Drugs, Health Technologies, Health Systems
Reimbursement Review
Venetoclax (Venclexta)
Sponsor: AbbVie Corporation
Therapeutic area: Chronic lymphocytic leukemia
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Clinical Review
Abbreviations
AE
adverse event
BEN + RIT
bendamustine plus rituximab
BTK
Bruton tyrosine kinase
CDA-AMC
Canada’s Drug Agency
CI
confidence interval
CIRS
Cumulative Illness Rating Scale
CLL
chronic lymphocytic leukemia
CR
complete response
CrCl
creatinine clearance
CrI
credible interval
CRir
complete response with incomplete recovery of the bone marrow
CTC
Common Toxicity Criteria
del(17p)
17p deletion
DIC
deviance information criterion
DSMB
Data and Safety Monitoring Board
ECOG PS
Eastern Cooperative Oncology Group Performance Status
FLU + CYC + RIT
fludarabine plus cyclophosphamide plus rituximab
HR
hazard ratio
HRQoL
health-related quality of life
IQR
interquartile range
ITT
intention to treat
iwCLL
International Workshop on Chronic Lymphocytic Leukemia
MRD
minimal residual disease
NICE
National Institute for Health and Care Excellence
NMA
network meta-analysis
OH-CCO
Ontario Health (Cancer Care Ontario)
OS
overall survival
pERC
pan-Canadian Oncology Drug Review Expert Review Committee
PFS
progression-free survival
RCT
randomized controlled trial
SLL
small lymphocytic lymphoma
TEAE
treatment-emergent adverse event
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Table 1: Background Information on Application Submitted for Review (Reassessment)
Item | Description |
|---|---|
Drug product | Venetoclax (Venclexta) 10 mg, 50 mg, and 100 mg oral tablets |
Sponsor | AbbVie Corporation |
Indication | Venetoclax (Venclexta), in combination with obinutuzumab, is indicated for the treatment of patients with previously untreated CLL |
Reimbursement request | As per indication. Clarifying note from the sponsor: This request is for the subgroup of patients with previously untreated CLL who are considered fit and potentially fludarabine-eligible, and who were not included in the reimbursement request and recommendation criteria in the previous CADTH review. Based on this request, the reimbursement criteria would be expanded for the treatment of patients with previously untreated CLL, aligned with the indication (i.e., irrespective of age or eligibility for fludarabine treatment). |
Health Canada approval status | Post-NOC |
Health Canada review pathway | Standard |
NOC date | April 28, 2020 |
Recommended dosage | Venetoclax (Venclexta) dose ramp-up schedule: The starting dose of Venclexta is 20 mg once daily for 7 days. The Venclexta dose must be administered according to a weekly ramp-up schedule to the daily dose of 400 mg over a period of 5 weeks as shown in Table 2. The 5-week ramp-up dosing schedule is designed to gradually reduce tumour burden (debulk) and decrease the risk of TLS. Venetoclax (Venclexta) in combination with obinutuzumab: On cycle 1, day 1, start obinutuzumab administration at 100 mg, followed by 900 mg that may be administered on day 1 or day 2. Administer 1,000 mg on day 8 and day 15 of cycle 1, and on day 1 of 5 subsequent cycles (for a total of 6 cycles, 28 days each). On cycle 1, day 22, start Venclexta according to the ramp-up schedule (Table 2), continuing through to cycle 2, day 28. After completing the ramp-up schedule, patients should continue Venclexta 400 mg once daily from cycle 3, day 1, of obinutuzumab to the end of cycle 12. Venclexta should be given for a total of 12 months as finite treatment: for six 28-day cycles in combination with obinutuzumab, followed by 6 months of Venclexta as a single drug. |
CLL = chronic lymphocytic leukemia; NOC = Notice of Compliance; TLS = tumour lysis syndrome.
Sources: Product monograph of venetoclax1 and Sponsor Summary of Clinical Evidence.2
Table 2: Dosing Schedule for Ramp-Up Phase in the Treatment of Chronic Lymphocytic Leukemia
Week | Venetoclax (Venclexta) daily dose (tablets) |
|---|---|
1 | 20 mg (2 × 10 mg) |
2 | 50 mg (1 × 50 mg) |
3 | 100 mg (1 × 100 mg) |
4 | 200 mg (2 × 100 mg) |
5 | 400 mg (4 × 100 mg) |
Note: The starting pack provides the first 4 weeks of venetoclax (Venclexta) according to the ramp-up schedule. The 400 mg dose is supplied in bottles of 100 mg tablets.
Sources: Product monograph of venetoclax1 and Sponsor Summary of Clinical Evidence.2
Introduction
Chronic lymphocytic leukemia (CLL) is a lymphoid neoplasm that is characterized by a progressive accumulation of monoclonal, mature, functionally impaired B lymphocytes. The pathologic and immunophenotypic features of the malignant cells are identical in CLL and small lymphocytic lymphoma (SLL). Although some patients might present with painless, swollen lymph nodes that wax and wane, most patients with CLL do not present with symptoms at the time of diagnosis.3
CLL is the most common leukemia in adults living in Canada — in 2019, 1,700 patients were diagnosed with CLL and in 2020 and 2022, 222 deaths and 554 deaths due to CLL were reported, respectively.4 CLL is considered incurable; the 5-year net survival for patients with CLL is estimated to be 83%.4 The estimated median life expectancy for patients with 17p deletion — also known as del(17p) — or TP53 mutation is less than 2 years to 3 years from the time of initial diagnosis;5 however, the clinical experts consulted by Canada’s Drug Agency (CDA-AMC) for the purposes of this review advised that this statistic likely reflects the prenovel therapy era and estimated the median life expectancy for this subset of patients to be longer than 3 years from initial diagnosis.
In symptomatic patients with previously untreated CLL with TP53 aberrations (del[17p] and/or TP53 mutation), the 2022 updated Canadian evidence-based guideline for the frontline treatment of CLL6 advised that continuous therapy with a Bruton tyrosine kinase (BTK) inhibitor (namely, ibrutinib and acalabrutinib) is the preferred therapy, while venetoclax plus obinutuzumab would be preferred in patients who would benefit from a time-limited therapy, if funded.
In symptomatic fit patients (as per the guideline,6 patients who are considered fit include those who are young and those who are eligible for treatment with fludarabine plus cyclophosphamide plus rituximab [FLU + CYC + RIT]) with previously untreated CLL without TP53 aberrations, the guideline advised that FLU + CYC + RIT is preferred for IGHV-mutated CLL, while a BTK inhibitor is an option for IGHV-mutated CLL and is the preferred option for IGHV-unmutated CLL. The guideline6 further advised that venetoclax plus obinutuzumab would become the preferred therapy in this subset of patients, regardless of IGHV mutation, if funded across Canada. Of note, the 2018 guideline7 had advised on bendamustine plus rituximab (BEN + RIT) for fit, older (65 years and older) patients with previously untreated CLL without TP53 aberrations but with mutated IGHV due to reduced toxicity concerns.
Patients with CLL and the clinical experts emphasized the importance of having additional treatment options available to better align with patient values, needs, and lifestyle, particularly for fit patients. The clinician groups and clinical experts identified 2 subsets of patients with CLL who have an unmet need for a treatment option that is not combined with chemotherapy and/or BTK inhibitor and who would benefit from targeted therapy (and thereby avoid the risk of bone marrow toxicities associated with FLU + CYC + RIT): young and fit patients with lower-risk disease and long life expectancy, and young and fit patients with high-risk genomic features.
In 2020, venetoclax in combination with obinutuzumab was first reviewed by the pan-Canadian Oncology Drug Review Expert Review Committee (pERC) for the treatment of adult patients with previously untreated CLL who are fludarabine-ineligible. pERC issued a recommendation that venetoclax plus obinutuzumab be listed for the indication under review in the reimbursement request, if the specified clinical criteria and conditions are met.8
The objective of the present reassessment is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of venetoclax 10 mg, 50 mg, and 100 mg oral tablets, in combination with obinutuzumab, in the treatment of patients with previously untreated CLL. The focus has been placed on the fit population (defined in the trial by a Cumulative Illness Rating Scale [CIRS] score of ≤ 6 and creatinine clearance [CrCl] of ≥ 70 mL per minute).
Perspectives of Patients, Clinicians, and Drug Programs
The information in this section is a summary of input provided by the patient and clinician groups that responded to the call for input and from clinical experts consulted for this review.
Patient Input
Two patient groups, Lymphoma Canada and CLL Canada, submitted joint input for the current review. The input includes results from 2 surveys conducted for past drug reimbursement reviews in CLL — 1 survey was for the original submission for venetoclax, in combination with obinutuzumab, reviewed in 2020, and 1 was the recent CLL survey conducted in 2023. For the 2023 survey, Lymphoma Canada collected information through an online survey that was distributed throughout Canada and to international locations from March 22 to May 2, 2023. A total of 87 people (49 from Canada, 12 from the US, 1 from Australia, and 25 from unknown locations) responded to the survey. Among the 87 respondents, 32 were female, 30 were male, and 25 skipped the question. Of the 87 respondents, most respondents (36 respondents) were diagnosed with CLL 9 years to 10 years ago, while other respondents were diagnosed with CLL 3 years to 5 years ago (15 respondents), 1 year to 2 years ago (10 respondents), 5 years to 8 years ago (8 respondents), and less than a year ago (4 respondents); 14 respondents skipped the question. The respondents reported various subtypes of CLL, including del(17p), deletion 13q, and deletion 11q; TP53 mutation; trisomy 12; and unmutated IGHV. The 2020 survey provided information on patients with CLL and SLL who had experience with frontline venetoclax plus obinutuzumab. Of the 33 survey respondents, 10 respondents were aged between 40 years and 59 years, 22 respondents were aged between 60 years and 79 years, 18 respondents were male, and 14 respondents were female; 1 respondent did not answer either question on age or sex. Survey respondents were from Canada (2 patients), the US (29 patients), and the UK (1 patient) (1 respondent did not answer the question).
Based on the 2023 survey, most patients with CLL are diagnosed through routine blood work and experience minor to no symptoms at the time of diagnosis. According to the 64 respondents who reported high negative impact at the time of diagnosis, fatigue (47%), high white blood cell counts (leukocytosis) (26%), body aches and pains (25%), enlarged lymph nodes (23%), and night sweats (20%) were the most frequent symptoms. Of the 71 respondents who reported on the psychosocial impact of CLL at the time of diagnosis, anxiety and worry (61%), the stress of diagnosis (59%), and difficulty sleeping (28%) were the most common concerns. According to the 70 respondents who reported high negative impact on their current health-related quality of life (HRQoL), fatigue (44%), body aches and pains (27%), and indigestion, abdominal pain, or bloating (17%) were the most frequently reported symptoms. Of the 87 respondents who reported on the psychosocial impact of CLL on their current HRQoL, anxiety and worry (42%), difficulty sleeping (31%), and the stress of diagnosis (28%) were the most common concerns. Of 87 respondents who indicated that CLL had a negative impact on their daily activities, fulfilling family obligations (51%) and spending time with family and friends (45%) were the most frequently affected activities.
Of the 68 respondents to the 2023 survey who provided information on their experience with CLL treatments, 21 respondents indicated that they have not received therapy, 26 respondents had received 1 line of treatment, and 19 respondents had completed 2 or more lines of treatments. According to the respondents, the most difficult to tolerate side effects include nausea, fatigue, joint pain, skin issues and bleeding, atrial fibrillation, diarrhea, inflammation, bodily aches and pain, headache, muscle weakness, heartburn, indigestion, night sweats, neuropathy, and frequent infections. Additionally, 26% of patient respondents reported that their CLL treatment had a negative impact on their HRQoL (due to side effects) (76%), their ability to travel (26%), and their ability to go to work or school, or to volunteer (19%). Based on patient respondent input, the most important considerations for a novel CLL treatment are a longer period of survival (81%), control of disease symptoms (75%), longer remission (71%), better HRQoL (66%), and fewer side effects (35%). Approximately half of all survey respondents emphasized the importance of having a choice in their treatment plan and having increased treatment options available to choose from. While some respondents to the 2023 survey indicated a preference for a fixed-duration therapy (24%), others stated a preference for a continuous therapy (10%); 66% of respondents reported that they were uncertain.
A total of 33 patient respondents from the 2020 survey reported experience with the current drug under review (i.e., they were either currently receiving venetoclax or had completed the treatment regimen). Among these patients, 2 reported not being able to complete the full course of obinutuzumab infusions due to side effects. While most respondents in the 2020 survey noted that side effects from this treatment had “no” or “some” impact on their HRQoL, 15% to 18% of respondents reported a “significant” or “very significant” impact on their HRQoL due to side effects. Most patient respondents (20 of 33 [61%] patients) reported that treatment managed all their symptoms. Symptoms that were not managed by treatment in more than 10% of respondents included fatigue or lack of energy (10 of 33 [30%] patients) and shortness of breath (4 of 33 [12%] patients). Overall, most respondents (31 of 33 [90%] patients) reported a positive experience with the drug under review, and 85% of respondents described their experience with treatment as “very good” or “excellent.”
Clinician Input
Input From Clinical Experts Consulted for the Present Review
The clinical experts indicated that alternative treatment options that are targeted, chemoimmunotherapy-free and/or BTK inhibitor-free, and time-limited are needed for fit patients with previously untreated CLL. Additionally, the clinical experts highlighted the importance of having alternative treatment regimens for patients to choose from (i.e., improving access and equity to care) to align with their values, needs, and lifestyle. The clinical experts indicated that venetoclax plus obinutuzumab would be considered as an option for frontline therapy in patients regardless of fitness, age, and high-risk cytogenetic markers. According to the clinical experts, the molecular profile (IGHV and TP53 mutation status) is the main criterion that informs discussions on selecting a treatment regimen. Other factors to consider when selecting a treatment regimen include accessibility to a local treatment centre and the availability of resources to implement the therapy and monitor for tumour lysis syndrome.
The clinical experts identified the following outcomes that are used to determine treatment response in practice: time to next treatment, clinical improvement in nodal burden or splenomegaly, and improvement in symptoms, HRQoL, and blood work as per International Workshop on Chronic Lymphocytic Leukemia (iwCLL) response criteria. The clinical experts advised on reassessing for treatment response every 6 months in the first year after completing therapy and annually thereafter. The clinical experts identified the following factors that would be considered for the discontinuation of venetoclax plus obinutuzumab: patients continue to present with AEs despite dose reductions and disease progression while on therapy. The clinical experts also presented a scenario where treatment response was demonstrated but treatment was discontinued due to AEs — the clinical experts advised switching to an alternative treatment when there is disease progression.
The clinical experts advised that hematologists and hematologist oncologists should diagnose, treat, and monitor patients who might receive venetoclax plus obinutuzumab. In consideration of the infusion-related reactions and tumour lysis syndrome, the clinical experts advised that a clinic with the resources to enable appropriate monitoring for laboratory abnormalities and access to advanced, complex care if needed are the most appropriate settings for treatment with venetoclax plus obinutuzumab.
Clinician Group Input
Two clinician groups provided input on the current review of venetoclax (in combination with obinutuzumab): Lymphoma Canada (represented by 6 clinicians) and Ontario Health (Cancer Care Ontario) (OH-CCO) Hematology Cancer Drug Advisory Committee (represented by 1 clinician). Note that Lymphoma Canada is a patient advocacy group that helped to facilitate their clinician group input submission by hematologists. The OH-CCO Hematology Cancer Drug Advisory Committee provides evidence-based, clinical, and health system guidance on drug-related issues in support of OH-CCO’s mandate, including the Provincial Drug Reimbursement Programs and the Systemic Treatment Program.
In consideration of the unmet needs, Lymphoma Canada highlighted that the younger patients with high-risk genomic features (e.g., unmutated IGHV) are only able to access the treatment under review by justifying that the poor-risk genomic features meet the definition for fludarabine ineligibility. The group felt that the current requested change in funding may reduce confusion and ensure fairness and equitable access across Canada for this subset of patients with CLL. Lymphoma Canada further suggested that expanded funding may allow the youngest and/or fittest patients with lower-risk disease and the longest life expectancy to benefit from targeted therapy and avoid the use of FLU + CYC + RIT and its associated risk of short-term and long-term bone marrow toxicities. The OH-CCO’s Hematology Cancer Drug Advisory Committee noted that the treatment under review provides an immunotherapy option that is not combined with chemotherapy.
Both clinician groups indicated that venetoclax plus obinutuzumab would be considered for first-line therapy in all patients with previously untreated CLL. Lymphoma Canada highlighted that the option of venetoclax plus obinutuzumab may encourage deferring BTK inhibitor-based therapy to the relapsed or refractory setting for most patients. Lymphoma Canada anticipates that this may reduce the budget impact of CLL therapy and would be in keeping with patient preference for frontline, fixed-duration, targeted therapy. Both clinician groups indicated that all patients with CLL who require a first-line therapy would benefit from treatment with venetoclax plus obinutuzumab. Lymphoma Canada suggested that the least suitable patients for the treatment under review are patients with del(17p) or TP53 mutation (these patients will typically receive BTK inhibitor monotherapy). Regardless, the group suggested that fixed-duration therapies should still be made available to this subset of patients on the rare occasion that a fixed-duration therapy is desired.
As per the OH-CCO’s Hematology Cancer Drug Advisory Committee, standard CLL response outcomes, improvement in progression-free survival (PFS), a reduction in symptoms, and improvement in HRQoL outcomes are used to determine whether a patient is responding to the treatment under review in clinical practice.
The OH-CCO Hematology Cancer Drug Advisory Committee advised considering treatment discontinuation in the setting of significant intolerance or disease progression, while Lymphoma Canada suggested considering treatment discontinuation if there is a lack of response or considering an abbreviated therapy in the setting of significant toxicity.
The clinician groups advised that any specialist physician who treats CLL or any prescribers familiar with CLL treatment should be able to provide and supervise therapy with the treatment under review. The OH-CCO Hematology Cancer Drug Advisory Committee also indicated that additional lab monitoring may be required during the venetoclax ramp-up period. Lymphoma Canada added that a physical exam and review of blood work are part of routine practice in response assessment.
Drug Program Input
Input was obtained from the drug programs that participate in the reimbursement review process. The following items were identified as key factors that could potentially impact the implementation of a recommendation of venetoclax plus obinutuzumab:
relevant comparators
considerations for the initiation of therapy
considerations for the prescribing of therapy
generalizability
funding algorithm
care provision issues
system and economic issues.
The clinical experts consulted for the purposes of the present review provided advice on the potential implementation issues raised by the drug programs. These are presented in Table 5.
Clinical Evidence
Systematic Review
Description of Study
The GAIA trial (also known as the CLL13 study and referred to hereafter as such) is an ongoing, phase III, multicentre, randomized, prospective, open-label clinical trial (N = 926).9 The primary objective of the study is to assess the efficacy of venetoclax plus obinutuzumab versus standard chemoimmunotherapy (BEN + RIT or FLU + CYC + RIT) on the negativity rate of minimal residual disease (MRD) in peripheral blood at month 15, and venetoclax plus obinutuzumab plus ibrutinib versus standard chemoimmunotherapy on PFS at predefined analysis time points in fit patients (defined in the CLL13 trial by a CIRS score of ≤ 6 and CrCl of ≥ 70 mL per minute) with previously untreated CLL and without del(17p) or TP53 mutation. Eligible patients were randomized in a 1:1:1:1 ratio to receive chemoimmunotherapy, venetoclax plus obinutuzumab, venetoclax plus obinutuzumab plus ibrutinib, and venetoclax plus rituximab. Randomization was stratified by Binet stage, age (with a cut-off of 65 years), and region study group. In the chemoimmunotherapy group, patients aged 65 years and younger received FLU + CYC + RIT while patients aged older than 65 years received BEN + RIT. The end of the trial was defined as the time point when 213 PFS events had been reached, which may take place approximately 73 months after the first patient was randomized.10 At the time of sponsor submission, results from the primary analysis of undetectable MRD; results from the interim analysis, which was also the primary analysis, of PFS; and results from a post hoc, exploratory, 4-year follow-up analysis were available of prespecified end points with all patients off treatment.9,11
Note that venetoclax plus rituximab is not approved by Health Canada for the population under review and that venetoclax plus obinutuzumab plus ibrutinib is also not approved by Health Canada. Therefore, data for these treatment groups from the CLL13 study are not presented in this Clinical Review Report for the purposes of this review.
The median age of patients was 62 years (range, 31 years to 83 years) in the venetoclax plus obinutuzumab group and 61 years (range, 29 years to 84 years) in the chemoimmunotherapy group. All patients in both groups had a CIRS score of 6 or less. The median CrCl was 86.3 mL per minute (range, 41.5 mL per minute to 180.2 mL per minute) in the venetoclax plus obinutuzumab group and 86.3 mL per minute (range, 39.5 mL per minute to 223.6 mL per minute) in the chemoimmunotherapy group. The distribution of patients by Rai staging was generally well balanced between groups, with most patients presenting with Rai stage I to stage IV. The median Eastern Cooperative Oncology Group Performance Status (ECOG PS) score was 0 (range, 0 to 2) in both groups. No patients in either group had del(17p) and all patients in both groups had unmutated TP53. The distribution of patients by IGHV mutation status was generally well balanced between groups, with most patients presenting with unmutated IGHV (approximately 57% of patients in each group).12
Efficacy Results
A summary of key efficacy results from the CLL13 study is presented in Table 3.
The median duration of follow-up in the full study population at the interim analysis (including the safety analysis), based on a data cut-off date of January 20, 2022, was 38.8 months (interquartile range [IQR], 32.7 months to 46.1 months).12 The median duration of follow-up in the full study population at the post hoc, exploratory, 4-year follow-up analysis, based on a data cut-off date of January 31, 2023, was 50.7 months (IQR, 44.6 months to 57.9 months).9
Progression-Free Survival
At the time of the interim analysis, the proportion of observed events (the first occurrence of progression or relapse or death) was 14.4% (33 events) in the venetoclax plus obinutuzumab group and 29.3% (67 events) in the chemoimmunotherapy group. The median PFS was not reached in the venetoclax plus obinutuzumab group and ████ ██████ ██████ ██████████ ████████ ████ ███ █████████ in the chemoimmunotherapy group (████████). Venetoclax plus obinutuzumab was favoured over chemoimmunotherapy (hazard ratio [HR] = 0.42 ███; 97.5% confidence interval [CI], 0.26 ███ to 0.68 ███). The PFS rates at 1 year, 2 years, 3 years, and 4 years were ██████ ██████ 87.7%, and ██████ respectively, in the venetoclax plus obinutuzumab group and ██████ ██████ 75.5%, and ██████ respectively, in the chemoimmunotherapy group.12
At the 4-year follow-up, the proportion of observed events was 24% (55 events) in the venetoclax plus obinutuzumab group and 39% (90 events) in the chemoimmunotherapy group. The median PFS had still not been reached in the venetoclax plus obinutuzumab group and was 59.4 months (95% CI not reported) in the chemoimmunotherapy group. The HR was 0.47 (97.5% CI, 0.32 to 0.69) following treatment with venetoclax plus obinutuzumab versus chemoimmunotherapy. The PFS survival rate at 4 years was 81.8% (97.5% CI, 75.8% to 87.8%) in the venetoclax plus obinutuzumab group and 62.0% (97.5% CI, 54.4% to 69.7%) in the chemoimmunotherapy group.9
Overall Survival
At the time of the interim analysis, the proportion of observed events (death due to any cause) was ████ ███ ███████ in the venetoclax plus obinutuzumab group and ████ ███ ███████ in the chemoimmunotherapy group. The median overall survival (OS) had not been reached in either group. The HR was █████ ██████ ███ █████ ██ ██████ following treatment with venetoclax plus obinutuzumab versus chemoimmunotherapy. The OS rates at 1 year, 2 years, 3 years, and 4 years were ██████ ██████ 96.3%, ███ █████, respectively, in the venetoclax plus obinutuzumab group and ██████ ██████ 95.0%, ███ ██████ respectively, in the chemoimmunotherapy group.12
At the 4-year follow-up, the proportion of observed events was 5% (11 events) in the venetoclax plus obinutuzumab group and 7% (17 events) in the chemoimmunotherapy group. The median OS had still not been reached in either group. The HR was 0.58 (97.5% CI, 0.24 to 1.38) following treatment with venetoclax plus obinutuzumab versus chemoimmunotherapy. The OS survival rate at 4 years was 95.1% (97.5% CI, 91.9% to 98.3%) in the venetoclax plus obinutuzumab group and 93.5% (97.5% CI, 89.6% to 97.4%) in the chemoimmunotherapy group.9
Duration of Response
At the time of the interim analysis, the proportion of observed events (the first occurrence of progression or relapse or death after the first documented response) was █████ ███ ███████ in the venetoclax plus obinutuzumab group and █████ ███ ███████ in the chemoimmunotherapy group. The median duration of response was ███ ███████ in either group. The HR was █████ ██████ ███ █████ ██ ██████ following treatment with venetoclax plus obinutuzumab versus chemoimmunotherapy. The event-free survival rates at 1 year, 2 years, 3 years, and 4 years were ██████ ██████ ██████ ██████ respectively, in the venetoclax plus obinutuzumab group and ██████ ██████ ██████ ███ ██████ respectively, in the chemoimmunotherapy group.12
Time to Next Treatment (From Randomization)
At the time of the interim analysis, the proportion of observed events (the initiation of the first subsequent treatment for CLL) was ████ ███ ███████ in the venetoclax plus obinutuzumab group and █████ ███ ███████ in the chemoimmunotherapy group. The median time to the next treatment was not reached in either group. The HR ███ █████ ██████ ███ █████ ██ ██████ following treatment with venetoclax plus obinutuzumab versus chemoimmunotherapy. The event-free survival rates at 1 year, 2 years, 3 years, and 4 years were ██████ ██████ ██████ ███ ██████ respectively, in the venetoclax plus obinutuzumab group and ██████ ██████ ██████ ███ ██████ respectively, in the chemoimmunotherapy group.12
At the 4-year follow-up, the proportion of observed events was 10.0% (23 events) in the venetoclax plus obinutuzumab group and 23.6% (54 events) in the chemoimmunotherapy group. The median time to the next treatment had still not been reached in either group. The HR was 0.34 (97.5% CI, 0.20 to 0.60) following treatment with venetoclax plus obinutuzumab versus chemoimmunotherapy. The event-free survival rate at 4 years was 90.4% (97.5% CI, 85.7% to 95.0%) in the venetoclax plus obinutuzumab group and 77.2% (97.5% CI, 70.2% to 84.1%) in the chemoimmunotherapy group.9
Undetectable MRD in Peripheral Blood
Venetoclax plus obinutuzumab was favoured over chemoimmunotherapy — at month 15, the undetectable MRD rate was 86.5% (97.5% CI, 80.6% to 91.1%) (198 of 229 patients) in the venetoclax plus obinutuzumab group compared with 52.0% (97.5% CI, 44.4% to 59.5%) (119 of 229 patients) in the chemoimmunotherapy group (P value < 0.0001). A total of 4.4% (10) of patients in the venetoclax plus obinutuzumab group and 14.8% (34) of patients in the chemoimmunotherapy group had a missing MRD status.13
Complete Response to Treatment
The median duration of follow-up in the full study population at month 15, based on a data cut-off date of February 28, 2021, was 27.9 months (IQR, 22.1 months to 35.3 months).13
At month 15, the complete response (CR) rate was 56.8% (130 of 229 patients) in the venetoclax plus obinutuzumab group compared with 31.0% (71 of 229 patients) in the chemoimmunotherapy group. A total of 3.1% (7) of patients in the venetoclax plus obinutuzumab group and 14.8% (34) of patients in the chemoimmunotherapy group had missing data for this parameter.13
Harms Results
The harms results from the CLL13 study are based on a data cut-off date of January 20, 2022 (interim analysis). A summary of key safety results from the CLL13 study is presented in Table 3.
Adverse Events
A total of █████ ████ ██ ███ █████████ in the venetoclax plus obinutuzumab group and █████ ████ ██ ███ █████████ in the chemoimmunotherapy group had at least 1 treatment-emergent adverse event (TEAE) of any Common Toxicity Criteria (CTC) grade 1 to grade 5. The most common TEAE in both groups was neutropenia and/or decreased neutrophil count based on a Standardized Medical Query — █████ ████ █████████ in the intervention group and █████ ████ █████████ in the comparator group. A total of █████ ████ █████████ in the venetoclax plus obinutuzumab group and █████ ███ █████████ in the chemoimmunotherapy group had an infusion-related reaction. A total of ████ ██ █████████ in the venetoclax plus obinutuzumab group and █████ ███ █████████ in the chemoimmunotherapy group had febrile neutropenia.12
Serious Adverse Events
A total of 102 (44.7%) patients in the venetoclax plus obinutuzumab group and 103 (47.7%) patients in the chemoimmunotherapy group had at least 1 serious TEAE of any CTC grade 1 to grade 5. The most common serious TEAEs in both groups were infections and infestations — █████ ███ ██ ███ ██████ in the intervention group and █████ ███ ██ ███ ██████ in the comparator group.12
Withdrawals Due to Adverse Events
A total of 13 (5.7%) patients in the venetoclax plus obinutuzumab group and 33 (15.3%) patients in the chemoimmunotherapy group had at least 1 TEAE leading to early treatment discontinuation.11 In the venetoclax plus obinutuzumab group, the most common TEAE leading to early treatment discontinuation was Richter syndrome — █████ ██ ██ ██ ██████ in the intervention group and ████ ██ ██ ██ ██████ in the comparator group. In the chemoimmunotherapy group, the most common TEAE leading to early treatment discontinuation was neutropenia — █████ ██ ██ ██ ██████ in the intervention group and █████ ███ ██ ██ ██████ in the comparator group.12
Treatment-Emergent Adverse Events With CTC Grade 5
In the venetoclax plus obinutuzumab group, a total of 9 patients had a CTC grade 5 adverse event (AE), of whom 1 patient had COVID-19 that was reported in the time frame between treatment period and until day 84 after the end of treatment, inclusive. The other 8 patients had a CTC grade 5 AE that was reported after day 84 after the end of treatment — secondary neoplasia (excluding Richter syndrome) in 3 patients, COVID-19 in 2 patients, and cardiac arrest or failure, Richter syndrome, and pneumonia in 1 patient each.11
In the chemoimmunotherapy group, a total of 10 patients had a CTC grade 5 AE, of whom 1 patient had an infection other than COVID-19 that was reported in the time frame between treatment period and until day 84 after end of treatment, inclusive. The other 9 patients had a CTC grade 5 AE that was reported after day 84 after the end of treatment — COVID-19 in 2 patients; Richter syndrome in 2 patients; bronchial obstruction, stroke, and respiratory failure in 2 patients; and secondary neoplasia (excluding Richter syndrome), cardiac arrest or failure, and pneumonia in 1 patient each.11
Notable Harms
Serious infections and infestations have been previously summarized.
At the interim analysis, there was a total of 27 cases of second primary malignances in the venetoclax plus obinutuzumab group, including 14 cases of nonmelanoma skin cancer and 13 cases of solid tumours. There was a total of 49 cases of second primary malignancies in the chemoimmunotherapy group, including 27 cases of nonmelanoma skin cancer, 18 cases of solid tumours, and 4 cases of hematological malignancies.11
At the 4-year follow-up, there was a total of 45 cases of second cancers in the venetoclax plus obinutuzumab group, including 16 cases of nonmelanoma skin cancer, 15 cases of solid tumours, 7 cases of benign tumours, and 7 cases of Richter syndrome. There was a total of 69 cases of second cancers in the chemoimmunotherapy group, including 33 cases of nonmelanoma skin cancer, 19 cases of solid tumours, 7 cases of benign tumours, 6 cases of Richter syndrome, and 4 cases of hematological malignancies (2 cases of plasma cell myeloma and 1 case each of myelodysplastic syndrome and cutaneous T-cell lymphoma).9
In the venetoclax plus obinutuzumab group, 1 case of cardiac arrest and 1 case of arrhythmia was reported. In the chemoimmunotherapy group, 1 case of arrhythmia was reported.12
Table 3: Summary of Key Efficacy and Safety Results From the CLL13 Study
Outcome | VEN + OBI (N = 229) | Chemoimmunotherapy (FLU + CYC + RIT or BEN + RIT) (N = 229) |
|---|---|---|
Time-to-event outcomes, per data cut-off at January 20, 2022 (ITT population) | ||
Follow-up time for all patients (months), median (IQR) | 38.8 (32.7 to 46.1) | |
Follow-up time (months), median (IQR) | ████ █████ ██ | ████ █████ ██ █████ |
PFS | ||
Events, n (%) | 33 (14.4) | 67 (29.3) |
PFS (months), median (97.5% CI) | Not reached | ████ ████ █████████ |
HR (97.5% CI) | 0.42 ████ (0.26 ████ to 0.68 ███) | |
P valuea | ████████ | |
PFS rate at 4 years, % | ████ | ████ |
OS | ||
Events, n (%) | ██ █████ | ██ █████ |
OS (months), median (97.5% CI) | Not reached | Not reached |
HR (97.5% CI) | █████ ██████ ██ ██████ | |
P value | Not reported | |
OS rate at 4 years, % | ████ | ████ |
DOR | ||
N of patients | ███ | ███ |
Events, n (%) | ██ ██████ | ██ ██████ |
DOR (months), median (95% CI) | ███ ███████ | ███ ███████ |
HR (97.5% CI) | █████ ██████ ██ ██████ | |
P value | ███ ████████ | |
Event-free survival rate at 4 years, % | ████ | ████ |
TTNT from randomization | ||
Events, n (%) | ██ █████ | ██ ██████ |
TTNT (months), median (95% CI) | Not reached | Not reached |
HR (97.5% CI) | █████ ██████ ██ ██████ | |
P value | ███ ████████ | |
Event-free survival rate at 4 years, % | ████ | ████ |
Undetectable MRD, per data cut-off at February 28, 2021 (ITT population) | ||
Follow-up time for all patients (months), median (IQR) | 27.9 (22.1 to 35.3) | |
Follow-up time (months), median (IQR) | 28.0 (23.2 to 35.4) | 27.1 (20.9 to 33.6) |
MRD in peripheral blood at month 15 | ||
Negative MRD status (< 10–4), n (%) | 198 (86.5) | 119 (52.0) |
97.5% CI by Clopper-Pearson | 80.6 to 91.1 | 44.4 to 59.5 |
P valuea | < 0.0001 | |
Missing MRD status, n (%) | 10 (4.4) | 34 (14.8) |
Response to treatment, per data cut-off at February 28, 2021 (ITT population) | ||
CR at month 15 | ||
Response, n (%) | ||
CR | 125 (54.6) | 63 (27.5) |
CRir | 5 (2.2) | 8 (3.5) |
Missing | 7 (3.1) | 34 (14.8) |
CR rate, n (%) | 130 (56.8) | 71 (31.0) |
Harms results, per data cut-off at January 20, 2022 (safety population) | ||
N of patients | 228 | 216 |
Patients with ≥ 1 TEAE of any CTC grade 1 to grade 5, n (%) | ███ ██████ | ███ ██████ |
Patients with ≥ 1 serious TEAE of any CTC grade 1 to grade 5, n (%) | 102 (44.7) | 103 (47.7) |
All cases of TEAE leading to treatment discontinuation, N | 13 | 45 |
Refer to the preceding text for a summary of TEAEs with CTC grade 5 and notable harms. | ||
BEN = bendamustine; CI = confidence interval; CR = complete response; CRir = complete response with incomplete recovery of the bone marrow; CTC = Common Toxicity Criteria; CYC = cyclophosphamide; DOR = duration of response; FLU = fludarabine; HR = hazard ratio; IQR = interquartile range; ITT = intention to treat; MRD = minimal residual disease; OBI = obinutuzumab; OS = overall survival; PFS = progression-free survival; RIT = rituximab; TEAE = treatment-emergent adverse event; TTNT = time to next treatment; VEN = venetoclax.
aThe P value was adjusted for multiple testing.
Sources: Interim analysis of the co-primary endpoint progression-free survival: CLL13 (GAIA) (data cut-off date of January 20, 2022),12 Co-Primary Endpoint Analysis of MRD negativity rate at month 15: CLL13 (GAIA) (data cut-off date of February 28, 2021),13 and Sponsor Summary of Clinical Evidence.2
Critical Appraisal
Internal Validity
The CLL13 study was generally appropriately designed and powered to evaluate the efficacy of venetoclax plus obinutuzumab relative to chemoimmunotherapy. Although the trial was open label and therefore susceptible to reporting and performance bias, this was considered justifiable in the context of CLL and the requirement of different study drug formulations and administration routes.
Relevant baseline characteristics were generally well balanced between the venetoclax plus obinutuzumab and chemoimmunotherapy groups. As such, it was concluded that the risk of bias arising from the randomization process is unlikely. While patients with unmutated IGHV were balanced between the treatment groups, this subset of patients would not typically receive chemoimmunotherapy in the frontline setting, as per the guideline.6 In consultation with the clinical experts, it was concluded that this subset of patients with unmutated IGHV randomized to receive chemoimmunotherapy was at a disadvantage when compared to venetoclax plus obinutuzumab, thereby introducing the potential for bias in favour of venetoclax plus obinutuzumab. However, the clinical experts noted that since chemoimmunotherapy was the standard of therapy when the trial was conducted, this issue is considered reasonable but specific bias remains.
In consultation with the clinical experts, it was concluded that a median follow-up of 38 months at the interim analysis is appropriate for evaluating the safety and efficacy of the study drugs and that the assessment time point at 15 months for MRD and response to treatment is standard in trials (i.e., 3 months post-treatment).
A total of 4.4% of patients in the venetoclax plus obinutuzumab group and 14.8% of patients in the chemoimmunotherapy group had missing data on MRD status. It was concluded that the imbalance observed in missing data and the relatively high rate of missing data in the chemoimmunotherapy group is a concern for the potential for biased results. Although patients without an MRD sample at month 15 were kept and indicated as non-negative in the analysis, missing data were not replaced or imputed in the primary efficacy analysis of undetectable MRD in peripheral blood at month 15. However, in consideration of the results (i.e., most patients had a negative MRD status in both treatment groups and there was an imbalance observed in missing data), there is a concern for the potential for biased results, likely in favour of venetoclax plus obinutuzumab, due to the approach for handling missing data.
Type I error was controlled only in the analyses of undetectable MRD and PFS, using a hierarchical testing sequence. A sensitivity analysis was not performed for the comparison of venetoclax plus obinutuzumab versus chemoimmunotherapy; therefore, no conclusions can be drawn on the robustness (or lack thereof) of the results. Since the study was not designed or powered to test specific hypotheses in all other secondary and exploratory analyses, these results are considered as supportive evidence only.
External Validity
The CLL13 study included a subset of the population of interest identified in the indication for venetoclax, in combination with obinutuzumab, that was not considered in the previous review — fit patients (defined in the trial by a CIRS score of ≤ 6 and CrCl of ≥ 70 mL per minute) with previously untreated CLL without TP53 aberrations.
In consultation with the clinical experts, it was concluded that the inclusion and exclusion criteria are standard in trials of CLL and are justifiable in the context of minimizing confounders and avoiding placing chemoimmunotherapy at a disadvantage in the comparisons made (i.e., excluded patients with del[17p] and TP53 mutation). However, the clinical experts noted that some criteria are not applicable to Canadian practice and are narrow when compared with patients with CLL seen in practice. Most of the patients excluded from the trial may still be considered in practice as candidates for venetoclax plus obinutuzumab by the clinical experts by working with the multidisciplinary team to resolve drug-drug interactions, control other pre-existing conditions, and dose-adjust accordingly. Overall, despite the narrow inclusion and exclusion criteria, the clinical experts had no concerns with generalizing the results to fit patients who were excluded from the trial — namely, patients with SLL and with del(17p) and TP53 mutation. Additionally, the baseline characteristics of the study population were generally representative of a fit patient population seen in practice that would be considered as a candidate for venetoclax plus obinutuzumab, as per clinical expert input.
Based on patient and clinician group input and in consultation with the clinical experts, it was concluded that the time-to-event outcomes are most meaningful to patients and clinicians. While treatment response and undetectable MRD are standard outcome measures in clinical trials of CLL, the clinical experts advised that they are of limited applicability to Canadian practice due to limitations in accessing relevant tests (MRD measurements, bone marrow biopsies, and scans for treatment response). Thus, while MRD levels might serve as a surrogate marker for OS and PFS in CLL according to literature,14 from a clinical practice perspective, response to treatment and undetectable MRD are relevant as supportive evidence for long-term outcomes.
According to the guidelines,6 FLU + CYC + RIT and BEN + RIT are appropriate comparators in fit patients without TP53 aberrations (del[17p] and TP53 mutation) and with mutated IGHV in the frontline setting, even though FLU + CYC + RIT is infrequently used and BEN + RIT is not used in practice as per clinician group and clinical expert input. As mentioned earlier, fit patients without TP53 aberrations and with unmutated IGHV do not typically receive chemoimmunotherapy in the frontline setting; instead, a BTK inhibitor would have been a more appropriate comparator in this subset of patients, as per the guidelines.6 Further, based on the guidelines,6 a BTK inhibitor would have been an appropriate comparator for fit patients with TP53 aberrations — a gap in the present systematic review evidence.
Long-Term Extension Study
No long-term extension studies were submitted by the sponsor.
Indirect Comparisons
Description of Sponsor-Submitted Network Meta-Analysis
The objective of the sponsor-submitted network meta-analysis (NMA) was to estimate the comparative effectiveness of venetoclax plus obinutuzumab versus relevant comparators in the treatment of patients who are fit, with previously untreated CLL, and without del(17p) or TP53 mutation, in terms of PFS, OS, time to next treatment, and undetectable MRD. Indirect comparisons of venetoclax plus obinutuzumab, venetoclax plus ibrutinib, FLU + CYC + RIT, BEN + RIT, obinutuzumab plus chlorambucil, acalabrutinib, zanubrutinib, and ibrutinib were made using a Bayesian NMA with Hamiltonian Monte Carlo, a Markov Chain Monte Carlo method.15
The population of interest is adult patients aged 18 years and older who are fit (defined in the included trials by a CIRS score of ≤ 6 and CrCl of ≥ 70 mL per minute), with previously untreated CLL, and without del(17p) or TP53 mutations. According to the authors of the NMA, an ███ ████ ████████ ███ ███████ ████ █████ ████████ ███ ███ ████████ ███ ██ ███ ███████ ████████ ███ ██████ ███ ████████. Hence, the base case included both fit and unfit patients without del(17p) or TP53 mutations (and whose blood sampling showed undetectable MRD).15
Efficacy Results
The evidence informing the NMA was based on a February 2024 literature search.16 After applying the more restrictive inclusion criteria used for the NMA, a total of ████ unique clinical trials were included in the feasibility assessment: ██████ ██████ ██████ ███████████ ████████ █████ █████████ ██████ ███ ████. The authors of the NMA indicated that the ████ trial was excluded from the analysis due to unclear reporting of outcomes as only conference abstracts were available at the time of the latest search, even though the interventions are relevant to the NMA. All studies were open-label, phase III, multinational randomized controlled trials (RCTs) (except for █████ █████ ███ █████████ ██ ███ ██████ ███████ ████) with a median follow-up ranging ████ ████ ██ ████ months. All studies included treatment-naive patients with CLL; the exception was ███████ in which patients with SLL were also included.15
Progression-Free Survival
Venetoclax plus obinutuzumab was favoured over ███ ███ █ █████ ███ ████████ ████████ ██████ ████ ██ █████ ███ ██ ███ █ █████ ███ ████ ████ ██ ██████ ██ █████████ was favoured between ██████████ ████ ████████████ ███ █████████████ ███ █ █████ ███ ████ ████ ██ █████████████ ███ █ █████ ███ ████ ████ ██ ██████ ████████████ ███ █ █████ ███ ████ ████ ██ ██████ ███ ██████████ ████ █████████ ███ █ █████ ███ ████ ████ ██ ████.
Overall Survival
██ █████████ was favoured based on comparisons between ██████████ ████ ████████████ ███ ███ ████████████ ███ ███ █ █████ ███ ████ ████ ██ ██████ ██ ███ █ █████ ███ ████ ████ ██ ██████ █████████████ ███ █ █████ ███ ████ ████ ██ ██████ █████████ ███ █ █████ ███ ████ ████ ██ ██████ ████████████ ███ █ █████ ███ ████ ████ ██ ██████ ███ ██████████ ████ █████████ ███ █ █████ ███ ████ ████ ██ █████.
Time to Next Treatment
Venetoclax plus obinutuzumab was favoured over ███ ███ █ █████ ███ ████ ████ ██ █████ ███ ██ ███ █ █████ ███ ████ ████ ██ ██████ ██ █████████ was favoured between ██████████ ████ ████████████ ███ ██████████ ████ █████████ ███ █ █████ ███ ████ ████ ██ █████.
Undetectable MRD
Venetoclax plus obinutuzumab was favoured between comparators: ███ █████ █████ ████ █ █████ ███ ████ ████ ██ ██████ ██ ███ █ ██████ ███ ████ ████ ██ ███████ █████████ ███ █ ████████ ███ ████ ██████ ██ ██████████ ███ ██████████ ████ █████████ ███ █ █████ ███ ████ ████ ██ ██████.
Harms Results
Harms results were not assessed in the NMA.
Critical Appraisal
Studies included in the NMA were selected from those identified by the systematic literature review. The systematic literature review was conducted using standard methods; a defined research question was specified a priori and multiple databases were searched with the last literature search conducted in ████████ ████. A narrowed set of criteria for the inclusion of studies for the NMA were provided and are consistent with the objective, including further restricting the eligible interventions to those that are relevant to Canadian practice for the first-line treatment of CLL in the population of interest based on the CLL13 trial population.
A Bayesian NMA was conducted that, according to the authors, was consistent with the National Institute for Health and Care Excellence (NICE) Decision Support Unit Technical Support Document 2.51 No major concerns with the statistical methods used were identified by the review team. Notably, no sensitivity analysis was performed to assess the sensitivity of model results against the informative priors used in the random-effects model. Further, assessment of consistency was not reported.
