Drugs, Health Technologies, Health Systems
Reimbursement Review
Abemaciclib (Verzenio)
Sponsor: Eli Lilly Canada Inc.
Therapeutic area: Adjuvant treatment of hormone receptor–positive, HER2-negative early breast cancer
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Clinical Review
Abbreviations
AE
adverse event
ALN
axillary lymph node
CBCN
Canadian Breast Cancer Network
CDA-AMC
Canada's Drug Agency
CDK
cyclin-dependent kinase
CI
confidence interval
DRFS
distant relapse–free survival
EBC
early breast cancer
ECOG PS
Eastern Cooperative Oncology Group Performance Status
ET
endocrine therapy
FACT-B
Functional Assessment of Cancer Therapy – Breast
FACIT-F
Functional Assessment of Chronic Illness Therapy – Fatigue
GRADE
Grading of Recommendations Assessment, Development, and Evaluation
HR
hormone receptor
HRQoL
health-related quality of life
IA
interim analysis
IDFS
invasive disease–free survival
IHC
immunohistochemistry
ILD
interstitial lung disease
ISH
in situ hybridization
ITT
intention to treat
LSM
least squares mean
MID
minimally important difference
OH-CCO
Ontario Health – Cancer Care Ontario
OFS
ovarian function suppression
OS
overall survival
RCT
randomized controlled trial
RR
relative risk
SAE
serious adverse event
SD
standard deviation
SOC
standard of care
TEAE
treatment-emergent adverse event
VTE
venous thromboembolic event
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Table 1: Background Information of Application Submitted for Review
Item | Description |
|---|---|
Drug product, strength, formulation | Abemaciclib (Verzenio), 50 mg, 100 mg, and 150 mg oral tablets |
Sponsor | Eli Lilly Canada Inc. |
Indication | In combination with endocrine therapy for the adjuvant treatment of adult patients with hormone receptor (HR)-positive, human epidermal growth factor receptor 2 (HER2)-negative, node-positive, early breast cancer at high risk of disease recurrence based on clinicopathological features. |
Reimbursement request | As per indication, where “high risk of disease recurrence based on clinicopathological features” refers to patients who satisfy 1 or more of the following:
|
Health Canada approval status | NOC |
Health Canada review pathway | Standard review |
NOC date | December 6, 2023 |
ALN = axillary lymph node; HER2 = human epidermal growth factor receptor 2; HR = hormone receptor; NOC = Notice of Compliance.
Introduction
Breast cancer is the most diagnosed cancer and the second leading cause of cancer-related death among females in Canada.1 In 2022, a total of 28,600 females were diagnosed with breast cancer and 5,500 females died of the disease (14% of cancer deaths among females).1 Breast cancer is a heterogeneous, phenotypically diverse disease composed of several biologic subtypes with distinct clinical behaviours.2 The most common subtype of breast cancer is hormone receptor (HR)-positive, human epidermal receptor 2 (HER2)-negative, which accounts for approximately 70% of breast cancers.3,4 Anatomical staging of breast cancer is defined using the American Joint Committee on Cancer (AJCC) staging system and is based on the size and extent of the breast tumour (T), the extent of regional lymph node involvement (N), and the presence or absence of distant metastases (M), collectively referred to as TNM staging.5 These features are assigned individual scores, which are then combined to identify the TNM stage.6 Early breast cancer (EBC) refers to invasive cancer that has not spread beyond the breast tissue or nearby lymph nodes. EBC includes ductal carcinoma in situ (stage 0) and stages I to III.7 Prognosis and treatment decisions for breast cancer have historically been guided by TNM staging. However, biological factors (e.g., histologic tumour grade, cell proliferation rate [mitotic count or Ki-67 expression], HR expression, HER2 expression, and gene expression prognostic panels [or multigene assays]) are now increasingly important in determining prognosis and response to treatment.5 More than 90% of patients with breast cancer are diagnosed with early-stage disease, which is potentially curable.8 In patients with HR-positive, HER2-negative EBC, the 5-year survival rate is greater than 90%.9 Although patients with EBC have a promising 5-year survival prognosis, a subset of up to 20% to 30% of patients will nonetheless experience disease recurrence in the first 10 years. Recurrences that are distant are described as metastatic disease that is incurable.10,11 Patients with high-risk clinicopathological features, particularly those with a high burden of nodal involvement, have been shown to be at a higher risk of disease recurrence.
A biopsy is routinely performed to evaluate the HR and HER2 status of the tumour.12,13 Immunohistochemistry (IHC) testing is used to test for HR14 and HER2.15 A tumour is considered HR-positive if at least 1% of the cells examined have estrogen receptors or progesterone receptors or both.13 Tumours are considered HER2-negative when they are IHC 0 or IHC 1+ or IHC 2+ with negative in situ hybridization (ISH).13 Ki-67 is a marker of cellular proliferation and may play a role as an independent prognostic factor for the risk of recurrence during the first 5 years after primary breast cancer treatment. Although there is no consensus on precise Ki-67 levels indicative of high versus low risk of recurrence, Ki-67 expression greater than 20% to 29% is generally considered appropriate for identifying a high-risk population.16-18 Ki-67 testing is currently required to identify those patients eligible for abemaciclib based on the initial Health Canada EBC indication and the CADTH recommendation for public reimbursement (i.e., for the cohort 1 “Ki-67–high” population in the monarchE trial, 2022)19 and as such has now become widely accessible nationally.
Adjuvant endocrine therapy (ET) is part of the standard of care (SOC) for the systemic treatment of patients with HR-positive, HER2-negative, node-positive EBC.20 Regimens may include tamoxifen and 1 of 3 aromatase inhibitors: anastrozole, letrozole, and exemestane.12,15 Patients diagnosed with HR-positive, HER2-negative, node-positive EBC are typically treated with surgery (lumpectomy or mastectomy), which may be preceded by neoadjuvant chemotherapy or ET or both and followed by a combination of adjuvant radiotherapy, chemotherapy, and ET or adjuvant ET alone. The type of adjuvant ET is guided by menopausal status. Ovarian suppression or ablation may also be used as part of ET for patients who are premenopausal with HR-positive breast cancer to improve disease outcomes. Ovarian function suppression (OFS) is required when used together with an aromatase inhibitor for patients who are premenopausal given the potential for aromatase inhibitors to stimulate ovarian function.20,21 Currently, abemaciclib in combination with ET (also, abemaciclib plus ET) is publicly reimbursed in the adjuvant setting for adult patients with HR-positive, HER2-negative, node-positive EBC at a high risk of disease recurrence based on clinicopathological features and a Ki-67 score of 20% or greater.20,22-30 However, a large proportion of patients remain ineligible to receive adjuvant abemaciclib based on current public reimbursement criteria, despite their known elevated risk of disease recurrence. These patients are faced with a scarcity of adjuvant treatment options to delay or prevent disease recurrence beyond what is offered by ET alone, despite existing evidence of benefit.
Abemaciclib is an inhibitor of cyclin D–dependent kinases 4 and 6 (CDK4 and CDK6) and was most active against cyclin D1/CDK4 complex in enzymatic assays. The recommended dose of abemaciclib is 150 mg taken orally, twice daily. For EBC, abemaciclib is continued until completion of either 2 years of treatment or until disease recurrence or unacceptable toxicity.31 On January 12, 2022, Health Canada–approved abemaciclib for use in combination with ET for the adjuvant treatment of adult patients with HR-positive, HER2-negative, node-positive EBC at high risk of disease recurrence based on clinicopathological features and a Ki-67 score of 20% or greater. That is, the initial indication was for a subpopulation with Ki-67 score of 20% or greater in cohort 1 (i.e., the cohort 1 Ki-67–high] in the monarchE trial).32 In 2022, CADTH recommended that abemaciclib in combination with ET be reimbursed for this population.33 In December 2023, Health Canada updated the indication based on a Supplement to a New Drug Submission (SNDS) to expand the use of abemaciclib plus ET for the adjuvant treatment of adult patients with HR-positive, HER2-negative, node-positive EBC at high risk of disease recurrence based on clinicopathological features.31
Patient and Clinician Group Perspectives
The information in this section is a summary of input provided by the patient and clinician groups who responded to the Canada's Drug Agency (CDA-AMC) call for input and from clinical expert(s) consulted for the purpose of this review.
Patient Input
CDA-AMC received 2 patient group submissions, 1 from the Canadian Breast Cancer Network (CBCN) and 1 from Rethink Breast Cancer (Rethink). CBCN is a leading, patient-directed, national health charity committed to ensuring the best quality of care for all people in Canada affected by breast cancer through the promotion of information, education, and advocacy activities. Rethink is a Canadian charity that educates, empowers, and advocates for system changes to improve the experience and outcomes of those with breast cancer, focusing on historically underserved groups: people diagnosed at a younger age, those with metastatic breast cancer, and those who are systemically marginalized due to race, income, or other factors.
CBCN gathered data via the 2022 Triple Negative Breast Cancer Patient Survey and the 2017 Breast Cancer Patient Survey. Of the 981 people who completed the English-only 2022 survey, 190 had early-stage HR-positive, HER2-negative breast cancer. Of the 216 patients who participated in CBCN’s 2017 survey, 32 had HR-positive, HER2-negative breast cancer. CBCN also conducted an interview in November 2023 with a person with HR-positive, HER2-negative breast cancer who was unable to receive abemaciclib treatment due to the requirement that a patient’s Ki-67 score be 20% or greater. CBCN also conducted a review of current studies and grey literature to identify the issues and experiences that are commonly shared among many women living with breast cancer as well as data from the clinical trial related to the treatment in question. Rethink also conducted telephone interviews in March 2022 with 2 patients who had experience with abemaciclib treatment for HR-positive, HER2-negative, high-risk EBC.
According to CBCN, a diagnosis of early-stage HR-positive, HER2-negative breast cancer has a significant impact on patients’ lives and breast cancer treatment has a significant impact on their emotional and physical well-being. CBCN further commented that most patients with early-stage breast cancer will undergo various treatments that may include surgery, chemotherapy, hormone therapy, targeted therapy, and radiation. These treatments significantly impact patients’ lives, not only due to the disruptions in their daily life caused by attending treatment appointments, but also due to the many side effects that breast cancer patients experience as a result of treatments. Rethink also highlighted that those diagnosed in their 20s, 30s, and early 40s face age-specific issues such as fertility or family-planning challenges, diagnosis during pregnancy, child care, impact on relationships, body image, dating and sexuality, feeling isolated from peers who do not have cancer, career hiatuses, and financial insecurity.
In terms of available treatments, both groups agreed that current treatment of patients with HR-positive, HER2-negative EBC depends on the details of the person’s diagnosis and the characteristics described in their pathology report. Treatment usually involves a combination of surgery, chemotherapy, radiation therapy, and hormonal therapy, which can reduce the risk of early-stage breast cancer coming back. Some patients opt for an oophorectomy. Responses to the 2022 CBCN survey showed that most of the patients with HR-positive, HER2-negative breast cancer had received or were currently receiving surgery (189 patients), hormone therapy (152 patients), and radiation therapy (135 patients); additional treatments included previous or current treatment with chemotherapy (89 patients) and biologics or targeted therapies (12 patients). Both the 2022 and the 2017 CBCN surveys indicated that efficacy of treatment was a high priority for patients. The proportion of survey respondents who rated treatment efficacy as an important, a very important, or the most important factor in treatment decision-making was 81% in the 2022 survey and 72% in the 2017 survey.
According to both groups, treatment efficacy, minimizing side effects, and reducing the risk of recurrence are the greatest concerns of patients with early-stage breast cancer, and patients expect treatment to result in a good quality of life.
Rethink conducted phone interviews with 2 patients with high-risk EBC who have experience with abemaciclib. Both patients accessed abemaciclib through the sponsor. They were willing to try treatment with abemaciclib because it can potentially lower the possibility of recurrence, and it is well-tolerated. CBCN did not interview any patients with experience with abemaciclib, but spoke with 1 patient who wanted to receive treatment with abemaciclib but was unable to because their Ki-67 index score was 18% instead of the required 20% or greater. The patient expressed their concern, “Being able to access the additional medication, the one that’s called Verzenio, that would mean a lot, especially mentally it’s going to help me just relax. Because right now I feel very stressed, and I don’t know what route to go to access that medication. What do I have to do to be able to take it? That’s stressful.”
Rethink emphasized that the removal of the requirement for a Ki-67 score of 20% or greater would remove a barrier to care for patients due to inequitable access to Ki-67 testing across Canada. The patients interviewed by Rethink indicated how critically important it was to them to be able to reduce their risk of recurrence, noting that by removing this barrier, more people in this patient population would have the choice to make treatment decisions based on their personal priorities and treatment goals.
Clinician Input
Input From Clinical Experts Consulted by CDA-AMC
The following input was provided by 2 clinical specialist(s) with expertise in the diagnosis and management of breast cancer.
The clinical experts indicated that the goal of the treatment is to decrease risk of recurrence. The most important goal is to improve overall survival (OS). Currently, the SOC of systemic adjuvant therapy can include chemotherapy, ET, and bisphosphonate treatment. The adjuvant ET includes tamoxifen and aromatase inhibitors (i.e., anastrozole, letrozole, and exemestane). The clinical experts indicated that the SOC of adjuvant therapies and the type of adjuvant ET is guided by menopausal status. The clinical experts indicated that for people with high-risk node-positive disease who are premenopausal, optimal ET is OFS plus aromatase inhibitor unless contraindicated or not tolerated.
The clinical experts indicated that despite these current treatments, many people develop metastatic disease, which is incurable once it occurs. Hence, there is an urgent need for new treatments to address this high risk of serious, life-threatening metastatic breast cancer. Furthermore, treatments that target the underlying mechanisms that drive breast cancer recurrence are needed.
Abemaciclib is in a class of medications called kinase inhibitors. It works by blocking the action of an abnormal protein that signals cancer cells to multiply. This helps slow or stop the spread of cancer cells. The clinical expert indicated that the mechanism of action of abemaciclib would be complementary and abemaciclib would be added to SOC with ET. The clinical experts indicated that abemaciclib is already in use through patient support programs for all patients who meet the inclusion criteria in the monarchE trial (i.e., for patients in both cohort 1 and cohort 2) in Canada. The treatment would be used for all patients who meet monarchE study criteria as long as there are no contraindications. It would not be appropriate for patients to try alternative therapies if they meet monarchE trial criteria. High-risk disease was defined as either 4 or more positive axillary lymph nodes (ALNs), or between 1 and 3 positive ALNs and either histologic grade 3 disease or tumour size of 5 cm or larger (cohort 1). Patients with high risk are at greater risk of recurrence or metastatic development. A smaller number of patients with between 1 and 3 positive ALNs and Ki-67 of at least 20% as an additional risk feature were also enrolled in the monarchE trial (cohort 2). Patients with metastatic (stage IV) disease would not receive abemaciclib as SOC but would move on to first-line metastatic treatment which would depend on their prior treatment exposure. The clinical experts indicated that Ki-67 testing would need to be made available for patients with 1 to 3 positive ALNs if they do not have a histologic grade 3 disease or tumour 5 cm or larger. Ki-67 testing is not reflexively conducted in Canada and may not be available in all jurisdictions. The clinical experts also indicated that misdiagnosis is unlikely given the SOC for pathological testing in breast cancer to date. It is not possible to confirm upfront who will respond to therapy.
As to the response assessment, the clinical experts indicated that for adjuvant therapies, the goal is to improve survival (preferably OS, but invasive disease–free survival [IDFS], distant relapse–free survival [DRFS] are also used). While OS is an important outcome, the clinical experts noted that most adjuvant trials do not power their analyses for OS and, given that patients with early-stage HR-positive, HER2-negative breast cancer have such a long survival duration with availability of life-prolonging options in the metastatic setting, it is probably not feasible to demonstrate OS benefit in a clinical trial setting.
The clinical experts indicated that the drug would be discontinued if a patient develops recurrence or metastatic disease while receiving adjuvant therapy.
The clinical experts noted that these treatments for breast cancer should be provided by medical oncology specialist outpatient clinics, general practitioner-oncologists with appropriate training, and community or academic medical oncology outpatient settings. Also, appropriate retail or specialty pharmacies for dispensing oral oncology agents are needed.
Clinician Group Input
CDA-AMC received 1 clinician group submission from the Ontario Health – Cancer Care Ontario (OH-CCO) Breast Cancer Drug Advisory Committee. OH-CCO’s Drug Advisory Committees (DAC) provide timely evidence-based clinical and health system guidance on drug-related issues in support of the OH-CCO mandate and the Provincial Drug Reimbursement Programs and the Systemic Treatment Program.
OH-CCO Drug Advisory Committees gathered information at a meeting. The Committee mentioned that standard treatment varies depending on risk of recurrence but includes combinations of surgery, radiotherapy, adjuvant and/or neoadjuvant chemotherapy, and ET. Adjuvant ET is standard treatment for HR-positive, HER2-negative EBC and has been associated with a significant reduction in risk of recurrence and death. The Drug Advisory Committee noted problems with access to Ki-67 testing in the 2022 submission to CADTH, and supports the inclusion of patients who are similar to patients in cohort 1 of the monarchE study. The DAC assumes that patients who are similar to patients in cohort 2 would continue to be eligible.
The OH-CCO Drug Advisory Committee recognized that abemaciclib is an oral, continuously dosed, CDK4 and CDK6 inhibitor approved for HR-positive, HER2-negative advanced breast cancer, and the efficacy and safety of abemaciclib in advanced breast cancer supported its evaluation in the adjuvant setting. The OH-CCO Drug Advisory Committee highlighted that the treatment goals would be improved survival and decrease risk of recurrence. The OH-CCO Drug Advisory Committee further commented that among people with BRCA1 or BRCA2 carrier status, both abemaciclib and olaparib are adjuvant choices; therefore, there may be downstream effects on subsequent agents in the event of relapse, which is addressed in the algorithm.
The OH-CCO Drug Advisory Committee agreed that despite the advances in treatment of patients with HR-positive, HER2-negative breast cancer, up to 50% of patients with high-risk clinical and/or pathologic features may experience distant recurrence. The OH-CCO Drug Advisory Committee stated that superior treatment options are therefore needed to prevent early recurrence and development of metastases in patients with high risk, and that abemaciclib could be used in addition to ET following surgery and chemotherapy (if applicable).
The OH-CCO Drug Advisory Committee indicated that the patients best suited for treatment with abemaciclib would be those with HR-positive, HER2-negative EBC at high risk of recurrence that is node positive and would align with the inclusion criteria of the monarchE clinical trial (i.e., both cohort 1 and cohort 2 of the trial).
The OH-CCO Drug Advisory Committees believed that no extra imaging would likely be needed to assess treatment response, but patients would need extra monitoring for hematologic toxicity and diarrhea as well as additional support from oncology pharmacists and nursing staff. Discontinuation factors for abemaciclib would be disease progression and toxicity.
The OH-CCO Drug Advisory Committee stated that the appropriate settings for treatment with abemaciclib would have clinicians with experience in treating patients with breast cancer, access to laboratory blood work, and pharmacy and nursing support in the management of oral agents.
Drug Program Input
The drug programs provide input on each drug being reviewed through the CDA-AMC Reimbursement Review processes by identifying issues that may impact their ability to implement a recommendation. The implementation input and corresponding responses from the clinical experts consulted by CDA-AMC are summarized in Table 3.
Clinical Evidence
Systematic Review
Description of Studies
One pivotal trial (monarchE trial) is included in the review. The monarchE trial was a multinational, ongoing, open-label, phase III randomized controlled trial (RCT) that compared the efficacy and safety of abemaciclib in combination with ET to ET alone in the adjuvant treatment of patients with HR-positive, HER2-negative, node-positive EBC who had completed definitive locoregional therapy and were at high risk of recurrence based on clinicopathological features or Ki-67 index. The monarchE trial had a screening period of up to 6 months, a 2-year treatment period, and a follow-up period of up to 10 years. A total of 5,637 patients (including ██ patients from Canada) in 38 countries, were randomized to treatment with either abemaciclib plus ET or ET alone. Patients were recruited into 2 cohorts; patients in cohort 1 (n = 5,120; 90.8%) were eligible based on high-risk clinicopathological features (i.e., ≥ 4 positive ALNs or 1 to 3 positive ALNs and at least 1 of the following: tumour size ≥ 5 cm or histologic grade 3 disease), and cohort 2 (n = 517; 9.2%) included patients with high risk of recurrence based on 1 to 3 positive ALNs and high levels of Ki-67 (Ki-67 index ≥ 20%). The primary efficacy end point was IDFS, and the secondary end points included DRFS, OS, health-related quality of life (HRQoL), and harms. Health care resource utilization (hospitalizations, transfusions) was analyzed and reported as exploratory outcomes. The results of IDFS, DRFS, and OS presented in this report are based on the OS interim analysis (IA) 3 data, after a median follow-up of 54 months. HRQoL measurements (e.g., Functional Assessment of Cancer Therapy – Breast [FACT-B]) and health care resource utilization are based on OS IA2 data, after a median follow-up of 42 months. Harms data reported in this review were based on either OS IA2 data (median follow-up of 42 months) or OS IA3 data (median follow-up of 54 months).
Efficacy Results
IDFS: In the intention-to-treat (ITT) population (cohort 1 + cohort 2 of the monarchE trial), a treatment benefit for IDFS was first observed at IA2 in an analysis that was controlled for multiplicity. At OS IA3 (median follow-up of 54 months), the median IDFS was not reached in either of the treatment arms. There were a total of 407 events (14.5%) in the abemaciclib plus ET arm and 585 (20.7%) in the ET arm (hazard ratio = 0.680; 95% CI, 0.599 to 0.772; P < 0.0001). The between-group differences in IDFS for abemaciclib plus ET versus ET alone were 2.8% (95% CI, 1.3% to 4.3%) at 24 months, 4.8% (95% CI, 3.0% to 6.6%) at 36 months, and 7.6% (95% CI, 5.2% to 10.0%) at 60 months. Subgroup analyses of OS were largely consistent with the primary analysis.
DRFS: The analysis of DRFS was uncontrolled for multiplicity. In the ITT population, at OS IA3 (median follow-up of 54 months), the median DRFS was not reached in either of the treatment arms. There were a total of 345 (12.3%) events in the abemaciclib plus ET arm and 501 (17.7%) in the ET arm (hazard ratio = 0.675; 95% CI, 0.588 to 0.774; P < 0.0001). The between-group differences in DRFS for abemaciclib plus ET versus ET alone were 2.5% (95% CI, 1.1% to 3.9%) at 24 months, 4.1% (95% CI, 2.4% to 5.8%) at 36 months, and 6.7% (95% CI, 4.5% to 9.0%) at 60 months. Subgroup analyses of DRFS were largely consistent with the primary analysis.
Based on the clinical experts CDA-AMC consulted for this review, these between-group differences observed for IDFS and DRFS are clinically meaningful.
It should be noted that patients enrolled in cohort 1 (N = 5,120; 90.8%) had high-risk EBC based on clinicopathological features including the number of positive lymph nodes, tumour size, and tumour grade.34-38 Patients were enrolled in cohort 2 (N = 517; 9.2%) based on clinicopathological features,35 or absence of high-risk clinicopathological features37 (i.e., no more than 3 nodes positive, tumour grade 1 or grade 2, and tumour size < 5 cm), with the additional risk factor of high cell proliferation defined as a Ki-67 score of at least 20%.34,35,37
OS: At a median follow-up of 54 months (OS IA3 data cut-off), OS results remained immature with 442 deaths in the ITT population, corresponding to a 68% information fraction of the 650 events required for the final OS analysis. The median OS was not reached in either of the treatment arms. The estimated hazard ratio was 0.903 (95% CI, 0.749 to 1.088; P = 0.284) for abemaciclib plus ET compared with ET alone. The between-group difference in OS probability for abemaciclib plus ET versus ET alone was 1.1% (95% CI, –0.8% to 3.0%) at 60 months.
HRQoL: At OS IA2 data cut-off (median follow-up: 42 months), the least squares mean (LSM) difference in change from baseline in FACT-B total score at 24 months was –2.60 points (95% CI, –3.5 to –1.69 points) for abemaciclib plus ET versus ET alone in the safety population. At 12 months following treatment discontinuation (also known as additional follow-up 2), the LSM difference in change from baseline was –0.79 (95% CI, –1.76 to 0.18 points.
Health care resource utilization: At OS IA2 (median follow-up: 42 months), more patients in the abemaciclib plus ET arm than in the ET arm experienced hospitalizations due to adverse events (AEs) (13.8% versus 8.8%). Patients were mostly hospitalized as a result of system organ class infections and infestations (196 [3.5%] patients), specifically pneumonia (23 [0.8%] in the abemaciclib plus ET arm and 15 [0.5%] in the ET arm). Also, numerically more patients in the abemaciclib plus ET arm than in the ET alone arm received transfusions (1.6% versus 0.4%), with anemia the most commonly reported AE requiring a transfusion (32 patients [1.1%] in the abemaciclib plus ET group and 7 [0.3%] patients in the ET group).
Harms Results
At OS IA3 (data cut-off date: July 3, 2023), most patients in both treatment arms experienced AEs (98.4% in the abemaciclib plus ET arm and 88.9% in the ET arm). The most common AEs (> 30%) were diarrhea, neutropenia, fatigue, leukopenia, and abdominal pain. These were experienced more frequently by patients in the abemaciclib plus ET arm than those in the ET arm. The most common AEs (> 20%), which occurred more often among patients in the ET arm than in the abemaciclib plus ET arm, were arthralgia and hot flush, and fatigue. Grade 5 treatment-emergent adverse events (TEAEs) were reported rarely (abemaciclib plus ET versus ET: 0.6% versus 0.4%). At OS IA3, numerically more patients in the abemaciclib plus ET arm than the ET arm experienced serious adverse events (SAEs) (15.6% versus 9.2%).
At OS IA2, the proportion of patients who discontinued treatment because of AEs was higher in the abemaciclib plus ET arm than in the ET arm (18.5% versus 1.1%). The AE that most commonly resulted in treatment discontinuation was diarrhea.
The clinical experts CDA-AMC consulted for this review indicated that, of the reported AEs of special interest, venous thromboembolic events (VTEs) and interstitial lung disease (ILD) and/or pneumonitis are most clinically important. Any grade of VTEs occurred among 2.5% of patients in the abemaciclib plus ET arm and 0.7% in the ET arm. Any grade of ILD/pneumonitis occurred in 3.3% of patients in the abemaciclib plus ET arm and 1.3% in the ET arm.
In summary, according to the clinical experts CDA-AMC consulted for this review, the harms results for abemaciclib plus ET in the monarchE trial were generally consistent with those previously reported for abemaciclib and ET in the locally advanced or metastatic breast cancer setting; no new or unexpected harms were identified in the monarchE trial. Overall, most AEs were predictable, low-grade, reversible, and clinically manageable with co-medications and/or dose modifications for most patients and were acceptable in the EBC curative setting.
Critical Appraisal
An appropriate method of randomization was reported. Sample size was adequate, and the study was powered (based on the ITT population) to test its primary end point. Objective outcomes and validated health-related outcomes were assessed. The statistical approach of gatekeeping to sequentially test the primary and secondary end points was acceptable to account for multiple testing across these analyses.
In terms of potential limitations, the trial was an open-label design. Performance and detection bias that may result from lack of blinding of patients and investigators to assigned study treatments cannot be ruled out. For example, a patient’s knowledge of their assigned treatment could result in overestimating or underestimating safety end points and patient-reported outcomes and HRQoL. However, there was minimal evidence of bias for the objective end points.
DRFS analysis was not controlled for multiple comparisons, and the analysis was at increased risk of type I error (i.e., false-positive findings).
IDFS and DRFS are considered early indicators of a patient’s survival, especially for less advanced conditions in which longer survival is expected. OS data in the monarchE trial remain immature, which is expected in this disease setting with longer survival prognosis. The efficacy of abemaciclib plus ET with regard to OS will require a larger number of events and a longer follow-up period. Considering that the OS data are not mature at OS IA3, it is unclear if improvements in IDFS and DRFS observed among patients in the abemaciclib plus ET arm of the monarchE trial would translate into clinically meaningful OS benefits. OS did not reach statistical significance; however, the lower number of deaths in the abemaciclib arm plus ET arm compared with the ET arm suggest that a survival signal favouring abemaciclib may be emerging.
Regarding the HRQoL (e.g., FACT-B), the sponsor noted that differences across treatment arms were evaluated based on numerical estimates and the interpretation should be viewed as exploratory. In addition, there was a substantial attrition rate for HRQoL (e.g., FACT-B) assessments over time, with 70.3% of patients contributing to the assessments at visit 27 and 64.3% to the assessments 12 months after treatment discontinuation. As a result, there is a risk of bias due to missing outcome data because the missing-at-random assumption underlying the analysis may not be plausible.
The clinical experts consulted by CDA-AMC noted that patients in the trial were about a decade younger than patients with EBC encountered in clinical practice, who are generally diagnosed and treated in their early to mid 60s. However, this may be explained by high-risk features being potentially more prevalent in younger patients. The clinical experts also noted that the inclusion of younger and healthier patients may have led to fewer harms and to a higher number of manageable and reversible AEs. In addition, a total of 98% patients in the trial had had prior chemotherapy (i.e., neoadjuvant or adjuvant chemotherapy). However, the clinical experts indicated that prior chemotherapy in this setting may not be used as much in current practice with the integration of genomic testing for patients with 1 to 3 nodes positive. Nevertheless, the clinical experts stated that inclusion of younger patients and the high proportion of patients with prior chemotherapy are unlikely to have a significant impact on the generalizability of the findings to Canadian clinical practice.
Overall, the clinical experts CDA-AMC consulted for this review indicated that the patients included in the monarchE trial are representative of patients in clinical practice in Canada. Generalizability of the results is unlikely to be a concern.
GRADE Summary of Findings and Certainty of the Evidence
Methods for Assessing the Certainty of the Evidence
For the 1 RCT included in the sponsor’s systematic review, Grading of Recommendations Assessment, Development, and Evaluation (GRADE) was used to assess the certainty of the evidence for outcomes considered most relevant to inform the CDA-AMC expert committee deliberations, and a final certainty rating was determined as outlined by the GRADE Working Group.39,40
High certainty: We are very confident that the true effect lies close to that of the estimate of the effect.
Moderate certainty: We are moderately confident in the effect estimate — The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. We use the word “likely” for evidence of moderate certainty (e.g., “X intervention likely results in Y outcome”).
Low certainty: Our confidence in the effect estimate is limited — The true effect may be substantially different from the estimate of the effect. We use the word “may” for evidence of low certainty (e.g., “X intervention may result in Y outcome”).
Very low certainty: We have very little confidence in the effect estimate — The true effect is likely to be substantially different from the estimate of effect. We describe evidence of very low certainty as “very uncertain.”
Following the GRADE approach, evidence from RCTs started as high-certainty evidence and could be rated down for concerns related to study limitations (which refers to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias.
When possible, certainty was rated in the context of the presence of an important (nontrivial) treatment effect; if this was not possible, certainty was rated in the context of the presence of any treatment effect (i.e., the clinical importance is unclear). In all cases, the target of the certainty of evidence assessment was based on the point estimate and where it was located relative to the threshold for a clinically important effect (when a threshold was available) or to the null.
Results of GRADE Assessments
Table 2 presents the GRADE summary of findings for abemaciclib plus ET versus ET alone for the adjuvant treatment of adult patients with HR-positive, HER2-negative, node-positive EBC at high risk of disease recurrence (the ITT population).
Long-Term Extension Studies
Not available.
Indirect Comparisons
Not available.
Studies Addressing Gaps in the Evidence From the Systematic Review
Not available.
Table 2: Summary of Findings of Abemaciclib Plus ET Combination Therapy Versus ET Monotherapy for Adult Patients With HR-Positive, HER2-Negative, Node-Positive Early Breast Cancer at High Risk of Disease Recurrence Based on Clinicopathological Features (ITT Population)
Outcome and follow-up | Patients (studies), N | Relative effect (95% CI) | Absolute effects (95% CI) | Certainty | What happens | ||
|---|---|---|---|---|---|---|---|
ET monotherapy | Abemaciclib + ET | Difference | |||||
IDFS at OS IA3 (data cut-off date: July 3, 2023) with a median follow-up of 54 months (IQR of 49.5 to 59.5 months in both arms) | |||||||
IDFS probability at 24 months | 5,637 (1 RCT) | NR | 89.9 per 100 | 92.7 per 100 (91.6 to 93.6 per 100) | 2.8 more per 100 (1.3 to 4.3 more per 100) | High | The combination of abemaciclib + ET results in little to no clinically important difference in IDFS compared with ET monotherapy at 24 months. |
IDFS probability at 36 months | 5,637 (1 RCT) | NR | 84.4 per 100 | 89.2 per 100 (88.0 to 90.4 per 100) | 4.8 more per 100 (3.0 to 6.6 more per 100) | Moderatea | The combination of abemaciclib + ET likely results in a clinically important increase in IDFS compared with ET monotherapy at 36 months. |
IDFS probability at 60 months | 5,637 (1 RCT) | NR | 76.0 per 100 | 83.6 per 100 (82.0 to 85.1 per 100) | 7.6 more per 100 (5.2 to 10.0 more per 100) | High | The combination of abemaciclib + ET results in a clinically important increase in IDFS when compared with ET monotherapy at 60 months. |
DRFS at OS IA3 (data cut-off date: July 3, 2023) with a median follow-up of 54 months (IQR of 49.5 to 59.5 months in both arms) | |||||||
DRFS probability at 24 months | 5,637 (1 RCT) | NR | 91.5 per 100 | 94.0 per 100 (93.1 to 94.9 per 100) | 2.5 more per 100 (1.1 to 3.9 more per 100) | High | The combination of abemaciclib + ET results in little to no clinically important difference in DRFS compared with ET monotherapy at 24 months. |
DRFS probability at 36 months | 5,637 (1 RCT) | NR | 86.7 per 100 | 90.9 per 100 (89.9 to 91.9 per 100) | 4.1 more per 100 (2.4 to 5.8 more per 100) | Moderatea | The combination of abemaciclib + ET likely results in a clinically important increase in DRFS compared with ET monotherapy at 36 months. |
DRFS probability at 60 months | 5,637 (1 RCT) | NR | 79.2 per 100 | 86.0 per 100 (84.5 to 87.4 per 100) | 6.7 more per 100 (4.5 to 9.0 more per 100) | High | The combination of abemaciclib + ET results in a clinically important increase in DRFS compared with ET monotherapy at 60 months. |
Overall survival at OS IA3 (data cut-off date: July 3, 2023) with a median follow-up of 54 months (IQR: 49.5 to 59.5 months in both arms) | |||||||
OS probability at 60 months | 5,637 (1 RCT) | NR | 89.6 per 100 | 90.7 per 100 (89.3 to 92.0 per 100) | 1.1 more per 100 (0.8 less to 3.0 more per 100) | Moderateb | The combination of abemaciclib + ET likely results in little to no clinically important difference in OS compared with ET monotherapy at 60 months. |
Health-related quality of life at OS IA2 with a median follow-up time of 42 months (IQR, 41.75 to 42.28 months) | |||||||
FACT-B total score (range, 0 [worst] to 148 [best]), LSM change from baseline to 24 months, points | 3,961 (1 RCT) | Not applicable | 0.08 (SE = 0.33) | –2.52 (SE = 0.33) | –2.60 (–3.5 to –1.69) | Lowc | The combination of abemaciclib + ET may result in little to no clinically important difference in FACT-B compared with ET monotherapy at 24 months. |
FACT-B total score (range, 0 [worst] to 148 [best]), LSM change from baseline to 12 months —after treatment discontinuation, points | 3,622 (1 RCT) | Not applicable | –0.10 (SE = 0.35) | –0.89 (SE = 0.35) | –0.79 (–1.76 to 0.18) | Lowc | The combination of abemaciclib + ET may result in little to no clinically important difference in FACT-B compared with ET monotherapy at 12 months post–treatment discontinuation. |
Notable harms (i.e., AEs of special interest) (OS IA2) with a median follow-up time: 42 months | |||||||
VTE (any grade) | 5,591 (1 RCT) | NR | 0.7 per 100 | 2.5 per 100 (NR) | NR | Moderated | The evidence of combination of abemaciclib + ET likely results in little to no clinically important difference on VTE compared with ET monotherapy. |
ILD/pneumonitis (any grade) | 5,591 (1 RCT) | NR | 1.3 per 100 | 3.3 per 100 (NR) | NR | Moderated | The evidence of combination of abemaciclib + ET likely results in little to no clinically important difference in ILD/pneumonitis compared with ET monotherapy. |
AE = adverse event; CI = Confidence interval; DRFS = distant relapse–free survival; ET = endocrine therapy; FACT-B = Functional Assessment of Cancer Therapy – Breast; HER2 = human epidermal growth factor receptor 2; HR = hormone receptor; IA = interim analysis; IDFS = invasive disease–free survival; ILD = interstitial lung disease; IQR = interquartile range; ITT = intention to treat; LSM = least squares mean; NR = not reported; OS = overall survival; RCT = randomized controlled trial; SE = standard error; VTE = venous thromboembolic event.
Notes: Study limitations (which refers to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias were considered when assessing the certainty of the evidence. All serious concerns in these domains that led to the rating down of the level of certainty are documented in the table footnotes.
The ITT population (N = 567) included cohort 1 (N = 5,120; 90.8%) and cohort 2 (N = 517; 9.2%). Therefore, results observed in the ITT population was primarily driven by the treatment effect in the cohort 1 population.
aRated down 1 level for serious imprecision. The lower bound of the 95% CI suggests little to no clinically important difference, based on clinical experts’ suggested clinically meaningful threshold of 3% to 5%.
bRated down 1 level for serious study limitations; the findings are from an IA; the findings might change at the final analysis once more events have accrued.
cRated down 2 levels for very serious study limitations: There is risk of bias in measurement of the outcome due to the open-level design and risk of bias due to missing outcome data (at least 30% patients were not included in the assessment at follow-up).
dRated down 1 level for serious imprecision. The difference between groups is informed by a small number of events.
Conclusions
Evidence from the monarchE trial shows that abemaciclib in combination with ET demonstrated a clinically meaningful benefit, compared with ET alone, in improving IDFS and DRFS when used for the adjuvant treatment of adult patients with HR-positive, HER2-negative, node-positive EBC at high risk of disease recurrence based on clinicopathological features. It is not yet clear whether IDFS and DRFS benefits will translate to improved OS benefit as the data remain immature at OS IA3. A longer follow-up time is needed to determine the OS benefit compared with ET alone in the Health Canada–indicated population given that patients with early-stage breast cancer usually have a long survival time. Abemaciclib in combination with ET may not result in a clinically meaningful difference in HRQoL assessed using FACT-B. In terms of harms, most AEs related to treatment with abemaciclib plus ET were predictable, reversible, and clinically manageable among most patients and acceptable in the EBC setting. The safety profile of abemaciclib plus ET in the monarchE trial was generally consistent with the known safety profiles previously reported for abemaciclib and ET, and the monarchE trial did not identify any new safety signals.
Introduction
Disease Background
Contents within this section have been informed by materials submitted by the sponsor and clinical expert input. The following have been summarized and validated by the CDA-AMC review team.
