Drugs, Health Technologies, Health Systems
Reimbursement Review
Quizartinib (Vanflyta)
Sponsor: Daiichi Sankyo Pharma Canada
Therapeutic area: Acute myeloid leukemia
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Clinical Review
Abbreviations
AE
adverse event
AESI
adverse event of special interest
AML
acute myeloid leukemia
ANC
absolute neutrophil count
CDA-AMC
Canada’s Drug Agency
CI
confidence interval
CIR
cumulative incidence of relapse
CLSG/CGEL
Canadian Leukemia Study Group/Groupe Canadien d'Étude Sur La Leucémie
CNS
central nervous system
CR
complete remission
CRc
composite complete remission
CRi
complete remission with incomplete hematologic recovery
CrI
credible interval
CTTC
Cell Transplant Therapy Canada
CYP
cytochrome P450
DIC
deviance information criterion
ECG
electrocardiogram
ECOG
Eastern Cooperative Oncology Group
EFS
event-free survival
ELN
European LeukemiaNet
ELPD
expected log predictive density
EORTC QLQ-C30
European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30
ESS
effective sample size
FLAG-IDA
a combination of fludarabine, cytarabine, idarubicin, and filgrastim
GHS
global health status
GRADE
Grading of Recommendations Assessment, Development and Evaluation
GVHD
graft-versus-host disease
HR
hazard ratio
HRQoL
health-related quality of life
HSCT
hematopoietic stem cell transplant
IPD
individual patient data
IRC
independent review committee
ITC
indirect treatment comparison
ITD
internal tandem duplication
ITF
induction treatment failure
KM
Kaplan-Meier
LLSC
Leukemia and Lymphoma Society of Canada
LOO
leave one out
LOOIC
leave-one-out information criterion
MAIC
matching adjusted indirect comparison
MID
minimally important difference
ML-NMR
multilevel network meta-regression
MRD
minimal or measurable residual disease
NE
not estimable
NGS
next-generation sequencing
OR
odds ratio
OS
overall survival
PCR
polymerase chain reaction
PH
proportional hazards
QoL
quality of life
QTc
corrected QT interval
QTcF
QT interval corrected using the Fridericia formula
RCT
randomized controlled trial
RFS
relapse-free survival
RMST
restricted mean survival time
RT-PCR
reverse transcription polymerase chain reaction
SAE
serious adverse event
SD
standard deviation
SR
systematic review
TEM
treatment effect modifier
TKD
tyrosine kinase domain
VAF
variant allele frequency
WBC
white blood cell
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Table 1: Background Information of Application Submitted for Review
Item | Description |
|---|---|
Drug product | Quizartinib (Vanflyta), 17.7 mg or 26.5 mg tablets, oral |
Sponsor | Daiichi Sankyo Pharma Canada |
Indication | In combination with standard cytarabine and anthracycline induction and standard cytarabine consolidation chemotherapy, followed by quizartinib maintenance monotherapy, for the treatment of adult patients with newly diagnosed acute myeloid leukemia that is FLT3 internal tandem duplication positive |
Reimbursement request | As per indication |
Health Canada approval status | NOC |
Health Canada review pathway | Standard review |
NOC date | June 9, 2025 |
Recommended dose | In combination with standard chemotherapy at a dose of 35.4 mg (two 17.7 mg doses) once daily for 2 weeks in each cycle of induction. For patients with complete remission or complete remission with incomplete hematologic recovery, quizartinib should be administered at 35.4 mg once daily for 2 weeks in each cycle of consolidation chemotherapy followed by quizartinib maintenance monotherapy initiated at 26.5 mg once daily. After 2 weeks, the maintenance dose should be increased to 53 mg (two 26.5 mg doses) once daily if the QT interval corrected using the Fridericia formula is ≤ 450 ms. |
NOC = Notice of Compliance.
Introduction
Acute myeloid leukemia (AML) is a heterogeneous hematologic malignancy with a rapid disease onset due to proliferation of abnormal blast cells.1 AML is one of the most aggressive forms of leukemia, with an estimated 5-year survival rate of 31.9%.2 In 2019, approximately 1,160 people in Canada were diagnosed with AML and in 2022, 1,286 died from the disease.3 Symptoms of AML include those associated with anemia (e.g., fatigue, weakness, shortness of breath, lightheadedness, dizziness, headaches), neutropenia (e.g., frequent infections, fever), and thrombocytopenia (e.g., easy bruising, petechiae, prolonged bleeding from minor cuts, frequent or severe nosebleeds, bleeding gums). Other symptoms may include loss of appetite, unexplained weight loss, discomfort in bones or joints, and fullness or swelling in the abdomen due to an enlarged spleen or liver.4
The FLT3 mutation can be found in approximately 30% of patients with newly diagnosed AML.5 The 2 main classes of FLT3 mutations are the internal tandem duplication (ITD) mutations within the receptor’s autoinhibitory juxtamembrane domain (approximately 25% of all AML cases) and the point mutations that occur within the tyrosine kinase domain (TKD) activation loop (5% to 10% of all AML cases).5,6 Compared with patients with the FLT3-TKD mutation and those without any FLT3 mutation, those with the FLT3-ITD mutation have a higher burden of disease at diagnosis, and poorer overall survival (OS) and relapse-free survival (RFS).5,7-12
Among patients with newly diagnosed AML that is FLT3-ITD positive, the goal of treatment is to control the disease and, whenever possible, provide a cure.13 Patients who are eligible for intensive chemotherapy receive standard induction therapy with cytarabine and an anthracycline (either daunorubicin or idarubicin) in combination with the FLT3 inhibitor, midostaurin. For patients with complete remission (CR) after 1 or 2 cycles, induction therapy is followed by allogeneic hematopoietic stem cell transplant (HSCT) and/or 1 to 4 cycles of consolidation therapy with either intermediate-dose or high-dose cytarabine plus midostaurin. This may be followed by maintenance treatment with oral azacitidine for patients not eligible for allogeneic HSCT.13-15
Quizartinib16 is a small molecule inhibitor of FLT3. It is approved by Health Canada in combination with standard cytarabine and anthracycline induction and standard cytarabine consolidation chemotherapy, followed by quizartinib maintenance monotherapy, for the treatment of adult patients with newly diagnosed AML that is FLT3-ITD positive. The sponsor’s submission to CDA-AMC was filed on a pre-Notice of Compliance basis. The Health Canada–approved indication includes clarifying statements stating that “improvement in overall survival has not been demonstrated for maintenance monotherapy following allogeneic hematopoietic stem cell transplantation,” and that “a validated test is required to confirm the FLT3-ITD status of AML.” The product monograph includes a Serious Warnings and Precautions Box, which states “do not initiate VANFLYTA therapy if the QT interval corrected by Fridericia’s formula (QTcF) is greater than 450 ms or in patients with severe hypokalemia, hypomagnesemia, or long QT syndrome.” The sponsor-requested reimbursement criteria align with the Health Canada–approved indication.
Midostaurin is currently the only drug specifically indicated for the treatment of patients with newly diagnosed FLT3-mutated AML in Canada. Although the addition of midostaurin to standard induction and consolidation therapy improves outcomes among these patients, there remains an important risk of relapse postremission and long-term survival may be limited.17 Evidence suggests that the use of FLT3 inhibitors as maintenance therapy presents an opportunity to prevent poor outcomes associated with relapsed postallogeneic HSCT.18
The objective of this clinical review report is to review and critically appraise the clinical evidence submitted by the sponsor on the beneficial and harmful effects of quizartinib in the treatment of adult patients with newly diagnosed AML that is FLT3-ITD positive. The focus will be placed on comparing quizartinib to relevant comparators and identifying gaps in the current evidence.
Perspectives of Patients, Clinicians, and Drug Programs
The information in this section is a summary of input provided by the patient and clinician groups who responded to the call for input and from clinical expert(s) consulted by for the purpose of this review.
Patient Input
Input for this review was submitted by 2 patient groups, Heal Canada and the Leukemia and Lymphoma Society of Canada (LLSC). Heal Canada gathered input through an online patient survey (N = 22). Information for the LLSC input was gathered through 2 patient surveys (N = 224 and N = 83, respectively).
Patients highlighted the profound impact of AML on their social lives, personal relationships, mental health, and independence. Nearly all patients reported needing caregiver support for daily tasks, which diminished their mental well-being by impeding independence and increasing the burden on caregivers. Patients also emphasized the impact of AML on their personal and home lives, reporting that symptoms, mental load, and frequent travel for appointments limit their ability to participate in social activities and maintain relationships. For many patients, current treatments can have severe adverse effects and limited long-term efficacy.
When evaluating new treatment options for AML, patients and caregivers indicated that they would prioritize improvements in long-term adverse effects and the impact of adverse effects on daily life, and a reduced risk of relapse. High importance was also placed on quality of life (QoL), maintaining independence, the severity and frequency of adverse effects, and the duration of and potential for sustained remission. When asked to elaborate on what desired improvements to QoL they would like to see from new treatments, patients noted longer remission, reduction in the fear and risk of reoccurrence, CR and a cure, resumption of regular daily activities, limited side effects, less time in hospital, a reduced need for transfusions, and better access to care in smaller communities.
In the Heal Canada input, 3 patients had experience with quizartinib and found the treatment to be well-tolerated. One patient reported improved response after switching from azacitidine, venetoclax, and gilteritinib. Another patient had CR during the first induction, received allogeneic HSCT, reported no residual disease post-transplant, and continued with quizartinib maintenance therapy. In the LLSC input, 13 respondents to the first survey had experience with quizartinib. Respondents reported the most severe adverse effects to be thrombocytopenia and anemia. Most respondents noted improved QoL, and all reported that they would choose quizartinib again and recommend it to others.
Clinician Input
Input From Clinical Experts Consulted for This Review
The clinical experts identified the need for evidence to support decision-making, including studies to inform the following: the efficacy and harms of FLT3-ITD inhibitors among patients aged older than 60 years; the comparative efficacy of midostaurin and more potent FLT3-ITD inhibitors, including quizartinib and gilteritinib; the role of minimal or measurable residual disease (MRD) assessment in determining which patients need more consolidative therapy and/or allogeneic HSCT; and the contribution of maintenance therapy to the efficacy of FLT3-ITD inhibitors, including among patients who have received allogeneic HSCT. The clinical experts also identified a need for an approved maintenance therapy for patients with newly diagnosed AML that is FLT3-ITD positive. Currently, only oral azacitidine is available, and patients are only eligible if they are in first-line CR, have intermediate-risk or adverse karyotype, and are not planned or have not received allogeneic HSCT. Azacitidine is associated with undesirable gastrointestinal effects.
According to the clinical experts, patients most likely to benefit from quizartinib are those with newly diagnosed AML that is FLT3-ITD positive and who are eligible for intensive induction and consolidation chemotherapy. These are the same patients who are currently treated with midostaurin. Midostaurin is also used for patients with FLT3-TKD mutations; however, these patients would not be treated with quizartinib. Although there is no direct evidence comparing quizartinib and midostaurin, the clinical experts indicated that most physicians would choose quizartinib over midostaurin, with the primary advantage being the option to administer it as maintenance therapy. According to the clinical experts, testing for FLT3-ITD mutations is currently performed as part of the standard of care for patients with newly diagnosed AML. Testing for FLT3-ITD mutations to determine treatment eligibility for quizartinib is not anticipated to pose any implementation issues.
According to the clinical experts, patients receiving quizartinib will be monitored for relapse based on clinical assessment and bloodwork at regular intervals, with a bone marrow assessment done when there is a concern for relapse. Patients will be discontinued from quizartinib upon disease relapse, the development of certain cardiac adverse events (AEs), death, or the completion of 3 years of maintenance therapy (per the protocol for the pivotal trial). Quizartinib may also be discontinued due to patient preference.
The clinical experts noted that MRD is being evaluated routinely for an increasing number of AML subtypes as a potential marker of prognosis and to inform treatment decision-making.14 Testing for FLT3-ITD MRD is being developed and validated at some Canadian centres, but is not currently funded or used in clinical practice.
According to the clinical experts, patients receiving quizartinib should be treated by a hematologist with experience in treating patients with acute leukemia in a centre with the appropriate resources. Consolidation chemotherapy may be administered in the outpatient setting provided certain institutional criteria are met. Quizartinib maintenance therapy would be administered as an outpatient under the supervision of a hematologist with experience in administering lower-intensity therapy in a centre with the appropriate resources.
Clinician Group Input
Input was submitted by 3 clinician groups, the Ontario Health (Cancer Care Ontario) Hematology Cancer Drug Advisory Committee and a joint input from the Canadian Leukemia Study Group/Groupe Canadien d'Étude Sur La Leucémie (CLSG/GCEL) and Cell Transplant Therapy Canada (CTTC). Input from the clinician groups about the current standard of care, unmet needs, patients most likely to benefit from quizartinib, measurements of response, and discontinuation criteria was aligned with the input from the clinical experts consulted for this review.
The clinician groups emphasized that there is currently no approved FLT3-ITD–specific maintenance therapy, highlighting this as a major cause of failure and death in patients with this mutation. The clinician groups also noted that currently available treatments are highly toxic and that patients have poor outcomes, including high relapse rates and short OS. As it is not possible to identify which FLT3-ITD–positive patients are most likely to respond to treatment, the clinician groups noted that all should receive it.
The clinician groups concurred that MRD response could be a surrogate; however, an appropriate FLT3-ITD MRD test is not available in Canada. The clinician groups suggested that depending on the patient’s disease phase, their treatment response could be reassessed weekly, every 2 weeks, monthly, or every 2 months to 3 months. Postinduction bone marrow is used to confirm remission. The clinician groups indicated that discontinuation of quizartinib should be considered in the event of relapse or intolerable toxicity. They noted that the optimal duration of quizartinib maintenance therapy is currently unclear; however, at least 3 years of maintenance therapy would be recommended, in the absence of disease relapse or intolerable toxicity, per the design of the pivotal trial.
The clinician groups agreed that treatment would be initiated and monitored at a university-associated academic leukemia centre, as an inpatient procedure for induction and outpatient for consolidation. The groups noted that during maintenance treatment, patients could be followed incrementally at a shared care site closer to home. Treatment would be initiated and monitored by specialists with expertise in leukemia, likely primarily hematologists, but also some oncologists.
Drug Program Input
Input was obtained from the drug programs that participate in the reimbursement review process for Canada’s Drug Agency (CDA-AMC). The input received and responses from the clinical experts consulted for this review are in Table 5. The following were identified as key factors that could potentially impact the implementation of the CDA-AMC recommendation for quizartinib:
considerations for the initiation of therapy
considerations for the continuation or renewal of therapy
considerations for the discontinuation of therapy
considerations for the prescribing of therapy
generalizability
funding algorithm (conditions under which quizartinib would be preferred over midostaurin).
Clinical Evidence
Systematic Review
Description of Studies
The sponsor’s systematic review (SR) identified 1 phase III, double-blind, multicentre randomized controlled trial (RCT), QuANTUM-First.19-22 The QuANTUM-First study compared the effects of quizartinib (n = 268) versus placebo (n = 271) (administered with standard induction and consolidation chemotherapy [and/or allogeneic HSCT], then administered as maintenance therapy for up to 36 cycles) among adult patients with newly diagnosed AML that is FLT3-ITD positive (N = 539). The sponsor’s SR did not identify any studies directly comparing the efficacy or harms of quizartinib and midostaurin.
The QuANTUM-First study was conducted in 193 sites in 26 countries, including 4 sites in Canada. The QuANTUM-First study consisted of 4 consecutive phases: induction, consolidation, continuation (hereafter termed “maintenance”), and long-term follow-up. The primary end point was OS. Secondary end points included event-free survival (EFS), CR rate, CR with FLT3-ITD MRD negativity rate, composite CR (CRc) rate (CR and CR with incomplete hematologic recovery [CRi]), and CRc with FLT3-ITD MRD negativity rate after induction. Relevant exploratory end points included RFS, duration of CR and CRc, transplant rate, and health-related quality of life (HRQoL), assessed via the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 (EORTC QLQ-C30) questionnaire. There were no interim analyses. The final data cut-off for efficacy analyses was August 13, 2021. At this time, the median duration of follow-up was 39.2 months in both groups. Updated safety data were provided up to a data cut-off of June 16, 2023.
Patients’ demographic and disease characteristics were generally balanced across groups. The median age of patients was 56 years and 40% were aged 60 years or older. Slightly more than half of patients were female (54.5%). Most patients were white (59.7%) or Asian (29.3%) and were recruited from Europe (60.5%). Most patients had de novo AML (92.4%), an Eastern Cooperative Oncology Group (ECOG) performance status of 0 or 1 (84.4%), and an intermediate cytogenetic risk status (72.4%). Approximately two-thirds of patients had a FLT3-ITD variant allele frequency (VAF) of more than 25%, half had a FLT3-ITD VAF more than 25% but less than 50%, and 10% had a FLT3-ITD VAF of 50% or more. Equal proportions of patients had a white blood cell (WBC) count at diagnosis of less than 40 × 109/L and 40 × 109/L or more. The mean bone marrow blast count at baseline was 66.91 to 67.60 across groups. The mean absolute neutrophil counts (ANCs) at baseline in the quizartinib and placebo groups were 0.60 (standard deviation [SD] = 1.827) and 0.44 (SD = 1.300), respectively, and mean platelet counts were 28.76 (SD = 22.137) and 31.27 (SD = 33.942), respectively. Approximately one-half and one-quarter of patients across groups had NPM1 and CEBPA mutations, respectively.
Of randomized patients, 265 of 268 (98.9%) in the quizartinib group and 268 of 271 (98.9%) in the placebo group were treated. Among these patients, all entered the induction phase. Sixty-five percent of patients in both groups entered the consolidation phase and 37.0% in the quizartinib group and 33.2% in the placebo group received allogeneic HSCT (with or without study drug plus chemotherapy). Forty-four percent of patients in the quizartinib group and 34.3% of patients in the placebo group entered the maintenance phase, including 70 of 98 (71.4%) patients in the quizartinib group and 49 of 89 (55.1%) patients in the placebo group who had received allogeneic HSCT during the consolidation phase. During the maintenance phase, an additional 4 (1.5%) and 2 (0.7%) patients in the quizartinib and placebo groups, respectively, received allogeneic HSCT. As of the time of the data cut-off, 84.9% of patients in the quizartinib group and 89.2% of patients in the placebo group had entered long-term follow-up.
Efficacy Results
Overall Survival
At the time of the data cut-off, 133 of 268 (49.6%) patients in the quizartinib group and 158 of 271 (58.3%) patients in the placebo group had died. The median OS was 31.9 months (95% confidence interval [CI], 21.0 months to not estimable [NE]) in the quizartinib group and 15.1 months (95% CI, 13.2 months to 26.2 months) in the placebo group. The hazard ratio (HR) was 0.776 (95% CI, 0.615 to 0.979), in favour of quizartinib (P = 0.0324). The Kaplan-Meier (KM)-estimated probability of OS at 12 months was 67.4% (95% CI, 61.3% to 72.7%) in the quizartinib group and 57.7% (95% CI, 51.6% to 63.4%) in the placebo group (difference = 9.6%; 95% CI, 1.4% to 17.8%). The KM-estimated probability of OS at 48 months was 48.4% (95% CI, 41.9% to 54.5%) in the quizartinib group and 37.0% (95% CI, 29.8% to 44.2%) in the placebo group (difference = 11.4%; 95% CI, 1.8% to 21.0%). Sensitivity analyses censoring patients who received allogeneic HSCT and using restricted mean survival time (RMST) to account for a possible plateau effect supported an OS benefit with quizartinib.
There was an apparent early OS detriment with quizartinib relative to placebo. During the first 30 days and 60 days of treatment, 15 (5.7%) and 20 (7.5%) patients in the quizartinib group died compared with 9 (3.4%) and 13 (4.9%) in the placebo group, respectively. Early deaths in the quizartinib versus placebo groups were attributed to AEs (6.4% versus 4.1%), AML disease progression (0.8% versus 0.7%), and other causes (0.4% versus 0%).
Results for OS among most prespecified subgroups were aligned with the main analysis; however, among patients aged 60 or older but aged younger than 65 years, patients from North America, patients with a WBC count less than 40 × 109/L at diagnosis, and patients without NPM1 mutational status, the point estimate for the HR of quizartinib versus placebo was near the null (i.e., no statistical difference). Among patients with a favourable AML cytogenetic risk score, the point estimate for the HR of quizartinib versus placebo favoured placebo. Across categories within each subgroup, the 95% CIs for the comparative effect estimates were overlapping.
Among the subgroup of patients who entered the consolidation (65% of patients in each group) and maintenance (43.3% in the quizartinib group and 33.9% in the placebo group) phases of treatment, the results were consistent with the main analysis. Among patients who entered the consolidation phase, the median OS was NE (95% CI, 48.6 months to NE) in the quizartinib group and 42.5 months (95% CI, 21.9 months to NE) in the placebo group. The HR was 0.703 (95% CI, 0.509 to 0.971). The KM-estimated probability of OS at 48 months was 60.2% (95% CI, 52.0% to 67.5%) in the quizartinib group and 46.5% (95% CI, 36.5% to 56.0%) in the placebo group. Among patients who entered the maintenance phase, the median OS was NE in both groups. The HR was 0.683 (95% CI, 0.395 to 1.183). The KM-estimated probability of OS at 48 months was 76.3% (95% CI, 66.2% to 83.7%) in the quizartinib group and 67.9% (95% CI, 55.3% to 77.6%) in the placebo group.
In a post hoc analysis among patients who received allogeneic HSCT and continued to the maintenance phase, the median OS was not reached in either group. The HR for OS in this subpopulation was 1.622 (95% CI, 0.623 to 4.220).23
Event-Free Survival
At the time of the data cut-off, 198 of 268 (73.9%) patients in the quizartinib group and 213 of 271 (78.6%) patients in the placebo group had an EFS event. The median EFS was 0.03 months (95% CI, 0.03 months to 0.95 months) in the quizartinib group and 0.71 months (95% CI, 0.03 months to 3.42 months) in the placebo group. The HR was 0.916 (95% CI, 0.754 to 1.114; P = 0.2371). The KM-estimated probability of EFS at 12 months was 34.2% (95% CI, 28.5% to 40.0%) in the quizartinib group and 25.0% (95% CI, 19.9% to 30.4%) in the placebo group (difference = 9.3%; 95% CI, 1.5% to 17.1%). The KM-estimated probability of EFS at 36 months was 24.1% (95% CI, 18.8% to 29.7%) in the quizartinib group and 19.2% (95% CI, 14.5% to 24.3%) in the placebo group (difference = 4.9%; 95% CI, −2.5% to 12.2%). Because no statistically significant difference between groups was observed, subsequent secondary end points were not tested statistically. Sensitivity analyses defining induction treatment failure (ITF) as no CR or CRc by the end of induction (day 56, per the original protocol definition of EFS), and censoring patients at the start date of the conditioning regimen for allogeneic HSCT (with ITF defined as not achieving CRc) favoured quizartinib. A sensitivity analysis censoring patients at the start date of the conditioning regimen for allogeneic HSCT and defining ITF as not achieving CR was aligned with the main analysis.
CR and CRc, With or Without MRD
At the end of the induction phase, 147 of 286 (54.9%; 95% CI, 48.7% to 60.9%) patients in the quizartinib group and 150 of 271 (55.4%; 95% CI, 49.2% to 61.4%) patients in the placebo group had CR (difference = −0.5%; 95% CI, −8.9% to 7.9%). Further, 71.6% (95% CI, 65.8% to 77.0%) and 64.9% (95% CI, 58.9% to 70.6%) of patients in the quizartinib and placebo groups, respectively, had CRc at the end of induction (difference = 6.7%; 95% CI, −1.1% to 14.5%).
Among patients in the quizartinib group versus placebo group, 20.1% (95% CI, 15.5% to 25.5%) and 18.8% (95% CI, 14.3% to 24.0%), respectively, had CR with FLT3-ITD MRD negativity (using a prespecified cut-off of 10-4 leukemic cells) at the end of induction. A respective 24.6% (95% CI, 19.6% to 30.2%) and 21.4% (95% CI, 16.7% to 26.8%) had CRc with FLT3-ITD MRD negativity at the end of induction.
Duration of CR and CRc
For patients with CR during induction, the median duration of CR was 38.6 months (95% CI, 21.9 months to NE) in the quizartinib group and 12.4 months (95% CI, 8.8 months to 22.7 months) in the placebo group (HR = 0.621; 95% CI, 0.451 to 0.857). For patients with CRc during induction, the median duration of CRc was 27.2 months (95% CI, 17.7 months to NE) in the quizartinib group and 12.4 months (95% CI, 8.7 months to 22.7 months) in the placebo group (HR = 0.742; 95% CI, 0.561 to 0.982).
Relapse-Free Survival
At the time of the data cut-off, among patients with CR during induction (147 of 268 [54.9%] in the quizartinib group and 150 of 271 [55.4%] in the placebo group), 44.2% in the quizartinib group and 58.7% in the placebo group had an RFS event. The median RFS was 39.3 months (95% CI, 22.6 months to NE) in the quizartinib group and 13.6 months (95% CI, 9.7 months to 23.7 months) in the placebo group. The HR was 0.613 (95% CI, 0.444 to 0.845) in favour of quizartinib, although this end point was not tested statistically. The KM-estimated probability of RFS at 6 months was 88.1% (95% CI, 81.6% to 92.5%) in the quizartinib group and 71.8% (95% CI, 63.8% to 78.4%) in the placebo group (difference = 16.3%; 95% CI, 7.3% to 25.3%). The KM-estimated probability of RFS at 36 months was 51.7% (95% CI, 42.5% to 60.1%) in the quizartinib group and 38.2% (95% CI, 30.0% to 46.4%) in the placebo group (difference = 13.5%; 95% CI, 1.4% to 25.6%).
Transplant Rate
At the time of the data cut-off, 102 of 268 (38.1%; 95% CI, 32.3% to 44.2%) patients in the quizartinib group and 91 of 271 (33.6%; 95% CI, 28.0% to 39.5%) patients in the placebo group underwent protocol-specified allogeneic HSCT (difference = 4.5%; 95% CI, −3.6% to 12.6%).
Health-Related Quality of Life
A total of 252 of 268 (94.0%) patients in the quizartinib group and 253 of 271 (93.4%) patients in the placebo group were included in the analysis of the global health status [GHS]/QoL scale of the EORTC QLQ-C30. Among these patients, all had baseline assessments. The proportion of patients available for assessment declined in both groups over time thereafter. In the quizartinib and placebo groups, 79.0% and 77.9% had assessments at day 28 of the first induction cycle, 40.9% and 42.3% had assessments at day 28 of the first consolidation cycle, and 39.7% and 33.2% had assessments at day 1 of the first maintenance cycle, respectively.
At baseline, the mean GHS/QoL scale score was similar across groups (45.9; SD = 24.4 in the quizartinib group and 48.1; SD = 24.9 in the placebo group). In the longitudinal (mixed-effects model of repeated measures) analysis summarizing the effect of quizartinib versus placebo over all time points, an improvement in GHS/QoL score was observed over time in both groups. The between-group difference in the least squares mean change from baseline was −2.0 points (95% CI, −4.8 points to 0.7 points). Results of a sensitivity analysis adjusting on additional covariates were aligned with the main analysis.
Harms Results
AEs occurred among nearly all patients in the quizartinib and placebo groups (99.6% and 98.9%, respectively). The most common AEs occurring among patients in the quizartinib versus placebo groups included febrile neutropenia (44.2% versus 42.2%), pyrexia (42.3% versus 40.7%), diarrhea (37.0% versus 35.1%), and hypokalemia (35.1% versus 35.8%).
Grade 3 to 4 AEs occurred among 80.8% of patients in the quizartinib group and 79.9% of patients in the placebo group. The most common grade 3 to 4 AEs in the quizartinib versus placebo groups included febrile neutropenia (43.4% versus 41.0%), hypokalemia (18.9% versus 16.4%), neutropenia (18.1% versus 8.6%), and pneumonia (11.3% versus 11.2%).
More patients in the quizartinib group (54.0%) than the placebo group (45.9%) experienced 1 or more serious AEs (SAEs). The most common SAEs occurring in the quizartinib versus placebo groups included febrile neutropenia (10.9% versus 8.2%), pneumonia (6.4% versus 5.6%), septic shock (4.2% versus 3.0%), and sepsis (3.8% versus 5.2%).
More patients in the quizartinib group (20.4%) than the placebo group (8.6%) stopped treatment due to AEs. There was no single AE that led to treatment discontinuation among more than 4% of patients across groups, although the most common occurring in the quizartinib versus placebo groups included septic shock (3.4% versus 0.4%), thrombocytopenia (1.1% versus 0%), and pneumonia (0.8% versus 1.1%).
AEs leading to death occurred among 11.3% of patients in the quizartinib group and 9.7% of patients in the placebo group. There was no single AE that led to death among more than 3% of patients across groups, although the most common occurring in the quizartinib versus placebo groups included septic shock (3.0% versus 1.1%), sepsis (1.1% versus 0.7%), and general physical health deterioration (0% versus 1.5%).
More patients in the quizartinib group versus the placebo group had an increase in the QT interval corrected using the Fridericia formula (QTcF) more than 30 ms from baseline (55.1% versus 32.5%) and/or a prolonged QT interval (13.6% versus 4.1%). Among patients in the quizartinib versus placebo groups, cardiac arrest with ventricular fibrillation (0.8% versus 0%) and ventricular tachycardia (0.4% versus 0.4%) were infrequent. Combined elevations of aspartate aminotransferase or alanine aminotransferase and total bilirubin occurred among 2.3% of patients in the quizartinib group and 3.4% of patients in the placebo group.
Among patients who underwent protocol-specified allogeneic HSCT, 57 of 102 (55.9%) in the quizartinib group and 43 of 91 (47.3%) in the placebo group had graft-versus-host disease (GVHD). In the quizartinib and placebo groups, 45.1% and 38.5% had acute GVHD and 29.4% and 19.8% had chronic GVHD, respectively. More patients in the quizartinib group (16.7%) than the placebo group (6.6%) had grade 3 to 4 GVHD.
Critical Appraisal
For all end points, there is low risk of bias arising from the randomization process. Due to the design of the QuANTUM-First study, the contribution of effects in each of the induction and consolidation phases and maintenance phase to the overall efficacy of quizartinib cannot be isolated.24
The QuANTUM-First study was double blind and there is a low risk of bias in the measurement of objective outcomes (OS and transplant rate). Risk of bias in the measurement of CR, CRc, EFS, and RFS is low as they were assessed by an independent review committee (IRC). If patients became aware of their assigned treatment (e.g., due to known harms of quizartinib) there would be risk of bias in HRQoL and subjective harms, but the risk is likely low.
Despite many major protocol violations, risk of bias due to deviations from the intended interventions is likely low, as these deviations were generally balanced across groups and unlikely to seriously impact efficacy results.
The QuANTUM-First study was powered to detect a statistically significant OS benefit. The family-wise type I error rate for the primary and secondary end points was adequately controlled for multiple testing. As the result for EFS (tested second in the hierarchy after OS) was not statistically significant, no other end points were tested statistically.
For the analyses of OS and EFS, there was a violation of the proportional hazards (PH) assumption so reliance on the HR alone to inform the effects of quizartinib versus placebo on these end points may be misleading. There was also a plateau in the KM curves for OS, so a comparison of median OS across groups may overestimate the benefit of quizartinib.
The certainty of evidence for OS and EFS was affected by imprecision. Although the point estimates for the between-group differences in KM-estimated probabilities of OS at 12 months and 48 months of follow-up suggested clinically important benefit with quizartinib, the 95% CIs included small differences that may not be considered clinically important. For EFS, although the point estimates for between-group differences in KM-estimated probabilities at 12 months and 36 months of follow-up suggested little to no clinically important difference, the 95% CIs included the potential for clinically important benefit with quizartinib.
Some variation in between-group effects on OS were noted across subgroups. However, the 95% CIs were wide and overlapping across categories within each subgroup, there were no statistical tests for treatment by subgroup interactions, and there were no adjustments for multiple testing, limiting credible conclusions about effect modification.25,26
Additional analyses of OS among patients who entered the consolidation and maintenance phases are at risk of bias as it is unlikely that prognostic balance was maintained across treatment groups among these subpopulations. The post hoc analysis of OS among patients who received allogeneic HSCT and continued to the maintenance phase was subject to the same limitation. Further, a small number of patients (n = 119) contributed to the analysis, the median was not reached in either group, and the effect estimate for the HR was affected by imprecision (the 95% CI included the potential that either group could be favoured).
The validity of EFS and RFS as surrogates for OS among patients with newly diagnosed FLT3-ITD–positive AML who are treated with kinase inhibitors as an add-on to standard chemotherapy remains uncertain.27-31
As RFS is evaluated only among patients with CR or CRc after induction, the results are at risk of bias as it is uncertain whether prognostic balance across treatment groups was maintained in this subpopulation of patients. The same limitation applies to the analysis of duration of CR and CRc.
Although the point estimate for the between-group difference in transplant rate suggested little to no clinically important difference between quizartinib and placebo, this estimate was affected by imprecision (i.e., the 95% CI included the potential for a clinically important increase).
For HRQoL, there is a high risk of bias due to missing outcome data. The proportion of evaluable patients who provided assessments decreased substantially over time. In the longitudinal analysis (mixed-effects model of repeated measures), missing data were handled under a missing at random assumption, which is unlikely to be reasonable.32
The comparison group was not directly relevant to clinical practice. According to the clinical experts, up to 10% of patients with FLT3-ITD–mutated AML and concomitant favourable-risk core binding factor or adverse-risk karyotype may receive intensive chemotherapy with gemtuzumab ozogamicin or an alternative regimen, such as fludarabine, cytarabine, idarubicin, and filgrastim (FLAG-IDA), rather than midostaurin. Of the remaining patients eligible for intensive induction and consolidation chemotherapy with midostaurin, less than 5% would not be treated with midostaurin, usually due to intolerance or gastrointestinal mucositis. Midostaurin was not yet approved at the start of the QuANTUM-First study.
GRADE Summary of Findings and Certainty of the Evidence
For the pivotal study (QuANTUM-First) identified in the sponsor’s SR, the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) framework was used to assess the certainty of the evidence for outcomes considered most relevant to inform expert committee deliberations, and a final certainty rating was determined as outlined by the GRADE Working Group (Table 2). Following the GRADE approach, evidence from the QuANTUM-First study started as high-certainty evidence and could be rated down for concerns related to study limitations (which refers to internal validity or risk of bias), indirectness, imprecision of effects, and publication bias.
Table 2: Summary of Findings for Quizartinib vs. Placeboa for Patients With Newly Diagnosed AML That Is FLT3-ITD Positive
Outcome and follow-up | Patients (studies), N | Relative effect (95% CI) | Absolute effects (95% CI) | Certainty | What happens | ||
|---|---|---|---|---|---|---|---|
Placebo | Quizartinib | Difference | |||||
Survival end points | |||||||
Probability of OS at 12 months Median follow-up: 39.2 months in both groups | 539 (1 RCT) | NA | 577 per 1,000 | 674 per 1,000 (613 to 727 per 1,000) | ██ more per 1,000 (██ ██ ███ more per 1,000) | Moderateb | Quizartinib likely results in a clinically important increase in the probability of OS at 12 months compared with placebo. |
Probability of OS at 48 months Median follow-up: 39.2 months in both groups | 539 (1 RCT) | NA | 370 per 1,000 | 484 per 1,000 (419 to 545 per 1,000) | ███ more per 1,000 (██ ██ ███ more per 1,000) | Moderateb | Quizartinib likely results in a clinically important increase in the probability of OS at 48 months compared with placebo. |
Probability of EFS at 12 months Median follow-up: 39.2 months in both groups | 539 (1 RCT) | NA | 250 per 1,000 | 342 per 1,000 (285 to 400 per 1,000) | ██ more per 1,000 (██ ██ ███ more per 1,000) | Moderatec | Quizartinib likely results in little to no clinically important difference in the probability of EFS at 12 months compared with placebo. |
Probability of EFS at 36 months Median follow-up: 39.2 months in both groups | 539 (1 RCT) | NA | 192 per 1,000 | 241 per 1,000 (188 to 297 per 1,000) | ██ more per 1,000 (██ █████ ██ ███ more per 1,000) | Moderatec | Quizartinib likely results in little to no clinically important difference in the probability of EFS at 36 months compared with placebo. |
Probability of RFS (among patients with CR after induction) at 6 months Median follow-up: 39.2 months in both groups | 297 (1 RCT) | NA | 718 per 1,000 | 881 per 1,000 (816 to 925 per 1,000) | ███ more per 1,000 (██ ██ ███ more per 1,000) | Lowd | Quizartinib may result in an increase in the probability of RFS at 6 months. The clinical importance of the increase is uncertain. |
Probability of RFS (among patients with CR after induction) at 36 months Median follow-up: 39.2 months in both groups | 297 (1 RCT) | NA | 382 per 1,000 | 517 per 1,000 (425 to 601 per 1,000) | ███ more per 1,000 (██ ██ ███ more per 1,000) | Lowd | Quizartinib may result in an increase in the probability of RFS at 36 months. The clinical importance of the increase is uncertain. |
Remission end points | |||||||
CR rate Follow-up: after induction | 539 (1 RCT) | NR | 554 per 1,000 | 549 per 1,000 (487 to 609 per 1,000) | ████ fewer per 1,000 (██ █████ ██ ██ more per 1,000) | Highe | Quizartinib results in little to no clinically important difference in CR rate compared with placebo. |
CRc (CR + CRi) rate Follow-up: after induction | 539 (1 RCT) | NR | 649 per 1,000 | 716 per 1,000 (658 to 770 per 1,000) | ██ more per 1,000 (██ █████ ██ ███ more per 1,000) | Highe | Quizartinib results in little to no clinically important difference in CRc rate compared with placebo. |
Transplant rate | |||||||
Patients undergoing allogeneic HSCT Median follow-up: 39.2 months in both groups | 539 (1 RCT) | NR | 336 per 1,000 | 381 per 1,000 (323 to 442 per 1,000) | ██ more per 1,000 (██ █████ ██ ███ more per 1,000) | Moderatef | Quizartinib likely results in little to no clinically important difference in transplant rate compared with placebo. |
HRQoL | |||||||
LS mean change from baseline EORTC QLQ-C30 GHS/QoL domain (0 [worse] to 100 [better]), summary effect, points Median follow-up: 39.2 months in both groups | 505 (1 RCT) | NA | NR | NR | (████████ ██ ███) | Lowg | Quizartinib may result in little to no clinically important difference in HRQoL compared with placebo. |
Harms | |||||||
Patients with ≥ 1 grade 3 to 5 AE Median follow-up: 39.2 months in both groups | 533 (1 RCT) | NR | 921 per 1,000 | 896 per 1,000 (853 to 929 per 1,000) | ██ more per 1,000 (██ █████ ██ ██ more per 1,000) | Lowh | Quizartinib may result in an increase in the proportion of patients with ≥ 1 grade 3 to 5 AEs compared with placebo. The clinical importance of the increase is uncertain. |
AE = adverse event; AML = acute myeloid leukemia; CI = confidence interval; CR = complete remission; CRc = composite complete remission; CRi = complete remission with incomplete hematologic recovery; EFS = event-free survival; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; GHS = global health status; HRQoL = health-related quality of life; HSCT = hematopoietic stem cell transplant; LS = least squares; MAR = missing at random; MID = minimally important difference; NA = not applicable; NR = not reported; OS = overall survival; QoL = quality of life; RCT = randomized controlled trial; RFS = relapse-free survival; vs.= versus.
Notes: Study limitations (which refer to internal validity or risk of bias), indirectness, imprecision of effects, and publication bias were considered when assessing the certainty of the evidence. All serious concerns in these domains that led to the rating down of the level of certainty are documented in the table footnotes. Between-group differences for all but the HRQoL end point were not part of the statistical analysis plan. These were provided by the sponsor in response to an additional information request.33
aIn combination with standard cytarabine and anthracycline induction and standard cytarabine consolidation chemotherapy, and as maintenance monotherapy following consolidation therapy.
bRated down 1 level for serious imprecision. The 95% CI for the between-group difference includes the possibility of little to no clinically important difference based on a threshold of 5% to 10%, as informed by the clinical experts consulted.
cRated down 1 level for serious imprecision. The 95% CI for the between-group difference includes the possibility of clinically important benefit with quizartinib based on a threshold of 10%, as informed by the clinical experts consulted.
dRated down 2 levels for very serious study limitations. RFS is measured only in the subpopulation of patients with CR after induction. It is uncertain whether prognostic balance across treatment groups is maintained in this subpopulation. The null was used as the threshold to inform the target of the certainty rating and the precision of the effect; hence, the clinical importance of the estimated effect is uncertain.
eA threshold of 10% to 15% for a clinically important between-group difference, as informed by the clinical experts consulted, was used to inform the target of the certainty rating and the precision of the effect estimate.
fRated down 1 level for serious imprecision. The 95% CI for the between-group difference includes the possibility of clinically important benefit with quizartinib based on a threshold of 10%, as informed by the clinical experts consulted.
gRated down 2 levels for very serious study limitations. The proportion of patients available for assessments diminished substantially over time. Missing data were handled under a MAR assumption, which is unlikely reasonable. A threshold of 10 points for a clinically important between-group difference, as adopted by the sponsor in their analyses of within-group improvement and detriment, was used to inform the target of the certainty rating and the precision of the effect estimate. There is uncertainty in this threshold. To the knowledge of the review team, no MID has been estimated in the literature specific to patients with AML.
hRated down 2 levels for very serious imprecision. The 95% CI for the between-group difference includes the possibility of benefit (i.e., reduced harms) and no difference. The null was used as the threshold to inform the target of the certainty rating and the precision of the effect; hence, the clinical importance of the estimated effect is uncertain. Results at the time of the updated safety addendum were identical.
Sources: Clinical Study Report for QuANTUM-First19 and sponsor-submitted additional trial data.33
When possible, certainty was rated in the context of the presence of an important (nontrivial) treatment effect; if this was not possible, certainty was rated in the context of the presence of any treatment effect (i.e., the clinical importance is unclear). In all cases, the target of the certainty of evidence assessment was based on the point estimate and where it was located relative to the threshold for a clinically important effect (when a threshold was available) or to the null. For OS, EFS, CR, CRc, transplant rate, and HRQoL, the target of the certainty of evidence assessment was the presence or absence of a clinically important effect. For RFS and grade 3 to 5 AEs, the target of the certainty of evidence assessment was the presence or absence of any (nonnull) effect.
The selection of outcomes for GRADE assessment was based on the sponsor’s summary of clinical evidence, consultation with clinical experts, and input received from patient and clinician groups and public drug plans. The following list of outcomes was finalized in consultation with expert committee members: OS, EFS, CR rate, CRc rate, RFS, transplant rate, HRQoL, and grade 3 to 5 AEs.
Long-Term Extension Studies
No long-term extension studies were submitted by the sponsor.
Indirect Comparisons
Description of ITCs
The QuANTUM-First study did not include a comparison to midostaurin plus chemotherapy, the current standard of care in Canada for patients with newly diagnosed AML that is FLT3-ITD positive. The sponsor submitted an anchored matching adjusted indirect comparison (MAIC) and multilevel network meta-regression (ML-NMR)34,35 to address this gap.
Two RCTs, the QuANTUM-First and RATIFY studies, were identified by the sponsor for inclusion in the indirect treatment comparisons (ITCs). The RATIFY study was a phase III, double-blind RCT comparing midostaurin and placebo as administered in combination with induction and consolidation chemotherapy in patients aged younger than 60 years with newly diagnosed AML with FLT3 mutations.17 The common placebo group across the 2 RCTs created an anchored network for the MAIC and ML-NMR. The sponsor undertook a feasibility assessment and identified multiple sources of heterogeneity across the 2 RCTs, justifying the chosen ITC methods. The sponsor identified treatment effect modifiers (TEMs) by reviewing available RCT publications and subgroups data, conducting univariate analyses of the QuANTUM-First study data, and consulting with clinical experts.
The objective of the MAIC was to compare the efficacy of quizartinib and midostaurin in combination with chemotherapy for the treatment of patients aged younger than 60 years with newly diagnosed AML that is FLT3-ITD positive. Restriction of the MAIC population to those aged younger than 60 years was necessary due to the narrow age criteria for the RATIFY study. Due to limitations in the external validity of the MAIC results and to inform the economic evaluation, the ML-NMR was then used to generate effect estimates of quizartinib and midostaurin relative to placebo among populations similar to the QuANTUM-First and RATIFY studies. Outcomes evaluated in the MAIC and ML-NMR included OS, CR, and cumulative incidence of relapse (CIR) for patients who relapse after CR.
Efficacy Results
Results of the Matching Adjusted ITC
Among patients aged 60 years or younger who were FLT3-ITD positive, the MAIC was insufficient to show a difference between quizartinib and midostaurin, in combination with chemotherapy, for OS (HR = ████ 95% CI, ████ to ████) and CR (odds ratio [OR] = ████ 95% CI, ████ to ████). Although the point estimates for the comparative effects favoured quizartinib for OS and midostaurin for CR, for both outcomes the 95% CIs were wide, including the possibility that either quizartinib or midostaurin could be favoured. Quizartinib was favoured over midostaurin for CIR (HR = ████ 95% CI, ████ to ████). Results of scenario analyses matching on alternative matching variables and defining CR as CR within 60 days were mostly aligned with the main analyses.
Results of the ML-NMR
In both the QuANTUM-First–like and RATIFY-like study populations, point estimates for the HR of OS favoured quizartinib and midostaurin compared with placebo, although the results were not statistically significant due to imprecision (i.e., the 95% credible interval [CrI] crossed the null). One exception was the comparison of midostaurin versus placebo in a RATIFY-like study population, where midostaurin was favoured (HR = ████ 95% CrI, ████ to ████). The predicted median OS with quizartinib was █████ months (95% CrI, █████ to █████) in a QuANTUM-First–like study population and █████ months (95% CrI, █████ to ██████) in a RATIFY-like study population. In a scenario analysis using data from patients aged younger than 60 years from the QuANTUM-First study, the results generally aligned with those from the main analysis.
In both the QuANTUM-First–like and RATIFY-like study populations, the analysis was insufficient to show a difference between quizartinib or midostaurin and placebo in CR, owing to imprecision (i.e., wide 95% CrIs including the possibility that either the active treatments or placebo could be favoured). One exception was the comparison of midostaurin versus placebo in a RATIFY-like study population, where midostaurin was favoured (OR = ████ 95% CI, ████ to ████). In a scenario analysis using data from patients aged younger than 60 years from the QuANTUM-First study, the analysis was insufficient to show a difference between quizartinib and placebo in any population, owing to imprecision (i.e., wide 95% CrIs including the possibility that either quizartinib or placebo could be favoured). Midostaurin was favoured over placebo in the both the QuANTUM-First–like and RATIFY-like study populations.
In both the QuANTUM-First–like and RATIFY-like study populations, quizartinib was favoured over placebo for CIR. The analysis was insufficient to show a difference between midostaurin and placebo in either population, owing to imprecision (i.e., wide 95% CrIs including the possibility that either midostaurin or placebo could be favoured). In a scenario analysis using data from patients aged younger than 60 years from the QuANTUM-First study, in all populations quizartinib was favoured over placebo. In this scenario, the analysis was insufficient to show a difference between midostaurin and placebo in any population, owing to imprecision.
Harms Results
No harms outcomes were evaluated in either of the ITCs.
Critical Appraisal
The risk of bias for the QuANTUM-First and RATIFY studies was considered low or unclear across all domains assessed by the sponsor. These risk of bias assessments were undertaken at the study level, which does not account for differences in risk of bias which may occur across the different effect estimates (for OS, CR, and CIR) used in the analyses.
As the RATIFY study had narrower eligibility criteria than the QuANTUM-First study for age, the MAIC was restricted to patients aged 60 years or younger. As such, the results cannot be generalized to patients aged older than 60 years who would be eligible for treatment with quizartinib. According to the clinical experts consulted, approximately 60% to 70% of patients in clinical practice are aged older than 60 years.
As neither the QuANTUM-First nor RATIFY studies were designed to inform on the contribution of the induction, consolidation, and maintenance phases of treatment to overall efficacy,24 the MAIC and ML-NMR also cannot inform on contributions of each of these distinct treatment phases. The maintenance regimen provided in the RATIFY study is not reflective of clinical practice in Canada, where midostaurin is not approved for this indication. The contribution of the maintenance phase in the RATIFY study to the overall efficacy of midostaurin and the impact on comparative effect estimates from the MAIC cannot be determined.
Unknown and known but unmeasured TEMs (e.g., race, ECOG performance status, demographic region, WBC, modified European LeukemiaNet [ELN] class, cytogenetic risk, karyotypes, and CEBPA mutations) could not be adjusted for in the analyses, representing a source of residual confounding. To maintain at least ███ effective sample size (ESS), FLT3-ITD allele frequency was not adjusted for, and remained imbalanced across groups after adjustment for other TEMs.
In the MAIC, patient characteristics before and after adjustment were provided only for the sponsor-identified TEMs. It is unknown whether additional patient characteristics were well balanced after adjustment. Imbalances in other baseline characteristics could represent an additional source of confounding.
For age and platelet count, sponsor-identified TEMs which were adjusted for in the analyses, only median values were available in the RATIFY study publications. These were used to impute the means required for analysis, under the assumption that these were equivalent. This assumption is not verifiable and could be a source of bias if it is not valid.
To confirm FLT3-ITD status among patients in the RATIFY study, next-generation sequencing (NGS) was used. Results were unavailable for ███ of patients, who were subsequently excluded from the MAIC analyses. It is unknown whether these results were missing completely at random, and whether their exclusion may have biased the comparative effect estimates.
