Drugs, Health Technologies, Health Systems
Reimbursement Review
Avapritinib (Ayvakyt)
Sponsor: Medison Pharma Canada Inc.
Therapeutic area: Advanced systemic mastocytosis
This multi-part report includes:
Clinical_Review
Pharmacoeconomic_Review
Clinical_Review
Abbreviations
AE
adverse event
AdvSM
advanced systemic mastocytosis
AdvSM-SAF
Advanced Systemic Mastocytosis Symptom Assessment Form
AHN
associated hematologic neoplasm
ASM
aggressive systemic mastocytosis
BAT
best available therapy
CDA-AMC
Canada’s Drug Agency
CI
confidence interval
CR
complete remission
CRh
complete remission with partial hematological recovery
ECOG PS
Eastern Cooperative Oncology Group Performance Status
EMA
European Medicines Agency
EORTC QLQ-C30
European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30
GRADE
Grading of Recommendations Assessment, Development and Evaluation
HR
hazard ratio
ICC
International Consensus Classification
IPD
individual patient-level data
IPTW
inverse probability of treatment weighting
IWG
International Working Group
IWG-MRT-ECNM
International Working Group - Myeloproliferative Neoplasms Research and Treatment - European Competence Network on Mastocytosis
LLSC
Leukemia & Lymphoma Society of Canada
MAIC
matching-adjusted indirect comparison
MCC
Mast Cell Connect
MCL
mast cell leukemia
MID
minimal important difference
NCCN
National Comprehensive Cancer Network
NICE
National Institute for Health and Care Excellence
ORR
overall response rate
OS
overall survival
PFS
progression-free survival
PGI-S
Patient Global Impression–Severity
PR
partial remission
RAC
Response Assessment Committee
RAC-RE
Response Assessment Committee–Response Evaluable
SAE
serious adverse event
SD
standard deviation
SM
systemic mastocytosis
SM-AHN
systemic mastocytosis with an associated hematologic neoplasm
TSS
total symptom score
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Table 1: Background Information on Application Submitted for Review
Item | Description |
|---|---|
Drug product | Avapritinib (Ayvakyt), 25 mg, 50 mg, 100 mg, and 200 mg film-coated tablets, oral |
Sponsor | Medison Pharma Canada Inc. |
Indication | For the treatment of adult patients with AdvSM. AdvSM includes patients with ASM, SM-AHN, and MCL. |
Reimbursement request | As per indication |
Health Canada approval status | Approved |
Health Canada review pathway | Standard review |
NOC date | September 18, 2024 |
Recommended dosage | 200 mg once daily |
AdvSM = advanced systemic mastocytosis; ASM = aggressive systemic mastocytosis; MCL = mast cell leukemia; NOC = Notice of Compliance; SM-AHN = systemic mastocytosis with an associated hematologic neoplasm.
Introduction
Systemic mastocytosis (SM) is a heterogenous group of rare disorders caused by a clonal, neoplastic proliferation of abnormal mast cells that accumulate typically in bone marrow and other extracutaneous tissues.1-3 Symptoms of SM are related to the release of mast cell mediators and mast cell tissue infiltration, which can vary widely from isolated symptoms to a constellation of symptoms, commonly including cutaneous involvement (e.g., skin flushing, pruritus, itching, hives, skin rash), wheezing and shortness of breath, dizziness, cardiovascular symptoms (e.g., rapid heart rate, chest pain, low blood pressure), gastrointestinal symptoms (e.g., diarrhea, nausea, vomiting, abdominal pain), fatigue, musculoskeletal symptoms (e.g., bone and/or muscle pain), and neuropsychiatric symptoms (e.g., headache, brain fog, cognitive dysfunction, anxiety, depression).4
SM is classified into distinct subtypes in order of increasing disease burden: indolent SM and bone marrow mastocytosis, smouldering SM, aggressive systemic mastocytosis (ASM), systemic mastocytosis with an associated hematologic neoplasm (SM-AHN), and mast cell leukemia (MCL).3-5 Advanced systemic mastocytosis (AdvSM) includes the disease variants of ASM, SM-AHN, and MCL.1 The prevalence rate of SM is estimated at 1 per 10,000 people of all ages.6 Based on estimates from the Danish incidence and German prevalence of adults with AdvSM, the estimated AdvSM incidence rate in Canada is 0.06 cases per 100,000 adults and the prevalence rate is 5.2 cases per million adults.7,8 Median overall survival (OS) has been estimated at 41 months for ASM,4,9 11 months to 42 months for SM-AHN depending on the type of AHN,4,10 and 2 months to 19.2 months for MCL.3,4
Cytoreduction is the principal treatment for AdvSM; it may improve quality of life, reverse or prevent organ damage, and prolong survival.4 Current available cytoreductive options in Canada for AdvSM include midostaurin, cladribine, interferons (e.g., peginterferon alfa-2a), and imatinib. The 2024 National Comprehensive Cancer Network (NCCN) clinical practice guidelines recommend enrolment in clinical trial, or KIT inhibitors — midostaurin or avapritinib — as first-line treatment for AdvSM.4
According to the clinical experts consulted for this review, there is a major treatment gap for patients with AdvSM in Canada. The off-label treatments currently available (cladribine and interferon) have low or unpredictable response rates, have a response of short duration, and may cause significant toxicity. Imatinib is suitable for a small minority of patients with AdvSM who do not have the KIT D816V mutation or have an unknown KIT mutational status. The targeted therapy, midostaurin, is approved for the treatment of AdvSM in Canada but is not publicly funded and therefore is inaccessible.
