Drugs, Health Technologies, Health Systems
Reimbursement Review
Osimertinib (Tagrisso)
Sponsor: AstraZeneca Canada Inc.
Therapeutic area: Non–small cell lung cancer
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Clinical Review
Abbreviations
AE
adverse event
AJCC
American Joint Committee on Cancer
BICR
blinded independent central review
CI
confidence interval
CNS
central nervous system
EGFRm
EGFR–mutated
EORTC QLQ-C30
European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30
EORTC QLQ-LC13
European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Lung Cancer Module
ex19del
exon 19 deletion
GRADE
Grading of Recommendations Assessment, Development, and Evaluation
HR
hazard ratio
HRQoL
health-related quality of life
ILD
interstitial lung disease
L858R
L858R substitution
LCC
Lung Cancer Canada
MID
minimal importance difference
NC
not calculable
NSCLC
non–small cell lung cancer
OH-CCO
Ontario Health (Cancer Care Ontario)
OS
overall survival
PFS
progression-free survival
PPS
post-progression survival
QoL
quality of life
RCT
randomized controlled trial
RECIST
Response Evaluation Criteria in Solid Tumors
RECIST 1.1
Response Evaluation Criteria in Solid Tumors Version 1.1
SAE
serious adverse event
TKI
tyrosine kinase inhibitor
TSST
time to second subsequent therapy
TTP
time to progression
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Table 1: Background Information of Application Submitted for Review
Item | Description |
|---|---|
Drug product | Osimertinib (Tagrisso) tablets, 40 mg and 80 mg (as osimertinib mesylate), oral |
Sponsor | AstraZeneca Canada Inc. |
Indication | In combination with pemetrexed and platinum-based chemotherapy for the first-line treatment of patients with locally advanced (not amenable to curative therapies) or metastatic NSCLC whose tumours have EGFR exon 19 deletions or exon 21 L858R substitution mutations |
Reimbursement request | As per indication |
Health Canada approval status | NOC |
Health Canada review pathway | Priority review and Project Orbis |
NOC date | July 10, 2024 |
Recommended dose | 80 mg tablet taken orally once a day |
NOC = Notice of Compliance; NSCLC = non–small cell lung cancer.
Source: Sponsor’s Summary of Clinical Evidence1 and product monograph.2
Introduction
Lung cancer is the most commonly diagnosed cancer and the leading cause of cancer deaths in Canada.3,4 In 2023, it was estimated that there would be 31,000 cases of lung cancer diagnosed and 20,600 deaths from lung cancer that year.4 It is estimated that 1 in 21 Canadians (4.8%) will die from lung cancer.4 Lung cancer is classified into non–small cell lung cancer (NSCLC) or small cell lung cancer, with NSCLC accounting for approximately 88% of cases in Canada.3 Approximately half of all lung cancer cases in Canada are stage I to III at diagnosis, defined by the American Joint Committee on Cancer (AJCC) staging criteria.3 Advanced disease, as defined by the AJCC, includes stage IV (metastatic) and unresectable stage IIIB and IIIC (locally advanced) cancer. Approximately 15% of patients in Canada with NSCLC have an EGFR-activating mutation in the region encoding the tyrosine kinase domain.5-7 EGFR mutations are more frequently observed in never-smokers, people of Asian ethnicity, patients with adenocarcinoma, and females.5,8 The most common EGFR mutations are the exon 19 deletion (ex19del) and L858R substitution (L858R).6,7 A common feature of EGFR–mutated (EGFRm) NSCLC is the development of central nervous system (CNS) metastases, which are detected in approximately 25% of patients at diagnosis and can affect approximately 50% of all patients within 3 years of diagnosis.9 Brain metastases are associated with a decreased quality of life (QoL) and poor prognosis, and are a significant cause of cancer-related mortality.10,11
For patients diagnosed with locally advanced or metastatic NSCLC who harbour EGFRm (i.e., an ex19del and/or L858R mutation), according to the clinical experts consulted by the review team, the current first-line treatment in Canada is osimertinib. Alternative treatment options in the first-line setting include first- and second-generation EGFR tyrosine kinase inhibitors (TKIs) (i.e., gefitinib, erlotinib, and afatinib) as well as platinum doublet chemotherapy. The clinical experts consulted by the review team also noted that patients would receive platinum doublet chemotherapy upon progressive disease after they had received osimertinib monotherapy. Since osimertinib became available, gefitinib, erlotinib and afatinib have had limited utilization in the first-line treatment setting in Canada and instead are reserved for the small number of patients whose tumours have noneligible EGFR mutations that cannot be treated with osimertinib.7
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of osimertinib (oral tablets, 40 mg and 80 mg) in combination with pemetrexed and platinum-based chemotherapy, for the first-line treatment of patients with locally advanced or metastatic NSCLC whose tumours have EGFR ex19del or L858R mutations. Osimertinib has been previously reviewed by the review team.
Perspectives of Patients, Clinicians, and Drug Programs
The information in this section is a summary of input provided by the patient and clinician groups that responded to our call for input and from clinical experts consulted by for the purpose of this review.
Patient Input
Two patient groups, Lung Cancer Canada (LCC) and the Lung Health Foundation (formerly the Ontario Lung Association), provided input for osimertinib in combination with pemetrexed and platinum-based chemotherapy (osimertinib plus chemotherapy) for the first-line treatment of patients with locally advanced or metastatic NSCLC whose tumours have EGFR ex19del or L858R mutations. Patient input was gathered from interviews and surveys, conducted in January 2021 and October 2023 by the Lung Health Foundation, and in December 2023 by LCC. The Lung Health Foundation conducted 2 interviews and gathered 15 responses from an online survey, and LCC conducted 13 interviews with patients and/or caregivers.
When asked about disease experience and its impact on day-to-day activities, respondents indicated that the disease has negative impacts on their day-to-day life, affecting their ability to participate in leisure activities and hobbies, use stairs, shop, and travel. Family members and caregivers of those living with lung cancer shared the same psychosocial burdens described by patients in this input. In addition, LCC reported that patients living with lung cancer have repeatedly stated in interviews that they desire a treatment that can improve their QoL while also effectively managing their disease.
Respondents from the Lung Health Foundation mentioned some benefits experienced with the currently available treatments, such as reduced coughing, reduced shortness of breath increased participation in daily activities, ability to exercise, prolonged life, delayed disease progression, and a reduction in the severity of other disease-related symptoms. The LCC input mentioned that, although chemotherapy and radiation may be clinically beneficial, they come with well-documented side effects that often reduce a patient’s QoL. The input added that osimertinib as a monotherapy has been well received by patients interviewed for this submission.
Respondents from the Lung Health Foundation reported that key treatment outcomes to consider when evaluating new therapies included stopping or slowing the progression of the disease with minimal side effects, as well as medications that are effective for advanced disease. When choosing a therapy, some of the most crucial outcomes that patients from the LCC input wanted to have include improved management of their symptoms of EGFR NSCLC, a full and worthwhile QoL, manageable side effects, longer lifespans, independence and functionality that minimizes the burden on their caregivers and loved ones, delayed disease progression, and the ability to settle into long-term management for improved survivorship.
Clinician Input
Input From Clinical Experts Consulted for This Review
According to the clinical experts consulted by the review team, the key treatment goals for patients with locally advanced or metastatic NSCLC whose tumours have EGFR ex19del or L858R mutations included improving overall survival (OS), controlling disease progression (including prevention and disease control of CNS metastasis), and maintaining QoL. The clinical experts consulted by the review team noted that needs are not met in patients who are younger, who present with significant disease burden, or who have CNS metastases.
The clinical experts consulted by the review team noted that osimertinib plus chemotherapy may be offered as an alternative to osimertinib monotherapy in the first-line setting to patients with locally advanced or metastatic NSCLC whose tumours have EGFR ex19del or L858R mutations. The clinical experts consulted by the review team also noted that osimertinib monotherapy should be a first-line treatment option. The clinical experts consulted by the review team further noted that if the osimertinib plus chemotherapy was adopted in the first line with maintenance pemetrexed, second-line treatment options would include rechallenge with platinum doublet chemotherapy or docetaxel.
The clinical experts consulted by the review team noted that osimertinib plus chemotherapy may preferentially be considered in younger patients with locally advanced or metastatic NSCLC whose tumours have EGFR ex19del or L858R mutations and in patients with CNS metastases. However, the clinical experts noted that older patients with fewer disease-related symptoms may choose not to receive osimertinib plus chemotherapy because of the additive toxicity associated with the combination.
According to the clinical experts consulted by the review team, outcomes to determine whether a patient is responding in clinical practice focus on functional status, disease-related symptoms, and radiographic imaging. Depending on local resources and time on treatment, radiographic imaging may be conducted every 2 to 4 months to confirm benefit.
The clinical experts consulted by the review team noted that, overall, it should be the clinician’s decision to discontinue the therapy based on a combination of factors, such as patient symptoms and conditions, radiographic imaging results, toxicities, and laboratory parameters, as well as the balance against clinical benefit for that patient. According to the clinical experts consulted by the review team, patients with progression defined by Response Evaluation Criteria in Solid Tumors (RECIST) may not necessarily indicate the deficiency of treatment, and in clinical practice, clinicians tend to make decisions regarding discontinuing treatment based on whether patients have clinically meaningful symptomatic disease progression.
The clinical experts consulted by the review team noted that the planned combination of osimertinib and chemotherapy would appropriately be delivered in any cancer treatment centre, academic institution, or community setting, and patients should be treated by medical oncologists well versed in the management of EGFR TKIs and platinum chemotherapy toxicity.
Clinician Group Input
Clinician group input on the review of osimertinib plus chemotherapy for the first-line treatment of patients with locally advanced or metastatic NSCLC whose tumours have EGFR ex19del or L858R mutations was received from 2 clinician groups: the Lung Cancer Drug Advisory Committee of Ontario Health (Cancer Care Ontario) (OH-CCO) and the LCC Medical Advisory Committee. A total of 28 clinicians provided input for this review.
The OH-CCO input mentioned that current treatments target shrinking the cancer, improvement in disease-related symptoms, and maximizing control of the disease to prevent or delay symptoms and prolong life. However, both clinician groups indicated that the current treatment options with osimertinib monotherapy and/or sequential therapy with osimertinib followed by chemotherapy are not curative. Both clinician groups emphasized need for improved therapies that result in longer control of the cancer, better QoL, and longer survival. Similar to the clinical experts consulted by the review team, the clinician groups mentioned the need for therapies that target specific patient populations, i.e., young patients and those with brain metastases. Both clinician groups noted that a treatment for brain metastases in EGFR-driven lung cancer is an urgent unmet need.
Both clinician groups noted that the combination of osimertinib and chemotherapy would be an option in patients with NSCLC with sensitizing EGFR mutations. The OH-CCO group emphasized the need for OS data before drawing any conclusions regarding the shift in the current treatment paradigm. They also mentioned that the addition of platinum-based chemotherapy to osimertinib is associated with an increase in chemotherapy-associated toxicities, which results in more inconvenience to patients, who are required to attend cancer centres more frequently because of the need for IV therapy. Similar to the input from the clinical experts consulted by the review team, both clinician groups noted that single-drug osimertinib would remain an option in first-line therapy.
The OH-CCO emphasized that all patients who have classic EGFR mutations would be suitable for osimertinib therapy if they can tolerate and have not had prior adjuvant osimertinib within the last several months. The group also mentioned that patients suitable for receiving the additional chemotherapy would be those for whom IV chemotherapy will be well tolerated or safe, and who have adverse features of their EGFR mutation–positive cancer. Similar to the input from the clinical experts consulted by the review team, the clinician groups noted that younger patients and patients with CNS metastases would benefit from the combination regimen. Both clinician groups agreed that treatment would be discontinued in cases of disease progression or undue toxicity.
Drug Program Input
Input was obtained from the drug programs that participate in the Reimbursement Review process. The following were identified as key factors that could potentially affect the implementation of a recommendation for osimertinib plus chemotherapy:
relevant comparators
consideration for initiation of therapy
consideration of discontinuation of therapy
consideration for prescribing of therapy
generalizability
funding algorithm
care provision issues
system and economic issues.
Clinical Evidence
Systematic Review
Description of Studies
One ongoing phase III, open-label randomized controlled trial (RCT), FLAURA2 (N = 557, including 13 patients in Canada), was included in the systematic literature search conducted by the sponsor. The FLAURA2 trial enrolled adult patients who were diagnosed with pathologically confirmed nonsquamous NSCLC that was locally advanced (clinical stage IIIB or IIIC), metastatic (clinical stage IVA or IVB), or recurrent (as defined by version 8 of the International Association for the Study of Lung Cancer Staging Manual in Thoracic Oncology) and whose tumours harboured an ex19del or L858R mutation, either alone or in combination with other EGFR mutations. Patients were randomized to the osimertinib plus chemotherapy group (n = 279) and the osimertinib monotherapy group (n = 278), stratified by race, WHO Performance Status, and methods used for tissue testing. The primary objective was to compare the treatment effect between osimertinib plus chemotherapy versus osimertinib monotherapy, measured by progression-free survival (PFS) according to investigator assessment. Other efficacy and safety outcomes included OS, European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Lung Cancer Module (EORTC QLQ-LC13), European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 (EORTC QLQ-C30), and harms (i.e., adverse events [AEs], serious adverse events [SAEs], withdrawal, deaths, and notable harms).
The median age of enrolled patients was 61.0 years (range = 26 to 85 years). The majority of enrolled patients were female (61.4%), Asian (63.7%), with a WHO PS of 1 (62.8%), an exon 19 deletion (53.1% by central cobas tissue test), and metastatic NSCLC at baseline (96.2%).
Efficacy Results
The FLAURA2 trial is ongoing, and the data cut-off date for all efficacy end points was April 3, 2023, except for OS, which was updated on January 8, 2024.
Overall Survival
As of the data cut-off date of January 8, 2024, the OS data had a data maturity of 40.6% and were adjusted for multiple statistical testing. There were 100 OS events (35.8%) in the osimertinib plus chemotherapy group and 126 OS events (45.3%) in the osimertinib monotherapy group. The hazard ratio (HR) for OS was 0.75 (95% confidence interval [CI], 0.57 to 0.97). The differences in the probability of being alive between osimertinib plus chemotherapy and osimertinib monotherapy at 24 and 36 months were 7.6 (95% CI, ███ to ████) and 13.5% (95% CI, ███ to ████), respectively. The median OS was 36.7 months in the osimertinib monotherapy group but it was not reached in the osimertinib plus chemotherapy group. There was a delayed separation of the Kaplan-Meier curves of the 2 treatment groups, which did not separate until about 16 months after randomization.
PFS According to Investigator Assessment
As the data cut-off date of April 3, 2023, with an overall data maturity of 51.3%, 120 PFS events (43.0%) according to investigator assessment were reported in the osimertinib plus chemotherapy group versus 166 PFS events (59.7%) according to investigator assessment in the osimertinib monotherapy group. The HR for PFS according to investigator assessment was 0.62 (95% CI, 0.49 to 0.79), in favour of osimertinib plus chemotherapy. The differences in the probability of being progression-free between osimertinib plus chemotherapy and osimertinib monotherapy 12 and 24 months were 14.2% (95% CI, ███ to ████) and 16.4% (95% CI, ███ to ████), respectively. The median PFS according to investigator assessment was 25.5 (95% CI, 24.7 to not calculable [NC]) months in the osimertinib and chemotherapy group versus 16.7 (95% CI, 14.1 to 21.3) in the osimertinib monotherapy group.
Results for PFS according to a blinded independent central review (BICR) assessment were generally consistent with the PFS results according to investigator assessment. Analysis of concordance between investigator and BICR assessment of PFS showed that there was an 82.1% agreement on progressions and nonprogressions in the osimertinib plus chemotherapy group, and a 75.6% agreement on progressions and nonprogressions in the osimertinib monotherapy group.
EORTC QLQ-LC13
The data cut-off date for EORTC QLQ-LC13 was April 3, 2023. The point estimates of difference in change from baseline scores of the coughing symptoms subscale between the osimertinib plus chemotherapy group and the osimertinib monotherapy group favoured osimertinib plus chemotherapy at week 52 and across all visits (i.e., average), while the point estimates of difference of the pain in chest subscale or the dyspnea symptom subscale favoured the osimertinib monotherapy group at week 52 and across all visits (i.e., average).
EORTC QLQ-C30
The data cut-off date for EORTC QLQ-C30 was April 3, 2023. The point estimates of difference in change from baseline scores of the Global Health Status/QoL between the osimertinib plus chemotherapy group and the osimertinib monotherapy group favoured osimertinib monotherapy at week 52 and across all visits (i.e., average).
Harms Results
The data cut-off date for harms data in the FLAURA2 trial was April 3, 2023. The proportions of patients experiencing at least 1 AE of any grade were similar between patients treated with osimertinib plus chemotherapy (100%) and patients treated with osimertinib monotherapy (97.5%). However, a higher proportion of patients treated with osimertinib plus chemotherapy experienced the most common AEs (those reported in ≥ 20% patients in either treatment group) compared with those treated with osimertinib monotherapy. Such AEs included anemia (46.4% versus 8.0%, respectively), nausea (43.1% versus 10.2%, respectively), and neutropenia (24.6% versus 3.3%). Moreover, a higher proportion of patients treated with osimertinib plus chemotherapy experienced AEs of grade 3 or higher compared with the proportion of patients treated with osimertinib monotherapy (63.8% versus 27.3%, respectively). The most common AE of grade 3 or higher in those treated with osimertinib plus chemotherapy was anemia (19.9%).
Higher percentages of patients in the osimertinib plus chemotherapy group experienced SAEs, compared to the percentages of patients in the osimertinib monotherapy group (37.7% versus 19.3%). Discontinuation of any study treatment occurred in 47.8% of the patients in the osimertinib plus chemotherapy group and 6.2% of the patients receiving osimertinib monotherapy. Within the osimertinib plus chemotherapy group, 45.3% of the patients discontinued chemotherapy, of whom 16.7% discontinued carboplatin or cisplatin treatment and 43.1% discontinued pemetrexed treatment.
Deaths were reported in 6.5% of the patients in the osimertinib plus chemotherapy group and 2.9% of the patients in the osimertinib monotherapy group. Of the patients in the osimertinib plus chemotherapy group 1.1% died due to pulmonary embolism, 1.11% due to pneumonia, and 0.7% due to cardiac failure.
The proportions of patients experiencing interstitial lung disease (ILD) or pneumonitis were similar between patients treated with osimertinib plus chemotherapy (3.3%) and those treated with osimertinib monotherapy (3.6%). A higher proportion of patients in the osimertinib plus chemotherapy group compared to patients in the osimertinib monotherapy group experienced cardiac failure (9.1% versus 3.6%, respectively), febrile neutropenia (4.0% versus 0.0%, respectively), and thrombocytopenia (18.5% versus 4.4%).
Critical Appraisal
The FLAURA2 trial used central randomization and concealed patient allocation during the randomization process.12 Overall, the baseline characteristics were balanced between the treatment groups. Generally, no serious concerns were identified in the protocol amendments and protocol deviations. As an open-label trial, investigators and patients were aware of the assigned treatment.12 The primary outcome in the FLAURA2 trial was PFS according to investigator assessment, which was susceptible to detection bias because of the open-label design. However, the potential risk of detection bias in PFS according to investigator assessment was considered relatively low by the review team because results were consistent with those of PFS according to BICR assessment, and the analysis of concordance between PFS according to investigator and PFS according to BICR showed an acceptable agreement. Similarly, for health-related quality of life (HRQoL) outcomes (EORTC QLQ LC-13 and EORTC QLQ-C30), which had unblinded assessment, the risk of performance bias was also considered relatively low as there was no evidence in the data indicating that knowledge of treatment assignment affected the results. However, it was more of a concern that the assessment of HRQoL outcomes at week 52 was based on a portion of randomized patients. For example, for EORTC QLQ-C30 assessment at week 52, 230 of 279 patients in the osimertinib plus chemotherapy group were expected to return a form, but only 180 forms were received and evaluated, for a compliance rate of 78.3%. It remains unclear how the missingness in data would affect the HRQoL assessment, resulting in increased uncertainty. The Kaplan-Meier curves for OS obtained from the April 3, 2023, data cut-off crossed several times, which violated the proportional hazards assumption for OS and affected the validity of the OS estimates as of April 3, 2023. A late divergence of the Kaplan-Meier curves of the updated OS (data cut-off date of January 8, 2024) was observed during visual inspection of the Kaplan-Meier curves (i.e., they did not separate until approximately 16 months after randomization). According to the clinical experts consulted by the review team, delayed separation of survival curves is acceptable in clinical practice as it is often seen in patients receiving a combination therapy including chemotherapy. However, the late divergence of survival curves may have implications for the statistical analysis used in the FLAURA2 trial (i.e., whether the proportional hazards assumption was violated), which introduced uncertainty to the OS evidence. When there is a delayed separation of survival curves, sensitivity analyses to assess whether the proportional hazards assumption was satisfied would have been appropriate (e.g., using survival analyses that do not rely on the proportional hazards assumption).
The generalizability of the FLAURA2 trial is subject to several considerations. The clinical experts consulted by the review team noted that the patient eligibility criteria of the FLAURA2 trials were appropriate overall in clinical trials involving patients with NSCLC and aligned with the selection criteria used in treatment settings in Canada when identifying suitable candidates for osimertinib plus chemotherapy. However, the clinical experts consulted by the review team noted that, in real-world settings, patients are generally sicker in terms of performance status. Second, the FLAURA2 trial did not allow eligible patients to have prior treatment with an EGFR TKI. Also, the FLAURA2 trial required eligible patients to be off other adjuvant and neoadjuvant therapies (e.g., chemotherapy, radiotherapy, immunotherapy, biologic therapy, and investigational drugs) at least 12 months before the development of recurrent disease. According to the clinical experts consulted by the review team, because osimertinib monotherapy has become a first-line treatment for EGFRm, patients who had received a prior EGFR TKI should also be considered for osimertinib plus chemotherapy. Third, the histology type of most patients enrolled in the FLAURA2 trial (> 98% for both groups) was adenocarcinoma. According to the clinical experts consulted by the review team, findings from the FLAURA2 trial could still be generalizable to patients with other histology types (e.g., adenosquamous carcinoma) because it is the existence of the driving mutation that determines whether osimertinib should be used. The clinical experts consulted by the review team noted that it is plausible that the treatment effects of osimertinib plus chemotherapy would likely not differ among patients with the same driving mutation but a different histology.
GRADE Summary of Findings and Certainty of the Evidence
Methods for Assessing the Certainty of the Evidence
For pivotal studies and RCTs identified in the sponsor’s systematic review, Grading of Recommendations Assessment, Development, and Evaluation (GRADE) was used to assess the certainty of the evidence for outcomes considered most relevant to inform our expert committee deliberations, and a final certainty rating was determined as outlined by the GRADE Working Group.13,14
Following the GRADE approach, evidence from RCTs started as high-certainty evidence and could be rated down for concerns related to study limitations (which refers to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias. When possible, certainty was rated in the context of the presence of an important (nontrivial) treatment effect; if this was not possible, certainty was rated in the context of the presence of any treatment effect (i.e., the clinical importance is unclear). In all cases, the target of the certainty-of-evidence assessment was based on the point estimate and where it was located relative to the threshold for a clinically important effect (when a threshold was available) or to the null.
The reference points for the certainty-of-evidence assessment for OS and PFS were set according to the presence of an important effect based on thresholds agreed upon by the clinical experts consulted by the review team for this review. The target of the certainty-of-evidence assessment was the presence of any (non-null) effect for EORTC QLQ-LC13 due to the lack of a formal estimate of the minimal important difference (MID). The MID for the Global Health Status/QoL of EORTC QLQ-C30 was based on estimates published in the literature.15 For harm events due to the unavailability of the absolute difference in effects, the certainty of evidence was summarized narratively.
The selection of outcomes for GRADE assessment was based on the sponsor’s Summary of Clinical Evidence, consultation with clinical experts, and input received from patient and clinician groups and public drug plans. The following list of outcomes was finalized in consultation with expert committee members:
survival outcomes (OS, PFS)
HRQoL outcome (coughing symptoms subscale of the EORTC QLQ-LC13, pain in chest subscale of the EORTC QLQ-LC13, dyspnea symptom subscale of the EORTC QLQ-LC13, and Global Health Status/QoL of the EORTC QLQ-C30)
harms (AEs of grade 3 or higher, SAEs, discontinuation of any treatment due to AEs, deaths, notable harms including ILD/pneumonitis, cardiac effects, hematological toxicities).
Results of GRADE Assessments
Table 2 presents the GRADE summary of findings for osimertinib plus chemotherapy versus osimertinib monotherapy in patients with locally advanced or metastatic NSCLC whose tumours have EGFR ex19del or L858R mutations.
Table 2: Summary of Findings for Osimertinib Plus Chemotherapy vs. Osimertinib Monotherapy for Patients With Locally Advanced (Not Amenable to Curative Therapies) or Metastatic NSCLC Whose Tumours Have EGFR Exon 19 Deletions or L858R Substitution Mutations
Outcome and follow-up | Patients (studies), N | Relative effect (95% CI) | Absolute effects | Certainty | What happens | ||
|---|---|---|---|---|---|---|---|
Osimertinib monotherapy | Osimertinib + chemotherapy (95% CI) | Difference (95% CI) | |||||
Overall survival — randomization phase, FAS (data cut-off date: January 8, 2024) | |||||||
Probability of being alive at 24 months Median follow-up duration (months): 31.7 for osimertinib + chemotherapy group; 30.5 for osimertinib monotherapy group | 557 (1 RCT) | NR | ███ per 1,000 | ███ per 1,000 (███ to ███ per 1,000) | ██ more per 1,000 (██ more to ███ more per 1,000) | Lowa | Osimertinib + chemotherapy may result in an increase in the probability of being alive at 24 months, compared to osimertinib monotherapy |
Probability of being alive at 36 months Median follow-up duration (months): 31.7 for osimertinib + chemotherapy group; 30.5 for osimertinib monotherapy group | 557 (1 RCT) | NR | ███ per 1,000 | ███ per 1,000 (███ to ███ per 1,000) | ███ more per 1,000 (██ more to ███ more per 1,000) | Lowb | Osimertinib + chemotherapy may result in an increase in the probability of being alive at 36 months, compared to osimertinib monotherapy |
PFS according to investigator assessment — randomization phase, FAS (data cut-off date: June 1, 2021) | |||||||
Probability of being progression-free at 12 months Median follow-up duration (months): 19.5 for osimertinib + chemotherapy group; 16.5 for osimertinib monotherapy group | 557 (1 RCT) | NR | ███ per 1,000 | ███ per 1,000 (███ to ███ per 1,000) | ███ more per 1,000 (██ more to ███ more per 1,000) | Moderatec | Osimertinib + chemotherapy likely results in an increase in the probability of being progression-free at 12 months, compared to osimertinib monotherapy |
Probability of being progression-free at 24 months Median follow-up duration (months): 19.5 for osimertinib + chemotherapy group; 16.5 for osimertinib monotherapy group | 557 (1 RCT) | NR | ███ per 1,000 | ███ per 1,000 (███ to ███ per 1,000) | ███ more per 1,000 (██ more to ███ more per 1,000) | Moderatec | Osimertinib + chemotherapy likely results in an increase in the probability of being progression-free at 24 months, compared to osimertinib monotherapy |
HRQoL — randomization phase, FAS (data cut-off date: June 1, 2021) | |||||||
Coughing symptoms subscale of the EORTC QLQ-LC13 (0 [best] to 100 [worst]) Follow-up: week 52 | 557 (1 RCT) | NR | −13.03 | −14.08 (−16.69 to −11.48) | −1.05 (−4.87 to 2.77) | Very lowd | The evidence is uncertain about the effect of osimertinib + chemotherapy on the coughing symptoms subscale of the EORTC QLQ-LC13 at week 52, compared to osimertinib monotherapy |
Pain in chest subscale of the EORTC QLQ-LC13 (0 [best] to 100 [worst]) Follow-up: week 52 | 557 (1 RCT) | NR | −7.03 | −6.65 (−8.92 to −4.38) | 0.38 (−2.96 to 3.72) | Very lowd | The evidence is uncertain about the effect of osimertinib + chemotherapy on the pain in chest subscale of EORTC QLQ-LC13 at week 52, compared to osimertinib monotherapy |
Dyspnea symptom subscale of the EORTC QLQ-LC13 (0 [best] to 100 [worst]) Follow-up: week 52 | 557 (1 RCT) | NR | −7.49 | −3.92 (−5.93 to −1.91) | 3.57 (0.65 to 6.48) | Very lowe | The evidence is uncertain about the effect of osimertinib + chemotherapy on the dyspnea symptom subscale of EORTC QLQ-LC13 at week 52, compared to osimertinib monotherapy |
Global Health Status/QoL of the EORTC QLQ-C30 (0 [worst] to 100 [best]) Follow-up: week 52 | 557 (1 RCT) | NR | 9.25 | 5.34 (3.17 to 7.51) | −3.91 (−7.04 to −0.77) | Very lowf | The evidence is uncertain regarding the effect of osimertinib + chemotherapy on the Global Health Status/QoL of EORTC QLQ-LC13 at week 52, compared to osimertinib monotherapy |
Harms, safety analysis set (data cut-off date: April 3, 2023) | |||||||
Anemia of grade 3 or higher | 551 (1 RCT) | Osimertinib + chemotherapy: 199 per 1,000 Osimertinib monotherapy: 4 per 1,000 | Highg | Osimertinib + chemotherapy results in an increase in anemia of grade 3 or higher, compared to osimertinib monotherapy | |||
SAEs | 551 (1 RCT) | Osimertinib + chemotherapy: 377 per 1,000 Osimertinib monotherapy: 193 per 1,000 | Highg | Osimertinib + chemotherapy results in an increase in SAEs, compared to osimertinib monotherapy | |||
Discontinuation of any treatment due to AEs | 551 (1 RCT) | Osimertinib + chemotherapy: 478 per 1,000 Osimertinib monotherapy: 62 per 1,000 | Highg | Osimertinib + chemotherapy results in an increase in discontinuation of any treatment due to AEs, compared to osimertinib monotherapy | |||
Deaths | 551 (1 RCT) | Osimertinib + chemotherapy: 65 per 1,000 Osimertinib monotherapy: 29 per 1,000 | Moderateh | Osimertinib + chemotherapy likely results in an increase in deaths, compared to osimertinib monotherapy | |||
ILD or pneumonitisi | 551 (1 RCT) | Osimertinib + chemotherapy: 33 per 1,000 Osimertinib monotherapy: 36 per 1,000 | Moderateh | Osimertinib + chemotherapy likely results in no or little difference in ILD or pneumonitis, compared to osimertinib monotherapy | |||
Cardiac failure | 551 (1 RCT) | Osimertinib + chemotherapy: 91 per 1,000 Osimertinib monotherapy: 36 per 1,000 | Moderateh | Osimertinib + chemotherapy likely results in an increase in cardiac effects, compared to osimertinib monotherapy | |||
AE = adverse event; CI = confidence interval; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; EORTC QLQ-LC13 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Lung Cancer Module; FAS = full analysis set; HRQoL = health-related quality of life; ILD = interstitial lung disease; MID = minimal important difference; NR = not reported; osimertinib + chemotherapy = osimertinib in combination with pemetrexed and platinum-based chemotherapy; NSCLC = non–small cell lung cancer; PFS = progression-free survival; RCT = randomized controlled trial; SAE = serious adverse event; vs. = versus.
Notes: The start point for the study design of the FLAURA2 trial (i.e., an RCT) was high certainty. Study limitations (which refer to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias were considered when assessing the certainty of the evidence. All serious concerns in these domains that led to the rating down of the level of certainty are documented in the table footnotes.
aCertainty was not rated down for risk of bias despite uncertainty about whether the proportional hazards assumption was met. Although the survival curves crossed over at earlier time points, there was clear separation at later time points. Indirectness was not rated down as the differences between patients in the indication and patients in the pivotal trial were not considered sufficient by the clinical experts consulted by the review team to result in important differences in the observed effect. Rated down 2 levels for very serious imprecision due to the following reasons. An empirically derived and validated between-group MID for overall survival was not identified. According to the clinical experts consulted by the review team, a between-group difference in the probability of being alive of between 5% and 10% may be clinically meaningful, and a difference of 10% or greater would indicate clinical significance. At 24 months, the point estimate of the between-group difference was between 5% and 10%, and the 95% CI for the between-group difference crossed both 5% and 10%, which indicated the possibility of both a benefit and no meaningful benefit. In addition, the overall survival data were not mature as of January 8, 2024 (40.6% maturity).
bCertainty was not rated down for risk of bias despite uncertainty about whether the proportional hazards assumption was met. Although the survival curves crossed over at earlier time points, there was clear separation at later time points. Indirectness was not rated down as the differences between patients in the indication and patients in the pivotal trial were not considered sufficient by the clinical experts consulted by the review team to result in important differences in the observed effect. Rated down 2 levels for very serious imprecision due to the following reasons. An empirically derived and validated between-group MID for overall survival was not identified. According to the clinical experts consulted by the review team, a between-group difference in the probability of being alive of between 5% and 10% may be clinically meaningful, and a difference of 10% or greater would indicate clinical significance. At 36 months, the point estimate of the between-group difference was greater than 10%; however, this was based on a large degree of uncertainty from few events and a high percentage of censoring (approximately 40% per group) between month 33 and month 36. The 95% CI for the between-group difference crossed both 5% and 10%, indicating the possibility of both a benefit and no meaningful benefit. In addition, the overall survival data were not mature as of January 8, 2024 (40.6% maturity).
cThe risk of bias was not rated down. Indirectness was not rated down as the differences between patients in the indication and patients in the pivotal trial were not considered sufficient by the clinical experts consulted by the review team to result in important differences in the observed effect. Rated down 1 level for serious imprecision. An empirically derived and validated between-group MID for PFS was not identified. According to the clinical experts consulted by the review team, a between-group difference of 10% or greater in the probability of being progression-free would indicate clinical significance. The 95% CI for the between-group difference included 10%, which indicated the possibility of both benefits and no meaningful benefit.
dRated 1 level down for risk of bias due uncertainty associated with missingness in data. For EORTC QLQ-LC13 assessments at week 52, out of 279 patients in the osimertinib plus chemotherapy group, 221 forms were expected, and 179 forms were received and evaluated, for a compliance rate of 81%. The type of data missing (e.g., completely at random, at random, or not at random) remains unclear, as does how the missingness in data would affect the HRQoL assessment. The risk of performance bias associated with the open-label design and the subjective nature of the measure was considered relatively low as no evidence in the data indicated that knowledge of treatment assignment affected the results. Indirectness was not rated down as the differences between patients in the indication and patients in the pivotal trial were not considered sufficient by the clinical experts consulted by the review team to result in important differences in the observed effect. Rated down 2 levels for very serious imprecision. An empirically derived and validated between-group MID for the coughing symptoms and chest pain subscales of the EORTC QLQ-LC13 was not identified. Because the clinical experts consulted by the review team were uncertain as to the exact threshold for clinical importance, the null was used as the threshold for clinical significance. The 95% CI of the between-group difference included the null or 0, indicating the possibility of both a benefit and little or no difference.
eRated 1 level down for risk of bias due to uncertainty associated with missingness in data. For EORTC QLQ-LC13 assessments at week 52, out of 279 patients in the osimertinib plus chemotherapy group, 221 forms were expected, and 179 forms were received and evaluated, for a compliance rate of 81%. The type of data missing (e.g., completely at random, at random, or not at random) remains unclear, as does how the missingness in data would affect the HRQoL assessment. The risk of performance bias associated with the open-label design and the subjective nature of the measure was considered relatively low as no evidence in the data indicated that knowledge of treatment assignment affected the results. Indirectness was not rated down as the differences between patients in the indication and patients in the pivotal trial were not considered sufficient by the clinical experts consulted by the review team to result in important differences in the observed effect. Rated down 2 levels for very serious imprecision. An empirically derived and validated between-group MID for the dyspnea symptom subscale of the EORTC QLQ-LC13 was not identified. Because the clinical experts consulted by the review team were uncertain as to the exact threshold for clinical importance, the null was used as the threshold for clinical significance. The lower bound of the 95% CI was greater than but close to the null, suggesting the magnitude of the effect was imprecisely estimated.
fRated 1 level down for serious risk of bias due to uncertainty associated with missingness in data. For EORTC QLQ-C30 assessments at week 52, out of 279 patients in the osimertinib plus chemotherapy group, 230 forms were expected, and 180 forms were received and evaluated, for a compliance rate of 78.3%. The type of data missing (e.g., completely at random, at random, or not at random) and how the missingness in data would affect the HRQoL assessment remain unclear. The risk of performance bias associated with the open-label design and the subjective nature of the measure was considered relatively low as no evidence in the data indicated that knowledge of treatment assignment affected the results. Indirectness was not rated down as the differences between patients in the indication and patients in the pivotal trial were not considered sufficient by the clinical experts consulted by the review team to result in important differences in the observed effect. Rated down 2 levels for very serious imprecision. An MID for the EORTC QLQ-C30 Global Health Status scale has not been definitively established, although a difference of 10 points is often cited. One review estimated the MID for the scale may be 5 points or greater in patients with lung cancer, and 5 points was adopted as the MID for this assessment.15 The between-group estimate is less than 5 points at week 52. The upper bound of the 95% CI crosses the null. Estimates therefore include both a trivial benefit and no benefit.
gRisk of bias was not rated down. Indirectness was not rated down as the differences between patients in the indication and patients in the pivotal trial were not considered sufficient by the clinical experts consulted by the review team to result in important differences in the observed effect. Imprecision was not rated down.
hRisk of bias was not rated down. Indirectness was not rated down as the differences between patients in the indication and patients in the pivotal trial were not considered sufficient by the clinical experts consulted by the review team to result in important differences in the observed effect. Rated down 1 level due to relatively smaller numbers of events.
iIncluded the following Medical Dictionary for Regulatory Activities Preferred Terms: interstitial lung disease, pneumonitis, acute interstitial pneumonitis, alveolitis, diffuse alveolar damage, idiopathic pulmonary fibrosis, lung disorder, organizing pneumonia, pulmonary toxicity, and pulmonary fibrosis.
