Drugs, Health Technologies, Health Systems
Reimbursement Review
Zolbetuximab for Injection (Vyloy)
Sponsor: Astellas Pharma Canada, Inc.
Therapeutic area: Gastric or gastroesophageal junction adenocarcinoma
This multi-part report includes:
Clinical Review
TPA Review
Pharmacoeconomic Review
Clinical Review
Abbreviations
ACT
anticancer treatment
ADCC
antibody-dependent cellular cytotoxicity
AE
adverse event
BOR
best overall response
CAPOX
capecitabine and oxaliplatin
CDA-AMC
Canada’s Drug Agency
CDC
complement-dependent cytotoxicity
CI
confidence interval
CLDN18.2
Claudin 18.2
CPS
combined positive score
CrI
credible interval
DCR
disease control rate
DIC
deviance information criterion
DOR
duration of response
ECOG
Eastern Cooperative Oncology Group
EMA
European Medicines Agency
EORTC GHS/QoL
European Organisation for Research and Treatment of Cancer Global Health Status/Quality of Life
EORTC QLQ-C30 PF
European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire – Core Questionnaire Physical Functioning
EORTC QLQ-OG25
European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Oesophago-Gastric 25
FAS
full analysis set
GEJ
gastroesophageal junction
GRADE
Grading of Recommendations, Assessment, Development, and Evaluations
HER2
human epidermal growth factor receptor 2
HR
hazard ratio
HRQoL
health-related quality of life
IHC
immunohistochemistry
IRC
independent review committee
IRR
infusion-related reaction
ITC
indirect treatment comparison
mFOLFOX6
leucovorin calcium (folinic acid), fluorouracil, and oxaliplatin
MMR
mismatch repair
NICE
National Institute for Health and Care Excellence
NMA
network meta-analysis
OH-CCO GI DAC
Ontario Health (Cancer Care Ontario) Gastrointestinal Cancer Drug Advisory Committee
ORR
objective response rate
OS
overall survival
PD
progressive disease
PD-L1
programmed death-ligand 1
PFS
progression-free survival
PFS2
progression-free survival following second-line anticancer treatment
RCT
randomized controlled trial
RECIST 1.1
Response Evaluation Criteria in Solid Tumours Version 1.1
SAE
serious adverse event
SAF
safety analysis set
TTCD
time to confirmed deterioration
TTP
time to progression
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Table 1: Background Information on the Application Submitted for Review
Item | Description |
|---|---|
Drug product | Zolbetuximab (Vyloy), 100-mg single-use vials, IV |
Sponsor | Astellas Pharma Canada, Inc. |
Indication | Zolbetuximab in combination with fluoropyrimidine- and platinum-containing chemotherapy is indicated for the first-line treatment of patients with locally advanced unresectable or metastatic human epidermal growth factor receptor 2–negative gastric or gastroesophageal junction adenocarcinoma whose tumours are Claudin 18.2 positive as determined by a validated test. |
Reimbursement request | As per indication |
Health Canada approval status | Approved |
Health Canada review pathway | Standard |
NOC date | December 13, 2024 |
Recommended dose | Loading dose: 800 mg/m2 IV on cycle 1, day 1 Maintenance dosage: 600 mg/m2 IV every 3 weeks or 400 mg/m2 IV every 2 weeks |
NOC = Notice of Compliance.
Introduction
Disease overview: Gastric cancers originate in the cells lining the stomach and are generally classified into 2 topographical subsites.1-3 Cardia gastric cancer arises in the upper part of the stomach near the gastroesophageal junction (GEJ), and noncardia gastric cancer arises in the more distal regions of the stomach.1 GEJ cancers occur in the cells lining the GEJ, the area where the esophagus joins the gastric cardia.2,3 In 2024, it was estimated that 4,000 people in Canada would be newly diagnosed with stomach cancer.4 The risk of developing gastric cancer increases with age and is greatest in people older than 50 years.5 Stomach cancer occurs more frequently in men than in women.5-7 Chronic infection with Helicobacter pylori is a major risk factor for noncardia gastric cancer; it is responsible for nearly 90% of these cancer cases worldwide.8,9 Early gastric cancers that are surgically curable are typically asymptomatic, and if symptoms are present at the early stage, these are usually nonspecific.10,11 As such, diagnosis of gastric or GEJ cancer frequently occurs when the disease is at an advanced, unresectable, or metastatic stage and is considered incurable.10,12,13 Quality of life in patients with gastric cancer is affected by emotional, physical, and social aspects of the disease and its treatment.14 Individuals may experience anxiety and depression as well as increasing symptom burden in advanced stages.12,14 In Canada from 2015 to 2017, the 5-year net survival rate for individuals diagnosed with stomach cancer was 29%, reflecting that diagnosis is often made at advanced-stage disease that is associated with poor prognosis.6,7,12,15 US data indicate that the 5-year relative survival rate for patients with metastatic gastric cancer is 7%.16 A clinical expert consulted by Canada’s Drug Agency (CDA-AMC) stated that, in clinical practice, the median survival duration for patients with metastatic gastric or GEJ cancer is approximately 1 year.
Greater than 90% of gastric cancers are histologically classified as adenocarcinomas.13 Various genetic aberrations can occur during the development of gastric cancer.17 Human epidermal growth factor receptor 2 (HER2) is overexpressed in approximately 20% of gastric or GEJ adenocarcinomas.18 Biomarker testing of cancer tissue may be performed to inform treatment decisions, including testing for HER2, programmed death-ligand 1 (PD-L1) combined positive score (CPS), and mismatch repair (MMR).19,20
Claudin 18.2 (CLDN18.2): CLDN18.2 is a membrane tight junction molecule that is inaccessible in normal gastric epithelial tissue. CLDN18.2 may become exposed on the surface of gastric or GEJ adenocarcinoma cells due to the disruption of cell polarity that occurs during carcinogenesis.21-23 Screening data from the SPOTLIGHT and GLOW trials suggest that 38% of patients with locally advanced unresectable or metastatic gastric or GEJ adenocarcinoma are CDLN18.2-positive (defined as expression with 2+ or 3+ intensity in ≥ 75% of tumour cells).24,25
Standard treatments: In patients with HER2-negative disease, the standard first-line treatment is nivolumab in combination with a platinum-fluoropyrimidine doublet, based on the results of the CheckMate-649 trial, which demonstrated that the addition of nivolumab to chemotherapy improved overall survival (OS) and progression-free survival (PFS).26-28 In addition, the combination of pembrolizumab and platinum-fluoropyrimidine doublet therapy is recommended as a standard first-line treatment for patients with advanced or metastatic HER2-negative GEJ adenocarcinoma and esophageal adenocarcinoma, based on the double-blind, phase III KEYNOTE-590 study.27,29 Standard first-line platinum-fluoropyrimidine doublet chemotherapy options in Canada include FOLFOX (leucovorin calcium [folinic acid], 5-fluorouracil, and oxaliplatin), CAPOX (capecitabine and oxaliplatin), FP (5-fluorouracil and cisplatin), or capecitabine-cisplatin. CDA-AMC issued a recommendation in September 2024 that pembrolizumab be reimbursed for use in combination with fluoropyrimidine- and platinum-containing chemotherapy for the first-line treatment of adult patients with locally advanced unresectable or metastatic HER2-negative gastric or GEJ adenocarcinoma.
Drug under review: Zolbetuximab is a monoclonal antibody that targets CLDN18.2. Zolbetuximab acts through antibody-dependent cellular cytotoxicity (ADCC) and complement-dependent cytotoxicity (CDC) to deplete CLDN18.2-positive cells. Cytotoxic drugs were shown to increase CLDN18.2 expression on human cancer cells and to improve the ADCC and CDC activities of zolbetuximab.21 Zolbetuximab is supplied in single-use vials containing zolbetuximab 100 mg as a lyophilized powder for concentrate for solution for IV infusion.21 The product monograph–recommended dosage consists of a single loading dose (800 mg/m2 IV) followed by a maintenance dosage of 600 mg/m2 IV once every 3 weeks or 400 mg/m2 IV once every 2 weeks. To align the administration schedule for zolbetuximab with the concomitant chemotherapy schedule, the product monograph recommends the 400 mg/m2 every 2 weeks maintenance dosage when used in combination with leucovorin calcium (folinic acid), fluorouracil, and oxaliplatin (mFOLFOX6) and the 600 mg/m2 every 3 weeks maintenance dosage when used in combination with CAPOX.21
Purpose of review: The objective of this clinical review report is to review and critically appraise the clinical evidence submitted by the sponsor on the beneficial and harmful effects of zolbetuximab, in combination with fluoropyrimidine- and platinum-containing chemotherapy, for the first-line treatment of patients with locally advanced unresectable or metastatic HER2-negative gastric or GEJ adenocarcinoma whose tumours are CLDN18.2-positive as determined by a validated test.
Perspectives of Patients, Clinicians, and Drug Programs
The information in this section is a summary of input provided by the patient and clinician groups who responded to the call for input and from the clinical experts consulted for the purpose of this review.
Patient Input
One patient group provided input for this review. My Gut Feeling – Stomach Cancer Foundation of Canada is a nonprofit organization providing support, awareness, education, information, and advocacy to patients with stomach cancer along with survivors and caregivers. My Gut Feeling conducted an international online survey of patients and caregivers affected by gastric, esophageal, and/or gastroesophageal cancer. A total of 35 respondents completed the survey, 14.3% of whom were caregivers and 85.7% of whom were patients; the majority of respondents resided in Canada (71.4%) or the US (25.7%).
Nearly all participants (97.2%) responded that their quality of life was significantly affected by the cancer diagnosis. Specifically, their physical and mental health, ability to eat, work life, finances, social life, identity, and personal image were all impacted. For example, respondents expressed the exhaustion of managing adequate daily nutrition and the toll of experiencing weight loss or weight gain, including its impact on body image. Patients and caregivers (particularly those affected by metastatic disease) communicated that the cancer diagnosis and its treatment had negative impacts on their mental health and caused anxiety surrounding finances (e.g., loss of income due to work absenteeism; additional expenses due to travel for medical care and specialized diet). Patients reported feeling anxiety, depression, and/or anger, and said that experiencing fatigue greatly impacted their daily activities.
Survey participants stated that many factors are considered when weighing treatment options, such as quality of life, survival benefits, side effects, convenience, and duration of therapy, recognizing that treatments have trade-offs that need to be considered on an individual basis. For example, most respondents (82.9%) would choose a treatment that prolongs life despite side effects. Patients also expressed a preference for the convenience of oral chemotherapy taken at home over IV chemotherapy administered in a hospital setting.
My Gut Feeling indicated that gastric and gastroesophageal cancers are rare in Canada, with few treatment options. This group expressed an unmet need for equitable access to therapies that prolong life, improve symptoms, reduce the risk of recurrence, and have improved tolerability. My Gut Feeling strongly supports the use of zolbetuximab in combination with chemotherapy as a first-line treatment for patients with locally advanced unresectable or metastatic HER2-negative gastric or GEJ adenocarcinoma whose tumours are CLDN18.2-positive and expressed that biomarker testing should be accessible at the onset of disease for all patients in Canada. The patient group believed that patients should have a choice of treatment options that are barrier-free and covered under the universal health care system in Canada.
Clinician Input
Input From the Clinical Experts Consulted by CDA-AMC
The clinical experts consulted for the purpose of this review emphasized that locally advanced and metastatic HER2-negative gastric or GEJ cancer is associated with considerable unmet needs. Treatment with nivolumab in combination with chemotherapy is the currently available first-line option for locally advanced metastatic HER2-negative gastric or GEJ cancer; however, OS outcomes remain poor (median OS = 13 months to 15 months). The clinical experts suggested that the addition of zolbetuximab to chemotherapy would represent an alternative to combination therapy with nivolumab plus chemotherapy in the first-line metastatic treatment setting for patients with locally advanced and metastatic HER2-negative gastric or GEJ cancer whose tumours are CLDN18.2-positive. Regulatory approval and reimbursement for nivolumab for patients with gastric or GEJ cancer is not limited based on a patient’s PD-L1 CPS; however, the clinical experts noted that there is some uncertainty in the clinical community regarding the effectiveness of nivolumab plus chemotherapy in patients with a PD-L1 CPS of less than 5. For example, a subgroup analysis from the pivotal CheckMate-649 study suggested a reduced effect of nivolumab in patients with a PD-L1 CPS of less than 5 (hazard ratio [HR] = 0.94; 95% confidence interval [CI], 0.78 to 1.13). As such, the clinical experts noted that zolbetuximab plus chemotherapy could be a preferred option for patients with CLDN18.2-positive tumours and a PD-L1 CPS of less than 5. For patients with both CLDN18.2-positive tumours and a PD-L1 CPS of greater than or equal to 5, it is currently unclear which option could offer the best outcomes.
The clinical experts noted that the following factors should be used to determine response to treatment: patient-reported symptoms and side effects, and response on cross-sectional imaging via CT or MRI scans. The clinical experts suggested that patients should be assessed by a clinician after every 2 to 3 cycles of treatment. Clinician assessment may occur more frequently if patients report the occurrence of bothersome symptoms or side effects. The clinical experts suggested that patients should undergo CT scans every 2 to 3 months. Tumour markers can be used, as per clinical judgment, to supplement a fulsome patient assessment. The clinical experts noted that the clinically meaningful end points across all oncology types are OS and quality of life, and that PFS has limited value in assessing clinical benefit for patients with metastatic disease and a relative short OS duration. The clinical experts suggested that the decision to discontinue treatment with zolbetuximab should be based on patient-reported symptoms, patient preference, side effects, and well-being, in combination with an assessment of treatment response and disease progression, either radiologic or clinical.
Clinician Group Input
Four clinicians from the Ontario Health (Cancer Care Ontario) Gastrointestinal Cancer Drug Advisory Committee (OH-CCO GI DAC) provided a joint clinician group input for this review. These committees provide timely, evidence-based clinical and health system guidance on drug-related issues in support of Cancer Care Ontario’s mandate, including the Provincial Drug Reimbursement programs and the Systemic Treatment Program.
Regarding current treatments for metastatic HER2-negative gastric cancer, the clinician group providing input stated that standard first-line therapy consists of chemotherapy (typically FOLFOX combined with immunotherapy [nivolumab, which is currently funded, or pembrolizumab, which is approved but not funded]). The goals of treatment are to prolong life, delay disease progression, and maintain quality of life. This clinician group expressed that there are currently no approved treatments that specifically target tumours overexpressing CLDN18.2, which represents an unmet need for this population. Clinical experts consulted by CDA-AMC also identified FOLFOX with or without nivolumab as a first-line therapy in this population, with goals of therapy that were aligned with those identified by the clinician group. These experts identified an unmet need for treatments with other biological targets and for new treatments that will increase survival.
The OH-CCO GI DAC remarked that patients best suited for treatment with zolbetuximab are those with HER2-negative, CLDN18.2-positive, advanced gastric or GEJ cancer. This clinician group stated that zolbetuximab would provide an alternative to nivolumab. For patients with CLDN18.2 overexpression and PD-L1-negative or -low disease, the clinician group suspects that zolbetuximab and chemotherapy would be the clear first-line choice of therapy, but acknowledges that the best first-line therapy (nivolumab, pembrolizumab or zolbetuximab) for patients with CLDN18.2 overexpression and a PD-L1 CPS greater than 5% is unclear. For the latter population, the choice of drug to add (i.e., zolbetuximab, nivolumab, or immunotherapy) would be at the physician’s discretion, based on comorbidities and toxicity profile and with consideration for maintaining good quality of life.
Drug Program Input
Input was obtained from the drug programs that participate in the reimbursement review process. The following were identified as key factors that could potentially impact the implementation of a reimbursement recommendation for zolbetuximab (refer to Table 4 for complete details):
Considerations for initiation of therapy: Drug programs are seeking advice on scenarios that may arise in which a patient’s biomarker status (i.e., HER2 or CLDN18.2) is delayed or uncertain; where a patient may not be eligible for platinum-based chemotherapy; or where a patient has previously been treated with nivolumab in the adjuvant setting.
Access to CLDN18.2 testing: The test is not widely available and would need to be implemented to evaluate patients for zolbetuximab eligibility.
Consideration for discontinuation of therapy: Drug programs are seeking advice on the potential continuation of therapy with zolbetuximab after a patient has been required to discontinue chemotherapy.
Prescribing considerations: Drug programs are seeking advice on considerations for potentially switching from other treatments used in the first-line metastatic setting (e.g., nivolumab plus chemotherapy) to zolbetuximab plus chemotherapy.
Provision funding algorithm: Drug programs identified the likely need for a provisional funding algorithm to support the implementation of zolbetuximab and other recently approved therapies for gastric or GEJ cancer.
Care provision issues: Drug programs noted that more health care resources (i.e., chair time, nursing time, and pharmacy time) could be required for zolbetuximab in comparison with nivolumab due to longer infusion times and a more complicated process to prepare the dosage for infusion.
Clinical Evidence
Systematic Review
Description of Studies
The systematic review included 2 multinational, double-blind, placebo-controlled, randomized studies of zolbetuximab in combination with fluoropyrimidine- and platinum-based chemotherapy compared with placebo in combination with fluoropyrimidine- and platinum-based chemotherapy for the first-line treatment of patients with locally advanced unresectable or metastatic HER2-negative gastric or GEJ adenocarcinoma whose tumours are CLDN18.2-positive (SPOTLIGHT trial [N = 565] and GLOW trial [N = 507]). In both trials, patients were randomized in a 1:1 ratio to zolbetuximab or placebo groups, with randomization stratified by region (Asia versus non-Asia), number of organs with metastatic sites (0 to 2 versus ≥ 3), and prior gastrectomy (yes or no). The chemotherapy backbones were mFOLFOX6 in the SPOTLIGHT trial and CAPOX in the GLOW trial.
The primary objective in both the SPOTLIGHT and GLOW trials was to assess the PFS benefit of zolbetuximab plus chemotherapy compared to placebo plus chemotherapy. Key secondary objectives were to evaluate OS and time to confirmed deterioration (TTCD) using the European Organisation for Research and Treatment of Cancer (EORTC) Global Health Status/Quality of Life (GHS/QoL) scale, the EORTC QLQ-C30 Physical Functioning (PF) scale, and the EORTC Quality of Life Questionnaire Oesophago-Gastric 25 (QLQ-OG25) scale on abdominal pain and discomfort. Additional secondary objectives were to evaluate objective response rate (ORR), duration of response (DOR), safety, tolerability, and additional patient-reported outcomes.
Efficacy Results
Table 2 summarizes results for the efficacy end points from the SPOTLIGHT and GLOW trials. The data cut-offs used in the report were from the primary analysis of PFS (September 9, 2022, and October 7, 2022, for the SPOTLIGHT and GLOW trials, respectively) and from the final analysis of OS (September 8, 2023, and January 12, 2024, for the SPOTLIGHT and GLOW trials, respectively).
OS: In the final analysis of OS in the SPOTLIGHT trial, treatment with zolbetuximab plus mFOLFOX6 demonstrated a statistically significant improvement in OS compared with placebo plus mFOLFOX6 treatment (HR = 0.78; 95% CI, 0.64 to 0.95; P = 0.0075). Median OS was 18.2 months (95% CI, 16.1 months to 20.6 months) in the zolbetuximab plus mFOLFOX6 arm and 15.6 months (95% CI, 13.7 months to 16.9 months) in the placebo plus mFOLFOX6 arm. In the GLOW trial, the final analysis of OS demonstrated that treatment with zolbetuximab plus CAPOX was associated with a statistically significant improvement in OS compared with placebo plus CAPOX (HR = 0.763; 95% CI, 0.622 to 0.936; P = 0.0047).
PFS: In the SPOTLIGHT trial, treatment with zolbetuximab plus mFOLFOX6 showed a statistically significant improvement in PFS compared with placebo plus mFOLFOX6 (HR = 0.751; 95% CI, 0.598 to 0.942; 1-sided P = 0.0066). The median PFS durations were 10.61 months (95% CI, 8.90 months to 12.48 months) and 8.67 months (95% CI, 8.21 months to 10.28 months) in the zolbetuximab plus mFOLFOX6 and placebo plus mFOLFOX6 groups, respectively. In the GLOW trial, treatment with zolbetuximab plus CAPOX demonstrated a statistically significant improvement in PFS compared with placebo plus CAPOX (HR = 0.687; 95% CI, 0.544 to 0.866; 1-sided P = 0.0007). The median PFS durations were 8.21 months (95% CI, 7.46 months to 8.84 months) and 6.80 months (95% CI, 6.14 months to 8.08 months) in the zolbetuximab plus CAPOX and placebo plus CAPOX groups, respectively.
ORR: There was no statistically significant difference between the zolbetuximab plus mFOLFOX6 or CAPOX and placebo plus mFOLFOX6 or CAPOX groups in either the SPOTLIGHT or GLOW trials. In the SPOTLIGHT trial, the ORRs were 47.7% (95% CI, 41.76% to 53.70%) in the group receiving zolbetuximab plus mFOLFOX6 and 47.5% (95% CI, 41.56% to 53.52%) in the group receiving placebo plus mFOLFOX6. In the GLOW trial, the ORRs per independent review committee (IRC) were 42.5% (95% CI, 36.36% to 48.85%) in the group receiving zolbetuximab plus CAPOX and 40.3% (95% CI, 34.22% to 46.64%) in the group receiving placebo plus CAPOX.
Disease control rate (DCR): Similar to ORR, there was no statistically significant difference in DCR between the zolbetuximab plus mFOLFOX6 or CAPOX group and the placebo plus mFOLFOX6 or CAPOX group in either the SPOTLIGHT or GLOW trial.
DOR: There was no statistically significant difference in DOR between the zolbetuximab plus mFOLFOX6 or CAPOX group and the placebo plus mFOLFOX6 or CAPOX group in either the SPOTLIGHT trial (HR = 0.876; 95% CI, 0.623 to 1.233; P = 0.2218) or the GLOW trial (HR = 0.758; 95% CI, 0.527 to 1.089; P = 0.0673).
Time to progression (TTP): In the SPOTLIGHT trial, the median TTPs were 17.81 months in the zolbetuximab plus mFOLFOX6 arm and 12.52 months in the placebo plus mFOLFOX6 arm (P = 0.0133). In the GLOW trial, the median TTPs, according to IRC, were 11.99 months (95% CI, 8.84 months to 20.80 months) in the zolbetuximab plus CAPOX arm and 8.31 months (95% CI, 8.11 months to 9.95 months) in the placebo plus CAPOX arm (P = 0.0002).
Progression-free survival following second-line anticancer treatment (ACT) (PFS2): In the SPOTLIGHT trial, treatment with zolbetuximab plus mFOLFOX6 was associated with reduced risk of a PFS2 event compared with placebo plus mFOLFOX6 treatment (HR = 0.782; 95% CI, 0.637 to 0.961). The median PFS2s were 14.23 months (95% CI, 12.12 months to 16.82 months) in the group receiving zolbetuximab plus mFOLFOX6 and 11.99 months (95% CI, 11.20 months to 13.40 months) in the group receiving placebo plus mFOLFOX6. In the GLOW trial, treatment with zolbetuximab plus CAPOX demonstrated a reduced risk of PFS2 event compared with placebo plus CAPOX (HR = 0.708; 95% CI, 0.575 to 0.871). The median PFS2s were 11.01 months (95% CI, 10.02 months to 13.11 months) in the group receiving zolbetuximab plus CAPOX and 9.03 months (95% CI, 8.28 months to 9.89 months) in the group receiving placebo plus CAPOX.
Harms Results
In the pooled analysis of safety from the SPOTLIGHT and GLOW trials, the AEs that were reported for at least 20% of patients in either group included (for zolbetuximab versus placebo, respectively) nausea (75.8% versus 55.8%), vomiting (66.8% versus 33.4%), decreased appetite (44.3% versus 33.6%), anemia (35.6% versus 37.0%), diarrhea (35.6% versus 39.5%), neutrophil count decrease (31.0% versus 28.5%), peripheral sensory neuropathy (30.4% versus 33.0%), neutropenia (28.5% versus 24.5%), constipation (25.9% versus 31.1%), fatigue (21.0% versus 25.2%), aspartate aminotransferase increase (21.0% versus 22.0%), abdominal pain (20.1% versus 25.8%), asthenia (20.1% versus 18.2%), and platelet count decrease (18.9% versus 20.7%). Serious adverse events (SAEs) were reported in 245 patients (46.0%) in the combined zolbetuximab group and in 245 patients (46.5%) in the combined placebo group. SAEs reported in at least 4% of patients in either group included (zolbetuximab versus placebo, respectively) vomiting (7.1% versus 4.6%), nausea (5.6% versus 3.2%), and malignant neoplasm progression (3.6% versus 4.7%). Adverse events (AEs) leading to permanent discontinuation of zolbetuximab or placebo were reported in 106 patients (19.9%) and 66 patients (12.5%), respectively. The most frequent AEs leading to permanent discontinuation of zolbetuximab or placebo (present in 2% or more of patients in either combined group) were vomiting (3.8% versus 0.6%) and nausea (3.4% versus 0.4%), respectively.
Critical Appraisal
Baseline and demographic characteristics were generally well balanced across the zolbetuximab and placebo groups in both the SPOTLIGHT and GLOW trials. The clinical experts consulted during this review had no concerns regarding the baseline characteristics of the SPOTLIGHT and GLOW trial populations. Both SPOTLIGHT and GLOW were double-blind clinical trials. Patients who received zolbetuximab more commonly reported AEs of nausea and vomiting as well as infusion-site reactions. The clinical experts consulted during this review noted that the AE profile in the trial could potentially allow some patients and investigators to infer the allocated treatment group. The objective end points (e.g., PFS, OS, and ORR) would not be subject to bias in the event that treatment groups could be inferred as a result of AEs; however, health-related quality of life (HRQoL), which requires subjective reporting, could potentially be biased. The primary and secondary end points of the SPOTLIGHT and GLOW trials were aligned with those recommended by regulatory authorities for gastric cancer trials in the metastatic setting. The clinical experts consulted by CDA-AMC noted that PFS is not a particularly useful end point in the context of metastatic disease, in which survival is typically limited to 1 year. However, the final analyses showing an improvement in OS were considered demonstrative of a clinically meaningful benefit compared with chemotherapy alone.
The clinical experts consulted during this review noted that the baseline and demographic characteristics for the SPOTLIGHT and GLOW trials are a reasonable reflection of the target patient population in Canada. There are no other drugs specifically indicated for use in the treatment of patients with CLDN18.2-positive gastric or GEJ cancer in Canada; therefore, the choice of placebo plus mFOLFOX6 or CAPOX was considered appropriate by regulatory authorities. However, the clinical experts consulted during this review noted that the comparator used in the SPOTLIGHT and GLOW trials (i.e., placebo plus mFOLFOX6 or CAPOX) is not reflective of routine practice in Canada, where patients would typically be offered nivolumab plus chemotherapy as the preferred treatment option. The SPOTLIGHT and GLOW trials began in 2018, predating the regulatory approval of nivolumab plus chemotherapy for gastric and GEJ cancer in Canada (in October 2021); however, nivolumab plus chemotherapy remains the most relevant comparator for the current review. In the absence of a direct comparison against nivolumab plus chemotherapy, the sponsor has provided an indirect comparison, which was reviewed by CDA-AMC. In October 2024, pembrolizumab received a recommendation in favour of reimbursement from the pan-Canadian Oncology Drug Review Expert Review Committee (pERC) for use in combination with fluoropyrimidine- and platinum-containing chemotherapy for the first-line treatment of adult patients with locally advanced unresectable or metastatic HER2-negative gastric or GEJ adenocarcinoma.
The SPOTLIGHT and GLOW trials involved the following zolbetuximab dosage regimen (single loading dose of 800 mg/m2 IV, followed by 600 mg/m2 IV every 3 weeks maintenance dosing). This is likely reflective of how zolbetuximab would be used in Canadian practice for patients receiving it in combination with CAPOX (which is administered every 3 weeks), but not when receiving it in combination with mFOLFOX6 (which is administered every 2 weeks). As such, the product monograph recommends the following regimen when zolbetuximab is used in combination with mFOLFOX6: 800 mg/m2 loading dose followed by 400 mg/m2 every 2 weeks. This was based on population pharmacokinetic modelling that predicted the 400 mg/m2 every 2 weeks maintenance dosage would have similar exposure as the 600 mg/m2 every 3 weeks regimen.
Zolbetuximab is the first drug to specifically target CLDN18.2. Routine screening for CLDN18.2 is not currently performed in Canada for patients with gastric or GEJ cancer (or any other cancer). The SPOTLIGHT and GLOW trials enrolled patients who had CLDN18.2-positive tumours, defined as at least 75% of tumour cells demonstrating moderate to strong membranous CLDN18.2 staining based on central immunohistochemistry (IHC) assessment using the companion diagnostic test (i.e., the CLDN18 RxDx Assay). The clinical experts consulted during this review supported the use a 75% threshold for concluding that a patient harbours CLDN18.2-positive tumours. The experts further noted that they would not anticipate any challenges with interpreting the results of the CLDN18 RxDx Assay (e.g., diagnosis would likely be consistent across different centres in Canada).
GRADE Summary of Findings and Certainty of the Evidence
The selection of outcomes for the Grading of Recommendations, Assessment, Development, and Evaluations (GRADE) assessment was based on the sponsor’s Summary of Clinical Evidence, consultation with clinical experts, and input received from patient and clinician groups and public drug plans. Table 2 provides the list of outcomes that was finalized in consultation with expert committee members.
Table 2: Summary of Findings for Zolbetuximab Plus Chemotherapy Versus Placebo Plus Chemotherapy
Outcome and follow-up | Patients (studies), N | Absolute effects (95% CI) | Certainty | What happens | ||
|---|---|---|---|---|---|---|
Placebo plus chemotherapy | Zolbetuximab plus chemotherapy | Difference | ||||
OS (SPOTLIGHT trial; mFOLFOX6 chemotherapy) | ||||||
Probability of survival at 12 months Median follow-up (months): Zolbetuximab: 33.28 Placebo: 31.38 | 1 RCT (N = 565) | 60.65 more per 100 (54.57 more per 100 to 66.19 more per 100) | 67.36 more per 100 (61.36 more per 100 to 72.64 more per 100) | 6.71 more per 100 (1.13 fewer per 100 to 14.55 more per 100) | Moderatea | The addition of zolbetuximab to chemotherapy likely results in a clinically important increase in OS compared to placebo plus chemotherapy at 12 months. |
Probability of survival at 36 months Median follow-up (months): Zolbetuximab: 33.28 Placebo: 31.38 | 1 RCT (N = 565) | 13.72 more per 100 (9.12 more per 100 to 19.26 more per 100) | 20.92 more per 100 (15.53 more per 100 to 26.87 more per 100) | 7.20 more per 100 (0.64 fewer per 100 to 15.04 more per 100) | Moderatea | The addition of zolbetuximab to chemotherapy likely results in a clinically important increase in OS compared to placebo plus chemotherapy at 12 months. |
OS (GLOW trial; CAPOX chemotherapy) | ||||||
Probability of survival at 12 months Median follow-up (months): Zolbetuximab: 31.70 Placebo: 32.95 | 1 RCT (N = 507) | 50.44 more per 100 (43.89 more per 100 to 56.61 more per 100) | 56.68 more per 100 (50.08 more per 100 to 62.75 more per 100) | 6.24 more per 100 (3.56 fewer per 100 to 16.04 more per 100) | Moderatea | The addition of zolbetuximab to chemotherapy likely results in a clinically important increase in OS compared to placebo plus chemotherapy at 12 months. |
Probability of survival at 36 months Median follow-up (months): Zolbetuximab: 31.70 Placebo: 32.95 | 1 RCT (N = 507) | 7.88 more per 100 (4.41 more per 100 to 12.63 more per 100) | 18.30 more per 100 (12.95 more per 100 to 24.39 more per 100) | 10.42 more per 100 (2.58 more per 100 to 18.26 more per 100) | Moderatea | The addition of zolbetuximab to chemotherapy likely results in a clinically important increase in OS compared to placebo plus chemotherapy at 12 months. |
PFS per RECIST 1.1 by IRC (SPOTLIGHT trial; mFOLFOX6 chemotherapy) | ||||||
Probability of PFS at 6 months Median follow-up (months): Zolbetuximab: 12.94 Placebo: 12.65 | 1 RCT (N = 565) | 71.95 more per 100 (66.03 more per 100 to 77.03 more per 100) | 78.05 more per 100 (72.43 more per 100 to 82.67 more per 100) | 6.1 more per 100 (1.74 fewer per 100 to 13.94 more per 100) | Moderatea | The addition of zolbetuximab to chemotherapy likely results in an increase in PFS compared to placebo plus chemotherapy at 6 months. The clinical importance of the increase is unclear. |
Probability of PFS at 12 months Median follow-up (months): Zolbetuximab: 12.94 Placebo: 12.65 | 1 RCT (N = 565) | 35.04 more per 100 (28.45 more per 100 to 41.69 more per 100) | 48.86 more per 100 (41.92 more per 100 to 55.43 more per 100) | 13.8 more per 100 (4.02 more per 100 to 23.62 more per 100) | High | The addition of zolbetuximab to chemotherapy results in an increase in PFS compared to placebo plus chemotherapy at 12 months. The clinical importance of the increase is unclear. |
Probability of PFS at 30 months Median follow-up (months): Zolbetuximab: 12.94 Placebo: 12.65 | 1 RCT (N = 565) | 13.01 more per 100 (7.07 more per 100 to 20.82 more per 100) | 24.41 more per 100 (17.36 more per 100 to 32.13 more per 100) | 11.4 more per 100 (1.60 more per 100 to 21.20 more per 100) | High | The addition of zolbetuximab to chemotherapy results in an increase in PFS compared to placebo plus chemotherapy at 30 months. The clinical importance of the increase is unclear. |
PFS per RECIST 1.1 by IRC (GLOW trial; CAPOX chemotherapy) | ||||||
Probability of PFS at 6 months Median follow-up (months): Zolbetuximab: 12.62 Placebo: 12.09 | 1 RCT (N = 507) | 61.47 more per 100 (54.82 more per 100 to 67.45 more per 100) | 70.20 more per 100 (63.42 more per 100 to 75.96 more per 100) | 8.7 more per 100 (1.07 fewer per 100 to 18.53 more per 100) | Moderateb | The addition of zolbetuximab to chemotherapy results in an increase in PFS compared to placebo plus chemotherapy at 6 months. The clinical importance of the increase is unclear. |
Probability of PFS at 12 months Median follow-up (months): Zolbetuximab: 12.62 Placebo: 12.09 | 1 RCT (N = 507) | 19.13 more per 100 (13.50 more per 100 to 25.51 more per 100) | 34.86 more per 100 (27.75 more per 100 to 42.05 more per 100) | 15.7 more per 100 (5.93 more per 100 to 25.53 more per 100) | Highc | The addition of zolbetuximab to chemotherapy results in an increase in PFS compared to placebo plus chemotherapy at 12 months. The clinical importance of the increase is unclear. |
Probability of PFS 30 months Median follow-up (months): Zolbetuximab: 12.62 Placebo: 12.09 | 1 RCT (N = 507) | 7.28 more per 100 (2.99 more per 100 to 14.16 more per 100) | Not reached | NE | NA | The addition of zolbetuximab to chemotherapy results in an increase in PFS compared to placebo plus chemotherapy at 30 months. The clinical importance of the increase is unclear. |
Time to first confirmed deterioration in health-related quality of life (SPOTLIGHT trial; mFOLFOX6 chemotherapy) | ||||||
Time to deterioration of 13 points in EORTC QLQ-C30 PF | 1 RCT (N = 565) | Median time to event: 12.32 months | Median time to event: 10.71 months | Absolute differences not reported by sponsor | Cannot evaluated | Based on relative estimates of effect, the evidence is uncertain about the effect of zolbetuximab added to chemotherapy on time to first confirmed deterioration, based on the EORTC QLQ-C30 PF, EORTC QLQ-OG25 Pain scale, and EORTC GHS/QoL scale. |
Time to deterioration of 16.7 in EORTC QLQ-OG25 Pain scale | 1 RCT (N = 565) | Median time to event: 8.48 months | Median time to event: 6.83 months | |||
Time to deterioration of 13 points in EORTC GHS/QoL scale | 1 RCT (N = 565) | Median time to event: 11.83 months | Median time to event: 15.44 months | |||
Time to first confirmed deterioration in health-related quality of life (GLOW trial; CAPOX chemotherapy) | ||||||
Time to deterioration of 13 points in EORTC QLQ-C30 PF scale | 1 RCT (N = 507) | Median time to event: 7.92 months | Median time to event: 8.31 months | Absolute differences not reported by sponsor | Cannot evaluated | Based on relative estimates of effect, the evidence is uncertain about the effect of zolbetuximab added to chemotherapy on time to first confirmed deterioration based on the EORTC QLQ-C30 PF scale, EORTC QLQ-OG25 Pain scale, and EORTC GHS/QoL scale. |
Time to deterioration of 16.7 points in EORTC QLQ-OG25 Pain scale | 1 RCT (N = 507) | Median time to event: 12.94 months | Median time to event: 19.81 months | |||
Time to deterioration of 13 points in EORTC GHS/QoL scale | 1 RCT (N = 507) | Median time to event: 7.49 months | Median time to event: 9.69 months | |||
Harms | ||||||
Nausea | 2 RCTs (N = 1,060) | 55.8 per 100 | 75.8 per 100 | NR | High | The addition of zolbetuximab to chemotherapy results in an increased risk of nausea, vomiting, and IRRs compared to placebo plus chemotherapy. The clinical experts consulted during this review noted that these events are manageable in clinical practice. |
Vomiting | 2 RCTs (N = 1,060) | 33.4 per 100 | 66.8 per 100 | NR | High | |
IRR | 2 RCTs (N = 1,060) | 11.0 per 100 | 40.3 per 100 | NR | High | |
CAPOX = capecitabine plus oxaliplatin; CDA-AMC = Canada’s Drug Agency; CI = confidence interval; EORTC GHS/QoL = European Organisation for Research and Treatment of Cancer Global Health Status/Quality of Life; EORTC QLQ-C30 PF = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire - Core Questionnaire Physical Functioning; EORTC QLQ-OG25 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Oesophago-Gastric 25; GRADE = Grading of Recommendations, Assessment, Development, and Evaluations; IRC = independent review committee; IRR = infusion-related reaction; mFOLFOX6 = modified 5-fluorouracil, folinic acid, and oxaliplatin; NA = not available; NE = not estimable; NR = not reported; OS = overall survival; PFS = progression-free survival; RCT = randomized controlled trial; RECIST 1.1 = Response Evaluation Criteria in Solid Tumours Version 1.1.
aRated down 1 level for serious imprecision. Although the point estimate suggests a clinically important benefit (exceeding the 5% to 10% threshold suggested by the clinical experts consulted on this review), the lower bound of the 95% CI is compatible with little to no difference in clinical benefit.
bRated down 1 level for serious imprecision because the lower bounds of the 95% CI were compatible with little to no difference in clinical benefit.
cThe clinical experts consulted on this review indicated a lack of clarity about a threshold of clinical importance; therefore, the null was used. Although the certainty of evidence was not rated down for serious indirectness, there were concerns about the clinical importance of PFS.
dCertainty of evidence cannot be evaluated because the sponsor did not report the absolute difference between groups and was not able provide this information upon request. In the absence of a reported absolute difference, CDA-AMC was unable to determine an appropriate target for the certainty assessment under the GRADE framework, given that the reported relative effects for these end points were not considered suitable for inferring whether a clinically meaningful difference was observed for these end points. Likewise, the ability to assess the imprecision of any target of the certainty assessment would have been limited if it were based on relative effect estimates alone. Although the certainty for these end points cannot be assessed, the results for these end points were noted to have a potential risk of bias because the sponsor reported that the results of the analyses are not mature enough to derive thresholds for clinically meaningful deterioration.
Long-Term Extension Studies
Not applicable.
Indirect Comparisons
In the absence of direct head-to-head trials evaluating the comparative efficacy of zolbetuximab versus relevant comparators for the first-line treatment of patients with locally advanced unresectable or metastatic HER2-negative gastric or GEJ adenocarcinoma whose tumours are CLDN18.2-positive, a review of indirect evidence was undertaken and submitted by the sponsor. The objective of this section is to summarize and critically appraise the sponsor-submitted indirect treatment comparison (ITC), and to inform the pharmacoeconomic model.
Description of Studies
In the sponsor-conducted systematic review, 174 publications reporting on 92 studies were included. After applying the network meta-analysis (NMA) inclusion and exclusion criteria, 21 randomized controlled trials (RCTs), including the GLOW and SPOTLIGHT trials, were deemed relevant for the sponsor’s NMA; these included 14 unique treatment regimens. After the removal of 1 study that did not include subgroup analysis based on CPS score, 20 studies were included in the analysis. The sponsor reported that the inclusion and exclusion criteria, including disease stage, age, and Eastern Cooperative Oncology Group (ECOG) Performance Status, were generally consistent across trials. The sample size across trials ranged from 38 patients to 1,581 patients, and the median follow-up durations ranged from 7 months to 26.6 months. Half of the included trials were only conducted in Asian countries. The dose schedule for the majority of treatment regimens appears consistent across studies, with some variation for fluorouracil-based regimens and tegafur/gimeracil/oteracil (S-1)–based regimens. OS and PFS were analyzed in the NMA, and the definitions were reported as mainly consistent across the trials.
Efficacy Results
The NMA was constructed using a fixed-effects model, and the sponsor reports that the trace and density plots, Gelman-Rubin plots, and Gelman-Rubin diagnostics showed that convergence of the results was generally achieved. For OS, results from the NMA are consistent with results of the pivotal evidence, in which zolbetuximab combined with CAPOX is superior to CAPOX alone (HR = 0.76; 95% credible interval [CrI], 0.62 to 0.94), and zolbetuximab combined with FOLFOX is superior to FOLFOX alone (HR = 0.78; 95% Crl, 0.64 to 0.95). The HRs for cross-comparisons with CAPOX and FOLFOX are also consistent. However, the wide CrIs may indicate heterogeneity between the studies that used CAPOX versus FOLFOX. CrIs for the comparisons of zolbetuximab plus chemotherapy versus nivolumab or pembrolizumab plus chemotherapy did not favour either comparator in OS; however, the HR was consistently higher with zolbetuximab plus FOLFOX compared to zolbetuximab plus CAPOX. For PFS, results are again consistent with results of the pivotal evidence, in which zolbetuximab combined with CAPOX is superior to CAPOX alone (HR = 0.69; 95% Crl, 0.55 to 0.86) and zolbetuximab combined with FOLFOX is superior to FOLFOX alone (HR = 0.73; 95% Crl, 0.59 to 0.91). The HRs for cross-comparisons with CAPOX and FOLFOX are also consistent; however, the wide CrIs may indicate heterogeneity between the studies that used CAPOX versus FOLFOX. The CrIs for the comparisons of zolbetuximab plus chemotherapy versus nivolumab or pembrolizumab plus chemotherapy did not favour either comparator in OS; however, the HR was consistently higher with zolbetuximab plus FOLFOX compared to zolbetuximab plus CAPOX.
Harms Results
Harms outcomes were not evaluated in the NMA.
Critical Appraisal
The sponsor-submitted NMA was based on studies identified from a systematic literature review of relevant evidence, based on a population, invention, comparator, and outcome (PICO) defined a priori. While the risk of bias of the comparator trials was assessed, it was not reported how many reviewers conducted the quality assessment; nor was the risk of bias assessed per outcome. The sponsor conducted 2 primary analyses: with CAPOX and FOLFOX as separate comparators and then with the 2 regimens combined as a single comparator. This was based on the sponsor’s assumption that CAPOX and FOLFOX were of equivalent efficacy, an assumption that was supported by the clinical experts consulted for this review. However, the results of the primary NMA analysis that keeps the comparators separate do not support combining these comparators because there are wide CrIs in the cross-comparisons between both treatments, indicating systematic heterogeneity between the studies that used CAPOX versus those that used FOLFOX. Therefore, the results of both analyses must be interpreted with caution.
The clinical experts consulted during this review noted that proactive screening for gastrointestinal cancers is more common in some Asian countries and that this tends to contribute to more favourable outcomes for some patients. Thus, the heterogeneity in the trial populations across the network likely introduced bias in the comparisons across the network. The sponsor conducted sensitivity analyses, excluding the Asia-only trials or focusing on Asia-only trials (or Asian subgroups of global trials), and the findings were similar to those of the primary NMA analysis; however, this sensitivity analysis was conducted only in the second primary analysis with CAPOX and FOLFOX combined and in which CDA-AMC has noted greater heterogeneity across studies.
The sponsor reports that differences in median follow-up durations (and, therefore, data maturity) could introduce bias because HRs tend to wane with longer follow-up times; yet the sponsor was unable to account for differences in data maturity in its analysis. With regards to patient baseline characteristics, the sponsor noted variations across trials in the median age, ECOG performance status, tumour location and type, disease stage, number of metastatic sites, mutation status, and prior surgery; however, it noted that it did not adjust for these variations in its analysis. Specifically for tumour location, the clinical experts noted that the trial data do not show benefits for patients with GEJ tumours; therefore, heterogeneity across the network in tumour location could be an important source of bias for these NMAs.
There were variations in the collection and reporting of mutation status across trials; therefore, the sponsor did not adjust for HER2 or CLDN18.2 expression status. The clinical experts consulted for this review noted that, while zolbetuximab plus chemotherapy could be a preferred option for patients with CLDN18.2-positive tumours and a PD-L1 CPS of less than 5, it is unclear which option would be best for patients with CLDN18.2-positive tumours and a PD-L1 CPS of greater than or equal to 5. In this NMA, the sponsor conducted 2 subgroup analyses with CPS greater than or equal 5 and CPS less than 5 in the 5 trials that reported CPS scores; however, these analyses used only CPS-specific HRs from the nivolumab and pembrolizumab trials and did not use the subgroup-specific data from the SPOTLIGHT and GLOW trials. The clinical review team considered this approach to be at risk for severe bias due to the existing evidence that has established CPS testing as a potential effect modifier in this disease area. Therefore, this subgroup analysis has significant limitations, and no definitive conclusions could be drawn for this subpopulation of patients.
NMA results were presented for OS and PFS only; harms outcomes and other outcomes of relevance to patients (e.g., HRQoL) were not reported. The treatment effects measured using HRs of OS or PFS assumed proportional hazards, which were confirmed in 3 trials but not reported in most included studies. The consistency test performed in the primary analysis using CAPOX and FOLFOX as combined treatments suggested evidence of inconsistency in the PFS network.
Studies Addressing Gaps in the Evidence From the Systematic Review
Not applicable.
Conclusions
Two randomized, double-blind, placebo-controlled, phase III trials (the SPOTLIGHT and GLOW trials) demonstrated that treatment with zolbetuximab in combination with fluoropyrimidine- and platinum-based chemotherapy (i.e., mFOLFOX6 or CAPOX) resulted in a clinically important improvement in OS compared with placebo in combination with fluoropyrimidine- and platinum-based chemotherapy for the first-line treatment of patients with locally advanced unresectable or metastatic HER2-negative gastric or GEJ cancer adenocarcinoma whose tumours are CLDN18.2-positive. The SPOTLIGHT and GLOW trials similarly demonstrated that treatment with zolbetuximab in combination with chemotherapy resulted in improvements in PFS compared with placebo in combination with chemotherapy. The results for time to deterioration based on changes in HRQoL scales were inconsistent across the SPOTLIGHT and GLOW trials.
The sponsor-submitted ITC suggested that there was little to no difference in treatment effect on OS and PFS between zolbetuximab and nivolumab in combination with chemotherapy; however, these comparisons were not limited to patients whose tumours were CLDN18.2-positive. However, the indirect evidence is associated with uncertainty due to clinical and methodological heterogeneity between the studies included in the network, with a potential to introduce bias to the ITC results.
Treatment with zolbetuximab in combination with chemotherapy is associated with an increased risk of nausea, vomiting, and infusion-related reactions (IRRs) compared with chemotherapy alone. The product monograph provides recommendations regarding pretreatment with medications to reduce the risk, as well as recommendations for treatment interruption and discontinuation (if required) for those who experience grade 2, 3, or 4 AEs. The clinical experts consulted during this review indicated that these events would be manageable in clinical practice and would not be expected to limit the usage of zolbetuximab. The sponsor’s submitted ITC did not include an evaluation of the comparative safety of zolbetuximab versus nivolumab or pembrolizumab. Acknowledging the absence of comparative evidence, the clinical experts noted that the AE profile for zolbetuximab in combination with chemotherapy is generally comparable to those of the alternative regimens that would be available for patients with metastatic gastric or GEJ cancer.
Introduction
The objective of this clinical review report is to review and critically appraise the clinical evidence submitted by the sponsor on the beneficial and harmful effects of zolbetuximab in combination with fluoropyrimidine- and platinum-containing chemotherapy for the first-line treatment of patients with locally advanced unresectable or metastatic HER2-negative gastric or GEJ adenocarcinoma whose tumours are CLDN18.2-positive as determined by a validated test. The focus will be on comparing zolbetuximab to relevant comparators and identifying gaps in the current evidence.
Disease Background
Contents within this section have been informed by materials submitted by the sponsor and clinical expert input. The following has been summarized and validated by CDA-AMC.
Gastric cancers originate in the cells lining the stomach and are generally classified into 2 topographical subsites.1-3 Cardia gastric cancer arises in the upper part of the stomach near the GEJ, and noncardia gastric cancer arises in the more distal regions of the stomach.1 GEJ cancers occur in the cells lining the GEJ, the area where the esophagus joins the gastric cardia.2,3
In 2024 in Canada, an estimated 4,000 people (2,600 males and 1,400 females) will be newly diagnosed with stomach cancer, and an estimated 2,000 individuals will die from this disease.4 The risk of developing gastric cancer increases with age and is greatest in people aged 50 years or older.5 Canadian statistics from 2019 showed that the lifetime probability of developing stomach cancer was higher among males (1.3%) than females (0.7%)5-7 and that the projected, estimated, age-standardized incidence rates for stomach cancer in 2022 were 12 per 100,000 and 5.6 per 100,000 for males and females, respectively.1 Chronic infection with Helicobacter pylori is a major risk factor for noncardia gastric cancer and is responsible for nearly 90% of these gastric cancer cases worldwide.8,9 Other risk factors for stomach cancer include smoking, heavy alcohol consumption, being overweight, and high consumption of foods preserved by nitrates and/or nitrites.30-32
Advanced, unresectable, or metastatic G/ GEJ cancers are considered incurable.13 Early gastric cancers that are surgically curable are typically asymptomatic.12 If symptoms are present at the early stage, these are usually nonspecific (e.g., indigestion, heartburn, bloating, mild nausea).10,11 Diagnosis of gastric or GEJ cancer frequently occurs when the disease is at an advanced, unresectable, or metastatic stage.10,12,13 According to data from the US, 36% of stomach cancers are diagnosed at the metastatic stage.16 Advanced gastric cancers are associated with symptoms such as unexplained weight loss, abdominal pain, early satiety, dysphagia, asthenia, nausea, vomiting, bleeding, anemia, ascites, and jaundice.11,12,14,28,33,34 Quality of life in patients with gastric cancer is affected by emotional, physical, and social aspects of the disease and its treatment.14 Individuals may experience anxiety and depression as well as increasing symptom burden in advanced stages.12,14 In Canada, from 2015 to 2017, the 5-year net survival rate for individuals diagnosed with stomach cancer was 29%, reflecting that diagnoses are often made at the advanced stages of the disease, a situation associated with poor prognosis.6,7,12,15 US data indicate that the 5-year relative survival rate for patients with metastatic gastric cancer is 7%.16 A clinical expert consulted by CDA-AMC stated that the median survival duration for patients with metastatic gastric or GEJ cancer is approximately 1 year.
Greater than 90% of gastric cancers are histologically classified as adenocarcinomas.13 Various genetic aberrations can occur during the development of gastric cancer.17 HER2 is overexpressed in approximately 20% of gastric or GEJ adenocarcinomas.18 Although the prognostic significance of HER2 status is not well established in gastric cancer, HER2 status can be applied clinically in individualizing treatment for advanced or metastatic gastric disease.17 Testing for HER2 expression is a routine part of clinical practice in Canada upon diagnosis of advanced gastric or GEJ cancer.35 CLDN18.2 is a membrane tight junction molecule that is inaccessible in normal gastric epithelial tissue. CLDN18.2 may become exposed on the surface of gastric or GEJ adenocarcinoma cells due to the disruption of cell polarity that occurs during carcinogenesis.21-23 The sponsor reported that, based on screening data from the SPOTLIGHT and GLOW trials, 38% of patients with locally advanced unresectable or metastatic gastric or GEJ adenocarcinoma are CDLN18.2-positive (defined as expression with 2+ or 3+ intensity in ≥ 75% of tumour cells).24,25
The diagnosis and staging of gastric or GEJ cancer are performed by an oncologist.19 Procedures include blood tests; imaging with upper gastrointestinal endoscopy; endoscopic ultrasound; CT, PET, and/or MRI scans; and tissue biopsy.2019,20 Biomarker testing of cancer tissue may also be performed to inform treatment decisions, including testing for HER2, PD-L1 CPS, and MMR.19,20 A clinical expert consulted by CDA-AMC expressed that upon approval of zolbetuximab, stomach cancers should be reflexively tested for HER2, CPS, MMR, and CLDN18.2 to inform treatment decisions.
Standards of Therapy
Contents within this section have been informed by materials submitted by the sponsor and clinical expert input. The following has been summarized and validated by CDA-AMC.
Drug Under Review
Indication and Requested Reimbursement Criteria
Zolbetuximab is approved for use in combination with fluoropyrimidine- and platinum-containing chemotherapy for the first-line treatment of patients with locally advanced unresectable or metastatic HER2-negative gastric or GEJ adenocarcinoma whose tumours are CLDN18.2-positive as determined by a validated test.21 The sponsor has requested reimbursement in accordance with the indication approved by Health Canada. Zolbetuximab has not been reviewed previously by CDA-AMC. Zolbetuximab was approved by the FDA on October 18, 2024.36 On July 25, 2024, the European Medicines Agency (EMA) Committee for Medicinal Products for Human Use recommended that market authorization be granted for zolbetuximab for the treatment of gastric or GEJ adenocarcinoma. The full indication is in alignment with the indication under review by CDA-AMC.37
Mechanism of Action
Zolbetuximab is a monoclonal antibody that targets CLDN18.2, a tight junction molecule that may become exposed on the surface of gastric or GEJ adenocarcinoma cells. Zolbetuximab acts through ADCC and CDC to deplete CLDN18.2-positive cells. Cytotoxic drugs were shown to increase the expression of CLDN18.2 on human cancer cells and to improve ADCC and CDC activities induced by zolbetuximab.21
Recommended Dosage
Zolbetuximab is supplied in single-use vials containing zolbetuximab 100 mg as a lyophilized powder for concentrate for solution for IV infusion.21 The product monograph–recommended dosage consists of a single loading dose (800 mg/m2 through IV) followed by a maintenance dosage of 600 mg/m2 through IV once every 3 weeks or 400 mg/m2 through IV once every 2 weeks. The recommended dose is administered by IV infusion over a minimum of 2 hours. As outlined in the product monograph, a slower rate is recommended at the start of each infusion to help minimize potential adverse reactions; in the absence of adverse reactions after 30 minutes to 60 minutes, the rate may be increased as tolerated.21 To align the administration schedule for zolbetuximab with the concomitant chemotherapy schedule, the product monograph recommends the 400 mg/m2 every 2 weeks maintenance dosage when used in combination with mFOLFOX6 and the 600 mg/m2 every 3 weeks maintenance dosage when used in combination with CAPOX.21
No dose reduction for zolbetuximab is recommended. Infusion rate reduction, interruption, and/or discontinuation is used for management of adverse reactions to zolbetuximab, as detailed in the product monograph.21 Patients should be monitored during and after infusion of zolbetuximab for signs and symptoms of hypersensitivity or IRRs.21 Premedication with antiemetics before each infusion of zolbetuximab is recommended for the prevention of nausea and vomiting; premedication may also be required for hypersensitivity or IRRs.21 Treatment with zolbetuximab should be initiated and supervised by a physician with experience in the use of ACTs.21
Proposed Place in Therapy
As shown in Figure 1, the sponsor is proposing that zolbetuximab be a preferred treatment option for the first-line treatment of patients with locally advanced unresectable or metastatic HER2-negative gastric or GEJ adenocarcinoma whose tumours are CLDN18.2-positive.
Figure 1: Sponsor’s Proposed Place in Therapy for Zolbetuximab
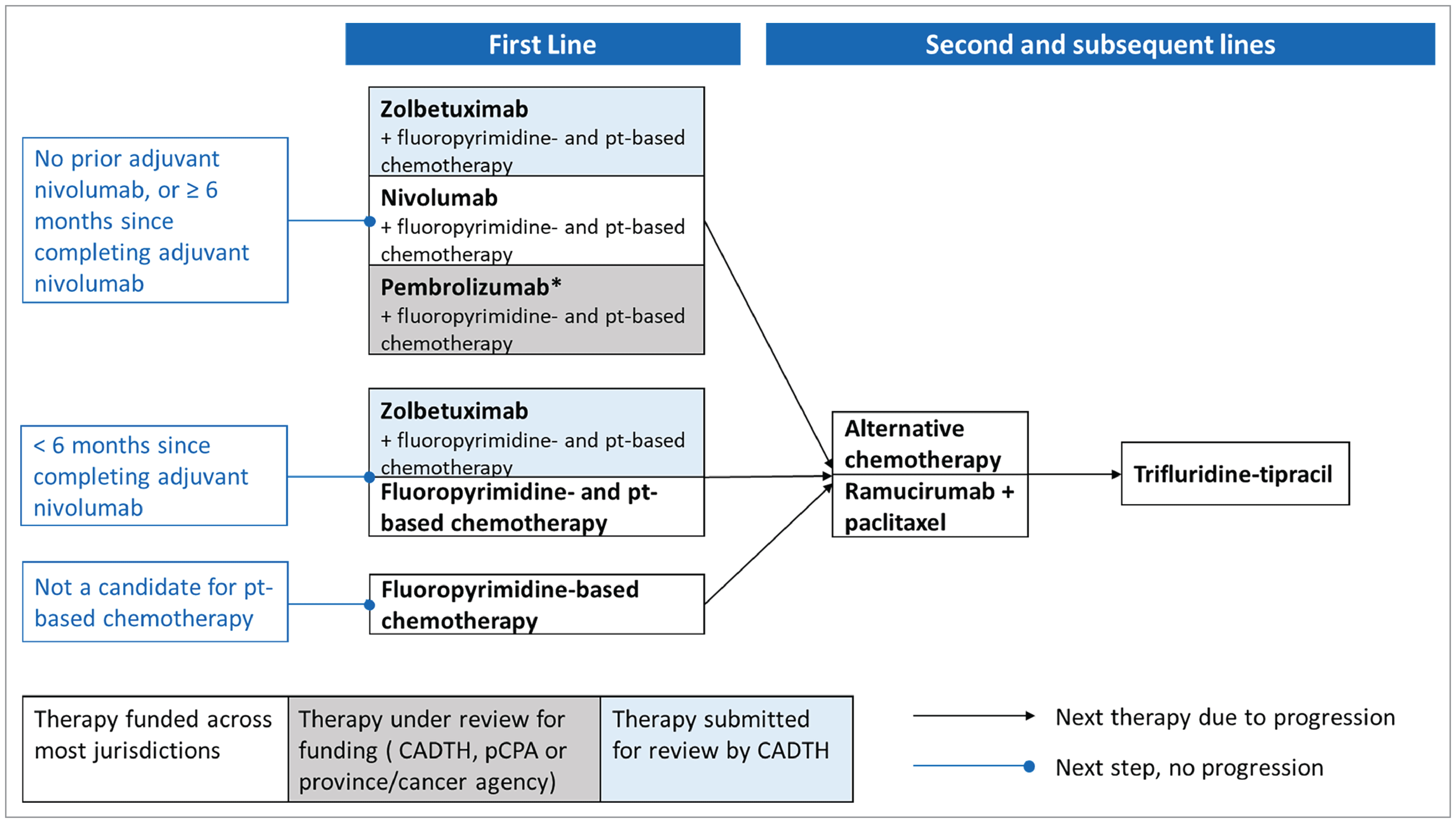
HER2 = human epidermal growth factor 2; pCPA = pan-Canadian Pharmaceutical Alliance; pt = platinum.
