Drugs, Health Technologies, Health Systems
Reimbursement Review
Alectinib (Alecensaro)
Sponsor: Hoffmann-La Roche Limited
Therapeutic area: Non–small cell lung cancer
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Clinical Review
Abbreviations
AE
adverse event
AJCC
American Joint Committee on Cancer
AUC
area under the concentration-time curve
BICR
blinded independent central review
CI
confidence interval
CNS
central nervous system
CNS-DFS
central nervous system disease–free survival
DAC
Drug Advisory Committee
DFS
disease-free survival
ECOG PS
Eastern Cooperative Oncology Group Performance Status
GRADE
Grading of Recommendations Assessment, Development and Evaluation
HR
hazard ratio
HRQoL
health-related quality of life
IHC
immunohistochemistry
ITT
intention to treat
LCC
Lung Cancer Canada
NSCLC
non–small cell lung cancer
OS
overall survival
RCT
randomized controlled trial
SAE
serious adverse event
SF-36 v2
Short Form (36) Health Survey version 2
SLR
systematic literature review
UICC
Union for International Cancer Control
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Table 1: Background Information of Application Submitted for Review
Item | Description |
|---|---|
Drug product | Alectinib (Alecensaro), 150 mg capsules, oral |
Sponsor | Hoffmann-La Roche Limited |
Indication | For adjuvant treatment following tumour resection for patients with stage IB (tumour ≥ 4 cm) to IIIAa ALK-positive NSCLC |
Reimbursement request | As adjuvant treatment following tumour resection in adult patients with stage IB (≥ 4 cm) to IIIA (according to AJCC/UICC staging manual) ALK-positive NSCLC |
Health Canada approval status | NOC |
Health Canada review pathway | Priority review, Project Orbis |
NOC date | June 27, 2024 |
Recommended dose | 600 mg (four 150 mg capsules) given orally twice daily with food (total daily dose of 1,200 mg) |
AJCC = American Joint Committee on Cancer; NOC = Notice of Compliance; NSCLC = non–small cell lung cancer; UICC = Union for International Cancer Control.
aAccording to American Joint Committee on Cancer (7th edition)
Source: Sponsor’s Summary of Clinical Evidence1 and product monograph.2
Introduction
Lung cancer is a leading cause of cancer-associated mortality for both males and females in Canada.3 In 2023, it was estimated that 20,600 people with lung cancer were expected to die.3-5 Non–small cell lung cancer (NSCLC) accounts for approximately 85% of lung cancer cases.3-5 Staging is used to identify the extent of disease, and utilizes the tumour, node, and metastasis system developed by the American Joint Committee on Cancer (AJCC) and Union for International Cancer Control (UICC).6-8 (Unless otherwise specified, all references in this report to staging use definitions from the AJCC/UICC staging manual, 7th edition.9) In Canada, approximately half of all lung cancer cases are stage I to III at diagnosis, and all such patients may be eligible for tumour resection.10,11 Some patients with NSCLC may possess an underlying pathogenic driver mutation, such as an ALK gene rearrangement within chromosome 2.12,13 Approximately 64% of patients with NSCLC will typically develop brain metastases during the course of their disease.14-16 Patients with ALK-positive disease are at a higher risk of developing brain metastases compared to those with ALK-negative disease.16 Generally, signs and symptoms of ALK-positive NSCLC, which are no different than other types of NSCLC, include shortness of breath, hemoptysis, and chest pain. Most patients with NSCLC also present with nonspecific systemic symptoms, such as fatigue, unexplained weight loss, and anorexia.
According to the clinical experts consulted for this review, the goal of treatment for adult patients with early-stage ALK-positive NSCLC is a cure. The first-line treatment option for these patients is therefore typically surgery, with the goal of complete resection.17 Both the sponsor and the clinical experts consulted by the review team noted that, following tumour resection, the standard of care for most patients is 4 cycles or 4 months of adjuvant platinum-based chemotherapy, depending on the regimen used.18 After adjuvant chemotherapy is complete, patients receive routine surveillance, and are observed for signs of disease progression. According to the clinical experts, routine surveillance typically consists of a medical history, physical examinations, and CT scans every 6 months for the first 2 years, then annually thereafter until year 5. According to the clinical experts, ALK gene rearrangement testing is currently performed as part of the standard of care for patients with resected NSCLC in Canada.
The objective of the Clinical Review is to review and critically appraise the clinical evidence submitted by the sponsor on the beneficial and harmful effects of alectinib, 150 mg capsules, orally administered, as adjuvant treatment following tumour resection for adult patients with stage IB (≥ 4 cm) to IIIA ALK-positive NSCLC. The focus is on comparing alectinib to relevant comparators and identifying gaps in the current evidence. Alectinib has been previously reviewed by the review team for other indications.
Perspectives of Patients, Clinicians, and Drug Programs
The information in this section is a summary of input provided by the patient and clinician groups who responded to the review team’s call for input and from 2 clinical experts consulted the purpose of this review.
Patient Input
Two patient groups, Lung Cancer Canada (LCC) and the Lung Health Foundation, submitted patient group input for this review. LCC gathered data through interviews with 17 patients and/or caregivers in Canada and other countries who had experience with alectinib, both in the early-stage (I to IIIB) ALK-positive setting and the stage IV setting. As of April 2024, 14 out of 17 patients interviewed for this submission were still being treated with alectinib. The Lung Health Foundation obtained input from patients with lung cancer via an online survey of 9 respondents (location not stated) conducted in April 2024, and interviews with 3 respondents living in Canada. Seven patients surveyed by the Lung Health Foundation had experience with alectinib.
Input from LCC noted that patients with ALK-positive NSCLC disease were most concerned about central nervous system (CNS) disease, as this type of lung cancer can aggressively spread to the brain, and current treatments with chemotherapy or radiation may not prevent metastases in the brain. Because the primary treatment goal of the current treatment paradigm is a cure, LCC emphasized that this may be particularly important for patients with early-stage resectable disease. The LCC input reported that patients in the early-stage setting prefer a treatment that can effectively treat their disease and manage their symptoms of lung cancer, delay disease progression, settle patients into long-term remission for improved survivorship, allow them to live longer and maintain their independence and functionality to minimize the burden on their caregivers and loved ones, allow them to have a fulfilling and worthwhile quality of life, and have manageable side effects. Similarly, input from the Lung Health Foundation indicated that desired treatment outcomes included stopping or slowing the progression of the disease with minimal side effects.
Clinician Input
Input From Clinical Experts Consulted by the Review Team
According to the clinical experts consulted by the review team, patients with early-stage ALK-positive NSCLC following tumour resection need effective treatments that are less toxic than adjuvant chemotherapy, can improve overall survival (OS), and can decrease the risk of recurrence more effectively than surgery alone or surgery plus adjuvant chemotherapy does.
According to the clinical experts, alectinib may replace chemotherapy in the adjuvant setting for some adult patients with stage IB (≥ 4 cm) to IIIA ALK-positive NSCLC. Th clinical experts added that chemotherapy should remain available in the adjuvant setting, and adjuvant alectinib could be used following adjuvant chemotherapy.
Both clinical experts consulted by the review team noted that patients with completely resected stage II to IIIA ALK-positive NSCLC would be best suited for alectinib. One of the clinical experts noted that patients with completely resected stage IB (≥ 4 cm) ALK-positive NSCLC would also be best suited for alectinib, whereas the other clinical expert noted that these patients may not be as suitable. Both experts agreed that patients with an Eastern Cooperative Oncology Group Performance Status (ECOG PS) of 0 to 2 could be eligible for treatment with alectinib. They added that patients who are least suitable for alectinib could be those who do not have a demonstrated ALK translocation. According to the clinical experts, OS, disease-free survival (DFS), and time to recurrence are meaningful outcomes that need to be assessed with regular imaging in adult patients with stage IB (≥ 4 cm) to IIIA ALK-positive NSCLC. According to the experts, alectinib should be discontinued in the event of unacceptable toxicity despite appropriate dose modifications, evidence of treatment failure (i.e., disease progression) or disease recurrence, or the patient’s withdrawal of consent.
According to the clinical experts, treatment with alectinib should occur in a medical oncology clinic and be supervised by a medical or pulmonary oncologist experienced in treating patients with lung cancer.
Clinician Group Input
Clinician group input on the review of alectinib was received from the LCC Medical Advisory Committee and the Ontario Health (Cancer Care Ontario) Lung Cancer Drug Advisory Committee (DAC). A total of 36 clinicians (30 from LCC and 6 from the DAC) provided input for this submission.
Similar to the clinical experts consulted by the review team, the DAC indicated that the treatment goals include improved survival, quality of life, and prevention of recurrence. LCC noted that the primary goal for treatment for stages IB to IIIA NSCLC is a cure (i.e., to improve 5-year OS).
The DAC emphasized that there is an unmet need because of poor outcomes with adjuvant chemotherapy alone among patients with lung cancer who are often young and healthy and who may have a high degree of brain tropism, with no known modifiable risk factors. The group noted that there is a need to improve central nervous system disease–free survival (CNS-DFS).
Similar to the clinical experts consulted by the review team, both the DAC and LCC indicated that, in practice, adjuvant alectinib would be expected to be either used alone or following adjuvant chemotherapy. The DAC noted that patients will be selected based on the presence of ALK rearrangement, which is applicable to patients with resected stage IIA or higher tumours, or any node positive for a T3/T4 or T2 tumour of 4.0 cm or larger. LCC stated that all patients with resected stage IB to IIIA ALK-positive NSCLC may benefit from adjuvant alectinib irrespective of clinical characteristics.
According to LCC, prevention of disease recurrence would be the only meaningful end point in the early-stage setting to determine if a patient is responding to treatment in clinical practice. Both clinician groups agreed that treatment discontinuation would be determined based on disease progression or recurrence, along with drug intolerance or severe complications.
Drug Program Input
Input was obtained from the drug programs that participate in the Reimbursement Review process. The following were identified as key factors that could affect implementation of a recommendation for alectinib:
relevant comparators
consideration for initiation of therapy
consideration of discontinuation of therapy
generalizability
funding algorithm
care provision issues.
Clinical Evidence
Systematic Review
Description of Studies
One ongoing phase III, open-label, randomized, active-controlled trial (ALINA, N = 257) was included in the sponsor-submitted systematic literature review (SLR). The ALINA trial enrolled adult patients who had complete resection of histologically confirmed stage IB (tumour ≥ 4 cm) to stage IIIA ALK-positive NSCLC. Patients were randomized to either the alectinib group (n = 130) or platinum-based chemotherapy group (n = 127), stratified by disease stage (IB [tumours ≥ 4 cm] versus II versus IIIA) and race (Asian versus non-Asian). The primary objective of the ALINA trial was to compare the efficacies of alectinib and chemotherapy, measured by DFS according to investigator assessment. Other efficacy and safety outcomes included OS, CNS-DFS, Short Form (36) Health Survey version 2 (SF-36 v2) mental and physical component scores, as well as harms, including adverse events (AEs), serious adverse events (SAEs), withdrawal, and deaths.
The median age of the intention-to-treat (ITT) population in the ALINA trial was 56 years (range = 26 to 87), and most (76.3% [196 of 257]) were aged younger than 65 years. Of the 257 patients enrolled, 47.9% were male, 55.6% were Asian, and 41.6% were white. Of the total patient population, 10.1% (26 of 257) had stage IB disease, 31.1% (80 of 257) had stage IIA disease, 3.9% (10 of 257) had stage IIB disease, and 54.9% (141 of 257) had stage IIIA disease. Most of the ITT population (96.5%, 248 of 257) had a nonsquamous histology, of which 96% (238 of 248) were adenocarcinoma.
Efficacy Results
The data cut-off date for efficacy results was June 26, 2023.
Overall Survival
In the ALINA trial’s ITT population, the median duration of survival follow-up was 27.8 months (range = 0 to 55.4). As of the data cut-off date (i.e., June 26, 2023), OS data were immature. There were 2 OS events (1.5%) in the alectinib group and 4 OS events (3.1%) in the chemotherapy group. The stratified hazard ratio (HR) for OS was 0.46 (95% confidence interval [CI], 0.08 to 2.52).
DFS According to Investigator Assessment
In the ALINA trial’s ITT population, the median duration of follow-up for DFS was 24.87 months (range = 0 to 55.4 months). As of June 26, 2023, 11.5% (15 of 130) of the patients in the alectinib group and 39.4% (50 of 127) in the chemotherapy group had experienced DFS events. The stratified HR was 0.24 (95% CI, 0.13 to 0.43; P < 0.0001), which met the prespecified stopping boundary (P ≤ 0.0077) in favour of alectinib. The difference in the probability of being disease–free between alectinib and chemotherapy was ██████ ████ ███ █████ ██ ██████ at 2 years, ██████ ████ ███ █████ ██ ██████ at 3 years, and ██████ ████ ███ █████ ██ ██████ at 4 years. The median DFS was not reached in the alectinib group and was 41.3 months (95% CI, 28.5 to not evaluable) in the chemotherapy group. The results in the subgroup classified by disease stage appeared to be consistent with the results for the ITT population in direction and magnitude, although there were few patients (n = 26) in the stage IB subgroup, resulting in a wide 95% CI.
A blinded independent central review (BICR) was used to assess DFS as a sensitivity analysis in the ITT population. The stratified HR was 0.30 (95% CI, 0.17 to 0.54, ██████). The difference in the probability of being disease–free between alectinib and chemotherapy was ██████ ████ ███ █████ ██ ██████ at 2 years, ██████ ████ ███ █████ ██ ██████ at 3 years, and ██████ ████ ███ ████ ██ ██████ at 4 years. The median DFS was not reached in either group. ███ ███████████ ████████ ███████ ███ ███ ████████████ ██████████ ███ ███ ███ ████ ███ ██████████ ████████ ████ █ ████████ ███ ██ █████ ███ █████████████ ██████████ ██████████ ██ ████ ████████████ ███ ████ ██ ███ ████ ██ ████ ███████ ██████ ████ ███ █████ ████ ██████████ █████████ ███ ████████████ ████████ █ ███████████ ████ ██ █████ ███ ████████ ██ ███ █████████ █████ ███ █████ ██ ███ ████████████ █████. Additional sensitivity analyses assessing the impact of missing disease assessments, stratification errors, and the Ukraine-Russia conflict had results similar to those of the primary analysis.
CNS Disease–Free Survival According to Investigator Assessment
In the ALINA trial’s ITT population, the median duration of follow-up for CNS-DFS was 25.07 months (range = 0 to 55.4). As of June 26, 2023, 3.8% (5 of 130) of the patients in the alectinib group and 14.2% (18 of 127) in the chemotherapy group had CNS-DFS events. The stratified HR was 0.22 (95% CI, 0.08 to 0.58), favouring the alectinib group. The difference in the probability of being CNS disease–free between alectinib and chemotherapy was ██████ ████ ███ ████ ██ ██████ at 2 years, ██████ ████ ███ ████ ██ ██████ at 3 years, and ██████ ████ ███ ████ ██ ██████ at 4 years. The median CNS-DFS was not reached for either group.
SF-36 v2 Mental Component Summary Score
The SF-36 v2 mental component summary scores ranged from 0 to 100, with a higher score indicating a better health-related quality of life (HRQoL). In the alectinib group, the mean change from baseline at week 12 was 3.65 (95% CI, 1.96 to 5.35), indicating an improvement. However, no improvement was observed in the chemotherapy group at week 12 (mean change from baseline = −2.24; 95% CI, −4.05 to −0.43). At week 12, the difference in mean change from baseline between the alectinib and chemotherapy groups was 5.89 (95% CI, 3.41 to 8.37).
SF-36 v2 Physical Component Summary Score
The SF-36 v2 physical component summary scores ranged from 0 to 100, with a higher score indicating a better HRQoL. In the alectinib group, the mean change from baseline at week 12 was 1.10 (95% CI, −0.02 to 2.21), indicating an improvement. However, no improvement was observed in the chemotherapy group at week 12 (mean change from baseline = −0.40; 95% CI, −1.59 to 0.78). At week 12, the difference in mean change from baseline between the alectinib group and the chemotherapy group was 1.50 (95% CI, −0.13 to 3.13).
Harms Results
The data cut-off date for harms outcomes was June 26, 2023. Among safety-evaluable patients, the median duration of safety follow-up was 24.8 months (range = 1.1 to 26.2) in the alectinib group, and 3.7 months (range = 1.6 to 5.3) in the chemotherapy group.
The proportion of patients who had at least 1 AE in the alectinib group was slightly higher than that of patients in the chemotherapy group (98.4% versus 93.3%, respectively). Increased blood creatine phosphokinase (43.0%), constipation (42.2%), increased aspartate transaminase (41.4%), increased alanine transaminase (33.6%), and increased blood bilirubin (33.6%) were among the most common AEs in the alectinib group. The proportions of patients who had at least 1 grade 3 to 5 AE were similar between the alectinib and chemotherapy groups (29.7%% versus 30.8%, respectively). The most common grade 3 to 5 AE in the alectinib group was increased blood creatine phosphokinase (6.3%), followed by appendicitis (3.1%). A higher percentage of patients in the alectinib group experienced SAEs, compared to the percentage of patients in the chemotherapy group (13.3% versus 8.3%, respectively). The most common SAE in the alectinib group was appendicitis (3.1%). Discontinuation of alectinib occurred in 5.5% of the patients in the alectinib group, which was lower than 12.5% in the chemotherapy group. Two deaths occurred in the alectinib group (1.6%) versus 5 in the chemotherapy group (4.2%).
Critical Appraisal
In the ALINA trial, a higher percentage of patients in the alectinib group were younger, female, and had a better performance status, without a history of smoking at baseline, which indicated a possibly improved prognosis for patients in the alectinib group compared with those in the chemotherapy group. The review team, in consultation with the clinical experts, determined that the bias introduced by the imbalance was likely trivial. The primary end point, DFS according to investigator assessment, could be vulnerable to detection bias because of the open-label design; however, the review team determined that the risk was low because the DFS results according to investigator assessment were relatively consistent with those of a BICR, and the analysis of concordance showed a relatively strong agreement between the ways of assessment. The risk of performance bias because of the open-label study design could not be ruled out for SF-36 v2, a self-reported HRQoL outcome, as well as for subjective harms outcomes. OS was immature at the current data cut-off time. The ALINA trial reported OS data up to 48 months. However, according to the clinical experts consulted by the review team, a follow-up of at least 60 months would likely be needed to allow for further understanding of the treatment effects of alectinib on OS. While DFS was adjusted for multiplicity, CNS-DFS was not. Additionally, DFS and CNS-DFS were assessed at an interim analysis, resulting in a potential overestimate of the true magnitude of the difference between alectinib and chemotherapy. There were minor concerns with the internal validity of the results of DFS and CNS-DFS. However, the impact of missing data on DFS estimates because of loss to follow-up or dropout remained unclear because relevant information for the review team to make the judgment was not provided. Based on patient disposition information, discontinuation of the study because of loss to follow-up and withdrawal by patients occurred among ████ ███████ of the alectinib group and ████ ████████ of the chemotherapy group. There was an imbalance between the 2 groups (████ ██████ ████). The review team determined that a potential bias from missing outcome data could not be ruled out but may be small because of the small imbalance. The missing data issue was also identified in HRQoL outcomes. Data were assumed to be missing at random, but this may not be plausible, and sensitivity analyses using different assumptions were not presented.
There are several considerations related to the generalizability of the ALINA trial. The clinical experts consulted by the review team noted that using adjuvant platinum-based chemotherapy as a comparator in the ALINA trial was appropriate, given that adjuvant chemotherapy is the standard of care in the Canadian setting for adult patients. In general, the clinical experts considered the patient eligibility criteria used in the ALINA trial appropriate and reflective of the criteria they would use to select patients in Canada. However, the clinical experts also commented that the eligibility criteria are restrictive, and patients who could benefit from alectinib but were excluded from the trial (e.g., those with a ECOG PS of 2, patients who are not eligible to receive a platinum-based chemotherapy regimen, patients who had prior adjuvant radiotherapy, patients who had prior systemic anticancer therapy, stage IIIA patients who received postoperative radiation therapy, patients with prior malignancies, patients who had a history of organ transplant, and those who tested positive for HIV).
GRADE Summary of Findings and Certainty of the Evidence
For pivotal studies and randomized controlled trials (RCTs) identified in the sponsor’s systematic review, Grading of Recommendations Assessment, Development and Evaluation (GRADE) was used to assess the certainty of the evidence for outcomes considered most relevant to inform the expert committee deliberations, and a final certainty rating was determined as outlined by the GRADE Working Group.19,20
Following the GRADE approach, evidence from RCTs started as high-certainty evidence and could be rated down in response to concerns related to study limitations (internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias.
When possible, certainty was rated in the context of the presence of an important (nontrivial) treatment effect; if this was not possible, certainty was rated in the context of the presence of any treatment effect (i.e., the clinical importance is unclear). In all cases, the target of the certainty of evidence assessment was based on the point estimate and where it was located relative to the threshold for a clinically important effect (when a threshold was available) or to the null.
The reference points for the certainty of evidence assessment for OS, DFS according to investigator assessment, and CNS-DFS were set according to the presence of an important effect based on thresholds agreed upon by the clinical experts consulted by the review team. The reference points for the certainty of evidence assessment for SF-36 v2 mental and physical component summary scores were set according to the presence of an important effect based on thresholds identified in the literature by the sponsor. For harm events, the certainty of evidence was summarized narratively.
The selection of outcomes for GRADE assessment was based on the sponsor’s Summary of Clinical Evidence, consultation with clinical experts, and input received from patient and clinician groups and public drug plans. The following list of outcomes was finalized in consultation with expert committee members:
survival outcomes (OS, DFS)
HRQoL outcome (SF-36 v2 mental and physical component summary scores)
harms (AEs of grade 3 or higher).
Results of GRADE Assessments
Table 2 summarizes the GRADE findings for alectinib versus platinum-based chemotherapy in patients with adult patients with stage IB (≥ 4 cm) to IIIA ALK-positive NSCLC.
Table 2: Summary of Findings for Alectinib Versus Platinum-Based Chemotherapy for Patients With Adult Patients With Stage IB (≥ 4 cm) to IIIA (AJCC/UICC Staging Manual, 7th Edition) ALK-positive NSCLC
Outcome and follow-up | Patients (studies), N | Relative effect (95% CI) | Absolute effects | Certainty | What happens | ||
|---|---|---|---|---|---|---|---|
Chemotherapy | Alectinib (95% CI) | Difference (95% CI) | |||||
OS — ITT (data cut-off date: June 26, 2023) | |||||||
Probability of being alive at 48 months Median follow-up duration (months): 27.8 for alectinib group; 28.4 for chemotherapy group | 257 (1 RCT) | NR | ███ per 1,000 | ███ per 1,000 (███ to █████ per 1,000) | ██ more per 1,000 ███ █████ to ███ ████ per 1,000) | Moderatea | Alectinib likely results in little or no difference in the probability of being alive at 48 months, compared to chemotherapy |
Probability of being alive at 60 months or more | NR | NR | NR | NR | NR | NA | There is no evidence about the effect of alectinib on the probability of being alive at 60 months or more (at present, OS data are immature) |
DFS according to investigator assessment — ITT population (data cut-off date: June 26, 2023) | |||||||
Probability of being disease–free at 24 months Median follow-up duration (months): █████ for alectinib group; █████ for chemotherapy group | 257 (1 RCT) | NR | 637 per 1,000 | 936 per 1,000 (894 to 979 per 1,000) | ███ ████ per 1,000 (███ ████ to ███ ████ per 1,000) | Moderateb | Alectinib likely results in a clinically important increase in the probability of being disease–free at 24 months, compared to chemotherapy |
Probability of being disease–free at 48 months Median follow-up duration (months): █████ for alectinib group; █████ for chemotherapy group | 257 (1 RCT) | NR | 462 per 1,000 | ███ per 1,000 (███ to ███ per 1,000) | ███ ████ per 1,000 (███ ████ to ███ ████ per 1,000) | Moderatec | Alectinib likely results in a clinically important increase in the probability of being disease–free at 48 months, compared to chemotherapy |
CNS-DFS — ITT population (data cut-off date: June 26, 2023) | |||||||
Probability of being CNS disease–free at 24 months Median follow-up duration (months): █████ for alectinib group; █████ for chemotherapy group | 257 (1 RCT) | NR | 858 per 1,000 | 984 per 1,000 (961 to 1,000 per 1,000) | ███ ████ per 1,000 (██ ████ to ███ ████ per 1,000) | Moderated | Alectinib likely results in a clinically important increase in the probability of being CNS disease–free at 24 months, compared to chemotherapy |
Probability of being CNS disease–free at 48 months Median follow-up duration (months): █████ for alectinib group; █████ for chemotherapy group | 257 (1 RCT) | NR | ███ per 1,000 | ███ per 1,000 (███ to ███ per 1,000) | ███ ████ per 1,000 (██ ████ to ███ ████ per 1,000) | Moderatee | Alectinib likely results in a clinically important increase in the probability of being CNS disease–free at 48 months, compared to chemotherapy |
HRQoL — ITT population (data cut-off date: June 26, 2023) | |||||||
SF-36 v2 mental component summary score (0 [worst] to 100 [best]) Follow-up: week 12 | 257 (1 RCT) | NR | −2.24 | 3.65 (NR) | 5.89 (3.41 to 8.37) | Lowf | Alectinib may result in a clinically important improvement in the SF-36 v2 mental component summary score at 12 weeks, compared to chemotherapy |
SF-36 v2 physical component summary score (0 [worst] to 100 [best]) Follow-up: week 12 | 257 (1 RCT) | NR | −0.40 | 1.10 (NR) | 1.50 (−0.13 to 3.13) | Very lowg | The evidence is uncertain about the effect of alectinib on the SF-36 v2 physical component summary score at 12 weeks, compared to chemotherapy |
Harms — safety-evaluable population (data cut-off date: June 26, 2023) | |||||||
AEs of grade 3 or higher | 248 (1 RCT) | RR: 0.963 (0.621 to 1.393) | 308 per 1,000 (NR) | 297 per 1,000 (NR) | 12 fewer per 1,000 (126 fewer to 103 more per 1,000) | Lowh | Alectinib may result in little or no difference in AEs of grade 3 or higher, compared to chemotherapy |
AE = adverse event; AJCC = American Joint Committee on Cancer; BICR = blinded independent central review; CI = confidence interval; CNS = central nervous system; CSN-DFS = central nervous system disease–free survival; DFS = disease-free survival; HRQoL = health-related quality of life; ITT = intention to treat; MID = minimal important difference; NA = not applicable; NR = not reported; NSCLC = non–small cell lung cancer; OS = overall survival; RCT = randomized controlled trial; SF-36 v2 = Short Form (36) Health Survey version 2; UICC = Union for International Cancer Control.
Note: The start point for the study design of the ALINA study (an RCT) was high certainty. Study limitations (which refer to internal validity or risk of bias), indirectness, imprecision of effects, and publication bias were considered when assessing the certainty of the evidence. All serious concerns in these domains that led to the rating down of the level of certainty are documented in the table footnotes. The between-group differences for SF-36 v2 mental and physical component summary scores and AEs of grade 3 or higher were not part of the sponsor’s statistical analysis plan and were requested by the review team to inform the interpretation of the findings.
aCertainty was not rated down for risk of bias. Compared with the chemotherapy group, a higher percentage of patients in the alectinib group were younger, female, and had a better performance status without a history of smoking at baseline, which indicated a possibly better prognosis of patients in the alectinib group. However, these imbalances in patient characteristics at baseline may have been the result of the relatively small sample size, which challenged achieving prognostic balance; as such, we did not rate down for risk of bias. Indirectness was not rated down, although the clinical experts consulted by the review team noted that year 5 was the earliest time point at which they would expect to see a meaningful between-group difference in probability of being alive. Rated down 1 level for imprecision. The point estimate suggests little to no difference while the upper bound of the 95% CI indicates benefits based on the clinical importance threshold of 5% to 10% suggested by the clinical experts.
bCertainty was not rated down for risk of bias. Although the assessment of DFS according to investigator assessment was prone to detection bias because of the open-label design, the risk was considered low because relatively consistent results were found using DFS according to a BICR; although absolute between-group differences by BICR were smaller in magnitude they remained clinically important. Rated down 1 level for imprecision. The clinical experts consulted by the review team suggested that the effect estimate and lower bound of the 95% CI were clinically important, but the result was informed by an interim analysis with a small number of events, resulting in the potential for overestimation of the true effect.
cCertainty was not rated down for risk of bias. Although the assessment of DFS according to investigator assessment was prone to detection bias because of the open-label design, the risk was considered low because relatively consistent results were found using DFS according to a BICR; although absolute between-group differences by BICR were smaller in magnitude, they remained clinically important. Rated down 1 level for imprecision. The clinical experts consulted by the review team suggested that the effect estimate and lower bound of the 95% CI were clinically important, but the result was informed by an interim analysis with a small number of events, resulting in the potential for overestimation of the true effect.
dCertainty was not rated down for risk of bias. Although the assessment of CNS-DFS was prone to detection bias because of the open-label design, the risk was considered relatively low (there may be some potential for overestimation, similar to DFS according to investigator). Rated down 1 level for imprecision. The point estimate suggests a benefit while the lower bound of the 95% CI suggests little to no difference based on a clinical importance threshold of 10% suggested by clinical experts.
eCertainty was not rated down for risk of bias. Although the assessment of CNS-DFS was prone to detection bias because of the open-label design, the risk was considered relatively low. Indirectness was not rated down (there may be some potential for overestimation, similar to DFS according to investigator). Rated down 1 level for imprecision. The point estimate suggests a benefit while the lower bound of the 95% CI suggests little to no difference based on a clinical importance threshold of 10% suggested by clinical experts.
fCertainty was rated down 2 levels for risk of bias because of imbalanced missing outcome data and a risk of performance bias associated to the open-label design and the subjective nature of the measure. Certainty was not rated down for imprecision. The 95% CI excludes the MID estimate of 3 provided by the sponsor.
gCertainty was rated down 2 levels for risk of bias because of imbalanced missing outcome data and a risk of performance bias associated with the open-label design and the subjective nature of the measure. Certainty was rated down 1 level for imprecision. The point estimate suggests little to no important difference but the upper bound of the 95% CI suggests a potential for benefit, based on the MID estimate of 2 points provided by the sponsor.
hRated down 2 levels for imprecision. The null was used as the threshold for clinical relevance. The point estimate suggested little to no important difference, but the 95% CI includes a potential for both benefit and harm.
