall Survival
In both data sources, OS was defined as the time between the index date and death from any cause. Patients still alive at the end of the study period were censored at the study end date. For patients who were alive or for whom their vital status was unknown, this interval was censored at the date the patient was last known to be alive.
Progression-Free Survival
PFS was defined as the time from index date to date of disease progression (as recorded in the database) or death (from any cause), whichever occurred first. Disease progression in the PAPILLON trail assessed by BICR was used. A definition for “progression” in the real-world data sources was not provided, but it was noted that the databases did not have a systematic capture of progressive disease or RECIST v.1.1 criteria.
Real-World PFS
As the real-world COTA and ConcertAI databases do not have a systematic capture of progressive disease or RECIST v1.1. criteria, which are not typically captured in the real-world, the start of subsequent treatment was also considered a progression event. Therefore, RW-PFS for COTA and ConcertAI was defined as the time from index date to date of disease progression, start date of subsequent treatment, or death (from any cause), whichever occurred first. Specifics of the estimation of RW-PFS in the PAPILLON trail were not provided.
Time to Next Treatment
In both data sources, TTNT was defined as the time between the index date and the start date of subsequent treatment or death, whichever came first. Patients without a record of subsequent therapy were censored at the date of last contact.
Nonrandomized Study Methods
Baseline Covariates
The identification of potential treatment effect modifiers and prognostic factors was based on an unpublished systematic review with expert input. Thereafter, selected variables for adjustment included prognostic factors that were mutually reported in both the PAPILLON trail as well as the COTA and ConcertAI real-world databases. Prognostic factors were assessed at baseline in the real-world databases, defined as 30 days before to 15 days after the start of therapy, and at baseline in the PAPILLON trial. It was not clear whether some information was missing for the covariate data in the sponsor’s analyses or how that might have been handled. The final list and ranking of covariates are outlined in Table 19, but it should be noted that not all covariates were used in all of the sponsor’s analyses, as described later in this report. Of the 9 factors identified as important for population adjustment, prior major surgery in the 4 weeks before index date was included as an exclusion criterion in the patient selection process instead of a prognostic factor for adjustment in the statistical models. While a sensitivity analysis of the full model including all 8 factors was conducted, the primary analysis of the base case only adjusted for the top 4 ranked factors.
Table 19: Final Ranking of Covariates and Usability
Covariate | Rank | Used in current analyses? | Categories |
|---|---|---|---|
Functional status ECOG at index date | 1 | Yes | 0 |
History of brain metastasesa | 2 | Yes | Yes |
History of liver metastasesa | 3 | Yes | Yes |
Age at index date | 4 | Yes | < 65 years ≥ 65 years |
Asian race | 5 | Yes | Yes No |
History of smokingb | 6 | Yes | Yes No |
Sex | 7 | Yes | Female Male |
History of other metastatic locationsa | 8 | Yes | Yes No |
Prior major surgeryc in the 4 weeks before index date | 9 | Yesd | Yes No |
ECOG = Eastern Cooperative Oncology Group.
aMetastatic disease time windows were anchored 30 days before to 15 days after the date of diagnosis of locally advanced or metastatic cancer.
bAny time before the index date.
cMajor surgery includes but is not limited to brain lobectomy, brain operation, brain tumour operation, cancer surgery, craniectomy, cranioplasty, craniotomy, lung lobectomy, lung neoplasm surgery, lung operation, lymphadenectomy, lymphadenopathy mediastinal, pleural decortication, pneumonectomy, pulmonary resection, thoracic operation, and thoracotomy.
dThis covariate was included as an exclusion criterion in the present analysis instead of a prognostic factor for adjustment.
Source: Sponsor’s ITC Report.81
Statistical Analysis
To improve the balance of baseline confounding variables between the PAPILLON trial and real-world comparator cohorts, IPTW was used to adjust for selected baseline characteristics, following recommendations of the National Institute for Health and Care Excellence Decision Support Unit Technical Support Document.48
IPTW with ATT weighting was used to adjust for baseline differences between the the PAPILLON trail and comparator cohorts. This method allowed the real-world cohorts to be reweighted to align with the PAPILLION cohort. It is important to note that IPTW with ATT weights may become unstable when the comparator arm sample size is small.
Propensity scores were derived with a multivariable logistic regression model using a binary treatment variable as the dependent variable and the following covariates: functional status ECOG at index date, history of brain metastases, history of liver metastases, and age at index date. These were ranked as the most important prognostic factors for adjustment. The estimated propensity scores were then used to derive weights for each patient, where patients in the PAPILLON trail group received a weight of 1, while patients in the real-world comparator groups were reweighted based on the probability of receiving treatment.
Population differences between the PAPILLON trial population and the comparator cohort populations were assessed before and after weighting, using SMDs. The sponsor considered an absolute SMD between 0 and 0.1 to be a small difference. The balance of covariates was also visually displayed by density plots of the propensity scores before and after weighting.
The ESS was calculated to reflect the impact of weighting on the available information in the individual patient data.
Outcome Analysis Methods
The comparative effectiveness of amivantamab plus carboplatin-pemetrexed versus the platinum plus IO and EGFR TKI comparator cohorts was determined for the following outcomes: OS, PFS, RW-PFS, and TTNT. Estimates of comparative effectiveness were derived for both the unadjusted comparison (i.e., amivantamab plus carboplatin-pemetrexed versus comparative treatment before IPTW) and the adjusted comparison (i.e., with IPTW).
A Cox proportional hazards model (with weights applied for the adjusted comparison) was used to derive an HR and its respective 95% CI. The variance was estimated using a robust sandwich estimator to account for the uncertainty in estimation of the weights.
Sensitivity Analysis
As summarized in Table 20, a number of sensitivity analyses were conducted using alternative weighting formulas. Average treatment effect in the control weighting and average treatment effect in the overlap (ATO) weighting were employed to improve the covariate balance and mitigate the limitations associated with the reduction in the ESS from the ATT weighting. Multivariable regression analysis using the same covariates was also conducted to assess the impact of an alternate analytical approach to adjusting for baseline differences between the 2 cohorts on the study’s results. All analyses were performed for all outcomes of interest (OS, PFS, RW-PFS, and TTNT).
IPTW with ATO weights were determined, where patients in both cohorts are reweighted to estimate the treatment effect in the overlap population between groups. ATO weights are less sensitive to extreme weights and can be considered when outliers may be a concern. ATO weighting may be beneficial when overlap between both cohorts is poor. ATO weights were derived, where patients in the PAPILLON trial group received a weight equal to the propensity score while the patients in the comparator treatment cohorts received a weight equal to 1 – propensity score. This estimated the treatment effect in the overlap population of the PAPILLON trial and comparator treatment cohorts.
A third sensitivity analysis was conducted using multivariable regression. This method requires overlap in covariate distribution, similar to IPTW. Unlike reweighting methods, however, regression models estimate the conditional average treatment effect and require a large sample size compared to the number of covariates in the model.
For each of the analytical approaches evaluated (e.g., ATT, average treatment effect in the control, ATO, and multivariable regression), adjusted comparisons were also conducted by sequentially adjusting for the remaining prognostic factors in order of importance, until the final model contained all prognostic covariates (referred to as the “full model”). The selected covariates were also adjusted for in the model to produce doubly robust results, as an additional sensitivity analysis.
Assessment of Proportional Hazards
Appropriateness of the proportional hazards assumption for survival outcomes was assessed based on visual inspection of the log-cumulative hazard plot, visual inspection of the Schoenfeld residuals plot, and performance of the Grambsch-Therneau test (with a P value less than 0.05 considered to indicate a violation of the assumption). For all analyses, patient numbers over time were reported.
Table 20: Sensitivity Analysis
Types of analyses | Analytic specification | ||
|---|---|---|---|
Outcomes | Covariates | Statistical method | |
Primary analysis | OS, PFS, RW-PFS, and TTNT | Base casea | IPTW with ATT weights |
Sensitivity analyses | |||
IPTW with ATT weights (doubly robust) | █████████ | █████████ | IPTW with ATT weights (doubly robust) |
IPTW with ATT weights — full model | █████████ | ████ ████ █ █████ █████ ███████ ██ ████████ ████ ███████ ██ █████ ██████████ | Unchanged |
IPTW with ATC weights | █████████ | █████████ | IPTW with ATC weights |
IPTW with ATC weights (doubly robust) | █████████ | █████████ | IPTW with ATC weights (doubly robust) |
IPTW with ATC weights — full model | ████████ | ████ ████ █ █████ █████ ███████ ██ ████████ ████ ███████ ██ █████ ██████████ | IPTW with ATC weights |
IPTW with ATO weights | █████████ | █████████ | IPTW with ATO weights (not doubly robust) |
IPTW with ATO weights (doubly robust) | █████████ | █████████ | IPTW with ATO weights (doubly robust) |
IPTW with ATO weights — full model | ████████ | ████ ████ █ █████ █████ ███████ ██ ████████ ████ ███████ ██ █████ ██████████ | IPTW with ATO weights |
Multivariable regression | █████████ | █████████ | Multivariable regression |
Multivariable regression — full model | ████████ | ████ ████ █ █████ █████ ███████ ██ ████████ ████ ███████ ██ █████ ██████████ | Multivariable regression |
ATC = average treatment effect in the control; ATO = average treatment effect in the overlap; ATT = average treatment effect in the treated; IPTW = inverse probability of treatment weighting; OS = overall survival; PFS = progression-free survival; RW- PFS = real-world progression-free survival; TTNT = time to next treatment.
Note: “Unchanged” indicates that the analytic specification was unchanged from the main analyses.
aECOG at index date, history of brain metastases, history of liver metastases, age at index date.
Source: Sponsor’s ITC Report.81
Results of the Nonrandomized Study
Selection of Participants
Of the 308 patients in the PAPILLON trial, the final cohort consisted of 153 patients that received amivantamab plus carboplatin-pemetrexed. Of the ██████ patients within the combined COTA and ConcertAI databases, the final RW comparator cohorts consisted of ██ ███ ██ patients who received first-line EGFR TKI or platinum plus IO treatment, respectively (Figure 3).
Figure 3: Patient Selection for the Nonrandomized Study [Redacted]

Source: Sponsor’s ITC Report81 — ITCs with individual patient data.
Treatment Regimens Received in the Real-world Cohorts
Following the application of inclusion criteria to align with the PAPILLON trial, sufficient sample size for comparison was only available for the EGFR TKI alone and platinum plus IO comparator cohorts, which were thus included as comparator groups in the analysis. A breakdown of the specific treatment regiments patients received in the EGFR TKI and platinum plus IO cohorts are included in Table 21 and Table 22.
Table 21: Specific Treatment Regimens Patients Received in the EGFR TKI Cohort
EGFR TKI treatments | Count |
|---|---|
████████ | ██ |
█████████ | ██ |
████████████ | ██ |
███████████ | ██ |
█████ | ██ |
TKI = tyrosine kinase inhibitor.
Sources: Sponsor’s ITC Report81 and indirect treatment comparisons with individual patient data.
Table 22: Specific Treatment Regimens Patients Received in the Platinum Plus IO Cohort
Platinum + IO treatments | Count |
|---|---|
████████████ ███████████ ███ █████████████ | ██ |
████████████ ██████████ ████████████ ██████████████ ███ █████████████ | ██ |
█████ | ██ |
IO = immunotherapy.
Source: Sponsor’s ITC Report.81
Summary of Baseline Population Characteristics
The population differences in baseline covariates between the PAPILLON trail and real-world comparator cohorts before and after adjustment with ATT weighting are shown in Table 23 and Table 24 for EGFR TKI and platinum + IO.
For the PAPILLON trial versus EGFR TKI comparison, before weighting, moderate differences (absolute SMD ████ ███ ████) were observed for ECOG at index date and history of smoking, and substantial differences (absolute SMD █████ seen for history of liver metastases, age, Asian race, sex, and history of other metastases. The PAPILLON trial cohort has a higher proportion of participants with ECOG PS 1, no history of liver metastases, history of other metastases, male sex, less than 65 years of age, and of Asian race. In the primary analysis, base-case ATT weighting balanced (SMD ████) all 4 covariates between cohorts, but race, sex, and history of metastases remained imbalanced. In the full model, however, all 8 of the included factors had absolute SMDs████, indicating lack of balance, with moderate differences observed for 6 factors (████ ██ █████ █████ ███████ ██ █████ ███████████ ████ ███████ ██ ████████ ████ ███████ ██ █████ ██████████), and substantial differences observed for the remaining 2 factors (███████ ██ █████ ███████████ █████ █████. The resulting ESS in the EGFR TKI cohort was ████ ███ ████ for the base-case and full model, respectively, compared to the original 18 observations.
For the PAPILLON trial versus platinum plus IO comparison, before weighting, substantial (absolute SMD ████) differences were observed for ████ ██ █████ █████ ███████ ██ █████ ███████████ ███████ ██ █████ ███████████ ████ █████ █████ ███ ███████ ██ █████ ███████████ ████ ███ ████████ ██████ ██████ █ ██████ ██████████ ██ ████████████ ████ ████ ██████ ████ ██ ███████ ██ █████ ██ █████ ███████████ ███████ ██ █████ ███████████ ████████ ████ ████ ██ █████ ██ ████ ███ ██ █████ ████. In the primary analysis, ATT weighting reduced the proportion of categories with absolute SMDs ████ ████ ████ ██████ ██ ███ ████) in the base case; however, differences remained in █████ ███████ ████████ ████ ███ ███████ ██ ██████████. The balance between populations in the full model, on the other hand, remained the same (6 of 8 factors balanced) following weighting, although moderate differences were observed for 3 factors (████ ██ █████ █████ ███████ ██ █████ ███████████ ███████ ██ ███████) and substantial differences observed for the remaining 3 factors (███████ ██ █████ ███████████ █████ █████ ███████ ██ █████ ██████████). The resulting ESS in the platinum plus IO cohort was █████ ███ ████ for the base case and full model, respectively, compared to the original ██ observations.
Table 23: Overview of Baseline Characteristics for Amivantamab Plus Carboplatin-Pemetrexed (PAPILLON) Versus EGFR TKI (COTA, ConcertAI) Before and After Adjustment With IPTW Using ATT
Variable | Categories | Unadjusted comparison | IPTW-ATT (base case) | IPTW-ATT (full model) | ||||
|---|---|---|---|---|---|---|---|---|
PAPILLON N = 153 (%) | EGFR TKI N = 18 (%) | SMD | EGFR TKI ESS = 15.08 (%) | SMD | EGFR TKI ESS = 7.17 (%) | SMD | ||
Functional status ECOG at index date | 0 | 35.3% | █████ | ████ | █████ | ████ | █████ | █████ |
1 | 64.7% | █████ | █████ | █████ | ||||
History of brain metastases | Yes | 22.9 | █████ | ████ | █████ | ████ | ████ | ████ |
No | 77.1 | █████ | █████ | █████ | ||||
History of liver metastases | Yes | █████ | █████ | █████ | █████ | ████ | ████ | ████ |
No | █████ | █████ | █████ | ███ | ||||
Age at index date | < 65 years | 63.4 | █████ | █████ | █████ | ████ | █████ | ████ |
≥ 65 years | 36.6 | █████ | █████ | █████ | ||||
Asian race | Yes | 63.4 | █████ | ████ | █████ | ████ | █████ | ████ |
No | 36.6 | █████ | █████ | █████ | ||||
History of smoking | Yes | 42.5 | █████ | █████ | █████ | ████ | █████ | ████ |
No | 57.5 | █████ | █████ | █████ | ||||
Sex | Male | 44.4 | █████ | █████ | █████ | ████ | █████ | █████ |
Female | 55.6 | █████ | █████ | █████ | ||||
History of other metastases | Yes | █████ | █████ | ████ | █████ | ████ | █████ | ████ |
No | █████ | █████ | █████ | █████ | ||||
ATT = average treatment effect in the treated; ECOG = Eastern Cooperative Oncology Group; ESS = effective sample size; IPTW = inverse probability of treatment weighting; SMD = standardized mean difference; TKI = tyrosine kinase inhibitor.
Note: Grey cells indicate that these variables were not adjusted for in the given analysis.
Source: Sponsor’s ITC Report.81
Table 24: Overview of Baseline Characteristics for Amivantamab Plus Carboplatin-Pemetrexed (PAPILLON) Versus Platinum Plus IO (COTA, ConcertAI) Before and After Adjustment With IPTW Using ATT
Variable | Categories | Unadjusted comparison | IPTW-ATT (base case) | IPTW-ATT (full model) | ||||
|---|---|---|---|---|---|---|---|---|
PAPILLON N = 153 (%) | Platinum + IO N = 27 (%) | SMD | Platinum + IO ESS = 16.27 (%) | SMD | Platinum + IO ESS = 9.42 (%) | SMD | ||
Functional status ECOG at index date | 0 | 35.3 | █████ | ████ | █████ | ████ | █████ | ████ |
1 | 64.7 | █████ | █████ | █████ | ||||
History of brain metastases | Yes | 22.9 | █████ | █████ | █████ | █████ | █████ | █████ |
No | 77.1 | █████ | █████ | █████ | ||||
History of liver metastases | Yes | █████ | █████ | █████ | █████ | ████ | ████ | ████ |
No | █████ | █████ | █████ | █████ | ||||
Age at index date | < 65 years | 63.4 | █████ | █████ | █████ | █████ | █████ | ████ |
≥ 65 years | 36.6 | █████ | █████ | █████ | ||||
Asian race | Yes | 63.4 | ████ | ████ | ████ | ████ | █████ | ████ |
No | 36.6 | █████ | █████ | █████ | ||||
History of smoking | Yes | 42.5 | █████ | █████ | █████ | ████ | █████ | ████ |
No | 57.5 | █████ | █████ | █████ | ||||
Sex | Male | 44.4 | █████ | █████ | █████ | █████ | █████ | █████ |
Female | 55.6 | █████ | █████ | █████ | ||||
History of other metastases | Yes | █████ | █████ | ████ | █████ | ████ | █████ | █████ |
No | █████ | █████ | ███ | █████ | ||||
ATT = average treatment effect in the treated; ECOG = Eastern Cooperative Oncology Group; ESS = effective sample size; IO = immunotherapy; IPTW = inverse probability of treatment weighting; SMD = standardized mean difference.
Note: Grey cells indicate that these variables were not adjusted for in the given analysis.
Source: Sponsor’s ITC Report.81
Summary of Results
Overall Survival
The unadjusted comparison of OS for the PAPILLON trail versus EGFR TKI produced an HR of ████ ████ ███ █████ █████ ███████), favouring amivantamab plus carboplatin-pemetrexed, as summarized in Table 25. The primary analysis, using base-case ATT weighting, produced results ██ ██████ ██ amivantamab plus carboplatin-pemetrexed, with an HR of ████ ████ ███ █████ █████ █████████. The results of the ATT full model produced results that were numerically in favour of amivantamab plus carboplatin-pemetrexed ███ ███ ██████████ ████████ ████████ ███ ████, with an HR of ████ ████ ███ █████ ██████.
The unadjusted comparison of OS for the PAPILLON trail versus platinum plus IO, produced an HR of ████ ████ ███ █████ █████ █████████, favouring amivantamab plus carboplatin-pemetrexed, as summarized in Table 26. In the primary analysis, using base-case ATT weighting, the point estimate favoured amivantamab plus carboplatin-pemetrexed ███ █████ ███ █ ████ ██ ████ ████████ ███ ████, with an HR of ████ ████ ███ █████ █████ ███████). The results of the ATT full model produced results that were in favour of amivantamab plus carboplatin-pemetrexed, with an HR of ████ ███████ █████ ████).
Results of the other sensitivity analyses (not shown) were mostly similar in direction of effect, with some results having CIs that ███████ ███ ████.
Table 25: Summary of Overall Survival Results for Amivantamab Plus Carboplatin-Pemetrexed (PAPILLON) Versus EGFR TKI
Variables | EGFR TKI | PAPILLON | PAPILLON versus EGFR TKI | |||||
|---|---|---|---|---|---|---|---|---|
IPTW | Doubly robust | |||||||
% events | Median TTE (95% CI) | % events | Median TTE (95% CI) | HR (95% CI) | P value | HR (95% CI) | P value | |
Unadjusted | ████ | ███████ | ████ | ██ | ███████ | █████ | █████████ | |
ATT weighting | ||||||||
Base case | ████ | ███████ | ████ | ██ | ███████ | █████ | ██████ | █████ |
Full model | ████ | ███████ | ████ | ██ | ███████ | █████ | ██████ | █████ |
ATT = average treatment effect in the treated; CI = confidence interval; HR = hazard ratio; IPTW = inverse probability of treatment weighting; NR = not reached; TKI = tyrosine kinase inhibitor; TTE = time to event.
Notes: Multivariable regression results: Base-case HR ████ ████ ███ █████ █████ ███████ ████ full model HR ████ ████ ███ █████ █████ ███████ ███.
The base-case results adjusted for ECOG at index date, history of brain metastases, history of liver metastases, and age at index date. The fully adjusted scenario adjusted for all the variables in the base case, plus Asian race, history of smoking, sex, and history of other metastases.
Source: Sponsor’s ITC Report.81
Table 26: Summary of Overall Survival Results for Amivantamab Plus Carboplatin-Pemetrexed (PAPILLON) Versus Platinum Plus IO
Variables | Platinum + IO | PAPILLON | PAPILLON versus platinum + IO | |||||
|---|---|---|---|---|---|---|---|---|
IPTW | Doubly robust | |||||||
% events | Median TTE (95% CI) | % events | Median TTE (95% CI) | HR (95% CI) | P value | HR (95% CI) | P value | |
Unadjusted | ████ | ██████ | ████ | ██ | ███████ | ████ | █████████ | |
ATT weighting | ||||||||
Base case | ████ | ██████ | ████ | ██ | ███████ | ████ | ██████ | █████ |
Full model | ████ | ██████ | ████ | ██ | ███████ | ████ | ██████ | █████ |
ATT = average treatment effect in the treated; CI = confidence interval; HR = hazard ratio; IO = immunotherapy; IPTW = inverse probability of treatment weighting; NA = not applicable; TTE = time to event.
Notes: Multivariable regression results: Base-case HR ████ ████ ███ █████ █████ ███████), full model HR ████ ████ ███ █████ █████ ████████.
The base-case results adjusted for ECOG at index date, history of brain metastases, history of liver metastases, and age at index date. The fully adjusted scenario adjusted for all the variables in the base case, plus Asian race, history of smoking, sex, and history of other metastases.