Overview of the Condition
Breast cancer is the most diagnosed cancer and the second leading cause of cancer-related death among females in Canada.1 In 2022, a total of 28,600 females were diagnosed with breast cancer and 5,500 females died of the disease (14% of cancer deaths among females).1 Breast cancer is a heterogeneous, phenotypically diverse disease composed of several biologic subtypes with distinct clinical behaviours.2 The most common subtype of breast cancer is HR-positive, HER2-negative, which accounts for approximately 70% of breast cancers.3,4 Anatomical staging of breast cancer is defined using the American Joint Committee on Cancer staging system and is based on the size and extent of the breast tumour (T), the extent of regional lymph node involvement (N), and the presence or absence of distant metastases (M), collectively referred to as TNM staging.5 These features are assigned individual scores, which are then combined to identify the TNM stage.6 EBC refers to invasive cancer that has not spread beyond the breast tissue or nearby lymph nodes. EBC includes ductal carcinoma in situ (stage 0) and stages I to III.7 Prognosis and treatment decisions for breast cancer have historically been guided by TNM staging, which remains valuable; however, biological factors (e.g., histologic tumour grade, cell proliferation rate [mitotic count or Ki-67 expression], HR expression, HER2 expression, and gene expression prognostic panels [or multigene assays]) are now increasingly important in determining prognosis and response to treatment.5
More than 90% of patients with breast cancer are diagnosed with early-stage disease, which is still potentially curable.8 For patients with HR-positive, HER2-negative EBC, the 5-year survival rate is greater than 90%.9 Although patients with EBC have a promising 5-year survival prognosis, and while standard therapies alone will be sufficient for many patients with HR-positive, HER2-negative disease to avoid local or distant recurrence, a subset of up to 20% to 30% of patients will nonetheless experience disease recurrence in the first 10 years. Recurrences that are distant are described as metastatic disease, which is incurable.10,11 Patients with high-risk clinicopathological features, particularly those with a high burden of nodal involvement, have been shown to be at a higher risk of disease recurrence, especially during the first few years of receiving adjuvant ET.41 For patients with EBC who do experience recurrence and progression to metastatic disease, 5-year survival rates drop dramatically to only 34.0% (for patients with HR-positive, HER2-negative disease).9 Breast cancer is the most prevalent form of cancer in Canada.42
A biopsy is routinely performed as part of assessment of the primary tumour and this is used to evaluate the HR and HER2 status of the tumour.12,13 According to American Society of Clinical Oncology (ASCO)/College of American Pathologists (CAP) criteria, a tumour is considered HR-positive if at least 1% of the cells examined have estrogen receptors or progesterone receptors or both.13 Biopsied tissue samples are IHC tested for estrogen and progesterone hormone receptors.14 IHC is used to measure the amount of HER2 protein in the cancer cell, and ISH or fluorescence in situ hybridization (FISH) testing identifies the number of copies of the HER2 gene in the cancer cell in the primary tumour.15 According to ASCO/CAP criteria, tumours are HER2-negative when they are IHC 0 or IHC 1+ or IHC 2+ with negative ISH.13 A subset of HER2-negative tumours can be considered HER2-low if they have an IHC score of 1+ or 2+ without HER2 gene amplification by ISH (i.e., ISH not amplified). Ki-67 is a marker of cellular proliferation and may play a role as an independent prognostic factor for the risk of recurrence during the first 5 years following primary breast cancer treatment. Although there is no consensus on precise Ki-67 levels indicative of high versus low risk of recurrence, Ki-67 expression greater than 20% to 29% is generally considered appropriate for identifying high risk.16-18 While Ki-67 testing was not previously routine clinical practice in Canada, it is currently required to identify those patients eligible for abemaciclib based on the initial Health Canada EBC indication and CADTH recommendation for public reimbursement (i.e., for the cohort 1 Ki-67–high population in the monarchE trial, 2022). As a result, Ki-67 testing has now become widely available nationally. The present reimbursement requirement does not require a Ki-67 testing result for the majority of patients eligible for the new Health Canada indication, that is, if a patient has 4 or more positive ALNs or 1 to 3 positive ALNs plus either histologic grade 3 disease or tumour size of 5 cm or larger, they qualify as being at “high risk of recurrence based on clinicopathological features.” However, for patients with tumour involvement of 1 to 3 ALNs, tumour grade less than 3, and tumour size less than 5 cm, a Ki-67 index score of 20% or greater is necessary to be selected for abemaciclib treatment in the adjuvant setting.
The new indication under review for abemaciclib is not expected to result in any change to current diagnostic workflow. The diagnostic tests for HR and HER2 status are widely available and funded in Canada as part of standard clinical practice. Ki-67 testing is performed to identify those patients eligible for public reimbursement for the earlier (2022) cohort 1 Ki-67–high EBC indication and is publicly reimbursed for EBC samples in all provinces where abemaciclib is currently reimbursed. Before starting abemaciclib treatment, patients should undergo complete blood cell counts (for hematologic toxicity) and liver function tests, including alanine aminotransferase, aspartate aminotransferase, and serum bilirubin (for hepatotoxicity).31 These required blood tests are routine, reimbursed procedures, ordered by a physician and typically performed at an outpatient laboratory clinic.
Standards of Therapy
Contents within this section have been informed by materials submitted by the sponsor and clinical expert input. The following have been summarized and validated by the CDA-AMC review team.
In the absence of Canadian guidelines, clinicians in Canada utilize international treatment guidelines for the adjuvant treatment of HR-positive, HER2-negative, node-positive EBC. These include those provided by the National Comprehensive Cancer Network (NCCN),20 the ASCO,43 and the European Society for Medical Oncology (ESMO).12 Patients diagnosed with HR-positive, HER2-negative, node-positive EBC are typically treated with curative intent (i.e., surgery [lumpectomy or mastectomy]), which may be preceded by neoadjuvant chemotherapy or ET or both, and followed by a combination of adjuvant radiotherapy, chemotherapy, and ET or adjuvant ET alone. The goal of treatments administered before breast cancer surgery (neoadjuvant) is to improve surgical outcomes, while the goal of treatments administered after breast cancer surgery (adjuvant) is to eradicate micrometastatic disease and prevent distant recurrence. Disease management is similar for both females and males.12,20 Adjuvant ET is part of the SOC for the systemic treatment of patients with HR-positive, HER2-negative, node-positive EBC.20 Regimens may include tamoxifen and 1 of 3 aromatase inhibitors: anastrozole, letrozole, or exemestane.12,15 Data from the publicly funded health care system in Ontario (between 2012 and 2016) indicate that 68.9% of patients with HR-positive, HER2-negative EBC received ET, with an aromatase inhibitor (42.5%) and/or tamoxifen (35.1%) being the most common treatments.44 The type of adjuvant ET is guided by menopausal status. Ovarian suppression or ablation may also be used as part of ET to improve disease outcomes for people with HR-positive breast cancer who are premenopausal.20,21 OFS is required when ET is used together with an aromatase inhibitor in the treatment of patients who are premenopausal given the potential for aromatase inhibitors to stimulate ovarian function. In addition, olaparib in combination with ET is also publicly reimbursed for the adjuvant treatment of adult patients with deleterious or suspected deleterious germline BRCA-mutated, HER2-negative, high-risk EBC (who have previously received neoadjuvant or adjuvant chemotherapy), representing a relatively small and targeted population defined by genetic mutation, as opposed to clinicopathological features.22-30
Currently, abemaciclib in combination with ET is publicly reimbursed in the adjuvant setting for adults patients with HR-positive, HER2-negative, node-positive EBC at a high risk of disease recurrence based on clinicopathological features and a Ki-67 score 20% or greater.20,22-30 Abemaciclib received a positive letter of intent from the pan-Canadian Pharmaceutical Alliance (pCPA) and is listed in most provinces for patients with HR-positive, HER2-negative EBC at a high risk of recurrence based on clinicopathological features and a Ki-67 score of 20% or greater. While standard therapies alone are sufficient to prevent locoregional or distant disease recurrence among most patients with HR-positive, HER2-negative EBC, previous SOCs leave up to 30% of patients with a markedly higher risk of cancer recurrence, often with incurable distant metastases.10,11 However, patients with high risk of recurrence based on clinicopathological features, but without a high Ki-67 score, remain ineligible to receive adjuvant abemaciclib based on current public reimbursement criteria, despite the known elevated risk of disease recurrence. These patients face a scarcity of adjuvant treatment options for delaying or preventing disease recurrence aside from ET alone.
Drug Under Review
Abemaciclib is an inhibitor of CDK4 and CDK6 and was most active against cyclin D1/CDK4 complex in enzymatic assays. Abemaciclib prevents retinoblastoma protein phosphorylation, blocking progression from G1 into S phase of the cell cycle, leading to suppression of tumour growth in preclinical models following short-duration target inhibition. In estrogen receptor–positive breast cancer cell lines, sustained target inhibition by abemaciclib prevents rebound of retinoblastoma protein phosphorylation and cell cycle re-entry, resulting in senescence and apoptosis. In breast cancer xenograft models, abemaciclib dosed daily without interruption at clinically relevant concentrations — as a single agent or in combination with antiestrogens — resulted in reduction of tumour size.31 The recommended dose of abemaciclib is 150 mg taken orally, twice daily. For EBC, abemaciclib may be continued until completion of either 2 years of treatment or until disease recurrence or unacceptable toxicity.31 Abemaciclib tablets should be swallowed whole and may be taken with or without food. Patients should be instructed to take their doses of abemaciclib at approximately the same times every day.31 There are no statements in the approved Canadian product monograph regarding restricting the prescribing and/or administration of abemaciclib to certain health care professionals. Abemaciclib was previously approved by Health Canada on January 12, 2022, with an initial indication for use in combination with ET for the adjuvant treatment of adult patients with HR-positive, HER2-negative, node-positive EBC at high risk of disease recurrence based on clinicopathological features and a Ki-67 score 20% or greater (i.e., indicated for a subpopulation with Ki-67 index score ≥ 20% in cohort 1 [i.e., the cohort 1 Ki-67–high ] in the monarchE trial).32 Abemaciclib has been previously reviewed by CADTH for this initial indication. In October 2022, CADTH recommended that abemaciclib in combination with ET be reimbursed with conditions for the adjuvant treatment of adult patients with HR-positive, HER2-negative, node-positive EBC at high risk of disease recurrence based on clinicopathological features and a Ki-67 score of at least 20%.33 In 2023, the sponsor filed an SNDS with Health Canada to expand the EBC indication for abemaciclib by removing the Ki-67 requirement, as for cohort 1, and including patients meeting cohort 2 criteria.38 In December 2023, Health Canada–approved an updated indication that abemaciclib be used in combination with ET for the adjuvant treatment of adult patients with HR-positive, HER2-negative, node-positive EBC at high risk of disease recurrence based on clinicopathological features.31 For this review, the sponsor’s reimbursement request indicates that, as per indication, where “high risk of disease recurrence based on clinicopathological features” refers to patients who satisfy 1 or more of the following:
Four or more positive ALNs OR
One to 3 positive ALNs plus histologic grade 3 disease OR
One to 3 positive ALNs plus tumour size of 5 cm or greater OR
One to 3 positive ALNs plus Ki-67 20% or greater.
Patient and Clinician Group Perspectives
Patient Group Input
This section was prepared by the CDA-AMC review team based on the input provided by patient groups. The full original patient input(s) received by CDA-AMC have been included in the Patient and Clinician Group Perspectives section of this report.
CDA-AMC received 2 patient group submissions, 1 from the CBCN and 1 from Rethink. CBCN is a leading, patient-directed, national health charity committed to ensuring the best quality of care for all people in Canada affected by breast cancer through the promotion of information, education, and advocacy activities. Rethink is a charity in Canada that educates, empowers, and advocates for system changes to improve the experience and outcomes of those with breast cancer, focusing on historically underserved groups: people diagnosed at a younger age, those with metastatic breast cancer, and those who are systemically marginalized due to race, income, or other factors.
CBCN gathered data via the 2022 Triple Negative Breast Cancer Patient Survey and 2017 Breast Cancer Patient Survey. A total of 981 people completed the English-only 2022 survey, of whom 190 had early-stage HR-positive, HER2-negative breast cancer. A total of 216 patients participated in the 2017 survey, of whom 32 had HR-positive, HER2-negative breast cancer. In November 2023, CBCN also interviewed a person with HR-positive, HER2-negative breast cancer who was unable to receive abemaciclib treatment due to the requirement that patients’ Ki-67 score must be 20% or greater at the time that they wanted to access the treatment. CBCN also reviewed current studies and grey literature to identify issues and experiences that are common to many people living with breast cancer as well as data from the clinical trial related to the treatment in question. Rethink also conducted telephone interviews in March 2022 with 2 patients who had experience with abemaciclib for HR-positive, HER2-negative, high-risk EBC.
According to CBCN, a diagnosis of early-stage HR-positive, HER2-negative breast cancer has a significant impact on patients’ lives, and treatment has a significant impact on their emotional and physical well-being. CBCN further commented that most patients with early-stage breast cancer will undergo a variety of treatments that may include surgery, chemotherapy, hormone therapy, targeted therapy, and radiation. These treatments significantly impact patients’ lives, not only due to the disruption caused by attending treatment appointments, but also due to the many treatment-related side effects that patients experience. Rethink also highlighted that those diagnosed in their 20s, 30s, and early 40s face age-specific issues such as fertility or family-planning challenges, diagnosis during pregnancy, child care, impact on relationships, body image, dating and sexuality, feelings of isolation from peers with no experience with cancer, career hiatuses, and financial insecurity.
In terms of available treatments, both groups agreed that current treatment of patients with HR-positive, HER2-negative EBC depends on the details of the person’s diagnosis and the characteristics described in their pathology report. Treatment usually involves a combination of surgery, chemotherapy, radiation therapy, and hormone therapy, which can reduce the risk of early-stage breast cancer coming back. Some patients opt for an oophorectomy. The results of the 2022 CBCN survey showed that most of the patients with HR-positive, HER2-negative breast cancer had received or were currently receiving surgery (189 patients), hormone therapy (152 patients), and radiation therapy (135 patients); additional treatments included previous or current treatment with chemotherapy (89 patients), and biologics or targeted therapies (12 patients). Both the 2022 and the 2017 CBCN surveys indicated that efficacy of treatment was a high priority for patients. The proportion of survey respondents who rated treatment efficacy as an important, very important, or the most important factor in treatment decision-making was 81% in the 2022 survey and 72% in the 2017 survey.
According to both groups, treatment efficacy, minimizing side effects, and reducing the risk of recurrence are the greatest concerns for patients with early-stage breast cancer, and patients expect treatment to result in a good quality of life.
Rethink conducted phone interviews with 2 patients with high-risk EBC who had experience with abemaciclib. Both these patients accessed abemaciclib through the sponsor; they were willing to try treatment with abemaciclib because it can potentially lower the possibility of recurrence and it is well-tolerated. CBCN did not interview any patients who had experience with abemaciclib, although they spoke with 1 patient who wanted to but was unable to receive abemaciclib treatment because their Ki-67 score at the time was 18% instead of 20% or greater. The patient expressed their concern, “Being able to access the additional medication, the one that’s called Verzenio, that would mean a lot, especially mentally it’s going to help me just relax. Because right now I feel very stressed, and I don’t know what route to go to access that medication. What do I have to do to be able to take it? That’s stressful.”
Rethink emphasized that the removal of the requirement for a Ki-67 score equal to or greater than 20% would remove a barrier to care for as a result of inequitable availability of Ki-67 testing across Canada. Patients interviewed by Rethink indicated how critically important it was to them to be able to reduce their risk of recurrence, noting that by removing this barrier, more people in this patient population will have the choice to make treatment decisions based on their personal priorities and treatment goals.
Clinician Input
Input From Clinical Experts Consulted by CDA-AMC
All CDA-AMC review teams include at least 1 clinical specialist with expertise regarding the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). The following input was provided by 2 clinical specialists with expertise in the diagnosis and management of breast cancer.
Unmet Needs
The clinical experts indicated that the goals of current treatments are to decrease risk of recurrence and distant recurrence, to prevent the development of stage IV disease, which is incurable, to improve survival rates, and to minimize long-term complications of current therapy. The most important goal is to improve OS. Current treatments attempt to eradicate micrometastatic disease by targeting cancer cells through different mechanisms. The SOC of adjuvant therapy currently includes chemotherapy, ET, and bisphosphonate treatment. Adjuvant ET includes tamoxifen and aromatase inhibitors (i.e., anastrozole, letrozole, and exemestane). The clinical experts indicated that the SOC of adjuvant therapies and the type of adjuvant ET can be guided by menopausal status. One clinical expert indicated that for people with high-risk node-positive disease and who are premenopausal, optimal ET should be OFS plus aromatase inhibitor unless contraindicated or not tolerated. The clinical experts indicated that the patients with BRCA1 or BRCA2 carrier status are eligible for adjuvant olaparib if they meet Olympia study45 criteria (accessible in Ontario via the Exceptional Access Program).
The clinical experts indicated that despite current treatments, not all individuals respond, and some people still develop metastatic disease. Once metastatic disease occurs, it is incurable. The current treatment can be used to control the disease for a period of time, but eventually it progresses and kills the patient. The other clinical expert indicated that the risk of metastatic recurrence of HR-positive, HER2-negative breast cancer is very high despite standard ET. Hence, there is an urgent need for new treatments to address this high risk of serious, life-threatening, metastatic breast cancer. In addition, as not all patients tolerate ET, other treatments are also needed. That abemaciclib can be used in combination with any endocrine option at the physician’s discretion is a strength; that is, if patients do not tolerate aromatase inhibitors and OFS, abemaciclib can be combined with tamoxifen with or without OFS. Furthermore, treatments that target underlying mechanisms are needed. Abemaciclib is in a class of medications called kinase inhibitors. It works by blocking the action of an abnormal protein that signals cancer cells to multiply, helping to slow or stop the spread of cancer cells.
Place in Therapy
The clinical expert indicated that the mechanism of action of abemaciclib complements ET. This is the first CDK inhibitor that would be used in the adjuvant setting. The clinical experts indicated that abemaciclib is already in use through patient support programs for all patients in Canada who meet the inclusion criteria in the monarchE trial (i.e., for both cohort 1 and cohort 2 patients). Abemaciclib would be used as adjuvant therapy with ET to modify the disease process and prevent metastases. One of the clinical experts indicated that abemaciclib has been shown to reduce the risk of distant relapse (i.e., of metastatic breast cancer) among patients in the monarchE trial in a clinically meaningful and statistically significant way. The treatment would be used for all patients who meet monarchE study criteria as long as there are no contraindications. The clinical experts indicated that once approved, this treatment would result in a shift in practice and become the new SOC. It would not be appropriate for patients to try alternative therapies if they meet monarchE criteria. One caveat may be for BRCA1 or BRCA2 carrier status and olaparib; however, clinical experts indicated that the proportion of patients who are HR-positive on Olympia were low so if patients are eligible for both olaparib and abemaciclib, they anticipate clinicians would prefer abemaciclib. One clinical expert also noted that for patients with a known pathogenic mutation in the BRCA1 and/or BRCA2 gene who meet criteria for both Olympia and monarchE trials, some clinicians may choose to use olaparib and abemaciclib in sequence (as recommended in the St. Gallen Expert Consensus meeting in 2023).46 This is technically possible because abemaciclib could start within 16 months postoperatively in the monarchE trial and the duration of adjuvant olaparib is 12 months. However, the efficacy of this approach has not been tested within the setting of a clinical trial.
Patient Population
The clinical experts indicated that treatment with abemaciclib would be appropriate for patients who meet monarchE criteria and for those with high-risk disease who need treatment intensification. High-risk disease was defined as either 4 or more positive ALNs or between 1 and 3 positive ALNs and either grade 3 disease or tumour size of 5 cm or larger (cohort 1). Also enrolled was a smaller group of patients with 1 to 3 positive ALNs and a Ki-67 index score of at least 20% as an additional risk feature (cohort 2). These patients are at greater risk of recurrence or metastatic development. Patients with metastatic (stage IV) disease would not receive abemaciclib as SOC but would receive a first-line treatment that would be chosen based on their prior treatment exposure. Patients would need to have a good performance status (0 or 1) and an absence of strong contraindications for abemaciclib usage. They would have to have intact renal, hepatic, and hematologic parameters before commencing treatment. The clinical experts indicated that Ki-67 testing would need to be available to patients with 1 to 3 nodes positive if they do not have a grade 3 disease or tumour size of 5 cm or greater. Ki-67 testing is not reflexively conducted in Canada and may not be available in all jurisdictions. In Ontario, it can be requested by oncologists. The clinical experts also indicated that misdiagnosis is unlikely given the SOC for pathological testing in breast cancer to date. It is not possible to confirm upfront who will respond to therapy.
Assessing the Response Treatment
The clinical experts indicated that for adjuvant therapies, the goal is to improve survival (preferably OS, but IDFS and DRFS are also goals). However, the clinical experts noted that most adjuvant trials do not power their analyses for OS because patients with early-stage HR-positive, HER2-negative breast cancer have such a long survival duration, and therefore it may be difficult to demonstrate OS benefit in the EBC clinical trial setting. In addition, adjuvant therapies are also assessed for toxicity to ensure patients can tolerate therapy for the required time (in this case, 2 years of abemaciclib) and live life as normally as possible during treatment (return to work; recover from chemotherapy, surgery, and/or radiation; carry out normal activities of daily living, and so on).
Discontinuing Treatment
The clinical experts indicated that development of recurrence or metastatic disease while patients are receiving adjuvant therapy would result in discontinuation of the drugs. Monthly assessments of tolerance (through lab work and clinical assessments) would be conducted to determine if dose reductions were needed or if the treatment should be discontinued. Main symptoms to monitor for include diarrhea, leukopenia, neutropenia, transaminitis, pneumonitis, and VTEs. One clinical expert indicated that most toxicities do not require treatment discontinuation, but could be handled via dose reduction or delay and/or supportive management (e.g., Imodium for diarrhea). Less common but potentially life-threatening toxicity, like pneumonitis, or severe toxicity (e.g., grade 4) of another nature, would result in treatment discontinuation.
Prescribing Considerations
The clinical experts noted that these treatments for breast cancer should be provided by medical oncology specialist outpatient clinics, general practitioner-oncologists with appropriate training, and community or academic medical oncology outpatient settings. There would need to be capacity from appropriate retail or specialty pharmacies for dispensing of oral oncology agents.
Clinician Group Input
This section was prepared by the CDA-AMC review team based on the input provided by clinician groups. The full original clinician group input(s) received by CDA-AMC have been included in the Patient and Clinician Group Perspectives section of this report.
CDA-AMC received 1 clinician group submission from the OH-CCO Breast Cancer Drug Advisory Committee. OH-CCO’s Drug Advisory Committees provide timely evidence-based clinical and health system guidance on drug-related issues in support of CCO’s mandate, including the Provincial Drug Reimbursement Programs and the Systemic Treatment Program.
The OH-CCO Breast Cancer Drug Advisory Committee gathered information at a committee meeting. The OH-CCO Drug Advisory Committee mentioned that standard treatment varies depending on risk of recurrence but includes combinations of surgery, radiotherapy, adjuvant and neoadjuvant chemotherapy, and ET. Adjuvant ET is standard treatment of patients with HR-positive, HER2-negative EBC and has been associated with a significant reduction in risk of recurrence and death. In their 2022 submission to CADTH, the OH-CCO Drug Advisory Committee noted problems with access to Ki-67 testing and support the inclusion of patients who are similar to cohort 1 in the monarchE study. The OH-CCO Drug Advisory Committee assumes that patients who are similar to cohort 2 would continue to be eligible.
The OH-CCO Drug Advisory Committee recognized that abemaciclib is an oral, continuously dosed, CDK4 and CDK6 inhibitor approved for HR-positive, HER2-negative advanced breast cancer, and the efficacy and safety of abemaciclib in the treatment of advanced breast cancer supported its evaluation in the adjuvant setting. The OH-CCO Drug Advisory Committee highlighted that the treatment goals would be improved survival and decreased risk of recurrence. The OH-CCO Drug Advisory Committee further commented that for people with BRCA1 or BRCA2 carrier status, both abemaciclib and olaparib are adjuvant choices; therefore, there may be downstream effects on subsequent agents in the event of a relapse, which is addressed in the algorithm.
The OH-CCO Drug Advisory Committee agreed that despite the advances in treatment of patients with HR-positive, HER2-negative breast cancer, up to 50% of patients with high-risk clinical and/or pathologic features may experience distant recurrence. The OH-CCO Drug Advisory Committee stated that superior treatment options are therefore needed to prevent early recurrence and development of metastases in this group of patients, and that abemaciclib could be used in addition to ET in patients with high risk following surgery and chemotherapy (if applicable).
The OH-CCO Drug Advisory Committee indicated that the patients best suited for treatment with abemaciclib would be those who have HR-positive, HER2-negative, node-positive EBC at high risk of recurrence and who align with the inclusion criteria of the monarchE clinical trial (i.e., both cohort 1 and cohort 2).
OH-CCO’s Drug Advisory Committees considered that no extra imaging is likely to be needed to assess treatment response, but patients would need extra monitoring for hematologic toxicity and diarrhea and that additional support from oncology pharmacists and nursing staff would be required. The discontinuation factors for abemaciclib would be disease progression and toxicity.
The OH-CCO Drug Advisory Committee stated that the appropriate settings for treatment with abemaciclib would have clinicians with experience treating patients with breast cancer, access to laboratory blood work, and pharmacy and nursing staff expert in the management of oral agents.
Drug Program Input
The drug programs provide input on each drug being reviewed through CDA-AMC Reimbursement Review processes by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CDA-AMC are summarized in Table 3.
Table 3: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical experts’ responses and comments |
|---|---|
2.1. Relevant comparators | |
Abemaciclib is currently funded in jurisdictions in this patient population. This submission represents a criteria modification or expanded eligible population which would remove the requirement for a Ki-67 score of 20% or greater. Therefore, the majority of PAG input for this submission provides current status for abemaciclib (based on the prior pERC recommendation). Removal of the Ki-67 requirement will not likely impact current funding or implementation processes for abemaciclib but would allow for more patients to be eligible. PAG notes that approximately 1 of 3 patients in the monarchE trial had Ki-67 of less than 20%. The current indication for abemaciclib for HR-positive, HER2-negative EBC requires initiation within 16 months of definitive surgery, as per monarchE. | Both clinical experts agree with this statement. Current processes would be used, but more patients would have access, and can potentially omit accessing Ki-67 for those who are ≥ 4 ALN nodes positive, or patients with 1 to 3 nodes positive with grade 3, or tumour size ≥ 5 cm. However, for patients who do not meet the above high-risk criteria (i.e., for smaller cohort 2 population in monarchE trial that represented ~10% of the full trial population) should have access to abemaciclib if their Ki67 ≥ 20%. One clinical expert indicated that although not accessible, ribociclib (NATALEE study)47 will eventually be a comparator. This study examined treatment with ribociclib 400 mg for 3 years. It also included patients with high-risk node-negative disease. In addition, not a direct comparator, but we are not sure what to do with BRCA mutation carriers who are also eligible for adjuvant olaparib. Most clinicians would use abemaciclib, but some could use olaparib, or try to sequence them. |
2.2. Considerations for initiation of therapy | |
a) Disease diagnosis, scoring, or staging for eligibility If recommended, implementation of this submission would remove the need to identify potential patient eligibility with additional Ki-67 testing of tumours. Ki-67 testing is not reflexively conducted in many jurisdictions. | Both clinical experts agreed that Ki-67 testing is not reflexively conducted, so removing this criterion would remove additional logistic steps from clinicians’ perspective and in terms of pathology. |
b) Eligibility to re-treatment CDK4 and CDK6 inhibitors are eligible for re-treatment in advanced and/or metastatic disease provided that there was at least a 6-month interval between any prior abemaciclib for HR-positive, HER2-negative EBC and the development of disease recurrence. | One clinical expert indicated that this is a reasonable approach and what many clinicians would use in practice, analogous with other adjuvant situations. |
2.7. Funding algorithm (oncology only) | |
Other aspects: Removal of Ki-67 requirement would be required. | Both clinical experts indicated that Ki-67 testing would not be completely removed as clinicians would still check Ki-67 index score to determine eligibility for treatment of patients with 1 to 3 positive lymph nodes, if not grade 3 disease or tumour size ˂ 5 cm (i.e., patients in cohort 2 in monarchE). There would be less testing, as there would be no need to test those with 4 positive lymph nodes, or 1 to 3 positive lymph nodes with grade 3 disease, or 1 to 3 positive lymph nodes with tumour size ≥ 5 cm. |
2.9. System and economic issues | |
a) Concerns regarding the anticipated budget impact and sustainability This expands the potentially eligible population for adjuvant abemaciclib, which represents an impact to the budget of uncertain magnitude. PAG notes that approximately 81% of patients on monarchE completed 2 years of abemaciclib and approximately 1 of 3 patients in the monarchE trial had Ki-67 score less than 20%. PAG is interested in knowing both the economic (i.e., cost-effectiveness) and budget impact to public drug plans by removing the Ki-67 requirement. | One clinical expert indicated that this is hard to quantify, but given a minimum 6.7% reduction in metastatic development at 5 years, treatment means these individuals do not develop metastatic disease or require subsequent palliative lines of therapy (including ADCs such as sacituzumab govitecan or Enhertu). Given that these patients live 5 years on average with metastatic disease and require treatment during that time, including CDK4 and CDK6 inhibitors, then later lines of therapy and supportive care, the total time on treatment is less in this adjuvant setting. The NATALEE study47 included all LN1 to 3 regardless of Ki-67 index score. The clinical expert’s concern was that patients who would derive a benefit would be excluded. It may be worthwhile to clarify the economic impact of Ki-67 testing. Removing Ki-67 testing as a criterion for treatment would assist with access through cohort 1 (particularly because that benefit was seen regardless of Ki-67 index score in cohort 1); but given that patients in cohort 2 also benefited, it would be valuable to find a way for those who with 1 to 3 positive lymph nodes, if not grade 3 disease or tumour size ˂ 5 cm and Ki-67 ≥ 20%, to receive the drug. The other clinical expert indicated that all patients who meet monarchE criteria should have access to abemaciclib irrespective of the budget. |
ADC = antibody drug conjugate; ALN = axillary lymph node; CDK = cyclin-dependent kinase; EBC = early breast cancer; ET = endocrine therapy; HER2 = human epidermal receptor 2; NA = not applicable; PAG = Provincial Advisory Group; pERC = pan-Canadian Oncology Review Expert Review Committee.
Clinical Evidence
The objective of this Clinical Review is to review and critically appraise the clinical evidence submitted by the sponsor on the beneficial and harmful effects of abemaciclib (150 mg, oral) in combination with ET for the adjuvant treatment of adult patients with HR-positive, HER2-negative, node-positive EBC at high risk of disease recurrence based on clinicopathologic features. The focus is on comparing abemaciclib in combination with ET to relevant comparators (i.e., ET) and identifying gaps in the current evidence.
A summary of the clinical evidence included by the sponsor in the review of abemaciclib is presented in 4 sections with the CDA-AMC critical appraisal of the evidence included at the end of each section. The first section, the systematic review, includes pivotal studies and RCTs that were selected according to the sponsor’s systematic review protocol. Assessment of the certainty of the evidence using the GRADE approach follows the critical appraisal of the evidence. The second section usually includes sponsor-submitted long-term extension studies, but none were available for this review. The third section usually includes indirect evidence from the sponsor, but none were available for this review. The fourth section includes additional studies that the sponsor considered as addressing important gaps in the systematic review evidence, but none were available for this review.
Included Studies
Clinical evidence from the following are included in the CDA-AMC review and appraised in this document:
One pivotal ongoing RCT (i.e., the monarchE trial) identified in systematic review.
Systematic Review
Contents within this section have been informed by materials submitted by the sponsor. The following have been summarized and validated by the CDA-AMC review team.
Description of Study
Key characteristics of the included study are summarized in Table 4 and Figure 1. The monarchE study is a multicentre, randomized, open-label, phase III trial that compares the efficacy and harms of abemaciclib plus standard adjuvant ET to ET alone in adult patients with HR-positive, HER2-negative, node-positive EBC at high risk of disease recurrence. The trial was conducted across 611 open sites (patients from different 603 sites participated in the monarchE trial) in 38 countries; 44 patients in Canada were randomized. Patients were randomized into 2 cohorts: cohort 1 (N = 5,120; 90.8%) included patients with a high risk of recurrence based on high-risk clinicopathological features and cohort 2 (N = 517; 9.2%) included patients with a high risk of recurrence based on high Ki-67 index (≥ 20%).34 In their submission, the sponsor focused on the ITT population. An interactive web-response system was used to randomly assign patients in a 1:1 ratio within each cohort to either up to 2 years of oral abemaciclib at 150 mg twice daily and ET or ET alone using the following stratification factors: prior treatment (neoadjuvant chemotherapy versus adjuvant chemotherapy versus no chemotherapy); menopausal status (premenopausal versus postmenopausal); and region (North America or Europe versus Asia versus other). A total of 5,637 patients were randomized to treatment with either abemaciclib plus ET (N = 2,808) or ET alone (N = 2,829). The primary end point was IDFS in the ITT population. The secondary efficacy end points were DRFS and OS in the ITT population. Other secondary or exploratory end points included HRQoL and health care resource utilization, assessed in the safety population. Participants in the study received treatment with abemaciclib for up to 2 years or until discontinuation criteria were met, whichever occurred first. The duration of 2 years was selected based on previous studies that showed patients with EBC receiving ET treatment experienced an initial peak of recurrence at 2 years of treatment; the goal of the monarchE trial was to treat through the first peak of recurrence. The choice of ET was at the investigator’s discretion and was taken as prescribed during the on-study treatment period, in year 1 and year 2. In year 3 and beyond, ET was continued for a total duration of at least 5 years and up to 10 years, if deemed medically appropriate. Patients receiving standard adjuvant ET at the time of study entry could not have received more than 12 weeks of standard adjuvant ET after completion of their last non-ET (surgery, chemotherapy, or radiation) before randomization. Randomization had to occur within a maximum of 16 months following the definitive breast cancer surgery.
Table 4: Details of Studies Included in the Systematic Review
Detail | MonarchE study |
|---|---|
Designs and populations | |
Study design | Phase III, open-label, multicentre RCT |
Locations | 611 open sites (603 sites entered patients into monarchE) in 38 countries: Argentina, Australia, Austria, Belgium, Brazil, Canada (███ patients randomized), China, Czech Republic, Denmark, Finland, France, Germany, Greece, Hong Kong, Hungary, India, Israel, Italy, Japan, South Korea, Mexico, the Netherlands, New Zealand, Poland, Portugal, Puerto Rico, Romania, Russia, Saudi Arabia, Singapore, South Africa, Spain, Sweden, Taiwan, Turkey (Türkiye), Ukraine, the UK, and the US |
Patient enrolment dates | Start date: July 12, 2017 End date: August 12, 2019 (The study is still in its follow-up period.) |
Randomized (N) | Randomized: N = 5,637 Abemaciclib + ET group: n = 2,808 ET group: n = 2,829 |
Inclusion criteria |
For cohort 1:
For cohort 2: eligible based on 1 to 3 positive axillary lymph nodes and high Ki-67 index (≥ 20%) as measured in untreated breast tumour tissue by a central laboratory. These patients would not have been eligible based on eligibility requirements for cohort 1.
|
Exclusion criteria |
|
Drugs | |
Intervention | Abemaciclib 150 mg orally twice daily with at least 6 hours between doses (up to 2 years or until discontinuation criteria are met) combined with standard adjuvant ET (the physician’s choice) until discontinuation criteria are met (≥ 5 years) |
Comparator(s) | Standard adjuvant ET (of physician’s choice, such as letrozole, anastrozole, exemestane, or tamoxifen with or without GnRH agonist) until discontinuation criteria are met (≥ 5 years) |
Study duration | |
Screening phase | Cohort 1 = 3 months; cohort 2 = 6 months |
Treatment phase | Standard adjuvant ET (of physician’s choice) until discontinuation criteria are met (≥ 5 years) in both treatment arms and abemaciclib daily in the abemaciclib plus ET arm (2 years) |
Follow-up phase | Visits every 6 months until year 5 and then annually from year 6 to year 10 |
Outcomes | |
Primary end point | IDFS in the ITT population (time frame: from date of randomization to the date of first occurrence of): 1. Ipsilateral invasive breast tumour recurrence — local recurrence, defined as invasive breast cancer in the ipsilateral breast parenchyma or invasive breast cancer in the skin of the breast or the chest wall occurring after a lumpectomy and/or mastectomy. 2. Regional invasive breast cancer recurrence — defined as the development of a tumour in the axilla, regional lymph nodes (internal mammary, supraclavicular, infraclavicular), and the soft tissue of the ipsilateral breast following surgery. 3. Distant recurrence — defined as evidence of tumour in all areas other than the ones qualifying for local or regional recurrence (as described previously). 4. Death attributable to any cause, including breast cancer, non-breast cancer, or unknown cause. 5. Contralateral invasive breast cancer. 6. Second primary non-breast invasive cancer. |
Secondary and exploratory end points | Secondary
|
Publication status | |
Publications | Rastogi et al. (2024)48 Tolaney (2024)49 Johnston et al. (2020)50 Harbeck et al. (2021)51 Rugo et al. (2022)52 Toi et al. (2023)36 Paluch-Shimon et al. (2023)53 Martin et al. (2022)54 Johnston et al. (2023)35 Hamilton et al. (2023)55 Harbeck et al. (2023)56 Clinicaltrials.gov entry57 |
AE = adverse event; CDK = cyclin-dependent kinase; CTCAE = Common Terminology Criteria for Adverse Events; DRFS = distant relapse–free survival; DVT = deep vein thrombosis; ECOG PS = Eastern Cooperative Oncology Group Performance Status; ET = endocrine therapy; EQ-5D-5L = 5-Level EQ-5D; FACIT = Functional Assessment of Chronic Illness Therapy; FACIT-F = Functional Assessment of Chronic Illness Therapy - Fatigue; FACT-B = Functional Assessment of Cancer Therapy – Breast; FACT-ES = Functional Assessment of Cancer Therapy – Endocrine Symptoms; GnRH = gonadotropin-releasing hormone; HR = hormone receptor; HRQoL = health-related quality of life; IDFS = invasive disease–free survival; ITT = intention to treat; OS = overall survival; PE = pulmonary embolism; RCT = randomized controlled trial; SAE = serious adverse event; TEAE = treatment-emergent adverse event; VTE = venous thromboembolic event.
Sources: MonarchE Clinical Study Report Addendum Amendment (May 20, 2020 report)58 and Clinical Study Report Addendum (July 1, 2022 report).59
The monarchE study was an open-label study; patients were aware of their assigned treatment group and all staff at each investigative site involved in treating and caring for study patients had full knowledge of each patient’s treatment assignment. According to the sponsor, an open-label design was chosen because toxicities and laboratory abnormalities related to abemaciclib treatment, such as diarrhea, neutropenia, and creatinine, increase, thus having the potential to unblind the study. The sponsor was blinded to treatment group assignment until the study reached a positive outcome. An independent data-monitoring committee was responsible for reviewing the unblinded safety and efficacy analyses.
The study has 3 phases: the screening phase lasted 3 months for cohort 1 and 6 months for cohort 2; the treatment phase started with the first dose of treatment following randomization (i.e., abemaciclib and ET in the intervention arm or ET alone in the control arm). The first dose of abemaciclib plus ET was initiated no later than 3 days following randomization. During year 1 and year 2 (the on-study treatment period), patients came to a clinic every 2 weeks (15 days ± 3 days) for the first 2 months, monthly (30 days ± 5 days) in month 3 to month 6, and every 3 months thereafter (every 90 days ± 10 days until visit 27, i.e., at 24 months). After a short-term follow-up visit that took place 30 days after discontinuation or after completion of the on-study treatment period, all patients entered the long-term follow-up period; this long-term follow-up period will continue for up to 10 years or until study completion, with long-term follow-up visits occurring approximately every 6 months until the completion of year 5 and then yearly starting in year 6.