Sources: FLAURA2 Clinical Study Report16 and Drug Reimbursement Review sponsor submission.17
Conclusions
The pivotal FLAURA2 trial is an ongoing, phase III, open-label RCT comparing the efficacy and safety of osimertinib plus chemotherapy and osimertinib monotherapy in patients with locally advanced, metastatic, or recurrent EGFRm (ex19del or L858R) NSCLC. Overall, efficacy evidence from the FLAURA2 trials suggests that osimertinib plus chemotherapy showed added clinical benefits in OS and PFS in the intention-to-treat trial population, compared with osimertinib monotherapy. Results of these clinically relevant efficacy end points were generally in favour of osimertinib plus chemotherapy over osimertinib monotherapy. Osimertinib plus chemotherapy may result in an increase in the probability of being alive at 24 and 36 months (low certainty) and likely lead to an increase in the probability of being progression-free at 12 and 24 months (moderate certainty), compared to osimertinib monotherapy. Because of the immaturity of the OS data (40.6%) and the fact that the median OS was not reached as of January 8, 2024, uncertainty remains in the OS results. The study subgroup analyses suggested the potential for greater benefit with osimertinib plus chemotherapy versus osimertinib monotherapy in patients with CNS metastases at baseline compared with patients without CNS metastases at baseline. However, uncertainty related to the trial design and analysis of these subgroups (including no formal interaction tests) prevented drawing a definitive conclusion. The review team concluded with moderate to high certainty that the combination use of osimertinib plus chemotherapy is associated with an increased frequency of grade 3 or higher AEs, SAEs, WDAEs, and deaths reported as AEs compared to osimertinib monotherapy.
Introduction
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of osimertinib (oral tablets, 40 mg and 80 mg), in combination with pemetrexed and platinum-based chemotherapy, for the first-line treatment of patients with locally advanced (not amenable to curative therapies) or metastatic NSCLC whose tumours have EGFR exon 19 deletions or L858R substitution mutations.
Disease Background
Contents within this section have been informed by materials submitted by the sponsor and clinical expert input. The following have been summarized and validated by the review team.
Lung cancer is the most commonly diagnosed cancer and the leading cause of cancer deaths in Canada.3,4 Survival rates from lung cancer of all stages and histologies are poor, with an overall 5-year net survival of 22%,4,18 and only 3% for those diagnosed with stage IV disease.4 In 2023, it was estimated that 31,000 cases of lung cancer would be diagnosed and 20,600 deaths from lung cancer would occur that year.4 It is estimated that 1 in 21 Canadians (4.8%) will die from lung cancer.4
Lung cancer is classified into NSCLC or small cell lung cancer, with NSCLC accounting for approximately 88% of cases in Canada.3 NSCLC is further classified into 3 main histologic subtypes: adenocarcinoma, squamous-cell carcinoma, and large-cell carcinoma.3 To determine a patient’s prognosis and treatment, NSCLC is staged using the AJCC criteria, which involves tumour-node-metastasis classification of the disease based on the size and spread of the primary tumour, lymph node involvement, and occurrence of metastasis.19 Approximately half of all lung cancer cases in Canada are stage I to III at diagnosis.3 Advanced disease as defined by the AJCC, includes stage IV (metastatic) and unresectable stage IIIB and IIIC (locally advanced) patients. NSCLC is often asymptomatic, and patients may live for several years before presentation due to its insidious nature.20 The most common symptoms include unspecific coughing, chest and shoulder pain, hemoptysis, weight loss, dyspnea, hoarseness, bone pain, fever, and recurring infections with bronchitis and pneumonia.20,21 Diagnostic procedures include imaging of the lungs, sputum cytology, and tissue biopsy.22 Approximately one-third of patients with NSCLC have operable disease.22
Approximately 15% of Canadians with NSCLC have an EGFR-activating mutation in the region of the genome encoding the tyrosine kinase domain.5-7 EGFR mutations are more frequently observed in never-smokers, people of Asian ethnicity, patients with adenocarcinoma, and females.5,8 The most common EGFR mutations are ex19del and L858R.6,7 A common feature of EGFRm NSCLC is the development of CNS metastases, which are detected in approximately 25% of patients at diagnosis and can affect approximately 50% of all patients within 3 years of diagnosis.9 Brain metastases are associated with decreased QoL and poor prognosis and are a significant cause of cancer-related mortality.10,11
Standards of Therapy
Contents within this section have been informed by materials submitted by the sponsor and clinical expert input. The following have been summarized and validated by the review team.
According to the clinical experts consulted by the review team, the goal of therapy in patients with advanced EGFRm NSCLC is to improve QoL and prolong survival while delaying disease progression.
For patients diagnosed with locally advanced or metastatic NSCLC who harbour EGFR mutations (i.e., ex19del and/or L858R), according to the clinical experts consulted by the review team, the current first-line treatment in Canada is osimertinib, which is a third-generation EGFR TKI. Alternative treatment options in the first-line setting include first- and second-generation EGFR TKIs (i.e., gefitinib, erlotinib, and afatinib) as well as platinum doublet chemotherapy. The clinical experts consulted by the review team also noted that patients would receive platinum doublet chemotherapy upon progressive disease after they had received osimertinib monotherapy.
Osimertinib is the preferred first-line treatment for EGFRm NSCLC based on a Canadian consensus and various provincial guidelines.7,23 Since osimertinib became available, gefitinib, erlotinib and afatinib have had limited utilization in the first-line treatment setting in Canada and instead are reserved for the small number of patients whose tumours have noneligible EGFR mutations that cannot be treated with osimertinib, as the Canadian consensus7 states “… gefitinib and erlotinib are not recommended in the first-line setting unless access to osimertinib is limited or unless they are combined with other drugs.”
The clinical experts consulted by the review team noted that amivantamab plus lazertinib could also be a first-line treatment option for patients with locally advanced or metastatic NSCLC who harbour EGFR mutations. However, amivantamab plus lazertinib is currently not available in Canada.
Drug Under Review
Key characteristics of osimertinib in combination with pemetrexed and platinum-based chemotherapy are summarized in Table 3, along with other treatments available for the first-line treatment of patients with locally advanced or metastatic NSCLC whose tumours have EGFR ex19del or L858R mutations. The recommended dose of osimertinib is 80 mg, once a day with pemetrexed and platinum-based chemotherapy.2
Osimertinib, is an irreversible TKI of both an EGFRm and T790M resistance mutation that has limited activity against wild-type EGFR.24 Osimertinib can readily cross the intact blood-brain barrier compared with earlier-generation EGFR TKIs.25-27
Table 3: Key Characteristics of Osimertinib Plus Chemotherapy and Osimertinib Monotherapy
Characteristic | Osimertinib + chemotherapy | Osimertinib monotherapy |
|---|---|---|
Mechanism of action | An irreversible TKI of both EGFRm and T790M resistance mutation that has limited activity against wild-type EGFR | Same |
Indicationa | For the first-line treatment of patients with locally advanced or metastatic NSCLC whose tumours have EGFR exon 19 deletions or L858R substitution mutations | For the first-line treatment of patients with locally advanced (not amenable to curative therapies), or metastatic NSCLC whose tumours have EGFR exon 19 deletions or L858R substitution mutations (either alone or in combination with other EGFR mutations) |
Route of administration | For osimertinib: oral; for pemetrexed + platinum-based chemotherapy: IV | Oral |
Recommended dose | For osimertinib: 80 mg tablet taken once a day, in combination with pemetrexed and platinum-based chemotherapy for 4 cycles, followed by osimertinib plus pemetrexed maintenance Dosing of pemetrexed + platinum-based chemotherapy: the recommended dose of pemetrexed is 500 mg/m2 administered over 10 minutes on day 1 of each 21-day cycle The recommended dose of cisplatin is 75 mg/m2 infused over 2 hours beginning approximately 30 minutes after completion of the pemetrexed administration; patients should receive appropriate hydration before and/or after receiving cisplatin The recommended dose of carboplatin is 5 mg/mL/min (AUC 5) | 80 mg tablet taken once a day |
Serious adverse effects or safety issues | Osimertinib: Interstitial lung disease (e.g., pneumonitis), including fatal cases; QTcF interval prolongation; left ventricular dysfunction and cardiomyopathy Chemotherapy Pemetrexed: Serious hepatobiliary toxicity and rare cases of fatal hepatic failure; gastrointestinal toxicity such as stomatitis, nausea, vomiting, and diarrhea; suppression of bone marrow function, as manifested by neutropenia, thrombocytopenia, and anemia (or pancytopenia); cases of hypersensitivity, including anaphylaxis; serious renal events, including acute renal failure; interstitial pneumonitis with respiratory insufficiency; rare cases of bullous epidermolysis including Stevens-Johnson syndrome and toxic epidermal necrolysis Platinum-based Cisplatin: Anaphylactic-like reactions; infections, such as sepsis; myelosupression such as neutropenia, leukopenia, thrombocytopenia; neurotoxicity (leukoencephalopathy; peripheral neuropathy; posterior reversible encephalopathy syndrome); renal toxicity; cardiovascular toxicity, such as venous thromboembolic events and pulmonary embolism Carboplatin: Highly toxic drug with a narrow therapeutic index; serious and fatal infections following administration of live or live-attenuated vaccines in patients treated with carboplatin; hypersensitivity reactions; bone marrow suppression; fatal veno-occlusive disease; fatal hemolytic anemia; fatal hemolytic-uremic syndrome | Osimertinib: Interstitial lung disease (e.g., pneumonitis), including fatal cases; QTcF interval prolongation; left ventricular dysfunction and cardiomyopathy |
Other | Chemotherapy Pemetrexed: May cause fetal harm when administered to a pregnant patient; contraindicated for concomitant yellow fever vaccine Cisplatin: Contraindicated in patients with pre-existing renal impairment and hearing impairment Carboplatin: Contraindicated in the following conditions: severe myelosuppression; pre-existing severe renal impairment; history of severe allergic reactions to carboplatin, or other platinum-containing compounds | NA |
AUC = area under the concentration-time curve during any dosing interval; EGFRm = EGFR–mutated; NSCLC = non–small cell lung cancer; osimertinib + chemotherapy = osimertinib in combination with pemetrexed and platinum-based chemotherapy; NA = not applicable; TKI = tyrosine kinase inhibitor.
aHealth Canada–approved indication.
Sources: Product monographs.2,28-30
Perspectives of Patients, Clinicians, and Drug Programs
Patient Group Input
The full patient and clinician group submissions received are available in the consolidated patient and clinician group input document for this review on the project website.
Two patient groups, LCC and the Lung Health Foundation (formerly the Ontario Lung Association), provided input on osimertinib plus chemotherapy for the first-line treatment of patients with locally advanced or metastatic NSCLC whose tumours have EGFR ex19del or L858R mutations. Patient input was gathered from interviews and surveys, conducted in January 2021 and October 2023 by the Lung Health Foundation, and in December 2023 by LCC. The Lung Health Foundation conducted 2 interviews and gathered 15 responses from online survey, while LCC conducted 13 interviews with patients and/or caregivers.
When asked about disease experience and its impact on day-to-day activities, respondents in the Lung Health Foundation input mentioned having varying experiences with their lung cancer diagnosis. Some symptoms and challenges these patients experienced because of their lung cancer were shortness of breath (80%), fatigue (60%), depression (25%), difficulty fighting infection (21%), and chest tightness (14%). Weight loss, diminished appetite, low mood, and challenges with physical and emotional intimacy were also noted by a few respondents. Respondents in this input indicated that the disease has negative impacts on their day-to-day life, affecting their ability to participate in leisure activities and hobbies, use stairs, shop, and travel. Family members and caregivers of those living with lung cancer shared the same psychosocial burdens as the patients in this input. In addition, LCC reported that patients living with lung cancer have repeatedly stated in interviews that their primary need is a treatment that improves their QoL while also managing their disease effectively.
Respondents from the Lung Health Foundation mentioned some benefits experienced with the currently available treatments, such as reduced coughing, reduced shortness of breath, increased participation in daily activities, ability to exercise, prolonged life, delayed disease progression, and a reduction in the severity of other disease-related symptoms. The input also noted that patients on oral drugs value the flexibility they provide in allowing them to work and travel without restrictions. Some patients from this input reported struggling with lingering side effects. Some of the side effects with medications mentioned in this input were extreme itching affecting sleep, brain fog, fatigue, nausea, vomiting, mood changes, diminished appetite, weight loss, hair loss, anemia, and neuropathy. The input also noted that side effects from chemotherapy severely affected the patients’ QoL, ability to work and in some cases, the ability to perform activities of daily living. Respondents who received surgery reported deconditioning and chronic fatigue. Some of the side effects reported from radiation were fatigue, skin changes, hair loss, and tissue scarring. When asked about challenges with access to treatment, the respondents from the Lung Health Foundation reported that they struggled with the cost associated with some treatments. They also found it challenging to navigate the health care system and, in some cases, they were unsure where to go for information and support. The LCC input mentioned that, although chemotherapy and radiation may be clinically beneficial, both come with well-documented side effects that often negatively affect a patient’s QoL. The input added that osimertinib as a monotherapy has been well received by patients interviewed for this submission.
Respondents from the Lung Health Foundation reported that key treatment outcomes to consider when evaluating new therapies included stopping or slowing the progression of the disease with minimal side effects, as well as medications that are effective for advanced disease. Patients in this input also expressed frustration with the speed at which treatments are approved in Canada, compared to other countries. Patients and caregivers perceive that fewer treatment options are available to them and that the drug approval process is a barrier to quick access. When choosing a therapy, some of the most crucial outcomes that patients in the LCC input wanted to have include improved management of their symptoms of EGFR NSCLC, a full and worthwhile QoL, manageable side effects, longer lives, independence and functionality to minimize the burden on their caregivers and loved ones, delayed disease progression, and the ability to settle into long-term management for improved survivorship.
Three patients from the Lung Health Foundation survey had experience with the drug under review. However, it was not clear if these patients were taking the drug as a monotherapy or in combination with chemotherapy. Some benefits reported by the patients include reduced coughing, reduced shortness of breath, improved ability to exercise, and increased participation in daily activities. Some of the side effects experienced on the drug by these patients include fatigue, appetite loss, low energy, nausea, and mild face rash. All 13 respondents from the LCC input had experience with osimertinib, 10 had received first-line and 3 had received second-line treatment. Respondents reported osimertinib to be effective at treating tumours and managing symptoms. Patients reported being able to maintain or improve their QoL, and function while on osimertinib. They also reported some frequent but manageable side effects. The most common side effects that patients interviewed by LCC recalled include diarrhea, muscle pain or spasms, lack of appetite, skin dryness or cracking, and fragile nails.
Clinician Input
Input From Clinical Experts Consulted for This Review
All CDA-AMC review teams include at least 1 clinical specialist with expertise regarding the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). The following input was provided by 2 clinical specialists with expertise in the diagnosis and management of patients with locally advanced or metastatic NSCLC whose tumours have EGFR ex19del or L858R mutations.
Unmet Needs
According to the clinical experts consulted by the review team, the key treatment goals for patients with locally advanced or metastatic NSCLC whose tumours have EGFR ex19del or L858R mutations included improving OS, controlling disease progression, and maintaining QoL. In addition, according to the clinical experts consulted by the review team, prevention and disease control of CNS metastasis are important aspects of the treatment goals. The clinical experts consulted by the review team noted that needs are not met in patients who are younger, present with significant disease burden, or have CNS metastases.
Place in Therapy
The clinical experts consulted by the review team noted that osimertinib plus chemotherapy may be offered as an alternative to osimertinib monotherapy as first-line treatment for patients with locally advanced or metastatic NSCLC whose tumours have EGFR ex19del or L858R mutations. The clinical experts consulted by the review team also noted that osimertinib monotherapy should remain as a first-line treatment option. The clinical experts consulted by the review team further noted that, if the osimertinib plus platinum chemotherapy was adopted in the first line with maintenance pemetrexed, second-line treatment options would include rechallenge with platinum doublet chemotherapy or docetaxel.
Patient Population
The clinical experts consulted by the review team noted that osimertinib plus chemotherapy may preferentially be considered in younger patients with locally advanced or metastatic NSCLC whose tumours have EGFR ex19del or L858R mutations. The clinical experts consulted by the review team noted that osimertinib plus chemotherapy may also be offered to patients with CNS metastases. However, according to the clinical experts consulted by the review team older patients with fewer disease-related symptoms may choose not to receive osimertinib plus chemotherapy because of the additive toxicity associated with osimertinib plus chemotherapy (compared to monotherapy).
Assessing the Response Treatment
According to the clinical experts consulted by the review team, outcomes to determine whether a patient is responding in clinical practice focus on functional status, disease-related symptoms, and radiographic imaging. Depending on local resources and time on treatment, radiographic imaging may be conducted every 2 to 4 months to confirm benefit. The clinical experts consulted by the review team noted that disease progression determined by RECIST would not necessarily result in a change in therapy, and patients may be considered for oligo-progression management with radiotherapy and continue on treatment. Alternatively, the patient and physician may discuss ongoing therapy, acknowledging that there is incomplete disease control. The clinical experts consulted by the review team noted that, in clinical practice patients may continue on osimertinib therapy for several months, even though they have met criteria for RECIST-determined progressive disease, if there is a good tolerance of osimertinib.
Discontinuing Treatment
According to the clinical experts consulted by the review team, overall, the decision to discontinue the therapy should be made jointly by the clinician and patient and be based on a combination of factors, such as patients’ symptoms and conditions, radiographic imaging results, toxicities, and laboratory parameters, as well as the balance against clinical benefit for that patient. The clinical experts consulted by the review team noted that it is reasonable to continue treatment as long as there is clinical benefit with respect to the targeted therapy component. In clinical practice, clinically meaningful symptomatic disease progression (rather than progression defined by RECIST) or toxicity would the rationale for stopping therapy.
Prescribing Considerations
The clinical experts consulted by the review team noted that the planned combination of osimertinib and chemotherapy would appropriately be delivered in any cancer treatment centre, academic facility, or community setting. According to the clinical experts consulted by the review team, patients should be treated by medical oncologists who are well versed in the management of EGFR TKIs and platinum chemotherapy toxicity.
Clinician Group Input
This section was prepared by the review team based on the input provided by clinician groups.
Clinician group input on the review of osimertinib plus chemotherapy for the first-line treatment of patients with locally advanced or metastatic NSCLC whose tumours have EGFR ex19del or L858R mutations, was received from 2 clinician groups: the OH-CCO Lung Cancer Drug Advisory Committee and LLC’s Medical Advisory Committee. A total of 28 clinicians provided input for this review.
The OH-CCO committee mentioned that current treatments target shrinking the cancer, improvement in disease-related symptoms, and maximizing control of the disease to prevent or delay symptoms and prolong life. However, both clinician groups indicated that the current treatment options with osimertinib monotherapy and/or sequential therapy with osimertinib followed by chemotherapy are not curative. Both clinician groups emphasized need for improved therapies that result in longer control of the cancer, better QoL and longer survival. The clinician groups mentioned the need to have therapies targeting specific patient populations, i.e., young patients and those with brain metastases, as did the clinical experts consulted by the review team. Both clinician groups described treatment for brain metastases in EGFR-driven lung cancer as an urgent unmet need.
Both clinician groups noted that the combination of osimertinib with chemotherapy would be an option in patients with NSCLC with sensitizing EGFR mutations. The OH-CCO group highlighted the need for OS data before drawing any conclusion regarding a shift in the current treatment paradigm. They also mentioned that the addition of platinum-based chemotherapy to osimertinib results in more inconvenience to patients due to the increase in chemotherapy-associated toxicities that require patients to attend a cancer centre more frequently for IV therapy. Similar to the clinical experts consulted by the review team, both clinician groups noted that single-drug osimertinib would remain an option in first-line therapy.
The OH-CCO committee pointed out that all patients who have classic EGFR mutations would be suitable for osimertinib therapy if they can tolerate and have not had prior adjuvant osimertinib within the last several months. They also mentioned that, for the addition of chemotherapy, suitable patients would be those for whom IV chemotherapy will be well tolerated or safe, and who have adverse features of their EGFR mutation–positive cancer. Similar to the clinical experts consulted by the review team, the clinician groups noted that there is a need for osimertinib plus chemotherapy among younger patients and patients with CNS metastases to gain survival benefits and improve QoL. Both clinician groups agreed that treatment would be discontinued in cases of disease progression or undue toxicity.
Drug Program Input
The drug programs provide input on each drug being reviewed the Reimbursement Review processes by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by the review team are summarized in Table 4.
Table 4: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Relevant comparators | |
The FLAURA-2 trial compared osimertinib-pemetrexed-platinum × 4 cycles followed by osimertinib and pemetrexed maintenance every 3 weeks with osimertinib alone, which is a relevant funded comparator in this setting. Other EGFR TKIs (erlotinib, gefitinib and afatinib) could potentially be used in this setting, but osimertinib is generally preferred, so there is no issue with the choice of comparator. No downstream treatment options would be affected. | This is a comment from the drug plans to inform pERC deliberations. |
Considerations for initiation of therapy | |
The FLAURA-2 trial enrolled patients with nonsquamous NSCLC, locally advanced (clinical stage IIIB, IIIC) or metastatic (clinical stage IVA or IVB), or recurrent NSCLC (according to version 8 of the IASLC staging manual), not amenable to curative surgery or radiotherapy.
| According to the clinical experts consulted by the review team, it is the driver mutation rather than histology that determines whether osimertinib should be used. The clinical experts indicated that it is plausible that the treatment effects of osimertinib + chemotherapy would likely not differ among patients with the same driving mutation but a different histology. According to the clinical experts consulted by the review team, osimertinib + chemotherapy should therefore be considered for patients with EGFR mutations in the proposed indication regardless of the histology of their lung cancer. According to the clinical experts consulted by the review team, some studies have demonstrated the effects of osimertinib in patients with NSCLC with uncommon EGFR mutations (e.g., L861q). The review team notes that these studies were not included in this submission and have not been reviewed in this report. In addition, the clinical experts consulted by the review team noted that to their knowledge, using osimertinib for patients with NSCLC with these uncommon EGFR mutations is not on-label in Canada. |
The FLAURA-2 trial allowed prior adjuvant and neoadjuvant therapies provided that the treatment was completed 12 months before the development of recurrent disease.
| The clinical experts consulted by the review team did not consider a 12-month interval before the development of recurrent disease is not appropriate in clinical practice. According to the clinical experts consulted by the review team, patients with a 6-month disease-free interval following completion of adjuvant chemotherapy alone or adjuvant osimertinib could be considered eligible for osimertinib + chemotherapy. The clinical experts consulted by the review team further noted that the clinicians should decide whether a patient with a disease-free interval of less than 6 months would be eligible for osimertinib + chemotherapy. |
Considerations for discontinuation of therapy | |
The FLAURA2 trial allowed treatment until disease progression or occurrence of unacceptable or clinically significant toxic effects. However, it was also noted that treatment beyond disease progression was permitted if the patient had a continued clinical benefit, according to the judgment of the investigator.
| Overall, it should be the clinician’s decision to discontinue the therapy based on a combination of factors, such as patients’ symptoms and conditions, radiographic imaging results, toxicities, and laboratory parameters, as well as the balance against clinical benefit for that patient. The clinical experts consulted by the review team noted that continuing on treatment as long as there is clinical benefit with the targeted therapy component is generally reasonable. In clinical practice, symptomatic disease progression or toxicity would be the rationale for stopping therapy. Of note, the clinical experts consulted by the review team clarified that patients with progression defined by RECIST may not necessarily indicate the deficiency of treatment and clinicians tend to make decisions regarding discontinuing treatment based on whether patients have clinically meaningful symptomatic disease progression. The clinical experts consulted by the review team noted that the decisions to stop osimertinib and chemotherapy should be dissociated, and it is not necessary to stop both osimertinib and chemotherapy at the same time. |
Generalizability | |
Should patients with a WHO PS > 1 be eligible? | The clinical experts consulted by the review team noted that rather than using rating of performance status to decide patient eligibility, a patient should be considered eligible if the patient has a good status in term of being suitable for chemotherapy. |
Funding algorithm | |
The drug plans noted the following items that may require the development of a provisional funding algorithm:
| This is a comment from the drug plans to inform pERC deliberations. |
Care provision issues | |
Additional toxicity is expected with the osimertinib-pemetrexed-platinum treatment (grade 3 or higher: 64% vs. 27%) (e.g., hematological toxicity 71% vs. 24%, cardiac toxicity 9% vs. 4%). | This is a comment from the drug plans to inform pERC deliberations. |
As EGFR mutation testing is part of routine clinical practice, it is not expected that there would be any incremental impact. | This is a comment from the drug plans to inform pERC deliberations. |
System and economic issues | |
Initial chemotherapy and maintenance pemetrexed require IV drug preparation and ambulatory treatment appointments every 3 weeks, which has an additional impact on resources. | This is a comment from the drug plans to inform pERC deliberations. |
There is a confidential negotiated prices for osimertinib, pemetrexed and cisplatin. | This is a comment from the drug plans to inform pERC deliberations. |
NSCLC = non–small cell lung cancer; osimertinib + chemotherapy = osimertinib in combination with pemetrexed and platinum-based chemotherapy; pERC = pan-Canadian Oncology Drug Review Expert Review Committee; RECIST = Response Evaluation Criteria in Solid Tumors; TKI = tyrosine kinase inhibitor; vs. = versus; WHO PS = WHO Performance Status.
Clinical Evidence
The objective of the Clinical Review Report is to review and critically appraise the clinical evidence submitted by the sponsor on the beneficial and harmful effects of osimertinib (oral tablets, 40 mg and 80 mg), in combination with pemetrexed and platinum-based chemotherapy, for the first-line treatment of patients with locally advanced (not amenable to curative therapies) or metastatic NSCLC whose tumours have EGFR ex19del or L858R mutations. The focus will be placed on comparing osimertinib plus chemotherapy to relevant comparators and identifying gaps in the current evidence.
A summary of the clinical evidence included by the sponsor in the review of osimertinib plus chemotherapy is presented in 1 section, with the critical appraisal of the evidence included at the end. The only section, a systematic review, includes pivotal studies and RCTs that were selected according to the sponsor’s systematic review protocol. Our assessment of the certainty of the evidence in this first section using the GRADE approach follows the critical appraisal of the evidence.
Included Studies
Clinical evidence from 1 phase III, open-label RCT, FLAURA2, is included in the review and appraised in this document.
Systematic Review
Contents within this section have been informed by materials submitted by the sponsor. The following summary was validated by the review team.
Description of Studies
One study conducted by the sponsor, FLAURA2,16,31 met the inclusion criteria of the sponsor-submitted systematic literature review. Characteristics of the included study are summarized in Table 5.
Table 5: Details of Studies Included in the Systematic Review
Detail | FLAURA2 |
|---|---|
Designs and populations | |
Study design | Multinational, open-label, randomized, phase III trial |
Locations | Patients were enrolled in 151 sites in 21 countries across Europe, Asia-Pacific, North America, South America, and Africa. There were 3 sites in Canada that enrolled a total of 13 patients in Canada. |
Key dates | Patient enrolment start date: May 15, 2020 Patient enrolment end date: November 30, 2021 |
Randomized (N) | Randomization phase: full analysis set, N = 557
|
Inclusion criteria |
|
Exclusion criteria |
|
Drugs | |
Intervention | Osimertinib 80 mg oral tablets once daily in combination with pemetrexed (500 mg/m2) and either cisplatin (75 mg/m2) or carboplatin (AUC of 5 mg/mL/min), with both treatments administered by IV infusion on day 1 of 21-day cycles for 4 cycles, followed by osimertinib 80 mg once daily plus pemetrexed maintenance (500 mg/m2) every 3 weeks, until disease progression as defined by RECIST 1.1, unacceptable toxicity, or until a treatment discontinuation criterion was met |
Comparator(s) | Osimertinib 80 mg oral tablets once daily, until disease progression as defined by RECIST 1.1, unacceptable toxicity, or until a treatment discontinuation criterion was met |
Study duration | |
Screening phase | 28 days |
Safety run-in phase | Until RECIST 1.1–defined progression or another discontinuation criterion was met; the safety run-in was conducted before the randomized period; patients included in the safety run-in were not included in the randomized phase |
Randomized phase | Until RECIST 1.1–defined progression by the investigator, or until another discontinuation criterion was met; following RECIST 1.1–defined progression, patients were followed for second progression on a subsequent treatment (according to local standard clinical practice) every 12 weeks, and for survival |
Follow-up phase | RECIST 1.1 assessment at 6 and 12 weeks, then every 12 weeks until RECIST 1.1–defined radiological disease progression or other withdrawal criteria were met. Brain imaging mandatory at baseline and progression for all patients, and at scheduled assessments until progression for patients with baseline CNS metastases |
Outcomes | |
Primary end point | PFS based on investigator assessment Time frame: until the date of objective disease progression (based on RECIST 1.1) or death (by any cause in the absence of progression), regardless of whether the patient withdrew from study treatment or received another anticancer therapy before progression |
Secondary and exploratory end points | Secondary:
HRQoL:
Safety:
Exploratory:
|
Publication status | |
Publications | 1 clinical trial registry entry (NCT04035486) |
AE = adverse event; ALT = alanine transaminase; AST = aspartate transaminase; AUC = area under the concentration-time curve; BICR = blinded independent central review; CLIA = Clinical Laboratory Improvement Amendments; CNS = central nervous system; CR = complete response; CTCAE = Common Terminology Criteria for Adverse Events; DCR = disease control rate; DoR = duration of response; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; EORTC QLQ-LC13 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Lung Cancer Module; HRQoL = health-related quality of life; LLN = lower limit of normal; NSCLC = non–small cell lung cancer; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; PFS2 = time to second progression; PR = partial response; PS = performance status; RECIST 1.1 = Response Evaluation Criteria in Solid Tumors Version 1.1; TFST = time to first subsequent therapy; TKI = tyrosine kinase inhibitor; TSST = time to second subsequent therapy; ULN = upper limit of normal.
Sources: FLAURA2 Clinical Study Protocol,39 FLAURA2 Clinical Study Reports.16,31 (Details included in the table are from the sponsor’s Summary of Clinical Evidence.1)
The FLAURA2 study is a phase III, open-label RCT investigating the use of osimertinib plus chemotherapy in patients with locally advanced, metastatic, or recurrent EGFRm (ex19del and/or L858R) NSCLC, not amenable to surgery or radiotherapy. The FLAURA2 trial was conducted in 557 patients from 21 countries worldwide, including patients in Canada. Patients were randomized to the osimertinib plus chemotherapy group (n = 279) or the osimertinib monotherapy group (n = 278), stratified by race, WHO PS, and methods used for tissue testing. The primary objective was to compare the treatment effect between osimertinib plus chemotherapy treatment versus osimertinib monotherapy, measured by PFS according to investigator assessment. Assessment of OS was a key secondary objective. The trial is ongoing, and the data cut-off date was April 3, 2023. Of note, OS data were updated on January 8, 2024, and assessed in this report. The schematic of the study design of the FLAURA2 trial is shown in Figure 1. Before randomization, there was a safety run-in period involving 30 patients with the aim of assessing the safety and tolerability of osimertinib plus chemotherapy. The safety run-in period has been completed with a data cut-off date of February 19, 2020.
Populations
Inclusion and Exclusion Criteria
The FLAURA2 trial included adult patients with pathologically confirmed nonsquamous NSCLC that was locally advanced (clinical stage IIIB, IIIC), metastatic (clinical stage IVA or IVB), recurrent (according to version 8 of the International Association for the Study of Lung Cancer Staging Manual in Thoracic Oncology), or not amenable to curative surgery or radiotherapy, including chemotherapy, biologic therapy, immunotherapy, or any investigational drug. The tumour of the eligible patients must harbour 1 of the 2 common EGFR mutations known to be associated with EGFR TKI sensitivity (i.e., ex19del or L858R), either alone or in combination with other EGFR mutations. Eligible patients should also have a WHO PS of 0 or 1. Prior adjuvant and neoadjuvant therapies (e.g., chemotherapy, radiotherapy, immunotherapy, biologic therapy, or investigational drugs), or definitive radiation and/or chemoradiation with or without regimens, including immunotherapy, biologic therapies, investigational drugs, were permitted as long as the treatment had been completed at least 12 months before the development of recurrent disease.