Source: Sponsor’s ITC Report.81
Assessment of Proportional Hazards
The proportional hazards assumption was assessed for the primary analysis (ATT, base case) populations of the PAPILLON trail versus EGFR TKI and platinum plus IO. Visual inspection of the log-cumulative hazard plots and Schoenfeld residual did not show any clear evidence of the proportional hazards assumption being violated before significant participant drop-off for EGFR TKI, but evidence of a potential violation was found for platinum plus IO. The Grambsch-Therneau test for proportional hazards assumption ███████████████ for both EGFR TKI (████████) and platinum plus IO █████████).
Progression-Free Survival
The unadjusted comparison of PFS for the PAPILLON trail versus EGFR TKI produced an HR of ████ ████ ███ █████ █████ ███████), favouring amivantamab plus carboplatin-pemetrexed (Table 27). The primary analysis, using base-case ATT weighting, produced a point estimate favouring amivantamab plus carboplatin-pemetrexed, but the 95% CI ████████ ███ ████, with an HR of ████ ████ ███ █████ █████ █████████ The results of the ATT full model produced results that were numerically favouring EGFR TKI, but the 95% CI ████████ ███ ████, with an HR of ████ ████ ███ █████ ██████.
The unadjusted comparison of PFS for the PAPILLON trail versus platinum plus IO produced an HR of ████ ████ ███ █████ █████ ███████), favouring amivantamab plus carboplatin-pemetrexed (Table 28). The primary analysis, using base-case ATT weighting, produced results in favour of amivantamab plus carboplatin-pemetrexed, with an HR ██ ████ ████ ███ █████ █████ ███████). The results of the ATT full model produced results that were numerically in favour of amivantamab plus carboplatin-pemetrexed, but the 95% CI ████████ ███ ████, with an HR of ████ ████ ███ █████ ██████
Results of the other sensitivity analyses (not shown) were mostly similar in direction of effect, with some results having CIs ████ ███████ ███ ████, while others had CIs ████ ████████ ███ ████.
Table 27: Summary of Progression-Free Survival Results for Amivantamab Plus Carboplatin-Pemetrexed (PAPILLON) Versus EGFR TKI
Variables | EGFR TKI | PAPILLON | PAPILLON versus EGFR TKI | |||||
|---|---|---|---|---|---|---|---|---|
IPTW | Doubly robust | |||||||
% events | Median TTE (95% CI) | % events | Median TTE (95% CI) | HR (95% CI) | P value | HR (95% CI) | P value | |
Unadjusted | ███ | ██████ | ████ | ██████ | ██████ | █████ | █████████ | |
ATT weighting | ||||||||
Base case | ███ | ██████ | ████ | ██████ | ██████ | █████ | ███████ | █████ |
Full model | ███ | ██████ | ████ | ██████ | ██████ | █████ | ███████ | █████ |
ATT = average treatment effect in the treated; CI = confidence interval; HR = hazard ratio; IPTW = inverse probability of treatment weighting; TKI = tyrosine kinase inhibitor; TTE = time to event.
Notes: Multivariable regression results: Base case HR ████ ████ ███ █████ █████ ███████), full model HR ████ ████ ███ █████ █████ ████████.
The base-case results adjusted for ECOG at index date, history of brain metastases, history of liver metastases, and age at index date. The fully adjusted scenario adjusted for all the variables in the base case, plus Asian race, history of smoking, sex, and history of other metastases.
Source: Sponsor’s ITC Report.81
Table 28: Summary of Progression-Free Survival Results for Amivantamab Plus Carboplatin-Pemetrexed (PAPILLON) Versus Platinum Plus IO
Variables | Platinum + IO | PAPILLON | PAPILLON versus platinum + IO | |||||
|---|---|---|---|---|---|---|---|---|
IPTW | Doubly robust | |||||||
% events | Median TTE (95% CI) | % events | Median TTE (95% CI) | HR (95% CI) | P value | HR (95% CI) | P value | |
Unadjusted | ████ | ██████ | ████ | ██████ | ██████ | █████ | █████████ | |
ATT weighting | ||||||||
Base Case | ████ | ██████ | ████ | ██████ | ██████ | █████ | ██████ | ██████ |
Full Model | ████ | ██████ | ████ | ██████ | ██████ | █████ | ██████ | █████ |
ATT = average treatment effect in the treated; CI = confidence interval; HR = hazard ratio; IO = immunotherapy; IPTW = inverse probability of treatment weighting; TTE = time to event.
Notes: Multivariable regression results: Base-case HR ████ ████ ███ █████ █████ ███████), full model HR ████ ████ ███ █████ █████ ████████.
The base-case results adjusted for ECOG at index date, history of brain metastases, history of liver metastases, and age at index date. The fully adjusted scenario adjusted for all the variables in the base case, plus Asian race, history of smoking, sex, and history of other metastases.
Source: Sponsor’s ITC Report.81
Assessment of Proportional Hazards
The proportional hazards assumption was assessed for the primary analysis (ATT, base case) populations of the PAPILLON trail versus EGFR TKI and platinum plus IO. Visual inspection of the log-cumulative hazard plots and Schoenfeld residual did not show any clear evidence of the proportional hazards assumption being violated before significant participant drop-off for EGFR TKI, but evidence of a potential violation was found for platinum plus IO. The Grambsch-Therneau test for proportional hazards assumption was nonsignificant for platinum plus IO (██████████. Conversely, the Grambsch-Therneau test for EGFR TKI indicated a potential violation of the proportional hazards assumption (███████████).
Real-World PFS
The unadjusted comparison of RW-PFS for the PAPILLON trail versus EGFR TKI produced an HR of ████ ████ ███ █████ █████ ███████), favouring amivantamab plus carboplatin-pemetrexed (Table 29). The primary analysis, using base-case ATT weighting, produced results in favour of amivantamab plus carboplatin-pemetrexed, with an HR of ████ ████ ███ █████ █████ █████████ The results of the ATT full model produced results that were numerically in favour of amivantamab plus carboplatin-pemetrexed, but the 95% CI ████████ ███ ████, with an ██ ██ ████ ████ ███ █████ ██████.
The unadjusted comparison of RW-PFS for the PAPILLON trail versus platinum plus IO produced an HR of ████ ████ ███ █████ █████ ████████, favouring amivantamab plus carboplatin-pemetrexed (Table 30). The primary analysis, using base-case ATT weighting, produced results in favour of amivantamab plus carboplatin-pemetrexed, with an HR of ████ ████ ███ █████ █████ ███████). The results of the ATT full model produced results that were numerically in favour of amivantamab plus carboplatin-pemetrexed, with an HR of ████ ████ ███ █████ ██████.
Results of the other sensitivity analyses (not shown) were mostly similar in direction of effect, with some results having CIs ████ ███████ ███ ████.
Table 29: Summary of Real-World Progression-Free Survival Results for Amivantamab Plus Carboplatin-Pemetrexed (PAPILLON) Versus EGFR TKI
Variables | EGFR TKI | PAPILLON | PAPILLON versus EGFR TKI | |||||
|---|---|---|---|---|---|---|---|---|
IPTW | Doubly robust | |||||||
% events | Median TTE (95% CI) | % events | Median TTE (95% CI) | HR (95% CI) | P value | HR (95% CI) | P value | |
Unadjusted | ████ | ██████ | ████ | ██████ | ██████ | █████ | █████████ | |
ATT weighting | ||||||||
Base case | ████ | ██████ | ████ | ██████ | ██████ | █████ | ██████ | ██████ |
Full model | ████ | ██████ | ████ | ██████ | ██████ | █████ | ██████ | ██████ |
ATT = average treatment effect in the treated; CI = confidence interval; HR = hazard ratio; IPTW = inverse probability of treatment weighting; TKI = tyrosine kinase inhibitor; TTE = time to event.
Notes: Multivariable regression results: Base-case ██ ████ ████ ███ █████ █████ ███████), full model HR ████ ████ ███ █████ █████ ████████.
The base-case results adjusted for ECOG at index date, history of brain metastases, history of liver metastases, and age at index date. The fully adjusted scenario adjusted for all the variables in the base case, plus Asian race, history of smoking, sex, and history of other metastases.
Source: Sponsor’s ITC Report.81
Table 30: Summary of Real-World Progression-Free Survival Results for Amivantamab Plus Carboplatin-Pemetrexed (PAPILLON) Versus Platinum Plus IO
Variables | Platinum + IO | PAPILLON | PAPILLON versus platinum + IO | |||||
|---|---|---|---|---|---|---|---|---|
IPTW | Doubly robust | |||||||
% events | Median TTE (95% CI) | % events | Median TTE (95% CI) | HR (95% CI) | P value | HR (95% CI) | P value | |
Unadjusted | ████ | ██████ | ████ | ██████ | ██████ | ████ | █████████ | |
ATT weighting | ||||||||
Base case | ████ | ██████ | ████ | ██████ | ██████ | █████ | ██████ | ██████ |
Full model | ████ | ██████ | ████ | ██████ | ██████ | █████ | ██████ | ██████ |
ATT = average treatment effect in the treated; CI = confidence interval; HR = hazard ratio; IO = immunotherapy; IPTW = inverse probability of treatment weighting; TTE = time to event.
Notes: Multivariable regression results: Base-case HR ████ ████ ███ █████ █████ ███████), full model HR ████ ████ ███ █████ █████ ███████).
The base-case results adjusted for ECOG at index date, history of brain metastases, history of liver metastases, and age at index date. The fully adjusted scenario adjusted for all the variables in the base case, plus Asian race, history of smoking, sex, and history of other metastases.
Source: Sponsor’s ITC Report.81
Assessment of Proportional Hazards
The proportional hazards assumption was assessed for the primary analysis (ATT, base case) populations of the PAPILLON trail versus EGFR TKI and platinum plus IO. Visual inspection of the log-cumulative hazard plots and Schoenfeld residual did not show any clear evidence of the proportional hazards assumption being violated before significant participant drop-off for EGFR TKI, but evidence of a potential violation was found for platinum plus IO. The Grambsch-Therneau test for proportional hazards assumption was nonsignificant for platinum plus IO (████████). Conversely, the Grambsch-Therneau test for EGFR TKI indicated a potential violation of the proportional hazards assumption (██████████).
Time to Next Treatment
The unadjusted comparison of TTNT for the PAPILLON trail versus EGFR TKI produced an HR of ████ ████ ███ █████ █████ ███████), favouring amivantamab plus carboplatin-pemetrexed (Table 31). The primary analysis, using base-case ATT weighting, produced results in favour of amivantamab plus carboplatin-pemetrexed, with an HR ██ ████ ████ ███ █████ █████ ███████). The results of the ATT full model produced results that favoured amivantamab plus carboplatin-pemetrexed, with an HR of ████ ████ ███ █████ ████).
The unadjusted comparison of TTNT for the PAPILLON trail versus platinum plus IO, produced an HR of ████ ████ ███ █████ █████ ████████ (Table 32). The primary analysis, using base-case ATT weighting, produced statistically significant results in favour of amivantamab plus carboplatin-pemetrexed, with an HR of ████ ████ ███ █████ █████ ████████. The results of the ATT full model produced results that were numerically in favour of amivantamab plus carboplatin-pemetrexed, with an HR of ████ ████ ███ █████ ████).
Results of the other sensitivity analyses (not shown) were mostly similar in direction of effect, with some results having CIs ████ ███████ ███ ████.
Table 31: Summary of Time to Next Treatment Results for Amivantamab Plus Carboplatin-Pemetrexed (PAPILLON) Versus EGFR TKI
Variables | EGFR TKI | PAPILLON | PAPILLON versus EGFR TKI | |||||
|---|---|---|---|---|---|---|---|---|
IPTW | Doubly robust | |||||||
% events | Median TTE (95% CI) | % events | Median TTE (95% CI) | HR (95% CI) | P value | HR (95% CI) | P value | |
Unadjusted | ████ | ██████ | ████ | ██████ | ██████ | █████ | █████████ | |
ATT weighting | ||||||||
Base case | ████ | ██████ | ████ | ██████ | ██████ | █████ | ██████ | ██████ |
Full model | ████ | ██████ | ████ | ██████ | ██████ | █████ | ██████ | ██████ |
ATT = average treatment effect in the treated; CI = confidence interval; HR = hazard ratio; IPTW = inverse probability of treatment weighting; TKI = tyrosine kinase inhibitor; TTE = time to event.
Notes: Multivariable regression results: Base-case HR ████ ████ ███ █████ █████ ███████), full model HR ████ ████ ███ █████ █████ ███████).
The base-case results adjusted for ECOG at index date, history of brain metastases, history of liver metastases, and age at index date. The fully adjusted scenario adjusted for all the variables in the base case, plus Asian race, history of smoking, sex, and history of other metastases.
Source: Sponsor’s ITC Report.81
Table 32: Summary of Time to Next Treatment Results for Amivantamab Plus Carboplatin-Pemetrexed (PAPILLON) Versus Platinum Plus IO
Variables | Platinum + IO | PAPILLON | PAPILLON versus platinum + IO | |||||
|---|---|---|---|---|---|---|---|---|
IPTW | Doubly robust | |||||||
% events | Median TTE (95% CI) | % events | Median TTE (95% CI) | HR (95% CI) | P value | HR (95% CI) | P value | |
Unadjusted | ████ | ██████ | ████ | ██████ | █████ | █████ | █████████ | |
ATT weighting | ||||||||
Base case | ████ | ██████ | ████ | ██████ | ██████ | █████ | ██████ | ██████ |
Full model | ████ | ██████ | ████ | ██████ | ██████ | █████ | ██████ | ██████ |
ATT = average treatment effect in the treated; CI = confidence interval; HR = hazard ratio; IO = immunotherapy; IPTW = inverse probability of treatment weighting; TTE = time to event.
Notes: Multivariable regression results: Base-case HR ████ ████ ███ █████ █████ ███████), full model HR ████ ████ ███ █████ █████ ███████).
The base-case results adjusted for ECOG at index date, history of brain metastases, history of liver metastases, and age at index date. The fully adjusted scenario adjusted for all the variables in the base case, plus Asian race, history of smoking, sex, and history of other metastases.
Source: Sponsor’s ITC Report.81
Assessment of Proportional Hazards
The proportional hazards assumption was assessed for the primary analysis (ATT, base case) populations of the PAPILLON trail versus EGFR TKI and platinum plus IO. Visual inspection of the log-cumulative hazard plots and Schoenfeld residual did not show any clear evidence of the proportional hazards assumption being violated before significant participant drop-off for EGFR TKI, but evidence of a potential violation was found for platinum plus IO. The Grambsch-Therneau test for proportional hazards assumption was nonsignificant for both EGFR TKI (█████████) and platinum plus IO (████████).
Critical Appraisal
There was no predefined protocol available, and the search and selection criteria, data extraction, and methods to appraise the risk of bias were not described. There was minimal information related to the real-world data source regarding data quality and completeness, suitability, and validity of any algorithms used to identify patients and classify outcomes. As a result of the lack of protocol, there is an increased risk of bias in the selection of the reported results (i.e., there is a possibility of these being chosen from multiple analyses based on magnitude, direction, or statistical significance). Additionally, the appropriateness of pooling the selected databases was not described. It is possible that heterogeneity in results across each database might have been obscured in the pooling. In a response to a request for additional information, the sponsor stated that a UK data source (National Cancer Registration Dataset) and a data source from France (Epidemiological Strategy and Medical Economics) were considered for the analysis. However, it is not clear how these would have been identified or whether any systematic process was used to make the database selection. The sponsor indicated that the National Cancer Registration Dataset data source was not selected because its sample size of patients treated with IOs plus platinum chemotherapy or EGFR TKIs was limited and these data were for a cohort of patients treated in the UK. The Epidemiological Strategy and Medical Economics data source was not selected for the analysis because only aggregated results were available, and the data were for a cohort of patients treated in France.
Propensity score–based methods aim to reduce the risk of bias due to confounding. However, it is important to note that no comparisons using data from randomized cohorts were used in the sponsor’s analysis. Lack of randomization in the datasets introduces the possibility of imbalance of patient characteristics, which could lead to comparing groups of patients who do not possess a similar prognostic risk. While the methods used by the sponsor serve to reduce confounding, the results indicate that a high risk of residual confounding is present in the analyses, even after the adjustments that were made on prognostic and effect-modifying covariates. While a sensitivity analysis of the full model including all 8 factors was conducted, the primary analysis of the base case only adjusted for 4 factors; it is unlikely that this represents all relevant prognostic and effect-modifying variables. In many cases, the full model was associated with high SMDs, indicating evidence of differences in baseline characteristics between the groups being compared. The base-case model, which used 4 factors, also had notable imbalances.
The use of real-world data has several limitations. Participants in the PAPILLON trial were monitored more strictly than were the patients from the real-world databases. There were some differences in the definitions and measurement of the outcomes. For example, it was noted that the databases did not have a systematic capture of progressive disease or RECIST v.1.1 criteria. Although an analysis of RW-PFS was included, this would not fully overcome the differences in the measurement of progression. OS measurements may include errors, including missing deaths, or censoring may differ between the clinical and real-world data sources. The sponsor suggested that missing deaths in real-world data may result in an overestimation of OS. The handling of missing data in the databases and in the analyses was not clearly described in the sponsor’s report.
The effective sample sizes were very small in the base case and in several of the full model analyses; for example, the ESS was ██ in the IPTW-ATT full model for the EGFR TKI group. The small ESS is expected to reduce the reliability of the results from the full model.
The sponsor employed several methods to test the proportionality assumption in the time-to-event analyses, and there was evidence to suggest that the proportional hazards assumption was not valid.
The relevance of EGFR TKIs as a comparator in these analyses is low, given that EGFR TKIs are generally not known to be efficacious in patients with exon 20ins, according to the clinical experts consulted for this review. Outcomes with IO are generally also expected to be poor in the patient target population, according to the clinical experts consulted for this review. Therefore, the selection of comparators in the analyses are of limited clinical relevance in the context of Canada. The relevance is also limited by the lack of analyses of patient-reported outcomes, such as HRQoL and harms.
Discussion
Summary of Available Evidence
One ongoing, phase III, multicentre, open-label RCT was included in this review. The PAPILLON trial was conducted in 131 centres across 25 countries, including 3 sites in Canada. Patients were 18 years of age or older, with treatment-naive EGFR exon 20ins mutated locally advanced or metastatic NSCLC. A total of 308 patients were randomized 1:1 to either the amivantamab plus carboplatin-pemetrexed or carboplatin-pemetrexed arm, from December 2020 to November 2022. The clinical cut-off date for data inclusion was May 2023. The treatment phase for each participant started at cycle 1 day 1 and continued in 21-day cycles until the end of treatment visit (approximately 30 days after discontinuation of study treatment). Patients in the carboplatin-pemetrexed group who progressed were allowed to cross over to amivantamab monotherapy. The primary outcome was PFS, with OS and ORR as key secondary outcomes included in the multiple testing procedure. The sponsor submitted an ITC report that included a nonrandomized study using propensity score weighting to reduce the impact of risk of bias due to confounding. This analysis used individual patient data from the PAPILLON trail for amivantamab plus carboplatin-pemetrexed and from real-world databases COTA and ConcertAI for EGFR TKI monotherapy and platinum chemotherapy plus IO. The analysis examined the outcomes of OS, PFS, real-world PFS, and TTNT.
Patients in the PAPILLON trail were 60 years of age, on average, and the majority (58%) were female. The majority of patients (61%) were Asian, and 36% were white. Nearly two-thirds of patients (65%) had ECOG PS 1, and the remainder had 0. Almost all patients (99%) had an adenocarcinoma that was either stage IVA or IVB (███) at screening.
Interpretation of Results
Efficacy
The OS data from the PAPILLON trail are not yet mature, and the large number of crossovers and the lack of precision suggest a low certainty of clinically important OS benefit when adding amivantamab to carboplatin-pemetrexed. Results from the PAPILLON trail show that the addition of amivantamab to carboplatin-pemetrexed results in a clinically important improvement in PFS over carboplatin-pemetrexed alone. However, the significance of an improvement in PFS in predicting a clinically important benefit on OS is less clear. The sponsor performed 3 sensitivity analyses, with the goal of accounting for the large number of crossovers. However, the conclusion that can be drawn from these analyses is limited due to the post hoc nature of the assessments and reliance on underlying assumptions that cannot be objectively verified and may not be plausible. The point estimates for these analyses were somewhat more favourable than the main analysis of the trial, but CIs were wide and came very close to or crossed the null. The final assessment of OS is planned to be conducted at a follow-up of about 48 months (current follow-up is just under 15 months), and crossovers will likely continue to be a confounder when analyzing OS results. Additionally, as the observed benefit of amivantamab on PFS becomes widely known, this will likely make it even more challenging to retain patients in the carboplatin-pemetrexed group of the trial. In the absence of OS data, results for PFS suggest a robust, clinically significant treatment effect for amivantamab plus carboplatin-pemetrexed over carboplatin-pemetrexed. A large methodological systematic review by Belin et al., submitted by the sponsor, attempted to draw a correlation between improvement in PFS and subsequent improvement in OS across various cancers, and the results were inconclusive.82 Additionally, the findings from this study are not specific to advanced NSCLC. Nevertheless, patients and clinicians, including the clinical experts consulted on this review, considered PFS to be an “intermediate end point,” with value on its own.
Another potential surrogate for OS is ORR. The ORR results from the PAPILLON trail demonstrated a robust, clinically significant treatment effect of amivantamab plus carboplatin-pemetrexed over carboplatin-pemetrexed. The sponsor submitted publications that were intended to inform the potential of ORR as a surrogate for OS. A paper by Hua et al. systematically reviewed phase II and III studies of patients with NSCLC, which reported OS with at least 1 of PFS or ORR.83 The authors, using Spearman’s rho, found a low correlation in the treatment effect on ORR and in the treatment effect on OS, a moderate correlation in the treatment effect on PFS and in the treatment effect on OS, and a high correlation in the treatment effect on ORR and the treatment effect on PFS. These findings support the notion that ORR serves as a better surrogate for PFS than it does for OS, and PFS is a better surrogate for OS than is ORR. The results from the PAPILLON trail would appear to support this observation, as a clear, clinically meaningful treatment effect for amivantamab plus carboplatin-pemetrexed over carboplatin-pemetrexed was observed for both PFS and ORR. The authors noted that performance of ORR (and PFS) as a surrogate was better in trials of first-line therapy. The findings of the analysis by Hua et al. are limited by the fact that the analysis was not conducted using patient-level data.