The focus of this submission is the OS IA3, with data cut-off on July 3, 2023. Of note, these new data became available after the SNDS submission to Health Canada. The SNDS was supported using data from OS IA2 (data cut-off on July 1, 2022).
A schematic of the study design is shown in Figure 1.
Figure 1: MonarchE Study Design
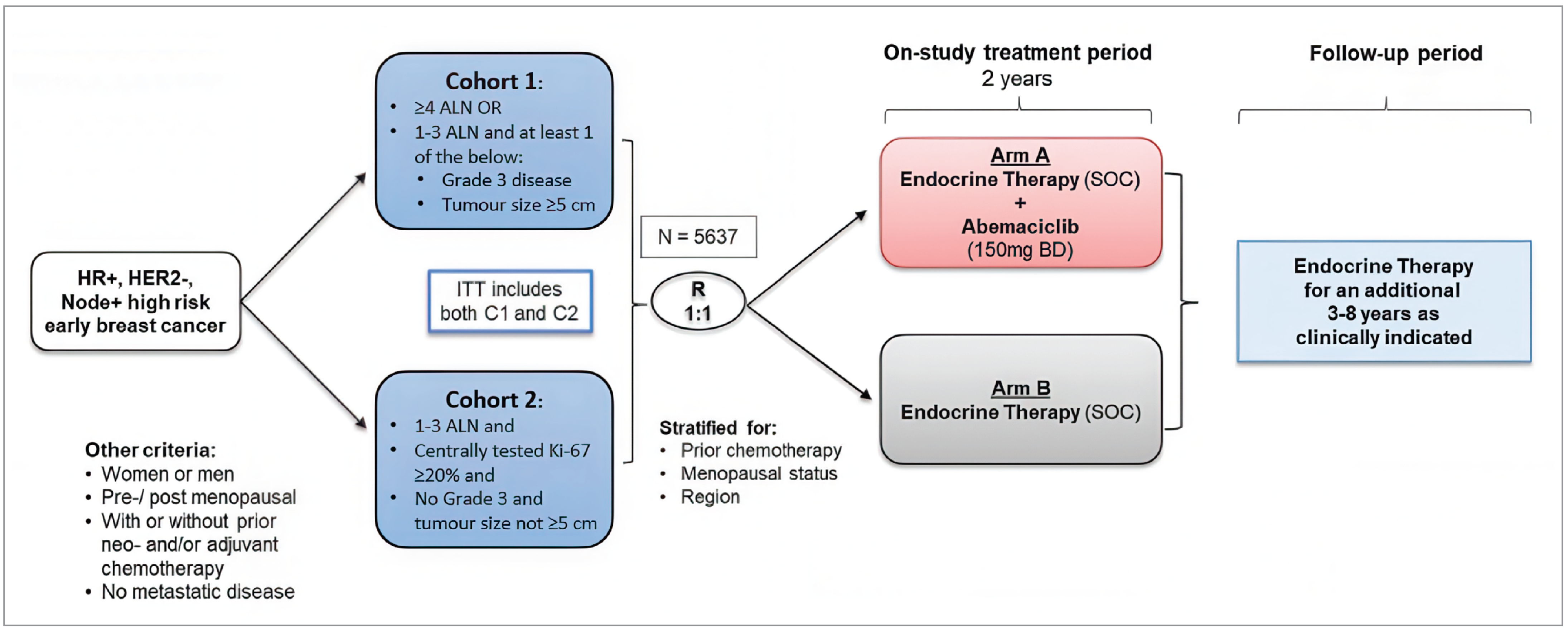
ALN = axillary lymph node; BD = twice daily; C1 = cohort 1; C2 = cohort 2; HER2- = HER2 negative; HR+ = hormone receptor positive; ITT = intention to treat; node+ = node-positive; R = randomization; SOC = standard of care.
Note: Details included in the figure are from the sponsor’s Summary of Clinical Evidence.
Source: MonarchE Clinical Study Report Addendum (July 3, 2023 report).34
Populations
Inclusion and Exclusion Criteria
Eligible patients were aged 18 years or older, with confirmed HR-positive, HER2-negative, resected invasive EBC without metastases, who had undergone definitive surgery of primary breast tumour and were randomized within 16 months of surgery, had an Eastern Cooperative Oncology Group (ECOG) Performance Status (PS) of 0 or 1, and adequate organ function. To be enrolled, patients had to fulfill 1 of the following criteria:
Cohort 1:
pathological tumour involvement in 4 or more positive ipsilateral ALNs, or
pathological tumour involvement in 1 ipsilateral ALN to 3 ipsilateral ALNs and at least 1 of
grade 3 disease, or
primary tumour size of 5 cm or larger
Cohort 2:
One to 3 positive ALNs and
centrally tested Ki-67 index score greater than or equal to 20% and
no grade 3 disease and tumour size not 5 cm or larger
Together, cohort 1 and cohort 2 represent the entirety of the randomized monarchE study population, referred to as the ITT population.
Patients with metastatic disease, node-negative or inflammatory breast cancer, a previous history of breast cancer (with the exception of ipsilateral ductal carcinoma in situ treated by locoregional therapy alone at least 5 years ago), a history of any other cancer (except nonmelanoma skin cancer or carcinoma in situ of the cervix), concurrent exogenous reproductive hormone therapy, prior ET for breast cancer, or raloxifene or previous exposure to CDK4 and CDK6 inhibitors were ineligible (refer to Table 4 for more detail).
The inclusion criteria for selecting the patient population at high risk of recurrence were based on unpublished efficacy outcome data from the West German Study Group PlanB trial and the National Surgical Adjuvant Breast and Bowel Project (NSABP) B-28 trial. Among a subset of the PlanB patient population that satisfied the monarchE criteria for high-risk disease, the estimated 5-year IDFS rate was 82.5% (95% CI, 77.8% to 87.2%), suggesting that approximately 17.5% of those patients who were at high risk of recurrence would develop invasive recurrence events within the first 5 years of primary breast cancer treatment.51
Patient population data from the more recent OS IA3 are presented in the following section, with the exception of some baseline characteristic and exposure data that were not updated since OS IA2.
Interventions
Abemaciclib Plus ET Arm
Treatment consisted of abemaciclib 150 mg administered orally, twice daily, with at least 6 hours between doses. Treatment with abemaciclib continued for up to 2 years or until discontinuation criteria were met. Standard adjuvant ET of a physician’s choice, such as letrozole, anastrozole, exemestane, or tamoxifen with or without gonadotropin-releasing hormone agonist, was taken as prescribed during the on-study treatment period (year 1 to year 2). Thereafter (in year 3 and beyond), standard adjuvant ET was continued for at least 5 years and up to 10 years, if medically appropriate. Treatment with ET continued until discontinuation criteria were met. Adjuvant treatment with fulvestrant was not allowed at any time during the study. If a patient discontinued only 1 of the combination drugs (abemaciclib or ET) before completion of the 2-year on-study treatment period for a reason other than an IDFS event, they had to continue the other drug until completion of the 2-year on-study treatment period or until other discontinuation criteria were met, whichever occurred first. The study protocol included instructions for mandated abemaciclib dose modifications (holds and reductions) to manage AEs, with a maximum of 2 dose reductions. Patients who required more than 2 dose reductions had to discontinue abemaciclib. Study treatment could be put on hold for up to 28 days to permit sufficient time for recovery from toxicity. For patients who did not recover from toxicity within 28 days, a delay of more than 28 days was permitted after agreement with the investigator and the sponsor; an abemaciclib dose adjustment was to be considered in this situation. Dose adjustment for ET was determined by the investigator and, if applicable, a switch to another ET regimen was permitted per the physician’s choice as part of SOC.
ET Arm
Standard adjuvant ET of a physician’s choice, such as letrozole, anastrozole, exemestane, or tamoxifen with or without gonadotropin-releasing hormone agonist, was given as prescribed during the on-study treatment period (year 1 to year 2). In year 3 and beyond, standard adjuvant ET was continued for at least 5 years and up to 10 years, if medically appropriate. Treatment with ET continued until discontinuation criteria were met. Adjuvant treatment with fulvestrant was not allowed at any time during the study. Dose adjustment for ET was determined by the investigator and, if applicable, a switch to another ET regimen was permitted per the physician’s choice as part of SOC.
All concomitant medications and supportive care therapies were documented at each visit. In general, the list of prohibited medications that affected patient eligibility or participation in the study were limited to ET for breast cancer prevention, concurrent exogenous reproductive hormone therapy, and recent experimental treatment in a clinical trial. Concurrent treatment with SOC bone-modifying drugs such as bisphosphonates and denosumab was permitted. With the exception of standard ET for breast cancer, no other anticancer therapy was permitted while patients were receiving on-study treatment. Patients could receive full supportive care to maximize quality of life (e.g., antiemetics, SOC bone-modifying drugs) based on the judgment of the treating physician. Patients in the abemaciclib plus ET arm received instructions on the management of diarrhea and were prescribed antidiarrheal therapy (e.g., loperamide) on their first visit. A list of concomitant medications is presented in Table 13.
Patients who discontinued the 2-year on-study treatment early were expected to continue on ET in follow-up or receive new systemic therapies at the physician’s discretion. After discontinuing or completing the 2-year on-study treatment, patients entered the study follow-up period; the systemic therapies patients received, including ET, were recorded as post-discontinuation therapies. If patients developed metastatic disease while participating in the study, they might receive anticancer therapies such as chemotherapies, ET, or targeted therapies in the metastatic setting. The post-discontinuation therapy is presented in the Table 14.
Outcomes
Efficacy
The primary end point was IDFS in the ITT population. Secondary efficacy end points were DRFS in the ITT population, OS in the ITT population, and IDFS in the Ki-67–high population (cohort 1 + cohort 2) and the Ki-67–high population (cohort 1). Other secondary end points included HRQoL and health care resource utilization, assessed in the safety population.
IDFS was defined using the standardized definitions for efficacy end points (STEEP) system60 and was measured from the date of randomization to the date of first occurrence of:
ipsilateral invasive breast tumour recurrence — local recurrence, defined as invasive breast cancer in the ipsilateral breast parenchyma or invasive breast cancer in the skin of the breast or the chest wall occurring after a lumpectomy and/or mastectomy
regional invasive breast cancer recurrence — defined as the development of a tumour in the axilla, regional lymph nodes (internal mammary, supraclavicular, infraclavicular), and the soft tissue of the ipsilateral breast following surgery
distant recurrence — defined as evidence of tumour in all areas other than the ones qualifying for local or regional recurrence (as described previously)
death attributable to any cause, including breast cancer, non-breast cancer, or unknown cause
contralateral invasive breast cancer
second primary non-breast invasive cancer.
Confirmation by biopsy or imaging was required, when possible. During treatment and follow-up, imaging was to be performed per the investigator’s judgment and according to routine standard practice. All imaging was done locally and, therefore, no central imaging assessments were performed. All patients who experienced local recurrence continued to be followed for distant recurrence. Patients for whom no event had been observed were censored at the date of their last postbaseline assessment for disease recurrence or date of randomization if no postbaseline assessment for disease recurrence had occurred. For patients who experienced an IDFS event other than distant recurrence or death, assessments continued to be performed until there was an event of distant recurrence, death, or study completion, whichever occurred first. According to the clinical experts consulted by CDA-AMC, a difference of 3% to 5% between groups would be considered clinically important.
DRFS was defined as the time from the date of randomization to distant recurrence or death attributable to any cause, whichever occurred first. Patients for whom no event was observed were censored on the day of their last assessment for recurrence or date of randomization if no postbaseline assessment for recurrence occurred. According to the clinical experts consulted by CDA-AMC, a difference of 3% to 5% between groups would be considered clinically important.
OS was defined as the time from the date of randomization to the date of death from any cause. For each patient who was not known to have died as of the data cut-off date for a particular analysis time point, OS was censored for that analysis at the date of the last contact before the data cut-off date. According to the clinical experts consulted by CDA-AMC, a difference of 3% to 5% between groups would be considered clinically important.
During year 1 and year 2 (the on-study treatment period), patients came to a clinic every 2 weeks (15 days ± 3 days) for the first 2 months, monthly (30 days ± 5 days) in month 3 to month 6, and every 3 months thereafter (every 90 days ± 10 days until visit 27). Phone visits were conducted monthly between the 3-monthly visits. A short-term follow-up visit took place approximately 30 days after 1 of the following time points, whichever occurred first: after the completion of the 2-year on-study treatment period, or after discontinuation criteria were met and a decision was made to discontinue all study treatment before the completion of the 2-year on-study treatment period. After this short-term follow-up visit, all patients entered the long-term follow-up period, which began the day after the short-term follow-up visit and will continue for up to 10 years or until study completion, whichever occurs first. Long-term follow-up visits occur approximately every 6 months until the completion of year 5 and then yearly starting in year 6.
The monarchE trial also assessed the effects of treatment on patient-reported HRQoL and AEs. The 37-item FACT-B questionnaire was used to evaluate the 2 treatment arms for general oncology–related and breast cancer–related self-reported HRQoL. The measurement properties of the FACT-B are described in Table 6. The summary scores are presented for the FACT-B total score (a score range of 0 to 148), the physical well-being (a score range of 0 to 28), social well-being (a score range of 0 to 28), emotional well-being (a score range of 0 to 24), and functional well-being (a score range of 0 to 28), as well as the breast cancer subscale (a score range of 0 to 40), and the trial outcome index (a score range of 0 to 96).61 Higher FACT-B scores indicate better quality of life.62 For patients with advanced breast cancer, a minimally important difference (MID) of 7-point to 8-point change in the total FACT-B score has been estimated using anchor and distribution-based methods. This MID was judged to be adequately applicable despite some differences in population.
A list of efficacy end points assessed in this Clinical Review is provided in Table 5, followed by descriptions of the outcome measures in Table 6. Summarized end points are based on outcomes included in the sponsor’s Summary of Clinical Evidence as well as any outcomes identified as important to this review according to the clinical expert(s) consulted by CDA-AMC and patient and clinician group input from patient and clinician groups and public drug plans. Using the same considerations, the CDA-AMC review team selected end points that were considered to be most relevant to inform CDA-AMC expert committee deliberations and finalized this list of end points in consultation with members of the expert committee. Important efficacy end points were assessed using GRADE. Select notable harms outcomes considered important for informing expert committee deliberations were also assessed using GRADE.
Harms
AEs were graded according to the Common Terminology Criteria for Adverse Events (CTCAE) version 4.0. TEAEs were defined as events that first occurred or worsened in severity while on therapy and continued until 30 days after treatment discontinuation, or serious events beyond 30 days of treatment discontinuation that were related to study treatment. SAEs were reported as treatment-emergent events on-study and during the long-term follow-up period (up to 5 years after randomization). SAEs included AEs with an outcome of death, initial or prolonged hospitalization, or life-threatening events. All SAEs in both arms were and will continue to be collected through year 5. AEs leading to dose adjustments, study treatment discontinuation, and death were also recorded. Second primary non-breast neoplasms were captured as AEs (in addition to being captured within the primary end point). Patients were followed up beyond 30 days post–study treatment discontinuation for SAEs, regardless of causality, to detect any long-term serious toxicities that are likely to be relevant for the adjuvant setting. Venous thromboembolism and ILD and/or pneumonitis were considered AEs of special interest for this review. According to the clinical experts consulted by CDA-AMC, a between-group difference of 5% to 10% for venous thromboembolism and 3% to 5% for ILD and/or pneumonitis would be considered clinically important.
Table 5: Outcomes Summarized From the Studies Included in the Systematic Review
Outcome | Time points | MonarchE |
|---|---|---|
IDFS (in ITT population) | 24, 36, and 60 months | Primarya |
DRFS (in ITT population) | 24, 36, and 60 months | Secondary |
OS (in ITT population) | 60 months | Secondarya |
HRQoL (FACT-B) | 24 months, 12 months after treatment discontinuation | Secondary |
Harms | Median 43 months | Secondary/harms |
DRFS = distant relapse–free survival; FACT-B = Functional Assessment of Cancer Therapy – Breast; HRQoL = health-related quality of life; IDFS = invasive disease–free survival; ITT = intention to treat; OS = overall survival.
Note: Details included in this table are from the sponsor’s Summary of Clinical Evidence.
aStatistical testing for these end points was adjusted for multiple comparisons via a sequential gatekeeping strategy, for type I error control. Refer to the Statistical Analysis section for more details.
Source: MonarchE Clinical Study Report Addendum.34
Table 6: Summary of Outcome Measures and Their Measurement Properties
Outcome measure | Type | Conclusion about measurement properties | MID |
|---|---|---|---|
Functional Assessment of Cancer Therapy –Breast (FACT-B); version 4 | Disease-specific HRQoL questionnaire including 27 items from the FACT-G related to physical, social/family, emotional, and functional well-being as well as a breast cancer–specific 10-item subscale.63 | Validity: In studies of breast cancer: moderate correlations between most FACT-B version 3 subscales and the Body Image Scale (r = –0.34 to –0.55);64 most subscales differentiated groups by ECOG PS rating or extent of disease indicating discriminant validity.65 Reliability: Good internal consistency reliability with alpha > 0.7 for most subscales in a study of patients with advanced breast cancer.64 Alpha coefficients ranged from 0.63 to 0.86 for all subscales and 0.90 for the total score, and test-retest reliability was good, with a correlation coefficient of 0.85 for the total score in a study of patients with breast cancer.65 Responsiveness: Among 47 patients with breast cancer tested at 2-month intervals, a significant sensitivity to change in ECOG PS rating was found for the FACT-B total score, the physical and functional well-being subscales, and the breast cancer subscale. Sensitivity to change, as measured by the Functional Living Index-Cancer, was found in the FACT-B and FACT-G total score and the physical, functional, and emotional well-being subscales.65 | In patients with advanced breast cancer, an MID has been estimated as a 7-point to 8-point change on the total FACT-B score using anchor and distribution-based methods.66 |
ECOG = Eastern Cooperative Oncology Group; FACT-B = Functional Assessment of Cancer Therapy – Breast; FACT-G = Functional Assessment of Cancer Therapy - General; HRQoL = health-related quality of life; MID = minimally important difference; PS = performance status.
Source: CADTH Reimbursement Review of Abemaciclib (2022).19
Statistical Analysis
A summary of statistical analyses for trial end points is presented in Table 7.
Sample Size and Power Calculation
Assuming a hazard ratio of 0.73 at a cumulative 2-sided alpha of 0.025, with a 5-year IDFS rate of 82.5% in the control arm, and a dropout probability rate of 10% over the first 5 years following randomization, the study would have to be powered at approximately 85% to detect the superiority of abemaciclib plus ET versus ET alone in terms of IDFS in the ITT population.35 This required approximately 390 events in the ITT population at the time of the primary analysis.
Statistical Testing
IDFS: The IDFS analysis to test the superiority of abemaciclib plus ET over ET alone was performed using the ITT population and with the log-rank test stratified by randomization factors. The 2 planned efficacy IAs and 1 planned final analysis for IDFS were to be performed after approximately 195 events, 293 events, and 390 events had been observed, respectively, in the ITT population. The second efficacy IA at approximately 293 IDFS events included both an efficacy criterion for statistical significance and a futility boundary. The cumulative 1-sided alpha was controlled at 0.025, with an alpha split of 0.00000001 for the first futility analysis and 0.02499999 for the planned efficacy analyses. The cumulative 1-sided type I error rate of 0.02499999 for the 2 planned efficacy IAs and 1 planned final analysis was maintained using the Lan-DeMets method.67 Specifically, the alpha spent at each efficacy IA was based on the exact number of IDFS events observed using the O’Brien-Fleming type stopping boundary.
A sequential gatekeeping strategy was used to control the family-wise type I error at 0.025 (1-sided) for IDFS in the ITT, Ki-67–high (cohort 1 + cohort 2), and cohort 1 Ki-67–high populations. IDFS was tested hierarchically in the order of the ITT, Ki-67–high (cohort 1 + cohort 2), then cohort 1 Ki-67–high populations, each gated after the former population. IDFS in the Ki-67–high (cohort 1 + cohort 2) population was tested only if IDFS in the ITT population was significant, and IDFS in the cohort 1 Ki-67–high population (cohort 1 + cohort 2) was tested only if IDFS in the Ki-67–high population was significant.
Table 7: Statistical Analysis of Efficacy End Points in the MonarchE Study
End point | Statistical model | Adjustment factors | Handling of missing data | Sensitivity analyses |
|---|---|---|---|---|
IDFS, as defined by STEEP system | Kaplan-Meier method was used to estimate the efficacy curves for each treatment arm. A stratified Cox proportional hazard model, with treatment as a factor, was used to estimate the hazard ratio between the 2 treatment arms and the corresponding CI and Wald P value. To test the superiority of abemaciclib plus ET to ET, IDFS analyses were performed on the ITT population and used the log-rank test. | Stratification factors included prior treatment (neoadjuvant chemotherapy vs. adjuvant chemotherapy vs. no chemotherapy), menopausal status (premenopausal vs. postmenopausal), and region (North America or Europe vs. Asia vs. other). If a patient received both neoadjuvant and adjuvant chemotherapy, the patient was stratified as having received neoadjuvant chemotherapy. Male patients were stratified as postmenopausal at the time of randomization. | Censored: Patients for whom no event had been observed were censored at the day of their last post baseline assessment for disease recurrence, as reported on the assessment for disease recurrence case report form, or the date of randomization if no post baseline assessment for disease recurrence occurred. |
|
DRFS | Analyses described for IDFS were repeated for DRFS | Stratification factors for DRFS were the same as for IDFS | Censored: Patients for whom no event had been observed were censored at the day of their last assessment for disease recurrence or date of randomization if no post baseline disease recurrence assessment occurred. DRFS events documented before the randomization date were censored at the date of randomization. DRFS events documented after more than 12 months ( + 28 days) following the last disease recurrence assessment or randomization were censored at the last assessment for disease recurrence before the documented DRFS event, or date of randomization, whichever is later. |
|
OS | Analyses described for IDFS were repeated for OS | Stratification factors for OS were the same as for IDFS | Censored: For each patient who is not known to have died as of the data-inclusion cut-off date for a particular analysis, OS was censored for that analysis at the date of last contact before the data-inclusion cut-off date. | Sensitivity analyses described for IDFS were repeated for OS. |
HRQoL | A mixed effects repeated measures model was applied to compare treatment arms | None | Implicit in the model. | None |
CDK = cyclin-dependent kinase; CI = confidence interval; DRFS = distant relapse–free survival; ET = endocrine therapy; HRQoL = health-related quality of life; IDFS = invasive disease–free survival; ITT = intention to treat; OS = overall survival; STEEP = standardized definitions for efficacy end points.
Notes: Population patient numbers are based on OS interim analysis 3.
Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Sources: MonarchE Clinical Study Report Addendum34 and Statistical Analysis Plan.68
The Kaplan-Meier method was used to estimate the IDFS curve for each treatment arm. The difference between IDFS rates for each arm was reported with 95% CIs estimated by normal approximation. A stratified Cox proportional hazards model with treatment as a factor was used to estimate the hazard ratio between the 2 treatment arms and the corresponding CI and Wald P value.
DRFS: Similar analyses as those described for IDFS were performed on DRFS but there was no alpha control to account for the risk of type I error.
OS: For OS, a sequential gatekeeping strategy was used to test treatment effect on OS in the ITT population, to maintain the experiment-wise type I error rate. That is, only if the tests of IDFS in the ITT, Ki-67–high (cohort 1 + cohort 2), and cohort 1 Ki-67–high populations were all significant, would OS (in the ITT population) be hierarchically tested. Of note, analyses of OS in other populations (i.e., cohort 1) were not part of the testing hierarchy and were not planned a priori. At each analysis, the treatment effect on OS was tested using a 1-sided log-rank test stratified by randomization factors. The Kaplan-Meier method was used to estimate the OS curve for each treatment arm. The OS rates for each arm were compared using a normal approximation for the difference between the rates. A stratified Cox proportional hazards model with treatment as a factor was used to estimate the hazard ratio between the 2 treatment arms and the corresponding confidence interval (CI) and Wald P values. The follow-up time for OS was defined from the date of randomization and used the inverse of censoring rules for OS. The median follow-up time was calculated using the Kaplan-Meier method. Per the last addendum to the statistical analysis plan, the final OS analysis was defined as observing approximately 650 OS events, or 10 years after the last patient is randomized, whichever occurs first. The cumulative 1-sided type I error rate of 0.025 was maintained using the Lan-DeMets method;67 the alpha spent at each IA was calculated based on the actual number of events using the O’Brien-Fleming type stopping boundary.
The stratification factors for the analysis of primary and secondary end points were prior treatment (neoadjuvant chemotherapy versus adjuvant chemotherapy versus no chemotherapy), menopausal status (premenopausal versus postmenopausal), and region (North America or Europe versus Asia versus other). If a patient received both neoadjuvant and adjuvant chemotherapy, the patient was stratified as neoadjuvant chemotherapy. Male patients were stratified as postmenopausal at the time of randomization.
HRQoL (FACT-B): For HRQoL scores, a mixed effects model for repeated measures was applied to compare treatment arms by assessment with respect to each of the summary scores and select items. Missing data were not imputed but were handled implicitly within the model.
Harms: AEs were summarized by maximum toxicity regardless of causality. TEAEs were summarized by system organ class and by decreasing frequency of preferred term within the system organ class. Preferred terms identified as clinically identical or synonymous were grouped together under a single consolidated preferred term. Descriptive statistics were used to summarize data on AEs, SAEs, withdrawals due to AEs, and deaths. With the exception of dates, missing data were not imputed.
Since all patients were no longer receiving the study treatment at OS IA2, some treatment exposure and harms data were considered final at OS IA2 and were not updated at OS IA3. Thus, OS IA2 data are presented for the interim, final, subgroup, and sensitivity analyses.
Interim and final analyses
There were or are 6 planned IAs and 1 final analysis to test the null hypothesis:
IDFS efficacy IA1 – approximately 195 IDFS events (data cut-off date: September 27, 2019)
IDFS efficacy IA2 – approximately 293 IDFS events (data cut-off date: March 16, 2020)
Final IDFS analysis – approximately 390 IDFS events (data cut-off date: July 8, 2020)
OS IA1 (an additional follow-up analysis conducted at regulatory request; data cut-off date: April 1, 2021)
OS IA2 (data cut-off date: July 1, 2022)
OS IA3 (data cut-off date: July 3, 2023)
Final OS analysis (event-driven; expected to occur after observing approximately 650 death events)
Subgroup Analyses
Subgroup analyses of IDFS in the ITT population were performed for preplanned subgroups according to menopausal status, primary tumour size, tumour grade, number of positive lymph nodes, progesterone receptor status, and ECOG PS at baseline; these were subgroups of interest identified in the systematic review protocol. A similar statistical analysis approach to the main IDFS analysis was used. There was no multiplicity control. As such, all subgroup analyses were exploratory in nature.
Sensitivity Analyses
A log-rank test without stratification by randomization factors was performed to test the superiority of abemaciclib plus standard ET to standard ET on the ITT population. An unstratified Cox proportional hazard model with treatment as a factor will be used to estimate the hazard ratio between the 2 treatment arms and the corresponding CI and Wald P value. An additional sensitivity analysis with censoring for control arm patients receiving CDK4 and CDK6 inhibitor was performed. If a patient in a control arm received a CDK4 and CDK6 inhibitor before their first IDFS event, IDFS was censored at the date of the last disease assessment before their CDK4 and CDK6 inhibitor start date. Sensitivity analyses were repeated for DRFS.
Analysis Populations
The analysis populations of relevance are presented in Table 8. The ITT population (N = 5,637) includes all randomized patients in cohort 1 (N = 5,120; 90.8%) and cohort 2 (N = 517; 9.2%). This was the primary analysis population for all efficacy analyses, including the primary end point (IDFS) and a key gated secondary end point (OS). The safety population included all patients in cohort 1 and cohort 2 who received any quantity of study treatment, regardless of the arm to which they were randomized. The safety population was used for the primary analysis of dosing and/or exposure, safety, and resource utilization. Other efficacy subpopulations (i.e., cohort 1, cohort 2, cohort 1 Ki-67–high, cohort 1 Ki-67–low, Ki-67–high [cohorts 1 and 2]) were reported but were not of direct interest to this review.
Table 8: Analysis Populations in the MonarchE Trial
Population (number of patients) | Definition | Application |
|---|---|---|
ITT (5,637 patients) | All randomized patients in cohort 1 and cohort 2. The ITT analysis of efficacy data considered allocation of patients to treatment groups as randomized and not by actual treatment received. | This population was used for baseline, efficacy, and health economics analyses. |
Safety (5,591 patients) | All randomized patients in cohort 1 and cohort 2 who received any quantity of study treatment, regardless of their eligibility for the study. The safety evaluation was performed based on the study regimen a patient actually received, regardless of the arm to which they were randomized. | This population was used for the primary analysis of dosing and/or exposure, safety, and resource utilization analyses. |
Efficacy subpopulationsa | ||
Cohort 1 (5,120 patients) | All randomized patients in cohort 1, which included patients who were considered high risk based on clinical and/or pathological features:
OR
| Cohort 1 is part of the ITT population and was used for baseline, efficacy, and health economics analyses. |
Cohort 1 Ki-67–high (2,003 patients) | All randomized patients in cohort 1 with a centrally assessed Ki-67 index ≥ 20% | Secondary efficacy analyses were performed on this population. |
Cohort 1 Ki-67–low (1,914 patients) | All randomized patients in cohort 1 with a centrally assessed Ki-67 index < 20% | Exploratory analyses were performed on this population. |
Cohort 2 (517 patients) | All randomized patients in cohort 2, which included patients based on the presence of 1 to 3 positive ALNs and Ki-67 index ≥ 20%; patients could not have tumour grade 3 or tumour size ≥ 5 cm. | Cohort 2 is part of ITT population that was used for baseline, efficacy, and health economics analyses. |
ITT = intention to treat; OS = overall survival.
Notes: Population patient numbers are based on OS interim analysis 3.
Details included in the table are from the sponsor’s Summary of Clinical Evidence.
aThe results for the subpopulations were not provided in the sponsor’s Summary of Clinical Evidence for this review, but were briefly reported in the Health Canada reviewer’s report (2023).38
Source: MonarchE Clinical Study Report Addendum (July 3, 2023 report).34
Results
Patient Disposition
Patient disposition of the ITT population as of the OS IA3 data cut-off on July 3, 2023, are shown in Table 9. Of 7,327 patients screened, 5,637 met the eligibility criteria and were randomized to abemaciclib plus ET (n = 2,808) or ET alone (n = 2,829). As of the OS IA3 data cut-off, all patients are no longer receiving treatment. The main reason for discontinuation was completion of the regimen in both study arms (> 80%). Other reasons were less common, with some imbalance in the proportion of patients discontinuing treatment due to AEs (5.9% in the abemaciclib plus ET arm versus 0.8% in the ET arm) and disease relapse (5.5% in the abemaciclib plus ET arm versus 8.7% in the ET arm). Most (> 85%) patients remained in post-discontinuation follow-up. Reasons for losses to follow-up were balanced across groups and mainly attributable to deaths.
Table 9: Summary of Patient Disposition From the MonarchE Study Included in the Systematic Review (OS IA3 — ITT Population)
Patient disposition | Abemaciclib + ET (N = 2,808) | ET (N = 2,829) |
|---|---|---|
Screened, N | 7,372 | |
Screening failure, N (%) | 1,872 | |
Rescreened and randomized | ███ | |
Randomized, N (%) | 2,808 | 2,829 |
Randomized but not treated | 14 (0.5) | 32 (1.1) |
Treated | 2,794 (99.5) | 2,797 (98.9) |
Patients on treatment, n (%) a | 0 (0.0) | 0 (0.0) |
Patients off treatment, n (%) a | 2,794 (99.5) | 2,797 (98.9) |
Reason for discontinuation, n (%) | ||
Completed | 2,284 (81.3) | 2,311 (81.7) |
Adverse event | 167 (5.9) | 22 (0.8) |
Disease relapse | 155 (5.5) | 247 (8.7) |
Withdrawal by patient | 141 (5.0) | 179 (6.3) |
█████ | ██ █████ | ██ █████ |
Physician decision | 12 (0.4) | 6 (0.2) |
Lost to follow-up | 8 (0.3) | 10 (0.4) |
██████████████ ████ █████ █ | █████ | █████ |
████████ █████████ | █████ | █████ |
█████ ██████████ ██ ███████ | █████ | █████ |
Post–treatment discontinuation follow-up,a,b n (%) | ||
No | 185 (6.6) | 187 (6.6) |
Yes | 2,623 (93.4) | 2,642 (93.4) |
██ ████████████████████████ | ████ ██████ | ████ ██████ |
███ ███████████████████████ | ███ ██████ | ███ ██████ |
Reasons for end of post-discontinuation follow-up, n (%) | ||
█████ | ███ █████ | ███ █████ |
Lost to follow-up | 42 (1.5) | 42 (1.5) |
Withdrawal by patient | 107 (3.8) | 114 (4.0) |
ET = endocrine therapy; IA = interim analysis; ITT = intention to treat; OS = overall survival.
Note: Details included in the table are from the sponsor’s Summary of Clinical Evidence.
aAt the time of OS IA3 data cut-off on July 3, 2023.
bIncludes patients who were off treatment as well as patients who were enrolled or randomly assigned, but never treated.
Source: MonarchE Clinical Study Report Addendum (July 3, 2023 report).34
Baseline Characteristics
Overall, baseline characteristics were well balanced between the treatment arms, as shown in Table 10.
Most of the 5,637 patients randomized were female (99.4%), with a mean age of 51.2 years (standard deviation [SD] = 11.2 years) and an ECOG PS of 0 (84.7%). More than half of the patients (56.5%) were postmenopausal. Most had received a diagnosis of invasive ductal breast carcinoma (68.3%), and 50.3% had a primary tumour size of 2 cm or greater but less than 5 cm, as determined by pathology. Almost all patients had positive ALNs (99.8%): 59.6% with 4 or more, and 40.1% with 1 to 3. The majority of patients (95.4%) had received prior radiotherapy; 36.4% of patients had received neoadjuvant chemotherapy and 61.5% of patients had received adjuvant chemotherapy.
Baseline characteristics from OS IA2 (data cut-off on July 1, 2022) are presented because baseline characteristics were not updated in OS IA3 (data cut-off on July 3, 2023).
Table 10: Summary of MonarchE Trial Patient Baseline Characteristics (OS IA2 Dataa — ITT Population)
Characteristics | Abemaciclib + ET (N = 2,808) | ET (N = 2,829) |
|---|---|---|
Age (years), mean (SD) | 52.2 (11.3) | 52.1 (11.2) |
Sex (female), n (%) | 2,787 (99.3) | 2,814 (99.5) |
Region, n (%) | ||
North America and Europe | 1,470 (52.4) | 1,479 (52.3) |
Asia | 574 (20.4) | 582 (20.6) |
Other | 764 (27.2) | 768 (27.1) |
Menopausal status, n (%) | ||
Premenopausal | 1,221 (43.5) | 1,232 (43.5) |
Postmenopausal | 1,587 (56.5) | 1,597 (56.5) |
Baseline ECOG PS, n (%) | ||
0 | 2,405 (85.7) | 2,369 (83.8) |
1 | 401 (14.3) | 455 (16.1) |
███████ ████████████ █████████ | ||
████████ ██████ ██████ █████████ | ████████ | ████████ |
██████ ██████ | ███ ██████ | ███ ██████ |
████████ ███████ ██████ █████████ | ███ ██████ | ███ ██████ |
████████ ██████ █████████ | ██ █████ | ██ █████ |
████████ █████████ ██████ █████████ | ██ █████ | ██ █████ |
████████████ █████████ ██ ███ ██████ | ██ █████ | ██ █████ |
█████████ █████████ ██ ███ ██████ | █████ | █████ |
███████ ██████ █████████ | █████ | █████ |
█████ ███████ ██ ██████ | █████ | █████ |
██████████ ██████ █████████ | █████ | █████ |
Primary tumour size by pathology after definitive surgery, n (%) | ||
< 20 mm | 780 (27.8) | 765 (27.0) |
≥ 20 mm but < 50 mm | 1,369 (48.8) | 1,419 (50.2) |
≥ 50 mm | 610 (21.7) | 612 (21.6) |
Number of positive lymph nodes, n (%) | ||
0 | 7 (0.2) | 7 (0.2) |
1 to 3 | 1,119 (39.9) | 1,143 (40.4) |
4 to 9 | 1,105 (39.4) | 1,125 (39.8) |
≥ 10 | 575 (20.5) | 554 (19.6) |
Histopathological diagnosis grade, n (%) | ||
G1: Favourable | 209 (7.4) | 215 (7.6) |
G2: Moderately favourable | 1,373 (48.9) | 1,395 (49.3) |
G3: Unfavourable | 1,090 (38.8) | 1,066 (37.7) |
GX: Cannot be assessed | 126 (4.5) | 140 (4.9) |
Disease stage at initial diagnosis, n (%) | ||
Stage IA | 2 (0.1) | 1 (0.0) |
Stage IIA | 323 (11.5) | 353 (12.5) |
Stage IIB | 389 (13.9) | 387 (13.7) |
Stage IIIA | 1,027 (36.6) | 1,024 (36.2) |
Stage IIIB | 104 (3.7) | 91 (3.2) |
Stage IIIC | 950 (33.8) | 962 (34.0) |
Progesterone receptor status, n (%) | ||
Positive | 2,421 (86.4) | 2,453 (86.8) |
Negative | 298 (10.6) | 294 (10.4) |
Unknown | 23 (0.8) | 21 (0.7) |
Missing | 61 (2.2) | 57 (2.0) |
Prior chemotherapy, n (%) | ||
Neoadjuvant chemotherapy | 1,026 (36.5) | 1,029 (36.4) |
Adjuvant chemotherapy | 1,734 (61.8) | 1,731 (61.2) |
No chemotherapy | – | – |
Prior radiotherapy, n (%) | 2,680 (95.4) | 2,700 (95.4) |
ECOG = Eastern Cooperative Oncology Group; ET = endocrine therapy; IA = interim analysis; ITT = intention to treat; OS = overall survival; PS = performance status; SD = standard deviation.
Note: Details included in the table are from the sponsor’s Summary of Clinical Evidence.
aThough OS IA3 was more recent (data cut-off on July 3, 2023), OS IA2 data (data cut-off on July 1, 2022) were used in this table because baseline characteristics were not updated in OS IA3.
Sources: Clinical Study Report Addendum Amendment (May 20, 2020 report),58 and Clinical Study Report Addendum (July 1, 2022 report).59
Exposure to Study Treatments
Study Treatments
The median duration of abemaciclib treatment was 23.7 months out of a maximum allowed abemaciclib treatment duration of 24 months. The median duration of ET received within the 2-year treatment period was 23.7 months in both arms. Thus, the addition of abemaciclib to ET did not decrease the exposure to ET treatment in the abemaciclib plus ET arm. Overall, the median duration of exposure to study treatment was similar in the abemaciclib plus ET and the ET groups, as shown in Table 11 and Table 12.
Among patients completing the 2-year on-study treatment, the actual duration of treatment may vary as a result of allowed protocol windows between visits. No patients remained on-study treatment at OS IA2 (data cut-off on July 1, 2022). Therefore, no updated exposure data were presented in OS IA3 (data cut-off on July 3, 2023).
