CADTH Reimbursement Review
Nivolumab (Opdivo)
Sponsor: Bristol Myers Squibb Canada
Therapeutic area: Stage IIB or IIC melanoma, adjuvant
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Clinical Review
Abbreviations
AACR
American Association for Cancer Research
AE
adverse event
AJCC
American Joint Committee on Cancer
ASIR
age-standardized incidence rate
ASMR
age-standardized mortality rate
BCC
basal cell carcinoma
BMS
Bristol Myers Squibb
CI
confidence interval
CrI
credible interval
DB
double blind
DMFS
distant metastases-free survival
ECOG
Eastern Cooperative Oncology Group
EMA
European Medicines Agency
ESMO
European Society of Medical Oncology
FACIT
Functional Assessment of Chronic Illness Therapy
FFR
freedom from relapse
GRADE
Grading of Recommendations Assessment, Development and Evaluation
HR
hazard ratio
HRQoL
health-related quality of life
IRT
interactive response technology
IMAE
immune-mediated adverse event
ITC
indirect treatment comparison
ITT
intention to treat
KM
Kaplan-Meier
LOCF
last observation carried forward
MID
minimal important difference
NOC
Notice of Compliance
NMA
network meta-analysis
ORR
objective response rate
OS
overall survival
PAG
Provincial Advisory Group
PET
positron emission tomography
PFS2
progression-free survival after the next line of subsequent therapy
PP
per protocol
PS
performance status
RCT
randomized controlled trial
RFS
recurrence-free survival
RR
relative risk
SAE
serious adverse event
SD
standard deviation
TFI
treatment-free interval
VAS
visual analogue scale
WDAE
withdrawal due to adverse event
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Table 1: Background Information of Application Submitted for Review
Item | Description |
|---|---|
Drug product | Drug product: Nivolumab (Opdivo) Strength: 40 mg nivolumab/4 mL (10 mg/mL) and 100 mg nivolumab/10 mL (10 mg/mL) Route of administration: IV infusion |
Sponsor | Bristol Myers Squibb |
Indication | Opdivo, as monotherapy, is indicated for the adjuvant treatment of adult patients with stage IIB or IIC melanoma following complete resection |
Reimbursement request | The reimbursement request for nivolumab is for the adjuvant treatment of adult patients with stage IIB or IIC melanoma following complete resection |
Health Canada approval status | NOC |
Health Canada review pathway | Standard |
NOC date | December 29, 2023 |
Recommended dose | Dosage: 240 mg every 2 weeks or 480 mg nivolumab every 4 weeks. Continue treatment as long as clinical benefit is observed or until treatment is no longer tolerated by the patient for up to 1 year. |
NOC = Notice of Compliance
Introduction
Melanoma originates from melanocytes, which are the pigment-producing cells of the skin, commonly present in cutaneous primary locations (cutaneous melanoma); but can also arise from melanocytes within the mucosal surfaces of the body (mucosal melanoma) and the uvea of the eye (uveal melanoma), or cutaneous locations in nonhair-bearing surfaces (acral melanoma). In Canada, melanoma is the fourth most common cancer in those aged 30 to 49 years (7% of all cancer cases).1
The estimated 25-year person-based prevalence of melanoma in Canada is estimated to be 1 in 399 persons (0.3% of the population in Canada).2 In 2018, 5.5% (93,890 cases) of all 25-year prevalent cancer cases diagnosed between 1993 and 2017 were melanoma.3 Based on the 25-year prevalence period, melanoma was the fourth and fifth most prevalent cancer among males and females in Canada, respectively.2 The estimated incidence of melanoma in Canada for 2022 is 23.5 per 100,000 persons.4
Surgical excision is the primary curative treatment for most cases of melanoma, which are identified.5-7 According to the Canadian Cancer Society, 10.4% of all new melanomas are stage III at diagnosis and 3.9% are stage IV (metastatic disease).6
Although there are no stage-specific survival statistics available in Canada for melanoma, the estimated US-based 5-year survival rate for stage IIB melanoma is 87% and decreases to 82% with stage IIC.8 Patients with stage IIB or IIC melanoma account for approximately half of patients with stage II melanoma and are at high risk of disease recurrence, with approximately one-third of patients with stage IIB and half of those with stage IIC experiencing recurrence within 5 years after surgery.9,10 In addition, some patients with stage IIB or IIC melanoma have worse survival outcomes than those with stage III, where adjuvant therapy is the standard of care.10 The decision to pursue adjuvant therapy requires assessment of an individual patient’s risk for recurrence. In stage II melanoma specifically, multivariate analysis found that the most relevant prognostic indicators were tumour thickness, presence of ulceration, and anatomic site of the tumour.8 The primary goal of adjuvant therapy in melanoma is to reduce risk of recurrence and improve overall survival (OS) in patients who have undergone complete surgical resection, but who are considered high risk for disease recurrence.11 Currently, pembrolizumab is the only active adjuvant therapy in Canada indicated for patients with stage IIB and IIC melanoma following complete resection and it is available through restricted benefit with specified criteria in most provinces and territoires.12
Nivolumab is administered as an IV infusion at a dose of 240 mg every 2 weeks or 480 mg every 4 weeks, until disease recurrence or unacceptable toxicity, up to 1 year. It is a humanized IgG4 monoclonal antibody immune checkpoint inhibitor that targets the PD-1 receptor, preventing PD-1 from inhibiting the immune response to tumours. This was a pre-Notice of Compliance (NOC) submission, and nivolumab received an NOC on December 29, 2023, for the adjuvant treatment of adult patients with stage IIB or IIC melanoma following complete resection, and the sponsor’s reimbursement request is consistent with the indication. Nivolumab is also indicated for melanoma with regional lymph node involvement or that is metastatic, as well as classical Hodgkin Lymphoma and various colorectal, renal, lung, head and neck, esophageal, gastric and urothelial carcinomas.
The objective of this report is to review and critically appraise the clinical evidence submitted by the sponsor on the beneficial and harmful effects of nivolumab in the adjuvant treatment of patients with stage IIB or IIC melanoma following complete resection in adults.
Stakeholder Perspectives
The information in this section is a summary of input provided by the patient and clinician groups who responded to CADTH’s call for input and from clinical experts consulted by CADTH for the purpose of this review.
Patient Input
Input was received from 2 patient groups, Melanoma Canada and Save Your Skin Foundation (SYSF), and both groups gathered data through online surveys, with a sample of 172 patients and 15 caregivers.
Patients describe a variety of impacts from their condition, including fear, anxiety, confusion, scarring and disfigurement of skin, disrupted sleep, as well as pain, fatigue and depression.
Patients identify a need for more treatment options, given that there is only 1 drug approved for this indication, pembrolizumab, and noting that the risk of recurrence with stage IIB or IIC is actually higher than with stage IIIA. A total of 22 patients, including 20 participants from the Melanoma Canada survey and 2 participants from the SYSF survey, indicated they had been treated with adjuvant therapy for stage IIB or IIC melanoma. A common issue reported by the Melanoma Canada survey participants was the length of time and cost of travel to get to a clinical trial site for treatment with nivolumab. Of those treated, 73% of 15 respondents indicated the side effects were worth the treatment and 27% indicated the side effects were not worth the treatment. One of the 2 patients from the SYSF survey who reported having experience with nivolumab stated that they believed the benefit from nivolumab was worth the side effects, but the other patient reported challenges with missing work due to travel requirements for accessing nivolumab.
Clinician Input
Input From the Clinical Experts Consulted by CADTH
The clinical experts consulted by CADTH on this review noted the need for other immunotherapies that have better efficacy. The clinical experts differed on their opinions of nivolumab, with 1 seeing it as a clear improvement over pembrolizumab, while the other saw it as being similar in efficacy and harms to pembrolizumab.
The clinical experts noted that the patients best suited for nivolumab would be those with low Eastern Cooperative Oncology Group (ECOG) performance status (PS), no comorbidities or active autoimmune conditions, and those who are at significant risk of relapse.
Response would be assessed through physical exam and periodic imaging (PET-CT or whole-body CT with MRI of the head). The decision to discontinue therapy would be prompted by evidence of recurrence, regional or distant metastases, or drug intolerance.
Clinician Group Input
CADTH received 1 clinician group submission from the Ontario Health (Cancer Care Ontario) Skin Cancer Drug Advisory Committee (OH-CCO’s DAC).
There were no significant areas of disagreement between the clinician group and the clinical experts consulted by CADTH on this review.
The clinician group and the clinical experts agreed that recurrence-free survival (RFS) and distant metastases-free survival (DMFS) are key outcomes for these patients, and it is important to have an additional drug for this population of patients, as pembrolizumab is the only current option. The clinician group noted the difference in dosing between nivolumab (every 2 or 4 weeks) and pembrolizumab (every 3 or 6 weeks). The clinician groups agreed with the clinical experts that the most appropriate patients to receive the drug would reflect those enrolled into CHECKMATE-76K.
Drug Program Input
In response to a question about the optimal time frame to initiate nivolumab, postsurgical resection, the clinical experts believed that in most circumstances, 12 weeks would be optimal.
The Provincial Advisory Group (PAG) asked whether the same principle that applies for other solid tumours, where patients are eligible for downstream PD-1 or PD-L1 inhibitors, provided disease recurrence occurs more than 6 months from the last dose of adjuvant PD-1 or PD-L1 inhibitor and the clinical experts agreed with this approach.
PAG asked about different examples of dose interruptions. Examples provided included a situation where a patient had to take 5 months off, 2 months into their regimen, and another patient 10 months into their regimen. One clinical expert believed that in the former scenario, the patient could get the remaining 10 months, and in the latter scenario, in most cases, the remaining 2 months would not be given. The other clinical expert did not believe that oncologists would be so focused on completing all of the planned treatments, and that treatment interruptions would like result in permanent discontinuation.
In response to a question about whether nivolumab should be used on noncutaneous melanoma, the clinical experts responded that it should not. In response to a question about whether patients with an ECOG PS of 2 or greater should be considered for nivolumab, 1 clinical expert believed that patients who have an ECOG PS of 2 should be considered, as long as they do not have comorbidities that are likely to be life-threatening in the immediate future, while in patients with an ECOG PS of 3, treatment would be unlikely due to this presentation on its own. The other clinical expert believed that patients with an ECOG PS of 2 or more are unlikely to tolerate nivolumab.
Clinical Evidence
Systematic Review
Description of Studies
CHECKMATE-76K is a phase III, randomized, double-blind, multicentre clinical trial designed to evaluate the efficacy and safety of nivolumab in completely resected stage IIB and IIC melanoma across 20 countries and 132 locations, including Canada.13 Adults and children 12 years and older were eligible for enrolment. A total of 790 patients were randomly assigned in a 2:1 ratio to receive 480 mg of nivolumab (n = 526) or placebo (n = 264). Patients in the treatment arm were treated with nivolumab 480 mg every 4 weeks via 30-minute IV infusions or a matched-administration placebo. Placebo-treated patients who experienced disease recurrence within 3 years after the last dose of placebo, and nivolumab-treated patients who experienced recurrence greater than 6 months and within 3 years after completing treatment, were eligible to receive on-study open-label nivolumab treatment. The primary objective of CHECKMATE-76K was to compare the efficacy, as measured by investigator-assessed RFS, provided by nivolumab monotherapy versus placebo in patients with completely resected stage IIB and IIC melanoma with no evidence of disease who are at high risk for recurrence.14 The secondary objectives were to compare OS and DMFS between the 2 treatment groups, assess the safety and toxicity of nivolumab, and evaluate investigator-assessed outcomes on next-line therapies.
Overall, the enrolled patient population was generally representative of a stage II melanoma population, with a median age of 62 years and more males (61.2%) than females (38.8%). The majority of patients had stage IIB melanoma (60.1%) (American Joint Committee on Cancer [AJCC], 8th edition). The mean time from local wide excision surgery to randomization was 10.3 weeks. Although patients aged 12 years or older were eligible for enrolment, no adolescents were randomized. Generally, baseline demographic and disease characteristics were well-balanced between the nivolumab and placebo groups.
Efficacy Results
Recurrence-Free Survival
At the data cut-off date of June 28, 2022, the median follow-up for all randomized patients was 15.84 months for the nivolumab arm and 15.93 months for the placebo arm. At the data cut-off date of February 21, 2023, the median follow-up for all randomized patients was 23.5 months for the nivolumab arm and 23.0 months for the placebo arm.
At the first interim analysis 1 (IA1) (data cut-off of June 28, 2022), a median RFS had not been reached in either group, for a hazard ratio (HR) of 0.42 (95% confidence interval [CI], 0.30 to 0.59), P < 0.0001. At the most recent data cut-off date of February 21, 2023, 186 RFS events had occurred (complete information fraction). The median RFS had not been reached in the nivolumab group and was 36.14 months (95% CI, 24.77 to NA) in the placebo group, for an HR of 0.53 (95% CI, 0.40 to 0.71).
At a data cut-off date of June 28, 2022, the RFS rate was 89.0% (95% CI, 85.6 to 91.6) and 79.4% (95% CI, 73.5 to 84.1) in nivolumab and placebo, respectively. At the February 21, 2023, data cut-off date, the RFS rate was largely unchanged from IA1, at 88.8% (95% CI, 85.6 to 91.2) and 81.1% (95% CI, 75.7 to 86.4) at 12 months, for nivolumab and placebo. At 24 months, which was only reported at IA2, the RFS rates were 76.5% (95% CI, |||| || ||||) and 60.6% (95% CI, |||| || ||||) in the nivolumab and placebo groups, respectively.
Overall Survival
At the time of the most recent February 21, 2023, data cut-off date, the prespecified number of events for the OS interim analysis had not been reached, and, as a result, there are no data reported.
Distant Metastases-Free Survival
At IA1, with a data cut-off date of June 28, 2022, a median DMFS had not been reached in either group, with 8.0% of patients in the nivolumab group having experienced an event, and 15.5% of patients experiencing an event in the placebo group, for an HR of 0.47 (95% CI, 0.30 to 0.72). The DMFS rate at 12 months was 92.3% (95% CI, 89.3 to 94.5) in the nivolumab group and 86.7% (95% CI, 81.4 to 90.5) in the placebo group. At the most recent data cut-off date, February 21, 2023, a median DMFS was still not reached in the nivolumab group, and was 36.14 months (95% CI, 32.85 to NA) in the placebo group, with 13.1% of patients in the nivolumab group and 19.3% of patients in the placebo group experiencing an event, for an HR of 0.62 (95% CI, 0.43 to 0.89). The DMFS rate at 12 months was 92.0% (95% CI, 89.3 to 94.1) with nivolumab and 88.5% (95% CI, 83.9 to 91.9) with placebo and at 24 months it was 84.0% (95% CI, |||| || ||||) with nivolumab and 76.5% (95% CI, |||| || ||||) with placebo.
Progression-Free Survival After the Next Line of Subsequent Therapy
A median progression-free survival (PFS) rate had not been reached as of the most recent data, February 21, 2023. In all randomized patients, 40 (7.6%) PFS after the next line of subsequent therapy (PFS2) events had occurred in the nivolumab arm and 31 (11.7%) PFS2 events had occurred in the placebo arm, for an HR of 0.63 (95% CI, 0.40 to 1.01).
Health-related quality of life (HRQoL) was an exploratory outcome in CHECKMATE-76K and was assessed using the EORTC QLQ-C30 and EQ-5D-5L instruments. None of the within-group changes from baseline over time in the study exceeded the minimal important difference (MID) for the instrument.
Harms Results
There were 96% of patients in the nivolumab group and 88% of patients in the placebo group who reported an adverse event (AE) (all-cause), with 23% and 12% of patients, respectively, reporting a grade 3 or 4 AE. The most common AEs, nivolumab versus placebo, were ||||||| |||| |||||| ||||| |||||||| |||| |||||| |||| ||| |||||||| |||| |||||| ||||. Hypothyroidism was reported in 12% of patients in the nivolumab group and no patients in the placebo group.
There were ||| of patients in the nivolumab group and ||| of patients in the placebo group who reported a serious adverse event (SAE). ||||| |||| || |||||||| |||| |||| |||||||| || || || |||| || |||||||||
There were 18% of patients in the nivolumab group and 4% of patients in the placebo group who discontinued due to an AE, and 7% versus 1% who withdrew due to a grade 3 or 4 AE, respectively. The most common reason for discontinuation was |||||||||| ||||| in the nivolumab group |||| with placebo).
Notable harms identified by the clinical experts consulted by CADTH on this review included diarrhea (particularly grade 3 or 4), diabetes mellitus, and arthritis. Grade 3 or 4 events of diarrhea and/or colitis occurred in |||| of nivolumab patients and |||| of placebo patients, while diabetes occurred in |||| of nivolumab patients and || placebo patients and arthritis in |||| of nivolumab and |||| placebo.
Critical Appraisal
With respect to internal validity, CHECKMATE-76K appears to have been a reasonably well-conducted trial, with adequate procedures for randomization and blinding. There was a relatively large number of patients who discontinued study treatment, and a difference in treatment discontinuations between the nivolumab (39%) and placebo (25%) groups, mostly accounted for by a difference in withdrawals due to AE, and this may have biased analysis of efficacy and harms.
With respect to external validity, CHECKMATE-76K was not of sufficient duration to assess OS, as the clinical experts believed that a follow-up of at least 5 years would be needed for such an analysis to occur. The clinical experts also were of the opinion that RFS, the primary outcome, is better assessed at a later time point than was reported in the trial. There was also no active comparator in CHECKMATE-76K, the most appropriate choice being pembrolizumab.
Table 2: Summary of Findings for Adjuvant Nivolumab vs. Placebo for Patients With Stage IIB or IIC Resected Melanoma
Outcome Measure | Patients (studies), N | Relative effect (95% CI) | Absolute effects (95% CI) | Difference | Certainty | What happens | |
|---|---|---|---|---|---|---|---|
Nivolumab | Placebo | ||||||
OS | |||||||
OS (secondary outcome) Follow-up: 5 years | 790 (1 RCT) | NR | NR | NR | NR | NAa | Cannot be assessed |
RFS | |||||||
RFS (primary outcome) Follow-up: 1 year Data cut-off: June 2022 | 790 (1 RCT) | 0.42 (0.30 to 0.59) | 89.0 (85.6 to 91.6) | 79.4 (73.5 to 84.1) | NR | Lowb | Nivolumab may result in an improvement in RFS when compared to placebo after 1 year follow-up |
Follow-up: 2 years Data cut-off: February 2023 | 790 (1 RCT) | 0.53 (0.40 to 0.71) | 76.5 ||||| || ||||| | 60.6 ||||| || ||||| | NR | Lowb | Nivolumab may result in an improvement in RFS when compared to placebo after 2 years follow-up |
Follow-up: 3 years Data cut-off: February 2023 | 790 (1 RCT) | |||| ||||| || ||||| | |||| ||||| || ||||| | |||| ||||| || ||||| | NR | Very lowc | The evidence is very uncertain about the effects of nivolumab on RFS when compared to placebo after 3 years follow-up |
DMFS | |||||||
DMFS (secondary outcome) Follow-up: 1 year Data cut-off: June 2022 | 790 (1 RCT) | 0.47 (0.30 to 0.72) | |||| ||||| || ||||| | |||| ||||| || ||||| | NR | Lowb | Nivolumab may result in an improvement in DFMS when compared to placebo after 1 year follow-up |
Follow-up: 2 years Data cut-off: February 2023 | 790 (1 RCT) | 0.62 (0.43 to 0.89) | |||| ||||| || ||||| | |||| ||||| || ||||| | NR | Lowb | Nivolumab may result in an improvement in DMFS when compared to placebo after 2 years follow-up |
Follow-up: 3 years Data cut-off: February 2023 | 790 (1 RCT) | |||| ||||| || ||||| | |||| ||||| || ||||| | |||| ||||| || ||||| | NR | Very lowc | The evidence is very uncertain about the effects of nivolumab on DMFS when compared to placebo after 3 years follow-up |
Harms | |||||||
Diarrhea (grade 3 or 4) Follow-up: within 100 days of last dose | 790 (1 RCT) | NR | 13 per 1,000 | None | NR | Very lowd | The evidence is very uncertain regarding whether nivolumab increases risk of Grade 3 to 4 diarrhea when compared to placebo |
Diabetes mellitus Follow-up: within 100 days of last dose | 790 (1 RCT) | NR | 6 per 1,000 | None | NR | Very lowd | The evidence is very uncertain regarding whether nivolumab increases risk of diabetes mellitus when compared to placebo |
Arthritis Follow-up: within 100 days of last dose | 790 (1 RCT) | NR | 25 per 1,000 | 4 per 1,000 | NR | Very lowd | The evidence is very uncertain regarding whether nivolumab increases risk of arthritis when compared to placebo |
CI = confidence interval; DMFS = distant metastasis-free survival; GRADE = Grading of Recommendations Assessment, Development and Evaluation; MID = minimal important difference; MTP = multiple testing procedure; NA = not available; NR = not reported; OS = overall survival; RCT = randomized controlled trial; RFS = recurrence-free survival; vs. = versus.
Note: In CHECKMATE-76K only OS and RFS were part of the multiple testing procedure, and none of the data points reported in this table were part of the MTP as they were specifically reported for the GRADE analysis.
aCould not be rated because no effect estimates were available for this time point.
bRated down 2 levels; once for serious concerns over imprecision as unable to conclusively determine whether between-group difference met the MID and once for serious concerns over risk of bias due to large difference in treatment discontinuations between groups.
cRated down 3 levels; twice for very serious concerns over imprecision, including low sample size and failure to meet MID and once for serious concerns over risk of bias due to large difference in treatment discontinuations between groups.
dRated down 3 levels; twice for very serious concerns over imprecision for not meeting the MID and unknown whether it reached null and once for serious concerns over risk of bias due to large difference in treatment discontinuations between groups.
GRADE Summary of Findings and Certainty of the Evidence
The selection of outcomes for Grading of Recommendations, Assessment, Development, and Evaluations (GRADE) assessment was based on the sponsor’s Summary of Clinical Evidence, consultation with clinical experts, and input received from patient and clinician groups and public drug plans. The following list of outcomes was finalized in consultation with expert committee members:
RFS (1, 2 and 3 years follow-up)
OS (5 years follow-up)
DMFS (1, 2 and 3 years follow-up).
Notable harms: diarrhea (grade 3 or 4), diabetes mellitus, arthritis (all reported within 100 days of last study dose).
Indirect Comparisons
Description of Studies
The sponsor conducted a systematic literature review in November 2022 to identify evidence for inclusion in a network meta-analysis (NMA) and a Bucher method indirect treatment comparison (ITC) in patients with nonmetastatic resected stage IIB or IIC cutaneous melanoma.
CHECKMATE-76K included 790 randomized patients and KEYNOTE-716 included 976 randomized patients. Both trials were double-blind, placebo controlled, and included an international, multicentre population.
Efficacy Results
For CHECKMATE-76K, data informing analyses were based on an updated analysis from April 2023 with a minimum follow-up of 15.6 months and a median follow-up of 23.0 months in both treatment arms (23.5 for nivolumab and 23.1 for placebo). One efficacy outcome, RFS, was included in these analyses. The assessment of proportional hazards demonstrated evidence of violation of the proportional hazards assumption and, therefore, the time-varying models are reported as the base case. There was no evidence for a difference in RFS between nivolumab and pembrolizumab at all time points.
Harms Results
In the results of the Bucher ITC for treatment-related AEs, there were no significant differences in the odds of treatment-related grade 3 or more AE incidence (odds ratio [OR] = 1.09; 95% CI, 0.41 to 2.94) or treatment-related any-grade AE incidence (OR = 1.55; 95% CI, 0.99 to 2.43) between nivolumab and pembrolizumab.
Critical Appraisal
The sponsor conducted an NMA and used a Bayesian approach with fixed effects models for the primary efficacy analysis, and a frequentist approach was applied using the Bucher method to estimate relative harms. Both these methods were appropriate given the limited availability of data.
The main limitation of the NMA is that it contained a very small amount of data, from only 2 studies. Efficacy assessment was limited to a single outcome (RFS) and it would have been informative to include other efficacy outcomes. Follow-up time was also limited to 23 months and 39 months in the CHECKMATE-76K and KEYNOTE-716 studies, respectively. Results beyond 23 months would therefore be less reliable and subject to increasingly greater extrapolation as time points become longer. In addition, the differential follow-up times for the studies exacerbates the uncertainty in the comparisons for later time points in the analyses. Efficacy assessment was limited to a single outcome (RFS) and it would have been informative to include other efficacy outcomes. A strength of the comparisons made within the NMA and the Bucher analyses was that the studies were similar in design and population characteristics.
Despite some differences in population characteristics between the 2 trials, the sponsor assumed that AJCC stage, administration frequency, and treatment history were not effect modifiers. The clinical experts consulted by CADTH for this review believed that this was a reasonable assumption.
To align definitions of recurrence between these 2 trials, an alternative definition of RFS was explored for CHECKMATE-76K, omitting malignant melanoma in situ and new primary invasive melanoma. The results of this sensitivity analysis were consistent with the base-case analysis.
There were no significant differences observed between nivolumab and pembrolizumab for RFS.
There were no significant differences observed between nivolumab and pembrolizumab for treatment-related adverse events (any grade, grade ≥ 3). The sponsor stated that all-cause adverse events were an outcome of interest, but no analyses of this outcome were provided and the sponsor did not provide an explanation for this omission. This would have been informative given the trends observed in the treatment-related adverse event analyses (Table 28).
Neither the NMA nor the Bucher analysis provided evidence of a difference in efficacy or harms outcomes for nivolumab compared to pembrolizumab in patients with nonmetastatic resected stage IIB or IIC cutaneous melanoma.
Conclusions
Evidence from 1 double-blind (DB) randomized controlled trial (RCT) suggests that after 1 year of adjuvant treatment with nivolumab in patients with resected stage IIB or IIC melanoma, the primary objective was met, demonstrating an improvement in RFS over placebo. After 1 and 2 years of follow-up, this improvement may be clinically significant, however, the clinical experts considered the results after 2 years of follow-up to be more clinically relevant. It is uncertain whether this improvement in RFS persists at 3 years of follow-up or longer, as there are not yet enough patients who have been followed for this long. OS could not be assessed yet in this ongoing trial, as this would require a longer follow-up. The clinical experts believed OS to be of critical importance in this setting, and therefore it is important that investigators plan to follow patients for survival for up to 8 years. Treatment with nivolumab also appeared to improve DMFS compared to placebo, however, the clinical significance of these results was less clear than they were for RFS. There was a relatively large percentage of patients who discontinued nivolumab due to an AE, and the clinical experts noted that patients with less advanced disease may be less likely to persist with therapy through tolerability issues, compared to patients with advanced melanoma. In their input to CADTH, a majority of patients believed that the benefits of nivolumab were worth the potential adverse effects. It is uncertain whether there is an increased risk of developing longer-term adverse effects such as diabetes mellitus and arthritis, and a longer follow-up than the current median of nearly 2 years in CHECKMATE-76K would likely be needed to adequately assess the risk in this population. Neither the NMA nor the Bucher analysis provided evidence to support a difference in efficacy or harms outcomes for nivolumab compared to pembrolizumab in patients with nonmetastatic resected stage IIB or IIC cutaneous melanoma; despite the limitations of the ITC, the claim of no difference between nivolumab compared to pembrolizumab is justified. Patients were clear that it is important to them to have another option aside from pembrolizumab to manage their condition.
Introduction
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of nivolumab 10 mg/mL IV infusion in the adjuvant treatment of stage IIB and IIC melanoma in adults.
Disease Background
Contents within this section have been informed by materials submitted by the sponsor and clinical expert input. The following have been summarized and validated by the CADTH review team.