While the base-case analysis of the mixed fit and unfit network was not according to protocol, the clinical experts had no concern with generalizing the NMA results that were based on the broader population to the fit population, regardless of del(17p) or TP53 mutation, as there are fewer concerns with comorbidities in the fit population. Nonetheless, it is important to note the differences in population fitness across the network that would represent a potential source of bias in the network. Notably, ██████ ████████ ████ ███ █████████ █████ █ ██████ ████████ ████ █████ ██ ██████ █████ ████████ █████████ ██ ████████ █████ ██ █████ █████ ███ ███. While exploring areas of uncertainty in the NMA results, the review team noted that ███ ██████████ █████ █████████ █████████████ ████ ██ ███████ ████████████ ██████ ████████████ ███ ████████████ ██ ████████ ████ ██ █████ ███ ██████ ██ █████ ████ ██ █████ ███ ███████ ████ ██ █████ ████ █████████████ █████ ██ ██ ██ ██ ██████ ████ ███ ██████████ █████ █ ███ ████ █████████ ████ ███ ████████ ██████ █████ █████████ █████████ ██████ █████████ ████ █████████ ███ ██ ██ ████████ ████ ██ █████ ███ ██████ ███ ███ ███████ ██████ █████ ████████ ████████████ ██████ ██ ██ ████████ ████ ██ █████ ███ █████ ██ ██████████████. These differences in eligibility criteria (i.e., fitness approximation) might have contributed to the difference observed in the direction of the results for the comparisons with the BTK inhibitors, suggesting fitness is an effect modifier; as such, this raises concerns for comparing the studies included in the NMA.
Heterogeneity in patient baseline characteristics was reported by the authors of the NMA as part of their feasibility assessment. Based on literature, del(17p) and TP53 mutation are predictive of worse clinical outcomes after treatment with chemoimmunotherapy compared with targeted therapies, and IGHV mutation is associated with prolonged durable remission after chemoimmunotherapy treatment, which was not observed in patients with IGHV-unmutated CLL or SLL;25 the clinical experts were in agreement. The base case excluded patients with del(17p) and TP53 mutation to align with the CLL13 trial population. However, these patients were included in the analyses where it was not possible for the investigators to exclude them. Therefore, differences in these treatment effect modifiers across the network would introduce bias in the NMA results.
Heterogeneity in study methodology was also reported by the authors of the NMA as part of their feasibility assessment. Across the included studies, the median follow-up ranged from ████ ██ ████ ██████. The clinical experts advised that a median follow-up of ██ ██████ is likely too short to evaluate treatment effect; the exception is upfront toxicities as CLL is not expected to progress until later. In contrast, a median follow-up of ██ ██████ is likely appropriate for assessing the treatment effect of time-limited therapies. The clinical experts further advised that a longer follow-up is likely advantageous for continuous therapies (i.e., there is a potential for biased results favouring BTK inhibitors with a long follow-up) as disease progression is expected to occur later with chronic therapy. Differential follow-up can also lead to bias when specifically comparing time-to-event outcomes such as PFS and OS since estimated HRs often wane with increased lengths of follow-up. Overall, these sources of clinical and methodological heterogeneity likely introduced bias in the results of the NMA.
Notably, the networks were sparse. The base case and the sensitivity analyses ████████ █ ██ █ ███████ which likely introduced uncertainty about the results. Due to the small number of studies included in the NMA, the authors deemed it was infeasible to account for heterogeneity using metaregression.
Study Addressing Gaps in the Evidence From the Systematic Review
No studies addressing gaps were submitted by the sponsor.
Conclusion
One phase III, multicentre, randomized, prospective, open-label clinical trial (the CLL13 study) was submitted for this reassessment to support the expansion of the reimbursement criteria for venetoclax plus obinutuzumab to include patients with previously untreated CLL who are considered fit and potentially fludarabine-eligible. At the primary data cut-off date, the CLL13 study demonstrated that venetoclax plus obinutuzumab results in an improvement in PFS, based on the estimated PFS rates at 4 years, when compared with FLU + CYC + RIT and BEN + RIT (chemoimmunotherapy). The results are also suggestive of an improvement with venetoclax plus obinutuzumab in the duration of response and time to next treatment, based on the estimated event-free survival rates at 4 years, when compared with chemoimmunotherapy. The benefit for PFS and time to next treatment was also consistently demonstrated at the updated data cut-off dates. In the absence of literature on the minimal important differences in these event-free survival rates in the target population, the clinical experts suggested that these results are clinically meaningful in the context of CLL being an incurable disease and that relapse is expected with time-limited therapies. The results for OS are difficult to interpret due to patients receiving second-line therapy. Notably, the potential for bias in favour of venetoclax plus obinutuzumab due to patients with unmutated IGHV receiving chemoimmunotherapy should be considered when interpreting the results for survival outcomes. The CLL13 study also demonstrated that treatment with venetoclax plus obinutuzumab results in an improvement in the rates of undetectable MRD in peripheral blood, measured by the proportion of patients with negative MRD status at month 15 (a coprimary end point), when compared with chemoimmunotherapy. Notably, the potential for bias due to the imbalance observed in missing data between groups and the handling of missing data in the primary efficacy analysis of undetectable MRD should be considered when interpreting the results. HRQoL was identified as an outcome of importance to patients and clinicians; however, relevant results were unavailable at the time of the sponsor’s submission. At the primary data cut-off, no major concern was identified in the safety profile of venetoclax plus obinutuzumab, although it was difficult to interpret for CTC grade 5 AEs, cardiac-specific TEAEs, and second primary malignancies due to the small number of events.
The NMA results showed a favourable treatment effect with venetoclax plus obinutuzumab compared with ██████████ ████ █████████ ██ ████████████ ███ ██ ██████████ █████. For all other indirect comparisons assessed in the NMA, there was uncertainty in the results primarily due to the 95% credible interval (CrI) including the null and the small number of studies included. Additionally, heterogeneity identified in population fitness and mutational status and the differential follow-up times likely introduced bias into the NMA results. No safety end point was evaluated in the NMA; therefore, no conclusions on safety can be drawn on the indirect comparison of venetoclax plus obinutuzumab versus other relevant comparators.
Introduction
The objective of the present reassessment is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of venetoclax 10 mg, 50 mg, and 100 mg oral tablets, in combination with obinutuzumab, in the treatment of patients with previously untreated CLL. The focus will be placed on the fit population (defined in the CLL13 trial by a CIRS score of ≤ 6 and a CrCl of ≥ 70 mL per minute).
Disease Background
Content in this section has been informed by materials submitted by the sponsor and clinical expert input. The following has been summarized and validated by the review team.
CLL is a lymphoid neoplasm that is characterized by a progressive accumulation of monoclonal, mature, functionally impaired B lymphocytes. The pathologic and immunophenotypic features of the malignant cells are identical in CLL and SLL. If the disease primarily presents in the blood, then the term CLL is used. If the disease primarily involves the lymph nodes, then the term SLL is used. Although some patients might present with painless, swollen lymph nodes that wax and wane, most patients with CLL do not present with symptoms at the time of diagnosis. A small proportion of patients with CLL might present with typical B symptoms of lymphoma, which include weight loss, fevers, fatigue, and night sweats. Signs of CLL might include enlargement of the lymph node (lymphadenopathy), spleen (splenomegaly), and liver (hepatomegaly) upon physical examination. In a variable proportion of patients, CLL can transform into another lymphoproliferative disorder or development of a second lymphoid malignancy. Richter syndrome refers to the transformation of CLL into a clinically aggressive lymphoma.3
Patients with CLL have been shown to have reduced HRQoL compared with healthy individuals.26 Moreover, patients with CLL receiving conventional therapy report poorer HRQoL compared with those not receiving treatment or with healthy individuals.27-29
CLL is more common in males, with a male to female ratio of approximately 1.2:1 to 1.8:1.3 CLL is often diagnosed in patients aged between 65 years and 70 years;30 however, at least 10% of CLL cases are diagnosed in patients aged younger than 55 years.31 CLL is the most common leukemia in adults living in Canada — in 2019, 1,700 patients were diagnosed with CLL (1,095 men and 605 women) and in 2020 and 2022, 222 deaths and 554 deaths due to CLL were reported, respectively.4 CLL is considered incurable; the 5-year net survival for CLL is estimated to be 83%.4 The estimated median life expectancy for patients with del(17p) or TP53 mutation is less than 2 years to 3 years from the time of initial diagnosis;5 however, the clinical experts advised that this statistic likely reflects the prenovel therapy era and estimated the median life expectancy for this subset of patients to be longer than 3 years from initial diagnosis.
Prognostic markers (associated with clinical outcomes independent of therapy received) include clinical staging (i.e., Rai and Binet), mutational status (i.e., IGHV and TP53), lymphocyte doubling time, beta2-microglobulin, and genetic abnormalities (e.g., del[17p], deletion 11q, deletion 13q, and trisomy 12).25 In addition to disease-related factors, the prognosis of patients with CLL is dependent on patient-related factors (e.g., age, sex, comorbidities, performance status) and treatment-related factors (e.g., type of treatment, response, MRD status).32 Mutational status is also a predictive marker (informs the likelihood of response to therapy received).25
The diagnosis of CLL in patients presenting with an absolute lymphocytosis (an increased B-lymphocyte count of at least 5 × 109/L) likely involves a complete blood count with differential, immunophenotypic analysis of lymphocytes (typically using flow cytometry), and the examination of a peripheral blood smear.3 The 2018 Canadian evidence-based guideline for the first-line treatment of CLL7 referred to the iwCLL guidelines for standardized criteria for the diagnosis of CLL.33 The Binet and Rai clinical staging methods are used to identify patients who require treatment and predict their survival; clinical staging is based on physical examination and standard laboratory tests.7 The 2022 updated Canadian evidence-based guideline for frontline treatment of CLL6 advised on IGHV mutation testing before the first treatment only, and del(17p) and TP53 mutation testing before each treatment.
Standards of Therapy
Content in this section has been informed by materials submitted by the sponsor and clinical expert input. The following has been summarized and validated by the review team.
According to the 2022 Canadian guideline,6 the selection of chemotherapy and/or chemoimmunotherapy is historically directed by patient age and/or comorbidities (also referred to as patient fitness). Since these factors continue to be used in inclusion criteria for phase III clinical trials on CLL, age and comorbidities are still considered when treatment decisions are being made, along with molecular testing results. The guideline6 advised that IGHV mutation status and TP53 aberrations, including del(17p) and TP53 mutation, are proven predictive markers for survival outcomes and should be used to guide the selection of therapy. Notably, the guideline6 indicated that patients with TP53 aberrations are associated with a negative prognosis (response rates, PFS, and OS) and in particular, with chemoimmunotherapy and novel drugs in the relapsed or refractory setting. Similarly, IGHV mutation status is predictive of outcomes following treatment with chemoimmunotherapy compared with targeted therapy (e.g., BTK or BCL-2 inhibitors). Specifically, patients with IGHV-mutated CLL or SLL treated with chemoimmunotherapy were associated with prolonged durable remissions, but this was not observed in patients with IGHV-unmutated CLL or SLL.25
In symptomatic patients with previously untreated CLL with TP53 aberrations (del[17p] and/or TP53 mutation), the guideline6 advised that continuous therapy with a BTK inhibitor (namely, ibrutinib and acalabrutinib) is the preferred therapy while venetoclax plus obinutuzumab would be preferred in patients who would benefit from a time-limited therapy, if funded. Of note, the guideline6 advised that second-generation covalent BTK inhibitors are preferred for their improved toxicity profile. The group hematologists who provided their input through Lymphoma Canada and the clinical experts highlighted that ibrutinib is associated with cardiac side effects (e.g., ventricular arrhythmias, including sudden deaths), the risk of bleeding, and skin and joint-related issues.
In symptomatic fit patients (as per the guideline,6 patients who are considered fit include those who are young and those who are eligible for treatment with FLU + CYC + RIT) with previously untreated CLL without TP53 aberrations, the guideline advised that FLU + CYC + RIT is preferred for IGHV-mutated CLL while a BTK inhibitor (namely, acalabrutinib) is an option for IGHV-mutated CLL and is the preferred option for IGHV-unmutated CLL. The clinical experts noted that zanubrutinib was not highlighted in the guideline due to a lack of funding at the time publication (2023). The guideline6 further advised that venetoclax plus obinutuzumab would become the preferred therapy in this subset of patients, regardless of IGHV mutation, if funded across Canada. Of note, the 2018 guideline7 had advised on BEN + RIT for fit, older (65 years and older) patients with previously untreated CLL without TP53 aberrations but with mutated IGHV due to reduced toxicity concerns.
The clinical experts stated that BEN + RIT is no longer used in practice while the group of hematologists who provided their input through Lymphoma Canada stated that FLU + CYC + RIT is infrequently used in practice. Nonetheless, the clinical experts noted that chemoimmunotherapy remains as an option for patients with intermediate (unmutated IGHV) and high-risk (TP53 aberrations) disease — for example, in scenarios where there are challenges in accessing preferred treatment regimens. However, the clinician group and the clinical experts highlighted that chemoimmunotherapy is commonly associated with treatment-related adverse effects, including the approximate 6% to 7% risk of myelodysplastic syndrome or acute myeloid leukemia with FLU + CYC + RIT in the young and fit patient population.34
While ibrutinib with venetoclax is currently under consideration for negotiation with the pan-Canadian Pharmaceutical Alliance,35 it is considered a relevant comparator as it previously received a pERC recommendation (November 2023) in favour of reimbursement for the indication under review. Ibrutinib with venetoclax is indicated for the treatment of adult patients with previously untreated CLL, including those with del(17p).36
According to the 2018 guideline,7 the goals of therapy include effective and durable disease control, measured by PFS and OS, while minimizing toxicity and maintaining acceptable HRQoL. The clinical experts further elaborated on the goals of therapy to include treatment-free periods (remission) in the population with low-risk cytogenetic markers (mutated IGHV) and disease control in the population with high-risk cytogenetic markers (TP53 mutation).
Drug Under Review
Key characteristics of venetoclax plus obinutuzumab are summarized in Table 4, along with other treatments available for the first-line treatment of fit and potentially fludarabine-eligible patients with CLL.
The starting dose of oral venetoclax is 20 mg once daily for 7 days followed by 50 mg daily in the second week, 100 mg daily in the third week, and 200 mg daily in the fourth week. The dose must be administered according to a weekly ramp-up schedule to the recommended daily dose of 400 mg over a period of 5 weeks. The recommended steady daily dose is 400 mg thereafter. The 5-week ramp-up dosing schedule is designed to gradually reduce tumour burden (debulk) and decrease the risk of tumour lysis syndrome.37
The obinutuzumab IV administration starts on cycle 1, day 1, at 100 mg, followed by 900 mg, which may be administered on day 1 or day 2. A dose of 1,000 mg is administered on day 8 and day 15 of cycle 1, and on day 1 of 5 subsequent cycles (a total of 6 cycles, 28 days each).37
Venetoclax is started on cycle 1, day 22, according to the ramp-up schedule, continuing through to cycle 2, day 28. After completing the ramp-up schedule, patients should continue on venetoclax 400 mg once daily from cycle 3, day 1, of obinutuzumab to the end of cycle 12. Venetoclax should be given for a total of 12 months as a finite treatment duration: for six 28-day cycles in combination with obinutuzumab, followed by 6 months of venetoclax as a single drug.37
Venetoclax is a selective small-molecule inhibitor of BCL-2, a protein that inhibits cells from programmed cell death (apoptosis). Venetoclax helps restore the process of apoptosis by binding directly to the BH3-binding groove of BCL-2, displacing BH3 motif-containing proapoptotic proteins like BIM, BAX, BAK, BAD, NOXA, and PUMA to initiate mitochondrial outer membrane permeabilization, the release of cytochrome c, and caspase activation, ultimately resulting in programmed cancer cell death (apoptosis).37
The reimbursement criteria requested for the current reassessment of venetoclax plus obinutuzumab is for the subgroup of previously untreated patients with CLL considered fit and potentially fludarabine-eligible, who were not included in the reimbursement request or recommendation criteria in the previous review by CADTH. Note that this request aims to expand the reimbursement criteria for venetoclax plus obinutuzumab to align with the Health Canada indication, which is for the “treatment of patients with previously untreated CLL” (i.e., irrespective of age or eligibility for fludarabine treatment).
Table 4: Key Characteristics of Comparator Regimens for Venetoclax Plus Obinutuzumab for the First-Line Treatment of Fit (Potentially Fludarabine-Eligible) Patients With CLL
Regimen | Mechanism of action | Indication(s) | Route and dosage | Serious adverse effects or safety issues |
|---|---|---|---|---|
Venetoclax plus obinutuzumab | Venetoclax: An oral selective small-molecule BCL-2 inhibitor (a protein that inhibits apoptosis). BCL-2 overexpression has been associated with resistance to chemotherapies. Obinutuzumab: A humanized recombinant type II anti-CD20 monoclonal antibody, which targets the CD20 transmembrane antigen on B lymphocytes and induces cell death via antibody-dependent cellular cytotoxicity | For the treatment of patients with previously untreated CLL | Cycle 1 (28 days):
Cycle 2 (28 days):
Cycle 3 to cycle 6 (28 days each):
| Venetoclax: TLS, myelosuppression ± infection, bleeding, dyspnea, and edema Obinutuzumab: Neutropenia, thrombocytopenia, infections, infusion-related reactions, and PML |
Ibrutinib plus venetoclax | Ibrutinib: A small molecule that forms a covalent bond with a cysteine residue (Cys-481) in the BTK active site, thereby inhibiting BTK activity. BTK is implicated in the pathogenesis of several B-cell malignancies, including CLL. Venetoclax: An oral selective small-molecule BCL-2 inhibitor (a protein that inhibits apoptosis). BCL-2 overexpression has been associated with resistance to chemotherapies. | For the treatment of adult patients with previously untreated CLL, including those with del(17p) | Cycle 1 to cycle 3 (28 days each):
Cycle 4 to cycle 15 (28 days each):
| Ibrutinib: Second primary malignancies, cardiac toxicity, cerebrovascular accidents, TLS, cytopenia, lymphocytosis, leukostasis, hemorrhage, hepatic impairment, infections, and teratogenic risk Venetoclax: TLS, myelosuppression ± infection, bleeding, dyspnea, and edema |
FLU + CYC + RIT | FLU: A synthetic fluorinated analogue of purine nucleoside antiviral, it prevents elongation of DNA strands through direct incorporation into DNA as a false nucleotide; inhibits DNA polymerase, primase, ligase, and ribonucleotide reductase; and partially inhibits RNA polymerase II. Induces cytotoxicity and/or apoptosis CYC: An alkylating drug, it prevents cell division primarily by cross-linking DNA and RNA strands. RIT: A chimeric mouse-human monoclonal IgG1k antibody, it binds to the CD20 antigen and depletes CD20-positive cells via antibody-dependent cell cytotoxicity and complement-mediated cell lysis. | Treatment of anti-CD20 antibody-naive previously untreated or second-line patients with RR CLL, in whom FLU-based therapy is considered appropriate | Cycle 1 (28 days):
Cycle 2 to cycle 6 (28 days each):
| FLU: Myelosuppression, neurotoxicity, immunosuppression or opportunistic infections, autoimmune hemolytic anemia, and pulmonary toxicities CYC: Immunosuppression, myelosuppression, infections, hemorrhagic cystitis, pulmonary toxicity, cardiac toxicity, secondary malignancies, and liver disease RIT: Neutropenia, infections, infusion-related symptoms, TLS, arterial thromboembolism, SJS or TEN, PRES, and PML |
BEN + RIT | BEN: Exact mechanism unknown, may cause apoptotic and nonapoptotic death of malignant cells by damaging DNA, increasing proapoptotic gene expression, inhibiting mitotic control RIT: A chimeric mouse-human monoclonal IgG1k antibody. It binds to the CD20 antigen expressed on B lymphocytes and depletes CD20-positive cells via antibody-dependent cell cytotoxicity and complement-mediated cell lysis. | For first-line treatment of CLL | Cycle 1 (28 days):
Cycle 2 to cycle 6 (28 days each):
| BEN: Cardiac toxicity, infusion reactions, myelosuppression, SJS or TEN, TLS, carcinogenicity, and mutagenicity RIT: Neutropenia, infections, infusion-related symptoms, TLS, arterial thromboembolism, SJS or TEN, PRES, and PML |
Zanubrutinib | Forms a covalent bond with a cysteine residue in the BTK active site, leading to inhibition of BTK activity | For the treatment of adults with CLL | Oral, 100 mg twice daily until disease progression or unacceptable toxicity | Serious hemorrhage, second primary malignancies (including nonskin carcinoma), atrial fibrillation and atrial flutter, serious and fatal infections (including bacterial, viral, or fungal) and opportunistic infections, and TLS |
Ibrutinib | A small molecule that forms a covalent bond with a cysteine residue (Cys-481) in the BTK active site, thereby inhibiting BTK activity. BTK is implicated in the pathogenesis of several B-cell malignancies, including CLL. | For the treatment of adult patients with previously untreated CLL, including those with del(17p) | Oral, 420 mg daily until disease progression or unacceptable toxicity | Second primary malignancies, cardiac arrhythmias and cardiac failure, PR interval prolongation, cerebrovascular accidents, TLS, cytopenia, lymphocytosis, leukostasis, hemorrhage, hepatic impairment, infections, and teratogenic risk |
Acalabrutinib | Acalabrutinib (a small molecule) and its active metabolite, ACP-5862, form a covalent bond with a cysteine residue in the BTK active site, leading to irreversible inactivation of BTK. | In combination with obinutuzumab or as monotherapy in patients with previously untreated CLL | Oral, 100 mg twice daily until disease progression or unacceptable toxicity | Atrial fibrillation, second primary malignancies, cytopenia, hemorrhage, (opportunistic) infections |
BEN = bendamustine; BTK = Bruton tyrosine kinase; CLL = chronic lymphocytic leukemia; CYC = cyclophosphamide; del(17p) = 17p deletion; FLU = fludarabine; IgG1k = immunoglobulin G1k; PML = progressive multifocal leukoencephalopathy; PR = partial response; PRES = posterior reversible leukoencephalopathy syndrome; RIT = rituximab; RNA = ribonucleic acid; RR = relapsed or refractory; SJS = Stevens-Johnson syndrome; TEN = toxic epidermal necrolysis; TLS = tumour lysis syndrome.
Sources: Ontario Health (Cancer Care Ontario)’s Drug Formulary 2023;38 BC Cancer;39 product monographs for venetoclax, acalabrutinib, zanubrutinib, obinutuzumab for injection, ibrutinib, and fludarabine phosphate;37,40-44 and Sponsor Summary of Clinical Evidence.2
Submission History
Initial Submission
In 2020, venetoclax in combination with obinutuzumab was first reviewed by pERC for the treatment of adult patients with previously untreated CLL who were fludarabine-ineligible. pERC issued a recommendation that venetoclax in combination with obinutuzumab be listed for the indication under review in the reimbursement request, if the specified clinical criteria and conditions were met. Patients were to have previously untreated CLL, be fludarabine-ineligible as indicated by either a CIRS score of greater than 6 or CrCl of less than 70 mL per minute, require treatment according to the iwCLL criteria, and have good performance status.8
The final recommendation issued by pERC and the Clinical Review Report for the previous review of venetoclax in combination with obinutuzumab, which contains the summary and appraisal of the CLL14 study that was used to inform the recommendation, are available on the publicly accessible project website.
Basis of Present Reassessment
Since the previous recommendation for venetoclax in combination with obinutuzumab, new clinical evidence has become available for the first-line treatment of patients with CLL considered fit and potentially fludarabine-eligible via the CLL13 trial.
Perspectives of Patients, Clinicians, and Drug Programs
The full patient and clinician group submissions received are available in the consolidated patient and clinician group input document for this review on the publicly accessible project website: Venetoclax.
Patient Group Input
This section was prepared by the review team based on the input provided by patient groups.
Two patient groups, Lymphoma Canada and CLL Canada, submitted a joint input for the current review. The input includes results from 2 surveys conducted for past drug reimbursement reviews in CLL — 1 survey was for the original submission for venetoclax in combination with obinutuzumab, reviewed in 2020, and 1 was a recent CLL survey conducted in 2023. For the 2023 survey, Lymphoma Canada collected information through an online survey that was distributed throughout Canada and to international locations from March 22 to May 2, 2023. A total of 87 people (49 from Canada, 12 from the US, 1 from Australia, and 25 from unknown locations) responded to the survey. Among the 87 respondents, 32 were female, 30 were male, and 25 skipped the question. Of the 87 respondents, most (36 respondents) were diagnosed with CLL 9 years to 10 years ago, while other respondents were diagnosed with CLL 3 years to 5 years ago (15), 1 year to 2 years ago (10), 5 years to 8 years ago (8), and less than a year ago (4); 14 respondents skipped the question. The respondents reported various subtypes of CLL, including del(17p), deletion 13q, or deletion 11q; TP53 mutation; trisomy 12; and unmutated IGHV. The 2020 survey provided information on patients with CLL and SLL who had experience with frontline venetoclax plus obinutuzumab. Of the 33 survey respondents, 10 respondents were aged between 40 years and 59 years, 22 respondents were aged between 60 years and 79 years, 18 respondents were male, and 14 respondents were female; 1 respondent did not answer either question on age or sex. Survey respondents were from Canada (2 patients), the US (29 patients), and the UK (1 patient) (1 respondent did not answer the question).
Based on the 2023 survey, most patients with CLL are diagnosed through routine blood work and experience minor to no symptoms at the time of diagnosis. According to the 64 respondents who reported high negative impact at the time of diagnosis, fatigue (47%), high white blood cell counts (leukocytosis) (26%), body aches and pains (25%), enlarged lymph nodes (23%), and night sweats (20%) were the most frequent symptoms. Of the 71 respondents who reported on the psychosocial impact of CLL at the time of diagnosis, anxiety and worry (61%), the stress of diagnosis (59%), and difficulty sleeping (28%) were the most common concerns. According to the 70 respondents who reported a high negative impact on their current HRQoL, fatigue (44%), body aches and pains (27%), and indigestion, abdominal pain, or bloating (17%) were the most frequently reported symptoms. Of the 87 respondents who reported on the psychosocial impact of CLL on their current HRQoL, anxiety and worry (42%), difficulty sleeping (31%), and the stress of diagnosis (28%) were the most common concerns. Of 87 respondents who indicated that CLL has a negative impact on their daily activities, fulfilling family obligations (51%) and spending time with family and friends (45%) were the most frequently affected activities.
Of the 68 respondents to the 2023 survey who provided information on their experience with CLL treatments, 21 respondents stated that they have not received therapy, 26 respondents had received 1 line of treatment, and 19 respondents had completed 2 or more lines of treatments. According to the respondents, the most difficult to tolerate side effects include nausea, fatigue, joint pain, skin issues and bleeding, atrial fibrillation, diarrhea, inflammation, bodily aches and pain, headache, muscle weakness, heartburn, indigestion, night sweats, neuropathy, and frequent infections. Additionally, 26% of patient respondents stated that their CLL treatment had a negative impact on their HRQoL (due to side effects) (76%), their ability to travel (26%), and their ability to go to work or school, or to volunteer (19%). Based on patient respondent input, the most important considerations for a novel CLL treatment are a longer period of survival (81%), control of disease symptoms (75%), longer remission (71%), better HRQoL (66%), and fewer side effects (35%). Approximately half of all survey respondents emphasized the importance of having a choice in their treatment plan and having increased treatment options available to choose from. While some respondents to the 2023 survey indicated preference for a fixed-duration therapy (24%), others indicated preference for a continuous therapy (10%); 66% of respondents indicated they were uncertain.
A total of 33 patient respondents from the 2020 survey reported experience with the current drug under review (i.e., they were either currently receiving venetoclax or had completed the treatment regimen). Among these patients, 2 reported not being able to complete the full course of obinutuzumab infusions due to side effects. While most respondents in the 2020 survey noted that side effects from this treatment had “no” or “some” impact on their HRQoL, 15% to 18% of respondents reported a “significant” or “very significant” impact on their HRQoL due to side effects. Most patient respondents (20 of 33 [61%] patients) reported that treatment managed all their symptoms. Symptoms that were not managed by treatment in more than 10% of respondents included fatigue or lack of energy (10 of 33 [30%] patients) and shortness of breath (4 of 33 [12%] patients). Overall, most respondents (31 of 33 [90%] patients) reported a positive experience with the drug under review, and 85% of respondents described their experience with treatment as “very good” or “excellent.”
Clinician Input
Input From Clinical Experts Consulted for the Present Review
All review teams include at least 1 clinical specialist with expertise regarding the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, providing guidance on the potential place in therapy). The following input was provided by 2 clinical specialists with expertise in the diagnosis and management of CLL.
Unmet Needs
The clinical experts indicated that alternative treatment options that are targeted, chemoimmunotherapy-free and/or BTK inhibitor-free, and time-limited are needed for fit patients with previously untreated CLL. Time-limited options include the drug under review and ibrutinib with venetoclax, which is currently under consideration for negotiation with the pan-Canadian Pharmaceutical Alliance.35
Additionally, the clinical experts consulted for the present review highlighted the importance of having alternative treatment regimens for patients to choose from (i.e., improving access and equity to care) to align with their values, needs, and lifestyle.
Place in Therapy
The clinical experts indicated that venetoclax plus obinutuzumab would be considered as an option for frontline therapy in patients regardless of fitness, age, and high-risk cytogenetic markers.
Patient Population
According to the clinical experts, the molecular profile (IGHV and TP53 mutation status) is the main criterion that informs discussions on selecting a treatment regimen. Other factors to consider when selecting a treatment regimen include accessibility to a local treatment centre and the availability of resources to implement the therapy.
The clinical experts identified the following group of patients who would be least suitable for treatment with venetoclax plus obinutuzumab: patients who are unable to access the treatment due to various reasons, including but not limited to scarce resources (i.e., cost of parking, being driven, and loss of independence), that lead to patients being unable to comply with monitoring for tumour lysis syndrome.
Assessing the Response Treatment
The clinical experts identified the following outcomes that are used to determine treatment response in practice: time to next treatment, clinical improvement in nodal burden or splenomegaly, and improvement in symptoms, HRQoL, and blood work as per iwCLL response criteria. The clinical experts noted that imaging is not typically part of routine practice in response assessment; instead, clinical or hematologic response is typically evaluated in practice.
The clinical experts advised on reassessing for treatment response every 6 months in the first year after completing therapy and annually thereafter.
Discontinuing Treatment
The clinical experts identified the following factors that would be considered for the discontinuation of venetoclax plus obinutuzumab: patients continue to present with AEs despite dose reductions and disease progression while on therapy.
The clinical experts also presented a scenario where treatment response was demonstrated but treatment was discontinued due to AEs — the clinical experts advised switching to an alternative treatment when there is disease progression.
Prescribing Considerations
The clinical experts advised that hematologists and hematologist oncologists should diagnose, treat, and monitor patients who might receive venetoclax plus obinutuzumab. Additionally, the clinical experts advised that having a multidisciplinary team with a nurse, nurse practitioner, physician assistants, and pharmacists would enhance monitoring.
In consideration of infusion-related reactions and tumour lysis syndrome, the clinical experts advised that a clinic with the resources to enable appropriate monitoring for laboratory abnormalities and access to advanced, complex care if needed are the most appropriate settings for treatment with venetoclax plus obinutuzumab.
Clinician Group Input
This section was prepared by the review team based on the input provided by clinician groups.
Two clinician groups provided input on the current review of venetoclax (in combination with obinutuzumab): Lymphoma Canada (represented by 6 clinicians) and the OH-CCO Hematology Cancer Drug Advisory Committee (represented by 1 clinician). Note that Lymphoma Canada is a patient advocacy group that helped to facilitate their clinician group input submission by hematologists. The OH-CCO Hematology Cancer Drug Advisory Committee provides evidence-based clinical and health system guidance on drug-related issues in support of OH-CCO’s mandate, including the Provincial Drug Reimbursement Programs and the Systemic Treatment Program.
In consideration of the unmet needs, Lymphoma Canada highlighted that younger patients with high-risk genomic features (e.g., unmutated IGHV) are only able to access the treatment under review by justifying that the poor-risk genomic features meet the definition for fludarabine ineligibility. The group felt that the current requested change in funding may reduce confusion and ensure fairness and equitable access across Canada for this subset of patients with CLL. Lymphoma Canada further suggested that expanded funding may allow the youngest and/or fittest patients with lower-risk disease and the longest life expectancy to benefit from targeted therapy and avoid the use of FLU + CYC + RIT and its associated risk of short-term and long-term bone marrow toxicities. The OH-CCO’s Hematology Cancer Drug Advisory Committee noted that the treatment under review provides an immunotherapy option that is not combined with chemotherapy.
Both clinician groups indicated that venetoclax plus obinutuzumab would be considered for first-line therapy in all patients with previously untreated CLL. Lymphoma Canada highlighted that the option of venetoclax plus obinutuzumab may encourage deferring BTK inhibitor-based therapy to the relapsed or refractory setting for most patients. Lymphoma Canada anticipates that this may reduce the budget impact of CLL therapy and would be in keeping with patient preference for frontline, fixed-duration, targeted therapy. Both clinician groups stated that all patients with CLL who require a first-line therapy would benefit from treatment with venetoclax plus obinutuzumab. Lymphoma Canada suggested that the least suitable patients for the treatment under review are patients with del(17p) or TP53 mutation (these patients will typically receive BTK inhibitor monotherapy). Regardless, the group suggested that fixed-duration therapies should still be made available to this subset of patients on the rare occasion that a fixed-duration therapy is desired.
As per the OH-CCO’s Hematology Cancer Drug Advisory Committee, standard CLL response outcomes, improvement in PFS, a reduction in symptoms, and improvement in HRQoL outcomes are used to determine whether a patient is responding to the treatment under review in clinical practice.
The OH-CCO Hematology Cancer Drug Advisory Committee advised considering treatment discontinuation in the setting of significant intolerance or disease progression, while Lymphoma Canada suggested considering treatment discontinuation if there is a lack of response or considering an abbreviated therapy in the setting of significant toxicity.
The clinician groups advised that any specialist physician who treats CLL or any prescribers familiar with CLL treatment should be able to provide and supervise therapy with the treatment under review. The OH-CCO Hematology Cancer Drug Advisory Committee also stated that additional lab monitoring may be required during venetoclax ramp-up. Lymphoma Canada added that a physical exam and a review of blood work are part of routine practice in response assessment.
Drug Program Input
The drug programs provide input on each drug being reviewed through the reimbursement review processes by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted for the present review are summarized in Table 5.
Table 5: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Relevant comparators | |
Relevant funded comparators include acalabrutinib, ibrutinib, zanubrutinib, FLU-based therapy, obinutuzumab plus chlorambucil, and other RIT-based chemotherapy combinations (e.g., BEN + RIT, chlorambucil + RIT). The comparators in the CLL13 trial were FLU + CYC + RIT or BEN + RIT. Ibrutinib plus venetoclax has received a positive recommendation for the treatment of adult patients with previously untreated CLL, including those with del(17p). This is currently being negotiated through pCPA. | This is a comment from the drug plans to inform pERC deliberations. |
Considerations for initiation of therapy | |
Venetoclax should be given for a total of 48 weeks as finite treatment for six 28-day cycles in combination with obinutuzumab, followed by 6 months of venetoclax as a single drug. For patients who do not experience progression, are there instances where these patients should be treated beyond the 48 weeks of treatment? | The clinical experts indicated that treatment with venetoclax plus obinutuzumab should be finite and advised that treatment beyond 48 weeks in patients who do not experience progression should be based on clinical judgment. For example, patients may be considered for treatment beyond 48 weeks if there was a delay in their therapy due to tumour lysis syndrome, difficulty in ramping up the dose, or potential cytopenia. |
For patients who have completed the 48 weeks of treatment, should these patients be re-treated with venetoclax plus obinutuzumab upon progression? | The clinical experts acknowledged that clinical trials on re-treatment upon progression that are anticipated to provide guidance on this situation were ongoing at the time of this review; however, the clinical experts do not foresee any concerns with re-treatment upon progression (i.e., the clinical experts suggested re-treatment is likely beneficial and safe, based on literature). |
Considerations for prescribing of therapy | |
If a patient experiences intolerance to venetoclax or obinutuzumab, can treatment with the other drug be continued as monotherapy? | The clinical experts advised that this scenario is reasonable and suggested dose adjustment is also possible and reasonable in this setting. The clinical experts advised that it is important to recognize that this may result in shorter remission periods. |
Venetoclax (oral) and obinutuzumab (IV) will be reimbursed through different programs. | This is a comment from the drug plans to inform pERC deliberations. |
Generalizability | |
Should patients currently on existing treatments (e.g., chemoimmunotherapy) be offered a time-limited switch to venetoclax plus obinutuzumab? | The clinical experts acknowledged that there is a lack of evidence for this scenario; however, in the setting of toxicity or progression with the patients’ current treatment, or if treatment decisions were previously based on access to existing treatments (in particular, to FLU + CYC + RIT), the clinical experts suggested it is reasonable to offer these patients a time-limited switch to venetoclax plus obinutuzumab. |
Should eligibility for venetoclax plus obinutuzumab be extended to fit patients with previously untreated SLL? | The clinical experts advised that eligibility for venetoclax plus obinutuzumab should be extended to fit patients with previously untreated SLL as SLL and CLL are different manifestations of the same disease. |
Funding algorithm | |
The drug under review may change place in therapy of relevant comparator drugs. | This is a comment from the drug plans to inform pERC deliberations. |
Please clarify on the eligible patient population for the drug under review (i.e., in reference to the fitness criteria used in the CLL13 study). | The clinical experts advised that all patients should be eligible for venetoclax plus obinutuzumab, regardless of fitness, age, and high-risk cytogenetic markers. The clinical experts noted that fitness and age criteria and the exclusion of del(17p) were designed for chemoimmunotherapy (the comparator in the CLL13 trial) and are not used with novel drugs. |
Under what clinical circumstances would venetoclax plus obinutuzumab be used over existing first-line options? | The clinical experts advised that the molecular profile, access to certain treatments, and patient values are considerations when selecting first-line treatment with venetoclax plus obinutuzumab. |
What will be the impact of the drug under review on the downstream sequencing from newly diagnosed CLL to relapsed and/or refractory CLL? | The clinical experts advised referring to the sequencing of treatment in the older adult population for which venetoclax plus obinutuzumab is already approved and funded. |
Care provision issues | |
Venetoclax has the potential for drug-drug, drug-food, and drug-herb interactions. | This is a comment from the drug plans to inform pERC deliberations. |
System and economic issues | |
There would be a budget impact for obinutuzumab given the increase in the venetoclax population. | This is a comment from the drug plans to inform pERC deliberations. |
BEN = bendamustine; CLL = chronic lymphocytic leukemia; CYC = cyclophosphamide; del(17p) = 17p deletion; FLU = fludarabine; pCPA = pan-Canadian Pharmaceutical Alliance; pERC = pan-Canadian Oncology Drug Review Expert Review Committee; RIT = rituximab; SLL = small lymphocytic lymphoma.
Clinical Evidence
The objective of the present Clinical Review Report is to review and critically appraise the clinical evidence submitted by the sponsor on the beneficial and harmful effects of venetoclax 10 mg, 50 mg, and 100 mg oral tablets, in combination with obinutuzumab, in the treatment of patients with previously untreated CLL. The focus will be placed on comparing venetoclax in combination with obinutuzumab to relevant comparators in the fit population (defined in the CLL13 trial by a CIRS score of ≤ 6 and CrCl of ≥ 70 mL per minute) and identifying gaps in the current evidence.
A summary of the clinical evidence included by the sponsor in the review of venetoclax in combination with obinutuzumab is presented in 2 sections, with the review team’s critical appraisal of the evidence included at the end of each section. The first section, the systematic review, includes the RCT that was selected according to the sponsor’s systematic review protocol. The second section includes indirect evidence from the sponsor.
Included Studies
Clinical evidence from the following is included in the present review and appraised in this document:
1 pivotal study identified in the systematic review
1 indirect treatment comparison.
Systematic Review
Content in this section has been informed by materials submitted by the sponsor. The following has been summarized and validated by the review team.
Description of CLL13 Study
Characteristics of the included study, the CLL13 trial, are summarized in Table 6.
Table 6: Details of CLL13 Study Included in the Systematic Review
Detail | CLL13 study |
|---|---|
Design and population | |
Study design | Phase III, multicentre, randomized, prospective, open-label clinical trial |
Locations | 159 sites across Germany, Austria, Switzerland, the Netherlands, Belgium, Denmark, Sweden, Finland, Israel, and Ireland11 |
Patient enrolment dates | Start date: December 13, 2016 End date: October 13, 2019 |
Randomized | A total of 926 patients were randomized 1:1:1:1 to the following treatment groups:
|
Key inclusion criteria |
|
Key exclusion criteria |
|
Drugs | |
Intervention | VEN + OBI: Treatment with VEN + OBI consisted of 6 cycles, followed by 6 additional cycles of venetoclax alone, each cycle with a duration of 28 days. |
Comparators |
|
Study duration | |
Screening phase | Screening assessments were performed within 42 days before randomization; the exception was CT and MRI scan results that were acceptable within 56 days before randomization. |
Treatment phase | Treatment started within 14 days after randomization. |
Follow-up phase | All patients had regular follow-ups until the end of the clinical trial, defined as the time point when 213 PFS events had been reached, which may take place 73 months after the first patient was randomized. Patients were informed about long-term follow-up within an appropriate national and/or international registry. |
Outcomes | |
Coprimary end points | The trial had 2 primary end points that were analyzed and interpreted independently:
|
Secondary and exploratory end points | Secondary end points:
Exploratory end points:
|
Publication status | |
ClinicalTrials.gov identifier | NCT02950051 |
Publications | Eichhorst et al.11 (primary undetectable MRD in peripheral blood analysis, as of data cut-off date of February 28, 2021; interim PFS analysis, as of data cut-off date of January 20, 2022) Fürstenau et al.9 (4-year PFS follow-up, as of data cut-off date of January 31, 2023) |
ALT = alanine aminotransferase; AST = aspartate aminotransferase; BEN = bendamustine; CIRS = Cumulative Illness Rating Scale; CLL = chronic lymphocytic leukemia; CR = complete response; CRir = complete response with incomplete recovery of the bone marrow; CYC = cyclophosphamide; del(17p) = 17p deletion; ECOG PS = Eastern Cooperative Oncology Group Performance Status; EFS = event-free survival; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; EORTC QLQ-CLL16 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Chronic Lymphocytic Leukaemia 16; FLU = fludarabine; GFR = glomerular filtration rate; HRQoL = health-related quality of life; IBRU = ibrutinib; IVIg = IV immunoglobulin; iwCLL = International Workshop on Chronic Lymphocytic Leukemia; MARS = Medication Adherence Report Scale; MRD = minimal residual disease; OBI = obinutuzumab; OS = overall survival; PFS = progression-free survival; PR = partial response; RIT = rituximab; RNA = ribonucleic acid; VEN = venetoclax; ULN = upper limit of normal; vs. = versus.
Sources: Trial protocol of CLL13 study,10 Statistical Analysis Plan - Primary Endpoints Analysis: CLL13,45 Statistical Analysis Plan - PFS Interim Analysis 2022: CLL13,46 and Sponsor Summary of Clinical Evidence.2
The CLL13 study is an ongoing, phase III, multicentre, randomized, prospective, open-label clinical trial conducted by the German CLL Study Group, the CLL Study Group of the Hemato-Oncology Foundation for Adults in the Netherlands, and the Nordic CLL Study Group (N = 926).9 The primary objective of the study is to assess the efficacy of venetoclax plus obinutuzumab versus standard chemoimmunotherapy (BEN + RIT or FLU + CYC + RIT) on the negativity rate of MRD in peripheral blood at month 15, and venetoclax plus obinutuzumab plus ibrutinib versus standard chemoimmunotherapy on PFS at predefined analysis time points in fit patients (defined in the CLL13 trial by a CIRS score of ≤ 6 and CrCl of ≥ 70 mL per minute) with previously untreated CLL and without del(17p) or TP53 mutation.10 A total of 159 sites across Germany, Austria, Switzerland, the Netherlands, Belgium, Denmark, Sweden, Finland, Israel, and Ireland were included in the trial.11
Screening assessments were performed within 42 days before randomization; the exceptions were CT and MRI scan results that were acceptable within 56 days before randomization. Patients underwent a central medical review for verification of trial eligibility, including confirmation of CLL diagnosis and exclusion of del(17p) or TP53 mutation. Patients who met all the inclusion criteria and none of the exclusion criteria were randomized in a 1:1:1:1 ratio to receive chemoimmunotherapy, venetoclax plus obinutuzumab, venetoclax plus obinutuzumab plus ibrutinib, or venetoclax plus rituximab. Randomization, using an interactive voice and web response system, was stratified by Binet stage, age (with a cut-off of 65 years), and region study group. In the chemoimmunotherapy group, patients aged 65 years and younger received FLU + CYC + RIT, while patients aged older than 65 years received BEN + RIT. Treatment was started within 14 days after randomization.10
After the end of treatment and initial response assessment and final restaging, patients are scheduled for regular follow-ups until the end of the trial. These consist of visits every 3 months until disease progression or month 15, whichever occurs later, and annual visits thereafter for the documentation of survival and the start of new CLL treatment. The end of the trial was defined as the time point when 213 PFS events have been reached, which may take place approximately 73 months after the first patient was randomized. Note that patients who discontinued all components of the study treatment before disease progression (e.g., for toxicity) continued the study and were followed for progressive disease and survival, regardless of receiving subsequent antileukemic therapy.10
An independent Data and Safety Monitoring Board (DSMB), consisting of 1 biometrician familiar with hematological trials and 3 experts in CLL from countries not participating in the conduct of the trial, was primarily responsible for the continual review of the study, including monitoring the safety data and advising the sponsor, and reviewing the interim PFS analysis.10
Venetoclax plus rituximab is not approved by Health Canada for the population under review and venetoclax plus obinutuzumab plus ibrutinib is also not approved by Health Canada. Therefore, data for these treatment groups from the CLL13 study are not presented in this Clinical Review Report for the purposes of this review.