Figure 1: Schematic of the FLAURA2 Study Design
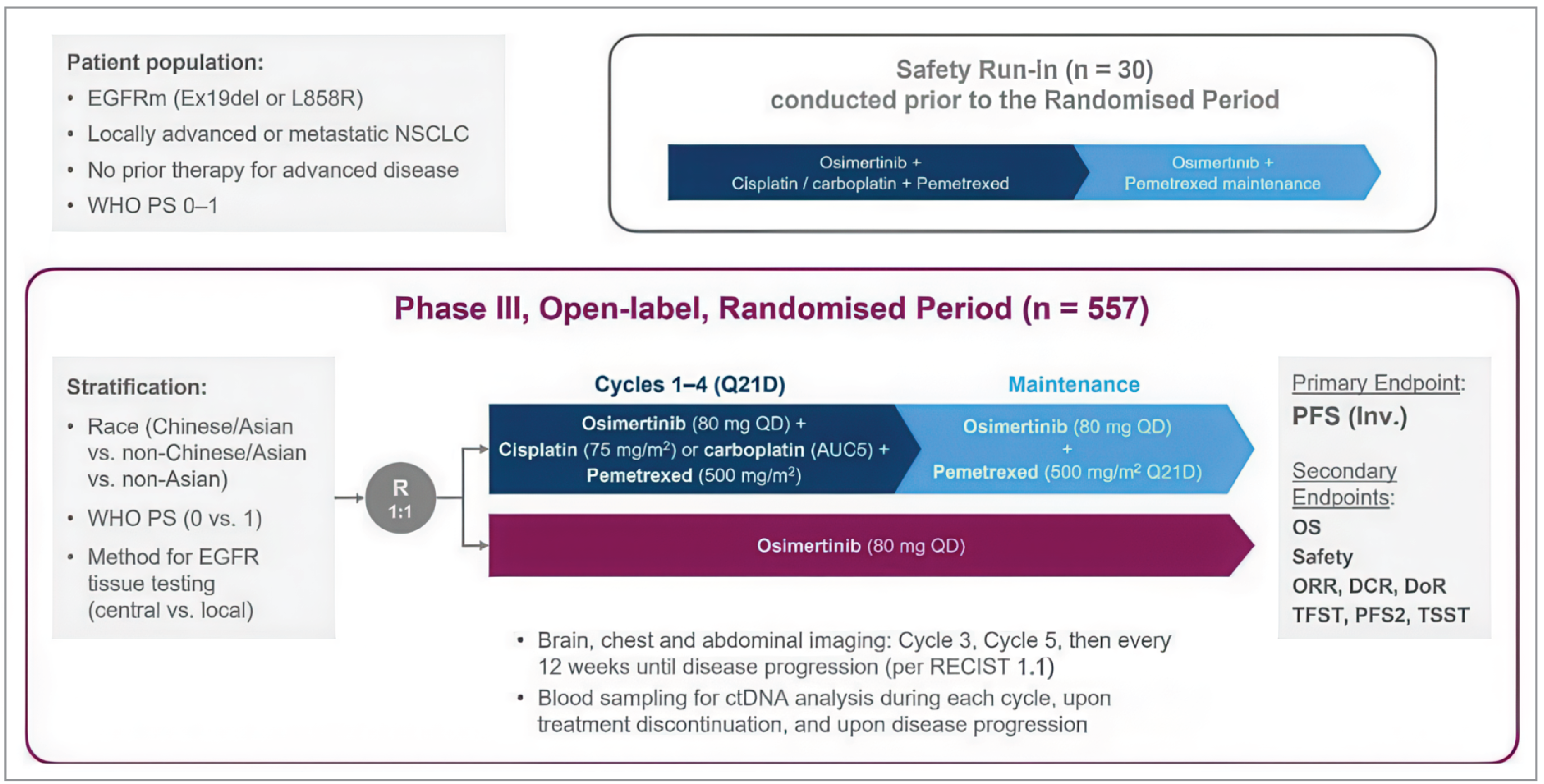
AUC5 = area under the concentration-time curve of 5 mg/mL/min; CNS = central nervous system; ctDNA = circulating tumour DNA; DCR = disease control rate; DoR = duration of response; EGFRm = eGFR–mutated; Inv. = investigator NSCLC = non–small cell lung cancer; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; PFS2 = time to second progression; Q21D = every 21 days; QD = once daily; RECIST 1.1 = Response Evaluation Criteria in Solid Tumors Version 1.1; TFST = time to first subsequent therapy; TSST = time to second subsequent therapy; WHO PS = WHO Performance Status.
Note: The safety run-in and randomized periods of the study were separate. Crossover between treatment groups was not permitted. Brain scans were performed in all patients at baseline and at progression. Patients with CNS metastases identified at baseline scan, or with a history of CNS metastases, had brain scans at each tumour assessment (baseline, 6 weeks, 12 weeks, and then every 12 weeks) until disease progression.
Sources: FLAURA2 Clinical Study Reports.16 (Details included in the table are from the sponsor’s Summary of Clinical Evidence.1)
Interventions
In the FLAURA2 trial, patients were randomized to 1 of 2 treatment groups:
osimertinib plus chemotherapy in the form of 80 mg oral tablets once daily with pemetrexed (500 mg/m2) and either cisplatin (75 mg/m2) or carboplatin (area under the concentration-time curve during any dosing interval of 5 mg/mL/min), with both treatments administered on day 1 of 21-day cycles for 4 cycles, followed by osimertinib 80 mg daily and pemetrexed maintenance (500 mg/m2), every 3 weeks
osimertinib monotherapy in the form of 80 mg oral tablets once daily.
In both treatment groups, osimertinib doses were to be taken approximately 24 hours apart at the same time each day. Doses were not to be missed. If a patient missed a scheduled dose, they could take the dose within a window of 12 hours. If the delay was more than 12 hours after the scheduled administration time, the missed dose was not to be taken, and the patient was advised to take the next dose at the next scheduled time. The initial dose of osimertinib 80 mg once daily could be reduced to 40 mg once daily to manage toxicities. However, once the dose of osimertinib was reduced to 40 mg once per day, the patient was to remain on the reduced dose until termination from study treatment. Rechallenge at 80 mg was not allowed.
In terms of chemotherapy (pemetrexed and platinum-based therapy), investigators could choose either carboplatin or cisplatin as the platinum-based therapy for patients according to local clinical practice, and patients could be switched to the alternative platinum drug.
Pemetrexed was administered at a dose of 500 mg/m2 as an IV infusion over 10 minutes on day 1 of each 21-day cycle according to local practice and labels until Response Evaluation Criteria in Solid Tumors Version 1.1 (RECIST 1.1)-defined progression or another discontinuation criterion was met. To reduce the severity of hematologic and gastrointestinal toxicity of pemetrexed, patients also received vitamin supplements. Patients were given oral folic acid or a multivitamin containing folic acid (350 mcg to 1,000 mcg) daily, and an intramuscular injection of vitamin B12 (1,000 mcg) in the week preceding the first dose of pemetrexed and once every 3 cycles thereafter. Subsequent vitamin B12 injections were given on the same day as pemetrexed. An oral corticosteroid (equivalent to 4 mg of dexamethasone administered orally twice a day) was given the day before, on the day of, and the day after pemetrexed administration to reduce the occurrence and severity of skin reactions.
Cisplatin was given at a dose of 75 mg/m2 as an IV infusion, according to local practice and labels approximately 30 minutes after the pemetrexed infusion, every 3 weeks for 4 cycles, and immediately preceded and followed by hydration.
Carboplatin was administered at a dose for a target area under the concentration-time curve during any dosing interval of 5 mg/mL/min over 15 to 60 minutes, after the pemetrexed infusion, every 3 weeks for 4 cycles, according to local practice and labels. Carboplatin dose was calculated using the Calvert formula. The carboplatin dose was not to exceed 750 mg.
Patients were to continue their randomized treatment until disease progression as defined by RECIST 1.1, unacceptable toxicity, or until a treatment discontinuation criterion was met. The criteria of discontinuation of study treatment included RECIST 1.1–defined progression if the patient was no longer receiving clinical benefit, patient decision, investigator decision, AEs, severe noncompliance with the study protocol, incorrect initiation on investigational product, and pregnancy. Patients were allowed to continue receiving their study treatment beyond RECIST 1.1–defined progression if, in the judgment of the investigator, they were receiving a clinical benefit and did not meet any of the discontinuation criteria. However, if the patient was deemed to have clinically significant unacceptable or irreversible toxicities, rapid tumour progression, or symptomatic progression requiring urgent medical intervention (e.g., CNS metastases, respiratory failure, spinal cord compression), the treatment was to be discontinued.
To maintain the dose intensity of osimertinib monotherapy and manage potential overlapping toxicities, it was recommended that, if clinically appropriate and where osimertinib interruption is not mandated, dose interruption or reduction of chemotherapy was prioritized above dose interruption or dose reduction of osimertinib. A maximum of 2 dose reductions for each component of chemotherapy treatment (i.e., cisplatin, carboplatin, or pemetrexed) was allowed. If a patient experienced toxicity that warranted a third dose reduction for any component of chemotherapy, that drug was to be discontinued. Only 1 dose reduction was permitted for osimertinib treatment. If a patient experienced a toxicity associated with osimertinib that would warrant a second dose reduction, osimertinib was to be discontinued. If a dose reduction for toxicity occurred with any drug, the dose of that drug might not have been re-escalated.
Outcomes
A list of efficacy end points assessed in this Clinical Review Report is provided in Table 6, followed by descriptions of the outcome measures. Summarized end points are based on outcomes included in the sponsor’s Summary of Clinical Evidence as well as any outcomes identified as important to this review according to the clinical expert(s) consulted for this review and input from patient and clinician groups and public drug plans. Using the same considerations, we selected end points that were considered to be most relevant to inform expert committee deliberations and finalized this list of end points in consultation with members of the expert committee. All summarized efficacy end points were assessed using GRADE. Select notable harms outcomes considered important for informing expert committee deliberations were also assessed using GRADE.
Table 6: Outcomes Summarized From FLAURA2
Outcome measure | Time point | FLAURA2 |
|---|---|---|
Overall survival:
| Time from the date of randomization until death due to any cause | Key secondary |
Progression-free survivala,b | Time from randomization until the date of objective disease progression or death (by any cause in the absence of progression) | Primary |
EORTC QLQ-LC13
| Week 52 posttreatment Week 82 posttreatment Averagec | Secondary |
EORTC QLQ-C30
| Week 52 posttreatment Week 82 posttreatment Averagec | Secondary |
BICR = blinded independent central review; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; EORTC QLQ-LC13 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Lung Cancer Module; MMRM = mixed-effects model for repeated measures; QoL = quality of life.
aStatistical testing for these end points was adjusted for multiple comparisons (e.g., hierarchal testing).
bPFS according to investigator assessment was prespecified as the primary outcome for FLAURA2; PFS according to BICR was presented as a sensitivity analysis.
cAverage included all patients contributing to the MMRM model over all visits (i.e., over 19 months or until progression disease). The score values are calculated by averaging across patients overall mean across all visits.
Sources: FLAURA2 Clinical Study Protocol version 2.0,39 FLAURA2 Statistical Analysis Plan version 2.0,40 FLAURA2 Clinical Study Report.16 (Details included in the table are from the sponsor’s Summary of Clinical Evidence.1)
Descriptions of efficacy and safety outcomes presented in FLAURA2 and appraised in the Clinical Review Report follow.16,39,40
Efficacy Outcomes
Overall Survival
Overall survival was defined as the time from the date of randomization until death due to any cause, regardless of whether the patient withdrew from study treatment or received another anticancer therapy (i.e., date of death or censoring – date of randomization + 1). Any patient not known to have died at the time of analysis was censored based on the last recorded date.
Progression-Free Survival
Progression-free survival according to investigator was specified as the primary outcome for the FLAURA2 trial, while PFS according to BICR was presented as a sensitivity analysis. PFS was defined as the time from randomization until the date of objective disease progression or death (by any cause in the absence of progression), regardless of whether the patient withdrew from randomized therapy or received another anticancer therapy before progression.
Patients who had not progressed or died at the time of analysis were censored at the time of the latest date of assessment from their last evaluable RECIST assessment. However, if the patient progressed or died after 2 or more missed visits, the patient was censored at the time of the latest evaluable RECIST assessment. Patients who had no evaluable visits or who did not have baseline RECIST data were censored at study day 1 unless they died within 2 visits of baseline, in which case their date of death was used as an event. The following rules were applied. First, the date of progression was determined based on the earliest of the dates of the component that triggered the progression; second, when censoring a patient for PFS, the patient was censored at the latest of the dates contributing to a particular overall visit assessment.
Details of censoring for primary PFS analysis are presented in Table 7.
Health-Related Quality of Life
A summary of EORTC QLQ-LC13 results is shown in Table 8.
Table 7: Censoring Rules for Primary PFS in FLAURA2
Situation | Event or censored | Event date or censored date |
|---|---|---|
No evaluable postbaseline visits or does not have baseline RECIST 1.1 data, and did not die within 2 visits of baseline | Censored | Randomization date (study day 1) |
No evaluable postbaseline visits or does not have baseline RECIST 1.1 data, and died within 2 visits of baseline | Event | Death date |
Progresses or died immediately after 2 or more consecutive missed visits | Censored | Latest evaluable RECIST 1.1 assessment before the 2 missed visits |
Disease progression or death (by any cause in the absence of progression) without 2 or more consecutive missed visits regardless of whether the patient withdrew from randomized therapy or received another anticancer therapy before progression | Event | Disease progression date, or death date if no progressive disease |
Not progressed or died at the time of analysis | Censored | Latest date of assessment from their last evaluable RECIST 1.1 assessment |
PFS = progression-free survival; RECIST 1.1 = Response Evaluation Criteria in Solid Tumors Version 1.1.
Source: FLAURA2 Statistical Analysis Plan version 2.0.40
Table 8: Summary of Outcome Measures and Their Measurement Properties
Outcome measure | Type | Conclusions about measurement properties | Minimal important difference |
|---|---|---|---|
EORTC QLQ-C30 | Cancer-specific self-reported measure of HRQoL 30-item questionnaire, consisting of 5 functional scales (physical, role, emotional, social, and cognitive), 9 symptom scales (fatigue, nausea/vomiting, pain, dyspnea, insomnia, appetite loss, constipation, diarrhea, and financial difficulties), and a Global Health Status scale A higher score for functional scales and for Global Health Status represents better functioning ability or HRQoL; a higher score for symptom scales represents a worsening of symptoms41 | In studies with lung cancer patients: Validity: Moderate to strong correlations between the 5 EORTC QLQ-C30 functioning scales (r = 0.41 to 0.77); FACT-G and EORTC QLQ-C30 scales (r = 0.64 to 0.76);42 HADS with all EORTC QLQ-C30 functioning scales (r = 0.28 to 0.75); BPI scales with all EORTC QLQ-C30 scales except for nausea/vomiting (r = 0.20 to 0.72),43 supporting convergent validity Known-groups approach: Able to differentiate across different measures of cancer severity: cancer stages (d = 0.49); ECOG PS (d = 0.65); and self-reported health status (d = 1.36)42 Reliability: Cronbach alpha ranging from 0.56 to 0.93 with 7 scales having acceptable internal consistency (alpha > 0.70)44 Responsiveness: Group differences (improved vs. deteriorated ECOG PS) over 28 days between pre- and on-treatment periods showed a statistically significant difference in global quality of life (P < 0.01) scale; no such difference was identified in patients whose ECOG PS remained unchanged41 | In a study with patients with NSCLC: MID estimates for improvement (deterioration) using the ECOG PS and weight change as anchors: Physical functioning: 9 and 5 (4 and 6) Role functioning: 14 and 7 (5 and 5) Social functioning: 5 and 7 (7 and 9) Global Health Status: 9 and 4 (4 and 4) Fatigue: 14 and 5 (6 and 11) Pain: 16 and 2 (3 and 7).45 In a study of lung cancer patients: an anchor-based approach in which patients who reported “a little” change on the SSQ had subsequent changes on a scale of the EORTC QLQ-C30 of 5 to 10 points46 The sponsor’s submission indicated a minimum clinically relevant change was defined as a change in the score from baseline of ≥ 10 for scales/items from the EORTC QLQ-C30 |
EORTC QLQ-LC13 | A tumour-specific questionnaire used to supplement the EORTC QLQ-C30 that contains 13 items related to lung cancer symptoms and treatment side effects including: a 3-item scale assessing dyspnea and 9 single items: pain in chest, pain in arm or shoulder, pain in other parts, coughing, hemoptysis, sore mouth or tongue, dysphagia, peripheral neuropathy, and alopecia41 Higher scores on the symptom scales indicate worse symptoms41 | Validity: Construct validity has been established between pain score and disease type (P < 0.001); based on ECOG PS, construct validity was confirmed in dyspnea, coughing, and pain (P < 0.001) scores;47 correlation between spirometry result and dyspnea score was found to be weak (r = 0.24); BPI intensity score and QLQ-LC13 pain score were found to be modestly correlated (r > 0.4)43 Reliability: Good internal consistency reliability for the dyspnea multi-item scale (alpha = 0.81);47 however, internal consistency was found to be unacceptable for pain scores (alpha = 0.53 to 0.54) when EORTC QLQ-LC13 was used alone without questionnaire pain items;47 reliability estimate for dyspnea scale has been confirmed to be acceptable, i.e., alpha = 0.76 in another study43 Responsiveness: Dyspnea, coughing, and pain scores improved significantly over time between pre-treatment and on-treatment period (P < 0.001 for all except for extrathoracic pain which showed P < 0.05); responsiveness of chest pain (P < 0.01), dyspnea (P < 0.001) and coughing (P < 0.001) to change in ECOG PS was also noted47 | No relevant studies identified in patients with NSCLC For the sponsor-submitted study, a minimum clinically relevant change was defined as a change in the score from baseline of ≥ 10 for scales/items from the EORTC QLQ-LC13 |
BPI = Brief Pain Inventory; ECOG PS = Eastern Cooperative Oncology Group Performance Status; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; EORTC QLQ-LC13 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Lung Cancer Module; FACT-G = Functional Assessment of Cancer Therapy–General; HADS = Hospital Anxiety and Depression Scale; HRQoL = health-related quality of life; MID = minimal important difference; NSCLC = non–small cell lung cancer; SSQ = subjective significance questionnaire; vs. = versus.
Harms Outcomes
The harms outcomes assessed in the FLAURA2 trial included AEs, SAEs, deaths, withdrawals due to AEs, and notable harms (e.g., ILD, pneumonitis, cardiac failure, and hematological toxicities).
An AE was defined as treatment-emergent if the onset or worsening (according to an investigator’s report of a change in intensity) occurred after the first dose of study treatment and within 28 days of discontinuation (i.e., the last dose of study treatment) but before or on the start date of a subsequent anticancer treatment). AEs were coded based on the Medical Dictionary for Regulatory Activities (version 25.1) and graded for severity according to the Common Terminology Criteria for Adverse Events (version 5.0).
An SAE is an AE occurring during any study phase (including treatment and follow-up) that fulfilled 1 or more of the following criteria: resulted in death, was immediately life-threatening, required inpatient hospitalization or prolongation of existing hospitalization, resulted in persistent or significant disability or incapacity, was a congenital abnormality or birth defect, was an important medical event that might jeopardize the patient or might require medical treatment to prevent 1 of the outcomes listed.
Statistical Analysis
Sample Size and Power Calculation
In the FLAURA2 trial, the sample size was estimated based on the primary end point of PFS according to investigator assessment, which was initially planned to be analyzed when approximately 278 PFS events (approximately 50% maturity) had occurred. This was expected to occur approximately 33 months after the first patient was randomized (under an assumed 15-month exponential recruitment). As such, an overall sample size of approximately 556 patients was planned for randomization in a 1:1 ratio.
Assuming the PFS HR for the comparison of osimertinib plus chemotherapy versus osimertinib monotherapy was 0.68, 278 progression events would provide 90% power to demonstrate a statistically significant difference in PFS at a 5% 2-sided significance level. This translates to an improvement in median PFS from 19 months to 28 months, assuming exponential distribution and proportional hazards. The minimum critical HR was 0.79, which translated to an approximate median PFS improvement from 19 months to 24 months.
Statistical Testing
Details of the statistical analysis of selected efficacy end points are summarized in Table 9.
The assumption of proportionality was assessed for OS, PFS according to investigator assessment, and PFS according to BICR. Proportional hazards were tested first by examining plots of complementary log-log (event times) versus log (time) and, if these raised concerns, by fitting a time-dependent covariate (adding a treatment-by-time or treatment-by-ln[time] interaction term) to assess the extent to which this represented random variation. If a lack of proportionality was evident, the variation in treatment effect could be described by presenting a piecewise HR calculated over distinct time periods (e.g., 0 to 6 months, 6 to 12 months). For nonproportionality, the HR was interpreted as an average over the observed extent of follow-up unless there was extensive crossing of the survival curves. Treatment-by-covariate interaction was investigated if a lack of proportionality was found.
To control the type I error rate (alpha = 0.05, 2-sided), OS and PFS were tested in sequential order. If the previous analysis in the sequence was not statistically significant, the alpha would not be transferred to subsequent analyses. At the time of the primary analysis of PFS, if the PFS analysis was statistically significant, then subsequent hypothesis testing for OS would be performed at an overall 2-sided alpha significance level of 0.05 using the O’Brien and Fleming spending function. If the results of the PFS analysis were not statistically significant at the time of the PFS analysis, then no hypothesis testing for OS would be performed. The OS was tested in a hierarchical procedure, at the time of the PFS analysis and after the primary PFS analysis when the OS data were approximately 60% mature (approximately 334 death events across both groups).
Table 9: Statistical Analysis of Efficacy End Points in FLAURA2
End point | Statistical model | Adjustment factors | Handling of missing data | Sensitivity and/or subgroup analyses |
|---|---|---|---|---|
OS |
| Stratified by race (Chinese/Asian vs. non-Chinese/Asian vs. non-Asian), WHO PS (0 vs. 1), and method used for tissue testing (central vs. local) | Any patient not known to have died at the time of analysis was censored based on the last recorded date from the survival case report form page only | Not performed |
PFS |
| Stratified by race (Chinese/Asian vs. non-Chinese/Asian vs. non-Asian), WHO PS (0 vs. 1), and method used for tissue testing (central vs. local) |
| Sensitivity analyses
Subgroup analyses
|
EORTC QLQ-LC13 | Change from baseline was analyzed using the MMRM analysis with all data from baseline up to progressive disease or 19 months posttreatment, whichever was earlier, of randomization | NA | Missing data were not imputed and handled through the mechanism of MMRM itself | Not performed |
EORTC QLQ-C30 | Change from baseline was analyzed using the MMRM analysis with all data from baseline up to progressive disease or 19 months posttreatment, whichever was earlier, of randomization | NA | Missing data were not imputed and handled through the mechanism of MMRM itself | Not performed |
BICR = blinded independent central review; CI = confidence interval; CNS = central nervous system; ctDNA = circulating tumour DNA; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; EORTC QLQ-LC13 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Lung Cancer Module; HR = hazard ratio; MMRM = mixed-effects model for repeated measures; NA = not applicable; OS = overall survival; PFS = progression-free survival; RECIST = Response Evaluation Criteria in Solid Tumors; vs. = versus; WHO PS = WHO Performance Status.
Sources: FLAURA2 Clinical Study Protocol version 2.0,39 FLAURA2 Statistical Analysis Plan version 2.0,40 FLAURA2 Clinical Study Report.16 (Details included in the table are from the sponsor’s Summary of Clinical Evidence.1)
Analysis Populations
Analysis populations of the FLAURA2 trial are summarized in Table 10.
Table 10: Analysis Populations of FLAURA2
Population | Definition | Application |
|---|---|---|
Full analysis set | The full analysis set includes all randomized patients | The FAS is used for all efficacy analyses, and treatment groups are compared based on randomized study treatment, regardless of the treatment actually received |
Safety analysis set | The safety analysis set consists of all randomized patients who received at least 1 dose of study treatment | Safety data are not formally analyzed but are summarized descriptively according to treatment actually received (e.g., a patient who was randomized to osimertinib + chemotherapy but who received only osimertinib was summarized under the osimertinib monotherapy group) |
CNS full analysis set | The CNS full analysis set includes all patients who undertook a brain scan in the screening/baseline period, had their scan sent for CNS BICR review, and were identified by that review as having nonmeasurable and/or measurable brain disease at baseline (i.e., at least 1 nonmeasurable and/or 1 measurable brain lesion noted at baseline) | The CNS full analysis set is used for all CNS efficacy analyses |
BICR = blinded independent central review; CNS = central nervous system; FAS = full analysis set; osimertinib + chemotherapy = osimertinib in combination with pemetrexed and platinum-based chemotherapy.
Sources: FLAURA2 Clinical Study Protocol version 2.0,39 FLAURA2 Statistical Analysis Plan version 2.0,40 FLAURA2 Clinical Study Report.16 (Details included in the table are from the sponsor’s Summary of Clinical Evidence.1)
Protocol Amendments and Deviations
In total, there were 2 versions of the clinical study protocol. The original study protocol was issued on March 19, 2019, and the amended protocol on August 26, 2021. In the amended protocol, the timing of the primary analysis was revised to include the requirement for at least a 16-month follow-up from the time of last participant in, in addition to approximately 278 PFS events. This was due to COVID-19, which had impacted study enrolment in non-Asian countries. The primary analysis was not conducted until at least 16-month follow-up had been reached to ensure a sufficient time frame to observe disease progression events.
A summary of protocol deviations in the FLAURA2 trial is presented in Table 11. Overall, 6.8% of randomized patients (38 of 557) had at least 1 protocol deviation. The most common reason was noncompliance with a RECIST 1.1 assessment (3.6%, 20 of 557).
Table 11: Summary of Protocol Deviations in FLAURA2 (Randomized Period — FAS)
Protocol deviation | Number (%) of patients | |
|---|---|---|
Osimertinib + chemotherapy | Osimertinib monotherapy | |
Number of patients with at least 1 protocol deviation | 19 (6.8) | 19 (6.8) |
Patient failed inclusion criteria | 1 (0.4) | 2 (0.7) |
Patient met exclusion criteria | 2 (0.7) | 2 (0.7) |
Incorrect investigational product administration and/or treatment | 3 (1.1) | 4 (1.4) |
Patient received prohibited concomitant therapy | 2 (0.7) | 3 (1.1) |
Noncompliance with RECIST 1.1 assessment | 11 (3.9) | 9 (3.2) |
FAS = full analysis set; osimertinib + chemotherapy = osimertinib in combination with pemetrexed and platinum-based chemotherapy; RECIST 1.1 = Response Evaluation Criteria in Solid Tumors Version 1.1.
Source: FLAURA2 Clinical Study Report.16
Results
Patient Disposition
A summary of patient disposition in the FLAURA2 trial is presented in Table 12. Of 887 participants screened, 330 (37.2%) were excluded. There were 279 and 278 eligible patients randomized to the osimertinib plus chemotherapy group and the osimertinib monotherapy group, respectively. The proportions of patients who discontinued from the FLAURA2 trial were 29.4% for the osimertinib plus chemotherapy group and 31.3% for the osimertinib monotherapy group, with death the most common reason for discontinuation from the trial (25.1% versus 27.7%, respectively).
Table 12: Summary of Patient Disposition in FLAURA2
Patient disposition | Osimertinib + chemotherapy | Osimertinib monotherapy |
|---|---|---|
Screened, N | 887 | |
Patients excluded, N (%) | 330 (37.2) | |
Reason for exclusion, N (%)a | ||
Screen failure | 319 (35.9) | |
Patient decision | 6 (0.7) | |
Death | 5 (0.6) | |
Randomized (FAS), N | 279 | 278 |
Patients ongoing study at data cut-off, N (%)b | 197 (70.6) | 191 (68.7) |
Patients who discontinued from study, N (%)b | 82 (29.4) | 87 (31.3) |
Death | 70 (25.1) | 77 (27.7) |
Lost to follow-up | 0 | 0 |
Withdrawal by patients | 11 (3.9) | 9 (3.2) |
Screen failure | 1 (0.4) | 1 (0.4) |
Patients who received any study treatment, N (%)b | 276 (98.9) | 275 (98.9) |
Patients ongoing any study treatment, N (%)c | 154 (55.8) | 123 (44.7) |
Patients who discontinued all study products, N (%)c | 122 (44.2) | 152 (55.3) |
Patients who discontinued any study products, N (%)c | 210 (76.1) | 152 (55.3) |
Patients who received osimertinib, N (%)c | 276 (100) | 275 (100) |
Patients ongoing osimertinib, N (%)d | 154 (55.8) | 123 (44.7) |
Patients who discontinued osimertinib, N (%)d | 122 (44.2) | 152 (55.3) |
Reason for osimertinib discontinuation, N (%)d | ||
Progression | 68 (24.6) | 118 (42.9) |
Adverse event | 30 (10.9) | 17 (6.2) |
Patient decision | 8 (2.9) | 6 (2.2) |
Study-specific discontinuation criteria | 2 (0.7) | 1 (0.4) |
Other | 14 (5.1) | 8 (2.9) |
Patients who received carboplatin/cisplatin treatment, N (%)c | 276 (100) | NA |
Patients who completed 4 cycles of carboplatin/cisplatin treatment, N (%)d | 212 (76.8) | NA |
Patients ongoing carboplatin/cisplatin treatment, N (%)d | 0 | NA |
Patients who discontinued carboplatin/cisplatin treatment, N (%)d | 64 (23.2) | NA |
Reason for carboplatin/cisplatin discontinuation, N (%)d | ||
Progression | 1 (0.4) | NA |
Adverse event | 47 (17.0) | NA |
Patient decision | 6 (2.2) | NA |
Study-specific discontinuation criteria | 2 (0.7) | NA |
Other | 8 (2.9) | NA |
Patients who received pemetrexed treatment, N (%)c | 276 (100) | NA |
Patients ongoing pemetrexed treatment, N (%)d | 68 (24.6) | NA |
Patients who discontinued pemetrexed treatment, N (%)d | 208 (75.4) | NA |
Reason for pemetrexed discontinuation, N (%)d | ||
Progression | 31 (11.2) | NA |
Adverse event | 119 (43.1) | NA |
Patient decision | 30 (10.9) | NA |
Study-specific discontinuation criteria | 11 (4.0) | NA |
Severe noncompliance to protocol | 1 (0.4) | NA |
Condition under investigation improved or patient recovered | 1 (0.4) | NA |
Other | 15 (5.4) | NA |
Patients ingoing study at data cut-off | ||
FAS, N | 279 | 278 |
Safety analysis set, N | 276 | 275 |
FAS = full analysis set; NA = not applicable; osimertinib + chemotherapy = osimertinib in combination with pemetrexed and platinum-based chemotherapy.
Note: Data cut-off: April 3, 2023.
aPercentages are based on the total number of patients enrolled.
bPercentages are based on the FAS.
cPercentages are based on the Safety analysis set. One patient was randomized to the osimertinib plus chemotherapy group, but only received osimertinib and was therefore included in the osimertinib group for the safety analysis set.
dPercentages are based on the number of patients who received one dose of the corresponding study drug.
Sources: FLAURA2 Clinical Study Report16 and Drug Reimbursement Review sponsor submission.17
Baseline Characteristics
The baseline characteristics outlined in Table 13 are limited to those that are most relevant to this review or were felt to affect the outcomes or interpretation of the study results. Baseline demographics and disease characteristics were generally balanced between the osimertinib plus chemotherapy group and the osimertinib monotherapy group. Overall, the median age of enrolled patients was 61.0 years (range = 26 to 85 years). In total, 30.5% of patients were aged 65 years or older to younger than 75 years, and 8.4% of patients were aged 75 years or older. The majority of enrolled patients were female (61.4%), Asian (63.7%), with a WHO PS of 1 (62.8%), an ex19del mutation (53.1% by central cobas tissue test), and metastatic NSCLC at baseline (96.2%).
Exposure to Study Treatments
Details on the extent of exposure to study treatments in the FLAURA2 trials are summarized in Table 14. As of April 3, 2023, the overall duration of exposure to any study treatment across treatment groups in the safety analysis set ranged from 0.1 months to 33.8 months (median = 21.09). Patients in the osimertinib plus chemotherapy group had a longer exposure than those in the osimertinib monotherapy group (e.g., total exposure = 455.3 treatment-years versus 415.3 treatment-years).
In the osimertinib plus chemotherapy group, the median number of cisplatin or carboplatin treatment cycles was 4 (range = 1 to 6); 76.4% (211 of 276) and 0.7% of patients (2 of 276) received 4 or more cycles of cisplatin or 5 or more cycles of carboplatin. The median number of pemetrexed treatment cycles was 12 (range = 1 to 48); 80.1% (221 of 276) and 24.6% of patients (68 of 276) received 4 or more or 30 or more cycles of pemetrexed treatment, respectively.