Sources: ALINA Clinical Study Report21 and Drug Reimbursement Review sponsor submission.22
Conclusions
The pivotal ALINA trial is an ongoing phase III, open-label, randomized trial comparing the efficacy and safety of adjuvant alectinib with that of platinum-based chemotherapy in adult patients who had complete resection of histologically confirmed stage IB (tumour ≥ 4 cm) to stage IIIA ALK-positive NSCLC. The ALINA trial demonstrated there were added clinical benefits of adjuvant alectinib in DFS and CNS-DFS in the ITT population. Compared to adjuvant chemotherapy, alectinib likely results in a clinically important increase in the probability of being disease–free at 24 and 48 months (moderate certainty of evidence) as well as in the probability of being free of CNS disease at 24 and 48 months (moderate certainty of evidence). The improvement in DFS was considered large by the clinical experts consulted by the review team and was observed consistently across the prespecified subgroups by disease stage (i.e., IB versus II versus IIIA); however, few patients had stage IB disease. Uncertainty remains in the OS results because of the data being immature. Compared to adjuvant chemotherapy, alectinib may improve SF-36 v2 mental component summary scores, but evidence for the SF-36 v2 physical component summary is uncertain. According to the clinical experts consulted by the review team, the safety profile of alectinib was consistent with their expectations for this drug.
Introduction
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of alectinib (Alecensaro), 150 mg capsules, administered orally, as adjuvant treatment following tumour resection for adult patients with stage IB (≥ 4 cm) to IIIA ALK-positive NSCLC.
Disease Background
Contents within this section were informed by materials submitted by the sponsor and clinical expert input. The following summary was validated by the review team.
Lung cancer is 1 of the leading causes of cancer-associated mortality for both males and females in Canada.3 In 2023, it is estimated that lung cancer accounted for approximately one-quarter of all cancer-related deaths in Canada, with NSCLC accounting for approximately 85% of cases.3-5 Staging is used to identify the extent of disease, based on the AJCC/UICC tumour, node, and metastasis system.6-8
In Canada, approximately half of all lung cancer cases are classified as stage I to III at diagnoses according to the AJCC/UICC staging manual,9 and all staging groups include subsets of patients who may be eligible for tumour resection.10,11 In early-stage NSCLC, patients are often asymptomatic, evading diagnosis until the cancer has spread enough to cause distinct symptomology.23 Survival in lung cancer is also inversely related to stage, with 5-year net survival estimates ranging from 3% to 62%.3,24
Some patients with NSCLC may possess an underlying pathogenic driver mutation, such as an ALK gene rearrangement within chromosome 2.12,13 This rearrangement may result in expression of an oncogenic ALK fusion protein mediating constitutive kinase activity.12,13 Compared to patients without ALK mutations, patients with ALK mutations are younger in age, more often employed with dependents, and more often never smokers.25-28 Patients with the ALK-positive disease are at a higher risk of developing brain metastases compared to those with ALK-negative disease.16 Approximately 64% of patients with NSCLC will typically develop brain metastases during the course of their disease.14-16 Signs and symptoms of ALK-positive NSCLC, which do not differ from other types of NSCLC, include shortness of breath, hemoptysis and chest pain. Most patients also present with nonspecific systemic symptoms such as fatigue, unexplained weight loss, and anorexia. Early-stage patients typically present with mild respiratory symptoms or are asymptomatic, often resulting in delayed diagnoses at later stages of the disease if not caught incidentally.29,30
Standards of Therapy
The goal of treatment for adult patients with early-stage ALK-positive NSCLC is a cure. The first-line treatment option for these patients is therefore typically surgery with the goal of complete resection.17 Both the sponsor and the clinical experts consulted by the review team noted that, following tumour resection, the standard of care for most patients is 4 cycles or 4 months of adjuvant platinum-based chemotherapy, depending on the regimen used.18 In clinical practice, cisplatin is typically the preferred platinum therapy, with carboplatin generally reserved for when cisplatin cannot be tolerated or comorbidities exist.31 The clinicians consulted by the review team and the sponsor agreed that the most common adjuvant chemotherapy regimens offered to patients across Canada are combinations of cisplatin and vinorelbine or cisplatin and pemetrexed. After adjuvant chemotherapy is complete, patients receive routine surveillance and are observed for signs of disease progression. According to the clinical experts, routine surveillance typically consists of a medical history, physical examinations, and CT scans every 6 months for the first 2 years followed by annual scans until year 5.
Drug Under Review
Key characteristics of alectinib and platinum-based chemotherapy doublets used for adjuvant treatment are summarized in Table 3.
The current reimbursement request for alectinib is as adjuvant treatment following tumour resection in adult patients with stage IB (≥ 4 cm) to IIIA ALK-positive NSCLC. The recommended dose of alectinib is 600 mg (four 150 mg capsules) given orally, twice daily with food (total daily dose of 1,200 mg).2
Alectinib is a highly selective and potent ALK and RET (REarranged during Transfection) tyrosine kinase inhibitor. Alectinib inhibits ALK phosphorylation and ALK-mediated downstream signalling pathways, including STAT 3 and PI3K/protein kinase B (also known as AKT), inducing tumour cell death (apoptosis).2
Table 3: Key Characteristics of Alectinib and Platinum-Based Chemotherapy Doublets
Characteristic | Alectinib | Platinum-based chemotherapy doublets | |||||
|---|---|---|---|---|---|---|---|
Cisplatin plus vinorelbine | Cisplatin plus pemetrexed | Cisplatin plus gemcitabine | Carboplatin plus vinorelbine | Carboplatin plus pemetrexed | Carboplatin plus gemcitabine | ||
Mechanism of action | Inhibits ALK phosphorylation and ALK-mediated downstream signalling pathways, including STAT 3 and PI3K/protein kinase B (also known as AKT), inducing tumour cell death (apoptosis) | Cisplatin: Has biochemical properties similar to those of bifunctional alkylating agents producing interstrand and intrastrand crosslinks in DNA Vinorelbine: Vinorelbine tartrate is a novel vinca alkaloid that interferes with microtubule assembly; the antitumour activity of vinorelbine is thought to be due primarily to inhibition of mitosis at metaphase through its interaction with tubulin | Cisplatin: Same as cisplatin plus vinorelbine Pemetrexed: Pemetrexed disodium is an antifolate antineoplastic drug that exerts its action by disrupting crucial folate-dependent metabolic processes essential for cell replication | Cisplatin: Same as cisplatin plus vinorelbine Gemcitabine: Cytotoxic effects are exerted through dFdCDP-assisted incorporation of dFdCTP into DNA, resulting in inhibition of DNA synthesis and induction of apoptosis | Carboplatin: Interferes with DNA intrastrands and interstrand crosslinks in cells exposed to the drug; DNA reactivity has been correlated with cytotoxicity Vinorelbine: Same as cisplatin plus vinorelbine | Carboplatin: Same as carboplatin plus vinorelbine Pemetrexed: Same as cisplatin plus pemetrexed | Carboplatin: Same as carboplatin plus vinorelbine Gemcitabine: Same as cisplatin plus gemcitabine |
Indicationa | For adjuvant treatment following tumour resection for patients with stage IB (tumour ≥ 4 cm) to IIIA (according to the AJCC/UICC staging manual, 7th edition) ALK-positive NSCLC | Cisplatin: Indication for lung cancer was not identified in the product monograph Vinorelbine: Indicated for the treatment of advanced NSCLC, as a single drug or in combination Regimen: Indication for lung cancer was not identified from the product monographs | Indicated for the initial treatment of patients with a good performance status and locally advanced or metastatic ██████ | Indicated for the treatment of patients with locally advanced or metastatic NSCLC as either a single drug or in combination with cisplatin | Carboplatin: An indication for lung cancer was not identified in the product monograph Vinorelbine: Indicated for the treatment of advanced NSCLC, as a single drug or in combination Regimen: Indication for lung cancer was not identified from the product monographs | Carboplatin: Indication for lung cancer was not identified in the product monograph Pemetrexed: Pemetrexed in combination with cisplatin therapy is indicated for the initial treatment of good performance status patients with locally advanced or metastatic nonsquamous NSCLC Regimen: Indication for lung cancer was not identified from the product monographs | Carboplatin: Indication for lung cancer was not identified in the product monograph Gemcitabine: Indicated for the treatment of patients with locally advanced or metastatic NSCLC as either a single drug or in combination with cisplatin Regimen: Indication for lung cancer was not identified from the product monographs |
Route of administration | Oral | IV | IV | IV | IV | IV | IV |
Recommended dosage | 600 mg (four 150 mg capsules) taken twice daily | Cisplatin: 50 to 75 mg/m2 as single dose every 3 to 4 weeks, or 15 to 20 mg/m2 daily for 5 days, every 3 to 4 weeks Vinorelbine: 30 mg/m2 administered weekly Cisplatin plus vinorelbine: No dosing listed in cisplatin or vinorelbine product monographs Otherb: Cisplatin 50 mg/m2 day 1, day 8 and vinorelbine 25 mg/m2 days 1, 8, 15, and 22 every 28 days | Cisplatin: 50 to 75 mg/m2 as single dose every 3 to 4 weeks, or 15 to 20 mg/m2 daily for 5 days, every 3 to 4 weeks Pemetrexed: 500 mg/m2 on day 1 of each 21-day cycle Cisplatin plus pemetrexed: Cisplatin 75 mg/m2 day 1, pemetrexed 500 mg/m2 on day 1 of each 21-day cycle | Cisplatin: 50 to 75 mg/m2 as single dose every 3 to 4 weeks, or 15 to 20 mg/m2 daily for 5 days, every 3 to 4 weeks Gemcitabine: 1,000 mg/m2 once weekly for 3 weeks Cisplatin plus gemcitabine: Cisplatin 100 mg/m2 day 1, gemcitabine 1,250 mg/m2 days 1 and 8 of each 21-day cycle (3-week schedule), gemcitabine 1,000 mg/m2 days 1, 8, and 15 of each 28-day cycle (4-week schedule) | Carboplatin: 400 mg/m2 given as single infusion Vinorelbine: 30 mg/m2 administered weekly Carboplatin plus vinorelbine: No dosing listed in carboplatin or vinorelbine product monographs | Carboplatin: 400 mg/m2 given as single infusion Pemetrexed: 500 mg/m2 on day 1 of each 21-day Carboplatin plus pemetrexed: No dosing was listed in carboplatin or pemetrexed product monographs | Carboplatin: 400 mg/m2 given as single infusion Gemcitabine: 1,000 mg/m2 once weekly for 3 weeks Carboplatin plus gemcitabine: No dosing listed in carboplatin or gemcitabine product monographs |
Serious adverse effects or safety issues | Gastrointestinal perforation, interstitial lung disease, hepatotoxicity, bradycardia | Cisplatin: Anaphylactic-like reactions; infections, such as sepsis; myelosupression such as neutropenia, leukopenia, thrombocytopenia; neurotoxicity (leuko-encephalopathy; peripheral neuropathy; posterior reversible encephalopathy syndrome); renal toxicity; cardiovascular toxicity, such as venous thromboembolic events and pulmonary embolism Vinorelbine: a cytotoxic drug; acute shortness of breath and severe bronchospasm; radiation recall reactions; should be used with extreme caution in patients whose bone marrow reserve may have been compromised by prior irradiation or chemotherapy, or whose marrow function is recovering from previous chemotherapy | Cisplatin: Same as cisplatin plus vinorelbine Pemetrexed: Serious hepatobiliary toxicity and rare cases of fatal hepatic failure; gastrointestinal toxicity such as stomatitis, nausea, vomiting, and diarrhea; suppression of bone marrow function, as manifested by neutropenia, thrombo-cytopenia, and anemia (or pancytopenia); cases of hypersensitivity, including anaphylaxis; serious renal events, including acute renal failure; interstitial pneumonitis with respiratory insufficiency; rare cases of bullous epidermolysis including Stevens-Johnson syndrome and toxic epidermal necrolysis | Cisplatin: Same as cisplatin plus vinorelbine Gemcitabine: A cytotoxic drug; can suppress bone marrow function manifested by leucopenia, thrombocytopenia and anemia; acute shortness of breath | Carboplatin: Highly toxic drug with a narrow therapeutic index; serious and fatal infections following administration of live or live-attenuated vaccines in patients treated with carboplatin; hypersensitivity reactions; bone marrow suppression; fatal veno-occlusive disease; fatal hemolytic anemia; fatal hemolytic-uremic syndrome. Vinorelbine: Same as cisplatin plus vinorelbine | Carboplatin: Same as carboplatin plus vinorelbine Pemetrexed: Same as cisplatin plus pemetrexed | Carboplatin: Same as carboplatin plus vinorelbine Gemcitabine: Same as cisplatin plus gemcitabine |
Other | NA | Cisplatin: Contraindicated in patients with pre-existing renal impairment and hearing impairment Vinorelbine: Contraindicated in patients who have drug-induced severe granulocytopenia or severe thrombocytopenia | Pemetrexed: May cause fetal harm when administered to a pregnant patient. Contraindicated for concomitant yellow fever vaccine | NA | Carboplatin: Contraindicated in the following conditions: severe myelosuppression; pre-existing severe renal impairment; history of severe allergic reactions to carboplatin, or other platinum-containing compounds | NA | NA |
AJCC = American Joint Committee on Cancer; dFdCDP = 2′,2'-difluoro-2′-deoxycytidine diphosphate; dFdCTP = 2′,2′-difluoro-2′-deoxycytidine triphosphate; NA = not applicable; NSCLC = non–small cell lung cancer; UICC = Union for International Cancer Control.
aHealth Canada–approved indication.
bThe dosing info was from clinical experts consulted by the review team, which was claimed to be used in clinical practice.
Sources: Product monographs2,32-36 and the sponsor’s Summary of Clinical Evidence.1
Testing Procedure Considerations
An estimated 3% to 5% of patients with NSCLC have ALK gene rearrangement.17,37 Reflex testing for ALK gene rearrangement upon diagnosis of NSCLC has been recommended as the standard of care in Canada.37,38 According to the clinical experts consulted by the review team, the use of patients’ resected tissue for ALK gene rearrangement testing following surgery is currently part of routine care for NSCLC.
One of 3 testing methods can be used to identify ALK gene rearrangement status in patients with NSCLC: immunohistochemistry (IHC), fluorescence in situ hybridization, or a next-generation sequencing panel.17 A Canadian study affirmed the acceptability of IHC testing for the ALK gene rearrangement in NSCLC,39 and the clinical experts consulted by the review team indicated that IHC is likely to currently be the most common mode of testing in Canada.
Potential impacts of ALK gene rearrangement testing to ascertain eligibility for adjuvant treatment with alectinib for stage IB to IIIA NSCLC following tumour resection were considered, including those to health systems, patients (including families and caregivers), and costs; these impacts are not anticipated to be substantial. Key considerations and relevant information available from materials submitted by the sponsor, input from the clinical experts consulted by the review team, and sources from the literature were validated by the review team and are summarized in Table 4.
Table 4: Considerations for ALK Gene Rearrangement Testing for Establishing Treatment Eligibility With Alectinib in NSCLC
Consideration | Criterion | Available information |
|---|---|---|
Health system | Availability of the testing procedure in jurisdictions across Canada | According to the clinical experts, biomarker testing for ALK gene rearrangement is broadly available for resected NSCLC. |
Number of individuals in Canada expected to require the test (e.g., per year) | Over the next 3 years, it is estimated that 2,590 to 2,698 patients per year will be tested for ALK gene rearrangement;22 however, because testing is already part of the standard of care for resected NSCLC, no additional impact on health systems is anticipated as part of establishing treatment eligibility. | |
Testing procedure as part of routine care | According to the clinical experts, ALK gene rearrangement testing is currently performed as part of the standard of care for resected NSCLC. | |
Repeat testing requirements | Testing for ALK gene rearrangement is generally not repeated; any need for repeat testing would likely be performed using resected tissue and would not require the patient to undergo any additional procedure(s) as part of establishing treatment eligibility. | |
Impact on health care human resources by provision of the testing procedure | Because testing for ALK gene rearrangement is currently part of the standard of care for resected NSCLC, use of the test to establish treatment eligibility is not anticipated to substantially affect health care human resources. | |
Patient-oriented | Accessibility of the testing procedure in jurisdictions across Canada | ALK gene rearrangement testing is part of the current standard of care for resected NSCLC in Canada. |
Expected wait times for the testing procedure | The turnaround time for ALK gene rearrangement testing is estimated to be between 2 and 4 weeks; however, because testing is currently part of the standard of care for resected NSCLC, no additional impact on wait times to patients is anticipated as part of establishing treatment eligibility. | |
Burden associated with the testing procedure for patients, families, and/or caregivers | Because testing for ALK gene rearrangement is currently part of the standard of care for resected NSCLC, no additional burden to patients, families, and/or caregivers is anticipated from the testing as part of establishing treatment eligibility. | |
Clinical | Clinical utility of the testing procedure | Evidence and guidance from Canada supports the diagnostic accuracy and clinical utility of IHC testing for ALK gene rearrangement.39,40 |
Risks of harm associated with the testing procedure | Because testing for ALK gene rearrangement is currently performed as part of the standard of care for resected NSCLC, no additional risk of harm is associated with the testing as part of establishing treatment eligibility. | |
Cost | Projected cost of the testing procedure | Because testing for ALK gene rearrangement is currently performed as part of the standard of care for resected NSCLC, no additional cost is anticipated from the testing as part of establishing treatment eligibility. |
IHC = immunohistochemistry; NSCLC = non–small cell lung cancer.
Perspectives of Patients, Clinicians, and Drug Programs
Patient Group Input
This section was prepared by the review team based on the input provided by patient groups. The full original patient inputs received by the review team are included in the Perspectives of Patients, Clinicians, and Drug Programs section of this report.
Two patient groups, LCC and the Lung Health Foundation, submitted patient group input for this review. LCC gathered data through interviews with 17 patients and/or caregivers in Canada and other countries who had experience with alectinib, both in the early-stage (I to IIIB) ALK-positive setting and stage IV setting. As of April 2024, of 17 patients interviewed for this submission, 14 were still being treated with alectinib. The Lung Health Foundation obtained input in April 2024 from patients with lung cancer via an online survey of 9 respondents (whose geographical locations were not collected) and from 3 interviews with respondents residing in Canada. Seven patients had experience with alectinib.
Input from LCC noted that almost half (47% [8 of 17]) of the patients interviewed had experience with chemotherapy before starting treatment with alectinib. Overall, patients agreed that chemotherapy reduced their quality of life and energy levels during treatment, more so than while on treatment with alectinib. Fatigue was the number 1 adverse effect reported by all patients, although the level varied by individual, with some feeling more severely debilitated than others. Input from LCC noted that patients with ALK-positive NSCLC disease were most concerned about CNS disease, because this type of lung cancer can be aggressive in spreading to the brain, and current treatments with chemotherapy or radiation may not prevent metastases in the brain. LCC further noted that alectinib may fill this gap in current treatment protocols for patients with stage I to III cancer by crossing the blood-brain barrier. Because the primary treatment goal is a cure, LCC emphasized that this may be particularly important for patients with early-stage resectable disease. The LCC input reported that patients in the early-stage setting prefer a treatment that may effectively treat their disease and manage their symptoms; delay disease progression and settle them into long-term remission for improved survivorship; allow patients to live longer and maintain their independence and functionality to minimize the burden on their caregivers and loved ones; allow patients to have a fulfilling and worthwhile quality of life; and involve manageable side effects.
Regarding their experience with alectinib, 7 of the patients interviewed by LCC reported showing no evidence of the disease at the time of the interview. The patients interviewed for this submission reported being treated with alectinib for a minimum of 5 months and an average of about 32 months. The patients in the LCC input reported a successful outcome in terms of extending their progression-free survival, reducing the risk of recurrence, and diminishing the need for traditional, systemic therapies that may have limited efficacy and harsh side effects. The most common AEs of alectinib reported by those interviewed by LCC were fatigue, increased skin sensitivity to sunlight, and gastrointestinal events (constipation or diarrhea). In comparison to AEs seen with other therapies, such as chemotherapy or radiation, these were described as relatively minor or manageable over time. Other side effects of alectinib that some patients noted in the LCC input included skin rash, changes in liver or kidney levels, changes in hormone levels, weight gain, and muscle weakness and/or pain. When the LCC asked patients to compare their experience with alectinib against other therapies on a scale of 1 to 10 (1 being worse and 10 being better), the average ranking was 9.7.
Respondents in the Lung Health Foundation input noted some benefits experienced with currently available treatments, such as reduced cough, reduced shortness of breath, increased participation in daily activities, ability to exercise, prolonged life, delayed disease progression and a reduction in the severity of other disease-related symptoms. Patients on oral drugs also emphasized the flexibility the drugs may provide in allowing them to work and travel without restrictions. Some patients from the Lung Health Foundation input reported struggling with the lingering side effects that come with currently available treatments. Respondents who received surgery reported deconditioning and chronic fatigue. Some of the side effects reported from radiation were fatigue, skin changes, hair loss, and tissue scarring. Side effects reported by patients taking medications included extreme itching affecting sleep, brain fog, fatigue, nausea, vomiting, mood changes, diminished appetite, weight loss, hair loss, anemia, and neuropathy. Patients also reported that side effects from chemotherapy severely reduced their quality of life, ability to work and in some cases, and ability to perform activities of daily living. When asked about challenges with access to treatment, respondents from the Lung Health Foundation input reported struggling with the cost associated with some treatments. They also found it challenging to navigate the health care system and, in some cases, where to go for information and support was not clear. Patients on targeted therapy also expressed their concern about access to the next line of treatment when their current treatment stops working. Key treatment outcomes for this group of patients with lung cancer included stopping or slowing the progression of the disease with minimal side effects. Patients included in the Lung Health Foundation input also expressed a desire for medications that are effective for advanced disease. Patients also described feeling very anxious about any sign or prospect of disease progression because of the poor outcomes associated with advanced disease. Patients considered the efficacy of the medication while choosing a therapy. One respondent commented that they would be more receptive to side effects if there was strong evidence that the medication would stop or slow the progression of their lung cancer.
Regarding their experience with the treatment under review, 7 patients in the Lung Health Foundation input reported some improvement in their quality of life and tangible benefits extending beyond symptom relief with alectinib. Patients also reported experiencing a notable reduction in debilitating symptoms, such as coughing and shortness of breath, coupled with an enhanced capacity to engage in daily activities and exercise. Patients in the Lung Health Foundation input described the side effects associated with alectinib as manageable and minor. However, some patients reported having difficulty with some side effects, such as fatigue, appetite loss, and mild nausea. The Lung Health Foundation input pointed to frustration among patients and caregivers regarding the lack of access to biomarker testing, the delays in getting biomarker testing, and inconsistencies in what biomarker testing is available where across Canada.
Clinician Input
Input From Clinical Experts Consulted by the Review Team
All review teams include at least 1 clinical specialist with expertise in the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). The following input was provided by 2 clinical specialists with expertise in the diagnosis and management of ALK-positive NSCLC.
Unmet Needs
According to the clinical experts consulted by the review team, the treatment goals for patients with early-stage ALK-positive NSCLC following tumour resection include improving OS as well as avoiding disease recurrence.
The clinical experts consulted by the review team noted that adjuvant chemotherapy is routinely offered to patients with completely resected stage II and stage III ALK-positive NSCLC and would be discussed with patients who have a tumour between 4 cm and 5 cm in size. According to the clinical experts, there is a need for an effective treatment following tumour resection that is less toxic than adjuvant chemotherapy, can improve OS, and can decrease the risk of disease recurrence compared to surgery alone or surgery plus adjuvant chemotherapy.
Place in Therapy
According to the clinical experts consulted by the review team, alectinib may replace chemotherapy in the adjuvant setting for some adult patients with stage IB (≥ 4 cm) to IIIA ALK-positive NSCLC. The clinical experts consulted by the review team also noted that chemotherapy should remain available in the adjuvant setting to be used before alectinib. The clinical experts further noted that alectinib will not be used in the adjuvant setting before chemotherapy because alectinib is usually given to patients for 2 years. Moreover, according to the clinical experts, there is currently no efficacy or safety evidence on the combination use of alectinib and platinum-based chemotherapy in the adjuvant setting for patients with stage IB (≥ 4 cm) to IIIA ALK-positive NSCLC.
Patient Population
Both clinical experts consulted by the review team noted that patients with completely resected stage II to IIIA ALK-positive NSCLC would be best suited for alectinib. For patients with completely resected stage IB (≥ 4 cm) ALK-positive NSCLC, 1 clinical expert noted that these patients with would also be best suited for alectinib, whereas the other clinical expert noted that these patients may not be as suitable. Both clinical consulted by the review team noted that patients with an ECOG PS of 0 to 2 could be eligible for alectinib. However, 1 of the clinical experts noted that patients who are most suitable for alectinib should have an ECOG PS of 0 or 1, whereas the other noted that all patients who are well enough to undergo tumour resection regardless of ECOG PS could be best suited for alectinib. In terms of patients who are least suitable for alectinib, the clinical experts noted that patients who do not have a demonstrated ALK translocation are unsuitable for alectinib, and patients who have a histology of squamous cell and with a demonstrated ALK translocation are least suitable for alectinib.
Assessing the Response Treatment
For adult patients with stage IB (≥ 4 cm) to IIIA ALK-positive NSCLC, the clinical experts consulted by the review team described OS, DFS, and time to recurrence as meaningful outcomes that need to be assessed with regular imaging. The clinical experts noted that there is as yet no consensus on the frequency of imaging, which may vary from every 3 months to every 6 months.
Discontinuing Treatment
According to the clinical experts consulted by the review team, alectinib should be discontinued in the event of unacceptable toxicity despite appropriate dose modifications, evidence of treatment failure (i.e., progression) or disease recurrence, or patient withdrawal of consent.
Prescribing Considerations
According to the clinical experts consulted by the review team, treatment with alectinib should occur in a medical oncology clinic, either in a community or academic/hospital setting, and be supervised by a medical or pulmonary oncologist who regularly treats patients with lung cancer and, in case of failure or toxicity, is knowledgeable about alternatives, and about metastatic treatment, to be able to counsel the patient properly regarding the potential implications of treatment or no treatment in the initial decision-making visit.
Clinician Group Input
This section was prepared by the review team based on the input provided by clinician groups. The full original clinician group inputs received by the review team are included in the Perspectives of Patients, Clinicians, and Drug Programs section of this report.
Clinician group input on the review of alectinib was received from the LCC Medical Advisory Committee and the Ontario Health Cancer Care Ontario Lung Cancer DAC. A total of 36 clinicians (30 from LCC and 6 from the DAC) provided input for this submission.
Aligned with the input provided by the clinical experts consulted by the review team, the DAC indicated that the treatment goals include improved survival, quality of life, and prevention of recurrence. LCC noted that the treatment for stages IB to IIIA NSCLC is both stage- and biomarker-dependent in Canada. They added that the primary goal of treatment of stages IB to IIIA NSCLC is a cure (i.e., to improve 5-year OS). LCC further noted that the standard treatment to achieve this goal is complete surgical resection for stage IB and stage II NSCLC. For stage IIIA NSCLC, the standard treatment depends on whether the primary tumour is considered resectable, balancing benefits and risks factors.
The DAC highlighted that there is an unmet need because of poor outcomes with adjuvant chemotherapy alone among patients with lung cancer, who are often young and healthy and who may have a very high degree of brain tropism and no known modifiable risk factors. The group further emphasized that there is a need to improve CNS-DFS. Input from LCC pointed out that recurrence rates are high with adjuvant chemotherapy. The group indicated that patients with ALK-positive NSCLC would not be candidates for neoadjuvant chemotherapy and nivolumab or adjuvant atezolizumab, which leads to an unmet need for these patients. LCC noted that prevention of a morbid complication such as CNS disease relapse has not been adequately addressed by adjuvant chemotherapy.
Both the DAC and LCC indicated that, despite not being tested in a trial, adjuvant alectinib would be expected to be used in practice, either alone or following adjuvant chemotherapy, which aligned with the input provided by the clinical experts consulted by the review team. LCC noted that alectinib could be used as the current postoperative management option for patients with resected stage IB to IIIA ALK-positive NSCLC, with the potential to become the standard of care for these patients. In regard to the patients best suited for treatment with alectinib, the DAC noted that patients will be selected based on the presence of ALK rearrangement, which is applicable to patients with resected stage IIA or higher, or any node positive for a T3/T4 or T2 tumour 4.0 cm or larger (the staging manual edition was not reported in the input). However, LCC stated that all patients with resected stage IB to IIIA ALK-positive NSCLC may benefit from adjuvant alectinib irrespective of clinical characteristics.
According to LCC, prevention of disease recurrence would be the only meaningful end point in the early-stage setting. Both clinician groups agreed that treatment discontinuation would be determined based on disease progression or recurrence, and drug intolerance or severe complications.
Drug Program Input
The drug programs provide input on each drug being reviewed through the Reimbursement Review processes by identifying issues that may affect their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by the review team are summarized in Table 5.