Concomitant Medications and Co-Interventions
A list of concomitant medications is presented in Table 13.
Table 11: Patient Exposure in the MonarchE Trial (OS IA2 Dataa — Safety Population)
Exposureb | Abemaciclib + ET (N = 2,791) | ET (N = 2,800) | |
|---|---|---|---|
Number of patients, n (%) | Abemaciclib 2,783 (99.7) | ET 2,791 (100.0) | ET 2,799 (100.0) |
Total patient-weeksc | █████████ | █████████ | █████████ |
Number of patients who received study treatment, n (%) | █████████ | █████████ | █████████ |
Complianced (%) | |||
Median | █████ | ██████ | ██████ |
IQR | █████ | ██████ | ██████ |
Minimum to maximum | █████ | ██████ | ██████ |
Mean (SD) | █████ ██ | █████ ██ | █████ ██ |
Cycles received per patiente | |||
Median | █████ | █████ | █████ |
IQR | █████ | ██████ | ██████ |
Minimum to maximum | █████ | ██████ | ██████ |
Mean (SD) | █████ | ██████ | ██████ |
Duration of therapy (weeks) | |||
Median | ███████ | ███████ | ███████ |
IQR | ███████ | ███████ | ███████ |
Minimum to maximum | ███████ | ███████ | ███████ |
Mean (SD) | ███████ | ███████ | ███████ |
ET = endocrine therapy; IA = interim analysis; OS = overall survival; IQR = interquartile range; SD = standard deviation.
Note: Details included in the table are from the sponsor’s Summary of Clinical Evidence.
aThough OS IA3 was more recent (data cut-off on July 3, 2023), OS IA2 data (data cut-off on July 1, 2022) were used in this table because patient exposure data were not updated in OS IA3.
bExposure data reflect drug received during the study treatment period of 2 years, and do not include ET treatment received during short- or long-term follow-up.
cTotal patient-weeks were calculated by multiplying the number of patients (n) by the median duration of therapy (weeks).
dAbemaciclib treatment compliance was measured using pill counts. Compliance was calculated as the ratio of total dose taken to the total prescribed dose (minus any dose adjustments and doses omitted or withheld). The total assigned dose for a patient with no modifications or omissions was 150 mg per dose × 2 doses per day × number of days on treatment. ET treatment compliance was calculated using the Exposure Compliance Endocrine Study Treatment form.
eA patient is considered to have received a treatment cycle after receiving at least 1 dose of study drug and/or ET, either partial or complete. Cycle duration was 30 days.
Source: MonarchE Clinical Study Report Addendum (July 1, 2022 report).59
Table 12: Summary of Endocrine Therapies in the MonarchE Trial (OS IA2 Dataa — Safety Population)
Drugs | Abemaciclib + ET (N = 2,791) | ET (N = 2,800) | ||
|---|---|---|---|---|
At start of study | Any time | At start of study | Any time | |
Aromatase inhibitors, n (%) | 1,928 (69.1) | 2,042 (73.2) | 1,891 (67.5) | 2,034 (72.6) |
Anastrozole | 610 (21.9) | 679 (24.3) | 616 (22.0) | 719 (25.7) |
Exemestane | 225 (8.1) | 296 (10.6) | 228 (8.1) | 353 (12.6) |
Letrozole | 1,093 (39.2) | 1,189 (42.6) | 1,047 (37.4) | 1,172 (41.9) |
██████████████ | ███ ██████ | ███ ██████ | ███ ██████ | ███ ██████ |
█████████ | ███ ██████ | ███ ██████ | ███ ██████ | ███ ██████ |
██████████ | █████ | ██ █████ | ██ █████ | ██ █████ |
████ █████████ | ██ | ███ ██████ | ██ | ███ ██████ |
█████████ | ██ | ███ ██████ | ██ | ███ ██████ |
███████████ | ██ | ███ █████ | ██ | ███ █████ |
███████████ | ██ | ██ █████ | ██ | ██ █████ |
ET = endocrine therapy; IA = interim analysis; OS = overall survival.
Note: Details included in the table are from the sponsor’s Summary of Clinical Evidence.
aThough OS IA3 was more recent (data cut-off on July 3, 2023), OS IA2 data (data cut-off on July 1, 2022) were used in this table because these data were not updated in OS IA3.
Source: MonarchE Clinical Study Report Addendum (July 1, 2022 report).59
Table 13: Concomitant Medications in the MonarchE Trial (ITT Population, May 20, 2020, Cut-Off Date)
Medications | Abemaciclib + ET (N = 2,808) | ET (N = 2,829) |
|---|---|---|
Concomitant bone-modifying agents (occurring in ≥ 0.5% of patients) | ||
Zoledronic acid | ███ █████ | ███ ██████ |
Denosumab | ██ █████ | ██ █████ |
Alendronic acid | ██ █████ | ██ █████ |
Ibandronic acid | ██ █████ | ██ █████ |
Risedronic acid | ██ █████ | ██ █████ |
███████████ ███████████ ███ ███████ ████ | ||
Medical history events | ████ ██████ | ████ ██████ |
Levothyroxine | ███ █████ | ███ █████ |
Metformin | ███ █████ | ███ █████ |
Paracetamol | ███ █████ | ███ █████ |
Amlodipine | ███ █████ | ███ █████ |
███████████ ███████████ ███ ███████ ████ | ||
Oxycodone | █████ | █████ |
Tramadol | █████ | █████ |
Anastrozole | █████ | █████ |
Tamoxifen | █████ | █████ |
Goserelin | █████ | █████ |
Hydrocodone; paracetamol | █████ | █████ |
Ibuprofen | █████ | █████ |
███████████ ███████████ ███ ███████ ██ | ||
Adverse event | ████ ██████ | ████ ██████ |
Loperamide | ████ ██████ | ██ █████ |
Paracetamol | ███ ██████ | ███ ██████ |
Ibuprofen | ███ █████ | ███ ████ |
Amoxicillin; clavulanic | ███ █████ | ███ █████ |
Amoxicillin | ███ █████ | ███ █████ |
Metoclopramide | ███ █████ | ██ █████ |
███████████ ███████████ ███ ███████████ ████ | ||
Prophylaxis | ████ ██████ | ████ ██████ |
Cholecalciferol | ███ █████ | ███ █████ |
Calcium carbonate; cholecalciferol | ███ █████ | ███ █████ |
Vitamin D | ███ █████ | ███ █████ |
Loperamide | ███ █████ | █████ |
ET = endocrine therapy; ITT = intention to treat.
Note: Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Source: MonarchE Clinical Study Report Addendum Amendment (May 20, 2020 report).58
Subsequent Treatment
The monarchE protocol defines study treatment as abemaciclib plus ET or ET during the first 2 years of the study (the 2-year on-study treatment period). Per protocol, physician’s choice of SOC ET was to be taken as prescribed during the 2-year on-study treatment period in both treatment arms unless ET discontinuation criteria were met. Thereafter, in year 3 and beyond, standard adjuvant ET was to be continued for at least 5 years. Discontinuation of all study treatment was defined as discontinuing from the 2-year on-study treatment period. Post-discontinuation therapies include all systemic treatments that patients received in their follow-up period in curative setting or therapies for metastatic disease or new second primaries.
At OS IA3, all patients had completed the study treatment period. In the follow-up period, the use of systemic therapies was balanced across treatment arms (2,567 [91.4%] in the abemaciclib plus ET arm and 2,580 [91.2%] in the ET arm), including the post-discontinuation ET, with numerically higher use of chemotherapy agents and CDK4 and CDK6 inhibitors (abemaciclib, palbociclib, and ribociclib) in the ET group. The most common systemic therapy received after discontinuation from the on-study treatment period was ET. This was expected; based on the monarchE trial protocol, patients should continue to receive adjuvant ET as SOC for at least 5 years.
Table 14 summarizes the post-discontinuation therapies started after the occurrence of distant metastatic disease in each treatment arm. Of note, this analysis does not reflect the patients who were receiving ET at the time of metastatic recurrence and continued receiving the same ET. Among patients who developed distant metastatic disease either before or after entering the post-discontinuation follow-up period (299 patients in the abemaciclib plus ET arm and 468 patients in the ET arm), the use of systemic therapies following diagnosis of metastatic disease was balanced between treatment arms (213 [74.7%] versus 331 [73.4%], respectively); however, the treatment choices varied between arms. A higher percentage of patients received chemotherapy in the abemaciclib plus ET arm than in the ET arm (131 [46%] versus 169 [37.5%]), while the use of CDK4 and CDK6 inhibitors in the metastatic setting was more common in the ET arm (11 [3.9%] versus 62 [13.7%] for abemaciclib, 39 [13.7%] versus 78 [17.3%] for palbociclib, 20 [7%] versus 52 [11.5%] for ribociclib).
Table 14: Post-Discontinuation Therapy in the MonarchE Trial for Patients With Distance Recurrence Who Entered the Post-Discontinuation Follow-Up Period (OS IA3 Data)
Drugs | Abemaciclib + ET (N = 299) | ET (N = 468) |
|---|---|---|
Patients with distant recurrence who entered post-discontinuation follow-up | ███ | ███ |
Systemic therapy | ||
Overall | ███ ██████ | ███ ██████ |
Chemotherapy | ███ ██████ | ███ ██████ |
ET | ███ ██████ | ███ ██████ |
Letrozole | ██ █████ | ██ ██████ |
Tamoxifen | ██ █████ | ██ █████ |
Anastrozole | ██ █████ | ██ █████ |
Exemestane | ██ █████ | ██ █████ |
Fulvestrant | ██ ██████ | ███ ██████ |
Targeted therapy | ███ ██████ | ███ ██████ |
Palbociclib | ██ ██████ | ██ ██████ |
Abemaciclib | ██ █████ | ██ ██████ |
Ribociclib | ██ █████ | ██ ██████ |
Other | ██ █████ | ██ █████ |
ET = endocrine therapy; IA = interim analysis; OS = overall survival.
Note: Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Source: MonarchE Clinical Study Report Addendum (July 3, 2023 report).34
Efficacy
Except for some safety and HRQoL results considered final at OS IA2 (median follow-up of 42 months), data from the more recent OS IA3 are presented in this section. At OS IA3, the median duration of follow-up was 54 months (IQR, 49 months to 59 months) in both the abemaciclib plus ET arm and the ET alone arm. A summary of data cut-off of key efficacy outcomes from the monarchE trial are presented in Table 15.
Table 15: Efficacy in the MonarchE Trial by Analysis Data Cut-Off (ITT Population)
Outcomes | Final IDFS | OS IA2 | OS IA3 |
|---|---|---|---|
Data cut-off date | July 8, 2020 | July 1, 2022 | July 3, 2023 |
Patients off the study treatment period, %a | 41.0 | 100 | 100 |
Patients completed 2-year study period, % | 25.5 | 81.5 | 81.5 |
Follow-up time in the abemaciclib + ET arm vs. ET arm (months), median | 19.1 vs. 19.2 | 42.0 vs. 42.2 | 53.9 vs. 53.9 |
IDFS | |||
Number of events in the abemaciclib + ET arm vs. the ET arm, n | 163 vs. 232 | 336 vs. 499 | 407 vs. 585 |
HR (95% CI)b | 0.713 (0.583 to 0.871) | 0.664 (0.578 to 0.762) | 0.680 (0.599 to 0.772) |
P value | 0.0009c | < 0.0001c | < 0.0001c |
DRFS | |||
Number of events in the abemaciclib + ET arm vs. the ET arm, n | 131 vs. 193 | 281 vs. 421 | 345 vs. 501 |
HR (95% CI)b | 0.687 (0.551 to 0.858) | 0.659 (0.567 to 0.767) | 0.675 (0.588 to 0.774) |
P value | 0.0009d | < 0.0001d | < 0.0001d |
OS | |||
Number of events in the abemaciclib + ET arm vs. the ET arm, n | 55 vs. 51 | 157 vs. 173 | 208 vs. 234 |
HR (95% CI)b | 1.093 (0.746 to 1.600) | 0.929 (0.748 to 1.153) | 0.903 (0.749 to 1.088) |
P value | 0.647 | 0.503 | 0.284 |
Data source | Final IDFS CSR Addendum | OS IA2 CSR Addendum | OS IA3 CSR Addendum |
CI = confidence interval; CSR = Clinical Study Report; DRFS = distant relapse–free survival; ET = endocrine therapy; HR = hazard ratio; IA = interim analysis; IDFS = invasive disease–free survival; ITT = intention to treat; IWRS = interactive web-response system; OS = overall survival; vs. = versus.
Note: Details included in the table are from the sponsor’s Summary of Clinical Evidence.
aExcludes 0.8% of patients who were randomized but never treated. All treated patients are off of the study treatment period or have discontinued.
bStratified by IWRS geographical region, IWRS prior treatment, and IWRS menopausal status.
cUncontrolled for multiplicity as statistical significance was achieved at IA2.
dUncontrolled for multiplicity as DRFS was not alpha-controlled for statistical significance testing.
Sources: MonarchE Clinical Study Report Addendum (July 1, 2022 report)59 and Clinical Study Report Addendum (July 3, 2023 report).34
Invasive Disease–Free Survival
The results for IDFS at OS IA3 in the ITT population are presented in Table 16. A treatment benefit for IDFS was first observed at IA2 (median follow-up 15.4 months for abemaciclib plus ET and 15.5 months for ET alone), in an analysis that was controlled for multiplicity. Thereafter, the data have continued to mature. A total of 992 (17.6%) IDFS events were observed, including 407 (14.5%) in the abemaciclib plus ET arm and 585 (20.7%) in the ET arm. The median IDFS was not reached. The hazard ratio was 0.680 (95% CI, 0.599 to 0.772; P < 0.0001) for abemaciclib plus ET compared with ET alone. The between-group difference in IDFS rate for abemaciclib plus ET versus ET alone was 2.8% (95% CI, 1.3% to 4.3%) at 24 months, 4.8% (95% CI, 3.0% to 6.6%) at 36 months, and 7.6% (95% CI, 5.2% to 10.0%) at 60 months. No detail of the prespecified sensitivity analysis with censoring for CDK4 and CDK6 inhibitor use was provided in the sponsor’s evidence summary.
Table 16: Summary of Investigator-Assessed IDFS in the MonarchE Study (OS IA3 — ITT Population)
Number of events, number of censored and time points | Abemaciclib + ET (N = 2,808) | ET (N = 2,829) |
|---|---|---|
Number of events, n (%) | 407 (14.5) | 585 (20.7) |
██████ ███████ ████████ ███████ | ██ █████ | ██ █████ |
████████ ███████ | ███ ██████ | ███ ██████ |
██████ ██ ████████ █████████ | ████ ██████ | ████ ██████ |
████████ ███████ █████ ██ ████████████ | █████ | █████ |
██████ ██ ████████ █████████ | ██ █████ | ██ █████ |
██ ██████████ ██ ████ ███████ ████████ | ████ ██████ | ████ ██████ |
███████ █████████ ████████ | ████████████████████ | |
██ ████ ███ | ████████████████████ | |
IDFS rate, % (95% CI)b | ||
12 months | 96.5 (95.8 to 97.2) | 95.7 (94.9 to 96.4) |
Treatment effect, 2-sided P valuec | 0.8 (–0.2 to 1.8) P = 0.1258 | |
24 months | 92.7 (91.6 to 93.6) | 89.9 (88.7 to 91.0) |
Treatment effect, 2-sided P valuec | 2.8 (1.3 to 4.3) P = 0.0003 | |
36 months | 89.2 (88.0 to 90.4) | 84.4 (83.0 to 85.8) |
Treatment effect, 2-sided P valuec | 4.8 (3.0 to 6.6) P < 0.0001 | |
48 months | 86.0 (84.6, 87.3) | 80.0 (78.5, 81.5) |
Treatment effect, 2-sided P valuec | 6.0 (3.9 to 8.0) P < 0.0001 | |
60 months | 83.6 (82.0 to 85.1) | 76.0 (74.1 to 77.8) |
Treatment effect, 2-sided P valuec | 7.6 (5.2 to 10.0) P < 0.0001 | |
CI = confidence interval; ET = endocrine therapy; IA = interim analysis; IDFS = invasive disease–free survival; ITT = intention to treat; IWRS = interactive web-response system; OS = overall survival.
Note: Details included in the table are from the sponsor’s Summary of Clinical Evidence.
aStratified by IWRS geographical region, IWRS prior treatment, and IWRS menopausal status.
b95% CIs and 2-sided P values for the difference between rates were calculated based on normal approximation.
cTreatment effect or difference and P values were computed based on comparator ET. Analyses are uncontrolled for multiplicity. The P values are not adjusted for multiplicity, but the log-rank test results met statistical significance at OS IA2.
Source: MonarchE Clinical Study Report Addendum (July 3, 2023 report).34
Figure 2 displays the Kaplan-Meier curves of IDFS in the ITT population. The inset shows the curves with a truncated y-axis (70% to 100%) without any censoring ticks to visualize the separation of curves more clearly.
Figure 2: Kaplan-Meier Plot of IDFS by Investigator Assessment (OS IA3 — ITT Population)
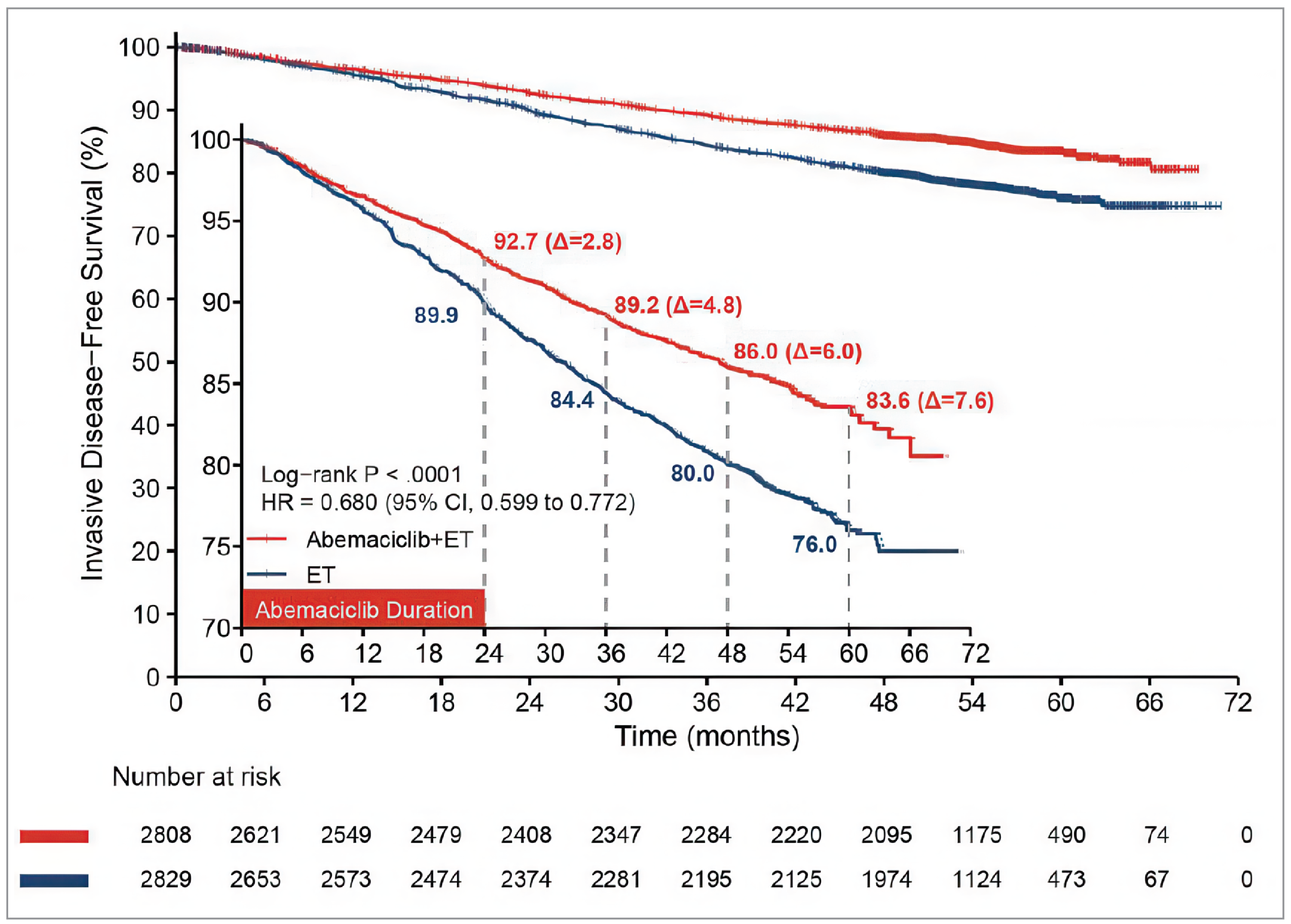
CI = confidence interval; ET = endocrine therapy; HR = hazard ratio; IA = interim analysis; IDFS = invasive disease–free survival; ITT = intention to treat; OS = overall survival.
Notes: P value is not adjusted for multiplicity; data cut-off date was July 3, 2023.
Details included in the figure are from the sponsor’s Summary of Clinical Evidence.
Source: MonarchE Clinical Study Report Addendum (July 3, 2023 report).34
Subgroup Analysis of IDFS
At OS IA3, there was a generally consistent direction of effect in IDFS for across all prespecified subgroups within the ITT population except for a few of the smaller subgroups (i.e., all other race groups [i.e., non-white and non-Asia (original wording from the source)], people with tumour stage IIB) (Figure 3).
Distant Relapse–Free Survival
The results for DRFS in the ITT population at OS IA3 are presented in Table 17; this end point was uncontrolled for multiplicity.
A total of 846 (15%) DRFS events were observed (345 [12.3%] in the abemaciclib plus ET and 501 [17.7%] in the ET arm). The median DRFS was not reached. The estimated hazard ratio was 0.675 (95% CI, 0.588 to 0.774, P < 0.00001). The between-group difference in DRFS rate for abemaciclib plus ET versus ET alone was 2.5% (95% CI, 1.1% to 3.9%) at 24 months, 4.1% (95% CI, 2.4% to 5.8%) at 36 months, and 6.7% (95% CI, 4.5% to 9.0%) at 60 months. No detail of the prespecified sensitivity analysis with censoring for CDK4 and CDK6 inhibitor use was provided in the sponsor’s evidence summary.
Figure 3: Subgroup Forest Plot of IDFS by Investigator Assessment (OS IA3 — ITT Population) [Redacted]

ET = endocrine therapy; IA = interim analysis; IDFS = invasive disease–free survival; ITT = intention to treat; OS = overall survival.
Note: This figure has been redacted at the request of the sponsor.
Source: MonarchE Clinical Study Report Addendum (July 3, 2023 report).34
Table 17: Summary of Investigator-Assessed DRFS in the MonarchE Trial (OS IA3 Data — ITT Population)
Number of events, number of censored and time points | Abemaciclib + ET (N = 2,808) | ET (N = 2,829) |
|---|---|---|
Number of events, n (%) | 345 (12.3) | 501 (17.7) |
██████ ███████ █ | ██ █████ | ██ █████ |
██████ | ███ ██████ | ███ ██████ |
██████ ██ ████████ | ████ ██████ | ████ ██████ |
███████ ███████ █████ | █████ | █████ |
███████ ███████ ██ ████ ██ | █████ | █████ |
██ █████████████ ███████ | ██ █████ | ██ █████ |
██ ██████████ ██ | ████ ██████ | ████ ██████ |
███████ █████████ ████████ | ██████████████████ | |
██ ████ ███ | █████████████ ███████ | |
DRFS rate, % (95% CI)c | ||
12 months | 97.4 (96.7 to 98.0) | 96.6 (95.8 to 97.2) |
Treatment effect, 2-sided P valued | 0.9 (–0.1 to 1.8) P = 0.0666 | |
24 months | 94.0 (93.1 to 94.9) | 91.5 (90.4 to 92.5) |
Treatment effect, 2-sided P valued | 2.5 (1.1 to 3.9) P = 0.0004 | |
36 months | 90.9 (89.7, 91.9) | 86.7 (85.4, 88.0) |
Treatment effect, 2-sided P valued | 4.1 (2.4 to 5.8) P < 0.0001 | |
48 months | 88.4 (87.1 to 89.6) | 83.1 (81.6 to 84.5) |
Treatment effect, 2-sided P valued | 5.3 (3.4 to 7.2) P < 0.0001 | |
60 months | 86.0 (84.5 to 87.4) | 79.2 (77.4 to 80.9) |
Treatment effect, 2-sided P valued | 6.7 (4.5 to 9.0) P < 0.0001 | |
CI = confidence interval; DRFS = distant relapse–free survival; ET = endocrine therapy; HR = hazard ratio; IA = interim analysis; ITT = intention to treat; IWRS = interactive web-response system; OS = overall survival.
Note: Details included in the table are from the sponsor’s Summary of Clinical Evidence.
aStratified by IWRS geographical region, IWRS prior treatment, and IWRS menopausal status.
bDRFS was not controlled for multiplicity.
c95% CIs and 2-sided P values for the difference between rates were calculated based on normal approximation.
dTreatment effect or difference and P values were computed based on comparator ET. Analyses were not controlled for multiplicity.
Source: MonarchE Clinical Study Report Addendum (July 3, 2023 report).34
Figure 4 shows the Kaplan-Meier curves of DRFS. The inset shows the curves with a truncated y-axis (70% to 100%) without any censoring ticks to visualize the separation of the curves more clearly.
Subgroup Analysis of DRFS
At OS IA3, there was a consistent direction of effect in DRFS across all prespecified subgroups within the ITT population except for a few of the smaller subgroups (i.e., patients aged ≥ 65 years, non-white and non-Asia race group [original wording from the source], patients with baseline ECOG PS of 1, patients with tumour grade 1, and patients with tumour stage IIB) (Figure 5).
Overall Survival
The results for OS in the ITT population at OS IA3 are shown in Table 18. A total of 442 (7.84%) deaths were observed (208 [7.4%] in the abemaciclib plus ET and 234 [8.3%] in the ET arm). The median OS was not reached. The estimated hazard ratio was 0.903 (95% CI, 0.749 to 1.088; P = 0.284). The between-group difference in the OS rate at 60 months was 1.1% (95% CI, –0.8% to 3.0%). It should be noted that most of the deaths of patients who received at least 1 dose of study treatment were due to the study disease, with fewer patients dying of study disease in the abemaciclib plus ET group (153 deaths) than in the ET alone group (186 deaths). There were 54 deaths due to AEs in the abemaciclib plus ET arm and 47 in the ET alone arm. In each arm, 1 randomly assigned patient died of the study disease before receiving study treatment, which accounts for the remaining 2 deaths. No subgroup analyses were presented, nor was the prespecified sensitivity analysis with censoring for CDK4 and CDK6 inhibitor use.
Figure 4: Kaplan-Meier Plot of DRFS by Investigator Assessment (OS IA3 — ITT Population)
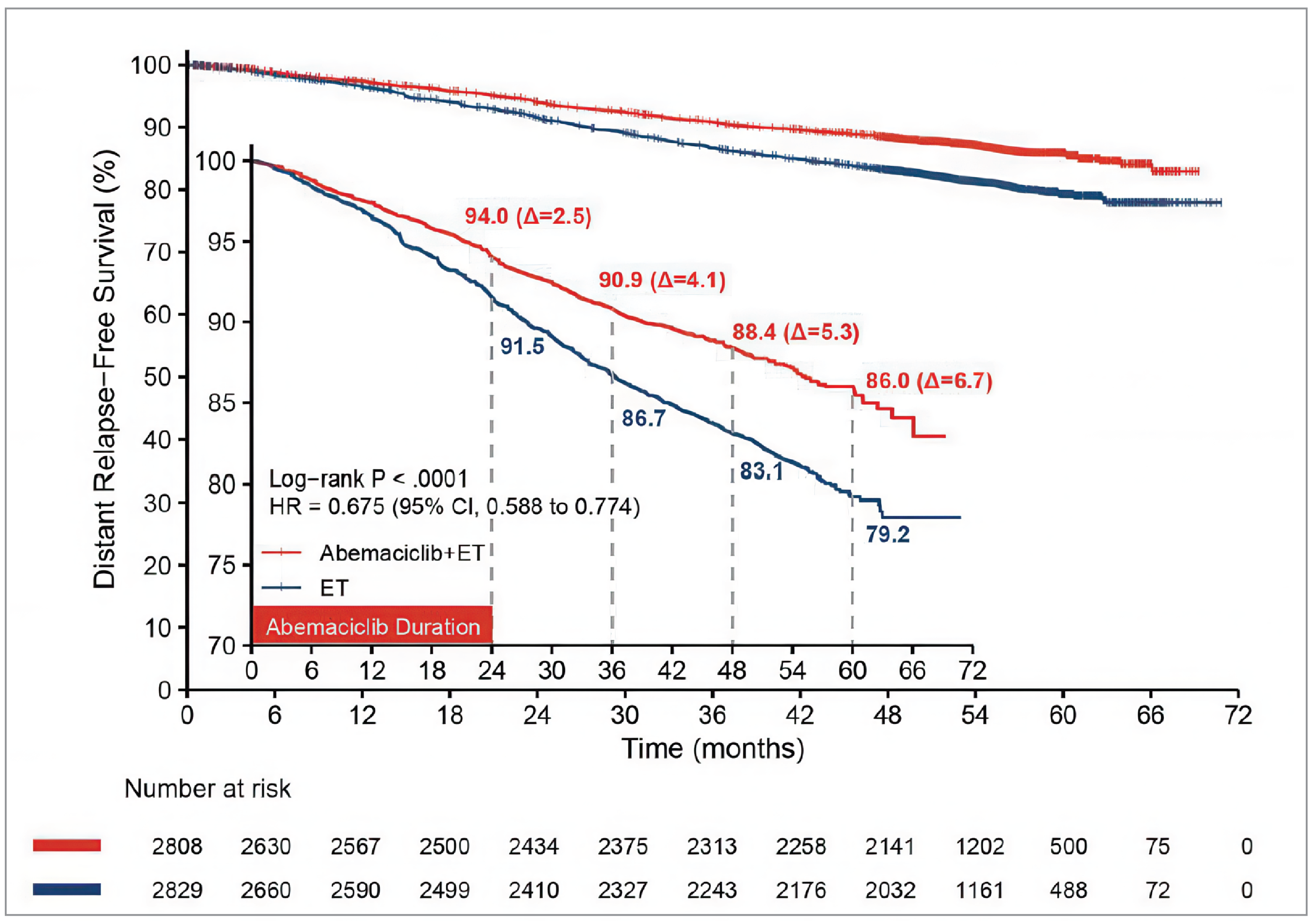
CI = confidence interval; DRFS = distant relapse–free survival; ET = endocrine therapy; HR = hazard ratio; IA = interim analysis; ITT = intention to treat; OS = overall survival.
Notes: P value is nominal. The absolute difference might slightly differ from the subtraction difference between estimated rates due to rounding.
Details included in the figure are from the sponsor’s Summary of Clinical Evidence.
Source: MonarchE Clinical Study Report Addendum (July 3, 2023 report).34
Figure 5: Subgroup Forest Plot of DRFS (OS IA3 — ITT Population) [Redacted]

DRFS = distant relapse–free survival; ET = endocrine therapy; IA = interim analysis; ITT = intention to treat; OS = overall survival.
Note: This figure has been redacted at the request of the sponsor.
Source: MonarchE Clinical Study Report Addendum (July 3, 2023 report).34
Table 18: Summary of OS in the MonarchE Trial (OS IA3 Data — ITT Population)
Description | Abemaciclib + ET (N = 2,808) | ET (N = 2,829) |
|---|---|---|
Number of deaths, n (%) | 208 (7.4) | 234 (8.3) |
██████ ██ ████████ ███████ | ████ ██████ | ████ ██████ |
██████ | ████ ██████ | ████ ██████ |
████ ██ ████ | ██ █████ | ██ █████ |
██████████ ██ █ | ███ █████ | ███ █████ |
███████ ███████ | ███████████████████████ | |
██ ███ | ████████████ ███████ █████████████ | |
OS rate, % (95% CI)b | ||
██ ████ | ████ ██████ █████ | ████ ██████ █████ |
█████████ ███████ | ████ ██████ ██████ █ ██████ | |
██ ████ | ████ ██████ █████ | ████ ██████ █████ |
█████████ ███████ | ███ ██████ ██████ █ ██████ | |
██ ████ | ████ ██████ █████ | ████ ██████ █████ |
█████████ ███████ | ████ ██████ ██████ █ ██████ | |
██ ████ | ████ ██████ █████ | ████ ██████ █████ |
█████████ ███████ | ███ ██████ ██████ █ ██████ | |
██ ████ | ████ ██████ █████ | ████ ██████ █████ |
█████████ ███████ | ███ ██████ ██████ █ ██████ | |
CI = confidence interval; ET = endocrine therapy; IA = interim analysis; ITT = intention to treat; IWRS = interactive web-response system; OS = overall survival.
Note: Details included in the table are from the sponsor’s Summary of Clinical Evidence.
aStratified by IWRS geographical region, IWRS prior treatment, and IWRS menopausal status.
b95% CIs and 2-sided P values for the difference between rates were calculated based on normal approximation.
cTreatment effect or difference and P values were computed based on comparator ET.
Source: MonarchE Clinical Study Report Addendum (July 3, 2023 report).34
HRQoL and Patient-Reported Outcomes
Health outcomes and quality-of-life evaluations were considered final at OS IA2 and not updated at OS IA3; therefore, the OS IA2 HRQoL results are outlined in this section. In the monarchE study, HRQoL data were assessed in the safety population. At baseline, completion rates of instruments used for patient-reported outcomes were greater than 96% in each treatment arm. At all on-treatment visits, more than 90% of available patients completed the instruments. At follow-up visits, approximately 80% of available patients completed the instruments. Patients did not complete the instruments because they refused to do so, because the study site failed to administer the instruments, because of lack of availability of translation, and for “other” or missing reasons. Of note, the most common reason for not completing the instruments at follow-up visits was characterized as “other” because patients were followed up over the telephone, rather than being seen in a clinic, mainly as a result of COVID-19 pandemic restrictions. Based on the input of the clinical experts CDA-AMC consulted for this review, the EQ-5D-5L and Functional Assessment of Chronic Illness Therapy - Fatigue (FACIT-F) scores are not presented and only the FACT-B scores are presented in this report.
Figure 6: Kaplan-Meier Plot of OS by Investigator Assessment (OS IA3 — ITT Population)
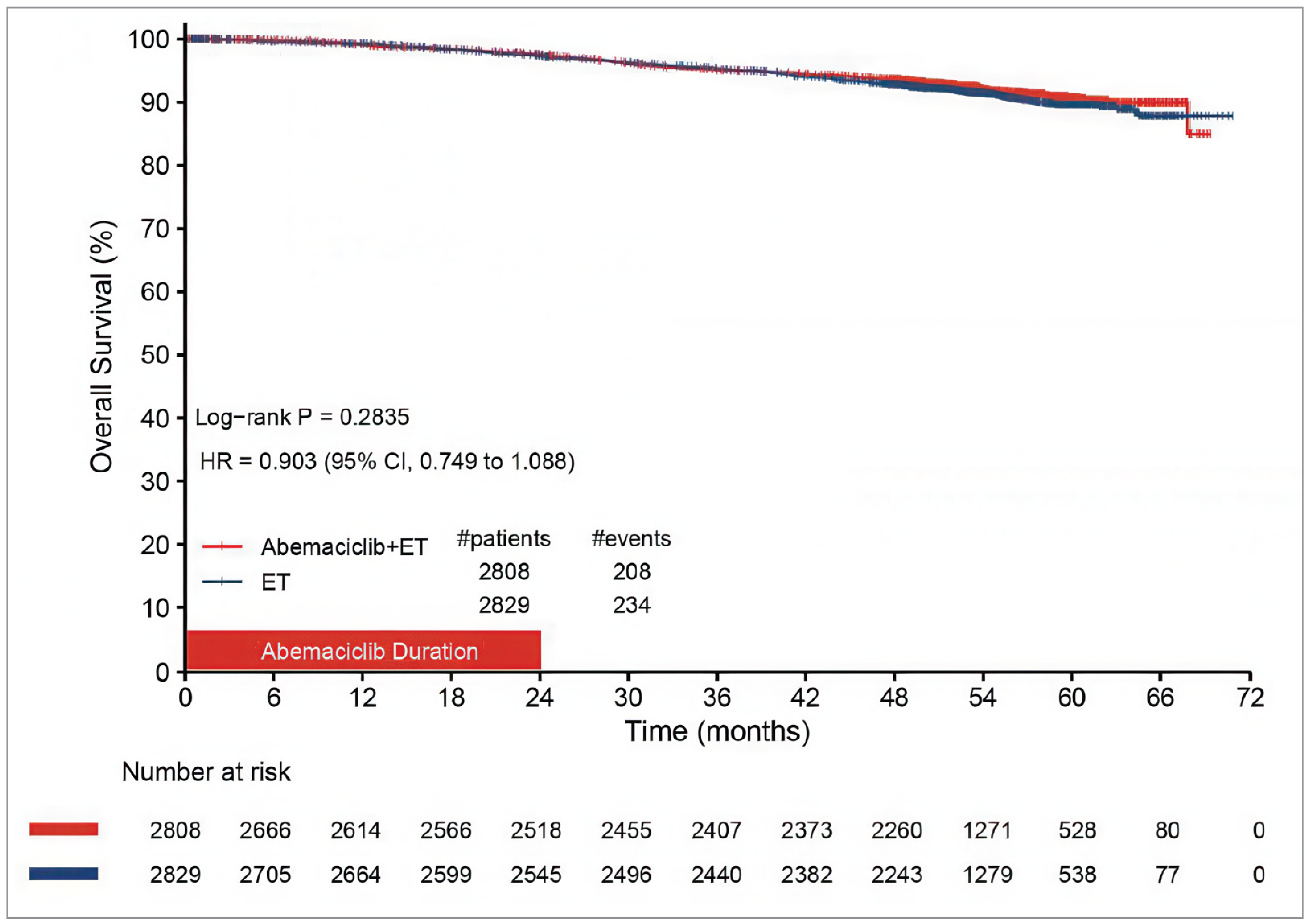
CI = confidence interval; ET = endocrine therapy; HR = hazard ratio; IA = interim analysis; ITT = intention to treat; OS = overall survival.
Notes: P value is nominal.
Details included in the figure are from the sponsor’s Summary of Clinical Evidence.
Source: MonarchE Clinical Study Report Addendum (July 3, 2023 report).34
Functional Assessment of Cancer Therapy – Breast
FACT-B summary scores are presented in Table 19. In the safety population, FACT-B total scores at baseline were 108.29 points (SD = 18.11 points) in the abemaciclib plus ET arm and 107.21 points (SD = 17.96 points) in the ET alone arm. At 24 months, the LSM changes from baseline in FACT-B scores were –2.52 (SE = 0.33) points in the abemaciclib plus ET arm and 0.08 (SE = 0.33) points in the ET arm. The between-group difference in change from baseline was –2.60 (95% CI, –3.5 to –1.69). At 12 months following treatment discontinuation (also known as additional follow-up 2), the FACT-B LSM changes from baseline scores were –0.89 (SE = 0.35) points in the abemaciclib plus ET arm and –0.10 (SE = 0.35) points in the ET arm. The between-group difference in LSM change from baseline was –0.79 points (95% CI, –1.76 points to 0.18 points).
