Drugs, Health Technologies, Health Systems
Reimbursement Review
Fruquintinib (Fruzaqla)
Sponsor: Takeda Canada Inc.
Therapeutic area: Metastatic colorectal cancer
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Clinical Review
Abbreviations
AE
adverse event
BSC
best supportive care
CCRAN
Colorectal Cancer Resource & Action Network
CDA-AMC
Canada's Drug Agency
CGOEN
Canadian GI Oncology Evidence Network
CI
confidence interval
CNS
central nervous system
CRC
colorectal cancer
dMMR
deficient mismatch repair
ECOG PS
Eastern Cooperative Oncology Group Performance Status
EORTC QLQ-C30
European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30
GRADE
Grading of Recommendations Assessment, Development and Evaluation
HR
hazard ratio
HRQoL
health-related quality of life
ITC
indirect treatment comparison
ITT
intention to treat
KM
Kaplan-Meier
mCRC
metastatic colorectal cancer
MID
minimally important difference
MSI-H
microsatellite instability-high
NMA
network meta-analysis
OS
overall survival
PFS
progression-free survival
pMMR
proficient mismatch repair
QoL
quality of life
RCT
randomized controlled trial
RECIST 1.1
Response Evaluation Criteria in Solid Tumours Version 1.1
SAE
serious adverse event
SD
standard deviation
TEAE
treatment-emergent adverse event
WDAE
withdrawal due to adverse event
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Table 1: Background Information of Application Submitted for Review
Item | Description |
|---|---|
Drug product | Fruquintinib (Fruzaqla),1 mg and 5 mg, oral capsules |
Sponsor | Takeda Canada Inc. |
Indication | For the treatment of adult patients with mCRC who have been previously treated with or are not considered candidates for available standard therapies, including fluoropyrimidine-, oxaliplatin-, and irinotecan-based chemotherapy, an anti-VEGF drug, an anti-EGFR drug (if RAS wild-type), and either trifluridine-tipiracil or regorafenib.a |
Reimbursement request | As per indication |
Health Canada approval status | NOC |
Health Canada review pathway | Standard review, Project Orbis, ACCESS Consortium (Australia, Canada, Singapore, Switzerland, UK) |
NOC date | September 10, 2024 |
Recommended dose | 5 mg orally once daily for 21 consecutive days, followed by a 7-day rest period to comprise a complete cycle of 28 days. Treatment with fruquintinib should be continued until disease progression or unacceptable toxicity occurs. |
mCRC = metastatic colorectal cancer; NOC = Notice of Compliance.
aThe proposed indication was revised during the review process. The original proposed indication was for the treatment of adult patients with mCRC who have been previously treated with or who are not considered candidates for available therapies including fluoropyrimidine, oxaliplatin, and irinotecan-based chemotherapy, an anti-VEGF therapy, and an anti-EGFR therapy.
Introduction
Colorectal cancer (CRC) collectively refers to malignant tumours that develop in the epithelial lining of the rectum or colon from polyps that progress into cancer.1 In Canada, CRC is the second leading cause of death from cancer in men and the third leading cause of death from cancer in women.2 The 5-year prevalence of CRC in Canada is estimated to be 79,009 (8.3 per 100,000).3 Metastatic colorectal cancer (mCRC) results when CRC cells become invasive and travel to other parts of the body, most commonly the liver, lungs, and bones.4,5 The most common symptoms of mCRC include altered bowel habits (such as diarrhea or constipation), blood in stool, fatigue, nausea, abdominal pain, loss of appetite, and unintentional weight loss. Prognosis is typically worse for patients who have progressed after multiple lines of therapy. Clinical trials of patients with mCRC receiving third-line or later treatment report a median overall survival (OS) that ranges from 6.4 months to 7.1 months.6-9
First-line and second-line treatments for mCRC consist of chemotherapy — which may be combined with molecular targeted therapies — with fluoropyrimidine-, oxaliplatin-, and/or irinotecan-based chemotherapy (e.g., folinic acid, fluorouracil, and oxaliplatin [FOLFOX]; folinic acid, fluorouracil, and irinotecan [FOLFIRI]; folinic acid, 5-fluorouracil, oxaliplatin, and irinotecan [FOLFOXIRI]; and capecitabine plus oxaliplatin [CAPOX]) being the most widely recommended chemotherapy treatments.10,11 Factors such as patient age, functional and nutritional status, comorbidities, predictive biomarkers, patient preference, and drug toxicity are considered in treatment selection.12 For patients who have progressed on available chemotherapy (i.e., third-line or later-line setting), trifluridine-tipiracil and regorafenib have been studied as single-drug treatments, but their benefits are modest and they are currently not publicly funded in Canada. Best supportive care (BSC) is offered in clinical practice to provide palliation of symptoms and maintain or improve quality of life (QoL) in patients who either do not have active treatment options or are not suitable candidates for such treatments. Trifluridine-tipiracil plus bevacizumab combination therapy has recently received a positive reimbursement recommendation from Canada's Drug Agency (CDA-AMC)13 and is currently under consideration for public funding as a third-line or later-line treatment. There is currently no approved treatment for patients with disease that progressed on standard chemotherapy, and either trifluridine-tipiracil or regorafenib (i.e., fourth-line or later-line setting); BSC is available to these patients in clinical practice.
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of fruquintinib 1 mg and 5 mg oral capsules in the treatment of adult patients with mCRC who have been previously treated with or are not considered candidates for available standard therapies, including fluoropyrimidine-, oxaliplatin-, and irinotecan-based chemotherapy, an anti–vascular endothelial growth factor (anti-VEGF) drug, an anti–epidermal growth factor receptor (anti-EGFR) drug (if RAS wild-type), and either trifluridine-tipiracil or regorafenib.
Perspectives of Patients, Clinicians, and Drug Programs
The information in this section is a summary of input provided by the patient and clinician groups that responded to a call for input by CDA-AMC and from clinical experts consulted by CDA-AMC for the purpose of this review.
Patient Input
CDA-AMC received 2 patient group submissions, from Colorectal Cancer Resource & Action Network (CCRAN) and Colorectal Cancer Canada. CCRAN is a national, not-for-profit patient advocacy group that champions the health and well-being of Canadians touched by CRC and those at risk of developing the disease by providing support, education, and advocacy to help improve the longevity and QoL of patients. Colorectal Cancer Canada is a not-for-profit CRC patient organization dedicated to CRC awareness and education, supporting patients and their caregivers, and advocating on their behalf.
CCRAN employed a multifaceted outreach approach that resulted in 3 patient interviews and a survey of patients with mCRC; of the 119 patients who responded from March 21 to April 17, 2024, 115 resided in Canada and the remaining 4 resided in the US. Data were gathered by Colorectal Cancer Canada using 4 online patient interviews, conducted between April 1 and May 15, 2024, and 1 online survey, conducted in August 2023, to which 15 patients and 1 caregiver in Canada and the US responded.
Most patients reported that abdominal cramps, gas, bloating, pain, fatigue, weakness, bloody stools, and diarrhea are common impacts of the disease that affect QoL and result in an inability to work, exercise, participate in social activities, fulfill family obligations, and concentrate. The caregiver also noted significant difficulties caring for patients with mCRC. Fluorouracil-based chemotherapy, capecitabine, bevacizumab, and panitumumab were cited as being the most frequently used treatments by the respondents, with the most common side effects being fatigue, hair loss, nausea, peripheral neuropathy, and diarrhea. Both patient groups reported that it is very important for a new therapy to improve the physical condition of patients (e.g., tumour shrinkage, tumour stability, reduction of pain, and improved breathing) and their QoL. Four respondents to CCRAN’s survey and 3 respondents to Colorectal Cancer Canada’s survey had experience with fruquintinib treatment; the patients’ main access to fruquintinib was through a clinical trial centre in the US. Patients reported that fruquintinib treatment helped stabilize their disease and was easy to administer as an oral therapy. Most patients experienced hand-foot syndrome associated with fruquintinib treatment, but noted that it was manageable. Both groups reported that access to fruquintinib for patients in the refractory mCRC setting is of utmost importance because it could provide these patients with an effective treatment option to stabilize their disease and improve their QoL.
Clinician Input
Input From Clinical Experts Consulted by CDA-AMC
The clinical experts noted that there is a need for effective mCRC treatments that provide more durable disease control and OS benefit, have fewer adverse effects, and could delay a decline in QoL related to the underlying cancer. The clinical experts also noted that comprehensive biomarker profiling and adaptive treatment strategies are required to personalize therapy more effectively. Equitable access to novel treatments remains a key barrier for many patients with mCRC, according to clinical expert input.
The clinical experts expect fruquintinib to be used in patients with mCRC in the fourth-line or later-line setting (i.e., in patients who have refractory disease or who have experienced intolerable toxicity to at least 2 lines of standard chemotherapy [including fluoropyrimidine, irinotecan, and oxaliplatin] and to trifluridine-tipiracil plus bevacizumab).
The clinical experts noted that fruquintinib would be most appropriate for patients with mCRC who have disease that progressed on or who experienced intolerable toxicity to all standard approved cytotoxic treatment (fluoropyrimidine, irinotecan, and oxaliplatin), an anti-VEGF drug, an anti-EGFR drug, as well as trifluridine-tipiracil plus bevacizumab or regorafenib. Appropriate patients should also have received prior immune checkpoint inhibitor and BRAF inhibitor targeted therapy, if indicated, according to the clinical experts. The clinical experts noted that patients with an Eastern Cooperative Oncology Group Performance Status (ECOG PS) score of 0 or 1 are suitable treatment candidates, and that patients with an ECOG PS score of 2 may be eligible for treatment at the treating physician’s discretion. However, for patients with an ECOG PS score of more than 2, the clinical experts felt it was inappropriate to prescribe fruquintinib given the absence of evidence and the likelihood that the harms would likely outweigh the benefits in these patients. The clinical experts noted that patients with untreated or unstable central nervous system (CNS) metastases would not be suitable candidates for fruquintinib treatment.
According to the clinical experts, a clinically meaningful response includes improved survival, significant reductions in the frequency and severity of disease-related symptoms, an enhanced ability to perform daily activities, and noticeable improvements in QoL. Patients are generally seen during each cycle (28 days in the case of fruquintinib), and blood work and a CT scan of chest, abdomen, and pelvis are performed every 2 to 3 cycles (8 to 12 weeks), according to the clinical experts. Treatment discontinuation would be considered upon disease progression and/or intolerable toxicity, the clinical experts noted, and fruquintinib should be prescribed by an oncologist with expertise in assessing and monitoring patients with mCRC.
Clinician Group Input
CDA-AMC received 1 clinician group submission from the Canadian GI Oncology Evidence Network (CGOEN), which is represented by 16 clinicians across Canada.
In general, CGOEN shared a consistent view on management of mCRC with the clinicians consulted by CDA-AMC. The clinician group stated that the main goals of treatment for mCRC are improvements in OS and QoL and the minimization of toxicities from treatment. In terms of unmet need, the clinician group noted that there are currently no publicly funded treatment options for patients with mCRC who have been previously treated with, or are intolerant to, standard chemotherapy. However, with recent a positive reimbursement recommendation for trifluridine-tipiracil used in combination with bevacizumab for treatment-refractory CRC, the clinician group indicated that fruquintinib could be considered in patients who would not be eligible for trifluridine-tipiracil plus bevacizumab and in patients who previously received trifluridine-tipiracil plus bevacizumab, which could provide the clinical flexibility required in this specific later-line setting.
Last, the clinician group indicated that fruquintinib would be used in patients with mCRC who have been treated with or who are intolerant of fluoropyrimidine, irinotecan, and oxaliplatin. Furthermore, fruquintinib would be considered after encorafenib-based therapy in patients with BRAF-mutant tumours, immunotherapy in patients with tumours that have deficient mismatch repair (dMMR), anti-EGFR therapies in patients with KRAS wild-type tumours, and anti-VEGF therapies, as well as in patients who have not received previous anti-VEGF therapy. The clinician group further commented that patients would undergo clinical evaluations on a regular basis for clinical response and toxicity, and a meaningful response would be patient preference, tolerability of treatment, QoL, and response on imaging. Moreover, fruquintinib should be discontinued upon disease progression (i.e., radiologic or clinical), toxicity, clinician discretion, or patient’s request. The clinician group also mentioned that fruquintinib could be reasonably given in any centre and by any specialist who is currently treating patients who have mCRC with systemic therapy.
Drug Program Input
Input was obtained from the drug programs that participate in the reimbursement review process. The following were identified as key factors that could potentially impact the implementation of a reimbursement recommendation for fruquintinib: relevant comparators, considerations for initiation and discontinuation of therapy, generalizability of the pivotal study results, funding algorithm, and system and economic issues.
In response to the drug programs’ questions on reimbursement criteria, the clinical experts noted that patients who have experienced disease progression on or who have been deemed not to be a candidate for trifluridine-tipiracil plus bevacizumab should be eligible for treatment with fruquintinib, and that fruquintinib treatment should be discontinued upon disease progression, severe or serious adverse events (SAEs) despite dose modification, and a decline in the patient’s clinical condition. The clinical experts also noted that patients with small bowel or appendiceal adenocarcinoma could be potential candidates for fruquintinib treatment, as could patients with microsatellite instability-high (MSI-H) and/or dMMR tumours and patients with BRAF V600E mutations after progression on immunotherapy or BRAF inhibitor. When considering the use of fruquintinib in patients with an ECOG PS of 2, the clinical experts felt that it would be reasonable to leave the decision to the treating physicians’ judgment. However, for patients with an ECOG PS score of more than 2, the clinical experts felt it would be inappropriate to prescribe fruquintinib, given the absence of evidence and the likelihood that the harms would likely outweigh the benefits in these patients.
Clinical Evidence
Systematic Review
Description of Studies
Two studies, the FRESCO (N = 416) and FRESCO-2 (N = 691) trials,14,15 met the inclusion criteria for the systematic review conducted by the sponsor. The FRESCO and FRESCO-2 trials were multicentre, randomized, double-blind, placebo-controlled, phase III trials that compared the efficacy and safety of fruquintinib plus BSC with placebo plus BSC in adult patients with metastatic colorectal adenocarcinoma. The FRESCO trial enrolled patients from 28 sites (all in China) who had progressed on or experienced intolerable toxicity to at least 2 lines of standard chemotherapy. The FRESCO-2 trial enrolled patients from 124 sites (in the Asia-Pacific region, Europe, and North America; there were no sites in Canada) who were previously treated with all standard chemotherapies, anti-VEGF therapy, and anti-EGFR therapy (if RAS is wild-type), and had progressed on, or been intolerant to, treatment with trifluridine-tipiracil and/or regorafenib. Patients in the FRESCO-2 trial also had received immune checkpoint inhibitors and/or BRAF inhibitors, if indicated.
In both trials, patients were randomized in a 2:1 ratio to receive fruquintinib (5 mg orally once daily for 3 weeks, followed by 1 week off, for a 28-day cycle) plus BSC or placebo plus BSC until disease progression or intolerable toxicity. The efficacy outcomes of interest to this review included OS (primary end point), progression-free survival (PFS) (secondary end point in the FRESCO trial and a key secondary end point in the FRESCO-2 trial), European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 (EORTC QLQ-C30) global health status/QoL score (in the FRESCO trial only, as a secondary end point).
In the FRESCO trial, at baseline, the majority of patients (78.8%) had received 3 or fewer lines of anticancer treatment for metastatic disease; 30.0% of patients had received anti-VEGF treatment, and 14.2% of patients had received anti-EGFR treatment. The proportion of patients that had received immune checkpoint inhibitors, BRAF inhibitors, trifluridine-tipiracil, or regorafenib was not reported. In the FRESCO-2 trial, at baseline, most patients (72.6%) had received more than 3 lines of anticancer treatment for metastatic disease, 96.4% of patients had received anti-VEGF treatment, and all patients had received treatment with trifluridine-tipiracil and/or regorafenib (52.2% received trifluridine-tipiracil alone and 39.4% received both trifluridine-tipiracil and regorafenib). Approximately one-third of patients had received anti-EGFR treatment. In both trials, the proportion of patients who had received trifluridine-tipiracil plus bevacizumab combination therapy was unknown.
Efficacy Results
Results presented here represent the final efficacy analysis, with data cut-off dates of January 17, 2017, for the FRESCO trial and June 24, 2022, for the FRESCO-2 trial.
Overall Survival
The FRESCO Trial: The median duration of follow-up was 13.3 months (95% confidence interval [CI], 12.1 to 14.7 months) in the fruquintinib plus BSC group and 13.2 months (95% CI, 10.6 to 19.6 months) in the placebo plus BSC group when a total of 297 deaths occurred. The Kaplan-Meier (KM) estimate for median OS (primary end point) was 9.30 months (95% CI, 8.18 to 10.45 months) in the fruquintinib plus BSC group and 6.57 months (95% CI, 5.88 to 8.11 months) in the placebo plus BSC group, with a stratified hazard ratio (HR) of 0.65 (95% CI, 0.51 to 0.83; P < 0.001). The between-group difference in the probability of survival at 6 months, 12 months, and 18 months was █████ ████ ███ ████ ██ ███████ █████ ████ ███ ████ ██ ███████ ███ ████ ████ ███ █████ ██ ███████ respectively. Results of the sensitivity analysis and the subgroup analyses of interest were, in general, consistent with those of the primary analysis.
The FRESCO-2 Trial: The median duration of follow-up was 11.3 months (95% CI, 10.6 to 12.4months) in the fruquintinib plus BSC group and 11.2 (95% CI, 9.9 to 12.0 months) in the placebo plus BSC group when a total of 490 deaths occurred. The KM estimate for median OS (primary end point) was 7.4 months (95% CI, 6.7 to 8.2 months) in the fruquintinib plus BSC group and 4.8 months (95% CI, 4.0 to 5.8 months) in the placebo plus BSC group, with a stratified HR of 0.66 (95% CI, 0.55 to 0.80; P < 0.001). The between-group difference in the probability of survival at 6 months, 12 months, and 18 months was █████ ████ ███ █████ ██ ███████ ████ ████ ███ █████ ██ ███████ ███ █████ ████ ███ █████ ██ █████), respectively. Results of the sensitivity analysis and the subgroup analyses of interest were, in general, consistent with those of the primary analysis. Of note, however, no effect was observed in the subgroup of patients who had received 3 or fewer lines (not specific to the stage of disease in which they were received) of chemotherapy treatments (HR = 0.94; 95% CI, 0.56 to 1.53), whereas a treatment effect was consistently observed in subgroups of patients by the number of prior lines of chemotherapy received in the metastatic setting.
Progression-Free Survival
The FRESCO Trial: The KM estimate for the median PFS (secondary end point) was 3.71 months (95% CI, 3.65 to 4.63 months) in the fruquintinib plus BSC group and 1.84 months (95% CI, 1.81 to 1.84 months) in the placebo plus BSC group, with a stratified HR of 0.26 (95% CI, 0.21 to 0.34; P < 0.001). The majority of PFS events in both treatment groups were attributed to disease progression. The between-group difference in the probability of surviving progression-free at 3 months, 6 months, and 9 months ███ █████ ████ ███ █████ ██ ██████ ███ █████ ████ ███ █████ ██ ███████ ███ █████ ████ ███ ████ ██ ██████, respectively. None of these end points were adjusted for multiplicity. Results of the subgroup analysis were consistent with those of the primary analysis.
The FRESCO-2 Trial: The KM estimate for median PFS (key secondary end point) was 3.7 months (95% CI, 3.5 to 3.8 months) in the fruquintinib plus BSC group and 1.8 months (95% CI, 1.8 to 1.9 months) in the placebo plus BSC group, with a stratified HR of 0.32 (95% CI, 0.27 to 0.39; P < 0.001); this end point was adjusted for multiplicity. The majority of PFS events in both treatment groups were attributed to disease progression. The between-group difference in the probability of survival at 3 months, 6 months, and 9 months was █████ ████ ███ █████ ██ ███████ █████ ████ ███ █████ ██ ███████ ███ █████ ████ ███ ████ ██ ██████, respectively. Results of the subgroup analysis were consistent with those of the primary analysis.
European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30
The FRESCO Trial: This outcome was not assessed in the FRESCO trial.
The FRESCO-2 Trial: EORTC QLQ-C30 questionnaire-based outcomes were secondary end points and not adjusted for multiplicity in the FRESCO-2 trial.
█████ ███████ ███████████ of 461 (██████ randomized patients) in the fruquintinib plus BSC group and ███ of 230 (██████ randomized patients) in the placebo plus BSC group were included in the analysis of patients with minimally important deterioration (i.e., at least a 6.38-point reduction) from baseline in EORTC QLQ-C30 global health status/QoL score at the final on-treatment visit. Of the patients analyzed, █████ in the fruquintinib plus BSC group and █████ in the placebo plus BSC group achieved this end point; the between-group difference was ████ ████ ███ █████ ██ ███████
Caregiver Burden
This outcome was not assessed in either of the trials.
Harms Results
Treatment-Emergent Adverse Events
The proportion of patients who reported at least 1 treatment-emergent adverse event (TEAE) was higher in the fruquintinib plus BSC group than in the placebo plus BSC group in both the FRESCO (98.6% versus 88.3%) and FRESCO-2 (98.9% versus 92.6%) trials. The most commonly reported TEAEs in the fruquintinib plus BSC group (reported in at least 30% of patients in at least 1 of the trials) were hand-foot syndrome, hypertension, dysphonia, proteinuria, and asthenia; all of these were more commonly reported in the fruquintinib plus BSC group than in the placebo plus BSC group.
TEAEs of grade 3 or higher were more commonly reported in the fruquintinib plus BSC group than in the placebo plus BSC group in both the FRESCO (61.2% versus 19.7%) and FRESCO-2 (62.7% versus 50.4%) trials. The most commonly reported TEAEs of grade 3 or higher in the fruquintinib plus BSC groups were hypertension, asthenia, and hand-foot syndrome. The frequencies of grade 3 or higher hypertension and hand-foot syndrome were consistently higher in the fruquintinib plus BSC group than in the placebo BSC group in both trials (hypertension rates were, respectively, 21.6% versus 2.2% in the FRESCO trial and 13.6% versus 0.9% in the FRESCO-2 trial, and hand-foot syndrome rates were, respectively, 10.8% versus 0.0% in the FRESCO trial and 6.4% versus 0.0% in the FRESCO-2 trial).
Serious Adverse Events
SAEs were more commonly reported in the fruquintinib plus BSC group than in the placebo plus BSC group in the FRESCO trial (15.5% versus 5.8%) but were similar between the 2 treatment groups in the FRESCO-2 trial (37.5% versus 38.3%). SAEs were not attributed to any specific TEAEs in either trial.
Withdrawals Due to Adverse Events
Withdrawals due to adverse events (WDAEs) were more commonly reported in the fruquintinib plus BSC group than in the placebo plus BSC group in the FRESCO trial (15.1% versus 5.8%) but were similar between the 2 treatment groups in the FRESCO-2 trial (20.4% versus 21.3%). WDAEs were not attributed to any specific TEAEs in either trial.
Mortality
Deaths were less commonly reported in the fruquintinib plus BSC group than in the placebo plus BSC group in both the FRESCO (67.6% versus 78.8%) and FRESCO-2 (68.9% versus 75.2%) trials.
Notable Harms
The incidences of thromboembolic events and gastrointestinal perforations were similarly low in the fruquintinib plus BSC group and the placebo plus BSC group in both trials (thromboembolic event rates were, respectively, 0.7% versus 0.7% in the FRESCO trial and 4.6% versus 2.2% in the FRESCO-2 trial, and gastrointestinal perforation rates were, respectively, 2.2% versus 1.7% in the FRESCO trial and 3.5% versus 0.4% in the FRESCO-2 trial). The proportions of patients with hand-foot syndrome, hemorrhage, hypertension, and proteinuria in the fruquintinib plus BSC group were reported to be between 43.2% and 57.2% in the FRESCO trial, and between 14.3% and 36.8% in the FRESCO-2 trial; these harms were notably more common in the fruquintinib plus BSC group than the placebo plus BSC group.
Critical Appraisal
The trials used adequate methods of randomization and allocation concealment. Baseline patient characteristics were generally balanced between treatment groups, with the exception of sex, although this was not expected to impact the study results. The trials were adequately blinded; however, there is a risk of bias in the measurement of subjective outcomes that are based on the inferred judgment of patients and investigators regarding treatment assignment because of adverse events (AEs) associated with the interventions (e.g., hypertension, hand-foot syndrome). This could potentially lead to results favouring fruquintinib plus BSC for health-related quality of life (HRQoL) outcomes and favouring placebo plus BSC for subjective harms outcomes. No multiplicity adjustment was in place for HRQoL outcomes in the FRESCO-2 trial or for PFS in the FRESCO trial, so statistically significant results were at an increased risk of type I error (false-positive results). In the FRESCO-2 trial, data were missing from a total of █████ of patients in the 2 treatment arms (with █████ ██ █████ completed data, fruquintinib plus BSC and placebo plus BSC, respectively) in the analysis of patients with minimally important deterioration from the baseline EORTC QLQ-C30 global health status/QoL score. Missing data could have biased the validity and interpretability of the HRQoL results. Sensitivity analyses for the change from baseline in score analysis using the mixed model for repeated measures (MMRM) were conducted to assess the impact of missing data; however, the underlying assumption that data were missing at random may not hold when, for example, missing data were more likely to occur in patients with end-stage disease and poor health status. There is the potential that the impact of the missing data ███████ could not be negligible in the analysis of proportion of patients with minimally important deterioration from baseline EORTC QLQ-C30 global health status/QoL score, particularly when the between-group difference was small █████ ████ ███ █████ ██ ████████.
Of note, in the FRESCO-2 trial, treatment exposure, measured as the mean duration of exposure (4.0 months versus 2.0 months), and the total number of treatment cycles received (4.3 versus 2.3) were almost doubled in the fruquintinib plus BSC group compared with the placebo plus BSC group. Patients discontinued the treatment largely due to disease progression, AEs, or investigator decision, yet the proportion of patients who discontinued treatment due to disease progression was not substantially different between the fruquintinib plus BSC and placebo plus BSC groups (59% versus 64%). According to the protocol, patients in the FRESCO-2 study were allowed to continue the study treatment after disease progression, determined by Response Evaluation Criteria in Solid Tumours Version 1.1 (RECIST 1.1), if the patient was deemed to be deriving clinical benefit by the investigator. Of the 461 patients randomized to fruquintinib plus BSC, 301 experienced disease progression; among these, 99 patients (32.9%) received at least 1 dose of fruquintinib after disease progression. It is unclear what proportion of patients in the placebo plus BSC group was allowed to continue treatment beyond radiographic progression. The decision to continue treatment beyond disease progression was made by the investigator in a blinded manner and, thus, unlikely to have introduced bias. The rate of subsequent anticancer treatments was lower in the fruquintinib plus BSC group than in the placebo plus BSC group (29.4% versus 34.3%), which could have biased the OS results in favour of placebo plus BSC.
For the prespecified OS and PFS subgroup analyses, there was a lack of consideration of sample size, control for multiplicity, and treatment-by-subgroup interaction, which precludes any firm conclusions on subgroup effects.
In terms of external validity, the clinical experts consulted by CDA-AMC anticipated that patients would have also received anti-VEGF drugs and, if indicated, an anti-EGFR drug, BRAF inhibitor, and immune checkpoint inhibitor (in addition to 2 lines of standard chemotherapy) before receiving fruquintinib treatment, in accordance with the current treatment approach in Canada. As well, the clinical experts noted that if trifluridine-tipiracil becomes publicly funded, fruquintinib would be used subsequently in the fourth-line or later-line setting in most patients. The FRESCO trial was designed for patients who had experienced treatment failure with at least 2 lines of chemotherapy and, hence, by inclusion criteria, the aforementioned prior therapies were not required. By baseline characteristics, the proportion of patients who had received these treatments was either small or unknown. This does not align with clinical expert input, which stated that in clinical practice, most patients eligible for fruquintinib treatment would have received these prior therapies. The FRESCO-2 trial included patients who had been heavily pretreated and received all standard chemotherapies, anti-VEGF drugs, anti-EGFR drugs, immune checkpoint inhibitors, and BRAF inhibitors, as indicated. Of note, patients were not required to have experienced disease progression on these treatments, which may increase uncertainty about the generalizability of the study results to the fourth-line or later-line setting. However, in the clinical experts’ opinions, the concern was minor because in clinical practice, typically, treatments are switched upon disease progression or poor tolerance. As well, most patients were expected to receive trifluridine-tipiracil plus bevacizumab combination therapy before fruquintinib treatment in clinical practice, per clinical expert input. Although the majority of patients in the FRESCO-2 trial previously received trifluridine-tipiracil (91.6%), the sponsor was unable to provide data on the proportion of patients who received trifluridine-tipiracil in combination with bevacizumab in the 2 trials, which could introduce uncertainty about the generalizability of the study results. The sponsor noted that the trials were completed during a time when there was limited clinical evidence for trifluridine-tipiracil plus bevacizumab therapy and no approved indications for the use of such combination therapy, which limits the ability to accurately characterize the proportion of patients who received trifluridine-tipiracil in combination with bevacizumab. In consultation with the clinical experts, the CDA-AMC review team considered that, compared to patients in the FRESCO trial, patients in the FRESCO-2 trial were more reflective of the patient population eligible for fruquintinib treatment, based on the inclusion criteria and baseline characteristics, albeit subject to the aforementioned generalizability concerns. In addition, the clinical experts noted that the use of chemotherapy as a common subsequent treatment in the trials did not align with clinical practice in Canada, given that patients in the trial populations were chemorefractory at baseline. As well, the FRESCO trial was conducted in China, so there is the potential for differences in the standard of care and the availability of BSC in different countries.
GRADE Summary of Findings and Certainty of the Evidence
For the pivotal studies and randomized controlled trials (RCTs) identified in the sponsor’s systematic review, the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach was used to assess the certainty of the evidence for outcomes considered to be most relevant to inform CDA-AMC expert committee deliberations, and a final certainty rating was determined as outlined by the GRADE Working Group. Following the GRADE approach, evidence from RCTs started as high-certainty evidence and could be rated down for concerns related to study limitations (which refer to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias.
The selection of outcomes for GRADE assessment was based on the sponsor’s Summary of Clinical Evidence, consultation with clinical experts, and input received from patient and clinician groups and public drug plans. The following list of outcomes was finalized in consultation with expert committee members:
OS (probability of OS at 6 months, 12 months, and 18 months)
PFS (probability of PFS at 3 months, 6 months, and 12 months)
HRQoL (EORTC QLQ-C30 global health status/score responder analysis)
harms (SAEs).
Table 2 presents the GRADE summary of findings for fruquintinib plus BSC and placebo plus BSC in patients with mCRC who had progressed on or who were intolerant to at least 2 lines of standard chemotherapy.
Table 3 presents the GRADE summary of findings for fruquintinib plus BSC and placebo plus BSC in patients with mCRC who had previously received standard chemotherapy, an anti-VEGF drug, and an anti-EGFR drug (if RAS wild-type), and had progressed on or been intolerant to trifluridine-tipiracil and/or regorafenib.