Melanoma, basal cell carcinoma, and squamous cell carcinoma are the 3 main types of skin cancer, accounting for 4% of all skin cancers.15,16 Melanoma originates from melanocytes, which are the pigment-producing cells of the skin, commonly present in cutaneous primary locations (cutaneous melanoma); but it can also arise from melanocytes within the mucosal surfaces of the body (mucosal melanoma) and the uvea of the eye (uveal melanoma), or cutaneous locations in nonhair-bearing surfaces (acral melanoma). In Canada, melanoma is the fourth most common cancer in those aged 30 to 49 years (7% of all cancer cases).1
Exposure to UV light from the sun, tanning beds, and a history of sunburn are well-established risk factors for cutaneous melanoma and have been shown to account for approximately 30% of all cutaneous melanoma cases in Canada.17,18 A family history of disease, phenotypic characteristics (e.g., fair hair, eye, and skin colouring, and likelihood to freckle), and a higher socioeconomic status have also been shown to be associated with a higher risk of melanoma.19
Melanoma accounts for 3.8% of new cancer cases and 1.4% of cancer deaths per year (1.7% of deaths for males and 1.1% of deaths in females).1,20 Over the past 4 decades (1984 to 2017), the incidence of melanoma in Canada has continued to rise (annual percent change in age-standardized incidence rates [ASIR] of 2.2% in males and 2.0% in females). An estimated 9,000 people were diagnosed with melanoma in 2022, with an ASIR of 23.1 per 100,000.1 Incidence is slightly higher in males than in females (25.9 vs 21.2 per 100,000).21,22
Between 1984 and 2017, the incidence rate of cutaneous malignant melanoma increased an average of 2.2% in males and 1.4% in females, annually, with the highest incidence rates reported in Nova Scotia and Prince Edward Island.4,20,21
In contrast, mortality rates are declining in Canada, likely due to the introduction of novel and effective targeted and immunotherapy treatments, and prevention initiatives. According statistics from the Canadian Cancer Society, an estimated 1,200 people in Canada died from melanoma in 2022, with an age-standardized mortality rate of 2.7 per 100,000.1 While it accounts for a minority of skin cancers, melanoma is responsible for approximately 65% of all skin cancer-related deaths due to its propensity to metastasize.23
Surgical excision is the primary curative treatment for most cases of melanoma, which are identified.5-7 According to the Canadian Cancer Society, 10.4% of all new melanomas are stage III at diagnosis and 3.9% are stage IV (metastatic disease).22 An ECOG PS of 2 or more, elevated lactate dehydrogenase (LDH), nodal involvement and metastases, increased tumour thickness, ulceration, and mitoses or 1/mm2 or more in thin T1 melanomas are all poor prognostic factors, leading to reduced survival.5,24 Although there are no stage-specific survival statistics available in Canada for melanoma, the estimated US-based 5-year survival rate for stage IIB melanoma is 87% and decreases to 82% with stage IIC.8 Patients with stage IIB or IIC melanoma account for approximately half of patients with stage II melanoma and are at high risk of disease recurrence, with approximately one-third of stage IIB and half of stage IIC patients experiencing recurrence within 5 years after surgery.9,10 In addition, some patients with stage IIB or IIC melanoma have worse survival outcomes than those with stage III, where adjuvant therapy is the standard of care.10
Statistics on the prevalence of melanoma in Canada as of January 1, 2018, are available from the Canadian Cancer Society, through the linkage of the Canadian Cancer Registry and Canadian Cancer Registry death-linked file.3,9,10 The estimated 25-year person-based prevalence of melanoma in Canada is estimated to be 1 in 399 persons (0.3% of the population in Canada).2 In 2018, 5.5% (93,890 cases) of all 25-year prevalent cancer cases diagnosed between 1993 and 2017 were melanoma.3 Based on the 25-year prevalence period, melanoma was the fourth and fifth most prevalent cancer among males and females in Canada, respectively.2
The estimated incidence of melanoma in Canada for 2022 is 23.5 per 100,000 persons.4 An estimated 6.1% of incident cases are stage IIB or IIC at diagnosis.25 These estimates reflect the incidence population used in the economic model. Incidence values presented have been estimated by Bristol Myers Squibb (BMS) Canada using incidence and population growth rates published by Statistics Canada.22,24 Using the average annual percent change [in the ASIR of melanoma of 2.2% for males and 1.4% for females reported by the Canadian Cancer Statistics (2021), rates were inflated to 2023.20 Adjuvant nivolumab will predominantly be used in patients who have not received prior systemic therapy and, therefore, incident cases are appropriate to determine the size of the patient population.
Skin examination, physical examination, skin and/or lymph node biopsy with pathologic assessment, genetic testing, and diagnostic imaging (i.e., CT)5,6,26,27 are all used as diagnostic tools for melanoma.
Guidelines in terms of follow-up care for resected melanoma differ by country.28 In Canada, guidelines suggest a history and physical examination including a review of systems, full skin examination, and lymph node examination every 3 to 6 months in years 1 to 3, then every 6 months in years 4 to 5. CT or PET scans should be considered every 6 to 12 months to screen for asymptomatic recurrence or metastatic disease in years 1 to 3, then annually in years 4 to 5.29
Eligibility for adjuvant nivolumab does not require any specific diagnostic technology outside of the standard assessments, which are routine for the diagnostic workup of melanoma.
The staging system developed by the AJCC, 8th edition is used to stage cutaneous melanoma in Canada.5,6 Staging is determined by the size and extent of the main tumour (T), noting whether the tumour has spread to nearby lymph nodes (N), and by assessing the presence of distant metastases (M). Once the T, N, and M are determined, an overall stage of 0, I, II, III, IV is assigned. Some stages are subdivided (i.e., IIB and IIC). In stage II, the melanoma is extending beyond the epidermis into the dermis layer of the skin, but there is no evidence of metastatic lymph nodes or distant metastases. Stage II is divided into 3 substages:
IIA where melanoma is greater than 1 mm to 2 mm thick with ulceration of the skin or greater than 2 mm to 4 mm thick without ulceration
IIB where the melanoma is greater than 2 mm to 4 mm thick with ulceration or greater than 4 mm without ulceration
IIC where the melanoma is thicker than 4 mm with ulceration.
Evaluating the architectural and cytologic features of a specimen is essential for the diagnosis and staging of melanoma.30 Several key distinctive features of melanoma are important hallmarks of prognosis and staging, including asymmetry, border irregularities, colour heterogeneity, and dynamics (i.e., changes in colour, elevation, or size).31 This ABCDE system (described in Table 3) is used to identify clinical features of malignant melanoma and can aid in the early detection of melanoma lesions.5,31
Table 3: The ABCDE of Melanoma
Letter | Description |
|---|---|
A | Asymmetry |
B | Border: irregular, ragged, notched, or blurred edges |
C | Colour: nonuniform |
D | Diameter: larger than 6 mm |
E | Evolving: changing in size, shape, or colour |
Source: Sundararajan et al. 202130
The decision to pursue adjuvant therapy requires assessment of an individual patient’s risk for recurrence. Four independent prognostic factors for recurrence (tumour thickness, ulceration, number of positive lymph nodes, and nodal type) are incorporated into the 8th edition AJCC melanoma staging system (Table 4). In stage II melanoma, specifically, multivariate analysis found that the most relevant prognostic indicators were tumour thickness, presence of ulceration, and anatomic site of the tumour.8
Table 4: Prognostic Factors for Melanoma Recurrence
Prognostic factors (description) | Relationship to relapse |
|---|---|
Primary tumour depth or Breslow thickness | Survival decreases commensurately with increasing thickness |
Ulceration (breakdown of the skin over the melanoma) | Ulceration of the melanoma tends to be associated with worse survival |
Regional metastatic burden (number of metastatic nodes and whether micro- or macro-metastatic) | Survival decreases the more lymph nodes (either microscopic or macroscopic) are involved |
Location and extent of distant metastatic disease | Distant skin, subcutaneous, and/or lymph node metastases have the best prognosis, while nonlung visceral metastases and tumours with elevated LDH level (M1c) have the worst prognosis |
LDH = lactate dehydrogenase.
The diagnostic tests described previously are available to all people in Canada under the public health care system. However, the availability of diagnostic tests varies among certain populations. People living in rural areas with limited access to health care services may have limited access to diagnostic testing and are less likely to have a regular primary care physician or use specialist physician services compared to those living in urban areas.32
People with lower socioeconomic status who live in more deprived health care regions of Canada have been shown to have an increased risk of presenting with advanced melanoma at diagnosis,33,34 suggesting that these populations have limited access to health care services that would enable timely diagnosis of melanoma. In addition, inequitable access to health care disproportionately affects Indigenous Peoples (Métis, First Nations, and Inuit populations), who are more likely to face challenges in accessing services for diagnosis compared to the general population in Canada.35
Access to radiologic PET-CT machines for diagnostic imaging varies by region in Canada.36 A report by the Canadian Medical Imaging Inventory conducted by CADTH in 2018 determined that a total of 51 PET-CT units across 45 sites were available in Canada. However, none were available in the territories and Prince Edward Island.36
In summary, there are health inequities and disparities across Canada in terms of access to the timely diagnosis of melanoma for those with lower socioeconomic status, people living in certain regions and rural areas, and First Nations and Inuit populations.34 These limitations are not specific to nivolumab adjuvant treatment. It is not expected that nivolumab adjuvant treatment will not impact the availability of diagnostic testing for patients with melanoma.
Standards of Therapy
Contents within this section have been informed by materials submitted by the sponsor and clinical expert input. The following have been summarized and validated by the CADTH review team.
The treatment algorithm presented in the following is designed to generally reflect clinical practice in Canada for the treatment of completely resected stage IIB and IIC melanoma based on publicly reimbursed treatments. The algorithm does not comprehensively capture all therapeutic and treatment sequencing options available to patients. Clinical practice may also vary by province.
Figure 1 presents the current treatment algorithm for resected melanoma in Canada. This algorithm has been adapted from the CADTH Provisional Funding Algorithm for Adjuvant Therapy for Melanoma published in February 2023, as this is the most relevant and up-to-date representation of the treatment landscape for resected melanoma in Canada.37 This algorithm is also based on reimbursement recommendations from the pan-Canadian Oncology Drug Review (pCODR) Expert Review Committee (pERC), Health Canada drug approvals, Canadian treatment guidelines, and consultation with Canadian clinical experts.
The primary goal of adjuvant therapy in melanoma is to reduce the risk of recurrence and improve OS in patients who have undergone complete surgical resection, but who are considered high risk for disease recurrence.11 Currently, pembrolizumab is the only active adjuvant therapy in Canada indicated for patients with stage IIB and IIC melanoma following complete resection.12
Figure 1: Current Provisional Funding Algorithm for Adjuvant Therapy for Melanoma in Canada
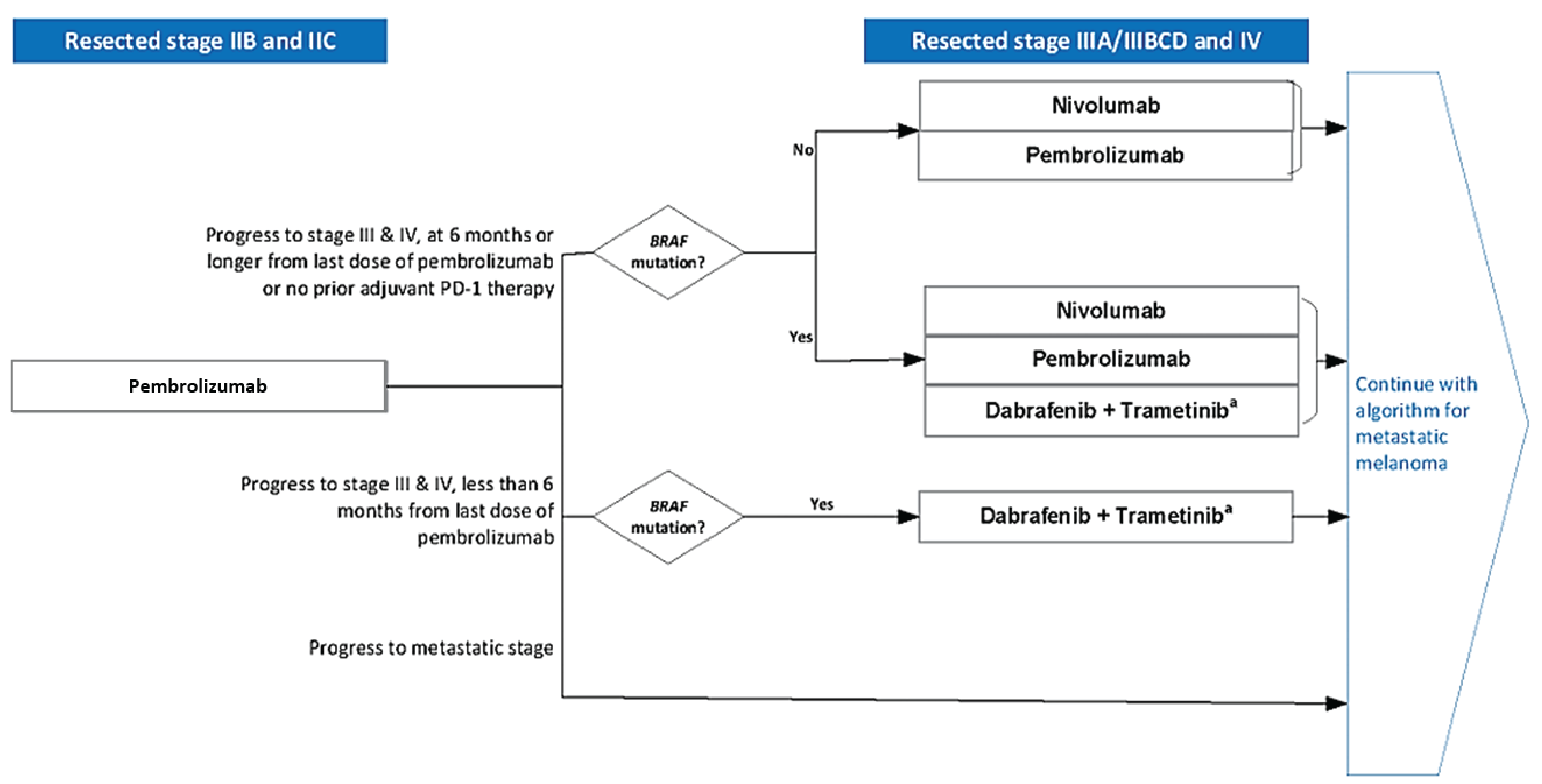
pCPA = pan-Canadian Pharmaceutical Alliance.
Note: Ocular melanoma is excluded.
a For cutaneous melanoma only. Excludes resected stage IV melanoma.
Sources: Adapted from the CADTH Provisional Funding Algorithm for Adjuvant Therapy for Melanoma48 and also based on pERC reimbursement recommendation for Keyruda (pembrolizumab).12
Drug Under Review
Nivolumab is administered as an IV infusion at a dose of 240 mg every 2 weeks or 480 mg every 4 weeks, until disease recurrence or unacceptable toxicity, up to 1 year. It is a humanized IgG4 monoclonal antibody immune checkpoint inhibitor that targets the PD-1 receptor, preventing PD-1 from inhibiting the immune response to tumours. This was a pre-NOC submission, and nivolumab received an NOC on December 29, 2023, for the adjuvant treatment of adult patients with stage IIB or IIC melanoma following complete resection, and the sponsor’s reimbursement request is consistent with the indication.
Key characteristics of nivolumab are summarized in Table 5 with other treatments available for adjuvant treatment of stage IIB or IIC melanoma following resection.
Table 5: Key Characteristics of Nivolumab and Pembrolizumab
Characteristic | nivolumab | pembrolizumab |
|---|---|---|
Mechanism of action | A humanized IgG4 monoclonal antibody (mAb) immune checkpoint inhibitor (ICI) that binds to the PD-1 receptor and blocks its interaction with PD-L1 and PD-L2, releasing PD-1 pathway-mediated inhibition of the immune response, including the antitumour immune response | An antibody with high affinity against anti-PD-1. PD-1 is an immune checkpoint receptor that limits the activity of T lymphocytes in peripheral tissues (active T-cell immune surveillance) |
Indicationa | Adjuvant treatment of adult patients with stage IIB or IIC melanoma following complete resection | Adjuvant treatment of adult and pediatric (12 years and older) patients with stage IIB or IIC melanoma following complete resection |
Route of administration | IV | IV |
Recommended dose | 480 mg q.4.w. or 240 mg, q.2.w. | 200 mg q.3.w. or 400 mg q.6.w. |
Serious adverse effects or safety issues | Pneumonitis, interstitial lung disease, encephalitis, myocarditis, Stevens-Johnson Syndrome (SJS), toxic epidermal necrolysis (TEN) and autoimmune hemolytic anemia | Immune-mediated reactions (colitis and pneumonitis), severe skin reactions (SJS and TEN), infusion-related reactions, and endocrine-related reaction |
Other | NA | Reviewed by CADTH with recommendation to reimburse with conditions on November 22, 2022 |
NA = not applicable; q.2.w. = every 2 weeks; q.3.w. = every 3 weeks, q.4.w. = every 4 weeks; q.6.w. = every 6 weeks; ROA = route of administration; SJS = Stevens-Johnson syndrome, TEN = toxic epidermal necrolysis.
aHealth Canada–approved indication.
Source: Product monographs.38,39
Stakeholder Perspectives
Patient Group Input
This section was prepared by the CADTH review team based on the input provided by patient groups. The full original patient input(s) received by CADTH have been included in the Stakeholder section of this report.
CADTH received 2 patient group submissions from Melanoma Canada and Save Your Skin Foundation (SYSF). Melanoma Canada is a national patient support organization, founded in 2009, advocating on behalf of patients to ensure timely and effective diagnosis and treatments are available to all patients across Canada and supporting people in Canada living with melanoma and skin cancer. SYSF is a national patient-led, not-for-profit group dedicated to the fight against non-melanoma skin cancers, melanoma, and ocular melanoma. It provides nationwide education, advocacy, and awareness initiatives by providing a community of oncology patient and caregiver support throughout the entire continuum of care, from prevention and diagnosis to survivorship.
Data were gathered by both groups via online surveys across social media, newsletters, and communications to registered networks of patients. Melanoma Canada conducted a survey from October 20, 2023, to November 17, 2023, and also combined this survey with results from 2 previous surveys; 1 conducted from November 28, 2018, to December 31, 2018, for adjuvant pembrolizumab for stage IIB and IIC and 1 conducted from August 1, 2018, to September 8, 2018, for adjuvant nivolumab. The survey conducted by Melanoma Canada was open to all patients and caregivers (172 patient and 15 caregiver), regardless of stage. Most respondents were early stage or did not know their staging. A total of 20 patients indicated they had been on adjuvant treatment pembrolizumab for stage IIB or IIC following complete resection and a total of 28 patients indicated they were on adjuvant therapy for stage III, treated with nivolumab. Two of the patients had been diagnosed at stage IIB or IIC initially. SYSF engaged 14 patients across all melanoma stages but focused on stage II cutaneous melanoma, and their data revealed that 2 participants were diagnosed with stage II and qualified for nivolumab. SYSF also included perspectives gathered from patients during fireside chats, support groups, and roundtables; one-on-one conversations; and other surveys over the past year to supplement the data collected in the survey.
A majority of these patients from 2 patient groups shared similar narratives and symptoms related to their diagnoses, with all acknowledging the impact of symptoms on their day-to-day lives, and most commonly shared experiences were fear, anxiety, confusion, scarring and disfigurement of skin, disrupted sleep as well as pain, fatigue, and depression. Caregivers who responded to Melanoma Canada also commented on the amount of time and additional costs of taking their family members to appointments and receiving outside care (home care), which affects the financial health and well-being of many families. Moreover, the emotional impact of the disease can be devastating for the entire family. A couple of caregivers also mentioned that it has permanently put them on social assistance and food banks, as the loss of income was significant. SYSF further emphasized that many of the patients were lacking knowledge about melanoma, its implications, and the subsequent steps in their journey. Cancer staging and lymph node dissection were unfamiliar concepts leading to a need for comprehensive information, seeking guidance from various sources.
In terms of currently available treatments, both patient groups emphasized that there is a need for more treatment options, since there is only 1 other drug-approved therapy, pembrolizumab, for treatment at this stage of disease (i.e., IIB or IIC). However, there is a higher risk of recurrence for this stage than for stage IIIA; therefore, there is an unmet need. A vast majority of patients from Melanoma Canada reported that lasting effects of surgery at this stage and the mental health issues associated with the diagnosis with little treatment beyond surgery were the most difficult and lasting impacts on their quality of life. If invasive surgeries could be minimized through use of an effective adjuvant therapy and the options for adjuvant treatment were available, it would go a long way to helping patients and their families. SYSF also acknowledged that travel to access treatment is a persistent issue in Canada's melanoma landscape.
Most patients indicated they are very willing to accept the side effect profile of nivolumab with good effectiveness and potential cancer elimination. Patients would like a therapy that allows them to function as best as possible. Patient responses to SYSF also mentioned new treatment options could bring them more options in case of recurrence, as well as more options in rural areas to negate the need for travel.
Regarding companion testing, SYSF mentioned that 2 respondents underwent testing, while 12 respondents were either told or found inapplicable. Notably, accessing companion testing posed no challenges for any respondent according to SYSF. However, 1 respondent faced treatment delays due to the testing process, with 3 respondents experiencing adverse effects. Additionally, 4 respondents were unsure about payment coverage, and 1 respondent confirmed substantial personal expenditure for testing.
A total of 20 patients from Melanoma Canada indicated that they had been treated with adjuvant therapy for stage IIB or IIC melanoma. A common issue was the length of time and cost of travel to get to a clinical trial site for treatment. Of those treated, 73% of 15 respondents indicated the side effects were worth the treatment and 27% indicated the side effects were not worth the treatment. Key values for patients and caregivers for nivolumab therapy include effectiveness in preventing recurrence of disease; tolerable side effects without long-term quality of life impacts; minimal impact on finances, including easily access without having to travel long distances and the possibility of continuation of work or daily activities without significant interruption. There were 2 respondents from SYSF who received nivolumab, and both indicated that they had only undergone surgery before starting nivolumab. Unfortunately, 1 respondent faced the challenge of missing work due to travel requirements for accessing nivolumab, which led them to disagree that benefits of nivolumab outweighed its side effects. However, the other respondent did affirm the benefit of nivolumab outweighed its side effects.
Both groups agreed that it is critically important to have more options for earlier treatment for this stage of disease. A majority of patients from both groups expressed a collective desire for new treatments that go beyond mere effectiveness. Patients commented that the emotional, physical, and societal impact of melanoma is significant and lasting, and they want to have new treatment options that eliminate cancer without negative side effects and increased resources in isolated or rural areas. It may also prevent unnecessary surgeries and radiation treatments impacting the quality of life and the burden to patients of ongoing treatment.
Clinician Input
Input From Clinical Experts Consulted by CADTH
All CADTH review teams include at least 1 clinical specialist with expertise regarding the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). The following input was provided by 2 clinical specialists with expertise in the diagnosis and management of stage IIB or IIC melanoma.
Unmet Needs
The clinical expert noted that although pembrolizumab is available as adjuvant therapy for this population, its efficacy in improving RFS are modest, therefore another immunotherapy with better efficacy is needed.
Place in Therapy
One clinical expert believed that nivolumab would complement current treatment strategies, and may in fact become the drug of choice due to superior efficacy than what has been documented with the current strategy with pembrolizumab.
One clinical expert believes that the drug could become first-line in this setting, and would result in a shift in the current treatment paradigm, while the other clinical expert believed nivolumab had a similar efficacy and harms profile to pembrolizumab, and therefore could be an alternative to pembrolizumab. One clinical expert noted that a distinguishing clinical feature between the 2 drugs could be chair time. Although pembrolizumab has been used every 3 weeks, it is licensed for every 6 weeks, while nivolumab is given every 4 weeks.
Patient Population
The clinical expert noted that the patients best suited for nivolumab would be those with low ECOG PS, no comorbidities or autoimmune conditions, and who are at significant risk of recurrence. According to the clinical expert, these patients are at significant risk for recurrence and death, hence the reason for being proactive when it comes to relapse.
Assessing the Response to Treatment
The clinical expert noted that patients are routinely assessed through physical exams and periodic imaging (PET-CT or whole-body CT with MRI of the head), based on the recommendations of the follow-up institution. According to the clinical expert, the physical exam is useful for assessing local recurrence or in-transit metastasis and nodal recurrences, while the imaging would primarily be done to exclude distant metastases. The clinical expert noted that the outcomes used to assess patients in clinical practice would be consistent with those used in clinical trials, with the predominant outcome being prevention of recurrence. This should be consistent across Canada.
Discontinuing Treatment
The clinical expert noted that factors that would be used to determine whether to discontinue therapy with nivolumab would be primarily relapse or recurrence or evidence of regional or distant metastasis or intolerability of therapy. Numerous side effects are associated with immunotherapy, many of which do not necessitate discontinuation of therapy; however, this is patient-dependent according to the clinical expert. At present, the clinical expert does not envision additional therapies being recommended for this subset of patients, although progression of disease would definitely necessitate additional therapies.
Prescribing Considerations
Nivolumab would be administered and managed by medical oncologists or cancer centre nurse practitioners who are expert in the management of immune oncology in a hospital setting, according to the clinical expert. The toxicities associated with immunotherapy are myriad and often require the expertise of multiple other disciplines including dermatologist, gastroenterologist, endocrinologist, rheumatologist cardiologist, and so forth.
Clinician Group Input
This section was prepared by the CADTH review team based on the input provided by clinician groups. The full original clinician group input(s) received by CADTH have been included in the Stakeholder section of this report.
CADTH received 1 clinician group submission from the Ontario Health (Cancer Care Ontario) Skin Cancer Drug Advisory Committee (OH-CCO’s Skin Cancer DAC). The OH-CCO’s Drug Advisory Committee provide timely evidence-based clinical and health system guidance on drug-related issues in support of CCO’s mandate, including the Provincial Drug Reimbursement Programs (PDRPs) and the Systemic Treatment Program.
Information was gathered through an OH-CCO Skin Cancer DAC meeting. The group stated that patients with stage IIB and stage IIC have high-risk for melanoma disease recurrence and mortality associated with this diagnosis, and the risk is higher compared to subgroups of stage III patients (stage IIIA). OH-CCO’s Skin Cancer DAC also stated that pembrolizumab is the only treatment currently available, and funding for nivolumab will provide additional options.
The clinician group emphasized that treatment for stage IIB and stage IIC melanoma is aimed at improving RFS and DMFS, as these are important end points for patients and possible surrogates for long-term overall survival.
OH-CCO Skin Cancer DAC mentioned that pembrolizumab is the only option for patients with stage IIB and stage IIC melanoma, so nivolumab will offer an additional choice. These 2 drugs have different dosing frequencies, with pembrolizumab being given every 3 or 6 weeks and nivolumab being given every 2 or 4 weeks. The clinician group noted that pembrolizumab’s vial size can sometimes limit the administration of dosing in satellite treatment centres, so that having an alternative drug option will ensure patients can receive their treatments close to home. Another unmet need noted by OH-CCO Drug Advisory Committees is that patients with infusion-related toxicity to 1 drug may be able to switch to another drug.
OH-CCO Skin Cancer DAC agreed that nivolumab would be an adjuvant treatment after appropriate surgical management. However, OH-CCO’s Skin Cancer DAC also emphasized that should patients experience an infusion reaction to nivolumab, they be allowed to switch to pembrolizumab, and vice versa.
OH-CCO Skin Cancer DAC indicated that patients best suited for nivolumab would align with the inclusion criteria of the study. Patients with stage IIB and stage IIC, and patients least suited for nivolumab would align with the exclusion criteria of the study. The clinician group expressed that treatment responses with nivolumab are based on lack of recurrence by physical exam and CT scans, as per clinical practice and that treatment discontinuation is based on toxicity and unresectable distant disease progression.
OH-CCO Skin Cancer DAC stated that nivolumab must be administered and monitored by medical oncologists who would need to diagnose and treat in an outpatient setting.
The clinician group believed that patients should have access to ipilimumab and nivolumab if patients have unresectable recurrent disease while on adjuvant nivolumab or relapsed within 6 months of adjuvant therapy. The clinician group also agreed that patients with resectable disease development during nivolumab adjuvant treatment would be able to complete the year of treatment following resection, and that if they recur more than 6 months following completion of therapy and have resectable disease, they could be considered for another year of adjuvant nivolumab. Finally, OH-CCO’s Skin Cancer DAC emphasized that patients who receive nivolumab “as potentially curative therapy and then relapse be eligible for downstream immunotherapy with nivolumab or pembrolizumab if equal or greater than 6 months have elapsed from the completion of adjuvant therapy,” which is to be consistent with the implementation advice for pembrolizumab according to CADTH.
Drug Program Input
The drug programs provide input on each drug being reviewed through CADTH’s Reimbursement Review processes by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CADTH are summarized in Table 6.