Table 13: Summary of Baseline Characteristics in FLAURA2 (Randomized Period — FAS)
Characteristic | FLAURA2 | |
|---|---|---|
Osimertinib + chemotherapy (N = 279) | Osimertinib monotherapy (N = 278) | |
Age (years)a | ||
Mean (SD) | 61.0 (10.03) | 60.7 (10.57) |
Median | 61.0 | 61.5 |
Minimum to maximum | 26 to 83 | 30 to 85 |
Sex, n (%) | ||
Male | 106 (38.0) | 109 (39.2) |
Female | 173 (62.0) | 169 (60.8) |
Race, n (%) | ||
Asian | 179 (64.2) | 176 (63.3) |
White | 74 (26.5) | 83 (29.9) |
American Indian or Alaska Native | 11 (3.9) | 6 (2.2) |
Black or African | 2 (0.7) | 3 (1.1) |
Other | 13 (4.7) | 10 (3.6) |
Body mass index, kg/m2 | ||
n | 275 | 271 |
Mean (SD) | 24.36 (4.403) | 24.39 (4.374) |
Smoking status, n (%) | ||
Never | 188 (67.4) | 181 (65.1) |
Smoker | 91 (32.6) | 97 (34.9) |
Current | 4 (1.4) | 4 (1.4) |
Former | 87 (31.2) | 93 (33.5) |
WHO PS, n (%) | ||
0 (Normal activity) | 104 (37.3) | 102 (36.7) |
1 (Restricted activity) | 174 (62.4) | 176 (63.3) |
2 (In bed ≤ 50% of the time)b | 1 (0.4) | 0 |
AJCC stage (8th edition) at initial diagnosis, n (%) | ||
Stage IIIB | 9 (3.2) | 4 (1.4) |
Stage IIIC | 4 (1.4) | 3 (1.1) |
Stage IVA | 98 (35.1) | 104 (37.4) |
Stage IVB | 168 (60.2) | 167 (60.1) |
EGFR testing method/mutation type, n (%) | ||
Central test | 123 (44.1) | 117 (42.1) |
Exon 19 deletion | 75 (26.9) | 67 (24.1) |
L858R | 47 (16.8) | 49 (17.6) |
Unknown or not detectedc | 1 (0.4) | 1 (0.4) |
Local test | 156 (55.9) | 161 (57.9) |
Exon 19 deletion | 94 (33.7) | 101 (36.3) |
L858R | 59 (21.1) | 58 (20.9) |
Both exon 19 deletion and L858R substitution | 3 (1.1) | 1 (0.4) |
Not detectedd | 0 | 1 (0.4) |
Overall extent of disease at study entry, n (%) | ||
Metastatice | 265 (95.0) | 271 (97.5) |
Locally advancedf | 14 (5.0) | 7 (2.5) |
Histology type, n (%) | ||
Adenocarcinomag | 275 (98.6) | 275 (98.9) |
Adenosquamous carcinoma | 2 (0.7) | 0 |
Other | 2 (0.7) | 3 (1.1) |
Number of patients with metastases (by location), n (%)h | ||
Central nervous system | 116 (41.6) | 110 (39.6) |
Liver | 43 (15.4) | 66 (23.7) |
Lung/pleura | 196 (70.3) | 216 (77.7) |
Lymph nodes | 160 (57.3) | 170 (61.2) |
Bone + locomotive | 132 (47.3) | 142 (51.1) |
Extrathoracic | 147 (52.7) | 149 (53.6) |
Other | 64 (22.9) | 58 (20.9) |
Time from initial diagnosis to the first dose, months | ||
n | 277 | 274 |
Mean (SD) | 3.6 (12.03) | 3.6 (16.20) |
Median | 1.1 | 1.1 |
Baseline target lesion tumour size, mmi | ||
n | 278 | 277 |
Mean (SD) | 65.1 (42.36) | 64.1 (38.87) |
Median | 57.0 | 57.0 |
AJCC = American Joint Committee on Cancer; ctDNA = circulating tumour DNA; EGFRm = EGFR–mutated; FAS = full analysis set; L816Q = exon 21 codon 816; osimertinib + chemotherapy = osimertinib in combination with pemetrexed and platinum-based chemotherapy; SD = standard deviation; WHO PS = WHO Performance Status.
Note: Data cut-off date: April 3, 2023.
aAge at study entry.
bThe patient had a WHO PS of 1 at the time of randomization but before study drug administration had a record of WHO PS 2.
cOne patient was randomized based on an invalid central tissue result (and was therefore categorized as having an EGFRm status of unknown); a retrospective baseline ctDNA result was exon 19 deletion–positive. The other patient was randomized based on a negative central tissue result (and was therefore categorized as EGFRm status not detected); a retrospective baseline ctDNA result was L858R-positive.
dThe patient was randomized based on local result of L858R substitution–positive, which was subsequently updated to exon 21 L861Q–positive and confirmed by central test result.
eMetastatic disease: patient had any metastatic site of disease.
fLocally advanced: patient had only locally advanced sites of disease.
gRepresents a combination of the following adenocarcinoma categories: not otherwise specified, acinar, papillary, bronchiolo-alveolar, and solid with mucous formation.
hThis is a programmatically derived composite end point with a list of contributing data sources.
iSum of longest diameters of target lesions at baseline.
Source: FLAURA2 Clinical Study Report.16 (Details included in the table are from the sponsor’s Summary of Clinical Evidence.1)
Concomitant Medications
Details about commonly reported concomitant medications (used in ≥ 20% of patients in either group) are shown in Table 15. As of April 3, 2023, most of the patients (549 patients [98.9%]) received at least 1 permitted concomitant medication during the study.
Table 14: Summary of Patient Exposure in FLAURA2 (Randomized Period — Safety Analysis Set)
Exposure | Osimertinib + chemotherapy (N = 279) | Osimertinib monotherapy (N = 278) | |||
|---|---|---|---|---|---|
Osimertinib (n = 276) | Carboplatin or cisplatin (n = 276) | Pemetrexed (n = 276) | Overall (n = 276)a | ||
Total exposure (months)b, c | |||||
Duration, mean (SD) | 19.67 (9.053) | 2.58 (0.742) | 12.06 (9.836) | 19.80 (9.016) | 18.12 (8.908) |
Duration, median | 22.26 | 2.76 | 8.28 | 22.31 | 19.32 |
Minimum to maximum | 0.1 to 33.8 | 0.7 to 4.1 | 0.7 to 33.8 | 0.7 to 33.8 | 0.1 to 33.8 |
Total treatment-yearsd | 452.3 | 59.3 | 277.3 | 455.3 | 415.3 |
Actual exposure (months)e | |||||
Duration, mean (SD) | 19.32 (9.032) | — | — | 19.36 (9.004) | 17.95 (8.904) |
Duration, median | 21.83 | — | — | 21.83 | 19.02 |
Minimum to maximum | 0.1 to 33.4 | — | — | 0.1 to 33.4 | 0.1 to 33.8 |
Total treatment-yearsd | 444.5 | — | — | 445.3 | 411.3 |
osimertinib + chemotherapy = osimertinib in combination with pemetrexed and platinum-based chemotherapy; SD = standard deviation.
Note: Data cut-off date: April 3, 2023.
aPatient received any of the study drugs (osimertinib, cisplatin, carboplatin, or pemetrexed).
bFor osimertinib, total exposure = (min [last dose date where dose > 0 mg, date of death, date of data cut-off] – first dose date + 1) / 30.4375.
cFor pemetrexed, cisplatin, and carboplatin, total exposure = (min [last dose date where dose > 0 mg, date of death, date of data cut-off] – first dose date + 21) / 30.4375.
dTotal treatment-years is the sum of treatment durations of all patients by treatment group.
eActual exposure = (total exposure – total duration of dose interruptions [i.e., number of days with dose = 0 mg]) / 30.4375.
Source: FLAURA2 Clinical Study Report.16 (Details included in the table are from the sponsor’s Summary of Clinical Evidence.1)
Table 15: Concomitant Medications (20% or More of Patients in Either Treatment Group) in FLAURA2 (Randomized Period — FAS)
Concomitant medication | Osimertinib + chemotherapy (N = 279) | Osimertinib monotherapy (N = 278) |
|---|---|---|
Number of patients with a concomitant medication, n (%) | 276 (98.9) | 273 (98.2) |
██████ ████ ██████████ | ███ ██████ | ██ ██████ |
████████ | ███ ██████ | ██ ██████ |
███████████ | ███ ██████ | ██ ██████ |
███████████████ | ███ ██████ | ██ ██████ |
█████████████ | ██ ██████ | ██ ██████ |
█████ █████ ████████ | ██ ██████ | ██ ██████ |
███████████ | ██ ██████ | ██ ██████ |
█████████ ███████████ | ███ ██████ | ██ █████ |
███████████████ | ██ ██████ | ██ ██████ |
████████████████ ██ | ██ ██████ | ██ ██████ |
█████ ███████████ | ██ ██████ | ██ █████ |
██████████████ █████████ | ██ ██████ | ██ ██████ |
█████ ██████████████ ██ | ██ ██████ | ██ ██████ |
███████████ ███ █████████ | ██ ██████ | ██ █████ |
███████████ ██████ ██████ | ██ ██████ | ██ ██████ |
██████ ███████████ █████ | ██ ██████ | █████ |
███████████ █████████ | ██ ██████ | ██ █████ |
FAS = full analysis set; osimertinib + chemotherapy = osimertinib in combination with pemetrexed and platinum-based chemotherapy.
Note: Data cut-off date: April 3, 2023.
Source: FLAURA2 Clinical Study Report.16 (Details included in the table are from the sponsor’s Summary of Clinical Evidence.1)
Subsequent Treatment
A summary of subsequent treatment in the FLAURA2 trial is shown in Table 16. As of the data cut-off date (April 3, 2023), 20.4% of the patients in the osimertinib plus chemotherapy group and 32.7%% of the patients in the osimertinib monotherapy group received any post-treatment anticancer therapy.
Efficacy
Key efficacy results in the FAS during the randomized period are presented in Table 17.
Table 16: Summary of Subsequent Treatment in FLAURA2 (Randomized Period — FAS)
Subsequent treatment | April 3, 2023 | January 8, 2024 | ||
|---|---|---|---|---|
Osimertinib + chemotherapy (N = 279) | Osimertinib monotherapy (N = 278) | Osimertinib + chemotherapy (N = 279) | Osimertinib monotherapy (N = 278) | |
Discontinued randomized study treatment, n (%) | 123 (44.1) | 151 (54.3) | 155 (55.6) | 187 (67.3) |
Any posttreatment anticancer therapy | 57 (20.4) | 91 (32.7) | 74 (26.5) | 115 (41.4) |
No posttreatment anticancer therapy | 66 (23.7) | 60 (21.6) | 81 (29.0) | 72 (25.9) |
Ongoing randomized study treatment, n (%) | 154 (55.2) | 123 (44.2) | 122 (43.7) | 87 (31.3) |
Did not receive study treatment, n (%) | 2 (0.7) | 4 (1.4) | 2 (0.7) | 4 (1.4) |
Types of posttreatment anticancer therapy received, n (%) [%]a | ||||
Cytotoxic chemotherapy | 41 (14.7) [33.3] | 81 (29.1) [53.6] | 51 (18.3) [32.9] | 100 (36.0) [53.5] |
Platinum compounds | 19 (6.8) [15.4] | 78 (28.1) [51.7] | 27 (9.7) [17.4] | 96 (34.5) [51.3] |
Folic acid analogues (pemetrexed) | 8 (2.9) [6.5] | 55 (19.8) [36.4] | 12 (4.3) [7.7] | 72 (25.9) [38.5] |
Taxanes | 26 (9.3) [21.1] | 39 (14.0) [25.8] | 34 (12.2) [21.9] | 48 (17.3) [25.7] |
Otherb | 14 (5.0) [11.4] | 16 (5.8) [10.6] | 20 (7.2) [12.9] | 18 (6.5) [9.6] |
EGFR TKI | 18 (6.5) [14.6] | 39 (14.0) [25.8] | 29 (10.4) [18.7] | 51 (18.3) [27.3] |
First- or second-generation EGFR TKI | 12 (4.3) [9.8] | 22 (7.9) [14.6] | 17 (6.1) [11.0] | 27 (9.7) [14.4] |
Third-generation EGFR TKI | 6 (2.2) [4.9] | 22 (7.9) [14.6] | 13 (4.7) [8.4] | 29 (10.4) [15.5] |
Osimertinib | 6 (2.2) [4.9] | 19 (6.8) [12.6] | 10 (3.6) [6.5] | 24 (8.6) [12.8] |
Aumolertinib | 0 | 3 (1.1) [2.0] | 1 (0.4) [0.6] | 1 (0.4) [ 0.5] |
Furmonertinib | 0 | 0 | 2 (0.7) [ 1.3] | 1 (0.4) [ 0.5] |
VEGF inhibitor — monoclonal antibody | 14 (5.0) [11.4] | 38 (13.7) [25.2] | 21 (7.5) [13.5] | 46 (16.5) [24.6] |
PD-1 or PD-L1 inhibitor — immunotherapy | 10 (3.6) [8.1] | 22 (7.9) [14.6] | 13 (4.7) [8.4] | 25 (9.0) [13.4] |
Radiotherapy | 13 (4.7) | 30 (10.8) | NR | NR |
Other | 11 (3.9) [8.9] | 19 (6.8) [12.6] | 17 (6.1) [11.0] | 24 (8.6) [12.8] |
FAS = full analysis set; NR = not reported; osimertinib + chemotherapy = osimertinib in combination with pemetrexed and platinum-based chemotherapy; TKI = tyrosine kinase inhibitor; VEGF = vascular endothelial growth factor.
Note: Treatment beyond progression was not counted as a subsequent anticancer therapy. A patient may be counted in multiple rows if they receive more than 1 posttreatment anticancer therapy. Includes anticancer therapies with a start date after the last dose date of study treatment.
aThe number of patients is shown with percentages calculated as the proportion of patients in the FAS and second as the proportion of patients who discontinued randomized study treatment. A patient may be counted in multiple rows if they receive more than 1 posttreatment anticancer therapy. Includes anticancer therapies with a start date after the last dose date of study treatment.
bIncluding pyrimidine analogues, vinca alcaloids, anthracyclines, podophyllotoxin derivatives.
Sources: FLAURA2 Clinical Study Report16 and Drug Reimbursement Review sponsor submission.17
Overall Survival
As of the data cut-off date of January 8, 2024, the OS data had a data maturity of 40.6% and were adjusted for multiple statistical testing. There were 100 OS events (35.8%) in the osimertinib plus chemotherapy group and 126 OS events (45.3%) in the osimertinib monotherapy group. The HR for OS was 0.75 (95% CI, 0.57 to 0.97). The differences in the probability of being alive between osimertinib plus chemotherapy and osimertinib monotherapy at 24 and 36 months were 7.6 (95% CI, ███ to ████) and 13.5% (95% CI, ███ to ████), respectively. The median OS was 36.7 months in the osimertinib monotherapy group, but it was not reached in the osimertinib plus chemotherapy group. The Kaplan-Meier curves of the 2 treatment groups did not separate until about 16 months after randomization (Figure 2).
Figure 2: Kaplan-Meier Plot of OS in FLAURA2 (Randomized Period — FAS, Data Cut-Off Date: January 8, 2024)
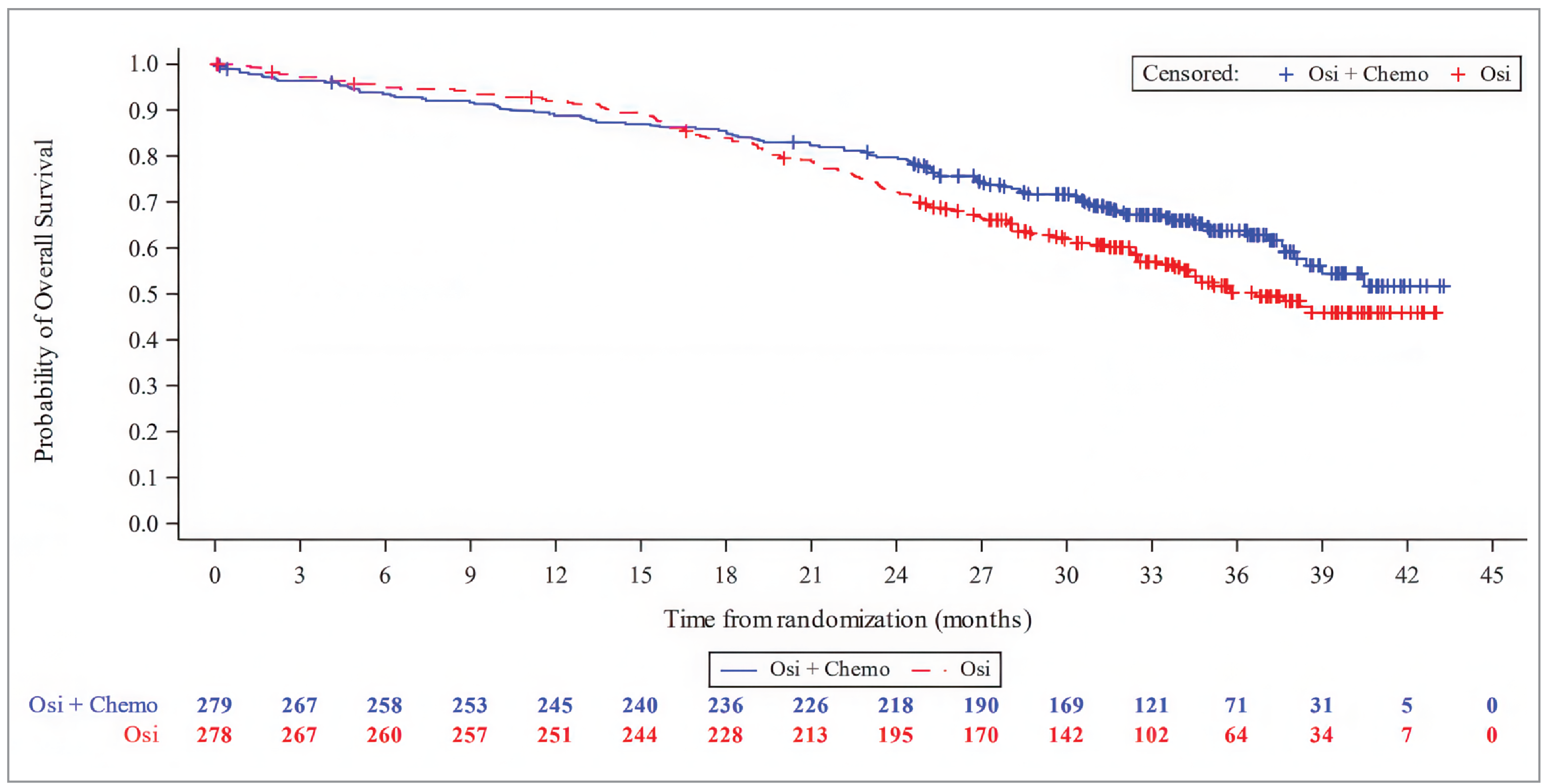
FAS = full analysis set; OS = overall survival; Osi = osimertinib; Osi + Chemo = osimertinib in combination with pemetrexed and platinum-based chemotherapy.
Note: The values at the base of the figure indicate number of patients at risk.
Source: Drug Reimbursement Review sponsor submission.17
Table 17: Summary of Key Efficacy Results in FLAURA2 (Randomized Period – FAS)
Efficacy outcome | Osimertinib + chemotherapy (N = 279) | Osimertinib monotherapy (N = 278) |
|---|---|---|
OS (data cut-off: January 8, 2024) | ||
Number (%) of deaths as of data cut-off date | 100 (35.8) | 126 (45.3) |
Median OS, months (95% CI)a | NC (38.0 to NC) | 36.7 (33.2 to NC) |
HR (95% CI) [2-sided P value]b | 0.75 (0.57 to 0.97) [0.0280] | |
Probability of being alive at 24 months, % (95% CI)a | 79.7 (74.5 to 84.0) | 72.1 (66.4 to 77.0) |
Difference in survival probability, % (95% CI) | 7.6 (███ to ████) | |
Probability of being alive at 36 months, % (95% CI)a | 63.7 (57.2 to 69.5) | 50.3 (43.4 to 56.7) |
Difference in survival probability, % (95% CI) | 13.5 (███ to ████) | |
Still in survival follow-up, n (%)c | 169 (60.6) | 143 (51.4) |
Terminated before death, n (%)d | 10 (3.6) | 9 (3.2) |
Completed | 0 | 0 |
Withdrawal by patient | 9 (3.2) | 8 (2.9) |
Lost to follow-up | 0 | 0 |
Other | 1 (0.4) | 1 (0.4) |
Median follow-up (minimum to maximum) for OS in all patients, months | 31.7 (0.1 to 43.3) | 30.5 (0.1 to 43.0) |
Median follow-up (minimum to maximum) for OS in censored patients, months | 34.0 (0.2 to 43.3) | 34.2 (0.1 to 43.0) |
PFS according to investigator assessment (data cut-off: April 3, 2023) | ||
Number (%) of PFS events | 120 (43.0) | 166 (59.7) |
Median PFS, months (95% CI)a | 25.5 (24.7 to NC) | 16.7 (14.1 to 21.3) |
HR (95% CI) [2-sided P value]e | 0.62 (0.49 to 0.79) [< 0.0001] | |
Probability of being progression-free at 12 months, % (95% CI)a | 79.7 (74.3 to 84.1) | 65.5 (59.5 to 70.8) |
Difference in survival probability, % (95% CI) | 14.2 (███ to ████) | |
Probability of being progression-free at 24 months, % (95% CI)a | 57.2 (50.4 to 63.3) | 40.8 (34.7 to 46.9) |
Difference in survival probability, % (95% CI) | 16.4 (███ to ████) | |
Progression, n (%) | 120 (43.0) | 166 (59.7) |
RECIST progressionf | 95 (34.1) | 158 (56.8) |
Target lesionsg | 51 (18.3) | 75 (27.0) |
Nontarget lesionsg | 31 (11.1) | 68 (24.5) |
New lesionsg | 46 (16.5) | 73 (26.3) |
Deathh | 25 (9.0) | 8 (2.9) |
No progression, n (%) | 159 (57.0) | 112 (40.3) |
Censored RECIST progression due to missing visitsi | 1 (0.4) | 0 |
Censored death due to missing visitsi | 6 (2.2) | 2 (0.7) |
Progression-free at time of analysisj | 143 (51.3) | 106 (38.1) |
Lost to follow-upk | 0 | 0 |
Withdrew consentk | 8 (2.9) | 3 (1.1) |
Discontinued study for other reasonsk | 1 (0.4) | 1 (0.4) |
Median follow-up (minimum to maximum) for PFS in all patients, months | 19.5 (0 to 33.3) | 16.5 (0 to 33.1) |
Median follow-up (minimum to maximum) for PFS in censored patients, months | 22.2 (0 to 33.1) | 23.7 (0 to 33.1) |
EORTC QLQ-LC13 (coughing symptoms subscale)l (data cut-off: April 3, 2023) | ||
Baseline | ||
n | 253 | 252 |
Mean (SD) | 32.4 (27.44) | 31.3 (28.55) |
Week 52 | ||
n | 169 | 139 |
Change from baseline LS mean (95% CI) | −14.08 (−16.69 to −11.48) | −13.03 (−15.83 to −10.23) |
LS mean difference [95% CI] | −1.05 (−4.87 to 2.77) | |
Averagem | ||
n | 253 | 251 |
Change from baseline LS mean (95% CI) | −13.23 (−14.85 to −11.62) | −11.19 (−12.83 to −9.55) |
LS mean difference [95% CI] | −2.04 (−4.35 to 0.26) | |
EORTC QLQ-LC13 (pain in chest subscale)l (data cut-off: April 3, 2023) | ||
Baseline | ||
n | 253 | 252 |
Mean (SD) | 16.9 (20.49) | 21.2 (25.46) |
Week 52 | ||
n | 169 | 139 |
Change from baseline LS mean (95% CI) | −6.65 (−8.92 to −4.38) | −7.03 (−9.47 to −4.59) |
LS mean difference (95% CI) | 0.38 (−2.96 to 3.72) | |
Averagem | ||
n | 253 | 252 |
Change from baseline LS mean (95% CI) | −6.33 (−7.66 to −4.99) | −6.61 (−7.98 to −5.25) |
LS mean difference (95% CI) | 0.29 (−1.62 to 2.20) | |
EORTC QLQ-LC13 (dyspnea symptom subscale)l (data cut-off: April 3, 2023) | ||
Baseline | ||
n | 258 | 256 |
Mean (SD) | 25.2 (26.27) | 29.8 (29.09) |
Week 52 | ||
n | 169 | 139 |
Change from baseline LS mean (95% CI) | −3.92 (−5.93 to −1.91) | −7.49 (−9.60 to −5.38) |
LS mean difference [95% CI] | 3.57 (0.65 to 6.48) | |
Averagem | ||
n | 253 | 251 |
Change from baseline LS mean (95% CI) | −3.09 (−4.70 to −1.49) | −5.67 (−7.30 to −4.04) |
LS mean difference (95% CI) | 2.57 (0.28 to 4.86) | |
EORTC QLQ-C30 (Global Health Status/QoL)n (data cut-off: April 3, 2023) | ||
Baseline | ||
n | 258 | 256 |
Mean (SD) | 65.7 (19.63) | 63.5 (21.72) |
Week 52 | ||
n | 170 | 143 |
Change from baseline LS mean (95% CI) | 5.34 (3.17 to 7.51) | 9.25 (6.99 to 11.51) |
LS mean difference (95% CI) | −3.91 (−7.04 to −0.77) | |
Averagem | ||
n | 253 | 253 |
Change from baseline LS mean (95% CI) | 3.32 (1.67 to 4.98) | 7.38 (5.70 to 9.07) |
LS mean difference (95% CI) | −4.06 (−6.42 to −1.69) | |
CI = confidence interval; EGFRm = EGFR–mutated; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; EORTC QLQ-LC13 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Lung Cancer Module; FAS = full analysis set; HR = hazard ratio; LS = least squares; MMRM = mixed-effects model for repeated measures; NC = not calculable; OS = overall survival; osimertinib + chemotherapy = osimertinib in combination with pemetrexed and platinum-based chemotherapy; PFS = progression-free survival; QoL = quality of life; RECIST = Response Evaluation Criteria in Solid Tumors; SD = standard deviation; vs. = versus.
aCalculated using the Kaplan-Meier method.
bThe analysis was performed using a log-rank test stratified by race (Chinese/Asian vs. non-Chinese/Asian vs. non-Asian), WHO Performance Status (0 vs. 1), and method used for EGFRm tissue testing (central vs. local). An HR of less than 1 favours osimertinib plus chemotherapy. The efficacy boundary for significance for the first interim OS analysis (data cut-off date: April 3, 2023) was 0.00158, and the efficacy boundary for significance for the second interim OS analysis (data cut-off date: January 8, 2024) was 0.000001.
cIncluded patients known to be alive at the data cut-off date.
dIncluded patients with unknown survival status or patients who were lost to follow-up.
eThe analysis was performed using a log-rank test stratified by race (Chinese/Asian vs. non-Chinese/Asian vs. non-Asian), WHO PS (0 vs. 1), and method used for EGFRm tissue testing (central vs. local). An HR of less than 1 favours osimertinib plus chemotherapy.
fOnly included progression events that occurred within 2 consecutive scheduled visits (plus visit window) of the last evaluable assessment (or randomization).
gTarget lesions, nontarget lesions, and new lesions were not necessarily mutually exclusive categories.
hDeath in absence of RECIST progression, within 2 visits of baseline or last RECIST assessment (not evaluable is not considered a missing visit).
iRECIST progression or death occurred more than 2 consecutive scheduled visits (plus visit window) after last previous evaluable RECIST assessment or baseline if no valid postbaseline assessment. Patients were censored at last previous evaluable RECIST assessment or randomization date.
jIncluded patients known to be alive with no evaluable baseline RECIST assessment (censored at day 1) or censored at last evaluable assessment.
kPatients censored at last evaluable RECIST assessment or randomization.
lEORTC QLQ-LC13 negative-change scores from baseline represented less symptom severity, and thus improvement on symptom status. As a result, a negative difference in change scores between osimertinib plus chemotherapy and osimertinib monotherapy on EORTC QLQ-LC13 would favour osimertinib plus chemotherapy, and a positive difference in change scores would favour osimertinib monotherapy.
mAverage included all patients contributing to the MMRM model over all visits (i.e., over 19 months or until progression disease). The score values were calculated by averaging across patients’ overall mean across all visits. The analysis was performed using an MMRM analysis on the change from baseline in patient-reported outcome symptom score or functional at each visit up to 19 months (579 days), including treatment (as a random effect), visit (as fixed effect and repeated measure), and treatment by visit interaction as explanatory variables, with the baseline patient-reported outcome score as a covariate along with the baseline patient-reported outcome score by assessment interaction.
nEORTC QLQ-C30 positive-change scores on the Global Health Status/QoL subscales indicate improvement on health status/function, and therefore improvement in symptom status. As a result, positive difference in change scores between osimertinib plus chemotherapy and osimertinib monotherapy on Global Health Status/QoL would favour osimertinib plus chemotherapy.
Sources: FLAURA2 Clinical Study Report16 and Drug Reimbursement Review sponsor submission.17
The OS was evaluated in patient subgroups by CNS metastases at baseline. As of January 8, 2024, in patients who had CNS metastases at baseline, the numbers of patients who had OS events were 44 of 116 (37.9%) patients treated with osimertinib plus chemotherapy and 62 of 110 (56.4%) patients treated with osimertinib monotherapy. The HR for OS in patients who had CNS metastases at baseline was 0.59 (95% CI, 0.40 to 0.87). In patients who did not have CNS metastases at baseline, the numbers of patients who had OS events were 56 of 163 (34.4%) treated with osimertinib plus chemotherapy and 64 of 168 (38.1%) treated with osimertinib monotherapy. The HR for OS in patients who did not have CNS metastases at baseline was 0.89 (95% CI, 0.62 to 1.28).
The OS results from the previous data cut-off date (i.e., April 3, 2023) are shown in Appendix 1. The OS data were immature (26.8% maturity of data) as of April 3, 2023, and tested following the hierarchical testing procedure. There were 71 OS events (25.4%) in the osimertinib plus chemotherapy group versus 78 (28.1%) in the osimertinib monotherapy group. The HR for OS was 0.90 (95% CI, 0.65 to 1.24). The differences in the probability of being alive between osimertinib plus chemotherapy and osimertinib monotherapy at 12 and 24 months were −3.2% and 5.9%, respectively (95% CIs were not reported). Median OS was not reached in either treatment group. The Kaplan-Meier curves of the 2 treatment groups crossed multiple times.
Progression-Free Survival According to Investigator Assessment
As the data cut-off date April 3, 2023, with an overall data maturity of 51.3%, 120 PFS events (43.0%) according to investigator assessment were reported in the osimertinib plus chemotherapy group versus 166 PFS events (59.7%) according to investigator assessment in the osimertinib monotherapy group. The HR for PFS according to investigator assessment was 0.62 (95% CI, 0.49 to 0.79), in favour of osimertinib plus chemotherapy. The differences in the probability of being progression-free between osimertinib plus chemotherapy and osimertinib monotherapy 12 and 24 months were 14.2% (95% CI, ███ to ████) and 16.4% (95% CI, ███ to ████), respectively. The median PFS according to investigator assessment was 25.5 months (95% CI, 24.7 to NC) in the osimertinib plus chemotherapy group versus 16.7 (95% CI, 14.1 to 21.3) in the osimertinib monotherapy group. The Kaplan-Meier plots of OS are shown in Figure 3.
The results for PFS according to BICR were assessed as a sensitivity analysis (Appendix 1). As of April 3, 2023 (data maturity of 43.1%), there were 102 PFS events (36.6%) according to BICR in the osimertinib plus chemotherapy group versus 138 PFS events (49.6%) according to BICR in the osimertinib monotherapy group. The HR for PFS according to BICR was 0.62 (95% CI, 0.48 to 0.80), favouring osimertinib plus chemotherapy. The differences in the probability of being progression-free between osimertinib plus chemotherapy and osimertinib monotherapy at 12 and 24 months were 12.5% and 14.8%, respectively (95% CIs were not reported). The median PFS value according to BICR was 29.4 (25.1 to NC) months in the osimertinib plus chemotherapy group versus 19.9 (16.6 to 25.3) in the osimertinib monotherapy group. For PFS according to BICR, the Kaplan-Meier curves showed an early separation and did not cross throughout the remaining duration of follow-up (plot not shown).
Analysis of concordance between investigator and BICR assessment of PFS revealed an 82.1% agreement on progressions and nonprogressions in the osimertinib plus chemotherapy group, and a 75.6% agreement on progressions and nonprogressions in the osimertinib monotherapy group.
The results for PFS according to investigator assessment were also evaluated in patient subgroups by CNS metastases at baseline. As of April 3, 2023, in patients who had CNS metastases at baseline, the numbers of patients who had PFS events were 52 of 116 (44.8%) treated with osimertinib plus chemotherapy and 79 of 110 (71.8%) treated with osimertinib monotherapy. The HR for PFS according to investigator assessment in patients who had CNS metastases at baseline was 0.47 (95% CI, 0.33 to 0.66). In patients who did not have CNS metastases at baseline, the numbers of patients who had PFS events were 68 of 163 (41.7%) treated with osimertinib plus chemotherapy and 87 of 168 (51.8%) treated with osimertinib monotherapy. The HR for PFS according to investigator assessment in patients who did not have CNS metastases at baseline was 0.75 (95% CI, 0.55 to 1.03).
Figure 3: Kaplan-Meier Plot of PFS According to Investigator Assessment in FLAURA2 (Randomized Period — FAS, Data Cut-Off Date: April 3, 2023)
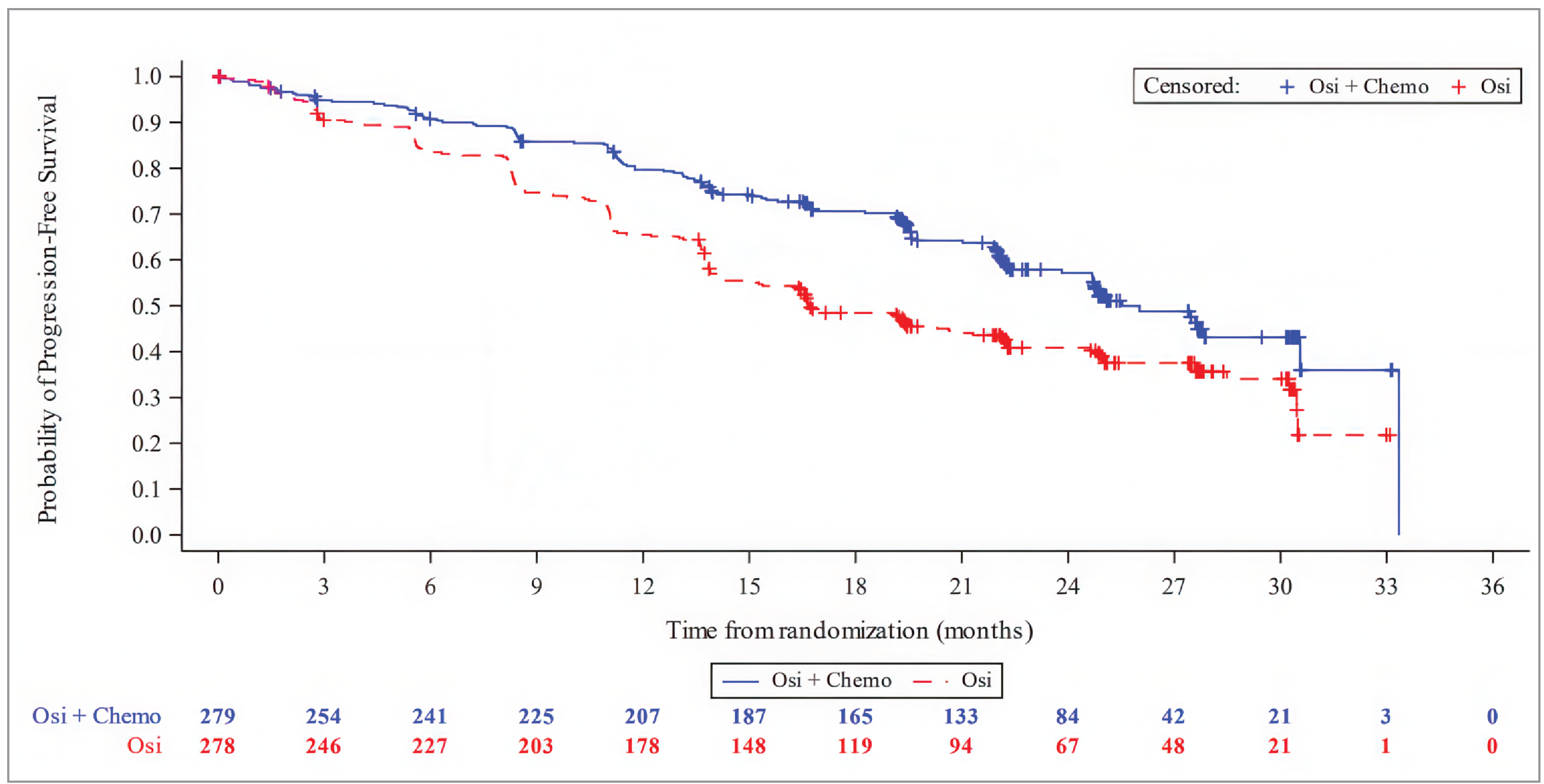
Chemo = pemetrexed and platinum-based chemotherapy; FAS = full analysis set; Osi = osimertinib; PFS = progression-free survival.