In the MAIC, the ESS was █████ of the original sample size of the QuANTUM-First study. This reduction in ESS contributes to a loss of precision and indicates a greater influence of subsets of patients in the QuANTUM-First study.36 In both the MAIC and ML-NMR, effect estimates were frequently imprecise, precluding conclusions as to which treatment was favoured (e.g., OS and CR in the MAIC and CR in the ML-NMR, for comparisons of quizartinib and midostaurin versus placebo in a QuANTUM-First–like study population).
As the definition of CIR was not reported in the RATIFY study publications, the sponsor noted that heterogeneity in the definitions of this outcome across the 2 RCTs could not be assessed. It is unknown whether differences in the definition across the RCTs could have biased the results, challenging credible conclusions on this outcome from the MAIC and ML-NMR.
Between-group effects comparing quizartinib versus midostaurin with 95% CrIs from the ML-NMR were not reported, precluding credible conclusions of their comparative efficacy among QuANTUM-First–like and RATIFY-like study populations.
Although the outcomes assessed in the MAIC and ML-NMR were relevant according to inputs received from interest holders, other relevant outcomes such as HRQoL were not investigated. No harms outcomes were investigated, precluding judgments regarding the balance of benefits and harms of quizartinib versus midostaurin.
Studies Addressing Gaps in the Evidence From the SR
No studies addressing gaps were submitted by the sponsor.
Conclusions
Among adult patients with newly diagnosed FLT3-ITD–positive AML who are eligible for intensive induction and consolidation chemotherapy, there is an unmet need for an approved and effective therapy that can also be used in the maintenance setting. The proposed goal of maintenance therapy is to reduce the risk of relapse, prolong remission, and extend OS. Results from the QuANTUM-First study suggest that quizartinib in combination with standard induction and consolidation chemotherapy (and/or allogeneic HSCT), then as maintenance therapy for up to 36 cycles, likely results in a clinically important increase in OS and may result in an increase in RFS compared to placebo. As patients were not re-randomized before the maintenance phase of treatment, it is not possible to determine the contribution of the maintenance phase to the observed OS and RFS benefits. There was little to no difference in the rates of CR and CRc, with or without MRD negativity across groups; however, responses seemed more durable with quizartinib. Results of the QuANTUM-First study also suggest that compared with placebo, quizartinib likely results in little to no difference in EFS or transplant rate and may result in little to no difference in HRQoL. The overall safety profile for quizartinib relative to placebo was acceptable to the clinical experts consulted for this review; however, due to the notable harms associated with quizartinib, they stated that they would not use it among patients with severe uncorrectable hypokalemia, severe uncorrectable hypomagnesemia, long QT syndrome, or a history of ventricular arrhythmias or torsades de pointes. Important limitations of the QuANTUM-First study include the lack of re-randomization before the maintenance phase and the limited applicability of the comparator in current practice. In the absence of re-randomization, the design of the QuANTUM-First study does not allow for isolation of the contribution of maintenance treatment to the overall efficacy of quizartinib, nor the efficacy of quizartinib as a maintenance therapy among patients who have received midostaurin during induction and consolidation. Population-adjusted ITCs were submitted by the sponsor to address the lack of direct evidence comparing quizartinib with midostaurin, the current standard of care. Due to important methodologic limitations and imprecision in the comparative effect estimates from the ITCs, the efficacy of quizartinib versus midostaurin is uncertain. As no harms were investigated in the ITCs, the comparative safety of quizartinib and midostaurin is not known.
Introduction
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of quizartinib (Vanflyta) in the treatment of adult patients with newly diagnosed AML that is FLT3-ITD positive.
Disease Background
Contents within this section have been informed by materials submitted by the sponsor and clinical expert input. The following have been summarized and validated by the review team.
AML is a heterogeneous hematologic malignancy with a rapid disease onset due to proliferation of abnormal blast cells.1 AML is one of the most aggressive forms of leukemia, with an estimated 5-year survival rate of 31.9%.2 Poorer prognosis is associated with older age,37,38 secondary AML (i.e., following prior diagnosis of myelodysplasia, myeloproliferative neoplasm, or aplastic anemia, as opposed to de novo AML in which there is no clinical history of myelodysplastic syndrome, myeloproliferative disorder, or exposure to potentially leukemogenic therapies or agents),39 and certain molecular subtypes.40 The prevalence of AML ranges from 0.6 to 11.0 per 100,000 persons for all age categories, genders, and ethnicities globally.41 In 2019, approximately 1,160 people in Canada were diagnosed with AML and in 2022, 1,286 died from the disease.3
Although the cause is not known, several factors are associated with an increased risk of AML, including older age, being male, smoking, exposure to certain chemicals (e.g., benzene, formaldehyde), previous treatment with certain chemotherapies (e.g., alkylating agents, topoisomerase II inhibitors), exposure to high-dose radiation, certain blood disorders (e.g., myelodysplastic syndrome), genetic factors, and having a family history of AML.42 Symptoms of AML include those associated with anemia (e.g., fatigue, weakness, shortness of breath, lightheadedness, dizziness, headaches), neutropenia (e.g., frequent infections, fever), and thrombocytopenia (e.g., easy bruising, petechiae, prolonged bleeding from minor cuts, frequent or severe nosebleeds, bleeding gums). Other symptoms may include loss of appetite, unexplained weight loss, discomfort in bones or joints, and fullness or swelling in the abdomen due to an enlarged spleen or liver.4
Mutation profiling studies reveal a wide spectrum of mutations in patients with AML.8,9,43,44 Driver mutations are present in most patients (97%), and co-mutations are common with a median of 4 mutations per patient.8 FLT3 is a member of the class III receptor tyrosine kinase family and plays a key role in controlling survival, proliferation, and differentiation of hematopoietic cells.45-49 The FLT3 mutation is the most frequent genetic alteration associated with a poor prognosis in patients with AML,50 and can be found in approximately 30% of newly diagnosed patients.5 The 2 main classes of FLT3 mutations are the ITD mutations within the receptor’s autoinhibitory juxtamembrane domain (approximately 25% of all AML cases) and the point mutations that occur within the TKD activation loop (5% to 10% of all AML cases).5,6 Compared with patients with the FLT3‑TKD mutation and those without any FLT3 mutation, those with the FLT3-ITD mutation have a higher burden of disease at diagnosis, and poorer OS and RFS.5,7-12
Assessments used to diagnose AML include bone marrow aspiration, biopsy, peripheral blood films, morphologic testing or immunophenotyping by flow cytometry, cytogenetic analysis including fluorescence in situ hybridization if applicable, and molecular genetic testing.51 These tests are usually performed in the outpatient or inpatient setting, and the diagnosis is often confirmed by a hematologist. These tests are commonly available in AML-treating hospitals across Canada, although capacity may vary by hospital and province.52 Molecular testing is considered standard of care for patients with AML and FLT3 mutations undergoing induction chemotherapy and is performed in accredited laboratories.51 The clinical utility of testing for FLT3 mutations is well established to determine prognosis and appropriate treatment, including the need for allogeneic HSCT among eligible patients.
Standards of Therapy
Contents within this section have been informed by materials submitted by the sponsor and clinical expert input. The following have been summarized and validated by the review team.
Among patients with newly diagnosed AML that is FLT3-ITD positive, the goal of treatment is to control the disease and, whenever possible, provide a cure.13 In Canada, the only publicly available and up-to-date clinical practice guidelines are those developed by Alberta Health Services.51 Recommendations available in international guidelines (National Comprehensive Cancer Network,15 MD Anderson Cancer Center,53 ELN,13 American Society of Hematology,54 Japanese Society of Hematology,55 and European Society of Medical Oncology14) are largely aligned with the current treatment paradigm in Canada.
First, patients are assessed for eligibility for intensive induction chemotherapy.43 Eligible patients receive standard induction therapy with cytarabine and an anthracycline (either daunorubicin or idarubicin) in combination with the FLT3 inhibitor, midostaurin. For patients with CR after 1 or 2 cycles, induction therapy is followed by 1 to 4 cycles of consolidation therapy with either intermediate-dose or high-dose cytarabine plus midostaurin and/or allogeneic HSCT. This may be followed by maintenance treatment with oral azacitidine for patients not eligible for allogeneic HSCT.13-15 Some guidelines also recommend a FLT3 inhibitor in the maintenance setting,13,15,53 but none are currently approved in Canada for this indication. In addition to cytarabine and an anthracycline, the treatment approach recommended by the MD Anderson Cancer Center prefers FLAG-IDA and a second generation FLT3 inhibitor (e.g., quizartinib) for patients in all settings, including maintenance for patients eligible and ineligible for allogeneic HSCT.53 FLAG-IDA is not reimbursed in all provinces in Canada.
Currently, midostaurin, a first generation FLT3 inhibitor, is the only drug specifically indicated for the treatment of patients with newly diagnosed FLT3-mutated AML in Canada. Although the addition of midostaurin to standard induction and consolidation therapy improves outcomes among these patients, there remains an important risk of relapse postremission and long-term survival may be limited.17 Results of the pivotal RATIFY trial, which investigated the efficacy and safety of midostaurin as an add-on to chemotherapy among patients aged younger than 60 years with newly diagnosed AML with FLT3 mutations, showed that the CIR was approximately 40% at 2 years and OS at 4 years was 51.4%.17 Avoiding relapse in FLT3-mutated AML is critical, as relapse is associated with a poor prognosis. The risk of relapse remains high even after aggressive treatments such as allogeneic HSCT.18
Evidence suggests that the use of FLT3 inhibitors in maintenance presents an opportunity to mitigate and prevent poor outcomes associated with relapse postallogeneic HSCT.18 Currently, there is no FLT3 inhibitor approved for maintenance therapy in Canada for patients with newly diagnosed AML that is FLT3-ITD positive. Azacitidine is the only approved treatment for maintenance therapy in AML; however, it is indicated only for patients who are not eligible or intended for allogeneic HSCT.56 Furthermore, the indication is not specific to patients with a FLT3 mutation.56 The availability of an effective FLT3 inhibitor in the maintenance setting would address an unmet need in the treatment of FLT3-mutated AML, particularly for patients with FLT3‑ITD–mutated AML who have worse survival outcomes.57
Drug Under Review
Key characteristics of quizartinib are summarized in Table 3 with other treatments available for adult patients with newly diagnosed AML that is FLT3-ITD positive.
Quizartinib16 is a small molecule inhibitor of FLT3. Quizartinib and its major circulating active metabolite AC886 competitively bind to the adenosine triphosphate binding pocket of FLT3 with high affinity, inhibiting FLT3 kinase activity and blocking FLT3-ITD–dependent cell proliferation downstream. At clinically relevant concentrations, quizartinib and AC886 also bind with less affinity to KIT and have little or no affinity for other receptor tyrosine kinases.
Quizartinib is currently being reviewed by Health Canada in combination with standard cytarabine and anthracycline induction and standard cytarabine consolidation chemotherapy, and as maintenance monotherapy following consolidation, for the treatment of adult patients with newly diagnosed AML that is FLT3-ITD positive. The sponsor-requested reimbursement criteria align with the Health Canada–approved indication.
Quizartinib is approved by the FDA in combination with standard cytarabine and anthracycline induction and cytarabine consolidation, and as maintenance monotherapy following consolidation chemotherapy, for the treatment of adult patients with newly diagnosed AML that is FLT3-ITD positive, as detected by an FDA–approved test.58 It is not indicated as maintenance monotherapy following allogeneic HSCT, noting that an OS benefit in this setting has not been demonstrated.58 Quizartinib in combination with standard induction and consolidation chemotherapy, and as maintenance monotherapy for adult patients with newly diagnosed AML that is FLT3-ITD positive is also approved by the European Medicines Agency, the National Institute for Health and Care Excellence, the Scottish Medicines Consortium, and the Haute Authorité de Santé, and recommended by the UK Medicines and Healthcare products Regulatory Agency.59 At the time of writing, quizartinib was under review by Institut national d’excellence en santé et en services sociaux (INESSS) for the same indication.59
Table 3: Key Characteristics of Quizartinib and Midostaurin
Characteristic | Quizartinib | Midostaurin |
|---|---|---|
Mechanism of action | Small molecule inhibitor of the receptor tyrosine kinase FLT3. | Inhibitor of multiple receptor tyrosine kinases, including FLT3 and KIT kinase, among others. |
Indicationa | In combination with standard cytarabine and anthracycline induction and cytarabine consolidation, followed by maintenance monotherapy, for the treatment of adult patients with newly diagnosed AML that is FLT3-ITD positive. | In combination with standard cytarabine and daunorubicin induction and cytarabine consolidation chemotherapy for the treatment of adult patients with newly diagnosed FLT3-mutated AML. |
Route of administration | Oral | Oral |
Recommended dose |
| Induction (up to 2 cycles of a minimum of 24 days) and consolidation (up to 4 cycles of a minimum of 28 days): 50 mg orally twice daily (2 weeks per cycle) on days 8 to 21 of each cycle of induction and on days 8 to 21 of each cycle of consolidation. |
Serious adverse effects or safety issues |
|
|
Other | None | Not indicated for maintenance therapy |
AML = acute myeloid leukemia; CYP = cytochrome P450; GVHD = graft-versus-host disease; HSCT = hematopoietic stem cell transplant; ITD = internal tandem duplication; QTcF = QT interval corrected using the Fridericia formula; WBC = white blood cells.
aHealth Canada–approved indication.
Sources: Draft product monograph for quizartinib16 and product monograph for midostaurin.60
Testing Procedure Considerations
Testing for FLT3-ITD mutations in patients with newly diagnosed AML is recommended as the standard of care in Canada and is currently part of routine care.61
NGS panels and polymerase chain reaction (PCR) testing can be used together or separately to identify FLT3-ITD mutations, using either bone marrow or peripheral blood samples.61 According to the clinical experts consulted for this review, reverse transcription PCR (RT-PCR) on RNA is the preferred method of PCR testing. The specific testing procedure used is dependent on the AML treatment centre; however, RT-PCR testing is the recommended because large internal duplications may not be detected with NGS, and the turnaround time for PCR testing is usually considerably shorter (3 days to 5 days) compared with NGS (2 weeks to 3 weeks).13,61
We considered the potential impacts of FLT3-ITD mutation testing to ascertain eligibility for treatment with quizartinib in adult patients with newly diagnosed AML, including those to health systems, patients (including families and caregivers), and costs; these impacts are not anticipated to be substantial. Key considerations and relevant information available from materials submitted by the sponsor, input from the clinical experts consulted by the review team, patient group input, and sources from the literature were validated by the review team when possible and are summarized in Table 4.
Table 4: Considerations for FLT3-ITD Mutation Testing for Establishing Treatment Eligibility With Quizartinib in Adult Patients With Newly Diagnosed AML
Consideration | Criterion | Available Information |
|---|---|---|
Health system-related | Number of individuals in Canada expected to require the test (e.g., per year) | According to the sponsor’s submission, all adult patients with newly diagnosed AML are tested for FLT3-ITD mutations, and this number was estimated to be 1,243 patients across Canada (excluding Quebec) for 2024. Because FLT3-ITD mutation testing is currently part of the standard of care across Canada, there is no additional impact on health systems anticipated as part of establishing treatment eligibility for quizartinib. |
Availability and reimbursement status of the testing procedure in jurisdictions across Canada | According to the clinical experts, testing for FLT3-ITD mutations is broadly available and funded as part of the current standard of care for newly diagnosed AML at AML treatment centres across Canada. | |
Testing procedure as part of routine care | According to the clinical experts, testing for FLT3-ITD mutations is currently performed as part of the standard of care for newly diagnosed AML across Canada. | |
Repeat testing requirements | According to the clinical experts, testing for FLT3-ITD mutations is conducted at diagnosis and repeated only in patients with refractory or relapsed disease. | |
Impacts on human and other health care resources by provision of the testing procedure | Because testing for FLT3-ITD mutations is currently available as part of the standard of care for patients with newly diagnosed AML and publicly funded at AML treatment centres across Canada, use of the test result to establish treatment eligibility for quizartinib is not anticipated to have any additional impact on human and other health care resources. | |
Patient-related | Accessibility of the testing procedure in jurisdictions across Canada | Testing for FLT3-ITD mutations is widely accessible in jurisdictions across Canada, because testing is currently available as part of the standard of care for newly diagnosed AML and publicly funded at AML treatment centres. |
Expected turnaround times for the testing procedure | Testing results would be needed in a timely manner (i.e., before quizartinib is to be initiated, on day 8 of induction chemotherapy).62 According to the clinical experts, expected turnaround times are 3 to 5 days for PCR testing results and 2 to 3 weeks for NGS results. According to patient group input that provided results from an online survey conducted by Heal Canada, 40% of patients received their mutation testing results within a week, and 33% of patients received them before treatment induction (although the exact timing was not defined). However, there is no additional impact on turnaround times anticipated as part of establishing treatment eligibility for quizartinib. | |
Burden associated with the testing procedure for patients, families, and/or caregivers | Because testing for FLT3-ITD mutations is currently part of the standard of care for newly diagnosed AML, there is no additional burden to patients, families, and/or caregivers anticipated from the testing as part of establishing treatment eligibility for quizartinib. | |
Clinical | Clinical utility and validity of the testing procedure | There is evidence from Canada to demonstrate the diagnostic accuracy and clinical utility of PCR fragment analysis and NGS testing for FLT3-ITD mutations in newly diagnosed AML.a, 61 PCR fragment analysis is best suited for detecting larger FLT3-ITD mutations, while NGS has clinical utility for the detection of additional mutations not detectable by PCR testing.61 Many AML treatment centres in Canada perform both tests but favour PCR testing for detecting FLT3-ITD mutations.61 According to the clinical experts, the test sensitivity of NGS panels is > 98% for the detection of substitutions and small insertions, duplications, and deletions. A Canadian consensus panel on the clinical utility of FLT3 mutation testing recommended PCR standardization so the lower limit of detection is between 1% and 5%.61 The clinical experts confirmed that their laboratories are meeting this threshold. |
Risks of harm associated with the testing procedure | According to the clinical experts, potential harms associated with retrieving bone marrow or peripheral blood samples include blood loss, pain, and risk of infection at the aspiration site. Because testing for FLT3-ITD mutations is currently part of the standard of care for newly diagnosed AML, there is no additional risk of harm associated with the testing as part of establishing treatment eligibility for quizartinib. | |
Cost | Projected cost of the testing procedure | Estimated costs for FLT3-ITD mutation testing range from $90 (for PCR testing) to $2,000 (for NGS panels);62,63 however, both are available and funded for patients with newly diagnosed AML across Canada. Therefore, there is no additional cost anticipated from the testing as part of establishing treatment eligibility for quizartinib. |
AML = acute myeloid leukemia; CDA-AMC = Canada's Drug Agency; ITD = internal tandem duplication; NGS = next-generation sequencing; PCR = polymerase chain reaction.
aCDA-AMC has not evaluated or critically appraised this evidence to determine its validity or reliability.
Perspectives of Patients, Clinicians, and Drug Programs
The full patient and clinician group submissions received are available in the consolidated patient and clinician group input document for this review on the project website.
Patient Group Input
This section was prepared by the review team based on the input provided by patient groups.
Input for this review was submitted by 2 patient groups, Heal Canada and LLSC. Heal Canada is a registered not-for-profit organization aiming to empower patients, improve health care outcomes, and advocate for equitable access to quality health care across Canada. LLSC is a national charity organization aiming to find a cure for blood cancers, as well as provide resources, education, and support to patients and caregivers affected by blood cancers. Information for the Heal Canada input was gathered through an online patient survey available between November 16 and December 16 (year not reported). Twenty-two patients living in Canada completed the survey, with representation from most of the provinces, including Ontario (38%), Quebec (18%), British Columbia (12%), Alberta (9%), Manitoba (3%), Nova Scotia (3%), New Brunswick (3%), and Saskatchewan (3%). Information for the LLSC input was gathered through 2 patient surveys. The first (survey 1) was available online from November 2024 to December 2024 and focused on patient and caregiver experiences with the drug under review. The second (survey 2) was gathered for a previous drug review submission. There were 224 respondents to the first survey and 83 respondents to the second survey.
When asked about their experience with AML, patients highlighted the profound impact on their social lives, personal relationships, mental health, and independence. Nearly all patients reported needing caregiver support for daily tasks, which LLSC noted diminishes patients’ mental well-being by impeding independence and increasing the burden on caregivers. Patients also emphasized the impact of AML on their personal and home lives, reporting that symptoms, mental load, and frequent travel for appointments limits their ability to participate in social activities and maintain relationships. Heal Canada highlighted that despite repeated emphasis by international expert consensus and the Canadian CLSG/GCEL 2023 guidelines on obtaining FLT3 mutation testing results before initiating treatment, 67% of survey 1 respondents had started treatment before receiving these results. Across inputs, most patients had received chemotherapy, stem cell transplant, and/or azacitidine plus venetoclax, with some also having received targeted therapy, immunotherapy, radiation, transfusions, or bone marrow transplant. However, for many patients, current treatments can have severe adverse effects and limited long-term efficacy. The top 5 most impactful adverse effects of AML treatments, as reported by survey 2 respondents, were fatigue (72%), neutropenia (57%), thrombocytopenia (54%), and anemia (43%). Patients highlighted their desire to live and hope of survival as key drivers in tolerating adverse effects of current treatments.
When evaluating new treatment options for AML, patients and caregivers indicated that they would prioritize improvements in long-term adverse effects and the impact of adverse effects on daily life, and a reduced risk of relapse. High importance was also placed on QoL, maintaining independence, severity and frequency of adverse effects, and the duration of and potential for sustained remission. When asked to elaborate on what desired improvements to QoL they would like to see from new treatments, patients noted longer remission, reduction in the fear and risk of reoccurrence, CR and a cure, resumption of regular daily activities, limited side effects, less time in hospital, a reduced need for transfusions, and better access to care in smaller communities.
Across both input submissions, respondents with experience with quizartinib (n = 3 in the Heal Canada input and n = 13 in the LLSC input) reported that adverse effects were minimal and mild. In the Heal Canada input, patients found quizartinib to be well-tolerated. One patient showed improved response after switching from azacitidine, venetoclax, and gilteritinib. Another patient had CR during the first induction, received allogeneic HSCT, reported no residual disease post-transplant, and continued with quizartinib maintenance therapy. In the LLSC input, most patients with experience with quizartinib had accessed it through the clinical trial (57%) or a compassionate use program (29%). Respondents reported the most severe adverse effects to be thrombocytopenia (with a weighted average severity of 2.3 of 5) and anemia (2.1 of 5). Compared to other treatments for AML, quizartinib was rated as the same or less difficult by 86% of survey 1 respondents, with more than 80% noting improved QoL. All stated that they would choose quizartinib again and recommend it to others.
Clinician Input
Input From Clinical Experts Consulted for This Review
All CDA-AMC review teams include at least 1 clinical specialist with expertise regarding the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). The following input was provided by 2 clinical specialists with expertise in the diagnosis and management of AML.
Unmet Needs
Although midostaurin is approved by Health Canada for adult patients with newly diagnosed FLT3-mutated AML without age restrictions, the pivotal trial was conducted in a population of patients aged 18 years to 59 years.17 As such, the population of patients in the pivotal trial was younger, on average, than those seen in clinical practice. Per the clinical experts consulted, there is a need for evidence of the efficacy and harms of FLT3-ITD inhibitors among older patients, who were excluded from earlier studies. The pivotal trial for quizartinib enrolled a population of patients aged 18 years to 75 years22 and is the first RCT to inform the efficacy and harms of a FLT3-ITD inhibitor in older patients.
There is an unmet need for an approved maintenance therapy for patients with newly diagnosed AML that is FLT3-ITD positive. At the current time, the only maintenance therapy available in Canada for patients with FLT3-ITD–mutated AML is oral azacitidine. Patients are only eligible if they are in first CR, have intermediate-risk or adverse-risk karyotype, and are not planned to receive or have not received allogeneic HSCT. Further, there is no RCT comparing maintenance therapy with oral azacitidine with FLT3-ITD inhibitors, like quizartinib or midostaurin. Ideally, such RCTs would re-randomize patients before maintenance therapy to inform on the contributions of the maintenance therapy to overall efficacy, including among patients who have received allogeneic HSCT. Per the clinical experts consulted, oral azacitidine is associated with adverse gastrointestinal effects, such as nausea and vomiting. Treatments used to control nausea often cause constipation, requiring laxatives. There is a need for an approved maintenance therapy with fewer adverse gastrointestinal effects.
Per the clinical experts consulted, to inform treatment decisions, there is a need for studies directly comparing midostaurin with more potent selective FLT3-ITD inhibitors, such as quizartinib and gilteritinib. There is also a need for studies to inform how MRD assessment may be used to determine which patients need more consolidative therapy before, or after allogeneic HSCT.
Place in Therapy
According to the clinical experts consulted, quizartinib would be administered to newly diagnosed treatment-naive patients with FLT3-ITD–mutated AML who are suitable for intensive chemotherapy. Patients with CR after standard anthracycline (daunorubicin or idarubicin) induction chemotherapy in combination with quizartinib would receive 1 to 4 consolidation therapies, consisting of intermediate or high-dose cytarabine plus quizartinib, followed by allogeneic HSCT for those patients who are eligible. Patients would receive quizartinib maintenance therapy after the completion of consolidation therapy and/or allogeneic HSCT.
There is no phase III RCT comparing maintenance therapy with oral azacitidine versus FLT3 inhibitors (like midostaurin and quizartinib), nor direct evidence comparing quizartinib and midostaurin as maintenance therapies. However, the clinical experts consulted indicated that most physicians will choose quizartinib over midostaurin, the current standard of care for patients with newly diagnosed, FLT3-ITD–positive AML. Per the clinical experts consulted, the primary advantage of quizartinib over midostaurin would be the ability to administer it as a maintenance therapy, with the goal of reducing the risk of relapse and prolonging OS after consolidation therapy and/or allogeneic HSCT.
Patient Population
According to the clinical experts consulted, patients most likely to benefit from quizartinib would be those with newly diagnosed AML that is FLT3-ITD positive and who are eligible for intensive induction and consolidation chemotherapy. These would be the same patients who are currently treated with midostaurin. Midostaurin is also used for patients with FLT3-TKD mutations; however, these patients would not be treated with quizartinib. The diagnosis of patients with FLT3-ITD–mutated AML follows an established standard of care, currently used to gain access to midostaurin.
The presence or absence of FLT3-ITD mutations is part of the standard of care work-up for newly diagnosed patients with AML and performed in laboratories accredited by Accreditation Canada Diagnostics. Per the clinical experts consulted, the presence or absence of FLT3-ITD mutations is assessed via NGS on DNA or RT-PCR on RNA. The choice of test is centre dependent. Details of mutation testing are discussed in the Testing Procedure Considerations.
Given the notable harms associated with quizartinib,16 the clinical experts consulted indicated that it would not be administered to patients with severe uncorrectable hypokalemia, severe uncorrectable hypomagnesemia, long QT syndrome, or with a history of ventricular arrhythmias or torsades de pointes.
Assessing the Response Treatment
According to the clinical experts consulted, patients receiving quizartinib will be monitored for relapse based on clinical assessment and bloodwork at regular intervals, with a bone marrow assessment done if there is a concern for relapse. The clinical experts noted that MRD is being evaluated routinely for an increasing number of AML subtypes as a potential marker of prognosis and to inform treatment decision-making.14 Testing for FLT3-ITD MRD is being developed and validated at some Canadian centres, but is not currently funded or used in clinical practice. The clinical experts stressed the need for FLT3-ITD MRD assessment, noting that it could be helpful to inform treatment decisions, including whether quizartinib maintenance therapy is indicated and when to stop therapy.22
Discontinuing Treatment
According to the clinical experts consulted, patients will be discontinued from quizartinib upon disease relapse, the development of certain AEs (specifically corrected QT interval [QTc] prolongation not controlled by dose reduction and correction of electrolytes, or the development of torsades de pointes, ventricular fibrillation, or cardiac arrest), death, or the completion of 3 years of maintenance therapy (as per the protocol for the pivotal trial). Quizartinib may also be discontinued due to patient preference.
Prescribing Considerations
According to the clinical experts consulted, patients receiving quizartinib should be treated by a hematologist with experience in treating patients with acute leukemia in a centre with the appropriate resources. Consolidation chemotherapy may be administered in the outpatient setting provided certain institutional criteria are met. Quizartinib maintenance therapy would be administered as an outpatient under the supervision of a hematologist with experience in administering lower intensity therapy in a centre with the appropriate resources.
Clinician Group Input
This section was prepared by the review team based on the input provided by clinician groups.
Input for this review was submitted by 3 clinician groups, 1 from the Ontario Health (Cancer Care Ontario) Hematology Cancer Drug Advisory Committee and a second joint input from the CLSG/GCEL and CTTC. The Ontario Health (Cancer Care Ontario) Drug Advisory Committees provide timely evidence-based clinical and health system guidance on drug-related issues. CLSG/GCEL is a national collective of acute leukemia-treating physicians representing all major leukemia centres across every Canadian province. CTTC is a member-led, Canada-wide, multidisciplinary professional organization providing leadership and promoting excellence in patient care, research, and education in the field of HSCT and cell therapy. Input for these submissions were gathered through relevant published literature and clinical disease experience.
According to clinician groups, since the pivotal trial for midostaurin in 2017, the standard of care for patients with FLT3-ITD–positive AML has consisted of midostaurin in combination with standard 7 + 3 induction chemotherapy (7 days of cytarabine and 3 days of anthracycline). CLSG/CGEL and CTTC noted that midostaurin is often not sufficient to prevent relapses or the need for allogeneic HSCT. Some patients are also ineligible for allogeneic HSCT due to age, comorbid illness, or a lack of suitable donors. For patients excluded from allogeneic HSCT, and transplant-eligible patients before and after allogeneic HSCT, CLSG/CGEL and CTTC emphasized there is currently no approved FLT3-ITD–specific maintenance therapy, highlighting this as a major cause of failure and death in these patients. Further, CLSG/CGEL and CTTC noted that currently available AML treatments typically have poor outcomes, with high relapse rates and low OS, and are highly toxic. CLSG/CGEL and CTTC noted that FLT3 inhibitors such as quizartinib target one of the most common AML driver mutations, thereby targeting and modifying the underlying disease mechanism.
Based on clinician group input, key goals of AML treatment are to improve OS, attain remission, and cure disease or palliate older patients. Additional treatment goals include reducing symptom severity, minimizing AEs, improving QoL, increasing the ability to maintain employment and independence, and reducing caregiver burden. The clinician groups anticipate that quizartinib will be used first-line as an alternative to midostaurin, in combination with 7 + 3 induction chemotherapy (i.e., cytarabine on days 1 through 7 and an anthracycline on days 1 through 3), as well as for consolidation and maintenance therapies. Patients identified by the clinician groups as best suited to quizartinib are those who have newly diagnosed AML with an FLT3-ITD mutation, noting that patients without this mutation are unlikely to respond to treatment. This patient group could be identified through up-front molecular testing, which is routinely performed at leukemia centres across Canada. As it is not possible to identify which FLT3-ITD–positive patients are most likely to respond to quizartinib, the clinician groups noted that all should receive treatment.
According to clinician groups, the outcome metrics used in the pivotal trial for quizartinib are identical to those used in clinical practice, and a meaningful response to therapy would include an absence of relapses, prolonged remission, and improved OS. CLSG/CGEL and CTTC suggested that MRD response could theoretically be used as a surrogate, but an appropriate FLT3-ITD MRD test is not currently available in Canada. CLSG/CGEL and CTTC suggested that, depending on the patient’s disease phase, their treatment response could be reassessed weekly, every 2 weeks, monthly, or every 2 months to 3 months. LLSC noted that postinduction bone marrow would be used to confirm remission. In the absence of relapses, CLSG/CGEL and CTTC indicated that QoL and patient performance would also be expected to improve. Clinician groups agreed that treatment would be initiated and monitored at a university-associated academic leukemia centre, as an inpatient procedure for induction and outpatient for consolidation. CLSG/CGEL and CTTC noted that for longer-term maintenance, patients could be followed incrementally at a shared care site closer to home. Treatment would be initiated and monitored by specialists with expertise in leukemia, likely primarily hematologists, but also some oncologists. Discontinuation of quizartinib should be considered in the event of relapse or intolerable toxicity. CLSG/CGEL and CTTC indicated that while the optimal duration of quizartinib treatment in the maintenance setting is currently unclear, the pivotal trial suggests that maintenance should be continued for 3 years.
Drug Program Input
The drug programs provide input on each drug being reviewed through the reimbursement review processes by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by for this review are summarized in Table 5.
Table 5: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Relevant comparators | |
The QuANTUM-First trial compared quizartinib to placebo in combination with chemotherapy for induction and consolidation and as a single drug for maintenance therapy. Midostaurin is currently funded, in combination with chemotherapy, for induction and consolidation of newly diagnosed FLT3-mutated AML. It is not currently indicated for maintenance therapy. Azacitidine is funded as maintenance for patients who are transplant ineligible. There is limited access to other agents for maintenance across Canadian jurisdictions (e.g., sorafenib in combination with azacitidine is available in British Columbia). | This was a comment from the drug programs to inform pERC deliberations. |
Considerations for initiation of therapy | |
FLT3 testing is standard across Canada. To be eligible, patients had to have a FLT3-ITD VAF of at least 3%. Should patients with a VAF < 3% be eligible for treatment? | Per the clinical experts, patients with VAF < 3% should be considered eligible for treatment with quizartinib. The clinical experts clarified that although FLT3 testing is standard in Canada, the method will differ by centre (i.e., NGS on DNA or RT-PCR on RNA). The sensitivity, specificity, and limitations of the FLT3-ITD assay will depend on the methodology and the laboratory. As such, the presence of FLT3-ITD should be used to inform eligibility, rather than a specific VAF threshold. |
Comment: FLT3 testing results will be required in a timely manner to begin treatment on day 8. | This was a comment from the drug programs to inform pERC deliberations. |
Considerations for continuation or renewal of therapy | |
The response criteria used in the study were adapted from Cheson et al.39 and Döhner et al. (2017):43 CR required bone marrow blasts < 5%, neutrophils > 1,000/mm3, and platelets > 100,000/mm3. Is this congruent with Canadian practice? | Per the clinical experts, achieving a strictly defined CR is not required in clinical practice for patients to continue to consolidation therapy. In clinical practice, patients with CR with partial hematological recovery, whereby these values may not be achieved, would be eligible for consolidation therapy. The clinical experts clarified that in the pivotal trial for quizartinib, patients with CR with incomplete hematologic recovery were eligible for consolidation therapy. They noted that this would align with clinical practice in Canada. |
To receive maintenance therapy, patients had to be able to start within 60 days of the first day of the last consolidation cycle or 30 to 180 days after allogeneic HSCT. Are there any reasons a patient might not be able to start treatment within these time frames and should remain eligible for maintenance with quizartinib? | Per the clinical experts, 60 days may be restrictive for some patients; for example, some older patients may take longer to recover, particularly after multiple rounds of consolidation chemotherapy. Per the clinical experts, the time frame for starting maintenance therapy postallogeneic HSCT is very wide. The wide time range reflects the multiple factors that would need to be considered to determine when a patient may be ready to begin maintenance therapy with quizartinib (e.g., active GVHD, organ comorbidities). |
Considerations for discontinuation of therapy | |
Quizartinib and placebo were discontinued for unacceptable toxicity, refractory disease, relapse, or upon completion of 36 cycles of maintenance therapy. Are there specific or standard definitions that should be used for discontinuation? | Per the clinical experts, there are no standard definitions used for discontinuation. However, the reasons listed are reflective of why patients would typically be discontinued from treatment. The clinical experts noted that in practice, patients may be continued beyond 36 cycles of maintenance therapy in certain circumstances. They underscored the potential role of FLT3-ITD MRD testing in informing treatment decisions, including when to discontinue or prolong quizartinib maintenance therapy. FLT3-ITD MRD testing is not currently funded or used in clinical practice in Canada. |
If a patient stops treatment with quizartinib for reasons other than progression, should they be able to resume quizartinib to complete 3 years total of maintenance therapy? | The clinical experts indicated patients should be allowed to resume treatment with quizartinib during maintenance if they needed to hold for a reason other than disease progression, such as to treat infections or other medical illnesses. |
Considerations for prescribing of therapy | |
In the trial, chemotherapy used for induction was 7 + 3 (7 days of cytarabine and 3 days of daunorubicin or idarubicin) and chemotherapy used for consolidation was high-dose cytarabine. Should patients using other chemotherapy regimens in induction and/or consolidation be eligible for treatment with quizartinib? | The clinical experts were not aware of any studies of quizartinib in combination with other chemotherapy regimens. Therefore, the clinical experts did not believe that patients using other chemotherapy regimens during induction and/or consolidation should be eligible for treatment with quizartinib. |
Generalizability | |
Should any of the following groups be considered for treatment with quizartinib?
| Except for patients < 18 years and those with BCR-ABL1-positive leukemia, the clinical experts asserted that all other subgroups listed should be eligible for treatment with quizartinib. The clinical experts clarified that decisions to administer intensive chemotherapy should be based not only on a patient’s performance status at the time of diagnosis of AML, but on their baseline performance status (i.e., before diagnosis of AML). The clinical experts highlighted that the quizartinib development program includes a phase I/II trial that is currently under way among pediatric and young adult patients with relapsed or refractory, FLT3-ITD–positive AML.64 As such, quizartinib is currently being used in pediatric patients in some centres on a trial basis. However, the clinical experts noted that they could not recommend its use in patients < 18 years at this time. |
Should patients currently receiving treatment for newly diagnosed AML with midostaurin be eligible to switch to quizartinib? If yes, in which phases of treatment? | The clinical experts noted that, in the absence of intolerance or toxicity from midostaurin (e.g., significant nausea or vomiting), there is no reason to switch from midostaurin to quizartinib during induction or consolidation therapy. Per the clinical experts, physicians would be more likely willing to provide quizartinib maintenance therapy to patients who received midostaurin during induction and consolidation. The clinical experts indicated that there is a lack of evidence demonstrating the degree of benefit in providing quizartinib maintenance to patients who received midostaurin during induction and consolidation. |
Should patients who recently completed treatment with midostaurin be eligible for quizartinib maintenance therapy? | Per the clinical experts, patients who have completed treatment with midostaurin should be eligible for maintenance therapy with quizartinib. |
Funding algorithm | |
Under what circumstances would quizartinib be preferred over midostaurin? | Per the clinical experts, the primary benefit of quizartinib would be that it can be used as a maintenance therapy after consolidation. Midostaurin is not approved for use as maintenance therapy. The clinical experts clarified that there is no direct evidence of the efficacy of midostaurin versus quizartinib; however, the practical aspect of being able to provide quizartinib during maintenance would likely result in most physicians choosing quizartinib over midostaurin. |
Care provision issues | |
Comment: There are 2 tablet strengths available, 17.7 mg and 26.5 mg (equivalent to 20 mg and 30 mg of quizartinib dihydrochloride respectively). Dose modifications were implemented for QTc prolongation, other nonhematological toxicities, and myelosuppression. | This was a comment from the drug programs to inform pERC deliberations. |
Comment: Quizartinib metabolism is impacted by the CYP3A4 pathway. Concomitant use of strong or moderate CYP3A4 inducers should be avoided. Dose modifications are required for concomitant use of strong CYP3A4 inhibitors. | This was a comment from the drug programs to inform pERC deliberations. |
Comment: In the maintenance phase, the dose of quizartinib was increased after ECG on cycle 1, day 15 or cycle 2, day 1 if the mean QTcF was ≤ 450 ms. | This was a comment from the drug programs to inform pERC deliberations. |
System and economic issues | |
Comment: This will potentially add 3 years of maintenance treatment for newly diagnosed patients with AML. | This was a comment from the drug programs to inform pERC deliberations. |
Comment: Increased workload to be expected for required QTc monitoring. | This was a comment from the drug programs to inform pERC deliberations. |
Confidential pricing exists for midostaurin. | This was a comment from the drug programs to inform pERC deliberations. |
AML = acute myeloid leukemia; CNS = central nervous system; CR = complete remission; CSF = cerebrospinal fluid; CYP = cytochrome P450; ECG = electrocardiogram; ECOG = Eastern Cooperative Oncology Group; GVHD = graft-versus-host disease; HSCT = hematopoietic stem cell transplant; ITD = internal tandem duplication; MRD = minimal or measurable residual disease; NGS = next-generation sequencing; pERC = pan-Canadian Oncology Drug Review Expert Committee; QTc = corrected QT interval; QTcF = QT interval corrected using the Fridericia formula; RT-PCR = reverse transcription polymerase chain reaction; VAF = variant allele frequency.
Clinical Evidence
The objective of this clinical review report is to review and critically appraise the clinical evidence submitted by the sponsor on the beneficial and harmful effects of quizartinib in the treatment of adult patients with newly diagnosed AML that is FLT3-ITD positive. The focus will be placed on comparing quizartinib to relevant comparators and identifying gaps in the current evidence. According to the clinical experts consulted for this review, midostaurin in combination with standard cytarabine and anthracycline induction and standard cytarabine consolidation chemotherapy, with or without allogeneic HSCT, is a relevant comparator. Patients who are ineligible for allogeneic HSCT may receive oral azacitidine as a maintenance therapy.
A summary of the clinical evidence included by the sponsor in the review of quizartinib is presented in 4 sections with the critical appraisal of the evidence included at the end of each section. The first section, the SR, includes pivotal studies and RCTs that were selected according to the sponsor’s SR protocol. The assessment of the certainty of the evidence in this first section using the GRADE approach follows the critical appraisal of the evidence. The second section would include sponsor-submitted long-term extension studies, but none were submitted. The third section includes indirect evidence from the sponsor. The fourth section would include additional studies that were considered by the sponsor to address important gaps in the SR evidence, but none were submitted.
Included Studies
Clinical evidence from the following is included in the review and appraised in this document:
Systematic Review
Contents within this section have been informed by materials submitted by the sponsor. The following have been summarized and validated by the review team.
Description of Studies
Characteristics of the included study are summarized in Table 6.
The QuANTUM-First study19-22 is a phase III, double-blind, multicentre RCT that aims to compare the effects of quizartinib versus placebo (administered with standard induction and consolidation chemotherapy [and/or allogeneic HSCT], then administered as maintenance therapy for up to 36 cycles) among adult patients with newly diagnosed AML that is FLT3-ITD positive (N = 539). The study was conducted in 193 sites in 26 countries, including 4 sites in Canada. Eligible patients were randomized in a 1:1 ratio via interactive web and voice response system to the quizartinib group (n = 268) or the placebo group (n = 271). Randomization was stratified by region (Europe; North America; or Asia, Australia, and South America), age (< 60 years; ≥ 60 years), and WBC count at diagnosis (< 40 × 109/L; ≥ 40 × 109/L). Neither the patients nor investigators were aware of the treatments received. Placebo was supplied to study sites as tablets matching the appearance of quizartinib dihydrochloride 20 mg and 30 mg tablets (equivalent to 17.7 mg and 26.5 mg quizartinib). Unblinding occurred only in case of emergency.
Table 6: Details of QuANTUM-First19-22
Detail | QuANTUM-First |
|---|---|
Designs and populations | |
Study design | Phase III, randomized, double-blind, placebo-controlled, multicentre, global study |
Locations | 193 sites in 26 countries in Asia, Australia, Europe, North America (including 4 sites in Canada), and South America |
Patient enrolment dates | Start date: September 27, 2016 End date: August 14, 2019 |
Randomized (N) | N = 539 Quizartinib group, n = 268 Placebo group, n = 271 |
Inclusion criteria |
|
Exclusion criteria |
|
Drugs | |
Interventionb | First induction cycle: standard 7 + 3 induction regimen with cytarabine 100 mg/m2 per day (200 mg/m2 per day allowed if institutional or local standard) by continuous IV infusion from day 1 to day 7 and an anthracycline (daunorubicin 60 mg/m2 per day or idarubicin 12 mg/m2 per day) by IV infusion on days 1, 2, and 3. On day 8, patients started quizartinib dihydrochloride 40 mg, orally once per day for 14 days. Consolidation (for patients with complete remission or complete remission with incomplete hematologic recovery during induction): high-dose cytarabine and quizartinib dihydrochloride (40 mg/day), allogeneic HSCT alone (from end of induction to within 3 months of starting maintenance), or treatment with high-dose cytarabine and quizartinib dihydrochloride (40 mg/day) then allogeneic HSCT. High-dose cytarabine was administered by IV infusion every 12 hour on days 1, 3, and 5 for a total of 6 doses. Maintenance: Quizartinib dihydrochloride, starting at 30 mg per day then increased to 60 mg per day if the mean QTcF of the triplicate echocardiogram was ≤ 450 ms on cycle 1, day 15. |
Comparator(s) | As per the intervention, except quizartinib is replaced with matched placebo |
Study duration | |
Screening phase | 7 days before the start of induction chemotherapy up to the day of randomization |
Treatment phase | Up to 42 cycles (inclusive of induction, consolidation, and maintenance phases) |
Follow-up phase |
|
Outcomes | |
Primary end point | Overall survival |
Secondary and exploratory end points | Secondary:
Exploratory:
Safety:
Other:
|
Publication status | |
Publications | Erba et al.22 ClinicalTrials.gov: NCT0266865321 |
AML = acute myeloid leukemia; CNS = central nervous system; CSF = cerebrospinal fluid; ECOG = Eastern Cooperative Oncology Group; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; HSCT = hematopoietic stem cell transplant; ITD = internal tandem duplication; MRD = minimal or measurable residual disease; QTc = corrected QT interval; QTcF = QT interval corrected using the Fridericia formula; VAF = variant allele frequency.
aDefined as bradycardia of < 50 beats per minute, unless the patient had a pacemaker; QTcF > 450 ms; diagnosis of or suspicion of long QT syndrome (including family history of long QT syndrome); systolic blood pressure ≥ 180 mm Hg or diastolic blood pressure ≥ 110 mm Hg; history of clinically relevant ventricular arrhythmias (e.g., ventricular tachycardia, ventricular fibrillation, or torsade de pointes); history of second-degree (Mobitz II) or third-degree heart block (patients with pacemakers were eligible if they had no history of fainting or clinically relevant arrhythmias while using the pacemaker); history of uncontrolled angina pectoris or myocardial infarction within 6 months before screening; history of New York Heart Association Class III or Class IV heart failure; left ventricular ejection fraction ≤ 45% or less than the institutional lower limit of normal per multigated acquisition scan or echocardiogram done within 30 days before randomization; or complete left bundle branch block.
bThe interventional drug was available as 20 mg and 30 mg tablets. Each 20 mg tablet contained 20 mg quizartinib dihydrochloride (equivalent to 17.7 mg quizartinib). Each 30 mg tablet contained 30 mg quizartinib dihydrochloride (equivalent to 26.5 mg quizartinib).
cDefined as complete remission or complete remission with incomplete neutrophil or platelet recovery.
Sources: Sponsor’s Summary of Clinical Evidence52 and Clinical Study Report for QuANTUM-First.19
The study consisted of 4 consecutive phases: induction (up to 2 cycles), consolidation, maintenance, and long-term follow-up (Figure 1). During induction, consolidation, and maintenance, each cycle was 28 days. The total duration of treatment with study drug is up to 42 cycles. The primary end point was OS. Secondary end points included EFS per IRC assessment, and CR rate: CR with FLT3-ITD MRD negativity rate, CRc rate, and CRc with FLT3 MRD negativity rate after induction. Exploratory end points included RFS, duration of CR, morphologic leukemia-free state rate after induction, transplant rate, HRQoL, general health status, health care resource utilization, and additional remission measures. Following induction and consolidation therapy, patients were followed for EFS and OS events. The total duration of patient participation was until death, withdrawal of consent, loss to follow-up, or study closure, whichever occurred first. The data cut-off for efficacy end points was August 13, 2021. Updated safety data were provided in an addendum to the Clinical Study Report to a data cut-off of June 16, 2023. No interim efficacy analyses were planned.
