Drugs, Health Technologies, Health Systems
Reimbursement Review
Trastuzumab Deruxtecan (Enhertu)
Sponsor: AstraZeneca Canada Inc.
Therapeutic area: Gastric or gastroesophageal junction adenocarcinoma
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Clinical Review
Abbreviations
AE
adverse event
AST
aspartate aminotransferase
CAPOX
capecitabine-oxaliplatin
CDA-AMC
Canada’s Drug Agency
CGOEN
Canadian Gastrointestinal Oncology Evidence Network
CI
confidence interval
CPS
combined positive score
CR
complete response
CrCl
creatinine clearance
ECOG PS
Eastern Cooperative Oncology Group Performance Status
ESS
effective sample size
FACT-Ga
Functional Assessment of Cancer Therapy – Gastric
FAS
full analysis set
FE
fixed effect
FOLFIRI
folinic acid–fluorouracil-irinotecan
FOLFOX
folinic acid–fluorouracil-oxaliplatin
GEJ
gastroesophageal junction
GRADE
Grading of Recommendations Assessment, Development, and Evaluation
HER2
human epidermal growth factor 2
HR
hazard ratio
HRQoL
health-related quality of life
ICR
independent central review
IHC
immunohistochemistry
ILD
interstitial lung disease
IRR
infusion-related reaction
ISH
in situ hybridization
ITC
indirect treatment comparison
ITT
intention to treat
KM
Kaplan-Meier
LV
left ventricular
LVEF
left ventricular ejection fraction
MAIC
matching-adjusted indirect comparison
NMA
network meta-analysis
NOC/c
Notice of Compliance with conditions
OH-CCO
Ontario Health (Cancer Care Ontario)
ORR
objective response rate
OS
overall survival
PD-L1
programmed death-ligand 1
PFS
progression-free survival
PR
partial response
RCT
randomized controlled trial
RE
random effect
RECIST 1.1
Response Evaluation Criteria in Solid Tumours Version 1.1
SLR
systematic literature review
TEAE
treatment-emergent adverse event
TESAE
treatment-emergent serious adverse event
TLR
time-limited reimbursement
ULN
upper limit of normal
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Table 1: Background Information on Application Submitted for Review
Item | Description |
|---|---|
Drug product | Trastuzumab deruxtecan (Enhertu), powder for concentrate for solution for infusion, 100 mg, IV infusion |
Sponsor | AstraZeneca Canada Inc. |
Indication | As monotherapy for the treatment of adult patients with unresectable, locally advanced or metastatic HER2-positive gastric or GEJ adenocarcinoma who have received a prior trastuzumab-based regimen |
Reimbursement request | As monotherapy for the second-line treatment of adult patients with unresectable locally advanced or metastatic HER2-positive gastric or GEJ adenocarcinoma who have received a prior anti–HER2-based regimen |
Health Canada approval status | NOC/c |
Health Canada review pathway | Advance consideration under NOC/c |
NOC date | January 17, 2025 |
Recommended dosage | 6.4 mg/kg given as an IV infusion once every 3 weeks (21-day cycle) until disease progression or unacceptable toxicity |
Eligible for consideration as a TLR recommendation? | Yes |
GEJ = gastroesophageal junction; HER2 = human epidermal growth factor 2; NOC = Notice of Compliance; NOC/c = Notice of Compliance with conditions; TLR = time-limited reimbursement.
Sources: Sponsor’s Summary of Clinical Evidence;1 draft product monograph;2 Drug Reimbursement Review sponsor submission for trastuzumab deruxtecan.3
Introduction
Gastric cancer is the fifth most common cancer and the fifth leading cause of cancer mortality worldwide, with approximately 968,000 incident cases and 659,853 associated deaths in 2022 (equating to 6.8% of all cancer-related deaths).4 Gastric adenocarcinoma is the most common histological type of gastric cancer, accounting for more than 95% of gastric cancer cases.5 In clinical trials, patients with advanced gastroesophageal junction (GEJ) adenocarcinoma are often included alongside patients with advanced gastric adenocarcinoma because of the similarities in tumour growth and patterns of disease spread between the 2 patient popualitons.6,7 In fact, gastric and GEJ adenocarcinoma have often been reviewed, investigated, or presented together in literature reviews, clinical trials, and clinical management guidelines.8-11 The projected incident rate of gastric cancer in Canada is 8.3 per 100,000 adults in 2024, with an estimated 1,400 cases in females and 2,600 cases in males.12 Signs and symptoms of gastric cancer include abdominal pain, heart burn, loss of appetite, bloating, nausea, vomiting, difficulty swallowing, blood in the stool, anemia, fatigue, ascites, and jaundice.13 The overall 5-year survival for all patients with gastric cancer is estimated to be 29%.14 Patients with distant metastases experience worse outcomes, with an estimated 5-year relative survival rate of 7%.15 Compared to patients with gastric adenocarcinoma, patients with GEJ adenocarcinoma might have worse disease-specific survival, with an approximately 10% higher cumulative incidence of recurrence.16 The prognostic role of human epidermal growth factor 2 (HER2) in gastric cancer remains controversial due to conflicting evidence.17-21 In a population of patients in Canada, an estimated 21% of all gastric and GEJ cancers showed HER2 positivity.22 All patients with advanced or metastatic gastric or GEJ cancer, including patients with both gastric and gastroesophageal adenocarcinomas, should undergo HER2 testing.23 HER2 testing is typically conducted at the time of diagnosis or at the onset of advanced or metastatic disease.23 Additionally, HER2 testing may be repeated if there is a need for re-evaluation due to disease progression or metastases.23 HER2 positivity is confirmed when test results show immunohistochemistry (IHC) 3+ or IHC 2+ followed by in situ hybridization (ISH) positivity.23,24
According to the clinical experts consulted by the review team, most patients with unresectable locally advanced or metastatic HER2-positive gastric or GEJ cancers are treated with palliative intent; the treatment goals of all therapies in this setting are to prolong overall survival (OS) and improve quality of life. The clinical experts consulted by the review team noted that the cornerstone of treatment for patients with unresectable locally advanced or metastatic HER2-positive gastric or GEJ cancers involves the sequential use of the best available systemic therapies. The clinical experts consulted by the review team noted that, in the first-line treatment setting, the standard of care for patients with locally advanced or metastatic HER2-positive gastric or GEJ cancers with a programmed death-ligand 1 (PD-L1) combined positive score (CPS) of less than 1 includes a fluoropyrimidine-platinum doublet chemotherapy (e.g., folinic acid–fluorouracil-oxaliplatin [FOLFOX], capecitabine-oxaliplatin [CAPOX], or cisplatin-capecitabine) in combination with trastuzumab. In the second-line treatment setting, according to the clinical experts consulted by the review team, the standard of care for locally advanced or metastatic HER2-positive gastric or GEJ cancers is treatment with ramucirumab-paclitaxel or with ramucirumab alone. However, the clinical experts consulted by the review team noted that, as a single drug, ramucirumab is not reimbursed in many jurisdictions across Canada, including Ontario. The clinical experts consulted by the review team also noted that the current second-line treatment of HER2-positive gastric or GEJ cancers is identical to that of HER2-negative gastroesophageal cancers. The sponsor noted that single-drug chemotherapy options, such as irinotecan, paclitaxel, or docetaxel, have been suggested in guidelines for patients who are not eligible for ramucirumab-paclitaxel.25,26 Further, according to the sponsor, relevant guidelines25,26 suggest the use a fluoropyrimidine and platinum combination, such as FOLFOX or CAPOX for patients previously treated with folinic acid–fluorouracil-irinotecan (FOLFIRI) in the first-line setting. In the third-line setting, the clinical experts consulted by the review team noted that the treatment options for patients with locally advanced or metastatic HER2-positive gastric or GEJ cancers include trifluridine-tipiracil (i.e., TAS-102), nivolumab, and pembrolizumab.
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of trastuzumab deruxtecan (Enhertu),100 mg, powder for concentrate for solution for IV infusion for the treatment of adult patients with unresectable locally advanced or metastatic HER2-positive gastric or GEJ adenocarcinoma who have received a prior trastuzumab-based regimen. Trastuzumab deruxtecan has been previously reviewed by the review team for other indications.
Of note, trastuzumab deruxtecan received an NOC/c from Health Canada on January 17, 2025. The sponsor filed for a time-limited reimbursement (TLR) recommendation on an NOC/c basis while awaiting results from the confirmatory, phase III DESTINY-Gastric04 study. More details on TLR recommendation eligibility are provided in the next section. The sponsor also requested a deviation from the Health Canada indication and limited the requested reimbursement criteria for trastuzumab deruxtecan monotherapy to the second-line treatment of adult patients with unresectable locally advanced or metastatic HER2-positive gastric or GEJ adenocarcinoma who have received a prior anti–HER2-based regimen.”3 The sponsor noted that this request was more aligned with both the DESTINY-Gastric02 study population and the trial design for the ongoing, confirmatory, phase III study, DESTINY-Gastric04. Of note, the proposed Health Canada indication targets patients who have received a prior trastuzumab-based regimen, while the reimbursement request targets those who have received a prior anti–HER2-based regimen (i.e., not necessarily a trastuzumab-based regimen). Trastuzumab is currently the only anti-HER2 drug that has been authorized for the first-line treatment of gastric or GEJ cancer in Canada.
Consideration for a TLR Recommendation
A TLR is a recommendation by the CDA-AMC expert committee to publicly fund a drug or drug regimen for a certain period of time on the condition that the sponsor will conduct 1 or more clinical studies that address uncertainty in the clinical evidence. CDA-AMC subsequently conducts a reassessment of the additional evidence and issues a final reimbursement recommendation within a defined period of time. Based on the preliminary assessment by CDA-AMC (Table 36 in Appendix 1), trastuzumab deruxtecan meets the requirements to be considered by the expert committee for a TLR recommendation.
The following paragraph describes these requirements and provides additional background on the reimbursement request.
Trastuzumab deruxtecan received an NOC/c from Health Canada on January 17, 2025, through Health Canada’s advance consideration process under the NOC/c policy. A phase III clinical trial (DESTINY-Gastric04) was being conducted at the time of the submission to CDA-AMC. The ongoing DESTINY-Gastric04 phase III study evaluates the efficacy and safety of trastuzumab deruxtecan relative to ramucirumab-paclitaxel for up to 3 years of follow-up in approximately 490 patients with HER2-positive gastric or GEJ adenocarcinoma. The DESTINY-Gastric04 study population targets the second-line treatment setting for patients with HER2-positive gastric or GEJ cancer, which aligns with the current reimbursement request proposed by the sponsor. However, the Health Canada indication targets a broader population, including not only patients in the second-line treatment setting, but also patients in the third-line and later settings. The DESTINY-Gastric04 trial population does not completely align with the patients in the third- and later-line settings described by the Health Canada indication. As a result, findings from the DESTINY-Gastric04 trial may not be generalizable to patients in the third and subsequent lines setting. According to the clinical experts consulted by the review team, the selection of ramucirumab-paclitaxel as a comparator in the phase III DESTINY-Gastric04 trial is appropriate because treatment with ramucirumab-paclitaxel is currently among the standard of care in the second-line setting for locally advanced or metastatic HER2-positive gastric or GEJ cancer, and will likely remain the standard of care in the second-line setting when the results of the DESTINY-Gastric04 trial become available. The results of the DESTINY-Gastric04 study are expected to be ready in the fourth quarter of 2025. The sponsor has expressed that it will commit to file a reassessment application with CDA-AMC in accordance with the time frames specified in the procedures for TLR recommendations.
Perspectives of Patients, Clinicians, and Drug Programs
The information in this section is a summary of the input provided by the patient and clinician groups who responded to our call for input and from clinical experts and drug programs consulted for the purpose of this review.
Patient Input
One input from My Gut Feeling – Stomach Cancer Foundation of Canada was received for this review. My Gut Feeling – Stomach Cancer Foundation of Canada is a nonprofit organization in Canada, dedicated to providing “support, awareness, education, information, and advocacy to stomach cancer patients, cancer survivors, caregivers, and family members.” The patient group gathered information from 30 respondents (75% patients, 25% caregivers) through an online survey conducted in September 2024.
According to the patient group input, 95% of respondents felt that their cancer diagnosis had a significant impact on their quality of life, and that cancer and its treatment affected their physical health, mental health, ability to eat, work, finances, social life, identity, psychosocial well-being, and self-image. Many respondents reported concerns about finances due to the inability to work because of their cancer diagnosis and/or treatment for cancer. Based on the input, patients and caregivers commented on the time and money spent for cancer treatment appointments, medications, driving and parking costs, and the costs of eating at the hospital as financial stressors.
The important outcomes reported by the respondents included quality of life, treatment side effects, cost of treatment, convenience of treatment, treatment access, duration of treatment, and the survival benefits.
My Gut Feeling – Stomach Cancer Foundation of Canada stated that there is an unmet patient and caregiver need to receive equitable access to therapies that may prolong life, improve symptoms, reduce the risk of recurrence, and improve treatment tolerability. The organization also noted that 4 respondents who had experience with trastuzumab deruxtecan were satisfied because trastuzumab deruxtecan had fewer side effects, was easier to tolerate, improved their quality of life, and better controlled their cancer.
Clinician Input
Input From Clinical Experts Consulted for This Review
According to the clinical experts consulted by the review team, the goals for the treatment of patients with unresectable locally advanced or metastatic HER2-positive gastric or GEJ adenocarcinoma who have received a prior anti–HER2-based regimen are to prolong OS and improve quality of life. The clinical experts consulted by the review team noted that there was a considerable unmet need for effective anti-HER2 therapies beyond the first-line treatment setting for patients with locally advanced unresectable or metastatic HER2-positive gastric or GEJ adenocarcinoma.
According to the clinical experts consulted by the review team, following disease progression on first-line, HER2-directed therapy, the current standard of care in the second-line setting for patients with HER2-negative gastric or GEJ adenocarcinoma is treatment with ramucirumab in combination with paclitaxel or treatment with ramucirumab alone. The clinical experts noted that trastuzumab deruxtecan would cause a shift in the current treatment paradigm for adult patients with locally advanced or metastatic HER2-positive gastric or GEJ adenocarcinoma who have received a prior trastuzumab-based regimen, such that all other current second-line treatment regimens would shift to the third and subsequent lines. According to the clinical experts consulted by the review team, in alignment with the eligible participants in the sponsor-submitted DESTINY-Gastric02 trial, the patients best suited for treatment with trastuzumab deruxtecan in the second-line treatment setting would be those who have all of the following criteria, unresectable or metastatic gastric or GEJ cancer with progressive disease on or after first-line therapy with a trastuzumab-containing regimen; HER2-positive gastric or GEJ cancer (defined as IHC 3+, or IHC 2+ and ISH-positive) confirmed by a repeat biopsy; a preserved Eastern Cooperative Oncology Group Performance Status (ECOG PS); and a preserved cardiac ejection.
According to the clinical experts consulted by the review team, key factors to determine response to treatment include patient-reported symptoms, side effects, and cross-sectional imaging (e.g., CT and/or MRI).
According to the clinical experts consulted by the review team, patient-reported symptoms, side effects, and the overall well-being of patients, in conjunction with assessment of treatment response, would be the major determinants for discontinuing treatment. In terms of toxicities, the clinical experts consulted by the review team noted that interstitial lung disease (ILD) is among the most important adverse events (AEs) to be aware of.
According to the clinical experts consulted by the review team, trastuzumab deruxtecan should only be prescribed by or under the supervision of a specialist in medical oncology with expertise in the diagnosis and management of immunotherapy-related side effects, including ILD. The clinical experts consulted by the review team noted that trastuzumab deruxtecan could be safely administered in a hospital or an outpatient clinic.
Clinician Group Input
Canada’s Drug Agency (CDA-AMC) received inputs from 2 clinician groups: the Ontario Health (Cancer Care Ontario) (OH-CCO) Gastrointestinal Cancer Drug Advisory Committee (5 clinicians) and the ad hoc group of physicians who treat adenocarcinoma and the Canadian Gastrointestinal Oncology Evidence Network (CGOEN), with contribution of 15 clinicians.
According to the clinician groups, the goals of treatment include improve symptoms, response rates, quality of life, and OS. Based on both clinician inputs, there is a gap in treatments for patients with HER2 positivity whose disease progresses after first-line standard therapy, and trastuzumab deruxtecan should be considered in the second-line setting. CGOEN added that efficacy outcomes, such as objective response rate (ORR), progression-free survival (PFS), and OS — along with safety and toxicity outcomes and quality of life — are important when assessing response to treatment. OH-CCO believes that response to treatment should be assessed every 2 months to 3 months.
According to the clinician inputs, factors to be considered to discontinue treatment would include disease progression and intolerance. Further, the outpatient setting under the care of a health care provider with training in oncology is appropriate for treatment.
Drug Program Input
Input was obtained from the drug programs that participate in the reimbursement review process. The following were identified as key factors that could potentially affect the implementation of a recommendation for trastuzumab deruxtecan:
relevant comparators
consideration for initiation of therapy
consideration for discontinuation of therapy
consideration for prescribing of therapy
generalizability
funding algorithm
care provision issues
system and economic issues.
Clinical Evidence
Systematic Review
Description of Studies
One relevant sponsor-conducted pivotal study, DESTINY-Gastric02 (N = 79), was included in the systematic review of this clinical report. The DESTINY-Gastric02 trial was a phase II, single-arm, open-label study investigating the use of trastuzumab deruxtecan as monotherapy for the treatment of patients (aged ≥ 18 years) who have unresectable or metastatic centrally confirmed HER2-positive gastric or GEJ cancer and have experienced disease progression during or after first-line therapy with a trastuzumab-containing regimen. Patients enrolled in the DESTINY-Gastric02 trial were from Europe and North America (no patients in Canada). The primary objective of the DESTINY-Gastric02 trial was to assess the efficacy of trastuzumab deruxtecan based on the confirmed ORR per independent central review (ICR) assessment (primary outcome). OS, PFS, health-related quality of life (HRQoL) outcomes (e.g., Functional Assessment of Cancer Therapy – Gastric [FACT-Ga]), and harms (e.g., ILD) were also assessed.
The median age in the DESTINY-Gastric02 trial population was 60.7 years (range, 20.3 years to 77.8 years), with 58.5% of patients aged younger than 65 years. The trial population was 27.8% female and 72.2% male. The race distribution of the trial population was 0% American Indian or Alaska Native, 5.1% Asian, 1.3% Black or African American, 1.3% Native Hawaiian or other Pacific Islander, and 87.3% white. The majority of patients in the trial population had an ECOG PS of 1 (63.3%), GEJ as the cancer location (65.8%), and a HER2 status of IHC 3+ (86.1%). Almost all the patients (78 out of 79 patients) had a histological subtype of adenocarcinoma.
Efficacy Results
Results submitted by the sponsor were from 2 data cut-off dates: April 9, 2021, and November 8, 2021. The median duration of follow-up was 5.9 months (range, 0.7 months to 15.4 months) as of the data cut-off date of April 9, 2021, and 10.2 months (range, 0.7 months to 22.1 months) as of the data cut-off date of November 8, 2021.
Overall Survival
As of the data cut-off date of November 8, 2021, the proportion of patients in the full analysis set (FAS) who had OS events was 58.2%. The median OS was 12.1 months (95% confidence interval [CI], 9.4 months to 15.4 months). The probability of being alive was 77.8% (95% CI, 66.8% to 85.6%) at 6 months, 50.6% (95% CI, 38.4% to 61.5%) at 12 months, and 35.1% (95% CI, 22.1% to 48.4%) at 18 months.
PFS per ICR Assessment
As of November 8, 2021, the proportion of patients in the FAS who had PFS events as determined by ICR was 64.6%. The median PFS was 5.6 months (95% CI, 4.2 months to 8.3 months). The probability of being progression-free was 70.5% (95% CI, 58.7% to 79.5%) at 3 months, 48.9% (95% CI, 36.6% to 60.2%) at 6 months, 36.3% (95% CI, 24.5% to 48.1%) at 9 months, and 20.0% (95% CI, 9.4% to 33.3%) at 12 months.
Confirmed ORR per ICR Assessment
As of November 8, 2021, the proportion of patients in the FAS who had achieved a confirmed ORR per ICR assessment was 41.8% (95% CI, 30.8% to 53.4%). There were 4 patients (5.1%) who achieved a best overall response of confirmed complete response (CR), and 29 patients (36.7%) who achieved a confirmed partial response (PR). The results of subgroup analyses on ORR were generally consistent with the results in the FAS.
FACT-Ga Total Score
A higher FACT-Ga total score indicates a better outcome. As of the data cut-off date of April 9, 2021, the mean FACT-Ga total score at baseline was █████ █████████ █████████ ████ █ ██████ The mean FACT-Ga total score at the end of treatment was █████ ███ █ ██████ with a mean change of ██████ ███ █ ███████
Harms Results
Treatment-Emergent AEs
The most commonly reported treatment-emergent adverse events (TEAEs) in the DESTINY-Gastric02 trial were nausea (67.1%), followed by fatigue (57.0%), vomiting (44.3%), and anemia (38.0%). The proportion of patients who had any TEAE of grade 3 or higher was 55.7%. The most commonly reported TEAE of grade 3 or higher was anemia (13.9%), followed by neutropenia (12.7%).
Treatment-Emergent Serious AEs
The proportion of patients who had any treatment-emergent serious adverse event (TESAE) was 41.8%. The most commonly reported TESAE was nausea (5.1%), followed by pneumonitis (3.8%) and vomiting (3.8%).
Treatment Discontinuation Due to TEAEs
The proportion of patients who discontinued trastuzumab deruxtecan was 19.0%. Discontinuation due to pneumonitis or ILD occurred in 7.6% and 2.5% of the trial population, respectively.
Mortality
As of the data cut-off date of November 8, 2021, the number of patients who had any TEAE associated with an outcome of death was 11 patients (13.9%); among these, 1 patient (1.3%) died due to ILD and 1 patient (1.3%) died due to pneumonitis.
Notable Harms
As of the data cut-off date of November 8, 2021, the proportion of patients who had ILD was ████%, and 10.5% of patients had a grade 2 left ventricular (LV) dysfunction (defined as the resting left ventricular ejection fraction [LVEF] ranges from 50% to 40%; and there is a 10% to 19% LVEF decrease from baseline). As of the data cut-off date of April 9, 2021, the proportion of patients who had experienced an infusion-related reaction (IRR) was 5.1%. QT prolongation was not reported in the DESTINY-Gastric02 trial.
Critical Appraisal
Overall, the absence of an internal comparison group in the single-arm DESTINY-Gastric02 trial is a key limitation. Moreover, a comparison between the trastuzumab deruxtecan group in the DESTINY-Gastric02 trial and an external control (e.g., a target value or historical study control) was not available. Lacking comparative data prevents the demonstration of the advantage of trastuzumab deruxtecan over therapies currently available in the second-line setting; in addition, inferences about the efficacy and safety of trastuzumab deruxtecan are challenging to make and cannot be established with certainty. The selection of the primary efficacy end point of confirmed ORR — defined as the sum of CR or PR, as determined by ICR based on the Response Evaluation Criteria in Solid Tumours Version 1.1 (RECIST 1.1) — was necessary for the single-arm DESTINY-Gastric02 trial for regulatory approval as a direct measure of a drug antitumour activity that can be assessed in a single-arm study.27 ORR does not always capture the effects of a treatment on patient survival and may not always correlate with symptoms or function.27 The DESTINY-Gastric02 trial addressed this limitation by examining time-to-event outcomes as secondary end points in the trial, including OS, which was considered the most important efficacy outcome for the trial population by the clinical experts consulted by the review team. Although OS was included in the statistical analysis plan and controlled for multiplicity, this outcome can be sensitive to natural history and progression of the disease as well as heterogeneity of patient characteristics; therefore, inference of treatment efficacy based on reported OS results can be prone to bias in the absence of a comparator.27-29
The DESTINY-Gastric02 trial targeted a second-line treatment setting for patients with HER2-positive gastric or GEJ cancer. This aligns with the treatment setting in the reimbursement request submitted by the sponsor. However, the Health Canada indication targets not only patients in the second-line treatment setting, but also in the third-line and later settings. The DESTINY-Gastric02 trial population does not align with the patients in the third-line and later settings described in the Health Canada indication. As a result, the findings from the DESTINY-Gastric02 trial may not be generalizable to patients in the third-line and subsequent lines setting, and there remains a gap in evidence. According to the clinical experts consulted by the review team, the eligibility criteria for the DESTINY-Gastric02 trial were generally aligned with the selection criteria in the Canadian setting when identifying eligible patients with HER2-positive gastric or GEJ cancer for the second-line use of trastuzumab deruxtecan.
GRADE Summary of Findings and Certainty of the Evidence
For the pivotal studies and randomized controlled trials (RCTs) identified in the sponsor’s systematic review, Grading of Recommendations Assessment, Development, and Evaluation (GRADE) was used to assess the certainty of the evidence for the outcomes considered most relevant to inform the expert committee deliberations; a final certainty rating was determined, as outlined by the GRADE Working Group.30,31
Although GRADE guidance is not available for noncomparative studies, the review team assessed the pivotal single-arm trials for study limitations (i.e., internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias to present these important considerations. Because the lack of a comparator arm does not allow for a conclusion to be drawn as to the effect of the intervention versus any comparator, the certainty of evidence for single-arm trials started at very low certainty with no opportunity for rating up.
When possible, certainty was rated in the context of the presence of an important (nontrivial) treatment effect; if this was not possible, certainty was rated in the context of the presence of any treatment effect (i.e., the clinical importance is unclear). In all cases, the target of the certainty of evidence assessment was based on the point estimate and its location relative to the threshold for a clinically important effect (when a threshold was available) or to the null.
Due to lack of comparators, certainty of evidence was summarized narratively for OS, PFS, ORR, FACT-Ga total score, and harms.
The selection of outcomes for the GRADE assessment was based on the sponsor’s Summary of Clinical Evidence, consultation with clinical experts, and input from patient and clinician groups and public drug plans. The following list of outcomes was finalized in consultation with expert committee members:
OS
PFS per ICR assessment
confirmed ORR per ICR assessment
HRQoL outcomes (FACT-Ga total score)
harms (ILD).
Results of GRADE Assessments
Table 2 presents the GRADE summary of findings for trastuzumab deruxtecan for the treatment of adult patients with unresectable or metastatic HER2-positive gastric or GEJ cancer who had disease progression during or after first-line therapy with a trastuzumab-containing regimen.
Table 2: Summary of Findings for Trastuzumab Deruxtecan for the Treatment of Adult Patients With Unresectable or Metastatic HER2-Positive Gastric or GEJ Cancer Who Had Disease Progression During or After First-Line Therapy With a Trastuzumab-Containing Regimen
Outcome and follow-up | Patients (studies), N | Effect | Certainty | What happens |
|---|---|---|---|---|
OS (data cut-off date: November 8, 2021) | ||||
OS Median follow-up duration: 10.2 months (range, 0.7 months to 22.1 months) | N = 79 (1 single-arm study) |
| Very lowa | The evidence is uncertain about the effect of trastuzumab deruxtecan on unresectable or metastatic HER2-positive gastric or GEJ cancer in the second-line treatment setting. |
PFS per ICR assessment (data cut-off date: November 8, 2021) | ||||
PFS per ICR assessment Median follow-up duration: 10.2 months (range, 0.7 months to 22.1 months) | N = 79 (1 single-arm study) |
| Very lowa | The evidence is uncertain about the effect of trastuzumab deruxtecan on unresectable or metastatic HER2-positive gastric or GEJ cancer in the second-line treatment setting. |
ORR (data cut-off date: November 8, 2021) | ||||
Confirmed ORR per ICR assessment Median follow-up duration: 10.2 months (range, 0.7 months to 22.1) months | N = 79 (1 single-arm study) | As of the data cut-off date, the confirmed ORR per ICR assessment was 41.8% (95% CI, 30.8% to 53.4%); among this proportion, 5.1% of patients had CR. | Very lowa | The evidence is uncertain about the effect of trastuzumab deruxtecan on unresectable or metastatic HER2-positive gastric or GEJ cancer in the second-line treatment setting. |
HRQoL (data cut-off date: April 9, 2021) | ||||
FACT-Ga total score Median follow-up duration: 5.9 months (range, 0.7 months to 15.4 months) | N = 27 (1 single-arm study) | At the end of treatment, the mean change from baseline in FACT-Ga total score was ██████ ███ █ ███████ | Very lowa | The evidence is uncertain about the effect of trastuzumab deruxtecan on unresectable or metastatic HER2-positive gastric or GEJ cancer in the second-line treatment setting. |
Harms (data cut-off date: November 8, 2021) | ||||
ILD Median follow-up duration: 10.2 months (range, 0.7 months to 22.1 months) | N = 79 (1 single-arm study) | The proportion of patients who had ILD was ████%. | Very lowa | The evidence is uncertain about the harmful effects of trastuzumab deruxtecan on patients with unresectable or metastatic HER2-positive gastric or GEJ cancer. |
CI = confidence interval; CR = complete response; FACT-Ga = Functional Assessment of Cancer Therapy – Gastric; GEJ = gastroesophageal junction; HER2 = human epidermal growth factor receptor 2; HRQoL = health-related quality of life; ICR = independent central review; ILD = interstitial lung disease; ORR = objective response rate; OS = overall survival; PFS = progression-free survival.
aIn the absence of a comparator arm, the certainty of evidence started at very low. There were no observed criteria that would warrant rating up.
Source: DESTINY-Gastric02 Clinical Study Report.32,33
Long-Term Extension Studies
No long-term extension studies were submitted by the sponsor for this review.
Indirect Comparisons
Description of Studies
In the absence of direct evidence comparing trastuzumab deruxtecan to other second-line treatments currently available in Canada (i.e., ramucirumab-paclitaxel, paclitaxel, FOLFIRI, irinotecan, and docetaxel), an indirect treatment comparison (ITC) was submitted by the sponsor to inform this gap. The sponsor-submitted ITC consisted of an unanchored, matching-adjusted indirect comparison (MAIC) and a network meta-analysis (NMA). The unanchored MAIC was used to connect the single-arm pivotal DESTINY-Gastric02 trial into the evidence network of the NMA. The relative treatment effect estimates between trastuzumab deruxtecan and ramucirumab-paclitaxel were generated based on this unanchored MAIC, while the relative treatment effect estimates between trastuzumab deruxtecan and other relevant comparators (including paclitaxel, FOLFIRI, irinotecan, and docetaxel) were generated from the NMA.
Efficacy Results
Overall Survival
Generated from the MAIC, the hazard ratio (HR) for OS was ████ ████ ████████ ████████ ██████ ████ ██ █████ between trastuzumab deruxtecan and ramucirumab-paclitaxel.
In the fixed-effects (FE) model of the NMA, the estimated base-case HRs for OS were ████ ████ ████ ████ ██ █████ between trastuzumab deruxtecan and paclitaxel, ████ ████ ████ ████ ██ █████ between trastuzumab deruxtecan and FOLFIRI, ████ ████ ████ ████ ██ █████ between trastuzumab deruxtecan and irinotecan, and ████ ████ ████ ████ ██ ████) between trastuzumab deruxtecan and docetaxel.
Progression-Free Survival
Generated from the MAIC, the HR for PFS was ████ ████ ████ ████ ██ █████ between trastuzumab deruxtecan and ramucirumab-paclitaxel.
In the FE model of the NMA, the estimated base-case HRs for PFS were ████ ████ ████ ████ ██ █████ between trastuzumab deruxtecan and paclitaxel, ████ ████ ████ ████ ██ █████ between trastuzumab deruxtecan and FOLFIRI, ████ ████ ████ ████ ██ █████ between trastuzumab deruxtecan and irinotecan, and ████ ████ ████ ████ ██ █████ between trastuzumab deruxtecan and docetaxel.
Harms Results
Harms were not addressed in the sponsor-submitted ITC.
Critical Appraisal
Through MAIC, the comparison was established between the cohort of patients treated with trastuzumab deruxtecan in the DESTINY-Gastric02 trial and the cohort of patients treated with ramucirumab-paclitaxel in the RAINBOW trial. There are concerns regarding patient comparability between the DESTINY-Gastric02 trial and the RAINBOW trial. There were differences in some of the important patient characteristics (e.g., HER2 status, time on first treatment) that were not involved in the weighting process due to lack of information or insufficient sample size. Currently, the prognostic role of HER2 in gastric cancer remains controversial due to conflicting evidence.17-21 With HER2 status being unavailable in the RAINBOW trial, there is increased uncertainty about the treatment effect estimates between trastuzumab deruxtecan and ramucirumab-paclitaxel, but the direction of bias is unclear. Additionally, only 5 out of 16 potential prognostic factors and treatment effect modifiers were involved in the propensity score weighting. Excluding potentially relevant prognostic factors from the analysis could bias the results; however, the magnitude of the residual bias in the relative treatment effect estimates remains uncertain. Furthermore, after reweighting, apparent differences were identified between the DESTINY-Gastric02 trial and RAINBOW trial in some of the patient characteristics, such as time to progressive disease on first-line therapy, histological subtype, and number of metastases sites, suggesting the possible existence of inadequate balance and increasing the uncertainty of the findings. After reweighting, there was also a marked reduction in effective sample size (ESS), from ██ to ████, indicating that the weights might be highly variable due to a lack of population overlap and that the treatment effect estimates yielded through the MAIC approach might be unstable. Other than heterogeneity in patient characteristics, there was significant design and methodological heterogeneity between the DESTINY-Gastric02 trial (a phase II, single-arm study without a hypothesis specified a priori, or a statistical test) and the RAINBOW trial (a phase III, double-blind RCT with formal hypothesis testing). The MAIC approach can correct only for bias that is directly related to differences in baseline patient characteristics; it does not correct heterogeneity caused by between-trial differences in study design or methods.
The limitations of the MAIC analyses also contributed to the uncertainty of the NMA findings because the NMA evidence network was constructed based on the MAIC, which connected the single-arm DESTINY-Gastric02 trial and the RAINBOW trial. On top of the heterogeneity sources in the MAIC analyses, additional sources of heterogeneity might have introduced uncertainty to the NMA estimates. For instance, in the MAIC, the sponsor assumed that geographical region and ethnicity were important prognostic factors, and that patients from Asia had a better prognosis than patients from Western countries. Subsequently, to limit the number of Asian patients in the MAIC, the sponsor selected only patients from Europe, Israel, Australia, and the US from the RAINBOW trial, and compared them with the study population of the DESTINY-Gastric02 trial of which the majority of participants were white (87.3%). However, in the NMA network, no included study reported on the distribution of ethnicity except for the DESTINY-Gastric02 trial and RAINBOW trials. Moreover, the KSCG/ST10-01 study, the Sym et al. (2013) study, and the WJOG 4007 study were conducted in Asia, while the Roy et al. (2013) study was conducted in both Western and Asian countries. Under the assumption made by the sponsor about geographic region and ethnicity being important prognostic factors, the potential heterogeneity regarding differences in geographical regions and ethnicity in the NMA network could not be ignored. However, the degree of uncertainty remains unknown. The rationale for reporting the results of an FE model is justified when the estimation of between-study variance using the random-effects (RE) model is very imprecise and unstable in situations that consider only a few studies.34,35 However, the FE model does not sufficiently account for heterogeneity between studies, leading to overly precise and narrow CIs.35 Given that various sources of heterogeneity existed in the sponsor-submitted ITC (described previously), the use of the FE model introduced uncertainty in the NMA treatment effect estimates.
Other Evidence
Description of Studies
The DESTINY-Gastric01 trial, conducted in Asia (i.e., Japan and South Korea), enrolled 188 patients with advanced HER2-positive gastric or GEJ adenocarcinoma who had progressed on or after at least 2 prior regimens including a fluoropyrimidine drug, a platinum drug, and a trastuzumab-containing regimen (i.e., in the third-line and later setting). The primary objective of the DESTINY-Gastric01 trial was to compare the efficacy of trastuzumab deruxtecan versus the physician’s choice of treatment (i.e., irinotecan 150 mg/m2 intravenously every 2 weeks or paclitaxel 80 mg/m2 intravenously every week), as measured by ORR per ICR assessment. Secondary end points included OS, PFS, FACT-Ga, and harms.
Rationale for the Inclusion of the DESTINY-Gastric01 Trial
The DESTINY-Gastric01 trial population is not aligned with the population described in sponsor’s reimbursement request because the DESTINY-Gastric01 trial focused on the third-line and later treatment settings, while the sponsor’s funding request is limited to the second-line treatment setting. Therefore, the DESTINY-Gastric01 trial was considered out of the scope for this Clinical Review Report.
Of note, the DESTINY-Gastric01 trial population (i.e., patients who received ≥ 2 prior regimens, including an anti-HER regimen) would be relevant for a group of patients who are implied in the broader Health Canada indication for trastuzumab deruxtecan, which is for use “as monotherapy in adult patients with unresectable locally advanced or metastatic HER2-positive gastric or GEJ adenocarcinoma who have received a prior trastuzumab-based regimen.” According to the clinical experts consulted by the review team, this group of patients who have received 2 or more prior regimens is small in number in the real-world setting, and will mainly include those patients who are on currently available second or later lines of therapy and may miss the window of opportunity for being considered eligible for treatment with trastuzumab deruxtecan under the current funding request for the second-line setting. Therefore, the results from the DESTINY-Gastric01 trial were considered supplementary evidence, and are summarized in this section.
Efficacy Results
Overall Survival
As of the data cut-off date of June 3, 2020, the proportion of patients in the intention-to-treat (ITT) population who had OS events in the DESTINY-Gastric01 trial was 67.2% for the trastuzumab deruxtecan group and 79.0% for the physician’s choice group. The median OS was 12.5 months (95% CI, 10.3 months to 15.2 months) in the trastuzumab deruxtecan group and 8.9 months (95% CI, 6.4 months to 10.4 months) in the physician’s choice group. The adjusted HR was 0.60 (95% CI, 0.42 to 0.86).
PFS per ICR Assessment
As of June 3, 2020, the proportion of patients in the ITT population who had PFS events was 65.1% in the trastuzumab deruxtecan group and 58.1% in the physician’s choice group. The median PFS was 5.6 months (95% CI, 4.3 months to 6.9 months) in the trastuzumab deruxtecan group and 3.5 months (95% CI, 2.0 months to 4.3 months) in the physician’s choice group. The adjusted HR was 0.47 (95% CI, 0.31 to 0.71).
Confirmed ORR per ICR Assessment
The confirmed ORRs per ICR assessment were █████ ████ ███ ████ ██ █████ in the trastuzumab deruxtecan group and 11.3% (95% CI, 4.7% to 21.9%) in the physician’s choice group. The proportion of patients who achieved a best overall response of confirmed CR in the trastuzumab deruxtecan group was 7.9%. No patients achieved CR in the physician’s choice group.
FACT-Ga Total Score
As of the data cut-off date of November 8, 2019, the mean FACT-Ga total scores at the end of treatment were █████ ███ █ ██████ for the trastuzumab deruxtecan group and █████ ███ █ ██████ for the physician’s choice group, with mean changes of █████ ███ █ ██████ and █████ ███ █ ███████ respectively.
Harms Results
The cut-off date for the harms data was June 3, 2020.
Treatment-Emergent AEs
All patients in the trastuzumab deruxtecan group and 98.4% of the patients in the physician’s choice group had TEAEs. The most commonly reported TEAE was neutropenia, reported in 64.8% of patients in the trastuzumab deruxtecan group versus 35.5% in the physician’s choice group.
The proportion of patients who had any TEAE of grade 3 or higher was 85.6% in the trastuzumab deruxtecan group, higher than the 56.5% reported in the physician’s choice group. The most commonly reported TEAE of grade 3 or higher was neutropenia (51.2% in the trastuzumab deruxtecan group versus 24.2% in the physician’s choice group), followed by anemia (38.4% in the trastuzumab deruxtecan group versus 22.6% in the physician’s choice group).
Treatment-Emergent Serious AEs
The proportion of patients who had any TESAE was 44.8% in the trastuzumab deruxtecan group, higher than the 25.8% reported in the physician’s choice group. The most commonly reported TESAE was decreased appetite (10.4% in the trastuzumab deruxtecan group versus 1.6% in the physician’s choice group), followed by ILD (5.6% in the trastuzumab deruxtecan group versus 0 in the physician’s choice group), anemia (3.2% in the trastuzumab deruxtecan group versus 3.2% in the physician’s choice group), and dehydration (3.2% in the trastuzumab deruxtecan group versus 0 in the physician’s choice group).
Treatment Discontinuation Due to TEAEs
The proportion of patients who discontinued study treatment was 17.6% in the trastuzumab deruxtecan group and 6.5% in the physician’s choice group. Discontinuation due to ILD occurred in 6.4% of patients in the trastuzumab deruxtecan group versus 0% in the physician’s choice group.
Mortality
The proportion of patients who had any TEAE associated with an outcome of death was 6.4% in the trastuzumab deruxtecan group, higher than the 3.2% reported in the physician’s choice group.
Notable Harms
The proportion of patients who had ILD was 12.8% in the trastuzumab deruxtecan group; of these, 5.6% occurred as TESAEs. No patients in the physician’s choice group had ILD. The proportion of patients who had IRR was 6.4% in the trastuzumab deruxtecan group and 3.2% in the physician’s choice group. The proportion of patients who had grade 2 LV dysfunction (defined as the resting LVEF ranges from 50% to 40%; and there is a 10% to 19% LVEF decrease from baseline) was 9.4% in the trastuzumab deruxtecan group. The proportion of patients who had QT prolongation events was 0.8% in the trastuzumab deruxtecan group and 3.2% in the physician’s choice group.
Critical Appraisal
The DESTINY-Gastric01 trial enrolled 188 patients, with 126 patients and 66 patients being randomized to the trastuzumab deruxtecan group and physician’s choice group (2:1 randomization), respectively. The randomization was done using an interactive web and voice response system and stratified based on region (Japan or South Korea), ECOG PS (0 or 1), and HER2 status (IHC 3+ or IHC 2+ and ISH-positive) to minimize potential imbalances between the study groups that might bias the results. Despite the relatively small sample size, the distribution of patients in baseline characteristics was generally balanced between the trastuzumab deruxtecan group and the physician’s choice group, indicating a low risk of bias in the randomization process. Despite the open-label study design, the review team determined that there is a low risk of detection bias when determining PFS or ORR, but that there is still increased uncertainty with respect to the treatment efficacy in this setting. The results of both the PFS per ICR assessment and the PFS per investigator assessment (data not shown) were generally consistent, as were the findings from unconfirmed and confirmed ORRs. However, there is a notable risk of performance bias for the FACT-Ga, which was associated with the open-label design and the subjective nature of the measure. The DESTINY-Gastric01 trial reported OS, which was considered by the clinical experts consulted by the review team to be the most important outcome for the study population. Multiplicity adjustment was carried out for unconfirmed ORR (i.e., the primary end point of the trial) and for OS to control for type I error; however, all the remaining efficacy end points (e.g., PFS, FACT-Ga) were not adjusted for multiplicity.
There are some concerns regarding whether the patient population in the DESTINY-Gastric01 trial was representative of the corresponding patient population in Canada. According to the clinical experts consulted by the review team, the inclusion and exclusion criteria of the DESTINY-Gastric01 trial were generally appropriate in terms of selecting eligible patients; however, the efficacies observed in the trastuzumab deruxtecan group and physician’s choice group were higher than the experts expected or have encountered in real-world third-line and later settings, in which patients are usually of poor status and efficacy. This suggests potential differences between the trial population and the real-world population in Canada.
There are additional concerns about generalizing the results from the DESTINY-Gastric01 trial population to the DESTINY-Gastric02 trial population due to obvious differences in patient characteristics. For instance, 87.3% of the patients in the DESTINY-Gastric02 trial were white and from North America, whereas all the patients in the DESTINY-Gastric01 trial were Asian and from Japan or South Korea. As noted in the sponsor-submitted ITC, geographical region and ethnicity were important prognostic factors, and Asian patients’ prognoses differed from those of patients in Western countries. Second, in the DESTINY-Gastric02 trial, 34.2% of patients had gastric cancer and 65.8% had GEJ cancer, whereas in the DESTINY-Gastric01 trial, 87.2% of patients had gastric cancer and 12.8% had GEJ cancer. These differences in patient characteristics may introduce treatment heterogeneity that increases the uncertainty of the results and their generalizability to the Canadian context.
The clinical experts consulted by the review team noted that the use of irinotecan or paclitaxel as comparators in the DESTINY-Gastric01 trial is not reflective of current clinical practice in Canada. According to the clinical experts consulted by the review team, when the DESTINY-Gastric01 trial was designed, irinotecan and paclitaxel were commonly used in the third-line and later settings. However, in current clinical practice, these drugs are rarely used — and if so, by a very small group of patients, such as those who experienced serious neuropathy from previous lines of therapy.