Table 5: Summary of Drug Plan Input and Clinical Expert Responses
Drug program implementation questions | Clinical expert response |
|---|---|
Relevant comparators | |
The ALINA trial compared adjuvant alectinib vs. platinum-based chemotherapy (cisplatin-vinorelbine, cisplatin-gemcitabine, cisplatin-pemetrexed, or, if intolerant to cisplatin, then carboplatin-vinorelbine, carboplatin-gemcitabine, carboplatin-pemetrexed). Do you have any comment on another relevant comparator that may be used in this setting — carboplatin-paclitaxel? | Both clinical experts noted that, in their own clinical practice, they would not offer carboplatin-paclitaxel in the adjuvant setting where chemotherapy will be used alone. |
Considerations for initiation of therapy | |
Who will be the eligible patient population based on the AJCC 8th edition staging system? | The ALINA trial included patients with stage IB (tumour ≥ 4 cm) to stage IIIA ALK-positive NSCLC (according to the AJCC/UICC staging manual, 7th edition), which could be converted to resected stage II and III NSCLC according to the 8th edition staging system. In the sponsor’s response to additional information requested on August 6, 2024,41 the sponsor noted that stage IB (tumour ≥ 4 cm) to stage IIIA ALK-positive NSCLC (according to the AJCC/UICC, 7th edition) could be converted to resected stage IB to IIIA and select IIIB NSCLC according to the 8th edition staging system. According to the sponsor, the ALINA study eligibility is based on the AJCC/UICC 7th edition staging and enrolled patients with stage IB (tumour ≥ 4 cm) to stage IIIA disease. According to the AJCC/UICC 8th edition, this would be classified as:
According to the sponsor, when the staging classification was changed, patients with IB disease > 4 cm according to the 7th edition became stage IIB according to the 8th edition. However, because ALINA enrolled some patients with stage IB ≥ 4 cm, some patients with stage IB according to the 8th edition were still taking part in the study. In ALINA, 11 patients had stage IB disease (8th edition). Nine patients had a tumour of 4 cm; the remaining 2 patients had tumours < 4 cm (major protocol deviations reported). When patients were restaged using the AJCC/UICC 8th edition, there were 13 patients with stage IIIB (8th edition). |
Can patients be re-treated with downstream ALK inhibitors provided that disease recurrence occurs 6 months or more from the last dose of adjuvant alectinib? Are there preferences on re-treatment with alectinib vs. other ALK inhibitors? | Both clinical experts agreed that patients can be re-treated with downstream ALK inhibitors provided that the disease recurs 6 months or more from the last dose of adjuvant alectinib. Three ALK inhibitors are funded as first-line therapy for metastatic disease (alectinib, brigatinib, and lorlatinib), and no data are available to facilitate the selection of a drug for the metastatic setting in patients who have received adjuvant alectinib. Both clinical experts agreed that clinicians may choose a different drug rather than receive alectinib again. One of the experts noted that, if the recurrence is soon (i.e., close to 6 months or less after the last dose of adjuvant treatment) in patients who have received adjuvant alectinib, in clinical practice many practitioners would likely move to a different ALK inhibitor rather than re-treating with alectinib. |
Considerations for discontinuation of therapy | |
In the trial, alectinib was given for 24 months or until the occurrence of disease recurrence or unacceptable toxicity, whichever occurred first. | This is a comment from the drug plans to inform pERC deliberations. |
Generalizability | |
The following patients were excluded from the ALINA trial. Should they be considered for alectinib?
| Patients with an ECOG PS of 2 could be considered for alectinib. However, patients with an ECOG PS of 3 or 4 would not be eligible for alectinib. Patients who are not eligible to receive platinum-based chemotherapy could still be eligible for alectinib. |
On a time-limited basis, should patients who are currently receiving adjuvant chemotherapy be eligible to switch to adjuvant alectinib? | Both clinical experts agreed that patients who are currently receiving adjuvant chemotherapy could switch to adjuvant alectinib. Sequentially adding alectinib after completing adjuvant chemotherapy could also be an option, although there is a lack evidence to either support or oppose the sequential use. |
Funding algorithm | |
Drug may change place in therapy of comparator drugs | This is a comment from the drug plans to inform pERC deliberations. |
Drug may change place in therapy of drugs reimbursed in subsequent lines | This is a comment from the drug plans to inform pERC deliberations. |
Care provision issues | |
Reflex testing must be in place. If adjuvant chemotherapy had to be started before ALK status is confirmed, should patients be given the option to switch to adjuvant alectinib once ALK positivity is confirmed? | Patients whose adjuvant chemotherapy started before ALK status is confirmed could switch to adjuvant alectinib once ALK positivity is confirmed. However, this situation would be rare because in current clinical practice reflex testing results should be available at time of medical oncology consultation. In other words, patients in Canada would normally not start adjuvant therapy before about 6 weeks after surgery, at which time testing results should be available. |
Should patients who have intolerable toxicities to platinum-based chemotherapy be switched to alectinib? | Both experts agreed that patients who have intolerable toxicities to platinum-based chemotherapy could be switched to alectinib as long as the patients meet other eligibility criteria (e.g., ALK-positive). |
AJCC = American Joint Committee on Cancer; ECOG PS = Eastern Cooperative Oncology Group Performance Status; NSCLC = non–small cell lung cancer; pERC = CADTH pan-Canadian Oncology Review Expert Review Committee; UICC = Union for International Cancer Control; vs. = versus.
Clinical Evidence
The objective of the Clinical Review is to review and critically appraise the clinical evidence submitted by the sponsor on the beneficial and harmful effects of alectinib (Alecensaro), 150 mg capsules, orally administered, as adjuvant treatment following tumour resection for adult patients with stage IB (≥ 4 cm) to IIIA ALK-positive NSCLC. The focus will be placed on comparing alectinib to relevant comparators and identifying gaps in the current evidence.
A summary of the clinical evidence included by the sponsor in the review of alectinib is presented in the Systematic Review section, with the review team’s critical appraisal of the evidence included at the end of the section. The section includes pivotal studies and RCTs that were selected according to the sponsor’s systematic review protocol. The review team’s assessment of the certainty of the evidence in this first section using the GRADE approach follows the critical appraisal of the evidence. No long-term extensions, indirect treatment comparisons, or studies addressing gaps were submitted.
Included Studies
Clinical evidence from 1 pivotal, phase III, multicentre, open-label, randomized active-controlled trial identified in the systematic review is included and appraised in this document.
Systematic Review
This section was informed by materials submitted by the sponsor. The following summary was validated by the review team.
Description of Study
One study (ALINA) was identified from the sponsor-submitted SLR. Characteristics of the ALINA trial are summarized in Table 6.
The ALINA study is a phase III, open-label, multicentre, randomized active-controlled trial, investigating the use of alectinib for the treatment of adult patients who had complete resection of histologically confirmed stage IB (tumour ≥ 4 cm) to stage IIIA ALK-positive NSCLC. A total of 257 participants from 113 sites across 26 countries (no sites in Canada) were randomized, via a central interactive voice or web-based response system, to the alectinib group (n = 130) and the chemotherapy group (n = 127). The randomization was stratified based on disease stage (IB [tumours ≥ 4 cm] versus II versus IIIA), and race (Asian versus non-Asian). The primary objective of the ALINA trial was to evaluate the efficacy of alectinib in patients with completely resected stage IB (tumours ≥ 4 cm) to stage IIIA ALK-positive NSCLC, compared to platinum-based chemotherapy. The primary end point was DFS according to investigator assessment. OS was 1 of the secondary end points.
The ALINA trial is ongoing. The cut-off date for the efficacy and safety data examined in the Clinical Review was June 26, 2023.
Table 6: Details of Studies Included in the Systematic Review
Detail | ALINA (BO40336) |
|---|---|
Designs and populations | |
Study design | Phase III, active-controlled, multicentre, open-label randomized controlled trial |
Locations | 113 sites across 26 countries |
Patient enrolment dates | Start: August 16, 2018 End: December 8, 2021 |
Randomized (N) | N = 257
|
Inclusion criteria |
|
Exclusion criteria |
|
Drugs | |
Intervention | Alectinib 600 mg (four 150 mg capsules) orally, twice daily for 2 years |
Comparator(s) | Platinum-based chemotherapy for 4 cycles x 21 days Regimens:
In case of intolerability to a cisplatin-based regimen, carboplatin could be administered instead in 1 of these combinations. Target dose: target AUC 5 mg/mL per min × (GFR [125 mL/min] + 25) day 1 IV. |
Study duration | |
Screening | Within 28 days before randomization |
Treatment | Alectinib group: 24 months Platinum-based chemotherapy group: 4 cycles, with each cycle lasting 21 days (total duration = 84 days) |
Follow-up | Approximately 5 years after last patient has enrolled |
Outcomes | |
Primary end point | DFS by investigator assessment assessed hierarchically:
|
Secondary and exploratory end points | Secondary:
Safety:
Exploratory:
|
Notes | |
Publications | NCT03456076 Solomon et al. (2023)42 Ahn et al. (2023)43 Barlesi et al. (2023)44 Solomon et al. (2019)45 Wu et al. (2024)46 |
AE = adverse event; AJCC = American Joint Committee on Cancer; ALT = alanine transaminase; AST = aspartate transaminase; AUC = area under the concentration-time curve; CNS-DFS = central nervous system disease–free survival; DFS = disease-free survival; ECOG PS = Eastern Cooperative Oncology Group Performance Status; EQ-5D-5L = 5-Level EQ-5D; GFR = glomerular filtration rate; HBcAb = hepatitis B core antibody; HBsAg = hepatitis B surface antigen; HBV = hepatitis B virus; HCV = hepatitis C virus; ITT = intention to treat; NSCLC = non–small cell lung cancer; OS = overall survival; PCR = polymerase chain reaction; SF-36 v2 = Short Form (36) Health Survey version 2; UICC = Union for International Cancer Control.
Sources: ALINA Clinical Study Report,21 ALINA Clinical Study Protocol version 6,47 and the sponsor’s Summary of Clinical Evidence.1
Populations
Inclusion and Exclusion Criteria
Eligible patients in ALINA were adults (aged ≥ 18 years) with an ECOG PS of 0 or 1, who had complete resection of histologically confirmed, stage IB (tumour ≥ 4 cm) to stage IIIA (T2 to T3 N0, T1 to T3 N1, T1 to T3 N2, T4 N0 to N1) ALK-positive NSCLC and were chemotherapy eligible. Patients who had previously been exposed to adjuvant radiotherapy, systemic anticancer therapy, or ALK inhibitors were excluded.
Interventions
Patients randomized to alectinib were to receive alectinib 600 mg (four 150 mg capsules), orally, twice daily with food, in the morning and evening. The first dose of the study drug was to be administered as soon as possible and no later than 7 days after randomization. Treatment was to continue until completion of the treatment period (24 months), disease recurrence, unacceptable toxicity, withdrawal of consent, or death, whichever occurred first. The dose could be reduced in steps of 150 mg up to 2 times for management of drug-related toxicities (i.e., from 600 mg twice daily to 450 mg twice daily and then from 450 mg twice daily to 300 mg twice daily). If a third dose reduction was indicated, the patient was required to discontinue alectinib. Administration of a dose below 300 mg twice daily was not allowed. Adjuvant chemotherapy was not offered to patients in the alectinib group.
Patients randomized to platinum-based chemotherapy received the treatment for 4 cycles, with each cycle lasting 21 days. The first dose of the study drug was to be administered as soon as possible after randomization, taking the required premedication into account, and no later than 7 days after randomization. Investigators could choose 1 of the permitted platinum-based chemotherapy regimens. Institutions were expected to follow their standard administration regimens (e.g., administration sequence or time) for the chemotherapy treatment. Patients must have received adequate premedications, antiemetic treatments, and IV hydration for platinum-based treatments according to the local standard of care and prescribing information. Platinum-based chemotherapy cycles may have been delayed for safety reasons; however, an interruption of more than 21 days (1 cycle) was considered a skipped cycle. This should not have prevented the investigator from completing 4 cycles.
Patients randomized to platinum-based chemotherapy received 1 of the following platinum-based chemotherapy regimens (in case of intolerability to a cisplatin-based regimen, carboplatin was administered instead):
cisplatin 75 mg/m2 IV over 6 to 8 hours on day 1 every 3 weeks, plus vinorelbine 25 mg/m2 on IV over 6 to 10 minutes on days 1 and 8 every 3 weeks (in case of intolerability, carboplatin area under the concentration-time curve (AUC) 5 mg/mL IV over approximately 30 to 60 minutes on day 1 every 3 weeks, plus vinorelbine 25 mg/m2 on IV over 6 to 10 minutes on days 1 and 8 every 3 weeks)
cisplatin 75 mg/m2 IV over 6 to 8 hours on day 1 every 3 weeks, plus gemcitabine 1,250 mg/m2 IV over 30 minutes on days 1 and 8 every 3 weeks (in case of intolerability, carboplatin AUC 5 IV over approximately 30 to 60 minutes on day 1 every 3 weeks, plus gemcitabine 1,000 mg/m2 IV over 30 minutes on days 1 and 8 every 3 weeks)
cisplatin 75 mg/m2 IV over 6 to 8 hours on day 1 every 3 weeks, plus pemetrexed 500 mg/m2 IV over approximately 10 minutes on day 1 every 3 weeks (in case of intolerability, carboplatin AUC 5 or 6 IV over approximately 30 to 60 minutes on day 1 every 3 weeks, plus pemetrexed 500 mg/m2 IV over approximately 10 minutes on day 1 every 3 weeks).
Outcomes
A list of efficacy end points assessed in this Clinical Review is provided in Table 7, followed by descriptions of the outcome measures. Summarized end points are based on outcomes included in the sponsor’s Summary of Clinical Evidence as well as any outcomes identified as important to this review by the clinical experts, patient and clinician groups, and public drug plans consulted by the review team. Using the same considerations, the review team selected end points most relevant to the expert committee deliberations and finalized this list of end points in consultation with members of the expert committee. All summarized efficacy end points were assessed using GRADE. Select notable harms outcomes considered important for informing the expert committee deliberations were also assessed using GRADE.
Table 7: Outcomes Summarized From ALINA
Outcome measure | Time point | ALINA |
|---|---|---|
OSa | Year 4 | Secondary |
DFS per investigator assessmenta | Year 2 Year 4 | Primary |
CNS-DFS per investigator assessment | Year 2 Year 4 | Exploratory |
SF-36 v2 mental component summary score | Week 12 | Secondary |
SF-36 v2 physical component summary score | Week 12 | Secondary |
CNS-DFS = central nervous system disease–free survival; DFS = disease-free survival; NSCLC = non–small cell lung cancer; OS = overall survival; SF-36 v2 = Short Form (36) Health Survey version 2.
aStatistical testing was adjusted for multiple comparisons (e.g., hierarchal testing).
Sources: ALINA Clinical Study Protocol version 647 and ALINA Statistical Analysis Plan version 7.48
Descriptions of efficacy and safety outcomes presented in the ALINA trial and appraised in the Clinical Review follow.
Efficacy Outcomes
Overall Survival
The time from the date of randomization to death because of any cause defined the OS period. Data for patients who were not reported as having died at the date of analysis were censored at the date when they were last known to be alive. If no postbaseline data were available, OS was censored at the date of randomization plus 1 day.
Disease-Free Survival
The primary efficacy end point in the ALINA trial, DFS according to investigator assessment, was defined as the time from randomization to the first documented recurrence of disease, new primary NSCLC, or death from any cause, whichever occurred first. DFS was determined by the investigator through an integrated assessment of radiographic data, biopsy sample results (if clinically feasible), and clinical status. Patients without an event were censored at the date of the last disease assessment. If no postbaseline data were available, DFS was censored at the date of randomization plus 1 day.
CNS Disease–Free Survival
The time from randomization to the first documented recurrence of disease in the CNS or death from any cause, whichever occurred first, was used to define CNS-DFS. Patients who were not reported as experiencing disease recurrence in the CNS or death would be censored at the date of the last disease assessment. Data for patients who experienced non-CNS recurrence before an eventual CNS recurrence would be censored at the date of non-CNS recurrence in this analysis. If no postbaseline data were available, data for these patients would be censored at the date of randomization plus 1 day.
Health-Related Quality of Life
Patients’ self-reported HRQoL was assessed using a generic measure, the SF-36 v2. Data were collected at baseline, every 3 weeks until week 12, and every 12 weeks thereafter until disease recurrence, death, withdrawal of consent, or end of follow-up (96 weeks). Measurement properties of the tool are presented in Table 8.
Table 8: Summary of Outcome Measures and Their Measurement Properties
Outcome measure | Type | Conclusions about measurement properties | MID |
|---|---|---|---|
SF-36 version 2 | A 36-item, generic, questionnaire using a Likert scale to collect self-reported HRQoL. It has a recall period of 4 weeks and consists of 8 subscales and 2 component summaries for physical and mental health. Subscale and summary scores range from 0 to 100 where a higher score indicates better HRQoL.49,50 | The sponsor provided the following information based on the SF-36 scoring manual, which was not supplied. Validity: The SF-36 has been previously validated for a variety of health states and diseases. Item-convergent validity was assessed using a population of adult patients differing in severity of medical and psychiatric conditions. The physical and mental components demonstrated correlation with their respective scales (0.77 to 0.88 and 0.71 to 0.90, respectively). Those scales measuring vitality and general health were moderately correlated to both physical and mental components (0.32 to 0.68).49 For item-discriminant validity, the physical components could not demonstrate correlation with the mental component subscales (0.12 to0.19) and vice versa (0.04 to 0.30).49 For discriminant validity, coefficients ranged from 0.09 to 0.62, showing correlation between an item and its hypothesized scale. For known-groups validity, the health domain scales and component summary measure that primarily assess mental health were found to be more valid in discriminating between groups of respondents differing in the presence of a mental condition than were the health domain scales and component summary measure that primarily assess physical health.49 Reliability: Internal consistency reliability for the MCS and PCS were 0.93 and 0.96, respectively. The Cronbach alpha coefficients for the 8 health scales ranged from 0.82 (general health) to 0.96 (role physical). The correlations between items and their scales (domains) was > 0.40.49 Responsiveness: No information on responsiveness was found from sponsor’s literature search. | General population MID:49
Not identified in populations with NSCLC. |
MCS = mental summary component; MID = minimal important difference; NSCLC = non–small cell lung cancer; PCS = physical component summary; SF-36 v2 = Short Form (36) Health Survey.
Harms Outcomes
The harms outcomes assessed in ALINA included AEs, SAEs, withdrawals because of AEs, and mortality. All safety events which occurred on or after the first dose of the study treatment were summarized by a mapped term using the Medical Dictionary for Regulatory Activities thesaurus, appropriate thesaurus level, and severity grade according to version 5.0 of the National Cancer Institute Common Terminology Criteria for Adverse Events. For events of varying severity, the highest grade was used in the summaries.
Statistical Analysis
Details of the statistical analysis of efficacy end points in ALINA are presented in Table 9.
Approximately 255 patients were planned to be randomized in a 1:1 ratio (alectinib to platinum-based chemotherapy) into the ALINA trial. The number of patients with stage IB disease would be capped at 25% to ensure that at least 75% of all randomized patients would be at stage II to IIIA. The sample size and the number of events required to demonstrate efficacy regarding the primary efficacy end point (DFS according to investigator assessment) at the primary analysis were based on the following assumptions: overall 2-sided significance level of 0.05 in the stage II to IIIA subpopulation and the ITT population; 80% power to detect an HR of 0.55, corresponding to an improvement in median DFS from 30 months to 55 months for patients receiving alectinib compared with chemotherapy in the stage II to IIIA subpopulation; 80% power to detect an HR of 0.58, corresponding to an improvement in median DFS from 36 months to 62 months for patients receiving alectinib compared with chemotherapy in the ITT population; and 1 interim analysis for DFS when approximately 67% of the total DFS events have occurred, with use of the Lan-DeMets approximation to the O’Brien-Fleming boundaries. Analysis timing in the ALINA trial was event-driven. Based on these assumptions, the primary DFS analysis was planned to occur after approximately 89 DFS events in the stage II to IIIA subpopulation had been observed. This was predicted to occur approximately 60 months (5 years) after the first patient was randomized.
The ALINA trial focused on testing the superiority of alectinib compared with chemotherapy with respect to DFS. A preplanned interim analysis of DFS was conducted after 59 events (about 67%) were observed in the stage II to IIIA subpopulation. A testing hierarchy was used to control the overall type I error rate at 5% with regard to DFS in the stage II to IIIA subpopulation and ITT population. The stopping boundaries for the DFS interim analysis were computed with use of the Lan-DeMets approximation to the O'Brien-Fleming boundaries. The stopping boundaries for early rejection of the null hypothesis for an overall 2-sided 5% significance level were P values of no more than 0.0118 (with 59 events) for stage II to IIIA subpopulation and no more than 0.0077 (with 65 events) for the ITT population. DFS was first tested in the stage II to IIIA subpopulation. Because a significant effect was observed in the stage II to IIIA subpopulation, DFS in the ITT population was then tested. Because the boundaries were crossed at the prespecified interim analysis, no further hypothesis testing was performed at later cut-off dates. This interim analysis became the primary analysis.
Other than DFS, the remaining outcomes were not adjusted for multiplicity.
Table 9: Statistical Analysis of Efficacy End Points in ALINA
End point | Statistical model | Adjustment factors | Handling of missing data | Sensitivity and subgroup analyses |
|---|---|---|---|---|
DFS according to investigator assessment |
|
| Data for patients who were not reported as experiencing disease recurrence, a new primary NSCLC, or death were censored at the date of the last disease assessment. If no postbaseline data were available, data for these patients were censored at the date of randomization plus 1 day. In addition, for patients with baseline disease, data were censored at the date of randomization plus 1 day. | Sensitivity analyses:
Subgroup analyses: The effects of demographics (e.g., disease stage) on duration of DFS were examined using unstratified HRs from Cox proportional hazards models and Kaplan-Meier estimates of medians. |
OS | Same as described for DFS per investigator assessment | Not performed | ||
CNS-DFS according to investigator assessment | Same as described for DFS per investigator assessment | Not performed | ||
SF-36 v2 |
| ████████████ ██████████ ██████ █████████ █████████ ██████████ █████ ███ █████████ ██ ████ ███████████ | █████████ ████████ ███████ ██ ██████ | Not performed |
BICR = blinded independent central review; CI = confidence interval; CNS-DFS = central nervous system disease–free survival; DFS = disease-free survival; eCRF = electronic case report form; HR = hazard ratio; ITT = intention to treat; NSCLC = non–small cell lung cancer; OS = overall survival; SF-36 v2 = Short Form (36) Health Survey version 2; vs. = versus.
aThis analysis was not in the sponsor’s statistical analysis plan but was requested by the review team to inform an appraisal of between-group differences.
Sources: ALINA Clinical Study Protocol version 6,47 ALINA Statistical Analysis Plan version 7,48 and sponsor’s Summary of Clinical Evidence.1
Analysis Populations
Analysis populations of the ALINA trial are summarized in Table 10.
Table 10: Analysis Populations of ALINA
Population | Definition | Application |
|---|---|---|
ITT | All randomized patients (stage IB [tumour ≥ 4 cm] to IIIA), whether or not the participant received the assigned treatment; participants grouped according to the treatment assigned at randomization by the IxRS | OS, DFS, CNS-DFS, SF-36 v2 |
Stage II to IIIA | All patients in the ITT population with stage II to IIIA NSCLC according to IxRS data | OS, DFS, CNS-DFS, SF-36 v2 |
Safety-evaluable | All patients who received at least 1 dose of study treatment; patients were assigned to treatment groups as treated, and all patients who received any dose of alectinib were included in the alectinib treatment group | Harms |
CNS-DFS = central nervous system disease–free survival; DFS = disease-free survival; ITT = intention to treat; IxRS = interactive voice or web-based response system; NSCLC = non–small cell lung cancer; OS = overall survival; SF-36 v2 = Short Form (36) Health Survey version 2.
Sources: ALINA Clinical Study Report,21 ALINA Clinical Study Protocol version 6,47 and the sponsor’s Summary of Clinical Evidence.1
Protocol Amendments and Deviations
In total, there were 7 versions of the clinical study protocol, including the original study protocol (issued on February 5, 2018) and 6 amendments (last amended on December 16, 2021). No major amendments were identified.
A higher proportion of patients in the alectinib group, compared to those in the chemotherapy group, caused major protocol deviations associated with study medication (11.5% versus 3.9%) and failing inclusion criteria (6.9% versus 3.1%). The details of major protocol deviations in the ALINA trial are presented in Table 11.
Table 11: Summary of Major Protocol Deviations in ALINA (ITT Population)
Protocol deviations | Alectinib (N = 130) | Chemotherapy (N = 127) |
|---|---|---|
Number of patients with at least 1 protocol deviation, n (%) | 46 (35.4) | 40 (31.5) |
Patient failed inclusion criteria | 9 (6.9) | 4 (3.1) |
ALK-positive disease | 1 (0.8) | 1 (0.8) |
Adequate renal function according to protocol | 2 (1.5) | 1 (0.8) |
Histologically confirmed stage IB to = stage IIIA NSCLC | 2 (1.5) | 1 (0.8) |
Pregnancy test not done within 3 days before first dose | 2 (1.5) | 1 (0.8) |
Use of contraception according to protocol | 2 (1.5) | 0 |
Patient met exclusion criteria | 0 | 2 (1.6) |
Any exclusion criteria for chemotherapy met | 0 | 2 (1.6) |
Medication related | 15 (11.5) | 5 (3.9) |
Continued treatment when should have discontinued | 2 (1.5) | 0 |
Received expired or quarantined study medication | 3 (2.3) | 0 |
Received incorrect dose of study medication | 8 (6.2) | 1 (0.8) |
Received incorrect study medication | 0 | 3 (2.4) |
Received prohibited concomitant medication | 1 (0.8) | 0 |
Treatment with prohibited procedure | 1 (0.8) | 1 (0.8) |
Procedural | 35 (26.9) | 34 (26.8) |
Contraception requirements not met | 1 (0.8) | 0 |
Delayed or nonreporting of SAE or AESI | 0 | 1 (0.8) |
Informed consent form amendment with new safety information not signed | 6 (4.6) | 8 (6.3) |
Missed disease assessment | 19 (14.6) | 23 (18.1) |
Omission of baseline assessment (not eligibility) | 3 (2.3) | 4 (3.1) |
Whole panel of lab assessment missed | 13 (10.0) | 9 (7.1) |
AESI = adverse event of special interest; ITT = intention to treat; NSCLC = non–small cell lung cancer; SAE = serious adverse event.
Source: ALINA Clinical Study Report.21
Results
Patient Disposition
A summary of patient disposition in the ALINA trial, as of June 26, 2023, is presented in Table 12. A total of 257 participants were randomized to either the alectinib group (n = 130) or the chemotherapy group (n = 127). The percentages of patients who discontinued from study were 5.4% for the alectinib group and 12.6% for the chemotherapy group. The percentages of patients who discontinued treatment were 14.1% for the alectinib group and 10.0% for the chemotherapy group; 6.3% of the patients in the alectinib group discontinued because of recurrence versus none for the patients in the chemotherapy group.
Table 12: Summary of Patient Disposition From ALINA
Patient disposition | Alectinib (N = 130) | Chemotherapy (N = 127) |
|---|---|---|
Screened, n | 1,642 | |
Randomized, n | 257 | |
Study ongoing, n (%) | 123 (94.6) | 111 (87.4) |
Discontinued study, n (%) | 7 (5.4) | 16 (12.6) |
Death | 2 (1.5) | 5 (3.9) |
Lost to follow-up | 0 | 1 (0.8) |
Protocol deviation | 0 | 1 (0.8) |
Withdrawal by patient | 5 (3.8) | 9 (7.1) |
Received treatment, n (%) | 128 (98.5) | 120 (94.5) |
Completed treatment, n (%)a | 84 (65.6) | 108 (90.0) |
Treatment ongoing, n (%)a | 26 (20.3) | 0 |
Discontinued treatment, n (%)a | 18 (14.1) | 12 (10.0) |
Adverse event | 7 (5.5) | 6 (5.0) |
Disease recurrence | 8 (6.3) | 0 |
Other | 0 | 1 (0.8) |
Physician decision | 0 | 1 (0.8) |
Protocol deviation | 2 (1.6) | 1 (0.8) |
Withdrawal by participants | 1 (0.8) | 3 (2.5) |
ITT population, n | 130 | 127 |
Stage II to IIIA subpopulation, n | 116 | 115 |
Safety-evaluable population, n | 128 | 120 |
ITT = intention to treat.
Note: Unless otherwise specified, the percentage referred to the proportions of the ITT population.
aProportion of the safety-evaluable population.
Sources: ALINA Clinical Study Report21 and the sponsor’s Summary of Clinical Evidence.1
Baseline Characteristics
The baseline characteristics listed in Table 13 are those most relevant to this review or assumed to affect the outcomes or interpretation of the study results. Overall, the median age of the ITT population in the ALINA trial was 56 years (range = 26 to 87), and most (76.3% [196 of 257]) were younger than 65 years. Of the total number of patients enrolled, 47.9% (123 of 257) were male, 55.6% (143 of 257) were Asian, and 41.6% (107 of 257) were white. According to the electronic case report forms, 10.1% (26 of 257) of patients had stage IB disease, 31.1% (80 of 257) had stage IIA disease, 3.9% (10 of 257) had stage IIB disease, and 54.9% (141 of 257) had stage IIIA disease. Most of the ITT population had a nonsquamous histology (96.5%, 248 of 257), of which 96% (238 of 248) were adenocarcinoma.
The alectinib group had more patients between 18 and 40 years old compared to the chemotherapy group (19.2% versus 10.2%, respectively), fewer patients aged older than 60 years (31.5% versus 40.9%), more females (57.5% versus 46.5%), and more patients who never used tobacco (64.6% versus 55.1%), as well as fewer with a history of tobacco use (31.5% versus 42.5%).
Table 13: Summary of Baseline Characteristics From ALINA
Characteristic | Alectinib (N = 130) | Chemotherapy (N = 127) |
|---|---|---|
Age, years | ||
Mean (SD) | 53.4 (12.5) | 56.6 (11.3) |
Median | 54.0 | 57.0 |
Minimum to maximum | 26, 80 | 33, 87 |
Age group, years, n (%) | ||
18 to 40 | 25 (19.2) | 13 (10.2) |
41 to 60 | 64 (49.2) | 62 (48.8) |
> 60 | 41 (31.5) | 52 (40.9) |
Sex, n (%) | ||
Male | 55 (42.3) | 68 (53.5) |
Female | 75 (57.7) | 59 (46.5) |
Race (eCRF), n (%) | ||
Asian | 72 (55.4) | 71 (55.9) |
Black or African American | 1 (0.8) | 0 |
White | 55 (42.3) | 52 (40.9) |
Unknown | 2 (1.5) | 4 (3.1) |
Weight (kg) at baseline | ||
Mean (SD) | 68.33 (16.05) | 70.96 (16.30) |
Median | 65.25 | 70.00 |
Minimum to maximum | 40.5 to 120.0 | 40.5 to 118.0 |
ECOG PS at baseline, n (%) | ||
0 | 72 (55.4) | 65 (51.2) |
1 | 58 (44.6) | 62 (48.8) |
Tobacco use history, n (%) | ||
Never | 84 (64.6) | 70 (55.1) |
Current | 5 (3.8) | 3 (2.4) |
Previous | 41 (31.5) | 54 (42.5) |
Time from initial diagnosis to randomization (months) | ||
n | 129 | 123 |
Mean (SD) | 2.21 (0.93) | 2.18 (1.28) |
Median | 2.04 | 1.94 |
Minimum to maximum | 0.6 to 7.0 | 0.4 to 13.1 |
Histology | ||
n | 130 | 127 |
Squamous | 6 (4.6) | 3 (2.4) |
Nonsquamous | 124 (95.4) | 124 (97.6) |
Initial diagnosis staging according to the AJCC 7th edition (eCRF) | ||
Stage IB | 17 (13.1) | 9 (7.1) |
Stage IIA | 38 (29.2) | 42 (33.1) |
Stage IIB | 5 (3.8) | 5 (3.9) |
Stage IIIA | 70 (53.8) | 71 (55.9) |
Initial diagnosis staging according to the AJCC 7th edition (IxRS) | ||
Stage IB | 14 (10.8) | 12 (9.4) |
Stage II | 47 (36.2) | 45 (35.4) |
Stage IIIA | 69 (53.1) | 70 (55.1) |
Primary tumour stage according to the AJCC 7th edition | ||
T1a | 30 (23.1) | 37 (29.1) |
T1b | 21 (16.2) | 22 (17.3) |
T2a | 59 (45.4) | 47 (37.0) |
T2b | 4 (3.1) | 10 (7.9) |
T3 | 15 (11.5) | 8 (6.3) |
T4 | 1 (0.8) | 3 (2.4) |
Regional lymph node stage, n (%) | ||
N0 | 21 (16.2) | 18 (14.2) |
N1 | 45 (34.6) | 43 (33.9) |
N2 | 64 (49.2) | 66 (52.0) |
Distant metastasis stage, n (%) | ||
M0 | 130 (100) | 127 (100) |
Prior surgical procedure, n (%) | ||
Lobectomy | 126 (96.9) | 117 (92.1) |
Sleeve lobectomy | 0 | 1 (0.8) |
Bilobectomy | 2 (1.5) | 5 (3.9) |
Pneumonectomy | 2 (1.5) | 4 (3.1) |
Time from last surgery to randomization (months) | ||
Mean (SD) | ████ ██████ | ████ ██████ |
Median | ████ | ████ |
Minimum to maximum | ████ ███ | ████ ███ |
AJCC = American Joint Committee on Cancer; ECOG PS = Eastern Cooperative Oncology Group Performance Status; eCRF = electronic case report form; IxRS = interactive voice or web-based response system; SD = standard deviation.