Figure 1: Study Design for QuANTUM-First
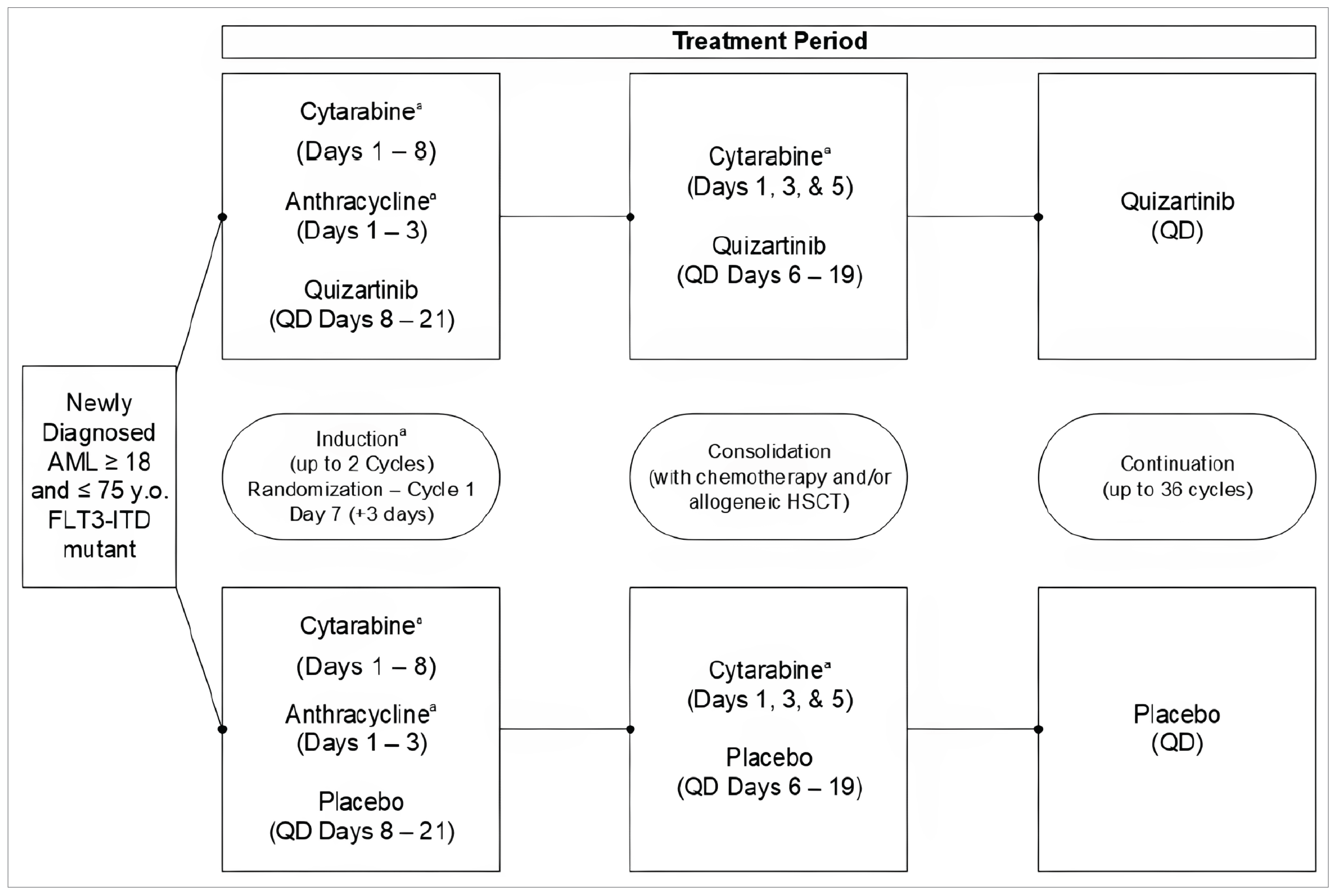
AML = acute myeloid leukemia; HSCT = hematopoietic stem cell transplant; ITD = internal tandem duplication; QD = once daily; y.o. = years old.
aDuring cycle 2 of induction, investigators may have chosen to administer the 7 + 3 chemotherapy regimen (7 days of cytarabine and 3 days of anthracycline) or the 5 + 2 chemotherapy regimen (5 days of continuous IV infusion of standard dose cytarabine and 2 days of the same anthracycline used during the first induction cycle), and study drug would therefore have started on day 8 or day 6, respectively.
Source: Clinical Study Report for QuANTUM-First.19
Populations
Inclusion and Exclusion Criteria
Adult patients (aged 18 years to 75 years) with newly diagnosed AML who were FLT3-ITD positive were eligible to be randomized (Table 6). FLT3-ITD mutation status from bone marrow and/or blood samples was determined via a previously developed clinical trial molecular assay using PCR and capillary electrophoresis technology. Eligible patients also needed an ECOG performance status of 0 to 2, adequate renal and hepatic function, and serum electrolytes within the institution’s normal limits. To be eligible for the consolidation phase, patients must have had CR or CRi based on local laboratory results at the end of the induction phase and been able to begin consolidation therapy within 60 days of the first day of the last induction cycle. To be eligible for the maintenance phase, patients must not have had active acute or grade 3 or higher GVHD and not initiated therapy for GVHD within 21 days; have confirmed less than 5% of blasts based on the most recent bone marrow aspirate; have an ANC less than 500/mm3 and a platelet count greater than 50,000/mm3 without platelet transfusion support; and have been able to begin maintenance therapy within 60 days of the first day of the last consolidation cycle received or 180 days after allogeneic HSCT.
Key exclusion criteria included a diagnosis of acute promyelocytic leukemia or BCR-ABL–positive leukemia, AML secondary to prior chemotherapy or radiotherapy for other neoplasms, a history of central nervous system (CNS) leukemia, and/or history of other malignancies, with some exceptions. Patients with active acute or chronic systemic fungal, bacterial, or viral infections, active clinically relevant liver disease, a history of HIV, and/or uncontrolled or significant cardiovascular disease were also excluded. Patients previously treated for AML were excluded, with some exceptions.
Interventions
Investigational Product
Throughout all phases of treatment, quizartinib was supplied as 20 mg and 30 mg tablets. Each 20 mg tablet contained 20 mg of quizartinib dihydrochloride, equivalent to 17.7 mg of quizartinib. Each 30 mg tablet contained 30 mg of quizartinib dihydrochloride, equivalent to 26.5 mg of quizartinib.
Induction Phase (Up to 2 Cycles)
During the first cycle of the induction phase, patients in both groups received cytarabine 100 mg/m2/day (or 200 mg/m2/day if this was the institutional or local standard) by continuous IV infusion for 7 days (day 1 through day 8). On days 1, 2, and 3, patients received 1 of 2 anthracycline regimens by IV infusion (per investigator’s choice): daunorubicin 60 g/m2/day or idarubicin 12 mg/m2/day. Following the end of the cytarabine infusion (usually day 8), patients received either quizartinib dihydrochloride 40 mg or placebo orally for 14 days. Among patients concomitantly receiving a strong cytochrome P450 (CYP) 3A4 inhibitor, the dose was 20 mg/day.
Patients could be eligible for a second induction cycle at the investigator’s discretion (to allow for blood counts to recover or for other reasons). The second induction cycle was to begin within 60 days of the first day of the first induction cycle. Patients could have received 1 of 2 regimens during the second induction cycle, decided by the investigator: 7 + 3 chemotherapy (7 days of continuous IV infusion of standard dose cytarabine and 3 days of the same anthracycline used during the first induction cycle) or 5 + 2 chemotherapy (5 days of continuous IV infusion of standard dose cytarabine and 2 days of the same anthracycline used during the first induction cycle). Patients received quizartinib or placebo orally following the end of the cytarabine infusion (usually day 6 or 8), per the dosing in the first induction cycle.
Consolidation Phase (Up to 4 Cycles)
There were 3 treatment options during the consolidation phase: consolidation chemotherapy followed by quizartinib or placebo for 14 days, allogeneic HSCT, or consolidation chemotherapy followed by quizartinib or placebo for 14 days followed by allogeneic HSCT. For regimens including consolidation chemotherapy, cytarabine was given on days 1, 3, and 5 with dosing dependent on age. Patients aged younger than 60 years and 60 years or older received cytarabine 3.0 g/m2 and 1.5 g/m2, respectively, by IV infusion every 12 hours for 6 doses. Patients could have received up to 4 cycles of consolidation chemotherapy and were not obligated to complete a full cycle in the case of intolerance. Patients received quizartinib dihydrochloride 40 mg or placebo orally once daily for 14 days starting on day 6. Among patients concomitantly receiving a strong CYP3A4 inhibitor, the dose was 20 mg/day.
Maintenance Phase (Up to 36 Cycles)
Maintenance therapy with quizartinib or placebo began after induction and consolidation therapy (including allogeneic HSCT) and following blood count recovery (ANC > 500/mm3 and platelet count > 50,000/mm3 without a platelet transfusion within 24 hours of drawing blood samples). For patients who underwent allogeneic HSCT, maintenance therapy began within 30 days to 180 days post-transplant.
During the maintenance phase, quizartinib or placebo was administered orally once daily starting on day 1, without breaks between cycles. Patients in the quizartinib group received 30 mg quizartinib dihydrochloride orally once daily on cycle 1, days 1 to 15. If the average QTcF of the triplicate electrocardiogram (ECG) was less than or equal to 450 ms on day 15 of cycle 1, then on day 16 the dose of quizartinib dihydrochloride was increased to 60 mg/day. Patients continued this dose so long as dose reduction was not needed. Among patients concomitantly receiving a strong CYP3A4 inhibitor, the dose was 20 mg/day during cycle 1, days 1 to 15. If the dose of quizartinib could not be increased on cycle 1, day 16, then it could later be increased on cycle 2, day 2, if the average QTcF of the triplicate ECG was less than or equal to 450 ms on day 1 of cycle 2.
Per the first version of the study protocol, maintenance therapy was to continue for up to 12 cycles after the induction and consolidation phases. This was changed to up to 36 cycles at the time of the third protocol amendment. Maintenance therapy continued until relapse, initiation of nonprotocol-specified treatment for AML, death, unacceptable toxicity, study closure, or completion of study drug, whichever occurred first.
Allogeneic HSCT
Patients could undergo allogeneic HSCT after achieving CR or CRi after the induction phase, any time during the consolidation phase, or within the first 3 months of the maintenance phase if the following criteria were met:
at the start of the consolidation phase, the plan was for the patients to undergo allogeneic HSCT as part of consolidation therapy
a donor was unable to be found during the consolidation phase, but became available after the start of the maintenance phase
the investigator discussed the case with the medical monitor
confirmed less than 5% of blasts based on the most recent bone marrow aspirate, based on local laboratory results
the transplant was performed within 3 months after day 1 of maintenance therapy.
Quizartinib or placebo were discontinued at least 7 days before the start of the conditioning regimen.
Patients who received any HSCT for other reasons (e.g., molecular relapse) or who received autologous HSCT were discontinued from the study drug, as these were considered nonprotocol-specified treatments for AML.
Concomitant Therapies
Concomitant chemotherapy, immunotherapy, radiotherapy, transplant, or any ancillary therapy for AML not specified in the protocol or considered to be investigational were prohibited during the study. Medications associated with QT or QTc interval prolongation were prohibited, except for antibiotics, antivirals, and antifungals used as standard of care for the prevention or treatment of infections or if the investigator considered that the QT-prolonging or QTc-prolonging medication was vital to the patient’s care. Coadministration of quizartinib with drugs that were substrates of P-glycoprotein was allowed with caution.
Strong CYP3A4 inhibitors were to be avoided, if possible, but allowed if vital to the patient’s care along with a reduction in quizartinib or placebo dosage. Moderate or weak CYP3A4 inhibitors were allowed, while strong or moderate CYP3A4 inducers were prohibited.
Donor lymphocyte infusion after allogeneic HSCT was permitted.
Dose Reductions or Interruptions and Permanent Discontinuation of Study Drug
During any treatment phase, doses of quizartinib or placebo could be reduced or interrupted for specific AEs (QTcF prolongation, other nonhematologic toxicities, or myelosuppression) and/or concomitant administration of a strong CYP3A4 inhibitor. At any time, the dose of quizartinib dihydrochloride or placebo could not be reduced to less than 30 mg/day (or 20 mg/day for patients receiving a strong CYP3A4 inhibitor). Interrupted doses were not made up.
During any treatment phase, quizartinib or placebo could be permanently discontinued for the following reasons: AEs, death, refractory disease, relapse, institution of nonprotocol-specified treatment for AML, pregnancy, patient decision, or study termination. Patients who permanently discontinued quizartinib or placebo because they completed 12 cycles of maintenance therapy (before the third protocol amendment) could restart at the discretion of the investigator following discussion with the medical monitor, in the group to which they were randomized. Patients who discontinued quizartinib or placebo remained in the study and continued to be followed for outcome data, unless they were withdrawn from the study.
Outcomes
A list of end points assessed in this clinical review report is provided in Table 7, followed by descriptions of the outcome measures. Summarized end points are based on outcomes included in the sponsor’s summary of clinical evidence as well as any outcomes identified as important to this review according to the clinical experts consulted for this review and input from patient and clinician groups and public drug plans. Using the same considerations, we selected end points that were considered most relevant to inform expert committee deliberations and finalized this list of end points in consultation with members of the expert committee.
Per the inputs received by the patient groups, clinician groups, and clinical experts consulted for this review, improving remission rates, prolonging the duration of remission, reducing the risk of relapse, extending OS, and maintaining HRQoL while limiting toxicity are important treatment goals among patients with newly diagnosed AML that is FLT3-ITD positive. The selected end points are reflective of these treatment goals. The following efficacy end points were assessed using GRADE: OS, EFS, CR rate, CRc rate, RFS among patients achieving CR during induction, transplant rate, and HRQoL. The remaining efficacy end points (RFS among patients achieving CRc during induction; CR and CRc with MRD negativity after induction; duration of CR and CRc) were summarized as supportive information. Grade 3 to 5 AEs, considered important for informing expert committee deliberations, was also assessed using GRADE.
Table 7: Efficacy Outcomes Summarized From QuANTUM-First
Outcome measure | Time point | QuANTUM-First |
|---|---|---|
Overall survival |
| Primarya |
Event-free survival |
| Secondarya |
Complete remission rate | At the end of the induction phase | Secondary |
Composite complete remission rate | At the end of the induction phase | Secondary |
Complete remission with FLT3-ITD MRD negativity rate | At the end of the induction phase | Secondary |
Composite complete remission with FLT3-ITD MRD negativity rate | At the end of the induction phase | Secondary |
Duration of complete remission and composite complete remission | At a median follow-up of 39.2 months | Exploratory |
Relapse-free survival |
| Exploratory |
Transplant rate | At a median follow-up of 39.2 months | Exploratory |
Health-related quality of life | At a median follow-up of 39.2 months | Exploratory |
CI = confidence interval; HR = hazard ratio; ITD = internal tandem duplication; KM = Kaplan-Meier; MRD = minimal or measurable residual disease.
aStatistical testing for these end points was adjusted for multiple comparisons via a serial hierarchically ordered gatekeeping strategy, beginning with overall survival, then event-free survival, followed by the other secondary end points. As the between-group difference in event-free survival was not statistically significant, the remaining end points (aside from overall survival) were not tested statistically.
Source: Clinical Study Report for QuANTUM-First.19
Overall Survival
The primary end point of OS was defined as the time from randomization until death from any cause. Patients who were alive or lost to follow-up at the time of the analysis were censored at the date when they were last known to be alive. During long-term follow-up, patients without and with an EFS event were assessed for survival every 4 weeks and 12 weeks, respectively.
According to the clinical experts consulted for this review, a 5% to 10% difference between the quizartinib and placebo groups in the KM-estimated probabilities of OS at 12 months and 48 months of follow-up could be considered clinically important.
Event-Free Survival
The secondary end point of EFS per IRC assessment was defined as the time from randomization until the date of refractory disease, relapse after CR or CRi, or death from any cause, whichever came first. Refractory disease (or ITF) as determined within 42 days of the start of the last cycle of induction, was defined as: no CR or CRi, blasts less than 5% if Auer rod positive, or the appearance of new or worsening extramedullary disease. For refractory disease, the EFS event date was set to day 1 at randomization. Relapse after CR or CRi was defined as 5% or less blasts in the bone marrow aspirate and/or biopsy not attributable to any other cause, the reappearance of leukemic blasts in the peripheral blood, and/or the new appearance of extramedullary leukemia, or the presence of Auer rods. Patients with CR and who were alive without relapse were censored at the date of the last response assessment. Patients alive and without postbaseline assessments were censored at the date of randomization minus 1.
During the induction phase, a bone marrow aspirate specimen and blood samples for hematology were collected on day 21 (or up to day 28) of cycle 1 and cycle 2. Response criteria were adapted from the study by Cheson and colleagues39 and the study by Döhner and colleagues (2017)43 and informed by FDA guidance.24 CR was defined by ANC more than 1,000/mm3, platelets more than 100,000/mm3, the absence of leukemic blasts in the peripheral blood by morphologic examination, no extramedullary disease, and no Auer rods. Patients with CRi were those who met the criteria for CR except for the platelet or neutrophil count.22 Starting on day 21, blood samples for hematology were also collected at least weekly to assess count recovery. If an accurate assessment of response could not be made based on the day 21 bone marrow aspirate, then it was to be repeated upon count recovery or day 56 (± 3 days), whichever occurred first.
During the consolidation phase, a bone marrow aspirate specimen for relapse assessment was to be collected during the first and last cycles, upon count recovery from day 21 to day 56 (± 3 days). Among patients who underwent allogeneic HSCT, every 4 weeks through the end of the allogeneic HSCT period (up to 180 days after the date of transplant) the investigator determined whether the patient had relapsed based on bone marrow aspirate and/or pathology reports.
During the maintenance phase, a bone marrow aspirate specimen for relapse assessment and blood samples for hematology were collected, and physical examination for signs and symptoms of relapse were performed at all study visits (days 1, 8, and 15 of cycle 1; days 1 and 15 of cycle 2; day 1 of cycle 3; day 1 of cycles 4, 7, 10, 13, 19, and 25; day 1 of subsequent cycles; and end of treatment).
Patients without an EFS event were followed every 4 weeks for relapse during long-term follow-up, except for patients who had permanently discontinued the study drug before or during the maintenance phase, who were followed every 12 weeks to 24 weeks.
According to the clinical experts consulted for this review, a 10% difference between the quizartinib and placebo groups in the KM-estimated probabilities of EFS at 12 months and 36 months of follow-up could be considered clinically important.
CR and CRc Rates, With or Without MRD Negativity
CR and CRc rates after induction, with or without MRD negativity, were secondary end points. The CR rate was based on IRC assessment and defined as the percentage of patients achieving CR after induction. The CRc rate was based on IRC assessment and was defined as the percentage of patients achieving either CR or CRi after induction. Response criteria and the schedule of assessments during the induction phase were as described for EFS. The duration of CR and CRc were defined as the time from the first documented CR or CRc until documented relapse or death from any cause, whichever came first. Patients who were alive without relapse or lost to follow-up were censored at their last response assessment.
MRD negativity was defined as the presence of a small number of leukemic cells in the bone marrow, below the level of detection using conventional morphologic assessment. Genomic DNA was isolated from bone marrow aspirates or peripheral blood after remission and analyzed with a FLT3-ITD PCR NGS assay. The cut-off for MRD analyses was 10-4 leukemic cells, corresponding to 0.01% VAF or 1 FLT3-ITD–positive leukemia cell/10,000 cells.22
According to the clinical experts consulted for this review, a 10% to 15% difference between the quizartinib and placebo groups in the rates of CR and CRc, with and without MRD negativity after induction could be considered clinically important.
Relapse-Free Survival
The exploratory end point of RFS was measured by IRC assessment among patients with CR or CRc during the induction phase. RFS was defined as the time from randomization until documented relapse or death from any cause, whichever came first. Patients who were alive without relapse or who were lost to follow-up at the time of the analysis were censored at the date of their last response assessment. Response criteria and the schedule of assessments for response/relapse were as described for EFS.
A threshold for a clinically important difference between the quizartinib and placebo groups in RFS could not be estimated.
Transplant Rate
The exploratory end point of transplant rate was defined as the percentage of patients undergoing allogeneic HSCT directly following protocol treatment with no intervening AML therapy (excluding conditioning regimens).
According to the clinical experts consulted for this review, a 10% difference between the quizartinib and placebo groups in transplant rate could be considered clinically important.
Health-Related Quality of Life
The exploratory end point of patient-reported HRQoL was measured via the EORTC QLQ-C30 and EQ-5D-5L. The disease-specific EORTC QLQ-C30 was selected for presentation herein, with a focus on the GHS/QoL scale. Baseline measurements were collected on day 8 of the first induction cycle, and repeated measurements were collected on day 28 of induction cycles 1 and 2, day 6 and 28 of consolidation cycles 1 through 4, and day 1 of maintenance cycles 1 through 34 at 3-cycle intervals. The questionnaire was self-administered with a recall period of 1 week.
The EORTC QLQ-C3065 is a 30-item instrument intended to assess various aspects that define the QoL of patients with cancer. The instrument includes 5 multi-item functional scales (physical, role, emotional, cognitive, social), 3 multi-item symptom scales (fatigue, pain, nausea and vomiting), a 2-item GHS/QoL scale, 5 single items assessing common cancer symptoms (dyspnea, loss of appetite, insomnia, constipation, diarrhea), and 1 item on the financial impact of the disease. Each item is evaluated using 4-point or 7-point Likert scales. Raw scores for each scale are computed as the average of the items that contribute to that scale. The raw scores are converted to standardized scores ranging from 0 to 100. Higher scores reflect better function on the function scales, greater symptoms on the symptom scales, and better HRQoL on the GHS/QoL scale.
Although the EORTC QLQ-C30 is commonly used in cancer trials66 (including trials of patients with AML),67-69 to the review team’s knowledge, its measurement properties have not been evaluated and a minimally important difference (MID) has not been estimated among patients with AML (Table 8). The sponsor submitted 1 study that investigated the validity of an EORTC QLQ-C30 summary score among patients with hematological malignancies70; however, this summary score was not used in the QuANTUM-First study. The sponsor used a 10-point within-group increase or decrease to infer a clinically important improvement or detriment, respectively, as this threshold has been used in previous studies of patients with hematologic cancers, including AML.67-69 Similar (or smaller) MID estimates, within and between groups, have been reported in the literature;71,72 however, none are specific to patients with AML.
Safety End Points
Safety end points of interest to this review included AEs, SAEs, grade 3 to 5 AEs, AEs of special interest (AESIs), withdrawals from treatment due to AEs, and deaths. Patients were assessed for AEs at all study visits during induction, consolidation, and maintenance phases, and every 30 days during long-term follow-up. AEs were coded using the latest version of the Medical Dictionary for Regulatory Activities and assigned grades based on National Cancer Institute Common Terminology Criteria for Adverse Events, version 4.03. AEs occurring before the first dose of quizartinib or placebo, or those recorded more than 30 days after the last dose of quizartinib or placebo were not considered unless they were thought to be related to the drug.
AESIs were based on the known safety profile of quizartinib, products in the same class, and events relevant for AML disease and/or its management. These included QTc prolongation, torsades de pointes and other ventricular arrhythmias, and combined elevations in aminotransferases and bilirubin. The AESIs were assessed using predefined MedDRA search criteria. The development of acute or chronic GVHD among patients who underwent allogeneic HSCT was also assessed during the maintenance phase.
Table 8: Summary of the EORTC QLQ-C30 and Measurement Properties
Type | Conclusions about measurement properties | MID |
|---|---|---|
EORTC QLQ-C30 | ||
A 30-item, cancer-specific, patient-reported measure of HRQoL65 including 5 multi-item functional scales (physical, role, emotional, cognitive, social), 3 multi-item symptom scales (fatigue, pain, nausea and vomiting), a 2-item GHS/QoL scale, 5 single items assessing common cancer symptoms (dyspnea, loss of appetite, insomnia, constipation, diarrhea), and 1 item on the financial impact of the disease. Each item is evaluated using 4-point or 7-point Likert scales. Raw scores for each scale are computed as the average of the items that contribute to that scale. The raw scores are converted to standardized scores ranging from 0 to 100. Higher scores reflect better function on the function scales, greater symptoms on the symptom scales, and better HRQoL on the GHS/QoL scale. | Not identified among patients with AML. | Not identified among patients with AML. Based on a systematic review, between-group MIDs for various cancers (solid tumours) were estimated as follows.72
A more recent study of 799 patients with various cancers (only solid tumours specified, 12% unspecified cancer type)71 estimated clinically important within-group improvement and deterioration to range from 2.44 to 6.31 and −3.41 to −7.11, respectively, across functional subscales. |
AML = acute myeloid leukemia; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; GHS = global health status; HRQoL = health-related quality of life; MID = minimally important difference; QoL = quality of life.
Statistical Analysis
Sample Size and Power Calculation
For the analysis of OS, the investigators used data from the RATIFY study,17 which investigated the efficacy and safety of midostaurin versus placebo among patients with newly diagnosed AML, and simulations to determine the sample size, timing of analysis, and power. In the RATIFY study, a plateau effect was observed after 30 months of treatment in the placebo group. Landmark survival rates of approximately 42% at 30 months and 38% at 60 months in the FLT3-ITD subgroup were observed in the placebo group. This resulted in a hazard rate of 0.029 in the first 30 months and 0.003 thereafter. Using this information and assuming HRs of 0.7 and 1 before and after 30 months, respectively, the assumed survival rates in the quizartinib group were 54% at 30 months and 50% at 60 months.
Simulations indicated that approximately 84% power and 287 events would be needed to achieve a statistically significant difference (via 2-sided log-rank test at an alpha level of 0.05) in OS with approximately 536 patients when analyzed 24 months after the last patient was randomized. Analyses were therefore planned for when the target 287 OS events were observed, and a minimum of 24 months had passed since the last patient was randomized. If 287 OS events were not observed by 24 months after the last patient was randomized, then the analyses would have been performed at a maximum of 30 months after the last patient was randomized.
Statistical Testing, Data Imputation Methods, and Sensitivity Analyses
Details of statistical testing, data imputation methods, and sensitivity and supplementary analyses for relevant end points are in Table 9.
Adjustment for Multiple Testing
The investigators used a serial hierarchically ordered gatekeeping strategy to control the family-wise type I error rate for the primary and secondary efficacy end points. The primary assessment of OS was evaluated first. If the result was statistically significant at a 2-sided alpha of 0.05, then the analysis of EFS by IRC was to be conducted. After the evaluation of EFS, the remaining secondary end points were to be tested in the following order: CR rate, CR with FLT3-ITD MRD negativity rate, CRc rate, and CRc with FLT3-ITD MRD negativity rate. Testing was to stop after any test in the sequence was not statistically significant. There were no multiplicity adjustments for the exploratory end points.
Subgroup Analyses
The investigators conducted prespecified subgroup analyses for efficacy and safety end points, as follows: age (< 60 years, 60 years to < 65 years, ≥ 65 years); sex (male, female); race (white, Black or African American, Asian, Other); region (North America, Europe, Asia/other regions); WBC count at the time of diagnosis of AML (< 40 × 109/L, ≥ 40 × 109/L); choice of anthracycline (daunorubicin, idarubicin); AML cytogenetic risk score (favourable, intermediate, unfavourable, unknown)73; ECOG performance status at baseline (0, 1, 2); FLT3-ITD VAF via central testing at randomization (< 3%, 3% to 25%, > 25% to ≤ 50%, > 50%); NPM1 mutational status (yes, no); concomitant use of a strong CYP3A4 inhibitor (yes, no) (for ECG analyses only); and concomitant use of QT-prolonging medication, per the Arizona Center for Education and Research on Therapeutics classification “known risk” (yes, no) (for ECG analyses only). Subgroup results for OS were considered relevant to the current report.
The investigators reported the median OS in each subgroup, as calculated via KM analysis. The HR and corresponding 2-sided 95% CI were obtained via an unstratified Cox PH model. P values were not reported and there were no adjustments for multiple testing. When there were less than 30 patients in any subgroup category, no analysis for that category was undertaken; instead, a summary was provided (i.e., number of events and number of patients in the category). When there were less than 5 patients in any subgroup category, no summary was provided.
Table 9: Statistical Analysis of Relevant Efficacy End Points in QuANTUM-First
End point | Statistical model | Adjustment factors | Handling of missing data | Sensitivity and supplementary analyses |
|---|---|---|---|---|
OS |
| The 3 stratification factors used for randomization.a | No imputations. Patients lost to follow-up were censored at the last date when they were known to be alive. |
|
EFS | As per the analyses of OS | As per the analyses of OS. | No imputations. Patients alive without postbaseline assessments were censored at the date of randomization minus 1. |
|
CR and CRc rates (and CR and CRc with MRD negativity rates) | Summarized by treatment group with the point estimate and associated 95% CI constructed via the Clopper-Pearson method | None. | No imputations. | None |
Duration of CR and CRc | Among patients with CR or CRc during induction:
| None. | No imputations. Patients who were lost to follow-up were censored at the date of their last response assessment. | None |
RFS | As per the analysis of duration of CR or CRc | None. | As per the analysis of duration of CR or CRc. | None |
Transplant rate | Summarized by treatment group with the point estimate and associated 95% CI constructed via the Clopper-Pearson method | None. | No imputations. | None |
HRQoL |
| None. |
| MMRM including additional covariates: age, sex, race/ethnicity, and ECOG performance status |
CI = confidence interval; CR = complete remission; CRc = composite complete remission; ECOG = Eastern Cooperative Oncology Group; EFS = event-free survival; HR = hazard ratio; HRQoL = health-related quality of life; HSCT = hematopoietic stem cell transplant; ITF = induction treatment failure; KM = Kaplan-Meier; MAR = missing at random; MRD = minimal or measurable residual disease; MMRM = mixed-effects model of repeated measures; OS = overall survival; PH = proportional hazards; RFS = relapse-free survival; RMST = restricted mean survival time.
aStratification factors included region (Europe; North America; or Asia, Australia, and South America), age (< 60 years; ≥ 60 years), and white blood cell count at diagnosis (< 40 × 109/L; ≥ 40 × 109/L).
bAs measured within 56 days from the start of the last cycle of induction chemotherapy.
Sources: Clinical Study Report for QuANTUM-First,19 statistical analysis plan for the QuANTUM-First study,74 and supplemental statistical analysis plan for the QuANTUM-First study.75
Analysis Populations
The relevant analysis populations are in Table 10.
Table 10: Analysis Populations of QuANTUM-First
Population | Definition | Application |
|---|---|---|
Intent-to-treat analysis set | All patients who were randomized, analyzed according to the treatment to which they were randomized | All efficacy analyses, except those for EQ-5D-5L and EORTC QLQ-C30 |
EQ-5D-5L and EORTC QLQ-C30 analysis set | All patients in the intent-to-treat analysis set who completed the relevant EQ-5D-5L and EORTC QLQ-C30 assessments at screening, at least partially in a manner that permitted imputation of missing responses post-treatment | All EQ-5D-5L and EORTC QLQ-C30 analyses |
Safety analysis set | All patients who received at least 1 dose of quizartinib or placebo, analyzed according to the treatment received | All safety analyses |
EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30.
Sources: Sponsor’s Summary of Clinical Evidence52 and Clinical Study Report for QuANTUM-First.19
Relevant Protocol Amendments
There were 7 versions of the clinical study protocol. In Protocol Amendment 3, the duration of double-blind therapy in the maintenance phase was changed from up to 12 cycles to up to 36 cycles. According to the sponsor, most AML relapses occur within 3 years after CR and an analysis of the pivotal trial for midostaurin showed that approximately 20% of patients who completed all 12 cycles of maintenance therapy relapsed within a few months of stopping therapy.76 Patients in the QuANTUM-First study were proactively seeking off-label FLT3 suppression therapy after completing 12 cycles of maintenance treatment.
In Protocol Amendment 5, the primary end point was changed from EFS to dual primary end points of EFS and OS. According to this amendment, the study would be considered positive if either EFS or OS were statistically significant. The rationale for this amendment was to ensure that OS would be tested, regardless of whether EFS was statistically significant. In Protocol Amendment 6, based on feedback from the FDA AML guidance,24 the primary end point was changed to OS and EFS became a secondary end point.
In Protocol Amendment 7, the definition of EFS was changed to align with the AML guidance (originally published in 2020 and not available at the start of the QuANTUM-First study)24 such that refractory disease would be determined within 42 days of the start of the last cycle of induction, rather than at the end of the induction phase (day 56). Per the sponsor, the original protocol-specified definition of EFS was intended to closely align with that for the pivotal trial for midostaurin. This definition was maintained as a sensitivity analysis.
Results
Patient Disposition
Details of the patient disposition at the August 13, 2021, data cut-off are in Table 11. Of 3,468 patients screened, 539 (15.5%) were eligible for inclusion and randomized to quizartinib (n = 268) or placebo (n = 271). The most common reason for screening failure was being FLT3-ITD negative (2,556 of 2,929 [87.3%]). All but 3 (1.1%) of the randomized patients in each group were treated.
Of the randomized patients, 212 (80.0%) in the quizartinib group and 219 (81.7%) in the placebo group discontinued the study drug during any phase. The most common reason for discontinuation in the quizartinib group was AEs among 58 (21.9%) patients compared to 23 (8.6%) patients in the placebo group. Reasons that were more common in the placebo group were refractory disease (41 [15.5%] patients in the quizartinib group versus 70 [26.1%] patients in the placebo group) and relapse (44 [16.6%] patients in the quizartinib group versus 65 [24.3%] patients in the placebo group). Approximately 9% of patients in both groups discontinued the study drug due to patient decision; other reasons were less common.
At the data cut-off, 148 (55.2%) patients in the quizartinib group and 168 (62.0%) patients in the placebo group had discontinued the study. The primary reason for study discontinuation was death among 133 (49.6%) patients in the quizartinib group and 158 (58.3%) patients in the placebo group.
Further details of the patient disposition for each phase of the study are in Table 12. During the induction phase, the same proportion of patients in each group (34.7%) discontinued the study drug. Approximately 20% of patients in each group received a second cycle of induction therapy. Sixty-five percent of patients in each group entered the consolidation phase, during which numerically more patients in the placebo group (31.0%) than the quizartinib group (21.5%) discontinued the study drug. Similar proportions of patients in the quizartinib versus placebo groups received study drug plus chemotherapy (28.3% versus 32.1%), allogeneic HSCT only (2.3% versus 2.2%), and study drug plus chemotherapy followed by allogeneic HSCT (34.7% versus 31.0%) during this phase. Numerically, more patients in the quizartinib group (43.8%) than the placebo group (34.3%) entered the maintenance phase. Few patients in each group received allogeneic HSCT during this phase (1.5% in the quizartinib group and 0.7% in the placebo group); however, 70 of 98 (71.4%) patients in the quizartinib group and 49 of 89 (55.1%) patients in the placebo group who received allogeneic HSCT during the consolidation phase entered the maintenance phase (26.4% and 18.3% of patients, respectively, in the safety analysis set). A respective 12.1% and 9.7% of patients in each group were ongoing in the maintenance phase at the data cut-off.
Patient disposition was overall similar at the time of the updated safety addendum (June 16, 2023, data cut-off). Since the August 13, 2021, data cut-off, 27 patients in the quizartinib group and 9 in the placebo group completed the maintenance phase. Five patients in the quizartinib group discontinued the study drug during the maintenance phase (2 due to AML, 2 due to an AE, and 1 due to investigator decision). Seventeen patients from the placebo group discontinued the study drug during the maintenance phase, mostly (94%) due to treatment unblinding.
Approximately half of patients in the quizartinib and placebo groups had major protocol deviations (52.6% and 50.2%, respectively). Reasons for protocol deviations were reasonably balanced across treatment groups. The most common reasons for major protocol deviations included not performing visits, assessments, or procedures per protocol in 21.0% of patients; not reporting SAEs within the 24-hour timeline among 14.1% of patients; and being enrolled without meeting the eligibility criteria in 9.6% of patients.
Table 11: Summary of Patient Disposition in QuANTUM-First, August 13, 2021, Data Cut-Off (All Screened Patients)
Patient disposition | Quizartinib | Placebo |
|---|---|---|
Screened, N | 3,468 | |
Screening failures, n (%) | 2,929 (84.5) | |
Reason for screening failure, n (%) | ||
FLT3-ITD negative | 2,556 (87.3) | |
FLT3-ITD positive but did not meet other eligibility criteria | 325 (11.1) | |
Not tested for FLT3-ITD status and did not meet other eligibility criteria | 48 (1.6) | |
Randomized, N | 268 | 271 |
Randomized but not treated, n (%) | 3 (1.1) | 3 (1.1) |
Discontinued the study drug during any phase, n (%)a | 212 (80.0) | 219 (81.7) |
Reason for discontinuation of the study drug, n (%)a | ||
Refractory disease | 41 (15.5) | 70 (26.1) |
Relapse | 44 (16.6) | 65 (24.3) |
Adverse event | 58 (21.9) | 23 (8.6) |
Patient decision | 25 (9.4) | 23 (8.6) |
Other | 16 (6.0) | 11 (4.1) |
Nonprotocol-specified AML therapy | 12 (4.5) | 6 (2.2) |
Investigator decision | 10 (3.8) | 7 (2.6) |
Failure to meet continuation criteria | 5 (1.9) | 12 (4.5) |
Lost to follow-up | 1 (0.4) | 0 |
Pregnancy | 0 | 1 (0.4) |
Death | 0 | 1 (0.4) |
Study status, n (%)b | ||
Ongoing with study drug | 32 (11.9) | 26 (9.6) |
Alive, continuing in long-term follow-up | 88 (32.8) | 77 (28.4) |
Discontinued | 148 (55.2) | 168 (62.0) |
Reason for discontinuation from study, n (%)b | ||
Death | 133 (49.6) | 158 (58.3) |
Withdrawal of consent | 13 (4.9) | 9 (3.3) |
Lost to follow-up | 2 (0.7) | 1 (0.4) |
ITT analysis set, N | 268 | 271 |
EQ-5D-5L and EORTC QLQ-C30 analysis set, N | 254 | 255 |
Safety analysis set, N | 265 | 268 |
AML = acute myeloid leukemia; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; ITD = internal tandem duplication; ITT = intent to treat.
aPercentages are based on the number of patients in the safety analysis set.
bPercentages are based on the number of patients in the ITT analysis set.
Sources: Sponsor’s Summary of Clinical Evidence52 and Clinical Study Report for QuANTUM-First.19
Table 12: Details of the Patient Disposition in Each Phase of QuANTUM-First, August 13, 2021, Data Cut-Off (Safety Analysis Set)
Patient disposition | Quizartinib N = 265 | Placebo N = 268 |
|---|---|---|
Entered induction phase, n (%) | 265 (100.0) | 268 (100.0) |
Received a second cycle of induction therapy | 54 (20.4) | 56 (20.9) |
Discontinued study drug during induction phase | 92 (34.7) | 93 (34.7) |
Entered consolidation phase, n (%) | 173 (65.3) | 175 (65.3) |
Study drug plus chemotherapy | 75 (28.3) | 86 (32.1) |
HSCT only | 6 (2.3) | 6 (2.2) |
Study drug plus chemotherapy followed by HSCT | 92 (34.7) | 83 (31.0) |
Discontinued study drug during consolidation phase | 57 (21.5) | 83 (31.0) |
Entered maintenance phase, n (%) | 116 (43.8) | 92 (34.3) |
Completed maintenance phase | 21 (7.9) | 23 (8.6) |
Discontinued study drug during maintenance phase | 63 (23.8) | 43 (16.0) |
Ongoing in maintenance phase | 32 (12.1) | 26 (9.7) |
Entered long-term follow-up phase, n (%) | 225 (84.9) | 239 (89.2) |
Received protocol-specified HSCT, n (%) | 102 (38.5) | 91 (34.0) |
Received protocol-specified HSCT in consolidation phase | 98 (37.0) | 89 (33.2) |
Received protocol-specified HSCT in consolidation phase and continued to maintenance phase | 70 (26.4) | 49 (18.3) |
Received protocol-specified HSCT in maintenance phase | 4 (1.5) | 2 (0.7) |
HSCT = hematopoietic stem cell transplant.
Source: Clinical Study Report for QuANTUM-First.19
Baseline Characteristics
The baseline characteristics outlined in Table 13 are limited to those that are most relevant to this review or were felt to affect the outcomes or interpretation of the study results.
Demographic and disease characteristics were mostly balanced across groups. The median age of randomized patients was 56 years; 60% of patients were aged younger than 60 years, while the remaining 40% were older. Approximately one-quarter of patients were aged older than 65 years. Slightly more than half of patients were female (54.5%). Most patients were white (59.7%) or Asian (29.3%) and were recruited from Europe (60.5%) or Asia (and other regions aside from North America) (33.2%).
Most patients had de novo AML (92.4%) and an ECOG performance status of 0 or 1 (84.4%). Most patients had an intermediate cytogenetic risk status (72.4%); data for cytogenetic risk status were unknown or missing for 12.8% of patients. The time from diagnosis to randomization was approximately 2 weeks. Numerically, more patients in the quizartinib group than the placebo group, respectively, received daunorubicin (46% versus 35%), and fewer received idarubicin (54% versus 64%, respectively) during induction. Approximately two-thirds of patients had a FLT3-ITD VAF of more than 25%, half had a FLT3-ITD VAF more than 25% but less than 50%, and 10% had a FLT3-ITD VAF of 50% or more. Equal proportions of patients had a WBC count at diagnosis of less than 40 × 109/L and 40 × 109/L or more. The mean bone marrow blast count at baseline was 66.91 to 67.60 across groups. Mean ANCs at baseline in the quizartinib and placebo groups, respectively, were 0.60 × 109/L (SD = 1.827) and 0.44 × 109/L (SD = 1.300); mean platelets counts were 28.76 × 109/L (SD = 22.137) and 31.27 × 109/L (SD = 33.942). Approximately one-half and one-quarter of patients across groups, respectively, had NPM1 and CEBPA mutations.
Table 13: Summary of Baseline Characteristics From QuANTUM-First, August 13, 2021, Data Cut-Off (ITT Analysis Set)
Characteristic | Quizartinib N = 268 | Placebo N = 271 |
|---|---|---|
Age (years), median (range) | 56.0 (23 to 75) | 56.0 (20 to 75) |
< 60 years, n (%) | 161 (60.1) | 162 (59.8) |
≥ 60 years, n (%) | 107 (39.9) | 109 (40.2) |
≥ 65 years, n (%) | 70 (26.1) | 65 (24.0) |
Sex, n (%) | ||
Female | 144 (53.7) | 150 (55.4) |
Male | 124 (46.3) | 121 (44.6) |
Race, n (%) | ||
American Indian or Alaska Native | 0 | 1 (0.4) |
Black or African American | 2 (0.7) | 5 (1.8) |
Asian | 80 (29.9) | 78 (28.8) |
White | 159 (59.3) | 163 (60.1) |
Other | 27 (10.1) | 24 (8.9) |
Region, n (%) | ||
North America | 16 (6.0) | 18 (6.6) |
Europe | 163 (60.8) | 163 (60.1) |
Asia and other regions | 89 (33.2) | 90 (33.2) |
ECOG performance status, n (%) | ||
0 | 87 (32.5) | 98 (36.2) |
1 | 134 (50.0) | 136 (50.2) |
2 | 47 (17.5) | 36 (13.3) |
Missing | 0 | 1 (0.4) |
Choice of anthracycline, n (%) | ||
Daunorubicin | 124 (46.3) | 95 (35.1) |
Daunorubicin, idarubicina | 0 | 2 (0.7) |
Idarubicin | 144 (53.7) | 173 (63.8) |
Missing | 0 | 1 (0.4) |
Time from diagnosis to randomization (weeks), mean (SD)b | 1.98 (0.79) | 1.96 (0.93) |
AML type, n (%) | ||
De novo AML | 243 (90.7) | 255 (94.1) |
Secondary AML | 25 (9.3) | 16 (5.9) |
Risk status with specific cytogenetic patterns, n (%)c | ||
Favourable | 14 (5.2) | 19 (7.0) |
Intermediate | 197 (73.5) | 193 (71.2) |
Unfavourable | 19 (7.1) | 27 (10.0) |
Unknown | 38 (14.2) | 31 (11.4) |
Missing | 0 | 1 (0.4) |
FLT3-ITD VAF by central laboratory testing (FLT3-ITD to total FLT3), n (%)d | ||
0 to < 3% | 0 | 0 |
≥ 3 to ≤ 25% | 94 (35.1) | 98 (36.2) |
> 25% to ≤ 50% | 143 (53.4) | 138 (50.9) |
> 50% | 30 (11.2) | 35 (12.9) |
> 25% | 173 (64.6) | 173 (63.8) |
Unknown | 1 (0.4) | 0 |
WBC count at diagnosis of AML, n (%) | ||
< 40 × 109/L | 135 (50.4) | 137 (50.6) |
≥ 40 × 109/L | 133 (49.6) | 134 (49.4) |
Bone marrow blast count at baseline (count), mean (SD)e | 66.91 (23.834) | 67.60 (23.749) |
ANC at baseline (count × 109/L), mean (SD) | 0.60 (1.827) | 0.44 (1.300) |
Platelet count at baseline (count × 109/L), mean (SD) | 28.76 (22.137) | 31.27 (33.942) |
Patients with NPM1 mutations, n (%) | 142 (53.0) | 140 (51.7) |
Patients with CEBPA mutations, n (%)f | 61 (22.8) | 65 (24.0) |
AML = acute myeloid leukemia; ANC = absolute neutrophil count; ECOG = Eastern Cooperative Oncology Group; ITD = internal tandem duplication; ITT = intent to treat; SD = standard deviation; VAF = variant allele frequency; WBC = white blood cell.
aIdarubicin in cycle 1 and daunorubicin in cycle 2.
bDuration of disease is defined as (randomization date – disease diagnosis date + 1)/7.
cFavourable risk is defined as inv(16), t(16;16), t(8;21), t(15;17); intermediate risk is defined as normal, + 8, + 6, -y; unfavourable risk is defined as deI5q, −5, del7q, −7, complex.73
dFLT3-ITD VAF refers to the allelic ratio of FLT3-ITD to total FLT3.
eBone marrow blast count taken at baseline as captured in electronic data capture using aspirate, if available, otherwise, from biopsy data.
fCEBPA mutation assessment as determined by all mutations present. In a post hoc analysis, 18 (6.7%) and 20 (7.4%) patients in the quizartinib and placebo groups, respectively, had CEBPA single mutations and 9 (3.4%) and 4 (1.5%) patients, respectively, had CEBPA double mutations.
Source: Clinical Study Report for QuANTUM-First.19
Exposure to Study Treatments
Overall Exposure
At the time of the August 13, 2021, data cut-off (analysis of efficacy end points), the mean treatment duration was 40.99 weeks (SD = 52.558) in the quizartinib group and 33.95 weeks (SD = 49.135) in the placebo group. The total patient-years of exposure were 208.16 and 174.38, respectively. At the time of the June 16, 2023, data cut-off (updated safety analysis), the mean treatment duration was 45.22 weeks (SD = 59.571) in the quizartinib group and 35.53 weeks (SD = 51.985) in the placebo group. The total patient-years of exposure were 229.64 and 182.48, respectively.
At the time of the August 13, 2021, data cut-off, the adjusted treatment duration in each phase and the median number of cycles patients received were similar across treatment groups. The median adjusted treatment durations of quizartinib and placebo, respectively, were 2.0 weeks (range, 0.1 weeks to 4.0 weeks) and 2.0 weeks (range, 0.3 weeks to 4.0 weeks) in induction, 4.0 weeks (range, 0.3 weeks to 8.0 weeks) and 4.0 weeks (range, 1.7 weeks to 8.0 weeks) in consolidation, and 67.4 weeks (range, 0.4 weeks, 164.1 weeks) and 67.7 weeks (range, 0.3 weeks to 150.4 weeks) in maintenance, respectively. For patients treated with quizartinib versus placebo, the median adjusted treatment durations during maintenance were 79.7 weeks (range, 0.4 weeks to 166.9 weeks) and 86.7 weeks (range, 0.3 weeks to 167.4 weeks), respectively, among those who underwent protocol-specified HSCT and 56.9 weeks (range, 1.6 weeks to 167.0 weeks) and 48.0 weeks (range, 2.1 weeks to 156.3 weeks), respectively, among those who did not undergo protocol-specified HSCT.33
In both treatment groups, the median numbers of cycles of treatment were 1 cycle (range, 1 cycle to 2 cycles) in induction and 2 cycles (range, 1 cycle to 4 cycles) in consolidation. During induction, mean relative dose intensities of the various chemotherapy options were 99% or more in both groups. During induction cycle 2, similar proportions of patients in the quizartinib versus placebo groups received the 7 + 3 chemotherapy regimen (7 days of cytarabine + 3 days of anthracycline) (16.6% versus 17.9%) and 5 + 2 chemotherapy regimen (5 days of continuous IV infusion of standard dose cytarabine and 2 days of the same anthracycline used during the first induction cycle) (3.8% versus 2.6%, respectively). During the consolidation phase, similar proportions of patients in the quizartinib versus placebo groups received 1 (95.4% versus 94.3%), 2 (60.7% versus 57.1%), 3 (31.2% versus 33.7%), and 4 (13.3% versus 12.0%) cycles of chemotherapy. The mean relative dose intensity was more than 98% in both groups. In maintenance, patients were treated for a median of 16.0 cycles (range, 1 cycle to 36 cycles) in the quizartinib group and 17.0 cycles (range, 1 cycle to 36 cycles) in the placebo group.
By the time of the June 16, 2023, data cut-off, the median treatment durations of quizartinib and placebo during the maintenance phase were 67.9 weeks (range, 0.4 weeks to 175.1 weeks) and 73.6 weeks (range, 0.3 weeks to 167.4 weeks), respectively. The mean number of cycles in the quizartinib and placebo groups was 19.9 (SD = 14.0) and 19.0 (SD = 13.3), respectively.
Treatment Modifications
Details of dose interruptions and dose reductions are in Table 14. At the time of the August 13, 2021, data cut-off, 49.4% of patients in the quizartinib group and 30.2% of patients in the placebo group experienced at least 1 dose interruption. Most dose interruptions were for AEs or “other” reasons. Numerically, more patients in the quizartinib group compared to the placebo group experienced at least 1 dose reduction (28.3% versus 13.8%, respectively). Most dose reductions were due to AEs and concomitant use of strong CYP3A4 inhibitors.
Table 14: Dose Interruptions and Dose Reductions in QuANTUM-First, August 13, 2021, Data Cut-Off (Safety Analysis Set)
Category | Quizartinib N = 265 | Placebo N = 268 |
|---|---|---|
Patients with at least 1 dose interruption, n (%) | 131 (49.4) | 81 (30.2) |
Reasons for dose interruption, n (%) | ||
Concomitant strong CYP3A4 inhibitor | 2 (0.8) | 0 |
QTcF prolongation | 8 (3.0) | 2 (0.7) |
AE | 106 (40.0) | 62 (23.1) |
Other | 47 (17.7) | 27 (10.1) |
Patients with at least 1 dose reduction, n (%) | 75 (28.3) | 37 (13.8) |
Reasons for dose reduction, n (%) | ||
Concomitant strong CYP3A4 inhibitor | 18 (6.8) | 22 (8.2) |
QTcF prolongation | 11 (4.2) | 3 (1.1) |
AE | 55 (20.8) | 15 (5.6) |
AE = adverse event; CYP = cytochrome P450; QTcF = QT interval corrected using the Fridericia formula.