Conclusions
DESTINY-Gastric02 (N = 79), a phase II, single-arm trial submitted by the sponsor, assessed the efficacy and safety of trastuzumab deruxtecan for the treatment of adult patients with unresectable or metastatic HER2-positive gastric or GEJ cancer in the second-line treatment setting. The clinical experts consulted by the review team noted that the results of some efficacy end points that were critical to decision-making (e.g., the probability of survival at 6 months or 12 months and the probability of being progression-free at 6 months) were clinically meaningful. However, the absence of a comparator group in the DESTINY-Gastric02 trial is a key limitation in the interpretation of the efficacy findings, resulting in very low certainty of evidence. The clinical experts consulted by the review team noted that the incidence of the key safety end point (ILD) in the DESTINY-Gastric02 trial met their expectations in terms of being consistent with the incidences reported in the literature. According to the experts, trastuzumab deruxtecan has an overall beneficial effect in the second-line treatment setting, warranting a confirmatory phase III clinical trial. The sponsor is currently conducting a phase III trial (the DESTINY-Gastric04 trial) to assess the efficacy and safety of trastuzumab deruxtecan relative to ramucirumab-paclitaxel in patients with HER2-positive gastric or GEJ adenocarcinoma in the second-line treatment setting. The trial results are anticipated to be ready in the fourth quarter of 2025.
In the absence of direct evidence comparing trastuzumab deruxtecan to other second-line treatments currently available in Canada (i.e., ramucirumab-paclitaxel, paclitaxel, FOLFIRI, irinotecan, and docetaxel), sponsor-submitted ITCs using an unanchored MAIC and NMA were reviewed. The ITC treatment effect estimates for OS and PFS favoured trastuzumab deruxtecan over all other comparators; however, several major limitations in the design and methods of the ITC preclude any definitive conclusion about the magnitude of effect. Specifically, missing prognostic factors (e.g., HER2 status), limited factors involved in the weighting process, residual imbalances in prognostic or effect-modifying factors, a significant reduction in ESS — as well as heterogeneity in study design, statistical analyses, geographical regions, and ethnicity distribution across the studies included in the NMA evidence network — can all result in biased estimates and overly precise credible intervals.
Introduction
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of trastuzumab deruxtecan (Enhertu), 100 mg, powder for concentrate for solution for IV infusion for the treatment of adult patients with unresectable locally advanced or metastatic HER2-positive gastric or GEJ adenocarcinoma who have received a prior trastuzumab-based regimen.
Disease Background
Contents within this section have been informed by materials submitted by the sponsor and clinical expert input. The following has been summarized and validated by the review team.
Gastric cancer is the fifth most common cancer and the fifth leading cause of cancer mortality worldwide, with approximately 968,000 incident cases and 659,853 associated deaths in 2022 (equating to 6.8% of all cancer-related deaths).4 Gastric adenocarcinoma is the most common histological type of gastric cancer, accounting for more than 95% of gastric cancer cases.5 Patients with advanced GEJ adenocarcinoma are often considered within the same clinical trial population as those with advanced gastric adenocarcinoma because of similarities in tumour growth and patterns of spread.6,7 In fact, gastric and GEJ adenocarcinoma have often been reviewed, investigated, or presented together in literature reviews, clinical trials, and clinical management guidelines.8-11
It is estimated that 1 in 98 people in Canada will have gastric cancer in their lifetime.36 In 2024, the projected incident rate of gastric cancer in Canada was 8.3 per 100,000 adults, with an estimated 1,400 cases in females and 2,600 cases in males.12 Signs and symptoms of gastric cancer include abdominal pain, heart burn, loss of appetite, bloating, nausea, vomiting, difficulty swallowing, blood in the stool, anemia, fatigue, ascites, and jaundice.13 The median survival duration for patients with advanced gastric cancer is low, approximately 10 months to 12 months, with a 5-year OS of 5% to 20%.37 The overall 5-year survival rate for all patients with gastric cancer is estimated to be 29%,14 and patients with distant metastases experience worse outcomes, with an estimated 5-year relative survival rate of 7%.15 Compared to patients with gastric adenocarcinoma, patients with GEJ adenocarcinoma may have worse disease-specific survival rates, with an approximately 10% higher cumulative incidence of recurrence.16
The prognostic role of HER2 in gastric cancer remains controversial due to conflicting evidence.17-21 Patients with HER2-positive gastric cancer account for 10% to 20.2% of all gastric cancer cases.38 In a population of patients in Canada between 2022 and 2023, an estimated 21% of all gastric and GEJ cancers showed HER2 positivity.22 All patients with advanced or metastatic gastric or GEJ cancer, including patients with both gastric and gastroesophageal adenocarcinomas, should undergo HER2 testing.23 HER2 testing should also be performed on biopsy or resection specimens.23 Recommended HER2 testing methods include IHC, which assesses HER2 protein expression levels, and ISH, which evaluates HER2 gene amplification.23 HER2 testing is typically conducted at the time of diagnosis or at the onset of advanced or metastatic disease.23 Additionally, HER2 testing may be repeated if there is a need for re-evaluation due to disease progression or metastases.23 HER2 positivity is confirmed when test results show IHC 3+ or IHC 2+ followed by ISH positivity.23,24
Standards of Therapy
Contents within this section have been informed by materials submitted by the sponsor and clinical expert input. The following has been summarized and validated by the review team.
According to the clinical experts consulted by the review team, most patients with unresectable locally advanced or metastatic HER2-positive gastric or GEJ cancers are treated with palliative intent; the treatment goals of all therapies in this setting are to prolong OS and improve quality of life. The clinical experts consulted by the review team noted that the cornerstone of treatment for patients with unresectable locally advanced or metastatic HER2-positive gastric or GEJ cancers involves the sequential use of the best available systemic therapies.
The clinical experts consulted by the review team noted that, in the first-line treatment setting, the standard of care for patients with locally advanced or metastatic HER2-positive gastric or GEJ cancers with a PD-L1 CPS of less than 1 includes a fluoropyrimidine-platinum doublet chemotherapy (e.g., FOLFOX, CAPOX, or cisplatin-capecitabine) in combination with trastuzumab. For patients with locally advanced or metastatic HER2-positive gastric or GEJ cancers who have a PD-L1 CPS greater than or equal to 1, according to the clinical experts consulted by the review team, the addition of pembrolizumab to the backbone of doublet chemotherapy and trastuzumab has been established as the standard of care first-line therapy.
According to the clinical experts consulted by the review team, in the second-line treatment setting, the standard of care for locally advanced or metastatic HER2-positive gastric or GEJ cancers is treatment with ramucirumab-paclitaxel or ramucirumab alone. However, the clinical experts noted that as a single-drug treatment, ramucirumab is not reimbursed in many jurisdictions across Canada, including Ontario. They also noted that the second-line treatment of HER2-positive gastric or GEJ cancers is identical to that of HER2-negative gastric or GEJ cancers at present.
The sponsor noted that single-drug chemotherapy options, such as irinotecan, paclitaxel, or docetaxel, have been suggested in guidelines for patients who are not eligible for ramucirumab-paclitaxel.25,26 Furthermore, according to the sponsor, relevant guidelines25,26 also suggest the use a fluoropyrimidine and platinum combination, such as FOLFOX or CAPOX, for patients previously treated with FOLFIRI in the first-line setting. According to the clinical experts consulted by the review team, FOLFIRI is often chosen for patients who have significant residual neuropathy from first-line therapy and for whom the use of paclitaxel would be relatively contraindicated.
The clinical experts consulted by the review team noted that in the third-line setting, treatment options for patients with locally advanced or metastatic HER2-positive gastric or GEJ cancers include trifluridine-tipiracil (i.e., TAS-102), nivolumab, and pembrolizumab.
Drug Under Review
The key characteristics of trastuzumab deruxtecan as monotherapy for the treatment of adult patients with unresectable locally advanced or metastatic HER2-positive gastric or GEJ adenocarcinoma who have received a prior trastuzumab-based regimen are summarized in Table 3.
The recommended dose of trastuzumab deruxtecan for locally advanced or metastatic gastric and GEJ cancer is 6.4 mg/kg, given as an IV infusion once every 3 weeks (21-day cycle) until disease progression or unacceptable toxicity.
Trastuzumab deruxtecan as a monotherapy is also indicated for:39
the treatment of adult patients with unresectable or metastatic HER2-positive breast cancer who have received at least 1 prior anti–HER2-based regimen, either in the metastatic setting or in the neoadjuvant or adjuvant setting, and have developed disease recurrence during or within 6 months of completing neoadjuvant or adjuvant therapy
the treatment of adult patients with unresectable or metastatic HER2-positive breast cancer who have received prior treatment with trastuzumab emtansine (T-DM1)
the treatment of adult patients with unresectable or metastatic HER2-low (i.e., IHC 1+ or IHC 2+ and ISH-negative) breast cancer who have received at least 1 prior line of chemotherapy in the metastatic setting or developed disease recurrence during or within 6 months of completing adjuvant chemotherapy.
Trastuzumab deruxtecan has not been previously reviewed for this indication (i.e., gastric or GEJ adenocarcinomas) by CDA-AMC.
Regarding the mechanism of action, trastuzumab deruxtecan is a HER2-targeted antibody-drug conjugate composed of 3 components: a humanized anti-HER2 immunoglobulin G1 monoclonal antibody with the same amino acid sequence as trastuzumab, covalently linked to a topoisomerase I inhibitor (an exatecan derivative) via a tetrapeptide-based cleavable linker. Deruxtecan is composed of the linker and the topoisomerase I inhibitor. Stability studies have demonstrated that less than 5% of the intact antibody-drug conjugate dissociates into the released topoisomerase inhibitor form within 21 days. After binding to HER2 on tumour cells, trastuzumab deruxtecan undergoes internalization and intracellular linker cleavage by lysosomal enzymes that are upregulated in cancer cells. Upon release, the membrane-permeable topoisomerase I inhibitor causes DNA damage and apoptotic cell death.
On January 15, 2021, the FDA approved trastuzumab deruxtecan for adult patients with locally advanced or metastatic HER2-positive gastric or GEJ adenocarcinoma who have received a prior trastuzumab-based regimen. Trastuzumab deruxtecan has been given “conditional” authorization by the European Medicines Agency. This means that the European Medicines Agency decided that the benefits of trastuzumab deruxtecan are greater than its risks. However, the manufacturer will have to provide additional evidence after authorization.
Trastuzumab deruxtecan received an NOC/c from Health Canada on January 17, 2025. The sponsor requested a TLR recommendation for trastuzumab deruxtecan on an NOC/c basis while awaiting results of the confirmatory phase III DESTINY-Gastric04 study. More details on TLR recommendation eligibility are provided in the next section.
Table 3: Key Characteristics of Trastuzumab Deruxtecan, Ramucirumab-Paclitaxel, Paclitaxel, Docetaxel, and Irinotecan
Characteristic | Trastuzumab deruxtecan | Ramucirumab-paclitaxel | Paclitaxel | Docetaxel | Irinotecan |
|---|---|---|---|---|---|
Mechanism of action | A HER2-targeted antibody that results in DNA damage and apoptotic cancer cell death | Ramucirumab is a recombinant, human receptor–targeted immunoglobulin G1 monoclonal antibody that binds VEGFR-2 specifically and blocks the binding of VEGF-A, VEGF-C, and VEGF-D. Ramucirumab inhibits ligand-stimulated activation of VEGFR-2 and its downstream signalling components, including p44 and p42 mitogen-activated protein kinases, neutralizing ligand-induced proliferation and the migration of human endothelial cells. | Paclitaxel promotes the assembly of microtubules and stabilizes these against depolymerization. This stability results in the inhibition of the normal dynamic reorganization of the microtubule network that is essential for vital interphase and mitotic cellular functions. | Docetaxel acts by disrupting the microtubular network in cells that is essential for cell division. It promotes the assembly of tubulin into stable microtubules while simultaneously inhibiting their disassembly. This leads to the stabilization of microtubules, resulting in the inhibition of mitosis in cells. | Irinotecan hydrochloride trihydrate belongs to the topoisomerase I inhibitor class. It is a semisynthetic derivative of camptothecin, an alkaloid extract from plants such as Camptotheca acuminata. Camptothecins interact with the enzyme topoisomerase I, which relieves torsional strain in DNA by inducing reversible single-strand breaks. Irinotecan and its active metabolite, SN-38, bind to the topoisomerase I DNA complex and prevent relegation of these single-strand breaks. |
Indicationa | As monotherapy for the treatment of adult patients with unresectable locally advanced or metastatic HER2-positive gastric or gastroesophageal junction adenocarcinoma who have received a prior trastuzumab-based regimen | As a single drug or in combination with paclitaxel for the treatment of patients with advanced or metastatic gastric cancer or gastroesophageal junction adenocarcinoma who experience disease progression on or after prior chemotherapy with platinum and fluoropyrimidine | For the treatment of metastatic breast cancer and the first-line treatment of metastatic adenocarcinoma of the pancreas in combination with gemcitabine | Breast cancer Non–small cell lung cancer Ovarian cancer Prostate cancer Squamous cell carcinoma of the head and neck | As a component of first-line therapy for patients with metastatic carcinoma of the colon or rectum As a single drug for the treatment of patients with metastatic carcinoma of the colon or rectum whose disease has recurred or progressed following 5-fluorouracil–based therapy |
Route of administration | IV | IV | IV | IV | IV |
Recommended dose | 6.4 mg/kg given as an IV infusion once every 3 weeks (i.e., in 21-day cycles) until disease progression or unacceptable toxicity | Ramucirumab: 8 mg/kg administered through IV over approximately 60 minutes on days 1 and 15 of 28-day cycles before paclitaxel infusion Paclitaxel: 80 mg/m2 through IV over approximately 60 minutes on days 1, 8, and 15 of 28-day cycles | In metastatic breast cancer: 260 mg/m2 administered through IV over 30 minutes every 3 weeks In metastatic pancreatic cancer: 125 mg/m2 administered through IV infusion over 30 minutes to 40 minutes on days 1, 8, and 15 of each 28-day cycle | In metastatic breast cancer, non–small cell lung cancer, ovarian cancer, and squamous cell carcinoma of the head and neck: 100 mg/m2 administered as a 1-hour infusion every 3 weeks When used in combination: 75 mg/m2 In prostate cancer: 75 mg/m2 as a 1-hour infusion every 3 weeks | Regimen 1, 6-week cycle Starting dose: 125 mg/m2 through IV over 90 minutes once weekly (days 1, 8, 15, 22), then 2-week rest 20 mg/m2 through IV bolus once weekly (days 1, 8, 15, 22), then 2-week rest 500 mg/ m2 IV bolus once weekly (days 1, 8, 15, 22), then 2-week rest Regimen 2, 6-week cycle Starting dose: 180 mg/ m2 through IV over 90 minutes once every 2 weeks (days 1, 15, 29), then 1-week rest 200 mg/m2 through IV over 2 hours on days 1 and 2 every 2 weeks (i.e., days 1, 2, 15, 16, 29, 30), then 1-week rest 400 mg/m2 through IV bolus followed immediately by 600 mg/m2 IV over 22 hours on days 1 and 2 every 2 weeks (i.e., days 1, 2, 15, 16, 29, 30), then 1-week rest |
Serious adverse effects or safety issues |
|
| Contraindicated in patients who have baseline neutrophil counts of < 1,500 cells/mm3 on day 1 of each treatment cycle
| Contraindicated in patients with neutrophil counts of < 1,500 cells/mm3 and in patients with severe liver impairment
| Coadministration of irinotecan hydrochloride trihydrate with azole antifungals (ketoconazole, fluconazole, itraconazole, which are known CYP3A4 inhibitors), is contraindicated
|
CYP3A4 = cytochrome P450 3A4; HER2 = human epidermal growth factor 2; p44 and p42 = extracellular signal-regulated kinase 1 and kinase 2; VEGF-A = vascular endothelial growth factor A; VEGF-C = vascular endothelial growth factor C; VEGF-D = vascular endothelial growth factor D; VEGFR-2 = vascular endothelial growth factor receptor 2.
aIndications approved by Health Canada.
Sources: Draft product monograph for trastuzumab deruxtecan;2 product monograph for ramucirumab;40 product monograph for docetaxel;41 product monograph for irinotecan.42
Consideration for a TLR Recommendation
A TLR is a recommendation by the CDA-AMC expert committee to publicly fund a drug or drug regimen for a certain period of time based on the condition that the sponsor will conduct 1 or more clinical studies that address uncertainty with the clinical evidence. CDA-AMC subsequently conducts a reassessment of the additional evidence and issues a final reimbursement recommendation within a defined period of time. Based on the preliminary assessment by CDA-AMC (Table 36 in Appendix 1), trastuzumab deruxtecan meets the criteria to be considered by the expert committee for a TLR recommendation. In accordance with the CDA-AMC Procedures for Reimbursement Reviews, this section of the report provides an assessment of the existing gaps in the evidence and the sponsor’s evidence-generation plans.
Eligibility Criteria for a TLR
Regulatory Status
Trastuzumab deruxtecan received an NOC/c from Health Canada on January 17, 2025.
Commitment to File for Reassessment
The sponsor has expressed a commitment to file a reassessment application with CDA-AMC in accordance with the time frames specified in the procedures for a TLR recommendation. The phase III trial, DESTINY-Gastric04, will be completed within a time frame that will not exceed 3 years from the target expert committee meeting date.
The sponsor has stated that primary completion of the DESTINY-Gastric04 trial is estimated to occur in the fourth quarter of 2025.43 This is within the 3-year period described within the CDA-AMC procedures for TLR recommendations.
Evidence-Generation Plans (Phase III DESTINY-Gastric04 Trial)
The DESTINY-Gastric04 trial (Table 4) meets the eligibility for a TLR recommendation because it is a phase III clinical trial conducted using trastuzumab deruxtecan as monotherapy in the target population for this review. Specifically, the following was noted by CDA-AMC.
Study design: Phase III trial that will be reported within the time frame specified in the CDA-AMC procedures.
Intervention: Trastuzumab deruxtecan will be intravenously administered as monotherapy at a dosage of 6.4 mg/kg every 3 weeks, which is the same dosage used in the phase II DESTINY-Gastric02 trial.
Patient population: Generally, the trial patient population is the same, with acceptable differences, specifically:
Tumour type and histology — These are the same for the indication reviewed by CDA-AMC and the pending phase III trial (i.e., HER2-positive gastric or GEJ adenocarcinoma).
Disease status — The pending phase III trial is being conducted in patients with unresectable locally advanced or metastatic disease. This is generally aligned with the indication that was initially submitted to CDA-AMC.
Line of therapy — The lines of therapy in the pending phase III trial appear to be the same as those in the reimbursement request that is under review by CDA-AMC (i.e., second-line therapy in the metastatic setting).
Required prior therapies — The prior therapies required to be eligible for treatment with trastuzumab deruxtecan are aligned between the funding request under review by CDA-AMC and the sponsor’s ongoing phase III trial (DESTINY-Gastric04). However, the patient population covered in the Health Canada indication (i.e., patients who have received a prior trastuzumab-based regimen) appears be broader than that of the phase III trial.
Comparator — Patients in the comparator group will receive IV infusion of ramucirumab-paclitaxel.
Outcomes — The primary end point is OS. Other end points include PFS, ORR, FACT-Ga, and harms.
Table 4: Pending Phase III Trial (the DESTINY-Gastric04 Trial)
Detail | DESTINY-Gastric04 trial |
|---|---|
Designs and populations | |
Study design | Phase III, multicentre, randomized, open-label study |
Locations | Approximately 148 study sites across Europe, Asia Pacific, and Latin America |
Patient enrolment dates | The study is ongoing, and the sponsor has stated that the primary completion of the DESTINY-Gastric04 trial is estimated to occur in the fourth quarter of 2025. It is anticipated that the study will provide up to 3 years of efficacy and safety follow-up data. |
Enrolled (N) | A total of approximately 490 patients will be randomized in a 1-to-1 ratio (245 patients to the trastuzumab deruxtecan group and 245 patients to the ramucirumab-paclitaxel group). |
Key inclusion criteria |
|
Key exclusion criteria |
|
Drugs | |
Intervention | Trastuzumab deruxtecan will be intravenously administered at a dosage of 6.4 mg/kg every 3 weeks |
Comparators | IV infusion of ramucirumab (8 mg/kg on days 1 and 15 of a 28-day cycle) plus paclitaxel (80 mg/m2 on days 1, 8, and 15 of a 28-day cycle) |
Study duration | |
Screening phase | NR |
Treatment phase | NR |
Follow-up phase | NR |
Outcomes | |
Primary end point | OS |
Secondary and exploratory end points |
|
Publication status | |
Publications | NR |
ASCP-CAP = American Society of Clinical Oncology – College of American Pathologists; CNS = central nervous system; DCR = disease control rate; DOR = duration of response; ECHO = echocardiogram; ECOG PS = Eastern Cooperative Oncology Group Performance Status; FACT-Ga = Functional Assessment of Cancer Therapy – Gastric; GEJ = gastroesophageal junction; HER2 = human epidermal growth factor 2; HRQoL = health-related quality of life; IHC = immunohistochemistry; ILD = interstitial lung disease; ISH = in situ hybridization; LVEF = left ventricular ejection fraction; MUGA = multigated acquisition; NR = not reported; NYHA = New York Heart Association; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; TTR = time to response.
Source: Sponsor’s Summary of Clinical Evidence.1
Assessment of Gaps in the Evidence
Gaps exist in the evidence derived from the pivotal DESTINY-Gastric02 trial currently under review by CDA-AMC. First, the DESTINY-Gastric02 trial was a single-arm study that lacked a comparator to determine the relative efficacy of trastuzumab deruxtecan on OS and evidence of a minimal important difference. Second, the DESTINY-Gastric02 trial was a phase II study designed to determine the efficacy and safety of trastuzumab deruxtecan for a comparatively short follow-up period in a small sample size (N = 79). The basis for the TLR and subsequent reassessment would be the ongoing DESTINY-Gastric04 phase III study that is evaluating efficacy and safety relative to ramucirumab-paclitaxel for up to 3 years of follow-up in approximately 490 patients with HER2-positive gastric or GEJ adenocarcinoma.
The study population of the DESTINY-Gastric04 trial targeted the second-line treatment setting for patients with HER2-positive gastric or GEJ cancer, which aligned with the current reimbursement request submitted by the sponsor. However, the Health Canada indication targets a broader population that includes not only patients in the second-line treatment setting, but also patients in the third-line and later settings. The DESTINY-Gastric04 trial population does not completely align with the patients in third-line and later settings, as described by the Health Canada indication. As a result, findings from the DESTINY-Gastric04 trial may not be generalizable to patients in the third-line and subsequent lines setting.
According to the clinical experts consulted by the review team, the selection of ramucirumab-paclitaxel as the comparator in the phase III, DESTINY-Gastric04 trial is appropriate because treatment with ramucirumab-paclitaxel is currently a standard of care in the second-line setting for locally advanced or metastatic HER2-positive gastric or GEJ cancer, and it will likely remain so in the second-line setting, when the results of the DESTINY-Gastric04 trial become available.
Perspectives of Patients, Clinicians, and Drug Programs
The full patient and clinician group submissions received are available in the consolidated patient and clinician group input document for this review on the project website.
Patient Group Input
This section was prepared by the review team based on the input provided by patient groups.
One input from My Gut Feeling – Stomach Cancer Foundation of Canada was received for this review. My Gut Feeling – Stomach Cancer Foundation of Canada is a nonprofit organization dedicated to providing “support, awareness, education, information and advocacy to stomach cancer patients, cancer survivors, caregivers, and family members.” Its mission is to improve the quality of life for people affected by gastric or GEJ cancers and to make systemic changes to reduce the incidence and mortality of GEJ cancers. The patient group gathered information from 30 respondents (75% patients, 25% caregivers) through an online survey conducted in September 2024. Respondents ranged in age from 20 years to 80 years, with 90% self-reporting as female and 10% as male; 95% were from Canada, and 5% were from the US.
The majority of respondents (90%) had a diagnosis of gastric cancer, and the remainder had GEJ cancer. The most common type of cancer was adenocarcinoma (85%), and most patients (40%) had been diagnosed with stage IV disease. Among the survey respondents,10% reported having HER2-positive disease; 10% had microsatellite instability–high disease; and 20% reported having a PD-L1 CPS score of greater than 5.
According to the patient group input, 95% of respondents felt that their cancer diagnosis had a significant impact on their quality of life, and that cancer and its treatment affected their physical health, mental health, ability to eat, work, finances, social life, identity, psychosocial well-being, and self-image. Many respondents reported concerns about finances due to the inability to work because of their cancer diagnosis and/or treatment. Patients and caregivers commented on the time and money they spent on cancer treatment appointments, medications, driving and parking, and eating at hospitals, describing these as financial stressors.
Based on the input, the most common symptoms reported by the respondents include reflux, abdominal pain, eating difficulties, poor appetite, weight loss, nausea, painful swallowing, and fatigue.
The survey respondents reported experience with a variety of treatment modalities, including chemotherapy, immunotherapy, targeted therapy, surgery, and radiation. Their satisfaction with their current or past treatment was evaluated on a scale of 1 to 10 (where 1 = “not satisfied” and 10 = “very satisfied”); 64% reported satisfaction of 8 or higher. The patient group added that, while current therapies lead to mixed satisfaction from respondents in terms of perceived efficacy and cancer control, these treatments have a variety of side effects that impair quality of life; all respondents identified at least 1 treatment-related side effect, with 88% reporting fatigue. This was followed by weight loss (80%), appetite changes (80%), nausea and/or vomiting (76%), “chemo brain” (64%), diarrhea (60%), taste changes (52%), neuropathy (52%), hair loss (48%), abdominal pain (44%), and insomnia (44%). The patient group reported that, based on the survey results, most of the patients were able to tolerate treatment as prescribed (40%). Another 16% had their systemic therapy dose reduced due to side effects; 16% had to delay or skip a cycle of their systemic therapy; 12% had to stop treatment due to side effects; and 8% were hospitalized due to the severity of an AE.
My Gut Feeling – Stomach Cancer Foundation of Canada noted that important outcomes reported by the respondents included quality of life, treatment side effects, cost of treatment, convenience of treatment, treatment access, duration of treatment, and survival benefits. According to the input, when respondents were asked if they would pay out of pocket for additional therapies, the majority were interested in discussing treatment options not covered by their current health care plans or universal health care; 48% said they would pay for therapies out of pocket. A total of 49% said “maybe” they would pay for these treatments: 16% said maybe they would pay if it improved their survival; 28% might pay depending on cost; and 5% might pay depending on the impact on their quality of life.
The patient group added that, while the survey found that most respondents (85%) did not have to pay directly out of pocket for specific treatments, the remainder (25%) had paid for targeted therapy or adjunct medications, either through private pay or insurance. Also, respondents mentioned that having more treatment options and access to first-line therapies were “extremely important” to them. The respondents noted that barriers to access included institutional and health care system barriers, limited availability of treatments, and speed of accessing treatment.
My Gut Feeling – Stomach Cancer Foundation of Canada noted that 4 respondents, including 3 patients from Canada, had experience with trastuzumab deruxtecan. At the time of the survey, 3 patients had been on trastuzumab deruxtecan for at least 1 month, but 1 patient had discontinued the treatment after disease progression. The patient group explained that these respondents were satisfied because trastuzumab deruxtecan had caused fewer side effects, was easier to tolerate, improved their quality of life, and better controlled their cancer. The most common side effects reported by the respondents included fatigue, nausea, vomiting, loss of appetite, and constipation.
My Gut Feeling – Stomach Cancer Foundation of Canada stated that there is an unmet patient and caregiver need to receive equitable access to therapies that may prolong life, improve symptoms, reduce risk of recurrence, and improve treatment tolerability.
Clinician Input
Input From Clinical Experts Consulted by the Review Team
All CDA-AMC review teams include at least 1 clinical specialist with expertise regarding the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the drug’s potential place in therapy). The following input was provided by 2 clinical specialists with expertise in the diagnosis and management of adult patients with unresectable locally advanced or metastatic HER2-positive gastric or GEJ adenocarcinoma who have received a prior trastuzumab-based regimen.
Unmet Needs
According to the clinical experts consulted by the review team, the goals for the treatment of patients with unresectable locally advanced or metastatic HER2-positive gastric or GEJ adenocarcinoma who have received a prior trastuzumab-based regimen are to prolong OS and improve quality of life.
The clinical experts consulted by the review team noted that there was a considerable unmet need for an effective anti-HER2 therapy beyond the first-line treatment setting for patients with unresectable locally advanced or metastatic HER2-positive gastric or GEJ adenocarcinoma.
Place in Therapy
According to the clinical experts consulted by the review team, following disease progression on first-line HER2-directed therapy, the current standard of care in the second-line setting is treatment with either ramucirumab in combination with paclitaxel or ramucirumab alone, similarly to how patients with HER2-negative cancer would be treated. The clinical experts noted that trastuzumab deruxtecan would cause a shift in the current treatment paradigm in adult patients with locally advanced or metastatic HER2-positive gastric or GEJ adenocarcinoma who have received a prior trastuzumab-based regimen: all other current second-line treatment regimens would shift to the third and subsequent lines.
Patient Population
According to the clinical experts consulted by the review team, in alignment with the eligible participants in the sponsor-submitted DESTINY-Gastric02 trial, the patients best suited for treatment with trastuzumab deruxtecan in the second-line setting would be those who have all the following criteria, unresectable or metastatic gastric or GEJ cancer with progressive disease on or after first-line therapy with a trastuzumab-containing regimen, a HER2-positive gastric or GEJ cancer (defined as IHC 3+ or IHC 2+ and ISH-positive) confirmed by a repeat biopsy, a preserved ECOG PS, and a preserved cardiac ejection.
Assessing the Response to Treatment
According to the clinical experts consulted by the review team, the key factors in determining response to treatment include patient-reported symptoms, side effects, and cross-sectional imaging (e.g., CT scan and/or MRI).
Discontinuing Treatment
According to the clinical experts consulted by the review team, patient-reported symptoms, side effects, and well-being, in conjunction with assessment of treatment response, would be the major determinants for discontinuing treatment. In terms of toxicities, the clinical experts consulted by the review team noted that ILD is among the most important AEs of which to be aware.
Prescribing Considerations
According to the clinical experts consulted by the review team, trastuzumab deruxtecan should be prescribed only by (or under the supervision of) a specialist in medical oncology with expertise in diagnosing and managing immunotherapy-related side effects, including ILD. The clinical experts noted that trastuzumab deruxtecan could be safely administered in a hospital or outpatient clinic.
Clinician Group Input
This section was prepared by the review team based on the input provided by clinician groups.
CDA-AMC received inputs from 2 clinician groups: the OH-CCO Gastrointestinal Cancer Drug Advisory Committee, and the ad hoc group of adenocarcinoma-treating physicians and the CGOEN.
OH-CCO’s Drug Advisory Committees provide timely, evidence-based clinical and health system guidance on drug-related issues in support of OH-CCO’s mandate, including the Provincial Drug Reimbursement Programs and the Systemic Treatment Program. The OH-CCO Gastrointestinal Cancer Drug Advisory Committee gathered information from 5 clinicians through videocall.
The CGOEN is a virtual and inclusive network of gastrointestinal oncology clinicians in Canada who contribute to the knowledge of gastrointestinal cancer and its treatments, including by participating in clinical trials, conducting observational research, and being involved in local, provincial, and/or national clinical guideline development and health technology assessment. A total of 15 clinicians contributed to the CGOEN submission.
According to the clinician groups, treatment is aimed at improving symptoms, response rates, quality of life, and OS. The clinician groups noted that the current treatment includes the anti–HER2-targeted therapy of trastuzumab with standard chemotherapy (mFOLFOX6), and added that the new standard of care involves adding the anti-PD1 drug, pembrolizumab, to the standard of care of trastuzumab and FOLFOX in tumours that have evidence of PD-L1 expression with a CPS of greater than 1.
Based on both clinician inputs, there is a gap in the treatment of patients with HER2-positive metastatic gastric and GEJ cancer whose disease progresses after first-line standard therapy, and trastuzumab deruxtecan should be considered in the second-line setting.
CGOEN clarified that all patients with metastatic HER2-positive gastric or GEJ cancer should be considered for treatment with trastuzumab deruxtecan if their cancer has progressed after first-line treatment with trastuzumab (plus pembrolizumab if CPS > 1) and chemotherapy (FOLFOX). Patients who have had pneumonitis in the past may not be eligible for trastuzumab deruxtecan, given that this was an exclusion criterion for the use of trastuzumab deruxtecan. Furthermore, if a patient’s cardiac ejection fraction is lower than 50%, a cardiologist would need to be involved to ensure safety, given the 3% cardiotoxicity rate and significant drop in ejection fraction associated with trastuzumab deruxtecan. CGOEN added that efficacy outcomes, such as ORR, PFS and OS — along with safety and toxicity outcomes and quality of life — are important when assessing response to treatment. OH-CCO believes that response to treatment should be assessed every 2 months to 3 months.
According to the clinician inputs, factors prompting the consideration of treatment discontinuation would include disease progression and intolerance. CGOEN added toxicities — including severe myelosuppression, liver toxicity, cardiac toxicity (with a significant drop in ejection fraction), and grade 2 or worse pneumonitis — and patient choice to the list.
OH-CCO stated that an outpatient setting in which the patient is under the care of a health care provider with training in oncology is appropriate for treatment. CGOEN’s view was that treatment with trastuzumab deruxtecan should be performed in an outpatient cancer clinic with health care providers who have experience in the delivery of cytotoxic therapy; these include pharmacists, oncology nurses, and medical oncologists who are aware of treatment side effects (i.e., toxicities). Furthermore, CGOEN noted that access to imaging (e.g., CT scans) and cardiac imaging (e.g., multigated acquisition or echocardiogram) is important for monitoring of both efficacy and toxicity.
Drug Program Input
The drug programs provide input on each drug being reviewed through the reimbursement review processes by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by the review team are summarized in Table 5.
Table 5: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Relevant comparators | |
DESTINY-Gastric01 evaluated the safety and efficacy of trastuzumab deruxtecan versus physician choice (single-drug irinotecan or paclitaxel) while DESTINY-Gastric02 was a single-arm trial of trastuzumab deruxtecan. Funded comparators include ramucirumab-paclitaxel, FOLFIRI, irinotecan, and paclitaxel. Question: How does trastuzumab deruxtecan compare against ramucirumab-paclitaxel and FOLFIRI? | According to the clinical experts consulted by the review team, the evidence from the sponsor-submitted ITC may shed light on the efficacy of trastuzumab deruxtecan relative to ramucirumab-paclitaxel or FOLFIRI. For the clinical review, an ITC was submitted by the sponsor and appraised by the CDA-AMC review team. The ITC aimed to determine the efficacy of trastuzumab deruxtecan relative to other second-line treatments currently available in Canada, including ramucirumab-paclitaxel, paclitaxel, FOLFIRI, irinotecan, and docetaxel. The ITC treatment effect estimates for OS and PFS favoured trastuzumab deruxtecan over all other comparators. However, several major limitations in the design and methods of the ITC preclude any definitive conclusion about the magnitude of effect. Specifically, missing prognostic factors (e.g., HER2 status), limited factors involved in the weighting process, residual imbalances in prognostic or effect-modifying factors, a significant reduction in ESS — as well as heterogeneity in study design, statistical analyses, geographical regions, and ethnicities across the NMA evidence network — can result in biased estimates and overly precise credible intervals. |
Considerations for initiation of therapy | |
The DESTINY-Gastric01 trial included patients who had progressed on or after at least 2 prior regimens that included a fluoropyrimidine, a platinum, and a (brand or approved biosimilar) trastuzumab-based regimen. The trastuzumab did not have to be the most recent regimen. The DESTINY-Gastric02 trial included patients who had progressive disease on or after a first-line (brand or approved biosimilar) trastuzumab-containing regimen. In both trials, prior adjuvant therapy could be counted as a line of therapy if disease progression occurred after or within 6 months of completing adjuvant therapy. The manufacturer’s submission is specific to the use of trastuzumab deruxtecan as a second-line option only (after failure of a trastuzumab-based therapy). Question: Should trastuzumab deruxtecan be considered for third or subsequent lines? | According to the clinical experts consulted by the review team, once reimbursed, trastuzumab deruxtecan will become the standard of care in the second-line setting for patients with HER2-positive gastric and GEJ cancer, and trastuzumab deruxtecan will not be rechallenged in the third-line and later settings when there is disease progression. However, the clinical experts consulted by the review team noted that, for a small number of patients who are on currently available, second or later lines of therapy and have never received trastuzumab deruxtecan (from present to the time when trastuzumab deruxtecan becomes the standard of care in the second-line setting), trastuzumab deruxtecan can be used in third-line and later settings. When it fails, trastuzumab deruxtecan should not be rechallenged. |
Question: Should trastuzumab deruxtecan be considered for patients with advanced HER2-positive esophageal adenocarcinoma who have received prior anti–HER2-targeted therapy? | According to the clinical experts consulted by the review team, any patient with esophageal, gastric, or GEJ HER2-positive cancer should be eligible for trastuzumab deruxtecan. The clinical experts consulted by the review team noted that the classification of “esophageal” versus “GEJ” is somewhat arbitrary, and that there is no preclinical or clinical rationale to suggest that the biology of HER2-positive disease and the response to HER2-directed therapies differ based on whether the disease is in the esophagus proper or the GEJ. According to the clinical experts consulted by the review team, an estimated 20% of all esophageal cancers (based on clinical experience in Ontario) are adenocarcinoma. The clinical experts consulted by the review team noted that the distribution of adenocarcinoma versus squamous cell carcinoma will differ between patient populations with different risk factors (e.g., patients with smoking and/or alcohol exposure are more likely to present with squamous cell carcinoma histology; patients with obesity, reflux, or metabolic syndrome are more likely to present with adenocarcinoma histology). |
Considerations for discontinuation of therapy | |
In DESTINY-Gastric01 and DESTINY-Gastric02, patients were allowed to continue the study drug even if the discontinuation criteria had been met, provided there was evidence of benefit (and after approval from the trial sponsor). Question: When should trastuzumab deruxtecan be discontinued? | The clinical experts consulted by the review team noted that trastuzumab deruxtecan should be discontinued when there is disease progression or significant toxicity. |
Considerations for prescribing of therapy | |
The recommended dosage of trastuzumab deruxtecan is 6.4mg/kg every 3 weeks, which is different from the starting dose for breast cancer (5.4 mg/kg); caution is needed to ensure that the appropriate dosage is given. | This is a comment from the drug plans to inform pERC deliberations. |
Generalizability | |
Question: Are the patients with the following eligible for trastuzumab deruxtecan:
| According to the clinical experts consulted by the review team, patients with an ECOG PS of 1 could be eligible for trastuzumab deruxtecan. However, the clinical experts consulted by the review team would exclude patients with an ECOG PS of 2 from receiving trastuzumab deruxtecan. The clinical experts consulted by the review team further noted that ECOG PS may not be used as a reimbursement criterion because the decision as to whether a patient is well enough to receive a treatment relies on the clinician’s interpretation of multiple factors and is not limited to ECOG PS. According to the clinical experts consulted by the review team, the scenario in which a patient with breast cancer receives trastuzumab deruxtecan and later develops gastric or GEJ cancer is very rare as to not merit any further consideration. The clinical experts consulted by the review team noted that, although there is currently no evidence regarding this scenario, such patients may not be eligible to be treated with trastuzumab deruxtecan again for gastric or GEJ cancer. |
Question:
| The clinical experts consulted by the review team noted that patients who have never been treated with trastuzumab deruxtecan, and are currently on other treatment regimens in second-line or subsequent settings, would be considered for treatment with trastuzumab deruxtecan. |
Funding algorithm (oncology only) | |
Request an initiation of a rapid provisional funding algorithm. Note that if the final reimbursement recommendation for this drug under review is “Do not Reimburse,” the project will be suspended indefinitely. | This is a comment from the drug plans to inform pERC deliberations. |
Drug may change place in therapy of comparator drugs. | This is a comment from the drug plans to inform pERC deliberations. |
Drug may change place in therapy of drugs reimbursed in subsequent lines. | This is a comment from the drug plans to inform pERC deliberations. |
Question: For patients with HER2-positive disease, under what circumstances would trastuzumab deruxtecan be preferred over ramucirumab-paclitaxel and vice versa? For patients who receive second-line trastuzumab deruxtecan, what therapies would be funded in subsequent lines? | According to the clinical experts consulted by the review team, once reimbursed, trastuzumab deruxtecan will become the standard of care in the second-line setting for patients with HER2-positive gastric and GEJ cancer. The clinical experts consulted by the review team noted that all therapies currently used in the second-line setting will move to the third line, and those currently in the third line to the fourth line, and so on, before considering Lonsurf as the last resort. The clinical experts consulted by the review team also noted that, despite these shifts, it remains the same in terms of the pathway or order of using these currently available therapies. According to the clinical experts consulted by the review team, once it becomes the standard of care in the second-line setting, trastuzumab deruxtecan will not be rechallenged in third-line and later settings when there is disease progression. |
Care provision issues | |
For dose reductions, the product monograph allows for a maximum of 2 dose reductions. Dose re-escalation after a dose reduction is not recommended. | This is a comment from the drug plans to inform pERC deliberations. |
Question: Is retesting of the tumour after progression on trastuzumab needed to confirm HER2 positivity (IHC 3+ or IHC 2+ and ISH-positive) for eligibility for trastuzumab deruxtecan? | According to the clinical experts consulted by the review team, a biopsy of the tumour after progression on trastuzumab to confirm HER2 positivity could be considered to determine whether trastuzumab deruxtecan is the best available treatment option for a patient; however, it should not be considered mandatory, especially if there is no easily accessible site to biopsy safely. |
System and economic issues | |
A confidential negotiated price exists for ramucirumab. | This is a comment from the drug plans to inform pERC deliberations. |
CDA-AMC = Canada’s Drug Agency; ECOG PS = Eastern Cooperative Oncology Group Performance Status; ESS = effective sample size; FOLFIRI = folinic acid–fluorouracil-irinotecan; GEJ = gastroesophageal junction; HER2 = human epidermal growth factor receptor 2; IHC = immunohistochemistry; ISH = in situ hybridization; ITC = indirect treatment comparison; NMA = network meta-analysis; OS = overall survival; pERC = pan-Canadian Oncology Drug Review Expert Review Committee; PFS = profession-free survival.
Clinical Evidence
The objective of the Clinical Review Report is to review and critically appraise the clinical evidence submitted by the sponsor on the beneficial and harmful effects of trastuzumab deruxtecan, 100 mg, powder for concentrate for solution for IV infusion, for the treatment of adult patients with unresectable locally advanced or metastatic HER2-positive gastric or GEJ adenocarcinoma who have received a prior trastuzumab-based regimen. The focus will be on comparing trastuzumab deruxtecan to relevant comparators and identifying gaps in the current evidence.
A summary of the clinical evidence included by the sponsor for the review of trastuzumab deruxtecan is presented in 2 sections, with the review team’s critical appraisal of the evidence included at the end of each. The first section, the systematic review, includes pivotal studies and RCTs that were selected according to the sponsor’s systematic review protocol. The review team’s assessment of the certainty of the evidence in this first section, using the GRADE approach, follows the critical appraisal of the evidence. The second section includes indirect evidence from the sponsor.
Included Studies
Clinical evidence from the following is included in the review and appraised in this document:
One phase II, single-arm study identified in the systematic review (i.e., the DESTINY-Gastric02 trial)
One ITC consisting of an unanchored MAIC and an NMA
One phase II RCT identified as other evidence (i.e., the DESTINY-Gastric01 trial).
Systematic Review
Contents within this section have been informed by materials submitted by the sponsor. The following has been summarized and validated by the review team.
Description of Studies
One study (the DESTINY-Gastric02 trial) was identified as the pivotal study. Characteristics of the DESTINY-Gastric02 study are summarized in Table 6.
The DESTINY-Gastric02 trial was a phase II, single-arm, open-label study investigating the use of trastuzumab deruxtecan as monotherapy for the treatment of patients (aged ≥ 18 years) who have unresectable or metastatic centrally confirmed HER2-positive gastric or GEJ cancer and have experienced disease progression during or after first-line therapy with a trastuzumab-containing regimen. A total of 79 patients from 24 sites across Europe and North America (no sites in Canada) were enrolled. The primary objective of the DESTINY-Gastric02 trial was to assess the efficacy of trastuzumab deruxtecan based on the confirmed ORR by ICR using RECIST 1.1. OS, PFS, HRQoL outcomes, and harms were also investigated in the DESTINY-Gastric02 trial.