Note: Values at the base of the figure indicate number of patients at risk.
Source: FLAURA2 Clinical Study Report16 and Drug Reimbursement Review sponsor submission.17
EORTC QLQ-LC13
EORTC QLQ-LC13 negative-change scores from baseline represented less symptom severity, and therefore improvement in symptom status. As a result, a negative difference in change scores between osimertinib plus chemotherapy and osimertinib monotherapy on EORTC QLQ-LC13 would favour osimertinib plus chemotherapy.
The point estimates of difference in change from baseline scores of the coughing symptoms subscale between the osimertinib plus chemotherapy group and the osimertinib monotherapy group favoured osimertinib plus chemotherapy at week 52 and across all visits (i.e., average), while the point estimates of difference of the pain in chest subscale or the dyspnea symptom subscale favoured the osimertinib monotherapy group at week 52 and across all visits (i.e., average).
EORTC QLQ-C30
EORTC QLQ-C30 positive-change scores on the Global Health Status/QoL subscales indicate improvement on health status/function, and therefore improvement on symptom status. As a result, a positive difference in change scores between osimertinib plus chemotherapy and osimertinib monotherapy on Global Health Status/QoL would favour osimertinib plus chemotherapy.
The point estimates of difference in change from baseline scores of the Global Health Status/QoL between the osimertinib plus chemotherapy and osimertinib monotherapy groups favoured osimertinib monotherapy at week 52 and across all visits (i.e., average).
Harms
During the safety run-in period (data cut-off date: February 19, 2020) of the FLAURA2 trial, 30 patients were involved, among whom 15 received osimertinib plus carboplatin-pemetrexed treatment and 15 received osimertinib plus cisplatin-pemetrexed treatment. AEs were reported in 90% (27 of 30) of the patients during the safety run-in period. All patients who received osimertinib plus carboplatin-pemetrexed had AEs, and 80% of the patients who received osimertinib plus cisplatin-pemetrexed treatment had AEs. The most common AEs were constipation (60%) for those on osimertinib plus carboplatin-pemetrexed treatment, and nausea (60%) for those on osimertinib plus cisplatin-pemetrexed. AEs of Common Terminology Criteria for Adverse Events grade 3 or higher were reported in 53.3% of the patients with osimertinib plus carboplatin-pemetrexed treatment and 20% of the patients with osimertinib plus cisplatin-pemetrexed treatment. SAEs were reported in 6 patients, 3 for each group. One patient with osimertinib plus carboplatin-pemetrexed treatment died. The cause was reported as suspected hypovolemic shock secondary to tumour-associated hemorrhage.
Harms data from the randomized period in the FLAURA2 trial are shown in Table 18. The data cut-off date was April 3, 2023.
Adverse Events
The proportions of patients experiencing AEs were similar between patients treated with osimertinib plus chemotherapy (100%) and patients treated with osimertinib monotherapy (97.5%). However, the proportion of patients experiencing the most common AEs (those reported in ≥ 20% patients in either treatment group), was greater among those treated with osimertinib plus chemotherapy compared with those treated with osimertinib monotherapy. Examples include anemia (46.4% versus 8.0%, respectively), nausea (43.1% versus 10.2%, respectively), and neutropenia (24.6% versus 3.3%, respectively). Moreover, a much higher proportion of patients treated with osimertinib plus chemotherapy experienced AEs of grade 3 or higher, compared with patients treated with osimertinib monotherapy (63.8% versus 27.3%, respectively). The most common AE of grade 3 and higher in patients treated with osimertinib plus chemotherapy was anemia (19.9%).
Serious Adverse Events
Higher percentages of patients in the osimertinib plus chemotherapy group experienced SAEs, compared to the percentages of patients in the osimertinib monotherapy group (37.7% versus 19.3%, respectively).
Discontinuation Due to Adverse Events
Discontinuation of osimertinib occurred in 10.9% of the patients in the osimertinib plus chemotherapy group and 6.2% of the patients in the osimertinib monotherapy. Within the osimertinib plus chemotherapy group, 45.3% of the patients discontinued chemotherapy, of whom 16.7% discontinued carboplatin or cisplatin treatment and 43.1% discontinued pemetrexed treatment.
Mortality
Deaths were reported in 6.5% of the patients in the osimertinib plus chemotherapy group and 2.9% of the patients in the osimertinib monotherapy group. Patients in the osimertinib plus chemotherapy group died due to pulmonary embolism (1.1%), pneumonia (1.1%), and cardiac failure (0.7%).
Notable Harms
The proportions of patients experiencing ILD or pneumonitis were similar between patients treated with osimertinib plus chemotherapy (3.3%) and patients treated with osimertinib monotherapy (3.6%). A higher proportion of patients in the osimertinib plus chemotherapy group compared to patients in the osimertinib monotherapy group experienced cardiac failure (9.1% versus 3.6%, respectively), febrile neutropenia (4.0% versus 0.0%, respectively), and thrombocytopenia (18.5% versus 4.4%).
Table 18: Summary of Harms Results in FLAURA2 (Randomized Period — Safety Analysis Set)
Adverse events | Osimertinib + chemotherapy (N = 276) | Osimertinib monotherapy (N = 275) |
|---|---|---|
Most common AEs, n (%) | ||
Patients with any AE (reported in ≥ 20% patients in either treatment group) | 276 (100) | 268 (97.5) |
Anemia | 128 (46.4) | 22 (8.0) |
Diarrhea | 120 (43.5) | 112 (40.7) |
Nausea | 119 (43.1) | 28 (10.2) |
Decreased appetite | 85 (30.8) | 26 (9.5) |
Constipation | 81 (29.3) | 28 (10.2) |
Rash | 77 (27.9) | 57 (20.7) |
Fatigue | 76 (27.5) | 26 (9.5) |
Vomiting | 73 (26.4) | 17 (6.2) |
Neutropenia | 68 (24.6) | 9 (3.3) |
Stomatitis | 68 (24.6) | 50 (18.2) |
Paronychia | 65 (23.6) | 73 (26.5) |
Decreased neutrophil count | 62 (22.5) | 16 (5.8) |
Increased alanine aminotransferase | 56 (20.3) | 21 (7.6) |
COVID-19 | 57 (20.7) | 39 (14.2) |
Patients with any AE of CTCAE grade 3 or higher (reported in ≥ 5% of patients in either treatment) | 176 (63.8) | 75 (27.3) |
Anemia | 55 (19.9) | 1 (0.4) |
Neutropenia | 37 (13.4) | 2 (0.7) |
Decreased neutrophil count | 31 (11.2) | 2 (0.7) |
Decreased platelet count | 21 (7.6) | 0 |
Thrombocytopenia | 19 (6.9) | 3 (1.1) |
SAEs, n (%) | ||
Patients with any SAE (reported in ≥ 2% of patients in either treatment group) | 104 (37.7) | 53 (19.3) |
Anemia | 9 (3.3) | 0 |
COVID-19 | 7 (2.5) | 2 (0.7) |
Pneumonia | 7 (2.5) | 6 (2.2) |
Febrile neutropenia | 6 (2.2) | 0 |
Platelet count decreased | 6 (2.2) | 0 |
Pulmonary embolism | 6 (2.2) | 2 (0.7) |
Patients who discontinued treatment due to AEs, n (%) | ||
Patients with any AE leading to discontinuation of any study treatment | 132 (47.8) | 17 (6.2) |
Patients with any AE leading to discontinuation of osimertinib | 30 (10.9) | 17 (6.2) |
Patients with any AE leading to discontinuation of chemotherapy | 125 (45.3) | NA |
Discontinuation of carboplatin/cisplatin treatment | 46 (16.7) | NA |
Discontinuation of pemetrexed treatment | 119 (43.1) | NA |
Deaths, n (%) | ||
Patients with AE with outcome of death (reported in ≥ 2 patients in either treatment group) | 18 (6.5) | 8 (2.9) |
Pulmonary embolism | 3 (1.1) | 0 |
Pneumonia | 3 (1.1) | 0 |
Cardiac failure | 2 (0.7) | 0 |
COVID-19 pneumonia | 0 | 4 (1.5) |
Notable harm, n (%) | ||
ILD or pneumonitisa | 9 (3.3) | 10 (3.6) |
Cardiac failure | 25 (9.1) | 10 (3.6) |
Hematological toxicities | ||
Febrile neutropenia | 11 (4.0) | 0 |
Thrombocytopenia | 51 (18.5) | 12 (4.4) |
AE = adverse event; CTCAE = Common Terminology Criteria for Adverse Events; ILD = interstitial lung disease; NA = not applicable; SAE = serious adverse event.
Note: Data cut-off date: April 3, 2023.
aIncluded the following Medical Dictionary for Regulatory Activities preferred terms: interstitial lung disease, pneumonitis, acute interstitial pneumonitis, alveolitis, diffuse alveolar damage, idiopathic pulmonary fibrosis, lung disorder, organizing pneumonia, pulmonary toxicity, and pulmonary fibrosis.
Source: FLAURA2 Clinical Study Report,16 Drug Reimbursement Review sponsor submission.17 (Details included in the table are from the sponsor’s Summary of Clinical Evidence.1)
Critical Appraisal
Internal Validity
The FLAURA2 trial investigated the use of osimertinib plus chemotherapy in patients with locally advanced, metastatic, or recurrent EGFRm (ex19del and/or L858R) NSCLC compared to osimertinib monotherapy. A total of 557 patients were randomized to the osimertinib plus chemotherapy group (n = 279) and the osimertinib monotherapy group (n = 278), stratified by race (Chinese/Asian versus non-Chinese/Asian versus non-Asian), WHO PS (0 versus 1), and methods used for tissue testing (central versus local EGFR method) to minimize potential imbalances between the study groups that might bias the results. The trial used central randomization and concealed patient allocation during the randomization process.12 Overall, the baseline characteristics presented in the Clinical Study Report were similar and balanced between the treatment groups.
Generally, no serious concerns were identified in protocol amendments and protocol deviations. According to the clinical experts consulted by the review team, the use of concomitant medications reflected the clinical practice settings, and the types of medications used were not expected to modify treatment effects. In the FLAURA2 trial, patients were allowed to receive subsequent anticancer treatment at the investigator’s discretion following discontinuation of the randomized treatment. Overall, 20.4% of patients in the osimertinib plus chemotherapy group and 32.7% of patients in the osimertinib monotherapy group received subsequent anticancer therapy, among whom 14.7% of the osimertinib plus chemotherapy group and 29.1% of the osimertinib monotherapy group received subsequent chemotherapy. According to the clinical experts consulted by the review team, these differences were not a concern because platinum chemotherapy is not typically expected to be used in patients who have received osimertinib plus chemotherapy. The review team also determined that, because the percentage of patients who had subsequent therapies was lower in the osimertinib plus chemotherapy group than in the osimertinib monotherapy group, the risk of bias leading to overestimation of treatment effects (the OS effect) was low.
Because the FLAURA2 trial was open-label, investigators and patients were aware of the assigned treatment.12 The primary outcome was PFS according to investigator assessment, which was prone to the impact of detection bias due to the open-label design. However, the potential risk of detection bias in PFS according to investigator assessment was considered relatively low by the review team. First, results of PFS according to investigator assessment were consistent with those of PFS according to BICR assessment. Second, the analysis of concordance between PFS according to investigator and according to BICR assessment showed that there was an 82.1% agreement on progressions and nonprogressions in the osimertinib plus chemotherapy group, and a 75.6% agreement on progressions and nonprogressions in the osimertinib monotherapy group, suggesting acceptable agreement between the ways of assessment. Similarly, for HRQoL outcomes (i.e., EORTC QLQ LC-13 and EORTC QLQ-C30), which had unblinded assessment, the risk of performance bias also was considered relatively low, and no evidence in the data indicated that knowledge of treatment assignment affected the results. However, it was more of a concern that the assessment of HRQoL outcomes at week 52 was based on a portion of randomized patients. For example, for EORTC QLQ-C30 assessment at week 52, out of 279 patients in the osimertinib plus chemotherapy group, 230 forms were expected and 180 forms were received and evaluated, for a compliance rate of 78.3%). The type of data missing (e.g., completely at random, at random, or not at random) is unclear, as is how the missingness in data would affect the HRQoL assessment, resulting in increased uncertainty.
The OS was considered by the clinical experts consulted by the review team as the most clinically relevant efficacy end point for patients with NSCLC. The OS data at the data cut-off dates of April 3, 2023 (26.8% maturity of data) and January 8, 2024 (40.6% maturity of data) were evaluated by the review team. Multiplicity was controlled using the hierarchal statistical testing for OS and PFS only. The efficacy boundary for statistical significance for the updated OS analysis (data cut-off date: January 8, 2024) was 0.000001. Although the P value was 0.028 for the HR of the updated OS analysis, there was therefore no statistical significance. The Kaplan-Meier curves of OS obtained from the April 3, 2023, data cut-off crossed several times, which violated the proportional hazards assumption for OS and made the OS estimates as of April 3, 2023, less valid. A late divergence of the Kaplan-Meier curves of the updated OS (data cut-off date: January 8, 2024) was observed during visual inspection of the Kaplan-Meier curves; the curves of the osimertinib plus chemotherapy group and the osimertinib monotherapy group did not separate until approximately 16 months after randomization. According to the clinical experts consulted by the review team, the delayed separation of survival curves reflected what they expected, as is often seen in patients receiving a combination therapy consisting of chemotherapy. However, the late divergence of survival curves may have implications for the statistical analysis used in the FLAURA2 trial (i.e., whether the proportional hazards assumption was violated), which introduced uncertainty to the OS evidence. Where there is a delayed separation of survival curves, a sensitivity analyses that assesses whether the proportional hazards assumption was satisfied would have been appropriate (e.g., using survival analyses that do not rely on the proportional hazards assumption).
External Validity
The clinical experts consulted by the review team noted that the chemotherapy protocols were appropriate and generally reflective of the standard dose schedules used for adult patients in Canada. The clinical experts also noted that, overall, the patient eligibility criteria of the FLAURA2 trial were appropriate in clinical trials for patients with NSCLC and aligned with the selection criteria in settings in Canada when identifying suitable candidates for osimertinib plus chemotherapy. However, the clinical experts noted that, in real-world settings, patients generally have a poorer performance status at the start of therapy. In other words, patients with a performance status of 2 could also be considered for osimertinib plus chemotherapy.
The FLAURA2 trial did not allow eligible patients to have prior treatment with an EGFR TKI. Also, the trial required eligible patients to be off other adjuvant and neoadjuvant therapies (e.g., chemotherapy, radiotherapy, immunotherapy, biologic therapy, and investigational drugs) at least 12 months before the development of recurrent disease. According to the clinical experts consulted by the review team, because osimertinib monotherapy has become first-line treatment for EGFRm, patients who had received prior EGFR TKI should also be considered for osimertinib plus chemotherapy. The clinical experts consulted by the review team also noted that, following completion of adjuvant chemotherapy alone or adjuvant osimertinib, patients with a 6-month disease-free interval before the development of recurrent disease could be considered eligible for osimertinib plus chemotherapy. The clinical experts consulted by the review team further noted that patients with a disease-free interval of less than 6 months may be eligible for osimertinib plus chemotherapy at the discretion of the treating physician.
The histology type of most patients enrolled in the FLAURA2 trial (> 98% for both groups) was adenocarcinoma. According to the clinical experts consulted by the review team, findings from the trial could still be generalizable to patients with other histology types (e.g., adenosquamous carcinoma) because it is the existence of the driving mutation that decides whether osimertinib should be used. The clinical experts consulted by the review team noted that it was plausible to believe that the treatment effects of osimertinib plus chemotherapy would likely not differ among patients with the same driving mutation but different histology.
GRADE Summary of Findings and Certainty of the Evidence
Methods for Assessing the Certainty of the Evidence
For pivotal studies and RCTs identified in the sponsor’s systematic review, GRADE was used to assess the certainty of the evidence for outcomes considered most relevant to inform our expert committee deliberations, and a final certainty rating was determined as outlined by the GRADE Working Group:13,14
High certainty: We are very confident that the true effect lies close to that of the estimate of the effect.
Moderate certainty: We are moderately confident in the effect estimate — the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. We use the word “likely” for evidence of moderate certainty (e.g., “X intervention likely results in Y outcome”).
Low certainty: Our confidence in the effect estimate is limited — the true effect may be substantially different from the estimate of the effect. We use the word “may” for evidence of low certainty (e.g., “X intervention may result in Y outcome”).
Very low certainty: We have very little confidence in the effect estimate — the true effect is likely to be substantially different from the estimate of effect. We describe evidence of very low certainty as “very uncertain.”
Following the GRADE approach, evidence from RCTs started as high-certainty evidence and could be rated down for concerns related to study limitations (which refers to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias.
When possible, certainty was rated in the context of the presence of an important (nontrivial) treatment effect; if this was not possible, certainty was rated in the context of the presence of any treatment effect (i.e., the clinical importance is unclear). In all cases, the target of the certainty-of-evidence assessment was based on the point estimate and where it was located relative to the threshold for a clinically important effect (when a threshold was available) or to the null.
The reference points for the certainty-of-evidence assessment for OS and PFS were set according to the presence of an important effect based on thresholds agreed upon by clinical experts consulted by the review team. The target of the certainty-of-evidence assessment was the presence of any (non-null) effect for EORTC QLQ-LC13 due to the lack of a formal MID estimate. The MID for the Global Health Status/QoL of EORTC QLQ-C30 was based on estimates published in the literature.15 For harm events due to the unavailability of the absolute difference in effects, the certainty of evidence was summarized narratively.
Results of GRADE Assessments
Table 2 presents the GRADE summary of findings for osimertinib plus chemotherapy versus osimertinib monotherapy in patients with locally advanced or metastatic NSCLC whose tumours have EGFR ex19del or L858R mutations.
Long-Term Extension Studies
No long-term extension studies were identified for this review.
Indirect Evidence
No indirect evidence was identified for this review.
Studies Addressing Gaps in the Systematic Review Evidence
No studies addressing gaps in the pivotal and RCT evidence were identified for this review.
Discussion
Summary of Available Evidence
One phase III, open-label RCT, FLAURA2, (N = 557, including 13 patients in Canada) was included in the systematic literature review conducted by the sponsor. FLAURA2 enrolled adult patients who were diagnosed with pathologically confirmed nonsquamous NSCLC that was locally advanced (clinical stage IIIB, IIIC), metastatic (clinical stage IVA or IVB), or recurrent (according to version 8 of the International Association for the Study of Lung Cancer Staging Manual in Thoracic Oncology) and whose tumour harboured 1 of the 2 common EGFR mutations — ex19del or L858R — either alone or in combination with other EGFR mutations. Patients were randomized to the osimertinib plus chemotherapy group (n = 279) and the osimertinib monotherapy group (n = 278), stratified by ethnicity, WHO PS, and methods used for tissue testing. The primary objective was to compare the treatment effect between osimertinib plus chemotherapy versus osimertinib monotherapy, measured by PFS according to investigator assessment. Other efficacy and safety outcomes included OS, EORTC QLQ-LC13, EORTC QLQ-C30, and harms (i.e., AEs, SAEs, withdrawal, deaths, notable harms). The FLAURA2 trial is ongoing, and the data cut-off date was April 3, 2023. OS data were updated on January 8, 2024, and assessed in this report. The median age of enrolled patients was 61.0 years (range = 26 to 85). The majority (61.4%) of enrolled patients were female, 63.7% were Asian, 62.8% had a WHO PS of 1, 53.1% had an ex19del mutation (as determined by a central cobas tissue test), and 96.2% had metastatic NSCLC at baseline.
Interpretation of Results
Efficacy
Prolonging life, controlling disease progression, and improving HRQoL were highlighted by both patients and clinicians as critical treatment goals in advanced NSCLC. In the FLAURA2 pivotal trial, these needs were captured by the evaluation of efficacy outcomes such as OS, PFS, EORTC QLQ LC-13, as well as EORTC QLQ LC-C30.
The OS was considered the most clinically relevant efficacy end point by the clinical experts consulted by the review team. The maturity of OS data as of the data cut-off date of April 3, 2023, was only 26.8%. As a small number of events can lead to unstable and unreliable estimates of OS, the review team did not consider these data at the first interim analysis for the outcome as interpretable. The clinical experts consulted by the review team agreed that the immature results limited the applicability to clinical practice.
██████ ██████ ██████ █ ██████ ██ ██████████ █████ ██ ███████ ███ ██████ ███ ███ ██ ███████████ ██ ███████████ ████ ██████████ ███ ██████████████ ████████████ ███ ███ █████████ ██ ████████ ████ ███████ ████████ ██ ██████████ █████ █████ ███████ ████ ████ ████ ██ █████████ ██ ████ ██ ███████ ████████████ ███████████████ █████████████ ████ ███ ███ ███████ ████████ ███ ██████████ █ ████████████ ███ ████ ████████ ██ ███████ ██ ██ ████████████ ██ ███ ██ ████ ██ ███ ███████ ████ ██ █████ ██ ██████ ██ ███ ███████ ██ ██ █████████ ████ ███ ████████ ███████ ██ ███ ███████████ █ ████████████ ███ ████████ ██ ███ ███████ ████ ██ ███████ ██ ████████ ██ ██████ ██ █████████ ███ ██████████ ████ ███████ ███ ████████ ██ ███ ███████ ██ ████ ███████████ █ █████████ █████████████ ██████ ███ ██████████ ███ ███████ █████ ████ ███ ███████ ██ ████████ █████ ███████ █████ ███████ ██ █████ ████ █████████ ██ ███ ████████ █████ ███ █ ████ ████████ ██ ██████. The HR for the updated OS was 0.75 (95% CI, 0.57 to 0.97; P = 0.028) in favour of osimertinib plus chemotherapy. The sponsor controlled for multiple statistical testing, and the efficacy boundary for statistical significance for the updated OS analysis was 0.000001; as a result, the updated analysis for OS did not reach statistical significance. The differences in the probability of being alive between the osimertinib plus chemotherapy group and the osimertinib monotherapy group at 24 and 36 months were 7.6 (95% CI, ███ to ████) and 13.5% (95% CI, ███ to ████), respectively. Although the sponsor did not submit an empirically validated MID for OS, the clinical experts consulted by the review team noted that a 10% or higher between-group difference in the probability of being alive at 24 and 36 months would be clinically significant, and a between-group difference between 5% and 10% would suggest that the treatment effect may be clinically relevant. Although the point estimate at 36 months exceeded 10% and the point estimate at 24 months fell between 5% and 10%, which favoured the osimertinib plus chemotherapy group, the certainty of OS evidence was affected by concerns about imprecision as the lower bound of the 95% CIs included the 5% threshold. The 36-month OS estimate had further imprecision associated with the reduction in the number of patients remaining at risk. For example, there was a high percentage of censoring (approximately 40% in each group) between month 33 and month 36. Moreover, according to the clinical experts consulted by the review team, although the OS findings were encouraging, a longer follow-up is warranted as the median OS for the osimertinib plus chemotherapy group was not reached.
The results of the primary efficacy end point in the FLAURA2 trial, PFS according to investigator assessment (data cut-off date: April 3, 2023; data maturity: 51.3%), revealed that osimertinib plus chemotherapy was more efficacious compared with osimertinib monotherapy in terms of delaying disease progression. The results of the sensitivity analysis of PFS according to BICR were generally consistent with the results of PFS according to investigator assessment. The HR for PFS according to investigator assessment was 0.62 (95% CI, 0.49 to 0.79; P < 0.0001), favouring osimertinib plus chemotherapy. The differences in the probability of being progression-free between osimertinib plus chemotherapy and osimertinib monotherapy 12 and 24 months were 14.2% (95% CI, ███ to ████) and 16.4% (95% CI, ███ to ████), respectively. According to the clinical experts consulted by the review team, the threshold to determine the clinical importance could be 10% or higher for the between-group difference in the probability of being progression-free at 24 and 36 months. Although the point estimates at 12 and 24 months were both higher than 10%, the lower bound of the 95% CIs crossed the threshold, indicating the possibility of both benefits and little to no benefit with osimertinib plus chemotherapy versus osimertinib monotherapy for PFS, thereby lowering the certainty of PFS evidence to moderate.
A closer examination of the PFS events identified other potential sources of uncertainty. In total, 43% and 59.7% of the patients had PFS events in the osimertinib plus chemotherapy group and the osimertinib monotherapy group, respectively. Out of these patients, 34.1% in the osimertinib plus chemotherapy group versus 56.8% in the osimertinib monotherapy group had RECIST-defined progression. However, a higher percentage of deaths in the osimertinib plus chemotherapy group contributed to PFS events compared with the osimertinib monotherapy group (9% versus 2.9%). Upon request, the sponsor provided further information on the patients who died during the follow-up of PFS (as of April 3, 2023). After examining the additional information (i.e., individual patient deaths), the review team in consultation with clinical experts noted that 9 deaths occurred within the 63 days since the start of the FLAURA2 trial in the osimertinib plus chemotherapy group versus only 1 death in the osimertinib monotherapy group during the same time period. However, the relatively small number of patients and limited information provided in the descriptions of the circumstances surrounding the deaths made it difficult to identify a clear association between treatment and an AE leading to death. The disparity in death occurrence at an early study stage between the osimertinib plus chemotherapy group and the osimertinib monotherapy group could not be explained with the available information. However, after weighing these deaths against the fewer total deaths with osimertinib plus chemotherapy versus osimertinib monotherapy, the review team determined that the results of the FLAURA2 trial suggest that the combination treatment likely leads to fewer PFS events.
Data on HRQoL were assessed based on the least squares mean change from baseline in EORTC QLQ-LC13 (e.g., coughing symptoms subscale, pain in chest subscale, and dyspnea symptom subscale) and EORTC QLQ-C30 (e.g., Global Health Status/QoL). The certainty of the HRQoL evidence from the FLAURA2 trial is considered very low, and the evidence is uncertain about the effect of osimertinib plus chemotherapy on the coughing symptoms subscale, pain in chest subscale, and dyspnea symptom subscale of EORTC QLQ-LC13 as well as on the Global Health Status/QoL of EORTC QLQ-LC13 at week 52, compared to osimertinib monotherapy. From a clinical perspective, the clinical experts consulted by the review team expected within-group improvement of HRQoL in both the osimertinib plus chemotherapy group and the osimertinib monotherapy group but they did not expect a between-group improvement. The HRQoL results generally met the expectation of the clinical experts. All within-group differences indicated improvements. In terms of between-group differences, only the point estimates of difference of the dyspnea symptom subscale of EORTC QLQ-LC13 and the Global Health Status/QoL of EORTC QLQ-C30 at week 52 and across all visits (i.e., average) showed non-null improvements, favouring the osimertinib monotherapy group.
According to the clinical experts consulted by the review team, CNS metastasis prevention and disease control in patients with NSCLC are important aspects of treatment goals as NSCLC is associated with CNS disease, resulting in morbidity and disease progression. In the FLAURA2 trial, 11 subgroups were prespecified, 1 of which was CNS metastases at baseline (yes or no). Both OS and PFS according to investigator assessment were evaluated in the CNS metastases subgroup, with the results suggesting that osimertinib plus chemotherapy is more efficacious than monotherapy in patients with CNS metastases than in those who do not have CNS metastases at baseline. For example, the HR for PFS according to investigator assessment in patients who had CNS metastases at baseline was 0.47 (95% CI, 0.33 to 0.66), whereas the HR for PFS in patients who did not have CNS metastases at baseline was 0.75 (95% CI, 0.55 to 1.03). However, despite differences in the percentages of events and point estimates for the HRs between the subgroups suggesting patients with CNS metastases may have greater benefit than those without CNS metastases, the subgroup results are inconclusive due to important uncertainties. The study was not adequately designed for subgroup analyses by CNS metastases at baseline (CNS metastases were not included in the sample size calculation and were not a stratification factor for randomization) and no formal testing for subgroup interaction was available. As a result, any difference identified may be due to chance and not a true difference in treatment effect.
Harms
The combination osimertinib plus chemotherapy in the first-line treatment setting likely results in an increase in the occurrence of harms outcomes among patients with NSCLC, compared to the osimertinib monotherapy. As of the April 3, 2023, data cut-off, the FLAURA2 trial showed that a higher percentage of patients treated with osimertinib plus chemotherapy experienced AEs of grade 3 or higher (63.8% versus 27.3%, respectively), SAEs (37.7% versus 19.3%, respectively), discontinuation of any study treatment (47.8% versus 6.2%, respectively), and death (6.5% versus 2.9%), compared to the percentage of patients treated with osimertinib monotherapy. ILD or pneumonitis, cardiac failure, and hematological toxicities (i.e., febrile neutropenia and thrombocytopenia) were considered notable harms. While the percentages of patients who had ILD or pneumonitis in the osimertinib plus chemotherapy group and the osimertinib monotherapy group were similar (3.3% versus 3.6%, respectively), higher proportions of patients in the osimertinib plus chemotherapy group experienced cardiac failure (9.1% versus 3.6%, respectively), febrile neutropenia (4.0% versus 0.0%, respectively), and thrombocytopenia (18.5% versus 4.4%).
The clinical experts consulted by the review team noted that the higher percentage of patients who discontinued any study treatment in the osimertinib plus chemotherapy group compared with the osimertinib monotherapy group was what they would expect to see in clinical practice, and therefore was not a serious concern. According to the clinical experts consulted by the review team, ILD or pneumonitis, which is a documented AE associated with osimertinib (the product monograph includes a serious warnings and precautions box), was similar between groups (3.3% versus 3.6%, respectively), as expected. The clinical experts consulted by the review team expressed concerns about anemia of grade 3 or higher (19.9% in the osimertinib plus chemotherapy group versus 0.4% in the osimertinib monotherapy group) as anemia-associated symptoms (e.g., feeling tired) would have a substantial impact on patients.
The patient input for this review noted that, in addition to being effective, osimertinib plus chemotherapy was also expected to have manageable side effects. After weighing the potential benefits and harms with the updated OS data, the clinical experts consulted by the review team noted that the AE profile in the osimertinib plus chemotherapy group was generally expected to be seen in clinical practice when using a combination therapy consisting of chemotherapy, there were no serious concerns with managing these AEs in clinical practice, and overall the evidence with updated OS data from the FLAURA2 trial suggests that the benefits of using osimertinib plus chemotherapy outweigh its potential harms. The clinical experts consulted by the review team also noted that patients who had received osimertinib monotherapy as first-line treatment typically would receive chemotherapy upon experiencing progressive disease in the second-line setting and would likely experience chemotherapy-associated harms at that time. Still, the clinical experts consulted by the review team noted that they predicted that the total harms would be similar between patients who received osimertinib plus chemotherapy as a combination therapy and patients who received osimertinib and chemotherapy in a sequential order. The clinical experts consulted by the review team further noted that, in clinical practice, clinicians need to determine patient eligibility with caution and on a case-by-case basis, particularly for patients who are more susceptible to the increased toxicity of osimertinib plus chemotherapy, such as older patients, patients with multiple comorbidities, and/or those with poorer performance status.
Conclusion
The pivotal FLAURA2 trial is an ongoing, phase III, open-label RCT comparing the efficacy and safety of osimertinib plus chemotherapy and osimertinib monotherapy in patients with locally advanced, metastatic, or recurrent EGFRm (ex19del or L858R) NSCLC. Overall, efficacy evidence from the FLAURA2 trials suggests that osimertinib plus chemotherapy showed added clinical benefits in OS and PFS in the intention-to-treat trial population, compared with osimertinib monotherapy. Results of these clinically relevant efficacy end points were generally in favour of osimertinib plus chemotherapy over osimertinib monotherapy. Osimertinib plus chemotherapy may result in an increase in the probability of being alive at 24 and 36 months (low certainty) and likely lead to an increase in the probability of being progression-free at 12 and 24 months (moderate certainty), compared to osimertinib monotherapy. Because of the immaturity of the OS data (40.6%) and the fact that the median OS was not reached as of January 8, 2024, uncertainty remains in the OS results. The study subgroup analyses suggested the potential for greater benefit with osimertinib plus chemotherapy versus osimertinib monotherapy in patients with CNS metastases at baseline compared with patients without CNS metastases at baseline. However, uncertainty related to the trial design and analysis of these subgroups (including no formal interaction tests) prevented drawing a definitive conclusion. The review team concluded with moderate to high certainty that the combination use of osimertinib plus chemotherapy is associated with an increased frequency of grade 3 or higher AEs, SAEs, WDAEs, and deaths reported as AEs compared to osimertinib monotherapy.
References
1.Sponsor's summary of clinical evidence [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Tagrisso (osimertinib) 40 mg and 80 mg oral tablets Mississauga (ON): AstraZeneca Canada Inc; 2023 Dec 11.
2.Tagrisso (osimertinib tabelets) 40 mg and 80 mg osimertinib (as osimertinib mesylate), oral tablets [product monograph]. Mississauga (ON): AstraZeneca Canada Inc; 2024 Jul 10.
3.Canadian Cancer Statistics Advisory Committee. Canadian cancer statistics: a 2020 special report on lung cancer. Toronto (ON): Canadian Cancer Society; 2020: https://cdn.cancer.ca/-/media/files/cancer-information/resources/publications/2020-canadian-cancer-statistics-special-report/2020-canadian-cancer-statistics-special-report-en.pdf?rev=15c66a0b05f5479e935b48035c70dca3&hash=3D51B0D0FB5C3F7E659F896D66495CE8. Accessed 2021 Apr 26.
4.Canadian Cancer Statistics Advisory in collaboration with the Canadian Cancer Society, Statistics Canada, Public Health Agency of Canada. Canadian cancer statistics 2023. Toronto (ON): Canadian Cancer Society; 2023: https://cancer.ca/Canadian-Cancer-Statistics-2023-EN. Accessed 2024 May 16.