Table 2: Summary of Findings for Fruquintinib Plus BSC Versus Placebo Plus BSC for Patients With mCRC Who Had Progressed on or Were Intolerant to at Least 2 Lines of Standard Chemotherapy
Outcome and follow-up | Patients (studies), N | Relative effect (95% CI) | Absolute effects (95% CI) | Certainty | What happens | ||
|---|---|---|---|---|---|---|---|
Fruquintinib plus BSC | Placebo plus BSC | Difference | |||||
Overall survival | |||||||
Probability of overall survival at 6 months, % (95% CI) Median follow-up: ████ ██ | ███ ██ | NR | ███ ███ | ███ ███ | ███ ███ | Lowa | Fruquintinib plus BSC may result in a clinically important increase in the probability of overall survival at 6 months compared to placebo plus BSC. |
Probability of overall survival at 12 months, % (95% CI) Median follow-up: ████ ██ | ███ ██ | NR | ███ ███ | ███ ███ | ███ ███ | Lowa | Fruquintinib plus BSC may result in a clinically important increase in the probability of overall survival at 12 months compared to placebo plus BSC. |
Probability of overall survival at 18 months, % (95% CI) Median follow-up: ████ ██ | ███ ██ | NR | ███ ███ | ███ ███ | ███ ███ | Very lowa,b,c | The evidence is very uncertain about the effect of fruquintinib plus BSC on the probability of overall survival at 18 months compared to placebo plus BSC. |
Progression-free survival | |||||||
Probability of progression-free survival at 3 months, % (95% CI) Median follow-up: ████ ███ | ███ ██ | NR | ███ ███ | ███ ███ | ███ ███ | Lowa | Fruquintinib plus BSC may result in a clinically important increase in the probability of progression-free survival at 3 months compared to placebo plus BSC. |
Probability of progression-free survival at 6 months, % (95% CI) Median follow-up: ████ ██ | ███ ██ | NR | ███ ███ | ███ ███ | ███ ███ | Lowa | Fruquintinib plus BSC may result in a clinically important increase in the probability of progression-free survival at 6 months compared to placebo plus BSC. |
Probability of progression-free survival at 9 months, % (95% CI) Median follow-up: ████ ███ | ███ ██ | NR | ███ ███ | ███ ███ | ███ ███ | Lowa,c | Fruquintinib plus BSC may result in a clinically important increase in the probability of progression-free survival at 9 months compared to placebo plus BSC. |
Health-related quality of life | |||||||
Health-related quality of life | NA | No data available | No data available | No data available | No data available | NA | There is no evidence for the effect of fruquintinib plus BSC on health-related quality of life compared with placebo plus BSC. |
Caregiver burden | |||||||
Caregiver burden | NA | No data available | No data available | No data available | No data available | NA | There is no evidence for the effect of fruquintinib plus BSC on caregiver burden compared with placebo plus BSC. |
Serious adverse events | |||||||
Proportion of patients with serious adverse events, % (95% CI) Follow-up: 4.47 months vs. 2.6 months | 415 (1 RCT) | NR | 155 per 1,000 | 58 per 1,000 | 96 more per 1,000 (38 more to 154 more per 1,000) | Lowd | Fruquintinib plus BSC may result in a clinically important increase in serious adverse events compared with placebo plus BSC. |
BSC = best supportive care; CI = confidence interval; mCRC = metastatic colorectal cancer; NA = not applicable; NR = not reported; OS = overall survival; PFS = progression-free survival; RCT = randomized controlled trial; vs. = versus.
Note: Study limitations (which refer to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias were considered when assessing the certainty of the evidence. All serious concerns in these domains that led to the rating down of the level of certainty are documented in the table footnotes.
aRated down 2 levels for very serious indirectness related to the trial population and subsequent anticancer treatment use. The clinical experts consulted by CDA-AMC anticipated that patients would have also received anti-VEGF drugs and, if indicated, an anti-EGFR drug, BRAF inhibitor, and immune checkpoint inhibitor (in addition to 2 lines of standard chemotherapy) before receiving fruquintinib treatment, in accordance with the current treatment approach in Canada. As well, the clinical experts noted that if trifluridine-tipiracil becomes publicly funded, fruquintinib would be used subsequently in the fourth-line or later-line setting in most patients. In the FRESCO trial, by inclusion criteria, these prior treatments were not required. By baseline characteristics, the proportion of patients who had received these treatments was either small or unknown. The clinical experts also noted that in the trial, the use of chemotherapy subsequent to the failure of fruquintinib did not align with the current treatment approach used in the target population (i.e., chemorefractory) in Canada.
bRated down 1 level for serious imprecision. Based on clinical expert input, 50 more to 100 more per 1,000 patients surviving could be considered clinically important. The 95% CI included the possibility of benefit and little to no difference.
cPer clinical expert input, the findings at later time points (i.e., at 18 months for OS and at 9 months for PFS) were less relevant because survival is generally limited for patients in late-line settings, and most patients were expected to have experienced disease progression or died by those time points.
dRated down 1 level for serious imprecision. Based on clinical expert input, 50 more to 100 more per 1,000 patients with serious adverse events could be considered clinically important. The 95% CI included the possibility of important harm and no difference. Rated down 1 level for indirectness. Clinical expert input indicated that patients eligible for fruquintinib treatment in clinical practice were expected to be more treatment experienced (i.e., received more prior anticancer treatments) than the population of the FRESCO trial and that the trial was conducted in single country, with all patients being Asian; both factors could limit the generalizability of the harms results to the patient population in Canada.
Sources: FRESCO Clinical Study Report,16 sponsor’s Summary of Clinical Evidence.17
Table 3: Summary of Findings for Fruquintinib Plus BSC Versus Placebo Plus BSC for Patients With mCRC Who Had Previously Received Standard Chemotherapy, an Anti-VEGF Drug, and an Anti-EGFR Drug (if RAS Wild-Type), and Had Progressed on or Been Intolerant to Trifluridine-Tipiracil and/or Regorafenib
Outcome and follow-up | Patients (studies), N | Relative effect (95% CI) | Absolute effects (95% CI) | Certainty | What happens | ||
|---|---|---|---|---|---|---|---|
Fruquintinib plus BSC | Placebo plus BSC | Difference | |||||
Overall survival | |||||||
Probability of overall survival at 6 months, % (95% CI) Median follow-up: █████ █ | ███ ███ | NR | ███ ███ | ███ ███ | ███ ███ | Moderatea | Fruquintinib plus BSC likely results in a clinically important increase in the probability of overall survival at 6 months compared to placebo plus BSC. |
Probability of overall survival at 12 months, % (95% CI) Median follow-up: ████ ███ | ███ ███ | NR | ███ ███ | ███ ███ | ███ ███ | Lowa,b | Fruquintinib plus BSC may result in little to no clinically important difference in the probability of overall survival at 12 months compared to placebo plus BSC. |
Probability of overall survival at 18 months, % (95% CI) Median follow-up: ████ ███ | ███ ███ | NR | ███ ███ | ███ ███ | ███ ███ | Lowa,c,d | Fruquintinib plus BSC may result in little to no clinically important difference in the probability of overall survival at 18 months compared to placebo plus BSC. |
Progression-free survival | |||||||
Probability of progression-free survival at 3 months, % (95% CI) Median follow-up: ████ ███ | ███ ███ | NR | ███ ███ | ███ ███ | ███ ███ | Moderatea | Fruquintinib plus BSC likely results in a clinically important increase in the probability of progression-free survival at 3 months compared to placebo plus BSC. |
Probability of progression-free survival at 6 months, % (95% CI) Median follow-up: ████ ██ | ███ ███ | NR | ███ ███ | ███ ███ | ███ ███ | Moderatea | Fruquintinib plus BSC likely results in a clinically important increase in the probability of progression-free survival at 6 months compared to placebo plus BSC. |
Probability of progression-free survival at 9 months, % (95% CI) Median follow-up: ████ ██ | ███ ███ | NR | ███ ███ | ███ ███ | ███ ███ | Moderatea,d | Fruquintinib plus BSC likely results in a clinically important increase in the probability of progression-free survival at 9 months compared to placebo plus BSC. |
EORTC QLQ-C30 | |||||||
Global health status score, (i.e., the proportion of patients with at least a 6.38-point deterioration from baseline at last on-treatment visit), % (95% CI) Median follow-up: ████ ███ | ███ ███ | NR | ███ ███ | ███ ███ | ███ ███ | Lowa,e | Fruquintinib plus BSC may result in little to no clinically important difference in the proportion of patients with at least a 6.38-point deterioration from baseline in global health status score compared to placebo plus BSC. |
Caregiver burden | |||||||
Caregiver burden | NA | No data available | No data available | No data available | No data available | NA | There is no evidence for the effect of fruquintinib plus BSC on caregiver burden compared with placebo plus BSC. |
Serious adverse events | |||||||
Proportion of patients with serious adverse events, % (95% CI) Follow-up: 3.71 months vs. 2.6 months | 686 (1 RCT) | NR | 375 per 1,000 | 383 per 1,000 | 8 fewer per 1,000 (85 fewer to 69 more per 1,000) | Moderatef | Fruquintinib plus BSC likely results in little to no clinically important difference in serious adverse events compared to placebo plus BSC. |
BSC = best supportive care; CI = confidence interval; EORTC = European Organization for Research and Treatment of Cancer; mCRC = metastatic colorectal cancer; NA = not applicable; NR = not reported; OS = overall survival; PFS = progression-free survival; RCT = randomized controlled trial; vs. = versus.
Note: Study limitations (which refer to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias were considered when assessing the certainty of the evidence. All serious concerns in these domains that led to the rating down of the level of certainty are documented in the table footnotes.
aRated down 1 level for serious indirectness related to the trial population and subsequent anticancer treatment use. The clinical experts consulted by CDA-AMC anticipate that in most patients, fruquintinib would be used in the fourth-line or later-line setting, subsequent to the failure of trifluridine-tipiracil plus bevacizumab combination therapy if this combination therapy becomes publicly funded. The proportion of patients who had previously received trifluridine-tipiracil plus bevacizumab was unknown in the FRESCO-2 trial. The clinical experts also noted that in the trial, the use of chemotherapy subsequent to the failure of fruquintinib did not align with the current treatment approach used in the target population (i.e., chemorefractory) in Canada.
bRated down 1 level for serious imprecision. Based on clinical expert input, 50 more to 100 more per 1,000 patients surviving could be considered clinically important. The 95% CI included the possibility of benefit and little to no difference.
cRated down 1 level for serious imprecision. Based on clinical expert input, 50 more to 100 more per 1,000 patients surviving could be considered clinically important. The 95% CI included the possibility of benefit and no difference. Was not rated down further, even though the lower bound of the 95% CI indicated the possibility for harm, given that it marginally crossed the threshold of 50 fewer per 1,000 patients.
dPer clinical expert input, the findings at later time points (i.e., at 18 months for OS and at 9 months for PFS) were less relevant because survival is generally limited for patients in late-line settings, and most patients were expected to have experienced disease progression or died by those time points.
eRated down 1 level for serious study limitation. There was a substantial amount of missing data (18.2%) in the treatment groups, which may have an impact on the prognostic balance of the groups. Was not rated down for imprecision. The lower limit of the 95% CI marginally crossed the threshold of 100 fewer per 1,000 patients with at least a 6.38-point deterioration from baseline in global health status score, based on clinical expert input. This outcome was not adjusted for multiplicity and was considered to be supportive evidence.
fRated down 1 level for serious imprecision. Based on clinical expert input, 50 more to 100 more per 1,000 patients with serious adverse events could be considered clinically important. The 95% CI included the possibility of both benefit and harm, based on the threshold of 50 more to 100 more per 1,000 patients threshold. Alternatively, if the threshold of 100 more per 1,000 patients was used, the point estimate and 95% CI would indicate little to no clinically important difference and, therefore, there would not be concerns about imprecision.
Sources: FRESCO-2 Clinical Study Report,18 sponsor’s Summary of Clinical Evidence.17
Long-Term Extension Studies
No long-term extension studies were submitted for review.
Indirect Comparisons
One sponsor-conducted indirect treatment comparison (ITC) that compared the efficacy of fruquintinib with alternative third-line or later-line treatments in patients with mCRC was included in the sponsor’s submission in anticipation of the approval of fruquintinib in third-line or later-line setting.19 Fruquintinib was subsequently granted a Notice of Compliance by Health Canada for use in fourth-line or later-line setting (i.e., after the failure of at least 2 lines of standard chemotherapy and either trifluridine-tipiracil or regorafenib). Direct evidence between fruquintinib and the relevant comparator (BSC) in fourth-line or later-line setting was available from the FRESCO-2 study. The sponsor-conducted ITC, which intended to provide indirect comparative evidence between fruquintinib and trifluridine-tipiracil plus bevacizumab in third-line or later-line setting, was therefore considered to have limited relevance for the purpose of this review and will not be further summarized. Refer to Appendix 2 for a summary of the sponsor-conducted ITC, along with a summary of a published ITC (Gao et al. [2023]20) that assessed the same population, intervention, comparison, and outcomes (PICO) identified in the sponsor’s submission.
Studies Addressing Gaps in the Evidence From the Systematic Review
No additional studies were submitted for review.
Conclusions
Direct evidence from 1 double-blind RCT (the FRESCO-2 trial) demonstrated a clinically meaningful improvement in OS and PFS with fruquintinib plus BSC over placebo plus BSC in patients with mCRC who had previously been treated with all standard chemotherapies, an anti-VEGF drug, and an anti-EGFR drug (if RAS is wild-type), and had progressed on or been intolerant to treatment with trifluridine-tipiracil and/or regorafenib. The evidence suggested that fruquintinib may result in little to no clinically important difference in deterioration of HRQoL; however, this is uncertain due to a notable amount of missing data. Fruquintinib had similar treatment effects on OS and PFS in another RCT (the FRESCO trial) that enrolled patients who had received less prior therapy for mCRC. Based on clinical expert input, the patient population in the FRESCO-2 trial was more reflective of the likely place in therapy of fruquintinib as a fourth-line or later-line treatment than the FRESCO trial. Nonetheless, there is uncertainty about whether results from the FRESCO-2 trial are generalizable to the fourth-line or later-line setting, based on treatment history and subsequent anticancer treatment. Fruquintinib plus BSC was associated with a higher frequency of all-grade TEAEs (including hand-foot syndrome, hypertension) than placebo plus BSC. The safety profile of fruquintinib was consistent with the known safety of VEGFR inhibitors, per clinical expert input.
Introduction
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of fruquintinib 1 mg and 5 mg oral capsules in the treatment of adult patients with mCRC who have been previously treated with or are not considered candidates for available standard therapies, including fluoropyrimidine-, oxaliplatin-, and irinotecan-based chemotherapy, an anti-VEGF drug, an anti-EGFR drug (if RAS wild-type), and either trifluridine-tipiracil or regorafenib.
Disease Background
Contents within this section have been informed by materials submitted by the sponsor and clinical expert input. The following has been summarized and validated by the CDA-AMC review team.
CRC arises when cells from a precancerous, benign polyp in the colon or rectum grow uncontrollably.4,21-23 CRC is a highly heterogeneous disease that can result from numerous types of genetic or epigenetic alterations, and can emerge in multiple anatomic sites, with each disease characteristic potentially impacting prognosis and treatment response.24,25 mCRC results when CRC cells become invasive and travel to other parts of the body, most commonly the liver, lungs, and bone.4,5 The National Cancer Institute broadly defines refractory cancer as cancer that is resistant before treatment or becomes resistant during treatment.26 Patients with refractory mCRC have limited treatment options because of their lack of response and/or resistance to upfront systemic therapies.27
CRC is the third-most common cancer type and has the second-highest mortality rate of all cancer types worldwide.5 Based on 2020 GLOBOCAN data and United Nations population data for 185 countries, CRC accounted for 10.7% of all cancer cases.28 The global CRC age-standardized incidence rate was 19.6 per 100,000 person-years (1,931,590 total cases).28 In 2020, patients with CRC contributed 9.5% of deaths among patients with cancer.28 The global age-standardized mortality rate was 9 per 100,000 person-years (935,173 total deaths).28 In Canada, 1 in 16 men and 1 in 18 women will develop CRC during their lifetime, with 1 in 38 men and 1 in 43 women dying from this disease.2
Between 19% and 31% of patients with CRC have metastatic disease at diagnosis, based on data from the US, Canada, Europe, and Japan.26,29-32 Additionally, up to half of all patients with localized disease eventually develop metastases.33 Symptoms of mCRC are more apparent than those at earlier stages of disease and can be attributed to both the disease and its treatment.22,34 The most common symptoms of mCRC include altered bowel habits, such as diarrhea or constipation, blood in stool, fatigue, nausea, abdominal pain, loss of appetite, and unintentional weight loss, per clinical expert input.
The prognosis of mCRC is poor, and patients with late-stage disease have substantially lower survival than those with earlier disease stages.26,29 Prognosis is also typically worse for patients who have progressed on multiple lines of therapy. Clinical trials of patients with mCRC receiving third-line or later-line treatment have reported median OS that ranges from 6.4 months to 7.1 months.6-9 Patients receiving third-line or later-line treatment setting represents individuals who were previously treated with or are not considered candidates for available therapies, including fluoropyrimidine-, oxaliplatin-, irinotecan-, anti-VEGF therapy, and anti-EGFR therapy (if RAS wild-type).35 Patients whose disease progressed on these therapies, as well as on either trifluridine-tipiracil or regorafenib, are eligible for treatment in a fourth-line or later-line setting.
In Canada, CRC is the second leading cause of death from cancer in men and the third leading cause of death from cancer in women.2 Approximately 24,000 Canadians were diagnosed with CRC in 2023, which represented 10% of all new cancer cases.2 In addition, approximately 9,300 patients died from CRC in Canada in 2023, representing 11% of all cancer deaths.2 According to the Global Cancer Observatory, the 5-year prevalence of CRC in Canada is estimated to be 79,009 (8.3 per 100,000).3 In addition, recent global and US epidemiological evidence suggests an alarming increase in early-onset CRC in adults younger than 50 years, who fall below the typical age for CRC screening eligibility criteria.36
Standards of Therapy
Contents within this section have been informed by materials submitted by the sponsor and clinical expert input. The following has been summarized and validated by the CDA-AMC review team.
First-line and second-line treatments for mCRC consist of chemotherapy, which may be combined with molecular targeted therapies. Factors such as patient age, functional and nutritional status, comorbidities, predictive biomarkers, patient preference, and drug toxicity are considered in treatment selection.12 The most widely recommended first-line and second-line treatments for low microsatellite instability or proficient mismatch repair (pMMR) mCRC include fluoropyrimidine-, oxaliplatin-, and/or irinotecan-based chemotherapy (e.g., folinic acid, fluorouracil, and oxaliplatin [FOLFOX]; folinic acid, fluorouracil, and irinotecan [FOLFIRI]; folinic acid, 5-fluorouracil, oxaliplatin, and irinotecan [FOLFOXIRI]; and capecitabine plus oxaliplatin [CAPOX]), which may be combined with targeted therapies.10,11 Unfortunately, most patients relapse or progress after first-line treatment and then receive second-line treatment (i.e., an alternative chemotherapy regimen from the remaining options).10,11,37,38
Based on the CDA-AMC provisional funding algorithm for mCRC treatments (published May 22, 2024)39 for patients with low microsatellite instability, microsatellite stable, or pMMR mCRC, the preferred first-line treatment is multidrug chemotherapy with or without either bevacizumab or panitumumab. Multidrug chemotherapy with panitumumab is listed as an alternative regimen, depending on tumour genetic biomarkers and location (Figure 1).
For patients who progress after first-line therapy, the provisional algorithm positions alternative chemotherapy as an option for second-line therapy, except in the case of a BRAF mutation, which may make a patient eligible for encorafenib plus an EGFR inhibitor.39 Furthermore, in the third-line and beyond, the algorithm includes alternative chemotherapy, encorafenib plus an EGFR inhibitor, an EGFR inhibitor with or without chemotherapy if not received previously, and trifluridine-tipiracil plus bevacizumab as treatment options (Figure 1).
Figure 1: CDA-AMC Provisional Funding Algorithm for mCRC (MSI-L, MSS, pMMR)
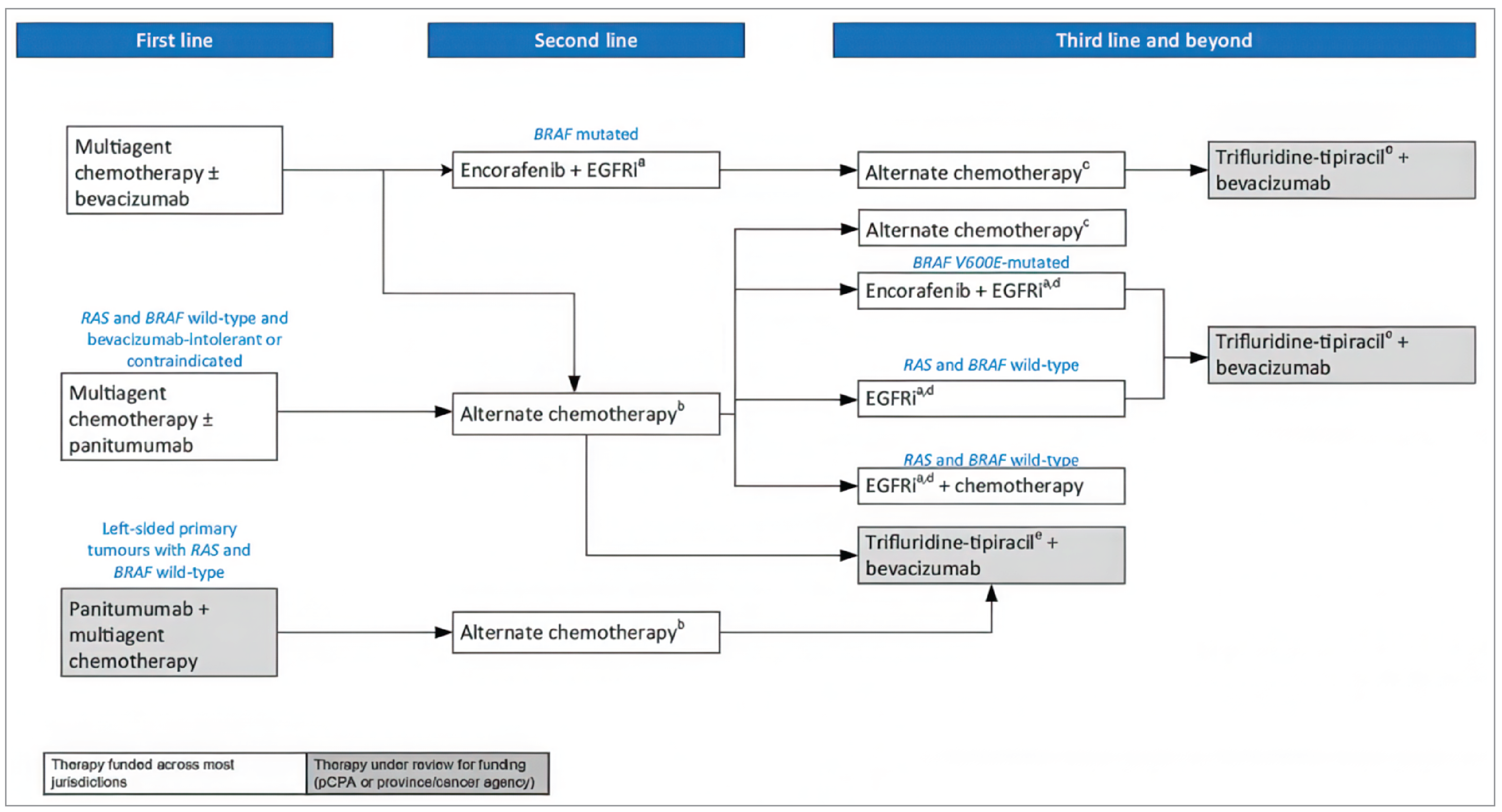
CDA-AMC = Canada's Drug Agency; EGFRi = epidermal growth factor receptor inhibitor; mCRC = metastatic colorectal cancer; MSI-L = low microsatellite instability; MSS = microsatellite stable; pCPA = pan-Canadian Pharmaceutical Alliance; pMMR = proficient mismatch repair.
Note: Encorafenib and EGFRis are classified as targeted therapies.
aEGFRis include cetuximab and panitumumab, where available.
bAlternate chemotherapy with or without bevacizumab. Bevacizumab may be available in some provinces in this setting if the patient did not receive a biologic combined with chemotherapy in previous lines.
cBevacizumab may be available in some provinces in this setting if the patient did not receive a biologic combined with chemotherapy in previous lines.
dThis would be the option if an EGFRi was not received in previous lines.
eTrifluridine-tipiracil in combination with bevacizumab is for patients who are refractory to chemotherapy and have been previously treated with fluoropyrimidine-, oxaliplatin-, and irinotecan-based chemotherapy, anti-VEGF biologics, and anti-EGFR drugs (if RAS is wild-type), and have disease progression or demonstrated intolerance to a maximum of 2 prior chemotherapy regimens for the treatment of advanced colorectal cancer. Patients who had received adjuvant and/or neoadjuvant chemotherapy and had a recurrence during treatment or in the 6 months after completion could count the adjuvant and/or neoadjuvant therapy as 1 of the maximum of 2 required prior chemotherapy regimens to qualify. Patients with small bowel or appendiceal adenocarcinoma are eligible for treatment with trifluridine-tipiracil in combination with bevacizumab.
Source: CDA-AMC Provisional Funding Algorithm for Metastatic Colorectal Cancer.39
In patients with MSI-H, dMMR mCRC, the preferred first-line treatment is pembrolizumab (Figure 2).39 For patients who progress after first-line therapy with pembrolizumab, multidrug chemotherapy with or without either bevacizumab or panitumumab or encorafenib plus an EGFR inhibitor are advised, depending on the molecular characteristics that guide treatment. For patients who progress after second-line therapy, the algorithm recommends alternative chemotherapy, unless encorafenib plus an EGFR inhibitor can be considered because of the presence of a BRAF mutation. Furthermore, in the fourth-line setting and beyond, the algorithm includes alternative chemotherapy, an EGFR inhibitor with or without chemotherapy, and trifluridine-tipiracil plus bevacizumab as treatment options, depending on the genetic and refractory status of the patient (Figure 2).39
Figure 2: CDA-AMC Provisional Funding Algorithm for mCRC (MSI-H, dMMR)
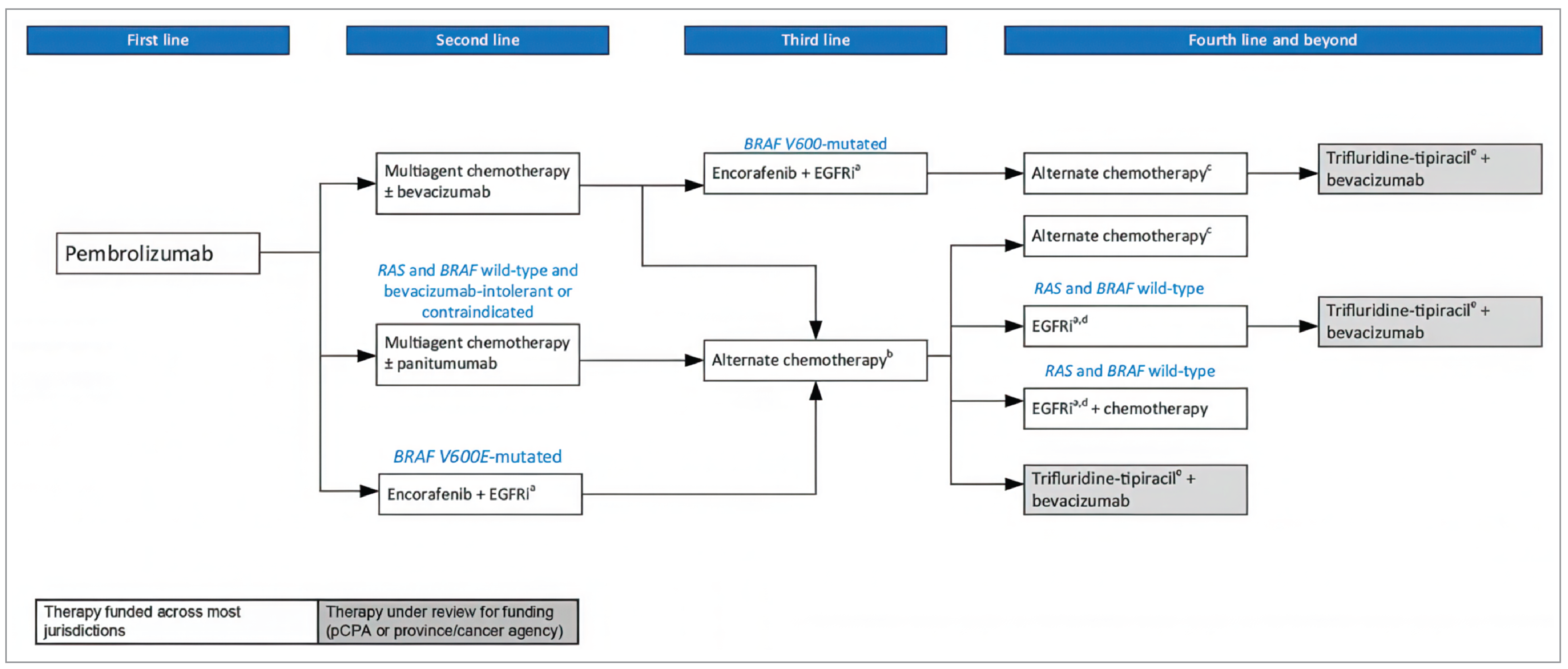
CDA-AMC = Canada's Drug Agency; dMMR = deficient mismatch repair; EGFRi = epidermal growth factor receptor inhibitor; mCRC = metastatic colorectal cancer; MSI-H = high microsatellite instability; pCPA = pan-Canadian Pharmaceutical Alliance.
Notes: Pembrolizumab is classified as an immunotherapy. Encorafenib and EGFRis are classified as targeted therapies.
aEGFRis include cetuximab and panitumumab, where available.
bAlternative chemotherapy with or without bevacizumab. Bevacizumab may be available in some provinces in this setting if the patient did not receive a biologic combined with chemotherapy in previous lines.
cBevacizumab may be available in some provinces in this setting if the patient did not receive a biologic combined with chemotherapy in previous lines.
dThis would be the option if an EGFRi was not received in previous lines.
eTrifluridine-tipiracil in combination with bevacizumab is for patients who are refractory to chemotherapy and have been previously treated with fluoropyrimidine-, oxaliplatin-, and irinotecan-based chemotherapy, anti-VEGF biologics, and anti-EGFR drugs (if RAS is wild-type), and have disease progression or demonstrated intolerance to a maximum of 2 prior chemotherapy regimens for the treatment of advanced colorectal cancer. Patients who had received adjuvant and/or neoadjuvant chemotherapy and had a recurrence during treatment or in the 6 months after completion could count the adjuvant and/or neoadjuvant therapy as 1 of the maximum of 2 required prior chemotherapy regimens to qualify. Patients with small bowel or appendiceal adenocarcinoma are eligible for treatment with trifluridine-tipiracil in combination with bevacizumab.
Source: CDA-AMC Provisional Funding Algorithm for Metastatic Colorectal Cancer.39
BSC encompasses interventions that provide palliation of symptoms and maintain or improve QoL for patients who either do not have active treatment options or are not suitable candidates for such treatments.39 In the third-line or later-line setting, BSC alone is offered to patients who have exhausted all active treatment options or when further active treatment is not appropriate due poor performance status or severe comorbid illness, per clinical expert input. Trifluridine-tipiracil and regorafenib have been studied as single-drug treatments in the third-line or later-line setting; their benefits are modest and they are currently not publicly funded in Canada. Trifluridine-tipiracil plus bevacizumab combination therapy has recently received a positive CDA-AMC reimbursement recommendation,13 and is currently under consideration for public funding as a third-line or later-line treatment. There is currently no approved treatment for patients with disease that has progressed on available standard chemotherapy and either trifluridine-tipiracil or regorafenib (i.e., fourth-line or later-line setting); BSC is available to these patients in clinical practice.
According to the clinical experts, the primary goals of treatment for patients with mCRC are to prolong survival, delay disease progression, and improve well-being and QoL. Symptom management and the minimization of treatment-related AEs are important for maintaining QoL and overall well-being. Specifically, in the context of last-line therapy, prolonging survival and improving QoL while minimizing treatment-related AEs and the burden of frequent treatment-related visits are meaningful goals for patients, per clinical expert input.
Drug Under Review
The key characteristics of fruquintinib are summarized in Table 4.
Fruquintinib is a highly selective, small-molecule tyrosine kinase inhibitor of VEGFR-1, VEGFR-2, and VEGFR-3, with antitumour effects that include the suppression of tumour angiogenesis and lymphangiogenesis.40-42 Fruquintinib is available as 1 mg and 5 mg oral capsules. The recommended dose is 5 mg administered orally once daily for 21 consecutive days, followed by a 7-day rest period, to comprise a complete cycle of 28 days. Treatment with fruquintinib should be continued until disease progression or unacceptable toxicity occurs. Dose reductions to 4 mg or 3 mg daily may be considered to manage AEs.