Sources: ALINA Clinical Study Report21 and the sponsor’s Summary of Clinical Evidence.1
Exposure to Study Treatments
Details on the extent of exposure to study treatments in the ALINA trial are summarized in Table 14.
Concomitant Medications
Details about commonly reported concomitant medications, which consisted of any medication received by the patient from 14 days before initiation of study drug to the study drug discontinuation visit, are shown in Table 15. Overall, as of June 26, 2023, the majority of patients in the ITT population received at least 1 concomitant medication (███████).
Table 14: Summary of Patient Exposure From ALINA (Safety-Evaluable Population)
Exposure | Alectinib (N = 128) | Chemotherapy (N = 120) | ||
|---|---|---|---|---|
Cisplatin-containing regimen (N = 119) | Carboplatin- containing regimen (N = 14) | Gemcitabine-pemetrexed-vinorelbine (N = 120) | ||
Treatment durationa (months) | ||||
Mean (SD) | 21.3 (6.3) | 2.0 (0.7) | 1.0 (0.6) | 2.2 (0.5) |
Median | 23.9 | 2.1 | 0.7 | 2.1 |
Minimum to maximum | 0 to 25 | 0 to 4 | 0 to 2 | 0 to 4 |
0 to ≤ 6 | 11 (8.6%) | — | — | — |
> 6 to ≤ 2 | 1 (0.8%) | — | — | — |
> 12 to ≤ 18 | 4 (3.1%) | — | — | — |
> 18 to ≤ 24 | 84 (65.6%) | — | — | — |
> 24 to ≤ 30 | 28 (21.9%) | — | — | — |
Dose intensityb (%) | ||||
Mean (SD) | 91.1 (14.8) | — | — | — |
Median | 99.4 | 100 | 100 | 100 |
Minimum to maximum | 47 to 100 | 86 to 101 | 83 to 100 | 91 to 101 |
Number of doses for alectinib or cycles for chemotherapy | ||||
Mean (SD) | 1,274.4 (380.7) | 3.6 (0.9) | 2.3 (0.8) | 3.8 (0.5) |
Median | 1,434.0 | 4.0 | 2.0 | 4.0 |
Minimum to maximum | 14 to 1,522 | 1 to 4 | 1 to 4 | 1 to 4 |
1 cycle | — | 8 (6.7%) | 2 (14.3%) | 3 (2.5%) |
2 cycles | — | 9 (7.6%) | 7 (50.0%) | 1 (0.8%) |
3 cycles | — | 5 (4.2%) | 4 (28.6%) | 8 (6.7%) |
4 cycles | — | 97 (81.5) | 1 (7.1%) | 108 (90.0%) |
Total cumulative dose (mg) for alectinib | ||||
Mean (SD) | 71,1029.30 (24,3018.85) | — | — | — |
Median | 834,300.00 | — | — | — |
Minimum to maximum | 8,400.0 to 91,3200.0 | — | — | — |
SD = standard deviation.
aTreatment duration is the date of the last study drug administration minus the date of the first study drug administration plus 1 day.
bDose intensity is the amount of study drug actually received divided by the expected amount to the time of the last administered dose.
Sources: ALINA Clinical Study Report21 and the sponsor’s Summary of Clinical Evidence.1
Table 15: Concomitant Medications in ALINA (ITT Population)
Concomitant medication | Alectinib (N = 130) | Chemotherapy (N = 127) |
|---|---|---|
Number of patients with at least 1 concomitant medication, n (%) | ███ ██████ | ███ ██████ |
█████████████████ | ██ ██████ | ███ ██████ |
██████████████ ████████████ | ██ ██████ | ███ ██████ |
████████ ███████████████ | ██ ██████ | ███ ████ |
█████ ███ ███████████ ██████ ████████ | ██ ██████ | ███ ██████ |
█████ ████████████ | ██ ██████ | ███ ██████ |
███████████ | ██ ██████ | ███ ██████ |
███████████████ | ██ ██████ | ███ ██████ |
██████████████ ██████████████ ████████ | ██ ██████ | ███ ██████ |
████████████████ ███ ██████████ ███████ | ██ ██████ | ███ ██████ |
███████████ ███ ██████████ ███████████ | ██ ██████ | ███ ██████ |
ITT = intention to treat.
Sources: ALINA Clinical Study Report21 and the sponsor’s Summary of Clinical Evidence.1
Subsequent Treatment
The summary of subsequent treatment in the ITT population of the ALINA trial is shown in Table 16. As of June 26, 2023, 21.4% of patients (55 of 257) received any subsequent follow-up anticancer systemic therapy after study treatment, among them 12.3% (16 of 130) were from the alectinib group and 30.7% (39 of 127) were from the chemotherapy group. Alectinib (including alectinib and alectinib hydrochloride) was the most commonly used drug by patients from both groups (3.8% [5 of 130] in the alectinib group and 22.8% [29 of 127] in the chemotherapy group).
In addition, 5.4% (14 of 257) received subsequent radiotherapy (3.8% [5 of 130] in the alectinib group versus 7.1% [9 of 127] in the chemotherapy group), with the brain the most common site (1.5% [2 of 130] in the alectinib group versus 3.9% [5 of 127] in the chemotherapy group), followed by the lymph nodes (1.5% [2 of 130] in the alectinib group versus 1.6% [2 of 127] in the chemotherapy group).
Subsequent cancer surgery was reported in 1.6% of patients (4 of 257) of the ITT population, of whom 0.8% (1 of 130) in the alectinib group underwent surgery at a location in bone, while 2.4% (3 of 127) in the chemotherapy group underwent surgery at locations reported as bone, brain, and lymph node (1 patient each).
Efficacy
Key efficacy results in the ALINA trial’s ITT population are presented in Table 17. The data cut-off date was June 26, 2023.
Table 16: Summary of Subsequent Treatment From ALINA (ITT Population)
Subsequent treatment | Alectinib (N = 130) | Chemotherapy (N = 127) |
|---|---|---|
Patients who received at least 1 subsequent anticancer systemic therapy, n (%) | 16 (12.3) | 39 (30.7) |
Alectinib | 5 (3.8) | 25 (19.7) |
Brigatinib | 4 (3.1) | 4 (3.1) |
Cisplatin | 4 (3.1) | 2 (1.6) |
Carboplatin | 4 (3.1) | 1 (0.8) |
Alectinib hydrochloride | 0 | 4 (3.1) |
Crizotinib | 0 | 4 (3.1) |
Pemetrexed | 3 (2.3) | 1 (0.8) |
Vinorelbine tartrate | 3 (2.3) | 0 |
Durvalumab | 1 (0.8) | 1 (0.8) |
Lorlatinib | 0 | 2 (1.6) |
Paclitaxel | 1 (0.8) | 1 (0.8) |
Ceritinib | 0 | 1 (0.8) |
Afatinib | 1 (0.8) | 0 |
Gimeracil; oteracil potassium; tegafur | 1 (0.8) | 0 |
Vinorelbine | 0 | 1 (0.8) |
Unspecified herbal and traditional medicine | 0 | 1 (0.8) |
Patients who received at least 1 subsequent radiotherapy, n (%) | 5 (3.8) | 9 (7.1) |
Patients who received at least 1 subsequent surgery, n (%) | 1 (0.8) | 3 (2.4) |
ITT = intention to treat.
Source: ALINA Clinical Study Report21 and the sponsor’s Summary of Clinical Evidence.1
Table 17: Summary of Key Efficacy Results From ALINA (ITT Population)
Efficacy outcome | Alectinib (N = 130) | Chemotherapy (N = 127) |
|---|---|---|
OS | ||
Patients with events, n (%) | 2 (1.5) | 4 (3.1) |
Patients alive, n (%) | 128 (98.5) | 123 (96.9) |
Median OS, months (95% CI) | NE (NE to NE) | NE (NE to NE) |
Stratified HR (95% CI) [P value] | 0.46 (0.08 to 2.52) [0.3603] | |
Probability of being alive at 2 years, % (95% CI) | █████ ██████ | █████ ██████ |
Patients remaining at risk at 2 years, n | 91 | 80 |
Difference in probability, % (95% CI) [P value] | ████ ██████ ██ █████ ████████ | |
Probability of being alive at 3 years, % (95% CI) | █████ ██████ | █████ ██████ |
Patients remaining at risk at 3 years, n | 43 | 45 |
Difference in probability, % (95% CI) [P value] | ████ ██████ ██ █████ ████████ | |
Probability of being alive at 4 years, % (95% CI) | █████ ██████ | █████ ██████ |
Patients remaining at risk at 4 years, n | ██ | ██ |
Difference in probability, % (95% CI) [P value] | ████ ██████ ██ ██████ ████████ | |
DFS according to investigator assessment | ||
Patients with events, n (%) | 15 (11.5) | 50 (39.4) |
Death | 0 (NR) | 1 (NR) |
Disease recurrence | 15 (NR) | 49 (NR) |
Patients without events (i.e., censored), n (%) | 115 (88.5) | 77 (60.6) |
Last tumour assessment | 112 (NR) | 69 (NR) |
Randomization | 3 (NR) | 8 (NR) |
Median DFS, months (95% CI), | NE (NE to NE) | 41.3 (28.5 to NE) |
Stratified HR (95% CI) [P value] | 0.24 (0.13 to 0.43) [< 0.0001] | |
Probability of being disease–free at 2 years, % (95% CI) | 93.64 (89.38 to 97.91) | 63.74 (54.59 to 72.90) |
Patients remaining at risk at 2 years, n | 74 | 55 |
Difference in probability, % (95% CI) [P value] | █████ ██████ ██ ██████ ██ ███████a | |
Probability of being disease–free at 3 years, % (95% CI) | 88.69 (81.76 to 95.63) | 53.97 (43.73 to 64.21) |
Patients remaining at risk at 3 years, n | 39 | 27 |
Difference in probability, % (95% CI) [P value] | █████ ██████ ██ ██████ ██ ███████ | |
Probability of being disease–free at 4 years, % (95% CI) | █████ ██████ | █████ ██████ |
Patients remaining at risk at 4 years, n | 10 | 11 |
Difference in probability, % (95% CI) [P value] | █████ ██████ ██ ██████ ████████ | |
CNS-DFS according to investigator assessment | ||
Patients with events (%) | 5 (3.8) | 18 (14.2) |
Death | ████ | ████ |
CNS disease recurrence | ██ | ██ ████ |
Patients without events (i.e., censored), n (%) | 125 (96.2) | 109 (85.8) |
Last tumour assessment | ███ ████ | ███ ████ |
Randomization | ███ | ████ |
Median time to CNS recurrence (95% CI), months | NE (NE to NE) | NE (NE to NE) |
Stratified HR (95% CI) | 0.22 (0.08 to 0.58) ████████a | |
Probability of being CNS disease–free at 2 years, % (95% CI) | 98.36 (96.11 to 100.00) | 85.82 (78.83 to 92.82) |
Patients remaining at risk at 2 years, n | 74 | 57 |
Difference in probability, % (95% CI) [P value] | █████ █████ ██ ██████ ████████ | |
Probability of being CNS disease–free at 3 years, % (95% CI) | 95.49 (90.99 to 99.99) | 79.73 (70.44 to 89.03) |
Patients remaining at risk at 3 years, n | 39 | 27 |
Difference in probability, % (95% CI) [P value] | █████ █████ ██ ██████ ████████ | |
Probability of being CNS disease–free at 4 years, % (95% CI) | █████ ██████ | █████ ██████ |
Patients remaining at risk at 4 years, n | ██ | ██ |
Difference in probability, % (95% CI) [P value] | █████ █████ ██ ██████ ████████ | |
SF-36 v2 mental component summary score | ||
Baseline | ||
Number of patients | ███ | ███ |
Mean (SE) | █████ ███████ | █████ ███████ |
Week 12 | ||
Number of patients | ███ | ██ |
Change from baseline, adjusted mean (SE) [95% CI] | 3.65 (0.861) [1.96 to 5.35] | −2.24 (0.917) [−4.05 to −0.43] |
Difference in adjusted means (95% CI) | 5.89 (3.41 to 8.37)a | |
SF-36 v2 physical component summary score | ||
Baseline | ||
Number of patients | ███ | ███ |
Mean (SE) | █████ ███████ | █████ ███████ |
Week 12 | ||
Number of patients | ███ | ██ |
Change from baseline, adjusted mean (SE) [95% CI] | 1.10 (0.564) [−0.02 to 2.21] | −0.40 (0.602) [−1.59 to 0.78] |
Difference in adjusted means (95% CI) | 1.50 (−0.13 to 3.13) | |
CI = confidence interval; CNS = central nervous system; CNS-DFS = central nervous system disease–free survival; DFS = disease-free survival; HR = hazard ratio; ITT = intention to treat; NE = not evaluable; NR = not reported; OS = overall survival; SE = standard error; SF-36 v2 = Short Form (36) Health Survey version 2.
aThese end points were not adjusted for multiple comparisons.
Sources: ALINA Clinical Study Report21 and the sponsor’s Summary of Clinical Evidence.1
Overall Survival
In the ALINA ITT population, the median duration of survival follow-up was 27.8 months (range = 0 to 55.4). As of the data cut-off date (June 26, 2023), OS was immature. Two OS events (1.5%) occurred in the alectinib group, and 4 OS events (3.1%) occurred in the chemotherapy group. The stratified HR for OS was 0.46 (95% CI, 0.08 to 2.52). The difference in the probability of being alive between alectinib and chemotherapy was █████ ██████ ██ █████ at 2 years, █████ ██████ ██ █████ at 3 years, and █████ ██████ ██ ██████ at 4 years. Median OS was not reached for either group. The Kaplan-Meier curves of the 2 treatment groups did not separate until after 30 months after randomization (Figure 1).
Figure 1: Kaplan-Meier Plot of Overall Survival in ALINA (ITT Population, Data Cut-off Date: June 26, 2023)
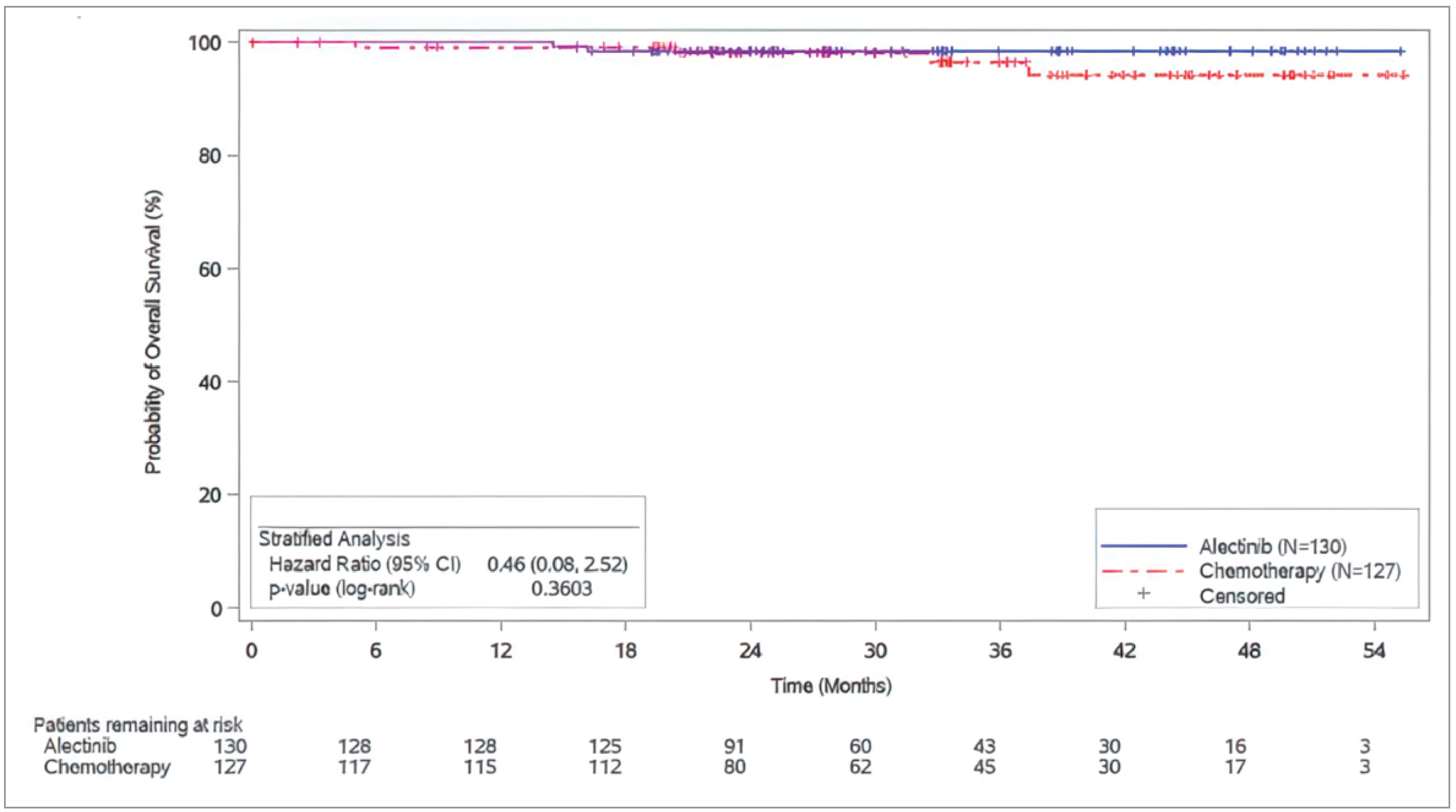
CI = confidence interval; ITT = intention to treat.
Source: ALINA Clinical Study Report.21
DFS According to Investigator Assessment
In the ALINA trial’s ITT population, the median duration of follow-up for DFS was 24.87 months (range = 0 to 55). As of June 26, 2023, 3.8% of the patients (15 of 130) in the alectinib group and 14.2% (50 of 127) in the chemotherapy group had DFS events. The stratified HR was 0.24 (95% CI, 0.13 to 0.43; P < 0.0001) in favour of alectinib, which met the prespecified stopping boundary (P ≤ 0.0077). The difference in the probability of being disease–free between alectinib and chemotherapy was ██████ ████ ███ █████ ██ ██████ at 2 years, ██████ ████ ███ █████ ██ ██████ at 3 years, and ██████ ████ ███ █████ ██ ██████ at 4 years. Median DFS was not reached in the alectinib group and was 41.3 months (95% CI, 28.5 to not evaluable) in the chemotherapy group. The Kaplan-Meier curves were separated at approximately 3 months after randomization in favour of alectinib (Figure 2).
Improvement in DFS according to investigator assessment in the subgroup classified by disease stage (i.e., stage IB versus stage II versus stage IIIA) was consistent with the results for the ITT population. The HR for DFS according to investigator assessment was 0.21 (95% CI, 0.02 to 1.84) for patients with stage IB disease, 0.24 (95% CI, 0.09 to 0.65) for patients with stage II disease, and 0.25 (95% CI, 0.12 to 0.53) for patients with stage IIIA disease. No formal testing for subgroup interaction was conducted.
A sensitivity analysis was used to assess DFS according to BICR in the ITT population as (Appendix 1). The stratified HR was 0.30 (95% CI, 0.17 to 0.54, ██████). The difference in the probability of being disease–free between alectinib and chemotherapy was ██████ ████ ███ █████ ██ ██████ at 2 years, ██████ ████ ███ █████ ██ ██████ at 3 years, and ██████ ████ ███ ████ ██ ██████ at 4 years. Median DFS was not reached in either group. ███ ███████████ ████████ ███████ ███ ███ ████████████ ██████████ ███ ███ ███ ████ ███ ██████████ ████████ ████ █ ████████ ███ ██ █████ ███ █████████████ ██████████ ██████████ ██ ████ ████████████ ███ ████ ██ ███ ████ ██ ████ ███████ ██████ ████ ███ █████ ████ ██████████ █████████ ███ ████████████ ████████ █ ███████████ ████ ██ █████ ███ ████████ ██ ███ █████████ █████ ███ █████ ██ ███ ████████████ ██████. Additional sensitivity analyses assessing the impact of missing disease assessments, stratification errors, and the Ukraine-Russia conflict has similar results as the primary analysis.
Figure 2: Kaplan-Meier Plot of DFS According to Investigator Assessment in ALINA (ITT Population, Data Cut-off Date: June 26, 2023)
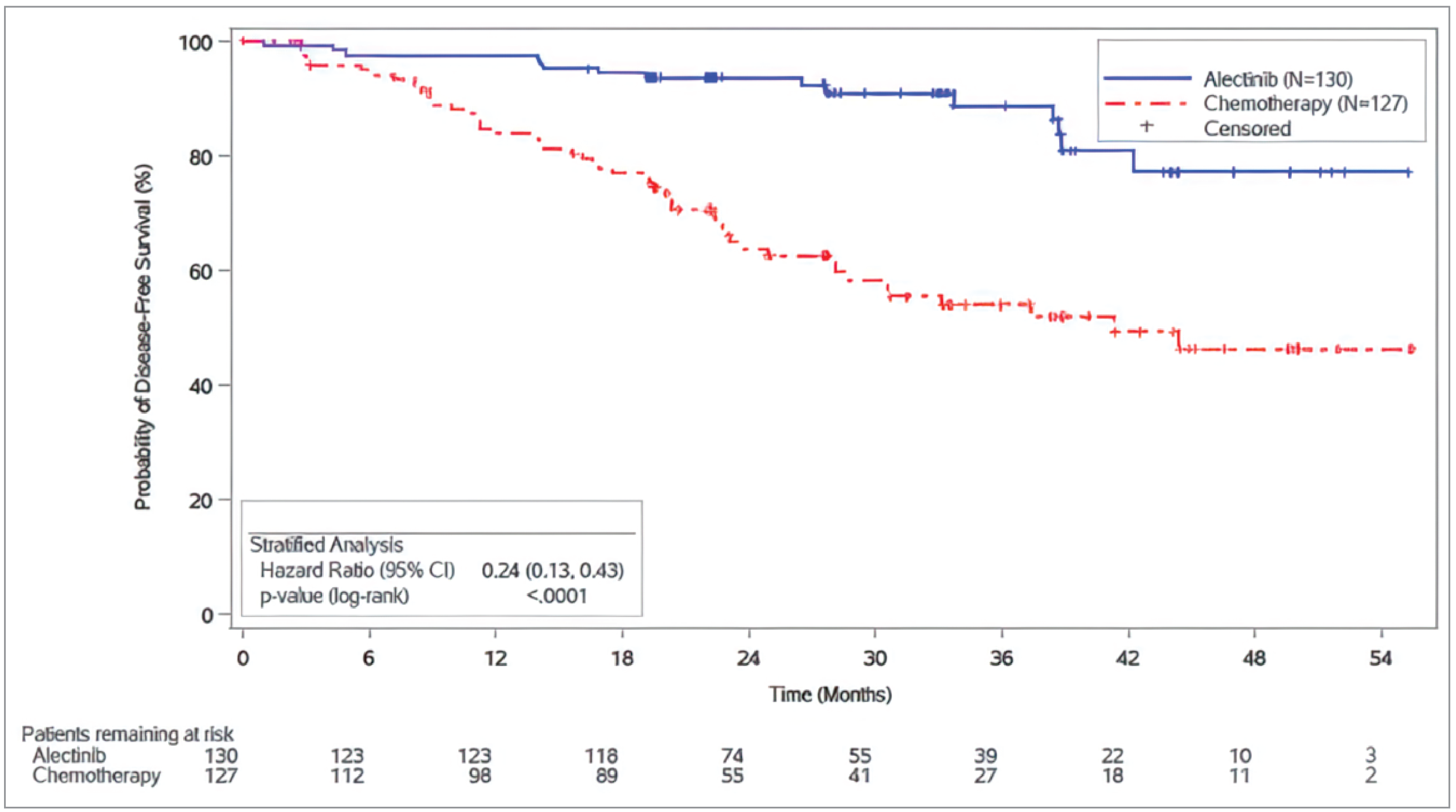
CI = confidence interval; DFS = disease-free survival; ITT = intention to treat.
Source: ALINA Clinical Study Report.21
CNS-DFS According to Investigator Assessment
In the ALINA trial’s ITT population, the median duration of follow-up for CNS-DFS was 25.07 months (range = 0 to 55.4). As of June 26, 2023, 11.5% of the patients (5 of 130) in the alectinib group and 39.4% (18 of 127) in the chemotherapy group had CNS-DFS events. The stratified HR was 0.22 (95% CI, 0.08 to 0.58), favouring the alectinib group. The difference in the probability of being CNS disease–free between alectinib and chemotherapy was ██████ ████ ███ ████ ██ ██████ at 2 years, ██████ ████ ███ ████ ██ ██████ at 3 years, and ██████ ████ ███ ████ ██ ██████ at 4 years. Median CNS-DFS was not reached for either group. The Kaplan-Meier curves are shown in Figure 3.
Figure 3: Kaplan-Meier Plot of CNS-DFS According to Investigator Assessment in ALINA (ITT Population, Data Cut-off Date: June 26, 2023)
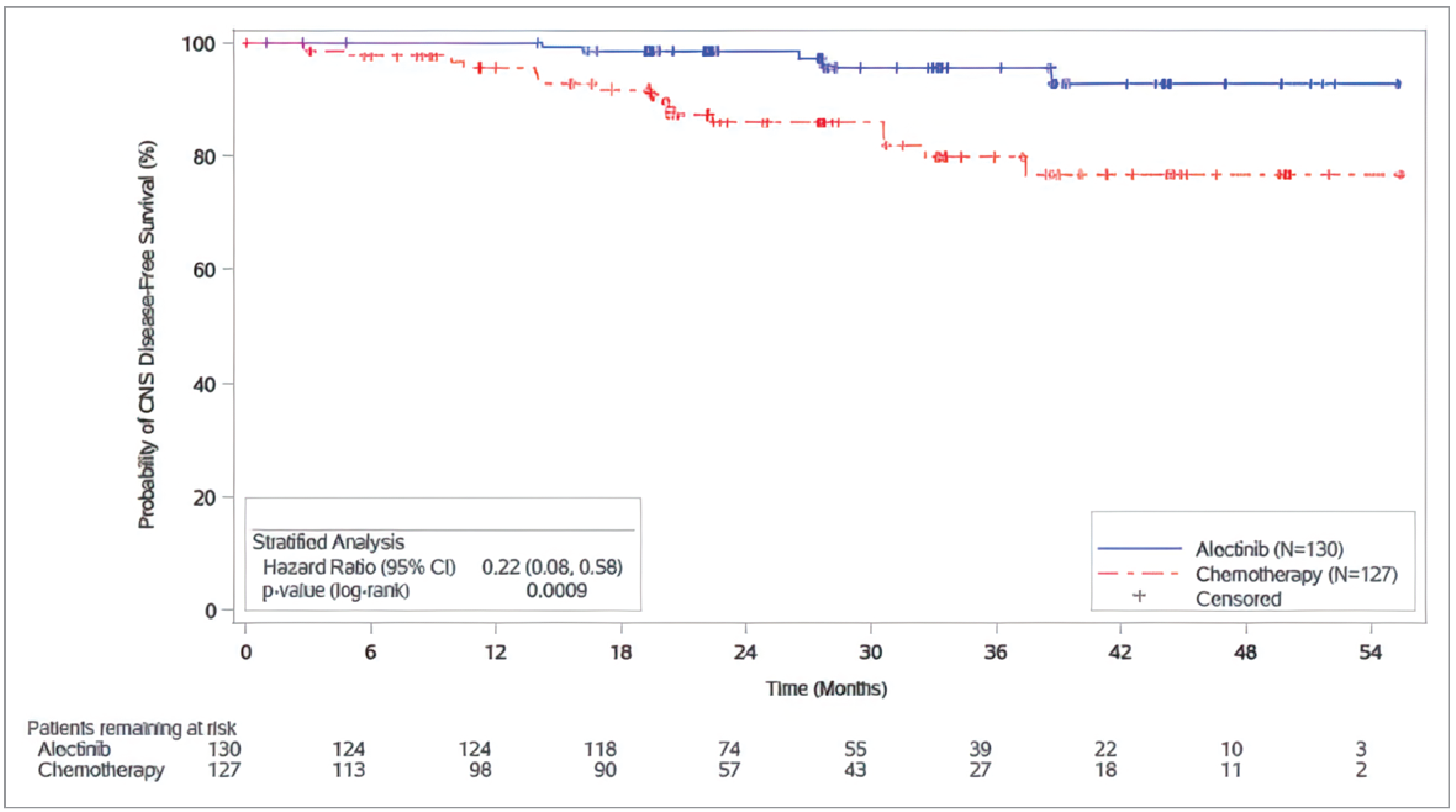
CI = confidence interval; CNS-DFS = central nervous system disease–free survival; ITT = intention to treat.