HRQoL is an important consideration in patients with locally advanced NSCLC, based on patient input received. Although HRQoL was assessed in the PAPILLON trail, the results suggested little to no difference between groups in change from baseline to 12 months. A key limitation of the analysis was that patients were not blinded. Lack of blinding is likely to bias results for any patient-reported outcomes. For example, a 2024 survey of meta-epidemiologic studies by Wang et al. found that lack of blinding likely results in an overestimation of the effect size for patient-reported outcomes.84 Additionally, there was a large amount of missing data, which may have biased the analysis of HRQoL results.
In the PAPILLON trial, both groups received a background of carboplatin-pemetrexed, which is standard for patients with NSCLC at this stage of their disease. The clinical experts consulted for this review did not expect that other EGFR TKI or IO would work in this population of patients with an EGFR exon 20ins mutation. The sponsor submitted a nonrandomized study using individual patient data from the PAPILLON trail and real-world databases aimed at determining the comparative efficacy of amivantamab plus carboplatin-pemetrexed versus EGFR TKI and chemotherapy plus IO for several efficacy outcomes (OS, PFS, RW-PFS, TTNT). This analysis was subject to several methodological limitations, including a lack of predefined methods or selection criteria for the real-world data sources; risk of residual confounding despite the application of IPTW methods; heterogeneity across study designs that could not be accounted for, including differences in outcome definitions; small ESS in the comparator arm; and, in some cases, imprecision (i.e., the null was not excluded). As a result, despite the analyses suggesting superiority of amivantamab plus carboplatin-pemetrexed over EGFR TKI and over chemotherapy plus IO for several efficacy outcomes, the evidence was insufficient to draw definitive conclusions on the relative efficacy of amivantamab plus carboplatin-pemetrexed compared to these treatments or on the precise magnitude of any potential difference. However, the clinical experts consulted by the review team indicated that superiority of amivantamab plus chemotherapy over EGFR TKI monotherapy or chemotherapy plus IO is plausible, given that the 2 comparators are not known to be efficacious in NSCLC patients with EGFR exon 20ins mutations. The nonrandomized study provided no information on HRQoL, an outcome of importance to patients.
Harms
Rash and infusion reactions likely occur more often with amivantamab plus carboplatin-pemetrexed than with carboplatin-pemetrexed, and the most common notable harm reported with amivantamab in the PAPILLON trail was rash. Rash has been a common AE associated with EGFR inhibitors since their appearance on the market and is likely due to targeting epidermal growth factor itself. According to the product monograph,57 the rash resulted in dose reductions in 18.5% of patients treated with amivantamab plus carboplatin-pemetrexed and discontinuation in 2% of patients. Rash usually developed within the first 3 weeks of therapy, with a median time to onset of 10 days. With monotherapy, according to the product monograph, rash occurred within the first 4 weeks, with a time to onset of 14 days. The product monograph also noted 1 case of toxic epidermal necrolysis, with instructions to permanently discontinue amivantamab if toxic epidermal necrolysis is confirmed. As far as management of rash or nail reactions, the product monograph recommends topical corticosteroids and topical and/or oral antibiotics. For grade 3 or poorly tolerated grade 2 events, systemic antibiotics and oral steroids are recommended, along with possible referral to a dermatologist, and, for grade 4 events, it is recommended that amivantamab be permanently discontinued.57
Other harms traditionally associated with EGFR inhibitors include gastrointestinal AEs (notably diarrhea) and interstitial lung disease.53-55 There were numerically more gastrointestinal TEAEs with amivantamab plus carboplatin-pemetrexed compared to carboplatin-pemetrexed. Both diarrhea (21% versus 13%) and constipation (40% versus 30%) were seen more frequently with amivantamab plus carboplatin-pemetrexed than carboplatin-pemetrexed. Pneumonitis was reported as a treatment-emergent SAE in 4 patients (2.6%) in the amivantamab plus carboplatin-pemetrexed group and none in the carboplatin-pemetrexed group, and all of these withdrawals were attributed to amivantamab and to pemetrexed. The product monograph advises that dosing of amivantamab should be withheld in patients with suspected pneumonitis or interstitial lung disease and permanently discontinued if these are confirmed.57
The most reported category of treatment-emergent SAEs in the PAPILLON trail was infections and infestations, occurring in ██ ███████ patients in the amivantamab plus carboplatin-pemetrexed group and ██ ██████ patients in the carboplatin-pemetrexed group, and there was also a large imbalance in TEAEs for infections and infestations between amivantamab plus carboplatin-pemetrexed, ███ █████ and carboplatin-pemetrexed, ██ █████ patients. Among TEAEs, by far the most common and the largest difference between groups was for paronychia, which occurred in 85 (56%) patients in amivantamab plus carboplatin-pemetrexed and no patients in the carboplatin-pemetrexed group. The mechanistic link between EGFR inhibitors and paronychia is similar to that seen for rash. Disruption of EGFR signalling pathways results in an inflammatory response, which then causes a disruption in the barrier function of the skin, and infection follows.85 Management of paronychia is as described in the previous paragraph on rash. Another infectious event that was numerically more common with amivantamab plus carboplatin-pemetrexed was pneumonia, reported as an AE in ██ patients (██████ with amivantamab plus carboplatin-pemetrexed and in ██ patients (█████ on carboplatin-pemetrexed and as an SAE in ██ patients (█████ in amivantamab plus carboplatin-pemetrexed and ██ patients ██████ in carboplatin-pemetrexed. Overall, the clinical experts consulted on this review believed the toxicity profile of amivantamab plus carboplatin-pemetrexed to be manageable.
The nonrandomized study that compared amivantamab plus chemotherapy to EGFR TKI monotherapy and chemotherapy plus IO did not assess harms.
Conclusion
There is evidence from 1 pivotal, phase III, open-label RCT (PAPILLON, n = 308) that amivantamab plus carboplatin-pemetrexed results in a clinically important improvement in PFS compared to carboplatin-pemetrexed alone, in patients with locally advanced NSCLC with an exon 20(ins) mutation. Evidence from the trial suggested that amivantamab plus carboplatin-pemetrexed may improve OS over carboplatin-pemetrexed alone. However, conclusions regarding OS are limited because the OS data are not yet mature, a large number of crossovers occurred in this trial, and the estimates are imprecise (i.e., 95% CIs included effects that may not be clinically important and crossed the null). The combination of amivantamab plus carboplatin-pemetrexed likely improves ORR compared to carboplatin-pemetrexed alone, although the clinical significance of this improvement is less clear, given that ORR is a surrogate outcome without strong evidence of a potential to predict the treatment effect on OS. Amivantamab plus carboplatin-pemetrexed may result in little to no difference in HRQoL; the results of this assessment were likely biased by the open-label design of the trial and patient attrition. Rash and infusion-related reactions are more likely to occur when amivantamab is added to carboplatin-pemetrexed. The most common notable harm associated with amivantamab was rash; however, this only rarely resulted in serious harm or prompted the patient to stop therapy.
A nonrandomized study using individual patient data from the PAPILLON trail and real-world databases, and IPTW methods to reduce the risk of bias due to confounding, aimed at determining the comparative efficacy of amivantamab plus carboplatin-pemetrexed versus EGFR TKI and chemotherapy plus IO for several efficacy outcomes (OS, PFS, RW-PFS, TTNT). Despite the analyses suggesting superiority of amivantamab plus carboplatin-pemetrexed for most outcomes, the evidence was insufficient to draw definitive conclusions on the relative efficacy of amivantamab plus carboplatin-pemetrexed or the precise magnitude of any potential difference. The clinical experts consulted by the review team suggested that superiority of amivantamab plus chemotherapy over EGFR TKI monotherapy or chemotherapy plus IO is plausible, given that the 2 comparators are not known to be efficacious in patients with NSCLC with EGFR exon 20ins mutations. The nonrandomized study provided no information on HRQoL, an outcome of importance to patients, or on harms.
References
1.Canadian cancer statistics Toronto (ON): Canadian Cancer Society; 2023: https://cancer.ca/Canadian-Cancer-Statistics-2023-EN. Accessed 2024 May 7.
2.Plunkett TA, Chrystal KF, Harper PG. Quality of life and the treatment of advanced lung cancer. Clin Lung Cancer. 2003;5(1):28-32. PubMed
3.Yang G, Li J, Xu H, et al. EGFR exon 20 insertion mutations in Chinese advanced non-small cell lung cancer patients: molecular heterogeneity and treatment outcome from nationwide real-world study. Lung Cancer. 2020;145:186-194. PubMed
4.Chouaid C, Filleron T, Debieuvre D, et al. A real-world study of patients with advanced non-squamous non-small cell lung cancer with EGFR exon 20 insertion: clinical characteristics and outcomes. Target Oncol. 2021;16(6):801-811. PubMed
5.Leal JL, Alexander M, Itchins M, et al. EGFR exon 20 insertion mutations: clinicopathological characteristics and treatment outcomes in advanced non-small cell lung cancer. Clin Lung Cancer. 2021;22(6):e859-e869. PubMed
6.Morita C, Yoshida T, Shirasawa M, et al. Clinical characteristics of advanced non-small cell lung cancer patients with EGFR exon 20 insertions. Sci Rep. 2021;11(1):18762. PubMed
7.Boyne DJ, Jarada TN, Yusuf A, et al. 51P testing patterns and outcomes of different EGFR-positive metastatic non-small cell lung cancer patients in a Canadian real-world setting. Ann Oncol. 2022;33(2):S56.
8.Burnett H, Emich H, Carroll C, Stapleton N, Mahadevia P, Li T. Epidemiological and clinical burden of EGFR exon 20 insertion in advanced non-small cell lung cancer: a systematic literature review. PLoS One. 2021;16(3):e0247620. PubMed
9.Forsythe ML, Alwithenani A, Bethune D, et al. Molecular profiling of non-small cell lung cancer. PLoS One. 2020;15(8):e0236580. PubMed
10.Gainor JF, Shaw AT, Sequist LV, et al. EGFR mutations and ALK rearrangements are associated with low response rates to PD-1 pathway blockade in non-small cell lung cancer: a retrospective analysis. Clin Cancer Res. 2016;22(18):4585-4593. PubMed
11.Amivantamb - scientific communication platform [sponsor supplied reference]. Toronto (ON): Janssen Inc; 2022.
12.ONCO CAPPS: EGFR positive and EGFR exon 20 mutations advanced non-squamous NSCLC [sponsor supplied reference]. Toronto (ON): Janssen Inc; 2022.
13.Li K, Bosdet I, Yip S, et al. Real-world clinical outcomes for patients with EGFR and HER2 exon 20 insertion-mutated non-small-cell lung cancer. Curr Oncol. 2023;30(8):7099-7111. PubMed
14.Melosky B, Banerji S, Blais N, et al. Canadian consensus: a new systemic treatment algorithm for advanced EGFR-mutated non-small-cell lung cancer. Curr Oncol. 2020;27(2):e146-e155. PubMed
15.Melosky B, Kambartel K, Häntschel M, et al. Worldwide prevalence of epidermal growth factor receptor mutations in non-small cell lung cancer: a meta-analysis. Mol Diagn Ther. 2022;26(1):7-18. PubMed
16.Mittal A, Hueniken K, Cheng S, et al. EP04.01-001 prevalence and outcomes of EGFR exon 20 insertion mutation in NSCLC: Princess Margaret Cancer Center experience. J Thorac Oncol. 2022;17(9 Supplement):S245.
17.Moulson R, Law J, Sacher A, et al. Real-world outcomes of patients with advanced epidermal growth factor receptor-mutated non-small cell lung cancer in Canada using data extracted by large language model-based artificial intelligence. Curr Oncol. 2024;31(4):1947-1960. PubMed
18.O'Sullivan DE, Jarada TN, Yusuf A, et al. Prevalence, treatment patterns, and outcomes of individuals with EGFR positive metastatic non-small cell lung cancer in a Canadian real-world setting: a comparison of exon 19 deletion, L858R, and exon 20 Insertion EGFR mutation carriers. Curr Oncol. 2022;29(10):7198-7208. PubMed
19.Vyse S, Huang PH. Targeting EGFR exon 20 insertion mutations in non-small cell lung cancer. Signal Transduct Target Ther. 2019;4:5. PubMed
20.Yusuf A, Boyne DJ, O'Sullivan DE, et al. Text analysis framework for identifying mutations among non-small cell lung cancer patients from laboratory data. BMC Med Res Methodol. 2024;24(1):63. PubMed
21.Canada's Drug Agency. Provisional funding algorithm: advanced or metastatic non-small cell lung cancer with activating epidermal growth factor receptor mutations. 2023; https://www.cadth.ca/non-small-cell-lung-cancer-nsclc-activating-epidermal-growth-factor-receptor-egfr-mutations-0. Accessed 2024 Jun 24.
22.CADTH reimbursement review: amivantamab (Rybrevant). Can J Health Technol. 2023;3(5). https://www.cadth.ca/sites/default/files/DRR/2023/PC0289-Rybrevant_combined.pdf. Accessed 2024 Jun 24.
23.Dersarkissian M, Bhak R, Lin HM, et al. Real-world treatment patterns and survival in non-small cell lung cancer patients with EGFR exon 20 insertion mutations. 2019.
24.Cardona AF, Rojas L, Zatarain-Barron ZL, et al. EGFR exon 20 insertion in lung adenocarcinomas among Hispanics (geno1.2-CLICaP). Lung Cancer. 2018;125:265-272. PubMed
25.Wu JY, Yu CJ, Shih JY. Effectiveness of treatments for advanced non-small-cell lung cancer with exon 20 insertion epidermal growth factor receptor mutations. Clin Lung Cancer. 2019;20(6):e620-e630. PubMed
26.Wang Y, Yang G, Li J, Hu H, Yang L, Xu F. Real-world treatment outcome of advanced Chinese NSCLC EGFR exon 20 insertion patients. J Clin Oncol. 2019;37(15 suppl):9043.
27.Udagawa H, Matsumoto S, Ohe Y, et al. OA07.03 clinical outcome of non-small cell lung cancer with EGFR/HER2 exon 20 insertions identified in the LC-SCRUM-Japan. J Thorac Oncol. 2019;14(10): S224.
28.Zhao C, Li X, Su C, Chen X, Ren S, Zhou C. P1. 01-111 EGFR exon20 insertion patients treated with first-line chemotherapy in non-small cell lung cancer. J Thorac Oncol. 2018;13(10):S507.
29.Coon CD, Schlichting M, Zhang X. Interpreting within-patient changes on the EORTC QLQ-C30 and EORTC QLQ-LC13. Patient. 2022;15(6):691-702. PubMed
30.Osoba D, Rodrigues G, Myles J, Zee B, Pater J. Interpreting the significance of changes in health-related quality-of-life scores. J Clin Oncol. 1998;16(1):139-144. PubMed
31.Rybrevant plus carboplatin-pemetrexed therapy for the treatment of patients with Epidermal Growth Factor Receptor (EGFR) Exon 20 insertion (exon 20 ins)-mutated locally advanced or metastatic Non-Small Cell Lung Cancer (NSCLC): 1,400 mg (1,750 mg if body weight is ≥ 80 kg) by intravenous (IV) infusion once weekly up to cycle 2 Day 1, then 1,750 mg (2,100 mg if body weight is ≥ 80 kg) on day 1 of each 21-day cycle, starting with cycle 3 [internal sponsor's report] In: Drug Reimbursement Review sponsor submission: Rybrevant (amivantamab), 350 mg/7 mL vial of liquid concentrate for intravenous infusion. Toronto (ON): Janssen Inc; 2024 Jun 21.
32.Canadian Cancer Society. Lung and bronchus cancer statistics. 2024; https://cancer.ca/en/cancer-information/cancer-types/lung/statistics. Accessed 2024 Sep 17.
33.Patient-reported outcomes supplemental analyses report. Clinical Study Report (Protocol): 61186372NSC3001. A randomized, open-label phase 3 study of combination amivantamab and carboplatin-pemetrexed therapy, compared with carboplatin-pemetrexed, in patients with EGFR Exon 20ins mutated locally advanced or metastatic non-small cell lung cancer (PAPILLON) [internal sponsor's report]. Raritan (NJ): Janssen Research & Development, LLC; 2023 Aug 16.
34.Pao W, Girard N. New driver mutations in non-small-cell lung cancer. Lancet Oncol. 2011;12(2):175-180. PubMed
35.Janne PA, Johnson BE. Effect of epidermal growth factor receptor tyrosine kinase domain mutations on the outcome of patients with non-small cell lung cancer treated with epidermal growth factor receptor tyrosine kinase inhibitors. Clin Cancer Res. 2006;12(14 Pt 2):4416s-4420s. PubMed
36.Arcila ME, Nafa K, Chaft JE, et al. EGFR exon 20 insertion mutations in lung adenocarcinomas: prevalence, molecular heterogeneity, and clinicopathologic characteristics. Mol Cancer Ther. 2013;12(2):220-229. PubMed
37.Oxnard GR, Lo PC, Nishino M, et al. Natural history and molecular characteristics of lung cancers harboring EGFR exon 20 insertions. J Thorac Oncol. 2013;8(2):179-184. PubMed
38.Bazhenova L, Minchom A, Viteri S, et al. Comparative clinical outcomes for patients with advanced NSCLC harboring EGFR exon 20 insertion mutations and common EGFR mutations. Lung Cancer. 2021;162:154-161. PubMed
39.Wang F, Li C, Wu Q, Lu H. EGFR exon 20 insertion mutations in non-small cell lung cancer. Transl Cancer Res. 2020;9(4):2982-2991. PubMed
40.Bell J, Roberts L, Jean-Baptiste M, et al. P3.15-03 capturing the patient experience for the treatment of EGFR exon 20 mutations in non-small cell lung cancer. J Thorac Oncol. 2018;13(10 Supplement):S991-S992.
41.Zhu Y, Jean-Baptiste M, Lenderking WR, et al. Identifying symptomatic adverse events using the patient-reported outcomes version of the common terminology criteria for adverse events in patients with non-small cell lung cancer with epidermal growth factor receptor exon 20 insertion mutations. Cancer Med. 2023;12(5):5494-5505. PubMed
42.Horn MK, Liu K, Mathias SD, et al. Evaluating the content validity, clarity, and relevance of two patient-reported outcomes for use with adults with EGFR-mutated NSCLC. JTO Clin Res Rep. 2021;2(8):100198. PubMed
43.Yu F, Han Y, Zhang R, Tou J, Ge Y. POSA347 an evaluation of the economic burden and quality of life for non-small cell lung cancer patients with exon 20 insertions in China. ISPOR. 2022;25(1 Supplement):S217.
44.Lababede O, Meziane MA. The eighth edition of TNM staging of lung cancer: reference chart and diagrams. Oncologist. 2018;23(7):844-848.
45.EGFR landscape summary: USA, UK, France, China, Japan & South Korea [sponsor supplied reference]. Toronto (ON): Janssen Inc; 2018.
46.Yang M, Xu X, Cai J, Ning J, Wery JP, Li QX. NSCLC harboring EGFR exon-20 insertions after the regulatory C-helix of kinase domain responds poorly to known EGFR inhibitors. Int J Cancer. 2016;139(1):171-176. PubMed
47.Ramalingam SS, Vansteenkiste J, Planchard D, et al. Overall survival with osimertinib in untreated, EGFR-mutated advanced NSCLC. N Engl J Med. 2020;382(1):41-50. PubMed
48.Owen DH, Singh N, Ismaila N, et al. Therapy for stage IV non-small-cell lung cancer with driver alterations: ASCO living guideline, version 2023.2. J Clin Oncol. 2023;41(24):e63-e72. PubMed
49.Hendriks LE, Kerr KM, Menis J, et al. Oncogene-addicted metastatic non-small-cell lung cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann Oncol. 2023;34(4):339-357. PubMed
50.CHRYSALIS (protocol amendment 7). A phase 1, first-in-human, open-label, dose escalation study of JNJ-61186372, a human bispecific EGFR and cMet antibody, in subjects with advanced non-small cell lung cancer [sponsor supplied reference]. Toronto (ON): Janssen Inc; 2019.
51.Cancer Care Ontario. Drug formulary: CRBPPEME. https://www.cancercareontario.ca/en/drugformulary/regimens/monograph/47031. Accessed 2024 Feb 29.
52.Pemetrexed for injection, for intravenous use [label]. Toronto (ON): Apotex; 2016: https://www.apotex.com/products/us/downloads/pre/peme_lyin_ins_750mg.pdf. Accessed 2024 Sep 13.
53.Gilotrif (afatinib): 20, 30 and 40 mg afatinib (as afatinib dimaleate) tablets [product monograph]. Burlington (ON): Boehringer Ingelheim (Canada) Ltd; 2019 June 6: https://pdf.hres.ca/dpd_pm/00051644.PDF. Accessed 2024 July 10.
54.Tarceva (erlotinib hydrochloride): 25, 100, 150 mg tablets [product monograph]. Mississauga (ON): Hoffmann-La Roche Limited; 2021 Sep 23: https://assets.roche.com/f/173850/x/46797b50c0/tarceva_pm_e.pdf. Accessed 2024 Jul 10.
55.Iressa (gefitinib): tablets, 250 mg, oral Use [product monograph]. Mississauga (ON): AstraZeneca Canada Inc; 2021 Mar 31 https://pdf.hres.ca/dpd_pm/00060650.PDF. Accessed 2024 Jul 10.
56.Keytruda (pembrolizumab): solution for infusion 100 mg/4 mL vial [product monograph]. Kirkland (QC): Merck Canada Inc; 2024 Jun 20: https://pdf.hres.ca/dpd_pm/00076054.PDF. Accessed 2024 Jul 10.
57.Rybrevant (amivantamab for injection): concentrate for solution for intravenous infusion 350 mg / 7 mL (50 mg/mL) single-use vial [product monograph]. Toronto (ON): Janssen Inc; 2024 Jun 28: https://pdf.hres.ca/dpd_pm/00076138.PDF. Accessed 2024 Jul 10.
58.Carboplatin Injection BP (carboplatin injection): sterile solution 10 mg / mL (50 mg, 150 mg, 450 mg, 600 mg of carboplatin per vial [product monograph]. 2019 Dec 16 https://pdf.hres.ca/dpd_pm/00054389.PDF. Accessed 2024 Aug 28.
59.Alimta (pemetrexed disodium for injection): 100 mg or 500 mg pemetrexed per vial [product monograph]. Toronto (ON): Eli Lilly Canada Inc; 2013 May 10: https://pdf.hres.ca/dpd_pm/00020514.PDF. Accessed 2024 Jul 10.
60.NCCN guidelines version 3.2024. Non-small cell lung cancer. Plymouth Meeting (PA): National Comprehensive Cancer Network (NCCN); 2024.