The DESTINY-Gastric02 trial has been completed. Results submitted by the sponsor are mainly from 2 data cut-off dates: April 9, 2021, and November 8, 2021. The median duration of follow-up was 5.9 months (range, 0.7 months to 15.4 months) as of the data cut-off date of April 9, 2021, and 10.2 months (range, 0.7 months to 22.1 months) as of the data cut-off date of November 8, 2021.
Table 6: Details of the DESTINY-Gastric02 Trial Included in the Systematic Review
Detail | DESTINY-Gastric02 trial |
|---|---|
Designs and populations | |
Study design | Phase II, multicentre, single-arm, open-label study |
Locations | Patients were enrolled at 24 sites in 5 countries across Europe and North America. There were no sites in Canada. |
Patient enrolment dates: | Start date: November 2019 Study completion date: April 2024 |
Randomized (N) | N = 79 |
Inclusion criteria |
|
Exclusion criteria |
|
Drugs | |
Intervention | Trastuzumab deruxtecan 6.4 mg/kg IV every 3 weeks |
Comparator | No comparator |
Study duration | |
Screening phase | Started on the day of signing the main informed consent form and had a maximum duration of 28 days |
Treatment phase | Started on cycle 1, day 1, with patients continuing treatment until disease progression or unacceptable toxicity |
Follow-up phase | Follow-up at 40 days (+ 7 days) after the last administration |
Outcomes | |
Primary end point | Confirmed ORR based on ICR per RECIST 1.1 |
Secondary and exploratory end points | Key secondary:
Secondary:
|
Publication status | |
Publications | Publications: Van Cutsem et al. (2023)44 Van Cutsem et at. (2021)45 Ku et al. (2022)46 ClinicalTrials.gov entry: |
CNS = central nervous system; DCR = disease control rate; DOR = duration of response; ECHO = echocardiogram; ECOG PS = Eastern Cooperative Oncology Group Performance Status; FACT-Ga = Functional Assessment of Cancer Therapy – Gastric; GEJ = gastroesophageal junction; HER2 = human epidermal growth factor 2; HRQoL = health-related quality of life; ICR = independent central review; IHC = immunohistochemistry; ILD = interstitial lung disease; ISH = in situ hybridization; LVEF = left ventricular ejection fraction; MUGA = multigated acquisition; NYHA = New York Heart Association; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; RECIST 1.1 = Response Evaluation Criteria in Solid Tumours Version 1.1; TTR = time to response.
Sources: Sponsor’s Summary of Clinical Evidence;1 DESTINY-Gastric02 Clinical Study Report;32,33 DESTINY-Gastric02 Clinical Study Protocol, Version 3.47
Populations
Inclusion and Exclusion Criteria
The DESTINY-Gastric02 trial enrolled patients who were aged 18 years and older with an ECOG PS of 0 or 1 and a diagnosis of unresectable or metastatic HER2-positive (defined as IHC 3+ or IHC 2+ and ISH-positive) gastric or GEJ cancer. Patients were considered eligible if their disease had progressed during or after first-line therapy with a trastuzumab-containing regimen. Patients were excluded if they had received anticancer therapy following a first-line treatment regimen containing trastuzumab.
Interventions
In the single-arm DESTINY-Gastric02 trial, all patients received 6.4 mg/kg of trastuzumab deruxtecan through IV on day 1 (± 2 days) of every 21-day treatment cycle (i.e., every 3 weeks) until disease progression, withdrawal by patient, physician decision, or death. Trastuzumab deruxtecan was administered in a hospital setting. The first infusion of trastuzumab deruxtecan took 90 minutes or greater. Subsequent infusions of trastuzumab were administered over 30 minutes or greater if there was no injection-related reaction after the first infusion.
Outcomes
A list of efficacy end points assessed in this Clinical Review Report is provided in Table 7, followed by descriptions of the outcome measures. Summarized end points are based on outcomes included in the sponsor’s Summary of Clinical Evidence as well as on any outcomes identified as important to this review by the clinical experts consulted by the review team, patient and clinician group inputs, and public drug plans. Using the same considerations, the review team selected end points that were considered most relevant to inform the expert committee deliberations and finalized this list of end points in consultation with members of the expert committee. All summarized efficacy end points were assessed using GRADE. Select notable harms outcomes considered important for informing the expert committee deliberations were also assessed using GRADE.
Table 7: Outcomes Summarized From the Studies Included in the Systematic Review
Efficacy outcome measure | Time point | DESTINY-Gastric02 trial |
|---|---|---|
OS | 6 months, 12 months (data cut-off date: November 8, 2021) | Secondary |
PFS per ICR assessment | 6 months (data cut-off date: November 8, 2021) | Key secondary |
Confirmed ORR per ICR assessment | As of the data cut-off date of November 8, 2021 | Primary |
FACT-Ga total score | End of treatment (data cut-off date: April 9, 2021) | Secondary |
FACT-Ga = Functional Assessment of Cancer Therapy – Gastric; ICR = independent central review; ORR = objective response rate; OS = overall survival; PFS = progression-free survival.
Sources: Sponsor’s Summary of Clinical Evidence;1 DESTINY-Gastric02 Clinical Study Report.32,33
Descriptions of the efficacy and safety outcomes presented in the DESTINY-Gastric02 trial32,33 and appraised in the Clinical Review Report follow.
Efficacy Outcomes
Overall Survival
In the DESTINY-Gastric02 trial, OS was defined as the time from the date of the first dose of study drug to the date of death due to any cause. If the patient was not known to have died by the analysis cut-off date, OS was censored at the date of last contact. The last contact date was defined as the last date on which the patient was known to be alive up to the data cut-off date.
PFS per ICR Assessment
PFS was defined as the time from the date of the first dose of the study drug to the date of radiographic disease progression (as measured by RECIST 1.1) or death due to any cause. The censoring rules are shown in Table 8.
Table 8: Censoring Rules for PFS Per ICR Assessment in the DESTINY-Gastric02 Trial
Scenario | Censoring date |
|---|---|
No baseline-evaluable tumour assessment | Date of first dose |
No postbaseline tumour assessment | Date of first dose |
Anticancer therapy started before disease progression, death, or analysis cut-off date | Date of last evaluable tumour assessment before anticancer therapy (other than study drug) |
Disease progression or death after missing assessments (i.e., more than 14 weeks) | Date of last evaluable tumour assessment (before earliest of death or progression date and analysis cut-off date) |
At least 1 postbaseline response assessment, patients with no death or objective documentation of radiographic disease progression (i.e., lost to follow-up; withdrawal of consent; ongoing without PFS event; adequate tumour assessment no longer available) | Date of last evaluable tumour assessment |
ICR = independent central review; PFS = progression-free survival.
Source: DESTINY-Gastric02 Statistical Analysis Plan, Version 2.48
Confirmed ORR Per ICR Assessment
Confirmed ORR per ICR assessment was defined as the proportion of patients who achieved a best overall response of confirmed CR or confirmed PR, as determined by ICR committee based on RECIST 1.1. The best overall response was defined as the best response (in the order of CR, PR, stable disease, and progressive disease) across all time points from the start of treatment until when patients were withdrawn from the study or started a new anticancer therapy. The best overall response of CR or PR could not be determined unless it was confirmed no earlier than 4 weeks (28 days) from the date on which a response of CR or PR was first acquired.
Health-Related Quality of Life
Patient-reported HRQoL was measured by FACT-Ga in the DESTINY-Gastric02 trial. The summary of measurement properties of FACT-Ga is shown in Table 9.
Table 9: Summary of Outcome Measures and Their Measurement Properties
Outcome measure | Type | Conclusions about measurement properties | MID |
|---|---|---|---|
FACT-Ga | The FACT-Ga is a 5-point, Likert-type instrument to measure the subjective QoL of patients with gastric cancer.49,50 A higher score indicates a better outcome. The subscale domains of FACT-Ga include physical well-being, social and family well-being, emotional well-being, functional well-being, and a gastric cancer subscale.49 | Validity: In terms of convergent and divergent validity, the FACT-Ga scores were associated with the SF-36, except for the social well-being subscale.50 In terms of criterion-related validity, cancer stage was significantly related to the FACT-Ga total score (F1, 81 = 5.00; P = 0.028).50 Reliability: The FACT-Ga total score and gastric subscale score both had good internal consistency with Cronbach alpha > 0.70.50 Sensitivity to change: Patients’ perception of QoL was correlated with FACT-Ga scores. For instance, the association between changes in FACT-Ga total score and patient-rated changes in global QoL was significant (F2,59 = 4.07; P = 0.022).50 | Validation of the FACT-Ga total score by Garland et al.50 proposes mean changes of:
|
FACT-Ga = Functional Assessment of Cancer Therapy – Gastric; MID = minimal important difference; QoL = quality of life; SF-36 = Short Form (36) Health Survey.
Harms Outcomes
The harms outcomes assessed in the DESTINY-Gastric02 trial mainly included TEAEs, TESAEs, withdrawal due to TEAEs, deaths, and notable harms (i.e., ILD, LV dysfunction, QT prolongation, and IRR).
A TEAE was defined as an occurring AE that was absent before the first dose of the study drug — or that worsened in severity or seriousness after initiating the study drug — up to 47 days after last dose of the study drug. Serious AEs with an onset or worsening 48 days or more after the last dose of study drug, if considered related to the study treatment, were also considered as TEAEs.
Statistical Analysis
The sample size was determined based on historical data related to the current standard of care, which suggested that Western patients with second-line gastric or GEJ cancer could have an ORR of up to 27%.48 Taking dropout into consideration, a sample size of approximately 80 patients would provide 90% power to achieve a lower limit of 95% CI for the ORR that exceeded 27% under a hypothesized alternative ORR of 45%.
Details on the statistical analysis of efficacy end points in the DESTINY-Gastric02 trial are presented in Table 10. The primary end point for the DESTINY-Gastric02 trial was confirmed ORR assessed per ICR assessment per RECIST 1.1. The estimate of ORR (along with the corresponding 95% exact CI) was calculated using the Clopper-Pearson method.51 For the key secondary end point in the DESTINY-Gastric02 trial (i.e., PFS per ICR assessment), the median event time and corresponding 95% CI were calculated using the Brookmeyer and Crowley method.52 OS, a secondary end point in the DESTINY-Gastric02 trial, was estimated using the Kaplan-Meier (KM) method; CIs for the rates at fixed time points were calculated using the delta method and a log-log transformation of the probabilities. KM estimates of survival curves are presented for PFS and OS. No statistical testing or inference was carried out in the DESTINY-Gastric02 trial.
Table 10: Statistical Analysis of Efficacy End Points in the DESTINY-Gastric02 Trial
End point | Statistical model | Adjustment factors | Handling of missing data | Sensitivity analyses |
|---|---|---|---|---|
OS |
| NR |
| None |
PFS per ICR assessment |
| NR |
|
|
Confirmed ORR per ICR assessment |
| NR |
|
|
FACT-Ga total score |
| NR |
| None |
CI = confidence interval; FACT-Ga = Functional Assessment of Cancer Therapy – Gastric; ICR = independent central review; KM = Kaplan-Meier; NR = not reported; ORR = objective response rate; OS = overall survival; PFS = progression-free survival.
Sources: Sponsor’s Summary of Clinical Evidence;1 DESTINY-Gastric02 Statistical Analysis Plan, Version 2.48
The following subgroups were examined in the DESTINY-Gastric02 trial for the primary end point of confirmed ORR based on ICR and the key secondary end point of PFS per ICR assessment:
region (North America, Europe)
age (< 65 years, ≥ 65 years; < 75 years, ≥ 75 years)
sex (female, male)
ECOG PS (0, 1)
HER2 status (IHC 3+ or IHC 2+ and ISH-positive)
primary tumour location (gastric, GEJ)
histological subtype (intestinal, diffuse, others)
number of metastatic sites (< 2, ≥ 2)
previous total gastrectomy (yes, no)
prior adjuvant or neoadjuvant therapy (yes, no)
prior nivolumab or pembrolizumab treatment (yes, no)
prior treatment with immune checkpoint inhibitor or other immuno-oncology therapy (yes, no)
presence of liver metastasis at baseline (yes, no)
renal function at baseline (normal, mild impairment, moderate impairment)
renal impairment status determined by baseline creatinine clearance (CrCl) (calculated using the Cockcroft-Gault equation):
hepatic impairment at baseline (normal, mild)
In each subgroup defined previously, the analysis was conducted using the same type of methodology as described for the corresponding end point. Results of the subgroup analyses were presented using descriptive summaries. Some subcategories were combined if the sample size within categories was too small (e.g., < 10 patients).
Analysis Populations
The analysis populations of the DESTINY-Gastric02 trial are summarized in Table 11.
Table 11: Analysis of Populations in the DESTINY-Gastric02 Trial
Study | Population | Definition | Application |
|---|---|---|---|
DESTINY-Gastric02 trial | FAS | Included all patients who received ≥ 1 dose of study drug | All efficacy analyses |
Response-evaluable set | Included all patients who received ≥ 1 dose of study drug and had measurable disease at baseline per ICR | Confirmed ORR | |
Safety analysis set | Included all patients who received ≥ 1 dose of study drug | Safety analyses |
FAS = full analysis set; ICR = independent central review; ORR = objective response rate.
Sources: Sponsor’s Summary of Clinical Evidence;1 DESTINY-Gastric02 Statistical Analysis Plan, Version 2.48
Protocol Amendments and Deviations
██ ██████ █████ ████ █ ████████ ██ ███ █████ █████████ ███ ███ █████████████████ ██████ █████████ ███ ███████ ████████ ██████ ███ █████ ███ █ ███████████47 ███ █████ █████████ ███ ████ ██ █████████ ███ █████ ████ ██████████ ████████ ████████ ███ █████████ ████████ ███████ ██ ████ ███ ██████ ████████ ██ ████████████ ██ ████████████ ██████████ ████████ █████████ ████████ ███████ ██ ███████████ ███████ ███████ ███ ███████ ██ ███████ █████████ ████ ██████ ██████████ ████ ███ ███ ███████ █████ ████████████ ███████████ ███████████ ██████ █████████ ████████ ███████ ██ ██████████ ██████ █████████ ██████████ ██████ █ ██████ ██ █████ ████ ███ ██ ██████████████ ███████ ██████ █ █████ ██ █████ █ ███ ██ ██ ████ ██ ████████ ███████ ████ ████████ ███████████ ████████████████████████ █████████ ████ ████ ██ ██████ ████████ ███ ████████ ████████ ██████████████████ ██ █████ ████████ ██████████ ██ ██ ███ ████ ███████ ████ ██ █████ ██ █████ ██ █████ ██ █████ ███
Table 12: Major Protocol Deviations in the DESTINY-Gastric02 Trial (FAS, Data Cut-Off Date: April 9, 2021)
Protocol deviation | Trastuzumab deruxtecan (N = 79) |
|---|---|
█████████████████████████████████ | ██ ██████ |
███████ █ ███ | |
███████████████ ████████ | ██ ██████ |
███████ | ██ ██████ |
██████████ ████████ | | ██████ |
████████ ███████ | | █████ |
██████████ | | █████ |
██████ █████████ | | █████ |
██████████████ | | █████ |
█████ ████████ | | █████ |
█████ | | █████ |
FAS = full analysis set.
Source: DESTINY-Gastric02 Clinical Study Report.32,33
Results
Patient Disposition
Patient disposition in the DESTINY-Gastric02 trial is summarized in Table 13. Of 89 patients screened, 79 were enrolled and treated with at least 1 dose of trastuzumab deruxtecan. As of November 8, 2021, 11 patients (13.9%) had discontinued trastuzumab deruxtecan due to AEs.
Baseline Characteristics
The baseline characteristics outlined in Table 14 are limited to those that are most relevant to this review or that were believed to affect the outcomes or interpretation of the study results. In the DESTINY-Gastric02 trial, the median age of the trial population was 60.7 years (range, 20.3 years to 77.8 years), with 58.5% of the patients being younger than 65 years. The majority of the trial population was male (72.2%), white (87.3%), presented with an ECOG PS of 1 (63.3%), had GEJ as the cancer location (65.8%), and had a HER2 status of IHC 3+ (86.1%). Almost all the patients (78 patients out of 79 patients) had a histological subtype of adenocarcinoma.
Exposure to Study Treatments
Treatment exposure is summarized in Table 15. As of the data cut-off date of November 8, 2021, the median treatment duration for the DESTINY-Gastric02 study was 4.3 months (range, 0.7 months to 22.1 months), and 10 patients (12.7%) were still on treatment with trastuzumab deruxtecan. The median dose intensity was 6.2 mg/kg per 3 weeks (range, 3.9 weeks to 6.7 weeks). The median relative dose intensity (i.e., the ratio of the amount of drug delivered to the planned dose delivered) was 96.6% (range, 60.3% to 104.1%).
Table 13: Summary of Patient Disposition in the DESTINY-Gastric02 Trial (Data Cut-Off Date: November 8, 2021)
Patient disposition | Trastuzumab deruxtecan |
|---|---|
Screened, n | 89 |
Excluded, n (%)a | 10 (11.2) |
Patients enrolled, n (%) | 79 |
Treated patients, n (%) | 79 (100.0) |
Discontinued from study drug, n (%) | 69 (87.3) |
Primary reason for discontinuation, n (%) | |
Progressive diseaseb | 48 (60.8) |
AE | 11 (13.9) |
Clinical progressionc | 4 (5.1) |
Death | 2 (2.5) |
Withdrawal by patient | 2 (2.5) |
Physician decision | 1 (1.3) |
Otherd | 1 (1.3) |
FAS, n | 79 |
Response-evaluable set, n | 78 |
Safety analysis set, n | 79 |
AE = adverse event; FAS = full analysis set.
aPercentage was based on the number of all-screened patients in the all-screened analysis set.
bDiscontinued based on objective evidence of disease progression.
cDiscontinued based on clinical manifestations, as judged by the investigator.
dThis was a drug hold for a treatment-emergent AE (preferred term for COVID-19 pneumonia) that exceeded the protocol-allowed time limit of 49 days from the last infusion date.
Sources: Sponsor’s Summary of Clinical Evidence;1 DESTINY-Gastric02 Clinical Study Report.32,33
Table 14: Summary of Baseline Characteristics in the DESTINY-Gastric02 Trial (FAS)
Characteristic | Trastuzumab deruxtecan |
|---|---|
Age (years), median (range) | 60.7 (20.3 to 77.8) |
Age group, n (%) | |
< 65 years | 46 (58.2) |
≥ 65 years | 33 (41.8) |
Sex | |
Female, n (%) | 22 (27.8) |
Male, n (%) | 57 (72.2) |
Race, n (%) | |
American Indian or Alaska Native | 0 |
Asian | 4 (5.1) |
Black or African American | 1 (1.3) |
Native Hawaiian or other Pacific Islander | 1 (1.3) |
White | 69 (87.3) |
Other | 3 (3.8) |
Missing | 1 (1.3) |
Baseline ECOG PS, n (%) | |
0 | 29 (36.7) |
1 | 50 (63.3) |
Lines of prior systemic therapy intended for locally advanced or metastatic disease, n (%) | |
0 | 6 (7.6)a |
1 | 73 (92.4) |
≥ 2 | 0 |
HER2 status (central laboratory), n (%) | |
IHC 3+ | 68 (86.1) |
IHC 2+ or ISH-positive | 10 (12.7) |
Not evaluable | 1 (1.3) |
Cancer location, n (%) | |
Gastric | 27 (34.2) |
Gastroesophageal junction | 52 (65.8) |
Histological subtype, n (%) | |
Adenocarcinoma | |
Intestinal | 19 (24.1) |
Diffuse | 1 (1.3) |
Mixed | 1 (1.3) |
Unknown | 57 (72.2) |
Other | 1 (1.3) |
Number of metastatic sites, n (%) | |
≥ 2 | 74 (93.7) |
< 2 | 5 (6.3) |
Prior adjuvant or neoadjuvant therapy, n (%) | |
Yes | 9 (11.4) |
No | 70 (88.6) |
Previous total gastrectomy, n (%) | |
No | 79 (100.0) |
Previous treatment, n (%) | |
Therapy containing trastuzumab | 79 (100.0) |
Immune checkpoint inhibitor | 7 (8.9) |
Presence of liver metastasis at baseline, n (%) | |
Yes | 50 (63.3) |
No | 29 (36.7) |
Time from initial diagnosis, months | |
Median | 14.2 |
Range | 3.6 to 88.5 |
ECOG PS = Eastern Cooperative Oncology Group Performance Status; FAS = full analysis set; HER2 = human epidermal growth factor receptor 2; IHC = immunohistochemistry; ISH = in situ hybridization.
Sources: Sponsor’s Summary of Clinical Evidence;1 DESTINY-Gastric02 Clinical Study Report.32,33
Table 15: Summary of Patient Exposure in the DESTINY-Gastric02 Trial (Safety Analysis Set; Data Cut-Off Date: November 8, 2021)
Exposure | Trastuzumab deruxtecan (N = 79) |
|---|---|
Total patient-years of exposure (years) | █████ |
Treatment duration (months),a median (range) | 4.3 (███ ██ ████) |
Duration of treatment, n (%) | |
≤ 3 months | ██ ██████ |
> 3 months to ≤ 6 months | ██ ██████ |
> 6 months to ≤ 9 months | | ██████ |
> 9 months to ≤ 12 months | ██ ██████ |
> 12 months to ≤ 24 months | | ██████ |
> 24 months | ██ |
Dose intensity,b mg/kg per 3 weeks, median (range) | ██████ ██ ███ |
Relative dose intensity,c %, median (range) | ████████ ██ █████ |
Total number of cycles treated, median (range) | ███| ██ ██ |
Number (%) of patients treated by cycles | |
≤ 2 cycles | ██ ██████ |
> 2 cycles to ≤ 4 cycles | ██ ██████ |
> 4 cycles to ≤ 6 cycles | | ██████ |
> 6 cycles to ≤ 8 cycles | | █████ |
> 8 cycles | ██ ██████ |
Patients with incomplete infusion, n (%) | | █████ |
Due to AEs | | █████ |
Due to technical difficulties | | █████ |
Patients with dose reduction, n (%) | ██ ██████ |
Due to AEs | ██ ██████ |
Other reasons | | █████ |
Patients with dose delay,d n (%) | ██ ██████ |
AE = adverse event; NR = not reported.
aTreatment duration (in months) was calculated as (date of last dose minus date of first dose + 21) divided by (365.25 × 12). For patients who were still on treatment at the data cut-off date, the last available date of dose was used.
bDose intensity (mg/kg per 3 weeks) = total amount of study drug taken during the treatment period (mg/kg) divided by (treatment duration in weeks divided by 3).
cRelative dose intensity (%) = dose intensity / planned dose intensity, where the planned dose intensity was 6.4 mg/kg per 3 weeks.
dDose delay was defined as at least 24 days (3 days later than scheduled) after the previous dose.
Source: DESTINY-Gastric02 Clinical Study Report.32,33
Prior Cancer Therapy
Details on prior cancer therapy in the DESTINY-Gastric02 trial are presented in Table 16. The majority of trial participants (96.2%) had received 1 prior regimen of cancer therapy.
Table 16: Prior Cancer Therapy in the DESTINY-Gastric02 Trial (FAS; Data Cut-Off Date: April 9, 2021)
Prior cancer therapy | Trastuzumab deruxtecan (N = 79) |
|---|---|
Number of regimens, median (range) | ███ ██ ██ ██ |
1 regimen, n (%) | ██ ██████ |
2 regimens, n (%) | | █████ |
Regimen intended for,a n (%) | |
Metastatic | ██ ██████ |
Maintenance | ██ ██████ |
Neoadjuvant | | ██████ |
Locally advanced | | █████ |
Adjuvant | | █████ |
Other | | █████ |
Prior gastric cancer surgery, n (%) | |
Yes | ██ ██████ |
No | ██ ██████ |
FAS = full analysis set.
aThe percentage for each subcategory was based on the number of patients with the corresponding prior cancer systemic therapy.
Source: DESTINY-Gastric02 Clinical Study Report.32,33
Concomitant Medications
Information about the use of concomitant medications in the DESTINY-Gastric02 trial is shown in Table 17.
Table 17: Concomitant Treatments Used in the DESTINY-Gastric02 Trial (FAS; Data Cut-Off Date: November 8, 2021)
Concomitant treatment | Trastuzumab deruxtecan (N = 79) |
|---|---|
██████████████████████████████████ | ██ ███████ |
███████████ ███ █████████████ | ██ ██████ |
██████████ | ██ ██████ |
███████████ | ██ ██████ |
████████████ █████████████ | | █████ |
███████████████ ███ ████████ ███ | ██ ██████ |
█████████████ | ██ ██████ |
█████████████ ██████ █████████ | | █████ |
█████ ███ ████ ███████ █████████ | ██ ██████ |
██████████ | ██ ██████ |
███████████ | ██ ██████ |
████████████████████████████████████████ | ██ ██████ |
████████████████████████████████████ | ██ ██████ |
█████ ███ ████████████ | ██ ██████ |
██████████████ ███ ████████ ███ | ██ ██████ |
██████████ ████████████ | ██ ██████ |
█████████████ | ██ ██████ |
█████████████████████████████████████ | ██ ██████ |
██████████ ███ ███████████ | | █████ |
██████████ | | █████ |
██████████████ ███ ████████ ███ | | ██████ |
██████████████ ██████ | ██ ██████ |
FAS = full analysis set.
Sources: Sponsor’s Summary of Clinical Evidence;1 DESTINY-Gastric02 Clinical Study Report.32,33
Subsequent Treatment
The summary of subsequent treatment in the DESTINY-Gastric02 trial is shown in Table 18. As of the data cut-off date of November 8, 2021, 49.4% patients had received subsequent anticancer treatment after the completion of trastuzumab deruxtecan. Paclitaxel was the most common subsequent treatment and was used by 17.7% of patients.
Table 18: Summary of Subsequent Treatment in the DESTINY-Gastric02 Trial (FAS; Data Cut-Off Date: November 8, 2021)
Exposure | Trastuzumab deruxtecan (N = 79) |
|---|---|
████████ ██████████ ████████ █ ███ | ██ ██████ |
██████████████ ██████ | ██ ██████ |
█████████ | | █████ |
██████████████████████ | | █████ |
██████████ | | █████ |
███████████ | ██ ██████ |
██████████ | ██ ██████ |
███████████ | | █████ |
█████████████████████████████████ | ██ |
██████████ ███████ | ██ |
███████████ | | █████ |
███████████████████████████████ | | █████ |
█████████ | | █████ |
████████████ | | █████ |
███████████ | ██ |
██████████ | | █████ |
███████ | ██ |
██████ | ██ |
████████ ████████ | ██ |
██████████ | ██ |
███ ███ | ██ |
████████ | ██ |
████████████ | | █████ |
█████████████ | | █████ |
██████████████████████ | | ██████ |
███████ | | █████ |
██████ | | █████ |
█████████████████ | | █████ |
█████████ | | █████ |
████████ | | █████ |
███████████ | | █████ |
████████ | | █████ |
███████████████ ██████████ | | █████ |
████████████ | | █████ |
██████████ | | █████ |
█████████ | | █████ |
█████ | | █████ |
███████████ | | █████ |
███ █████ ███████████ ████████ | | █████ |
███████ ████████ | ██ |
███████ ████████████ | ██ |
███████ ████ | | █████ |
███████████ ████ | | █████ |
██████████ ██████ | ██ |
██████████ | ██ |
███████████████ ████ | ||| |
FAS = full analysis set.
Source: Sponsor’s Summary of Clinical Evidence.1
Efficacy
Key efficacy results in the DESTINY-Gastric02 FAS are presented in Table 19. The median duration of follow-up was 10.2 months (range, 0.7 months to 22.1 months) as of the data cut-off date of November 8, 2021, and 5.9 months (range, 0.7 months to 15.4 months) as of the data cut-off date of April 9, 2021. The data cut-off date for efficacy results was November 8, 2021, unless otherwise specified.
Table 19: Summary of Key Efficacy Results in the DESTINY-Gastric02 Trial (FAS; Data Cut-Off Date: November 8, 2021)
Efficacy | Trastuzumab deruxtecan (N = 79) |
|---|---|
OS | |
Patients with OS events, n (%) | 46 (58.2) |
Patients censored, n (%) | 33 (41.8) |
Alive | 26 (32.9) |
Lost to follow-upa | 7 (8.9) |
OS (months),b median (95% CI) | 12.1 (9.4 to 15.4) |
Probability of being alive at 6 months,b % (95% CI) | 77.8 (66.8 to 85.6) |
Probability of being alive at 12 months,b % (95% CI) | 50.6 (38.4 to 61.5) |
Probability of being alive at 18 months,b % (95% CI) | 35.1 (22.1 to 48.4) |
PFS per ICR assessment | |
Patients with PFS events, n (%) | 51 (64.6) |
Progressive disease | 44 (55.7) |
Death | 7 (8.9) |
Patients censored, n (%) | ██ ██████ |
New anticancer therapy | ██ ██████ |
Ongoing without progression | | █████ |
Adequate assessment no longer available | | █████ |
Missed 2 consecutive tumour assessments | | █████ |
PFS (months),b median (95% CI) | 5.6 (4.2 to 8.3) |
Probability of being progression-free at 3 months,b % (95% CI) | 70.5 (58.7 to 79.5) |
Probability of being progression-free at 6 months,b % (95% CI) | 48.9 (36.6 to 60.2) |
Probability of being progression-free at 9 months,b % (95% CI) | 36.3 (24.5 to 48.1) |
Probability of being progression-free at 12 months,b % (95% CI) | 20.0 (9.4 to 33.3) |
ORR per ICR assessment | |
Confirmed ORR, n (%; 95% CI) | 33 (41.8; 30.8 to 53.4) |
CR, n (%) | 4 (5.1) |
PR, n (%) | 29 (36.7) |
FACT-Ga total scorec | |
Baseline | — |
n (%) | ██ ██████ |
Mean (SD) | █████ ██████ |
End of treatment | — |
nd (%) | ██ ██████ |
Mean change from baseline (SD) | ██████ ███████ |
CI = confidence interval; CR = complete response; FACT-Ga = Functional Assessment of Cancer Therapy – Gastric; FAS = full analysis set; ICR = independent central review; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; PR = partial response; SD = standard deviation.
aLost to follow-up was defined as the time interval between the last contact date and analysis cut-off date being longer than the protocol-defined 3-month interval of survival follow-up plus 2 weeks.
bEstimated using Kaplan-Meier.
cData on FACT-Ga scores were based on the data cut-off date of April 9, 2021.
dThe n for the change from baseline section was the number of patients who had the patient-reported outcome assessment values at both baseline and the specified visit.
Sources: Sponsor’s Summary of Clinical Evidence;1 DESTINY-Gastric02 Clinical Study Report;32,33 Drug Reimbursement Review Sponsor Submission for trastuzumab deruxtecan.3
Overall Survival
As of the data cut-off date of November 8, 2021, the proportion of patients in the FAS who had OS events was 58.2%. The median OS was 12.1 months (95% CI, 9.4 months to 15.4 months). The probability of being alive was 77.8% (95% CI, 66.8% to 85.6%) at 6 months, 50.6% (95% CI, 38.4% to 61.5%) at 12 months, and 35.1% (95% CI, 22.1% to 48.4%) at 18 months. The KM plot for OS is presented in Figure 1.
Figure 1: KM Plot of OS in the DESTINY-Gastric02 Trial (FAS; Data Cut-Off Date: November 8, 2021)
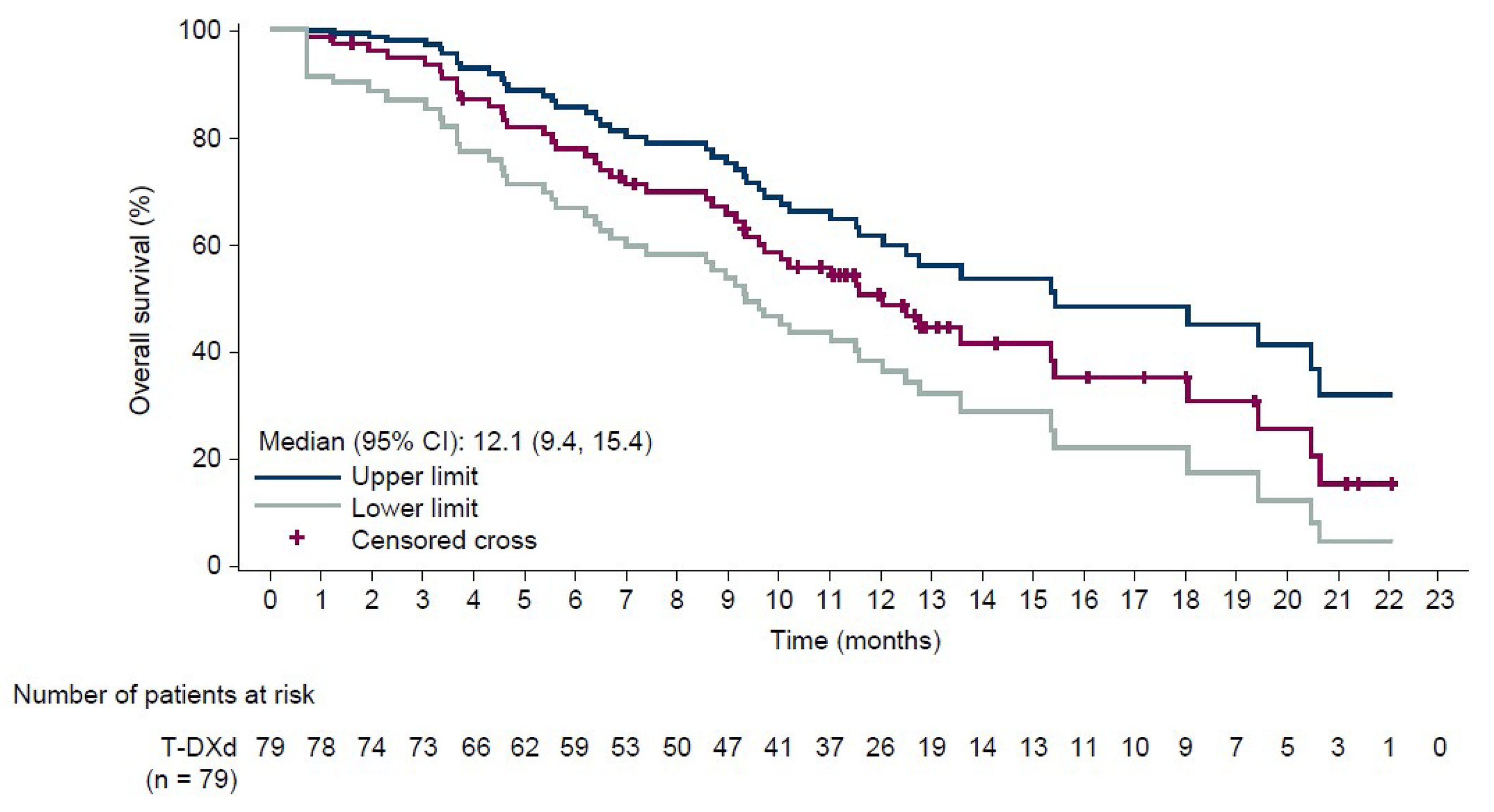
CI = confidence interval; FAS = full analysis set; KM = Kaplan-Meier; OS = overall survival; T-DXd = trastuzumab deruxtecan.
Sources: DESTINY-Gastric02 Clinical Study Report,32,33 Summary of Clinical Evidence.1
PFS per ICR Assessment
As of the data cut-off date of November 8, 2021, the proportion of patients in the FAS who had PFS events as determined by ICR was 64.6%. The median PFS was 5.6 months (95% CI, 4.2 months to 8.3 months). The probabilities of being progression-free were 70.5% (95% CI, 58.7% to 79.5%) at 3 months, 48.9% (95% CI, 36.6% to 60.2%) at 6 months, 36.3% (95% CI, 24.5% to 48.1%) at 9 months, and 20.0% (95% CI, 9.4% to 33.3%) at 12 months. The KM plot for PFS per ICR assessment is presented in Figure 2.
Figure 2: KM Plot of PFS per ICR Assessment in the DESTINY-Gastric02 Trial (FAS; Data Cut-Off Date: November 8, 2021)
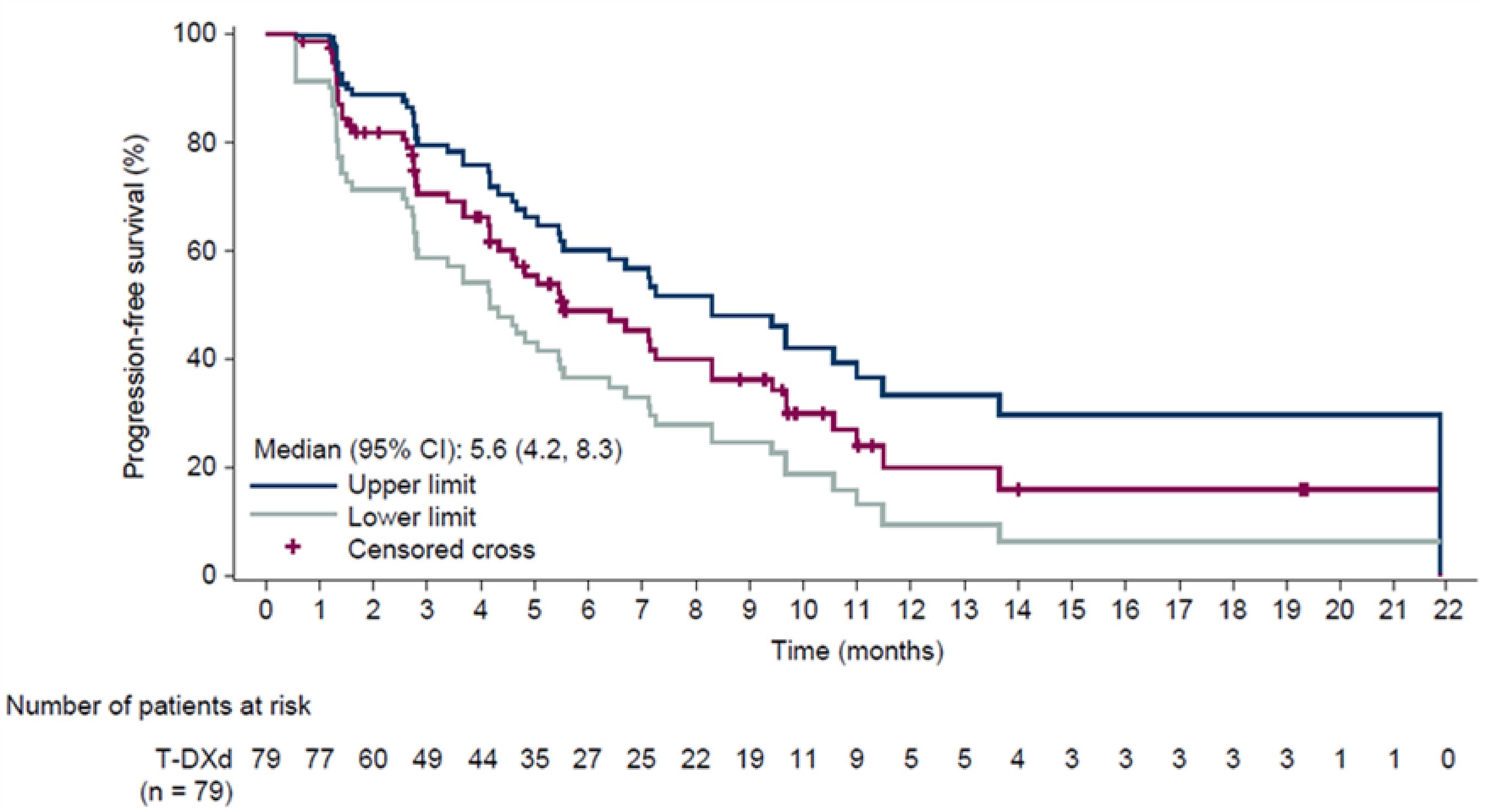
CI = confidence interval; FAS = full analysis set; ICR = independent central review; KM = Kaplan-Meier; PFS = progression-free survival; T-DXd = trastuzumab deruxtecan.
Sources: DESTINY-Gastric02 Clinical Study Report;32,33 Summary of Clinical Evidence.1
Confirmed ORR per ICR Assessment
As of November 8, 2021, the proportion of patients in the FAS who achieved confirmed ORR per ICR assessment was 41.8% (95% CI, 30.8 to 53.4). There were 4 patients (5.1%) who achieved a best overall response of confirmed CR, and 29 patients (36.7%) who achieved confirmed PR. The results of subgroup analyses on ORR were generally consistent with the results in the FAS.
FACT-Ga Total Score
The FACT-Ga total scores were based on the data as of April 9, 2021. A higher FACT-Ga total score indicates a better outcome.
The mean FACT-Ga total score at baseline was █████ ███ █ █████. The mean FACT-Ga total score at the end of treatment was █████ ███ █ █████, with a mean change of ██████ ███ █ ██████.
Harms
Harms data from the DESTINY-Gastric02 trial are shown in Table 20.
Treatment-Emergent AEs
The most commonly reported TEAE in the DESTINY-Gastric02 trial was nausea (67.1%), followed by fatigue (57.0%), vomiting (44.3%), and anemia (38.0%).
The proportion of patients who had any TEAE of grade 3 or higher was 55.7%. The most commonly reported TEAE of grade 3 or higher was anemia (13.9%), followed by neutropenia (12.7%).
Treatment-Emergent SAEs
The proportion of patients who had any TESAE was 41.8%. The most commonly reported TESAE was nausea (5.1%), followed by pneumonitis (3.8%) and vomiting (3.8%).
Treatment Discontinuation Due to TEAEs
The proportion of patients who discontinued trastuzumab deruxtecan was 19.0%. Discontinuation due to pneumonitis or ILD occurred in 7.6% and 2.5% of the trial population, respectively.
Mortality
As of the data cut-off date of November 8, 2021, the number of patients who had any TEAE associated with an outcome of death was 11 patients (13.9%), among whom 1 patient (1.3%) died due to ILD and 1 patient (1.3%) died due to pneumonitis.
Notable Harms
Interstitial Lung Disease
As of the data cut-off date of November 8, 2021, the proportion of patients who had ILD was ████%.
Infusion-Related Reaction
As of the data cut-off date of April 9, 2021, the proportion of patients who had IRR was ███%. No results were reported as of the data cut-off date of November 8, 2021.
LV Dysfunction
As of the data cut-off date of November 8, 2021, 10.5% of patients had a grade 2 LV dysfunction (defined as the resting LVEF ranges from 50% to 40%; and there is a 10% to 19% LVEF decrease from baseline).
QT Prolongation
QT prolongation was not reported in the DESTINY-Gastric02 trial.
Table 20: Summary of Harms Results in the DESTINY-Gastric02 Trial (Safety Analysis Set; Data Cut-Off Date: November 8, 2021)
Harms | Trastuzumab deruxtecan (N = 79) |
|---|---|
TEAE | |
Number of patients with any TEAE, n (%) | 79 (100.0) |
TEAEs (reported in ≥ 20% of patients), n (%) | |
Nausea | 53 (67.1) |
Fatigue | ██ ██████ |
Vomiting | 35 (44.3) |
Anemia | 30 (38.0) |
Diarrhea | 29 (36.7) |
Weight decrease | 28 (35.4) |
Decreased appetite | 26 (32.9) |
Constipation | 23 (29.1) |
Neutropenia | ██ ██████ |
Alopecia | 19 (24.1) |
Thrombocytopenia | ██ ██████ |
Abdominal pain | ██ █████ |
Number of patients with any TEAE of grade 3 or higher, n (%) | 44 (55.7) |
TEAEs of grade 3 or higher (reported in ≥ 10% of patients), n (%) | |
Anemia | 11 (13.9) |
Neutropenia | ██ ██████ |
TESAE | |
Number of patients with any TESAE, n (%) | 33 (41.8) |
TESAEs reported in ≥ 2% of patients, n (%) | |
Nausea | | █████ |
Pneumonitis | | █████ |
Vomiting | | █████ |
Abdominal pain | | █████ |
Acute kidney injury | | █████ |
COVID-19 | | █████ |
Disease progression | | █████ |
Malignant neoplasm progression | | █████ |
Pneumonia | | █████ |
Urinary tract infection | | █████ |
Treatment discontinuation due to TEAEs | |
Number of patients with ≥ 1 TEAE leading to study treatment discontinuation, n (%) | 15 (19.0) |
TEAE leading to study treatment discontinuation reported in ≥ 2% patients, n (%) | |
Pneumonitis | 6 (7.6) |
ILD | 2 (2.5) |
Death | |
Number of patients who had any TEAE associated with an outcome of death (%) | 11 (13.9) |
Reason for death, n (%) | |
Disease progression | 2 (2.5) |
COVID-19 | 2 (2.5) |
Malignant neoplasm progression | 2 (2.5) |
Cerebrovascular accident | 1 (1.3) |
ILD | 1 (1.3) |
Intestinal obstruction | 1 (1.3) |
Lymphangiosis carcinomatosa | 1 (1.3) |
Pneumonitis | 1 (1.3) |
Notable harms, n (%) | |
ILD | ██ ██████ |
IRRa | | █████ |
LV dysfunction (grade 2)b | | ██████ |
QT prolongation | NR |
ILD = interstitial lung disease; IRR = infusion-related reaction; LV = left ventricular; NR = not reported; TEAE = treatment-emergent adverse event; TESAE = treatment-emergent serious adverse event.
aAs of the data cut-off date of April 9, 2021.
bThe percentage was calculated using 57 as the denominator. This was the number of patients who had both baseline and postbaseline data.