This is the first reimbursement review of fruquintinib conducted by CDA-AMC. The Health Canada indication for fruquintinib is for the treatment of adult patients with mCRC who have been previously treated with or are not considered candidates for available standard therapies, including fluoropyrimidine-, oxaliplatin-, and irinotecan-based chemotherapy, an anti-VEGF drug, an anti-EGFR drug (if RAS wild-type), and either trifluridine-tipiracil or regorafenib. The sponsor is seeking reimbursement of fruquintinib as per the indication. The sponsor characterized the patient population of interest as follows:
patients who have shown disease progression despite receiving the aforementioned standard treatments; disease progression can be identified through radiological imaging or clinical deterioration
previously treated patients include those who have received the aforementioned standard therapies or are intolerant to associated toxicities
patients who have preexisting medical conditions or comorbidities that preclude the use of standard therapies could be considered as not being candidates for these standard therapies.
Table 4: Key Characteristics of Fruquintinib
Characteristic | Fruquintinib |
|---|---|
Mechanism of action | A highly selective, small-molecule tyrosine kinase inhibitor of VEGFR-1, VEGFR-2, and VEGFR-3, with antitumour effects that include the suppression of tumour angiogenesis and lymphangiogenesis |
Indicationa | For the treatment of adult patients with mCRC who have been previously treated with or who are not considered candidates for available standard therapies, including fluoropyrimidine-, oxaliplatin-, and irinotecan-based chemotherapy, an anti-VEGF drug, an anti-EGFR drug (if RAS wild-type), and either trifluridine-tipiracil or regorafenib |
Route of administration | Orally |
Recommended dose | 5 mg once daily for the first 21 days of every 28-day treatment cycle |
Serious adverse effects or safety issues | Hypertension, hemorrhagic events, influence on the ability to drive and use machines, gastrointestinal perforation, arterial thromboembolic events, posterior reversible encephalopathy syndrome, proteinuria, impaired wound healing, palmar-plantar erythrodysesthesia, and embryo-fetal toxicity |
Other | NA |
mCRC = metastatic colorectal cancer; NA = not applicable.
aHealth Canada–approved indication.
Source: Product monograph for fruquintinib.43
Perspectives of Patients, Clinicians, and Drug Programs
Patient Group Input
This section was prepared by the CDA-AMC review team based on the input provided by patient groups. The full patient and clinician group submissions received are available in the consolidated patient and clinician group input document for this review on the project website here.
CDA-AMC received 2 patient group submissions from CCRAN and Colorectal Cancer Canada. CCRAN is a national, not-for-profit patient advocacy group championing the health and well-being of patients in Canada touched by CRC and those at risk of developing the disease by providing support, education, and advocacy to help improve patient longevity and QoL. Colorectal Cancer Canada is a not-for-profit CRC patient organization dedicated to CRC awareness and education, supporting patients and their caregivers and advocating on their behalf.
CCRAN employed a multifaceted outreach approach that resulted in 3 patient interviews and a survey of patients with mCRC; of the 119 patients who responded from March 21 to April 17, 2024, 115 resided in Canada and the remaining 4 resided in the US. Data were gathered by Colorectal Cancer Canada using 4 online patient interviews, conducted between April 1 and May 15, 2024, and 1 online survey, conducted in August 2023, to which 15 patients and 1 caregiver responded.
Most patients reported that abdominal cramps, gas, bloating, and pain, fatigue, weakness, bloody stools, and diarrhea are common impacts of the disease that affect QoL and result in an inability to work, exercise, participate in social activities, fulfill family obligations, and concentrate. The caregivers also noted significant difficulties caring for patients with mCRC. Fluorouracil-based chemotherapy, capecitabine, bevacizumab and panitumumab were cited as being the most frequently used treatments by the respondents, with the most common side effects being fatigue, hair loss, nausea, peripheral neuropathy, and diarrhea. Both patient groups reported that it is very important for a new therapy to improve the physical condition of patients (e.g., tumour shrinkage, tumour stability, reduction of pain, and improved breathing) and their QoL. Four respondents from CCRAN’s and 3 respondents from Colorectal Cancer Canada’s survey had experience with fruquintinib treatment; the patients’ main access to fruquintinib was through a clinical trial centre in the US Patients reported that fruquintinib treatment helped stabilize their disease and was easy to administer as an oral therapy. Most patients experienced hand-foot syndrome associated with fruquintinib treatment, but noted that it was manageable. Both groups reported that access to fruquintinib for patients in the refractory mCRC setting is of utmost importance because it could provide these patients with an effective treatment option to stabilize their disease and improve their QoL.
Clinician Input
Input From Clinical Experts Consulted by CDA-AMC
All CDA-AMC review teams include at least 1 clinical specialist with expertise in the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). The following input was provided by 2 clinical specialists with expertise in the diagnosis and management of mCRC.
Unmet Needs
The clinical experts consulted by CDA-AMC noted that despite advancements in the treatment of patients with mCRC, several gaps exist. The clinical experts noted that while treatments have extended OS, the median OS remains short, and survival beyond 5 years is still uncommon for most patients. Many patients experience progression despite initial responses to therapy, according to the clinical experts. As well, the clinical experts noted that the toxicity and side effects related to available treatments could significantly diminish QoL, underscoring the need for more effective treatments with durable disease control, fewer adverse effects, and that can delay declines in QoL from the underlying cancer. They also noted that comprehensive biomarker profiling and adaptive treatment strategies are required to personalize therapy more effectively. Furthermore, equitable access to novel treatments remains a key barrier for many patients with mCRC, per the clinical experts.
Place in Therapy
The clinical experts said they expect fruquintinib to be used in patients with mCRC in the fourth-line or later-line setting (i.e., have disease refractory to or intolerable toxicity to at least 2 lines of standard chemotherapy [including fluoropyrimidine, irinotecan, and oxaliplatin], and to trifluridine-tipiracil plus bevacizumab). The clinical experts also noted that trifluridine-tipiracil plus bevacizumab combination therapy is currently under consideration for public funding as a third-line or later-line treatment; in the event that trifluridine-tipiracil plus bevacizumab is not publicly funded, the use fruquintinib as a third-line treatment after the failure of all standard chemotherapies may be considered.
The clinical experts also noted that most patients would have also received targeted therapy and immunotherapy, if indicated, before receiving fruquintinib or trifluridine-tipiracil plus bevacizumab, per the current treatment approach in Canada.
Patient Population
The clinical experts noted that fruquintinib would be most appropriate for patients with mCRC who have good performance status and have disease that has progressed on or intolerable toxicity to all standard approved cytotoxic treatments, targeted therapies, and immunotherapies, as well as trifluridine-tipiracil plus bevacizumab or regorafenib. The clinical experts noted that patients, typically in the later lines of therapy, have limited treatment options and are in urgent need of effective treatment. The clinical experts noted that patients with severe comorbid illnesses that may contraindicate the use of VEGFR inhibitors, such as significant cardiovascular disease, poorly controlled hypertension, or poor performance status, would not be appropriate candidates for fruquintinib treatment (a VEGFR inhibitor). They clinical experts noted that no companion diagnostic test is required for fruquintinib treatment.
The clinical experts noted patients with an ECOG PS score of 0 or 1 are potential candidates for fruquintinib. When considering the use of fruquintinib in patients with an ECOG PS of 2 (who were excluded from the clinical trials), the clinical experts stated that it would be reasonable to leave the decision to the treating physicians’ judgment, based on patient-specific factors, recognizing that an ECOG PS score of 2 does not necessarily preclude eligibility for treatment in clinical practice. However, for patients with an ECOG PS score of more than 2, the clinical experts noted that it would be inappropriate to prescribe fruquintinib in the absence of evidence and that the benefit would likely outweigh the harms.
The clinical experts also noted that patients with untreated or unstable CNS metastases would not be suitable candidates for fruquintinib treatment.
Assessing the Response to Treatment
The clinical experts noted that in clinical practice, disease control and treatment tolerance are 2 important outcomes used to determine if a patient is responding to treatment. According to the clinical experts, a clinically meaningful response includes improved survival, significant reductions in the frequency and severity of disease-related symptoms, an enhanced ability to perform daily activities, and noticeable improvements in QoL. These outcomes are typically evaluated with periodic assessments, blood work, and imaging scans, per clinical expert input. The clinical experts noted that patients are generally seen in each cycle (28 days in the case of fruquintinib), with blood work and a CT scan of chest, abdomen, and pelvis performed every 2 to 3 cycles (8 to 12 weeks).
Discontinuing Treatment
The clinical experts noted that treatment discontinuation would be considered upon disease progression, severe or serious AEs despite dose modification, and a decline in the patient’s clinical condition. The clinical experts noted that, typically, treatment discontinuation is indicated upon clinical and radiographic progression; however, in some cases, when there is significant discordance between clinical improvement and radiographic changes, treatment may be continued for a few more cycles, at the treating oncologist’s discretion, until a lack of benefit is confirmed by the clinician.
Prescribing Considerations
The clinical experts noted that fruquintinib should be prescribed by an oncologist with expertise in assessing and monitoring patients with mCRC, given the complexities of managing mCRC and the potential for AEs with fruquintinib.
Clinician Group Input
This section was prepared by the CDA-AMC review team based on the input provided by a clinician group. The full clinician group submission received is available in the consolidated patient and clinician group input document for this review on the project website here.
CDA-AMC received 1 clinician group submission from the CGOEN, represented by 16 clinicians in Canada.
In general, CGOEN shared a consistent view on the management of mCRC with the clinicians consulted by CDA-AMC. The clinician group stated that the main goals of treatment for mCRC are improving OS and QoL while minimizing toxicities from treatment. In terms of unmet need, the clinician group noted that there are currently no publicly funded treatment options for patients with mCRC who have been previously treated with, or are intolerant to, standard chemotherapy. However, with recent a positive reimbursement recommendation for trifluridine-tipiracil in combination with bevacizumab for treatment-refractory CRC, the clinician group indicated that fruquintinib could be considered in patients who would not be eligible for trifluridine-tipiracil plus bevacizumab or in patients who previously received trifluridine-tipiracil plus bevacizumab, which could provide the clinical flexibility required in this specific later-line setting.
Last, the clinician group indicated that fruquintinib would be used in patients with mCRC who have been treated with or who are intolerant of fluoropyrimidine, irinotecan, and oxaliplatin. Furthermore, it would be considered after encorafenib-based therapy in patients with BRAF-mutant tumours, immunotherapy in patients with dMMR tumours, anti-EGFR therapies in patients with KRAS wild-type tumours, and anti-VEGF therapies as well as patients who have not received previous anti-VEGF therapy. The clinician group further commented that patients would undergo clinical evaluations on a regular basis for clinical response and toxicity, and a meaningful response would be patient preference, tolerability of treatment, QoL, and response on imaging. Moreover, fruquintinib should be discontinued upon disease progression (i.e., radiologic or clinical), toxicity, clinician discretion, or patient’s request. The clinician group also mentioned that fruquintinib could be reasonably given in any centre and by any specialist who is currently treating patients with mCRC with systemic therapy.
Drug Program Input
The drug programs provide input on each drug being reviewed through the CDA-AMC Reimbursement Review processes by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CDA-AMC are summarized in Table 5.
Table 5: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Considerations for initiation of therapy | |
Given the negative CDA-AMC recommendation for trifluridine-tipiracil monotherapy and the fact regorafenib is not publicly funded, can pERC confirm whether eligible patients must have progressed on or been deemed not a candidate for trifluridine-tipiracil plus bevacizumab? | The clinical experts noted that results favoured fruquintinib plus BSC over placebo plus BSC in the FRESCO-2 trial, in which the majority of patients had previously received trifluridine-tipiracil. In the opinion of the clinical experts, it would be reasonable for patients who experienced disease progression on or who are not candidates for trifluridine-tipiracil plus bevacizumab to receive fruquintinib treatment. |
Considerations for discontinuation of therapy | |
In the FRESCO-2 trial, patients who experienced progressive disease were able to continue treatment if the investigator deemed that there could be further clinical benefit. What discontinuation criteria should be used for fruquintinib? | The clinical experts noted that, typically, treatment discontinuation is indicated upon clinical and radiographic progression; however, in some cases, when there is a significant discordance between clinical improvement and radiographic changes (e.g., when there is doubt about progression or when there is no clinical progression), treatment may be continued for a few more cycles, at the treating oncologist’s discretion, until a lack of benefit is confirmed. The clinical experts noted that treatment discontinuation would be considered upon disease progression, severe or serious AEs despite dose modification, and a decline in a patient’s clinical condition. |
Generalizability | |
Should fruquintinib be used in patients with:
| The clinical experts agreed that patients with small bowel or appendiceal adenocarcinoma could be potential candidates for fruquintinib treatment, as could be in patients with MSI-H/dMMR and patients with BRAF V600E mutation after progression on immunotherapy or a BRAF inhibitor, respectively. The clinical experts noted patients with an ECOG PS of 0 or 1 are potential candidates for fruquintinib. When considering the use of fruquintinib in patients with an ECOG PS of 2 (who were excluded from the clinical trials), the clinical experts stated that it is reasonable to leave the decision to the treating physicians’ judgment based on patient-specific factors, recognizing that an ECOG PS score of 2 does not necessarily preclude eligibility for treatment in clinical practice. However, for patients with an ECOG PS greater than 2 (excluded from the trials), the clinical experts felt it would be inappropriate to prescribe fruquintinib in the absence of evidence, and that the harms would likely outweigh the benefits in these patients. |
Funding algorithm | |
Provisional funding algorithm to be updated to include fruquintinib. | For pERC consideration. |
System and economic issues | |
Trifluridine-tipiracil with bevacizumab will be negotiated by pCPA. | For pERC consideration. |
AE = adverse event; BSC = best supportive care; CDA-AMC = Canada's Drug Agency; dMMR = deficient mismatch repair; ECOG PS = Eastern Cooperative Oncology Group Performance Status; MSI-H = microsatellite instability-high; pCPA = pan-Canadian Pharmaceutical Alliance; pERC = pan-Canadian Oncology Drug Review Expert Review Committee.
Clinical Evidence
The objective of CDA-AMC’s Clinical Review Report is to review and critically appraise the clinical evidence submitted by the sponsor on the beneficial and harmful effects of fruquintinib 1 mg and 5 mg oral capsules in the treatment of adult patients with mCRC who have been previously treated with or are not considered candidates for available standard therapies, including fluoropyrimidine-, oxaliplatin-, and irinotecan-based chemotherapy, an anti-VEGF drug, an anti-EGFR drug (if RAS wild-type), and either trifluridine-tipiracil or regorafenib. The focus will be placed on comparing fruquintinib to relevant comparators and identifying gaps in the current evidence.
A summary of the clinical evidence included by the sponsor in the review of fruquintinib is presented in 4 sections, with the CDA-AMC critical appraisal of the evidence included at the end of each section. The first section, the Systematic Review, includes pivotal studies and RCTs selected according to the sponsor’s systematic review protocol. The CDA-AMC’s assessment of the certainty of the evidence in this first section, using the GRADE approach, follows the critical appraisal of the evidence. The second section typically includes sponsor-submitted long-term extension studies, but no such evidence was submitted for this review. The third section includes indirect evidence from the sponsor. The fourth section typically includes additional studies that were considered by the sponsor to address important gaps in the systematic review evidence, but such studies were not submitted.
Included Studies
Clinical evidence from the following is included in the CDA-AMC review and appraised in this document:
2 RCTs identified in the sponsor-conducted systematic review (the FRESCO and FRESCO-2 trials)
1 sponsor-conducted ITC and 1 published ITC (Gao et al. [2023]20). Note that the relevance of the ITCs was considered by the review team to be limited because they aimed to assess patients with mCRC in the third-line or later-line setting (after the failure of at least 2 lines of standard chemotherapy). A summary of the results and critical appraisal of the ITCs is presented in Appendix 2.
Systematic Review
Contents within this section have been informed by materials submitted by the sponsor. The following has been summarized and validated by the CDA-AMC review team.
Description of Studies
Characteristics of the included studies are summarized in Table 6.
Two multicentre, randomized, double-blind, placebo-controlled, phase III trials (the FRESCO trial, N = 416; the FRESCO-2 trial, N = 691)14,15 that compared the efficacy and safety of fruquintinib plus BSC with placebo plus BSC in patients with metastatic colorectal adenocarcinoma were identified in the sponsor-conducted systematic review. The FRESCO trial enrolled patients who had progressed on or experienced intolerable toxicity to at least 2 lines of standard chemotherapy. The FRESCO-2 trial enrolled patients who were previously treated with standard chemotherapy, anti-VEGF therapy, and anti-EGFR therapy (if RAS wild-type), and had progressed on or been intolerant to treatment with trifluridine-tipiracil and/or regorafenib. The FRESCO trial was conducted in 28 study sites in China. The FRESCO-2 trial was conducted in 124 sites in the Asia-Pacific region, Europe, and North America (there were no sites in Canada). The FRESCO and FRESCO-2 trials were initiated on December 8, 2014, and August 14, 2020, respectively. The final analysis is complete for both trials. This report presents the final efficacy analysis at the data cut-off on January 17, 2017 (FRESCO trial), and June 24, 2022 (FRESCO-2 trial).
The FRESCO trial consisted of 3 study phases: screening, treatment, and follow-up. After a 21-day screening phase to assess study eligibility, eligible patients entered the treatment phase, in which they were randomized in a 2:1 ratio to receive fruquintinib plus BSC or placebo plus BSC in a double-blinded manner. Randomization was stratified by previous use of VEGF inhibitors (yes versus no) and KRAS gene status (wild-type versus mutant) using the Interactive Web Response System. Patients received study interventions until disease progression or intolerable toxicity. They were subsequently monitored in the post- end of treatment follow-up period for 30 days and followed for survival every 2 months.
The study design of the FRESCO-2 trial was similar to that of the FRESCO trial, except that screening occurred in the 28 days before randomization and that randomization was stratified based on prior therapy (trifluridine-tipiracil versus regorafenib versus both trifluridine-tipiracil and regorafenib), KRAS status (wild-type versus mutant), and duration of metastatic disease (18 months or less versus more than 18 months). As well, the follow-up period of the FRESCO-2 trial consisted of an end-of-treatment visit 7 days after the last dose of the intervention drug, a safety follow-up 30 days after the end-of-treatment visit), and survival follow-up that occurred every 12 weeks.
Populations
Inclusion and Exclusion Criteria
The key inclusion and exclusion criteria for the FRESCO and FRESCO-2 trials are summarized in Table 6.
The studies enrolled adults with metastatic colorectal adenocarcinoma who had measurable disease or lesions by RECIST 1.1 and had an ECOG PS of 0 or 1. In the FRESCO trial, enrolled patients had a history of disease progression or intolerable toxicity to at least 2 lines of standard chemotherapy, including fluorouracil, oxaliplatin, and irinotecan. In the FRESCO-2 trial, enrolled patients had previously received standard fluoropyrimidine-, oxaliplatin-, and irinotecan-based chemotherapy; an anti-VEGF therapy; and an anti-EGFR therapy (if RAS is wild-type). In addition, patients in the FRESCO-2 trial had disease that progressed on or experienced intolerably toxicity to treatment with trifluridine-tipiracil and/or regorafenib. As well, patients had received immune checkpoint inhibitor treatment (if MSI-H or dMMR tumours) or a BRAF inhibitor (if BRAF-mutant positive) if eligible.
The FRESCO trial excluded patients with current CNS metastasis or prior brain metastases. The FRESCO-2 study excluded patients with untreated brain metastases and/or spinal cord compression, patients with no evidence of stable disease of the CNS for 14 days or longer, and patients who required steroid treatment in the previous 4 weeks.
Table 6: Details of Studies Included in the Systematic Review
Detail | FRESCO | FRESCO-2 |
|---|---|---|
Designs and populations | ||
Study design | Phase III, multicentre, randomized, double-blind, placebo-controlled trial | Phase III, multicentre, randomized, double-blind, placebo-controlled trial |
Locations | 28 study sites (all in China) | 124 sites (in Asia-Pacific, Europe, and North America; 0 sites in Canada) |
Patient enrolment dates | Start date: December 8, 2014 Data cut-off date: January 17, 2017 | Start date: August 14, 2020 Data cut-off: June 24, 2022 |
Randomized | Total N = 416 (for fruquintinib plus BSC, n = 278; for placebo plus BSC, n = 138) | Total N = 691 (fruquintinib + BSC, n = 461; placebo + BSC, n = 230) |
Key inclusion criteria |
|
|
Key exclusion criteria |
|
|
Drugs | ||
Intervention | Fruquintinib 5 mg once daily, orally, in combination with BSC, for 3 consecutive weeks followed by 1 week off treatment (28-day cycle). The 28-day treatment cycles continue until disease progression or intolerable toxicity. | Fruquintinib 5 mg once daily, orally, in combination with BSC, for 3 consecutive weeks followed by 1 week off treatment (28-day cycle). The 28-day treatment cycles continue until disease progression or intolerable toxicity. Study treatment could be continued beyond radiographic progression until loss of clinical benefit if the patient was believed to be deriving clinical benefit by the investigator. |
Comparator(s) | Placebo once daily, orally, in combination with BSC, for 3 consecutive weeks followed by 1 week off treatment (28-day cycle). The 28-day treatment cycles continue until disease progression or intolerable toxicity. | Placebo once daily, orally, in combination with BSC, for 3 consecutive weeks followed by 1 week off treatment (28-day cycle). The 28-day treatment cycles continue until disease progression or intolerable toxicity. |
Study duration | ||
Screening phase | 21 days | 28 days |
Treatment phase | Until disease progression or intolerable toxicity | |
Follow-up phase |
|
|
Outcomes | ||
Primary end point | OS | OS |
Secondary and exploratory end points | Secondary:
Safety:
| Key secondary:
Secondary:
Exploratory:
|
Publication status | ||
Publications | Li et al. (2018)14 (NCT02314819). | Dasari et al. (2023)15 (NCT04322539). |
BSC = best supportive care; CNS = central nervous system; DCR = disease control rate; dMMR = deficient mismatch repair; DOR = duration of response; ECG = electrocardiogram; ECOG PS = Eastern Cooperative Oncology Group Performance Status; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; EQ-5D-5L = 5-Level EQ-5D; MSI-H = microsatellite instability-high; ORR = objective response rate; PFS = progression-free survival; RECIST 1.1 = Response Evaluation Criteria in Solid Tumours Version 1.1; TEAE = treatment-emergent adverse event.
aThe criterion pertaining to prior standard chemotherapy was not specific to metastatic disease.
bOr ≥ age 20 years in Japan.
cWith documented RAS, BRAF, and microsatellite instability/mismatch repair status.
dThe criterion pertaining to prior standard chemotherapy was not specific to metastatic disease. Patients were required to have been previously treated with standard chemotherapies, but progression on or intolerance to standard chemotherapy was not specifically required by the protocol eligibility criteria.
ePatients who received oxaliplatin in the adjuvant setting and developed metastatic disease during treatment or within 6 months of completing adjuvant therapy, was considered eligible without receiving oxaliplatin in the metastatic setting. Patients who developed metastatic disease more than 6 months after completion of oxaliplatin-containing adjuvant treatment must have been treated with oxaliplatin-based therapy in the metastatic setting to be eligible.
fUntreated with surgery or radiotherapy.
Sources: Clinical Study Reports for FRESCO and FRESCO-2 trials,16,18 sponsor’s Summary of Clinical Evidence.17
Interventions
In both trials, patients received either fruquintinib 5 mg or placebo capsules, orally on an empty stomach, daily for 3 consecutive weeks followed by 1 week off treatment (28-day cycle). Patients continued treatment cycles along with BSC until the occurrence of progressive disease, death, intolerance to toxicity, or until other criteria for the termination of treatment were met. In the FRESCO-2 study, treatment could be continued beyond radiographic progression until the loss of clinical benefit if the patient was believed to be deriving clinical benefit by the investigator. When clinically significant toxicities were present, dose reductions of fruquintinib to 4 mg or 3 mg daily were allowed.
The sponsor noted that BSC encompassed symptom management (e.g., pain control, nausea and vomiting, fatigue, or other symptoms), psychological support, nutritional support, and certain palliative care. Sites were permitted to implement their own institutional protocols for BSC to ensure that patients received care aligned with established standards and practices.
Anticoagulants, prophylactic antiemetic, granulocyte colony-stimulating factors, granulocyte macrophage colony-stimulating factors, platelet-simulating factors, or erythropoietin were permitted as clinically indicated. The concomitant use of anticancer treatments, such as chemotherapy, radiotherapy, biologic therapy, and hormonal therapy, were prohibited. Palliative radiation was allowed to control symptoms, provided it did not compromise tumour assessments of target lesions.
Double-blinding was in place so the investigators and patients were not aware of the treatment assignment. Fruquintinib and placebo capsules were identical in appearance. If a dose adjustment was required, 1 mg fruquintinib or matching placebo capsules were used.
Outcomes
A list of efficacy and safety end points assessed in this Clinical Review Report is provided in Table 7, followed by descriptions of the outcome measures. Summarized end points are based on outcomes included in the sponsor’s Summary of Clinical Evidence, as well as any outcomes identified as important to this review by the clinical experts consulted by CDA-AMC and input from patient and clinician groups and public drug plans. Using the same considerations, the CDA-AMC review team selected end points that were considered to be most relevant to inform CDA-AMC expert committee deliberations and finalized this list of end points in consultation with members of the expert committee. All summarized efficacy end points were assessed using the GRADE approach. Select notable harms outcomes considered important for CDA-AMC’s expert committee deliberations were also assessed using GRADE.
Considerations that informed the selection of efficacy outcomes to be summarized and assessed using the GRADE approach include the following:
OS and PFS were noted to be important outcomes, according to input from patient and clinician groups and the clinician experts consulted by CDA-AMC, and were used to inform the sponsor’s pharmacoeconomic model. The probabilities of OS and PFS at specific time points (6 months, 12 months, and 18 months for OS; 3 months, 6 months, and 9 months for PFS) were selected in consultation with the clinical experts.
Tumour response outcomes (objective response rate, disease control rate, duration of response, duration of stable disease) were excluded, as per clinical expert input that tumour response outcomes were not as meaningful as survival outcomes in the population under review, in which most patients are expected to receive fruquintinib as the last line of therapy.
HRQoL was identified as an important outcome in patients with mCRC, as per input from patient and clinician groups and the clinical experts. EORTC QLQ-C30 is a cancer-specific HRQoL instrument; the responder analysis based on the proportion of patients with at least a 6.38-point deterioration from baseline in global health status, specifically, was included in the GRADE assessment. The 5-Level EQ-5D is a generic HRQoL measure and was excluded from the GRADE assessment.
Harms were considered important outcomes, according to input from patient and clinician groups and the clinical experts. SAEs were selected for GRADE assessment.
Table 7: Outcomes Summarized From the FRESCO and FRESCO-2 Trials
Outcome measure | Time point | FRESCO | FRESCO-2 |
|---|---|---|---|
Efficacy | |||
OS | Months 6, 12, and 18 | Primary | Primarya |
PFS | Months 3, 6, and 9 | Secondary | Key secondarya |
EORTC QLQ-C30 | Last on-treatment visit | Not measured | Secondary |
Harms | |||
Serious adverse event | Throughout the study | Safety | Secondary |
Outcome not assessed | |||
Caregiver burden | Not measured | Not measured | Not measured |
EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; OS = overall survival; PFS = progression-free survival.
aStatistical testing for these end points was adjusted for multiple comparisons (e.g., hierarchal testing).
Sources: Clinical Study Reports for FRESCO and FRESCO-2 trials,16,18 sponsor’s Summary of Clinical Evidence.17
Efficacy Outcomes
Overall Survival
OS was the primary end point in both trials, and was defined as the time between the date of randomization and the date of death from any cause. Based on consensus from Colorectal Cancer Canada, an improvement of 2 months or more in median OS or a HR for survival of 0.75 or lower are the thresholds for a clinically meaningful benefit.44
Based on input from the clinical experts consulted by CDA-AMC, a difference of 5% to 10% between the fruquintinib plus BSC group and the placebo plus BSC group is likely to be clinically important with respect to the probability of survival at 6 months, 12 months, and 18 months.
Progression-Free Survival
PFS was a secondary end point in the FRESCO trial and a key secondary end point in the FRESCO-2 trial. It was defined as the time from randomization until the first radiographic documentation of objective progressive disease (as assessed by the investigator using RECIST 1.1) or death from any cause, whichever was earlier.
Based on input from the clinical experts consulted by CDA-AMC, a difference of 5% to 10% between the fruquintinib plus BSC group and the placebo plus BSC group is likely to be clinically important with respect to the probability of survival at 3 months, 6 months, and 9 months.
European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30
The EORTC QLQ-C30 is a patient-reported outcome instrument designed to assess the HRQoL of patients with cancer by evaluating functional, symptom, and global health status or QoL domains. Scores range from 0 to 100 after linear transformation. Higher scores for global health status or QoL and functioning scales represent higher functioning (i.e., a better state) or higher levels of symptoms (i.e., a worse state).
The proportion of patients with at least a 6.38-point reduction from baseline in global health status score was assessed as a secondary outcome in the FRESCO-2 trial. The minimally important difference (MID) threshold of a 6.38-point deterioration was selected by the sponsor based on a study of patients with ovarian cancer.45 A study of patients with advanced CRC treated with chemotherapy was used to estimate the anchor-based MIDs for between-group differences in change in global health status score, which ranged from 5.53 to 6.36 (weighted value of 5.86) for improvement and ranged from –9.21 to –6.81 (weighted value of –8.13) for deterioration.46
Based on input from the clinical experts consulted by CDA-AMC, a difference of at least 10% between the fruquintinib plus BSC group and the placebo plus BSC group is likely to be clinically important with respect to the proportion of patients with at least a 6.38-point reduction from baseline in global health status score.
Harms Outcomes
Harms outcomes, including TEAEs, SAEs, WDAEs, death, and notable harms (hypertension, proteinuria, palmar-plantar erythrodysesthesia syndrome, hemorrhage, thromboembolic events, gastrointestinal perforations), were assessed. Based on input from the clinical experts consulted by CDA-AMC, a difference of 5% to 10% between the fruquintinib plus BSC group and the placebo plus BSC group is likely to be clinically important with respect to the proportion of patients with SAEs.
Outcomes Not Assessed
Caregiver burden was not an outcome assessed in either of the trials.
Statistical Analysis
Sample Size and Power Calculations
Sample size and power calculations were not reported in the FRESCO trial. The FRESCO-2 trial was designed to randomize approximately 687 patients over approximately 15 months in the intention-to-treat (ITT) population, and achieve at least 480 death events, to detect an HR of 0.73 (fruquintinib plus BSC versus placebo plus BSC) with respect to OS at a 1-sided alpha of 0.025 and with a power of 90%, using a stratified log-rank test, based on the following assumptions:
an enrolment rate of 30 patients per month during the first 3 months, and 50 patients per month thereafter
a yearly dropout rate of 10%
the randomization of patients to fruquintinib and placebo in a 2:1 ratio
data maturity at 70%.
Interim and Final Analyses
No formal interim analysis was performed during the FRESCO trial. The planned final analysis was to occur after approximately 280 OS events in the trial. In the FRESCO-2 trial, 1 planned interim analysis for futility and 1 planned final analysis were to occur after 160 and 480 OS events, respectively. The independent data monitoring committee was instructed to recommend discontinuation of the study for futility at the interim analysis if the 1-sided P value from a stratified long-rank test was at least 0.772 (corresponding to an observed HR of 1.133).
Statistical Analysis
In the primary analysis of OS and PFS in both trials, the between-group difference was tested using a stratified log-rank test with a 2-sided alpha of 0.05 in the intention-to-treat population. In the FRESCO trial, stratifications by prior use of VEGF inhibitor and KRAS gene state were applied. In the FRESCO-2 trial, stratifications by prior therapy, RAS status, and duration of metastatic disease were applied. In both trials, the HRs and 95% CIs were based on a stratified Cox proportional hazards model. Median OS and median PFS, survival rates at various time points, and their 95% CIs were estimated for each treatment group using the KM method. An exploratory sensitivity analysis of OS using alternative stratification factors to the Cox proportional hazards model was conducted in the FRESCO trial and of interest to this review. The proportion of patients with a minimally important deterioration (i.e., at least a 6.38-point reduction) from baseline in EORTC QLQ-C30 global health status/QoL score was summarized using descriptive statistics by visit and treatment group.