Source: Clinical Study Report for QuANTUM-First.19
Concomitant Medications
At the time of the August 13, 2021, data cut-off, all patients in both treatment groups had used concomitant medications. Overall, the use of various concomitant medications was comparable across treatment groups. The most common (≥ 80% of patients) classes of concomitant medications included antibacterials for systemic use (99.8%), antimycotics for systemic use (96.1%), drugs for acid-related disorders (89.9%), analgesics (85.9%), antiemetics and antinauseants (85.7%), and blood substitutes and perfusion solutions (81.2%). Overall, the most common medications (≥ 50% of patients) included paracetamol (73.0%), furosemide (64.2%), piperacillin sodium/tazobactam sodium (59.1%), acyclovir (53.8%), and allopurinol (52.5%).
Similar proportions of patients in the quizartinib versus placebo groups, respectively, used any concomitant strong CYP3A4 inhibitor (62.6% versus 60.4%), the most common being posaconazole (40.4% versus 41.8%) and voriconazole (28.7% versus 22.8%). Few patients in either group used a concomitant strong or moderate CYP3A4 inducer (1.5% in both groups).
All patients in both treatment groups used concomitant QT-prolonging medications. The use of specific medications was comparable across treatment groups. The most common QT-prolonging medications with known risks, conditional risks, and possible risks were fluconazole (42.8%), furosemide (64.2%), and granisetron (21.2%), respectively.
More than 99% of patients in both groups received blood product transfusions during the study. Platelets (98.5% in the quizartinib group and 98.1% in the placebo group) and packed red blood cells (98.1% in the quizartinib group and 97.0% the placebo group) were the most common blood transfusion products received.
Subsequent Treatments
Among treated patients, at the time of the August 13, 2021, data cut-off, 42 of 265 (15.8%) patients in the quizartinib group and 87 of 268 (32.5%) patients in the placebo group went on to use subsequent nonprotocol-specified AML therapies, most of which were drug therapies. The most common nonprotocol-specified AML therapy was cytarabine (10.9% in the quizartinib group versus 21.3% in the placebo group). Across groups, 20 patients received FLT3 inhibitors. In the quizartinib versus placebo groups, 3 (1.1%) versus 6 (2.2%) patients received sorafenib, 2 (0.8%) versus 3 (1.1%) received gilteritinib, and 1 (0.4%) versus 5 (1.9%) received midostaurin.
Efficacy
As of the August 13, 2021, data cut-off, the median follow-up time was 39.2 months (95% CI, 37.2 months to 41.5 months) in the quizartinib group and 39.2 months (95% CI, 36.6 months to 41.2 months) in the placebo group.
Overall Survival
Results for the primary analysis of OS are in Table 15. At the time of the data cut-off, 133 of 268 (49.6%) patients in the quizartinib group and 158 of 271 (58.3%) patients in the placebo group had died. The median OS was 31.9 months (95% CI, 21.0 months to NE) in the quizartinib group and 15.1 months (95% CI, 13.2 months to 26.2 months) in the placebo group. The HR was 0.776 (95% CI, 0.615 to 0.979), in favour of quizartinib (P = 0.0324). The KM-estimated probability of OS at 12 months was 67.4% (95% CI, 61.3% to 72.7%) in the quizartinib group and 57.7% (95% CI, 51.6% to 63.4%) in the placebo group (difference = 9.6%; 95% CI, 1.4% to 17.8%). The KM-estimated probability of OS at 48 months was 48.4% (95% CI, 41.9% to 54.5%) in the quizartinib group and 37.0% (95% CI, 29.8% to 44.2%) in the placebo group (difference = 11.4%; 95% CI, 1.8% to 21.0%).
The KM plot for the primary analysis of OS is in Figure 2. There was an apparent early OS detriment with quizartinib relative to placebo. During the first 30 days and 60 days of treatment 15 (5.7%) and 20 (7.5%) patients in the quizartinib group died compared with 9 (3.4%) and 13 (4.9%) in the placebo group, respectively. Early deaths in the quizartinib versus placebo groups were attributed to AEs (6.4% versus 4.1%), AML disease progression (0.8% versus 0.7%), and other causes (0.4% versus 0%). Between approximately 3 months and 6 months, the KM curves crossed and there was a sustained separation thereafter.
A prespecified sensitivity analysis of OS that censored patients who received allogeneic HSCT at any time and an unstratified supplementary analysis were both consistent with the primary analysis (HR = 0.752; 95% CI, 0.562 to 1.008 and HR = 0.774; 95% CI, 0.614 to 0.975, respectively). An additional sensitivity analysis was undertaken using the RMST to account for a possible plateau effect. The difference in RMST at a cut-off time of 55.8 months for quizartinib versus placebo was 4.53 months (95% CI, 0.55 months to 8.51 months), favouring quizartinib.
Results for OS among most prespecified subgroups were aligned with the primary analysis; however, among patients aged 60 years to younger than 65 years, patients from North America, patients with a WBC count less than 40 × 109/L at diagnosis, and patients without NPM1 mutational status, the point estimate for the HR of quizartinib versus placebo was near the null (i.e., no statistical difference). Among patients with a favourable AML cytogenetic risk score, the point estimate for the HR of quizartinib versus placebo favoured placebo. Across categories within each subgroup, the 95% CIs for the effect estimates were overlapping. Detailed subgroup data are in Appendix 1, Figure 7.
Among patients who entered the consolidation (65% of patients in each group) and maintenance (43.3% in the quizartinib group and 33.9% in the placebo group) phases of treatment, the results were consistent with the main analysis. Among patients who entered the consolidation phase, the median OS was NE (95% CI, 48.6 months to NE) in the quizartinib group and 42.5 months (95% CI, 21.9 months to NE) in the placebo group. The HR was 0.703 (95% CI, 0.509 to 0.971). The KM-estimated probability of OS at 48 months was 60.2% (95% CI, 52.0% to 67.5%) in the quizartinib group and 46.5% (95% CI, 36.5% to 56.0%) in the placebo group. Among patients who entered the maintenance phase, the median OS was NE in both groups. The HR was 0.683 (95% CI, 0.395 to 1.183). The KM-estimated probability of OS at 48 months was 76.3% (95% CI, 66.2% to 83.7%) in the quizartinib group and 67.9% (95% CI, 55.3% to 77.6%) in the placebo group.
In a post hoc analysis among patients who received allogeneic HSCT and continued to the maintenance phase, the median OS was not reached in either group. The HR for OS in this subpopulation was 1.622 (95% CI, 0.623 to 4.220).23
Event-Free Survival
Results for the primary analysis of EFS by IRC assessment are in Table 15. At the time of the data cut-off, 198 of 268 (73.9%) patients in the quizartinib group and 213 of 271 (78.6%) patients in the placebo group had an EFS event. The median EFS was 0.03 months (95% CI, 0.03 months to 0.95 months) in the quizartinib group and 0.71 months (95% CI, 0.03 months to 3.42 months) in the placebo group. The HR was 0.916 (95% CI, 0.754 to 1.114; P = 0.2371). The KM-estimated probability of EFS at 12 months was 34.2% (95% CI, 28.5% to 40.0%) in the quizartinib group and 25.0% (95% CI, 19.9% to 30.4%) in the placebo group (difference = 9.3%; 95% CI, 1.5% to 17.1%). The KM-estimated probability of EFS at 36 months was 24.1% (95% CI, 18.8% to 29.7%) in the quizartinib group and 19.2% (95% CI, 14.5% to 24.3%) in the placebo group (difference = 4.9%; 95% CI, −2.5% to 12.2%). Because no statistically significant difference between treatment groups was observed for EFS, subsequent secondary end points in the statistical hierarchy were not tested statistically.
The KM plot for the primary analysis of EFS is in Figure 3. There was an early EFS detriment with quizartinib versus placebo before the KM curves crossed between 3 months and 6 months, remaining separated thereafter. Due to the stringent definition of ITF (42-day window), a large (50.7% and 48.3% of patients in the quizartinib and placebo groups, respectively) proportion of patients in each group were classified as having refractory disease (i.e., EFS events on day 1). Results for sensitivity analyses where ITF was defined as not achieving CR or CRc by the end of induction (i.e., day 56, per the original protocol-specified definition of EFS) favoured quizartinib (HR = 0.818; 95% CI, 0.669 to 0.999 and HR = 0.729; 95% CI, 0.592 to 0.897, respectively).
In sensitivity analyses where patients were censored at the start date of the conditioning regimen for allogeneic HSCT, the HR for quizartinib versus placebo was 0.830 (95% CI, 0.669 to 1.030) when ITF was defined as not achieving CR and 0.703 (95% CI, 0.557 to 0.887) when ITF was defined as not achieving CRc. Results for EFS per investigator assessment favoured quizartinib (HR = 0.780; 95% CI, 0.635 to 0.959).
Table 15: Summary of Results for OS and EFS by IRC Assessment From QuANTUM-First, August 13, 2021, Data Cut-Off (ITT Analysis Set)
Variable | Quizartinib N = 268 | Placebo N = 271 |
|---|---|---|
OSa | ||
Events, n (%) | 133 (49.6) | 158 (58.3) |
Censored, n (%) | 135 (50.4) | 113 (41.7) |
Alive at data cut-off date | 120 (44.8) | 103 (38.0) |
Withdrawal of consent | 13 (4.9) | 9 (3.3) |
Lost to follow-up | 2 (0.7) | 1 (0.4) |
Median OS (months), 95% CIb | 31.9 (21.0 to NE) | 15.1 (13.2 to 26.2) |
HR (95% CI)c | 0.776 (0.615 to 0.979) | Reference |
P valued | 0.0324 | Reference |
OS rate (%) (95% CI)e | ||
6 months | 82.3 (77.1 to 86.4) | 79.1 (73.7 to 83.5) |
12 months | 67.4 (61.3 to 72.7) | 57.7 (51.6 to 63.4) |
24 months | 54.7 (48.4 to 60.5) | 44.7 (38.7 to 50.6) |
36 months | 49.9 (43.7 to 55.9) | 41.1 (35.0 to 47.0) |
48 months | 48.4 (41.9 to 54.5) | 37.0 (29.8 to 44.2) |
EFSf | ||
Events, n (%) | 198 (73.9) | 213 (78.6) |
Refractory disease | 136 (50.7) | 131 (48.3) |
Relapse | 30 (11.2) | 53 (19.6) |
Death | 32 (11.9) | 29 (10.7) |
Censored, n (%) | ||
No postbaseline response assessment, no death date | 1 (0.4) | 1 (0.4) |
Had CR, no relapse, no death | 69 (25.7) | 57 (21.0) |
Median EFS (months), 95% CIb | 0.03 (0.03 to 0.95) | 0.71 (0.03 to 3.42) |
HR (95% CI)c | 0.916 (0.754 to 1.114) | Reference |
P valued | 0.2371 | Reference |
EFS rate (%) (95% CI)e | ||
2 months | 43.1 (37.1 to 48.9) | 48.5 (42.4 to 54.3) |
6 months | 40.0 (34.1 to 45.8) | 35.5 (29.7 to 41.2) |
12 months | 34.2 (28.5 to 40.0) | 25.0 (19.9 to 30.4) |
18 months | 30.5 (24.9 to 36.1) | 22.9 (17.9 to 28.2) |
24 months | 26.9 (21.6 to 32.5) | 20.7 (15.9 to 25.9) |
30 months | 25.4 (20.2 to 31.0) | 20.2 (15.5 to 25.4) |
36 months | 24.1 (18.8 to 29.7) | 19.2 (14.5 to 24.3) |
AML = acute myeloid leukemia; CI = confidence interval; CR = complete remission; EFS = event-free survival; HR = hazard ratio; IRC = independent review committee; ITT = intention to treat; NE = not estimable; OS = overall survival.
aDefined as the time from randomization to the date of death from any cause.
bPer Kaplan-Meier analysis. CI for the median is computed using the Brookmeyer-Crowley method.
cCox regression analysis stratified by region (Europe; North America; or Asia, Australia, and South America), age (< 60 years; ≥ 60 years), and white blood cell count at diagnosis (< 40 × 109/L; ≥ 40 × 109/L).
dTwo-sided log-rank test stratified by region (Europe; North America; or Asia, Australia, and South America), age (< 60 years; ≥ 60 years), and white blood cell count at diagnosis (< 40 × 109/L; ≥ 40 × 109/L). Statistical testing was adjusted for multiple testing via a serial hierarchically ordered gatekeeping strategy.
eEstimated using the Kaplan-Meier method.
fDefined as the time from randomization to the date of refractory disease, relapse, or death from any cause, whichever occurred first. The primary analysis for EFS was based on the response assessment by IRC with response of CR only, using a 42-day window from the start of the last cycle in induction for CR evaluation as defined in the AML guidance.24
Source: Clinical Study Report for QuANTUM-First.19
CR and CRc Rates, With or Without MRD Negativity
Results for the secondary remission end points by IRC assessment are in Table 16. In the quizartinib and placebo groups, 18 of 268 (6.7%) and 8 of 271 (3.0%) patients could not be assessed for CR or MRD negativity, respectively, as they had insufficient bone marrow for biopsy or aspiration to conduct an assessment. An additional 5 patients in each group (1.9% versus 1.8%, respectively) were not evaluated for CR or MRD negativity. These patients had sufficient bone marrow and it was biopsied or aspirated, but they were not evaluated for other reasons.77
At the end of the induction phase, 54.9% (95% CI, 48.7% to 60.9%) of patients in the quizartinib group and 55.4% (95% CI, 49.2% to 61.4%) of patients in the placebo group had CR (difference = −0.5%; 95% CI, −8.9% to 7.9%). Further, 71.6% (95% CI, 65.8% to 77.0%) and 64.9% (95% CI, 58.9% to 70.6%) of patients in the quizartinib and placebo groups, respectively, had CRc at the end of induction (difference = 6.7%; 95% CI, −1.1% to 14.5%).
Figure 2: Kaplan-Meier Plot of OS, August 13, 2021, Data Cut-Off (ITT Analysis Set)
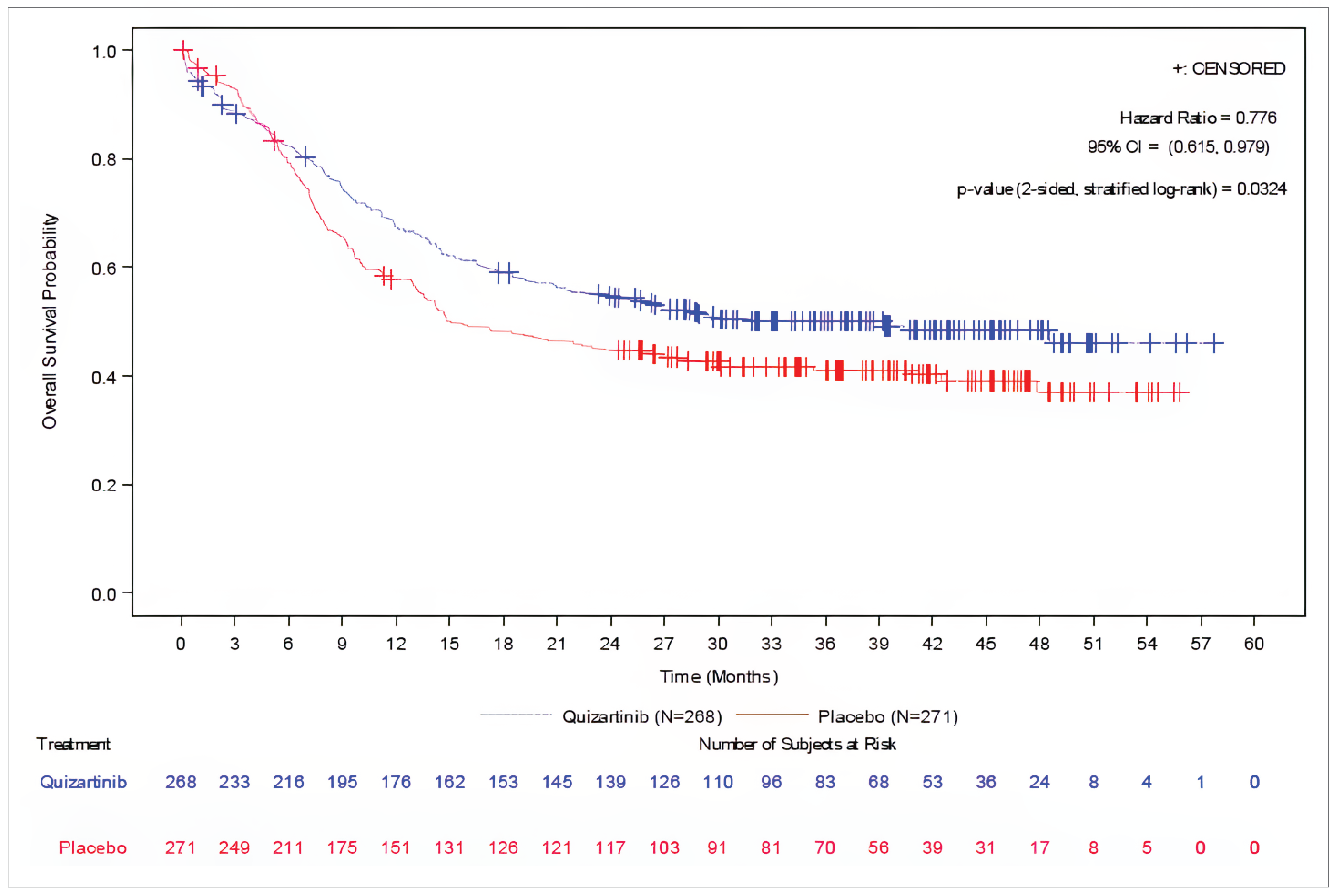
CI = confidence interval; HR = hazard ratio; ITT = intent to treat; OS = overall survival.
Note: A stratified Cox proportional hazard model and stratified log-rank test were used to calculate the HR and P value, respectively. Stratification factors included region (Europe; North America; or Asia, Australia, and South America), age (< 60 years; ≥ 60 years), and white blood cell count at diagnosis (< 40 × 109/L; ≥ 40 × 109/L).
Source: Clinical Study Report for QuANTUM-First.19
Among patients in the quizartinib group versus placebo group, 20.1% (95% CI, 15.5% to 25.5%) and 18.8% (95% CI, 14.3% to 24.0%), respectively, had CR with FLT3-ITD MRD negativity at the end of induction. Further, 24.6% (95% CI, 19.6% to 30.2%) and 21.4% (95% CI, 16.7% to 26.8%), respectively, had CRc with FLT3-ITD MRD negativity at the end of induction.
Because the primary analysis of EFS per IRC was not statistically significant, secondary remission end points (with or without MRD negativity) were not tested statistically.
Figure 3: Kaplan-Meier Plot of EFS (42-Day Window) by IRC Assessment, August 13, 2021, Data Cut-Off (ITT Analysis Set)
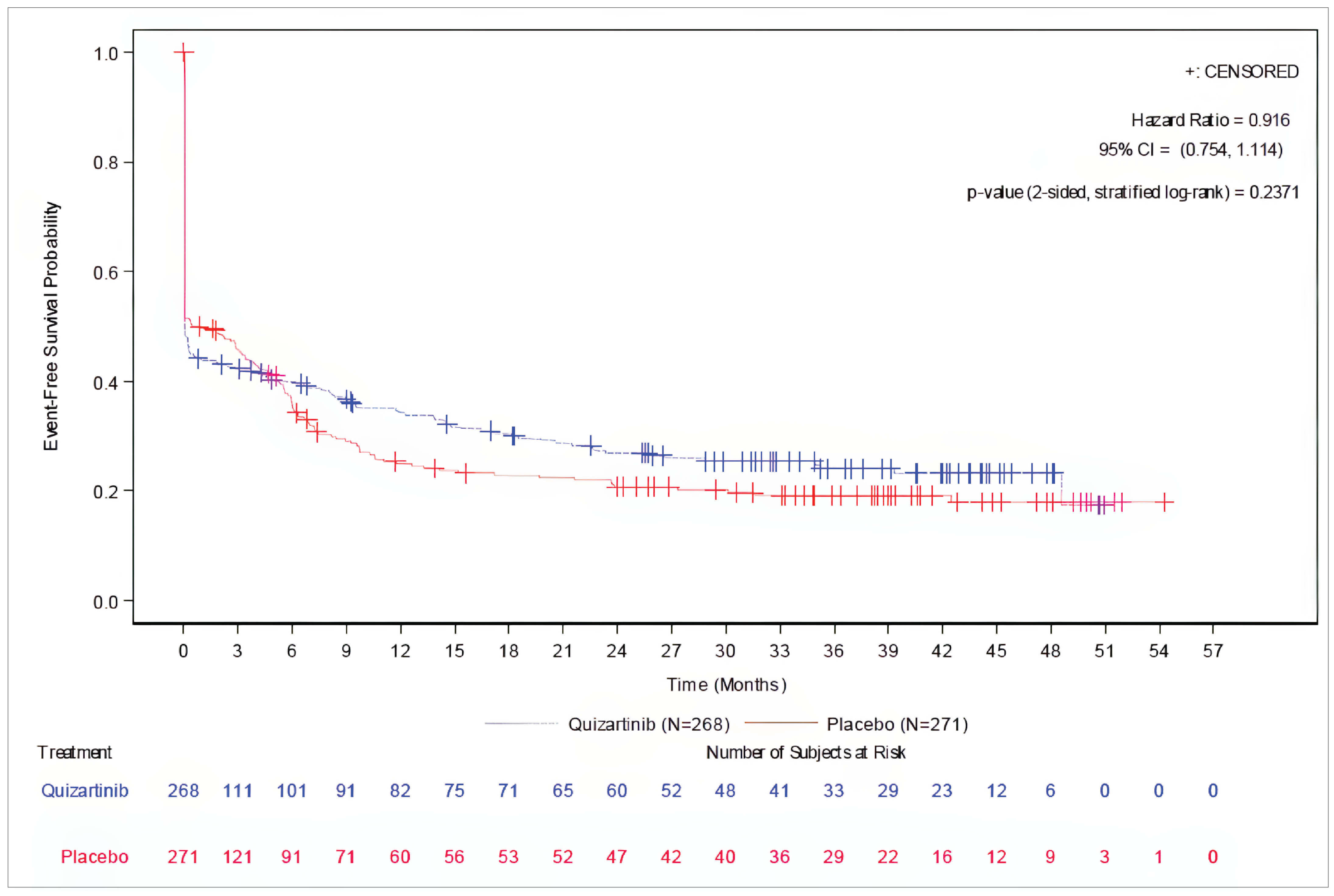
CI = confidence interval; EFS = event-free survival; HR = hazard ratio; IRC = independent review committee; ITT = intent to treat.
Notes: A stratified Cox proportional hazard model and stratified log-rank test were used to calculate the HR and P value, respectively. Stratification factors included region (Europe; North America; or Asia, Australia, and South America), age (< 60 years; ≥ 60 years), and white blood cell count at diagnosis (< 40 × 109/L; ≥ 40 × 109/L).
Source: Clinical Study Report for QuANTUM-First.19
Duration of CR and CRc
For patients with CR by IRC assessment during induction, the median duration of CR was 38.6 months (95% CI, 21.9 months to NE) in the quizartinib group and 12.4 months (95% CI, 8.8 months to 22.7 months) in the placebo group (HR = 0.621; 95% CI, 0.451 to 0.857). For patients with CRc by IRC assessment during induction, the median duration of CRc was 27.2 months (95% CI, 17.7 months to NE) in the quizartinib group and 12.4 months (95% CI, 8.7 months to 22.7 months) in the placebo group (HR = 0.742; 95% CI, 0.561 to 0.982).
Table 16: Summary of Results for Secondary Remission End Points by IRC Assessment From QuANTUM-First, August 13, 2021, Data Cut-Off (ITT Analysis Set)
Variable | Quizartinib N = 268 | Placebo N = 271 |
|---|---|---|
CR | ||
Patients with CR, n | 147 | 150 |
Patients with CR (%) (95% CI)a | 54.9 (48.7 to 60.9) | 55.4 (49.2 to 61.4) |
Difference (%) (95% CI) | −0.5 (−8.9 to 7.9) | Reference |
CR with FLT3-ITD MRD negativity | ||
Patients with CR with FLT3-ITD MRD negativity, n | 54 | 51 |
Patients with CR with FLT3-ITD MRD negativity (%) (95% CI)a | 20.1 (15.5 to 25.5) | 18.8 (14.3 to 24.0) |
Difference (%) (95% CI) | NR | Reference |
CRc (CR + CRi) | ||
Patients with CRc, n | 192 | 176 |
Patients with CRc (%) (95% CI)a | 71.6 (65.8 to 77.0) | 64.9 (58.9 to 70.6) |
Difference (%) (95% CI) | 6.7 (−1.1 to 14.5) | Reference |
CRc with FLT3-ITD MRD negativity | ||
Patients with CRc with FLT3-ITD MRD negativity, n | 66 | 58 |
Patients with CRc with FLT3-ITD MRD negativity (%) (95% CI)a | 24.6 (19.6 to 30.2) | 21.4 (16.7 to 26.8) |
Difference (%) (95% CI) | NR | Reference |
CI = confidence interval; CR = complete remission; CRc = composite complete remission; CRi = complete remission with incomplete hematologic recovery; IRC = independent review committee; ITD = internal tandem duplication; ITT = intent to treat; MRD = minimal or measurable residual disease; NR = not reported.
Notes: Based on assessments by the end of induction. Denominator for percentages is the number of subjects in the ITT analysis set.
aBased on the Clopper-Pearson method.
Sources: Clinical Study Report for QuANTUM-First19 and sponsor-submitted additional trial data.33
Relapse-Free Survival
Results for the analysis of RFS by IRC assessment among patients with CR or CRc during induction are in Table 17. At the time of the data cut-off, among patients with CR during induction (147 of 268 [54.9%] in the quizartinib group and 150 of 271 [55.4%] in the placebo group), 44.2% in the quizartinib group and 58.7% in the placebo group had an RFS event. The median RFS was 39.3 months (95% CI, 22.6 months to NE) in the quizartinib group and 13.6 months (95% CI, 9.7 months to 23.7 months) in the placebo group. The HR was 0.613 (95% CI, 0.444 to 0.845) in favour of quizartinib, although this end point was not tested statistically. The KM-estimated probability of RFS at 6 months was 88.1% (95% CI, 81.6% to 92.5%) in the quizartinib group and 71.8% (95% CI, 63.8% to 78.4%) in the placebo group (difference = 16.3%; 95% CI, 7.3% to 25.3%). The KM-estimated probability of RFS at 36 months was 51.7% (95% CI, 42.5% to 60.1%) in the quizartinib group and 38.2% (95% CI, 30.0% to 46.4%) in the placebo group (difference = 13.5%; 95% CI, 1.4% to 25.6%). The KM plot for the RFS among patients who had CR during induction is in Figure 4.
Among patients with CRc during induction (192 of 268 [71.6%] in the quizartinib group and 176 of 271 [64.9%] in the placebo group), 49.5% in the quizartinib group and 58.0% in the placebo group had an RFS event. The median RFS was 28.5 months (95% CI, 18.5 months to NE) in the quizartinib group and 12.6 months (95% CI, 9.7 months to 23.7 months) in the placebo group. The HR was 0.733 (95% CI, 0.554 to 0.969) in favour of quizartinib, although this end point was not tested statistically. The KM-estimated probability of RFS at 6 months was 83.5% (95% CI, 77.4% to 88.1%) in the quizartinib group and 71.4% (95% CI, 64.0% to 77.6%) in the placebo group (difference = 12.1%; 95% CI, 3.5% to 20.7%). The KM-estimated RFS rate at 36 months was 46.4% (95% CI, 38.6% to 53.9%) in the quizartinib group and 39.1% (95% CI, 31.5% to 46.7%) in the placebo group (difference = 7.3%; 95% CI, −1.3% to 18.1%). The KM plot for the RFS among patients with CRc during induction is in Figure 5.
Table 17: Summary of Results for RFS by IRC Assessment From QuANTUM-First Among Patients With CR or CRc During Induction, August 13, 2021, Data Cut-Off (ITT Analysis Set)
Variable | Quizartinib N = 268 | Placebo N = 271 |
|---|---|---|
RFS among patients with CR during inductiona | ||
Patients with CR, nb | 147 | 150 |
Patients with events, n (%) | 65 (44.2) | 88 (58.7) |
Relapse | 44 (29.9) | 63 (42.0) |
Death | 21 (14.3) | 25 (16.7) |
Censored, n (%) | 82 (55.8) | 62 (41.3) |
Still on study drug | 27 (10.1) | 19 (7.0) |
Continuing in follow-up | 46 (17.1) | 38 (14.0) |
Lost to follow-up | 1 (0.4) | 1 (0.4) |
Withdrawal by patient | 8 (3.0) | 4 (1.5) |
Median RFS (months) (95% CIc) | 39.3 (22.6 to NE) | 13.6 (9.7 to 23.7) |
HR (95% CI)d | 0.613 (0.444 to 0.845) | Reference |
RFS rate (%) (95% CI)e | ||
6 months | 88.1 (81.6 to 92.5) | 71.8 (63.8 to 78.4) |
12 months | 73.4 (65.2 to 80.0) | 52.4 (43.9 to 60.2) |
18 months | 65.0 (56.4 to 72.4) | 46.4 (37.9 to 54.4) |
24 months | 57.8 (48.9 to 65.7) | 40.9 (32.7 to 49.0) |
30 months | 54.3 (45.3 to 62.4) | 40.1 (31.8 to 48.2) |
36 months | 51.7 (42.5 to 60.1) | 38.2 (30.0 to 46.4) |
RFS among patients with CRc during inductionb | ||
Patients with CRc, nb | 192 | 176 |
Patients with events, n (%) | 95 (49.5) | 102 (58.0) |
Relapse | 61 (31.8) | 75 (42.6) |
Death | 34 (17.7) | 27 (15.3) |
Censored, n (%) | 97 (50.5) | 74 (42.0) |
Still on study drug | 31 (11.6) | 25 (9.2) |
Continuing in follow-up | 56 (20.9) | 44 (16.2) |
Lost to follow-up | 1 (0.4) | 1 (0.4) |
Withdrawal by patient | 9 (3.4) | 4 (1.5) |
Median RFS (months), 95% CIc | 28.5 (18.5 to NE) | 12.6 (9.7 to 23.7) |
HR (95% CI)d | 0.733 (0.554 to 0.969) | Reference |
RFS rate (%) (95% CI)e | ||
6 months | 83.5 (77.4 to 88.1) | 71.4 (64.0 to 77.6) |
12 months | 68.0 (60.7 to 74.2) | 51.8 (44.0 to 59.1) |
18 months | 58.7 (51.1 to 65.5) | 46.1 (38.3 to 53.5) |
24 months | 51.9 (44.3 to 59.0) | 41.5 (33.9 to 48.9) |
30 months | 48.4 (40.8 to 55.7) | 40.8 (33.1 to 48.2) |
36 months | 46.4 (38.6 to 53.9) | 39.1 (31.5 to 46.7) |
CI = confidence interval; CR = complete remission; CRc = composite complete remission; HR = hazard ratio; IRC = independent review committee; ITT = intent to treat; NE = not estimable; RFS = relapse-free survival.
aRFS is the time from randomization, for patients who had CR or CRc during induction, until the date of documented relapse or death from any cause, whichever comes first.
bUsed as denominator for percentage calculation. Patients without a documented CR or CRc during induction are excluded from the analysis.
cMedian RFS is from Kaplan-Meier analysis. The CI for the median is computed using the Brookmeyer-Crowley method.
dUnstratified Cox regression analysis.
eEstimated using the Kaplan-Meier method.
Sources: Clinical Study Report for QuANTUM-First19 and sponsor-submitted additional trial data.77
Transplant Rate
At the time of the data cut-off, 102 of 268 (38.1%; 95% CI, 32.3% to 44.2%) patients in the quizartinib group and 91 of 271 (33.6%; 95% CI, 28.0% to 39.5%) patients in the placebo group underwent protocol-specified allogeneic HSCT (difference = 4.5%; 95% CI, −3.6% to 12.6%). Among patients in the quizartinib and placebo groups who did not undergo allogeneic HSCT, 0.7% and 0.4% were lost to follow-up and 3.7% and 2.6% withdrew from the study, respectively. The timing of these losses to follow-up and withdrawals was not reported.
Figure 4: Kaplan-Meier Plot of RFS by IRC Assessment Among Patients With CR During Induction, August 13, 2021, Data Cut-Off (ITT Analysis Set)
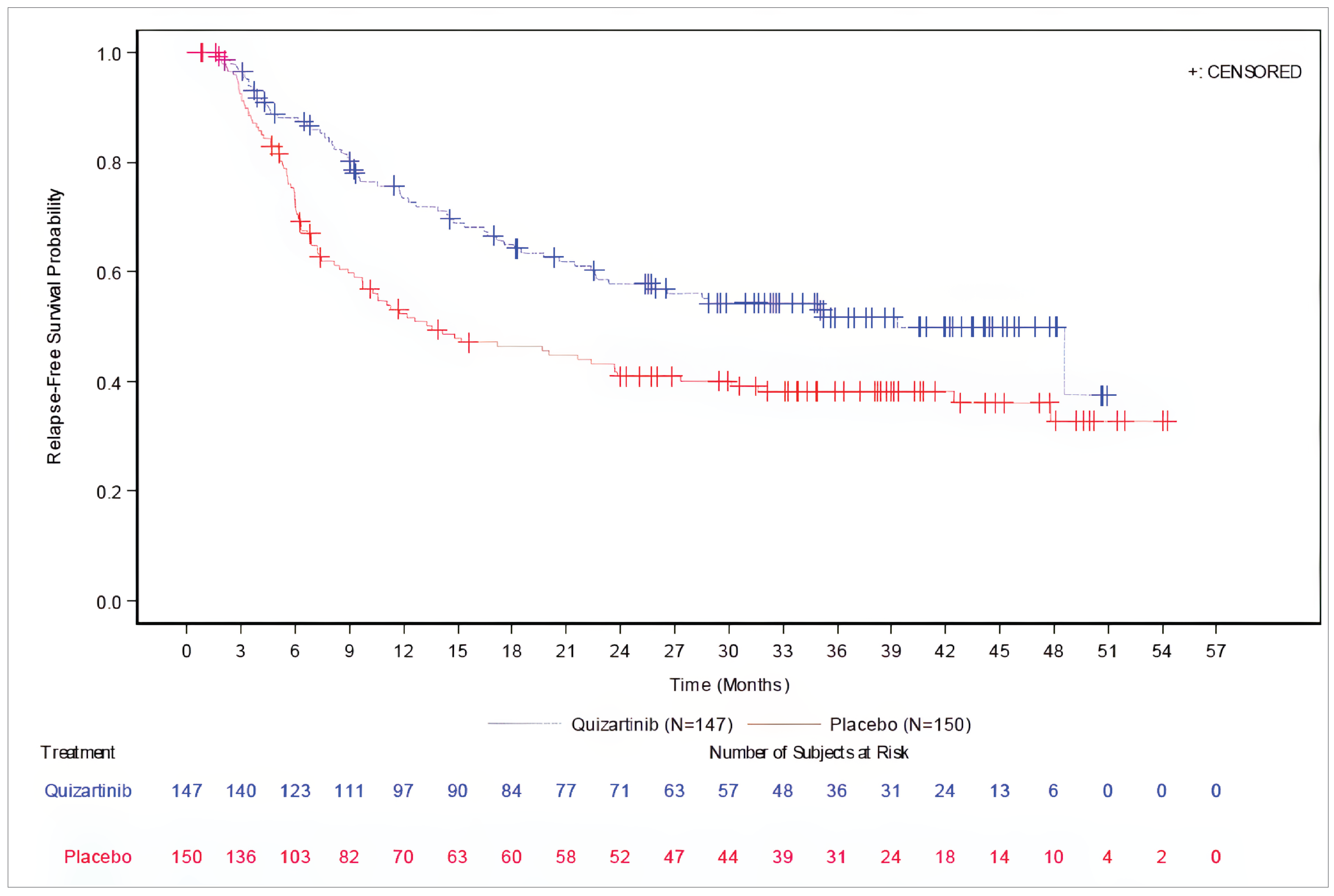
CR = complete remission; IRC = independent review committee; ITT = intent to treat; RFS = relapse-free survival.
Note: Patients without a documented response of CR are excluded from the analysis. RFS is the time from randomization, for patients with CR during induction, until the date of documented relapse or death from any cause, whichever comes first.
Source: Clinical Study Report for QuANTUM-First.19
Health-Related Quality of Life
A total 252 of 268 (94.0%) patients in the quizartinib group and 253 of 271 (93.4%) patients in the placebo group were included in the analysis of the GHS/QoL scale of the EORTC QLQ-C30. Among these patients, all had results available at baseline. The proportion of patients available for assessment declined in both groups over time thereafter. In the quizartinib and placebo groups, 79.0% and 77.9% had assessments at day 28 of the first induction cycle; 40.9% and 42.3% had assessments at day 28 of the first consolidation cycle; 7.9% and 7.1% had assessments at day 28 of the fourth consolidation cycle; 39.7% and 33.2% had assessments at day 1 of the first maintenance cycle; and 7.5% and 5.5% had assessments at day 1 of the 34th maintenance cycle, respectively.
Figure 5: Kaplan-Meier Plot of RFS by IRC Assessment Among Patients With CRc During Induction, August 13, 2021, Data Cut-Off (ITT Analysis Set)
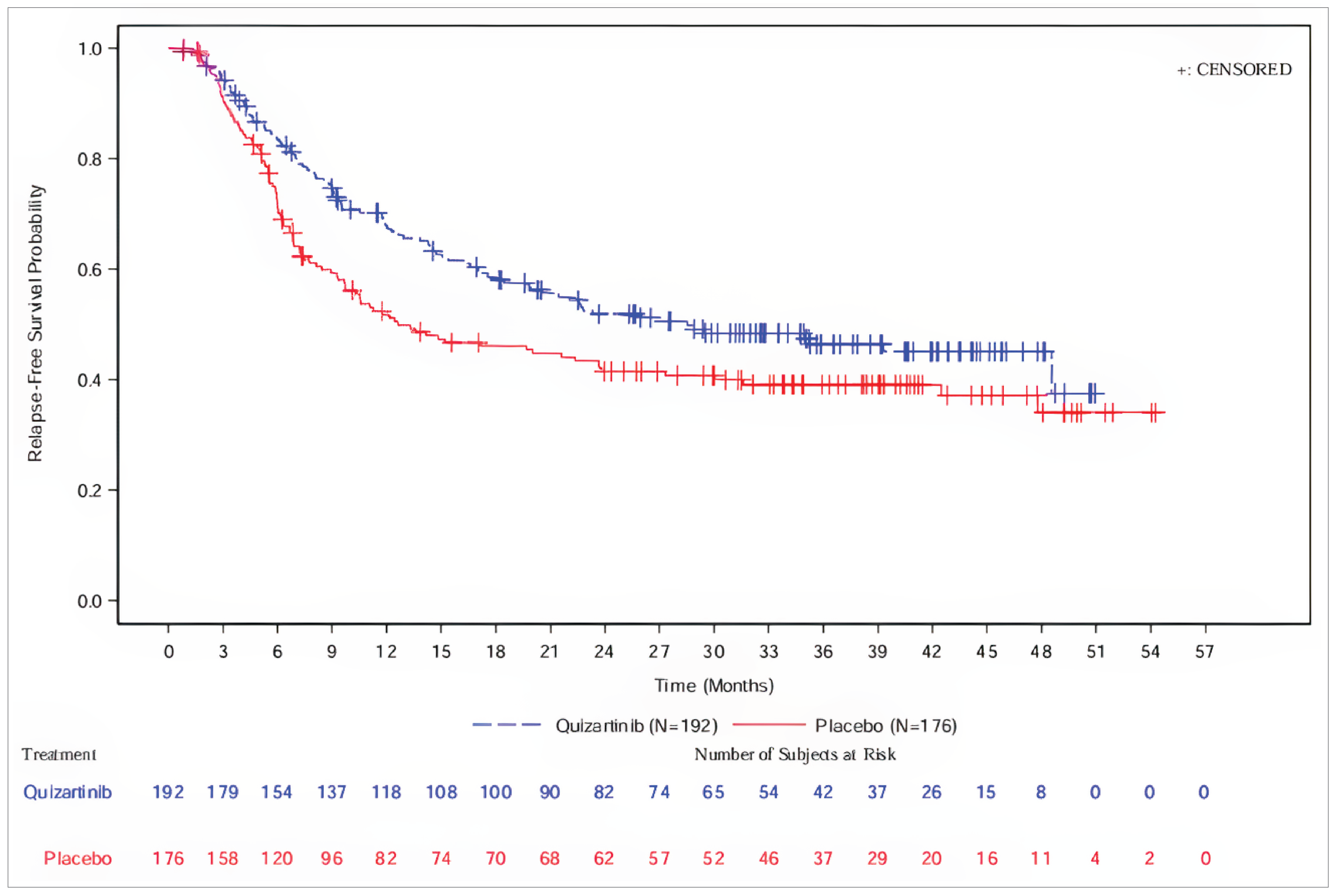
CRc = composite complete remission; IRC = independent review committee; ITT = intent to treat; RFS = relapse-free survival.
Notes: Patients without a documented response of CRc are excluded from the analysis. RFS is the time from randomization, for patients with CRc during induction, until the date of documented relapse or death from any cause, whichever comes first.
Source: Clinical Study Report for QuANTUM-First.19
At baseline, the mean GHS/QoL scale score was similar across groups (45.9 [SD = 24.4]) in the quizartinib group and 48.1 [SD = 24.9] in the placebo group). Among evaluable patients in the quizartinib and placebo groups, 91 of 199 (45.7%) versus 93 of 197 (47.2%) at the end of the first induction cycle, 58 of 103 (56.3%) versus 57 of 107 (53.3%) at the end of the first consolidation cycle, 12 of 20 (60.0%) versus 7 of 18 (38.9%) at the end of the fourth consolidation cycle, 72 of 100 (72.0%) versus 65 of 84 (77.4%) at the beginning of the first maintenance cycle, and 16 of 19 (84.2%) versus 12 of 14 (85.7%) at the beginning of the 34th maintenance cycle, respectively, had improved GHS/QoL scores based on the 10-point threshold adopted by the sponsor.
In the longitudinal (mixed-effects model of repeated measures) analysis summarizing the effect of quizartinib versus placebo over all time points, an improvement in GHS/QoL score was observed over time in both groups, with a between-group difference in the least squares mean change from baseline of −2.0 points (95% CI, −4.8 points to 0.7 points). Results of a sensitivity analysis adjusting on additional covariates were aligned with the main analysis. The overall trajectory of this end point across treatment phases is in Figure 6.
Figure 6: EORTC QLQ-C30 GHS/QoL Change From Baseline Score Across Treatment Phases in QuANTUM-First, MMRM Analysis, August 13, 2021, Data Cut-Off (EQ-5D-5L and EORTC QLQ-C30 Analysis Set)
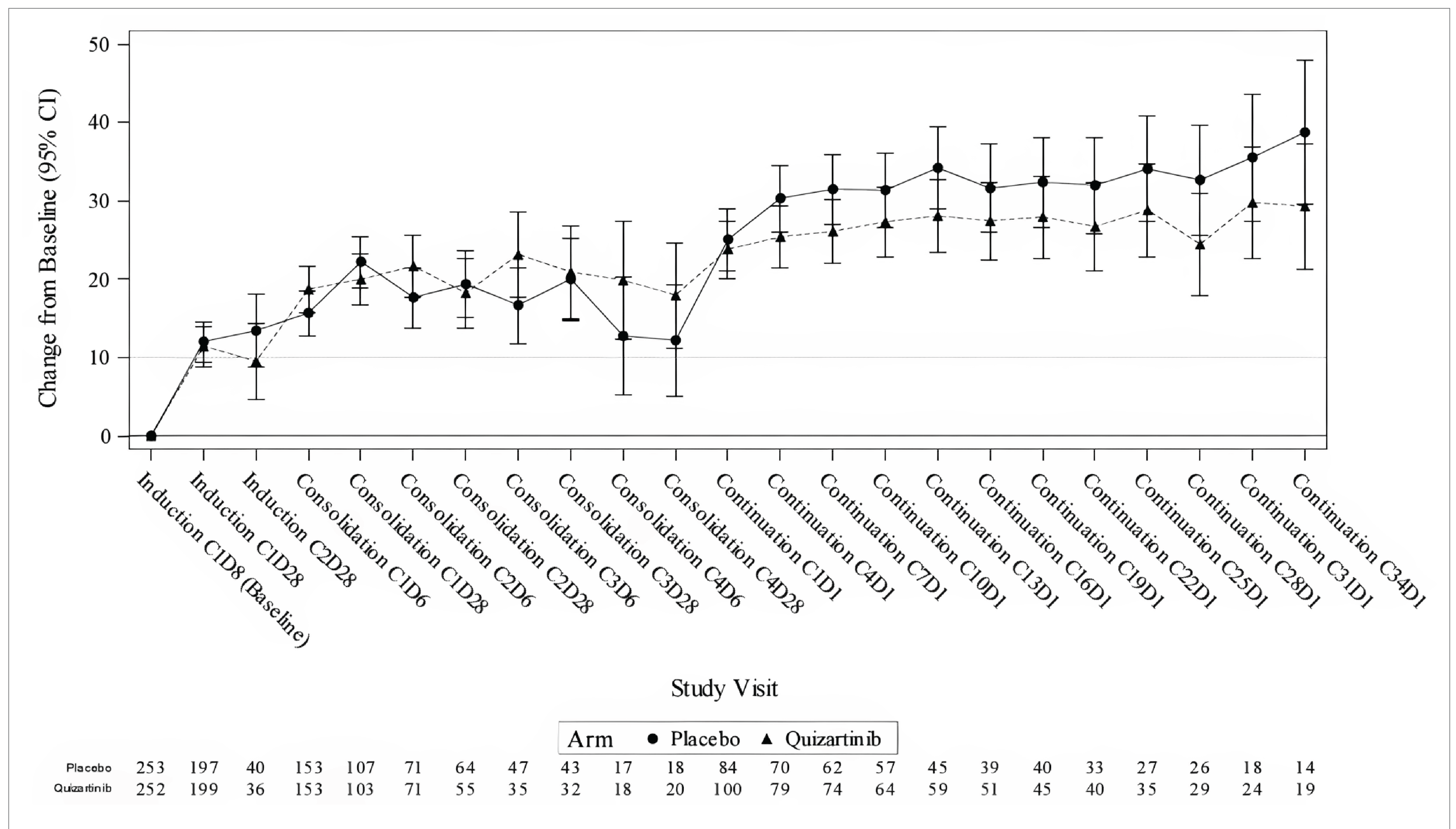
C = cycle; CI = confidence interval; D = day; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; GHS = global health status; MMRM = mixed-effects model of repeated measures; QoL = quality of life.
Note: MMRM includes variables for baseline score, treatment, time, and treatment by time interaction.
Source: Clinical Study Report for QuANTUM-First, Quality of Life Analysis.78
Harms
Detailed safety data are in Table 18. Unless otherwise specified, all safety data are from the August 13, 2021, data cut-off. These are supplemented with results from the June 16, 2023, safety addendum as available.
Adverse Events
AEs occurred among nearly all patients in the quizartinib and placebo groups (264 of 265 [99.6%] and 265 of 268 [98.9%], respectively). The most common AEs occurring among patients in the quizartinib versus placebo groups included febrile neutropenia (44.2% versus 42.2%), pyrexia (42.3% versus 40.7%), diarrhea (37.0% versus 35.1%), and hypokalemia (35.1% versus 35.8%). At the time of the June 16, 2023, data cut-off, there were 24 (9.1%) patients in the quizartinib group and 4 (1.5%) patients in the placebo group with new AEs. According to the investigators, no new safety signals were detected.
Grade 3 to 4 AEs
Grade 3 to 4 AEs occurred among 80.8% of patients in the quizartinib group and 79.9% of patients in the placebo group. The most common grade 3 to 4 AEs in the quizartinib versus placebo groups included febrile neutropenia (43.4% versus 41.0%), hypokalemia (18.9% versus 16.4%), neutropenia (18.1% versus 8.6%), and pneumonia (11.3% versus 11.2%). Grade 3 to 5 AEs occurred among 92.1% of patients in the quizartinib group and 89.6% of patients in the placebo group (refer Deaths Due to Adverse Events in the following).
Serious Adverse Events
Numerically, a larger proportion of patients in the quizartinib group (54.0%) than the placebo group (45.9%) experienced 1 or more SAE. The most common SAEs occurring in the quizartinib versus placebo groups included febrile neutropenia (10.9% versus 8.2%), pneumonia (6.4% versus 5.6%), septic shock (4.2% versus 3.0%), and sepsis (3.8% versus 5.2%). At the time of the June 16, 2023, data cut-off, there were 3 new SAEs in the quizartinib group and 1 in the placebo group.
Withdrawals Due to AEs
Numerically, a larger proportion of patients in the quizartinib group (20.4%) than the placebo group (8.6%) stopped treatment due to AEs. There was no single AE that led to treatment discontinuation among more than 4% of patients across groups. The most common AEs resulting in treatment discontinuation in the quizartinib versus placebo groups included septic shock (3.4% versus 0.4%), thrombocytopenia (1.1% versus 0%), and pneumonia (0.8% versus 1.1%). At the time of the June 16, 2023, data cut-off, there were 2 additional patients who discontinued quizartinib due to AEs, both due to neutropenia.