Note: The asterisk indicates that pembrolizumab is reimbursed only for patients with gastroesophageal junction cancer. (It is also indicated for esophageal cancer, but these patients are not included in this diagram.) It remains under review by Canada’s Drug Agency for the entire population of patients with HER2-negative gastric or gastroesophageal junction adenocarcinoma. Although technically funded, pembrolizumab is not currently used in patients with gastroesophageal junction adenocarcinoma.
Source: Sponsor’s submission.
Characteristics of Drugs for Gastric or GEJ Adenocarcinoma
The key characteristics of zolbetuximab are summarized in Table 3, along with those of other treatments available for gastric or GEJ adenocarcinoma.
Table 3: Key Characteristics of First-Line Treatments for Gastric or GEJ Adenocarcinoma
Characteristic | Zolbetuximab plus fluoropyrimidine- and platinum-containing chemotherapy | Pembrolizumab plus platinum-fluoropyrimidine doublet chemotherapy | Platinum-fluoropyrimidine doublet chemotherapy | Nivolumab plus platinum-fluoropyrimidine doublet chemotherapy |
|---|---|---|---|---|
Mechanism of action | Zolbetuximab: Monoclonal antibody directed against the tight junction molecule CLDN18.2. Zolbetuximab depletes CLDN18.2-positive cells through ADCC and CDC. Cytotoxic drugs were shown to increase CLDN18.2 expression on human cancer cells and to improve zolbetuximab-induced ADCC and CDC activities. Chemotherapy: Antineoplastic (i.e., slows cancer growth or stops the growth of tumours [neoplasms]) or cytotoxic (i.e., kills tumour cells) | Pembrolizumab: Releases PD-1 pathway-mediated inhibition of the immune response and restores T-cell proliferation and cytokine production. Chemotherapy: Antineoplastic (i.e., slows cancer growth or stops the growth of tumours [neoplasms]) or cytotoxic (i.e., kills tumour cells) | Chemotherapy: Antineoplastic (i.e., slows cancer growth or stops the growth of tumours [neoplasms]) or cytotoxic (i.e., kills tumour cells) | Nivolumab: Blockade of PD-1:PD-L1 and PD-L2 interaction and release of antitumour T-cell responses Chemotherapy: Antineoplastic (i.e., slows cancer growth or stops the growth of tumours [neoplasms]) or cytotoxic (i.e., kills tumour cells) |
Indicationa | Proposed indication: In combination with fluoropyrimidine- and platinum-containing chemotherapy, indicated for the first-line treatment of patients with locally advanced unresectable or metastatic HER2-negative gastric or GEJ adenocarcinoma whose tumours are CLDN18.2-positive as determined by a validated test. | First-line treatment, in combination with fluoropyrimidine- and platinum-containing chemotherapy, of adult patients with locally advanced unresectable or metastatic HER2-negative gastric or GEJ adenocarcinoma | Not reviewed by Health Canada, but standard of care in clinical practice in Canada | HER2-negative advanced or metastatic gastric cancer, GEJ cancer, or esophageal adenocarcinoma, in combination with fluoropyrimidine- and platinum- containing chemotherapy38 |
Recommended dose and route of administration | Zolbetuximab:
AND Fluoropyrimidine- and platinum-containing chemotherapy:
OR
Alternative regimens that may be used in clinical practice:
OR
| Pembrolizumab: 200 mg IV over 30 minutes every 3 weeks or 400 mg IV every 6 weeks AND Fluoropyrimidine- and platinum-containing chemotherapy:
OR
Alternative regimens that may be used in clinical practice:
OR
| Fluoropyrimidine- and platinum-containing chemotherapy:
OR
OR
OR
| Nivolumab: 360 mg IV over 30 minutes (every 3 weeks) or 240 mg IV (every 2 weeks) AND Fluoropyrimidine- and platinum-containing chemotherapy:
OR
OR
OR
|
Serious adverse effects or safety issues | Zolbetuximab: Warnings and precautions for immune-mediated adverse reactions, infusion-related reactions, and nausea and vomiting | Pembrolizumab in combination with chemotherapy: Fatigue and/or asthenia, nausea, constipation, diarrhea, decreased appetite, rash, vomiting, cough, dyspnea, pyrexia, alopecia, peripheral neuropathy, mucosal inflammation, stomatitis, headache, weight loss, abdominal pain, arthralgia, myalgia, and insomnia Chemotherapy: Hair loss, nausea, vomiting, anemia, bone loss, constipation, diarrhea, fatigue, depression, anxiety, hand-foot syndrome, low platelets, low WBCs, mouth problems | Chemotherapy: Hair loss, nausea, vomiting, anemia, bone loss, constipation, diarrhea, fatigue, depression, anxiety, hand-foot syndrome, low platelets, low WBCs, mouth problems | Nivolumab: Severe and/or fatal immune-mediated adverse reactions Chemotherapy: Hair loss, nausea, vomiting, anemia, bone loss, constipation, diarrhea, fatigue, depression, anxiety, hand-foot syndrome, low platelets, low WBCs, mouth problems |
Other | Under review | Draft recommendation in favour of reimbursement (May 2024) | Not reviewed by CDA-AMC | Recommendation in favour of reimbursement (March 2022) |
5-FU = 5-fluorouracil; ADCC = antibody-dependent cellular cytotoxicity; CAPECISP = capecitabine plus cisplatin; CAPOX = capecitabine plus oxaliplatin; CDA-AMC = Canada’s Drug Agency; CDC = complement-dependent cytotoxicity; CLDN18.2 = Claudin 18.2; FOLFOX = leucovorin calcium (folinic acid), fluorouracil, and oxaliplatin; FP = 5-fluorouracil and cisplatin; GEJ = gastroesophageal junction; HER2 = human epidermal growth factor receptor 2; PD-1 = programmed death protein 1; PD-L1 = programmed death-ligand 1; PD-L1 = programmed death-ligand 2; WBC = white blood cell.
aHealth Canada–approved indication.
Source: Product monographs.
Perspectives of Patients, Clinicians, and Drug Programs
Patient Group Input
This section was prepared by CDA-AMC based on the input provided by patient groups. The full original patient group input received by CDA-AMC is available on the project webpage.
One patient group provided input for this review. My Gut Feeling – Stomach Cancer Foundation of Canada is a nonprofit organization providing support, awareness, education, information, and advocacy to patients with (and survivors of) stomach cancer and their caregivers. Individuals with gastroesophageal and esophageal cancer receive support and are included in service programs. The mission of this organization is to improve the quality of life for people affected by gastroesophageal cancers and to make systemic changes to reduce the incidence and mortality of gastroesophageal cancers.
From June 21 to July 2, 2024, My Gut Feeling – Stomach Cancer Foundation of Canada conducted an international online survey of patients and caregivers affected by gastric, esophageal, and/or gastroesophageal cancer. The survey was shared through the social media platforms and email distribution lists of My Gut Feeling and other organizations (e.g., the Gastrointestinal Society). A total of 35 respondents completed the survey, 14.3% of whom were caregivers and 85.7% of whom were patients. Of the participants, 17.1% were currently receiving treatment and 68.6% had completed treatment; 68.6% and 31.4% of respondents identified as female and male, respectively, and their ages at initial diagnosis ranged from 20 to 80 years. The majority of respondents resided in Canada (71.4%) or the US (25.7%); survey results were presented for the overall population surveyed. Most participants had gastric cancer (88.6%); the remainder had gastroesophageal cancer (11.4%). The stage at diagnosis ranged from I to IV; 71.4% of patients were reported to have adenocarcinoma, while 20% did not know the type of cancer they had. Regarding biomarker testing, 51% of participants confirmed having been tested; 8.6% reported being CLDN18.2-positive, 20% reported being HER2-negative, and 34.3% reported that the results were not shared with them.
Nearly all participants (97.2%) responded that their quality of life was significantly affected by the cancer diagnosis. Specifically, their physical and mental health, ability to eat, work, finances, social life, identity, and personal image were all impacted. For example, respondents expressed the exhaustion of managing adequate daily nutrition and the toll of experiencing weight loss or weight gain, including its impact on body image. Patients and caregivers (particularly those affected by metastatic disease) communicated that the cancer diagnosis and its treatment had negative impacts on their mental health and caused anxiety surrounding finances (e.g., loss of income due to work absenteeism, additional expenses due to travel for medical care and/or specialized diets). Patients reported feeling anxiety, depression, and/or anger, and said that experiencing fatigue greatly impacted their daily activities.
Regarding previously received and current treatments, patients reported receiving fluorouracil, leucovorin, oxaliplatin, and docetaxel (FLOT) (45.7%), chemotherapy consisting of either FOLFOX or leucovorin calcium (folinic acid), fluorouracil, and irinotecan hydrochloride (FOLFIRI) alone (8.6%), or combined chemotherapy and immunotherapy (8.6%). A combination of various treatments (e.g., 5-fluorouracil plus radiation, surgery, capecitabine, pembrolizumab) were received by the remainder of patients. Participants reported experiencing a wide range of side effects during treatment, with fatigue (91.4%) and weight loss (77.1%) being most frequently mentioned. Regarding the effectiveness of controlling cancer and symptoms, 62.9% and 31.5% of respondents felt that their treatment had been very effective or moderately effective, respectively, while the remainder of respondents (5.6%) felt there was little or no efficacy. None of the survey participants had experience with zolbetuximab.
Participants stated that many factors are considered when weighing treatment options (such as quality of life, survival benefits, side effects, convenience, and duration of therapy), recognizing that treatments have trade-offs that need to be considered. For example, most respondents (82.9%) would choose a treatment that prolongs life despite side effects. Patients also expressed a preference for the convenience of oral chemotherapy taken at home over IV chemotherapy administered in a hospital setting.
My Gut Feeling indicated that gastric and gastroesophageal cancers are rare in Canada, with few treatment options. The organization expressed an unmet need for equitable access to therapies that prolong life, improve symptoms, reduce the risk of recurrence, and have improved tolerability. My Gut Feeling strongly supports the use of zolbetuximab in combination with chemotherapy as first-line treatment for patients with locally advanced unresectable or metastatic HER2-negative gastric or GEJ adenocarcinoma whose tumours are CLDN18.2-positive. The organization also expressed the view that biomarker testing should be accessible at the onset of disease for all patients in Canada. This patient group believes that there should be a choice in treatment options that are available barrier-free and covered under the universal health care system in Canada for the benefit of these patients.
Clinician Input
Input From Clinical Experts Consulted by CDA-AMC
All review teams include at least 1 clinical specialist with expertise regarding the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). The input described in this section was provided by 2 clinical specialists with expertise in the diagnosis and management of gastric or GEJ adenocarcinoma.
Unmet Needs
The clinical experts consulted for the purpose of this review emphasized that locally advanced and metastatic HER2-negative gastric or GEJ cancers are associated with considerable unmet needs. Treatment with nivolumab in combination with chemotherapy is the only available first-line option for locally advanced metastatic HER2-negative gastric or GEJ cancer; however, OS outcome remains poor (with a median OS of 13 months to 15 months).
Place in Therapy
The clinical experts suggested that the addition of zolbetuximab to chemotherapy would represent an alternative to combination therapy with nivolumab plus chemotherapy in the first-line metastatic treatment setting for patients with locally advanced and/or metastatic HER2-negative gastric or GEJ cancer whose tumours are CLDN18.2-positive.
Patient Population
Regulatory approval and reimbursement for nivolumab for patients with gastric or GEJ cancer is not limited based on a patient’s PD-L1 CPS; however, the clinical experts noted that there is some uncertainty in the clinical community regarding the effectiveness of nivolumab plus chemotherapy in patients with a PD-L1 CPS of less than 5. As such, the clinical experts noted that zolbetuximab plus chemotherapy could be a preferred option for patients with CLDN18.2-positive tumours and a PD-L1 CPS of less than 5. For patients with CLDN18.2-positive tumours and a PD-L1 CPS of at least 5, it is currently unclear which option could offer the best outcomes.
Assessing the Response Treatment
The clinical experts noted that the clinically meaningful end points across all oncology types are OS and quality of life, and that PFS has limited value when assessing clinical benefit for patients with metastatic disease and a relative short OS duration. The clinical experts noted that the following factors should be used to determine response to treatment: patient-reported symptoms and side effects and response on cross-sectional imaging with CT or MRI. The clinical experts suggested that patients should be assessed by a clinician after every 2 to 3 cycles of treatment. Clinician assessment may occur more frequently if a patient reports the occurrence of bothersome symptoms or side effects. The clinical experts suggested that patients should undergo CT scans every 2 to 3 months. Tumour markers can be used as per clinical judgment to supplement a fulsome patient assessment.
Discontinuing Treatment
The clinical experts suggested that the decision to discontinue treatment with zolbetuximab should be based on patient-reported symptoms, patient preference, side effects, and well-being, in combination with an assessment of treatment response and disease progression, either radiological or clinical.
Prescribing Considerations
The clinical experts suggested that zolbetuximab should be prescribed only by (or under the supervision of) a medical oncologist with expertise in the management of immunotherapy side effects. The clinical experts noted that immunotherapy and chemotherapy are currently delivered as standard of care in all oncology centres. Accordingly, these therapies, with the addition of zolbetuximab, can be safely administered in all centres approved for oncology care.
Clinician Group Input
This section was prepared by CDA-AMC based on the input provided by clinician groups. The full original clinician group input received by CDA-AMC is available on the project webpage.
Four clinicians from the OH-CCO GI DAC provided input for this review. These committees provide timely, evidence-based clinical and health system guidance on drug-related issues in support of Cancer Care Ontario’s mandate, including the Provincial Drug Reimbursement programs and the Systemic Treatment Program.
Regarding currently available treatments for metastatic HER2-negative gastric cancer, the clinician group stated that standard first-line therapy consists of chemotherapy (typically FOLFOX) combined with immunotherapy (nivolumab, which is currently funded, or pembrolizumab, which is approved but not funded). The goals of treatment are to prolong life, delay disease progression, and maintain quality of life. The OH-CCO GI DAC expressed that there are currently no approved treatments that specifically target tumours overexpressing CLDN18.2; therefore, there is an unmet need in this population. Clinical experts consulted by CDA-AMC also identified FOLFOX with or without nivolumab as a first-line therapy in this population, with the goals of therapy including to improve symptoms, delay progression, improve quality of life, and prolong survival. These experts identified an unmet need for treatments with other biological targets and for new treatments that will increase survival.
The OH-CCO GI DAC remarked that the patients best suited for treatment with zolbetuximab are those with HER2-negative, CLDN18.2-positive advanced gastric or GEJ cancer. This clinician group stated that zolbetuximab would provide an alternative to nivolumab, noting that zolbetuximab and nivolumab in the first-line setting have not been compared head-to-head. For patients with CLDN18.2 overexpression and a negative or low PD-L1 CPS, the clinician group suspects that zolbetuximab and chemotherapy would be the clear first-line choice of therapy, but acknowledges that the best first-line therapy (i.e., nivolumab, pembrolizumab or zolbetuximab) for patients with CLDN18.2 overexpression and a PD-L1 CPS of greater than 5 is unclear. For the latter population of patients, the choice of drug to add (i.e., zolbetuximab, nivolumab, or immunotherapy) would be at the physician’s discretion based on comorbidities and toxicity profile and with consideration for maintaining good quality of life. Clinical experts consulted by CDA-AMC also indicated that zolbetuximab would be offered to patients with HER2-negative, CLDN18.2-positive metastatic or locally advanced unresectable gastric or GEJ cancer One expert noted that treatment would be based on clinical decision-making by the treating physician for patients who are both HER2-positive and CLDN18.2-positive; another expert reported that the choice of FOLFOX plus zolbetuximab versus FOLFOX plus nivolumab would be unclear for patients with HER2-negative, CLDN18.2-positive disease and a PD-L1 CPS of 5 or greater.
The clinician group communicated that, upon approval of zolbetuximab, upfront CLDN18.2 testing will be required in all patients (in addition to HER2 and PD-L1 CPS testing, which are already mandated). The group noted that while the testing is inexpensive, assays will need to be developed and standardized.
The clinician group stated that, in clinical practice, CT scans are performed regularly at clinician discretion to determine response to treatment and that the decision to discontinue treatment with zolbetuximab would consider disease response, immune-related toxicities, and overall functional status. Similarly, disease progression and symptoms and adverse effects were identified as considerations for discontinuing treatment by clinical experts consulted by CDA-AMC. Patients treated with zolbetuximab should be under the care of a medical oncologist.
Drug Program Input
The drug programs provide input on each drug being reviewed through the reimbursement review processes by identifying issues that may affect their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted during this review are summarized in Table 4.
Table 4: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Relevant comparators | |
No questions identified | Not applicable |
Considerations for initiation of therapy | |
Recipients of adjuvant nivolumab: Should patients who have received adjuvant treatment with nivolumab, but who relapse less than 6 months after completing adjuvant treatment, be eligible for treatment with zolbetuximab plus chemotherapy? Patients were eligible for SPOTLIGHT and GLOW if they had received either neoadjuvant or adjuvant immunotherapy, as long as it was completed at least 6 months before randomization, but no patients were identified as having received prior treatment with nivolumab. | The clinical experts consulted during this review suggested that these patients would likely be relatively rare in clinical practice, and that those who could be considered candidates for zolbetuximab (based on CLDN18.2 biomarker status, ECOG Performance Status, and other eligibility criteria) should be offered the treatment. |
Performance status: Patients with ECOG Performance Status of 0 or 1 were included in the SPOTLIGHT and GLOW clinical trials. Should patients with ECOG Performance Status greater than 1 be eligible for zolbetuximab? | The clinical experts consulted during this review noted that there could be interest from prescribers in Canada to administer zolbetuximab for patients with an ECOG Performance Status of 2. |
Delayed confirmation of HER2-negative status: Patients are required to be HER2-negative to be eligible for zolbetuximab plus chemotherapy. Should patients who have initiated chemotherapy and whose disease has unknown HER2 status be eligible to add zolbetuximab upon confirmation of HER2-negative status? | The clinical experts consulted during this review noted that patients who have initiated chemotherapy and whose disease has unknown HER2 status should be eligible to add zolbetuximab upon confirmation of HER2-negative status. It was noted that this already occurs on occasion in routine practice; the patient would receive the initial doses of chemotherapy and subsequently receive add-on therapy with nivolumab upon confirmation of HER2-negative status. |
Unknown HER2 status: Should patients be eligible for zolbetuximab if they meet the criteria for CLDN18.2 expression, but their HER2 status cannot be determined? | The clinical experts consulted during this review noted that this would be a small minority of patients and that unknown HER2 status should not prevent access to zolbetuximab if the patient has been confirmed as meeting the criterion for CLDN18.2 expression. |
Consistency with prior recommendations: The participating drug programs noted that nivolumab plus chemotherapy and pembrolizumab plus chemotherapy have previously been recommended for reimbursement by CDA-AMC for use as first-line options in patients with gastric or GEJ adenocarcinoma. The drug programs noted that consistency with initiation criteria in the same therapeutic space can be beneficial from a formulary management perspective. | For consideration by expert committee. The clinical experts consulted during this review did not identify any issues or concerns with the existing criteria that have been recommended by the pan-Canadian Oncology Drug Review Expert Review Committee for treatment regimens indicated for use in the treatment of gastric or GEJ cancer. |
Chemotherapy-ineligible: The Health Canada–approved indication for zolbetuximab states that the drug should be provided in combination with fluoropyrimidine- and platinum-containing chemotherapy. Should patients be eligible for treatment with zolbetuximab if they are not able to receive concomitant chemotherapy? | The clinical experts consulted during this review stated that patients who are unable to initiate treatment with chemotherapy would likely not be considered candidates for zolbetuximab. |
Considerations for discontinuation of therapy | |
Discontinuation of chemotherapy: The product monograph states that cytotoxic drugs were shown to increase CLDN18.2 expression in cancer cells and improve zolbetuximab-induced antibody-dependent cellular cytotoxicity or complement-dependent cytotoxicity. Can zolbetuximab be continued if chemotherapy must be stopped due to intolerance? | The clinical experts consulted during this review noted that all patients will eventually have to discontinue chemotherapy due to toxicity, and that these patients should still be considered candidates for treatment with zolbetuximab, provided they are continuing to benefit from the therapy and have not demonstrated disease progression. |
Considerations for prescribing of therapy | |
Switching (clinical preference): If zolbetuximab is reimbursed by public drug programs, should patients who are currently receiving treatment with nivolumab plus chemotherapy be eligible to switch to zolbetuximab plus chemotherapy? | The clinical experts consulted during this review noted that patients who are currently receiving treatment with nivolumab plus chemotherapy should be considered eligible to switch to zolbetuximab plus chemotherapy upon confirmation of CLDN18.2 status. |
Switching (intolerance): If zolbetuximab is reimbursed by public drug programs, should patients who have unacceptable toxicity to nivolumab plus chemotherapy be eligible to switch to zolbetuximab plus chemotherapy (or vice versa)? | The clinical experts consulted during this review noted that patients who are currently receiving treatment with nivolumab plus chemotherapy should be considered eligible to switch to zolbetuximab plus chemotherapy upon confirmation of CLDN18.2 status. |
Generalizability | |
No issues identified | Not applicable |
Funding algorithm (oncology only) | |
Provisional funding algorithm: The participating drug programs noted that gastric and GEJ is a complex and evolving therapeutic space, with multiple lines of therapy, subpopulations, and emerging therapies. If recommended for reimbursement, the implementation of a recommendation for zolbetuximab may require an updated provisional funding algorithm from CDA-AMC. | For information to inform expert committee, patient groups, and clinician groups. |
Care provision issues | |
Increased nursing and chair time: The product monograph states that zolbetuximab should be administered over a minimum of 2 hours, whereas the administration of nivolumab and pembrolizumab (2 relevant comparators for this review) occurs over 30 minutes. As such, zolbetuximab would require additional nursing resources and chair time. | For consideration in economic evaluations and feasibility of adoption. |
Increased preparation time: Zolbetuximab is available in 100 mg vials and must be reconstituted with 5 mL of diluent. The dose is then drawn up and added to an infusion bag. Nivolumab and pembrolizumab are available as a solution; therefore, zolbetuximab will take more time for health care professionals to prepare. In addition, there will be the requirement to use:
This adds significant additional preparation time compared to nivolumab (3 vials to 6 vials, depending on dose) and pembrolizumab (2 vials to 4 vials, depending on dose). | For consideration in economic evaluations and feasibility of adoption. |
Shorter stability: Once reconstituted, the vial stability is 5 hours at room temperature. There is no preservative. The final preparation in the infusion bag is stable for 6 hours at room temperature or 24 hours in the refrigerator (including time for infusion). If the infusion time exceeds 6 hours from time of preparation, then the infusion bag must be discarded and a new infusion bag prepared. | For consideration in economic evaluations and feasibility of adoption. |
System and economic issues | |
None identified | Not applicable |
CDA-AMC = Canada’s Drug Agency; CLDN18.2 = Claudin 18.2; ECOG = Eastern Cooperative Oncology Group; GEJ = gastroesophageal junction; HER2 = human epidermal growth factor receptor 2.
Clinical Evidence
The objective of this clinical review report is to review and critically appraise the clinical evidence submitted by the sponsor on the beneficial and harmful effects of zolbetuximab in combination with fluoropyrimidine- and platinum-containing chemotherapy for the first-line treatment of patients with locally advanced unresectable or metastatic HER2-negative gastric or GEJ adenocarcinoma whose tumours are CLDN18.2-positive as determined by a validated test. The focus will be on comparing zolbetuximab to relevant comparators and identifying gaps in the current evidence.
A summary of the clinical evidence included by the sponsor in the review of zolbetuximab is presented in 4 sections, with critical appraisal of the evidence included at the end of each. The first section, the Systematic Review, includes pivotal studies and RCTs that were selected according to the sponsor’s systematic review protocol. The CDA-AMC assessment of the certainty of the evidence in this first section, using the GRADE approach, follows the critical appraisal of the evidence. The second section includes sponsor-submitted long-term extension studies (not submitted). The third section includes indirect evidence from the sponsor. The fourth section includes additional studies that were considered by the sponsor to address important gaps in the systematic review evidence (not submitted).
Included Studies
Clinical evidence from the following studies is included in the review and appraised in this document:
two pivotal studies RCTs identified in systematic review (i.e., the SPOTLIGHT and GLOW trials)
one ITC.
Systematic Review
Contents within this section are informed by materials submitted by the sponsor. The following have been summarized and validated by CDA-AMC.
Description of Studies
Key characteristics of the SPOTLIGHT and GLOW trials are summarized in Table 5.
The SPOTLIGHT and GLOW trials are both ongoing, multinational, double-blind, placebo-controlled, randomized studies of zolbetuximab in combination with fluoropyrimidine- and platinum-based chemotherapy compared with placebo in combination with fluoropyrimidine- and platinum-based chemotherapy for the first-line treatment of patients with locally advanced unresectable or metastatic HER2-negative gastric or GEJ adenocarcinoma whose tumours are CLDN18.2-positive. In both trials, patients were randomized 1:1 into zolbetuximab or placebo arms, with randomization stratified by region (Asia versus non-Asia), number of organs with metastatic sites (0 to 2 versus ≥ 3), and prior gastrectomy (yes or no). The chemotherapy backbone used in the SPOTLIGHT trial was mFOLFOX6, while the backbone used in the GLOW trial was CAPOX.24,25 Notably, the SPOTLIGHT trial enrolled more patients from Japan and South Korea, whereas the GLOW trial enrolled more patients from mainland China, whose disease course tends to be more similar to that of patients from western countries, with a lower OS than patients from Japan.10,39,41
Table 5: Details of Studies Included in the Systematic Review
Characteristics | SPOTLIGHT Trial (NCT03504397) | GLOW Trial (NCT03462719) |
|---|---|---|
Designs and populations | ||
Study design | Multicentre, phase III, double-blind, placebo-controlled RCT | Multicentre, phase III, double-blind, placebo-controlled RCT |
Locations | 232 sites in 20 countries (215 sites screened ≥ 1 patient): Australia (5 sites), Belgium (10 sites), Brazil (12 sites), Canada (5 sites), Chile (4 sites), China (8 sites), Colombia (6 sites), France (13 sites), Germany (11 sites), Israel (6 sites), Italy (18 sites), Japan (15 sites), Korea (8 sites), Mexico (8 sites), Peru (5 sites), Poland (5 sites), Spain (13 sites), Taiwan (7 sites), UK (10 sites), and US (46 sites) | 176 sites in 18 countries (166 sites screened ≥ 1 patient): Argentina (5 sites), Canada (4 sites), China (40 sites), Croatia (3 sites), Greece (7 sites), Ireland (2 sites), Japan (12 sites), South Korea (13 sites), Malaysia (5 sites), Netherlands (2 sites), Portugal (10 sites), Romania (9 sites), Spain (13 sites), Taiwan (4 sites), Thailand (11 sites), Turkey (11 sites), UK (4 sites), and US (11 sites) |
Patient enrolment dates | First patient screened: June 21, 2018 Primary completion date: September 9, 2022 | First patient screened: November 28, 2018 Primary completion date: October 7, 2022 |
Randomized (N) | 565 | 507 |
Inclusion criteria |
| |
Exclusion criteria |
| |
Drugs | ||
Interventions | Zolbetuximab:
mFOLFOX6:
| Zolbetuximab:
CAPOX:
|
Comparators | Placebo in combination with mFOLFOX6 | Placebo in combination with CAPOX |
Study durations | ||
Screening period | 45 days | |
Treatment period | From the time of first treatment with either zolbetuximab or placebo until the patient meets study treatment discontinuation criteria | |
Safety follow-up | 90 days after last dose of zolbetuximab or placebo | |
Posttreatment follow-up for PFS | If a patient discontinued all study treatments before disease progression, the patient entered the posttreatment follow-up period and continued to undergo scheduled imaging assessments every 9 weeks (± 7 days) (or every 12 weeks [± 7 days] if they had been on study over 54 weeks) until radiologic disease progression (i.e., PFS event) per IRC, or until they started any other anticancer treatment, whichever occurred earlier. | |
Long-term follow-up for PFS2 | Following disease progression on first-line treatment or start of any other anticancer treatment, patients were followed up in the long term and survival follow-up periods (per institutional guidelines), but not less than every 12 weeks. Subsequent anticancer treatment details, progression status, and survival status were collected until PD following subsequent anticancer therapy (i.e., PFS2) was documented, or until the patient started another systemic anticancer treatment, whichever occurred earlier. | |
Survival follow-up for OS | Patients continued to be followed for survival status (OS) in the survival follow-up period until death (from any cause). | |
Outcomes | ||
Primary end point | PFS, defined as the time from the date of randomization until the date of radiological PD (per RECIST 1.1 by IRC) or death from any cause, whichever is earliest | |
Secondary and exploratory end points | Key secondary:
Secondary:
Exploratory:
Safety and tolerability:
| |
Publication status | ||
Publications | Shitara et al. (2023)39 Shitara et al. (2024) (final OS analysis poster)40 Clinicaltrials.gov Identifier: NCT03504397 | Shah et al. (2023)41 Clinicaltrials.gov Identifier: NCT03653507 |
5-FU = 5-fluorouracil; AE = adverse event; b.i.d. = twice daily; CAPOX = capecitabine and oxaliplatin; CLDN18.2 = Claudin 18.2; CR = complete response; DCR = disease control rate; DOR = duration of response; ECG = electrocardiogram; ECOG = Eastern Cooperative Oncology Group; EORTC GHS/QoL = European Organisation for Research and Treatment of Cancer Global Health Status/Quality of Life; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; EORTC QLQ-OG25 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Oesophago-Gastric 25; GEJ = gastroesophageal junction; GP = Global Pain; HER2 = human epidermal growth factor receptor 2; HRQoL = health-related quality of life; IHC = immunohistochemistry; IRC = independent review committee; mFOLFOX6 = modified 5-fluorouracil, folinic acid, and oxaliplatin; ORR = objective response rate; OS = overall survival; PD = progressive disease; PFS = progression-free survival; PFS2 = progression-free survival following second-line anticancer treatment; PR = partial response; q.2.w. = every 2 weeks; q.3.w. = every 3 weeks; RCT = randomized controlled trial; RECIST 1.1 = Response Evaluation Criteria in Solid Tumours Version 1.1; SAE = serious adverse event; STO22 = EORTC Quality of Life Questionnaire - Gastric Cancer Module; TTCD = time to confirmed deterioration; TTP = time to progression.
Sources: SPOTLIGHT trial Primary Analysis Clinical Study Report (2023);24 GLOW trial Primary Analysis Clinical Study Report (2023).25
The primary objective in both the SPOTLIGHT and GLOW trials was to assess the PFS benefit of zolbetuximab plus chemotherapy compared to placebo plus chemotherapy. Key secondary objectives were to evaluate OS and TTCD using the EORTC GHS/QoL scale, the EORTC QLQ-OG25 scale, and EORTC QLQ-C30 PF. Additional secondary objectives were to evaluate ORR, DOR, safety, tolerability, and additional patient-reported outcomes.
Each study consisted of the following periods: screening, treatment, safety follow-up, posttreatment follow-up for PFS, long-term follow-up for PFS2, and survival follow-up for OS. During the screening period, formalin-fixed, paraffin-embedded tumour tissue was collected for central testing to determine CLDN18.2 and HER2 status. Confirmation of CLDN18.2 status was to be obtained before patients proceeded to any other screening procedures. If the specimen was insufficient or unavailable, a biopsy may have been performed to obtain a tumour sample. Patients who were screened out could be rescreened 1 time after consultation with the medical monitor. In these cases, a new patient number was assigned, and patients had to reconsent to the study and all screening procedures (with the exception CLDN18.2 and HER2 testing and radiological imaging procedure to confirm eligibility, if the scan was within 28 days before the first dose of study treatment).
Figure 2: SPOTLIGHT Study Schema
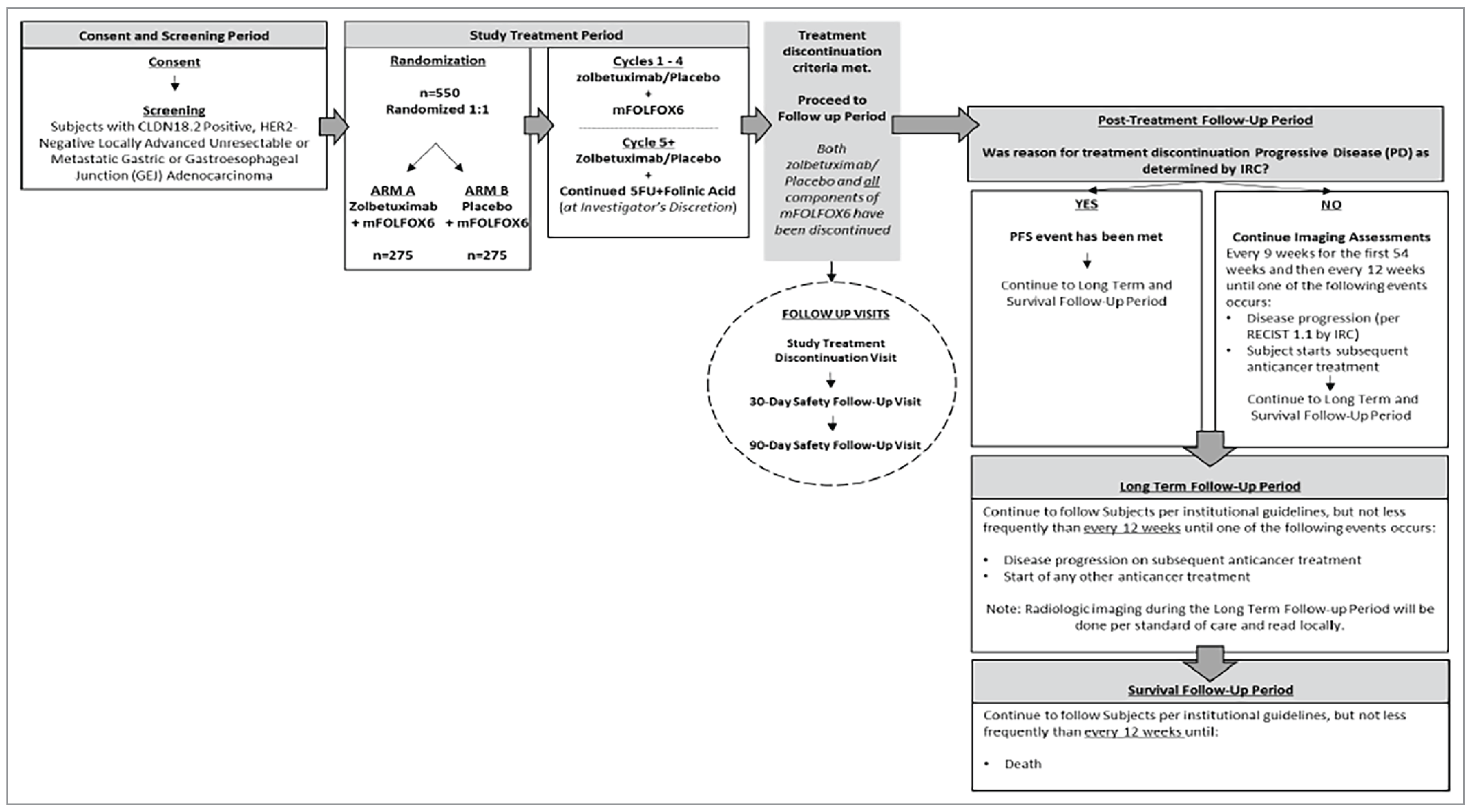
5FU = 5-fluorouracil; CLDN18.2 = Claudin 18.2; GEJ = gastroesophageal junction; HER2 = human epidermal growth factor receptor 2; IRC = independent review committee; mFOLFOX6 = modified 5-fluorouracil, folinic acid, and oxaliplatin; PFS = progression-free survival; RECIST 1.1 = Response Evaluation Criteria in Solid Tumours Version 1.1.
Note: Sample size in the figure (n = 550) represents the planned total. In the SPOTLIGHT trial, 565 patients were randomized 1:1 to arm A (n = 283) and arm B (n = 282).
Source: SPOTLIGHT trial Primary Analysis Clinical Study Report (2023).24
The recruitment period for the SPOTLIGHT trial was from October 29, 2018 (first patient randomized) to April 1, 2022 (last patient randomized). The data cut-off for the primary analysis of PFS and interim analysis of OS occurred on September 9, 2022.24 The data cut-off for the final analysis of OS occurred on September 8, 2023.42 The recruitment period for the GLOW trial was from January 21, 2019 (first patient randomized), to February 18, 2022 (last patient randomized). The data cut-off for the primary analysis of PFS and interim analysis of OS occurred on October 7, 2022.25 The data cut-off for the final analysis of OS occurred on January 12, 2024.
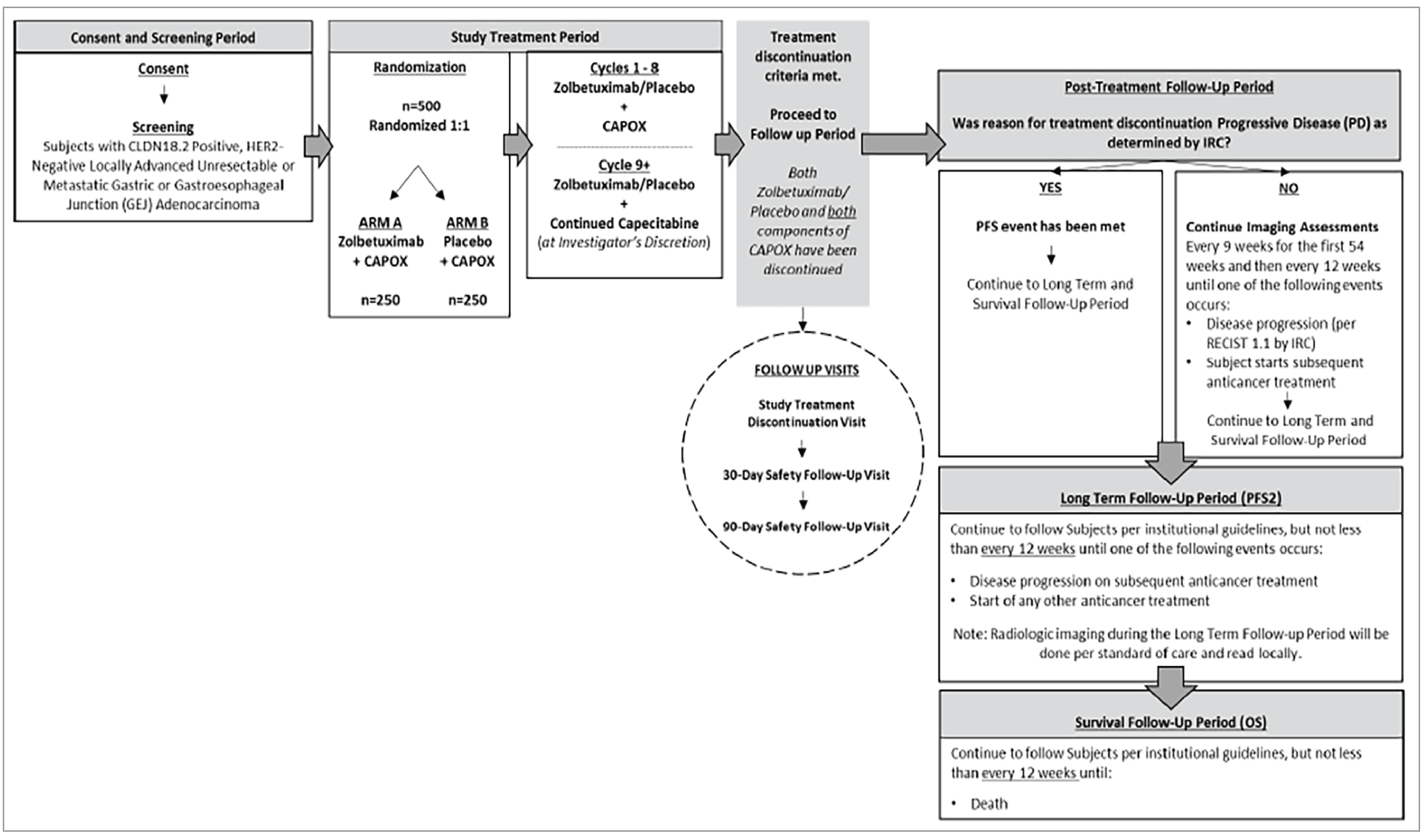
CAPOX = capecitabine and oxaliplatin; CLDN18.2 = Claudin 18.2; GEJ = gastroesophageal junction; HER2 = human epidermal growth factor receptor 2; IRC = independent review committee; OS = overall survival; PFS = progression-free survival; PFS2 = progression-free survival following subsequent anticancer treatment; RECIST 1.1 = Response Evaluation Criteria in Solid Tumours Version 1.1.
Note: Sample size in the figure (n = 500) represents the planned total. In the GLOW trial, 507 patients were randomized 1:1 to arm A (n = 254) and arm B (n = 253).
Source: GLOW trial Primary Analysis Clinical Study Report (2023).25
Populations
Inclusion and Exclusion Criteria
Key inclusion criteria were aligned in the SPOTLIGHT and GLOW trials. Eligible patients were aged 18 years or older with CLDN18.2-positive (defined as ≥ 75% of tumour cells showing moderate to strong membranous CLDN18.2 staining, as determined by central IHC using the investigational VENTANA CLDN18 [43-14A] RxDx Assay [Roche Diagnostic Solutions; Tucson, AZ, US]), HER2-negative (based on local or central evaluation), previously untreated, locally advanced unresectable or metastatic gastric or GEJ adenocarcinoma with radiologically evaluable disease (measurable or nonmeasurable) according to Response Evaluation Criteria in Solid Tumours Version 1.1 (RECIST 1.1); patients were also required to have an ECOG Performance Status score of 0 or 1 and adequate organ function.24,25,39 Differences in the exclusion criteria between the SPOTLIGHT and GLOW trials included treatment with herbal medications that had known antitumour activity less than or equal to 28 days before randomization (excluded in the GLOW trial only), as well as prior severe allergic reaction or intolerance to any component of mFOLFOX6 (SPOTLIGHT trial only) or CAPOX (GLOW trial only).24,25
Interventions
In the SPOTLIGHT and GLOW trials, 565 patients and 507 patients, respectively, were randomized in a 1:1 ratio to 2 treatment arms, with dosing and administration summarized in Table 6. In real-world practice, zolbetuximab and all chemotherapy components, with the exception of capecitabine, are administered in an outpatient hospital setting or infusion centre. Capecitabine is administered at home or in a community setting. Both of the chemotherapy backbones used in the SPOTLIGHT and GLOW trials (mFOLFOX6 and CAPOX, respectively) are used in Canada as part of routine clinical practice.
Prophylactic Medications Used in the SPOTLIGHT and GLOW Trials
Prophylactic antiemetics were given to patients before administration of the chemotherapy backbones in accordance with institutional standard of care, published guidelines, and the respective product package insert(s):43,44
All antiemetic premedications were to be given at minimum 30 minutes before treatment.
On days when zolbetuximab or placebo and the chemotherapy backbone were administered together, the antiemetic premedication was to be given before zolbetuximab or placebo administration.
It was recommended that the prophylactic antiemetic regimen include (but not be limited to) neurokinin-1 and 5-hydroxytryptamine type 3 receptor blockers.
Table 6: Treatment Groups and Dosing Regimens in the SPOTLIGHT and GLOW Trials
Study treatment | SPOTLIGHT (N = 565) | GLOW (N = 507) |
|---|---|---|
Zolbetuximab | 800 mg/m2 IV loading dose at C1D1 followed by subsequent doses of 600 mg/m2 IV q.3.w. until study discontinuation criteria were met | 800 mg/m2 IV loading dose at C1D1 followed by subsequent doses of 600 mg/m2 IV q.3.w. until study discontinuation criteria were met |
Chemotherapy backbone (both groups) | mFOLFOX6:
| CAPOX:
|
Placebo | 0.9% sodium chloride solution; timing and administration matched to zolbetuximab | 0.9% sodium chloride solution; timing and administration matched to zolbetuximab |
5-FU = 5-fluorouracil; b.i.d. = twice daily; C1D1 = cycle 1, day 1; CAPOX = capecitabine oxaliplatin; mFOLFOX6 = modified 5-fluorouracil, folinic acid, and oxaliplatin; q.2.w. = once every 2 weeks; q.3.w. = every 3 weeks.
Sources: SPOTLIGHT trial and GLOW trial Clinical Study Reports.24,25
Table 7: Outcomes Summarized From the Studies Included in the Systematic Review
Outcome measure | Time point | SPOTLIGHT and GLOW trials |
|---|---|---|
PFS | Time from date of randomization to date of radiological PD (per RECIST 1.1 by IRC) or death from any cause, whichever is earliest | Primarya |
OS | Time from date of randomization to date of death from any cause | Key secondary a |
TTCD (measured by the EORTC QLQ-C30 and EORTC QLQ-OG25 plus the EORTC QLQ-STO22 belching subscale) | Time from randomization to first clinically meaningful deterioration that is confirmed at the next scheduled visit | Key secondary a |
ORR | NA (determined by IRC per RECIST 1.1) | Secondary |
DOR | Time from date of first response (CR or PR) to date of PD, as assessed by IRC per RECIST 1.1, or date of death from any cause | Secondary |
EORTC QLQ-C30 | HRQoL questionnaires collected at screening, every 3 weeks, at study treatment discontinuation, and at 30 days and 90 days after zolbetuximab or placebo treatment | Secondary |
EORTC QLQ-OG25 | ||
Global Pain | ||
EQ5D-5L | ||
TTP | Time from date of randomization to date of PD as assessed by IRC per RECIST 1.1 | Exploratory |
PFS2 | Time from date of randomization to date of radiological PD (per investigator) following subsequent anticancer therapy or death from any cause, whichever was earliest | Exploratory |
DCR | NA (determined by IRC per RECIST 1.1) | Exploratory |
HRU questionnaire | Collected every 3 weeks, at study treatment discontinuation, and at 30 days and 90 days after zolbetuximab or placebo treatment | Exploratory |
AEs | NA | Harms |
AE = adverse event; DCR = disease control rate; DOR = duration of response; EORTC GHS/QoL = European Organisation for Research and Treatment of Cancer Global Health Status/Quality of Life; EORTC QLQ-C30 PF = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Physical Functioning; EORTC QLQ-OG25 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Oesophago-Gastric 25; EORTC QLQ-STO22 = EORTC Quality of Life Questionnaire - Gastric Cancer Module; HRQoL = health-related quality of life; HRU = health resource utilization; IRC = independent review committee; NA = not applicable; ORR = objective response rate; OS = overall survival; PD = progressive disease; PFS = progression-free survival; PFS2 = second progression-free survival; PF = Physical Functioning; RECIST 1.1 = Response Evaluation in Solid Tumours Version 1.1; TTCD = time to first clinically meaningful deterioration; TTP = time to progression.
aStatistical testing for these end points was adjusted for multiple comparisons using a gatekeeping testing strategy to address multiplicity.
Sources: SPOTLIGHT trial and GLOW trial Clinical Study Protocols.43,44
Outcomes
A list of efficacy end points assessed in this clinical review report is provided in Table 7, followed by descriptions of the outcome measures. Summarized end points are based on outcomes included in the sponsor’s Summary of Clinical Evidence as well as on any outcomes identified as important to this review, according to the clinical experts consulted during this review and input from patient and clinician groups and public drug plans. Using the same considerations, the review team selected end points that were most relevant to inform the expert committee deliberations and finalized this list of end points in consultation with members of the expert committee. All summarized efficacy end points were assessed using GRADE. Select notable harms outcomes considered important for informing the expert committee deliberations were also assessed using GRADE.
Progression-Free Survival
PFS was the primary end point of both the SPOTLIGHT and GLOW trials and was assessed by the blind IRC. PFS was defined as the time from randomization until the date of radiological disease progression assessed by IRC, or until death due to any cause, whichever was earlier. If a patient had neither progressed nor died, they were censored at the date of last radiological assessment. Patients who received new anticancer therapy before radiological progression were censored at the date of the last radiological assessment before the new anticancer therapy started. If progression or death occurred after a patient missed 2 or more scheduled radiological assessments, the patient was censored at the date of the last radiological assessment or at the date of randomization, if no postbaseline radiological assessment was available.43,44
Overall Survival
OS was a key secondary end point in both the SPOTLIGHT and GLOW trials. It was defined as the time from the date of randomization until the documented date of death from any cause. Patients still alive at the time of the analysis were censored at the last date known to be alive.43,44
Objective Response Rate
Best overall response (BOR) was classified based on RECIST 1.1 criteria. For BOR of stable disease, stable disease had to be documented as present at least once after study entry and at least 8 weeks after the first dose. ORR was defined as the proportion of patients with a BOR of complete or partial response based on IRC per RECIST 1.1.43,44
Duration of Response
DOR was defined as the time from first complete or partial response (whichever was first recorded) as assessed by IRC to the date of radiological progression or death, whichever was earlier. If a patient had not progressed, the patient was censored at the date of the last radiological assessment or at the date of first complete or partial response if no postbaseline radiological assessment was available. Other censoring used for the PFS analysis applied to DOR as well. The distribution of DOR was estimated for each treatment arm using Kaplan-Meier methodology and compared using the log-rank test stratified by the same factors used for PFS. A stratified Cox proportional hazard model was used to estimate the HR and corresponding 95% CI.43,44
Time to Confirmed Deterioration
TTCD was defined as the duration of time from the date of randomization to the date of the first deterioration in patient-reported outcome scores of at least 1 threshold unit compared to the baseline score, if the deterioration (of at least 1 threshold unit compared to the baseline score) is also observed at the next consecutive scheduled visit (e.g., after the first deterioration was observed) or if the patient dropped out or died after deterioration, resulting in missing data.43,45 Given the absence of reliable and well-accepted thresholds for within-patient clinically meaningful change, the clinically meaningful threshold denoting a deterioration was defined based on anchor-based analyses performed on the same trial data.
Health-Related Quality of Life
HRQoL end points were summarized using descriptive statistics with respect to change from baseline for each treatment arm. Completion rate for each questionnaire was summarized by time point.43,44
Time to Progression
TTP is defined as the time from the date of randomization until the date of progressive disease (PD) (per RECIST 1.1, as determined by IRC). TTP did not include deaths as events. For deaths before the first documented PD by IRC, patients were censored at the time of their last radiological assessment. Kaplan-Meier and log-rank methods were applied to TTP end point.43,44
Progression-Free Survival Following Second-Line Anticancer Treatment (PFS2)
PFS2 is defined as the time from the date of randomization until the date of PD (per investigator) following subsequent anticancer therapy, death from any cause, or start of any other anticancer therapy, whichever is earliest. In cases where PFS2 could not reliably be determined, discontinuation of subsequent ACT could be used as the event date. Patients who were alive and for whom a PFS2 event date had not been observed were to be censored at the last time known to be alive and without second objective disease progression.43,44
Disease Control Rate
DCR was defined as the proportion of patients with a BOR of complete response, partial response, or stable disease, based on RECIST 1.1 by IRC.43,44
Adverse Events
An AE was defined as any untoward medical occurrence. It did not necessarily have to have a causal relationship with the study treatment. SAEs were considered events that the investigator or sponsor concluded resulted in death; life-threatening events; persistent or significant disability or incapacity; substantial disruption of the ability to conduct normal life functions; congenital anomaly; or inpatient hospitalization. AEs of special interest included nausea, vomiting, and hypersensitivity or IRRs.43,44
Statistical Analysis
Sample size and power calculation: In the SPOTLIGHT trial, the sponsor planned to randomize approximately 550 patients 1:1 to zolbetuximab plus mFOLFOX6 or placebo plus mFOLFOX6. Three hundred PFS events during the study would provide 93.4% power to detect a difference in PFS between the treatment groups, with the assumption of 9 months’ median PFS time for zolbetuximab and 6 months median PFS time for placebo (HR = 0.67) at the 1-sided 0.025 significance level. The planned 396 OS events during the study would provide 81% power to detect a difference in OS between the treatment groups, with the assumption of 14.7 months’ median survival time with zolbetuximab and 11 months’ median survival time (HR = 0.75) with placebo at the 1-sided 0.025 significance level.24
In the GLOW trial, the sponsor planned to randomize approximately 500 patients 1:1 to receive zolbetuximab plus CAPOX or placebo plus CAPOX. Three hundred PFS events during the study would provide 93.4% power to detect a difference in PFS between the treatment groups, with assumptions of 9 months’ and 6 months’ median PFS in the zolbetuximab and placebo groups, respectively (HR = 0.67) at the overall 1-sided 0.025 significance level. The planned 386 OS events during the study would provide 80% power to detect a difference in OS between the treatment groups, with the assumption of 14.7 months’ and 11 months’ median OS in the zolbetuximab and placebo groups, respectively (HR = 0.75) at the overall 1-sided 0.025 significance level.25
Data imputation methods: Missing variable values were not imputed in the SPOTLIGHT and GLOW trials.
Subgroup analyses: For both the SPOTLIGHT and GLOW trials, PFS, ORR, and DOR — based on IRC assessments — and OS were summarized for the following subgroups:45,46 age group 1 (≤ 65 years versus > 65 years); age group 2 (≤ 75 years versus > 75 years); sex (male versus female); race (white versus Asian); tobacco history (never, current, or former); region (Asia versus non-Asia); number of organs with metastatic sites (0 to 2 versus greater than or equal to 3); prior gastrectomy (no versus yes [total or partial]); histology (tumour type) (diffuse versus intestinal versus mixed or other); tumour location (gastric versus GEJ; gastric proximal versus gastric distal; GEJ proximal versus GEJ distal); country (Japan versus non-Japan; China versus non-China). These subgroup analyses were not controlled for multiplciticity.45,46
Sensitivity analyses: Sensitivity analyses performed in the SPOTLIGHT and GLOW trials and summarized in Table 8.
Statistical Testing
Primary End Point
The primary analysis of PFS used radiological assessment of PD by the IRC and performed using the full analysis set (FAS). The comparisons of zolbetuximab and placebo were tested at a 1-sided significance level of 0.025.45,46 The distribution and median of PFS were estimated using Kaplan-Meier methodology. PFS rates at 6 months, 12 months, and 18 months were also presented. In addition, numbers of patients who had PFS events and were censored — and 95% CIs for median PFS and PFS rates — were presented.45,46 Hypotheses testing for zolbetuximab versus placebo was performed using log-rank test stratified by region (Asia versus non-Asia); number of organs with metastatic sites (0 to 2 versus ≥ 3); and prior gastrectomy (yes versus no).
A stratified Cox proportional hazards model was used to estimate the HR and corresponding 95% CI. Evaluable radiological assessments included all except those assessed by IRC as not evaluable.45,46
Secondary End Points
To maintain the overall type I error rate at the 0.025 significance level, the hypothesis testing for OS interim and OS final analyses was performed only if the null hypothesis in PFS primary analysis was rejected at the overall 1-sided 0.025 significance level.45,46
The formal OS interim analysis was planned when the final PFS analysis occurred with the prespecified number of PFS events. A group sequential design using the O’Brien-Fleming–type alpha-spending function was utilized to control the overall 1-sided 0.025 significance level for the OS analysis. In the case of favourable results, the 1-sided significance levels for superiority were 0.0074 for the interim OS analysis and 0.0228 for the final OS analysis. These alpha boundaries were based on an information factor of 70% and were subject to adjustment if the observed information factor deviated from 70%. If the 1-sided P value of the interim analysis was less than 0.0074, the Independent Data Monitoring Committee (IDMC) could recommend terminating the trial for success without the need to conduct the final OS analysis. If the study was not stopped after the interim analysis, the final OS analysis was planned to occur after 100% of the planned number of deaths had been observed.45,46
The distribution and median of OS, as well as OS rates at 12 months, 18 months, 24 months, 30 months, and 36 months, were estimated for each treatment arm using Kaplan-Meier methodology. The 95% CIs for median OS and milestone OS rates were presented. Zolbetuximab and placebo were compared using the log-rank test stratified by the same stratification factors used for the PFS analysis.45,46 A stratified Cox proportional hazard model was used to estimate the HR and corresponding 95% CI.45,46
The median of time on study using reverse Kaplan-Meier approach and range were provided. Patients who were alive up to the cut-off date were considered as events, and deaths of patients on or before the data cut-off date were censored in the reverse Kaplan-Meier approach for the estimation of median of time on study.45,46
The key secondary TTCD end points of the EORTC QLQ-C30 PF scale, EORTC QLQ-OG25 Pain scale, and EORTC GHS/QoL scale scores were analyzed using the same method as for OS and PFS. To maintain the overall type I error rate at the 0.025 significance level, the hypothesis testing of TTCD end points was to be performed only if the null hypothesis on the OS was rejected at the 1-sided 0.025 significance level.24,25 If the null hypothesis on the OS was rejected at the overall 1-sided 0.025 significance level, then TTCD would be tested using the gatekeeping procedure, using the following order:
noninferiority testing for TTCD in EORTC QLQ-C30 PF scale at the 0.025 significance level
noninferiority testing for TTCD in the EORTC QLQ-OG25 Pain scale at the 0.025 significance level
noninferiority testing for TTCD in the EORTC GHS/QoL scale at the 0.025 significance level
superiority testing for TTCD in the EORTC QLQ-C30 PF scale at the 0.025 significance level
superiority testing for TTCD in the EORTC QLQ-OG25 Pain scale at the 0.025 significance level
superiority testing for TTCD in the EORTC GHS/QoL scale at the 0.025 significance level.