Subgroup Analyses
In both trials, prespecified subgroup analyses with respect to OS and PFS were conducted using an unstratified Cox proportional hazards model.
The subgroups that were assessed in the FRESCO trial and of interest to this review included:
prior treatment (number of lines of prior treatment lines in the metastatic disease setting, VEGF inhibitors, EGFR inhibitors, targeted treatment)
ECOG PS
KRAS gene mutation status
primary tumour site at first diagnosis.
The subgroups that were assessed in the FRESCO-2 trial and of interest to this review included:
prior treatment (trifluridine-tipiracil and/or regorafenib; VEGF inhibitors; EGFR inhibitors; targeted treatment; immune checkpoint inhibitors for patients with MSI-H/dMMR; BRAF V600E)
ECOG PS
gene mutation status (RAS, BRAF, microsatellite/mismatch repair status)
primary tumour site at first diagnosis.
No adjustment for type I error was involved and no statistical testing was performed for treatment-by-subgroup interaction in the subgroup analyses.
Multiplicity Adjustment
No multiplicity adjustments were made in the FRESCO trial.
In the FRESCO-2 trial, a hierarchal testing procedure was used to control type I error. The primary end point of OS was first tested with a 2-sided alpha of 0.05 using a stratified log-rank test. If the null hypothesis of OS was rejected, the key secondary end point of PFS was tested next using the same significance level. No other end points were included in the statistical testing hierarchy.
Handling of Missing Data
No imputations were performed to account for missing data in any efficacy analysis in either trial.
Harms Outcomes
Harms outcomes were analyzed using descriptive statistics.
Analysis Populations
A summary of analysis sets defined in the FRESCO and FRESCO-2 trials is presented in Table 9.
Results
Results presented here are from the final efficacy analysis as of the data cut-off date of January 17, 2017, in the FRESCO trial and June 24, 2022, in the FRESCO-2 trial.
Table 8: Statistical Analysis of Efficacy End Points
End point | Statistical model | Adjustment factors | Handling of missing data | Sensitivity analyses |
|---|---|---|---|---|
OS PFS | Estimated using the KM methods; 2-sided stratified log-rank test used to assess between-group differences; stratified Cox proportional hazards model used to estimate hazard ratio and 95% CI | FRESCO: Prior use of VEGF inhibitor and KRAS gene state FRESCO-2: Prior therapy, RAS status, and duration of metastatic disease | No imputation | FRESCO: Stratification using alternative factors (OS analysis only)a |
Proportion of patients with a minimally important deterioration (i.e., at least a 6.38-point reduction) from baseline in EORTC QLQ-C30 global health status/QoL score (FRESCO-2 trial only) | Descriptive statistics | NA | No imputation | NA |
CI = confidence interval; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; KM = Kaplan-Meier; NA = not applicable; OS = overall survival; PFS = progression-free survival; QoL = quality of life.
aStratified by the presence of liver metastasis, the time interval between the first confirmed diagnosis of metastasis and randomization, the primary site during the first diagnosis, the site of metastasis, prior targeted therapy, and history of tumours.
Sources: Clinical Study Reports for FRESCO and FRESCO-2 trials,16,18 sponsor’s Summary of Clinical Evidence.17
Table 9: Analysis Populations of the FRESCO and FRESCO-2 Trials
Population | Definition | Application |
|---|---|---|
ITT | Included all randomized patients. Patients were grouped according to the intervention patients were assigned to at randomization. | Efficacy analyses. Demographic data and baseline characteristics. |
SAS in the FRESCO trial; safety population in the FRESCO-2 trial | Included all randomized patients who received at least 1 dose of the study drug or placebo. Patients were grouped according to the actual treatment they received. | Safety analyses. |
ITT = intention to treat; SAS = safety analysis set.
Note: The trials included additional analysis sets, but they were not of interest to this review and are not summarized in the table.
Sources: Clinical Study Reports for FRESCO and FRESCO-2 trials,16,18 sponsor’s Summary of Clinical Evidence.17
Patient Disposition
Patient dispositions in the FRESCO and FRESCO-2 trials are summarized in Table 10.
In the FRESCO and FRESCO-2 trials, 19.8% and 26.0% of patients were excluded during the screening period, respectively, mostly because of a failure to meet the eligibility criteria. In the FRESCO trial, 416 enrolled patients were randomized to fruquintinib plus BSC (n = 278) or placebo plus BSC (n = 138). In the FRESCO-2 trial, 691 enrolled patients were randomized to fruquintinib plus BSC (n = 461) or placebo plus BSC (n = 230). Study treatment discontinuation was numerically lower in the fruquintinib plus BSC group than in the placebo plus BSC group (91.4% versus 98.6%) in the FRESCO trial, as it was in the FRESCO-2 trial (95.0% versus 98.7%). Disease progression was the most common reason for treatment discontinuation in the fruquintinib plus BSC group and in the placebo plus BSC group in the FRESCO trial (70.9% versus 80.4%) and in the FRESCO-2 trial (58.8% versus 63.9%), followed by AEs in the FRESCO trial (11.9% versus 4.3%) and in the FRESCO-2 trial (19.7% versus 17.4%).
The ITT population consisted of all randomized patients in the 2 treatment groups, and the safety analysis set in the FRESCO trial and the safety population in the FRESCO-2 trial consisted of all or close to all randomized patients in the 2 treatment groups (98.9% to 100.0%).
Table 10: Patient Disposition in the FRESCO and FRESCO-2 Trials
Patient disposition | FRESCO | FRESCO-2 | ||
|---|---|---|---|---|
Fruquintinib + BSC | Placebo + BSC | Fruquintinib + BSC | Placebo + BSC | |
Screened, N | 519 | 934 | ||
Screening failure, n (%) | 103 (19.8) | 243 (26.0) | ||
Reason for screening failure, n (%) | ||||
Did not meet inclusion/exclusion criteria | 102 (19.7) | 201 (21.5) | ||
Consent withdrawn | 1 (0.2) | 13 (1.4) | ||
Investigator decision | 0 (0.0) | 8 (0.9) | ||
Adverse event | 0 (0.0) | 5 (0.5) | ||
Other | 0 (0.0) | 16 (1.7) | ||
Randomized, N (%) | 278 (100.0) | 138 (100.0) | 461 (100.0) | 230 (100.0) |
Treatment discontinuation, n (%) | 254 (91.4) | 136 (98.6) | 438 (95.0) | 227 (98.7) |
Reason for treatment discontinuation, n (%) | ||||
Adverse events | 33 (11.9) | 6 (4.3) | 91 (19.7) | 40 (17.4) |
Consent withdrawal | 5 (1.8) | 13 (9.4) | 6 (1.3) | 2 (0.9) |
Lost to follow-up | 0 (0.0) | 0 (0.0) | 1 (0.2) | 0 (0.0) |
Disease progression | 197 (70.9) | 111 (80.4) | 271 (58.8) | 147 (63.9) |
Death | 4 (1.4) | 2 (1.4) | 4 (0.9) | 4 (1.7) |
Patient decision | 0 (0.0) | 0 (0.0) | 16 (3.5) | 3 (1.3) |
Investigator decision | 15 (5.4) | 4 (2.9) | 31 (6.7) | 18 (7.8) |
Other | 0 (0.0) | 0 (0.0) | 18 (3.9) | 13 (5.7) |
ITT, N (%) | 278 (100.0) | 138 (100.0) | 461 (100.0) | 230 (100.0) |
SAS in the FRESCO trial and safety population in the FRESCO-2 trial, N (%) | 278 (100.0) | 137 (99.3) | 456 (98.9) | 230 (100.0) |
BSC = best supportive care; ITT = intention to treat; SAS = safety analysis set.
Sources: Clinical Study Reports for FRESCO and FRESCO-2 trials,16,18 sponsor’s Summary of Clinical Evidence.17
Baseline Characteristics
The baseline characteristics outlined in Table 11 are limited to those that are most relevant to this review or are likely to affect the outcomes or interpretation of the study results.
Patients in the FRESCO trial were younger (mean age = 54.6 years; standard deviation [SD] = not reported) than patients in the FRESCO-2 trial (mean age = 62.2 years; SD = 10.16]). In both the FRESCO and FRESCO-2 trials, the majority of patients were male (61.3% and 55.7%). All patients in the FRESCO trial were Asian, whereas most patients in the FRESCO-2 trial were white (80.9%). The FRESCO-2 trial had a higher proportion of patients with an ECOG PS of 0 than the FRESCO trial (43.1% versus 27.4%), more patients who had been diagnosed with metastatic disease for at least 18 months (92.8% versus 42.8%), and more patients with a RAS mutation (63.1% versus 44.5%). In the FRESCO-2 trial, the majority of patients in the fruquintinib plus BSC and the placebo plus BSC groups had tumours with BRAF wild-type (87.0% versus 86.1%) and tumours with microsatellite stability /pMMR (92.6% versus 93.5%). The majority of patients (72.6%) in the FRESCO-2 trial received more than 3 lines of prior anticancer treatment for metastatic disease, whereas only 21.2% of patients in the FRESCO trial did. Prior anti-VEGF therapy was reported in 30.0% of patients in the FRESCO trial and almost all patients in the FRESCO-2 trial (96.4%). Prior anti-EGFR therapy was reported in 14.2% and 37.8% of patients in the FRESCO and FRESCO-2 trials, respectively. In the FRESCO-2 trial, the proportion of patients who previously received trifluridine-tipiracil, regorafenib, or both treatments was 52.2%, 8.4%, and 39.4%, respectively (data not reported in the FRESCO trial). The proportion of patients who received prior trifluridine-tipiracil plus bevacizumab combination therapy was unknown in both trials.
No notable imbalances were noted between treatment groups in the 2 trials, except the proportion of male patients was consistently higher in the placebo plus BSC (FRESCO trial, 70.3%; FRESCO-2 trial, 60.9%), group than the fruquintinib plus BSC group (FRESCO trial, 56.8%; FRESCO-2 trial, 53.1%)
Table 11: Baseline Characteristics in the FRESCO and FRESCO-2 Trials (ITT Population)
Characteristic | FRESCO | FRESCO-2 | ||
|---|---|---|---|---|
Fruquintinib + BSC (N = 278) | Placebo + BSC (N = 138) | Fruquintinib + BSC (N = 461) | Placebo + BSC (N = 230) | |
Demographic | ||||
Age, years, mean (SD) | 54.3 (10.7) | 55.1 (10.5) | 62.2 (10.4) | 62.4 (9.7) |
Male, n (%) | 158 (56.8) | 97 (70.3) | 245 (53.1) | 140 (60.9) |
Region, n (%) | ||||
Asia | 278 (100.0) | 138 (100.0) | 0 (0.0) | 0 (0.0) |
Europe | 0 (0.0) | 0 (0.0) | 329 (71.4) | 166 (72.2) |
North America | 0 (0.0) | 0 (0.0) | 82 (17.8) | 42 (18.3) |
Japan | 0 (0.0) | 0 (0.0) | 40 (8.7) | 16 (7.0) |
Australia | 0 (0.0) | 0 (0.0) | 10 (2.2) | 6 (2.6) |
Race, n (%) | ||||
Asian | 278 (100.0) | 138 (100.0) | 43 (9.3) | 18 (7.8) |
White | 0 (0.0) | 0 (0.0) | 367 (79.6) | 192 (83.5) |
Other | 0 (0.0) | 0 (0.0) | 51 (11.1) | 20 (8.7) |
ECOG PS, n (%) | ||||
0 | 77 (27.7) | 37 (26.8) | 196 (42.5) | 102 (44.3) |
1 | 201 (72.3) | 101 (73.2) | 265 (57.5) | 128 (55.7) |
Disease characteristics | ||||
Duration of metastatic disease, n (%) | ||||
< 18 months | 163 (58.6) | 75 (54.3) | 37 (8.0) | 13 (5.7) |
≥ 18 months | 115 (41.4) | 63 (45.7) | 424 (92.0) | 217 (94.3) |
Number of metastatic sites, n (%) | ||||
Single | 13 (4.7) | 4 (2.9) | 61 (13.2) | 41 (17.8) |
Multiple | 265 (95.3) | 134 (97.1) | 400 (86.8) | 189 (82.2) |
RAS status, n (%) | ||||
Wild-type | 157 (56.5) | 74 (53.6) | 170 (36.9) | 85 (37.0) |
Mutant | 121 (43.5) | 64 (46.4) | 291 (63.1) | 145 (63.0) |
BRAF status, n (%) | ||||
Wild-type | NR | NR | 401 (87.0) | 198 (86.1) |
V600E | NR | NR | 7 (1.5) | 10 (4.3) |
Other | NR | NR | 53 (11.5) | 22 (9.6) |
Microsatellite or mismatch repair status, n (%) | ||||
MSS/pMMR | NR | NR | 427 (92.6) | 215 (93.5) |
MSI-H/dMMR | NR | NR | 5 (1.1) | 4 (1.7) |
Unknown | NR | NR | 29 (6.3) | 11 (4.8) |
Cancer treatment history | ||||
Number of prior treatment lines for metastatic disease, n (%) | ||||
≤ 3 lines | 221 (79.5) | 107 (77.5) | 125 (27.1) | 64 (27.8) |
> 3 lines | 57 (20.5) | 31 (22.5) | 336 (72.9) | 166 (72.2) |
Fluoropyrimidine, oxaliplatin, and irinotecan-based chemotherapy | 278 (100.0) | 138 (100.0) | NR | NR |
Fluoropyrimidine | NR | NR | 460 (99.8) | 230 (100.0) |
Oxaliplatin | NR | NR | 460 (99.8) | 228 (99.1) |
Irinotecan | NR | NR | 459 (99.6) | 229 (99.6) |
VEGF inhibitor, n (%) | 84 (30.2) | 41 (29.7) | 445 (96.5) | 221 (96.1) |
EGFR inhibitor, n (%) | 40 (14.4) | 19 (13.8) | 180 (39.0) | 88 (38.3) |
VEGF inhibitor, EGFR inhibitor, or both | 111 (39.9) | 55 (39.9) | 457 (99.1) | 225 (97.8) |
Immune checkpoint inhibitor, n (%) | NR | NR | 21 (4.6) | 11 (4.8) |
BRAF inhibitor, n (%) | NR | NR | 9 (2.0) | 7 (3.0) |
Prior therapy with trifluridine-tipiracil and/or regorafenib | NR | NR | 461 (100.0) | 230 (100.0) |
Trifluridine-tipiracil alone, n (%) | NR | NR | 240 (52.1) | 121 (52.6) |
Regorafenib alone, n (%) | NR | NR | 40 (8.7) | 18 (7.8) |
Trifluridine-tipiracil and regorafenib, n (%) | NR | NR | 181 (39.3) | 91 (39.6) |
Time since last chemotherapy and medication to randomization, months, mean (SD) | 1.9 (1.8) | 2.0 (1.4) | NR | NR |
BSC = best supportive care; dMMR = deficient mismatch repair; ECOG PS = Eastern Cooperative Oncology Group Performance Status; ITT = intention to treat; MSI-H = microsatellite instability-high; MSS = microsatellite stable; NR = not reported; pMMR = proficient mismatch repair; SD = standard deviation.
Sources: Clinical Study Reports for FRESCO and FRESCO-2 trials,16,18 sponsor’s Summary of Clinical Evidence.17
Exposure to Study Treatments
Patient exposure to study treatments is summarized in Table 12. The mean duration of treatment exposure was higher in the fruquintinib plus BSC group than in the placebo plus BSC group in the FRESCO trial (4.9 months [SD = 4.0 months] versus 1.9 months [SD = 1.5 months]) and in the FRESCO-2 trial (4.0 months [SD = 3.1 months] versus 2.0 months [SD = 1.4 months]). As well, a higher proportion of patients required a dose reduction in the fruquintinib plus BSC group than in the placebo plus BSC group in the FRESCO trial (24.8% versus 4.4%) and in the FRESCO-2 trial (26.5% versus 4.3%).
According to the protocol, patients in the FRESCO-2 study who were randomized to the fruquintinib plus BSC group were allowed to continue study treatment after disease progression determined by RECIST 1.1. Of the 461 patients randomized to the fruquintinib plus BSC group, 301 experienced disease progression. Among these, 99 patients (32.9%) received at least 1 dose of fruquintinib after disease progression.
Table 12: Patient Exposure to Treatments in the FRESCO Trial (SAS) and the FRESCO-2 Trial (Safety Population)
Exposure | FRESCO | FRESCO-2 | ||
|---|---|---|---|---|
Fruquintinib + BSC (N = 278) | Placebo + BSC (N = 137) | Fruquintinib + BSC (N = 456) | Placebo + BSC (N = 230) | |
Duration, months, mean (SD) | 4.9 (4.0) | 1.9 (1.5) | 4.0 (3.1) | 2.0 (1.4) |
Number of treatment cycles received, mean (SD) | NR | NR | 4.3 (3.2) | 2.3 (1.4) |
Relative dose intensitya | 0.92 (0.14) | 0.98 (0.13) | 0.95 (0.18) | 0.89 (0.17) |
Number of patients with a dose reduction, n (%) | 69 (24.8) | 6 (4.4) | 121 (26.5) | 10 (4.3) |
Reduction from 5 mg to 4 mg | 69 (24.8) | 6 (4.4) | 121 (26.5) | 10 (4.3) |
Reduction from 4 mg to 3 mg | 23 (8.3) | 1 (0.7) | 45 (9.9) | 0 (0.0) |
BSC = best supportive care; NR = not reported; SAS = safety analysis set; SD = standard deviation.
aRelative dose intensity = dose intensity (mg/day)/planned dose intensity (mg/day); planned dose intensity was 3.75 mg/day, per protocol.
Sources: Clinical Study Reports for FRESCO and FRESCO-2 trials,16,18 sponsor’s Summary of Clinical Evidence.17
Concomitant Treatments
In the FRESCO trial, the fruquintinib plus BSC group, in comparison to placebo plus BSC group, had a higher proportion of patients who received psycholeptics (█████ ██████ ██████ anti-inflammatory and antirheumatic drugs ██████ ██████ ███████ drugs for functional gastrointestinal disorders (█████ ██████ ███████ blood substitute or perfusion solutions (█████ ██████ ███████ and appetite stimulants (█████ ██████ ██████. In the FRESCO-2 trial, no notable between-group imbalance was observed for any BSC treatments.
Table 13: BSC Treatment in the FRESCO and FRESCO-2 Trials (ITT Population)
BSC | FRESCO | FRESCO-2 | ||
|---|---|---|---|---|
Fruquintinib + BSC (N = 278) | Placebo + BSC (N = 138) | Fruquintinib + BSC (N = 461) | Placebo + BSC (N = 230) | |
Analgesics | ███ ██████ | ██ ██████ | ███ ██████ | ███ ████ |
Psycholeptics | ██ ██████ | ██ █████ | ███ ██████ | ██ █████ |
Systemic corticosteroids | ██ ██████ | ██ ██████ | ███ ██████ | ██ █████ |
Anti-inflammatory and antirheumatic drugs | ██ ██████ | ██ ██████ | ███ ██████ | ██ █████ |
Drugs for constipation | ██ ██████ | ██ ██████ | ███ ██████ | ██ █████ |
Antiemetics and antinauseants | ██ ██████ | ██ ██████ | ███ ██████ | ██ █████ |
Diuretics | ██ ██████ | ██ ██████ | ███ ██████ | ██ █████ |
Mineral supplements | ██ █████ | █████ | ██ ██████ | ██ █████ |
Vitamins | ██ █████ | ██ ██████ | ██ ██████ | ██ █████ |
Drugs for functional gastrointestinal disorders | ██ ██████ | ██ ██████ | ██ ██████ | ██ █████ |
Blood substitutes, perfusion solutions | ██ ██████ | ██ ██████ | ██ ██████ | ██ █████ |
Psychoanaleptics | █████ | ███ | ██ ██████ | ██ █████ |
Antianemia preparations | ██ █████ | █████ | ██ █████ | ██ █████ |
General nutrients | ██ █████ | █████ | ██ █████ | █████ |
Appetite stimulants | ██ ██████ | █████ | ██ █████ | █████ |
BSC = best supportive care; ITT = intention to treat.
Sources: Clinical Study Reports for FRESCO and FRESCO-2 trials,16,18 sponsor’s Summary of Clinical Evidence.17
Subsequent Anticancer Treatment
A lower proportion of patients in the fruquintinib plus BSC group than in the placebo plus BSC group received subsequent anticancer therapy in the FRESCO trial (42.4% versus 50.7%) and in the FRESCO-2 trial (29.4% versus 34.3%). The most common subsequent anticancer therapy was chemotherapy in both trials.
Table 14: Subsequent Anticancer Treatment in the FRESCO (ITT Population) and FRESCO-2 (Safety Population) Trials
Subsequent treatment | FRESCO | FRESCO-2 | ||
|---|---|---|---|---|
Fruquintinib + BSC (N = 278) | Placebo + BSC (N = 138) | Fruquintinib + BSC (N = 456) | Placebo + BSC (N = 230) | |
≥ 1 subsequent anticancer therapy, n (%) | 118 (42.4) | 70 (50.7) | 134 (29.4) | 79 (34.3) |
VEGF inhibitor or VEGFR inhibitor | 30 (10.8) | 22 (15.9) | 25 (5.5) | 20 (8.7) |
EGFR inhibitor | 8 (2.9) | 6 (4.3) | 17 (3.7) | 8 (3.5) |
Regorafenib | NR | NR | 34 (7.5) | 18 (7.8) |
Tipiracil-trifluridine | NR | NR | 15 (3.3) | 6 (2.6) |
Chemotherapy | 90 (32.4) | 61 (44.2) | NR | NR |
Fluoropyrimidine | NR | NR | 68 (14.9) | 45 (19.6) |
Oxaliplatin | NR | NR | 35 (7.7) | 25 (10.9) |
Irinotecan | NR | NR | 31 (6.8) | 16 (7.0) |
BSC = best supportive care; ITT = intention to treat; NR = not reported.
Sources: Clinical Study Reports for FRESCO and FRESCO-2 trials,16,18 sponsor’s Summary of Clinical Evidence.17
Efficacy
Key efficacy outcomes from the FRESCO and FRESCO-2 trials are summarized in Table 15. The results presented are based on the data cut-off date of January 17, 2017, in the FRESCO trial and June 24, 2022, in the FRESCO-2 trial, representing the final efficacy analysis.
Overall Survival
The FRESCO Trial
The median duration of follow-up was 13.3 months (95% CI, 12.1 to 14.7 months) in the fruquintinib plus BSC group and 13.2 months (95% CI, 10.6 to 19.6 months) in the placebo plus BSC group when a total of 297 deaths occurred. The KM estimate for the median OS (primary end point) was 9.30 months (95% CI, 8.18 to 10.45 months) in the fruquintinib plus BSC group and 6.57 months (95% CI, 5.88 to 8.11 months) in the placebo plus BSC group, with a stratified HR of 0.65 (95% CI, 0.51 to 0.83; P < 0.001) (Figure 3). The between-group difference in the probability of survival at 6 months, 12 months, and 18 months was █████ ████ ███ ████ ██ ███████████ ████ ███ ████ ██ █████), and ████ ████ ███ █████ ██ █████), respectively.
Results of the sensitivity analysis (which used alternative stratification factors) and the subgroup analyses of interest (prior treatment [number of lines of prior treatment lines in the metastatic disease setting, VEGF inhibitors, EGFR inhibitors, targeted treatment], ECOG PS, KRAS gene mutation status, primary tumour site at first diagnosis) were, in general, consistent with those of the primary analysis. Forest plots of the subgroup analyses are presented in Figure 5 in Appendix 1.
Figure 3: KM Curves for OS in the FRESCO Trial (ITT Population)
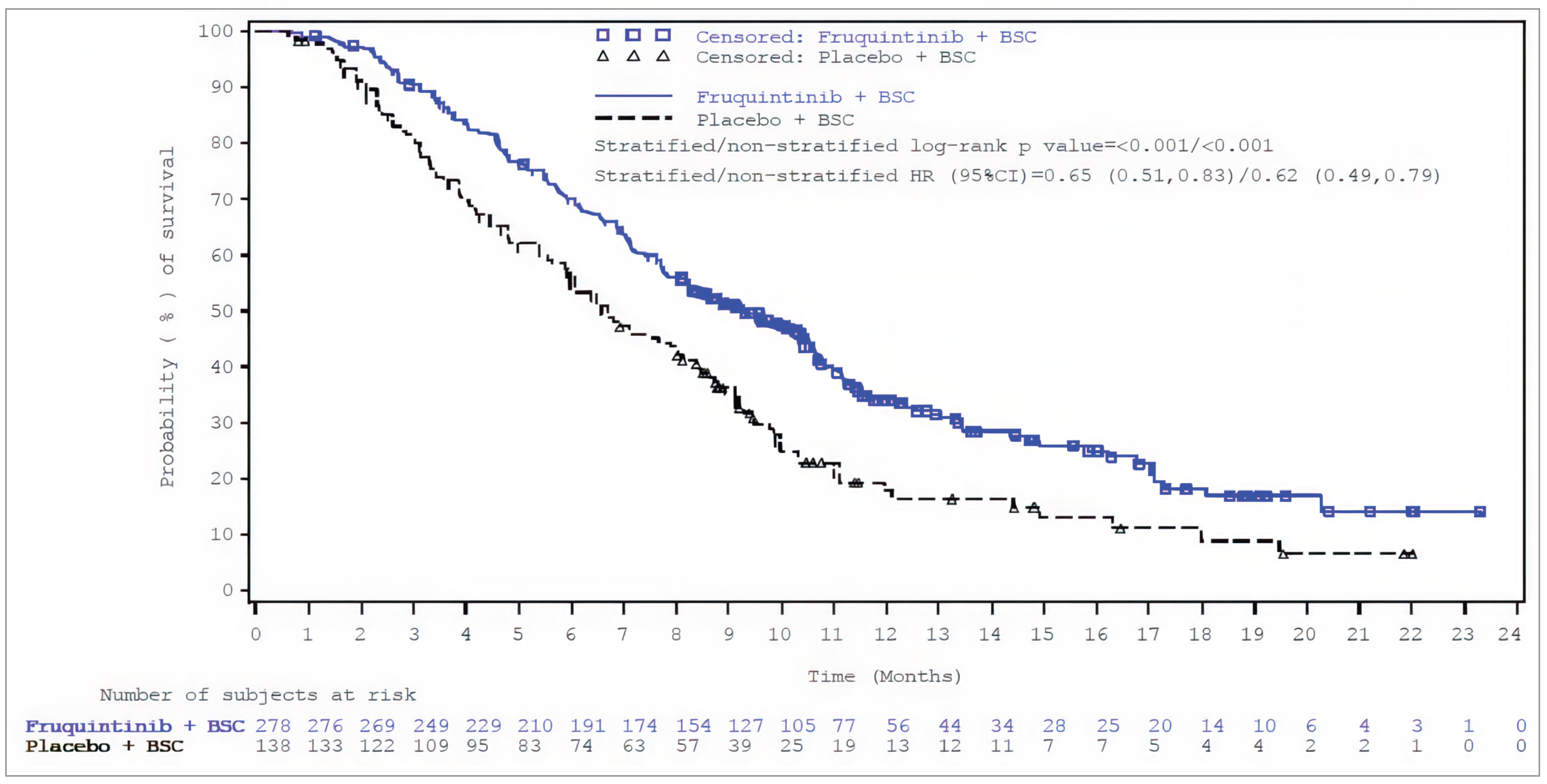
BSC = best supportive care; CI = confidence interval; HR = hazard ratio; ITT = intention to treat; KM = Kaplan-Meier; OS = overall survival.
Source: FRESCO Clinical Study Report.16
The FRESCO-2 Trial
The median duration of follow-up was 11.3 months (95% CI, 10.6 to 12.4 months) in the fruquintinib plus BSC group and 11.2 months (95% CI, 9.9 to 12.0 months) in the placebo plus BSC group when a total of 490 deaths occurred. The KM estimate for median OS (primary end point) was 7.4 months (95% CI, 6.7 to 8.2 months) in the fruquintinib plus BSC group and 4.8 months (95% CI, 4.0 to 5.8 months) in the placebo plus BSC group, with a stratified HR of 0.66 (95% CI, 0.55 to 0.80; P < 0.001) (Figure 4). The between-group difference in the probability of survival at 6 months, 12 months, and 18 months was █████ ████ ███ █████ ██ ████), ████ ████ ███ █████ ██ ████), and █████ ████ ███ █████ ██ █████), respectively.
Results of the subgroup analyses of interest (prior treatment [trifluridine-tipiracil and/or regorafenib; VEGF inhibitors; EGFR inhibitors; targeted treatment; immune checkpoint inhibitors for MSI-H/dMMR; BRAF V600E], ECOG PS, gene mutation status [RAS, BRAF, microsatellite/mismatch repair status], primary tumour site at first diagnosis) were, in general, consistent with those of the primary analysis. Of note, however, no effect was observed in patients who had received 3 or fewer prior chemotherapies treatment lines (HR = 0.94; 95% CI, 0.56 to 1.53), whereas the treatment effect was consistent across subgroups by the number of prior lines of chemotherapy specific to the metastatic setting. Forest plots of the subgroup analyses are presented in Figure 6 in Appendix 1.
Figure 4: KM Curves for OS in the FRESCO-2 Trial (ITT Population)
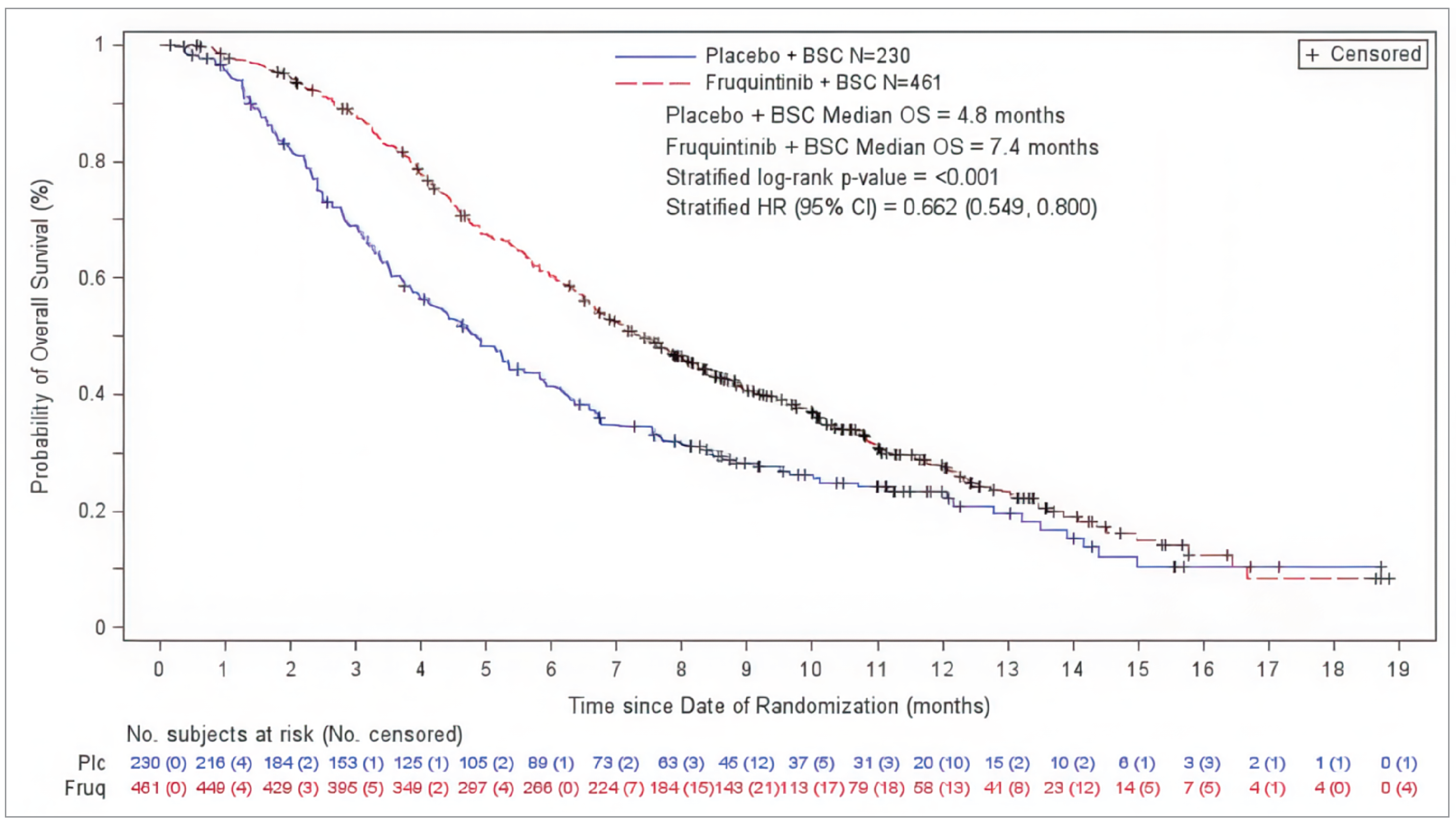
BSC = best supportive care; CI = confidence interval; Fruq = fruquintinib; HR = hazard ratio; ITT = intention to treat; KM = Kaplan-Meier; Plc = placebo; OS = overall survival.