Table 6: Summary of Drug Plan Input and Clinical Expert Response
Additional implementation questions from the drug programs | |
|---|---|
Implementation issues | Response from clinical experts |
Relevant comparators | |
Phase III, global, double-blind, randomized, CHECKMATE-76K Trial compared nivolumab to placebo, appropriate at the time. Pembrolizumab is now indicated for this population. Nivolumab will be positioned as an additional adjuvant therapy option in this space, there will be no shift in the current treatment paradigm. | No response from Clinical Experts required. For pERC consideration. |
Considerations for initiation of therapy | |
PAG notes CHECKMATE-76K references the American Joint Committee on Cancer Cancer Staging Manual, 8th edition for disease staging. Would other classification systems be applicable? In CHECKMATE-76K, patients were randomized to receive either nivolumab or placebo within 12 weeks after surgery. What is considered the maximum time frame postsurgical resection to initiate nivolumab? | No, the clinical expert did not believe that other classification systems would apply, as this 8th edition is the current standard. The maximum time frame, according to the clinical experts, would be 12 weeks, although one clinical expert noted that occasionally there may be extenuating circumstances that may prompt a physician to still offer treatment beyond this time frame with the understanding that the evidence is based on treatment being initiated within 12 weeks postop. |
In CHECKMATE-76K placebo-treated patients who experienced disease recurrence within 3 years after the last dose of placebo and nivolumab-treated patients who experienced recurrence greater than 6 months and within 3 years after completing treatment, were eligible to cross over or rechallenge with nivolumab. Patients with recurrent, resectable disease were offered nivolumab for a maximum duration of 12 months. In other solid tumours (e.g., lung, melanoma), patients are eligible for a downstream PD-1 or PD-L1 inhibitor, provided that disease recurrence (whether locoregional or distant) occurs more than 6 months from the last dose of adjuvant PD-1 or PD-L1 inhibitor. Can the same principle be applied in this setting? | Yes, the clinical experts believed that the same principle could be applied in this case. One clinical expert noted that the rechallenge would be with a combination of nivolumab and ipilimumab. |
Considerations for discontinuation of therapy | |
If treatment interruptions occur, should the remainder of the doses be given even if it will take more than a calendar year to deliver the treatments, provided there has been no disease progression in between? For example:
| One clinical expert agreed with this approach; however, the other clinical expert did not believe oncologists would be so focused on getting in all the planned treatments, and if there were treatment interruptions this would likely result in permanent discontinuation. One clinical expert believed that this would depend on the clinical circumstances and a discussion of the pros and cons with the patient, however in most cases would probably not restart. The other clinical expert believed that a wait and see approach would be taken, and emphasized that in this setting, there is no active disease being treated, rather the theoretical presence of disease. Response from clinical experts: One clinical expert believed that this depends on the clinical circumstances, and noted that the principle of adjuvant therapy is to start and complete the treatment in a timely and uninterrupted manner. The other clinical expert reiterated that a wait and see approach would be taken, and emphasized that in this setting, there is no active disease being treated, rather the theoretical presence of disease. |
Considerations for prescribing of therapy | |
PAG would like to inform pERC that jurisdictions will implement weight-based dosing up to a cap, similar to other immunotherapy policies (i.e., nivolumab 3mg/kg up to 240mg every 2 weeks or nivolumab 6mg/kg up to 480mg every 4 weeks. | No response from Clinical Experts required. For pERC consideration. Note that the pivotal trial used flat dosing rather than weight-based dosing so the latter has not been reviewed. |
Generalizability | |
Should patients with noncutaneous melanoma be considered for treatment with nivolumab for this indication? (current Pembrolizumab indication for this population allows stage IIB and IIC cutaneous or mucosal melanoma, and excludes ocular or uveal melanoma) Should patients with ECOG PS of 2 or greater be eligible for nivolumab for this indication? | Response from clinical experts: The clinical experts believed that patients with uveal and ocular melanoma should be excluded. One clinical expert added that nivolumab might be used as treatment but not as adjuvant therapy. Response from clinical experts: One clinical expert believed that yes, patients should be eligible if they have other comorbidities that are unlikely to be life-threatening in the foreseeable future, while in patients who have an ECOG PS of 3, treatment would be unlikely for this presentation on its own. The other clinical expert believed that patients who have an ECOG PS of 2 or more are unlikely to tolerate nivolumab and emphasized that this is adjuvant therapy and no active disease is being treated. |
PAG notes that pembrolizumab is currently available for this population. | No response from Clinical Experts required. For pERC consideration. |
Care provision issues | |
Nivolumab is already prepared and administered at facilities throughout Canada. Health care professionals have extensive experience with it. Preparation and administration time for nivolumab are relatively reasonable and would not be expected to create a significant increase to health system resources. | No response from Clinical Experts required. For pERC consideration. |
System and economic issues | |
PAG notes that there is confidential pricing for pembrolizumab. | No response from Clinical Experts required. For pERC consideration. |
ECOG = Eastern Cooperative Oncology Group; PAG = Provincial Advisory Group; PS = performance status.
Clinical Evidence
The objective of CADTH’s Clinical Review Report is to review and critically appraise the clinical evidence submitted by the sponsor on the beneficial and harmful effects of nivolumab in the adjuvant treatment of patients with stage IIB or IIC melanoma following complete resection in adults. The focus will be placed on comparing nivolumab to relevant comparators and identifying gaps in the current evidence.
A summary of the clinical evidence included by the sponsor in the review of nivolumab is presented in 4 sections with CADTH’s critical appraisal of the evidence included at the end of each section. The first section, the systematic review, includes pivotal studies and RCTs that were selected according to the sponsor’s systematic review protocol. CADTH’s assessment of the certainty of the evidence in this first section using the GRADE approach follows the critical appraisal of the evidence. The second section normally includes sponsor-submitted long-term extension studies; however, none were submitted. The third section includes indirect evidence from the sponsor. The fourth section normally includes additional studies that were considered by the sponsor to address important gaps in the systematic review evidence, however none were submitted.
Included Studies
Clinical evidence from the following are included in the CADTH review and appraised in this document:
1 pivotal study
1 indirect treatment comparison.
Systematic Review
Contents within this section have been informed by materials submitted by the sponsor. The following have been summarized and validated by the CADTH review team.
Description of Studies
Characteristics of the included studies are summarized in Table 7.
Table 7: Details of Studies Included in the Systematic Review
Criteria | CHECKMATE-76K |
|---|---|
Designs and populations | |
Study design | Phase III, randomized, double-blind study of adjuvant immunotherapy with nivolumab vs. placebo after complete resection of stage IIB or IIC melanoma |
Locations | This study was conducted at 129 sites in 20 countries (Australia, Austria, Belgium, Canada, Czech Republic, Denmark, Finland, France, Germany, Greece, Italy, Netherlands, Norway, Poland, Romania, Spain, Sweden, Switzerland, UK, and the US) |
Patient enrolment dates | Start date: April 28, 2019 End date: Study is ongoing |
Randomized (N) | Total: N = 790 Opdivo (nivolumab): n = 526 Placebo: n = 264 |
Inclusion criteria |
|
Exclusion criteria |
|
Drugs | |
Intervention | Nivolumab 480 mg IV q.4.w. until disease progression, treatment discontinuation, unacceptable toxicity, withdrawal of consent, or end of study |
Comparator(s) | Nivolumab-matched placebo IV (0.9% sodium chloride and 5% dextrose) every 4 weeks until disease progression, treatment discontinuation, withdrawal of consent, or end of study |
Study duration | |
Screening phase | 14 days |
Treatment phase | Treatment was given until disease progression, treatment discontinuation, unacceptable toxicity, withdrawal of consent, or end of study. Data presented are based on a database lock date of April 20, 2023, after a median follow-up of 23 months |
Follow-up phase | The first follow-up visit was conducted 30 ± 7 days after the last dose of study treatment, and the second follow-up visit was conducted 100 ± 7 days from the last dose of treatment. Clinical examinations continued every 12 weeks for 12 months following the second follow-up visit |
Outcomes | |
Primary end point | Investigator-assessed RFS (final RFS analysis conducted after a median follow-up of 23.5 months in the nivolumab arm and 23.0 months in the placebo arm months [database cut-off February 21, 2023]) |
Secondary and exploratory end points | Secondary:
Exploratory:
|
Safety | Rate of AEs, SAEs, select AEs, IMAEs, OESIs, AEs leading to treatment discontinuation, deaths, and laboratory abnormalitiesc |
Publication status | |
Publications | Studies identified from databases:
Identified from conference searches:
Identified from trial registries:
Internal data on file from Bristol-Myers Squibb (BMS):
Published following completion of SLR:
|
AEs = Adverse events; DMFS = distant metastases-free survival; EORTC QLQ-C30 = European Organization for Research and Treatment of Care (EORTC) QLQ-C30 Global Health Status score; FACT-GP5 = Functional Assessment of Cancer Therapy; FFR = freedom from relapse; FFPE = formalin-fixed paraffin embedded; IMAE = immune-mediated adverse event; OESI = other event of special interest; ORR = objective response rate; OS = overall survival; PFS2 = progression-free survival after the next line of subsequent therapy; PS = performance status; q.4.w. = every 4 weeks; RFS = recurrence-free survival; SAEs = serious adverse events; TFI = treatment-free interval; VAS = visual analogue scale; vs. = versus.
aWith the exception of endocrine events, most select AEs and IMAEs were considered resolved at time of data cut-off of the primary Clinical Study Report (June 28, 2022).
Source: BMS 2022 Study Protocol,14 BMS 2022 Primary Clinical Study Report,13 BMS 2023 Addendum 01 – Primary Clinical Study Report,43 BMS 2022 Statistical Analysis Plan44
CHECKMATE-76K is a phase III, randomized, double-blind, multicentre clinical trial to evaluate the efficacy and safety of nivolumab in completely resected stage IIB and IIC melanoma across 20 countries and 132 locations, including Canada.13
Adults and children aged 12 years or older were eligible for enrolment. A total of 790 patients were randomly assigned in a 2:1 ratio to receive 480 mg of nivolumab (n = 526) or placebo (n = 264).43 All but 2 (n = 788) patients randomized received at least 1 dose of study drug. Patients in the treatment arm were treated with nivolumab 480 mg every 4 weeks via 30-minute IV infusions. Nivolumab-matched placebo (0.9% sodium chloride for injection and 5% dextrose for injection) was administered via IV over approximately 30 minutes every 4 weeks.
Placebo-treated patients who experienced disease recurrence within 3 years after the last dose of placebo, and nivolumab-treated patients who experienced recurrence greater than 6 months and within 3 years after completing treatment, were eligible to receive on-study open-label nivolumab treatment. Patients with recurrent, resectable disease were offered nivolumab for a maximum duration of 12 months, whereas patients with recurrent unresectable or metastatic disease were offered nivolumab for a maximum of 24 months.14
The primary objective of CHECKMATE-76K was to compare the efficacy, as measured by investigator-assessed RFS, provided by nivolumab monotherapy versus placebo in patients with completely resected stage IIB and IIC melanoma with no evidence of disease who are at high risk for recurrence.14 The secondary objectives were to compare OS and DMFS between the 2 treatment groups, assess the safety and toxicity of nivolumab and evaluate investigator-assessed outcomes on next-line therapies.
Note: The main results presented for the primary and secondary end points, as well as respective subgroup analyses, focus on the final analysis time points as prespecified in the statistical hierarchy (based on the June 28, 2022, data cut-off13 and February 21, 2023, data cut-off,43 respectively). For the most recent data cut-off date of February 21, 2023, the median follow-up (date of randomization to the last known date alive or death date) for all randomized patients was 23.49 months for the nivolumab arm and 23.05 months for the placebo arm.
Analyses from the February 21, 2023, data cut-off date addresses the primary objective, secondary objectives (aside from OS) and a subset of exploratory objectives in all randomized (efficacy), as well as all treated (safety) populations, previously reported as part of an interim analysis based on the data cut-off date of June 28, 2022, when approximately 123 RFS events had been reached. At the time of the most recent data cut-off date (February 21, 2023), BMS remained blinded to the OS results of the study (a key secondary end point) as the prespecified number of events for the OS interim analysis have not been reached. The February 21, 2023, data cut-off date includes patients who are on-study but for whom the treatment period is complete, and the follow-up period is ongoing.
![This figure describes the design of CHECKMATE-76K, which begins with a blinded phase that compares nivolumab to placebo and then transitions to an open-label phase as described in the Study Design section; Source: BMS 2021 [CSR].](https://canjhealthtechnol.ca/index.php/cjht/article/download/PC0339r/version/992/2164/8399/PC0339CL-fig02.png)
DMFS = distant metastases-free survival; NIVO = Nivolumab; OS = Overall survival; PBO = Placebo; RFS = recurrence-free survival; PFS2 = progression-free survival after the next line of subsequent therapy; Q4W = every 4 weeks.
Populations
Inclusion and Exclusion Criteria
Patients included in CHECKMATE-76K were aged 12 years or older with completely resected stage IIB or IIC cutaneous melanoma (AJCC Staging, 8th edition), with no evidence of disease.14 Patients must have had an ECOG PS of 0 or 1 and have not been previously treated for melanoma beyond surgical resection for melanoma lesion.14 Participants must have had disease-free status documented by a complete physical examination (within 14 days) and imaging studies within 4 weeks (28 days) before randomization and a negative sentinel lymph node biopsy. Tumour tissue from the primary diagnostic biopsy (minimum of 15 stained slides, freshly cut or 1 formalin-fixed paraffin-embedded block) must be provided (see Table 7 for details of the inclusion and exclusion criteria CHECKMATE-76K).14
Interventions
Patients were randomized 2:1 to receive either nivolumab monotherapy (480 mg) or placebo. Both treatments were administered as an IV infusion every 4 weeks over 30 minutes in a clinic or hospital setting.14 Adolescents aged 12 to 17 years weighing less than 40 kg were to receive weight-based therapy (nivolumab 6 mg/kg up to a maximum of 240 mg) yet, no adolescents were enrolled in the study. Adult and pediatric patients in the placebo arm received nivolumab-matched placebo (0.9% sodium chloride for injection and 5% dextrose for injection) IV over 30 minutes every 4 weeks). Treatment continued until disease progression, treatment discontinuation, unacceptable toxicity, withdrawal of consent, or end of study.14
CHECKMATE-76K was double-blinded to minimize bias arising from differences in thresholds for classification of recurrence between the treatment arms, which could subsequently affect treatment duration between the arms and have an impact on the primary end point of RFS. In addition, blinding reduced bias in reporting, classification, and management of adverse events. Some participants with recurrence who discontinued required knowledge of which treatment arm they were assigned to to appropriately select any postrecurrence subsequent therapy (including treatment in the optional open-label nivolumab portion of the trial). In these cases, the participant’s treatment assignment was unblinded via interactive response technology (IRT) to inform the appropriate subsequent treatment.
Note that designated staff of BMS could be unblinded (obtain the randomization codes) before database lock to facilitate the bioanalytical analysis of pharmacokinetic samples and immunogenicity. In addition, there was an unblinded pharmacist/designee at each trial site to provide oversight of drug supply and other unblinded study documentation.14
Dose reductions or escalations were not permitted for either treatment arm. Administration of study treatment was allowed to be delayed but not skipped.44
Treatment details for adults and pediatric patients in the open-label phase were the same as in the blinded phase, except that the use of a placebo was not applicable to the open-label nivolumab portion of the trial.14 In addition, nivolumab 480 mg will be administered day 1 of each treatment cycle until unacceptable toxicity, withdrawal of consent, completion of 12 months (arm 1: resectable disease) or 24 months (arm 2: unresectable or metastatic disease) of treatment (from first dose of open-label nivolumab), disease progression, or the study ends, whichever occurs first. Patients receiving open-label nivolumab treatment after recurrence must have not received any other systemic anticancer therapy (including investigational anticancer therapy) or locoregional anticancer therapy (other than surgery for complete resection of the recurrence and radiation therapy administered with a palliative intent) between the last dose of blinded study treatment and the first dose of open-label study treatment.14
Outcomes
The primary end point was investigator-assessed RFS, defined as the time between the date of randomization and the date of first recurrence by the investigator (local, regional, or distant metastasis), new primary melanoma (including melanoma in situ), or death (due to any cause), whichever occurs first. For patients who remained alive and whose disease had not recurred, RFS was censored on the date of last evaluable disease assessment. For those patients who remained alive and had no recorded postrandomization tumour assessment, RFS was censored on the day of randomization.14
The per-protocol analysis for RFS was conducted at the June 28, 2022, data cut-off after a median follow-up of ||||| |||||| for the nivolumab arm and ||||| |||||| for the placebo arm.13
The following were secondary end points in the CHECKMATE-76 trial:14
OS was defined as the time between the date of randomization and the date of death, from any cause. For patients that were alive, their survival time was censored at the date of last contact (or “last known alive date”). OS was censored at the date of randomization for patients who were randomized. No follow-up has been formally assessed. At the time of the February 21, 2023 data cut-off, the prespecified number of events for the OS interim analysis had not been reached. Per-protocol amendment 3, a formal interim analysis of OS was added, to occur at an information fraction of 60%, which is expected to be approximately 8 years since the first patient was treated.13
DMFS was determined based on the first date of distant metastasis provided by the investigator and was defined as the time between the date of randomization and the date of first distant recurrence or the date of death (due to any cause), whichever occurred first.
PFS2 was defined as the time from randomization to recurrence/objective disease progression after the start of next-line of systemic anticancer therapy, or to the start of second next-line systemic therapy, or to death from any cause, whichever occurred first.
Objective response rate (ORR) on next-line therapy was defined as the number of randomized patients who achieve a best overall response of complete response or partial response after next-line therapy based on investigator assessments (using RECIST v1.1) divided by the number of all randomized patients. Note that because an analysis of OS was not yet feasible, ORR could not be formally tested.
Duration of treatment on next-line therapy was defined as the time from first dose date of next-line therapy to last dose date of next-line therapy. Patients who did not stop the next-line therapy were censored.
Safety assessments included the rate of AEs, serious adverse events (SAEs), select AEs, AEs leading to study treatment discontinuation, immune-mediated AEs (IMAEs), other events of special interest (OESI), abnormalities in clinical laboratory assessments, and death.13
IMAEs were assessed to further evaluate AEs of clinical interest.44 They were defined as specific events, or groups of preferred terms (PTs) describing specific events, considered by the investigator as being potentially immune-mediated and that met the following criteria:44
occurred within 100 days of the last dose
regardless of causality
treated with immune-modulating medication
had no clear alternate etiology or had an immune-mediated component.
Several exploratory end points were assessed in CHECKMATE-76K, including:
Freedom from relapse (FFR) was defined as the time from randomization to recurrence (as per RFS definition); however, patients who died from causes other than melanoma or treatment-related toxic effects were censored.
Treatment-free interval (TFI) was defined as the time from last dose of study treatment to the start of subsequent systemic therapy or the last known alive date (for those who never received subsequent cancer therapy).
The FACT-GP581,82, EQ-5D-3L83, and EORTC QLQ-C3084 patient-reported measures are validated instruments that were evaluated in CHECKMATE-76K to assess the impact of treatment on HRQoL.
EQ-5D-5L
The EQ-5D-5L measure assessed patient-reported overall health status and comprised the following:
EQ-5D-5L descriptive system, which generated utility index (UI) scores
EQ-5D-5L visual analogue scale (VAS).
The EQ-5D-5L descriptive system involves 5 domains of mobility, self-care, usual activities, pain/discomfort, and anxiety/depression, each with 5 levels, ranging from no problems, slight problems, moderate problems, severe problems and extreme problems.48
The EQ-5D-5L VAS assessed general health on a vertical VAS, with scores ranging from 0 (worst health imaginable) to 100 (best health imaginable; the MID for the EQ-5D-5L was predefined in the statistical analysis plan as a change from baseline of 0.08 in health UI scores, and a change of 7 for the EQ-5D-5L VAS.44,49
A list of efficacy end points assessed in this Clinical Review Report is provided in Table 8 followed by descriptions of the outcome measures. Summarized end points are based on outcomes included in the sponsor’s Summary of Clinical Evidence, as well as any outcomes identified as important to this review according to the clinical expert(s) consulted by CADTH and stakeholder input from patient and clinician groups and public drug plans.
For the purpose of conducting a GRADE assessment, the CADTH review team selected end points that were considered to be most relevant to inform CADTH’s expert committee deliberations and finalized this list of end points in consultation with members of the expert committee. The following outcomes were assessed using GRADE: OS at 5 years, RFS and DMFS at 1, 2 and 3 years. Select notable harms outcomes considered important for informing CADTH’s expert committee deliberations were also assessed using GRADE (grade 3 to 4 diarrhea, diabetes mellitus, and arthritis that occurred within 100 days of the final dose).
Table 8: Outcomes Summarized From the Studies Included in the Clinical Report
Outcome Measure | Time point | CHECKMATE-76K |
|---|---|---|
RFS | Year 1, 2, and 3 | Primary end point |
DMFS | Year 1, 2, and 3 | Secondary end point |
PFS2 | Final analysis conducted at the February 21, 2023, data cut-off (median follow-up of 23.5 months for nivolumab arm and 23.0 months for placebo arm) | Secondary end point |
OS | The prespecified number of events for the OS interim analysis have not been reached | Secondary end point |
EQ-5D-5L, FACIT-GP, EORTC QLQ-C30 | The most recent analyses for patient-reported measures are available from the data cut-off of June 28, 2022 (median follow-up of 15.8 months for nivolumab arm and 15.9 months for placebo arm). Note that only baseline results are available for the FACIT-5P and the EORTC QLQ-C3 | Exploratory end point |
FFR and TFI | Data reported are based on the data cut-off of June 28, 2022 (median follow-up of 15.8 months for nivolumab arm and 15.9 months for placebo arm) | Exploratory end point |
Safety and tolerability | Data are based on the February 21, 2023, data cut-off (median follow-up of 23.5 months for nivolumab arm and 23.0 months for placebo arm) | Safety assessment |
DMFS = distant metastasis-free survival; EORTC QLQ-C30 = EORTC Core Quality of Life questionnaire; FACIT-GP = Functional Assessment of Chronic Illness Therapy - General Population; FFR = Freedom from relapse; OS = overall survival; PFS2 = progression-free survival after the next line of subsequent therapy; RFS = Regression-free survival; TFI = treatment-free interval.
Sources: BMS 2022 Study Protocol,14 BMS 2022 Primary Clinical Study Report,13 BMS 2023 Addendum 01 – Primary Clinical Study Report,43 BMS 2022 Statistical Analysis Plan.44
Table 9: Summary of Outcome Measures and Their Measurement Properties
Outcome measure | Type | Conclusions about measurement properties | MID |
|---|---|---|---|
RFS | Time between the date of randomization and the date of first recurrence by the investigator (local, regional, or distant metastasis), new primary melanoma (including melanoma in situ), or death (due to any cause), whichever occurs first | The clinical experts noted that although RFS is of primary importance for this indication, the relationship between OS and RFS is uncertain | The clinical experts believed that a between-group MID at 1 year would be 10%, at 2 years would be 15%, and this may increase with time |
DMFS | Determined based on the first date of distant metastasis provided by the investigator and was defined as the time between the date of randomization and the date of first distant recurrence or the date of death (due to any cause), whichever occurred first. | The clinical experts believed DMFS to be an important outcome to assess, along the same lines as RFS | The clinical experts believed that the between-group MID for DMFS would be similar to those for DMFS |
OS | Time between the date of randomization and the date of death, from any cause. | The clinical experts noted that due to the relatively low mortality rate in this population, OS data may not be attainable within the typical follow-up of an RCT | The clinical experts did not define an MID for OS, noting that the data are not yet mature enough to obtain OS data |
PFS2 | Time from randomization to recurrence/objective disease progression after the start of next-line of systemic anticancer therapy, or to the start of second next-line systemic therapy, or to death from any cause, whichever occurred first | The clinical experts did not believe this to be a key clinical outcome | NA |
EQ-5D-5L utility index | Five domains: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression Each has 5 levels, ranging from no problems, slight problems, moderate problems, severe problems and extreme problems | This is a well-established and validated generic HRQoL instrument | change from baseline of 0.08 in health UI scores |
EQ-5D-5L VAS | Vertical VAS, with scores ranging from 0 (worst health imaginable) to 100 (best health imaginable | This is a well-established and validated generic HRQoL instrument | Change of 7 for the EQ-5D-5L VAS |
EORTC QLQ-C30 | 30 items Divided among:
| This is a well-established and validated instrument for assessing HRQoL in oncology | Not reported |
Notable harms: diarrhea, diabetes mellitus, arthritis | As described | NA | NA |
DMFS = distant metastasis-free survival; HRQoL = health-related quality of life; OS = overall survival; PFS2 = progression-free survival after the next line of subsequent therapy; RFS = Regression-free survival; VAS = visual analogue scale.
Statistical Analysis
Sample Size and Power Calculation
The study sample size for CHECKMATE-76K was based on the primary end point of investigator-assessed RFS.44 Simulation models incorporating aspects of immunotherapy, such as delayed separation (observed as late separation of survival curves between the experimental and placebo arms) and long-term survival benefits (observed as a long-lasting plateau toward the tail of the survival curve) were developed for sample size estimation. The sample size was calculated to compare RFS between nivolumab and placebo in all randomized patients. Approximately 154 RFS events were required for a 2-sided experiment-wise alpha = 0.05 log-rank test, to show a statistically significant difference in RFS between the treatment arms with at least 90% power when the average HR of the nivolumab arm to the placebo arm is 0.573.44
Given the estimated accrual rate, the accrual of 780 patients (i.e., 520 patients in the nivolumab arm and 260 patients in the placebo arm) would take approximately 29.6 months. Under the assumptions for accrual, an assumed delayed treatment effect of 6 months as per the Sunbelt Melanoma Trial and assumed HR as stated previously (HR = 1 for the first 6 months, HR = 0.537 after 6 months, HR = 1 from year 10 [plateau effect]), it would take approximately 68.1 months from the randomization of the first patient to observe the required number of RFS events. An observed HR of 0.707 or less would result in a statistically significant improvement at the final analysis of RFS.44
An interim RFS analysis was conducted when approximately 123 RFS events had been reached (June 28, 2022, cut-off). For this interim analysis, the type I error was 0.024 (2-sided) with a power of 62.8%. An observed HR of 0.65 or less would result in a statistically significant improvement. The 2-sided type I error used for final RFS analysis was 0.0043 (Table 20).44 Statistical Test or Model.
The primary RFS analysis was conducted using a stratified 2-sided log-rank test. The stratification factor that was used in the analysis was AJCC T category at study entry (as recorded per IRT). The 2-sided stratified log-rank P value was reported. A stratified Cox proportional hazards model, with treatment as the sole covariate, stratified by the previously noted stratification factor, was used to estimate the RFS HR of nivolumab to placebo. Ties were handled using the exact method.44
The RFS function for each treatment group was estimated using Kaplan-Meier (KM) product-limit method and displayed graphically. Median RFS along with 95% CIs were estimated based on a log-log transformed CI for the survivor function. Rates at fixed time points (depending on the minimum follow-up) were derived from the KM estimate and the corresponding CI was be derived based on the Greenwood50 formula for variance derivation and on log-log transformation applied on the survivor function.44,51
For those participants who remained alive and had no recorded postrandomization tumour assessment, RFS will be censored on the day of randomization. Censoring rules for the primary definition of RFS are presented in Table 10.
Table 10: Censoring Scheme for Primary Definition of PFS
Situation | Date of progression or censoring | Outcome |
|---|---|---|
Recurrence (local, regional, distant, new primary melanoma, including melanoma in situ) | Date of first recurrence | Event |
Death without recurrence | Date of death | Event |
Disease at baseline | Date of randomization | Event |
No baseline disease assessment | Date of randomization | Censored |
No on-study disease assessments and no death | Date of randomization | Censored |
No recurrence and no deatha | Date of last evaluable disease assessment | Censored |
New anticancer therapy,b tumour-directed radiotherapy, or tumour-directed surgery received without recurrence reported before or on the same day of disease assessment | Date of last evaluable disease assessment before or on the same date of initiation of subsequent therapy | Censored |
Second non-melanoma primary cancer (excluding BCC) reported prior or on the same day of disease assessment | Date of last evaluable disease assessment before or on the same date of diagnosis of second nonmelanoma primary cancer | Censored |
BCC = basal cell carcinoma.
aDisease assessments and death if any, occurring after start of subsequent anticancer therapy are not considered.
bOpen-label nivolumab treatment considered as a new anticancer therapy.
Source: BMS 2022, Statistical Analysis Plan.44
Multiple Testing Procedure
For the interim analyses, RFS and OS were tested using a hierarchical procedure, with RFS compared first in all randomized participants with an alpha allocation of 0.05 (2-sided). If significant, OS was then compared in all randomized participants with an alpha allocation of 0.05 (2-sided).
Table 11: Conventions Used for Imputing Partial Dates in Efficacy and Safety Analyses
Outcome measure | Convention |
|---|---|
AEs and safety | For missing and partial AE onset dates, imputation was planned to be performed using the Adverse Event Domain Requirements Specification For missing and partial AE resolution dates, imputation was planned to be performed as follows: If only the day of the month was missing, the last day of the month was used to replace the missing day. If the imputed date was after the death date or the last known alive date, then the latest known alive date or death date was considered as the resolution date If the day and month were missing or a date was completely missing, it was considered as missing For death dates, the following conventions were planned for imputing partial dates:
|
Disease progression | Patients with 2 consecutive missing images were censored at the last assessment date before the 2 missing assessments for RFS For date of recurrence/progression after the start of study therapy, the following conventions were planned for imputing partial dates:
For date of recurrence or progression to prior therapies, the following conventions were planned for imputing partial dates:
For other partial/missing dates, the following conventions were used:
|
HRQoL | EORTC QLQ-C30: Missing values will be imputed for missing items by “assuming that the missing items have values equal to the average of those items which are present” for any scale in which at least half the items are completed. A scale in which less than half of the items are completed will be treated as missing. For missing responses on any single-item measures, the score is set to missing. EQ-5D-5L: In the event where the patient has no valid assessment at all in a specific window, the observation will be treated as missing for that time point. |
Conversion factors | The following conversion factors were used to convert days to months or years:
Duration (e.g., time-to-onset, time-to-resolution) was calculated as follows:
|
AE = adverse event; CRF = case report form; EORTC QLQ-C30 = EORTC Core Quality of Life questionnaire; HRQoL = health-related quality of life; RFS = recurrence-free survival.
Source: BMS 2022, Statistical Analysis Plan.44
Subgroup Analyses
Subgroup analyses of RFS reported median RFS based on the Kaplan-Meier product-limit method along with 2-sided 95% CIs derived based on the Greenwood formula for variance derivation and on log-log transformation applied on the survivor function.