5.Midha A, Dearden S, McCormack R. EGFR mutation incidence in non–small-cell lung cancer of adenocarcinoma histology: a systematic review and global map by ethnicity (mutMapII). Am J Cancer Res. 2015;5(9):2892-2911. PubMed
6.Graham RP, Treece AL, Lindeman NI, et al. Worldwide frequency of commonly detected EGFR mutations. Arch Pathol Lab Med. 2018;142(2):163-167. PubMed
7.Melosky B, Banerji S, Blais N, et al. Canadian consensus: a new systemic treatment algorithm for advanced EGFR-mutated non–small-cell lung cancer. Curr Oncol. 2020;27(2):e146-e155. PubMed
8.Ellis PM, Verma S, Sehdev S, Younus J, Leighl NB. Challenges to implementation of an epidermal growth factor receptor testing strategy for non–small-cell lung cancer in a publicly funded health care system. J Thorac Oncol. 2013;8(9):1136-1141. PubMed
9.Rangachari D, Yamaguchi N, VanderLaan PA, et al. Brain metastases in patients with EGFR-mutated or ALK-rearranged non–small-cell lung cancers. Lung Cancer. 2015;88(1):108-111. PubMed
10.Roughley A, Damonte E, Taylor-Stokes G, Rider A, Munk VC. Impact of brain metastases on quality of life and estimated life expectancy in patients with advanced non–small cell lung cancer. Value Health. 2014;17(7):A650. PubMed
11.Peters S, Bexelius C, Munk V, Leighl N. The impact of brain metastasis on quality of life, resource utilization and survival in patients with non–small-cell lung cancer. Cancer Treat Rev. 2016;45:139-162. PubMed
12.Planchard D, Jänne PA, Cheng Y, et al. Osimertinib with or without chemotherapy in EGFR-mutated advanced NSCLC. N Engl J Med. 2023. PubMed
13.Balshem H, Helfand M, Schünemann HJ, et al. GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol. 2011;64(4):401-406. PubMed
14.Santesso N, Glenton C, Dahm P, et al. GRADE guidelines 26: informative statements to communicate the findings of systematic reviews of interventions. J Clin Epidemiol. 2020;119:126-135. PubMed
15.Musoro JZ, Coens C, Singer S, et al. Minimally important differences for interpreting European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 scores in patients with head and neck cancer. Head Neck. 2020;42(11):3141-3152. PubMed
16.Clinical Study Report: D5169C00001. A phase III, open-label, randomised study of osimertinib with or without platinum plus pemetrexed chemotherapy, as first-line treatment in patients with epidermal growth factor receptor mutation positive, locally advanced or metastatic non–small cell lung cancer (FLAURA2) - randomised period [internal sponsor's report]. Mississauga (ON): AstraZeneca Canada Inc; 2023 Aug 4.
17.Drug Reimbursement Review sponsor submission: Tagrisso (osimertinib) 40 mg and 80 mg oral tablets [internal sponsor's package]. Mississauga (ON): AstraZeneca Canada; 2023 Dec 11.
18.Cancer-specific stats 2022: snapshot of incidence, mortality and survival estimates by cancer type. Toronto (ON): Canadian Cancer Society: https://cdn.cancer.ca/-/media/files/research/cancer-statistics/2022-statistics/2022_cancer-specific-stats.pdf. Accessed 2024 May 16.
19.Detterbeck FC, Boffa DJ, Kim AW, Tanoue LT. The eighth edition lung cancer stage classification. Chest. 2017;151(1):193-203.
20.Canadian Cancer Society. What is lung cancer? https://www.cancer.ca/en/cancer-information/cancer-type/lung/lung-cancer/?region=on. Accessed 2024 May 16.
21.Birring SS, Peake MD. Symptoms and the early diagnosis of lung cancer. Thorax. 2005;60(4):268-269. PubMed
22.BC Cancer. Lung. 2013; http://www.bccancer.bc.ca/health-professionals/clinical-resources/cancer-management-guidelines/lung/lung#Management. Accessed 2021 Jun 3.
23.Recommendations summary, non–small cell lung cancer. A consensus of the Alberta Provincial Lung Tumour Team. Edmonton (AB): Cancer Care Alberta; 2023: https://www.albertahealthservices.ca/assets/info/hp/cancer/if-hp-cancer-guide-lu-nsclc-summary.pdf. Accessed 2024 May 16.
24.Cross DA, Ashton SE, Ghiorghiu S, et al. AZD9291, an irreversible EGFR TKI, overcomes T790M-mediated resistance to EGFR inhibitors in lung cancer. Cancer Discov. 2014;4(9):1046-1061. PubMed
25.Ballard P, Yates JW, Yang Z, et al. Preclinical comparison of osimertinib with other EGFR-TKIs in EGFR-mutant NSCLC brain metastases models, and early evidence of clinical brain metastases activity. Clin Cancer Res. 2016;22(20):5130-5140. PubMed
26.Ramalingam SS, Vansteenkiste J, Planchard D, et al. Overall survival with osimertinib in untreated, EGFR-mutated advanced NSCLC. N Engl J Med. 2020;382(1):41-50. PubMed
27.Reungwetwattana T, Nakagawa K, Cho BC, et al. CNS response to osimertinib versus standard epidermal growth factor receptor tyrosine kinase inhibitors in patients with untreated EGFR-mutated advanced non–small-cell lung cancer. J Clin Oncol. 2018:Jco2018783118. PubMed
28.Cisplatin Injection BP (cisplatin injection): 1 mg / mL (50 mg and 100 mg cisplatin per vial) [product monograph] Kirkland (QC): Pfizer Canada ULC 2018 Dec 7.
29.Pemetrexed (pemetrexed disodium for injection): 100 mg or 500 mg pemetrexed per vial [product monograph]. Toronto (ON): Apotex Inc; 2016 Jun 1.
30.Carboplatin Injection BP (carboplatin injection): 10 mg / mL (50 mg, 150 mg, 450 mg, 600 mg of carboplatin per vial) [product monograph]. Kirkland (QC): Pfizer Canada ULC; 2019 Dec 16.
31.Clinical Study Report: D5169C00001. A phase III, open-label, randomised study of osimertinib with or without platinum plus pemetrexed chemotherapy, as first-line treatment in patients with epidermal growth factor receptor mutation positive, locally advanced or metastatic non–small cell lung cancer (FLAURA2) - safety run-in period [internal sponsor's report]. Mississauga (ON): AstraZeneca Canada Inc; 2020 Nov 26.
32.Janne P, Planchard D, Cheng Y, et al. PL03.13 osimertinib with/without platinum-based chemotherapy as first-line treatment in patients with EGFRm advanced NSCLC (FLAURA2). J Thorac Oncol. 2023;18(11):S36-S37.
33.Jänne P, Planchard D, Howarth P, Todd A, Kobayashi K. OA07.01 osimertinib plus platinum/pemetrexed in newly-diagnosed advanced EGFRm-positive NSCLC; the phase 3 FLAURA2 study. J Thorac Oncol. 2019;14(10):S222-S223.
34.Jänne PA, Planchard D, Kobayashi K, et al. CNS efficacy of osimertinib with or without chemotherapy in epidermal growth factor receptor-mutated advanced non–small-cell lung cancer. J Clin Oncol. 2023:Jco2302219. PubMed
35.Kim SW, Planchard D, Feng PH, et al. 366MO osimertinib plus platinum/pemetrexed in newly diagnosed EGFR mutation (EGFRm)-positive advanced NSCLC: safety run-in results from the FLAURA2 study. Ann Oncol. 2020;31:S1382.
36.Planchard D, Feng PH, Karaseva N, et al. Osimertinib plus platinum-pemetrexed in newly diagnosed epidermal growth factor receptor mutation-positive advanced/metastatic non–small-cell lung cancer: safety run-in results from the FLAURA2 study. ESMO Open. 2021;6(5):100271. PubMed
37.Planchard D, Feng PH, Karaseva N, et al. 1401P osimertinib plus platinum/pemetrexed in newly-diagnosed EGFR mutation (EGFRm)-positive advanced NSCLC: safety run-in results from the FLAURA2 study. Ann Oncol. 2020;31:S888.
38.Planchard D, Jänne PA, Cheng Y, et al. LBA68 FLAURA2: safety and CNS outcomes of first-line (1L) osimertinib (osi) ± chemotherapy (CTx) in EGFRm advanced NSCLC. Ann Oncol. 2023;34:S1311-S1312.
39.Clinical Study Protocol version 2.0: D5169C00001. A phase III, open-label, randomised study of osimertinib with or without platinum plus pemetrexed chemotherapy, as first-line treatment in patients with epidermal growth factor receptor mutation positive, locally advanced or metastatic non–small cell lung cancer (FLAURA2) [internal sponsor's report]. Södertälje (SE): AstraZeneca AB; 2021 Aug 26.
40.Statistical analysis plan version 2.0: D5169C00001. A phase III, open-label, randomised study of osimertinib with or without platinum plus pemetrexed chemotherapy, as first-line treatment in patients with epidermal growth factor receptor mutation positive, locally advanced or metastatic non–small cell lung cancer (FLAURA2) [internal sponsor's report]. Mississauga (ON): AstraZeneca Canada Inc; 2023 Jan 9.
41.Aaronson NK, Ahmedzai S, Bergman B, et al. The European Organisation for Research and Treatment of Cancer QLQ-C30: a quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst. 1993;85(5):365-376. PubMed
42.Teckle P, Peacock S, McTaggart-Cowan H, et al. The ability of cancer-specific and generic preference-based instruments to discriminate across clinical and self-reported measures of cancer severities. Health & Quality of Life Outcomes. 2011;9:106. PubMed
43.Nicklasson M, Bergman B. Validity, reliability and clinical relevance of EORTC QLQ-C30 and LC13 in patients with chest malignancies in a palliative setting. Qual Life Res. 2007;16(6):1019-1028. PubMed
44.Ozturk A, Sarihan S, Ercan I, Karadag M. Evaluating quality of life and pulmonary function of long-term survivors of non–small cell lung cancer treated with radical or postoperative radiotherapy. Am J Clin Oncol. 2009;32(1):65-72. PubMed
45.Maringwa JT, Quinten C, King M, et al. Minimal important differences for interpreting health-related quality of life scores from the EORTC QLQ-C30 in lung cancer patients participating in randomized controlled trials. Support Care Cancer. 2011;19(11):1753-1760. PubMed
46.Osoba D, Rodrigues G, Myles J, Zee B, Pater J. Interpreting the significance of changes in health-related quality-of-life scores. J Clin Oncol. 1998;16(1):139-144. PubMed
47.Bergman B, Aaronson NK, Ahmedzai S, Kaasa S, Sullivan M. The EORTC QLQ-LC13: a modular supplement to the EORTC Core Quality of Life Questionnaire (QLQ-C30) for use in lung cancer clinical trials. EORTC Study Group on Quality of Life. Eur J Cancer. 1994;30a(5):635-642. PubMed
48.AstraZeneca Canada Inc. response to January 10, 2024 CADTH request for additional information regarding Osimertinib review [internal sponsor's report]. Mississauga (ON): AstraZeneca Canada Inc; 2024 Jan 18.
49.Hayashi H, Okamoto I, Morita S, Taguri M, Nakagawa K. Postprogression survival for first-line chemotherapy of patients with advanced non–small-cell lung cancer. Ann Oncol. 2012;23(6):1537-1541. PubMed
50.Hotta K, Kiura K, Fujiwara Y, et al. Role of survival post-progression in phase III trials of systemic chemotherapy in advanced non–small-cell lung cancer: a systematic review. PLoS One. 2011;6(11):e26646. PubMed
51.Imai H, Kaira K, Mori K, et al. Post-progression survival is highly linked to overall survival in patients with non–small-cell lung cancer harboring sensitive EGFR mutations treated with first-line epidermal growth factor receptor-tyrosine kinase inhibitors. Thorac Cancer. 2019;10(12):2200-2208. PubMed
52.Yoshino R, Imai H, Mori K, et al. Surrogate endpoints for overall survival in advanced non–small-cell lung cancer patients with mutations of the epidermal growth factor receptor gene. Mol Clin Oncol. 2014;2(5):731-736. PubMed
53.Hotta K, Fujiwara Y, Matsuo K, et al. Time to progression as a surrogate marker for overall survival in patients with advanced non–small cell lung cancer. J Thorac Oncol. 2009;4(3):311-317. PubMed
54.Johnson KR, Ringland C, Stokes BJ, et al. Response rate or time to progression as predictors of survival in trials of metastatic colorectal cancer or non–small-cell lung cancer: a meta-analysis. Lancet Oncol. 2006;7(9):741-746. PubMed
55.Grigore B, Ciani O, Dams F, et al. Surrogate endpoints in health technology assessment: an international review of methodological guidelines. Pharmacoeconomics. 2020;38(10):1055-1070. PubMed
56.Fleming TR, DeMets DL. Surrogate end points in clinical trials: are we being misled? Ann Intern Med. 1996;125(7):605-613. PubMed
57.Bujkiewicz S, Achana F, Papanikos T, Riley RD, Abrams KR. NICE DSU technical support document 20: multivariate meta-analysis of summary data for combining treatment effects on correlated outcomes and evaluating surrogate endpoints. Sheffield (GB): University of Sheffield; 2019: https://www.sheffield.ac.uk/sites/default/files/2022-02/TSD20-mvmeta-final.pdf. Accessed 2024 May 23.
58.Welton NJ, Phillippo DM, Owen R, et al. CHTE2020 sources and synthesis of evidence; update to evidence synthesis methods. 2020; https://www.sheffield.ac.uk/nice-dsu/methods-development/chte2020-sources-and-synthesis-evidence. Accessed 2024 May 23.
59.Endpoints used in relative effectiveness assessment of pharmaceuticals- surrogate endpoints. Diemen (NL): EUnetHTA; 2013: https://www.eunethta.eu/wp-content/uploads/2018/01/Surrogate-Endpoints.pdf. Accessed 2024 May 23.
60.Ciani O, Manyara AM, Davies P, et al. A framework for the definition and interpretation of the use of surrogate endpoints in interventional trials. EClinicalMedicine. 2023;65:102283. PubMed
61.Hayashi H, Okamoto I, Taguri M, Morita S, Nakagawa K. Postprogression survival in patients with advanced non–small-cell lung cancer who receive second-line or third-line chemotherapy. Clin Lung Cancer. 2013;14(3):261-266. PubMed
62.Imai H, Takahashi T, Mori K, et al. Individual-level data on the relationships of progression-free survival, post-progression survival, and tumor response with overall survival in patients with advanced non-squamous non–small cell lung cancer. Neoplasma. 2014;61(2):233-240. PubMed
63.Kotake M, Miura Y, Imai H, et al. Post-progression survival associated with overall survival in patients with advanced non–small-cell lung cancer receiving docetaxel monotherapy as second-line chemotherapy. Chemotherapy. 2017;62(4):205-213. PubMed
64.Imai H, Mori K, Ono A, et al. Individual-level data on the relationships of progression-free survival and post-progression survival with overall survival in patients with advanced non-squamous non–small cell lung cancer patients who received second-line chemotherapy. Med Oncol. 2014;31(8):88. PubMed
65.Liu G, Zhang J, Zhou ZY, Li J, Cai X, Signorovitch J. Association between time to progression and subsequent survival inceritinib-treated patients with advanced ALK-positive non–small-cell lung cancer. Curr Med Res Opin. 2016;32(11):1911-1918. PubMed
66.Giroux Leprieur E, Lavole A, Ruppert AM, et al. Factors associated with long-term survival of patients with advanced non–small cell lung cancer. Respirology. 2012;17(1):134-142. PubMed
67.Khozin S, Miksad RA, Adami J, et al. Real-world progression, treatment, and survival outcomes during rapid adoption of immunotherapy for advanced non–small cell lung cancer. Cancer. 2019;125(22):4019-4032. PubMed
68.Griffith SD, Miksad RA, Calkins G, et al. Characterizing the feasibility and performance of real-world tumor progression end points and their association with overall survival in a large advanced non–small-cell lung cancer data set. JCO Clin Cancer Inform. 2019;3:1-13. PubMed
69.Berghmans T, Pasleau F, Paesmans M, et al. Surrogate markers predicting overall survival for lung cancer: ELCWP recommendations. Eur Respir J. 2012;39(1):9-28. PubMed
Appendix 1: Detailed Outcome Data
Please note that this appendix has not been copy-edited.
Table 19: OS in FLAURA2 (Randomized Period — FAS, Data Cut-off Date: April 3, 2023)
Efficacy outcome | FLAURA2 | |
|---|---|---|
Osimertinib + chemotherapy (N = 279) | Osimertinib monotherapy (N = 278) | |
OS (data cut-off: April 3, 2023) | ||
Number (%) of deaths as of data cut-off date | 71 (25.4) | 78 (28.1) |
Median OS (months) (95% CI)a | NC (31.9 to NC) | NC (NC to NC) |
HR (95% CI) [2-sided P value]b | 0.90 (0.65 to 1.24) [0.5238] | |
Still in survival follow-up, n (%)c | 197 (70.6) | 191 (68.7) |
Terminated before death, n (%)d | 11 (3.9) | 9 (3.2) |
Completed | 0 | 0 |
Withdrawal by patients | 10 (3.6) | 8 (2.9) |
Lost to follow-up | 0 | 0 |
Other | 1 (0.4) | 1 (0.4) |
Median (min, max) follow-up for OS in all patients, months | 23.9 (0.1 to 34.1) | 23.7 (0.1 to 33.9) |
Median (min, max) follow-up for OS in censored patients, months | 25.0 (0.2 to 34.1) | 25.1 (0.1 to 33.9) |
CI = confidence interval; FAS = full analysis set; HR = hazard ratio; NC = not calculable; NR = not reported; OS = overall survival; osimertinib + chemotherapy = osimertinib in combination with pemetrexed and platinum-based chemotherapy
aCalculated using the Kaplan-Meier method.
bThe analysis was performed using a log-rank test stratified by race (Chinese/Asian vs. Non-Chinese/Asian vs. Non Asian), WHO PS (0 vs. 1), and method used for EGFRm tissue testing (central vs. local). An HR < 1 favours osimertinib plus chemotherapy. The efficacy boundary for significance for the first interim OS analysis (data cut-off date: April 3, 2023) was 0.00158, and the efficacy boundary for significance for the second interim OS analysis (data cut-off date: January 8, 2024) was 0.000001.
cIncluded patients known to be alive at the data cut-off date.
dIncluded patients with unknown survival status or patients who were lost to follow-up.
Source: FLAURA2 Clinical Study Report,16 Drug Reimbursement Review sponsor submission.17
Table 20: Sensitivity Analysis of PFS According to BICR in FLAURA2 (Randomized Period — FAS, Data Cut-off Date: April 3, 2023)
Efficacy outcome | FLAURA2 | |
|---|---|---|
Osimertinib + chemotherapy (N = 279) | Osimertinib (N = 278) | |
PFS according to BICR in FAS | ||
Number (%) of PFS events | 102 (36.6) | 138 (49.6) |
Median PFS (months) (95% CI)a | 29.4 (25.1 to NC) | 19.9 (16.6 to 25.3) |
HR (95% CI) [2-sided P value]b,c | 0.62 (0.48 to 0.80) [0.0002] | |
Probability of being progression-free at 12 months (%) (95% CI)a | 79.8 (74.5 to 84.2) | 67.3 (61.2 to 72.6) |
Difference in probability (%) (95% CI) | 12.5 (NR) | |
Probability of being progression-free at 24 months (%) (95% CI)a | 61.6 (54.8 to 67.7) | 46.8 (40.2 to 53.2) |
Difference in probability (%) (95% CI) | 14.8 (NR) | |
Progression, n (%) | 102 (36.6) | 138 (49.6) |
RECIST progressiond | 75 (26.9) | 124 (44.6) |
Target lesionse | 48 (17.2) | 79 (28.4) |
Nontarget lesionse | 21 (7.5) | 34 (12.2) |
New lesionse | 23 (8.2) | 47 (16.9) |
Deathf | 27 (9.7) | 14 (5.0) |
No progression, n (%) | 177 (63.4) | 140 (50.4) |
Censored RECIST progression due to missing visitsg | 1 (0.4) | 0 |
Censored death due to missing visitsg | 11 (3.9) | 16 (5.8) |
Progression-free at time of analysish | 154 (55.2) | 119 (42.8) |
Lost to follow-upi | 0 | 0 |
Withdrawn consenti | 10 (3.6) | 4 (1.4) |
Discontinued study for other reasonsi | 1 (0.4) | 1 (0.4) |
BICR = blinded independent central review; CI = confidence interval; FAS = full analysis set; HR = hazard ratio; NC = not calculable; NR = not reported; osimertinib + chemotherapy = osimertinib in combination with pemetrexed and platinum-based chemotherapy; PFS = progression-free survival; RECIST = Response Evaluation Criteria in Solid Tumors.
aCalculated using the Kaplan-Meier method.
bThe analysis was performed using a log-rank test stratified by race (Chinese/Asian vs. non-Chinese/Asian vs. non-Asian), WHO PS (0 vs. 1), and method used for EGFRm tissue testing (central vs. local). An HR < 1 favours osimertinib plus chemotherapy.
cNominal P value.
dOnly included progression events that occurred within 2 consecutive scheduled visits (plus visit window) of the last evaluable assessment (or randomization).
eTarget lesions, nontarget lesions, and new lesions were not necessarily mutually exclusive categories.
fDeath in the absence of RECIST progression, within 2 visits of baseline or last RECIST assessment (Not Evaluable is not considered as missing visit).
gRECIST progression or death occurred more than 2 consecutive scheduled visits (plus visit window) after last previous evaluable RECIST assessment or baseline if no valid postbaseline assessment. Patients are censored at last previous evaluable RECIST assessment or randomization date.
hIncluded patients, known to be alive, with no evaluable baseline RECIST assessment (censored at Day 1) or censored at last evaluable RECIST assessment.
iPatients censored at last evaluable RECIST assessment or randomization.
Sources: FLAURA2 Clinical Study Report16 and Drug Reimbursement Review sponsor submission.17
Figure 4: Kaplan-Meier Plot of OS in FLAURA2 (Randomized Period — FAS, Data Cut-off Date: April 3, 2023)
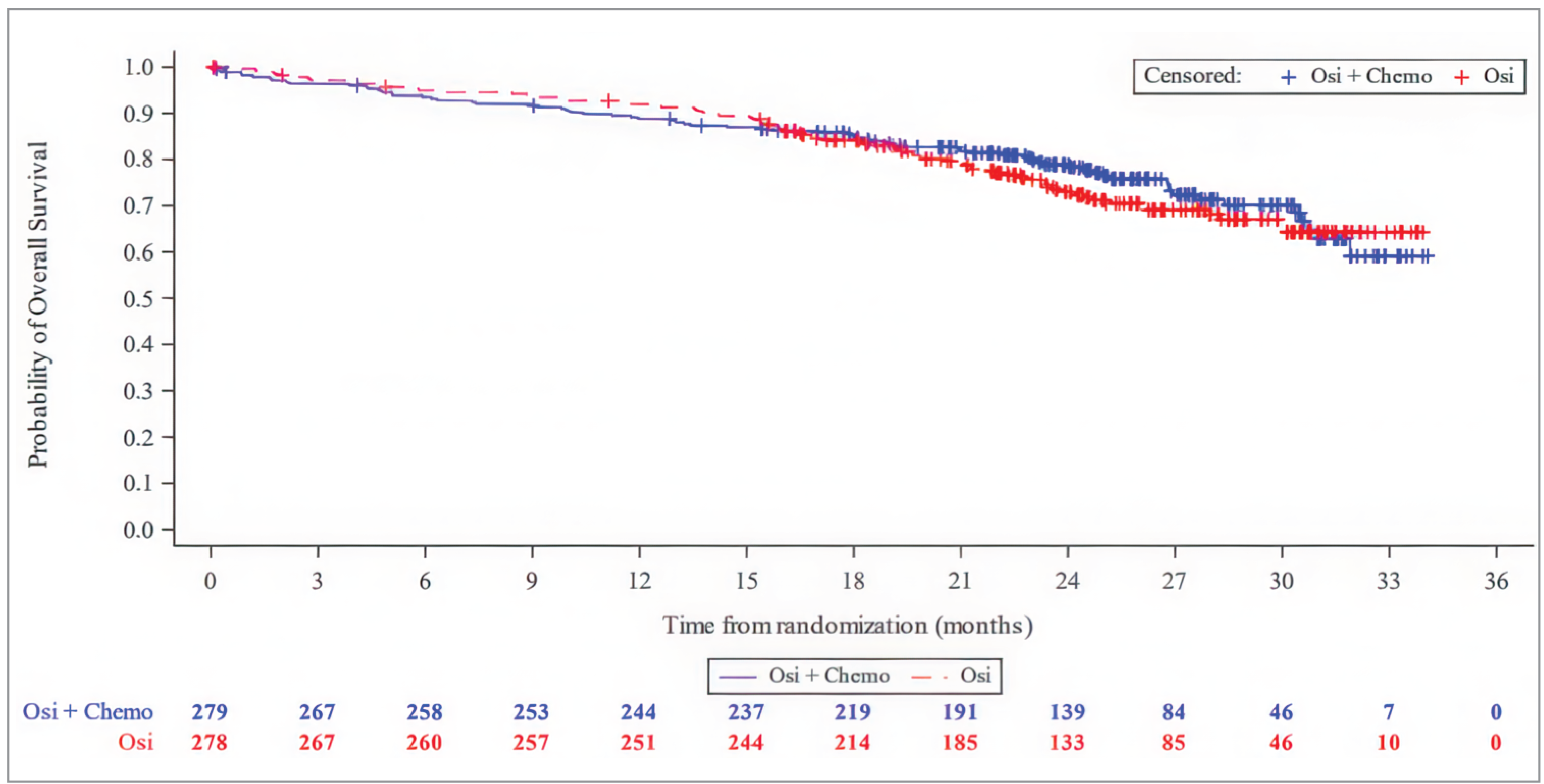
Note: Osimertinib + chemotherapy was denoted as Osi + Chemo, and osimertinib monotherapy as Osi in sponsor’s Clinical Study Report. The values at the base of the figure indicate number of patients at risk.
OS = overall survival; osimertinib + chemotherapy = osimertinib in combination with pemetrexed and platinum-based chemotherapy
Source: FLAURA2 Clinical Study Report,16 Drug Reimbursement Review sponsor submission17
Figure 5: Kaplan-Meier Plot of PFS According to BICR in FLAURA2 (Randomized Period — FAS, Data Cut-Off Date: April 3, 2023)
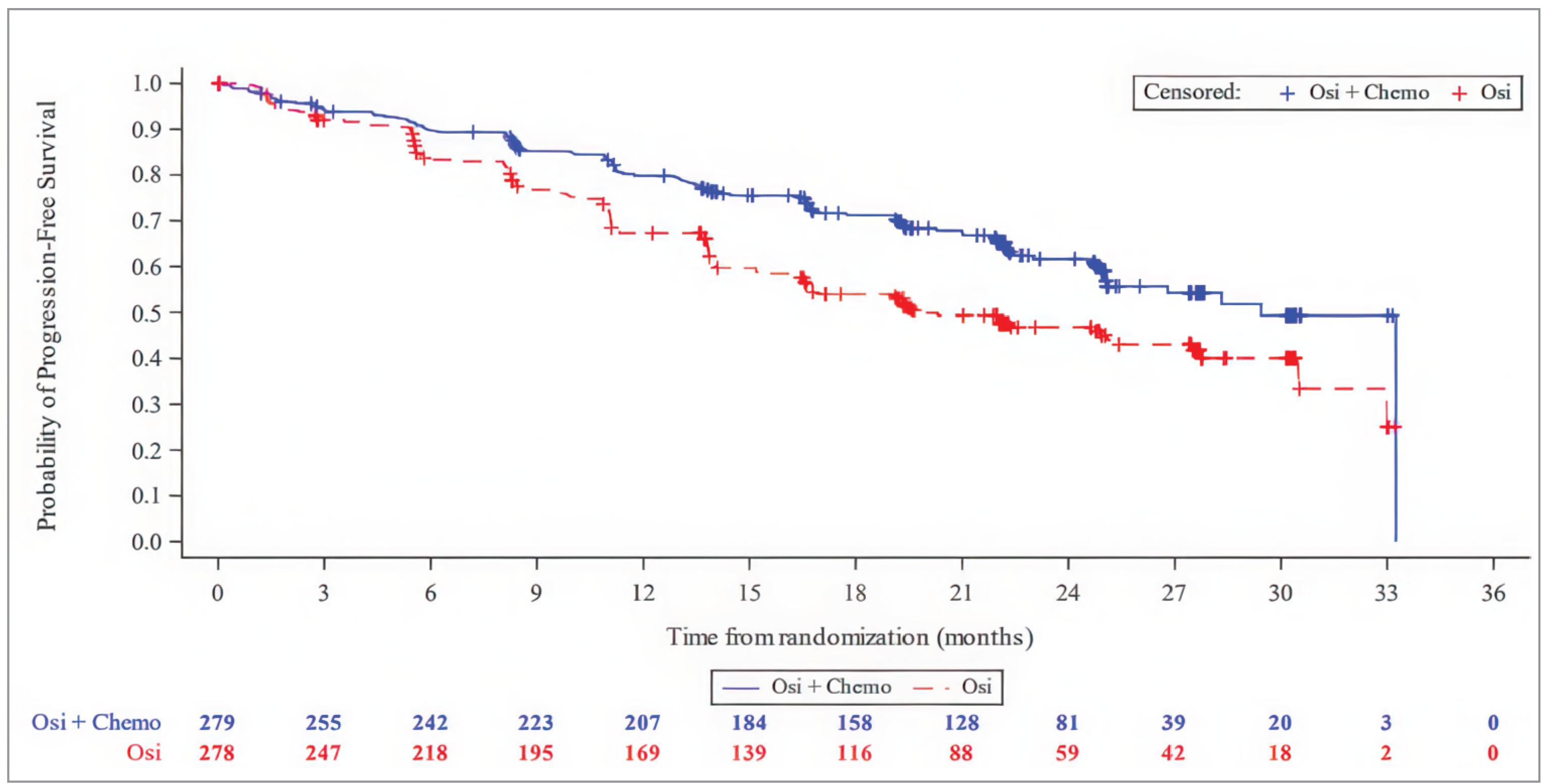
BICR = blinded independent central review; osimertinib + chemotherapy = osimertinib in combination with pemetrexed and platinum-based chemotherapy; PFS = progression-free survival.
Note: Osimertinib + chemotherapy was denoted as Osi + Chemo, and osimertinib monotherapy as Osi in sponsor’s Clinical Study Report. The values at the base of the figure indicate number of patients at risk.
Sources: FLAURA2 Clinical Study Report16 and Drug Reimbursement Review sponsor submission.17
Appendix 2: Post-Progression Survival and Time to Progression
Please note that this appendix has not been copy-edited.
In the correspondence with the review team,48 the sponsor provided 2 systematic reviews with meta-analyses49,50 and 2 retrospective studies51,52 that suggested a correlation (r > 0.8) between post-progression survival (PPS) and OS in patients in first-line setting for advanced or metastatic NSCLC. Two meta-analyses53,54 indicated that time to progression (TTP) accounted for only one-fifth to one-third (R2 = 0.19 and R2 = 0.33) of the variance in OS in patients with advanced NSCLC.
The methods used in the provided studies aligned with those that are recommended. For example, meta-analytic approaches that provide estimates of trial level correlation (often measured using r and R2) are recommended by several HTA agencies as part of determining end point surrogacy,55 but there is no consensus – currently – on what values of these measures constitute strong evidence or that an end point is a “good surrogate.” As well, establishing an end point as a surrogate for a patient important clinical outcome is multidimensional and there is increasingly emphasis to not rely on statistical correlation alone.56-60 Hotta et al.53 in discussing the results of their meta-analysis on the correlation between TTP and OS acknowledged the need for studies that specifically study the interplay between causal pathways of NSCLC, the mechanism of action of the treatment of interest, and the links between intermediate and terminal outcomes.
Additionally, correlation and regression methods do not comprehensively account for relevant uncertainty, including the variability and other sources of uncertainty associated with the treatment effect on the surrogate end point.57 This limitation was acknowledged in some of the provided articles. Moreover, assessing the certainty and precision of the correlation results was hampered by the lack of reporting of confidence intervals in most of the published articles. Thus, the reported values represent a summary statistic and do not provide information on the distribution of the correlations. This is important given the variability in the correlation between each of PPS and TTP with OS based on the subgroups and factors analyzed in the reviewed studies. For example, 1 meta-analysis reported an overall R2 for the correlation between the median TTP ratio (between trial arms) and the median OS ratio of 0.33, but the estimate varied across subgroups (R2 = 0.16 in trials with no description of the primary end point definition to 0.51 in studies53 that used cisplatin as part of the initial treatment).
Other important limitations with the provided evidence for surrogacy of PPS and TTP include, but are not limited to:
Retrospective design of the individual studies that were set at a single cancer centre in Japan with relatively smaller sample sizes (N < 100 patients).51,52
It was difficult to assess the systematic reviews and meta-analytic methods due to limited reporting of the search strategies, eligibility criteria (including intervention, intervention, comparison, outcome, study design [PICOS]), and statistical analyses including assessments of the robustness of the results (e.g., lack of assessments for publication bias). Reviewers could not conclude with confidence that the methods used aligned with those that are accepted.
Most of the analyses did not (or could not for lack of information) account for differences in and the effects of therapies received after progression, which could impact PPS and its association with OS.
The studies were published between 2006 and 2019 and therefore the evidence is likely more representative of the situation at those time frames, including patients’ risk of progression and/or response to first-line treatment. Moreover, the systematic reviews (all published before 2013) included studies from previous decades. The meta-analyses that examined the effects of trial initiation or publication date on the association between PPS and OS49,50 and TTP and OS53 reported this factor had an important impact on the correlations, generally with the older trials associated with weaker correlations.
There were also the weaker correlations in targeted therapy trials than in chemotherapy regimen trials which indicates initial treatment type is an important factor. It is acknowledged that the number of trials on targeted therapies was smaller than for chemotherapy regimens, likely related to the dates the trials were conducted.
Each of the meta-analyses identified variation in outcome definitions and assessments. As well, trials often did not report definitions of outcomes. For example, Hotta et al.53 noted that 44% of the 54 included trials did not describe the definition of TTP and 65% of the trials provided a definition of OS. In addition, the retrospective studies identified the potential for bias related to variation on the date on which a tumour response was recorded by each physician. While, as the authors identify, this was not unique to their studies it is a key limitation especially because the determination of the duration of PPS would be based on this date (i.e., OS = PFS + PPS). The impact of outcome definition on the results of the meta-analyses and retrospective studies was not reported, except by Hayashi et al.49 who only reported on their assumption to consider TTP and PFS as the same outcome from the trials.
Some of the analyses adjusted for potentially confounding factors such as (but not limited to) patient age, performance status, tumour histology, molecular biomarkers, year of trial, and subsequent lines of therapy. However, there was variation in which covariates were modelled and the choice of these was not well-described. There is a potential for the failure to account for confounding variables to influence the relationship between PPS and OS or TTP and OS.
The included populations impact the accuracy of the estimates for the relationship between the surrogate end points and OS, but also the generalizability. As mentioned, there was limited information provided about the PICOS in the systematic reviews and the eligibility criteria for the retrospective studies. The meta-analyses included patients with advanced or metastatic NSCLC who received first-line therapy, generally either with cytotoxic chemotherapy or molecular targeted drugs. Patients with EGFR mutations were not specifically selected for these analyses. The retrospective studies, however, specifically included patients with EGFR mutation–positive advanced or metastatic NSCLC. The sponsor provided studies61-68 in other patient populations (e.g., anaplastic lymphoma kinase–positive NSCLC and/or later lines of therapy) as supportive evidence. The studies had similar limitations as those already described in addition the uncertainty of how the results in these increasingly heterogeneous populations apply to the target population for this review. Therefore, there is limited evidence for the strength of the surrogacy of PPS and TTP with OS in the population of interest.