Source: FRESCO-2 Clinical Study Report.18
Progression-Free Survival
The FRESCO Trial
The KM estimate for median PFS (secondary end point) was 3.71 months (95% CI, 3.65 to 4.63 months) in the fruquintinib plus BSC group and 1.84 months (1.81 to 1.84 months) in the placebo plus BSC group, with a stratified HR of 0.26 (95% CI, 0.21 to 0.34; P < 0.001). The majority of PFS events in the 2 treatment groups were attributed to disease progression. The between-group difference in the probability of surviving progression-free at 3 months, 6 months, and 9 months was █████ ████ ███ █████ ██ ██████ ███ █████ ████ ███ █████ ██ ███████ ███ █████ ████ ███ ████ ██ ██████, respectively. None of these end points were adjusted for multiplicity. Results of the subgroup analysis were consistent with those of the primary analysis.
The FRESCO-2 Trial
The KM estimate for median PFS (key secondary end point) was 3.7 months (95% CI, 3.5 to 3.8 months) in the fruquintinib plus BSC group and 1.8 months (95% CI, 1.8 to 1.9 months) in the placebo plus BSC group, with a stratified HR of 0.32 (95% CI, 0.27 to 0.39; P < 0.001); this end point was adjusted for multiplicity. The majority of PFS events in the 2 treatment groups were attributed to disease progression. The between-group difference in the probability of survival at 3 months, 6 months, and 9 months was █████ ████ ███ █████ ██ ███████ █████ ████ ███ █████ ██ ███████ ███ █████ ████ ███ ████ ██ ██████, respectively. Results of the subgroup analysis were consistent with those of the primary analysis.
Health-Related Quality of Life
The FRESCO Trial
This outcome was not assessed in the FRESCO trial.
The FRESCO-2 Trial
Outcomes assessed with the EORTC QLQ-C30 were secondary end points and not adjusted for multiplicity in the FRESCO-2 trial.
█████ ███████ ███████████ of 461 ███████ randomized patients in the fruquintinib plus BSC group and ███ of 230 (██████) randomized patients in the placebo plus BSC group were included in the analysis of proportion of patients with minimally important deterioration (i.e., at least a 6.38-point reduction) from baseline in EORTC QLQ-C30 global health status/QoL score at the last on-treatment visit. Of the patients analyzed, █████ in the fruquintinib plus BSC group and █████ in the placebo plus BSC group achieved this end point; the between-group difference was █████ ████ ███ ██████ ██ █████.
███ ███████ █████████ of 461 (██████) randomized patients in the fruquintinib plus BSC group and ██ of 230 (██████) randomized patients in the placebo plus BSC group were included in the analysis of change from baseline in EORTC QLQ-C30 global health status/QoL score at cycle 4. The between-group difference in change from baseline in EORTC QLQ-C30 global health status/QoL score at the cycle 4 visit was ████ ████ ███ ████ ██ ██████████
The proportion of patients with a minimally important deterioration (based on the sponsor-identified MID) from baseline at the last on-treatment visit was similar between groups with respect to role functioning (MID = ██████), emotional functioning (MID = ██), and fatigue (MID = █████). The proportion was numerically higher in the fruquintinib plus BSC group than in the placebo plus BSC group with respect to physical functioning (MID = ████) (█████ ██████ ████%) and pain (MID = ██) (█████ ██████ ███████ The difference between the fruquintinib plus BSC group and the placebo plus BSC group in change from baseline in EORTC QLQ-C30 score at the cycle 4 visit with respect to physical functioning, role functioning, emotional functioning, pain, and fatigue was ████ ████ ███ ████ ██ ██████████ ████ ████ ███ █████ ██ ██████████ ████ ████ ███ ████ ██ ██████████ ███ ████ ███ ████ ██ ██████████ ███ ███ ████ ███ ████ ██ ██████████ respectively.
Caregiver Burden
This outcome was not assessed in either of the trials.
Table 15: Key Efficacy Results From the FRESCO and FRESCO-2 Trials (ITT Population)
Outcome | FRESCO | FRESCO-2 | |||
|---|---|---|---|---|---|
Fruquintinib + BSC (N = 278) | Placebo + BSC (N = 138) | Fruquintinib + BSC (N = 461) | Placebo + BSC (N = 230) | ||
OS | |||||
Events (death), n (%) | 188 (67.6) | 109 (79.0) | 317 (68.8) | 173 (75.2) | |
OS, months, median (95% CI)a | 9.30 (8.18 to 10.45) | 6.57 (5.88 to 8.11) | 7.4 (6.7 to 8.2) | 4.8 (4.0 to 5.8) | |
Hazard ratiob | 0.65 (0.51 to 0.83) | 0.66 (0.55 to 0.80) | |||
P valuec | < 0.001 | < 0.001 | |||
Follow-up time, months, median (95% CI) | 13.3 (12.1 to 14.7) | 13.2 (10.6 to 19.6) | 11.3 (10.6 to 12.4) | 11.2 (9.9 to 12.0) | |
Survival probability,d % (95% CI) | |||||
6 months | ████ ████ | ████ ████ | ████ ████ | ████ ████ | |
Difference between groups (%), (95% CI) | ████ ████ | ████ ████ | |||
12 months | ████ ████ | ████ ████ | ████ ████ | ████ ████ | |
Difference between groups (%), (95% CI) | ████ ████ | ████ ████ | |||
18 months | ████ ████ | ████ ████ | ████ ████ | ████ ████ | |
Difference between groups (%), (95% CI) | ████ ████ | ████ ████ | |||
PFS | |||||
Events (death or disease progression), n (%) | 235 (84.5) | 125 (90.6) | 392 (85.0) | 213 (92.6) | |
Disease progression | 214 (77.0) | 110 (79.7) | 301 (65.3) | 167 (72.6) | |
Death | 21 (7.6) | 15 (10.9) | 91 (19.7) | 46 (20.0) | |
PFS, months,a median (95% CI) | 3.71 (3.65 to 4.63) | 1.84 (1.81 to 1.84) | 3.7 (3.5 to 3.8) | 1.8 (1.8 to 1.9) | |
Hazard ratiob | 0.26 (0.21 to 0.34) | 0.32 (0.27 to 0.39) | |||
P valuec | < 0.001e | < 0.001 | |||
PFS probability,d % (95% CI) | |||||
3 months | ████ ████ | ████ ████ | ████ ████ | ████ ████ | |
Difference between groups (%), (95% CI) | ████ ████ | ████ ████ | |||
6 months | ████ ████ | ████ ████ | ████ ████ | ████ ████ | |
Difference between groups (%), (95% CI) | ████ ████ | ████ ████ | |||
9 months | ████ ████ | ████ ████ | ████ ████ | ████ ████ | |
Difference between groups (%), (95% CI) | ████ ████ | ████ ████ | |||
EORTC QLQ-C30 global health status/QoL | |||||
Number of patients contributing to this analysis, N | NA | NA | ████ ████ | ████ ████ | |
Proportion of patients with a ≥ 6.38-point reduction (i.e., deterioration) in score from baseline at last on-treatment assessment visit, n (%) | NA | NA | ████ ████ | ████ ████ | |
Difference between groups (%), (95% CI) | NA | ████ ██████ ██ ████ | |||
BSC = best supportive care; CI = confidence interval; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; ITT = intention to treat; NA = not assessed; OS = overall survival; PFS = progression-free survival; QoL = quality of life.
aEstimated based on the Kaplan-Meier method.
bThe hazard ratio and 95% CI were estimated using the stratified Cox proportional hazards model. The adjustment factors included prior use of a VEGF inhibitor and KRAS gene state in the FRESCO trial, and prior therapy, RAS status, and duration of metastatic disease in the FRESCO-2 trial.
cThe P value was calculated using the stratified log-rank test.
dThe survival probabilities and corresponding 95% CIs were calculated using a linear transformation based on the Brookmeyer-Crowley method.
eThe P value was not adjusted for multiplicity.
Sources: Clinical Study Reports for FRESCO and FRESCO-2 trials,16,18 sponsor’s Summary of Clinical Evidence.17
Harms
Key harms outcomes from the FRESCO and FRESCO-2 trials are summarized in Table 16.
Treatment-Emergent Adverse Events
The proportion of patients who reported at least 1 TEAE was higher in the fruquintinib plus BSC group than in the placebo plus BSC group in both the FRESCO (98.6% versus 88.3%) and the FRESCO-2 (98.9% versus 92.6%) trials. The most common TEAEs (reported in at least 30% of patients in at least 1 of the trials) were (fruquintinib plus BSC versus placebo plus BSC) hand-foot syndrome (49.3% versus 2.9% in the FRESCO trial and 19.3% versus 2.6% in the FRESCO-2 trial), hypertension (57.2% versus 15.3% and 36.8% versus 8.7%, respectively), dysphonia (37.8% versus 1.5% and 16.2% versus 5.2%, respectively), proteinuria (43.2% versus 24.8% and 17.3% versus 5.2%, respectively), and asthenia (12.6% versus 2.2% and 34.0% versus 22.6%, respectively); all were more commonly reported in the fruquintinib plus BSC group than in the placebo plus BSC group. The incidence of these TEAEs, except asthenia, was notably higher in the fruquintinib plus BSC group than in the placebo plus BSC group in the FRESCO trial than in the FRESCO-2 trial (hand-foot syndrome, 49.3% versus 19.3%; hypertension, 57.2% versus 36.8%; dysphonia, 37.8% versus 16.2%; proteinuria, 43.2% versus 17.3%).
Grade 3 or higher TEAEs were more commonly reported in the fruquintinib plus BSC group than the placebo plus BSC group in both the FRESCO (61.2% versus 19.7%) and the FRESCO-2 (62.7% versus 50.4%) trials. The most commonly reported grade 3 or higher TEAEs in the fruquintinib plus BSC group of the FRESCO and FRESCO-2 trials were (fruquintinib plus BSC versus placebo plus BSC) hypertension (21.6% versus 2.2% and 13.6% versus 0.9%, respectively), asthenia (0.7% versus 0.0% and 7.7% versus 3.9%, respectively), and hand-foot syndrome (10.8% versus 0.0% and 6.4% versus 0.0%, respectively).
Serious Adverse Events
SAEs were more commonly reported in the fruquintinib plus BSC group than in the placebo plus BSC group in the FRESCO trial (15.5% versus 5.8%), but the rate of SAEs was similar in the fruquintinib plus BSC and placebo plus BSC groups in the FRESCO-2 trial (37.5% versus 38.3%). In the FRESCO trial, the most common TEAEs in the fruquintinib plus BSC group were (fruquintinib plus BSC versus placebo plus BSC) intestinal obstruction (2.5% versus 0.7%) and lung infections (1.1% versus 0%). In the FRESCO-2 trial, the most common TEAEs in the fruquintinib plus BSC group were (fruquintinib plus BSC versus placebo plus BSC) pneumonia (1.8% versus 0.4%), intestinal obstruction (1.5% versus 2.6%), and ileus (1.5% versus 0.9%).
Withdrawals Due to Adverse Events
WDAEs were more commonly reported in the fruquintinib plus BSC group than in the placebo plus BSC group (15.1% versus 5.8%) in the FRESCO trial, but the rate of WDAEs was similar in the fruquintinib plus BSC and placebo plus BSC groups in the FRESCO-2 trial (20.4% versus 21.3%). No specific TEAEs were identified to account for the majority of WDAEs in either group in either trial.
Mortality
Deaths were less common in the fruquintinib plus BSC group than in the placebo plus BSC group in both the FRESCO trial (67.6% versus 78.8%) and the FRESCO-2 trial (68.9% versus 75.2%). The majority of deaths (fruquintinib plus BSC versus placebo plus BSC) were attributed to progressive disease in both the FRESCO trial (70.4% versus 76.9%) and the FRESCO-2 trial (58.8% versus 64.3%) trials. No specific TEAEs were identified to account for the majority of deaths in either group in either trial.
Notable Harms
The incidence of thromboembolic events and gastrointestinal perforations was similarly low in the fruquintinib plus BSC group (between 0.7% and 4.6%) and the placebo plus BSC group (from 0.7% to 2.2%) in both trials. The proportion of patients with hand-foot syndrome, hemorrhage, hypertension, and proteinuria in the fruquintinib plus BSC group was between 43.2% and 57.2% in the FRESCO trial and between 14.3% and 36.8% in the FRESCO-2 trial; these harms were notably more common in the fruquintinib plus BSC group than in the placebo plus BSC group.
Critical Appraisal
Internal Validity
The FRESCO and FRESCO-2 trials were randomized, double-blind, placebo-controlled trials. The methods of randomization, which involved stratification by prior therapy, KRAS gene status, and duration of metastatic disease (FRESCO-2 only), and interactive response technology for concealment of the randomized assignment, were appropriate. The baseline patient demographics and disease characteristics were, in general, balanced between treatment groups, except that the proportion of males was consistently higher in the placebo plus BSC group than in the fruquintinib plus BSC group in both trials; the clinical experts consulted by CDA-AMC stated that such an imbalance would not likely introduce bias into the study results.
Blinding of patients and study personnel was appropriately maintained. However, given that placebo was used as the control drug in the trials, patients may have been able to infer treatment assignment based on AEs associated with the study intervention (hand-foot syndrome, hypertension). Subjective outcomes reported by patients, such as HRQoL (assessed by the EORTC QLQ-C30) and AEs, might be subject to bias in the measurement of outcomes, potentially leading to results favouring fruquintinib plus BSC for HRQoL outcomes and favouring placebo plus BSC for subjective harms outcomes.
Table 16: Key Harms Results From the FRESCO Trial (SAS) and the FRESCO-2 Trial (Safety Population)
Adverse events, n (%) | FRESCO | FRESCO-2 | ||
|---|---|---|---|---|
Fruquintinib + BSC (N = 278) | Placebo + BSC (N = 137) | Fruquintinib + BSC (N = 456) | Placebo + BSC (N = 230) | |
TEAEs | ||||
Patients with ≥ 1 TEAE | 274 (98.6) | 121 (88.3) | 451 (98.9) | 213 (92.6) |
Most common TEAEsa | ||||
Hand-foot syndrome | 137 (49.3) | 4 (2.9) | 88 (19.3) | 6 (2.6) |
Hypertension | 159 (57.2) | 21 (15.3) | 168 (36.8) | 20 (8.7) |
Dysphonia | 105 (37.8) | 2 (1.5) | 74 (16.2) | 12 (5.2) |
Proteinuria | 120 (43.2) | 34 (24.8) | 79 (17.3) | 12 (5.2) |
Asthenia | 35 (12.6) | 3 (2.2) | 155 (34.0) | 52 (22.6) |
Grade 3 or higher TEAEs | ||||
Patients with ≥ 1 grade 3 or higher TEAE | 170 (61.2) | 27 (19.7) | 286 (62.7) | 116 (50.4) |
Most common grade 3 or higher TEAEsb | ||||
Hypertension | 60 (21.6) | 3 (2.2) | 62 (13.6) | 2 (0.9) |
Asthenia | 2 (0.7) | 0 (0.0) | 35 (7.7) | 9 (3.9) |
Hand-foot syndrome | 30 (10.8) | 0 (0.0) | 29 (6.4) | 0 (0.0) |
Increased blood bilirubin | 7 (2.5) | 7 (5.1) | 11 (2.4) | 6 (2.6) |
SAEs | ||||
Patients with ≥ 1 SAE | 43 (15.5) | 8 (5.8) | 171 (37.5) | 88 (38.3) |
WDAEs | ||||
Patients who withdrew treatment due to AEs | 42 (15.1) | 8 (5.8) | 93 (20.4) | 49 (21.3) |
Deaths | ||||
Deaths | 188 (67.6) | 108 (78.8) | 314 (68.9) | 173 (75.2) |
Notable harms,c n (%) | ||||
Hand-foot syndrome | 137 (49.3) | 4 (2.9) | 88 (19.3) | 6 (2.6) |
Hemorrhage | 123 (44.2) | 30 (21.9) | 65 (14.3) | 22 (9.6) |
Thromboembolic events | 2 (0.7) | 1 (0.7) | 21 (4.6) | 5 (2.2) |
Gastrointestinal perforations | 6 (2.2) | 1 (0.7) | 16 (3.5) | 1 (0.4) |
Hypertension | 159 (57.2) | 21 (15.3) | 168 (36.8) | 20 (8.7) |
Proteinuria | 120 (43.2) | 34 (24.8) | 79 (17.3) | 12 (5.2) |
AE = adverse event; BSC = best supportive care; SAE = serious adverse event; SAS = safety analysis set; TEAE = treatment-emergent adverse event; WDAE = withdrawal due to adverse event.
Note: Unless otherwise specified, the AEs were based on MedDRA preferred terms.
aReported in ≥ 30% of patients in any group.
bReported in ≥ 5% of patients in any group.
cReported by adverse event of special interest category.
Sources: Clinical Study Reports for FRESCO and FRESCO-2 trials,16,18 sponsor’s Summary of Clinical Evidence.17
OS was an objective outcome and was unlikely to be influenced by knowledge of the treatment assignment. PFS was investigator-assessed; no independent blinding committee was involved in the assessment process. Therefore, there is a risk of bias associated with the measurement of PFS, although the extent and direction of that bias are unclear. Of note, survival follow-up was conducted once every 2 months (FRESCO trial) to every 3 months (FRESCO-2 trial), which could have potentially biased the estimate of OS due to inaccurate recording of survival time, although the direction of that bias is difficult to predict.
The results presented correspond to those from the final efficacy analysis, which was conducted as planned a priori, based on the number of death events that occurred. Efficacy analyses were conducted in the ITT population, which is the ideal approach to assess the effect of assignment to the intervention. A hierarchal testing procedure was used to account for multiplicity in PFS outcomes in the FRESCO-2 trial. No multiplicity adjustment was in place for HRQoL outcomes in the FRESCO-2 trial or for PFS outcomes in the FRESCO trial. Outcomes that were not adjusted for multiplicity were at increased risk for type I error (false-positive results) and should be considered to be supporting evidence. For the prespecified OS and PFS subgroup analyses, there was a lack of sample-size consideration, control for multiplicity, and treatment-by-subgroup interaction analysis, which precludes any firm conclusions about subgroup effects. The stratified Cox proportional hazards model was checked for underlying assumptions; a visual inspection of the KM plots indicates that there do not appear to be any major violations of the proportional hazards assumptions.
Of note, in the FRESCO-2 trial, the mean duration of treatment exposure (4.0 months versus 2.0 months) and the total number of treatment cycles received (4.3 versus 2.3) were almost twice as high in the fruquintinib plus BSC group as in placebo plus BSC group. Patients discontinued treatment largely because of disease progression, AEs, or investigator decision, yet the proportion of patients who discontinued due to disease progression was not substantially different in the 2 groups (59% versus 64%). According to the protocol, patients in the FRESCO-2 study were allowed to continue the study treatment after disease progression that met the RECIST criteria. Of the 461 patients randomized to the fruquintinib plus BSC group, 301 experienced disease progression; of these, ██ ████████ ███████ received at least 1 dose of fruquintinib after disease progression. It is unclear what proportion of patients in the placebo plus BSC group was allowed to continue treatment beyond radiographic progression. The decision to continue treatment beyond disease progression was made by the investigator in a blinded manner, so is unlikely to have introduced bias. Subsequent anticancer treatments were lower in the fruquintinib plus BSC group than in the placebo plus BSC group (29.4% versus 34.3%), which could have introduced bias into the OS results in favour of placebo plus BSC.
In the analysis of proportion of patients with minimally important deterioration from baseline EORTC QLQ-C30 global health status/QoL score at the last on-treatment visit in the FRESCO-2 trial, data were missing from ████% of patients in the fruquintinib plus BSC group and the placebo plus BSC group (with █████ ██ █████ completed data in the fruquintinib plus BSC and placebo plus BSC groups, respectively). No data imputation was involved in this analysis. Missing data could have biased the validity and interpretability of HRQoL results. Sensitivity analyses were conducted for the change from baseline in score analysis, using the mixed model for repeated measures to assess the impact of the missing data; however, the underlying assumption that data were missing at random may not hold when, for example, missing data were more likely to occur in patients with end-stage disease and poor health status. There is the potential that the impact of the missing data (████%) would not be negligible in the analysis of the proportion of patients with minimally important deterioration from baseline EORTC QLQ-C30 global health status/QoL score, particularly when the between-group difference was small (████ ████ ███ █████ ██ ████████).
The sponsor selected the MID threshold for deterioration of 6.38 points based on a study in patients with ovarian cancer. Evidence from a study patients with advanced CRC treated with chemotherapy suggested higher MID estimates, which ranged from 9.21 to 6.81 points of deterioration. The sponsor’s choice of thresholds was considered less conservative, but unlikely to be a significant concern for bias due to the proximity of the estimates.
External Validity
The clinical experts consulted by CDA-AMC said they expect fruquintinib to be used as a fourth-line or later-line treatment (i.e., upon disease progression on or intolerance to all standard chemotherapies and tipiracil-trifluridine plus bevacizumab therapy if this combination [currently under consideration for public funding as a third-line or later-line treatment] becomes publicly reimbursed). In light of the clinical experts’ input about the anticipated place in therapy of fruquintinib, the CDA-AMC review team noted important considerations regarding the generalizability of the study results on efficacy and safety to the population and clinical practice setting in Canada.
In the FRESCO trial, patients were required to have progressed on or been intolerant to all standard chemotherapy; however, they were not required to have received prior targeted therapy, immunotherapy, or trifluridine-tipiracil (alone or in combination with bevacizumab). At baseline, approximately 40% of patients had received prior anti-VEGF drugs, anti-EGFR drugs, or both; as well, the proportion of patients who received prior immune checkpoint inhibitors, BRAF inhibitors, and trifluridine-tipiracil (alone or in combination with bevacizumab) could not be provided the sponsor. This introduces uncertainty to the generalizability of the findings; clinical expert input indicated that in clinical practice, most patients would have received these therapies (if indicated) before receiving fruquintinib treatment. In the FRESCO-2 trial, by inclusion criteria, patients had received all standard chemotherapy, anti-VEGF drugs, anti-EGFR drugs, immune checkpoint inhibitors, or BRAF inhibitors, as indicated; however, progression on or intolerance to these treatments was not specifically required, according to the sponsor. This may increase uncertainty about the generalizability of the study results to fourth-line or later-line setting. However, in the opinion of the clinical experts, the concern was likely to be minor, because in clinical practice typically, treatments are switched upon disease progression or poor tolerance. As well, most patients were expected to receive trifluridine-tipiracil plus bevacizumab combination therapy before fruquintinib treatment in clinical practice, per clinical expert input. Although the majority of patients in the FRESCO-2 trial previously received trifluridine-tipiracil (91.6%), the sponsor was unable to provide data on the proportion of patients who received trifluridine-tipiracil in combination with bevacizumab in either trial, which could introduce uncertainty into the generalizability of the study results.
The sponsor noted that these trials were completed during a time when there was limited clinical evidence on trifluridine-tipiracil plus bevacizumab therapy (results from the SUNLIGHT trial supporting the use of this combination were published in 2023) and no approved indications for the use of such combination therapy, which limit the ability to accurately characterize the proportion of patients who receive trifluridine-tipiracil in combination with bevacizumab. In addition, neither the FRESCO trial nor the FRESCO-2 trial specified in the inclusion criteria whether prior standard chemotherapy was specific to the metastatic setting, although the clinical experts had no major concerns about the generalizability of the study populations as a result. The clinical experts noted that standard chemotherapy is used in the metastatic setting, and could also be used in the adjuvant or neoadjuvant setting, although patients would typically be considered to have disease refractory to chemotherapy and be eligible for fruquintinib regardless of the setting in which disease progression occurs. Overall, in consultation with the clinical experts, the CDA-AMC review team considered that, compared to patients in the FRESCO trial, those in the FRESCO-2 trial were more reflective of the patient population expected to be eligible for fruquintinib treatment in Canada, based on the inclusion criteria and baseline characteristics, albeit subject to the generalizability concerns previously noted.
Other generalizability considerations with respect to the study populations were identified. Both trials included patients with an ECOG PS of 0 or 1, which, according to the clinical experts, is reflective of most patients who would be eligible for fruquintinib in clinical practice; however, some patients could potentially receive fruquintinib treatment despite having an ECOG PS of 2 if deemed clinically appropriate by the treating physician. As well, the FRESCO trial excluded patients with current CNS metastasis; the clinical experts noted that such patients would not necessarily be excluded from treatment, as long as they had been treated for CNS metastasis and are stable. The impact of these exclusions pertaining to ECOG PS and CNS metastasis on generalizability was expected to be low, per clinical expert input.
The dosing regimen of fruquintinib in the trials aligns with the product monograph. The FRESCO-2 trial allowed the continuation of fruquintinib treatment beyond radiographic progression until loss of clinical benefit, per the investigator’s discretion, which aligns with the anticipated use of fruquintinib in clinical practice. The clinical experts noted that the list of allowed concomitant medications in the trials was consistent with clinical practice. In regard to subsequent treatment use, between 29.4% and 50.7% of patients received at least 1 subsequent anticancer treatment; chemotherapy was the most common one. The clinical experts noted that the use of chemotherapy subsequent to fruquintinib does not align with clinical practice because these patients were chemorefractory. The clinical experts noted that most patients would be expected to receive BSC after the failure of fruquintinib treatment if fruquintinib was used as a fourth-line therapy (i.e., after the failure of 2 lines of standard chemotherapy and then trifluridine-tipiracil plus bevacizumab).
Outcomes assessed in the trials (OS, PFS, HRQoL, and harms) are important to patients and clinicians. The EORTC QLQ-C30 captured some aspects of HRQoL that were identified by patients and clinicians to be important, such as symptoms, functioning, pain, and fatigue, although this questionnaire is typically used in a clinical trial setting, not in clinical practice. Caregiver burden and the time required for treatment-related clinician visits, which were identified as important outcomes in input from the patient groups and clinical experts, were not assessed.
Of note, the FRESCO trial was conducted in China, whereas the FRESCO-2 trial was a global study conducted in Asia-Pacific, Europe, and North America (there were no sites in Canada). In consultation with the clinical experts, the CDA-AMC review team noted that, given that there is a potential for differences in the standard of care and availability of BSC across countries, there is high uncertainty about whether results from the FRESCO trial, in particular, would be generalizable to patients in Canada.
In consultation with the clinical experts, the CDA-AMC review team considered the most relevant comparators of fruquintinib to be BSC in the fourth-line or later-line setting (i.e., progression on at least 2 lines of standard chemotherapy and trifluridine-tipiracil plus bevacizumab). The FRESCO-2 trial provided direct evidence comparing fruquintinib plus BSC with placebo plus BSC in the fourth-line or later-line setting.
GRADE Summary of Findings and Certainty of the Evidence
Methods for Assessing the Certainty of the Evidence
For the pivotal studies and RCTs identified in the sponsor’s systematic review, GRADE was used to assess the certainty of the evidence for outcomes considered most relevant to inform CDA-AMC’s expert committee deliberations, and a final certainty rating was determined as outlined by the GRADE Working Group.47,48
High certainty: We are very confident that the true effect lies close to that of the estimate of the effect.
Moderate certainty: We are moderately confident in the effect estimate. The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. We use the word “likely” for evidence of moderate certainty (e.g., “X intervention likely results in Y outcome”).
Low certainty: Our confidence in the effect estimate is limited — The true effect may be substantially different from the estimate of the effect. We use the word “may” for evidence of low certainty (e.g., “X intervention may result in Y outcome”).
Very low certainty: We have very little confidence in the effect estimate — The true effect is likely to be substantially different from the estimate of effect. We describe evidence of very low certainty as “very uncertain.”
Following the GRADE approach, evidence from RCTs started as high-certainty evidence and could be rated down for concerns related to study limitations (which refers to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias.
When possible, certainty was rated in the context of the presence of an important (nontrivial) treatment effect; if this was not possible, certainty was rated in the context of the presence of any treatment effect (i.e., the clinical importance is unclear). In all cases, the target of the certainty of evidence assessment was based on the point estimate and where it was located relative to the threshold for a clinically important effect (when a threshold was available) or to the null. For this review, the target of the certainty of evidence assessment was based on presence or absence of an important effect as informed by thresholds identified based on clinical expert input (OS, PFS, EORTC QLQ-C30, SAEs).
Findings from the FRESCO and FRESCO-2 trials were assessed individually because these studies were conducted in different patient populations. The FRESCO-2 trial included patients who had received all standard chemotherapy, and who progressed on or were intolerant to trifluridine-tipiracil plus bevacizumab, which is likely reflective of the use of fruquintinib in the fourth-line or later-line setting, per clinical expert input. The FRESCO trial included patients who had progressed on or were intolerant to all standard chemotherapy alone, which is reflective of the use of fruquintinib in the third-line or later-line setting. In addition, patients in the FRESCO-2 trial had previously received an anti-VEGF drug, and if indicated, an anti-EGFR drug, BRAF inhibitor, and immune checkpoint inhibitor, whereas patients in the FRESCO trial were not required to have received these treatments before study enrolment.
Results of GRADE Assessments
Table 2 presents the GRADE summary of findings for fruquintinib plus BSC versus placebo plus BSC in patients with mCRC who had progressed on or were intolerant to at least 2 lines of standard chemotherapy.
Table 3 presents the GRADE summary of findings for fruquintinib plus BSC versus placebo plus BSC in patients with mCRC who had previously received standard chemotherapy, an anti-VEGF drug, and an anti-EGFR drug (if RAS wild-type), and had progressed on or been intolerant to trifluridine-tipiracil and/or regorafenib.
Long-Term Extension Studies
No long-term extension studies were submitted for review.
Indirect Evidence
One sponsor-conducted ITC comparing the efficacy of fruquintinib with alternative third-line or later-line treatments in patients with mCRC was included in the sponsor’s submission in anticipation of the approval of fruquintinib in the third-line or later-line setting.19 Fruquintinib was subsequently granted a Notice of Compliance by Health Canada for use in the fourth-line or later-line setting (i.e., after the failure of at least 2 lines of standard chemotherapy and either trifluridine-tipiracil or regorafenib). Direct evidence on the use of fruquintinib and a relevant comparator (BSC) in the fourth-line or later-line setting was available from the FRESCO-2 study. The sponsor-conducted ITC, which was intended to provide indirect comparative evidence between fruquintinib to trifluridine-tipiracil in combination with bevacizumab in the third-line or later-line setting, was therefore considered to have limited relevance for the purpose of this review and will not be further summarized in this section. Refer to Appendix 2 for a summary of the sponsor-conducted ITC, along with a summary of a published ITC (Gao et al. [2023]20) assessing the same population, intervention, comparison, and outcomes (PICO) identified in the sponsor’s submission.
Studies Addressing Gaps in the Systematic Review Evidence
No additional studies were submitted for review.
Discussion
This report summarizes the evidence for fruquintinib for the treatment of adult patients with mCRC based on 2 phase III RCTs and 2 ITCs.