Sensitivity Analyses
Prespecified sensitivity analyses were conducted to assess the robustness of the primary RFS analysis, as follows:44
adjustment for treatment by time in the Cox regression model
comparison of RFS between treatment groups via 2-sided Max-Combo test and the restricted mean survival time generalized linear model to test assess delayed effect of immunotherapy
adjustment for potentially important covariates
stratified analysis using factors obtained from baseline
an unstratified analysis
test for interaction between treatment and strata
censoring for 2 or more consecutively missing disease assessments before RFS event (In case a patient has 2 or more consecutively missing disease assessments, the patient will be censored at the last evaluable disease assessment before the missing assessments prior the RFS event).
In addition, median RFS based on KM product-limit method along with 2-sided 95% CIs were produced by age category, gender, race, disease stage category, T stage and ragion.44 Forest plots of the RFS hazard ratios (along with 95% CIs) were produced for subgroup.
The currentness of follow-up for RFS, defined as the time from last evaluable tumour assessment to cut-off date in months are summarized descriptively (median, min, max, etc.) by treatment group and overall for all randomized patients. Patients who have an RFS event are considered as current for this analysis. The currentness of follow-up is categorized into categories: 0, greater than 0 to less than 3 months, 3 to less than 6 months, 6 to less than 9 months, 9 to less than 12 months, 12 to less than 18 months, 18 to less than 24 months, 24 to less than 30 months, 30 to less than 36 months, and 36 or more months.44
Secondary Outcomes of the Studies
A 2-sided log-rank test, stratified by AJCC T stage at study entry was used to analyze DMFS. The estimate of the DMFS hazard ratio (with 95% Cis), of nivolumab to placebo, was calculated using a stratified Cox proportional hazards model, with treatment as the single covariate. The DMFS distribution for each treatment group was estimated using KM techniques. Median DMFS with 95% CIs was estimated based on a log-log transformed CI for the survivor function. Rates at fixed time points were derived from the KM estimate and corresponding CIs were derived using the methods previously presented for RFS previously.44
The source of DMFS event was categorized by disease at baseline, distant metastasis or death. The status of participants who are censored in the DMFS KM analysis were tabulated using the following categories:44
censored on randomization date
no baseline disease assessment
no on-study disease assessment and no distant metastasis or death
censored on date of last disease assessment on-study
still on treatment
in follow-up
off study
lost to follow-up
participant withdrew consent
other.
Sensitivity and subgroup analyses of DMFS were also conducted. These analyses were the same as those specified previously for RFS.44
Censoring rules for the analysis of DMFS are presented in Table 12.
Table 12: Censoring Scheme for Primary Definition of DMFS
Situation | Date of progression or censoring | Outcome |
|---|---|---|
Recurrence (distant metastasis) | Date of first recurrence | Event |
Death without recurrence | Date of death | Event |
Disease at baseline | Date of randomization | Event |
No baseline disease assessment | Date of randomization | Censored |
No on-study disease assessments and no death | Date of randomization | Censored |
No recurrence and no deatha | Date of last evaluable disease assessment | Censored |
aDisease assessments and death if any, occurring after start of subsequent anticancer therapy are not considered.
Source: BMS 2022, Statistical Analysis Plan.44
The hazard ratio and corresponding 95% CIs were estimated using a Cox proportional hazards model, with treatment group as a single covariate.44 The PFS2 distribution for each treatment group estimated using KM and the median PFS2 with 95% CIs were derived using the methods previously presented for RFS previously.44 Reason for event or censoring on and through next-line systemic therapy (primary and substitute event definition) and PFS per investigator on next-line systemic therapy (primary and substitute event definition) were also analyzed.44
Table 13: Statistical Analysis of Efficacy End Points
End point | Statistical model | Adjustment factors | Sensitivity analyses |
|---|---|---|---|
RFS (Primary) |
|
|
|
OS (Secondary) |
| NA | Sensitivity analyses for OS mimicked those presented for RFS |
DMFS (Secondary) |
| NA | Sensitivity analyses for DMFS mimicked those presented for RFS |
PFS2 (Secondary) |
| NA | NA |
Safety (Safety) |
| NA | NA |
FFR and TFI (Tertiary or exploratory) |
| NA | NA |
HRQoL | |||
EORTC QLQ-C30 (Exploratory) |
| NA | NA |
EuroQoL 5Q-5D-5L (Exploratory) |
| NA | NA |
FACIT GP5 (Exploratory) | Descriptive statistics (mean, median, count and proportion of responses) of the one-item FACIT GP5 included the questionnaire completion rate by time point and treatment group, and the frequency and percentage of patients who endorsed each FACIT GP5 response option at each assessment time point | NA | NA |
AE = adverse event; AJCC = American Joint Committee on Cancer; CI = confidence interval; CRF = case report form; DMFS = distant metastases-free survival: EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Core Quality of Life questionnaire; FACIT = Functional Assessment of Cancer Therapy; FFR = freedom from relapse; HRQoL = health-related quality of life; IMAE = immune-mediated adverse event; IRT = interactive response technology; KM = Kaplan-Meier; MedDRA v5.0 = Medical Dictionary for Regulatory Activities version 5.0; MID = minimally important difference; NA = not applicable; NCI-CTCAE v25.0 = National Cancer-Institute Common Terminology Criteria for Adverse Events version 25.0; OESI = other event of special interest; OS = overall survival; PT = preferred term; RFS = recurrence-free survival; SAE = serious adverse event; SD = standard deviation; SOC = system organ class; TFI = treatment-free interval; UI = utility index; VAS = visual analogue scale.
aPrespecified in the statistical analysis plan based on Pickard et al. (2007).49
Sources: BMS 2022 Study Protocol,14 BMS 2022 Primary Clinical Study Report,13 BMS 2023 Addendum 01 – Primary Clinical Study Report,43 BMS 2022 Statistical Analysis Plan.44
Analysis Populations
Table 14: Analysis Populations of CHECKMATE-76K
Population | Definition | Application |
|---|---|---|
Enrolled patients | All patients who sign informed consent and obtained a patient number | Patient disposition |
Randomized | All patients who were randomized through the IRT. Analyses used the treatment arm as randomized, unless otherwise specified | Baseline demographic and disease characteristics, efficacy analyses, PRO analyses |
PK | All randomized patients with available serum time concentration data | PK analyses |
Treatment and safety | All randomized patients who received at least one dose of any study medication | Safety analyses |
Immunogenicity | All treated participants with baseline and at least 1 postbaseline preinfusion nivolumab immunogenicity assessment | Analysis of immunogenicity data |
Biomarker | All randomized patients with available biomarker data | Biomarker analyses |
Patients enrolled in the open-label treatment group | All patients who signed the informed consent form for the open-label treatment and obtained a patient number | Open-label patient disposition |
Patients included in the open-label treatment group | All patients who received at least one dose of Nivolumab during the open-label treatment medication | All open-label anlayses |
IRT = interactive response technology; PK = pharmacokinetic; PRO = patient-reported outcomes.
Source: BMS 2022, Statistical Analysis Plan.44
Results
Patient Disposition
At data cut-off date, June 28, 2022, the median follow-up (date of randomization to the last known date alive or death date) for all randomized patients was 15.84 months for the nivolumab arm and 15.93 months for the placebo arm. At data cut-off date February 21, 2023, the median follow-up for all randomized patients was 23.5 months for the nivolumab arm and 23.0 months for the placebo arm.13,43
A total of 790 patients were randomized 2:1 in the nivolumab and placebo arms — 526 to the nivolumab arm and 264 to the placebo arm. Of those, 788 patients were treated: 524 with nivolumab and 264 with placebo. The most common reason for discontinuation of treatment was study drug toxicity in the nivolumab arm and disease progression in the placebo arm.
Patient disposition in CHECKMATE-76K for interim RFS analysis (June 28, 2022, data cut-off) and completed treatment period patient population (February 21, 2023, data cut-off) is described in Table 15.
Table 15: Summary of Patient Disposition From Studies Included in the Systematic Review [Redacted]
Characteristic | Interim RFS analysis (June 28, 2022, data cut-off) | Completed treatment period patient population (February 21, 2023, data cut-off) | ||
|---|---|---|---|---|
Nivolumab (n = 524) | Placebo (n = 264) | Nivolumab (n = 524) | Placebo (n = 264) | |
Treated, n (%)a | ||| |||||| | ||| ||||||| | ||| |||||| | ||| ||||||| |
Not treated | ||||| | ||||| | ||||| | ||||| |
Reason for not treated | ||||| | ||||| | ||||| | |
Patient no longer meets study criteria | ||||| | ||||| | ||||| | ||||| |
Other | ||||| | ||||| | ||||| | ||||| |
Not treated due to Covid-19 | ||||| | ||||| | ||||| | ||||| |
Ongoing treatment, n (%) | || |||||| | ||||| | ||||| | ||||| |
Completed treatment, n (%) | ||| |||||| | ||| |||||| | ||| |||||| | ||| |||||| |
Discontinued from study, n (%) | ||| |||||| | || |||||| | ||| |||||| | || |||||| |
Reason for treatment discontinuation, n (%) | ||||
Study drug toxicity | || |||||| | ||||| | ||||| | ||||| |
Disease recurrence | || ||||| | ||||| | ||||| | ||||| |
Patient request to discontinue study treatment | || ||||| | ||||| | ||||| | ||||| |
Patient withdrew consent | ||||| | ||||| | ||||| | ||||| |
Adverse event unrelated to study drug | ||||| | ||||| | ||||| | ||||| |
Death | ||||| | ||||| | ||||| | ||||| |
Maximum clinical benefit | ||||| | ||||| | ||||| | ||||| |
Lost to follow-up | ||||| | ||||| | ||||| | ||||| |
Patient no longer meets study criteria | ||||| | ||||| | ||||| | ||||| |
Poor or noncompliance | ||||| | ||||| | ||||| | ||||| |
Other | ||||| | ||||| | ||||| | ||||| |
Discontinued treatment due to COVID-19, n (%)b | ||||| | ||||| | ||||| | ||||| |
Reason for discontinuation of treatment due to COVID-19, n (%) | ||||
Patient request to discontinue study treatment | ||||| | ||||| | ||||| | ||||| |
Patient withdrew consent | ||||| | ||||| | ||||| | ||||| |
Death | ||||| | ||||| | ||||| | ||||| |
Study drug toxicity | ||||| | ||||| | ||||| | ||||| |
Adverse event unrelated to study drug | ||||| | ||||| | ||||| | ||||| |
Ongoing study, n (%) | ||||| | ||||| | ||||| | ||||| |
Discontinued study, n (%) | ||||| | ||||| | ||||| | ||||| |
Reason for discontinuation of study, n (%) | ||||
Patient withdrew consent | ||||| | ||||| | ||||| | ||||| |
Death | ||||| | ||||| | ||||| | ||||| |
Lost to follow-up | ||||| | ||||| | ||||| | ||||| |
Other | ||||| | ||||| | ||||| | ||||| |
Reason for discontinuation of treatment due to COVID-19, n (%) | ||||
Death | ||||| | ||||| | ||||| | ||||| |
Patient withdrew consent | ||||| | ||||| | ||||| | ||||| |
Note: Percentages based on patients entering period. Data before the open-label first dose date is being reported. For patients receiving open-label nivolumab, the treatment period for the original arm is considered to have stopped.
aTwo patients were found to be ineligible after randomization and, therefore, were not treated. One patient was found to have suspected autoimmune disease (sarcoidosis) and the other was found to have elevated hepatic enzymes.
bThese discontinuations are part of overall reasons for the treatment discontinuations noted previously, but were also assigned a secondary reason of having a relationship to COVID-19.
Source: BMS 2022, Primary Clinical Study Report;13 BMS 2023, Primary Clinical Study Report, Addendum 01.43
Baseline Characteristics
Overall, the enrolled patient population was generally representative of a stage II melanoma population, with a median age of 62 years and more males (61.2%) than females (38.8%). The majority of patients had stage IIB melanoma (60.1%) (AJCC, 8th edition). The mean time from local wide excision surgery to randomization was 10.3 weeks. Although patients 12 years or older were eligible for enrolment, no adolescents were randomized. Generally, baseline demographic and disease characteristics were well-balanced between the nivolumab and placebo groups.
The baseline characteristics outlined in Table 16 are limited to those that are most relevant to this review or were felt to affect the outcomes or interpretation of the study results.
Table 16: Baseline Characteristics From Studies Included in the Systematic Review [Redacted]
Characteristic | CHECKMATE-76K | ||
|---|---|---|---|
Nivolumab (n = 526) | Placebo (n = 264) | Total (N = 790) | |
Median age (range), years | |||| |||||| | |||| |||||| | |||| |||||| |
Mean age (SD), years | |||| |||||| | |||| |||||| | |||| |||||| |
Age group, years, n (%) | |||
< 65 | ||| |||||| | ||| |||||| | ||| |||||| |
≥ 65 | ||| |||||| | ||| |||||| | ||| |||||| |
< 18 | |||| |||||| | |||| |||||| | |||| |||||| |
≥ 18 and < 65 | |||| |||||| | |||| |||||| | |||| |||||| |
≥ 65 and < 75 | |||| |||||| | |||| |||||| | |||| |||||| |
≥ 75 and < 85 | |||| |||||| | |||| |||||| | |||| |||||| |
≥ 85 | |||| |||||| | |||| |||||| | |||| |||||| |
Male sex, n (%) | |||| |||||| | |||| |||||| | |||| |||||| |
Female sex, n (%) | |||| |||||| | |||| |||||| | |||| |||||| |
Race, n (%) | |||
White | ||| |||||| | ||| |||||| | ||| |||||| |
Black or African American | |||| |||||| | |||| |||||| | |||| |||||| |
Asian | |||| |||||| | |||| |||||| | |||| |||||| |
Other | |||| |||||| | |||| |||||| | |||| |||||| |
Not reported | |||| |||||| | |||| |||||| | |||| |||||| |
Ethnicity, n (%) | |||
Hispanic or Latino | |||| |||||| | |||| |||||| | |||| |||||| |
Not Hispanic or Latino | |||| |||||| | |||| |||||| | |||| |||||| |
Not reported | |||| |||||| | |||| |||||| | |||| |||||| |
Country by geographic region, n (%) | |||
US and Canada | |||| |||||| | |||| |||||| | |||| |||||| |
Canada | |||| |||||| | |||| |||||| | |||| |||||| |
US | |||| |||||| | |||| |||||| | |||| |||||| |
Western Europe | |||| |||||| | |||| |||||| | |||| |||||| |
Eastern Europe | |||| |||||| | |||| |||||| | |||| |||||| |
Australia | |||| |||||| | |||| |||||| | |||| |||||| |
Melanoma subtype, n (%) | |||
Superficial spreading | |||| |||||| | |||| |||||| | |||| |||||| |
Nodular | |||| |||||| | |||| |||||| | |||| |||||| |
Lentigo malignaa | |||| |||||| | |||| |||||| | |||| |||||| |
Acral lentiginous | |||| |||||| | |||| |||||| | |||| |||||| |
Desmoplastic | |||| |||||| | |||| |||||| | |||| |||||| |
Other | |||| |||||| | |||| |||||| | |||| |||||| |
Not reported | |||| |||||| | |||| |||||| | |||| |||||| |
Disease stage at study entry (per CRF), n (%) | |||
IIB | |||| |||||| | |||| |||||| | |||| |||||| |
IIC | |||| |||||| | |||| |||||| | |||| |||||| |
Other | |||| |||||| | |||| |||||| | |||| |||||| |
Unknown | |||| |||||| | |||| |||||| | |||| |||||| |
T stage at study entry (per CRF), n (%) | |||
Stage II patients | ||| ||||||| | ||| ||||||| | ||| ||||||| |
T3B | ||| |||||| | ||| |||||| | ||| |||||| |
T4A | ||| |||||| | || |||||| | ||| |||||| |
T4B | ||| |||||| | ||| |||||| | ||| |||||| |
Baseline ECOG PS, n (%) | |||
0 | ||| |||||| | ||| |||||| | ||| |||||| |
1 | || ||||| | || ||||| | || ||||| |
Baseline LDH I, n (%) | |||
≤ ULN | |||| |||||| | |||| |||||| | |||| |||||| |
> ULN | |||| |||||| | |||| |||||| | |||| |||||| |
Not reported | |||| |||||| | |||| |||||| | |||| |||||| |
Baseline LDH II, n (%) | |||
≤ 2 × ULN | |||| |||||| | |||| |||||| | |||| |||||| |
> 2 × ULN | |||| |||||| | |||| |||||| | |||| |||||| |
Not reported | |||| |||||| | |||| |||||| | |||| |||||| |
Weight | |||| |||||| | |||| |||||| | |||| |||||| |
Mean, kg (SD) | |||| |||||| | |||| |||||| | |||| |||||| |
Median, kg (range) | |||| |||||| | |||| |||||| | |||| |||||| |
Time from wide local excision surgery to randomization, weeks (%) | ||||||| | ||||||| | ||||||| |
Mean (SD) | ||||| |||||| | ||||| |||||| | ||||| |||||| |
Median (range) | |||| |||||| | |||| |||||| | |||| |||||| |
< 3 | |||| |||||| | |||| |||||| | |||| |||||| |
3 to < 6 | |||| |||||| | |||| |||||| | |||| |||||| |
6 to < 9 | |||| |||||| | |||| |||||| | |||| |||||| |
9 to < 12 | |||| |||||| | |||| |||||| | |||| |||||| |
12 to < 15 | |||| |||||| | |||| |||||| | |||| |||||| |
15 to < 18 | |||| |||||| | |||| |||||| | |||| |||||| |
18 to < 21 | |||| |||||| | |||| |||||| | |||| |||||| |
≥ 21 | |||| |||||| | |||| |||||| | |||| |||||| |
Not reported | |||| |||||| | |||| |||||| | |||| |||||| |
Time from sentinel lymphadenectomy surgery to randomization, weeks (%) | |||| |||||| | |||| |||||| | |||| |||||| |
Mean (SD) | |||| |||||| | |||| |||||| | |||| |||||| |
Median (range) | |||| |||||| | |||| |||||| | |||| |||||| |
< 3 | |||| |||||| | |||| |||||| | |||| |||||| |
3 to < 6 | |||| |||||| | |||| |||||| | |||| |||||| |
6 to < 9 | |||| |||||| | |||| |||||| | |||| |||||| |
9 to < 12 | |||| |||||| | |||| |||||| | |||| |||||| |
12 to < 15 | |||| |||||| | |||| |||||| | |||| |||||| |
15 to < 18 | |||| |||||| | |||| |||||| | |||| |||||| |
18 to < 21 | |||| |||||| | |||| |||||| | |||| |||||| |
≥ 21 | |||| |||||| | |||| |||||| | |||| |||||| |
Not reported | |||| |||||| | |||| |||||| | |||| |||||| |
CRF = case report form; ECOG = Eastern Cooperative Oncology Group; LDH = lactate dehydrogenase; PS = performance status; SD = standard deviation; ULN = upper limit of normal.
aRefers to lentigo malignant melanoma, a primary invasive melanoma.
Source: BMS 2022, Primary Clinical Study Report.13
Exposure to Study Treatments
At both data cut-off dates (June 28, 2022, and February 21, 2023), the majority of patients had received 90% or more of the planned nivolumab dose intensity (89.7% and 90.1% respectively). In the blinded phase, 97.5% of all treated patients in the nivolumab arm received the first dose of treatment within 0 to 3 days of randomization.13,43 The median duration of therapy was 11.04 months and 11.07 months for the June 28, 2022, data cut-off and 11.07 and 11.20 months for the February 21, 2023, data cut-off, in the nivolumab and placebo arms, respectively.
There was no meaningful difference observed in the number of doses received between the nivolumab and placebo groups at the data cut-off dates (June 28, 2022, and February 21, 2023): at the June 28, 2022, data cut-off, the mean number of doses received in the nivolumab and placebo group were 12.0 and 13.0 respectively and at the February 21, 2023, data cut-off, the mean number of doses received in the nivolumab and placebo group were 13.0 in both groups.13,43
Patient exposure in CHECKMATE-76K, described as cumulative and relative dose intensity is provided in Table 17 for interim RFS analysis (June 28, 2022, data cut-off) and completed treatment period patient population (February 21, 2023, data cut-off).13,43
Table 17: Summary of Patient Exposure From Studies Included in the Systematic Review [Redacted]
Exposure | Interim RFS analysis (Jun 28, 2022, data cut-off) | Completed treatment period patient population (February 21, 2023, data cut-off) | ||
|---|---|---|---|---|
Nivolumab (n = 524) | Placebo (n = 264) | Nivolumab (n = 524) | Placebo (n = 264) | |
Number of doses received, mean (SD) | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| |
Number of doses received, median (range) | |||| || || ||| | |||| || || ||| | |||| || || ||| | |||| || || ||| |
Cumulative dose (mg), mean (SD) | |||||| ||||||||| | ||| | |||||| ||||||||| | ||| |
Cumulative dose (mg), median (range) | |||||| |||||||||| | ||| | |||||| ||||||||||| | ||| |
Relative dose intensity, n (%) | ||||
≥ 110% | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| |
90% to < 110% | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| |
70% to < 90% | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| |
50% to < 70% | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| |
< 50% | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| |
NA = not available; SD = standard deviation.
Sources: BMS 2022, Primary Clinical Study Report;13 BMS 2023, Primary Clinical Study Report, Addendum 01.43
Table 18: Summary of Subsequent Treatment From Studies Included in the Systematic Review [Redacted]
Exposure | CHECKMATE-76K | |
|---|---|---|
Nivolumab (n = 526) | Placebo (n = 264) | |
Patients with any subsequent therapy, n (%)a | |||| |||||| | |||| |||||| |
Patients who received subsequent radiotherapy, n (%) | |||| |||||| | |||| |||||| |
Curative | |||| |||||| | |||| |||||| |
Palliative | |||| |||||| | |||| |||||| |
Other | |||| |||||| | |||| |||||| |
Patients who received subsequent surgery, n (%) | |||| |||||| | |||| |||||| |
Tumour resection curative | |||| |||||| | |||| |||||| |
Tumour resection palliative | |||| |||||| | |||| |||||| |
Other | |||| |||||| | |||| |||||| |
Patients who received subsequent systemic therapy, n (%)b | |||| |||||| | |||| |||||| |
Anti-CTLA4 | |||| |||||| | |||| |||||| |
Ipilimumab | |||| |||||| | |||| |||||| |
Anti-PD-1 or Anti-PD-L1 | |||| |||||| | |||| |||||| |
Nivolumabb | |||| |||||| | |||| |||||| |
Pembrolizumab | |||| |||||| | |||| |||||| |
Retifanlimab | |||| |||||| | |||| |||||| |
Combination therapy Anti-CTLA4 + Anti-PD-1, or Anti-CTLA4 + Anti-PD-L1 | |||| |||||| | |||| |||||| |
Ipilimumab; Nivolumab | |||| |||||| | |||| |||||| |
Combination therapy BRAF MEK NRAS inhibitor | |||| |||||| | |||| |||||| |
Binimetinib; Encorafenib | |||| |||||| | |||| |||||| |
Dabrafenib; Trametinib | |||| |||||| | |||| |||||| |
Combination therapy Anti-PD1 and Anti-LAG3 | |||| |||||| | |||| |||||| |
Nivolumab; Relatlimab | |||| |||||| | |||| |||||| |
Investigational antineoplastic | |||| |||||| | |||| |||||| |
Investigational drug | |||| |||||| | |||| |||||| |
Investigational antineoplastic drugs | |||| |||||| | |||| |||||| |
Investigational antineoplastic drugs | |||| |||||| | |||| |||||| |
Nemvaleukin Alfa | |||| |||||| | |||| |||||| |
NL 101 | |||| |||||| | |||| |||||| |
MEK NRAS inhibitor | |||| |||||| | |||| |||||| |
Trametinib | |||| |||||| | |||| |||||| |
Other systemic anticancer drugs | |||| |||||| | |||| |||||| |
Imatinib mesylate | |||| |||||| | |||| |||||| |
Other systemic anticancer chemotherapy | |||| |||||| | |||| |||||| |
Cyclophosphamide | |||| |||||| | |||| |||||| |
Dacarbazine | |||| |||||| | |||| |||||| |
Dacarbazine citrate | |||| |||||| | |||| |||||| |
Fotemustine | |||| |||||| | |||| |||||| |
Paclitaxel | |||| |||||| | |||| |||||| |
Platinum compounds | |||| |||||| | |||| |||||| |
Carboplatin; Paclitaxel | |||| |||||| | |||| |||||| |
Cisplatin; Etopside | |||| |||||| | |||| |||||| |
VEGFR Targeted therapy | |||| |||||| | |||| |||||| |
Cabozantinib S-Malate | |||| |||||| | |||| |||||| |
Patients who received next-line open-label nivolumab treatment | |||| |||||| | |||| |||||| |
VEGFR = Vascular endothelial growth factor receptor.
aPatient may have received more than one type of subsequent therapy. Subsequent therapy was defined as therapy started on or after first dosing date (randomization date if patient never treated).
bOpen-label treatment (nivolumab monotherapy) is considered a subsequent therapy in this summary.
Source: BMS 2023, Primary Clinical Study Report, Addendum 01.43
Efficacy
Recurrence-Free Survival
At the data cut-off date of June 28, 2022, the median follow-up for all randomized patients was 15.84 months for the nivolumab arm and 15.93 months for the placebo group. At the data cut-off date of February 21, 2023, the median follow-up for all randomized patients was 23.5 months for the nivolumab group and 23.0 months for the placebo group.
At IA1 (data cut-off of June 28, 2022), a median RFS had not been reached in either group, for a HR of 0.42 (95% CI, 0.30 to 0.59), P < 0.0001 (Table 19). At the most recent data cut-off date of February 21, 2023, 186 RFS events had occurred (complete information fraction), and the median RFS had not been reached in the nivolumab group and was 36.14 months (95% CI, 24.77 to NA) in the placebo group, for a HR of 0.53 (95% CI, 0.40 to 0.71).
At a data cut-off date of June 28, 2022, the RFS rate was 89.0% (95% CI, 85.6 to 91.6) and 79.4% (95% CI, 73.5 to 84.1) in nivolumab and placebo, respectively. At the February 21, 2023, data cut-off, the RFS rate was largely unchanged from IA1, 88.8% (95% CI, 85.6 to 91.2) and 81.1% (95% CI, 75.7 to 86.4) at 12 months, for nivolumab and placebo. At 24 months, which was only reported at IA2, the RFS rates were 76.5% (95% CI, |||| || ||||) and 60.6% (95% CI, |||| || ||||) in the nivolumab and placebo groups, respectively.
Detailed subgroup data are provided in Figure 6 in Appendix 1. In a prespecified subgroup analysis for all randomized patients, RFS HRs for all subgroups were greater than 1 (Figure 6). Although the HR was not significant for the 65 or older and younger than 75 years, 75 or older and younger than 85 years at the data cut-off of February 21 2023, the overall direction of effect is consistent with the intention-to-treat (ITT) and the 95% CI includes the ITT unstratified HR of 0.43 and 0.54 at the 2 data cut-off dates.13,43 RFS by T stage was reported for T3b (HR = 0.45; 95% CI, 0.26 to 0.77), T4a (HR = 0.49; 95% CI, 0.26 to 0.92) and T4b (HR = 0.59; 95% CI, 0.39 to 0.89).