Sources: Sponsor’s Summary of Clinical Evidence;1 DESTINY-Gastric02 Clinical Study Report.32,33
Critical Appraisal
Internal Validity
One phase II, single-arm clinical trial, the DESTINY-Gastric02 trial, was appraised by the CDA-AMC review team as the pivotal evidence to assess the second-line use of trastuzumab deruxtecan in patients who have unresectable or metastatic HER2-positive gastric or GEJ cancer.
Overall, the absence of an internal comparison group in the single-arm DESTINY-Gastric02 trial is a key limitation. Moreover, a comparison between the trastuzumab deruxtecan group in the DESTINY-Gastric02 trial and an external control (e.g., a target value or historical study control) was not available. The lack of comparative data prevents the demonstration of the advantage of trastuzumab deruxtecan over current therapies available in the second-line setting. Inferences about the efficacy and safety of trastuzumab deruxtecan are challenging to make and cannot be established with certainty.
The DESTINY-Gastric02 trial involved a small sample size of 72 patients. The sample size was calculated based on historical data that suggested that patients with gastric or GEJ cancer in Western countries have a best ORR of up to 27% in the second-line setting. According to the clinical experts consulted by the review team, the ORR of up to 27% used to calculate sample size was reasonable.
The selection of the primary efficacy end point, confirmed ORR (defined as the sum of CR or PR, as determined by ICR based on RECIST 1.1), was necessary for the single-arm DESTINY-Gastric02 trial from the regulatory perspective because ORR is considered by some regulatory bodies as a direct measure of a drug’s antitumour activity — an end point that can be assessed in a single-arm study.27 Of note, there was no a priori hypothesis with a target value of treatment effect prespecified for ORR to establish a clinically meaningful superiority threshold in the DESTINY-Gastric02 trial. Therefore, the significance of the findings is nominal; as such, the interpretation of the results is uncertain.
The DESTINY-Gastric02 trial addressed the limitation of relying solely on ORR by examining time-to-event end points, including OS, which was considered the most important efficacy outcome for the trial population by the clinical experts consulted by the review team. Although OS was included in the statistical analysis plan and controlled for multiplicity, this outcome can be sensitive to natural history and disease progression as well as to heterogeneity in patient characteristics; therefore, the inference of treatment efficacy based on the reported OS results in the absence of a comparator can be prone to bias.27-29
External Validity
The DESTINY-Gastric02 trial used trastuzumab deruxtecan in the second-line treatment setting for patients with HER2-positive gastric or GEJ cancer, which aligns with the treatment setting in the reimbursement request proposed by the sponsor. However, the indication currently under review by Health Canada is for patients with unresectable locally advanced or metastatic HER2-positive gastric GEJ adenocarcinoma who have received a prior trastuzumab-based regimen. The sponsor confirmed that the indication is not limited to patients in the second-line treatment setting but also includes patients in the third-line and later settings. The DESTINY-Gastric02 trial population does not completely align with the patients in the third-line and later settings described by the Health Canada indication. Consequently, results from the DESTINY-Gastric02 trial may not be generalizable to patients in the third-line setting and beyond; there remains a gap in evidence.
According to the clinical experts consulted by the review team, the eligibility criteria of the DESTINY-Gastric02 trial were generally aligned with the selection criteria in the Canadian setting when identifying eligible patients with HER2-positive gastric or GEJ cancer for the second-line use of trastuzumab deruxtecan.
GRADE Summary of Findings and Certainty of the Evidence
Methods for Assessing the Certainty of the Evidence
For the pivotal studies and RCTs identified in the sponsor’s systematic review, GRADE was used to assess the certainty of the evidence for the outcomes considered most relevant to inform the expert committee deliberations, and a final certainty rating was determined as outlined by the GRADE Working Group:30,31
High certainty — We are very confident that the true effect lies close to that of the estimate of the effect.
Moderate certainty — We are moderately confident in the effect estimate. The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. We use the word “likely” for evidence of moderate certainty (e.g., “X intervention likely results in Y outcome”).
Low certainty — Our confidence in the effect estimate is limited. The true effect may be substantially different from the estimate of the effect. We use the word “may” for evidence of low certainty (e.g., “X intervention may result in Y outcome”).
Very low certainty — We have very little confidence in the effect estimate. The true effect is likely to be substantially different from the estimate of effect. We describe evidence of very low certainty as “very uncertain.”
Although GRADE guidance is not available for noncomparative studies, the review team assessed the pivotal single-arm trials for study limitations (i.e., internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias to present these important considerations. Because the lack of a comparator arm does not allow for a conclusion to be drawn on the effect of the intervention versus any comparator, the certainty of evidence started at very low, with no opportunity for rating up.
When possible, certainty was rated in the context of the presence of an important (nontrivial) treatment effect; if this was not possible, certainty was rated in the context of the presence of any treatment effect (i.e., the clinical importance is unclear). In all cases, the target of the certainty of evidence assessment was based on the point estimate and its location relative to the threshold for a clinically important effect (when a threshold was available) or to the null.
Due to lack of comparators, certainty of evidence was summarized narratively for OS, PFS, ORR, FACT-Ga total score, and harms.
Results of GRADE Assessments
Table 2 presents the GRADE summary of findings for trastuzumab deruxtecan for the treatment of adult patients with unresectable or metastatic HER2-positive gastric or GEJ cancer who had disease progression during or after first-line therapy with a trastuzumab-containing regimen.
Long-Term Extension Studies
No long-term extension studies were submitted by the sponsor for this review.
Indirect Evidence
Contents within this section have been informed by materials submitted by the sponsor. The following information has been summarized and validated by the review team.
Objectives for the Summary of Indirect Evidence
The DESTINY-Gastric02 pivotal trial was a single-arm study. The efficacy of trastuzumab deruxtecan relative to other treatments that are currently available in the second-line setting in Canada is unclear. Therefore, an ITC is warranted to address this evidence gap.
Of note, according to the sponsor, although results of the DESTINY-Gastric01 trial were included in the systematic review section as pivotal evidence, it was not appropriate to include the DESTINY-Gastric01 trial in the ITC, given that this trial provided head-to-head comparisons between trastuzumab deruxtecan and physician’s choice of irinotecan or paclitaxel in a patient population that has already progressed through at least 2 lines of therapy (i.e., third-line and later settings).
Description of the ITC
The sponsor-submitted ITC included a Bayesian NMA in which an unanchored MAIC was used to establish a connection between the single-arm DESTINY-Gastric02 pivotal trial and the rest of the evidence network.
Of note, the NMA focused on comparisons between trastuzumab deruxtecan and ramucirumab-paclitaxel, docetaxel, paclitaxel monotherapy, irinotecan, and FOLFIRI. Although there were available studies in the literature investigating best supportive care, ramucirumab plus best supportive care, ramucirumab-FOLFIRI, and irinotecan-cisplatin, these studies were not included in the NMA for this reimbursement request because the sponsor considered these comparators irrelevant in the Canadian landscape. The sponsor also noted an exception for PEP02, which was not considered by the sponsor as a relevant comparator in Canada but was included in the NMA base-case analysis. The sponsor claimed that the inclusion would ensure all available evidence was incorporated within the NMA and enhance the robustness and credibility of the results.
ITC Design
Objectives
The NMA submitted by the sponsor aimed to answer the following review question: what is the comparative effectiveness of trastuzumab deruxtecan versus guideline-recommended, second-line treatments for advanced or metastatic gastric cancer, based on the currently available literature evidence?
Study Selection Methods
The criteria for study selection and methods for the ITC submitted by the sponsor are shown in Table 21. Relevant studies serving as an evidence base for the ITC were identified from 3 major sources, including a sponsor-conducted systematic literature review (SLR) in 2021, a grey literature search in 2022, and a targeted search between September 2021 and April 2024.
The SLR searches, performed initially in May 2020 and updated on September 9, 2021, were conducted in multiple electronic databases (i.e., MEDLINE, MEDLINE In-Process, Embase, and Cochrane Library), conference proceedings, and submissions to health technology assessment regulatory bodies.
To identify relevant single-arm trials, the grey literature search was carried out by searching the reference lists of the 2016 European Society for Medical Oncology (ESMO) and 2022 National Comprehensive Cancer Network (NCCN) guidelines as well as the records of Clinicaltrials.gov (performed in March 2022).
The targeted searches, which aimed to identify relevant long-term studies, subgroup analyses, and phase III studies, were conducted in MEDLINE, MEDLINE In-Process, Embase, and the reference lists of the updated 2022 ESMO and 2024 NCCN guidelines from September 2021 to April 2024.
Study screening and selection from the SLR were conducted by 2 independent reviewers. Potentially eligible studies selected from the SLR and the records retrieved from the grey literature search were further screened by 1 reviewer to determine eligibility for the NMA. Data extraction was carried out by 1 reviewer, with a second independent reviewer responsible for quality checks for the handsearch. The quality of the selected studies was also assessed by 2 independent reviewers using version 2 of the Cochrane risk-of-bias tool. Any disputes between reviewers were resolved by a third independent reviewer.
Table 21: Study Selection Criteria and Methods for the ITC Submitted by the Sponsor
Characteristics | Indirect comparison |
|---|---|
Population | Adult (aged ≥ 18 years) patients with advanced or metastatic gastric or GEJ cancer who have received at least 1 previous treatment |
Intervention | Trastuzumab deruxtecan 6.4 mg/kg every 3 weeks until disease progression |
Comparator |
|
Outcome |
|
Study designs | Clinical trials (RCTs and single-arm trials) |
Publication characteristics | Publications in the English language |
Exclusion criteria | Population:
Interventions and outcomes:
Study designs
Publication types
Languages
|
Databases searched |
|
Selection process | All records identified from the SLR were screened based on a review of the title and abstract by 2 independent reviewers, then further screened and selected based on the full texts by 2 independent reviewers. Any disagreements were resolved through discussion with a third reviewer. A single reviewer then assessed the studies selected from the SLR and the records from the grey literature search to determine the included studies for the NMA. |
Data extraction process |
|
Quality assessment | Version 2 of the Cochrane risk-of-bias tool for randomized trials was used to assess the quality of the full-text articles associated with the RCTs. Judgments were largely summarized as “low” or “high” risk of bias, though these could also be expressed as “high” or “some concerns.” |
ESMO = European Society for Medical Oncology; FOLFIRI = folinic acid–fluorouracil-irinotecan; GEJ = gastroesophageal junction; HTA = health technology assessment; ITC = indirect treatment comparison; KM = Kaplan-Meier; NCCN = National Comprehensive Cancer Network; NMA = network meta-analysis; OS = overall survival; PFS = progression-free survival; RCT = randomized controlled trial; SLR = systematic literature review.
Sources: Sponsor’s Summary of Clinical Evidence;1 sponsor-submitted ITC report.43
ITC Analysis Methods
Unanchored MAIC Analysis Methods
The single-arm DESTINY-Gastric02 pivotal trial was the only eligible study containing the intervention of interest for this reimbursement request (trastuzumab deruxtecan). To include trastuzumab deruxtecan in the NMA, the sponsor used an unanchored MAIC to connect the treatment to the network.
The details regarding the analysis methods of the unanchored MAIC are shown in Table 22.
Table 22: Unanchored MAIC Analysis Methods
Methods | Description |
|---|---|
Analysis methods | An unanchored MAIC was used to align with NICE DSU TSD 18.53 The outcomes of interest included in the MAIC were PFS and OS. The unanchored MAIC used IPD from the sponsor’s trial (i.e., the DESTINY-Gastric02 trial in this setting) and aggregate data for the comparator group from the competitor’s trial (e.g., published studies). Relevant baseline characteristics from the sponsor’s trial were reweighted to exactly match those in the target population in the comparator trial. The propensity score weights were estimated under a logistic regression model in which a weight assigned to an individual represents the odds of being included in the comparator trial. |
Selection of comparator trial | Among 5 studies in the NMA evidence network — including RAINBOW,54 KCSG ST10-01,55 Sym et al. (2013),56 WJOG 4007,57 and Roy et al. (2013)58 — the RAINBOW trial was selected by the sponsor to serve as the comparator trial against the DESTINY-Gastric02 pivotal trial in the unanchored MAIC. The sponsor claimed that the KCSG ST10-01 trial, Sym et al. (2013), and the WJOG 4007 trial were not appropriate to serve in the MAIC because these trials focused on Asian populations and did not align with the population investigated in the DESTINY-Gastric02 trial, whose participants were from Europe and the US. According to the sponsor, Asian versus Western ethnicity is a main prognostic factor for gastric cancer, and it is more reasonable to conduct the unanchored MAIC in the population with the same ethnicity (e.g., in the DESTINY-Gastric02 trial). Roy et al. (2013) was also considered inappropriate for the MAIC by the sponsor because it reported limited baseline characteristics that did not allow adequate adjustment for the treatment effect modifiers and prognostic factors in the unanchored MAIC. |
Preliminary steps | 1. IPD from the DESTINY-Gastric02 trial were used to select only the participants treated with trastuzumab deruxtecan who could have been included in the competitor’s trial (i.e., the RAINBOW trial).
2. Baseline descriptive statistics from the restricted trastuzumab deruxtecan group and the competitor’s treatment group were generated and compared to assess imbalances between populations.
|
Implementation steps | The weights for participants enrolled in the trastuzumab deruxtecan group were calculated to match those reported in the treatment group of the competitor’s trial (i.e., the RAINBOW trial). Each patient’s weight equalled their estimated odds of enrolment in the DESTINY-Gastric02 trial versus the competitor’s trial. All prognostic factors and treatment effect modifiers were considered as potential adjustment variables. A comparison between the baseline characteristics of the trastuzumab deruxtecan group and each relevant group of the comparator trial was reported. The weights reported for each individual patient treated with trastuzumab deruxtecan were the log odds for each patient to be included in the trastuzumab deruxtecan group versus the relevant group of the comparator trial: 𝑙𝑜𝑔(𝑤𝑖) = 𝛼₀+ 𝛼₁𝛸𝑖 in which 𝛸𝑖 is the covariate vector for the i-th patient in the trastuzumab deruxtecan group and 𝑤𝑖 is the weight attributed to the i-th patient treated with trastuzumab deruxtecan. The method of moments was used to estimate the regression parameters so that the weights balance the mean characteristics between the reweighted trastuzumab deruxtecan population and the relevant group of the comparator trial. |
Validation of the MAIC | The distribution of weights was inspected to detect overly influential individuals and study the populations’ overlap. The ESS was estimated as an indicator of the quality of the weighting process. It was additionally used to detect whether few individuals were driving the results due to influential weights. In general, if the ESS was substantially reduced, the initial set of adjustment variables was revisited and modified (if possible). The ESS was calculated as:
Descriptive statistics were generated from the competitor’s trial baseline characteristics and the reweighted characteristics of the trastuzumab deruxtecan group and compared to assess whether the previously observed imbalances between populations were reduced by the weighting process. |
Conducted MAICs | Cox model59 HRs of time-to-event outcomes were calculated using the weights estimated in the MAIC for the trastuzumab deruxtecan group and reconstructed IPD for the treatment group of the RAINBOW trial based on KM curves using the Guyot algorithm.60 MAIC outputs included PFS and OS HRs and associated 95% CIs. |
 in which 𝑤𝑖 is the weight attributed to the i-th patient treated with trastuzumab deruxtecan.
in which 𝑤𝑖 is the weight attributed to the i-th patient treated with trastuzumab deruxtecan.CI = confidence interval; ESS = effective sample size; HR = hazard ratio; IPD = individual patient data; ITC = indirect treatment comparison; KM = Kaplan-Meier; MAIC = matching-adjusted indirect comparison; NICE DSU TSD = National Institute for Health and Care Excellence Decision Support Unit Technical Support Document; NMA = network meta-analysis; OS = overall survival; PFS = progression-free survival.
Sources: Sponsor’s Summary of Clinical Evidence;1 sponsor-submitted ITC report.43
NMA Analysis Methods
After the MAIC of DESTINY-Gastroic02 and the RAINBOW trial were completed, a hypothetical population including the RAINBOW trial and the reweighted trastuzumab deruxtecan groups was connected to the existing network of interventions to perform a Bayesian NMA. The details of the NMA analysis methods are shown in Table 23.
Table 23: NMA Analysis Methods
Methods | Description |
|---|---|
Analysis methods | The Bayesian NMAs used MCMC to estimate the posterior distribution of the OS and PFS HRs, in accordance with NICE DSU TSDs 2 and 3.61,62 Both FE and RE models were fit. |
Priors | Vague or uninformative prior distributions were adopted. Following the recommendations from the NICE DSU TSD 2,62 a normal distribution with a mean of 0 and variance of 10,000 was assumed for the treatment effect difference and nuisance parameters, and a uniform distribution (0 to 5) was assumed for the SD of the between-trial heterogeneity parameter. No sensitivity analyses were conducted to assess the impact of the selected priors. |
Assessment of model fit | Given the geometry of the constructed networks (i.e., sparse treatment comparisons, usually 1 or 2 trials informing them), it was anticipated that the RE models would not provide a good fit to the data; thus, the FE results are considered as final outputs. |
Assessment of consistency | For the analyses, a closed loop was present in the network. Therefore, loop-specific inconsistency checks were additionally performed using the Bucher method.63 |
Assessment of convergence | The parameters of the FE and RE models were estimated using an MCMC implemented in WinBUGS V1.4. In the FE analyses, a series of 20,000 iterations were discarded as “burn-in,” and the inferences were based on a subsequent 20,000 iterations (3 chains). In the RE analyses, 100,000 iterations were used as burn-in and 100,000 for parameters’ inference. Convergence was confirmed by evaluating the 3 chains and visually inspecting Brooks-Gelman-Rubin plots.64 |
Outcomes’ likelihood and statistical assumptions | Time-to-event outcomes, including PFS and OS, were considered in the NMA; the logarithm of the HR was modelled assuming normal likelihood. |
Outputs | The output of the Bayesian NMA is a posterior distribution of all relative treatment effects between the treatments forming the network of evidence. The posterior distribution per relative treatment effect is summarized by a median as well as the 2.5th and 97.5th percentiles, which constitute a 95% CrI. |
Construction of nodes | No assumption was made to create the nodes. |
Base-case analysis | Trastuzumab deruxtecan was linked to the NMA network through an unanchored MAIC comparing it to the ramucirumab plus paclitaxel arm of the RAINBOW trial using the November 2021 data cut-off for the DESTINY-Gastric02 pivotal trial. |
Sensitivity analyses | The following sensitivity analyses were performed:
Both the FE and RE models were fitted and compared for each sensitivity analysis. |
Methods for pairwise meta-analysis | To assess the potential heterogeneity in pairwise treatment comparisons informed by more than 1 trial was assessed by performing FE and RE meta-analyses of direct evidence. |
CrI = credible interval; FE = fixed effect; HR = hazard ratio; ITC = indirect treatment comparison; MAIC = matching-adjusted indirect comparison; MCMC = Markov chain Monte Carlo; NICE DSU TSD = National Institute for Health and Care Excellence Decision Support Unit Technical Support Document; NMA = network meta-analysis; OS = overall survival; PFS = progression-free survival; RE = random effect; SD = standard deviation.
Sources: Sponsor’s Summary of Clinical Evidence;1 sponsor-submitted ITC report.43
In the unanchored MAIC, 5 treatment effect modifiers or prognostic factors, including age, gender, previous surgery, ECOG PS, and primary tumour location, were included as adjustment variables. The list of treatment effect modifiers or prognostic factors adjusted or not adjusted in the unanchored MAIC is presented in Table 24.
Table 24: List of Treatment Effect Modifiers and Prognostic Factors for the Unanchored MAIC
Treatment effect modifiers or prognostic factors | Details |
|---|---|
Factors adjusted | |
Age | Adjustment made on proportion of patients younger than 65 years |
Sex | Adjustment made on proportion of male patients |
Previous surgery | Adjustment made on proportion of patients with prior gastric cancer surgery |
ECOG PS (≥ 1 versus 0) | Adjustment made on proportion of patients with ECOG PS of 0 |
Primary tumour location (GEJ versus gastric) | Adjustment made on proportion of patients with gastric location |
Factors not adjusted | |
Number of metastatic sites | Rationale for nonadjustment: Approach was too restrictive, resulting in a very small ESS |
Time to progressive disease on first-line therapy (≥ 6 months versus < 6 months) | Rationale for nonadjustment: Approach was too restrictive, resulting in a very small ESS |
Presence of metastases (yes versus no) | Rationale for nonadjustment: Not available in the RAINBOW trial |
HER2 expression (high versus low) | Rationale for nonadjustment: Not available in the RAINBOW trial |
Geographical region | Rationale for nonadjustment: Not available in the RAINBOW trial |
PD-L1 combined positive score (patients with a score of ≥ 10 versus all patients) | Rationale for nonadjustment: Not available in the DESTINY-Gastric02 trial |
Disease measurability (measurable versus nonmeasurable) | Rationale for nonadjustment: Not available in the DESTINY-Gastric02 trial |
Previous weight loss (< 10% versus ≥ 10%) | Rationale for nonadjustment: Not available in the DESTINY-Gastric02 trial |
Peritoneal metastases (no versus yes) | Rationale for nonadjustment: Not available in the DESTINY-Gastric02 trial |
Ethnicity (Western versus Asian) | Rationale for nonadjustment: Both studies were conducted in Western populations |
Histological subtype (diffuse versus intestinal) | Rationale for nonadjustment: Only 1 patient had a diffuse histological subtype in the DESTINY-Gastric02 trial |
ECOG PS = Eastern Cooperative Oncology Group Performance Status; ESS = effective sample size; GEJ = gastroesophageal junction; HER2 = human epidermal growth factor 2; ITC = indirect treatment comparison; PD-L1 = programmed death-ligand 1.
Source: Sponsor-submitted ITC report.43
The distribution of baseline characteristics before and after weighting adjustment is shown in Table 25. The ESS of the weighted trastuzumab deruxtecan group was ████, reduced from ██ before weighting.
Table 25: Baseline Characteristics Before and After Weighting Adjustment in the Unanchored MAIC
Treatment effect modifiers or prognostic factors | Characteristics | Before adjustment | After adjustment | |
|---|---|---|---|---|
Ramucirumab-paclitaxel in the RAINBOW trial (N = 198), n (%) | Trastuzumab deruxtecan in the DESTINY-Gastric02 trial (N = 77a), n (%) | Trastuzumab deruxtecan (ESS = ████), % | ||
Age | < 65 years | 123 (62.1) | 45 (58.4) | 62.1 |
Sex | Male | 140 (70.7) | 55 (71.4) | 70.7 |
Previous surgery | Yes | 70 (35.4) | 21 (27.3) | 35.4 |
ECOG PS | ECOG PS of 0 | 68 (34.3) | 28 (36.4) | 34.3 |
ECOG PS of 1 | 130 (65.7) | 49 (63.6) | 65.7 | |
Primary tumour location | Gastric | 139 (70.2) | 26 (33.8) | 70.2 |
GEJ | 59 (29.8) | 51 (66.2) | 29.8 | |
Number of metastatic sites | 0 to 2 | 110 (55.6) | 15 (19.5) | 26.8 |
≥ 3 | 88 (44.4) | 62 (80.5) | 73.2 | |
Time to progressive disease on first-line therapy | ≥ 6 months | 72 (36.4) | 56 (72.7) | 84.3 |
Presence of metastases | Yes | 88 (44.9) | NR | NA |
HER2 expression | HER2-positive | NR | 77 (100) | 100 |
Geographical region | Europe | NR | 44 (57.1) | 57.7 |
US | NR | 33 (42.9) | 42.3 | |
PD-L1 combined positive score | Patients with a score ≥ 10 | NR | NR | NA |
Disease measurability | Measurable | 164 (82.8) | NR | NA |
Previous weight loss | < 10% | 168 (84.8) | NR | NA |
≥ 10% | 30 (15.2) | NR | NA | |
Peritoneal metastases | Yes | 89 (44.9) | NR | NA |
Ethnicity | Western | 198 (100) | 77 (100) | 100 |
Histological subtype | Intestinal | 92 (46.5) | 18 (23.4) | 33.1 |
Diffuse | 62 (31.3) | 1 (1.3) | 0.6 | |
Unknown | 44 (22.2) | 58 (75.3) | 66.3 | |
ECOG PS = Eastern Cooperative Oncology Group Performance Status; ESS = effective sample size; FAS = full analysis set; GEJ = gastroesophageal junction; HER2 = human epidermal growth factor 2; ITC = indirect treatment comparison; MAIC = matching-adjusted indirect comparison; NA = not applicable; NR = not reported; PD-L1 = programmed death-ligand 1.
Note: Because of data privacy issues, the FAS population comprising 79 patients in the DESTINY-Gastric02 trial was reduced to 77.
Source: Sponsor-submitted ITC report.43
Results of the ITC
Summary of Studies Included in the NMA
In total, 6 studies were included in the NMA, including the DESTINY-Gastric02 pivotal trial,32,33 the RAINBOW trial,54 the KCSG ST10-01 trial,55 the Sym et al. (2013) trial,56 the WJOG 4007 trial,57 and the Roy et al. (2013) trial.58 According to the ITC report submitted by the sponsor, these included trials assessed the second-line use of treatments. These studies investigated trastuzumab deruxtecan, ramucirumab-paclitaxel, docetaxel, paclitaxel monotherapy, irinotecan, and FOLFIRI, which were considered by the sponsor as relevant therapies in Canada. The characteristics of the 6 included studies are presented in Table 26.
Table 26: Characteristics of Studies Included in the Sponsor-Submitted NMA
Studies included in NMA | Trial design | Intervention and comparator (N) | Median follow-up durations | Definitions of OS and PFS |
|---|---|---|---|---|
DESTINY-Gastric02 trial33 | Phase II, single-arm, open-label, multicentre trial |
| 10.2 months |
|
KCSG ST10-01 trial55 | Phase III, randomized, parallel-assignment, open-label, multicentre trial |
| NR |
|
WJOG 4007 trial57 | Phase III, randomized, parallel-assignment, open-label, multicentre trial |
| 17.6 months |
|
RAINBOW trial54 | Phase III, randomized, parallel-assignment, double-blind, multicentre trial |
| 7.9 months |
|
Sym et al. (2013) trial56 | Phase II, randomized, parallel-assignment, open-label, multicentre trial |
| NR |
|
Roy et al. (2013) trial58 | Phase II, randomized, parallel-assignment, open-label, multicentre trial |
| NR |
|
FOLFIRI = folinic acid–fluorouracil-irinotecan; ITC = indirect treatment comparison; NMA = network meta-analysis; NR = not reported; OS = overall survival; PFS = progression-free survival; RECIST 1.1 = Response Evaluation Criteria in Solid Tumours Version 1.1.
Source: Sponsor-submitted ITC report.43
In terms of risk of bias, the sponsor claimed that the majority of studies included in the NMA were of low risk; this conclusion was determined by using version 2 of the Cochrane risk-of-bias tool for randomized trials.65 According to the sponsor, the majority of included studies were at low risk of bias. The Sym et al. (2013) trial failed to meet its primary end point; therefore, risk-of-bias assessment was not performed for this trial.
The assessment of homogeneity in the sponsor-submitted ITC is shown in Table 27.
Table 27: Assessment of Homogeneity in the Sponsor-Submitted ITC
Characteristics | Description and handling of potential treatment effect modifiers and prognostic factors |
|---|---|
Treatment history |
|
HER2 status |
|
Trial eligibility criteria |
|
Patient characteristicsa |
|
Dosages of comparators | There were some differences in the treatment regimens among the comparators. For example, 2 irinotecan studies had varying dosage regimens: the Sym et al. (2013) trial had irinotecan IV infusion every 2 weeks at a dose of 150 mg/m2, while the Roy et al. (2013) trial used irinotecan IV infusion every 3 weeks at a dose of 300 mg/m2 until progression or unacceptable toxicity as well as docetaxel IV infusion every 3 weeks at a dose of 75 mg/m2 until progression or unacceptable toxicity. |
Study design | Among the 6 studies included in the NMA, 3 studies were phase II trials, including the DESTINY-Gastric02, Sym et al. (2013), and Roy et al. (2013) trials. The remaining 3 were phase III trials. All 6 were RCTs with a parallel treatment assignment except for the DESTINY-Gastric02 trial, which was a single-arm trial. All 6 trials were open-label, except for the RAINBOW trial, which was double-blinded. All 6 trials were multicentre, except for the Sym et al. (2013) trial, which was conducted in a single centre in South Korea. |
GEJ = gastroesophageal junction; HER2 = human epidermal growth factor receptor 2; ITC = indirect treatment comparison; NMA = network meta-analysis; RCT = randomized controlled trial.
aUnless specified otherwise, the values reported for patient characteristics were summarized from 12 studies identified in the SLR, including 6 studies analyzed in this sponsor-submitted NMA and 6 studies that were not analyzed in the NMA because the interventions used were considered by the sponsor to be irrelevant to the Canadian setting.
Sources: Sponsor’s Summary of Clinical Evidence;1 sponsor-submitted ITC report.43
Results
The NMA base-case network diagram is the same for OS and PFS and is presented in Figure 3.
Figure 3: Network Diagram for the Sponsor-Submitted NMA (OS and PFS, Base-Case Analysis)
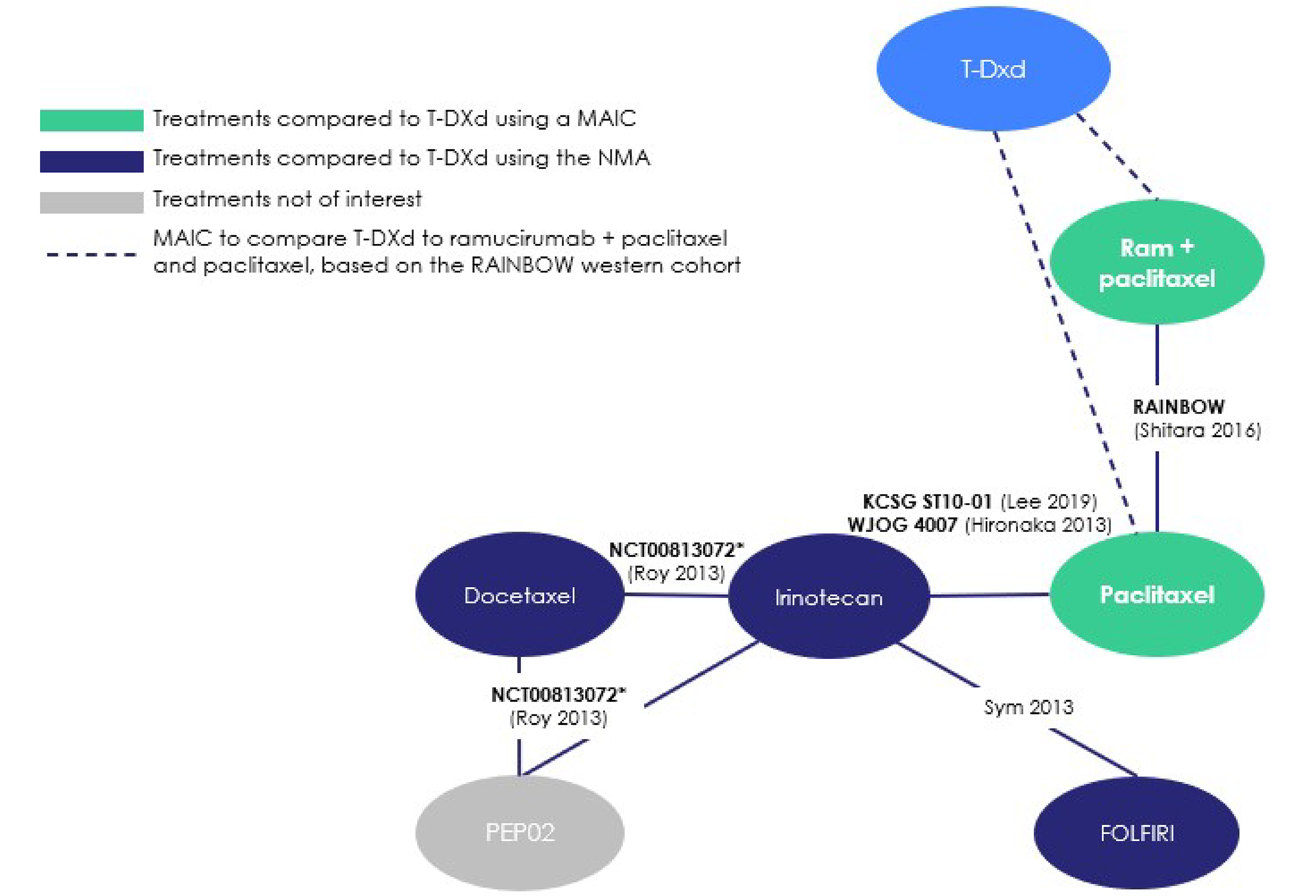
FOLFIRI = folinic acid–fluorouracil-irinotecan; ITC = indirect treatment comparison; MAIC = matching-adjusted indirect comparison; NMA = network meta-analysis; OS = overall survival; PFS = progression-free survival; Ram = ramucirumab; T-DXd = trastuzumab deruxtecan.
Sources: Sponsor’s Summary of Clinical Evidence;1 sponsor-submitted ITC report.43
The summary of the results for OS and PFS in the base-case analyses and sensitivity analyses is shown in Table 28. In the base-case analysis, trastuzumab deruxtecan was linked to the NMA network through an unanchored MAIC comparing it to the ramucirumab plus paclitaxel arm of the RAINBOW trial using the November 2021 data cut-off in the DESTINY-Gastric02 pivotal trial. In sensitivity analysis 1, trastuzumab deruxtecan was linked to the NMA network through a MAIC connecting it to the RAINBOW trial using the April 2021 data cut-off in the DESTINY-Gastric02 trial. In sensitivity analysis 2, the PEP02 arm from the Roy et al. (2013) trial was removed from the network.
Of note, according to the sponsor, the reweighted population of the DESTINY-Gastric02 trial via MAIC was considered as a third arm to the competitor’s trial (i.e., the RAINBOW trial) by using the initial HR of the RAINBOW trial (i.e., ramucirumab-paclitaxel versus placebo-paclitaxel) and the HR between trastuzumab deruxtecan and ramucirumab-paclitaxel, which was calculated through the unanchored MAIC.
Overall Survival
Generated from the MAIC, the HR for OS was ████ ████ ████ ████ ██ █████ between trastuzumab deruxtecan and ramucirumab-paclitaxel.
In the FE model of the NMA, the estimated base-case HRs for OS were ████ ████ ████ ████ ██ █████ between trastuzumab deruxtecan and paclitaxel, ████ ████ ████ ████ ██ █████ between trastuzumab deruxtecan and FOLFIRI, ████ ████ ████ ████ ██ █████ between trastuzumab deruxtecan and irinotecan, and ████ ████ ████ ████ ██ █████ between trastuzumab deruxtecan and docetaxel.
In the RE model of the NMA, the estimated HRs for OS were ████ ████ ████ ████ ██ ██████ between trastuzumab deruxtecan and ramucirumab-paclitaxel, ████ ████ ████ ████ ██ ██████ between trastuzumab deruxtecan and paclitaxel, ███ ████ ████ █ ██ ███████ between trastuzumab deruxtecan and FOLFIRI, ████ ████ ████ █ ██ ██████ between trastuzumab deruxtecan and irinotecan, and ████ ████ ████ █ ██ ███████ between trastuzumab deruxtecan and docetaxel.
In both sensitivity analyses, the HR estimates for OS obtained from the FE model were generally consistent with the results from the base-case analysis.
Progression-Free Survival
Generated from the MAIC, the HR for PFS was ████ ████ ████ ████ ██ █████ between trastuzumab deruxtecan and ramucirumab-paclitaxel.
In the FE model of the NMA, the estimated base-case HRs for PFS were ████ ████ ████ ████ ██ █████ between trastuzumab deruxtecan and paclitaxel | ████ ████ ████ ████ ██ █████ between trastuzumab deruxtecan and FOLFIRI, ████ ████ ████ ████ ██ █████ between trastuzumab deruxtecan and irinotecan, and ████ ████ ████ ████ ██ █████ between trastuzumab deruxtecan and docetaxel.
In the RE model of the NMA, the estimated base-case HRs for PFS were ████ ████ ████ ████ ██ ██████ between trastuzumab deruxtecan and ramucirumab-paclitaxel, ████ ████ ████ ████ ██ ██████ between trastuzumab deruxtecan and paclitaxel, ████ ████ ████ ████ ██ ███████ between trastuzumab deruxtecan and FOLFIRI, ████ ████ ████ ████ ██ ██████ between trastuzumab deruxtecan and irinotecan, and ████ ████ ████ ████ ██ ███████ between trastuzumab deruxtecan and docetaxel.
In both sensitivity analyses, the HR estimates for PFS obtained from the FE model were consistent with the results from the base-case analysis for PFS except that the HR between trastuzumab deruxtecan and ramucirumab-paclitaxel was no longer statistically significant.
Table 28: Summary of Results of the Sponsor-Submitted NMA
Analysis (model) | Comparison | OS HR (95% CrI) | PFS HR (95% CrI) |
|---|---|---|---|
Base case (FE model) | Trastuzumab deruxtecan versus ramucirumab-paclitaxel | ████ █████ ██ █████ | ████ █████ ██ █████ |
Trastuzumab deruxtecan versus paclitaxel | ████ █████ ██ █████ | ████ █████ ██ █████ | |
Trastuzumab deruxtecan versus FOLFIRI | ████ █████ ██ █████ | ████ █████ ██ █████ | |
Trastuzumab deruxtecan versus irinotecan | ████ █████ ██ █████ | ████ █████ ██ █████ | |
Trastuzumab deruxtecan versus docetaxel | ████ █████ ██ █████ | ████ █████ ██ █████ | |
Sensitivity analysis 1 (FE model) | Trastuzumab deruxtecan versus ramucirumab-paclitaxel | ████ █████ ██ █████ | ████ █████ ██ █████ |
Trastuzumab deruxtecan versus paclitaxel | ████ █████ ██ █████ | ████ █████ ██ █████ | |
Trastuzumab deruxtecan versus FOLFIRI | ████ █████ ██ █████ | ████ █████ ██ █████ | |
Trastuzumab deruxtecan versus irinotecan | ████ █████ ██ █████ | ████ █████ ██ █████ | |
Trastuzumab deruxtecan versus docetaxel | ████ █████ ██ █████ | ████ █████ ██ █████ | |
Sensitivity analysis 2 (NR) | Trastuzumab deruxtecan versus ramucirumab-paclitaxel | ████ █████ ██ █████ | ████ █████ ██ █████ |
Trastuzumab deruxtecan versus paclitaxel | ████ █████ ██ █████ | ████ █████ ██ █████ | |
Trastuzumab deruxtecan versus FOLFIRI | ████ █████ ██ █████ | ████ █████ ██ █████ | |
Trastuzumab deruxtecan versus irinotecan | ████ █████ ██ █████ | ████ █████ ██ █████ |
CrI = credible interval; FE = fixed effect; FOLFIRI = folinic acid–fluorouracil-irinotecan; HR = hazard ratio; ITC = indirect treatment comparison; MAIC = matching-adjusted indirect comparison; NMA = network meta-analysis; NR = not reported; OS = overall survival; PFS = progression-free survival.
Note: In sensitivity analysis 1, trastuzumab deruxtecan was connected to the NMA network through an unanchored MAIC comparing it to the ramucirumab plus paclitaxel arm of the RAINBOW trial using data from the DESTINY-Gastric02 trial as of the April 2021 cut-off. This sensitivity analysis aimed to assess the impact of the data cut-off change. Sensitivity analysis 2 removed the PEP02 arm from the Roy et al. (2013) trial. This sensitivity analysis aimed to assess the impact of PEP02.
Sources: Sponsor’s Summary of Clinical Evidence;1 sponsor-submitted ITC report.43
Critical Appraisal of Sponsor-Submitted ITC
In the absence of direct evidence comparing trastuzumab deruxtecan to other second-line treatments currently available in Canada (i.e., ramucirumab-paclitaxel, paclitaxel, FOLFIRI, irinotecan, and docetaxel), an ITC was submitted by the sponsor. The clinical experts consulted by the review team noted that the selection of the comparators was appropriate and reflective of clinical practice in Canada. The sponsor-submitted ITC comprised 2 components: an unanchored MAIC and an NMA. The unanchored MAIC was used to connect the single-arm, pivotal DESTINY-Gastric02 trial into the evidence network of the NMA using the RAINBOW trial as a comparator. The relative treatment effect estimates between trastuzumab deruxtecan and ramucirumab-paclitaxel were generated based on this unanchored MAIC.
A typical unanchored MAIC involves an index trial for which the individual patient data are available and a comparator trial for which aggregate-level data are available. In the sponsor-conducted MAIC, the pivotal, single-arm DESTINY-Gastric02 trial served as the index trial, and the RAINBOW trial served as the comparator trial. Through the MAIC, the comparison was established between the cohort of patients treated with trastuzumab deruxtecan in the DESTINY-Gastric02 trial and the cohort of patients treated with ramucirumab-paclitaxel in the RAINBOW trial. To ensure the comparability of these 2 cohorts in terms of patient characteristics considered to be potential treatment effect modifiers or prognostic factors, a propensity score weighting approach adjusted for these patient characteristics.
There are concerns regarding patient comparability between the DESTINY-Gastric02 trial and the RAINBOW trial. First, there were differences in some of the important patient characteristics (e.g., HER2 status, time on first treatment) that were not involved in the weighting process due to lack of information or insufficient sample size. The RAINBOW trial did not report HER2 status, stating only that “up to 9% of the trial population received prior targeted therapies including anti-HER2, antiepidermal growth factor receptor, or other targeted therapies.” Currently, although HER2 positivity seems to be correlated with poor prognosis in gastric cancer, there is conflicting evidence for the prognostic role of HER2 in gastric cancer.17-21 With HER2 status unavailable in the RAINBOW trial, there is increased uncertainty about the treatment effect estimates between trastuzumab deruxtecan and ramucirumab-paclitaxel, and the direction of bias is unclear. Second, a list containing more than 16 potential prognostic factors and treatment effect modifiers was prespecified by the sponsor. These were considered relevant and comprehensive by the clinical experts consulted by the review team. However, only 5 of these factors were involved in the propensity score weighting. The rationale for not including the remaining factors is reasonable, given that the information was unavailable in either the DESTINY-Gastric02 trial or the RAINBOW trial. However, the exclusion of potentially relevant factors from the analysis could bias the results, with the magnitude of the residual bias in the relative treatment effect estimates remaining uncertain. Third, after reweighting, apparent differences were identified between the DESTINY-Gastric02 trial and the RAINBOW trial in some patient characteristics, such as time to progressive disease on first-line therapy, histological subtype, and number of metastases sites. These differences suggest the possible existence of inadequate balance and increase the uncertainty of the findings.
ESS is heuristically used to reflect the amount of heterogeneity between studies among the variables included in the weighting process. There was a marked reduction from ██ (i.e., the actual number of patients involved in the reweighting process from the DESTINY-Gastric02 trial) to ████ (i.e., the ESS of the DESTINY-Gastric02 trial after reweighting), indicating that the weights might be highly variable due to a lack of population overlap and that the treatment effect estimates yielded using the MAIC approach might be unstable. Moreover, the MAIC excluded time to progressive disease on first-line therapy from the weighting process because it would have made the ESS very small. This suggests post hoc selection of prognostic factors or treatment effect modifiers, which is inappropriate given that prognostic factors and treatment effect modifiers should be selected before analysis. Excluding a relevant factor from the weighting process would increase the risk of producing biased treatment effect estimates.