Source: ALINA Clinical Study Report.21
SF-36 v2 Mental Component Summary Score
The SF-36 v2 mental component summary scores range from 0 to 100, with a higher score indicating a better HRQoL. The ITT population included 130 and 127 patients in the alectinib and chemotherapy groups, respectively. At week 12, there were 122 patients in the alectinib group, and 106 patients in the chemotherapy group were expected to complete the instrument. Data from ███ patients in the alectinib group (accounting for ███ of the ITT population) and ██ patients (accounting for ███ of the ITT population) in the chemotherapy group contributed to the analysis.
In the alectinib group, the mean change from baseline at week 12 was 3.65 (95% CI, 1.96 to 5.35), indicating an improvement. However, no improvement was observed in the chemotherapy group at week 12 (mean change from baseline = −2.24; 95% CI, −4.05 to −0.43). The difference in mean change from baseline at week 12 between the alectinib group and the chemotherapy group was 5.89 (95% CI, 3.41 to 8.37).
SF-36 v2 Physical Component Summary Score
The SF-36 v2 physical component summary scores range from 0 to 100, with a higher score indicating a better HRQoL. The ITT population included 130 and 127 patients in the alectinib and chemotherapy groups, respectively. At week 12, 122 patients in the alectinib group and 106 patients in the chemotherapy group were expected to complete the instrument. Data from ███ patients in the alectinib group (accounting for ███ of the ITT population) and ██ patients (accounting for ███ of the ITT population) in the chemotherapy group contributed to the analysis.
In the alectinib group, the mean change from baseline at week 12 was 1.10 (95% CI, −0.02 to 2.21), indicating an improvement. However, no improvement was observed in the chemotherapy group at week 12 (mean change from baseline: −0.40; 95% CI, −1.59 to 0.78). The difference in mean change from baseline at week 12 between the alectinib group and the chemotherapy group was 1.50 (95% CI, −0.13 to 3.13).
Harms
Harms data from the ALINA trial are shown in Table 18. The data cut-off date was June 26, 2023. Among patients in the safety-evaluable population, the median duration of safety follow-up was 24.8 months (range = 1.1 to 26.2) for the alectinib group, and 3.7 months (range = 1.6 to 5.3) for the chemotherapy group. Duration of safety follow-up referred to the time from first study drug administration to the end of the AE reporting period which was the earliest among:
date of study completion or discontinuation
last treatment date + 28 days for alectinib or day 1 of last cycle + 21 days + 28 days for chemotherapy (28 days after end of last cycle of chemotherapy, i.e., 7 weeks after day 1 of last cycle)
the clinical cut-off date.
Adverse Events
The proportion of patients who had at least 1 AE in the alectinib group was slightly higher than that of patients in the chemotherapy group (98.4% versus 93.3%, respectively). Increased blood creatine phosphokinase (43.0%), constipation (42.2%), increased aspartate transaminase (41.4%), increased alanine transaminase (33.6%), and increased blood bilirubin (33.6%) were among the most common AEs in the alectinib group.
The proportions of patients who had at least 1 grade 3 to 5 AE were similar between the alectinib and chemotherapy groups (29.7% versus 30.8%, respectively). The most common grade 3 to 5 AE in the alectinib group was increased blood creatine phosphokinase (6.3%), followed by appendicitis (3.1%).
Serious Adverse Events
A higher percentage of patients in the alectinib group experienced SAEs compared to the patients in the chemotherapy group (13.3% versus 8.3%, respectively). The most common SAE in the alectinib group was appendicitis (3.1%).
Withdrawals Due to Adverse Events
Discontinuation of alectinib occurred in 5.5% of the patients in the alectinib group, which was lower than 12.5% in the chemotherapy group.
Mortality
Two deaths occurred in the alectinib group (1.6%) versus 5 in the chemotherapy group (4.2%).
Table 18: Summary of Harms Results From ALINA (Safety-Evaluable Population)
Harms | Alectinib (N = 128) | Chemotherapy (N = 120) |
|---|---|---|
AEs | ||
Total number of patients with at least 1 AE, n (%) | 126 (98.4) | 112 (93.3) |
Most common AEs reported in ≥ 20% patients in either treatment group, n (%) | ||
Nausea | 10 (7.8) | 87 (72.5) |
Constipation | 54 (42.2) | 30 (25.0) |
Vomiting | 9 (7.0) | 30 (25.0) |
Increased AST | 53 (41.4) | 6 (5.0) |
Increased blood creatine phosphokinase | 55 (43.0) | 1 (0.8) |
Increased ALT | 43 (33.6) | 11 (9.2) |
Increased blood bilirubin | 43 (33.6) | 1 (0.8) |
Increased blood alkaline phosphatase | 32 (25.0) | 4 (3.3) |
COVID-19 | 37 (28.9) | 1 (0.8) |
Decreased appetite | 7 (5.5) | 35 (29.2) |
Anemia | 30 (23.4) | 31 (25.8) |
Myalgia | 36 (28.1) | 2 (1.7) |
Grade 3 to Grade 5 AEs, n (%) | 38 (29.7) | 37 (30.8) |
Most common grade 3 to 5 AEs reported in ≥ 2% patients in either treatment group, n (%) | ||
Decreased neutrophil count | 0 | 12 (10.0) |
Increased blood creatine phosphokinase | 8 (6.3) | 1 (0.8) |
Decreased white blood cell count | 0 | 4 (3.3) |
Nausea | 0 | 5 (4.2) |
Appendicitis | 4 (3.1) | 0 |
Neutropenia | 0 | 10 (8.3) |
Asthenia | 0 | 3 (2.5) |
SAEs | ||
Total number of patients with SAEs, n (%) | 17 (13.3) | 10 (8.3) |
Most common SAEs reported in ≥ 2% patients in either treatment group, n (%) | ||
Appendicitis | 4 (3.1) | 0 |
Pneumonia | 3 (2.3) | 1 (0.8) |
Patients who discontinued treatment due to AEs | ||
Patients with any AE leading to discontinuation of treatment | 7 (5.5) | 15 (12.5) |
Death | ||
Patients who died, n (%) | 2 (1.6) | 5 (4.2) |
███████ ██████████ | █████ | █████ |
█████████ █████████ | █████ | █████ |
████████ | █████ | █████ |
███████ | █████ | █████ |
AE = adverse event; ALT = alanine aminotransferase; AST = aspartate aminotransferase; SAE = serious adverse event.
Source: ALINA Clinical Study Report.21
Critical Appraisal
Internal Validity
Randomization was performed using a central interactive voice or web-based response system and stratified based on disease stage (IB [tumours ≥ 4 cm] versus II versus IIIA) and race (Asian versus non-Asian) to minimize potential imbalances between the study groups that might bias the results. The review team noted that, compared with the chemotherapy group, a higher percentage of patients in the alectinib group were younger and female, with a better performance status and without a history of smoking at baseline, which indicated a possibly improved prognosis for patients in the alectinib group. The clinical experts consulted by the review team noted that this imbalance was small and not expected to significantly bias treatment-effect estimates. The review team, in agreement with the clinical experts, determined that such an imbalance may be caused by the relatively small sample size of the ALINA trial (N = 257), which may not enable full prognostic balance, but any bias introduced by the imbalance was likely trivial.
Because the ALITA was open-label, investigators and patients were aware of the assigned treatment. On the 1 hand, the review team recognized that it was not feasible to conduct blinding because of the nature of the interventions. On the other hand, DFS according to investigator assessment (the primary efficacy end point) was susceptible to the impact of detection bias because of the open-label design, although the review team determined that the risk of detection bias in DFS according to investigator assessment was low. First, the results of DFS according to investigator assessment were generally consistent with those of DFS according to BICR, although the magnitude of absolute between-group differences at relevant time points was somewhat smaller in the analyses of DFS according to BICR compared to investigator assessment. ███████ ███ ████████ ██ ███████████ ██████ █ ██████████ ████ █████████ ███████ ███ ████ ██ ██████████ ██████ █ ███████████ ████ ██ █████ ██ ███ █████████ █████ ███ █████ ██ ███ ████████████ ███████ The risk of performance bias because of the open-label study design could not be ruled out for SF-36 v2, a self-reported HRQoL outcome, or for subjective harms outcomes.
No major concerns were raised about protocol amendments and deviations in the ALINA trial. For each category of the concomitant medications, a higher percentage of patients in the chemotherapy group received concomitant treatment compared with that in the alectinib group. According to the clinical experts consulted by the review team, the difference in concomitant medications was in general reasonable and expected from a clinical perspective because patients treated with chemotherapy usually need more supportive medications. In terms of postrecurrence subsequent anticancer therapy, 12.3% of the patients in the alectinib group versus 30.7% in the chemotherapy group received a postrecurrence therapy. As a result, the effect of the difference in subsequent anticancer therapy on OS would be considered as a combination of the alectinib or chemotherapy in addition to the subsequent treatments. The clinical experts consulted by the review team also noted that the difference in postrecurrence subsequent treatments in general aligns with their clinical practice, and the difference may have reflected the differential efficacy in preventing DFS events between alectinib and chemotherapy. Overall, the review team determined that the risk of deviation from the intended interventions caused by concomitant medications or postrecurrence subsequent anticancer therapy was low.
Data on OS, reported up to 48 months in the ALINA trial, were immature at the current data cut-off time (June 26, 2023). Few OS events occurred in either the alectinib group (2 events) or the chemotherapy group (4 events). According to the clinical experts consulted by the review team, a follow-up of at least 60 months will likely be needed to detect a meaningful between-group difference in OS and allow for further understanding the treatment effects of alectinib on OS. The ALINA trial is ongoing, and the planned follow-up duration for survival follow-up analysis was about 60 months after enrolment of the last patient. Altogether, no definitive conclusion could be drawn based on the immature OS data as of June 26, 2023.
In the ALINA trial, DFS, not CNS-DFS, was adjusted for multiplicity. Both DFS and CNS-DFS were assessed at an interim analysis, resulting in a potential overestimate of the true magnitude of the difference between alectinib and chemotherapy.51 There were minor concerns with the internal validity of the results of DFS and CNS-DFS. The proportional hazards assumption for DFS and CNS-PFS was evaluated, with visual inspection of the Kaplan-Meier curves indicating that the assumption was met. The Kaplan-Meier curves began to separate at an early stage (around 3 months after randomization) and did not cross thereafter. Sensitivity analyses addressing missing scheduled tumour assessments were carried out for DFS according to investigator assessment and produced results similar to those of the primary analysis. However, the impact of missing data on DFS estimates because of loss to follow-up or dropout remained unclear because relevant information for the review team to make the judgment was not provided. Based on the patient disposition information, discontinuation of the study because of loss to follow-up and withdrawal by patients occurred among ████ ███████ of the alectinib group and ████ ████████ of the chemotherapy group. There was an imbalance between the 2 groups █████ ██████ █████. The review team determined that a potential bias because of missing outcome data could not be ruled out but may be small because of the small imbalance. The missing-data issue was also identified in HRQoL outcomes; the missingness was imbalanced between groups and relatively large in the chemotherapy group. For example, SF-36 v2 mental and physical component summary scores ███ out of 130 (███) patients in the alectinib group and ██ out of 127 (███) patients in the chemotherapy group were evaluated at week 12. The statistical model for HRQoL end points assumed that the data were missing at random; however, this assumption may not be plausible, and no sensitivity analyses were conducted to assess robustness of the findings to different missingness mechanisms.
External Validity
The clinical experts consulted by the review team noted that using adjuvant platinum-based chemotherapy as a comparator in the ALINA trial was appropriate given that adjuvant chemotherapy is the standard of care in the Canadian setting for adult patients. However, the clinical experts identified some differences in the regimen, dosing, and schedule of chemotherapy between the ALINA trial and clinical practice in Canada. The clinical experts noted that the difference was not a concern because regimens, dosing, and schedules of chemotherapy often change in clinical practice depending on patient conditions. According to the clinical experts, overall, the regimen, dosing, and schedule of the adjuvant platinum-based chemotherapy used in the ALINA trial were reasonably representative of those in the Canadian setting, and the results generated from the chemotherapy group in the ALINA trial were generalizable to the patient population in Canada.
In general, the clinical experts consulted by the review team considered the patient eligibility criteria used in the ALINA trial appropriate and reflective of the criteria they would use to select patients in Canada. However, the clinical experts also pointed out that the eligibility criteria are restrictive, and a small number who might benefit from alectinib may have been excluded. These patients included those with an ECOG PS of 2, those not eligible to receive a platinum-based hemotherapy regimen, those who had prior adjuvant radiotherapy, those who had prior systemic anticancer therapy, stage IIIA patients who received postoperative radiation therapy, patients with prior malignancies, patients who had a history of organ transplant, and patients who are HIV-positive.
The clinical experts consulted by the review team noted that the treatment duration of approximately 2 months for patients receiving chemotherapy was shorter than what they would expect, as 4 cycles of chemotherapy would take about 3 months. However, the clinical experts determined that shorter duration was likely not a concern as that most patients received 4 cycles of chemotherapy.
GRADE Summary of Findings and Certainty of the Evidence
Methods for Assessing the Certainty of the Evidence
In pivotal studies and RCTs identified in the sponsor’s systematic review, GRADE was used to assess the certainty of the evidence for outcomes considered most relevant to inform the expert committee deliberations, and a final certainty rating was determined as outlined by the GRADE Working Group:19,20
High certainty: We are very confident that the true effect lies close to that of the estimate of the effect.
Moderate certainty: We are moderately confident in the effect estimate — The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. We use the word “likely” for evidence of moderate certainty (e.g., “X intervention likely results in Y outcome”).
Low certainty: Our confidence in the effect estimate is limited — The true effect may be substantially different from the estimate of the effect. We use the word “may” for evidence of low certainty (e.g., “X intervention may result in Y outcome”).
Very low certainty: We have very little confidence in the effect estimate — The true effect is likely to be substantially different from the estimate of effect. We describe evidence of very low certainty as “very uncertain.”
Following the GRADE approach, evidence from RCTs started as high-certainty evidence and could be rated down for concerns related to study limitations (which refers to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias.
When possible, certainty was rated in the context of the presence of an important (nontrivial) treatment effect; if this was not possible, certainty was rated in the context of the presence of any treatment effect (i.e., the clinical importance is unclear). In all cases, the target of the certainty of evidence assessment was based on the point estimate and its location relative to the threshold for a clinically important effect (when a threshold was available) or to the null.
The reference points for the certainty of evidence assessment for OS, DFS according to investigator assessment, and CNS-DFS were set according to the presence of an important effect based on thresholds agreed upon by clinical experts consulted by the review team for this review. The reference points for the certainty of evidence assessment for SF-36 v2 mental and physical component summary scores were set according to the presence of an important effect based on minimal important difference estimates identified from the literature by the sponsor. For harm events, the certainty of evidence was summarized narratively.
Results of GRADE Assessments
Table 2 presents the GRADE summary of findings for alectinib versus platinum-based chemotherapy in patients with adult patients with stage IB (≥ 4 cm) to IIIA ALK-positive NSCLC.
Long-Term Extension Studies
No long-term extension studies were identified for this review.
Indirect Evidence
No indirect evidence was identified for this review.
Studies Addressing Gaps in the Systematic Review Evidence
No studies addressing gaps in the pivotal and RCT evidence were identified for this review.
Discussion
Summary of Available Evidence
One phase III, open-label RCT (ALINA, N = 257) was included in the sponsor-submitted SLR. The ALINA trial enrolled adult patients who had complete resection of histologically confirmed stage IB (tumour ≥ 4 cm) to stage IIIA ALK-positive NSCLC. Patients were randomized to the adjuvant alectinib group (n = 130) or the adjuvant platinum-based chemotherapy group (n = 127), stratified by disease stage (IB [tumours ≥ 4 cm] versus II versus IIIA) and race (Asian versus non-Asian). The primary objective of the ALINA trial was to evaluate the efficacy of alectinib relative to chemotherapy, measured by DFS according to investigator assessment. Other efficacy and safety outcomes included OS, CNS-DFS, and SF-36 v2 mental and physical component scores, as well as harms (i.e., AEs, SAEs, withdrawal, and deaths). The ALINA trial is ongoing, and the data cut-off date for this review was June 26, 2023. The median age of the ITT population in ALINA was 56 years (range = 26 to 87) and most were younger than 65 years (76.3% [196 of 257]). Of the 257 patients enrolled, 47.9% were male, 55.6% were Asian, and 41.6% were white. There were 10.1% patients (26 of 257) with stage IB disease, 31.1% (80 of 257) with stage IIA disease, 3.9% (10 of 257) with stage IIB disease, and 54.9% (141 of 257) with stage IIIA disease. Most of the ITT population had a nonsquamous histology (96.5%, 248 of 257), of which 96% (238 of 248) were adenocarcinoma.
Interpretation of Results
Efficacy
Patient group input emphasized that the key treatment goals for patients with early-stage NSCLC were prolonging life, stopping or delaying disease progression, and preventing metastasis in the brain, as well as improving HRQoL. These goals were captured in the ALINA trial by assessment of efficacy end points, including OS, DFS, CNS-DFS, and SF-36 v2 mental and physical component summary scores.
Current evidence suggests that OS, which was considered by the clinical experts consulted by the review team to be the most clinically important outcome, likely results in little to no difference in the probability of being alive at 48 months, compared to chemotherapy. However, currently available OS data were immature in the ALINA trial, precluding any conclusion on the efficacy of alectinib for OS relative to platinum-based chemotherapy. After a median follow-up duration of 27.8 months, only a small number of OS events occurred (2 in the alectinib group versus 4 in the chemotherapy group). According to the clinical experts, a follow-up of at least 5 years will likely be needed to detect a meaningful between-group difference in OS. The final survival follow-up analysis in ALINA is planned for approximately 5 years after the last patient is enrolled.
Both DFS and CNS-DFS were considered by the clinical experts consulted by the review team as clinically important outcomes for patients with early-stage NSCLC. The results of the primary efficacy end point in the ALINA trial — DFS according to investigator assessment (data cut-off date: June 26, 2023) — demonstrated that alectinib was likely more efficacious compared with platinum-based chemotherapy in terms of delaying disease recurrence. The HR for DFS according to investigator assessment was 0.24 (95% CI, 0.13 to 0.43; P < 0.0001), favouring alectinib. The differences in the probability of being disease–free between alectinib and chemotherapy at 24 and 48 months were █████ ████ ███ █████ ██ ██████ and ██████ ████ ███ █████ ██ ██████, respectively, in favour of alectinib. The clinical experts noted that the absolute effect estimates and entire confidence interval at each time point were clinically important. However, there was some uncertainty in the magnitude of benefit because the results were informed by an interim analysis with relatively few events, and the true effect may have been overestimated. When DFS was assessed by BICR, the HR and its 95% CI were similar. The magnitudes of the absolute between-group differences at 24 and 48 months were somewhat smaller but remained clinically important. The HRs for DFS according to investigator assessment were 0.21 (95% CI, 0.02 to 1.84) for patients with stage IB disease, 0.24 (95% CI, 0.09 to 0.65) for patients with stage II disease, and 0.25 (95% CI, 0.12 to 0.53) for those with stage IIIA disease. Although improvement in DFS according to investigator assessment was observed consistently in the prespecified subgroups by disease stage (i.e., IB versus II versus IIIA), caution is warranted in interpreting the results in stage IB because there were few patients in this group.
It was necessary to determine how well the benefits of DFS would translate into improvements in OS for patients with NSCLC, given that current OS evidence from the ALINA trial was immature. A 2023 study52 analyzed data from the Surveillance, Epidemiology, and End Results–Medicare database for 2007 to 2019 and investigated the patient-level correlation between DFS and OS in patients with newly diagnosed stage IB (tumour size ≥ 4 cm) to IIIA NSCLC who underwent surgery for primary NSCLC. It showed that postsurgery real-world DFS was significantly correlated with OS in patients with early-stage NSCLC (estimated normal scores rank correlation = 0.58; 95% CI, 0.54 to 0.62; P < 0.001).52 A reanalysis of meta-analyses of individual patient-level data involving 15,071 patients from RCTs suggested that, at the trial level, DFS is strongly correlated with OS in studies of adjuvant chemotherapy involving patients with NSCLC (R2 = 0.92; 95% CI, 0.88 to 0.95 in trials without radiotherapy and R2 = 0.99, 95% CI, 0.98 to 1.00 in trials with radiotherapy).53 However, the trial-level validation of surrogate end points is specific to the population and type of therapy under study.54 This evidence may therefore not be generalizable to treatment with alectinib, and the ability of DFS to predict the treatment effect on OS in this particular setting remains uncertain.
Similar to DFS, evidence on CNS-DFS was also considered of moderate certainty and suggested that alectinib likely results in an increase in the probability of being CNS disease–free at 24 and 48 months, compared to chemotherapy. The certainty of evidence was lower mainly because of imprecision as the lower bound of the 95% CI for the difference in the probability of being CNS disease–free at 24 and 48 months was below the 10% threshold that the clinical experts consulted by the review team suggested would be considered clinically important. Additionally, the small number of events at the interim analysis in the alectinib group adds uncertainty, which may have overestimated the true effect and affected the precision and stability of the treatment-effect estimates.
The certainty of evidence on HRQoL outcomes was determined to be low for an improvement in the SF-36 v2 mental component summary score and very low for the SF-36 v2 physical component summary score. The SF-36 v2 instrument is a generic measure of health status for a wide range of medical conditions55 and has been used by several studies56,57 to examine the change in HRQoL over time in patients with NSCLC. However, as a generic health status questionnaire, the SF-36 has the potential drawback of lacking condition-specificity for NSCLC. Information provided by generic HRQoL instruments may be less clinically useful, compared to disease-specific instruments, because generic instruments do not focus on any specific condition. There is evidence suggesting that generic quality-of-life instruments are less responsive than disease-specific instruments.58 In addition to the potential risk of performance bias associated with the open-label design and the subjective nature of the measure, there was also a potential risk of bias because of imbalanced missing data for both the SF-36 v2 mental and physical component summary scores. At the week 12 assessment, ███ out of 130 patients in the alectinib group and ██ out of 127 patients in the chemotherapy group were evaluated. The type of data missing (e.g., missing completely at random, missing at random, or missing not at random) and how the missingness in data would affect the HRQoL assessment remain unclear.
Harms
The proportions of patients who had at least 1 grade 3 to 5 AE were similar between the alectinib and chemotherapy groups (29.7% versus 30.8%, respectively). A slightly higher percentage of patients in the alectinib group experienced SAEs, compared to the chemotherapy group (13.3% versus 8.3%, respectively). The most common SAE in the alectinib group was appendicitis. According to the clinical experts consulted by the review team, appendicitis is not an expected side effect of treatment with alectinib, and the number of observed events was low. Discontinuation of assigned treatment occurred in 5.5% of the patients in the alectinib group and was lower than the 12.5% reported in the chemotherapy group. Two deaths occurred in the alectinib group (1.6%) versus 5 in the chemotherapy group (4.2%).
According to the clinical experts consulted by the review team, alectinib and chemotherapy have different safety profiles (i.e., cause different types of side effects) as their mechanisms of action are different. In other words, the clinical experts expected to see higher percentages of patients with alectinib-associated side effects (e.g., increased aspartate transaminase and myalgia) in the alectinib group and a higher percentage of patients who had chemotherapy-associated side effects in the chemotherapy group. The clinical experts reported that the overall safety profile of alectinib is consistent with their expectations for this drug.
Conclusion
The pivotal ALINA trial is an ongoing phase III, open-label RCT comparing the efficacy and safety of adjuvant alectinib and platinum-based chemotherapy in adult patients who had complete resection of histologically confirmed stage IB (tumour ≥ 4 cm) to stage IIIA ALK-positive NSCLC (according to the 7th edition of the AJCC/UICC staging manual). The ALINA trial demonstrated there were added clinical benefits of adjuvant alectinib in DFS and CNS-DFS in the ITT population. Compared to adjuvant chemotherapy, alectinib likely results in a clinically important increase in the probability of being disease–free at 24 and 48 months (moderate certainty of evidence) as well as in the probability of being CNS disease–free at 24 and 48 months (moderate certainty of evidence). The improvement in DFS was considered large by the clinical experts consulted by the review team and consistent across the prespecified subgroups by disease stage (i.e., IB versus II versus IIIA); however, few patients had stage IB disease. Uncertainty remains in the OS results because of the immaturity of the data. Compared to adjuvant chemotherapy, alectinib may improve SF-36 mental component summary scores, but the evidence regarding physical component summary scores is uncertain. According to the clinical experts consulted by the review team, the safety profile of alectinib is consistent with their expectations for this drug.
References
1.Clinical Evidence for the ALECENSARO® (alectinib) as adjuvant treatment following tumour resection in adult patients with stage IB (≥4 cm) to IIIA anaplastic lymphoma kinase (ALK)-positive non–small cell lung cancer [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Alectinib, 150 mg capsules, oral. Mississauga (ON): Hoffmann-La Roche Limited; 2024.
2.Alectinib (Alecensaro), 150 mg capsules, oral [product monograph]. Mississauga (ON): Hoffmann-La Roche Limited; June 27, 2024.
3.Canadian Cancer Society. Canadian Cancer Statistics 2023. Ottawa (ON): Government of Canada; 2023: https://cdn.cancer.ca/-/media/files/research/cancer-statistics/2023-statistics/2023_PDF_EN.pdf. Accessed 2024 Aug.
4.Sharma R. Mapping of global, regional and national incidence, mortality and mortality-to-incidence ratio of lung cancer in 2020 and 2050. Int J Clin Oncol. 2022;27(4):665-675. PubMed
5.Reck M, Rabe KF. Precision Diagnosis and Treatment for Advanced Non–small-Cell Lung Cancer. N Engl J Med. 2017;377(9):849-861. PubMed
6.Lababede O, Meziane MA. The Eighth Edition of TNM Staging of Lung Cancer: Reference Chart and Diagrams. Oncologist. 2018;23(7):844-848.
7.Detterbeck FC, Boffa DJ, Kim AW, Tanoue LT. The Eighth Edition Lung Cancer Stage Classification. Chest. 2017;151(1):193-203.
8.Goldstraw P, Chansky K, Crowley J, et al. The IASLC Lung Cancer Staging Project: Proposals for Revision of the TNM Stage Groupings in the Forthcoming (Eighth) Edition of the TNM Classification for Lung Cancer. J Thorac Oncol. 2016;11(1):39-51. PubMed
9.Canadian Cancer Society. Canadian Cancer Statistics: A 2020 special report on lung cancer. Ottawa (ON): Government of Canada; 2020: https://cdn.cancer.ca/-/media/files/cancer-information/resources/publications/2020-canadian-cancer-statistics-special-report/2020-canadian-cancer-statistics-special-report-en.pdf. Accessed 05 June 2024.
10.O'Reilly D, Botticella A, Barry S, et al. Treatment Decisions for Resectable Non–Small-Cell Lung Cancer: Balancing Less With More? American Society of Clinical Oncology Educational Book. 2023:43:e389950. PubMed
11.Subramanian J, Velcheti V, Gao F, Govindan R. Presentation and stage-specific outcomes of lifelong never-smokers with non–small cell lung cancer (NSCLC). J Thorac Oncol. 2007;2(9):827-830. PubMed
12.Shin SH, Lee H, Jeong BH, et al. Anaplastic lymphoma kinase rearrangement in surgically resected stage IA lung adenocarcinoma. J Thorac Dis. 2018;10(6):3460-3467. PubMed
13.Soda M, Choi YL, Enomoto M, et al. Identification of the transforming EML4-ALK fusion gene in non–small-cell lung cancer. Nature. 2007;448(7153):561-566. PubMed
14.Schütte W, Gütz S, Nehls W, et al. [Prevention, Diagnosis, Therapy, and Follow-up of Lung Cancer - Interdisciplinary Guideline of the German Respiratory Society and the German Cancer Society - Abridged Version]. Pneumologie. 2023;77(10):671-813. PubMed
15.Lassman AB, DeAngelis LM. Brain metastases. Neurol Clin. 2003;21(1):1-23, vii. PubMed
16.Griesinger F, Roeper J, Pöttgen C, Willborn KC, Eberhardt WEE. Brain metastases in ALK-positive NSCLC - time to adjust current treatment algorithms. Oncotarget. 2018;9(80):35181-35194. PubMed
17.NCCN Clinical Practice Guidelines in Oncology: Non–small Cell Lung Cancer. Vol Version 1. Plymouth Meeting (PA): National Comprehensive Cancer Network; 2023.
18.Pignon JP, Tribodet H, Scagliotti GV, et al. Lung adjuvant cisplatin evaluation: a pooled analysis by the LACE Collaborative Group. J Clin Oncol. 2008;26(21):3552-3559. PubMed
19.Balshem H, Helfand M, Schünemann HJ, et al. GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol. 2011;64(4):401-406. PubMed
20.Santesso N, Glenton C, Dahm P, et al. GRADE guidelines 26: informative statements to communicate the findings of systematic reviews of interventions. J Clin Epidemiol. 2020;119:126-135. PubMed
21.Clinical Study Report: BO40336. A Phase III, open-label, randomized study to evaluate the efficacy and safety of adjuvant alectinib versus adjuvant platinum-based chemotherapy in patients with completely resected StageIB (tumors ≥4 cm) to Stage IIIA anaplastic lymphoma kinase-positivenon–small-cell lung cancer. [internal sponsor's report]. Mississauga (ON): Hoffmann-La Roche Limited 2023.
22.Drug Reimbursement Review sponsor submission: Alectinib, 150 mg capsules, oral [internal sponsor's package]. Mississauga (ON): Hoffmann-La Roche Limited; 2024.
23.Birring SS, Peake MD. Symptoms and the early diagnosis of lung cancer. Thorax. 2005;60(4):268-269. PubMed
24.Ellison LF, Saint-Jacques N. Five-year cancer survival by stage at diagnosis in Canada. Health Rep. 2023;34(1):3-15. PubMed
25.Shaw AT, Yeap BY, Mino-Kenudson M, et al. Clinical features and outcome of patients with non–small-cell lung cancer who harbor EML4-ALK. J Clin Oncol. 2009;27(26):4247-4253. PubMed
26.Chia PL, Mitchell P, Dobrovic A, John T. Prevalence and natural history of ALK positive non–small-cell lung cancer and the clinical impact of targeted therapy with ALK inhibitors. Clin Epidemiol. 2014;6:423-432. PubMed
27.Ho C, Lefresne S, Liberman M, et al. Lung Cancer in Canada. J Thorac Oncol. 2019;14(7):1128-1133. PubMed
28.Mori M, Hayashi H, Fukuda M, et al. Clinical and computed tomography characteristics of non–small cell lung cancer with ALK gene rearrangement: Comparison with EGFR mutation and ALK/EGFR-negative lung cancer. Thoracic Cancer. 2019;10(4):872-879. PubMed
29.Beckles MA, Spiro SG, Colice GL, Rudd RM. Initial Evaluation of the Patient With Lung Cancer: Symptoms, Signs, Laboratory Tests, and Paraneoplastic Syndromes. Chest. 2003;123:97S-104S. PubMed
30.Polanco D, Pinilla L, Gracia-Lavedan E, et al. Prognostic value of symptoms at lung cancer diagnosis: a three-year observational study. J Thorac Dis. 2021;13(3):1485-1494. PubMed
31.Smit E, Moro-Sibilot D, Carpeno Jde C, et al. Cisplatin and carboplatin-based chemotherapy in the first-line treatment of non–small cell lung cancer: Analysis from the European FRAME study. Lung Cancer. 2016;92:35-40. PubMed
32.PrCISPLATIN injection BP: 1 mg / mL (50 mg and 100 mg cisplatin per vial) [Product Monograph]. Kirkland (QC): Pfizer Canada ULC 2018.