Figure 3: KM Analysis of RFS Results From CHECKMATE-76K
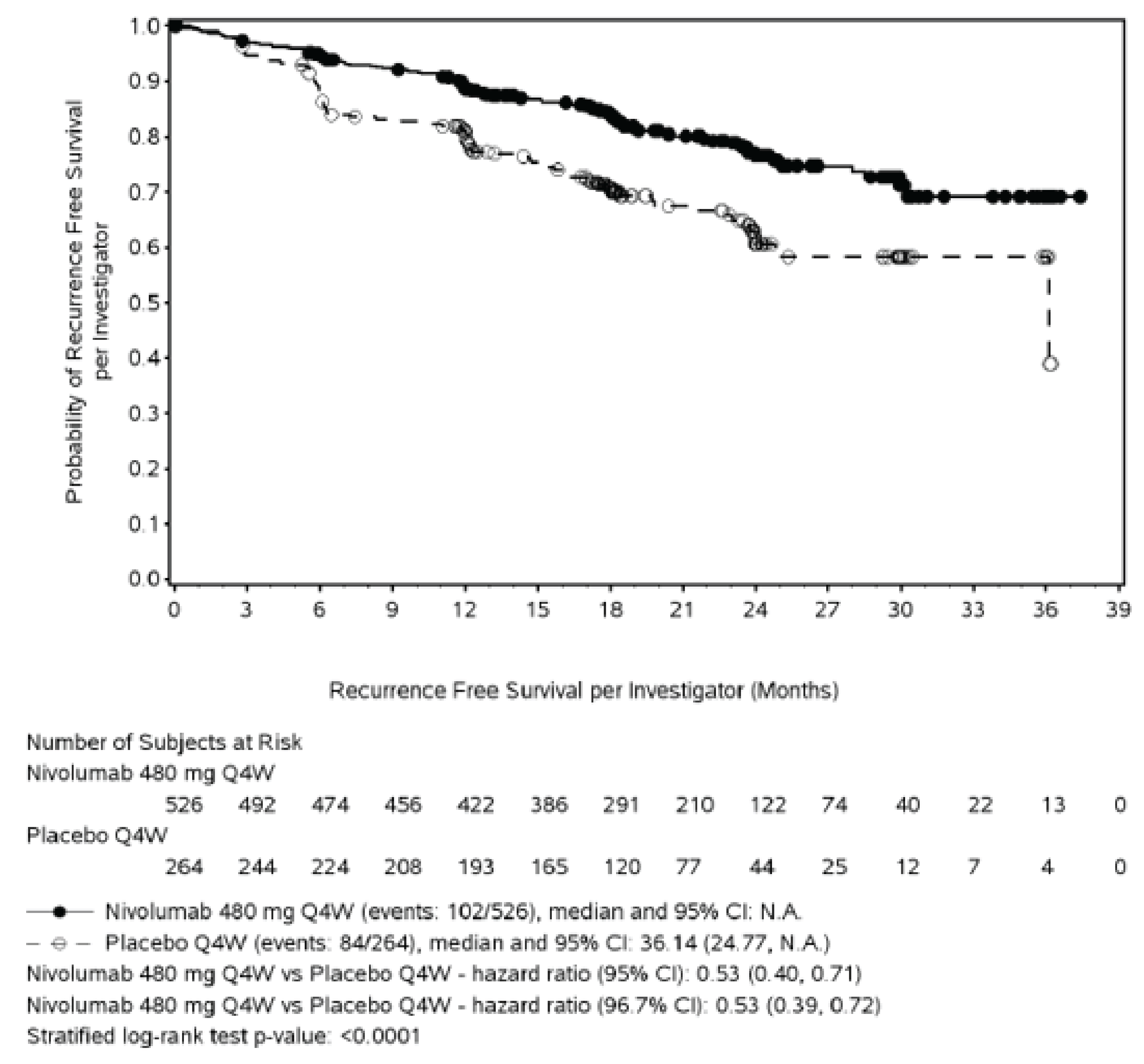
Source: Summary of Clinical Efficacy provided by sponsor.
Overall Survival
At the time of the February 21, 2023, data cut-off, the prespecified number of events for the OS interim analysis had not been reached.
Distant Metastases-Free Survival
At IA1, with a data cut-off of June 28, 2022, a median DMFS had not been reached in either group, with 8.0% of patients in the nivolumab group having experienced an event, and 15.5% of patients experiencing an event in the placebo group, for a HR of 0.47 (95% CI, 0.30 to 0.72). The DMFS rate at 12 months was 92.3% (95% CI, 89.3 to 94.5) in the nivolumab group and 86.7% (95% CI, 81.4 to 90.5) in the placebo group. At the most recent data cut-off, February 21, 2023, a median DMFS was still not reached in the nivolumab group, and was 36.14 months (95% CI, 32.85, NA) in the placebo group, with 13.1% of patients in the nivolumab group and 19.3% of patients in the placebo group experiencing an event, for a HR of 0.62 (95% CI, 0.43 to 0.89). The DMFS rate at 12 months was 92.0% (95% CI, 89.3 to 94.1) with nivolumab and 88.5% (95% CI, 83.9 to 91.9) with placebo and at 24 months was 84.0% (95% CI, |||| || ||||) with nivolumab and was 76.5% (95% CI, |||| || ||||) with placebo (Table 19).
Progression-Free Survival Through Next-line Therapy
Relatively few PFS2 events (n = 71) had occurred at the data cut-off of February 21, 2023. In all randomized patients, 40 (7.6%) PFS2 events had occurred in the nivolumab arm and 31 (11.7%) events had occurred in the placebo arm. PFS2 results are descriptive. Median PFS2 was not reached in either treatment arm at the time of analysis (data cut-off February 2023) (Table 19).
Health-Related Quality of Life
HRQoL was an exploratory outcome in CHECKMATE-76K and was assessed using the EORTC QLQ-C30 and EQ-5D-5L instruments. None of the within-group changes from baseline over time in the study exceeded the MID for the instrument. See Appendix 1 Figure 9, Figure 10, Figure 11, Figure 12, and Figure 13 for further details regarding HRQoL results.
Table 19: Summary of Key Efficacy Results From Studies Included in the Systematic Review
Characteristic | Nivolumab (n = 526) | Placebo (n = 264) |
|---|---|---|
RFS per investigator (primary end point) data cut-off June 28, 2022 | ||
Events, n/N (%) | 66/526 (12.5) | 69/264 (26.1) |
Median RFSc (95% CI), months | NA (28.52 to NA) | NA (21.62 to NA) |
HRa (95% CI) | 0.42 (0.30 to 0.59) | |
log-rank P valueb | < 0.0001 | |
Rate at 12 months,c % (95% CI) | 89.0 (85.6 to 91.6) | 79.4 (73.5 to 84.1) |
RFS per investigator (primary end point) data cut-off February 21, 2023 | ||
Events, n/N (%) | 102/526 (19.4) | 84/264 (31.8) |
Median RFSc (95% CI), months | NA (NA) | 36.14 (24.77 to NA) |
HRa (95% CI) | 0.53 (0.40 to 0.71) | |
log-rank P valueb | < 0.0001 | |
Rate at 12 months,c % (95% CI) | 88.8 (85.6 to 91.2) | 81.1 (75.7 to 86.4) |
Rate at 24 months,c % (95% CI) | 76.5 (|||| || ||||) | 60.6 (|||| || ||||) |
Rate at 36 months,c % (95% CI) | |||| ||||| || ||||| | |||| ||||| || ||||| |
DMFS per investigator (secondary end point) data cut-off June 28, 2022 | ||
Events/number of patients, n/N (%) | 42/526 (8.0) | 41/264 (15.5) |
Median DMFSc (95% CI), months | NA (28.52 to NA) | NA |
HRa (95% CI) | 0.47 (0.30 to 0.72) | |
Rate at 12 months,b % (95% CI) | 92.3 (89.3 to 94.5) | 86.7 (81.4 to 90.5) |
DMFS per investigator (secondary end point) data cut-off February 21, 2023 | ||
Events/number of patients, n/N (%) | 69/526 (13.1) | 51/264 (19.3) |
Median DMFSc (95% CI), months | NA (NA) | 36.14 (32.85 to NA) |
HRa (95% CI) | 0.62 (0.43 to 0.89) | |
Rate at 12 months,b % (95% CI) | 92.0 (89.3 to 94.1) | 88.5 (83.9 to 91.9) |
Rate at 24 months,b % (95% CI) | 84.0 (|||| || ||||) | 76.5 (|||| || ||||) |
Rate at 36 months,b % (95% CI) | |||| ||||| || ||||| | |||| ||||| || ||||| |
PFS2 per investigator (secondary end point) data cut-off June 28, 2022 | ||
Events/number of patients, n (%) | 23/526 (4.4) | 17/264 (6.4) |
Medianc PFS2 (95% CI), months | NA | NA |
HRa (95% CI) | 0.68 (0.36 to 1.27) | |
PFS2 per investigator (secondary end point) data cut-off February 21, 2023 | ||
Events/number of patients, n (%) | 40/526 (7.6) | 31/264 (11.7) |
Medianc PFS2 (95% CI), months | NA | NA |
HRa (95% CI) | 0.63 (0.40 to 1.01) | |
CI = confidence interval; DMFS = distant metastasis-free survival; HR = hazard ratio; NA = not available (i.e., not reached), median or limit of CI not estimable; PFS2 = progression-free survival through next-line therapy; RFS = recurrence-free survival.
Note: Data cut-off: June 28, 2022; Minimum follow-up: nivolumab arm 7.8 months, placebo arm 8.7 months. Median follow-up: nivolumab arm 15.8 months, placebo arm 15.9 months. Data cut-off: February 21, 2023; Minimum follow-up: nivolumab arm 7.8 months, placebo arm 8.7 months. Median follow-up: nivolumab arm 23.5 months, placebo arm 23.0 months.
aHR is nivolumab over placebo from Cox proportional hazard model stratified by AJCC T stage at study entry (T3b vs T4a vs T4b) as entered into the interactive response technology (IRT).
b2-sided log-rank test stratified by the same factor as used in the Cox proportional hazard model. Boundary for statistical significance P value < 0.033.
cBased on Kaplan-Meier estimates.
Sources: BMS 2022, Primary Clinical Study Report;13 BMS 2023, Primary Clinical Study Report, Addendum 01.43
Harms
Refer to Table 20 for harms data.
Adverse Events
There were 96% of patients in the nivolumab group and 88% of patients in the placebo group who reported an AE, with 23% and 12% of patients, respectively, reporting a grade 3 or 4 AE. The most common AE, nivolumab versus placebo, were ||||||| |||| |||||| ||||| |||||||| |||| |||||| |||| ||| |||||||| |||| |||||| ||||. Hypothyroidism was reported in 12% of nivolumab patients and no patients in the placebo group.
Serious Adverse Events
There were ||| of patients in the nivolumab group and ||| of patients in the placebo group who reported a SAE. ||||| |||| || |||||||| |||| |||| |||||||| || || || |||| || ||||||||.
Withdrawals Due to Adverse Events
There were 18% of patients in the nivolumab group and 4% of patients in the placebo group who discontinued due to an AE, and 7% versus 1% who withdrew due to a grade 3 or 4 AE, respectively. Results for discontinuations due to drug-related AE were generally similar/identical to those for all-cause discontinuations due to AE for the most common AE, such as arthralgia and diarrhea.
Notable Harms
Notable harms where there were differences between the nivolumab and placebo groups included diarrhea/colitis (5.0% versus 0.8%), hepatitis (4.2% versus 0.4%), rash (8.6% versus 1.5%), hypothyroidism or thyroiditis (13.0% versus 0.4%), and hyperthyroidism (7.6% versus 1.1%).
Table 20: Summary of Harms Results From Studies Included in the Systematic Review
AEs | Nivolumab (n = 524) | Placebo (n = 264) | ||
|---|---|---|---|---|
Adverse event of any grade | Grade 3 or 4 adverse event | Any grade adverse event | Grade 3 or 4 adverse event | |
Total all-causality AEs, n (%) | ||| |||||| | ||| |||||| | ||| |||||| | || |||||| |
Most common (≥ 10%) AEs, n (%) | ||||
Fatigue | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| |
Diarrhea | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| |
Pruritus | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| |
Arthralgia | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| |
Nausea | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| |
Rash | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| |
Hypothyroidism | 63 (12.0) | 0 | 0 | 0 |
Asthenia | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| |
Headache | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| |
Blood creatine phosphokinase increased | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| |
All-causality select AEs, n (%) | ||||
Endocrine | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| |
Gastrointestinal | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| |
Hepatic | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| |
Pulmonary | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| |
Renal | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| |
Skin | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| |
Hypersensitivity/Infusion Reactions | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| |
Deaths, n (%) | ||||
Patients who died | 21 (4.0) | 16 (6.1) | ||
Primary Reason for Death | ||||
Disease | |||| |||||| | |||| |||||| | ||
Study drug toxicitya | |||| |||||| | |||| |||||| | ||
Unknown | |||| |||||| | |||| |||||| | ||
Otherb | |||| |||||| | |||| |||||| | ||
All-causality SAEs, n (%) | 76 (14.5) | 57 (10.9) | 29 (11.0) | 20 (7.6) |
Most common SAEs in any treatment arm, n (%) | ||||
COVID-19 | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| |
ALT increased | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| |
AST increased | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| |
Melanoma recurrent | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| |
Breast carcinoma | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| |
All-causality AEs leading to discontinuation, n (%) | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| |
Musculoskeletal and connective tissue | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| |
Arthralgia | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| |
Gastrointestinal disorders | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| |
Diarrhea | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| |
Colitis | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| |
Investigations | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| |
ALT increased | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| |
AST increased | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| |
Skin and subcutaneous tissue disorders | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| |
Rash | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| |
AESIs, n (%) | ||||
All-cause IMAEs within 100 days of last dose Treated with immune modulation medication | ||||
Diarrhea/Colitis | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| |
Arthritis | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| |
Hepatitis | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| |
Pneumonitis | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| |
Nephritis or renal dysfunction | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| |
Rash | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| |
Hypersensitivity/infusion reactions | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| |
All-cause Endocrine IMAEs within 100 days of last dose With or without immune modulation medication | ||||
Adrenal insufficiency | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| |
Hypophysitis | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| |
Hypothyroidism/thyroiditis | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| |
Hyperthyroidism | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| |
Diabetes mellitus | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| |
Total all-cause OESIs within 100 days of last dose (> 1.5%) — with or without immune-modulating medication Data cut-off June 28,2022 | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| |
Myositis | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| |
Pancreatitis | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| |
Rhabdomyolysis | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| |
AEs = adverse events; AESIs = adverse events of special interest; ALT = alanine aminotransferase; IMAE = immune-mediated adverse event; OESI = other event of special interest; SAEs = serious adverse events.
aThe causes of death per investigator was heart failure and acute kidney failure.
bThe causes of death due to “other” reasons were as follows: in the nivolumab arm: COVID-19 lung infection, diverticulitis, circulatory failure, suicide, pulmonary embolism, HSV-1 encephalitis, potential allergic reaction during TEP scanner, acute cardiac ischemic event not related to therapy, stroke, and brain hemorrhage from dementia and fall with no evidence of melanoma at the time of death (1 patient each); in the placebo arm: multiorgan failure, sudden death, and COVID-19 infection (1 patient each).
Sources: BMS 2022, Primary Clinical Study Report,13 Primary Clinical Study Report, Addendum 01.43
Critical Appraisal
Internal Validity
CHECKMATE-76K appears to have been a well-conducted trial, with steps taken to maintain allocation concealment throughout the randomization process, and facilitate blinding through use of a matching-administration placebo infusion. The study also met its primary objective. There was a notable difference in diarrhea between nivolumab and placebo groups, and given that this is a known side effect of nivolumab, there is a risk that this may have resulted in unblinding for those patients experiencing those events. Unblinding is more likely to impact patient-reported outcomes, such as HRQoL, and there was limited emphasis on these outcomes in CHECKMATE-76K. Therefore, if unblinding did occur, it is less likely to bias results for key outcomes such as RFS and DMFS.
There was a large percentage of patients who withdrew from treatment in CHECKMATE-76K and a large difference in treatment discontinuations between nivolumab and placebo groups (39% versus 25% at the June 28, 2022, data cut-off). |||||| |||| ||||| of discontinuations in the nivolumab group were due to ||||| |||||||||, while the most common reason for withdrawal in the placebo group was |||||||| ||||||||||| |||||||. The high withdrawal rate may compromise stratification achieved during randomization, so, for example, if there are now imbalances between groups in important prognostic factors, then this may bias results. The differential rate of withdrawals may bias assessment of efficacy, as patients who stop treatment may be counted as treatment failures, regardless of the reason they discontinue. On the other hand, if these early treatment discontinuations are not accounted for at all, we do not know whether the treatment benefit seen for RFS, for example, is due to the drug. In any event, informative censoring is an issue in CHECKMATE-76K that may have biased results in either direction, and this is important to consider when drawing conclusions about results for outcomes such as RFS. The difference in withdrawals may also have impacted interpretation of harms, as patients in the nivolumab group may have had less exposure to study drug, and therefore this may have biased results in favour of finding fewer harms with nivolumab.
RFS was the primary outcome of CHECKMATE-76K. Although there was a multiple testing procedure in place, it focused only on RFS and OS, and, as noted in the next section, CHECKMATE-76K did not have sufficient duration of follow-up to assess OS, and it may not be feasible to assess OS at all in this population. The clinical experts consulted by CADTH on this review did not believe that other outcomes, like PFS2 and HRQoL, are important for making decisions about the clinical utility of this drug; therefore, the relatively limited multiple testing procedure in CHECKMATE-76K may not be an important limitation of this review. RFS was identified as the most important efficacy outcome by the clinical experts consulted by CADTH on this review; however, the precise nature of the impact of RFS on subsequent OS is uncertain.
External Validity
The clinical experts consulted by CADTH on this review believed that the patients enrolled in CHECKMATE-76K were generally representative of the patients who would be expected to use nivolumab in Canada. The clinical experts did note that excluding patients who have autoimmune disease seemed too conservative, as these patients are now often being treated with immunotherapy in practice.
The primary outcome of CHECKMATE-76K was RFS, and this is an appropriate outcome to prioritize according to the clinical experts consulted by CADTH on this review. The clinical experts were of the opinion, however, that RFS is optimally assessed at a later time point, more like 3 to 5 years, than the median follow-up of less than 16 months used for the primary analysis. The clinical experts noted that the treatment effect for survival analysis seemed to change with time, growing from 12 to 24 months and then possibly shrinking thereafter, further emphasizing the importance of longer follow-up for RFS.
Although OS was identified as a secondary outcome in CHECKMATE-76K, the follow-up was not of sufficient duration to assess this outcome. The clinical experts believed that OS would need to be assessed a minimum of 5 years post-treatment, and likely much longer than that to adequately assess OS.
There is no direct comparison of nivolumab to an active comparator, most notably pembrolizumab, for this indication. Pembrolizumab is the natural comparator for nivolumab, as both drugs act by the same mechanism of action, and pembrolizumab is a publicly funded first-line systemic therapy in this space. Although the approval of pembrolizumab for the indication under review predated that of nivolumab, it is unlikely that it predated it enough to reasonably expect a trial to have been designed and implemented with nivolumab as the comparator. In their comments on the clinical review, the sponsor confirmed that at the time CHECKMATE-76K was planned, observation was the standard of care.
GRADE Summary of Findings and Certainty of the Evidence
Methods for Assessing the Certainty of the Evidence
For pivotal studies and RCTs identified in the sponsor’s systematic review, GRADE was used to assess the certainty of the evidence for outcomes considered most relevant to inform CADTH’s expert committee deliberations, and a final certainty rating was determined as outlined by the GRADE Working Group:52,53
High certainty: We are very confident that the true effect lies close to that of the estimate of the effect.
Moderate certainty: We are moderately confident in the effect estimate — The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. We use the word “likely” for evidence of moderate certainty (e.g., “X intervention likely results in Y outcome”).
Low certainty: Our confidence in the effect estimate is limited — The true effect may be substantially different from the estimate of the effect. We use the word “may” for evidence of low certainty (e.g., “X intervention may result in Y outcome”).
Very low certainty: We have very little confidence in the effect estimate — The true effect is likely to be substantially different from the estimate of effect. We describe evidence of very low certainty as “very uncertain.”
For RCTs: Following the GRADE approach, evidence from RCTs started as high-certainty evidence and could be rated down for concerns related to study limitations (which refers to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias.
When possible, certainty was rated in the context of the presence of an important (nontrivial) treatment effect; if this was not possible, certainty was rated in the context of the presence of any treatment effect (i.e., the clinical importance is unclear). In all cases, the target of the certainty of evidence assessment was based on the point estimate and where it was located relative to the threshold for a clinically important effect (when a threshold was available) or to the null.
Results of GRADE Assessments
Table 2 presents the GRADE summary of findings for nivolumab versus placebo.
Long-Term Extension Studies
Contents within this section have been informed by materials submitted by the sponsor. The following have been summarized and validated by the CADTH review team.
No long-term extension studies were submitted for nivolumab adjuvant therapy in the proposed indication.
Indirect Evidence
Contents within this section have been informed by materials submitted by the sponsor. The following have been summarized and validated by the CADTH review team.
Objectives for the Summary of Indirect Evidence
The objective of this section is to summarize and critically appraise the methods and findings of the sponsor-submitted review of the literature and NMA comparing nivolumab and pembrolizumab for patients aged 12 years or older with resected stage IIB and IIC melanoma.
Description of Indirect Evidence
The sponsor conducted a systematic literature review in November 2022 to identify evidence for inclusion in the NMA (Table 21). A feasibility assessment was conducted to gauge the appropriateness of proceeding with an NMA given the nature of the available evidence. Two trials were included in the systematic literature review and were subsequently considered sufficiently similar and were included in the NMA. The same 2 trials were also used in a Bucher method indirect comparison to analyze harms. CHECKMATE-76K included 790 randomized patients and KEYNOTE-716 included 976 randomized patients. Both trials were double-blind, placebo controlled, and included an international, multicentre population.
Encorafenib in combination with binimetinib was included as a comparator in the systematic literature review; however, no trials on encorafenib in combination with binimetinib for resected stage IIB and IIC met inclusion criteria, and therefore none were included in the NMA.
Information from this section comes from 3 sources: the sponsor’s main NMA report, which focused on efficacy,54 the sponsor’s brief analysis of harms using the Bucher method,55 and the sponsor’s Summary of Clinical Evidence.
Table 21: Study Selection Criteria and Methods for Indirect Comparisons
Characteristics | Indirect comparison |
|---|---|
Population | Patients aged 12 years and older with non-metastatic resected stage IIB or IIC cutaneous melanomaa |
Intervention | Eligible interventions include adjuvant treatment (given after surgery) with one of the following:
|
Comparator | Eligible comparators include the following:
|
Outcome | Studies must report recurrence-free survival The following safety and tolerability outcomes are of interest:b
|
Study designs | Randomized controlled trials |
Publication characteristics |
|
Exclusion criteria |
|
Databases searched | Relevant studies were identified by searching (search date: November 22, 2022) the following databases from inception through the Ovid platform:
Hand searches for relevant materials from the following scientific conferences were conducted from 2011 to 2022:
A manual search of the US National Institutes of Health Clinical Trial Registry was conducted |
Selection process | Study selection followed a 2-stage screening process based on the review of titles and abstracts (stage I) and then full-text articles (stage II) by 2 independent investigators. Any disagreements were resolved by discussion between investigators, including a third, more senior researcher, if needed. |
Data extraction process | Data from the included studies were extracted into a standardized table template in Microsoft Excel. Data were captured by a single investigator and independently validated by a second investigator. Any discrepancies were resolved by discussion between investigators, including a third, more senior researcher, if needed. In cases where multiple publications on the same trial were included, the most comprehensive publication (e.g., reporting detailed methods and results for all/most outcomes of interest in the target population(s)) was designated as the “principal” publication, and remaining publications were designated as “related”. The related publications reported either additional or duplicative data. Relevant additional data were extracted from the related publications. Conflicting data were considered on a case-by-case basis. Generally, values from more recently published full-text articles were prioritized. |
Quality assessment | Two independent researchers assessed study quality. Following reconciliation between the 2 researchers, a third researcher was included to reach consensus for any remaining discrepancies. The Cochrane Collaboration’s Risk of Bias tool was used to assess risk of bias in included clinical trial. |
aStudies were required to present data on patients with stage IIB or IIC.
bStudies were not screened for these outcomes (i.e., if a study only presented a safety/tolerability outcome, it was not included in the systematic literature review).
Source: Sponsor’s Summary of Clinical Evidence.
Network Meta-Analysis
Objectives
Upon completion of the systematic literature review of trials in stage IIB or IIC melanoma, the evidence was synthesized by means of a Bayesian NMA. The NMA evaluated the relative efficacy of nivolumab versus pembrolizumab. The outcomes analyzed in the network included 3 outcomes: recurrence-free survival (RFS), treatment-related adverse events (≥ grade 3), and treatment-related adverse events of any grade.
Study Selection Methods
The sponsor searched MEDLINE, Embase and the Cochrane Register of Controlled Trials for relevant literature, using a search date of November 22, 2022. Manual searches were performed of material from annual meetings of relevant oncology associations. Relevant studies were identified by 2 independent reviewers. Data were extracted by 1 reviewer and verified by a second reviewer.
NMA Analysis Methods
Feasibility Assessment
A feasibility assessment was conducted to gauge the appropriateness of proceeding with an NMA. The feasibility assessment process included: A) a determination of whether the RCT evidence for the interventions of interest formed 1 connected network for the overall population and each outcome of interest, and an assessment of the distribution of trial characteristics across the network; B) an assessment of the distribution of treatments; C) an exploration of the distribution of baseline patient characteristics both within and between comparisons to identify factors that may bias indirect estimates (i.e., identify effect modifiers); and D) an assessment of outcome definitions and reporting. The sponsor stated that they attempted to align their approach with the International Society for Pharmacoeconomics and Outcomes Research (ISPOR), National Institute for Health and Care Excellence (NICE), and Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines. Potentially important treatment-effect modifiers were identified based on subgroup results of studies included in the evidence base, and included: age, race, baseline ECOG PS, AJCC stage, and BRAF mutation status.
NMA Methods
The methods used by the sponsor are summarized in Table 22. All analyses were performed in a Bayesian framework and involved a model with parameters, data and a likelihood distribution, and prior distributions. Analyses of RFS were conducted assuming both a constant hazard ratio over time and allowing for time-varying hazard ratios. Testing of the proportional hazards assumption was conducted for RFS using Schoenfeld residual plots, hazards over time, and log-cumulative hazard plots, according to the guidelines provided in NICE TSD 14. Schoenfeld residual plots were visually inspected for evidence of whether the proportional hazards assumption was valid (parallel with horizontal axis) or not (not parallel with horizontal axis). The Grambsch-Therneau test was conducted to provide a statistical measure of violation or validation of the proportional hazards assumption for the Schoenfeld residuals, with a statistically significant P value (< 0.05) suggesting violation. The hazards over time plot and log-cumulative hazard plots were visually inspected to provide evidence for whether the proportional hazards assumption was valid (were parallel between treatment arms) or violated (not parallel or crossing between treatment arms). Collectively, these tests were used to assess if the proportional hazards assumption was valid or not. Proportional hazards testing was conducted for both CHECKMATE 76K and KEYNOTE-716.
Table 22: Indirect Comparison Analysis Methods
Methods | Description | |
|---|---|---|
Analysis methods | Analyses were performed in a Bayesian framework for the constant HR. Standard parametric models were employed for the time-varying HR (parametric NMA). A frequentist approach was used for safety outcomes. Whenever possible, fixed and random-effects models were considered. However, only fixed effects models were employed given that there was insufficient evidence available to estimate the between-study heterogeneity required to run the random-effects models. The insufficiency was due to the availability of only a single trial for each treatment comparison in the evidence networks. All analyses were performed using R version 4.2.1 and JAGS version 4.3.1. | |
Time-to-event outcomes | The proportional hazard assumption regarding time-to-event outcomes for each individual trial was assessed using the Grambsch and Therneau test plots of hazards over time and log-cumulative hazard plots. Pseudo IPD was extracted from digitized Kaplan-Meir curves using DigitizeIt and an algorithm described by Jansen and Cope. Standard and flexible parametric functions were fit to each treatment arm individually using the flexsurv package in R (version 2.2.2). Constant HR NMA (used for RFS constant HR analysis): Fixed-effect NMA of the constant HRs using the generalized linear model framework described by Dias et al., with a contrast-based normal likelihood for the log HRand identity link. Time-varying HR NMA (used for RFS time-varying HR analysis): Fixed-effect NMA using the generalized gamma (fixed Q) parametric model. Data are presented up until the maximum follow-up of the included trials. Results are also presented as survival at landmark time points (12, 36, 60, and 120 months). | |
Safety outcomes | NMAs were based on the frequentist approach using the Bucher method. For binary safety end points, Odds Ratios (ORs) and their corresponding log scale standard errors were used as inputs, and the indirect comparisons were analyzed on the natural log scale. | |
Priors | Normal non-informative prior distributions (0,1002) were used for the relative treatment effect parameters. | |
NMA model selection | Time-to-event outcomes | Constant HR NMA: No model comparison was required (only fixed effects NMA models were applied since there was insufficient evidence available to estimate the between-study heterogeneity required to run random-effects models). Time-varying HR NMA: Parametric distributions tested included exponential, Weibull, Gompertz, log-logistic, log normal, gamma, and generalized gamma. Models were assessed for goodness of fit based on the Akaike information criterion (AIC). Bayesian information criterion (BIC) values were used to confirm goodness of fit by AIC. |
Safety outcomes | Standard Bucher frequentist approach was used without the need to select models. No model selection necessary. | |
Assessment of model fit | Constant HR NMA: Model fit was assessed by comparing the total residual deviance to the number of data points contributing to the model. In a well-fitting model, the number of data points and total residual deviance will be similar. Time-varying HR NMA: In the initial step, goodness of fit at the arm-level for each model was evaluated based on the AIC and visual inspection of the smoothed hazards and survival curves in the short-term (maximum follow-up for each trial) and long-term to assess plausibility. At the network-level, assessment for each distribution was driven by the full network of evidence, based on the plausibility of underlying assumptions, plausibility of model fits with priority given to key trials in the network, and goodness of fit across trials | |
Assessment of heterogeneity | The presence of clinical and methodological heterogeneity was assessed through a feasibility assessment, in which the population, interventions/comparators, outcome, and study characteristics were compared. The feasibility assessment process aligned with ISPOR, NICE, and PRISMA guidelines. | |
Assessment of consistency | Not performed due to a lack of closed loops in the network. | |
Assessment of convergence | Convergence of Bayesian models was assessed through visual inspection of trace, autocorrelation, Gelman-Rubin statistic, and posterior density plots. | |
Outcomes | Time-to-event outcomes | RFS |
Binary outcomes | Treatment-related grade ≥ 3 AE Treatment-related any-grade AE | |
Follow-up time points | Constant HR NMA: The HR with the shortest follow-up was used as reported in primary publications where possible. In cases where no HR was reported but the trial reported KM curves, HRs were derived using the Guyot algorithm. Time-varying HR NMA: The time-specific HRs are presented for all times between 0 and 82 months in graphical format, as well as in tabular format at 3-month intervals for the first year (12 months) and 6-month intervals thereafter, up until 54 months. The maximum value of 54 months reflects the maximum follow-up of CHECKMATE-76K in the most recent data cut-off. Results are also presented at landmark time points including 60 and 120 months. | |
Sensitivity analyses | Within CHECKMATE-76K, RFS is defined as comprising distant recurrences, local recurrences, regional node recurrences, malignant melanoma in situ, and new primary invasive melanoma. Malignant melanoma in situ or new primary invasive melanoma is not included in the KEYNOTE-716 definition of RFS. To align definitions of recurrence between these 2 trials, an alternative definition of RFS was explored for CHECKMATE-76K omitting malignant melanoma in situ and new primary invasive melanoma. | |
Subgroup analysis | None | |
AE = adverse event; HR = hazard ration; IPD = individual participant data; ISPOR = International Society for Pharmacoeconomics and Outcomes Research; NMA = network meta-analysis; NICE = National Institute for Health and Care Excellence; PRISMA = Preferred Reporting Items for Systematic Reviews and Meta-Analysis; RFS = recurrence-free survival.