The sponsor provided The European Lung Cancer Working Party (ELCWP) 2012 guidelines that reported on surrogate markers as adequate predictive of OS in patients with lung cancer.69 It was highlighted that the ELCWP issued a strong recommendation (based on “moderate quality evidence”) about TTP as a surrogate end point for OS based on the results of the aforementioned meta-analyses.53,54 The recommendation was: “TTP is an intermediate marker for overall survival in advanced NSCLC treated with first-line chemotherapy.”69 It is notable that Hotta et al. concluded based on their meta-analysis that:
“…our findings indicate that TTP in our collection of relevant trials is too weakly correlated with survival to use as a surrogate for survival in first-line chemotherapy for advanced NSCLC. With the increasing number of active compounds available for the treatment of NSCLC, even in second-line or later settings, the role of surrogate markers, including TTP, should be investigated extensively.”53
Another important consideration, relating to the use of PPS and TTP in the health economic model, is that both were determined post hoc.
In summary, while the studies provided by the sponsor suggest PPS and TTP as surrogate end points for OS in advanced NSCLC, the limitations and multiple sources of uncertainty complicate the interpretation of the results. The review team determined that currently available evidence is not a strong support for the sponsor’s claim of surrogacy.
Pharmacoeconomic Review
Abbreviations
AE
adverse event
BSA
body surface area
CDA-AMC
Canada’s Drug Agency
ex19del
exon 19 deletion
ICER
incremental cost-effectiveness ratio
L858R
L858R substitution
LCC
Lung Cancer Canada
NSCLC
non–small cell lung cancer
OH-CCO
Ontario Health (Cancer Care Ontario)
OS
overall survival
PD
progressed disease
PF
progression-free
PFS
progression-free survival
PPS
post-progression survival
QALY
quality-adjusted life-year
RECIST
Response Evaluation Criteria in Solid Tumors
TTD
time to treatment discontinuation
TTP
time to progression
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Osimertinib (Tagrisso) oral tablets, 40 mg and 80 mg |
Indication | In combination with pemetrexed and platinum-based chemotherapy for the first-line treatment of patients with locally advanced (not amenable to curative therapies) or metastatic NSCLC whose tumours have EGFR exon 19 deletions or exon 21 L858R substitution mutations. |
Health Canada approval status | NOC |
Health Canada review pathway | Priority review and Project Orbis |
NOC date | July 10, 2024 |
Reimbursement request | As per indication |
Sponsor | AstraZeneca Canada Inc. |
Submission history | Previously reviewed: Yes Indication: Adjuvant therapy after tumour resection in patients with stage IB-IIIA NSCLC whose tumours have EGFR exon 19 deletions or L858R substitution mutations
Indication: NSCLC (first line)
Indication: NSCLC
|
NOC = Notice of Compliance; NSCLC = non–small cell lung cancer.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Markov model |
Target population | Patients with locally advanced (not amenable to curative therapies) or metastatic NSCLC whose tumours have EGFR exon 19 deletions or exon 21 L858R substitution mutations |
Treatment | Osimertinib in combination with pemetrexed and platinum-based chemotherapy |
Dose regimen | Osimertinib plus chemotherapy:
|
Submitted price | Per tablet (80 mg), $322.13 |
Submitted treatment cost | The 21-day per patient cost of osimertinib plus chemotherapy is $10,704 during the induction phase (assuming a 50:50 split between cisplatin and carboplatin) and $10,114 during the maintenance phase |
Comparator | Osimertinib monotherapy (80 mg once daily) |
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs, life-years |
Time horizon | Lifetime (15 years) |
Key data source | FLAURA2: multinational, open-label, randomized phase III trial evaluating the efficacy of osimertinib with or without pemetrexed and platinum-based chemotherapy |
Submitted results | ICER = $146,769 per QALY gained (incremental costs = $59,009; incremental QALYs = 0.40) |
Key limitations |
|
CDA-AMC reanalysis results |
|
AUC = area under the concentration-time curve during any dosing interval; CDA-AMC = Canada’s Drug Agency; HRQoL = health-related quality of life; ICER = incremental cost-effectiveness ratio; OS = overall survival; PD = progressed disease; PF = progression-free; PPS = post-progression survival; QALY = quality-adjusted life-year; TTP = time to progression.
Conclusions
Our Clinical Review found that no conclusions could be drawn about the effect of osimertinib plus chemotherapy on overall survival (OS) because of the immaturity of the data from the FLAURA2 trial (26.8% overall data maturity). Despite these limitations, clinical experts consulted by the review team noted that the findings appear to be favourable and may be clinically important. These data were used to inform the economic analysis, and the underlying uncertainties in the clinical findings translate to uncertainty within the economic results, most specifically the interpretation of the survival benefit estimated by the sponsor’s model. While the difference in OS at the data cut point was not statistically significant, the sponsor’s model predicted 0.44 additional years of life for patients receiving osimertinib plus chemotherapy. More than 100% of incremental survival in the sponsor’s model was generated by extrapolating beyond the observation period of the FLAURA2 trial.
The review team identified several limitations in the economic analyses submitted by the sponsor, beyond the uncertainty regarding the impact of osimertinib plus chemotherapy on OS. In the review team’s base case, osimertinib plus chemotherapy is associated with an incremental cost of $57,897 and 0.246 incremental quality-adjusted life-years (QALYs) compared to osimertinib monotherapy, resulting in an incremental cost-effectiveness ratio (ICER) of $235,123 per QALY gained. These findings were broadly similar to the sponsor’s, insofar as osimertinib plus chemotherapy was expected to yield higher quality-adjusted survival at a higher cost compared to osimertinib monotherapy. If the price of osimertinib was reduced to $0, the resulting ICER would be $75,865 due to the fact that the price of osimertinib is reduced in both modelled treatment arms, while the cost of chemotherapy remains in the osimertinib plus chemotherapy arm.
Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, clinician groups, and drug plans that participated in the review conducted by Canada’s Drug Agency (CDA-AMC).
Patient input was received by 2 patient groups: Lung Cancer Canada (LCC) and the Ontario Lung Association (now the Lung Health Foundation). Patient input was gathered from interviews and surveys conducted in January 2021 and October 2023 by the Lung Health Foundation and December 2023 by LCC. The Lung Health Foundation conducted 2 interviews and gathered 15 responses from online surveys and LCC conducted 13 interviews with patients and/or caregivers. Respondents indicated that the disease negatively affected their ability to participate in leisure activities, hobbies, shopping, and travel. Respondents in the LCC interviews reported that patients living with lung cancer require a treatment that improves their quality of life while also managing their disease effectively. Some benefits from currently available treatments included reduced coughing and shortness of breath, ability to exercise, delayed disease progression, reduction in disease-related symptoms, and prolonged life, as reported by the Lung Health Foundation. Input from the LCC patient group emphasized that respondents had experience with osimertinib, noting that the treatment has been effective at treating patients’ tumours and managing symptoms, and that side effects such as diarrhea, muscle pain and spasms, skin issues, and lack of appetite were frequent at treatment onset, but are generally manageable. Patients noted they were able to maintain or improve their quality of life and functionality while on osimertinib. One respondent from the Lung Health Foundation noted that, while the treatment is effective, it is costly, and they hope that the next treatment option is approved and funded.
Clinician input was received from the Ontario Health (Cancer Care Ontario) (OH-CCO) Lung Cancer Drug Advisory Committee and LCC, with a total of 28 clinicians providing input on osimertinib plus chemotherapy. The OH-CCO committee mentioned that current treatments target shrinking the cancer, improvement in disease-related symptoms, and maximizing control of the disease to prevent or delay symptoms and prolong life. However, both clinician groups indicated that the current treatment options with osimertinib monotherapy and/or sequential therapy with osimertinib followed by chemotherapy are not curative. Both clinician groups emphasized the need for improved therapies that result in longer control of the cancer, a better quality of life, and longer survival. Both clinician groups noted that the combination of osimertinib and chemotherapy would be an option in patients with non–small cell lung cancer (NSCLC) with sensitizing EGFR mutations. The OH-CCO group highlighted the need for OS data before drawing any conclusion regarding a shift in the current treatment paradigm. They further mentioned that the addition of platinum-based chemotherapy to osimertinib is associated with more inconvenience to patients due to an increase in chemotherapy-associated toxicities, which require the patients to attend cancer centres more frequently for IV therapy. Both clinician groups noted that single-drug osimertinib would remain an option for first-line therapy, as did the clinical experts consulted by the review team.
Drug plan input received by the review team noted that initial chemotherapy and maintenance of pemetrexed requires IV drug preparation and ambulatory treatment appointments every 3 weeks, which will have an additional impact on resources and may increase incremental costs. The plans questioned if patients with an Eastern Cooperative Oncology Group Performance Status greater than 1 should be eligible for treatment, an inclusion that may affect overall drug costs. Plans noted that EGFR mutation testing is a part of routine clinical practice for this reimbursement population and therefore is not expected to result in an incremental difference in costs.
Several of these concerns were addressed in the sponsor’s model:
Health-state utilities that captured lung cancer symptoms and quality of life were included.
Adverse events (AEs) associated with osimertinib plus chemotherapy were included.
The cost of chemotherapy and associated costs related to administration, disease management, and monitoring were included.
The review team was unable to address the following concerns raised from patient and clinician group input:
No conclusions could be drawn about the effect of osimertinib plus chemotherapy on OS because of the immaturity of the data.
The inconvenience experienced by patients receiving osimertinib plus chemotherapy due to more frequent visits to a cancer centre for IV therapy was not captured in the analysis.
Economic Review
The current review is for osimertinib (Tagrisso) in combination with pemetrexed and platinum-based chemotherapy for the first-line treatment of patients with locally advanced (not amenable to curative therapies) or metastatic NSCLC whose tumours have EGFR exon 19 deletion (ex19del) or L858R substitution (L858R) mutations.
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted a cost-utility analysis of osimertinib in combination with pemetrexed and platinum-based chemotherapy (osimertinib plus chemotherapy), for the first-line treatment of adult patients (aged ≥ 18 years) with locally advanced or metastatic NSCLC whose tumours have EGFR ex19del or L858R mutations, compared with osimertinib monotherapy.1 The model population comprised the same target population and was aligned with the Health Canada indication.2
Osimertinib is available as a 40 mg or 80 mg tablet. The recommended dose is 80 mg, to be taken orally once daily until disease progression or unacceptable toxicity.2 Patients in both the intervention and comparator arm of the model receive osimertinib via once-daily oral administration until treatment discontinuation. At the sponsor’s submitted price of $322.13 per 80 mg tablet, the 21-day cost of osimertinib monotherapy is $6,764.69. In the osimertinib plus chemotherapy arm, chemotherapy treatment consists of an induction phase and maintenance phase. During the induction phase patients either receive cisplatin (75 mg/m2) or carboplatin (area under the concentration-time curve during any dosing interval of 5 mg/mL/min) in combination with pemetrexed (500 mg/m2) on day 1 of each 21-day cycle (every 3 weeks) for 4 cycles, with both treatments administered via IV infusion. This is followed by a maintenance phase during which pemetrexed (500 mg/m2) is administered every 3 weeks. The dosing of the chemotherapy regimens was based on the patient’s body surface area (BSA), which was assumed to be consistent with target population observed in the FLAURA2 trial (BSA = 1.71 m2).3 In the base case, the sponsors assumed a 50:50 split of patients receiving cisplatin or carboplatin during the induction chemotherapy phase. The treatment-acquisition costs of chemotherapy per 21-day treatment cycle included wastage and were estimated by the sponsor to be $405.00 for cisplatin, $775.00 for carboplatin, and $450.00 for pemetrexed. At the sponsor’s submitted price for osimertinib and the public price for the chemotherapy regiments, the 21-day cost of osimertinib plus chemotherapy is $10,703.84 during the induction phase (assuming a 50:50 split between cisplatin and carboplatin) and $10,113.84 during the maintenance phase.
The model also included subsequent (second- and third-line) treatment-acquisition costs following treatment discontinuation of osimertinib in both study arms. Patients were assumed to receive either platinum doublet chemotherapy, pemetrexed, docetaxel, or immuno-oncology therapies.
The clinical outcomes of interest were QALYs and life-years. The economic analysis was undertaken over a lifetime time horizon of 15 years from the perspective of a Canadian public health care payer. Discounting at 1.5% annually was applied to both costs and outcomes.1
Model Structure
The sponsor submitted a Markov model with 3 mutually exclusive states: progression-free (PF), progressed disease (PD), and dead. Transitions between states occurred on a monthly cycle (Figure 1, Appendix 3). From the PF state, patients could transition to the PD state, the dead state, or remain PF. Patients in the PD state could remain in the PD state or transition to the dead state. In the model the proportion of patients on treatment (first-line and subsequent treatment) are determined according to time to treatment discontinuation (TTD) curves, regardless of statement membership.
Model Inputs
The model’s baseline population characteristics and clinical efficacy parameters were characterized by the FLAURA2 trial, a multinational, open-label, randomized phase III trial evaluating the efficacy of osimertinib with or without pemetrexed and platinum-based chemotherapy in patients with previously untreated EGFR-mutated (ex19del or L858R) locally advanced or metastatic NSCLC.3 The sponsor assumed that the FLAURA2 population (baseline characteristics: mean age = 60.8 years; proportion male = 38.6%) reflected the Canadian population.1
All transition probabilities in the model were derived from the FLAURA2 trial, using the April 3, 2023, data cut-off date. Investigator-assessed progression-free survival (PFS) was the primary outcome in the FLAURA2 trial. PFS was defined as objective disease progression (according to Response Evaluation Criteria in Solid Tumors [RECIST]) or death (by any cause in the absence of progression), regardless of whether the patient withdrew from study treatment or received another anticancer therapy before progression. OS was the secondary end point in the FLAURA2 trial and was defined as the time from the date of randomization until death due to any cause. As OS maturity was not observed (the overall maturity of data was 26.8% and the median OS was not reached) the modelled transition probabilities were assumed to be aligned with the data reported in post hoc analyses of the FLAURA2 trial. Specifically, transitions from PF to PD were modelled using time to progression (TTP) data, PD to dead was modelled using post-progression survival (PPS) data, and PF to dead was modelled using a combination of PFS and TTP data. TTP was defined as disease progression according to RECIST only, while PPS was defined as a patient experiencing death, with prior record of disease progression according to RECIST.
Parametric survival modelling was used to extrapolate health-state transition probabilities beyond the trial period (30 months of follow-up). Survival distributions were selected based on clinical plausibility of long-term projections, visual inspection of fit, and the Akaike information criterion and Bayesian information criterion.1
Because of the limited number of mortality events in the available FLAURA2 data and associated uncertainty in the relative extrapolated hazards, the hazards for PPS were assumed to be identical in both study arms. The sponsors used the PPS data in the osimertinib monotherapy arm to estimate the transition from PD to dead in the model for both study arms. Kaplan-Meier estimates of OS data from the FLAURA trial were used to guide selection of clinically plausible curves fitted to the FLAURA2 post-progression data.4
The grade 3 or greater AEs observed in the FLAURA2 trial were incorporated into the model with an associated cost and disutility.3 These were applied for the first month (i.e., model cycle); after 1 month, no additional AEs were applied.
Health-state utility values were sourced from EQ-5D-5L data collected in the FLAURA2 trial and published estimates. The EQ-5D-5L data collected in the FLAURA2 trial were used to derive utility values for the PF (█████) and PD (█████) health states. EQ-5D scores were converted to a utility value using the Canadian value set for the EQ-5D-5L questionnaire.5 However, in its base-case analysis the sponsor used a PD utility of 0.70, which was sourced from a real-world study of health-state utilities in patients in Canada with lung cancer.6 Scenario analyses were also conducted to explore the impact of alternative sets of health-state utility values on the resulting ICERs. An age adjustment was also applied to each health-state utility by applying a multiplier based on general population utilities.7 Disutilities for AEs were either sourced from the literature or based on assumptions and incorporated as a single disutility as a one-off in the first cycle.1
The model incorporated treatment-acquisition costs for osimertinib, chemotherapy, and subsequent therapies. Dosing details were sourced from Health Canada product monographs, with acquisition costs for osimertinib derived from the sponsor's submitted price1 and IQVIA Delta Price for other treatments.8 The dosage of treatments, including chemotherapy regimens, were estimated from the average BSA estimates (1.71 m2) from the FLAURA2 trial’s patient population.3 IV treatment vial sizes were chosen based on the lowest monthly acquisition cost and assumed wastage in the base case.
In the model treatment duration, for all treatments, was determined regardless of state membership. Treatment duration was determined by treatment discontinuation data from the FLAURA2 trial, which was available separately for osimertinib and pemetrexed. Extrapolations of this data were used to estimate the proportion of patients on treatment in each model cycle. In the base case, no treatment stopping rules were applied in either study arm, although the model allows for application of stopping rules.
In both study arms, the cost of subsequent treatments was applied upon discontinuation of osimertinib, regardless of state membership. Subsequent treatments included both second- and third-line therapies. The distribution of patients across these treatments was based on reported estimates from the FLAURA2 study, and it was assumed that all treatments had the same duration in both second- and third-line settings. The total cost of subsequent treatment was estimated by calculating a weighted average cost for each arm, accounting for the proportion of patients receiving subsequent treatments and the duration of those treatments.
Other costs included those for monitoring, treatment administration, disease management, central nervous system metastases-related expenses, AEs, and end-of-life costs. Monitoring costs related solely to chemotherapy treatments were applied only in the osimertinib plus chemotherapy arm. Administration costs were included for each treatment based on administration frequency according to the respective product monographs.
Resources for disease management of patients in the PF and PD states were sourced from studies conducted in the UK,9-12 while unit costs were primarily informed by the Ontario Ministry of Health and Long-Term Care Schedule of Benefits.13 Disease management costs for patients with central nervous system metastases were assumed to be 1.2 times higher.14 Additionally, the model included a one-off end-of-life cost valued at $17,334.08 and costs associated with managing AEs for each study arm.15
Summary of Sponsor’s Economic Evaluation Results
The base-case analysis was run probabilistically (2,000 iterations). The deterministic and probabilistic results were similar. The probabilistic findings are presented in the following section.
Base-Case Results
Osimertinib plus chemotherapy was associated with a gain of 0.402 QALYs at an additional cost of $59,009, resulting in an ICER of $146,769 compared with osimertinib monotherapy. Compared with osimertinib monotherapy, osimertinib plus chemotherapy was cost-effective at a willingness-to-pay threshold of $50,000 per QALY in approximately 16% of iterations. Drug acquisition contributed to 90% (67% for osimertinib, 23% chemotherapy) of the incremental costs. In both study arms, more than half of the accrued QALYs were derived within the observed trial period of 30 months. Because of the increased mortality due to chemotherapy-associated AEs observed in the FLAURA2 trial data, incremental life-years were 0.4% lower for osimertinib plus chemotherapy (i.e., osimertinib monotherapy was associated with more life-years) during the observed period of the trial, and 11.49% of the incremental QALYs accrued during the observed trial period.
Table 3: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER vs. osimertinib monotherapy ($ per QALY) |
|---|---|---|---|---|---|
Osimertinib monotherapy | 327,912 | Reference | 2.67 | Reference | Reference |
Osimertinib plus chemotherapy | 386,921 | 59,009 | 3.07 | 0.40 | 146,770 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; vs. = versus.
Source: Sponsor’s pharmacoeconomic submission.1
Additional results from the sponsor’s submitted economic evaluation base case are presented in Appendix 3.
Sensitivity and Scenario Analysis Results
The sponsor assessed several model parameters in deterministic sensitivity and scenario analyses. The model results were most sensitive to assumptions around the choice of extrapolated curves for TTD for osimertinib monotherapy and alternative utility values used in the PD and PF states. No scenario analysis used a perspective other than that of the health care payer.
Appraisal of the Sponsor’s Economic Evaluation
The review team identified several key limitations to the sponsor’s economic analysis that have notable implications.
The impact of osimertinib plus chemotherapy on long-term OS is uncertain: The FLAURA2 data used within the sponsor’s submitted model did not include statistical significantly different estimates of OS between patients receiving osimertinib plus chemotherapy compared to those receiving osimertinib monotherapy. Transition probabilities between the model states was informed by a post hoc analysis of TTP data and PPS data available from the FLAURA2 trial in each study arm. Further, the sponsor’s model assumed that the PPS in the osimertinib plus chemotherapy arm is identical to the PPS in the osimertinib monotherapy arm.
As the available trial follow-up data at the time of this analysis was 30 months and data maturity was not reached, the sponsor relied on parametric survival modelling to extrapolate the TTP and PPS beyond the observed time points in the trial. The sponsor fitted separate gamma distributions to the observed TTP Kaplan-Meier curves to determine the time spent in the PF state over the 15-year time horizon for combination therapy relative to monotherapy. Transitions between PF and dead were calculated from PFS and TTP data, assuming that preprogression survival data are approximated by the difference between PFS and TTP. This approach was used because the preprogression survival data from the FLAURA2 trial were less than ██% mature. The sponsor's model therefore assumes that the probability of death is lower in the PF state, and that a longer time spent in the PF state leads to an increased survival time. Although the updated OS data from January 8, 2024, from the FLAURA2 trial (not included in the model) generally favoured osimertinib plus chemotherapy over osimertinib alone, uncertainty remains in the OS results, as the median OS was not reached as of January 8, 2024, and the OS data were 40.6% mature.
Other important considerations include the use of TTP and PPS as surrogate end points for OS in advanced NSCLC, and the post hoc estimation of TTP and PPS. The Clinical Review, which assessed the sponsor’s submitted studies in support of this claim, determined that there is limited evidence for the strength of the surrogacy of PPS and TTP with OS in the population of interest. Furthermore, post hoc estimation of these outcomes could have introduced an additional layer of bias, which is of concern as these data were used to extrapolate TTP and PPS for the entire lifetime horizon in the model. Together, these limitations add another source of uncertainty when interpreting the evidence used in the model.
According to the clinical experts consulted for this review and the most recent OS data (i.e., those available at January 8, 2024), a benefit with combination therapy was deemed plausible. However, the magnitude of such a benefit was uncertain without more robust evidence. Alternative parametric distributions for TTP and PPS, along with assumptions about different PPS between the study arms, were considered more plausible.
Given these limitations, and consistent with clinical expert opinion, the review team’s reanalysis adopted alternate assumptions for OS and PFS extrapolation. The team selected the Weibull distribution for TTP in both modelled cohorts (i.e., patients receiving osimertinib plus chemotherapy and those receiving osimertinib monotherapy). Additionally, it was assumed that PPS would differ between the study arms, with the Weibull distribution selected in both modelled cohorts.
The impact of healthy-participant bias on the observed benefits is uncertain: The sponsor’s model predicted an additional 0.56 PF life-years, which translates to 0.44 additional predicted life-years for patients receiving osimertinib plus chemotherapy compared to those receiving osimertinib monotherapy over the 15-year lifetime horizon. These estimated survival benefits are not realized until 22 months in the modelled time horizon. Instead, based on the clinical data, a higher number of deaths were observed for patients receiving combination treatment over the first 22 months (refer to Figure 2). This observation arises given the increased harms and deaths reported from AEs for patients receiving osimertinib plus chemotherapy compared to those receiving osimertinib monotherapy.
The clinical experts consulted for this review described the harms observed in the FLAURA2 trial as what they would expect for the addition of chemotherapy to osimertinib. A higher number of deaths observed in the combination therapy arm relative to the monotherapy arm during the early months of the trial could suggest that “sicker” patients experience mortality due to chemotherapy AEs. The remaining “healthier” patients would then be left to experience the long-term survival benefit of the treatment. Assuming perfect randomization, meaning the percentage of “sicker” individuals was equal in both study arms, continued survival of the “sicker” individuals in the monotherapy arm of FLAURA2 could indicate that the benefits of osimertinib plus chemotherapy are overestimated compared to the outcomes that would occur in the general population. This phenomenon would introduce a bias of unknown size into the economic model that favours osimertinib plus chemotherapy.
CDA-AMC was not able to address this limitation, as quantifying the exact impact of the healthy-participant bias on the incremental benefits was not possible.
Utility in the PD state lacks face validity: The sponsor’s base case assumed that patients’ health-related utility decreases at disease progression, from a utility of ████ in the PF state to 0.70 in the PD state. Data from FLAURA2 trial suggest a smaller utility drop of ████ when transitioning from PF to PD. The sponsors used utilities obtained from 2 different sources to inform the health-state utility value of PF and PD states in the model. This is methodologically inappropriate and limits comparability of the utility measures across studies, as it is unclear if they measure the same construct and are derived from similar patient populations using similar methodologies. Differences in measurement tools, populations studied, and valuation techniques can lead to inconsistencies and bias in the model. According to the clinical experts consulted for this review, the decline in utility may not be as pronounced, particularly considering that patients continue treatment post-progression.
The review team’s reanalysis used the utility estimates from the FLAURA2 trial for both PF and PD states.
Additionally, the following key assumptions were made by the sponsor and have been appraised by CDA-AMC (Table 4).
Table 4: Key Assumptions of the Submitted Economic Evaluation (Not Noted as Limitations to the Submission)
Sponsor’s key assumption | CDA-AMC comment |
|---|---|
Treatment duration occurs regardless of state membership. | According to the clinicians consulted, patients continue taking osimertinib following disease progression. The sponsor's approach to modelling TTD is therefore appropriate. The clinicians also indicated that the TTD curves used were in line with their expectations for this clinical population. |
AEs were assumed to occur only in the first month of treatment. | AEs were incorporated in the sponsor’s model as a one-off cost, and the disutility was applied only during the first cycle of the model. With this approach the sponsor is assuming that the patients on osimertinib plus chemotherapy do not have ongoing toxicity associated with chemotherapy. When considered over the model’s time horizon, and the proportion of patients who continue treatment on pemetrexed, this assumption is not likely to have a significant impact on overall cost-effectiveness. |
AE = adverse event; CDA-AMC = Canada’s Drug Agency; TTD = time to treatment discontinuation.
CDA-AMC Reanalyses of the Economic Evaluation
Base-Case Results
The CDA-AMC base case was derived by making changes in model parameter values and assumptions, in consultation with clinical experts. The review team undertook a stepped analysis, incorporating each change detailed in Table 5 into the sponsor’s model to highlight the impact of each change. The summary results of the CDA-AMC reanalyses for the weighted population are presented in Table 6.
Table 5: CDA-AMC Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CDA-AMC value or assumption |
|---|---|---|
Changes to derive the CDA-AMC base case | ||
1. Parametric extrapolation of TTP and OS | Parametric distribution of TTP:
| Parametric distribution of TTP:
|
2. Assumption of equal relationship of PPS between osimertinib plus chemotherapy and osimertinib monotherapy | Assumed equivalence of osimertinib monotherapy for PPS: Yes Parametric distribution of PPS:
| Assumed equivalence of osimertinib monotherapy for PPS: No Parametric distribution of PPS:
|
3. Health utility in PF state | Health-state utilities: PF: ████ PD: 0.70 | Health-state utilities: PF: ████ PD: 0.80 |
CDA-AMC base case | ― | Reanalysis 1 + 2 + 3 |
CDA-AMC = Canada’s Drug Agency; PD = progressed disease; PF = progression-free; OS = overall survival; PPS = post-progression survival; TTP = time to progression.
Results from the CDA-AMC reanalysis demonstrate that osimertinib plus chemotherapy was associated with $57,897 in incremental costs and an incremental gain of 0.246 QALYs compared to osimertinib monotherapy, resulting in an ICER of $235,123 per QALY gained. Selecting the Weibull distribution for TTP in both study arms resulted in the largest change to the sponsor’s base case (Table 7). Based on results from the review team’s reanalysis, 91% of the total costs for osimertinib plus chemotherapy are related to treatment acquisition (67% osimertinib, 24% chemotherapy). Approximately −7% of the incremental life-years and less than 1% of the incremental QALYs accrued during the observed trial period. The probability that osimertinib plus chemotherapy is cost-effective at a willingness-to-pay threshold of $50,000 per QALY is 10.35%.
Table 6: Summary of the Stepped Analysis of the CDA-AMC Reanalysis Results
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($ per QALY) |
|---|---|---|---|---|
Sponsor’s base case (deterministic) | Osimertinib + chemotherapy | 382,430 | 3.08 | Reference |
Osimertinib monotherapy | 328,530 | 2.73 | 150,081 | |
CDA-AMC reanalysis 1 | Osimertinib + chemotherapy | 381,711 | 2.90 | Reference |
Osimertinib monotherapy | 327,515 | 2.68 | 247,249 | |
CDA-AMC reanalysis 2 | Osimertinib + chemotherapy | 382,323 | 3.07 | Reference |
Osimertinib monotherapy | 328,530 | 2.73 | 155,210 | |
CDA-AMC reanalysis 3 | Osimertinib + chemotherapy | 382,430 | 3.22 | Reference |
Osimertinib monotherapy | 328,530 | 2. 88 | 156,165 | |
CDA-AMC base case 1 + 2 + 3 (deterministic) | Osimertinib + chemotherapy | 381,606 | 3.02 | Reference |
Osimertinib monotherapy | 327,515 | 2.83 | 282,754 | |
CDA-AMC base case 1 + 2 + 3 (probabilistic) | Osimertinib + chemotherapy | 383,306 | 3.03 | Reference |
Osimertinib monotherapy | 325,408 | 2.78 | 235,123 |
CDA-AMC = Canada's Drug Agency; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Note: The CDA-AMC reanalysis is based on publicly available prices of the comparator treatments. The results of all steps are presented deterministically unless otherwise indicated, while the cumulative CDA-AMC base case is always presented both deterministically and probabilistically.
Scenario Analysis Results
A scenario analysis was conducted in which the TTP curves were assumed to reach equivalence between osimertinib plus chemotherapy and osimertinib monotherapy after 60 months. This analysis resulted in an ICER of $260,330 per QALY gained.
The review team undertook price-reduction analyses based on the CDA-AMC base case. At a 100% price reduction, osimertinib plus chemotherapy reached an ICER of $75,585 compared to osimertinib monotherapy. This occurred because any reduction in the price of osimertinib will necessarily result in a corresponding decrease in the cost of osimertinib monotherapy. There remained an additional $19,033 of additional costs, due primarily to the additional cost of chemotherapy. A scenario analysis was conducted in which the price of osimertinib and the price of chemotherapy were both reduced. In this scenario, a 91% reduction in the price of all drugs was necessary to achieve an ICER below a willingness-to-pay threshold of $50,000 per QALY.
Table 7: CDA-AMC Price-Reduction Analyses
Analysis | Unit drug cost ($) | ICERs for osimertinib plus chemotherapy vs. osimertinib monotherapy ($ per QALY) | |
|---|---|---|---|
Price reduction | $ | Sponsor base case | CDA-AMC reanalysis |
No price reduction | 322.13 | 146,769 | 235,123 |
10% | 289.92 | 136,765 | 214,474 |
20% | 257.71 | 127,359 | 192,334 |
30% | 225.49 | 116,312 | 180,115 |
40% | 193.28 | 107,063 | 172,451 |
50% | 161.07 | 99,010 | 149,582 |
60% | 128.85 | 87,620 | 134,010 |
70% | 96.64 | 77,859 | 122,208 |
80% | 64.43 | 68,257 | 107,706 |
90% | 32.21 | 58,941 | 91,916 |
100% | 0 | 47,913 | 75,585 |
vs. = versus; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; vs. = versus.
Issues for Consideration
Osimertinib has been previously reviewed by CADTH for the treatment of patients with locally advanced or metastatic NSCLC that is positive for the amino acid substitution from a threonine to a methionine at position 790 in EGFR (the EGFR T790M mutation) that has progressed on or after therapy with an EGFR tyrosine kinase inhibitor,16 for the first-line treatment of patients with locally advanced or metastatic NSCLC whose tumours have other EGFR mutations,10 and as adjuvant therapy after tumour resection in patients with stage IB to stage III NSCLC whose tumours have EGFR ex19del or L858R mutations.17 These reviews were at the submitted price of $294.68 per 40 mg or 80 mg tablet. All reviews received a recommendation for reimbursement with clinical criteria and/or conditions.9,10,17 These conditions included improvement of the cost-effectiveness of osimertinib.9,10,17
As in all CDA-AMC pharmacoeconomic reports, the economic evaluation presented in this report is based on publicly available list prices for all comparators, including osimertinib and all chemotherapy drugs. Negotiated prices are in place for all drugs in this evaluation. The finding that osimertinib plus chemotherapy is not cost-effective at a 100% price reduction may be sensitive to changes in the cost of chemotherapy, if negotiated prices are meaningfully lower than the list prices.
Overall Conclusions
Based on the evidence from the FLAURA2 trial, osimertinib plus chemotherapy showed added clinical benefits in OS and PFS in the intention-to-treat trial population compared with osimertinib monotherapy. However, because of the interim nature of the analyses (i.e., the OS data were immature at 40.6% and the median OS was not reached as of January 8, 2024), uncertainty remains in the OS results. This is concerning as these data were used in the post hoc analysis to estimate the surrogate outcomes used in the model (i.e., PPS and TTP), which were then extrapolated over the lifetime horizon. No conclusions could be drawn about the effect of osimertinib plus chemotherapy on OS because of data immaturity. Despite these limitations, the clinical experts consulted for this review noted that the findings appear to be favourable and may be clinically important. While there was no statistically significant difference in OS at the data cut point, the sponsor’s model predicted 0.44 additional years of life for patients receiving osimertinib plus chemotherapy. More than 100% of incremental survival in the sponsor’s model was generated by extrapolating beyond the observation period of the FLAURA2 trial.
The review team identified several limitations in the economic analyses submitted by the sponsor, beyond the uncertainty regarding the impact of osimertinib plus chemotherapy on OS. These key limitations included uncertainty about the use of surrogate outcomes (PPS and TTP) to inform model transitions, the unknown impact of healthy-participant bias on the observed benefits, the misalignment of the assumed utility drop from PF to PD with trial data or clinical expert opinion, and the potential for introducing bias because of differences in utility measurement sources. In its reanalysis, the review team included changes to TTP extrapolations, different rates of PPS in study arms, and the use of FLAURA2 utility estimates. The reanalysis found that osimertinib plus chemotherapy is $57,898 more costly and yields 0.246 more QALYs compared with osimertinib monotherapy, resulting in an ICER of $235,123 per QALY gained. If the price of osimertinib was reduced to $0, the resulting ICER would be $75,865 because the price of osimertinib is reduced in both modelled treatment arms, while the cost of chemotherapy remains in the osimertinib plus chemotherapy arm.