Summary of Available Evidence
Two studies, FRESCO (N = 416) and FRESCO-2 (N = 691), met the inclusion criteria for the systematic review conducted by the sponsor. The FRESCO and FRESCO-2 trials were multicentre, randomized, double-blind, placebo-controlled, phase III trials that compared the efficacy and safety of fruquintinib plus BSC with placebo plus BSC in adult patients with metastatic colorectal adenocarcinoma. The FRESCO trial enrolled patients who had progressed on or experienced intolerable toxicity to at least 2 lines of standard chemotherapy. The FRESCO-2 trial enrolled patients who were previously treated with all standard chemotherapies, anti-VEGF therapy, and anti-EGFR therapy (if RAS is wild-type), and had progressed on or been intolerant to treatment with trifluridine-tipiracil and/or regorafenib. Patients in the FRESCO-2 trial also had received immune checkpoint inhibitors and/or BRAF inhibitors, if indicated. The efficacy outcomes of interest to this review included OS (primary end point), PFS (secondary end point in the FRESCO trial; key secondary end point in the FRESCO-2 trial), EORTC QLQ-C30 global health status/QoL score (FRESCO-2 trial only, secondary end point). In the FRESCO trial, at baseline, the majority of patients (78.8%) had received 3 or fewer lines of prior anticancer treatment for metastatic disease, 30.0% of patients received prior anti-VEGF treatment, and 14.2% of patients received prior anti-EGFR treatment. The proportion of patients who had previously received immune checkpoint inhibitors, BRAF inhibitors, trifluridine-tipiracil, and regorafenib was not reported. In the FRESCO-2 trial, at baseline, most patients had received more than 3 lines of prior anticancer treatment for metastatic disease (72.6%) and prior anti-VEGF treatment (96.4%). All patients received prior treatment with trifluridine-tipiracil and/or regorafenib (including 52.2% who received trifluridine-tipiracil alone, and 39.4% who received both trifluridine-tipiracil and regorafenib). Approximately one-third of patients had received prior anti-EGFR treatment. In both trials, the proportion of patients who received prior trifluridine-tipiracil plus bevacizumab combination therapy was unknown.
Interpretation of Results
Efficacy
Improving survival and delaying disease progression were outcomes identified to be important by patients and clinicians. The primary end point of OS was met in the FRESCO and FRESCO-2 trials, supporting the superiority of fruquintinib plus BSC over placebo plus BSC in patients with mCRC who were chemorefractory. The clinical experts considered the extension of median OS by close to 3 months to be clinically meaningful in both trials. Point estimates of the between-group difference in the probability of OS also favoured fruquintinib plus BSC, and the magnitude of benefit was considered by the clinical experts consulted by CDA-AMC to be clinically meaningful at 6 months and 12 months in the FRESCO trial, and similarly, at 6 months in the FRESCO-2 trial. Point estimates at later time points in both trials suggested little to no clinically important difference, although the results were of low to very low certainty. Findings for PFS (median PFS and probability of PFS at 3 months, 6 months, and 9 months) in both studies also favoured fruquintinib plus BSC over placebo plus BSC, and the magnitude of benefits was clinically meaningful, per clinical expert input, further supporting the benefits of fruquintinib in delaying disease progression and improving survival. Of note, per clinical expert input, the findings at later time points (i.e., 18 months for OS and 9 months for PFS) were less relevant because survival is generally limited for patients in late-line settings, and most patients were expected to have experienced disease progression or died at those time points. Prespecified subgroup analyses were conducted for OS and PFS to assess the subgroup effects of prior treatment, ECOG PS, gene mutation status, and primary tumour site at first diagnosis, which were potential effect modifiers of treatments for mCRC, per clinical expert input. Results were, in general, consistent with the primary analyses across all subgroups of interest. Of note, however, no effect on OS was observed in the subgroup of patients who had received 3 or fewer lines of prior chemotherapy (not specific to the stage of disease in which they were given) in the FRESCO-2 trial (HR = 0.94; 95% CI, 0.56 to 1.53), whereas the treatment effect was consistently observed across subgroups by the number of prior lines of chemotherapy specific to the metastatic setting. However, due to a lack of sample-size consideration, control for multiplicity, and treatment-by-subgroup interaction analysis, no firm conclusions can be drawn regarding subgroup effects.
The clinical experts emphasized that maintenance of HRQoL was a key treatment goal in patients with chemorefractory disease, in whom survival is typically short. The importance of maintaining HRQoL was similarly noted in patient group and clinician group inputs. The impact of fruquintinib on HRQoL was not assessed in the FRESCO trial, but was assessed as supporting evidence using the EORTC QLQ-C30 in the FRESCO-2 trial. The point estimate and 95% CI suggested little to no clinically important difference in the responder analysis, based on a 6.38-point threshold of deterioration from baseline in global health status score; moreover, there is a large amount of missing data (██████ in the treatment groups, so the benefit of fruquintinib on HRQoL is uncertain. In addition, due to the subjective nature of this outcome, there is a potential for bias in the measurement of this outcome, leading to inflated efficacy of fruquintinib, based on the inferred judgment of patients and investigators regarding treatment assignment related to associated AEs. Of note, the threshold of 6.38-point deterioration in this analysis was selected by the sponsor based on a study of patients with ovarian cancer. Based on evidence available in patients with advanced CRC (MID estimates range from 9.21 to 6.81 points of deterioration), the choice of MID by the sponsor was considered less conservative, but unlikely to be a concern for bias because of the proximity of the values. Results for other aspects of HRQoL, including role functioning, emotional functioning, and physical functioning, pain, and fatigue, in general, were consistent with the global health status score analysis. Caregiver burden was highlighted as being an important aspect in caring for patients with mCRC, although this outcome was not assessed in the trials so the effect of fruquintinib on that is unknown.
The sponsor requested that fruquintinib be reimbursed as per the Health Canada indication (i.e., for the treatment of adult patients with mCRC who have been previously treated with or are not considered candidates for available standard therapies, including fluoropyrimidine-, oxaliplatin-, and irinotecan-based chemotherapy, an anti-VEGF drug, an anti-EGFR drug (if RAS wild-type), and either trifluridine-tipiracil or regorafenib. The sponsor clarified that the population of interest included patients who have shown disease progression on, are intolerant to toxicities to, or have contraindications to, the standard treatments. This is generally consistent with clinical expert input received by CDA-AMC that the anticipated place of therapy of fruquintinib is as a fourth-line or later-line treatment, upon disease progression on or intolerance to standard chemotherapy, and tipiracil-trifluridine plus bevacizumab combination therapy, if this combination (currently under consideration for public funding as a third-line or later-line treatment) becomes publicly reimbursed. In consultation with the clinical experts, the CDA-AMC review team considered the FRESCO-2 trial to be more reflective of the likely place in therapy of fruquintinib (i.e., fourth-line or later-line treatment) than the FRESCO trial, based on the inclusion criteria and baseline patient characteristics. Nonetheless, the generalizability of the FRESCO-2 trial could potentially be limited, because the proportion of patients who received prior trifluridine-tipiracil plus bevacizumab is unknown (the sponsor was unable to provide such data). As well, although patients were required to have been previously treated with standard chemotherapy, progression on or intolerance to standard chemotherapy was not specifically required, according to the sponsor. This may increase uncertainty about the generalizability of the study results to fourth-line or later-line setting, although in the opinion of the clinical experts, the concern is likely to be low because in clinical practice, typically, treatments are switched upon disease progression or poor tolerance. It should also be noted that the use of chemotherapy as a common subsequent anticancer treatment in the trials did not align with clinical practice in Canada, per clinical expert input, which could potentially limit the generalizability of the study results.
The FRESCO and FRESCO-2 trials were the only phase III, RCTs of fruquintinib to date. The CDA-AMC review team considered the most relevant comparators of fruquintinib to be BSC in the fourth-line or later-line setting. The FRESCO-2 trial provided direct evidence comparing fruquintinib plus BSC with placebo plus BSC in the fourth-line or later-line setting.
Harms
Direct comparative evidence from the FRESCO and FRESCO-2 trials showed that fruquintinib plus BSC was associated with a higher frequency of all-grade TEAEs than placebo plus BSC. The most frequently reported all-grade TEAEs of fruquintinib were hand-foot syndrome, hypertension, dysphonia, proteinuria, and asthenia; all of these were more commonly reported in the fruquintinib plus BSC group than in the placebo plus BSC group. Hypertension and hand-foot syndrome of grade 3 or higher were more commonly reported in the fruquintinib plus BSC group than in the placebo plus BSC in both trials; the clinical experts noted that these TEAEs are generally manageable in clinical practice, although hand-foot syndrome, in particular, can be distressing for patients. The frequency of SAEs and WDAEs was comparable between treatment groups in the FRESCO-2 trial, but was higher in the fruquintinib plus BSC group than in the placebo plus BSC group in the FRESCO trial, although they were not attributed to any specific TEAE. Overall, the clinical experts had no major concerns about the safety profile of fruquintinib, and noted that the AEs reported were consistent with the known safety of VEGFR inhibitors.
Conclusion
Direct evidence from 1 double-blind RCT (the FRESCO-2 trial) demonstrated a clinically meaningful improvement in OS and PFS with fruquintinib plus BSC over placebo plus BSC in patients with mCRC who had previously been treated with all standard chemotherapies, an anti-VEGF drug, and an anti-EGFR drug (if RAS is wild-type), and had progressed on or been intolerant to treatment with trifluridine-tipiracil and/or regorafenib. The evidence suggested that fruquintinib may result in little to no clinically important difference in deterioration of HRQoL; however, this is uncertain due to a notable amount of missing data. Fruquintinib had similar treatment effects on OS and PFS in another RCT (the FRESCO trial) that enrolled patients who had received less prior therapy for mCRC. Based on clinical expert input, the patient population in the FRESCO-2 trial was more reflective of the likely place in therapy of fruquintinib as a fourth-line or later-line treatment than the FRESCO trial. Nonetheless, there is uncertainty about whether results from the FRESCO-2 trial are generalizable to the fourth-line or later-line setting, based on treatment history and subsequent anticancer treatment. Fruquintinib plus BSC was associated with a higher frequency of all-grade TEAEs (including hand-foot syndrome, hypertension) than placebo plus BSC. The safety profile of fruquintinib was consistent with the known safety of VEGFR inhibitors, per clinical expert input.
References
1.Canadian Cancer Society. Colorectal Cancer. 2024: https://cancer.ca/en/cancer-information/cancer-types/colorectal. Accessed 2024 Jul 25.
2.Canada Cancer Society. Colorectal cancer statistics. 2024; https://cancer.ca/en/cancer-information/cancer-types/colorectal/statistics. Accessed 2024 Jul 25.
3.Ferlay J EM, Lam F, Laversanne M, Colombet M, Mery L, Piñeros M, Znaor A, Soerjomataram I, Bray F. Global Cancer Observatory: Cancer Today (version 1.1). Lyon (FR): International Agency for Research on Cancer; 2024: https://gco.iarc.who.int/today. Accessed 2024 Jul 25.
4.Hossain MS, Karuniawati H, Jairoun AA, et al. Colorectal Cancer: A Review of Carcinogenesis, Global Epidemiology, Current Challenges, Risk Factors, Preventive and Treatment Strategies. Cancers (Basel). 2022;14(7). PubMed
5.Shin AE, Giancotti FG, Rustgi AK. Metastatic colorectal cancer: mechanisms and emerging therapeutics. Trends Pharmacol Sci. 2023;44(4):222-236. PubMed
6.Grothey A, Van Cutsem E, Sobrero A, et al. Regorafenib monotherapy for previously treated metastatic colorectal cancer (CORRECT): an international, multicentre, randomised, placebo-controlled, phase 3 trial. Lancet. 2013;381(9863):303-312. PubMed
7.Hamers PAH, Elferink MAG, Stellato RK, et al. Informing metastatic colorectal cancer patients by quantifying multiple scenarios for survival time based on real-life data. Int J Cancer. 2021;148(2):296-306. PubMed
8.Mayer RJ, Van Cutsem E, Falcone A, et al. Randomized trial of TAS-102 for refractory metastatic colorectal cancer. N Engl J Med. 2015;372(20):1909-1919. PubMed
9.Shen C, Tannenbaum D, Horn R, et al. Overall Survival in Phase 3 Clinical Trials and the Surveillance, Epidemiology, and End Results Database in Patients With Metastatic Colorectal Cancer, 1986-2016: A Systematic Review. JAMA Netw Open. 2022;5(5):e2213588. PubMed
10.Cervantes A, Adam R, Rosello S, et al. Metastatic colorectal cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann Oncol. 2023;34(1):10-32. PubMed
11.Grothey A, Marshall JL, Bekaii-Saab T. Sequencing beyond the second-line setting in metastatic colorectal cancer. Clin Adv Hematol Oncol. 2019;17 Suppl 7(3):1-19.
12.Sanchez-Gundin J, Fernandez-Carballido AM, Martinez-Valdivieso L, Barreda-Hernandez D, Torres-Suarez AI. New Trends in the Therapeutic Approach to Metastatic Colorectal Cancer. Int J Med Sci. 2018;15(7):659-665. PubMed
13.Reimbursement Recommendation Trifluridine-Tipiracil (Lonsurf). Ottawa (ON): Canada’s Drug Agency/l’Agence des médicaments du Canada; 2024: https://www.cadth.ca/sites/default/files/DRR/2024/PC0330%20Lonsurf%20-%20Confidential%20CADTH%20Final%20Rec.pdf. Accessed 2024 Jul 25.
14.Li J, Qin S, Xu RH, et al. Effect of fruquintinib vs placebo on overall survival in patients with previously treated metastatic colorectal cancer: the FRESCO randomized clinical trial. JAMA. 2018;319(24):2486-2496. PubMed
15.Dasari A, Lonardi S, Garcia-Carbonero R, et al. Fruquintinib versus placebo in patients with refractory metastatic colorectal cancer (FRESCO-2): an international, multicentre, randomised, double-blind, phase 3 study. Lancet. 2023;402(10395):41-53. PubMed
16.Clinical Study Report: FRESCO. Fruquintinib Clinical Study Report. A Randomized, Double-blind and Placebo-controlled Phase III Trial Comparing Fruquintinib Efficacy and Safety vs Best Support Care (BSC) in Advanced Colorectal Cancer Patients Who Have Failed at Least Second Lines of Chemotherapies [internal sponsor's report]. Shanghai (CN): Hutchison MediPharma Limited; 2017 May 27.
17.Canada’s Drug Agency/l’Agence des médicaments du Canada (CDA-AMC) Reimbursement Review: Summary of Clinical Evidence Template [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: fruquintinib, 1 mg and 5 mg capsules, for oral administration. Toronto (ON): Takeda Canada Inc.; 2024 May 21.
18.Clinical Study Report: FRESCO-2. A Global, Multicenter, Randomized, Placebo-controlled Phase 3 Trial to Compare the Efficacy and Safety of Fruquintinib Plus Best Supportive Care to Placebo Plus Best Supportive Care in Patients With Refractory Metastatic Colorectal Cancer (FRESCO-2) Final Analysis Clinical Study Report [internal sponsor's report]. Shanghai (CN): Hutchison MediPharma Limited; 2023 Feb 03.
19.Metastatic Colorectal Cancer Previously Treated with Fluoropyrimidine-, Oxaliplatin-, and Irinotecan-based Chemotherapy, an Anti-VEGF Therapy, and if RAS Wild Type, an Anti-EGFR Therapy. Indirect Treatment Comparison. Final Report v3.1 [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: fruquintinib, 1 mg and 5 mg, oral capsules. Toronto (ON): Takeda Canada Inc.; 2023 Dec 19.
20.Gao L, Tang L, Hu Z, Peng J, Li X, Liu B. Comparison of the efficacy and safety of third-line treatments for metastatic colorectal cancer: a systematic review and network meta-analysis. Front Oncol. 2023;13:1269203. PubMed
21.American Gastroenterological Association. Colorectal cancer (CRC). 2024; https://patient.gastro.org/colorectal-cancer-crc/. Accessed 2023 May 4.
22.Centers for Disease Control and Prevention. Colorectal Cancer Basics. 2024: https://www.cdc.gov/colorectal-cancer/about/?CDC_AAref_Val=https://www.cdc.gov/cancer/colorectal/basic_info/. Accessed 2024 Jul 25.
23.Meseeha M, Attia M. Colon Polyps. StatPearls. Treasure Island (FL): 2023: https://www.ncbi.nlm.nih.gov/pubmed/28613512. Accessed 2024 Jul 25.
24.Baran B, Mert Ozupek N, Yerli Tetik N, Acar E, Bekcioglu O, Baskin Y. Difference Between Left-Sided and Right-Sided Colorectal Cancer: A Focused Review of Literature. Gastroenterology Res. 2018;11(4):264-273. PubMed
25.Holch JW, Ricard I, Stintzing S, Modest DP, Heinemann V. The relevance of primary tumour location in patients with metastatic colorectal cancer: A meta-analysis of first-line clinical trials. Eur J Cancer. 2017;70:87-98. PubMed
26.National Cancer Institute. Cancer Stat Facts: Colorectal Cancer. https://seer.cancer.gov/statfacts/html/colorect.html. Accessed 2024 Jul 25.
27.Dekker E, Tanis PJ, Vleugels JLA, Kasi PM, Wallace MB. Colorectal cancer. Lancet. 2019;394(10207):1467-1480. PubMed
28.Morgan E, Arnold M, Gini A, et al. Global burden of colorectal cancer in 2020 and 2040: incidence and mortality estimates from GLOBOCAN. Gut. 2023;72(2):338-344. PubMed
29.Centers for Disease Control and Prevention. United States Cancer Statistics: Data Visualizations. 2024; https://gis.cdc.gov/Cancer/USCS/. Accessed 2023 May 5.
30.Bouvier AM, Jooste V, Sanchez-Perez MJ, et al. Differences in the management and survival of metastatic colorectal cancer in Europe. A population-based study. Dig Liver Dis. 2021;53(5):639-645. PubMed
31.Chen Y, Qiu Z, Kamruzzaman A, Snodgrass T, Scarfe A, Bryant HE. Survival of metastatic colorectal cancer patients treated with chemotherapy in Alberta (1995-2004). Support Care Cancer. 2010;18(2):217-224. PubMed
32.Tamakoshi A, Nakamura K, Ukawa S, et al. Characteristics and prognosis of Japanese colorectal cancer patients: The BioBank Japan Project. J Epidemiol. 2017;27(3S):S36-S42. PubMed
33.Ciardiello F, Ciardiello D, Martini G, Napolitano S, Tabernero J, Cervantes A. Clinical management of metastatic colorectal cancer in the era of precision medicine. CA Cancer J Clin. 2022;72(4):372-401. PubMed
34.Guillemin I, Darpelly M, Wong B, Ingelgard A, Griebsch I. Development of a disease conceptual model of patient experience with metastatic colorectal cancer: identification of the most salient symptoms and impacts. J Cancer Surviv. 2022:1-11. PubMed
35.Takeda. Global Value Dossier – Clinical Value: Fruquintinib, Late-Line Metastatic Colorectal Cancer. Data on file. In: Drug Reimbursement Review sponsor submission: fruquintinib, 1 mg and 5 mg capsules, for oral administration. 2023 Nov 9 (version 1.0).
36.Akimoto N, Ugai T, Zhong R, et al. Rising incidence of early-onset colorectal cancer - a call to action. Nat Rev Clin Oncol. 2021;18(4):230-243. PubMed
37.Neugut AI, Lin A, Raab GT, et al. FOLFOX and FOLFIRI Use in Stage IV Colon Cancer: Analysis of SEER-Medicare Data. Clin Colorectal Cancer. 2019;18(2):133-140. PubMed
38.Souglakos J, Androulakis N, Syrigos K, et al. FOLFOXIRI (folinic acid, 5-fluorouracil, oxaliplatin and irinotecan) vs FOLFIRI (folinic acid, 5-fluorouracil and irinotecan) as first-line treatment in metastatic colorectal cancer (MCC): a multicentre randomised phase III trial from the Hellenic Oncology Research Group (HORG). Br J Cancer. 2006;94(6):798-805. PubMed
39.Provisional Funding Algorithm Indication: Metastatic Colorectal Cancer. Ottawa (ON): Canada’s Drug Agency/l’Agence des médicaments du Canada; 2024: https://www.cadth.ca/sites/default//files/DRR/2024/PH0044%20Metastatic%20Colorectal%20Cancer%20Rapid%20Algorithm%20Report.pdf. Accessed 2024 Jul 24.
40.U.S. Cancer Statistics Working Group. Cancer Statistics At a Glance. 2024; https://www.cdc.gov/cancer/dataviz. Accessed 2024 Jul 25.
41.Takeda Pharmaceuticals. What is fruquintinib? 2024; https://www.fruzaqla.com/#:~:text=full%20Prescribing%20Information.-,What%20is%20FRUZAQLA%C2%AE%20(fruquintinib)%3F,with%20certain%20anti%2Dcancer%20medicines. Accessed 2024 Jul 25.
42.Sun Q, Zhou J, Zhang Z, et al. Discovery of fruquintinib, a potent and highly selective small molecule inhibitor of VEGFR 1, 2, 3 tyrosine kinases for cancer therapy. Cancer Biol Ther. 2014;15(12):1635-1645. PubMed
43.Fruzaqla (fruquintinib capsules): capsules, 1 mg and 5 mg, Oral [product monograph]. Toronto (Ontario): Takeda Canada Inc.; 2024.
44.Ko YJ, Abdelsalam M, Kavan P, et al. What is a clinically meaningful survival benefit in refractory metastatic colorectal cancer? Curr Oncol. 2019;26(2):e255-e259. PubMed
45.Musoro JZ, Coens C, Greimel E, et al. Minimally important differences for interpreting European Organisation for Research and Treatment of Cancer (EORTC) Quality of life Questionnaire core 30 scores in patients with ovarian cancer. Gynecol Oncol. 2020;159(2):515-521. PubMed
46.Musoro JZ, Sodergren SC, Coens C, et al. Minimally important differences for interpreting the EORTC QLQ-C30 in patients with advanced colorectal cancer treated with chemotherapy. Colorectal Dis. 2020;22(12):2278-2287. PubMed
47.Balshem H, Helfand M, Schünemann HJ, et al. GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol. 2011;64(4):401-406. PubMed
48.Santesso N, Glenton C, Dahm P, et al. GRADE guidelines 26: informative statements to communicate the findings of systematic reviews of interventions. J Clin Epidemiol. 2020;119:126-135. PubMed
Appendix 1: Detailed Outcomes Data
Please note that this appendix has not been copy-edited.


Appendix 2: Summary of Sponsor-Conducted and Published ITCs
Please note that this appendix has not been copy-edited.
Description of Studies
One sponsor-conducted network meta-analysis (NMA)19 and 1 published NMA (Gao et al. [2023]20), which indirectly compared fruquintinib to available treatments (with BSC as background therapy for all interventions) with respect to OS and PFS in patients with mCRC in the third- or later-line setting (i.e., progression on or intolerance to all standard chemotherapy) via a Bayesian NMA, was included in this report. The Gao et al. NMA also assessed the comparative effects on grade 3 or higher AEs.
Efficacy Results
Overall Survival
The base-case OS analysis of the sponsor-conducted NMA was based on a total of 8 studies. There was insufficient evidence to show a difference in OS between fruquintinib versus trifluridine-tipiracil plus bevacizumab because the credible interval (CrI) for HR was wide ███ █ █████ ███ ███ ████ ██ ████). The HR of OS for the comparison of fruquintinib versus placebo was ████ ████ ████ ████ ██ ██████ in favour of fruquintinib.
The Gao et al. NMA was based on a total of 9 studies. The HR of OS for the comparison of fruquintinib versus trifluridine-tipiracil plus bevacizumab was 1.60 (95% CrI, 1.13 to 2.25), in favour of trifluridine-tipiracil plus bevacizumab. The HR of OS for the comparison of fruquintinib versus BSC was 0.65 (95% CrI, 0.51 to 0.83), in favour of fruquintinib.
Progression-Free Survival
In the base-case PFS analysis of the sponsor-conducted NMA. There was insufficient evidence to show a difference in PFS between fruquintinib versus trifluridine-tipiracil plus bevacizumab because the Crl for HR was wide ███ █ █████ ███ ████ ████ ██ ██████. The HR of PFS for the comparison of fruquintinib versus placebo was ████ ████ ████ ████ ██ █████, in favour of fruquintinib.
In the Gao et al. NMA, the point estimate for the difference in PFS between trifluridine-tipiracil plus bevacizumab versus fruquintinib was in favour of trifluridine-tipiracil plus bevacizumab but the CrI included the null (HR = 0.76; 95% CrI, 0.55 to 1.05). The HR of PFS for the comparison of BSC versus fruquintinib was 3.74 (95% CrI, 2.94 to 4.67), in favour of fruquintinib.
Harms Results
Grade 3 or Higher AEs
This outcome was not assessed in the sponsor-conducted NMA. In the Gao et al. NMA, the relative risk of trifluridine-tipiracil plus bevacizumab versus fruquintinib in the incidence rate of grade 3 or higher AEs was 0.54 (95% CrI, 0.36 to 0.79), in favour of trifluridine-tipiracil plus bevacizumab. The relative risk of BSC versus fruquintinib in the incidence rate of grade 3 or higher AEs was 0.61 (95% CrI, 0.53 to 0.70), in favour of BSC.
Critical Appraisal
The validity of the results from both NMAs were overall uncertain because there is evidence that the exchangeability assumptions have been violated due to heterogeneity across included studies in study design (blinding, study location), and patient population by inclusion criteria (number of prior treatment lines, prior anticancer treatment, ECOG PS) and by baseline patient characteristics identified as potential treatment effect modifiers by the clinical experts (proportion of older adults, number of metastatic sites, number of lines of prior therapy for metastatic disease, time since diagnosis of metastatic disease, RAS mutation status). As well, the networks were sparse and without a close loop connecting fruquintinib which render an assessment of consistency impossible. Based on results from their NMA, the sponsor concluded that there was no difference in OS and PFS between fruquintinib and trifluridine-tipiracil plus bevacizumab. However, the results were imprecise with wide 95% CrIs, which preclude definitive conclusions on the comparative efficacy between the interventions. Of note, OS and PFS findings from the published NMA by Gao et al. were in favour of trifluridine-tipiracil plus bevacizumab over fruquintinib. An important distinction of the methods between the NMAs is that the Gao et al. NMA was conducted using the fixed-effect model, while the sponsor’s NMA was conducted using the random-effect model. In the case of a sparse network, a fixed-effect model would generally yield results with narrower 95% CrIs than a random-effect model and is deemed more appropriate by the review team. Results based on different NMA model selections (fixed versus random) was not available in both the sponsor’s NMA and the published NMA. Of note, findings of statistical significance for OS were inconsistent between NMAs, as although point estimates were aligned in favour of trifluridine-tipiracil plus bevacizumab, a smaller credible interval (not crossing the null) was generated in the published ITC due to the use of a fixed-effects model (versus random-effects model in the sponsor-conducted NMA in which the CrIs were wide and crossed the null). This further hinders our ability to draw firm conclusions from the sponsor-conducted NMA. In addition, the research questions of the NMAs were almost identical yet there is a slight difference in study selection. There is a risk of bias in the findings of both NMAs due to missing results in the synthesis.
Conclusions
The comparative efficacy between fruquintinib and trifluridine-tipiracil plus bevacizumab in patients remains largely uncertain in the treatment of patients with mCRC in the third- or later-line setting based the sponsor-conducted NMA and the published NMA. No definitive conclusions can be drawn due to important limitations of the NMAs, including significant heterogeneity across included studies, a sparse network, and imprecise results in the sponsor-conducted NMA. Comparative harms were not assessed in the sponsor-conducted ITC. The published ITC suggested that fruquintinib may have inferior safety profile (grade 3 or higher AEs) relative to trifluridine-tipiracil plus bevacizumab but this cannot be concluded based on the overall evidence and uncertainties associated with the NMAs.
Pharmacoeconomic Review
Abbreviations
AE
adverse event
BSC
best supportive care
CDA-AMC
Canada's Drug Agency
HR
hazard ratio
ICER
incremental cost-effectiveness ratio
ITC
indirect treatment comparison
mCRC
metastatic colorectal cancer
NMA
network meta-analysis
OS
overall survival
PD
progressed disease
PF
progression free
PFS
progression-free survival
PSM
partitioned survival model
QALY
quality-adjusted life-year
WTP
willingness to pay
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Fruquintinib (Fruzaqla), 1 mg or 5 mg capsule |
Indication | For the treatment of adult patients with metastatic colorectal cancer who have been previously treated with or are not considered candidates for available standard therapies, including fluoropyrimidine, oxaliplatin, and irinotecan-based chemotherapy, an anti-VEGF agent, an anti-EGFR agent (if RAS wild type), and either trifluridine-tipiracil or regorafenib.a |
Health Canada approval status | NOC |
Health Canada review pathway | Standard review, Project Orbis, ACCESS Consortium (Australia, Canada, Singapore, Switzerland, UK) |
NOC date | September 10, 2024 |
Reimbursement request | Per indication |
Sponsor | Takeda Canada Inc. |
Submission history | Previously reviewed: No |
NOC = Notice of Compliance.
aThe proposed indication was revised during the review process. The original indication was as follows: for the treatment of adult patients with metastatic colorectal cancer who have been previously treated with or are not considered candidates for available therapies, including fluoropyrimidine-based chemotherapy, oxaliplatin-based chemotherapy, and irinotecan-based chemotherapy, an anti-VEGF therapy, and an anti-EGFR therapy.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis PSM |
Target population | Adult patients with mCRC who have been previously treated with or are not considered candidates for available therapies, including fluoropyrimidine-based chemotherapy, oxaliplatin-based chemotherapy, and irinotecan-based chemotherapy, an anti-VEGF therapy, and an anti-EGFR therapya |
Treatment | Fruquintinib |
Dose regimen | 5 mg daily for 21 days, followed by 7 days off treatment, to comprise a complete cycle of 28 days. Treatment should be continued until disease progression or unacceptable toxicity |
Submitted price | Fruquintinib:
|
Submitted treatment cost | 28-day cycle cost = $6,321 |
Comparators |
|
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs, LYs |
Time horizon | Lifetime (10 years) |
Key data source | FRESCO phase III trial, FRESCO-2 phase III trial, sponsor submitted NMA |
Submitted results | Based on a sequential analysis, fruquintinib is not on the cost-effectiveness frontier (extendedly dominated by BSC and trifluridine-tipiracil plus bevacizumab). Fruquintinib was more costly (incremental costs = $38,292) and more effective (incremental QALYs = 0.24) than BSC, but less costly (incremental costs = –$19,813) and less effective (incremental QALYs = –0.45) than trifluridine-tipiracil plus bevacizumab. |
Key limitations |
|
CDA-AMC reanalysis results |
|
BSC = best supportive care; CDA-AMC = Canada's Drug Agency; ICER = incremental cost-effectiveness ratio; LY = life-year; mCRC = metastatic colorectal cancer; NMA = network meta-analysis; OS = overall survival; PFS = progression-free survival; PSM = partitioned survival model; QALY = quality-adjusted life-year.
aThe indication was revised during the review process. The target population described here was aligned with the original proposed indication, although the sponsor’s economic evaluation could be modified to consider a target population aligned with the revised indication. This also required a change in the primary comparator, from tipiracil-trifluridine plus bevacizumab to BSC. The population for the budget impact analysis was also aligned with the original proposed indication.
Conclusions
The CDA-AMC clinical review determined that fruquintinib is associated with prolonged overall survival (OS) and progression-free survival (PFS) relative to BSC for the treatment of metastatic colorectal cancer (mCRC) in patients who had previously been treated with all standard chemotherapies, an anti-VEGF drug, and an anti-EGFR drug (if RAS is wild-type), and had progressed on or been intolerant to treatment with trifluridine-tipiracil and/or regorafenib, based on the FRESCO-2 trial. According to clinical expert input, the FRESCO-2 trial was more reflective of the likely place in therapy of fruquintinib as a fourth-line or later-line treatment than the FRESCO trial. Clinical reviewers noted there is some uncertainty as to whether the results from either study are generalizable to the setting in Canada.
CADTH conducted reanalyses based on the FRESCO population, and the findings were aligned with the sponsor’s base case results. Fruquintinib was more costly and more effective than BSC, but it was also less costly (incremental costs: –$20,828) and less effective (incremental QALYs: −0.44) than trifluridine/tipiracil plus bevacizumab. As such, fruquintinib was subject to extended dominance through BSC and trifluridine-tipiracil plus bevacizumab.