Source: Sponsor’s Summary of Clinical Evidence.
Results of NMA
Summary of Included Studies
CHECKMATE-76K and KEYNOTE-716 were the 2 trials included in the evidence base for which placebo was the common comparator. The network diagram is presented in Figure 4.
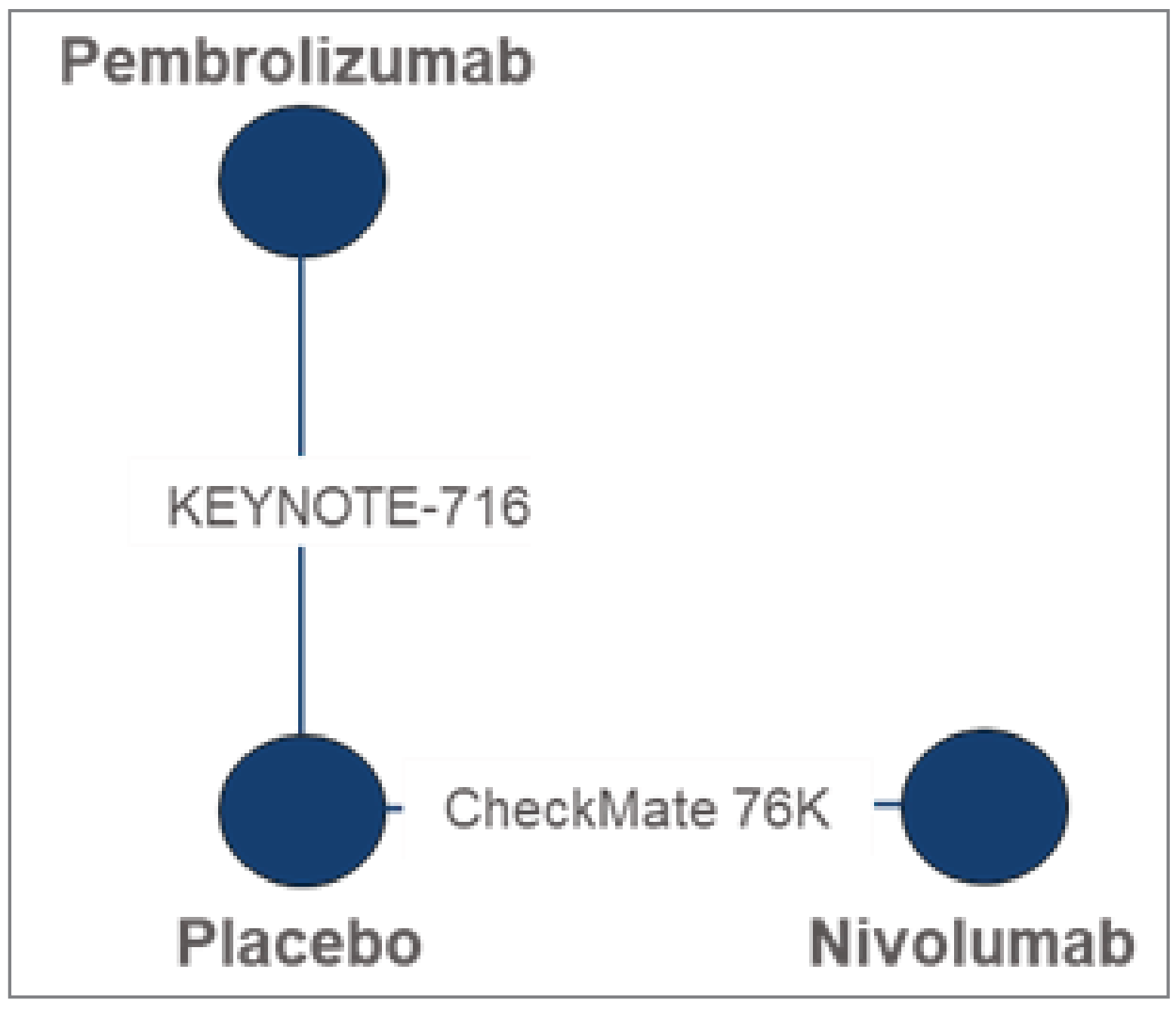
Table 23: Summary of Key Baseline and Trial Characteristics of CHECKMATE-76K and KEYNOTE-716
Trial name (NCT) | Treatment Arm | Sample size | At baseline | Follow-up duration (months), median | Treatment duration (months) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
Age (years), median (IQR) | Male, n (%) | White, n (%) | ECOG PS, n (%) | Disease stage, n (%) | |||||||
0 | 1 | IIB | IIC | ||||||||
CHECKMATE-76K (NCT04099251) | NIVO | 526 | 62 (51 to 71) | 322 (61.2) | 515 (97.9) | 495 (94.1) | 31 (5.9) | 316 (60.1) | 210 (39.9) | 15.84 | 11.04 |
Placebo | 264 | 61 (51 to 69) | 161 (61) | 262 (99.2) | 245 (92.8) | 19 (7.2) | 163 (61.7)a | 101 (38.3) | 15.93 | 11.07 | |
KEYNOTE-716 (NCT03553836) | PEM | 487 | 60 (51 to 68) | 300 (62) | 435 (89) | 454 (93) | 32 (7) | 309 (63) | 171 (35) | 20.9 | 11.1 |
Placebo | 489 | 61 (53 to 69) | 289 (59) | 439 (90) | 452 (92) | 35 (7) | 316 (65) | 169 (35) | 20.9 | 11.1 | |
ECOG PS = Eastern Cooperative Oncology Group; IQR = interquartile range; NIVO = nivolumab; PEM = pembrolizumab; PS = performance status.
aStage IIB includes a patient incorrectly categorized as stage IIB instead of stage IIC.
Source: Sponsor’s Summary of Clinical Evidence.
Table 24: Assessment of Homogeneity
Characteristics | Description and handling of potential effect modifiers |
|---|---|
Age, sex, race, ECOG PS | The median age of patients enrolled in CHECKMATE-76K was 62 years in the NIVO arm and 61 years in the placebo arm; the median age of patients enrolled in KEYNOTE-716 was 60 years in the PEM arm and 61 in the placebo arm. The proportion of male patients was 61.2% among patients receiving NIVO and 61% among patients receiving placebo in CHECKMATE-76K, and 62% among patients receiving PEM and 59% among patients receiving placebo in KEYNOTE-716. The proportion of Caucasian patients was slightly higher in CHECKMATE-76K, with 97.9% and 99.2% of Caucasian patients in the NIVO and placebo arms compared to 89% and 90% of Caucasian patients in the PEM and placebo arms in KEYNOTE-716. Both trials reported high proportions of patients, with an ECOG PS of 0: 94.1% in the NIVO arm and 92.8% in the placebo arm in CHECKMATE-76K, and 93% in the PEM arm and 92% in the placebo arm in KEYNOTE-716. The proportion of patients with an ECOG PS of 1 was 5.9% in the NIVO arm and 7.2% in the placebo arm in CHECKMATE-76K and 7% in the PEM and placebo arms in KEYNOTE-716. Due to sufficient similarity in median age, race, sex distribution, and distribution of ECOG PS across the 2 trials, it was assumed that differences in these patient characteristics do not act as a treatment effect modifiers. |
AJCC cancer stage | Both trials had a higher proportion of patients with stage IIB melanoma than IIC. Proportions of stage IIB patients were: 60.1% in the NIVO arm and 61.6% of patients in the placebo arm in CHECKMATE-76K compared to 63% in the PEM arm and 65% in the placebo arm in KEYNOTE-716. CHECKMATE-76K had a slightly higher proportion of stage IIC patients, with 39.9% in the NIVO arm and 38.3% in the placebo arm compared to 35% of stage IIC patients in the PEM and placebo arms in KEYNOTE-716. It was assumed that differences in AJCC stage does not act as a treatment effect modifier. |
Dosing | CHECKMATE-76K evaluated NIVO 480 mg dose for adult patients and a 6 mg/kg dose for pediatric patients once every 4 weeks for 12 months. KEYNOTE-716 evaluated a PEM 200 mg dose for adults and a 2mg/kg dose for pediatric patients once every 3 weeks for 17 cycles. Therefore, patients in CHECKMATE-76K received 12 doses of NIVO compared to 17 doses of PEM in KEYNOTE-716. Median treatment duration was 11.04 months for NIVO and 11.1 months for PEM. Placebo was administered for a median of 11.07 months in CHECKMATE-76K and 11.1 months in KEYNOTE-716. It was assumed that the difference in administration frequency does not act as a treatment effect modifier. |
Treatment history | Prior adjuvant treatment with interferon (for melanoma other than study entry melanoma) was permitted in CHECKMATE-76K only (not KEYNOTE-716) if it was completed 6 or more months before randomization. It was assumed that this difference in treatment history does not act as a treatment effect modifier. |
Definition of end point | Within CHECKMATE-76K, RFS is defined as comprising distant recurrences, local recurrences, regional node recurrences, malignant melanoma in situ, and new primary invasive melanoma. Malignant melanoma in situ or new primary invasive melanoma is not included in the KEYNOTE-716 definition of RFS. To align definitions of recurrence between these 2 trials, an alternative definition of RFS was explored for CHECKMATE-76K, omitting malignant melanoma in situ and new primary invasive melanoma. |
AJCC = American Joint Committee on Cancer; mutation-positive; ECOG = Eastern Cooperative Oncology Group; NIVO = nivolumab; NMA = network meta-analysis; PEM = pembrolizumab; PS = performance status; RCT = randomized controlled trial; RFS = regression-free survival; SLR = systematic literature review.
Source: Sponsor’s Summary of Clinical Evidence.
Summary of Outcomes
Efficacy
One efficacy outcome, RFS, was included in these analyses. No analyses were conducted to estimate comparative efficacy with respect to OS between nivolumab and pembrolizumab given lack of reporting on this outcome. Analyses of RFS were conducted assuming constant HRs and also allowing for time-varying HRs. The assessment of proportional hazards demonstrated evidence of violation of the proportional hazards assumption and, therefore, the time-varying models are reported as the base case and the results of the constant HR analysis were briefly summarized.
For CHECKMATE-76K, data informing analyses were based on an updated analysis from April 2023 with a minimum follow-up of 15.6 months and a median follow-up of 23.0 months in both treatment arms (23.5 for nivolumab and 23.1 for placebo).54 For KEYNOTE-716, data informing analyses were based on the fourth interim analysis from January 4, 2023 with a median follow-up of 39.4 months in both treatment arms.
RFS Recurrence
The generalized gamma (fixed Q) was assessed to be the best fitting model for the time-varying HR NMA based on the AIC and observed fit (lowest total Akaike information criterion across studies). The sponsor included additional models that are not reported here. Results of the time-varying NMA of RFS supported the pivotal study results that nivolumab RFS was superior to placebo but did not provide evidence to support differences with pembrolizumab at all time points (Table 25). Results beyond 30 months are considered less reliable because they include extrapolations of existing data.
Table 25: Results of the Fixed-Effect Generalized Gamma Model NMA for RFS, Presented as Hours Over Time for Nivolumab vs. Comparators [Redacted]
NIVO vs. | Time-varying HR (95% CrI) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
3 months | 6 months | 9 months | 12 months | 18 months | 24 months | 30 months | 36 months | 42 months | 48 months | 54 months | |
Placebo | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| |
PEM | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| |
CrI = credible interval; HR = hazard ratio; NIVO = nivolumab; PEM = pembrolizumab; vs. = versus.
Note: Cells shaded in dark grey indicate estimates based on model extrapolations. All bolded values are statistically significant at the 0.05 significance level.
Source: Sponsor’s Summary of Clinical Evidence.
Figure 5: Network Meta-Analysis Using Standard Parametric Models Results for Recurrence-Free Survival as Reported in the Trial; Estimated Survival Over Time, Generalized Gamma Model
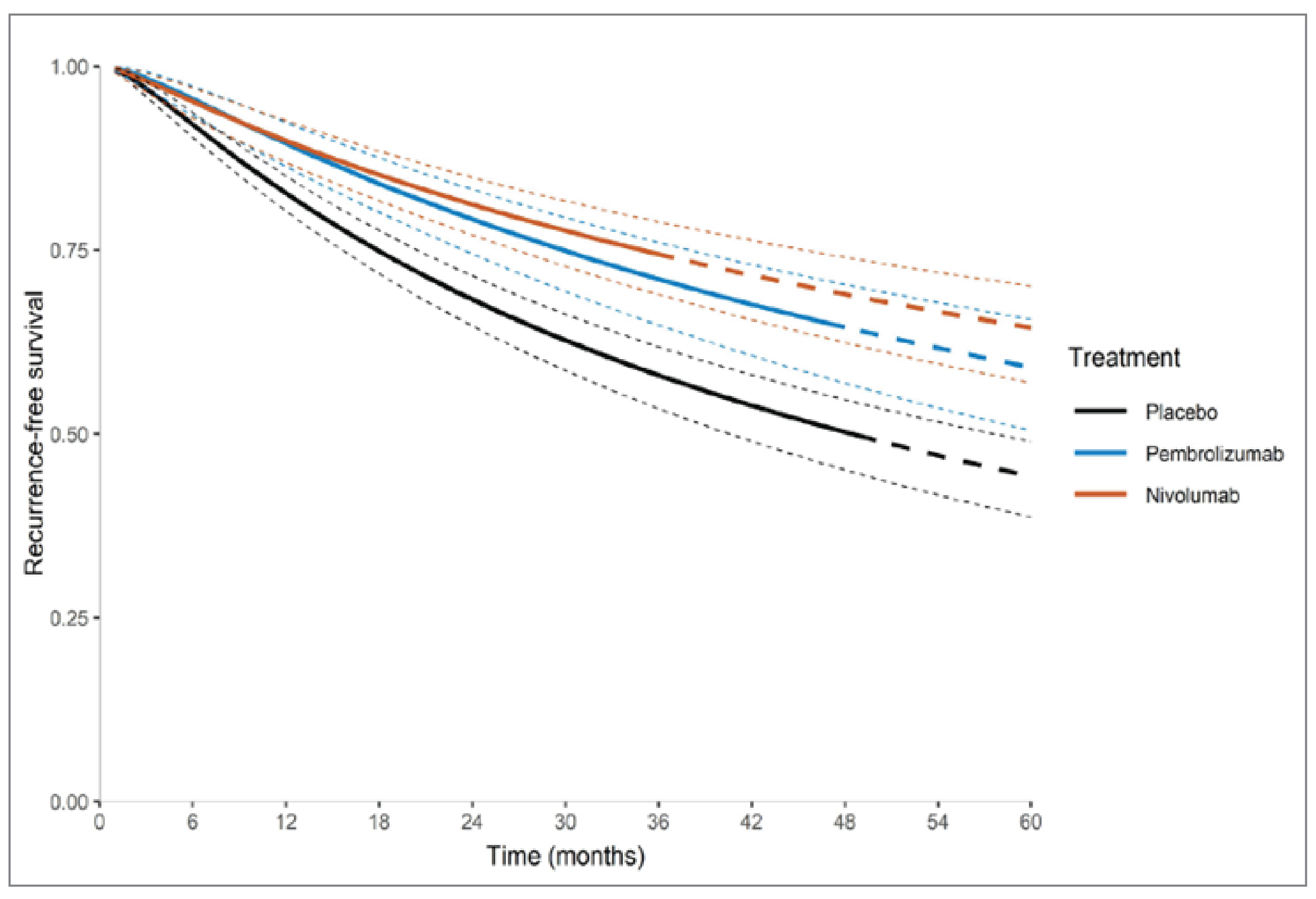
Source: Sponsor’s Full Network Meta-Analysis Report.
Table 26: Network Meta-Analysis Results Using Standard Parametric Models for Recurrence-Free Survival as Reported in The Trial; Survival at Landmark Times, Generalized Gamma Model [Redacted]
Treatment | Survival proportion at 12 months (95% CI) | Survival proportion at 36 months (95% CI) | Survival proportion at 60 months (95% CI) | Survival proportion at 120 months (95% CI) |
|---|---|---|---|---|
Placebo | |||| |||||||||||| | |||| ||||||||||| | |||| ||||||||||| | |||| ||||||||||| |
Pembrolizumab | |||| ||||||||||| | |||| ||||||||||| | |||| ||||||||||| | ||||| ||||||||||| |
Nivolumab | |||| ||||||||||| | |||| ||||||||||| | |||| ||||||||||| | |||| ||||||||||| |
Source: Sponsor’s full network meta-analysis report.
RFS Scenario Analysis
As described in Table 26, the definition used for RFS was not consistent between CHECKMATE-76K and KEYNOTE-716. Therefore, a scenario analysis was conducted using the definition of RFS as reported in KEYNOTE-716 (i.e., not including malignant melanoma in situ or new primary invasive melanoma). Consistent with the main RFS analysis, the generalized gamma (fixed Q) model was assessed to be the best fitting model for the time-varying HR NMA based on the AIC and observed fit. Using the KEYNOTE-716 RFS definition, a total of 89 and 76 recurrence events were reported for nivolumab and placebo, respectively.
Results of the time-varying NMA of RFS using the KEYNOTE-716 RFS definition indicated that at all time points, treatment with nivolumab had comparable RFS to pembrolizumab (the null effect was not excluded from credible intervals [CrIs] for any time point comparing nivolumab to pembrolizumab; Table 27).
Results assuming constant HRs were consistent with the time-varying analyses; nivolumab was associated with comparable RFS compared to pembrolizumab (HR = |||| ; 95% CrI, |||||| ||||). This hazard ratio was similar to the hazard ratio results when the original definitions of RFS were used (HR = |||| ; 95% CrI, |||||| ||||).
Table 27: Results of the Fixed-Effect Generalized Gamma Model NMA For RFS as Defined In KEYNOTE-716; Presented as Hours Over Time for Nivolumab vs. Comparators [Redacted]
NIVO vs. | Time-varying HR (95% CrI) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
3 months | 6 months | 9 months | 12 months | 18 months | 24 months | 30 months | 36 months | 42 months | 48 months | 54 months | |
Placebo | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| |
PEM | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| |
CrI = credible interval; HR = hazard ratio; NIVO = nivolumab; PEM = pembrolizumab; vs. = versus.
Note: Cells shaded in dark grey indicate estimates based on model extrapolations. All bolded values are statistically significant at the 0.05 significance level.
Source: Sponsor’s Summary of Clinical Evidence.
Harms
The results of the Bucher ITC for treatment-related AEs are presented in Table 28. There were no significant differences in the odds of treatment-related grade 3 or higher AE incidence ||| |||| ||| |||| |||||| |||||| or treatment-related any-grade AE incidence ||||| |||||| |||||| between nivolumab and pembrolizumab.
Table 28: Treatment-Related Adverse Events — Summary Data and Indirect Comparison [Redacted]
Trial | AE definition | Intervention n/N (%) | Placebo n/N (%) | OR (95% CI) |
|---|---|---|---|---|
CHECKMATE-76K | Treatment-related grade ≥ 3 AE | |||| |||||| | |||| |||||| | |||| |||||| |
KEYNOTE-716 | Treatment-related grade ≥ 3 AE | |||| |||||| | |||| |||||| | |||| |||||| |
CHECKMATE-76K | Treatment-related any-grade AE | |||| |||||| | |||| |||||| | |||| |||||| |
KEYNOTE-716 | Treatment-related any-grade AE | |||| |||||| | |||| |||||| | |||| |||||| |
Indirect comparisons: NIVO vs PEMBRO: OR (95% CI) | ||||
Treatment-related grade ≥ 3 AE | |||| |||||| ||||| | |||
Treatment-related any-grade AE | |||| |||||| ||||| | |||
AE = adverse event; CI = confidence interval; NIVO = nivolumab; OR = odds ratio; PEM = pembrolizumab.
Source: Sponsor’s Summary of Clinical Evidence.
Critical Appraisal of the NMA
The sponsor conducted an NMA using a Bayesian approach with fixed effects models for the primary efficacy analyses. These were reasonable methods to apply for this NMA, given the common placebo comparator and sparse network of studies. The NMA was informed by a systematic review of relevant databases. For the harms outcomes, a frequentist approach was applied using the Bucher method. Study selection was based on appropriate criteria and 2 reviewers were involved with the study selection and data extraction. Quality assessment of the included studies was performed but it was not clear if the results of this were incorporated into the ITC analyses.
The main limitation of the NMA is that it contained a very small amount of data from 2 studies. Follow up time was also limited to 23 months and 39 months in the CHECKMATE-76K and KEYNOTE-716 studies, respectively. Results at later time points would therefore be less reliable and subject to extrapolation. The shorter follow-up for the CHECKMATE-76K trial, compared the KEYNOTE-716 follow-up will likely have led to overestimation of the hazards ratio and this would impact on the time points after approximately 18 months. In addition, the use of time-varying effect would have increased uncertainty in the comparisons based on extrapolated data. Non–time-varying effects are not reliable in this analysis because they would be influenced by later time frames. Efficacy assessment was limited to a single outcome (RFS) and it would have been informative to include other efficacy outcomes. A strength of the comparisons made within the NMA and the Bucher analyses was that the studies were similar in design and population characteristics. Due to similarity in median age, race sex distribution, and distribution of ECOG PS across the 2 trials, the sponsor assumed that differences in these patient characteristics do not act as a treatment effect modifiers. Although BRAF mutation status was not reported across either trial, it is assumed that it does not act as a treatment effect modifier based on evidence for immunotherapies in adjuvant treatment of metastatic melanoma. The clinical experts consulted by CADTH agreed with this approach.
The following differences were observed between the 2 trials:
CHECKMATE-76K had a slightly higher proportion of stage IIC patients than KEYNOTE-716.
Median treatment durations were similar between 2 trials, however, cycle lengths differed, resulting in patients in CHECKMATE-76K receiving more doses of NIVO compared to PEM doses in KEYNOTE-716.
Despite these differences, the sponsor assumed that AJCC stage, administration frequency, treatment history were not effect modifiers. The clinical experts consulted by CADTH for this review believed that these were reasonable assumptions.
To align definitions of recurrence between these 2 trials, an alternative definition of RFS was explored for CHECKMATE-76K, omitting malignant melanoma in situ and new primary invasive melanoma. The results of this sensitivity analysis were consistent with the base case analysis.
There were no significant differences observed between nivolumab and pembrolizumab for RFS.
There were no significant differences observed between nivolumab and pembrolizumab for treatment-related adverse events (any grade, grade ≥ 3). The sponsor stated that all-cause adverse events were an outcome of interest, but no analyses of this outcome was provided. This would have been informative given the trends observed in the treatment-related adverse event analyses (Table 28).
Neither the NMA nor the Bucher analysis provided evidence of a difference in efficacy or harms outcomes for nivolumab compared to pembrolizumab in patients with non-metastatic resected stage IIB or IIC cutaneous melanoma.
Studies Addressing Gaps in the Systematic Review Evidence
Contents within this section have been informed by materials submitted by the sponsor. The following have been summarized and validated by the CADTH review team.
No important gaps were identified of nivolumab adjuvant therapy in resected stage IIB and IIC melanoma.
Discussion
Summary of Available Evidence
One pivotal, phase III, sponsor-funded DB RCT was included in this review. The primary objective of CHECKMATE-76K was to compare the efficacy, as measured by investigator-assessed RFS, provided by nivolumab monotherapy versus placebo in patients with completely resected stage IIB and IIC melanoma with no evidence of disease who are at high-risk for recurrence. The secondary objectives were to compare OS and DMFS between the 2 treatment groups, assess the safety and toxicity of nivolumab and evaluate investigator-assessed outcomes on next-line therapies. A total of 790 patients were randomly assigned in a 2:1 ratio to receive 480 mg of nivolumab (n = 526) or placebo (n = 264). The sponsor also conducted an NMA used a Bayesian approach with fixed effects models for the primary efficacy analysis and a frequentist approach was applied using the Bucher method to estimate relative harms. Both these methods were appropriate given the limited availability of data. The limitations of the NMA were that it contained very small amount of data from 2 studies and differences in follow-up time between the 2 included studies.
Overall, the enrolled patient population had a median age of 62 years and more males (61.2%) than females (38.8%). The majority of patients had stage IIB melanoma (60.1%) (AJCC, 8th edition). The mean time from local wide excision surgery to randomization was 10.3 weeks. Although patients aged 12 years or older were eligible for enrolment, no adolescents were randomized, and this is not surprising given how rare melanoma is in this age group.
Interpretation of Results
Efficacy
As of the February 2023 data cut-off, there were not enough events for the sponsor to analyze OS data. Therefore, the impact of nivolumab on mortality cannot be ascertained, and given how few events there have been thus far, this is not likely to change in the future. According to the clinical experts consulted by CADTH on this review, mortality would not be expected to be high in this population, particularly over the intermediate term. Therefore, the optimal time point to assess OS would be at a minimum of 5 years, and this length of follow-up is not available from CHECKMATE-76K. Therefore, although it seems reasonable to assume that a reduction in recurrence due to adjuvant treatment with nivolumab will ultimately lead to an improvement in OS in the long-term, there may be no way to confirm this in a controlled trial. One of the clinical experts noted that OS is a critical outcome in this indication.
The clinical experts consulted by CADTH on this review believed RFS to be a key outcome in this population, and CHECKMATE-76K met its primary objective. They noted that a between-group difference in RFS of 10% at 1 year would be considered clinically significant, and they would expect a clinically important effect to increase with time, to 15% at 2 years and perhaps even greater at 3 years, for example. Although the sponsor did not provide between-group differences for any time points, the percentage of patients who had not had an RFS event at 12 months was 88.8% (95% CI, 85.6 to 91.2) in the nivolumab group and 81.1% (95% CI, 75.7 to 86.4) in the placebo group, suggesting that the between-group difference at this time point may not be clinically significant. The between-group difference appeared to widen at 2 years, as 76.5% (95% CI, |||| || ||||) of patients in the nivolumab group and 60.6% (95% CI, |||| || ||||) of patients in the placebo group had not had an event, suggesting that perhaps the benefits of nivolumab for RFS are delayed in appearing. On the other hand, at 3 years, the percentage of patients who had not had an event was ||||| (95% CI, |||| || ||||) with nivolumab and ||||| (95% CI, |||| || ||||) with placebo, which suggests that the treatment effect may peak at 2 years, then diminish with longer follow-up. It is important to note that this sample at the 3-year time point may only represent a small fraction of the original ITT, as many patients have not reached this time point in the trial, therefore caution must be exercised when interpreting these data. There is other evidence suggesting a potential diminished effect over time when looking at the HR for the June 2022 data cut-off (HR = 0.42; 95% CI, 0.30 to 0.59) versus the more recent February 2023 data cut-off (HR = 0.53; 95% CI, 0.40 to 0.71). The clinical experts are not aware of a diminishing effect with PD-1 inhibitors in this adjuvant setting. An important confounder to keep in mind when trying to compare RFS and DMFS results between nivolumab and placebo is the differential rate of treatment discontinuations between the 2 groups. As noted in the assessment of bias, there were considerably more patients who stopped treatment in the nivolumab group versus the placebo group, and therefore there is the potential for the treatment effect to be exaggerated due to informative censoring.
The clinical experts believed that PFS2 is not as relevant in assessing the efficacy of nivolumab in this population. The clinical experts noted that the most important opportunity to have a large impact with treatment is up front, and the PD-1 inhibitors are, at present, likely the best option for these patients. On that note, the clinical experts also mentioned that there are a number of new therapies in the pipeline that would also complicate the assessment of PFS2 in this trial, as this is a rapidly evolving therapeutic picture.