61.Ionescu DN, Stockley TL, Banerji S, et al. Consensus recommendations to optimize testing for new targetable alterations in non-small cell lung cancer. Curr Oncol. 2022;29(7):4981-4997. PubMed
62.Sebastião MM, Ho RS, de Carvalho JPV, Nussbaum M. Diagnostic accuracy of next generation sequencing panel using circulating tumor DNA in patients with advanced non-small cell lung cancer: a systematic review and meta-analysis. J Health Econ Outcomes Res. 2020;7(2):158-163. PubMed
63.Brenner DR, Gillis J, Demers AA, et al. Projected estimates of cancer in Canada in 2024. CMAJ. 2024;196(18):E615-E623. PubMed
64.Zou D, Ye W, Hess LM, et al. Diagnostic value and cost-effectiveness of next-generation sequencing–based testing for treatment of patients with advanced/metastatic non-squamous non–small-cell lung cancer in the US. J Mol Diagn. 2022;24(8):901-914. PubMed
65.PAPILLON clinical summary [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Rybrevant (amivantamab), 350 mg/7 mL vial of liquid concentrate for intravenous infusion. Toronto (ON): Janssen Inc; 2024 Jun 21.
66.Zhou C, Tang J, Liu B, et al. Amivantamab plus chemotherapy vs chemotherapy as a first-line treatment among asian patients with EGFR exon 20 insertion–mutated advanced Non-small Cell Lung Cancer (NSCLC): PAPILLON subgroup analysis. 2023.
67.Fayers P, Aaronson, N. K., Bjordal K, Groenvold M, Curran D, Bottomley A. EORTC QLQ-C30 scoring manual. Third edition, 2001 ed. Brussels (BE): EORTC Data Center; 2001: https://www.eortc.org/app/uploads/sites/2/2018/02/SCmanual.pdf. Accessed 2024 Aug 8.
68.Montazeri A, Gillis CR, McEwen J. Quality of life in patients with lung cancer: a review of literature from 1970 to 1995. Chest. 1998;113(2):467-481. PubMed
69.Aaronson NK, Ahmedzai S, Bergman B, et al. The European Organization for Research and Treatment of Cancer QLQ-C30: a quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst. 1993;85(5):365-376. PubMed
70.Osoba D, Aaronson N, Zee B, Sprangers M, te Velde A. Modification of the EORTC QLQ-C30 (version 2.0) based on content validity and reliability testing in large samples of patients with cancer. The Study Group on Quality of Life of the EORTC and the Symptom Control and Quality of Life Committees of the NCI of Canada Clinical Trials Group. Qual Life Res. 1997;6(2):103-108. PubMed
71.Osoba D, Zee B, Pater J, Warr D, Kaizer L, Latreille J. Psychometric properties and responsiveness of the EORTC quality of Life Questionnaire (QLQ-C30) in patients with breast, ovarian and lung cancer. Qual Life Res. 1994;3(5):353-364. PubMed
72.Kluetz PG, Slagle A, Papadopoulos EJ, et al. Focusing on core patient-reported outcomes in cancer clinical trials: symptomatic adverse events, physical function, and disease-related symptoms. Clin Cancer Res. 2016;22(7):1553-1558. PubMed
73.HealthMeasures. PROMIS physical function scoring manual. 2022; https://staging.healthmeasures.net/score-and-interpret/calculate-scores/223-promis-scoring-manuals. Accessed 2024 May 16.
74.Jensen RE, Potosky AL, Reeve BB, et al. Validation of the PROMIS physical function measures in a diverse US population-based cohort of cancer patients. Qual Life Res. 2015;24(10):2333-2344. PubMed
75.Houts CR, Savord A, Gardner M, et al. PCR172 patient-reported outcomes in non-small cell lung cancer: psychometric evaluation of the PROMIS PF-SF 8C and NSCLC-SAQ in phase 3 clinical trials. Value Health. 2024;27(6):S328.
76.Peipert JD, Chapman R, Shaunfield S, Kallen MA, Schalet BD, Cella D. Do you recall?: Results from a within-person recall study of the Patient-Reported Outcomes Measurement Information System (PROMIS) short form v2.0 - physical function 8c. Value Health. 2022;25(2):161-166. PubMed
77.Clinical Study Report (Primary Analysis): 61186372NSC3001. A randomized, open-label phase 3 study of combination amivantamab and carboplatin-pemetrexed therapy, compared with carboplatin-pemetrexed, in patients with EGFR Exon 20ins mutated locally advanced or metastatic non-small cell lung cancer (PAPILLON) [internal sponsor's report]. Raritan (NJ): Janssen Research & Development, LLC; 2023 Sep 5. Accessed 5 September 2023.
78.Question and answer on adjustment for cross-over in estimating effects in oncology trials. Amsterdam (NL): European Medicines Agency; 2018: https://www.ema.europa.eu/en/documents/scientific-guideline/question-and-answer-adjustment-cross-over-estimating-effects-oncology-trials_en.pdf. Accessed 2024 Aug 9.
79.Balshem H, Helfand M, Schünemann HJ, et al. GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol. 2011;64(4):401-406. PubMed
80.Santesso N, Glenton C, Dahm P, et al. GRADE guidelines 26: informative statements to communicate the findings of systematic reviews of interventions. J Clin Epidemiol. 2020;119:126-135. PubMed
81.Indirect treatment comparisons with individual patient data from PAPILLON and two real-world data sources report [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Rybrevant (amivantamab), 350 mg/7 mL vial of liquid concentrate for intravenous infusion. Toronto (ON): Janssen Inc; 2024 May 28.
82.Belin L, Tan A, De Rycke Y, Dechartres A. Progression-free survival as a surrogate for overall survival in oncology trials: a methodological systematic review. Br J Cancer. 2020;122(11):1707-1714. PubMed
83.Hua T, Gao Y, Zhang R, Wei Y, Chen F. Validating ORR and PFS as surrogate endpoints in phase II and III clinical trials for NSCLC patients: difference exists in the strength of surrogacy in various trial settings. BMC Cancer. 2022;22(1):1022. PubMed
84.Wang Y, Parpia S, Couban R, et al. Compelling evidence from meta-epidemiological studies demonstrates overestimation of effects in randomized trials that fail to optimize randomization and blind patients and outcome assessors. J Clin Epidemiol. 2024;165:111211. PubMed
85.Guggina LM, Choi AW, Choi JN. EGFR inhibitors and cutaneous complications: a practical approach to management. Oncol Ther. 2017;5(2):135-148.
86.Clinical Study Report (Crossover Phase): 61186372NSC3001. A randomized, open-label phase 3 study of combination amivantamab and carboplatin-pemetrexed therapy, compared with carboplatin-pemetrexed, in patients with EGFR Exon 20ins mutated locally advanced or metastatic non-small cell lung cancer (PAPILLON) [internal sponsor's report]. Raritan (NJ): Janssen Research & Development, LLC; 2023 Sep 5.
Appendix 1: Detailed Outcome Data
Please note that this appendix has not been copy-edited.
Table 33: Change From Baseline in PROMIS PF Total Score
Variable | Amivantamab + CP N = 153 | CP N = 155 |
|---|---|---|
PROMIS Physical Function Total score | ||
Mean (SD) baseline | █████ █████████████ | █████ █████████████ |
Mean change from baseline to 12 months (cycle 17 day 1) (95% CI)a | ████ ██████ █████ ████ | ████ ██████ ████ ████ |
Mean change from baseline to 18 months (cycle 25 day 1) (95% CI)a | ████ ██████ █████ ████ | ████ ██████ ████ ███ |
CI = confidence interval; CP = carboplatin-pemetrexed; SD = standard deviation.
aLeast squares means are derived based on the mixed-effects model with repeated measures, in which the dependent variable is change from baseline in score, and independent variables are baseline, visit, treatment, and visit by treatment interaction as fixed effects and individual patient as random effect.
Source: Papillon PRO CSR.33
Table 34: Forest Plot of PFS by BICR for Subgroups Defined by Baseline Clinical Disease Characteristics; Full Analysis Set [Redacted]
█████ | █████ | █████ |
|---|---|---|
███████████ | █████████████ | ████████████████ |
████████████ | ████████████ | █████████████ |
█████████████ | ████████████ | ██████████████ |
Source: Details included in the table are from the sponsor’s Summary of Clinical Evidence.31
Papillon: Crossover Phase
Table 35: Analysis Populations (Crossover Phase)
Study | Population | Analysis | Number Analyzed | Definition | Application |
|---|---|---|---|---|---|
PAPILLON: Crossover Phase | Crossover analysis set | Study population Efficacy Safety | N = 65 | Enrolled participants who entered the crossover phase and received at least 1 (1) dose of study treatment | Used to summarize the population, efficacy, and safety data of the crossover population. |
Source: PAPILLON Crossover CSR.86
Patient Population
Baseline Characteristics
Baseline demographic and clinical characteristics of the PAPILLON trial crossover phase are summarized in Table 36.
Table 36: Summary of Baseline Characteristics in PAPILLON (Crossover Phase)
Characteristic | PAPILLON: Crossover Phase Amivantamab monotherapy |
|---|---|
Age, years | N = 65 |
Mean (SD) | ████ ███████ |
Median | ████ |
Range | ████ ███ |
18 to 25 | | ██████ |
26 to 50 | ██ ███████ |
51 to 64 | ██ ███████ |
65 to 74 | ██ ███████ |
≥ 75 | | ██████ |
Sex | N = 65 |
Female | ██ ███████ |
Male | ██ ███████ |
Racea | N = 65 |
Asian | ██ ███████ |
White | ██ ███████ |
Ethnicity | N = 65 |
Hispanic or Latino | | ██████ |
Not Hispanic or Latino | ██ ███████ |
Weight, kg | N = 65 |
Mean (SD) | ████ ████████ |
Median | ████ |
Range | ████ ████ |
< 80 kg | ██ ███████ |
≥ 80 kg | | ███████ |
Height, cm | N = 65 |
Mean (SD) | █████ ██████ |
Median | █████ |
Range | ████ ███ |
Body mass index, kg/m2 | N = 65 |
Mean (SD) | ████ ██████ |
Median | ████ |
Range | ████ ███ |
Baseline ECOG score | N = 65 |
0 | ██ ███████ |
1 | ██ ███████ |
History of smoking | N = 65 |
Yes | ██ ███████ |
No | ██ ███████ |
ECOG = Eastern Cooperative Oncology Group; kg = kilogram; m = metre; SD = standard deviation
aIn some regions reporting of Race is not required
Source: PAPILLON Crossover CSR.86
Patient Disposition
Table 37: Patient Disposition in PAPILLON (Crossover Phase)
Patient disposition | PAPILLON: Crossover phase Amivantamab monotherapy |
|---|---|
Analysis set: Crossover, N (%) | ██ ████████ |
Subjects ongoing, N (%) | ██ ███████ |
Discontinued from amivantamab, N (%) | ██ ███████ |
Reason for discontinuation, N (%) | |
Progressive disease | ██ ███████ |
Adverse event | | ███████ |
Source: PAPILLON Crossover CSR.86
Exposure to Interventions
Study Treatments
A summary of exposure to study treatments in the PAPILLON trial crossover phase is presented in Table 38. The median duration of amivantamab monotherapy was ████ months, and the median number of treatment cycles was ||.
Table 38: Patient Exposure to Study Treatments in PAPILLON (Crossover Phase)
Exposure | PAPILLON: Crossover Phase amivantamab monotherapy (N = 65) |
|---|---|
Total patient-years* | ████ |
Duration of study treatment (months) | |
Mean (SD) | ████ ███████ |
Median | ████ |
Range | █████ █████ |
< 1 | ██ ███████ |
1- < 2 | | ██████ |
2- < 3 | | ███████ |
3- < 4 | | ██████ |
4- < 5 | | ███████ |
5- < 6 | | ██████ |
6- < 7 | | ██████ |
7- < 8 | | ██████ |
8- < 9 | | ██████ |
9- < 10 | | ██████ |
10- < 11 | | ██████ |
11- < 12 | | ██████ |
12- < 13 | | ██████ |
13- < 14 | | ██████ |
14- < 15 | | ██████ |
15- < 16 | | ██████ |
16- < 17 | | ██████ |
17- < 18 | | ██████ |
18- < 19 | | ██████ |
Total number of treatment cycles | |
Mean (SD) | ████ ███████ |
Median | ████ |
Range | █████ █████ |
1 to 4 | ██ ███████ |
5 to 8 | ██ ███████ |
9 to 12 | ██ ███████ |
13 to 16 | | ███████ |
17 to 20 | | ██████ |
21 to 24 | | ██████ |
25 to 28 | | ██████ |
Amivantamab Relative Dose Intensitya | |
Mean (SD) | ██████ ███████ |
Median | ██████ |
Range | ███████ ██████ |
SD = standard deviation
*Total exposure is the sum of treatment duration for each patient.
aRelative dose intensity (%) is calculated as the ratio of total received dose versus total prepared dose.
Note: Amivantamab is administered once weekly (with the first dose split over days 1 and 2) up to cycle 2 day 1 and then administered once every 2 weeks.
Source: PAPILLON Crossover CSR.86
Concomitant Medications and Co-interventions
In the PAPILLON trial crossover phase, a total of 65 subjects (100%) took 1 or more concomitant medications during the trial. The most common medication classes taken concomitantly during the trial were antibacterials. Concomitant medications taken by > 10% of subjects are presented in Table 39.
Table 39: Patient Exposure to Key Concomitant Medications in PAPILLON (Crossover Phase)
Exposure to Concomitant Medication Classes Taken by > 10% of Subjects | PAPILLON: Crossover Phase amivantamab monotherapy (N = 65) |
|---|---|
Patients taking any concomitant medications [n (%)] | ██ ███████ |
Antibacterials for Systemic Use | ██ ███████ |
Corticosteroids for Systemic Use | ██ ███████ |
Corticosteroids, Dermatological Preparations | ██ ███████ |
Analgesics | ██ ███████ |
Antibiotics and Chemotherapeutics for Dermatological Use | ██ ███████ |
Drugs for Acid-Related Disorders | ██ ███████ |
Antihistamines for Systemic Use | ██ ███████ |
Blood Substitutes and Perfusion Solutions | ██ ███████ |
Anti-inflammatory and Antirheumatic Products | ██ ███████ |
Cough and Cold Preparations | ██ ███████ |
Antithrombotic Agents | ██ ███████ |
Ophthalmologicals | ██ ███████ |
Throat Preparations | ██ ███████ |
Unspecified Herbal and Traditional Medicine | ██ ███████ |
All Other Therapeutic Products | ██ ███████ |
Diuretics | ██ ███████ |
Drugs for Obstructive Airway Diseases | ██ ███████ |
Drugs for Treatment of Bone Disease | ██ ███████ |
Drugs for Constipation | ██ ███████ |
Psycholeptics | ██ ███████ |
Mineral Supplements | | ███████ |
Antiseptics and Disinfectants | | ███████ |
Emollients and Protectives | | ███████ |
Antiacne Preparations | | ███████ |
Antianemic Preparations | | ███████ |
Drugs for Functional Gastrointestinal Disorders | | ███████ |
Immunostimulants | | ███████ |
Vaccines | | ███████ |
Source: PAPILLON Crossover CSR.86
Subsequent Treatment
Subsequent therapy data were not reported for the PAPILLON trial crossover phase.
Results
Efficacy
Summary of Efficacy Outcomes
A summary of key efficacy outcomes for the PAPILLON trial crossover phase is presented in Table 40.
Objective Response Rate
Based on investigator assessment in subjects with measurable disease at baseline who entered the crossover phase, there were ██ responders at CCO, yielding an ORR of █████ ████ ███ ██████ ███████ An additional ██ patients (██████ had stable disease.
PFS (by Investigator)
PFS in the crossover phase was defined as the time from first administration of amivantamab monotherapy until the date of objective disease progression (using RECIST v1.1) or death (by any cause), whichever occurred first. Analyses were performed after ██ events had occurred during a median follow-up of ████ months. The median PFS by investigator was ████ months (95% CI, █████ ████).
Overall Survival
At CCO, there was a median follow-up of ████ months and a total of ██ ███████ death events reported in the crossover arm. Median OS was █████ ████ ███ ██████ ██) months.
Time to Subsequent Therapy
At CCO, ██ subjects in the crossover phase had not initiated subsequent system anticancer therapy. The median TTST was 9.██ months (95% CI, █████ ███████
Time to Treatment Discontinuation
At CCO, ██ subjects (██████ in the crossover phase had discontinued treatment. The median TTD was 9███ months (95% CI, █████ ██████.
Table 40: Summary of Key Efficacy Outcomes in PAPILLON (Crossover Phase)
Outcome | PAPILLON: Crossover Phase amivantamab monotherapy (N = 65) |
|---|---|
ORR | |
Number of subjects with 2 or more disease assessmentsa | ██ |
Responders (CR + PR) | ██ |
ORR | █████ |
95% CI | ███████ ██████ |
Best Overall Response | |
Complete response | | ██████ |
Partial response | ██ ███████ |
Stable disease | ██ ███████ |
Progressive disease | | ███████ |
Not evaluable | | ██████ |
12-month | ████ ██████ █████ |
PFS | |
Event | ██ ███████ |
Censored | ██ ███████ |
Time to event (months) | |
25th percentile (95% CI) | ████ ██████ █████ |
Median (95% CI) | ████ ██████ █████ |
75th percentile (95% CI) | █████ ██████ ███ |
Range | ██████ ██████ |
Event-free rate (95% CI) | |
6-month | ████ ██████ █████ |
12-month | ████ ██████ █████ |
OS | |
Event | ██ ███████ |
Censored | ██ ███████ |
Time to event (months) | |
25th percentile (95% CI) | ████ ██████ ██████ |
Median (95% CI) | █████ ███████ ███ |
75th percentile (95% CI) | █████ ███████ ███ |
Range | ██████ █████ |
Event-free rate (95% CI) | |
6-month | ████ ██████ █████ |
12-month | ████ ██████ █████ |
18-month | ████ ██████ █████ |
CI = confidence interval; CR = complete response; DOR = duration of response; NE = not estimable; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; PR = partial response; TTD = time to treatment discontinuation; TTST = time to subsequent therapy
aSubjects with 2 or more disease assessments include subjects who received at least one dose of study drug and either had a t least 2 postbaseline efficacy disease assessments, or discontinues treatment for any reason, or had disease progression/death before the second postbaseline disease assessment
Note: + = censored observation
Source: PAPILLON Crossover CSR.86
Harms
Safety Evaluation Plan
Safety data for the PAPILLON trial crossover phase were analyzed using the crossover analysis set, which comprised the 65 participants who entered the crossover phase and had received at least 1 dose of amivantamab through the CCO. TEAEs were defined as any AE occurring at or after the initial administration of amivantamab in the crossover phase through 30 days after last dose of amivantamab (or > 30 days if the AE was considered related to amivantamab). As crossover subjects could not initiate treatment with amivantamab earlier than 21 days or later than 90 days after their last dose of chemotherapy in the main study, AEs occurring after 30 days of last dose of chemotherapy in the main study and before the first dose of amivantamab in the crossover phase were not considered treatment-emergent.
Overview of Safety
A summary of key harms data for the PAPILLON trial crossover phase is presented in Table 41. The 3 most common AEs were rash (███████ paronychia ███████ and infusion-related reaction (███████ Seventeen patients died during the study period.
Table 41: Summary of Key Harms Data in PAPILLON (Crossover Phase)
Adverse events | PAPILLON: Crossover phase amivantamab monotherapy |
|---|---|
Most common treatment-emergent adverse events (≥ 5% subjects), N (%) | |
Analysis set: Crossover | 65 |
Subjects with 1 or more AEs | ██ ███████ |
Skin and subcutaneous tissue disorders | ██ ███████ |
Rash | ██ ███████ |
Dermatitis acneiform | ██ ███████ |
Dry skin | | ██████ |
Infections and infestations | ██ ███████ |
Paronychia | ██ ███████ |
COVID-19 | ██ ███████ |
Pneumonia | | ██████ |
Rash pustular | | ██████ |
Gastrointestinal disorders | ██ ███████ |
Constipation | ██ ███████ |
Gingival bleeding | | ███████ |
Stomatitis | | ███████ |
Nausea | | ██████ |
Vomiting | | ██████ |
Mouth ulceration | | ██████ |
Metabolism and nutrition disorders | ██ ███████ |
Hypoalbuminemia | ██ ███████ |
Decreased appetite | ██ ███████ |
Hypoproteinemia | | ███████ |
Hypocalcemia | | ██████ |
Hypokalemia | | ██████ |
Injury, poisoning, and procedural complications | ██ ███████ |
Infusion-related reaction | ██ ███████ |
Investigations | ██ ███████ |
Aspartate aminotransferase increased | ██ ███████ |
Alanine aminotransferase increased | ██ ███████ |
Blood alkaline phosphatase increased | | ███████ |
Gamma-glutamyltransferase increased | | ███████ |
Weight decreased | | ██████ |
General disorders and administration site conditions | ██ ███████ |
Edema peripheral | ██ ███████ |
Asthenia | | ██████ |
Malaise | | ██████ |
Pyrexia | | ██████ |
Respiratory, thoracic, and mediastinal disorders | ██ ███████ |
Dyspnea | | ███████ |
Cough | | ██████ |
Pleural effusion | | ██████ |
Blood and lymphatic system disorders | ██ ███████ |
Neutropenia | | ███████ |
Anemia | | ███████ |
Leukopenia | | ███████ |
Thrombocytopenia | | ██████ |
Musculoskeletal and connective tissue disorders | ██ ███████ |
Back pain | | ███████ |
Arthralgia | | ██████ |
Nervous system disorders | ██ ███████ |
Dizziness | | ██████ |
Psychiatric disorders | | ███████ |
Insomnia | | ██████ |
Hepatobiliary disorders | | ███████ |
Hyperbilirubinemia | | ██████ |
Most common treatment-emergent serious adverse events (≥ 1% subjects), N (%) | |
Analysis set: Crossover | 65 |
Subjects with 1 or more SAEs | ██ ███████ |
Respiratory, thoracic, and mediastinal disorders | | ██████ |
Pleural effusion | | ██████ |
Dyspnea | | ██████ |
Interstitial lung disease | | ██████ |
Organizing pneumonia | | ██████ |
Pneumonitis | | ██████ |
Pulmonary embolism | | ██████ |
Infections and infestations | | ██████ |
Pneumonia | | ██████ |
Cellulitis | | ██████ |
Gastrointestinal disorders | | ██████ |
Abdominal pain | | ██████ |
Vomiting | | ██████ |
Musculoskeletal and connective tissue disorders | | ██████ |
Back pain | | ██████ |
Nervous system disorders | | ██████ |
Dizziness | | ██████ |
Spinal cord compression | | ██████ |
Eye disorders | | ██████ |
Retinal detachment | | ██████ |
Injury, poisoning, and procedural complications | | ██████ |
Infusion-related reaction | | ██████ |
Skin and subcutaneous tissue disorders | | ██████ |
Rash | | ██████ |
Treatment-emergent adverse events leading to discontinuation of study drug (≥ 1% subjects in either treatment group), N (%) | |
Analysis set: Crossover | 65 |
Subjects with 1 or more AE leading to discontinuation of any study treatment | | ███████ |
Respiratory, thoracic, and mediastinal disorders | | ██████ |
Interstitial lung disease | | ██████ |
Pleural effusion | | ██████ |
Pneumonitis | | ██████ |
General disorders and administration site conditions | | ██████ |
Performance status decreased | | ██████ |
Infections and infestations | | ██████ |
Pneumonia | | ██████ |
Injury, poisoning, and procedural complications | | ██████ |
Infusion-related reaction | | ██████ |
Skin and subcutaneous tissue disorders | | ██████ |
Dermatitis acneiform | | ██████ |
Deaths during treatment and follow-up, N (%) | |
Analysis set: Crossover | 65 |
Deaths during study | ██ ███████ |
Progressive disease | ██ ███████ |
Adverse event | | ██████ |
Deaths within 30 days of last dosea | | ██████ |
Adverse event | | ██████ |
Progressive disease | | ██████ |
Treatment-emergent adverse events of special interest, N (%) | |
Analysis set: Crossover | 65 |
Subjects with 1 or more AEs of special interest | ██ ███████ |
Rash | ██ ███████ |
Rash | ██ ███████ |
Dermatitis acneiform | ██ ███████ |
Rash pustular | | ██████ |
Dermatitis | | ██████ |
Dermatitis infected | | ██████ |
Erythema | | ██████ |
Rash maculo-papular | | ██████ |
Skin exfoliation | | ██████ |
Skin lesion | | ██████ |
Infusion-related reaction | ██ ███████ |
Infusion-related reaction | ██ ███████ |
Pneumonitis/ILD | | ██████ |
Interstitial lung disease | | ██████ |
Pneumonitis | | ██████ |
AE = adverse event; ILD = interstitial lung disease; SAE = serious adverse event
aSubjects who died within 30 days will be counted in both categories
Note: Subjects are counted only once for any given event, regardless of the number of times they actually experienced the event. Adverse events are coded using MedDRA Version 25.0
Source: PAPILLON Crossover CSR.86
Adverse Events
An overall summary of TEAEs for the PAPILLON trial crossover phase is presented in Table 42. Most patients reported at least 1 TEAE (███████ with the majority classified as toxicity grade 2 or 3 ██████ ███ ██████ respectively). A low frequency of TEAEs leading to death were observed (██████ and there were no study-related deaths. Seven participants (██████ discontinued the study drug due to an AE. Four (█████ participants discontinued amivantamab due to AEs considered to be related to amivantamab.