The secondary HRQoL end points collected through the EORTC QLQ Core 30, EORTC QLQ-OG25, Global Pain, and EQ-5D-5L were analyzed with summary of change from baseline.24,25
Exploratory End Points
TTP and PFS2 were analyzed in a similar manner to PFS; however, in the TTP analysis, deaths were censored instead of being counted as events. DCR was analyzed similarly to ORR. The health resource utilization variables were summarized by treatment arm.
Multiple Testing Procedure
To address multiplicity, a gatekeeping testing strategy was used for PFS (the primary efficacy end point) and OS (the key secondary end point). PFS was tested once at a 1-sided significance level of 0.025. Only if PFS was significant, hypothesis testing for the OS interim and final analyses was performed. An O’Brien-Fleming–type alpha-spending function was utilized to control the overall 1-sided 0.025 significance level for the OS interim and final analyses.47 Other secondary end points’ tests results were not multiplicity adjusted.45,46
Analysis Populations
Analysis populations, including the FAS, safety analysis set (SAF), pharmacokinetic analysis set, and per-protocol analysis set, were defined the same way in the SPOTLIGHT and GLOW trials, as summarized in Table 9.24,25
Table 8: Statistical Analysis of Efficacy End Points in the SPOTLIGHT and GLOW Trials
End point | Statistical model | Adjustment factors | Handling of missing data | Sensitivity analyses |
|---|---|---|---|---|
SPOTLIGHT and GLOW trials (statistical methods aligned between studies) | ||||
PFS | Stratified log-rank test; stratified Cox proportional hazards model was used to estimate the HR and 95% CI | Stratified by adjustment factors employed in randomization: region (Asia vs. non-Asia), number of organs with metastatic sites (0 to 2 vs. ≥ 3), and prior gastrectomy (yes vs. no) | Patients with no baseline imaging assessments or no evaluable postbaseline imaging assessment If radiological PD or death occurred after missing 2 or more scheduled radiological assessments, patients were censored at the date of the last radiological assessment. Did not receive new ACT Patients with neither documented radiological PD nor death were censored at the date of the last radiological assessment. Received new ACT Patients with radiological PD documented only after the start of new ACT were censored at the date of last radiological assessment before the start of the new ACT. Patients with neither documented radiological PD nor death were censored at the date of the last radiological assessment before ACT. | The following sensitivity analyses were performed:
|
OS | Stratified log-rank test; the stratified Cox proportional hazards model was used to estimate the HR and 95% CI | Stratified by adjustment factors employed in randomization | Patients with last known alive date before the cut-off date were censored at the last known alive date. Patients with death after the analysis cut-off date were censored at the analysis cut-off date. Patients with last known alive date after the cut-off date were censored at the analysis cut-off date. | Not performed |
TTCD (EORTC GHS/QOL scale, EORTC QLQ-C30 PF scale, and EORTC QLQ-OG25 Pain scale) | Stratified log-rank test; the stratified Cox proportional hazards model was used to estimate the HR and 95% CI | Stratified by adjustment factors employed in randomization | Patients with no baseline assessment, without a postbaseline PRO questionnaire, or whose baseline cores did not allow for further deterioration were censored at randomization. Deaths or progressions were not considered deterioration events. Instrument completion rate at each analysis visit was reported for each instrument. | None prespecified; additional analyses based on sensitivity thresholds were presented |
ORR | The comparison was performed using a stratified CMH test. ORR for each arm was estimated, and 95% CI was be constructed using the Clopper-Pearson method. | Stratified by adjustment factors employed in randomization | If all time point overall responses were NE, then BOR was NE. For BOR of SD, SD had to be documented as present at least once and at least 8 weeks after randomization. If the first assessment of SD did not meet the minimum “8 weeks from randomization” time window, that assessment of SD was treated as NE in the analysis. Time point responses after the start of new ACT were not to be used in determining BOR. | Analysis of ORR with confirmation ORR per investigator assessment for both confirmed and unconfirmed response |
DOR | Stratified log-rank test; the stratified Cox proportional hazards model was used to estimate the HR and 95% CI | Stratified by adjustment factors employed in randomization | If a patient had not progressed, they were censored at the date of last evaluable radiological assessment or at the date of first CR or PR, if no later evaluable radiological assessment was available. Other censoring used for the PFS analysis applied to DOR too. | Analysis for confirmed responses Responses per investigator assessment for both confirmed and unconfirmed response |
HRQoL collected through the EORTC QLQ-C30 scale, QLQ-OG25 scale, GP scale, and EQ5D-5L | Descriptive analyses: scores and change from baseline were summarized for each visit where 10 patients were evaluable in either treatment arm. | Not applicable | Instrument completion rate at each analysis visit was reported for each instrument. | Not performed |
TTP | Kaplan-Meier and log-rank methods were applied to the TTP end point. | Not applicable | Patients with no baseline imaging assessments were censored at the date of randomization. Patients with no evaluable postbaseline imaging assessments were censored at the date of randomization. Patients with radiological progression occurring after 2 or more scheduled radiological assessments were censored at the date of the last radiological assessment. | Per investigator assessment |
PFS2 | PFS2 was estimated using KM methodology and compared using stratified log-rank test. Stratified Cox proportional hazard model was used to estimate the HR and 95% CI. | Same stratification factors as used for the PFS analysis | For patients with no record of second-line therapy or start date of third-line therapy were censored at the last known alive date. | Not performed |
HRU | Variables were measured by visit and sums over visits and summarized by treatment arms. | Not applicable | Not reported | Not performed |
ACT = anticancer treatment; BOR = best overall response; CI = confidence interval; DOR = duration of response; EORTC GHS/QoL = European Organisation for Research and Treatment of Cancer Global Health Status/Quality of Life; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; EORTC QLQ-C30 PF = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 Physical Functioning; EORTC QLQ-OG25 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Oesophago-Gastric 25; GP = Global Pain; HR = hazard ratio; HRQoL = health-related quality of life; HRU = health resource utilization; KM = Kaplan-Meier; NE = not evaluable; ORR = objective response rate; OS = overall survival; PD = progressive disease; PFS = progression-free survival; PFS2 = progression-free survival following second-line anticancer treatment; PRO = patient-reported outcome; SD = stable disease; TTCD = time to first clinically meaningful deterioration; TTP = time to progression; vs. = versus.
Sources: SPOTLIGHT trial and GLOW trial Statistical Analysis Plans.45,46
Table 9: Analysis Populations in the SPOTLIGHT and GLOW Trials
Population | Definition | Application |
|---|---|---|
Full analysis set | All randomized patients | Baseline characteristics; all efficacy analyses |
Safety analysis set | All patients who received at least 1 dose of any study drug (zolbetuximab, chemotherapy, or placebo) | Used for summaries of demographic and baseline characteristics and all safety- and tolerability-related variables |
Per-protocol analysis set | All randomized patients who did not receive study treatment or who lacked sufficient study drug exposure and/or an imaging assessment — this excluded patients who were not adherent to the study protocol | Analyses of PFS and OS in the per-protocol set population were presented for the final analysis of SPOTLIGHT (data cut-off: September 8, 2023) |
OS = overall survival; PFS = progression-free survival.
Sources: SPOTLIGHT trial and GLOW trial Primary Analysis Clinical Study Reports.24,25
Results
Patient Disposition
In the SPOTLIGHT trial, of the 2,767 patients (including rescreened patients), 2,403 unique patients had valid CLDN18.2 IHC results, and 38.4% (n = 922) of screened patients had tumours that were CLDN18.2-positive (defined as ≥ 75% of tumour cells demonstrating moderate to strong membranous CLDN18.2 staining).24 In total, 2,735 patients were screened, and 565 patients were randomized to receive either zolbetuximab plus mFOLFOX6 (n = 283) or placebo plus mFOLFOX6 (n = 282). (Of the 922 patients with a positive CLDN18.2 result, 357 patients failed screening for other reasons, including withdrawal by patient, laboratory findings, HER2-expression status, and ECOG Performance Status).39
In the GLOW trial, of the 2,333 patients screened, 2,104 unique patients had valid CLDN18.2 IHC results, and 38.4% of patients (n = 808) had tumours that were CLDN18.2-positive (defined as ≥ 75% of tumour cells demonstrating moderate to strong membranous CLDN18.2 staining).25 In total, 507 patients were randomized to receive either zolbetuximab plus CAPOX (n = 254) or placebo plus CAPOX (n = 253). The recruitment period was from January 21, 2019 (first patient randomized) to February 18, 2022 (last patient randomized).
Table 10: Summary of Patient Disposition in the SPOTLIGHT and GLOW Trials
Patient disposition | SPOTLIGHT | GLOW | ||
|---|---|---|---|---|
Zolbetuximab plus mFOLFOX6 | Placebo plus mFOLFOX6 | Zolbetuximab plus CAPOX | Placebo plus CAPOX | |
Screened, N | 2,735 | 2,333 | ||
Screened out, N (%) | 2,170 (79.3%) | 1,826 (78.3) | ||
Reason for being screened out, N (%) | ||||
CLDN18.2 status not available | 332 (15.3) | 229 (12.5) | ||
CLDN18.2-negative* | 1,481 (68.2) | 1,296 (71.0) | ||
Other | 357 (16.5) | 301 (16.5) | ||
Randomized, N | 283 | 282 | 254 | 253 |
Received at least 1 dose of study drug, N | 279 | 278 | 253 | 250 |
Discontinued from study drug, N (%) | 232 (82.3) | 236 (84.9) | 224 (88.2) | 231 (92.8) |
Reason for discontinuation, N (%) | ||||
Adverse event | 40 (14.3) | 14 (5.0) | 34 (13.4) | 14 (5.6) |
Lost to follow-up | 1 (0.4) | 0 | 24 (9.4) | 22 (8.8) |
Progressive disease | 133 (47.7) | 177 (63.7) | 103 (40.6) | 156 (62.7) |
Protocol deviation | 1 (0.4) | 0 | 2 (0.8) | 21 (8.4) |
Withdrawal by patient | 28 (10.0) | 16 (5.8) | 35 (13.8) | 21 (8.4) |
Pregnancy | 0 | 0 | 0 | 0 |
Other | 16 (5.7) | 14 (5.0) | 25 (9.8) | 16 (6.4) |
If progressive disease or death | ||||
Radiographic progression | 101 (36.2) | 133 (47.8) | 85 (33.5) | 138 (55.4) |
Clinical progression | 54 (19.4) | 74 (26.6) | 38 (15.0) | 62 (24.9) |
FAS, N | 283 | 282 | 254 | 253 |
SAF, N | 279 | 278 | 254 | 249 |
CAPOX = capecitabine plus oxaliplatin; CLDN18.2 = Claudin 18.2; FAS = full analysis set; mFOLFOX6 = modified 5-fluorouracil, folinic acid, and oxaliplatin; SAF = safety analysis set.
Source: Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Baseline Characteristics
The baseline characteristics outlined in Table 11 are limited to those that are most relevant to this review or were believed to affect the outcomes or interpretation of the study results.
Table 11: Summary of Baseline Characteristics in the SPOTLIGHT and GLOW Trials
Characteristic | SPOTLIGHT | GLOW | ||
|---|---|---|---|---|
Zolbetuximab plus mFOLFOX6 (N = 283) | Placebo plus mFOLFOX6 (N = 282) | Zolbetuximab plus CAPOX (N = 254) | Placebo plus CAPOX (N = 253) | |
Sex, n (%) | ||||
Female | 107 (37.8) | 107 (37.9) | 95 (37.4) | 97 (38.3) |
Male | 176 (62.2) | 175 (62.1) | 159 (62.6) | 156 (61.7) |
Race, n (%) | ||||
American Indian, Alaska Native | 9 (3.4) | 8 (3.2) | 0 | 0 |
Asian | 96 (36.8) | 97 (38.3) | 158 (62.7) | 158 (63.7) |
Black, African American | 5 (1.9) | 2 (0.8) | 0 | 0 |
Native Hawaiian, other Pacific Islander | 0 | 0 | 0 | 0 |
White | 140 (53.6) | 134 (53.0) | 94 (37.3) | 90 (36.3) |
Other | 11 (4.2) | 12 (4.7) | 0 | 0 |
Missing | 22 | 29 | 2 | 5 |
Age (years) | ||||
Mean (SD) | 59.7 (11.7) | 58.8 (13.0) | 58.6 (12.1) | 56.7 (13.0) |
Median (range) | 62.0 (27 to 83) | 60.0 (20 to 86) | 61.0 (22 to 82) | 59.0 (21 to 83) |
Age group 1 (years), n (%) | ||||
≤ 65 | 181 (64.0) | 181 (64.2) | 176 (69.3) | 180 (71.1) |
> 65 | 102 (36.0) | 101 (35.8) | 78 (30.7) | 73 (28.9) |
Age group 2 (years), n (%) | ||||
≤ 75 | 267 (94.3) | 260 (92.2) | 242 (95.3) | 239 (94.5) |
> 75 | 16 (5.7) | 22 (7.8) | 12 (4.7) | 14 (5.5) |
ECOG Performance Status at baseline, n (%) | ||||
0 | 125 (44.8) | 115 (41.4) | 108 (42.7) | 108 (43.2) |
1 | 153 (54.8) | 163 (58.6) | 145 (57.3) | 142 (56.8) |
2 | 1 (0.4) | 0 | 0 | 0 |
Missing | 4 | 4 | 1 | 3 |
Weight (kg) | ||||
Mean (SD) | 64.66 (14.47) | 65.43 (16.39) | 61.60 (13.60) | 60.17 (12.73) |
Median (range) | 63.00 (38.0 to 110.6) | 64.80 (28.5 to 128.3) | 60.50 (35.5 to 111.2) | 59.55 (29.1 to 100.0) |
BMI (kg/m2) | ||||
N | 279 | 277 | 253 | 250 |
Mean (SD) | 23.19 (4.19) | 23.47 (4.55) | 22.79 (4.32) | 22.05 (3.79) |
Median (range) | 22.98 (15.6 to 41.8) | 23.18 (13.4 to 43.1) | 22.12 (14.9 to 44.3) | 21.77 (13.1 to 34.0) |
BSA (m2) | ||||
Mean (SD) | 1.73 (0.23) | 1.74 (0.25) | 1.67 (0.20) | 1.65 (0.20) |
Median (range) | 1.73 (1.2 to 2.4) | 1.73 (1.1 to 2.5) | 1.67 (1.2 to 2.3) | 1.63 (1.1 to 2.3) |
Tobacco history, n (%) | ||||
Never | 142 (50.5) | 137 (48.9) | 128 (51.2) | 132 (53.0) |
Current | 26 (9.3) | 25 (8.9) | 32 (12.8) | 33 (13.3) |
Former | 113 (40.2) | 118 (42.1) | 90 (36.0) | 84 (33.7) |
Missing | 2 | 2 | 4 | 4 |
Primary diagnosis | ||||
Gastric adenocarcinoma | 219 (77.4) | 210 (74.5) | 219 (86.2) | 209 (82.6) |
GEJ adenocarcinoma | 64 (22.6) | 72 (25.5) | 35 (13.8) | 44 (17.4) |
Duration since initial diagnosis (days) | ||||
Mean (SD) | 270.4 (478.5) | 297.6 (675.2) | 230.2 (462.0) | 243.0 (609.5) |
Median (range) | 56 (2 to 3,010) | 56 (7 to 5,366) | 44.0 (12 to 2,396) | 43.5 (2 to 6,010) |
Tumour location | ||||
Gastric | ||||
N | 219 | 210 | 219 | 209 |
Proximal | 73 (33.6) | 59 (28.1) | 73 (33.3) | 73 (34.9) |
Distal | 91 (41.9) | 87 (41.4) | 90 (41.1) | 83 (39.7) |
Unknown | 53 (24.4) | 64 (30.5) | 56 (25.6) | 53 (25.4) |
Missing | 2 | 0 | 0 | 0 |
GEJ | ||||
N | 64 | 72 | 35 | 44 |
Proximal | 30 (47.6) | 26 (36.6) | 15 (42.9) | 21 (47.7) |
Distal | 19 (30.2) | 31 (43.7) | 10 (28.6) | 13 (29.5) |
Unknown | 14 (22.2) | 14 (19.7) | 10 (28.6) | 10 (22.7) |
Missing | 1 | 1 | 0 | 0 |
Tumour type | ||||
Diffuse | 82 (29.1) | 117 (42.1) | 87 (34.4) | 100 (39.5) |
Intestinal | 70 (24.8) | 66 (23.7) | 36 (14.2) | 41 (16.2) |
Mixed | 31 (11.0) | 13 (4.7) | 20 (7.9) | 21 (8.3) |
Unknown | 49 (17.4) | 40 (14.4) | 76 (30.0) | 64 (25.3) |
Other | 50 (17.7) | 42 (15.1) | 34 (13.4) | 27 (10.7) |
Missing | 1 | 4 | 1 | 0 |
Primary tumour | ||||
TX | 62 (22.1) | 46 (16.4) | 65 (25.6) | 47 (18.6) |
T0 | 0 | 0 | 1 (0.4) | 0 |
Tis | 1 (0.4) | 2 (0.7) | 0 | 0 |
T1 | 2 (0.7) | 4 (1.4) | 1 (0.4) | 1 (0.4) |
T1a | 2 (0.7) | 1 (0.4) | 0 | 2 (0.8) |
T1b | 2 (0.7) | 6 (2.1) | 1 (0.4) | 2 (0.8) |
T2 | 15 (5.3) | 16 (5.7) | 20 (7.9) | 12 (4.7) |
T3 | 86 (30.6) | 98 (34.9) | 63 (24.8) | 63 (24.9) |
T4 | 32 (11.4) | 35 (12.5) | 36 (14.2) | 44 (17.4) |
T4a | 56 (19.9) | 56 (19.9) | 47 (18.5) | 62 (24.5) |
T4b | 23 (8.2) | 17 (6.0) | 20 (7.9) | 20 (7.9) |
Missing | 2 | 1 | 0 | 0 |
Regional lymph nodes | ||||
NX | 66 (23.7) | 60 (21.4) | 82 (32.3) | 64 (25.3) |
N0 | 40 (14.3) | 38 (13.6) | 23 (9.1) | 25 (9.9) |
N1 | 56 (20.1) | 66 (23.6) | 48 (18.9) | 39 (15.4) |
N2 | 44 (15.8) | 51 (18.2) | 45 (17.7) | 51 (20.2) |
N3 | 42 (15.1) | 32 (11.4) | 31 (12.2) | 47 (18.6) |
N3a | 17 (6.1) | 19 (6.8) | 15 (5.9) | 14 (5.5) |
N3b | 14 (5.0) | 14 (5.0) | 10 (3.9) | 13 (5.1) |
Missing | 4 | 2 | 0 | 0 |
Distant metastasisa | ||||
M0 | 85 (30.4) | 70 (24.8) | 59 (23.3) | 56 (22.1) |
M1 | 195 (69.6) | 212 (75.2) | 194 (76.7) | 197 (77.9) |
Missing | 3 | 0 | 1 | 0 |
Tumour metastatica | ||||
No | 44 (15.5) | 44 (15.6) | 32 (12.6) | 31 (12.3) |
Yes | 239 (84.5) | 238 (84.4) | 222 (87.4) | 222 (87.7) |
Metastasis location (≥ 5% patients in any treatment group)b | ||||
Abdominal cavity | 19 (6.7) | 17 (6.0) | 16 (6.3) | 9 (3.6) |
Bone | 28 (9.9) | 23 (8.2) | 18 (7.1) | 26 (10.3) |
Liver | 62 (21.9) | 75 (26.6) | 73 (28.7) | 57 (22.5) |
Lung | 36 (12.7) | 33 (11.7) | 18 (7.1) | 21 (8.3) |
Lymph node | 101 (35.7) | 109 (38.7) | 131 (51.6) | 119 (47.0) |
Ovary | 16 (5.7) | 19 (6.7) | 21 (8.3) | 21 (8.3) |
Peritoneum | 94 (33.2) | 76 (27.0) | 83 (32.7) | 91 (36.0) |
History of Helicobacter pylori infection | ||||
No | 139 (49.1) | 136 (48.2) | 102 (40.2) | 114 (45.1) |
Yes | 31 (11.0) | 45 (16.0) | 44 (17.3) | 35 (13.8) |
Unknown | 113 (39.9) | 101 (35.8) | 108 (42.5) | 104 (41.1) |
Barrett’s esophagus diagnosed | ||||
No | 166 (58.7) | 173 (61.3) | 150 (59.1) | 163 (64.4) |
Yes | 7 (2.5) | 11 (3.9) | 4 (1.6) | 3 (1.2) |
Unknown | 110 (38.9) | 98 (34.8) | 100 (39.4) | 87 (34.4) |
CLDN18.2 testing result | ||||
< 75% | 0 | 0 | 0 | 0 |
≥ 75% | 283 (100) | 282 (100) | 254 (100) | 253 (100) |
Not applicable | 0 | 0 | 0 | 0 |
Measurable disease based on central imaging (yes) | 211 (74.6) | 211 (74.8) | 206 (81.1) | 209 (82.6) |
Measurable disease based on local imaging (yes) | 235 (83.0) | 227 (80.5) | 83 (32.7) | 91 (36.0) |
BMI = body mass index; BSA = body surface area; CAPOX = capecitabine plus oxaliplatin; CLDN18.2 = Claudin 18.2; ECOG = Eastern Cooperative Oncology Group; FAS = full analysis set; GEJ = gastroesophageal junction; HER2 = human epidermal growth factor receptor 2; mFOLFOX6 = modified 5-fluorouracil, folinic acid, and oxaliplatin; SD = standard deviation.
Note: Data cut-offs were on September 9, 2022 (SPOTLIGHT trial) and October 7, 2022 (GLOW trial).
aDistant metastases (M1) and tumour metastatic (Y) may differ depending on date of initial diagnosis.
bOther metastasis locations (reported in < 5% of patients) were omentum (3.9%), retroperitoneum (2.8%), adrenal gland (2.3%), esophagus (1.2%), mediastinum (1.2%), stomach (1.8%), pleura (1.6%), pancreas (1.1%), chest (0.9%), colon (0.9%), pelvis (0.9%), spleen (0.9%), heart (0.5%), rectum (0.5%), kidney (0.4%), bladder (0.2%), brain (0.2%), breast (0.2%), gallbladder (0.2%), neck (0.2%), pericardium (0.2%), skin (0.2%), and/or other (7.1%).
Sources: SPOTLIGHT trial and GLOW trial Clinical Study Reports.24,25
Exposure to Study Treatments
In the SPOTLIGHT trial, the mean duration of treatment with zolbetuximab was 260.6 days in the zolbetuximab plus mFOLFOX6 arm (SAF). The majority of patients had cumulative zolbetuximab exposure of more than 6 weeks (239 patients [85.7%]) or more than 12 weeks (206 patients [73.8%]). Exposure to chemotherapy was similar between the 2 arms. All patients received mFOLFOX6. In the SAF, the mean duration of treatment with the components of mFOLFOX6 was similar between the arms.24 In the GLOW trial, the mean duration of treatment with zolbetuximab was 194.8 days. A total of 170 patients (66.9%) had cumulative zolbetuximab exposure of more than 12 weeks. All patients in the SAF received CAPOX. The mean durations of treatment with the components of CAPOX were similar between the treatment groups.25
Patient exposure to study treatment in the SPOTLIGHT and GLOW trials is summarized in Table 12.
Table 12: Summary of Patient Exposure in the SPOTLIGHT and GLOW Trials
Exposure | SPOTLIGHT | GLOW | ||
|---|---|---|---|---|
Zolbetuximab plus mFOLFOX6 (n = 279) | Placebo plus mFOLFOX6 (n = 278) | Zolbetuximab plus CAPOX (n = 254) | Placebo plus CAPOX (n = 249) | |
Exposure to zolbetuximab or placebo | ||||
Duration of zolbetuximab or placebo (days) | ||||
Duration, mean (SD) | 260.6 (242.0) | 237.0 (182.1) | 194.8 (191.9) | 176.7 (148.4) |
Median (range) | 190.0 (1 to 1,246) | 195 (1 to 1,016) | 134.0 (1 to 933) | 148.0 (1 to 848) |
Relative dose intensity (%) | ||||
N | 278 | 278 | 253 | 249 |
Mean (SD) | 92.336 (19.002) | 98.474 (4.797) | 96.094 (15.619) | 99.591 (6.315) |
Median (range) | 100.000 (9.64 to 184.18) | 100.000 (64.43 to 112.50) | 100.000 (6.40 to 146.78) | 100.000 (3.49 to 114.29) |
Number of infusions administered | ||||
N | 279 | 278 | 254 | 249 |
Mean (SD) | 12.2 (10.7) | 11.1 (8.0) | 9.3 (8.5) | 8.5 (6.4) |
Median (range) | 9.0 (1 to 60) | 9.0 (1 to 46) | 6.0 (1 to 40) | 7.0 (1 to 38) |
Exposure to mFOLFOX6 components | ||||
Duration of oxaliplatin (days) | ||||
Duration, mean (SD) | 131.3 (56.5) | 130.0 (51.7) | NA | NA |
Median (range) | 150.0 (1 to 267) | 148.0 (1 to 253) | NA | NA |
Duration of leucovorin (days) | ||||
Duration, mean (SD) | 234.2 (233.2) | 204.0 (176.9) | NA | NA |
Median (range) | 180.5 (1 to 1,254) | 169.0 (1 to 1,030) | NA | NA |
Duration of levofolinic acid (days) | ||||
Duration, mean (SD) | 245.5 (214.5) | 218.5 (179.0) | NA | NA |
Median (range) | 183.0 (1 to 911) | 178.5 (1 to 919) | NA | NA |
Duration of 5-fluorouracil bolus (days) | ||||
Duration, mean (SD) | 204.8 (203.6) | 185.0 (163.5) | NA | NA |
Median (range) | 160.0 (1 to 1,212) | 149.0 (1 to 962) | NA | NA |
Duration of 5-fluorouracil infusion (days) | ||||
Duration, mean (SD) | 267.0 (225.4) | 225.9 (175.2) | NA | NA |
Median (range) | 198.0 (2 to 1,256) | 178 (3 to 1,032) | NA | NA |
mFOLFOX6 (24 weeks) treatment completed, N (%) | 103 (36.9%) | 99 (35.6%) | NA | NA |
Exposure to CAPOX components | ||||
Duration of oxaliplatin (days) | ||||
Duration, mean (SD) | NA | NA | 110.2 (61.9) | 110.4 (58.9) |
Median (range) | NA | NA | 123.5 (1 to 240) | 118.0 (1 to 223) |
Duration of capecitabine (days) | ||||
Duration, mean (SD) | NA | NA | 189.6 (166.9) | 170.7 (134.7) |
Median (range) | NA | NA | 141.5 (1 to 757) | 141.0 (1 to 862) |
CAPOX (24 weeks) treatment completed, N (%) | NA | NA | 70 (27.6%) | 69 (27.7%) |
CAPOX = capecitabine plus oxaliplatin; mFOLFOX6 = modified 5-fluorouracil, folinic acid, and oxaliplatin; NA = not applicable; SD = standard deviation.
Source: Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Prior Medications
In the SPOTLIGHT trial, 119 patients (21.1%) had received prior chemotherapy. The mean duration of medication was 5.33 months. Prior radiation therapy was received by 41 patients (7.3%). Of the randomized patients, 245 patients (43.4%) had undergone prior procedures for primary cancer.24 In the GLOW trial, 93 patients (18.3%) had received prior chemotherapy. The mean duration of medication was 5.5 months. Prior radiation therapy had been received by 20 patients (3.9%). A total of 182 patients (35.9%) had undergone prior procedures for primary cancer.25
Concomitant Medications
In both the SPOTLIGHT and GLOW trials, the frequency of concomitant medication use was similar across treatment groups (Table 14).24,25
Table 13: Prior Cancer Therapy (FAS)
Medication | SPOTLIGHT | GLOW | ||
|---|---|---|---|---|
Zolbetuximab plus mFOLFOX6 (n = 283) | Placebo plus mFOLFOX6 (n = 282) | Zolbetuximab plus CAPOX (n = 254) | Placebo plus CAPOX (n = 253) | |
Platinum-based chemotherapy | 13 (4.6) | 9 (3.2) | 3 (1.2) | 10 (4.0) |
Oxaliplatin-based chemotherapy | 35 (12.4) | 28 (9.9) | 21 (8.3) | 21 (8.3) |
Irinotecan | 0 | 0 | 0 | 0 |
S1 | 10 (3.5) | 6 (2.1) | 6 (2.4) | 6 (2.4) |
Docetaxel | 15 (5.3) | 9 (3.2) | 7 (2.8) | 6 (2.4) |
Ramucirumab | 0 | 0 | 0 | 0 |
Paclitaxel | 3 (1.1) | 6 (2.1) | 1 (0.4) | 5 (2.0) |
Ramucirumab with paclitaxel | 1 | (0.4) | 0 | 0 |
Nivolumab | 0 | 0 | 0 | 0 |
Pembrolizumab | 1 (0.4) | 0 | 0 | 0 |
Atezolizumab | 0 | 0 | 0 | 0 |
Herceptin | 0 | 0 | 0 | 0 |
Other | 39 (13.8) | 29 (10.3) | 38 (15.0) | 28 (11.1) |
CAPOX = capecitabine plus oxaliplatin; FAS = full analysis set; mFOLFOX6 = modified 5-fluorouracil, folinic acid, and oxaliplatin; S1 = oral 5-fluorouracil (5-FU) anticancer agent.
Note: Data cut-offs were September 9, 2022 (SPOTLIGHT trial) and October 7, 2022 (GLOW trial).
Sources: SPOTLIGHT trial Primary Analysis Clinical Study Report;25 GLOW trial Primary Analysis Clinical Study Report.25
Table 14: Concomitant Medications Used by at Least 20% of Patients in Any Group of Either Study (FAS)
Chemical subgroup (ATC fourth level) Preferred WHO name (ingredients) | SPOTLIGHT trial | GLOW trial | ||
|---|---|---|---|---|
Zolbetuximab plus mFOLFOX6 (n = 283) | Placebo plus mFOLFOX6 (n = 282) | Zolbetuximab plus CAPOX (n = 254) | Placebo plus CAPOX (n = 253) | |
Received concomitant medications, n (%) | 278 (98.2) | 277 (98.2) | 247 (97.2) | 246 (97.2) |
Anilides | 120 (42.4) | 126 (44.7) | 63 (24.8) | 56 (22.1) |
Paracetamol | 119 (42.0) | 126 (44.7) | 61 (24.0) | 54 (21.3) |
Other antiemetics | 125 (44.2) | 100 (35.5) | 112 (44.1) | 114 (45.1) |
Aprepitant | 86 (30.4) | 72 (25.5) | 86 (33.9) | 98 (38.7) |
Antiemetics and antinauseants | 9 (3.2) | 5 (1.8) | 148 (58.3) | 109 (43.1) |
Metoclopramide | 4 (1.4) | 2 (0.7) | 73 (28.7) | 61 (24.1) |
Metoclopramide hydrochloride | 1 (0.4) | 1 (0.4) | 71 (28.0) | 39 (15.4) |
Serotonin (5-HT3) antagonists | 147 (51.9) | 139 (49.3) | 128 (50.4) | 97 (38.3) |
Ondansetron | 88 (31.1) | 79 (28.0) | 40 (15.7) | 29 (11.5) |
Glucocorticoids | 116 (41.0) | 88 (31.2) | 100 (39.4) | 71 (28.1) |
Dexamethasone | 92 (32.5) | 63 (22.3) | 68 (26.8) | 49 (19.4) |
Proton pump inhibitors | 202 (71.4) | 183 (64.9) | 172 (67.7) | 157 (62.1) |
Omeprazole | 60 (21.2) | 61 (21.6) | 52 (20.5) | 49 (19.4) |
Propulsives | 199 (70.3) | 144 (51.1) | 59 (23.2) | 43 (17.0) |
Metoclopramide | 92 (32.5) | 66 (23.4) | 5 (2.0) | 5 (2.0) |
Metoclopramide hydrochloride | 95 (33.6) | 51 (18.1) | 0 | 3 (1.2) |
Colony-stimulating factors | 90 (31.8) | 90 (31.9) | 58 (22.8) | 39 (15.4) |
Filgrastim | 56 (19.8) | 56 (19.9) | 15 (5.9) | 17 (6.7) |
5-HT3 = 5-hydroxytryptamine type 3; ATC = anatomical therapeutic chemical; CAPOX = capecitabine plus oxaliplatin; FAS = full analysis set; mFOLFOX6 = modified 5-fluorouracil, folinic acid, and oxaliplatin.
Note: Data cut-offs were on September 9, 2022 (SPOTLIGHT trial) and October 7, 2022 (GLOW trial).
Sources: SPOTLIGHT trial Primary Analysis Clinical Study Report;25 GLOW trial Primary Analysis Clinical Study Report.25
Subsequent Treatment: New ACTs
In the SPOTLIGHT trial, a total of 135 patients (47.7%) in the zolbetuximab plus mFOLFOX6 arm and 148 patients (52.5%) in the placebo plus mFOLFOX6 arm received a new ACT after discontinuation of study treatment. The most frequently received new ACTs (at least 10% of patients) in both arms were (shown by preferred WHO name) paclitaxel (17.0% of patients in the zolbetuximab plus mFOLFOX6 arm and 19.5% of patients in the placebo plus mFOLFOX6 arm) and ramucirumab (12.4% of patients in the zolbetuximab plus mFOLFOX6 arm and 12.1% of patients in the placebo plus mFOLFOX6 arm).24
In the GLOW trial, a total of 118 patients (46.5%) in the zolbetuximab plus CAPOX arm and 140 patients (55.3%) in the placebo plus CAPOX arm received a new systemic anticancer therapy. The most frequently received (i.e., by at least 10% of patients in either arm) new ACTs in both arms were (shown by preferred WHO name) paclitaxel (18.1% of patients in the zolbetuximab plus CAPOX arm and 20.2% of patients in the placebo plus CAPOX arm) and ramucirumab (8.3% of patients in the zolbetuximab plus CAPOX arm and 11.1% of patients in the placebo plus CAPOX arm).25
Efficacy
Table 15 summarizes the efficacy end points from the SPOTLIGHT and GLOW trials.
Overall Survival
In the SPOTLIGHT trial final analysis of OS (September 8, 2023, data cut-off), treatment with zolbetuximab plus mFOLFOX6 demonstrated a statistically significant improvement compared with placebo plus mFOLFOX6 (P = 0.0075). The HR was 0.78 (95% CI, 0.64 to 0.95), and the median OS was 18.2 months (95% CI, 16.1 months to 20.6 months) in the zolbetuximab plus mFOLFOX6 arm and 15.6 months (95% CI, 13.7 months to 16.9 months) in the placebo plus mFOLFOX6 arm. In the GLOW trial, the final analysis of OS (January 12, 2024, data cut-off) demonstrated that treatment with zolbetuximab plus CAPOX was associated with a statistically significant improvement in OS compared with placebo plus CAPOX (P = 0.0047). The HR was 0.763 (95% CI, 0.622 to 0.936).
Kaplan-Meier plots of OS for the SPOTLIGHT and GLOW trials are provided in Figure 4 and Figure 5, respectively.
Table 15: Summary of Key Efficacy Results in the SPOTLIGHT and GLOW Trials
Analysis | SPOTLIGHT trial | GLOW trial | ||
|---|---|---|---|---|
Zolbetuximab plus mFOLFOX6 (n = 283) | Placebo plus mFOLFOX6 (n = 282) | Zolbetuximab plus CAPOX (n = 254) | Placebo plus CAPOX (n = 253) | |
PFS by IRC (per RECIST 1.1) (primary analysis) | ||||
PFS events, n (%) | 146 (51.6) | 167 (59.2) | 137 (53.9) | 172 (68.0) |
Median follow-up (months)a (95% CI) | 12.94 (11.63 to 15.28) | 12.65 (10.71 to 15.24) | 12.62 (10.32 to 15.21) | 12.09 (10.25 to 15.05) |
Median PFS (months) (95% CI)b | 10.61 (8.90 to 12.48) | 8.67 (8.21 to 10.28) | 8.21 (7.46 to 8.84) | 6.80 (6.14 to 8.08) |
HR (95% CI)a | 0.751 (0.598 to 0.942) | 0.687 (0.544 to 0.866) | ||
1-sided P valuec | 0.0066k | 0.0007k | ||
PFS rate, % (95% CI)d | ||||
At 6 months | 78.05 (72.43 to 82.67) | 71.95 (66.03 to 77.03) | 70.20 (63.42 to 75.96) | 61.47 (54.82 to 67.45) |
Difference (95% CI) | 6.10 (–1.74 to 13.94) | 8.73 (–1.07 to 18.53) | ||
At 12 months | 48.86 (41.92 to 55.43) | 35.04 (28.45 to 41.69) | 34.86 (27.75 to 42.05) | 19.13 (13.50 to 25.51) |
Difference (95% CI) | 13.82 (4.02 to 23.62) | 15.73 (5.93 to 25.53) | ||
At 18 months | 30.93 (23.83 to 38.28) | 20.82 (14.48 to 27.96) | 23.91 (17.09 to 31.38) | 10.62 (5.68 to 17.33) |
Difference (95% CI) | 10.11 (0.31 to 19.91) | 13.29 (3.49 to 23.09) | ||
At 24 months | 24.41 (17.36 to 32.13) | 14.87 (8.78 to 22.47) | 14.49 (6.17 to 26.19) | 7.28 (2.99 to 14.16) |
Difference (95% CI) | 9.54 (–0.26 to 19.34) | 7.21 (–4.55 to 18.97) | ||
At 30 months | 24.41 (17.36 to 32.13) | 13.01 (7.07 to 20.82) | NE (NE to NE) | 7.28 (2.99 to 14.16) |
Difference (95% CI) | 11.40 (1.60 to 21.20) | NE (NE to NE) | ||
OS (final analysis) | ||||
Deaths, n (%) | 197 (69.6) | 217 (77.0) | 180 (70.9) | 207 (81.8) |
Median follow-up time (months) (95% CI)a | 33.28 (29.27 to 37.59) | 31.38 (28.68 to 36.17) | 31.70 (28.19 to 33.71) | 32.95 (29.70 to 35.91) |
Median OS (months) (95% CI)b | 18.23 (16.13 to 20.63) | 15.57 (13.67 to 16.92) | 14.32 (12.09 to 16.39) | 12.16 (10.28 to 13.67) |
HR (95% CI)a | 0.784 (0.644 to 0.954) | 0.763 (0.622 to 0.936) | ||
1-sided P valuec | 0.0075k | 0.0047k | ||
OS rate, % (95% CI)d | ||||
At 12 months | 67.36 (61.36 to 72.64) | 60.65 (54.57 to 66.19) | 56.68 (50.08 to 62.75) | 50.44 (43.89 to 56.61) |
Difference (95% CI) | 6.71 (–1.13 to 14.55) | 6.24 (–3.56 to 16.04) | ||
At 24 months | 37.71 (31.68 to 43.71) | 29.45 (23.99 to 35.10) | 29.02 (23.21 to 35.06) | 18.81 (14.01 to 24.16) |
Difference (95% CI) | 8.26 (0.42 to 16.10) | 10.21 (2.37 to 18.05) | ||
At 36 months | 20.92 (15.53 to 26.87) | 13.72 (9.12 to 19.26) | 18.30 (12.95 to 24.39) | 7.88 (4.41 to 12.63) |
Difference (95% CI) | 7.20 (–0.64 to 15.04) | 10.42 (2.58 to 18.26) | ||
At 48 months | 15.55 (10.07 to 22.13) | 11.40 (6.89 to 17.16) | 16.77 (11.28 to 23.20) | 7.88 (4.41 to 12.63) |
Difference (95% CI) | 4.15 (–3.69 to 11.99) | 8.89 (1.05 to 16.73) | ||
Time to first confirmed deterioration | ||||
EORTC QLQ-C30 PF (deterioration threshold = 13) | ||||
Total patients, n (%) | 283 (100.0) | 282 (100.0) | 254 (100.0) | 253 (100.0) |
Deterioration events, n (%) | 115 (40.6) | 102 (36.2) | 99 (39.0) | 109 (43.1) |
Median TTCD (months) (95% CI) | 10.71 (6.01 to NE) | 12.32 (9.26 to NE) | 8.31 (5.88 to 19.81) | 7.92 (6.47 to 11.10) |
Stratified HR (95% CI)e | 1.309 (1.000 to 1.713) | 0.999 (0.759 to 1.315) | ||
Stratified 1-sided P valuec | 0.0252 | 0.4980 | ||
EORTC QLQ-OG25 Pain scale (deterioration threshold = 16.7) | ||||
Total patients, n (%) | 283 (100.0) | 282 (100.0) | 254 (100.0) | 253 (100.0) |
Deterioration events, n (%) | 13 (13.4) | 54 (19.1) | 99 (39.0) | 109 (43.1) |
Median TTCD (months) (95% CI) | NYR | NYR (15.08 to NE) | NYR | 25.82 (NE to NE) |
Stratified HR (95% CI)e | 0.679 (0.446 to 1.034) | 1.066 (0.692 to 1.642) | ||
Stratified 1-sided P valuec | 0.0345 | 0.3880 | ||
EORTC GHS/QoL scale (deterioration threshold = 13) | ||||
Total patients, n (%) | 283 (100.0) | 282 (100.0) | 254 (100.0) | 253 (100.0) |
Deterioration events, n (%) | 111 (39.2) | 105 (37.2) | 85 (33.5) | 111 (43.9) |
Median TTCD (months) (95% CI) | 15.44 (6.90 to 22.83) | 11.83 (8.74 to 15.08) | 9.69 (7.39 to NE) | 7.49 (6.11 to 9.86) |
Stratified HR (95% CI)e | 1.68 (0.890 to 1.533) | 0.847 (0.636 to 1.129) | ||
Stratified 1-sided P valuec | 0.1321 | 0.1299 | ||
Objective response rate by IRC (per RECIST 1.1) | ||||
Best overall response, n (%)f | 256 (90.5) | 266 (94.3) | 210 (82.7) | 226 (89.3) |
CR | 19 (6.7) | 10 (3.5) | 9 (3.5) | 5 (2.0) |
PR | 116 (41.0) | 124 (44.0) | 99 (39.0) | 97 (38.3) |
Stable disease | 45 (15.9) | 52 (18.4) | 46 (18.1) | 57 (22.5) |
Non-CR/non-PD | 52 (18.4) | 59 (20.9) | 40 (15.7) | 33 (13.0) |
Progressive disease | 15 (5.3) | 17 (6.0) | 11 (4.3) | 28 (11.1) |
Not evaluable | 4 (1.4) | 3 (1.1) | 1 (0.4) | 5 (2.0) |
No disease | 5 (1.8) | 1 (0.4) | 4 (1.6) | 1 (0.4) |
Not availableg | 27 | 16 | 44 | 27 |
ORR, n (%) (95% CI) | 135 (47.7) | 134 (47.5) | 108 (42.5) | 102 (40.3) |
Difference, % (95% CI) | 0.2 (–8.14 to 8.53) | 2.2 (–6.43 to 10.83) | ||
Odds ratio | NR | NR | ||
95% CI for ORR | (41.76 to 53.70) | (41.56 to 53.52) | (36.36 to 48.85) | (34.22 to 46.64) |
Stratified 1-sided P valueh | 0.4875l | 0.3104l | ||
DCR, n (%)i | 232 (82.0) | 245 (86.9) | 194 (76.4) | 192 (75.9) |
Difference, % (95% CI) | –4.9 (NR) | 0.4 (NR) | ||
Odds ratio | NR | NR | ||
95% CI for DCR | (77.00 to 86.28) | (82.37 to 90.59) | (70.67 to 81.46) | (70.13 to 81.03) |
Stratified 1-sided P valueh | 0.0569l | 0.4609l | ||
Duration of response by IRC (per RECIST 1.1) | ||||
Events, n (%) | 67 (49.6) | 77 (57.5) | 66 (61.1) | 67 (65.7) |
Censored, n (%) | 68 (50.4) | 57 (42.5) | 42 (38.9) | 35 (34.3) |
Median DOR, months (95% CI)b | 9.00 (6.87 to 10.25) | 8.05 (6.47 to 10.81) | 6.14 (5.03 to 8.08) | 6.08 (4.44 to 6.34) |
Stratified 1-sided P valuec,j | 0.2218l | 0.0673l | ||
HR (95% CI) | 0.876 (0.623 to 1.233) | 0.758 (0.527 to 1.089) | ||
CAPOX = capecitabine plus oxaliplatin; CI = confidence interval; CR = complete response; DCR = disease control rate; DOR = duration of response; EORTC QLQ-C30 PF = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 Physical Functioning; EORTC GHS/QoL = European Organisation for Research and Treatment of Cancer Global Health Status/Quality of Life; EORTC QLQ-OG25 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Oesophago-Gastric 25; HR = hazard ratio; IRC = independent review committee; mFOFLOX6 = modified 5-fluorouracil, folinic acid, and oxaliplatin; NE = not evaluable; NR = not reported; NYR = not yet reached; ORR = objective response rate; OS = overall survival; PD = partial disease; PFS = progression-free survival; PR = partial response; RECIST 1.1 = Response Evaluation Criteria in Solid Tumours Version 1.1; TTCD = time to confirmed deterioration.
aBased on a Cox proportional hazards model with treatment, region, number of organs with metastatic sites, and prior gastrectomy as the explanatory variables. Assuming proportional hazards, an HR < 1 indicates a reduction in the rate in favour of the treatment arm.
bBased on Kaplan-Meier estimate.
cBased on 1-sided log-rank test; P values for the TTCD end points are not suitable to support inference because the test for noninferiority failed for these end points.
dRate and 95% CI were estimated using the Kaplan-Meier method and Greenwood formula.
eBased on stratified Cox proportional hazard model with region, number of organs with metastatic sites, and prior gastrectomy as the explanatory variables. Assuming proportional hazards, an HR < 1 indicates a reduction in the hazard rate in favour of the treatment arm.
fThe definition of best overall response followed RECIST 1.1. When stable disease (or non-CR/non-PD) is believed to be best response, the assessment should be at least 8 weeks after randomization. For calculation of percentages, the denominator includes the total number of patients in each arm.
gNo postbaseline imaging assessment.
hBased on a 1-sided Cochran-Mantel-Haenszel test. Stratification factors were region, number of organs with metastatic sites, and prior gastrectomy.
iDCR was defined as the proportion of patients who have a best overall response of CR, PR, stable disease, or non-CR or non-PD (≥ 8 weeks).
jStratification factors were region, number of organs with metastatic sites, and prior gastrectomy from interactive response technology.
kP value adjusted for multiplicity.
lP value not adjusted for multiplicity.
Sources: SPOTLIGHT trial and GLOW trial Primary Analysis Clinical Study Reports;24,25 final OS analysis for the SPOTLIGHT trial from Shitara et al. (2024);40 SPOTLIGHT trial Final Analysis Clinical Study Report;42 final OS analysis for the GLOW trial.
Progression-Free Survival
In the SPOTLIGHT trial, treatment with zolbetuximab plus mFOLFOX6 showed a statistically significant improvement in PFS compared with placebo plus mFOLFOX6 (HR = 0.75; 95% CI, 0.598 to 0.942; 1-sided P = 0.0066). In the zolbetuximab plus mFOLFOX6 group, 146 patients (51.6%) had either progressed or died by the cut-off date, with a median PFS of 10.61 months (95% CI, 8.90 months to 12.48 months). In the placebo plus mFOLFOX6 group, 167 patients (59.2%) had disease progression or died, with a median PFS duration of 8.67 months (95% CI, 8.21 months to 10.28 months). The PFS rates at 12 months were 48.9% and 35.0% in the zolbetuximab plus mFOLFOX6 group and placebo plus mFOLFOX6 group, respectively. Median follow-up times were similar, with 12.94 months (95% CI, 11.63 months to 15.28 months) in the zolbetuximab plus mFOLFOX6 arm and 12.65 months (95% CI, 10.71 months to 15.24 months) in the placebo plus mFOLFOX6 arm.24
Figure 4: Kaplan-Meier Plot of OS in the SPOTLIGHT trial (FAS; Final Analysis)
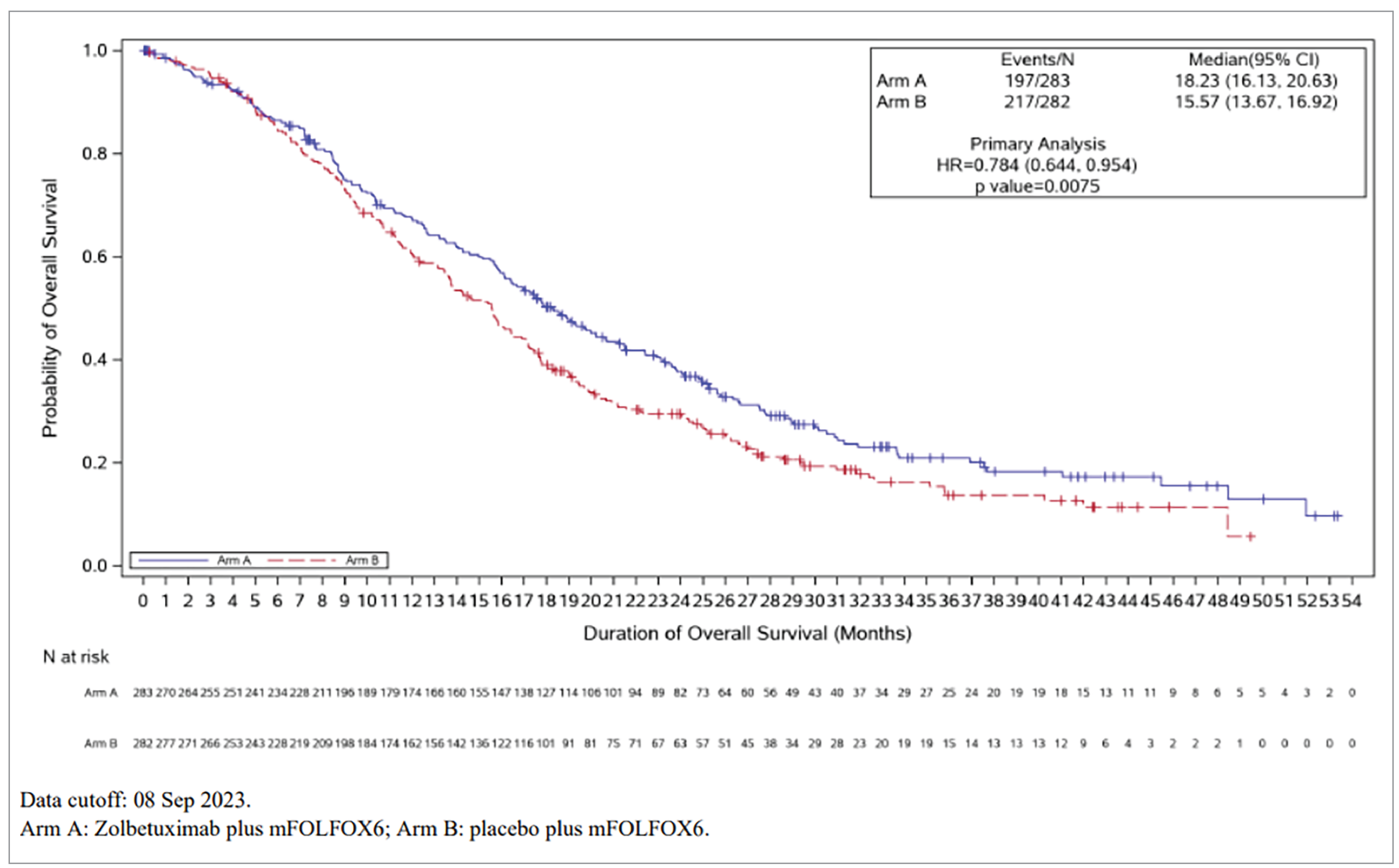
CI = confidence interval; FAS = full analysis set; HR = hazard ratio; OS = overall survival.
Source: SPOTLIGHT trial Clinical Study Report.48
In the GLOW trial, treatment with zolbetuximab plus CAPOX demonstrated a statistically significant improvement in PFS compared with placebo plus CAPOX (HR = 0.687; 95% CI, 0.544 to 0.866; 1-sided P = 0.0007). In the zolbetuximab plus CAPOX group, 137 patients (53.9%) had disease progression or died, with a median PFS of 8.21 (95% CI, 7.46 to 8.84) months. In the arm receiving placebo plus CAPOX, 172 patients (68.0%) had either progressed or died, with a median PFS of 6.80 months (95% CI, 6.14 months to 8.08 months). The PFS rates at 12 months were 34.86% (95% CI, 27.75% to 42.05%) and 19.13% (95% CI, 13.50% to 25.51%) in the zolbetuximab and placebo groups, respectively. The median follow-up times were 12.62 months (95% CI, 10.32 months to 15.21 months) in the zolbetuximab plus CAPOX arm and 12.09 months (95% CI, 10.25 months to 15.05 months) in the placebo plus CAPOX arm.25 Kaplan-Meier plots of PFS for the SPOTLIGHT and GLOW trials are provided in Figure 6 and Figure 7, respectively.
Figure 5: Kaplan-Meier Plot of OS in the GLOW trial (FAS; Final Analysis)
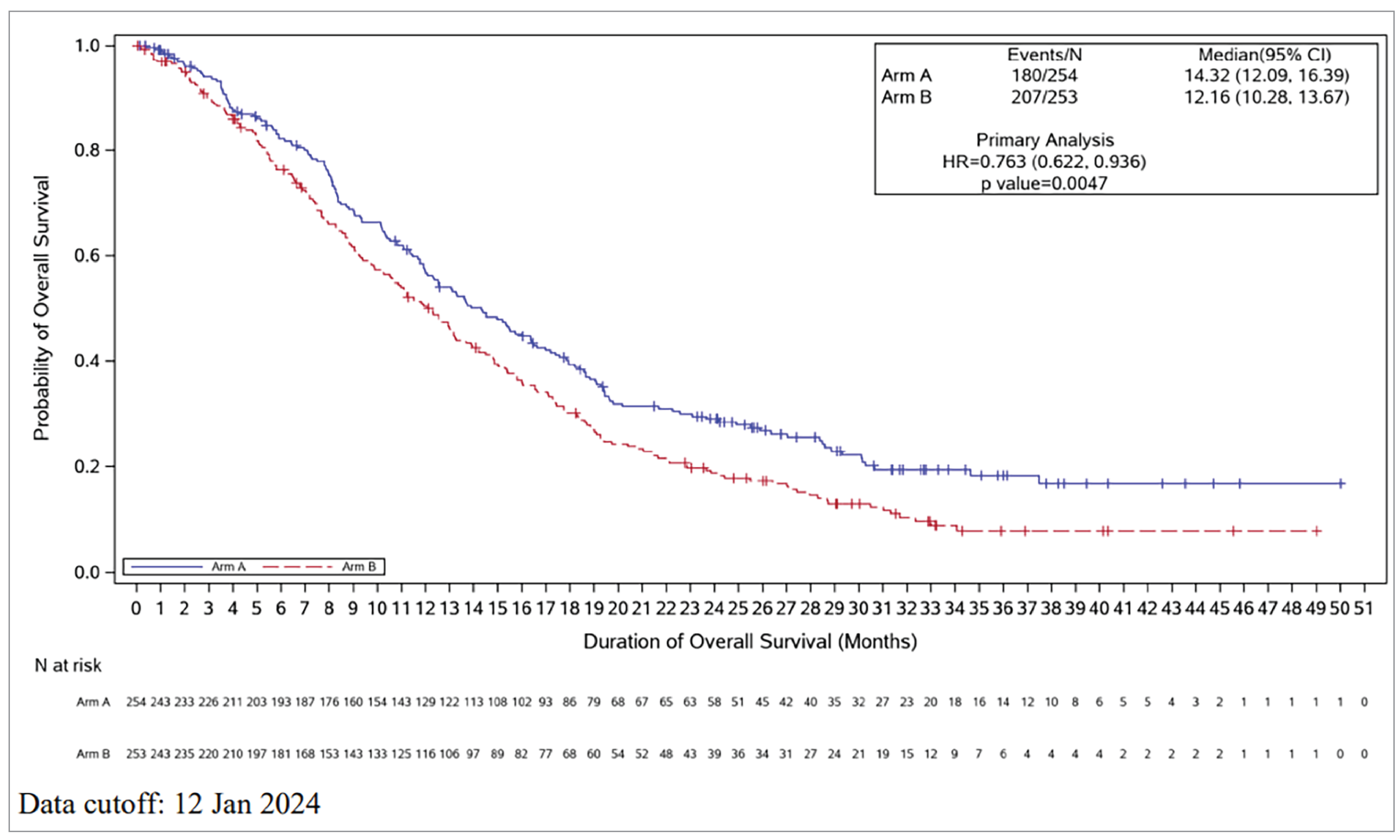
CI = confidence interval; FAS = full analysis set; HR = hazard ratio; OS = overall survival.