There was significant design and methodological heterogeneity between the DESTINY-Gastric02 and RAINBOW trials. The DESTINY-Gastric02 trial was a phase II, single-arm, open-label study without a hypothesis specified a priori or a statistical test, whereas the RAINBOW trial was a phase III, double-blind, randomized, active-controlled trial with formal hypothesis testing. The MAIC approach can correct only for bias directly related to differences in baseline patient characteristics, not for heterogeneity caused by between-trial differences in study design or methods. Therefore, uncertainty exists in the MAIC results; the exact impacts remain unclear based on the currently available information submitted by the sponsor. Due to the weighting process, the results of the MAIC are specific to the baseline characteristics of the population of the comparator trial (i.e., the RAINBOW trial). Consequently, there was uncertainty with respect to generalizing the MAIC results to the target population described in the Health Canada indication and reimbursement request. For instance, the indicated population requires eligible patients to be HER2-positive, whereas HER2 status in the population of the RAINBOW trial is unknown. Additionally, the indicated population requires eligible patients to have received a prior trastuzumab-based regimen, while the RAINBOW trial required the study population to have received first-line platinum and fluoropyrimidine doublet with or without anthracycline.
The treatment effect estimates from the MAIC analyses served as the basis for generating the NMA that includes the DESTINY-Gastric02 trial connected to the evidence network of relative treatment effect estimates between trastuzumab deruxtecan and other relevant comparators, including paclitaxel, FOLFIRI, irinotecan, and docetaxel. This means all the potential limitations of the MAIC analyses discussed previously apply to the NMA results. On top of the sources of heterogeneity existing in the MAIC analyses, additional sources of heterogeneity might have introduced uncertainty to the NMA estimates. For instance, in the MAIC, the sponsor assumed that geographical region and ethnicity were important prognostic factors and that Asian patients had better prognoses than patients from Western countries. Subsequently, to limit the number of Asian patients in the MAIC, the sponsor selected only RAINBOW trial patients from Australia, Europe, Israel, and the US (excluding patients from Argentina, Brazil, Chile, Hong Kong, Japan, Mexico, Singapore, South Korea, and Taiwan), and compared them with the study population of the DESTINY-Gastric02 trial, the majority of whom were white (87.3%). However, in the NMA network, all included studies did not report on the distribution of ethnicity except for the DESTINY-Gastric02 and RAINBOW trials. Moreover, the KSCG/ST10-01, Sym et al. (2013), and WJOG 4007 trials were conducted in Asia, while the Roy et al. (2013) trial was conducted in both Western and Asian countries. Under the assumption made by the sponsor about geographic region and ethnicity being important prognostic factors, the potential heterogeneity regarding differences in geographical regions and ethnicity in the NMA network could not be ignored; the degree of uncertainty remains unknown. The rationale for reporting the results of an FE model is justified when estimation of between-study variance using the RE model is very imprecise and unstable in situations that consider only a few studies.34,35 However, the FE model does not sufficiently account for heterogeneity between studies, leading to overly precise and narrow CIs.35 Given that various sources of heterogeneity existed in the sponsor-submitted ITC (described previously), use of the FE model introduced uncertainty in the NMA treatment effect estimates.
Other Evidence
The contents of this section have been informed by materials submitted by the sponsor. The following information has been summarized and validated by the review team.
Table 29: Summary of Gaps in the Systematic Review Evidence
Evidence gap | Studies that address gaps | |
|---|---|---|
Study description | Summary of key results | |
Population: Patients with HER2-positive (defined as IHC 3+ or IHC 2+ and ISH-positive), advanced gastric or GEJ adenocarcinoma who have progressed on or after at least 2 prior regimens that included fluoropyrimidine, platinum, and trastuzumab | Study design: Phase II, multicentre, open-label, randomized, active-controlled trial Location: 66 sites in Japan and South Korea Sample size: 188 patients randomized Intervention: Trastuzumab deruxtecan (n = 126) Comparator: Physician’s choice (n = 62) of irinotecan (n = 55) or paclitaxel (n = 7) Outcomes: OS, PFS, ORR per ICR assessment, FACT-Ga, harms |
|
CI = confidence interval; FACT-Ga = Functional Assessment of Cancer Therapy – Gastric; GEJ = gastroesophageal junction; HER2 = human epidermal growth factor 2; ICR = independent central review; IHC = immunohistochemistry; ILD = interstitial lung disease; ISH = in situ hybridization; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; TEAE = treatment-emergent adverse event; TESAE = treatment-emergent serious adverse event.
Source: Sponsor’s Summary of Clinical Evidence.43
Description of Studies
The DESTINY-Gastric01 trial was a phase II, multicentre RCT. Evidence generated from the primary cohort of the DESTINY-Gastric01 trial is the focus of this section. The primary cohort of the DESTINY-Gastric01 trial included 188 patients with HER2-positive (i.e., IHC 3+ or IHC 2+ and ISH-positive), advanced gastric or GEJ adenocarcinoma who had progressed on or after at least 2 prior regimens that included a fluoropyrimidine drug, a platinum drug, and a trastuzumab-containing regimen. The primary objective of the DESTINY-Gastric01 trial was to compare the efficacy of trastuzumab deruxtecan versus the physician’s choice of treatment (i.e., irinotecan 150 mg/m2 through IV every 2 weeks or paclitaxel 80 mg/m2 through IV every week) in the primary cohort, as measured by ORR per ICR assessment using RECIST 1.1. Secondary end points included OS, PFS, FACT-Ga, and harms.
Characteristics of the DESTINY-Gastric01 trial are summarized in Table 30.
Table 30: Details of the DESTINY-Gastric01 Trial
Detail | DESTINY-Gastric01 trial |
|---|---|
Designs and populations | |
Study design | Phase II, multicentre, randomized, open-label, active-controlled study |
Locations | Patients were enrolled in 66 sites in Japan and South Korea. |
Patient enrolment dates | Start date: November 2017 Study completion date: January, 2021 |
Randomized (N) | N = 188 (primary cohort)
|
Inclusion criteria |
|
Exclusion criteria |
|
Drugs | |
Intervention | Trastuzumab deruxtecan 6.4 mg/kg IV every 3 weeks |
Comparators |
|
Study duration | |
Screening phase | Started on the day of signing the informed consent form and had a maximum duration of 28 days |
Treatment phase | Started on cycle 1, day 1, with patients continuing treatment until disease progression or unacceptable toxicity |
Follow-up phase | Follow-up at 40 days (+ 7 days) after the last administration |
Outcomes | |
Primary end point | Unconfirmed ORR per ICR assessment per RECIST 1.1 |
Secondary and exploratory end points | Secondary:
|
Publication status | |
Publications | Publications: Shitara et al. (2020)68 Yamaguchi et al. (2024)69 Yamaguchi et al. (2022)70 Yamaguchi et al. (2021)71 Shitara et al. (2024)72 ClinicalTrials.gov entry: |
CNS = central nervous system; DCR = disease control rate; DOR = duration of response; ECHO = echocardiogram; ECOG PS = Eastern Cooperative Oncology Group Performance Status; FACT-Ga = Functional Assessment of Cancer Therapy – Gastric; GEJ = gastroesophageal junction; HER2 = human epidermal growth factor 2; HRQoL = health-related quality of life; ICR = independent central review; IHC = immunohistochemistry; ILD = Interstitial lung disease; ISH = in situ hybridization; LVEF = left ventricular ejection fraction; MUGA = multigated acquisition; NYHA = New York Heart Association; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; RECIST 1.1 = Response Evaluation Criteria in Solid Tumours Version 1.1; TTF = time to treatment failure; TTR = time to response.
Sources: Sponsor’s Summary of Clinical Evidence;1 DESTINY-Gastric01 Clinical Study Report.66,67
Populations
Patients in the primary cohort of the DESTINY-Gastric01 trial were enrolled across 66 study cites in Japan and South Korea. Eligible patients were adults (aged at least 20 years) who had been diagnosed with locally advanced or metastatic HER2-positive (defined as IHC 3+ or IHC 2+ and ISH-positive) gastric or GEJ adenocarcinoma and who had an ECOG PS of 0 or 1. Eligible patients must have progressed on or after at least 2 prior regimens that included a fluoropyrimidine drug, a platinum drug, and trastuzumab.
Interventions
Trastuzumab deruxtecan was administered intravenously on day 1 of every 21-day treatment cycle (i.e., every 3 weeks) until disease progression, withdrawal by patient, physician decision, or death. The starting dose was 6.4 mg/kg. Trastuzumab deruxtecan was provided as a lyophilized powder in a single-use glass vial to be reconstituted. The first infusion was administered over approximatively 90 minutes. Subsequent infusions were administered over approximatively 30 minutes if there was no injection-related reaction after the first infusion. Trastuzumab deruxtecan was administered in a hospital setting.
Patients who were enrolled in the physician’s choice treatment arm received either irinotecan monotherapy or paclitaxel monotherapy. Irinotecan was administered intravenously biweekly, with a starting dose of 150 mg/m2. Paclitaxel was administered through IV on days 1, 8, and 15, then every 4 weeks, with a starting dose of 80 mg/m2.
Outcomes
ORR per ICR assessment, the primary efficacy end point of the DESTINY-Gastric01 trial, was defined as the proportion of patients who achieved a best overall response of CR or PR, as determined by ICR committee based on RECIST 1.1.
OS was defined as the time from the date of randomization to the date of death due to any cause. If there was no death reported for a patient before the OS data cut-off time point, OS was censored at the last contact date on which the patient was known to be alive.
PFS assessed by ICR assessment was defined as the time from the date of randomization to the earliest date of the first objective documentation of progressive disease or death due to any cause.
FACT-Ga is a quality-of-life instrument specific to gastric cancer. The details of the FACT-Ga measurement instrument are shown in Table 9.
The harms outcomes assessed in the DESTINY-Gastric01 trial mainly included TEAEs, TESAEs, withdrawal due to TEAEs, deaths, and notable harms (i.e., ILD, LV dysfunction, QT prolongation, and IRRs).
Statistical Analysis
The target sample size for the primary cohort of the DESTINY-Gastric01 trial was approximately 180 patients (120 patients in the trastuzumab deruxtecan group and 60 patients in the physician’s choice group). The trial would have 92.9% power to detect a difference in the primary end point between the 2 groups at a 2-sided significance level of 0.05 under the assumed ORRs of 40% in the trastuzumab deruxtecan group and 15% in the physician’s choice group.
Approximately 133 OS events would be needed to have 80% power to reject a null hypothesis of no difference under an assumed alternative HR of 0.61 (a 64% improvement in median OS, from 5.5 months in the physician’s choice group to 9.0 months in the trastuzumab deruxtecan group) at a 2-sided significance level of 0.05. This is assuming a 10-month enrolment period and a 12-month follow-up period after randomization of the last patient.
To compare ORR per ICR assessment between treatment groups, a Cochran-Mantel-Haenszel test with region as a stratification factor was used. An ORR estimate and its 2-sided 95% exact CI were provided for each group.
OS and PFS was compared between the treatment groups using stratified log-rank tests with region as a stratification factor. To control the family-wise type I error rate for the primary and secondary efficacy end points of ORR and OS, a serial, hierarchically ordered gatekeeping strategy was applied. The tests were performed in the following order: ORR per ICR assessment, followed by OS. The sequence of tests continued until the test did not meet the significance level of the 2-sided alpha of 0.05. The testing procedure followed the steps shown here:
Test the primary end point, ORR, at a 2-sided, 5% significance level. If positive, continue to step 2; otherwise, stop.
Test OS (interim and final analyses) at an overall 2-sided, 5% significance level.
The first analysis of OS occurred at the time of the primary analyses for ORR (based on ICR) only if the ORR met the significance level of a 2-sided alpha of 0.05. The ORR (based on ICR) analysis and prespecified interim analysis of OS were conducted after all the patients completed tumour assessments at approximately 24 weeks (or discontinued the study); the final analysis of OS was to be performed after approximately 133 OS events had occurred. A Lan-DeMets alpha-spending function with the O’Brien-Fleming stopping boundary was used to determine the significance levels for the OS analyses.73,74 The HR and 95% CIs were estimated using stratified Cox proportional hazards regression models with region as a stratification factor for the analyses of OS and PFS. KM-estimated survival curves of OS and PFS were presented for each treatment group. The median, with a 2-sided 95% CI, was calculated using the Brookmeyer and Crowley method.52
Results
Patient Disposition
Patient disposition in the DESTINY-Gastric01 trial is summarized in Table 31. In the DESTINY-Gastric01 trial, 561 patients were screened, and a total of 188 patients were enrolled in the primary cohort. The ITT population is defined as the complete enrolled patient population in the primary cohort. The FAS population excluded 1 patient in the ITT population who did not receive the study drug because informed consent was not obtained before study procedures were performed. As of June 3, 2020, 17.6% of patients in the trastuzumab deruxtecan group and 6.5% of patients in the physician’s choice group discontinued their assigned treatments due to AEs.
Table 31: Summary of Patient Disposition in the DESTINY-Gastric01 Trial (Data Cut-Off Date: June 3, 2020)
Patient disposition | DESTINY-Gastric01 trial | |
|---|---|---|
Trastuzumab deruxtecan | Physician’s choice | |
Screened, n | 561 | |
Excluded, n | 327 | |
Patients enrolled, n | 126 | 62 |
Patients who received treatments, n (%) | 125 (99.2) | 62 (100.0) |
Discontinued study drug, n (%) | 115 (92.0) | 62 (100.0) |
Primary reason for discontinuing study treatment, n (%) | ||
Progressive disease | 82 (65.6) | 50 (80.6) |
AE | 22 (17.6) | 4 (6.5) |
Clinical progression | 6 (4.8) | 5 (8.1) |
Death | 2 (1.6) | 0 (0.0) |
Withdrawal by patient | 2 (1.6) | 3 (4.8) |
Physician decision | 1 (0.8) | 0 (0.0) |
ITT, n | 126 | 62 |
FAS, N | 125 | 62 |
Safety analysis set, N | 125 | 62 |
AE = adverse event; FAS = full analysis set; ITT = intention to treat; NR = not reported.
Sources: Sponsor’s Summary of Clinical Evidence;1 DESTINY-Gastric01 Clinical Study Report.66,67
Baseline Characteristics
The baseline characteristics of the patients in the DESTINY-Gastric01 trial are summarized in Table 32. The median age of patients was 66.0 years (range, 28 years to 82 years). All patients were Asian; 79.2% of patients in the trastuzumab deruxtecan group and 80.6% of patients in the physician’s choice group were Japanese. The majority of patients had gastric adenocarcinoma (86.4% in the trastuzumab deruxtecan group and 88.7% in the physician’s choice group).
Table 32: Summary of Patient Baseline Characteristics in the DESTINY-Gastric01 Trial (FAS)
Characteristic | DESTINY-Gastric01 trial | |
|---|---|---|
Trastuzumab deruxtecan (N = 125) | Physician’s choice (N = 62) | |
Age (years), median (range) | 65.0 (34 to 82) | 66.0 (28 to 82) |
Age group, n (%) | ||
65 years | 55 (44.0) | 27 (43.5) |
≥ 65 years | 70 (56.0) | 35 (56.5) |
Sex | ||
Female, n (%) | 30 (24.0) | 15 (24.2) |
Male, n (%) | 95 (76.0) | 47 (75.8) |
Race | ||
Asian | 125 (100.0) | 62 (100.0) |
Baseline ECOG PS, n (%) | ||
0 | 62 (49.6) | 30 (48.4) |
1 | 63 (50.4) | 32 (51.6) |
Lines of prior systemic therapy intended for locally advanced or metastatic disease, n (%) | ||
0 | NA | NA |
1 | NA | NA |
2 | 66 (52.8) | 38 (61.3) |
3 | 34 (27.2) | 18 (29.0) |
≥ 4 | 25 (20.0) | 6 (9.7) |
HER2 status (central laboratory), n (%) | ||
IHC 3+ | 96 (76.8) | 47 (75.8) |
IHC 2+ or ISH-positive | 29 (23.2) | 15 (24.2) |
Cancer location, n (%) | ||
Gastric | 108 (86.4) | 55 (88.7) |
Gastroesophageal junction | 17 (13.6) | 7 (11.3) |
Adenocarcinoma subtype, n (%) | ||
Intestinal | 89 (71.2) | 38 (61.3) |
Diffuse | 28 (22.4) | 18 (29.0) |
Others | 8 (6.4) | 6 (9.7) |
Number of metastatic sites, n (%) | ||
< 2 | 23 (18.4) | 10 (16.1) |
≥ 2 | 102 (81.6) | 52 (83.9) |
Previous total gastrectomy, n (%) | ||
Yes | 22 (17.6) | 9 (14.5) |
No | 103 (82.4) | 53 (85.5) |
Previous treatment, n (%) | ||
Therapy containing trastuzumab | 125 (100.0) | 62 (100.0) |
Immune checkpoint inhibitor | 44 (35.2) | 17 (27.4) |
Presence of liver metastasis at baseline, n (%) | ||
Yes | 68 (54.4) | 34 (54.8) |
No | 57 (45.6) | 28 (45.2) |
Time from initial diagnosis (months), median (range) | 22.7 (4.6 to 156.3) | 20.3 (4.5 to 233.4) |
ECOG PS = Eastern Cooperative Oncology Group Performance Status; FAS = full analysis set; HER2 = human epidermal growth factor receptor 2; IHC = immunohistochemistry; ISH = in situ hybridization; NA = not applicable.
Sources: Sponsor’s Summary of Clinical Evidence;1 DESTINY-Gastric01 Clinical Study Report.66,67
Exposure to Study Treatments
Treatment exposure in the DESTINY-Gastric01 trial is summarized in Table 33. As of the data cut-off date of June 3, 2020, the treatment duration was 4.6 months (range, 0.7 months to 29.7 months) for the trastuzumab deruxtecan group and 2.76 months (range, 0.5 months to 13.1 months) for the physician’s choice group.
Table 33: Summary of Patient Exposure in the DESTINY-Gastric01 Trial (Safety Analysis Set; Data Cut-Off Date: June 3, 2020)
Exposure | Trastuzumab deruxtecan (N = 125) | Physician’s choice (N = 62) | |
|---|---|---|---|
Irinotecan (N = 55) | Paclitaxel (N = 7) | ||
Total patient-years of exposure (years) | ████ | ████ | ███ |
Treatment duration (months), median (range) | ███████ ██ ████ | ███████ ██ ████ | ███████ ██ ████ |
Duration of treatment, n (%) | |||
≤ 3 months | ██ ██████ | ██ ██████ | | ██████ |
> 3 months to ≤ 6 months | ██ ██████ | ██ ██████ | | ██████ |
> 6 months to ≤ 9 months | ██ ██████ | | █████ | | ██████ |
> 9 months to ≤ 12 months | | █████ | | █████ | ██ |
> 12 months to ≤ 24 months | ██ ██████ | ██ | | ██████ |
> 24 months | | █████ | ██ | ██ |
Dose intensitya, median (range) | ███████ ██ ███ | ███████ ██ █████ | ████████ ██ █████ |
Relative dose intensity (%)b, median (range) | █████████ ██ █████ | █████████ ██ █████ | █████████ ██ ████ |
Total number of cycles treated, median (range) | ███| ██ ██ | ████ | ████ |
AE = adverse event; NA = not applicable; NR = not reported.
aDose intensity: Trastuzumab deruxtecan (mg/kg per 3 weeks) = cumulative dose level divided by duration of treatment (days) divided by 21; irinotecan (mg/m2 per 2 weeks) = cumulative dose level divided by the duration of treatment (days) divided by 14; paclitaxel (mg/m2 per 4 weeks) = cumulative dose level divided by duration of treatment (days) divided by 28.
bRelative dose intensity: Trastuzumab deruxtecan = dose intensity divided by 6.4 mg/kg per 3 weeks; irinotecan = dose intensity divided by 150 mg/m2 per 2 weeks; paclitaxel = dose intensity divided by 240 mg/m2 per 4 weeks.
Sources: Sponsor’s Summary of Clinical Evidence;1 DESTINY-Gastric01 Clinical Study Report.66,67
Efficacy
Results of the DESTINY-Gastric01 trial (Table 34) provided by the sponsor were from 2 data cut-off dates: November 8, 2019, and June 3, 2020. Data from the former date were used in the final analysis of PFS and ORR. The latter date, which was also the final data cut-off date, was used in the final OS analysis and harms analysis. Efficacy results were based on the ITT population, which included all patients in the primary cohort. Harms results were based on the safety analysis set, which excluded 1 patient in the ITT population who did not receive the study drug.
Table 34: Summary of Key Efficacy Results from the DESTINY-Gastric01 Trial (ITT Population)
Exposure | Trastuzumab deruxtecan (N = 126) | Physician’s choice (N = 62) |
|---|---|---|
OSa | ||
Patients with OS events, n (%) | ██ ██████ | ██ ██████ |
Patients censored, n (%) | ██ ██████ | ██ ██████ |
Alive | NR | NR |
Lost to follow-up | NR | NR |
OSb (months), median (95% CI) | 12.5 (████ ██ █████ | ███ ████ ██ ████) |
Adjusted HRc (95% CI; P value) | ████ ██████ ██ █████ ███████ | |
Probability of being alive at 3 months,b % (95% CI) | 92.7 (86.5 to 96.2) | 90.0 (79.1 to 95.4) |
Between-group difference | NR | |
Probability of being alive at 6 months,b % (95% CI) | 80.7 (72.5 to 86.6) | 65.0 (51.5 to 75.6) |
Between-group difference | NR | |
Probability of being alive at 9 months,b % (95% CI) | 63.7 (54.6 to 71.5) | 50.0 (36.8 to 61.8) |
Between-group difference | NR | |
Probability of being alive at 12 months,b % (95% CI) | 52.2 (43.1 to 60.6) | 29.7 (18.7 to 41.5) |
Between-group difference | NR | |
PFS per ICR assessment | ||
Patients with PFS events, n (%) | ██ ██████ | 36 (58.1) |
Progressive disease | ██ ██████ | 34 (54.8) |
Death | 11 (8.7) | 2 (3.2) |
Patients censored, n (%) | ██ ██████ | 26 (41.9) |
No baseline tumour assessments | | ███ | 2 (3.2) |
No postbaseline tumour assessments | | █████ | 3 (4.8) |
New anticancer therapy | ██ ██████ | ██ ██████ |
Missed 2 consecutive tumour assessments | | █████ | 1 (1.6) |
No progression or death | 23 (18.3) | 6 (9.7) |
PFSb (months), median (95% CI) | 5.6 (4.3 to 6.9) | 3.5 (2.0 to 4.3) |
Adjusted HRc (95% CI; P value) | 0.47 (0.31 to 0.71; 0.0003) | |
Probability of being progression-free at 3 months,b % (95% CI) | 71.9 (63.0 to 79.1) | 50.3 (35.5 to 63.5) |
Between-group difference | NR | |
Probability of being progression-free at 6 months,b % (95% CI) | 43.0 (33.6 to 52.0) | 20.6 (8.9 to 35.6) |
Between-group difference | NR | |
Probability of being progression-free at 9 months,b % (95% CI) | 33.3 (24.4 to 42.4) | NR |
Between-group difference | NR | |
Probability of being progression-free at 12 months,b % (95% CI) | 30.4 (21.5 to 39.7) | NR |
Between-group difference | NR | |
ORR per ICR assessment | ||
Unconfirmed ORR, n (%; 95% CI) | 61 (█████ ████ ██ ████) | 8 (█████ ███ ██ ████) |
CR, n (%) | 11 (███) | 0 (0) |
PR, n (%) | 50 (████) | 8 (████) |
Confirmed ORR, n (%; 95% CI) | ██ ██████ ████ ██ █████ | 7 (█████ ███ ██ ████) |
CR, n (%) | 10 (7.9) | 0 (0) |
PR, n (%) | ██ █████) | 7 (████) |
FACT-Ga total score | ||
Baseline | ||
n (%) | NR | NR |
Mean (SD) | █████ ███████ | █████ ███████ |
End of treatment | ||
n (%)c | NR | NR |
Mean (SD) | █████ ███████ | █████ ███████ |
Change from baseline, mean (SD) | █████ ███████ | █████ ███████ |
CI = confidence interval; CR = complete response; FACT-Ga = Functional Assessment of Cancer Therapy – Gastric; ICR = independent central review; HR = hazard ratio; ITT = intention to treat; NR = not reported; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; PR = partial response; SD = standard deviation.
aAs of the data cut-off date of June 3, 2020, the median duration of survival follow-up was 10.4 months (range, 0.3 months to 29.7 months).
bEstimated using Kaplan-Meier.
cRegion as a stratification factor.
Sources: Sponsor’s Summary of Clinical Evidence;1 DESTINY-Gastric01 Clinical Study Report.66,67
Overall Survival
As of the data cut-off date of June 3, 2020, the proportion of patients in the ITT population who had OS events was 67.2% in the trastuzumab deruxtecan group and 79.0% in the physician’s choice group. The median OS duration was 12.5 months (95% CI, 10.3 months to 15.2 months) in the trastuzumab deruxtecan group and 8.9 months (95% CI, 6.4 months to 10.4 months) in the physician’s choice group. The adjusted HR was 0.60 (95% CI, 0.42 to 0.86). The KM curves for OS are presented in Figure 4.
PFS per ICR Assessment
As of June 3, 2020, the proportion of patients in the ITT population who had PFS events was 65.1% in the trastuzumab deruxtecan group and 58.1% in the physician’s choice group. The median PFS was 5.6 months (95% CI, 4.3 months to 6.9 months) in the trastuzumab deruxtecan group and 3.5 months (95% CI, 2.0 months to 4.3 months) in the physician’s choice group. The estimated HR was 0.47 (95% CI, 0.31 to 0.71). The KM plots for PFS per ICR assessment are presented in Figure 5.
Figure 4: KM Plot of OS in the DESTINY-Gastric01 Trial (ITT; Data Cut-Off Date: June 3, 2020)
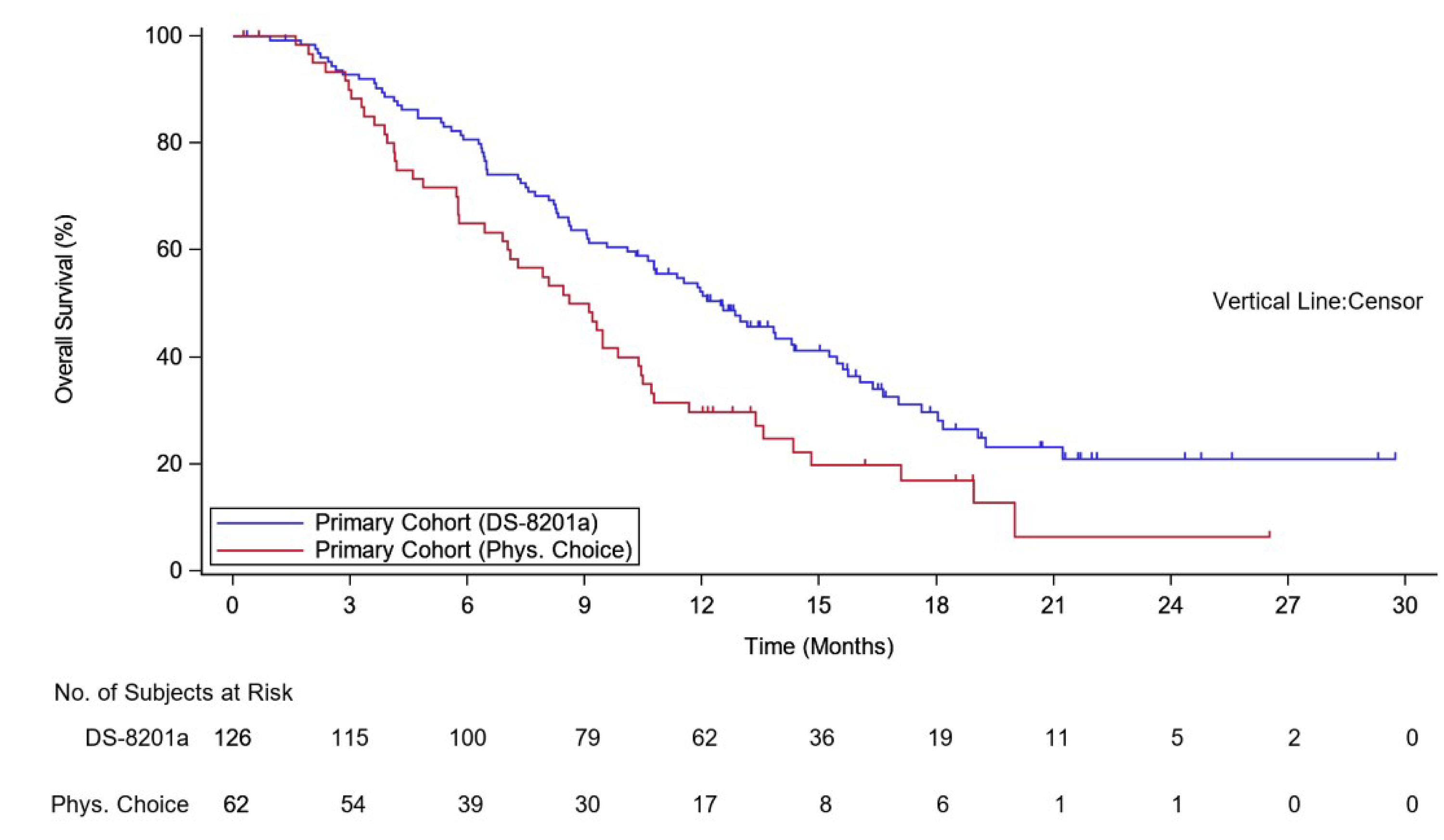
DS-8201a = trastuzumab deruxtecan; ITT = intention to treat; KM = Kaplan-Meier; OS = overall survival; Phys. = physician’s.
Figure 5: KM Plot of PFS per ICR Assessment in the DESTINY-Gastric01 Trial (ITT; Data Cut-Off Date: June 3, 2020)
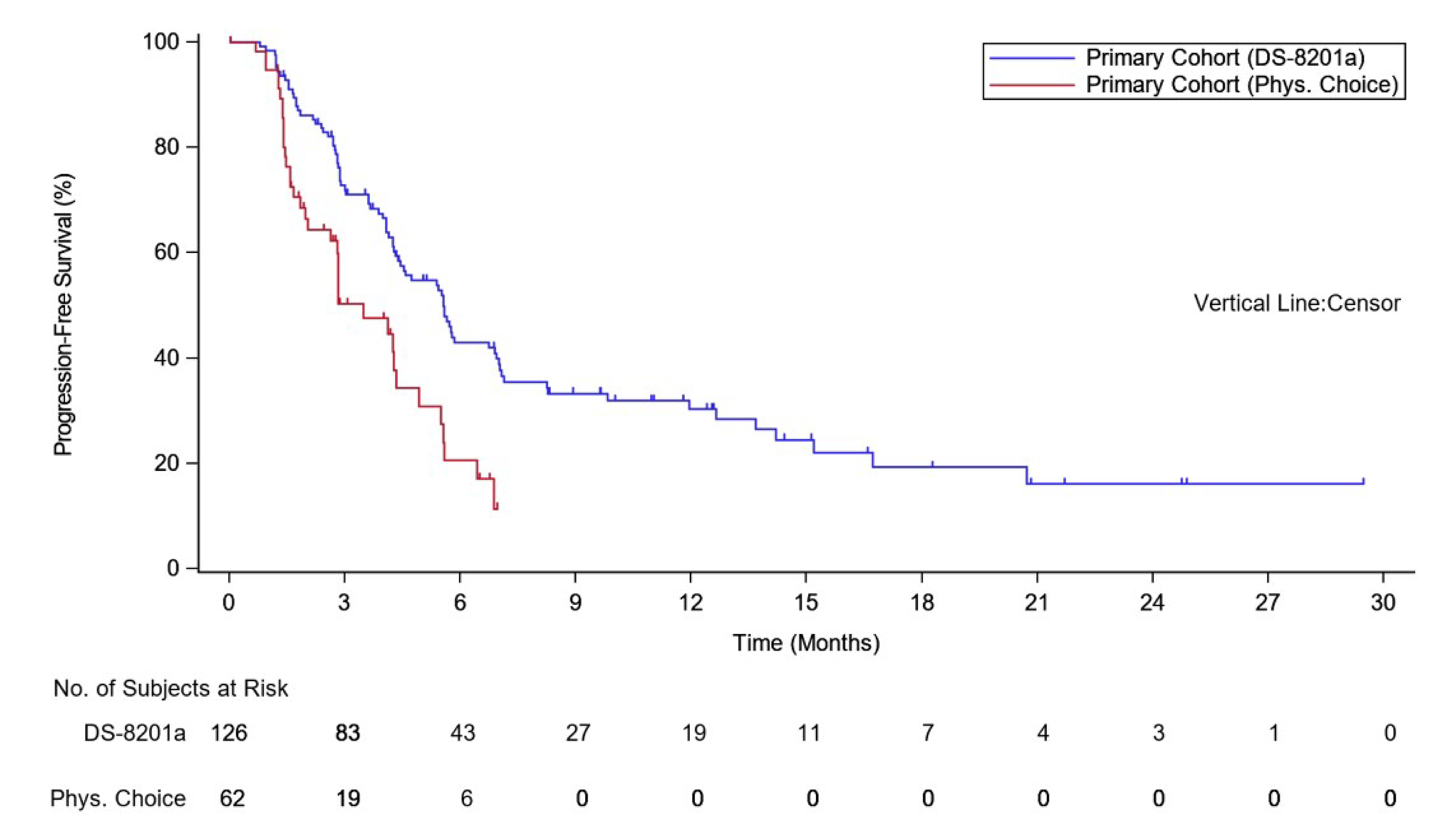
DS-8201a = trastuzumab deruxtecan; ITT = intention to treat; ICR = independent central review; KM = Kaplan-Meier; PFS = progression-free survival; Phys. = physician’s.
ORR per ICR Assessment
As of June 3, 2020, the unconfirmed ORRs per ICR assessment were █████ ████ ███ ████ ██ █████ in the trastuzumab deruxtecan group and █████ ████ ███ ███ ██ █████ in the physician’s choice group. The proportion of patients who achieved a best overall response of unconfirmed CR in the trastuzumab deruxtecan group was █████ while no patients achieved CR in the physician’s choice group.
Of note, according to the sponsor’s response to Health Canada, in the study protocol of the DESTINY-Gastric01 trial, the primary end point was unconfirmed ORR, and no confirmation of ORR was required because the trial design included a randomized control group. The confirmed ORR was defined, as was a supportive end point, not formally specified as a key secondary end point.
As of June 3, 2020, the confirmed ORRs per ICR assessment were █████ ████ ███ ████ ██ ████) in the trastuzumab deruxtecan group and █████ ████ ███ ███ ██ ████) in the physician’s choice group. The proportion of patients who achieved a best overall response of confirmed CR in the trastuzumab deruxtecan group was 7.9%, while no patients achieved CR in the physician’s choice group.
FACT-Ga Total Score
The FACT-Ga total scores were based on the data available as of November 8, 2019.
The mean FACT-Ga total score at the end of treatment was █████ ███ █ █████) in the trastuzumab deruxtecan group and █████ (██ █ █████) in the physician’s choice group, with a mean change of █████ ███ █ ██████ and █████ ███ █ █████), respectively.
Harms
Harms data from the DESTINY-Gastric01 trial are shown in Table 35. The cut-off date for the harms data was June 3, 2020.
Treatment-Emergent AEs
All the patients in the trastuzumab deruxtecan group and 98.4% of the patients in the physician’s choice group had TEAEs. The most commonly reported TEAE was neutropenia, reported by 64.8% of patients in the trastuzumab deruxtecan group and 35.5% of patients in the physician’s choice group.
The proportion of patients who had any TEAE of grade 3 or higher was 85.6% in the trastuzumab deruxtecan group, which was higher than the 56.5% reported in the physician’s choice group. The most commonly reported TEAE of grade 3 or higher was neutropenia (51.2% in the trastuzumab deruxtecan group versus 24.2% in the physician’s choice group). This was followed by anemia (38.4% in the trastuzumab deruxtecan group versus 22.6% in the physician’s choice group).
Treatment-Emergent Serious AEs
The proportion of patients who had any TESAE in the trastuzumab deruxtecan group was 44.8%, which was higher than the 25.8% in the physician’s choice group. The most commonly reported TESAE was decreased appetite (10.4% in the trastuzumab deruxtecan group versus 1.6% in the physician’s choice group). This was followed by ILD (5.6% in the trastuzumab deruxtecan group versus 0% in the physician’s choice group), anemia (3.2% in the trastuzumab deruxtecan group versus 3.2% in the physician’s choice group), and dehydration (3.2% in the trastuzumab deruxtecan group versus 0% in the physician’s choice group).
Treatment Discontinuation Due to TEAEs
The proportion of patients who discontinued the study treatment was 17.6% in the trastuzumab deruxtecan group and 6.5% in the physician’s choice group. Discontinuation due to ILD occurred in 6.4% of patients in the trastuzumab deruxtecan group versus 0% in the physician’s choice group.
Mortality
The proportion of patients who had any TEAE associated with an outcome of death was 6.4% in the trastuzumab deruxtecan group, which was higher than the 3.2% reported in the physician’s choice group.
Notable Harms
Interstitial Lung Disease
The proportion of patients who had ILD was 12.8% in the trastuzumab deruxtecan group; 5.6% of cases occurred as TESAEs. No patients in the physician’s choice group had ILD.
Infusion-Related Reactions
The proportion of patients who had IRRs was ███% in the trastuzumab deruxtecan group and ███% in the physician’s choice group.
LV Dysfunction
The proportion of patients who had grade 2 LV dysfunction (defined as the resting LVEF ranges from 50% to 40%; and there is a 10% to 19% LVEF decrease from baseline) was 9.4% in the trastuzumab deruxtecan group.
QT Prolongation
The proportion of patients who had QT prolongation events was ███% in the trastuzumab deruxtecan group and ███% in the physician’s choice group.
Table 35: Summary of Harms Results in the DESTINY-Gastric01 Trial (Safety Analysis Set; Data Cut-Off Date: June 3, 2020)
Harms | Trastuzumab deruxtecan (N = 125) | Physician’s choice (N = 62) |
|---|---|---|
TEAEs | ||
Number of patients with any TEAE (%) | 125 (100.0) | 61 (98.4) |
TEAEs (reported in ≥ 20% of patients), n (%) | ||
Neutropenia | 81 (64.8) | 22 (35.5) |
Nausea | 79 (63.2) | 29 (46.8) |
Decreased appetite | 76 (60.8) | 28 (45.2) |
Anemia | 72 (57.6) | 19 (30.6) |
Thrombocytopenia | 50 (40.0) | 4 (6.5) |
Leukopenia | 48 (38.4) | 22 (35.5) |
Malaise | 43 (34.4) | 10 (16.1) |
Diarrhea | 41 (32.8) | 20 (32.3) |
Vomiting | 33 (26.4) | 5 (8.1) |
Constipation | 31 (24.8) | 15 (24.2) |
Pyrexia | 31 (24.8) | 10 (16.1) |
Lymphopenia | 29 (23.2) | 2 (3.2) |
Alopecia | 28 (22.4) | 9 (14.5) |
Fatigue | 28 (22.4) | 18 (29.0) |
Number of patients with any TEAE of grade 3 or higher | 107 (85.6) | 35 (56.5) |
TEAEs of grade 3 or higher reported in ≥ 10% of patients, n (%) | ||
Neutropenia | ██ ██████ | ██ ██████ |
Anemia | ██ ██████ | ██ ██████ |
Leukopenia | ██ ██████ | | ██████ |
Decreased appetite | ██ ██████ | | ██████ |
Lymphopenia | ██ ██████ | | █████ |
Thrombocytopenia | ██ ██████ | | █████ |
TESAEs | ||
Number of patients with any TESAE (%) | ██ ██████ | ██ ██████ |
TESAEs reported in ≥ 2% patients, n (%) | ██ | ██ |
Decreased appetite | ██ ██████ | | █████ |
ILD | | █████ | | ███ |
Anemia | | █████ | | █████ |
Dehydration | | █████ | | ███ |
Cholangitis | | █████ | | █████ |
Disease progression | | █████ | | █████ |
Jaundice, cholestatic | | █████ | | █████ |
Pneumonia | | █████ | | ███ |
Pyrexia | | █████ | | █████ |
Tumour hemorrhage | | █████ | | ███ |
Fatigue | | █████ | | █████ |
Blood creatinine increase | | ███ | | █████ |
Neutropenia | | ███ | | █████ |
Treatment discontinuation due to TEAEs | ||
Number of patients with ≥ 1 TEAE leading to study treatment discontinuation (%) | 22 (17.6) | 4 (6.5) |
TEAEs leading to study treatment discontinuation reported in ≥ 2% patients, n (%) | ||
ILD | | █████ | | ███ |
Neutropenia | | ███ | | █████ |
Death | ||
Number of patients who had any TEAE associated with an outcome of death (%) | 8 (6.4) | 2 (3.2) |
Reason for death, n (%) | ||
Disease progression | | █████ | | █████ |
Neoplasm progression | | █████ | | █████ |
Disseminated intravascular coagulation | | █████ | | ███ |
Large intestine perforation | | █████ | | ███ |
Pneumonia | 1 (0.8) | 0 (0) |
Notable harms, n (%) | ||
ILD | ██ ██████ | 0 (0) |
IRR | | █████ | | █████ |
LV dysfunction | ██ █████| | ██ |
QT prolongation | █████ | █████ |
ILD = interstitial lung disease; IRR = infusion-related reaction; LV = left ventricular; NR = not reported; TEAE = treatment-emergent adverse event; TESAE = treatment-emergent serious adverse event.
aThe percentage was calculated by using 117 as the denominator because that was the number of patients who had both baseline and postbaseline data.
Sources: Sponsor’s Summary of Clinical Evidence;1 DESTINY-Gastric01 Clinical Study Report.66,67
Critical Appraisal
Internal Validity
The DESTINY-Gastric01 trial enrolled 188 patients, randomizing 126 patients and 66 patients to the trastuzumab deruxtecan group and physician’s choice group (i.e., 2 to 1 randomization), respectively. The randomization was done using an interactive web and voice response system and stratified based on region (Japan or South Korea), ECOG PS (0 or 1), and HER2 status (IHC 3+ or IHC 2+ and ISH-positive) to minimize potential imbalances between the study groups that might bias the results. Despite the relatively small sample size, the distribution of baseline characteristics among patients was generally balanced between the trastuzumab deruxtecan group and the physician’s choice group, indicating a low risk of bias in the randomization process.
The review team determined that, despite the open-label study design, there was a low risk of detection bias in PFS or ORR, but still increased uncertainty with respect to treatment efficacy in this setting. Results for both PFS per ICR assessment and PFS per investigator assessment (data not shown) were consistent in general, as were the findings for unconfirmed and confirmed ORR. However, there is a notable risk of performance bias for the FACT-Ga. This risk was associated with the open-label design and subjective nature of the measure.
The DESTINY-Gastric01 trial reported OS, which was considered by the clinical experts consulted by the review team as the most important outcome for the study population. Multiplicity adjustment was carried out for unconfirmed ORR (i.e., the primary end point of the trial) and OS to control for type I error; however, the remaining efficacy end points (e.g., PFS and FACT-Ga) were not adjusted for multiplicity.
External Validity
The DESTINY-Gastric01 trial population is not aligned with the population described in the sponsor’s reimbursement request because the DESTINY-Gastric01 trial focused on the third-line and later treatment settings, whereas the reimbursement request involves only the second-line treatment setting. However, the DESTINY-Gastric01 trial population aligns with a group of patients who are implied in the Health Canada indication, the trial included adult patients with locally advanced or metastatic HER2-positive gastric or GEJ adenocarcinoma who have received greater than or equal to 2 prior treatment regimens, including an anti-HER regimen. According to the clinical experts consulted by the review team, this group of patients is small in number in the real-world setting and mainly includes those who are on their second or later lines of therapy.
There are some concerns regarding whether the patient population in the DESTINY-Gastric01 trial was representative of the corresponding patient population in Canada. According to the clinical experts consulted by the review team, the inclusion and exclusion criteria of the DESTINY-Gastric01 trial were generally appropriate in terms of selecting eligible patients; however, the efficacy observed in the trastuzumab deruxtecan group and physician’s choice group were higher than the experts expected or have encountered in real-world, third-line and later settings, in which patients tend to be of poor status and efficacy, suggesting the potential differences between the trial population and the real-world population in Canada.
In addition to the concern about the difference in lines of treatment, there are concerns about generalizing the results from the DESTINY-Gastric01 trial population to the DESTINY-Gastric02 trial population due to differences in patient characteristics. For instance, 87.3% of the patients in the DESTINY-Gastric02 trial were white and from North America, whereas all the patients in the DESTINY-Gastric01 trial were Asian and from Japan or South Korea. As noted in the sponsor-submitted ITC, geographical region and ethnicity were important prognostic factors, and Asian patients had different prognoses than patients in Western countries. Second, in the DESTINY-Gastric02 trial, 34.2% of patients had gastric cancer and 65.8% had GEJ cancer, whereas in the DESTINY-Gastric01 trial, 87.2% had gastric cancer and 12.8% had GEJ cancer. These differences in patient characteristics may introduce treatment heterogeneity that increases the uncertainty of the results and their generalizability to the Canadian context.