33.PrVinorelbine Injection, USP: 10 mg/mL vinorelbine (as vinorelbine tartrate) [product monograph]. Etobicoke (ON): Mylan Pharmaceuticals ULC 2014.
34.PrPEMETREXED: 100 mg or 500 mg pemetrexed per vial [Product Monograph]. Toronto (ON): APOTEX INC.; 2016.
35.PrGemcitabine for Injection: 1 g and 2 g gemcitabine (as gemcitabine hydrochloride) per vial [Product Monograph]. Kirkland (QC): Accord Healthcare Inc.; 2020.
36.PrCARBOPLATIN injection; BP: 10 mg / mL (50 mg, 150 mg, 450 mg, 600 mg of carboplatin per vial) [Product Monograph]. Kirkland (QC): Pfizer Canada ULC 2019.
37.Melosky B, Blais N, Cheema P, et al. Standardizing biomarker testing for Canadian patients with advanced lung cancer. Current Oncology. 2018;25(1):73-82. PubMed
38.Ionescu DN, Stockley TL, Banerji S, et al. Consensus Recommendations to Optimize Testing for New Targetable Alterations in Non–small Cell Lung Cancer. Curr Oncol. 2022;29(7):4981-4997. PubMed
39.Cutz JC, Craddock KJ, Torlakovic E, et al. Canadian anaplastic lymphoma kinase study: a model for multicenter standardization and optimization of ALK testing in lung cancer. J Thorac Oncol. 2014;9(9):1255-1263. PubMed
40.Melosky B, Agulnik J, Albadine R, et al. Canadian consensus: inhibition of ALK-positive tumours in advanced non–small-cell lung cancer. Curr Oncol. 2016;23(3):196-200. PubMed
41.Hoffmann-La Roche Limited response to August 6, 2024, 2024, Request for additional information regarding Alectinib review [internal additional sponsor's information]. Mississauga (ON): Hoffmann-La Roche Limited 2024.
42.Solomon BJ, Ahn JS, Dziadziuszko R, et al. LBA2 ALINA: Efficacy and safety of adjuvant alectinib versus chemotherapy in patients with early-stage ALK+ non–small cell lung cancer (NSCLC). Ann Oncol. 2023;34:S1295-S1296.
43.Ahn JS, Wu Y-L, Dziadziuszko R, et al. Efficacy and safety of adjuvant alectinib vs platinum-based chemotherapy in patients from Asia with resected, early-stage ALK+ NSCLC: a subanalysis of ALINA. ESMO Asia; 2023; Singapore, Republic of Singapore.
44.Barlesi F, Solomon BJ, Ahn JS, et al. Alectinib vs Chemotherapy in Non-Asian Patients with Resected ALK+ Non–small Cell Lung Cancer from the ALINA trial. IASLC 2023 North America Conference on Lung Cancer (NACLC); Dec 1-3, 2023; Chicago, Illinois.
45.Solomon BJ, Ahn JS, Barlesi F, et al. ALINA: A phase III study of alectinib versus chemotherapy as adjuvant therapy in patients with stage IB–IIIA anaplastic lymphoma kinase-positive (ALK+) non–small cell lung cancer (NSCLC). ASCO; 2019; Chicago, Illinois.
46.Wu Y-L, Dziadziuszko R, Ahn Jin S, et al. Alectinib in Resected ALK-Positive Non–Small-Cell Lung Cancer. N Engl J Med. 2024;390(14):1265-1276. PubMed
47.Clinical Study Protocol version 6: BO40336. A Phase III, Open-Label, Randomized Study To Evaluate The Efficacy And Safety Of Adjuvant Alectinib Versus Adjuvant Platinum-Based Chemotherapy In Patients With Completely Resected Stage Ib (Tumors >= 4 cm) To Stage IIIa Anaplastic Lymphoma Kinase-Positive Non–small-Cell Lung Cancer. [internal sponsor's report]. Mississauga (ON): Hoffmann-La Roche Limited; 2021.
48.Statistical Analysis Plan version 7: BO40336. A Phase III, Open-Label, Randomized Study To Evaluate The Efficacy And Safety Of Adjuvant Alectinib Versus Adjuvant Platinum-Based Chemotherapy In Patients With Completely Resected Stage Ib (Tumors >= 4 cm) To Stage IIIa Anaplastic Lymphoma Kinase-Positive Non–small-Cell Lung Cancer [internal sponsor's report]. Mississauga (ON): Hoffmann-La Roche Limited; 2021.
49.Maruish ME. User's Manual for the SF-36v2 Health Survey. Johnson (RI): Quality Metric Incorporated; 2011.
50.Jenkinson C, Stewart-Brown S, Petersen S, Paice C. Assessment of the SF-36 version 2 in the United Kingdom. J Epidemiol Community Health. 1999;53(1):46-50. PubMed
51.Bassler D, Briel M, Montori VM, et al. Stopping Randomized Trials Early for Benefit and Estimation of Treatment Effects: Systematic Review and Meta-regression Analysis. JAMA. 2010;303(12):1180-1187. PubMed
52.West H, Hu X, Zhang S, et al. Evaluation of disease-free survival as a predictor of overall survival and assessment of real-world burden of disease recurrence in resected early-stage non–small cell lung cancer. J Manag Care Spec Pharm. 2023;29(7):749-757. PubMed
53.Mauguen A, Pignon JP, Burdett S, et al. Surrogate end points for overall survival in chemotherapy and radiotherapy trials in operable and locally advanced lung cancer: a re-analysis of meta-analyses of individual patients' data. Lancet Oncol. 2013;14(7):619-626. PubMed
54.End points used in relative effectiveness assessment of pharmaceuticals Surrogate End points. Diemen (NL): European network for Health Technology Assessment; 2013: https://www.eunethta.eu/wp-content/uploads/2018/01/Surrogate-End points.pdf. Accessed 2024 Jul.
55.Pompili C, Koller M, Velikova G. Choosing the right survey: the lung cancer surgery. J Thorac Dis. 2020;12(11):6892-6901. PubMed
56.Majem M, Goldman JW, John T, et al. Health-Related Quality of Life Outcomes in Patients with Resected Epidermal Growth Factor Receptor-Mutated Non–small Cell Lung Cancer Who Received Adjuvant Osimertinib in the Phase III ADAURA Trial. Clin Cancer Res. 2022;28(11):2286-2296. PubMed
57.Fukai R, Nishida T, Sugimoto H, et al. Perioperative Evaluation of the Physical Quality of Life of Patients with Non–small Cell Lung Cancer: A Prospective Study. Cancers (Basel). 2024;16(8). PubMed
58.Wiebe S, Guyatt G, Weaver B, Matijevic S, Sidwell C. Comparative responsiveness of generic and specific quality-of-life instruments. J Clin Epidemiol. 2003;56(1):52-60. PubMed
59.Hoffmann-La Roche Limited response to May 17, 2024, Request for additional information regarding Alectinib review [internal additional sponsor's information]. Mississauga (ON): Hoffmann-La Roche Limited 2024.
Appendix 1: Detailed Outcome Data
Please note that this appendix has not been copy-edited.
Table 19: According to BICR From ALINA (ITT Population; Sensitivity Analysis)
Efficacy outcome | Alectinib (N = 130) | Chemotherapy (N = 127) |
|---|---|---|
DFS according to BICR | ||
████████ ████ ███████ █ ███ | ██ ██████ | ██ ██████ |
█████ | ████ | ████ |
███████ ██████████ | ██ ████ | ██ ████ |
████████ ███████ ███████ █ ███ | ███ ██████ | ██ ██████ |
██████ ███ ████ ████ ██████ | █████ ███ | █████ ███ |
██████████ ██ ████ ███ ██ ██████ | ████ █████ ██ █████ ██ ███ | |
███████████ ██ █████ ████████████ | █████ ███ | █████ ███ |
████████ ███████ ███████ █ ███ | ██████ | ██████ |
████████ ███████ ███████ █ ███ | █████ ███ | |
████████ ███████ ███████ █ ███ | █████ ███ | █████ ███ |
████████ ███████ ███████ █ ███ | ██████ | ██████ |
████████ ███████ ███████ █ ███ | █████ ███ | |
████████ ███████ ███████ █ ███ | █████ ███ | █████ ███ |
████████ ███████ ███████ █ ███ | ██████ | ██████ |
████████ ███████ ███████ █ ███ | █████ █████ ██ ██████ ███ | |
BICR = blinded independent central review; CI = confidence interval; DFS = disease-free survival; ITT = intent to treat; NE = not evaluable; NR = not reported.
Source: Sponsor’s response to request for additional information.59
Pharmacoeconomic Review
Abbreviations
AE
adverse event
AJCC
American Joint Committee on Cancer
BIA
budget impact analysis
ChT
platinum-based chemotherapy
CNS
central nervous system
DFS
disease-free survival
ICER
incremental cost-effectiveness ratio
IPD
independent patient-level data
ITT
intention to treat
LY
life-year
NSCLC
non–small cell lung cancer
OS
overall survival
QALY
quality-adjusted life-year
SLR
systematic literature review
UICC
Union for International Cancer Control
WTP
willingness to pay
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Alectinib (Alecensaro), 150 mg oral capsule |
Indication | For adjuvant treatment following tumour resection for patients with stage IB (tumours ≥ 4 cm) to IIIA (according to the AJCC/UICC staging manual, 7th edition) ALK-positive NSCLC |
Health Canada approval status | NOC |
Health Canada review pathway | Priority review, Project Orbis |
NOC date | June 27, 2024 |
Reimbursement request | As adjuvant treatment following tumour resection in adult patients with stage IB (≥ 4 cm) to IIIA (according to the AJCC/UICC staging manual, 7th edition) ALK-positive NSCLC |
Sponsor | Hoffmann-La Roche Limited |
Submission history | Previously reviewed: Yes Indication: Locally advanced or metastatic ALK-positive NSCLC with CNS metastases Recommendation date: May 4, 2017 Recommendation: Do not reimburse Indication: Locally advanced or metastatic ALK-positive NSCLC (second line) Recommendation date: March 29, 2018 Recommendation: Reimburse with clinical criteria and/or conditions Indication: Locally advanced or metastatic ALK-positive NSCLC (first line) Recommendation date: July 25, 2018 Recommendation: Reimburse with clinical criteria and/or conditions |
AJCC = American Joint Committee on Cancer; CNS = central nervous system; NOC = Notice of Compliance; NSCLC = non–small cell lung cancer; UICC = Union for International Cancer Control.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Semi-Markov model |
Target population | Adult patients with stage IB (≥ 4 cm) to IIIA (according to the AJCC/UICC staging manual, 7th edition) ALK-positive NSCLC, following tumour resection |
Treatment | Alectinib as adjuvant treatment |
Dosage regimen | 600 mg twice daily (total daily dose of 1,200 mg) for 24 months |
Submitted price | Alectinib: $44.28 per 150 mg capsule |
Submitted treatment cost | Annual drug acquisition cost of $129,372 per patient 28-day drug acquisition cost of $9,918 per patient |
Comparator | Platinum-based ChT:
|
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs, LYs |
Time horizon | Lifetime (40 years) |
Key data source | ALINA trial; data cut-off date: June 26, 2023 (ITT population). |
Submitted results | Alectinib was dominant compared with ChT (−$2,454 in incremental costs and 3.54 incremental QALYs) |
Key limitations |
|
CDA-AMC reanalysis results |
|
AJCC = American Joint Committee on Cancer; ChT = platinum-based chemotherapy; DFS = disease-free survival; ICER = incremental cost-effectiveness ratio; ITT = intention to treat; LY = life-year; NSCLC = non–small cell lung cancer; OS = overall survival; QALY = quality-adjusted life-year; UICC = Union for International Cancer Control.
Conclusions
Evidence from the ongoing phase III, open-label, randomized ALINA trial comparing the efficacy and safety of alectinib and platinum-based chemotherapy (ChT) revealed added clinical benefits of adjuvant alectinib in disease-free survival (DFS) among adult patients who had complete resection of histologically confirmed stage IB (tumour ≥ 4 cm) to stage IIIA ALK-positive non–small cell lung cancer (NSCLC) as defined by the 7th edition of the American Joint Committee on Cancer (AJCC) and Union for International Cancer Control (UICC) staging manual (all further references in this review to staging use definitions from this manual). Specifically, the Clinical Review found that alectinib likely results in an increase in the probability of being disease-free at 24 and 48 months compared to ChT, with moderate certainty of evidence. The Clinical Review further noted that it is not yet clear whether DFS benefits will translate to improved overall survival (OS) as the interim analysis (which had a data cut-off date of June 26, 2023, and median follow-up at 27.8 months) is too early for an effect to be observed. Clinical experts consulted by the review team also noted that a longer follow-up time would be required to determine the OS benefit of alectinib relative to ChT.
As part of its base-case reanalysis, the review team assembled by CDA-AMC adopted alternative parametric survival extrapolations of DFS for alectinib and ChT, assumed that 90% of patients who are disease-free 5 years after treatment initiation and 95% of patients who are disease-free 10 years after treatment initiation would be considered cured, assumed treatment would begin to wane at 28 months and end at 60 months, used pooled trial data to inform the type of first disease recurrence, and applied health state–specific utility values.
The review team’s base-case results align with those of the sponsor’s submitted analysis, indicating that alectinib is cost-effective at a willingness-to-pay (WTP) threshold of $50,000 per quality-adjusted life-year (QALY) gained, relative to ChT. In the base case, adjuvant treatment with alectinib was associated with an incremental cost-effectiveness ratio (ICER) of $37,154 per QALY gained compared to ChT ($87,506 in incremental costs and 2.36 incremental QALYs). The estimated ICER was driven by the selection of alternative distributions for extrapolating DFS, and assumptions about treatment waning. The base-case results rely on patients treated with alectinib experiencing an OS benefit of 3.9 life-years (LYs) compared to those treated with ChT.
The cost-effectiveness of alectinib was sensitive to assumptions about the persistence of long-term treatment effect and cure among patients who remain disease-free, for which evidence is pending. Assuming no further effect beyond treatment discontinuation (i.e., 24 months) increased the ICER for alectinib to $107,457 per QALY gained compared to ChT. By assuming a lower proportion of patients with NSCLC (65%) would be cured after remaining disease-free for 10 years, which aligns with published literature, following complete primary tumour resection, the ICER for alectinib increased to $55,735 per QALY gained relative to ChT. Given this clinical uncertainty, price reductions may be required to achieve cost-effectiveness at a WTP threshold of $50,000 per QALY gained.
The review team was unable to address limitations related to the sponsor’s inflexible modelling approach, which forces the assumption of hazard proportionality for DFS and time-invariant extrapolations across all postprogression health states and complicates assessment of their impacts on the cost-effectiveness of alectinib. Given the extent of limitations associated with the sponsor’s submitted model, considerable uncertainty remains in the cost-effectiveness results. Moreover, when comparing the duration of follow-up in the ALINA trial to the model’s time horizon (55 months versus 40 years), it is important to note that the majority of the QALY and LY benefits (70% and 75%, respectively) realized by patients treated with alectinib in the CDA-AMC base case accrued in the posttrial period of the model on the basis of extrapolation. In the absence of long-term evidence, the comparative impact of alectinib on DFS and OS relative to ChT remains highly uncertain. Should the long-term effectiveness of alectinib be lower than predicted, the ICER would be higher than the review team’s base case, requiring price reductions to achieve cost-effectiveness.
Input Relevant to the Economic Review
This section summarizes feedback from the patient groups, clinician groups, and drug plans that participated in this review.
Two patient groups, the Ontario Lung Association and Lung Cancer Canada, provided input for this review. Information was collected from respondents in Canada and other countries through surveys and included patients with experience with alectinib. Overall, patients’ disease experiences were influenced by the physical symptoms associated with lung cancer (e.g., fatigue, shortness of breath, and cough), the psychosocial effect associated with fear of death and poor disease prognosis (e.g., anxiety, distress, depression), and the adverse side effects of treatment with chemotherapy and radiation (e.g., nausea, vomiting, neuropathy, and lung injury). The most important outcomes for patients included delaying disease progression and achieving long-term remission, with the ultimate objective of improving survival; experiencing minimal side effects from treatments; preserving independence to minimize the burden on caregivers; and maintaining an optimal quality of life. The current standard of treatment for patients with resectable ALK-positive NSCLC is surgical resection, followed by adjuvant chemotherapy. Survey respondents treated with alectinib reported the drug successfully extended progression-free survival, reduced the risk of recurrence, and diminished the need for traditional systemic therapies that have limited efficacy and severe side effects.
Registered clinician input was received from 2 groups: Lung Cancer Canada and the Ontario Health (Cancer Care Ontario) Drug Advisory Committee. According to clinician input, the current pathway of care includes surgical resection and adjuvant platinum doublet chemotherapy. There is an unmet need because of the high recurrence rates experienced with adjuvant chemotherapy, as well as the high degree of brain tropism with no known modifiable risk factors associated with the disease. Patients are typically young and otherwise healthy and have limited treatment options beyond chemotherapy. Clinician input noted that patients would have the option of adjuvant alectinib or chemotherapy followed by alectinib in clinical practice. Clinician input noted that alectinib provided clear and significant DFS and central nervous system (CNS) disease relapse benefit over the platinum doublet control arm.
Drug plans participating in this review noted considerations related to treatment eligibility. Specifically, they expressed concerns regarding re-treatment with downstream ALK inhibitors, provided that disease recurrence is 6 months or more from the last dose of adjuvant alectinib. Drug plans also expressed concerns surrounding preferences on re-treatment with alectinib versus other ALK inhibitors (e.g., lorlatinib). Drug plans further noted that carboplatin plus paclitaxel was excluded as a treatment option for ChT, but it may be relevant in this treatment setting. Finally, drug plans asked whether patients who are currently receiving adjuvant chemotherapy should be eligible to switch to adjuvant alectinib.
Several of these concerns were addressed in the sponsor’s model:
DFS and OS were included in the model.
Subsequent treatment following disease recurrence after the last dose of adjuvant alectinib was modelled by the sponsor.
Costs and utility decrements related to adverse events (AEs) were included in the model.
The review team was unable to address 2 concerns raised in input:
The exclusion of adjuvant carboplatin plus paclitaxel as an option for ChT could not be addressed.
The sponsor’s model did not capture the impact of treatment on CNS disease relapse.
Economic Review
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted a cost-utility analysis of alectinib as adjuvant therapy after complete tumour resection compared with ChT.1 The model population comprised adult patients with completely resected stage IB (tumour size ≥ 4cm) to IIIA ALK-positive NSCLC. The target population aligns with the reimbursement request and the population in the ALINA pivotal trial. The modelled cohort aligns with the Health Canada indication, as the conditionality on tumour resection effectively excludes patients with stage IV NSCLC.
Alectinib is available as 150 mg oral capsules.2 The recommended dosage of alectinib is 600 mg (four 150 mg capsules) taken twice daily for 24 months, for a total daily dose of 1,200 mg.2 The submitted price of alectinib is $44.28 per capsule, or $9,918 per 28-day cycle.1 The comparator for this analysis was a ChT regimen administered once every 3 weeks for 4 cycles, based on the control arm of the ALINA trial. Patients receiving ChT could receive 1 of 3 cisplatin-based regimens (cisplatin plus vinorelbine, cisplatin plus gemcitabine, or cisplatin plus pemetrexed) but could substitute carboplatin for cisplatin if required. The drug acquisition cost per administration of ChT ranged from $712 (cisplatin plus vinorelbine) to $4,765 (carboplatin plus pemetrexed) based on the regimen received.1
Outcomes of interest included QALYs and LYs. The economic evaluation was conducted over a lifetime horizon of 40 years, from the perspective of the Canadian public health care payer. Discounting at 1.5% per year was applied for both costs and outcomes, and a cycle length of 1 month was used with a half-cycle correction applied.
Model Structure
The sponsor submitted a semi-Markov model consisting of 8 health states: “DFS,” “nonmetastatic recurrence (treatment and no treatment),” “metastatic recurrence (first-line: treatment and no treatment),” “metastatic recurrence (second-line: treatment and no treatment)” and “death.”1 All patients start in the DFS health state, receiving either alectinib or ChT, and can experience disease recurrence (nonmetastatic or metastatic) or death or remain disease-free. Patients experiencing nonmetastatic recurrence could receive either treatment with chemoradiotherapy or no treatment. Patients experiencing metastatic recurrence must progress through first-line health states before becoming eligible to progress to second-line health states. Those experiencing first-line metastatic occurrence either received no treatment or were assumed to receive 1 of 4 treatment options (alectinib, crizotinib, brigatinib, or lorlatinib). The choice of treatment varied based on whether a relapse occurred within 24 months of alectinib treatment. Those experiencing second-line metastatic occurrence received either no treatment or ChT. Patients could transition to the death state from any other health state.
Model Inputs
The target population was based on the intention-to-treat (ITT) population of the phase III, active-controlled, open-label ALINA trial, which enrolled adult patients with stage IB to IIIA NSCLC who have undergone tumour resection and whose tumours have ALK gene rearrangement mutations (N = 257; mean age = 56 years; proportion male = 47.9%).3
Clinical efficacy parameters were derived from the ITT patient population of the ALINA trial (data cut-off date: June 26, 2023). The ALINA trial compared the efficacy and safety of alectinib with those of ChT. Parametric survival modelling was used to estimate health-state transition probabilities from the observed survival data from the ALINA trial (median follow-up = 28 months; maximum follow-up = 55 months) to extrapolate transition probabilities for the entire lifetime horizon of the model (40 years). The sponsor’s parametric survival analysis pooled patients across study arms and included a covariate to model the effect of adjuvant alectinib on the location parameters of each distribution (i.e., a dependent parametric model with a treatment coefficient). The sponsor did not conduct the survival analysis independently by treatment arm, claiming that it cannot be concluded that the proportional hazards assumption was violated. The selection of parametric survival models used in the base case was based on the clinical plausibility of long-term survival projections and a visual inspection of model fit, as well as Akaike and Bayesian information criteria of statistical fit.1
A log-logistic curve was selected in the sponsor’s base case to parameterize investigator-assessed DFS based on the best statistical fit. The sponsor further assumed that the 95% and 100% of patients achieving 5 and 10 years of DFS, respectively, were considered cured.1 For patients assumed to be cured at 5- and 10-year landmarks, their risk of mortality was assumed to be equivalent to that of the general population. Additionally, the sponsor assumed no waning of treatment effect with alectinib, implying that the benefit associated with alectinib would be maintained throughout the lifetime horizon of the model.
The proportion of patients experiencing nonmetastatic recurrence, metastatic recurrence, and death were based on the number of events occurring in each treatment arm of the ALINA trial.3 All subsequent efficacy data and parameters used to inform disease progression after first recurrence were based on studies identified in the sponsor’s systematic literature review (SLR).1,4-7 The sponsor used published literature to digitize the reported Kaplan-Meier estimates of progression-free survival (PFS) and OS for nonmetastatic and metastatic recurrence to obtain synthetic independent patient-level data (IPD). Parametric survival modelling was used to extrapolate transition probabilities over the lifetime model horizon. It was assumed that all outcomes would follow an exponential distribution across all health states and treatments. The model adjusts any mortality rates generated from the projected curves that exceed the age- and sex-matched general population mortality rates to be equal to general population mortality. Patients were assumed to discontinue adjuvant treatment if they experienced recurrence or death, or for reasons including intolerable toxicity and AEs. Discontinuation rates for both treatment arms were informed by the ALINA trial.3 Discontinuation after recurrence for reasons other than disease progression or death were treatment-specific and based on sources identified in the SLR to inform efficacy after recurrence.4-7
Rates of AEs for both alectinib and ChT were informed by the ALINA trial and modelled as a monthly probability. Only grade 3 or 4 AEs in either treatment arm were included in the analysis, as they were assumed to be treatment-related and require intervention. Treatment-specific AEs after recurrence were informed by the same sources used to inform discontinuation and efficacy, with the exception of ChT in the nonmetastatic setting, which was informed by the ALINA trial.4-7
Health-state utility values in the model were informed by data from 5-Level EQ-5D questionnaires collected in the ALINA trial and estimated through a Canada-specific algorithm and linear mixed-effects model.1 Utility values were treatment-specific to alectinib and ChT, and dependent on whether patients were on or off treatment (Table 9). Published literature was used to inform utility values for patients after experiencing nonmetastatic and metastatic recurrences.8
Costs included those for drug acquisition, subsequent treatment, administration, health state and disease management, AEs, ALK testing, and end-of-life care. Drug acquisition costs and subsequent treatment costs were taken from DeltaPA.9 Administration costs were included for oral treatments (i.e., physician visit to obtain prescription and dispensing costs) and IV treatments (based on chair time). Chair time was calculated using the infusion time for each regimen, the number of treatment cycles for each regimen, and the cost per hour of chair time reported in the literature and by Cancer Care Ontario.10,11 Health state and disease management costs included those for radiotherapy and follow-up care for routine CT scans.12,13 Nonmetastatic recurrence costs included those for hospitalization, oncologist and physician visits, and nontherapeutic costs related to X-rays, bronchoscopy, thoracoscopy, MRI, and PET scans.14 Metastatic recurrence costs, which included those for complex continuing care, hospitalization, inpatient admissions, emergency department visits, inpatient rehabilitation, homecare services, and surgery, were sourced from the literature.15 Costs associated with AE management were sourced from the Canadian Institute for Health Information Patient Cost Estimator.16 The sponsor assumed that immunohistochemistry testing was the primary method of choice in current Canadian clinical practice. End-of-life costs were sourced from published literature.17
Summary of Sponsor’s Economic Evaluation Results
The sponsor conducted its base case via a probabilistic sensitivity analysis with 5,000 iterations. The deterministic and probabilistic results were similar. The probabilistic findings are presented in the following section.
Base-Case Results
The results of the sponsor’s probabilistic base-case analysis suggested that adjuvant alectinib was associated with an additional 3.54 QALYs at a decreased cost of $2,454 relative to ChT (Table 3). Alectinib was dominant over ChT; that is, the use of adjuvant alectinib resulted in an additional health benefit at a decreased cost.
The sponsor’s analysis predicted that alectinib was associated with a longer duration of life compared with ChT (5.94 incremental LYs). Based on the sponsor’s results, the near entirety (92%) of the incremental QALYs for alectinib accrued in the DFS health state. Furthermore, given the duration of the ALINA trial (median follow-up = 28 months) in contrast to the model’s lifetime horizon (40 years), it is important to note that the majority (84%) of incremental QALYs realized by patients receiving alectinib relative to ChT were derived during the period beyond which there are no observed trial data (i.e., the extrapolated period).
The probability that alectinib was cost-effective at a threshold of $50,000 per QALY gained was 99%.
Table 3: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER vs. ChT ($ per QALY) |
|---|---|---|---|---|---|
ChT | 417,946 | Reference | 8.99 | Reference | Reference |
Alectinib | 415,470 | −2,454 | 12.53 | 3.54 | Dominant |
ChT = platinum-based chemotherapy; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; vs. = versus.
Note: The submitted analysis is based on publicly available prices of comparator treatments.
Source: Sponsor’s pharmacoeconomic submission.1
Additional results from the sponsor’s submitted economic evaluation base case are presented in Appendix 3.
Sensitivity and Scenario Analysis Results
The sponsor conducted several scenario analyses, including alternative extrapolations informing DFS, alternative cure assumptions, inclusion of a treatment-waning effect, inclusion of excess mortality among cured patients, ALK-testing assumptions, varying proportions of patients initiating treatment upon recurrence, alternative time horizons, applying alectinib utility values to both treatment arms, and increasing health care costs. Across all scenario analyses, alectinib remained dominant or resulted in an ICER ranging from $1,928 to $20,781 per QALY gained. The ICER was most sensitive to the introduction of a treatment-waning effect beginning at 32 months, resulting in an ICER of $20,781 per QALY gained.
The sponsor conducted a scenario analysis from a societal perspective that included additional costs associated with productivity losses. In this analysis, alectinib remained dominant relative to ChT. The results were similar to the sponsor’s base-case analysis using a health care payer perspective.
Appraisal of the Sponsor’s Economic Evaluation
We identified several key limitations to the sponsor’s analysis that have notable implications on the economic analysis:
The proportional hazards assumption for DFS is improbable. The sponsor selected a dependent log-logistic model to extrapolate DFS for alectinib and ChT (a single parametric model with treatment coefficient). In using a dependent proportional hazards model to characterize the comparative efficacy of alectinib and ChT alone, the sponsor assumed that the hazard rates for alectinib and ChT would remain proportional across the lifetime horizon of the model. The review team noted that it is not ideal to apply a dependent model to Kaplan-Meier data for 2 treatment groups when the pivotal trial assesses the efficacy of treatments with different mechanisms of action and, consequently, different patterns of event hazards over time.18 Alectinib represents a different class of therapy with a unique mechanism of action relative to ChT. It is therefore unlikely that a single functional form will effectively match both alectinib and ChT, and a dependent model may introduce bias to the estimated DFS in both arms, given that the parameter estimates inevitably deviate from the best fit for either arm.19
The sponsor presented a log-cumulative hazard plot for DFS and conducted a Schoenfeld test to assess the proportionality assumption for DFS between patients treated with alectinib and those treated with ChT alone in the ALINA trial. The review team noted that, because Schoenfeld residuals represent the difference between the observed and expected values of the treatment covariate at each failure time point, they should be flat and centred around zero to support proportionality. The Schoenfeld residuals presented in the sponsor’s report indicate a nonlinear pattern and departure from zero over time. In addition, the sponsor conducted a Schoenfeld residual test that was not statistically significant. There is therefore insufficient evidence to reject the null hypothesis of no difference between the hazards of alectinib and those of ChT.