Source: GLOW trial Clinical Study Report.49
Objective Response Rate
In both the SPOTLIGHT and GLOW trials, there was no statistically significant difference between the zolbetuximab plus mFOLFOX6 (or CAPOX) group and the placebo plus mFOLFOX6 (or CAPOX group). In the SPOTLIGHT trial, 135 patients (47.7%) in the zolbetuximab plus mFOLFOX6 group and 134 patients (47.5%) in the placebo plus mFOLFOX6 group had an objective response. In the zolbetuximab plus mFOLFOX6 arm, the ORR per IRC was 47.7% (95% CI, 41.76% to 53.70%), and the DCR was 82.0% (95% CI, 77.00% to 86.28%). In the placebo plus mFOLFOX6 group, the ORR per IRC was 47.5% (95% CI, 41.56% to 53.52%), and the DCR was 86.9% (95% CI, 82.37% to 90.59%).24 In the GLOW trial, the ORRs per IRC were 42.5% (95% CI, 36.36% to 48.85%) in the zolbetuximab plus CAPOX group and 40.3% (95% CI, 34.22% to 46.64%) in the placebo plus CAPOX group. The DCRs were 76.4% (95% CI, 70.67% to 81.46%) in the zolbetuximab plus CAPOX group and 75.9% (95% CI, 70.13% to 81.03%) in the placebo plus CAPOX group.
Figure 6: Kaplan-Meier Plot of PFS by IRC per RECIST 1.1 in the SPOTLIGHT Trial (FAS)
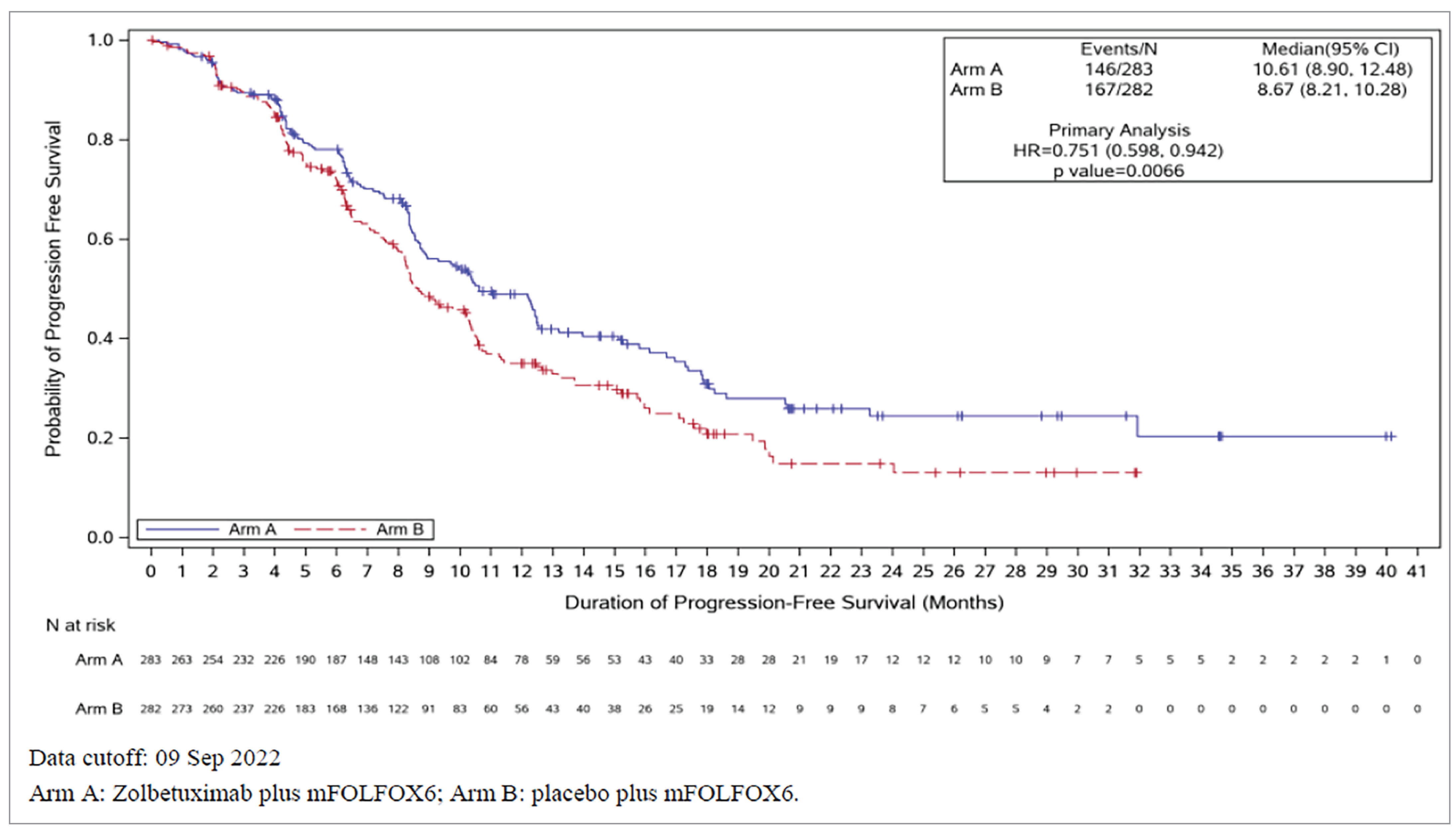
CI = confidence interval; FAS = full analysis set; HR = hazard ratio; IRC = independent review committee; mFOFLOX6 = modified 5-fluorouracil, folinic acid, and oxaliplatin; PFS = progression-free survival; RECIST 1.1 = Response Evaluation Criteria in Solid Tumours Version 1.1.
Source: SPOTLIGHT trial Primary Analysis Clinical Study Report.24
Disease Control Rate
Similarly to ORR, there was no statistically significant difference in DCR between the zolbetuximab plus mFOLFOX6 (or CAPOX) group and the placebo plus mFOLFOX6 (or CAPOX) group in either the SPOTLIGHT trial or the GLOW trial. In the SPOTLIGHT trial, the DCRs were 82.0% (95% CI, 77.00% to 86.28%) in the zolbetuximab plus mFOLFOX6 group and 86.9% (95% CI, 82.37% to 90.59%) in the placebo plus mFOLFOX6 group (P = 0.0569). In the GLOW trial, the DCRs were 76.4% (95% CI, 70.67% to 81.46%) in the zolbetuximab plus CAPOX group and 75.9% (95% CI, 70.13% to 81.03%) in the placebo plus CAPOX group (P = 0.4609).
Duration of Response
There were no statistically significant differences in DOR between the zolbetuximab plus mFOLFOX6 (or CAPOX) group and the placebo plus mFOLFOX6 (or CAPOX) group in either the SPOTLIGHT trial (HR = 0.876; 95% CI, 0.623 to 1.233; P = 0.2218) or the GLOW trial (HR = 0.758; 95% CI, 0.527 to 1.089; P = 0.0673).
Figure 7: Kaplan-Meier Plot of PFS by IRC per RECIST 1.1 in the GLOW Trial (FAS)
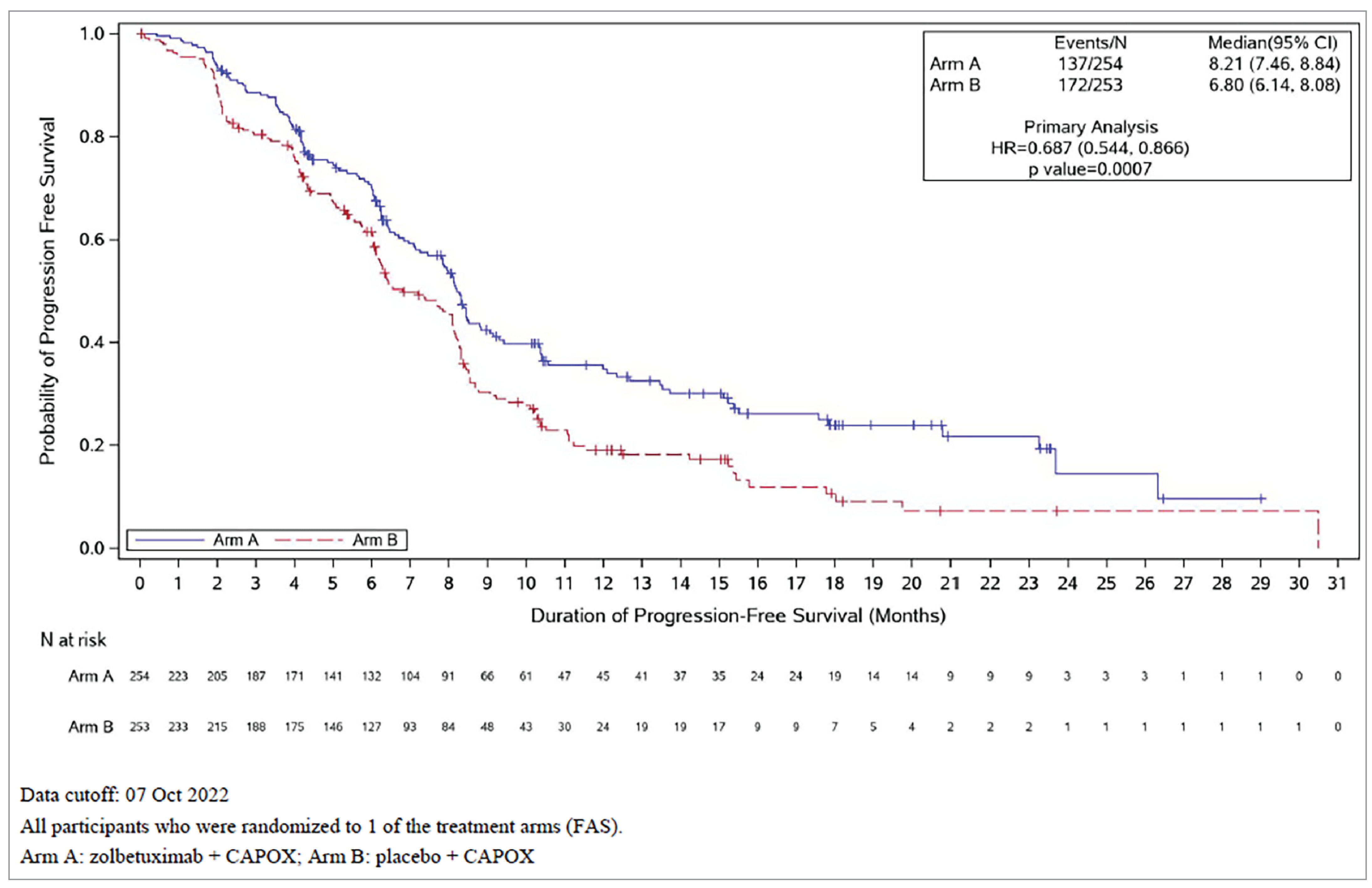
CAPOX = capecitabine plus oxaliplatin; CI = confidence interval; FAS = full analysis set; HR = hazard ratio; IRC = independent review committee; PFS = progression-free survival; RECIST 1.1 = Response Evaluation Criteria in Solid Tumours Version 1.1.
Source: GLOW trial Primary Analysis Clinical Study Report.25
Health-Related Quality of Life
TTCD in EORTC QLQ-C30 PF
In the SPOTLIGHT trial, based on a total of 217 deterioration events in EORTC QLQ-C30 PF scale score, the median (95% CI) TTCDs for EORTC QLQ-C30 PF scale score were 10.71 months (6.01 months to NE) for patients who received zolbetuximab plus mFOLFOX6 and 12.32 months (9.26 months to NE) for patients who received placebo plus mFOLFOX6 (HR = 1.309; 95% CI, 1.000 to 1.713).24 In the GLOW trial, based on a total of 208 deterioration events in EORTC QLQ-C30 PF scale score, the median TTCDs for EORTC QLQ-C30 PF scale score were 8.31 months (95% CI, 5.88 months to 19.81 months) for patients who received zolbetuximab plus CAPOX and 7.92 months (95% CI, 6.47 months to 11.10 months) for patients who received placebo plus CAPOX (HR = 0.999; 95% CI, 0.759 to 1.315).25
Figure 8: Forest Plot of PFS Assessed by IRC in the SPOTLIGHT Trial — Subgroup Analysis (FAS)
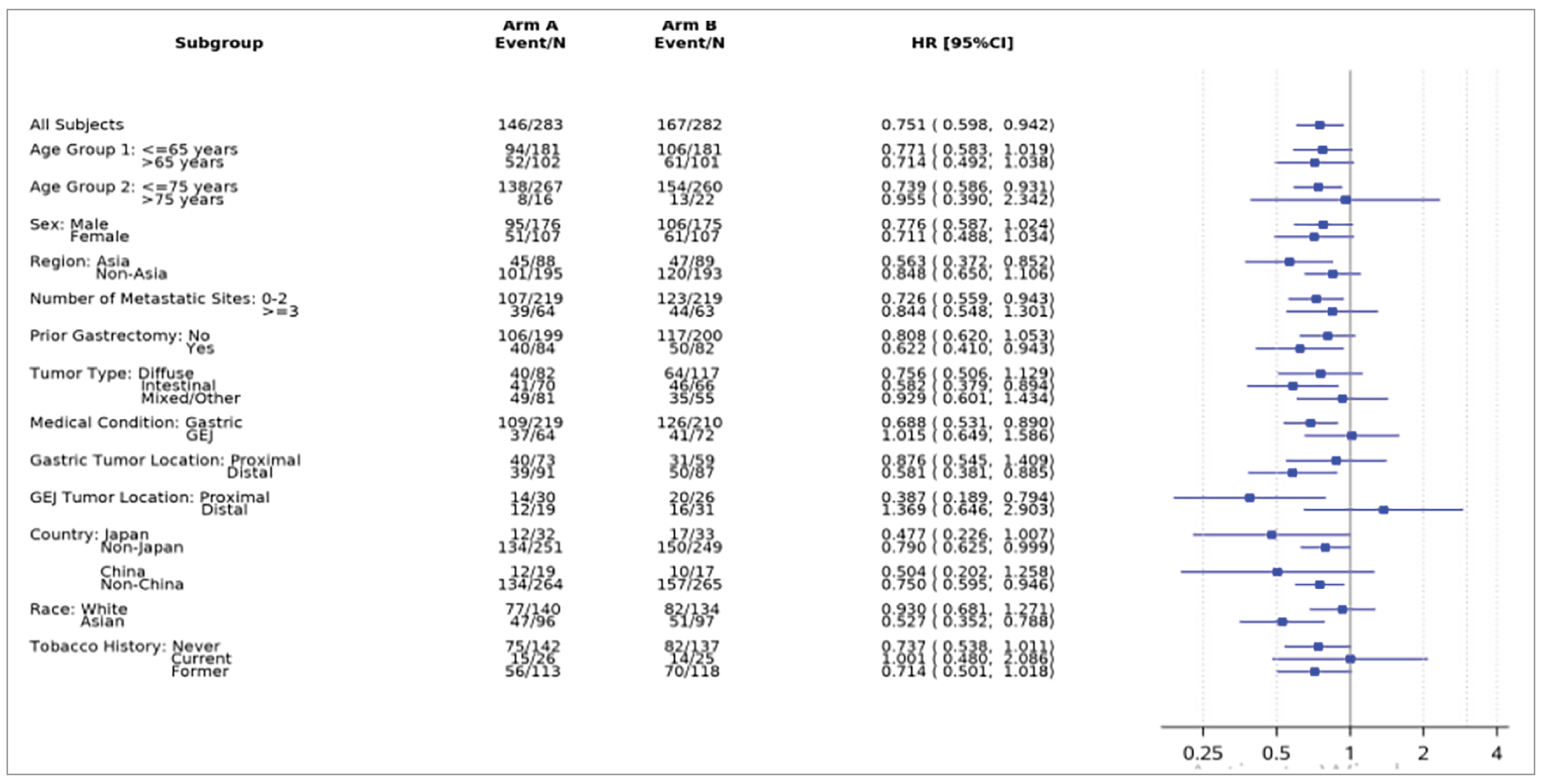
CI = confidence interval; FAS = full analysis set; GEJ = gastroesophageal junction; HR = hazard ratio; IRC = independent review committee; PFS = progression-free survival.
Source: SPOTLIGHT trial Primary Analysis Clinical Study Report.24
TTCD in EORTC QLQ-OG25 Pain Scale
In the SPOTLIGHT trial, based on a total of 92 deterioration events in the EORTC QLQ-OG25 Pain scale, the median TTCD for pain was not yet reached for patients who received zolbetuximab plus mFOLFOX6 or placebo plus mFOLFOX6 (HR = 0.679; 95% CI, 0.446 to 1.034).24 In the GLOW trial, based on a total of 84 deterioration events in pain score, the median TTCD for pain was not yet reached for patients who received zolbetuximab plus CAPOX; it was 25.82 months (95% CI, not estimable) for patients who received placebo plus CAPOX (HR = 1.066; 95% CI, 0.692 to 1.642).25
Figure 9: Forest Plot of PFS Assessed by IRC in the GLOW Trial — Subgroup Analysis (FAS)
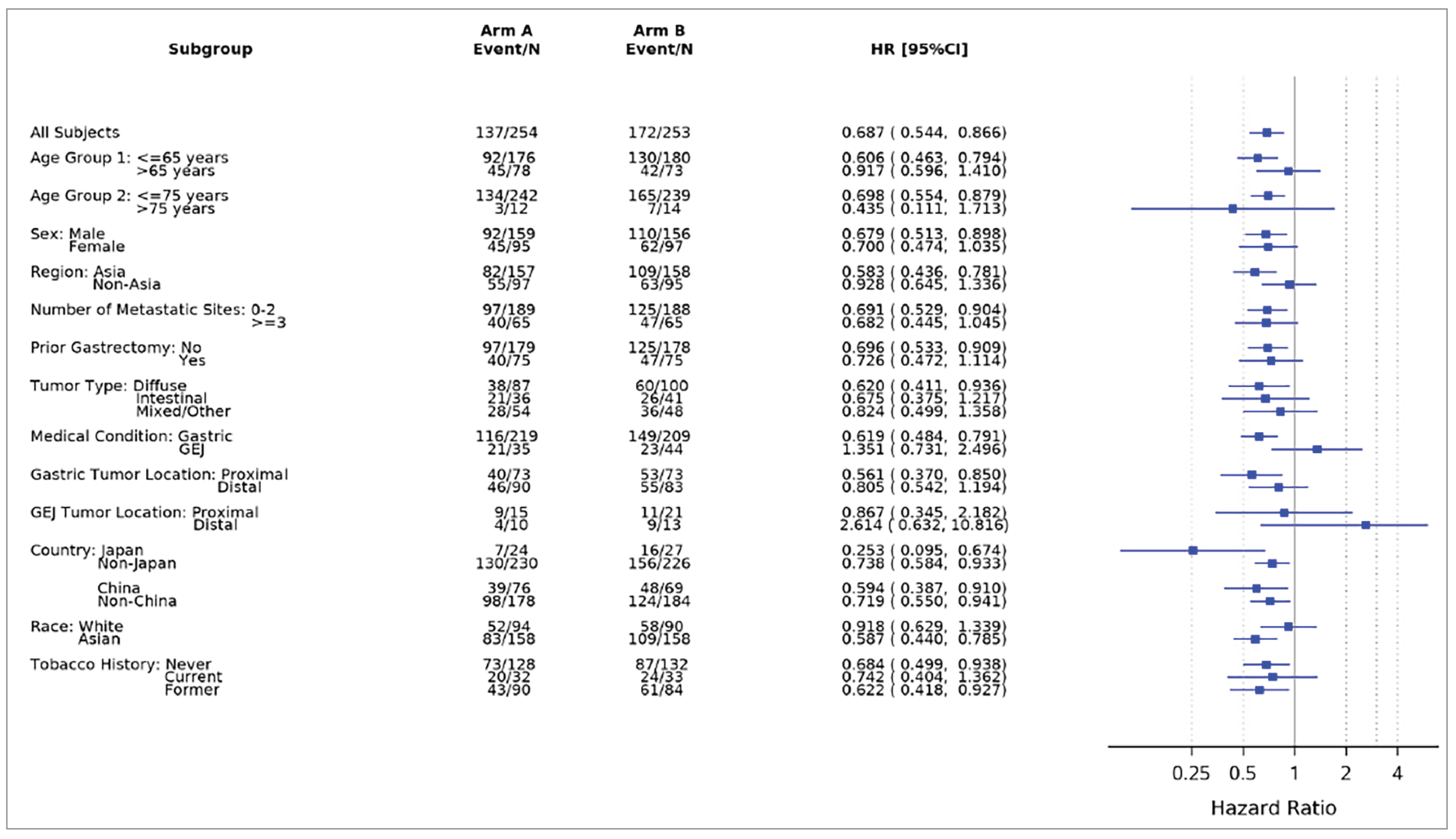
CI = confidence interval; FAS = full analysis set; GEJ = gastroesophageal junction; HR = hazard ratio; IRC = independent review committee; PFS = progression-free survival.
Source: GLOW trial Primary Analysis Clinical Study Report.25
TTCD in Global Health Status/Quality of Life
In the SPOTLIGHT trial, based on a total of 216 deterioration events in EORTC GHS/QoL scale score, the median (95% CI) TTCDs for the EORTC GHS/QoL scale were 15.44 months (95% CI, 6.90 months to 22.83 months) for patients who received zolbetuximab plus mFOLFOX6 and 11.83 months (95% CI, 8.74 months to 15.08 months) for patients who received placebo plus mFOLFOX6 (HR = 1.168; 95% CI, 0.890 to 1.533).24 In the GLOW trial, based on a total of 196 deterioration events in EORTC GHS/QoL scale scores, the median TTCDs for the EORTC GHS/QoL scale were 9.69 months (95% CI, 7.39 months to NE) months for patients who received zolbetuximab plus CAPOX and 7.49 months (95% CI, 6.11 months to 9.86 months) for patients who received placebo plus CAPOX (HR = 0.847; 95% CI, 0.636 to 1.129).25
Time to Progression
In the SPOTLIGHT trial, 87 patients (30.7%) in the zolbetuximab plus mFOLFOX6 arm and 98 patients (34.8%) in the placebo plus mFOLFOX6 arm had progression events. The median TTPs were 17.81 months in the zolbetuximab plus mFOLFOX6 arm and 12.52 months in the placebo plus mFOLFOX6 arm (P = 0.0133). In the GLOW trial, 77 patients (30.3%) in the zolbetuximab plus CAPOX arm and 103 patients (40.7%) in the placebo plus CAPOX arm had progression events. The median TTPs, according to IRC, were 11.99 months (95% CI, 8.84 months to 20.80 months) in the zolbetuximab plus CAPOX arm and 8.31 months (95% CI, 8.11 months to 9.95 months) in the placebo plus CAPOX arm (P = 0.0002).
Table 16: Estimates of TTP Assessed by IRC in the SPOTLIGHT and GLOW Trials (FAS)
Analyses | SPOTLIGHT | GLOW | ||
|---|---|---|---|---|
Zolbetuximab plus mFOLFOX6 (n = 283) | Placebo plus mFOLFOX6 (n = 282) | Zolbetuximab plus CAPOX (n = 254) | Placebo plus CAPOX (n = 253) | |
Progression events, n (%) | 87 (30.7) | 98 (34.8) | 77 (30.3) | 103 (40.7) |
Radiographical progression, n (%) | 87 (30.7) | 98 (34.8) | 77 (30.3) | 103 (40.7) |
Censored, n (%) | 196 (69.3) | 184 (65.2) | 177 (69.7) | 150 (59.3) |
TTP, monthsa | ||||
Median TTP (95% CI) | 17.81 (12.48 to 23.26) | 12.52 (10.22 to 17.97) | 11.99 (8.84 to 20.80) | 8.31 (8.11 to 9.95) |
Stratified analysisb | ||||
1-sided P valuec | 0.0133 | 0.0002 | ||
Hazard ratio (95% CI) | NR | NR | ||
Event-free rates at time points | NR | NR | ||
CAPOX = capecitabine plus oxaliplatin; CI = confidence interval; FAS = full analysis set; IRC = independent review committee; IRT = interactive response technology; mFOLFOX6 = modified 5-fluorouracil, folinic acid, and oxaliplatin; NR = not reported; TTP = time to progression.
Notes: Data cut-offs were September 9, 2022 (SPOTLIGHT trial) and October 7, 2022 (GLOW trial).
aBased on Kaplan-Meier estimate.
bStratification factors were region, number of organs with metastatic sites, and prior gastrectomy from IRT.
cBased on 1-sided log-rank test; not adjusted for multiple comparisons.
Sources: SPOTLIGHT trial Primary Analysis Clinical Study Report24 and GLOW trial Primary Analysis Clinical Study Report.2.5
PFS After Subsequent Therapy
In both the SPOTLIGHT and GLOW trials, PFS2 was defined as the time from the date of randomization until the date of radiological or objective PD (per patient’s local physician) following subsequent (second-line) ACT or death from any cause, whichever was earliest. In cases where PFS2 could not be reliably determined, the end date of subsequent (second-line) ACT or the start date of third-line ACT was used as the event date. Otherwise, patients were censored.24,25
In the SPOTLIGHT trial, based on a total 388 PFS2 events at the data cut-off date, treatment with zolbetuximab plus mFOLFOX6 showed a 22% reduction in the risk of a patient experiencing a PFS2 event compared with placebo plus mFOLFOX6 (HR = 0.782; 95% CI, 0.637 to 0.961). A total of 79 patients (27.9%) in the zolbetuximab plus mFOLFOX6 arm and 71 patients (25.2%) in the placebo plus mFOLFOX6 arm had progressed after starting new ACT. The median PFS2s were 14.23 months (95% CI, 12.12 months to 16.82 months) in the zolbetuximab plus mFOLFOX6 arm and 11.99 months (11.20 months to 13.40 months) in the placebo plus mFOLFOX6 arm.24
In the GLOW trial, based on a total of 376 PFS2 events at the data cut-off date, treatment with zolbetuximab plus CAPOX demonstrated a 29.2% reduction in the risk of a patient experiencing a PFS2 event compared with placebo plus CAPOX (HR = 0.708; 95% CI, 0.575 to 0.871). A total of 44 patients (17.3%) in the zolbetuximab plus CAPOX arm and 64 patients (25.3%) in the placebo plus CAPOX arm had progressed after starting new anticancer therapy. The median PFS2s were 11.01 months (95% CI, 10.02 months to 13.11 months) in the zolbetuximab plus CAPOX arm and 9.03 months (95% CI, 8.28 months to 9.89 months) in the placebo plus CAPOX arm.25
Table 17: Summary of PFS2 by Investigator Assessment in the SPOTLIGHT and GLOW Trials (FAS)
Analysis | SPOTLIGHT | GLOW | ||
|---|---|---|---|---|
Zolbetuximab plus mFOLFOX6 (n = 283) | Placebo plus mFOLFOX6 (n = 282) | Zolbetuximab plus CAPOX (n = 254) | Placebo plus CAPOX (n = 253) | |
PFS2 events, n (%) | 185 (65.4) | 203 (72.0) | 171 (67.3) | 205 (81.0) |
Progression of disease after new ACT | 79 (27.9) | 71 (25.2) | 44 (17.3) | 65 (25.3) |
Death after new ACT | 29 (10.2) | 46 (16.3) | 41 (16.1) | 50 (19.8) |
Death from any cause without new ACT | 64 (22.6) | 71 (25.2) | 69 (27.2) | 71 (28.1) |
No PD, no death, ended second-line or started third-line ACT | 13 (4.6) | 15 (5.3) | 17 (6.7) | 20 (7.9) |
Censored, n (%) | 98 (34.6) | 79 (28.0) | 83 (32.7) | 48 (19.0) |
Duration of PFS2, monthsa | ||||
Median (95% CI) | 14.23 (12.12 to 16.82) | 11.99 (11.20 to 13.40) | 11.01 (10.02 to 13.11) | 9.03 (8.28 to 9.89) |
Stratified analysisb | ||||
1-sided P valuec | 0.0095 | 0.0005 | ||
Hazard ratio (95% CI)d | 0.782 (0.637 to 0.961) | 0.708 (0.575 to 0.871) | ||
Event-free rates at time points | NR | NR | ||
ACT = anticancer therapy; CAPOX = capecitabine and oxaliplatin; CI = confidence interval; FAS = full analysis set; IRT = interactive response technology; mFOLFOX6 = modified 5-fluorouracil, folinic acid, and oxaliplatin; NR = not reported; PFS2 = progression-free survival following second-line anticancer treatment.
aBased on Kaplan-Meier estimate.
bStratification factors were region, number of organs with metastatic sites, and prior gastrectomy from IRT.
cBased on 1-sided log-rank test; P value was not adjusted for multiple comparisons.
dBased on Cox proportional hazards model with treatment, region, number of organs with metastatic sites, and prior gastrectomy as the explanatory variables. Assuming proportional hazards, a hazard ratio of less than 1 indicates a reduction in the hazard rate in favour of the treatment arm.
Sources: SPOTLIGHT trial Primary Analysis Clinical Study Report24 and GLOW trial Primary Analysis Clinical Study Report.25
Harms
All harms data reported here reflect the integrated SPOTLIGHT and GLOW trials analysis. Refer to Table 18 for harms data.
Adverse Events
Nearly all patients had at least 1 treatment-emergent AE. AEs reported for at least 20% of patients in either group included (zolbetuximab versus placebo, respectively): nausea (75.8% versus 55.8%), vomiting (66.8% versus 33.4%), decreased appetite (44.3% versus 33.6%), anemia (35.6% versus 37.0%), diarrhea (35.6% versus 39.5%), neutrophil count decrease (31.0% versus 28.5%), peripheral sensory neuropathy (30.4% versus 33.0%), neutropenia (28.5% versus 24.5%), constipation (25.9% versus 31.1%), fatigue (21.0% versus 25.2%), aspartate aminotransferase increase (21.0% versus 22.0%), abdominal pain (20.1% versus 25.8%), asthenia (20.1% versus 18.2%), and platelet count decrease (18.9% versus 20.7%). Nausea, vomiting, and decreased appetite were reported with at least a 10% higher incidence in the combined zolbetuximab group than in the combined placebo group.
Serious AEs
SAEs were reported in 245 patients (46.0%) in the combined zolbetuximab group and 245 patients (46.5%) in the combined placebo group.42 SAEs reported in at least 4% of patients in either group included (zolbetuximab versus placebo, respectively): vomiting (7.1% versus 4.6%), nausea (5.6% versus 3.2%), and malignant neoplasm progression (3.6% versus 4.7%).42
Withdrawals Due AEs
AEs leading to permanent discontinuation of at least 1 component of any study drug were reported in 199 patients (37.3%) in the combined zolbetuximab group and 169 patients (32.1%) in the combined placebo group.42 AEs leading to permanent discontinuation of zolbetuximab or placebo were reported in 106 patients (19.9%) and 66 patients (12.5%), respectively. The most frequent AEs leading to permanent discontinuation of zolbetuximab or placebo (present in ≥ 2% of patients in either combined group) were vomiting (3.8% versus 0.6%) and nausea (3.4% versus 0.4%), respectively.
Notable Harms
Nausea
Nausea (any grade) was reported in 404 patients (75.8%) in the combined zolbetuximab group and 294 patients (55.8%) in the combined phase III control group. In most patients, the first event occurred within the first 21 days after the start of the first infusion in cycle 1 (62.5% and 37.2% in the zolbetuximab and placebo groups, respectively).42 Grade 3 events were reported in 12.6% and 4.6% of patients in the zolbetuximab and placebo groups, respectively.42
Vomiting
Vomiting (any grade) was reported in 357 patients (67.0%) in the combined zolbetuximab group and 178 patients (33.8%) in the combined placebo group. In most patients, the first event occurred within the first 21 days after the start of the first infusion in cycle 1 (51.8% and 17.1% of patients in the zolbetuximab and placebo groups, respectively). Grade 3 events were reported for 14.3% and 4.7% of patients, respectively.42
Table 18: Summary of Harms Results in the SPOTLIGHT AND GLOW Trials
MedDRA v25.0 system organ class Preferred term, n (%) | Integrated SPOTLIGHT and GLOW trial results | |
|---|---|---|
Zolbetuximab plus mFOLFOX6 or CAPOX (N = 533) | Placebo plus mFOLFOX6 or CAPOX (N = 527) | |
Most common TEAEs, n (%) (reported in ≥ 10% patients in any treatment arm) | ||
Any TEAE | 529 (99.2) | 521 (98.9) |
Blood and lymphatic system disorders | 297 (55.7) | 293 (55.6) |
Anemia | 190 (35.6) | 195 (37.0) |
Neutropenia | 152 (28.5) | 129 (24.5) |
Thrombocytopenia | 56 (10.5) | 76 (14.4) |
Gastrointestinal disorders | 498 (93.4) | 449 (85.2) |
Nausea | 404 (75.8) | 294 (55.8) |
Vomiting | 356 (66.8) | 176 (33.4) |
Diarrhea | 190 (35.6) | 208 (39.5) |
Constipation | 138 (25.9) | 164 (31.1) |
Abdominal pain | 107 (20.1) | 136 (25.8) |
Abdominal pain upper | 70 (13.1) | 45 (8.5) |
Stomatitis | 66 (12.4) | 64 (12.1) |
General disorders and administration-site conditions | 346 (64.9) | 327 (62.0) |
Fatigue | 112 (21.0) | 133 (25.2) |
Asthenia | 107 (20.1) | 96 (18.2) |
Pyrexia | 88 (16.5) | 71 (13.5) |
Edema, peripheral | 75 (14.1) | 32 (6.1) |
Malaise | 52 (9.8) | 31 (5.9) |
Investigations | 335 (62.9) | 321 (60.9) |
Neutrophil count decrease | 165 (31.0) | 150 (28.5) |
AST increase | 112 (21.0) | 116 (22.0) |
Weight decrease | 105 (19.7) | 79 (15.0) |
Platelet count decrease | 101 (18.9) | 109 (20.7) |
White blood cell count decrease | 101 (18.9) | 85 (16.1) |
ALT increase | 82 (15.4) | 99 (18.8) |
Metabolism and nutrition disorders | 343 (64.4) | 297 (56.4) |
Decreased appetite | 236 (44.3) | 177 (33.6) |
Hypoalbuminemia | 100 (18.8) | 52 (9.9) |
Hypokalemia | 86 (16.1) | 77 (14.6) |
Hypocalcemia | 43 (8.1) | 21 (4.0) |
Musculoskeletal and connective tissue disorders | 112 (21.0) | 138 (26.2) |
Back pain | 42 (7.9) | 50 (9.5) |
Nervous system disorders | 347 (65.1) | 351 (66.6) |
Peripheral sensory neuropathy | 162 (30.4) | 174 (33.0) |
Dysgeusia | 59 (11.1) | 52 (9.9) |
Paresthesia | 57 (10.7) | 57 (10.8) |
Dizziness | 50 (9.4) | 38 (7.2) |
Hypoesthesia | 41 (7.7) | 41 (7.8) |
Headache | 39 (7.3) | 43 (8.2) |
Psychiatric disorders | 79 (14.8) | 69 (13.1) |
Insomnia | 56 (10.5) | 41 (7.8) |
Respiratory, thoracic, and mediastinal disorders | 158 (29.6) | 173 (32.8) |
Cough | 39 (7.3) | 42 (8.0) |
Dyspnea | 35 (6.6) | 45 (8.5) |
Skin and subcutaneous tissue disorders | 203 (38.1) | 187 (35.5) |
Palmar-plantar erythrodysesthesia syndrome | 65 (12.2) | 68 (12.9) |
Vascular disorders | 130 (24.4) | 94 (17.8) |
Hypertension | 46 (8.6) | 29 (5.5) |
Serious TEAEs, n (%) (reported in ≥ 1% patients in any treatment arm) | ||
Any serious TEAE | 245 (46.0) | 245 (46.5) |
Blood and lymphatic system disorders | 29 (5.4) | 24 (4.6) |
Anemia | 10 (1.9) | 10 (1.9) |
Neutropenia | 10 (1.9) | 5 (0.9) |
Febrile neutropenia | 8 (1.5) | 4 (0.8) |
Thrombocytopenia | 4 (0.8) | 2 (0.4) |
Gastrointestinal disorders | 109 (20.5) | 92 (17.5) |
Vomiting | 38 (7.1) | 24 (4.6) |
Nausea | 30 (5.6) | 17 (3.2) |
Diarrhea | 15 (2.8) | 14 (2.7) |
Intestinal obstruction | 10 (1.9) | 4 (0.8) |
Upper gastrointestinal hemorrhage | 10 (1.9) | 4 (0.8) |
Abdominal pain | 8 (1.5) | 15 (2.8) |
Dysphagia | 5 (0.9) | 5 (0.9) |
Obstruction gastric | 5 (0.9) | 1 (0.2) |
Ascites | 4 (0.8) | 5 (0.9) |
Ileus | 3 (0.6) | 6 (1.1) |
Haematemesis | 2 (0.4) | 5 (0.9) |
Gastric hemorrhage | 1 (0.2) | 5 (0.9) |
General disorders and administration-site conditions | 42 (7.9) | 35 (6.6) |
Pyrexia | 12 (2.3) | 8 (1.5) |
Asthenia | 7 (1.3) | 4 (0.8) |
Fatigue | 7 (1.3) | 6 (1.1) |
General physical health deterioration | 2 (0.4) | 6 (1.1) |
Hepatobiliary disorders | 17 (3.2) | 20 (3.8) |
Hepatic function abnormal | 3 (0.6) | 3 (0.6) |
Cholecystitis | 2 (0.4) | 5 (0.9) |
Infections and infestations | 54 (10.1) | 44 (8.3) |
Pneumonia | 12 (2.3) | 13 (2.5) |
Sepsis | 6 (1.1) | 3 (0.6) |
COVID-19 | 3 (0.6) | 5 (0.9) |
Pneumonia aspiration | 3 (0.6) | 2 (0.4) |
Investigations | 19 (3.6) | 19 (3.6) |
Platelet count decrease | 8 (1.5) | 6 (1.1) |
Neutrophil count decrease | 2 (0.4) | 5 (0.9) |
Metabolism and nutrition disorders | 31 (5.8) | 24 (4.6) |
Decreased appetite | 11 (2.1) | 5 (0.9) |
Hypokalemia | 11 (2.1) | 8 (1.5) |
Musculoskeletal and connective tissue disorders | 3 (0.6) | 6 (1.1) |
Myalgia | 0 | 3 (0.6) |
Neoplasms, benign, malignant, and unspecified | 24 (4.5) | 34 (6.5) |
Malignant neoplasm progression | 19 (3.6) | 25 (4.7) |
Nervous system disorders | 17 (3.2) | 16 (3.0) |
Syncope | 4 (0.8) | 1 (0.2) |
Renal and urinary disorders | 13 (2.4) | 14 (2.7) |
Acute kidney injury | 4 (0.8) | 3 (0.6) |
Hydronephrosis | 3 (0.6) | 1 (0.2) |
Urinary tract obstruction | 1 (0.2) | 3 (0.6) |
Respiratory, thoracic, and mediastinal disorders | 23 (4.3) | 37 (7.0) |
Pulmonary embolism | 8 (1.5) | 12 (2.3) |
Respiratory failure | 4 (0.8) | 2 (0.4) |
Acute respiratory failure | 3 (0.6) | 0 |
Dyspnea | 3 (0.6) | 10 (1.9) |
Pleural effusion | 3 (0.6) | 10 (1.9) |
Vascular disorders | 15 (2.8) | 6 (1.1) |
Hypotension | 5 (0.9) | 1 (0.2) |
Deep vein thrombosis | 4 (0.8) | 1 (0.2) |
Patients who stopped treatment due to adverse events, n (%) (reported in ≥ 1 patient in any treatment arm) | ||
TEAE leading to permanent discontinuation | 106 (19.9) | 66 (12.5) |
Blood and lymphatic system disorders | 5 (0.9) | 3 (0.6) |
Disseminated intravascular coagulation | 2 (0.4) | 0 |
Anemia | 1 (0.2) | 2 (0.4) |
Cardiac disorders | 4 (0.8) | 4 (0.8) |
Acute myocardial infarction | 2 (0.4) | 1 (0.2) |
Cardiac arrest | 0 | 2 (0.4) |
Gastrointestinal disorders | 46 (8.6) | 17 (3.2) |
Vomiting | 20 (3.8) | 3 (0.6) |
Nausea | 18 (3.4) | 2 (0.4) |
Upper gastrointestinal hemorrhage | 4 (0.8) | 2 (0.4) |
Diarrhea | 3 (0.6) | 1 (0.2) |
Dysphagia | 3 (0.6) | 2 (0.4) |
Intestinal obstruction | 3 (0.6) | 0 |
Abdominal pain | 2 (0.4) | 0 |
Obstruction gastric | 2 (0.4) | 0 |
Hematemesis | 0 | 2 (0.4) |
General disorders and administration-site conditions | 14 (2.6) | 6 (1.1) |
Malaise | 4 (0.8) | 0 |
Fatigue | 3 (0.6) | 0 |
Asthenia | 2 (0.4) | 1 (0.2) |
Chest discomfort | 2 (0.4) | 0 |
Death | 2 (0.4) | 1 (0.2) |
Immune system disorders | 2 (0.4) | 1 (0.2) |
Anaphylactic reaction | 2 (0.4) | 0 |
Infections and infestations | 10 (1.9) | 10 (1.9) |
Pneumonia | 5 (0.9) | 2 (0.4) |
Septic shock | 1 (0.2) | 2 (0.4) |
Injury, poisoning, and procedural complications | 4 (0.8) | 0 |
Infusion-related reaction | 2 (0.4) | 0 |
Investigations | 10 (1.9) | 5 (0.9) |
Blood bilirubin increase | 2 (0.4) | 1 (0.2) |
Gamma-glutamyltransferase increase | 2 (0.4) | 0 |
Platelet count decrease | 2 (0.4) | 0 |
Weight decrease | 2 (0.4) | 0 |
Aspartate aminotransferase increase | 1 (0.2) | 2 (0.4) |
Ejection fraction decrease | 0 | 2 (0.4) |
Metabolism and nutrition disorders | 9 (1.7) | 4 (0.8) |
Decreased appetite | 4 (0.8) | 0 |
Hypokalemia | 2 (0.4) | 0 |
Neoplasms, benign, malignant, and unspecified (including cysts and polyps) | 7 (1.3) | 11 (2.1) |
Malignant neoplasm progression | 6 (1.1) | 6 (1.1) |
Metastases to meninges | 1 (0.2) | 2 (0.4) |
Tumour hemorrhage | 0 | 2 (0.4) |
Nervous system disorders | 7 (1.3) | 5 (0.9) |
Intracranial pressure increased | 2 (0.4) | 0 |
Renal and urinary disorders | 3 (0.6) | 3 (0.6) |
Acute kidney injury | 1 (0.2) | 2 (0.4) |
Respiratory, thoracic, and mediastinal disorders | 4 (0.8) | 7 (1.3) |
Acute respiratory distress syndrome | 0 | 2 (0.4) |
Pleural effusion | 0 | 3 (0.6) |
Vascular disorders | 4 (0.8) | 0 |
Flushing | 2 (0.4) | 0 |
Deaths, n (%) (reported in ≥ 2 patients in any treatment arm) | ||
TEAEs leading to death | 49 (9.2) | 56 (10.6) |
Malignant neoplasm progression | 16 (3.0) | 25 (4.7) |
Death | 3 (0.6) | 2 (0.4) |
Pneumonia | 3 (0.6) | 3 (0.6) |
Septic shock | 3 (0.6) | 2 (0.4) |
Upper gastrointestinal hemorrhage | 3 (0.6) | 1 (0.2) |
Cerebral hemorrhage | 2 (0.4) | 1 (0.2) |
Disseminated intravascular coagulation | 2 (0.4) | 0 |
Respiratory failure | 2 (0.4) | 1 (0.2) |
Sepsis | 2 (0.4) | 0 |
Cardio-respiratory arrest | 1 (0.2) | 2 (0.4) |
Adverse events of special interest, n (%) | ||
Nausea event | 404 (75.8) | 294 (55.8) |
Vomiting event | 357 (67.0) | 178 (33.8) |
Abdominal pain event | 181 (34.0) | 192 (36.4) |
Hypersensitivity reaction events | 191 (35.8) | 170 (32.3) |
Infusion-related reactions | 215 (40.3) | 58 (11.0) |
Potential infusion-related reaction events | 369 (69.2) | 151 (28.7) |
Anemia event | 193 (36.0) | 196 (37.2) |
Neutropenia event | 305 (57.2) | 274 (52.0) |
AST = aminotransferase; CAPOX = capecitabine plus oxaliplatin; ISS = integrated summary of safety; MedDRA = Medical Dictionary for Regulatory Activities; mFOLFOX6 = modified 5-fluorouracil, folinic acid, and oxaliplatin; PT = preferred term; SAF = safety analysis set; TEAE = treatment-emergent adverse event.
Note: Data cut-offs were September 9, 2022 (SPOTLIGHT trial) and October 7, 2022 (GLOW trial).
Source: Common Technical Document 2.7.4 (contains integrated analysis).42
Infusion-Related Reactions
IRRs (any grade) were reported in 215 patients (40.3%) in the combined zolbetuximab group and 58 patients (11.0%) in the combined placebo group.42 Grade 3 events were reported in 6.8% and 0.4% of patients in the zolbetuximab and placebo groups, respectively. A grade 4 investigator-assessed IRR event was reported in 1 patient (0.2%) in the combined zolbetuximab group and in 1 patient (0.2%) in the combined placebo group.42
Critical Appraisal
Internal Validity
Baseline characteristics: Randomization in the SPOTLIGHT and GLOW trials was performed using an appropriate methodology with adequate allocation concealment (i.e., interactive response technology). Randomization was stratified by region (Asia versus non-Asia); number of organs with metastatic sites (0 to 2 versus ≥ 3); and prior gastrectomy (yes or no). The clinical experts consulted during this review noted that the stratification variables were reasonable for the target patient population. It was noted that proactive screening for gastrointestinal cancers is more common in some Asian countries (e.g., Japan and Korea) and that this can translate to an increase in OS for newly diagnosed patients with gastric or GEJ cancer if the disease is identified at an earlier stage compared with western nations that do not screen as aggressively. The clinical experts consulted during this review noted that the proactive screening is commendable and has contributed to more favourable outcomes for some patients, but that this would not limit the generalizability of the trial findings to the target population in Canada (i.e., those with newly diagnosed metastatic disease). Overall, baseline and demographic characteristics were generally well balanced across the zolbetuximab and placebo groups in both the SPOTLIGHT and GLOW trials. Between-group imbalances were noted for the subset of patients with GEJ in the SPOTLIGHT trial for tumour location (e.g., proximal [47.6% versus 36.6%] and distal [30.2% versus 43.7%] for zolbetuximab and placebo, respectively) and tumour type (e.g., diffuse [29.1% versus 42.1% for zolbetuximab and placebo, respectively]). The clinical experts consulted during this review had no concerns regarding the baseline characteristics of the SPOTLIGHT and GLOW trial populations.
Treatment masking: Both the SPOTLIGHT and GLOW trials were double-blind clinical trials. Patients who received zolbetuximab more commonly reported AEs of nausea and vomiting as well as infusion-site reactions. The clinical experts consulted during this review noted that the AE profile in the trial could potentially allow some patients and investigators to infer the allocated treatment group. The objective end points (e.g., PFS, OS, and ORR) would not be subject to bias in the event that treatment allocation could be inferred as a result of AEs; however, HRQoL, which requires subjective reporting, could potentially be biased.
Concomitant supportive therapies: Supportive cancer therapies were generally well balanced across the groups.
Subsequent ACTs: The most frequent postprogression therapies were paclitaxel (17% versus 19.5% and 18.1% versus 20.2% for zolbetuximab versus placebo in the SPOTLIGHT and GLOW trials) and ramucirumab (12.4% versus 12.1% and 8.3% versus 11.1% for zolbetuximab versus placebo in the SPOTLIGHT and GLOW trials). The clinical experts consulted by CDA-AMC felt that the overall proportion of patients who did not receive any subsequent ACT (approximately 50% of patients in both trials) was a reasonable reflection of the target population in Canada, where survival is often limited to 1 year. The experts noted that the distribution of therapies seemed appropriate for the Canadian setting and that the EMA had concluded that OS results did not seem to have been impacted by differences in the use of subsequent (i.e., postprogression) therapies.50
Patient disposition: In general, patient disposition in the SPOTLIGHT and GLOW trials highlights the poor prognosis for those in the target patient population (e.g., across all treatment groups, more than 80% of patients discontinued therapy).50 Acknowledging that there is little experience with zolbetuximab in Canadian clinical practice, the clinical experts consulted during this review noted that the patient disposition appears to be a reasonable reflection of what would be anticipated in Canadian practice for a regimen that includes the use of cytotoxic chemotherapy.
End points: The primary and secondary end points of the SPOTLIGHT and GLOW trials were aligned with those recommended by regulatory authorities for gastric cancer trials in the metastatic setting. The clinical experts consulted by CDA-AMC noted that PFS is not a particularly useful end point in the context of metastatic disease in which survival is typically limited to 1 year. However, the final analyses showing an improvement in OS were considered demonstrative of a clinically meaningful benefit in comparison with chemotherapy alone. The EMA noted that the choice of PFS as the primary end point and OS as the secondary end point was reflective of its scientific advice to the sponsor.50
Sample size and statistical testing: The SPOTLIGHT and GLOW trials had adequate statistical power to detect differences between the zolbetuximab and placebo groups for PFS and OS. Statistical testing for the primary end point (i.e., PFS) and key secondary end point (i.e., OS) were adjusted for multiple testing. (That is, to maintain the type I error rate at the 0.025 significance level, the hypothesis testing for the interim and final analyses of OS were performed only if the null hypothesis in the PFS primary analysis was rejected at the overall 1-sided 0.025 significance level.) Reviewers for the National Institute for Health and Care Excellence (NICE) and the EMA noted that the statistical analyses were appropriate in these trials.50,51 The EMA further noted that the sponsor’s prespecified sensitivity analyses of PFS to address likely informative censoring showed overall consistency with the primary analyses and were supportive of the robustness of the results from both the SPOTLIGHT and GLOW studies.50
The key secondary TTCD end points of the EORTC QLQ-C30 PF, EORTC QLQ-OG25 Pain, and EORTC GHS/QoL scales were also analyzed using a statistical testing hierarchy to control type I error. The test for noninferiority failed; therefore, the P values reported by the sponsor should be interpreted with caution. All other end points were considered exploratory, and there was no control for multiplicity. The sponsor noted that no concrete conclusions should be drawn from the results for the subgroup analyses because no formal statistical tests of hypotheses were performed for any of the subgroup analyses.
External Validity
Patient population: The clinical experts consulted during this review stated that the baseline and demographic characteristics for the SPOTLIGHT and GLOW trials are a reasonable reflection of the target patient population in Canada. The EMA similarly concluded that the trial populations were acceptable and that the selection of patients with good ECOG Performance Status and adequate organ function is common in oncology clinical trials and not a serious limitation of the studies.50 Only a single patient with an ECOG Performance Status of 2 was enrolled in the SPOTLIGHT and GLOW trials. The clinical experts consulted during this review noted that there could be interest from prescribers in Canada in administering zolbetuximab for patients with an ECOG Performance Status of 2.
Median survival: The median survival duration in the placebo plus chemotherapy group was 15.57 months (95% CI, 13.67 months to 16.92 months). It was 12.16 months (95% CI, 10.28 months to 13.67 months) in the SPOTLIGHT and GLOW trials, respectively. The clinical experts consulted by CDA-AMC noted that this may be slightly greater than would be expected for typical patients in Canada, where average survival for those with previously untreated metastatic gastric or GEJ cancer would be approximately 1 year. It was noted that OS time is often longer in a clinical trial setting because the enrolment criteria can result in a study population that is heathier than that found in routine practice. The clinical experts further noted that it was unclear why OS was longer in the SPOTLIGHT trial in comparison with the GLOW trial, noting that the enrolment criteria were the same and that the background chemotherapy regimen (i.e., mFOLFOX6 or CAPOX) would not be expected to result in a difference in OS of 3 months.
Concomitant supportive therapies: The clinical experts consulted during this review indicated that the concomitant medications used in the SPOTLIGHT and GLOW trials were a reasonable reflection of what would be expected in routine Canadian practice for the target patient population.
Subsequent cancer therapies: After the end-of-treatment visit, patients were allowed to take any type of ACT at the discretion of their local physician and in their best interest (including medications that were not permitted during the treatment phase). The most frequently received new ACTs were paclitaxel and ramucirumab.
Comparator: There are no other drugs specifically indicated for use in the treatment of patients with CLDN18.2-positive gastric or GEJ cancer in Canada; therefore, the choice of placebo plus mFOLFOX6 (or CAPOX) was considered appropriate by regulatory authorities. However, the clinical experts consulted during this review noted that the comparator used in the SPOTLIGHT and GLOW trials (i.e., placebo plus mFOLFOX6 or CAPOX) is not reflective of routine practice in Canada, where patients would typically be offered nivolumab plus chemotherapy as the preferred treatment option (an assumption that is also reflected in the sponsor’s budget impact analysis). The experts noted that only patients with a contraindication or intolerance to nivolumab would receive chemotherapy alone. The SPOTLIGHT and GLOW trials began in 2018, predating the 2021 regulatory approval of nivolumab plus chemotherapy for gastric and GEJ cancer in Canada; however, this remains the most relevant comparator for the current review. In the absence of a direct comparison against nivolumab plus chemotherapy, the sponsor provided an ITC. The ITC was reviewed by CDA-AMC (refer to the Indirect Evidence section).
Withdrawals: The clinical experts consulted during this review noted that the distributions and reasons for discontinuation from zolbetuximab in the SPOTLIGHT and GLOW trials were a reasonable reflection of what would likely be observed in routine clinical practice; however, it was noted that discontinuation due to AEs could occur more frequently in the real-world setting (e.g., patients in the real-world setting may be less healthy than those enrolled in the trial, and there would be no pressure to try to have patients complete the treatment regimen, as specified in a trial protocol).
Dosing: Both the SPOTLIGHT and GLOW trials involved a zolbetuximab dosage regimen that included a single loading dose of 800 mg/m2 IV followed by a maintenance dose of 600 mg/m2 IV every 3 weeks. This is likely reflective of how zolbetuximab would be used in Canadian practice for patients receiving it in combination with CAPOX (which is administered once every 3 weeks); however, it would not reflect its administration in combination with mFOLFOX6 (which is administered once every 2 weeks). As such, when zolbetuximab is used in combination with mFOLFOX6, the product monograph recommends an 800 mg/m2 loading dose followed by 400 mg/m2 every 2 weeks. This is based on population pharmacokinetic modelling that predicted that the maintenance dosage of 400 mg/m2 every 2 weeks would have similar exposure to the regimen of 600 mg/m2 every 3 weeks. These data were reviewed and accepted by Health Canada for inclusion in the product monograph. The clinical experts consulted during this review indicated that the dose distributions reported in the SPOTLIGHT and GLOW trials were likely to be an accurate reflection of what would occur with patients in Canada. The experts noted that the dosing of zolbetuximab would occur in accordance with the timing of the chemotherapy regimen selected by the patient and clinician.
Study locations: The SPOTLIGHT and GLOW trials were multinational, with relatively few patients enrolled at Canadian sites (e.g., n = 2 in the GLOW trial and n = 8 in the SPOTLIGHT trial). The clinical experts consulted during this review noted that the study locations (e.g., primarily in the US) would not be expected to limit the generalizability of the results to the Canadian setting. As is common in oncology trials for metastatic disease, the usage of subsequent therapies can be different in the US compared with Canada and Europe, where public drug programs may have stricter reimbursement criteria.
Treatment setting: Zolbetuximab was administered in an outpatient manner in the SPOTLIGHT and GLOW trials, which is reflective of how it would be used in Canadian practice.
CLDN18.2 screening: Zolbetuximab is the first drug to specifically target CLDN18.2. Routine screening for CLDN18.2 is not currently performed in Canada for patients with gastric or GEJ cancer (or any other cancer). The SPOTLIGHT and GLOW trials enrolled patients who had CLDN18.2-positive tumours, defined as at least 75% of tumour cells demonstrating moderate to strong membranous CLDN18.2 staining based on central IHC assessment using the companion diagnostic test (i.e., the CLDN18 RxDx Assay). The clinical experts consulted during this review supported the use of a 75% threshold for concluding that a patient harbours CLDN18.2-positive tumours. The experts further noted that they would not anticipate any challenges with interpreting the results of the CLDN18 RxDx Assay (e.g., diagnosis would likely be consistent across different centres in Canada).
GRADE Summary of Findings and Certainty of the Evidence
Methods for Assessing the Certainty of the Evidence
For pivotal studies and RCTs identified in the sponsor’s systematic review, GRADE was used to assess the certainty of the evidence for outcomes considered most relevant to inform the expert committee deliberations; a final certainty rating was determined as outlined by the GRADE Working Group based on the following criteria:52,53
High certainty: CDA-AMC is very confident that the true effect lies close to that of the estimate of the effect.
Moderate certainty: CDA-AMC is moderately confident in the effect estimate. The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. The word “likely” is used for evidence of moderate certainty (e.g., “X intervention likely results in Y outcome”).
Low certainty: Confidence in the effect estimate is limited. The true effect may be substantially different from the estimate of the effect. The word “may” is used for evidence of low certainty (e.g., “X intervention may result in Y outcome”).
Very low certainty: CDA-AMC has very little confidence in the effect estimate. The true effect is likely to be substantially different from the estimate of effect. Evidence of very low certainty is described as “very uncertain.”
Following the GRADE approach, evidence from RCTs started as high-certainty evidence and could be rated down for concerns related to study limitations (i.e., internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, or publication bias.
When possible, certainty was rated in the context of the presence of an important (nontrivial) treatment effect; if this was not possible, certainty was rated in the context of the presence of any treatment effect (i.e., the clinical importance is unclear). In all cases, the target of the certainty of evidence assessment was based on the point estimate and where it was located relative to the threshold for a clinically important effect (when a threshold was available) or to the null.
Results of GRADE Assessments
Table 2 presents the GRADE summary of findings for zolbetuximab plus chemotherapy versus placebo plus chemotherapy.
Long-Term Extension Studies
No long-term extension studies were submitted to CDA-AMC.
Indirect Evidence
The contents within this section have been informed by materials submitted by the sponsor. The following has been summarized and validated by CDA-AMC.
Objectives for the Summary of Indirect Evidence
In the absence of direct head-to-head trials evaluating the comparative efficacy of zolbetuximab versus relevant comparators for the first-line treatment of patients with locally advanced unresectable or metastatic HER2-negative gastric or GEJ adenocarcinoma whose tumours are CLDN18.2-positive, a review of indirect evidence was undertaken and submitted by the sponsor.54 The objective of this section is to summarize and critically appraise the sponsor-submitted ITC and to inform the pharmacoeconomic model.
Description of Indirect Comparison
Objectives
The objective of the sponsor-submitted NMA was to evaluate the comparative efficacy of zolbetuximab versus relevant comparators for the first-line treatment of patients with locally advanced unresectable or metastatic HER2-negative gastric or GEJ adenocarcinoma whose tumours are CLDN18.2-positive.