The clinical experts consulted by the review team noted that the use of irinotecan or paclitaxel as comparators in the DESTINY-Gastric01 trial is not well reflective of current clinical practice in Canada. According to the clinical experts consulted by the review team, it is understandable that at the time of designing the DESTINY-Gastric01 trial irinotecan and paclitaxel were commonly used in the third-line and later settings; however, in current clinical practice, irinotecan and paclitaxel are rarely used, and generally only in a very small group of patients, such as those who had serious neuropathy during previous lines of therapy.
Discussion
Summary of Available Evidence
One sponsor-conducted pivotal study, DESTINY-Gastric02, was included in the systematic review of this clinical report. The DESTINY-Gastric02 trial was a phase II, single-arm, open-label study investigating the use of trastuzumab deruxtecan as monotherapy for the treatment of patients (aged ≥ 18 years) who had unresectable or metastatic centrally confirmed HER2-positive gastric or GEJ cancer and who had experienced disease progression during or after first-line therapy with a trastuzumab-containing regimen. The DESTINY-Gastric02 trial enrolled 79 patients from 24 sites across Europe and North America (no sites in Canada). The primary objective of the DESTINY-Gastric02 trial was to assess the efficacy of trastuzumab deruxtecan based on confirmed ORR per ICR assessment. OS, PFS, HRQoL-related outcomes (e.g., FACT-Ga), and harms were also investigated in the DESTINY-Gastric02 trial. The median age of patients in the DESTINY-Gastric02 trial population was 60.7 years (range, 20.3 years to 77.8 years), with 58.5% of patients being younger than 65 years. The trial population was 27.8% female and 72.2% male. The race distribution of the trial population was 0% American Indian or Alaska Native, 5.1% Asian, 1.3% Black or African American, 1.3% Native Hawaiian or other Pacific Islander, and 87.3% white. The majority of patients in the trial population had an ECOG PS of 1 (63.3%), GEJ adenocarcinoma (65.8%), and a HER2 status of IHC 3+ (86.1%).
An ITC consisting of 1 unanchored MAIC and 1 NMA was submitted by the sponsor. The ITC aimed to assess the comparative efficacy of trastuzumab deruxtecan versus currently available treatments that are relevant in Canada (i.e., ramucirumab-paclitaxel, docetaxel, paclitaxel monotherapy, irinotecan, and FOLFIRI) for patients with advanced or metastatic HER2-positive gastric cancer in the second-line treatment setting. Because the DESTINY-Gastric02 trial is a single-arm study, the unanchored MAIC was used to establish a connection between the trial and the rest of the NMA evidence network through the RAINBOW trial. In total, 6 studies were involved in the base-case analysis of the NMA. Efficacy was measured by OR and PFS. Safety was not evaluated.
The sponsor also submitted a phase II RCT (the DESTINY-Gastric01 trial) that enrolled 188 patients with HER2-positive advanced gastric or GEJ adenocarcinoma who had progressed on or after at least 2 prior regimens including a fluoropyrimidine drug, a platinum drug, and a trastuzumab-containing regimen (i.e., in the third-line and later settings). The primary objective of the DESTINY-Gastric01 trial was to compare the efficacy of trastuzumab deruxtecan versus the physician’s choice of treatment (i.e., irinotecan 150 mg/m2 intravenously every 2 weeks or paclitaxel 80 mg/m2 intravenously every week), as measured by ORR per ICR assessment. Secondary end points included OS, PFS, FACT-Ga, and harms.
Interpretation of Results
Efficacy
Among the many treatment goals, survival benefits and quality of life were highlighted as top priorities by both patients and the clinical experts consulted by the review team. These needs were well-captured by the pivotal DESTINY-Gastric02 trial, which assessed OS, PFS per ICR assessment, confirmed ORR per ICR assessment, and FACT-Ga. Despite the inclusion of these end points in the trial, the review team was unable to draw a definitive conclusion as to the beneficial effect of trastuzumab deruxtecan based on efficacy end points. The primary limitation is that, according to a GRADE framework, the certainty of evidence for these end points is very low due to the lack of either an internal control group or an external control.
According to the clinical experts consulted by the review team, assessing the probability of OS until 6 months or 12 months after treatment and assessing the probability of PFS at 6 months are critical to decision-making. The results from the DESTINY-Gastric02 trial showed that the probabilities of being alive were 77.8% (95% CI, 66.8% to 85.6%) at 6 months and 50.6% (95% CI, 38.4% to 61.5%) at 12 months; the probability of being progression-free at 6 months was 48.9% (95% CI, 36.6% to 60.2%). There were no thresholds identified from the literature, yet the clinical experts consulted by the review team noted that a 20% improvement in OS probability and a 10% improvement in PFS could be adopted to determine a minimal clinical benefit. The clinical experts noted that, in their experience, the observed OS and PFS probabilities may meet these thresholds; however, the experts were cautious in their interpretations due to the lack of a control group in the DESTINY-Gastric02 trial. Consequently, although the results suggest a promising treatment effect of trastuzumab deruxtecan on OS and PFS in the second-line setting, comparative evidence from properly designed and executed clinical trials is required to ascertain the existence and magnitude of such benefits.
Confirmed ORR per ICR assessment was the primary efficacy end point of the DESTINY-Gastric02 trial. The results showed a beneficial effect that 41.8% (95% CI, 30.8% to 53.4%) of the patients had ORR, with 5.1% having CR, suggesting a response to trastuzumab deruxtecan. As discussed previously, ORR might be a key end point of a clinical trial with a single-arm study design for regulatory purposes;27 however, based on input from the clinical experts consulted, ORR is considered less relevant and informative than OS or PFS in the clinical setting.
The results of the DESTINY-Gastric02 trial did not show a within-group improvement from baseline by the end of treatment in FACT-Ga total score (mean change from baseline: ██████ ██ █ █████). This aligned with the experience of the clinical experts consulted by the review team, according to whom the cessation of trastuzumab deruxtecan treatment would usually suggest either progression or intolerable side effects that negatively affect a patient’s quality of life. Furthermore, the clinical experts noted that the relative effect of trastuzumab deruxtecan on FACT-Ga could not be determined due to the lack of a comparator group.
An ITC was submitted by the sponsor to determine the efficacy of trastuzumab deruxtecan relative to other second-line treatments currently available in Canada, including ramucirumab-paclitaxel, paclitaxel, FOLFIRI, irinotecan, and docetaxel. A MAIC was used to connect the single-arm DESTINY-Gastric02 trial to the NMA evidence network and yield estimates of the relative treatment effect estimate between trastuzumab deruxtecan and ramucirumab-paclitaxel and the remaining comparators. Findings from the ITC showed that the treatment effect estimates for OS and PFS favoured trastuzumab deruxtecan over all the comparators included. However, the findings from the ITC should be interpreted with caution because the evidence is uncertain due to several major limitations. In the unanchored MAIC, patient comparability between the DESTINY-Gastric02 trial and the RAINBOW trial might not be adequate, given that information about some important prognostic factors (e.g., HER2 status) was missing; only 5 of 16 factors were involved in the weighting process, and imbalances remained after weighting in certain key factors (e.g., time to progressive disease on first-line therapy). A marked reduction in the MAIC ESS (from ██ to ████) suggests that the weights are highly variable due to a lack of population overlap across trials, and that the treatment effect estimates may be imprecise. Furthermore, other sources of heterogeneity in study design and statistical analyses existed that could not be addressed by the MAIC weighting process. The limitations of the MAIC analyses also contributed to uncertainty in the NMA findings because the NMA evidence network was constructed based on the MAIC, which connected the single-arm DESTINY-Gastric02 trial and the RAINBOW trial. One limitation specific to the NMA that can bias the estimate is the heterogeneity of the geographical regions and ethnicities observed between studies across the NMA evidence network.
Findings from the DESTINY-Gastric01 trial favoured trastuzumab deruxtecan over physician’s choice of irinotecan or paclitaxel in third-line and later settings. Until the results of a well-conducted confirmatory phase III trial are available, the positive findings from the DESTINY-Gastric01 trial should be interpreted with caution. In addition, there are concerns with respect to generalizing the results from the DESTINY-Gastric01 trial population to the patient population observed in third-line and later settings in Canada or to the DESTINY-Gastric02 trial population, due to differences in patient characteristics (e.g., cancer location, race) and/or the representativeness of the comparators (e.g., irinotecan or paclitaxel).
Harms
In the single-arm DESTINY-Gastric02 trial, the proportion of patients who had any TEAE of grade 3 or higher was 55.7%, with anemia (13.9%) being the most commonly reported. The proportion of patients who had any TESAE was 41.8%; 19.0% had at least 1 TEAE leading to the discontinuation of trastuzumab deruxtecan, and 13.9% had any TEAE associated with an outcome of death.
Overall, despite the challenge presented by the lack of a comparator group, most of the AEs reported in the DESTINY-Gastric02 trial, such as nausea, vomiting, anemia, and neutropenia, were not contrary to the expectation of the clinical experts consulted by the review team. According to the clinical experts consulted by the review team, trastuzumab deruxtecan associated lung toxicity – ILD, was a key safety end point upon which they would focus in this setting. Results showed that ████% of patients in the DESTINY-Gastric02 safety analysis set had ILD, with 2 events leading to trastuzumab deruxtecan discontinuation and 1 event leading to death. The clinical experts consulted by the review team noted that the incidence of ILD in the DESTINY-Gastric02 trial was consistent with the incidences reported in existing studies of patients who received trastuzumab deruxtecan to treat breast cancer. The clinical experts consulted by the review team also noted that clinicians are still learning about how to address lung toxicity associated with trastuzumab deruxtecan, given that trastuzumab deruxtecan is a relatively new drug. Nonetheless, the clinical experts consulted by the review team determined that the benefits of trastuzumab deruxtecan still outweighed its harms. Harms were not addressed in the sponsor-submitted ITC.
In the DESTNITY-Gastric01 trial, a higher proportion of patients in the trastuzumab deruxtecan group than in the control group had at least 1 TEAE of grade 3 or higher (85.6% versus 56.5%), at least 1 TESAE (44.8% versus 25.8%), at least 1 TEAE leading to the discontinuation of trastuzumab deruxtecan (17.6% versus 6.5%), and any TEAE associated with an outcome of death (6.4% versus 3.2%). The proportion of patients who had ILD was 12.8% in the trastuzumab deruxtecan group versus 0% in the control group. According to the clinical experts consulted by the review team, the use of trastuzumab deruxtecan requires careful attention, especially to ILD and other effects that can result in changes in a patient’s quality of life (e.g., diarrhea).
Consideration for a TLR Recommendation
A TLR recommendation is a recommendation by the CDA-AMC expert committee to publicly fund a drug or drug regimen for a certain period of time based on the condition that the sponsor will conduct 1 or more clinical studies that address uncertainty with the clinical evidence. CDA-AMC will subsequently conduct a reassessment of the additional evidence and issue a final reimbursement recommendation within a defined period of time. Based on the preliminary assessment by CDA-AMC (Table 36 in Appendix 1), trastuzumab deruxtecan meets the requirements to be considered by the expert committee for a TLR recommendation because:
Trastuzumab deruxtecan received an NOC/c from Health Canada on January 17, 2025, through Health Canada’s advance consideration process under the NOC/c policy.
A phase III clinical trial (the DESTINY-Gastric04 trial) is currently being conducted. This ongoing study will evaluate the efficacy and safety of trastuzumab deruxtecan relative to ramucirumab-paclitaxel for up to 3 years of follow-up in approximately 490 patients with HER2-positive gastric or GEJ adenocarcinoma. In terms of study population, the DESTINY-Gastric04 trial targets the second-line treatment setting for patients with HER2-positive gastric or GEJ cancer, in alignment with the current reimbursement request proposed by the sponsor. However, the indication currently under review by Health Canada targets a broader population, which includes not only patients in the second-line treatment setting, but also those in third-line and later settings. Therefore, the DESTINY-Gastric04 trial population does not completely align with the settings described in the Health Canada indication. As a result, the findings from the DESTINY-Gastric04 trial may not be generalizable to patients in the third-line setting and beyond. According to the clinical experts consulted by the review team, the selection of ramucirumab-paclitaxel as a comparator in the DESTINY-Gastric04 trial is appropriate because treatment with ramucirumab-paclitaxel is currently part of the standard of care in the second-line setting for locally advanced or metastatic HER2-positive gastric or GEJ cancer, and will likely remain as the standard of care in the second-line setting, when the results of the DESTINY-Gastric04 trial become available.
The results of the DESTINY-Gastric04 trial are expected to be ready in the fourth quarter of 2025.
The sponsor has expressed that it will commit to filing a reassessment application with CDA-AMC in accordance with the time frames specified in the procedures for TLR recommendations.
Conclusion
The DESTINY-Gastric02 trial (N = 79), a phase II, single-arm trial submitted by the sponsor, assessed the efficacy and safety of trastuzumab deruxtecan for the treatment of adult patients with unresectable or metastatic HER2-positive gastric or GEJ cancer in the second-line treatment setting. The clinical experts consulted by the review team noted that the results of some efficacy end points that were critical to decision-making (e.g., the probability of survival at 6 months or 12 months and of being progression-free at 6 months) were clinically meaningful. However, the absence of a comparator group in DESTINY-Gastric02 is a key limitation in the interpretation of the efficacy findings, resulting in very low certainty of evidence. The clinical experts consulted by the review team noted that the incidence of the key safety end point in the trial (i.e., ILD) met their expectations in terms of being consistent with the incidences reported in literature. According to the clinical experts, trastuzumab deruxtecan has an overall beneficial effect in the second-line treatment setting, warranting a confirmatory phase III clinical trial. The sponsor is currently conducting a phase III DESTINY-Gastric04 trial assessing the efficacy and safety of trastuzumab deruxtecan relative to ramucirumab-paclitaxel in patients with HER2-positive gastric or GEJ adenocarcinoma in the second-line treatment setting. The trial results are anticipated to be ready in the fourth quarter of 2025.
In the absence of direct evidence comparing trastuzumab deruxtecan to other second-line treatments currently available in Canada (i.e., ramucirumab-paclitaxel, paclitaxel, FOLFIRI, irinotecan, and docetaxel), sponsor-submitted ITCs using an unanchored MAIC and NMA were reviewed. The ITC treatment effect estimates for OS and PFS favoured trastuzumab deruxtecan over all other comparators; however, several major limitations in the design and methods of the ITC preclude any definitive conclusion about the magnitude of effect. Specifically, missing prognostic factors (e.g., HER2 status), the limited number of factors involved in the weighting process, residual imbalances in prognostic or effect-modifying factors, a significant reduction in ESS — and heterogeneity in study design, statistical analyses, geographical regions, and ethnicities across the NMA evidence network — can all result in biased estimates and overly precise credible intervals.
References
1.Summary of Clinical Evidence: ENHERTU (trastuzumab deruxtecan) as monotherapy for the treatment of adult patients with locally advanced or metastatic human epidermal growth factor 2 (HER2)-positive gastric or gastroesophageal junction (GEJ) adenocarcinoma who have received a prior anti-HER2-based regimen [internal sponsor's report]. Mississauga (ON): AstraZeneca Canada Inc.; 2024.
2.Pr ENHERTU®(Trastuzumab deruxtecan for injection). Powder for concentrate for solution for infusion, 100 mg, Intravenous infusion [draft product monograph]. Mississauga (ON): AstraZeneca; 2024. Accessed 2024/05/01/.
3.Drug Reimbursement Review sponsor submission: Trastuzumab deruxtecan (Enhertu), powder for concentrate for solution for infusion, 100 mg, intravenous infusion [internal sponsor's package]. Mississauga (ON): AstraZeneca Canada Inc.; 2024.
4.Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229-263. PubMed
5.Ajani JA, D'Amico TA, Bentrem DJ, et al. Gastric Cancer, Version 2.2022, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw. 2022;20(2):167-192. PubMed
6.Barra WF, Moreira FC, Pereira Cruz AM, et al. GEJ cancers: gastric or esophageal tumors? searching for the answer according to molecular identity. Oncotarget. 2017;8(61):104286-104294. PubMed
7.Curea FG, Hebbar M, Ilie SM, et al. Current Targeted Therapies in HER2-Positive Gastric Adenocarcinoma. Cancer Biother Radiopharm. 2017;32(10):351-363. PubMed
8.Al-Batran SE, Homann N, Pauligk C, et al. Perioperative chemotherapy with fluorouracil plus leucovorin, oxaliplatin, and docetaxel versus fluorouracil or capecitabine plus cisplatin and epirubicin for locally advanced, resectable gastric or gastro-oesophageal junction adenocarcinoma (FLOT4): a randomised, phase 2/3 trial. Lancet. 2019;393(10184):1948-1957. PubMed
9.Shapiro J, van Lanschot JJB, Hulshof M, et al. Neoadjuvant chemoradiotherapy plus surgery versus surgery alone for oesophageal or junctional cancer (CROSS): long-term results of a randomised controlled trial. Lancet Oncol. 2015;16(9):1090-1098. PubMed
10.Systemic Therapy for Advanced Gastric and Gastro-Esophageal Carcinoma. Toronto (ON): Cancer Care Ontario; 2022: https://www.cancercareontario.ca/en/guidelines-advice/types-of-cancer/366. Accessed 2024 Nov 18.
11.Taieb J, Bennouna J, Penault-Llorca F, Basile D, Samalin E, Zaanan A. Treatment of gastric adenocarcinoma: A rapidly evolving landscape. Eur J Cancer. 2023;195:113370. PubMed
12.Brenner DR, Gillis J, Demers AA, et al. Projected estimates of cancer in Canada in 2024. CMAJ. 2024;196(18):E615-E623. PubMed
13.Symptoms of stomach cancer. Toronto (ON): Canadian Cancer Society; 2019: https://cancer.ca/en/cancer-information/cancer-types/stomach/signs-and-symptoms. Accessed 2024 Oct 14.
14.Canadian Cancer Society, Canadian Cancer Statistics Advisory Committee. Canadian Cancer Statistics 2023. Ottawa (ON): Government of Canada; 2023: https://cdn.cancer.ca/-/media/files/research/cancer-statistics/2023-statistics/2023_pdf_en.pdf. Accessed 2024 Jun 25.
15.Stomach (Gastric) Cancer Survival Rates. Washington (DC): American Cancer Society; 2024: https://www.cancer.org/cancer/types/stomach-cancer/detection-diagnosis-staging/survival-rates.html. Accessed 2024 Jan 17.
16.Nakauchi M, Vos EL, Carr RA, et al. Distinct Differences in Gastroesophageal Junction and Gastric Adenocarcinoma in 2194 Patients: In Memory of Rebecca A. Carr, February 24, 1988-January 19, 2021. Ann Surg. 2023;277(4):629-636. PubMed
17.Jorgensen JT, Hersom M. HER2 as a Prognostic Marker in Gastric Cancer - A Systematic Analysis of Data from the Literature. J Cancer. 2012;3:137-144. PubMed
18.Barros-Silva JD, Leitao D, Afonso L, et al. Association of ERBB2 gene status with histopathological parameters and disease-specific survival in gastric carcinoma patients. Br J Cancer. 2009;100(3):487-493. PubMed
19.Zhou F, Li N, Jiang W, et al. Prognosis significance of HER-2/neu overexpression/amplification in Chinese patients with curatively resected gastric cancer after the ToGA clinical trial. World J Surg Oncol. 2012;10:274. PubMed
20.Ma C, Wang X, Guo J, Yang B, Li Y. Challenges and future of HER2-positive gastric cancer therapy. Front Oncol. 2023;13:1080990. PubMed
21.Roviello G, Catalano M, Iannone LF, et al. Current status and future perspectives in HER2 positive advanced gastric cancer. Clin Transl Oncol. 2022;24(6):981-996. PubMed
22.Holland P, Rafiq R, Matheson K, et al. Population based assessment of HER-2 and PD-L1 positivity in gastric and gastroesophageal junction adenocarcinomas in a Canadian population. J Clin Oncol. 2024;42(16_suppl):e16038-e16038.
23.Bartley AN, Washington MK, Ventura CB, et al. HER2 Testing and Clinical Decision Making in Gastroesophageal Adenocarcinoma: Guideline From the College of American Pathologists, American Society for Clinical Pathology, and American Society of Clinical Oncology. Arch Pathol Lab Med. 2016;140(12):1345-1363. PubMed
24.HER2 status test. Ottawa (ON): Canadian Cancer Society; 2023: https://cancer.ca/en/treatments/tests-and-procedures/her2-status-test#ci_her2_status_test_89_8823_00. Accessed 2024 Nov 18.
25.Guideline Resource Unit. Gastric Cancer. Clinical Practice Guideline GI-008– Version 6. Edmonton (AB): Alberta Health Services; 2021: https://www.albertahealthservices.ca/assets/info/hp/cancer/if-hp-cancer-guide-gi008-gastric.pdf. Accessed 2024 May 17.
26.Asmis T, Souter L, Agbassi C, et al. Systemic Therapy for Advanced Gastric and Gastro-Esophageal Carcinoma. 2022.
27.Food and Drug Administration. Clinical trial endpoints for the approval of cancer drugs and biologics: Guidance for industry. Silver Spring (MD): U.S. Department of Health and Human Services; 2018: https://www.fda.gov/media/71195/download. Accessed 2024 Nov 4.
28.Committee for Medicinal Products for Human Use. Guideline on the evaluation of anticancer medicinal products in man. Amsterdam (NL): European Medicines Agency; 2017: https://www.ema.europa.eu/en/documents/scientific-guideline/guideline-evaluation-anticancer-medicinal-products-man-revision-5_en.pdf. Accessed 2024 Nov 6.
29.Zhou H, Sun L, Wang M. Statistical considerations of designs for single-arm proof-of-concept oncology trial with time-to-event endpoint. Contemp Clin Trials. 2023;129:107200. PubMed
30.Balshem H, Helfand M, Schünemann HJ, et al. GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol. 2011;64(4):401-406. PubMed
31.Santesso N, Glenton C, Dahm P, et al. GRADE guidelines 26: informative statements to communicate the findings of systematic reviews of interventions. J Clin Epidemiol. 2020;119:126-135. PubMed
32.Clinical Study Report: DESTINY-Gastric02 (data cut-off date: April 9, 2021). A Phase 2, Open-label, Single-arm Trial of Trastuzumab Deruxtecan (DS-8201a) in HER2- positive, Unresectable or Metastatic Gastric or Gastroesophageal Junction (GEJ) Adenocarcinoma Subjects Who Have Progressed On or After a Trastuzumab containing Regimen [internal sponsor's report]. Mississuaga (ON): AstraZeneca Canada Inc.; 2022.
33.Clinical Study Report: DESTINY-Gastric02 (data cut-off date: Nov 8, 2021). A Phase 2, Open-label, Single-arm Trial of Trastuzumab Deruxtecan (DS-8201a) in HER2- positive, Unresectable or Metastatic Gastric or Gastroesophageal Junction (GEJ) Adenocarcinoma Subjects Who Have Progressed On or After a Trastuzumab containing Regimen [internal sponsor's report]. Mississuaga (ON): AstraZeneca Canada Inc.; 2022.
34.Higgins JP, Thompson SG, Spiegelhalter DJ. A re-evaluation of random-effects meta-analysis. J R Stat Soc Ser A Stat Soc. 2009;172(1):137-159. PubMed
35.Murad MH, Montori VM, Ioannidis JPA, Prasad K, Cook DJ, Guyatt G. Fixed-Effects and Random-Effects Models. In: Guyatt G, Rennie D, Meade MO, Cook DJ, eds. Users' Guides to the Medical Literature: A Manual for Evidence-Based Clinical Practice, 3rd ed. New York, NY: McGraw-Hill Education; 2015.
36.Cattelan L, Ghazawi FM, Le M, et al. Geographic and Socioeconomic Disparity of Gastric Cancer Patients in Canada. Curr Oncol. 2021;28(3):2052-2064. PubMed
37.Kahraman S, Yalcin S. Recent Advances in Systemic Treatments for HER-2 Positive Advanced Gastric Cancer. Onco Targets Ther. 2021;14:4149-4162. PubMed
38.Hu HH, Wang SQ, Zhao H, Chen ZS, Shi X, Chen XB. HER2(+) advanced gastric cancer: Current state and opportunities (Review). Int J Oncol. 2024;64(4). PubMed
39.Pr Enhertu®(Trastuzumab deruxtecan for injection). Powder for concentrate for solution for infusion, 100 mg, Intravenous infusion [product monograph]. Mississauga (ON): AstraZeneca; 2024: https://pdf.hres.ca/dpd_pm/00076260.PDF. Accessed 2024 Nov 27.
40.Pr CYRAMZA® (ramucirumab). Intravenous injection 10 mg ramucirumab / mL [product monograph]. Toronto (ON): Eli Lilly Canada, Inc; 2022: https://pi.lilly.com/ca/cyramza-ca-pm.pdf. Accessed 2024 May 17.
41.TAXOTERE (docetaxel): Concentrated Solution 80 mg/2.0 mL, 20 mg/0.5 mL injection [product monograph]. Laval (Québec) sanofi-aventis Canada Inc.; 2017: https://pdf.hres.ca/dpd_pm/00041993.PDF. Accessed 2024 Oct 13.
42.PrIrinotecan Hydrochloride Injection (Irinotecan hydrochloride trihydrate). Sterile solution: 20 mg/mL. House standard: 40 mg / 2 mL, 100 mg / 5 mL, 300 mg / 15 mL and 500 mg / 25 mL IV [product monograph]. Woodbridge (Ontario): Auro Pharma Inc; 2020: https://pdf.hres.ca/dpd_pm/00056704.PDF. Accessed 2024 Oct 13.
43.Clinical Evidence Summary for trastuzumab deruxtecan (Enhertu) as second-line treatment for gastric cancer: Indirect treatment comparison [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Trastuzumab deruxtecan (Enhertu), powder for concentrate for solution for infusion, 100 mg, intravenous infusion. Mississauga (ON): AstraZeneca Canada Inc.; 2024.
44.Van Cutsem E, di Bartolomeo M, Smyth E, et al. Trastuzumab deruxtecan in patients in the USA and Europe with HER2-positive advanced gastric or gastroesophageal junction cancer with disease progression on or after a trastuzumab-containing regimen (DESTINY-Gastric02): primary and updated analyses from a single-arm, phase 2 study. Lancet Oncol. 2023;24(7):744-756. PubMed
45.van Cutsem E, Di Bartolomeo M, Smyth E, et al. LBA55 Primary analysis of a phase II single-arm trial of trastuzumab deruxtecan (T-DXd) in western patients (Pts) with HER2-positive (HER2+) unresectable or metastatic gastric or gastroesophageal junction (GEJ) cancer who progressed on or after a trastuzumab-containing regimen. Ann Oncol. 2021;32:S1332.
46.Ku GY, Bartolomeo MD, Smyth E, et al. 1205MO - Updated analysis of DESTINY-Gastric02: A phase II single-arm trial of trastuzumab deruxtecan (T-DXd) in western patients (Pts) with HER2-positive (HER2+) unresectable/metastatic gastric/gastroesophageal junction (GEJ) cancer who progressed on or after trastuzumab-containing regimen. Ann Oncol. 2022;33(suppl_7):S555-S580.
47.Clinical Study Protocol for DESTINY-Gastric02 version 3: A Phase 2, Open-Label, Single-Arm Trial Of Trastuzumab Deruxtecan (DS-8201A) In HER2-Positive, Unresectable Or Metastatic Gastric Or Gastro-Esophageal Junction (GEJ) Adenocarcinoma Subjects Who Have Progressed On Or After A Trastuzumab-Containing Regimen [internal sponsor's report]. Mississuaga (ON): AstraZeneca Canada Inc.; 2020.
48.Statistical Analysis Plan for DESTINY-Gastric02 version 2: A Phase 2, Open-Label, Single-Arm Trial Of Trastuzumab Deruxtecan (DS-8201A) In HER2-Positive, Unresectable Or Metastatic Gastric Or Gastro-Esophageal Junction (GEJ) Adenocarcinoma Subjects Who Have Progressed On Or After A Trastuzumab-Containing Regimen [internal sponsor's report]. Mississuaga (ON): AstraZeneca Canada Inc.; 2021.
49.FACT-Ga. Functional Assessment of Cancer Therapy – Gastric. Broomfield (CO): FACIT Group: https://www.facit.org/measures/fact-ga. Accessed 2024 Oct 27.
50.Garland SN, Pelletier G, Lawe A, et al. Prospective evaluation of the reliability, validity, and minimally important difference of the functional assessment of cancer therapy-gastric (FACT-Ga) quality-of-life instrument. Cancer. 2011;117(6):1302-1312. PubMed
51.Clopper CJ, Pearson ES. The Use of Confidence or Fiducial Limits Illustrated in the Case of the Binomial. Biometrika. 1934;26(4):404-413.
52.Brookmeyer R, Crowley J. A Confidence Interval for the Median Survival Time. Biometrics. 1982;38(1):29-41.
53.Phillippo D, Ades T, Dias S, Palmer S, Abrams KR, Welton N. NICE DSU Technical Support Document 18: Methods for population-adjusted indirect comparisons in submissions to NICE. Vol 18. Decision Support Unit, ScHARR, University of Sheffield: NICE Decision Support Unit; 2016.
54.Wilke H, Muro K, Van Cutsem E, et al. Ramucirumab plus paclitaxel versus placebo plus paclitaxel in patients with previously treated advanced gastric or gastro-oesophageal junction adenocarcinoma (RAINBOW): a double-blind, randomised phase 3 trial. Lancet Oncol. 2014;15(11):1224-1235. PubMed
55.Lee KW, Maeng CH, Kim TY, et al. A Phase III Study to Compare the Efficacy and Safety of Paclitaxel Versus Irinotecan in Patients with Metastatic or Recurrent Gastric Cancer Who Failed in First-line Therapy (KCSG ST10-01). Oncologist. 2019;24(1):18-e24. PubMed
56.Sym SJ, Hong J, Park J, et al. A randomized phase II study of biweekly irinotecan monotherapy or a combination of irinotecan plus 5-fluorouracil/leucovorin (mFOLFIRI) in patients with metastatic gastric adenocarcinoma refractory to or progressive after first-line chemotherapy. Cancer Chemother Pharmacol. 2013;71(2):481-488. PubMed
57.Hironaka S, Ueda S, Yasui H, et al. Randomized, open-label, phase III study comparing irinotecan with paclitaxel in patients with advanced gastric cancer without severe peritoneal metastasis after failure of prior combination chemotherapy using fluoropyrimidine plus platinum: WJOG 4007 trial. J Clin Oncol. 2013;31(35):4438-4444. PubMed
58.Roy AC, Park SR, Cunningham D, et al. A randomized phase II study of PEP02 (MM-398), irinotecan or docetaxel as a second-line therapy in patients with locally advanced or metastatic gastric or gastro-oesophageal junction adenocarcinoma. Ann Oncol. 2013;24(6):1567-1573. PubMed
59.Cox DR. Regression Models and Life-Tables. Journal of the Royal Statistical Society Series B: Statistical Methodology. 1972;34(2):187-202.
60.Guyot P, Ades AE, Ouwens MJ, Welton NJ. Enhanced secondary analysis of survival data: reconstructing the data from published Kaplan-Meier survival curves. BMC Med Res Methodol. 2012;12(1):9. PubMed
61.Dias S, Sutton AJ, Welton NJ, Ades AE. NICE DSU Technical Support Document 3: Heterogeneity: Subgroups, Meta-Regression, Bias and Bias-Adjustment. National Institute for Health and Clinical Excellence; 2011.
62.Dias S, Welton NJ, Sutton AJ, Ades AE. NICE DSU Technical Support Document 2: A Generalised Linear Modelling Framework for Pairwise and Network Meta-Analysis of Randomised Controlled Trials. 2014.
63.Bucher HC, Guyatt GH, Griffith LE, Walter SD. The results of direct and indirect treatment comparisons in meta-analysis of randomized controlled trials. J Clin Epidemiol. 1997;50(6):683-691. PubMed
64.Brooks SP, Gelman A. General Methods for Monitoring Convergence of Iterative Simulations. Journal of Computational and Graphical Statistics. 1998;7(4):434-455.
65.Sterne JAC, Savovic J, Page MJ, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366:l4898. PubMed
66.Clinical Study Report: DESTINY-Gastric01 (data cut-off date: November 8, 2019). A Phase 2, Multicenter, Open-Label Study of DS-8201a in Subjects with HER2 Expressing Advanced Gastric or Gastroesophageal Junction Adenocarcinoma [internal sponsor's report]. Mississuaga (ON): AstraZeneca Canada Inc.; 2020.
67.Clinical Study Report: DESTINY-Gastric01 (data cut-off date: June 30, 2020). A Phase 2, Multicenter, Open-Label Study of DS-8201a in Subjects with HER2 Expressing Advanced Gastric or Gastroesophageal Junction Adenocarcinoma [internal sponsor's report]. Mississuaga (ON): AstraZeneca Canada Inc.; 2021.
68.Shitara K, Bang YJ, Iwasa S, et al. Trastuzumab Deruxtecan in Previously Treated HER2-Positive Gastric Cancer. N Engl J Med. 2020;382(25):2419-2430. PubMed
69.Yamaguchi K, Bang YJ, Iwasa S, et al. Trastuzumab Deruxtecan in Anti-Human Epidermal Growth Factor Receptor 2 Treatment-Naive Patients With Human Epidermal Growth Factor Receptor 2-Low Gastric or Gastroesophageal Junction Adenocarcinoma: Exploratory Cohort Results in a Phase II Trial. J Clin Oncol. 2023;41(4):816-825. PubMed
70.Yamaguchi K, Bang Y-J, Iwasa S, et al. Trastuzumab deruxtecan (T-DXd; DS-8201) in patients with HER2–positive advanced gastric or gastroesophageal junction (GEJ) adenocarcinoma: Final overall survival (OS) results from a randomized, multicenter, open-label, phase 2 study (DESTINY-Gastric01). J Clin Oncol. 2022;40(4_suppl):242-242.
71.Yamaguchi K, Bang Y-J, Iwasa S, et al. Trastuzumab deruxtecan (T-DXd; DS-8201) in patients with HER2-positive advanced gastric or gastroesophageal junction (GEJ) adenocarcinoma: Final overall survival (OS) results from a randomized, multicenter, open-label, phase 2 study (DESTINY-Gastric01). J Clin Oncol. 2021;39(15_suppl):4048-4048.
72.Shitara K, Yamaguchi K, Muro K, et al. Trastuzumab deruxtecan in patients with locally advanced or metastatic HER2-positive gastric cancer: a multicenter, open-label, expanded-access study. Int J Clin Oncol. 2024;29(1):27-35. PubMed
73.DeMets DL, Gordon Lan KK. Lan‐DeMetsAlpha‐Spending Function. Wiley StatsRef: Statistics Reference Online: John Wiley & Sons, Inc; 2014: https://onlinelibrary.wiley.com/doi/10.1002/9781118445112.stat06962. Accessed 2024 Nov 15.
74.O'Brien PC, Fleming TR. A multiple testing procedure for clinical trials. Biometrics. 1979;35(3):549-556. PubMed
Appendix 1: CDA-AMC Preliminary Assessment for TLR Eligibility
Please note that this appendix has not been copy-edited.
Table 36: Preliminary CDA-AMC Assessment of Eligibility for a TLR
Eligibility for TLR | CDA-AMC assessment |
|---|---|
Regulatory status | |
The drug has been issued an NOC/c by Health Canada or is undergoing review through Health Canada’s advance consideration process under the NOC/c policy. | Criterion has been met: The sponsor has noted that Health Canada has accepted the file for review through the advanced consideration under the NOC/c pathway with approval anticipated in Q1 2025. |
Evidence generation | |
A phase III clinical trial is being planned and/or conducted at the time of the submission to CDA-AMC. | Criterion has been met: Sponsor is currently conducting the phase III DESTINY-Gastric04 trial as part of the anticipated NOC/c postmarket requirements for the indication that will be reviewed by CDA-AMC. |
The phase III trial is being or will be conducted in a patient population that is reflective of the indication being reviewed by CDA-AMC | Criterion has been met:
Overall, CDA-AMC concludes that is acceptable and meets the criterion for a TLR recommendation. |
The phase III trial is being or will be conducted using the intervention at dosages and/or combination regimens that are reflective of the intervention that will be reviewed by CDA-AMC. | Criterion has been met: The intervention in the pending phase III trial is identical to the regimen that would be initially submitted to CDA-AMC and is consistent across the phase II and phase III studies (i.e., Enhertu as monotherapy administered at a dose of 6.4 mg/kg every 3 weeks). |
The phase III trial will be completed within a time frame that will not exceed 3 years from the target expert committee meeting date. | Criterion has been met: The target date for completion of the phase III trial is well within the 3-year window from the February 2025 expert committee meeting. The sponsor has stated that the primary completion of the DESTINY-Gastric04 trial is estimated to occur in the fourth quarter of 2025. |
Commitment to file for reassessment | |
Sponsor is willing to commit to file a reassessment application with CDA-AMC in accordance with the time frames specified in the procedures for TLR recommendations. | Criterion has been met: AstraZeneca has expressed that it will commit to file a reassessment application with CDA-AMC in accordance with the time frames specified in the procedures for TLR recommendations. |
HER2 = human epidermal growth factor 2; NOC/c = Notice of Compliance with conditions; Q1 = first quarter; Q4 = fourth quarter; TLR = time-limited reimbursement.
aAt the time of assessment, the indication proposed to Health Canada was as monotherapy, indicated for the treatment of adult patients with locally advanced or metastatic HER2-positive gastric or gastroesophageal junction adenocarcinoma who have received a prior anti-HER2-based regimen.
Pharmacoeconomic Review
Abbreviations
AE
adverse event
BIA
budget impact analysis
BSA
body surface area
CDA-AMC
Canada’s Drug Agency
CUA
cost-utility analysis
ESS
effective sample size
FOLFIRI
folinic acid–fluorouracil-irinotecan
GEJ
gastroesophageal junction
HER2
human epidermal growth factor receptor 2
HR
hazard ratio
ICER
incremental cost-effectiveness ratio
ITC
indirect treatment comparison
KM
Kaplan-Meier
MAIC
matching-adjusted indirect comparison
NMA
network meta-analysis
OS
overall survival
PFS
progression-free survival
QALY
quality-adjusted life-year
TTD
time to treatment discontinuation
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Trastuzumab deruxtecan (Enhertu), powder for concentrate for solution for infusion, 100 mg, IV infusion |
Indication | As monotherapy for the treatment of adult patients with unresectable, locally advanced or metastatic HER2-positive gastric or gastroesophageal junction adenocarcinoma who have received a prior trastuzumab-based regimen |
Health Canada approval status | NOC/c |
Health Canada review pathway | Advance consideration under NOC/c |
NOC date | January 18, 2025 |
Reimbursement request | As monotherapy for the second-line treatment of adult patients with unresectable locally advanced or metastatic HER2-positive gastric or gastroesophageal junction adenocarcinoma who have received a prior anti–HER2-based regimen |
Sponsor | AstraZeneca Canada Inc. |
Submission history | Previously reviewed: Yes Indication: Trastuzumab deruxtecan as monotherapy for the treatment of adult patients with unresectable or metastatic HER2-low (IHC 1+ or IHC 2+/ISH-) breast cancer who have received at least 1 prior line of chemotherapy in the metastatic setting or developed disease recurrence during or within 6 months of completing adjuvant chemotherapy. Patients with hormone receptor (HR positive) breast cancer should have received at least 1 and be no longer considered eligible for endocrine therapy. Recommendation date: June 29, 2023 Recommendation: Reimburse with clinical criteria and/or conditions Indication: Trastuzumab deruxtecan for the treatment of adult patients with unresectable or metastatic HER2-positive breast cancer who have received a prior treatment with an anti–HER2-based regimen in the metastatic setting or developed disease recurrence during or within 6 months of completing neoadjuvant or adjuvant therapy Recommendation date: September 28, 2022 Recommendation: Reimburse with clinical criteria and/or conditions |
HER2 = human epidermal growth factor receptor 2; HR = hormone receptor positive; IHC = immunohistochemistry; ISH = in situ hybridization; NOC = Notice of Compliance; NOC/c = Notice of Compliance with Conditions.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis PSM |
Target population | As second-line treatment in adult patients with locally advanced or metastatic HER2-positive gastric or GEJ adenocarcinoma who have progressed on or after 1 anti–HER2-containing regimena |
Treatment | Trastuzumab deruxtecan |
Dose regimen | 6.4 mg/kg every 21 days until disease progression or unacceptable toxicity |
Submitted price | Trastuzumab deruxtecan: $2,440.00 per 100 mg single-use vial for IV infusion |
Submitted treatment cost | $13,083.50 every 21 days (considers wastage, relative dose intensity, and average dose assumptions) |
Comparator | Ramucirumab-paclitaxelb |
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs, LYs |
Time horizon | 5 years |
Key data sources | Sponsor-submitted MAIC in which efficacy inputs for trastuzumab deruxtecan were informed by DESTINY-Gastric02, (NCT04014075; data cut-off date: November 2021), a phase II, open-label, single-arm trial, and RAINBOW (NCT01170663) for ramucirumab-paclitaxel.c |
Submitted results | ICER = $179,945 per QALY gained (incremental costs = $57,330; incremental QALYs = 0.32)d |
Key limitations |
|
CDA-AMC reanalysis results |
|
CDA-AMC = Canada’s Drug Agency; FOLFIRI = folinic acid–fluorouracil-irinotecan; GEJ = gastroesophageal junction; HER2 = human epidermal growth factor receptor 2; ICER = incremental cost-effectiveness ratio; LY = life-year; MAIC = matching-adjusted indirect comparison; NMA = network meta-analysis; OS = overall survival; PFS = progression-free survival; PSM = partitioned survival model; QALY = quality-adjusted life-year; QoL = quality of life; TTD = time to treatment discontinuation.
aIn line with the sponsor’s reimbursement request and the rationale for going through the time-limited reimbursement recommendation process, the sponsor’s economic analysis was restricted to the second-line population; thus, it did not consider evidence from the DESTINY-Gastric01 trial.
bThe sponsor included comparisons of trastuzumab deruxtecan with paclitaxel, docetaxel, irinotecan, and FOLFIRI in scenario analyses. Ramucirumab-paclitaxel was considered standard of care by the sponsor and deemed the primary comparator.
cThe comparisons of trastuzumab deruxtecan with paclitaxel, docetaxel, irinotecan, and FOLFIRI were derived through a sponsor-submitted NMA, in which trastuzumab deruxtecan was incorporated into the NMA via the adjusted results from the MAIC.
dScenario analysis results suggested that trastuzumab deruxtecan is associated with more QALYs and higher costs compared with each of paclitaxel, docetaxel, irinotecan, and FOLFIRI. The pairwise ICERs for trastuzumab deruxtecan versus each comparator range from $228,558 per QALY gained to $302,654 per QALY gained.
Conclusions
The sponsor submitted evidence from 2 phase II trials assessing the efficacy and safety of trastuzumab deruxtecan in adult patients with unresectable or metastatic human epidermal growth factor receptor 2 (HER2)-positive gastric or gastroesophageal junction (GEJ) cancer. Only 1 of these studies (DESTINY-Gastric02) was conducted in the patient population under review. DESTINY-Gastric02 was a single-arm trial that assessed the efficacy and safety of trastuzumab deruxtecan as a second-line treatment. The clinical experts consulted by the review team noted that the results of some efficacy end points that were critical to decision-making (e.g., probability of survival at 6 months or 12 months and probability of being progression-free at 6 months) were clinically meaningful. However, the absence of a comparator group in the DESTINY-Gastric02 trial is a key limitation in interpreting the efficacy findings, resulting in a very low certainty of evidence. In the absence of direct evidence comparing trastuzumab deruxtecan to other second-line treatments currently available in Canada (i.e., ramucirumab-paclitaxel; folinic acid–fluorouracil-irinotecan [FOLFIRI]; paclitaxel, irinotecan, and docetaxel), an indirect treatment comparison (ITC) was conducted using an unanchored matching-adjusted indirect comparison (MAIC) that informed the comparative efficacy of trastuzumab deruxtecan versus ramucirumab-paclitaxel and a network meta-analysis (NMA) that informed the comparative efficacy of trastuzumab deruxtecan versus paclitaxel, docetaxel, irinotecan, and FOLFIRI. The indirect evidence suggests that trastuzumab deruxtecan may offer superior overall survival (OS) and progression-free survival (PFS) compared to other second-line treatments. However, Canada’s Drug Agency (CDA-AMC) identified several major limitations in the MAIC and NMA. The sponsor acknowledged the uncertainty of the NMA in its submission and stated that results reliant on the NMA should be interpreted with caution. In the absence of randomized evidence or robust ITCs, it is uncertain to what degree the differences in PFS and OS benefits between trastuzumab deruxtecan and other second-line treatments are driven by confounding rather than treatment effect. The conclusions from the economic analysis are contingent on the submitted indirect evidence associated with methodological limitations, as noted in the clinical review. Therefore, the economic analysis may not accurately reflect the true incremental difference between trastuzumab deruxtecan and other second-line treatments.