The coprimary end point of undetectable MRD was analyzed using a data cut-off date of February 28, 2021, while the primary analysis of the coprimary end point PFS was analyzed using a data cut-off date of January 20, 2022, following the recommendation of the DSMB and the statistically significant results of the planned interim analysis.11 Additionally, a post hoc, exploratory, 4-year follow-up analysis of prespecified end points in the CLL13 study was conducted with all patients off treatment based on a data cut-off date of January 31, 2023.9
Populations
Inclusion and Exclusion Criteria
A summary of key inclusion and exclusion criteria for the CLL13 trial is presented in Table 6. The CLL13 study included patients aged 18 years and older with CLL who warranted treatment according to the 2008 iwCLL criteria. The trial included patients with a life expectancy of 6 months and greater, a glomerular filtration rate of 70 mL per minute and greater, and an ECOG PS score of 0 to 2.10
The CLL13 study excluded patients with experience with any prior CLL-specific therapies; the exception was corticosteroid treatment indicated for immediate intervention within the last 10 days before the start of study treatment and only at dose equivalents up to 20 mg of prednisolone. The trial excluded patients with any comorbidity or organ system impairment rated with a single CIRS score of 4 (excluding the eyes, ears, nose, throat, and larynx organ system) or a total CIRS score greater than 6. The CIRS ranges from 0 to 56, with higher scores indicating greater impaired function of organ systems. Notably, the trial excluded patients with del(17p) or TP53 mutation.10
Interventions
Venetoclax Plus Obinutuzumab
Treatment with venetoclax plus obinutuzumab consisted of 6 cycles, followed by 6 additional cycles of venetoclax alone, with each cycle having a duration of 28 days.10
The dosing schedule for obinutuzumab IV infusion in the trial is presented in Table 7. Obinutuzumab was intravenously administered on day 1 (and possibly day 2), day 8, and day 15 of the first cycle as well as on day 1 of cycle 2 to cycle 6. If the infusion of the test dose of 100 mg was well tolerated by the patient, then the first infusion of obinutuzumab could be administered at the full dose of 1,000 mg on day 1 of the first cycle. Alternatively, if the infusion of the test dose was not well tolerated, then the remaining 900 mg of the first dose was to be administered on day 2. Obinutuzumab was administered at an inpatient or outpatient clinical setting and only after the intake of the oral study drug, when applicable.10
The dosing schedule for venetoclax oral administration in the CLL13 trial is presented in Table 8. The continuous daily administration with a slow dose escalation of venetoclax started on day 22 of the first cycle. After completing the ramp-up schedule in a clinic, patients continued venetoclax 400 mg once daily from cycle 3, day 1, of obinutuzumab to the end of cycle 12 at home.10
The first 50 patients enrolled and not at an increased risk of developing tumour lysis syndrome were included in an assessment of compliance to dosing at home. This subset of patients received their dose escalation to venetoclax 50 mg in a clinic or outpatient department. Subsequent dose escalations to venetoclax 400 mg were dispensed to the patients to take at home. If compliance was deemed adequate, dosing at home was extended to the first 2 weeks of venetoclax dose escalation to 20 mg and 50 mg for all patients who were not at an increased risk of tumour lysis syndrome.10
Table 7: Dosing Schedule for Obinutuzumab IV Infusion in the CLL13 Study
Cycle | Day | Obinutuzumab dose |
|---|---|---|
1 | 1 | 100 mg |
1 (or 2)a | 900 mg | |
8 | 1,000 mg | |
15 | 1,000 mg | |
2 to 6 | 1 | 1,000 mg |
aIf the infusion of the test dose of 100 mg was well tolerated by the patient, then the first infusion of obinutuzumab could be administered at the full dose of 1,000 mg on day 1 of the first cycle. Alternatively, if the infusion of the test dose was not well tolerated, then the remaining 900 mg of the first dose was to be administered on day 2.
Sources: Trial protocol of CLL13 study10 and Sponsor Summary of Clinical Evidence.2
Table 8: Dosing Schedule for Venetoclax Oral Administration in the CLL13 Study
Cycle | Day | Venetoclax dose |
|---|---|---|
1 | 22 to 28 | 20 mg |
2 | 1 to 7 | 50 mg |
8 to 14 | 100 mg | |
15 to 21 | 200 mg | |
22 to 28 | 400 mg | |
3 to 12 | 1 to 28 | 400 mg |
Sources: Trial protocol of CLL13 study10 and Sponsor Summary of Clinical Evidence.2
Standard Chemoimmunotherapy
Before the application of chemotherapy, rituximab was intravenously administered at a dose of 375 mg/m2 in the first cycle and at a dose of 500 mg/m2 in cycle 2 to cycle 6, with premedication according to the clinical practice of the participating sites.10
Fludarabine Plus Cyclophosphamide Plus Rituximab
Patients aged 65 years and younger received 6 cycles of FLU + CYC + RIT, each cycle with a duration of 28 days. Fludarabine 25 mg/m2 and cyclophosphamide 250 mg/m2 were intravenously administered over 15 minutes to 30 minutes (they can be administered immediately 1 after the other) on day 1 to day 3 of cycle 1 to cycle 6.10
After cycle 3, patients were assessed for response before proceeding to cycle 4. If a patient had stable disease or appeared to be responding to therapy and toxicity was acceptable, then the patient continued therapy.10
Bendamustine Plus Rituximab
Patients aged older than 65 years received 6 cycles of BEN + RIT, each cycle with a duration of 28 days. Bendamustine 90 mg/m2 was intravenously administered over 30 minutes on day 1 and day 2 of cycle 1 to cycle 6.10
Dose and Schedule Modifications
Treatment may be held, postponed, reduced, or permanently discontinued depending on the results of complete blood counts and analyses of serum chemistry as well as reports of serious AEs and active infections. Detailed guidance on dose and schedule modifications as well as the possible resumption in various possible scenarios are provided in the protocol.10
Permitted Comedications
The following standard supportive care therapies were permitted during the CLL13 trial:10
hydration and antiemetics
prophylaxis of tumour lysis syndrome (e.g., uric acid–reducing drugs)
prophylaxis of infusion-related reactions (e.g., corticosteroids, acetaminophen, antihistamines)
prophylaxis of infections (e.g., antibiotic, antiviral, antifungal) — guidance on possible venetoclax dose reduction and subsequent resumption was provided in the protocol if a concomitant strong or moderate CYP3A inhibitor was required
any other standard supportive care therapies required as prophylaxis or for the management of symptoms, as clinically indicated.
Dose equivalents of 20 mg and lower of prednisolone (except for premedication before antibody application) may be administered during study treatment.10
Hematopoietic growth factors (granulocyte colony-stimulating factor) may be administered during the study according to the American Society of Clinical Oncology, the European Organisation for Research and Treatment of Cancer, and the European Society for Medical Oncology guidelines, but are advised for neutropenia CTC grade 4, even as prophylaxis for the following cycles.10
Continuous anticoagulant therapy with phenoprocoumon, warfarin, or any other vitamin K antagonist may be administered with venetoclax, under close monitoring. Switching to an alternative anticoagulant, such as heparin or factor Xa inhibitors, was suggested in the protocol.10
Prohibited Medications
The following mediations were prohibited during study treatment:10
any other chemotherapy, anticancer immunotherapy, or radiotherapy
any other investigational drugs
continuous use of corticosteroids at dosages of 20 mg or greater per day of prednisone or equivalent
immunization with a live vaccine.
Outcomes
A list of efficacy and safety end points assessed in this Clinical Review Report is provided in Table 9, followed by descriptions of the outcome measures. Summarized end points are based on outcomes included in the Sponsor Summary of Clinical Evidence2 as well as any outcomes identified as important to this review according to the clinical experts consulted and input from patient and clinician groups and public drug plans. Using the same considerations, the review team selected end points and notable harms outcomes that were considered to be most relevant to inform the expert committee deliberations and finalized this list of end points in consultation with members of the expert committee.
Table 9: Outcomes Summarized for the Comparison of VEN + OBI and Chemoimmunotherapy From the CLL13 Study
Outcome measure | Time point | CLL13 study |
|---|---|---|
Time-to-event end points | ||
Progression-free survival | Data cut-off date of January 20, 2022 | Secondary end pointa,b |
Overall survival | Secondary end point | |
Duration of response | Secondary end point | |
Time to next treatment for CLL | Secondary end point | |
Undetectable minimal residual disease | ||
Undetectable minimal residual disease in peripheral blood | At month 15 | Coprimary end pointa,c |
Response to treatment | ||
Complete response rate | At month 15 | Secondary end point |
Notable harms | ||
Serious infections (may lead to hospitalization or death) | At month 61 | Secondary end points (safety parameters) |
Second primary malignancies | At month 61 and 4-year follow-up | |
Sudden cardiac deaths | At month 61 | |
Ventricular arrhythmias | At month 61 | |
CDA-AMC = Canada’s Drug Agency; CLL = chronic lymphocytic leukemia; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; EORTC QLQ-CLL16 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Chronic Lymphocytic Leukaemia 16; HRQoL = health-related quality of life; IBRU = ibrutinib; OBI = obinutuzumab; PFS = progression-free survival; VEN = venetoclax.
Notes: Response was assessed based on the 2008 International Workshop on Chronic Lymphocytic Leukemia criteria.
HRQoL was identified as an outcome of importance in the patient and clinician group input as well as in input from the clinical experts consulted by CDA-AMC. Although HRQoL was measured by EORTC QLQ-C30 and EORTC QLQ-CLL16 in the CLL13 study, results were unavailable at the time of sponsor submission.
aStatistical testing for these end points was adjusted for multiple comparisons (e.g., hierarchical testing).
bThe comparison of VEN + OBI vs. chemoimmunotherapy for PFS was tested after the comparison of VEN + OBI + IBRU vs. chemoimmunotherapy.
cThe coprimary end point is the comparison of VEN + OBI + IBRU vs. chemoimmunotherapy for PFS, which is not included in this review.
Sources: Trial protocol of CLL13 study,10 Statistical Analysis Plan – Primary Endpoints Analysis: CLL13,45 Statistical Analysis Plan – PFS Interim Analysis 2022: CLL13,46 and Sponsor Summary of Clinical Evidence.2
Time-to-Event End Points
Progression-Free Survival
PFS (investigator-assessed) was measured from the date of randomization until the first occurrence of progression or relapse, according to the 2008 iwCLL guidelines, or death from any cause, whichever occurs first.10
Overall Survival
OS was measured from the date of randomization to the date of death due to any cause.46
Duration of Response
The duration of response was measured from the date of the first documented, investigator-assessed response to the first occurrence of progression or relapse according to the criteria in the 2008 iwCLL guidelines, or death by any cause, whichever occurred first. Duration of response was calculated for patients with CR or complete response with incomplete recovery of the bone marrow (CRir), clinical CR or clinical CRir, or PR (with or without lymphocytosis) as their best response until month 15, inclusive. A clinical CR and CRir fulfills the same criteria as a CR and CRir, respectively, but are yet to be confirmed by a bone marrow examination.10 Best response was determined by the global principal investigator and coordinating physician.46
Time to Next Treatment
Time to next treatment was measured from the date of randomization to the date of initiation of the first subsequent treatment for CLL. Additionally, time to next treatment in the safety population was measured from the date of the last treatment exposure to the date of initiation of the first subsequent treatment for CLL.46
Undetectable MRD
MRD Measured in Peripheral Blood
MRD status was centrally analyzed using 4-colour flow cytometry. Undetectable (negative) MRD was defined as at least less than 1 CLL cell in 10,000 leukocytes analyzed (i.e., < 10–4).10 Values above this threshold (i.e., ≥ 10–4 and < 10–2; ≥ 10–2) were considered MRD-intermediate and MRD-positive, respectively. The negativity rate of MRD measured in peripheral blood at a specific time point was defined as the proportion of patients with MRD-negative status at the specific time point.45
Response to Treatment
CR Rate
CR rate was defined as the proportion of patients with (investigator-assessed) CR or CRir, according to 2008 iwCLL guidelines, at month 15. Responses after final restaging are based on the assessment by the German CLL Study Group.45
Safety
TEAEs are defined as AEs that develop after or at the initiation of study treatment and before the end of study therapy, plus 84 days or the start of the first subsequent therapy, whichever occurs first. The exceptions are benign, malignant, and unspecified neoplasms (including cysts and polyps) and AEs with CTC grade 5, which are indicated as TEAEs without time limits after the initiation of study treatment. TEAEs are classified according to the Medical Dictionary for Regulatory Activities classification system, reported by the Medical Dictionary for Regulatory Activities system organ class and preferred terms. The severity of AEs is graded according to the National Cancer Institute’s Common Terminology Criteria for Adverse Events version 4.45
Statistical Analysis
Sample Size and Power Calculation
The sample size was determined to enable a hypothesis testing for superiority of venetoclax plus obinutuzumab over chemoimmunotherapy with regard to the coprimary end point analyzed first — the negativity rate of MRD measured in peripheral blood at month 15 — and the superiority of venetoclax plus obinutuzumab plus ibrutinib over chemoimmunotherapy with regard to the coprimary end point analyzed second — PFS — in the target population. A 2-sided significance level of 5.0% was allocated equally to these 2 hypotheses (i.e., alpha split into 0.025 for each testing); thus, the interpretation of the coprimary end point analyses can be made independent of each other. Accordingly, the inferiority of chemoimmunotherapy compared to a chemo-free regimen can be concluded if at least 1 null hypothesis was rejected.10
For testing the second coprimary end point, PFS, the following assumptions were made:10
the log-rank test was at the 2-sided 0.025 significance level
the median PFS was assumed to be 48 months with standard chemoimmunotherapy, based on the CLL10 trial
there was 80% power to detect an HR of 0.649, with median PFS for venetoclax plus obinutuzumab plus ibrutinib increased to 74 months
there was exponential distribution of PFS
one formal interim analysis of investigator-assessed PFS was planned (details can be found as follows).
Based on the aforementioned assumptions, a total of 213 PFS events are required for the final PFS analysis. Assuming nonlinear accrual of 460 patients over 33 months (230 patients each for standard chemoimmunotherapy and venetoclax plus obinutuzumab plus ibrutinib), the 213 PFS events would be reached 73 months after the first patient was randomized. In terms of timely completion, the final PFS analysis would be conducted when either 213 PFS events had occurred or 73 months had passed since the first patient was randomized.10
In the scenario where the final PFS analysis is conducted at the time point of 73 months after the first patient is randomized with less than 213 PFS events observed, the significance boundaries of the final PFS analysis would be determined using the Lan-DeMets alpha spending function with an O’Brien-Fleming boundary based on the actual total number of PFS events (information fraction) observed at the interim analysis and final analysis to maintain the overall 2-sided type I error at the 0.025 level.10
For testing the first coprimary end point, the MRD negativity rate, the following assumptions were made:10
the MRD negativity rate in peripheral blood at month 15 was assumed to be 30% with standard chemoimmunotherapy, based on the CLL10 trial
venetoclax plus obinutuzumab was assumed to improve this rate to at least 50%, resulting in an increase of the absolute difference to at least 20%.
Given the estimated 33-month recruitment period, the time point of the final MRD analysis was projected at month 49, when the last patient randomized reaches the time point of month 15 and all MRD samples have been analyzed. Based on these assumptions, a 2-sided 2-sample chi-square test of rates with an overall significance level of 2.5% would provide 98.7% power to detect a difference of 20% if the total number of patients was 460 — 230 patients each for standard chemoimmunotherapy and venetoclax plus obinutuzumab.10
Equal recruitment in each group was considered to enable balanced comparisons between all treatments; hence, the total number of patients to be randomized was 920. A failure rate of 20% by screening was assumed; therefore, 1,100 patients were estimated to be screened for the study.10
According to the CLL10 trial, there are 2 subgroups of fit patients with CLL: patients aged 65 years and younger and eligible for FLU + CYC + RIT versus patients aged older than 65 years and not eligible for FLU + CYC + RIT. For the latter subset of patients, BEN + RIT is considered the standard chemoimmunotherapy in the frontline setting. Based on previous study data, a mixed control group for the trial with 50% FLU + CYC + RIT and 50% BEN + RIT was assumed. A lower limit of 35% and an upper limit of 65% were implemented at recruitment to meet the assumptions; accordingly, each subgroup included at least 322 patients. Once the lower limit is reached for both subgroups, the remaining 276 patients can be flexibly recruited. Recruitment for a subgroup closes once 598 patients are randomized, after which patients can only be randomized according to the other age group.10
Statistical Test
The statistical analyses of the efficacy end points in the CLL13 study for the comparison of venetoclax plus obinutuzumab versus chemoimmunotherapy (BEN + RIT or FLU + CYC + RIT) are summarized in Table 10.
Negativity Rate of MRD in Peripheral Blood
The negativity rates of MRD for venetoclax plus obinutuzumab versus chemoimmunotherapy were compared using the Cochran-Mantel-Haenszel test, stratified by age (with a cut-off of 65 years) and Binet stage. Numbers, rates, and associated 97.5% CIs were reported for each treatment group.10
For the primary efficacy analysis, missing data were not replaced or imputed. MRD response assessments after starting the first subsequent CLL therapy were not taken into account. Patients without an MRD sample at month 15 were kept and indicated as MRD non-negative in the analysis.45 More specifically, patients without an MRD sample at month 15 and who had disease progression or died before month 15 were indicated as MRD-positive. All patients without an MRD sample at month 15 and who were free from progression and alive were indicated as not evaluable. In the analysis, these were counted for patients with positive MRD.10
Progression-Free Survival
PFS for venetoclax plus obinutuzumab plus ibrutinib versus chemoimmunotherapy were compared using a 2-sided stratified log-rank test, adjusted for the interim analysis and stratified by age and Binet stage. Median PFS and associated 97.5% CI were estimated using Kaplan-Meier survival methodology, with the Kaplan-Meier survival curve presented to provide a visual description. PFS rates at 1 year, 2 years, 3 years, and so on after randomization, as well as the number of patients at risk, were reported. Estimates of the treatment effect were expressed as HR, including a 97.5% CI estimated through a stratified Cox proportional hazards analysis, stratified by age and Binet stage.10
Interim Analysis
One formal interim analysis of investigator-assessed PFS was planned for the comparison of venetoclax plus obinutuzumab plus ibrutinib versus chemoimmunotherapy. The purpose of this interim analysis was to decide whether the study might be stopped early for either efficacy or futility. The futility boundary was implemented as nonbinding. The interim analysis was performed either after 65% of the total 213 PFS events were observed (i.e., 138 PFS events projected at month 49 after the first patient was randomized) or 61 months after the first patient was randomized, whichever occurred first.10
PFS would be tested at the significance level determined by the Lan-DeMets alpha spending function with an O’Brien-Fleming boundary. The significance level of the final PFS analysis would then be adjusted to incorporate the alpha spent at the interim analysis, so that the overall 2-sided type I error rate would be maintained at the 0.025 level. Detailed, unblinded reports would be forwarded to the independent DSMB for review. The study could be stopped early for efficacy if the DSMB advised that the results of the interim analysis were statistically significant, robust, and reliable, based on the stopping boundaries. If these conditions were met, then the primary analysis of PFS, including PFS comparisons for all treatment groups and secondary time-to-event end point analyses for all treatment groups, could be conducted at the time of the PFS interim analysis.10
Subgroup Analyses
Prespecified exploratory subgroup analyses for the correlations between MRD (and PFS) and the following clinical and genetic parameters were performed for all treatment groups:45,46
age used for stratification with a cut-off of 65 years
Binet stage used for stratification
cytogenetic subgroups by hierarchical order
IGHV mutation status
International Prognostic Index for Chronic Lymphocytic Leukemia risk group
complex karyotype.
In consultation with the clinical experts, it was concluded that the subgroups listed previously are not relevant to the present review of venetoclax plus obinutuzumab. Notably, the clinical experts advised that TP53 aberrations and IGHV mutation status are treatment effect modifiers specific to chemoimmunotherapy, that the International Prognostic Index for Chronic Lymphocytic Leukemia, and Binet staging are not commonly used in Canadian practice, and that testing for complex karyotype is not widely available in Canada.
Secondary Outcomes
Analysis of PFS
PFS treatment comparisons of other treatment groups were performed and presented as specified for the second coprimary end point, PFS, as described earlier. To control for type I error, a hierarchical test sequence, based on Lehmacher et al.,47 was considered. The a priori–ordered sequence of comparisons is as follows:10
venetoclax plus obinutuzumab plus ibrutinib versus chemoimmunotherapy (a coprimary end point)
venetoclax plus obinutuzumab versus chemoimmunotherapy
venetoclax plus rituximab versus chemoimmunotherapy
venetoclax plus obinutuzumab versus venetoclax plus obinutuzumab plus ibrutinib
venetoclax plus rituximab versus venetoclax plus obinutuzumab
venetoclax plus rituximab versus venetoclax plus obinutuzumab plus ibrutinib.
Subsequent to the first PFS comparison, each comparison was performed as confirmatory, considering an alpha of 2.5%, if the P value of the previous comparison was significant; otherwise, it was to be considered exploratory without reporting the corresponding P value.10
If the DSMB advises on conducting the primary analysis of the second coprimary end point, PFS, at the time of the interim analysis, then the secondary PFS end points would be performed at the time of the PFS interim analysis.46
Analysis of CR Rate
Frequencies and corresponding percentages were presented for the assessment of CR rate at month 15. For the primary efficacy analysis, missing data were not replaced or imputed. Patients with missing response assessment were kept and indicated as non-CR or non-CRir in the analysis.45
Analysis of OS, Duration of Response, and Time to Next Treatment
Analyses of OS, duration of response, and time to next treatment were performed using the Kaplan-Meier method. Kaplan-Meier estimates of median times and rates at 12 months, 24 months, 36 months, and so on after randomization (or after the first documented response for duration of response, or after randomization or last treatment exposure for time to next treatment) and the number of patients at risk were reported. Kaplan-Meier survival curves were presented to provide a visual description. Estimates of the treatment effect were expressed as HR and associated 97.5% CI, estimated through a nonstratified Cox proportional hazards analysis. P values of secondary time-to-event end points were not calculated.46
If the DSMB advises on conducting the primary analysis of the second coprimary end point, PFS, at the time of the interim analysis, then the secondary time-to-event end points would be performed at the time of the PFS interim analysis.46
Information on Censoring
For the primary efficacy analysis, missing data were not replaced or imputed, but possibly censored.
If there was no documented event for the time-to-event outcome at the time of analysis, then patients were censored on the date of their last study observation visit (or last tumour assessment) that they were assessed to be event-free. If no visit was documented after randomization (or screening), then patients were censored at the time of randomization plus 1 day (or censored at the time of first documented response plus 1 day for the duration of response outcome). For time to next treatment, deceased patients were censored on the date of death. If an antileukemic treatment was initiated without documentation of disease progression, then patients were censored at their last tumour assessment before the start of the subsequent therapy.46
Post Hoc Exploratory 4-Year Follow-Up Analysis by Fürstenau et al.9
A post hoc exploratory 4-year follow-up analysis of prespecified end points in the CLL13 study was conducted with all patients off treatment. All statistical tests were 2-sided and P values were descriptive without adjustments for multiple testing.9
Table 10: Statistical Analysis of Efficacy End Points for the Comparison of VEN + OBI and Chemoimmunotherapy in the CLL13 Study
End point | Statistical model | Adjustment factors | Handling of missing data |
|---|---|---|---|
Undetectable MRD in peripheral blood at month 15 | Cochran-Mantel-Haenszel test | Stratified by age (with a cut-off of 65 years) and Binet stage | For the primary efficacy analysis, missing data were not replaced or imputed. MRD response assessments after starting the first subsequent CLL therapy were not taken into account. Patients without an MRD sample at month 15 were kept and indicated as non-negative in the analysis. Patients without an MRD sample at month 15 and who had disease progression or died before month 15 were indicated as MRD-positive. All patients without an MRD sample at month 15 and who were free from progression and alive were indicated as not evaluable. In the analysis, these patients were counted for patients with positive MRD. |
CR | Descriptive only Frequencies and corresponding percentages were presented. | Not applicable | For the primary efficacy analysis, missing data were not replaced or imputed. Patients with missing response assessment were kept and indicated as non-CR or non-CRir in the analysis. |
Progression-free survival | 2-sided stratified log-rank test Estimates of the treatment effect were expressed as HR, including 97.5% CI, estimated through a stratified Cox proportional hazards analysis. | Stratified by age (with a cut-off of 65 years) and Binet stage | For the primary efficacy analysis, missing data were not replaced or imputed, but possibly censored. If there was no documented event for the time-to-event outcome at the time of analysis, then patients were censored on the date of their last study observation visit (or last tumour assessment) that they were assessed to be event-free. If no visit was documented after randomization (or screening), then patients were censored at the time of randomization plus 1 day (or censored at the time of the first documented response plus 1 day for the duration of response outcome). For time to next treatment, deceased patients were censored on the date of death. If an antileukemic treatment was initiated without documentation of disease progression, then patients were censored at their last tumour assessment before the start of the subsequent therapy. |
Overall survival Duration of response Time to next treatment | Descriptive only Kaplan-Meier method Estimates of the treatment effect were expressed as HR, including 97.5% CI, estimated through a nonstratified Cox proportional hazards analysis. | Not applicable |
CI = confidence interval; CLL = chronic lymphocytic leukemia; CR = complete response; CRir = complete response with incomplete recovery of the bone marrow; HR = hazard ratio; MRD = undetectable minimal residual disease; vs. = versus.
Note: No sensitivity analysis was conducted for the comparison of venetoclax plus obinutuzumab vs. standard chemoimmunotherapy.
Sources: Trial protocol of CLL13 study,10 Statistical Analysis Plan – Primary Endpoints Analysis: CLL13,45 Statistical Analysis Plan – PFS Interim Analysis 2022: CLL13,46 and Sponsor Summary of Clinical Evidence.2
Kaplan-Meier estimates were presented along with associated 97.5% and 95% CIs, estimated using the Greenwood formula. Estimates of treatment effect were expressed as HR, estimated through log-rank tests and Cox proportional hazards regression modelling (only when the proportional hazards assumption was satisfied based on Schoenfeld residuals). Censoring was assumed to be noninformative based on the censoring criteria. Analysis of PFS considered stratification factors of age (with a cut-off of 65 years) and Binet stage while analyses of OS and time to next treatment did not.9
Analysis Populations
Definitions of the intention-to-treat (ITT) and safety analysis populations of the CLL13 study are presented in Table 11. All efficacy analyses were conducted using the ITT population and all safety end points were evaluated using the safety population.10
Table 11: Analysis Populations of the CLL13 Study
Population | Definition | Application |
|---|---|---|
Intention-to-treat population | All randomized patients, regardless of whether they received any of the study treatment or not. Patients were assigned to treatment groups and analyzed as randomized. | For analysis of all study end points except safety |
Safety population | All patients enrolled in the study, receiving at least 1 dose of any component of the study treatment. Patients were analyzed according to the treatment received. | For evaluating the safety end points |
Sources: Trial protocol of CLL13 study10 and Sponsor Summary of Clinical Evidence.2
Results
Patient Disposition
A summary of patient disposition from the CLL13 study, based on a data cut-off date of January 20, 2022, is presented in Table 12.
A total of 1,080 patients were screened, of whom 154 patients were not eligible for randomization in the study following screening. Notably, 29 patients were screened but not randomized due to presenting with another hematologic malignancy (mantle cell lymphoma, SLL, or B-cell prolymphocytic leukemia).
Table 12: Summary of Patient Disposition From the CLL13 Study, per Data Cut-Off at January 20, 2022
Patient disposition | VEN + OBI | Chemoimmunotherapy (FLU + CYC + RIT or BEN + RIT) |
|---|---|---|
Screened (all treatment groups), N | 1,080 | |
Reason for ineligibility following screening (all treatment groups), N | 154 | |
Del(17p) and/or TP53 mutation | 46 | |
Other hematologic malignancy (MCL, SLL, or B-PLL) | 29 | |
Creatinine clearance < 70 mL per minute | 26 | |
Patient decision | 14 | |
Other inclusion or exclusion criterion | 12 | |
CIRS score > 6 or single CIRS score > 4 | 11 | |
No treatment indication | 9 | |
Physician decision | 4 | |
HBV DNA PCR-positive | 1 | |
Active infection | 1 | |
Received prohibited concomitant medication | 1 | |
Randomized, N | 926 | |
Assigned treatment, N | 229 | 229 |
Early study treatment discontinuation, n (%) | 14 (6.1) | 40 (17.5) |
Reason for early study treatment discontinuation, n (%) | ||
Adverse event or intercurrent illness | 9 (3.9) | 32 (14.0) |
Progressive disease | 3 (1.3) | 2 (0.9) |
Refusal of treatment | 1 (0.4) | 2 (0.9) |
Death | 1 (0.4) | 0 |
Other reason | 0 | 4 (1.7) |
Early study termination, n (%) | 13 (5.7) | 33 (14.4) |
Reason for early study termination, n (%) | ||
Death | 11 (4.8) | 12 (5.2) |
Withdrawal of consent | 2 (0.9) | 16 (7.0) |
Other | 0 | 5 (2.2) |
In follow-up phase at data cut-off date of January 20, 2022, N | 216 | 196 |
ITT, N | 229 | 229a |
Safety, N | 228 | 216b |
B-PLL = B-cell prolymphocytic leukemia; BEN = bendamustine; CIRS = Cumulative illness rating scale; CYC = cyclophosphamide; del(17p) = 17p deletion; FLU = fludarabine; HBV = hepatitis B virus; ITT = intention to treat; MCL = mantle cell lymphoma; OBI = obinutuzumab; PCR = polymerase chain reaction; RIT = rituximab; SLL = small lymphocytic lymphoma; VEN = venetoclax.
aA total of 150 patients were allocated to FLU + CYC + RIT and 79 patients were allocated to BEN + RIT.
bA total of 137 (63.4%) patients were allocated to FLU + CYC + RIT and 79 (36.6%) patients were allocated to BEN + RIT.
Sources: Interim analysis of the co-primary endpoint progression-free survival: CLL13 (GAIA) (data cut-off date of January 20, 2022)12 and Sponsor Summary of Clinical Evidence.2
A total of 926 patients were randomized in the study — 229 patients who were randomized to receive venetoclax plus obinutuzumab and 229 patients who were randomized to receive chemoimmunotherapy (150 patients were allocated to FLU + CYC + RIT and 79 patients were allocated to BEN + RIT). Of those randomized to each group, 14 (6.1%) patients in the venetoclax plus obinutuzumab group and 40 (17.5%) patients in the chemoimmunotherapy group discontinued their study treatment early. The most common reason for early study treatment discontinuation in both groups was due to an AE or intercurrent illness (9 [3.9%] patients in the intervention group and 32 [14.0%] patients in the comparator group). Of those randomized to each group, 13 (5.7%) patients in the venetoclax plus obinutuzumab group and 33 (14.4%) patients in the chemoimmunotherapy group discontinued the study early. While the most common reason for early study termination was death in the venetoclax plus obinutuzumab group (11 [4.8%] patients in the intervention group and 12 [5.2%] patients in the comparator group), the most common reason was withdrawal of consent in the chemoimmunotherapy group (2 [0.9%] patients in the intervention group and 16 [7.0%] patients in the comparator group).
A total of 216 patients in the venetoclax plus obinutuzumab group and 196 patients in the chemoimmunotherapy group were in a follow-up phase based on a data cut-off date of January 20, 2022.12 As of the data cut-off date of January 31, 2023, a total of 215 patients in the venetoclax plus obinutuzumab group and 188 patients in the chemoimmunotherapy group were in the follow-up phase.9
Baseline Characteristics
The baseline characteristics outlined in Table 13 are limited to those that are most relevant to this review or were felt to affect the outcomes or interpretation of the study results.
The median age of patients was 62 years (range, 31 years to 83 years) in the venetoclax plus obinutuzumab group and 61 years (range, 29 years to 84 years) in the chemoimmunotherapy group. The distribution of patients by age based on a cut-off of 65 years was well balanced between groups, with most patients being aged 65 years and younger. The median CIRS score was 2 (range, 0 to 6) in both groups (a higher CIRS score indicates greater impaired function of organ systems); all patients in both groups had a CIRS score of 6 or less. The median CrCl was 86.3 mL per minute (range, 41.5 mL per minute to 180.2 mL per minute) in the venetoclax plus obinutuzumab group and 86.3 mL per minute (range, 39.5 mL per minute to 223.6 mL per minute) in the chemoimmunotherapy group. The distribution of patients by CrCl based on a cut-off of 70 mL per minute was well balanced between groups, with most patients being in the 70 mL per minute and greater category. Note that patients with CrCl of less than 70 mL per minute were eligible if a central review confirmed that impaired renal function was due to abdominal lymphadenopathy.
The median time between CLL diagnosis and randomization was 27.7 months (IQR, 8.3 months to 62.0 months) in the venetoclax plus obinutuzumab group and 26.7 months (IQR, 9.2 months to 59.1 months) in the chemoimmunotherapy group. The distribution of patients by Rai staging was generally well balanced between groups, with most patients presenting with Rai stage I to stage IV. The median ECOG PS score was 0 (range, 0 to 2) in both groups (a higher performance status score indicates greater disability). The distribution of patients by ECOG PS score based on a cut-off of 0 was well balanced between groups, with most patients having an ECOG PS score of 0.
No patient in either group had del(17p) and all patients in both groups had unmutated TP53. The distribution of patients by IGHV mutation status was generally well balanced between groups, with most patients having unmutated IGHV.
Table 13: Summary of Baseline Characteristics From the CLL13 Study (ITT Population)
Characteristic | VEN + OBI (N = 229) | Chemoimmunotherapy (N = 229) |
|---|---|---|
Age (years), median (range) | 62 (31 to 83) | 61 (29 to 84) |
Age, n (%) | ||
≤ 65 years | 147 (64.2) | 150 (65.5) |
> 65 years | 82 (35.8) | 79 (34.5) |
Gender, n (%) | ||
Female | 58 (25.3) | 66 (28.8) |
Male | 171 (74.7) | 163 (71.2) |
Time between diagnosis and randomization (months), median (IQR) | 27.7 (8.3 to 62.0) | 26.7 (9.2 to 59.1) |
Binet stage used for stratification, n (%) | ||
A | 60 (26.2) | 61 (26.6) |
B | 90 (39.3) | 85 (37.1) |
C | 79 (34.5) | 83 (36.2) |
Rai stage, n (%) | ||
N of patients | 228 | 227 |
0 | 13 (5.7) | 7 (3.1) |
I | 56 (24.6) | 53 (23.3) |
II | 66 (28.9) | 60 (26.4) |
III | 54 (23.7) | 57 (25.1) |
IV | 39 (17.1) | 50 (22.0) |
Missing information | 1 (0.4) | 2 (0.9) |
ECOG PS, median (range) | 0 (0 to 2) | 0 (0 to 2) |
ECOG PS, n (%) | ||
0 | 165 (72.1) | 164 (71.6) |
> 0 | 64 (27.9) | 65 (28.4) |
CIRS score, median (range) | 2 (0 to 6) | 2 (0 to 6) |
CIRS score, n (%) | ||
Score ≤ 6 | 229 (100.0) | 229 (100.0) |
Creatinine clearance (mL per minute), median (range) | 86.3 (41.5 to 180.2) | 86.3 (39.5 to 223.6) |
Creatinine clearance, n (%) | ||
< 70 mL per minutea | 47 (20.6) | 41 (17.9) |
≥ 70 mL per minute | 181 (79.4) | 188 (82.1) |
Missing information | 1 (0.4) | 0 |
Cytogenetic subgroup by hierarchical order, n (%) | ||
Deletion 17p | 0 | 0 |
Deletion 11q | 44 (19.2) | 41 (17.9) |
Trisomy 12 | 47 (20.5) | 34 (14.8) |
Deletion 13q | 94 (41.0) | 101 (44.1) |
No abnormalities | 44 (19.2) | 53 (23.1) |
IGHV region mutation status, n (%) | ||
N of patients | 228 | 229 |
Unmutated | 130 (57.0) | 131 (57.2) |
Mutated | 89 (39.0) | 95 (41.5) |
Not evaluable | 9 (3.9) | 3 (1.3) |
Missing information | 1 (0.4) | 0 |
TP53 unmutated, n (%) | 229 (100.0) | 229 (100.0) |
CLL-IPI risk group, n (%) | ||
N of patients | 217 | 225 |
Low | 32 (14.7) | 36 (16.0) |
Intermediate | 76 (35.0) | 67 (29.8) |
High | 109 (50.2) | 122 (54.2) |
Very high | 0 | 0 |
Missing information | 12 (5.2) | 4 (1.7) |
Serum beta2-microglobulin (mg/L), median (range) | 4.0 (2.0 to 16.2) | 4.2 (1.4 to 15.5) |
Complex karyotype, n (%) | ||
N of patients | 218 | 223 |
< 3 aberrations | 182 (83.5) | 177 (79.4) |
≥ 3 and < 5 aberrations | 25 (11.5) | 30 (13.5) |
≥ 5 aberrations | 11 (5.0) | 16 (7.2) |
Missing information | 11 (4.8) | 6 (2.6) |
Tumour lysis syndrome risk category, n (%) | ||
N of patients | 211 | 214 |
Low | 31 (14.7) | 31 (14.5) |
Intermediate | 127 (60.2) | 132 (61.7) |
High | 53 (25.1) | 51 (23.8) |
Missing information | 18 (7.9) | 15 (6.6) |
BEN = bendamustine; CIRS = Cumulative Illness Rating Scale; CLL = chronic lymphocytic leukemia; CLL-IPI = International Prognostic Index for Chronic Lymphocytic Leukemia; CYC = cyclophosphamide; ECOG PS = Eastern Cooperative Oncology Group Performance Status; FLU = fludarabine; IQR = interquartile range; OBI = obinutuzumab; RIT = rituximab; VEN = venetoclax.
Notes: Binet stage indicates CLL advancement based on organ and lymph node involvement, hemoglobin levels, and platelet counts.11
Rai stage 0 indicates low-risk disease, Rai stage I or stage II indicates intermediate-risk disease, and Rai stage III or stage IV indicates high-risk disease.11
An ECOG PS score ranges from 0 to 5, with higher scores indicating greater disability.11
A CIRS score ranges from 0 to 56, with higher scores indicating greater impaired function of organ systems.11
Creatinine clearance was measured according to the Cockcroft-Gault equation.11
CLL-IPI categorizes risk according to the following weighted individual risk factors: 17p deletion, TP53 and IGHV region mutation status, serum beta2-microglobulin level (cut-off of 3.5 mg/L), age, and clinical stage.11
Low tumour lysis syndrome risk is defined as an absolute lymphocyte count of less than 25 multiplied by 103 per cubic millimetre and the largest diameter of all measurable lymph nodes of less than 5 cm. Intermediate risk is defined as an absolute lymphocyte count of 25 or more multiplied by 103 per cubic millimetre or the largest diameter of any measurable lymph node of 5 cm or more and less than 10 cm. High risk is defined as an absolute lymphocyte count of 25 or more multiplied by 103 per cubic millimetre and the largest diameter of any measurable lymph node of 5 cm or more and less than 10 cm, or the largest diameter of any measurable lymph node of 10 cm or more, regardless of absolute lymphocyte count.11
aPatients with a creatinine clearance of less than 70 mL per minute were eligible if a central review confirmed impaired renal function was due to abdominal lymphadenopathy.
Sources: Interim analysis of the co-primary endpoint progression-free survival: CLL13 (GAIA) (data cut-off date of January 20, 2022)12 and Sponsor Summary of Clinical Evidence.2
Exposure to Study Treatments
The median number of treatment cycles was 12 (IQR, 2 to 12) in the venetoclax plus obinutuzumab group and 6 (IQR, 1 to 6) in the chemoimmunotherapy group. In total, 214 of 228 (93.9%) patients in the venetoclax plus obinutuzumab group and 176 of 216 (81.5%) patients in the chemoimmunotherapy group received the full number of treatment cycles for their respective treatment per protocol in the safety population.11
A dose reduction of greater than 20% in any study drug was reported in 48 of 228 (21.2%) patients in the venetoclax plus obinutuzumab group and 32 of 216 (14.8%) patients in the chemoimmunotherapy group in the safety population.11
Concomitant Medication
A total of ███ ██ ███ ████████ ███████ in the venetoclax plus obinutuzumab group and ███ ██ ███ ████████ ███████ in the chemoimmunotherapy group received at least 1 administration of granulocyte colony-stimulating factor as concomitant therapy in the safety population.12
First Documented Subsequent Treatment
A summary of the first documented subsequent antileukemic treatment from the CLL13 study, based on a data cut-off date of January 20, 2022, is presented in Table 14. A total of ██ patients in the venetoclax plus obinutuzumab group and ██ patients in the chemoimmunotherapy group received subsequent antileukemic therapies. The most common (> 1 patient) subsequent treatments reported in the intervention group were ibrutinib (████████) and venetoclax plus obinutuzumab (████████). The most common subsequent treatments reported in the comparator group were ibrutinib (██ ████████), venetoclax plus rituximab (████████), venetoclax plus obinutuzumab, acalabrutinib, and venetoclax plus ibrutinib (████████ ████).
At the 4-year follow-up (with a data cut-off date of January 31, 2023), a total of 111 patients across all treatment groups reported subsequent therapies for CLL-type progression. For their second-line treatment, 60 (54%) patients received a BTK inhibitor, 30 (37%) patients received a venetoclax-based therapy, 12 (11%) patients received a BTK inhibitor and venetoclax-based combination, and 5 (5%) patients received chemoimmunotherapy. Across all treatment groups, a total of 6 patients received a second-line therapy after stopping their assigned study drug without disease progression. A total of 12 patients received a second-line therapy for Richter syndrome.9
Table 14: Summary of First Documented Subsequent Treatment From the CLL13 Study, per Data Cut-Off at January 20, 2022 (ITT Population)
First documented subsequent antileukemic treatment | Venetoclax + obinutuzumab (N = 229) | Chemoimmunotherapy (fludarabine + cyclophosphamide + rituximab or bendamustine + rituximab) (N = 229) |
|---|---|---|
All patients receiving subsequent treatment, N | ██ | ██ |
Subsequent treatment, n (%) | ||
Ibrutinib | ██████ | ██ ██████ |
Obinutuzumab + venetoclax | ██████ | ██████ |
Allogeneic stem cell transplant | ██████ | ██████ |
Bendamustine + rituximab | ██████ | ██████ |
Acalabrutinib + bendamustine + obinutuzumab + venetoclax | ██████ | ██ ██████ |
Acalabrutinib + obinutuzumab + venetoclax | ██████ | ██ ██████ |
Acalabrutinib + venetoclax | ██████ | ██ ██████ |
Bleomycin + dacarbazine + doxorubicin + vinblastine | ██████ | ██ ██████ |
Cyclophosphamide + doxorubicin + obinutuzumab + prednisone + vincristine | ██████ | ██ ██████ |
Cyclophosphamide + doxorubicin + prednisone + rituximab + vincristine | ██████ | ██ ██████ |
Dexamethasone + doxorubicin + vincristine | ██████ | ██ ██████ |
Rituximab + venetoclax | ██ ██████ | ██████ |
Acalabrutinib | ██ ██████ | ██████ |
Ibrutinib + venetoclax | ██ ██████ | ██████ |
Acalabrutinib + cytarabine + methotrexate + rituximab | ██ ██████ | ██████ |
Acalabrutinib + navtemadlin | ██ ██████ | ██████ |
Bendamustine + rituximab + venetoclax | ██ ██████ | ██████ |
Cyclophosphamide + fludarabine + rituximab | ██ ██████ | ██████ |
Ibrutinib + rituximab + venetoclax | ██ ██████ | ██████ |
Obinutuzumab + zanubrutinib | ██ ██████ | ██████ |
Rituximab | ██ ██████ | ██████ |
Rituximab + prednisolone | ██ ██████ | ██████ |
ITT = intention to treat.
Sources: Interim analysis of the co-primary endpoint progression-free survival: CLL13 (GAIA) (data cut-off date of January 20, 2022)12 and Sponsor Summary of Clinical Evidence.2
Efficacy
A summary of key efficacy results from the CLL13 study is presented in Table 15.