Table 42: Summary of Key Harms Data in PAPILLON (Crossover Phase)
Harms | PAPILLON: Crossover Phase amivantamab monotherapy |
|---|---|
Analysis set: Crossover, N | 65 |
Subjects with 1 or more: | |
AEs | ██ ███████ |
Related AEsa | ██ ███████ |
Related nonserious AEsa | ██ ███████ |
Grade 3 or greater AEs | ██ ███████ |
Related grade 3 or greater AEsa | ██ ███████ |
Maximum toxicity grade | |
Grade 1 | | ██████ |
Grade 2 | ██ ███████ |
Grade 3 | ██ ███████ |
Grade 4 | | ██████ |
Grade 5 | | ██████ |
Serious AEs | ██ ███████ |
AEs leading to discontinuation of study drug | | ███████ |
AEs leading to drug interruption of study drugb | ██ ███████ |
AEs leading to dose reduction of study drug | | ███████ |
AEs leading to deathc | | ██████ |
COVID-19 associated AEsd | ██ ███████ |
COVID-19 associated serious AEsd | | ██████ |
COVID-19 associated nonserious AEsd | ██ ███████ |
COVID-19 associated grade 3 or greater AEsd | | ██████ |
COVID-19 associated AEs leading to deathb,c | | ██████ |
AE = adverse event, COVID-19 = coronavirus disease 2019
aAn AE is assessed by the investigator as related to study treatment.
bExcludes infusion-related reactions.
cAEs leading to death are based on AE outcome of Fatal. Per protocol, all deaths within 30 days of last dose were required to have an associated AE reported, even if due to progressive disease.
dCOVID-19 associated AEs are based on events that code to a COVID-19 MedDRA term and events that are identified via the COVID-19 Case of AEs form.
Source: PAPILLON Crossover CSR.86
Serious Adverse Events
Treatment-emergent SAEs were reported in ██ patients (███████ The most common SAE system organ class was ████████████ ████████ ███ ███████████ ██████████ The most common SAEs were █████████ ██ ████████ ████████ ███████ ████████ ██ ████████ ███████ ███ ████ ████ ██ ████████ ████████ All other SAEs had an incidence of ██████
Withdrawals Due to Adverse Events
TEAEs leading to dose interruption of amivantamab monotherapy occurred in ██ patients ████████ and COVID-19 was the most common cause (████████ ████████ TEAEs leading to dose reduction occurred in ██ subjects ████████ and paronychia was the most common cause (████████ ████████ From study initiation through the CCO, a total of ██ participants (██████ had TEAEs leading to discontinuation of amivantamab monotherapy, of which ██████ were considered to be related to the study drug.
Adverse Events of Special Interest
There was a total of ██ patients (██████ in the crossover phase who experienced at least 1 AESI. ████ ███ ████████ █████████ ████████ ███████ ████████ ███ ████████ ████████ ███ ██████████ █████████ ███ ████████ █████████ were the most commonly reported AESIs.
Figure 4: Kaplan-Meier Plot of OS; Full Analysis Set
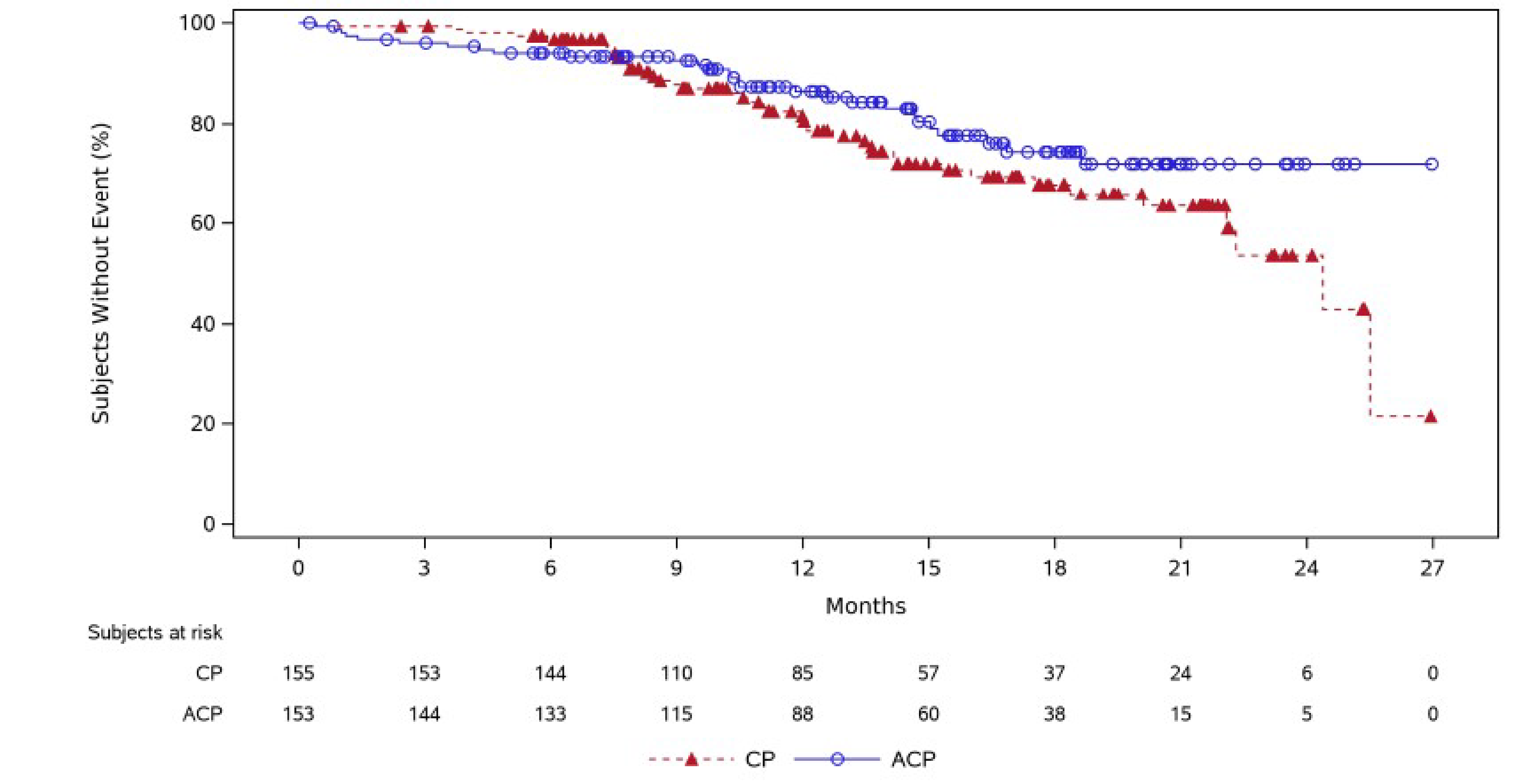
CP = carboplatin plus pemetrexed; ACP = amivantamab plus carboplatin plus pemetrexed.
Source: PAPILLON Clinical Summary.65
Pharmacoeconomic Review
Abbreviations
20ins
20 insertion
AE
adverse event
CDA-AMC
Canada’s Drug Agency
CHT
platinum-based chemotherapy
ICER
incremental cost-effectiveness ratio
IO
immuno-oncology drug
IRR
infusion-related reactions
NSCLC
non–small cell lung cancer
OS
overall survival
PFS
progression-free survival
QALY
quality-adjusted life-year
RPSFT
rank-preserving structural failure time
TKI
tyrosine kinase inhibitor
TTD
time to treatment discontinuation
WTP
willingness to pay
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Amivantamab (Rybrevant), 350 mg/7 mL (50 mg/mL) single-use vial for IV infusion |
Indication | In combination with carboplatin and pemetrexed for the first-line treatment of adult patients with locally advanced (not amenable to curative therapy) or metastatic non–small cell lung cancer with activating epidermal growth factor receptor exon 20 insertion mutations. |
Health Canada approval status | NOC |
Health Canada review pathway | Standard |
NOC date | June 28, 2024 |
Reimbursement request | As per indication |
Sponsor | Janssen Inc. |
Submission history | Previously reviewed: Yes Indication: For the treatment of adult patients with locally advanced or metastatic non–small cell lung cancer with activating epidermal growth factor receptor exon 20 insertion mutations whose disease has progressed on, or after platinum-based chemotherapy. Recommendation date: March 20, 2023 Recommendation: Recommended with clinical conditions and price reduction |
exon 20ins = exon 20 insertion; NSCLC = non–small cell lung cancer; NOC = Notice of Compliance.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Partitioned survival model |
Target population | Adult patients with locally advanced (not amenable to curative therapy) or metastatic NSCLC with activating EGFR exon 20ins mutations receiving first-line treatment |
Treatment | Amivantamab plus CP |
Dose regimen | Amivantamab (Rybrevant) 1,400 mg (1,750 mg if body weight is ≥ 80 kg) by IV infusion once weekly for 4 weeks (first dose split on days 1 and 2), then 1,750 mg (2,100 mg if body weight is ≥ 80 kg) on day 1 of each 21-day cycle, starting with cycle 3 Administer with carboplatin (target AUC 5 maximum dose 750 mg for carboplatin for 4 cycles) and pemetrexed (500 mg/m2 IV until disease progression) on a 21-day cycle |
Submitted price | Amivantamab, 350 mg/7 mL vial: $1,676 |
Submitted treatment cost | First 28 days: $21,481 (less than 80 kg) to $27,606 (80 kg or more) Thereafter, per 21 days: $6,713 (less than 80 kg) to $8,282 (80 kg or more) Amivantamab is administered in combination with carboplatin ($1,099 per 21-day cycle for 4 cycles) and pemetrexed ($372 per 21-day cycle until disease progression). The annual cost of amivantamab plus CP was $116,093 in year 1 and $49,295 afterwards, as calculated by the sponsor (accounting for discontinuation, dose reductions, and dose skipping). |
Comparators |
|
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs, LYs |
Time horizon | Lifetime (15 years) |
Key data source | PAPILLON trial, phase III, open-label RCT |
Submitted results |
|
Key limitations |
|
CDA-AMC reanalysis results |
|
AUC = area under the curve; CDA-AMC = Canada’s Drug Agency; CHT = platinum-based chemotherapy; CP = carboplatin-pemetrexed; exon 20ins = exon 20 insertion; ICER = incremental cost-effectiveness ratio; IO = immune-oncology drug; LY = life-year; NSCLC = non–small cell lung cancer; OS = overall survival; QALY = quality-adjusted life-year, RCT = randomized controlled trial; TKI = tyrosine kinase inhibitor; WTP = willingness to pay.
Conclusions
The Canada’s Drug Agency (CDA-AMC) clinical review concluded that evidence from the phase III, open-label, randomized controlled trial (PAPILLON) supports that amivantamab plus carboplatin-pemetrexed improves progression-free survival (PFS) compared to carboplatin-pemetrexed alone in patients with locally advanced non–small cell lung cancer (NSCLC) with an exon 20 insertion (20ins) mutation. Amivantamab plus carboplatin-pemetrexed likely improves overall survival (OS) compared with carboplatin-pemetrexed alone. However, conclusions regarding OS are limited by the fact that the data are not yet mature, the large number of crossovers that occurred in this trial, and by imprecision in the estimates (i.e., 95% confidence intervals included effects that may not be clinically important and crossed the null). Amivantamab plus carboplatin-pemetrexed may result in little to no difference in health-related quality of life, and the results of this assessment were likely biased by the open-label design of the trial and patient attrition. A nonrandomized study using individual patient data from the PAPILLON trial and real-world databases suggested that amivantamab plus carboplatin-pemetrexed is superior to EGFR tyrosine kinase inhibitors (TKIs) and immune-oncology drugs (IOs) plus platinum-based chemotherapy (CHT) for most outcomes, although the analysis was subject to numerous methodological limitations that precluded definitive conclusions. Despite this, clinical expert feedback obtained by CDA-AMC suggested that the superiority of amivantamab plus carboplatin-pemetrexed over EGFR TKIs or IOs plus CHT is plausible, given that these 2 comparators are not known to be efficacious in this patient population. Given the methodological limitations of the nonrandomized study, it was not possible to precisely quantify the magnitude of potential benefit over these comparators. The comparative clinical efficacy of CHT alone versus EGFR TKIs and IOs plus CHT is unknown and was not assessed in the nonrandomized study. Clinical expert feedback obtained by CDA-AMC indicated that CHT alone is the standard of care in clinical practice, as it is known to be more efficacious than EGFR TKIs and IOs plus CHT.
The CDA-AMC base-case results align with those of the sponsor’s submitted analysis, indicating that amivantamab plus carboplatin-pemetrexed is not cost-effective at a willingness-to-pay (WTP) threshold of $50,000 per quality-adjusted life-year (QALY) gained, relative to CHT alone. Results from the CDA-AMC base case suggest that the incremental cost-effectiveness ratio (ICER) for amivantamab plus carboplatin-pemetrexed, compared with CHT alone, is $233,922 per QALY gained. At the submitted price, amivantamab would require a price reduction of 83% for amivantamab plus carboplatin-pemetrexed to be considered cost-effective at a WTP threshold of $50,000 per QALY.
The cost-effectiveness of amivantamab plus carboplatin-pemetrexed was sensitive to alternative assumptions exploring treatment waning (after 5 years) and alternative methods of crossover adjustment for OS for those receiving CHT alone (rank-preserving structural failure time [RPSFT] models). The ICERs ranged from $245,355 and $308,627 per QALY gained relative to CHT alone in these respective scenario analyses, suggesting that higher price reductions may be required to ensure the cost-effectiveness of treatment with amivantamab plus carboplatin-pemetrexed (e.g., 88% price reduction if the RPSFT method for cross-adjustment is considered more robust).
CDA-AMC was unable to address uncertainty related to the comparative clinical data or the relevance of the modelled comparators. The clinical and cost-effectiveness of amivantamab plus carboplatin-pemetrexed compared with osimertinib are unknown. Due to the limitations associated with the evidence base and model structure, the CDA-AMC base case was restricted to results generated from the deterministic analysis of the revised model and focused on the comparison with CHT alone. CDA-AMC was unable to address limitations related to the lack of long-term clinical evidence, and results were largely driven by the predicted survival benefit, favouring amivantamab plus carboplatin-pemetrexed over CHT alone (approximately 1 year). In the absence of robust, long-term clinical evidence, the extent of survival benefit for amivantamab plus carboplatin-pemetrexed compared to CHT alone remains uncertain. Higher price reductions may therefore be required for amivantamab plus carboplatin-pemetrexed to be cost-effective at a WTP threshold of $50,000 per QALY gained.
Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, clinician groups, and drug plans that participated in the CDA-AMC review process.
Patient input was received from 3 groups: the Lung Health Foundation, the Canadian Cancer Survivor Network, and Lung Cancer Canada. Lung Cancer Canada and the Canadian Cancer Survivor Network conducted interviews with 9 patients with NSCLC, 7 of whom are in Canada. Of the interviewed patients, 3 accessed amivantamab through the PAPILLON clinical trial. Patients reported previous treatment with surgery, radiation, chemotherapy, targeted therapy, and immunotherapy. The input indicated that most patients struggled with lingering side effects, including fatigue, nausea, weight loss, and hair loss, and side effects from chemotherapy were specifically noted to impact patients’ quality of life, ability to work, and daily activities. The patient input noted a specific unmet need for therapy targeted to the exon 20ins mutation, which current treatment options do not address. Patients with experience with amivantamab reported experiencing shrinkage or stability in tumours and metastases while on amivantamab. The most common adverse events (AEs) reported by patients were skin-related, including rashes, acne, and dry and sensitive skin. Other common AEs included eye dryness, sun sensitivity, fatigue, and nausea. All patients noted that side effects are manageable and the potential benefits outweigh the negatives.
Clinician input was received from 2 groups, Ontario Health (Cancer Care Ontario) Lung Cancer Drug Advisory Committee and Lung Cancer Canada Medical Advisory Committee. Clinicians indicated that the current standard of care for patients is first-line platinum-based doublet chemotherapy. EGFR TKIs may also be used for patients with EGFR mutations, but patients with EGFR exon 20ins are resistant to EGFR TKIs and have a low response rate to immunotherapy. Clinician input suggested that amivantamab plus platinum-based doublet chemotherapy would be used in the first-line setting for patients with NSCLC with EGFR exon 20ins mutation and would become the standard of care.
Drug plan input received for this review noted uncertainty in evidence to inform the use of amivantamab in combination with alternate platinum-doublet chemotherapy options, other than that used in the PAPILLON trial (carboplatin-pemetrexed). The plans also highlighted that additional resource use would be required with amivantamab, due to its split first dose and escalating infusion rate schedule. Additional labour will be required for drug preparation, and premedications are required to prevent infusion-related reactions. The plans noted that additional therapies may be required for the management of skin toxicities with amivantamab. Drug plan input also highlighted uncertainty with discontinuation criteria in clinical practice and confidential prices of comparators.
Several of these concerns were addressed in the sponsor’s model:
Costs (including administration costs and premedication) and utility decrements related to AEs were included in the model.
CDA-AMC was unable to address the following concerns raised from input relevant to the economic review:
CDA-AMC was unable to incorporate the presence of confidential, negotiated prices for comparator treatments.
Economic Review
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted a cost-utility analysis of amivantamab plus carboplatin-pemetrexed compared with CHT alone, EGFR TKIs, and IOs plus CHT.1 The modelled population is consistent with the Health Canada indication and the reimbursement request, and these populations are aligned with the sponsor’s PAPILLON trial population.
Amivantamab is supplied in single-use vials containing 350 mg amivantamab in 7 mL solution (50 mg/mL).2 The recommended dose of amivantamab is 1,400 mg (4 vials) for patients weighing less than 80 kg and 1,750 mg (5 vials) for patients weighing greater than or equal to 80 kg.2 The recommended dosing schedule for amivantamab is once weekly for the first 4 weeks (first dose split on days 1 and 2) and every 3 weeks starting at week 7.2 Amivantamab should be reconstituted and administered by a health care professional with appropriate medical support to manage infusion-related reactions (IRRs) if they occur.2 Premedications consisting of antihistamines, antipyretics, and glucocorticoids should be administered to reduce IRRs.2 Amivantamab should be administered until disease progression or unacceptable toxicity. The cost for amivantamab is $1,676.00 per vial, leading to costs for the first 28-day cycle of $21,481 for patients weighing less than 80 kg and $27,606 for patients weighing greater than or equal to 80 kg; the cost in subsequent 21-day cycles is $6,713 and $8,282, respectively, as estimated by the sponsor.1 Amivantamab is administered in combination with carboplatin (21-day cycles for 4 cycles) and pemetrexed (21-day cycles until disease progression). As assumed by the sponsor, the cost of pemetrexed is $372 per 21-day cycle and the cost of carboplatin is $1,099 per 21-day cycle.1 The sponsor’s estimated costs considered discontinuation, dose reductions, and dose skipping, as observed in the PAPILLON trial for amivantamab plus carboplatin-pemetrexed. The annual cost of amivantamab plus carboplatin-pemetrexed was $116,093 in year 1 and $49,295 afterwards, as calculated by the sponsor.