The base-case analyses are presented relative to ramucirumab-paclitaxel because the clinical expert input received by CDA-AMC deemed this regimen to be the most relevant comparator in the indicated population; however, CDA-AMC also considered a scenario analysis comparing trastuzumab deruxtecan with FOLFIRI. The results and conclusions that can be drawn from the economic evaluation are similar between the sponsor’s analysis and CDA-AMC’s reanalysis. In the CDA-AMC base case, trastuzumab deruxtecan was associated with an incremental cost-effectiveness ratio (ICER) of $242,356 per quality-adjusted life-year (QALY) gained relative to ramucirumab-paclitaxel. Results from the CDA-AMC base case suggest that a price reduction of approximately 31% is required for trastuzumab deruxtecan to achieve an ICER of $50,000 per QALY gained relative to ramucirumab-paclitaxel. This ICER assumes that there is a notable clinical benefit in terms of both PFS and OS associated with trastuzumab deruxtecan compared with ramucirumab-paclitaxel, based on the results of the MAIC (i.e., 0.41 life-years gained). Because the comparative clinical evidence is highly uncertain, if these benefits are not borne out, then a higher price reduction would be required to achieve cost-effectiveness.
Because the economic analysis was restricted to the use of trastuzumab deruxtecan for the second-line treatment of adult patients with locally advanced or metastatic HER2-positive gastric or GEJ adenocarcinoma and did not consider evidence from the DESTINY-Gastric01 trial, the cost-effectiveness of trastuzumab deruxtecan in third-line treatment or later is unknown.
This review of trastuzumab deruxtecan was conducted as a review eligible for a time-limited reimbursement recommendation by CDA-AMC, pending additional clinical studies to address uncertainty in the clinical evidence. When this information becomes available, CDA-AMC will subsequently conduct a reassessment of the additional clinical and economic evidence and issue a final recommendation.
Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, clinician groups, and drug plans that participated in the CDA-AMC review process.
Patient and caregiver input was collected by My Gut Feeling – Stomach Cancer Foundation of Canada through an international online survey. Ninety-five percent of respondents resided in Canada. Respondents reported they had experience with a variety of treatment modalities, including chemotherapy, immunotherapy, targeted therapy, surgery, and radiation. While current therapies led to mixed satisfaction from respondents in terms of perceived efficacy and cancer control, all respondents experienced at least 1 treatment-related side effect with previous treatments. The survey found that current systemic therapy to treat gastroesophageal cancers has a significant impact on patient morbidity and quality of life. Patients and caregivers who were less satisfied with current treatment options cited recurrence, lack of alternative treatment options, side effect burden, or treatment not working as the primary reasons of dissatisfaction. When evaluating their treatment options, patients and caregivers identified multiple factors that are important to them, such as quality of life, treatment side effects, cost of treatment, convenience of treatment, duration of treatment, and survival benefits. Additionally, barriers to access were identified; these included institutional and health care system barriers, limited availability of treatment, and how quickly treatment could be accessed. Patients and caregivers commented on the time and money lost to attending cancer treatment appointments, citing money spent on medications, driving and parking costs, and costs of eating at the hospital as financial stressors. Four respondents had experience with trastuzumab deruxtecan. Participants commented that they were satisfied with this drug primarily because it had fewer side effects or slowed their disease.
Clinician input was received from the Canadian Gastrointestinal Oncology Evidence Network and Cancer Care Ontario. These groups commented that, following disease progression after HER2-targeted therapy in the first line, there is no further targeted therapy available for patients who are HER2 positive because improvements in objective response rate and OS have not been demonstrated by currently used treatments in previous clinical trials. Thus, standard systemic therapies are used in the second- and third-line settings. It was noted that paclitaxel (with or without ramucirumab) is currently the standard of care for second-line therapy. Clinician groups commented that trastuzumab deruxtecan would likely be the new standard of care for second-line treatment of metastatic HER2-positive gastric or GEJ cancer disease due to the current lack of effective treatment options. The clinician input commented that lung toxicity with pneumonitis is the most concerning adverse event (AE) and should be monitored with algorithms and frequent CT imaging. Input suggested that trastuzumab deruxtecan should be discontinued in the event of grade 2 or worse pneumonitis. Clinician group input indicated that approximately 160 patients in Canada per year who have metastatic HER2-positive gastric or GEJ cancer would be eligible for treatment with trastuzumab deruxtecan, should it be reimbursed by public drug plans for use as a second-line therapy.
The drug plan input stated that funded comparators in the second-line setting include ramucirumab-paclitaxel, FOLFIRI, irinotecan, and paclitaxel. Additionally, the plans noted that a confidential negotiated price exists for ramucirumab. Participating drug plans noted that while the sponsor’s proposed place in therapy is use in the second-line setting, the DESTINY-Gastric01 trial suggests it may also be used in later-line settings. The drug plan input noted that reimbursement of trastuzumab deruxtecan may change the place in therapy of comparators, including the place in therapy of treatments reimbursed in subsequent lines. As such, it is unclear what therapies would be funded for subsequent lines of therapy for patients who were treated with trastuzumab deruxtecan in second-line setting.
Several of these concerns were addressed in the sponsor’s model:
The sponsor conducted a scenario analysis that considered additional costs associated with out-of-pocket expenses and travel time as well as those incurred due to lost productivity or income for patients younger than 65 years.
The impact of disease and treatment on patient quality of life was captured with utility values. AEs were incorporated as disutilities within the analysis.
Ramucirumab-paclitaxel, FOLFIRI, irinotecan, and paclitaxel were included as comparators.
CDA-AMC was unable to address the following concerns raised from patient group, clinician group, and drug plan input:
CDA-AMC was unable to determine the cost-effectiveness of trastuzumab deruxtecan in the third-line or later setting owing to a lack of comparative data and the submitted model structure.
CDA-AMC was unable to consider the cost of subsequent therapy in reanalyses because these were highly uncertain.
Economic Review
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted a cost-utility analysis assessing trastuzumab deruxtecan compared with ramucirumab-paclitaxel.1 Paclitaxel, docetaxel, irinotecan, and FOLFIRI were considered relevant comparators in the scenario analyses. The modelled population comprised adults with locally advanced or metastatic HER2-positive gastric or GEJ adenocarcinoma who had progressed on or after receiving 1 trastuzumab-containing regimen (i.e., second-line treatment); this population aligned with the submitted reimbursement request and the population enrolled in the DESTINY-Gastric02, a phase II, open-label, single-arm trial.2 The modelled population and reimbursement request are narrower than the proposed Health Canada indication, which does not restrict use to the second-line setting.3
Trastuzumab deruxtecan is available as a 100-mg single-use vial of powder to be reconstituted for IV infusion at a submitted price of $2,440.00.1,3 The recommended dosage of trastuzumab deruxtecan is 6.4 mg/kg once every 3 weeks (i.e., in 21-day cycles) until disease progression or unacceptable toxicity.3 Assuming wastage (i.e., no vial sharing), a relative dose intensity of 100%, and a mean dose of ███ ██ (calculated assuming a patient weight of ████ ██) per administration, the sponsor estimated drug acquisition costs for trastuzumab deruxtecan to be $13,083.50 every 21 days.
The sponsor assumed the following dosing schedule for ramucirumab-paclitaxel: ramucirumab is administered twice per 28-day cycle at a dosage of 8 mg/kg (mean dose of ███ ██), and paclitaxel is administered 3 times per 28-day cycle at a dose of 80 mg/m2 (mean dose of ███ ██ assuming a patent body surface area [BSA] of ████|). Both drugs were assumed to be administered until progression. The sponsor assumed ramucirumab costs to be $626.88 per 100-mg vial (or $3,134.40 per 500-mg vial) and paclitaxel costs of $300.00 per 30-mg vial, $1,196.80 per 100-mg infusion bag, and $3,740.00 per 300-mg infusion bag. Assuming wastage and a relative dose intensity of 100%, the sponsor estimated drug acquisition costs for ramucirumab-paclitaxel to be $10,210.20 every 21 days.
The sponsor’s base case only includes ramucirumab-paclitaxel as a comparator. Scenario analyses include docetaxel, FOLFIRI, paclitaxel alone, and irinotecan as comparators. Relevant cost and recommended dosage information, as assumed by the sponsor, for treatments considered in the scenario analyses are described in Appendix 3, Table 10.
The clinical outcomes modelled were OS, PFS, and time to treatment discontinuation (TTD). The model simulated life-years, QALYs, and costs for each treatment over a lifetime time horizon (i.e., 5 years), discounted at a rate of 1.5% per annum. The analysis was undertaken from the perspective of the Canadian public health care payer.
Model Structure
The sponsor submitted a partitioned survival model with 3 health states: alive and progression-free (preprogression), alive with progressed disease (postprogression), and dead.1 The proportion of patients who were preprogression, postprogression, or dead at any time over the model horizon were derived from non–mutually exclusive survival curves for each intervention. All patients entered the model in the preprogression health state, where they received either trastuzumab deruxtecan or ramucirumab-paclitaxel. The proportion of patients in each state was tracked each cycle (cycle length = 1 week). Disease progression was determined by investigator assessment according to Response Evaluation Criteria in Solid Tumours Version 1.1 (RECIST 1.1). Once a patient experienced disease progression, they could not subsequently be considered progression-free. Patients could discontinue treatment before or after disease progression based on the estimated TTD, after which time the cost of first-line treatment would no longer be incurred. Patients could remain on treatment while in the postprogression disease state. Dead was modelled as an absorbing state.
Model Inputs
This section describes the relevant model inputs for trastuzumab deruxtecan and all comparators considered by the sponsor in base-case and scenario analyses.
Baseline patient characteristics in the model reflected patients enrolled in the DESTINY-Gastric02 trial.2 The average patient in the modelled cohort, which the sponsor assumed reflected the patient population in Canada, was aged 60.7 years, weighed ████ ██, had a mean BSA of ███ ██, and was more likely to be male (72.2%). Weight and BSA were used to calculate treatment costs for treatments with weight- or BSA-based dosing. Age and the proportion of the population who were male were used to assign age- and sex-specific mortality and to cap the lower bound for all-cause mortality in the model.
Key clinical efficacy inputs for trastuzumab deruxtecan, including OS, PFS, and TTD, were derived from Kaplan-Meier (KM) data from the DESTINY-Gastric02 trial (data cut-off: November 8, 2021). KM estimates of OS, PFS, and TTD from the trial period were used to fit parametric survival curves to extrapolate the treatment effect beyond the observed trial data (median follow-up = 10.2 months; maximum follow-up = 22.1 months) over the entire model time horizon (5 years). Several parametric functions were fitted to the OS and PFS data to select candidate distributions based on diagnostic plots, goodness-of-fit statistics, and clinical plausibility of long-term projections, as determined by clinical experts consulted by the sponsor. The chosen parametric survival distributions for OS, PFS, and TTD for trastuzumab deruxtecan were gamma, log-normal, and generalized gamma, respectively.
Efficacy inputs for OS and PFS for ramucirumab-paclitaxel were based on the results of the sponsor’s MAIC4 using data from the DESTINY-Gastric02 trial2 and the RAINBOW trial.5 The sponsor estimated PFS and OS for trastuzumab deruxtecan from the DESTINY-Gastric02 trial and extrapolated the curves to derive PFS and OS for ramucirumab-paclitaxel by applying the hazard ratio (HR) for each outcome (OS = ████; PFS = ████) from the MAIC to the reference trastuzumab deruxtecan curve. This approach implies a proportional hazards assumption. Similarly, efficacy inputs for OS and PFS for paclitaxel, docetaxel, irinotecan, and FOLFIRI were derived by applying the HR for each outcome to the reference trastuzumab deruxtecan curve (Appendix 3, Table 10). However, the HRs were based on the results of an NMA. Data from the unanchored MAIC were used to connect the single-arm, pivotal DESTINY-Gastric02 trial into the evidence network of the NMA. TTD for all comparators was derived by applying the PFS HR to the reference trastuzumab deruxtecan TTD curve.
The sponsor’s base case assumed no waning of treatment effect, implying that the predicted clinical benefits associated with trastuzumab deruxtecan would be maintained indefinitely throughout the lifetime horizon of the model. Postprogression treatment outcomes were not explicitly modelled; thus, it was implicitly assumed that the OS data reflected the survival benefit of subsequent therapies. As such, subsequent therapies affect only costing. The sponsor assumed 19.94% of patients received a subsequent line of treatment, irrespective of the treatment received in the second-line setting. Subsequent therapies modelled were FOLFIRI, paclitaxel, ramucirumab-paclitaxel, and trifluridine and tipiracil. The sponsor assumed no re-treatment was permitted. The subsequent therapy received was based on clinical expert opinion (described in Appendix 3, Table 11). The duration of subsequent therapy was sourced from the DESTINY-Gastric02 trial,2 except for trifluridine and tipiracil which were sourced from the TAGS clinical trial.6
Health state utility values applied in the economic model (preprogression = █████; postprogression = █████) were derived from EQ-5D-5L data collected in the DESTINY-Gastric02 trial and mapped to EQ-5D-3L using an algorithm by Hernández Alava et al.7,8 A relative utility decrement was applied to the health state utility values in each cycle to account for the deterioration in health-related quality of life associated with aging.9
AEs in the model were restricted to grade 3 or 4 events, which occurred in at least 5% of patients in the DESTINY-Gastric02 trial.10 The incidences of AEs were obtained from the RAINBOW trial for ramucirumab-paclitaxel and paclitaxel alone,5 from the COUGAR-02 trial for docetaxel,11 and from published literature for FOLFIRI and irinotecan.12,13 The modelled AEs included anemia, leukopenia, nausea, decreased neutrophil count, decreased appetite, interstitial lung disease, fatigue, anorexia, febrile neutropenia, abdominal pain, hypertension, pain, diarrhea, neuropathy, vomiting, infection, and mucositis. Utility decrements for treatment-related AEs included in the model were sourced from gastric cancer, non–small cell lung cancer, and metastatic breast cancer literature and applied as a 1-time utility decrement in the first model cycle.14-18 The duration of each AE was sourced from patients treated with trastuzumab deruxtecan in the DESTINY-Gastric02 trial.10
The sponsor’s base case included costs for drug acquisition, administration, subsequent therapy, AEs, resource utilization, and end-of-life care. Drug unit costs were sourced from DeltaPA for all treatments, including subsequent therapies.19 Administration costs were sourced from Ontario’s Schedule of Benefits for Physician Services.20 Administration costs associated with chair time ($216.05 per hour) were sourced from Tam et al. and account for the preparation of the regimen, hourly wages for the pharmacist and chemotherapy nurse, and overhead costs.21 Treatment infusion times were sourced from Rugo et al. for trastuzumab deruxtecan,22 from Cancer Care Ontario for ramucirumab-paclitaxel23 and FOLFIRI,24 and from other published literature for docetaxel, irinotecan, and paclitaxel alone.25-27 Additionally, an administration cost associated with the insertion and removal of an IV pump was included for FOLFIRI ($107.55).20,28 AE unit costs were derived from the Canadian Institute for Health Information Patient Cost Estimator for patients aged 60 years to 79 years and applied as a one-time cost in the first model cycle.29 Health care resource use unit costs that were applied irrespective of treatment type were sourced from Ontario’s Schedule of Benefits for Physician Services, with the frequency of use obtained from a previous National Institute for Health and Care Excellence (NICE) appraisal.18,20 However, patients treated with trastuzumab deruxtecan were assumed to require an echocardiogram every 12 weeks and more frequent CT scans (every 9 weeks versus every 12 weeks for comparators). Lastly, a one-time terminal care cost was included, encompassing expenses related to end-of-life care based on estimates from the literature.30
Summary of Sponsor’s Economic Evaluation Results
The base-case analysis was run probabilistically (1,000 iterations); sensitivity analyses were conducted deterministically. The deterministic and probabilistic results were similar. The probabilistic findings are presented here.
Base-Case Results
The submitted analysis was based on publicly available prices of the comparator treatments. Results from the base case of the submitted economic evaluation are presented in Table 3. Additional results from the sponsor’s submitted economic evaluation base case are presented in Appendix 3.
In the sponsor’s submitted base case, the expected total costs and QALYs over a lifetime horizon (i.e., 5 years) for trastuzumab deruxtecan were $244,817 and 0.93, respectively. Approximately 0.25% of the population of patients treated with trastuzumab deruxtecan were alive at the end of the modelled time horizon (i.e., 5 years). Trastuzumab deruxtecan was associated with an ICER of $179,945 per QALY gained relative to ramucirumab-paclitaxel (incremental costs = $57,330; incremental QALYs = 0.32). Approximately 29.2% of the incremental QALYs for trastuzumab deruxtecan relative to ramucirumab-paclitaxel were gained after the maximum follow-up time of 22.1 months observed in the DESTINY-Gastric02 trial. In the sponsor’s analysis, trastuzumab deruxtecan had a 2% probability of being cost-effective at a willingness-to-pay threshold of $50,000 per QALY gained. Trastuzumab deruxtecan was more costly and more effective than ramucirumab-paclitaxel in 100% of the probabilistic iterations. The key drivers of the results were QALYs gained in the preprogression health state and drug acquisition costs.
Table 3: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER versus reference ($/QALY) |
|---|---|---|---|---|---|
Ramucirumab-paclitaxel | 187,487 | Reference | 0.61 | Reference | Reference |
Trastuzumab deruxtecan | 244,817 | 57,330 | 0.93 | 0.32 | 179,945 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Source: Sponsor’s pharmacoeconomic submission.1
Sensitivity and Scenario Analysis Results
The sponsor conducted scenario analyses for the comparison of trastuzumab deruxtecan with ramucirumab-paclitaxel, encompassing considerations such as alternative time horizons, discount rates, parametric distributions for OS, PFS, and TTD, utility values, and the inclusion of relative dose intensities. The sponsor’s results for all scenario analyses were aligned with the base case, in that trastuzumab deruxtecan had higher costs and higher QALYs compared to ramucirumab-paclitaxel.
Additionally, the sponsor conducted a scenario analysis from a societal perspective. This analysis included additional costs associated with out-of-pocket expenses, travel time, and costs incurred due to lost productivity or income for patients younger than 65 years. In this analysis, relative to ramucirumab-paclitaxel, the ICER was $179,969 per QALY gained. The results were similar to the sponsor’s base-case analysis using a health care payer perspective.
Furthermore, the sponsor included alternative sequential and pairwise analyses in which paclitaxel, docetaxel, irinotecan, and FOLFIRI were considered comparators. As noted by the sponsor, results from these analyses are to be interpreted with caution due to limitations associated with the NMA. In sequential analyses, all the treatments were either dominated or extendedly dominated by docetaxel, except for trastuzumab deruxtecan. Because efficacy inputs were informed by the MAIC analysis, in which patient-level data from the DESTINY-Gastric02 trial were reweighted to match the RAINBOW trial, a sequential analysis may not be appropriate. The results of the pairwise analyses indicate that trastuzumab deruxtecan is more costly and more expensive than paclitaxel, docetaxel, irinotecan, and FOLFIRI (Appendix 3, Table 13); the ICERs ranged from $228,558 per QALY gained to $302,654 per QALY gained.
CDA-AMC Appraisal of the Sponsor’s Economic Evaluation
CDA-AMC identified several key limitations to the sponsor’s analysis that have notable implications for the economic analysis.
Comparative clinical efficacy (OS and PFS) is highly uncertain: There is a lack of direct, head-to-head evidence comparing the efficacy of trastuzumab deruxtecan to that of other second-line treatments currently available in Canada (i.e., ramucirumab-paclitaxel, paclitaxel, FOLFIRI, irinotecan, and docetaxel). The DESTINY-Gastric02 trial was a single-arm trial lacking a comparator or external control. As such, an ITC was submitted by the sponsor to inform this evidence gap. The ITC comprised 2 components: an unanchored MAIC and an NMA. The unanchored MAIC was used to connect the single-arm DESTINY-Gastric02 trial into the evidence network of the NMA using the RAINBOW trial as a comparator. HRs for ramucirumab-paclitaxel were derived from the MAIC, while HRs for paclitaxel, FOLFIRI, irinotecan, and docetaxel were derived from the NMA.
Although the results of the indirect evidence suggest that trastuzumab deruxtecan may offer superior OS and PFS compared to ramucirumab-paclitaxel, paclitaxel, FOLFIRI, irinotecan, and docetaxel, the clinical review notes that several major limitations in the MAIC and NMA preclude any definitive conclusion about the magnitude of effect, including missing prognostic factors (e.g., HER2 status), limited factors involved in the weighting process, residual imbalances in prognostic or effect-modifying factors, a significant reduction in effective sample size (ESS), and heterogeneity in study design, statistical analyses, geographical regions, and ethnicities across the NMA evidence network. Notably, the sponsor commented in its pharmacoeconomic submission that results reliant on the results of the NMA (i.e., trastuzumab deruxtecan versus paclitaxel, FOLFIRI, irinotecan, and docetaxel) should be interpreted with caution due to limitations associated with the NMA. While the sponsor limits its statement to treatments reliant on the NMA, results reliant on the MAIC analyses (i.e., trastuzumab deruxtecan versus ramucirumab-paclitaxel) are highly uncertain. The only aforementioned limitation specific to the NMA is the heterogeneity of geographical region and ethnicity observed between studies across the NMA evidence network.
Furthermore, CDA-AMC notes that, despite a marked reduction in the ESS from the DESTINY-Gastric02 trial to conduct the MAIC (i.e., from ██ patients, the actual number of patients involved in the reweighting process in the DESTINY-Gastric02 trial, to ████ patients, the ESS of the DESTINY-Gastric02 trial after reweighting), the sponsor estimated OS and PFS for trastuzumab deruxtecan using KM data from all patients treated with trastuzumab deruxtecan in the DESTINY-Gastric02 trial (N = 79). It was inappropriate to use KM data from the full DESTINY-Gastric02 trial population to apply HRs from the MAIC because the HRs represented an adjusted population from the DESTINY-Gastric02 trial. The sponsor’s approach potentially biases the effect estimates in an unknown direction.
CDA-AMC was unable to address the limitations associated with the currently available evidence in reanalyses.
Model structure may overestimate comparative efficacy: Results from the sponsor’s model suggested that trastuzumab deruxtecan was associated with additional survival benefits after progression (i.e., life-years for trastuzumab deruxtecan in the postprogression health state were 36% greater than for ramucirumab-paclitaxel). However, clinical experts consulted by CDA-AMC noted that there is no rationale to support this because there is no clear mechanism by which trastuzumab deruxtecan would continue to provide a survival benefit after progression versus ramucirumab-paclitaxel. The sponsor’s use of a partitioned survival model introduces structural assumptions about the relationship between PFS and OS that likely do not accurately reflect causal relationships within the disease pathway (for example, that PFS and OS can be assumed to be independent). These assumptions may produce a biased postprogression survival benefit for trastuzumab deruxtecan, as observed in the sponsor’s base case.
CDA-AMC was unable to address this limitation in reanalyses.
The chosen OS and PFS distributions produce results that lack face validity: Parametric extrapolations were fit to OS and PFS KM data from the DESTINY-Gastric02 trial for trastuzumab deruxtecan (data cut-off: November 8, 2021) to extrapolate the treatment effect beyond the observed trial data (median follow-up = 10.2 months; maximum follow-up = 22.1 months) over the entire model time horizon (i.e., 5 years). For all other comparators, HRs from the sponsor’s submitted indirect evidence were applied to the reference trastuzumab deruxtecan curve. The parametric extrapolations chosen by the sponsor for OS (gamma) and PFS (log-normal) result in PFS exceeding OS, but it is clinically implausible for more patients to be at risk of progression than alive. The sponsor artificially capped PFS so that if PFS exceeds OS, PFS is set equal to OS. CDA-AMC explored alternative parametric distributions of OS and PFS for trastuzumab deruxtecan but was unable to identify suitable alternative parametric distributions due to a poor visual fit with the KM data from the DESTINY-Gastric02 trial.
CDA-AMC was unable to address this limitation in reanalyses.
Subsequent therapy costs are highly uncertain: The inclusion of subsequent therapies only affects costing; it was implicitly assumed that the OS data reflected the survival benefit of subsequent therapies. The sponsor assumed, citing Starling et al.,31 that 19.94% of patients were treated with a subsequent line of therapy, irrespective of the second-line treatment received. However, in Starling et al., only 6.6% of patients were treated in the third-line setting. Furthermore, in the DESTINY-Gastric02 trial, 49.4% of patients were treated with subsequent therapy. This range of patients treated with third-line therapy highlights the uncertainty of this parameter. The clinical expert input noted that although the sponsor’s assumption that nearly 20% of patients received third-line treatment is reasonable, it is currently rare for a patient to make it to third-line treatment. Given this, the decision as to what treatment a patient is offered in the third-line setting would depend on their clinical status. Furthermore, the use of trastuzumab in the third-line setting was not considered by the sponsor, and it is unclear whether subsequent use differed in the trials for the comparator treatments.
As there is uncertainty in both the proportion of patients treated with third-line therapy and the relative distribution of subsequent therapy received, and because trastuzumab deruxtecan was not considered as a subsequent therapy in the third-line setting, subsequent therapy costs are highly uncertain.
In the CDA-AMC base case, subsequent therapy costs were excluded. If trastuzumab deruxtecan is considered more effective than comparators, this change biases the results in its favour. The cost-effectiveness of trastuzumab deruxtecan in the third-line or later population is unknown.
Health state utility values are uncertain: The sponsor derived health state utility values from EQ-5D-5L data collected in the DESTINY-Gastric02 trial. The sponsor’s derived utility value for the preprogression health state implies that patients with locally advanced or metastatic HER2-positive gastric or GEJ adenocarcinoma who have had a prior anti-HER2-containing regimen and have not yet progressed on their second-line treatment have a similar quality of life as an average person in Canada. The clinical expert input noted that the preprogression utility value exceeded expectations, given that patients being treated with second-line therapy are generally symptomatic, have alterations in their ability to eat and maintain a healthy body weight, and may experience some side effects from treatment. Moreover, the clinical expert input commented that the incremental difference between the preprogression and postprogression health states was markedly smaller than expected. The sponsor noted that, because the EQ-5D data were not collected following treatment discontinuation in the DESTINY-Gastric02 trial, the impact of disease progression on health-related quality of life may not be fully captured. The sponsor provided alternative utility values sourced from the RAINBOW trial (preprogression = 0.737; postprogression = 0.587) and used in a previous National Institute for Health and Care Excellence submission.32 The clinical expert input found the alternative utility values to be more reasonable for the indicated patient population.
In the CDA-AMC base case, health state utility values derived from the RAINBOW trial were adopted.
TTD is uncertain: The sponsor modelled TTD for trastuzumab deruxtecan by fitting a generalized gamma distribution to KM data from the DESTINY-Gastric02 trial to extrapolate the treatment effect beyond the observed trial data. TTD for all comparators was derived by applying the PFS HR to the reference trastuzumab deruxtecan TTD curve. The sponsor’s chosen approach assumes that patients discontinue treatment before experiencing disease progression. As noted in the respective product monographs, treatment should be discontinued upon disease progression or unacceptable toxicity.3,23,24,33-35 The clinical expert input obtained by CDA-AMC for this review indicated that, while some patients may discontinue treatment before progression due to AEs or unacceptable toxicity, the majority discontinue treatment due to progression.
In the CDA-AMC base case, TTD was set as equal to PFS for all comparators. CDA-AMC acknowledges that this assumption is conservative and may overestimate drug acquisition costs for all treatments.
Drug acquisition costs are uncertain: First, while the sponsor indicated that drug unit costs were sourced from DeltaPA,19 CDA-AMC notes that there were numerous discrepancies between the unit costs calculated by CDA-AMC (based on DeltaPA prices) and the unit costs calculated by the sponsor.19 These differences were attributed to factors such as jurisdiction-specific pricing (i.e., ramucirumab and irinotecan), inaccurate pricing data (paclitaxel), reliance on only the most expensive vial sizes in cost estimates (i.e., docetaxel), and incorrect cost calculations (leucovorin). Nonetheless, all prices were based on publicly available list prices and may not reflect the actual prices paid by public drug plans. Ramucirumab concluded negotiations with the pan-Canadian Pharmaceutical Alliance with a Letter of Intent and any potential confidential rebates are not reflected.36
Second, CDA-AMC notes that, for treatments with a recommended dose that is dependent on patient characteristics (i.e., body weight and BSA), drug acquisition costs are sensitive to the assumed patient characteristics because wastage of unused product is assumed. For example, based on a patient weight of █████ ██ in the DESTINY-Gastric02 trial, a dose of ███ ██ per administration is required for ramucirumab. The sponsor assumes that an additional 100 mg vial of ramucirumab will be required to achieve the recommended dose and that 93 mg will be wasted. It is unlikely that an additional vial would be opened to provide approximately 1% of the target dose. The issue of product wastage is not solely attributed to ramucirumab, given that all treatments included in this review depend on patient characteristics (i.e., either weight or BSA). The direction and magnitude of the impact is sensitive to the assumed patient characteristics and the number of vials required to achieve the recommended dosage.
Third, the wastage of unused product was inappropriately considered for fluorouracil and leucovorin. Costs for fluorouracil and leucovorin were based on the prices of bulk pharmacy vials. Bulk pharmacy vials are intended to be used for multiple doses, as detailed by the respective product monographs;37,38 thus, the inclusion of wastage for the unused product of bulk pharmacy vials is not aligned with the intended use of the products. The sponsor’s assumptions pertaining to wastage overestimate the amount of product wasted and may overestimate drug acquisition costs for FOLFIRI.
Lastly, the sponsor assumed that fluorouracil, administered as part of the FOLFIRI regimen, was provided at a dose of 3,000 mg/m2 every 14 days. Cancer Care Ontario states that the recommended dose is 400 mg/m2 on day 1, then 2,400 mg/m2 by continuous infusion over 46 hours every 14 days starting on day 1 (i.e., simplified to 2,800 mg/m2 every 14 days).24 The clinical experts confirmed that the recommended dose listed by Cancer Care Ontario is used in clinical practice.
In the CDA-AMC base case, unit drug costs for ramucirumab, paclitaxel, docetaxel, and irinotecan were corrected. Additionally, CDA-AMC assumed no wastage of unused product for fluorouracil and leucovorin and corrected the dose of fluorouracil administered. CDA-AMC was unable to consider the impact of alternative patient characteristics on product wastage.
Poor modelling practices were employed: When executing probabilistic analyses with random seeding for the CDA-AMC base case, the generated results lacked face validity. As noted in CDA-AMC’s Procedures for Reimbursement Reviews, if seeding is used with a model, the functionality to easily revise or disable this feature must be included to aid in verifying the stability of the probabilistic analysis.39 Because CDA-AMC was restricted to using a fixed seeding, this criterion was not met. Furthermore, the sponsor’s submitted model included numerous IFERROR statements which led to situations in which the parameter value is overwritten with an alternative value without alerting the user to the automatized overwriting. The systematic use of IFERROR statements makes thorough auditing of the sponsor’s model impractical because it remains unclear whether the model is running inappropriately by overriding errors.
CDA-AMC was unable to address this limitation and notes that a thorough validation of the sponsor’s model was not possible. As a result of the seeding issue, CDA-AMC considered only the deterministic analysis results.
Additionally, the following key assumptions were made by the sponsor and have been appraised by CDA-AMC (refer to Table 4).
Table 4: Key Assumptions of the Submitted Economic Evaluation
Sponsor’s key assumption | CDA-AMC comment |
|---|---|
Ramucirumab-paclitaxel is the only relevant comparator. | Unlikely to be appropriate. While the clinical expert feedback agreed that ramucirumab-paclitaxel was the most relevant comparator, the feedback also agreed that FOLFIRI is a relevant comparator and is used in approximately 25% of patients (per the sponsor’s BIA). However, the clinical expert feedback noted that the large differences in clinical outcomes assumed between FOLFIRI and ramucirumab-paclitaxel did not align with clinical expectations. CDA-AMC undertook a scenario analysis considering the cost-effectiveness of trastuzumab deruxtecan compared with FOLFIRI. This analysis resulted in an ICER of $300,592 per QALY gained for trastuzumab deruxtecan. Given the clinical expert feedback, this estimate may underestimate the ICER for trastuzumab deruxtecan. As per the CDA-AMC cost table, FOLFIRI is much less costly than ramucirumab-paclitaxel. |
The incidence rates of AEs are expected to reflect those observed in clinical trials. | Not appropriate. The incidence rates of grade 3 and 4 AEs for trastuzumab deruxtecan and other second-line treatments currently available in Canada (i.e., ramucirumab-paclitaxel, paclitaxel, FOLFIRI, irinotecan, and docetaxel) were based on naive comparisons, without adjusting or accounting for differences in patient characteristics. The rate of AEs is used to calculate AE costs in the sponsor’s base case. Owing to the direct use of clinical trial data, it is not possible to determine if any observed differences between the therapies are solely due to the treatment or, rather, to bias or confounding factors. Furthermore, no safety end point was evaluated in the NMA; therefore, no conclusions on safety can be drawn on the indirect comparison of trastuzumab deruxtecan to ramucirumab-paclitaxel, paclitaxel, FOLFIRI, irinotecan, and docetaxel. |
EQ-5D-5L scores were mapped to EQ-5D-3L index values using an algorithm by Hernández Alava et al.8 | Uncertain. Mapping from EQ-5D-5L to EQ-5D-3L is unnecessary and adds uncertainty to both the precision and validity of the utility estimates. |
All treatments are administered at a dose intensity of 100%. | Reasonable. Assuming a dose intensity of 100% is a conservative assumption that only impacts treatment acquisition costs. CDA-AMC notes that the respective product monographs for trastuzumab deruxtecan and ramucirumab-paclitaxel outline dose interruption and reduction criteria for patients experiencing adverse reactions.3,23 |
AE = adverse event; BIA = budget impact analysis; CDA-AMC = Canada’s Drug Agency; FOLFIRI = folinic acid–fluorouracil-irinotecan; ICER = incremental cost-effectiveness ratio; NMA = network meta-analysis; QALY = quality-adjusted life-year.
CDA-AMC Reanalyses of the Economic Evaluation
Base-Case Results
CDA-AMC undertook the reanalyses outlined in Table 5 to address, where possible, the limitations within the sponsor’s submitted economic model. The CDA-AMC base case was derived by making changes in model parameter values and assumptions in consultation with clinical experts.
Table 5: CDA-AMC Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CDA-AMC value or assumption |
|---|---|---|
Changes to derive the CDA-AMC base case | ||
1. TTD |
| TTD equals PFS for all treatments |
2. Subsequent therapy costs | Included | Excluded |
3. Health state utility values |
|
|
4. Unit drug costs |
|
|
5. Fluorouracil dose | 3,000 mg/m2 per 14-day cycle | 2,800 mg/m2 per 14-day cycle |
6. Bulk pharmacy vial wastage | Assumes no vial sharing for bulk pharmacy vials of leucovorin (500 mg) and fluorouracil (5,000 mg) | Assumes vial sharing for bulk pharmacy vials of leucovorin (500 mg) and fluorouracil (5,000 mg) |
CDA-AMC base case | ― | Reanalysis 1 + 2 + 3 + 4 + 5 + 6 |
CDA-AMC = Canada’s Drug Agency; HR = hazard ratio; PFS = progression-free survival; TTD = time to treatment discontinuation.
The CDA-AMC base case was based on publicly available prices of the comparator treatments. Results from the CDA-AMC base case are presented in Table 6. Additional results from the CDA-AMC base case are presented in Appendix 4. Due to the limitations with the sponsor’s model coding and implausible results from the random seeding for the probabilistic analysis, CDA-AMC considered only the deterministic results.
In the CDA-AMC base case, the expected total costs and QALYs over a lifetime horizon (i.e., 5 years) for trastuzumab deruxtecan were $265,114 and 0.81, respectively. Trastuzumab deruxtecan was associated with an ICER of $242,356 per QALY gained relative to ramucirumab-paclitaxel (incremental costs = $69,457; incremental QALYs = 0.29). Approximately 29% of the incremental QALYs for trastuzumab deruxtecan relative to ramucirumab-paclitaxel were gained after the maximum follow-up time of 22.1 months observed in the DESTINY-Gastric02 trial. The key drivers of the results were QALYs gained in the preprogression health state and drug acquisition costs.
Table 6: Summary of the Stepped Analysis of the CDA-AMC Reanalysis Results
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALY) |
|---|---|---|---|---|
Sponsor’s base case | Ramucirumab-paclitaxel | 185,426 | 0.60 | Reference |
Trastuzumab deruxtecan | 243,769 | 0.92 | 179,408 | |
CDA-AMC reanalysis 1: TTD | Ramucirumab-paclitaxel | 196,998 | 0.60 | Reference |
Trastuzumab deruxtecan | 271,456 | 0.92 | 228,963 | |
CDA-AMC reanalysis 2: subsequent therapy costs | Ramucirumab-paclitaxel | 182,574 | 0.60 | Reference |
Trastuzumab deruxtecan | 237,428 | 0.92 | 168,678 | |
CDA-AMC reanalysis 3: health state utility values | Ramucirumab-paclitaxel | 185,426 | 0.52 | Reference |
Trastuzumab deruxtecan | 243,769 | 0.81 | 203,573 | |
CDA-AMC reanalysis 4: unit drug costs | Ramucirumab-paclitaxel | 187,709 | 0.60 | Reference |
Trastuzumab deruxtecan | 244,175 | 0.92 | 173,637 | |
CDA-AMC reanalysis 5: fluorouracil dose | Ramucirumab-paclitaxel | 185,426 | 0.60 | Reference |
Trastuzumab deruxtecan | 243,769 | 0.92 | 179,408 | |
CDA-AMC reanalysis 6: bulk pharmacy vial wastage | Ramucirumab-paclitaxel | 185,324 | 0.60 | Reference |
Trastuzumab deruxtecan | 243,731 | 0.92 | 179,605 | |
CDA-AMC base case (reanalysis 1 + 2 + 3 + 4 + 5 + 6) | Ramucirumab-paclitaxel | 195,657 | 0.52 | Reference |
Trastuzumab deruxtecan | 265,114 | 0.81 | 242,356 |
CDA-AMC = Canada’s Drug Agency; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; TTD = time to treatment discontinuation.
Note: Results are based on deterministic analyses, given the probabilistic analysis limitation identified in the CDA-AMC Appraisal of the Sponsor’s Economic Evaluation section.
Scenario Analysis Results
CDA-AMC undertook price reduction analyses based on the sponsor’s base case and CDA-AMC’s base case (Table 7). The CDA-AMC base case suggested that a price reduction of approximately 30.6% would be required for trastuzumab deruxtecan to achieve an ICER of $50,000 per QALY gained.
Table 7: CDA-AMC Price Reduction Analyses
Analysis | Unit drug cost ($) | ICERs for trastuzumab deruxtecan versus ramucirumab-paclitaxel ($/QALY) | |
|---|---|---|---|
Price reduction | $ | Sponsor’s base case | CDA-AMC reanalysis |
No price reduction | 2,440 | 179,945 | 242,356 |
10% | 2,196 | 134,616 | 175,495 |
20% | 1,952 | 89,287 | 114,595 |
30% | 1,708 | 43,958 | 53,696 |
40% | 1,464 | Trastuzumab deruxtecan is dominant | Trastuzumab deruxtecan is dominant |
50% | 1,220 | Trastuzumab deruxtecan is dominant | Trastuzumab deruxtecan is dominant |
60% | 976 | Trastuzumab deruxtecan is dominant | Trastuzumab deruxtecan is dominant |
70% | 732 | Trastuzumab deruxtecan is dominant | Trastuzumab deruxtecan is dominant |
80% | 488 | Trastuzumab deruxtecan is dominant | Trastuzumab deruxtecan is dominant |
90% | 244 | Trastuzumab deruxtecan is dominant | Trastuzumab deruxtecan is dominant |
CDA-AMC = Canada’s Drug Agency; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
CDA-AMC considered an analysis using the lowest public price of ramucirumab ($65.133 per mL; approximately 6% lower than the price used in the CDA-AMC base case). Using this price, the deterministic ICER for trastuzumab deruxtecan increases to $253,149 per QALY gained, and a price reduction of approximately 34% would be required for trastuzumab deruxtecan to achieve an ICER of $50,000 per QALY gained.
CDA-AMC also undertook a scenario analysis considering the cost-effectiveness of trastuzumab deruxtecan compared with FOLFIRI, which resulted in an ICER of $300,592 per QALY gained for trastuzumab deruxtecan. A price reduction of at least 69% is required to achieve an ICER of $50,000 per QALY gained. The clinical expert feedback noted that the large differences in clinical outcomes assumed between FOLFIRI and ramucirumab-paclitaxel did not align with clinical expectations. Given the clinical expert feedback, this estimate may underestimate the ICER for trastuzumab deruxtecan versus FOLFIRI. As a result, the price reduction may also be underestimated.
Issues for Consideration
DESTINY-Gastric04 (NCT04704934): A Phase 3, Multicenter, 2-Arm Randomized, Open-Label Study of Trastuzumab Deruxtecan in Subjects With HER2-Positive Metastatic and/or Unresectable Gastric or Gastro-Esophageal Junction (GEJ) Adenocarcinoma Subjects Who Have Progressed on or After a Trastuzumab-Containing Regimen is currently under way to assess trastuzumab deruxtecan versus ramucirumab-paclitaxel, and it will likely address uncertainty within the clinical evidence submitted in this review. The trial is expected to be completed by February 1, 2026.40 Thus, this review of trastuzumab deruxtecan was conducted as a time-limited reimbursement recommendation by CDA-AMC on the basis that the sponsor has expressed a commitment to filing a reassessment application with CDA-AMC within the time frames specified in the procedures for time-limited reimbursement recommendations. CDA-AMC notes that the studied population for the confirmatory trial differs slightly from the population for trastuzumab deruxtecan currently under review by Health Canada.
The sponsor’s reimbursement request is for trastuzumab deruxtecan as monotherapy for the second-line treatment of adult patients with locally advanced or metastatic HER2-positive gastric or GEJ adenocarcinoma who have received a prior anti–HER2-based regimen. This population is narrower than the proposed Health Canada indication, which does not restrict use to the second-line setting. The clinical experts consulted by CDA-AMC anticipated that the majority of patients would be treated with trastuzumab deruxtecan in the second-line setting because there are no other HER2-directed therapies available for these patients. As the sponsor’s economic analysis was restricted to the second-line population, the cost-effectiveness of trastuzumab deruxtecan in the third-line or later setting is unknown.
CDA-AMC has previously reviewed trastuzumab deruxtecan for 2 breast cancer indications.41,42 The cost-effectiveness results of these evaluations may not be directly comparable to those in the current review, owing to differences in model structure, clinical effectiveness parameters, health state utility values, and cost inputs.
CDA-AMC–participating drug plans indicated that the sponsor’s primary comparator, ramucirumab, has a negotiated price. Therefore, the costs associated with the ramucirumab-paclitaxel regimen are overestimated.