Deaths Due to AEs
AEs leading to death occurred among 11.3% of patients in the quizartinib group and 9.7% of patients in the placebo group. There was no single AE that led to death among more than 3% of patients across groups. The most common AEs leading to death in the quizartinib versus placebo groups included septic shock (3.0% versus 1.1%), sepsis (1.1% versus 0.7%), and general physical health deterioration (0% versus 1.5%). Of note, 1 patient in the quizartinib group died of cardiac arrest and another died of ventricular dysfunction during the induction phase. At the time of the June 16, 2023, data cut-off, there were no additional deaths with AE as the primary cause.
There was an apparent early OS detriment with quizartinib compared to placebo. Numerically, a larger proportion of patients in the quizartinib group than the placebo group died within 30 days (5.7% versus 3.4%) and 60 days (7.5% versus 4.9%) of study drug initiation. Within 30 days of study drug administration, 5.3% of patients in the quizartinib group and 3.0% of patients in the placebo group had an AE that resulted in death. During the first 60 days of study drug administration, 6.4% of patients in the quizartinib group and 4.1% of patients in the placebo group had an AE that resulted in death. Causes of early deaths in the quizartinib group were sepsis (n = 3), klebsiella sepsis (n = 3), septic shock (n = 2), pulmonary edema (n = 1), cerebral hematoma (n = 1), febrile neutropenia (n = 1), pneumonia (n = 1), cerebral infarction (n = 1), acute respiratory distress syndrome (n = 1), mucormycosis (n = 1), brain edema (n = 1), and unknown (n = 1). Causes of early deaths in the placebo group were sepsis, pneumonia, respiratory failure, pulmonary hemorrhage, encephalitis, disease progression, intracranial hemorrhage, candida sepsis, and cerebrovascular accident, all occurring in 1 patient each.
Notable Harms
Numerically, more patients in the quizartinib group versus the placebo group had a QTcF increase of more than 30 ms from baseline (55.1% versus 32.5%) and/or a prolonged QT interval (13.6% versus 4.1%). Among patients in the quizartinib versus placebo groups cardiac arrest with ventricular fibrillation (0.8% versus 0%) and ventricular tachycardia (0.4% versus 0.4%) were infrequent. Combined elevations of aspartate aminotransferase or alanine aminotransferase and total bilirubin occurred among 2.3% of patients in the quizartinib group and 3.4% of patients in the placebo group.
Among patients who underwent protocol-specified allogeneic HSCT, 57 of 102 (55.9%) in the quizartinib group and 43 of 91 (47.3%) in the placebo group had GVHD. In the quizartinib versus placebo groups, 45.1% versus 38.5% had acute GVHD and 29.4% versus 19.8% had chronic GVHD. Numerically, a larger proportion of patients in the quizartinib group (n = 17; 16.7%) than the placebo group (n = 6; 6.6%) had grade 3 to 4 GVHD.
Table 18: Summary of Harms Results From QuANTUM-First, August 13, 2021, Data Cut-Off (Safety Analysis Set)
Adverse events | Quizartinib N = 265 | Placebo N = 268 |
|---|---|---|
Adverse events, n (%) | ||
≥ 1 adverse event | 264 (99.6) | 265 (98.9) |
Most common adverse events (≥ 15%) | ||
Febrile neutropenia | 117 (44.2) | 113 (42.2) |
Pyrexia | 112 (42.3) | 109 (40.7) |
Diarrhea | 98 (37.0) | 94 (35.1) |
Hypokalemia | 93 (35.1) | 96 (35.8) |
Nausea | 90 (34.0) | 84 (31.3) |
Headache | 73 (27.5) | 53 (19.8) |
Rash | 69 (26.0) | 66 (24.6) |
Vomiting | 65 (24.5) | 53 (19.8) |
Stomatitis | 57 (21.5) | 56 (20.9) |
Constipation | 56 (21.1) | 69 (25.7) |
Neutropenia | 54 (20.4) | 27 (10.1) |
Cough | 50 (18.9) | 44 (16.4) |
Abdominal pain | 46 (17.4) | 38 (14.2) |
Decreased appetite | 46 (17.4) | 36 (13.4) |
Alanine aminotransferase increased | 42 (15.8) | 27 (10.1) |
Epistaxis | 40 (15.1) | 29 (10.8) |
Pneumonia | 39 (14.7) | 41 (15.3) |
Grade 3 to 4 adverse events, n (%) | ||
Patients with ≥ 1 grade 3 to 4 adverse event | 214 (80.8) | 214 (79.9) |
Most common grade 3 to 4 adverse events (≥ 10%) | ||
Febrile neutropenia | 115 (43.4) | 110 (41.0) |
Hypokalemia | 50 (18.9) | 44 (16.4) |
Neutropenia | 48 (18.1) | 23 (8.6) |
Pneumonia | 30 (11.3) | 30 (11.2) |
Serious adverse events, n (%) | ||
Patients with ≥ 1 serious adverse event | 143 (54.0) | 123 (45.9) |
Most common serious adverse events (≥ 2%) | ||
Febrile neutropenia | 29 (10.9) | 22 (8.2) |
Pneumonia | 17 (6.4) | 15 (5.6) |
Septic shock | 11 (4.2) | 8 (3.0) |
Sepsis | 10 (3.8) | 14 (5.2) |
Pyrexia | 8 (3.0) | 5 (1.9) |
Klebsiella sepsis | 7 (2.6) | 1 (0.4) |
Thrombocytopenia | 2 (0.8) | 8 (3.0) |
Patients who stopped treatment due to adverse events, n (%) | ||
Patients who stopped | 54 (20.4) | 23 (8.6) |
Most common adverse events leading to stopping (≥ 1%) | ||
Septic shock | 9 (3.4) | 1 (0.4) |
Thrombocytopenia | 3 (1.1) | 0 |
Pneumonia | 2 (0.8) | 3 (1.1) |
Patients who died due to adverse events, n (%) | ||
Patients who died | 30 (11.3) | 26 (9.7) |
Most common adverse events leading to death (≥ 1%) | ||
Septic shock | 8 (3.0) | 3 (1.1) |
Sepsis | 4 (1.5) | 2 (0.7) |
General physical health deterioration | 0 | 4 (1.5) |
Patients with early deaths, n (%) | ||
Patients who died within 30 days of study drug initiation | 15 (5.7) | 9 (3.4) |
Adverse event | 14 (5.3) | 8 (3.0) |
Other | 1 (0.4) | 0 |
AML disease progression | 0 | 1 (0.4) |
Patients who died within 60 days of study drug initiation | 20 (7.5) | 13 (4.9) |
Adverse event | 17 (6.4) | 11 (4.1) |
AML disease progression | 2 (0.8) | 2 (0.7) |
Other | 1 (0.4) | 0 |
Notable harms, n (%) | ||
QTcF | ||
New > 450 and ≤ 480 ms | 73 (27.5) | 43 (16.0) |
New > 480 and ≤ 500 ms | 15 (5.7) | 4 (1.5) |
New > 500 ms | 6 (2.3) | 2 (0.7) |
Increase from baseline > 30 ms | 146 (55.1) | 87 (32.5) |
Increase from baseline > 60 ms | 27 (10.2) | 13 (4.9) |
ECG QT prolonged | 36 (13.6) | 11 (4.1) |
Cardiac arrest with ventricular fibrillation | 2 (0.8) | 0 |
Ventricular tachycardia | 1 (0.4) | 1 (0.4) |
Combined elevations of AST or ALT and total bilirubin | 6 (2.3) | 9 (3.4) |
ALT = alanine aminotransferase; AML = acute myeloid leukemia; AST = aspartate aminotransferase; ECG = electrocardiogram; QTcF = QT interval corrected using the Fridericia formula.
Source: Clinical Study Report for QuANTUM-First.19
Critical Appraisal
Internal Validity
The QuANTUM-First study was overall well-conducted, but not without limitations that could introduce bias and/or uncertainty. For all end points, there is low risk of bias arising from the randomization process. Patients were randomized via interactive web and voice response system using a stratified permuted block procedure, which is adequate for concealing allocation until the time of randomization. Patient characteristics were generally well balanced across treatment groups, except for a slight imbalance by ECOG performance status. This imbalance was judged by the review team to be likely attributable to chance and therefore unlikely to introduce bias.79 There was also an imbalance in the choice of anthracycline during induction (daunorubicin or idarubicin). The clinical experts consulted for this review advised that this imbalance was unlikely to introduce bias as the 2 treatments are used interchangeably and have comparable efficacy.
The study included 4 consecutive phases; however, the effects of the induction, consolidation, and maintenance phases were tested together, without re-randomization before the maintenance phase. In this design, the contribution of effects in each of the induction and consolidation phases, and the maintenance phase to the overall efficacy of quizartinib cannot be isolated.24 The QuANTUM-First study was considered positive on the primary end point of OS, but it should be noted that the primary end point changed twice during the trial (from EFS, to co-primary EFS and OS, and finally to OS). The rationale for the protocol amendments that resulted in changes to the primary end point were considered reasonable to the clinical review team. Results for the primary analysis of EFS were not statistically significant.
The QuANTUM-First study was double blind and there is a low risk of bias in the measurement of objective outcomes, such as OS and transplant rate. There is some risk that patients could have become aware of the treatment group to which they were assigned due to differences in treatment-related AEs. If such were to have occurred, there would be some concerns for risk of bias in subjective outcomes, such as HRQoL. Risk of bias in the measurement of CR, CRc, EFS, and RFS is low because these end points were assessed by an IRC. Although there were many major protocol violations, risk of bias due to deviations from the intended interventions is likely low, as these deviations were balanced across groups and unlikely to have a serious impact on the efficacy results. Dose interruptions and reductions, although numerically more frequent in the quizartinib group, were considered as expected in clinical practice per the clinical experts consulted, and therefore not considered a source of bias.
Per the sample size calculation, the QuANTUM-First study was powered to detect a statistically significant OS benefit. Analyses of efficacy end points were based on the intention-to-treat principle, which is appropriate for measuring the effect of assignment to the intervention. The family-wise type I error rate for the primary and secondary end points was controlled via serial, hierarchically ordered gatekeeping strategies. The result for EFS, which was tested second in the hierarchy (after OS), was not statistically significant. As such, the remaining secondary end points (i.e., remission end points) were not tested statistically. These and the exploratory end points (RFS, transplant rate, and HRQoL) are considered as supportive evidence. The results for RFS, where the 95% CI for the between-group difference excluded the null, are at increased risk of type I error.
For the analysis of OS, there was a violation of the PH assumption as evidenced by an early survival detriment with quizartinib relative to placebo. As such, the ratio of the hazard functions is not constant over time and reliance on the HR alone to inform the OS benefit may be misleading. As is common in trials for AML treatments that aim to be curative,24 the KM plot for OS showed an initial drop followed by a plateau in the curves just above and below the median. As such, comparisons of median survival across the groups may overestimate the OS benefit of quizartinib. Between-group differences in KM-estimated probabilities of OS at clinically relevant follow-up times, which were used herein to judge the certainty of evidence for this end point, are not affected by these limitations. A sensitivity analysis at a survival cut-off time of 55.8 months showed an increase in RMST with quizartinib compared with placebo, supporting a beneficial effect of quizartinib on OS. As is common in oncology trials,80 the results for OS are reflective of the effects of quizartinib versus placebo, and any subsequent nonprotocol-specified antileukemic treatments received in each group (rather than each treatment in isolation). Although the effects of quizartinib versus placebo are confounded by subsequent treatments (used more frequently in the placebo group), the comparison is of direct relevance as, per the clinical experts consulted, these treatments are reflective of those used in practice. Further, the clinical experts noted that up-front therapy provides the best chance for a cure.
The subgroup analyses of OS were preplanned. Although the estimated effects in most groups appeared aligned with the primary analysis, there were some exceptions. Among patients aged 60 years or older and younger than 65 years, patients from North America, patients with a WBC count less than 40 × 109/L at diagnosis, and patients without NPM1 mutational status, the point estimate for the HR of quizartinib versus placebo was near the null (i.e., no statistical difference). Among patients with a favourable AML cytogenetic risk score, the point estimate for the HR of quizartinib versus placebo favoured placebo. As the QuANTUM-First study was not designed or powered to detect subgroup differences, the 95% CIs were wide and overlapping across categories within each subgroup. Further, there were no statistical tests for treatment by subgroup interactions and no adjustments for multiple testing, limiting credible conclusions about effect modification.25,26 Additional analyses of OS among patients who entered the consolidation and maintenance phases of treatment are at risk of bias as it is unlikely that prognostic balance was maintained across treatment groups among these subpopulations. The post hoc analysis of OS among patients who received allogeneic HSCT and continued to the maintenance phase was subject to the same limitation. Further, a small number of patients (n = 119) contributed to the analysis, the median was not reached in either group, and the effect estimate for the HR was affected by imprecision (the 95% CI included the potential that either group could be favoured), rendering the analysis inconclusive. The QuANTUM-First study was not designed to inform the effect of quizartinib compared with placebo among patients who received allogeneic HSCT and maintenance treatment.
The definition of EFS was aligned with FDA guidance for trials of drugs for AML,24 whereby day 1 of treatment was assigned as the event date for patients with ITF (i.e., no CR or CRc within 42 days). The lack of statistical significance for this end point may be attributed, in part, to the stringent definition of ITF. Per this definition, approximately half (50.7% and 48.3% of patients in the quizartinib and placebo groups, respectively) of patients in each group were assigned an EFS date of baseline. Results of sensitivity analyses defining ITF as not achieving CR or CRc by the end of induction (i.e., day 56, per the original protocol definition of EFS) favoured quizartinib, but these analyses were not adjusted for multiple testing so there is an increased risk of type I errors. As per the analyses of OS, there was a violation of the PH assumption as evidenced by an early EFS detriment with quizartinib compared with placebo. As such, the ratio of the hazard functions is not constant over time and reliance on the HR alone to inform the effect of quizartinib relative to placebo on EFS may be misleading. This limitation does not apply to the interpretation of the KM-estimated probabilities of EFS at clinically relevant follow-up times, which were used to judge the certainty of evidence for this end point.
As of the time of writing, EFS and RFS are accepted by the FDA as end points that represent clinical benefit for traditional approval for treatments for AML with curative intent.24 However, evidence submitted by the sponsor and identified by the review team suggests that the validity of EFS and RFS as surrogates for OS among patients with newly diagnosed FLT3-ITD–positive AML who are treated with kinase inhibitors as an add-on to standard chemotherapy remains uncertain. Analyses of trial-based data have suggested modest correlations between EFS and OS for patients with AML.27-29 However, none of these analyses were specific to the patient population or treatment type under review, and the strength of correlation was affected by the definition of EFS used across trials. Other studies have suggested that EFS is not a reliable surrogate for OS in trials of drugs for AML.30,31 Indeed, in the QuANTUM-First study, a clinically relevant and statistically significant OS benefit with quizartinib relative to placebo was observed, in the absence of clinically relevant or statistically significant differences in EFS. As RFS was evaluated only among patients with CR or CRc during induction, the results are at risk of bias as it is uncertain whether prognostic balance across treatment groups was maintained in this subpopulation of patients. The same limitation applies to the analyses of duration of CR and CRc.
Few patients were lost to follow-up and for the time-to-event end points (OS, EFS, and RFS), there were no indications of informative censoring. Data were mostly complete for the remission end points and transplant rate, so there is low risk of bias due to missing outcome data. For HRQoL, there is a high risk of bias due to missing outcome data for all time points assessed. Although most patients had baseline assessments, the proportion of evaluable patients who provided assessments decreased substantially thereafter. Missing data were not imputed in the bivariate comparison of the proportion of patients with clinically important improvements in HRQoL. This complete case analysis assumes that the data are missing completely at random, which is unrealistic.32 In the longitudinal analysis (mixed-effects model of repeated measures), missing data were handled under a missing at random assumption. This assumption implies that the recorded characteristics can account for differences in the distribution of missing data for observed and missing cases, which is unlikely to be reasonable.32 Sensitivity analyses testing different assumptions about the missing data were not undertaken.
The certainty of evidence for the between-group effect estimates for OS, EFS, and transplant rate were affected by imprecision. Although the point estimates for the between-group differences in KM-estimated probabilities of OS at 12 months and 48 months of follow-up suggested clinically important benefit with quizartinib, the 95% CIs included small differences that may not be considered clinically important. For EFS, although the point estimates for between-group differences in KM-estimated probabilities at 12 months and 36 months of follow-up suggested little to no clinically important difference, the 95% CIs included the potential for clinically important benefit with quizartinib. Finally, although the point estimate for the between-group difference in transplant rate suggested little to no clinically important difference between quizartinib and placebo, the 95% CI included the potential for a clinically important increase.
To the knowledge of the review team, the measurement properties of the EORTC QLQ-C30 instrument have not been studied among patients with AML; however, it is commonly used to measure patient-reported HRQoL in cancer trials66 (including trials of patients with AML).67-69 A literature-based MID estimate was not identified for patients with AML. A SR by Musoro and colleagues72 reported MID estimates for between-group differences across 21 clinical trials involving 9 cancer types. Clinically important improvement and deterioration in the GHS/QoL scale varied by cancer type, ranging from 3 points to 11 points and −4 points to −13 points for clinically important improvement and deterioration, respectively. A more recent study71 of 799 patients with various cancers estimated values for clinically important within-group improvement and deterioration ranging from 2.44 to 6.31 and −3.41 to −7.11, respectively, across scales. As all (or most) patients analyzed in these studies had solid tumours, it is uncertain whether these estimates can be generalized to patients with AML. There is also uncertainty in the 10-point threshold used by the sponsor, which was not substantiated in the literature but selected based on a value used in previous trials of hematologic cancers, including AML.67-69 It is possible that within and between-group differences smaller than 10 points may have been clinically important; however, in the absence of evidence for an estimated MID among patients with AML it is challenging to identify these differences.
External Validity
According to the clinical experts consulted, the characteristics of the patients enrolled in the QuANTUM-First study were mostly reflective of those in clinical practice who would be eligible for treatment with quizartinib, with a few exceptions. Notably, few patients from North America were enrolled and nearly all were white or Asian. As such, the patients enrolled are unlikely to be completely representative of the racial or ethnic diversity of patients seen in clinical practice in Canada. Although patients aged older than 75 years, with ECOG performance status greater than 2, with AML secondary to prior chemotherapy or radiotherapy for other neoplasms, and/or with a history of known CNS leukemia (including cerebrospinal fluid positive for AML blasts) were excluded, per the clinical experts consulted, these patients could be treated with quizartinib in clinical practice. Per the clinical experts, decisions to administer intensive chemotherapy should be based not only on patients’ performance status at the time of diagnosis of AML, but on their baseline performance status before diagnosis. The clinical experts specifically noted that patients aged older than 75 years would still be eligible for induction therapy in clinical practice.
According to the clinical experts consulted, the background chemotherapy regimens provided during the induction and consolidation phases were reflective of those used in practice for newly diagnosed patients who are eligible for intensive chemotherapy. The comparison group in the QuANTUM-First study, however, was not directly relevant to clinical practice. For newly diagnosed patients who are FLT3-ITD positive and eligible for intensive chemotherapy, midostaurin is currently funded by all public drug programs in Canada and has been the standard of care since being approved by Health Canada in 2017.60 According to the clinical experts consulted, up to 10% of patients with FLT3-ITD–mutated AML and concomitant favourable-risk core binding factor or adverse-risk karyotype may receive intensive chemotherapy with gemtuzumab ozogamicin or an alternative regimen, like FLAG-IDA, rather than midostaurin. Of the remaining patients eligible for intensive chemotherapy with midostaurin, less than 5% would not receive midostaurin, namely due to intolerance or gastrointestinal mucositis. Midostaurin was not yet approved at the start of the QuANTUM-First study in 2016. The data monitoring committee reviewed data from the pivotal trial for midostaurin17 and recommended that the QuANTUM-First study be continued as originally planned.22 As such, there is no direct evidence from RCTs to inform on the comparative efficacy and harms of quizartinib and midostaurin. Although midostaurin is not approved for maintenance therapy in Canada, per the clinical experts, in clinical practice some patients who are ineligible for allogeneic HSCT may receive oral azacitidine, which was also not an option in the QuANTUM-First study.
The end points assessed in the QuANTUM-First study were aligned with those advised by the FDA for confirmatory trials of treatments for AML.24 Further, the selected end points were considered relevant to interest holders, including patients and clinicians, who underscored the need for treatments that improve remission rates, prolong the duration of remission, reduce the risk of relapse, extend OS, and maintain HRQoL while limiting toxicity. While MRD negativity is emerging as a potentially important biomarker to inform prognosis and guide clinical decision-making,81 per the clinical experts, testing for FLT3-ITD MRD is being developed and validated in some Canadian centres, but is neither funded nor currently used in clinical practice. Although maintaining HRQoL is important for patients, the results from the QuANTUM-First study do not allow for the review team to confidently conclude on the effect of quizartinib versus placebo on this end point due to risk of bias due to attrition.
GRADE Summary of Findings and Certainty of the Evidence
Methods for Assessing the Certainty of the Evidence
For the pivotal study (QuANTUM-First) identified in the sponsor’s SR, GRADE was used to assess the certainty of the evidence for outcomes considered most relevant to inform expert committee deliberations, and a final certainty rating was determined as outlined by the GRADE Working Group.82,83
High certainty: We are very confident that the true effect lies close to that of the estimate of the effect.
Moderate certainty: We are moderately confident in the effect estimate — the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. We use the word “likely” for evidence of moderate certainty (e.g., “X intervention likely results in Y outcome”).
Low certainty: Our confidence in the effect estimate is limited — the true effect may be substantially different from the estimate of the effect. We use the word “may” for evidence of low certainty (e.g., “X intervention may result in Y outcome”).
Very low certainty: We have very little confidence in the effect estimate — the true effect is likely to be substantially different from the estimate of effect. We describe evidence of very low certainty as “very uncertain.”
Following the GRADE approach, evidence from the QuANTUM-First study started as high-certainty evidence and could be rated down for concerns related to study limitations (which refers to internal validity or risk of bias), indirectness, imprecision of effects, and publication bias.
When possible, certainty was rated in the context of the presence of an important (nontrivial) treatment effect; if this was not possible, certainty was rated in the context of the presence of any treatment effect (i.e., the clinical importance is unclear). In all cases, the target of the certainty of evidence assessment was based on the point estimate and where it was located relative to the threshold for a clinically important effect (when a threshold was available) or to the null. For OS, EFS, CR, CRc, transplant rate, and HRQoL, the target of the certainty of evidence assessment was the presence or absence of a clinically important effect. For RFS and grade 3 to 5 AEs, the target of the certainty of evidence assessment was the presence or absence of any (nonnull) effect.
Results of GRADE Assessments
Table 2 presents the GRADE summary of findings for quizartinib versus placebo.
Quizartinib likely results in a clinically important increase in the probability OS at 12 months and 48 months of follow-up compared with placebo (moderate certainty due to serious imprecision).
Quizartinib likely results in little to no clinically important difference in the probability of EFS at 12 months and 36 months of follow-up compared with placebo (moderate certainty due to serious imprecision).
Quizartinib may result in an increase in the probability of RFS (among patients with CR after induction) at 6 months and 36 months of follow-up compared with placebo (low certainty due to very serious study limitations). The clinical importance of the increase is uncertain.
Quizartinib results in little to no clinically important difference in the rates of CR and CRc after induction compared with placebo (high certainty).
Quizartinib likely results in little to no clinically important difference in transplant rate at a median 39.2 months of follow-up compared with placebo (moderate certainty due to serious imprecision).
Quizartinib may result in little to no clinically important difference in the change from baseline in HRQoL at a median 39.2 months of follow-up compared with placebo (low certainty due to very serious study limitations).
Quizartinib may result in an increase in the proportion of patients with 1 or more grade 3 to 5 AEs at a median 39.2 months of follow-up compared with placebo (low certainty due to very serious imprecision). The clinical importance of the increase is uncertain.
Long-Term Extension Studies
No long-term extension studies were submitted by the sponsor.
Indirect Evidence
Contents within this section have been informed by materials submitted by the sponsor. The following have been summarized and validated by the review team.
Objectives for the Summary of Indirect Evidence
As the QuANTUM-First study did not include a comparison to midostaurin plus chemotherapy, the current standard of care in Canada for patients with newly diagnosed AML that is FLT3-ITD positive, the sponsor submitted 2 ITCs.34,35 These included an anchored MAIC and a ML-NMR. The objective of the MAIC was to compare the efficacy of quizartinib to midostaurin in combination with chemotherapy for the treatment of patients aged younger than 60 years with newly diagnosed AML that is FLT3-ITD positive. Restriction of the MAIC population to those aged younger than 60 years was necessary due to the narrower age criteria for the comparator trial, to which the QuANTUM-First study population was matched. Due to limitations in the external validity of the MAIC results and to inform the economic evaluation, the ML-NMR was then used to generate effect estimates of quizartinib and midostaurin relative to placebo among the target population of interest (i.e., those meeting the Health Canada–approved indication, including patients aged older than 60 years).
Description of the Matching Adjusted ITC
Study Identification, Data Extraction, and Critical Appraisal Methods
The sponsor conducted a SR in February 2022 in alignment with a predetermined protocol (Table 19).84 First, a search of electronic databases and other sources was undertaken for RCTs published in English comparing first-line treatments, either to each other or to placebo, among patients with newly diagnosed, FLT3-ITD–positive AML. Relevant outcomes included OS, CR, and CIR. Records retrieved by the searches were screened by 1 reviewer, with adjudication by another review as needed. One reviewer extracted data and assessed the risk of bias of the included studies, with adjudication of a random selection of extracted data and risk of bias assessments by another reviewer. Risk of bias at the study level (rather than outcome level) was assessed using a SR-specific tool, which included items for randomization, allocation concealment, blinding, missing outcome data, and selective outcome reporting.
Table 19: Study Selection Criteria and Methods for ITCs Submitted by the Sponsor
Characteristics | Indirect comparison |
|---|---|
Population | Adult patients with newly diagnosed AML that is FLT3-ITD positive |
Intervention | Any first-line treatment |
Comparator | Any (including placebo) or none |
Outcome | OS, CR, CIR |
Study designs | RCTs |
Publication characteristics | Published in English from January 1, 2011, to February 2022 |
Sources searched | Databases: Embase, MEDLINE Grey literature: Google, Google Scholar, Tufts CEA Registry |
Selection process | 1 reviewer with adjudication by another reviewer as needed |
Data extraction process | 1 reviewer with adjudication of a random selection of extracted data by another reviewer |
Quality assessment | 1 reviewer with adjudication of a random selection of appraisals by another reviewer, using a review-specific tool including items for randomization, allocation concealment, blinding, missing outcome data, and selective outcome reporting |
AML = acute myeloid leukemia; CEA = cost-effectiveness analysis; CIR = relapse after complete remission in patients who previously had complete remission; CR = complete remission; ITC = indirect treatment comparison; ITD = internal tandem duplication; MAIC = matching adjusted indirect treatment comparison; OS = overall survival; RCT = randomized controlled trial; SR = systematic review.
Sources: Sponsor’s SR Protocol84 and sponsor’s MAIC report.34
Nine hundred and fifty-five unique records were identified via the searches, of which 704 were excluded during title and abstract screening. Following full text screening, 2 RCTs, the QuANTUM-First and RATIFY studies, were included. As described herein, the QuANTUM-First study was a pivotal, phase III, double-blind RCT comparing quizartinib and placebo as administered in combination with induction and consolidation chemotherapy, and as maintenance therapy in patients aged 18 years to 75 years with newly diagnosed AML that is FLT3-ITD positive. The RATIFY study was a phase III, double-blind RCT comparing midostaurin and placebo as administered in combination with induction and consolidation chemotherapy in patients aged younger than 60 years with newly diagnosed AML with FLT3 mutations.17 The common placebo group across these 2 RCTs created an anchored network for the MAIC. Both RCTs were considered at low risk of bias in all domains assessed by the sponsor, except for “other” sources, where the risk of bias was considered unclear for both RCTs, and missing outcome data where the risk of bias was considered unclear for the RATIFY study.
Among patients aged younger than 60 years in the QuANTUM-First study, baseline characteristics were reasonably balanced across the groups and aligned with the overall population, as described in the SR section. There were imbalances across the midostaurin versus placebo groups, at baseline in the FLT3-ITD subgroup of the RATIFY study by sex (female, 50.4% versus 58.6%), cytogenetic risk (favourable, 25.2% versus 32.3%; intermediate, 33.3% versus 37.6%; and adverse, 41.5% versus 30.1%), and NPM1 mutation status (positive, 50.0% versus 64.3%).
Feasibility Assessment
The sponsor carried out a feasibility assessment to investigate alignment of the eligibility criteria of the 2 RCTs and heterogeneity in patient baseline characteristics and TEMs; the outcomes measured, the timing of outcome measures, and the length of follow-up; and in study design and conduct.
The feasibility assessment identified similarities and differences across the RCTs in design and patient characteristics. Both RCTs were phase III, placebo-controlled trials. Both enrolled more than 500 FLT3-ITD–positive patients (N = 539 in the QuANTUM-First study and N = 555 in the RATIFY study) with newly diagnosed AML. OS was the primary end point in both RCTs, with CR as a secondary end point. These were defined and measured similarly across the 2 RCTs, although the definition of CR was slightly more stringent in the QuANTUM-First study (requiring the absence of blasts with Auer rods [versus no requirement in the RATIFY study] and absence of extramedullary disease [versus < 5% blasts in the bone marrow or extramedullary disease in the RATIFY study]). In both RCTs, CR was measured at approximately 60 days and 120 days.
Sources of heterogeneity across the 2 RCTs are detailed in Table 20. The QuANTUM-First study enrolled patients aged 18 years to 75 years, whereas the RATIFY study enrolled only patients aged younger than 60 years. As such, patients in the QuANTUM-First study were older, on average, as compared with those enrolled in the RATIFY study. The QuANTUM-First study enrolled only patients who were FLT3-ITD positive, whereas the RATIFY study enrolled patients positive for either FLT3-ITD or FLT3-TKD. There were imbalances across RCTs in patient characteristics including race, FLT3-ITD allelic ratio, platelet count, and ANC. The reporting of other patient characteristics was insufficient to inform a comparison. As such, it is unknown whether the patients in the 2 RCTs differed on any additional characteristics. Stratification factors differed across the 2 RCTs. There were also differences across the 2 RCTs in terms of the induction treatments received, the protocol for providing allogeneic HSCT (and proportions of patients who underwent allogeneic HSCT), and the protocol-specified number of maintenance therapy cycles. With respect to outcomes, in the QuANTUM-First study, CIR was defined by: 5% or more blasts in bone marrow aspirate and/or biopsy not attributable to any other cause, or the reappearance of leukemic blasts in the peripheral blood, and/or the new appearance of extramedullary leukemia, or the presence of Auer rods. The definition of CIR was not reported in the RATIFY study. RFS was defined differently across the 2 RCTs and therefore not considered within the MAIC. The median follow-up time was numerically shorter in the QuANTUM-First study compared with the RATIFY study.
Table 20: Sources of Heterogeneity Across the QuANTUM-First and RATIFY Trials
Characteristics | Sources of heterogeneity |
|---|---|
Eligible patients |
|
Stratification factors | Randomization was stratified by age, region, and WBC in the QuANTUM-First study and by subtype of FLT3 mutation in the RATIFY study. |
Patient baseline characteristics |
|
Treatments investigated |
|
Median follow-up time | The median follow-up time was numerically shorter in the QuANTUM-First study compared with the RATIFY study (39 months vs. 59 months, respectively). |
Outcome definitions |
|
AML = acute myeloid leukemia; ANC = absolute neutrophil count; CIR = relapse after complete remission in patients who previously had complete remission; CR = complete remission; ECOG = Eastern Cooperative Oncology Group; ELN = European LeukemiaNet; HSCT = hematopoietic stem cell transplant; ITD = internal tandem duplication; RCT = randomized controlled trial; TKD = tyrosine kinase domain; vs. = versus; WBC = white blood cell.
Sources: Sponsor’s matching adjusted indirect treatment comparison report34 and Stone et al. (2017).17
Identification of Treatment Effect Modifiers
To provide unbiased effect estimates, anchored MAICs must be adjusted for all TEMs.36 To identify TEMs, the sponsor reviewed available trial publications and subgroups data, conducted univariate analyses of the QuANTUM-First study data, and consulted with clinical experts. First, publications of the RATIFY study were evaluated for the reporting of subgroups across which the estimated treatment effect varied based on statistical significance. Next, individual patient data (IPD) from the QuANTUM-First study were leveraged to conduct univariate regression analyses to identify characteristics affecting the treatment effect of quizartinib versus placebo (both added to chemotherapy) by introducing interaction terms of baseline characteristics with treatment in the model. Patient characteristics with a level of statistical significance of a P value of 0.25 or less without a “great deal” (not further defined by the sponsor) of missing values were flagged for consideration. Finally, 3 clinical experts were consulted by the sponsor to inform whether all relevant TEMs had been identified and to rank them in order of importance.
Of subgroup analyses presented in the RATIFY study (sex, age, FLT3 subtype, ELN risk, NPM1 mutation, and WBC), age, NPM1 mutation, and ELN risk were statistically considered potential TEMs. Statistical results for these subgroups were not considered robust by the sponsor, as the sample sizes contributing to each subgroup were small. The analyses of IPD from the QuANTUM-First study showed a statistically significant treatment by subgroup interaction for FLT3-ITD allelic ratio, cytogenetic risk, and bone marrow blasts for OS.
The 3 clinical experts consulted by the sponsor indicated that the TEMs identified in the literature were plausible and that from a clinical perspective, age, gender, FLT3 mutation status, platelet count, and ANC were TEMs for the outcomes of interest. The clinical experts noted that race and bone marrow blasts were also relevant, but less important. Further, cytogenetic risk, WBC, patients’ geographic region, and NPM1 mutation status were flagged by the clinical experts as being important, with cytogenetic risk and WBC being most impactful. These 2 variables could not be considered in the MAIC due to not being collected and/or reported in either of the contributing RCTs. As such, key TEMs identified by the sponsor for matching and adjustment in the MAIC comparing with the FLT3-ITD population in the RATIFY study included age, gender, FLT3-ITD allelic ratio, NPM1 mutation status, platelet count, and bone marrow blasts.
Analysis Methods
The MAIC used IPD from the QuANTUM-First study based on the August 13, 2021, data cut-off. The HR for OS was assessed using the Cox PH model as in the RATIFY study. A logistic model was used to estimate the OR for CR. The HR of CIR was assessed using the Fine-Gray competing risk model considering death as a competing risk. All patients who were alive and had not relapsed at the last evaluation were censored. Two MAIC analyses were undertaken, comparing the RATIFY study’s overall population and the subgroup of RATIFY study patients who were FLT3-ITD positive, with the subgroup of the QuANTUM-First study patients aged younger than 60 years. Only the comparison of FLT3-ITD–positive patients was relevant to the Health Canada–approved indication for quizartinib and therefore reported herein. FLT3-ITD mutation status in the RATIFY study was verified by NGS, which was unavailable for 19% of patients in the FLT3-ITD subgroup; these patients were excluded from the analyses. Competing risk model–based HRs were extracted from relevant RATIFY study publications for the analyses. Unadjusted comparisons of the QuANTUM-First and RATIFY studies were also conducted. The results are not reported herein owing to the high risk of bias associated with unadjusted comparisons.
To conduct the MAIC analysis, first propensity score weighting was used to estimate inverse odds for each QuANTUM-First study patient, representing the probability of being part of the RATIFY study’s population. Propensity score weights were estimated using the method of moments approach. Matching variables for the MAIC were included via stepwise forward inclusion, starting with the highest-ranking TEM. Additional TEMs were added until the ESS of the adjusted QuANTUM-First study population reached 50% of the initial sample size. The sponsor cited the National Institute for Health and Care Excellence Decision Support Unit technical support document on the methods for population-adjusted indirect comparisons as justification for the 50% threshold.36 This resulted in matching for age, sex, platelet count, and NPM1 mutation status. FLT3-ITD allelic ratio could not be matched, as the ESS fell below ███. In the absence of reported means for age and platelet count in the RATIFY study publications, medians were assumed equivalent by the sponsor and used to impute the means. Relative treatment effects of OS and CIR for quizartinib versus midostaurin post matching were estimated via log HRs and standard errors. The log OR and standard error were used for CR.
The sponsor conducted the following additional scenario analyses.
Scenario 1 (OS): Analysis of OS, matching on an alternative set of matching variables (including age, sex, platelet count, and FLT3-ITD allelic ratio)
Scenario 1 (CR): Analysis of CR, defining CR as CR within 60 days
Scenario 1 (CIR): Analysis of CIR, defining CR as CR within 60 days
Scenario 2: Analysis of OS, CR, and CIR using all sponsor-identified matching variables, except for age and sex (including platelet count, NPM1 mutation status, and FLT3-ITD allelic ratio)
Scenario 3: Analysis of OS, CR, and CIR using all sponsor-identified matching variables (age, sex, platelet count, NPM1 mutation status, and FLT3-ITD allelic ratio)
Scenario 4: Analysis of OS, CR, and CIR using age, sex, platelet count, NPM1 mutation status, and baseline bone marrow blasts as matching variables
Results of the MAIC
Patient Characteristics Before and After Matching
Baseline characteristics of patients aged 60 years and younger in the QuANTUM-First study (N = 331) and patients who were FLT3-ITD positive in the RATIFY study (N = 452) before and after matching are in Table 21. Only information for the sponsor-selected TEMs were reported by the sponsor. Other baseline characteristics before and after matching were not reported.
Before adjustment, there were imbalances by platelet count, NPM1 mutation status, and FLT3-ITD allelic ratio. The mean and median age of patients and distribution by sex were relatively balanced. Following adjustment, there was balance across the RCTs in the sponsor-selected TEMs, except for median platelet count (34 × 109/L; range, 3 to 203 in the QuANTUM-First study compared with 50 × 109/L; range, 2 to 461 in the RATIFY study) and the proportion of patients with FLT3-ITD with high allelic ratio greater than 0.5 (████% in the QuANTUM-First study compared ████ ████% in the RATIFY study). After matching, the ESS was ██████ (████% of the original sample size of the QuANTUM-First study).
Distribution of Weights
Most propensity score weights were centred around 1, with a median of 0.80 (range, 0.39 to 11.68; interquartile range, 0.59 to 1.07) and mean of 1.00. There were 4 outliers with weights greater than 5. Due to the higher median and maximum platelet count among patients in the RATIFY study, patients with high platelet counts were under-represented in the QuANTUM-First trial population up to age 60 years and received higher weights during matching.
Table 21: Patient Baseline Characteristics Included in the MAIC Comparing Quizartinib (Patients From QuANTUM-First Aged ≤ 60 Years) and Midostaurin (Patients From RATIFY Who Were FLT3-ITD Positive) Before and After Matching
Matching variable | QuANTUM-First unadjusted N = 331 | QuANTUM-First adjusted █████ ██ | RATIFY FLT3-ITD positive N = 452 |
|---|---|---|---|
Sponsor-specified TEMs used for matching | |||
Age (years), meana | 46.1 | █████ ██ | 47a |
Age (years), median (range) | 48 (20 to 60) | █████ ██ | 47 (18 to 60) |
Sex (male), n (%) | 150 (45.3) | █████ ██ | 206 (45.6) |
Platelet count (× 109/L), meana | 30.3 | █████ ██ | 50a |
Platelet count (× 109/L), median (range) | 23 (3 to 203) | █████ ██ | 50 (2 to 461) |
NPM1 mutation status (positive), n (%) | 155 (46.8) | █████ ██ | 203 (56.7) |
Sponsor-specified TEMs not used for matching | |||
Subtype of FLT3-ITD with high allelic ratio > 0.5, n (%) | 161 (48.6) | █████ ██ | 290 (64.3) |
ESS = effective sample size; ITD = internal tandem duplication; MAIC = matching adjusted indirect comparison; TEM = treatment effect modifier.
aGiven only the median was available from the RATIFY study, but the matching approach uses the mean, it was assumed that the median and mean were equal. Matching was conducted on the assumed mean from the RATIFY study, but medians are presented for comparison.
Source: Sponsor’s MAIC report.34
Efficacy Results
Primary Analysis (Base Case)
Detailed efficacy results for the MAIC are in Table 22. Among patients up to age 60 who were FLT3-ITD positive, the MAIC was insufficient to show a difference between quizartinib and midostaurin, in combination with chemotherapy, for OS (HR = ████ 95% CI, ████ ██ ████) and CR (OR = ████ 95% CI, ████ ██ ████). Although the point estimates for the comparative effects favoured quizartinib for OS and midostaurin for CR, the 95% CIs were wide, including the possibility that either quizartinib or midostaurin could be favoured. Quizartinib was favoured over midostaurin for CIR (HR = ████ 95% CI, ████ ██ ████).
Table 22: Efficacy Results for the MAIC Comparing Quizartinib (QuANTUM-First Patients Aged ≤ 60 Years) and Midostaurin (RATIFY Patients Who Were FLT3-ITD Positive)
Method | Comparison | Effect estimate |
|---|---|---|
OS, HR (95% CI) | ||
QuANTUM-First unadjusteda | Quizartinib vs. placebo | ████ █████ ██ |
QuANTUM-First adjustedb | Quizartinib vs. placebo | ████ █████ ██ |
RATIFYc | Midostaurin vs. placebo | ████ █████ ██ |
MAICd | Quizartinib vs. midostaurin | ████ █████ ██ |
CR, OR (95% CI) | ||
QuANTUM-First unadjusted | Quizartinib vs. placebo | ████ █████ ██ |
QuANTUM-First adjustede | Quizartinib vs. placebo | ████ █████ ██ |
RATIFYf | Midostaurin vs. placebo | ████ █████ ██ |
MAICd | Quizartinib vs. midostaurin | ████ █████ ██ |
CIR, HR (95% CI) | ||
QuANTUM-First unadjustedg | Quizartinib vs. placebo | ████ █████ ██ |
QuANTUM-First adjustedh | Quizartinib vs. placebo | ████ █████ ██ |
RATIFYi | Midostaurin vs. placebo | ████ █████ ██ |
MAICd | Quizartinib vs. midostaurin | ████ █████ ██ |
CI = confidence interval; CIR = relapse after complete remission in patients who previously had complete remission; CR = complete remission; HR = hazard ratio; ITD = internal tandem duplication; MAIC = matching adjusted indirect comparison; OR = odds ratio; OS = overall survival; PH = proportional hazards; vs. = versus.
aHR and 95% CI from a stratified Cox PH model.
bHR from a weighted Cox PH model. CI was computed using the robust sandwich variance estimation.
cHR and 95% CI from a Cox PH model per Rücker et al. (2022) (refer to Table 3 and Figure 4).85
dCI was computed using the robust sandwich variance estimation. A MAIC HR or OR of < 1 favours quizartinib.
eOR based on weighted logistic regression with binomial link. CI was computed using the robust sandwich variance estimation.
fBased on Figure 2 in Rücker et al. (2022).85
gHR and 95% CI from competing risk model with death as competing risk.
hHR from weighted competing risk model with death as competing risk. CI was computed using the robust sandwich variance estimation.
iHR and 95% CI from competing risk model with death as a competing risk based on Table 3 in Rücker et al.85
Source: Sponsor’s MAIC report.34
Scenario Analyses
Results of the scenario analyses are detailed in Appendix 1, Table 27. The ESS was █████ of the original QuANTUM-First study sample size for Scenario 1 (OS), █████ for Scenario 2, █████ for Scenario 3, and █████ for Scenario 4. For all outcomes, results of the scenario analyses were overall aligned with those of the primary analysis (base case), except for CR in Scenario 4. In Scenario 4, whereby CR was analyzed using age, sex, platelet count, NPM1 status, and baseline bone marrow blasts as matching variables, the OR for quizartinib versus midostaurin was ████ (95% CI, ████ ██ ████). Although the point estimate for the between-groups effect favoured quizartinib, the 95% CI included the possibility that either quizartinib or midostaurin could be favoured.
Description of the ML-NMR
Included Studies and Identification of TEMs
The ML-NMR analysis leveraged the same SR as for the MAIC, yielding 2 relevant RCTs for inclusion. The same TEMs were also considered.
Analysis Methods
Using a Bayesian framework, an individual-level regression model was fit directly to the IPD of the QuANTUM-First study, underlying the aggregate RATIFY study population characteristics of interest. The individual-level model was then integrated over the RATIFY study population to form an aggregate-level model. This aggregate-level model was then fitted to the summary outcomes of interest. The model was implemented using Markov Chain Monte Carlo. Scenario analyses were run in patients aged younger than 60 years to align with the RATIFY study population. The analyses relied on published summary statistics for OS (HR), CR (OR), and CIR (HR) for the RATIFY study. For OS and CIR, KM curves were digitized.
For OS and CIR, parametric survival models (m-spline, exponential, Weibull, and log-normal) were used to fit the pseudo IPD. The survival models included both PH and accelerated failure time models. The regression model was specified with 4 covariates — sex, age, platelet count, and NMP1 mutation status. These were specified as both prognostic factors and TEMs. Model comparison was done using approximate leave-one-out (LOO) cross validation. The expected log predictive density (ELPD), a measure of the expected predictive performance of the model, was calculated. Among candidate models, the model with the greatest ELPD was selected. The LOO information criterion (LOOIC) was defined as minus 2 times the ELPD thus transforming the ELPD onto the deviance scale to be used analogous to the deviance information criterion (DIC), whereby lower values were considered better. For survival analysis, the ELPD was calculated via pareto-smoothed importance sampling LOO, where the model with the lowest LOOIC was considered to have the best fit. The m-spline baseline hazard model had the lowest LOOIC for both OS and CIR and was selected.
For CR, both fixed effect and random effects ML-NMR models were fitted. The regression model was specified with the same 4 covariates as for OS and CIR, as both prognostic factors and TEMs. To assess for model fit, the integrand was simplified so that the aggregate-level likelihood was available in a closed form. The residual deviance and effective number of parameters, and hence the DIC were calculated and used for model comparison, as in conventional Bayesian network meta-analysis. Lower DIC values were considered better. The DIC for the fixed effect and random effects models were similar, yet divergent transition errors occurred under the random-effects model. As such, the fixed effect model was selected.
Results of the ML-NMR
Baseline Patient Characteristics
Baseline patient characteristics from the QuANTUM-First study (all patients and patients aged < 60 years) and the FLT3-ITD–positive subgroup of the RATIFY study used in the ML-NMR are in Table 23.
For the analysis of OS and CR, the QuANTUM-First study patients were older and had lower mean platelet counts, on average, compared with those in the FLT3-ITD–positive subgroup of the RATIFY study (54.0 years versus 47.1 years and 30.0 × 109/L versus 44.6 × 109/L, respectively). Numerically fewer QuANTUM-First study patients were NPM1 positive compared with those in the FLT3-ITD–positive subgroup of the RATIFY study (52% versus 57%, respectively). Patients aged younger than 60 years in QuANTUM-First study also had lower mean platelet counts (30.3 × 109/L) and numerically fewer were NPM1 positive (47%) compared with those in the FLT3-ITD–positive subgroup of RATIFY.
For the analysis of CIR, QuANTUM-First study patients were older and had lower mean platelet counts compared with those in the FLT3-ITD–positive subgroup of the RATIFY study (54.0 years versus 47.1 years and 29.8 × 109/L versus 44.6 × 109/L, respectively). Numerically more QuANTUM-First study patients were NPM1 positive compared with those in the FLT3-ITD–positive subgroup of the RATIFY study (68% versus 57%, respectively). Patients aged younger than 60 years in the QuANTUM-First study also had lower mean platelet counts (31.1 × 109/L) and numerically more were NPM1 positive (63%) compared with those in the FLT3-ITD–positive subgroup of the RATIFY study.
The distribution by sex was relatively consistent for all populations and outcomes; 40% to 45% were male.
Table 23: Patient Baseline Characteristics Used in the ML-NMR for OS, CR, and CIR
Baseline characteristic | QuANTUM-First (all patients) | QuANTUM-First (patients aged < 60 years) | RATIFY (FLT3-ITD–positive patients) |
|---|---|---|---|
OS and CR | |||
Age (years), mean (SD) | 54.0 (12.9) | 46.2 (10.3) | 47.1 (NR) |
Sex (male), % | 45 | 45 | 45 |
Platelet count (× 109/L), mean (SD) | 30.0 (28.7) | 30.3 (24.7) | 44.6 (NR) |
NPM1 mutation status, % positive | 52 | 47 | 57 |
CIR | |||
Age (years), mean (SD) | 54.0 (12.6) | 46.2 (9.8) | 47.1 (NR) |
Sex (male), % | 41 | 40 | 45 |
Platelet count (× 109/L), mean (SD) | 29.8 (23.1) | 31.1 (24.6) | 44.6 (NR) |
NPM1 mutation status, % positive | 68 | 63 | 57 |
CIR = relapse after complete remission in patients who previously had complete remission; CR = complete remission; ITD = internal tandem duplication; ML-NMR = multilevel network meta-regression; NR = not reported; OS = overall survival; SD = standard deviation.
Source: Sponsor’s ML-NMR report.35
Efficacy Results
Overall Survival
Population-average conditional HR estimates for OS in a QuANTUM-First–like study population, QuANTUM-First–like study population aged younger than 60 years, and RATIFY-like study population from the ML-NMR are in Table 24.
In both QuANTUM-First–like and RATIFY-like study populations, point estimates favoured quizartinib and midostaurin compared with placebo, although the results were not statistically significant due to imprecision (i.e., the 95% CrI crossed the null). One exception was the comparison of midostaurin versus placebo in a RATIFY-like study population, where midostaurin was favoured (HR = ████ 95% CrI, ████ ██ ████). The predicted median OS with quizartinib was █████ months (95% CrI, █████ ██ █████) in a QuANTUM-First–like study population and █████ months (95% CrI, █████ ██ ██████) in a RATIFY-like study population.