Functional Assessment of Chronic Illness Therapy – Fatigue
Fatigue experienced during treatment was evaluated using the FACIT-F subscale score. At the OS IA2 data cut-off, the changes from baseline FACIT-F scores were less than MID of 0.5 of the baseline SD in both arms. Changes from baseline are less than the MID of 7 to 8 points.
Health Care Resource Utilization
Although hospitalizations due to an AE, regardless of causality, are reported as SAEs up to year 5, additional details on these hospitalizations were collected in a dedicated form only while patients were receiving on-study treatment and within 30 days of study discontinuation. Thus, data on hospitalizations were considered final at OS IA2 as all patients were no longer receiving study treatment. A total of 633 patients reported at least 1 hospitalization, including 386 patients (13.8%, based on the safety population) in the abemaciclib plus ET arm and 247 patients (8.8%) in the ET arm. Patients were mostly hospitalized as a result of system organ class infections and infestations (196 [3.5%] patients), specifically pneumonia (23 [0.8%] in the abemaciclib plus ET arm and 15 [0.5%] in the ET arm). The median duration of hospitalization was 6 days for those in the abemaciclib plus ET arm and 5 days for those in the ET arm. Data on transfusions were also considered final at OS IA2. Altogether 56 patients received transfusions during the study treatment period and within 30 days following study treatment discontinuation, including 44 patients (1.6%) in the abemaciclib plus ET group and 12 patients (0.4%) in the ET group. AEs were the most frequently reported reason for the transfusions (44 [1.6%] in the abemaciclib plus ET arm and 12 [0.4%] in the ET arm), with anemia the most commonly reported AE requiring a transfusion (32 patients [1.1%] in the abemaciclib plus ET group and 7 [0.3%] patients in the ET group). The most common transfusion blood product was packed red blood cells (35 [1.3%] in the abemaciclib plus ET arm and 10 [0.4%] in the ET arm).
Harms
Only those harms identified in the sponsor’s evidence summary review protocol are reported subsequently. Refer to Table 20 for detailed harms data.
Adverse Events
After a median follow-up of 54 months at OS IA3, a total of 98.4% of patients in the abemaciclib plus ET arm and 88.9% in the ET arm experienced at least 1 TEAE (Table 20). The most common AEs (≥ 35% in either of the groups) were diarrhea (abemaciclib plus ET versus ET: 83.6% versus 8.8%), neutropenia (45.9% versus 5.6%), fatigue (40.8% versus 18.1%), leukopenia (37.8% versus 6.6%), and abdominal pain (35.7% versus 9.9%). The overall rate of grade 5 TEAEs was low, but higher in the abemaciclib plus ET arm than in the ET arm (0.6% versus 0.4%).
Table 19: Summary of FACT-B Total Score at Selected Visits (OS IA2 — Safety Population)
Time points of the visits | Abemaciclib + ET (N = 2,791) | ET (N = 2,800) | Abemaciclib + ET vs. ET alone | ||||
|---|---|---|---|---|---|---|---|
N | FACT-B total score,a mean (SD) | Change from baseline, LSM (SE) | N | FACT-B total score,a mean (SD) | Change from baseline, LSM (SE) | LSM difference in change from baseline (SE) | |
Baseline | 2,438 | 108.29 (18.11) | NA | 2,436 | 107.21 (17.96) | NA | NA |
Visit 6 (3 months) | 2,304 | 106.68 (19.00) | –1.64 (0.26) | 2,322 | 107.66 (18.51) | 0.24 (0.26) | –1.88 (0.36) |
Visit 15 (12 months) | 2,133 | 107.01 (19.58) | –1.70 (0.30) | 2,147 | 108.31 (18.66) | 0.70 (0.30) | –2.40 (0.42) |
Visit 27 (24 months) | 1,995 | 106.47 (19.86) | –2.52 (0.33) | 1,966 | 108.22 (19.28) | 0.08 (0.33) | –2.60 (0.46) (95% CI, –3.5 to –1.69) |
Additional follow-up 1 (median follow-up of 27 months)b | 1,997 | 107.57 (19.63) | –1.35 (0.33) | 1,944 | 107.98 (19.24) | 0.00 (0.33) | –1.35 (0.47) (95% CI, –2.26 to –0.44) |
Additional follow-up 2b | 1,837 | 107.84 (20.11) | –0.89 (0.35) | 1,785 | 107.67 (19.63) | –0.10 (0.35) | –0.79 (0.49) (95% CI, –1.76 to 0.18) |
ET = endocrine therapy; FACT-B = Functional Assessment of Cancer Therapy – Breast; LSM = least squares mean; NA = not applicable; NE = not evaluated; SD = standard deviation; SE = standard error; vs. = versus.
Notes:: Health outcomes and quality of life evaluations were considered final at OS IA2 and were not updated in the OS IA3 analysis; thus, OS IA2 data are presented here.
Details included in the table are from the sponsor’s Summary of Clinical Evidence.
aFACT-B total score (score range 0 to 148), physical well-being (score range 0 to 28), social well-being (score range 0 to 28), emotional well-being (score range 0 to 24), functional well-being (score range 0 to 28) breast cancer subscale (score range 0 to 40), and the trial outcome index (physical well-being + functional well-being + breast cancer subscale; score range 0 to 96).
bAdditional follow-up 1 occurred 6 months following treatment discontinuation. The median follow-up was 27 months.53 Additional follow-up 2 occurred 12 months following treatment discontinuation.
Source: MonarchE Clinical Study Report Addendum (July 1, 2022 report).59
Serious Adverse Events
After a median follow-up of 54 months, at OS IA3, 15.6% of patients in the abemaciclib plus ET arm and 9.2% in the ET arm experienced at least 1 SAE (Table 20). The most common SAE (≥ 1.0% in either of the arms) was pneumonia (abemaciclib plus ET versus ET alone: 1.0% versus 0.6%).
Deaths
At OS IA3, there were 207 deaths in the abemaciclib plus ET arm (7.4%) and 233 in (8.3%) in ET alone arm (Table 20). The majority of deaths were due to the study disease (153 in the abemaciclib plus ET arm versus 186 in the ET alone arm). Fifteen (0.5%) patients in the abemaciclib plus ET arm and 11 (0.4%) patients in the ET alone arm died as a result of AEs while receiving study therapy or within 30 days of study treatment discontinuation. Thirty-nine (1.4%) patients in the abemaciclib plus ET arm and 36 (1.3%) patients in the ET arm died due to AEs more than 30 days after study treatment discontinuation.
Adverse events | Abemaciclib + ET (N = 2,791) | ET (N = 2,800) |
|---|---|---|
Most common AEs (≥ 15% of patients receiving abemaciclib + ET with a ≥ 2% difference to ET alone arm) at OS IA3 | ||
Patients with any TEAE, n (%) | ████ ██████ | ████ ██████ |
Diarrhea | ████ ██████ | ███ █████ |
Neutropenia | ████ ██████ | ███ █████ |
Fatigue | ████ ██████ | ███ ██████ |
Leukopenia | ████ ██████ | ███ █████ |
Abdominal pain | ███ ██████ | ███ █████ |
Nausea | ███ ██████ | ███ █████ |
Arthralgia | ███ ██████ | ████ ██████ |
Anemia | ███ ██████ | ███ █████ |
Headache | ███ ██████ | ███ ██████ |
Vomiting | ███ ██████ | ███ █████ |
Hot flush | ███ ██████ | ███ ██████ |
Patients with grade 5 TEAE, n (%) | ██ █████ | ██ █████ |
SAEs (occurring in ≥ 0.5% patients in any arm) at OS IA3 | ||
Patients with any serious TEAE, n (%) | ███ ██████ | ███ █████ |
Pneumonia | ██ █████ | ██ █████ |
Cellulitis | ██ █████ | ██ █████ |
Urinary tract infection | ██ █████ | █████ |
Diarrhea | ██ █████ | █████ |
Pulmonary embolism | ██ █████ | █████ |
Patients who stopped abemaciclib or all study treatment due to AEs | ||
Patients discontinued abemaciclib or all treatment due to AE, n (%) | 515 (18.5) | 30 (1.1) |
Diarrhea | 146 (5.2) | 0 (0.0) |
Abdominal pain | 20 (0.7) | 0 (0.0) |
Fatigue | 56 (2.0) | 0 (0.0) |
Neutropenia | 25 (0.9) | 0 (0.0) |
Alanine aminotransferase increase | 16 (0.6) | 0 (0.0) |
Pneumonitis | 13 (0.5) | 0 (0.0) |
Deaths, n (%) | ||
All deaths at OS IA3 | 207 (7.4) | 233 (8.3) |
██████ ██ ███████ ██ ███ | ██ █████ | ██ █████ |
█████ █████ | █████ | █████ |
███████ ███ | ██ █████ | ██ █████ |
██████ █████████ ████ ██ | ███ █████ | ███ █████ |
█████ ███████ | ███ █████ | ███ █████ |
███████ ██████ | ██ █████ | ██ █████ |
Patients with TEAE of special interest at OS IA2, n (%) | ||
Neutropenia (any grade) | 1,281 (45.9) | 158 (5.6) |
█████ | ███ ██████ | ██ █████ |
█████ | █████ | █████ |
███████ ████████████ █████ ██ | █████ | █████ |
█████████ ████ ██████ | ████ ██████ | ████ ██████ |
█████ | ███ █████ | ██ █████ |
█████ | █████ | █████ |
█████ | █████ | █████ |
████████ ████ ██████ | ████ ██████ | ███ █████ |
█████ | ███ █████ | █████ |
█████ | █████ | █████ |
█████ | █████ | █████ |
███ █████████ ████ ██████ | ███ ██████ | ███ █████ |
████ | ██ █████ | ██ █████ |
█████ | █████ | █████ |
███ █████████ ████ ██████ | ███ ██████ | ███ █████ |
█████ | ██ █████ | ██ █████ |
█████ | █████ | █████ |
███ ████ ██████ | ██ █████ | ██ █████ |
█████ | █████ | █████ |
█████ | █████ | █████ |
█████ | █████ | █████ |
████ ███████████ ████ ██████ | ██ █████ | ██ █████ |
█████ | ██ █████ | █████ |
█████ | █████ | █████ |
█████ | █████ | █████ |
AE = adverse event; AST = aspartate aminotransferase; ET = endocrine therapy; IA = interim analysis; ILD = interstitial lung disease; OS = overall survival; PE = pulmonary embolism; SAE = serious adverse event; TEAE = treatment-emergent adverse event; VTE = venous thromboembolic event.
Notes: Because all patients were no longer receiving on-study treatment at OS IA2 (data cut-off on July 1, 2022), AEs leading to treatment discontinuation and AEs of special interest were considered final at OS IA2 and were not updated in OS IA3. As such, OS IA2 data are presented for these results.
Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Source: MonarchE Clinical Study Report Addendum (July 3, 2023 report).34
Withdrawals Due to Adverse Events
At OS IA2 (median follow-up: 42 months), 515 patients (18.5%) had discontinued abemaciclib due to AEs. The most common (> 1%) AEs that resulted in discontinuing abemaciclib were diarrhea (5.2%) and fatigue (2.0%). In addition, 180 patients (6.4%) discontinued both abemaciclib and the study treatment ET due to AEs. In the ET arm, 30 patients (1.1%) discontinued ET treatment due to AEs.
Notable Harms
AEs of special interest for abemaciclib were neutropenia, infections, diarrhea, hepatic events, VTEs, and ILD/pneumonitis. Neutropenia was defined as the preferred term for neutropenia or neutrophil count decreased and laboratory neutrophil count decreases. Hepatic events were confined to increased alanine aminotransferase and increased aspartate aminotransferase levels. At OS IA2 (median follow-up of 42 months), any grade of neutropenia was reported in 45.9% of patients in the abemaciclib plus ET arm and 5.6% in the ET arm. Any grade of infection was reported in 51.5% of patients in the abemaciclib plus ET arm and 39.6% in the ET arm. Any grade of diarrhea was reported in 83.6% of patients in the abemaciclib plus ET arm and 8.7% in the ET arm. Any grade of hepatic event was reported in 24.6% of patients in the abemaciclib plus ET arm and 10.6% in the ET arm. Any grade of VTE was reported in 2.5% of patients in the abemaciclib plus ET arm and 0.7% in the ET arm. Any grade of ILD/pneumonitis was reported in 3.3% of patients in the abemaciclib plus ET arm and 1.3% of patients in the ET arm (Table 20).
Critical Appraisal
Internal Validity
In monarchE trial, the randomization method was adequate with treatment assignment based on a central randomization scheme, which would ensure concealment of the randomized groups until allocation. Baseline characteristics were well balanced across the treatment groups, suggesting that the randomization was successful. The clinical experts CDA-AMC consulted for this review indicated that the high-risk criteria used in the monarchE trial appeared reasonable. The primary and secondary efficacy end points of IDFS, OS, and DRFS are considered appropriate for the disease setting. The statistical approach of gatekeeping to sequentially test the primary and secondary end points was acceptable to account for multiple testing across these analyses (IDFS and OS). The analysis of DRFS was not controlled for multiple comparisons, so it was at increased risk of type I error (i.e., false-positive findings).
A total of 7 (0.2%) patients in each arm were lymph node–negative, and did not meet the inclusion criteria. However, it is unlikely that this small proportion would not have a significant impact on the findings. The trial was an open-label design. Although the sponsor noted that patient blinding would have been impractical and challenging given the differences in the 2 study treatment regimens and different known harms, performance and detection bias that may result from lack of blinding of patients and investigators to assigned study treatments cannot be ruled out. For example, a patient’s knowledge of their assigned treatment could result in overestimation or underestimation of subjectively reported harms and patient-reported symptoms and HRQoL; patient-reported outcomes are particularly susceptible to bias from a lack of blinding of patients to their treatment. Investigator knowledge of the treatment group could have also resulted in different concomitant supportive care being offered to patients in the 2 treatment arms. However, the main difference in concomitant treatments was loperamide use in the abemaciclib plus ET arm (56.5% versus 1.4% in the ET arm). Loperamide is used to manage diarrhea, which is a known AE related to abemaciclib treatment. In addition, the prespecified outcomes in the study (IDFS, DRFS, and OS) are objective measures, which were unlikely to be significantly affected by the lack of investigator blinding. Furthermore, an independent data-monitoring committee assessed safety and efficacy data, and the sponsor remained blinded to the aggregate data before the positive efficacy outcome.69
IDFS and DRFS are considered early indicators of a patient’s survival, especially for less advanced conditions in which longer survival is expected. OS data in the monarchE trial remain immature, which is expected in this disease setting with longer survival prognosis. The trial was not powered to detect an OS benefit. The efficacy of abemaciclib and ET with regard to OS will require a larger number of events and a longer follow-up. The correlation of disease-free survival surrogates (e.g., IDFS or DRFS) with OS remains debatable and requires further investigation. Evidence from the literature is limited, with some studies suggesting that the correlation with disease-free survival may not be strong enough to be used as a predictor of OS in adjuvant breast cancer trials.70 Considering the OS data are not yet mature at OS IA3, it is unclear if improvements in IDFS and DRFS observed among patients in the abemaciclib plus ET arm of the monarchE trial would translate into clinically meaningful OS benefits. The analysis of OS is a reflection of the effect of both the study treatments as well as subsequent treatments used after disease recurrence. However, the subsequent treatments are largely balanced in the 2 treatment arms. The clinical experts CDA-AMC consulted for this review mentioned that these subsequent treatments seemed reflective of what might occur in practice, with decisions being patient-specific and based on which treatments were received previously.
There was a substantial attrition rate for HRQoL (e.g., FACT-B) assessments over time, with just 70.3% of patients contributing to the assessments at visit 27 and 64.3% to the assessments 12 months after treatment discontinuation. This results in a risk of bias due to missing outcome data, but the direction of potential bias cannot be predicted. Missing data were implicitly handled within the mixed model for repeated measures, which assumed that the data are missing at random. However, no sensitivity analyses were conducted to confirm whether this assumption about the missing data was appropriate.
External Validity
The monarchE trial included a heterogenous population of patients with EBC, and a wide range of clinical presentations were well-represented. Although ████ ██ patients from Canada were included in the monarchE trial, the clinical experts consulted by CDA-AMC indicated that the results of this trial are generalizable to Canadian clinical practice. The clinical experts consulted noted that patients in the trial are about a decade younger than patients with EBC encountered in clinical practice, where patients are generally diagnosed and treated in their early to mid 60s, although this may be explained by high-risk features potentially being more prevalent in younger patients. The clinical experts consulted for this review indicated that the inclusion of younger and healthier patients may have led to a more favourable harms profile where more AEs were manageable or reversible. A total of 98% patients had prior chemotherapy (i.e., neoadjuvant or adjuvant chemotherapy) in both treatment arms. The clinical experts indicated that prior chemotherapy in this setting is not used as much as used to be in current clinical practice. Nevertheless, the clinical experts consulted for this review stated that inclusion of younger patients and the high proportion of patients with prior chemotherapy would be unlikely to have an impact on the generalizability of the findings to clinical practice.
In terms of the clinicopathological features used for eligibility, the clinical experts noted that for patients who received neoadjuvant therapy, the monarchE trial allowed the tumour size to be based on imaging; however, all imaging was done locally and no central imaging assessments were performed, which could have resulted in potential inconsistency in assessment across study sites. In addition, lymph node involvement could have been assessed cytologically and may have produced different results. If multiple lymph nodes were sampled in the trial to determine eligibility, this is not done in routine clinical practice. Nevertheless, the clinical experts CDA-AMC consulted for this review indicated that the potential inconsistency of imaging or cytological assessment is unlikely to have a significant impact on the generalizability of the findings to Canadian clinical practice. The clinical experts consulted for this review indicated that the 2-year monarchE trial was conducted during 2017 to 2019 (i.e., 5 to 7 years ago), and the proportion of patients with prior chemotherapy (i.e., neoadjuvant or adjuvant chemotherapy) was high in both groups (i.e., about 98%). However, the clinical experts indicated that the prior chemotherapy in this setting is likely not used to the same proportion in current practice given the introduction of genomic testing to safely omit chemotherapy with those with 1 to 3 nodes positive. The clinical experts noted that the ET regimens used in the trial and their distribution are representative of ET regimens used in the Canadian clinical setting. The extent to which the evidence is applicable to males is unclear given the very small number of male patients in the trial. This would be expected given the rate of occurrence among males. Overall, the clinical experts consulted for this review indicated that the patients included in the monarchE trial are representative of patients in Canadian clinical practice, and generalizability is unlikely to be a concern.
GRADE Summary of Findings and Certainty of the Evidence
Methods for Assessing the Certainty of the Evidence
For pivotal studies and RCTs identified in the sponsor’s systematic review, GRADE was used to assess the certainty of the evidence for outcomes considered most relevant to inform CDA-AMC expert committee deliberations, and a final certainty rating was determined as outlined by the GRADE Working Group.39,40
High certainty: We are very confident that the true effect lies close to that of the estimate of the effect.
Moderate certainty: We are moderately confident in the effect estimate — The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. We use the word “likely” for evidence of moderate certainty (e.g., “X intervention likely results in Y outcome”).
Low certainty: Our confidence in the effect estimate is limited — The true effect may be substantially different from the estimate of the effect. We use the word “may” for evidence of low certainty (e.g., “X intervention may result in Y outcome”).
Very low certainty: We have very little confidence in the effect estimate — The true effect is likely to be substantially different from the estimate of effect. We describe evidence of very low certainty as “very uncertain.”
Following the GRADE approach, evidence from RCTs started as high-certainty evidence and could be rated down for concerns related to study limitations (which refers to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias.
When possible, certainty was rated in the context of the presence of an important (nontrivial) treatment effect; if this was not possible, certainty was rated in the context of the presence of any treatment effect (i.e., the clinical importance is unclear). In all cases, the target of the certainty of evidence assessment was based on the point estimate and where it was located relative to the threshold for a clinically important effect (when a threshold was available) or to the null.
Results of GRADE Assessments
Table 2 presents the GRADE summary of findings for abemaciclib plus ET versus ET alone for the adjuvant treatment of adult patients with HR-positive, HER2-negative, node-positive EBC at high risk of disease recurrence based on clinicopathological features.
Long-Term Extension Studies
Not available.
Indirect Evidence
Not available.
Studies Addressing Gaps in the Systematic Review Evidence
Not available.
Discussion
Summary of Available Evidence
This Clinical Review included input from patient groups, clinician groups, clinical experts, and drug programs, as well as evidence from 1 pivotal trial (monarchE). The monarchE trial was a multinational, ongoing, open-label, phase III RCT that compared the efficacy and harms of abemaciclib in combination with ET and those of ET alone in the adjuvant treatment of patients with HR-positive, HER2-negative, node-positive EBC at high risk of recurrence based on clinicopathological features or Ki-67 index score and who had completed definitive locoregional therapy. The monarchE trial had a screening period of up to 6 months, a treatment period of 2 years, and a follow-up period of up to 10 years. A total of 5,637 patients in 38 countries, including ██ patients from Canada, were randomized to receive treatment with either abemaciclib plus ET or ET alone. Patients were recruited into 2 cohorts: patients in cohort 1 (n = 5,120; 90.8%) were eligible based on high-risk clinicopathological features (i.e., ≥ 4 positive ALNs or 1 to 3 positive ALNs and at least 1 of the following: tumour size ≥ 5 cm or histologic grade 3 disease), and cohort 2 (n = 517; 9.2%) included patients with high risk of recurrence based on 1 to 3 positive ALNs and a Ki-67 index score of 20% or higher. The primary efficacy end point was IDFS, and the secondary end points included DRFS, OS, HRQoL (e.g., FACT-B), and the harms outcomes. The results of IDFS, DRFS, and OS presented in this report are based on the OS IA3 data after a median follow-up of 54 months. HRQoL measurements (e.g., FACT-B) and health care resource utilization (hospitalizations, transfusions) are based on OS IA2 data after a median follow-up of 42 months. Harms data reported in this review are based on either OS IA2 or OS IA3 data.
Interpretation of Results
Efficacy
At OS IA3 (median follow-up of 54 months), the median IDFS and the median DRFS were not reached in either of the treatment arms. However, the clinical experts CDA-AMC consulted for this review indicated that, compared with ET monotherapy, the benefits of treatment with abemaciclib plus ET were clinically meaningful for both the IDFS and DRFS outcomes.
IDFS: The Kaplan-Meier analysis of IDFS based on the ITT population (cohort 1 + cohort 2) showed that the relative risk of developing an IDFS event was clinically meaningfully reduced by 32% (hazard ratio = 0.680; 95% CI, 0.599 to 0.772; nominal P value < 0.00001) in the abemaciclib plus ET arm compared to the ET alone arm. The absolute risk differences were 2.8% (95% CI, 1.3% to 4.3%; P = 0.0003) at 24 months, 4.8% (95% CI, 3.0% to 6.6%; P < 0.0001) at 36 months, 6.0% (95% CI, 3.9% to 8.0%; P < 0.0001) at 48 months, and 7.6% (95% CI, 5.2% to 10.0%; P < 0.0001) at 60 months. Compared with the ET arm, the abemaciclib plus ET arm showed a statistically significant and clinically meaningful higher IDFS rate from 36 months to 60 months. Subgroup analyses of OS were largely consistent with the primary analysis. However, the prespecified sensitivity analysis results were not provided in full in the sponsor’s evidence summary.
DRFS: The Kaplan-Meier analysis of DRFS based on the ITT population (cohort 1 + cohort 2) showed that the relative risk of developing a DRFS event was statistically significantly and clinically meaningfully reduced by 32.5% (hazard ratio = 0.675; 95% CI, 0.588 to 0.774; nominal P value < 0.0001) in the abemaciclib plus ET arm compared to the ET alone arm. The absolute risk differences were 2.5% (95% CI, 1.1% to 3.9%; P = 0.0004) at 24 months, 4.1% (95% CI, 2.4% to 5.8%; P < 0.0001) at 36 months, 5.3% (95% CI, 3.4% to 7.2%; P < 0.0001) at 48 months, and 6.7% (95% CI, 4.5% to 9.0%; P < 0.0001) at 60 months. Compared with the ET arm, the abemaciclib plus ET arm showed a statistically significant and clinically meaningful higher DRFS rate from 36 months to 60 months. Subgroup analyses of DRFS were largely consistent with the primary analysis. However, the prespecified sensitivity analysis results were not provided in full in the sponsor’s evidence summary.
OS: Based on the patient and clinician group input (patient group, clinical group, and the clinical experts CDA-AMC consulted for this review), 1 of the most important treatment goals of the adjuvant abemaciclib plus ET is to increase OS rate. However, at OS IA3 (median follow-up of 54 months), OS results remained immature with 442 deaths in the ITT population, corresponding to a 68% information fraction of the 650 events required for the final OS analysis. The median OS was not reached in either of the treatment arms. The Kaplan-Meier analysis of OS based on the ITT population (cohort 1 + cohort 2) showed that the threshold for declaring an OS benefit was not met, with a hazard ratio of 0.903 (95% CI, 0.749 to 1.088; P = 0.284) for abemaciclib plus ET compared with ET alone. Based on the Kaplan-Meier probabilities at 60 months, treatment with abemaciclib plus ET is likely to result in little to no clinically important difference in OS. Subgroup analyses and the prespecified sensitivity analysis results of OS were not provided in the sponsor’s evidence summary. The clinical experts CDA-AMC consulted for this review indicated that OS is important outcome but that it is likely too early to determine the OS benefit at 60 months, given the risk of late relapse in this patient population and difficulty showing OS benefit in adjuvant trials. Furthermore, it is difficult to assess OS in this type of early-stage breast cancer setting given that patients have a long survival time and that multiple effective postprogression therapies exist. The clinical experts were of the opinion that the lack of a signal of detriment is encouraging. A longer follow-up is needed to establish whether there is an OS benefit of abemaciclib plus ET over ET alone. The final OS analysis has been scheduled to occur in December 2024, that is, a 1-year longer follow-up than the OS IA3 data used in this review.
HRQoL: Patients expect treatment will offer them a good quality of life. HRQoL was analyzed as a secondary outcome in the monarchE trial using FACT-B, a disease-specific HRQoL assessment for patients with breast cancer. After a median follow-up of 42 months (OS IA2 data cut-off), abemaciclib plus ET was found to result in little to no clinically important difference in FACT-B total score when compared with ET monotherapy at 24 months and at 12 months after treatment discontinuation. The certainty of evidence was reduced due to risk of bias associated with the open-label design and missing outcome data. The clinical experts CDA-AMC consulted for this review indicated that these results were expected and reasonable, because the worsening FACT-B total score at 24 months might be due to potential AEs that occur over up to 2 years of study treatment.
Health care resource utilization: At OS IA2, more patients in the abemaciclib plus ET arm than in the ET arm experienced hospitalizations due to AEs ██████ █. Also, more patients experienced ████████████ ████ ██. The clinical experts CDA-AMC consulted for this review indicated that proportion of patients who experienced hospitalization in both arms appeared higher than that seen in clinical practice.
Harms
At OS IA3 (data cut-off date: July 3, 2023), most patients in both treatment arms experienced AEs (98.4% in the abemaciclib plus ET arm and 88.9% in the ET arm). The most common AEs (experienced by > 30%), which occurred more often in the abemaciclib plus ET arm than in ET arm, were diarrhea, neutropenia, fatigue, leukopenia, and abdominal pain. The most common AEs (experienced by > 20%), which occurred more often among patients in the ET arm than in the abemaciclib plus ET arm, were arthralgia and hot flush. Grade 5 TEAEs were reported rarely (abemaciclib plus ET versus ET: 0.6% versus 0.4%). At OS IA3, more patients in the abemaciclib plus ET arm than in the ET arm experienced SAEs (15.6% versus 9.2%). The clinical experts consulted indicated that, overall, the type and distribution of AEs observed in the monarchE trial were not unexpected compared to those observed in clinical practice.
At OS IA2, the proportion of patients who discontinued treatment because of AEs was higher in the abemaciclib plus ET arm than in the ET arm (18.5% versus 1.1%). Diarrhea was the most common AE that caused treatment discontinuation. The clinical experts consulted indicated that diarrhea is a known AE of abemaciclib treatment and is mostly managed effectively in clinical practice.
In terms of the AEs of special interest for this review, the AEs of special interest also appeared to be higher in the abemaciclib plus ET arm than in the ET arm. The clinical experts CDA-AMC consulted for this review indicated that, of the reported AEs of special interest, VTEs and ILD and/or pneumonitis are the most clinically important. Incidence of VTEs of any grade occurred at a higher rate in the abemaciclib plus ET arm than in the ET arm (2.5% versus 0.7%). ILD/pneumonitis of any grade also appeared to occur at a higher rate in the abemaciclib plus ET arm than in the ET arm (3.3% versus 1.3%). However, the between-group difference did not meet the threshold for a clinically important difference suggested by the clinical experts consulted by CDA-AMC, suggesting that the combination of abemaciclib plus ET likely results in little to no clinically important difference in VTE and in ILD/pneumonitis when compared with ET monotherapy.
In summary, according to the clinical experts CDA-AMC consulted for this review, the harms profile of abemaciclib plus ET in the monarchE trial was generally consistent with that previously reported for abemaciclib and ET in the locally advanced or metastatic breast cancer setting; with no new safety signals or adverse drug reactions identified. Overall, most AEs were predictable, low-grade, reversible, and clinically manageable with co-medications and/or dose modifications in most patients and acceptable in the EBC curative setting.
Conclusion
Evidence from the monarchE trial showed that abemaciclib in combination with ET demonstrated a clinically meaningful benefit compared to ET alone in improving IDFS and DRFS for the adjuvant treatment of adult patients with HR-positive, HER2-negative, node-positive EBC at high risk of disease recurrence based on clinicopathological features. It is not yet clear whether these IDFS and DRFS benefits will translate to improved OS benefit as the data remain immature at OS IA3. A longer follow-up time is needed to determine the OS benefit compared with ET alone in the Health Canada–indicated population given that patients with early-stage breast cancer usually have a long survival time. Treatment with abemaciclib in combination with ET may not result in a clinically meaningful difference in HRQoL as assessed using FACT-B. In terms of harms, most AEs of abemaciclib and ET treatment were predictable, reversible, and clinically manageable among most patients and acceptable in the EBC setting. The safety profile of abemaciclib plus ET in the monarchE trial was generally consistent with the known safety profiles previously reported for abemaciclib and ET, and the monarchE trial did not identify any new safety signals.
References
1.Brenner DR, Poirier A, Woods RR, et al. Projected estimates of cancer in Canada in 2022. CMAJ. 2022;194(17):E601-e607. PubMed
2.Weigelt B, Geyer FC, Reis-Filho JS. Histological types of breast cancer: how special are they? Mol Oncol. 2010;4(3):192-208. PubMed
3.Howlader N, Altekruse SF, Li CI, et al. US incidence of breast cancer subtypes defined by joint hormone receptor and HER2 status. J Natl Cancer Inst. 2014;106(5):dju055. PubMed
4.Seung SJ, Traore AN, Pourmirza B, Fathers KE, Coombes M, Jerzak KJ. A population-based analysis of breast cancer incidence and survival by subtype in Ontario women. Curr Oncol. 2020;27(2):e191-e198. PubMed
5.Giuliano AE, Edge SB, Hortobagyi GN. Eighth edition of the AJCC Cancer Staging Manual: breast cancer. Ann Surg Oncol. 2018;25(7):1783-1785.
6.Giuliano AE, Connolly JL, Edge SB, et al. Breast Cancer-major changes in the American Joint Committee on Cancer eighth edition cancer staging manual. CA Cancer J Clin. 2017;67(4):290-303.
7.Vaidya JS, Patkar VN. Fast facts: early breast cancer. London (UK): Health Press; 2017.
8.Harbeck N, Penault-Llorca F, Cortes J, et al. Breast cancer. Nat Rev Dis Primers. 2019;5(1):66. PubMed
9.Surveillance, Epidemiology, and End Results Program (SEER). Cancer stat facts: female breast cancer subtypes. Bethesda (MD): National Cancer Institute: https://seer.cancer.gov/statfacts/html/breast-subtypes.html. Accessed by sponsor, no date provided.
10.Early Breast Cancer Trialists' Collaborative Group (EBCTCG). Aromatase inhibitors versus tamoxifen in early breast cancer: patient-level meta-analysis of the randomised trials. Lancet. 2015;386(10001):1341-1352. PubMed
11.Cheng L, Swartz MD, Zhao H, et al. Hazard of recurrence among women after primary breast cancer treatment--a 10-year follow-up using data from SEER-Medicare. Cancer Epidemiol Biomarkers Prev. 2012;21(5):800-809. PubMed
12.Cardoso F, Kyriakides S, Ohno S, et al. Early breast cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up†. Ann Oncol. 2019;30(8):1194-1220. PubMed
13.Wolff AC, Somerfield MR, Dowsett M, et al. Human epidermal growth factor receptor 2 testing in breast cancer. Arch Pathol Lab Med. 2023;147(9):993-1000. PubMed
14.Canadian Cancer Society. Hormone receptor status test. 2023; https://cancer.ca/en/treatments/tests-and-procedures/hormone-receptor-status-test. Accessed by sponsor, no date provided.
15.Canadian Cancer Society. HER2 status test. 2023; https://cancer.ca/en/treatments/tests-and-procedures/her2-status-test. Accessed by sponsor, no date provided.
16.Burstein HJ, Curigliano G, Loibl S, et al. Estimating the benefits of therapy for early-stage breast cancer: the St. Gallen International Consensus Guidelines for the primary therapy of early breast cancer 2019. Ann Oncol. 2019;30(10):1541-1557. PubMed
17.Liang Q, Ma D, Gao RF, Yu KD. Effect of Ki-67 expression levels and histological grade on breast cancer early relapse in patients with different immunohistochemical-based subtypes. Sci Rep. 2020;10(1):7648. PubMed
18.Vasconcelos I, Hussainzada A, Berger S, et al. The St. Gallen surrogate classification for breast cancer subtypes successfully predicts tumor presenting features, nodal involvement, recurrence patterns and disease free survival. Breast. 2016;29:181-185. PubMed
19.Drug Reimbursement Review clinical review and pharmacoeconomic review: abemaciclib (Verzenio) for adjuvant treatment of hormone receptor–positive, human epidermal growth factor receptor 2–negative early breast cancer. Can J Health Technol. 2022;2(12). https://www.canjhealthtechnol.ca/index.php/cjht/article/view/PC0282r/PC0282r. Accessed 2024 Apr 14.
20.NCCN Guidelines. Breast cancer, version 4.2023 - March 23, 2023. Plymouth Meeting (PA): National Comprehensive Cancer Network; 2023: https://www.nccn.org/. Accessed 2023 Oct 23.
21.Francis PA, Regan MM, Fleming GF, et al. Adjuvant ovarian suppression in premenopausal breast cancer. N Engl J Med. 2015;372(5):436-446. PubMed
22.BC Cancer Drug Benefit List. Vancouver (BC): BC Cancer; 2024: http://www.bccancer.bc.ca/systemic-therapy-site/Documents/Policy%20and%20Forms/Benefit%20Drug%20List.pdf. Accessed by sponsor, no date provided.
23.Alberta Health Services. Outpatient Cancer Drug Benefit Program. 2024; https://www.albertahealthservices.ca/services/page2328.aspx. Accessed by sponsor, no date provided.
24.Saskatchewan Cancer Agency. Drug Formulary. 2024; https://saskcancer.ca/health-care-professionals/drug-formulary. Accessed by sponsor, no date provided.
25.Exceptional Access Program (EAP). Toronto (ON): Ontario Ministry of Health; Ontario Ministry of Long-Term Care; 2024: http://www.health.gov.on.ca/en/pro/programs/drugs/odbf/odbf_except_access.aspx. Accessed by sponsor, no date provided.
26.Government of New Brunswick. New Brunswick Drug Plans Formulary. https://www2.gnb.ca/content/gnb/en/departments/health/DrugPlans/NBDrugPlan/ForHealthCareProfessionals/NewBrunswickDrugPlansFormulary.html. Accessed by sponsor, no date provided.
27.Government of Nova Scotia. Nova Scotia Pharmacare Formulary. 2024; https://novascotia.ca/dhw/pharmacare/formulary.asp. Accessed by sponsor, no date provided.
28.Health and Community Services, Newfoundland and Labrador. NLPDP Drug Database. https://www.health.gov.nl.ca/health/prescription/newformulary.asp. Accessed by sponsor, no date provided.
29.Express Scripts Canada. Non-Insured Health Benefits Program Drug Benefit List. 2024; https://nihb-ssna.express-scripts.ca/en/0205140506092019/16/160407. Accessed by sponsor, no date provided.
30.Health PEI Formulary Drugs: Oncology. Charlottetown (PE): Health PEI; 2024: https://www.princeedwardisland.ca/sites/default/files/publications/oncologyformulary.pdf. Accessed by sponsor, no date provided.
31.Verzenio (abemaciclib tablets); 50 mg, 100 mg, 150 mg, 200 mg oral tablets [product monograph]. Toronto (ON): Eli Lilly Canada Inc.; 2023 Dec 01.
32.Verzenio (abemaciclib): 50 mg, 100 mg, 150 mg, or 200 mg oral tablets [product monograph]. Toronto (ON): Eli Lilly Canada Inc.; 2022 Jan 01.
33.Drug Reimbursement Expert Review Committee final recommendation: abemaciclib (Verzenio - Eli Lilly Canada Inc.). Can J Health Technol. 2022;2(10). https://www.canjhealthtechnol.ca/index.php/cjht/article/view/PC0282r/PC0282r. Accessed 2024 Apr 30.
34.Clinical Study Report Addendum: I3Y-MC-JPCF. monarchE: a randomized, open-label, phase 3 study of abemaciclib combined with standard adjuvant endocrine therapy versus standard adjuvant endocrine therapy alone in patients with high risk, node positive, early stage, hormone receptor positive, human epidermal receptor 2 negative, breast cancer [internal sponsor's report]. Indianapolis (IN): Eli Lilly and Company; 2023 Oct 11.
35.Johnston SRD, Toi M, O'Shaughnessy J, et al. Abemaciclib plus endocrine therapy for hormone receptor-positive, HER2-negative, node-positive, high-risk early breast cancer (monarchE): results from a preplanned interim analysis of a randomised, open-label, phase 3 trial. Lancet Oncol. 2023;24(1):77-90. PubMed
36.Toi M, Boyle F, Im YH, et al. Adjuvant abemaciclib combined with endocrine therapy: efficacy results in monarchE Cohort 1. Oncologist. 2023;28(1):e77-e81. PubMed
37.Health Canada reviewer's report: Verzenio (abemaciclib) [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Verzenio (abemaciclib), 50 mg, 100 mg, 150 mg, or 200 mg oral tablets. Toronto (ON): Eli Lilly Canada Inc.; 2022 Apr 07.
38.Health Canada reviewer's report: Verzenio (abemaciclib) [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Verzenio (abemaciclib), 50 mg, 100 mg, 150 mg, or 200 mg oral tablets. Toronto (ON): Eli Lilly Canada Inc.; 2023 Nov 24.
39.Balshem H, Helfand M, Schünemann HJ, et al. GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol. 2011;64(4):401-406. PubMed
40.Santesso N, Glenton C, Dahm P, et al. GRADE guidelines 26: informative statements to communicate the findings of systematic reviews of interventions. J Clin Epidemiol. 2020;119:126-135. PubMed
41.Mamounas EP, Tang G, Paik S, et al. 21-Gene Recurrence Score for prognosis and prediction of taxane benefit after adjuvant chemotherapy plus endocrine therapy: results from NSABP B-28/NRG Oncology. Breast Cancer Res Treat. 2018;168(1):69-77. PubMed
42.Canadian Cancer Statistics Advisory in collaboration with the Canadian Cancer Society, Statistics Canada, Public Health Agency of Canada. Canadian Cancer Statistics: a 2022 special report on cancer prevalence. Toronto (ON): Canadian Cancer Society; 2022: https://cdn.cancer.ca/-/media/files/research/cancer-statistics/2022-statistics/2022-special-report/2022_prevalence_report_final_en.pdf. Accessed by sponsor, no date provided.