Study Selection Methods
The studies eligible for inclusion in the sponsor-submitted NMA were selected according to a sponsor-conducted systematic literature review.54 The sponsor’s systematic literature review was defined by the relevant PICOs described in Table 19. The scope of the systematic literature review included RCT evidence of adult patients with pathologically confirmed, metastatic, locally advanced unresectable or recurrent gastric or GEJ adenocarcinoma who had not received any previous first-line treatment for gastric or GEJ cancer and who had HER2-negative status.
Clinical evidence for the systematic literature review was identified using multiple electronic databases, as listed in Table 20, along with additional searches using forward citation, searches in relevant conference proceedings, and additional searching of relevant websites.
Table 19: PICOS for the Sponsor-Conducted Systematic Literature Review
PICOS | Inclusion criteria |
|---|---|
Population | Adult patients (≥ 18 years) with pathologically confirmed metastatic or locally advanced unresectable or recurrent gastric or GEJ adenocarcinoma who:
|
Intervention |
|
Comparator |
|
Outcome | Efficacy outcomes:
Safety outcomes:
|
Study designs | RCTs, any duration (irrespective of treatment masking) |
5-FU = 5-fluorouracil; AE = adverse event; CAPOX = capecitabine plus oxaliplatin; DOR = duration of response; FOLFIRI = folinic acid, 5-fluorouracil, irinotecan; GEJ = gastroesophageal junction; HER2 = human epidermal growth factor receptor 2; mFOLFOX6 = leucovorin calcium (folinic acid), fluorouracil, and oxaliplatin; OS = overall survival; PFS = progression-free survival; PICOS = population, intervention, comparators, outcomes, and study design; SAE = severe adverse event; TREA = treatment-related adverse event; TTP = time to progression.
Source: Network Meta-Analysis Technical Study Report.54
Table 20: Study Selection Criteria and Methods for the NMA Submitted by the Sponsor
Characteristics | Indirect comparison |
|---|---|
Population | Adult patients (≥ 18 years) with pathologically confirmed metastatic, locally advanced, unresectable, or recurrent gastric or GEJ adenocarcinoma who:
|
Intervention | Zolbetuximab plus CAPOX Zolbetuximab plus mFOLFOX6 |
Comparator | Comparators of interests included:
|
Outcome | Studies reporting at least 1 of the following efficacy outcomes:
|
Study designs | Randomized, phase II, phase III, or phase unknown trials with at least 2 treatment arms of interest |
Publication characteristics | English language publications, no geographical restrictions, 2000 to present. Published studies and additional searches were conducted using reference lists of included publications, relevant conference proceedings, and additional searching of relevant websites. |
Exclusion criteria |
|
Databases searched | Embase, MEDLINE (R), MEDLINE In-Process, MEDLINE ePub Ahead of Print, the Cochrane Library, up to March 4, 2024 |
Selection process | Articles screened independently by 2 researchers |
Data extraction process | Relevant information was extracted into the data extraction template by a reviewer. A second reviewer checked the data extraction, and any inconsistencies were resolved through discussion or by a third reviewer. |
Quality assessment | Quality assessment of RCTs was conducted using the 7-criteria checklist provided in section 2.5 of the NICE single-technology appraisal user guide. |
CAPOX = capecitabine plus oxaliplatin; CF = fluorouracil plus cisplatin; HER2 = human epidermal growth factor receptor 2; KM = Kaplan-Meier; mFOLFOX6 = leucovorin calcium (folinic acid), fluorouracil, and oxaliplatin; NICE = National Institute for Health and Care Excellence; RCT = randomized clinical trial; OS = overall survival; PFS = progression-free survival; SOX = tegafur, gimeracil, and oteraci (S-1) plus oxaliplatin.
aComparators not included in the pharmacoeconomic analysis.
Source: Network Meta-Analysis Technical Study Report.54
ITC Design
ITC Analysis Methods
An indirect comparison of zolbetuximab versus other first-line treatments was conducted using a Bayesian NMA. The sponsor conducted a primary NMA, with data taken as is from the studies, and conducted a second primary NMA that combined CAPOX and mFOLFOX6 The sponsor provided the following considerations for the assumed equivalent efficacy of CAPOX and mFOLFOX6: oxaliplatin-based therapies were considered to be equivalent, based on prior NICE and CADTH submissions of nivolumab and clinical inputs; the efficacy outcomes of CAPOX and mFOLFOX6 in historical studies were generally similar; this increased the stability of the network. The clinical experts consulted for this review agree with the sponsor’s assumptions of equivalency.
Details of the ITC analysis methods are summarized in Table 21. Treatment effect was measured using reported HRs of OS or PFS in the RCT publications. When HR was not reported, HR was reconstructed based on the Kaplan-Meier curve. Both fixed-effects and random-effects models were fitted to account for assumptions regarding heterogeneity of treatment effects; however, a fixed-effects model was used as the primary analysis because more than half the links in the network had only 1 contributing study.
The Bayesian NMA was conducted using 50,000 burn-in iterations, with an additional 50,000 sampling iterations to generate posterior distributions for the treatment effects. Three chains were run based on the NICE Decision Support Unit guidance, and autocorrelation was assessed visually through autocorrelation plots.
Log HR was modelled as a continuous outcome using normal distributions for the likelihood function (rescaling of results). Vague priors for the treatment effects and between-study variation (relevant for the random-effects model only) were considered based on guidance from the NICE Decision Support Unit for indirect comparison. Model fit was assessed using the posterior mean of residual deviance and deviance information criterion (DIC), and 1 final model with the lowest DIC was chosen. A probability distribution was generated for each parameter of interest (i.e., the HR of OS and PFS) for pairwise comparisons of the treatment regimens. The comparative estimates were summarized using posterior medians and their associated 95% CrIs, and both means and medians were reported in the NMA results.
Relative rankings for each study drug based on its efficacy were estimated based on ranking probabilities. To determine convergence of the results, the Gelman-Rubin diagnostics approach was used.
During the feasibility assessment, the sponsor attempted to ensure that the included trials were similar in terms of patient populations, outcome measures, and definitions. For networks with loops, the sponsor used an approach (suggested in NICE Technical Support Document 4) to detect inconsistency in the network, in which comparison between the posterior means of the residual deviance and DIC statistics of the consistency and inconsistency models provided an “omnibus” test of consistency. If the deviance and DIC were lower than or similar to the consistency model, this suggested no evidence of inconsistency in the network. The sponsor used Cochran Q statistics to assess the heterogeneity of outcomes in trials comparing all pairs of treatments that were compared in 2 or more trials. Subgroup analyses using different CPS score cut-offs were conducted, and sensitivity analyses excluding Asia-only trials or focusing on Asia-only trials were also explored.
Table 21: ITC Analysis Methods
Methods | Description |
|---|---|
Analysis methods | The NMA was conducted using a Bayesian model; both fixed-effects and random-effects models were constructed, but a fixed-effects model was used. Log HR was used to estimate the treatment effect. |
Priors | Vague priors for the treatment effects and between-study variation (relevant only for the random-effects model) were considered. |
Assessment of model fit | Model fit was assessed using the posterior mean of residual deviance and DIC, and 1 final model with the lowest DIC was chosen. |
Assessment of consistency | For networks with loops, the sponsor used an approach (suggested in NICE Technical Support Document 4) to detect inconsistency in the network, in which comparison between the posterior means of the residual deviance and DIC statistics of the consistency and inconsistency models provided an “omnibus” test of consistency. If the deviance and DIC were lower than or similar to the consistency model. |
Assessment of convergence | Gelman-Rubin diagnostics |
Outcomes | OS or PFS |
Follow-up time points | Median follow-up across trials ranged from 7 months to 54.3 months |
Construction of nodes | Each chemotherapy comparator was a node in the NMA. |
Sensitivity analyses |
|
Subgroup analysis |
|
Methods for pairwise meta-analysis | Using Cochran Q statistics |
CAPOX = capecitabine and oxaliplatin; CPS = combined positive score; CX = capecitabine and cisplatin; DIC = deviance information criterion; HR = hazard ratio; ITC = indirect treatment comparison; mFOLFOX6 = leucovorin calcium (folinic acid), fluorouracil, and oxaliplatin; NMA = network meta-analysis; OS = overall survival; PFS = progression-free survival.
Source: Network Meta-Analysis Technical Study Report.54
Results
Summary of Included Studies
In the sponsor’s systematic review, 174 publications reporting on 92 studies were included. After applying the NMA inclusion and exclusion criteria, 21 RCTs, including the GLOW and SPOTLIGHT trials, were deemed relevant for the sponsor’s NMA, including 14 unique treatment regimens. After removal of 1 study (the KEYNOTE-062 study) that did not include any prespecified subgroup analysis based on CPS score or CLDN18.2 expression level, 20 studies were included in the analysis. Risk of bias was assessed for all studies in the sponsor’s systematic review, and a high risk of bias related to treatment masking was reported in more than half of the included studies. No additional details on the risk of bias in the studies included in the NMA were available. An assessment of homogeneity conducted by the sponsor is summarized in Table 22.
The sponsor reported that the inclusion and exclusion criteria, including disease stage, age, and ECOG Performance Status, were generally consistent across the trials. Of the 21 RCTs that met the NMA inclusion criteria, 1 (KEYNOTE-062 study) was removed from the analysis because it required patients to be all-comers, with no restrictions on CPS score or CLDN18.2 expression level. The majority were phase III trials; only 6 trials were phase II. Almost half of the included trials (10 of 21) were conducted in Asian countries only; therefore, the sponsor conducted sensitivity analyses excluding Asia-only trials or focusing only on Asia (including an Asian subgroup of global trials) in the primary analysis of CAPOX or FOLFOX combined. The dosing schedules in the majority of treatment regimens appeared to be consistent across studies, with some variation for 5-fluorouracil-based regimens and Tegafur/gimeracil/oteracil (S-1)–based regimens. The sponsor reported that the impact of this variation was expected to be small.
The sample size across trials ranged from 38 patients in ATTRACTION-4 trial (Part 1) to 1,581 patients in the CheckMate 649 trial.
The median follow-up durations ranged from 7 months in the Popov (2008) trial to 26.6 months in the ATTRACTION-4 trial (Part 2) (and 54.3 months in the KEYNOTE 062 study). The median age of patients ranged from 55 years to 57 years in the Popov (2008) trial to 64 years to 68 years in the HERBIS-4A trial. An assessment of homogeneity conducted by the sponsor is summarized in Table 22.
OS and PFS were analyzed in the NMA, and the definitions were reported as mainly consistent across the trials. All trials reported OS, defined as time from randomization to death due to any cause in most trials that defined OS; 17 trials reported HRs only or both HRs and Kaplan-Meier curves, and 4 trials reported only Kaplan-Meier curves. PFS was reported in 16 out of 21 trials, defined as time from randomization to PD or death due to any cause in most trials that defined PFS; 15 trials reported HRs only or both HRs and Kaplan-Meier curves, and 3 trials reported only Kaplan-Meier curves. The sponsor noted some variation in how PD and censoring were defined across the trials.
Table 22: Assessment of Homogeneity
Characteristics | Description and handling of potential effect modifiers |
|---|---|
Trial design | Trial design was evaluated for each trial and compared with trials for zolbetuximab (i.e., the GLOW and SPOTLIGHT trials). Most included trials (14 out of 20) were phase III trials. Only 6 trials were phase II. |
Inclusion and exclusion criteria | The sponsor reported that the inclusion and exclusion criteria, including disease stage, age, and ECOG Performance Status, were generally consistent across trials. Of the 21 RCTs that met the NMA inclusion criteria, 1 (the KEYNOTE-062 trial) was removed from the analysis because it required patients to be all-comers, with no restriction on CPS score or CLDN18.2 expression level (i.e., it did not include any prespecified subgroup analysis based on CPS score or CLDN18.2 expression level). |
Geographic distribution | Almost half (10 out of 21) of the included trials were conducted in Asian countries only; therefore, the sponsor conducted sensitivity analyses excluding Asia-only trials or focusing only on Asia and included a subgroup of global trials conducted in Asia in the primary analysis with CAPOX or mFOLFOX6 combined. |
Dosing schedule | The dosing schedule of the majority of treatment regimens appears to be consistent across studies, with some variation for 5-fluorouracil-based regimens and Tegafur/gimeracil/oteracil (S-1)–based regimens. The sponsor reported that the impact of this variation was expected to be small, and the clinical experts consulted for the purpose of this review agreed with the sponsor’s assessment. |
Sample size | The sample size across trials ranged from 38 patients in ATTRACTION-4 trial (Part 1) to 1,581 patients in the CheckMate 649 trial. The sponsor noted that, while this heterogeneity was not likely to affect the robustness of results, it may have induced a larger risk of bias in the primary analysis of PFS (with CAPOX and mFOLFOX6 separate) because the smallest trial (ATTRACTION-4 Part 1) established a link by itself in the network for certain comparisons. |
Median follow-up | The median follow-up times ranged from 7 months in the Popov (2008) trial to 26.6 months in ATTRACTION-4 (Part 2) (and 54.3 months in the excluded KEYNOTE 062 trial). The sponsor acknowledged that differences in data maturity could introduce bias but reported that it was infeasible to account for differences in data maturity in its analysis. |
Age | The median ages of patients ranged from 55 to 57 years in the Popov (2008) trial to 64 years to 68 years in the HERBIS-4A trial. The sponsor did not adjust for differences in median age and reported that data from 4 trials (including the SPOTLIGHT and GLOW trials) suggest that age (< 65 years and ≥ 65 years) will not remarkably affect the treatment. The clinical experts agreed with the sponsor’s assessment. |
Race | Most trials (13 out of 21) did not explicitly report the race or ethnicity of participants. For the trials that reported race or ethnicity information, 4 trials enrolled predominantly white patients, including the SPOTLIGHT trial (48% to 49%), and the other 4 trials enrolled predominantly Asian patients, including the GLOW trial (62%). The sponsor conducted the sensitivity analyses described earlier, excluding and focusing on patients in Asian trials. |
ECOG Performance Status | Out of the 20 studies that enrolled patients based on ECOG PS, 10 studies (including the GLOW and SPOTLIGHT trials) enrolled patients with an ECOG PS of 0 to 1, and 10 studies enrolled patients with an ECOG PS of 0 to 2 (however, the sponsor reports that it enrolled predominantly patients with ECOG PS 0 to 1). Only 1 study (Kang [2009]) enrolled patients based on KPS information (patients with KPS ≥ 70 scores). Based on evidence from 2 trials, the sponsor did not adjust for differences in baseline PS. The clinical experts agreed with the sponsor’s assessment. |
Tumour location and tumour type | More than half of the included trials (13 out of 21) reported data on tumour location (gastric versus GEJ), while the remaining trials reported combined data (gastric and GEJ) and did not report specific subgroup data on tumour location. Based on data availability and clinical input, the sponsor did not adjust for tumour location or tumour type. The clinical experts agreed with the sponsor’s assessment but noted that the trial data do not show benefits for patients with GEJ tumours, and that this may influence clinicians’ decision-making. |
Disease stage and number of metastatic sites | All trials enrolled patients with locally advanced or metastatic GC or GEJ; only 12 trials reported information on metastatic disease status, and only 8 of those 12 trials enrolled predominantly patients with metastatic GC or GEJ (i.e., higher than 90%). The number of metastatic sites was reported in 9 trials, and the proportion of parents with 3 or more metastatic sites was reported to be comparable among the 4 trials that reported this information (ranging from 17% to 26%). Based on data from the GLOW and SPOTLIGHT trials regarding subgroups of patients by number of metastatic sites, the sponsor did not adjust for the number of metastatic sites in the analysis. The clinical experts agreed with the sponsor’s assessment. |
Mutation status | Ten studies enrolled patients with HER2-negative status but allowed the inclusion of patients with unknown HER2 status. Moreover, CLDN18.2 expression status was reported only in the GLOW and SPOTLIGHT trials. Therefore, the sponsor did not adjust for HER2 or CLDN18.2 expression status. However, it did conduct subgroup analyses assessing the impact of CPS scores, including the 5 trials (6 trials, if including KEYNOTE-062) that reported information on PD-L1 CPS scores. These analyses only used CPS-specific HRs from the nivolumab and pembrolizumab trials and did not use the subgroup-specific data from the SPOTLIGHT and GLOW trials. |
Prior surgery | Information on prior surgery was reported in 12 trials. However, based on data from the SPOTLIGHT and GLOW trials on the subgroups of patients with and without prior gastrectomy, the sponsor did not adjust for prior surgery. |
End point definition | PFS and OS were analyzed in the NMAs. These outcomes were extracted by treatment arm for each trial. The definitions for each end point were mainly consistent across the trials, with some variability in how disease progression and censoring were defined across trials. |
CAPOX = capecitabine plus oxaliplatin; CLDN18.2 = Claudin 18.2; CPS = combined positive score; ECOG PS = Eastern Cooperative Oncology Group Performance Status; GEJ = gastroesophageal junction; HER2 = human epidermal growth factor receptor 2; KPS = Karnofsky Performance Score; mFOLFOX6 = leucovorin calcium (folinic acid), fluorouracil, and oxaliplatin; NMA = network meta-analysis; OS = overall survival; PD-L1 = programmed death-ligand 1; PFS = progression-free survival; RCT = randomized controlled trial.
Source: Network Meta-Analysis Technical Study Report.54
Evidence Networks
The evidence network for the primary analysis of OS is presented in Figure 10, with studies separated according to use of CAPOX and FOLFOX. It is also presented in Appendix 2 with CAPOX and FOLFOX combined into a single analysis.
Primary NMA
Of the 21 trials deemed relevant after applying the NMA inclusion and exclusion criteria, 1 trial (the KEYNOTE-062 trial) was removed because it required patients to be all-comers (e.g., no restriction on CPS score or CLDN18.2 expression level). The 20 included trials, comprising 14 unique regimens, were included in the primary NMA (as presented in Figure 10) for the analysis of OS.
Results
The NMA was constructed using a fixed-effects model, and the sponsor reported that the trace and density plots, Gelman-Rubin plots, and Gelman-Rubin diagnostics showed that convergence of the results was generally achieved. In the primary analysis, the sponsor reported only consistency test results in the primary analysis with CAPOX and FOLFOX combined. This discussion presents the results of the primary analysis with CAPOX and FOLFOX presented separately. The results of the primary analysis with CAPOX and FOLFOX combined are presented in Appendix 2.
Figure 10: Evidence Network of OS for the Primary NMA
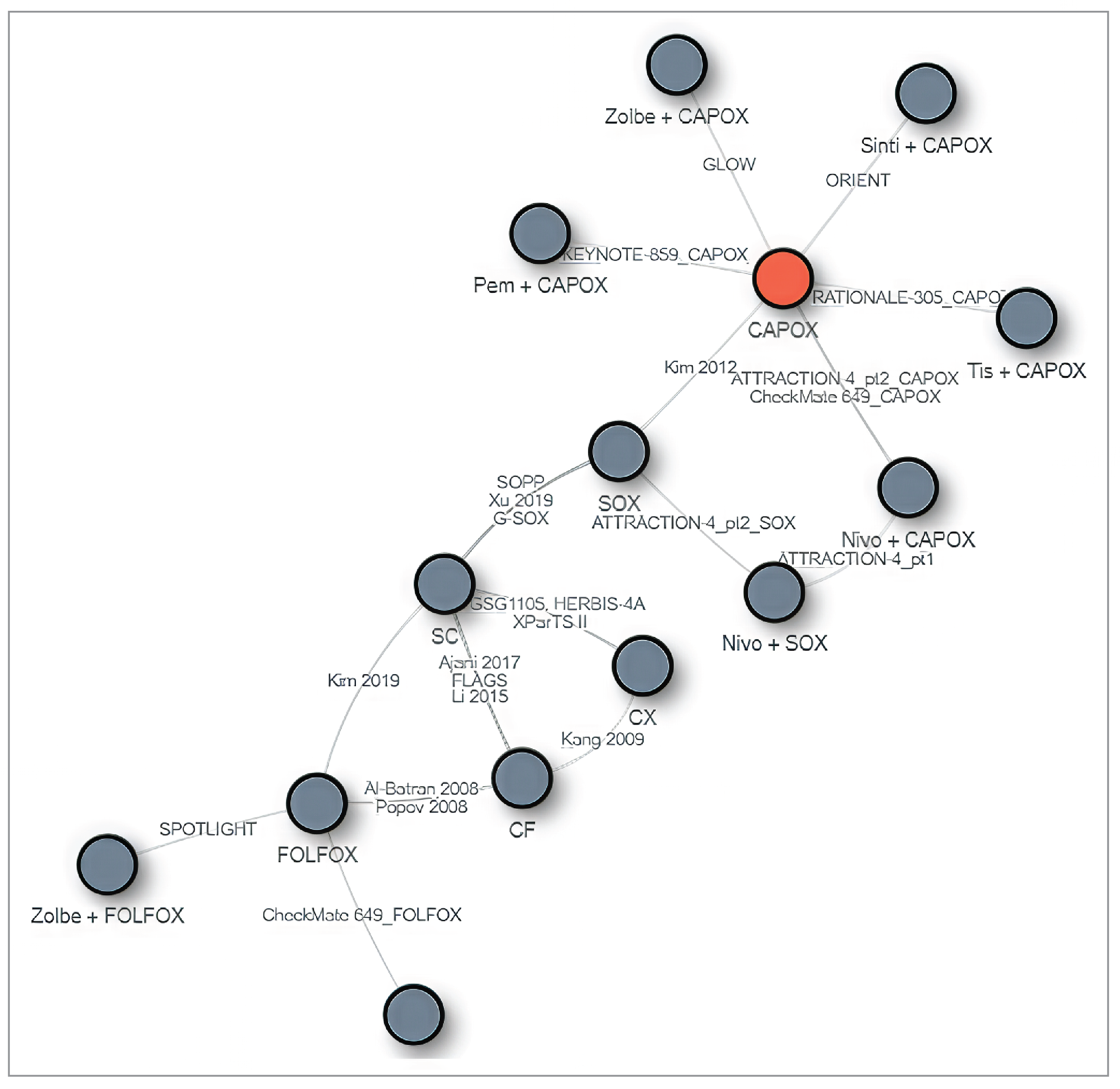
CAPOX = capecitabine plus oxaliplatin; CF = 5-fluorouracil and cisplatin; CX = capecitabine and cisplatin; FOLFOX = leucovorin calcium (folinic acid), fluorouracil, and oxaliplatin; Nivo = nivolumab; Pem = pembrolizumab; SC = tegafur, gimeracil, and oteracil (S-1) plus cisplatin; Sinti = sintilimab; SOX = tegafur, gimeracil, and oteracil (S-1) plus oxaliplatin; Tis = tislelizumab; Zolbe = zolbetuximab.
Source: Network Meta-Analysis Technical Study Report.54
Overall Survival
Primary analysis: The HRs and 95% Crls across various comparisons for OS are summarized in Table 23. Results from the NMA are consistent with results of the pivotal evidence, in which zolbetuximab combined with CAPOX is superior to CAPOX alone (HR = 0.76; 95% Crl; 0.62 to 0.94) and zolbetuximab combined with FOLFOX is superior to FOLFOX alone (HR = 0.78; 95% Crl, 0.64 to 0.95). The HR for cross-comparisons with CAPOX and FOLFOX are also consistent; however, the wide CrIs may indicate heterogeneity between studies that used CAPOX versus FOLFOX. CrIs for the comparisons of zolbetuximab plus chemotherapy versus nivolumab or pembrolizumab plus chemotherapy did not favour either comparator in OS; however, the HR was consistently higher with zolbetuximab plus FOLFOX compared to zolbetuximab plus CAPOX.
Table 23: Pairwise Comparisons of OS for Zolbetuximab Plus Chemotherapy Versus Relevant Comparators in the Primary NMA, Median HR (95% Crl)
Zolbetuximab regimens | CAPOX | FOLFOX | Nivo plus CAPOX | Nivo plus FOLFOX | Pembro plus CAPOX | Capecitabine and Cisplatin | CF |
|---|---|---|---|---|---|---|---|
Zolbetuximab plus CAPOX | 0.76 (0.62 to 0.94) | 0.68 (0.42 to 1.11) | 0.94 (0.73 to 1.20) | 0.88 (0.54 to 1.47) | 0.98 (0.78 to 1.23) | 0.61 (0.38 to 0.99) | 0.57 (0.37 to 0.88) |
Zolbetuximab plus FOLFOX | 0.88 (0.54 to 1.41) | 0.78 (0.64 to 0.95) | 1.09 (0.66 to 1.76) | 1.02 (0.80 to 1.30) | 1.13 (0.69 to 1.83) | 0.71 (0.50 to 1.01) | 0.66 (0.49 to 0.88) |
CAPOX = capecitabine plus oxaliplatin; CF = 5-fluorouracil and cisplatin; CrI = credible interval; HR = hazard ratio; mFOLFOX6 = leucovorin calcium (folinic acid), fluorouracil, and oxaliplatin; Nivo = nivolumab; NMA = network meta-analysis; OS = overall survival, pembro = pembrolizumab.
Note: Each cell represents the comparison (HR and 95% Crl) of the row-defined treatment versus the column treatment.
Source: Network Meta-Analysis Technical Study Report.54
Progression-Free Survival
Primary analysis: The HRs and 95% Crls across various comparisons for PFS are summarized in Table 24. Results from the NMA are again consistent with the results of the pivotal evidence, in which zolbetuximab combined with CAPOX is superior to CAPOX alone (HR = 0.69; 95% Crl, 0.55 to 0.86) and zolbetuximab combined with FOLFOX is superior to FOLFOX alone (HR = 0.73; 95% Crl, 0.59 to 0.91). The HRs for cross-comparisons with CAPOX and FOLFOX are also consistent; however, the wide CrIs may indicate heterogeneity between the studies that used CAPOX versus FOLFOX. CrIs for the comparisons of zolbetuximab plus chemotherapy versus nivolumab or pembrolizumab plus chemotherapy did not favour either comparator in OS; however, the HR was consistently higher with zolbetuximab plus FOLFOX compared to zolbetuximab plus CAPOX.
Table 24: Pairwise Comparisons of PFS for Zolbetuximab Plus CAPOX or FOLFOX Versus Relevant Comparators in the Primary NMA, Median HR (95% Crl)
Zolbetuximab regimens | CAPOX | FOLFOX | Nivolumab plus CAPOX | Nivolumab plus FOLFOX | Pembrolizumab plus CAPOX | Capecitabine and cisplatin | CF |
|---|---|---|---|---|---|---|---|
Zolbetuximab plus CAPOX | 0.69 (0.55 to 0.86) | 0.53 (0.21 to 1.25) | 0.88 (0.69 to 1.13) | 0.66 (0.26 to 1.59) | 0.91 (0.71 to 1.16) | 0.6 (0.24 to 1.41) | 0.51 (0.21 to 1.19) |
Zolbetuximab plus FOLFOX | 0.96 (0.41 to 2.42) | 0.73 (0.59 to 0.91) | 1.23 (0.52 to 3.07) | 0.93 (0.73 to 1.19) | 1.26 (0.53 to 3.20) | 0.83 (0.57 to 1.22) | 0.71 (0.52 to 0.98) |
CAPOX = capecitabine plus oxaliplatin; CF = fluorouracil and cisplatin; CrI = credible interval; CX = capecitabine and cisplatin; FOLFOX = leucovorin calcium (folinic acid), fluorouracil, and oxaliplatin; HR = hazard ratio; NMA = network meta-analysis; PFS = progression-free survival.
Note: Each cell represents the comparison (HR and 95% Crl) of the row-defined treatment versus the column treatment.
Source: Network Meta-Analysis Technical Study Report.54
Harms
Harms outcomes were not evaluated in the NMA.
Critical Appraisal of the ITC
The sponsor-submitted NMA was based on studies identified in a systematic literature review of relevant evidence, based on a PICO-defined a priori. The systematic literature review involved searches in multiple electronic databases, clinical registries, and supplementary sources. Given that the search and selection of relevant studies were restricted to trials published in English, relevant non-English publications may have been excluded. Selection was conducted by 2 independent reviewers, with discrepancies resolved by a third reviewer; the reasons for exclusion were reported. Data extraction criteria were predefined in a template, and data were extracted by 1 review and checked by a second. While the risk of bias of the comparator trials was assessed, the number of reviewers who conducted the quality assessment was not reported, and the risk of bias was not assessed per outcome.
Out of 21 eligible trials, 20 were included in the NMA, comprising 14 unique treatment regimens. The sponsor noted that 1 trial (the KEYNOTE-062 trial) was excluded because it included patients with no restriction on CPS score or CLDN18.2 expression level. The clinical review team assessed this trial’s publication and found that no subgroup analysis based on CPS score or CLDN18.2 expression level was reported; therefore, the exclusion of this trial was deemed appropriate.
The sponsor conducted 2 primary analyses: 1 with CAPOX and FOLFOX treated as separate comparators and another with the 2 regimens combined as a single comparator. This was based on the sponsor’s assumption that CAPOX and FOLFOX were of equivalent efficacy (an assumption that was supported by the clinical experts consulted for this review). However, the results of the primary NMA that kept the comparators separate do not support combining these because there are wide CrIs in the cross-comparisons of both treatments, indicating systematic heterogeneity between the studies that used CAPOX versus those that used FOLFOX. Therefore, the results of both analyses must be interpreted with caution. Three studies included patients in Canada (the SPOTLIGHT, GLOW, and CheckMate 649 trials), but nearly half of included trials (10 of 22) were conducted in Asian countries only. The clinical experts consulted during this review noted that proactive screening for gastrointestinal cancers is more common in some Asian countries and that this tends to contribute to more favourable outcomes for some patients. Thus, this heterogeneity in the trial populations across the network likely introduced bias in the comparisons across the network. In addition, most trials (14 of 22) did not explicitly report the race or ethnicity of participants. Of the trials that reported race or ethnicity, 4 trials enrolled predominantly white patients, and the other 4 enrolled predominantly patients categorized as “Asian.” The clinical experts did not note any concerns regarding the racial differences in populations between trials. The sponsor conducted sensitivity analyses excluding the Asia-only trials or focusing on Asia-only trials (or Asian subgroups of global trials), and the findings were similar to those of the primary NMA analysis. However, this sensitivity analysis was conducted only in the second primary analysis with CAPOX and FOLFOX combined, for which CDA-AMC has noted greater heterogeneity across studies.
The sponsor reported on potential sources of heterogeneity across trials, including dosing schedules and sample size; it reported that the impact of this variation was expected to be small. The sponsor also reported that differences in median follow-up (and, as a result, data maturity) could introduce bias because HRs tend to wane with longer follow-up times, yet it was unable to account for differences in data maturity in its analysis. With regards to patient baseline characteristics, the sponsor noted variations across trials in median age, ECOG Performance Status, tumour location and type, disease stage, number of metastatic sites, mutation status, and prior surgery; however, it noted that it did not adjust for these variations in its analysis. Specifically for tumour location, the clinical experts noted that the trial data do not show benefits for patients with GEJ tumours; therefore, heterogeneity across the network in tumour location could be an important source of bias for these NMAs.
There were variations in the collecting and reporting of mutation status across trials; therefore, the sponsor did not adjust for HER2 or CLDN18.2 expression status. The clinical experts consulted for this review have noted that, while zolbetuximab plus chemotherapy could be a preferred option for patients with CLDN18.2-positive tumours and a PD-L1 CPS of less than 5, it is unclear which option would be best for patients with both CLDN18.2-positive tumours and a PD-L1 CPS of greater than or equal to 5. The sponsor reported that CPS is not considered a treatment-effect modifier for zolbetuximab; thus, CPS testing was not routinely conducted in the SPOTLIGHT and GLOW trials. In this NMA, the sponsor conducted 2 subgroup analyses (with CPS ≥ 5 and CPS < 5) in the 5 trials that reported CPS scores; however, these analyses only used CPS-specific HRs from the nivolumab and pembrolizumab trials and did not use the subgroup-specific data from the SPOTLIGHT and GLOW trials. The clinical review team considered this approach to be at risk for bias due to the existing evidence that has established CPS testing as a potential effect modifier in this disease area; this would make it inappropriate to assume this factor is an effect modifier for only some comparators and not others without additional evidence to support this claim. Furthermore, even if such evidence existed for some comparators, other sources of heterogeneity in the network that are related to CPS testing could artificially modify effects that would also introduce bias into the assessment by not using CPS-specific results for all comparators in the network. Therefore, this subgroup analysis has significant limitations, and no definitive conclusions could be drawn for this subpopulation of patients.
NMA results were presented for OS and PFS only; harms outcomes and other outcomes of relevance to patients (e.g., HRQoL) were not reported. The treatment effects measured by HRs of OS or PFS assumed proportional hazards, which were held in 3 trials but not reported in most included studies. The consistency test performed in the primary analysis treating CAPOX and FOLFOX as combined suggested evidence of inconsistency in the PFS network.
Summary
The SPOTLIGHT and GLOW trials began screening patients on June 21, 2018, and November 28, 2018, respectively. At that time, fluoropyrimidine- and platinum-based chemotherapy represented standard of care for the treatment of patients with locally advanced or metastatic HER2-negative gastric or GEJ adenocarcinoma; therefore, these were used in combination with placebo in the control arms of these studies. In the absence of direct head-to-head trials evaluating the comparative efficacy of zolbetuximab versus currently relevant comparators, a review of indirect evidence was undertaken and submitted by the sponsor. The NMA included 20 relevant trials comprising 14 unique treatment regimens. Overall, the results were consistent with the pivotal evidence, in which the treatment effect on OS and PFS of adding zolbetuximab to chemotherapy appeared to consistently be favoured over chemotherapy alone. The comparisons of zolbetuximab plus chemotherapy versus nivolumab or pembrolizumab plus chemotherapy presented little to no difference in OS or PFS between the treatments. However, there are sources of clinical and methodological heterogeneity across trials that may have biased the effect estimates of the ITC. Specifically, there were sources of heterogeneity identified in the networks between trials that used CAPOX versus those that used FOLFOX that are likely to have introduced systematic bias in both primary analyses. However, it is unclear in which direction; therefore, the results should be interpreted with extreme caution.
Studies Addressing Gaps in the Systematic Review Evidence
Contents within this section have been informed by materials submitted by the sponsor. The following has been summarized and validated by CDA-AMC.
No studies addressing gaps in the systematic review evidence were submitted by the sponsor.
Discussion
Summary of Available Evidence
The clinical evidence included in the review consisted of 2 pivotal RCTs (the SPOTLIGHT trial [N = 565] and the GLOW trial [N = 507]) as well as 1 ITC. No long-term extension studies or studies addressing gaps in the systematic review were submitted by the sponsor.
Pivotal trials: The SPOTLIGHT and GLOW trials are both ongoing, multinational, double-blind, placebo-controlled, randomized studies of zolbetuximab combined with fluoropyrimidine- and platinum-based chemotherapy compared with placebo combined with fluoropyrimidine- and platinum-based chemotherapy for the first-line treatment of patients with locally advanced unresectable or metastatic HER2-negative gastric or GEJ adenocarcinoma whose tumours are CLDN18.2-positive. The chemotherapy backbone used in the SPOTLIGHT trial was mFOLFOX6, while the backbone used in the GLOW trial was CAPOX.24,25 The sponsor reported that the SPOTLIGHT trial enrolled more patients from Japan and South Korea, whereas the GLOW trial enrolled more patients from mainland China, whose disease course tends to be more similar to that of patients from western countries, with a lower OS duration than patients from Japan.10,39,41 The primary objective in both the SPOTLIGHT and GLOW trials was to assess the PFS benefit of zolbetuximab plus chemotherapy compared to placebo plus chemotherapy. OS was a key secondary end point of both the SPOTLIGHT and GLOW trials, and the sponsor provided final analyses for OS in the application. Eligible patients were randomized 1:1 to receive zolbetuximab or placebo, with both treatments provided in combination with fluoropyrimidine- and platinum-based chemotherapy (mFOLFOX6 in the SPOTLIGHT trial and CAPOX in the GLOW trial).
Indirect comparison: The SPOTLIGHT and GLOW trials began screening patients in June 2018 and November 2018, respectively. At that time, fluoropyrimidine- and platinum-based chemotherapy was considered the standard treatment for patients with locally advanced or metastatic HER2-negative gastric or GEJ adenocarcinoma; therefore, the use of these chemotherapy regimens in combination with placebo was considered an appropriate comparator when trials were initiated. However, the use of chemotherapy alone is no longer reflective of routine practice in Canada, where patients would typically be offered nivolumab plus chemotherapy as the preferred treatment option. Only patients with a contraindication or intolerance to nivolumab would receive chemotherapy alone. The sponsor has acknowledged this evolution in the treatment landscape and included an ITC in its application. The sponsor’s NMA compared zolbetuximab in combination with chemotherapy against the 2 most relevant comparators in the current treatment setting (i.e., nivolumab and pembrolizumab, both in combination with chemotherapy).
Interventions: Zolbetuximab was studied with FOLFOX and CAPOX as the chemotherapy backbone. In this review, CAPOX and FOLFOX were assumed to have the same efficacy, based on input from clinical experts. This aligned with the EMA review of zolbetuximab, which noted that the extrapolation of efficacy data from the SPOTLIGHT and GLOW trials to the broader indication of “in combination with fluoropyrimidine- and platinum-containing chemotherapy” is appropriate, given that cisplatin and oxaliplatin have been shown to be equally effective in clinical trials. However, the EMA noted that the safety profile of the combination of zolbetuximab with a cisplatin-containing regimen could be emetogenic compared to the oxaliplatin combinations studied in the SPOTLIGHT and GLOW trials.50
Interpretation of Results
Efficacy
Evidence from the pivotal phase III trials, the SPOTLIGHT and GLOW trials, showed that first-line treatment with zolbetuximab combined with fluoropyrimidine- and platinum-containing chemotherapy (mFOLFOX6 or CAPOX) in adult patients with locally advanced unresectable or metastatic HER2-negative gastric or GEJ adenocarcinoma whose tumours are CLDN18.2-positive resulted in improved OS and PFS compared to placebo in combination with fluoropyrimidine- and platinum-containing chemotherapy.
Based on input from the clinical experts consulted for the purpose of this review, improvement in OS is the main outcome of importance for any treatment in oncology. The clinical experts noted that an increase of 5% to 10% in the proportion of patients alive at 12 months and 36 months could be considered clinically meaningful. While the observed probability of increased survival at 12 months and 36 months met the threshold for a clinically meaningful improvement in OS, the lower bound of the 95% CI was compatible with little to no clinically important difference for all the analyses. The GRADE standard suggests moderate certainty of this benefit at 12 months and 36 months. Overall, the clinical experts consulted during this review noted that the improvement in OS reported in the SPOTLIGHT and GLOW trials compared with chemotherapy alone is clinically important in (while noting that few patients in the target population in Canada would receive chemotherapy alone, given that nivolumab plus chemotherapy is now the preferred treatment option for the first-line, metastatic setting). The EMA similarly concluded that the SPOTLIGHT and GLOW trials demonstrated a clinically meaningful improvement versus chemotherapy alone.50
Median OS was lower in the GLOW study compared to the SPOTLIGHT study for both treatment groups. The EMA also noted that directly comparing the outcome of placebo-treated participants between 2 different studies presents challenges, and that the higher proportion of Asian participants in the GLOW study could be a contributing factor. The agency noted that the preplanned subgroup analysis showed that the survival of placebo-treated participants in China was lower than that of the overall study population in both the SPOTLIGHT and GLOW trials, which might have contributed to the differences.
The subgroup analysis of OS suggested the potential for differential treatment effects by tumour type. In both the SPOTLIGHT and GLOW trials, the impact of zolbetuximab on OS was reduced in patients with GEJ cancer (HR = 1.022 [95% CI, 0.694 to 1.505] and HR = 1.046 [95% CI, 0.634 to 1.726], respectively) than in those who had gastric cancer (HR = 0.725 [95% CI, 0.579 to 0.907] and HR = 0.713 [0.573 to 0.888], respectively). This suggested that the difference in OS observed in the overall study population was driven primarily by patients with gastric cancer. This issue was investigated in detail by the EMA, which noted that the observed reduction in efficacy was in patients with distal GEJ (given that those with proximal GEJ had an even more favourable outcome compared to the overall study population).50 Additional analyses provided by the sponsor suggested that exposure to zolbetuximab and oxaliplatin was lower in the GEJ versus the gastric cancer subgroups and lower in the subgroup of patients with GEJ distal cancer versus GEJ proximal cancer. The EMA noted that this suggests that the reduction in efficacy in these subgroups is likely due to differences in exposure to zolbetuximab and/or oxaliplatin (including an increase in dose interruptions and slightly higher rates of early discontinuation).50
In the CDA-AMC assessment of PFS, there was high certainty that the addition of zolbetuximab to chemotherapy resulted in an increase in PFS at 12 months and 30 months compared with placebo plus chemotherapy.
Patients were eligible for the SPOTLIGHT and GLOW trials if they had received either neoadjuvant or adjuvant immunotherapy, as long as it was completed at least 6 months before randomization; however, no patients were identified as having received prior treatment with nivolumab, and only a single patient had received prior treatment with pembrolizumab. Hence, there is no evidence from the SPOTLIGHT or GLOW trials to inform the sequential use of zolbetuximab plus chemotherapy after receiving adjuvant treatment with nivolumab. The clinical experts consulted during this review suggested that these patients would likely be relatively rare in clinical practice, and that those who could be considered candidates for zolbetuximab based on CLDN18.2 biomarker status, ECOG Performance Status, and other eligibility criteria could be offered the treatment because they may benefit if the disease has progressed to the locally advanced or metastatic setting.
HRQoL was considered an important and meaningful outcome to both patients and clinicians. Results for time to deterioration based on changes in HRQoL scales were inconsistent across the SPOTLIGHT and GLOW trials. The EMA similarly noted that there was no meaningful difference in the secondary objective, TTCD — as measured by the EORTC QLQ-C30 PF, EORTC QLQ-OG25 Pain, and EORTC GHS/QoL scales — among treatment groups in the SPOTLIGHT and GLOW trials.50
No direct comparative evidence between zolbetuximab and relevant comparators used in the Canadian practice setting were identified (i.e., nivolumab or pembrolizumab). To address this gap, the sponsor submitted an NMA comparing zolbetuximab in combination with chemotherapy against nivolumab and pembrolizumab (both in combination with chemotherapy). The indirect comparative evidence from the results of the NMA suggested little to no difference in treatment effect on OS for zolbetuximab versus nivolumab (median HR = 0.97; 95% CrI, 0.81 to 1.16) or pembrolizumab (median HR = 0.99; 95% CrI, 0.83 to 1.19) in the overall patient population. It is important to note that these comparisons were not limited to patients whose tumours were CLDN18.2-positive.
A key subgroup of interest for this review is patients with a CPS score of less than 5, given that the clinical experts who provided input into this review noted uncertainty regarding the added clinical benefit of treatment with nivolumab in these patients. Of note, the EMA has approved nivolumab for use only in patients with a CPS score greater than 5. The sponsor also submitted subgroup analyses with the NMA based on patients’ baseline CPS. The subgroup analysis for patients with CPS of less than 5 supported the opinions of the clinical experts because it demonstrated a more favourable treatment effect with zolbetuximab plus chemotherapy in comparison with nivolumab plus chemotherapy for PFS (median HR = 0.76; 95% CrI, 0.60 to 0.98) and numerically lower for OS (median HR = 0.81; 95% CrI, 0.66 to 1.01). Although these results, at face value, were consistent with the perspective of the clinical experts consulted during this review (i.e., that zolbetuximab may be the preferred therapeutic option for patients who have a CPS score less than 5), the clinical review team did not consider this analysis suitable for supporting this conclusion due to the risk of bias associated with these results from potential effect-modifier factors that were unaccounted for as well as potential differences in patient populations (e.g., subgroup data from nivolumab and pembrolizumab trials and the full trial populations in the SPOTLIGHT and GLOW trials).51 In its comments on the draft report, the sponsor objected to the appraisal of the NMA based on PD-L1 subgroup analyses, noting that: “The CPS based subgroup analyses used the prespecified CPS-specific HRs from the nivolumab and pembrolizumab trials, and the full study population from the SPOTLIGHT and GLOW trials. This approach was appropriate because CPS testing was not required for enrolment into the SPOTLIGHT or GLOW trials.”
As is common with NMAs, the results for the sponsor’s ITC are associated with uncertainty due to clinical and methodological heterogeneity between the studies included in the network, with a potential to introduce bias to the ITC results. The potential risk of bias is even greater when the analyses are conducted using subgroup data, and in this specific case, the analytical approach to the NMA was not considered to be consistent with best practices for assessing subgroup effects in an NMA setting. Therefore, the results are not sufficient to support the conclusion that zolbetuximab is more efficacious than nivolumab for patients with a CPS score of less than 5.
As previously described, patient and clinician groups and the clinical experts consulted for this review stated that there is an unmet need for more treatment options associated with improved survival and quality of life for patients with locally advanced and metastatic HER2-negative gastric and GEJ adenocarcinoma. The addition of zolbetuximab to chemotherapy would represent an additional first-line standard of care treatment for the subset of patients whose tumours are CLDN18.2-positive, for whom it is likely to result in a clinically important OS benefit. However, it is uncertain whether improved quality of life could be met. Finally, it is unknown whether the treatment effect on OS could be generalizable to patients excluded from the trial, especially those with an ECOG Performance Status of 2 who, in clinical practice, are managed in a similar manner to patients with an ECOG Performance Status of 0 or 1.
Harms
The product monograph includes a warning regarding the risk of nausea and vomiting following treatment with zolbetuximab in combination with mFOLFOX6 or CAPOX. Nausea and vomiting occurred more often during the first cycle of treatment but decreased in incidence with subsequent cycles of treatment. To reduce the occurrence of nausea and vomiting, the product monograph includes recommendations for pretreatment with antiemetics before each infusion with zolbetuximab. The product monograph similarly provides recommendations regarding treatment interruption and discontinuation (if required) for those who experience grade 2, 3, or 4 AEs of nausea and vomiting. The clinical experts consulted during this review indicated that these events would be manageable in clinical practice and would not be expected to limit the usage of zolbetuximab.
The product monograph also includes a warning about IRRs with zolbetuximab (e.g., nausea, vomiting, abdominal pain, salivary hypersecretion, pyrexia, chest discomfort, chills, back pain, cough, and hypertension). The monograph advises that patients should be monitored for signs and symptoms of IRRs, and it provides recommendations concerning interruption or discontinuation of treatment. Patients who experience IRRs should be pretreated with antihistamines before the next infusion, receive the drug in accordance with reduced infusion rates, and be closely monitored for symptoms and signs of an IRR. The clinical experts consulted during this review indicated that these events would be manageable in clinical practice and would not be expected to limit usage of zolbetuximab.
The sponsor’s submitted ITC did not include an evaluation of the comparative safety of zolbetuximab versus nivolumab or pembrolizumab. Acknowledging the absence of comparative evidence, the clinical experts noted that the AE profile for zolbetuximab plus chemotherapy is generally comparable to those of the alternative regimens available for patients with metastatic gastric or GEJ cancer.
Other Considerations
The product monograph states that zolbetuximab can be administered until disease progression or unacceptable toxicity. This is different from the maximum number of cycles recommended in the product monographs for nivolumab for this indication and similar to the recommendations for pembrolizumab (i.e., 24 months or 35 doses of 200 mg or 18 doses of 400 mg, whichever is longer). The clinical experts noted that, given the prognosis for the target patient population, few patients are likely to reach the maximum number of cycles for nivolumab or pembrolizumab before disease progression or death occurs.
Conclusion
Two randomized, double-blind, placebo-controlled, phase III trials (the SPOTLIGHT and GLOW trials) demonstrated that treatment with zolbetuximab in combination with fluoropyrimidine- and platinum-based chemotherapy (mFOLFOX6 or CAPOX) resulted in a clinically important improvement in OS compared with placebo in combination with fluoropyrimidine- and platinum-based chemotherapy for the first-line treatment of patients with locally advanced unresectable or metastatic HER2-negative gastric or GEJ adenocarcinoma whose tumours are CLDN18.2-positive. The SPOTLIGHT and GLOW trials similarly demonstrated that treatment with zolbetuximab in combination with chemotherapy resulted in improvements in PFS compared with placebo in combination with chemotherapy. Results for time to deterioration based on changes in HRQoL scales were inconsistent across the SPOTLIGHT and GLOW trials.
The sponsor-submitted ITC suggested that there was little to no difference in treatment effect on OS and PFS between zolbetuximab and nivolumab in combination with chemotherapy, although these comparisons were not limited to patients whose tumours were CLDN18.2-positive. However, the indirect evidence is associated with uncertainty due to clinical and methodological heterogeneity between the studies included in the network, with a potential to introduce bias to the ITC results.
Treatment with zolbetuximab in combination with chemotherapy is associated with an increased risk of nausea, vomiting, and IRRs compared with chemotherapy alone. The product monograph provides recommendations regarding pretreatment with medications to reduce the risk as well as recommendations for treatment interruption and discontinuation (if required) for those who experience grade 2, 3, or 4 AEs. The clinical experts consulted during this review indicated that these events would be manageable in clinical practice and would not be expected to limit usage of zolbetuximab. The sponsor’s submitted ITC did not include an evaluation of the comparative safety of zolbetuximab versus nivolumab or pembrolizumab. Acknowledging the absence of comparative evidence, the clinical experts noted that the AE profile for zolbetuximab in combination with chemotherapy is generally comparable to the alternative regimens available for patients with metastatic gastric or GEJ cancer.
References
1.Arnold M, Ferlay J, van Berge Henegouwen MI, Soerjomataram I. Global burden of oesophageal and gastric cancer by histology and subsite in 2018. Gut. 2020;69(9):1564-1571. PubMed
2.National Cancer Institute. What is Stomach Cancer. https://www.cancer.gov/types/stomach#:~:text=Stomach%20(gastric)%20cancer%20is%20cancer,the%20mouth%20to%20the%20anus. Accessed 2023 Dec 20.
3.Canadian Cancer Society. The Stomach. https://cancer.ca/en/cancer-information/cancer-types/stomach/what-is-stomach-cancer/the-stomach. Accessed 2024 Jul 29.
4.Brenner DR, Gillis J, Demers AA, et al. Projected estimates of cancer in Canada in 2024. CMAJ. 2024;196(18):E615-E623. PubMed
5.Canadian Cancer Society. Risks for stomach cancer. https://cancer.ca/en/cancer-information/cancer-types/stomach/risks. Accessed 2023 Dec 20.
6.Brenner DR, Poirier A, Woods RR, et al. Projected estimates of cancer in Canada in 2022 (Appendix 2 - Supplementary Table 3). Can Med Assoc J. 2022;194(17):E601-E607.
7.Canadian Cancer Statistics Advisory Committee. Canadian Cancer Statistics. 2023; https://cancer.ca/en/cancer-information/cancer-types/stomach/statistics. Accessed 2023 Dec 20.
8.Moss SF. The Clinical Evidence Linking Helicobacter pylori to Gastric Cancer. Cell Mol Gastroenterol Hepatol. 2017;3(2):183-191. PubMed
9.National Cancer Institute. Stomach Cancer Causes and Risk Factors. https://www.cancer.gov/types/stomach/causes-risk-factors. Accessed 2024 Jul 29.
10.Van Cutsem E, Sagaert X, Topal B, Haustermans K, Prenen H. Gastric cancer. Lancet. 2016;388(10060):2654-2664. PubMed
11.National Cancer Institute. Stomach Cancer Symptoms. https://www.cancer.gov/types/stomach/symptoms. Accessed 2024 Jul 29.
12.Mansfield PF. Clinical features, diagnosis, and staging of gastric cancer. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2024: http://www.uptodate.com. Accessed 2024 Jul 3.
13.Yoon HH. Initial systemic therapy for metastatic esophageal and gastric cancer. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2024: http://www.uptodate.com. Accessed 2024 Jul 3.
14.Rupp SK, Stengel A. Influencing Factors and Effects of Treatment on Quality of Life in Patients With Gastric Cancer-A Systematic Review. Front Psychiatry. 2021;12:656929. PubMed
15.CADTH reimbursement review: nivolumab (Opdivo). Can J Health Technol. 2022;2(7). https://www.cadth.ca/sites/default/files/DRR/2022/PC0259-Opdivo-combinedReport.pdf. Accessed 2023 Oct 30.
16.National Cancer Institute. Surveillance, Epidemiology, and End Results Program. Cancer Stat Facts: Stomach Cancer. https://seer.cancer.gov/statfacts/html/stomach.html. Accessed 2023 Jul 10.
17.National Comprehensive Cancer Network. NCCN Guidelines. Gastric Cancer Version 1.2023. https://www.nccn.org/professionals/physician_gls/pdf/gastric.pdf. Accessed 2023 Jul 10.
18.pCODR Final Clinical Guidance Report. Trifluridine-Tipiracil (Lonsurf) for Gastric Cancer. Toronto, ON, Canada: pan-Canadian Oncology Drug Review; Canada’s Drug and Health Technology Agency;2020 [sponsor submitted reference].
19.National Cancer Institute. Stomach Cancer Diagnosis. https://www.cancer.gov/types/stomach/diagnosis. Accessed 2024 Jul 29.
20.Canadian Cancer Society. Diagnosis of Stomach Cancer. https://cancer.ca/en/cancer-information/cancer-types/stomach/diagnosis. Accessed 2024 Jul 29.
21.Vyloy (zolbetuximab): zolbetuximab for injection lyophilised powder for concentrate for solution for intravenous infusion 100 mg/vial [product monograph]. Markham (ON): Astellas Pharma Canada Inc.; 2024 Dec 13.
22.Grizzi G, Venetis K, Denaro N, et al. Anti-Claudin Treatments in Gastroesophageal Adenocarcinoma: Mainstream and Upcoming Strategies. J Clin Med. 2023;12(8). PubMed
23.Wang DW, Zhang WH, Danil G, Yang K, Hu JK. The role and mechanism of claudins in cancer. Front Oncol. 2022;12:1051497. PubMed
24.SPOTLIGHT (8951-CL0302) Primary analysis CSR. March 28, 2023. In: Drug Reimbursement Review sponsor submission: Vyloy (zolbetuximab): lyophilised powder for concentrate for solution for intravenous infusion, 100 mg zolbetuximab single-use vials. Markham (ON): Astellas Pharma Canada, Inc.; 2024 Jun 27.
25.GLOW (8951-CL-0302) Primary Analysis CSR. March 27, 2023. In: Drug Reimbursement Review sponsor submission: Vyloy (zolbetuximab): lyophilised powder for concentrate for solution for intravenous infusion, 100 mg zolbetuximab single-use vials. Markham (ON): Astellas Pharma Canada, Inc.; 2024 Jun 27.
26.Janjigian YY, Shitara K, Moehler M, et al. First-line nivolumab plus chemotherapy versus chemotherapy alone for advanced gastric, gastro-oesophageal junction, and oesophageal adenocarcinoma (CheckMate 649): a randomised, open-label, phase 3 trial. Lancet. 2021;398(10294):27-40. PubMed
27.CADTH Provisional Funding Algorithm for HER2-Negative Gastric, Gastroesophageal Junction (GEJ), or Esophageal Cancer. 2022; https://www.cadth.ca/sites/default/files/pdf/PH0010-EC%20GEJC%20GC-Final-Report.pdf. Accessed 2024 Feb 7.
28.pCODR Final Recommendation for Nivolumab for Advanced/Metastatic HER2-Negative gastric/GEJ/Esophageal Adenocarcinoma. 2022 [sponsor submitted reference].
29.Sun JM, Shen L, Shah MA, et al. Pembrolizumab plus chemotherapy versus chemotherapy alone for first-line treatment of advanced oesophageal cancer (KEYNOTE-590): a randomised, placebo-controlled, phase 3 study. Lancet. 2021;398(10302):759-771. PubMed
30.Joshi SS, Badgwell BD. Current treatment and recent progress in gastric cancer. CA Cancer J Clin. 2021;71(3):264-279. PubMed
31.Morgan E, Arnold M, Camargo MC, et al. The current and future incidence and mortality of gastric cancer in 185 countries, 2020-40: A population-based modelling study. EClinicalMedicine. 2022;47:101404. PubMed
32.Canadian Cancer Society. Risks for stomach cancer. https://cancer.ca/en/cancer-information/cancer-types/stomach/risks. Accessed 2024 Jul 29.
33.Lordick F, Carneiro F, Cascinu S, et al. Gastric cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann Oncol. 2022;33(10):1005-1020. PubMed
34.Saltzman JR, Gibson MK. Clinical manifestations, diagnosis, and staging of esophageal cancer. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2024: https://www.uptodate.com/. Accessed 2024 Jul 3.
35.Canadian Cancer Society. HER2 Status Test. 2023; https://cancer.ca/en/treatments/tests-and-procedures/her2-status-test#:~:text=HER2%20status%20testing%20is%20also,gastroesophageal%2C%20or%20GE%20junction. Accessed 2024 Jul 3.
36.Astellas. U.S. FDA acknowledges Astellas’ resubmission of biologics license application for zolbetuximab and sets new action date. 2024; https://www.astellas.com/en/news/29186. Accessed 2023 Jul 24.
37.European Medicines Agency. Summary of opinion (initial authorisation) Vyloy zolbetuximab. https://www.ema.europa.eu/en/documents/smop-initial/chmp-summary-positive-opinion-vyloy_en.pdf. Accessed 2024 Jul 31.
38.Opdivo (nivolumab): intravenous infusion, 10 mg nivolumab /mL 40 mg and 100 mg single-use vials [product monograph]. Montreal (QC): Bristol-Myers Squibb Canada; 2023: https://pdf.hres.ca/dpd_pm/00073986.PDF.
39.Shitara K, Lordick F, Bang Y-J, et al. Zolbetuximab plus mFOLFOX6 in patients with CLDN18.2-positive, HER2-negative, untreated, locally advanced unresectable or metastatic gastric or gastro-oesophageal junction adenocarcinoma (SPOTLIGHT): a multicentre, randomised, double-blind, phase 3 trial. The Lancet. 2023;401(10389):1655-1668. PubMed
40.Shitara K, Cutsem EV, Lordick F, et al. Final overall survival results from phase 3 SPOTLIGHT study evaluating zolbetuximab + mFOLFOX6 as first-line (1L) treatment for patients (pts) with claudin 18 isoform 2 (CLDN18.2)+, HER2−, locally advanced (LA) unresectable or metastatic gastric or gastroesophageal junction (mG/GEJ) adenocarcinoma. J Clin Oncol. 2024;42(16_suppl):4036-4036.