In the scenario analysis using data from patients aged younger than 60 years from the QuANTUM-First study, the results generally aligned with those from the primary analysis (base case). Point estimates favoured both quizartinib and midostaurin over placebo in all populations, although the results were only statistically significant in a QuANTUM-First–like study population.
Table 24: Population-Average Conditional HR Estimates of OS, ML-NMR Fixed Effect M-Spline Models
Comparison | Analysis with all QuANTUM-First patients | Analysis with QuANTUM-First patients aged < 60 years |
|---|---|---|
In a QuANTUM-First–like population, HR (95% CrI)a | ||
Quizartinib vs. placebo | ████ █████ ██ | ████ █████ ██ |
Midostaurin vs. placebo | ████ █████ ██ | ████ █████ ██ |
In a QuANTUM-First–like population aged < 60 years, HR (95% CrI)a | ||
Quizartinib vs. placebo | NA | ████ █████ ██ |
Midostaurin vs. placebo | NA | ████ █████ ██ |
In a RATIFY-like population, HR (95% CrI)a | ||
Quizartinib vs. placebo | ████ █████ ██ | ████ █████ ██ |
Midostaurin vs. placebo | ████ █████ ██ | ████ █████ ██ |
CrI = credible interval; HR = hazard ratio; ML-NMR = multilevel network meta-regression; NA = not applicable; OS = overall survival; vs. = versus.
aPopulation-average conditional estimates.
Source: Sponsor’s ML-NMR report.35
Complete Remission
Population-average OR estimates for CR in a QuANTUM-First–like study population, QuANTUM-First–like study population aged younger than 60 years, and RATIFY-like study population from the ML-NMR are in Table 25.
In both QuANTUM-First–like and RATIFY-like study populations, the analysis was insufficient to show a difference between quizartinib or midostaurin and placebo, owing to imprecision (i.e., wide 95% CrIs including the possibility that either the active treatments or placebo could be favoured). One exception was the comparison of midostaurin versus placebo in a RATIFY-like study population, where midostaurin was favoured over placebo (OR = ████ 95% CI, ████ ██ ████).
In the scenario analysis using data from patients aged younger than 60 years from the QuANTUM-First study, the analysis was insufficient to show a difference between quizartinib and placebo in any population, owing to imprecision (i.e., wide 95% CrIs including the possibility that either quizartinib or placebo could be favoured). Midostaurin was favoured over placebo in the both QuANTUM-First–like and RATIFY-like study populations.
Table 25: Population-Average OR Estimates of CR, ML-NMR Fixed Effects Models
Comparison | Analysis with all QuANTUM-First patients | Analysis with QuANTUM-First patients aged < 60 years |
|---|---|---|
In a QuANTUM-First–like population, OR (95% CrI)a | ||
Quizartinib vs. placebo | ████ █████ ██ | ████ █████ ██ |
Midostaurin vs. placebo | ████ █████ ██ | ████ █████ ██ |
In a QuANTUM-First–like population aged < 60 years, OR (95% CrI)a | ||
Quizartinib vs. placebo | NA | ████ █████ ██ |
Midostaurin vs. placebo | NA | ████ █████ ██ |
In a RATIFY-like population, OR (95% CrI)a | ||
Quizartinib vs. placebo | ████ █████ ██ | ████ █████ ██ |
Midostaurin vs. placebo | ████ █████ ██ | ████ █████ ██ |
CR = complete remission; CrI = credible interval; ML-NMR = multilevel network meta-regression; NA = not applicable; OR = odds ratio; vs. = versus.
aPopulation-average estimates.
Source: Sponsor’s ML-NMR report.35
Relapse After CR
Population-average conditional HR estimates for CIR in a QuANTUM-First–like study population, QuANTUM-First–like study population aged younger than 60 years, and RATIFY-like study population from the ML-NMR are in Table 26.
In both QuANTUM-First–like and RATIFY-like study populations, quizartinib was favoured over placebo. The analysis was insufficient to show a difference between midostaurin and placebo in either population, owing to imprecision (i.e., wide 95% CrIs including the possibility that either the midostaurin or placebo could be favoured).
In the scenario analysis using data from patients aged younger than 60 years from the QuANTUM-First study, in all populations quizartinib was favoured over placebo. The analysis was insufficient to show a difference between midostaurin and placebo in any population, owing to imprecision.
Critical Appraisal of the Sponsor-Submitted ITCs
Matching Adjusted Indirect Comparison
The sponsor used a SR to identify relevant studies for inclusion in the MAIC, with methods outlined in a prespecified protocol. The search methods were overall adequate to identify relevant studies; however, the methods for study selection, data extraction, and risk of bias assessment may not have been adequate to minimize the risk of error and bias in these processes. Study selection was performed by 1 reviewer with adjudication “as necessary,” whereas data extraction and risk of bias assessments were undertaken by 1 reviewer with adjudication of a random selection. These methods fall short of current standards for SRs of health care interventions, which suggest that these processes ideally be undertaken by 2 independent reviewers. At minimum, a pilot testing round with an acceptable level of agreement is recommended before proceeding with single-reviewer methods.86-88 The risk of bias of the included studies was considered low or unclear in all domains as assessed by the sponsor; however, risk of bias was assessed at the study level, rather than at the level of the reported effects (i.e., for each end point of interest). This methodology ignores that risk of bias can vary depending on the effect estimate being evaluated, particularly for such domains as performance, detection, attrition, and reporting bias.79 As such, the risk of bias reported by the sponsor for each study may not universally apply to OS, CR, and CIR.
Table 26: Population-Average Conditional HR Estimates of CIR, ML-NMR Fixed Effect M-Spline Models
Comparison | Analysis with all QuANTUM-First patients | Analysis with QuANTUM-First patients aged < 60 years |
|---|---|---|
In a QuANTUM-First–like population, HR (95% CrI)a | ||
Quizartinib vs. placebo | ████ █████ ██ | ████ █████ ██ |
Midostaurin vs. placebo | ████ █████ ██ | ████ █████ ██ |
In a QuANTUM-First–like population aged < 60 years, HR (95% CrI)a | ||
Quizartinib vs. placebo | NA | ████ █████ ██ |
Midostaurin vs. placebo | NA | ████ █████ ██ |
In a RATIFY-like population, HR (95% CrI)a | ||
Quizartinib vs. placebo | ████ █████ ██ | ████ █████ ██ |
Midostaurin vs. placebo | ████ █████ ██ | ████ █████ ██ |
CIR = relapse after complete remission in patients who previously had complete remission; CrI = credible interval; HR = hazard ratio; ML-NMR = multilevel network meta-regression; NA = not applicable; vs. = versus.
aPopulation-average conditional estimates.
Source: Sponsor’s ML-NMR report.35
The rationale for the anchored MAIC was valid. Only 2 RCTs were available for inclusion. There was heterogeneity across these 2 RCTs in patients’ baseline characteristics (e.g., allelic ratio, platelet counts, NPM1 mutations) that precluded unbiased results from a Bucher ITC or network meta-analysis.36 There were also differences across the 2 RCTs in their design, namely in terms of the induction chemotherapies used and protocols for providing allogeneic HSCT (with a lower transplant rate in the QuANTUM-First study compared with the RATIFY study). These differences in design cannot be adjusted for using a MAIC36; however, the clinical experts consulted for this review noted that these differences were unlikely to affect efficacy and therefore were not considered a source of bias. As the RATIFY study had narrower eligibility criteria than the QuANTUM-First study for age, the analysis was restricted to patients aged 60 years or younger. As such, the results cannot be generalized to patients aged older than 60 years. According to the clinical experts consulted, approximately 60% to 70% of patients who would be treated with quizartinib would be aged older than 60 years.
The MAIC compares the total follow-up of patients in the 2 RCTs. As neither the QuANTUM-First nor RATIFY studies were designed to inform on the contribution of the induction and consolidation, and maintenance phases of treatment to overall efficacy (i.e., patients were not re-randomized before the maintenance phase),24 the MAIC also cannot inform on comparative contribution of each of these distinct treatment phases. Further, the maintenance regimen provided in the RATIFY study is not reflective of clinical practice in Canada. Although the RATIFY study allowed for 12 cycles of maintenance therapy, midostaurin is not approved in Canada for this indication. The contribution of the maintenance phase in the RATIFY study to the overall efficacy of midostaurin and impact on the comparative effect estimates from the MAIC cannot be determined.
The definitions of OS and CR were comparable across the 2 RCTs, although the length of follow-up was longer in the RATIFY study. As the definition of CIR was not reported in the RATIFY publications, the sponsor noted that heterogeneity in the definitions of this outcome across the 2 RCTs could not be assessed. It is unknown whether differences in the definition across the RCTs could have biased the results, challenging credible conclusions on this outcome in the absence of additional information. Because CIR was measured among the subpopulation of patients who had CR during induction, it is uncertain whether prognostic balance across treatment groups was maintained for this outcome in either RCT. If it was not, this would be a source of bias.
To provide unbiased effect estimates, anchored MAICs should adjust for all TEMs.36 The identification of TEMs by the sponsor followed a 3-stage approach, starting by investigating trial-based data from the QuANTUM-First and RATIFY studies, followed by input from clinical experts. The initial identification of TEMs in the 2 RCTs was based on the statistical significance of subgroups effects and regression analyses. These analyses may have missed important TEMs, as the RCTs were not powered to detect subgroup effects. Further, such analyses ignore the potential for clinically relevant differences that may not have reached statistical significance.89 Additional TEMs were suggested by the sponsors’ clinical experts; however, no literature was cited to inform the list of TEMs and it is unclear whether the list is comprehensive. As per all MAICs, the sponsor could only adjust for known and measured TEMs.36 Unknown and known but unmeasured TEMs (e.g., race, ECOG performance status, demographic region, WBC, ELN class, genetic risk, karyotypes, and CEBPA mutations) could not be adjusted for, representing a source of residual confounding. This includes WBC and cytogenetic risk which were characterized as most impactful by the 3 clinical experts consulted by the sponsor. The clinical experts consulted for this review agreed that cytogenetic risk and WBC are important TEMs and that the variables included in the MAIC analyses were unlikely comprehensive.
Patient characteristics before and after adjustment were provided only for the sponsor-identified TEMs. The balance of other baseline characteristics before and after adjustment were not reported. As such, it is unknown whether these were well balanced after adjustment. Imbalances in additional baseline characteristics could represent a source of confounding. In the primary analysis (base case), the ESS was ████% of the original sample size of the QuANTUM-First study. This reduction in ESS contributes to a loss of precision and indicates a greater influence of subsets of patients in the QuANTUM-First study.36 To maintain at least 50% of the original sample size, the sponsor did not include all known and measured TEMs in their primary analysis (FLT3-ITD allelic ratio was omitted). There remained an imbalance in FLT3-ITD allelic ratio after adjustment, representing a source of confounding. ESS was further reduced in the scenario analyses using different matching variables. The effect estimates for OS and CR were imprecise; that is, the 95% CIs were wide and included the potential that either quizartinib or midostaurin could be favoured. Irrespective of other limitations, this imprecision rendered the MAIC inconclusive for these outcomes.
There were imbalances across the midostaurin and placebo groups, respectively, at baseline in the RATIFY study’s FLT3-ITD subgroup by sex, cytogenetic risk, and NPM1 mutation status, suggesting that the randomization may not have been maintained in this subgroup. As such, results from this RCT are at risk of bias. To confirm FLT3-ITD status among RATIFY study patients, NGS was used. Results were unavailable for 19% of patients, who were subsequently excluded from the MAIC analyses. The reason for the missing NGS results was not reported, but per the sponsor the RCT publication noted that it was unknown whether the missingness was completely at random. As such, it is unknown if or how these patients differed from those with NGS results, and whether their exclusion may have biased the comparative effect estimates.
For age and platelet count, only median values were available in the RATIFY study publications. These were used to impute the means required for the MAIC analysis, under the assumption that these were equivalent. This assumption is not verifiable and could be a source of bias if it is not valid. Analyses of OS relied on HRs from Cox PH models. In both RCTs, there was an apparent early OS detriment with the experimental interventions before the KM curves crossed, indicating a violation of the PH assumption. Evidence of the validity of the PH assumption in the analysis of CIR was not reported. Reliance on these HRs in the analyses may have resulted in biased comparative effect estimates.
Although the outcomes assessed in the MAIC were relevant according to inputs received from the patient and clinician groups and the clinical experts consulted, other relevant outcomes such as HRQoL were not investigated. No harms outcomes were investigated, precluding judgments regarding the balance of benefits and harms of quizartinib versus midostaurin.
Multilevel Network Meta-Regression
The rationale for the ML-NMR was justified. Although the MAIC allowed for an indirect comparison of the efficacy of quizartinib versus midostaurin in the absence of direct evidence from RCTs, its external validity is limited. As the RATIFY study had stricter age criteria for enrolment, the results of the MAIC apply only to patients aged younger than 60 years. The ML-NMR allowed for comparisons of both quizartinib and midostaurin with placebo in QuANTUM-First–like and RATIFY-like study populations.
As the ML-NMR analyses leveraged the same 2 RCTs as the anchored MAIC, and investigated the same outcomes, some of the same limitations apply (refer to the previously discussed limitations). Briefly, these included the following:
the SR methods may not have been adequate to minimize the risk of bias and error in study selection, data extraction, and risk of bias assessment
risk of bias assessments were undertaken at the study level, which does not account for differences in risk of bias which may occur across the different effect estimates used in the analyses
the analysis cannot inform on the specific contributions of the induction and consolidation, and maintenance phases of treatment
the maintenance regimen provided in the RATIFY study is not reflective of clinical practice in Canada
the definition of CIR was not reported in the RATIFY study publications, so consistency in the definitions across RCTs could not be assessed
there were imbalances across groups in baseline characteristics for the FLT3-ITD subgroup of the RATIFY study
medians were used to impute missing means for age and platelet count in the RATIFY study
CIR was measured among the subpopulation of patients who had CR during induction and it is uncertain whether prognostic balance across treatment groups was maintained for this outcome
some important outcomes, such as HRQoL and harms, were not investigated.
As per the MAIC, an underlying assumption of the ML-NMR is that the relative effects are constant given all TEMs are adjusted for. In a network of 2 RCTs, this assumption is not verifiable;90 however, only 4 TEMs were adjusted for in the analyses and per the clinical experts consulted for this review, the list was unlikely comprehensive. Other known but unmeasured sponsor-identified TEMs could not be adjusted for, representing a source of residual confounding. For CR and CIR, effect estimates for quizartinib and midostaurin versus placebo were frequently imprecise, with wide 95% CrIs precluding conclusions as to whether the active treatments or placebo were favoured.
Between-group effects comparing quizartinib versus midostaurin with 95% CrIs were not reported, precluding conclusions of their comparative efficacy among QuANTUM-First–like and RATIFY-like study populations. For example, although the effect estimates for quizartinib versus placebo and midostaurin versus placebo for OS appeared similar in each of the populations, without a comparative effect estimate and measure of precision, it is not possible to assert similarity of the active treatments for this outcome.
Studies Addressing Gaps in the SR Evidence
No studies addressing gaps were submitted by the sponsor.
Discussion
Summary of Available Evidence
The clinical evidence submitted by the sponsor included 1 pivotal RCT (QuANTUM-First) and 2 population-adjusted ITCs. The QuANTUM-First study (N = 539) is a phase III, double-blind, multicentre RCT that aims to compare the effects of quizartinib and placebo, administered with standard induction and consolidation chemotherapy (and/or allogeneic HSCT), then administered as maintenance therapy for up to 36 cycles, among adult patients with newly diagnosed AML that is FLT3-ITD positive. The QuANTUM-First study consisted of 4 consecutive phases including induction, consolidation, maintenance, and long-term follow-up, without re-randomization before any phase. The primary end point was OS. Secondary end points included EFS, and CR and CRc with or without MRD negativity. Relevant exploratory end points included RFS, transplant rate, and patient-reported HRQoL assessed via the EORTC QLQ-C30.
The median age of randomized patients was 56 years. Approximately 40% of patients were aged 60 years or older and 25% were aged older than 65 years. Slightly more than half of patients were female (54.5%), and most were white (59.7%) or Asian (29.3%) and enrolled from Europe (60.5%). Most patients had de novo AML (92.4%) and an ECOG performance status of 0 or 1 (84.4%). Nearly three-quarters of patients had an intermediate cytogenetic risk status. Approximately two-thirds of patients had a FLT3-ITD VAF of more than 25%, half had a FLT3-ITD VAF more than 25% but less than 50%, and 10% had a FLT3-ITD VAF of 50% or more. Equal proportions of patients had a WBC count at diagnosis of less than 40 × 109/L and 40 × 109/L or more. The mean bone marrow blast count at baseline was 66.91 to 67.60 across groups. Mean ANCs at baseline in the quizartinib and placebo groups, respectively, were 0.60 and 0.44; mean platelet counts were 28.76 and 31.27. Approximately one-half and one-quarter of patients across groups, respectively, had NPM1 and CEBPA mutations. Although patients aged older than 75 years, those with an ECOG performance status greater than 2, those with AML secondary to prior chemotherapy or radiotherapy for other neoplasms, and those with a known history of CNS leukemia, including cerebrospinal fluid positive for AML blasts, were excluded from the QuANTUM-First study, the clinical experts consulted informed that these patients could be treated with quizartinib in clinical practice.
When the QuANTUM-First study began in 2016, there was no approved FLT3 inhibitor for newly diagnosed patients with FLT3-mutated AML. In 2017, midostaurin was approved by Health Canada in combination with standard induction and consolidation chemotherapy for these patients,60 and subsequently became the standard of care. The sponsor submitted an anchored MAIC and a ML-NMR to address the lack of direct evidence for the comparative efficacy of quizartinib and midostaurin. The MAIC leveraged IPD from the QuANTUM-First study and aggregate data from the RATIFY study (the pivotal trial for midostaurin), anchored on a common placebo group, to compare the efficacy of quizartinib and midostaurin for patients with newly diagnosed, FLT3-ITD–positive AML aged younger than 60 years. Restriction of the MAIC analysis to patients aged younger than 60 years was necessary due to the narrower age criteria for the RATIFY study. Given the limitations to the external validity of the MAIC results and to inform the economic evaluation, the ML-NMR was used to generate effect estimates of quizartinib and midostaurin versus placebo among QuANTUM-First–like and RATIFY-like study populations. The outcomes evaluated in the ITCs included OS, CR, and CIR.
Interpretation of Results
Efficacy
Patient and clinician groups noted that extending OS is an important goal of treatment for patients with newly diagnosed, FLT3-ITD–positive AML. Further, the clinical experts consulted indicated that for patients who are eligible for intensive chemotherapy, the goal of treatment is to provide a cure. The QuANTUM-First study was declared positive on its primary end point of OS. Approximately 10% and 11% more patients in the quizartinib group than the placebo group were alive at 12 months and 48 months of follow-up, respectively, suggesting a likely clinically important OS benefit. The extent to which this OS benefit can be attributed to the induction and consolidation, and maintenance phases of treatment is unclear. There was an apparent early OS detriment with quizartinib, with more patients dying within 60 days of starting induction therapy compared with the placebo group. Most early deaths were attributed to infections. According to the clinical experts consulted, this apparent early OS detriment would not affect who would be treated with quizartinib but highlights that patients should be closely monitored for infections and other AEs during induction therapy. One clinical expert suggested that postmarket real-world evidence may help to inform the nature of the AEs resulting in early deaths. Results of the prespecified subgroup analyses of OS were suggestive of smaller benefit among patients aged 60 years or older and younger than 65 years, from North America, with a WBC count less than 40 × 109/L at diagnosis, and without NPM1 mutational status. Among patients with a favourable AML cytogenetic risk score, the point estimate for the HR of quizartinib versus placebo favoured placebo. Although credible effect modification could not be inferred from these analyses, the results raise uncertainty as to whether the magnitude of benefit observed in the QuANTUM-First study can be generalized to these groups.
Patient and clinician groups, and the clinical experts consulted, highlighted improving remission rates, prolonging the duration of remission, and reducing the risk of relapse as important treatment goals. Results from the QuANTUM-First study suggest that there is likely little to no clinically important difference between quizartinib and placebo in the probability of EFS at 12 months and 48 months follow-up. The primary analysis of EFS, whereby patients who did not have CR or CRi by day 42 (approximately half of patients in both groups) were assigned an event time of baseline, was not statistically significant. This definition of EFS was aligned with FDA guidance for confirmatory trials of treatments for AML (published in 2020, before the start of the QuANTUM-First study).24 Sensitivity analyses wherein patients who did not have CR or CRc by day 56 (per the original protocol definition of EFS, which was intended to align with the pivotal trial of midostaurin) were assigned an event time of baseline was statistically significant in favour of quizartinib; however, these analyses were not adjusted for multiple testing so there is an increased risk that the results are false positives. As a composite end point (including ITF, relapse after CR or CRi, or death) that is defined differently across trials,28 the clinical experts consulted noted that EFS is challenging to interpret and may best inform early toxicities rather than efficacy. Indeed, evidence suggests that the validity of EFS as a surrogate for OS among patients with AML is uncertain27-31 and the review team identified no studies specific to patients with FLT3 mutations being treated with a kinase inhibitor. At its inception, EFS was the primary end point of the QuANTUM-First study; it later became a secondary end point following 2 protocol amendments, allowing for the testing of OS regardless of the statistical significance of EFS. In adherence with the statistical analysis plan, as the primary analysis of EFS was not statistically significant, the other secondary end points were not tested statistically and were considered as supportive evidence.
There was little to no difference between the quizartinib and placebo groups in the rates of CR and CRc, with or without MRD negativity after induction therapy; however, the durations of CR and CRc were longer in the quizartinib group, suggesting more durable responses. These results are at risk of bias as it is uncertain whether prognostic balance was maintained among the subpopulations of patients achieving CR or CRc. The clinical experts consulted indicated that CR or CRi are required for patients to ultimately be cured, and to proceed to allogeneic HSCT. They noted that the array of remission end points (i.e., CR, CR with MRD negativity, CRc, CRc with MRD negativity) tested in the QuANTUM-First study is reflective of uncertainty as to the most appropriate end points and the degree of response required to predict a favourable long-term prognosis. There remains uncertainty as to the optimal duration of maintenance therapy, with few patients in the QuANTUM-First study receiving the full 36 cycles; although the clinical experts noted that in some circumstances, treatment may be continued for longer. MRD negativity is increasingly being recognized as a potentially important biomarker to inform prognosis and guide clinical decision-making.14 Per the clinical experts consulted, MRD negativity may help to determine when therapy can be discontinued (during the maintenance phase) by informing when the harms of continuing may outweigh the benefits. Although testing for FLT3-ITD MRD is being developed and validated at some Canadian centres, it is neither funded nor currently used in clinical practice. Results of the QuANTUM-First study suggested that there may be an RFS benefit with quizartinib versus placebo among patients who had CR or CRc during induction; however, the clinical relevance of this benefit is uncertain. These results are at risk of bias as it is uncertain that prognostic balance was maintained in these subpopulations. The analysis of this end point was also not adjusted for multiple testing, so there is an increased risk that the results are false positives (although not tested statistically). According to the clinical experts, RFS would not be a deciding factor in judging the efficacy of quizartinib. However, preventing relapses is important, as in this disease area frontline treatment provides the best chance for a cure.
Patient and clinician groups indicated that maintaining or improving HRQoL is an important goal of treatment for AML. The results of the QuANTUM-First study suggest that there is likely little to no difference between quizartinib and placebo in the rate of protocol-specified allogeneic HSCT. The clinical experts explained that this result provides confidence that quizartinib does not result in increased toxicities that would preclude patients being fit for allogeneic HSCT; however, there is no direct evidence to support this assertion. Results of the patient-reported EORTC QLQ-C30 assessments suggested that HRQoL improved in both groups during treatment and that there may be little to no difference between groups in the change from baseline. These results are at risk of bias due to attrition, as the proportion of patients who were available to provide assessments diminished substantially over time. Further, there is uncertainty in the threshold used to infer a clinically important benefit or detriment, both within and between groups. The sponsor adopted a 10-point threshold, as this has been used in previous trials of treatments for hematological malignancies, including AML.67-69 However, there is no evidence to substantiate this threshold. Other studies71,72 have suggested that smaller between-group differences may be clinically relevant; however, these estimates were for patients with solid tumours and may not be generalizable to patients with AML.
Important limitations of the QuANTUM-First study include the lack of re-randomization before the maintenance phase, and the limited applicability of the comparison group. FDA guidance notes that for confirmatory trials with multiple treatment phases, re-randomization before maintenance treatment is required to isolate the treatment effect during this phase.24 Although the clinical experts identified a need for approved maintenance therapies, the beneficial effects of quizartinib relative to placebo (e.g., for OS and RFS) cannot be attributed to any phase of treatment but are instead reflective of the overall treatment regimen investigated. Per the clinical experts, the optimal duration of maintenance therapy also remains uncertain. Relevant to the comparator in the QuANTUM-First study, the clinical experts estimated that up to 10% of patients with FLT3-ITD–mutated AML and concomitant favourable-risk core binding factor or adverse-risk karyotype may receive intensive chemotherapy with gemtuzumab ozogamicin or an alternative regimen, such as FLAG-IDA, rather than with midostaurin. Of the remaining patients eligible for intensive chemotherapy with midostaurin, less than 5% would not receive midostaurin, usually due to intolerance or gastrointestinal mucositis.
The sponsor-submitted ITCs aimed to provide indirect evidence of the efficacy of quizartinib relative to midostaurin. The MAIC was insufficient to demonstrate superiority of quizartinib over midostaurin on either OS or CR among patients aged younger than 60 years. Notwithstanding other limitations, the between-group effect estimates were too imprecise to inform which treatment may be favoured. Although the MAIC suggested a benefit of quizartinib over midostaurin on CIR, credible conclusions could not be drawn for this outcome owing to multiple methodological limitations. The most important of these likely included the inability to adjust for unmeasured TEMs, uncertainty in the definition of CIR in the RATIFY study, and the potential that prognostic balance was not maintained in either study for this outcome, among others. The ML-NMR aimed to address the limited generalizability of the MAIC by estimating the efficacy of quizartinib and midostaurin versus placebo in QuANTUM-First–like and RATIFY-like study populations. The ML-NMR was subject to many of the same limitations as the MAIC, including the inability to adjust for unmeasured TEMs. Although point estimates for between-group differences versus placebo for OS were suggestive of similar benefit of quizartinib and midostaurin, the absence of between-group effect estimates for the active treatments precluded any credible conclusions about their comparative efficacy for any outcome assessed. Nevertheless, the clinical experts noted that most physicians would choose quizartinib over midostaurin, under the assumption that maintenance therapy could reduce the risk of relapses and prolong OS.
Harms
Patient and clinician groups, and the clinical experts consulted, identified limiting toxicities as an important treatment goal. Nearly all patients in both treatment groups in the QuANTUM-First study were reported to have 1 or more AEs, with the most common including febrile neutropenia, pyrexia, diarrhea, and hypokalemia. Numerically more patients in the quizartinib group than the placebo group (54.0% versus 45.9%) were reported to have 1 or more SAEs, with the most common including febrile neutropenia, pneumonia, septic shock, and sepsis. Approximately 80% of patients in both groups were reported to have 1 or more grade 3 to 4 AEs, with the most common including febrile neutropenia, pneumonia, septic shock, and sepsis. According to the clinical experts consulted, these harms were as expected and would not alter clinical practice or the decision to treat a patient with quizartinib. However, evidence of known harms could help inform strategies to mitigate toxicity and needs for supportive care. Results of the QuANTUM-First study were suggestive of an increased risk of grade 3 to 4 GVHD among patients in the quizartinib group who underwent protocol-specified allogeneic HSCT compared with those in the placebo group (16.7% versus 6.6%). The magnitude and clinical relevance of the increase is uncertain owing to the small number of events contributing to this analysis.
Numerically, a larger proportion of patients withdrew from treatment due to AEs in the quizartinib group compared with the placebo group (20.4% versus 8.6%). There was no single AE that led to treatment discontinuation among more than 4% of patients in any group. Similar proportions of patients in each group (11.3% in the quizartinib group and 9.7% in the placebo group) died due to AEs. As previously noted, more patients in the quizartinib group than the placebo group died during the first 60 days of study drug administration, mostly due to infections.
Warnings and precautions listed in the draft product monograph for quizartinib include QT interval prolongation, which may increase the risk of ventricular arrhythmias or torsades de pointes. In the QuANTUM-First study, more patients in the quizartinib group than the placebo group were reported with a QTcF increase more than 30 ms from baseline (55.1% versus 32.5%) and/or a prolonged QT interval (13.6% versus 4.1%). Two patients died due to cardiac AEs (1 event each of cardiac arrest and ventricular dysfunction), both in the quizartinib group. The clinical experts noted that QT interval prolongation is expected and that it is encouraging that few patients died from cardiac AEs. They indicated that patients with severe uncorrectable hypokalemia, severe uncorrectable hypomagnesemia, long QT syndrome, or a history of ventricular arrhythmias or torsades de pointes would not be treated with quizartinib.
In the absence direct or indirect evidence, no conclusion can be drawn about the harms of quizartinib compared with midostaurin.
Conclusion
Among adult patients with newly diagnosed FLT3-ITD–positive AML who are eligible for intensive induction and consolidation chemotherapy, there is an unmet need for an approved and effective therapy that can also be used in the maintenance setting. The proposed goal of maintenance therapy is to reduce the risk of relapse, prolong remission, and extend OS. Results from the QuANTUM-First study suggest that quizartinib in combination with standard induction and consolidation chemotherapy (and/or allogeneic HSCT), then as maintenance therapy for up to 36 cycles, likely results in a clinically important increase in OS and may result in an increase in RFS compared to placebo. As patients were not re-randomized before the maintenance phase of treatment, it is not possible to determine the contribution of the maintenance phase to the observed OS and RFS benefits. There was little to no difference in the rates of CR and CRc, with or without MRD negativity across groups; however, responses seemed more durable with quizartinib. Results of the QuANTUM-First study also suggest that compared with placebo, quizartinib likely results in little to no difference in EFS or transplant rate and may result in little to no difference in HRQoL. The overall safety profile for quizartinib relative to placebo was acceptable to the clinical experts consulted for this review; however, due to the notable harms associated with quizartinib, they stated that they would not use it among patients with severe uncorrectable hypokalemia, severe uncorrectable hypomagnesemia, long QT syndrome, or a history of ventricular arrhythmias or torsades de pointes. Important limitations of the QuANTUM-First study include the lack of re-randomization before the maintenance phase and the limited applicability of the comparator in current practice. In the absence of re-randomization, the design of the QuANTUM-First study does not allow for isolation of the contribution of maintenance treatment to the overall efficacy of quizartinib, nor the efficacy of quizartinib as a maintenance therapy among patients who have received midostaurin during induction and consolidation. Population-adjusted ITCs were submitted by the sponsor to address the lack of direct evidence comparing quizartinib with midostaurin, the current standard of care. Due to important methodologic limitations and imprecision in the comparative effect estimates from the ITCs, the efficacy of quizartinib versus midostaurin is uncertain. As no harms were investigated in the ITCs, the comparative safety of quizartinib and midostaurin is not known.
References
1.Döhner H, Weisdorf DJ, Bloomfield CD. Acute Myeloid Leukemia. N Engl J Med. 2015;373(12):1136-52. doi: 10.1056/NEJMra1406184 PubMed
2.National Cancer Institute. Cancer stat facts: Leukemia - acute myeloid leukemia (AML). Accessed January 16, 2025. https://seer.cancer.gov/statfacts/html/amyl.html
3.Canadian Cancer Society. Acute myeloid leukemia statistics. 2024. Accessed January 16, 2025. https://cancer.ca/en/cancer-information/cancer-types/acute-myeloid-leukemia-aml/statistics
4.Leukemia & Lymphoma Society. Acute Myeloid Leukemia. Signs and Symptoms. Accessed January 16, 2025. https://www.lls.org/leukemia/acute-myeloid-leukemia/signs-and-symptoms
5.Fedorov K, Maiti A, Konopleva M. Targeting FLT3 Mutation in Acute Myeloid Leukemia: Current Strategies and Future Directions. Cancers (Basel). 2023;15(8):2312. doi: 10.3390/cancers15082312 PubMed
6.Bacher U, Haferlach C, Kern W, Haferlach T, Schnittger S. Prognostic relevance of FLT3-TKD mutations in AML: the combination matters--an analysis of 3082 patients. Blood. 2008;111(5):2527-37. doi: 10.1182/blood-2007-05-091215 PubMed
7.Levis M. FLT3 mutations in acute myeloid leukemia: what is the best approach in 2013? Hematology Am Soc Hematol Educ Program. 2013;2013:220-6. doi: 10.1182/asheducation-2013.1.220 PubMed
8.Metzeler KH, Herold T, Rothenberg-Thurley M, et al. Spectrum and prognostic relevance of driver gene mutations in acute myeloid leukemia. Blood. 2016;128(5):686-98. doi: 10.1182/blood-2016-01-693879 PubMed
9.Patel JP, Gonen M, Figueroa ME, et al. Prognostic relevance of integrated genetic profiling in acute myeloid leukemia. N Engl J Med. 2012;366(12):1079-89. doi: 10.1056/NEJMoa1112304 PubMed
10.Ravandi F, Kantarjian H, Faderl S, et al. Outcome of patients with FLT3-mutated acute myeloid leukemia in first relapse. Leuk Res. 2010;34(6):752-6. doi: 10.1016/j.leukres.2009.10.001 PubMed
11.Santos FP, Jones D, Qiao W, et al. Prognostic value of FLT3 mutations among different cytogenetic subgroups in acute myeloid leukemia. Cancer. 2011;117(10):2145-55. doi: 10.1002/cncr.25670 PubMed
12.Tallman MS. New strategies for the treatment of acute myeloid leukemia including antibodies and other novel agents. Hematology Am Soc Hematol Educ Program. 2005:143-50. doi: 10.1182/asheducation-2005.1.143 PubMed
13.Dohner H, Wei AH, Appelbaum FR, et al. Diagnosis and management of AML in adults: 2022 recommendations from an international expert panel on behalf of the ELN. Blood. 2022;140(12):1345-1377. doi: 10.1182/blood.2022016867 PubMed
14.Heuser M, Ofran Y, Boissel N, et al. Acute myeloid leukaemia in adult patients: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2020;31(6):697-712. doi: 10.1016/j.annonc.2020.02.018 PubMed
15.National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology: Acute Myeloid Leukemia [accessed by sponsor]. 2023. Accessed 2023. https://www.nccn.org/
16.Daiichi Sankyo Pharma Canada Ltd. Vanflyta (quizartinib): tablets, 17.7 mg and 26.5 mg, oral use [draft product monograph]. 2024.
17.Stone RM, Mandrekar SJ, Sanford BL, et al. Midostaurin plus Chemotherapy for Acute Myeloid Leukemia with a FLT3 Mutation. N Engl J Med. 2017;377(5):454-464. doi: 10.1056/NEJMoa1614359 PubMed
18.Bazarbachi A, Bug G, Baron F, et al. Clinical practice recommendation on hematopoietic stem cell transplantation for acute myeloid leukemia patients with FLT3-internal tandem duplication: a position statement from the Acute Leukemia Working Party of the European Society for Blood and Marrow Transplantation. Haematologica. 2020;105(6):1507-1516. doi: 10.3324/haematol.2019.243410 PubMed
19.Daiichi Sankyo Pharma Canada. Clinical Study Report: AC220-A-U302. A phase 3, double-blind, placebo-controlled study of quizartinib administered in combination with induction and consolidation chemotherapy, and administered as continuation therapy in subjects 18 to 75 years old with newly diagnosed FLT3-ITD (+) acute myeloid leukemia (QuANTUM-First) [internal sponsor's report]. 2022.
20.Daiichi Sankyo Pharma Canada. Clinical Study Report Addendum: AC220-A-U302. A Phase 3, Double-Blind, Placebo-Controlled Study of Quizartinib Administered in Combination with Induction and Consolidation Chemotherapy, and Administered as Continuation Therapy in Subjects 18 to 75 Years Old with Newly Diagnosed FLT3-ITD (+) Acute Myeloid Leukemia (QuANTUM-First) [internal sponsor's report]. 2024.
21.Daiichi Sankyo. NCT02668653: A Phase 3, Double-Blind, Placebo-controlled Study of Quizartinib Administered in Combination With Induction and Consolidation Chemotherapy, and Administered as Continuation Therapy in Subjects 18 to 75 Years Old With Newly Diagnosed FLT3-ITD (+) Acute Myeloid Leukemia (QuANTUM First). ClinicalTrials.gov. Accessed December 13, 2024. https://clinicaltrials.gov/study/NCT02668653
22.Erba HP, Montesinos P, Kim HJ, et al. Quizartinib plus chemotherapy in newly diagnosed patients with FLT3-internal-tandem-duplication-positive acute myeloid leukaemia (QuANTUM-First): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet. 2023;401(10388):1571-1583. doi: 10.1016/S0140-6736(23)00464-6 PubMed
23.Sekeres MA, Erba H, Montesinos P, et al. QuANTUM-First: Efficacy in newly diagnosed patients with FMS-like tyrosine kinase 3-internal tandem duplication-positive (FLT3-ITD+) acute myeloid leukemia (AML) who received continuation therapy. Presented at the European Hematology Association Congress. 2024. Accessed March 11, 2025. https://library.ehaweb.org/eha/2024/eha2024-congress/422246/mikkael.a.sekeres.quantum-first.efficacy.in.newly.diagnosed.patients.with.html
24.US Department of Health and Human Services, Food and Drug Administration, Oncology Center of Excellence, Center for Drug Evaluation and Research, Center for Biologics Evaluation and Research. Acute myeloid leukemia: developing drugs and biological products for treatment. Guidance for industry. 2022. Accessed January 7, 2025. https://www.fda.gov/media/162362/download
25.Schandelmaier S, Briel M, Varadhan R, et al. Development of the Instrument to assess the Credibility of Effect Modification Analyses (ICEMAN) in randomized controlled trials and meta-analyses. CMAJ. 2020;192(32):E901-E906. doi: 10.1503/cmaj.200077 PubMed
26.European Medicines Agency. Guideline on the investigation of subgroups in confirmatory clinical trials. 2019. Accessed January 28, 2025. https://www.ema.europa.eu/en/documents/scientific-guideline/guideline-investigation-subgroups-confirmatory-clinical-trials_en.pdf
27.Othus M, van Putten W, Lowenberg B, et al. Relationship between event-free survival and overall survival in acute myeloid leukemia: a report from SWOG, HOVON/SAKK, and MRC/NCRI. Haematologica. 2016;101(7):e284-6. doi: 10.3324/haematol.2015.138552 PubMed
28.Assouline S, Wiesinger A, Spooner C, Jovanovic J, Schlueter M. Validity of event-free survival as a surrogate endpoint in haematological malignancy: Review of the literature and health technology assessments. Crit Rev Oncol Hematol. 2022;175:103711. doi: 10.1016/j.critrevonc.2022.103711 PubMed
29.Norsworthy KJ, Gao X, Ko CW, et al. Response Rate, Event-Free Survival, and Overall Survival in Newly Diagnosed Acute Myeloid Leukemia: US Food and Drug Administration Trial-Level and Patient-Level Analyses. J Clin Oncol. 2022;40(8):847-854. doi: 10.1200/JCO.21.01548 PubMed
30.Sasine JP, Schiller GJ. Acute Myeloid Leukemia: How Do We Measure Success? Curr Hematol Malig Rep. 2016;11(6):528-536. doi: 10.1007/s11899-016-0346-x PubMed
31.Estey E, Othus M, Lee SJ, Appelbaum FR, Gale RP. New drug approvals in acute myeloid leukemia: what's the best end point? Leukemia. 2016;30(3):521-5. doi: 10.1038/leu.2015.262 PubMed
32.Little RJ, D'Agostino R, Cohen ML, et al. The prevention and treatment of missing data in clinical trials. N Engl J Med. 2012;367(14):1355-60. doi: 10.1056/NEJMsr1203730 PubMed
33.Daiichi Sankyo Pharma Canada. Daiichi Sankyo Pharma Canada response to January 21, 2025 request for additional information regarding Vanflyta (quizartinib) review: additional data for QuANTUM-First [internal additional sponsor's information]. February 10, 2025.
34.Daiichi Sankyo Pharma Canada. Matching adjusted indirect treatment comparison of quizartinib vs midostaurin [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Vanflyta (quizartinib), 17.7 mg or 26.5 mg oral tablets. 2024.
35.Daiichi Sankyo Pharma Canada. Multi-level network meta-regression quizartinib [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Vanflyta (quizartinib), 17.7 mg or 26.5 mg oral tablets. 2024.
36.Phillippo DM, Ades AE, Dias S, Palmer S, Abrams KR, Welton NJ. Methods for Population-adjusted Indirect Comparisons in Submissions to NICE (NICE DSU Technical Support Document 18). Decision Support Unit, ScHARR, University of Sheffield; 2016. Accessed January 14, 2025. https://www.sheffield.ac.uk/media/34216/download?attachment
37.Klepin HD, Rao AV, Pardee TS. Acute myeloid leukemia and myelodysplastic syndromes in older adults. J Clin Oncol. 2014;32(24):2541-52. doi: 10.1200/JCO.2014.55.1564 PubMed
38.Statistics Canada. Age-specific five-year net survival estimates for primary sites of cancer, by sex, three years combined. 2020. Accessed January 16, 2025. https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310015801
39.Cheson BD, Bennett JM, Kopecky KJ, et al. Revised recommendations of the International Working Group for Diagnosis, Standardization of Response Criteria, Treatment Outcomes, and Reporting Standards for Therapeutic Trials in Acute Myeloid Leukemia. J Clin Oncol. 2003;21(24):4642-9. doi: 10.1200/JCO.2003.04.036 PubMed
40.Papaemmanuil E, Gerstung M, Bullinger L, et al. Genomic Classification and Prognosis in Acute Myeloid Leukemia. N Engl J Med. 2016;374(23):2209-2221. doi: 10.1056/NEJMoa1516192 PubMed
41.Lubeck DP, Danese M, Jennifer D, Miller K, Richhariya A, Garfin PM. Systematic Literature Review of the Global Incidence and Prevalence of Myelodysplastic Syndrome and Acute Myeloid Leukemia. Blood. 2016;128(22):5930-5930. doi: 10.1182/blood.V128.22.5930.5930
42.American Cancer Society. Risk factors for acute myeloid leukemia. 2025. Accessed January 16, 2025. https://www.cancer.org/cancer/types/acute-myeloid-leukemia/causes-risks-prevention/risk-factors.html
43.Dohner H, Estey E, Grimwade D, et al. Diagnosis and management of AML in adults: 2017 ELN recommendations from an international expert panel. Blood. 2017;129(4):424-447. doi: 10.1182/blood-2016-08-733196 PubMed
44.Grimwade D, Ivey A, Huntly BJ. Molecular landscape of acute myeloid leukemia in younger adults and its clinical relevance. Blood. 2016;127(1):29-41. doi: 10.1182/blood-2015-07-604496 PubMed
45.Grafone T, Palmisano M, Nicci C, Storti S. An overview on the role of FLT3-tyrosine kinase receptor in acute myeloid leukemia: biology and treatment. Oncol Rev. 2012;6(1):e8. doi: 10.4081/oncol.2012.e8 PubMed
46.Rosnet O, Buhring HJ, deLapeyriere O, et al. Expression and signal transduction of the FLT3 tyrosine kinase receptor. Acta Haematol. 1996;95(3-4):218-23. doi: 10.1159/000203881 PubMed
47.van der Geer P, Hunter T, Lindberg RA. Receptor protein-tyrosine kinases and their signal transduction pathways. Annu Rev Cell Biol. 1994;10:251-337. doi: 10.1146/annurev.cb.10.110194.001343 PubMed
48.Wander SA, Levis MJ, Fathi AT. The evolving role of FLT3 inhibitors in acute myeloid leukemia: quizartinib and beyond. Ther Adv Hematol. 2014;5(3):65-77. doi: 10.1177/2040620714532123 PubMed
49.Zhou F, Ge Z, Chen B. Quizartinib (AC220): a promising option for acute myeloid leukemia. Drug Des Devel Ther. 2019;13:1117-1125. doi: 10.2147/DDDT.S198950 PubMed
50.Kiyoi H, Kawashima N, Ishikawa Y. FLT3 mutations in acute myeloid leukemia: Therapeutic paradigm beyond inhibitor development. Cancer Sci. 2020;111(2):312-322. doi: 10.1111/cas.14274 PubMed
51.Alberta Health Services. Cancer Guidelines. Accessed February 12, 2024. https://www.albertahealthservices.ca/info/cancerguidelines.aspx
52.Daiichi Sankyo Pharma Canada. Daiichi Sankyo Clinical Evidence Template: Vanflyta (R) (quizartinib) [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Vanflyta (quizartinib), 17.7 mg or 26.5 mg oral tablets. 2023.
53.Daver N, Venugopal S, Ravandi F. FLT3 mutated acute myeloid leukemia: 2021 treatment algorithm. Blood Cancer J. 2021;11(5):104. doi: 10.1038/s41408-021-00495-3 PubMed
54.Sekeres MA, Guyatt G, Abel G, et al. American Society of Hematology 2020 guidelines for treating newly diagnosed acute myeloid leukemia in older adults. Blood Adv. 2020;4(15):3528-3549. doi: 10.1182/bloodadvances.2020001920 PubMed
55.Maeda Y. JSH practical guidelines for hematological malignancies, 2023: I. Leukemia-1. Acute myeloid leukemia (AML). Int J Hematol. 2024;119(4):347-373. doi: 10.1007/s12185-024-03730-2 PubMed
56.Dr. Reddy's Laboratories Limited. Reddy-azacitidine: azacitidine for injection, 100 mg azaciticine per vial [product monograph]. April 18, 2017. Accessed January 17, 2025. https://pdf.hres.ca/dpd_pm/00041872.PDF
57.Short NJ, Nguyen D, Ravandi F. Treatment of older adults with FLT3-mutated AML: Emerging paradigms and the role of frontline FLT3 inhibitors. Blood Cancer J. 2023;13(1):142. doi: 10.1038/s41408-023-00911-w PubMed
58.U.S. Food and Drug Administration. Vanflyta (quizartinib): tablets, 17.7 mg or 26.5 mg, for oral use [prescribing information]. 2023. Accessed January 16, 2025. https://www.accessdata.fda.gov/drugsatfda_docs/label/2023/216993s000lbl.pdf
59.Daiichi Sankyo Pharma Canada. Drug Reimbursement Review sponsor submission: quizartinib, 17.7 mg and 26.5 mg tablets, oral use [internal sponsor's package]. 2025.
60.Novartis Pharmaceuticals Canada Inc. RYDAPT (midostaurin): capsule, 25 mg, oral [product monograph]. July 21, 2017. Updated March 31, 2023. Accessed January 15, 2025. https://pdf.hres.ca/dpd_pm/00070168.PDF
61.Bergeron J, Capo-Chichi JM, Tsui H, et al. The Clinical Utility of FLT3 Mutation Testing in Acute Leukemia: A Canadian Consensus. Curr Oncol. 2023;30(12):10410-10436. doi: 10.3390/curroncol30120759 PubMed
62.pan-Canadian Oncology Drug Review Final Clinical Guidance Report: Midostaurin (Rydapt) for Acute Myeloid Leukemia. CADTH; 2017. Accessed January 27, 2025. https://www.cda-amc.ca/sites/default/files/pcodr/pcodr_midostaurin_rydapt_all_fn_cgr.pdf
63.Institut national d'excellence en santé et services sociaux. Stratification prognostique des leucémies myéloïdes aiguës par sécençage de nouvelle génération: Panel de gènes. 2016. Accessed January 27, 2025. https://www.inesss.qc.ca/fileadmin/doc/INESSS/Analyse_biomedicale/Juin_2016/INESSS-Avis_analyses_bm-juin16_8_Stratification_pronostique_leucemies_myeloides_aigues_sequencage_nouv_gen_panel_genes.pdf
64.Zwaan CM, Kolb EA, Mires DE, et al. A Phase 1/2 Study of Quizartinib (Q) in Combination with Re-Induction Chemotherapy and As Single-Agent Continuation Therapy in Pediatric and Young Adult Patients with Relapsed/Refractory (R/R) FLT3-ITD Acute Myeloid Leukemia (AML). Blood. 2019;134(Supplement_1):3937-3937. doi: 10.1182/blood-2019-121736
65.Aaronson NK, Ahmedzai S, Bergman B, et al. The European Organization for Research and Treatment of Cancer QLQ-C30: a quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst. 1993;85(5):365-76. doi: 10.1093/jnci/85.5.365 PubMed
66.Fayers P, Bottomley A, EORTC Quality of Life Group, Quality of Life Unit. Quality of life research within the EORTC-the EORTC QLQ-C30. European Organisation for Research and Treatment of Cancer. Eur J Cancer. 2002;38 Suppl 4:S125-33. doi: 10.1016/s0959-8049(01)00448-8 PubMed
67.Deschler B, Binek K, Ihorst G, et al. Prognostic factor and quality of life analysis in 160 patients aged > or =60 years with hematologic neoplasias treated with allogeneic hematopoietic cell transplantation. Biol Blood Marrow Transplant. 2010;16(7):967-75. doi: 10.1016/j.bbmt.2010.02.004 PubMed
68.Montesinos P, Recher C, Vives S, et al. Ivosidenib and Azacitidine in IDH1-Mutated Acute Myeloid Leukemia. N Engl J Med. 2022;386(16):1519-1531. doi: 10.1056/NEJMoa2117344 PubMed
69.Pratz KW, Panayiotidis P, Recher C, et al. Venetoclax combinations delay the time to deterioration of HRQoL in unfit patients with acute myeloid leukemia. Blood Cancer J. 2022;12(4):71. doi: 10.1038/s41408-022-00668-8 PubMed
70.Efficace F, Cottone F, Sommer K, et al. Validation of the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 Summary Score in Patients With Hematologic Malignancies. Value Health. 2019;22(11):1303-1310. doi: 10.1016/j.jval.2019.06.004 PubMed
71.Bourke S, Bennett B, Oluboyede Y, et al. Estimating the minimally important difference for the EQ-5D-5L and EORTC QLQ-C30 in cancer. Health Qual Life Outcomes. 2024;22(1):81. doi: 10.1186/s12955-024-02294-3 PubMed
72.Musoro JZ, Coens C, Sprangers MAG, et al. Minimally important differences for interpreting EORTC QLQ-C30 change scores over time: A synthesis across 21 clinical trials involving nine different cancer types. Eur J Cancer. 2023;188:171-182. doi: 10.1016/j.ejca.2023.04.027 PubMed
73.Grimwade D, Walker H, Harrison G, et al. The predictive value of hierarchical cytogenetic classification in older adults with acute myeloid leukemia (AML): analysis of 1065 patients entered into the United Kingdom Medical Research Council AML11 trial. Blood. 2001;98(5):1312-20. doi: 10.1182/blood.v98.5.1312 PubMed
74.Daiichi Sankyo Pharma. Statistical Analysis Plan (SAP). A Phase 3, Double-blind, Placebo-controlled Study of Quizartinib Administered in Combination with Induction and Consolidation Chemotherapy, and Administered as Continuation Therapy in Subjects 18 to 75 Years old With Newly Diagnosed FLT3-ITD (+) Acute Myeloid Leukemia [internal sponsor's report]. 2021.