Issues with the Schoenfeld residual test in terms of statistical hypothesis testing have been acknowledged elsewhere,20 prompting recommendations to employ multiple methods concurrently to assess hazards proportionality.21-23 Specifically, the P value of the Schoenfeld residual test is influenced by sample size, meaning a large sample size could yield high significance with minimal assumption violation, whereas a small sample size could result in a nonsignificant apparent violation of the assumption. Moreover, as Schoenfeld residual tests are often not sufficiently powered to detect differences between the observed and expected values, the absence of evidence (i.e., a nonstatistically significant test) does not conclusively prove hazards proportionality. Given that the Schoenfeld residual test yielded inconclusive results, assuming proportionality in the within-trial period is not supported by evidence.
Finally, the assessments submitted by the sponsor do not inform how the pattern of event hazards between patients treated with alectinib and those treated with ChT may evolve in the extrapolated period. According to the CDA-AMC Methods and Guidelines for Extrapolating Clinical Evidence Within Economic Evaluations,24 the relevance of constant proportional hazards over the modelled lifetime horizon should be considered, rather than only the short-term clinical trial period. The assumption of proportional hazards is unlikely to persist in the context of the lifetime horizon.25 This becomes particularly pertinent when considering heterogeneous study populations, for which the relative treatment effects may vary based on patient characteristics, leading to a situation in which proportional hazards cannot be maintained because of the evolving characteristics of the surviving population over time.19 Consequently, assuming hazard proportionality and employing a dependent model with a covariate adjusting for treatment effect is unsuitable for extrapolating DFS.
We could not address this limitation because of the structure of the model and the sponsor’s decision to exclude independently fitted parametric distributions from the submitted model.
The impact of alectinib on long-term DFS is highly uncertain. The sponsor used parametric modelling to extrapolate DFS beyond the observable time points in the ALINA trial (the median follow-up period for the ITT population is 28 months and the maximum follow-up period is 55 months) to a lifetime horizon of 40 years. The parametric distribution chosen by the sponsor (in addition to other modelling assumptions, such as excluding treatment waning, the subsequent limitation applies) resulted in an incremental gain of 4.99 QALYs in the DFS health state among patients treated with alectinib, which exceeds the total incremental QALYs accrued over the total model time horizon of 3.54 QALYs. This is because alectinib resulted in incremental QALY losses across all postprogression health states because of more patients receiving ChT occupying the postprogression health state compared with patients receiving alectinib. The gains in predicted incremental QALYs accrued through extrapolation. Notably, 84% of the total incremental QALYs were accrued by patients from the time period beyond which there are no observed clinical data (i.e., the extrapolated period).
The sponsor selected parametric distributions based on goodness-of-fit criteria, visual inspection, and clinical plausibility, following guidance from the National Institute for Health and Care Excellence Decision Support Unit.26 However, while the review team agreed that models should be compared based on their statistical fit, this pertains only to the observed trial period, not to the extrapolation period. The weight given to the comparative fit of alternative parametric models to the observed data depends on the extent to which extrapolation is required and the degree of censoring present. Considering the short duration of available trial data relative to the extrapolation period, the clinical plausibility of the predicted long-term DFS associated with alectinib is highly uncertain. Clinical experts consulted for this review confirmed that, although the ALINA trial findings concerning DFS appeared favourable and clinically important, the magnitude and durability of such a benefit were highly uncertain in the absence of longer-term evidence. Clinical experts indicated that the predicted DFS for alectinib, based on the log-normal distribution, was clinically plausible.
We selected the log-normal distribution to extrapolate the long-term DFS for alectinib and ChT alone.
We performed a scenario analysis to explore the impact of using the log-logistic distribution to extrapolate DFS for alectinib.
The impact of alectinib on long-term OS and modelling of treatment after first recurrence is highly uncertain. The sponsor’s base case predicts a survival advantage with alectinib compared to ChT (an incremental gain of 5.94 LYs). As noted in the Clinical Review, uncertainty remains in the OS results (very low certainty of evidence) as very few OS events occurred within a median follow-up duration of 27.8 months, which was considered inadequate by the clinical experts consulted by the review team. The clinical experts indicated that it is uncertain whether delayed disease recurrence (reflected by DFS as observed in the ALINA trial), will translate to gains in OS.
Furthermore, additional uncertainty is associated with the predicted OS for alectinib because of the modelling approach adopted by the sponsor. Data informing disease progression after first recurrence were not collected in the ALINA trial, and therefore OS data identified in the sponsor’s SLR were used in the model and extrapolated to the lifetime horizon.1 Studies identified in the SLR did not allow for access to IPD, and the sponsor therefore digitized reported Kaplan-Meier estimates and transformed PFS and OS estimates to synthetic IPD. The sponsor selected an exponential distribution to model OS across all health states and treatments (e.g., alectinib, crizotinib, brigatinib, lorlatinib, ChT, and no treatment), making the estimated transition probabilities time-invariant. As noted by the sponsor, this restriction is not appropriate from a statistical or clinical standpoint and the subsequent analysis may incorrectly model the amount of time that patients remain in these health states after disease progression. The predicted incremental gain in LYs associated with alectinib is therefore highly uncertain, given the limitations of the immature OS data observed in the ALINA trial, the lack of available long-term efficacy data for alectinib and comparators, and the sponsor’s modelling approach when extrapolating OS.
We were unable to address this limitation because of the structure of the sponsor’s model.
The assumptions regarding a cure are highly uncertain. The model assumed that 95% and 100% of patients who remain disease-free for 5 years and 10 years, respectively, are considered cured and not at risk of a DFS event. This was based on clinical expert input obtained by the sponsor indicating that patients who remain disease-free for 5 years could be considered cured, but up to 5% of them may still experience recurrence. The sponsor referenced previous CDA-AMC reviews for adjuvant treatments in NSCLC, noting that the goal of treatment is maximizing the chance of a cure.27,28 These reviews indicate that the 5-year DFS is considered the gold-standard metric of treatment success and serves as a landmark time point for assessing a cure.27,28 The clinical experts consulted for this review confirmed that the assumption of a cure within a proportion of disease-free patients to be appropriate in the context of NSCLC, given that the therapeutic target following surgical resection is curative. However, the clinical experts indicated that the cure assumptions proposed by the sponsor were overly optimistic, particularly regarding the assumed cure fraction at the 10-year landmark (100%). The review team acknowledged the uncertainty regarding the risk of late recurrence that patients with NSCLC may experience beyond the 5-year landmark for DFS. Furthermore, evidence points to the magnitude of the late-recurrence risk in patients who remain recurrence-free 10 years after resection, which demonstrates that the recurrence-free probability can vary between 65% and 89%.29
We adjusted the cure assumption to reflect clinical expert input that 90% of patients be considered cured if disease-free at year 5 and 95% of patients be considered cured if disease-free at year 10.
We performed a scenario analysis to explore the impact of assuming a 65% cure fraction at the 10-year landmark, consistent with the literature.
The durability of treatment effect is highly uncertain. The sponsor assumed no waning of the treatment effect for alectinib. In the submitted model, patients remaining on treatment experienced the treatment effect of alectinib indefinitely. This assumption implies that the treatment effect of alectinib will persist for 38 years after discontinuation (in patients who are not cured). The clinical experts consulted for this review indicated that they are unaware of evidence supporting this assumption and that it is plausible for treatment-effectiveness to wane earlier than assumed by the sponsor. The clinical experts also indicated that a 5-year follow-up would be necessary to observe meaningful differences in the treatment effect between alectinib and ChT, rendering the current trial’s follow-up duration insufficient. In the absence of evidence to support the long-term effectiveness of alectinib, the review team assumed treatment would begin to wane at the median follow-up time observed in the alectinib arm of the ALINA trial (i.e., 27.8 months) and last until year 5. That is, the treatment effect of alectinib would continue to be experienced for approximately 3 years after treatment discontinuation. A high degree of uncertainty remains, and, according to Methods and Guidelines for Extrapolating Clinical Evidence Within Economic Evaluations,24 including waning of a treatment effect is appropriate where long-term clinical data are lacking.
In the CDA-AMC reanalysis, treatment-effect waning begins at 27.8 months and ends at 60 months.
Considering the limited duration of trial data, in circumstances where treatment is assumed to have a continued effect on event rates postdelivery, it is necessary to investigate assumptions regarding the persistence of long-term treatment effects.24 The review team performed 2 scenario analyses: 1 that assumes no waning of treatment effect (i.e., indefinite relative effectiveness) and another that assumes treatment-effect waning following discontinuation of alectinib (i.e., after 24 months). Although each is improbable, these proposed scenarios offer upper- and lower-bound estimates to examine the impact of treatment-effect waning on the cost-effectiveness of alectinib.
The distribution of patients with disease recurrence who have nonmetastatic and metastatic recurrence is uncertain. Based on data from the ALINA trial, the sponsor estimated the proportion of patients who experience nonmetastatic and metastatic recurrence using treatment-specific data, citing notable differences across treatment arms according to the clinical experts consulted by the sponsor. This distribution was applied for the entire lifetime horizon of the submitted model. In doing so, the model assumed that most patients who received alectinib develop nonmetastatic recurrence as the first DFS event (64%), while most patients who receive ChT develop metastatic recurrence as the first DFS event (54%). The review team noted the absence of formal statistical testing regarding the sites of disease recurrence and the observed differences between patients treated with alectinib and patients treated with ChT. Furthermore, there is no evidence to inform how the proportion of recurrences evolve throughout the duration of patients’ lifetimes, particularly beyond the maximum follow-up duration of 55 months observed in the ALINA trial. The potential benefit of a greater proportion of recurrences being nonmetastatic in patients treated with alectinib in comparison with ChT is therefore associated with considerable uncertainty.
In reanalysis, we used the pooled data provided by the sponsor for alectinib and ChT. Pooled proportions were assumed to remain constant over the model time horizon.
Use of treatment-specific health-state utility values is inappropriate. The sponsor incorporated treatment-specific utility values for alectinib and ChT for the preprogression health state based on 5-Level EQ-5D data from the ALINA trial, with a greater utility applied for alectinib (i.e., increment ranging between 0.01 and 0.02). The estimated utility values also differed depending on whether patients were on or off treatment (i.e., receiving either alectinib or ChT, or not being treated). According to the CDA-AMC Guidelines for the Economic Evaluation of Health Technologies,30 utilities should reflect the health states included in the model and not be specific to treatment. The review team further noted that the sponsor did not justify its decision to use treatment-specific utility values within the DFS health state. The use of treatment-specific utilities in the submitted model overestimated the incremental QALYs associated with alectinib relative to ChT. Clinical expert input noted that there is no clinical justification to support the assumption that patients in the same health state should have a different quality of life, with the exception of being on or off treatment.
In reanalysis, equal utility values were applied in the DFS health state for alectinib and ChT (0.87 for on-treatment and 0.89 for off-treatment).
Additionally, the following key assumptions were made by the sponsor and appraised by the review team (Table 4).
Table 4: Key Assumptions of the Submitted Economic Evaluation
Sponsor’s key assumption | CDA-AMC comment |
|---|---|
Patients receive alectinib adjuvant therapy for 24 months (or until disease recurrence or unacceptable toxicity). | Reasonable. Aligned with product monograph and confirmed by clinical expert feedback. |
Costs of ALK testing were based on IHC, which was assumed to be the primary testing method in the submission. | Likely reasonable. The majority of patients in the ALINA trial (84%) were confirmed to be ALK-positive through IHC. Clinical expert feedback indicated that assuming ALK testing was based on IHC was likely reasonable. |
All patients who switched from cisplatin to carboplatin in the trial were assumed to initiate treatment on carboplatin within the model. | Likely reasonable. Patients enrolled in the ALINA trial started treatment on a cisplatin-based regimen but were able to switch to carboplatin as needed. Clinical expert feedback stated that it was likely reasonable to assume similar efficacy between cisplatin- and carboplatin-base regimens. |
Adjuvant immunotherapy was excluded from the model as a comparator. | Reasonable. According to the clinical experts, adjuvant immunotherapies such as osimertinib, atezolizumab, and pembrolizumab would not be used to treat adult patients with completely resected stage IB to IIIA ALK-positive NSCLC. |
Patients with nonmetastatic recurrence were assumed to be treated with ChT, patients with first-line metastatic recurrence were assumed to receive ALK inhibitors, and patients with second-line metastatic recurrence were assumed to receive ChT. | Likely reasonable. According to clinical expert input, several assumptions made by the sponsor regarding subsequent treatment did not meet face validity. The sponsor estimates that 64% of patients would receive treatment with alectinib after experiencing first-line metastatic recurrence when previously treated with ChT or relapsing after 24 months of treatment with alectinib (at least 6 months posttreatment). The clinical experts indicated that these patients would likely receive lorlatinib instead of alectinib in clinical practice, citing 2024 guidance from the American Society of Clinical Oncology.31 Furthermore, the experts indicated that between 50% and 60% of patients experiencing second-line metastatic recurrence would be treated with ChT in clinical practice. The sponsor’s assumptions were conservative and resulted in additional incremental costs associated with alectinib relative to ChT. |
ChT = platinum-based chemotherapy; IHC = immunohistochemistry.
CDA-AMC Reanalyses of the Economic Evaluation
Base-Case Results
The review team’s base case was derived by making changes in model parameter values and assumptions, in consultation with clinical experts. We undertook a stepped analysis by sequentially incorporating each change detailed in Table 5 into the sponsor’s model to illustrate the impact of each. These included: adopting alternative parametric survival extrapolations of DFS for alectinib and ChT; assuming that 90% of patients who are disease-free 5 years after treatment initiation and 95% of patients who are disease-free 10 years after treatment initiation would be considered cured; assuming treatment waning would begin at 28 months and end at 60 months; using pooled trial data to inform the type of first disease recurrence; and applying health state–specific utility values.
A summary of the results of the CDA-AMC reanalyses for the weighted population is presented in Table 6.
Table 5: CDA-AMC Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CDA-AMC value or assumption |
|---|---|---|
Changes to derive the CDA-AMC base case | ||
1. Extrapolation of DFS |
|
|
2. Cure assumption |
|
|
3. Treatment waning | Not included | Treatment waning begins after 27.8 months, the median follow-up duration of the ITT population receiving alectinib from the ALINA trial; treatment effect is assumed to be null at 60 months |
4. Treatment-specific utilities | Treatment-specific preprogression utility values:
| Health state–specific preprogression utility values:
|
5. Distribution of patients who experience nonmetastatic and metastatic recurrence | Distribution varies by treatment:
| Pooled distribution across treatments:
|
CDA-AMC base case | ― | Reanalysis 1 + 2 + 3 + 4 + 5 |
ChT = platinum-based chemotherapy; DFS = disease-free survival; ITT = intention to treat; vs. = versus.
In the CDA-AMC base case, adjuvant treatment with alectinib was associated with an ICER of $37,154 per QALY gained compared to ChT ($87,506 in incremental costs: and 2.36 QALYs) (Table 6). The probability that alectinib was cost-effective at a WTP threshold of $50,000 per QALY gained was 76%. The CDA-AMC base case is based on publicly available prices of the comparator treatments. A detailed breakdown of the disaggregated results is available in Appendix 4.
The CDA-AMC base-case results align with those of the sponsor’s submitted analysis, indicating that alectinib is cost-effective at a WTP threshold of $50,000 per QALY gained, relative to ChT. Consistent with the sponsor’s analysis, the CDA-AMC reanalysis estimates that the majority of incremental QALYs realized by patients receiving alectinib relative to ChT were derived in the model on the basis of extrapolation.
Table 6: Summary of the Stepped Analysis of the CDA-AMC Reanalysis Results
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($ per QALY) |
|---|---|---|---|---|
Sponsor’s base case | ChT | 416,740 | 8.70 | Reference |
Alectinib | 411,352 | 12.48 | −1,429 | |
CDA-AMC reanalysis 1 — disease-free survival | ChT | 385,661 | 9.17 | Reference |
Alectinib | 411,671 | 12.47 | 7,876 | |
CDA-AMC reanalysis 2 — cure assumption | ChT | 435,397 | 8.56 | Reference |
Alectinib | 436,811 | 12.31 | 377 | |
CDA-AMC reanalysis 3 — treatment waning | ChT | 416,740 | 8.70 | Reference |
Alectinib | 485,107 | 11.40 | 25,374 | |
CDA-AMC reanalysis 4 — treatment-specific utilities | ChT | 416,740 | 8.7052a | Reference |
Alectinib | 411,352 | 12.48 | −1,429 | |
CDA-AMC reanalysis 5 — distribution of patients experiencing nonmetastatic and metastatic recurrence | ChT | 417,514 | 8.71 | Reference |
Alectinib | 409,816 | 12.48 | −2,042 | |
CDA-AMC base case (reanalysis 1 + 2 + 3 + 4 + 5) | ChT | 405,486 | 9.03 | Reference |
Alectinib | 491,278 | 11.50 | 34,841 | |
CDA-AMC base case (reanalysis 1 + 2 + 3 + 4 + 5) (probabilistic) | ChT | 408,764 | 9.26 | Reference |
Alectinib | 496,270 | 11.62 | 37,154 |
ChT = platinum-based chemotherapy; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Note: The reanalysis is based on publicly available prices of the comparator treatments. The results of all steps are presented deterministically unless otherwise indicated, while the cumulative base case is always presented both deterministically and probabilistically.
aReanalysis 4 resulted in a slightly higher total QALYs estimated for ChT relative to the sponsor’s base case (8.7052 vs. 8.7049).
Scenario Analysis Results
Although the review team’s reanalysis indicates that a price reduction may not be necessary for alectinib to be considered cost-effective at a WTP threshold of $50,000 per QALY gained, uncertainty remains in the analysis (Table 12). The review team conducted a series of scenario analyses to determine the impact of alternative assumptions on the cost-effectiveness of alectinib:
adopting an alternative parametric distribution to extrapolate DFS (log-logistic), aligned with the sponsor’s base case
assuming a 65% cure fraction at the 10-year landmark, consistent with the literature
assuming no waning of treatment effect (i.e., assuming that the effect of alectinib persists for the remaining 38-year lifetime horizon of the model among uncured patients)
assuming no additional treatment effect beyond treatment discontinuation of alectinib (i.e., 24 months).
Results of the CDA-AMC scenario analyses are presented in Table 13 of Appendix 4. The cost-effectiveness of alectinib was sensitive to assumptions concerning the persistence of long-term treatment effect and cure among patients who remain disease-free. When assuming no waning of treatment effect (i.e., indefinite relative effectiveness), the ICER for alectinib decreased to $7,988 per QALY gained compared to ChT. Conversely, when assuming treatment-effect waning following discontinuation, the ICER for alectinib increased to $107,457 per QALY gained compared to ChT. In this scenario, a price reduction of 29% would be required for alectinib to be cost-effective at a WTP threshold of $50,000 per QALY gained relative to ChT. Additionally, when assuming a lower proportion of patients would be cured after remaining disease-free for 10 years, the ICER for alectinib increased to $55,735 per QALY gained relative to ChT. In this scenario a price reduction of 5% would be required for alectinib to be cost-effective at the WTP threshold of $50,000 per QALY gained relative to ChT.
Issues for Consideration
Alectinib was previously reviewed by CDA-AMC for locally advanced or metastatic ALK-positive NSCLC as a first-line and second-line treatment. The final recommendations (July 25, 2018, and March 29, 2018, respectively) state that alectinib is recommended for reimbursement conditional on improved cost-effectiveness.32,33 Alectinib was also previously reviewed specifically for locally advanced or metastatic ALK-positive NSCLC for the treatment of patients with CNS metastases. The final recommendation (issued May 4, 2017) states that alectinib is not recommended for reimbursement because of uncertainty in the clinical evidence submitted.34
Overall Conclusions
Evidence from the ongoing phase III, open-label, randomized ALINA trial comparing the efficacy and safety of alectinib and ChT revealed added clinical benefits of adjuvant alectinib in DFS among adult patients who had complete resection of histologically confirmed stage IB (tumour ≥ 4 cm) to stage IIIA ALK-positive NSCLC (according to the AJCC/UICC staging manual, 7th edition). The Clinical Review found that alectinib likely results in an increase in the probability of being disease-free at 24 and 48 months compared to ChT, with moderate certainty of evidence. The Clinical Review found that it is not yet clear whether DFS benefits will translate to improved OS, as the interim analysis (data cut-off date: June 26, 2023; median follow-up: 27.8 months) is too early for an effect to be observed. The clinical experts consulted by the review team suggested that a longer follow-up time would be required to determine the OS benefit of alectinib relative to ChT.
In addition to the limitations with the clinical evidence, we identified several limitations with the sponsor’s economic submission: exclusion of independently fitted parametric distributions for DFS from the submitted model; uncertainty regarding the long-term impact of alectinib on OS and DFS; additional uncertainty surrounding predicted OS because of the use of time-invariant extrapolations across all postprogression health states; uncertainty regarding the assumption of a cure among patients who remain disease-free; uncertainty regarding the assumption that the treatment effect of alectinib is sustained indefinitely; uncertainty regarding the distribution of nonmetastatic and metastatic recurrences among patients treated with alectinib and ChT; and inappropriate use of treatment-specific utility values. As part of the base-case reanalysis, we adopted alternative parametric survival extrapolations of DFS for alectinib and ChT; assumed that 90% of patients who are disease-free 5 years after treatment initiation and 95% of patients who are disease-free 10 years after treatment initiation would be considered cured; assumed treatment would begin to wane at 28 months and end at 60 months; used pooled trial data to inform the type of first disease recurrence, and applied health state–specific utility values.
The review team’s base-case results align with the sponsor’s submitted analysis, indicating that alectinib is cost-effective at a WTP threshold of $50,000 per QALY gained, relative to ChT. In our base case, adjuvant treatment with alectinib was associated with an ICER of $37,154 per QALY gained compared to ChT ($87,506 in incremental costs and 2.36 incremental QALYs). The estimated ICER was driven by the selection of alternative distributions for extrapolating DFS, and assumptions about treatment waning. The base case results rely on patients treated with alectinib experiencing an OS benefit of 3.9 LYs compared to those treated with ChT. When compared to the sponsor’s analysis, our base case estimated a reduced QALY benefit with alectinib (i.e., 2.36 incremental QALYs [CDA-AMC base case] versus 3.54 [sponsor’s analysis]) at a higher cost (i.e., $87,506 in incremental costs: [CDA-AMC base case] versus −$2,454 [sponsor’s analysis]). The cost-effectiveness of alectinib was sensitive to assumptions concerning the persistence of the long-term treatment effect and cure among patients who remain disease-free, for which evidence is still pending. When assuming no further effect beyond treatment discontinuation (i.e., 24 months), the ICER for alectinib increased to $107,457 per QALY gained compared to ChT. Additionally, when assuming a lower proportion of patients (65%) would be cured after remaining disease-free for 10 years, which aligns with published literature for patients with NSCLC following complete primary tumour resection, the ICER for alectinib increased to $55,735 per QALY gained relative to ChT. Given this clinical uncertainty, price reductions may be required to achieve cost-effectiveness at a WTP threshold of $50,000 per QALY gained.
We were unable to address limitations related to the sponsor’s inflexible modelling, which forced us to assume hazard proportionality for DFS and time-invariant extrapolations across all postprogression health states, complicating the assessment of their impacts on the cost-effectiveness of alectinib. Given the extent of limitations associated with the sponsor’s submitted model, considerable uncertainty remains in the cost-effectiveness results. Moreover, when comparing the duration of follow-up in the ALINA trial to the model’s time horizon (55 months versus 40 years), it is important to note that most of the QALY and LY benefits (70% and 75%, respectively) realized by patients treated with alectinib in the CDA-AMC base case accrued in the posttrial period of the model on the basis of extrapolation. In the absence of long-term evidence, the comparative impact of alectinib on DFS and OS relative to ChT remains highly uncertain. Should the long-term effectiveness of alectinib be lower than predicted, the ICER would be higher than the CDA-AMC base case, requiring price reductions to achieve cost-effectiveness.
References
1.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Alecensaro (alectinib), 150 mg capsule. Mississauga (ON): Hoffmann-La Roche Limited; 2024.
2.Alecensaro (alectinib): 150 mg capsule [DRAFT product monograph]. Mississauga (ON): Hoffmann-La Roche Limited; 2023 Dec 22.
3.Clinical Study Report: BO40336. A Phase III, open-label, randomized study to evaluate the efficacy and safety of adjuvant alectinib versus adjuvant platinum-based chemotherapy in patients with completely resected StageIB (tumors ⌑4 cm) to Stage IIIA anaplastic lymphoma kinase-positivenon-small-cell lung cancer [internal sponsor's report]. Mississauga (ON): Hoffmann-La Roche Limited 2023.
4.Nakamichi S, Horinouchi H, Asao T, et al. Comparison of Radiotherapy and Chemoradiotherapy for Locoregional Recurrence of Non–small-cell Lung Cancer Developing After Surgery. Clin Lung Cancer. 2017;18(6):e441-e448. PubMed
5.Wong ML, McMurry TL, Stukenborg GJ, et al. Impact of age and comorbidity on treatment of non-small cell lung cancer recurrence following complete resection: A nationally representative cohort study. Lung Cancer. 2016;102:108-117. PubMed
6.Solomon BJ, Bauer TM, Mok TSK, et al. Efficacy and safety of first-line lorlatinib versus crizotinib in patients with advanced, ALK-positive non-small-cell lung cancer: updated analysis of data from the phase 3, randomised, open-label CROWN study. Lancet Respir Med. 2023;11(4):354-366. PubMed
7.Camidge DR, Kim HR, Ahn M-J, et al. Brigatinib Versus Crizotinib in ALK Inhibitor-Naive Advanced ALK-Positive NSCLC: Final Results of Phase 3 ALTA-1L Trial. J Thorac Oncol. 2021;16(12):2091-2108. PubMed
8.Chouaid C, Agulnik J, Goker E, et al. Health-Related Quality of Life and Utility in Patients with Advanced Non–Small-Cell Lung Cancer: A Prospective Cross-Sectional Patient Survey in a Real-World Setting. J Thorac Oncol. 2013;8(8):997-1003. PubMed
9.DeltaPA [sponsor supplied reference]. Ottawa (ON): IQVIA; 2024.
10.Drug Formulary [sponsor supplied reference]. Toronto (ON): Cancer Care Ontario; 2024: https://www.cancercareontario.ca/en/drugformulary/drugs; https://app.readcube.com/library/532bb15e-caff-4a0d-9126-d561508e450d/item/7ccbad21-464a-45cc-b8d5-c35593ce85ad.
11.Tam VC, Ko YJ, Mittmann N, et al. Cost-Effectiveness of Systemic Therapies for Metastatic Pancreatic Cancer. Current Oncology. 2013;20(2):90-106. PubMed
12.Ministry of Health. Ontario Schedule of Benefits: Physician Services Under the Health Insurance Act [sponsor supplied reference]. Toronto (ON): Government of Ontario; 2023: https://www.ontario.ca/files/2024-01/moh-ohip-schedule-of-benefits-2024-01-24.pdf; https://app.readcube.com/library/532bb15e-caff-4a0d-9126-d561508e450d/item/9a15106d-f6a1-4ed9-bf41-edd329fb363c.
13.Cancer Care Ontario. Lung Cancer Follow-up Care Pathway Map [sponsor supplied reference]. Version 2023.04. Toronto (ON): Ontario Health; 2023: https://www.cancercareontario.ca/sites/ccocancercare/files/assets/LungCancerFollowupCarePathwayMap.pdf.
14.Mahar AL, Coburn NG, Johnson AP. A population-based study of the resource utilization and costs of managing resectable non-small cell lung cancer. Lung Cancer. 2014;86(2):281-287. PubMed
15.Seung SJ, Hurry M, Hassan S, Walton RN, Evans WK. Cost-of-illness study for non-small-cell lung cancer using real-world data. Curr Oncol. 2019;26(2):102-107. PubMed
16.Canadian Institute for Health Information. Patient Cost Estimator [sponsor supplied reference]. Ottawa (ON): CIHI; 2024: https://www.cihi.ca/en/patient-cost-estimator.
17.Walker H, Anderson M, Farahati F, et al. Resource Use and costs of End-Of-Life/Palliative Care: Ontario Adult Cancer Patients Dying during 2002 and 2003. J Palliat Care. 2010;27(2):79-88. PubMed
18.Royston P, Parmar MK. Restricted mean survival time: an alternative to the hazard ratio for the design and analysis of randomized trials with a time-to-event outcome. BMC Med Res Methodol. 2013;13:152. PubMed
19.Bagust A, Beale S. Survival analysis and extrapolation modeling of time-to-event clinical trial data for economic evaluation: an alternative approach. Med Decis Making. 2014;34(3):343-351. PubMed
20.In J, Lee DK. Survival analysis: part II - applied clinical data analysis. Korean J Anesthesiol. 2019;72(5):441-457. PubMed
21.Hancock MJ, Maher CG, Costa Lda C, Williams CM. A guide to survival analysis for manual therapy clinicians and researchers. Man Ther. 2014;19(6):511-516. PubMed
22.Kleinbaum DG D, Klein M. Survival analysis a self-learning text [sponsor supplied reference]. Springer; 1996.
23.Grambsch PM, Therneau TM. Proportional hazards tests and diagnostics based on weighted residuals. Biometrika. 1994;81(3):515-526.
24.Coyle D, Haines A, Lee K. Extrapolating Clinical Evidence Within Economic Evaluations: CADTH Methods and Guidelines. Can J Health Technol. 2023;3(5). PubMed
25.Guyot P, Ades AE, Beasley M, Lueza B, Pignon JP, Welton NJ. Extrapolation of Survival Curves from Cancer Trials Using External Information. Med Decis Making. 2017;37(4):353-366. PubMed
26.National Institute for Health and Care Excellence. NICE DSU Technical Support Document 14: Survival Analysis For Economic Evaluations Alongside Clinical Trials - Extrapolation With Patient-Level Data [sponsor supplied reference]. London (GB): NICE; 2011: https://www.ncbi.nlm.nih.gov/books/NBK395885/pdf/Bookshelf_NBK395885.pdf. Accessed 2024 July 4.
27.CADTH Reimbursement Recommendation: Osimertinib (Tagrisso - AstraZeneca Canada Inc.) [sponsor supplied reference). Clinical Review, Pharmacoeconomic Review. Ottawa (ON): CADTH; 2022: https://www.cadth.ca/sites/default/files/DRR/2022/PC0246-Tagrisso.pdf.