Health-related quality of life was assessed in CHECKMATE-76K, but only as an exploratory outcome, and this limits any conclusions that can be drawn from these data. In their input to CADTH on this review, patients identified a wide range of HRQoL issues, such as anxiety or fear, scarring or disfigurement and pain from the excision site, and time and money spent travelling to appointments and the need for home care. It is difficult to directly determine the impact of nivolumab on many of these concerns, however, presumably reducing the risk of recurrence may be of benefit with respect to the impact of their condition on their mental health, as well as reducing risk of pain and disfigurement from future surgical excision. Most patients indicated that they are very willing to accept the side effect profile of nivolumab if it would potentially mean that they would not have to deal with a recurrence. Both pembrolizumab and nivolumab need to be administered intravenously, and therefore both require patients to travel for administration of the drug, however, pembrolizumab dosing allows for a longer interval between doses (either every 3 or 6 weeks, depending on dose) compared to nivolumab (every 2 or 4 weeks, depending on dose). Additionally, approximately one-quarter of patients indicated that side effects they experienced from adjuvant treatment were not worth any benefit they might receive from the drug, and this is consistent with the opinions of the clinical experts consulted by CADTH on this review, who believed that patients who have stage IIB or IIC melanoma might be less inclined to tolerate adverse effects than patients with more advanced disease, due to the different prognoses between the 2.
In the sponsor’s ITC, there were no significant differences observed between nivolumab and pembrolizumab for RFS. Efficacy assessment was limited to a single outcome (RFS). Follow-up time was limited to 23 months and 39 months in the CHECKMATE-76K and KEYNOTE-716 studies, respectively. Results beyond 23 months would therefore be less reliable and subject to increasingly greater extrapolation as time points become longer. In addition, differential follow-up times would likely have exacerbated any bias in the extrapolated data.
Harms
The notable harms of most importance according to the clinical experts include diarrhea, arthritis and type 1 diabetes mellitus. The clinical experts noted that grade 3 and 4 events of diarrhea are most important, as these are the events that often leave patients essentially housebound, and may precipitate a trip to the hospital to receive IV fluids. These grade 3 and 4 diarrhea events were infrequent, but did occur in 1% of patients in the nivolumab group versus 0% in the placebo group. The product monograph for nivolumab does list diarrhea, particularly grade 3 to 4 diarrhea, under warnings and precautions, and does provide guidance as to management, including discontinuation of therapy for patients with grade 4 diarrhea. The product monograph recommends that nivolumab be held and corticosteroids initiated for patients with grade 2 or 3 diarrhea.38 Generally speaking, the clinical experts consulted by CADTH on this review were confident that the adverse effects of nivolumab are manageable, given that oncologists have more than a decade of experience using immunotherapy.
Diabetes mellitus also appears to be a class effect of PD-1 inhibitors, and is believed to be caused by immune activation that results in destruction of pancreatic beta cells.56 The clinical experts consulted by CADTH on this review identified diabetes mellitus and arthritis as important harms because both have long-term consequences. In CHECKMATE-76K there were 0.6% of patients in the nivolumab group and no patients in the placebo group who reported diabetes as an AE.
In the sponsor’s ITC, there were no significant differences observed between nivolumab and pembrolizumab for treatment-related adverse events (any grade, grade ≥ 3). The clinical experts consulted for the review stated that adverse event profiles of nivolumab and pembrolizumab would not typically be a factor for treatment selection where 1 of these 2 drugs are needed.
Conclusion
Evidence from 1 DB RCT suggests that after 1 year of adjuvant treatment with nivolumab, in patients with resected stage IIB or IIC melanoma, the primary objective was met, demonstrating an improvement in RFS over placebo. After 1 and 2 years of follow-up, this improvement may be clinically significant; however, the clinical experts considered the results after 2 years of follow-up to be more clinically relevant. It is uncertain whether this improvement in RFS persists at 3 years of follow-up or longer, as there are not yet enough patients who have been followed for this long. OS could not be assessed yet in this ongoing trial, as this would require a longer follow-up. The clinical experts believed OS to be of critical importance in this setting, and therefore it is important that investigators plan to follow patients for survival for up to 8 years. Treatment with nivolumab also appeared to improve DMFS compared to placebo, however, the clinical significance of these results was less clear than they were for RFS. There was a relatively large percentage of patients who discontinued nivolumab due to an AE, and the clinical experts noted that patients with less advanced disease may be less likely to persist with therapy through tolerability issues, compared to patients with advanced melanoma. In their input to CADTH, a majority of patients believed that the benefits of nivolumab were worth the potential adverse effects. It is uncertain whether there is an increased risk of developing longer-term adverse effects such as diabetes mellitus and arthritis, and a longer follow-up than the current median of nearly 2 years in CHECKMATE-76K would likely be needed to adequately assess the risk in this population. Neither the NMA nor the Bucher analysis provided evidence to support a difference in efficacy or harms outcomes for nivolumab compared to pembrolizumab in patients with non-metastatic resected stage IIB or IIC cutaneous melanoma; despite the limitations of the ITC, the claim of no difference between nivolumab compared to pembrolizumab is justified. Patients were clear that it is important to them to have another option aside from pembrolizumab to manage their condition.
References
1.Brenner DR, Poirier A, Woods RR, et al. Projected estimates of cancer in Canada in 2022. Can Med Assoc J. 2022;194(17):E601-E607. PubMed
2.Canadian Cancer Society. Canadian cancer statistics: a 2022 special report on cancer prevalence. Resources - supplementary online data 2022; https://cancer.ca/en/research/cancer-statistics/canadian-cancer-statistics. Accessed by sponsor, no date provided.
3.Canadian cancer statistics: a 2022 special report on cancer prevalence. Toronto (ON): Canadian Cancer Society; 2022: https://cdn.cancer.ca/-/media/files/research/cancer-statistics/2022-statistics/2022-special-report/2022_prevalence_report_final_en.pdf. Accessed by sponsor, no date provided.
4.Conte S, Ghazawi FM, Le M, et al. Population-based study detailing cutaneous melanoma incidence and mortality trends in Canada. Front Med (Lausanne). 2022;9:830254. PubMed
5.Princess Margaret Cancer Centre clinical practice guidelines (melanoma). Toronto (ON): Princess Margaret Cancer Centre; 2015: https://www.uhn.ca/PrincessMargaret/Health_Professionals/Programs_Departments/Documents/CPG_Melanoma.pdf. Accessed by sponsor, no date provided.
6.Burns D, George J, Aucoin D, et al. The pathogenesis and clinical management of cutaneous melanoma: an evidence-based review. J Med Imaging Radiat Sci. 2019;50(3):460-469.e461. PubMed
7.Gwadry-Sridhar F, McConkey H, Teng X, Ernst DS. The national melanoma research registry: a fundamental for disease characterization and epidemiology. Ann Oncol. 2018;29:viii460.
8.Keung EZ, Je G. The eighth edition American Joint Committee on Cancer (AJCC) melanoma staging system: implications for melanoma treatment and care. Expert Rev Anticancer Ther. 2018;18(8):775-784.
9.Jang S, Poretta T, Bhagnani T, Harshaw Q, Burke M, Rao S. Real-world recurrence rates and economic burden in patients with resected early-stage melanoma. Dermatol Ther (Heidelb). 2020;10(5):985-999. PubMed
10.Poklepovic AS, Luke JJ. Considering adjuvant therapy for stage II melanoma. Cancer. 2020;126(6):1166-1174. PubMed
11.Michielin O, van Akkooi A, Lorigan P, et al. ESMO consensus conference recommendations on the management of locoregional melanoma: under the auspices of the ESMO Guidelines Committee. Ann Oncol. 2020;31(11):1449-1461. PubMed
12.CADTH reimbursement recommendation - pembrolizumab (Keytruda). Can J Health Technol. 2022;2(11). 10.51731/cjht.2022.506. Accessed by sponsor, no date provided.
13.Primary clinical study report for study CA20976K: A phase 3, randomized, double-blind study of adjuvant immunotherapy with nivolumab versus placebo after complete resection of stage IIB/C melanoma [internal sponsor's report]. Uxbridge (GB): Bristol-Myers Squibb; 2023.
14.Clinical Protocol: CA20976K. A phase 3, randomized, double-blind study of adjuvant immunotherapy with nivolumab versus placebo after complete resection of stage IIB/C melanoma [internal sponsor's report]. Lawrenceville (NJ): Bristol-Myers Squibb; 2019.
15.Joshua AM. Melanoma prevention: are we doing enough? A Canadian perspective. Curr Oncol. 2012;19(6):e462-467. PubMed
16.Curti BD, Leachman S, Wj U. Chapter 72: cancer of the skin. In: Jameson J, Fauci AS, Kasper DL, Hauser SL, Longo DL, Loscalzo J, eds. Harrison's Principles of Internal Medicine. 20th ed. New York, (NY): McGraw-Hill; 2019.
17.O'Sullivan DE, Brenner DR, Villeneuve PJ, et al. Estimates of the current and future burden of melanoma attributable to ultraviolet radiation in Canada. Prev Med. 2019;122:81-90. PubMed
18.Berman-Rosa M, Logan J, Ghazawi FM, et al. Analysis of geographic and environmental factors and their association with cutaneous melanoma incidence in Canada. Dermatology. 2022;238(6):1006-1017. PubMed
19.Obrador E, Liu-Smith F, Dellinger RW, Salvador R, Meyskens FL, Estrela JM. Oxidative stress and antioxidants in the pathophysiology of malignant melanoma. Biol Chem. 2019;400(5):589-612. PubMed
20.Canadian cancer statistics 2021. Toronto (ON): Canadian Cancer Society; 2021: https://cdn.cancer.ca/-/media/files/research/cancer-statistics/2021-statistics/2021-pdf-en-final.pdf. Accessed by sponsor, no date provided.
21.Ghazawi FM, Cyr J, Darwich R, et al. Cutaneous malignant melanoma incidence and mortality trends in Canada: a comprehensive population-based study. J Am Acad Dermatol. 2019;80(2):448-459. PubMed
22.Statistics Canada. Table: 13-10-0111-01. Number and rates of new cases of primary cancer, by cancer type, age group and sex. 2023; https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310011101&pickMembers%5B0%5D=2.1&pickMembers%5B1%5D=3.1&pickMembers%5B2%5D=4.26&cubeTimeFrame.startYear=2015&cubeTimeFrame.endYear=2019&referencePeriods=20150101%2C20190101. Accessed by sponsor, no date provided.
23.Davey MG, Miller N, McInerney NM. A review of epidemiology and cancer biology of malignant melanoma. Cureus. 2021;13(5):e15087. PubMed
24.Rigo R, Doherty J, Koczka K, et al. Real world outcomes in patients with advanced melanoma treated in Alberta, Canada: a time-era based analysis. Curr Oncol. 2021;28(5):3978-3986. PubMed
25.Orlow I, Sadeghi KD, Edmiston SN, et al. InterMEL: an international biorepository and clinical database to uncover predictors of survival in early-stage melanoma. PLoS One. 2023;18(4):e0269324. PubMed
26.Canadian Cancer Society. Diagnosis of melanoma skin cancer. https://cancer.ca/en/cancer-information/cancer-types/skin-melanoma/diagnosis. Accessed 2023 Feb 22.
27.BC Cancer. Melanoma; 4. Diagnosis. 2014; http://www.bccancer.bc.ca/health-professionals/clinical-resources/cancer-management-manual/skin/melanoma#Diagnosis. Accessed by sponsor, no date provided.
28.Trotter SC, Sroa N, Winkelmann RR, Olencki T, Bechtel M. A global review of melanoma follow-up guidelines. J Clin Aesthet Dermatol. 2013;6(9):18-26. PubMed
29.A quality initiative of the Program in Evidence-Based Care (PEBC), Ontario Health (Cancer Care Ontario), Surveillance of patients with stage I, II, III, or resectable IV melanoma who were treated with curative intent. Toronto (ON): Cancer Care Ontario; 2023: https://www.cancercareontario.ca/en/file/44496/download?token=voOcEGEC. Accessed by sponsor, no date provided.
30.Sundararajan S, Thida AM, Badri T. Metastatic melanoma. StatPearls. Treasure Island (FL): StatPearls Publishing LLC; 2021.
31.Rigel DS, Russak J, Friedman R. The evolution of melanoma diagnosis: 25 years beyond the ABCDs. CA Cancer J Clin. 2010;60(5):301-316. PubMed
32.Sibley LM, Weiner JP. An evaluation of access to health care services along the rural-urban continuum in Canada. BMC Health Serv Res. 2011;11(1):20. PubMed
33.Mavor ME, Richardson H, Miao Q, Asai Y, Hanna TP. Disparities in diagnosis of advanced melanoma: a population-based cohort study. CMAJ Open. 2018;6(4):E502-E512. PubMed
34.Li HO-Y, Bailey AJ-M, Grose E, et al. Socioeconomic status and melanoma in Canada: a systematic review. J Cutan Med Surg. 2021;25(1):87-94. PubMed
35.Access to health services as a social determinant of First Nations, Inuit and Métis health. Prince George (BC): National Collaborating Centre for Indigenous Health; 2019.
36.Lee CW, McKinnon JG, Davis N. Canadian Melanoma Conference recommendations on high-risk melanoma surveillance: a report from the 14th annual Canadian Melanoma Conference; Banff, Alberta; 20-22 February 2020. Curr Oncol. 2021;28(3):2040-2051. PubMed
37.Provisional funding algorithm. Indication: melanoma. Ottawa (ON): CADTH; 2023: https://cadth.ca/sites/default/files/DRR/2023/PH0022%20Rapid%20Algorithm%20Report%20for%20Melanoma_with%20CAPCA%20Endorsement_FINAL.pdf. Accessed by sponsor, no date provided.
38.Opdivo (nivolumab): intravenous infusion, 10 mg nivolumab /mL, 40 mg and 100 mg single-use vials [DRAFT product monograph]. Montreal (QC): Bristol-Myers Squibb Canada; 2015.
39.pembrolizumab (Keytruda): solution for infusion 100 mg/4 mL vial [product monograph]. Kirkland (QC): Merck Canada; 2023.
40.Kirkwood J, Del Vecchio M, Weber J, et al. Adjuvant nivolumab in resected stage IIB/C melanoma: primary results from the randomized, phase 3 CheckMate 76K trial. Nat Med. 2023;29(11):2835-2843. PubMed
41.Long GV, Del Vecchio M, Weber J, Hoeller C, Grob JJ, Mohr P. Adjuvant therapy with nivolumab versus placebo in patients with resected stage IIB/C melanoma (CheckMate 76K). Pigment Cell Melanoma Res. 2022;35(1):1-184.
42.Bristol-Myers Squibb. Phase 3 study of nivolumab or nivolumab plus ipilimumab versus ipilimumab alone in previously untreated advanced melanoma (Checkmate 067). ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2013.
43.Addendum 01 to the primary clinical study report for study CA20976K. A phase 3, randomized, double-blind study of adjuvant immunotherapy with nivolumab versus placebo after complete resection of stage IIB/C melanoma. Supplementary figures [internal sponsor's report]. Uxbridge (GB): Bristol-Myers Squibb.
44.Statistical analysis plan for CSR: Study CA20976K. A Phase 3, randomized, double-blind study of adjuvant immunotherapy with nivolumab versus placebo after complete resection of stage IIB/C melanoma V2.0 [internal sponsor's report]. Uxbridge (GB): Bristol-Myers Squibb; 2022.
45.Gastman B, Long GV, Kirkwood JM, et al. Adjuvant therapy with nivolumab versus placebo in patients with resected stage IIB/C melanoma (Checkmate 76K). Ann Surg Oncol. 2023;30(suppl_26).
46.Long GV, Del Vecchio M, Weber J, et al. Adjuvant therapy with nivolumab versus placebo in patients with resected stage IIB/C melanoma (CheckMate 76K). SKIN The Journal of Cutaneous Medicine. 2023;7(2):s163.
47.Long GV, Kirkwood JMM, Hoeller C, et al. Association of biomarkers (BMs) with efficacy of adjuvant nivolumab (NIVO) vs placebo (PBO) in patients with resected stage IIB/C melanoma (CA209-76K). J Clin Oncol. 2023;41(suppl_16):9504-9504.
48.Herdman M, Gudex C, Lloyd A, et al. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual Life Res. 2011;20(10):1727-1736. PubMed
49.Pickard AS, Neary MP, Cella D. Estimation of minimally important differences in EQ-5D utility and VAS scores in cancer. Health Qual Life Outcomes. 2007;5:70. PubMed
50.Greenwood M. The errors of sampling of the survivorship table. Ministry of Health Reports on Public Health and Medical Subjects. 1926;33(Appendix 1).
51.Kalbfleisch JD, Prentice RL. The statistical analysis of failure time data. Hoboken (N.J): John Wiley & Sons; 2011.
52.Balshem H, Helfand M, Schünemann HJ, et al. GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol. 2011;64(4):401-406. PubMed
53.Santesso N, Glenton C, Dahm P, et al. GRADE guidelines 26: informative statements to communicate the findings of systematic reviews of interventions. J Clin Epidemiol. 2020;119:126-135. PubMed
54.Nivolumab for the adjuvant treatment of stage IIB/C melanoma: network meta-analysis report v1.0 [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Opdivo (nivolumab for injection) intravenous infusion, 10 mg /mL, 40 mg and 100 mg single-use vials. Montreal (QC): Bristol Myers Squibb Canada; 2023.
55.Systematic literature review of treatments for resected stage IIB/C cutaneous melanoma: Technical report V1.0. In: Drug Reimbursement Review sponsor submission: Opdivo (nivolumab), intravenous infusion, 10 mg nivolumab /mL; 40 mg and 100 mg single-use vials. Montreal (QC): Bristol-Myers Squibb Canada; 2023. Accessed 2023.
56.Clotman K, Janssens K, Specenier P, Weets I, De Block CEM. Programmed cell death-1 inhibitor-induced type 1 diabetes mellitus. J Clin Endocrinol Metab. 2018;103(9):3144-3154. PubMed
Appendix 1: Detailed Outcome Data
Note this appendix has not been copy-edited.
Subgroup Analyses Related to Primary Outcome (RFS)
Figure 6: Plot of Treatment Effect on RFS per Investigator in Predefined Subsets — All Randomized Patients, Data Cut-Off February 21, 2023 [Redacted]

Source: BMS 2023, Primary Clinical Study Report, Addendum 01.43
Freedom From Relapse (FFR) and Treatment-Free Interval (TFI, Exploratory End Points)
In all randomized patients at the 28-June-2022 data cut-off, FFR appeared to be longer in the nivolumab arm than in the placebo arm (Figure 7). Median FFR was not reached in either the nivolumab or placebo arms. Twelve month FFR rates were numerically higher in the nivolumab arm compared with the placebo arm: 90.4% vs 80.2%.13
Figure 7: Kaplan-Meier Plot of Freedom From Relapse In CHECKMATE-76K — All Randomized Patients, Data Cut-Off Date June 28, 2022 [Redacted]

Source: BMS 2023, Primary Clinical Study Report13
In all randomized patients, at the June 28, 2022 data cut-off, improvement in TFI was observed in the nivolumab arm compared with the placebo arm (Figure 8). Median TFI was not reached in either the nivolumab or placebo arms. 12-month TFI rates were numerically higher in the nivolumab arm compared with the placebo arm: 91.6% vs 71.1%.13
Figure 8: Kaplan-Meier Plot of Treatment-Free Interval in CHECKMATE-76K — All Randomized Patients, Data Cut-Off Date June 28, 2022 [Redacted]

Source: BMS 2023, Primary Clinical Study Report13
HRQoL (Exploratory End Point)
HRQoL results in CHECKMATE-76K are based on the June 28, 2022 data cut-off after a median follow-up of 15.8 months in the nivolumab arm and 15.9 months in the placebo arm. HRQoL analyses were not updated at the subsequent data cut-off February 21, 2023.
EORTC QLQ-C30
Questionnaire completion rates of EORTC QLQ-C30 at baseline were 97.5% (513/526) in the nivolumab arm and 97.0% (256/264) in the placebo arm. Completion rates for the nivolumab and placebo arms met or exceeded 94.4% and 91.4%, respectively, at all assessments through week 53. Completion rates for Follow-up Visits 1 and 2 for the nivolumab and placebo arms met or exceeded 79.8% and 87.4%, respectively. Available data rates for questionnaires, were slightly lower for the nivolumab arm than the placebo arm, reflecting a slightly higher dropout rate for the nivolumab patients through week 49.
At baseline, mean EORTC QLQ-C30 summary scores for all domains and all randomized patients were comparable between treatment arms with generally high functioning and quality of life and low bother from symptoms.
Quality of life through week 53, as measured by the EORTC QLQ-C30 Global Health Status subscale, was similar in both treatment arms showing a slight average deterioration from baseline but no group mean change in score reaching the MID at any time point in either treatment arm (Figure 9).
Figure 9: Mean Changes in EORTC QLQ-C30 Global Health Status/QoL Score From Baseline — All Randomized Adult Patients, Data Cut-Off June 28, 2022 [Redacted]

Source: BMS 2022, Primary Clinical Study Report.13
Quality of life through week 53 as measured by the EORTC QLQ-C30 Physical Functioning subscale is presented in Figure 10. EORTC QLQ-C30 Physical Functioning subscale remained stable in both treatment arms, with no group mean change in score from baseline reaching the MID at any time point in either treatment arm. In global health and physical functioning there were drops in both arms after treatment discontinuation, which did not surpass the MID and seemed to stabilize or improve from follow-up 1 to follow-up 2.13
Figure 10: Mean Changes in EORTC QLQ-C30 Physical Functioning Score From Baseline — All Randomized Adult Patients, Data Cut-Off June 28, 2022 [Redacted]

Source: BMS 2022, Primary Clinical Study Report.13
Quality of life through week 53 as measured by the EORTC QLQ-C30 Role Functioning subscale based on cut-off date June 28, 2022, is presented in Figure 11. The EORTC QLQ-C30 Role Functioning subscale remained stable in both treatment arms with patients in the nivolumab arm generally showing slightly lower functioning than placebo patients but with no mean change in score from baseline reaching the MID at any time point in either treatment arm.13
Figure 11: Mean Changes in EORTC QLQ-C30 Role Functioning Score From Baseline — All Randomized Adult Patients, Data Cut-Off June 28, 2022 [Redacted]

Source: BMS 2022, Primary Clinical Study Report for Study CHECKMATE-76K.13
EQ-5D-5L
Questionnaire completion rates of the EQ-5D-5L at baseline for patients were similar to the EORTC QLQ-C30 with 97.3% (512 out of 526) and 97.7% (258 out of 264) completed for the nivolumab and placebo arms, respectively. During treatment, questionnaire completion rates were 94.3% or more in the nivolumab arm and 91.4% or more in the placebo arm. As with the EORTC QLQ-C30, available data rates for questionnaires were slightly lower for the nivolumab arm than the placebo arm due to drop out.
At baseline, mean mapped EQ-5D-5L utility index and mean VAS scores for all patients were comparable between treatment arms and demonstrated good general health status. Mapped EQ-5D-5L UI and VAS scores through week 53 remained stable in both arms during treatment. There was a slight deterioration in both arms during follow-up visits, but no group mean change in score from baseline reached the MID at any time point in either treatment arm (Figure 12 and Figure 13).13
Figure 12: Mean Changes in Mapped EQ-5D-3L UI Score From Baseline — All Randomized Patients, Data Cut-Off June 28, 2022 [Redacted]

Source: BMS 2022, Primary Clinical Study Report for Study CHECKMATE-76K13
Figure 13: Mean Changes in Mapped EQ-5D-3L VAS Score From Baseline — All Randomized Patients, Data Cut-Off June 28, 2022 [Redacted]

Source: BMS 2022, Primary Clinical Study Report for Study CHECKMATE-76K13
FACIT GP5
Questionnaire completion rates for the FACIT GP5 at baseline were 83.7% (440/526) and 87.9% (232/264) for the nivolumab and placebo arms, respectively. The lower completion rates compared to the other HRQoL questionnaires is likely due to the FACIT GP5 asks about side effects on treatment and the study treatment has not yet been initiated at baseline.13 During treatment, questionnaire completion rates were 93.2% or more in the nivolumab arm and 91.4% or more in the placebo arm. As with the other PROs, available data rates for questionnaires were slightly lower for the nivolumab arm than the placebo arm due to drop out.13
In responding to FACIT GP5 (“I am bothered by side effects of treatment”), the proportion of patients who responded “Quite a Bit” or “Very Much” in the nivolumab and placebo arms were low at all postbaseline treatment visits up to week 53. In the nivolumab arm, the proportion of patients who responded “Quite a Bit” or “Very Much” was 3.1% or less and 1.0% or less, respectively, through week 53. In the placebo arm, the proportion of patients who responded “Quite a Bit” or “Very Much” was 2.5% or less and 0.6% or less, respectively, through week 53. For both treatment arms, the highest proportion of patients responding “Quite a Bit” or “Very Much” to bother by side effects of treatment came after treatment ended, during Follow-Up Visits 1 and 2, where the nivolumab arm had a combined rate of 10.8% and 8.6% at FU1 and FU2, respectively, and the placebo arm had a combined rate of 4.4% and 2.2%, respectively. Overall, few patients on nivolumab reported a lot of bother (“Quite a Bit” or “Very Much”) from side effects during treatment and the proportions were similar to placebo patients.13
Pharmacoeconomic Review
Abbreviations
AE
adverse event
BIA
budget impact analysis
ITC
indirect treatment comparison
NMA
network meta-analysis
RFS
recurrence-free survival
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Nivolumab (Opdivo), 10 mg/mL injection for IV use |
Indication | Opdivo, as monotherapy, is indicated for the adjuvant treatment of adult patients with stage IIB or IIC melanoma following complete resection. |
Health Canada approval status | NOC |
Health Canada review pathway | Standard |
NOC date | December 29, 2023 |
Reimbursement request | As per indication |
Sponsor | Bristol Myers Squibb Canada |
Submission history | Yesa Indication: Melanoma with regional lymph node involvement, in transit metastases/satellites without metastatic nodes, or distant metastases, as adjuvant therapy after complete resection. Recommendation date: March 7, 2019 Recommendation: Reimburse with clinical criteria and/or conditions Indication: For the treatment of patients with unresectable or metastatic melanoma, regardless of BRAF status. Recommendation date: April 1, 2016 Recommendation: Reimburse with clinical criteria and/or conditions |
NOC = Notice of Compliance.
aNivolumab as an individual drug has been reviewed by CADTH for multiple oncology indications; only reviews for melanoma indications have been included in this table.
Table 2: Summary of Economic Information
Component | Description |
|---|---|
Type of economic evaluation | Cost-minimization analysis |
Target population | As adjuvant treatment in patients with stage IIB or IIC resected melanoma |
Treatment | Nivolumab as adjuvant treatment to resection. |
Dose regimen | 3 mg/kg (maximum 240 mg) every 14 days or 6 mg/kg (maximum 480 mg) every 28 days.a |
Submitted price | Nivolumab, 40 mg/4 mL vial: $782.22 Nivolumab, 100 mg/10 mL vial: $1,955.56 |
Submitted treatment cost | $9,387 per patient per 28-days |
Comparator | Pembrolizumab as adjuvant treatment to resection |
Perspective | Canadian publicly funded health care payer |
Time horizon | 1 year |
Key data source | CHECKMATE-76K double-blind, randomized controlled trial comparing nivolumab to placebo One sponsor-conducted network meta-analysis comparing nivolumab to pembrolizumab |
Costs considered | Drug acquisition costs, administration costs, subsequent treatment costs, subsequent treatment administration costs Monitoring costs and adverse event costs were considered in a scenario analysis |
Submitted results | Incremental savings = $7,234 per patient |
Key limitations |
|
CADTH reanalysis results |
|
NMA = network meta-analysis.
aThe dosing in the product monograph recommends a fixed dose of 240 mg every 14 days or 480 mg every 28 days. As noted by the sponsor and CADTH-participating public drug plans, weight-based dosing is implemented in Canada.
Conclusions
The CADTH clinical review concluded that nivolumab demonstrated an improvement in recurrence-free survival (RFS) compared with placebo based on 1 year of adjuvant treatment in patients with resected stage IIB or IIC melanoma. There was no direct evidence comparing nivolumab to the primary comparator, pembrolizumab. The sponsor-submitted indirect comparison did not provide evidence to support a difference in efficacy or safety between nivolumab and pembrolizumab. Despite the limitations of the indirect treatment comparison (ITC), CADTH considered that the claim of no difference between nivolumab compared to pembrolizumab is justified.
The sponsor’s cost-minimization analysis is based on the assumption of clinical similarity between nivolumab and pembrolizumab. This is in line with the CADTH clinical review, as nivolumab is considered to have similar clinical efficacy and safety to pembrolizumab, and treatment with nivolumab is less costly than pembrolizumab at public list prices. No revisions were undertaken to the sponsor’s base case, which indicated that nivolumab was associated with a cost saving of $7,234 per patient compared with pembrolizumab. CADTH explored scenario analyses that indicated that nivolumab remained cost saving.