41.Shah MA, Shitara K, Ajani JA, et al. Zolbetuximab plus CAPOX in CLDN18.2-positive gastric or gastroesophageal junction adenocarcinoma: the randomized, phase 3 GLOW trial. Nat Med. 2023;29(8):2133-2141. PubMed
42.SPOTLIGHT (8951-CL0302) Final Analysis CSR. Data on file. In: Drug Reimbursement Review sponsor submission: Vyloy (zolbetuximab): lyophilised powder for concentrate for solution for intravenous infusion, 100 mg zolbetuximab single-use vials. Markham (ON): Astellas Pharma Canada, Inc.; 2024 Jun 27.
43.GLOW Clinical Study Protocol. Data on file. In: Drug Reimbursement Review sponsor submission: Vyloy (zolbetuximab): lyophilised powder for concentrate for solution for intravenous infusion, 100 mg zolbetuximab single-use vials. Markham (ON): Astellas Pharma Canada, Inc.; 2024 Jun 27.
44.SPOTLIGHT Clinical Study Protocol. Data on file. In: Drug Reimbursement Review sponsor submission: Vyloy (zolbetuximab): lyophilised powder for concentrate for solution for intravenous infusion, 100 mg zolbetuximab single-use vials. Markham (ON): Astellas Pharma Canada, Inc.; 2024 Jun 27.
45.SPOTLIGHT Statistical Analysis Plan. Data on file. In: Drug Reimbursement Review sponsor submission: Vyloy (zolbetuximab): lyophilised powder for concentrate for solution for intravenous infusion, 100 mg zolbetuximab single-use vials. Markham (ON): Astellas Pharma Canada, Inc.; 2024 Jun 27.
46.GLOW Statistical Analysis Plan. Data on file. In: Drug Reimbursement Review sponsor submission: Vyloy (zolbetuximab): lyophilised powder for concentrate for solution for intravenous infusion, 100 mg zolbetuximab single-use vials. Markham (ON): Astellas Pharma Canada, Inc.; 2024 Jun 27.
47.Gordon Lan KK, Demets DL. Discrete sequential boundaries for clinical trials. Biometrika. 1983;70(3):659-663.
48.SPOTLIGHT (8951-CL0302) Final analysis CSR. March 6, 2024. In: Drug Reimbursement Review sponsor submission: Vyloy (zolbetuximab): lyophilised powder for concentrate for solution for intravenous infusion, 100 mg zolbetuximab single-use vials. Markham (ON): Astellas Pharma Canada, Inc.; 2024 Jun 27.
49.GLOW (8951-CL-0302) Final Analysis CSR. July 19, 2024. In: Drug Reimbursement Review sponsor submission: Vyloy (zolbetuximab): lyophilised powder for concentrate for solution for intravenous infusion, 100 mg zolbetuximab single-use vials. Markham (ON): Astellas Pharma Canada, Inc.; 2024 Jun 27.
50.Committee for Medicinal Products for Human Use. Assessment report: Vyloy (zolbetuximab). (European public assessment report). Amsterdam (Netherlands): European Medicines Agency; 2024: https://www.ema.europa.eu/en/documents/assessment-report/vyloy-epar-public-assessment-report_en.pdf. Accessed 2024 Sep 25.
51.National Institute for Health and Care Excellence. Zolbetuximab with chemotherapy for untreated claudin 18.2-positive HER2 negative unresectable advanced gastric or gastro-oesophageal junction adenocarcinoma [ID5123]. [NICE single technology appraisal] 2024: https://www.nice.org.uk/guidance/gid-ta11316/documents/committee-papers. Accessed 2024 Sep 21.
52.Balshem H, Helfand M, Schünemann HJ, et al. GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol. 2011;64(4):401-406. PubMed
53.Santesso N, Glenton C, Dahm P, et al. GRADE guidelines 26: informative statements to communicate the findings of systematic reviews of interventions. J Clin Epidemiol. 2020;119:126-135. PubMed
54.Network Meta-Analysis (NMA) of First-Line Treatments for Locally Advanced or Metastatic Gastric and Gastroesophageal Junction Cancer. In: Drug Reimbursement Review sponsor submission: Vyloy (zolbetuximab): lyophilised powder for concentrate for solution for intravenous infusion, 100 mg zolbetuximab single-use vials. Markham (ON): Astellas Pharma Canada, Inc.; 2024 Jun 27.
Appendix 1: Detailed Outcomes Data
Please note that this appendix has not been copy-edited.
Figure 11: Forest Plot of OS in the SPOTLIGHT Trial — Subgroup Analysis (FAS)
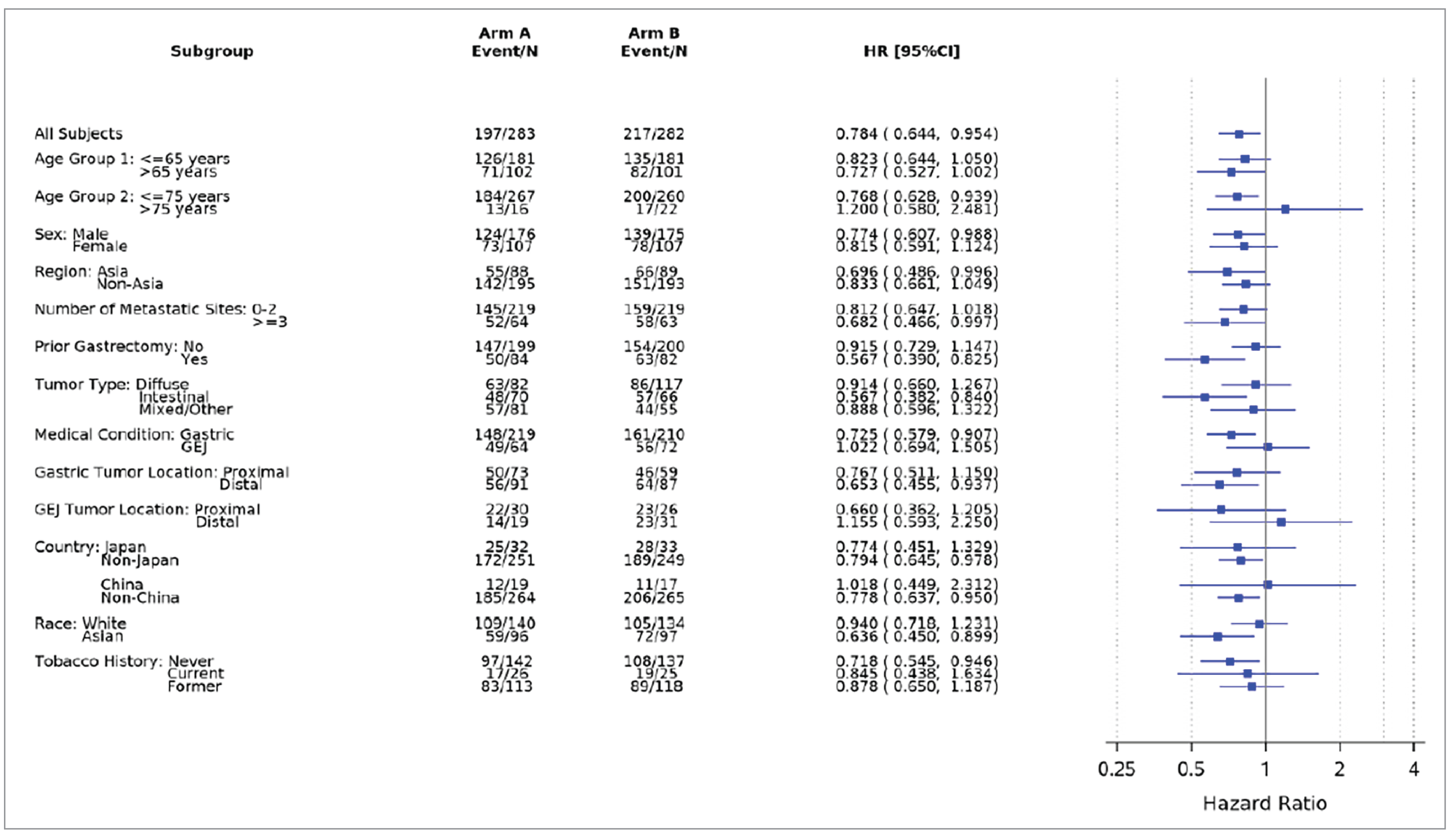
Source: Clinical Study Report for SPOTLIGHT
Figure 12: Forest Plot of OS in the GLOW Trial — Subgroup Analysis (FAS)
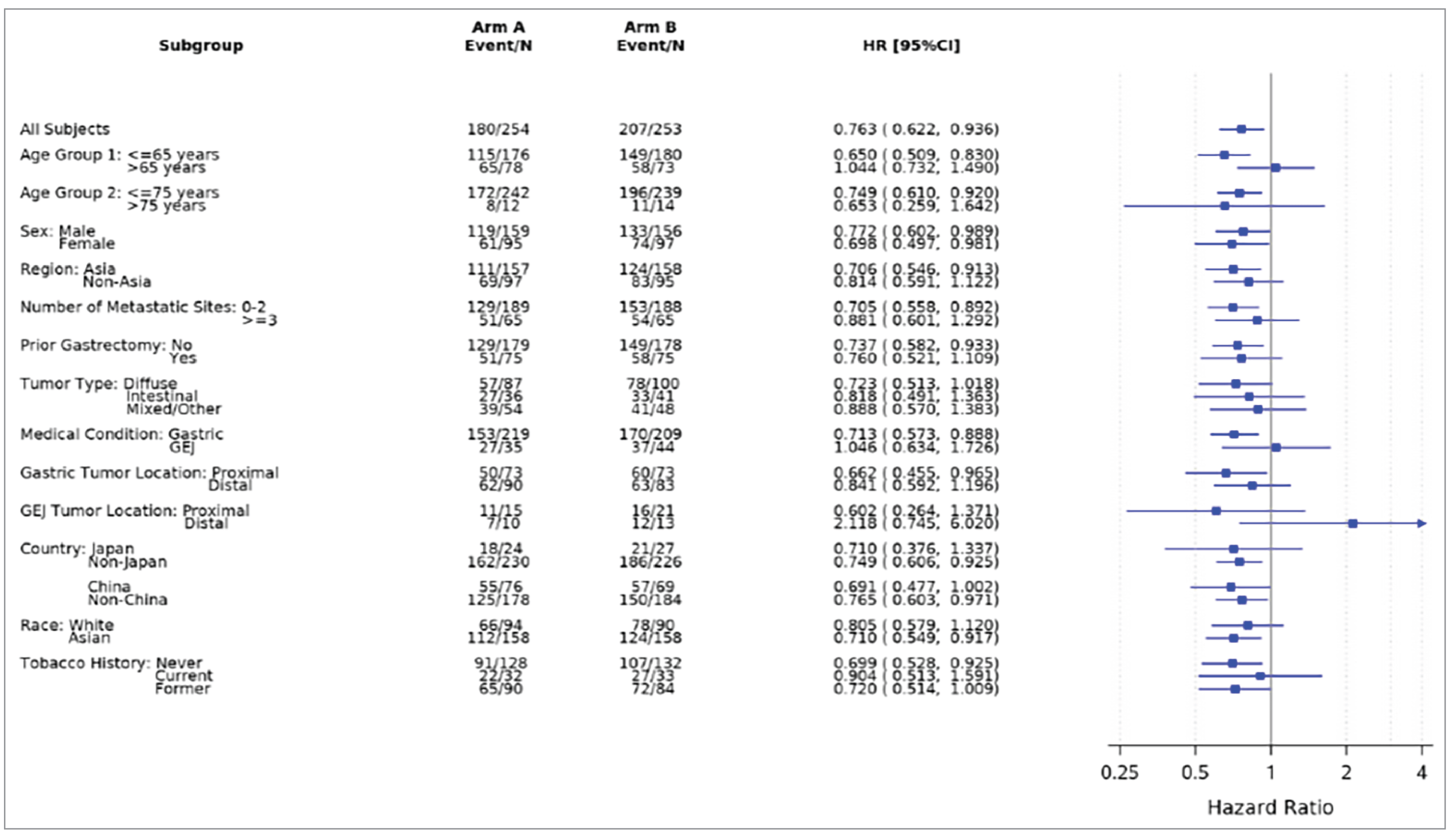
Source: Clinical Study Report for GLOW.
Table 25: New ACTs in the SPOTLIGHT and GLOW Trials (FAS)
Preferred WHO name (ingredients) | SPOTLIGHT, n (%) | GLOW, n (%) | ||
|---|---|---|---|---|
Zolbetuximab + mFOLFOX6 (n = 283) | Placebo + mFOLFOX6 (n = 282) | Zolbetuximab + CAPOX (n = 254) | Placebo + CAPOX (n = 253) | |
Received new anticancer therapy | 135 (47.7) | 148 (52.5) | 118 (46.5) | 140 (55.3) |
All other therapeutic products | 9 (3.2) | 6 (2.1) | 5 (2.0) | 4 (1.6) |
ALPN 202 | 0 | 1 (0.4) | 0 | 0 |
AL2846 | 0 | 0 | 0 | 1 (0.4) |
Amivantamab | 1 (0.4) | 0 | 0 | 0 |
Antineoplastic drugs | 2 (0.7) | 1 (0.4) | 2 (0.8) | 1 (0.4) |
Antineoplastic monoclonal antibodies | 0 | 1 (0.4) | 1 (0.4) | 1 (0.2) |
Astragalus mongholicus root; isatis tinctoria leaf; panax notoginseng root; paris | 1 (0.4) | 0 | 0 | 0 |
polyphylla var. chine bemarituzumab | 0 | 1 (0.4) | 0 | 0 |
BI 836880 | 0 | 1 (0.4) | 0 | 0 |
blind therapy | 0 | 0 | 3 (1.2) | 1 (0.4) |
brucea javanica oil | 1 (0.4) | 0 | 1 (0.4) | 0 |
calcium folinate | 2 (0.7) | 0 | 4 (1.6) | 6 (2.4) |
calcium folinate; fluorouracil | 0 | 1 (0.4) | 3 (1.2) | 8 (3.2) |
calcium folinate; fluorouracil; irinotecan HCl | 21 (7.4) | 21 (7.4) | 0 | 0 |
calcium levofolinate | 1 (0.4) | 0 | 0 | 0 |
calcium levofolinate pentahydrate | 1 (0.4) | 0 | 1 (0.4) | 0 |
camrelizumab | 1 (0.4) | 0 | 3 (1.2) | 1 (0.4) |
Capecitabine | 3 (1.1) | 3 (1.1) | 12 (4.7) | 17 (6.7) |
capecitabine; irinotecan | 0 | 1 (0.4) | 0 | 0 |
capecitabine; oxaliplatin | 2 (0.7) | 0 | 4 (1.6) | 3 (1.2) |
capecitabine; oxaliplatin; trastuzumab | 0 | 0 | 1 (0.4) | 0 |
Carboplatin | 1 (0.4) | 1 (0.4) | 3 (1.2) | 0 |
Catequentinib HCl | 1 (0.4) | 1 (0.4) | 0 | 4 (1.6) |
catumaxomab | 0 | 0 | 1 (0.4) | 0 |
cinobufagin | 0 | 0 | 0 | 1 (0.4) |
cisplatin | 0 | 2 (0.7) | 9 (3.5) | 8 (3.2) |
cisplatin; fluorouracil | 1 (0.4) | 1 (0.4) | 0 | 1 (0.4) |
CMG 901 | 0 | 0 | 1 (0.4) | 3 (1.2) |
coix lacryma-jobi subsp. ma-yuen seed | 0 | 0 | 0 | 1 (0.4) |
combinations of antineoplastic drugs | 7 (2.5) | 7 (2.5) | 1 (0.4) | 2 (0.8) |
DKN | 0 | 0 | 0 | 1 (0.2) |
datopotamab deruxtecan | 1 (0.4) | 0 | 0 | 0 |
docetaxel | 6 (2.1) | 8 (2.8) | 10 (3.9) | 14 (5.5) |
durvalumab | 1 (0.4) | 0 | 0 | 0 |
endostatin | 0 | 0 | 1 (0.4) | 1 (0.4) |
epirubicin HCl | 0 | 0 | 1 (0.4) | 0 |
Etoposide | 0 | 0 | 0 | 1 (0.4) |
Ezabenlimab | 0 | 1 (0.4) | 0 | 0 |
Fluorouracil | 9 (3.2) | 10 (3.5) | 15 (5.9) | 18 (7.1) |
fluorouracil; folinic acid | 2 (0.7) | 0 | 0 | 0 |
fluorouracil; folinic acid; irinotecan | 1 (0.4) | 0 | 0 | 1 (0.4) |
fluorouracil; folinic acid; oxaliplatin | 12 (4.2) | 8 (2.8) | 4 (1.6) | 2 (0.8) |
fluorouracil; irinotecan; oxaliplatin | 0 | 1 (0.4) | 0 | 0 |
folinic acid | 1 (0.4) | 4 (1.4) | 1 (0.4) | 2 (0.8) |
fruquintinib | 0 | 0 | 1 (0.4) | 1 (0.4) |
gemcitabine | 0 | 0 | 1 (0.4) | 0 |
gemtuzumab | 0 | 1 (0.4) | 0 | 0 |
gimeracil; oteracil potassium; tegafur | 6 (2.1) | 4 (1.4) | 7 (2.8) | 9 (3.6) |
herbal anticancer remedies | 0 | 0 | 2 (0.8) | 2 (0.8) |
immunotherapy | 2 (0.7) | 0 | 1 (0.4) | 0 |
INCB 086550 | 1 (0.4) | 0 | 0 | 0 |
investigational antineoplastic drugs | 4 (1.4) | 4 (1.4) | 1 (0.4) | 1 (0.4) |
irinotecan | 8 (2.8) | 13 (4.6) | 16 (6.3) | 19 (7.5) |
irinotecan HCl | 0 | 1 (0.4) | 3 (1.2) | 4 (1.6) |
irinotecan HCl trihydrate | 0 | 1 (0.4) | 0 | 1 (0.4) |
irinotecan HCl trihydrate liposomal | 0 | 0 | 1 (0.4) | 0 |
lenvatinib | 0 | 0 | 1 (0.4) | 0 |
levofolinic acid | 0 | 0 | 0 | 1 (0.4) |
methotrexate | 0 | 1 (0.4) | 0 | 2 (0.8) |
mitomycin | 1 (0.4) | 1 (0.4) | 1 (0.4) | 0 |
nimotuzumab | 0 | 0 | 1 (0.4) | 0 |
nivolumab | 18 (6.4) | 22 (7.8) | 17 (6.7) | 12 (4.7) |
olaparib | 1 (0.4) | 0 | 0 | 0 |
oxaliplatin | 8 (2.8) | 6 (2.1) | 15 (5.9) | 13 (5.1) |
paclitaxel | 48 (17.0) | 55 (19.5) | 46 (18.1) | 51 (20.2) |
paclitaxel nanoparticle albumin-bound | 11 (3.9) | 5 (1.8) | 14 (5.5) | 17 (6.7) |
paclitaxel; pembrolizumab | 0 | 0 | 1 (0.4) | 0 |
paclitaxel; ramucirumab | 8 (2.8) | 6 (2.1) | 8 (3.1) | 10 (4.0) |
pembrolizumab | 8 (2.8) | 6 (2.1) | 5 (2.0) | 4 (1.6) |
penpulimab | 0 | 0 | 0 | 4 (1.6) |
prednisolone sodium succinate | 0 | 0 | 0 | 1 (0.4) |
radiotherapy | 4 (1.4) | 14 (5.0) | 7 (2.8) | 13 (5.1) |
raltitrexed | 2 (0.7) | 0 | 1 (0.4) | 1 (0.4) |
ramucirumab | 35 (12.4) | 34 (12.1) | 21 (8.3) | 28 (11.1) |
regorafenib | 0 | 2 (0.7) | 0 | 1 (0.4) |
rivoceranib | 0 | 1 (0.4) | 3 (1.2) | 3 (1.2) |
rivoceranib mesylate | 1 (0.4) | 1 (0.4) | 5 (2.0) | 3 (1.2) |
sintilimab | 0 | 1 (0.4) | 6 (2.4) | 11 (4.3) |
sodium folinate | 1 (0.4) | 0 | 1 (0.4) | 0 |
spartalizumab | 1 (0.4) | 0 | 0 | 0 |
taxanes | 0 | 1 (0.4) | 0 | 0 |
tegafur | 0 | 0 | 1 (0.4) | 1 (0.4) |
THOR 707 | 1 (0.4) | 0 | 0 | 1 (0.4) |
tipiracil | 1 (0.4) | 1 (0.4) | 0 | 0 |
tipiracil HCl; trifluridine | 1 (0.4) | 6 (2.1) | 1 (0.4) | 4 (1.6) |
tipiracil; trifluridine | 1 (0.4) | 0 | 0 | 0 |
tislelizumab | 1 (0.4) | 0 | 1 (0.4) | 2 (0.8) |
toripalimab | 1 (0.4) | 0 | 2 (0.8) | 1 (0.4) |
TQ B2450 | 0 | 0 | 0 | 1 (0.4) |
trifluridine | 1 (0.4) | 1 (0.4) | 0 | 1 (0.4) |
zimberelimab | 0 | 0 | 0 | 1 (0.4) |
zoledronic acid | 0 | 1 (0.4) | 0 | 0 |
CAPOX = capecitabine plus oxaliplatin; FAS = full analysis set; mFOLFOX6 = modified 5-fluorouracil, folinic acid, and oxaliplatin.
Note: Data cut-offs were on September 9, 2022 (SPOTLIGHT trial), and October 7, 2022 (GLOW trial).
Sources: SPOTLIGHT trial Primary Analysis Clinical Study Report (Table 9.2.2.6.2);25 GLOW trial Primary Analysis Clinical Study Report (Table 9.2.2.6.2).25
Table 26: Summary of Included RCTs
Trial | Phase | Median follow-up | Treatment arm | Dosing | Outcome |
|---|---|---|---|---|---|
GLOW | 3 | 12.1 to 12.6 months | Zolbetuximab + CAPOX (n = 254) CAPOX (n = 253) |
| OS, PFS |
SPOTLIGHT | 3 | 12.7 to 12.9 months | Zolbetuximab + FOLFOX (n = 283) FOLFOX (n = 282) |
| OS, PFS |
FLAGS | 3 | 18.3 monthsa | SC (n = 521) CF (n = 508) |
| OS, PFS |
Ajani 2017 | 3 | 18.4 months | SC (n = 239) CF (n = 112) |
| OS, PFS |
Al-Batran, 2008 | 3 | 14.0 months | FOLFOX (n = 112) CF (n = 106) |
| OS, PFS |
Kang, 2009 | 3 | CX: 21.5 months CF: 21.4 months | CX (n = 160) CF (n = 156) |
| OS, PFS |
HERBIS-4A | 2 | 11.3 months | SC (n = 41) CX (n = 43) |
| OS, PFS |
Kim, 2019 | 2 | 12.4 months | SC (n = 45) FOLFOX (n = 44) |
| OS, PFS |
Kim, 2012 | 2 | 13.0 months | SOX (n = 65) CAPOX (n = 64) |
| OS only |
SOPP | 3 | 15.6 months | SOX (n = 173) SC (n = 164) |
| OS, PFS |
Li 2015 | 3 | NR | SC (n = 120) CF (n = 116) |
| OS only |
XParTS II | 2 | 1.5 years | SC (n = 55) CX (n = 55) |
| OS, PFS |
Popov, 2008 | 2 | 7 months | FOLFOX (n = 36) CF (n = 36) |
| OS only |
Xu, 2019 | 3 | NR | SOX (n = 279) SC (n = 279) |
| OS, PFS |
G-SOX | 3 | 25.9 months | SOX (n = 318) SC (n = 324) |
| OS, PFS |
CheckMate 649 | 3 | 24 months | Nivolumab + CAPOX/FOLFOX (n = 789; Nivo + CAPOX n = 363; Nivo + FOLFOX n = 426) CAPOX/FOLFOX (n = 792; CAPOX n = 372; FOLFOX n = 420)) |
| OS, PFS |
ORIENT | 3 | 18.8 months | Sintilimab + CAPOX (n = 323) CAPOX (n = 327) |
| OS, PFS |
ATTRACTION4 Part 1 | 2 | 13.2 months | Nivolumab + SOX (n = 21) Nivolumab + CAPOX (n = 17) |
| OS, PFS |
ATTRACTION4 Part 2 | 3 | 26.6 months | Nivolumab + CAPOX/SOX (n = 362) CAPOX/SOX (n = 362) |
| OS, PFS |
KEYNOTE-859 | 3 | NR | Pembro + CAPOX/CF (n = 790; Pembro + CAPOX n = 682; Pembro + CF n = 108) CAPOX/CF (n = 789; CAPOX n = 681; CF n = 108) |
| OS, PFS |
RATIONALE305 | 3 | 11.7 to 11.8 months | Tis + CAPOX/CF (n = 501; Tis + CAPOX n = 466; Tis + CF n = 35) CAPOX/CF (n = 496; CAPOX n = 465; CF n = 31) |
| OS, PFS |
FOLFOX = leucovorin calcium (folinic acid), fluorouracil, and oxaliplatin; FP = 5-fluorouracil and cisplatin.
Source: Network Meta-Analysis Technical Study Report.54
Appendix 2: Additional ITC Evidence
Please note that this appendix has not been copy-edited.
Primary NMA Using CAPOX and FOLFOX as Combined
A second primary NMA including all trials identified for the first primary NMA was conducted. In this analysis, CAPOX and FOLFOX were assumed to have the same efficacy based on clinical inputs and were combined in the NMA. A total of 11 unique regimens were included in the analysis. presented in Figure 13 and Figure 14. Two subgroup analyses were noted as clinically relevant by the clinical experts consulted for this review: CPS 5 or greater and CPS less than 5. Evidence networks for these subgroup analyses are presented in Figure 15 and Figure 16. However, the sponsor notes that the subgroup analysis did not use the subgroup-specific data from GLOW and SPOTLIGHT as CPS testing was not routinely conducted in those trials. CPS-specific HRs were utilized for nivolumab and pembrolizumab but not for zolbetuximab.
Figure 13: Evidence Network of OS for the Primary NMA Using CAPOX and FOLFOX Combined
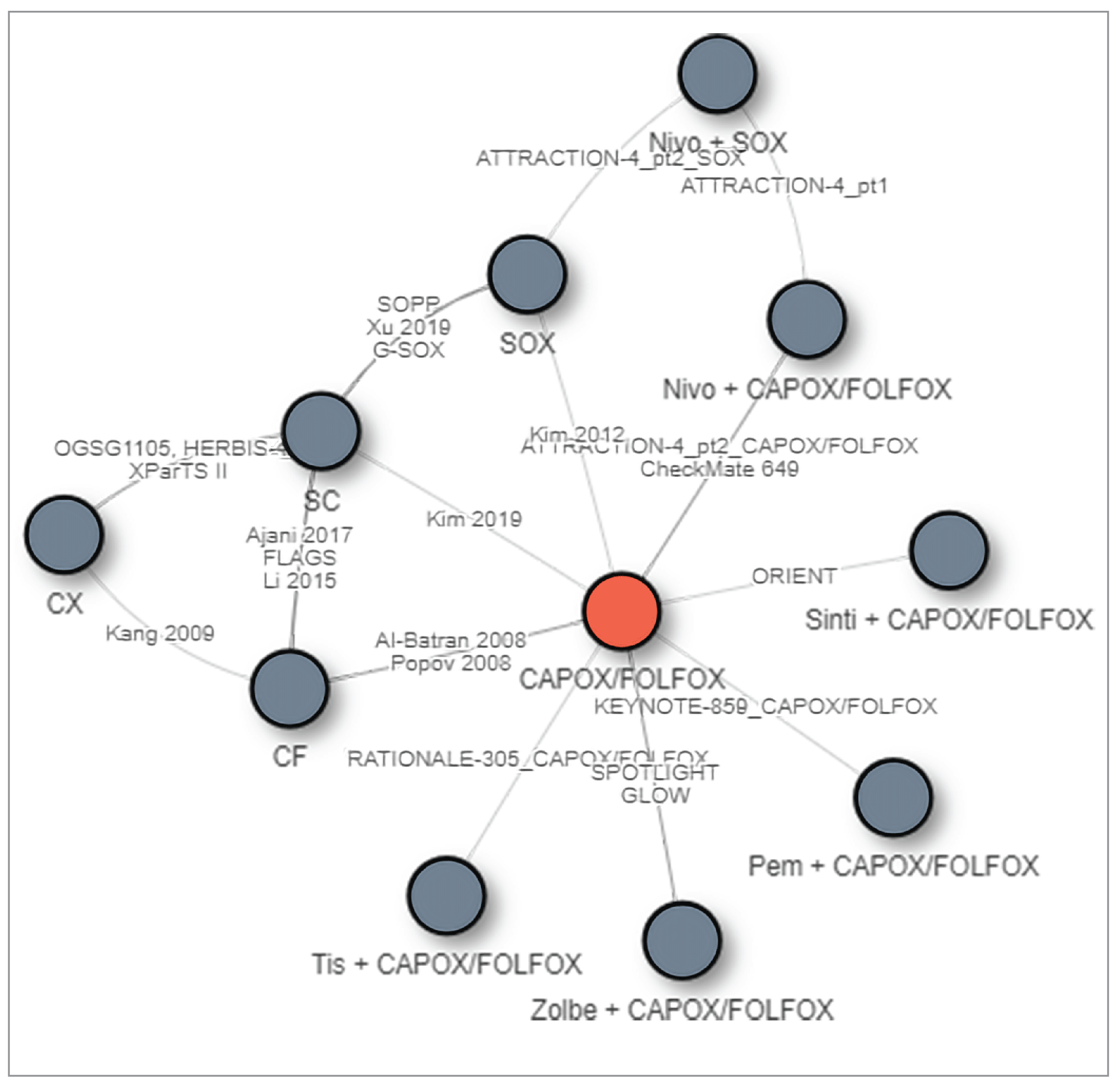
Source: Network Meta-Analysis Technical Study Report.54
Figure 14: Evidence Network of PFS for the Primary NMA Using CAPOX and FOLFOX as Combined
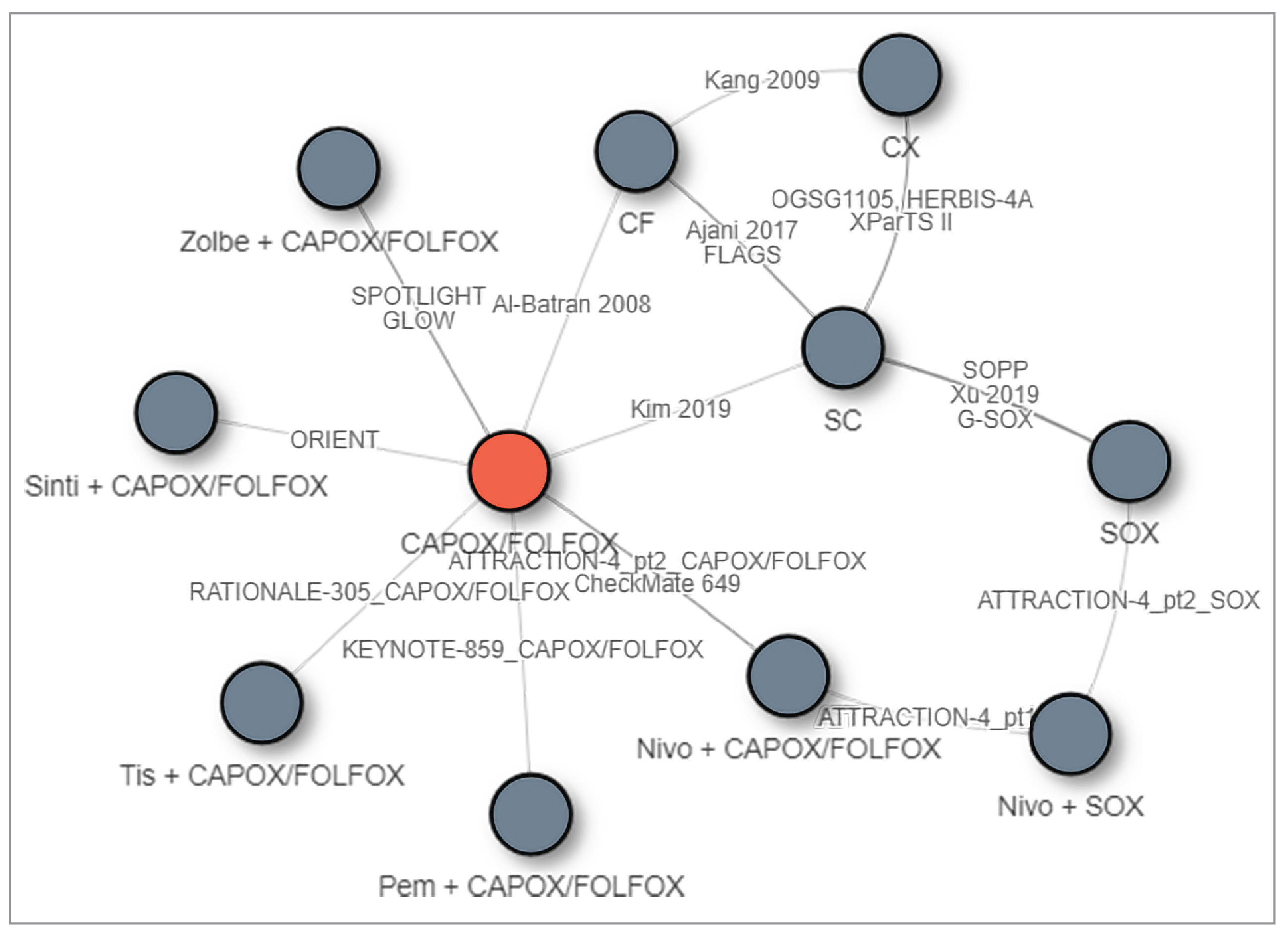
Source: Network Meta-Analysis Technical Study Report.54
Figure 15: Evidence Network of OS for Subgroup Analysis of Patients With CPS of 5 or More Using CAPOX and FOLFOX as Combined
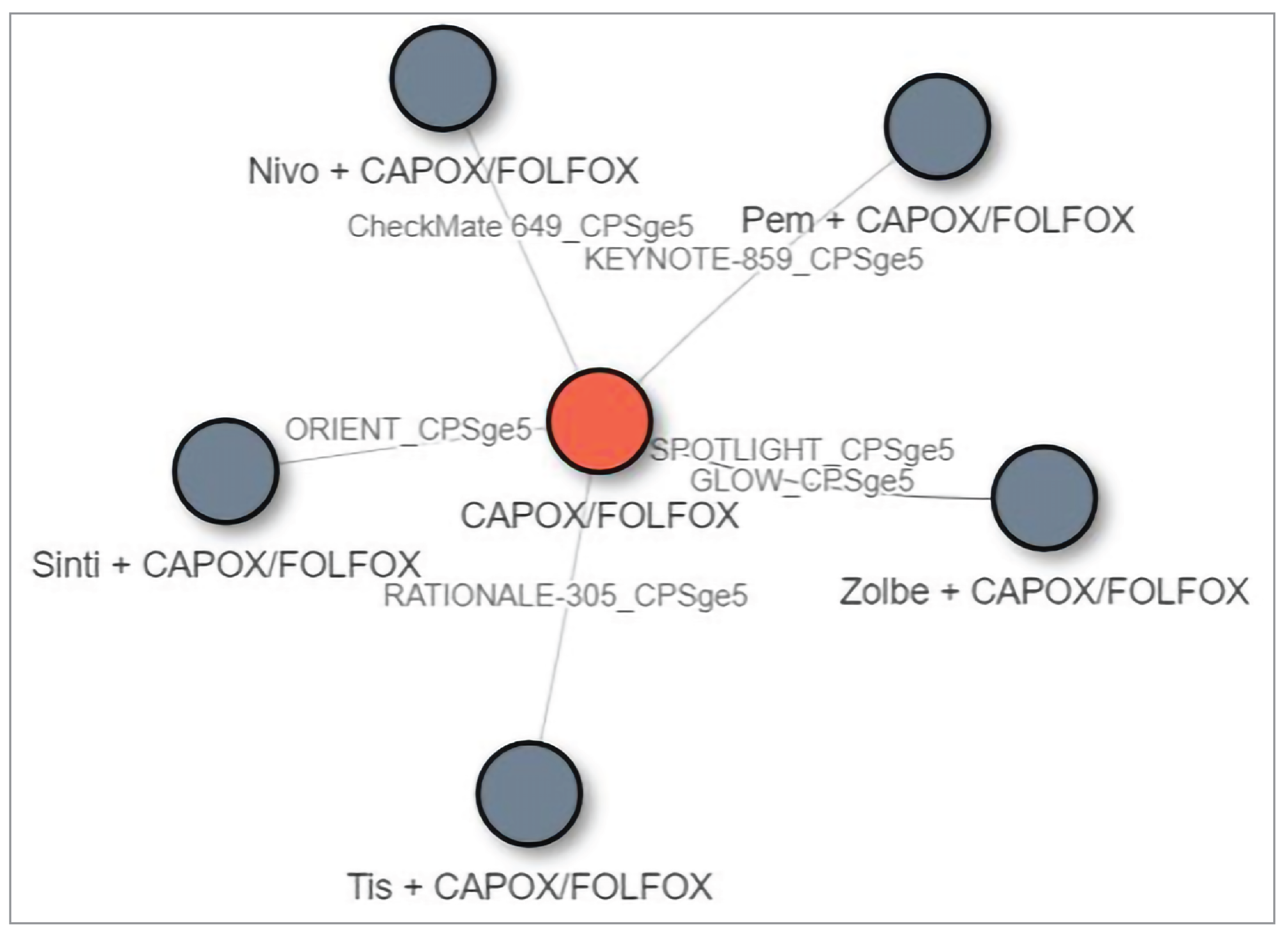
Source: Network Meta-Analysis Technical Study Report.54
Figure 16: Evidence Network of OS for Subgroup Analysis of Patients With CPS of Less Than 5 Using CAPOX and FOLFOX as Combined
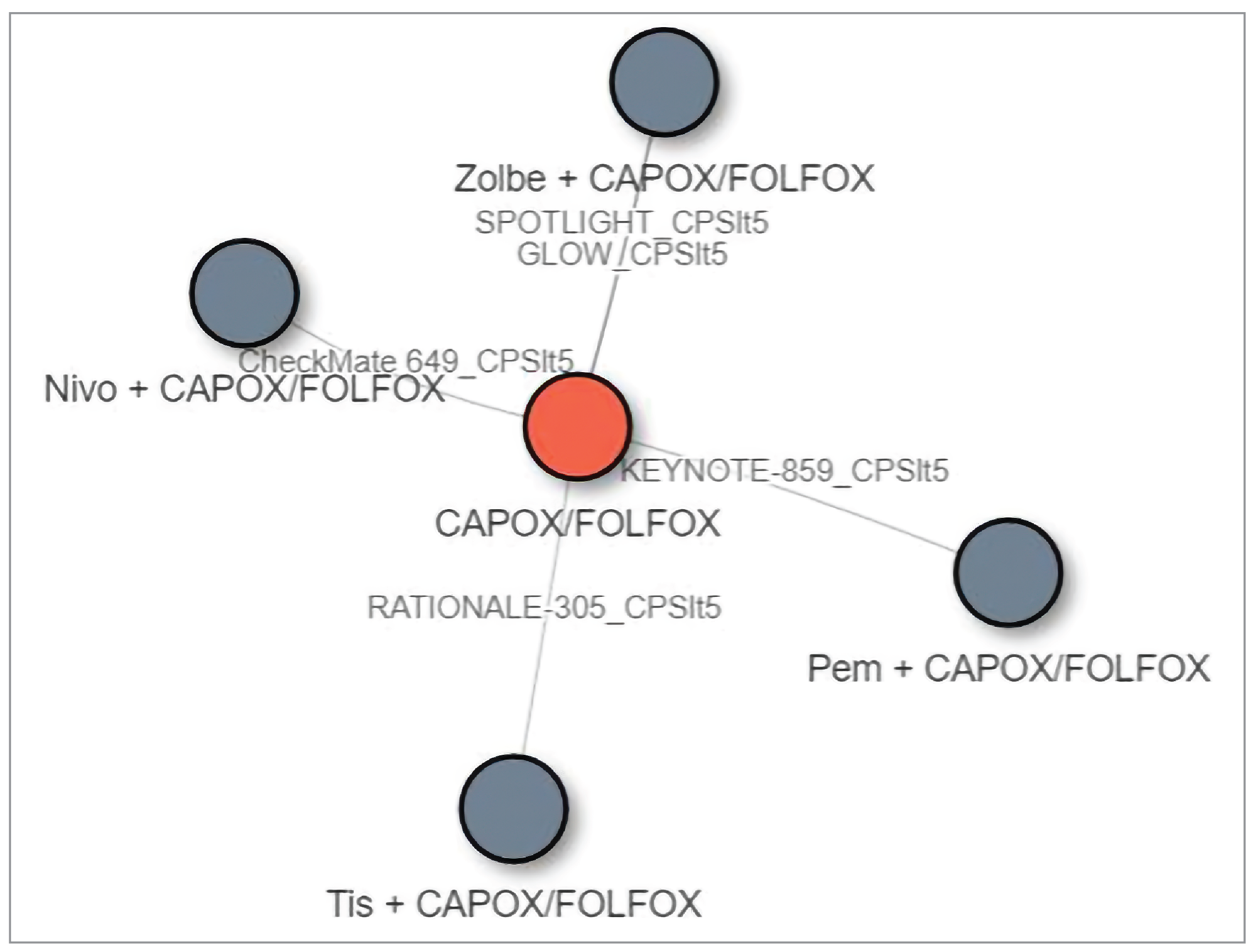
Source: Network Meta-Analysis Technical Study Report.54
Results
Primary Analysis, Using CAPOX and FOLFOX as Combined
Overall survival: The HRs and the 95% Crls across various comparisons for OS are summarized in Table 27. Results from the NMA are consistent with results of the pivotal evidence, where zolbetuximab combined with CAPOX or FOLFOX is superior to CAPOX/FOLFOX alone (HR: 0.77 [95% Crl: 0.67 to 0.89]). CrIs for the comparisons of zolbetuximab plus chemotherapy versus nivolumab or pembrolizumab plus chemotherapy presented little to no difference in OS between the treatments. In the sensitivity analyses excluding and including Asia-only trials and Asian subgroup of global trials for select regimens of interest using SOX, CAPOX and FOLFOX as combined, the findings were similar to the findings from the primary NMA.
Table 27: Pairwise Comparisons of OS for Zolbetuximab Versus Relevant Comparators in the Primary NMA With CAPOX and FOLFOX Combined, Median HR (95% Crl)
Zolbetuximab + CAPOX/FOLFOX | CAPOX/FOLFOX | Nivolumab + CAPOX/FOLFOX | Pembrolizumab + CAPOX / FOLFOX | CAPE CISP (CX) | FP (CF) |
|---|---|---|---|---|---|
Reference | 0.77 (0.67 to 0.89) | 0.97 (0.81 to 1.16) | 0.99 (0.83 to 1.19) | 0.68 (0.50 to 0.93) | 0.63 (0.50 to 0.80) |
CAPOX = capecitabine plus oxaliplatin; CF = fluorouracil and cisplatin; CrI = credible interval; CX = capecitabine and cisplatin; FOLFOX = leucovorin calcium (folinic acid), fluorouracil, and oxaliplatin; HR = hazard ratio; NR = not reported; OS = overall survival; vs. = versus.
Note: Each cell represented the comparison (HR and 95% Crl) of the row-defined treatment vs. column treatment.
Source: Network Meta-Analysis Technical Study Report.54
Progression-free survival: The HRs and the 95% Crls across various comparisons for PFS are summarized in Table 28. Results from the NMA are consistent with results of the pivotal evidence, where zolbetuximab combined with CAPOX or FOLFOX is superior to CAPOX/FOLFOX alone (HR: 0.71 [95% Crl: 0.61 to 0.83]). CrIs for the comparisons of zolbetuximab plus chemotherapy versus nivolumab or pembrolizumab plus chemotherapy presented little to no difference in PFS between the treatments. In the sensitivity analyses excluding and including Asia-only trials and Asian subgroup of global trials for select regimens of interest using SOX, CAPOX and FOLFOX as combined, the findings were similar to the findings from the primary NMA.
Table 28: Pairwise Comparisons of PFS for Zolbetuximab Versus Relevant Comparators in the Primary NMA With CAPOX and FOLFOX Combined, Median HR (95% Crl)
Zolbetuximab + CAPOX/FOLFOX | CAPOX / FOLFOX | Nivolumab + CAPOX / FOLFOX | Pembrolizumab + CAPOX / FOLFOX | CAPE CISP (CX) | FP (CF) |
|---|---|---|---|---|---|
Reference | 0.71 (0.61 to 0.83) | 0.9 (0.75 to 1.08) | 0.94 (0.78 to 1.13) | 0.79 (0.56 to 1.10) | 0.68 (0.51 to 0.89) |
CAPOX = capecitabine plus oxaliplatin; CF = fluorouracil and cisplatin; CrI = credible interval; CX = capecitabine and cisplatin; FOLFOX = leucovorin calcium (folinic acid), fluorouracil, and oxaliplatin; HR = hazard ratio
Source: Network Meta-Analysis Technical Study Report54
TPA Review
Abbreviations
CLDN18.2
Claudin 18.2
CPS
combined positive score
FFPE
formalin-fixed, paraffin-embedded
GEJ
gastroesophageal junction
GI
gastrointestinal
HER2
human epidermal growth factor receptor 2
IHC
immunohistochemistry
PD-L1
programmed death-ligand 1
Objective
The objective of this Testing Procedure Assessment is to identify and describe the health system implications of companion diagnostic testing for Claudin 18.2 (CLDN18.2) status in patients with locally advanced unresectable or metastatic human epidermal growth factor receptor 2 (HER2)-negative gastric or gastroesophageal junction (GEJ) adenocarcinoma to determine their eligibility for treatment with zolbetuximab as a first-line therapy.
Methods
The contents of this report have been informed by materials submitted by the sponsor, a literature search, and clinical expert input, as well as by input from patient and clinician groups collected as part of the review.
Materials submitted by the sponsor related to the companion diagnostic test were reviewed and summarized by the review team.
An information specialist conducted a literature search of key resources — including MEDLINE, the Cochrane Database of Systematic Reviews, the International HTA Database, and the websites of Canadian and major international health technology agencies — as well as a focused internet search. The search approach was customized to retrieve a limited set of results, balancing comprehensiveness with relevancy. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were CLDN18.2 testing and gastric or GEJ cancers. Secondary searches were conducted with search filters applied to limit retrieval to citations related to economics and equity considerations. The search was completed on July 29, 2024, and limited to English-language documents. The literature search results were screened for relevance by 1 reviewer, with relevant sources selected to support and inform this report.
Clinical expert input was provided by 2 clinical specialists with expertise in the diagnosis and management of locally advanced unresectable or metastatic gastric and GEJ adenocarcinoma.
Context
What Is CLDN18.2 Positivity in Locally Advanced Unresectable or Metastatic Gastric and GEJ Adenocarcinoma?
In the gastrointestinal (GI) tract, tight cell junctions provide a protective intestinal barrier while ensuring that water and nutrients can be absorbed by the body.1,2 Claudins are a group of transmembrane proteins that form essential components of these tight cell junctions.3 CLDN18.2 is an isoform of the Claudin family that is dominant within the GI tract.4 In healthy GI cells, CLDN18.2 is generally found deep within the tight junctions, inaccessible to antibodies, whereas in cancerous cells, CLDN18.2 may become exposed and detectable.3,4
In the sponsor-submitted SPOTLIGHT and GLOW trials of zolbetuximab, CLDN18.2 positivity was defined as greater than or equal to 75% of cells demonstrating moderate to strong membranous CLDN18.2-staining using a newly developed assay.5,6 The clinical experts consulted for the review agreed that this threshold was likely to be appropriate. CLDN18.2 positivity has been identified in up to 38% of patients with metastatic gastric and GEJ cancer.4,7,8
How Is CLDN18.2 Positivity Identified in Locally Advanced Unresectable or Metastatic Gastric and GEJ Adenocarcinoma?
CLDN18.2 positivity can be identified using molecular testing of tissue samples. These samples are collected during a biopsy performed using an endoscope, which currently occurs as part of routine diagnostic care of patients with gastric and GEJ adenocarcinoma.3,8 To verify whether a patient with locally advanced unresectable or metastatic gastric or GEJ cancer is eligible for treatment with zolbetuximab as first-line therapy, testing for CLDN18.2 positivity could be carried out when similar testing for HER2 status is performed (i.e., as part of routine care). The clinical experts consulted for the review agreed that the optimal timing of testing for CLDN18.2 status would be at the time of diagnosis, concurrently with testing for HER2 status. Testing for CLDN18.2 status could also be performed on previously collected samples for patients who have already been diagnosed to help establish their eligibility for treatment with zolbetuximab.
To date, the assessment of CLDN18.2 status has relied primarily on immunohistochemistry (IHC) testing, although other techniques — including whole transcriptome sequencing — are undergoing investigation.9
What Is Immunohistochemistry?
IHC is a staining method performed in laboratories using tissue samples collected during biopsy.10 The tissue is generally used to prepare formalin-fixed, paraffin-embedded (FFPE) samples to which an antibody is applied so it binds to and stains its antigen, allowing the biomarker of interest to be detectable using a microscope.10,11 The findings are interpreted by a pathologist, and a report is produced.3 In locally advanced unresectable or metastatic gastric and GEJ adenocarcinoma, IHC is currently used in Canada to detect HER2 status at the time of diagnosis, to provide prognostic information, and to identify therapeutic targets.12
What Is the Current Testing Practice for Gastric and GEJ Junction Adenocarcinoma in Canada?
In Canada, tissue biopsy is already part of the current standard of care for patients with suspected gastric or GEJ adenocarcinoma to confirm diagnosis and ascertain HER2 status. Tissue samples collected during biopsy are prepared using FFPE and may be saved for up to 20 years13 (which could enable their use for any future testing). Tissue samples collected through biopsy are sent to an in-house molecular pathology laboratory or centralized laboratory for processing. The results are then reviewed and interpreted by a registered pathologist.
A multidisciplinary group of health care practitioners in Canada has recommended biomarker testing in locally advanced unresectable or metastatic gastric and GEJ adenocarcinoma, including the investigation of mismatch repair proteins and programmed death-ligand 1 (PD-L1); the latter is measured by the combined positive score (CPS).8 While investigation of CLDN18.2 status in locally advanced unresectable or metastatic gastric or GEJ adenocarcinoma is not a current standard of care in Canada, the multidisciplinary group recommended reflexive testing for CLDN18.2 status as part of the standard of care.8 To implement IHC testing for CLDN18.2 status, samples collected during biopsy (or samples that were previously collected) could be used. There is currently no finite period during which the results of IHC testing are considered valid; the use of archived patient biopsy tissue for testing is considered acceptable.14
Testing Procedure Considerations
What Are Some Health System Considerations?
How Many Individuals in Canada Could Be Expected to Require IHC Testing for CLDN18.2 Status?
Gastric cancers are the fifth most common cancer type across the world.3,8 In Canada, the estimated incidence of stomach cancers (including gastric and GEJ adenocarcinomas) in 2023 was 8.6 per 100,000,8 with additional estimates indicating that 3,080 incident cases were expected in 2024 (excluding Quebec, and with no data available for the territories).15 According to a 2018 Canadian Cancer Statistics special report, approximately 90% of gastric cancer cases are adenocarcinomas, and 43.5% of gastric cancer cases are metastatic.16
If zolbetuximab were to be approved for funding in Canada, all patients with locally advanced unresectable or metastatic gastric or GEJ adenocarcinoma would be expected to require IHC testing for CLDN18.2 status — alongside IHC testing for HER2 status in newly diagnosed patients, and only for those with established HER2-negative status among previously diagnosed patients (who comprise an estimated 77% of all patients17). Using an epidemiological approach, the sponsor projected that, on average, an estimated 3,645 patients per year in Canada could require testing for CLDN18.2 status in the first 3 years if zolbetuximab were approved for funding.18 This estimate accounted for projected testing uptake during the first 3 years of implementing zolbetuximab therapy, which was estimated to reach a maximum of 85.4% of eligible patients.18
Of note, the clinical experts consulted by Canada’s Drug Agency indicated that there may be uncertainty with regard to the optimal place in therapy for zolbetuximab, given current practice and available data concerning the management of locally advanced unresectable or metastatic gastric and GEJ adenocarcinoma when based on levels of PD-L1 as measured by CPS. Specifically, while patients do not require CPS testing to obtain treatment with nivolumab (a currently available treatment option), the clinical experts expressed some uncertainty regarding the clinical effectiveness of nivolumab for patients with a CPS of less than 5. As such, it is possible that some clinicians could seek information regarding both CLDN18.2 and CPS status to guide treatment decisions, given that they could consider zolbetuximab as a preferred option for patients with CLDN18.2-positive tumours and a CPS of less than 5. Consequently, it is unclear whether this could affect the volume (e.g., require an increase) of testing for PD-L1 alongside the expected increase in IHC testing for CLDN18.2 status, if zolbetuximab were to be approved for funding.
What Is the Availability of IHC Testing for CLDN18.2 Status in Canada?
Availability
According to both the sponsor and the clinical experts consulted for the review, IHC testing is widely available in Canadian jurisdictions, including for HER2 status in locally advanced unresectable or metastatic gastric and GEJ adenocarcinoma; however, IHC testing for CLDN18.2 status is not.19 Similarly, both the sponsor and the clinical experts indicated that IHC testing for CLDN18.2 status to ascertain eligibility for treatment with zolbetuximab would best be conducted alongside standard IHC testing for HER2 status in all patients with newly diagnosed locally advanced unresectable or metastatic gastric or GEJ adenocarcinoma.19 Testing could also be conducted for previously diagnosed patients using existing samples, as available.
The sponsored clinical trials designed to assess the efficacy of zolbetuximab used a newly developed assay from Roche Diagnostics to detect CLDN18.2 positivity (i.e., the VENTANA CLDN18 [43-14A] RxDx IHC Assay, processed using the VENTANA platform).20 At the time of this review, this new assay was still under review by Health Canada. A recent sponsor-conducted assessment of 23 laboratories in Canada that currently test for HER2 status found that 12 have access to the VENTANA platform. Nonetheless, the sponsor indicated that if zolbetuximab is introduced into health systems in Canada, only a minority of patients with gastric and GEJ adenocarcinoma would be expected to receive IHC testing for CLDN18.2 status using this platform; it is anticipated that many pathology laboratories in Canada would rely on the use of lab-developed tests to detect CLDN18.2 positivity in gastric and GEJ adenocarcinoma. This is because of the anticipated upfront costs associated with investment in the newly developed VENTANA platform and/or the implementation of the VENTANA CLDN18 (43-14A) RxDx IHC Assay.21
Ensuring the availability of IHC testing for CLDN18.2 status in locally advanced unresectable or metastatic gastric and GEJ adenocarcinoma in Canada would have impacts on clinical systems and protocols, health care providers, and laboratory services. The clinical experts consulted for the review agreed that making IHC testing for CLDN18.2 status in locally advanced unresectable or metastatic gastric and GEJ adenocarcinoma available in Canada is feasible, but that impacts on pathology departments are likely, including the need for assay development or purchase and training for pathologists and laboratory staff.
Funding
IHC testing for CLDN18.2 status in locally advanced unresectable or metastatic gastric and GEJ adenocarcinoma is currently not funded across provincial and territorial health systems in Canada.
Sponsor Support for the Implementation of IHC Testing for CLDN18.2 Status in Gastric and GEJ Adenocarcinoma
To support the availability of IHC testing for CLDN18.2 status in gastric and GEJ adenocarcinoma, the sponsor has described needs assessment activities and ongoing educational initiatives to ensure awareness among health care providers across Canada. These educational initiatives consist of 4 components. The first is a global “train the trainer” program, which would include pathologists in Canada and be designed to ensure that pathology departments are prepared to implement IHC testing for CLDN18.2 status. Once trained, trainers would provide local training opportunities to colleagues within Canadian jurisdictions and institutions. The second component is access to an expert pathologist for virtual consultations to support the implementation of CLDN18.2 testing at pathology departments. Third, the sponsor has developed a digital hub designed to support the development and implementation of CLDN18.2 testing in pathology laboratories, including information to support assay interpretation and complex case management. Finally, the sponsor has committed to providing a testing proficiency program to support concordance in CLDN18.2 testing across pathology laboratories in Canada if zolbetuximab were to be approved for funding.21
What Is the Expected Timing and Frequency of IHC Testing for CLDN18.2 Status?
According to the sponsor and the clinical experts consulted for the review, testing for CLDN18.2 status would ideally be performed reflexively at the time of gastric or GEJ adenocarcinoma diagnosis for most patients. In addition to reflex testing in newly diagnosed patients, there may be opportunities and benefits to testing existing samples from patients previously diagnosed with HER2-negative gastric or GEJ adenocarcinoma to help establish eligibility for treatment with zolbetuximab.
There is some evidence indicating that CLDN18.2 status remains stable across time in most patients,14,22 which suggests that repeat testing is unlikely to be required in most cases. There is also some evidence to indicate that previously collected FFPE samples can reliably be used to test for CLDN18.2 status (although data remain limited).3 It is possible that a new sample could be required in specific circumstances, such as if a previously collected tissue sample were to be unavailable, inaccessible, or of poor quality.
What Are Some Expected Impacts of IHC Testing for CLDN18.2 Status to Health Care Infrastructure and Human Resources?
While impacts to health systems of implementing IHC testing for CLDN18.2 status in locally advanced unresectable or metastatic gastric or GEJ adenocarcinoma are anticipated if zolbetuximab were to be approved for funding, these are not expected to be substantial or disruptive, according to the clinical experts consulted for the review. Impacts on health care infrastructure could include revisions to clinical protocols for those patients who are newly diagnosed or previously diagnosed with locally advanced unresectable or metastatic gastric or GEJ adenocarcinoma to ensure that IHC testing for CLDN18.2 status would be ordered when appropriate. Impacts would be expected for pathology laboratories, where assays would have to be selected and developed; the need for additional laboratory equipment and/or resources may have to be assessed.