43.Visvanathan K, Fabian CJ, Bantug E, et al. Use of endocrine therapy for breast cancer risk reduction: ASCO clinical practice guideline update. J Clin Oncol. 2019;37(33):3152-3165. PubMed
44.Brezden-Masley C, Fathers KE, Coombes ME, Pourmirza B, Xue C, Jerzak KJ. A population-based comparison of treatment patterns, resource utilization, and costs by cancer stage for Ontario patients with hormone receptor-positive/HER2-negative breast cancer. Breast Cancer Res Treat. 2021;185(2):507-515. PubMed
45.Tutt ANJ, Garber JE, Kaufman B, et al. Adjuvant olaparib for patients with BRCA1- or BRCA2-mutated breast cancer. N Engl J Med. 2021;384(25):2394-2405. PubMed
46.Curigliano G, Burstein HJ, Gnant M, et al. Understanding breast cancer complexity to improve patient outcomes: the St Gallen International Consensus Conference for the Primary Therapy of Individuals with Early Breast Cancer 2023. Ann Oncol. 2023;34(11):970-986. PubMed
47.Slamon D, Lipatov O, Nowecki Z, et al. Ribociclib plus endocrine therapy in early breast cancer. N Engl J Med. 2024;390(12):1080-1091. PubMed
48.Rastogi P, O'Shaughnessy J, Martin M, et al. Adjuvant abemaciclib plus endocrine therapy for hormone receptor–positive, human epidermal growth factor receptor 2–negative, high-risk early breast cancer: results from a preplanned monarchE overall survival interim analysis, including 5-year efficacy outcomes. J Clin Oncol. 2024;42(9):987-993. PubMed
49.Tolaney SM, Guarneri V, Seo JH, et al. Long-term patient-reported outcomes from monarchE: abemaciclib plus endocrine therapy as adjuvant therapy for HR+, HER2-, node-positive, high-risk, early breast cancer. Eur J Cancer. 2024;199:113555. PubMed
50.Johnston SRD, Harbeck N, Hegg R, et al. Abemaciclib combined with endocrine therapy for the adjuvant treatment of HR+, HER2-, node-positive, high-risk, early breast cancer (monarchE). J Clin Oncol. 2020;38(34):3987-3998. PubMed
51.Harbeck N, Rastogi P, Martin M, et al. Adjuvant abemaciclib combined with endocrine therapy for high-risk early breast cancer: updated efficacy and Ki-67 analysis from the monarchE study. Ann Oncol. 2021;32(12):1571-1581. PubMed
52.Rugo HS, O'Shaughnessy J, Boyle F, et al. Adjuvant abemaciclib combined with endocrine therapy for high-risk early breast cancer: safety and patient-reported outcomes from the monarchE study. Ann Oncol. 2022;33(6):616-627. PubMed
53.Paluch-Shimon S, Neven P, Huober J, et al. Efficacy and safety results by menopausal status in monarchE: adjuvant abemaciclib combined with endocrine therapy in patients with HR+, HER2-, node-positive, high-risk early breast cancer. Ther Adv Med Oncol. 2023;15:17588359231151840. PubMed
54.Martin M, Hegg R, Kim SB, et al. Treatment with adjuvant abemaciclib plus endocrine therapy in patients with high-risk early breast cancer who received neoadjuvant chemotherapy: a prespecified analysis of the monarchE randomized clinical trial. JAMA Oncol. 2022;8(8):1190-1194. PubMed
55.Hamilton EP, Kim JH, Eigeliene N, et al. Efficacy and safety results by age in monarchE: adjuvant abemaciclib combined with endocrine therapy (ET) in patients with HR+, HER2-, node-positive, high-risk early breast cancer (EBC). J Clin Oncol. 2023;41(16_suppl):501-501.
56.Harbeck N, Rastogi P, O'Shaughnessy J, et al. LBA17 Adjuvant abemaciclib plus endocrine therapy for HR+, HER2-, high-risk early breast cancer: Results from a preplanned monarchE overall survival interim analysis, including 5-year efficacy outcomes. Ann Oncol. 2023;34(Supplement 2):S1256.
57.Eli Lilly and Company. NCT03155997: endocrine therapy with or without abemaciclib (LY2835219) following surgery in participants with breast cancer (monarchE). ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2024: https://classic.clinicaltrials.gov/ct2/show/NCT03155997. Accessed 2024 Mar 12.
58.Clinical Study Report Addendum Amendement: I3Y-MC-JPCF. monarchE: a randomized, open-label, phase 3 study of abemaciclib combined with standard adjuvant endocrine therapy versus standard adjuvant endocrine therapy alone in patients with high risk, node positive, early stage, hormone receptor positive, human epidermal receptor 2 negative, breast cancer [internal sponsor's report]. Indianapolis (IN): Eli Lilly and Company; 2021 Mar 02.
59.Clinical Study Report Addendum: I3Y-MC-JPCF. monarchE: a randomized, open-label, phase 3 study of abemaciclib combined with standard adjuvant endocrine therapy versus standard adjuvant endocrine therapy alone in patients with high risk, node positive, early stage, hormone receptor positive, human epidermal receptor 2 negative, breast cancer [internal sponsor's report]. Indianapolis (IN): Eli Lilly and Company; 2022 Nov 09.
60.Hudis CA, Barlow WE, Costantino JP, et al. Proposal for standardized definitions for efficacy end points in adjuvant breast cancer trials: the STEEP system. J Clin Oncol. 2007;25(15):2127-2132. PubMed
61.FACIT.org. FACT-B: Functional Assessment of Cancer Therapy – Breast. 2024; https://www.facit.org/measures/FACT-B. Accessed by sponsor, no date provided.
62.Kim J, Jo MW, Lee HJ, et al. Validity and reliability of the Health-Related Quality of Life Instrument with 8 Items (HINT-8) in Korean breast cancer patients. Osong Public Health Res Perspect. 2021;12(4):254-263. PubMed
63.Webster K, Cella D, Yost K. The Functional Assessment of Chronic Illness Therapy (FACIT) Measurement System: properties, applications, and interpretation. Health Qual Life Outcomes. 2003;1:79. PubMed
64.Hahn EA, Segawa E, Kaiser K, Cella D, Smith BD. Validation of the Functional Assessment of Cancer Therapy-Breast (FACT-B) quality of life instrument. J Clin Oncol. 2015;33(15_suppl):e17753-e17753.
65.Brady MJ, Cella DF, Mo F, et al. Reliability and validity of the Functional Assessment of Cancer Therapy-Breast quality-of-life instrument. J Clin Oncol. 1997;15(3):974-986. PubMed
66.Eton DT, Cella D, Yost KJ, et al. A combination of distribution- and anchor-based approaches determined minimally important differences (MIDs) for four endpoints in a breast cancer scale. J Clin Epidemiol. 2004;57(9):898-910. PubMed
67.DeMets DL, Lan KK. Interim analysis: the alpha spending function approach. Stat Med. 1994;13(13-14):1341-1352; discussion 1353-1346. PubMed
68.Statistical Analysis Plan I3Y-MC-JPCF, version 5: a randomized, open-label, phase 3 study of abemaciclib combined with standard adjuvant endocrine therapy versus standard adjuvant endocrine therapy alone in patients with high risk, node positive, early stage, hormone receptor positive, human epidermal receptor 2 negative, breast cancer [internal sponsor's report]. Indianapolis (IN): Eli Lilly and Company; 2020 Jun 05.
69.Drug Reimbursement Review sponsor submission: Verzenio (abemaciclib), tablets, 50 mg, 100 mg, 150 mg, 200 mg oral [internal sponsor's package]. Toronto (ON): Eli Lilly Canada Inc; 2024 Feb 9.
70.Gyawali B, Hey SP, Kesselheim AS. Evaluating the evidence behind the surrogate measures included in the FDA's table of surrogate endpoints as supporting approval of cancer drugs. EClinicalMedicine. 2020;21:100332. PubMed
Pharmacoeconomic Review
Abbreviations
AE
adverse event
AIC
Akaike information criterion
ALN
axillary lymph node
BIA
budget impact analysis
BIC
Bayesian information criterion
CDA-AMC
Canada’s Drug Agency
CDK
cyclin-dependent kinase
ET
endocrine therapy
HER2
human epidermal growth factor receptor 2
HR
hormone receptor
IA
interim analysis
ICER
incremental cost-effectiveness ratio
IDFS
invasive disease–free survival
ITT
intention to treat
LY
life-year
NICE
National Institute for Health and Care Excellence
OS
overall survival
QALY
quality-adjusted life-year
TTD
time to treatment discontinuation
WTP
willingness to pay
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Abemaciclib (Verzenio), 50 mg, 100 mg, and 150 mg oral tablets. |
Indication | In combination with ET for the adjuvant treatment of adult patients with HR-positive, HER2-negative, node-positive, early breast cancer at high risk of disease recurrence based on clinicopathological features. |
Health Canada approval status | NOC |
Health Canada review pathway | Standard review |
NOC date | December 6, 2023 |
Reimbursement request | As per indication, where “high risk of disease recurrence based on clinicopathological features” refers to patients who satisfy 1 or more of the following:
|
Sponsor | Eli Lilly Canada Inc. |
Submission history | Previously reviewed: Yes Indication: In combination with ET for the adjuvant treatment of adult patients with HR-positive, HER2-negative, node-positive early breast cancer at high risk of disease recurrence based on clinicopathological features and a Ki-67 score ≥ 20%.
Indication: For the treatment of HR-positive, HER2-negative, advanced, or metastatic breast cancer. In combination with an aromatase inhibitor in postmenopausal women as initial endocrine-based therapy. In combination with fulvestrant in women with disease progression following ET.
|
ALN = axillary lymph node; ET = endocrine therapy; HER2 = human epidermal growth factor receptor 2; HR = hormone receptor; NOC = Notice of Compliance.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Markov model |
Target population | Patients with HR-positive, HER2-negative, node-positive early breast cancer at high risk of recurrence |
Treatment | Adjuvant abemaciclib in combination with ET (abemaciclib plus ET). ET comprises a combination of physicians’ choice therapies, including anastrozole (22%), exemestane (8%), letrozole (38%), or tamoxifen (33%). |
Dose regimen | The recommended dose of abemaciclib is 150 mg twice daily, when taken in combination with ET, until the completion of either 2 years of therapy or until disease recurrence or unacceptable toxicity. |
Submitted pricea | Abemaciclib 50 mg: $112.58 per tablet 100 mg: $111.54 per tablet 150 mg: $111.86 per tablet |
Submitted treatment cost | The 28-day cost of abemaciclib is $6,264 per patient. When used in combination with ET, the 28-day costs per patient are as follows: abemaciclib plus anastrozole ($6,291); abemaciclib plus exemestane ($6,301); abemaciclib plus letrozole ($6,302); and abemaciclib plus tamoxifen ($6,274). |
Comparator | Adjuvant ET |
Perspective | Publicly funded health care payer in Canada |
Outcomes | QALYs, LYs |
Time horizon | Lifetime (49 years) |
Key data source | monarchE trial (intention-to-treat, overall survival interim analysis 3 data cut-off date: July 3, 2023) |
Submitted results | ICER = $63,959 per QALY gained (incremental costs = $71,038; incremental QALYs = 1.11) |
Key limitations |
|
CDA-AMC reanalysis results |
|
ALN = axillary lymph node; CDA-AMC = Canada's Drug Agency; CDK = cyclin-dependent kinase; ET = endocrine therapy; HER2 = human epidermal growth factor receptor 2; ICER = incremental cost-effectiveness ratio; IDFS = invasive disease–free survival; LY = life-year; OS = overall survival; QALY = quality-adjusted life-year.
aThe sponsor did not provide the submitted price for the abemaciclib 200 mg tablet as this strength is not relevant given the recommended dosage for this indication.
Conclusions
Evidence from monarchE suggests that abemaciclib in combination with endocrine therapy (ET; henceforth, abemaciclib plus ET) resulted in a statistically significant and clinically important improvement in invasive disease–free survival (IDFS) when compared with ET alone in the adjuvant treatment of patients with hormone receptor (HR)–positive, human epidermal growth factor receptor 2 (HER2)–negative, node-positive early breast cancer at high risk of disease recurrence based on clinicopathological features. The CDA-AMC Clinical Review noted that it is not yet clear whether IDFS benefits will translate to improved overall survival (OS) because the data remain immature and evidence at the OS interim analysis 3 (OS IA3) data cut (median follow-up: 54 months) suggests little to no clinically significant difference between the 2 treatments. Clinical experts consulted by CDA-AMC noted that a longer follow-up time would be required to determine the OS benefit of abemaciclib plus ET relative to ET alone considering the risk of late relapse in this patient population.
In addition to the aforementioned limitations with the clinical evidence, CDA-AMC identified several limitations with the sponsor’s economic submission: lack of transparency of the “fixed payoff” modelling approach; uncertainty regarding the long-term impact of abemaciclib plus ET on OS and IDFS; uncertainty regarding the waning of treatment effectiveness; misalignment of the sponsor’s assumptions regarding the use of cyclin-dependent kinase (CDK) 4 and CDK6 inhibitors in the metastatic setting in Canadian clinical practice; and omission of adjuvant olaparib as a relevant comparator. As part of the base-case reanalysis, CDA-AMC used independent models and adopted alternative distributions to extrapolate IDFS; revised treatment effectiveness waning parameters; and updated the proportion of patients with metastatic ET-sensitive disease who receive CDK4 and CDK6 inhibitors in the metastatic setting.
As adjunctive therapy for the adjuvant treatment of adult patients with HR-positive, HER2-negative, node-positive early breast cancer at high risk of disease recurrence based on clinicopathological features, abemaciclib plus ET was associated with an incremental cost-effectiveness ratio (ICER) of $133,903 per quality-adjusted life-year (QALY) gained compared to ET alone (incremental costs = $103,572; incremental QALYs = 0.77). CDA-AMC was unable to determine the probability that abemaciclib plus ET is cost-effective at a willingness-to-pay (WTP) threshold because of structural limitations in the sponsor’s model. As such, CDA-AMC analyses are deterministic and do not reflect uncertainty. The estimated ICER was higher than the sponsor’s base-case value, driven by the selection of alternative distributions for extrapolating IDFS, and assumptions about treatment waning. A price reduction of 51% for abemaciclib would be required for abemaciclib plus ET to be cost-effective compared with ET alone at a WTP threshold of $50,000 per QALY gained. This would reduce the price of abemaciclib from $111.86 to $54.81 (per 150 mg tablet).
The cost-effectiveness of abemaciclib plus ET was sensitive to assumptions concerning the persistence of long-term treatment effects. When assuming no waning of treatment effect, the ICER of abemaciclib plus ET decreased to $122,027 per QALY gained relative to ET alone. When assuming no further effect beyond the duration of the monarchE trial, the ICER of abemaciclib plus ET increased to $167,833 per QALY gained relative to ET alone. CDA-AMC was unable to address limitations related to the modelling approach and the omission of adjuvant olaparib from the economic analysis. Therefore, the cost-effectiveness of abemaciclib plus ET versus olaparib plus ET is unknown. Finally, it is important to note that the entirety of the QALY benefit realized by patients in the CDA-AMC base case was accrued in the post-trial period of the model on the basis of extrapolation.
Patient, Clinician, and Drug Plan Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, clinician groups, and drug plans that participated in the CDA-AMC review process.
Two patient groups, the Canadian Breast Cancer Network and Rethink Breast Cancer provided input for this review. The Canadian Breast Cancer Network collected responses, through its 2017 and 2022 online surveys, from 222 patients with early-stage HR-positive, HER2-negative breast cancer living in Canada, and conducted a key informant interview in 2023. Rethink Breast Cancer conducted interviews in 2022 with 2 patients with HR-positive, HER2-negative, high-risk early-stage breast cancer who had experience with abemaciclib. Overall, patients’ disease experience was influenced by the physical symptoms associated with early-stage breast cancer (e.g., fatigue), psychosocial effects associated with fear of death and risk of recurrence (e.g., anxiety, distress, depression), and adverse side effects associated with chemotherapy and radiation (e.g., nausea, vomiting, neuropathy). Patients noted that important outcomes of treatment include delaying disease recurrence, achieving long-term remission, and improving survival, as well as reducing side effects, preserving independence, and maintaining productivity and quality of life. Patients noted the lack of adjuvant therapeutic options that could be used in combination with ET to reduce the risk of recurrence following surgical resection and chemotherapy. The 2 patients previously treated with abemaciclib described mild to moderate side effects, including fatigue, diarrhea, cramping, and bloating.
Registered clinician input was received from the Ontario Health – Cancer Care Ontario (OH-CCO) Breast Cancer Drug Advisory Committee. The clinicians indicated that the current pathway of care for patients with HR-positive, HER2-negative early-stage breast cancer varies depending on risk of recurrence but includes combinations of surgery, radiotherapy, adjuvant or neoadjuvant chemotherapy, and ET. The clinicians noted that adjuvant ET is standard treatment of HR-positive, HER2-negative early-stage breast cancer; however, a proportion of patients with high-risk clinical and/or pathologic features may experience distant recurrence, and additional treatment options are needed to prevent early recurrence and development of metastases. The clinicians also noted that adjuvant abemaciclib plus ET would supplement the current management of HR-positive, HER2-negative early-stage breast cancer following surgery but would not replace current therapies. The clinicians indicated that treatment goals include improved survival and decreased risk of recurrence. Of note, the clinician input highlighted that olaparib is a relevant adjuvant therapy for the subset of patients with deleterious or suspected deleterious germline BRCA1 or BRCA2-mutated disease.
Participating drug plans noted considerations related to re-treatment eligibility. Specifically, patients currently treated with CDK4 and CDK6 inhibitors are eligible for re-treatment in subsequent lines of therapy provided that there is at least a 6-month interval between any prior treatment with a CDK4 and CDK6 inhibitor and the development of disease recurrence. The participating drug plans initially highlighted that the indication under review would broaden the eligible patient population by eliminating the requirement for Ki-67 testing, which is not universally conducted across jurisdictions. Hence, participating drug plans considered that the removal of a testing barrier would introduce a potential budget impact of indeterminate magnitude.
Several of these concerns were addressed in the sponsor’s model:
IDFS and OS were included in the model.
The use of a cost-utility approach accounts for some issues related to health-related quality of life; however, it is unclear if all quality-of-life concerns noted to be important to patients were captured in the health state utility values adopted by the sponsor.
Costs and utility decrements related to adverse events (AEs) were included in the model.
CDA-AMC addressed some of these concerns as follows:
In reanalysis, CDA-AMC adopted alternative assumptions regarding re-treatment with CDK4 and CDK6 inhibitors among patients with metastatic recurrence.
CDA-AMC was unable to address the following concerns raised from patient and clinician group input:
The exclusion of adjuvant olaparib plus ET as relevant comparator could not be addressed.
The sponsor’s modelling approach precludes full validation of the model findings related to OS.
Economic Review
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted a cost-utility analysis of abemaciclib plus ET compared with ET alone.1 The model population comprised patients with HR-positive, HER2-negative, and node-positive early breast cancer at high risk of recurrence. This population includes patients with either 4 or more positive axillary lymph nodes (ALNs), or between 1 and 3 positive ALNs and either grade 3 disease or tumour size 5 cm or larger (cohort 1 of the monarchE trial) as well as patients with between 1 and 3 positive ALNs and Ki-67 of at least 20% as an additional risk feature (cohort 2 of the monarchE trial).1
Abemaciclib is a reversible small-molecule CDK inhibitor. Abemaciclib is available as 50 mg, 100 mg, 150 mg, and 200 mg oral tablets.2 The recommended dosage of abemaciclib when taken in combination with ET for early-stage breast cancer is 150 mg twice daily, until the completion of either 2 years of therapy or until disease recurrence or unacceptable toxicity.2 ET comprises a combination of physicians’ choice therapies, including anastrozole, exemestane, letrozole, and tamoxifen. At the sponsor’s submitted price of $111.86 per 150 mg tablet,1 the 28-day cost of abemaciclib is $6,264 per patient (annual cost: $81,710). In combination with ET, the 28-day costs per patient are as follows: abemaciclib plus anastrozole, $6,291 (anastrozole monotherapy = $27); abemaciclib plus exemestane, $6,301 (exemestane monotherapy = $37); abemaciclib plus letrozole, $6,302 (letrozole monotherapy = $39); and abemaciclib plus tamoxifen, $6,274 (tamoxifen monotherapy = $10). The 28-day cost per patient of ET alone, amounting to $27 (annual cost = $347), was determined by considering the observed utilization rates of physicians’ choice of therapy in the monarchE study: anastrozole (22%), exemestane (8%), letrozole (38%), and tamoxifen (33%). Wastage was not included in the submitted base case given the oral administration route of the intervention and comparator treatments.
The clinical outcomes modelled were IDFS, time to treatment discontinuation (TTD), OS (without distant relapse), remission, metastatic disease recurrence, and nonmetastatic disease recurrence.1 The economic outcomes of interest were QALYs and life-years (LYs).1 The economic evaluation was conducted over a lifetime horizon (i.e., 49 years), from the perspective of the Canadian public health care payer.1 Costs and QALYs were discounted at 1.5% annually, while LYs were undiscounted.
Model Structure
The sponsor submitted a Markov model with 5 health states: invasive disease–free, nonmetastatic recurrence, metastatic recurrence, remission, and death (Figure 1).1 Metastatic recurrence and death were modelled as absorbing states. Patients entered the model in the invasive disease–free state and received abemaciclib plus ET or ET alone. Abemaciclib (in combination with ET) could be received for a maximum of 2 years, and ET (in both arms) could be received for up to 5 years, with discontinuation prior to 2 years (abemaciclib plus ET arm) or 5 years (ET alone arm) based on TTD in the monarchE trial.1 In each 28-day cycle, patients could remain in the invasive disease–free state or experience metastatic recurrence, nonmetastatic recurrence, or death. Patients with metastatic recurrence transitioned to either the ET-resistant or the ET-sensitive substates of the metastatic recurrence health state, depending on the timing of recurrence (≤ 12 months or > 12 months of completing adjuvant ET, respectively).1 Patients in the metastatic recurrence health state were assigned a fixed number of LYs based on external models developed by the sponsor for other submissions (i.e., the fixed payoff approach).1 These LYs were multiplied by costs and utilities to determine total costs and QALYs for patients in the metastatic recurrence state. Patients who experienced nonmetastatic recurrence transitioned to the nonmetastatic recurrence health state and were assumed to have either a second primary neoplasm or locoregional or contralateral disease.1 Those with a second primary neoplasm were assumed to only incur the cost of diagnosis, following which they leave the model to receive treatment for that specific neoplasm (i.e., the cost of treating the secondary primary neoplasm was not included in the model).1 Patients with nonmetastatic locoregional or contralateral recurrence were assumed to receive treatment (based on type and location of the disease) for 12 months (unless death occurred prior to 12 months), and to subsequently move to the remission health state.1 Patients in the remission state were at risk of death from non-early breast cancer, remained at risk of metastatic recurrence, and were assumed to remain in remission unless a recurrence occurred.1
Model Inputs
Baseline patient characteristics were derived from monarchE, a randomized, open label, phase III trial designed to evaluate the efficacy and safety of abemaciclib plus ET versus ET alone in patients with HR-positive, HER2-negative, node-positive early breast cancer at high risk of recurrence (intention-to-treat [ITT] population: n = 5,637; cohort 1: n = 5,120; and cohort 2: n = 517)).3 On average, patients in the modelled cohort (assumed by the sponsor to reflect the patient population in Canada) were aged ██ years, weighed ██ kg, had a mean body surface area of ███ m2, and were more likely to be female (██%).1 These characteristics were derived from the monarchE trial and used to inform the drug dosage regimens, as well as the age- and sex-specific distribution of the general population mortality risk.
Clinical efficacy parameters used to characterize abemaciclib plus ET and ET alone, including IDFS, TTD, and OS without distant recurrence, were derived from the ITT OS IA3 of the monarchE trial using the July 3, 2023 data cut-off date (median follow-up of 54 months for cohort 1 and of 51 months for cohort 2).3 Parametric distributions were derived for abemaciclib plus ET and ET alone using Kaplan-Meier curves of IDFS, TTD, and OS (excluding distant recurrence) from the monarchE trial, enabling the extrapolation of observed trial data to the lifetime model horizon. Dependent parametric models were explored statistically through the assessment of the proportional hazard assumption (i.e., constant treatment effect on the hazards) and the accelerated failure time assumption (i.e., constant treatment effect on the time scales).1 The sponsor tested the correlation of scaled Schoenfeld residuals with rank-ordered time, and used plots of the log(cumulative hazard) against log(time) to assess hazards proportionality over time. In addition to the standard parametric distributions, Weibull spline models with 1 and 2 intermediate knots were examined. Candidate distributions were selected based on clinical plausibility of long-term survival projections, visual inspection of model fit, as well as Akaike information criterion (AIC) and Bayesian information criterion (BIC). The sponsor opted for a dependent log-logistic model to extrapolate IDFS and a dependent exponential model to extrapolate OS (without distant relapse) for patients receiving abemaciclib plus ET and patients receiving ET alone.1 Moreover, the sponsor used Kaplan-Meier data to model TTD for abemaciclib in the abemaciclib plus ET group (i.e., no extrapolation needed) and selected independent models with a hazard spline 2-knot distribution to extrapolate TTD for ET across intervention groups.
The sponsor used external data sources to derive clinical effectiveness estimates for outcomes not observed in the monarchE trial. The probability of transitioning from the remission health state to the metastatic recurrence health state was sourced from a previous early-stage breast cancer model submitted to the National Institute for Health and Care Excellence (NICE) for trastuzumab.4 As noted in the Model Structure section, the sponsor adopted a fixed payoff approach to determine LYs, QALYs, and costs for patients with metastatic recurrence. The disease course for patients with ET-resistant and ET-sensitive metastatic recurrence was based on data from the MONARCH 2 and MONARCH 3 models.5,6 The MONARCH 2 trial included patients with HR-positive, HER2-negative locally advanced or metastatic breast cancer that progressed while patients were receiving or immediately after receiving prior ET; the MONARCH 3 trial included patients with HR-positive, HER2-negative locoregionally recurrent or metastatic disease who had not received prior systemic therapy.1
Health state utility values were adopted from multiple sources. For the invasive disease–free health state, utility values (0.813) were derived from an analysis of EQ-5D index data collected from the monarchE trial, with Canadian tariffs applied.1 For the first 3 months of nonmetastatic recurrence health state occupancy, utilities were adopted from the NICE appraisal of neratinib,7 which adopted values from the literature (0.696).8 For the last 9 months of nonmetastatic recurrence health state occupancy, utilities were assumed to be equal to the invasive disease–free health state (0.813). For the metastatic recurrence health state, utility estimates for patients in the ET-resistant sub–health state were based on EQ-5D data from the MONARCH 2 trial (0.748 for patients who are progression-free and 0.706 for patients with progressed disease),6 while utility estimates for patients with ET-sensitive disease were based on EQ-5D data collected in the MONARCH 3 trial (0.724 for patients who are progression-free and 0.505 for patients with progressed disease).5 Utility values for patients in the premetastatic states were age-adjusted.9 The sponsor incorporated disutilities associated with AEs (qualified as greater than or equal to grade 3), with greater than or equal to 1% incidence in any of the interventions considered.1 Treatment-related AE prevalence was informed by the monarchE trial, and AE-specific marginal disutilities were estimated from multiple sources, including the MONARCH 3 trial and the literature. Disutilities were applied as a 1-time decrement during the first model cycle, assuming that serious AEs likely occurred at the time of treatment initiation. Treatment-related total mean utility decrements were calculated as the weighted sum of the treatment-specific prevalence of each AE and its associated disutility.
Costs captured in the model included those associated with drug acquisition, drug administration, disease monitoring and medical follow-up, AE management, subsequent treatment, and terminal care costs. Drug acquisition costs for abemaciclib were based on the sponsor’s submitted price,1 while acquisition costs for anastrozole, exemestane, letrozole, and tamoxifen (as part of ET) were obtained from the Ontario Drug Benefit Formulary.10 The dosing modelled for abemaciclib plus ET is consistent with that described in the Overview section. Dosages for drugs included as part of ET were based on their respective product monographs. TTD curves, which capture treatment discontinuation due to any cause, were used alongside drug acquisition costs to determine treatment costs in the intervention and comparator groups. No administration costs were applied for oral drugs; administration costs for chemotherapy received in the nonmetastatic recurrence health state were obtained from the Ontario Ministry of Health and Long-Term Care.10 For patients in the invasive disease–free health state, disease management costs included general practitioner visits and mammograms, with the frequency of each obtained from the NICE technology appraisal guidance of pertuzumab.11 The costs were based on the Ontario Schedule of Benefits for Physician Services Under the Health Insurance Act.12 For patients in the nonmetastatic recurrence health state, resource use included oncologist visits, mammograms, echocardiography, radionuclide lymphangiography, CT scans, mastectomy, breast reconstruction, and radiotherapy; the costs were sourced from the Ontario Case Costing Initiative13 and the Ontario Schedule of Benefits for Physician Services Under the Health Insurance Act.12 Patients with a second primary neoplasm were assumed to incur the cost of 1 multidisciplinary team meeting for diagnosis (sourced from the Ontario Schedule of Benefits for Physician Services Under the Health Insurance Act12); no further costs were applied. Patients in the remission health state incurred costs related to oncologist and general practitioner visits, mammograms, echocardiography, and radionuclide lymphangiography. For patients in the metastatic recurrence health state, costs were based on whether the patient had ET-resistant or ET-sensitive recurrence. The per-cycle cost of each resource used in the ET-resistant and ET-sensitive substates was multiplied by the applicable number of cycles, calculated based on mean progression-free survival, postprogression survival, and time on treatment derived from data in the MONARCH 2 and MONARCH 3 models.5,6 The cost of terminal care ($19,957) per patient was obtained from the literature.14 Costs associated with the management of AEs were applied as a 1-time cost in the first model cycle, based on the incidence in the monarchE trial (the ITT population) and costs obtained from the Ontario Case Costing Initiative.13
Summary of Sponsor’s Economic Evaluation Results
The sponsor conducted the base case via a probabilistic sensitivity analysis with 1,000 simulations.1 The deterministic and probabilistic results were similar. The probabilistic findings are presented subsequently.
Base Case Results
In the sponsor’s base case, abemaciclib plus ET was associated with an incremental cost of $71,038 and an incremental QALY gain of 1.11 compared with ET alone, resulting in an ICER of $63,959 per QALY gained.
The sponsor’s analysis predicted that abemaciclib plus ET was associated with a longer duration of life than that associated with ET alone (i.e., incremental undiscounted LYs = 2.19). Given the duration of the monarchE trial (median follow-up of 54 months) in contrast to the model’s time horizon (49 years), it is important to note that the totality of the incremental QALYs realized by patients receiving abemaciclib plus ET relative to ET alone were derived from the period beyond which there are observed trial data (i.e., extrapolated period). In fact, abemaciclib plus ET resulted in an incremental QALY loss of –0.10 (relative to ET alone) in the interpolated period. This is because in the first 4 years of the model (approximately aligned with the median follow-up time of the monarchE trial), more QALYs were accrued by patients who received ET alone (3.44 QALYs) than by those who received abemaciclib plus ET (3.34 QALYs). Indeed, while patients treated with abemaciclib plus ET accrued more QALYs than patients treated with ET alone in the invasive disease–free state (3.07 versus 2.96), they also accrued fewer QALYs in the metastatic recurrence state (0.24 versus 0.44).
The key cost driver among patients receiving abemaciclib plus ET was drug acquisition, accounting for 75% of the total cost incurred. The primary cost driver among patients receiving ET alone was the payoff cost incurred by patients with metastatic recurrence, which accounted for 74% of the total estimated cost.
The probability that abemaciclib plus ET was cost-effective at a $50,000 per QALY gained threshold was 17%.1 The sponsor’s submitted analysis is based on the publicly available prices for all drug treatments. Additional results from the sponsor’s submitted economic evaluation base case are presented in Appendix 3.
Table 3: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER vs. ET alone ($/QALY) |
|---|---|---|---|---|---|
ET alone | 101,973 | Reference | 13.67 | Reference | Reference |
Abemaciclib + ET | 173,011 | 71,038 | 14.78 | 1.11 | 63,959 |
ET = endocrine therapy; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; vs. = versus.
Source: Sponsor’s pharmacoeconomic submission.1
Sensitivity and Scenario Analysis Results
The sponsor assessed several model parameters and assumptions in deterministic scenario analyses. These included considering different model time horizons; using alternative discount rates for costs and QALYs; applying a hybrid model for IDFS that uses Kaplan-Meier curves from the monarchE trial for the interpolated period and parametric distributions for the extrapolated period across interventions; and applying a hybrid model to extrapolate TTD among patients receiving ET alone.1 The most influential parameter was time horizon, particularly as regards the selection of 10- and 20-year horizons. When adopting a 10-year model horizon, the ICER increased to $3,284,682 per QALY gained. When applying a 20-year model horizon, the ICER increased to $171,161 per QALY gained. All other scenarios resulted in ICERs ranging between $45,330 and $92,292 per QALY gained. No scenario analysis was conducted using a perspective other than the health care payer.
CDA-AMC Appraisal of the Sponsor’s Economic Evaluation
CDA-AMC identified several key limitations to the sponsor’s analysis that have notable implications on the economic analysis:
Modelling approach lacks transparency. The sponsor’s model included health states in which patients were assumed to have no invasive disease (the invasive disease–free state) or to have a metastatic or nonmetastatic recurrence. For the invasive disease–free and nonmetastatic recurrence states, the sponsor adopted a typical Markov cohort approach in which patients accrue costs, LYs, and QALYs based on the duration of time spent in each health state. In contrast, for the metastatic recurrence state, the sponsor adopted a fixed payoff approach. Using this approach, the sponsor assigned each patient who entered this state a fixed number of LYs and multiplied this by costs and utility values to determine total costs and QALYs. To determine the LYs (and hence costs and QALYs), the sponsor used previous economic models built to assess the cost-effectiveness of abemaciclib in the metastatic breast cancer setting.5,6 Clinical experts consulted by the sponsor described this fixed payoff approach as a “black box approach to modelling.”1 CDA-AMC agrees with this assessment, as the models used by the sponsor to estimate LYs, QALYs, and costs for patients with metastatic disease were not provided to CDA-AMC as part of the review process. Thus, CDA-AMC was unable to validate the model’s predicted outcomes for patients in the metastatic recurrence health state. CDA-AMC also notes that these external models were partitioned survival models, which are subject to inherent modelling limitations, and any assumptions made during the development of these models are carried through to the current submission.
CDA-AMC further notes that the models used to determine the payoff for patients in the metastatic recurrence health state were informed by data from the MONARCH 2 trial (which assessed abemaciclib in combination with fulvestrant after progression on or after prior ET) and the MONARCH 3 trial (which assessed abemaciclib in the first-line metastatic setting). Because individual patient data were not used in the current model, the sponsor incorporated an assumption that all patients in the metastatic recurrence state would remain alive until the mean LY point was reached in the MONARCH 2 and MONARCH 3 trial populations. This may lead to underestimating or overestimating the survival outcomes of the modelled population. Because the MONARCH 2 and MONARCH 3 trials were not submitted to CDA-AMC as part of this review, the data incorporated in the economic models from these trials have not been appraised by CDA-AMC as part of this submission.
Finally, the sponsor’s submitted model included numerous IFERROR statements, which lead to situations in which the parameter value is overwritten with another value without alerting the user to the automatized overwriting. The systematic use of IFERROR statements makes thorough auditing of the sponsor’s model impractical, as it remains unclear whether the model is running inappropriately by overriding errors.
CDA-AMC was unable to thoroughly validate the sponsor’s model, particularly in regard to predicting outcomes for patients in the metastatic recurrence health state. Due to this limitation, CDA-AMC was unable to validate the predicted incremental LYs, QALYs, and costs for abemaciclib plus ET relative to ET alone. Therefore, the resulting ICER should be considered to be highly uncertain.
Impact of abemaciclib on OS is highly uncertain. The sponsor’s base case predicts a survival advantage to treatment with abemaciclib plus ET compared to treatment with ET alone (incremental undiscounted gain of 2.19 LYs). As noted in the CDA-AMC clinical report, the monarchE trial was not powered to detect differences in OS between the abemaciclib plus ET and the ET alone arms. As of OS IA3 (data cut-off on July 3, 2023), the OS data remain immature, and there was no significant difference in OS between the abemaciclib plus ET and ET alone treatment arms (hazard ratio = 0.90; 95% CI, 0.75 to 1.09) for patients in the ITT population. The clinical experts consulted by CDA-AMC indicated that it is uncertain whether delayed disease recurrence (reflected by IDFS), as observed in Cohorts 1 and 2 of the monarchE trial, will translate to gains in OS.
There is additional uncertainty associated with the predicted OS associated with abemaciclib plus ET owing to the modelling approach adopted by the sponsor. The sponsor’s model incorporates OS data from the monarchE trial only for patients without distance recurrence, while a fixed payoff approach was adopted for patients with metastatic recurrence. This approach is subject to extensive limitations (refer to the “Modelling approach lacks transparency” limitation). For the OS data incorporated in the current model, the sponsor selected a dependent exponential model (i.e., single model with treatment coefficient) to extrapolate OS (without distant recurrence) for patients receiving abemaciclib plus ET and patients receiving ET alone, based on AIC and BIC values. However, statistical fit speaks only to the fit of the predicted data to the observed data within the interpolated period, and not to the validity of predicted data for the extrapolated period. CDA-AMC notes that there were several parametric distributions with comparable AIC and BIC values; however, selecting alternative curves for OS for patients without distant recurrence had little impact on the ICER, likely owing to the modelling approach adopted by the sponsor.
CDA-AMC was unable to address this limitation because of the structure of the sponsor’s model.