The interim analysis of PFS, including analysis of further time-to-event end points and safety, were conducted at month 61 after the first patient was randomized (with a data cut-off date of January 20, 2022). Since venetoclax plus obinutuzumab plus ibrutinib met the PFS significance level at the interim analysis and the independent DSMB advised on conducting the full analysis of the primary and secondary end points, the interim analysis for venetoclax plus obinutuzumab was considered to be the primary analysis for evaluation.11
The median duration of follow-up in the full study population at the interim analysis, based on a data cut-off date of January 20, 2022, was 38.8 months (IQR, 32.7 months to 46.1 months). More specifically, it was ████ ██████ ████ █ ████ ██ ████ ███████ for patients in the venetoclax plus obinutuzumab group and ████ ██████ ████ █ ████ ██ ████ ██████ in the chemoimmunotherapy group.12 The median duration of follow-up in the full study population at the 4-year follow-up analysis, based on a data cut-off date of January 31, 2023, was 50.7 months (IQR, 44.6 months to 57.9 months).9
Table 15: Summary of Key Efficacy Results From the CLL13 Study (ITT Population)
Efficacy outcome | VEN + OBI (N = 229) | Chemoimmunotherapy (FLU + CYC + RIT or BEN + RIT) (N = 229) |
|---|---|---|
Time to event (data cut-off date: January 20, 2022) | ||
Follow-up time for all patients (months), median (IQR) | 38.8 (32.7 to 46.1) | |
Follow-up time (months), median (IQR) | ████ █████ ██ | ████ █████ ██ █████ |
PFS | ||
Events, n (%) | 33 (14.4) | 67 (29.3) |
PFS (months), median (97.5% CI) | Not reached | ████ ████ █████████ |
HR (97.5% CI) | 0.42 ██ (0.26 ██ to 0.68 ██) | |
P valuea | ████████ | |
PFS rate at 1 year, % | ████ | ████ |
PFS rate at 2 years, % | ████ | ████ |
PFS rate at 3 years, % | 87.7 | 75.5 |
PFS rate at 4 years, % | ████ | ████ |
OS | ||
Events, n (%) | ██ █████ | ██ █████ |
OS (months), median (97.5% CI) | Not reached | Not reached |
HR (97.5% CI) | █████ ██████ ██ ██████ | |
P value | ███ ████████ | |
OS rate at 1 year, % | ████ | ████ |
OS rate at 2 years, % | ████ | ████ |
OS rate at 3 years, % | 96.3 | 95.0 |
OS rate at 4 years, % | ████ | ████ |
DOR | ||
N of patients | ███ | ███ |
Events, n (%) | ██ ██████ | ██ ██████ |
DOR (months), median (95% CI) | ███ ███████ | ███ ███████ |
HR (97.5% CI) | █████ ██████ ██ ██████ | |
P value | ███ ████████ | |
Event-free survival rate at 1 year, % | ████ | ████ |
Event-free survival rate at 2 years, % | ████ | ████ |
Event-free survival rate at 3 years, % | ████ | ████ |
Event-free survival rate at 4 years, % | ████ | ████ |
TTNT from randomization | ||
Events, n (%) | ██ █████ | ██ ██████ |
TTNT (months), median (95% CI) | Not reached | Not reached |
HR (97.5% CI) | █████ ██████ ██ ██████ | |
P value | ███ ████████ | |
Event-free survival rate at 1 year, % | ████ | ████ |
Event-free survival rate at 2 years, % | ████ | ████ |
Event-free survival rate at 3 years, % | ████ | ████ |
Event-free survival rate at 4 years, % | ████ | ████ |
Undetectable MRD (data cut-off date: February 28, 2021) | ||
Follow-up time for all patients (months), median (IQR) | 27.9 (22.1 to 35.3) | |
Follow-up time (months), median (IQR) | ████ █████ ██ | ████ █████ ██ █████ |
MRD in peripheral blood at month 15 | ||
Negative MRD status (< 10–4), n (%) | 198 (86.5) | 119 (52.0) |
97.5% CI by Clopper-Pearson | 80.6 to 91.1 | 44.4 to 59.5 |
P valuea | < 0.0001 | |
Intermediate MRD status (≥ 10–4 and < 10–2), n (%) | 21 (9.2) | 47 (20.5) |
Positive MRD status (≥ 10–2), n (%) | 0 | 29 (12.7) |
Missing MRD status, n (%) | 10 (4.4) | 34 (14.8) |
Response to treatment (data cut-off date: February 28, 2021) | ||
CR at month 15 | ||
Response, n (%) | ||
CR | 125 (54.6) | 63 (27.5) |
CRir | 5 (2.2) | 8 (3.5) |
Missing | 7 (3.1) | 34 (14.8) |
CR rate, n (%) | 130 (56.8) | 71 (31.0) |
BEN = bendamustine; CI = confidence interval; CR = complete response; CRir = complete response with incomplete recovery of the bone marrow; CYC = cyclophosphamide; DOR = duration of response; FLU = fludarabine; HR = hazard ratio; IQR = interquartile range; ITT = intention to treat; MRD = minimal residual disease; OBI = obinutuzumab; OS = overall survival; PFS = progression-free survival; RIT = rituximab; TTNT = time to next treatment; VEN = venetoclax.
aThe P value was adjusted for multiple testing.
Sources: Interim analysis of the co-primary endpoint progression-free survival: CLL13 (GAIA) (data cut-off date of January 20, 2022),12 Co-Primary Endpoint Analysis of MRD negativity rate at month 15: CLL13 (GAIA) (data cut-off date of February 28, 2021),13 and Sponsor Summary of Clinical Evidence.2
Progression-Free Survival
At the time of the interim analysis, the proportion of observed events (the first occurrence of progression or relapse or death) was 14.4% (33 events) in the venetoclax plus obinutuzumab group and 29.3% (67 events) in the chemoimmunotherapy group. The median PFS was not reached in the venetoclax plus obinutuzumab group and ████ ██████ ██████ ██ ███ █████████ in the chemoimmunotherapy group (████████). Venetoclax plus obinutuzumab was favoured over chemoimmunotherapy (HR = 0.42 ███; 97.5% CI, 0.26 ████ to 0.68 ███). The PFS rates at 1 year, 2 years, 3 years, and 4 years were ██████ █████, 87.7%, and ██████ respectively, in the venetoclax plus obinutuzumab group and ██████ ██████ 75.5%, and █████, respectively, in the chemoimmunotherapy group.12
At the 4-year follow-up, the proportion of observed events was 24% (55 events) in the venetoclax plus obinutuzumab group and 39% (90 events) in the chemoimmunotherapy group. The median PFS had still not been reached in the venetoclax plus obinutuzumab group and was 59.4 months (95% CI not reported) in the chemoimmunotherapy group. The HR was 0.47 (97.5% CI, 0.32 to 0.69) following treatment with venetoclax plus obinutuzumab versus chemoimmunotherapy. The PFS survival rate at 4 years was 81.8% (97.5% CI, 75.8% to 87.8%) in the venetoclax plus obinutuzumab group and 62.0% (97.5% CI, 54.4% to 69.7%) in the chemoimmunotherapy group.9
The results from the analysis of PFS, stratified by chemoimmunotherapy and age based on a cut-off of 65 years, at the 4-year follow-up were used to inform the accompanying pharmacoeconomic analysis; a summary of the results are presented Table 22 and Table 23 in Appendix 1.
Overall Survival
At the time of the interim analysis, the proportion of observed events (death due to any cause) was ████ ███ ███████ in the venetoclax plus obinutuzumab group and ████ ███ ███████ in the chemoimmunotherapy group. The median OS had not been reached in either group. The HR was █████ ██████ ███ █████ ██ ██████ following treatment with venetoclax plus obinutuzumab versus chemoimmunotherapy. The OS rates at 1 year, 2 years, 3 years, and 4 years were ██████ ██████ 96.3%, and ██████ respectively, in the venetoclax plus obinutuzumab group and ██████ ██████ 95.0%, and ██████ respectively, in the chemoimmunotherapy group.12
At the 4-year follow-up, the proportion of observed events was 5% (11 events) in the venetoclax plus obinutuzumab group and 7% (17 events) in the chemoimmunotherapy group. The median OS had still not been reached in either group. The HR was 0.58 (97.5% CI, 0.24 to 1.38) following treatment with venetoclax plus obinutuzumab versus chemoimmunotherapy. The OS survival rate at 4 years was 95.1% (97.5% CI, 91.9% to 98.3%) in the venetoclax plus obinutuzumab group and 93.5% (97.5% CI, 89.6% to 97.4%) in the chemoimmunotherapy group.9
Duration of Response
At the time of the interim analysis, the proportion of observed events (the first occurrence of progression or relapse or death after the first documented response) was █████ ███ ███████ in the venetoclax plus obinutuzumab group and █████ ███ ███████ in the chemoimmunotherapy group. The median duration of response was ███ ███████ in either group. The HR was █████ ██████ ███ █████ ██ ██████ following treatment with venetoclax plus obinutuzumab versus chemoimmunotherapy. The event-free survival rates at 1 year, 2 years, 3 years, and 4 years were ██████ ██████ ██████ ██████ respectively, in the venetoclax plus obinutuzumab group and ██████ ██████ ██████ ███ ██████ respectively, in the chemoimmunotherapy group.12
Time to Next Treatment (From Randomization)
At the time of the interim analysis, the proportion of observed events (the initiation of the first subsequent treatment for CLL) was ████ ███ ███████ in the venetoclax plus obinutuzumab group and █████ ███ ███████ in the chemoimmunotherapy group. The median time to the next treatment had not been reached in either group. The HR was █████ ██████ ███ █████ ██ ██████ following treatment with venetoclax plus obinutuzumab versus chemoimmunotherapy. The event-free survival rates at 1 year, 2 years, 3 years, and 4 years were ██████ ██████ ██████ ███ ██████ respectively, in the venetoclax plus obinutuzumab group and ██████ ██████ ██████ ███ █████, respectively, in the chemoimmunotherapy group.12
At the 4-year follow-up, the proportion of observed events was 10.0% (23 events) in the venetoclax plus obinutuzumab group and 23.6% (54 events) in the chemoimmunotherapy group. The median time to the next treatment had still not been reached in either group. The HR was 0.34 (97.5% CI, 0.20 to 0.60) following treatment with venetoclax plus obinutuzumab versus chemoimmunotherapy. The event-free survival rate at 4 years was 90.4% (97.5% CI, 85.7% to 95.0%) in the venetoclax plus obinutuzumab group and 77.2% (97.5% CI, 70.2% to 84.1%) in the chemoimmunotherapy group.9
The results from the analysis of time to next treatment, stratified by chemoimmunotherapy and age based on a cut-off of 65 years, at the 4-year follow-up were used to inform the accompanying pharmacoeconomic analysis; a summary of the results are presented in Table 24 and Table 25 in Appendix 1.
Undetectable MRD in Peripheral Blood
Venetoclax plus obinutuzumab was favoured over chemoimmunotherapy — at month 15, the undetectable MRD rate was 86.5% (97.5% CI, 80.6% to 91.1%) (198 of 229 patients) in the venetoclax plus obinutuzumab group compared with 52.0% (97.5% CI, 44.4% to 59.5%) (119 of 229 patients) in the chemoimmunotherapy group (P value < 0.0001). A total of 4.4% (10 patients) in the venetoclax plus obinutuzumab group and 14.8% (34 patients) in the chemoimmunotherapy group had a missing MRD status.13
CR to Treatment
The median duration of follow-up in the full study population at month 15, based on a data cut-off date of February 28, 2021, was 27.9 months (IQR, 22.1 months to 35.3 months). More specifically, it was ████ ██████ ████ █ ████ ██ ████ ███████ for patients in the venetoclax plus obinutuzumab group and ████ ██████ ████ █ ████ ██ ████ ██████ in the chemoimmunotherapy group.13
At month 15, the CR rate was 56.8% (130 of 229 patients) in the venetoclax plus obinutuzumab group compared with 31.0% (71 of 229 patients) in the chemoimmunotherapy group. A total of 3.1% (7) of patients in the venetoclax plus obinutuzumab group and 14.8% (34) of patients in the chemoimmunotherapy group had missing data for this parameter.13
Harms
A summary of harms results from the CLL13 study based on a data cut-off date of January 20, 2022 (interim analysis) is presented in Table 16.
Adverse Events
A total of █████ ████ ██ ███ █████████ in the venetoclax plus obinutuzumab group and █████ ████ ██ ███ ████████) in the chemoimmunotherapy group had at least 1 TEAE of any CTC grade 1 to grade 5. The most common TEAE in both groups was neutropenia and/or decreased neutrophil count based on Standardized Medical Query — █████ ████ █████████ in the intervention group and █████ ████ █████████ in the comparator group. A total of █████ ████ █████████ in the venetoclax plus obinutuzumab group and █████ ███ █████████ in the chemoimmunotherapy group had an infusion-related reaction. A total of ████ ██ █████████ in the venetoclax plus obinutuzumab group and █████ ███ █████████ in the chemoimmunotherapy group had febrile neutropenia.12
Serious AEs
A total of 44.7% (102) of patients in the venetoclax plus obinutuzumab group and 47.7% (103) of patients in the chemoimmunotherapy group had at least 1 serious TEAE of any CTC grade 1 to grade 5. The most common serious TEAEs in both groups were infections and infestations — █████ ███ ██ ███ ██████ in the intervention group and █████ ███ ██ ███ ██████ in the comparator group.12
Withdrawals Due to AEs
A total of 5.7% (13) of patients in the venetoclax plus obinutuzumab group and 15.3% (33) of patients in the chemoimmunotherapy group had at least 1 TEAE leading to early treatment discontinuation.11 In the venetoclax plus obinutuzumab group, the most common TEAE leading to early treatment discontinuation was Richter syndrome — █████ ██ ██ ██ ██████ in the intervention group and ████ ██ ██ ██ ██████ in the comparator group. In the chemoimmunotherapy group, the most common TEAE leading to early treatment discontinuation was neutropenia — █████ ██ ██ ██ ██████ in the intervention group and █████ ███ ██ ██ ██████ in the comparator group.12
Treatment-Emergent AEs With CTC Grade 5
In the venetoclax plus obinutuzumab group, a total of 9 patients had a CTC grade 5 AE, of whom 1 patient had COVID-19 that was reported in the time frame between treatment period and until day 84 after the end of treatment, inclusive. The other 8 patients had a CTC grade 5 AE that was reported after day 84 after the end of treatment — secondary neoplasia (excluding Richter syndrome) in 3 patients, COVID-19 in 2 patients, and cardiac arrest or failure, Richter syndrome, and pneumonia in 1 patient each.11
In the chemoimmunotherapy group, a total of 10 patients had a CTC grade 5 AE, of whom 1 patient had an infection other than COVID-19 that was reported in the time frame between treatment period and until day 84 after the end of treatment, inclusive. The other 9 patients had a CTC grade 5 AE that was reported after day 84 after the end of treatment — COVID-19 in 2 patients; Richter syndrome in 2 patients; bronchial obstruction, stroke, and respiratory failure in 2 patients; and secondary neoplasia (excluding Richter syndrome), cardiac arrest or failure, and pneumonia in 1 patient each.11
Notable Harms
Serious Infections and Infestations
Refer to the previous Serious AEs section.
Second Primary Malignancies
At the interim analysis, there was a total of 27 cases of second primary malignances in the venetoclax plus obinutuzumab group, including 14 cases of nonmelanoma skin cancer and 13 cases of solid tumours. There was a total of 49 cases of second primary malignancies in the chemoimmunotherapy group, including 27 cases of nonmelanoma skin cancer, 18 cases of solid tumours, and 4 cases of hematological malignancies.11
At the 4-year follow-up, there was a total of 45 cases of second cancers in the venetoclax plus obinutuzumab group, including 16 cases of nonmelanoma skin cancer, 15 cases of solid tumours, 7 cases of benign tumours, and 7 cases of Richter syndrome. There was a total of 69 cases of second cancers in the chemoimmunotherapy group, including 33 cases of nonmelanoma skin cancer, 19 cases of solid tumours, 7 cases of benign tumours, 6 cases of Richter syndrome, and 4 cases of hematological malignancies (2 cases of plasma cell myeloma and 1 case each of myelodysplastic syndrome and cutaneous T-cell lymphoma).9
Cardiac-Related AEs
In the venetoclax plus obinutuzumab group, 1 case of cardiac arrest and 1 case of arrhythmia was reported. In the chemoimmunotherapy group, 1 case of arrhythmia was reported.12
Table 16: Summary of Harms Results From the CLL13 Study, per Data Cut-Off at January 20, 2022 (Safety Population)
Adverse event | VEN + OBI (N = 228) | Chemoimmunotherapy (FLU + CYC + RIT or BEN + RIT) (N = 216) |
|---|---|---|
Most common (> 10%) TEAEs by PT | ||
████████ ███████ ██ ███ ███ █████ █ ██ ██ █ ███ | ███ ██████ | ███ ██████ |
███████████ ██████ ██████████ █████ █████████ █████ | ███ ██████ | ███ ██████ |
████████ ███████ ████████ | ███ ██████ | ██ ██████ |
███████████ | ███ ██████ | ███ ██████ |
█████ ███████████ █████ ██████████ █████ | ██ ██████ | ██ ██████ |
███████ | ██ ██████ | ██ ██████ |
████████ | ██ ██████ | ██ ██████ |
██████ | ██ ██████ | ██ ██████ |
███████████████ | ██ ██████ | ██ █████ |
███████ | ██ ██████ | ██ ██████ |
████████████████ ██████ ████████ █████ █████████ █████ | ██ ██████ | ██ ██████ |
████████████████ | ██ ██████ | ██ ██████ |
█████ | ██ ██████ | ██ ██████ |
████████ | ██ ██████ | ██ ██████ |
██████████ █████ █████████ | ██ ██████ | ██ █████ |
██████████ | ██ ██████ | █████ |
████████████ | ██ ██████ | ██ ██████ |
████ | ██ ██████ | ██ ██████ |
█████████ █████ | ██ ██████ | ██ █████ |
██████ █████ ████████ | ██ ██████ | ██ █████ |
█████████████ █████████████ █████ ████████ ████████████ ████ ██████ | ██ ██████ | ██ ██████ |
██████████ | ██ █████ | ██ ██████ |
██████ | ██ █████ | ██ ██████ |
████████ | ██ █████ | ██ ██████ |
███████ ███████████ | █████ | ██ ██████ |
Serious TEAEs | ||
Patients with ≥ 1 serious TEAE of any CTC grade 1 to grade 5, n (%) | 102 (44.7) | 103 (47.7) |
Most common (> 10%) serious TEAEs by SOC | ||
███ █████ ██ ███████ █████ | ███ | ███ |
██████████ ███ ████████████ █████████████ █ ███ | ██ ██████ | ██ ██████ |
█████████ ███████ ██████████ ███ ███████████ ██████████ █████ ███ ███████ █████████████ █ ███ | ██ ██████ | ██ ██████ |
███████ ██████████ ███ ██████████ █████████████ █████████ ████████ ███████ ██████████ █████████████ | ██ ██████ | ██ █████ |
█████ ███ █████████ ██████ █████████ █████████████ █ ███ | ██ ██████ | ██ ██████ |
Most common (> 10%) TEAEs by PT leading to treatment discontinuation | ||
All cases of TEAEs leading to treatment discontinuation, N | 13 | 45 |
RS (case level), n (%) | ██████ | █████ |
Neutropenia (case level), n (%) | ██████ | ██ ██████ |
Notable harms | ||
Refer to the preceding text for a summary of notable harms. | ||
BEN = bendamustine; CTC = Common Toxicity Criteria; CYC = cyclophosphamide; FLU = fludarabine; HLT = high-level term according to Medical Dictionary for Regulatory Activities; MedDRA = Medical Dictionary for Regulatory Activities; OBI = obinutuzumab; PT = preferred term; RIT = rituximab; RS = Richter syndrome; SMQ = standardized medical query; SOC = system organ class; TEAE = treatment-emergent adverse event; VEN = venetoclax.
Note: Standardised MedDRA Queries are validated, standard sets of MedDRA terms used to support signal detection and monitoring, and represent a variety of safety topics of regulatory interest. Standardised MedDRA Queries include narrow and/or broad terms; narrow terms are highly likely to represent the condition of interest.48
Sources: Interim analysis of the co-primary endpoint progression-free survival: CLL13 (GAIA) (data cut-off date of January 20, 2022)12 and Sponsor Summary of Clinical Evidence.2
Critical Appraisal
Internal Validity
The CLL13 study was generally appropriately designed and powered to evaluate the efficacy of venetoclax plus obinutuzumab relative to chemoimmunotherapy. Although the trial was open label and therefore susceptible to reporting and performance bias, this was considered justifiable in the context of CLL and the requirement of different formulations and administration routes for each study drug. Nonetheless, disease progression and response to treatment were based on investigator assessment (without an independent review committee), which can introduce the potential for biased results when evaluating efficacy (e.g., favouring venetoclax plus obinutuzumab if the assessor believes the study drug is likely to provide benefit). However, safety data and unblinded reports for the interim PFS analysis were reviewed by an independent DSMB, thereby reducing the potential for biased results.
Based on clinical expert input, patients receiving BEN + RIT are more likely to die in remission before evaluations are made or disease progresses, compared with patients receiving FLU + CYC + RIT, due to a difference in age. Since randomization was stratified by age (with a cut-off of 65 years), Binet stage, and region study group, there was less concern for this potential impact on the interpretation of the results. Relevant baseline characteristics were generally well balanced between the venetoclax plus obinutuzumab and chemoimmunotherapy groups. As such, it was concluded that the risk of bias arising from the randomization process is unlikely. While patients with unmutated IGHV were balanced between the treatment groups, this subset of patients would not typically receive chemoimmunotherapy in the frontline setting, as per the 2022 Canadian guideline.6 In consultation with the clinical experts, it was concluded that this subset of patients with unmutated IGHV randomized to receive chemoimmunotherapy were at a disadvantage when compared to venetoclax plus obinutuzumab, thereby introducing the potential for bias in favour of venetoclax plus obinutuzumab. However, the clinical experts noted that since chemoimmunotherapy was the standard of therapy when the trial was conducted, this issue is considered reasonable but specific bias remains.
The clinical experts advised that without knowing the specific AEs or intercurrent illnesses, it is difficult to conclude whether the imbalance observed in early study treatment discontinuation due to AEs or intercurrent illness between treatment groups has an impact on the interpretation of the results. In consideration of febrile neutropenia and infection-related complications that are associated with chemoimmunotherapy based on previous studies, it was concluded that this imbalance is not a major concern.
Detailed information on protocol amendments and protocol deviations as well as a breakdown of events and censoring for the time-to-event end points were not available from the sponsor; therefore, their impact on the interpretation of the results is unknown.
Notably, the evaluation of PFS was based on results at the interim analysis where 100 events were observed for venetoclax plus obinutuzumab and chemoimmunotherapy, combined. This represents approximately 47% of the expected events planned for the final analysis (i.e., 100 of 213 events) and as such, there is an increased risk of overestimating the treatment effect on PFS based on the interim analysis. Note that this is only an approximation since the study did not specify the target number of PFS events for this treatment comparison of interest (i.e., 213 events were expected for the final analysis comparing venetoclax plus obinutuzumab plus ibrutinib and chemoimmunotherapy). However, it was concluded that this is not a major concern because the 4-year follow-up results were generally consistent with the interim analysis results, suggesting that it is unlikely that the effect observed in the interim analysis was an inflated effect observed by chance.
In consultation with the clinical experts, it was concluded that a median follow-up of 38 months at the interim analysis is appropriate for evaluating the safety and efficacy of the study drugs and that the assessment time point at 15 months for MRD and response to treatment is standard in trials (i.e., 3 months post-treatment).
A total of 4.4% of patients in the venetoclax plus obinutuzumab group and 14.8% of patients in the chemoimmunotherapy group had missing data on MRD status. It was concluded that the imbalance observed in missing data and the relatively high rate of missing data in the chemoimmunotherapy group is a concern for the potential for biased results. Although patients without an MRD sample at month 15 were kept and indicated as non-negative in the analysis, missing data were not replaced or imputed in the primary efficacy analysis of undetectable MRD in peripheral blood at month 15. However, in consideration of the results (i.e., most patients had a negative MRD status in both treatment groups and the imbalance observed in missing data), there is a concern for the potential for biased results, likely in favour of venetoclax plus obinutuzumab, due to the approach for handling missing data.
Type I error was controlled only in the analyses of undetectable MRD and PFS, using a hierarchical testing sequence. A sensitivity analysis was not performed for the comparison of venetoclax plus obinutuzumab versus chemoimmunotherapy; therefore, no conclusions can be drawn on the robustness (or lack thereof) of the results. Since the study was not designed or powered to test specific hypotheses in all other secondary and exploratory analyses, these results are considered as supportive evidence only.
External Validity
The CLL13 study included a subset of the population of interest identified in the indication for venetoclax plus obinutuzumab that was not considered in the previous review — fit patients (defined in the trial by a CIRS score of ≤ 6 and CrCl of ≥ 70 mL per minute) with previously untreated CLL without TP53 aberrations.
In consultation with the clinical experts, it was concluded that the inclusion and exclusion criteria are standard in trials of CLL and are justifiable in the context of minimizing confounders and avoiding placing chemoimmunotherapy at a disadvantage in the comparisons made (i.e., excluded patients with del[17p] and TP53 mutation). However, the clinical experts noted that some criteria are not applicable to Canadian practice and are narrow when compared with patients with CLL seen in practice. For example, 24-hour urine collection is not used in practice to estimate glomerular filtration rate. Most of the patients excluded from the trial may still be considered as candidates for venetoclax plus obinutuzumab in practice by the clinical experts by working with the multidisciplinary team to resolve drug-drug interactions (e.g., patients requiring therapy with strong CYP3A inhibitors or inducers), control other pre-existing conditions (e.g., patients with a known infection of HIV), and dose-adjust accordingly (e.g., patients with varying ECOG PS scores). In other cases, such as pregnancy, the appropriateness of therapy is determined by having a discussion with the patient. Overall, despite the narrow inclusion and exclusion criteria used in the trial, the clinical experts had no concerns with generalizing the results to fit patients who were excluded from the trial — namely, patients with SLL and with del(17p) and TP53 mutation.
The baseline characteristics of the study population are generally representative of the fit patient population seen in practice that would be considered as a candidate for venetoclax plus obinutuzumab, as per clinical expert input. Of note, Rai staging is more commonly used in Canadian practice compared with Binet staging. The median age of the study population is younger than the patient population seen in practice, which is likely between 70 years and 75 years based on clinical expert input; however, no major concern was identified because the study population included patients aged 80 years.
Based on patient and clinician group input and in consultation with the clinical experts, it was concluded that the time-to-event end points (the duration of response, time to next treatment, PFS, and OS) are most meaningful to patients and clinicians. While treatment response and undetectable MRD are standard outcome measures in clinical trials of CLL, the clinical experts advised that they are limited in applicability to Canadian practice due to limitations in accessing relevant tests (MRD measurements, bone marrow biopsies, and scans for treatment response). Thus, while MRD levels might serve as a surrogate marker for OS and PFS in CLL according to literature,14 from a clinical practice perspective, response to treatment and undetectable MRD are relevant as supportive evidence for long-term outcomes.
Standard protocols of supportive care therapies for the delivery of venetoclax plus obinutuzumab, similar to those that were permitted in the trial, have already been established in Canadian practice, as per clinical expert input.
According to the guideline,6 FLU + CYC + RIT and BEN + RIT are appropriate comparators in fit patients without TP53 aberrations (del[17p] and TP53 mutation) and with mutated IGHV in the frontline setting, even though FLU + CYC + RIT is infrequently used and BEN + RIT is not used in practice as per clinician group and clinical expert input. As mentioned earlier, fit patients without TP53 aberrations and with unmutated IGHV do not typically receive chemoimmunotherapy in the frontline setting; instead, a BTK inhibitor would have been a more appropriate comparator in this subset of patients, as per the guideline.6 Further, based on the guideline,6 a BTK inhibitor would have been an appropriate comparator for fit patients with TP53 aberrations — a gap in the present systematic review evidence.
Indirect Evidence
Content in this section has been informed by materials submitted by the sponsor. The following has been summarized and validated by the review team.
Objectives for the Summary of Indirect Evidence
Direct comparative evidence of venetoclax plus obinutuzumab versus chemoimmunotherapy (FLU + CYC + RIT and BEN + RIT) was available from the CLL13 trial. In the absence of direct head-to-head trials evaluating the comparative efficacy of venetoclax plus obinutuzumab versus other relevant comparators for the first-line treatment of CLL in the Canadian practice setting, 1 indirect treatment comparison in the form of an NMA was submitted by the sponsor.
Indirect Treatment Comparison Design
Objectives
The objective of the sponsor-submitted NMA was to estimate the comparative effectiveness of venetoclax plus obinutuzumab versus relevant comparators in the treatment of patients who are fit, with previously untreated CLL, and without del(17p) or TP53 mutation, in terms of PFS, OS, time to next treatment, and undetectable MRD.15
Study Selection Methods
To capture all relevant evidence, the systematic literature review was broad in its scope. The objectives of the systematic literature review were to identify all eligible interventional and observational evidence on relevant treatments for adult patients with previously untreated CLL. Additional criteria listed in Table 17 were then applied to select studies to inform the sponsor-submitted NMA.15,16
The authors reported that the systematic literature review was in line with the guidelines set out by Cochrane and the Centre for Reviews and Dissemination49 and the 27-item PRISMA statement checklist. The systematic literature review was initiated ██ ████████ ███ █████ ████ ███████ ███ ██ ████ ██ █████ █████████ ███ █████ ████████ ██ █████ ███ ████████ ███ █████ ████ ████ ████ ███ ██████ ██ ███ ██████ ████████ █ ████████ ████ ██ ████████ ████████ ███ ███████ ███ █████ ███ █████ ███ ██ ████ ████. Screening was performed by 2 independent reviewers according to the prespecified Population, Interventions, Comparators, Outcomes, and Study design criteria presented in Table 17, along with the methods used.16
The sponsor indicated that ████████████ ████ ████████████ ██ ███ ██████████ █ ████████ ██████████ ██ ███ ████████ ███████ ██ ██ █████ ███ ██ ████████ ██ ██ ████████████ ██ ███ ███ ███████████ ████████ ██ ███ ████████ ██ ███ ███ ██ ██ ███ ████ ██ ██████ comparison in the full desired evidence network.2
Table 17: Study Selection Criteria and Methods for the Sponsor-Submitted NMA
Characteristics | Indirect comparison |
|---|---|
Population | Based on the CLL13 trial:
|
Intervention | Venetoclax plus obinutuzumab administered as per the CLL13 trial. |
Comparators |
|
Outcomes |
|
Study designs | Clinical trials and observational studies |
Publication characteristics |
|
Exclusion criteria |
|
Databases searched | Embase, MEDLINE (including MEDLINE In-Process), Cochrane, the Centre for Reviews and Dissemination database (including the Database of Abstracts of Reviews of Effects), and conference databases for 2016 to 2023 (ASCO, ASH, BSH, EHA, ESMO, ISPOR, and iWCLL) |
Selection process | The identified citations from the search were compiled into an Excel file and titles and abstracts were screened. Subsequently, the full texts of the title and/or abstract inclusions were screened by 2 reviewers. In case of any conflicts, consensus was reached by the 2 reviewers. |
Data extraction process | After the full-text selection phase, data of interest from all included publications were extracted in a prespecified data extraction template by 1 researcher. A second reviewer checked all extracted data. |
Quality assessment | Following the data extraction process, a critical appraisal of the quality of selected studies was performed by 1 researcher using the quality assessment checklist presented in the NICE single technology assessment sponsor submission template for RCTs.50 |
ASCO = American Society of Clinical Oncology; ASH = American Society of Hematology; BEN = bendamustine; BSH = British Society for Haematology; CIRS = Cumulative Illness Rating Scale; CLL = chronic lymphocytic leukemia; CrCl = creatinine clearance; CYC = cyclophosphamide; del(17p) = 17p deletion; ECOG PS = Eastern Cooperative Oncology Group Performance Status; EHA = European Hematology Association; ESMO = European Society for Medical Oncology; FLU = fludarabine; ISPOR = International Society of Pharmacoeconomics and Outcomes Research; iwCLL = International Workshop on Chronic Lymphocytic Leukemia; NICE = National Institute for Health and Care Excellence; NMA = network meta-analysis; RCT = randomized controlled trial; RIT = rituximab.
Note: Venetoclax plus ibrutinib and zanubrutinib were added to the inclusion criteria in the September 2020 update and onward to acknowledge their increased relevance.
aStudies were excluded if the average age of the population was younger than 18 years; however, the inclusion of individual patients aged younger than 18 years in an otherwise adult population did not make the article ineligible for inclusion.
bAny corrections of relevant data were included.
cThese were checked for bibliographic references only.
Sources: Systematic Literature Review of Clinical Evidence for Previously Untreated Chronic Lymphocytic Leukaemia (CLL) (sponsor’s report),16 Indirect Treatment Comparison (ITC) for venetoclax plus obinutuzumab in untreated patients with chronic lymphocytic leukemia (sponsor’s report),15 and Sponsor Summary of Clinical Evidence.2
NMA Methods
A feasibility assessment of the studies identified from the systematic literature review was performed by the authors of the NMA before a final selection was made on the studies relevant for the NMA. The similarity assumption was assessed by comparing the studies according to population characteristics, intervention and comparators, outcomes, and study design.15
Indirect comparisons of venetoclax plus obinutuzumab, venetoclax plus ibrutinib, FLU + CYC + RIT, BEN + RIT, obinutuzumab plus chlorambucil, acalabrutinib, zanubrutinib, and ibrutinib were made using a Bayesian NMA with Hamiltonian Monte Carlo, a Markov Chain Monte Carlo method. Each treatment was a node in the NMA. The NMA considered both fixed-effects and random-effects models with uninformative and informative priors. For continuous outcomes, HRs for PFS, OS, and time to next treatment were estimated using generalized linear models with a normal likelihood and identity link. For dichotomous outcomes, the log ORs were estimated using a logistic regression model with a binomial likelihood and logit link.15 Methods of the sponsor-submitted NMA are summarized in Table 18.
The population of interest is adult patients aged 18 years and older who are fit (defined in the trials by a CIRS score of ≤ 6 and CrCl of ≥ 70 mL per minute), with previously untreated CLL and without del(17p) or TP53 mutations. According to the authors, ██ ███ ████ ████████ ███ ███████ ████ █████ ████████ ███ ███ ████████ ███ ██ ███ ███████ ████████ ███ ██████ ███ █████████. Hence, the base case included both fit and unfit patients without del(17p) or TP53 mutations (and whose blood sampling showed undetectable MRD). A number of sensitivity analyses listed in Table 18 were performed to explore the impact of heterogeneity observed in the trials. The authors indicated that no sensitivity analysis that excludes outlier trials was conducted as this would have removed relevant comparators from the NMA. A subgroup analysis was conducted according to age based on a cut-off of 65 years ███ ██████ ██ █████ ███ ███ ██████ ████████ ████ ██ █████ ███ ███████ ███████████ ██ ██ █████████████ ██ ███ ████████████████████ ███████ ███████████. Due to limitations in data availability, the only outcome that could be tested in this subgroup was PFS.15
The authors indicated that the NMAs were conducted in accordance with the NICE Decision Support Unit Technical Support Document 2.51 Model fit was assessed based on the deviance information criterion (DIC) and in consideration of heterogeneity. Convergence was assessed through visual diagnostic plots and Gelman-Rubin Ȓ and Monte Carlo standard error. The NMA protocol specified that statistical heterogeneity in pairwise comparisons would be examined using the I2 statistic and Cochran’s Q test. However, the authors indicated that statistical heterogeneity was instead assessed by evaluating the posterior distribution for the between-study standard deviation output under the Bayesian approach due to the shape of the network and the limited number of pairwise comparisons with multiple studies. Additionally, the authors noted that metaregression would not be feasible for addressing any statistical heterogeneity due the small number of studies. The assessment of consistency was not reported.15
Table 18: Methods of the Sponsor-Submitted NMA
Methods | Description |
|---|---|
Analysis methods | A Bayesian NMA using the Hamiltonian MCMC method was conducted; both fixed- and random-effects models were considered. Four simulation chains at 10,000 iterations with 5,000 burn-ins were used per model run.
Models were constructed following the NICE DSU Technical Support Document 251 and implemented in Stan software,52 using the multinma package developed by Phillippo et al.53 |
Priors | Both uninformative and informative priors were considered. |
Assessment of model fit | The model with the lowest DIC was preferred, which was interpreted as the model with better prediction. A difference > 3 in the DIC across models was considered meaningful. Additionally, heterogeneity was considered to determine the use of random or fixed effects for each model. |
Assessment of consistency | Not reported. |
Assessment of convergence | Visual diagnostic plots, including trace, density, and autocorrelation plots, were generated. Additionally, convergence was assessed using Gelman-Rubin Ȓ values, comparing estimates between chain and within chain variances for each model parameter (convergence can be assumed if Ȓ < 1.1), and the Monte Carlo standard error of the mean of the posterior draws (convergence can be assumed if the Monte Carlo standard error is no greater than 5%). If there was nonconvergence and model instability, the following approaches were applied:
|
Assessment of heterogeneity | Given the shape of the network and the limited number of pairwise comparisons with multiple studies, statistical heterogeneity was assessed by evaluating the posterior distribution for the between-study standard deviation (tau) output under the Bayesian approach, which according to the authors was in alignment with the NICE DSU Technical Support Document 2.56 A tau value of 0 can be interpreted as no evidence of heterogeneity and that the homogeneity assumption holds.57 Given the small number of studies, metaregression to address statistical heterogeneity was not feasible. |
Outcomes | PFS, OS, TTNT (antileukemic), and undetectable MRD |
Follow-up time points | Median follow-up ranged from ████ ██ ████ ███████ |
Rescaling of results | Median HRs were presented on the log scale, with FLU + CYC + RIT chosen as the reference treatment based on Canadian and ESMO treatment guidelines6,58 for fit patients without del(17p) and TP53 mutations. |
Construction of nodes | Each treatment was a node in the NMA. |
Sensitivity analyses | Base case: This comprised fit and unfit patients without del(17p) or TP53 mutations (and whose blood sampling showed undetectable MRD). Due to the limited evidence for solely fit patients, an NMA excluding all studies with unfit patients was not feasible. The following sensitivity analyses were performed to explore the impact of heterogeneity observed in the trials:
|
Subgroup analysis | Subgroup analysis was conducted according to age based on a cut-off of 65 years ███ ██████ ██ █████ ███ ███ ██████ ████████ ████ ██ █████ ███ ███████ ███████████ ██ ██ █████████████ ██ ███ ████████████████████. |
Methods for pairwise meta-analysis | Not reported. |
BEN = bendamustine; CIRS = Cumulative Illness Rating Scale; CYC = cyclophosphamide; del(17p) = 17p deletion; DIC = deviance information criterion; DSU = Decision Support Unit; ESMO = European Society for Medical Oncology; FLU = fludarabine; HR = hazard ratio; ITT = intention to treat; MCMC = Markov Chain Monte Carlo; MRD = minimal residual disease; NICE = National Institute for Health and Care Excellence; NMA = network meta-analysis; OBI = obinutuzumab; OR = odds ratio; OS = overall survival; PFS = progression-free survival; Ȓ = Rhat; RIT = rituximab; TTNT = time to next treatment; VEN = venetoclax.
Sources: Indirect Treatment Comparison (ITC) for venetoclax plus obinutuzumab in untreated patients with chronic lymphocytic leukemia (CLL) (sponsor’s report)15 and Sponsor Summary of Clinical Evidence.2
Results
Summary of Included Studies
The evidence informing the NMA was based on the ████████ ████ literature search. A █████ ██ ███ ████████████ ███ ████████ ████████ ███ ██████████ █████████ ██ ████ ███ ███ █████████ ████████ ██ ███ ██████████ ███████ ██ █████ ███ ████████████ ████████ ██ ██ ██████ ████ ███ ███ ████████████ █████████ ████████ ██ ██████████████ ███████ ██████ ████████ ██████ ███ █████████████ ████████.
After applying the more restrictive inclusion criteria used for the NMA, a █████ ██ █ ██████ ████████ ██████ ████ ████████ ██ ███ ███████████ ███████████ ██████ ██████ ██████ ███████████ ████████ █████ █████████ ██████ ███ ████. The authors of the NMA indicated that the ████ █████ ███ ████████ ████ ███ ████████ ███ ██ ███████ █████████ ██ ████████ ██ ████ ██████████ █████████ ████ █████████ ██ ███ ████ ██ ███ ██████ ███████ ██████ ███ █████████████ ███ ████████ ██ ███ ████ ███ ███████ ██████ ████ ███ █████████ ██ ████ ████ ████████ ███████ ███ ███████████ ████ ███ ████████ ███ ███ ████.
All studies were open-label, phase III, multinational RCTs (██████ ███ █████ █████ ███ █████████ ██ ███ ██████ ███████ ████) with a median follow-up ranging from ████ ██ ████ ███████ ███████ ████████ ███████████████ ████████ ████ ████ ███ █████████ ███ ███████ ██ █████ ████████ ████ ███ ████ ████ █████████
Sources of heterogeneity identified by the authors are presented in Table 19. The authors concluded █████ █████████████ ███ ████████ ██ ██████████ ████████████ ████████ ████ ███ █████████ █████ █ ██████ ████████ ████ █████ ██ ██████ █████ ████████ █████████ ██ ████████ █████ ██ █████ ██████████ ██████████ ███ ████ ███ ██ ███ ███████ ████████ ███ ██████ ███ █████████ ██ ███ █████████ ████ ██ ███ ██████████ ██ ███████ ███████ ████ █████ ████████ ████ ███ ████.
The authors also concluded major heterogeneity was observed in the mutational status of patients for del(17p) and TP53 — ██████ ████████ ████████ ████ █ ██████ ████ ████████ ████████ ███████████████ █ █████ ████████ ████████ ████ ████████ ████████ ██ ███████ ████ ███ ██ ███ ██████ ███ ████ ████████ ██ ███ █████████ █ ██████ ███ ████████ ██████████████ ██████ ███████ ███ ██████████ ██ ████████ ████ ███████████████████ ████ ███ ██ ████. The NMA base case excluded patients with del(17p) and TP53 mutation to align with the CLL13 study population.
███ ███████ ████ █████████ █████ █████████████ ███ ████████ ██ ████ ███████████ ███████ █████ ████████ ███ ████████ █████████ ████████ ██ ██████████ ████ ██████████ ██ ████ ██ ████████ █████████████ ███ ████████ ██ █████ ██████ ██████████████ ████████ ██ █████ █████████ ██████ █████████ ███ ███ █████████.
Notably, no risk of bias assessment was reported for the trials by the authors of the NMA.
Table 19: Assessment of Homogeneity for the Sponsor-Submitted NMA
Characteristics | Description and handling of potential effect modifiers |
|---|---|
Available comparators in included studies | CLL13 study (N = 458): VEN + OBI, FLU + CYC + RIT, and BEN + RIT ██████ █ █████ ████ █████████ █ █████ █████ ██████████████ █ █████ ████ █████████████ █ █████ ███ ██████████ █ █████ █████ ██████████████ █ █████ ███ ██████████ █ █████ ████ |
Disease | ███ ███████ ████████ ███████████████ ████████ ████ ████████████ ████ ████████ ████████ ████ ████ |
Age | ███ ███████ ██ ███ ███ █████████ █████ █████████████ ███ ████████ ██ ████████ ██████ ███ ██████████████████ ██ █████ ██ ██████ ██████ ███ █████ ███████ ███ ███ ██ ██████ ██ █████ ███ █████████████████████ ██ █████ █ |
Sex | ███ ███████ █████████ █████ █████████████ ███ ████████ ██ ███████████ ███████ ███ ██████████ ██ ████ ████████ ██████ ████ ███ ██ ███ ██ ████ ██ ███ ██ ███ ██ ██████ ███ ██ ███ ██ ██████ ███ ███ ██ ███ ██ ██████ |
Population fitness | ███ ███████ █████████ █████ █████████████ ███ ████████ ██ ██████████ ███████████████ ██████ ███ █████ ████████ ████ ███ ████████████████ ███████████ ████████ █████ ████████ ████████ ████ █████ ██ ██████ █████ ████████ █████████ ██ ████ ████ ██████ ███████████ ██ ███ ████████ ███████████████ █████ ██████ ██████ ████ ███████ ████ ████████ ██ ██████████ █████ ██ ██████████ ████ █████ ████ ████████ ██ █████ ██████ ███ ████████ █████ ██ ██████████ █████████████ ████ █████ ██████ ██████ ████ ████ ██████ ██ ███ ████ █████ ████ ████ ██ ████ ██████ ██ ███ ███ █████ ████ ██████ ████ ███ ███ ████████ ██ █████████████████ ██ █████████ ██████ ████████ ██ ███ █████████ ██ ███ ███████ ████████ ███ ██████ ███ █████████ ██ ███ ██████████ ██ ███████ █████ ████████ ████ ███ █████████ |
Mutational status | ███ ███████ █████████ █████ █████████████ ███ ████████ ██ ███ ████████ ██ ████████ █████████████████████ ██████ ███ ████ ████████ ████████ ████ ███████████████ ███ █████ ████ ████████ ████████ █████████████████████ ████████ ████████ ███████████ ██ █ ███ ██ ███ ██████████ ██████████ ██ ████████ ████ ████████ ██████ ████ ██ ██ ██ ██ ██████ ██████████ ███ █████████████ ██████████ ██ ████████ ███████████████ ██████ ████ ████ ██ █████ ██ ██████ ██████ ███████████ ████████ █████ ████████████ ███████ ███ ██████████ ██ ████████ ████ ██████████████████ ████ ███ ██ █████████████ ██ █████████ ██████ ████████ ██ ███ ██████████ ███ ████████ ████████ ████ ████████ ██████████████ █████ █████████ ██ █████████ ████ ███ █████ ███████████ |
ECOG PS | ███ ███████ █████████ █████ █████████████ ███ ████████ ██ ████ ███████████ ███████████ ████████ ██████████ ██ ████████ ████ █ █████ ██ █ ███ ████████ ██ █████ ████ ██ ████ ███ █████ ████ ██ ████████ ███████████ ███ ██████████ ██ ████████ ████ █ █████ ██ █ ██ █ ███ ███ ██ ████████ ██████████ ██ ████████ ████ █ █████ ██ █ ██ █ ██████ ███ ██ ██████ ███ ██ █████ ███ █████████ ███ ██ ██████ ██████ ███ █████ |
Binet stage | ███ ███████ █████████ █████ █████████████ ███ ████████ ██ █████ ████████████ ██████████ ██ ████████ ████ █████ █████ █ ███████ ██████ ████ ██ ██ ████ ██ ███ ██ ████████ |
Rai stage | The authors concluded that major heterogeneity was observed in Rai staging.
|
Serum beta2-microglobulin | The authors concluded moderate heterogeneity was observed in beta2-microglobulin. ███ ██████████ ██ ████████ ████ █████████ ██████ █████████████ ███ ███ ██ ███ ██ ██████ ████████ ██ ███ ██ ███ ██ ████████ ██ █████ ███████ |
Dosing of comparators | The authors concluded no heterogeneity was observed in VEN + OBI █████ ███ ██ █████ ████ ████████ ██ ████ ████ █ █████ █ █████████ ███████ ███ ████████ ████ █████████ ██████ ███████████ █████ ████ ███████ ███████ ████████ ████ █████ ███████████ ████████ ████████████ ███ ████████████ ██████ ██ ██ █████ ███████ ██ █████████████ ██ ██ ██████ █████ ███ ███████████████████████ ███ ████████████ ██ ███ ███████ ██ ████ █ ██ █ ███████ ███ ████████ █████████████ ██ ███ █████ █ ████ ██ ████ █████ ██ █████ ███ ██████████ ███████ █████████ █████ █████████████ ███ ████████ ███ █████████ █████████ ████████ ██ ████ ██ █████ ███ █ █████ ████████ ██ ██ ██████ ██ █████ ██████ ████████ █████ ████ ████ |
Definitions of end points | The authors reported consistent definitions for PFS, OS, and TTNT were found across trials. Undetectable MRD or negative MRD was defined as detecting < 1 tumour cell in 10,000 cells, which was consistent across trials. ██ ██████ ███ ███ ████ ████████ ██ ████████ ████ ████████ ████████ █████████ ██ ███ ███████ ████████ ██████████████ █████████ ████ ███ ██████████ ██ ████████ ████ ████████████ ███ ███ ████████ ██████ ██ ███████████ ██ ███████ █████████ ███████████ ███ ████████████ ████ ██████ █████████ ████ █████ ████████████ ██████ ██████ █████ ███ ██████ ███ ██████████ ██ ████████ ████ █████████████ ███████████ ███ ███████ ███ ████████████ ████ █████████ |
Outcome assessment | PFS and OS were primarily based on investigator assessment ██████ ███ ███████ █████ ███ ███ ████████ ██ ██ ███████████ ██████ ██████████ The assessment of TTNT was conducted by the investigators in all included trials. |
Follow-up time | Median follow-up ranged from ████ ██ ████ ██████. |
Study design and clinical trial setting | The authors concluded that minor differences were reported in study designs.
|
███ █ ██████████████ ██ █ ████████████ ████ █████████; BEN = bendamustine; CIRS = Cumulative Illness Rating Scale; CLL = chronic lymphocytic leukemia; CrCl = creatinine clearance; CYC = cyclophosphamide; ECOG PS = Eastern Cooperative Oncology Group Performance Status; FLU = fludarabine; ███ █ ████████████ █████████████████ ███ ██████████ ███ █ ██████████ MRD = minimal residual disease; NMA = network meta-analysis; ████ █ ████████████ ████ ████████████; OBI = obinutuzumab; OS = overall survival; PFS = progression-free survival; RCT = randomized controlled trial; SLL = small lymphocytic lymphoma; RIT = rituximab; TTNT = time to next (antileukemic) treatment; VEN = venetoclax; ████ █ ██████████ ████ ██████████ ████ █ ██████████ ████ █████████████ ████ █ █████████████
Note: Only comparators relevant to the NMA analysis conducted are listed in Table 19. Listed sample sizes are informed by relevant comparators only.