Overall Conclusions
The sponsor submitted evidence from 2 phase II trials assessing the efficacy and safety of trastuzumab deruxtecan in adult patients with unresectable or metastatic HER2-positive gastric or GEJ cancer, DESTINY-Gastric02, a single-arm trial assessing the efficacy and safety of trastuzumab deruxtecan as a second-line treatment; and the DESTINY-Gastric01 trial, a randomized controlled trial assessing the efficacy and safety of trastuzumab deruxtecan in the third-line or later treatment. In line with the sponsor’s reimbursement request and the rationale for going through the time-limited reimbursement recommendation process, the sponsor’s economic analysis was restricted to the second-line population; thus, it did not consider evidence from the DESTINY-Gastric01 trial. The clinical experts consulted by the review team noted that the results of some efficacy end points in the DESTINY-Gastric02 trial that were critical to decision-making (e.g., the probability of survival at 6 months or 12 months and of being progression-free at 6 months) were clinically meaningful. However, the absence of a comparator group in the DESTINY-Gastric02 trial is a key limitation in the interpretation of the efficacy findings, resulting in very low certainty of evidence. In the absence of direct evidence comparing trastuzumab deruxtecan to other second-line treatments currently available in Canada (i.e., ramucirumab-paclitaxel, FOLFIRI, paclitaxel, irinotecan, and docetaxel), an ITC was conducted using an unanchored MAIC that informed the comparative efficacy of trastuzumab deruxtecan versus ramucirumab-paclitaxel as well as an NMA that informed the comparative efficacy of trastuzumab deruxtecan versus paclitaxel, docetaxel, irinotecan, and FOLFIRI. The indirect evidence suggests that trastuzumab deruxtecan may offer superior OS and PFS compared to other second-line treatments. However, CDA-AMC identified several major limitations in the MAIC and NMA. The sponsor acknowledged the uncertainty of the NMA in its submission and stated that results reliant on the NMA should be interpreted with caution. In the absence of randomized evidence or robust indirect comparisons, it is uncertain to what degree the differences in PFS and OS benefits between trastuzumab deruxtecan and other second-line treatments are driven by confounding rather than treatment effect. The conclusions from the economic analysis are contingent on the submitted indirect evidence, which is associated with methodological limitations, as noted in the clinical review. Therefore, the economic analysis may not accurately reflect the true incremental difference between trastuzumab deruxtecan and other second-line treatments.
In addition to the comparative efficacy of trastuzumab deruxtecan versus other second-line treatments being uncertain, CDA-AMC identified several limitations in the sponsor’s economic submission: the cost-effectiveness of trastuzumab deruxtecan in the third-line or later population is unknown; the model structure potentially overestimates the survival benefit attributed to trastuzumab deruxtecan; the chosen OS and PFS distributions produce results that lack face validity; and there is uncertainty with respect to subsequent therapy costs, health state utilities, drug acquisition costs, and TTD. The CDA-AMC base case was derived by assuming that TTD equals PFS for all treatments, excluding subsequent therapy costs, adopting health state utility values from the RAINBOW trial, correcting unit drug costs and the dose of fluorouracil, and assuming that bulk pharmacy vials are shared.
The base-case analyses are presented relative to ramucirumab-paclitaxel because the clinical expert input received by CDA-AMC deemed this regimen to be the most relevant comparator in the indicated population; however, CDA-AMC also considered a scenario analysis comparing trastuzumab deruxtecan with FOLFIRI. The results and conclusions that can be drawn from the economic evaluation are similar between the sponsor’s analysis and CDA-AMC’s reanalysis. In the CDA-AMC base case, trastuzumab deruxtecan was associated with an ICER of $242,356 per QALY gained relative to ramucirumab-paclitaxel (incremental costs = $69,457; incremental QALYs = 0.29). Results from the CDA-AMC base case suggest that a price reduction of approximately 31% is required for trastuzumab deruxtecan to achieve an ICER of $50,000 per QALY gained relative to ramucirumab-paclitaxel. This ICER assumes a notable clinical benefit in both PFS and OS associated with trastuzumab deruxtecan compared with ramucirumab-paclitaxel, based on the results of the MAIC (i.e., 0.41 life-years gained). As the comparative clinical evidence is highly uncertain, if these benefits are not borne out, a higher price reduction would be required to achieve cost-effectiveness.
Because the economic analysis was restricted to the use of trastuzumab deruxtecan for the second-line treatment of adult patients with locally advanced or metastatic HER2-positive gastric or GEJ adenocarcinoma and did not consider evidence from the DESTINY-Gastric01 trial, the cost-effectiveness of trastuzumab deruxtecan in the third-line or later setting is unknown.
This review of trastuzumab deruxtecan was conducted as a review eligible for a time-limited recommendation by CDA-AMC, pending additional clinical studies to address uncertainty in the clinical evidence. When this information becomes available, CDA-AMC will subsequently conduct a reassessment of the additional clinical and economic evidence and issue a final recommendation.
References
1.AstraZeneca Canada Inc. Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Enhertu (trastuzumab deruxtecan), 6.4 mg/kg intravenous (IV) infusion. September 16, 2024.
2.Daiichi Sankyo, Inc. Clinical Study Report Addendum: DESTINY-Gastric02. November DCO. A Phase 2, Open-label, Single-arm Trial of Trastuzumab Deruxtecan (DS-8201a) in HER2-positive, Unresectable or Metastatic Gastric or Gastroesophageal Junction (GEJ) Adenocarcinoma Subjects Who Have Progressed On or After a Trastuzumab containing Regimen. Version 1.0 [internal sponsor's report]. October 12, 2022.
3.AstraZeneca Canada Inc. Enhertu (trastuzumab deruxtecan): powder for concentrate for solution for infusion, 100 mg, Intravenous infusion [DRAFT product monograph]. May 1, 2024.
4.AstraZeneca Canada Inc. Trastuzumab deruxtecan (Enhertu®) as second-line treatment for gastric cancer: Indirect treatment comparison [internal sponsor’s report]. In: Drug Reimbursement Review sponsor submission: Trastuzumab deruxtecan, 100 mg single-use vial for intravenous infusion. November 12, 2024.
5.Wilke H, Muro K, Van Cutsem E, et al. Ramucirumab plus paclitaxel versus placebo plus paclitaxel in patients with previously treated advanced gastric or gastro-oesophageal junction adenocarcinoma (RAINBOW): A double-blind, randomised phase 3 trial. Lancet Oncol. 2014;15(11):1224-35. doi: 10.1016/S1470-2045(14)70420-6 PubMed
6.Shitara K, Doi T, Dvorkin M, et al. Trifluridine/tipiracil versus placebo in patients with heavily pretreated metastatic gastric cancer (TAGS): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2018;19(11):1437-1448. doi: 10.1016/S1470-2045(18)30739-3 PubMed
7.Daiichi Pharmaceuticals LP. In House Data, Daiichi Pharmaceuticals LP. Utility report [sponsor supplied reference]. October 3, 2022.
8.Hernandez Alava M, Wailoo A, Pudney S. Methods for mapping between the EQ 5D 5L and the 3L. NICE Decision Support Unit report [accessed by sponsor]. Decision Support Unit, ScHARR, University of Sheffield; 2017. https://drive.google.com/file/d/1ehLw3-Mo7WyHFiwyijI4Ur5kCAPTEAPe/view
9.Guertin JR, Feeny D, Tarride JE. Age- and sex-specific Canadian utility norms, based on the 2013-2014 Canadian Community Health Survey. CMAJ. 2018;190(6):E155-E161. doi: 10.1503/cmaj.170317 PubMed
10.Daiichi Sankyo, Inc. Clinical Study Report: DESTINY-Gastric02. April DCO. A Phase 2, Open-label, Single-arm Trial of Trastuzumab Deruxtecan (DS-8201a) in HER2-positive, Unresectable or Metastatic Gastric or Gastro-esophageal Junction (GEJ) Adenocarcinoma Subjects Who Have Progressed On or After a Trastuzumab-containing Regimen. Version 2.0 [internal sponsor’s report]. April 8, 2022.
11.Ford HE, Marshall A, Bridgewater JA, et al. Docetaxel versus active symptom control for refractory oesophagogastric adenocarcinoma (COUGAR-02): An open-label, phase 3 randomised controlled trial. Lancet Oncol. 2014;15(1):78-86. doi: 10.1016/S1470-2045(13)70549-7 PubMed
12.Maugeri-Sacca M, Pizzuti L, Sergi D, et al. FOLFIRI as a second-line therapy in patients with docetaxel-pretreated gastric cancer: A historical cohort. J Exp Clin Cancer Res. 2013;32(1):67. doi: 10.1186/1756-9966-32-67 PubMed
13.Thuss-Patience PC, Kretzschmar A, Bichev D, et al. Survival advantage for irinotecan versus best supportive care as second-line chemotherapy in gastric cancer: A randomised phase III study of the Arbeitsgemeinschaft Internistische Onkologie (AIO). Eur J Cancer. 2011;47(15):2306-14. doi: 10.1016/j.ejca.2011.06.002 PubMed
14.National Institute for Health and Care Excellence. Trifluridine–tipiracil for treating metastatic gastric cancer or gastro-oesophageal junction adenocarcinoma after 2 or more therapies. (NICE technology appraisal TA669). Accessed December 12, 2024. https://www.nice.org.uk/guidance/TA669
15.Nafees B, Stafford M, Gavriel S, Bhalla S, Watkins J. Health state utilities for non small cell lung cancer. Health Qual Life Outcomes. 2008;6:84. doi: 10.1186/1477-7525-6-84 PubMed
16.National Institute for Health and Care Excellence. Trastuzumab deruxtecan for treating HER2-positive unresectable or metastatic breast cancer after 2 or more anti-HER2 therapies. (NICE technology appraisal TA704) [accessed by sponsor]. https://www.nice.org.uk/guidance/ta704
17.National Institute for Health and Care Excellence. Ramucirumab for previously treated locally advanced or metastatic non-small-cell lung cancer. (NICE technology appraisal TA403) [accessed by sponsor]. https://www.nice.org.uk/guidance/ta403
18.National Institute for Health and Care Excellence. Ramucirumab for treating advanced gastric cancer or gastro–oesophageal junction adenocarcinoma previously treated with chemotherapy. (NICE technology appraisal TA378). Accessed August 11, 2022. https://www.nice.org.uk/guidance/TA378
19.IQVIA. DeltaPA. 2023. Accessed October 17, 2024. https://www.iqvia.com/
20.Government of Ontario. Schedule of Benefits - Physician Services - Under the Health Insurance Act (February 20, 2024 (effective April 1, 2024) [accessed by sponsor].
21.Tam VC, Ko YJ, Mittmann N, et al. Cost-effectiveness of systemic therapies for metastatic pancreatic cancer. Curr Oncol. 2013;20(2):e90-e106. doi: 10.3747/co.20.1223 PubMed
22.Rugo HS, Bianchini G, Cortes J, Henning JW, Untch M. Optimizing treatment management of trastuzumab deruxtecan in clinical practice of breast cancer. ESMO Open. 2022;7(4):100553. doi: 10.1016/j.esmoop.2022.100553 PubMed
23.Cancer Care Ontario. Drug formulary: PACL(W)+RAMU. Accessed November 22, 2024. https://www.cancercareontario.ca/en/drugformulary/regimens/monograph/47456
24.Cancer Care Ontario. Drug formulary: FOLFIRI. Accessed November 22, 2024. https://www.cancercareontario.ca/en/drugformulary/regimens/monograph/49306
25.Pfizer Inc. CAMPTOSAR (irinotecan hydrochloride): injection, for intravenous use [highlights of prescribing information]. Accessed June 13, 2024. https://labeling.pfizer.com/showlabeling.aspx?id=533
26.U.S. Food and Drug Administration. Prescribing information: Docetaxel injection, solution for intravenous infusion. Accessed June 13, 2024. https://www.accessdata.fda.gov/drugsatfda_docs/label/2012/201525s002lbl.pdf
27.BC Cancer. BC Cancer Protocol summary for second or third line palliative combination chemotherapy for metastatic gastric or esophageal adenocarcinoma or esophageal squamous cell carcinoma using irinotecan, fluorouracil and leucovorin. Accessed April 8, 2024. http://www.bccancer.bc.ca/chemotherapy-protocols-site/Documents/Gastrointestinal/GIGFOLFIRI_Protocol.pdf
28.Employment and Social Development Canada. Wages: Registered Nurse (R.N.) in Ontario. Accessed August 14, 2024. https://www.jobbank.gc.ca/marketreport/wages-occupation/993/ON
29.Canadian Institute for Health Information. Patient Cost Estimator. Accessed June 13, 2024. https://www.cihi.ca/en/patient-cost-estimator
30.De Oliveira C, Pataky R, Bremner KE, et al. Estimating the Cost of Cancer Care in British Columbia and Ontario: A Canadian Inter-Provincial Comparison. Healthc Policy. 2017;12(3):95-108. doi: 10.12927/hcpol.2017.25024 PubMed
31.Starling N, Zhang L, Dunton K, et al. 1586P Characteristics, treatment (Tx) patterns and outcomes of patients with advanced/metastatic gastric cancer (GC) or gastro-esophageal junction (GEJ) adenocarcinoma previously treated with anti-HER2 therapy in an English national registry. Ann Oncol. 2023;34:S883. doi: 10.1016/j.annonc.2023.09.1498
32.National Institute for Health and Care Excellence. Ramucirumab for treating advanced gastric cancer or gastro-oesophageal junction adenocarcinoma previously treated with chemotherapy. (NICE technology appraisal TA378 supporting evidence: committee papers). Accessed November 26, 2024. https://www.nice.org.uk/guidance/TA378/documents/gastric-cancer-metastatic-ramucirumab-after-chemotherapy-id741-committee-papers2
33.Cancer Care Ontario. Drug formulary: Paclitaxel. Accessed November 22, 2024. https://www.cancercareontario.ca/en/drugformulary/regimens/monograph/49036
34.Cancer Care Ontario. Drug formulary: Docetaxel. Accessed November 22, 2024. https://www.cancercareontario.ca/en/drugformulary/regimens/monograph/46836
35.Cancer Care Ontario. Drug formulary: Irinotecan. Accessed November 22, 2024. https://www.cancercareontario.ca/en/drugformulary/regimens/monograph/49276
36.pan-Canadian Pharmaceutical Alliance. Cyramza (ramucirumab). Accessed November 26, 2024. https://www.pcpacanada.ca/negotiation/20850
37.Accord Healthcare Inc. Fluorouracil injection USP: 50 mg/mL (5 g/100 mL) [product mongraph]. Updated October 30, 2019. Accessed September 18, 2024. https://pdf.hres.ca/dpd_pm/00053796.PDF
38.Pfizer Canada ULC. LEUCOVORIN CALCIUM INJECTION USP: Leucovorin calcium solution, 10 mg/mL, intravenous and intramuscular [product monograph]. Accessed November 26, 2024. https://pdf.hres.ca/dpd_pm/00068748.PDF
39.Canada's Drug Agency. Procedures for Reimbursement Reviews. Accessed November 28, 2024. https://www.cda-amc.ca/sites/default/files/Drug_Review_Process/Drug_Reimbursement_Review_Procedures.pdf
40.Daiichi Sankyo. NCT04704934: Trastuzumab Deruxtecan for Subjects With HER2-Positive Gastric Cancer or Gastro-Esophageal Junction Adenocarcinoma After Progression on or After a Trastuzumab-Containing Regimen (DESTINY-Gastric04). ClinicalTrials.gov. Accessed November 25, 2024. https://clinicaltrials.gov/study/NCT04704934
41.CADTH Reimbursement Recommendation: Trastuzumab Deruxtecan (Enhertu). Can J Health Technol. 2023;3(7). doi:10.51731/cjht.2023.695
42.CADTH Reimbursement Recommendation: Trastuzumab Deruxtecan (Enhertu). Can J Health Technol. 2022;2(10). doi:10.51731/cjht.2022.472
43.Mahar AL, Zagorski B, Kagedan D, et al. Evaluating TNM stage prognostic ability in a population-based cohort of gastric adenocarcinoma patients in a low-incidence country. Can J Public Health. 2018;109(4):480-488. doi: 10.17269/s41997-018-0102-1 PubMed
44.Spolverato G, Ejaz A, Kim Y, et al. Rates and patterns of recurrence after curative intent resection for gastric cancer: A United States multi-institutional analysis. J Am Coll Surg. 2014;219(4):664-75. doi: 10.1016/j.jamcollsurg.2014.03.062 PubMed
45.Holland P, Rafiq R, Matheson K, et al. Population based assessment of HER-2 and PD-L1 positivity in gastric and gastroesophageal junction adenocarcinomas in a Canadian population. J Clin Oncol. 2024;42(16_suppl):e16038-e16038. doi: 10.1200/JCO.2024.42.16_suppl.e16038
46.Statistics Canada. Accessed April 8, 2024. https://www.statcan.gc.ca/en/start
47.AstraZeneca Canada Inc. AstraZeneca Canada Inc. response to Canada's Drug Agency request for additional information regarding trastuzumab deruxtecan review on October 17, 2024 [internal additional sponsor's information]. October 23, 2024.
Appendix 1: Cost Comparison Table
Please note that this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical expert(s) and drug plans. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 8: CDA-AMC Cost Comparison Table for Locally Advanced or Metastatic HER2-Positive Gastric or GEJ Adenocarcinoma
Treatment | Strength | Forma | Price ($) | Recommended dosage | Daily cost ($) | Average 28-day cycle cost |
|---|---|---|---|---|---|---|
Trastuzumab deruxtecan (Enhertu) | 20 mg/mL | 5 mL (100 mg) | 2,440.0000b | 6.4 mg/kg once every 21-daysc | 580.95 | 16,267 |
Ramucirumab-paclitaxel | ||||||
Ramucirumab (Cyramza) | 10 mg/mL | 10 mL (100 mg) 50 mL (500 mg) | 690.6300 3,453.1600 | 8 mg/kg on days 1 and 15 of a 28-day cycle | 295.98 | 8,288 |
Paclitaxel (generic) | 6 mg/mL | 5 mL (30 mg) 16.7 mL (100 mg) 25 mL (150 mg) 50 mL (300 mg) | 300.0000 1,002.0000 1,500.0000 3,000.0000 | 80 mg/m2 on days 1, 8, and 15 of a 28-day cycle | 192.86 | 5,400 |
Ramucirumab-paclitaxel | 488.84 | 13,688 | ||||
FOLFIRI | ||||||
Leucovorin (generics) | 10 mg/mL | 5 mL (50 mg) 50 mL (500 mg) | 68.9400 689.0000 | 400 mg/m2 every 14 days | 74.81 | 2,095 |
Fluorouracil (generics) | 50 mg/mL | 100 mL (5,000 mg) | 160.9000 | 400 mg/m2 on Day 1, then 2,400 mg/m2 by continuous infusion over 46 hours starting Day 1 every 14 days | 12.23 | 342 |
Irinotecan (generics) | 20 mg/mL | 2 mL (40 mg) 5 mL (100 mg) 25 mL (500 mg) | 208.3500 520.8500 2,600.0000 | 180 mg/m2 on days 1 and 15 of a 28-day cycle | 141.38 | 3,959 |
FOLFIRI | 228.41 | 6,395 | ||||
Single-drug chemotherapies | ||||||
Docetaxel (generic) | 10 mg/mL | 8 mL (80 mg) 16 mL (160 mg) | 970.2000 1,850.0000 | 75 mg/m2 every 21 days | 35.40 | 990 |
20 mg/mL | 4 mL (80 mg) 8 mL (160 mg) | 497.0000 990.0000 | ||||
Paclitaxel (generic) | 6 mg/mL | 5 mL (30 mg) 16.7 mL (100 mg) 25 mL 150 mg 50 mL (300 mg) | 300.0000 1,002.0000 1,500.0000 3,000.0000 | 80 mg/m2 on days 1, 8, and 15 of a 28-day cycle | 192.86 | 5,400 |
Note: All prices are IQVIA Delta PA wholesale list prices (accessed October 2024), unless otherwise indicated, and do not include dispensing fees. For weight- or BSA-based dosing, a patient weight of 75 kg or a BSA of 1.90 m2 was assumed. Except for fluorouracil and the 500 mg vial of leucovorin, which are available in bulk pharmacy vials, wastage was included. Recommended dosages were retrieved from Cancer Care Ontario,23,24,33-35 unless otherwise indicated.
aAll drug interventions are vials for IV infusion or infusion bags.
bSponsor-submitted price.1
cDose is as specified in sponsor-submitted product monograph.3
Appendix 2: Submission Quality
Please note that this appendix has not been copy-edited.
Description | Yes or No | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | No | As the sponsor’s economic analysis was restricted to the second-line population, and the proposed Health Canada indication does not restrict to second-line therapy only, the cost-effectiveness of trastuzumab deruxtecan in the third-line or later population is unknown. |
Model has been adequately programmed and has sufficient face validity | No | Refer to the ‘Chosen OS and PFS distributions produce results that lack face validity’ and ‘Poor modelling practices were employed’ limitations in CDA-AMC’s Appraisal of the Sponsor’s Economic Evaluation. |
Model structure is adequate for decision problem | No | Refer to the ‘Model structure may overestimate comparative efficacy’ limitation in CDA-AMC’s Appraisal of the Sponsor’s Economic Evaluation. |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | No | Refer to the ‘Poor modelling practices were employed’ limitation in CDA-AMC’s Appraisal of the Sponsor’s Economic Evaluation. |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | No | Refer to the ‘Poor modelling practices were employed’ limitation in CDA-AMC’s Appraisal of the Sponsor’s Economic Evaluation. |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | No | Refer to the ‘Poor modelling practices were employed’ limitation in CDA-AMC’s Appraisal of the Sponsor’s Economic Evaluation. |
Appendix 3: Additional Information on the Submitted Economic Evaluation
Please note that this appendix has not been copy-edited.
Table 10: Overview of Key Inputs
Treatment | Modelled Dosage | 21-day cost ($) | OS HRa | PFS HRa |
|---|---|---|---|---|
Trastuzumab deruxtecan | 6.4 mg/kg once per 21-day cycle | 13,084 | Reference | Reference |
Ramucirumab-paclitaxel |
| 10,210 | █████████ | █████████ |
Docetaxel | 75 mg/m2 once per 21-day cycle | 1,940 | █████████ | █████████ |
FOLFIRI |
| 3,337 | █████████ | █████████ |
Paclitaxel | 80 mg/m2 3 times per 28-day cycle | 4,043 | █████████ | █████████ |
Irinotecan | 150 mg/m2 once per 14-day cycle | 2,344 | █████████ | █████████ |
FOLFIRI = folinic acid, fluorouracil, and irinotecan; HR = hazard ratio.
aHazard ratio for trastuzumab deruxtecan versus each comparator treatment.
Table 11: Distribution of Subsequent Therapies
Third-line treatment | Second-line treatment | |||||
|---|---|---|---|---|---|---|
Trastuzumab deruxtecan | Ramucirumab-paclitaxel | FOLFIRI | Paclitaxel | Irinotecan | Docetaxel | |
FOLFIRI | 30% | 80% | 0% | 40% | 0% | 30% |
Paclitaxel | 10% | 0% | 20% | 0% | 20% | 10% |
Ramucirumab-paclitaxel | 50% | 0% | 70% | 50% | 70% | 50% |
Trifluridine and tipiracil | 10% | 20% | 10% | 10% | 10% | 10% |
FOLFIRI = folinic acid, fluorouracil, and irinotecan.
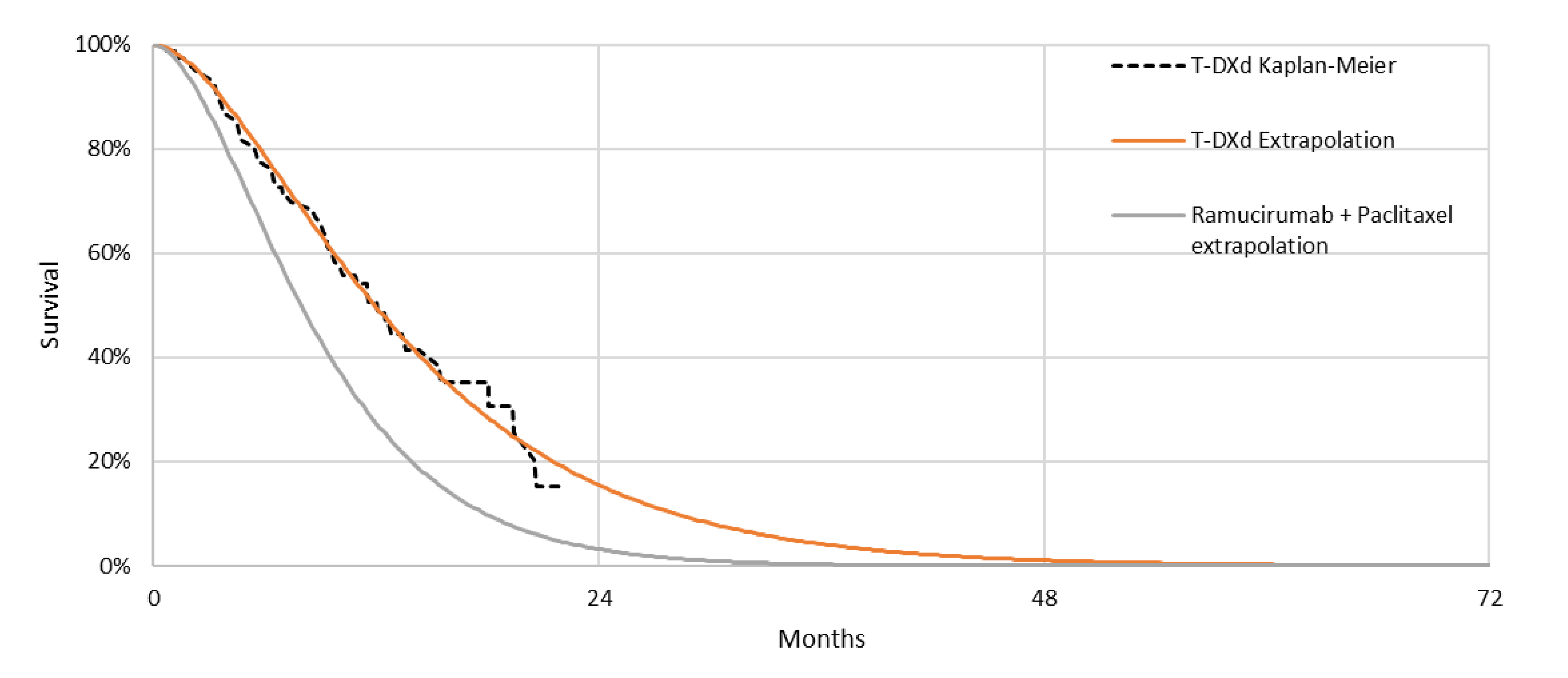
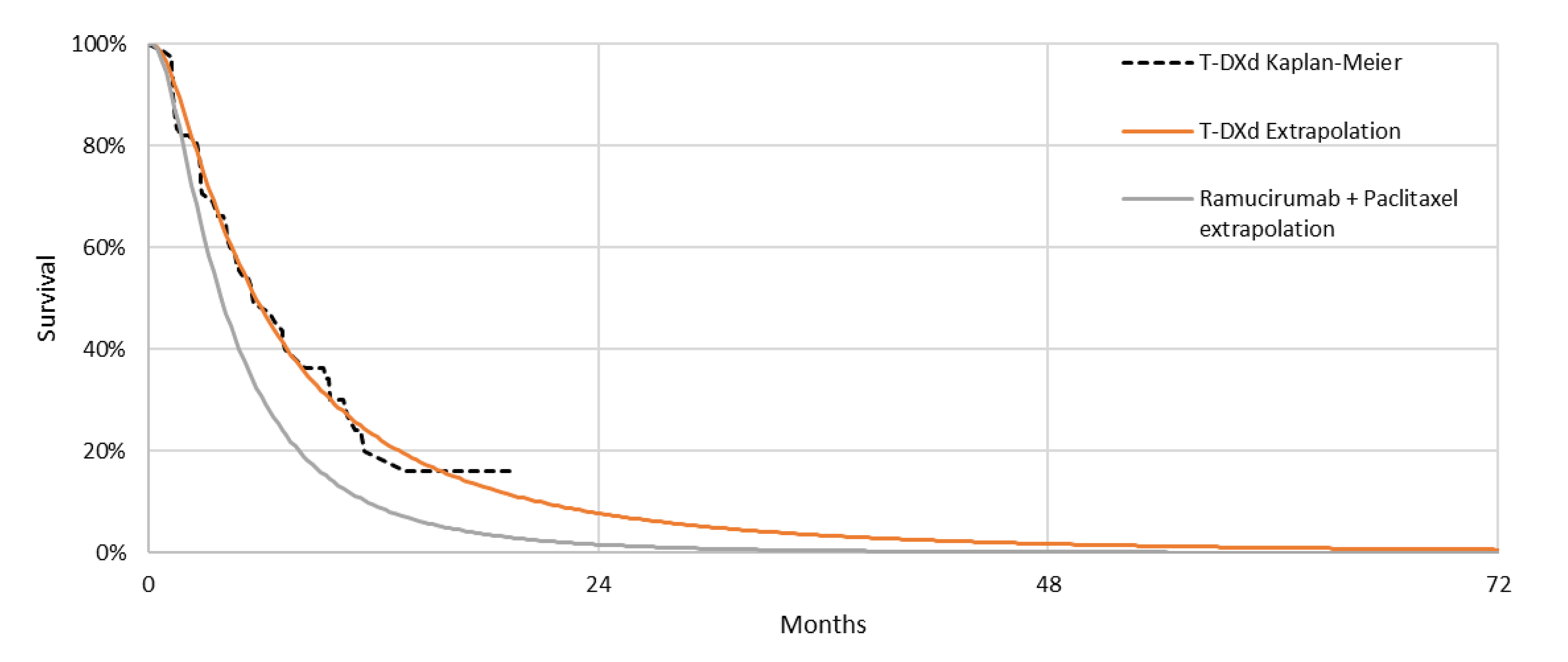
Table 12: Disaggregated Summary of the Sponsor’s Economic Evaluation Results
Parameter | Base case | Additional comparators considered in alternative analysesa | ||||
|---|---|---|---|---|---|---|
Trastuzumab deruxtecan | Ramucirumab-paclitaxel | Docetaxel | FOLFIRI | Paclitaxel | Irinotecan | |
Discounted LYs | ||||||
Total | 1.19 | 0.79 | 0.63 | 0.50 | 0.63 | 0.57 |
Preprogression | 0.75 | 0.46 | 0.24 | 0.31 | 0.31 | 0.27 |
Postprogression | 0.45 | 0.33 | 0.40 | 0.20 | 0.32 | 0.30 |
Discounted QALYs | ||||||
Total | 0.93 | 0.61 | 0.48 | 0.39 | 0.48 | 0.43 |
Preprogression | 0.61 | 0.38 | 0.19 | 0.25 | 0.25 | 0.22 |
Postprogression | 0.32 | 0.24 | 0.29 | 0.14 | 0.23 | 0.22 |
AE disutility | −0.0019 | −0.0045 | −0.0029 | −0.0020 | −0.0020 | −0.0014 |
Discounted costs ($) | ||||||
Total | 244,817 | 187,487 | 108,188 | 122,189 | 123,138 | 114,229 |
Drug acquisition (second line) | 145,641 | 73,744 | 7,329 | 16,682 | 19,767 | 10,111 |
Sub. tx, drug acquisition | 5,345 | 2,342 | 5,382 | 6,686 | 5,363 | 6,695 |
Administration (second line) | 2,037 | 13,238 | 1,099 | 5,417 | 5,575 | 2,446 |
Subsequent treatment, administration | 1,000 | 509 | 1,007 | 1,181 | 1,008 | 1,183 |
Disease management | 1,905 | 775 | 550 | 531 | 596 | 538 |
AE | 3,884 | 11,064 | 6,813 | 5,561 | 4,810 | 7,173 |
Terminal care | 85,005 | 85,815 | 86,007 | 86,132 | 86,018 | 86,083 |
Societal costs | 0 | 0 | 0 | 0 | 0 | 0 |
AE = adverse event; FOLFIRI = folinic acid, fluorouracil, and irinotecan.
aThe sponsor’s alternative analysis includes paclitaxel, docetaxel, irinotecan, and FOLFIRI as comparators in addition to the treatments considered in base-case analyses (i.e., trastuzumab deruxtecan and ramucirumab-paclitaxel).
Source: Sponsor’s pharmacoeconomic submission.1
Table 13: Summary of the Sponsor’s Alternative Economic Evaluation Results, Pairwise
Drug | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER versus reference ($/QALY) |
|---|---|---|---|---|---|
Trastuzumab deruxtecan vs. Docetaxel | |||||
Docetaxel | 108,188 | Reference | 0.48 | Reference | Reference |
Trastuzumab deruxtecan | 244,817 | 136,630 | 0.93 | 0.45 | 302,654 |
Trastuzumab deruxtecan vs. Irinotecan | |||||
Irinotecan | 114,229 | Reference | 0.43 | Reference | Reference |
Trastuzumab deruxtecan | 244,817 | 130,589 | 0.93 | 0.49 | 264,187 |
Trastuzumab deruxtecan vs. FOLFIRI | |||||
FOLFIRI | 122,189 | Reference | 0.39 | Reference | Reference |
Trastuzumab deruxtecan | 244,817 | 122,628 | 0.93 | 0.54 | 228,558 |
Trastuzumab deruxtecan vs. Paclitaxel | |||||
Paclitaxel | 123,138 | Reference | 0.48 | Reference | Reference |
Trastuzumab deruxtecan | 244,817 | 121,679 | 0.93 | 0.44 | 273,696 |
FOLFIRI = folinic acid, fluorouracil, and irinotecan; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Note: In sequential analyses, all the treatments were either dominated or extendedly dominated by docetaxel, except for trastuzumab deruxtecan.
Source: Sponsor’s pharmacoeconomic submission.1
Appendix 4: Additional Details on the CDA-AMC Reanalyses and Sensitivity Analyses of the Economic Evaluation
Please note that this appendix has not been copy-edited.
Detailed Results of CDA-AMC Base Case
Table 14: Disaggregated Summary of CDA-AMC’s Economic Evaluation Results, Deterministic
Parameter | Trastuzumab deruxtecan | Ramucirumab-paclitaxel |
|---|---|---|
Discounted LYs | ||
Total | 1.18 | 0.78 |
Preprogression | 0.75 | 0.46 |
Postprogression | 0.43 | 0.32 |
Discounted QALYs | ||
Total | 0.81 | 0.52 |
Preprogression | 0.56 | 0.34 |
Postprogression | 0.25 | 0.19 |
AE disutility | −0.0019 | −0.0045 |
Discounted costs ($) | ||
Total | 265,114 | 195,657 |
Drug acquisition (second line) | 171,529 | 83,198 |
Subsequent treatment, drug acquisition | 0 | 0 |
Administration (second line) | 2,400 | 14,676 |
Subsequent treatment administration | 0 | 0 |
Disease management | 2,070 | 779 |
AE | 3,886 | 11,061 |
Terminal care | 85,231 | 85,942 |
Societal costs | 0 | 0 |
AE = adverse event; FOLFIRI = folinic acid, fluorouracil, and irinotecan.
Scenario Analyses
Table 15: CDA-AMC Scenario Analysis Results, Deterministic
Scenario analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALY) |
|---|---|---|---|---|
FOLFIRI as a relevant comparator | FOLFIRI | 123,047 | 0.33 | Reference |
Trastuzumab deruxtecan | 265,114 | 0.81 | 300,592 |
Note: in this analysis, if undertaken sequentially, ramucirumab-paclitaxel is extendedly dominated through FOLFIRI and trastuzumab deruxtecan. Based on this analysis, a price reduction of at least 69% is required for trastuzumab deruxtecan to achieve an ICER of $50,000 per QALY gained compared to FOLFIRI.
Appendix 5: Submitted Budget Impact Analysis and CDA-AMC Appraisal
Please note that this appendix has not been copy-edited.
Table 16: Summary of Key Take-Aways
Key take-aways of the budget impact analysis |
|---|
|
Summary of Sponsor’s Budget Impact Analysis
In the submitted budget impact analysis (BIA), the sponsor assessed the introduction of trastuzumab deruxtecan for the second-line treatment of adults with locally advanced or metastatic HER2-positive gastric and/or GEJ adenocarcinoma who have progressed on or after receiving a trastuzumab-containing regimen. The BIA was undertaken from the perspective of a Canadian public payer over a 3-year time horizon (Q4 2025 to Q4 2028) using an epidemiological approach. The sponsor compared a reference scenario in which patients received either ramucirumab-paclitaxel, FOLFIRI, paclitaxel, irinotecan, or docetaxel to a new drug scenario in which trastuzumab deruxtecan was reimbursed. The sponsor’s submission only considered annual drug acquisition costs and subsequent therapy costs which were obtained from IQVIA DeltaPA.19 Data informing key parameters of the budget impact model were obtained from various sources including published literature,43-45 Statistics Canada,46 clinical expert input, and assumption.
Key inputs to the BIA are documented in Table 17.
Trastuzumab deruxtecan will be listed on the Canadian public drug plans in Q4 2025.
The percentage of patients receiving an anti-HER2-based regimen in the first line is 90.00%.
Market shares in the refence scenario remain constant over the 3-year time horizon.
Relative dose intensity for all treatments is 100%.
No vial sharing (i.e., complete wastage of unused product) for all treatments.
The OS, PFS, and TTD data used in the submitted CUA represent survival, progression, and treatment duration patterns in Canada.
Table 17: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as year 1 / year 2 / year 3 if appropriate) |
|---|---|
Target population | |
Total population in Pan-Canada without Quebec46 | 25,748,814 |
Annual population growth46 | 1.80% |
G/GEJ annual incidence46 | 0.0116% |
Average annual G/GEJ incidence change46 | −0.2350% |
Proportion of patients with de novo locally advanced or metastatic G/GEJ43 | 66.30% |
Proportion of patients recurring/progressing to locally advanced or metastatic G/GEJ44 | 25.63% |
Proportion of patients with HER2+ locally advanced or metastatic G/GEJ adenocarcinoma45 | 20.65% |
Proportion of patients receiving anti-HER2-based regimen in first linea | 90.00% |
Percentage who receive therapy after trastuzumab31 | 33.00% |
Number of patients eligible for drug under review | 139 / 142 / 144 |
Market Uptake (3 years) | |
Uptake (reference scenario) Ramucirumab-paclitaxel FOLFIRI Paclitaxel Irinotecan Docetaxel | 62.00% / 62.00% / 62.00% 26.00% / 26.00% / 26.00% 8.00% / 8.00% / 8.00% 2.00% / 2.00% / 2.00% 2.00% / 2.00% / 2.00% |
Uptake (new drug scenario) Trastuzumab deruxtecan Ramucirumab-paclitaxel FOLFIRI Paclitaxel Irinotecan Docetaxel | ████████████████████ ████████████████████ ██████████████████ █████████████████ █████████████████ █████████████████ |
Cost of treatment (per patient, per year) | |
Name of drug under review Trastuzumab deruxtecan Ramucirumab-paclitaxel FOLFIRI Paclitaxel Irinotecan Docetaxel | $226,780.75 $176,976.86 $57,835.96 $70,075.20 $40,626.30 $33,633.60 |
FOLFIRI = folinic acid, fluorouracil, and irinotecan; G/GEJ = gastric and gastroesophageal junction; HER2 = human epidermal growth factor receptor 2.
aBased on sponsor assumption.
Summary of the Sponsor’s BIA Results
The sponsor estimated that the 3-year budget impact of reimbursing trastuzumab deruxtecan for the second-line treatment of adults with locally advanced or metastatic HER2-positive gastric or GEJ adenocarcinoma who have progressed on or after receiving a trastuzumab-containing regimen to be $22,572,044 (Year 1: $4,518,314; Year 2: $8,704,420; Year 3: $9,349,311).
CDA-AMC Appraisal of the Sponsor’s BIA
CDA-AMC identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
The number of eligible patients is likely underestimated: The sponsor estimated that 33% of patients receive second-line therapy after treatment with trastuzumab, based on a study of data from an English national registry.31 Clinical expert input commented that the sponsor’s estimate was reasonable as it is expected that less than 50% of patients would be treated with second-line therapy. It was noted that the proportion of patients currently treated with second-line therapy is partially due to current therapies in the second-line offering a very modest benefit. Clinical expert input suggested that should a more effective second-line therapy become available, the proportion of patients treated in the second-line setting will likely increase. Furthermore, the sponsor’s BIA is restricted to the second-line treatment of adults with locally advanced or metastatic HER2-positive gastric or GEJ adenocarcinoma who have progressed on or after receiving a trastuzumab-containing regimen. However, the proposed Health Canada indication which does not restrict the use of trastuzumab deruxtecan to the second-line setting.3 The sponsor noted trastuzumab deruxtecan would be “an option in the second and subsequent line setting…[as] there could be a time-limited period where a small number of patients on existing second-line agents who missed the opportunity to have Enhertu in the second-line could benefit from it in a third-line or later setting.”47 Clinical experts consulted by CDA-AMC anticipated that majority of patients would be treated with trastuzumab deruxtecan in the second-line setting as there are no other HER2-directed therapies available for patients. However, due to the exclusion of patients in the third-line and beyond, the sponsor’s estimated budget impact is underestimated. Clinical experts noted that the absolute number of patients eligible for trastuzumab deruxtecan may be underestimated in the sponsor’s budget impact analysis and the number of eligible patients could be several times greater than estimated by the sponsor. However, CDA-AMC was unable to identify alternative sources of information to validate this estimate.
CDA-AMC was unable to address this limitation owing to the sponsor’s model structure and a lack of alternative data.
TTD is uncertain: The sponsor estimated TTD based on the mean TTD in the submitted CUA. As such, the sponsor has assumed that 100% of patients are on treatment until the mean TTD at which point it is assumed all patients discontinue treatment. This approach resulted in all patients, irrespective of treatment, discontinuing therapy in the first year of treatment which is inappropriate. CDA-AMC explored alternative methods to align TTD in the BIA with TTD in the CDA-AMC CUA base case, however, other issues with programming in the BIA were identified that precluded CDA-AMC from adequately aligning the BIA with the CUA. The alternative methods explored by CDA-AMC resulted had minimal impact on the total budget impact, but it is uncertain whether this is due to issues related to the model programming.
CDA-AMC did not adjust for this limitation in reanalyses.
Drug acquisition costs are uncertain: As noted in CDA-AMC’s Appraisal of the Sponsor’s Economic Evaluation, numerous discrepancies were identified between the unit costs calculated by CDA-AMC and the unit costs calculated by the sponsor;19 ramucirumab concluded negotiations with the pan-Canadian Pharmaceutical Alliance with a Letter of Intent and any potential confidential rebates are not reflected in the BIA,36 drug acquisition costs are sensitive to the assumed patient characteristics due to the assumption of no vial sharing; wastage of unused product was inappropriately considered for fluorouracil and leucovorin as the unit prices are for bulk pharmacy vials which are intended to be used for multiple doses, overestimating drug acquisition costs for FOLFIRI; and the sponsor assumed the incorrect dose for fluorouracil, administered as part of the FOLFIRI regimen. CDA-AMC explored the impact of correcting drug unit costs, excluding wastage for bulk pharmacy vials, and correcting the dose of FOLFIRI and found the impact to be minimal as the 3-year total budget impact estimate decreased by less than 2.5%.
CDA-AMC did not adjust for this limitation in reanalyses.
The market uptake of trastuzumab deruxtecan is likely underestimated: The sponsor’s submitted budget impact analysis indicated that trastuzumab deruxtecan would result in a market uptake of ███ in year 1, █████ in year 2, and ███ in year 3 based on internal forecasting. However, CDA-AMC obtained clinical expert feedback indicating that the market uptake in all 3 years is likely underestimated as there are currently no other HER2-directed therapies available for patients in the second-line and beyond. Clinical expert input suggested that uptake of trastuzumab deruxtecan among eligible patients may be 40% in year 1, 50% to 60% in year 2, and 75% in year 3. CDA-AMC explored uncertainty aligning the market uptake with clinical expert input but found the impact to be minimal as the 3-year total budget impact estimate decreased by less than 2%.
CDA-AMC did not adjust for this limitation in reanalyses.
Subsequent therapy costs are uncertain: As noted in CDA-AMC’s Appraisal of the Sponsor’s Economic Evaluation, the proportion of patients treated with third-line therapy and the relative use of each subsequent therapy is associated with notable uncertainty. Furthermore, input highlighted that the treatment pathway would likely shift should trastuzumab deruxtecan be reimbursed for the indicated population. CDA-AMC explored the impact of excluding subsequent and found the impact to be minimal as the 3-year total budget impact estimate decreased by less than 1%.
CDA-AMC did not adjust for this limitation in reanalyses.
CDA-AMC Reanalyses of the BIA
The limitations identified by CDA-AMC had minimal impact on the results of the BIA. Furthermore, in the absence of more reliable estimates to inform the key parameters of the BIA (i.e., the number of eligible patients), the sponsor’s submitted base case was maintained.
Table 18: Detailed Breakdown of the Sponsor’s Submitted BIA
Stepped analysis | Scenario | Year 0 (current situation) ($) | Year 1 ($) | Year 2 ($) | Year 3 ($) | Three-year total ($) |
|---|---|---|---|---|---|---|
Submitted base case | Reference | 7,655,764 | 7,775,253 | 7,896,607 | 8,019,855 | 23,691,715 |
New drug | 7,655,764 | 12,293,567 | 16,601,027 | 17,369,166 | 46,263,759 | |
Budget impact | 0 | 4,518,314 | 8,704,420 | 9,349,311 | 22,572,044 |
BIA = budget impact analysis.
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.