The results are contingent on TTP and PPS extrapolation from the observed trial data and whether this translates into improvement in OS. Although the sponsor’s approach to modelling the relationship between TTP and OS is appropriate, longer-term evidence is required to validate OS for patients receiving osimertinib plus chemotherapy. The CDA-AMC reanalysis adopted a conservative assumption that osimertinib plus chemotherapy would confer more modest long-term TTP and corresponding PFS and OS benefits relative to osimertinib monotherapy. The clinical experts consulted for this review deemed the parametric extrapolations used in the CDA-AMC base case to model transition probabilities from TTP and PPS more plausible than those used in the sponsor’s base case. As such, relative to the sponsor’s base case, the CDA-AMC reanalysis resulted in a reduction of life-year gains from 3.8 to 3.6 in this patient population. However, due to the small magnitude of the incremental benefits, the cost-effectiveness of osimertinib plus chemotherapy varied significantly when more optimistic and pessimistic TTP extrapolations were considered.
CDA-AMC was unable to address limitations related to the use of surrogate outcomes and the potential impact of healthy-participant bias on model outcomes. However, even without accounting for these uncertainties, the sponsor’s submitted base case was not cost-effective at a willingness-to-pay threshold of $50,000 per QALY.
References
1.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Tagrisso (osimertinib) 40 mg and 80 mg tablets. Mississauga (ON): AstraZeneca Canada; 2023 Dec 11.
2.Tagrisso (osimertinib tabelets) 40 mg and 80 mg osimertinib (as osimertinib mesylate), oral tablets [product monograph]. Mississauga (ON): AstraZeneca Canada; 2024 Jul 10.
3.Clinical Study Report: D5169C00001. A phase III, open-label, randomised study of osimertinib with or without platinum plus pemetrexed chemotherapy, as first-line treatment in patients with epidermal growth factor receptor mutation positive, locally advanced or metastatic non-small cell lung cancer (FLAURA2) - randomised period [internal sponsor's report]. Mississauga (ON): AstraZeneca Canada Inc; 2023 Aug 4.
4.Ramalingam SS, Vansteenkiste J, Planchard D, et al. Overall survival with osimertinib in untreated, EGFR-mutated advanced NSCLC. N Engl J Med. 2020;382(1):41-50. PubMed
5.Xie F, Pullenayegum E, Gaebel K, et al. A time trade-off-derived value set of the EQ-5D-5L for Canada. Med Care. 2016;54(1):98-105. PubMed
6.Labbé C, Leung Y, Silva Lemes JG, et al. Real-world EQ5D health utility scores for patients with metastatic lung cancer by molecular alteration and response to therapy. Clin Lung Cancer. 2017;18(4):388-395.e384. PubMed
7.Yan J, Xie S, Johnson JA, et al. Canada population norms for the EQ-5D-5L. Eur J Health Econ. 2023. PubMed
8.DeltaPA. Ottawa (ON): IQVIA; 2023: https://www.iqvia.com/. Accessed 2024 Jun 1.
9.pan-Canadian oncology drug review: osimertinib (Tagrisso) for non-small cell lung cancer (post TKI). Ottawa (ON): CADTH; 2017.
10.pan-Canadian oncology drug review: osimertinib (Tagrisso) for non-small cell lung cancer (first line). Ottawa (ON): CADTH; 2019.
11.pan-Canadian oncology drug review: dacomitinib (Vizimpro) for non-small cell lung cancer. Ottawa (ON): CADTH; 2019.
12.Brown T, Pilkington G, Bagust A, et al. Clinical effectiveness and cost-effectiveness of first-line chemotherapy for adult patients with locally advanced or metastatic non-small cell lung cancer: a systematic review and economic evaluation. Health Technol Assess. 2013;17(31):1-278. PubMed
13.Canadian Institute for Health Information. Patient cost estimator. https://www.cihi.ca/en/patient-cost-estimator. Accessed 2023 Nov.
14.Kong AM, Pavilack M, Huo H, et al. Real-world impact of brain metastases on healthcare utilization and costs in patients with non-small cell lung cancer treated with EGFR-TKIs in the US. J Med Econ. 2021;24(1):328-338. PubMed
15.Hollander MJ. Costs of end-of-life care: findings from the province of Saskatchewan. Healthc Q. 2009;12(3):50-58. PubMed
16.pan-Canadian Oncology Drug Review Committee (pERC) final recommendation: osimertinib (Tagrisso - AstraZeneca Canada). Ottawa (ON): CADTH; 2017: https://www.cda-amc.ca/sites/default/files/pcodr/pcodr_osimertinib_tagrisso_nsclc_fn_rec.pdf. Accessed 2024 June 1.
17.CADTH reimbursement review: osimertinib (Tagrisso) adjuvant. Ottawa (ON): CADTH; 2022.
18.Cancer Care Ontario. Funded evidence-informed regimens. 2023; https://www.cancercareontario.ca/en/drugformulary/regimens. Accessed 2024 Jun 1.
19.Wu Y-L, Zhou Q. Combination therapy for EGFR-mutated lung cancer. N Engl J Med. 2023;389(21):2005-2007. PubMed
20.Canadian Cancer Statistics Advisory in collaboration with the Canadian Cancer Society, Statistics Canada, Public Health Agency of Canada. Canadian cancer statistics 2023. Toronto (ON): Canadian Cancer Society; 2023: https://cancer.ca/en/cancer-information/resources/publications/canadian-cancer-statistics-2023. Accessed 2024 Jun 1.
21.Cancer Care Ontario. Ontario cancer facts: lung cancer incidence higher in First nations people than other people in Ontario. 2024; https://www.cancercareontario.ca/en/cancer-facts/lung-cancerincidence-higher-first-nations-people-other-people-ontario. Accessed 2024 Jun 1.
22.Canadian Cancer Statistics Advisory in collaboration with the Canadian Cancer Society, Statistics Canada, Public Health Agency of Canada. Canadian cancer statistics 2021. Toronto (ON): Canadian Cancer Society; 2021: https://cdn.cancer.ca/-/media/files/research/cancer-statistics/2021-statistics/2021-pdf-en-final.pdf. Accessed 2024 Jun 1.
23.Canadian Partnership Against Cancer. Figure 3.7 Distribution of cases by stage at diagnosis for non-small cell lung cancer – 2013 diagnosis year.
24.Karacz CM, Yan J, Zhu H, Gerber DE. Timing, sites, and correlates of lung cancer recurrence. Clin Lung Cancer. 2020;21(2):127-135. e123.
25.Boyne DJ, Jarada T, Yusuf A, et al. 51P Testing patterns and outcomes of different EGFR-positive metastatic non-small cell lung cancer (NSCLC) patients in a Canadian real-world setting. Ann Oncol. 2022;33:56.
26.CADTH. CADTH Reimbursement Review Reports. Amivantamab (Rybrevant-Janssen Inc.) Can J Health Technol. 2023;3(5). https://www.cadth.ca/sites/default/files/DRR/2023/PC0289-Rybrevant_combined.pdf. Accessed 2024 Jun 1.
27.O’Sullivan DE, Jarada TN, Yusuf A, et al. Prevalence, treatment patterns, and outcomes of individuals with EGFR positive metastatic non-small cell lung cancer in a Canadian real-world setting: a comparison of Exon 19 deletion, L858R, and Exon 20 insertion EGFR mutation carriers. Curr Oncol. 2022;29(10):7198-7208. PubMed
28.Sutherland G, Dihn T. Understanding the gap: a pan-Canadian analysis of prescription drug insurance coverage. Ottawa (ON): The Conference Board of Canada; 2017: https://www.conferenceboard.ca/e-library/abstract.aspx?did=9326. Accessed 2024 Jun 1.
Appendix 1: Cost-Comparison Table
Please note that this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical experts and drug plan. Comparators may be recommended (appropriate) practice or actual practice. Existing product listing agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 8: CDA-AMC Cost-Comparison Table for First-Line Treatment of Patients With Locally Advanced or Metastatic Non–Small Cell Lung Cancer
Treatment | Strength / concentration | Form | Price ($) | Recommended dosage | Daily cost ($) | 21-day cost ($) |
|---|---|---|---|---|---|---|
Osimertinib (Tagrisso) | 80 mg | Tablet | 322.1320a | 80 mg daily until disease progression or unacceptable toxicity | 322.13 | 6,765 |
CISPPME + osimertinib | 362.84 | 7,620 | ||||
CRBPPME + osimertinib | 390.46 | 8,200 | ||||
CISPPME | ||||||
Cisplatin (Generic) | 50 mg/50 mL 100 mg/100 mL | Vial for IV infusion | 135.0000 270.0000 | 75 mg/m2 q.3.w. | 19.29 | 405 |
Pemetrexed (Generic) | 100 mg 500 mg 1,000 mg | Powder for solution for infusion | 50.0000 250.0000 4,290.0000 | 500 mg/m2 q.3.w. | 21.43 | 450 |
CISPPME | 40.71 | 855 | ||||
CRBPPME | ||||||
Carboplatin (Generic) | 50 mg/5 mL 150 mg/15 mL 450 mg/45 mL 600 mg/60 mL | Vial for IV infusion | 70.0000 210.0000 599.9985 775.0020 | Target AUC 5 on day 1 q.3.w., 750 mg/mL | 46.90 | 985 |
Pemetrexed (Generic) | 100 mg 500 mg 1,000 mg | Powder for solution for infusion | 50.0000 250.0000 4,290.0000 | 500 mg/m2 q.3.w. | 21.43 | 450 |
CRBPPME | 68.33 | 1,435 | ||||
CISPPME = cisplatin and pemetrexed regimen; CRBPPME = carboplatin and pemetrexed regimen; q.3.w. = every 3 weeks.
Note: All prices are from IQVIA Delta PA (accessed January 2024),8 unless otherwise indicated, and do not include dispensing fees. Dosing is based on Cancer Care Ontario product monographs.18 For treatments using weight-based or GFR-based dosing, CDA-AMC assumed 64.8 kg, 1.71m2 and 125 mL/min based on the FLAURA2 trial.3
aSponsor-submitted pricing.1
Appendix 2: Submission Quality
Please note that this appendix has not been copy-edited.
Description | Yes or No | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | Yes | No comment |
Model has been adequately programmed and has sufficient face validity | Yes | No comment |
Model structure is adequate for decision problem | Yes | No comment |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | Yes | No comment |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | Yes | No comment |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | Yes | No comment |
Appendix 3: Additional Information on the Submitted Economic Evaluation
Please note that this appendix has not been copy-edited.
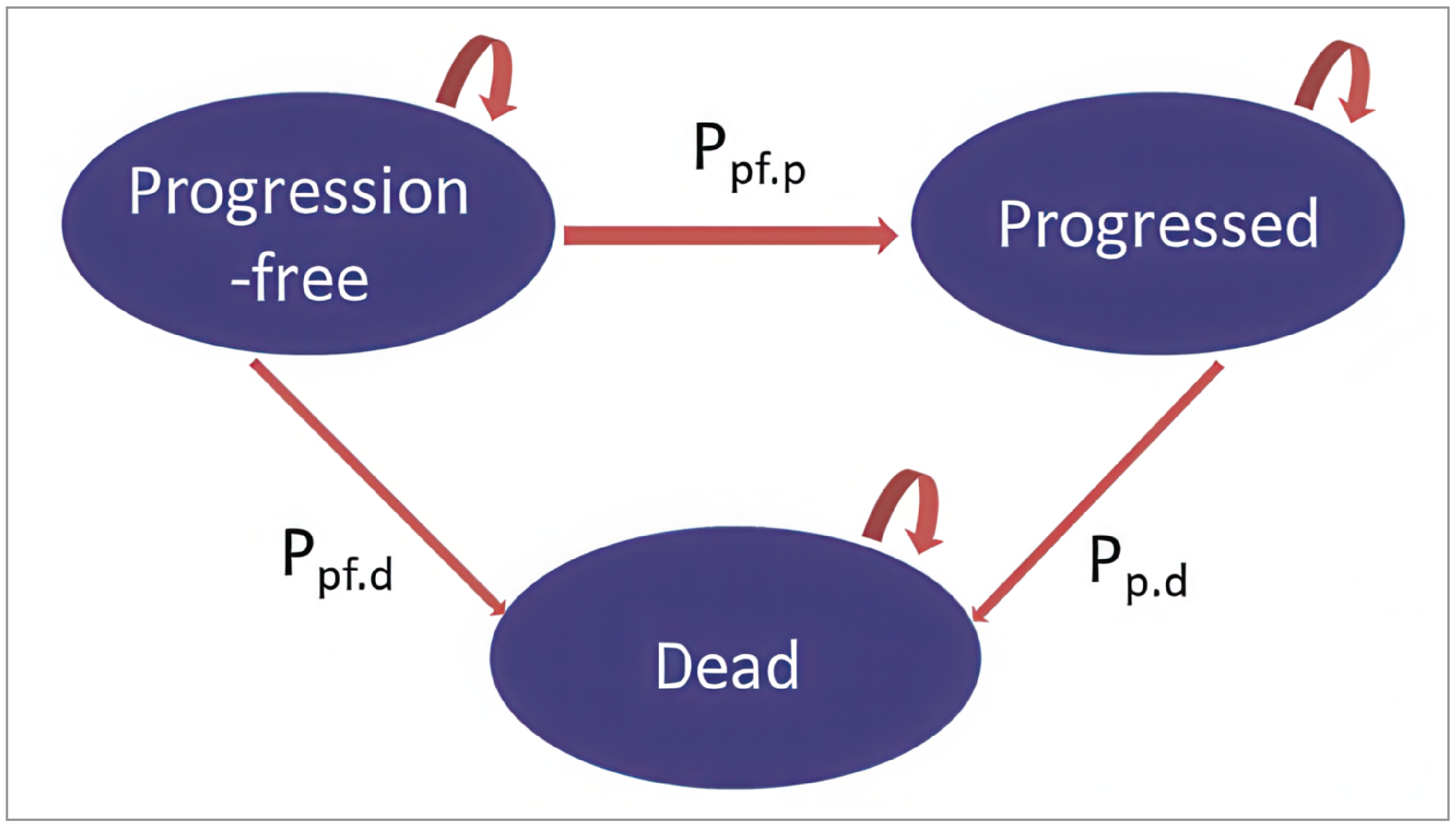
PD = progressed disease; PF = progression-free; STM = state transition model; Pff.p = transition probability PF to PD; Pp.d = transition probability PD to Death; Pfd.d = transition probability PF to Death.
Source: Sponsor’s pharmacoeconomic submission.1
Figure 2: Predicted Overall Survival Outcomes Based on Sponsor’s Parametric Survival Extrapolation Choices for TTP (Gamma)
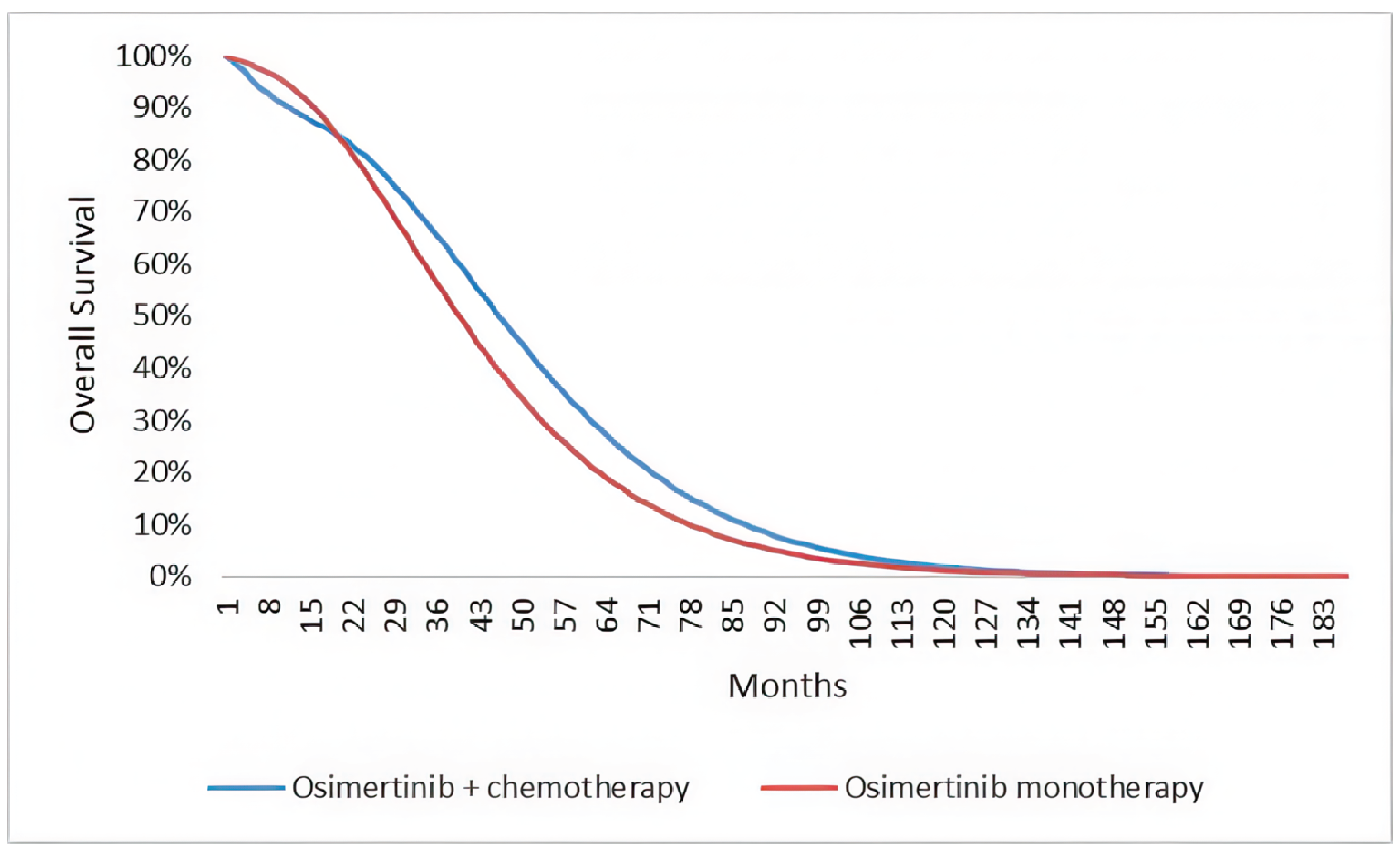
TTP = Time to progression.
Source: Sponsor’s pharmacoeconomic submission.1
Figure 3: Predicted Progression-Free Survival Outcomes Based on Sponsor’s Parametric Survival Extrapolation Choices for PFS (Gamma)
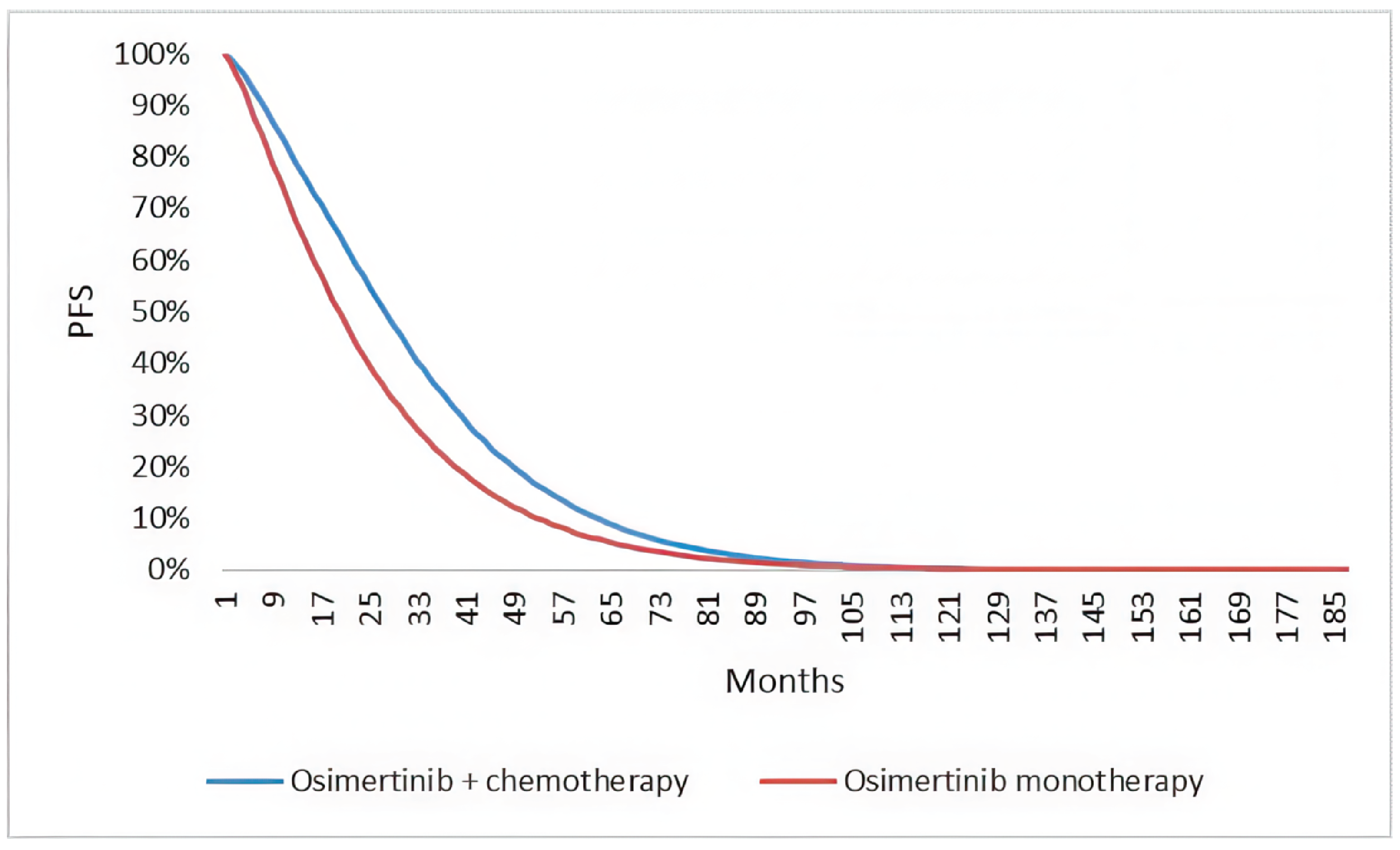
PFS = Progression-free survival.
Source: Sponsor’s pharmacoeconomic submission.1
Table 10: Benefits Accrued in the Extrapolated vs. Observed Data Period
Benefit accrued | Osimertinib plus chemotherapy | Osimertinib monotherapy |
|---|---|---|
Discounted Lys | ||
Total | 3.84 | 3.44 |
PF observed period | 1.81 | 1.53 |
PF extrapolated period | 0.70 | 0.44 |
PD observed period | 0.36 | 0.64 |
PD extrapolated period | 0.97 | 0.83 |
Discounted QALYs | ||
Total | 3.08 | 2.73 |
PF observed period | 1.55 | 1.31 |
PF extrapolated period | 0.60 | 0.38 |
PD observed period | 0.25 | 0.45 |
PD extrapolated period | 0.69 | 0.59 |
PD = progressed disease; PF = progression-free; AE = adverse event; LY = life-year; QALY = quality-adjusted life-year; vs. = versus.
Table 11: Disaggregated Summary of the Sponsor’s Probabilistic Base Case
Parameter | Osimertinib + chemotherapy | Osimertinib monotherapy |
|---|---|---|
Discounted Lys | ||
Total | 3.82 | 3.37 |
Progression-free | 2.49 | 1.93 |
Progressed disease | 1.33 | 1.44 |
Discounted QALYs | ||
Total | 3.70 | 2.67 |
Progression-free | 2.13 | 1.65 |
Progressed disease | 0.94 | 1.01 |
AE | −0.00 | −0.00 |
Discounted costs ($) | ||
Total | $386,921 | $327,912 |
Primary Treatment Acquisition-Total cost | $343,073 | $289,970 |
Osimertinib | $329,381 | $289,970 |
carboplatin + cisplatin | $2,432 | — |
Pemetrexed | $11,260 | — |
Administration – Total cost | $5,991 | $289 |
Administration (osimertinib) | $340 | $289 |
Administration (carboplatin + cisplatin) | $928 | — |
Administration (pemetrexed) | $4,724 | — |
Subsequent Treatment Acquisition costs | $2,069 | $5,034 |
Disease management -Total cost | $33,489 | $32,207 |
Progression-free | $9,242 | $7,170 |
Progressed disease | $7,761 | $8,431 |
Terminal care | $16,486 | $16,606 |
Monitoring | $310 | — |
AE | $1,990 | $412 |
AE = Adverse events; ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year.
Source: Sponsor’s pharmacoeconomic submission.1
Appendix 4: Additional Details on the CDA-AMC Reanalyses and Sensitivity Analyses of the Economic Evaluation
Please note that this appendix has not been copy-edited.
Detailed Results of CDA-AMC Base Case
Table 12: Disaggregated Summary of CDA-AMC Economic Evaluation Probabilistic Results
Parameter | Osimertinib + chemotherapy | Osimertinib monotherapy |
|---|---|---|
Discounted LYs | ||
Total | 3.61 | 3.33 |
Progression-free | 2.28 | 1.33 |
Progressed disease | 1.88 | 1.45 |
Discounted QALYs | ||
Total | 3.03 | 2.78 |
Progression-free | 1.94 | 1.61 |
Progressed disease | 1.08 | 1.17 |
AE | −0.00 | −0.00 |
Discounted costs | ||
Total | $383,306 | $325,408 |
Primary Treatment Acquisition-Total cost | $340,205 | $287,656 |
Osimertinib | $326,501 | $287,656 |
carboplatin + cisplatin | $2,432 | — |
Pemetrexed | $11,272 | — |
Subsequent Treatment Aquisition costs | $2,073 | $5,033 |
Administration — Total cost | $6,002 | $285 |
Administration (osimertinib) | $335 | $285 |
Administration (carboplatin + cisplatin) | $931 | — |
Administration (pemetrexed) | $4,736 | — |
Disease management -Total cost | $32,725 | $32,021 |
Progression-free | $8,438 | $6,971 |
Progressed disease | $7,779 | $8,462 |
Terminal care | $16,509 | $16,588 |
Monitoring | $311 | — |
AE | $1,989 | $412 |
AE = adverse event; ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year.
A scenario analysis was performed to examine the impact of reductions in the price of osimertinib and chemotherapy. The results of this scenario analysis are described in Table 13. These results suggest that osimertinib plus chemotherapy would be considered cost-effective at a willingness-to-pay threshold of $50,000 per QALY if the price of osimertinib and the price of chemotherapy drugs were reduced by 91%.
Table 13: Price-Reduction Scenario Analysis for all Therapies
Analysis | Unit drug cost ($) | ICERs for osimertinib plus chemotherapy vs. osimertinib monotherapy ($ per QALY) | ||||
|---|---|---|---|---|---|---|
Price reduction | Osimertinib | Cisplatin | Carboplatin (AUC5) | Pemetrexed | Sponsor base case | CDA-AMC reanalysis |
No price reduction | $322.13 | $135.00 | $775.00 | $50.00 | $150,081 | $282,754 |
10% | $290 | $122 | $698 | $45 | $136,679 | $257,158 |
20% | $258 | $108 | $620 | $40 | $123,277 | $231,562 |
30% | $225 | $95 | $543 | $35 | $109,874 | $206,801 |
40% | $193 | $81 | $465 | $30 | $96,472 | $180,370 |
50% | $161 | $68 | $388 | $25 | $83,070 | $154,774 |
60% | $129 | $54 | $310 | $20 | $69,667 | $129,178 |
70% | $97 | $41 | $233 | $15 | $56,265 | $103,581 |
80% | $64 | $27 | $155 | $10 | $42,863 | $77,985 |
90% | $32 | $14 | $78 | $5 | $29,461 | $52,389 |
100% | $0 | $0 | $0 | $0 | $16,058 | $26,793 |
QALY = quality-adjusted life-year; vs. = versus.
A second scenario analysis was performed to estimate the impact of negotiation on the price of osimertinib, compared to the current price of osimertinib. This scenario recognizes that osimertinib currently has a negotiated price that is unlikely to be renegotiated. While the CDA-AMC standard approach to price reduction considers the reduction in price on ‘both sides’ of the decision problem (i.e., both in the comparator arm and in the new drug arm), this review presents the unusual circumstance in which a drug is being compared to itself in the identical setting. Accordingly, this scenario analysis considers an osimertinib price reduction in the new drug arm, but keeps the price of osimertinib the same in the comparator arm.
In this analysis, a 14% reduction in the price of osimertinib was required to reach an ICER of $50,000 per QALY gained. At an 18% price reduction, the total health care system costs associated with osimertinib plus chemotherapy were lower than the total health care system costs associated with osimertinib monotherapy (i.e., osimertinib plus chemotherapy was dominant).
Table 14: Price-Reduction Scenario Analysis for Osimertinib Alone
Analysis | Unit drug cost ($) | ICERs for osimertinib plus chemotherapy vs. osimertinib monotherapy ($ per QALY) | ||
|---|---|---|---|---|
Price reduction | Osimertinib (in new drug arm) | Osimertinib (in comparator arm) | Sponsor base case | CDA-AMC reanalysis |
No price reduction | 322.13 | 322.13 | 150,081 | 235,123 |
10% | 290 | 322.13 | 59,656 | 102,531 |
12% | 283 | 322.13 | 41,570 | 76,013 |
14% | 277 | 322.13 | 23,485 | 49,495 |
18% | 264 | 322.13 | Osimertinib plus chemotherapy dominates osimertinib monotherapy | Osimertinib plus chemotherapy dominates osimertinib monotherapy |
Appendix 5: Submitted Budget Impact Analysis and CDA-AMC Appraisal
Please note that this appendix has not been copy-edited.
Table 15: Summary of Key Take-Aways
Key take-aways of the budget impact analysis |
|---|
|
Summary of Sponsor’s Budget Impact Analysis
The sponsor’s submitted budget impact analysis (BIA) assessed the impact resulting from reimbursing osimertinib in combination with pemetrexed and platinum-based chemotherapy for first-line treatment of patients with locally advanced or metastatic NSCLC whose tumours have EGFR ex19del or L858R mutations. The BIA was conducted from the perspective of the Canadian public drug plans over a 3-year (2025 to 2027) time horizon with 2024 as the base year, using an epidemiologic approach. The sponsor’s pan-Canadian estimates reflect the aggregated results from provincial budgets (excluding Quebec) as well as the Non-Insured Health Benefits (NIHB) program. Adjustments were made to the provincial populations to remove NIHB patients to estimate the provincial public plan population. The sponsor’s base case included drug acquisition costs only and no mark-ups or dispensing fees were included in the cost calculations. TTD curves from the FLAURA2 trial were applied to each cycle to determine the proportion of patient who discontinued treatment. Patients who discontinued from osimertinib + chemotherapy and osimertinib monotherapy were eligible to receive subsequent treatment. Market share inputs were estimated based on sponsor-submitted patient and physician preferences published in a FLAURA2 editorial.19 Key inputs to the BIA are documented in Table 16.
The following key assumptions were made by the sponsor:
An average BSA of 1.71m2 was used in the drug acquisition calculations and was derived from the FLAURA2 trial.
The sponsor assumed that 100% of patients in the reference scenario would receive osimertinib monotherapy.
Table 16: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as year 1 / year 2 / year 3 if appropriate) |
|---|---|
Target population | |
Annual incidence of lung cancer Proportion of NSCLC Stage IIB, IIC or IV at diagnosis Incident population with early-stage disease Annual recurrence to metastatic disease Total patients with de novo metastasis or distance recurrence Proportion tested for EGFR mutations Proportion positive for EGFR mutations Proportion with exon 19 deletions or exon 21 L858R mutations Proportion receiving first-line systemic treatment Drug plan eligibility | 88.0%22 52.7%23 47.3%22 5.1%24 10,796 15.2%27 18.3%27 87.6%27 77.9%28 |
Number of patients eligible for drug under review | 740 / 752 / 764 |
Market uptake (3 years) | |
Uptake (reference scenario) Osimertinib monotherapy | 100% / 100% / 100% |
Uptake (new drug scenario) Osimertinib + chemotherapy Osimertinib monotherapy | ███ █ ███ / 27% ███ █ ███ / 73% |
Cost of treatment (per patient, per 21-day cycle)a | |
Osimertinib + chemotherapy [induction] Osimertinib + chemotherapy [maintenance] Osimertinib monotherapyb | $7,653 $7,265 $6,765 |
NSCLC = non–small cell lung cancer.
aCosts of treatment were calculated per 21-day cycle to align with the dosing cycles for platinum induction and pemetrexed.
bOsimertinib monotherapy does not differ in cost between induction and maintenance.
Summary of the Sponsor’s BIA Results
The sponsor’s base case reported that the reimbursement for osimertinib + chemotherapy for the treatment for first-line treatment of patients with locally advanced or metastatic NSCLC whose tumours have EGFR ex19del or L858R mutations would result in an incremental budget impact of $589,350 in year 1, $2,162,331 in year 2, $4,379,040 in year 3. The total 3-year incremental cost of reimbursing osimertinib + chemotherapy is $7,130,721.
CDA-AMC Appraisal of the Sponsor’s BIA
CDA-AMC identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
The proportion of patients eligible for public coverage is uncertain. The sponsor’s base case used age and jurisdiction-specific public coverage rates for all medications. IV oncology drugs are likely to be fully covered. Depending on the jurisdiction, oral oncology drugs may be fully reimbursed or may only be reimbursed by regular public drug plans, as assumed in the sponsor’s base case.
To address uncertainty regarding the proportion eligible for public drug coverage, CDA-AMC assumed 100% coverage across jurisdictions and age as a scenario analysis.
CDA-AMC Reanalyses of the BIA
CDA-AMC Did not undertake a base-case reanalysis and accepted the sponsor’s submitted base case.
Table 17: CDA-AMC Revisions to the Submitted Budget Impact Analysis
Stepped analysis | Sponsor’s value or assumption | CDA-AMC value or assumption |
|---|---|---|
Changes to derive the CDA-AMC base case | ||
No changes. | — | — |
CDA-AMC conducted the following scenario analyses to address remaining uncertainty, using the CDA-AMC base case (results are provided in Table 18):
Assuming 100% drug plan coverage.
Table 18: Detailed Breakdown of the CDA-AMC Reanalyses of the Budget Impact Analysis
Stepped analysis | Scenario | Year 0 (current situation) ($) | Year 1 ($) | Year 2 ($) | Year 3 ($) | Three-year total ($) |
|---|---|---|---|---|---|---|
Submitted base case | Reference | 41,159,894 | 102,891,320 | 144,461,484 | 171,833,373 | 419,186,177 |
New drug | 41,159,894 | 103,480,670 | 146,623,815 | 176,212,413 | 426,316,898 | |
Budget impact | 0 | 589,350 | 2,162,331 | 4,379,040 | 7,130,721 | |
CDA-AMC scenario analysis 1: 100% Drug Plan Coverage | Reference | 53,114,451 | 132,775,086 | 186,413,877 | 221,726,395 | 540,915,358 |
New drug | 53,114,451 | 133,538,718 | 189,212,449 | 227,395,190 | 550,146,357 | |
Budget impact | 0 | 763,631 | 2,798,573 | 5,668,796 | 9,230,999 |
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.