According to the sponsor, there could also be impacts to some health care personnel, such as workflow integration of the test for CLDN18.2 status, including training and awareness among oncologists and associated health care providers. Incorporating routine testing for CLDN18.2 status in locally advanced unresectable or metastatic gastric and GEJ adenocarcinoma would also necessitate conversations between patients and their care providers to ensure understanding of the nature of any test results.23 According to the sponsor, there are no expected increases in demand for genetic counselling services if zolbetuximab were to be approved for funding because CLDN18.2 positivity in locally advanced unresectable or metastatic gastric and GEJ adenocarcinoma is not understood to be a hereditary condition. Health administrative staff could be involved in the initial setup of revised workflows to ensure that medical records capture testing for CLDN18.2 status in patients with locally advanced unresectable or metastatic gastric and GEJ adenocarcinoma. Impacts on workload are expected for pathology laboratories, where pathologists, lab technicians, and bioinformaticians may have to undergo training to incorporate the new test for CLDN18.2 status into their work. In addition, there could be an increase in the time necessary to analyze and interpret samples for CLDN18.2.24
What Are Some Patient-Oriented Considerations?
Patient-oriented considerations for biomarker testing in locally advanced unresectable or metastatic gastric and GEJ adenocarcinoma include equitable access to testing, informed decision-making regarding testing, any potential burden associated with the procedure(s) necessary to perform the test (e.g., collection of tissue samples), the need to ensure that the implications of a positive result are clear and comprehensible, and the need to facilitate effective communication with patients and/or families.23 Because IHC testing for HER2 status is already performed as part of routine care for locally advanced unresectable or metastatic gastric and GEJ adenocarcinoma — and the clinical experts consulted for the review agree that testing for CLDN18.2 status could feasibly be incorporated within these existing testing processes (including biopsy) — the impact on patients and their families would be expected to be low.
If zolbetuximab is approved for funding, during the initial phases of introducing the therapy into health systems in Canada, there may be variable levels of patient access to testing for CLDN18.2 status. Testing may be centralized (e.g., limited to major centres only) in some or all jurisdictions, particularly during the initial phases of implementing the new treatment regimen with zolbetuximab. This could introduce challenges in access for patients living in rural and/or remote areas or for those living with socioeconomic barriers.23
Concerning sample collection, both the sponsor and clinical experts consulted for the review agreed it is unlikely that any additional procedure(s) or tissue collection would be necessary to process the test for CLDN18.2 status; therefore, testing would not impose additional burdens on patients and/or families if zolbetuximab were to be approved for funding. Notably, a recent study that investigated the addition of molecular tests in gastric cancer (including for CLDN18.2 status) using standard endoscopic samples found that, while the addition of tests was feasible, ensuring that there was a sufficient amount of tissue available was an important consideration.24
Finally, clear and effective communication and messaging for patients with locally advanced unresectable or metastatic gastric or GEJ adenocarcinoma concerning testing for CLDN18.2 status would be important. It would be incumbent upon health care providers and institutions to ensure that patients continue to have access to clear, comprehensible information to support decision-making and effective treatment during the implementation of any new testing and treatment protocols.23
What Are the Clinical Considerations?
Clinical Utility
In locally advanced unresectable or metastatic gastric and GEJ adenocarcinoma, biomarker testing can provide prognostic information, identify therapeutic targets, and support treatment response monitoring.8 The sponsor-conducted SPOTLIGHT and GLOW trials were critically appraised by Canada’s Drug Agency as part of the review, and the appraisal suggested that there is clinical utility to CLDN18.2 testing in locally advanced unresectable or metastatic gastric and GEJ adenocarcinoma because of the demonstration of a clinically meaningful benefit of the CLDN18.2-targeted therapy (zolbetuximab) compared to chemotherapy alone.5,6 Although no additional studies (outside of the sponsor-conducted studies) were found reporting direct evidence of the clinical utility of CLDN18.2 testing, best practice recommendations advise that biomarker testing in gastric or GEJ adenocarcinoma — including for CLDN18.2 status — should be part of the standard of care in Canada, based on its clinical utility in guiding effective, targeted therapy and improving patient outcomes.8
As described previously, if zolbetuximab were to be approved for funding, there may be impacts on clinical decision-making regarding optimal therapy for patients with CLDN18.2-positive tumours who have a CPS greater than or equal to 5 because it is currently unclear whether nivolumab or zolbetuximab could offer the best outcomes for these patients.
Diagnostic Accuracy
To assess concordance between various available IHC testing assays and platforms for CLDN18.2, a sponsor-funded, international, comparative study of 3 assays across 3 testing platforms among 27 laboratories (1 of which is in Canada) was conducted.20 Although Canada’s Drug Agency has not critically appraised the study, the authors concluded that a range of antibodies and platforms can reliably be used for the assessment of CLDN18.2 status in patients with gastric and GEJ adenocarcinoma.20 This conclusion supports the use of lab-developed tests. The study authors also highlighted the importance of appropriate methodology and selection of primary antibodies to ensure reliability.20 As described previously, the sponsor has committed resources to supporting the diagnostic accuracy of testing for CLDN18.2 status in Canada by providing a testing proficiency program.
What Are the Cost Considerations?
What Is the Cost of IHC Testing for CLDN18.2 Status?
The sponsor estimated the unit cost of IHC at $100 per test, based on the highest listed cost for currently funded IHC tests by Cancer Care Ontario (Schedule V).25 However, it is not yet certain whether the cost of IHC testing for CLDN18.2 status would be consistent with this estimate, and the clinical experts consulted for the review suggested that the unit cost per test could be higher. The sponsor also acknowledged that the unit cost of IHC tests for CLDN18.2 status is likely to vary across jurisdictions in Canada, depending on the assays and platforms selected by individual laboratories.
The approximate number of patients needed to test to identify 1 patient eligible for zolbetuximab was calculated by the sponsor as 3; thus, the cost of IHC testing to identify 1 patient with CLDN18.2 positivity who would be eligible for treatment with zolbetuximab was estimated at $260.63.26 However, any variability in the unit cost per test would accordingly affect the estimated cost associated with the number needed to test.
In addition to the unit cost per test, upfront costs are anticipated to support the development and establishment of IHC testing for CLDN18.2 status across jurisdictions in Canada. These anticipated costs were not quantified by the sponsor; however, the clinical experts consulted for the review suggested that costs associated with clinical workflow integration (including changes to forms and administrative health care infrastructure as well as training and awareness among treating oncologists) and costs associated with ensuring readiness among pathology departments (including awareness, training, equipment, and assay development) may be incurred as well. There may also be additional costs associated with the time needed for laboratories to process samples undergoing testing for CLDN18.2 status.24 As described previously, the sponsor has committed to initiatives that could mitigate some of these anticipated costs. However, the clinical experts consulted for the review also highlighted the opportunity for biomarker testing in gastric and GEJ adenocarcinomas to reduce overall health care costs in the longer term by helping to ensure that patients who could benefit most from a biomarker-targeted therapy can receive it while patients who are not likely to experience a particular benefit from that therapy do not.
References
1.Lee SH. Intestinal Permeability Regulation by Tight Junction: Implication on Inflammatory Bowel Diseases. Intest Res. 2015;13(1):11-18. PubMed
2.Singh AB, Sharma A, Dhawan P. Claudin family of proteins and cancer: an overview. J Oncol. 2010;2010:541957. PubMed
3.Angerilli V, Ghelardi F, Nappo F, et al. Claudin-18.2 testing and its impact in the therapeutic management of patients with gastric and gastroesophageal adenocarcinomas: A literature review with expert opinion. Pathol Res Pract. 2024;254:155145. PubMed
4.Pellino A, Brignola S, Riello E, et al. Association of CLDN18 Protein Expression with Clinicopathological Features and Prognosis in Advanced Gastric and Gastroesophageal Junction Adenocarcinomas. J Pers Med. 2021;11(11). PubMed
5.Shitara K, Lordick F, Bang YJ, et al. Zolbetuximab plus mFOLFOX6 in patients with CLDN18.2-positive, HER2-negative, untreated, locally advanced unresectable or metastatic gastric or gastro-oesophageal junction adenocarcinoma (SPOTLIGHT): a multicentre, randomised, double-blind, phase 3 trial. Lancet. 2023;401(10389):1655-1668. PubMed
6.Shah MA, Shitara K, Ajani JA, et al. Zolbetuximab plus CAPOX in CLDN18.2-positive gastric or gastroesophageal junction adenocarcinoma: the randomized, phase 3 GLOW trial. Nat Med. 2023;29(8):2133-2141. PubMed
7.Dai J, Zheng H, Jin J, Cheng Y, Xu H. Claudin18.2 expression and clinicopathological features in cytology effusion specimens from gastric adenocarcinoma: A comparative study with tissue specimens. Cancer Cytopathol. 2023;131(6):365-372. PubMed
8.Snow S, Gabrielson D, Lim H, Tehfe M, Brezden-Masley C. Best Practices for Managing Patients with Unresectable Metastatic Gastric and Gastroesophageal Junction Cancer in Canada. Curr Oncol. 2024;31(5):2552-2565. PubMed
9.Hashimoto T, Nakamura Y, Mishima S, et al. Whole-transcriptome sequencing in advanced gastric or gastroesophageal cancer: A deep dive into its clinical potential. Cancer Sci. 2024;115(5):1622-1633. PubMed
10.Magaki S, Hojat SA, Wei B, So A, Yong WH. An Introduction to the Performance of Immunohistochemistry. Methods Mol Biol. 2019;1897:289-298. PubMed
11.National Cancer Institute. Immunohistochemistry. NCI Dictionary of Cancer Terms; n.d.: https://www.cancer.gov/publications/dictionaries/cancer-terms/def/immunohistochemistry. Accessed 2024 Jul 29.
12.Canadian Cancer Society. HER2 status test. 2023: https://cancer.ca/en/treatments/tests-and-procedures/her2-status-test. Accessed 2024 Sep 10.
13.Canadian Association of Pathologists. The Retention and Use of Human Biologic Material. 2014: https://www.cap-acp.org/guide_retention-human-biologic-material.php. Accessed 2024 Aug 23.
14.Waters R, Sewastjanow-Silva M, Yamashita K, et al. Retrospective Study of Claudin 18 Isoform 2 Prevalence and Prognostic Association in Gastric and Gastroesophageal Junction Adenocarcinoma. JCO precis. 2024;8:e2300543.
15.Canadian Cancer Statistics Dashboard. Projected Cancer Cases by Geographic Region, Canada, 2024 Both Sexes, Stomach. n.d.: https://cancerstats.ca/Incidence/Region. Accessed 2024 Aug 26.
16.Canadian Cancer Statistics Advisory Committee. Canadian Cancer Statistics. 2018: https://cdn.cancer.ca/-/media/files/research/cancer-statistics/2018-statistics/canadian-cancer-statistics-2018-en.pdf. Accessed 2024 Aug 26.
17.Van Cutsem E, Bang YJ, Feng-Yi F, et al. HER2 screening data from ToGA: targeting HER2 in gastric and gastroesophageal junction cancer. Gastric Cancer. 2015;18(3):476-484. PubMed
18.Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Vyloy (zolbetuximab): lyophilised powder for concentrate for solution for intravenous infusion, 100 mg zolbetuximab single-use vials. Markham (ON): Astellas Pharma Canada, Inc.; 2024 Jun 27.
19.Clinical summary [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Vyloy (zolbetuximab): lyophilised powder for concentrate for solution for intravenous infusion, 100 mg zolbetuximab single-use vials. Markham (ON): Astellas Pharma Canada, Inc.; 2024 Jun 27.
20.Jasani B, Taniere P, Schildhaus HU, et al. Global Ring Study to Investigate the Comparability of Total Assay Performance of Commercial Claudin 18 Antibodies for Evaluation in Gastric Cancer. Lab Invest. 2024;104(1):100284. PubMed
21.Astellas Pharma Canada, Inc. response to August 6, 2024 CDA-AMC request for additional information regarding zolbetuximab CDA-AMC review. Markham (ON): Astellas Pharma Canada, Inc.; 2024 Aug 6.
22.Kubota Y, Kawazoe A, Mishima S, et al. Comprehensive clinical and molecular characterization of claudin 18.2 expression in advanced gastric or gastroesophageal junction cancer. ESMO Open. 2023;8(1):100762. PubMed
23.Snow S, Brezden-Masley C, Carter MD, et al. Barriers and Unequal Access to Timely Molecular Testing Results: Addressing the Inequities in Cancer Care Delays across Canada. Curr Oncol. 2024;31(3):1359-1375. PubMed
24.Costache S, Baltan A, Diaz McLynn S, et al. Implementing an integrated molecular classification for gastric cancer from endoscopic biopsies using on-slide tests. Rom J Morphol Embryol. 2024;65(2):257-265. PubMed
25.Schedule 5 – cancer programs. Toronto (ON): Ontario Health; n.d.: https://www.ontariohealth.ca/sites/ontariohealth/files/2020-09/7.%20CCO%20Schedule%205%20-%20Cancer%20Programs%20EN.pdf. Accessed 2024 Aug 26.
26.Key Sources and Assumptions for Economic Model Inputs Regarding the Companion Diagnostic [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Vyloy (zolbetuximab): lyophilised powder for concentrate for solution for intravenous infusion, 100 mg zolbetuximab single-use vials. Markham (ON): Astellas Pharma Canada, Inc.; 2024 Jun 27.
Pharmacoeconomic Review
Abbreviations
AE
adverse event
BIA
budget impact analysis
BSA
body surface area
CAPOX
capecitabine and oxaliplatin
CDA-AMC
Canada’s Drug Agency
CLDN18.2
Claudin 18.2
CPS
combined positive score
CUA
cost-utility analysis
DOT
duration of treatment
GEJ
gastroesophageal junction
HER2
human epidermal growth factor receptor 2
HR
hazard ratio
ICER
incremental cost-effectiveness ratio
ITT
intention to treat
KM
Kaplan-Meier
mFOLFOX6
modified leucovorin calcium (folinic acid), 5-fluorouracil, and oxaliplatin
NMA
network meta-analysis
OS
overall survival
PD-L1
programmed death-ligand 1
PFS
progression-free survival
QALY
quality-adjusted life-year
WTP
willingness to pay
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Zolbetuximab for injection (Vyloy), 100-mg single-use vial for IV infusion |
Indication | Zolbetuximab, in combination with fluoropyrimidine- and platinum-containing chemotherapy, is indicated for the first-line treatment of adult patients with locally advanced unresectable or metastatic HER2-negative gastric or GEJ adenocarcinoma whose tumours are CLDN18.2-positive, as determined by a validated test. |
Health Canada approval status | Approved |
Health Canada review pathway | Standard |
NOC date | December 13, 2024 |
Reimbursement request | As per indication |
Sponsor | Astellas Pharma Canada, Inc. |
Submission history | Previously reviewed: No |
CLDN18.2 = Claudin 18.2; GEJ = gastroesophageal junction; HER2 = human epidermal growth factor receptor 2.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Partitioned survival model |
Target population | Adult patients with locally advanced unresectable or metastatic HER2-negative, CLDN18.2-positive gastric or GEJ adenocarcinoma |
Treatment | Zolbetuximab plus mFOLFOX6a |
Dose regimen |
|
Submitted price | Zolbetuximab: $638.00 per 100 mg vial |
Submitted treatment cost | Assuming a maintenance dose of 600 mg/m2 every 3 weeks for zolbetuximab, the sponsor estimated drug acquisition costs per 21-day cycle for zolbetuximab plus mFOLFOX6 to be $10,091 in cycle 1, $7,887 in cycles 2 to 8, and $7,724 thereafter (first year: $142,250; subsequent years: $131,542). |
Comparators |
|
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs, Lys |
Time horizon | Lifetime (17 years) |
Key data sources |
|
Submitted results |
|
Key limitations |
|
CDA-AMC reanalysis results |
|
CAPOX = capecitabine plus oxaliplatin; CDA-AMC = Canada’s Drug Agency; CCO = Cancer Care Ontario; CLDN18.2 = Claudin 18.2; DOT = duration of therapy; mFOLFOX6 = modified leucovorin calcium (folinic acid), 5-fluorouracil, and oxaliplatin; GEJ = gastric or gastroesophageal junction; HER2 = human epidermal growth factor receptor 2; ICER = incremental cost-effectiveness ratio; LY = life-year; NMA = network meta-analysis; OS = overall survival; PFS = progression-free survival; q.2.w. = every 2 weeks; QALY = quality-adjusted life-year; QoL = quality of life; vs. = versus.
aThe sponsor also considered analyses using costs associated with CAPOX. The indirect treatment comparison included clinical evidence for different backbone treatment individually and combined. For the purposes of the economic evaluation, the sponsor considered mFOLFOX6 to be equivalent to CAPOX in terms of efficacy.
bAll modelled treatments (i.e., mFOLFOX6, nivolumab plus mFOLFOX6, and zolbetuximab plus mFOLFOX6) were on the cost-effectiveness frontier.
Conclusions
The sponsor submitted evidence from 2 randomized, double-blind, placebo-controlled, phase III trials (the SPOTLIGHT trial and the GLOW trial) that demonstrated that treatment with zolbetuximab for injection (subsequently referred to as zolbetuximab) in combination with fluoropyrimidine- and platinum-based chemotherapy (modified 5-fluorouracil, leucovorin, and oxaliplatin [mFOLFOX6] or capecitabine plus oxaliplatin [CAPOX]) resulted in a clinically important improvement in overall survival (OS) and progression-free survival (PFS) compared with placebo in combination with fluoropyrimidine- and platinum-based chemotherapy for the first-line treatment of patients with locally advanced unresectable or metastatic human epidermal growth factor 2 (HER2)-negative gastric or gastroesophageal junction (GEJ) adenocarcinoma whose tumours are positive for Claudin 18.2 (CLDN18.2). The sponsor considered the most relevant chemotherapy in the setting in Canada to be mFOLFOX6, which aligned with clinical expert input.
Based on clinical expert input, nivolumab plus chemotherapy was identified as the most relevant comparator. In the absence of direct evidence, the sponsor submitted a network meta-analysis (NMA) to assess the relative efficacy of zolbetuximab plus chemotherapy (i.e., mFOLFOX6, CAPOX, and a combination of the 2 chemotherapies) relative to nivolumab plus chemotherapy in the indicated population. The indirect evidence suggests there is little to no difference in treatment effect on OS and PFS between zolbetuximab and nivolumab in combination with mFOLFOX6. However, the indirect evidence is associated with uncertainty due to clinical and methodological heterogeneity between the studies included in the network, with a potential to introduce bias in the NMA results. The sponsor’s NMA is used to model OS and PFS for both zolbetuximab plus mFOLFOX6 and nivolumab plus mFOLFOX6.
The results of the CDA-AMC reanalysis are similar to the results of the sponsor’s analysis in that zolbetuximab plus mFOLFOX6 is associated with greater cost and a small number of incremental, quality-adjusted life-years (QALYs) compared with nivolumab plus mFOLFOX6. In sequential analysis, zolbetuximab plus mFOLFOX6 was associated with an incremental cost-effectiveness ratio (ICER) of $1,611,078 per QALY gained relative to nivolumab plus mFOLFOX6 (incremental cost = $56,474; incremental QALYs = 0.035). In alignment with the sponsor’s analysis, zolbetuximab plus mFOLFOX6 had a 0% probability of being cost-effective at a willingness-to-pay (WTP) threshold of $50,000 per QALY gained. The key drivers of the results were time spent in the preprogression health state and drug acquisition costs. The difference in QALYs between zolbetuximab- and nivolumab-based regimens was small, with most of the difference occurring beyond the trial period. Given that the sponsor-submitted NMA suggests that there may be little to no difference in treatment effect on OS and PFS between zolbetuximab and nivolumab in combination with mFOLFOX6, there is insufficient evidence to suggest that zolbetuximab should be priced higher than currently available immunotherapies for adult patients with locally advanced unresectable or metastatic HER2-negative gastric or GEJ adenocarcinoma.
Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, clinician groups, and drug plans that participated in the CDA-AMC review process.
Patient group input was gathered by My Gut Feeling – Stomach Cancer Foundation of Canada through an international survey of patients and caregivers affected by gastric, esophageal, and/or gastroesophageal cancer. Seventy-one percent of respondents resided in Canada. Respondents had experience with fluorouracil, leucovorin, oxaliplatin, and docetaxel (FLOT); mFOLFOX6; leucovorin calcium (folinic acid), fluorouracil, and irinotecan hydrochloride (FOLFIRI); immunotherapy in combination with chemotherapy; radiation; and surgery. The majority of respondents felt their treatment had been effective. They noted a preference for a treatment that offers a longer life and survival rate despite the side effects. Some respondents favoured treatment options that reduced the number of hospital visits. The most frequently reported adverse events (AEs) during treatment were fatigue and weight loss. None of the survey respondents had experience with zolbetuximab.
Clinician group input was received from the Ontario Health (Cancer Care Ontario) Gastrointestinal Cancer Drug Advisory Committee. The group commented that there are currently no approved treatments specifically targeting tumours that overexpress CLDN18.2. As such, standard first-line chemotherapy for metastatic, HER2-negative gastric cancer consists of chemotherapy (typically mFOLFOX6) combined with immunotherapy (nivolumab is currently funded; pembrolizumab is approved, but unfunded). The clinician group input highlighted that there has been no direct head-to-head evidence comparing first-line zolbetuximab and first-line nivolumab in the indicated population; thus, it is unclear which immunotherapy would be the preferred treatment option among select patients (e.g., CLDN18.2 overexpression and programmed death-ligand 1 [PD-L1] combined positive score [CPS] of less than 5). Clinician group input commented that treatment goals include prolonging life, delaying disease progression, and maintaining quality of life.
CDA-AMC participating drug plans commented that both nivolumab and pembrolizumab in combination with chemotherapy are relevant comparators in patients who have had no prior adjuvant nivolumab or greater than or equal to 6 months since completing adjuvant treatment but there are currently no specific treatments available for patients who are CLDN18.2 positive. Drug plans noted all incident patients eligible for zolbetuximab would require a greater than or equal to 75% expression to test positive for CLDN18.2 and treatment eligibility is dependent on a positive test. It was commented that labs across Canada will need to prepare for the CLDN18.2 test because there is currently no need for this test. Plans are anticipating that approximately 38.4% of patients will test positive for CLDN18.2 and 50% of patients will have CLDN18.2 testing routinely done at diagnosis by the time the final recommendation from CDA-AMC is available. The drug plans highlighted that zolbetuximab, relative to nivolumab and pembrolizumab, will require significant additional time to prepare, has a longer administration time, and has a shorter stability, such that if the infusion time exceeds 6 hours from the time of preparation, the infusion bag must be discarded and a new bag prepared. The drug plans also commented that the management of AEs, specifically hypersensitivity and infusion-related reactions, will need to be considered.
Several of these concerns were addressed in the sponsor’s model:
Nivolumab plus mFOLFOX6 was included as a comparator.
AEs were included.
Testing costs associated with CLDN18.2 were included.
CDA-AMC was unable to address the following concerns raised in the patient, clinician, and drug plan input:
CDA-AMC was unable to consider pembrolizumab in the cost-utility analysis (CUA) owing to model structure and a lack of data.
CDA-AMC was unable to consider all relevant administration costs (i.e., nursing resources, pharmacist resources, and chair time).
CDA-AMC was unable to consider the impact of hypersensitivity and infusion-related reactions.
Economic Review
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted a CUA comparing zolbetuximab in combination with mFOLFOX6 (zolbetuximab plus mFOLFOX6) to nivolumab in combination with mFOLFOX6 (nivolumab plus mFOLFOX6) and mFOLFOX6 alone for adult patients with locally advanced unresectable or metastatic HER2-negative, CLDN18.2-positive gastric or gastric or GEJ adenocarcinoma. The modelled population was aligned with the intention-to-treat (ITT) population in the SPOTLIGHT trial and the proposed Health Canada–indicated population.1-3
Zolbetuximab is available as a 100 mg, single-use vial for IV infusion at a submitted price of $638.00 per vial.1 The recommended dose of zolbetuximab is 800 mg/m2 on day 1 of cycle 1 followed by 600 mg/m2 every 3 weeks or 400 mg/m2 every 2 weeks through IV until disease progression or unacceptable toxicity.4 The sponsor assumed that mFOLFOX6 is administered intravenously per the SPOTLIGHT trial as follows: 85 mg/m2 of oxaliplatin every 2 weeks (up to 24 weeks), 400 mg/m2 of folinic acid every 2 weeks, 400 mg/m2 of 5-fluorouracil (bolus) every 2 weeks, and 2,400 mg/m2 of 5-fluorouracil (infuser) every 2 weeks.5 Zolbetuximab is infused over a minimum of 2 hours, regardless of how frequently it is administered.4 Based on a previous CDA-AMC reimbursement review,6 the sponsor assumed the following costs for oxaliplatin, folinic acid, 5-fluorouracil as $36.27 per 50 mg vial; $74.41 per 500 mg vial; and $160.90 per 5,000 mg vial, respectively.1 Assuming no wastage (i.e., perfect vial-sharing) and a maintenance dose of 600 mg/m2 every 3 weeks, the sponsor estimated drug acquisition costs per 21-day cycle for zolbetuximab plus mFOLFOX6 to be $10,090.86 in cycle 1, $7,887.15 in cycles 2 to 8, and $7,723.93 thereafter (first year cost = $142,250 [zolbetuximab = $131,542]; subsequent years’ cost = $121,919 [zolbetuximab = $119,306]).1
The sponsor assumed that nivolumab was administered intravenously at a dosage of 240 mg every 2 weeks for a maximum of 2 years or until disease progression or unacceptable toxicity.1,6,7 The recommended dosage for mFOLFOX6 is the same across the modelled treatments (i.e., zolbetuximab plus mFOLFOX6, nivolumab plus mFOLFOX6, and mFOLFOX6). Nivolumab is infused over 30 minutes.8 Assuming wastage, the sponsor estimated drug acquisition costs per 21-day cycle for nivolumab plus mFOLFOX6 and mFOLFOX6 to be $7,909.13 and $869.15, respectively, in cycles 1 to 8, and $7,745.91 and $705.93, respectively, thereafter (nivolumab plus mFOLFOX6 year 1 and subsequent year costs = $140,732 and $134,262, respectively; mFOLFOX6 year 1 and subsequent year costs = $14,012 and $12,236, respectively).1
The clinical outcomes modelled were OS, PFS, and duration of treatment (DOT). The model simulated life-years, QALYs, and costs for each treatment over a lifetime time horizon (17 years), discounted at a rate of 1.5% per annum. The analysis was undertaken from the perspective of the Canadian public health care payer.
Model Structure
The sponsor submitted a partitioned survival model with 3 health states: preprogression, postprogression, and death, with transitions between health states occurring on a weekly cycle length (refer to Appendix 3, Figure 1).1 The proportion of patients in each health state was estimated over time based on the OS and PFS curves for each intervention. All patients entered the model in the preprogression health state, at which time they received either zolbetuximab plus mFOLFOX6, nivolumab plus mFOLFOX6, or mFOLFOX6 alone, with state occupancy defined by PFS. During each cycle, patients remained progression-free, transitioned to the postprogression state, or progressed to death. Death was modelled as an absorbing state. The proportion of patients in the postprogression state was calculated by subtracting the proportion of patients alive and progression-free (based on the PFS curve) from the proportion of patients alive (based on the OS curve). Patients in the postprogression state could either remain in this state or transition to death (i.e., patients could not return to the preprogression state).
Model Inputs
Baseline patient characteristics in the model reflected patients enrolled in the SPOTLIGHT trial. The average patient in the modelled cohort, which the sponsor assumed reflected the population of patients in Canada, was aged 59.3 years, weighed 65.04 kg, had a mean body surface area (BSA) of 1.74 m2, and was more likely to be male (62.12%). Weight and BSA were used to calculate treatment costs for treatments with weight- or BSA-based dosing. Age and the proportion of the population who were male were used to assign age- and sex-specific mortality and to cap the lower bound for all-cause mortality in the model.
The key clinical efficacy inputs (i.e., OS and PFS) for mFOLFOX6 were based on individual patient data from the ITT population of the SPOTLIGHT trial (final data cut-off September 8, 2023). Efficacy inputs for zolbetuximab plus mFOLFOX6 and nivolumab plus mFOLFOX6 were based on the results of the sponsor’s NMA, which incorporated data from the ITT population from the SPOTLIGHT trial (final data cut-off September 8, 2023) and the CHECKMATE 649 trial (nivolumab plus mFOLFOX6 versus mFOLFOX6) (data cut-off May 27, 2020).9
The sponsor used a piecewise extrapolation approach, modelling survival using the Kaplan-Meier (KM) curve from the clinical study up to the switch point and applying parametric estimation beyond the Kaplan-Meier curve. The sponsor selected a switch point based on criterion 1 specified by Gebski et al.10 The chosen parametric survival distribution for OS and PFS for mFOLFOX6 was KM plus log-logistic (OS switch point = 190 weeks; PFS switch point = 139 weeks). Several parametric functions were fitted to the OS and PFS data to select candidate distributions based on diagnostic plots, goodness-of-fit statistics, visual inspection, and the clinical plausibility of long-term projections, as determined by clinical experts and external data sources. The sponsor suggested that the proportional hazards assumption was not violated, based on a nonsignificant relationship between residuals and time in the Schoenfeld residuals plot and because the treatment curves are approximately parallel in the log-cumulative hazard plot. As a result, the sponsor applied hazard ratios (HRs) for each outcome from the NMA to the reference mFOLFOX6 curve. For OS, the sponsor reported HRs of 0.77 for zolbetuximab plus mFOLFOX6 and ████ for nivolumab plus mFOLFOX6. For PFS, the sponsor reported HRs of 0.71 for zolbetuximab plus mFOLFOX6 and ████ for nivolumab plus mFOLFOX6. The sponsor’s base case assumed no waning of treatment effect, implying that the predicted benefit associated with zolbetuximab would be maintained indefinitely throughout the lifetime horizon of the model. Postprogression treatment outcomes were not explicitly modelled. The sponsor assumed that the OS data reflected the survival benefit of subsequent therapies.
The sponsor modelled DOT for zolbetuximab plus mFOLFOX6 and mFOLFOX6 based on individual patient-level data from the SPOTLIGHT trial. In the model, patients received preprogression treatments (i.e., either zolbetuximab plus mFOLFOX6, nivolumab plus mFOLFOX6, or mFOLFOX6) based on the modelled DOT curve. DOT was capped by PFS (i.e., DOT could not be greater than PFS). For mFOLFOX6, the sponsor chose a KM plus log-logistic distribution (switch point: 187 weeks). For zolbetuximab plus mFOLFOX6 and nivolumab plus mFOLFOX6, DOT was modelled as 2 separate components, with 1 DOT curve for the immunotherapy and 1 DOT curve for the mFOLFOX6 component of the regimen. For the zolbetuximab component of zolbetuximab plus mFOLFOX6 DOT, the sponsor chose a KM plus gamma distribution (switch point: 187 weeks). For the mFOLFOX6 component of zolbetuximab plus mFOLFOX6 DOT, the sponsor chose a KM plus Gompertz distribution (switch point: 187 weeks). The sponsor modelled DOT for nivolumab plus mFOLFOX6 based on the median DOT reported in the CHECKMATE 649 trial7 and assuming an exponential distribution (i.e., constant risk of discontinuation). The median DOT for the nivolumab component of nivolumab plus mFOLFOX6 was 6.7 months.1 The median DOT for the mFOLFOX6 component of nivolumab plus mFOLFOX6 was 5.9 months.1
Health state utility values applied in the economic model were based on the results of the EQ-5D-5L administered to the population in the SPOTLIGHT trial. The sponsor applied Canadian preference weights based on Xie et al.11 Utility values for the preprogression and postprogression health states were █████ and █████, respectively. The sponsor adjusted health state utility values by age- and sex-matched general population utility values from Yan et al.12 Disutilities for AEs were sourced from the literature and applied as a one-time utility decrement in the first model cycle.13-15 AEs in the model were restricted to grade 3 or 4 events that occurred in at least 5% of patients in the SPOTLIGHT trial or the nivolumab plus chemotherapy arm of the CHECKMATE 649 trial.5,7 Modelled AEs were nausea, diarrhea, vomiting, anemia, decreased appetite, platelet count decrease, neutrophil count decrease, neutropenia, lipase increase, asthenia, white blood cell count decrease, and peripheral sensory neuropathy.
The sponsor’s base case included costs for drug acquisition (preprogression and postprogression), drug administration, AEs, disease management, CLDN18.2 testing, and terminal care. Drug acquisition costs for zolbetuximab were based on sponsor-submitted prices.1 All other treatment costs were sourced from a previous CADTH Reimbursement Report.16 A proportion of patients were assumed to receive subsequent therapy, informed by the SPOTLIGHT trial, incurring a lump-sum postprogression treatment cost at the point of progression. The sponsor assumed postprogression therapy would consist of ramucirumab with paclitaxel and paclitaxel monotherapy.1 The distribution of subsequent treatments, derived from the SPOTLIGHT trial, was assumed to be the same, irrespective of the previous treatment received.2,5 The sponsor assumed that the proportion of patients receiving subsequent treatment after nivolumab plus mFOLFOX6 was the same as the proportion receiving zolbetuximab plus mFOLFOX6. The duration of subsequent therapy was derived from median PFS, as reported by Gomez-Ulloa et al.17 Drug administration costs were derived from the Ontario Schedule of Benefits (oral = $25.75; IV = $105.15; subcutaneous = $3.89).18 AE costs were derived from the Canadian Institute for Health Information Patient Cost Estimator.19 Disease management resource use was sourced from the literature13,20-22 and multiplied by costs sourced from the Ontario Schedule of Benefits for Physician Services and Closing the Gap Healthcare.23,24 Patients receiving zolbetuximab plus mFOLFOX6 were assumed to incur a one-off CLDN18.2 testing cost. Based on the proportion of screened patients with CLDN18.2-positive expression in the SPOTLIGHT trial (38.4%),2 the sponsor assumed that 3 CLDN18.2 tests were required to identify 1 patient with CLDN18.2-positive expression. Using the highest immunohistochemistry test cost from Cancer Care Ontario ($100),25 the sponsor estimated that it costs $260.63 to detect 1 patient with CLDN18.2-positive expression. Lastly, a 1-time terminal care cost was included, encompassing expenses related to end-of-life care based on estimates from the literature.26 All costs were reported in 2024 Canadian dollars; prices were inflated using the Consumer Price Index, where required.27,28
Summary of Sponsor’s Economic Evaluation Results
All analyses were run probabilistically (2,000 iterations for the base-case and scenario analyses). The deterministic and probabilistic results were similar. The probabilistic findings are presented here.
Base-Case Results
The submitted analysis was based on publicly available prices of the comparator treatments. Results from the base case of the submitted economic evaluation are presented in Table 3. Additional results from the sponsor’s submitted economic evaluation base case are presented in Appendix 3.
In the sponsor’s submitted base case, the expected total costs and QALYs over a lifetime horizon (i.e., 17 years) for zolbetuximab plus mFOLFOX6 were $247,004 and 2.03 QALYs, respectively. All modelled treatments (zolbetuximab plus mFOLFOX6, nivolumab plus mFOLFOX6, and mFOLFOX6 alone) were on the cost-effectiveness frontier, representing optimal treatment strategies. In sequential analysis, zolbetuximab plus mFOLFOX6 was associated with an ICER of $481,803 per QALY gained relative to nivolumab plus mFOLFOX6 (incremental cost = $40,988; incremental QALYs = 0.09) (Table 3). Approximately 60.6% of the incremental QALYs for zolbetuximab plus mFOLFOX6 relative to nivolumab plus mFOLFOX6 — and 50% of the incremental QALYs for zolbetuximab plus mFOLFOX6 relative to mFOLFOX6 alone — were gained during the extrapolated period of the model (i.e., beyond the maximum follow-up time of 4.5 years observed in the SPOTLIGHT trial). In the sponsor’s analysis, zolbetuximab plus mFOLFOX6 had a 0% probability of being cost-effective at a WTP threshold of $50,000 per QALY gained. The key drivers of the results were time spent in the preprogression health state and drug acquisition costs.
Table 3: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total costs ($) | Total QALYs | Sequential ICER ($/QALY) |
|---|---|---|---|
mFOLFOX6 | 119,949 | 1.51 | Reference |
Nivolumab plus mFOLFOX6 | 206,016 | 1.95 | 196,669 vs. mFOLFOX6 |
Zolbetuximab plus mFOLFOX6 | 247,004 | 2.03 | 481,803 vs. nivolumab plus mFOLFOX6 |
mFOLFOX6 = modified leucovorin calcium (folinic acid), 5-fluorouracil, and oxaliplatin; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; vs. = versus.
Source: Sponsor’s pharmacoeconomic submission.1
Sensitivity and Scenario Analysis Results
The sponsor conducted various scenario analyses to assess the following considerations: factoring in relative dose intensities and treatment waning; adopting a shorter time horizon (15 years); applying discount rates for comparators (mFOLFOX6 or CAPOX, zolbetuximab plus mFOLFOX6 or CAPOX, nivolumab plus mFOLFOX6 or CAPOX); applying parametric distributions for mFOLFOX6 PFS and switch points for the mFOLFOX6 alone KM plus parametric extrapolations; excluding wastage, postprogression treatment costs, and the utility age adjustment; and informing zolbetuximab efficacy (PFS and OS) relative to mFOLFOX6 based on the per-protocol set population. No scenario analysis was conducted using a perspective other than the health care payer.
The sponsor’s results for the conducted scenario analyses were aligned with the sponsor’s base case in that zolbetuximab plus mFOLFOX6 was more costly and more effective than mFOLFOX6 alone and nivolumab plus mFOLFOX6. In the scenario that only modelled mFOLFOX6 or CAPOX, zolbetuximab plus mFOLFOX6 or CAPOX, and nivolumab plus mFOLFOX6 or CAPOX, zolbetuximab plus CAPOX or mFOLFOX6 was associated with an ICER of $400,093 per QALY gained relative to nivolumab plus CAPOX or mFOLFOX6.
CDA-AMC Appraisal of the Sponsor’s Economic Evaluation
CDA-AMC identified several key limitations to the sponsor’s analysis that have notable implications on the economic analysis:
The comparative efficacy of zolbetuximab plus mFOLFOX6 relative to nivolumab plus mFOLFOX6 is uncertain: There is a lack of direct head-to-head evidence comparing zolbetuximab plus mFOLFOX6 and nivolumab plus mFOLFOX6. To estimate OS and PFS for zolbetuximab plus mFOLFOX6 and nivolumab plus mFOLFOX6, the sponsor first extrapolated the available OS and PFS data for mFOLFOX6 from the SPOTLIGHT trial. The sponsor then applied the findings of the sponsor-submitted NMA in previously untreated adults with pathologically confirmed metastatic or locally advanced unresectable or recurrent gastric or GEJ adenocarcinoma who are HER2-negative.9 The sponsor assumed proportional hazards and applied the relevant HR for each outcome and treatment from the NMA to the reference mFOLFOX6 curve to derive OS and PFS for zolbetuximab plus mFOLFOX6 and nivolumab plus mFOLFOX6. The CDA-AMC Clinical Review Report noted that the comparisons of zolbetuximab plus mFOLFOX6 versus nivolumab plus mFOLFOX6 suggested little to no difference in treatment effect on OS or PFS. There are sources of clinical and methodological heterogeneity across trials included in the NMA that may have biased the effect estimates of the NMA, but the magnitude and direction of potential bias cannot be predicted. As such, no robust comparative evidence was provided to support a price premium for zolbetuximab compared with nivolumab. CDA-AMC notes that uncertainty in the sponsor’s NMA directly translates into uncertainty in the modelled OS and PFS curves for zolbetuximab plus mFOLFOX6 and nivolumab plus mFOLFOX6 because these are directly modelled using the HRs derived in the NMA.
CDA-AMC was unable to address this limitation in reanalyses owing to a lack of data.
The long-term efficacy of zolbetuximab plus mFOLFOX6 is uncertain: In the sponsor’s base case, approximately 60% of incremental QALYs and incremental life-years for zolbetuximab plus mFOLFOX6 relative to nivolumab plus mFOLFOX6 (and 50% of these for zolbetuximab plus mFOLFOX6 relative to mFOLFOX6 alone) were gained in the extrapolated period of the model (i.e., beyond the maximum follow-up time of 4.5 years observed in the SPOTLIGHT trial). Therefore, because a large proportion of the incremental benefit associated with zolbetuximab plus mFOLFOX6 was gained in the extrapolated period of the model, the sponsor’s assumptions related to the durability of zolbetuximab’s treatment effect (i.e., parametric survival curve selected, the assumption of proportional hazards, and treatment waning) are highly influential. Furthermore, the proportion of patients informing the KM curves in the SPOTLIGHT trial beyond 36 months were low (i.e., < 10% of the baseline population), and there was notable censoring of patients. As a result, while the results were clinically meaningful, there is uncertainty regarding the magnitude of the longer-term treatment effects. Although the sponsor assumed a log-logistic distribution for the parametric portions of both the mFOLFOX6 PFS and OS curves (i.e., the reference curve to which the HR derived from the sponsor-submitted NMA was applied), the clinical expert input noted that all the alternative distributions for the mFOLFOX6 reference curve were clinically plausible. Thus, the distributions selected by the sponsor are associated with uncertainty. For example, the sponsor’s modelling of OS estimates that approximately 12% of the cohort treated with zolbetuximab plus mFOLFOX6 would be alive 5 years after initiating treatment. However, the alternative curves deemed reasonable by clinical experts estimate that approximately 4% of the cohort would remain alive. The clinical expert input noted that the shapes of the parametric curves were uncertain because there is a lack of long-term evidence on the durability of zolbetuximab’s treatment effect.
In the submitted model, the sponsor assumed that the treatment effect of zolbetuximab plus mFOLFOX6 was experienced indefinitely among patients remaining on treatment and that the proportional hazards assumption is valid (i.e., the assumption that the relative hazard remains constant over time across the intervention groups in both the observed and extrapolated periods). The clinical experts consulted by CDA-AMC for this review noted that there is currently a lack of long-term evidence available to substantiate the sponsor’s assumptions. They indicated that targeted therapies, such as zolbetuximab, do not provide the same durability of effect as more broadly used immunotherapies (such as nivolumab and pembrolizumab); their experience has been that patients eventually develop a resistance to targeted therapy. As such, the experts noted that zolbetuximab plus mFOLFOX6 is unlikely to maintain the treatment effect indefinitely and that the treatment effect of zolbetuximab plus mFOLFOX6 is likely to wane toward mFOLFOX6 alone after 3 to 5 years. Thus, the proportional hazards assumption is likely violated in the long term because proportional hazards can be assumed only if a credible argument based on the epidemiology of disease and the mechanism of action of the interventions is provided.29 Additionally, CDA-AMC notes that, based on visual observation of the log-cumulative hazard plots for zolbetuximab plus mFOLFOX6 relative to mFOLFOX6, the proportional hazards assumption is imperfect in the short term as well. The clinical experts emphasized that they do not expect the treatment effect of zolbetuximab to be maintained as well as that of nivolumab.
Lastly, CDA-AMC notes that the sponsor employed a piecewise extrapolation approach, modelling survival using the clinical study KM data up to week 190 for mFOLFOX6 OS, week 130 for mFOLFOX6 PFS, and week 187 for mFOLFOX6 and zolbetuximab plus mFOLFOX6 DOT, with parametric estimation utilized exclusively thereafter. By fitting the parametric curve to all observed data, a more realistic hazard rate is derived by effectively mitigating the “stepped” characteristic observed in a KM curve, which is generally preferred. CDA-AMC notes that the sponsor applied an HR to the mFOLFOX6 curve to extrapolate both zolbetuximab plus mFOLFOX6 and nivolumab plus mFOLFOX6 rather than independently modelling the KM data. Consequently, the adoption of a fully parametric curve in the sponsor's base case has marginal influence.
The CDA-AMC base case assumed that the treatment effect for zolbetuximab plus mFOLFOX6 wanes to match the efficacy of mFOLFOX6 alone at 5 years. Additionally, the full parametric survival curves for OS, PFS, and DOT were used for all treatments.
CDA-AMC conducted a scenario analysis assuming that the treatment effect for zolbetuximab plus mFOLFOX6 wanes to match the efficacy of mFOLFOX6 alone at 3 years. The time point selected was based on the clinical expert input received during the review process.
Drug acquisition and administration costs are uncertain: First, the sponsor assumed that nivolumab is administered at a fixed dose of 240 mg every 2 weeks, in alignment with both the Health Canada product monograph–recommended dosing and the dosing used in the CHECKMATE-649 pivotal trial.8,30 However, per the product monograph listed by Cancer Care Ontario and as noted by CDA-AMC participating drug plans, weight-based dosing is commonly used across Canada (i.e., 3 mg/kg up to a maximum of 240 mg every 2 weeks). Based on the baseline patient characteristics utilized in the model, the use of a fixed dose of 240 mg for nivolumab overestimated the costs for nivolumab and biased the relative costs in favour of zolbetuximab.
Second, the sponsor assumed that the maintenance dose of zolbetuximab was 600 mg/m2 every 3 weeks when used in combination with mFOLFOX6, in alignment with the dosage in the SPOTLIGHT trial.5 The submitted product monograph provides 2 maintenance dose schedules: 600 mg/m2 every 3 weeks and 400 mg/m2 every 2 weeks.4 Additionally, the product monograph states that “the cycle duration of [zolbetuximab] is determined based on the respective chemotherapy backbone.”4 While zolbetuximab was administered every 3 weeks in the SPOTLIGHT trial, the sponsor submitted additional evidence stating that:
“…The proposed dosing regimen of 800/400 mg/m2 every 2 weeks will be comparable to the dosing regimen of 800/600 mg/m2 every 3 weeks used in the phase III studies in terms of efficacy and safety and will be a valuable alternative regimen that can be used in combination with mFOLFOX6. An every 2 week dosing regimen for zolbetuximab will facilitate synchronous dosing with mFOLFOX6 thereby reducing the hospital visit burden for the patient.”31
Clinical experts consulted by CDA-AMC for this review agreed that zolbetuximab is likely to be administered every 2 weeks to reduce the number of overall visits required for treatment. CDA-AMC notes that the annual cost of zolbetuximab is impacted when assuming administration every 3 weeks versus every 2 weeks. The direction and magnitude of impact are highly sensitive to the assumed BSA and the number of vials required to achieve the recommended dosage. Because zolbetuximab is packaged as single-use vials, wastage of unused product may be associated with considerable costs. CDA-AMC notes that the impact of patient characteristics (i.e., body weight and BSA) on product wastage is not an issue that is solely attributed to zolbetuximab; it may also be relevant to the other modelled treatments included in this review.
Third, the sponsor assumed that all regimens administered intravenously have an administration cost of $105.15.1,18 The sponsor did not consider all relevant administration costs (i.e., nursing resources, pharmacist resources, and chair time). Input from participating drug plans noted that the product monograph for zolbetuximab states that zolbetuximab should be administered over a minimum of 2 hours, whereas the administration of nivolumab (and pembrolizumab) occurs over 30 minutes. As such, zolbetuximab would require additional nursing resources and chair time. Furthermore, it was noted that zolbetuximab is associated with increased preparation time because it is available in 100 mg vials and must be reconstituted with 5 mL of diluent; the mixture must then be drawn up and added to an infusion bag. However, both nivolumab and pembrolizumab are available as solutions. Therefore, zolbetuximab will take more time for health care professionals to prepare; and depending on the number of vials required to achieve the recommended dose, the preparation time may be substantial and may lead to wastage of the product. As a result, administration costs are underestimated and likely biased in favour of zolbetuximab.
Fourth, wastage of unused product was inappropriately considered for fluorouracil and folinic acid (i.e., leucovorin). Costs for fluorouracil were based on the price of bulk pharmacy vials (50 g/100 mL). CDA-AMC notes that bulk pharmacy vials are intended to be used for multiple doses, as detailed by the fluorouracil product monograph;32 thus, the inclusion of wastage for unused product did not align with its intended use. Additionally, the sponsor considered only the largest vial size of folinic acid (i.e., 500 mg/50 mL) in cost calculations and assumed wastage of unused product, despite a smaller vial size (i.e., 50 mg/5 mL) being available. The sponsor’s assumptions pertaining to wastage overestimate the amount of product wasted and the treatment acquisition costs.
Lastly, CDA-AMC notes that the list price of oxaliplatin informing the sponsor’s analysis, retrieved from a previous CDA-AMC Reimbursement Review Report,6 is now out of date. The list price, per IQVIA DeltaPA, has increased.33
The CDA-AMC base case assumed a weight-based dose of 3 mg/kg up to a maximum of 240 mg every 2 weeks for nivolumab and a maintenance dose of 400 mg/m2 every 2 weeks for zolbetuximab. Additionally, CDA-AMC corrected the sponsor’s assumption of wastage for the bulk pharmacy vial of fluorouracil, considered the smallest vial size of folinic acid (50 mg/5 mL) in cost calculations, and revised the price of oxaliplatin from $36.27 to $45.00 per 50 mg/10mL vial.
CDA-AMC was unable to consider all relevant administration costs (i.e., nursing resources, pharmacist resources, and chair time) owing to the model structure and notes that administration costs are underestimated and likely biased in favour of zolbetuximab.
Health state utility values are associated with uncertainty: The health state utility values applied in the economic model were derived from the results of the EQ-5D-5L administered to the population in the SPOTLIGHT trial, with Canadian preference weights sourced from Xie et al. applied.11 The sponsor further adjusted health state utility values by age- and sex-matched general population utility values from Yan et al.12 Based on the sponsor’s derived utility value for the preprogression health state (█████), patients who have not yet progressed on treatment have a quality of life that is similar to the average health utility for individuals aged 55 years to 59 years in Canada, at 0.840 (the median age in the SPOTLIGHT trial was 59.3 years).34 However, the clinical experts indicated that it was unlikely for patients with gastric or GEJ adenocarcinoma who have not yet progressed to have the same quality of life as someone who is healthy, given the severity of the cancer. The clinical experts added that in general, patients with cancer do not have the same quality of life as someone who is healthy.
Additionally, the sponsor’s derived utility value for the postprogression health state (█████) signals that there is little difference in terms of quality of life between those who have not yet progressed on treatment and those who have progressed disease. The clinical expert input noted that patients who have progressed disease will have a markedly worse quality of life. The input highlighted that the severity of the cancer, emphasized by the low OS rates, is suggestive of the notion that quality of life among patients who have progressed is likely notably worse than that of patients who have not yet progressed.
In consultation with clinical experts, the utility values derived from the CHECKMATE 649 trial (preprogression = 0.797; postprogression = 0.577) — used previously as inputs in economic evaluations published for the treatment of gastric or GEJ adenocarcinoma in the first-line setting — were deemed more reflective of the quality of life for the indicated population.35-37
The CDA-AMC base case adopted utility values derived from the CHECKMATE 649 trial (preprogression = 0.797; postprogression = 0.577).
Additional limitations were identified, but were not considered to be key limitations. These limitations are outlined subsequently.
The model lacked transparency: The sponsor’s submitted model included numerous IFERROR statements, which lead to situations in which the parameter value is overwritten with an alternative value without alerting the user to the automatized overwriting. The systematic use of IFERROR statements makes thorough auditing of the sponsor’s model impractical, because it remains unclear whether the model is running inappropriately by overriding errors.
CDA-AMC was unable to address this limitation and notes that a thorough validation of the sponsor’s model was not possible.
Additionally, the following key assumptions were made by the sponsor and have been appraised by CDA-AMC (refer to Table 4).
Table 4: Key Assumptions of the Submitted Economic Evaluation (Not Noted as Limitations to the Submission)
Sponsor’s key assumption | CDA-AMC comment |
|---|---|
The patient demographics from the SPOTLIGHT trial were assumed to be generalizable to the population of patients in Canada. | Reasonable. The clinical experts consulted during this review commented that the baseline and demographic characteristics for the SPOTLIGHT trial were a reasonable reflection of the target patient population in Canada. |
The treatment effects modelled are homogenous among the indicated population. | Uncertain. As noted in the CDA-AMC Clinical Review Report, subgroup analysis of OS suggested potential for differential treatment effects by tumour type. In both the SPOTLIGHT and GLOW trials, the impact of zolbetuximab on OS was reduced in patients with GEJ cancer in comparison with those who had gastric cancer, suggesting that the difference in OS observed in the overall study population was driven primarily by patients with gastric cancer. CDA-AMC notes that the sponsor’s submitted CUA did not permit subgroup analysis; thus, CDA-AMC is unable to comment on the cost-effectiveness of zolbetuximab in patients with gastric cancer relative to those with GEJ cancer. |
mFOLFOX6 alone is a relevant comparator. | Uncertain. Clinical experts consulted during this review noted that mFOLFOX6 alone is not a relevant comparator because it is not reflective of routine practice in Canada, where patients would typically be offered nivolumab plus chemotherapy as the preferred treatment option. The experts noted that only patients with a contraindication or intolerance to nivolumab would receive chemotherapy alone. CDA-AMC notes that the inclusion of mFOLFOX6 has minimal impact on the interpretation of the cost-effectiveness of zolbetuximab plus mFOLFOX6 because the ICER for zolbetuximab plus mFOLFOX6 is presented as relative to nivolumab plus mFOLFOX6. |
mFOLFOX6 and CAPOX have similar efficacy. | Likely appropriate. Clinical expert input agreed that it is reasonable to assume that mFOLFOX6 and CAPOX have similar efficacy. The CDA-AMC Clinical Review Report noted that there was systematic heterogeneity between studies that used CAPOX and mFOLFOX in the submitted NMA. |
Grade ≥ 3 AEs are captured as 1-time costs and QALY loss in the first model cycle, based on the assumption that most AEs happen soon after treatment starts. | Uncertain. Clinical expert input noted that, while AEs associated with zolbetuximab are likely to occur within the first 3 months of treatment, AEs associated with nivolumab are likely to occur within the first year of treatment. |
The incidence rate of AEs is expected to reflect the rates observed in clinical trials. | Not appropriate. The incidence rate of grade 3 and higher AEs for nivolumab plus mFOLFOX6 was based on naive comparisons to zolbetuximab plus mFOLFOX6 and mFOLFOX6, without adjusting or accounting for differences in patient characteristics. The rate of AEs is used to calculate AE costs in the sponsor’s base case. Owing to the direct use of clinical trial data, it is not possible to determine if any observed differences between the therapies are due solely to treatment or, rather, due to bias or confounding factors. Furthermore, no safety end point was evaluated in the NMA; therefore, no conclusions on safety can be drawn on the indirect comparison of zolbetuximab plus mFOLFOX6 and nivolumab plus mFOLFOX6. |
CPS testing costs were not included because these were assumed to be standard of care for all patients. | Uncertain. The clinical experts consulted during this review noted that patients do not currently require CPS testing. However, CPS testing may be performed more frequently to guide treatment decisions in patients with CLDN18.2-positive tumours and a CPS of less than 5. Therefore, testing costs are likely underestimated. However, CDA-AMC notes that the impact on the cost-effectiveness of zolbetuximab plus mFOLFOX6 is likely minimal. |
The unit cost for the CLDN18.2 test is $100. | Uncertain. The sponsor estimated the unit cost of IHC at $100 per test, based on the highest listed cost for currently funded IHC tests by Cancer Care Ontario (Schedule V).25 However, it is not yet certain whether the cost of IHC testing for CLDN18.2 status would be consistent with this estimate, and the clinical experts consulted for the review suggested that the unit cost per test could be higher. The sponsor also acknowledged that the unit cost of IHC tests for CLDN18.2 status is likely to vary across jurisdictions in Canada, based on the assay and platform selected by individual laboratories. |
AE = adverse event; CAPOX = capecitabine and oxaliplatin; CDA-AMC = Canada’s Drug Agency; CLDN18.2 = Claudin 18.2; CPS = combined positive score; CUA = cost-utility analysis; GEJ = gastroesophageal junction; ICER = incremental cost-effectiveness ratio; IHC = immunohistochemistry; mFOLFOX6 = modified leucovorin calcium (folinic acid), 5-fluorouracil, and oxaliplatin; NMA = network meta-analysis; OS = overall survival; QALY = quality-adjusted life-year.
CDA-AMC Reanalyses of the Economic Evaluation
Base-Case Results
CDA-AMC undertook the reanalyses outlined in Table 5 to address, where possible, the limitations within the sponsor’s submitted economic model. The CDA-AMC base case was derived by making changes in model parameter values and assumptions in consultation with clinical experts.
Table 5: CDA-AMC Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CDA-AMC value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
1. Drug acquisition costs | Oxaliplatin = $36.27 per 50 mg/10mL vial | Oxaliplatin = $45.00 per 50 mg/10mL vial |
2. Drug wastage |
|
|
Changes to derive the CDA-AMC base case | ||
1. Nivolumab dosage | 240 mg q.2.w. | 3 mg/kg (maximum of 240 mg) q.2.w. |
2. Zolbetuximab maintenance dosage | 600 mg/m2 q.3.w. | 400 mg/m2 q.2.w. |
3. Health state utilities | Derived from the SPOTLIGHT trial:
| Derived from the CHECKMATE649 trial:
|
4. Use of KM data when modelling OS, PFS, and DOT | Applied KM data up to:
| No KM data applied; full parametric survival analysis curve used |
5. Treatment waning | No treatment waning | Zolbetuximab plus mFOLFOX6 OS will wane to match mFOLFOX6 OS at 5 years |
CDA-AMC base case | ― | Reanalysis 1 + 2 + 3 + 4 + 5 |
CDA-AMC = Canada’s Drug Agency; DOT = duration of therapy; KM = Kaplan-Meier; mFOLFOX6 = modified leucovorin calcium (folinic acid), 5-fluorouracil, and oxaliplatin; OS = overall survival; PFS = progression-free survival; q.2.w. = every 2 weeks; q.3.w. = every 3 weeks.
aThe sponsor applied a price of $74.41 for the 500 mg/50 mL vial of folinic acid (leucovorin). CDA-AMC notes that, should the 500 mg/50 mL vial be used to determine costs in the model, the price should be corrected to $689.00 per 500 mg/50 mL vial of folinic acid. A correction was not made to the vial price because the 500 mg/50 mL vial is no longer a relevant input in the CDA-AMC base case.
The CDA-AMC base case was based on publicly available prices of the comparator treatments. Results from the CDA-AMC base case are presented in Table 6. Additional results from the CDA-AMC base case, including the results of the step-wise analyses, are presented in Appendix 4.