The sponsor selected 3 therapy classes as comparators: CHT alone, consisting of carboplatin-pemetrexed (70%) and cisplatin-pemetrexed (30%); EGFR TKIs, consisting of afatinib (85%), erlotinib (5%) and gefitinib (10%); and IO plus CHT, consisting of pembrolizumab plus carboplatin-pemetrexed (70%) and pembrolizumab plus cisplatin-pemetrexed (30%).1 Costs and effects for these comparators were weighted by these proportions, which were derived based on market share estimates in Canada and clinician input.1 The 21-day cycle costs, as calculated by the sponsor, were $792 to $1,529 for CHT, $1,308 to 1,627 for EGFR TKIs, and $9,655 to $10,417 for IO agents plus CHT.1 The sponsor’s estimated costs assumed dose reductions and dose skipping, as observed in the PAPILLON trial for CHT alone, and assumed no dose reductions or dose skipping for the other comparators.
The clinical outcomes of interest were QALYs and life-years over a lifetime horizon (15 years). Discounting (1.5% per annum) was applied to both costs and outcomes, and a cycle length of 1 week was used along with a half-cycle correction. The base-case perspective was that of the Canadian publicly funded health care payer.
Model Structure
The sponsor submitted a partitioned survival model consisting of 3 mutually exclusive health states: preprogression, postprogression, and death.1 All patients entered the model in the preprogression state and received amivantamab plus carboplatin-pemetrexed or a comparator. The allocation of patients into health states is based on treatment-specific PFS and OS functions. The proportions of patients in the preprogression health state were derived from the respective PFS curves from the PAPILLON trial (for patients treated with amivantamab plus carboplatin-pemetrexed and CHT alone) or by applying hazard ratios to the amivantamab plus carboplatin-pemetrexed PFS curve (for those treated with EGFR TKIs and IOs plus CHT).1 The proportion of patients in the postprogression health state was equal to the difference between the OS and the PFS curves, and patients discontinued first-line treatment upon disease progression. Patients in the postprogression state can receive a subsequent line of therapy consisting of amivantamab monotherapy, CHT alone, non–platinum-based chemotherapy, EGFR TKIs, or IOs. Patients transitioning into the death state remained there until the end of the model time horizon. The sponsor’s model structure is available in Figure 1, Appendix 3.
Model Inputs
The target population of the economic evaluation was based on the phase III, open-label PAPILLON trial, which included patients with NSCLC with activating EGFR exon 20ins mutation receiving first-line treatment. The mean age of the population was 59.6, the mean weight was 65.8 kg, and 57.8% of patients were female.3
The key clinical inputs (i.e., PFS, OS, and treatment discontinuation) for amivantamab plus carboplatin-pemetrexed and CHT alone were obtained from the May 3, 2023, PAPILLON trial data cut with a median follow-up of 14.9 months.3 Kaplan-Meier curves were generated and used to estimate median time to event for each treatment group. Extrapolations of the PFS, OS, and time to treatment discontinuation (TTD) data were performed, and the base case applied the inverse probability of censoring weighting adjustment method to account for crossover in the pivotal trial. For amivantamab plus carboplatin-pemetrexed, the PFS, OS, and TTD data were fit with a log-logistic, Weibull, and gamma parametric distribution, respectively. For CHT alone, the PFS, OS, and TTD data were fit with gamma parametric distributions.
In the absence of direct comparative evidence versus EGFR TKIs and IOs plus CHT, comparative effectiveness data were derived from a sponsor-commissioned nonrandomized study using individual patient data from the PAPILLON trial versus a real-world evidence cohort from the US (ConcertAI and COTA).4 The adjusted treatment comparison used inverse probability of treatment weights derived from a propensity score model to account for covariates. The covariates used to estimate the weights included the functional status Eastern Cooperative Oncology Group at index date, history of brain metastases, history of liver metastases, and age at index date.4 It was assumed that unobserved confounders did not have an impact on the comparator treatment effect estimate. For OS, PFS, real-world PFS, and time to next treatment, time-to-event analyses were performed using weighted Cox proportional hazards models. PFS, OS, and TTD were modelled using hazard ratios derived from the nonrandomized study applied to their respective curves of the amivantamab plus carboplatin-pemetrexed treatment arm in the model.
Regarding the safety of amivantamab plus carboplatin-pemetrexed, the model included Grade 3 or 4 AEs occurring in 5% or more of patients in the PAPILLON trial, as well as Grade 1 to 4 IRRs.3 Safety data for each included comparator was informed by their respective pivotal trial, with AE incidence rates for selected index drugs used to represent the corresponding treatment class.
Health state utility values in the model were informed by the 5-Level EQ-5D data collected in the PAPILLON trial, valued using a Canada-specific tariff and calculated by combining both treatment arms.1 The estimated values were ████ for progression-free disease and ████ for progressed disease. Disutilities due to AEs were derived from various sources and were also applied in the model as a one-time disutility decrement.1
Costs included were related to drug acquisition, drug administration, premedication, AEs, monitoring and disease management, subsequent treatment, and terminal care. Dosing for amivantamab plus carboplatin-pemetrexed was as described earlier, with weighted acquisition costs for the initial and subsequent cycles calculated based on data from the PAPILLON trial, which found that 84.4% of patients weighed less than 80 kg at baseline.3 The sponsor included dose skipping (number of administered versus expected doses) and dose reductions (total dose prepared versus total expected doses) for amivantamab plus carboplatin-pemetrexed and CHT alone, based on the planned trial dosing in the pivotal trial. Administration costs were included for any treatments administered as IV infusion. Premedication costs were sourced from the Ontario Drug Benefit formulary.5 Monitoring and disease management costs consisted of costs for outpatient visits, chest radiography, CT scans, nurse visits, and routine blood work, which were obtained from the Ontario Schedule of Benefits for Physician and Laboratory Services.6 Resource utilization frequency was assumed to be the same across all treatments but differed for patients in the pre- and postprogression health states.1 Costs for most AEs were derived from the Ontario Case Costing Initiative, while the cost of IRRs and febrile neutropenia came from published sources.7-9 A one-off terminal care cost was applied based on a published study.10
Summary of Sponsor’s Economic Evaluation Results
All analyses were run probabilistically (1,000 iterations for the base-case and scenario analyses). The deterministic and probabilistic results were similar. The probabilistic findings are presented in this section.
Base-Case Results
In the sponsor’s base case, amivantamab plus carboplatin-pemetrexed was associated with an estimated cost of $280,942 and 3.51 QALYs over a lifetime horizon. In sequential analysis, amivantamab plus carboplatin-pemetrexed was associated with an ICER of $96,774 compared to CHT alone (incremental costs: $195,847; incremental QALYs: 2.02). Amivantamab plus carboplatin-pemetrexed had a 0.9% probability of being cost-effective at a WTP threshold of $50,000 per QALY. The key cost driver among patients receiving amivantamab plus carboplatin-pemetrexed was drug acquisition, accounting for 70% of the total cost incurred. The sponsor’s analysis predicted that approximately 56% of the incremental benefit was obtained after the trial period based on extrapolations (i.e., 1.94 of the incremental QALYs were accrued after the maximum follow-up in the PAPILLON trial of 27 months). IOs plus CHT and EGFR TKIs were extendedly dominated by CHT alone and amivantamab plus carboplatin-pemetrexed. Additional results from the sponsor’s submitted economic evaluation base case are available in Appendix 3.
Table 3: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total costs ($) | Total QALYs | Sequential ICER($/QALY) |
|---|---|---|---|
CHT alone | 85,095 | 1.49 | Reference |
Amivantamab plus CP | 280,942 | 3.51 | 96,774 |
Dominated treatments | |||
EGFR TKIs | 121,106 | 1.57 | Extendedly dominated |
IOs plus CHT | 207,762 | 1.99 | Extendedly dominated |
CHT = platinum-based chemotherapy; CP = carboplatin-pemetrexed; ICER = incremental cost-effectiveness ratio; IO = immune-oncology drug; QALY = quality-adjusted life-year; TKI = tyrosine kinase inhibitor.
Note: The submitted analysis is based on publicly available prices of comparator treatments.
Source: Sponsor’s pharmacoeconomic submission.1
Sensitivity and Scenario Analysis Results
The sponsor conducted several scenario analyses, including alternate discount rates, time horizons, crossover adjustment methods (RPSFT, 2-stage, no adjustment), alternative methods of weighting the nonrandomized study results, UK-specific utility weights, inclusion of vial sharing, exclusion of amivantamab monotherapy as a second-line treatment (from subsequent therapies), and exclusion of dose skipping and dose reductions. Across all scenario analyses, the ICER comparing amivantamab plus carboplatin-pemetrexed versus CHT alone ranged from $93,856 to $121,961 per QALY gained and it was most sensitive to the exclusion of dose skipping and dose reductions.
The sponsor conducted a scenario analysis from a societal perspective that included additional costs associated with caregiver costs and patient sick leave, as well as caregiver disutilities for progressed patients. In this analysis, the ICER per QALY gained was $166,426 relative to CHT alone, higher than the sponsor’s base-case analysis using a health care payer perspective.
CDA-AMC Appraisal of the Sponsor’s Economic Evaluation
CDA-AMC identified several key limitations to the sponsor’s analysis that have notable implications on the economic analysis:
The OS extrapolations of the PAPILLON trial data are uncertain for both amivantamab plus carboplatin-pemetrexed and CHT alone and lack plausibility. As stated in the CDA-AMC clinical review, evidence from the trial suggested that amivantamab plus carboplatin-pemetrexed may improve OS over carboplatin-pemetrexed alone. However, conclusions regarding OS are limited by the fact that the data are not yet mature (final assessment for OS is planned to be done at 48 months), by the large number of crossovers that occurred in this trial, and by the imprecision in the estimates despite the sponsor’s attempt to adjust for crossover (i.e., 95% CIs included effects that may not be clinically important and crossed the null). When the sponsor extrapolated the OS data from the PAPILLON trial (maximum follow-up 27 months) to the 15-year model time horizon using independent parametric distributions, the sponsor’s model predicted a median survival of 19 months for patients treated with CHT alone. Clinical expert feedback obtained by CDA-AMC indicated that these estimates were higher than expected in clinical practice. They explained that patients in clinical trials are generally healthier than the patient population treated in clinical practice, which further contributes to the higher-than-expected OS observed with carboplatin-pemetrexed alone; combined with the allowed crossover in the trial, it makes the results uncertain and difficult to interpret. Additionally, the sponsor’s model predicted a substantially higher median survival for amivantamab plus carboplatin-pemetrexed, resulting in an incremental gain of approximately 2 QALYs versus CHT alone, with 56% of this incremental gain accruing in the extrapolated period (beyond 27 months), for which there are no observed clinical data. Clinical expert feedback obtained by CDA-AMC deemed that survival estimates for amivantamab plus carboplatin-pemetrexed based on the Gompertz distribution would be more clinically plausible (median OS 34 months, 5-year OS of 10.5%) than the sponsor-selected Weibull distribution (median OS 42 months, 5-year OS of 35.9%). The sponsor selected parametric distributions based on goodness-of-fit criteria, visual inspection, and clinical plausibility, following Decision Support Unit guidance.11 While CDA-AMC agrees that parametric models should be compared based on their statistical fit, this pertains only to the observed trial period, not to the extrapolation period. The weight given to the comparative fit of alternative parametric models to the observed data depends on the extent to which extrapolation is required and the degree of censoring present. Considering the short duration of available trial data relative to the extrapolation period, the clinical plausibility of the predicted long-term OS associated with amivantamab plus carboplatin-pemetrexed or CHT alone, as well as the magnitude and durability of such a benefit as predicted by the sponsor’s extrapolation are therefore highly uncertain.
CDA-AMC selected the Gompertz distribution to extrapolate long-term OS for amivantamab plus carboplatin-pemetrexed in the base case, which was deemed more reasonable by clinical experts. CDA-AMC was unable to address the uncertainty in OS extrapolations for CHT alone, as no other available parametric distributions meaningfully shorten the median OS. Therefore, the relative survival benefit of amivantamab plus carboplatin-pemetrexed versus CHT alone remains uncertain.
CDA-AMC included 2 scenario analyses to explore the impact of treatment waning and alternative methods to adjust OS for crossover for those treated with CHT alone.
The comparative clinical efficacy of amivantamab plus carboplatin-pemetrexed versus EGFR TKIs and IOs plus CHT is highly uncertain and produces model results that lack face validity. Due to the lack of head-to-head evidence from randomized controlled trials comparing amivantamab plus carboplatin-pemetrexed with EGFR TKIs and IOs plus CHT, the sponsor submitted a nonrandomized study against these active comparators to inform the pharmacoeconomic model (PFS, OS, TTD). The analysis used individual patient data from the PAPILLON trial and real-world databases, and inverse probability of treatment weights methods to reduce the risk of bias due to confounding. Although the CDA-AMC clinical review of the nonrandomized study suggests superiority of amivantamab plus carboplatin-pemetrexed for most efficacy outcomes, the precise quantification of benefit over these comparators could not be determined due to the numerous methodological limitations, including lack of protocol and methods to appraise the risk of bias and suitability of the data sources, potential heterogeneity across databases, lack of randomization, small sample sizes, and low relevance of EGFR TKIs and IOs as comparators in the analyses. The nonrandomized study provided no information on health-related quality of life or harms. When using results from the nonrandomized study, the sponsor’s model resulted in EGFR TKIs and IOs plus CHT being more efficacious than CHT alone. The relative efficacy of CHT alone versus EGFR TKIs and IOs plus CHT was not assessed, and it was not included in the analysis. Despite this, clinical expert feedback obtained by CDA-AMC for this review suggested that superiority of amivantamab plus carboplatin-pemetrexed over EGFR TKIs and IOs plus CHT is plausible as they are known to be futile treatments for NSCLC in patients with EGFR exon 20ins mutations and, therefore, not expected to be more efficacious than CHT alone. Hence, CHT alone remains the standard of care in clinical practice in Canada. Therefore, the comparative evidence from the nonrandomized study remains highly uncertain, and the model estimates for EGFR TKIs and IOs plus CHT do not meet face validity, according to clinical expert feedback obtained by CDA-AMC.
CDA-AMC was unable to address the limitations associated with the sponsor’s nonrandomized study.
Modelled comparators did not reflect clinical practice. The sponsor included IOs (pembrolizumab) plus CHT, EGFR TKIs (afatinib, erlotinib, and gefitinib), and CHT alone as comparators in the analysis. However, clinical experts consulted by CDA-AMC indicated that access to pembrolizumab is limited due to a lack of Health Canada approval for patients with EGFR mutation and limited funding (e.g., restricted benefit in some provinces to patients without EGFR mutations). Additionally, EGFR TKIs in general are considered futile for patients with exon 20ins mutation due to lack of efficacy. As a result, both IOs plus CHT (i.e., pembrolizumab) and EGFR TKIs are less relevant comparators in this patient population, as submitted by the sponsor. Furthermore, the sponsor excluded osimertinib from the EGFR TKI options without adequate justification. Osimertinib is only considered in the submitted model as a possible treatment in the second-line setting or later. However, clinical expert feedback received by CDA-AMC indicated that, for the very few patients who would be considered for treatment with EGFR TKI, osimertinib would be the only EGFR TKI used in clinical practice in Canada, as it is better tolerated. As such, osimertinib may remain a relevant comparator for patients but, in the absence of comparative data, the cost-effectiveness of amivantamab plus carboplatin-pemetrexed versus osimertinib in this population remains unknown. Clinical experts consulted by CDA-AMC indicated that the standard of care is currently CHT alone, which is clinically superior to both EGFR TKIs and IOs plus CHT. Notably, however, the sponsor assumes that CHT alone comprises 70% carboplatin-pemetrexed regimen and 30% cisplatin-pemetrexed regimen, although the PAPILLON trial included the carboplatin-based regimen only. Based on publicly available list prices for carboplatin and cisplatin, the incremental costs of amivantamab plus carboplatin-pemetrexed versus CHT alone may have been slightly underestimated by the sponsor, if cisplatin is less likely to be used in clinical practice.
CDA-AMC was unable to address this limitation in reanalysis.
Decision uncertainty cannot be accurately characterized. Consistent with the CDA-AMC guidelines,12 the sponsor’s base case used a Monte Carlo simulation to characterize the uncertainty of relevant input parameters. However, in the submitted model, the probabilistic results demonstrated considerable instability in OS when using the only clinically plausible parametric distribution for OS extrapolation of amivantamab plus carboplatin-pemetrexed (i.e., 10% of patients alive after 5 years, 0% alive after 10 years). The probabilistic results differed substantially from the deterministic results ($152,169 per QALY gained versus $233,922 per QALY gained, respectively). When reviewing each probabilistic iteration, implausible scenarios were noted where the average patient receiving amivantamab plus carboplatin-pemetrexed experienced nearly 9 years of additional survival relative to CHT. Given these iterations were not considered clinically plausible, based on the evidence presented, the probabilistic analysis generated a biased estimate. Given the immaturity of the OS data in the PAPILLON trial (with a maximum follow-up of 27 months) and the absence of long-term evidence to support this magnitude of the superiority of amivantamab plus carboplatin-pemetrexed over CHT alone, CDA-AMC opted to report the results deterministically.
CDA-AMC could not address this limitation in reanalysis. The CDA-AMC base case and reanalysis reported deterministic analysis results.
Additionally, the following key assumptions were made by the sponsor and have been appraised by CDA-AMC (refer to Table 4).
Table 4: Key Assumptions of the Submitted Economic Evaluation (Not Noted as Limitations to the Submission)
Sponsor’s key assumption | CDA-AMC comment |
|---|---|
Dose skipping and dose reductions were included for patients receiving amivantamab plus CP and CHT alone, based on the total prepared and expected doses observed in the PAPILLON trial.13 However, dose skipping and reductions were not included for EGFR TKIs and IOs plus CHT. | Uncertain and likely inappropriate. CDA-AMC notes that it is uncertain whether the trial-based proportion of doses skipped may reflect real-world clinical practice. Clinical expert feedback obtained by CDA-AMC deemed the proportions observed in the pivotal trial to be reasonable for amivantamab plus CP and CHT alone. However, results are biased in favour of amivantamab plus CP versus EGFR TKIs and IOs plus CHT. Clinical expert feedback found it inappropriate to exclude dose skipping and dose reductions for IOs plus CHT, as it would be expected to at least be similar to those receiving CHT alone due to adverse events related to the CHT. Similarly, a proportion of dose skipping or dose reductions would be expected with EGFR TKIs, albeit at lower rates, as treatment with osimertinib is known to be better tolerated than CHT alone. However, as there is low relevance of EGFR TKIs and IOs as comparators in the analyses as submitted by the sponsor, this is not expected to significantly impact the results. |
Safety outcomes were based on a naive comparison versus EGFR TKIs and IOs plus CHT. | Uncertain. The sponsor included Grade 3 or 4 AEs occurring in 5% of more of patients in the safety population of the PAPILLON trial along with Grade 1 to 4 IRRs.3 However, as safety was not captured in the RWE study, data from the respective pivotal trials of individual comparator treatments were used to inform safety data, which were compared directly to AE rates in the PAPILLON trial. This represents an uncontrolled, naive comparison of safety, as rates of AEs were not included in the adjusted treatment comparison. It is uncertain whether the metric used to define adverse events (e.g., treatment-emergent or treatment-related) would be similar across all trials. |
The proportion of patients who require subsequent therapy is uncertain. | Uncertain and likely inappropriate. The sponsor assumed that no patients treated with amivantamab plus CP would receive amivantamab as second-line treatment but assumed that a large proportion of patients progressing on EGFR TKIs and IOs plus CHT would receive amivantamab monotherapy as second-line treatment, which did not meet face validity according to clinical feedback obtained by CDA-AMC. They indicated that a proportion of patients would be expected to continue treatment with amivantamab plus CP despite disease progression in clinical practice, depending on the severity of the progression. Furthermore, access to amivantamab monotherapy in second-line treatment is restricted (i.e., negotiations were concluded without an agreement) and therefore is not a relevant subsequent treatment at the present time. However, due to the low relevance of IOs plus CHT and EGFR TKIs as comparators for this patient population, and the small impact of any cost savings due to delay or avoidance of subsequent therapy (versus CHT alone), this is not expected to significantly impact the results. |
AE = adverse event; CHT = platinum-based chemotherapy; CP = carboplatin-pemetrexed; IO = immune-oncology drug; RWE = real-world evidence; TKI = tyrosine kinase inhibitor.
CDA-AMC Reanalyses of the Economic Evaluation
Base-Case Results
The CDA-AMC base case was derived by making changes in model parameter values and assumptions, in consultation with clinical experts. A summary of the changes applied to the submitted economic evaluation is presented in Table 5. Due to the limitations associated with the evidence base and model structure, the CDA-AMC base case was restricted to results generated from the deterministic analysis of the revised model. The summary results of the CDA-AMC reanalysis are presented in Table 6.
Table 5: CDA-AMC Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CDA-AMC value or assumption |
|---|---|---|
Changes to derive the CDA-AMC base case | ||
1. Amivantamab plus CP OS parametric extrapolation | Weibull | Gompertz |
CDA-AMC base case | ― | Reanalysis 1 |
CP = carboplatin-pemetrexed; OS = overall survival.
Results from the CDA-AMC base case estimated that amivantamab plus carboplatin-pemetrexed was associated with incremental costs of $193,368 and an incremental QALY gain of 0.83 versus CHT alone, resulting in an ICER of $233,922 per QALY gained. Owing to structural limitations of the sponsor’s model (probabilistic and deterministic results do not align), all CDA-AMC analyses are deterministic and do not reflect uncertainty. The CDA-AMC base case is based on publicly available prices of the comparator treatments. In contrast with the sponsor’s analysis, the CDA-AMC results suggest that 0.77 of total QALYs were accrued after the maximum follow-up in the PAPILLON trial (27 months), corresponding to approximately 34% of the incremental benefit being obtained from extrapolation.
Table 6: Summary of the Stepped Analysis of the CDA-AMC Reanalysis Results
Stepped analysis | Drug | Total costs ($) | Total QALYs | Sequential ICER ($/QALY) |
|---|---|---|---|---|
Sponsor base case (deterministic) | CHT alone | 85,614 | 1.48 | Reference |
Amivantamab plus CP | 282,040 | 3.48 | 98,593 | |
EGFR TKIs | 123,412 | 1.47 | Dominated by CHT alone | |
IOs plus CHT | 208,960 | 1.85 | Extendedly dominated | |
1. CDA-AMC reanalysis 1 — overall survival for amivantamab plus CP | CHT alone | 85,614 | 1.48 | Reference |
Amivantamab plus CP | 278,982 | 2.31 | 233,922 | |
EGFR TKIs | 123,285 | 1.27 | Dominated by CHT alone | |
IOs plus CHT | 208,666 | 1.51 | Extendedly dominated | |
CDA-AMC base case (deterministic) (reanalysis 1) | CHT alone | 85,614 | 1.48 | Ref. |
Amivantamab plus CP | 278,982 | 2.31 | 233,922 | |
EGFR TKIs | 123,285 | 1.27 | Dominated by CHT alone | |
IOs plus CHT | 208,666 | 1.51 | Extendedly dominated |
CHT = platinum-based chemotherapy; CP = carboplatin-pemetrexed; TKI = tyrosine kinase inhibitor; ICER = incremental cost-effectiveness ratio; IO = immuno-oncology drug; QALY = quality-adjusted life-year.