Sources: Indirect Treatment Comparison (ITC) for venetoclax plus obinutuzumab in untreated patients with chronic lymphocytic leukemia (CLL) (sponsor’s report)15 and Sponsor Summary of Clinical Evidence.2
Evidence Networks
Model Fit and Diagnostics
An inspection of statistics for model fit and diagnostics plots demonstrated that the fixed-effects and random-effects models with informative priors fit equally well. Monte Carlo standard error was no greater than 5% and the Gelman-Rubin Ȓ was less than 1.1, indicating convergence could be assumed successful for all parameters in both models across outcomes. The effective number of parameters was sometimes marginally smaller for the fixed-effects model.15
In consideration of the heterogeneity observed among the trials based on the feasibility assessment, the random-effects model with a half-normal informative prior (tau = 0.25) was preferred by the investigators for all analyses with a normal likelihood and identity link. For the binomial models, the model with the informative log-normal prior was preferred by the investigators. When fitting the random-effects model with informative priors, few divergent transitions were present and moderate heterogeneity was observed (tau > 0.1 and < 0.6).15
Evidence Network for PFS and OS
The networks of evidence for PFS and OS are presented in Figure 1. For the base-case analysis of PFS and OS, the ITT population from a total of ███████ ███████ ██████ ██████ ██████ ███████████ ████████ █████ ███ █████████ ███ █ ██████████ ██████████████ ██████████ ████ ███ ██████████ ████ █████████████ ██████████ ████ ██████████ ████████████ ████ █████████████ ███ ██████████████ ████ ████████ ██ ███ ███████ ██ ███ ███ █████ ████████ ███████ ████████ ███████████ ████████ ███ ████████ ████████ ████████ ████ ████████ ████████████████ ████ ████ ██████ █████ ███ ████████ ██ ████████.
Figure 1: Network of Evidence for Progression-Free Survival and Overall Survival [Redacted]

Sources: Indirect Treatment Comparison (ITC) for venetoclax plus obinutuzumab in untreated patients with chronic lymphocytic leukemia (CLL) (sponsor’s report)15 and Sponsor Summary of Clinical Evidence.2
Evidence Network for Time to Next Treatment
The networks of evidence for time to next treatment are presented in Figure 2. ███ ███ ████ ████ ████████ ██ ████ ██ ████ ██████████ ███ ███ ██████████ ████ █ █████ ██ █ ███████ ███████ ██████ ██████ █████ ███ █ ██████████ █████ ███ ██████████ ████ █████████████ ██████████ ████ ██████████ ███ ████████████ ████ █████████████ ████ ████████ ██ ███ ███████ ██ ███ ███ █████ ████████ ███████ ████████ ██████████ ████████ ███ ████████ ████████ ████████ ██████████████ ████ █████.
Figure 2: Network of Evidence for Time to Next Treatment [Redacted]

Sources: Indirect Treatment Comparison (ITC) for venetoclax plus obinutuzumab in untreated patients with chronic lymphocytic leukemia (CLL) (sponsor’s report)15 and Sponsor Summary of Clinical Evidence.2
Evidence Network for Undetectable MRD
The networks of evidence for time to next treatment are presented in Figure 3. ███ ███ ████ ████ ████████ ██ ████████████ ███ ████████ ██ █████ █████████ ███ ███ ██████████ ████ █ █████ ██ █ ███████ ███████ ██████ █████ ███ ██████ ███ █ ██████████ █████ ███ ██████████ ████ █████████████ ██████████ ████ ██████████ ████████████ ████ █████████████ ███ ██████████ ████ ████████ ██ ███ ███████ ██ ███ ███ █████ ████████ ███████ ████████ ██ ███████████ ████████ ███ ████████ ████████ ████████ █████████████ ████ ███████ ███ ███ █████ ██ █████ ████ █████████ ███ ███████████ ████ ██████ █████████ ████████ ███ █████ ███ ███████ ████████████ ████████ ████ ███ █████ ██ ███ ███████ ████ ███ ███ █████████ ██████ ███ ███████ ████████████ █████████ ██ ███ ████████ ████ ████████ ███ ████ ██ █████ ███ █████████ ██ █████████████ ████████ █████ ████████████ ████████████ █████████ ███████ ███ ███████
Efficacy Results
A summary of the NMA base-case results of pairwise treatment comparisons for PFS, OS, time to next treatment, and undetectable MRD is presented in Table 20.
Figure 3: Network of Evidence for Undetectable Minimal Residual Disease [Redacted]

Sources: Indirect Treatment Comparison (ITC) for venetoclax plus obinutuzumab in untreated patients with chronic lymphocytic leukemia (CLL) (sponsor’s report)15 and Sponsor Summary of Clinical Evidence.2
Progression-Free Survival
██████████ ████ ████████████ ███ ████████ ████ ███ ███ █ █████ ███ ████ ████ ██ █████ ███ ██ ███ █ █████ ███ ████ ████ ██ ██████ ██ █████████ ███ ████████ ███████ ██████████ ████ ████████████ ███ █████████████ ███ █ █████ ███ ████ ████ ██ ██████ █████████ ███ █ █████ ███ ████ ████ ██ ██████ ████████████ ███ █ █████ ███ ████ ████ ██ ██████ ███ ██████████ ████ █████████ ███ █ █████ ███ ████ ████ ██ ██████████ ███████████ ████████ ██ ███ ████████ ███ ████████ ████████████ ██ ███ ███ ████ █████ ████ ███████ ████████ █████████████ ███ █████ ████████ ████ █ ██ █████ ██ ████ █████ █ ███ █████ ███████ ███ ██████████ ██. Table 21 ███ ███████ ███ ███ ██████████ ██ ██████████ ████ ████████████ ██████ ████ ███ ██████████████ ███ █████████ ████ ██████████ ████ ███ ███████ ████ ███ ████ █████ █████ ██ █████████ ███ ████████ ███████ ██████████ ████ ████████████ ███ █████████████ ███ █████████ ██ ███ ██████ ████████ ███ ████████████ ████ ███ ████ ████ ███████ ███ █ █████ ███ ████ ████ ██ ██████ ██ ████████ ██ ███ ████ ████ ████████ ██████████ ████ █████████ ███ ████████ ████ ██████████ ████ ████████████ ███ █ █████ ███ ████ ████ ██ ██████████ ███ ████████ ████████ ███████ ███ ███ █████████ ██ ████████ ████ ██ █████ ███ ███████ ████ ████ ██ ██████ ███ ████████████ ████████████████ ████████; a summary of the results is presented in Table 26 in Appendix 1.
Table 20: NMA Efficacy Results of Pairwise Treatment Comparisons for PFS, OS, TTNT, and uMRD (Base Case)
Detail | PFS | OS | TTNT | uMRD |
|---|---|---|---|---|
VEN + OBI vs. comparator | VEN + OBI vs. comparator | |||
Number of studies, N | ██ ██ ███ | ██ ██ ███ | ██ ██ | ██ ██ ███ |
Sample size of treatment group, range | ██ ██ ███ | ██ ██ ███ | ██ ██ | ██ ██ ███ |
Model | RE | RE | RE | RE |
██ ██ ███ | ██ ██ ███ | ██ ██ ███ | ██ ██ | ██ ██ ███ |
██ ██ ███ | ██ ██ ███ | ██ ██ ███ | ██ ██ | ██ ██ ███ |
██ ██ ███ | ██ ██ ███ | ██ ██ ███ | ██ ██ | ██ ██ ███ |
██ ██ ███ | ██ ██ ███ | ██ ██ ███ | ██ ██ | ██ ██ ███ |
██ ██ ███ | ██ ██ ███ | ██ ██ ███ | ██ ██ | ██ ██ ███ |
██ ██ ███ | ██ ██ ███ | ██ ██ ███ | ██ ██ | ██ ██ ███ |
███ █ ██████████████ ██ █ ████████████ ███ █████████; CrI = credible interval; ███ █ ████████████ █████████████████ ███ ██████████ ███ █ █████████; HR = hazard ratio; NA = not applicable; NMA = network meta-analysis; OBI = obinutuzumab; OR = odds ratio; OS = overall survival; PFS = progression-free survival; RE = random effects; TTNT = time to next treatment ████ █ ██████████ ████ ██████████ ████ █ ██████████ ████ ████████████; uMRD = undetectable minimal residual disease; VEN = venetoclax; vs. = versus; ████ █ █████████████
Note: The data in Table 20 presents the pairwise HRs and ORs for posterior medians. HR values below 1 are in favour of VEN + OBI while HR values above 1 are in favour of the reference treatment. OR values above 1 are in favour of VEN + OBI while OR values below 1 are in favour of the reference treatment. Statistically significant results are shaded in grey and indicated in bold text.
Source: Indirect Treatment Comparison (ITC) for venetoclax plus obinutuzumab in untreated patients with chronic lymphocytic leukemia (CLL) (sponsor’s report).15
Table 21: NMA Sensitivity Analysis Results for PFS (Fitness Approximation by Age or CIRS Score)
Detail | PFS |
|---|---|
VEN + OBI vs. comparator | |
Number of studies, N | 8 |
Sample size of treatment group, range | 24 to 282 |
Model | RE |
███ | ████ █████ ██ █████ |
███ | ████ █████ ██ █████ |
██ | ████ █████ ██ █████ |
███ | ████ █████ ██ █████ |
████ | ████ █████ ██ █████ |
████ | ████ █████ ██ █████ |
███ █ ██████████████ ██ █ ████████████ ███ ██████████ CIRS = Cumulative Illness Rating Scale; CrI = credible interval; del(17p) = 17p deletion; HR = hazard ratio; ███ █ ████████████ █████████████████ ███ ███████████ █ ██████████ NMA = network meta-analysis; OBI = obinutuzumab; OR = odds ratio; PFS = progression-free survival; RE = random-effects; VEN = venetoclax; vs. = versus; ████ █ ██████████ ████ ██████████ ████ █ ██████████ ████ █████████████ ████ █ █████████████
Notes: Due to the limited evidence for solely fit patients, an NMA excluding all studies with unfit patients was not feasible. A sensitivity analysis was performed to explore the impact of heterogeneity observed in the trials: fitness approximation by age and CIRS score (fit without del[17p] and TP53 mutations [excluded where possible] and unfit patients aged ≤ 65 years or with a CIRS score of ≤ 6). This was only available for PFS.
The data in Table 21 presents the pairwise HRs and ORs for posterior medians. HR values below 1 are in favour of VEN + OBI while HR values above 1 are in favour of the reference treatment. OR values above 1 are in favour of VEN + OBI while OR values below 1 are in favour of the reference treatment. Statistically significant results are shaded in grey and indicated in bold text.
Source: Indirect Treatment Comparison (ITC) for venetoclax plus obinutuzumab in untreated patients with chronic lymphocytic leukemia (CLL) (sponsor’s report).15
Overall Survival
██ █████████ ███ ████████ █████ ██ ███████████ ███████ ██████████ ████ ████████████ ███ ███ ████████████ ███ ███ █ █████ ███ ████ ████ ██ ██████ ██ ███ █ █████ ███ ████ ████ ██ ██████ █████████████ ███ █ █████ ███ ████ ████ ██ ██████ █████████ ███ █ █████ ███ ████ ████ ██ ██████ ████████████ ███ █ █████ ███ ████ ████ ██ ██████ ███ ██████████ ████ █████████ ███ █ █████ ███ ████ ████ ██ ██████.
Time to Next Treatment
Venetoclax plus obinutuzumab was favoured over ███ ███ █ █████ ███ ████ ████ ██ █████ ███ ██ ███ █ █████ ███ ████ ████ ██ ██████ ██ █████████ ███ ████████ ███████ ██████████ ████ ████████████ ███ ██████████ ████ █████████ ███ █ █████ ███ ████ ████ ██ ██████.
Undetectable MRD
Venetoclax plus obinutuzumab was favoured ███████ ████████████ ███ ███ █ █████ ███ ████ ████ ██ ██████ ██ ███ █ ██████ ███ ████ ████ ██ ███████ █████████ ███ █ ████████ ███ ████ ██████ ██ ██████████ ███ ██████████ ████ █████████ ███ █ █████ ███ ████ ████ ██ ███████.
Critical Appraisal
The systematic literature review was conducted using standard methods, a defined research question was specified a priori, multiple databases were searched with the last literature search conducted in ████████ ████, and at least 2 independent reviewers were involved in study selection and data extraction. The authors of the systematic literature review performed a quality assessment of the included studies using the checklist presented in the NICE single technology assessment manufacturer submission template for RCTs. Several categories in the checklist for each of the trials included in the NMA were rated as unclear or not reported; however, the implications of these ratings were not discussed.
Studies included in the NMA were selected from those identified by the systematic literature review. A narrowed set of criteria for the inclusion of studies for the NMA were provided and are consistent with the objective, including further restricting the eligible interventions to those that are relevant to Canadian practice for first-line treatment of CLL in the population of interest based on the CLL13 trial population. ███ █████████ ███ ████████████ ████ ████████████ ███ █████ █████████ █████ ███ ████████ ██ ███ ███ ██ ██████ ██████████ ██ ███ ████ ███████ ████████ ████████ ████ ████████ ████████ ████████ ████ █████████████ ███ ███ ████ █████ ███ ██████ ███ ██████ ████ ███ █████████
While the base-case analysis of the mixed fit and unfit network was not according to protocol, the clinical experts had no concern with generalizing the NMA results that were based on the broader population to the fit population, regardless of del(17p) or TP53 mutation, as there are fewer concerns with comorbidities in the fit population. Nonetheless, it is important to note the differences in population fitness across the network that would represent a potential source of bias in the network. ████████ █ ██████ ████████ ████ ███ █████████ █████ █ ██████ ████████ ████ █████ ██ ██████ █████ ████████ █████████ ██ ████████ █████ ██ █████ █████ ███ ████ █████ █████████ █████ ██ ███████████ ██ ███ ███ ████████ ███ ██████ ████ █████ ████ ███ ██████████ █████ █████████ █████████████ ████ ██ ███████ ████████████ ██████ ████████████ ███ ████████████ ██ ████████ ████ ██ █████ ███ ██████ ██ █████ ████ ██ █████ ███ ███████ ████ ██ █████ ████ █████████████ █████ ██ ██ ██ ██ ██████ ████ ███ ██████████ █████ █ ███ ████ █████████ ████ ███ ████████ ██████ █████ █████████ █████████ ██████ █████████ ████ █████████ ███ ██ ██ ████████ ████ ██ █████ ███ ██████ ███ ███ ███████ ██████ █████ ████████ ████████████ ██████ ██ ██ ████████ ████ ██ █████ ███ █████ ██ ███████████████. These differences in eligibility criteria (i.e., fitness approximation) might have contributed to the difference observed in the direction of the results for the comparisons with the BTK inhibitors, suggesting fitness is an effect modifier and as such, raises concerns for comparing the studies included in the NMA.
Heterogeneity in patient baseline characteristics was reported by the authors of the NMA as part of their feasibility assessment. Differences in age, clinical staging, ECOG PS scores, and beta2-microglobulin levels across studies included in the NMA were reported by the authors; however, these are identified in the literature as prognostic markers in CLL and SLL.25,32 Based on literature, del(17p) and TP53 mutation are predictive of worse clinical outcomes after treatment with chemoimmunotherapy, compared with targeted therapies, and IGHV mutation is associated with prolonged durable remission after chemoimmunotherapy treatment, which was not observed in patients with IGHV-unmutated CLL or SLL;25 the clinical experts were in agreement. The base case excluded patients with del(17p) and TP53 mutation to align with the CLL13 trial population; however, these patients were included in the analyses of PFS, OS, time to next treatment, and undetectable MRD where it was not possible for the investigators to exclude them. Therefore, differences in these treatment effect modifiers across the network would introduce bias in the NMA results.
Heterogeneity in study methodology was also reported by the authors of the NMA as part of their feasibility assessment. Across the included studies, the median follow-up ranged from ████ ██ ████ ██████. The clinical experts advised that a median follow-up of ██ ██████ is likely too short to evaluate treatment effect; the exception is upfront toxicities as CLL is not expected to progress until later. In contrast, a median follow-up of ██ ██████ is likely appropriate for assessing the treatment effect of time-limited therapies. The clinical experts further advised that a longer follow-up is likely advantageous for continuous therapies (i.e., the potential for biased results favouring BTK inhibitors with a long follow-up) as disease progression is expected to occur later with chronic therapy. ████████ ███ █████████ ████████ ██ ██████████ ████ █████████ ██ █████ ███ █ █████ ████████ ██ ██ ██████ ██ ████. Differential follow-up can also lead to bias when specifically comparing time-to-event outcomes such as PFS and OS since estimated HRs often wane with increased lengths of follow-up. Overall, these sources of clinical and methodological heterogeneity likely introduced bias in the results of the NMA.
A Bayesian NMA was conducted that, according to the authors, was consistent with the NICE Decision Support Unit Technical Support Document 2.51 No major concerns with the statistical methods used were identified by the review team. Both fixed-effects and random-effects models as well as uninformative and informative priors were considered. Model selection was based on goodness-of-fit using DIC — the random-effects model with informative priors was selected based on the DIC and was preferred by the investigators due to expected heterogeneity identified in the feasibility assessment. Notably, no sensitivity analysis was performed to assess the sensitivity of model results to the informative priors used in the random-effects model. Further, assessment of consistency was not reported.
Notably, the networks were sparse. The base case and the sensitivity analyses ████████ █ ██ █ ███████ which likely introduced uncertainty about the results. Due to the small number of studies included in the NMA, the authors deemed it was infeasible to account for heterogeneity using metaregression. Although a sensitivity analysis was conducted to explore the impact of heterogeneity in fitness observed in the trials, it should be noted that fitness was approximated by age (≤ 65 years) or CIRS score (≤ 6) in the unfit patients (instead of by CIRS score and CrCl), patients with del(17p) and/or TP53 mutation were excluded only where possible, and results were only available for PFS. As such, it was concluded that the results from this particular sensitivity analysis would not reduce the concern for the potential for biased results due to the presence of unfit patients in the network for the primary analysis.
Discussion
Summary of Available Evidence
The CLL13 study is an ongoing, phase III, multicentre, randomized, prospective, open-label clinical trial (N = 926). The primary objective of the study is to assess the efficacy of venetoclax plus obinutuzumab versus standard chemoimmunotherapy (BEN + RIT or FLU + CYC + RIT) on the negativity rate of MRD in peripheral blood at month 15, and venetoclax plus obinutuzumab plus ibrutinib versus standard chemoimmunotherapy on PFS at predefined analysis time points in fit patients (defined in the trial by a CIRS score of ≤ 6 and CrCl of ≥ 70 mL per minute) with previously untreated CLL and without del(17p) or TP53 mutation. Eligible patients were randomized in a 1:1:1:1 ratio to receive chemoimmunotherapy, venetoclax plus obinutuzumab, venetoclax plus obinutuzumab plus ibrutinib, and venetoclax plus rituximab. Randomization was stratified by Binet stage, age (with a cut-off of 65 years), and region study group. In the chemoimmunotherapy group, patients aged 65 years and younger received FLU + CYC + RIT while patients aged older than 65 years received BEN + RIT. The median age of patients was 62 years (range, 31 years to 83 years) in the venetoclax plus obinutuzumab group and 61 years (range, 29 years to 84 years) in the chemoimmunotherapy group. All patients in both groups had a CIRS score of 6 or less. The median CrCl was 86.3 mL per minute (range, 41.5 mL per minute to 180.2 mL per minute) in the venetoclax plus obinutuzumab group and 86.3 mL per minute (range, 39.5 mL per minute to 223.6 mL per minute) in the chemoimmunotherapy group. The distribution of patients by Rai staging was generally well balanced between groups, with most patients presenting with Rai stage I to stage IV. The median ECOG PS score was 0 (range, 0 to 2) in both groups. No patient in either group had del(17p) and all patients in both groups had unmutated TP53. The distribution of patients by IGHV mutation status was generally well balanced between groups, with most patients presenting with unmutated IGHV (approximately 57% of patients in each group). The median duration of follow-up in the full study population at the interim analysis (including safety), based on a data cut-off date of January 20, 2022, was 38.8 months (IQR, 32.7 months to 46.1 months). The median duration of follow-up in the full study population at the 4-year follow-up analysis, based on a data cut-off date of January 31, 2023, was 50.7 months (IQR, 44.6 months to 57.9 months).
The objective of the sponsor-submitted NMA was to estimate the comparative effectiveness of venetoclax plus obinutuzumab versus relevant comparators in the treatment of patients who are fit, with previously untreated CLL, and without del(17p) or TP53 mutation, in terms of PFS, OS, time to next treatment, and undetectable MRD. Indirect comparisons of venetoclax plus obinutuzumab, venetoclax plus ibrutinib, FLU + CYC + RIT, BEN + RIT, obinutuzumab plus chlorambucil, acalabrutinib, zanubrutinib, and ibrutinib were made using a Bayesian NMA with Hamiltonian Monte Carlo, a Markov Chain Monte Carlo method. The population of interest is adult patients aged 18 years and older who are fit (defined by a CIRS score of ≤ 6 and CrCl of ≥ 70 mL per minute), with previously untreated CLL and without del(17p) or TP53 mutations. According to the authors, ██ ███ ████ ████████ ███ ███████ ████ █████ ████████ ███ ███ ████████ ███ ██ ███ ███████ ████████ ███ ██████ ███ █████████. Hence, the base case included both fit and unfit patients without del(17p) or TP53 mutations (and whose blood sampling showed undetectable MRD).
Interpretation of Results
Patients with CLL and the clinical experts consulted by CDA-AMC emphasized the importance of having additional treatment options available to better align with patient values, needs, and lifestyle, particularly for fit patients. When considering novel CLL therapies, patients identified the following factors that are considered in their decision-making: a longer period of survival, longer remission, control of disease symptoms, improved HRQoL, and fewer side effects. The clinical experts advised that disease progression does not always indicate treatment (i.e., this might return to a watchful waiting phase) — hence, the importance of duration of response and time to next treatment in decision-making in the frontline treatment setting.
The clinician groups and clinical experts identified 2 subsets of patients with CLL who have an unmet need for a treatment option that is not combined with chemotherapy and/or a BTK inhibitor and who would benefit from targeted therapy (and thereby avoid the risk of bone marrow toxicities associated with FLU + CYC + RIT): young and fit patients with lower-risk disease (i.e., with mutated IGHV and no TP53 aberrations as per guidelines6) and long life expectancy, and young and fit patients with high-risk genomic features (i.e., unmutated IGHV and TP53 aberrations). However, the available evidence from the CLL13 trial and the sponsor-submitted NMA excluded patients with high cytogenetic risk, specifically del(17p) and TP53 mutation. Despite the lack of evidence for this subset of patients, the clinical experts had no concern with generalizing the findings to patients with TP53 aberrations in practice; the clinical experts suggested referring to the relevant evidence in the CLL14 trial.18
Efficacy
At the primary data cut-off, the CLL13 study demonstrated that 6 cycles of treatment with venetoclax plus obinutuzumab followed by 6 additional cycles of venetoclax alone (each cycle with a duration of 28 days) result in an improvement in PFS, based on the estimated PFS rates at 4 years, when compared with chemoimmunotherapy (6 cycles of FLU + CYC + RIT or BEN + RIT). This benefit was consistently demonstrated at the updated data cut-off date. Additionally, results from the CLL13 study are suggestive of an improvement with venetoclax plus obinutuzumab in the duration of response and time to next treatment, based on the estimated event-free survival rates at 4 years, when compared with chemoimmunotherapy. This finding was also consistently demonstrated at the updated data cut-off date for time to next treatment. In the absence of literature on the minimal important differences in these event-free survival rates in patients with previously untreated CLL, the clinical experts suggested that these results are clinically meaningful in the context of CLL being an incurable disease and that relapse is expected with time-limited therapies.
In consultation with the clinical experts, it was concluded that the results for OS are difficult to interpret as patients received second-line (salvage) therapy, which is appropriate from an ethics perspective. Regarding first documented subsequent treatment, the clinical experts indicated that a BTK inhibitor (or venetoclax plus rituximab as a time-limited option) is a reasonable second-line therapy. Of note, triplet and quadruplet therapies are not available in Canada unless through clinical trials. The clinical experts advised that it is important to acknowledge re-treatment with venetoclax plus obinutuzumab due to the evolving landscape, especially in patients with disease who had a durable response.
At the primary and updated data cut-off dates, the median PFS (for the venetoclax plus obinutuzumab group only), duration of response, time to next treatment, and OS were not reached. Therefore, the magnitude of benefit with venetoclax plus obinutuzumab based on those time-to-event end points is currently unknown. Notably, the potential for bias in favour of venetoclax plus obinutuzumab due to patients with unmutated IGHV receiving chemoimmunotherapy should be considered when interpreting the results for survival outcomes and, in particular, for PFS.
The CLL13 study also demonstrated that treatment with venetoclax plus obinutuzumab results in an improvement in the rates of undetectable MRD in peripheral blood, measured by the proportion of patients with negative MRD status at month 15, when compared with chemoimmunotherapy. Additionally, the results from the CLL13 study are suggestive of an improvement with venetoclax plus obinutuzumab in the rates of treatment response, based on the proportion of patients with CR at month 15, when compared with chemoimmunotherapy. Notably, the potential for bias likely in favour of venetoclax plus obinutuzumab due to the imbalance observed in missing data between groups and the handling of missing data in the primary efficacy analysis of undetectable MRD should be considered when interpreting the results. Further, it is important to acknowledge that patients in the venetoclax plus obinutuzumab group received treatment that was twice as long as that of patients in the chemoimmunotherapy group (12 cycles versus 6 cycles). In consultation with the clinical experts, it was concluded that there is a concern for possible disease progression between the time at which treatment with chemoimmunotherapy is completed and the assessment time point at month 15 (i.e., > 3 months post-treatment compared with the venetoclax plus obinutuzumab group). Hence, the clinical experts suggested extrapolating the benefit of venetoclax plus obinutuzumab observed in the CLL14 trial18 where chemoimmunotherapy (chlorambucil plus obinutuzumab) was also administered for 12 cycles, each cycle with a duration of 28 days, in unfit patients (defined in the trial by a CIRS score of > 6 or CrCl of < 70 mL per minute) with previously untreated CLL.
While the effect estimates are suggestive of a favourable treatment effect with venetoclax plus obinutuzumab compared with █████████ ███ ████████████ ██ ███ ███ ████████ ████ █████████ ██ █████ ██ ████████████ ███ ██ ██████████ █████, there is uncertainty in the NMA results as the 95% CrI included the null and due to the wide 95% CrI, respectively. While exploring areas of uncertainty in the NMA results, the review team noted that ██ ████████ ██ ███ █████████ █████ ████ ███ █████ █████ ███ ████████████ ███, which might have contributed to the wide CrI. While the effect estimate is suggestive of a favourable treatment effect with █████████████ ████████ ████ ██████████ ████ ████████████ ██ ████ there is uncertainty in the NMA results as the 95% CrI included the null. As concluded for the CLL13 trial results, OS results are difficult to interpret as patients received second-line antileukemic therapy. Further, the authors of the NMA noted that there was a small number of OS events across included studies.
While the effect estimates are suggestive of a favourable treatment effect with ██████████ ████ █████████ ████████ ████ ██████████ ████ ████████████ on PFS and time to next treatment, there is uncertainty in the NMA results as the 95% CrI included the null. In contrast, the NMA results showed a favourable treatment effect with venetoclax plus obinutuzumab ████████ ████ ██████████ ████ █████████ on undetectable MRD in peripheral blood.
In consultation with the clinical experts, it was concluded that differences observed in the potential effect modifiers is primarily the result of including studies with a chemoimmunotherapy group in the NMA. Differences in age, fitness, and mutational status across studies are to enable the administration of the FLU + CYC + RIT, BEN + RIT, and obinutuzumab plus chlorambucil groups. A difference in the ECOG PS score across studies was expected because each study used a threshold to limit heterogeneity in the trial; moreover, the clinical experts advised that dose adjustments could be made accordingly. A difference in serum beta2-microglobulin level across studies was also expected as it reflects renal function that can fluctuate. As well, a difference in staging across studies was expected as it reflects 1 of the many factors that go into consideration for the initiation of therapy.
Nonetheless, it is important to consider the sources of clinical and methodological heterogeneity across studies included in the NMA — namely, the inclusion of fit and unfit patients, differences in the patient population according to TP53 aberrations and IGHV mutation status, and differential follow-up times — which likely introduced bias into the NMA results. Notably, ██████ ████████ ████ ███ █████████ █████ █ ██████ ████████ ████ █████ ██ ██████ █████ ████████ █████████ ██ ████████ █████ ██ █████ █████ ███ ████ █████ █████████ █████ ██ ███████████ ██ ███ ███ ████████ ███ ██████ ████ █████ ████ ███ ██████████ █████ █████████ █████████████ ████ ██ ███████ ████████████ ██████ ████████████ ███ ████████████ ██ ████████ ████ ██ █████ ███ ██████ ██ █████ ████ ██ █████ ███ ███████ ████ ██ █████ ████ █████████████ █████ ██ ██ ██ ██ ██████ ████ ███ ██████████ █████ █ ███ ████ █████████ ████ ███ ████████ ██████ █████ █████████ █████████ ██████ █████████ ████ █████████ ███ ██ ██ ████████ ████ ██ █████ ███ ██████ ███ ███ ███████ ██████ █████ ████████ ████████████ ██████ ██ ██ ████████ ████ ██ █████ ███ █████ ██ ███████████████ . These differences in eligibility criteria (i.e., fitness approximation) might have contributed to the difference observed in the direction of the results for the comparisons with the BTK inhibitors, suggesting fitness is an effect modifier and as such, raises concerns for comparing the studies included in the NMA. Additionally, the networks were sparse as the base case and the sensitivity analyses included ██ █ ███████, thereby introducing uncertainty about the results. Further, it was concluded that the sensitivity analysis results that approximated fitness by age or CIRS score would not reduce the concern about the potential for biased results due to the presence of unfit patients in the network for the primary analysis.
HRQoL was identified as an outcome of importance in the patient and clinician group input as well as in input from the clinical experts. Although HRQoL was measured by the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 (EORTC QLQ-C30) and by European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Chronic Lymphocytic Leukaemia 16 (EORTC QLQ-CLL16) in the CLL13 study, results were unavailable at the time of sponsor submission. No HRQoL end point was evaluated in the NMA; therefore, no conclusions on HRQoL can be drawn on the indirect comparison of venetoclax plus obinutuzumab versus other relevant comparators.
Harms
The proportions of patients with at least 1 TEAE of any CTC grade were similar between venetoclax plus obinutuzumab and chemoimmunotherapy. Although the proportion of patients with infusion-related reactions was numerically greater in the venetoclax plus obinutuzumab group compared with the chemoimmunotherapy group, this is aligned with clinical expert expectations as the AE is known to be associated with obinutuzumab administration. The proportions of patients with at least 1 serious TEAE of any CTC grade were similar between groups. The proportion of patients who discontinued their treatment early due to any TEAE was numerically less in the venetoclax plus obinutuzumab group compared with the chemoimmunotherapy group. Results for CTC grade 5 AEs are difficult to interpret due to the small number of events reported in both groups.
In consultation with the clinical experts, it was concluded that febrile neutropenia, serious infections, hematological malignancies (as second primary malignancies), and cardiac-specific TEAEs (specifically, sudden cardiac deaths and ventricular arrhythmias) are important considerations in treatment decisions. Reports of febrile neutropenia were numerically less in the venetoclax plus obinutuzumab group compared with the chemoimmunotherapy group. Reports of serious infections and infestations were similar between groups. Results for cardiac-specific TEAEs, reported as cardiac arrest and arrhythmia, are difficult to interpret due to the small number of events reported in both groups.
Regarding second primary malignancies, results for hematological malignancies at both the interim analysis and 4-year follow-up, including myelodysplastic syndrome, and Richter syndrome at the 4-year follow-up are difficult to interpret due to the small number of events reported in both groups. The clinical experts advised that the monitoring of second primary malignancies following treatment is lifelong as it can present at any time in untreated and treated patients, with a greater risk in patients receiving chemoimmunotherapy or radiotherapy. The clinical experts also advised that Richter syndrome is unpredictable and not often associated with therapy — it can be pre-existing before therapy, due to progression of disease despite therapy, or a consequence of therapy.
No safety end point was evaluated in the NMA; therefore, no conclusions on safety can be drawn on the indirect comparison of venetoclax plus obinutuzumab versus other relevant comparators.
Conclusion
One phase III, multicentre, randomized, prospective, open-label clinical trial (the CLL13 study) was submitted for this reassessment to support the expansion of the reimbursement criteria for venetoclax plus obinutuzumab to include patients with previously untreated CLL who are considered fit and potentially fludarabine-eligible. At the primary data cut-off date, the CLL13 study demonstrated that venetoclax plus obinutuzumab results in an improvement in PFS, based on the estimated PFS rates at 4 years, when compared with FLU + CYC + RIT and BEN + RIT (chemoimmunotherapy). The results are also suggestive of an improvement with venetoclax plus obinutuzumab in duration of response and time to next treatment, based on the estimated event-free survival rates at 4 years, when compared with chemoimmunotherapy. The benefit for PFS and time to next treatment was also consistently demonstrated at the updated data cut-off dates. In the absence of literature on the minimal important differences in these event-free survival rates in the target population, the clinical experts consulted by CDA-AMC suggested that these results are clinically meaningful in the context of CLL being an incurable disease and relapse is expected with time-limited therapies. The results for OS are difficult to interpret due to patients receiving second-line therapy. Notably, the potential for bias in favour of venetoclax plus obinutuzumab due to patients with unmutated IGHV receiving chemoimmunotherapy should be considered when interpreting the results for survival outcomes. The CLL13 study also demonstrated that treatment with venetoclax plus obinutuzumab results in an improvement in the rates of undetectable MRD in peripheral blood, measured by the proportion of patients with negative MRD status at month 15 (a coprimary end point), when compared with chemoimmunotherapy. Notably, the potential for bias due to the imbalance observed in missing data between groups and the handling of missing data in the primary efficacy analysis of undetectable MRD should be considered when interpreting the results. HRQoL was identified as an outcome of importance to patients and clinicians; however, relevant results were unavailable at the time of sponsor submission. At the primary data cut-off date, no major concern was identified in the safety profile of venetoclax plus obinutuzumab, although it was difficult to interpret for CTC grade 5 AEs, cardiac-specific TEAEs, and second primary malignancies due to the small number of events.
The NMA results showed a favourable treatment effect with venetoclax plus obinutuzumab compared ████ ██████████ ████ █████████ on undetectable MRD in peripheral blood. For all other indirect comparisons assessed in the NMA, there was uncertainty in the results primarily due to the 95% CrI including the null and the small number of studies included. Additionally, heterogeneity identified in population fitness and mutational status and the differential follow-up times likely introduced bias in the NMA results. No safety end point was evaluated in the NMA; therefore, no conclusions on safety can be drawn on the indirect comparison of venetoclax plus obinutuzumab versus other relevant comparators.
References
1.Venclexta (venetoclax): tablets, 10 mg, 50 mg and 100 mg, oral [product monograph]. St-Laurent (QC): AbbVie Corporation; 2022.
2.Sponsor Summary of Clinical Evidence [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Venclexta (venetcolax), in combination with obinutuzumab. Saint-Laurent (QC): AbbVie Corporation; 2023.
3.Rai KR, Stilgenbauer S, Aster JC. Clinical features and diagnosis of chronic lymphocytic leukemia/small lymphocytic lymphoma. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2024: http://www.uptodate.com. Accessed 2024 July 8.
4.Canadian Cancer Society. Chronic lymphocytic leukemia. 2024; https://www.cancer.ca/en/cancer-information/cancer-type/leukemia-chronic-lymphocytic-cll/statistics/?region=on. Accessed 2024 July 02.
5.Schnaiter A, Stilgenbauer S. 17p deletion in chronic lymphocytic leukemia: risk stratification and therapeutic approach. Hematol Oncol Clin North Am. 2013;27(2):289-301. PubMed
6.Owen C, Banerji V, Johnson N, et al. Canadian evidence-based guideline for frontline treatment of chronic lymphocytic leukemia: 2022 update. Leuk Res. 2023;125:107016. PubMed
7.Owen C, Gerrie AS, Banerji V, et al. Canadian evidence-based guideline for the first-line treatment of chronic lymphocytic leukemia. Curr Oncol. 2018;25(5):e461-e474. PubMed
8.CADTH pCODR Expert Review Committee final recommendation: venetoclax (Venclexta - AbbVie Corporation). Ottawa (ON): CADTH; 2020 Nov 17: https://www.cadth.ca/sites/default/files/pcodr/Reviews2020/10212VenetoclaxObinutuzumabCLL_fnRec_EC_Post17Nov2020_final.pdf. Accessed 2024 July 25.
9.Furstenau M, Kater AP, Robrecht S, et al. First-line venetoclax combinations versus chemoimmunotherapy in fit patients with chronic lymphocytic leukaemia (GAIA/CLL13): 4-year follow-up from a multicentre, open-label, randomised, phase 3 trial. Lancet Oncol. 2024;25(6):744-759. PubMed
10.Trial protocol: CLL13. A phase 3 multicenter, randomized, prospective, open-label trial of standard chemoimmunotherapy (FCR/BR) versus rituximab plus venetoclax (RVe) versus obinutuzumab (GA101) plus venetoclax (GVe) versus obinutuzumab plus ibrutinib plus venetoclax (GIVe) in fit patients with perveiously untreated chronic lymphocytic leukemia (CLL) without del(17p) or TP53 mutation [internal sponsor's report]. Cologne (DE): Deutsche CLL Studiengruppe; 2021.
11.Eichhorst B, Niemann CU, Kater AP, et al. First-Line Venetoclax Combinations in Chronic Lymphocytic Leukemia. N Engl J Med. 2023;388(19):1739-1754. PubMed
12.Giza A, Robrecht S, Zahng C. Interim analysis of the co-primary endpoint progression-free survival: CLL13 (GAIA). A phase 3 multicenter, randomized, prospective, open-label trial of standard chemoimmunotherapy (FCR/BR) versus rituximab plus venetoclax (RVe) versus obinutuzumab (GA101) plus venetoclax (GVe) versus obinutuzumab plus ibrutinib plus venetoclax (GIVe) in fit patients with perveiously untreated chronic lymphocytic leukemia (CLL) without del(17p) or TP53 mutation. Data cut-off January 20, 2022 [internal sponsor's report]. Cologne (DE): Deutsche CLL Studiengruppe; 2022.
13.Braun G, Giza A, Robrecht S, Zahng C. Co-Primary Endpoint Analysis of MRD negativity rate at month 15: CLL13 (GAIA). A phase 3 multicenter, randomized, prospective, open-label trial of standard chemoimmunotherapy (FCR/BR) versus rituximab plus venetoclax (RVe) versus obinutuzumab (GA101) plus venetoclax (GVe) versus obinutuzumab plus ibrutinib plus venetoclax (GIVe) in fit patients with perveiously untreated chronic lymphocytic leukemia (CLL) without del(17p) or TP53 mutation. Data cut-off February 28, 2021 [internal sponsor's report]. Cologne (DE): Deutsche CLL Studiengruppe; 2022.
14.Böttcher S, Ritgen M, Fischer K, et al. Minimal residual disease quantification is an independent predictor of progression-free and overall survival in chronic lymphocytic leukemia: a multivariate analysis from the randomized GCLLSG CLL8 trial. J Clin Oncol. 2012;30(9):980-988. PubMed
15.Indirect Treatment Comparison (ITC) for venetoclax plus obinutuzumab in untreated patients with chronic lymphocytic leukemia (CLL) - Report [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Venetoclax plus obinutuzumab. St-Laurent (QC): AbbVie; 2024 April 26.
16.Systematic Literature Review of Clinical Evidence for Previously Untreated Chronic Lymphocytic Leukaemia [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Venetoclax plus obinutuzumab. St-Laurent (QC): AbbVie; 2024 May 17.
17.Eichhorst B, Fink AM, Bahlo J, et al. First-line chemoimmunotherapy with bendamustine and rituximab versus fludarabine, cyclophosphamide, and rituximab in patients with advanced chronic lymphocytic leukaemia (CLL10): an international, open-label, randomised, phase 3, non-inferiority trial. Lancet Oncol. 2016;17(7):928-942. PubMed
18.Fischer K, Al-Sawaf O, Bahlo J, et al. Venetoclax and Obinutuzumab in Patients with CLL and Coexisting Conditions. N Engl J Med. 2019;380(23):2225-2236. PubMed
19.Woyach JA, Ruppert AS, Heerema NA, et al. Ibrutinib Regimens versus Chemoimmunotherapy in Older Patients with Untreated CLL. N Engl J Med. 2018;379(26):2517-2528. PubMed
20.Tam CS, Brown JR, Kahl BS, et al. Zanubrutinib versus bendamustine and rituximab in untreated chronic lymphocytic leukaemia and small lymphocytic lymphoma (SEQUOIA): a randomised, controlled, phase 3 trial. Lancet Oncol. 2022;23(8):1031-1043. PubMed
21.Kater AP, Owen C, Moreno C, et al. Fixed-Duration Ibrutinib-Venetoclax in Patients with Chronic Lymphocytic Leukemia and Comorbidities. NEJM Evid. 2022;1(7):EVIDoa2200006.
22.Sharman JP, Egyed M, Jurczak W, et al. Acalabrutinib with or without obinutuzumab versus chlorambucil and obinutuzmab for treatment-naive chronic lymphocytic leukaemia (ELEVATE TN): a randomised, controlled, phase 3 trial. Lancet. 2020;395(10232):1278-1291. PubMed
23.Munir T, Cairns DA, Bloor A, et al. Chronic Lymphocytic Leukemia Therapy Guided by Measurable Residual Disease. N Engl J Med. 2024;390(4):326-337. PubMed
24.Quinquenel A, Letestu R, Le Garff-Tavernier M, et al. Preliminary Results of the Filo Phase 2 Trial for Untreated Fit Patients with Intermediate Risk Chronic Lymphocytic Leukemia Comparing Ibrutinib Plus Venetoclax (IV) Versus FCR: Results of the Month 15 MRD Evaluation. Blood. 2022;140(Supplement 1):7007-7009.
25.Rai KR, Stilgenbauer S. Staging and prognosis of chronic lymphocytic leukemia. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2023: http://www.uptodate.com. Accessed 2024 July 8.
26.Kutsch N, Busch R, Bahlo J, et al. FCR front-line therapy and quality of life in patients with chronic lymphocytic leukemia. Leuk Lymphoma. 2017;58(2):399-407. PubMed
27.Holtzer-Goor KM, Schaafsma MR, Joosten P, et al. Quality of life of patients with chronic lymphocytic leukaemia in the Netherlands: results of a longitudinal multicentre study. Qual Life Res. 2015;24(12):2895-2906. PubMed
28.van den Broek EC, Oerlemans S, Nijziel MR, Posthuma EF, Coebergh JW, van de Poll-Franse LV. Impact of active surveillance, chlorambucil, and other therapy on health-related quality of life in patients with CLL/SLL in the Netherlands. Ann Hematol. 2015;94(1):45-56. PubMed
29.Kosmas CE, Shingler SL, Samanta K, et al. Health state utilities for chronic lymphocytic leukemia: importance of prolonging progression-free survival. Leuk Lymphoma. 2015;56(5):1320-1326. PubMed
30.Abrisqueta P, Pereira A, Rozman C, et al. Improving survival in patients with chronic lymphocytic leukemia (1980-2008): the Hospital Clinic of Barcelona experience. Blood. 2009;114(10):2044-2050. PubMed
31.Parikh SA, Rabe KG, Kay NE, et al. Chronic lymphocytic leukemia in young (≤ 55 years) patients: a comprehensive analysis of prognostic factors and outcomes. Haematologica. 2014;99(1):140-147. PubMed
32.Oscier D, Dearden C, Eren E, et al. Guidelines on the diagnosis, investigation and management of chronic lymphocytic leukaemia. Br J Haematol. 2012;159(5):541-564. PubMed
33.Hallek M, Cheson BD, Catovsky D, et al. Guidelines for the diagnosis and treatment of chronic lymphocytic leukemia: a report from the International Workshop on Chronic Lymphocytic Leukemia updating the National Cancer Institute-Working Group 1996 guidelines. Blood. 2008;111(12):5446-5456. PubMed
34.Thompson PA, Bazinet A, Wierda WG, et al. Sustained remissions in CLL after frontline FCR treatment with very-long-term follow-up. Blood. 2023;142(21):1784-1788. PubMed
35.pan-Canadian Pharmeutical Alliance. Imbruvica (ibrutinib). 2024; https://www.pcpacanada.ca/negotiation/22489. Accessed 2024 Jul 8.