75.Daiichi Sankyo Pharma. Supplemental Statistical Analysis Plan (SAP) for Healthcare Resource Utilization and Quality of Life Endpoints. A Phase 3, Double-blind, Placebo-controlled Study of Quizartinib Administered in Combination with Induction and Consolidation Chemotherapy, and Administered as Continuation Therapy in Subjects 18 to 75 Years old With Newly Diagnosed FLT3-ITD (+) Acute Myeloid Leukemia [internal sponsor's report]. 2021.
76.Larson RA, Mandrekar SJ, Sanford BL, et al. An Analysis of Maintenance Therapy and Post-Midostaurin Outcomes in the International Prospective Randomized, Placebo-Controlled, Double-Blind Trial (CALGB 10603/RATIFY [Alliance]) for Newly Diagnosed Acute Myeloid Leukemia (AML) Patients with FLT3 Mutations. Blood. 2017;130:145. doi: https://doi.org/10.1182/blood.V130.Suppl_1.145.145
77.Daiichi Sankyo Pharma Canada. Daiichi Sankyo Pharma Canada response to January 31, 2025 request for additional information regarding Vanflyta (quizartinib) review: missing outcome data and censoring reasons [internal additional sponsor's information]. February 10, 2025.
78.Daiichi Sankyo Pharma. Clinical Study Report for Quality of Life Analysis: AC220-A-U302. A phase 3, double-blind, placebo-controlled study of quizartinib administered in combination with induction and consolidation chemotherapy, and administered as continuation therapy in subjects 18 to 75 years old with newly diagnosed FLT3-ITD (+) acute myeloid leukemia [internal sponsor's report]. 2022.
79.Sterne JAC, Savovic J, Page MJ, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366:l4898. doi: 10.1136/bmj.l4898 PubMed
80.US Department of Health and Human Services, Food and Drug Administration, Oncology Center of Excellence, Center for Drug Evaluation and Research, Center for Biologics Evaluation and Research. Clinical Trial Endpoints for the Approval of Cancer Drugs and Biologics: Guidance for Industry. 2018. Accessed January 28, 2025. https://www.fda.gov/media/71195/download
81.Heuser M, Freeman SD, Ossenkoppele GJ, et al. 2021 Update on MRD in acute myeloid leukemia: a consensus document from the European LeukemiaNet MRD Working Party. Blood. 2021;138(26):2753-2767. doi: 10.1182/blood.2021013626 PubMed
82.Balshem H, Helfand M, Schunemann HJ, et al. GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol. 2011;64(4):401-6. doi: 10.1016/j.jclinepi.2010.07.015 PubMed
83.Santesso N, Glenton C, Dahm P, et al. GRADE guidelines 26: informative statements to communicate the findings of systematic reviews of interventions. J Clin Epidemiol. 2020;119:126-135. doi: 10.1016/j.jclinepi.2019.10.014 PubMed
84.Systematic literature review of clinical, economic, and humanistic evidence associated with FLT3m AML 1st line treatment [internal sponsor's report], v2.1. Pharmerit - an OPEN Health Company; 2021.
85.Rucker FG, Du L, Luck TJ, et al. Molecular landscape and prognostic impact of FLT3-ITD insertion site in acute myeloid leukemia: RATIFY study results. Leukemia. 2022;36(1):90-99. doi: 10.1038/s41375-021-01323-0 PubMed
86.Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. doi: 10.1136/bmj.j4008 PubMed
87.Whiting P, Savovic J, Higgins JP, et al. ROBIS: A new tool to assess risk of bias in systematic reviews was developed. J Clin Epidemiol. 2016;69:225-34. doi: 10.1016/j.jclinepi.2015.06.005 PubMed
88.Higgins JPT, Thomas J, Chandler J, et al, eds. Cochrane Handbook for Systematic Reviews of Interventions version 6.5 (updated August 2024). Cochrane; 2024. Accessed January 28, 2025. https://training.cochrane.org/handbook/
89.Sedgwick P. Clinical significance versus statistical significance. BMJ. 2014;348(mar14 11):g2130-g2130. doi: 10.1136/bmj.g2130
90.Phillippo DM, Dias S, Ades AE, et al. Multilevel network meta-regression for population-adjusted treatment comparisons. J R Stat Soc Ser A Stat Soc. 2020;183(3):1189-1210. doi: 10.1111/rssa.12579 PubMed
91.Stone Richard M, Mandrekar Sumithra J, Sanford Ben L, et al. Midostaurin plus Chemotherapy for Acute Myeloid Leukemia with a FLT3 Mutation. N Engl J Med. 377(5):454-464. doi: 10.1056/NEJMoa1614359 PubMed
Appendix 1: Detailed Outcome Data
Please note that this appendix has not been copy-edited.
Figure 7: Forest Plot of Overall Survival Subgroup Analyses From QuANTUM-First, August 13, 2021, Data Cut-off (ITT Analysis Set) [Redacted]

██████████████████████████████████████████████.
Source: Clinical Study Report for QuANTUM-First.19
Table 27: Scenario Analysis Results for the MAIC Comparing Quizartinib (QuANTUM-First Patients up to Age 60) and Midostaurin (RATIFY Patients Who Were FLT3-ITD Positive)
Method | Comparison | Effect estimate | |||
|---|---|---|---|---|---|
Scenario 1 | Scenario 2 | Scenario 3 | Scenario 4 | ||
OS, HR (95% CI) | |||||
QuANTUM-First unadjusteda | Quizartinib vs. placebo | ████ | ████ | ████ | ████ |
QuANTUM-First adjustedb | Quizartinib vs. placebo | ████ | ████ | ████ | ████ |
RATIFYc | Midostaurin vs. placebo | ████ | ████ | ████ | ████ |
MAICd | Quizartinib vs. midostaurin | ████ | ████ | ████ | ████ |
CR, OR (95% CI) | |||||
QuANTUM-First unadjusted | Quizartinib vs. placebo | ████ | ████ | ████ | ████ |
QuANTUM-First adjustede | Quizartinib vs. placebo | ████ | ████ | ████ | ████ |
RATIFYf | Midostaurin vs. placebo | ████ | ████ | ████ | ████ |
MAICd | Quizartinib vs. midostaurin | ████ | ████ | ████ | ████ |
CIR, HR (95% CI) | |||||
QuANTUM-First unadjustedg | Quizartinib vs. placebo | ████ | ████ | ████ | ████ |
QuANTUM-First adjustedh | Quizartinib vs. placebo | ████ | ████ | ████ | ████ |
RATIFYi | Midostaurin vs. placebo | ████ | ████ | ████ | ████ |
MAICd | Quizartinib vs. midostaurin | ████ | ████ | ████ | ████ |
CI = confidence interval; CIR = relapse after complete remission in patients who previously had complete remission; CR = complete remission; HR = hazard ratio; IPD = individual patient data; ITD = internal tandem duplication; MAIC = matching adjusted indirect comparison; OR = odds ratio; OS = overall survival; PH = proportional hazards.
aHR and 95% CI from a stratified Cox PH model.
bHR from a weighted Cox PH model. CI was computed using the robust sandwich variance estimation.
cHR and 95% CI from a Cox PH model per Stone et al. (2017).91
dCI was computed using the robust sandwich variance estimation. A MAIC HR or OR of < 1 favours quizartinib.
eOR based on weighted logistic regression with binomial link. CI was computed using the robust sandwich variance estimation.
fBased on Stone et al. (2017).91
gHR and 95% CI from competing risk model with death as competing risk.
hHR from weighted competing risk model with death as competing risk. CI was computed using the robust sandwich variance estimation.
IHR and 95% CI from competing risk model with death as a competing risk based on digitized IPD from Stone et al. (2017).91
Note: In Scenario 1 the analysis of OS was matched on age, sex, platelet count, and FLT3-ITD mutation status. The analysis of CR and CIR defined CR as CR within 60 days. In Scenario 2, all sponsor-identified matching variables were used, except age and sex (platelet count, NPM1 mutation status, and FLT3-ITD mutation status). In Scenario 3, analyses were matched on age, sex, platelet count, NPM1 mutation status, and FLT3-ITD mutation status. In Scenario 4, analyses were matched on age, sex, platelet count, NPM1 mutation status, and baseline bone marrow blasts.
Source: Sponsor’s MAIC Report.34
Pharmacoeconomic Review
Abbreviations
AE
adverse event
AML
acute myeloid leukemia
BIA
budget impact analysis
CDA-AMC
Canada's Drug Agency
CI
confidence interval
CIR
cumulative incidence of relapse
CR
complete remission
CR1
complete remission in the first line
CR2
complete remission in the second line
FLAG-IDA
a combination of fludarabine, cytarabine, idarubicin, and filgrastim
HSCT
hematopoietic stem cell transplant
ICER
incremental cost-effectiveness ratio
ITC
indirect treatment comparison
ITD
internal tandem duplication
KM
Kaplan-Meier
LY
life-year
MAIC
matching-adjusted indirect comparison
ML-NMR
multilevel network meta-regression
NICE
National Institute for Health and Care Excellence
OS
overall survival
QALY
quality-adjusted life-year
QTcF
QT interval corrected using the Fridericia formula
RFS
relapse-free survival
WTP
willingness to pay
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Quizartinib (Vanflyta), 17.7 mg and 26.5 mg oral tablets |
Indication | Quizartinib in combination with standard cytarabine and anthracycline induction and standard cytarabine consolidation chemotherapy, followed by quizartinib maintenance monotherapy, for the treatment of adult patients with newly diagnosed AML that is FLT3-ITD positive. Improvement in overall survival has not been demonstrated for maintenance monotherapy following allogeneic hematopoietic stem cell transplantation. A validated test is required to confirm the FLT3-ITD status of AML. |
Health Canada approval status | Under review |
Health Canada review pathway | Standard |
NOC date | June 9, 2025 |
Reimbursement request | As per indication |
Sponsor | Daiichi Sankyo Pharma Canada |
Submission history | Previously reviewed: No |
AML = acute myeloid leukemia; ITD = internal tandem duplication; NOC = Notice of Compliance.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Semi-Markov model |
Target population | Adult patients with newly diagnosed AML with the presence of FLT3-ITD–activating mutation |
Treatments | Quizartinib plus chemotherapya |
Dose regimen | Induction (up to two 28-day cycles)
Consolidation (up to four 28-day cycles)
Maintenance (up to thirty-six 28-day cycles)
|
Submitted price | Quizartinib: $388.29 per 17.7 mg tablet or 26.5 mg tablet |
Submitted treatment cost | Year 1: $237,970 (quizartinib = $211,617; chemotherapy = $26,352) Year 2 and beyond: $282,675 (quizartinib = $282,675; chemotherapy = $0) |
Comparator | Midostaurin plus chemotherapyb |
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs and LYs |
Time horizon | Lifetime (53 years) |
Key data sources | Sponsor-submitted MAIC in which the efficacy for quizartinib plus chemotherapy was determined from a subset of the QuANTUM-First trial who were matched to patients from the RATIFY trial (midostaurin plus chemotherapy) |
Submitted results | ICER = $33,415 per QALY gained (incremental costs = $133,317; incremental QALYs = 3.99) |
Key limitations |
|
CDA-AMC reanalysis results |
|
AML = acute myeloid leukemia; CDA-AMC = Canada's Drug Agency; CR1 = complete remission in first line; HSCT 1L = allogeneic hematopoietic stem cell transplant in the first line; ICER = incremental cost-effectiveness ratio; ITC = indirect treatment comparison; ITD = internal tandem duplication; KM = Kaplan-Meier; LY = life-year; MAIC = matching-adjusted indirect comparison; ML-NMR = multilevel network meta-regression; QALY = quality-adjusted life-year; QTcF = QT interval corrected using the Fridericia formula; vs. = versus.
aChemotherapy consists of cytarabine, and idarubicin or daunorubicin.
bChemotherapy consists of cytarabine and daunorubicin. Midostaurin is not indicated for use in the maintenance phase. In the maintenance phase, 15% of patients are assumed to receive azacitidine, 85% of patients are assumed to receive no maintenance treatment.
Conclusions
According to the CDA-AMC clinical review, results from the QuANTUM-First study suggest that when used in combination with standard induction and consolidation chemotherapy (and/or allogeneic hematopoietic stem cell transplant [HSCT]), then as maintenance therapy for up to 36 cycles, quizartinib likely results in a clinically important increase in overall survival (OS) and may result in an increase in relapse-free survival (RFS) compared to placebo. The overall safety profile for quizartinib was acceptable to the clinical experts consulted for this review, although the notable harms may restrict its use in patients with some comorbid conditions. Important limitations of the QuANTUM-First study include the lack of re-randomization before the maintenance phase and the limited applicability of the comparator. In the absence of re-randomization, the design of the QuANTUM-First study does not allow for isolation of the contribution of maintenance treatment to the overall efficacy of quizartinib. However, the relevant comparator in the induction and consolidation phases is midostaurin plus chemotherapy (midostaurin is not indicated for the maintenance phase). Population-adjusted indirect treatment comparisons (ITCs) were submitted by the sponsor to address the lack of direct evidence comparing quizartinib with midostaurin, the current standard of care. Due to important methodologic limitations and imprecision in the comparative effect estimates from the ITCs, the clinical reviewers concluded that the comparative efficacy and harms of quizartinib versus midostaurin is uncertain. The clinical experts consulted by CDA-AMC indicated that the primary benefit for quizartinib is the availability to use the treatment in the maintenance phase with the goal of reducing the risk of relapse and prolonging OS. However, there was no robust evidence to validate this information. In practice in Canada, a small proportion of individuals may receive azacitidine in the maintenance phase; there is no comparative evidence assessing quizartinib and azacitidine as maintenance therapy.
CDA-AMC undertook reanalyses to address some of the key limitations in the sponsor’s analysis which included: selecting multilevel network meta-regression (ML-NMR) to inform the clinical inputs of the model, assuming death and relapse rates postallogeneic HSCT for patients receiving midostaurin plus chemotherapy to be same as those receiving quizartinib plus chemotherapy, assuming transition probabilities in induction and consolidation phases to be same across 2 arms, and defining patients staying in complete remission in the first line (CR1) and allogeneic HSCT in the first line health states for 5 years as cured. The CDA-AMC reanalysis resulted in an increment cost-effectiveness ratio (ICER) for quizartinib plus chemotherapy versus midostaurin plus chemotherapy of $104,121 per quality-adjusted life-year (QALY) gained (incremental cost = $112,992; incremental QALYs = 1.09; incremental life-years [LYs] = 1.09). A price reduction of 33.3% (from $388.29 to $258.99 per 17.7 mg and 26.5 mg per oral tablet, respectively) was necessary for quizartinib to be considered cost-effective at a willingness-to-pay (WTP) threshold of $50,000 per QALY gained.
The cost-effectiveness of quizartinib plus chemotherapy is driven by an assumed benefit in RFS for quizartinib plus chemotherapy compared with midostaurin plus chemotherapy, as well as the drug acquisition cost for an FLT3 inhibitor in CR1. However, given analyses by both the sponsor and CDA-AMC were limited by the lack of head-to-head clinical evidence to inform relative treatment effects, the cost-effectiveness of quizartinib and price reduction estimates are highly uncertain. Further price reductions may be warranted to address this uncertainty.
Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, clinician groups, and drug plans that participated in the CDA-AMC review process.
Patient input was gathered from 2 sources: The Leukemia and Lymphoma Society of Canada conducted an online survey with 245 respondents (72% patients with acute myeloid leukemia [AML], 27% caregivers), while Heal Canada surveyed 22 patients with AML. More than 90% of respondents reside in Canada. It was noted that most patients with AML start treatment before mutation results, despite guidelines recommending waiting for personalized treatment. AML significantly impacts patients' mental health and personal life, often requiring substantial caregiver support for daily tasks. Treatment options are limited, and even those who undergo intensive therapy face high relapse rates and poor long-term survival. Current treatments also cause severe side effects, impair daily functioning, and often require long-distance travel for specialized care, adding to patient burden. The drug under review is expected to improve long-term outcomes, reduce relapse risk, and enhance quality of life, aligning with patients’ preference for extended remission and manageable side effects. Respondents who used quizartinib tolerated it well, with mild side effects, and reported improved quality of life compared to other AML treatments.
Clinician input was received from the Cancer Care Ontario Hematology Cancer Drug Advisory Committee. Clinicians indicated that the current standard of care for AML includes midostaurin with 7 + 3 induction chemotherapy (7 days of cytarabine and 3 days of anthracycline) and allogeneic HSCT. It is noted that quizartinib offers an alternative to midostaurin with the added benefit of use in maintenance therapy, potentially improving survival and remission rates. It is expected to integrate into first-line treatment alongside 7 + 3 induction, consolidation, and maintenance, addressing unmet needs in current treatment options.
The drug plans raised considerations about eligibility criteria, particularly FLT3 testing thresholds and response monitoring. Questions were noted on treatment discontinuation criteria, interruptions, and whether patients switching from midostaurin should be eligible. The use of quizartinib in combination with different chemotherapy regimens outside those specified in the trial was also questioned, along with its eligibility for specific patient populations, such as those with Eastern Cooperative Oncology Group Perform Status greater than 2, pediatric patients, older patients, and those with secondary AML. Concerns about dose modifications due to cytochrome P450 3A4 interactions or corrected QT interval prolongation were also raised. Lastly, concerns about the anticipated budget impact were highlighted, as quizartinib introduces a 3-year maintenance phase, along with the additional resource burden of corrected QT interval monitoring and clinical workload.
Several of those concerns were addressed in the sponsor’s model.
The time-to-treatment discontinuation of quizartinib were modelled based on the data from the QuANTUM-First trial where quizartinib was discontinued for unacceptable toxicity, refractory disease, relapse, or upon completion of 36 cycles of maintenance therapy.
A subset of the QuANTUM-First study population (adults aged < 60 years, matching the RATIFY study’s FLT3 internal tandem duplication [ITD]–positive population) was modelled, while patients aged younger than 18 years, older than 60 years, or with specific exclusions (e.g., central nervous system leukemia, BCR-ABL–positive AML, secondary AML) were not included.
CDA-AMC was unable to address the following concerns raised from the input relevant to the economic review.
No information was available for patients outside of the trial’s inclusion criteria for quizartinib treatment. The cost-effectiveness in the additional populations of interest to the drug plans cannot be assessed.
Economic Review
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted a cost-utility analysis assessing quizartinib plus chemotherapy compared with midostaurin plus chemotherapy in adult patients with newly diagnosed AML that is FLT3-ITD positive. The modelled population was aligned with the population enrolled in the QuANTUM-First study and the Health Canada–indicated population.1,2
Quizartinib is available as 17.7 mg and 26.5 mg oral tablets at a submitted price of $388.29 per tablet.3 The recommended dose of quizartinib during the induction (up to two 28-day cycles) and consolidation periods (up to four 28-day cycles) is 35.4 mg once daily for 14 days. The recommended dose of quizartinib in the maintenance period (up to thirty-six 28-day cycles) is 26.5 mg once daily for 14 days and 53 mg once daily thereafter if QTcF is less than or equal to 450 ms.1 During the induction period in the economic model, quizartinib is used in combination with standard cytarabine and anthracycline. Standard cytarabine is administered at a dose of 200 mg/m2 per day by continuous IV infusion from day 1 to day 7 of a 28-day cycle and anthracycline is administered by IV infusion on days 1, 2, and 3 of a 28-day cycle at a dose of 60 mg/m2 per day of daunorubicin or 12 mg/m2 per day of idarubicin. During the consolidation period, quizartinib is used in combination with high-dose cytarabine in which cytarabine is administered by IV infusion on days 1, 3, and 5 of a 28-day cycle at a dose of 3,000 mg/m2 every 12 hours for patients aged younger than 60 years and 1,500 mg/m2 every 12 hours for patients aged 60 years and older. In the maintenance period, quizartinib is administered as a monotherapy. When including wastage, assuming 46.4% of anthracycline use is daunorubicin and 53.6% of anthracycline use is idarubicin during the induction period, and a relative dose intensity of 100%, aligned with the QuANTUM-First trial, the sponsor estimated the 28-day cost of quizartinib plus chemotherapy to be $13,904 during the induction period (quizartinib = $10,872; chemotherapy = $3,032), $15,944 during the consolidation period (quizartinib = $10,872; chemotherapy = $5,072), and $15,920 to $21,744 during the maintenance period (quizartinib = $15,920 to $21,744; chemotherapy = $0).1
The sponsor assumed the following dose schedule for midostaurin plus chemotherapy: midostaurin is administered at a dose of 50 mg orally twice daily on days 8 through 21 of the induction and consolidation periods.1 The induction period is up to two 28-day cycles and the consolidation period is up to four 28-day cycles. During the induction phase, midostaurin is administered in combination with cytarabine and daunorubicin at the same dose and frequency, as described previously. During the consolidation phase, midostaurin is administered in combination with high-dose cytarabine, as described previously. Including wastage and relative dose intensity of 95% for midostaurin, the sponsor estimated the 28-day cost of midostaurin plus chemotherapy to be $11,432 during the induction period (midostaurin = $9,184; chemotherapy = $2,248) and $14,256 during the consolidation period (midostaurin = $9,184; chemotherapy = $5,072).1
The clinical outcomes modelled were OS, RFS, and complete remission (CR). The model simulated LYs, QALYs, and costs for each treatment over a lifetime time horizon (53 years), discounted at a rate of 1.5% per annum. The analysis was undertaken from the perspective of the Canadian public health care payer.1
Model Structure
The sponsor submitted a semi-Markov model with 12 health states (induction, CR1, allogeneic HSCT in the first line, post allogeneic HSCT relapse in the first line, refractory, relapse in the first line, CR in second line [CR2], allogeneic HSCT in second line, postallogeneic HSCT in the second line recovery, postallogeneic HSCT maintenance in the second line, relapse in the second line, and death) (Figure 1).1 The cycle length in the model was 28 days. Patients enter the model in the induction health state where they receive either quizartinib plus chemotherapy or midostaurin plus chemotherapy and remain in induction for a maximum of 2 cycles before transitioning to either CR1, relapse in the first line, refractory, or death. Patients who fail to achieve CR in response to induction therapy move to the refractory health state where they will receive second-line therapy (a combination of fludarabine, cytarabine, idarubicin, and granulocyte colony-stimulating factor [FLAG-IDA] or gilteritinib). Patients who achieve CR1 but whose response wanes will transition to remission in the first line (R1) where they will receive second-line therapy. If patients in relapse in the first line experience a response to second-line therapy, they transition to CR2. Patients who do not experience a response to induction therapy or whose response has waned (e.g., those with refractory or relapse in the first line health states) but experience response to second-line treatment will enter CR2 where they will remain until they die, receive allogeneic HSCT, or relapse. Patients in the CR2 health state or who have an allogeneic HSCT in the second line and whose response subsequently wanes are assumed to receive salvage therapy, transitioning to relapse in the second line where they will remain until death. Patients can only transition to allogeneic HSCT in the first line from CR1 and to allogeneic HSCT in the second line from CR2. Patients who receive allogeneic HSCT remain in an allogeneic HSCT health state until they experience relapse or die.1
Model Inputs
The baseline patient characteristics in the model reflect patients enrolled in the QuANTUM-First trial.2 The average patient in the modelled cohort, which the sponsor assumed reflected the population of patients living in Canada, was 47 years old, weighed 73.39 kg, had a mean body surface area of 1.83 m2, and was more likely to be female (54.4%). Body surface area was used to calculate treatment costs for treatments with body surface area–based dosing. Age and the proportion of the population who were female were used to assign age-specific and sex-specific mortality and to cap the lower bound for all-cause mortality in the model.
Key clinical efficacy inputs (i.e., OS, RFS, and CR) for quizartinib plus chemotherapy and midostaurin plus chemotherapy were based on the results of the sponsor-submitted ITC, specifically, a matching-adjusted indirect comparison (MAIC).4 In the MAIC, efficacy for quizartinib plus chemotherapy was determined by the QuANTUM-First trial, and efficacy for midostaurin plus chemotherapy was determined by the RATIFY trial.5 Placebo plus standard induction chemotherapy and consolidation chemotherapy were used as an anchor to enable the comparison between quizartinib plus chemotherapy and midostaurin plus chemotherapy. In addition to the MAIC, the sponsor conducted a ML-NMR and used the output to inform a scenario analysis.
Transition probabilities from the induction health state to CR, refractory, and death for quizartinib plus chemotherapy were estimated using individual patient data from the MAIC-adjusted population (i.e., a subset of the QuANTUM-First study’s intention-to-treat population [aged < 60 years, matched to the RATIFY FLT3-ITD–positive study population]). For the same transition probabilities, the sponsor used alternative methods to estimate the comparative efficacy of midostaurin plus chemotherapy. For the transitions from induction to CR, the sponsor applied an odds ratio of ████ (95% lower confidence interval [CI], ████; 95% upper CI, ████) to the quizartinib plus chemotherapy transition probability. For the transitions from induction to refractory and induction to death, the sponsor assumed equivalence between midostaurin plus chemotherapy and quizartinib plus chemotherapy.
The transition probabilities for CR1 to death, CR1 to relapse, and allogeneic HSCT to death relied on evidence from the sponsor’s submitted MAIC for OS, RFS, and survival after allogeneic HSCT, respectively. To model the aforementioned transition probabilities for quizartinib plus chemotherapy, the sponsor used Kaplan-Meier (KM) data from the MAIC-adjusted QuANTUM-First trial population.4 Several parametric functions were fit to the KM data to select candidate distributions based on diagnostic plots, goodness-of-fit statistics, and visual inspection. For OS and RFS, the sponsor chose a log-normal parametric distribution (Appendix 3, Figure 2 and Figure 3), and for survival after allogeneic HSCT, the sponsor chose a Gompertz distribution (Appendix 3, Figure 4). For midostaurin plus chemotherapy, the sponsor assumed proportional hazards but acknowledged that the criteria required to assume proportional hazards were not satisfied. Under this assumption, the sponsor applied the hazard ratio of ████ (95% lower CI, ████; 95% upper CI, ████), as estimated in the MAIC, to the reference OS curve for quizartinib plus chemotherapy to estimate the transition probabilities for CR1 to death for midostaurin plus chemotherapy. A hazard ratio of ████ (95% lower CI, ████; 95% upper CI, ████) was applied to the reference RFS curve for quizartinib plus chemotherapy to estimate the transition probabilities for relapse after CR in patients who previously achieved CR (i.e., CR1 to relapse; termed in the clinical review as the cumulative incidence of relapse [CIR]) for midostaurin plus chemotherapy. Efficacy for survival after allogeneic HSCT for midostaurin plus chemotherapy was assumed to be the same as the adjusted population treated with placebo plus chemotherapy in the QuANTUM-First trial.
The probability of transitioning between the remaining health states was largely informed by the ADMIRAL trial,6 and assumed equal efficacy across comparators. Exceptions to this — where transitions differ between comparators — include the transitions from allogeneic HSCT in the first line to postallogeneic HSCT relapse in the first line and postallogeneic HSCT relapse 1 to death. For the aforementioned transitions, probabilities were estimated using individual patient data for patients treated with quizartinib plus chemotherapy in QuANTUM-First study for quizartinib plus chemotherapy and patients treated with placebo plus chemotherapy for midostaurin plus chemotherapy.
The sponsor applied a cure assumption which assumed that patients who remained in the CR1 and allogeneic HSCT in the first line health states for 3 years would be considered cured and have twice the risk of death as the age-adjusted and sex-adjusted general population of Canada (standardized mortality rate = 2.0). Cured patients do not accrue disease management costs and have utilities equal to those of the general population.7
Time on treatment for quizartinib (induction, consolidation, and maintenance) was sourced from the QuANTUM-First trial.8 For midostaurin, the treatment durations in induction and consolidation were assumed to match those of quizartinib due to lack of public data. Additionally, midostaurin was not assumed to be used for postallogeneic HSCT, as it is not approved in that setting. During maintenance, according to Canadian expert opinion, 15% of patients in the midostaurin arm were assumed to receive azacitidine. Furthermore, the costs of midostaurin in the maintenance phase were not accounted in the model to reflect the indication approved in Canada.
Health state utility values applied in the economic model for the first line health states were based on a previous National Institute for Health and Care Excellence (NICE) review for midostaurin plus chemotherapy for untreated AML.9 Utility values for allogeneic HSCT health states in the first line setting were based on European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 data from Grulke and colleagues and mapped to EQ-5D values.10,11 In the second-line setting, allogeneic HSCT health relied on the assumption that health-related quality of life was 90% of the respective allogeneic HSCT value in the first-line setting. The sponsor adjusted health state utility values by age-matched and sex-matched general population utility values from the study by Guertin and colleagues.12 Except for graft-versus-host disease, adverse event (AE) disutilities are assumed to be captured by health state utility values. Graft-versus-host disease disutilities were sourced from the study by Peric and colleagues, as used in a previous NICE review and applied to a proportion of patients in the postallogeneic HSCT (first line and second line) health states.9,13
The sponsor’s base case included costs for drug acquisition and administration, treatment monitoring, disease monitoring, AEs, and terminal care. Drug acquisition costs for quizartinib were based on sponsor-submitted prices.1 All other treatment costs were sourced from IQVIA Delta PA.7 Relative dose intensity was considered in the sponsor’s base case with estimates sourced from the QuANTUM-First trial for quizartinib plus chemotherapy and a previous NICE review for midostaurin plus chemotherapy.8,14 Relative dose intensity in the second-line setting was based on assumption and the ADMIRAL trial.6 Based on clinical expert input, the sponsor assumed that 27% of patients being treated with second-line therapy receive FLAG-IDA and 73% receive gilteritinib. Administration costs for treatments administered intravenously or subcutaneously were sourced from Stewart et al.,15 assuming a 1-hour administration time for IV treatments and 0.5 hours for subcutaneous treatments. Treatment monitoring, allogeneic HSCT, AE, and disease monitoring costs were sourced from published literature, previous CADTH Reimbursement Review Reports, and publicly available costing and pricing data from Canada.16-24 The frequency of AEs was based on grade 3, 4, or 5 treatment-emergent AEs occurring in at least 5% of the respective trial populations (in the QuANTUM-First and RATIFY studies) and costs were applied as a 1-time cost in the first model cycle.5,8 Lastly, a 1-time terminal care cost was included, encompassing expenses related to end-of-life care based on estimates from the literature.16 All costs were reported in 2024 Canadian dollars; prices were inflated using the Consumer Price Index where required.
Summary of Sponsor’s Economic Evaluation Results
The base-case analysis was run probabilistically (5,000 iterations). The deterministic and probabilistic results were similar. The probabilistic findings are presented in the following.
Base-Case Results
The submitted analysis was based on publicly available prices of the comparator treatments. Results from the base case of the submitted economic evaluation are presented in Table 3. Additional results from the sponsor’s submitted economic evaluation base case are presented in Appendix 3.
In the sponsor’s submitted base case, the expected total costs and QALYs over a lifetime horizon (53 years) for quizartinib plus chemotherapy were $621,798 and 11.05, respectively. Quizartinib plus chemotherapy was associated with an ICER of $33,415 per QALY gained relative to midostaurin plus chemotherapy (incremental costs = $133,317; incremental QALYs = 3.99). Approximately 79% of the incremental QALYs for quizartinib plus chemotherapy were gained in the extrapolated period of the model (i.e., beyond the maximum follow-up time of 3.7 years observed in the QuANTUM-First trial). In the sponsor’s analysis, quizartinib plus chemotherapy had a 71% probability of being cost-effective at a WTP threshold of $50,000 per QALY gained. The key drivers of the results were the RFS hazard ratio (i.e., QALYs gained in the CR1 health state) and first-line drug acquisition costs.
Table 3: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER vs. midostaurin plus chemotherapy ($/QALY) |
|---|---|---|---|---|---|
Midostaurin plus chemotherapy | 488,481 | Reference | 7.06 | Reference | Reference |
Quizartinib plus chemotherapy | 621,798 | 133,317 | 11.05 | 3.99 | 33,415 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; vs. = versus.
Source: Sponsor’s pharmacoeconomic submission.1
Sensitivity and Scenario Analysis Results
The sponsor conducted various scenario analyses encompassing considerations such as alternative discount rates, time horizons, utility values, parametric survival curve distributions, AE frequencies, cure points, comparators, and adopting alternative rates of death, relapse rates postallogeneic HSCT, and CR. Additionally, the sponsor conducted an analysis in which clinical inputs were derived using the ML-NMR approach rather than the MAIC used in the sponsor’s base case. The most influential scenarios were the analyses comparing quizartinib plus chemotherapy to standard chemotherapy only (ICER = $106,303 per QALY gained), adopting a shorter 10-year time horizon (ICER = $105,411 per QALY gained), and using the ML-NMR ITC approach to inform clinical efficacy (ICER = $58,179 per QALY gained).1
Lastly, the sponsor conducted a scenario analysis from a societal perspective; this analysis included additional costs associated with productivity loss for patients and caregivers. In this analysis, relative to midostaurin plus chemotherapy, the ICER was $33,669 per QALY gained. This was similar to the sponsor’s base-case analysis using a health care payer perspective.
CDA-AMC Appraisal of the Sponsor’s Economic Evaluation
CDA-AMC identified several key limitations to the sponsor’s analysis that have notable implications for the economic analysis.
Comparative efficacy of quizartinib and midostaurin is highly uncertain: Because there was no head-to-head comparison between quizartinib and midostaurin, which is the current standard of care in Canada for patients with newly diagnosed AML that is FLT3-ITD positive in the induction and consolidation phase, the sponsor submitted an anchored MAIC, supported by a ML-NMR to address this gap.4,25 However, both ITCs are associated with limitations. The ITCs compared quizartinib and midostaurin based on data in which the treatments were used in the induction, consolidation, and maintenance phases (albeit with differing durations of maintenance use; a maximum of 12 cycles for midostaurin and 36 cycles for quizartinib). However, midostaurin is not indicated for use in maintenance treatment in Canada. Neither the QuANTUM-First trial nor the RATIFY trial were designed to inform on the contribution of the maintenance phase to the overall efficacy, thus the MAIC cannot inform on the contribution of each treatment phase separately. Furthermore, the MAIC did not adequately adjust for important treatment-effect modifiers so as to maintain at least 50% of the original sample size; this resulted in residual confounding, and the effective sample size of 53.7% reduced precision in the estimates. Additionally, differences in outcome reporting between the 2 trials could introduce bias; the definition of CIR was not reported in the RATIFY study publications, and it is unknown whether differences in the definition across the randomized controlled trials could have biased the results. Moreover, the MAIC only included a cohort aged 60 years or younger, which does not adequately reflect the population in Canada likely to receive quizartinib; the ML-NMR is potentially more reflective of the population in Canada, although it is associated with its own limitations. Further limitations on the comparative evidence are outlined in the CDA-AMC clinical review.
The CDA-AMC clinical review noted that most of the results from both ITCs did not show a statistically significant improvement with quizartinib over midostaurin (i.e., the 95% credible interval crossed the null), except for the MAIC result for CIR (hazard ratio = 0.42; 95% CI, 0.20 to 0.91). In the sponsor’s base case, the MAIC was selected to inform the clinical inputs of the model. This input was the key driver of the differences between quizartinib and midostaurin. However, because the RATIFY study had narrower eligibility criteria than the QuANTUM-First study, the generalizability of the results is highly impacted by this restricted population in the ITC, considering the large proportion of patients aged older than 60 years in this indication (60% to 70% according to the clinical experts consulted). The CDA-AMC clinical review appraisal noted that the results for this outcome were too uncertain to determine given limitations specific to the CIR outcome (it was measured only in the subpopulation of patients who experienced complete response, so randomization is not maintained, resulting in a high risk of bias; and the definition of CIR could not be ascertained for the RATIFY trial, so it is unknown whether the definition of this end point was similar across the 2 trials). According to the CDA-AMC clinical review and clinical experts consulted, the evidence from these ITCs was insufficient to demonstrate superiority of quizartinib over midostaurin, particularly in the induction and consolidation phases.
To obtain transition probabilities for the midostaurin arm, the sponsor assumed proportional hazards and thus applied a hazard ratio for midostaurin to the reference survival curves. This assumption implied that the relative risk reduction due to treatment remains constant throughout the lifetime horizon of the model. However, the sponsor acknowledged that the conditions for assuming proportional hazards were not met, yet they maintained this assumption in their model.
Finally, in the sponsor’s base case, it was assumed that the death and relapse rates for postallogeneic HSCT in the midostaurin plus chemotherapy arm were the same as standard of care, which were higher than those for the quizartinib plus standard of care arm. However, clinical experts consulted by CDA-AMC indicated that there is no evidence to support this assumption.
In the CDA-AMC reanalysis, ML-NMR was selected to inform the clinical inputs of the model, as it was deemed more applicable to the population that are eligible for quizartinib. CDA-AMC acknowledges the limitations with the ML-NMR and as a result, taking into consideration feedback from the clinical experts consulted, the postallogeneic HSCT death and relapse rates in the midostaurin arm were assumed to be the same as those in the quizartinib arm and the transition probabilities in the induction and consolidation phases were assumed to be the same across the 2 arms to explore the contribution of benefit in the maintenance phase. This aligned with the clinical expert feedback which noted that there is not expected to be a difference in the induction and consolidation phases, and that the incremental benefit for quizartinib would be in the maintenance phase in which they hope to see a reduction in relapses and increase in OS.
CDA-AMC undertook a scenario analysis in which all comparative benefits of quizartinib over midostaurin were assumed to be equivalent, given the lack of robust evidence to determine a benefit for quizartinib over midostaurin. The incremental costs will differ based on the duration of treatment with quizartinib.
CDA-AMC was unable to address the limitation of lack of disaggregated results by distinct treatment phases due to the inflexibility of the model structure.
Long-term efficacy of quizartinib is uncertain. The follow-up period of the QuANTUM-First trial was 3.7 years, while the time horizon of the economic model was lifetime (53 years). The sponsor extrapolated the time-varying data beyond the time horizon of the trial by using survival modelling. With the parametric function selected by the sponsor, approximately 79% of the incremental QALYs for quizartinib plus chemotherapy were accrued in the extrapolated period of the model, which contributes to the uncertainty in the long-term clinical benefits. Additionally, visual inspection indicated poor fit between the survival curves by selected parametric function and the KM curves, further increasing uncertainty regarding the long-term efficacy of quizartinib.
The sponsor applied a “cure model” approach to estimate the proportion of patients who are “cured.” Cured patients were defined as those remaining in the CR1 and allogeneic HSCT in the first line health states beyond 3 years and followed a survival function that was in line with the general population with an additional risk of excess mortality. According to the clinical experts consulted by CDA-AMC, given the probability of relapse for CR1 and allogeneic HSCT in the first line, it would be more appropriate to define cured patients as those who remain in the CR1 and allogeneic HSCT in the first line health states for at least 5 years.
Finally, the maintenance regimen provided in the RATIFY study is not reflective of clinical practice in Canada. Although the RATIFY study allowed for 12 cycles of maintenance therapy, midostaurin is not approved in Canada for this indication. The contribution of the maintenance phase in the RATIFY study to the overall efficacy of midostaurin and impact on the comparative effect estimates from the MAIC cannot be determined.
In the CDA-AMC reanalysis, patients who remain in the CR1 and allogeneic HSCT in the first line health states for 5 years were assumed to be “cured.”
CDA-AMC was unable to address the uncertainty in the extrapolated data, and the uncertainty in results of the maintenance phase caused by the inappropriate use of comparator cannot be solved.
Drug acquisition costs are uncertain. The clinical inputs in the model were sourced from the MAIC which used data from the QuANTUM-First and RATIFY trials. However, because both trials were not designed to inform on the contribution of the induction, consolidation, and maintenance phases of treatment independent of the overall efficacy of the treatment, the MAIC conducted by the sponsor cannot inform the contribution of each of these distinct treatment phases. This limitation poses a challenge in determining the optimal duration of quizartinib maintenance therapy and introduces uncertainty in the cost estimate. Additionally, clinical data from the RATIFY study were used to estimate the efficacy of midostaurin in maintenance therapy, but the drug acquisition costs for midostaurin maintenance were not included in the model as midostaurin is not indicated for maintenance use in Canada. Instead, the sponsor assumed that 15% of patients would receive azacitidine as a maintenance treatment. This discrepancy in sources between clinical efficacy data and economic inputs introduces uncertainty in the overall cost estimates.
CDA-AMC was unable to address the uncertainty in the drug acquisition costs discussed previously due to the inherent limitation of the trial design and the inflexibility of the model structure.
Poor modelling practices were employed. As described previously, the model submitted by the sponsor did not report or provide the flexibility to obtain the disaggregated results for clinical benefit and costs in each treatment phase. This limitation is particularly relevant given the overall ITC results compared quizartinib and midostaurin based on data in which the treatments were used in the induction, consolidation, and maintenance phases (albeit with differing durations of maintenance use; a maximum of 12 cycles for midostaurin and 36 cycles for quizartinib). The CDA-AMC clinical review appraisal of the indirect evidence identified significant limitation with the comparative evidence, such that credible conclusions could not be drawn or that there is evidence of similar efficacy.
CDA-AMC conducted a reanalysis to explore the clinical benefit generated in the maintenance phase as described previously.
Additionally, the following key assumptions were made by the sponsor and have been appraised by CDA-AMC (refer to Table 4).
Table 4: Key Assumptions of the Submitted Economic Evaluation
Sponsor’s key assumption | CDA-AMC comment |
|---|---|
15% of patients treated with midostaurin plus chemotherapy were assumed to receive azacitidine as maintenance therapy. | Potentially appropriate. According to clinical experts consulted by CDA-AMC, azacitidine is the only approved drug for maintenance therapy in patients with intermediate-risk or poor-risk AML in CR1 who are not eligible for allogeneic HSCT. |
In the 2L setting, 73% of patients will receive gilteritinib, and 27% will receive FLAG-IDA. | Potentially appropriate. The assumption aligns with the clinical expert feedback obtained by CDA-AMC regarding 2L treatment. |
Patients who do not achieve CR or CRi, even those who experience a partial response to treatment, are assumed to be equivalent to refractory patients (i.e., patients who do not achieve CR). | Potentially appropriate. The assumption aligns with the clinical expert feedback obtained by CDA-AMC. However, the clinical expert consulted by CDA-AMC also noted that patients who do not achieve CR or CRi would be eligible to receive salvage therapy with gilteritinib and would have a better outcome when they get to allogeneic HSCT after salvage therapy. |
Health utilities in health states of CR, maintenance, allogeneic HSCT recovery, and postallogeneic HSCT 1L maintenance were assumed to be similar to those of the general population in Canada. | Inappropriate but unlikely to be a key model driver. According to clinical experts consulted by CDA-AMC, quality of life after allogeneic HSCT may be deteriorated by long-term complications such as cognitive dysfunction. |
2L = second line; AML = acute myeloid leukemia; CDA-AMC = Canada's Drug Agency; CR = complete remission; CR1 = complete remission in first line; CRi = complete remission with incomplete hematologic recovery; FLAG-IDA = a combination of fludarabine, cytarabine, idarubicin, and filgrastim; HSCT = hematopoietic stem cell transplant; HSCT 1L = allogeneic hematopoietic stem cell transplant in first line.
CDA-AMC Reanalyses of the Economic Evaluation
Base-Case Results
The CDA-AMC base case was derived by making changes in model parameter values and assumptions, in consultation with clinical experts. Changes to the sponsor’s analyses are summarized in Table 5 and include replacing the sponsor’s MAIC with ML-NMR to inform model inputs, adjusting the postallogeneic HSCT survival assumption for the midostaurin arm, revising the assumption of comparative efficacy for quizartinib plus chemotherapy over midostaurin plus chemotherapy in the induction and consolidation phases, and modifying the definition of cured patients.
Table 5: CDA-AMC Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CDA-AMC value or assumption |
|---|---|---|
Changes to derive the CDA-AMC base case | ||
1. Source of comparative efficacy | MAIC | ML-NMR |
2. Postallogeneic HSCT survival for midostaurin | Same as SoC arm | Same as quizartinib arm |
3. Transition probabilities for CR1 to dead and CR1 to relapse in 2 arms during induction and consolidation phases | Sourced from MAIC | Transition probabilities for CR1 to dead and CR1 to relapse for quizartinib arm were assumed to be same as those in midostaurin arm in induction and consolidation phase |
4. Definition of cured patients | Patients who remain in the CR1 and allogeneic HSCT 1L health states for 3 years | Patients who remain in the CR1 and allogeneic HSCT 1L health states for 5 years |
CDA-AMC base case | Reanalysis 1 + 2 + 3 + 4 | |
CDA-AMC = Canada's Drug Agency; CR1 = complete remission in first line; HSCT = hematopoietic stem cell transplant; HSCT 1L = allogeneic hematopoietic stem cell transplant in first line; ITC = indirect treatment comparison; MAIC = matching-adjusted indirect comparison; ML-NMR = multilevel network meta-regression; SoC = standard of care.
In the CDA-AMC base case, quizartinib plus chemotherapy was associated with a total cost of $626,377 and 6.43 QALYs, compared to $513,385 and 5.35 QALYs for the midostaurin plus chemotherapy (Table 6). The resulting ICER for quizartinib plus chemotherapy compared to midostaurin plus chemotherapy was $104,121 per QALY, with a 7% probability of cost-effectiveness at a WTP threshold of $50,000 per QALY.
Results of the CDA-AMC reanalysis were driven by the RFS hazard ratio for quizartinib plus chemotherapy over midostaurin plus chemotherapy, as well as the drug acquisition cost in CR1. In the CDA-AMC base case, 84% of the incremental costs were accrued by FLT3 inhibitor drug acquisition cost, and incremental QALYs were only accrued in the CR 1 health state. Further details and disaggregated outcomes are available in Table 12.
Table 6: Summary of the Stepped Analysis of the CDA-AMC Reanalysis Results
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALY) |
|---|---|---|---|---|
Sponsor’s base case | Midostaurin plus chemotherapy | 488,481 | 7.06 | Reference |
Quizartinib plus chemotherapy | 621,798 | 11.05 | 33,415 | |
CDA-AMC reanalysis 1: Source of comparative efficacy | Midostaurin plus chemotherapy | 480,863 | 6.10 | Reference |
Quizartinib plus chemotherapy | 608,578 | 8.30 | 58,179 | |
CDA-AMC reanalysis 2: Postallogeneic HSCT survival for midostaurin plus chemotherapy | Midostaurin plus chemotherapy | 487,928 | 8.53 | Reference |
Quizartinib plus chemotherapy | 627,651 | 11.66 | 44,851 | |
CDA-AMC reanalysis 3: Transition probabilities in 2 arms during induction and consolidation phases | Midostaurin plus chemotherapy | 490,378 | 7.73 | Reference |
Quizartinib plus chemotherapy | 617,131 | 10.67 | 43,297 | |
CDA-AMC reanalysis 4: Definition of cured patients | Midostaurin plus chemotherapy | 523,029 | 6.02 | Reference |
Quizartinib plus chemotherapy | 665,735 | 10.03 | 35,541 | |
CDA-AMC base case (reanalyses 1 + 2 + 3 + 4) | Midostaurin plus chemotherapy | 516,927 | 5.36 | Reference |
Quizartinib plus chemotherapy | 629,225 | 6.59 | 91,581 | |
CDA-AMC base case (reanalyses 1 + 2 + 3 + 4) (probabilistic) | Midostaurin plus chemotherapy | 513,385 | 5.35 | Reference |
Quizartinib plus chemotherapy | 626,377 | 6.43 | 104,121 |
CDA-AMC = Canada's Drug Agency; HSCT = hematopoietic stem cell transplant; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Scenario Analysis Results
CDA-AMC conducted price analyses based on the sponsor’s base case and the CDA-AMC base-case reanalysis. Based on the CDA-AMC base case, a price reduction of approximately 33.3% would be required to achieve cost-effectiveness at a WTP threshold of $50,000 per QALY (Table 7).
CDA-AMC conducted a scenario analysis to assess the impact on the cost-effectiveness of quizartinib if approval were limited to induction and consolidation therapy only. In this analysis, all comparative benefit for quizartinib plus chemotherapy over midostaurin plus chemotherapy was assumed to be zero, and the costs in the maintenance phase for quizartinib plus chemotherapy were assumed to be same as those in the maintenance phase for midostaurin plus chemotherapy.