Note: The submitted analysis is based on publicly available prices of comparator treatments. The CDA-AMC base case was restricted to deterministic results due to the limitations associated with the evidence base and model structure (discrepancy between probabilistic and deterministic results, and implausible incremental OS survival).
Scenario Analysis Results
CDA-AMC undertook price reduction analyses based on the sponsor’s submitted results and the CDA-AMC base-case reanalysis. The CDA-AMC base case suggests that an 83% price reduction for amivantamab is required for amivantamab plus carboplatin-pemetrexed to be considered cost-effective at a WTP threshold of $50,000 per QALY gained versus CHT alone. This would reduce the price of amivantamab from $1,676.00 to $285 (per 350 mg vial).
Table 7: CDA-AMC Price Reduction Analyses
Analysis: Price reduction | Unit drug cost ($) | ICERs for amivantamab plus CP versus CHT alone ($/QALY) | |
|---|---|---|---|
Sponsor base case | CDA-AMC reanalysis | ||
No price reduction | 1,676 | 98,593 | 233,922 |
10% | 1,508 | 89,319 | 211,661 |
20% | 1,341 | 80,046 | 189,399 |
30% | 1,173 | 70,772 | 167,138 |
40% | 1,006 | 61,498 | 144,876 |
50% | 838 | 52,225 | 122,615 |
60% | 670 | 42,951 | 100,353 |
70% | 503 | 33,677 | 78,092 |
80% | 335 | 24,403 | 55,830 |
90% | 168 | 15,130 | 33,569 |
CHT = platinum-based chemotherapy; CP = carboplatin-pemetrexed; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
CDA-AMC conducted a series of scenario analyses to explore the impact of alternative assumptions on the cost-effectiveness of amivantamab plus carboplatin-pemetrexed:
assuming treatment waning (i.e., assuming that the effect of amivantamab plus carboplatin-pemetrexed is equivalent to CHT alone after 5 years)
adopting the RPSFT method for OS crossover adjustment.
Results of the CDA-AMC scenario analyses are available in Table 12, Appendix 4. The cost-effectiveness of amivantamab plus carboplatin-pemetrexed was sensitive to assumptions regarding long-term treatment effect and the crossover adjustment method applied. When assuming no difference in treatment effect between amivantamab plus carboplatin-pemetrexed versus CHT alone after 5 years, the ICER increased to $245,355 per QALY gained. When adopting the RPSFT crossover adjustment method, the ICER for amivantamab plus carboplatin-pemetrexed increased to $308,627 per QALY gained relative to CHT alone. In this later scenario, a price reduction of 88% would be required for amivantamab plus carboplatin-pemetrexed to be cost-effective at the WTP threshold of $50,000 per QALY gained relative to CHT alone.
Issues for Consideration
CDA-AMC previously reviewed amivantamab monotherapy for the treatment of adult patients with locally advanced or metastatic NSCLC with activating EGFR exon 20ins mutations whose disease has progressed on or after CHT.14 The committee recommended reimbursement of amivantamab with conditions, including a price reduction of at least 77%. However, negotiations were concluded without an agreement.15 The submitted price was consistent across both submissions ($1,676 per 350 mg vial), and results from the current review of amivantamab plus carboplatin-pemetrexed used as a first-line treatment were similar, indicating that this drug is not cost-effective at the submitted price and would require a substantial price reduction.
Drug plan input highlighted the additional resource use required with amivantamab due to its split first dose and escalating infusion rate schedule. Additional labour will also be required for drug preparation, and premedications are required to prevent IRRs. This may put a strain on resources (e.g., staff, pharmacists, overhead) in some settings.
Other targeted therapies — poziotinib, mobocertinib, and furmonertinib — have been submitted to the FDA for adult patients with NSCLC with activating EGFR exon 20ins mutations and may be relevant in the future.16-18 The cost-effectiveness of amivantamab plus carboplatin-pemetrexed versus these other agents is unknown.
Overall Conclusions
The CDA-AMC clinical review concluded that evidence from the phase III, open-label, randomized controlled trial (PAPILLON) supports that amivantamab plus carboplatin-pemetrexed improves PFS compared to carboplatin-pemetrexed alone in patients with locally advanced NSCLC with an exon 20ins mutation. Amivantamab plus carboplatin-pemetrexed likely improves OS compared with carboplatin-pemetrexed alone. However, conclusions regarding OS are limited by the fact that the data are not yet mature, the large number of crossovers that occurred in this trial, and by imprecision in the estimates (i.e., 95% confidence intervals included effects that may not be clinically important and crossed the null). Amivantamab plus carboplatin-pemetrexed may result in little to no difference in health-related quality of life, and the results of this assessment was likely biased by the open-label design of the trial and patient attrition. A nonrandomized study using individual patient data from the PAPILLON trial and real-world databases suggested that amivantamab plus carboplatin-pemetrexed is superior to EGFR TKIs and IOs plus CHT for several efficacy outcomes, although the analysis was subject to numerous methodological limitations that precluded definitive conclusions. Despite this, clinical expert feedback obtained by CDA-AMC suggested that the superiority of amivantamab plus carboplatin-pemetrexed over EGFR TKIs or IOs plus CHT is plausible, given that these 2 comparators are not known to be efficacious in this patient population. Given the methodological limitations of the nonrandomized study, it was not possible to precisely quantify the magnitude of potential benefit over these comparators. The comparative clinical efficacy of CHT alone versus EGFR TKIs and IOs plus CHT is unknown and was not assessed in the nonrandomized study. Clinical expert feedback obtained by CDA-AMC indicated that CHT alone is the standard of care in clinical practice, as it is known to be more efficacious than EGFR TKIs and IOs plus CHT.
Therefore, EGFR TKIs and IOs plus CHT, as considered by the sponsor in their economic evaluation, are of low relevance for this patient population. Further, when using results from the nonrandomized study, the sponsor’s model estimates results that lack face validity (i.e., EGFR TKIs and IOs plus CHT being more efficacious than CHT alone). The CDA-AMC base case was derived by adopting a Gompertz distribution to extrapolate OS for amivantamab plus carboplatin-pemetrexed.
The CDA-AMC base-case results align with those of the sponsor’s submitted analysis, indicating that amivantamab plus carboplatin-pemetrexed is not cost-effective at a WTP threshold of $50,000 per QALY gained, relative to CHT alone. Results from the CDA-AMC base case suggest that the ICER for amivantamab plus carboplatin-pemetrexed, compared with CHT alone, is $233,922 per QALY gained. At the submitted price, amivantamab would require a price reduction of 83% for amivantamab plus carboplatin-pemetrexed to be considered cost-effective at a WTP threshold of $50,000 per QALY.
The cost-effectiveness of amivantamab plus carboplatin-pemetrexed was sensitive to alternative assumptions exploring treatment waning (after 5 years) and alternative methods of crossover adjustment for OS for those receiving CHT alone (RPSFT models). The ICERs ranged from $245,355 and $308,627 per QALY gained relative to CHT alone in these respective scenario analyses, suggesting that higher price reductions may be required to ensure the cost-effectiveness of treatment with amivantamab plus carboplatin-pemetrexed (e.g., 88% price reduction if the RPSFT method for cross-adjustment is considered more robust).
CDA-AMC was unable to address uncertainty related to the comparative clinical data or the relevance of the modelled comparators. The clinical and cost-effectiveness of amivantamab plus carboplatin-pemetrexed compared with osimertinib are unknown. Due to the limitations associated with the evidence base and model structure, the CDA-AMC base case was restricted to results generated from the deterministic analysis of the revised model and focused on the comparison with CHT alone. CDA-AMC was unable to address limitations related to the lack of long-term clinical evidence, and results were largely driven by the predicted survival benefit favouring amivantamab plus carboplatin-pemetrexed over CHT alone (approximately 1 year). In the absence of robust, long-term clinical evidence, the extent of the survival benefit for amivantamab plus carboplatin-pemetrexed compared to CHT alone remains uncertain. Higher price reductions may therefore be required for amivantamab plus carboplatin-pemetrexed to be cost-effective at a WTP threshold of $50,000 per QALY gained.
References
1.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Rybrevant (amivantamab), 350 mg/7 mL vial of liquid concentrate for intravenous infusion. Toronto (ON): Janssen Inc; 2024 Jun 21.
2.Rybrevant (amivantamab): 350 mg/7 mL vial of liquid concentrate for intravenous infusion [product monograph]. Toronto (ON): Janssen Inc; 2024 Jun 12.
3.Clinical Study Report (Primary Analysis): 61186372NSC3001. A randomized, open-label phase 3 study of combination amivantamab and carboplatin-pemetrexed therapy, compared with carboplatin-pemetrexed, in patients with EGFR Exon 20ins mutated locally advanced or metastatic non-small cell lung cancer (PAPILLON) [internal sponsor's report]. Raritan (NJ): Janssen Research & Development, LLC; 2023 Sep 5.
4.Indirect treatment comparisons with individual patient data from papillon and two real-world data sources report [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Rybrevant (amivantamab), 350 mg/7 mL vial of liquid concentrate for intravenous infusion. Toronto (ON): Janssen Inc; 2024 May 28.
5.Ontario Ministry of Health, Ontario Ministry of Long-Term Care. Ontario drug benefit formulary/comparative drug index [sponsor supplied reference]. https://www.formulary.health.gov.on.ca/formulary/. Accessed 2024 April 22.
6.Ontario Ministry of Health. Schedule of Benefits. Physician services under the Health Insurance Act (February 20, 2024 (effective April 1, 2024)) [sponsor supplied reference]. 2024: https://www.ontario.ca/files/2024-04/moh-schedule-benefit-2024-02-20.pdf. Accessed 2024 April 18.
7.Ontario Ministry of Health. OCCI tool (2017-2018). 2018.
8.CIHI. Patient cost estimator (2021-2022) 2022; https://www.cihi.ca/en/patient-cost-estimator. Accessed 2024 Apr 23.
9.Tam VC, Ko YJ, Mittmann N, Cheung MC, Kumar K, et al. Cost-effectiveness of systemic therapies for metastatic pancreatic cancer. Curr Oncol. 2013;20(2):e90-e106. PubMed
10.De Oliveira C, Pataky R, Bremner KE, Rangrej J, Chan KKW, et al. Estimating the cost of cancer care in British Columbia and Ontario: a Canadian inter-provincial comparison. Appendix Table 2. Healthc Policy. 2017;12(3):95-108. PubMed
11.NICE DSU technical support document 14: survival analysis for economic evaluations alongside clinical trials - extrapolation with patient-level data. Sheffield (GB): Decision Support Unit, ScHARR, University of Sheffield; 2011.
12.Guidelines for the economic evaluation of health technologies: Canada. 4th ed. Ottawa (ON): CADTH; 2017: https://www.cadth.ca/guidelines-economic-evaluation-health-technologies-canada-4th-edition. Accessed 2024 Sep 5.
13.PAPILLON dose skipping and dose reductions [sponsor supplied reference]. Toronto (ON): Janssen Inc; 2024.
14.CADTH reimbursement recommendation: amivantamab (Rybrevant). Can J Health Technol. 2023;3(3). https://www.cadth.ca/sites/default/files/DRR/2023/PC0289%20Rybrevant%20-%20Confidential%20CADTH%20Final%20Recommendation.pdf. Accessed 2024 Sep 5.
15.pan-Canadian Pharmaceutical Alliance. Rybrevant (amivantamab). 2023; https://www.pcpacanada.ca/index.php/negotiation/22311. Accessed 2024 Sep 9.
16.U.S. Food & Drug Administration (FDA). FDA grants accelerated approval to mobocertinib for metastatic non-small cell lung cancer with EGFR exon 20 insertion mutations. 2021; https://www.fda.gov/drugs/resources-information-approved-drugs/fda-grants-accelerated-approval-mobocertinib-metastatic-non-small-cell-lung-cancer-egfr-exon-20. Accessed 2024 Sep 5.
17.U.S. Food & Drug Administration (FDA). Poziotinib for HER2 exon 20 insertion mutation positive non-small cell lung cancer (NSCLC. 2022; https://www.fda.gov/media/161759/download. Accessed 2024 Sep 5.
18.ArriVent Biopharma Inc. ArriVent receives FDA breakthrough therapy designation for furmonertinib for first-line treatment of advanced or metastatic non-small cell lung cancer with EGFR Exon 20 insertion mutations. 2023; https://ir.arrivent.com/news-releases/news-release-details/arrivent-receives-fda-breakthrough-therapy-designation. Accessed 2024 Sep 5.
19.DeltaPA. Ottawa (ON): IQVIA; 2023: https://www.iqvia.com/. Accessed 2024 Jul 15.
20.Cancer Care Ontario. Funded evidence-informed regimens. 2024; https://www.cancercareontario.ca/en/drugformulary/regimens. Accessed 2024 Jul 15.
21.Exceptional Access Program (EAP). Toronto (ON): Ontario Ministry of Health; Ontario Ministry of Long-Term Care; 2024: http://www.health.gov.on.ca/en/pro/programs/drugs/odbf/odbf_except_access.aspx. Accessed 2024 Jul 15.
22.Ontario Ministry of Health, Ontario Ministry of Long-Term Care. Ontario drug benefit formulary/comparative drug index. 2024; https://www.formulary.health.gov.on.ca/formulary/. Accessed 2024 Jul 15.
23.Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Rybrevant (amivantamab), 350 mg/7 mL vial of liquid concentrate for intravenous infusion. Toronto (ON): Janssen Inc; 2024 Jun 21.
24.Brenner DR, Gillis J, Demers AA, et al. Projected estimates of cancer in Canada in 2024. CMAJ. 2024;196(18):E615-E623. PubMed
25.Canadian cancer statistics: a 2020 special report on lung cancer. Toronto (ON): Canadian Cancer Society; 2020: https://cdn.cancer.ca/-/media/files/cancer-information/resources/publications/2020-canadian-cancer-statistics-special-report/2020-canadian-cancer-statistics-special-report-en.pdf?rev=15c66a0b05f5479e935b48035c70dca3&hash=3D51B0D0FB5C3F7E659F896D66495CE8&_ga=2.1870065.1988674510.1635847835-1688650972.1629385192. Accessed 2024 Jun 6.
26.Burnett H, Emich H, Carroll C, Stapleton N, Mahadevia P, Li T. Epidemiological and clinical burden of EGFR Exon 20 insertion in advanced non-small cell lung cancer: a systematic literature review. PLoS One. 2021;16(3):e0247620. PubMed
27.Melosky B, Banerji S, Blais N, et al. Canadian consensus: a new systemic treatment algorithm for advanced EGFR-mutated non-small-cell lung cancer. Curr Oncol. 2020;27(2):e146-e155. PubMed
28.Graham RP, Treece AL, Lindeman NI, et al. Worldwide frequency of commonly detected EGFR mutations. Arch Pathol Lab Med. 2018;142(2):163-167. PubMed
29.Midha A, Dearden S, McCormack R. EGFR mutation incidence in non-small-cell lung cancer of adenocarcinoma histology: a systematic review and global map by ethnicity (mutMapII). Am J Cancer Res. 2015;5(9):2892-2911. PubMed
30.Boyne DJ, Jarada TN, Yusuf A, et al. 51P Testing patterns and outcomes of different EGFR-positive metastatic non-small cell lung cancer (NSCLC) patients in a Canadian real-world setting. Ann Oncol. 2022;33(2 Suppl):S56.
31.O'Sullivan DE, Jarada TN, Yusuf A, et al. Prevalence, treatment patterns, and outcomes of individuals with EGFR positive metastatic non-small cell lung cancer in a Canadian real-world setting: a comparison of Exon 19 deletion, L858R, and Exon 20 insertion EGFR mutation carriers. Curr Oncol. 2022;29(10):7198-7208. PubMed
Appendix 1: Cost Comparison Table
Please note that this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical experts. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 8: CDA-AMC Cost Comparison Table for Locally Advanced or Metastatic NSCLC
Treatment | Strength / concentration | Form | Price | Recommended dosage | Daily cost ($) | 21-day cost ($)a |
|---|---|---|---|---|---|---|
Amivantamab + CP | ||||||
Amivantamab (Rybrevant) | 50 mg/mL | 7 mL (350 mg) Liquid concentrate for IV infusion | 1,676.0000a | Body weight < 80 kg: 1,400 mg weekly for 4 weeks, then 1,750 mg every 3 weeks starting at Week 7 onwards Body weight ≥ 80 kg: 1,750 mg weekly for 4 weeks, then 2,100 mg every 3 weeks starting at Week 7 onwards | Body weight < 80 kg: First 28-day cycle: 957.71 21-day cycles thereafter: 399.05 Body weight ≥ 80 kg: First 28-day cycle 1,197.14 21-day cycle thereafter:478.86 | Body weight < 80 kg: First 28-day cycle: 26,816 21-day cycles thereafter: 8,380 Body weight ≥ 80 kg: First 28-day cycle: $33,520 21-day cycles thereafter: 10,056 |
Carboplatin (generic) | 50 mg 150 mg 450 mg 600 mg | 10 mg/mL vial for injection | 70.0000 210.0000 599.9985 775.0020 | 21-day cycles: Target AUC 5 on Day 1, maximum dose for AUC 5 is 750 mgd up to 12 weeks | 46.90 | 985 |
Pemetrexed (generic) | 100 mg vial 500 mg vial | 10 mg/mL IV solution | 50.0000 250.0000 | 21-day cycles: 500 mg/m2 IV on Day 1 until disease progression | 21.43 | 450 |
Amivantamab + CRBPPEME regimen cost | Cycles 1 and 2: 765.88 Cycles 3 and 4: 479.83 Cycles 5 and beyond: 432.93 | Cycles 1 and 2: 16,083 Cycles 3 and 4: 10,076 Cycles 5 and beyond: 9,091 | ||||
CHT alone | ||||||
CISPPEME | ||||||
Cisplatin (generic) | 50 mg vial 100 mg vial | 1 mg/mL IV solution | 135.0000 270.0000 | 21-day cycles: 75 mg/m2 IV on Day 1 until disease progression | 19.29 | 405 |
Pemetrexed (generic) | 100 mg vial 500 mg vial | 10 mg/mL IV solution | 50.0000 250.0000 | 21-day cycles: 500 mg/m2 IV on Day 1until disease progression | 21.43 | 450 |
CISPPEME regimen cost | 40.72 | 855 | ||||
CRBPPEME | ||||||
Carboplatin (generic) | 50 mg 150 mg 450 mg 600 mg | 10 mg/mL vial for injection | 70.0000 210.0000 599.9985 775.0020 | 21-day cycles: Target AUC 5 on Day 1, maximum dose for AUC 5 is 750 mgd up to 12 weeks | 46.90 | 985 |
Pemetrexed (generic) | 100 mg vial 500 mg vial | 10 mg/mL IV solution | 50.0000 250.0000 | 21-day cycles: 500 mg/m2 IV on Day 1 until disease progression | 21.43 | 450 |
CRBPPEME regimen cost | Cycles 1 to 4: 68.33 Cycles 5 and beyond: 21.43 | Cycles 1 to 4: 1,435 Cycles 5 and beyond: 450 | ||||
EGFR TKIs | ||||||
Afatinib | 20 mg 30 mg 40 mg | Tablet | 77.4784b | 40 mg once daily | 77.48 | 1,627 |
Erlotinib | 25 mg 100 mg 150 mg | Tablet | 11.8667c 47.4667 71.2000 | 150 mg once daily | 71.20 | 1,495 |
Gefitinib | 250 mg | Tablet | 62.3050c | 250 mg once daily | 62.31 | 1,308 |
Osimertinib | 40 mg 80 mg | Tablet | 322.1280 | 80 mg once daily | 332.13 | 6,975 |
IOs plus CHT | ||||||
PEMBRO + CISPPEME | ||||||
Pembrolizumab | 25 mg/mL | 4 mL (100 mg) Solution for IV injection | 4,400.0000 | 200 mg every 3 weeks; or, 400 mg every 6 weeks until disease progression, unacceptable toxicity, or up to 24 months or 35 doses for 200 mg or 18 doses for 400 mg | 419.05 | 8,800 |
Cisplatin (generic) | 50 mg vial 100 mg vial | 1 mg/mL IV solution | 135.0000 270.0000 | 21-day cycles: 75 mg/m2 IV on Day 1 until disease progression | 19.29 | 405 |
Pemetrexed (generic) | 100 mg vial 500 mg vial | 10 mg/mL IV solution | 50.0000 250.0000 | 21-day cycles: 500 mg/m2 IV on Day 1 until disease progression | 21.43 | 450 |
PEMBRO + CISPPEME regimen cost | 459.76 | 9,655 | ||||
PEMBRO + CRBPPEME | ||||||
Pembrolizumab | 25 mg/mL | 4 mL (100 mg) Solution for IV injection | 4,400.0000 | 200 mg every 3 weeks; or, 400 mg every 6 weeks until disease progression, unacceptable toxicity, or up to 24 months or 35 doses for 200 mg or 18 doses for 400 mg | 419.05 | 8,800 |
Carboplatin (generic) | 50 mg 150 mg 450 mg 600 mg | 10 mg/mL vial for injection | 70.0000 210.0000 599.9985 775.0020 | 21-day cycles: Target AUC 5 on Day 1, maximum dose for AUC 5 is 750 mgd up to 12 weeks | 46.90 | 985 |
Pemetrexed (generic) | 100 mg vial 500 mg vial | 10 mg/mL IV solution | 50.0000 250.0000 | 21-day cycles: 500 mg/m2 IV on Day 1 until disease progression | 21.43 | 450 |
PEMBRO + CRBPPEME regimen cost | Cycles 1 to 4: 483.38 Cycles 5 and beyond: 440.48 | Cycles 1 to 4: 10,235 Cycles 5 and beyond: 9,250 | ||||
CHT = platinum-based chemotherapy; IOs = immune-oncology agents; NSCLC = non–small cell lung cancer; TKIs = tyrosine kinase inhibitors.