36.CADTH Drug Reimbursement Expert Review Committee final recommendation: Ibrutinib (Imbruvica - Janssen Inc.). Can J Health Technol. 2023;3(11). https://www.cadth.ca/sites/default/files/DRR/2023/PC0317REC-Imbruvica-Final-Recommendation-meta.pdf. Accessed 2024 July 25.
37.Venclexta (venetoclax): tablets, 10 mg, 50 mg and 100 mg, oral [product monograph; sponsor-supplied reference]. St-Laurent (QC): AbbVie Corporation; 2022: https://pdf.hres.ca/dpd_pm/00065382.PDF. Accessed 2024 Jul 25.
38.Cancer Care Ontario. Drug Formulary 2023; https://www.cancercareontario.ca/en/cancer-treatments/chemotherapy/drug-formulary. Accessed 2024 July 02.
39.BC Cancer. 2023; http://www.bccancer.bc.ca/. Accessed 2024 Jul 02.
40.Calquence (acalabrutinib): capsules, 100 mg, oral [product monograph; sponsor-supplied reference]. Mississauga (ON): AstraZeneca Canada, Inc; 2019: https://pdf.hres.ca/dpd_pm/00054129.PDF. Accessed 2024 Jul 25.
41.Brukinsa (zanubrutinib): capsules, 80 mg, oral [product monograph; sponsor-supplied reference]. Basel (CH): BeiGene Switzerland Gmb, H.; 2021: https://pdf.hres.ca/dpd_pm/00062218.PDF. Accessed 2024 Jul 25.
42.Gazyva (obinutuzumab for injection): 25 mg/mL concentrate for solution for infusion [product monograph; sponsor-supplied reference]. Mississauga (ON): Hoffmann-La Roche, Limited; 2022: https://assets.roche.com/f/173850/x/0c07cb9986/gazyva_pm_e.pdf. Accessed 2024 Jul 25.
43.Imbruvica (ibrutinib): capsules, 140 mg [product monograph; sponsor-supplied reference]. Toronto (ON): Janssen, Inc; 2018: https://pdf.hres.ca/dpd_pm/00046525.PDF. Accessed 2024 Jul 25.
44.Fludarabine phosphate: injection, 25 mg/mL [product monograph; sponsor-supplied reference]. Montreal (QC): Omega Laboratories, Ltd; 2013: https://pdf.hres.ca/dpd_pm/00022717.PDF. Accessed 2024 Jul 25.
45.Statistical Analysis Plan - Primary Endpoints Analysis: CLL13. A phase 3 multicenter, randomized, prospective, open-label trial of standard chemoimmunotherapy (FCR/BR) versus rituximab plus venetoclax (RVe) versus obinutuzumab (GA101) plus venetoclax (GVe) versus obinutuzumab plus ibrutinib plus venetoclax (GIVe) in fit patients with perveiously untreated chronic lymphocytic leukemia (CLL) without del(17p) or TP53 mutation [internal sponsor's report]. Cologne (DE): Deutsche CLL Studiengruppe; 2021.
46.Statistical Analysis Plan - PFS Interim Analysis 2022: CLL13. A phase 3 multicenter, randomized, prospective, open-label trial of standard chemoimmunotherapy (FCR/BR) versus rituximab plus venetoclax (RVe) versus obinutuzumab (GA101) plus venetoclax (GVe) versus obinutuzumab plus ibrutinib plus venetoclax (GIVe) in fit patients with perveiously untreated chronic lymphocytic leukemia (CLL) without del(17p) or TP53 mutation [internal sponsor's report]. Cologne (DE): Deutsche CLL Studiengruppe; 2022.
47.Lehmacher W, Kieser M, Hothorn L. Sequential and Multiple Testing for Dose-Response Analysis. Drug Inf J. 2000;34(2):591-597.
48.Medical Dictionary for Regulatory Activities (MedDRA). Standardised MedDRA Queries (SMQs). [date unknown]: https://www.meddra.org/how-to-use/tools/smqs. Accessed 2024 Jul 25.
49.CRD’s guidance for undertaking reviews in health care. York (GB): Centre for Reviews and Dissemination, University of York; 2008: https://www.york.ac.uk/media/crd/Systematic_Reviews.pdf. Accessed 2024 Aug 6.
50.National Institute for Health and Care Excellence. Appendix F Quality appraisal checklist – quantitative intervention studies [sponsor-supplied reference]. 2012; https://www.nice.org.uk/process/pmg4/chapter/appendix-f-quality-appraisal-checklist-quantitative-intervention-studies.
51.Dias N, Welton N, Sutton A, Ades A. NICE DSU Technical Support Document 2: A generalised linear modelling framework for pairwise and network meta-analysis of randomised controlled trials [sponsor-supplied reference]. Sheffield (GB): NICE Decision Support Unit; 2014: https://www.ncbi.nlm.nih.gov/books/NBK310366/pdf/Bookshelf_NBK310366.pdf.
52.Stan Development Team. Stan Modeling Language Users Guide and Reference Manual. [date unknown]; https://mc-stan.org.
53.Phillippo DM, Dias S, Ades AE, et al. Multilevel network meta-regression for population-adjusted treatment comparisons. J R Stat Soc Ser A Stat Soc. 2020;183(3):1189-1210. PubMed
54.Städler N, Shang A, Bosch F, et al. A Systematic Review and Network Meta-Analysis to Evaluate the Comparative Efficacy of Interventions for Unfit Patients with Chronic Lymphocytic Leukemia. Adv Ther. 2016;33(10):1814-1830. PubMed
55.Turner RM, Davey J, Clarke MJ, Thompson SG, Higgins JP. Predicting the extent of heterogeneity in meta-analysis, using empirical data from the Cochrane Database of Systematic Reviews. Int J Epidemiol. 2012;41(3):818-827. PubMed
56.Dias N, Welton N, Sutton A, Ades A. NICE DSU technical support document 2: a generalised linear modelling framework for pairwise and network meta-analysis of randomised controlled trials. Sheffield (GB): Decision Support Unit, ScHARR, University of Sheffield; 2011: https://www.sheffield.ac.uk/sites/default/files/2022-02/TSD2-General-meta-analysis-corrected-2Sep2016v2.pdf. Accessed 2024 Aug 6.
57.Ren S, Oakley JE, Stevens JW. Incorporating Genuine Prior Information about Between-Study Heterogeneity in Random Effects Pairwise and Network Meta-analyses. Med Decis Making. 2018;38(4):531-542. PubMed
58.Eichhorst B, Robak T, Montserrat E, et al. Chronic lymphocytic leukaemia: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2015;26 Suppl 5:v78-84. PubMed
59.Giza A, Ligtvoet R, Robrecht S. Priority 1 analyses for AbbVie: CLL13 (GAIA). v1.0 (Data cut-off January 31, 2023) [internal sponsor's report]. Cologne (DE): Deutsche CLL Studiengruppe; 2024.
Appendix 1: Detailed Outcome Data
Please note that this appendix has not been copy-edited.
Table 22: Analysis of PFS From the CLL13 Study, Stratification by Chemoimmunotherapy, per Data Cut-Off at January 31, 2023 (ITT Population)
Outcome | VEN + OBI (N = 229) | Chemoimmunotherapy | |
|---|---|---|---|
FLU + CYC + RIT (N = 150) | BEN + RIT (N = 79) | ||
Follow-up time (months) for all patients, median (IQR) | 50.7 (44.6 to 57.9) | ||
Events, n (%) | 55 (24.0) | 47 (31.3) | 43 (54.4) |
PFS (months), median (95% CI) | Not reached | 61.5 (NE) | 45.5 (34.1 to 56.9) |
HR for VEN + OBI vs. CIT (95% CI) | — | █████ █ | █████ |
Log-rank P value (descriptive) | — | █████ | █████ |
PFS rate at month 12, % | 97.4 | 93.3 | 93.7 |
PFS rate at month 24, % | 92.5 | 87.2 | 74.4 |
PFS rate at month 36, % | 88.5 | 84.2 | 61.6 |
PFS rate at month 48, % | 81.8 | 69.8 | 48.9 |
BEN = bendamustine; CI = confidence interval; CIT = chemoimmunotherapy; CYC = cyclophosphamide; FLU = fludarabine; IQR = interquartile range; NE = not evaluable; OBI = obinutuzumab; PFS = progression-free survival; RIT = rituximab; VEN = venetoclax; vs. = versus.
Sources: Priority 1 analyses for AbbVie Corporation: CLL13 (GAIA) (data cut-off date of January 31, 2023)59 and Sponsor Summary of Clinical Evidence.2
Table 23: Analysis of PFS From the CLL13 Study, Stratification by Age, per Data Cut-Off at January 31, 2023 (ITT Population)
Outcome | VEN + OBI (≤ 65 years) (N = 147) | FLU + CYC + RIT (N = 150) |
|---|---|---|
Follow-up time (months) for all patients, median (IQR) | 50.7 (44.6 to 57.9) | |
Events, n (%) | ██ ██████ | 47 (31.3) |
PFS (months), median (95% CI) | ████ ████ | 61.5 (NE) |
HR (95% CI) | █████ ██████ ██ ██████ | |
Log-rank P value (descriptive) | █████ | |
PFS rate at month 12, % | ████ | 93.3 |
PFS rate at month 24, % | ████ | 87.2 |
PFS rate at month 36, % | ████ | 84.2 |
PFS rate at month 48, % | ████ | 69.8 |
CI = confidence interval; CYC = cyclophosphamide; FLU = fludarabine; IQR = interquartile range; NE = not evaluable; OBI = obinutuzumab; PFS = progression-free survival; RIT = rituximab; VEN = venetoclax.
Sources: Priority 1 analyses for AbbVie Corporation: CLL13 (GAIA) (data cut-off date of January 31, 2023)59 and Sponsor Summary of Clinical Evidence.2
Table 24: Analysis of TTNT From the CLL13 Study, Stratification by Chemoimmunotherapy, per Data Cut-Off at January 31, 2023 (ITT Population)
Outcome | VEN + OBI (N = 229) | Chemoimmunotherapy | |
|---|---|---|---|
FLU + CYC + RIT (N = 150) | BEN + RIT (N = 79) | ||
Follow-up time (months) for all patients, median (IQR) | 50.7 (44.6 to 57.9) | ||
Events, n (%) | 23 (10.0) | 33 (22.0) | 21 (26.6) |
TTNT (months), median (95% CI) | Not reached | Not reached | Not reached |
HR for VEN + OBI vs. CIT (95% CI) | — | █████ █████ | █████ ████ |
Log-rank P value (descriptive) | — | █████ | █████ |
Event-free survival rate at month 12, % | 98.7 | 97.0 | 98.7 |
Event-free survival rate at month 24, % | 97.8 | 92.5 | 94.8 |
Event-free survival rate at month 36, % | 94.6 | 88.7 | 84.1 |
Event-free survival rate at month 48, % | 90.4 | 78.7 | 74.4 |
BEN = bendamustine; CI = confidence interval; CIT = chemoimmunotherapy; CYC = cyclophosphamide; FLU = fludarabine; IQR = interquartile range; NE = not evaluable; OBI = obinutuzumab; RIT = rituximab; TTNT = time to next treatment; VEN = venetoclax; vs. = versus.
Source: Priority 1 analyses for AbbVie Corporation: CLL13 (GAIA) (data cut-off date of January 31, 2023).59
Table 25: Analysis of TTNT From the CLL13 Study, Stratification by Age, per Data Cut-Off at January 31, 2023 (ITT Population)
Outcome | VEN + OBI (≤ 65 years) (N = 147) | FLU + CYC + RIT (N = 150) |
|---|---|---|
Follow-up time (months) for all patients, median (IQR) | 50.7 (44.6 to 57.9) | |
Events, n (%) | ██ ██████ | 33 (22.0) |
TTNT (months), median (95% CI) | ███ ███████ | Not reached |
HR (95% CI) | █████ ██████ ██ ██████ | |
Log-rank P value (descriptive) | █████ | |
Event-free survival rate at month 12, % | ████ | 97.0 |
Event-free survival rate at month 24, % | ████ | 92.5 |
Event-free survival rate at month 36, % | ████ | 88.7 |
Event-free survival rate at month 48, % | ████ | 78.7 |
CI = confidence interval; CYC = cyclophosphamide; FLU = fludarabine; IQR = interquartile range; NE = not evaluable; OBI = obinutuzumab; RIT = rituximab; TTNT = time to next treatment; VEN = venetoclax.
Source: Priority 1 analyses for AbbVie Corporation: CLL13 (GAIA) (data cut-off date of January 31, 2023).59
Table 26: Network Meta-Analysis Subgroup Analysis Results for PFS (Patients Aged 65 Years and Younger) [Redacted]
█████████████████████ | ███████████████ |
|---|---|
██████ ██ ████████ | ██ ██ ███ |
██████ ████ ██ █████████ ██████ █████ | ██ ██ ███ |
█████ | ██ |
████ ███ ███████████ ██ ████ ████ | |
███ | ████ █████ ██ █████ |
███ | ████ █████ ██ █████ |
██ | ████ █████ ██ █████ |
████ | ████ █████ ██ █████ |
████ | ████ █████ ██ █████ |
ACA = acalabrutinib; BR = bendamustine and rituximab; CrI = credible interval; FCR = fludarabine, cyclophosphamide, and rituximab; IBRU = ibrutinib; NA = not applicable; NMA = network meta-analysis; OBI = obinutuzumab; OR = odds ratio; PFS = progression-free survival; RE = random-effects; VEN = venetoclax; ZANU = zanubrutinib.
Note: The data in Table 26 presents the pairwise hazard ratios for posterior medians. HR values below 1 are in favour of VEN + OBI while HR values above 1 are in favour of the reference treatment. OR values above 1 are in favour of VEN + OBI while OR values below 1 are in favour of the reference treatment. Statistically significant results are shaded in grey and indicated in bold text.
Source: Indirect Treatment Comparison (ITC) for venetoclax plus obinutuzumab in untreated patients with chronic lymphocytic leukemia (CLL) (sponsor’s report).15
Pharmacoeconomic Review
Abbreviations
1L
first line
2L
second line
AE
adverse event
BIA
budget impact analysis
BEN + RIT
bendamustine plus rituximab
BSA
body surface area
BTKi
Bruton tyrosine kinase inhibitor
CDA-AMC
Canada’s Drug Agency
CLL
chronic lymphocytic leukemia
CUA
cost-utility analysis
del(17p)
17p deletion
FLU + CYC + RIT
fludarabine plus cyclophosphamide plus rituximab
HR
hazard ratio
ICER
incremental cost-effectiveness ratio
ITT
intention to treat
KM
Kaplan-Meier
LY
life-year
NIHB
Non-Insured Health Benefits
NMA
network meta-analysis
ODB
Ontario Drug Benefit
OS
overall survival
PFS
progression-free survival
QALY
quality-adjusted life-year
TLS
tumour lysis syndrome
ToT
time on treatment
TTNT
time to next treatment
VEN + IBRU
venetoclax plus ibrutinib
VEN + OBI
venetoclax plus obinutuzumab
WTP
willingness to pay
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Venetoclax (Venclexta), 10 mg, 50 mg, and 100 mg oral tablets |
Indication | Venetoclax, in combination with obinutuzumab, is indicated for the treatment of patients with previously untreated CLL. |
Health Canada approval status | NOC |
Health Canada review pathway | Standard |
NOC date | April 28, 2020 |
Reimbursement request | As per indication. Clarifying note from the sponsor: For the subgroup of previously untreated patients with CLL considered fit and potentially fludarabine-eligible, and who were not included in the reimbursement request and recommendation criteria in the previous CADTH review Note that based on this request, the reimbursement criteria would be expanded for the treatment of patients with previously untreated CLL, aligned with the indication (i.e., irrespective of age or eligibility for fludarabine treatment). |
Sponsor | AbbVie Corporation |
Submission history | Previously reviewed: Yes, venetoclax (Venclexta) has been reviewed for AML and CLL by CADTH as per the following details. In combination with azacitidine for the treatment of patients with newly diagnosed AML who are 75 years or older, or who have comorbidities that preclude use of intensive induction chemotherapy Recommendation date: August 20, 2021 Recommendation: Reimburse with clinical criteria and/or conditions In combination with low-dose cytarabine for the treatment of patients with newly diagnosed AML who are 75 years or older, or who have comorbidities that preclude use of intensive induction chemotherapy Recommendation date: August 23, 2021 Recommendation: Do not reimburse In combination with obinutuzumab for the treatment of adult patients with previously untreated CLL who are fludarabine-ineligible Recommendation date: November 17, 2020 Recommendation: Reimburse with clinical criteria and/or conditions In combination with rituximab for the treatment of adult patients with CLL who have received at least 1 prior therapy Recommendation date: May 31, 2019 Recommendation: Reimburse with clinical criteria and/or conditions As monotherapy for the treatment of patients with CLL who have received at least 1 prior therapy and who did not experience improvement with a BCRi Recommendation date: March 2, 2018 Recommendation: Reimburse with clinical criteria and/or conditions |
AML = acute myeloid leukemia; BCRi = B-cell receptor inhibitor; CLL = chronic lymphocytic leukemia; NOC = Notice of Compliance.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis PSM |
Target population | Previously untreated patients with CLL, including those who are FLU-eligible (i.e., ≤ 65 years who received FLU + CYC + RIT in the CLL13 trial) and those who are FLU-ineligible (i.e., > 65 years who received BEN + RIT in the CLL13 trial) |
Treatments | VEN + OBI |
Dosage regimen | The recommended dose of VEN is 400 mg daily. This dose is achieved according to a weekly ramp-up schedule over a period of 5 weeks: 20 mg daily during week 1, 50 mg daily during week 2, 100 mg daily during week 3, 200 mg daily during week 4, and 400 mg daily during week 5. VEN is started on day 22 of the first cycle and should be given for six 28-day cycles in combination with OBI, followed by 6 months of VEN as monotherapy. The recommended dose for OBI is 1,000 mg on day 1, day 8, and day 15 of the first 28-day cycle, followed by 1,000 mg on day 1 of the 5 subsequent cycles (a total of 6 cycles, 28 days each). |
Submitted price | VEN: $7.08 per 10 mg oral tablet VEN: $35.40 per 50 mg oral tablet VEN: $70.80 per 100 mg oral tablet |
Submitted treatment cost | $17,354 in cycle 1, $9,469 in cycle 2, $13,681 in cycle 3 to cycle 6, and $7,930 in cycle 7 to cycle 12a |
Comparators |
|
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs, LYs |
Time horizon | Lifetime (40 years) |
Key data source |
|
Submitted results |
|
Key limitations |
|
CDA-AMC reanalysis results |
|
2L = second line; BEN = bendamustine; BTKi = Bruton tyrosine kinase inhibitor; CDA-AMC = Canada’s Drug Agency; CLL = chronic lymphocytic leukemia; CrI = credible interval; CYC = cyclophosphamide; FLU = fludarabine; IBRU = ibrutinib; ICER = incremental cost-effectiveness ratio; LY = life-year; NMA = network meta-analysis; OBI = obinutuzumab; OS = overall survival; PFS = progression-free survival; PSM = partitioned survival model; QALY = quality-adjusted life-year; RIT = rituximab; TTNT = time to next treatment; VEN = venetoclax; vs. = versus; WTP = willingness to pay.
aSubmitted treatment cost with the price of OBI corrected from $5,477.84 to $5,751.73 per 1,000 mg vial.
Conclusions
The new evidence in the CLL13 trial was submitted to support the expansion of the reimbursement criteria to include patients with previously untreated chronic lymphocytic leukemia (CLL) who are considered fit and potentially fludarabine-eligible, and who were not included in the reimbursement request and recommendation criteria in the previous submission. Based on the clinical review by Canada’s Drug Agency (CDA-AMC), the CLL13 trial demonstrated that venetoclax plus obinutuzumab (VEN + OBI) results in an improvement in progression-free survival (PFS) and may provide an improvement in time to next treatment (TTNT), relative to fludarabine plus cyclophosphamide plus rituximab (FLU + CYC + RIT) and bendamustine plus rituximab (BEN + RIT). Results for overall survival (OS) were difficult to interpret as patients received second-line (2L) salvage therapy. Notably, the potential for bias in favour of VEN + OBI due to patients with unmutated immunoglobin heavy-chain variable (IGHV) receiving chemotherapy should be considered when interpreting the results for survival outcomes. The magnitude of benefit with VEN + OBI based on time-to-event end points in the CLL13 study is currently unknown as the median PFS (for the VEN + OBI group only), TTNT, and OS were not reached at the updated data cut-off date of January 31, 2023.
The comparative clinical efficacy of VEN + OBI, venetoclax plus ibrutinib (VEN + IBRU), and Bruton tyrosine kinase inhibitor (BTKi)–based therapies (acalabrutinib, ibrutinib, and zanubrutinib) is uncertain due to the lack of head-to-head evidence and limitations with the sponsor's network meta-analysis (NMA). The CDA-AMC clinical review noted uncertainty associated with the NMA results due to 95% credible intervals including the null and heterogeneity in population fitness and mutational status. This clinical uncertainty is propagated in the submitted economic analysis given that the sponsor extrapolated OS, PFS, and TTNT for the lifetime horizon of the model using parametric distributions fitted to clinical data from the CLL13 study. Moreover, since the sponsor’s NMA included both fit and unfit patients, while the CLL13 trial included only fit patients (used to model efficacy for BEN + RIT, FLU + CYC + RIT, and VEN + OBI), incorporating the sponsor’s NMA results into the economic model introduces an efficacy bias favouring VEN + OBI, BEN + RIT, and FLU + CYC + RIT over VEN + IBRU and BTKi-based therapies.
In the CDA-AMC base case, FLU + CYC + RIT is among the optimal treatments (on the cost-effectiveness frontier). As such, VEN + OBI is compared to FLU + CYC + RIT in sequential analyses and is associated with an incremental cost-effectiveness ratio (ICER) of $167,257 per quality-adjusted life-year (QALY) gained (incremental QALYs = 0.49; incremental costs = $82,007). The estimated ICER is driven by higher total costs for VEN + OBI and the adoption of more plausible assumptions about the prolonged benefit of VEN + OBI in delaying TTNT. Additionally, the CDA-AMC base case estimated higher total QALYs for FLU + CYC + RIT and BEN + RIT based on more plausible extrapolations of PFS and OS for these treatments. Based on the CDA-AMC base-case reanalysis, a 75% price reduction for venetoclax is required for VEN + OBI to be considered cost-effective relative to FLU + CYC + RIT at a willingness-to-pay (WTP) threshold of $50,000 per QALY gained. This would reduce the price of venetoclax from $7.08 to $1.77 (per 10 mg tablet), $35.40 to $8.85 (per 50 mg tablet), and $70.80 to $17.70 (per 100 mg tablet). With this price reduction, the per-patient 28-day drug acquisition costs for VEN + OBI would be $17,280 for the first cycle and from $1,982 to $7,734 for each subsequent cycle.
The CDA-AMC base case relies on a sustained OS benefit for VEN + OBI, where patients receiving VEN + OBI gain 0.5 additional life-years (LYs) compared to those treated with FLU + CYC + RIT. In the absence of long-term clinical evidence, the extent of this survival benefit is highly uncertain. Should the long-term effectiveness of VEN + OBI be lower than predicted, the ICER would be higher than the CDA-AMC base case, requiring larger price reductions to achieve cost-effectiveness. Moreover, when comparing the duration of follow-up in the CLL13 trial to the model’s time horizon (67 months [approximately 5.5 years] versus 40 years), it is important to note that most of the QALY benefit and the entirety of the LY benefit predicted by the model for patients treated with VEN + OBI are accrued in the post-trial period of the model on the basis of extrapolation.
The cost-effectiveness of VEN + OBI is sensitive to assumptions concerning TTNT and subsequent therapy costs. When assuming a Weibull distribution for the TTNT extrapolation of VEN + OBI, the ICER for VEN + OBI decreased to $88,275 per QALY gained relative to FLU + CYC + RIT. However, this is dependent on the relative risk of TTNT between VEN + OBI and BEN + RIT or FLU + CYC + RIT remaining constant for 25 years, which is considered optimistic given the lack of evidence supporting a prolonged benefit of VEN + OBI in delaying TTNT. When excluding subsequent therapy costs, to capture the cost-effectiveness of VEN + OBI among the small subset of patients who may not go on to receive 2L therapy, VEN + OBI was extendedly dominated by a combination of FLU + CYC + RIT and VEN + IBRU.
Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, clinician groups, and drug plans that participated in the CDA-AMC review process.
Patient input was received from a joint submission by Lymphoma Canada and CLL Canada. Input provided was based on 2 surveys of patients with CLL, which included patients in Canada. Input commented that due to the nature of CLL, many patients undergo a period of watchful waiting before needing to start treatment and 20% to 30% of patients in “watch and wait” mode will not require treatment. Of the survey respondents who provided information on their CLL treatment, 30% had not received treatment, 38% had received 1 line of treatment, and 28% had completed 2 or more treatments. The majority of patients received ibrutinib in the first-line (1L) setting. Other treatment options that patients had experience within the 1L setting included VEN + IBRU, acalabrutinib, chlorambucil plus obinutuzumab plus venetoclax monotherapy, BEN + RIT, and venetoclax plus acalabrutinib. Fewer than half of respondents were satisfied with the management of their CLL symptoms. Treatment factors deemed important to patients were extended life expectancy, symptom control, longer remission, an improved quality of life, and fewer adverse events (AEs). Thirty-three patients with CLL or small lymphocytic lymphoma had experience with VEN + OBI. Two patients did not complete the full course of treatment due to AEs. More than half of patients with VEN + OBI experience noted that VEN + OBI managed all their symptoms. Approximately 20% of patients noted that the AEs associated with treatment with VEN + OBI had a “significant” or “very significant” impact on their quality of life.
Clinician group input was received from Lymphoma Canada and Ontario Health (Cancer Care Ontario) Hematology Cancer Drug Advisory Committee. Input indicated that current treatment options included VEN + OBI, VEN + IBRU, and indefinite BTKi monotherapy (ibrutinib, acalabrutinib, or zanubrutinib). Clinician input noted that FLU + CYC + RIT is used infrequently in Canada. Clinician input also commented that while no data currently exists to determine if VEN + OBI is better, worse, or equivalent to VEN + IBRU, some clinicians may favour VEN + OBI until longer-term data are available given that it is expected to reduce resistance to BTKis in the relapsed setting and decrease the risk of cardiac events associated with VEN + IBRU. Input indicated that all patients with CLL who require 1L therapy would benefit from treatment with VEN + OBI but suggested that the least suitable patients for VEN + OBI are patients with 17p deletion — or del(17p) in short — or TP53 mutation. Input noted that fixed-duration therapies should still be available to this subset of patients when such therapies are desired. Input additionally noted that the indication under review would allow patients with CLL to have equitable access to VEN + OBI, deferring indefinite BTKi-based therapy to the relapsed or refractory setting for most patients. Based on this, input from clinician groups highlighted the expectation that the budget impact of CLL therapy would decrease. This aligns with patient preferences for accessing frontline, fixed-duration, targeted therapy.
Drug plan input commented that relevant funded comparators include acalabrutinib, ibrutinib, zanubrutinib, fludarabine-based therapy, obinutuzumab plus chlorambucil, and other rituximab-based chemotherapy combinations (e.g., BEN + RIT, chlorambucil plus rituximab). Additionally, it was noted that VEN + IBRU is currently in negotiations with the pan-Canadian Pharmaceutical Alliance for the indicated population. Plan input highlighted that venetoclax (oral) and obinutuzumab (IV) will be reimbursed through different drug programs. It was also noted that venetoclax has the potential for drug-drug, drug-food, and drug-herb interactions.
Several of these concerns were addressed in the sponsor’s model:
PFS and OS were included in the model.
The impact of disease and treatment on a patient’s quality of life was captured with utility values. AEs were incorporated as disutilities within the analysis.
VEN + IBRU, BEN + RIT, FLU + CYC + RIT, and BTKi-based therapies were included as comparators in the cost-utility analysis (CUA).
CDA-AMC was unable to address the following concerns raised from input relevant to the economic review:
The reimbursement of venetoclax (oral) and obinutuzumab (IV) though different drug programs could not be reflected in the budget impact analysis (BIA).
Economic Review
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted a CUA assessing VEN + OBI compared with BEN + RIT, FLU + CYC + RIT, acalabrutinib, ibrutinib, zanubrutinib, and VEN + IBRU for previously untreated patients with CLL, aligned with the CLL13 clinical trial and the Health Canada–indicated population. The modelled population includes fit patients who are fludarabine-eligible (who received FLU + CYC + RIT in the CLL13 trial) and fit patients who are fludarabine-ineligible (who received BEN + RIT in the CLL13 trial). By including the subgroup of patients considered fit and potentially fludarabine-eligible, the current reimbursement request expands the reimbursement criteria of VEN + OBI to capture the full Health Canada indication of patients with previously untreated CLL (i.e., irrespective of eligibility for fludarabine treatment).1
Venetoclax is available as 10 mg, 50 mg, and 100 mg oral tablets at submitted prices of $7.08, $35.40, and $70.80 per oral tablet, respectively.1,2 The recommended dose of venetoclax is 400 mg daily.2 This dose is achieved according to a weekly ramp-up schedule over a period of 5 weeks: 20 mg daily during week 1, 50 mg daily during week 2, 100 mg daily during week 3, 200 mg daily during week 4, and 400 mg daily during week 5.2 Venetoclax is started on day 22 of the first cycle and should be given for six 28-day cycles in combination with obinutuzumab, followed by 6 months of venetoclax as a monotherapy.2 The recommended dose for obinutuzumab, available in 1,000 mg vials at a price of $5,477.84 as assumed by the sponsor, is 1,000 mg on day 1, day 8, and day 15 of the first 28-day cycle, followed by 1,000 mg on day 1 of the 5 subsequent cycles (a total of 6 cycles, 28 days each).1,2 Assuming no wastage, the sponsor estimated VEN + OBI drug acquisition costs as $16,533 in cycle 1, $9,195 in cycle 2, $13,407 in cycle 3 to cycle 6, and $7,930 in cycle 7 to cycle 12.1
The clinical outcomes modelled were OS, PFS, time on treatment (ToT), and TTNT. The model simulated LYs, QALYs, and costs for each treatment over a lifetime time horizon (40 years), discounted at a rate of 1.5% per annum. The analysis was undertaken from the perspective of the Canadian public health care payer.
Model Structure
The sponsor submitted a partitioned survival model with 3 health states: progression-free, postprogression, and dead, whereby transitions between health states occurred on a 28-day cycle length (Appendix 3, Figure 1).1 The proportion of patients in each health state was estimated over time based on the OS and PFS curves for each intervention. All patients entered the model in the progression-free health state, where they received either VEN + OBI, FLU + CYC + RIT, BEN + RIT, VEN + IBRU, acalabrutinib, ibrutinib, or zanubrutinib, with state occupancy defined by PFS. During each cycle, patients either remained progression-free, transitioned to the postprogression state, or progressed to death. The dead state was modelled as an absorbing state. The proportion of patients in the postprogression state was calculated by subtracting the proportion of patients alive and progression-free (based on the PFS curve) from the proportion of patients alive (based on the OS curve). Patients in the postprogression state could either remain in this state or transition to death (i.e., patients could not return to the progression-free state).
Model Inputs
Baseline patient characteristics in the model were reflective of the CLL13 trial’s intention-to-treat (ITT) population (N = 458). The average patient in the modelled cohort, which the sponsor assumed reflected the Canadian patient population, was aged 62 years, weighed ██ kg, had a mean body surface area (BSA) of ███ m2, and was more likely to be male (75%). These characteristics were used to inform the drug dosage regimens as well as the age- and sex-specific distribution of the general population mortality risk, which the sponsor used to cap the lower bound for all-cause mortality in the model.
Key clinical efficacy inputs, including OS, PFS, ToT, and TTNT, for VEN + OBI, FLU + CYC + RIT, and BEN + RIT were derived from digitized Kaplan-Meier (KM) data from the CLL13 clinical trial (with a data cut-off date of January 31, 2023). KM estimates of OS, PFS, ToT, and TTNT from the trial period were used to fit parametric survival curves to extrapolate the treatment effect beyond the observed trial data (median follow-up = 51 months; maximum follow-up = 67 months) over the entire model time horizon (40 years). Several parametric functions were fitted to the OS, PFS, ToT, and TTNT data to select candidate distributions based on diagnostic plots, goodness-of-fit statistics, visual inspection, and the clinical plausibility of long-term projections as determined by clinical experts in Canada. For the ITT population, the sponsor’s chosen parametric survival distributions of OS for VEN + OBI, FLU + CYC + RIT, and BEN + RIT were exponential, gamma, and log-normal, respectively. The sponsor’s chosen parametric survival distribution of PFS for VEN + OBI, FLU + CYC + RIT, and BEN + RIT were Weibull, generalized gamma, and log-logistic, respectively. As FLU + CYC + RIT and BEN + RIT are administered for 6 cycles and VEN + OBI is administered for 12 cycles, ToT was entirely informed by KM data from the CLL13 study and capped by their respective TTNT curves. The sponsor’s chosen parametric survival distribution of TTNT for VEN + OBI, FLU + CYC + RIT, and BEN + RIT was exponential, Weibull, and gamma, respectively. The efficacy of subsequent treatments is assumed to be implicitly captured by OS and PFS and as such, TTNT is assumed to only affect costing.
Efficacy inputs for VEN + IBRU and BTKi-based treatments (i.e., acalabrutinib, ibrutinib, and zanubrutinib) were based on median random-effects model hazard ratios (HRs) derived from an NMA conducted by the sponsor and applied to the reference VEN + OBI time-to-event curves. For OS, the sponsor reported HRs of ████ for VEN + IBRU, ████ for acalabrutinib, ████ for ibrutinib, and ████ for zanubrutinib, each relative to VEN + OBI. For PFS, the sponsor reported HRs of ████ for VEN + IBRU, ████ for acalabrutinib, ████ for ibrutinib, and ████ for zanubrutinib, each relative to VEN + OBI. For the aforementioned treatments, the sponsor assumed that ToT was equal to PFS and in the absence of comparative TTNT data, the sponsor further assumed that patients would transition to the next antileukemic treatment in the postprogression survival state.
Subsequent therapies modelled included acalabrutinib, ibrutinib, zanubrutinib, venetoclax plus rituximab, and venetoclax monotherapy. Subsequent treatment usage frequencies and the maximum subsequent treatment duration for acalabrutinib, ibrutinib, and venetoclax plus rituximab were informed by clinical expert opinion. The maximum subsequent treatment duration for zanubrutinib was assumed to equal that of ibrutinib. The median venetoclax monotherapy duration from Study VENICE-1 was used to proxy the maximum subsequent treatment duration for venetoclax monotherapy.3 To calculate the complete subsequent treatment costs, the sponsor calculated the difference between the modelled OS and TTNT curves. However, if this calculation was greater than the maximum estimates previously detailed, the maximum estimate was used instead. Monitoring costs for subsequent therapy, as well as oral administration costs, are assumed to be captured in the resource usage costs associated with the postprogression health state.
Health state utility values applied in the economic model were retrieved from Hancock et al.4 and utility values of 0.80 and 0.60 were assigned to the progression-free and postprogression health states, respectively. A relative utility decrement was applied to the health state utility values in each cycle to account for the deterioration in health-related quality of life associated with aging.5 Additionally, disutilities for AEs were sourced from the literature and applied as a 1-time utility decrement in the first model cycle.6-11
AEs in the model were restricted to grade 3 or grade 4 events, which occurred in at least 5% of patients in the CLL13 trial or were included in a previous National Institute for Health and Care Excellence review for CLL (TA891).6 The incidence of AEs for VEN + OBI, FLU + CYC + RIT, and BEN + RIT was obtained from the CLL13 study while the incidence of AEs for VEN + IBRU, acalabrutinib, ibrutinib, and zanubrutinib was obtained from the respective pivotal trials for each treatment.12-16 AEs modelled included anemia, diarrhea, urinary tract infections, infusion-related reactions, leukocytopenia, lymphocyte count decreases, febrile neutropenia, pneumonia, thrombocytopenia, atrial fibrillation, cardiac failure, cataract, hypertension, hyponatremia, musculoskeletal tissue, myocardial infarction, and tumour lysis syndrome (TLS).
The sponsor’s base case included costs for drug acquisition, drug administration, subsequent treatments, resource usage and monitoring, AEs, and terminal care. Drug acquisition costs for venetoclax were based on the sponsor-submitted prices.1 The dosing modelled for VEN + OBI is consistent with that described in the overview section. The prices of obinutuzumab, fludarabine, cyclophosphamide, and bendamustine were retrieved from previous CDA-AMC reimbursement review reports.17,18 The prices of rituximab were retrieved from the Ontario Drug Benefit (ODB) Formulary and the prices for BTKi-based treatments were retrieved from the ODB Exceptional Access Program.19,20 Drug administration costs for IV treatments were derived from the literature (IV = $199.14; rapid IV = $102.61) and encompassed the cost of administration as well as the cost of pharmacist time for IV drug dispensation.9 Administration costs for subcutaneous treatments ($13.38) were derived from the Ontario Schedule of Benefits: Physician Services Under the Health Insurance Act (February 20, 2024) (or Ontario Schedule of Benefits: Physician Services, in short) and the Government of Canada Job Bank.21,22 Administration costs for oral treatments ($1.23 per administration) were derived from the Ontario Schedule of Benefits: Physician Services.21 Resource usage frequencies were derived from a previous National Institute for Health and Care Excellence review for CLL and costs were derived from the Ontario Schedule of Benefits for Laboratory Services, the Ontario Schedule of Benefits: Physician Services, and the Canadian Institute for Health Information.6,21,23 Additionally, laboratory TLS prophylaxis costs were included and applied as a 1-time monitoring cost with cost inputs sourced from a multitude of sources.19,21,22,24-26 To estimate the TLS prophylaxis frequencies, the sponsor used data from the CLL13 trial for VEN + OBI, FLU + CYC + RIT, and BEN + RIT and assumed all other treatments have the same TLS prophylaxis frequency as VEN + OBI. AE unit costs were derived from the Canadian Institute for Health Information Patient Cost Estimator for patients aged 60 years or older.23 The sponsor assumed all AEs (grade 3 or higher) were treated in an inpatient setting. Lastly, a 1-time terminal care cost was included, encompassing expenses related to end-of-life care based on estimates from the literature.27
Summary of Sponsor’s Economic Evaluation Results
Base-case analyses for the ITT population and scenario analyses for the fludarabine-eligible subpopulation were run probabilistically (1,000 iterations); sensitivity analyses were conducted deterministically. The deterministic and probabilistic results were similar. The probabilistic findings are presented as follows.
Base-Case Results
The submitted analysis was based on publicly available prices of the comparator treatments. Results from the base case of the submitted economic evaluation are presented in Table 3. Additional results from the sponsor’s submitted economic evaluation base case are presented in Appendix 3.
In the sponsor’s submitted base case, the expected total costs and QALYs over a lifetime horizon for VEN + OBI were $276,217 and 11.91, respectively. The cost-effectiveness frontier consisted of BEN + RIT, VEN + OBI, and VEN + IBRU, representing the optimal treatment strategies. In sequential analysis, VEN + OBI was associated with an ICER of $19,316 relative to BEN + RIT (incremental costs = $119,326; incremental QALYs = 6.18) (Table 3). Approximately 93% of incremental QALYs for VEN + OBI, relative to BEN + RIT, were gained in the extrapolated period of the model (i.e., beyond the 5.6 years observed in the CLL13 trial). In the sponsor’s analysis, VEN + OBI had a 90% probability of being cost-effective at a WTP threshold of $50,000 per QALY gained compared with BEN + RIT. Results were largely driven by QALYs gained in the progression-free health state and subsequent treatment costs.
Table 3: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total costs ($) | Total QALYs | Sequential ICER ($/QALY) |
|---|---|---|---|
Sponsor’s base case (deterministic) | |||
BEN + RIT | 160,390 | 5.66 | Reference |
VEN + OBI | 281,080 | 11.96 | 19,160 vs. BEN + RIT |
VEN + IBRU | 573,644 | 12.68 | 408,798 vs. VEN + OBI |
Dominated treatments | |||
FLU + CYC + RIT | 365,965 | 11.30 | Dominated by VEN + OBI |
Zanubrutinib | 1,020,379 | 9.48 | Dominated by VEN + OBI, FLU + CYC + RIT, and VEN + IBRU |
IBRU | 1,064,621 | 9.09 | Dominated by VEN + OBI, FLU + CYC + RIT, VEN + IBRU, and zanubrutinib |
Acalabrutinib | 1,426,661 | 12.54 | Dominated by VEN + IBRU |
Sponsor’s base case (probabilistic) | |||
BEN + RIT | 156,890 | 5.73 | Reference |
VEN + OBI | 276,217 | 11.91 | 19,316 vs. BEN + RIT |
VEN + IBRU | 559,588 | 12.68 | 367,252 vs. VEN + OBI |
Dominated treatments | |||
FLU + CYC + RIT | 310,841 | 10.44 | Dominated by VEN + OBI |
Zanubrutinib | 987,794 | 9.32 | Dominated by VEN + OBI, FLU + CYC + RIT, and VEN + IBRU |
IBRU | 1,038,364 | 8.97 | Dominated by VEN + OBI, FLU + CYC + RIT, VEN + IBRU, and zanubrutinib |
Acalabrutinib | 1,434,255 | 12.09 | Dominated by VEN + IBRU |
BEN = bendamustine; CYC = cyclophosphamide; FLU = fludarabine; IBRU = ibrutinib; ICER = incremental cost-effectiveness ratio; OBI = obinutuzumab; QALY = quality-adjusted life-year; RIT = rituximab; VEN = venetoclax; vs. = versus.
Source: Sponsor’s pharmacoeconomic submission.1
Sensitivity and Scenario Analysis Results
The sponsor conducted a scenario analysis for the subpopulation of previously untreated patients with CLL who were considered fludarabine-eligible (i.e., aged 65 or under). In the fludarabine-eligible subpopulation, the cost-effectiveness frontier consisted of FLU + CYC + RIT, VEN + OBI, and VEN + IBRU. VEN + OBI was associated with an ICER of $7,186 per QALY gained (incremental costs = $29,778; incremental QALYs = 1.01) compared with FLU + CYC + RIT. Note that only FLU + CYC + RIT, VEN + IBRU, zanubrutinib, and acalabrutinib were considered comparators in the subpopulation analysis due to data restrictions.
The sponsor conducted further scenario analyses for both the ITT population and the fludarabine-eligible subpopulation, encompassing considerations such as alternative time horizons, discount rates, subsequent treatment distributions, AE costing, OS distributions (fludarabine-eligible subpopulation only), and TTNT distributions, and excluding age-adjusted utilities and subsequent treatment costs. The sponsor’s results for all scenario analyses were aligned with the base case in that VEN + OBI was cost-effective at a WTP threshold of $50,000 per QALY gained.
Additionally, the sponsor conducted a scenario analysis from a societal perspective. This analysis included additional costs associated with productivity losses and travel expenses for both patients and caregivers. In this analysis, relative to BEN + RIT, the ICER of VEN + OBI was $26,187 per QALY gained. This was similar to the sponsor’s base-case analysis using a health care payer perspective.
CDA-AMC Appraisal of the Sponsor’s Economic Evaluation
CDA-AMC identified several key limitations to the sponsor’s analysis that have notable implications for the economic analysis.
The comparative clinical efficacy (OS, PFS, and TTNT) of VEN + OBI, VEN + IBRU, and BTKi-based therapies is highly uncertain: There is a lack of direct head-to-head evidence comparing VEN + OBI to VEN + IBRU, and BTKi-based therapies (i.e., acalabrutinib, ibrutinib, and zanubrutinib). To inform efficacy in the pharmacoeconomic model (i.e., OS and PFS), the sponsor conducted NMAs to estimate the relative efficacy of VEN + OBI in previously untreated patients with CLL.28 HRs derived from the sponsor’s NMA were applied to the VEN + OBI reference curves to derive the OS and PFS curves for VEN + IBRU and BTKi-based therapies. The CDA-AMC clinical review highlighted the uncertainty associated with the results of the sponsor’s NMA, primarily due to inclusion of the null in the 95% credible interval, heterogeneity in population fitness and mutational status, and small number of studies included. CDA-AMC notes that uncertainty in the sponsor’s NMA directly translates into uncertainty in the modelled OS and PFS curves for VEN + IBRU and BTKi-based therapies. Additionally, while the sponsor’s NMA included both fit and unfit patients, the CLL13 study only included fit patients. Consequently, fit patients inform the efficacy for VEN + OBI, BEN + RIT, and FLU + CYC + RIT but a mix of fit and unfit patients inform the efficacy for VEN + IBRU, acalabrutinib, ibrutinib, and zanubrutinib. This may result in a modelled efficacy bias favouring VEN + OBI, BEN + RIT, and FLU + CYC + RIT. CDA-AMC notes that the inclusion of unfit patients in the submitted NMA was required to enable a comparison to all relevant comparators. Clinical experts consulted by CDA-AMC were not concerned with generalizing the NMA results based on the broader population to the fit population, as there are fewer concerns with comorbidities in the fit population.
Furthermore, the relative efficacy between VEN + OBI and acalabrutinib is highly uncertain. Clinical expert input indicated that while the HRs suggest ██████████ █████████ ██████ ███ █████████████ ████████ ████ █████ (OS = ████; PFS = ████), this outcome did not align with clinical expectations. The experts anticipated that the direction of acalabrutinib’s HRs would be consistent with those of ibrutinib (OS = ████; PFS = ████) and zanubrutinib (OS = ████; PFS = ████). As noted by the CDA-AMC clinical review, differences in fitness eligibility criteria across trials may explain the direction of acalabrutinib’s HRs, highlighting the uncertainty in the sponsor’s NMA.
Lastly, CDA-AMC notes that while TTNT was evaluated in the sponsor’s NMA, the findings were not used in the pharmacoeconomic model due to data availability limitations resulting in incomplete TTNT networks. Instead, the sponsor assumed that patients receiving VEN + IBRU or BTKi-based therapy would transition to the next antileukemic treatment upon progression. Clinical expert input deemed this assumption reasonable for continuous BTKi-based therapies but not for VEN + IBRU, as it is a time-limited treatment. It is uncommon for patients on time-limited treatments to start subsequent therapy immediately after progression. Hence, the subsequent therapy costs associated with VEN + IBRU may be overestimated, introducing a bias in favour of VEN + OBI.