Table 7: CDA-AMC Price Reduction Analyses
Analysis: price reduction | Unit drug cost 17.7 mg and 26.5 mg tablet ($) | ICERs for quizartinib plus chemotherapy vs. midostaurin plus chemotherapy ($/QALY) | |
|---|---|---|---|
Sponsor base case | CDA-AMC reanalysis | ||
No price reduction | 388.29 | 35,729 | 104,121 |
10% | 349.46 | 30,084 | 87,867 |
20% | 310.62 | 24,439 | 71,594 |
30% | 271.80 | 18,794 | 55,322 |
33.3% | 258.99 | 16,931 | 50,000 |
40% | 232.97 | 13,148 | 39,049 |
CDA-AMC = Canada's Drug Agency; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; vs. = versus.
In the CDA-AMC scenario analysis, where quizartinib was assumed to be approved only for induction and consolidation therapy, there was no comparative benefit in QALYs, and quizartinib plus chemotherapy was associated with incremental costs of $10,467.
Issues for Consideration
The clinical experts highlighted that there is a phase I/II trial currently under way among pediatric and young adult patients with relapsed or refractory, FLT3-ITD–positive AML.26 As such, quizartinib is currently being used in pediatric patients in some centres on a trial basis. However, the clinical experts noted that they could not recommend its use in patients aged younger than 18 years at this time given the lack of published evidence in this population.
Although testing for FLT3-ITD mutations is currently performed as part of the standard of care for patients with newly diagnosed AML, testing for FLT3-ITD minimal or measurable residual disease is not currently funded or used in clinical practice. This may limit its clinical utility, as it is being evaluated routinely for an increasing number of AML subtypes as a potential marker of prognosis and to inform treatment decision-making.27
In 2024, NICE reviewed quizartinib for adults with newly diagnosed FLT3-ITD–positive AML when used with standard cytarabine and anthracycline chemotherapy as induction treatment, then with standard cytarabine chemotherapy as consolidation treatment, then alone as maintenance treatment. The NICE reviewers identified several limitations with the sponsor’s economic evaluation, relating to the uncertainty in the comparative evidence, the way clinical data had been applied in the economic model, and that the results from the sponsor’s base case were highly unreliable and lacked face validity. NICE reviewers revised the structure of the model and revised several assumptions and data sources to arrive at their base case. Ultimately the NICE committee agreed that it was uncertain whether quizartinib improved the rate of relapse, because of the lack of statistical significance in the ITC results. But it also agreed that the point estimates were improved with quizartinib and so a small incremental QALY could be plausible.28
Overall Conclusions
According to the CDA-AMC clinical review, results from the QuANTUM-First study suggest that when used in combination with standard induction and consolidation chemotherapy (and/or allogeneic HSCT), then as maintenance therapy for up to 36 cycles, quizartinib likely results in a clinically important increase in OS and may result in an increase in RFS compared to placebo. The overall safety profile for quizartinib was acceptable to the clinical experts consulted for this review, although the notable harms may restrict its use in patients with some comorbid conditions. Important limitations of the QuANTUM-First study include the lack of re-randomization before the maintenance phase and the limited applicability of the comparator. In the absence of re-randomization, the design of the QuANTUM-First study does not allow for isolation of the contribution of the maintenance treatment to the overall efficacy of quizartinib. However, the relevant comparator in the induction and consolidation phases is midostaurin plus chemotherapy (midostaurin is not indicated for the maintenance phase). Population-adjusted ITCs were submitted by the sponsor to address the lack of direct evidence comparing quizartinib with midostaurin, the current standard of care. Due to important methodologic limitations and imprecision in the comparative effect estimates from the ITCs, the clinical reviewers concluded that the comparative efficacy and harms of quizartinib versus midostaurin are uncertain. The clinical experts consulted by CDA-AMC indicated that the primary benefit for quizartinib is the availability to use the treatment in the maintenance phase with the goal of reducing the risk of relapse and prolonging OS. However, there was no robust evidence to validate this information. In practice in Canada, a small proportion of individuals may receive azacitidine in the maintenance phase; there is no comparative evidence assessing quizartinib and azacitidine as maintenance therapy.
CDA-AMC undertook reanalyses to address some of the key limitations in the sponsor’s analysis which included: selecting ML-NMR to inform the clinical inputs of the model, assuming death and relapse rates postallogeneic HSCT for patients receiving midostaurin plus chemotherapy to be same as those receiving quizartinib plus chemotherapy, assuming transition probabilities in induction and consolidation phases to be same across 2 arms, and defining patients staying in the CR1 and allogeneic HSCT in the first line health states for 5 years as cured. The CDA-AMC reanalysis resulted in an ICER for quizartinib plus chemotherapy versus midostaurin plus chemotherapy of $104,121 per QALY gained (incremental cost = $112,992; incremental QALYs = 1.09; incremental LYs = 1.09). A price reduction of 33.3% (from $388.29 to $258.99 per 17.7 mg and 26.5 mg per oral tablet) was necessary for quizartinib to be considered cost-effective at a WTP threshold of $50,000 per QALY gained.
The cost-effectiveness of quizartinib plus chemotherapy is driven by an assumed benefit in RFS for quizartinib plus chemotherapy compared with midostaurin plus chemotherapy, as well as the drug acquisition cost for an FLT3 inhibitor in CR1. However, given both the sponsor and CDA-AMC analyses were limited by the lack of head-to-head clinical evidence to inform relative treatment effects, the cost-effectiveness of quizartinib and price reduction estimates are highly uncertain. Further price reductions may be warranted to address this uncertainty.
References
1.Daiichi Sankyo Canada. Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Quizartinib, 17.7 mg and 26.5 mg oral tablets. December 2024.
2.Erba HP, Montesinos P, Kim HJ, et al. Quizartinib plus chemotherapy in newly diagnosed patients with FLT3-internal-tandem-duplication-positive acute myeloid leukaemia (QuANTUM-First): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet. 2023;401(10388):1571-1583. doi: 10.1016/S0140-6736(23)00464-6 PubMed
3.Daiichi Sankyo Pharma Canada Ltd. Quizartinib: 17.7 mg and 26.5 mg tablets [product monograph]. 2024.
4.Daiichi Sankyo Inc. Matching Adjusted Indirect Treatment Comparison of Quizartinib vs Midostaurin, version 3 [sponsor supplied reference]. 2024.
5.Stone RM, Mandrekar SJ, Sanford BL, et al. Midostaurin plus Chemotherapy for Acute Myeloid Leukemia with a FLT3 Mutation. N Engl J Med. 2017;377(5):454-464. doi: 10.1056/NEJMoa1614359 PubMed
6.Perl AE, Martinelli G, Cortes JE, et al. Gilteritinib or Chemotherapy for Relapsed or Refractory FLT3-Mutated AML. N Engl J Med. 2019;381(18):1728-1740. doi: 10.1056/NEJMoa1902688 PubMed
7.IQVIA RWS Canada. Primary Market Research in Acute Myeloid Leukemia (AML) to Support Economic Evaluation of Quizartinib [sponsor supplied reference]. 2024.
8.Daiichi Sankyo, Inc. Clinical Study Report: AC220-A-U302. A Phase 3, Double-blind, Placebo-controlled Study of Quizartinib Administered in Combination with Induction and Consolidation Chemotherapy, and Administered as Continuation Therapy in Subjects 18 to 75 Years Old with Newly Diagnosed FLT3-ITD (+) Acute Myeloid Leukemia (QuANTUM-First) [internal sponsor's report]. 2022.
9.National Institute for Health and Care Excellence. Midostaurin for untreated acute myeloid leukaemia (NICE Technology appraisal guidance TA523) [accessed by sponsor]. 2018. https://www.nice.org.uk/guidance/ta523/resources/midostaurin-for-untreated-acute-myeloid-leukaemia-pdf-82606838794693
10.Grulke N, Albani C, Bailer H. Quality of life in patients before and after haematopoietic stem cell transplantation measured with the European Organization for Research and Treatment of Cancer (EORTC) Quality of Life Core Questionnaire QLQ-C30. Bone Marrow Transplant. 2012;47(4):473-82. doi: 10.1038/bmt.2011.107 PubMed
11.Crott R, Briggs A. Mapping the QLQ-C30 quality of life cancer questionnaire to EQ-5D patient preferences. Eur J Health Econ. 2010;11(4):427-34. doi: 10.1007/s10198-010-0233-7 PubMed
12.Guertin JR, Feeny D, Tarride JE. Age- and sex-specific Canadian utility norms, based on the 2013-2014 Canadian Community Health Survey. CMAJ. 2018;190(6):E155-E161. doi: 10.1503/cmaj.170317 PubMed
13.Peric Z, Desnica L, Durakovic N, et al. Which questionnaires should we use to evaluate quality of life in patients with chronic graft-vs-host disease? Croat Med J. 2016;57(1):6-15. doi: 10.3325/cmj.2016.57.6 PubMed
14.National Institute for Health and Care Excellence. Quizartinib for induction, consolidation and maintenance treatment of newly diagnosed FLT3-ITD-positive acute myeloid leukaemia [accessed by sponsor]. 2024. https://www.nice.org.uk/guidance/ta1013
15.Stewart DA, Boudreault JS, Maturi B, Boras D, Foley R. Evaluation of subcutaneous rituximab administration on Canadian systemic therapy suites. Curr Oncol. 2018;25(5):300-306. doi: 10.3747/co.25.4231 PubMed
16.Guinan K, Mathurin K, Au Y, et al. Venetoclax in Combination with Azacitidine for the Treatment of Newly Diagnosed Acute Myeloid Leukemia: A Canadian Cost-Utility Analysis. Curr Oncol. 2022;29(10):7524-7536. doi: 10.3390/curroncol29100592 PubMed
17.Ontario Ministry of Health. Schedule of benefits for laboratory services [accessed by sponsor]. 2023. https://www.ontario.ca/files/2024-01/moh-ohip-schedule-of-benefits-laboratory-services-2024-01-24.pdf
18.Ontario Ministry of Health and Long-Term Care. Schedule of Benefits, Physician Services Under the Health Insurance Act [accessed by spopnsor]. 2024. https://www.ontario.ca/files/2024-08/moh-schedule-benefit-2024-08-30.pdf
19.Hu Y, Charaan M, van Oostrum I, Heeg B, Bell T. The cost-effectiveness of glasdegib in combination with low-dose cytarabine, for the treatment of newly diagnosed acute myeloid leukemia in adult patients who are not eligible to receive intensive induction chemotherapy in Canada. J Med Econ. 2021;24(1):150-161. doi: 10.1080/13696998.2021.1875743 PubMed
20.pCODR Final Economic Guidance Report - Midostaurin (Rydapt) for Acute Myeloid Leukemia [accessed by sponsor]. 2017. https://www.cda-amc.ca/sites/default/files/pcodr/pcodr_midostaurin_rydapt_all_fn_egr.pdf
21.Furzer J, Gupta S, Nathan PC, et al. Cost-effectiveness of Tisagenlecleucel vs Standard Care in High-risk Relapsed Pediatric Acute Lymphoblastic Leukemia in Canada. JAMA Oncol. 2020;6(3):393-401. doi: 10.1001/jamaoncol.2019.5909 PubMed
22.Canadian Institute for Health Information. Patient Cost Estimator [accessed by sponsor]. https://www.cihi.ca/en/patient-cost-estimator
23.Common Drug Review Pharmacoeconomic Review Report for Signifor [accessed by sponsor]. 2015. https://www.cda-amc.ca/sites/default/files/cdr/pharmacoeconomic/SR0372_Signifor_PE_Report.pdf
24.Wehler E, Zhao Z, Pinar Bilir S, Munakata J, Barber B. Economic burden of toxicities associated with treating metastatic melanoma in eight countries. Eur J Health Econ. 2017;18(1):49-58. doi: 10.1007/s10198-015-0757-y PubMed
25.Daiichi Sankyo Pharma Canada. Multi-level network meta-regression quizartinib [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Vanflyta (quizartinib), 17.7 mg or 26.5 mg oral tablets. March 2024.
26.Zwaan CM, Kolb EA, Mires DE, et al. A Phase 1/2 Study of Quizartinib (Q) in Combination with Re-Induction Chemotherapy and As Single-Agent Continuation Therapy in Pediatric and Young Adult Patients with Relapsed/Refractory (R/R) FLT3-ITD Acute Myeloid Leukemia (AML). Blood. 2019;134(Supplement_1):3937-3937. doi: 10.1182/blood-2019-121736
27.Heuser M, Ofran Y, Boissel N, et al. Acute myeloid leukaemia in adult patients: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2020;31(6):697-712. doi: 10.1016/j.annonc.2020.02.018 PubMed
28.National Institute for Health and Care Excellence. Quizartinib for induction, consolidation and maintenance treatment of newly diagnosed FLT3-ITD-positive acute myeloid leukaemia (NICE Technology appraisal guidance TA1013) [accessed by sponsor]. 2024. https://www.nice.org.uk/guidance/ta1013
29.IQVIA. DeltaPA. 2025. Accessed February 20, 2025. https://www.iqvia.com/
30.Statistics Canada. Table 17-10-0005-01 Population estimates on July 1, by age and gender [accessed by sponsor]. https://doi.org/10.25318/1710000501-eng
31.Statistics Canada. Number and rates of new cases of primary cancer, by cancer type, age group and sex [accessed by sponsor]. https://doi.org/10.25318/1310011101-eng
32.Tefferi A, Gangat N, Al-Kali A, et al. A dynamic 3-factor survival model for acute myeloid leukemia that accounts for response to induction chemotherapy. Am J Hematol. 2022;97(9):1127-1134. doi: 10.1002/ajh.26630 PubMed
33.Dohner H, Wei AH, Appelbaum FR, et al. Diagnosis and management of AML in adults: 2022 recommendations from an international expert panel on behalf of the ELN. Blood. 2022;140(12):1345-1377. doi: 10.1182/blood.2022016867 PubMed
34.Patented Medicine Prices Review Board. Markup Policies in Public Drug Plans, 2020/21 [accessed by sponsor]. 2023. https://www.canada.ca/en/patented-medicine-prices-review/services/npduis/analytical-studies/supporting-information/markup-policies-public-drug.html
Appendix 1: Cost Comparison Table
Please note that this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical experts and CDA-AMC participating drug plans. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 8: CDA-AMC Cost Comparison Table for FLT3-Mutated AML
Treatment | Strength / concentration | Form | Price ($) | Recommended dosage | Daily cost ($) | 28-day cost ($) |
|---|---|---|---|---|---|---|
Quizartinib | 17.7 mg 26.5 mg | Film-coated tablet | 388.2900a | Induction and consolidation: 35.4 mg once daily for 14 days in each 28-day cycle Maintenance: starting dose of 26.5 mg once daily for 14 days if QTcF ≤ 450 ms; then increase to 53 mg once daily if QTcF ≤ 450 ms; with no break between cycles | Induction and consolidation: 388.29 Maintenance: 582.44 for the first 28 days; 776.58 for the following cycles | Induction and consolidation: 10,872 Maintenance: 16,308 for the first 28 days; 21,744 for the following cycles |
Induction therapy (7 + 3 with quizartinib or midostaurin) | ||||||
Cytarabine | 100 mg/mL (5 mL vial) 100 mg/mL (20 mL vial) | Injectable solution | 306.5000 (15.3250 per mL) 76.8500 (15.37 per mL) | 100 mg/m2/day continuous IV infusion days 1 to 7 (≥ 60 years of age) 200 mg/m2/day continuous IV infusion days 1 to 7 (< 60 years of age) | 19.21 | 538 |
Daunorubicin | 20 mg/20mL vial 1 mg/mL (5 mL vial) | IV powdered solution | 95.0000 (4.7500 per mg) 211.5200 (42.304 per mL) | 60 mg/m2 IV days 1 to 3 | 61.07 | 1,710 |
Idarubicin | 1 mg/mL vial | IV solution (5 mL vial) | 211.5200 (42.3040 per mL in 5 mL vial) | 12mg/m2 days 1 to 3 | 113.31 | 3,173 |
Quizartinib | 17.7 mg and 26.5 mg per tablet | Film-coated tablet | 388.2900a | 35.4 mg once daily for 14 days in each cycle (up to 2 28-day cycles) | 388.29 | 10,872 |
Midostaurin | 25 mg | Capsule | 167.9248 | 50 mg twice daily on days 8 to 21 (up to 2 28-day cycles) | 335.85 | 9,404 |
7 + 3 induction therapy (quizartinib + cytarabine + daunorubicin) | 468.57 | 13,120 | ||||
7 + 3 induction therapy (quizartinib + cytarabine + idarubicin) | 520.72 | 14,538 | ||||
7 + 3 induction therapy (midostaurin + cytarabine + daunorubicin) | 416.13 | 11,652 | ||||
Consolidation therapy (high-dose cytarabine with quizartinib or midostaurin) | ||||||
Cytarabine | 100 mg/mL (5 mL vial) 100 mg/mL (20 mL vial) | Injectable solution | 306.5000 (15.3250 per mL) 76.8500 (15.37 per mL) | 1,500 mg/m2 every 12 hours on days 1, 3, 5 for age ≥ 60 years and 3,000 mg/m2 every 12 hours on days 1, 3, 5 for age < 60 years High-dose cytarabine: 3,000 mg every 12 hours on days 1, 3, and 5 | 181.15 | 5,072 |
Quizartinib | 17.7 mg and 26.5 mg per tablet | Film-coated tablet | 388.2900a | 35.4 mg once daily for 14 days in each cycle (up to 4 28-day cycles) | 388.29 | 10,872 |
Midostaurin | 25 mg | Capsule | 167.9248 | 50 mg twice daily on days 8 to 21 (up to 4 28-day cycles) | 335.85 | 9,404 |
Consolidation therapy (quizartinib + high-dose cytarabine) | 569.44 | 15,944 | ||||
Consolidation therapy (midostaurin + high-dose cytarabine) | 517.00 | 14,476 | ||||
Maintenance therapy | ||||||
Quizartinib | 17.7 mg 26.5 mg | Film-coated tablet | 388.2900a | Starting dose of 26.5 mg once daily for 14 days if QTcF ≤ 450 ms; then increase to 53 mg once daily if QTcF ≤ 450 ms; with no break between cycles (up to 36 28-day cycles) | Induction and consolidation: 388.29 Maintenance: 582.44 for the first 28 days; 776.58 for the following cycles | Induction and consolidation: 10,872 Maintenance: 16,308 for the first 28 days; 21,744 for the following cycles |
Azacitidine | 100 mg | Vial | 599.9900 | 75 mg/m2 IV or SC once daily on days 1 to 7 of each 28-day cycle | 300.00 | 8,400 |
QTcF = Fridericia's Heart Rate Correction Formula; IV = IV; SC = subcutaneous.
Note: All prices are from the IQVIA (accessed February 20 2025),29 unless otherwise indicated, and do not include dispensing fees. Assuming body surface area of 1.80 m2. No vial sharing.
aSponsor-submitted price. The price was the same for both the 17.7 mg and 26.5 mg tablets.
Appendix 2: Submission Quality
Please note that this appendix has not been copy-edited.
Description | Yes or No | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | No | Refer to key limitations discussed previously. The population in the MAIC was restricted by the narrower eligibility criteria in RATIFY than in QuANTUM-First. Additionally, the MAIC compared quizartinib and midostaurin based on data in which the treatments were used in the induction, consolidation, and maintenance phases, but midostaurin is not indicated for use in maintenance treatment in Canada. |
Model has been adequately programmed and has sufficient face validity | No | Refer to key limitations discussed previously. The model submitted by the sponsor did not report or provide the flexibility to obtain the disaggregated results for clinical benefit and costs in each treatment phase. |
Model structure is adequate for decision problem | No | It is partly adequate, but does not adequately capture the impact of differences in phases of treatment, given the lack of robust evidence to identify a difference between quizartinib and midostaurin. |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | Yes | No comment. |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | Yes | No comment. |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | Yes | No comment. |
MAIC = matching-adjusted indirect comparison.
Appendix 3: Additional Information on the Submitted Economic Evaluation
Please note that this appendix has not been copy-edited.
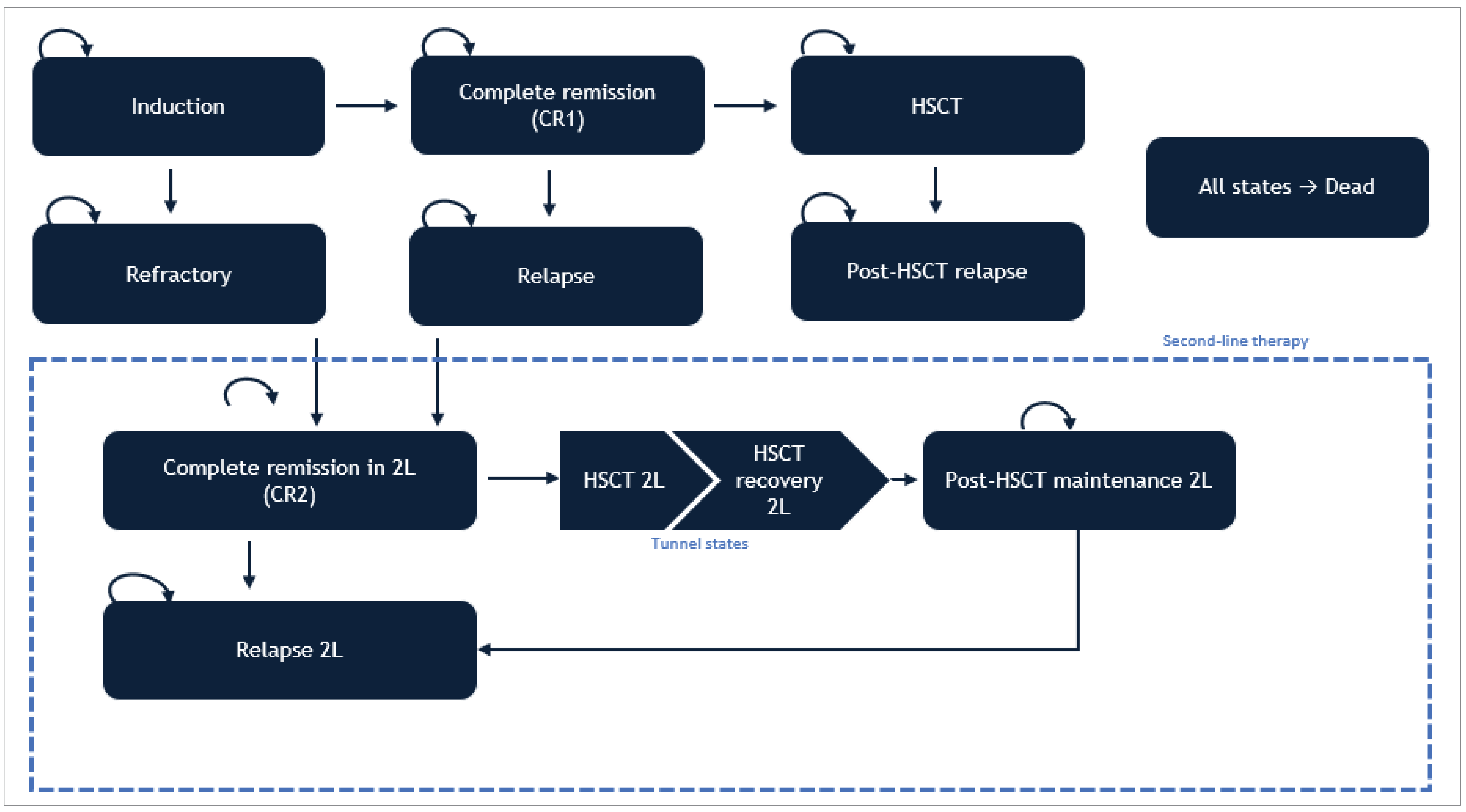
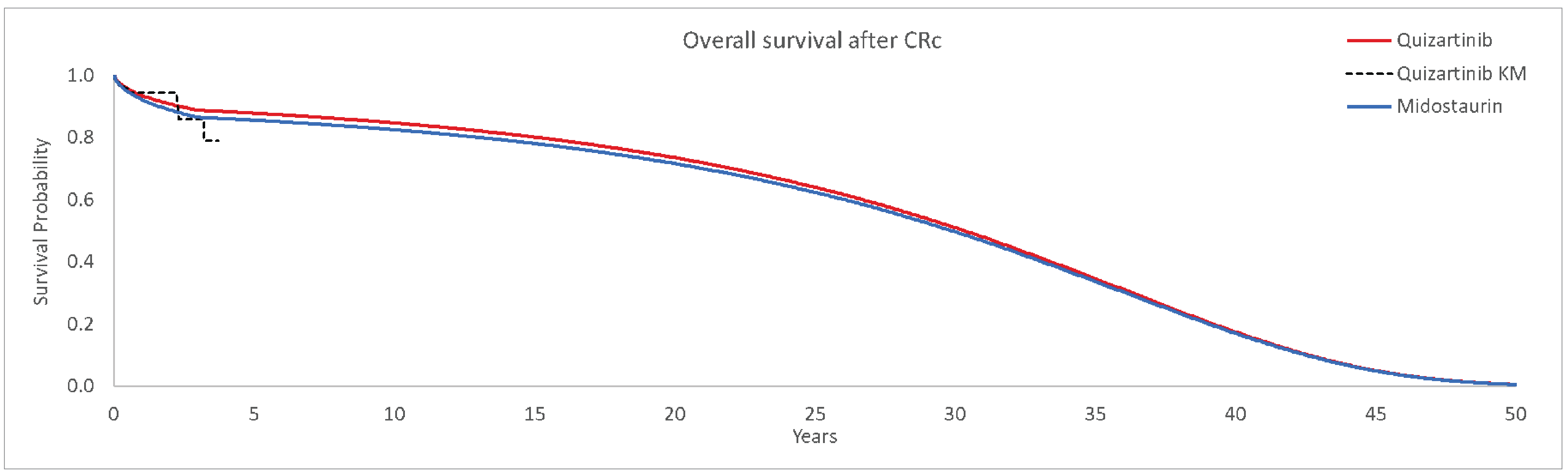
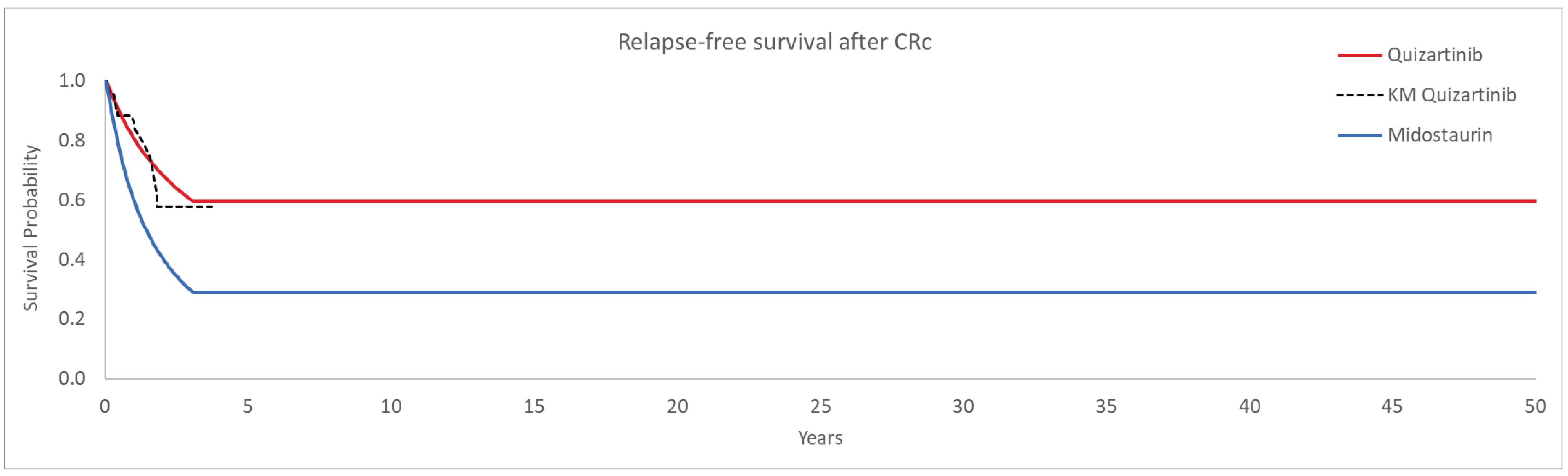
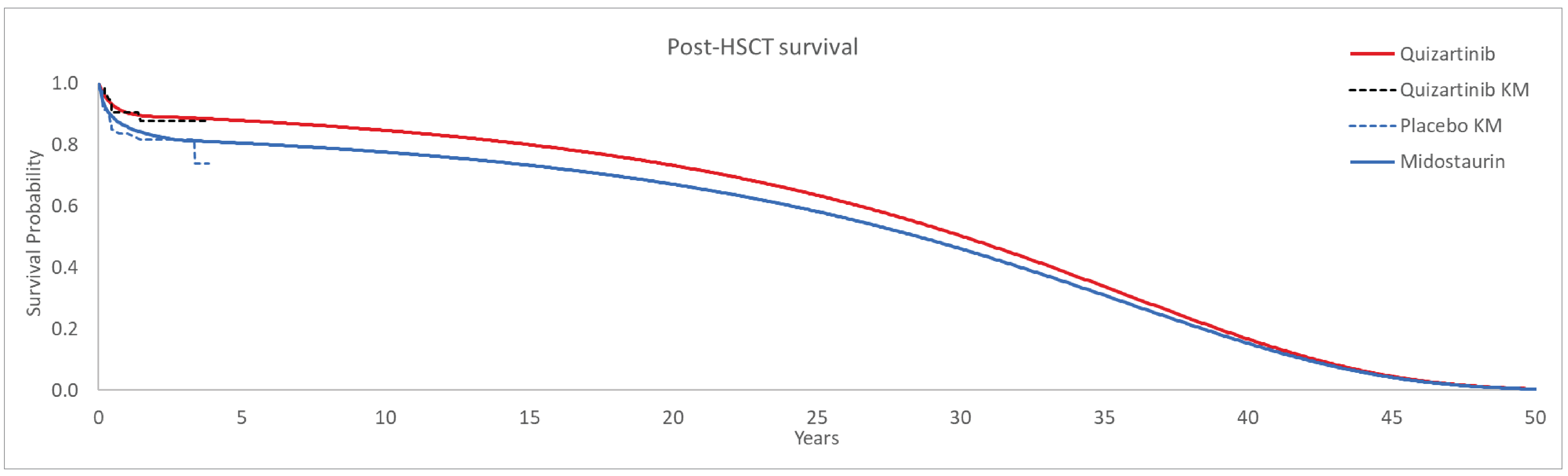
Detailed Results of the Sponsor’s Base Case
Table 10: Disaggregated Summary of the Sponsor’s Economic Evaluation Results
Parameter | Quizartinib plus chemotherapy | Midostaurin plus chemotherapy |
|---|---|---|
Discounted LYs | ||
Total | 11.74 | 7.77 |
Induction | 0.11 | 0.11 |
Refractory | 0.06 | 0.07 |
First CR | 6.33 | 3.09 |
Relapse | 0.04 | 0.06 |
Second CR | 0.28 | 0.40 |
Relapse 2 | 0.09 | 0.13 |
Allogeneic HSCT 1L | 4.47 | 3.42 |
Relapse after allogeneic HSCT 1L | 0.02 | 0.03 |
Allogeneic HSCT 2L | 0.02 | 0.03 |
Allogeneic HSCT recovery 2L | 0.05 | 0.07 |
Postallogeneic HSCT 2L maintenance | 0.25 | 0.36 |
Discounted QALYs | ||
Total | 11.05 | 7.06 |
Induction | 0.07 | 0.07 |
Refractory | 0.03 | 0.04 |
First CR | 6.11 | 2.94 |
Relapse | 0.02 | 0.03 |
Second CR | 0.21 | 0.30 |
Relapse 2 | 0.03 | 0.04 |
Allogeneic HSCT 1L | 4.33 | 3.30 |
Relapse after allogeneic HSCT 1L | 0.01 | 0.02 |
Allogeneic HSCT 2L | 0.01 | 0.02 |
Allogeneic HSCT recovery 2L | 0.04 | 0.05 |
Postallogeneic HSCT 2L maintenance | 0.19 | 0.27 |
AEs | −0.0063 | −0.0028 |
Discounted costs ($) | ||
Total | 621,798 | 488,481 |
1L drug acquisition | 229,137 | 55,705 |
1L admin and monitoring | 59,753 | 51,759 |
2L drug acquisition | 27,998 | 48,245 |
2L admin and monitoring | 15,128 | 22,764 |
Disease management | 189,094 | 201,068 |
FLT3-ITD testing | 87 | 87 |
AEs | 21,365 | 23,985 |
Terminal care | 79,236 | 84,868 |
Source: Sponsor’s pharmacoeconomic submission.1
Appendix 4: Additional Details on the CDA-AMC Reanalyses and Sensitivity Analyses of the Economic Evaluation
Please note that this appendix has not been copy-edited.
Detailed Results of CDA-AMC Base Case
Table 11: Disaggregated Summary of the CDA-AMC Economic Evaluation Results
Parameter | Quizartinib plus chemotherapy | Midostaurin plus chemotherapy |
|---|---|---|
Discounted LYs | ||
Total | 7.27 | 6.19 |
Induction | 0.10 | 0.10 |
Refractory | 0.08 | 0.08 |
First CR | 3.18 | 2.00 |
Relapse | 0.05 | 0.07 |
Second CR | 0.36 | 0.44 |
Relapse 2 | 0.13 | 0.15 |
Allogeneic HSCT 1L | 2.85 | 2.85 |
Relapse after allogeneic HSCT 1L | 0.03 | 0.03 |
Allogeneic HSCT 2L | 0.03 | 0.03 |
Allogeneic HSCT recovery 2L | 0.08 | 0.08 |
Postallogeneic HSCT 2L maintenance | 0.38 | 0.39 |
Discounted QALYs | ||
Total | 6.43 | 5.35 |
Induction | 0.07 | 0.07 |
Refractory | 0.04 | 0.04 |
First CR | 2.96 | 1.79 |
Relapse | 0.03 | 0.04 |
Second CR | 0.27 | 0.33 |
Relapse 2 | 0.03 | 0.04 |
Allogeneic HSCT 1L | 2.66 | 2.66 |
Relapse after allogeneic HSCT 1L | 0.02 | 0.02 |
Allogeneic HSCT 2L | 0.02 | 0.02 |
Allogeneic HSCT recovery 2L | 0.06 | 0.06 |
Postallogeneic HSCT 2L maintenance | 0.28 | 0.29 |
AEs | −0.0064 | −0.0028 |
Discounted costs ($) | ||
Total | 626,377 | 513,385 |
1L drug acquisition | 189,962 | 53,375 |
1L admin and monitoring | 53,884 | 49,972 |
2L drug acquisition | 37,655 | 51,869 |
2L admin and monitoring | 22,170 | 24,821 |
Disease management | 214,435 | 221,966 |
FLT3-ITD testing | 87 | 87 |
AEs | 22,533 | 24,183 |
Terminal care | 85,652 | 87,112 |
ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year; vs. = versus; CR = complete remission; HSCT = hematopoietic stem cell transplant; AE = adverse event; FLT3-ITD = FMS-like tyrosine kinase 3 internal tandem duplication.
Scenario Analyses
Table 12: Summary of CDA-AMC Scenario Analysis
Scenarios | Treatment | Total costs ($) | Total QALYs | ICER ($ per QALY) |
|---|---|---|---|---|
CDA-AMC base case | Midostaurin plus chemotherapy | 513,385 | 5.35 | Reference |
Quizartinib plus chemotherapy | 626,377 | 6.43 | 104,121 | |
CDA-AMC Scenario Analysis 1: Assuming quizartinib is only approved for induction and consolidation therapy | Midostaurin plus chemotherapy | 494,778 | 7.10 | Reference |
Quizartinib plus chemotherapy | 505,245 | 7.09 | Dominated |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Note: the scenario analysis was presented deterministically. The difference in QALYs is due to slight differences in AE profiles, which resulted in a greater QALY decrement for quizartinib compared with midostaurin (refer to Table 11 for further information).
Appendix 5: Submitted Budget Impact Analysis and CDA-AMC Appraisal
Please note that this appendix has not been copy-edited.
Table 13: Summary of Key Take-Aways
Key Take-aways of the budget impact analysis |
|---|
|
FLT-3-ITD = FMS-like tyrosine kinase 3 internal tandem duplication; FLAG-IDA = a combination of fludarabine, cytarabine, idarubicin, and filgrastim; BIA = budget impact analysis; AML = acute myeloid leukemia.
Summary of Sponsor’s Budget Impact Analysis
In the submitted budget impact analysis (BIA), the sponsor assessed the introduction of quizartinib plus chemotherapy for adult patients with newly diagnosed AML that is FLT3-ITD-mutated that are eligible/fit for intensive chemotherapy. The BIA was undertaken from the perspective of a Canadian public payer over a 3-year time horizon (2026 to 2028) using an epidemiological approach. The sponsor compared a reference scenario in which patients received midostaurin plus chemotherapy to a new drug scenario in which patients received either midostaurin plus chemotherapy or quizartinib plus chemotherapy. The sponsor’s submission only considered drug acquisition costs administered in an outpatient setting whereby unit drug costs were obtained from IQVIA DeltaPA.7 Data informing key parameters of the budget impact model were obtained from various sources including Statistics Canada,30,31 published literature,32 the QuANTUM-First and RATIFY clinical trials,5,8 a previous NICE review,9 published guidelines,33 internal estimates, the Patented Medicine Prices Review Board,34 clinical expert feedback, market research,7 and assumption. Key inputs to the BIA are documented in Table 14.
Key assumptions included:
All patients with newly diagnosed AML were assumed to undergo genetic testing for an FLT3-ITD mutation.
70% of patients are eligible to receive intensive chemotherapy.
Only drugs administered in an outpatient setting were included. It was assumed that in the induction phase, 8% of administrations occur in an outpatient setting. In the consolidation phase, 69% of administrations for midostaurin or quizartinib are in an outpatient setting and 89% of cytarabine administrations. In the maintenance phase, 100% of administrations occur in an outpatient setting.
Midostaurin is not used in the maintenance phase. Costs accrued for the regimen during this phase include the cost of azacitidine only. The mean time on treatment in the maintenance phase is set equal to quizartinib plus chemotherapy.
Duration of treatment for those initiating quizartinib was assumed to be 1.11 months in the induction phase, 1.23 months in the consolidation phase, and 4.95 months (year 1), 3.04 months (year 2) and 1.37 months (year 3) in the maintenance phase. Duration of treatment for those initiating midostaurin was assumed to be 1.08 months in the induction phase, 1.73 months in the consolidation phase, and 4.95 months (year 1), 3.04 months (year 2) and 1.37 months (year 3) months in the maintenance phase.
Dosing for cytarabine is 200 mg/m2 per day during the induction period and 3,000 mg/m2 per day during the maintenance phase.
The QuANTUM-First trial is representative of clinical practice for the proportion of patients who receive daunorubicin (46.4%) or idarubicin (56.3%) during the induction phase of patients treated with quizartinib plus chemotherapy.
Wastage of unused product in vials.
Table 14: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as year 1 / year 2 / year 3 if appropriate) | ||
|---|---|---|---|
Target population | |||
Population of people living in Canada (excluding Quebec) | 25,153,92430 | ||
AML incidence rate | 0.0049%31 | ||
Proportion tested for FLT3-ITD+ mutation | 100%a | ||
Proportion of patients with an FLT3-ITD+ mutation | 25%32 | ||
Proportion of patients eligible to receive intensive chemotherapy | 70%a | ||
Number of patients eligible for drug under review | 220 / 223 / 226 | ||
Market uptake (3 years) | |||
Uptake (reference scenario) Midostaurin plus chemotherapy | ████ █ ████ █ ████ | ||
Uptake (new drug scenario) Quizartinib plus chemotherapy Midostaurin plus chemotherapy | █████ █ █████ █ █████ █████ █ █████ █ █████ | ||
Cost of treatment (per patient, per month) | |||
Quizartinib plus chemotherapy Midostaurin plus chemotherapy | Induction $1,209.14 $1,036.18 | Consolidation $14,322.95 $13,157.02 | Maintenance $20,886.28 $3,259.86b |
AML = acute Myeloid Leukemia; FLT3-ITD+ = FMS-like tyrosine kinase 3 internal tandem duplication positive
aBased on expert opinion.
bNo patients receive midostaurin but assuming 15% of patients receive azacitidine in the maintenance phase
Summary of the Sponsor’s BIA Results
The sponsor estimated that the 3-year budget impact of reimbursing quizartinib plus chemotherapy for adult patients with newly diagnosed AML that is FLT3-ITD-mutated that are eligible/fit for intensive chemotherapy is expected to result in a cost of $21,469,962 (year 1 = $1,907,015; year 2 = $6,071,562; year 3 = $13,491,386).
CDA-AMC Appraisal of the Sponsor’s BIA
CDA-AMC identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
The market share before and after quizartinib is publicly reimbursed for the indication under review is uncertain. The sponsor assumed that before reimbursement, midostaurin would hold ████ of the market. After reimbursement, quizartinib’s market share was projected to be ███, ███, and ███ over 3 years. According to clinical experts consulted by CDA-AMC, up to 4% of patients with FLT3-ITD-mutated AML have a complex or poor-risk karyotype and would receive FLAG-IDA/MEC for induction chemotherapy. Additionally, if quizartinib is funded for maintenance therapy, its usage may exceed 50%, as physicians would prefer to administer it postallogeneic HSCT in the hope of reducing relapse and increasing OS. However, if quizartinib is not funded for maintenance, its market share would be significantly lower, as physicians would likely continue using midostaurin for induction and consolidation due to their familiarity with the medication.
CDA-AMC conducted a reanalysis by assuming a 4% market share for FLAG-IDA both before and after public funding of quizartinib and increased the market share of quizartinib in year 3 to 60%.
A scenario analysis was also conducted to assess market share if the indication for quizartinib does not include use in the maintenance phase. In this scenario, CDA-AMC assumed the market share for quizartinib would be 5%, 10%, and 20% based on clinical expert feedback, and maintenance therapy regimens in quizartinib arm were assumed to be the same as those in the comparator arm.
The proportion of patients eligible to receive intensive chemotherapy is uncertain. In the base case, the sponsor assumed that 70% of patients with FLT3-ITD-mutated AML would be eligible, resulting in an estimated 217 target patients for the indication under review in Canada (excluding Quebec). According to clinical experts consulted by CDA-AMC, this assumption is likely overestimated. Many patients are older with comorbidities and may not be suitable for intensive chemotherapy, while some (typically older patients with or without poor-risk/complex karyotype) may receive venetoclax plus azacitidine instead.
CDA-AMC conducted a reanalysis assuming that 60% of patients with FLT3-ITD mutated AML are eligible for intensive chemotherapy.
The treatment durations in induction and consolidation phases were uncertain. In the base case, the sponsor assumed a different treatment duration for midostaurin compared to quizartinib in the induction phase. In the consolidation phase, the treatment durations for midostaurin, chemotherapy, and FLAG-IDA differed from that of quizartinib. This assumption is inappropriate as it is not aligned with the economic evaluation.
CDA-AMC conducted a reanalysis assuming the same treatment duration for midostaurin and quizartinib in the induction and consolidation phases, and the same treatment duration for chemotherapy and FLAG-IDA as quizartinib in the consolidation phase.
CDA-AMC acknowledges that the duration of treatment by phase does not align with what was reported for the economic evaluation but was unable to revise the sponsor budget impact model to reflect these numbers to the lack of flexibility in the model.
The costs of subsequent treatment were not included. In base case, the sponsor excluded costs associated with subsequent treatment for patients who failed or relapsed after first-line therapy, such as FLAG-IDA and gilteritinib. This assumption was inappropriate, as both treatments are funded through the drug formulary, and the reimbursement of quizartinib would influence subsequent treatment use and impact the overall drug formulary budget due to the difference in efficacy from midostaurin. Additionally, only drugs administered in an outpatient setting were included (e.g., 8% of administrations occur in induction phase, 69% of administrations for midostaurin or quizartinib and 89% of cytarabine administrations in consolidation phase, and 100% of administrations in maintenance phase). Because some jurisdictions may cover the drug costs in both inpatient and outpatient settings, this assumption may underestimate the overall costs.
CDA-AMC conducted a scenario analysis to include costs for subsequent treatment
CDA-AMC was unable to explore the impact on BIA under the assumption of 100% drug coverage due to the lack of flexibility of the model.
The population modelled in BIA was inconsistent with that in economic evaluation. In the base-case BIA, newly diagnosed adults with FLT3-ITD-mutated AML (aged > 18 years) were modelled, aligning with the Health Canada indication. However, in the economic evaluation, efficacy data for midostaurin were derived from the RATIFY trial, which included a more restricted age group (18 to 59 years) compared to the QuANTUM-First trial (18 to 75 years). Therefore, only data from QuANTUM-First patients under 60 years weighted for the RATIFY population were used in the model base case.
Refer to the appraisal of economic evaluation discussed previously.
CDA-AMC Reanalyses of the BIA
Table 15: CDA-AMC Revisions to the Submitted Budget Impact Analysis
Stepped analysis | Sponsor’s value or assumption | CDA-AMC value or assumption |
|---|---|---|
Changes to derive the CDA-AMC base case | ||
1. Market share before after quizartinib is publicly reimbursed | FLAG-IDA: Baseline: ██; Year 1: ██; Year 2: ██; Year 3: ██ Quizartinib: Baseline: ██; Year 1: ███; Year 2: ███; Year 3: ███ Midostaurin: Baseline: ████; Year 1: ███; Year 2: ███; Year 3: ███ | FLAG-IDA: Baseline: 4%; Year 1: 4%; Year 2: 4%; Year 3: 4% Quizartinib: Baseline: 0%; Year 1: 15%; Year 2: 30%; Year 3: 60% Midostaurin: Baseline: 96%; Year 1: 81%; Year 2: 66%; Year 3:36% |
2. Proportion of patients eligible to receive intensive chemotherapy | 70% | 60% |
3. Treatment durations in induction and consolidation phases | Induction phase:
Consolidation phase:
| Induction phase:
Consolidation phase:
|
CDA-AMC base case | 1 + 2 + 3 | |
FLAG-IDA = a combination of fludarabine, cytarabine, idarubicin, and filgrastim.
The results of the CDA-AMC step-wise reanalysis are presented in summary format in Table 16 and a more detailed breakdown is presented in Table 17.
Based on CDA-AMC reanlayses, the expected budget impact for funding quizartinib for adult patients with newly diagnosed FLT3-ITD mutated AML to be $24,393,381 over the 3-year time horizon (Year 1: $2,630,407; Year 2: $6,948,421; Year 3: $14,814,553). The increased budget impact was primarily driven by the alternative assumptions for market share.
As quizartinib is more costly than midostaurin (refer to Table 14 and Table 8) and CDA-AMC could not address limitations that would increase the use of treatments (treatment duration, and number of individuals treated in the outpatient setting), the budget impact of reimbursing quizartinib may be underestimated.
Table 16: Summary of the CDA-AMC Reanalyses of the Budget Impact Analysis
Stepped analysis | Three-year total ($) |
|---|---|
Submitted base case | 21,469,962 |
CDA-AMC reanalysis 1 | 26,876,739 |
CDA-AMC reanalysis 2 | 18,402,825 |
CDA-AMC reanalysis 3 | 22,779,454 |
CDA-AMC base case (1 + 2 + 3) | 24,393,381 |
CDA-AMC conducted the following scenario analyses to address remaining uncertainty, using the CDA-AMC base case (results are provided in Table 17):
Assumed quizartinib is not funded for maintenance therapy (maintenance therapy regimens in quizartinib arm were assumed to be the same as those in the comparator arm).
Included costs for subsequent treatment.
Table 17: Detailed Breakdown of the CDA-AMC Reanalyses of the BIA
Stepped analysis | Scenario | Year 0 (current situation) ($) | Year 1 ($) | Year 2 ($) | Year 3 ($) | Three-year total ($) |
|---|---|---|---|---|---|---|
Submitted base case | Reference | 9,150,524 | 11,537,885 | 12,714,337 | 12,880,506 | 46,283,253 |
New drug | 9,150,524 | 13,444,900 | 18,785,899 | 26,371,891 | 67,753,215 | |
Budget impact | 0 | 1,907,015 | 6,071,562 | 13,491,386 | 21,469,962 | |
CDA-AMC base case | Reference | 6,498,044 | 8,526,383 | 9,516,800 | 9,641,260 | 34,182,487 |
New drug | 6,498,044 | 11,156,791 | 16,465,221 | 24,455,813 | 58,575,868 | |
Budget impact | 0 | 2,630,407 | 6,948,421 | 14,814,553 | 24,393,381 | |
CDA-AMC scenario analysis 1: Assumed quizartinib is not funded for maintenance therapy | Reference | 6,498,044 | 8,526,383 | 9,516,800 | 9,641,260 | 34,182,487 |
New drug | 6,498,044 | 8,542,531 | 9,549,522 | 9,707,554 | 34,297,651 | |
Budget impact | 0 | 16,148 | 32,721 | 66,294 | 115,164 | |
CDA-AMC scenario analysis 2: Included costs for subsequent treatment | Reference | 11,631,705 | 15,256,078 | 18,256,505 | 19,974,128 | 65,118,417 |
New drug | 11,631,705 | 17,736,541 | 24,830,018 | 33,946,305 | 88,144,569 | |
Budget impact | 0 | 2,480,463 | 6,573,512 | 13,972,177 | 23,026,153 |
BIA = budget impact analysis.
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.