In the CDA-AMC base case, the expected total costs and QALYs over a lifetime horizon (17 years) for zolbetuximab plus mFOLFOX6 were $259,623 and 1.82 QALYs, respectively. All modelled treatments (i.e., zolbetuximab plus mFOLFOX6, nivolumab plus mFOLFOX6, and mFOLFOX6) were on the cost-effectiveness frontier, representing the optimal treatment strategies. In sequential analysis, zolbetuximab plus mFOLFOX6 was associated with an ICER of $1,611,078 per QALY gained relative to nivolumab plus mFOLFOX6 (incremental cost = $56,474; incremental QALYs = 0.035) (Table 3). Approximately 44% of incremental QALYs for zolbetuximab plus mFOLFOX6, relative to nivolumab plus mFOLFOX6, were gained in the extrapolated period of the model (i.e., beyond the maximum follow-up time of 4.5 years observed in the SPOTLIGHT trial). In alignment with the sponsor’s analysis, zolbetuximab plus mFOLFOX6 had a 0% probability of being cost-effective at a WTP threshold of $50,000 per QALY gained, and the key drivers of the results were time spent in the preprogression health state and drug acquisition costs.
Table 6: Summary of the CDA-AMC Reanalysis Results
Drug | Total costs ($) | Total QALYs | Sequential ICER ($/QALY) |
|---|---|---|---|
Sponsor’s base case (probabilistic) (corrected) | |||
mFOLFOX6 | 135,110 | 1.52 | Reference |
Nivolumab plus mFOLFOX6 | 218,284 | 1.96 | 189,070 vs. mFOLFOX6 |
Zolbetuximab plus mFOLFOX6 | 265,588 | 2.04 | 551,573 vs. nivolumab plus mFOLFOX6 |
CDA-AMC base case (probabilistic) | |||
mFOLFOX6 | 136,072 | 1.36 | Reference |
Nivolumab plus mFOLFOX6 | 203,149 | 1.78 | 159,683 vs. mFOLFOX6 |
Zolbetuximab plus mFOLFOX6 | 259,623 | 1.82 | 1,611,078 vs. nivolumab plus mFOLFOX6 |
CDA-AMC = Canada’s Drug Agency; ICER = incremental cost-effectiveness ratio; mFOLFOX6 = modified leucovorin calcium (folinic acid), 5-fluorouracil, and oxaliplatin; QALY = quality-adjusted life-year; vs. = versus.
Scenario Analysis Results
CDA-AMC undertook price reduction analyses based on the sponsor’s corrected base case and the CDA-AMC base case. The CDA-AMC base case suggested that an 87.9% price reduction for zolbetuximab would be required for zolbetuximab plus mFOLFOX6 to achieve cost-effectiveness relative to mFOLFOX6 at a WTP threshold of $50,000 per QALY gained (Table 7).
Table 7: CDA-AMC Price Reduction Analyses
Analysis | Unit drug cost | ICERs for zolbetuximab plus mFOLFOX6 vs. comparator (as indicated) ($/QALY) | |
|---|---|---|---|
Price reduction | ($) | Sponsor’s corrected base case | CDA-AMC reanalysis |
No price reduction | 638.00 | 551,573 (vs. nivolumab plus mFOLFOX6) | 1,611,078 (vs. nivolumab plus mFOLFOX6) |
10% | 574.20 | 406,287 (vs. nivolumab plus mFOLFOX6) | 1,283,795 (vs. nivolumab plus mFOLFOX6) |
20% | 510.40 | 261,001 (vs. nivolumab plus mFOLFOX6) | 956,513 (vs. nivolumab plus mFOLFOX6) |
30% | 446.60 | 177,103 (vs. mFOLFOX6) | 629,230 (vs. nivolumab plus mFOLFOX6) |
40% | 382.80 | 153,400 (vs. mFOLFOX6) | 301,948 (vs. nivolumab plus mFOLFOX6) |
50% | 319.00 | 129,698 (vs. mFOLFOX6) | 145,432 (vs. mFOLFOX6) |
60% | 255.20 | 105,995 (vs. mFOLFOX6) | 120,225 (vs. mFOLFOX6) |
70% | 191.40 | 82,292 (vs. mFOLFOX6) | 95,017 (vs. mFOLFOX6) |
80% | 127.60 | 58,590 (vs. mFOLFOX6) | 69,809 (vs. mFOLFOX6) |
90% | 121.22 | 34,887 (vs. mFOLFOX6) | 44,602 (vs. mFOLFOX6) |
CDA-AMC = Canada’s Drug Agency; ICER = incremental cost-effectiveness ratio; mFOLFOX6 = modified leucovorin calcium (folinic acid), 5-fluorouracil, and oxaliplatin; QALY = quality-adjusted life-year; vs. = versus; WTP = willingness to pay.
Note: A price reduction of 47.4% for zolbetuximab would be required for zolbetuximab plus mFOLFOX6 to achieve cost-effectiveness relative to nivolumab plus mFOLFOX6 at a WTP threshold of $50,000 per QALY gained, based on the CDA-AMC reanalysis.
CDA-AMC conducted a scenario analysis to explore the impact of alternative assumptions regarding the waning of treatment effect for zolbetuximab plus mFOLFOX6 on the cost-effectiveness of zolbetuximab plus mFOLFOX6. Results of the scenario analysis are presented in Appendix 4, Table 13.
First, CDA-AMC explored the impact of assuming that the treatment effect of zolbetuximab plus mFOLFOX6 wanes to match the efficacy of mFOLFOX6 alone at 3 years, based on the clinical expert input received. This scenario assumes that the treatment effect associated with zolbetuximab plus mFOLFOX6 dissipates faster than assumed in the CDA-AMC base case and results in zolbetuximab plus mFOLFOX6 being dominated by nivolumab plus mFOLFOX6.
Issues for Consideration
During the review period, a potentially relevant comparator, pembrolizumab (in combination with fluoropyrimidine- and platinum-containing chemotherapy), received a positive recommendation from the pan-Canadian Oncology Drug Review Expert Review Committee (pERC).38 The sponsor did not include pembrolizumab plus chemotherapy in the CUA as a comparator, in line with the deviation request accepted by CDA-AMC. However, while pembrolizumab was included in the submitted NMA, CDA-AMC would like to highlight that, as noted in the CDA-AMC Clinical Review Report, the comparisons of zolbetuximab plus chemotherapy versus pembrolizumab plus chemotherapy presented little to no difference in OS or PFS between the treatments. The clinical expert feedback obtained by CDA-AMC suggested that pembrolizumab may not be the most relevant comparator for zolbetuximab.
CDA-AMC has previously reviewed nivolumab in combination with fluoropyrimidine- and platinum-containing chemotherapy for the treatment of adult patients with advanced or metastatic gastric or GEJ adenocarcinoma.16 The cost-effectiveness results of the evaluation may not be directly comparable to those in the current review owing to differences in model structure, clinical effectiveness parameters, health state utility values, and cost inputs.
The clinical experts suggested that there is some uncertainty in the clinical community regarding the effectiveness of nivolumab plus chemotherapy in patients with a PD-L1 CPS of less than 5. As such, the clinical experts noted that zolbetuximab plus chemotherapy could be a preferred option for patients with CLDN18.2-positive tumours and a PD-L1 CPS of less than 5. For patients with both CLDN18.2-positive tumours and a PD-L1 CPS greater than or equal to 5, it is currently unclear which option could offer the best outcomes. The model did not have the flexibility to assess the cost-effectiveness of zolbetuximab in these subgroups. The sponsor noted that this flexibility was not incorporated because these subgroups were not defined in the SPOTLIGHT or GLOW trials.
The administration of zolbetuximab is highly resource-intensive. Zolbetuximab is available in 100 mg vials and must be reconstituted with 5 mL of diluent; this mixture is then drawn up and added to an infusion bag, with multiple vial reconstitutions required for a single dose. In contrast, nivolumab and pembrolizumab (2 relevant comparators for this review) are available as solutions; as a result, zolbetuximab will take more time for health care professionals to prepare. Additionally, the product monograph states that zolbetuximab should be administered over a minimum of 2 hours, whereas the administration of nivolumab and pembrolizumab occurs over 30 minutes. As such, zolbetuximab would require additional nursing resources and chair time.
The final product stability of zolbetuximab is very short. If the infusion time exceeds 6 hours from the time of preparation, then the infusion bag must be discarded and a new infusion bag prepared.
Overall Conclusions
The sponsor submitted evidence from 2 randomized, double-blind, placebo-controlled, phase III trials (SPOTLIGHT and GLOW) that demonstrated that treatment with zolbetuximab in combination with fluoropyrimidine- and platinum-based chemotherapy (i.e., mFOLFOX6 or CAPOX) resulted in a clinically important improvement in OS and PFS compared with placebo in combination with fluoropyrimidine- and platinum-based chemotherapy for the first-line treatment of adult patients with locally advanced unresectable or metastatic HER2-negative gastric or GEJ adenocarcinoma whose tumours are CLDN18.2-positive. The sponsor considered the most relevant chemotherapy in the setting in Canada to be mFOLFOX6, which aligned with clinical expert input.
Based on clinical expert input, nivolumab plus chemotherapy was identified as the most relevant comparator. In the absence of direct evidence, the sponsor submitted an NMA to assess the relative efficacy of zolbetuximab plus chemotherapy (i.e., mFOLFOX6, CAPOX, and a combination of the 2 chemotherapies) relative to nivolumab plus chemotherapy in the indicated population. The indirect evidence suggests there is little to no difference in treatment effect on OS and PFS between zolbetuximab and nivolumab in combination with mFOLFOX6. However, the indirect evidence is associated with uncertainty due to clinical and methodological heterogeneity between the studies included in the network, with a potential to introduce bias in the NMA results. The sponsor’s NMA is used to model OS and PFS for both zolbetuximab plus mFOLFOX6 and nivolumab plus mFOLFOX6.
In addition to the uncertainty concerning the comparative efficacy of zolbetuximab plus mFOLFOX6 relative to nivolumab plus mFOLFOX6, CDA-AMC identified several limitations with the sponsor’s economic submission. These included uncertainty in the long term efficacy of zolbetuximab plus mFOLFOX6; uncertainty in drug acquisition and administration costs; and uncertainty in the health state utility values derived from the SPOTLIGHT trial. The CDA-AMC base case was derived by adopting a weight-based dose for nivolumab, adopting an every-2-week maintenance dosing schedule for zolbetuximab, adopting utility values from the CHECKMATE 649 trial, adopting full parametric survival analysis curves for OS, PFS, and DOT, and assuming that the treatment effect of zolbetuximab plus mFOLFOX6 wanes toward that of mFOLFOX6 alone after 5 years. Additionally, CDA-AMC corrected the drug unit price for oxaliplatin and the assumptions of drug wastage for folinic acid and fluorouracil.
The results of the CDA-AMC reanalysis are similar to the results of the sponsor’s analysis in that zolbetuximab plus mFOLFOX6 is associated with greater costs and a small number of incremental QALYs compared with nivolumab plus mFOLFOX6. In sequential analysis, zolbetuximab plus mFOLFOX6 was associated with an ICER of $1,611,078 per QALY gained relative to nivolumab plus mFOLFOX6 (incremental cost = $56,474; incremental QALYs = 0.035). In alignment with the sponsor’s analysis, zolbetuximab plus mFOLFOX6 had a 0% probability of being cost-effective at a WTP threshold of $50,000 per QALY gained, and the key drivers of the results were the time spent in the preprogression health state and drug acquisition costs. The difference in QALYs between zolbetuximab- and nivolumab-based regimens was small, with most of the difference occurring beyond the trial period. Given that the sponsor-submitted NMA suggests that there may be little to no difference in treatment effect on OS and PFS between zolbetuximab and nivolumab in combination with mFOLFOX6, there is insufficient evidence to suggest that zolbetuximab should be priced higher than currently available immunotherapies for adult patients with locally advanced unresectable or metastatic HER2-negative gastric or GEJ adenocarcinoma.
While the cost of testing for the CLDN18.2 mutation was included in the economic evaluation, there was limited information to support the cost inputs included, and the scope of the test costs included was likely underestimated (e.g., equipment, infrastructure, and training). Furthermore, other potentially relevant diagnostic test costs (e.g., CPS testing) were not included in the analysis. Test costs are unlikely to be a key driver of the treatment costs in this patient population; however, CDA-AMC could not fully test this assumption.
References
1.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Vyloy (zolbetuximab): lyophilised powder for concentrate for solution for intravenous infusion, 100 mg zolbetuximab single-use vials. Markham (ON): Astellas Pharma Canada, Inc.; 2024 Jun 27.
2.Shitara K, Lordick F, Bang YJ, et al. Zolbetuximab plus mFOLFOX6 in patients with CLDN18.2-positive, HER2-negative, untreated, locally advanced unresectable or metastatic gastric or gastro-oesophageal junction adenocarcinoma (SPOTLIGHT): a multicentre, randomised, double-blind, phase 3 trial. Lancet. 2023;401(10389):1655-1668. PubMed
3.Al-Batran S-E, Schuler MH, Zvirbule Z, et al. FAST: An international, multicenter, randomized, phase II trial of epirubicin, oxaliplatin, and capecitabine (EOX) with or without IMAB362, a first-in-class anti-CLDN18.2 antibody, as first-line therapy in patients with advanced CLDN18.2+ gastric and gastroesophageal junction (GEJ) adenocarcinoma. J Clin Oncol. 2016;34(18_suppl).
4.Vyloy (zolbetuximab): lyophilised powder for concentrate for solution for intravenous infusion, 100 mg zolbetuximab single-use vials [product monograph]. Markham (ON): Astellas Pharma Canada, Inc.; 2024 Dec 13.
5.SPOTLIGHT (8951-CL0302). Final analysis clinical study report. In: Drug Reimbursement Review sponsor submission: Vyloy (zolbetuximab): lyophilised powder for concentrate for solution for intravenous infusion, 100 mg zolbetuximab single-use vials. Markham (ON): Astellas Pharma Canada, Inc.; 2024 Jun 27.
6.CADTH reimbursement review: Nivolumab (Opdivo). Ottawa (ON): CADTH [sponsor submitted reference].
7.Janjigian YY, Ajani JA, Moehler M, et al. First-Line Nivolumab Plus Chemotherapy for Advanced Gastric, Gastroesophageal Junction, and Esophageal Adenocarcinoma: 3-Year Follow-Up of the Phase III CheckMate 649 Trial. J Clin Oncol. 2024;42(17):2012-2020. PubMed
8.Opdivo (nivolumab for injection): intravenous Infusion, 10 mg nivolumab /mL 40 mg and 100 mg single-use vials [product monograph]. Montreal (QC): Bristol-Myers Squibb Canada; 2024 May 17: https://pdf.hres.ca/dpd_pm/00075707.PDF.
9.Sponsor's NMA [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Vyloy (zolbetuximab): lyophilised powder for concentrate for solution for intravenous infusion, 100 mg zolbetuximab single-use vials. Markham (ON): Astellas Pharma Canada, Inc.; 2024 Jun 27.
10.Gebski V, Gares V, Gibbs E, Byth K. Data maturity and follow-up in time-to-event analyses. Int J Epidemiol. 2018;47(3):850-859. PubMed
11.Xie F, Pullenayegum E, Gaebel K, et al. A Time Trade-off-derived Value Set of the EQ-5D-5L for Canada. Med Care. 2016;54(1):98-105. PubMed
12.Yan J, Xie S, Johnson JA, et al. Canada population norms for the EQ-5D-5L. Eur J Health Econ. 2024;25(1):147-155. PubMed
13.National Institute for Health Care Excellence. Nivolumab in combination with chemotherapy for untreated advanced gastric or gastro-oesophageal junction cancer [TA857, ID1465]. [sponsor submitted reference].
14.National Institute for Health Care Excellence. Pixantrone monotherapy for the treatment of relapsed or refractory aggressive non-Hodgkin’s lymphoma [TA306]. [sponsor submitted reference].
15.Shah BD, Smith NJ, Feng C, et al. Cost-Effectiveness of KTE-X19 for Adults with Relapsed/Refractory B-Cell Acute Lymphoblastic Leukemia in the United States. Adv Ther. 2022;39(8):3678-3695. PubMed
16.CADTH Reimbursement Review. Nivolumab for gastroesophageal junction or esophageal adenocarcinoma. https://www.cadth.ca/nivolumab-0. [sponsor submitted reference].
17.Gomez-Ulloa D, Amonkar M, Kothari S, et al. Real-world treatment patterns, healthcare resource use and clinical outcomes of patients receiving second line therapy for advanced or metastatic gastric cancer. BMC Gastroenterol. 2020;20(1):133. PubMed
18.Schedule of benefits for physician services under the Health Insurance Act: (June 29, 2023 (effective July 24, 2023)). Toronto (ON): Ontario Ministry of Health; 2023: https://www.health.gov.on.ca/en/pro/programs/ohip/sob/physserv/sob_master.pdf. Accessed 2024 Jun 13.
19.Patient cost estimator. 2024; https://www.cihi.ca/en/patient-cost-estimator. Accessed 2024 Jun 13.
20.Mahar AL, Coburn NG, Kagedan DJ, Viola R, Johnson AP. Regional variation in the management of metastatic gastric cancer in Ontario. Curr Oncol. 2016;23(4):250-257. PubMed
21.Rider A, Calvo E, Bertwistle D, Hall J, Higson O, Moon R. Pcn293 Real-World Productivity, Healthcare Resource Utilization (Hcru) and Quality of Life (Qol) in Patients Receiving First-Line Treatment for Advanced Gastric Cancer (Gc) in Canada and Europe. Value Health. 2019;22.
22.Fuldeore R, Chaves LP, Feng Q, Rozario N, Nimke D, Braun S. Treatment patterns, healthcare resource utilization and costs of HER2-negative gastric/gastroesophageal junction cancer. Future Oncol. 2023;19(8):575-586. PubMed
23.Ontario Ministry of Health. Schedule of Benefits. Physician Services Under the Health Insurance Act. https://www.ontario.ca/files/2024-01/moh-ohip-schedule-of-benefits-2024-01-24.pdf. [sponsor submitted reference].
24.Closing the Gap Healthcare. Home care costs in Ontario—a complete breakdown. [sponsor submitted reference].
25.Ontario Health. Schedule 5 – cancer programs. n.d.: https://www.ontariohealth.ca/sites/ontariohealth/files/2020-09/7.%20CCO%20Schedule%205%20-%20Cancer%20Programs%20EN.pdf. Accessed 2024 Aug 26.
26.de Oliveira C, Pataky R, Bremner KE, et al. Phase-specific and lifetime costs of cancer care in Ontario, Canada. BMC Cancer. 2016;16(1):809. PubMed
27.Statistics Canada. Table 18-10-0005-01 Consumer price index, annual average, not seasonally adjusted. [sponsor submitted reference].
28.Statistics Canada. Table 18-10-0004-01 Consumer price index, monthly, not seasonally adjusted. [sponsor submitted reference].
29.Coyle D, Haines A, Le K. CADTH methods and guidelines: Extrapolating clinical evidence within economic evaluations. Can J Health Technol. 2023;3(5). https://www.cda-amc.ca/sites/default/files/attachments/2023-05/MH0011-Extrapolating%20Clinical%20Evidence%20Within%20Economic%20Evaluations_0.pdf. PubMed
30.Janjigian YY, Shitara K, Moehler M, et al. First-line nivolumab plus chemotherapy versus chemotherapy alone for advanced gastric, gastro-oesophageal junction, and oesophageal adenocarcinoma (CheckMate 649): a randomised, open-label, phase 3 trial. Lancet. 2021;398(10294):27-40. PubMed
31.CTD Module 2.7.4. Zolbetuximab (IMAB362) Intravenous Infusion. Summary of Clinical Safety. Data on File. In: Drug Reimbursement Review sponsor submission: Vyloy (zolbetuximab): lyophilised powder for concentrate for solution for intravenous infusion, 100 mg zolbetuximab single-use vials. Markham (ON): Astellas Pharma Canada, Inc.; 2024 Jun 27.
32.Fluorouracil injection USP, 50mg/mL [product monograph]. Kirkland (QC): Accord Healthcare Inc.; 2019 Oct 30: https://pdf.hres.ca/dpd_pm/00053796.PDF. Accessed 2024 Sep 18.
33.DeltaPA. Ottawa (ON): IQVIA; 2023: https://www.iqvia.com/. Accessed 2024 Jun 13.
34.Guertin JR, Feeny D, Tarride JE. Age- and sex-specific Canadian utility norms, based on the 2013-2014 Canadian Community Health Survey. CMAJ. 2018;190(6):E155-e161. PubMed
35.Cao X, Zhang M, Li N, et al. First-line nivolumab plus chemotherapy versus chemotherapy alone for advanced gastric cancer, gastroesophageal junction cancer, and esophageal adenocarcinoma: a cost-effectiveness analysis. Ther Adv Med Oncol. 2023;15:17588359231171038. PubMed
36.Zhang PF, Shi XQ, Li Q. Nivolumab plus chemotherapy versus chemotherapy alone as first-line treatment for advanced gastric, gastroesophageal junction, and esophageal adenocarcinoma: a cost-effectiveness analysis. Cost Eff Resour Alloc. 2023;21(1):65. PubMed
37.Shu Y, Ding Y, Zhang Q. Cost-Effectiveness of Nivolumab Plus Chemotherapy vs. Chemotherapy as First-Line Treatment for Advanced Gastric Cancer/Gastroesophageal Junction Cancer/Esophagel Adenocarcinoma in China. Front Oncol. 2022;12:851522. PubMed
38.CADTH Reimbursement Recommendation (Draft): pembrolizumab (Keytruda) in combination with fluoropyrimidine- and platinum-containing chemotherapy, is indicated for the firstline treatment of adult patients with locally advanced unresectable or metastatic HER2-negative gastric or gastroesophageal junction adenocarcinoma. Ottawa (ON): CADTH: https://www.cda-amc.ca/sites/default/files/DRR/2024/PC0356_Draft%20Recommendation.pdf. Accessed 2024 Sep 16.
39.Cancer Care Ontario. MFOLFOX6+NIVL. https://www.cancercareontario.ca/fr/drugformulary/regimens/monograph/70331. Accessed 2024 Jul 24.
40.Cancer Care Ontario. XELOX+NIVL. https://www.cancercareontario.ca/en/drugformulary/regimens/monograph/70336. Accessed 2024 Jul 24.
41.Cancer Care Ontario. XELOX+PEMB. https://www.cancercareontario.ca/en/drugformulary/regimens/monograph/70491. Accessed 2024 Jul 24.
42.Cancer Care Ontario. MFOLFOX6+PEMB. https://www.cancercareontario.ca/en/drugformulary/regimens/monograph/70496. Accessed 2024 Jul 24.
43.Cancer Care Ontario. MFOLFOX6. https://www.cancercareontario.ca/en/drugformulary/regimens/monograph/47941. Accessed 2024 Jul 24.
44.Cancer Care Ontario. XELOX. https://www.cancercareontario.ca/en/drugformulary/regimens/monograph/47936. Accessed 2024 Jul 24.
45.Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Vyloy (zolbetuximab): lyophilised powder for concentrate for solution for intravenous infusion, 100 mg zolbetuximab single-use vials. Markham (ON): Astellas Pharma Canada, Inc.; 2024 Jun 27.
46.Ontario Ministry of Health. Ontario Drug Benefit Formulary / Comparative Drug Index, effective from November 30, 2023. https://www.formulary.health.gov.on.ca/formulary. [sponsor submitted reference].
47.Statistics Canada. Population estimates on July 1, by age and gender. Table: 17-10-0005-01 (formerly CANSIM 051-0001). Release date: 2024-02-21.: https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1710000501. [sponsor submitted reference].
48.Shah MA, Shitara K, Ajani JA, et al. Zolbetuximab plus CAPOX in CLDN18.2-positive gastric or gastroesophageal junction adenocarcinoma: the randomized, phase 3 GLOW trial. Nat Med. 2023;29(8):2133-2141. PubMed
49.Van Cutsem E, Bang YJ, Feng-Yi F, et al. HER2 screening data from ToGA: targeting HER2 in gastric and gastroesophageal junction cancer. Gastric Cancer. 2015;18(3):476-484. PubMed
50.Brenner DR, Gillis J, Demers AA, et al. Projected estimates of cancer in Canada in 2024. CMAJ. 2024;196(18):E615-E623. PubMed
51.Canadian Cancer Statistics. A 2018 special report on cancer incidence by stage. https://cdn.cancer.ca/-/media/files/research/cancer-statistics/2018-statistics/canadian-cancer-statistics-2018-en.pdf. [sponsor submitted reference].
52.Canadian Cancer Statistics Advisory in collaboration with the Canadian Cancer Society SCatPHAoC. Canadian Cancer Statistics: A 2022 special report on cancer prevalence. Toronto (ON): Canadian Cancer Society; 2022: cancer.ca/Canadian-Cancer-Statistics-2022-EN. Accessed 2023 Sep 21.
53.Spolverato G, Ejaz A, Kim Y, et al. Rates and patterns of recurrence after curative intent resection for gastric cancer: a United States multi-institutional analysis. J Am Coll Surg. 2014;219(4):664-675. PubMed
54.Sanjeevaiah A, Cheedella N, Hester C, Porembka MR. Gastric Cancer: Recent Molecular Classification Advances, Racial Disparity, and Management Implications. J Oncol Pract. 2018;14(4):217-224. PubMed
55.Shankaran V, Xiao H, Bertwistle D, et al. A Comparison of Real-World Treatment Patterns and Clinical Outcomes in Patients Receiving First-Line Therapy for Unresectable Advanced Gastric or Gastroesophageal Junction Cancer Versus Esophageal Adenocarcinomas. Adv Ther. 2021;38(1):707-720. PubMed
56.CADTH Reimbursement Review for Nivolumab (Opdivo) for Gastric, gastroesophageal junction, or esophageal adenocarcinoma. https://www.cadth.ca/sites/default/files/DRR/2022/PC0259-Opdivo-combinedReport.pdf/ [sponsor submitted reference].
57.Cancer Care Ontario. MFOLFOX6+NIVL. https://www.cancercareontario.ca/fr/drugformulary/regimens/monograph/70331. Accessed 2024 Sep 16.
58.Cancer Care Ontario. CAPECRBP+NIVL. https://www.cancercareontario.ca/en/drugformulary/regimens/monograph/70541.
59.European Medicines Agency. Assessment Report. OPDIVO (nivolumab). Procedure No. EMEA/H/C/003985/II/0096. [sponsor submitted reference].
60.GLOW (8951-CL0302). Final analysis clinical study report. In: Drug Reimbursement Review sponsor submission: Vyloy (zolbetuximab): lyophilised powder for concentrate for solution for intravenous infusion, 100 mg zolbetuximab single-use vials. Markham (ON): Astellas Pharma Canada, Inc.; 2024 Jun 27.
Appendix 1: Cost Comparison Table
Please note that this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical expert(s) and drug plans. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 8: CDA-AMC Cost Comparison Table for Locally Advanced Unresectable or Metastatic HER2-Negative Gastric or GEJ Adenocarcinoma
Treatment | Strength/ concentration | Form | Price ($) | Recommended dosage | Average daily cost ($) | Average 28-day cycle cost ($)a |
|---|---|---|---|---|---|---|
Zolbetuximab for injection | 20 mg/mL | 5 mL vial | 638.0000a | 800 mg/m2 on day 1 of cycle 1 followed by 600 mg/m2 every 21 days or 400 mg/m2 every 14 days thereafterb | Cycle 1: 478.50 to 569.64 Cycle 2+: 250.64 to 501.29 | Cycle 1: 13,398 to 15,950 Cycle 2+: 7,018 to 14,036 |
Zolbetuximab plus CAPOX | Cycle 1: 498.68 to 598.82 Cycle 2+: 270.82 to 521.46 | Cycle 1: 13,963 to 16,515 Cycle 2+: 7,583 to 14,601 | ||||
Zolbetuximab plus mFOLFOX6 | Cycle 1: 571.54 to 662.68 Cycle 2+: 343.68 to 594.32 | Cycle 1: 16,003 to 18,555 Cycle 2+: 9,623 to 16,641 | ||||
CAPOX | ||||||
Capecitabine (generic) | 150 mg 500 mg | Tablet | 0.4575 1.5250 | 1,000 mg/m2 twice daily on days 1 through 14 every 21-days | 7.32 | 205 |
Oxaliplatin (generic) | 5 mg/mL | 10 mL vial 20 mL vial 40 mL vial | 45.0000 90.0000 180.0000 | 130 mg/m2 every 21-days | 12.86 | 360 |
CAPOX | 20.18 | 565 | ||||
mFOLFOX6 | ||||||
Fluorouracil (generic) | 50 mg/mL | 100 mL vial | 160.9000 | 400 mg/m2 by IV bolus and 2,400 mg/m2 by continuous IV infusion every 14-days | 11.26 | 315 |
Leucovorin (generic) | 10 mg/mL | 5 mL vial 50 mL vial | 68.9400 689.0000 | 400 mg/m2 every 14-days | 68.91 | 1,930 |
Oxaliplatin (generic) | 5 mg/mL | 10 mL vial 20 mL vial 40 mL vial | 45.0000 90.0000 180.0000 | 85 mg/m2 every 14-days | 12.86 | 360 |
mFOLFOX6 | 93.03 | 2,605 | ||||
Immune checkpoint inhibitors | ||||||
Nivolumab (Opdivo) | 10 mg/mL | 4 mL vial 10 mL vial | 782.2200 1,955.5600 | 3 mg/kg (max 240 mg) every 14-days or 4.5 mg/kg (max 360 mg) every 21-days cycle for up to 2 yearsc | 279.37 | 7,822 |
Pembrolizumab (Keytruda) | 25 mg/mL | 4 mL vial | 4,400.0000 | 2 mg/kg (max 200 mg) every 21 days or 4 mg/kg (max 400 mg) every 42 days for up to 2 yearsc | 314.29 to 419.05 | 8,800 to 11,733 |
Nivolumab plus CAPOX | 299.54 | 8,387 | ||||
Nivolumab plus mFOLFOX6 | 372.40 | 10,427 | ||||
Pembrolizumab plus CAPOX | 334.46 to 439.22 | 9,365 to 12,298 | ||||
Pembrolizumab plus mFOLFOX6 | 407.32 to 512.08 | 11,405 to 14,388 | ||||
Note: All prices were retrieved from IQVIA Delta PA (accessed June 2024),33 unless otherwise indicated, and do not include dispensing fees. For weight- or BSA-based dosing, a patient weight of 65 kg or a BSA of 1.75 m2 was assumed. Except for fluorouracil, which is available in bulk pharmacy vials, wastage was included. Recommended dosages were retrieved from Cancer Care Ontario,39-44 unless otherwise indicated. Treatments in vial form are for IV infusion.
aSponsor-submitted price.1
bThe cycle duration of zolbetuximab is determined based on the chemotherapy backbone it is used in combination with (CAPOX or mFOLFOX6).4
cThe Health Canada recommended dosage is fixed. Drug plans indicated the weight-based dosage, as listed by Cancer Care Ontario, was funded.
Appendix 2: Submission Quality
Please note that this appendix has not been copy-edited.
Description | Yes or No | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | Yes | No comment. |
Model has been adequately programmed and has sufficient face validity | No | Refer to the ‘Model lacked transparency’ limitation in the CDA-AMC Appraisal of the Sponsor’s Economic Evaluation. |
Model structure is adequate for decision problem | Yes | No comment. |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | Yes | No comment. |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | Yes | No comment. |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | Yes | No comment. |
Appendix 3: Additional Information on the Submitted Economic Evaluation
Please note that this appendix has not been copy-edited.
Detailed Results of the Sponsor’s Base Case
Table 10: Disaggregated Summary of the Sponsor’s Economic Evaluation Results
Parameter | Zolbetuximab plus mFOLFOX6 | mFOLFOX6 | Nivolumab plus mFOLFOX6 |
|---|---|---|---|
Discounted LYs | |||
Total | 2.461 | 1.843 | 2.364 |
Preprogression | 1.890 | 1.246 | 1.681 |
Postprogression | 0.571 | 0.597 | 0.683 |
Discounted QALYs | |||
Total | 2.033 | 1.510 | 1.948 |
Preprogression | 1.581 | 1.039 | 1.405 |
Postprogression | 0.455 | 0.474 | 0.544 |
Decrement due to adverse events | −0.003 | −0.002 | −0.001 |
Discounted costs ($) | |||
Total | 247,004 | 119,949 | 206,016 |
Preprogression | 142,535 | 14,251 | 105,262 |
Postprogression | 21,402 | 23,786 | 21,711 |
Adverse events | 9,007 | 7,249 | 4,502 |
Preprogression disease management | 2,761 | 1,946 | 2,291 |
Postprogression disease management | 4,756 | 4,972 | 5,706 |
Testing | 260 | 0 | 0 |
Terminal care | 66,282 | 67,745 | 66,543 |
LY = life-year; mFOLFOX6 = modified leucovorin calcium (folinic acid), 5-fluorouracil, and oxaliplatin; QALY = quality-adjusted life-year.
Source: Sponsor’s pharmacoeconomic submission.1
Appendix 4: Additional Details on the CDA-AMC Reanalyses and Sensitivity Analyses of the Economic Evaluation
Please note that this appendix has not been copy-edited.
Detailed Results of CDA-AMC Base Case
Table 11: Summary of the Stepped Analysis of the CDA-AMC Base-Case Results
Stepped analysis | Drug | Total costs ($) | Total QALYs | Sequential ICER ($/QALY) |
|---|---|---|---|---|
Sponsor base case | mFOLFOX6 | 119,661 | 1.52 | Reference |
Nivolumab plus mFOLFOX6 | 205,387 | 1.95 | 196,213 vs. mFOLFOX6 | |
Zolbetuximab plus mFOLFOX6 | 245,884 | 2.05 | 431,029 vs. nivolumab+ | |
Sponsor’s corrected base case | mFOLFOX6 | 134,884 | 1.52 | Reference |
Nivolumab plus mFOLFOX6 | 218,041 | 1.95 | 190,333 vs. mFOLFOX6 | |
Zolbetuximab plus mFOLFOX6 | 263,989 | 2.05 | 489,046 vs. nivolumab+ | |
1. CDA-AMC reanalysis 1: Nivolumab dosage | mFOLFOX6 | 134,884 | 1.52 | Reference |
Nivolumab plus mFOLFOX6 | 202,524 | 1.95 | 154,817 vs. mFOLFOX6 | |
Zolbetuximab plus mFOLFOX6 | 263,989 | 2.05 | 654,199 vs. nivolumab+ | |
2. CDA-AMC reanalysis 2: Zolbetuximab maintenance dosage | mFOLFOX6 | 134,884 | 1.52 | Reference |
Nivolumab plus mFOLFOX6 | 218,041 | 1.95 | 190,333 vs. mFOLFOX6 | |
Zolbetuximab plus mFOLFOX6 | 258,844 | 2.05 | 434,284 vs. nivolumab+ | |
3. CDA-AMC reanalysis 3: Health state utilities | mFOLFOX6 | 134,884 | 1.35 | Reference |
Nivolumab plus mFOLFOX6 | 218,041 | 1.75 | 204,690 vs. mFOLFOX6 | |
Zolbetuximab plus mFOLFOX6 | 263,989 | 1.87 | 388,632 vs. nivolumab+ | |
4. CDA-AMC reanalysis 4: Use of KM data when modelling OS, PFS, and DOT | mFOLFOX6 | 135,805 | 1.54 | Reference |
Nivolumab plus mFOLFOX6 | 218,456 | 1.99 | 183,160 vs. mFOLFOX6 | |
Zolbetuximab plus mFOLFOX6 | 259,553 | 2.08 | 430,184 vs. nivolumab+ | |
5. CDA-AMC reanalysis 5: Treatment waning | mFOLFOX6 | 134,884 | 1.52 | Reference |
Nivolumab plus mFOLFOX6 | 218,041 | 1.95 | 190,333 vs. mFOLFOX6 | |
Zolbetuximab plus mFOLFOX6 | 264,094 | 1.96 | 4,852,918 vs. nivolumab+ | |
CDA-AMC base case (deterministic) (Reanalysis 1 + 2 + 3 + 4 + 5) | mFOLFOX6 | 135,805 | 1.36 | Reference |
Nivolumab plus mFOLFOX6 | 202,939 | 1.78 | 161,740 vs. mFOLFOX6 | |
Zolbetuximab plus mFOLFOX6 | 254,667 | 1.83 | 1,006,146 vs. nivolumab+ | |
CDA-AMC base case (probabilistic) (Reanalysis 1 + 2 + 3 + 4 + 5) | mFOLFOX6 | 136,072 | 1.36 | Reference |
Nivolumab plus mFOLFOX6 | 203,149 | 1.78 | 159,683 vs. mFOLFOX6 | |
Zolbetuximab plus mFOLFOX6 | 259,623 | 1.82 | 1,611,078 vs. nivolumab+ |
DOT = duration of therapy; mFOLFOX6 = modified leucovorin calcium (folinic acid), 5-fluorouracil, and oxaliplatin; ICER = incremental cost-effectiveness ratio; KM = Kaplan-Meier; OS = overall survival; PFS = progression-free survival; QALY = quality-adjusted life-year; vs. = versus.
Note: to ensure the table is not too long, the comparators for the sequential analysis in column 5 have been abbreviated to “versus primary treatment+” to represent the full regimen (e.g., nivolumab+” to represent nivolumab plus mFOLFOX6) where relevant.
Table 12: Disaggregated Summary of the CDA-AMC Economic Evaluation Results
Parameter | Zolbetuximab plus mFOLFOX6 | mFOLFOX6 | Nivolumab plus mFOLFOX6 |
|---|---|---|---|
Discounted LYs | |||
Total | 2.419 | 1.880 | 2.427 |
Preprogression | 1.890 | 1.257 | 1.698 |
Postprogression | 0.529 | 0.623 | 0.729 |
Discounted QALYs | |||
Total | 1.820 | 1.365 | 1.785 |
Preprogression | 1.516 | 1.005 | 1.361 |
Postprogression | 0.307 | 0.362 | 0.425 |
Decrement due to adverse events | −0.003 | −0.002 | −0.001 |
Discounted costs ($) | |||
Total | 259,623 | 136,072 | 203,149 |
Preprogression | 155,472 | 30,530 | 102,749 |
Postprogression | 21,468 | 23,880 | 21,495 |
Adverse events | 8,939 | 7,233 | 4,501 |
Preprogression disease management | 2,723 | 1,993 | 2,323 |
Postprogression disease management | 4,433 | 5,204 | 6,110 |
Testing | 259 | 0 | 0 |
Terminal care | 66,328 | 67,231 | 65,971 |
mFOLFOX6 = modified leucovorin calcium (folinic acid), 5-fluorouracil, and oxaliplatin; LY = life-year; QALY = quality-adjusted life-year.
Scenario Analyses
Table 13: Summary of the Scenario Analysis of the CDA-AMC Base-Case Results
Stepped analysis | Drug | Total costs ($) | Total QALYs | Sequential ICER ($/QALY) |
|---|---|---|---|---|
CDA-AMC base case | mFOLFOX6 | 136,072 | 1.36 | Reference |
Nivolumab plus mFOLFOX6 | 203,149 | 1.78 | 159,683 vs. mFOLFOX6 | |
Zolbetuximab plus mFOLFOX6 | 259,623 | 1.82 | 1,611,078 vs. nivolumab+ | |
CDA-AMC scenario 1: treatment effect for zolbetuximab plus mFOLFOX6 wanes to the efficacy of mFOLFOX6 at 3 years | mFOLFOX6 | 136,072 | 1.36 | Reference |
Nivolumab plus mFOLFOX6 | 203,149 | 1.78 | 159,683 vs. mFOLFOX6 | |
Zolbetuximab plus mFOLFOX6 | 259,252 | 1.75 | Dominated |
mFOLFOX6 = modified leucovorin calcium (folinic acid), 5-fluorouracil, and oxaliplatin; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; vs. = versus.
Note: results are presented probabilistically. Also, to ensure the table is not too long, the comparators for the sequential analysis in column 5 have been abbreviated to “versus primary treatment+” to represent the full regimen (e.g., nivolumab+” to represent nivolumab plus mFOLFOX6) where relevant.
Appendix 5: Submitted Budget Impact Analysis and CDA-AMC Appraisal
Please note that this appendix has not been copy-edited.
Table 14: Summary of Key Take-Aways
Key take-aways of the budget impact analysis |
|---|
|
Summary of Sponsor’s Budget Impact Analysis
In the submitted budget impact analysis (BIA), the sponsor assessed the introduction of zolbetuximab, in combination with mFOLFOX6 and CAPOX for the first-line treatment of adult patients with locally advanced unresectable or metastatic HER2-negative, CLDN18.2-positive gastric or GEJ adenocarcinoma.45 The BIA was undertaken from the perspective of a Canadian public payer over a 3-year time horizon (2026 to 2028) using an epidemiological approach. The sponsor compared a reference scenario in which patients received either zolbetuximab plus chemotherapy (mFOLFOX6 or CAPOX), nivolumab plus chemotherapy (mFOLFOX6 or CAPOX), mFOLFOX6, or CAPOX to a new drug scenario in which zolbetuximab plus chemotherapy was reimbursed. The sponsor’s submission only considered annual drug acquisition costs in which the costs were obtained from a previous CDA-AMC Reimbursement Review and the Ontario Drug Benefit Formulary (ODB).16,46 Data informing key parameters of the budget impact model were obtained from various sources including Statistics Canada,47 published literature (sources detailed in Table 15), SPOTLIGHT and GLOW,2,48 internal estimates, clinical expert feedback, and assumption. Key inputs to the BIA are documented in Table 15.
Key assumptions included:
Zolbetuximab plus chemotherapy will be initially reimbursed in 2026.
A HER2-negativity rate of 77.0% was assumed, derived from the Trastuzumab for Gastric cancer (ToGA) study.49
80% of patients are platinum-eligible, derived from the market shares of a previous CDA-AMC Reimbursement Review.16
Epidemiological data for patients with metastatic disease are assumed to be representative of all patients with locally advanced unresectable or metastatic disease.
The stomach cancer prevalence (0.023%) and incidence (0.012%) were assumed to be representative of gastric or GEJ cancer.
The relative use between zolbetuximab plus CAPOX and zolbetuximab plus mFOLFOX6 was 65% and 35%, respectively.
Pembrolizumab plus chemotherapy is not used to treat the indicated population (i.e., 0% market share).
85% and 15% of the market capture for zolbetuximab plus chemotherapy shares were expected to come from nivolumab plus chemotherapy and chemotherapy alone (i.e., CAPOX or mFOLFOX6), respectively.
All incident patients with gastric or GEJ cancer would be eligible for CLDN18.2 testing upon diagnosis.
The cost of testing for CLDN18.2 is $100 in all jurisdictions.
The detection rate for CLDN18.2 testing is 100% (i.e., no false-negative results).
Table 15: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as year 1 / year 2 / year 3 if appropriate) |
|---|---|
Target population | |
Pan-Canadian population 18 years and older47 | 26,308,344 |
Incident population with de novo metastasis Annual incidence of gastric or GEJ cancer50 Proportion with de novo metastasis51 | 0.012% 43.5% |
Population with recurrent metastatic disease 5-year prevalence52 Proportion of prevalent patients that are early stage47,51,52 Annual rate of recurrence53 Proportion with distant recurrence (i.e., metastatic disease)53 | 0.023% 77.6% 14.8% 75.8% |
Total new CLDN18.2+, HER2- metastatic gastric or GEJ adenocarcinoma patients Proportion of patients with adenocarcinoma54 Proportion of patients with HER2-negative disease49 Proportion receiving first-line systemic therapy55 Platinum-eligible56 CLDN18.2+2 CLDN18.2 testing ratea CLDN18.2 detection rateb | 90.0% 77.0% 75.5% 80.0% 38.4% 63.3% / 77.3% / 85.4% 100% |
Number of patients eligible for drug under review | 197 / 245 / 276 |
Market uptake (3 years) | |
Uptake (reference scenario) Nivolumab plus CAPOX Nivolumab plus mFOLFOX6 CAPOX mFOLFOX6 | 29.8% / 29.8% / 29.8% 55.3% / 55.3% / 55.3% 5.3% / 5.3% / 5.3% 9.8% / 9.8% / 9.8% |
Uptake (new drug scenario) Zolbetuximab plus CAPOX Zolbetuximab plus mFOLFOX6 Nivolumab plus CAPOX Nivolumab plus mFOLFOX6 CAPOX mFOLFOX6 | 3.6% / 12.5% / 14.1% 6.8% / 23.2% / 26.3% 26.7% / 19.1% / 17.7% 49.5% / 35.5% / 32.9% 4.7% / 3.4% / 3.1% 8.7% / 6.3% / 5.8% |
Cost of treatment (per patient, per year) | |
Zolbetuximab plus CAPOX Zolbetuximab plus mFOLFOX6 Nivolumab plus CAPOX Nivolumab plus mFOLFOX6 CAPOX mFOLFOX6 | Year 1: $91,525.78; Year 2+: $0 Year 1: $94,339.91; Year 2+: $0 Year 1: $83,530.02; Year 2+: $0 Year 1: $92,684.79; Year 2+: $0 Year 1: $2,372.17; Year 2+: $0 Year 1: $5,940.75; Year 2+: $0 |
CAPOX = capecitabine and oxaliplatin; CLDN18.2+ = Claudin 18.2-positive; mFOLFOX6 = modified leucovorin calcium (folinic acid), 5-fluorouracil, and oxaliplatin; GEJ = gastroesophageal junction; HER2 = human epidermal growth factor receptor 2.
Note: Pembrolizumab plus CAPOX and pembrolizumab plus mFOLFOX6 were included as comparators in the submitted BIA but market uptake was assumed to be 0% in the reference and new drug scenarios.
aBased on the sponsor’s internal estimates.
bBased on sponsor assumption.
Summary of the Sponsor’s BIA Results
The sponsor estimated that the 3-year budget impact of reimbursing zolbetuximab, in combination with fluoropyrimidine- and platinum-containing chemotherapy, for the first-line treatment of adult patients with locally advanced unresectable or metastatic HER2-negative, CLDN18.2-positive gastric or GEJ adenocarcinoma to be $3,640,283 (Year 1: $339,428; Year 2: $1,450,959; Year 3: $1,849,897).
The sponsor provided an estimate of the impact on testing costs. In line with the information in Table 15, the sponsor assumed there are individuals currently being tested for CLDN18.2 and that public payers are funding testing, indicating a 3-year budget impact of $516,955 in the reference scenario, increasing to $822,396 if zolbetuximab is funded, resulting in a 3-year budget impact of CLDN18.2 testing of $305,441 (Year 1: $49,787; Year 2: $89,152; Year 3: $166,502). When added to the drug acquisition cost, the total 3-year budget impact of reimbursing zolbetuximab is estimated to be $3,945,724.
CDA-AMC Appraisal of the Sponsor’s BIA
CDA-AMC identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
Drug acquisition and administration costs are uncertain: First, the sponsor assumed nivolumab was administered with a fixed dose of 240 mg every 2 weeks in combination with mFOLFOX6 and 360 mg every 3 weeks in combination with CAPOX. While fixed dosing for nivolumab is aligned with the Health Canada product monograph–recommended dosing, and the dosing used in the CHECKMATE-649 pivotal trial,8,30 input received by CDA-AMC participating drug plans noted that nivolumab is likely to be administered with a weight-based dose, aligned with the product monographs listed by Cancer Care Ontario.57,58 As such, the recommended dose of nivolumab is 3 mg/kg, up to a maximum of 240 mg, every 2 weeks when administered with mFOLFOX6 and 4.25 mg/kg, up to a maximum of 360 mg, every 3 weeks when administered with CAPOX. As noted in the CDA-AMC Appraisal of the Sponsor’s Economic Evaluation, as the sponsor assumed nivolumab was administered with a fixed dose, the costs associated with nivolumab were likely overestimated and biased in favour of zolbetuximab.
Second, the assumed DOT was equal to the mean exposure to therapy from various clinical trials. The DOT for zolbetuximab + mFOLFOX6 was sourced from SPOTLIGHT.5 The DOT for nivolumab + mFOLFOX6 and nivolumab + CAPOX were sourced from CHECKMATE 649.59 The zolbetuximab and oxaliplatin DOT for zolbetuximab + CAPOX were sourced from SPOTLIGHT as the patient characteristics were deemed more reflective of the indicated population in Canada;5 the remaining components of the regimen were sourced from GLOW.60 CDA-AMC notes that the sponsor’s approach results in all drug acquisition costs being borne in the first year of treatment such that there are zero costs attributed to subsequent years on therapy. CDA-AMC compared the year 1 costs in the BIA (as all treatment costs are borne in the first year) to the 3-year undiscounted preprogression costs calculated in the CDA-AMC base case (calculated by setting the time horizon in the CDA-AMC base case to 3 years) to determine the magnitude of difference and the direction of bias, if possible. CDA-AMC determined that in general, the sponsor’s submitted BIA underestimated costs and the magnitude of difference was biased in favour of zolbetuximab. The impact on the estimated budget impact is likely minor. For reference, the drug acquisition costs for the first-line treatment of zolbetuximab + mFOLFOX6 in the CUA were $140,491 over 3 years ($94,272 attributed to year 1, $32,167 attributed to year 2, and $14,051 attributed to year 3); total drug costs for the first-line treatment of zolbetuximab + mFOLFOX6 in the BIA were $94,340. Therefore, while costs for the first year of treatment are similar between the 2 analyses, as the BIA assumes there are no patients on treatment in year 2, drug acquisition costs for zolbetuximab + mFOLFOX6 were underestimated by approximately $45,000 over 3 years in the BIA. Compare this to treatment costs for nivolumab + mFOLFOX6 which were $103,024 over 3 years in the CUA ($81,034 attributed to year 1, $20,972 attributed to year 2, and $1,018 attributed to year 3); total drug costs in the BIA were $92,685. Drug acquisition costs for nivolumab + mFOLFOX6 were underestimated by approximately $10,000 over 3 years in the BIA. CDA-AMC notes that the sponsor’s BIA model structure does not permit the user to enter drug costs beyond year 2.
Lastly, as commented in the CDA-AMC Appraisal of the Sponsor’s Economic Evaluation, wastage of unused product was inappropriately considered for fluorouracil and folinic acid (leucovorin) and the list price of oxaliplatin informing the sponsor’s analysis, retrieved from a previous CDA-AMC Reimbursement Review Report,6 is now out of date as the list price, per IQVIA DeltaPA, has increased.33
In the CDA-AMC base case, CDA-AMC assumed a weight-based dose of 3 mg/kg up, to a maximum of 240 mg, every 2 weeks when used in combination with mFOLFOX6 and a weight-based dose of 4.5 mg/kg up, to a maximum of 360 mg, every 3 weeks when used in combination with CAPOX. Aligned with the CDA-AMC CUA, CDA-AMC corrected the sponsor’s assumption of wastage for the bulk pharmacy vial of fluorouracil, considered the smallest vial size of folinic acid (50 mg/5 mL) in cost calculations, and revised the price of oxaliplatin from $36.27 to $45.00 per 50 mg/10mL vial.
CDA-AMC was unable to address all drug acquisition costs being borne in the first year of treatment (i.e., zero costs attributed to subsequent years on therapy) owing to the sponsor’s model structure. CDA-AMC notes that drug acquisition costs are underestimated and underestimate the incremental budget impact of reimbursing zolbetuximab.
The number of eligible patients is uncertain: The sponsor used an epidemiologic approach to estimate the number of patients eligible for zolbetuximab should it become publicly reimbursed by drug plans for the first-line treatment of patients with locally advanced unresectable or metastatic HER2-negative gastric or GEJ adenocarcinoma whose tumours are CLDN18.2-positive. While clinical expert input found the estimated number of eligible patients in 2026 (year 1 in the BIA) to be reasonable, it was noted that the eligible population size may change over time as the annual incidence rate has been increasing due to improved scoping and diagnosing among other variables and as more data becomes available regarding the effectiveness of zolbetuximab in the GEJ subpopulation. CDA-AMC notes that should the CLDN18.2 testing rates increase from the sponsor’s assumed rates in the BIA (63.3% in year 1 [2026], 77.3% in year 2, and 85.4% in year 3), the eligible population size will increase, and thus the sponsor’s calculated budget impact may be underestimated.
CDA-AMC was unable to address this limitation in reanalyses owing to a lack of alternative data.
Market shares are uncertain: As noted in the CDA-AMC Issues for Consideration, pembrolizumab, in combination with fluoropyrimidine- and platinum-containing chemotherapy, received a positive recommendation from the pan-Canadian Oncology Drive Review Expert Review Committee for the first-line treatment of adult patients with locally advanced unresectable or metastatic HER2-negative gastric or GEJ adenocarcinoma.38 This sponsor assumed that pembrolizumab held zero market share. Clinical experts consulted by CDA-AMC noted that pembrolizumab uptake is likely to be lower than the market share attributed to nivolumab (85% in the reference scenario) as nivolumab has a more convenient dosing interval but that pembrolizumab will gain a notable market share in the immunotherapy space. CDA-AMC notes that should the negotiated price for pembrolizumab be less than the sponsor-submitted price for zolbetuximab, the budget impact associated with reimbursing zolbetuximab is likely underestimated.
CDA-AMC was unable to address this limitation in reanalyses owing to a lack of data.
The market uptake of zolbetuximab is uncertain: The sponsor’s submitted base case assumed that 10.4%, 35.7%, and 40.4% of eligible patients would receive zolbetuximab in year 1, year 2, and year 3, respectively, based on clinician input elicited by the sponsor. Clinical expert input elicited by CDA-AMC for this review suggests that the sponsor’s estimates may underestimate the uptake of zolbetuximab in year 1 (2026) as clinicians noted there is a high proportion of patients who are CPS-low and CLDN18.2-positive, they are likely to receive zolbetuximab should the treatment be publicly reimbursed. Clinician input suggested that the size of the aforementioned patient is likely to be at least 20% of the eligible patient population and thus uptake in year 1 should reflect the size of this population.
CDA-AMC explored uncertainty in the uptake of zolbetuximab in scenario analyses.
CDA-AMC Reanalyses of the BIA
The CDA-AMC base case was derived by adopting a weight-based dose for nivolumab and correcting the drug unit price for oxaliplatin and the assumptions of drug wastage for folinic acid and fluorouracil.
The results of the CDA-AMC step-wise reanalysis are presented in summary format in Table 17 and a more detailed breakdown is presented in Table 18. Based on publicly list prices, CDA-AMC estimated the 3-year budget impact of reimbursing zolbetuximab, in combination with fluoropyrimidine- and platinum-containing chemotherapy, for the first-line treatment of adult patients with locally advanced unresectable or metastatic HER2-negative, CLDN18.2-positive gastric or GEJ adenocarcinoma to be $6,410,018 (Year 1: $597,683; Year 2: $2,554,931; Year 3: $3,257,404). Consistent with the sponsor’s analysis, estimated costs for CLDN18.2 testing results in a 3-year budget impact of $305,441 (Year 1: $49,787; Year 2: $89,152; Year 3: $166,502). When added to the drug acquisition cost, the total 3-year budget impact of reimbursing zolbetuximab is estimated to be $6,715,459.
Table 16: CDA-AMC Revisions to the Submitted BIA
Stepped analysis | Sponsor’s value or assumption | CDA-AMC value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
1. Drug acquisition costs | Oxaliplatin = $36.27 per 50 mg/10mL vial | Oxaliplatin = $45.00 per 50 mg/10mL vial |
2. Drug wastage |
|
|
Changes to derive the CDA-AMC base case | ||
1. Nivolumab dosage |
|
|
CDA-AMC base case | ― | Reanalysis 1 |
CAPOX = capecitabine and oxaliplatin; mFOLFOX6 = modified leucovorin calcium (folinic acid), 5-fluorouracil, and oxaliplatin; q.2.w. = every 2 weeks; q.3.w. = every 3 weeks.
aThe sponsor applied a price of $74.41 for the 500 mg/50 mL vial of folinic acid (leucovorin). CDA-AMC notes that should the 500 mg/50 mL vial be used to determine costs in the model, the price should be corrected to $689.00 per 500 mg/50 mL vial of folinic acid. A correction was not made to the vial price as the 500 mg/50 mL vial is no longer a relevant input under the CDA-AMC base case.
bCDA-AMC assumed three 100 mg vials of nivolumab were required to achieve the required dose of 293 mg as this combination of vials is both the least costly combination of vials, and the combination that uses the fewest vials and is thus most likely to be used in clinical practice.
Table 17: Summary of the CDA-AMC Reanalyses of the BIA
Stepped analysis | Three-year total ($) |
|---|---|
Submitted base case (drug plan perspective) | 3,640,283 |
Submitted base case (drug plan perspective plus testing costs) | 3,945,724 |
Sponsor’s corrected base case | 3,787,155 |
CDA-AMC reanalysis 1: nivolumab dosage | 6,410,018 |
CDA-AMC base case (drug plan perspective) | 6,410,018 |
CDA-AMC base case (drug plan perspective plus testing costs) | 6,715,459 |
CDA-AMC conducted the following scenario analyses to address remaining uncertainty, using the CDA-AMC base case (results are provided in Table 18:
Assuming the uptake of zolbetuximab in year 1 is 20%.
Table 18: Detailed Breakdown of the CDA-AMC Reanalyses of the BIA
Stepped analysis | Scenario | Year 0 (current situation) ($) | Year 1 ($) | Year 2 ($) | Year 3 ($) | Three-year total ($) |
|---|---|---|---|---|---|---|
Submitted base case | Reference | 11,695,480 | 15,098,900 | 18,802,619 | 21,183,496 | 55,085,016 |
New drug | 11,695,480 | 15,438,328 | 20,253,578 | 23,033,393 | 58,725,299 | |
Budget impact | 0 | 339,428 | 1,450,959 | 1,849,897 | 3,640,283 | |
CDA-AMC base case | Reference | 11,129,431 | 14,368,129 | 17,892,592 | 20,158,237 | 52,418,959 |
New drug | 11,129,431 | 14,965,813 | 20,447,523 | 23,415,641 | 58,828,977 | |
Budget impact | 0 | 597,683 | 2,554,931 | 3,257,404 | 6,410,018 | |
CDA-AMC scenario analysis 1: uptake of zolbetuximab in year 1 is 20% | Reference | 11,129,431 | 14,368,129 | 17,892,592 | 20,158,237 | 52,418,959 |
New drug | 11,129,431 | 15,517,521 | 20,447,523 | 23,415,641 | 59,380,685 | |
Budget impact | 0 | 1,149,391 | 2,554,931 | 3,257,404 | 6,961,726 |
BIA = budget impact analysis.
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.