CDA-AMC was unable to address this limitation in reanalyses owing to a lack of clinical data.
The long-term efficacy (OS and PFS) is uncertain: The sponsor used parametric modelling to extrapolate OS and PFS for VEN + OBI, FLU + CYC + RIT, and BEN + RIT beyond the observable time points in the CLL13 trial (maximum follow-up = 67 months) to a lifetime time horizon (40 years). The parametric distributions chosen by the sponsor resulted in 93% of the incremental QALYs and 97% of the incremental LYs for VEN + OBI, relative to BEN + RIT, being gained in the extrapolated period of the model (i.e., beyond the 5.6 years observed in the CLL13 trial). The magnitude of benefit with VEN + OBI based on time-to-event end points in the CLL13 study is currently unknown as the median PFS (for the VEN + OBI group only) and OS were not reached at the updated data cut-off date of January 31, 2023. Evidence suggests that the clinical benefit of cancer drugs demonstrated in primary publications is often different compared with updated mature data.29 Hence, CDA-AMC contends that, in the absence of mature OS and PFS data, the extent to which the extrapolations of VEN + OBI overestimate or underestimate the true incremental LYs and QALYs is uncertain.
The sponsor selected parametric distributions based on diagnostic plots, goodness-of-fit statistics, visual inspection, and the clinical plausibility of long-term projections as determined by clinical experts in Canada. While CDA-AMC agrees that models should be compared based on their statistical fit, this pertains only to the observed trial period, not to the extrapolation period. The weight given to the comparative fit of alternative parametric models to the observed data depends on the extent to which extrapolation is required and the degree of censoring present. Given the length of time required for extrapolation, the clinical plausibility of the extrapolated portion of alternative models is of greater importance than the statistical fit to the observed data.30
First, the sponsor’s chosen extrapolation of OS for BEN + RIT (log-normal) predicts that 74%, 29%, and 10% of patients are alive at year 5 (cohort age = 67 years), year 10 (cohort age = 72 years), and year 15 (cohort age = 77 years), respectively. In contrast, the sponsor’s chosen extrapolations of OS for FLU + CYC + RIT (gamma) and VEN + OBI (exponential) predict that 94%, 85%, and 73% of FLU + CYC + RIT–treated patients and 97%, 87%, and 77% of VEN + OBI–treated patients are alive at year 5, year 10, and year 15, respectively. Clinical expert input indicated that survival estimates for BEN + RIT were likely underestimated, as BEN + RIT–treated patients are anticipated to access the same salvage therapy as FLU + CYC + RIT–treated and VEN + OBI–treated patients. In consultation with clinical experts, CDA-AMC selected an exponential distribution to extrapolate BEN + RIT; it predicts that 81%, 65%, and 53% of patients are alive at year 5, year 10, and year 15, respectively. Additionally, clinical experts noted that patients with previously untreated CLL may have a risk of death similar to the age- and sex-adjusted population in Canada, irrespective of the 1L therapy received as the opportunity for salvage is equivalent across treatments.
Second, the long-term efficacy of VEN + OBI, FLU + CYC + RIT, and BEN + RIT in the economic model is uncertain due to the reliance on extrapolated PFS data. Most of the predicted benefits of VEN + OBI relative to FLU + CYC + RIT and BEN + RIT occur beyond the observed trial period. Given this reliance on extrapolation, it is important to note that the sponsor’s chosen extrapolations of PFS for BEN + RIT (log-logistic) and FLU + CYC + RIT (generalized gamma) generate long-term survival estimates that do not align with clinical practice. The sponsor’s extrapolations predict that in the short-term, patients who were treated with FLU + CYC + RIT will have a lower risk of progression than patients who were treated with BEN + RIT but in the long-term, patients who were treated with BEN + RIT will have a lower risk of progression than patients who were treated with FLU + CYC + RIT and VEN + OBI. Clinical expert input noted that the PFS estimates for BEN + RIT and FLU + CYC + RIT should be more closely aligned than what the sponsor modelled, following a similar pattern of progression risk while recognizing that BEN + RIT is generally not as effective as FLU + CYC + RIT. In consultation with clinical experts, CDA-AMC explored alternative PFS distributions for FLU + CYC + RIT and BEN + RIT. It was determined that applying a Weibull distribution to model PFS for BEN + RIT and FLU + CYC + RIT generated extrapolations that were more reflective of clinical practice but that likely underestimated VEN + OBI’s PFS benefit relative to BEN + RIT and FLU + CYC + RIT.
In the CDA-AMC base case, CDA-AMC adopted an alternative extrapolation of OS (exponential) for BEN + RIT and an alternative extrapolation of PFS (Weibull) for FLU + CYC + RIT and BEN + RIT.
CDA-AMC conducted a scenario analysis assuming an equal risk of death across all modelled treatments.
CDA-AMC also conducted a scenario analysis using the generalized gamma distribution originally selected by the sponsor for the PFS curve of FLU + CYC + RIT; this resulted in an increased relative benefit of VEN + OBI relative to FLU + CYC + RIT.
The impact of VEN + OBI on TTNT is uncertain: The sponsor derived TTNT from digitized KM data from the CLL13 clinical trial (with a data cut-off date of January 31, 2023) and extrapolated the treatment effect beyond the observed trial data (median follow-up = 51 months; maximum follow-up = 67 months) over the entire model time horizon (40 years). TTNT was assumed to only affect costing as the efficacy of subsequent treatments was assumed to be implicitly captured by OS and PFS. CDA-AMC notes that the exponential parametric distribution chosen by the sponsor to extrapolate TTNT for VEN + OBI results in a 14.6-year lag between median PFS and median TTNT. As such, 50% of patients progress within 7 years of initiating VEN + OBI but may wait up to 15 years before starting their next line of antileukemic therapy. In contrast, using the sponsor’s chosen parametric distributions to extrapolate TTNT for FLU + CYC + RIT and BEN + RIT, the resulting lag between median PFS and median TTNT is 1.7 years and 2.2 years, respectively. Clinical expert input commented that the sponsor’s assumptions do not reflect clinical practice, as the expected difference between median TTNT and median PFS is anticipated to range between 4 years and 8 years, depending on the patients’ molecular profile. Clinical experts commented that whether a patient receives subsequent therapy will largely depend on their risk stratification; older low-risk patients receiving 1L therapy may not live long enough to receive 2L therapy. However, young patients with unmutated IGHV will likely require 2L therapy (unmutated IGHV patients comprised 58% of the ITT population in the CLL13 trial). Patients with mutated IGHV have a greater risk of experiencing a sustained response to 1L therapy and are more likely to experience a longer lag between progression and initiating 2L therapy. Clinical experts commented that only a small subset of patients with good prognosis would experience a more substantial lag between the time of progression and the start of 2L treatment.
In consultation with clinical experts, CDA-AMC determined that a hazard spline (1 knot) distribution and Weibull distribution produced more clinically plausible TTNT estimates. However, use of the Weibull distribution resulted in the relative risk of TTNT between VEN + OBI and BEN + RIT and FLU + CYC + RIT remaining relatively constant for 25 years (Appendix 4, Figure 2). CDA-AMC notes that there must be sufficient evidence to support the assumption that VEN + OBI has a sustained long-term benefit associated with delaying TTNT. Per CADTH Methods and Guidelines: Extrapolating Clinical Evidence Within Economic Evaluations,31 any deviations from the U-shaped relationship between the relative effects and time would necessitate a compelling argument.32 In the absence of sufficient evidence to support the sustained treatment benefit associated with VEN + OBI when a Weibull distribution is assumed for TTNT, CDA-AMC deemed the hazard spline (1 knot) distribution most likely to produce the most plausible TTNT projections. The hazard spline (1 knot) distribution allows for the treatment effect of VEN + OBI on TTNT to wane over time, producing a U-shaped relationship between the relative risk of TTNT and time such that the relative risk for TTNT declines monotonically during the period covered by the CLL13 trial and trends to 1 over the extrapolated period (Appendix 4, Figure 2).
In the CDA-AMC base case, a hazard spline (1 knot) distribution was used to extrapolate TTNT for VEN + OBI. This results in a 3.4-year lag between median PFS and median TTNT. To explore the uncertainty associated with TTNT, CDA-AMC conducted a scenario analysis that uses a Weibull distribution to extrapolate TTNT for VEN + OBI, which assumes a 6.3-year lag between median PFS and median TTNT.
CDA-AMC conducted a scenario analysis in which subsequent therapy costs were excluded to capture the cost-effectiveness of patients who do not require subsequent therapy. CDA-AMC notes that this scenario is not applicable to the majority of patients as most patients will be treated with subsequent therapy.
Poor modelling practices were employed: First, CDA-AMC notes that the submitted economic model fails to execute probabilistically when selecting the hazard spline (1 knot) distribution to extrapolate TTNT for VEN + OBI. CDA-AMC was unable to determine the probability that VEN + OBI is cost-effective at a WTP threshold (e.g., of $50,000 per QALY) owing to structural limitations of the sponsor’s model (that is, all CDA-AMC analyses are deterministic and do not reflect uncertainty). Second, when including wastage, CDA-AMC was unable to produce deterministic results owing to an error on 1 of the calculation sheets. Moreover, estimated wastage costs lacked face validity as the wastage costs attributed to VEN + IBRU were negative when the option to include wastage was selected. Lastly, the sponsor’s submitted model included numerous IFERROR statements, which lead to situations in which the parameter value is overwritten with an alternative value without alerting the user to the automatized overwriting. The systematic use of IFERROR statements makes thorough auditing of the sponsor’s model impractical, as it remains unclear whether the model is running inappropriately by overriding errors.
CDA-AMC opted to present the CDA-AMC base case and scenario analyses deterministically and notes that due to the use of IFERROR statements, a thorough validation of the sponsor’s model was not possible. CDA-AMC was unable to consider the impact of wastage due to the errors identified in the sponsor’s calculations.
Additionally, the following key assumptions were made by the sponsor and have been appraised by CDA-AMC (refer to Table 4).
Table 4: Key Assumptions of the Submitted Economic Evaluation
Sponsor’s key assumption | CDA-AMC comment |
|---|---|
The patient population in the model reflects the baseline characteristics of patients from the CLL13 trial expected to be treated in Canadian clinical practice. | Uncertain. Clinical expert input received by CDA-AMC noted that baseline characteristics, specifically age, were not reflective of the average patient expected to be treated in Canada. While the cohort starting age in the model is aged ██ years, clinical expert input suggested that the average age of patients who receive 1L treatment for CLL in Canada is likely between 70 years and 75 years. |
Treatment duration for BTKi-based therapies is equal to PFS. | Not appropriate. While the BTKi therapies are treat-until-progression therapies, clinical expert input noted that patients may discontinue treatments for reasons unrelated to progression such as intolerance, AEs, or toxicities. Clinical expert input commented that approximately 10% to 30% of patients receiving a BTKi therapy discontinue before progression. As such, the sponsor is overestimating BTKi treatment costs as they have assumed no patients discontinue BTKi-based therapy before progression. CDA-AMC notes that while the sponsor’s assumption introduces a bias in favour of VEN + OBI, adjusting the proportion of patients discontinuing BTKi-based therapy before progression, in alignment with clinical expert opinion, does not impact the relative cost-effectiveness of VEN + OBI as BTKi-based therapies (i.e., acalabrutinib, IBRU, and zanubrutinib) are not on the cost-effectiveness frontier. |
Fifty-five percent of patients who received acalabrutinib in the 1L setting received zanubrutinib as their 2L treatment and 55% of patients who received zanubrutinib in the 1L setting received acalabrutinib as their 2L treatment. | Not appropriate. The sponsor estimated the proportion of patients who receive each subsequent therapy based on clinical expert opinion, with the caveat that patients are assumed to not receive the same treatment in the 2L as they did in the 1L. Clinical expert input found the sponsor’s relative use estimates for acalabrutinib and zanubrutinib in the 2L setting unreasonable as the resistant patterns for BTKis are similar such that unless the BTKi was stopped due to toxicities, and did not progress on therapy, there is no biologic reason for another covalent BTKi monotherapy to be considered for 2L therapy. Expert input noted that this does not hold true if the BTKi is combined with VEN as patients who have progressed on a BTKi can respond to combination therapy. CDA-AMC notes that adjusting the subsequent therapy distributions for acalabrutinib and zanubrutinib does not impact the relative cost-effectiveness of VEN + OBI as neither treatment is on the cost-effectiveness frontier. |
The incidence rate of AEs are expected to reflect those observed in clinical trials. | Not appropriate. The incidence rate of grade 3 and grade 4 AEs for VEN + OBI, VEN + IBRU, acalabrutinib, IBRU, and zanubrutinib were based on naive comparisons, without adjustment or accounting for differences in patient characteristics. The rate of AEs was used to calculate AE costs in the sponsor’s base case. Owing to the direct use of clinical trial data, it is not possible to determine if any observed differences between the therapies are solely due to the treatment or, rather, due to bias or confounding factors. Furthermore, no safety end point was evaluated in the NMA; therefore, no conclusions on safety can be drawn on the indirect comparison of VEN + OBI to VEN + IBRU, and BTKis. |
1L = first line; 2L = second line; AE = adverse event; BTKi = Bruton tyrosine kinase inhibitor; CDA-AMC = Canada’s Drug Agency; CLL = chronic lymphocytic leukemia; IBRU = ibrutinib; NMA = network meta-analysis; OBI = obinutuzumab; PFS = progression-free survival; VEN = venetoclax.
CDA-AMC Reanalyses of the Economic Evaluation
Base-Case Results
CDA-AMC undertook the reanalyses outlined in Table 5 to address, where possible, the limitations within the sponsor’s submitted economic model. The CDA-AMC base case was derived by making changes in model parameter values and assumptions, in consultation with clinical experts.
Table 5: CDA-AMC Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CDA-AMC value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
1. Unit drug prices |
|
|
Changes to derive the CDA-AMC base case | ||
1. OS parametric distribution | OS for BEN + RIT was modelled using a log-normal distribution. | OS for BEN + RIT was modelled using an exponential distribution. |
2. PFS parametric distribution |
| PFS for BEN + RIT and FLU + CYC + RIT were modelled using a Weibull distribution. |
3. TTNT parametric distribution | TTNT for VEN + OBI was modelled using an exponential distribution. | TTNT for VEN + OBI was modelled using a hazard spline (1 knot) distribution. |
CDA-AMC base case | ― | Reanalysis 1 + 2 + 3 |
BEN = bendamustine; CDA-AMC = Canada’s Drug Agency; CYC = cyclophosphamide; FLU = fludarabine; OBI = obinutuzumab; OS = overall survival; PFS = progression-free survival; RIT = rituximab; TTNT = time to next treatment; VEN = venetoclax.
Note: CDA-AMC notes that the sponsor sourced the price of BEN from a previous CADTH report in which the price was transcribed incorrectly. The corrections made to the prices of OBI and CYC are due to changes in the publicly available prices.
The CDA-AMC base case was based on publicly available prices of the comparator treatments. Results from the CDA-AMC base case are presented in Table 6. Additional results from the CDA-AMC base case, including the results of the stepwise analyses, are presented in Appendix 4.
In the CDA-AMC base case, the expected total costs and QALYs over a lifetime time horizon for VEN + OBI were $446,335 and 11.96, respectively. The cost-effectiveness frontier consisted of BEN + RIT, FLU + CYC + RIT, VEN + OBI, and VEN + IBRU, representing the optimal treatment strategies. In sequential analysis, VEN + OBI was associated with an ICER of $167,257 relative to FLU + CYC + RIT (incremental costs = $82,007; incremental QALYs = 0.49). Approximately 88% of incremental QALYs for VEN + OBI, relative to FLU + CYC + RIT, were gained in the extrapolated period of the model (i.e., beyond the 5.6 years observed in the CLL13 trial). Results were largely driven by drug acquisition costs and QALYs gained in the progression-free health state.
Table 6: Summary of the CDA-AMC Reanalysis Results
Drug | Total costs ($) | Total QALYs | Sequential ICER ($/QALY) |
|---|---|---|---|
Sponsor’s corrected base case (deterministic) | |||
BEN + RIT | 182,401 | 5.66 | Reference |
VEN + OBI | 283,260 | 11.96 | 16,740 vs. BEN + RIT |
VEN + IBRU | 573,644 | 12.68 | 405,753 vs. VEN + OBI |
Dominated treatments | |||
FLU + CYC + RIT | 366,016 | 11.30 | Dominated by VEN + OBI |
Zanubrutinib | 1,020,379 | 9.48 | Dominated by VEN + OBI, FLU + CYC + RIT, and VEN + IBRU |
IBRU | 1,064,621 | 9.09 | Dominated by VEN + OBI, FLU + CYC + RIT, VEN + IBRU, and zanubrutinib |
Acalabrutinib | 1,426,661 | 12.54 | Dominated by VEN + IBRU |
CDA-AMC base case (deterministic) | |||
BEN + RIT | 339,878 | 9.01 | Reference |
FLU + CYC + RIT | 364,328 | 11.47 | 9,924 vs. BEN + RIT |
VEN + OBI | 446,335 | 11.96 | 167,257 vs. FLU + CYC + RIT |
VEN + IBRU | 573,644 | 12.68 | 177,889 vs. VEN + OBI |
Dominated treatments | |||
Zanubrutinib | 1,020,379 | 9.48 | Dominated by VEN + OBI, FLU + CYC + RIT, and VEN + IBRU |
IBRU | 1,064,621 | 9.09 | Dominated by VEN + OBI, FLU + CYC + RIT, VEN + IBRU, and zanubrutinib |
Acalabrutinib | 1,426,661 | 12.54 | Dominated by VEN + IBRU |
BEN = bendamustine; CDA-AMC = Canada’s Drug Agency; CYC = cyclophosphamide; FLU = fludarabine; HR = hazard ratio; IBRU = ibrutinib; ICER = incremental cost-effectiveness ratio; NMA = network meta-analysis; OBI = obinutuzumab; QALY = quality-adjusted life-year; RIT = rituximab; VEN = venetoclax; vs. = versus.
Note: Should the direction of NMA HRs for acalabrutinib align with those for IBRU and zanubrutinib, as anticipated by clinical experts, acalabrutinib would also be dominated by VEN + OBI in all aforementioned analyses.
Scenario Analysis Results
CDA-AMC undertook price reduction analyses based on the sponsor’s corrected base case and the CDA-AMC base case. The CDA-AMC base case suggested that a 75% price reduction for venetoclax would be required for VEN + OBI to achieve cost-effectiveness relative to FLU + CYC + RIT at a WTP threshold of $50,000 per QALY gained (Table 7).
Table 7: CDA-AMC Price Reduction Analyses
Analysis: price reduction | Unit drug cost ($) | ICERs for VEN + OBI vs. comparator (as indicated) ($/QALY) | |||
|---|---|---|---|---|---|
10 mg | 50 mg | 100 mg | Sponsor’s corrected base case | CDA-AMC reanalysis | |
No price reduction | 7.08 | 35.40 | 70.80 | 16,740 (vs. BEN + RIT) | 167,257 (vs. FLU + CYC + RIT) |
10% | 6.37 | 31.86 | 63.72 | 15,571 (vs. BEN + RIT) | 151,676 (vs. FLU + CYC + RIT) |
20% | 5.66 | 28.32 | 56.64 | 14,402 (vs. BEN + RIT) | 136,095 (vs. FLU + CYC + RIT) |
30% | 4.96 | 24.78 | 49.56 | 13,233 (vs. BEN + RIT) | 120,514 (vs. FLU + CYC + RIT) |
40% | 4.25 | 21.24 | 42.48 | 12,065 (vs. BEN + RIT) | 104,933 (vs. FLU + CYC + RIT) |
50% | 3.54 | 17.70 | 35.40 | 10,896 (vs. BEN + RIT) | 89,352 (vs. FLU + CYC + RIT) |
60% | 2.83 | 14.16 | 28.32 | 9,727 (vs. BEN + RIT) | 73,771 (vs. FLU + CYC + RIT) |
70% | 2.12 | 10.62 | 21.24 | 8,558 (vs. BEN + RIT) | 58,190 (vs. FLU + CYC + RIT) |
80% | 1.42 | 7.08 | 14.16 | 7,389 (vs. BEN + RIT) | 42,609 (vs. FLU + CYC + RIT) |
90% | 0.71 | 3.54 | 7.08 | 6,221 (vs. BEN + RIT) | 27,028 (vs. FLU + CYC + RIT) |
BEN = bendamustine; CDA-AMC = Canada’s Drug Agency; CYC = cyclophosphamide; FLU = fludarabine; ICER = incremental cost-effectiveness ratio; OBI = obinutuzumab; QALY = quality-adjusted life-year; RIT = rituximab; VEN = venetoclax; vs. = versus.
Note: Price reduction estimates use deterministic analysis results.
CDA-AMC conducted scenario analyses to explore the impact of alternative assumptions on the cost-effectiveness of VEN + OBI. Results of the scenario analyses are presented in Appendix 4, Table 13.
First, CDA-AMC explored the impact of assuming a Weibull distribution for VEN + OBI’s TTNT, which clinical experts identified as a clinically plausible alternative to the hazard spline (1 knot) curve used in the CDA-AMC base case. When assuming a Weibull distribution for VEN + OBI’s TTNT, the ICER for VEN + OBI decreased to $88,275 per QALY gained relative to FLU + CYC + RIT. CDA-AMC notes that using the Weibull distribution resulted in the relative risk of TTNT between VEN + OBI and BEN + RIT or FLU + CYC + RIT remaining stable for 25 years. However, due to the lack of evidence supporting a sustained long-term benefit of VEN + OBI in delaying TTNT, this scenario is viewed as optimistic.
Second, CDA-AMC explored the impact of assuming the risk of death was equal across treatments as clinical experts noted that patients with previously untreated CLL may have a risk of death similar to the age- and sex-adjusted population in Canada, irrespective of the 1L therapy received as the opportunity for salvage is equivalent across treatments. When an equal risk of death is assumed across treatments, VEN + OBI is extendedly dominated by a combination of FLU + CYC + RIT and VEN + IBRU. This scenario is driven by the assumption that VEN + OBI and FLU + CYC + RIT have an equal risk of death.
Third, CDA-AMC explored the impact of excluding subsequent therapy costs to capture the cost-effectiveness of patients who do not require subsequent therapy. CDA-AMC notes that this scenario is not applicable to the majority of patients as most patients will be treated with subsequent therapy. Similar to the results of the second scenario analysis, VEN + OBI was extendedly dominated by a combination of FLU + CYC + RIT and VEN + IBRU.
Fourth, CDA-AMC evaluated the impact of using a generalized gamma distribution for the PFS curve of FLU + CYC + RIT, as originally assumed by the sponsor, increasing the relative benefit of VEN + OBI relative to FLU + CYC + RIT. When assuming a generalized gamma distribution for FLU + CYC + RIT’s PFS curve, the ICER for VEN + OBI decreased to $121,340 per QALY gained relative to FLU + CYC + RIT.
Issues for Consideration
VEN + IBRU is currently in negotiations with the pan-Canadian Pharmaceutical Alliance; should negotiations conclude with a letter of intent,33 the price of VEN + IBRU paid by drug plans may be lower than the price incorporated into the sponsor’s pharmacoeconomic model.
The sponsor is requesting that VEN + OBI be reimbursed for patients with previously untreated CLL. However, VEN + OBI may be used off-label for other conditions that relevant comparator products are also indicated for, such as small lymphocytic lymphoma. The potential for off-label use of VEN + OBI may be associated with additional costs to the drug plans. However, it should be noted that the possibility of off-label use is not unique to VEN + OBI and applies to the other available treatments on the market in Canada and used in the indicated population.
CDA-AMC has previously reviewed venetoclax, in combination with obinutuzumab and in combination with ibrutinib, for previously untreated patients with CLL.34,35 The cost-effectiveness results of these evaluations may not be directly comparable to those in the current review, owing to differences in model structure, clinical effectiveness parameters, health state utility values, and cost inputs.
Clinical expert input indicated that alternative treatment options that are targeted, chemoimmunotherapy-free and/or BTKi-free, and time-limited are needed for fit patients with previously untreated CLL.
Overall Conclusions
The new evidence in the CLL13 trial was submitted to support the expansion of the reimbursement criteria to include patients with previously untreated CLL who are considered fit and potentially fludarabine-eligible, and who were not included in the reimbursement request and recommendation criteria in the previous submission. Based on the CDA-AMC clinical review, the CLL13 study demonstrated that VEN + OBI results in an improvement in PFS and may provide an improvement in TTNT, relative to FLU + CYC + RIT and BEN + RIT. Results for OS were difficult to interpret as patients received 2L salvage therapy. Notably, the potential for bias in favour of VEN + OBI due to patients with unmutated IGHV receiving chemotherapy should be considered when interpreting the results for survival outcomes. The magnitude of benefit with VEN + OBI based on time-to-event end points in the CLL13 study is currently unknown as the median PFS (for the VEN + OBI group only), TTNT, and OS were not reached at the updated data cut-off date of January 31, 2023.
The comparative clinical efficacy of VEN + OBI, VEN + IBRU, and BTKi-based therapies (acalabrutinib, ibrutinib, and zanubrutinib) is uncertain due to the lack of head-to-head evidence and limitations with the sponsor's NMA. The CDA-AMC clinical review noted uncertainty associated with the NMA results due to 95% credible intervals including the null and heterogeneity in population fitness and mutational status. This clinical uncertainty is propagated in the submitted economic analysis given that the sponsor extrapolated OS, PFS, and TTNT for the lifetime time horizon of the model using parametric distributions fitted to clinical data from the CLL13 study. Moreover, since the sponsor’s NMA included both fit and unfit patients while the CLL13 trial included only fit patients (used to model efficacy for BEN + RIT, FLU + CYC + RIT, and VEN + OBI), incorporating the sponsor’s NMA results into the economic model introduces an efficacy bias favouring VEN + OBI, BEN + RIT, and FLU + CYC + RIT over VEN + IBRU and BTKi-based therapies.
In addition to the aforementioned limitations with the clinical evidence, CDA-AMC identified several limitations with the sponsor’s economic submission. These limitations included uncertainty with the comparative clinical efficacy of VEN + OBI, VEN + IBRU, and BTKi-based therapies; uncertainty with the long-term OS and PFS of VEN + OBI, FLU + CYC + RIT, and BEN + RIT; and uncertainty regarding the impact of VEN + OBI on long-term TTNT. As part of the base-case reanalysis, CDA-AMC adopted alternative parametric distributions to extrapolate OS for BEN + RIT, adopted alternative parametric distributions to extrapolate PFS for BEN + RIT and FLU + CYC + RIT, and adopted alternative parametric distributions to extrapolate TTNT for VEN + OBI. CDA-AMC additionally corrected the sponsor’s submitted base case by revising the unit prices for obinutuzumab, bendamustine, and cyclophosphamide, which were incorrectly programmed in the submitted model.
In the CDA-AMC base case, FLU + CYC + RIT is among the optimal treatments (on the cost-effectiveness frontier). As such, VEN + OBI is compared to FLU + CYC + RIT in sequential analyses and is associated with an ICER of $167,257 per QALY gained (incremental QALYs = 0.49; incremental costs = $82,007). The estimated ICER is driven by higher total costs for VEN + OBI and the adoption of more plausible assumptions about the prolonged benefit of VEN + OBI in delaying TTNT. Additionally, the CDA-AMC base case estimated higher total QALYs for FLU + CYC + RIT and BEN + RIT based on more plausible extrapolations of PFS and OS for these treatments. Based on the CDA-AMC base-case reanalysis, a 75% price reduction for venetoclax is required for VEN + OBI to be considered cost-effective relative to FLU + CYC + RIT at a WTP threshold of $50,000 per QALY gained. This would reduce the price of venetoclax from $7.08 to $1.77 per 10 mg tablet, $35.40 to $8.85 per 50 mg tablet, and $70.80 to $17.70 per 100 mg tablet. With this price reduction, the per-patient 28-day drug acquisition costs for VEN + OBI would be $17,280 for the first cycle and from $1,982 to $7,734 for each subsequent cycle.
The CDA-AMC base case relies on a sustained OS benefit for VEN + OBI, where patients receiving VEN + OBI gain 0.5 additional LYs compared to those treated with FLU + CYC + RIT. In the absence of long-term clinical evidence, the extent of this survival benefit is highly uncertain. Should the long-term effectiveness of VEN + OBI be lower than predicted, the ICER would be higher than the CDA-AMC base case, requiring larger price reductions to achieve cost-effectiveness. Moreover, when comparing the duration of follow-up in the CLL13 trial to the model’s time horizon (67 months [approximately 5.5 years] versus 40 years), it is important to note that most of the QALY benefit and the entirety of the LY benefit predicted by the model for patients treated with VEN + OBI are accrued in the post-trial period of the model on the basis of extrapolation.
The cost-effectiveness of VEN + OBI is sensitive to assumptions concerning TTNT and subsequent therapy costs. When assuming a Weibull distribution for VEN + OBI’s TTNT extrapolation, the ICER for VEN + OBI decreased to $88,275 per QALY gained relative to FLU + CYC + RIT. However, this is dependent on the relative risk of TTNT between VEN + OBI and BEN + RIT or FLU + CYC + RIT remaining constant for 25 years, which is considered optimistic given the lack of evidence supporting a prolonged benefit of VEN + OBI in delaying TTNT. When excluding subsequent therapy costs, to capture the cost-effectiveness of VEN + OBI among the small subset of patients who may not go on to receive 2L therapy, VEN + OBI was extendedly dominated by a combination of FLU + CYC + RIT and VEN + IBRU.
References
1.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Venclexta® (venetoclax), 10 mg, 50 mg, and 100 mg oral tablets. St-Laurent (QC): AbbVie Corporation; 2024 May 22.
2.Venclexta (venetoclax): 10 mg, 50 mg and 100 mg tablets [product monograph; sponsor-supplied reference]. St-Laurent (QC): AbbVie Corporation; 2020 Jan 13: https://pdf.hres.ca/dpd_pm/00054630.PDF.
3.Kater AP, Arslan O, Demirkan F, et al. Activity of venetoclax in patients with relapsed or refractory chronic lymphocytic leukaemia: analysis of the VENICE-1 multicentre, open-label, single-arm, phase 3b trial. Lancet Oncol. 2024;25(4):463-473. PubMed
4.Hancock S, Wake B, Hyde C. Fludarabine as first line therapy for chronic lymphocytic leukaemia: A West Midlands Health Technology Assessment Collaboration report [sponsor-supplied reference]. Birmingham (GB): University of Birmingham; 2003: https://www.birmingham.ac.uk/Documents/college-mds/haps/projects/WMHTAC/REPreports/2002/Fludarabine.pdf.
5.Guertin JR, Feeny D, Tarride JE. Age- and sex-specific Canadian utility norms, based on the 2013-2014 Canadian Community Health Survey. CMAJ. 2018;190(6):E155-E161. PubMed
6.National Institute for Health and Care Excellence. Ibrutinib with venetoclax for untreated chronic lymphocytic leukaemia [sponsor-supplied reference]. (Technology appraisal guidance TA891) 2023; https://www.nice.org.uk/guidance/ta891.
7.Herring W, Pearson I, Purser M, et al. Cost-Effectiveness of Ofatumumab Plus Chlorambucil in First Line Chronic Lymphocytic Leukemia in Canada. Value Health. 2014;17(7):A633. PubMed
8.Ball G, Lemieux C, Cameron D, Seftel MD. Cost-Effectiveness of Brexucabtagene Autoleucel versus Best Supportive Care for the Treatment of Relapsed/Refractory Mantle Cell Lymphoma following Treatment with a Bruton's Tyrosine Kinase Inhibitor in Canada. Curr Oncol. 2022;29(3):2021-2045. PubMed
9.Chatterjee A, van de Wetering G, Goeree R, et al. A Probabilistic Cost-Effectiveness Analysis of Venetoclax and Obinutuzumab as a First-Line Therapy in Chronic Lymphocytic Leukemia in Canada. Pharmacoecon Open. 2023;7(2):199-216. PubMed
10.Guinan K, Mathurin K, Au Y, et al. Venetoclax in Combination with Azacitidine for the Treatment of Newly Diagnosed Acute Myeloid Leukemia: A Canadian Cost-Utility Analysis. Curr Oncol. 2022;29(10):7524-7536. PubMed
11.Jones GL, Will A, Jackson GH, Webb NJ, Rule S, British Committee for Standards in Haematology. Guidelines for the management of tumour lysis syndrome in adults and children with haematological malignancies on behalf of the British Committee for Standards in Haematology. Br J Haematol. 2015;169(5):661-671. PubMed
12.Eichhorst B, Niemann CU, Kater AP, et al. First-Line Venetoclax Combinations in Chronic Lymphocytic Leukemia. N Engl J Med. 2023;388(19):1739-1754. PubMed
13.Kater AP, Owen C, Moreno C, et al. Fixed-Duration Ibrutinib-Venetoclax in Patients with Chronic Lymphocytic Leukemia and Comorbidities. NEJM Evid. 2022;1(7):EVIDoa2200006.
14.Sharman JP, Egyed M, Jurczak W, et al. Acalabrutinib with or without obinutuzumab versus chlorambucil and obinutuzmab for treatment-naive chronic lymphocytic leukaemia (ELEVATE TN): a randomised, controlled, phase 3 trial. Lancet. 2020;395(10232):1278-1291. PubMed
15.Tam CS, Brown JR, Kahl BS, et al. Zanubrutinib versus bendamustine and rituximab in untreated chronic lymphocytic leukaemia and small lymphocytic lymphoma (SEQUOIA): a randomised, controlled, phase 3 trial. Lancet Oncol. 2022;23(8):1031-1043. PubMed
16.Woyach JA, Ruppert AS, Heerema NA, al e. Ibrutinib Regimens Versus Chemoimmunotherapy in Older Patients With Untreated CLL. N Engl J Med. 2018;379(26):2517- 2528. PubMed
17.CADTH Reimbursement Recommendation: Ibrutinib (Imbruvica) in combination with venetoclax for the treatment of adult patients with previously untreated chronic lymphocytic leukemia, including those with 17p deletion [sponsor-supplied reference]. Can J Health Technol. 2023;3(11). https://www.cadth.ca/sites/default/files/DRR/2023/PC0317REC-Imbruvica-Final-Recommendation-meta.pdf.
18.CADTH Reimbursement Recommendation: Zanubrutinib (Brukinsa) for the treatment of adult patients with chronic lymphocytic leukemia [sponsor-supplied reference]. Can J Health Technol. 2023;3(9). https://www.cadth.ca/sites/default/files/DRR/2023/PC0310REC-Brukinsa_KT%20-%20MFJ_KT-meta.pdf#page=2.15.
19.Government of Ontario. Ontario Drug Benefit Formulary/Comparative Drug Index [sponsor-supplied reference]. 2024; https://www.formulary.health.gov.on.ca/formulary/.
20.Ontario Ministry of Health. Ontario Exceptional Access Program (EAP) product prices [sponsor-supplied reference]. https://www.ontario.ca/page/exceptional-access-program-product-prices.
21.Ontario Ministry of Health. Schedule of Benefits: Physician Services Under the Health Insurance Act (Februrary 20, 2024) [sponsor-supplied reference]. 2024; https://www.ontario.ca/files/2024-04/moh-schedule-benefit-2024-02-20.pdf.
22.Government of Canada Job Bank. Wages for Registered nurses and registered psychiatric nurses [sponsor-supplied reference]. 2024; https://www.jobbank.gc.ca/wagereport/occupation/993.
23.Canadian Institute for Health Information. Patient Cost Estimator [sponsor-supplied reference]. 2022; https://www.cihi.ca/en/patient-cost-estimator.
24.Ontario Ministry of Health. Schedule of Benefits for Laboratory Services [sponsor-supplied reference]. 2023; https://www.ontario.ca/files/2024-01/moh-ohip-schedule-of-benefits-laboratory-services-2024-01-24.pdf.
25.Ngo JS, Ho MHM. Evaluation of Rasburicase Use in the Fraser Health Authority: A Retrospective Review. Can J Hosp Pharm. 2019;72(4):311-319. PubMed
26.Bruera E, Pruvost M, Schoeller T, Montejo G, Watanabe S. Proctoclysis for hydration of terminally ill cancer patients. J Pain Symptom Manage. 1998;15(4):216-219. PubMed
27.Truong J, Cheung M, Seung SJ, al e. Phase-specific costs of care in diffuse large B-cell lymphoma in Ontario, Canada. J Clin Oncol. 2022;40.
28.Indirect Treatment Comparison (ITC) for venetoclax plus obinutuzumab in untreated patients with chronic lymphocytic leukemia (CLL) - Report [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Venclexta® (venetoclax), 10 mg, 50 mg, and 100 mg oral tablets. St-Laurent (QC): AbbVie Corporation; 2024 Apr 26.
29.Everest L, Blommaert S, Chu RW, Chan KKW, Parmar A. Parametric Survival Extrapolation of Early Survival Data in Economic Analyses: A Comparison of Projected Versus Observed Updated Survival. Value Health. 2022;25(4):622-629. PubMed
30.Latimer NR. Survival analysis for economic evaluations alongside clinical trials--extrapolation with patient-level data: inconsistencies, limitations, and a practical guide. Med Decis Making. 2013;33(6):743-754. PubMed
31.Coyle D, Haines A, Lee K. CADTH Methods and Guidelines: Extrapolating Clinical Evidence Within Economic Evaluations. Can J Health Technol. 2023;3(5). https://www.cda-amc.ca/sites/default/files/attachments/2023-05/MH0011-Extrapolating%20Clinical%20Evidence%20Within%20Economic%20Evaluations_0.pdf. Accessed 2024 Jun 1. PubMed
32.Guyot P, Ades AE, Beasley M, Lueza B, Pignon JP, Welton NJ. Extrapolation of Survival Curves from Cancer Trials Using External Information. Med Decis Making. 2017;37(4):353-366. PubMed
33.pan-Canadian Pharmaceutical Alliance (pCPA). Imbruvica (ibrutinib). 2024; https://www.pcpacanada.ca/negotiation/22489. Accessed 2024 Aug 2.
34.CDA-AMC. Drug Reimbursement Review: Venetoclax (Venclexta) in combination with obinutuzumab for the treatment of adult patients with previously untreated chronic lymphocytic leukemia (CLL) who are fludarabine ineligible. 2020; https://www.cadth.ca/venetoclax-venclexta-combo-obinutuzumab-cll-details. Accessed 2024 Aug 2.
35.CDA-AMC. Drug Reimbursement Review: ibrutinib (Imbruvica) with venetoclax for the treatment of adult patients with previously untreated chronic lymphocytic leukemia (CLL), including those with 17p deletion. 2024; https://www.cadth.ca/ibrutinib-0. Accessed 2024 Aug 2.
36.Ontario Ministry of Health, Ontario Ministry of Long-Term Care. Ontario drug benefit formulary/comparative drug index. 2024; https://www.formulary.health.gov.on.ca/formulary/. Accessed 2024 Jun.
37.DeltaPA. Ottawa (ON): IQVIA; 2023: https://www.iqvia.com/. Accessed 2024 Jun 13.
38.Exceptional Access Program (EAP). Toronto (ON): Ontario Ministry of Health; Ontario Ministry of Long-Term Care; 2024: http://www.health.gov.on.ca/en/pro/programs/drugs/odbf/odbf_except_access.aspx. Accessed 2024 Jun 11.
39.Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Venclexta® (venetoclax), 10 mg, 50 mg, and 100 mg oral tablets. St-Laurent (QC): AbbVie Corporation; 2024 May 22.
40.CADTH Reimbursement Review: Ibrutinib (Imbruvica) for the treatment of chronic lymphocytic leukemia [sponsor-supplied reference]. Can J Health Technol. 2024;4(2). https://www.cadth.ca/sites/default/files/DRR/2024/PC0317-Imbruvica_combined.pdf.
41.CADTH Reimbursement Review: Ibrutinib (Imbruvica) for the treatment of Waldenström macroglobulinemia [sponsor-supplied reference]. Can J Health Technol. 2024;4(4). https://www.cadth.ca/sites/default/files/DRR/2024/PC0328-Imbruvica-Combined-Report.pdf.
42.CADTH Reimbursement Review: Zanubrutinib (Brukinsa) for the treatment of chronic lymphocytic leukemia [sponsor-supplied reference]. Can J Health Technol. 2023;3(11). https://www.cadth.ca/sites/default/files/DRR/2023/PC0310-Brukinsa_combined.pdf.
43.Statistics Canada. Number of prevalent cases and prevalence proportions of primary cancer, by prevalence duration, cancer type, attained age group and sex [sponsor-supplied reference]. 2022: https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310075101&pickMembers%5B0%5D=2.1&pickMembers%5B1%5D=3.1&pickMembers%5B2%5D=4.51&pickMembers%5B3%5D=5.2&cubeTimeFrame.startYear=2014&cubeTimeFrame.endYear=2018&referencePeriods=20140101%2C20180101.
44.Statistics Canada. Number and rates of new cases of primary cancer, by cancer type, age group and sex [sponsor-supplied reference]. 2024: https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310011101&pickMembers%5B0%5D=2.1&pickMembers%5B1%5D=3.1&pickMembers%5B2%5D=4.51&cubeTimeFrame.startYear=2017&cubeTimeFrame.endYear=2021&referencePeriods=20170101%2C20210101.
45.Sutherland G, Dihn T. Understanding the gap: a pan-Canadian analysis of prescription drug insurance coverage [sponsor-supplied reference]. Ottawa (ON): The Conference Board of Canada; 2017: https://www.conferenceboard.ca/e-library/abstract.aspx?did=9326.
46.Fischer K, Al-Sawaf O, Bahlo J, et al. Venetoclax and Obinutuzumab in Patients with CLL and Coexisting Conditions. N Engl J Med. 2019;380(23):2225-2236. PubMed
47.American Cancer Society. Cancer Facts & Figures (2022) [sponsor-supplied reference]. 2022; https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/annual-cancer-facts-and-figures/2022/2022-cancer-facts-and-figures.pdf.
48.Canadian Institute for Health Information. Prescribed Drug Spending in Canada, 2019: A Focus on Public Drug Programs [sponsor-supplied reference]. Ottawa (ON): CIHI; 2019.
49.Drug Intelligence. ONCO-CAPPS Q4 2023. Data on File [sponsor-supplied reference]. 2024.
50.Statistics Canada. Table 17-10-0005-01 Population estimates on July 1st, by age and sex [sponsor-supplied reference]. https://doi.org/10.25318/1710000501-eng.
51.Non-Insured Health Benefits Program. First Nations and Inuit Health Branch: Annual report 2021 to 2022 [sponsor-supplied reference]. https://www.sac-isc.gc.ca/eng/1683039690813/1683039973755.
52.Non-Insured Health Benefits Program. First Nations and Inuit Health Branch: Annual report 2018/19 [sponsor-supplied reference]. https://www.sac-isc.gc.ca/DAM/DAM-ISC-SAC/DAM-HLTH/STAGING/texte-text/nihb-Annual_Report_2018-19_1589921777815_eng.pdf.
53.Non-Insured Health Benefits Program. First Nations and Inuit Health Branch: Annual report 2019 to 2020 [sponsor-supplied reference]. https://www.sac-isc.gc.ca/eng/1624462613080/1624462663098.
54.Non-Insured Health Benefits Program. First Nations and Inuit Health Branch: Annual report 2020 to 2021 [sponsor-supplied reference]. https://www.sac-isc.gc.ca/eng/1645718409378/1645718500555.
55.Barr PM, Owen C, Robak T, et al. Up to 8-year follow-up from RESONATE-2: first-line ibrutinib treatment for patients with chronic lymphocytic leukemia Blood Advances. 2022;6(11):3440-3450. PubMed
56.Munir T, Shadman M, Robak T, et al. P639: Zanubrutinib (Zanu) Vs Bendamustine + Rituximab (Br) in Patients (Pts) with Treatment-NaÏve Chronic Lymphocytic Leukemia/Small Lymphocytic Lymphoma (Cll/Sll): Extended Follow-up of the Sequoia Study. HemaSphere. 2023;7(S3).
57.Byrd JC, Woyach JA, Furman RR, et al. Acalabrutinib in treatment-naive chronic lymphocytic leukemia. Blood. 2021;137(24):3327-3338. PubMed
58.Alignment Among Public Formularies in Canada, Part 2: Oncology Medicines. Ottawa (ON): Patented Medicine Prices Review Board; 2021: https://www.canada.ca/content/dam/pmprb-cepmb/documents/npduis/analytical-studies/formularies/PMPRB-P2-Formularies-en.pdf. Accessed 2023 Oct 27.