In the CDA-AMC base case based on the FRESCO-2 population, fruquintinib was more costly (incremental costs = $28,034) and more effective (incremental QALYs = 0.08) than BSC, resulting in an incremental cost-effectiveness ratio (ICER) of $325,989 per QALY gained. This population was considered to better reflect the setting in which fruquintinib will be used in Canada. In FRESCO-2, more than half of the population had received trifluridine-tipiracil previously, and 98% had received a VEGF inhibitor and/or EGFR inhibitor. As a result, trifluridine-tipiracil plus bevacizumab (a VEGF inhibitor) was not considered a relevant comparator. A price reduction of at least 87% ($803 per 28-day treatment cycle) is needed for fruquintinib to be considered cost-effective at a $50,000 per quality-adjusted life-year (QALY) gained threshold.
Patient, Clinician, and Drug Plan Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, clinician groups, and drug plans that participated in the CDA-AMC review process.
Patient input was received from Colorectal Cancer Resource and Action Network and Colorectal Cancer Canada. Both submissions collected information from patient interviews and online surveys. All participants were residents of Canada. Respondents’ treatment experience included fluorouracil-based chemotherapy, capecitabine, bevacizumab, and panitumumab. Common side effects included fatigue, hair loss, nausea, peripheral neuropathy, and diarrhea. Patients expressed a desire for a treatment that could bring improvements to their quality of life and physical condition (tumour shrinkage, tumour stability, pain reduction, and improved breathing). A total of 7 respondents across both submissions reported experience with fruquintinib. It was reported that fruquintinib helped stabilize their illness and was easy to administer as an oral therapy. Although most respondents experienced hand-foot syndrome, the symptoms were reported to be manageable.
Clinical input was received from the Canadian Gastrointestinal Oncology Evidence Network. The submission stated that the main goal of treatment is the improvement of OS and quality of life. This involves the use of fluoropyrimidine, irinotecan, oxaliplatin, bevacizumab, and anti-EGFR therapy (in KRAS wild-type tumours). Patients with BRAF mutations, which represent a small subset of patients, are also eligible for treatment with pembrolizumab. It was noted that an ideal treatment would improve OS with manageable toxicity, which would result in quality-of-life benefits. In addition, outside of Quebec, there are no publicly funded treatment options for patients with mCRC who have been treated with any of the prior therapies. It was noted that even though most patients could tolerate further treatment with trifluridine-tipiracil or regorafenib, the lack of public coverage results in patients transitioning to supportive and palliative care. The submission stated that fruquintinib would be expected as an option for patients who are not eligible for, or after treatment with, trifluridine-tipiracil plus bevacizumab.
CDA-AMC-participating drug plans noted that there are no publicly funded treatment options for the indicated population. Although trifluridine-tipiracil monotherapy plus bevacizumab did receive a positive reimbursement recommendation, it had not completed price negotiations with pan-Canadian Pharmaceutical Alliance at the time of this writing. Nevertheless, the drug plans expressed a desire to understand the efficacy of fruquintinib relative to trifluridine-tipiracil plus bevacizumab. Of additional interest was whether patients should be eligible for fruquintinib after disease progression on trifluridine-tipiracil plus bevacizumab.
Several of these concerns were addressed in the sponsor’s model:
The effectiveness of fruquintinib relative to trifluridine-tipiracil plus bevacizumab was obtained in the sponsor’s indirect treatment comparison (ITC). This estimate was used to incorporate trifluridine-tipiracil as a comparator in the economic evaluation.
The economic evaluation incorporated evidence related to OS and quality of life.
CDA-AMC addressed some of these concerns, as follows:
To consider the possibility that patients would be eligible for fruquintinib after the discontinuation of trifluridine-tipiracil plus bevacizumab, the FRESCO-2 trial was used as the source of treatment effectiveness in the CDA-AMC base case. In this study, more than 50% of patients had previously received trifluridine-tipiracil and 98% of patients had received anti-VEGF treatment (e.g., bevacizumab) or anti-EGFR treatment.
Economic Review
Note: The sponsor’s application was filed on a pre–Notice of Compliance basis, and the pharmacoeconomic submission is reflective of the proposed indication and information incorporated into the draft product monograph that was submitted to Health Canada and CDA-AMC. The sponsor’s submission focused on the use of fruquintinib in an earlier line of therapy than recommended in the final indication. However, the sponsor’s economic evaluation was flexible so could assess the use of fruquintinib in the population indicated by Health Canada. The sponsor’s budget impact analysis reflected the originally proposed indication and was not flexible enough to assess fruquintinib as a fourth-line or later treatment.
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted an economic evaluation that compared fruquintinib with existing alternatives for the treatment of adults with mCRC who have been previously treated with or are not considered candidates for available therapies, including fluoropyrimidine-based chemotherapy, oxaliplatin-based chemotherapy, irinotecan-based chemotherapy, anti-VEGF therapy, and anti-EGFR therapy.1 This target population was aligned with the proposed Health Canada indication and the reimbursement request.
Fruquintinib is available as an oral capsule at strengths of 1 mg and 5 mg, with unit costs of $75 and $301, respectively. The recommended dose is 5 mg daily for 21 days, followed by 7 days off treatment. Patients continue the 28-day cycles until disease progression or unacceptable toxicity.2 At the submitted price, fruquintinib will cost $6,321 every 28-days.1
Two comparators were included in the economic evaluation. The first was a regimen of trifluridine-tipiracil plus bevacizumab. Trifluridine-tipiracil is available as an oral tablet, at strengths of 15 mg of trifluridine and 6.14 mg of tipiracil (15 mg/6.14 mg) and 20 mg of trifluridine and 8.19 mg of tipiracil (20 mg/8.19 mg), with unit costs of $76 and $79. respectively. The recommended dose from the Cancer Care Ontario regimen monograph is 35 mg/m2 once daily on days 1 to 5 and days 8 to 12, and patients remain off treatment until the end of the 28-day cycle.1,3 The calculated dose for a patient with a body surface area of 1.70 m2 would be 59.5 mg, which corresponds to a 28-day cycle cost of $4,673. Bevacizumab is available as a vial for IV infusion at a concentration of 25 mg/mL and a price of $86.75 per 25 mg. The recommended dose from the Cancer Care Ontario regimen monograph is 5 mg/kg on day 1 and day 15 of a 28-day cycle.1,3 A patient weighing 63.72 kg would receive a calculated dose of 318.6 mg, which corresponds to a 28-day cycle cost of $2,559. The combined cost for the trifluridine-tipiracil plus bevacizumab regimen was calculated to be $7,232. The second comparator was assumed to be best supportive care (BSC). This was defined as interventions that provide palliation of symptoms and improved quality of life. The cost of BSC was assumed to be $0.1
Modelled outcomes included life-years and QALYs. Costs were estimated from the perspective of the Canadian public health care payer. Model outputs were generated over a lifetime horizon of 10 years, with a cycle length of 1 week. Costs and outcomes were discounted at 1.5%.1
Model Structure
The costs and effects for each alternative were estimated using a partitioned survival model (PSM).1 As illustrated in Figure 1, the model comprised 3 mutually exclusive health states: progression free (PF), progressed disease (PD), and death. State membership was estimated using an area under the curve approach from 2 independent survival curves (PFS and OS).1
Model Inputs
Costs and effects were estimated using a homogeneous baseline population. All data summarizing baseline characteristics were obtained from the FRESCO trial. This was a randomized, phase III trial that involved the direct comparison of fruquintinib and placebo in patients with mCRC in China.1,4,5 Baseline characteristics of interest were obtained from the fruquintinib arm of the trial, and included age (mean = 54.33 years, standard deviation = 10.70), sex (56.8% male), body surface area (████ █ ██████ █ ████), and weight (████ █ █████ ███ ██ █ █████).1,4,5
Estimates of relative efficacy comparators excluded from the FRESCO trial were obtained from the sponsor-submitted systematic review and network meta-analysis (NMA).1,6 The NMA was conducted using 9 of the identified trials of treatments for patients with mCRC who have been previously treated with or are not considered candidates for available therapies.4,6-14 These trials formed a network comprised of the following comparators: fruquintinib, trifluridine-tipiracil, trifluridine-tipiracil plus bevacizumab, regorafenib, and placebo. The outcome of interest from the NMA, as it related to the economic evaluation, was the estimated hazard ratio (HR) for OS and PFS. For OS, the HR between fruquintinib and trifluridine-tipiracil plus bevacizumab was estimated to be ████ ████ ███ ████ ██ █████. For PFS, the HR for the same comparison was estimated to be ████ ████ ███ ████ ██ █████.1,6
Direct and indirect approaches were used to estimate the treatment-specific survival probabilities needed to estimate state membership. For fruquintinib and BSC, 2 parametric survival models were fit: PFS and OS. Treatment-dependent and treatment-independent models were fit using the exponential, log-logistic, log-normal, Weibull, Gompertz, gamma, and generalized gamma distributions. Selection of the base-case configuration was informed by visual inspection of the Kaplan-Meier curve, assessment of model fit statistics, and clinical plausibility. In the base case, the sponsor selected the treatment-dependent OS model, which followed the generalized gamma distribution. To estimate PFS, treatment-independent models that followed log-normal (fruquintinib) and log-logistic (BSC) distributions were selected. For trifluridine-tipiracil plus bevacizumab, both OS and PFS were estimated indirectly by applying the corresponding HR estimated in the NMA, with fruquintinib as the reference curve.1
To ensure that the risk of death would not fall below that of the general population, the predicted values for OS could not fall below the corresponding general-population mortality risk.1 Age-specific and sex-specific mortality risks were obtained from life tables published by Statistics Canada.15 Similarly, the sponsor assumed that the predicted values for PFS could not exceed the corresponding OS value.1
In addition, the sponsor sought to distinguish patients in the PF state by treatment status. For each treatment, the time on treatment was used to determine the proportion of patients on or off treatment in each cycle of the model.1 This was assumed to be 21.43 weeks for fruquintinib and 21.74 weeks for trifluridine-tipiracil plus bevacizumab.1,5,14
In addition to tracking the proportion of the cohort in each health state, the model also tracked the occurrence of adverse events (AEs). This was restricted to grade 3 or 4 AEs that occurred in at least 5% of patients in any arm of the FRESCO or SUNLIGHT trials.1,5,14 The identified AEs included anemia, asthenia, diarrhea, fatigue, hand-foot syndrome, hypertension, leukopenia, neutropenia, rash, thrombocytopenia, and laboratory abnormalities.1 Each event was assumed to last for 1 week, and patients remained at risk for each AE for the duration of treatment.
Health-related quality of life was captured in the model by calculating health-state utility values in a 3-step process. Health-state utility values were predicted from a prespecified linear regression model of data from the FRESCO-2 trial. Preferences in this trial were measured indirectly, using the EQ-5D questionnaire. Before fitting the regression, the sponsor calculated EQ-5D utilities using Canadian population tariffs.1,16 The regression assumed that utility values were affected by 3 independent covariates: progression status (PF versus PD), whether a patient was experiencing an AE (yes versus no), and whether the patient was within 28 days of death (yes versus no). In other words, health-state utility values were predicted as a function of health state, AE status, and the proportion of the cohort within 28 days of death. Subsequently, the sponsor’s submission included the option (applied in the base case) to adjust the predicted health-state utility value for age.1,17 In the absence of Canadian-specific utility values, the adjustment was made using estimates reflecting the general population of the UK.1
Costs in the model included acquisition and administration costs, health-state monitoring costs, the management of AEs, and end-of-life care. Treatment-acquisition costs were calculated from the price per unit consumed, based on the recommended dosage for each alternative. The price of fruquintinib represented the sponsor’s submitted price, whereas all other drug prices were obtained from the Ontario Exceptional Access Program (bevacizumab, trifluridine-tipiracil).18 Treatment-administration costs were applied for any treatment that required IV administration and comprised the physician billing code for IV administration and the hourly chair time ($217.51 per hour). The was obtained from a Canadian cost-effectiveness study of systemic therapies for pancreatic cancer, which priced chair time at $178 per hour in 2013 Canadian dollars.1,19 Management costs related to AEs were incurred as a one-time event at the start of treatment. The specific costs incurred were obtained from the Ontario Schedule of Benefits: Physician Services and the Canadian Institute for Health Information.20,21 These costs were calculated as a product of each identified medical service cost with the incidence rate of each AE.1 Treatment-monitoring costs reflected resource use associated with routine patient monitoring, such as consultation, imaging, and laboratory testing. In the base case, a micro-costing approach was used to capture costs associated with oral outpatient chemotherapy, home consultations by a family physician, community nurse specialist visits, palliative care specialists, CT scans, and a complete blood counts.1 Estimates for the frequency of service use were obtained from clinical experts consulted by the sponsor and a National Institute for Health and Care Excellence (NICE) technology appraisal for regorafenib.1,22 The corresponding costs were obtained from the Ontario Schedules of Physician Services and Laboratory Services.1,23,24 End-of-life care ($40,489.03) was assumed to represent palliative care costs for patients with colorectal cancer in Ontario from 1997 to 2007, inflated to 2024 Canadian dollars.1,25 It was incorporated into the model as a one-time cost upon entry to the death state.1
Summary of Sponsor’s Economic Evaluation Results
The costs and QALYs for each alternative were generated in a Monte Carlo simulation of 1,000 iterations. Overall findings from the probabilistic base case were aligned with the deterministic analysis, although there were numeric differences. The probabilistic findings are presented here.
Base-Case Results
The submitted analysis was based on publicly available prices of the comparator treatments. Results from the base case of the submitted economic evaluation are presented in Table 3. Fruquintinib was extendedly dominated by trifluridine-tipiracil plus bevacizumab and BSC and, as a result, was the only alternative that did not lie on the cost-effectiveness frontier. This means that fruquintinib is not cost-effective because QALYs are produced at a higher incremental cost than the other available option(s) (i.e., trifluridine-tipiracil plus bevacizumab).26 As a result, fruquintinib had a 0% probability of being cost-effective at a willingness-to-pay (WTP) threshold of $50,000 per QALY. In other words, relative to BSC, one is better off choosing trifluridine-tipiracil plus bevacizumab over fruquintinib, as the former offers a lower incremental cost per QALY. Approximately 55% of the incremental QALYs for fruquintinib compared with BSC were derived beyond the median follow-up period in the FRESCO trial.
Table 3: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total costs ($) | Total QALYs | ICER ($/QALY) |
|---|---|---|---|
BSC | 42,971 | 0.536 | Reference |
Trifluridine-tipiracil plus bevacizumab | 101,436 | 1.222 | 85,246 vs. BSC |
Dominated treatments | |||
Fruquintinib | 81,623 | 0.774 | Extendedly dominated by trifluridine-tipiracil plus bevacizumab |
BSC = best supportive care; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; vs. = versus.
Source: Sponsor’s pharmacoeconomic submission.1
Additional results from the sponsor’s submitted economic evaluation base case are presented in Appendix 3.
Sensitivity and Scenario Analysis Results
In addition to the submitted base case, the sponsor considered 12 distinct scenario analyses. These scenarios considered alternate inputs or assumptions related to the time horizon, discount rates, AE costs, AE disutilities, the approach to calculate health-state utility values, vial sharing, eligibility for subsequent therapy, the approach to treatment discontinuation, and the selected parametric survival functions for OS and PFS. Although each scenario had a slight impact on the expected costs and benefits, none had a meaningful effect on the conclusion for the cost-effectiveness of fruquintinib.
No scenario analysis was conducted using any perspective other than the health care payer.
CDA-AMC Appraisal of the Sponsor’s Economic Evaluation
CDA-AMC identified several key limitations of the sponsor’s analysis that have notable implications for the economic analysis.
The efficacy of fruquintinib relative to relevant comparators is uncertain: The submitted economic evaluation compared fruquintinib with relevant alternatives that could be used for the third-line or fourth-line therapy of adult patients with mCRC. For third-line therapy, estimates of relative efficacy were obtained from the FRESCO trial, as well as from the sponsor-submitted systematic review and NMA. Using the results from the FRESCO trial, the CDA-AMC clinical review showed that fruquintinib may be associated with prolonged OS and PFS relative to BSC. For fourth-line therapy, estimates of relative efficacy were obtained from the FRESCO-2 trial. For this evidence, the CDA-AMC clinical review concluded that fruquintinib may be associated with prolonged OS and PFS relative to BSC. No other alternatives were considered for fourth-line therapy, due to the absence of alternatives authorized or recommended at this stage of treatment.
Evidence from 2 ITCs suggested that trifluridine-tipiracil may be more effective than fruquintinib for the treatment of mCRC in the third-line or later-line setting, based on the point estimates for OS and PFS. However, the CDA-AMC review team indicated that no definitive conclusion could be reached due to important limitations of the indirect comparisons (the study design of the included trials and the associated patient characteristics were cited as important sources of heterogeneity, as was the sparse network) and imprecise results in the sponsor-commissioned NMA (█████ ███ ██ █ ████ ██ ████ ███ █████ ███ ██ █ ████ ██ ████).
The limitations in the underlying clinical evidence could not be addressed through reanalysis.
The submitted model did not consider the entire population of interest: In the submitted base case, the population of interest was based on the population from the FRESCO trial (i.e., patients with mCRC who had disease that failed at least 2 lines of standard chemotherapy). The sponsor considered this population to be representative of the population eligible for third-line treatment, as evidenced by the selection of comparators and the population included in the NMA. The sponsor used the FRESCO trial as the source for the parametric survival models used to estimate state occupancy. In the FRESCO study, 80% of patients had received 3 or fewer lines of therapy, and 40% had received a VEGF inhibitor and/or an EGFR inhibitor previously. As a result, the FRESCO trial was not consistent with the Health Canada indication or the reimbursement request, it did not consider all of the evidence that might be relevant to the decision problem. This is reflected by the availability of data from the FRESCO-2 trial, which sought to evaluate the safety and efficacy of fruquintinib as therapy in the fourth-line and beyond for patients with refractory mCRC who progressed or were intolerant to trifluridine-tipiracil or regorafenib.1,27 In the FRESCO-2 trial, more than 70% of patients had received at least 3 prior lines of therapy, 98% of patients had received a VEGF inhibitor and/or an EGFR inhibitor, and more than 50% had received trifluridine-tipiracil. The sponsor justified the exclusion of the FRESCO-2 data on the basis that the requisite third-line therapies (trifluridine-tipiracil or regorafenib) were not publicly reimbursed at the time of the submission.1 This rationale is insufficient for 2 reasons. First, CDA-AMC guidelines encourage the development of decision models that consider all evidence relevant to the target population for which the intervention will be used. Both the FRESCO and FRESCO-2 trials are relevant to the decision problem because the proposed indication captures patients eligible for third-line and fourth-line treatment. Second, the sponsor did not explain why the funding status of a preceding third-line treatment should result in the exclusion of evidence for fourth-line therapy. Trifluridine-tipiracil in combination with bevacizumab (a VEGF inhibitor) received a positive recommendation from the pan-Canadian Oncology Drug Review Expert Review Committee before the fruquintinib submission and, therefore, it was reasonable to consider it a relevant third-line treatment. Although the CDA-AMC clinical review noted some uncertainty as to whether results from the FRESCO-2 trial were generalizable on the basis of prior treatment history and subsequent anticancer treatment use, based on the evidence submitted by the sponsor, the clinical experts consulted by CDA-AMC noted that the FRESCO-2 trial was more representative of the likely place in therapy of fruquintinib in Canada as a fourth-line or later-line treatment option.
CDA-AMC undertook the base-case analysis that focused on data from the FRESCO-2 trial as the source for the parametric survival models needed to estimate state occupancy, in line with feedback from the clinical experts consulted by CDA-AMC regarding the likely place in therapy for fruquintinib.
CDA-AMC considered a scenario analysis using data from the FRESCO trial.
Improper methods were used to calculate state membership: When estimating state membership with a PSM, the estimates for each mutually exclusive health state (PF, PD, death) must be calculated from a series of non–mutually exclusive survival functions.28 In the submitted model, this requirement was not satisfied due to the decision to cap the predicted OS curves at the general-population mortality risk. This is problematic because the 2 types of probabilities are not interchangeable. The general-population mortality risk refers to the probability of death at a specific age. In contrast, survival probability refers to the probability that death will not occur after a specific point in time. Given that the general-population mortality risk is not a survival probability, it cannot be used to estimate state membership in a PSM.
CDA-AMC modified the economic evaluation to remove the assumption capping the OS curve at the general-population mortality risk.
Decision uncertainty cannot be accurately characterized: Consistent with CDA-AMC guidelines, the sponsor’s base case used a Monte Carlo simulation to characterize parameter uncertainty. However, the mechanism by which state membership is estimated in a PSM limits the usefulness of this approach.28 This is attributed to the fact that the survival functions for OS and PFS are fitted independently, even though progression can be conceptualized as an intermediate end point that affects (increases) the risk of death. As a result, there is a risk that some simulation trials represent scenarios in which PFS exceeds OS, which is clinically implausible. Conditional statements that replace PFS with OS at times when PFS exceeds OS are problematic, as they prevent the simulation from considering the full range of possible values that PFS may hold over the simulated time horizon. One way to avoid this problem would be to generate estimates of state occupancy using a Markov chain. In the context of a PSM, one would need to produce a series of correlated parametric survival models for PFS and OS by resampling the trial data using bootstrapping. Regardless of the approach, concerns related to the accuracy of the extrapolated predictions will persist.28
CDA-AMC was unable to address this limitation.
The methods for the age adjustment of health-state utility values were inappropriate: After the calculation of health-state utilities, the sponsor implemented a procedure to adjust the values by age. The intent of this procedure was to reflect the fact that quality of life for the general population declines with age.1,17 In the absence of Canadian-specific data, the sponsor applied age adjustment using utility values that reflect the general population of the UK.1 This was inappropriate because the sponsor took great care to ensure that the unadjusted health-state utility values reflected the preferences of people living in Canada. Therefore, the correct implementation of the age adjustment required a comparison using EQ-5D utility values of the general population in Canada, matched by age to the simulated cohort. In light of this limitation, it should be noted that the removal of the age adjustment had no impact on the conclusions of the economic evaluation. Results from a scenario analysis submitted by the sponsor were nearly identical to results from the submitted base case.1 Despite a very small reduction in expected QALYs for each alternative, fruquintinib remained subject to extended dominance by trifluridine-tipiracil plus bevacizumab.
CDA-AMC modified the economic evaluation to remove the age adjustment.
The sponsor did not consider the effects of subsequent lines of treatment: The sponsor focused on third-line treatment in the submitted model and assumed that the amount of time spent on treatment would affect the acquisition costs, but not the estimates of state occupancy. Patients were assumed to switch to fourth-line therapy after 21.4 weeks (fruquintinib) and 21.7 weeks (trifluridine-tipiracil plus bevacizumab) of treatment. At this point in the model, 60% of patients were assumed to receive BSC. The remaining 40% initiated the alternative active therapy (patients received fourth-line fruquintinib if they received third-line trifluridine-tipiracil plus bevacizumab). This resulted in a mismatch, in which the sponsor assumed that evidence related to third-line therapy would apply to use of a regimen as a fourth-line treatment. Given the availability of fourth-line treatment-effectiveness data from the FRESCO-2 trial, the sponsor had the opportunity to track costs and effects using evidence specific to the line of therapy. Doing so would have necessitated changes to the conceptualized model, as the PSM is not well suited to decision problems in which consideration of treatment sequences is necessary. Instead, the sponsor relied on a method that considered the costs but not the benefits of fourth-line therapy. As a result, the model mischaracterized the trade-off between the alternatives.
CDA-AMC modified the economic evaluation, removing the costs related to subsequent therapy.
CDA-AMC Reanalyses of the Economic Evaluation
Base-Case Results
CDA-AMC undertook reanalyses that addressed the key limitations of the submitted economic model, as summarized in Table 5. The CDA-AMC base case was derived by making changes in model parameter values and assumptions, in consultation with clinical experts. CDA-AMC was unable to address limitations related to relative treatment effectiveness or the characterization of parameter uncertainty. Consistent with the sponsor’s base case, the costs and effects for each alternative were generated from a Monte Carlo simulation of 1,000 iterations.
Table 4: CDA-AMC Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CDA-AMC value or assumption |
|---|---|---|
1. Predicted values for OS | Parametric OS curve capped at the general-population mortality risk. | Removed. State membership was estimated using unmodified survival probabilities. |
2. Age-adjusted utility values | General population utilities from the UK are interchangeable with those from Canada. | Age adjustment removed. Canadian-specific utility values are required for the sponsor’s age adjustment. |
3. Treatment switching | The model considered the costs but not the effects associated with fourth-line therapy. | Costs related to treatment switching were removed. |
4. Exclusion of relevant subpopulation | To reflect alternative third-line therapies, the FRESCO trial was used as the source for the parametric survival functions. | To reflect alternative fourth-line therapies, the FRESCO-2 trial was used as the source for the parametric survival functions. |
CDA-AMC base case | ― | 1 + 2 + 3 + 4 |
CDA-AMC scenario analysis | — | 1 + 2 + 3 |
CDA-AMC = Canada's Drug Agency; OS = overall survival.
Results from the CDA-AMC base case are presented in Table 5. As with the sponsor’s base case, the results were generated using publicly available prices of the comparator treatments. In contrast to the submitted base case, the population of interest represented a homogeneous cohort of patients eligible for fourth-line therapy in the treatment of mCRC. The clinical experts consulted by CDA-AMC indicated that trifluridine-tipiracil plus bevacizumab was unlikely to be considered as an option for fourth-line therapy. In addition, the submitted evidence synthesis did not include any trials that considered trifluridine-tipiracil plus bevacizumab as a fourth-line therapy. As a result, BSC was the only relevant comparator for this analysis (refer to Appendix 4 for stepped analysis results).
In the CDA-AMC base case, fruquintinib was more costly (incremental costs = $28,076) and more effective (incremental QALYs = 0.09) than BSC. This corresponded to an ICER of $325,989 per QALY relative to BSC, and a 0% probability of fruquintinib being cost-effective at a WTP threshold of $50,000 per QALY gained.
Table 5: Summary of the CDA-AMC Reanalysis Results
Drug | Total costs ($) | Total QALYs | ICER ($/QALY) |
|---|---|---|---|
Sponsor base case (probabilistic) | |||
BSC | 42,971 | 0.536 | Reference |
Trifluridine-tipiracil plus bevacizumab | 101,436 | 1.222 | 85,246 vs. BSC |
Dominated treatments | |||
Fruquintinib | 81,623 | 0.774 | Extendedly dominated by trifluridine-tipiracil plus bevacizumab |
CDA-AMC base case (probabilistic)a | |||
BSC | 42,877 | 0.513 | Reference |
Fruquintinib | 70,953 | 0.599 | 325,989 vs. BSC |
BSC = best supportive care; CDA-AMC = Canada's Drug Agency; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-years; vs. = versus.
aDue to the absence of evidence related to the fourth-line use of trifluridine-tipiracil plus bevacizumab and the place in therapy for trifluridine-tipiracil plus bevacizumab in Canada, the comparators for this reanalysis were restricted to BSC and fruquintinib.
Source: Sponsor’s pharmacoeconomic submission.1
Scenario Analysis Results
CDA-AMC conducted a scenario analysis to explore the cost-effectiveness of fruquintinib for the third-line treatment of adult patients with mCRC. Consistent with the sponsor’s base case, the FRESCO trial served as the source for the parametric survival models of OS and PFS. This enabled the inclusion of trifluridine-tipiracil plus bevacizumab as a comparator, in addition to BSC. Costs and benefits were generated using a Monte Carlo simulation of 1,000 iterations.
Results from the scenario analysis of third-line or later therapy are presented in Table 12. Fruquintinib was extendedly dominated by trifluridine-tipiracil plus bevacizumab. As a result, it was the only alternative that did not lie on the cost-effectiveness frontier. This means that fruquintinib is not expected to be cost-effective because QALYs are produced at a higher incremental cost than necessary. In other words, relative to BSC, one is better off choosing trifluridine-tipiracil plus bevacizumab over fruquintinib, as the former offers a lower incremental cost per QALY gained. This result corresponds to a 0% probability of being cost-effective at a WTP threshold of $50,000 per QALY gained.
Table 6: CDA-AMC Price-Reduction Analyses
Analysis | Fruquintinib cost per 5 mg vial ($) | ICER ($/QALY) | ||
|---|---|---|---|---|
Price reduction | Sponsor base case (third-line or later) | CDA-AMC base case (fourth-line) | CDA-AMC third-line or later scenario | |
None | 301 | Extendedly dominated | 325,989 (vs. BSC) | Extendedly dominated (through BSC and trifluridine-tipiracil plus bevacizumab) |
10% | 271 | Extendedly dominated | 294,363 (vs. BSC) | Extendedly dominated |
20% | 241 | Extendedly dominated | 262,737 (vs. BSC) | Extendedly dominated |
30% | 211 | Extendedly dominated | 231,111 (vs. BSC) | Extendedly dominated |
40% | 181 | Extendedly dominated | 199,485 (vs. BSC) | Extendedly dominated |
50% | 151 | Extendedly dominated | 167,860 (vs. BSC) | 78,646 (vs. BSC)a |
60% | 120 | 74,080 (vs. BSC)b | 136,234 (vs. BSC) | 64,119 (vs. BSC) |
70% | 90 | 59,373 (vs. BSC) | 104,608 (vs. BSC) | 49,593 (vs. BSC)c |
80% | 60 | 44,667 (vs. BSC)d | 72,982 (vs. BSC) | 35,067 (vs. BSC) |
90% | 30 | 29,960 (vs. BSC) | 41,356 (vs. BSC) | 20,541 (vs. BSC) |
BSC = best supportive care; CDA-AMC = Canada's Drug Agency; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; vs. = versus.
aThe ICER for trifluridine-tipiracil plus bevacizumab vs. fruquintinib is $87,035 per QALY gained.
bThe ICER for trifluridine-tipiracil plus bevacizumab vs. fruquintinib is $91,185 per QALY gained.
cThe ICER for trifluridine-tipiracil plus bevacizumab vs. fruquintinib is $102,935 per QALY gained.
dThe ICER for trifluridine-tipiracil plus bevacizumab vs. fruquintinib is $106,829 per QALY gained.
Note: Costs are to the nearest dollar.
In addition to the third-line scenario, CDA-AMC undertook price-reduction analyses based on the sponsor’s results and the CDA-AMC base case. As detailed in Table 6, a 60% price reduction is required for fruquintinib to lie on the cost-effectiveness frontier using the sponsor’s base case. For the CDA-AMC scenario analysis in the third-line or later population, a 50% price reduction is needed for fruquintinib to lie on the cost-effectiveness frontier; however, trifluridine-tipiracil plus bevacizumab remains a more effective option (in terms of QALYs) for this patient population based on the economic model. Further price reductions will be necessary for fruquintinib to be considered the most cost-effective third-line therapy.
In the CDA-AMC base case, a price reduction of 87% (i.e., a price of $38.23 per 5 mg fruquintinib tablet and $9.56 per 1 mg tablet, or $802.80 per 28-day cycle) is needed for fruquintinib to be considered cost-effective at a threshold of $50,000 per QALY gained.
Issues for Consideration
Fruquintinib and trifluridine-tipiracil are the only advanced therapies that can be orally administered. However, trifluridine-tipiracil is used in combination with bevacizumab, which is administered intravenously. Ease of administration may be an important aspect of treatment for patients.
Overall Conclusions
The CDA-AMC clinical review determined that fruquintinib is associated with prolonged OS and PFS relative to BSC for the treatment of mCRC in patients who had previously been treated with all standard chemotherapies, an anti-VEGF drug, and an anti-EGFR drug (if RAS is wild-type), and had progressed on or been intolerant to treatment with trifluridine-tipiracil and/or regorafenib, based on the FRESCO-2 trial. According to clinical expert input, the FRESCO-2 trial was more reflective of the likely place in therapy of fruquintinib as a fourth-line or later-line treatment than the FRESCO trial. Clinical reviewers noted that there is some uncertainty as to whether the results from either study are generalizable to the setting in Canada.