Proportional hazards assumption for IDFS is improbable. The sponsor selected a dependent log-logistic model to extrapolate IDFS for treatment with abemaciclib plus ET and treatment with ET alone (i.e., single parametric model with treatment coefficient). In using a dependent proportional hazards model to characterize the comparative efficacy of abemaciclib plus ET and ET alone, the sponsor assumed that the hazard rates for abemaciclib plus ET and for ET alone would remain proportional for the first 8 years of the model. CDA-AMC notes that it is not ideal to apply a dependent model to Kaplan-Meier data for 2 treatment groups when the pivotal trial assesses the efficacy of treatments with different mechanisms of action and, consequently, different patterns of event hazards over time.15 As the only CDK4 and CDK6 inhibitor approved for the adjuvant treatment of HR-positive, HER2-negative early breast cancer, abemaciclib represents a different class of therapy with a unique mechanism of action relative to ET. Therefore, it is unlikely that a single functional form will effectively match both the abemaciclib plus ET and ET alone intervention groups, and the utilization of a dependent model may introduce bias to the estimated IDFS in both arms given that the parameter estimates inevitably deviate from the best fit for either arm.16
The sponsor presented a log-log hazard plot and tested the correlation of scaled Schoenfeld residuals with rank-ordered time to assess the proportionality assumption for IDFS between patients treated with abemaciclib plus ET and ET alone in the monarchE trial. The log-log hazard plot depicting IDFS against time reveals multiple instances where the hazard curves of abemaciclib plus ET and ET alone intersect.1 This suggests a departure from the assumption of proportional hazards and implies that the hazard ratios fluctuate during the observation period of the monarchE trial rather than remain constant. In addition, the Schoenfeld residual plot conducted for IDFS shows a distinct nonlinear hazard pattern between abemaciclib plus ET and ET alone when ranked by event time.1 CDA-AMC notes that since Schoenfeld residuals represent the difference between the observed and expected values of the treatment covariate in each failure time point, they should be flat and centred around zero to support proportionality. In addition, the sponsor conducted a Schoenfeld residual test that was not statistically significant. Hence, there is insufficient evidence to reject the null hypothesis of no difference between the hazards of abemaciclib plus ET and ET alone. CDA-AMC further notes that issues with the Schoenfeld residual test in terms of statistical hypothesis testing have been acknowledged elsewhere,17 prompting recommendations to employ multiple methods concurrently to assess hazards proportionality.18-20 Specifically, the P value of the Schoenfeld residual test is influenced by sample size, meaning a large sample size might yield high significance with minimal assumption violation, whereas a small sample size could result in a nonsignificant apparent violation of the assumption. Moreover, as it is often the case that Schoenfeld residual tests are not sufficiently powered to detect differences between the observed and expected values, CDA-AMC cautions that the absence of evidence (i.e., a nonstatistically significant test) does not conclusively prove hazards proportionality. Given that the log-log hazard plot demonstrates a violation of proportional hazards (while the Schoenfeld residual test yields inconclusive results), CDA-AMC notes that assuming proportionality in the within-trial period is not supported by evidence.
Finally, the assessments submitted by the sponsor do not inform how the pattern of event hazards between patients treated with abemaciclib plus ET and patients treated with ET alone may evolve in the extrapolated period. According to CADTH Methods and Guidelines for Extrapolating Clinical Evidence Within Economic Evaluations,21 it is essential to consider the relevance of constant proportional hazards over the modelled lifetime horizon, rather than solely the short-term clinical trial period. Indeed, the assumption of proportional hazards is unlikely to persist for the long term in most cases.22 This becomes particularly pertinent when considering heterogeneous study populations, where the relative treatment effects may vary based on patient characteristics, leading to a situation where proportional hazards cannot be maintained because of the evolving characteristics of the surviving population over time.16 Therefore, assuming hazard proportionality and employing a dependent model with an adjustment factor for treatment effect is considered unsuitable for extrapolating IDFS.
CDA-AMC applied independent parametric models to estimate the IDFS benefit of treatment with abemaciclib plus ET versus treatment with ET alone.
Impact of abemaciclib plus ET on long-term IDFS is highly uncertain. The sponsor used parametric modelling to extrapolate IDFS beyond the observable time points in the monarchE trial (median follow-up of 54 months) to a lifetime horizon (49 years). The parametric distribution chosen by the sponsor (along with other modelling assumptions, such as treatment effectiveness waning (refer to the “Waning of treatment effectiveness of abemaciclib plus ET is highly uncertain” limitation) resulted in an incremental gain of 1.62 QALYs in the invasive disease–free health state among patients treated with abemaciclib plus ET, which exceeds the total incremental QALYs accrued over the model horizon (1.11 QALYs). This is because abemaciclib plus ET treatment resulted in incremental QALY losses across postprogression health states (–0.51). CDA-AMC further notes that the gains in predicted incremental QALYs are generated primarily through extrapolation. Notably, 94% of the incremental QALYs realized by patients in the invasive disease–free health state were derived from the period beyond which there are observed trial data (i.e., extrapolated period).
The sponsor selected parametric distributions based on goodness-of-fit criteria, visual inspection, and clinical plausibility, following NICE Decision Support Unit guidance.23 While CDA-AMC agrees that models should be compared based on their statistical fit, this pertains only to the observed trial period, not to the extrapolation period. The weight given to the comparative fit of alternative parametric models to the observed data depends on the extent to which extrapolation is required and the degree of censoring present. Given the length of time required for extrapolation and the size of the censored population (82%), the clinical plausibility of the extrapolated portion of alternative models is of greater importance than the statistical fit to the observed data.24 According to the clinical experts consulted by CDA-AMC for this review, although the monarchE trial findings concerning IDFS appeared favourable and clinically important, the magnitude and durability of such a benefit were highly uncertain in the absence of longer-term evidence.
By characterizing the long-term IDFS benefits of treatment with abemaciclib plus ET and with ET alone using a dependent log-logistic model, the sponsor implicitly assumed that the IDFS benefit of abemaciclib plus ET treatment continues to increase in the extrapolated period, for which there are no data. In the submitted base case, the incremental benefit in IDFS achieved with abemaciclib plus ET treatment is 6.8 percentage points in year 5 and 9.8 percentage points in year 15. The clinical experts consulted by CDA-AMC for this review noted a lack of evidence to substantiate the assumption that abemaciclib plus ET would continue to increase in effectiveness after patients have stopped treatment (i.e., when patients are not receiving any treatment from year 5 onwards). Following clinical expert input, CDA-AMC selected alternative distributions to extrapolate the long-term IDFS benefits of abemaciclib plus ET (Weibull) and of ET alone (Weibull spline model with 2 intermediate knots), which resulted in more plausible survival projections.
Furthermore, following CADTH Methods and Guidelines for Extrapolating Clinical Evidence Within Economic Evaluations,21 CDA-AMC performed an analysis of the sponsor’s submitted data for time to invasive disease to assess the plausibility of the implied relative effects (Figure 2, Appendix 3). As per the guidelines, a U-shaped relationship between the relative effects and time would be anticipated, and any deviations would necessitate a compelling argument.22 In the CDA-AMC base case, the relative risk of invasive disease over time reveals the expected U-shaped relationship: (1) in the immediate post–treatment commencement stage, the choice of treatment had little effect on the relative risk of invasive disease; (2) in the main period covered by the monarchE trial, the relative risk of invasive disease declined monotonically; and (3) over the extrapolated period, the relative risk of invasive disease progressively trended to 1. This further confirms that the independent distributions selected in the CDA-AMC base case, in concordance with clinical expert input, reflect the expectation that the relative risk of invasive disease would exhibit an acceleration pattern during the interpolated period and a deceleration pattern throughout the extrapolated lifetime horizon of the model.
CDA-AMC selected alternative distributions to extrapolate the long-term IDFS benefit of treatment with abemaciclib plus ET (Weibull) and with ET alone (Weibull spline model with 2 intermediate knots). Clinical experts considered the magnitude of IDFS benefit resulting from these extrapolations to be more plausible; however, they emphasized that the persistence of this benefit over the patients’ lifetime remained highly uncertain in the absence of longer-term evidence.
Waning of treatment effectiveness of abemaciclib plus ET is highly uncertain. In the pharmacoeconomic model, the sponsor assumes that treatment waning for abemaciclib plus ET will start at year 8 and gradually wane until year 27. Because the maximum duration of abemaciclib treatment in the monarchE trial was 2 years, implicit in this assumption is that the treatment effect of abemaciclib will continue to be experienced for at least 6 years after abemaciclib discontinuation and that, when waning starts, it will take approximately 19 years for the effect of abemaciclib plus ET to fully dissipate. The clinical experts consulted by CDA-AMC for this review indicated that they are unaware of any data that support these assumptions and that it is plausible that treatment effectiveness will start waning earlier. The clinical experts also considered it unlikely that waning would last for 19 years. The sponsor’s assumptions about when waning would start were based on data from the ATAC trial,25 which reported follow-up data for anastrozole and tamoxifen for up to 10 years among patients who were HR-positive (their HER2 status was not reported). The clinical experts indicated that differences in study populations, alongside differences in the mechanisms of action of the interventions assessed in the ATAC and monarchE trials, restrict the degree to which conclusions drawn from the ATAC trial can be generalized to predict the prolonged efficacy of abemaciclib plus ET compared to ET alone. The clinical experts also noted that assuming a 19-year waning period was overly optimistic and unlikely to occur in clinical practice, and therefore lacked face validity. In the absence of data to support the long-term effectiveness waning for abemaciclib plus ET, the experts considered it equally likely that waning would start at year 7 and to last until year 10 (i.e., a total of 3 years).
In the CDA-AMC reanalysis, the effectiveness of abemaciclib plus ET persists for 8 years after discontinuing abemaciclib, in contrast with the 25 years assumed by the sponsor.
Considering the limited duration of trial data, in circumstances where treatment is assumed to have a continued effect on event rates post delivery, it is necessary to investigate assumptions regarding the persistence of long-term treatment effects. CDA-AMC performed 2 scenario analyses: the first assumed no waning of treatment effect over time, while the second assumed no further effect beyond the duration of the monarchE trial. Although each is improbable, the CDA-AMC proposed scenarios offer upper and lower bound estimates to examine the impact of treatment effect waning on the cost-effectiveness of abemaciclib plus ET.
Costs associated with metastatic recurrence are highly uncertain. The sponsor’s model predicts that abemaciclib plus ET will generate cost savings in the metastatic recurrence health state (incremental costs are –$59,902 versus ET). Given the sponsor’s use of a fixed payoff approach, this value is highly uncertain. The method for calculating total costs in the model lacks transparency in its description. The per-cycle cost of each drug (stratified by, for example, progression-free or postprogression status, first or second line of treatment) was multiplied by a set number of cycles, which was informed by the mean number of LYs accrued in the progression-free state or the postprogression state, as predicted by the sponsor’s external MONARCH 2 (for ET-resistant disease) and MONARCH 3 (for ET-sensitive disease) models,5,6 as well as on the primary publications used in a network meta-analysis.1 Moreover, the sponsor assumed that patients treated with abemaciclib plus ET in the adjuvant setting who experience metastatic recurrence more than 12 months after completing adjuvant ET or while in remission (i.e., ET-sensitive) would not be treated with a CDK4 and CDK6 inhibitor in the metastatic setting. The clinical experts consulted by CDA-AMC for this review indicated that the proportion of patients with metastatic ET-sensitive disease assumed by the sponsor to receive a CDK4 and CDK6 inhibitor (0%) does not align with Canadian clinical practice and that patients whose disease recurred at least 6 months after completing adjuvant treatment would be considered for a CDK4 and CDK6 inhibitor because these are standard of care for primary treatment of metastatic breast cancer. Input received from participating drug plans also confirmed this. Given the higher price of CDK4 and CDK6 inhibitors, compared with the other included treatments for metastatic recurrence, and the incremental difference in CDK4 and CDK6 inhibitor usage assumed for patients who initially received abemaciclib plus ET (0%) or ET alone (79%), the sponsor’s assumption underestimates incremental costs, biasing cost-effectiveness in favour of abemaciclib plus ET.
CDA-AMC was unable to validate the costs predicted by the sponsor’s analysis owing to the use of a fixed payoff approach that relied on outputs from external models.
CDA-AMC conducted a reanalysis that adopted alternative assumptions regarding the use of CDK4 and CDK6 inhibitors among patients with metastatic recurrence. Following clinical expert input, CDA-AMC revised the parameter to indicate that 60% of patients with metastatic ET-sensitive disease receive CDK4 and CDK6 inhibitors in the abemaciclib plus ET model arm.
Selection of relevant comparators is misaligned with current clinical practice. The sponsor omitted adjuvant olaparib from the base-case analysis. During the review process, participating drug plan input, clinician group input, and clinical expert feedback indicated that adjuvant olaparib is prescribed in Canada for the treatment of patients with HR-positive, HER2-negative, node-positive early breast cancer at high risk of recurrence with deleterious or suspected deleterious germline BRCA1- or BRCA2-mutated disease, which is a subset of the Health Canada–indicated population for abemaciclib. The sponsor indicated that adjuvant olaparib was excluded as a pertinent comparator due to its funding eligibility is limited to a specific subgroup of patients for whom treatment with olaparib is preferred over treatment with abemaciclib.26 The Provisional Funding Algorithm for HR-positive, HER2-negative breast cancer recommends either of the following adjuvant treatment options based on individual patient characteristics: olaparib plus ET or abemaciclib plus ET. Moreover, the clinical experts consulted by CDA-AMC for this review indicated that if patients with BRCA1 or BRCA2 pathogenic mutations were eligible to receive adjuvant olaparib and abemaciclib, clinicians would generally prefer to treat with abemaciclib rather than olaparib. Hence, the omission of adjuvant olaparib as a relevant comparator for this indication does not reflect current clinical practice in Canada. CDA-AMC notes the absence of head-to-head trials comparing olaparib and abemaciclib in the adjuvant early breast cancer setting. Since both drugs have been studied in high-risk patient populations, each defined differently, any indirect treatment comparison between their respective trials would be of low methodological quality and thus provide limited utility as inputs for an economic model. The cost-effectiveness of abemaciclib plus ET versus olaparib plus ET is unknown.
CDA-AMC could not address this limitation because this comparator was excluded from the submitted model.
Model does not execute probabilistically in every case. CDA-AMC notes that the submitted economic model fails to execute probabilistically when selecting the Weibull distribution to extrapolate IDFS for abemaciclib plus ET and the Weibull spline 2-knot distribution to extrapolate OS for ET alone. CDA-AMC was unable to determine the probability that abemaciclib plus ET is cost-effective at a WTP threshold (e.g., of $50,000 per QALY) owing to structural limitations in the sponsor’s model (that is, all the CDA-AMC analyses are deterministic and do not reflect uncertainty).
CDA-AMC opted to present the CDA-AMC base case deterministically.
Additionally, the key assumptions in Table 4 were made by the sponsor and have been appraised by CDA-AMC).
Table 4: Key Assumptions of the Submitted Economic Evaluation
Sponsor’s key assumption | CDA-AMC comment |
|---|---|
Patients enrolled in the monarchE trial were assumed to be representative of patients in Canada who would be eligible for abemaciclib plus ET (age ██ years, ██% female, ██ kg, body surface area ███ m2). | Reasonable, although clinical experts noted that the patients enrolled in the monarchE trial were generally younger than patients typically seen in Canadian clinical practice by approximately 10 years. |
The probability of having a metastatic recurrence for patients in the remission health state was assumed to be equal to the risk of having a second primary malignancy. | Uncertain. The sponsor based the probability of a metastatic recurrence for patients in remission on a retrospective cohort study of secondary malignancy after adjuvant therapy among women with stage I or stage II breast cancer.27 The clinical experts consulted for this review indicated that secondary malignancy is conceptually distinct from disease recurrence and that it may be inappropriate to assume the same risk. |
Health state utility values were acquired from multiple sources. | Uncertain. The sponsor adopted utility values from (1) the monarchE trial for the invasive disease–free health state; (2) published sources for the nonmetastatic health state; (3) the MONARCH 2 and MONARCH 3 trials for the ET-resistant and ET-sensitive metastatic recurrence sub–health states. Moreover, a mapping algorithm28 was used to transform EQ-5D-3L value sets from the MONARCH 2 and MONARCH 3 trials into EQ-5D-5L index values. CDA-AMC notes that incorporating utilities from a variety of sources, which were measured and valued in different ways in different patient populations, adds uncertainty to the analysis. |
Adverse events were assumed to occur once during the first model cycle. | Inappropriate. The sponsor’s model included grade ≥ 3 adverse events (≥ 1% incidence) based on the observed frequency in the monarchE trial (ITT population), applied in the first model cycle. The sponsor selected an arbitrary threshold to capture the impact of adverse events rather than selecting the most clinically meaningful adverse events to include within the model. This approach may underestimate the impact of rare adverse events, and it is uncertain whether patients are at risk of AEs only once. |
CDA-AMC = Canada's Drug Agency; EQ-5D-3L = 3-Level EQ-5D; EQ-5D-5L = 5-Level EQ-5D; ET = endocrine therapy; ITT = intention to treat.
CDA-AMC Reanalyses of the Economic Evaluation
Base Case Results
CDA-AMC reanalyses addressed several limitations within the economic model. The CDA-AMC base case was derived by making changes in model parameter values and assumptions, in consultation with clinical experts. These included the following: using independent models to extrapolate IDFS; adopting alternative distributions to extrapolate IDFS for patients treated with abemaciclib plus ET (Weibull) and ET alone (Weibull spline 2-knot distribution); assuming treatment effectiveness waning starts at year 7 and continues until year 10; and revising the proportion of patients with metastatic ET-sensitive disease who receive CDK4 and CDK6 inhibitors in the abemaciclib plus ET model arm. CDA-AMC also corrected the sponsor’s submitted base case by adjusting the price of abemaciclib 150 mg tablet, which was incorrectly programmed in the submitted model. These changes are summarized in Table 5.
Table 5: CDA-AMC Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CDA-AMC value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
1. Price of abemaciclib 150 mg tablet | $112.5818 | $111.8550 |
Changes to derive the CDA-AMC base case | ||
1. Proportional hazards assumption | Dependent model | Independent model |
2. IDFS distribution |
|
|
3. Treatment waning |
|
|
4. Distribution of subsequent treatment regimens for patients with ET-sensitive disease who were previously treated with abemaciclib plus ET |
|
|
CDA-AMC base case | ― | Reanalysis 1 + 2 + 3 + 4 |
CDA-AMC = Canada’s Drug Agency; CDK = cyclin-dependent kinase; ET = endocrine therapy; IDFS = invasive disease–free survival; ITT = intention to treat; NSAI = nonsteroidal aromatase inhibitor.
In the CDA-AMC base case, abemaciclib plus ET was associated with an ICER of $133,903 per QALY gained compared with ET alone (incremental costs = $103,572; incremental QALYs = 0.77) (Table 6). Owing to structural limitations in the sponsor’s model, all CDA-AMC analyses are deterministic and do not reflect uncertainty. The CDA-AMC base case is based on publicly available prices of the comparator treatments. A detailed breakdown of the disaggregated results is available in Appendix 4.
The CDA-AMC estimated ICER was higher than the sponsor’s base-case value, primarily due to the selection of alternative distributions for extrapolating IDFS and assumptions about treatment waning. Consistent with the sponsor’s analysis, the CDA-AMC reanalysis estimates that the entirety of incremental QALYs were accrued in the post-trial period of the model on the basis of extrapolation.
Table 6: Summary of the Stepped Analysis of the CDA-AMC Reanalysis Results
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALY) |
|---|---|---|---|---|
Sponsor’s base case (deterministic) | ET alone | 102,139 | 13.69 | Reference |
Abemaciclib plus ET | 172,959 | 14.80 | 63,736 | |
Sponsor’s corrected base case (deterministic) | ET alone | 102,139 | 13.69 | Reference |
Abemaciclib plus ET | 172,129 | 14.80 | 62,989 | |
CDA-AMC reanalysis 1 – independent IDFS models | ET alone | 103,872 | 13.50 | Reference |
Abemaciclib plus ET | 172,680 | 14.93 | 48,069 | |
CDA-AMC reanalysis 2 – IDFS distributions | ET alone | 102,490 | 13.75 | Reference |
Abemaciclib plus ET | 173,999 | 14.45 | 101,992 | |
CDA-AMC reanalysis 3 – treatment waning | ET alone | 102,139 | 13.69 | Reference |
Abemaciclib plus ET | 173,769 | 14.47 | 91,676 | |
CDA-AMC reanalysis 4 – subsequent treatment | ET alone | 102,139 | 13.69 | Reference |
Abemaciclib plus ET | 203,137 | 14.94 | 80,687 | |
CDA-AMC base case reanalyses 1 + 2 + 3 + 4 (deterministic) | ET alone | 102,490 | 13.75 | Reference |
Abemaciclib plus ET | 206,063 | 14.52 | 133,903 |
CDA-AMC = Canada's Drug Agency; ET = endocrine therapy; ICER = incremental cost-effectiveness ratio; IDFS = invasive disease–free survival; QALY = quality-adjusted life-year.
Note: The CDA-AMC reanalysis is based on publicly available prices of the comparator treatments. The results of all steps are presented deterministically unless otherwise indicated.
Scenario Analysis Results
CDA-AMC undertook price reduction analyses based on the sponsor’s corrected results and the CDA-AMC base case. The CDA-AMC base case suggests that a 51% price reduction for abemaciclib would be required for abemaciclib plus ET to be considered cost-effective at a WTP threshold of $50,000 per QALY gained relative to ET alone (Table 7).
Table 7: CDA-AMC Price Reduction Analyses
Analysis | Unit drug cost ($) | ICERs for abemaciclib + ET vs. ET alone ($/QALY) | |
|---|---|---|---|
Price reduction | $ | Sponsor base casea | CDA-AMC reanalysis |
No price reduction | 111.86 | 62,989 | 133,903 |
10% | 100.67 | 51,500 | 117,399 |
20% | 89.48 | 40,011 | 100,894 |
30% | 78.30 | 28,523 | 84,390 |
40% | 67.11 | 17,034 | 67,886 |
50% | 55.93 | 5,545 | 51,381 |
60% | 44.74 | Abemaciclib plus ET is dominant | 34,877 |
70% | 33.56 | Abemaciclib plus ET is dominant | 18,373 |
80% | 22.37 | Abemaciclib plus ET is dominant | 1,868 |
90% | 11.19 | Abemaciclib plus ET is dominant | Abemaciclib plus ET is dominant |
CDA-AMC = Canada's Drug Agency; ET = endocrine therapy; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; vs. = versus.
aCDA-AMC used the sponsor’s corrected base case, whereby the price of abemaciclib 150 mg tablet was set to $111.8550. All analyses were performed deterministically.
CDA-AMC conducted a series of scenario analyses to explore the impact of alternative assumptions on the cost-effectiveness of abemaciclib plus ET
Assuming no waning of treatment effect over time
Assuming no further effect beyond the duration of the monarchE trial.
Results of these scenarios are presented in Appendix 4 (Table 12).
Scenarios 1 and 2 represent upper and lower bound estimates of cost-effectiveness for abemaciclib plus ET, derived from exploring the impact of assumptions regarding the persistence of long-term treatment effects. When assuming no waning of treatment effect, the ICER of abemaciclib plus ET decreased to $122,027 per QALY gained relative to ET alone. When assuming no further effect beyond the duration of the monarchE trial, the ICER of abemaciclib plus ET increased to $167,833 per QALY gained relative to ET alone.
Issues for Consideration
CDA-AMC previously reviewed abemaciclib in combination with ET for the adjuvant treatment of adult patients with HR-positive, HER2-negative, node-positive early breast cancer at high risk of disease recurrence based on clinicopathological features and a Ki-67 score of 20%. The pan-Canadian Oncology Review Expert Review Committee (pERC) recommended that abemaciclib be reimbursed for this indication with clinical criteria and conditions on September 29, 2022.29 The criteria for initiation in the 2022 recommendation only includes patients with between 1 and 3 positive ALNs and Ki-67 score of at least 20% who present with histologic grade 3 disease or tumour size of 5 cm or larger. Therefore, the sponsor’s inclusion of cohort 2 in the current reimbursement request and Health Canada–approved indication will continue to impact Ki-67 testing capacity across the health system.
CDA-AMC also reviewed abemaciclib for the treatment of HR-positive, HER2-negative advanced or metastatic breast cancer. The pan-Canadian Oncology Review Expert Review Committee (pERC) recommended that abemaciclib be reimbursed for this indication with clinical criteria and conditions on July 5, 2019.30
Overall Conclusions
Evidence from the monarchE trial suggests that, when compared with ET alone, abemaciclib plus ET resulted in a statistically significant and clinically important improvement in IDFS in the adjuvant treatment of patients with HR-positive, HER2-negative, node-positive early breast cancer at high risk of disease recurrence based on clinicopathological features. The CDA-AMC Clinical Review noted that it is not yet clear whether IDFS benefits will translate to improved OS as the data remain immature at the time of the OS IA3 data cut-off (median follow-up of 54 months). Clinical experts consulted by CDA-AMC noted that a longer follow-up time would be required to determine the OS benefit of abemaciclib plus ET relative to ET alone considering the risk of late relapse in this patient population. This uncertainty is propagated into the submitted economic analysis as the sponsor extrapolated IDFS and OS without distant recurrence for the lifetime horizon of the model using parametric distributions fitted to Kaplan-Meier data from the monarchE trial. Indeed, the sponsor’s base case predicts a survival advantage with abemaciclib plus ET compared with ET alone (incremental LYs = 2.19) over a 49-year horizon, notwithstanding evidence from the monarchE trial indicating little to no clinically significant difference in OS at 5 years between the 2 treatments.
In addition to the aforementioned limitations with the clinical evidence, CDA-AMC identified several limitations with the sponsor’s economic submission. These limitations included the following: lack of transparency of the fixed payoff modelling approach adopted by the sponsor; uncertainty regarding the long-term impact of abemaciclib plus ET on OS and IDFS; uncertainty regarding the waning of treatment effectiveness of abemaciclib plus ET; misalignment of the sponsor’s assumptions regarding the use of CDK4 and CDK6 inhibitors in the metastatic setting with Canadian clinical practice; and omission of adjuvant olaparib as a relevant comparator in the current treatment landscape. As part of the base case reanalysis, CDA-AMC used independent models to extrapolate IDFS; adopted alternative distributions to extrapolate IDFS for patients treated with abemaciclib plus ET and ET alone; revised treatment effectiveness waning parameters to reflect clinical plausibility; and updated the proportion of patients with metastatic ET-sensitive disease who receive CDK4 and CDK6 inhibitors in the abemaciclib plus ET model arm. CDA-AMC also corrected the sponsor’s submitted base case by adjusting the price of abemaciclib 150 mg tablet.
As adjunctive therapy for the adjuvant treatment of adult patients with HR-positive, HER2-negative, node-positive early breast cancer at high risk of disease recurrence based on clinicopathological features, abemaciclib plus ET was associated with an ICER of $133,903 per QALY gained compared with ET alone (incremental costs = $103,572; incremental QALYs = 0.77). CDA-AMC was unable to determine the probability that abemaciclib plus ET is cost-effective at a WTP threshold because of structural limitations in the sponsor’s model. As such, CDA-AMC analyses are deterministic and do not reflect uncertainty. The estimated ICER was higher than the sponsor’s base case value, driven by the selection of alternative distributions for extrapolating IDFS and assumptions about treatment waning. When compared with the sponsor’s analysis, the CDA-AMC base case estimated a reduced QALY benefit with abemaciclib plus ET (i.e., incremental QALYs of 0.77 according to the CDA-AMC base case versus 1.11 according to the sponsor’s analysis) at a higher cost (i.e., incremental costs of $103,572 according to the CDA-AMC base case versus $69,991 according to the sponsor’s analysis). A price reduction for abemaciclib of 51% would be required for abemaciclib plus ET to be cost-effective, compared with ET alone, at a WTP threshold of $50,000 per QALY gained. This would reduce the price of abemaciclib from $111.86 to $54.81 (per 150 mg tablet).
The cost-effectiveness of abemaciclib plus ET was sensitive to assumptions concerning the persistence of long-term treatment effects. When assuming no waning of treatment effect, the ICER of abemaciclib plus ET decreased to $122,027 per QALY gained relative to ET alone. When assuming no further effect beyond the duration of the monarchE trial, the ICER of abemaciclib plus ET increased to $167,833 per QALY gained relative to ET alone. CDA-AMC was unable to address limitations related to the modelling approach, which relies on data from external models to predict outcomes for patients with metastatic recurrence, and the omission of adjuvant olaparib from the economic analysis. Therefore, the cost-effectiveness of abemaciclib plus ET versus olaparib plus ET is unknown. Given the extent of limitations associated with the sponsor’s submitted model, there remains considerable uncertainty in the cost-effectiveness results. Moreover, when comparing the duration of follow-up in the monarchE trial to the model’s time horizon (54 months versus 49 years), it is important to note that the entirety of the QALY benefit realized by patients in the CDA-AMC base case was accrued in the post-trial period of the model on the basis of extrapolation. In the absence of long-term evidence, the true comparative impact of abemaciclib plus ET on IDFS and OS relative to ET alone remains highly uncertain. Should the long-term effectiveness of abemaciclib plus ET be lower than predicted, the ICER would be higher than the CDA-AMC base case, requiring more substantial price reductions to achieve cost-effectiveness.
References
1.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Verzenio (abemaciclib), tablets, 50 mg, 100 mg, 150 mg, 200 mg oral. Toronto (ON): Eli Lilly Canada Inc; 2024 Feb 9.
2.Devlin N, Shah K, Y. F, Mulhern B, Van Hout B. Valuing health-related quality of life: an EQ-5D-5L value set for England. Vol 16/01. London (GB): Office of Health Economics Research; 2016.
3.Clinical Study Report Addendum: I3Y-MC-JPCF. monarchE: a randomized, open-label, phase 3 study of abemaciclib combined with standard adjuvant endocrine therapy versus standard adjuvant endocrine therapy alone in patients with high risk, node positive, early stage, hormone receptor positive, human epidermal receptor 2 negative, breast cancer [internal sponsor's report]. Indianapolis (IN): Eli Lilly and Company; 2022.
4.National Institute for Health Care Excellence. Trastuzumab emtansine for adjuvant treatment of HER2-positive early breast cancer. (Technology appraisal guidance TA632) 2020.
5.A cost-effectiveness analysis of abemaciclib in the treatment of advanced breast cancer in the MONARCH 3 indication: Canadian pCODR technical report [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Verzenio (abemaciclib), 50 mg, 100 mg, 150 mg, or 200 mg oral tablets. Toronto (ON): Eli Lilly Canada Inc; 2018 Nov 09.
6.A cost-effectiveness analysis of abemaciclib in the treatment of advanced or metastatic breast cancer in the MONARCH 2 indication: pCODR technical report [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Verzenio (abemaciclib), 50 mg, 100 mg, 150 mg, or 200 mg oral tablets. Toronto (ON): Eli Lilly Canada Inc; 2018 Nov 27.
7.National Institute for Health and Care Excellence. Neratinib for extended adjuvant treatment of hormone receptor-positive, HER2-positive early stage breast cancer after adjuvant trastuzumab. (Technology appraisal guidance TA612) 2019; https://www.nice.org.uk/guidance/ta612. Accessed 2022 Jun 6.
8.Lidgren M, Wilking N, Jönsson B, Rehnberg C. Health related quality of life in different states of breast cancer. Qual Life Res. 2007;16(6):1073-1081. PubMed
9.Ara R, Brazier JE. Using health state utility values from the general population to approximate baselines in decision analytic models when condition-specific data are not available. Value Health. 2011;14(4):539-545. PubMed
10.Ontario Ministry of Health, Ontario Ministry of Long-Term Care. Ontario drug benefit formulary/comparative drug index. 2024; https://www.formulary.health.gov.on.ca/formulary/. Accessed 2024 Mar 22.
11.National Institute for Health Care Excellence. Pertuzumab for adjuvant treatment of HER2-positive early stage breast cancer. (Technology appraisal guidance TA569) 2019.
12.Schedule of benefits for physician services under the Health Insurance Act: (June 29, 2023 (effective July 24, 2023)). Toronto (ON): Ontario Ministry of Health; 2023: https://www.health.gov.on.ca/en/pro/programs/ohip/sob/physserv/sob_master.pdf. Accessed 2024 Mar 22.
13.Government of Ontario. Ontario case costing initiative. 2018.
14.Yu M, Guerriere D, Coyte P. Societal costs of home and hospital end-of-life care for palliative care patients in Ontario, Canada. Health Soc Care Community. 2015;23(6):605-618. PubMed
15.Royston P, Parmar MK. Restricted mean survival time: an alternative to the hazard ratio for the design and analysis of randomized trials with a time-to-event outcome. BMC Med Res Methodol. 2013;13(152). PubMed
16.Bagust A, Beale S. Survival analysis and extrapolation modeling of time-to-event clinical trial data for economic evaluation: an alternative approach. Med Decis Making. 2014;34(3):343-351. PubMed
17.In J, Lee DK. Survival analysis: part II - applied clinical data analysis. Korean J Anesthesiol. 2019;72(5):441-457. PubMed
18.Hancock MJ, Maher CG, Costa Lda C, Williams CM. A guide to survival analysis for manual therapy clinicians and researchers. Man Ther. 2014;19(6):511-516. PubMed
19.Kleinbaum DG, Klein M. Survival analysis a self-learning text. New York (NY): Springer; 1996.
20.Grambsch PM, Therneau TM. Proportional hazards tests and diagnostics based on weighted residuals. Biometrika. 1994;81(3):515-526.
21.Coyle D, Haines A, Lee K. CADTH health technology review: extrapolating clinical evidence within economic evaluations: CADTH methods and guidelines. Can J Health Technol. 2023;3(5).
22.Guyot P, Ades AE, Beasley M, Lueza B, Pignon JP, Welton NJ. Extrapolation of survival curves from cancer trials using external information. Med Decis Making. 2017;37(4):353-366. PubMed
23.NICE DSU Technical support document 14: Survival analysis for economic evaluations alongside clinical trials - extrapolation with patient-level data. Sheffield (GB): University of Sheffield; 2011.
24.Latimer N. Survival analysis for economic evaluations alongside clinical trials—extrapolation with patient-level data: inconsistencies, limitations, and a practical guide. Med Decis Making. 2013;33(6):743-754. PubMed
25.Cuzick J, Sestak I, Baum M, et al. Effect of anastrozole and tamoxifen as adjuvant treatment for early-stage breast cancer: 10-year analysis of the ATAC trial. Lancet Oncol. 2010;11(12):1135-1141. PubMed
26.CADTH reimbursement review: provisional funding algorithm indication: breast cancer with hormone receptor (HR) positive, human epidermal growth factor receptor 2 (HER2) negative, with inclusion of HER2 low. Ottawa (ON): CADTH; 2024: https://www.cadth.ca/sites/default/files/DRR/2024/PH0041%20HR%2B%20HER2-%20Breast%20Cancer%20Rapid%20Algorithm%20Report%20DRAFT%20for%20Stakeholder%20Feedback%20Feb%2023%202024.pdf. Accessed 2024 Mar 22.
27.Hamilton SN, Tyldesley S, Li D, Olson R, McBride M. Second malignancies after adjuvant radiation therapy for early stage breast cancer: is there increased risk with addition of regional radiation to local radiation? Int J Radiat Oncol Biol Phys. 2015;91(5):977-985. PubMed
28.van Hout B, Janssen MF, Feng YS, et al. Interim scoring for the EQ-5D-5L: mapping the EQ-5D-5L to EQ-5D-3L value sets. Value Health. 2012;15(5):708-715. PubMed
29.CADTH reimbursement recommendation: abemaciclib (Verzenio). Ottawa (ON): CADTH; 2022.
30.pCODR Expert Review Committee (pERC) final recommendation:abemaciclib (Verzenio - Eli Lilly Canada Inc.) Ottawa (ON): CADTH; 2019: https://www.cadth.ca/sites/default/files/pcodr/Reviews2019/10161AbemaciclibMBC_fnRec_ApprovedbyChair_v01_2019-07-04_Post_05Jul2019_final.pdf. Accessed 2024 May 4.
31.Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Verzenio (abemaciclib), tablets, 50 mg, 100 mg, 150 mg, 200 mg oral. Toronto (ON): Eli Lilly Canada Inc; 2024 Feb 9.
32.Stastistics Canada. Five-year cancer survival by stage at diagnosis in Canada. https://www150.statcan.gc.ca/n1/pub/82-003-x/2023001/article/00001-eng.htm. Accessed 2024 May 10.
33.Pan H, Gray R, Braybrooke J, et al. 20-year risks of breast-cancer recurrence after stopping endocrine therapy at 5 years. N Engl J Med. 2017;377(19):1836-1846. PubMed
34.Lee J, Lee YJ, Bae SJ, et al. Ki-67, 21-gene recurrence score, endocrine resistance, and survival in patients with breast cancer. JAMA Netw Open. 2023;6(8):e2330961. PubMed
Appendix 1: Cost Comparison Table
Please note that this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical experts and drug plans. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 8: CDA-AMC Cost Comparison Table for Adjuvant Treatment of Hormone Receptor–Positive, Human Epidermal Growth Factor Receptor 2–Negative, Early Breast Cancer
Treatment | Strength | Form | Price ($) | Recommended Dosage | Daily Cost ($) | 28-day Cost ($) |
|---|---|---|---|---|---|---|
Cyclin-dependent kinase (CDK) inhibitor + Endocrine Therapy | ||||||
Abemaciclib (Verzenio) | 150 mg | Tablet | 111.8550a | 150 mg, twice dailya,b | 223.71 | 6,264 |
Abemaciclib + Anastrozole | 224.66 | 6,291 | ||||
Abemaciclib + Exemestane | 225.04 | 6,301 | ||||
Abemaciclib + Letrozole | 225.09 | 6,302 | ||||
Abemaciclib + Tamoxifen | 224.06 | 6,274 | ||||
Endocrine Therapy | ||||||
Anastrozolec (Arimidex) | 1 mg | Tablet | 0.9522 | 1 mg, once dailyb | 0.95 | 27 |
Exemestanec (Aromasin) | 25 mg | Tablet | 1.3263 | 25 mg, once dailyb | 1.33 | 37 |
Letrozolec (Femara) | 2.5 mg | Tablet | 1.3780 | 2.5 mg, once dailyb | 1.38 | 39 |
Tamoxifen (Nolvadex) | 20 mg | Tablet | 0.3500 | 20 mg, once dailyb | 0.35 | 10 |
CDA-AMC = Canada’s Drug Agency.
Note: All prices are from the Ontario Drug Benefit Formulary (accessed February 2024), unless otherwise indicated, and do not include dispensing fees.
Olaparib (Lynparza) has been noted by CDA-AMC as a comparator to abemaciclib for this review for a subset of the patient population (those with deleterious or suspected deleterious germline BRCA1- or BRCA2-mutated disease). The olaparib unit cost is $69.9482 per 150 mg tablet, the daily cost is $279.79, and the 28-day cost is $7,834 at a recommended dose of 300 mg twice a day (sourced from IQVIA).
aSponsor’s submitted price and recommended dosage.
bCancer Care Ontario Formulary.
cNot recommended for people who are premenopausal according to the Cancer Care Ontario Formulary.
Appendix 2: Submission Quality
Please note that this appendix has not been copy-edited.
Description | Yes or No | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | No | The sponsor omitted adjuvant olaparib from the base-case analysis. Refer to the CDA-AMC appraisal regarding selection of relevant comparators. |
Model has been adequately programmed and has sufficient face validity | No | The sponsor adopted a “fixed payoff” modelling approach and included numerous IFERROR statements. Refer to the CDA-AMC appraisal regarding the lack of transparency of the modelling approach. |
Model structure is adequate for decision problem | No | While the model structure is generally adequate (i.e., the included health states are appropriate for the indication), the sponsor has adopted a “fixed payoff” approach to modelling costs, LYs, and QALYs for the Metastatic Recurrence health state. Refer to the CDA-AMC appraisal regarding the lack of transparency of the modelling approach. |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | Yes | In probabilistic sensitivity analyses, each model parameter was assigned a specific distribution, with the mean of the distribution equal to the point estimate. The standard error was determined based on any distributional information provided in the original source; if none is available, the standard error was assumed to be 20% of the mean estimate. |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | Yes | Parameter uncertainty was adequately assessed. |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | No | The model is poorly organized and difficult to maneuver. Refer to the CDA-AMC appraisal regarding the lack of transparency of the modelling approach. |
CDA-AMC = Canada’s Drug Agency; LY = life-year; QALY = quality-adjusted life-year.
Appendix 3: Additional Information on the Submitted Economic Evaluation
Please note that this appendix has not been copy-edited.