CADTH notes that the magnitude of cost savings associated with nivolumab, relative to pembrolizumab, is highly dependent on patient weight, with drug acquisition costs being equal when patients weigh 80 kg or less. All costs and incremental savings are based on publicly available list prices and may not reflect actual prices paid by public drug plans in Canada.
Economic Review
The current review is for nivolumab (Opdivo) for adjuvant treatment of adult patients with stage IIB or IIC melanoma following complete resection.
Economic Information
Summary of Sponsor’s Economic Information
The sponsor submitted a cost-minimization analysis for nivolumab compared with pembrolizumab for the adjuvant treatment of adult patients with stage IIB or IIC melanoma, following complete resection.1,2 The sponsor’s reimbursement request is consistent with the indication.
To support the assumption of clinical similarity inherent to a cost-minimization analysis, the sponsor submitted a network meta-analysis (NMA) comparing nivolumab as assessed in the CHECKMATE-76K trial and pembrolizumab as assessed in the KEYNOTE-716 trial for the outcomes of RFS and treatment-related adverse events (AEs).3 The analysis was conducted from the perspective of a public health payer and includes drug acquisition and administration costs for both adjuvant and subsequent therapies in the base case. The time horizon of the analysis was 1 year and thus no discounting of future costs was considered.
Nivolumab is available as a 10 mg/mL injection for IV infusion in 40 mg and 100 mg vials, with a recommended dose for this indication of 240 mg every 2 weeks or 480 mg every 4 weeks, continuing treatment for as long as clinical benefit is observed or until treatment is no longer tolerated, for up to 1 year.2 The submitted price of nivolumab is $782.22 for the 40 mg/4 mL vials and $1,955.56 for the 100 mg/10 mL vials.1 When used at the recommended dose, the cost of nivolumab is $9,387 per 28 days. The cost of pembrolizumab, when used as in the KEYNOTE-716 trial4 and as recommended in the product monograph, is $11,733 per 28 days.
The sponsor used weight-based dosing for both comparators, with nivolumab dosed at 6 mg/kg (maximum 480 mg) every 4 weeks and pembrolizumab dosed at 2 mg/kg (maximum 200 mg) every 3 weeks, consistent with typical use in practice in Canada. Patients were assumed to receive 10.9 months of adjuvant therapy, regardless of treatment group, based on time to treatment discontinuation of nivolumab in the CHECKMATE-76K trial.5,6 The sponsor assumed a mean body weight of 84.7 kg5 and included 5% wastage. Additional included costs were those associated with administration ($105 per infusion),7 as well as subsequent therapy costs for patients experiencing a local or distal recurrence, including costs for surgery and radiotherapy7 and drug acquisition and administration costs for subsequent systemic therapies.7-9 Subsequent therapies included within the analysis could exceed the 1-year time horizon, but as they were identical between treatment options, there were no differences between treatments. All analyses were deterministic. The sponsor’s base case estimated that as adjuvant therapy in adult patients with stage IIB or IIC melanoma following complete resection, nivolumab was associated with a total cost of $125,989 per patient (Table 3), while pembrolizumab was associated with a total cost of $133,223 per patient. The use of nivolumab was therefore predicted to result in a saving of $7,234 per patient, relative to pembrolizumab.
Table 3: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total drug costs ($) | Incremental drug costs ($) | Total costs ($) | Incremental costs ($) |
|---|---|---|---|---|
Pembrolizumab | 123,617 | Reference | 133,223 | Reference |
Nivolumab | 116,799 | −6,818 | 125,989 | −7,234 |
Source: Sponsor’s economic submission.1
The sponsor also conducted a number of scenario analyses, including those assuming: flat dosing of 480 mg of nivolumab every 4 weeks and 200 mg of pembrolizumab every 3 weeks (incremental savings with nivolumab = $29,615 per patient), no wastage of medication (incremental savings with nivolumab = $6,909 per patient), full wastage of excess medication in vials (incremental savings with nivolumab = $28,225 per patient), or assuming the mean number of doses received by patients within each product’s pivotal trial4-6 (incremental savings with nivolumab = $4,824 per patient). All analyses assumed publicly available prices for comparators and may not represent prices paid by public plans.
CADTH Appraisal of the Sponsor’s Economic Information
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the economic analysis:
The sponsor’s claim of clinical similarity between nivolumab and pembrolizumab as analyzed is associated with some uncertainty: The assumption of clinical similarity was based on a sponsor-conducted NMA,3 including the CHECKMATE-76K10 (nivolumab) and KEYNOTE-716 (pembrolizumab)4 trials. The NMA assessed RFS and treatment-related AEs (any grade and grade 3 or higher). As noted in the CADTH clinical report, the limitations of the sponsor’s NMA were the very small amount of data contained from 2 studies, the inclusion of only 1 efficacy outcome, the limited follow-up times, differences in follow-up time between the 2 studies, and the lack of analysis for all-cause AEs. The NMA did not provide evidence of a difference in efficacy or harms outcomes for nivolumab compared to pembrolizumab in this population. Despite the identified limitations, CADTH considered that it is likely that the claim of clinical similarity is justifiable. However, the included trials used flat dosing of 480 mg every 4 weeks for nivolumab, and 200 mg every 3 weeks for pembrolizumab. While clinical expert opinion obtained by CADTH, drug plan input, and the sponsor’s model all agreed that weight-based dosing will be used in clinical practice (typically 6 mg/kg up to 480 mg every 4 weeks for nivolumab, 2 mg/kg every 3 weeks up to 200 mg for pembrolizumab), it is unclear whether this weight-based dosing will remain as clinically similar between treatments as indicated by the NMA, particularly for patients weighing in between 80 kg (where nivolumab reaches its maximum dose) and 100 kg (where pembrolizumab reaches its maximum dose).
CADTH was unable to address this limitation in reanalysis.
Uncertainty that all patients will receive nivolumab every 4 weeks: Clinical expert input obtained by CADTH indicated, based on experience in other indications where nivolumab is already funded, that some patients may benefit from lower, more frequent dosing to reduce toxicity. This input estimated that approximately 10% of patients use the more frequent dosing regimen. Additionally, the recommended dosing of pembrolizumab includes a dosing regimen every 6 weeks, which may be preferable, if funded, for patients experiencing limited toxicity.
CADTH included a scenario where 10% of patients treated with nivolumab received 3 mg/kg (maximum 240 mg) every 2 weeks and 10% of patients treated with pembrolizumab received 4 mg/kg (maximum 400 mg).
Savings associated with nivolumab are highly dependent on patient weight: As the maximum dose of nivolumab is reached when patients weigh 80 kg, while the maximum dose of pembrolizumab is reached when patients weigh 100 kg, the incremental savings associated with nivolumab compared to pembrolizumab is higher for patients weighing more than 80 kg than for those weighing 80 kg or less. At 80 kg, the drug acquisition costs of pembrolizumab and nivolumab are the same, with only administration costs differing. The sponsor’s base case assumes a mean body weight of 84.7 kg.5
CADTH explored patient body weight assumptions of 80 kg and 100 kg in scenario analyses.
Confidential pricing agreements: The sponsor’s analyses use pricing available from IQVIA’s Delta PA for pembrolizumab,11 consistent with the price submitted to CADTH during the review of pembrolizumab as adjuvant therapy of stage IIB or IIC melanoma following resection.12 The submitted price of nivolumab is also consistent with publicly available pricing as well as that submitted for a previous CADTH review of nivolumab for adjuvant therapy for stage III/IV melanoma following resection.13 However, confidential pricing agreements exist for both products for these indications.14,15 Therefore, the submitted price of nivolumab may require a price reduction to avoid incurring additional costs relative to pembrolizumab.
CADTH was unable to address this limitation in reanalysis, as the negotiated price of pembrolizumab is unknown.
CADTH Reanalyses of the Economic Information
CADTH did not conduct a base-case reanalysis and accepted the sponsor’s submitted base case and scenarios.
CADTH conducted an additional scenario where 10% of patients receiving nivolumab received 3 mg/kg (maximum 240 mg) every 2 weeks and 10% of patients receiving pembrolizumab received 4 mg/kg (maximum 400 mg) every 6 weeks. This scenario had limited impact on results, with nivolumab (total cost = $126,114) associated with a savings of $7,026 per patient compared to pembrolizumab (total cost = $133,140). CADTH also explored alternate assumptions for patient body weight. For patients weighing 80 kg or less, the incremental savings associated with nivolumab compared to pembrolizumab would be $416 per patient, while for patients weighing 100 kg or more, the incremental savings would be $29,615 per patient. Refer to Table 5.
Conclusions
The CADTH clinical review concluded that nivolumab demonstrated an improvement in RFS compared with placebo based on 1 year of adjuvant treatment in patients with resected stage IIB or IIC melanoma. There was no direct evidence comparing nivolumab to the primary comparator, pembrolizumab. The sponsor-submitted indirect comparison did not provide evidence to support a difference in efficacy or safety between nivolumab and pembrolizumab. Despite the limitations of the ITC, CADTH considered that the claim of no difference between nivolumab compared to pembrolizumab is justified.
The sponsor’s cost-minimization analysis is based on the assumption of clinical similarity between nivolumab and pembrolizumab. In line with the CADTH clinical review, as nivolumab is considered to have similar clinical efficacy and safety to pembrolizumab, treatment with nivolumab is less costly than pembrolizumab at public list prices. No revisions were undertaken to the sponsor’s base case, which indicated that nivolumab was associated with a cost saving of $7,234 per patient compared with pembrolizumab. CADTH explored scenario analyses which indicated that nivolumab remained cost saving.
CADTH notes that the magnitude of cost savings associated with nivolumab, relative to pembrolizumab, is highly dependent on patient weight, with drug acquisition costs being equal when patients weigh 80 kg or less. All costs and incremental savings are based on publicly available list prices and may not reflect actual prices paid by public drug plans in Canada.
References
1.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Opdivo (nivolumab), intravenous infusion, 10 mg nivolumab /mL; 40 mg and 100 mg single-use vials. Montreal (QC): Bristol-Myers Squibb Canada; 2023.
2.Opdivo (nivolumab): intravenous infusion, 10 mg nivolumab /mL, 40 mg and 100 mg single-use vials [DRAFT product monograph]. Montreal (QC): Bristol-Myers Squibb Canada; 2015.
3.Nivolumab for the adjuvant treatment of stage IIB/C melanoma: network meta-analysis report [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Opdivo (nivolumab), intravenous infusion, 10 mg nivolumab /mL; 40 mg and 100 mg single-use vials. Montreal (QC): Bristol-Myers Squibb Canada; 2023.
4.Long GV, Luke JJ, Khattak MA, et al. Pembrolizumab versus placebo as adjuvant therapy in resected stage IIB or IIC melanoma (KEYNOTE-716): distant metastasis-free survival results of a multicentre, double-blind, randomised, phase 3 trial. Lancet Oncol. 2022;23(11):1378-1388. PubMed
5.Clinical Protocol: CA20976K. A phase 3, randomized, double-blind study of adjuvant immunotherapy with nivolumab versus placebo after complete resection of stage IIB/C melanoma [internal sponsor's report]. Lawrenceville (NJ): Bristol-Myers Squibb; 2019.
6.Clinical Study Report Addendum: CA20976K. A phase 3, randomized, double-blind study of adjuvant immunotherapy with nivolumab versus placebo after complete resection of stage IIB/C melanoma [internal sponsor's report]. Uxbridge (GB): Bristol-Myers Squibb; 2023.
7.Ontario Ministry of Health. Ontario Schedule of Benefits and Fees. 2023; https://www.health.gov.on.ca/en/pro/programs/ohip/sob/. Accessed 2023 Dec 9.
8.pan-Canadian oncology drug review. Final economic guidance report - nivolumab (Opdivo) plus Ipilimumab (Yervoy) for metastatic melanoma. Ottawa (ON): CADTH; 2017 Nov 30: https://www.cadth.ca/sites/default/files/pcodr/pcodr_opdivo_yervoy_metmela_fn_egr.pdf. Accessed 2024 May 23.
9.CADTH reimbursement recommendation - encorafenib (Braftovi) in combination with binimetinib (Mektovi) Can J Health Technol. 2021;1(7). https://www.cadth.ca/sites/default/files/pcodr/Reviews2021/PC0232%20Braftovi%20and%20Mektovi%20Final.pdf. Accessed 2024 May 23.
10.Primary clinical study report for study CA224047: a randomized, double-blind phase 2/3 study of relatlimab combined with nivolumab versus nivolumab in participants with previously untreated metastatic or unresectable melanoma. 2021 [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Opdivo (nivolumab for injection) intravenous infusion, 10 mg /mL, 40 mg and 100 mg single-use vials. Montreal (QC): Bristol Myers Squibb Canada; 2023.
11.DeltaPA. Ottawa (ON): IQVIA; 2023: https://www.iqvia.com/. Accessed 2023 Dec 09.
12.CADTH reimbursement review: pembrolizumab (Keytruda) Can J Health Technol. 2023;3(2). https://www.cadth.ca/sites/default/files/DRR/2023/PC0286-Keytruda-Melanoma_combined.pdf. Accessed 2023 Dec 10.
13.pan-Canadian oncology drug review. Final economic guidance report: nivolumab (Opdive) for adjuvant melanoma. Ottawa (ON): CADTH; 2019 Mar 7: https://www.cadth.ca/sites/default/files/pcodr/Reviews2019/10147NivolumabMAT_FnEGR_NOREDACT-ABBREV_POST07Mar2019_Final.pdf. Accessed 2024 Jan 21.
14.pan-Canadian Pharmaceutical Alliance. Opdivo (nivolumab): melanoma adjuvant therapy. 2019; https://www.pcpacanada.ca/negotiation/21111. Accessed 2024 Jan 21.
15.pan-Canadian Pharmaceutical Alliance. Keytruda (pembrolizumab): for the adjuvant treatment of adult and pediatric (12 years and older) patients with stage IIB or IIC melanoma following complete resection. 2023; https://www.pcpacanada.ca/negotiation/22073. Accessed 2024 Jan 21.
16.Cancer Care Ontario. Funded evidence-informed regimens. 2023; https://www.cancercareontario.ca/en/drugformulary/regimens. Accessed 2024 Jan 21.
17.Outpatient cancer drug benefit program. Edmonton (AB): Alberta Health Services; 2023: https://www.albertahealthservices.ca/assets/programs/ps-1025651-drug-benefit-list.pdf. Accessed 2024 Feb 07.
18.Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Opdivo (nivolumab), intravenous infusion, 10 mg nivolumab /mL; 40 mg and 100 mg single-use vials. Montreal (QC): Bristol-Myers Squibb Canada; 2023.
19.Statistics Canada. Table: 13-10-0111-01. Number and rates of new cases of primary cancer, by cancer type, age group and sex. 2022; https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310011101&pickMembers%5B0%5D=2.1&pickMembers%5B1%5D=3.1&pickMembers%5B2%5D=4.26&cubeTimeFrame.startYear=2015&cubeTimeFrame.endYear=2019&referencePeriods=20150101%2C20190101. Accessed 2023 Mar 10.
20.Statistics Canada. Table: 17-10-0059-01. Estimates of the components of natural increase, quarterly. 2023; https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1710005901. Accessed 2023 Aug 1.
21.Statistics Canada. Table: 17-10-0009-01. Population estimates, quarterly. 2023; https://www150.statcan.gc.ca/t1/tbl1/en/cv.action?pid=1710000901. Accessed 2024 Jan 22.
Appendix 1: Additional Economic Information
Note this appendix has not been copy-edited.
Cost Comparison Table
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical experts and drug plans. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 4: CADTH Cost Comparison Table for Adjuvant Treatment of Stage IIB or IIC Melanoma
Treatment | Concentration | Form | Price | Recommended dosage | Daily cost ($) | Cost per 28-days ($) |
|---|---|---|---|---|---|---|
Fixed dosing (as per Health Canada product monographs) | ||||||
Nivolumab (Opdivo) | 10 mg/mL | 40 mg 100 mg Vials for IV infusion | 782.2200a 1,955.5600a | 240 mg every 2 weeks or 480 mg every 4 weeks for up to 1 year as long as clinical benefit is observed or until treatment is no longer tolerated. | 335 | 9,387 |
Pembrolizumab (Keytruda) | 25 mg/mL | 50 mg 100 mg Vials for IV infusion | 2,200.0000 4,400.0000 | 200 mg every 3 weeks or 400 mg every 6 weeks for up to 12 months, or until disease progression or unacceptable toxicity. | 419 | 11,733 |
Weight-based dosingb | ||||||
Nivolumab (Opdivo) | 10 mg/mL | 40 mg 100 mg Vials for IV infusion | 782.2200a 1,955.5600a | 3 mg/kg (maximum: 240 mg) every 2 weeks or 6 mg/kg (maximum: 480 mg) every 4 weeks for up to 1 year as long as clinical benefit is observed or until treatment is no longer tolerated. | 335 | 9,387 |
Pembrolizumab (Keytruda) | 25 mg/mL | 50 mg 100 mg Vials for IV infusion | 2,200.0000 4,400.0000 | 2 mg/kg (maximum: 200 mg) every 3 weeks or 4 mg/kg (maximum: 400 mg) every 6 weeks for up to 12 months, or until disease progression or unacceptable toxicitya | 356 | 9,973 |
Note: All prices are wholesale prices as reported by IQVIA Delta PA (accessed December 2023),11 unless otherwise indicated, and do not include dispensing fees. Costs assume an 85kg patient and perfect vial sharing.c
aSponsor’s submitted price.1
bClinical expert opinion obtained by CADTH, drug plan input, cancer formularies (e.g., Ontario and Alberta)16,17 and the sponsor’s submission all suggest that weight-based dosing up to a maximum is typically used for pembrolizumab and will be used for nivolumab, if funded.
cClinical expert input obtained by CADTH indicated that most treatment centres share vials where possible, thus minimizing wastage. This input also noted that treatment centres are reimbursed by public payers based on patient weight, and thus any wastage of excess medication is not directly paid by public plans. When full wastage of excess medication in vials is assumed and at a patient weight of 85 kg, the cost per patient of nivolumab would be $335 per day or $9,387 per 28-days, and the cost per patient of pembrolizumab would be $419 per day or $11,733 per 28-days. Of note, as the maximum dose for nivolumab is reached when patients weigh 80 kg while the maximum dose for pembrolizumab is reached when patients weigh 100 kg, savings associated with the use of nivolumab are substantially reduced when patients weigh 80 kg or less.
Additional Details on the Sponsor’s Submission
No additional information from the sponsor’s submitted pharmacoeconomic evaluation was considered in the review of nivolumab.
Additional Details on the CADTH Reanalyses and Additional Analyses
Table 5: Scenario Analyses Conducted by CADTH on the Sponsor’s Base Case
Scenario analysis | Drug | Total drug costs ($) | Incremental drug costs ($) | Total costs ($) | Incremental costs ($) |
|---|---|---|---|---|---|
Sponsor’s base case | Pembrolizumab | 123,617 | Reference | 133,223 | Reference |
Nivolumab | 116,799 | −6,818 | 125,989 | −7,234 | |
CADTH Scenario 1: 10% use alternatea dosing regimen | Pembrolizumab | 123,617 | Reference | 133,140 | Reference |
Nivolumab | 116,799 | −6,818 | 126,114 | −7,026 | |
CADTH Scenario 2: Patient weight 80kg | Pembrolizumab | 116,799 | Reference | 126,295 | Reference |
Nivolumab | 116,799 | $0 | 125,879 | −415 | |
CADTH Scenario 3: Patient weight 100 kg | Pembrolizumab | 145,999 | Reference | 155,966 | Reference |
Nivolumab | 116,799 | −29,200 | 126,351 | −29,615 |
a10% of patients receiving nivolumab are assumed to receive 3 mg/kg (maximum 240 mg) every 2 weeks and 10% of patients receiving pembrolizumab are assumed to receive 4 mg/kg (maximum 400 mg).
Appendix 2: Submitted BIA and CADTH Appraisal
Note this appendix has not been copy-edited.
Table 6: Summary of Key Take-Aways
Key Take-aways of the BIA |
|---|
|
Summary of Sponsor’s BIA
In the submitted budget impact analysis (BIA), the sponsor assessed the introduction of nivolumab as adjuvant treatment of adult patients with stage IIB or IIC melanoma following complete resection.18 The BIA was undertaken from the perspective of a Canadian public drug plan payer over a 3-year time horizon (2024 to 2026) using an epidemiological approach. The sponsor’s analysis included drug acquisition costs for both adjuvant and subsequent therapies as well as administration costs; dispensing fees and markups were not included. Data from the model were obtained from various sources including Statistics Canada,19,20 the CADTH review of pembrolizumab for a similar indication,12 IQVIA Delta PA for drug list prices, and the sponsor’s internal projections. Key inputs to the BIA are documented in Table 7.
Key assumptions used to inform the sponsor’s base case included:
The population of adults with stage IIB or IIC melanoma at diagnosis can be approximated by the total number of patients with stage IIB or IIC melanoma at diagnosis.
The proportion of patients requiring subsequent therapies and the types and proportions of subsequent therapies received will not differ by choice of adjuvant therapy.
All patients eligible to receive pembrolizumab in the reference case will do so.
Table 7: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as Year 1 / Year 2 / Year 3 if appropriate) |
|---|---|
Target population | |
Population of Canada, excluding Quebec (base year) | 30,700,265a |
Annual population growth rate | 1.01%20 |
Incidence of melanoma | 23.5 per 100,00019 |
Proportion with stage IIB or IIC at diagnosis | 6.10%12 |
Proportion stage IIB or IIC with surgically resectable melanoma | 90%12 |
Proportion of resected patients referred to a medical oncologist | 90%12 |
Number of patients eligible for drug under review | 360 / 364 / 367 |
Market uptake (reference scenario, 3 years)b | |
Nivolumab | 0% / 0% / 0% |
Pembrolizumab | 100% / 100% / 100% |
Market uptake (new drug scenario, 3 years)b | |
Nivolumab | ||||% / ||||% / ||||% |
Pembrolizumab | ||||% / ||||% / ||||% |
Cost of treatment (per patient per 10.9 month course) | |
Nivolumab | $116,799 |
Pembrolizumab | $123,617 |
Note: Cost of treatment as listed here includes drug acquisition costs11 only and include 5% drug wastage. When administration and subsequent therapy costs are included, as in the sponsor’s base case, the total cost per patient associated with nivolumab is $125,989 while the total cost associated with is $133,223.
aCited as from Statistics Canada Table 17-10-0059-01. Estimates of the components of natural increase, quarterly,20 however it is unclear how the total population of Canada, excluding Quebec, was derived from this source. CADTH deemed the sponsor’s as similar enough to other estimates21 to be left uncorrected.
bBased on the sponsor’s internal projections, not provided.
Summary of the Sponsor’s BIA Results
The sponsor estimated that the 3-year budget impact of reimbursing nivolumab for as adjuvant treatment of adult patients with stage IIB or IIC melanoma following complete resection would be a savings of $2,424,037 (savings in year 1: $573,033; year 2: $920,852, year 3: $930,152).
CADTH Appraisal of the Sponsor’s BIA
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
Health care payer perspective was inappropriate: CADTH submissions guideline stipulate that the BIA base case should reflect a drug program perspective. Administration costs should therefore not be included in the submitted base case but may be presented within a scenario.
CADTH excluded administration costs from its base-case reanalysis. As this is the only change made by CADTH to inform its base case, a scenario analysis reintroducing administration costs would be the same as the sponsor’s submitted base case.
Market share of pembrolizumab and nivolumab may be overestimated: Public funding of pembrolizumab as adjuvant treatment of adult patients with stage IIB or IIC melanoma following complete resection is relatively new, with successful negotiations through the pan-Canadian Pharmaceutical Alliance concluding in March 202315 followed by entry onto jurisdictional cancer agency formularies thereafter (e.g., Cancer Care Ontario16). Pembrolizumab is therefore still in the process of entering the publicly funded market for this indication. According to clinical expert input obtained by CADTH, adjuvant nivolumab is expected to only be received by patients who would otherwise receive adjuvant pembrolizumab and that choice of adjuvant therapy is unlikely to affect choice of subsequent therapy, if required. However, this expert input also noted that the proportion of otherwise eligible patients currently receiving adjuvant pembrolizumab varies by jurisdiction but is not yet approaching 100%.
CADTH did not have sufficient information on the proportion of patients still receiving routine surveillance rather than adjuvant treatment to make a change to its base-case analysis. In a scenario analysis, CADTH assumed the market share of pembrolizumab in the reference case was 80% in year 1, 85% in year 2, and 90% in year 3, and that nivolumab would take its sponsor-forecasted market share of ||||% in year 1 and ||||% in years 2 and 3 from these proportions.
Uptake of nivolumab is uncertain: Clinical expert input obtained by CADTH indicated that given the reduced frequency of administration with nivolumab (every 4 weeks) compared to the typically funded pembrolizumab regimen (every 3 weeks), uptake of nivolumab may be higher than the sponsor’s estimated ||||% of the eligible market by year 3. However, the same input also noted that uptake of nivolumab in place of pembrolizumab in other indications varies substantially by jurisdiction. As such, the extent to which nivolumab will displace pembrolizumab for the indication under review is uncertain and likely to vary by jurisdiction.
CADTH did not have sufficient information on the likelihood of nivolumab uptake by jurisdiction to adjust for this limitation in reanalysis. In jurisdictions with a low uptake of nivolumab in place of pembrolizumab, the extent of savings is likely to be lower than estimated by the sponsor.
The price of drugs paid by public drug plans is uncertain: Both the sponsor’s and CADTH’s analyses are based on publicly available list prices. As pembrolizumab has gone through negotiations at the pan-Canadian Pharmaceutical Alliance for this indication,15 the price paid by public plans is not known.
CADTH was unable to address this limitation in reanalysis. A confidential negotiated price for pembrolizumab may limit or eliminated estimated budgetary savings associated with nivolumab.
CADTH Reanalyses of the BIA
CADTH revised the sponsor’s submitted analysis by removing administration costs to reflect a drug payer perspective. The change made to derive the CADTH base case is described in Table 8.
Table 8: CADTH Revisions to the Submitted BIA
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Correctionsa to sponsor’s base case | ||
None | — | — |
Changes to derive the CADTH base case | ||
1. Administration costs | Included | Excluded |
CADTH base case | 1 | |
aCorrections are minor errors (e.g., transcription errors between report and model, misapplication of distributions or standard errors in probabilistic analyses) that are not identified as limitations.
The results of the CADTH step-wise reanalysis are presented in summary format in Table 9 and a more detailed breakdown is presented in Table 10. In the CADTH base case, the 3-year budget impact of reimbursing nivolumab as adjuvant treatment of adult patients with stage IIB or IIC melanoma following complete resection is expected to be a savings of $2,284,851 (savings in year 1: $540,130, year 2: $867,977, and year 3: $876,743).
Table 9: Summary of the CADTH Reanalyses of the BIA
Stepped analysis | 3-year total |
|---|---|
Submitted base case | -$2,424,037 |
CADTH reanalysis 1: Administration costs excluded | -$2,284,851 |
CADTH base case | -$2,284,851 |
BIA = budget impact analysis; [add as required].
CADTH conducted an additional scenario analysis to explore remaining uncertainty associated with the potential budget impact, using the CADTH base case. Results are provided in Table 10.
The market share of pembrolizumab in the reference case was assumed to be 80% in year 1, 85% in year 2, and 90% in year 3, with nivolumab taking ||||% of this share in year 1 and ||||% in years 2 and 3. Remaining eligible patients are assumed to receive active surveillance (annual cost = $0).
Table 10: Detailed Breakdown of the CADTH Reanalyses of the BIA
Stepped analysis | Scenario | Year 0 (current situation) | Year 1 | Year 2 | Year 3 | Three-year total |
|---|---|---|---|---|---|---|
Submitted base case | Reference | $47,490,309 | $47,969,961 | $48,454,457 | $48,943,847 | $145,368,265 |
New drug | $47,490,309 | $47,396,927 | $47,533,606 | $48,013,695 | $142,944,228 | |
Budget impact | $0 | -$573,033 | -$920,852 | -$930,152 | -$2,424,037 | |
CADTH base case | Reference | $46,877,019 | $47,350,477 | $47,828,717 | $48,311,787 | $143,490,981 |
New drug | $46,877,019 | $46,810,347 | $46,960,740 | $47,435,044 | $141,206,131 | |
Budget impact | $0 | -$540,130 | -$867,977 | -$876,743 | -$2,284,851 | |
CADTH scenario 1: active surveillance included | Reference | $35,176,388 | $37,899,680 | $40,674,394 | $43,501,291 | $122,075,365 |
New drug | $35,176,388 | $37,467,576 | $39,936,614 | $42,712,222 | $120,116,411 | |
Budget impact | $0 | -$432,104 | -$737,780 | -$789,069 | -$1,958,954 |
BIA = budget impact analysis.
Note: Due to the exclusion of administration costs, a scenario assuming that 10% of nivolumab patients receive treatment every 2 weeks while 10% of pembrolizumab patients receive treatment every 6 weeks would result in an identical budgetary impact as the CADTH base case and was thus not included.
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.