CDA-AMC identified several additional limitations of the sponsor’s economic submission. These included improper methods to calculate state membership, the improper characterization of uncertainty, inappropriate methods to calculate age-adjusted utility values, and a failure to consider the effects of fourth-line treatment. CDA-AMC attempted to resolve some of these limitations through reanalysis. In the CDA-AMC base case, this involved removing the cap on OS, using correct treatment-acquisition costs, removing age-adjusted utility values, removing costs associated with treatment switching, and using clinical evidence from the FRESCO-2 trial, which reflects the fourth-line treatment population. CDA-AMC also conducted a scenario analysis based on the FRESCO population that was more representative of a third-line treatment population.
The findings from the CDA-AMC reanalyses based on the FRESCO population were aligned with the sponsor’s base-case results. Fruquintinib was more costly and more effective than BSC, but it was also less costly (incremental costs = –$20,828) and less effective (incremental QALYs = –0.44) than trifluridine-tipiracil plus bevacizumab. As such, fruquintinib was subject to extended dominance by BSC and trifluridine-tipiracil plus bevacizumab.
In the CDA-AMC base case based on the FRESCO-2 population, fruquintinib was more costly (incremental costs = $28,034) and more effective (incremental QALYs = 0.08) than BSC, resulting in an ICER of $325,989 per QALY gained. This population was considered to better reflect the setting in which fruquintinib will be used in Canada. In the FRESCO-2 trial, more than half of the population had received trifluridine-tipiracil previously, and 98% had received a VEGF inhibitor and/or an EGFR inhibitor. As a result, trifluridine-tipiracil plus bevacizumab (a VEGF inhibitor) was not considered a relevant comparator. A price reduction of at least 87% ($803 per 28-day treatment cycle) is needed for fruquintinib to be considered cost-effective at a $50,000 per QALY gained threshold.
References
1.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Fruzaqla (fruquintinib), capsules, 1 mg and 5 mg, oral. Toronto (ON): Takeda Canada Inc; 2024 May 21.
2.Fruzaqla (fruquintinib): capsules, 1 mg and 5 mg, oral [product monograph]. Toronto (ON): Takeda Canada Inc.; 2024 Sep 10.
3.Cancer Care Ontario. Trifluridine-tipiracil + Bevacizumab Regimen. https://www.cancercareontario.ca/en/drugformulary/regimens/monograph/74806. Accessed 2024 Jan 20.
4.Li J, Qin S, Xu RH, et al. Effect of fruquintinib vs placebo on overall survival in patients with previously treated metastatic colorectal cancer: the FRESCO randomized clinical trial. JAMA. 2018;319(24):2486-2496. PubMed
5.Hutchison MediPharma Limited. Clinical Study Report: 2013-013-00CH1. FRESCO [internal sponsor's report]. Shanghai (CN): Hutchison MediPharma Limited; 2017.
6.Sponsor's NMA report title [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Fruzaqla (fruquintinib), capsules, 1 mg and 5 mg, oral. Toronto (ON): Takeda Canada Inc; 2024 May 21.
7.Xu R-H, Li J, Bai Y, et al. Safety and efficacy of fruquintinib in patients with previously treated metastatic colorectal cancer: a phase Ib study and a randomized double-blind phase II study. J Hematol Oncol. 2017;10:1-8. PubMed
8.Li J, Qin S, Xu R, et al. Regorafenib plus best supportive care versus placebo plus best supportive care in Asian patients with previously treated metastatic colorectal cancer (CONCUR): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2015;16(6):619-629. PubMed
9.Grothey A, Van Cutsem E, Sobrero A, et al. Regorafenib monotherapy for previously treated metastatic colorectal cancer (CORRECT): an international, multicentre, randomised, placebo-controlled, phase 3 trial. Lancet. 2013;381(9863):303-312. PubMed
10.Yoshino T, Mizunuma N, Yamazaki K, et al. TAS-102 monotherapy for pretreated metastatic colorectal cancer: a double-blind, randomised, placebo-controlled phase 2 trial. Lancet Oncol. 2012;13(10):993-1001. PubMed
11.Mayer RJ, Van Cutsem E, Falcone A, et al. Randomized trial of TAS-102 for refractory metastatic colorectal cancer. N Engl J Med. 2015;372(20):1909-1919. PubMed
12.Xu J, Kim TW, Shen L, et al. Results of a Randomized, Double-Blind, Placebo-Controlled, Phase III Trial of Trifluridine/Tipiracil (TAS-102) Monotherapy in Asian Patients With Previously Treated Metastatic Colorectal Cancer: The TERRA Study. J Clin Oncol. 2018;36(4):350-358. PubMed
13.Pfeiffer P, Yilmaz M, Möller S, et al. TAS-102 with or without bevacizumab in patients with chemorefractory metastatic colorectal cancer: an investigator-initiated, open-label, randomised, phase 2 trial. Lancet Oncol. 2020;21(3):412-420. PubMed
14.Prager GW, Taieb J, Fakih M, et al. Trifluridine–tipiracil and bevacizumab in refractory metastatic colorectal cancer. N Engl J Med. 2023;388(18):1657-1667. PubMed
15.Table: 13-10-0114-01. Life expectancy and other elements of the life table, Canada, all provinces except Prince Edward Island. Ottawa (ON): Statistics Canada; 2023: https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310011401. Accessed 2024 Jun 6.
16.Xie F, Pullenayegum E, Gaebel K, et al. A Time Trade-off-derived Value Set of the EQ-5D-5L for Canada. Med Care. 2016;54(1):98-105. PubMed
17.Hernandez Alava M, Pudney S, Wailoo A. Estimating EQ-5D by Age and Sex for the UK. NICE DSU Report. 2022; https://www.sheffield.ac.uk/nice-dsu/methods-development/estimating-eq-5d, 2023 Dec 20 [sponsor submitted reference].
18.Government of Ontario. Exceptional Access Program product prices. 2024: https://www.ontario.ca/page/exceptional-access-program-product-prices. [sponsor submitted reference].
19.Tam VC, Ko YJ, Mittmann N, et al. Cost-effectiveness of systemic therapies for metastatic pancreatic cancer. Curr Oncol. 2013;20(2):e90-e106. PubMed
20.Canadian Institute for Health Information. https://www.cihi.ca/en. [sponsor submitted reference].
21.Ontario. OHIP Schedule of Benefits and fees: Physician Services Under the Health Insurance Act. 2024 [sponsor submitted reference].
22.National Institute for Health Care Excellence. Regorafenib for previously treated metastatic colorectal cancer [ID4002]. 2022 [sponsor submitted reference].
23.Schedule of benefits for physician services under the Health Insurance Act: (June 29, 2023 (effective July 24, 2023)). Toronto (ON): Ontario Ministry of Health; 2023: https://www.health.gov.on.ca/en/pro/programs/ohip/sob/physserv/sob_master.pdf. Accessed 2024 Jun 10.
24.Schedule of benefits for laboratory services. (Effective July 24, 2023). Toronto (ON): Ontario Ministry of Health; 2023: https://www.health.gov.on.ca/en/pro/programs/ohip/sob/lab/sob_lab_2023.pdf. Accessed 2024 Jun 10.
25.de Oliveira C, Pataky R, Bremner KE, et al. Phase-specific and lifetime costs of cancer care in Ontario, Canada. BMC Cancer. 2016;16(1):809. PubMed
26.Karlsson G, Johannesson M. The decision rules of cost-effectiveness analysis. Pharmacoeconomics. 1996;9(2):113-120. PubMed
27.Dasari A, Sobrero A, Yao J, et al. FRESCO-2: a global Phase III study investigating the efficacy and safety of fruquintinib in metastatic colorectal cancer. Future Oncol. 2021;17(24):3151-3162. PubMed
28.Woods B, Sideris E, Palmer S, Latimer N, Soares M. Partitioned survival analysis for decision modelling in health care: a critical review. (NICE DSU Technical Support Document 19). Sheffield (UK): Decision Support Unit, ScHARR, University of Sheffield; 2017: http://nicedsu.org.uk/wp-content/uploads/2017/06/Partitioned-Survival-Analysis-final-report.pdf. Accessed 2024 Jun 6.
29.DeltaPA. Ottawa (ON): IQVIA; 2023: https://www.iqvia.com/. Accessed 2024 Jun 6.
30.Canadian Cancer Society. Canadian Cancer Statistics 2023. 2023; https://cancer.ca/en/cancer-information/resources/publications/canadian-cancer-statistics-2023. Accessed 2024 Jan 15.
31.Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Fruzaqla (fruquintinib), capsules, 1 mg and 5 mg, oral. Toronto (ON): Takeda Canada Inc; 2024 May 21.
32.Government of Canada. Non-Insured Health Benefits program: First Nations and Inuit Health Branch: Annual report 2020 to 2021. 2021: https://www.sac-isc.gc.ca/eng/1645718409378/1645718500555. Accessed 2024 Jan 15.
33.Government of Canada. Non-Insured Health Benefits program: First Nations and Inuit Health Branch: Annual report 2021 to 2022. https://www.sac-isc.gc.ca/eng/1683039690813/1683039973755. Accessed 2024 Apr 15.
34.Government of Canada. Non-Insured Health Benefits program: First Nations and Inuit Health Branch: Annual report 2017 to 2018. https://www.sac-isc.gc.ca/eng/1581294869253/1581294905909. Accessed 2024 Apr 15.
35.Government of Canada. Non-Insured Health Benefits program: First Nations and Inuit Health Branch: Annual report 2019 to 2020. https://www.sac-isc.gc.ca/eng/1624462613080/1624462663098. Accessed 2024 Apr 15.
36.Government of Canada. Non-Insured Health Benefits program: First Nations and Inuit Health Branch: Annual report 2018 to 2019. https://www.sac-isc.gc.ca/DAM/DAM-ISC-SAC/DAM-HLTH/STAGING/texte-text/nihb-Annual_Report_2018-19_1589921777815_eng.pdf. Accessed 2024 Apr 15.
37.Siegel RL, Wagle NS, Cercek A, Smith RA, Jemal A. Colorectal cancer statistics, 2023. CA Cancer J Clin. 2023;73(3):233-254. PubMed
38.Boyne DJ, Ngan E, Carbonell C, et al. Real-World Study to Assess Patterns of Treatment Practices and Clinical Outcomes in Metastatic Colorectal Cancer Patients with RAS Wild-Type Left-Sided Tumours in Canada. Curr Oncol. 2023;30(9):8220-8232. PubMed
39.Clarivate Primary Research. Colorectal cancer physician surveys and KOL interviews. 2022 [sponsor submitted reference].
40.Kennecke H, Berry S, Maroun J, et al. A retrospective observational study to estimate the attrition of patients across lines of systemic treatment for metastatic colorectal cancer in Canada. Curr Oncol. 2019;26(6):e748-e754. PubMed
41.Iqvia. OncoMAX mCRC Patient Chart Audit Report. 2023 [sponsor submitted reference].
42.Morris V, Overman MJ, Jiang ZQ, et al. Progression-free survival remains poor over sequential lines of systemic therapy in patients with BRAF-mutated colorectal cancer. Clin Colorectal Cancer. 2014;13(3):164-171. PubMed
43.CADTH Reimbursement Recommendation Trifluridine-Tipiracil (Lonsurf). Ottawa (ON): CADTH; 2024: https://www.cadth.ca/sites/default/files/DRR/2024/PC0330%20Lonsurf%20-%20Confidential%20CADTH%20Final%20Rec.pdf. Accessed 2024 Mar 22.
44.Trifluridine-Tipiracil (Lonsurf). Can J Health Technol. 2024;4(6). https://canjhealthtechnol.ca/index.php/cjht/article/view/PC0330r. Accessed 2024 Jun 13.
45.Budget Impact Analysis Guidelines: Guidelines for Conducting Pharmaceutical Budget Impact Analysis for Submission to Public Drug Plans in Canada. Ottawa (ON): Patented Medicine Prices Review Board; 2020: https://www.canada.ca/content/dam/pmprb-cepmb/documents/reports-and-studies/budget-impact-analysis-guidelines/PMPRB-BIA-Guidlines-en.pdf. Accessed 2024 Jul 25.
Appendix 1: Cost Comparison Table
Please note that this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical expert(s). Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 7: CDA-AMC Cost Comparison for Third-Line or Later-Line Metastatic Colorectal Cancer
Treatment | Strength / concentration | Form | Price | Recommended dosage | Daily cost ($) | 28-day cost ($) |
|---|---|---|---|---|---|---|
Fruquintinib (Fruzaqla) | 1 mg | Capsule | 75.2381a | 5 mg daily for 21 days, followed by 7 days off treatment. Repeat until disease progression or unacceptable toxicity. | 225.75 | 6,321 |
Trifluridine-tipiracil plus bevacizumab | ||||||
Trifluridine- (Lonsurf) | 15 mg/6.14 mg | Tablet | 76.2500 | 35 mg/m2 twice daily on days 1 to 5 and 8- to 12. Repeat 28-day cycle until disease progression or unacceptable toxicity.c | 168.30 | 4,713 |
Bevacizumab | 25 mg/mL | 4 mL vial | 347.0000b | 5 mg/kg on days 1 and 15 of a 28-day cycle. Repeat until disease progression or unacceptable toxicity.c | 99.14 | 2,776 |
Trifluridine-tipiracil plus bevacizumab (biosimilar) | 267.44 | 7,488 | ||||
Note: All prices are from the Ontario Exceptional Access Program (accessed May 2024), unless otherwise indicated, and do not include dispensing fees. Costs were calculated assuming a hypothetical patient weighing █████ ██ with a body surface area of ████.
aFruquintinib supplied as a bottle containing 21 capsules, with a submitted price of $1,580 per bottle of 1 mg capsules and $6,321 per bottle of 5 mg capsules.
bIQVIA DELTA-PA Wholesale Price (accessed June 2024).29 Wholesale prices: bevacizumab (Aybintio / MVASI / Zirabev) = 86.7500 per 25 mg; bevacizumab (Abevmy) = 86.9625 per mg.
cCancer Care Ontario Regimen Monograph: Trifluridine/Tipiracil-Bevacizumab (TRIFTIPIplusBEVA).3
Appendix 2: Submission Quality
Please note that this appendix has not been copy-edited.
Description | Yes or no | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | No | Refer to limitations. The submitted model did not consider the entire population of interest. |
Model has been adequately programmed and has sufficient face validity | Yes | No comment. |
Model structure is adequate for decision problem | No | Refer to limitations. The submitted model did not consider the entire population of interest. Additionally, the model did not consider the effects of fourth-line treatment. |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | No | Refer to limitations. Improper methods were used to calculate state membership. Decision uncertainty cannot be accurately characterized. Inappropriate data were used to adjust utility values for age. |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | No | Refer to limitations. Decision uncertainty cannot be accurately characterized. |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | Yes | No comment. |
Appendix 3: Additional Information on the Submitted Economic Evaluation
Please note that this appendix has not been copy-edited.
Detailed Results of the Sponsor’s Base Case
Table 9: Disaggregated Summary of the Sponsor’s Economic Evaluation Results
Parameter | Fruquintinib | Trifluridine-tipiracil plus bevacizumab | BSC |
|---|---|---|---|
Discounted LYs | |||
Total | 1.012 | 1.601 | 0.708 |
By health state or data source | |||
Progression-free | 0.439 | 0.633 | 0.165 |
Post-progression | 0.573 | 0.969 | 0.543 |
Discounted QALYs | |||
Total | 0.774 | 1.222 | 0.536 |
By health state or data source | |||
Progression-free | 0.346 | 0.500 | 0.130 |
Post-progression | 0.429 | 0.724 | 0.406 |
QALY loss: AE disutility | –0.00067 | –0.00111 | –0.00010 |
Discounted costs ($) | |||
Total | 81,623 | 101,136 | 42,971 |
Acquisition | 35,110 | 49,117 | 0 |
Administration | 0 | 3,975 | 0 |
AE management | 31 | 529 | 5 |
Disease management | 4,590 | 7,136 | 2,918 |
Subsequent treatment | 2,041 | 1,579 | 0 |
Terminal care | 39,851 | 39,100 | 40,048 |
BSC = best supportive care; AE = adverse event; QALY = quality-adjusted life-year.
Source: Sponsor’s pharmacoeconomic submission.1
Appendix 4: Additional Details on the CDA-AMC Reanalyses and Sensitivity Analyses of the Economic Evaluation
Please note that this appendix has not been copy-edited.
Detailed Results of CDA-AMC Base Case
Table 10: Summary of the Stepped Analysis of the CDA-AMC Base-Case Results
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALY) |
|---|---|---|---|---|
Sponsor base case | BSC | 42,971 | 0.536 | Reference |
Trifluridine-tipiracil plus bevacizumab | 101,436 | 1.222 | 85,246 | |
Dominated treatments | ||||
Fruquintinib | 81,623 | 0.774 | Extendedly dominated by trifluridine-tipiracil plus bevacizumab | |
1. CDA-AMC reanalysis 1 | BSC | 42,952 | 0.533 | Reference |
Trifluridine-tipiracil plus bevacizumab | 105,329 | 1.179 | 96,483 | |
Dominated treatments | ||||
Fruquintinib | 81,535 | 0.771 | Extendedly dominated by trifluridine-tipiracil plus bevacizumab | |
2. CDA-AMC reanalysis 2 | BSC | 42,952 | 0.533 | Reference |
Trifluridine-tipiracil plus bevacizumab | 105,329 | 1.184 | 95,837 | |
Dominated treatments | ||||
Fruquintinib | 81,535 | 0.772 | Extendedly dominated by trifluridine-tipiracil plus bevacizumab | |
3. CDA-AMC reanalysis 3 | BSC | 42,952 | 0.533 | Reference |
Trifluridine-tipiracil plus bevacizumab | 103,644 | 1.179 | 93,877 | |
Dominated Treatments | ||||
Fruquintinib | 79,480 | 0.771 | Extendedly dominated by trifluridine-tipiracil plus bevacizumab | |
4. CDA-AMC reanalysis 4a | BSC | 42,868 | 0.511 | Reference |
Fruquintinib | 73,011 | 0.596 | 353,874 | |
CDA-AMC base case (deterministic) 1 + 2 + 3 + 4 | BSC | 42,868 | 0.512 | Reference |
Fruquintinib | 70,902 | 0.596 | 331,086 | |
CDA-AMC base case (probabilistic) 1 + 2 + 3 + 4 | BSC | 42,877 | 0.513 | Reference |
Fruquintinib | 70,953 | 0.599 | 325,989 | |
BSC = best supportive care; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
aDue to the absence of evidence relating to the fourth-line use of trifluridine-tipiracil plus bevacizumab, the comparators for this stepped reanalysis (and the corresponding base-case analysis) were restricted to BSC and fruquintinib.
Note: The CDA-AMC reanalysis is based on publicly available prices of the comparator treatments. The results of all steps are presented deterministically unless otherwise indicated, while the cumulative CDA-AMC base case is always presented both deterministically and probabilistically. The deterministic ICER for the sponsor’s base case was aligned with CDA-AMC reanalysis 1 (i.e., $96,483 per QALY gained).
Table 11: Disaggregated Summary of the CDA-AMC Economic Evaluation Results
Parameter | Base case | Scenario analysis | |||
|---|---|---|---|---|---|
Fruquintinib | BSC | Fruquintinib | Trifluridine-tipiracil plus bevacizumab | BSC | |
Discounted LYs | |||||
Total | 0.780 | 0.676 | 1.013 | 1.587 | 0.706 |
By health state or data source | |||||
Progression free | 0.384 | 0.178 | 0.437 | 0.636 | 0.164 |
Post-progression | 0.396 | 0.498 | 0.576 | 0.951 | 0.542 |
Discounted QALYs | |||||
Total | 0.599 | 0.513 | 0.776 | 1.217 | 0.535 |
By health state or data source | |||||
Progression free | 0.303 | 0.140 | 0.345 | 0.502 | 0.130 |
Post-progression | 0.297 | 0.373 | 0.432 | 0.715 | 0.405 |
Discounted costs ($) | |||||
Total | 70,953 | 42,887 | 79,436 | 100,264 | 42,996 |
Acquisition | 27,274 | 0 | 34,961 | 49,516 | 0 |
Administration | 0 | 0 | 0 | 4,007 | 0 |
AE management | 32 | 6 | 31 | 527 | 5 |
Disease management | 3,640 | 2,830 | 4,595 | 7,094 | 2,912 |
Subsequent treatment | 0 | 0 | 0 | 0 | 0 |
Terminal care | 40,007 | 40,041 | 39,850 | 39,121 | 40,049 |
AE = adverse event; BSC = best supportive care; LY = life-year; NA = not applicable; QALY = quality-adjusted life-year.
Scenario Analyses
CDA-AMC conducted a single scenario analysis which explored the relative cost-effectiveness of fruquintinib. Consistent with the submitted base case, the population of interest represented a homogeneous cohort of patients eligible for third-line or later therapy in the treatment of metastatic CRC. As a result, the FRESCO trial and sponsor-submitted NMA served as the sources of evidence for treatment effectiveness. This allowed trifluridine-tipiracil plus bevacizumab and BSC to be included as comparators.
Table 12: CDA-AMC Scenario Analysis Results — Third-Line or Later-Line Treatment
Analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALY) |
|---|---|---|---|---|
CDA-AMC scenario (deterministic) 1 + 2 + 3 | BSC | 42,952 | 0.533 | Reference |
Trifluridine-tipiracil plus bevacizumab | 86,627 | 1.184 | 67,103 | |
Dominated treatments | ||||
Fruquintinib | 79,480 | 0.772 | Extendedly dominated by trifluridine-tipiracil plus bevacizumab | |
CDA-AMC scenario (probabilistic) 1 + 2 + 3 | BSC | 42,966 | 0.535 | Reference |
Trifluridine-tipiracil plus bevacizumab | 100,264 | 1.217 | 84,067 | |
Dominated treatments | ||||
Fruquintinib | 79,436 | 0.776 | Extendedly dominated by trifluridine-tipiracil plus bevacizumab | |
BSC = best supportive care; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Appendix 5: Submitted Budget Impact Analysis and CDA-AMC Appraisal
Note that this appendix has not been copy-edited.
Table 13: Summary of Key Take-Aways
Key take-aways of the budget impact analysis |
|---|
|
Summary of Sponsor’s Budget Impact Analysis
The sponsor submitted a budget impact analysis (BIA) for the introduction of fruquintinib for the treatment of adults with mCRC who have been previously treated with or are not considered candidates for available therapies including fluoropyrimidine-, oxaliplatin-, and irinotecan-based chemotherapy, an anti-VEGF therapy, and an anti-EGFR therapy. Estimates were generated from the perspective of pCODR-participating drug plans (all but Quebec) and the results were aggregated into pan-Canadian totals over a 3-year time horizon (2025 to 2027). Alternatives to fruquintinib considered in the BIA included: trifluridine-tipiracil plus bevacizumab and BSC. An epidemiological approach was used to estimate the eligible population size for the analysis. Key inputs to the BIA are documented in Table 14.
In the reference scenario, it was assumed that patients eligible for treatment would receive 1 of the comparators. In the new drug scenario, it was assumed the fruquintinib would displace market share from the treatments available in the reference scenario.
The sponsor’s BIA included the following key assumptions:
In the base year of the BIA, it was assumed that there would be 24,100 cases of colorectal cancer. This was based on the estimated incident cases (males = 13,500; females = 10,600) in 2023 estimated by the Canadian Cancer Society.30,31
The incidence of colorectal cancer will not change over time.31
The number of cases of colorectal cancer were assumed to increase proportionally with the population. The growth rate for all plans was calculated as the average annual growth rate from 2018 to 2023 and 2018 to 2022 for the Non-Insured Health Benefits population.31-36
The incidence of metastatic colorectal cancer was assumed to be 60%. The estimate was obtained from an observational study of American patients and was assumed to be generalizable to the population in Canada.31,37
80% of patients with metastatic colorectal cancer will receive first-line therapy.31,38,39 Progression rates to second- and third-line therapy were assumed to be consistent with findings from a multisite retrospective chart review across Canada.31,40
2.3% of patients eligible were assumed to be ineligible for fruquintinib due to a diagnosis with BRAF V600E mutated metastatic colorectal cancer.31,41 This estimate was viewed to be consistent with other evidence that BRAF mutations will be identified among 5% to 10% of patients.31,42
In the reference scenario, it was assumed that patients would not receive any fourth-line therapy. In the new drug scenario, it was assumed 40% of patients who progressed on third-line fruquintinib or trifluridine-tipiracil plus bevacizumab would be eligible to receive the alternate active therapy as fourth-line treatment. The remaining 60% of patients received BSC. The average per-patient cost of fourth-line therapy was calculated as the product of the annual treatment cost, the mean duration of treatment (4 weeks), and the proportion of patients eligible for fourth-line therapy.
Table 14: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (year 1 / year 2 / year 3) |
|---|---|
Target population | |
CRC incidencea | 18,641 / 19,003 / 19,371 |
mCRC incidence | 60% |
Eligible for first-line treatment | 80% |
Eligible for second-line treatment | 69.5% |
Eligible for third-line+ treatment | 43.2% |
Without BRAF V600E mutated mCRC | 97.7% |
Received third-line+ treatment | 100% |
Number of patients eligible for drug under review | 2,625 / 2,676 / 2,727 |
Market uptake: third-line therapy (3 years) | |
Uptake (reference scenario) | |
BSC | 10% / 10% / 10% |
Trifluridine-tipiracil plus bevacizumab | 90% / 90% / 90% |
Uptake (new drug scenario) | |
Fruquintinib | 9% / 17% / 20% |
BSC | 5.5% / 5.5% / 5.5% |
Trifluridine-tipiracil plus bevacizumab | 85.5% / 77.5% / 74.5% |
Cost of treatment (per patient, per 1 year)b | |
Fruquintinib | $82,455.19 |
BSC | $0 |
Trifluridine-tipiracil plus bevacizumab | $94,332.25 |
BSC = best supportive care; CRC = colorectal cancer; mCRC = metastatic colorectal cancer.
aCalculated assuming an average annual growth rate of 1.95% for the pan-Canadian population (excluding Quebec).
bCalculated by adjusting annual costs of treatment (fruquintinib = $82,455.19; trifluridine-tipiracil plus bevacizumab = $94,332.25) by the assumed mean time on treatment. For third-line therapy, estimates of mean time on treatment (fruquintinib = 0.41 years; trifluridine-tipiracil plus bevacizumab = 0.42 years). Estimates of mean time on were obtained from the FRESCO and SUNLIGHT trials.4,14 For fourth-line therapy, the mean time on treatment was assumed to be 4 weeks (0.8 years).31
Summary of the Sponsor’s BIA Results
The sponsor estimated that the 3-year budget impact of reimbursing fruquintinib for the treatment of adult patients with mCRC would be $27,142,807 (year 1: $9,725,263; year 2: $8,830,251; year 3: $8,587,293).31
CDA-AMC Appraisal of the Sponsor’s BIA
CDA-AMC identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
The size of the eligible population is uncertain: The sponsor adopted an epidemiologic approach to estimate the size of the population eligible for third-line therapy. This involved the iterative application of relevant epidemiologic data to a starting population of interest. For the submitted model, the number of eligible beneficiaries were forecasted to be 2,625 (year 1), 2,676 (year 2), and 2,727 (year 3). CDA-AMC did not identify any key limitations with respect to the nature of the evidence used to obtain these estimates. Nevertheless, they remain considerably different from the corresponding values forecasted in the CDA-AMC review of a different product for the same indication.43,44 In that report, published in June 2024, adoption of an epidemiologic approach resulted in forecasted market sizes of 1,059 (year 1), 1,066 (year 2), and 1,073 (year 3).43,44 The differences in the number of eligible beneficiaries can be attributed to the selection (and size) of the starting population and alternate sources of epidemiologic evidence. The uncertainty arises from the fact that both approaches may represent valid implementations of the epidemiologic approach to estimate market size for a BIA.45 As the net budget impact is affected by the sources and assumptions used for the market shares of each alternative, this uncertainty will impact magnitude of the forecasted expenditures in each year of the BIA. However, the degree to which it affects the net budget impact will be minimal, unless changes in the market share assumptions are also required.
The assumption that 40% of patients who progressed on third-line fruquintinib or trifluridine-tipiracil plus bevacizumab would be eligible to receive the alternate active therapy as fourth-line treatment was unable to validated. Thus, the estimation of the budget impact for patients receiving fruquintinib in the fourth-line is highly uncertain.
CDA-AMC was unable to address this limitation.
CDA-AMC Reanalyses of the BIA
In the absence of more reliable estimates to inform the parameters of the BIA, the sponsor’s base case was maintained. CDA-AMC expects that the budget impact of fruquintinib will be sensitive to more reliable inputs which may affect the market size calculation. CDA-AMC undertook a scenario analysis to explore the impact of an 87% price reduction to the submitted price for fruquintinib. The selected value reflects price at which fruquintinib is no longer subject to any form of dominance in the economic evaluation. Results of the CDA-AMC step-wise reanalysis, disaggregated by line of therapy, are presented in Table 15 and summarized in Table 16.
Table 15: Detailed Breakdown of the BIA Results
Scenario | Year 0 ($) | Year 1 ($) | Year 2 ($) | Year 3 ($) | Three-year total ($) |
|---|---|---|---|---|---|
Submitted base case | |||||
Initial (third-line) treatment | |||||
Reference | 50,634,550 | 92,907,358 | 94,707,803 | 96,544,243 | 284,159,404 |
New drug | 50,634,550 | 96,270,895 | 96,975,037 | 98,411,436 | 291,657,368 |
Budget impact | 0 | 3,363,537 | 2,227,233 | 1,867,194 | 7,497,964 |
Subsequent (fourth-line) treatment | |||||
Reference | 0 | 0 | 0 | 0 | 0 |
New drug | 0 | 6,361,726 | 6,563,018 | 6,720,099 | 19,644,843 |
Budget impact | 0 | 6,361,726 | 6,563,018 | 6,720,099 | 19,644,843 |
Combined | |||||
Reference | 50,634,550 | 92,907,358 | 94,707,803 | 96,544,243 | 284,159,404 |
New drug | 50,634,550 | 102,632,621 | 103,539,055 | 105,131,536 | 311,302,211 |
Budget impact | 0 | 9,725,263 | 8,830,251 | 8,587,293 | 27,142,807 |
CDA-AMC scenario analysis: 87% price reduction | |||||
Initial (third-line) treatment | |||||
Reference | 50,634,550 | 92,907,358 | 94,707,803 | 96,544,243 | 284,159,404 |
New drug | 50,634,550 | 89,279,121 | 83,512,421 | 82,265,950 | 255,057,491 |
Budget impact | 0 | –3,628,237 | –11,195,383 | –14,278,293 | –29,101,913 |
Subsequent (fourth-line) treatment | |||||
Reference | 0 | 0 | 0 | 0 | 0 |
New drug | 0 | 1,404,871 | 1,982,892 | 2,231,895 | 5,619,658 |
Budget impact | 0 | 1,404,871 | 1,982,892 | 2,231,895 | 5,619,658 |
Combined | |||||
Reference | 50,634,550 | 92,907,358 | 94,707,803 | 96,544,243 | 284,159,404 |
New drug | 50,634,550 | 90,683,992 | 85,495,313 | 84,497,844 | 260,677,149 |
Budget impact | 0 | –2,223,366 | –9,212,491 | –12,046,399 | –23,482,255 |
BIA = budget impact analysis.
Table 16: Summary of the CDA-AMC Reanalyses of the BIA
Stepped analysis | Scenario | Year 0 (current situation) ($) | Year 1 ($) | Year 2 ($) | Year 3 ($) | Three-year total ($) |
|---|---|---|---|---|---|---|
Submitted base case | Reference | 50,634,550 | 92,907,358 | 94,707,803 | 96,544,243 | 284,159,404 |
New drug | 50,634,550 | 102,632,621 | 103,538,055 | 105,131,536 | 311,302,211 | |
Budget impact | 0 | 9,725,263 | 8,830,251 | 8,587,293 | 27,142,807 | |
CDA-AMC scenario analysis: 87% price reduction | Reference | 50,634,550 | 92,907,358 | 94,707,803 | 96,544,243 | 284,159,404 |
New drug | 50,634,550 | 90,683,992 | 85,495,313 | 84,497,844 | 260,677,149 | |
Budget impact | 0 | –2,223,366 | –9,212,491 | –12,046,399 | –23,482,255 |
BIA = budget impact analysis.
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.