Appendix 1: Cost Comparison Table
Table 8: CDA-AMC Cost Comparison Table for Adult Patients With Chronic Lymphocytic Leukemia
Treatment | Strength / concentration | Form | Price ($) | Recommended dosage | Daily cost ($) | 28-day cycle cost ($) |
|---|---|---|---|---|---|---|
Bcl-2 inhibitor + CD20 monoclonal antibody | ||||||
Venetoclax (Venclexta) | 10 mg 50 mg 100 mg | Tablet | 7.0800a 35.4000a 70.8000a | 5-week dose ramp up to 400 mg starting day 22 of cycle 1 (1 week each of 20 mg daily, 50 mg daily, 100 mg daily, 200 mg daily, and 400 mg daily); 400 mg once daily thereafter for a total of 12 28-day cycles. | Cycle 1: 3.54 Cycle 2: 132.75 Cycle 3 to 12: 283.20 | Cycle 1: 99 Cycle 2: 3,717 Cycle 3 to 12: 7,930 |
Obinutuzumab (Gazyva) | 1,000 mg | 25 mg/mL vial for IV infusion | 5,751.7300b | 100 mg on day 1, cycle 1, followed by 900 mg on day 1 or day 2, and 1,000 mg on day 8 and day 15 of a 28-day cycle; 1,000 mg on day 1 of 5 subsequent 28-day cycles | Cycle 1: 616.26 Cycle 2 to 6: 205.42 | Cycle 1: 17,255 Cycle 2 to 6: 5,752 |
Venetoclax + Obinutuzumab | Cycle 1: 619.80 Cycle 2: 338.17 Cycle 3 to 6: 488.62 Cycle 7 to 12: 283.20 | Cycle 1: 17,354 Cycle 2: 9,469 Cycle 3 to 6: 13,681 Cycle 7 to 12: 7,930 | ||||
Bcl-2 inhibitor + Bruton tyrosine kinase inhibitor | ||||||
Venetoclax (Venclexta) | 10 mg 50 mg 100 mg | Tablet | 7.0800a 35.4000a 70.8000a | 5-week dose ramp up to 400 mg starting in cycle 4 (1 week each of 20 mg daily, 50 mg daily, 100 mg daily, 200 mg daily, and 400 mg daily); 400 mg once daily thereafter for a total of 12 28-day cycles. | Cycle 4: 65.49 Cycle 5 to 15: 283.20 | Cycle 4: 1,834 Cycle 5 to 15: 7,930 |
Ibrutinib (Imbruvica) | 140 mg | Capsule | 99.8350c | 420 mg once daily for a total of 15 28-day cycles. | 299.51 | 8,386 |
Venetoclax + ibrutinib | Cycle 1 to 3: 299.51 Cycle 4: 365.00 Cycle 5 to 15: 582.71 | Cycle 1 to 3: 8,386 Cycle 4: 10,220 Cycle 5 to 15: 16,316 | ||||
Chemoimmunotherapy | ||||||
Bendamustine (Generics) | 25 mg 100 mg | 5 mg/mL vial for IV infusion | 250.0000b 1,000.0000b | 90 mg/m2 day 1 and day 2 for six 28-day cycles. | 125.00 | 3,500 |
Rituximab (Subsequent entry biologics) | 100 mg 500 mg | 10 mg/mL vial for IV infusion | 297.0000 1,485.0000 | 375 mg/m2 on day 1 of cycle 1; 500 mg/m2 on day 1 for 5 subsequent 28-day cycles. | Cycle 1: 74.25 Cycle 2 to 6: 95.46 | Cycle 1: 2,079 Cycle 2 to 6: 2,673 |
Bendamustine + rituximab (subsequent entry biologics) | Cycle 1: 199.25 Cycle 2 to 6: 220.46 | Cycle 1: 5,579 Cycle 2 to 6: 6,173 | ||||
Fludarabine | 10 mg | Tablet | 41.8940 | 25 mg/m2 day 1 to day 3 for 6 cycles (28 days per cycle) | 22.44 | 628 |
Cyclophosphamide | 500 mg 1,000 mg 2,000 mg | 20 mg/mL vial for IV infusion | 101.7100b 184.36000b 339.2000b | 250 mg/m2 day 1 to day 3 for 6 cycles (28 days per cycle) | 10.90 | 305 |
Rituximab (subsequent entry biologics) | 100 mg 500 mg | 10 mg/mL vial for IV infusion | 297.0000 1,485.0000 | 375 mg/m2 day 1 of cycle 1; 500 mg/m2 on day 1 for 5 subsequent 28-day cycles. | Cycle 1: 74.25 Cycle 2 to 6: 95.46 | Cycle 1: 2,079 Cycle 2 to 6: 2,673 |
Fludarabine + cyclophosphamide + rituximab (subsequent entry biologics) | Cycle 1: 107.59 Cycle 2 to 6: 128.81 | Cycle 1: 3,013 Cycle 2 to 6: 3,607 | ||||
Bruton tyrosine kinase inhibitors | ||||||
Acalabrutinib (Calquence) | 100 mg | Capsule | 142.7738c | 100 mg twice daily. | 285.55 | 7,995 |
Ibrutinib (Imbruvica) | 140 mg | Capsule | 99.8350c | 420 mg once daily until disease progression or no longer tolerated by the patient. | 299.51 | 8,386 |
Zanubrutinib (Brukinsa) | 80 mg | Capsule | 67.9833c | 320 mg once daily or 160 mg twice daily. | 271.93 | 7,614 |
CDA-AMC = Canada’s Drug Agency.
Notes: This table has not been copy-edited.
The comparators presented in the above table have been deemed to be appropriate based on feedback from clinical expert(s) and drug plans. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
All prices are from the Ontario Drug Benefit Formulary (accessed June 11 2024),36 unless otherwise indicated, and do not include dispensing fees. Costs assume a body surface area of 1.8m2 and include wastage of unused medication in vials. Unless otherwise specified, all treatments are to be administered for the specified treatment length or until disease progression or unacceptable toxicity. Recommended dosages were retrieved from Cancer Care Ontario.
aSponsor-submitted price.
bIQVIA DeltaPA (accessed June 13, 2024).37
cOntario EAP (accessed June 11, 2024).38
Appendix 2: Submission Quality
Please note that this appendix has not been copy-edited.
Description | Yes or no | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | Yes | No comment. |
Model has been adequately programmed and has sufficient face validity | No | Refer to the ‘Poor modelling practices were employed’ limitation in the CDA-AMC Appraisal of the Sponsor’s Economic Evaluation. |
Model structure is adequate for decision problem | Yes | No comment. |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | No | Refer to the ‘Poor modelling practices were employed’ limitation in the CDA-AMC Appraisal of the Sponsor’s Economic Evaluation. |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | No | The model was unable to execute probabilistically and thus parameter and structural uncertainty were not assessed in the CDA-AMC base case. |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | No | Refer to the ‘Poor modelling practices were employed’ limitation in the CDA-AMC Appraisal of the Sponsor’s Economic Evaluation. |
CDA-AMC = Canada’s Drug Agency.
Appendix 3: Additional Information on the Submitted Economic Evaluation
Please note that this appendix has not been copy-edited.
Detailed Results of the Sponsor’s Base Case
Table 10: Disaggregated Summary of the Sponsor’s Economic Evaluation Results
Parameter | VEN + OBI | FLU + CYC + RIT | BEN + RIT | VEN + IBRU | ACA | IBRU | ZANU |
|---|---|---|---|---|---|---|---|
Discounted LYs | |||||||
Total | 18.63 | 15.89 | 8.10 | 18.82 | 17.91 | 13.40 | 14.06 |
Progression-free | 7.47 | 7.45 | 4.86 | 11.23 | 10.52 | 6.54 | 6.46 |
Postprogression | 11.16 | 8.43 | 3.23 | 7.59 | 7.39 | 6.86 | 7.60 |
Discounted QALYs | |||||||
Total | 11.909 | 10.444 | 5.732 | 12.681 | 12.089 | 8.973 | 9.321 |
Progression-free | 5.904 | 5.834 | 3.846 | 8.671 | 8.145 | 5.168 | 5.112 |
Postprogression | 6.007 | 4.612 | 1.888 | 4.012 | 3.945 | 3.808 | 4.210 |
Adverse events | –0.002 | –0.001 | –0.002 | –0.003 | –0.001 | –0.003 | –0.001 |
Discounted costs ($) | |||||||
Total | 276,217 | 310,841 | 156,890 | 559,588 | 1,434,255 | 1,038,364 | 987,794 |
Acquisition | 124,757 | 19,210 | 15,359 | 212,813 | 1,097,018 | 715,748 | 641,921 |
Administration | 1,966 | 1,150 | 3,272 | 17 | 4,755 | 2,948 | 2,911 |
Wastage | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
Monitoring | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
Disease management | 52,765 | 42,850 | 19,817 | 46,226 | 44,328 | 35,763 | 38,114 |
Subsequent treatment | 86,780 | 237,475 | 106,743 | 286,870 | 279,677 | 269,883 | 296,094 |
One-time costsa | 500 | 346 | 622 | 498 | 498 | 498 | 498 |
Terminal care | 5,801 | 6,124 | 7,047 | 5,779 | 5,886 | 6,417 | 6,338 |
Adverse events | 3,648 | 3,685 | 4,030 | 7,385 | 2,094 | 7,109 | 1,918 |
ACA = acalabrutinib; BEN = bendamustine; CYC = cyclophosphamide; FLU = fludarabine; IBRU = ibrutinib; LY = life-year; OBI = obinutuzumab; QALY = quality-adjusted life-year; RIT = rituximab; VEN = venetoclax; ZANU = zanubrutinib.
aIncludes 1-time drug, administration, and monitoring costs.
Source: Sponsor’s pharmacoeconomic submission.1
Appendix 4: Additional Details on the CDA-AMC Reanalyses and Sensitivity Analyses of the Economic Evaluation
Please note that this appendix has not been copy-edited.
Detailed Results of CDA-AMC Base Case
Figure 2: Relative Risk of Next Treatment for VEN + OBI Versus FLU + CYC + RIT and BEN + RIT
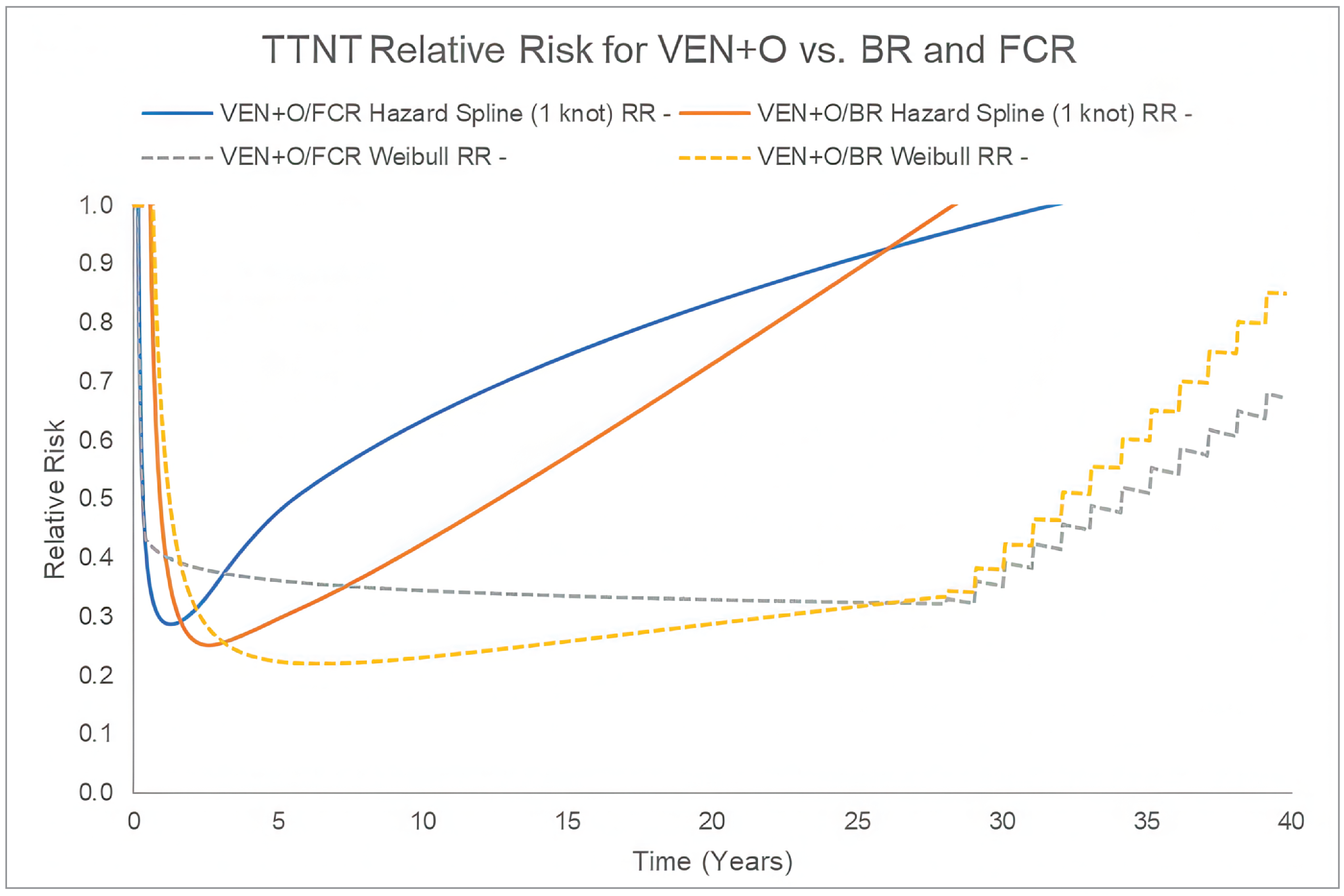
Source: CDA-AMC calculation was based on Kaplan-Meier data from the CLL13 study and parametric extrapolations presented in the sponsor’s pharmacoeconomic model.
Table 11: Summary of the Stepped Analysis of the CDA-AMC Base-Case Results
Stepped analysis | Drug | Total costs ($) | Total QALYs | Sequential ICER ($/QALY) |
|---|---|---|---|---|
Sponsor base case | BEN + RIT | 160,390 | 5.66 | Reference |
VEN + OBI | 281,080 | 11.96 | 19,160 vs. BEN + RIT | |
VEN + IBRU | 573,644 | 12.68 | 408,798 vs. VEN + OBI | |
Dominated treatments | ||||
FLU + CYC + RIT | 365,965 | 10.44 | Dominated by VEN + OBI | |
Zanubrutinib | 1,020,379 | 9.48 | Dominated by VEN + OBI, FLU + CYC + RIT, VEN + IBRU | |
IBRU | 1,064,621 | 9.09 | Dominated by VEN + OBI, FLU + CYC + RIT, VEN + IBRU, zanubrutinib | |
Acalabrutinib | 1,426,661 | 12.54 | Dominated by VEN + IBRU | |
Sponsor’s corrected base case | BEN + RIT | 177,815 | 5.66 | Reference |
VEN + OBI | 283,260 | 11.96 | 16,740 vs. BEN + RIT | |
VEN + IBRU | 573,644 | 12.68 | 405,753 vs. VEN + OBI | |
Dominated treatments | ||||
FLU + CYC + RIT | 366,016 | 11.30 | Dominated by VEN + OBI | |
Zanubrutinib | 1,020,379 | 9.48 | Dominated by VEN + OBI, FLU + CYC + RIT, VEN + IBRU | |
IBRU | 1,064,621 | 9.09 | Dominated by VEN + OBI, FLU + CYC + RIT, VEN + IBRU, zanubrutinib | |
Acalabrutinib | 1,426,661 | 12.54 | Dominated by VEN + IBRU | |
1. CDA-AMC reanalysis 1: OS for BEN + RIT was modelled using an exponential distribution | VEN + OBI | 283,260 | 11.96 | Reference |
VEN + IBRU | 573,644 | 12.68 | 405,753 vs. VEN + OBI | |
Dominated treatments | ||||
BR | 338,374 | 9.15 | Dominated by VEN + OBI | |
FLU + CYC + RIT | 366,016 | 11.30 | Dominated by VEN + OBI | |
Zanubrutinib | 1,020,379 | 9.48 | Dominated by VEN + OBI, FLU + CYC + RIT, VEN + IBRU | |
IBRU | 1,064,621 | 9.09 | Dominated by VEN + OBI, FLU + CYC + RIT, BEN + RIT, VEN + IBRU, zanubrutinib | |
Acalabrutinib | 1,426,661 | 12.54 | Dominated by VEN + IBRU | |
2. CDA-AMC reanalysis 2: PFS for BEN + RIT and FLU + CYC + RIT were modelled using a Weibull distribution | BEN + RIT | 179,294 | 5.52 | Reference |
VEN + OBI | 283,260 | 11.96 | 16,137 vs. BEN + RIT | |
VEN + IBRU | 573,644 | 12.68 | 405,753 vs. VEN + OBI | |
Dominated treatments | ||||
FLU + CYC + RIT | 364,328 | 11.47 | Dominated by VEN + OBI | |
Zanubrutinib | 1,020,379 | 9.48 | Dominated by VEN + OBI, FLU + CYC + RIT, VEN + IBRU | |
IBRU | 1,064,621 | 9.09 | Dominated by VEN + OBI, FLU + CYC + RIT, VEN + IBRU, zanubrutinib | |
Acalabrutinib | 1,426,661 | 12.54 | Dominated by VEN + IBRU | |
3. CDA-AMC reanalysis 3: TTNT for VEN + OBI was modelled using a hazard spline (1 knot) distribution | BEN + RIT | 177,815 | 5.66 | Reference |
FLU + CYC + RIT | 366,016 | 11.30 | 33,386 vs. BEN + RIT | |
VEN + OBI | 446,335 | 11.96 | 121,340 vs. FLU + CYC + RIT | |
VEN + IBRU | 573,644 | 12.68 | 177,889 vs. VEN + OBI | |
Dominated treatments | ||||
Zanubrutinib | 1,020,379 | 9.48 | Dominated by VEN + OBI, FLU + CYC + RIT, VEN + IBRU | |
IBRU | 1,064,621 | 9.09 | Dominated by VEN + OBI, FLU + CYC + RIT, VEN + IBRU, zanubrutinib | |
Acalabrutinib | 1,426,661 | 12.54 | Dominated by VEN + IBRU | |
CDA-AMC base case (reanalysis 1 + 2 + 3) | BEN + RIT | 339,878 | 9.01 | Reference |
FLU + CYC + RIT | 364,328 | 11.47 | 9,924 vs. BEN + RIT | |
VEN + OBI | 446,335 | 11.96 | 167,257 vs. FLU + CYC + RIT | |
VEN + IBRU | 573,644 | 12.68 | 177,889 vs. VEN + OBI | |
Dominated treatments | ||||
Zanubrutinib | 1,020,379 | 9.48 | Dominated by VEN + OBI, FLU + CYC + RIT, VEN + IBRU | |
IBRU | 1,064,621 | 9.09 | Dominated by VEN + OBI, FLU + CYC + RIT, VEN + IBRU, zanubrutinib | |
Acalabrutinib | 1,426,661 | 12.54 | Dominated by VEN + IBRU | |
BEN = bendamustine; CDA-AMC = Canada’s Drug Agency; CYC = cyclophosphamide; FLU = fludarabine; IBRU = ibrutinib; ICER = incremental cost-effectiveness ratio; OBI = obinutuzumab; OS = overall survival; PFS = progression-free survival; QALY = quality-adjusted life-year; RIT = rituximab; TTNT = time to next treatment; VEN = venetoclax; vs. = versus.
Note: The CDA-AMC reanalysis is based on publicly available prices of the comparator treatments. All results are presented deterministically.
Table 12: Disaggregated Summary of the CDA-AMC Economic Evaluation Results
Parameter | VEN + OBI | FLU + CYC + RIT | BEN + RIT | VEN + IBRU | ACA | IBRU | ZANU |
|---|---|---|---|---|---|---|---|
Discounted LYs | |||||||
Total | 18.73 | 18.22 | 14.48 | 18.88 | 18.82 | 13.51 | 14.26 |
Progression-free | 7.45 | 6.30 | 4.18 | 10.84 | 10.21 | 6.50 | 6.49 |
Post progression | 11.29 | 11.92 | 10.30 | 8.04 | 8.61 | 7.01 | 7.77 |
Discounted QALYs | |||||||
Total | 11.963 | 11.473 | 9.009 | 12.679 | 12.536 | 9.088 | 9.483 |
Progression-free | 5.914 | 5.015 | 3.342 | 8.464 | 8.007 | 5.177 | 5.167 |
Post progression | 6.051 | 6.459 | 5.669 | 4.217 | 4.530 | 3.914 | 4.317 |
Adverse events | –0.002 | –0.001 | –0.002 | –0.003 | –0.001 | –0.003 | –0.001 |
Discounted costs ($) | |||||||
Total | 446,335 | 364,328 | 339,878 | 573,644 | 1,426,661 | 1,064,621 | 1,020,379 |
Acquisition | 126,974 | 19,262 | 32,785 | 213,047 | 1,065,350 | 711,175 | 644,376 |
Administration | 1,963 | 1,149 | 3,270 | 17 | 4,575 | 2,912 | 2,906 |
Wastage | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
Monitoring | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
Disease management | 53,352 | 53,683 | 44,229 | 47,420 | 48,409 | 36,338 | 39,045 |
Subsequent treatment | 550 | 366 | 741 | 550 | 550 | 550 | 550 |
One-time costsa | 5,766 | 5,826 | 6,267 | 5,749 | 5,756 | 6,381 | 6,293 |
Terminal care | 446,335 | 364,328 | 339,878 | 573,644 | 1,426,661 | 1,064,621 | 1,020,379 |
Adverse events | 126,974 | 19,262 | 32,785 | 213,047 | 1,065,350 | 711,175 | 644,376 |
ACA = acalabrutinib; BEN = bendamustine; CDA-AMC = Canada’s Drug Agency; CYC = cyclophosphamide; FLU = fludarabine; IBRU = ibrutinib; LY = life-year; OBI = obinutuzumab QALY = quality-adjusted life-year; RIT = rituximab; VEN = venetoclax; ZANU = zanubrutinib.
aIncludes 1-time drug, administration, and monitoring costs.
Scenario Analyses
Table 13: Scenario Analyses Conducted on the CDA-AMC Base Case
Stepped analysis | Drug | Total costs ($) | Total QALYs | Sequential ICER ($/QALY) |
|---|---|---|---|---|
CDA-AMC base case | BEN + RIT | 339,878 | 9.01 | Reference |
FLU + CYC + RIT | 364,328 | 11.47 | 9,924 vs. BEN + RIT | |
VEN + OBI | 446,335 | 11.96 | 167,257 vs. FLU + CYC + RIT | |
VEN + IBRU | 573,644 | 12.68 | 177,889 vs. VEN + OBI | |
Dominated treatments | ||||
Zanubrutinib | 1,020,379 | 9.48 | Dominated by VEN + OBI, FLU + CYC + RIT, VEN + IBRU | |
IBRU | 1,064,621 | 9.09 | Dominated by VEN + OBI, FLU + CYC + RIT, VEN + IBRU, zanubrutinib | |
Acalabrutinib | 1,426,661 | 12.54 | Dominated by VEN + IBRU | |
CDA-AMC Scenario 1: TTNT for VEN + OBI was modelled using a Weibull distribution | BEN + RIT | 339,878 | 9.01 | Reference |
FLU + CYC + RIT | 364,328 | 11.47 | 9,924 vs. BEN + RIT | |
VEN + OBI | 407,610 | 11.96 | 88,275 vs. FLU + CYC + RIT | |
VEN + IBRU | 573,644 | 12.68 | 231,999 vs. VEN + OBI | |
Dominated treatments | ||||
Zanubrutinib | 1,020,379 | 9.48 | Dominated by VEN + OBI, FLU + CYC + RIT, VEN + IBRU | |
IBRU | 1,064,621 | 9.09 | Dominated by VEN + OBI, FLU + CYC + RIT, VEN + IBRU, zanubrutinib | |
Acalabrutinib | 1,426,661 | 12.54 | Dominated by VEN + IBRU | |
CDA-AMC Scenario 2: OS is equal across treatments | FLU + CYC + RIT | 369,405 | 11.74 | Reference |
VEN + IBRU | 572,984 | 12.60 | 237,332 vs. FLU + CYC + RIT | |
Dominated treatments | ||||
BEN + RIT | 403,686 | 11.32 | Dominated by FLU + CYC + RIT | |
VEN + OBI | 446,335 | 11.96 | Extendedly dominated by a combination of FLU + CYC + RIT and VEN + IBRU | |
Zanubrutinib | 1,038,276 | 11.78 | Dominated by VEN + OBI, VEN + IBRU | |
IBRU | 1,086,662 | 11.78 | Dominated by VEN + OBI, VEN + IBRU | |
Acalabrutinib | 1,425,638 | 12.49 | Dominated by VEN + IBRU | |
CDA-AMC Scenario 3: Excluding subsequent therapy costs | FLU + CYC + RIT | 83,961 | 11.47 | Reference |
VEN + IBRU | 274,070 | 12.68 | 157,640 vs. FLU + CYC + RIT | |
Dominated treatments | ||||
BEN + RIT | 91,327 | 9.01 | Dominated by FLU + CYC + RIT | |
VEN + OBI | 192,242 | 11.96 | Extendedly dominated by a combination of FLU + CYC + RIT and VEN + IBRU | |
Zanubrutinib | 695,072 | 9.48 | Dominated by VEN + OBI, FLU + CYC + RIT, VEN + IBRU | |
IBRU | 764,454 | 9.09 | Dominated by VEN + OBI, FLU + CYC + RIT, VEN + IBRU, Zanubrutinib | |
Acalabrutinib | 1,126,727 | 12.54 | Dominated by VEN + IBRU | |
CDA-AMC Scenario 4: PFS for FLU + CYC + RIT was modelled using a generalized gamma distribution | BEN + RIT | 339,878 | 9.01 | Reference |
FLU + CYC + RIT | 366,016 | 11.30 | 11,404 | |
VEN + OBI | 446,335 | 11.96 | 121,340 | |
VEN + IBRU | 573,644 | 12.68 | 177,889 | |
Dominated treatments | ||||
Zanubrutinib | 1,020,379 | 9.48 | Strictly dominated by VEN + OBI, FLU + CYC + RIT, VEN + IBRU | |
IBRU | 1,064,621 | 9.09 | Strictly dominated by VEN + OBI, FLU + CYC + RIT, VEN + IBRU, Zanubrutinib | |
Acalabrutinib | 1,426,661 | 12.54 | Strictly dominated by VEN + IBRU | |
BEN = bendamustine; CDA-AMC = Canada’s Drug Agency; CYC = cyclophosphamide; FLU = fludarabine; IBRU = ibrutinib; ICER = incremental cost-effectiveness ratio; OBI = obinutuzumab; OS = overall survival; PFS = progression-free survival; QALY = quality-adjusted life-year; RIT = rituximab; TTNT = time to next treatment; VEN = venetoclax; vs. = versus.
Note: The CDA-AMC reanalysis is based on publicly available prices of the comparator treatments. All results are presented deterministically. Should the direction of NMA HRs for acalabrutinib align with those for IBRU and zanubrutinib, as anticipated by clinical experts, acalabrutinib would also be dominated by VEN + OBI in all aforementioned analyses.
Appendix 5: Submitted BIA and CDA-AMC Appraisal
Please note that this appendix has not been copy-edited.
Table 14: Summary of Key Take-Aways
Key take-aways of the budget impact analysis |
|---|
|
CDA-AMC = Canada’s Drug Agency; NIHB = Non-Insured Health Benefits.
Summary of Sponsor’s BIA
In the submitted BIA, the sponsor assessed the budget impact of reimbursing VEN + OBI for previously untreated adult patients with CLL considered fit and potentially fludarabine-eligible.39 The BIA was undertaken from the perspective of a Canadian public payer over a 3-year time horizon (Q2 2025 to Q1 2028) using an epidemiologic approach. The sponsor’s pan-Canadian estimates reflect the aggregated results from provincial budgets (excluding Quebec), as well as the Non-Insured Health Benefits (NIHB) program. The sponsor’s analysis included drug acquisition costs, assuming wastage. Data informing the model were obtained from various sources, including previous CDA-AMC Pharmacoeconomic reports,40-42 Statistics Canada,43,44 published literature,12,45-48 the sponsor’s internal data,49 and input from clinical experts consulted by the sponsor. Key inputs to the BIA are documented in Table 15.
The sponsor’s BIA also included the following key assumptions:
100% dose intensity and adherence were assumed for all treatments
Average patient body weight and BSA from the CLL14 clinical trial are reflective of the Canadian population
For fixed-duration treatments (VEN + OBI, VEN + IBRU, FLU + CYC + RIT, and BEN + RIT), all patients complete the full course of treatment; for the remaining treatments (acalabrutinib, zanubrutinib, and ibrutinib), treatment duration was assumed to equal the mean ToT from the submitted pharmacoeconomic analysis
The costs of all IV products were set to $0 for the NIHB Program
50% of prevalent patients are not actively receiving treatment (i.e., “watchful waiting”) and 50% of newly diagnosed patients receive 1L systemic therapy annually
The annual mortality rate for patients with CLL is 2.8%, derived from the 5-year survival rate of 87% for CLL reported by the American Cancer Society.47
Table 15: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as year 1 / year 2 / year 3 if appropriate) |
|---|---|
Target population | |
Pan-Canadian population | |
Population growth | 1.36%a |
Prevalent cases Prevalence Proportion of prevalent cases on watchful waiting Proportion of watchful waiting cases switching to 1L treatment Proportion of fit patients (i.e., potentially FLU-eligible) | 0.027%43 57.0%b 50.0%b 17.0%b |
Incident cases Incidence Proportion treated at diagnosis Proportion of fit patients (i.e., potentially FLU-eligible) | 0.0054%44 50.0%b 17.0%b |
Public drug plan eligibility | |
Number of patients eligible for drug under review | 350 / 295 / 269 |
Market uptake (3 years) | |
Uptake (reference scenario) VEN + OBI VEN + IBRU Acalabrutinib Zanubrutinib IBRU BEN + RIT FLU + CYC + RIT | █████ █ ██ █████ █ ██ █████ █ ██ █████ █ ██ █████ █ ██ █████ █ ██ █████ █ ██ |
Uptake (new drug scenario) VEN + OBI VEN + IBRU Acalabrutinib Zanubrutinib IBRU BEN + RIT FLU + CYC + RIT | █████ █ ██ █████ █ ██ █████ █ ██ █████ █ ██ █████ █ ██ █████ █ ██ █████ █ ██ |
Cost of treatment (per patient, per year) | |
VEN + OBI VEN + IBRU IBRU Acalabrutinib Zanubrutinib BEN + RIT FLU + CYC + RIT | Year 1: $126,934.84; year 2+: $0 Year 1: $182,948.32; year 2: $31,903.10; year 3+: $0 Year 1+: $109,394.20 Year 1+: $104,296.26 Year 1+: $99,323.60 Year 1: $16,494.00; year 2+: $0 Year 1: $24,328.37; year 2+: $0 |
1L = first-line therapy; BEN = bendamustine; CDA-AMC = Canada’s Drug Agency; CYC = cyclophosphamide; FLU = fludarabine; IBRU = ibrutinib; OBI = obinutuzumab; RIT = rituximab; VEN = venetoclax.
Note: For target population parameters with text in brackets, the point estimate is a weighted average from CDA-AMC participating jurisdictions and the text in brackets indicates the range in values across jurisdictions.
aSponsor calculated the average population growth from 2018 to 2023 using Statistics Canada population estimates.50
bBased on clinical expert input obtained by the sponsor.
Summary of the Sponsor’s BIA Results
The sponsor estimated that the 3-year budget impact of reimbursing VEN + OBI for previously untreated adult patients with CLL considered fit and potentially fludarabine-eligible is expected to result in cost savings of $6,473,033 (Year 1 costs: $455,805; Year 2 savings: $1,728,609; Year 3 savings: $5,200,230).
CDA-AMC Appraisal of the Sponsor’s BIA
CDA-AMC identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
Drug acquisition costs for BTKi-based therapies may be overestimated: The duration of treatment for BTKi-based therapies (acalabrutinib, ibrutinib, and zanubrutinib) was assumed equal to the mean ToT from the sponsor’s submitted CUA. In the BIA, patients receiving acalabrutinib are on treatment for an average of 11.3 years and patients receiving ibrutinib or zanubrutinib are on treatment for an average of 7 years. As such, the sponsor is assuming all patients receiving a BTKi-based therapy remain on treatment in Years 1 to 3 of the BIA despite a proportion of patients discontinuing treatment, as reflected in the CUA. For reference, in the submitted CUA, 99%, 96%, and 93% of patients remain on acalabrutinib at the end of Year 1, 2, and 3, respectively, and 97%, 91%, and 83% of patients remain on ibrutinib and zanubrutinib at the end of Year 1, 2, and 3, respectively. Additionally, as noted in the CDA-AMC Appraisal of the Sponsor’s Economic Evaluation, while the BTKi therapies are treat-until-progression therapies, clinical expert input noted that patients may discontinue treatments for reasons unrelated to progression such as intolerance, AEs, or toxicities. Clinical expert input commented that approximately 10% to 30% of patients receiving a BTKi therapy discontinue before progression. CDA-AMC notes that the RESONATE-255 study reported a discontinuation rate due to AEs of 16.3% over 3 years for patients treated with ibrutinib; the discontinuation rate due to AEs for patients treated with zanubrutinib in the SEQUOIA56 trial was 14.9% at a median follow-up of 43.7 months for patients without del(17p) and 13.5% for patients with del(17p); the discontinuation rate due to AEs was 6% at a median follow-up time of 53 months for patients treated with acalabrutinib in the ACE-CL-00157 trial. As such, the sponsor overestimated BTKi treatment costs in each year of the BIA as it was assumed that no patients discontinue BTKi-based therapy.
In the CDA-AMC base case, CDA-AMC derived annual treatment costs for acalabrutinib, ibrutinib, and zanubrutinib by retrieving the proportion of patients on treatment at the end of Years 1, 2, and 3 from the CDA-AMC CUA base case and multiplied the respective proportions by annual treatment costs in the sponsor’s submitted BIA.
CDA-AMC conducted scenario analyses by assuming that 10% and 30% of patients receiving BTKi-based therapies discontinue treatment before progression, in alignment with clinical expert opinion.
Market shares in the reference scenario are uncertain: The sponsor derived market shares in the reference scenario from ONCO-CAPPS, a real-world oncology database.49 First, data from ONCO-CAPPS ████████ ████ ███ █████████ ██████████ ███ ██ █████████ █████ ██████████ ███████ █████ ███ █████ ██████ ██ ███████████████████ ████ █████ ███ ███ █████████ ██████████ ██████████ ███████ ████████ █████ █████ █████ ███ █████████ ████ █████████ ██████████ ██ ███████ ██ ████████████████████████. The sponsor acknowledged that VEN + OBI uptake was potentially overestimated in ONCO-CAPPS as the data may have included patients for which VEN + OBI is currently reimbursed for (i.e., fludarabine-ineligible patients). As such, the sponsor reduced base year market shares for VEN + OBI, as estimated by ONCO-CAPPS, by a factor of 0.6 and redistributed the market share to VEN + IBRU which the sponsor assumed would be listed in the base year.
In the sponsor’s base-case reference scenario, ██ patients, ██ patients, and ██ patients in Years 1, 2, and 3, respectively, were assumed to be treated with VEN + OBI. However, CDA-AMC notes that the ONCO-CAPPS data used by the sponsor did not differentiate between patients who accessed treatment through a public drug plan from those using private insurance or out-of-pocket payments. As such, the data includes an unknown proportion of patients who access VEN + OBI privately.
Second, clinical experts consulted by CDA-AMC for this review commented that access to FLU + CYC + RIT and ibrutinib may vary by jurisdiction and use of both treatments may be declining at rates higher than estimated by the sponsor. Clinical experts commented market shares for zanubrutinib may be underestimated as zanubrutinib should have a market share similar to acalabrutinib. Lastly, clinical experts noted that market shares for VEN + IBRU may be overestimated due to the limited access of VEN + IBRU and clinician preference to avoid the use of ibrutinib.
In the CDA-AMC base case, the raw 2024 ONCO-CAPPS market share data for VEN + OBI was reduced by 50% as CDA-AMC assumed 50% of eligible patients were currently accessing VEN + OBI via a public drug plan. The sponsor’s market share estimates for the unmutated IGHV population in British Columbia were maintained. In the CDA-AMC base case, the number of patients assumed to be treated with VEN + OBI in the reference scenario was reduced to 54 patients, 46 patients, and 42 patients in Years 1, 2, and 3, respectively.
Uptake of VEN + OBI is uncertain: The sponsor’s submitted base case assumed that should VEN + OBI become publicly reimbursed for the indicated population, ██████ ██████ ███ ██% of eligible patients would receive VEN + OBI in Year 1, Year 2, and Year 3, respectively (███ ██████████████ ██████). As VEN + OBI is funded in British Columbia for unmutated IGHV patients, regardless of fitness or fludarabine eligibility, the sponsor assumed uptake of VEN + OBI in British Columbia would be ██████ ██████ ███ ███ ██ ████ ██ ████ ██ ███ ██ |, respectively. First, clinical expert input noted that uptake of VEN + OBI may vary by jurisdiction, with lower uptake in smaller communities due to the requirement of a treatment room and monitoring of infusion-related reactions for the obinutuzumab component of the regimen. Lastly, the sponsor assumed that VEN + OBI would displace all comparators proportionate to their respective market shares in the reference scenario. CDA-AMC notes that per the CDA-AMC Clinical Review Report, the sponsor’s submitted NMA suggests that in comparison to ██████ █████████████ ███ █████ ████ █ ██████████ █████████ ██████ ██ ███. Should clinicians agree with this finding, which is associated with uncertainty as the 95% credible interval includes the null, ██ ██ ████████ ████ █████ █████ ███ ███████ █ █████ ██████ █████ ████ █████ ██ █████████████ ██ ██████████ ███ ████████ ███ ██████ █████████████ ███ █████ ███ ██ █████ ██ ███.
CDA-AMC did not adjust for this limitation in reanalyses.
The estimated proportion of patients that would be eligible for public coverage is uncertain: The sponsor calculated drug plan eligibility across CDA-AMC participating jurisdictions based on province-specific data from the Canadian Institute for Health Information and the Conference Board of Canada,45,48 in conjunction with age demographics from the CLL13 trial.12 As the regimen under review includes both an oral (venetoclax) and an IV (obinutuzumab) treatment, coverage rates may differ between venetoclax and obinutuzumab within a jurisdiction. Generally, IV treatments have 100% coverage, but take-home oncology medications (e.g., oral medications) are not covered using a consistent approach.58 For example, in Ontario and Atlantic provinces, these medications are funded for the subset of the population eligible for public coverage and eligibility may depend on factors such as age and income.58
CDA-AMC did not adjust for this limitation owing to a lack of data.
The NIHB population was inappropriately calculated: First, the sponsor assumed the cost of all IV products was $0 for the NIHB population therefore limiting NIHB costs to oral products only. This was inappropriate as it effectively assumes NIHB patients will not be able to access IV oncology treatments and underestimates total treatment costs. Additionally, the provinces of Saskatchewan and Alberta fund all oncology products for patients residing within their borders, including those who would otherwise be reimbursed by the NIHB, as does Ontario for patients under 25 years of age and 65 years of age and older. NIHB clients of the appropriate ages who are living within the borders of these 3 jurisdictions should therefore be considered clients of the provincial plan for the purpose of modelling the budget impact of reimbursing VEN + OBI. Lastly, NIHB clients residing within Ontario who are under 25 years of age and 65 years of age and older are eligible for reimbursement by ODB and thus should be counted as ODB clients and included in the Ontario population estimates rather than NIHB clients for the purpose of modelling the budget impact of reimbursing VEN + OBI.
In the CDA-AMC base case, CDA-AMC assumed the NIHB population would fund IV oncology treatments for the purpose of estimating the total budget impact. CDA-AMC did not adjust the NIHB population size in in reanalysis; the impact on pan-Canadian model results is expected to be minimal.
Misalignment of model inputs between the sponsor-submitted CUA and BIA. Several model inputs and assumptions in the BIA were not aligned with the CUA submitted by the sponsor. First, the sponsor sourced patient body weight and BSA from the CLL14 trial rather than the CLL13 trial, the data source used in the CUA. Second, the sponsor considered wastage in the BIA for FLU + CYC + RIT and BEN + RIT, however no wastage (i.e., no vial sharing) was assumed in the CUA.
In the CDA-AMC base case, CDA-AMC aligned the baseline characteristics for patient body weight and patient BSA with the CUA and excluded drug wastage for all treatments.
CDA-AMC Reanalyses of the BIA
CDA-AMC revised the sponsor’s base case by correcting the price of obinutuzumab, bendamustine, and cyclophosphamide, aligning the baseline characteristics for patient body weight and patient BSA with the CUA, excluding drug wastage for all treatments, including annual costs for IV treatments in the NIHB population, and adjusting the duration of BTKi-based therapies to align with the CUA.
The results of the CDA-AMC stepwise reanalysis are presented in summary format in Table 17 and a more detailed breakdown is presented in Table 18.
In the CDA-AMC base case, the 3-year budget impact of reimbursing VEN + OBI for previously untreated adult patients with CLL considered fit and potentially fludarabine-eligible is expected to result in cost savings of $8,371,343 (Year 1 costs: $1,158,251; Year 2 savings: $2,535,407; Year 3 savings: $6,994,187).
Table 16: CDA-AMC Revisions to the Submitted Budget Impact Analysis
Stepped analysis | Sponsor’s value or assumption | CDA-AMC value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
Unit drug prices |
|
|
Changes to derive the CDA-AMC base case | ||
1. Baseline characteristics |
|
|
2. Drug wastage | Drug wastage was considered for BEN + RIT and FLU + CYC + RIT. | In alignment with the CUA, drug wastage was not considered for any treatment. |
3. NIHB annual costsa |
|
|
4. Discontinuation of BTKi-based therapy | No patients discontinued acalabrutinib, zanubrutinib, and ibrutinib in Y1, Y2, and Y3 | The proportion of patients remaining on therapy at the end of Y1, Y2, and Y3 was aligned with the CUA:
|
5. VEN + OBI market shares in reference scenario (aggregated) | Year 1 = ████% Year 2 = ████% Year 3 = ████% | Year 1 = 15.5% Year 2 = 15.6% Year 3 = 15.7% |
CDA-AMC base case | Reanalysis 1 + 2 + 3 + 4 + 5 | |
BEN = bendamustine; BSA = body surface area; BTKi = Bruton tyrosine kinase inhibitor; CDA-AMC = Canada’s Drug Agency; CUA = cost-utility analysis; CYC = cyclophosphamide; FLU = fludarabine; NIHB = Non-Insured Health Benefits; RIT = rituximab; Y1 = year 1; Y2 = year 2; Y3 = year 3.
Note: CDA-AMC notes that the sponsor sourced the price of a 25 mg vial of BEN from a previous CDA-AMC report in which the price was transcribed incorrectly. The corrections made to the prices of obinutuzumab and CYC and 100 mg vial of BEN are due to changes in the publicly available prices. The proportion of patients on treatment was rounded to 2 decimal places in the table; however, 13 decimal places were used in the stepped analysis.
aWhile NIHB does not fund IV treatments, CDA-AMC assumed the NIHB population would fund IV oncology treatments for the purposes of estimating the total budget impact.
Table 17: Summary of the CDA-AMC Reanalyses of the Budget Impact Analysis
Stepped analysis | Three-year total ($) |
|---|---|
Sponsor’s submitted base case | –6,473,033 |
Sponsor’s corrected base case | –6,474,557 |
CDA-AMC reanalysis 1: Baseline characteristics | –6,491,031 |
CDA-AMC reanalysis 2: Drug wastage | –6,446,099 |
CDA-AMC reanalysis 3: NIHB annual costs | –6,219,962 |
CDA-AMC reanalysis 4: Discontinuation of BTKi-based therapy | –5,714,038 |
CDA-AMC reanalysis 5: VEN + OBI market shares in reference scenario | –9,970,942 |
CDA-AMC base case | –8,371,343 |
BTKi = Bruton tyrosine kinase inhibitor; CDA-AMC = Canada’s Drug Agency; NIHB = Non-Insured Health Benefits; OBI = obinutuzumab; VEN = venetoclax.
CDA-AMC conducted the following scenario analyses to address remaining uncertainty, using the CDA-AMC base case (results are provided in Table 18:
Assuming the proportion of patients discontinuing BTKi-therapy before progression is increased by 10%.
Assuming the proportion of patients discontinuing BTKi-therapy before progression is increased by 30%.
Assuming the price of venetoclax is reduced by 75% (the CDA-AMC estimated price reduction from the CUA).
Table 18: Detailed Breakdown of the CDA-AMC Reanalyses of the BIA
Stepped analysis | Scenario | Year 0 (current situation) ($) | Year 1 ($) | Year 2 ($) | Year 3 ($) | Three-year total ($) |
|---|---|---|---|---|---|---|
Submitted base case | Reference | 48,597,560 | 65,842,897 | 81,446,129 | 97,247,179 | 244,536,205 |
New drug | 48,597,560 | 66,298,702 | 79,717,520 | 92,046,950 | 238,063,171 | |
Budget impact | 0 | 455,805 | –1,728,609 | –5,200,230 | –6,473,033 | |
CDA-AMC base case | Reference | 45,718,680 | 65,172,596 | 81,313,358 | 101,099,572 | 247,585,526 |
New drug | 45,718,680 | 66,330,847 | 78,777,951 | 94,105,385 | 239,214,183 | |
Budget impact | 0 | 1,158,251 | –2,535,407 | –6,994,187 | –8,371,343 | |
CDA-AMC scenario analysis 1: Discontinuation of BTKi-therapy before progression is increased by 10% | Reference | 42,901,059 | 60,122,432 | 74,443,227 | 95,031,629 | 229,597,289 |
New drug | 42,901,059 | 61,654,411 | 72,768,085 | 89,537,942 | 223,960,439 | |
Budget impact | 0 | 1,531,979 | –1,675,142 | –5,493,687 | –5,636,850 | |
CDA-AMC scenario analysis 2: Discontinuation of BTKi-therapy before progression is increased by 30% | Reference | 37,265,816 | 50,022,105 | 60,702,964 | 82,895,744 | 193,620,814 |
New drug | 37,265,816 | 52,301,540 | 60,748,353 | 80,403,057 | 193,452,949 | |
Budget impact | 0 | 2,279,434 | 45,388 | –2,492,687 | –167,865 | |
CDA-AMC scenario analysis 3: 75% price reduction | Reference | 39,279,033 | 59,587,890 | 76,428,945 | 96,564,760 | 232,581,595 |
New drug | 39,279,033 | 58,117,102 | 70,621,299 | 85,257,021 | 213,995,422 | |
Budget impact | 0 | –1,470,788 | –5,807,647 | –11,307,739 | –18,586,174 |
BTKi = Bruton tyrosine kinase inhibitor; CDA-AMC = Canada’s Drug Agency.
Results from the CDA-AMC scenario analyses demonstrate that the budget impact is sensitive to assumptions regarding the proportion of patients who discontinue BTKi-based therapies (acalabrutinib, ibrutinib, and zanubrutinib) before progression. Increasing the proportion of patients who discontinue BTKi-based therapy before progression due to intolerance, AEs, or toxicities decreases the cost savings associated with reimbursing VEN + OBI, as demonstrated by the 2 scenario analyses. CDA-AMC notes that if greater than 31% of patients discontinue BTKi-therapy before progression, VEN + OBI would no longer be cost-saving.
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.