28.CADTH Reimbursement Recommendation: Atezolizumab (Tecentriq - Hoffman-La Roche Ltd.) [sponsor supplied reference). Clinical Review, Pharmacoeconomic Review, Stakeholder Input. Ottawa (ON): CADTH; 2022: https://www.cadth.ca/sites/default/files/DRR/2022/PC0277-Tecentriq-SCLC_combined.pdf.
29.Maeda R, Yoshida J, Hishida T, et al. Late recurrence of non-small cell lung cancer more than 5 years after complete resection: incidence and clinical implications in patient follow-up. Chest. 2010;138(1):145-150. PubMed
30.Guidelines for the economic evaluation of health technologies: Canada. 4th ed. Ottawa (ON): CADTH; 2017: https://www.cadth.ca/guidelines-economic-evaluation-health-technologies-canada-4th-edition.
31.[sponsor supplied reference]. Paper presented at: ASCO Annual Meeting; May 31, 2024 - June 4, 2024, 2024; Chicago, IL.
32.pan-Canadian Oncology Drug Review Committee (pERC) final recommendation: Alectinib (2L). Ottawa (ON): CADTH; 2018: https://www.cadth.ca/sites/default/files/pcodr/pcodr_alectinib_alecensaro_nsclc_2ln_fn_rec.pdf. Accessed 2024 July 4.
33.pan-Canadian Oncology Drug Review Committee (pERC) final recommendation: Alectinib (1L). Ottawa (ON): CADTH; 2018: https://www.cadth.ca/sites/default/files/pcodr/pcodr_alectinib_alecensaro_nsclc_1stln_fn_rec.pdf. Accessed 2024 July 4.
34.pan-Canadian Oncology Drug Review Committee (pERC) final recommendation: Alectinib. Ottawa (ON): CADTH; 2017: https://www.cadth.ca/sites/default/files/pcodr/pcodr_alectinib_alecensaro_nsclc_fn_rec.pdf. Accessed 2024 July 4.
35.Clinical Study Protocol version 6: BO40336. A Phase III, Open-Label, Randomized Study To Evaluate The Efficacy And Safety Of Adjuvant Alectinib Versus Adjuvant Platinum-Based Chemotherapy In Patients With Completely Resected Stage Ib (Tumors >= 4 cm) To Stage IIIa Anaplastic Lymphoma Kinase-Positive Non-Small-Cell Lung Cancer [internal sponsor's report]. Mississauga (ON): Hoffmann-La Roche Limited; 2021.
36.Budget Impact Analysis [internal sponsor'’s report]. In: Drug Reimbursement Review sponsor submission: Alecensaro (alectinib), 150 mg capsule. Mississauga (ON): Hoffmann-La Roche Limited; 2024 Apr 18.
37.Evans W W, Flanagan C., Gauvreau P., et al. How in the real world are lung cancer patients treated? The Ontario, Canada Experience. J Thorac Oncol. 2018;13(10).
38.Chen Mf CJE. Early-stage anaplastic lymphoma kinase (ALK)-positive lung cancer: a narrative review. Transl Lung Cancer Res. 2023;12:337-345. PubMed
39.Pharmastat Claims Dataset - November 2023 [sponsor supplied reference]. Vol IQVIA: Ottawa (ON); 2023.
Appendix 1: Cost-Comparison Table
Please note that this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical expert(s) and drug plan. Comparators may be recommended (appropriate) practice or actual practice. Existing product listing agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 7: CDA-AMC Cost-Comparison Table for Resectable Stage IB to IIIA ALK-Positive NSCLC
Treatment | Strength / concentration | Form | Price ($) | Recommended dosage | Cost per cycle ($) | 28-day cost ($) |
|---|---|---|---|---|---|---|
Adjuvant therapy | ||||||
Alectinib (Alecensaro) | 150 mg | Oral capsule | 44.2750a | 600 mg given orally, twice daily with food (total daily dose of 1,200 mg) | 354.20b | 9,918 |
Cisplatin-based regimens | ||||||
CISPPEME | ||||||
Cisplatin (generic) | 50 mg vial 100 mg vial | 1 mg/mL IV solution | 135.0000 270.0000 | 21-day cycles: 75 mg/m2 IV on Day 1 | 405 | 540 |
Pemetrexed (generic) | 100 mg vial 500 mg vial 1,000 mg vial | 10 mg/mL IV solution | 2,145.00 4,290.00 | 21-day cycles: 500 mg/m2 IV on Day 1 | 3,861 | 5,148 |
CISPPEME regimen cost (21-day cycle) | 4,266 | 5,688 | ||||
CISPGEMC | ||||||
Cisplatin (generic) | 50 mg vial 100 mg vial | 1 mg/mL IV solution | 135.0000 270.0000 | 21-day cycles: 75 mg/m2 IV on Day 1 | 405 | 540 |
Gemcitabine (generic) | 200 mg vial 1,000 mg vial 2,000 mg vial | 40 mg/mL IV solution | 54.0600 270.3000 540.6000 | 21-day cycles: 1,250 mg/m2 IV on Day 1 and Day 8 | 1,297 | 1,730 |
CISPGEMC regimen cost (21-day cycle) | 1,702 | 2,270 | ||||
CISPVINO | ||||||
Cisplatin (generic) | 50 mg vial 100 mg vial | 1 mg/mL IV solution | 135.0000 270.0000 | 21-day cycles: 75 mg/m2 IV on Day 1 | 405 | 540 |
Vinorelbine (generic) | 10 mg vial 50 mg vial | 10 mg/mL IV solution | 80.0000 400.0000 | 21-day cycles: 25 mg/m2 on Day 1 and Day 8 | 800 | 1,067 |
CISPVINO regimen cost (21-day cycle) | 1,205 | 1,607 | ||||
Carboplatin-based regimens | ||||||
CRBPPEME | ||||||
Carboplatin (generic) | 50 mg 150 mg 450 mg 600 mg | 10 mg/mL vial for injection | 70.0000 210.0000 599.9985 775.0020 | 21-day cycles: Target AUC 5 on Day 1, maximum dose for AUC 5 is 750 mgb | 985 | 1,313 |
Pemetrexed (generic) | 100 mg vial 500 mg vial 1,000 mg vial | 10 mg/mL IV solution | 2,145.00 4,290.00 | 21-day cycles: 500 mg/m2 IV on Day 1 | 3,861 | 5,148 |
CRBPPEME regimen cost (21-day cycle) | 4,846 | 6,461 | ||||
CRBPGEMC | ||||||
Carboplatin (generic) | 50 mg 150 mg 450 mg 600 mg | 10 mg/mL vial for injection | 70.0000 210.0000 599.9985 775.0020 | 21-day cycles: Target AUC 5 on Day 1, maximum dose for AUC 5 is 750 mgb | 985 | 1,313 |
Gemcitabine (generic) | 200 mg vial 1,000 mg vial 2,000 mg vial | 40 mg/mL IV solution | 54.0600 270.3000 540.6000 | 21-day cycles: 1,250 mg/m2 IV on Day 1 and Day 8 | 1,297 | 1,730 |
CRBPGEMC regimen cost (21-day cycle) | 2,282 | 3,043 | ||||
CRBPVINO | ||||||
Carboplatin (generic) | 50 mg 150 mg 450 mg 600 mg | 10 mg/mL vial for injection | 70.0000 210.0000 599.9985 775.0020 | 21-day cycles: Target AUC 5 on Day 1, maximum dose for AUC 5 is 750 mgb | 985 | 1,313 |
Vinorelbine (generic) | 10 mg vial 50 mg vial | 10 mg/mL IV solution | 80.0000 400.0000 | 21-day cycles: 25 mg/m2 on Day 1 and Day 8 | 800 | 1,067 |
CRBPVINO regimen cost (21-day cycle) | 1,785 | 2,380 | ||||
NSCLC = non–small cell lung cancer.
Note: All prices are wholesale from IQVIA Delta PA (accessed June 2024), unless otherwise indicated, and do not include dispensing fees. Calculations assume a patient body weight of 69.63 kg and a body surface area of 1.77 m2 as per the ALINA trial.3 Vial wastage was assumed (i.e., no vial sharing). All recommended dosages are retrieved from Cancer Care Ontario Drug Formulary Regimens.10 Adjuvant alectinib consists of 24 months. Adjuvant platinum-based chemotherapy consists of 4 full cycles.
aSponsor’s submitted price.1
bDaily cost.
cDose [mg] = Target AUC * [GFR + 25]; AUC = product of serum concentration (mg/mL) and time (min); GFR (glomerular filtration rate) expressed as measured Creatinine Clearance or estimated from Serum Creatinine (by Cockcroft and Gault method or Jelliffe method).1 Maximum Carboplatin Dose (mg) = Target AUC (mg/mL per min) x (125 mL/min + 25). Target AUC was assumed to be 5, aligned with the ALINA protocol.35
Appendix 2: Submission Quality
Please note that this appendix has not been copy-edited.
Description | Yes or no | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | Yes | No comment. |
Model has been adequately programmed and has sufficient face validity | No | Refer to key limitations “Proportional hazards assumption for DFS is improbable” and “Impact of alectinib on long-term OS and modelling of treatment after first recurrence is highly uncertain.” |
Model structure is adequate for decision problem | No | Refer to key limitations “Proportional hazards assumption for DFS is improbable” and “Impact of alectinib on long-term DFS is highly uncertain.” |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | Yes | No comment. |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | Yes | No comment. |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | Yes | No comment. |
DFS = disease-free survival; OS = overall survival.
Appendix 3: Additional Information on the Submitted Economic Evaluation
Please note that this appendix has not been copy-edited.
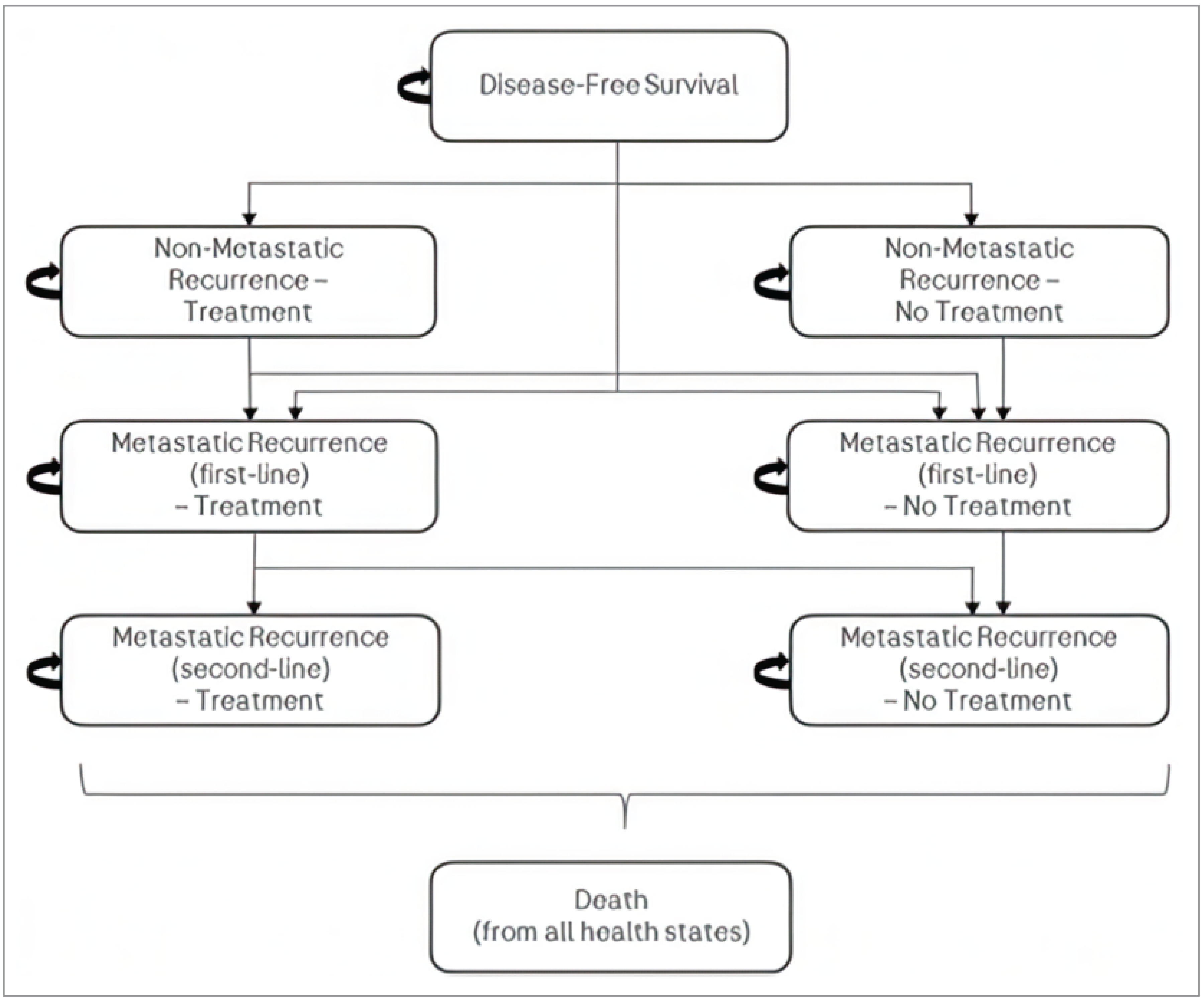
Table 9: Health-State Utility Values in the Submitted Model
Parameter | Alectinib | ChT |
|---|---|---|
DFS: On treatment | 0.87 | 0.85 |
DFS: Off treatment | 0.89 | 0.88 |
Progressed disease (nonmetastatic recurrence) | 0.77 | 0.77 |
Progressed disease (metastatic recurrence) | 0.71 | 0.71 |
ChT = platinum-based chemotherapy; DFS = disease-free survival.
Source: Sponsor’s pharmacoeconomic submission.1
Detailed Results of the Sponsor’s Base Case
Table 10: Disaggregated Summary of the Sponsor’s Economic Evaluation Results
Parameter | Alectinib | ChT |
|---|---|---|
Discounted LYs | ||
Total | 19.11 | 13.17 |
Disease-free survival | 17.55 | 9.62 |
Nonmetastatic recurrence | 0.38 | 0.66 |
Metastatic recurrence/progression (1L) | 0.95 | 2.28 |
Metastatic progression (2L) | 0.23 | 0.62 |
Discounted QALYs | ||
Total | 12.53 | 8.99 |
Disease-free survival | 11.44 | 6.45 |
Nonmetastatic recurrence | 0.27 | 0.47 |
Metastatic recurrence/progression (1L) | 0.66 | 1.63 |
Metastatic progression (2L) | 0.16 | 0.43 |
Discounted costs ($) | ||
Total | 415,470 | 417,946 |
Disease-free survival | 258,807 | 37,094 |
Nonmetastatic recurrence | 21,874 | 38,036 |
Metastatic recurrence/progression (1L) | 113,845 | 278,827 |
Metastatic progression (2L) | 17,840 | 47,268 |
End of life | 3,103 | 16,721 |
1L = first line; 2L = second line; ChT = platinum-based chemotherapy; LY = life-year; QALY = quality-adjusted life-year.
Note: Costs for each health state include costs of treatment, AE management, and follow-up health care.
Source: Sponsor’s pharmacoeconomic submission.1
Appendix 4: Additional Details on the CDA-AMC Reanalyses and Sensitivity Analyses of the Economic Evaluation
Please note that this appendix has not been copy-edited.
Detailed Results of CDA-AMC Base Case
Table 11: Disaggregated Summary of the CDA-AMC Economic Evaluation Results
Parameter | Alectinib | ChT |
|---|---|---|
Discounted LYs | ||
Total | 17.49 | 13.62 |
Disease-free survival | 15.22 | 10.15 |
Nonmetastatic recurrence | 0.44 | 0.70 |
Metastatic recurrence/progression (1L) | 1.46 | 2.18 |
Metastatic progression (2L) | 0.37 | 0.59 |
Discounted QALYs | ||
Total | 11.62 | 9.26 |
Disease-free survival | 10.06 | 6.81 |
Nonmetastatic recurrence | 0.31 | 0.50 |
Metastatic recurrence/progression (1L) | 1.00 | 1.54 |
Metastatic progression (2L) | 0.25 | 0.41 |
Discounted costs ($) | ||
Total | 496,270 | 408,764 |
Disease-free survival | 261,499 | 39,568 |
Nonmetastatic recurrence | 25,545 | 40,393 |
Metastatic recurrence/progression (1L) | 176,658 | 267,408 |
Metastatic progression (2L) | 28,078 | 45,283 |
End of life | 4,490 | 16,113 |
1L = first line; 2L = second line; ChT = platinum-based chemotherapy; LY = life-year; QALY = quality-adjusted life-year.
Note: Costs for each health state include costs of treatment, AE management, and follow-up health care.
Scenario Analyses
Table 12: CDA-AMC Price-Reduction Analyses
Analysis | Unit drug cost ($) | ICERs for alectinib vs. ChT ($ per QALY) | |
|---|---|---|---|
Price reduction | $ | Sponsor base case | CDA-AMC reanalysis |
No price reduction | 44 | Alectinib is dominant | 37,154 |
10% | 40 | Alectinib is dominant | 25,908 |
20% | 35 | Alectinib is dominant | 14,736 |
30% | 31 | Alectinib is dominant | 3,565 |
40% | 27 | Alectinib is dominant | Alectinib is dominant |
50% | 22 | Alectinib is dominant | Alectinib is dominant |
60% | 18 | Alectinib is dominant | Alectinib is dominant |
70% | 13 | Alectinib is dominant | Alectinib is dominant |
80% | 9 | Alectinib is dominant | Alectinib is dominant |
90% | 4 | Alectinib is dominant | Alectinib is dominant |
ChT = platinum-based chemotherapy; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; vs. = versus.
Table 13: Scenario Analysis Conducted on the CDA-AMC Base Case
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($ per QALY) |
|---|---|---|---|---|
CDA-AMC base case | ChT | 408,764 | 9.26 | Reference |
Alectinib | 496,270 | 11.62 | 37,154 | |
CDA-AMC scenario 1: Log-logistic DFS extrapolation | ChT | 434,253 | 8.84 | Reference |
Alectinib | 516,144 | 11.30 | 33,315 | |
CDA-AMC scenario 2: 65% of patients considered cured at year 10 | ChT | 464,191 | 8.97 | Reference |
Alectinib | 585,121 | 11.14 | 55,735 | |
CDA-AMC scenario 3: No treatment waning | ChT | 407,063 | 9.26 | Reference |
Alectinib | 432,536 | 12.45 | 7,988 | |
CDA-AMC scenario 4: No additional treatment effect beyond treatment discontinuation of alectinib | ChT | 406,962 | 9.27 | Reference |
Alectinib | 555,021 | 10.65 | 107,457 |
ChT = platinum-based chemotherapy; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Note: All analyses were run probabilistically.
Appendix 5: Submitted Budget Impact Analysis and CDA-AMC Appraisal
Please note that this appendix has not been copy-edited.
Table 14: Summary of Key Take-Aways
Key take-aways of the budget impact analysis |
|---|
|
Summary of Sponsor’s Budget Impact Analysis
In the submitted budget impact analysis (BIA),36 the sponsor assessed the budget impact of reimbursing alectinib as adjuvant treatment for completely resected stage IB (tumour size ≥ 4cm) to IIIA (according to AJCC/UICC 7th edition) ALK-positive NSCLC. The analysis took the perspective of CDA-AMC-participating Canadian public drug plans using a top-down, epidemiological approach over a 3-year time horizon. Data to inform the model were obtained from various sources, including the published literature, the sponsor’s internal data, and input from clinical experts consulted by the sponsor. Key inputs to the BIA are documented in Table 15.
Key assumptions included:
Distribution of resectable NSCLC staging was derived from a retrospective study of Ontario NSCLC patients and was assumed to be reflective of real-world staging observed in Canadian clinical practice.37
100% biomarker testing rate based on clinical expert opinion in Canada.
Chemotherapy costs weighted from the ALINA trial and assumed to be reflective of Canadian clinical practice.
Market shares of alectinib informed by previous values assumed by the review team in a prior biomarker-directed adjuvant therapy in NSCLC and validated by Canadian clinician input.27
Figure 2: Sponsor’s Estimation of the Size of the Eligible Population
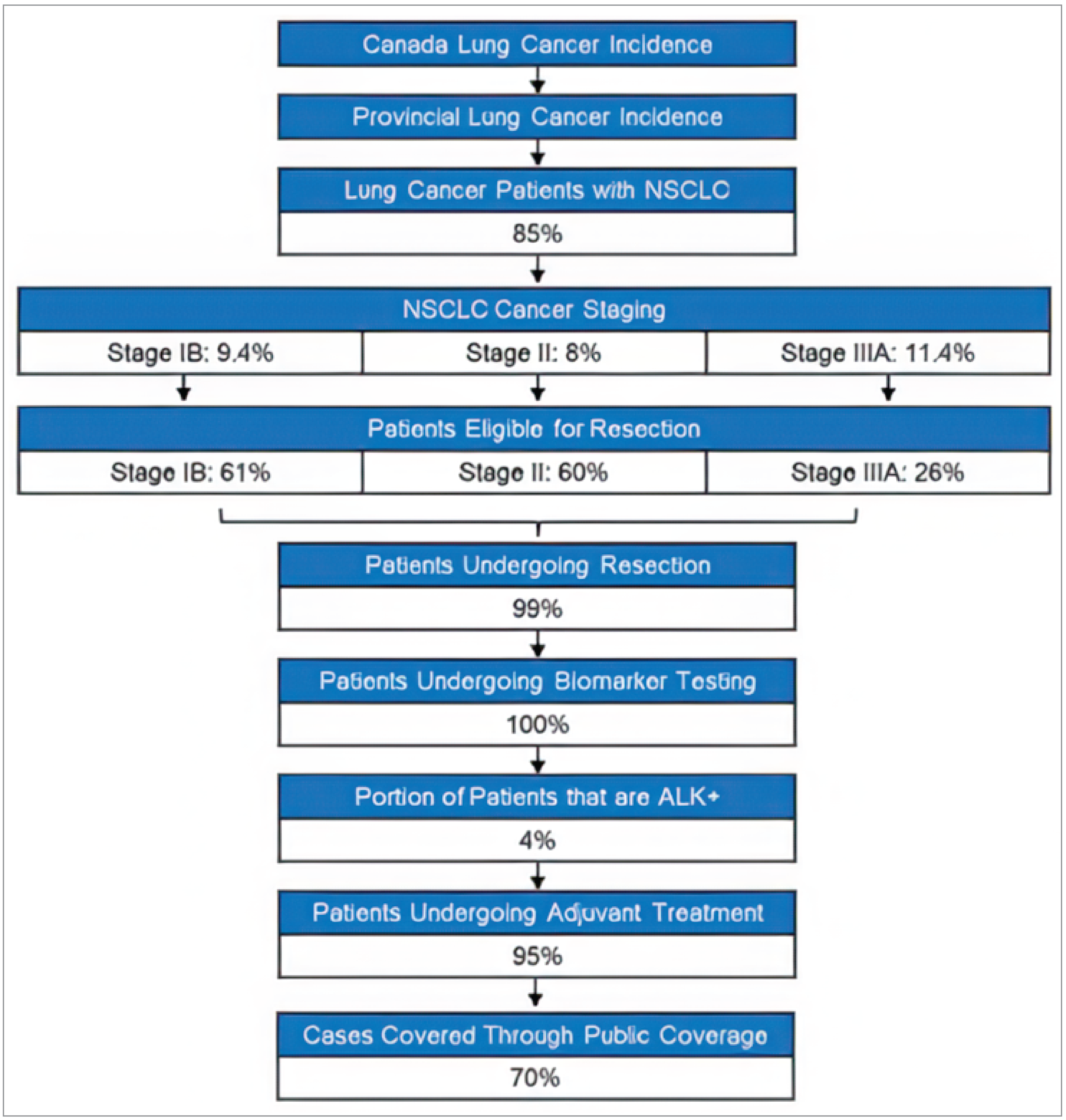
Source: Sponsor’s pharmacoeconomic submission.1
Table 15: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as year 1 / year 2 / year 3 if appropriate) |
|---|---|
Target population | |
Number of patients eligible for drug under review | 70 / 71 / 72 |
Market uptake (3 years) | |
Uptake (reference scenario) ChTa | 100% / 100% / 100% |
Uptake (new drug scenario) Alectinib ChTa | 25% / 20% / 15% 75% / 80% / 85% |
Cost of treatment (per patient)b | |
Alectinib Cisplatin + pemetrexed Cisplatin + vinorelbine Cisplatin + gemcitabine Carboplatin + pemetrexed Carboplatin + vinorelbine Carboplatin + gemcitabine | $258,743 $16,620 $4,266 $6,213 $19,062 $6,707 $8,654 |
ChT = platinum-based chemotherapy.
aPlatinum-based chemotherapy regimens included cisplatin or carboplatin in combination with pemetrexed, vinorelbine, or gemcitabine. Proportion of use for each regimen was based on the ALINA trial and was estimated to be 70% cisplatin + pemetrexed, 17.5% cisplatin + vinorelbine, 0.8% cisplatin + gemcitabine, 10.0% carboplatin + pemetrexed, 1.7% carboplatin + vinorelbine, and 0.0% carboplatin + gemcitabine.
bDuration of treatment for alectinib was the recommended 24 months. Duration of treatment for all ChT regimens was 4 cycles, each consisting of 21 days.
Summary of the Sponsor’s Budget Impact Analysis Results
The sponsor estimated that the budget impact of reimbursing alectinib as adjuvant treatment for completely resected stage IB (tumour size ≥ 4cm) to IIIA (according to AJCC/UICC 7th edition) ALK-positive NSCLC would be $6,022,741 in year 1, $13,292,716 in year 2, and $14,343,161 in year 3, for a three-year total of $33,658,618.
CDA-AMC Appraisal of the Sponsor’s Budget Impact Analysis
CDA-AMC identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
Uncertainty regarding the estimated size of the eligible population: Although most inputs were deemed to be plausible based on clinical expert feedback obtained by the review team, it was noted that some uncertainty remains in the sponsor’s estimates, specifically in the ALK positivity rate in NSCLC, which was found to range between 2% and 7% across the literature.38 It is uncertain whether the estimates sourced from literature are representative of the population in Canada, as the sponsor’s cited systematic review includes data from international countries in addition to Canada. However, as noted by the sponsor, standardized biomarker testing has historically not been routinely performed in Canada or globally for early-stage NSCLC and there remains uncertainty surrounding prevalence in this disease setting. The sponsor assumed a 4% ALK positivity rate in the submitted base case. The estimated size of the eligible population remains a key driver in determining budget impact estimates. Hence, underestimating this parameter would result in an underestimated budgetary impact.
CDA-AMC conducted a scenario analysis to evaluate the budgetary impact of assuming a 7% ALK positivity rate.
Uncertainty regarding market shares of alectinib: The market uptake of alectinib was assumed to be 75% in year 1, 80% in year 2, and 85% in year 3 based on clinical expert input and alignment with values assumed by the review team in a previous review of a biomarker-directed adjuvant therapy in patients with NSCLC.27 The sponsor’s market share estimates were deemed to be plausible based on clinical expert feedback obtained by the review team; however, clinical experts also noted that market shares may be slightly higher because of clinicians’ familiarity with the use of Tyrosine Kinase Inhibitors in clinical practice. Uncertainty remains in these estimates and increases in the projected market shares will increase the anticipated budget impact associated with the reimbursement of alectinib.
We conducted a scenario analysis to evaluate the budgetary impact of assuming a higher market uptake for alectinib (80% in year 1, 85% in year 2, and 90% in year 3).
Target population is potentially underestimated by excluding patients who are not covered by drug plans: The sponsor assumed that 70% of patients would be eligible for public coverage by drug plans according to IQVIA Pharmastat.39
We conducted a scenario analysis to evaluate the budgetary impact of assuming 100% public coverage.
Drug prices paid by public drug plans is uncertain: Both the sponsor’s and the CDA-AMC analyses are based on publicly available list prices for all comparators. Actual costs paid by public drug plans are unknown.
We could not address this limitation in reanalysis.
CDA-AMC Reanalyses of the Budget Impact Analysis
We did not undertake a base case reanalysis. Instead, we conducted several scenario analyses which included:
Assuming 7% ALK positivity rate.
Assuming that the market shares for alectinib would reach 80% in year 1, 85% in year 2, and 90% in year 3.
Assuming 100% public coverage.
Results are presented in Table 16. Assuming a higher ALK positivity rate of 7% resulted in a three-year total budget impact of $58,902,582. Assuming greater market shares for alectinib reaching 80% in year 1, 85% in year 2, and 90% in year 3 resulted in a three-year total budget impact of $35,789,849. Assuming 100% public coverage resulted in a three-year total budget impact of $48,083,741.
Table 16: Detailed Breakdown of the CDA-AMC Reanalyses of the Budget Impact Analysis
Stepped analysis | Scenario | Year 0 (current situation) ($) | Year 1 ($) | Year 2 ($) | Year 3 ($) | Three-year total ($) |
|---|---|---|---|---|---|---|
Submitted base case | Reference | 1,127,300 | 1,143,369 | 1,159,102 | 1,174,494 | 3,476,965 |
New drug | 1,127,300 | 7,166,111 | 14,451,818 | 15,517,655 | 37,135,583 | |
Budget impact | 0 | 6,022,741 | 13,292,716 | 14,343,161 | 33,658,618 | |
CDA-AMC scenario 1: ALK positivity rate | Reference | 1,873,978 | 1,900,691 | 1,926,844 | 1,952,431 | 5,779,967 |
New drug | 1,873,978 | 12,440,489 | 25,189,097 | 27,052,963 | 64,682,549 | |
Budget impact | 0 | 10,539,798 | 23,262,253 | 25,100,532 | 58,902,582 | |
CDA-AMC scenario 2: Market uptake | Reference | 1,127,300 | 1,143,369 | 1,159,102 | 1,174,494 | 3,476,965 |
New drug | 1,127,300 | 7,567,627 | 15,310,863 | 16,388,325 | 39,266,814 | |
Budget impact | 0 | 6,424,258 | 14,151,761 | 15,213,831 | 35,789,849 | |
CDA-AMC scenario 3: Public coverage | Reference | 1,553,973 | 1,576,125 | 1,597,811 | 1,619,030 | 4,792,966 |
New drug | 1,553,973 | 10,180,041 | 20,587,406 | 22,109,260 | 52,876,706 | |
Budget impact | 0 | 8,603,916 | 18,989,594 | 20,490,230 | 48,083,741 |
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.