Note: All prices are wholesale from IQVIA Delta PA (accessed July 2024),19 unless otherwise indicated, and do not include dispensing fees. Calculations assume a patient body weight of 65.8 kg and a body surface area of 1.71 m2 as per the PAPILLON trial.3 Regimen costs assume that 84.4% of patients were < 80 kg as per the PAPILLON trial.3 Vial wastage was assumed (i.e., no vial sharing). All recommended dosages are retrieved from Cancer Care Ontario Drug Formulary Regimens.20
aSponsor’s submitted price.1
bPrice from Ontario Exceptional Access Program (accessed July 2024).21
cPrice from Ontario Drug Benefit formulary (accessed July 2024).22
dDose [mg] = Target AUC * [GFR + 25]; AUC = product of serum concentration (mg/mL) and time (min); GFR (glomerular filtration rate) expressed as measured Creatinine Clearance or estimated from Serum Creatinine (by Cockcroft and Gault method or Jelliffe method). Maximum Carboplatin Dose (mg) = Target AUC (mg/mL per min) x (125 mL/min + 25). Target AUC was assumed to be 5, aligned with the PAPILLON trial.3
Appendix 2: Submission Quality
Please note that this appendix has not been copy-edited.
Description | Yes or No | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | No | Refer to CDA-AMC critical appraisal section “Modelled comparators did not reflect clinical practice.” |
Model has been adequately programmed and has sufficient face validity | No | Refer to CDA-AMC critical appraisal section. The sponsor’s base-case survival estimates for amivantamab plus CP and CHT alone were likely overestimated based on clinical expert opinion. The probabilistic and deterministic results were discrepant when choosing certain OS extrapolations. The comparative clinical efficacy of amivantamab plus CP versus EGFR TKIs and IOs plus CHT produce model results that lack face validity: |
Model structure is adequate for decision problem | No | Refer to CDA-AMC critical appraisal section “Decision uncertainty cannot be accurately characterized.” |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | Yes | No comment. |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | No | Refer to CDA-AMC critical appraisal section “Decision uncertainty cannot be accurately characterized.” |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | Yes | No comment. |
CHT = platinum-based chemotherapy.
Appendix 3: Additional Information on the Submitted Economic Evaluation
Please note that this appendix has not been copy-edited.
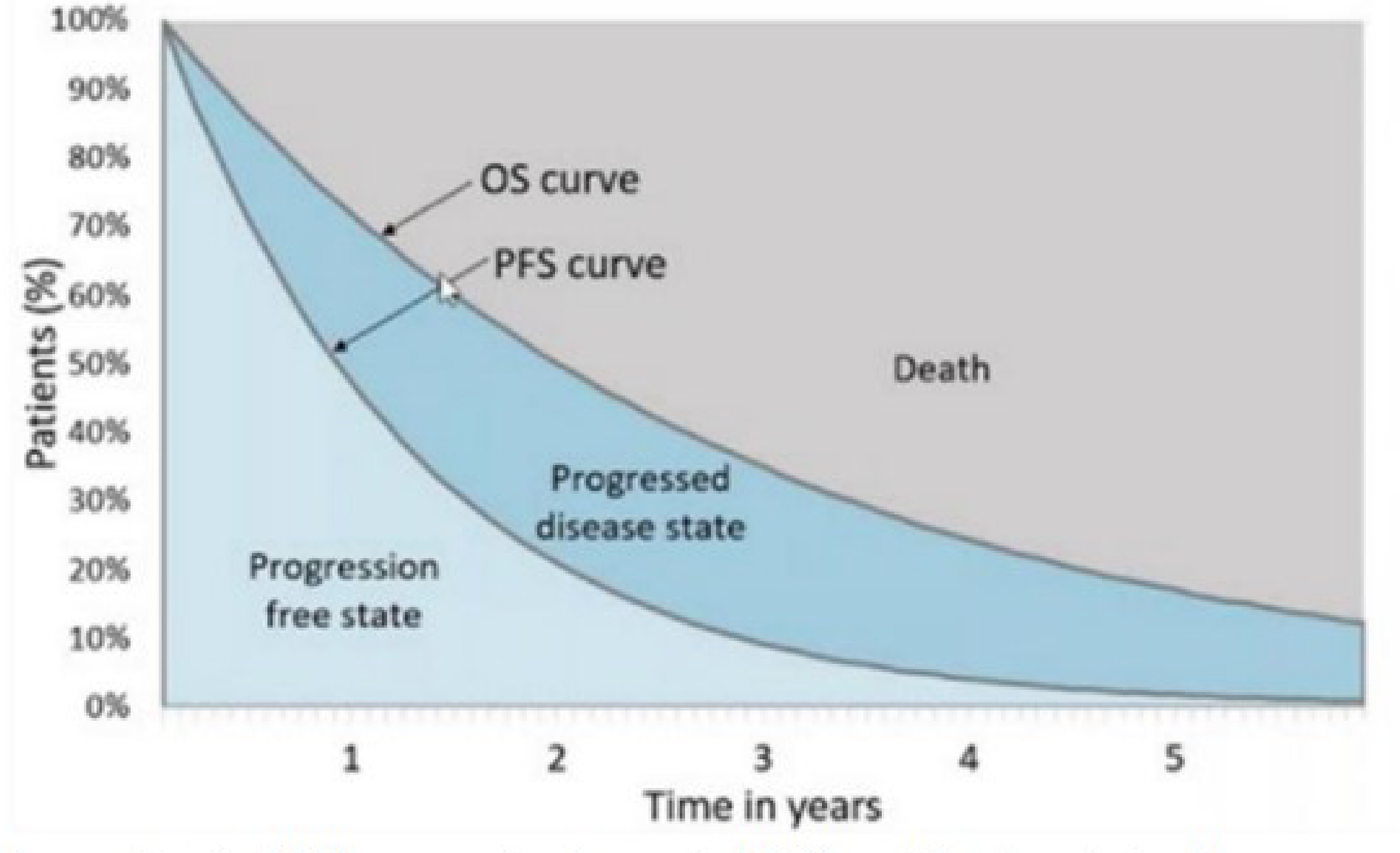
OS = overall survival; PFS = progression-free survival.
Source: Sponsor’s pharmacoeconomic submission.1
Detailed Results of the Sponsor’s Base Case
Table 10: Disaggregated Summary of the Sponsor’s Economic Evaluation Results
Parameter | Amivantamab + CP | CHT alone | EGFR TKIs | IOs plus CHT |
|---|---|---|---|---|
Discounted LYs | ||||
Total | 4.42 | 1.85 | 1.94 | 2.48 |
Progression-free LYs | 1.55 | 0.64 | 0.82 | 0.96 |
Postprogression LYs | 2.87 | 1.20 | 1.12 | 1.52 |
Discounted QALYs | ||||
Total | 3.51 | 1.49 | 1.57 | 1.99 |
Progression-free QALYs | 1.31 | 0.55 | 0.70 | 0.82 |
Postprogression QALYs | 2.20 | 0.94 | 0.87 | 1.17 |
Disutilities due to AEs | 0.00 | 0.00 | 0.00 | 0.00 |
Discounted costs ($) | ||||
Total | 280,942 | 85,095 | 121,106 | 207,762 |
Drug acquisition | 199,015 | 8,638 | 18,654 | 97,646 |
Administration | 3,424 | 859 | 0 | 764 |
Premedication | 154 | 56 | 0 | 48 |
Monitoring | 435 | 219 | 201 | 238 |
Subsequent treatment | 11,022 | 12,671 | 38,784 | 46,010 |
Disease management — preprogression | 3,969 | 1,644 | 2,103 | 2,459 |
Disease management — postprogression | 6,545 | 2,748 | 2,550 | 3,470 |
Terminal care | 51,636 | 56,052 | 55,802 | 55,066 |
Adverse events | 4,742 | 2,208 | 3,012 | 2,061 |
AE = adverse event; CHT = platinum-based chemotherapy; ICER = incremental cost-effectiveness ratio; IO = immuno-oncology agents; LY = life-year; QALY = quality-adjusted life-year; TKI = tyrosine kinase inhibitor.
Source: Sponsor’s pharmacoeconomic submission.1
Appendix 4: Additional Details on the CDA-AMC Reanalyses and Sensitivity Analyses of the Economic Evaluation
Please note that this appendix has not been copy-edited.
Detailed Results of CDA-AMC Base Case
Table 11: Disaggregated Summary of the CDA-AMC Economic Evaluation Results
Parameter | Amivantamab + CP | CHT alone | EGFR TKIs | IOs plus CHT |
|---|---|---|---|---|
Discounted LYs | ||||
Total | 2.84 | 1.84 | 1.56 | 1.85 |
Progression-free LYs | 1.41 | 0.64 | 0.78 | 0.93 |
Postprogression LYs | 1.44 | 1.20 | 0.78 | 0.92 |
Discounted QALYs | ||||
Total | 2.31 | 1.48 | 1.27 | 1.51 |
Progression-free QALYs | 1.20 | 0.55 | 0.66 | 0.79 |
Postprogression QALYs | 1.12 | 0.94 | 0.61 | 0.72 |
Disutilities due to AEs | 0.00 | 0.00 | 0.00 | 0.00 |
Discounted costs ($) | ||||
Total | 278,982 | 85,614 | 123,285 | 208,666 |
Drug acquisition | 197,695 | 8,601 | 18,338 | 96,870 |
Administration | 3,402 | 859 | 0 | 757 |
Premedication | 153 | 55 | 0 | 48 |
Monitoring | 432 | 219 | 198 | 236 |
Subsequent treatment | 10,425 | 13,164 | 41,634 | 48,134 |
Disease management — preprogression | 3,588 | 1,637 | 1,979 | 2,363 |
Disease management — postprogression | 3,289 | 2,748 | 1,786 | 2,107 |
Terminal care | 55,253 | 56,120 | 56,338 | 56,095 |
Adverse events | 4,746 | 2,211 | 3,013 | 2,055 |
AE = adverse event; CHT = platinum-based chemotherapy; ICER = incremental cost-effectiveness ratio; IO = immuno-oncology agents; LY = life-year; QALY = quality-adjusted life-year; Ref. = reference; TKI = tyrosine kinase inhibitor.
Note: Results are presented deterministically due to discrepancies between probabilistic and deterministic results.
Scenario Analyses
Table 12: Scenario Analysis Conducted on the CDA-AMC Base Case
Stepped analysis | Drug | Total costs ($) | Total QALYs | Sequential ICER ($/QALY) |
|---|---|---|---|---|
Sponsor base case (deterministic) | CHT alone | 85,614 | 1.48 | Reference |
Amivantamab plus CP | 282,040 | 3.48 | 98,593 | |
EGFR TKIs | 123,412 | 1.47 | Dominated | |
IOs plus CHT | 208,960 | 1.85 | Extendedly dominated | |
CDA-AMC Scenario 1: Treatment waning effect (no difference between treatments after 5 years) | CHT alone | 85,614 | 1.48 | Reference |
Amivantamab plus CP | 277,635 | 2.27 | 245,355 | |
EGFR TKIs | 123,285 | 1.27 | Dominated | |
IOs plus CHT | 208,666 | 1.51 | Extendedly dominated | |
CDA-AMC Scenario 2: RPSFT crossover adjustment | CHT alone | 86,416 | 1.69 | Ref. |
Amivantamab plus CP | 278,982 | 2.31 | 308,627 | |
EGFR TKIs | 123,285 | 1.27 | Dominated | |
IOs plus CHT | 208,666 | 1.51 | Extendedly dominated |
CHT = platinum-based chemotherapy; CP = carboplatin-pemetrexed; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Note: Results are presented deterministically due to discrepancies between probabilistic and deterministic results.
Appendix 5: Submitted Budget Impact Analysis and CDA-AMC Appraisal
Please note that this appendix has not been copy-edited.
Table 13: Summary of Key Take-Aways
Key take-aways of the budget impact analysis |
|---|
|
Summary of Sponsor’s Budget Impact Analysis
The submitted budget impact analysis (BIA) assessed the introduction of amivantamab plus carboplatin-pemetrexed for the first-line treatment of adult patients with locally advanced (not amenable to curative therapy) or metastatic NSCLC with activating EGFR exon 20ins mutations.23 The analysis was taken from the perspective of the Canadian public drug plans using an epidemiology-based approach, with drug acquisition and administration costs included in the base case. A three-year time horizon was used, from 2026 to 2028, with 2025 as a base year. The population size was estimated starting with incident lung cancer cases followed by a series of attritions. Key inputs to the BIA are documented in Table 14.
The reference case scenario included CHT alone, EGFR TKIs, and IOs plus CHT. The new drug scenario included the same comparators along with amivantamab plus carboplatin-pemetrexed. The market share estimates were derived from chart review in Canada and input from clinical experts in Canada.
Table 14: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as year 1 / year 2 / year 3 if appropriate) | |
|---|---|---|
Target population | ||
Incidence of lung cancer | 63.8 per 100,00024 | |
Proportion of new cases that are NSCLC | 88%25 | |
Proportion of NSCLC cases that are locally advanced or metastatic | 63.6%25 | |
Proportion of locally advanced/metastatic NSCLC cases that are nonsquamous | 83.1%26 | |
Proportion of patients tested for EGFR mutations | 81.6%27 | |
Proportion of patients that are EGFR positive | 14.3%27 | |
Proportion of patients with EGFR exon 20ins mutations | ||
Proportion of patients initiating first-line treatment | 83.1%28 | |
Number of patients eligible for drug under review | 79 / 81 / 82 | |
Market Uptake (3 years) | ||
Uptake (reference scenario) CHT alone EGFR TKIs IOs plus CHT | 50% / 50% / 50% 20% / 20% / 20% 30% / 30% / 30% | |
Uptake (new drug scenario) Amivantamab plus CP CHT alone EGFR TKIs IOs plus CHT | 45% / 55% / 65% 25% / 20% / 15% 10% / 5% / 5% 20% / 20% / 15% | |
Duration of treatment in months (based on median PFS)a | ||
Amivantamab plus CP CHT alone EGFR TKIs IOs plus CHT | 11.37 6.70 6.85 8.01 | |
Cost of treatment (per patient) | ||
Amivantamab plus CP CHT alone EGFR TKIs IOs plus CHT | $171,175 Year 1; $0 Maintenance $6,356 Year 1; $0 Maintenance $15,772 Year 1; $0 Maintenance $113,330 Year 1; $0 Maintenance | |
CHT = platinum-based chemotherapy; IO = immuno-oncology; NSCLC = non–small cell lung cancer; PFS = progression-free survival; TKI = tyrosine kinase inhibitors.
Note: Cost of treatment per patient per year assumed the following proportion of use across comparator treatments: CHT (comprising 70% carboplatin + pemetrexed and 30% cisplatin + pemetrexed), EGFR TKIs (comprising 85% afatinib, 5% erlotinib, and 10% gefitinib), IOs + CHT (comprising 70% pembrolizumab + carboplatin + pemetrexed and 30% pembrolizumab + cisplatin + pemetrexed)23
aMedian PFS values for each regimen were used as a proxy for the duration of treatment, as per their respective pivotal trial data.23
Summary of the Sponsor’s BIA Results
The estimated budget impact of funding amivantamab plus carboplatin-pemetrexed for the first-line treatment of adult patients with locally advanced (not amenable to curative therapy) or metastatic NSCLC with activity EGFR exon 20ins mutations was $4,939,830 in Year 1, $6,361,788 in Year 2, and $7,353,249 in Year 3, for a three-year total of $18,654,867.
CDA-AMC Appraisal of the Sponsor’s BIA
CDA-AMC identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
The market uptake of amivantamab plus carboplatin-pemetrexed and the base year market share of comparators are uncertain. The sponsor assumed market uptake for amivantamab plus carboplatin-pemetrexed of 45%, 55%, and 65% in years 1, 2, and 3 of the BIA, respectively. Clinical expert feedback obtained by CDA-AMC and input from clinician groups suggest that the estimated market uptake of amivantamab plus carboplatin-pemetrexed appeared to be underestimated. Clinicians expect almost full displacement of CHT alone and a shift toward amivantamab plus carboplatin-pemetrexed becoming the standard of care due to the benefit versus CHT alone, and the known lack of efficacy associated with EGFR TKIs and IOs plus CHT in this patient population. There are limited reasons to not administer amivantamab to a patient if they are well enough and willing to receive CHT alone. Furthermore, clinical expert feedback obtained by CDA-AMC noted that the base year market shares of IOs plus CHT and EGFR TKIs appeared to be overestimated given their minimal use in clinical practice in Canada due to their known lack of efficacy, lack of Health Canada approval for IOs plus CHT use in patients with EGFR mutations and limited funding.
CDA-AMC adjusted the base year market shares of comparators to reflect the use of CHT alone as the current standard of care in this patient population; and assumed a market uptake for amivantamab plus carboplatin-pemetrexed reaching 70% in Year 1, 80% in Year 2, and stabilizing at 80% by year 3, aligned with clinical input obtained by CDA-AMC. Amivantamab plus carboplatin-pemetrexed was assumed to also heavily displace IOs plus CHT and EGFR TKIs, yet maintaining a small share (5% across all 3 years in reanalysis) to account for the remaining utilization of EGFR TKIs due to the convenience of their oral route of administration despite their lack of efficacy in this patient population; or some residual utilization of IOs plus CHT for heavy smoker patients.
The number of eligible patients is uncertain. The sponsor derived the population for the BIA using an epidemiology-based approach with a series of attritions, eventually resulting in approximately 75 incident patients that would potentially be eligible for amivantamab plus carboplatin-pemetrexed in 2024. This number was considered lower than the estimated annual incidence of 200 to 1,000 patients provided by the clinician input from the LCC Medical Advisory Committee.
Additionally, clinical expert feedback obtained by CDA-AMC, noted that the sponsor assumed that only a proportion of patients with nonsquamous NSCLC are tested for EGFR mutations, after which EGFR and exon20ins mutations are determined in the submitted model, which did not meet face validity. According to clinical input obtained by CDA-AMC and the CDA-AMC Testing Procedure Considerations, testing for EGFR exon20ins mutations is currently done as routine care in all patients with locally advanced or metastatic NSCLC.
CDA-AMC adjusted the EGFR testing rate to 100% to reflect clinical expert input and the current standard of care.
As part of a scenario analysis, CDA-AMC increased the population size to 200 incident cases per year.
Subsequent therapy was not considered. The sponsor did not consider subsequent therapy in the BIA, despite including assumptions regarding subsequent therapy in their pharmacoeconomic model. This was of concern according to the clinical experts, who noted that patients would most likely receive either CHT alone after being treated with EGFR TKIs or IOs plus CHT. For those receiving amivantamab plus carboplatin-pemetrexed, a proportion of patients may continue treatment with amivantamab despite disease progression in clinical practice depending on individual patients’ disease severity. The budget impact of amivantamab plus carboplatin-pemetrexed may likely be underestimated with the exclusion of subsequent therapy costs after disease progression.
CDA-AMC could not address this limitation in reanalysis.
Drug prices paid by public drug plans are uncertain. Both the sponsor and the CDA-AMC analyses are based on publicly available list prices for all comparators. Actual costs paid by public drug plans are unknown.
CDA-AMC could not address this limitation in reanalysis.
CDA-AMC Reanalyses of the BIA
Table 15: CDA-AMC Revisions to the Submitted Budget Impact Analysis
Stepped analysis | Sponsor’s value or assumption | CDA-AMC value or assumption |
|---|---|---|
Changes to derive the CDA-AMC base case | ||
1. Market shares (Years 0 through 3) | Amivantamab + CP: 0% / 45% / 55% / 65% CHT alone: 50% / 25% / 20% / 15% IOs + CHT: 30% / 20% / 20% / 15% EGFR TKIs: 20% / 10% / 5% / 5% | Amivantamab + CP: 0% / 70% / 80% / 80% CHT alone: 70% / 20% / 10% / 10% IOs + CHT: 20% / 5% / 5% / 5% EGFR TKIs: 10% / 5% / 5% / 5% |
2. Proportion of patients with NSCLC tested for EGFR mutations | 81.6% | 100% |
CDA-AMC base-case | Reanalysis 1 + 2 | |
NSCLC = non–small cell lung cancer.
The results of the CDA-AMC step-wise reanalysis are presented in summary format in Table 16 and a more detailed breakdown is presented in Table 17. The CDA-AMC reanalysis of the BIA suggests that the estimated budget impact of funding amivantamab plus carboplatin-pemetrexed for the first-line treatment of adult patients with locally advanced (not amenable to curative therapy) or metastatic NSCLC with activity EGFR exon 20ins mutations was $9,490,208 in Year 1, $11,418,486 in Year 2, and $11,649,162 in Year 3, for a three-year total of $32,557,856.
Scenario analyses conducted by CDA-AMC indicate that the BIA results are sensitive to the population size, with the scenario assuming 200 incident patients per year resulting in a three-year budget impact of 65,906,562. Thus, the sponsor’s base-case results may have underestimated the true budget impact (Table 17).
Table 16: Summary of the CDA-AMC Reanalyses of the Budget Impact Analysis
Stepped analysis | Three-year total ($) |
|---|---|
Submitted base case | 18,654,867 |
CDA-AMC reanalysis 1 | 26,609,783 |
CDA-AMC reanalysis 2 | 22,835,401 |
CDA-AMC base case | 32,557,856 |
BIA = budget impact analysis.
Table 17: Detailed Breakdown of the CDA-AMC Reanalyses of the BIA
Stepped analysis | Scenario | Year 0 (current situation) ($) | Year 1 ($) | Year 2 ($) | Year 3 ($) | Three-year total ($) |
|---|---|---|---|---|---|---|
Submitted base case | Reference | 3,105,517 | 8,126,009 | 9,628,630 | 10,660,422 | 28,415,062 |
New drug | 3,105,517 | 3,186,179 | 3,266,842 | 3,307,174 | 9,760,195 | |
Budget impact | 0 | 4,939,830 | 6,361,788 | 7,353,249 | 18,654,867 | |
CDA-AMC base case | Reference | 2,697,076 | 12,244,669 | 14,259,024 | 14,547,085 | 41,050,777 |
New drug | 2,697,076 | 2,754,461 | 2,840,538 | 2,897,922 | 8,492,921 | |
Budget impact | 0 | 9,490,208 | 11,418,486 | 11,649,162 | 32,557,856 | |
CDA-AMC scenario analysis 1: 200 incident patients per year | Reference | 5,738,460 | 25,509,727 | 28,806,108 | 28,806,108 | 83,121,943 |
New drug | 5,738,460 | 5,738,460 | 5,738,460 | 5,738,460 | 17,215,381 | |
Budget impact | 0 | 19,771,267 | 23,067,648 | 23,067,648 | 65,906,562 |
BIA = budget impact analysis
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.