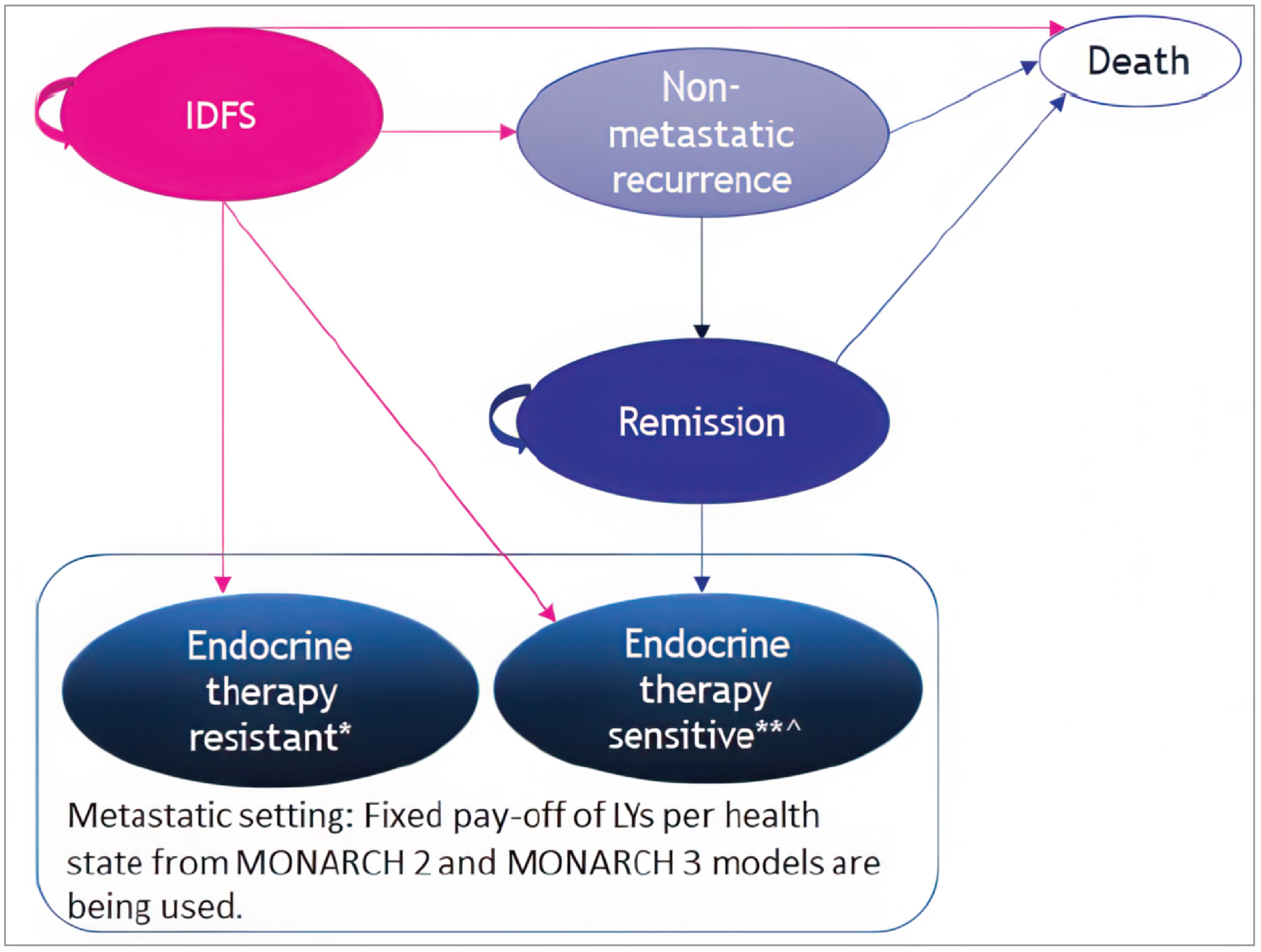
IDFS = invasive disease–free survival; LY = life-year.
Source: Sponsor’s pharmacoeconomic submission.1
Detailed Results of the Sponsor’s Base Case
Table 10: Disaggregated Summary of the Sponsor’s Economic Evaluation Results
Parameter | Abemaciclib + ET | ET alone |
|---|---|---|
Undiscounted LYs | ||
Total | 25.11 | 22.92 |
IDFS | 21.55 | 18.60 |
NMR | 0.13 | 0.13 |
Remission | 0.95 | 1.02 |
MR (ET-Resistant) | 0.48 | 0.82 |
MR (ET-Sensitive) | 1.99 | 2.35 |
Discounted QALYs | ||
Total | 14.78 | 13.67 |
IDFS | 12.97 | 11.35 |
NMR | 0.07 | 0.08 |
Remission | 0.50 | 0.56 |
MR (ET-Resistant) | 0.33 | 0.57 |
MR (ET-Sensitive) | 0.91 | 1.12 |
Adverse events | −0.0007 | −0.0004 |
Discounted costs ($) | ||
Total | 173,011 | 101,973 |
Total drug-related costs pre-MR | 135,080 | 5,068 |
Drug acquisition | 129,747 | 1,314 |
Drug administration | 0 | 0 |
Treatment-specific costs | 4,176 | 2,586 |
Background therapy | 1,057 | 1,063 |
Drug-related costs in NMR (ET) | 100 | 106 |
Total disease management pre-MR | 4,084 | 4,076 |
IDFS | 1,548 | 1,354 |
NMR | 1,733 | 1,835 |
Remission | 803 | 888 |
Total costs in MR | 15,064 | 74,966 |
MR (ET-Resistant) | 4,521 | 25,232 |
MR (ET-Sensitive) | 10,543 | 49,734 |
Terminal care | 13,463 | 14,123 |
Adverse events | 5,320 | 3,739 |
ET = endocrine therapy; IDFS = invasive disease–free survival; MR = metastatic disease; NMR = nonmetastatic disease; LY = life-year; QALY = quality-adjusted life-year.
Source: Sponsor’s pharmacoeconomic submission.1
Figure 2: Relative Risk of Invasive Disease Progression for Abemaciclib Plus ET Compared with ET Alone
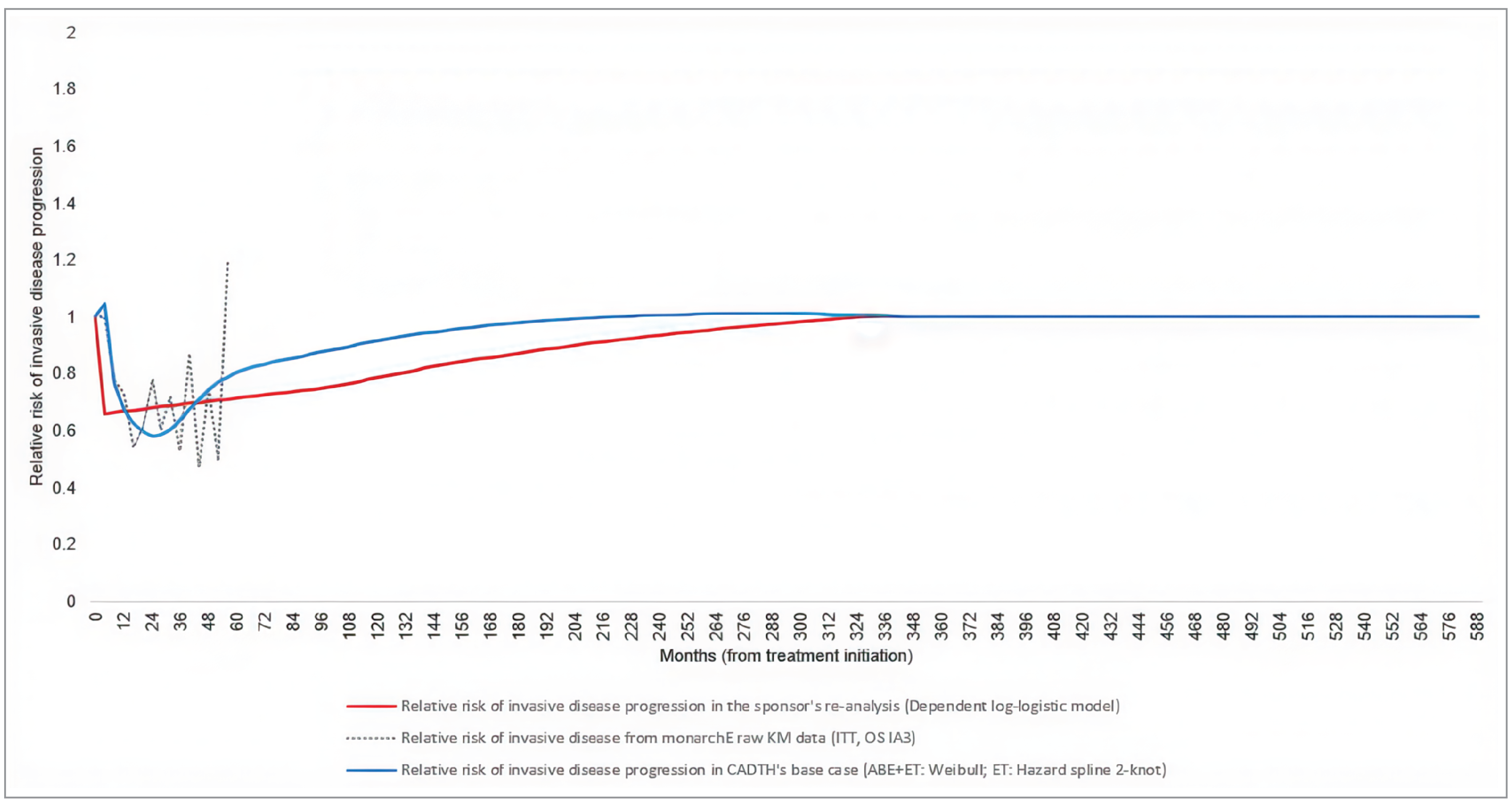
ABE = abemaciclib; ET = endocrine therapy; IA = interim analysis; ITT = intention to treat; KM = Kaplan-Meier; OS = overall survival; RR = relative risk.
Note: The dashed line represents the RR of invasive disease with abemaciclib + ET versus ET alone over 4-month periods, based on the raw data from the monarchE trial. Data shown in the figure are simply “1 – IDFS at time t + 1/IDFS at time t.” The data are shown until month 56 as they closely approximate the median follow-up time of 54 months in cohort 1. The raw Kaplan-Meier trial data suggested that (1) up to month 16, the RR of invasive disease for patients treated with abemaciclib + ET compared with ET alone decreases steadily; (2) from months 16 to 52, the risk of invasive disease is lower among patients treated with abemaciclib + ET compared with ET alone (RR fluctuating between 0.5 and 0.9); until (3) the risk increases above 1 at the end of month 56. This suggests a U-shape relationship between the RR of invasive disease and time in the within-trial period. The blue line represents the RR of invasive disease in the CDA-AMC base case, revealing the expected U-shaped relationship. The red line represents the RR of invasive disease in the sponsor’s submission.
Source: CDA-AMC calculation based on the monarchE trial Kaplan-Meier data and parametric extrapolations presented in the sponsor’s pharmacoeconomic model.
Appendix 4: Additional Details on the CDA-AMC Reanalyses and Sensitivity Analyses of the Economic Evaluation
Please note that this appendix has not been copy-edited.
Detailed Results of CDA-AMC Base Case
Table 11: Disaggregated Summary of the CDA-AMC Economic Evaluation Results
Parameter | Abemaciclib + ET | ET alone |
|---|---|---|
Undiscounted LYs | ||
Total | 24.43 | 22.96 |
IDFS | 20.39 | 18.61 |
NMR | 0.14 | 0.13 |
Remission | 1.00 | 1.01 |
MR (ET-Resistant) | 0.47 | 0.80 |
MR (ET-Sensitive) | 2.42 | 2.41 |
Discounted QALYs | ||
Total | 14.52 | 13.75 |
IDFS | 12.44 | 11.41 |
NMR | 0.08 | 0.08 |
Remission | 0.53 | 0.55 |
MR (ET-Resistant) | 0.33 | 0.56 |
MR (ET-Sensitive) | 1.15 | 1.15 |
Adverse events | −0.0008 | −0.0004 |
Discounted costs ($) | ||
Total | 206,063 | 102,490 |
Total drug-related costs pre-MR | 134,251 | 5,119 |
Drug acquisition | 128,920 | 1,339 |
Drug administration | 0 | 0 |
Treatment-specific costs | 4,207 | 2,655 |
Background therapy | 1,017 | 1,019 |
Drug-related costs in NMR (ET) | 106 | 107 |
Total disease management pre-MR | 4,166 | 4,073 |
IDFS | 1,481 | 1,357 |
NMR | 1,831 | 1,838 |
Remission | 853 | 878 |
Total costs in MR | 47,416 | 75,504 |
MR (ET-Resistant) | 4,482 | 24,592 |
MR (ET-Sensitive) | 42,934 | 50,911 |
Terminal care | 13,603 | 14,047 |
Adverse events | 6,627 | 3,747 |
CDA-AMC = Canada’s Drug Agency; ET = endocrine therapy; IDFS = invasive disease–free survival; MR = metastatic disease; NMR = non = metastatic disease; LY = life-year; QALY = quality-adjusted life-year.
Scenario Analyses
Table 12: Scenario Analyses Conducted on the CDA-AMC Base Case
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALYs) |
|---|---|---|---|---|
Sponsor’s base case (deterministic)a | ET alone | 102,139 | 13.69 | Reference |
Abemaciclib + ET | 172,129 | 14.80 | 62,989 | |
CDA-AMC base case (Deterministic)b | ET alone | 102,490 | 13.75 | Reference |
Abemaciclib + ET | 206,063 | 14.52 | 133,903 | |
CDA-AMC Scenario 1: No treatment waning (Deterministic) | ET alone | 102,490 | 13.75 | Reference |
Abemaciclib + ET | 205,692 | 14.59 | 122,027 | |
CDA-AMC Scenario 2: No effect beyond the within-trial period (Deterministic) | ET alone | 102,490 | 13.75 | Reference |
Abemaciclib + ET | 206,598 | 14.37 | 167,833 |
CDA-AMC = Canada’s Drug Agency; ET = endocrine therapy; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
aCDA-AMC used the sponsor’s corrected base case, whereby the price of abemaciclib 150 mg tablet was set to $111.8550.
bThe CDA-AMC base case results shown deterministically as the probabilistic model failed to execute in this instance.
Appendix 5: Submitted Budget Impact Analysis and CDA-AMC Appraisal
Please note that this appendix has not been copy-edited.
Table 13: Summary of Key Take-Aways
Key take-aways of the budget impact analysis |
|---|
|
BIA = budget impact analysis; CDA-AMC = Canada’s Drug Agency; CDK = cyclin-dependent kinase.
Summary of Sponsor’s Budget Impact Analysis
Abemaciclib previously received a NOC from Health Canada on January 21, 2022, for the adjuvant treatment of adult patients with HR-positive, HER2-negative, node-positive, early breast cancer at high risk of disease recurrence based on clinicopathological features and a Ki-67 score ≥ 20%. The current submitted BIA assessed the expected budgetary impact resulting from reimbursing adjuvant abemaciclib for the expanded Health Canada indication for use in combination with ET, for the adjuvant treatment of adult patients with HR-positive, HER2-negative, early breast cancer at high risk of disease recurrence based on clinicopathological features (i.e., for patients meeting criteria for Cohort 1 or Cohort 2 of the MonarchE trial in the new drug scenario), compared with the current reimbursement criteria (i.e., based on Cohort 1 clinicopathological features and a Ki-67 score ≥ 20% in the reference scenario). The BIA was undertaken from the perspective of the Canadian public drug plans over a 3-year horizon (Q3 2024 – Q2 2027) using an epidemiological approach. The sponsor’s analysis included drug acquisition costs, wholesaler mark-up, and dispensing fees. Data to inform the model were obtained from various sources, including the published literature, the sponsor’s internal data, and input from clinical experts consulted by the sponsor.31
In the model, abemaciclib (150 mg twice daily) was assumed to be received for a maximum of 2 years, after which time patients were assumed to receive ET alone for the remainder of the model horizon. Discontinuation of abemaciclib prior to 2 years was based on discontinuation rates from the MonarchE trial, with 69% of patients assumed to receive 2 full years of abemaciclib treatment in the new drug scenario, and 41% of patients to receive 2 full years of abemaciclib treatment in the reference scenario. ET was assumed to comprise anastrozole (22.2%), exemestane (8.3%), letrozole (37.7%), and tamoxifen (31.8%), and was assumed to be administered for the full BIA time horizon. Drug costs were obtained from the sponsor’s submission for abemaciclib or from the Ontario Drug Benefit Formulary.10 In the new drug scenario, the drug uptake was based on internal forecast data and market research.31 Key inputs to the BIA are documented in Table 16.
Table 14: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as year 1 / year 2 / year 3 if appropriate) |
|---|---|
Target Population | |
Cohort 1 | |
Active beneficiaries | 11,161,206 |
Incidence of BC | 0.09% |
Diagnosis rate | 95.0% |
Local Disease (Stage I-III) | 94.9% |
HR-positive, HER2-negative | 68.2% |
High risk of recurrence | 12.0% |
CDK4/6 inhibitor penetrance | 68.0% [A] |
Cohort 2 | |
Relative Incidence versus Cohort 1 | 10.1% [applied to A] |
Ki-67 testing rate | 75.0% [D] |
Target Population (MonarchE Intent-to-treat) | |
Cohort 1 + Cohort 2 | A+D |
Cohort 1, Ki-67 High Subgroup | |
Ki-67 High (Score ≥ 20%) | 50% |
Ki-67 Testing Rate | 75% |
Number of patients in Reference Scenario | 118 / 160 / 201 |
Number of patients in New Drug Scenario | 183 / 379 / 580 |
Market Uptake (Reference Scenario, 3 years) | |
ABE + ET | 17.3% / 17.4% / 17.4% |
ET | 82.7% / 82.6% / 82.6% |
Market Uptake (New Drug Scenario, 3 years) | |
ABE + ET | 40.7% / 48.4% / 49.7% |
ET | 59.3% / 51.6% / 50.3% |
Cost of treatment (per patient, per year) | |
ABE + ET | $82,022 $82,022 $348 |
ET | $348 $348 $348 |
ABE = abemaciclib: ET = endocrine therapy.
Note: [A] represents the number of individuals in cohort 1 who are eligible for CDK4/6 inhibitor treatment, calculated by applying the CDK4/6 inhibitor penetration rate (68.0%) to the active beneficiaries within cohort 1. [D] represents the number of individuals in cohort 2 who are eligible for CDK4/6 inhibitor treatment, determined by applying the Ki-67 testing rate (75.0%) to the active beneficiaries within cohort 2.
aAssumed to comprise anastrozole (22.2%), exemestane (8.3%), letrozole (37.7%), and tamoxifen (31.8%).
bAbemaciclib was assumed to be received for a maximum of 2 years, after which time costs for ET alone were incurred. The cost of abemaciclib was based on the sponsor’s submitted price for the 150 mg tablet ($111.8550). The sponsor’s base case assumes 100% usage of the 150 mg tablet.
Source: Sponsor’s budget impact analysis submission.31
Key assumptions included:
12% of the total HR-positive, HER2-negative early breast cancer population are at high risk of disease recurrence based on clinicopathological features, as per monarchE inclusion criteria (i.e., those with ≥ 4 positive lymph nodes; or 1 to 3 positive lymph nodes with Grade 3 disease or tumour size ≥ 5cm).
The CDK 4/6 inhibitor penetrance was assumed to be 68%.
The relative incidence of patients with early breast cancer at high risk of recurrence based on Cohort 2 enrolment criteria compared with the incidence of early breast cancer based on Cohort 1 criteria was assumed to be proportional to the Cohort 2 to Cohort 1 ratio in the randomly sampled MonarchE ITT population (517 patients in Cohort 2 / 5,120 patients in Cohort 1 = 10.1%). This rate was applied to the calculated Cohort 1 population to estimate the incident Cohort 2 population. A Ki-67 testing rate of 75% was applied to further narrow this population.
50% of the patients are assumed to have a high Ki-67 (≥ 20%) and the Ki-67 testing rate is assumed to be 75% (for Cohort 1 in the reference scenario).
The base case market share estimates for abemaciclib + ET in the Reference and New Drug Scenarios were provided by Eli Lilly by applying uptake curve assumptions to an estimated peak market share of 50% in the respective eligible population.
The peak market share estimates were based on market research from the US and assumed to be representative of the Canadian context.
In the Reference Scenario, abemaciclib market shares were assumed to immediately reach month 13 of the uptake curve upon first listing in August 2023 to account for patients transitioning from patient support programs to public coverage.
It was assumed that market shares in the New Drug Scenario would never be lower than the Reference Scenario for the same time point. Therefore, market shares for abemaciclib + ET were assumed to be at a minimum of the shares in the Reference Scenario.
Summary of the Sponsor’s BIA Results
Results of the sponsor’s analysis suggest that the reimbursement of abemaciclib for the adjuvant treatment of adult patients with HR-positive, HER2-negative, node-positive, early breast cancer at high risk of disease recurrence based on clinicopathological features will be associated with a 3-year cost of $38,582,820 (Year 1: $1,830,977; Year 2: $12,607,303; $24,144,538).31
CDA-AMC Appraisal of the Sponsor’s BIA
CDA-AMC identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
Proportion of patients with a high risk of recurrence in Cohort 1 is underestimated: In the sponsor’s BIA, 12% of the total HR-positive, HER2-negative early breast cancer population were assumed to be at high risk of disease recurrence based on clinicopathological features, as per MonarchE inclusion criteria (i.e., those with ≥ 4 positive ALNs; or 1 to 3 positive ALNs with Grade 3 disease or tumour size ≥ 5cm). However, the study cited by the sponsor references 12.2% of patients being triple-negative (HR(-)/HER2(-)) and 12% had unknown HR/HER2 status, which does not align with the definition of high risk of disease recurrence based on clinicopathological features. Furthermore, clinical experts consulted by CDA-AMC for this review indicated that the sponsor’s assumption (12%) seems underestimated compared to their clinical experience (30%). They noted that, according to Stats Canada, 12% to 20% of patients present with stage III at the time of diagnosis (and typically with ≥ 4 positive ALNs) and would, at a minimum, represent the high-risk population.32 Additionally, a proportion of stage I-II (1 to 3 ALNs) would also be eligible. Alternatively, Pan et al.33 report that the risk of distant recurrence was strongly correlated with the original nodal status. In this study, patients who have ER-positive T1-T2 breast cancer with 4 to 9 positive ALNs represented 16.6% of the study population; and ER-positive T1-T2 patients with 1 to 3 positive ALNs represented 43.0% of the study population (with the caveat that this study excludes patients who have T3 and does not assess HER2 status and tumour grade). In the absence of a study that can provide the proportion of patients with a high risk of recurrence based on the MonarchE trial Cohort 1 criteria in the population in Canada, clinical experts consulted by CDA-AMC recommended the results from Pan et al. as the best available evidence to derive the proportion of patients who are at high risk.
In concordance with clinical expert input, the CDA-AMC base-case reanalysis assumed the midpoint (29.8%) between the proportion of patients with T1-T2 4 to 9 positive ALNs (16.6%) and the proportion of patients with T1-T2 1 to 3 positive ALNs (43%) from Pan et al.33 to estimate the proportion of patients in Cohort 1 with a high risk of recurrence based on clinicopathological features. However, CDA-AMC notes that uncertainty remains concerning the proportion of patients with a high risk of recurrence in Cohort 1 due to the lack of good supporting data combining all features.
In addition, CDA-AMC conducted scenario analyses where the Cohort 1 high-risk of recurrence proportion is set to 26.08% to remove the patients who were HER2-negative based on the SEER data, and a scenario analysis where it is 12% based on the sponsor’s original estimates.
Proportion of patients potentially eligible as Cohort 2 is highly uncertain: In the sponsor’s BIA, Cohort 2 is estimated by applying the relative incidence (calculated as the ratio of patients randomized into Cohort 2 patients (517)/Cohort 1 patients (5,120) = 10.1% in the MonarchE trial) to the calculated number of eligible patients in Cohort 1, and then applying the Ki-67 testing rate (refer to Table 14). However, the enrolment for Cohort 2 was small, with the accrual starting approximately 1 year after accrual initiated for Cohort 1. The Cohort 2 population is less mature and more uncertain. Additionally, the size of clinical trials is arbitrarily calculated to explore a certain outcome and does not necessarily represent the prevalence of those clinicopathological features in the Stage I-III, HR-positive, HER2-negative breast cancer population. Furthermore, the estimated proportion of patients with high risk of recurrence in Cohort 1, which was used to derive the number of patients in Cohort 2 was deemed underestimated (refer to the limitation “Proportion of patients with a high risk of recurrence in Cohort 1 is underestimated”).36 In Pan et al.,33 43% of patients with T1-T2 presented with 1 to 3 positive ALNs at diagnosis. Clinical experts consulted by CDA-AMC noted that clinicians would test any patients that meet the study criteria for Cohort 2 (1 to 3 ALNs) but not all would need Ki-67 testing if they meet Cohort 1 eligibility criteria in other ways (grade 3 or tumour size > 5cm). They estimated that 25% to 30% of patients with Stage I to III, HR-positive, HER2-negative early breast cancer would meet the Cohort 2 eligibility criteria based on the MonarchE trial (1 to 3 ALNs + Ki-67 ≥ 20%).
The CDA-AMC base case assumed 27.5% as the proportion of patients with Stage I to III, HR-positive, HER2-negative early breast cancer who would be referred for Ki-67 testing and potentially eligible as Cohort 2 (i.e., 1 to 3 positive ALNs but NOT grade 3 nor tumour size less than 5cm).
The proportion of patients who score high on the Ki-67 test for Cohort 2 is uncertain. The number of patients that would be eligible for treatment as Cohort 2 patients was estimated by the sponsor as the enrolment ratio of patients into Cohort 2 and Cohort 1 of the monarchE trial (10.1%) and assumed to account for the probability of testing Ki-67 score ≥ 20. Clinical experts consulted by CDA-AMC note that the proportion of patients scoring high on the Ki-67 test should be lower for Cohort 2 compared to Cohort 1. This is because the more advanced the tumour presentation at diagnosis, the higher the likelihood of a Ki-67 score ≥ 20. Lee et al.34 reported 37.9% of the patients with breast cancer had a high Ki-67 score, which was deemed by the clinical experts consulted by CDA-AMC as a better representation of the proportion of Cohort 2 patients who would score ≥ 20% on Ki-67 testing, and therefore, further considered for treatment with abemaciclib.
The CDA-AMC base case assumed that 37.9% of the Cohort 2 patients tested would have a high Ki-67 score (≥ 20%).
The market share estimates in the reference scenario do not align with clinical expectations and the market uptake is uncertain. In the reference scenario and new drug scenario, the sponsor assumed the peak market share was 50% (i.e., 50% of the eligible patients would be treated with abemaciclib + ET over the time horizon of the model). The peak market share was applied to the ratio of the number of eligible patients in the reference scenario to the number of eligible patients in the new drug scenario in the base year (to allow for consistent comparison between scenarios). The resulting reference scenario market share was 16.8%, 17.3%, 17.4%, and 17.4% in the base, first, second, and third years, respectively. In the new drug scenario, the sponsor assumed a 50% peak market share and used an uptake curve to estimate the market share. The resulting new drug scenario market share was 40.7%, 48.4%, and 49.7% among eligible patients in the base, first, second, and third year, respectively. The peak market share was based on internal market data from the US (not provided for validation) and assumed to represent the same treatment patterns in Canada. Clinical experts consulted by CDA-AMC suggested the peak market share in the sponsor’s BIA is likely underestimated because all patients who meet the current reimbursement criteria will be offered abemaciclib (unless there are contraindications) and the majority of these patients agree to proceed with treatment as it is not as toxic as chemotherapy. Clinical experts consulted by CDA-AMC estimated that the current uptake of abemaciclib among eligible patients is approximately 70% to 80% in current clinical practice.
CDA-AMC reanalysis adjusted the market shares of abemaciclib +ET to peak at 75% in the reference and the new drug scenarios.
Proportion of patients anticipated to receive CDK4/6 inhibitors in the eligible population is underestimated. The sponsor’s BIA estimates that the CDK4/6 inhibitor penetrance rate was 68% in the eligible population based on internal assumptions. Clinical experts consulted by CDA-AMC noted that clinicians would offer therapy with CDK4/6 inhibitors (if available) to anyone who meets study criteria so long as there are no contraindications. In their experience, 80% to 90% of eligible patients would be recommended treatment with CDK4/6 inhibitors.
The CDA-AMC base case reanalysis assumed 85% CDK4/6 inhibitor penetrance in the eligible population, aligned with clinical expert input.
In addition, CDA-AMC conducted a scenario analysis where the CDK4/6 inhibitor penetrance is maintained at the sponsor’s estimates of 68%.
Testing rate is likely underestimated. The sponsor’s BIA assumed a 75% Ki-67 testing rate in the reference scenario for Cohort 1 and the new drug scenario for Cohort 2. Clinical experts consulted by CDA-AMC stated that the testing rate is expected to increase as clinicians become aware of the recommendations and testing becomes more routine practice.
In a scenario analysis, CDA-AMC explored the impact of assuming a higher Ki-67 testing rate of 90%.
Ki-67 testing cost was not included. The sponsor did not include the costs of Ki-67 testing for patients who still require test results to be eligible to receive abemaciclib. This includes Cohort 1 patients in the reference scenario and Cohort 2 patients in the new drug scenario. It is uncertain how the forgone costs of exempting patients who meet eligibility criteria as Cohort 1 from Ki-67 testing in the new drug scenario, may or may not offset the costs of testing patients who have Stage I-III, HR-positive, HER2-negative early breast cancer who would meet the Cohort 2 eligibility criteria based on the monarchE trial (1 to 3 ALNs) but do not meet Cohort 1 eligibility criteria in other ways (grade 3 or tumour size > 5cm), due to uncertainty with the size of this population (addressed in the limitation above “Proportion of patients potentially eligible as Cohort 2 is highly uncertain). Therefore, any estimated BIA results remain highly uncertain.
CDA-AMC was unable to address this limitation in reanalysis.
The ET basket of treatments does not represent current Canadian clinical practice. The sponsor omitted adjuvant olaparib from the base-case analysis. During the review process, participating drug plan input, clinician group input, and clinical expert feedback indicated that adjuvant olaparib is prescribed in Canada for the treatment of patients with HR-positive, HER2-negative, node-positive early breast cancer at high risk of recurrence with deleterious or suspected deleterious germline BRCA1- or BRCA2-mutated disease, which is a subset of the Health Canada–indicated population for abemaciclib. The sponsor indicated that adjuvant olaparib was excluded as a pertinent comparator due to its funding eligibility being limited to a specific subgroup of patients, in whom olaparib would be preferred over abemaciclib.26 CDA-AMC notes that the Provisional Funding Algorithm for breast cancer with HR-positive, HER2-negative recommends both of the following adjuvant treatment options: olaparib + ET or abemaciclib + ET based on patient individual characteristics. Moreover, clinical experts consulted by CDA-AMC for this review indicated that if patients with BRCA1 or BRCA2 pathogenic mutations were eligible to receive adjuvant olaparib and abemaciclib, clinicians would generally prefer to treat with the latter. Hence, the omission of adjuvant olaparib as a relevant comparator for this indication does not reflect current clinical practice in Canada. The inclusion of olaparib as a comparator would likely reduce the budget impact for this subset of patients with BRCA1 or BRCA2 pathogenic mutations, thus the estimated overall budget impact may be conservative.
CDA-AMC was unable to address this limitation in reanalysis.
CDA-AMC Reanalyses of the BIA
Table 15: CDA-AMC Revisions to the Submitted Budget Impact Analysis
Stepped analysis | Sponsor’s value or assumption | CDA-AMC value or assumption |
|---|---|---|
Changes to derive the CDA-AMC base case | ||
1. Cohort 1 high risk of recurrence | 12% | 29.8% |
2. Cohort 2 estimated size | Relative incidence (10.1% of the Cohort 1 size) | (1) the proportion of patients with stage I to III, HR-positive, HER2-negative breast cancer eligible to be tested based on the MonarchE Cohort 2 criteria (1 and 3 positive lymph nodes, tumour size less than 5 cm, and not Grade 3) assumed as 27.5%, and (2) 37.9% of those tested would present with high Ki-67 (≥ 20%) results.a |
3. Cohort 1 and Cohort 2 CDK 4/6 inhibitor penetrance | 68% | 85% |
4. Peak Market Share | Reference scenario: 50% New drug scenario: 50% | Reference scenario: 75% New drug scenario: 75% |
CDA-AMC base case | Reanalysis 1 + 2 + 3 + 4 | |
CDA-AMC = Canada’s Drug Agency; CDK = cyclin-dependent kinase.
aCDK 4/6 inhibitor penetrance value changed in Stepped analysis #3, hence value is still the same as the sponsor’s original estimate in Stepped analysis #2.
The results of the CDA-AMC step-wise reanalysis are presented in summary format in Table 16 and a more detailed breakdown is presented in Table 17. In the CDA-AMC base case, the 3-year budget impact is expected to be $227,985,601 (Year 1: $11,905,600; Year 2: $75,275,792; Year 3: $140,804,210) should abemaciclib be reimbursed as per Health Canada’s indication (i.e., for patients meeting criteria for Cohort 1 or Cohort 2 of the MonarchE trial).
Table 16: Summary of the CDA-AMC Reanalyses of the Budget Impact Analysis
Stepped analysis | Three-year total ($) |
|---|---|
Sponsor’s base case | 38,582,820 |
CDA-AMC reanalysis 1 (Size of Cohort 1) | 95,813,455 |
CDA-AMC reanalysis 2 (Size of Cohort 2) | 70,849,511 |
CDA-AMC reanalysis 3 (CDK penetrance) | 48,228,249 |
CDA-AMC reanalysis 4 (market share) | 57,873,899 |
CDA-AMC base case (Reanalysis 1 + 2 + 3 + 4) | 227,985,601 |
CDA-AMC = Canada’s Drug Agency; CDK = cyclin-dependent kinase.
CDA-AMC conducted the following scenario analyses to address remaining uncertainty, using the CDA-AMC base case (results are provided in Table 17):
Assuming Ki-67 testing rate is 90%
Assuming Cohort 2 is excluded from the reimbursed population
Assuming the market share for the reference scenario remains the same as the sponsor’s submitted BIA (peak market share of 50%) but the new drug scenario market share would be increased by increasing the peak market share to 75%
Assuming 26.08% of Cohort 1 is at high risk of recurrence to exclude any patients with HER2-positive breast cancer from the CDA-AMC base case estimates (87.5% of the patients with HR-positive breast cancer are HER2 negative based on SEER data)
Assuming CDK 4/6 inhibitor penetrance is the sponsor’s estimated value of 68%
Assuming 12% of Cohort 1 is at high risk of recurrence as per sponsor’s original assumptions
Results of the CDA-AMC scenario analyses demonstrate that the budget impact is sensitive to assumptions regarding the proportion of Cohort 1 patients with a high risk of recurrence based on clinicopathological characteristics independently of Ki-67 score, the size of Cohort 2 and whether Cohort 2 patients (patients with early breast cancer with Stage I to III, HR-positive, HER2-negative, 1 to 3 positive ALNs, NOT grade 3, and tumour size less than 5cm) would be referred for Ki-67 testing and be included in the reimbursed population.
CDA-AMC reanalysis suggests that the potential budget impact of the indication for an expanded population may lie between $132,842,833 (if the percentage of patients at high risk of recurrence for Cohort 1 is converted back to the sponsor’s estimates: 12%) and $262,255,762 (if the reference scenario peak market share remains at the sponsor’s estimates of 50% and the new peak market share is increased to 75%). These estimates remain uncertain as testing costs were not included in the analysis.
Table 17: Detailed Breakdown of the CDA-AMC Reanalyses of the BIA
Stepped analysis | Scenario | Year 0 (current situation) ($) | Year 1 ($) | Year 2 ($) | Year 3 ($) | Three-year total ($) |
|---|---|---|---|---|---|---|
Sponsor’s base case | Reference | 3,090,063 | 8,687,033 | 11,468,010 | 12,089,510 | 32,244,553 |
New drug | 3,090,063 | 10,518,010 | 24,075,313 | 36,234,049 | 70,827,372 | |
Budget impact | — | 1,830,977 | 12,607,303 | 24,144,538 | 38,582,820 | |
CDA-AMC base case | Reference | 14,237,948 | 40,019,340 | 52,684,507 | 55,290,283 | 147,994,130 |
New drug | 14,237,948 | 51,924,939 | 127,960,300 | 196,094,493 | 375,979,731 | |
Budget impact | — | 11,905,600 | 75,275,792 | 140,804,210 | 227,985,601 | |
CDA-AMC scenario analysis 1: higher Ki-67 testing rate | Reference | 17,000,049 | 47,778,593 | 62,815,244 | 65,778,162 | 176,372,000 |
New drug | 17,000,049 | 58,426,134 | 135,364,767 | 204,317,420 | 398,108,321 | |
Budget impact | — | 10,647,541 | 72,549,522 | 138,539,258 | 221,736,321 | |
CDA-AMC scenario analysis 2: Cohort 2 excluded | Reference | 14,125,825 | 39,698,514 | 52,151,800 | 54,542,463 | 146,392,777 |
New drug | 14,125,825 | 46,902,155 | 104,177,345 | 155,542,287 | 306,531,786 | |
Budget impact | — | 7,203,640 | 52,025,545 | 100,909,823 | 160,139,009 | |
CDA-AMC scenario analysis 3: Market share | Reference | 9,671,820 | 27,194,192 | 35,977,515 | 38,059,757 | 101,231,464 |
New drug | 9,671,820 | 43,342,212 | 124,123,036 | 196,021,978 | 363,487,226 | |
Budget impact | — | 16,148,020 | 88,145,521 | 157,962,221 | 262,255,762 | |
CDA-AMC scenario analysis 4: 26.08% high risk of recurrence for Cohort 1 (HR-positive, HER2-negative, SEER data) | Reference | 12,474,590 | 35,063,686 | 46,174,283 | 48,481,626 | 129,719,595 |
New drug | 12,474,590 | 46,119,631 | 115,005,249 | 176,696,547 | 337,821,427 | |
Budget impact | — | 11,055,945 | 68,830,967 | 128,214,920 | 208,101,832 | |
CDA-AMC scenario analysis 5: CDK 4/6 inhibitor penetrance returns to sponsor estimate (68%) | Reference | 11,390,358 | 32,015,472 | 42,147,606 | 44,232,226 | 118,395,304 |
New drug | 11,390,358 | 41,539,951 | 102,368,240 | 156,875,594 | 300,783,785 | |
Budget impact | — | 9,524,480 | 60,220,634 | 112,643,368 | 182,388,481 | |
CDA-AMC scenario analysis 6: High risk of recurrence for Cohort 1 as per sponsor’s assumptions (12%) | Reference | 5,800,374 | 16,306,804 | 21,533,432 | 22,711,228 | 60,551,464 |
New drug | $5,800,374 | 24,146,852 | $65,971,081 | $103,276,364 | 193,394,297 | |
Budget impact | — | 7,840,048 | 44,437,649 | 80,565,136 | 132,842,833 |
BIA = budget impact analysis; CDA-AMC = Canada’s Drug Agency; CDK = cyclin-dependent kinase; HR = hormone receptor; SEER = Surveillance, Epidemiology, and End Results.
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.