The objective of this report is to review and critically appraise the clinical evidence submitted by the sponsor on the beneficial and harmful effects of avapritinib 25 mg, 50 mg, 100 mg, and 200 mg oral tablets in the treatment of adult patients with AdvSM, including ASM, SM-AHN, and MCL. The recommended starting dose of avapritinib is 200 mg daily.
Perspectives of Patients, Clinicians, and Drug Programs
The information in this section is a summary of input provided by the patient and clinician groups who responded to the call by Canada’s Drug Agency (CDA-AMC) for input and from clinical experts consulted for this review.
Patient Input
CDA-AMC received 2 patient group submissions from Heal Canada and the Leukemia & Lymphoma Society of Canada (LLSC). Heal Canada is a not-for-profit organization that aims to empower patients, provide patient education and awareness, improve health care outcomes, and advocate for equitable access to quality health care. LLSC is a national charitable organization dedicated to finding a cure and improving quality of life for people and their families affected by blood cancers through research, educational resources, services, and support. Heal Canada conducted an online survey of patients living with blood cancer (from February to May 2024); however, no patient with AdvSM was recruited and no patient was identified to have had experience with avapritinib, so the submitted information was based on the Mast Cell Connect (MCC) patient registry data and its publications. LLSC conducted 1-on-1 interviews with 3 patients with SM (1 patient each with AdvSM, indolent SM, and an unknown SM subtype) and 1 caregiver whose father had AdvSM. One interviewed patient with ASM and a caregiver of a patient with ASM reported on experience with avapritinib. The caregiver reported that their father’s skin issues and itching dissipated and his quality of life improved while receiving avapritinib, with no major adverse effects. The patient who received avapritinib via compassionate care access expressed its life-changing impact in alleviating symptom burden and mental strain due to the disease, with no observable adverse effects.
Both Heal Canada and LLSC reported SM to be a rare disease with a complex and variable clinical presentation that can lead to misdiagnosis or delays in diagnosis. Patients with AdvSM frequently reported symptoms of fatigue, concentration difficulties, body pain, sleep disturbances, nausea, vomiting, skin irritations (e.g., rashes, itching, hives), and anxiety and depression. The onset of symptoms is unpredictable, and may be triggered by temperature, stress, exercise, food, medication, and other factors. Patients are at risk of life-threatening anaphylaxis due to SM. The frequency and intensity of symptoms can vary widely, with some patients chronically disabled while others may lead relatively normal lives.
There is a lack of accessible and effective treatments for patients with AdvSM in Canada. Patients seek better treatments that address the underlying disease, provide symptom relief, have tolerable adverse effects, allow the restoration of daily activities, and improve physical and mental well-being.
Clinician Input
Input From Clinical Experts Consulted by CDA-AMC
According to the clinical experts consulted for this review, there is a major treatment gap for patients with AdvSM in Canada. The off-label treatments currently available have low or unpredictable response rates, have a response of short duration, and may cause significant toxicity. The clinical experts stated that avapritinib would be used as first-line monotherapy in patients with AdvSM, except for patients who present very acutely and need rapid debulking with cladribine or those patients with a platelet count of less than 50 multiplied by 109/L. In these patients, avapritinib may be used as second-line therapy, after debulking or once platelet counts have increased. The experts identified that the patients most suitable for treatment are those who meet the WHO diagnostic criteria for AdvSM, who are treatment-naive, or who have received prior therapy for AdvSM. The experts anticipated that patients with all subtypes of AdvSM (ASM, SM-AHN, and MCL) would benefit from treatment with avapritinib monotherapy.
According to the clinical experts consulted, assessment of a clinically meaningful response requires the integration of patients’ goals of treatment with clinical and histopathological factors. Improvement in a patient’s symptoms is a critical part of the response assessment. Treatment response also requires a reduction in abnormal mast cell burden in bone marrow, and improvement in clinical signs of organ damage due to infiltration by neoplastic mast cells. This may include a normalization of complete blood counts and liver function enzymes, a reduction in spleen or liver volume, a reduction or an absence of transfusion requirements, and a reduction in the need for diuretics and/or therapeutic paracentesis.
As per the pivotal trials and input from the clinical experts, avapritinib should be discontinued in patients who are no longer getting clinical benefit from a symptom or quality-of-life perspective, in patients who experience intracranial bleeding or have a platelet count less than 50 multiplied by 109/L, in patients with persistent severe treatment-related adverse events (AEs) that cannot be managed with dose interruptions or dose reduction, in patients where there is evidence of progressive disease of either the SM or associated hematologic neoplasm (AHN) disease component, or in patients who are pregnant.
Clinician Group Input
Two clinician groups provided input for this review: the Ontario Health (Cancer Care Ontario) Hematology Cancer Drug Advisory Committee (based on 2 clinicians) and the LLSC Clinician Network and Myeloproliferative Neoplasms Canada Clinician Group (based on 6 clinicians).
In general, the clinician groups’ input was consistent with the input provided by the clinical experts consulted for this review. The clinician groups agreed that there is a significant unmet need for patients with AdvSM in Canada who have poor outcomes and a high symptomatic burden. The experts anticipated that avapritinib would be used as first-line monotherapy in Canada for adults with all subtypes of AdvSM. The clinician groups agreed that patients with AdvSM should be managed by hematologists or medical teams with expertise in diagnosis, treatment, and response evaluation. Input from clinician groups indicated that standardized response criteria are evolving and may be used in conjunction with evaluations of clinical benefit, including patient-reported symptoms and health-related quality of life. The clinician groups agreed that treatment with avapritinib should be discontinued among patients whose health-related quality of life is impacted by a lack of clinical benefit, and those with a platelet count of less than 50 multiplied by 109/L, detectable disease progression, or significant adverse effects.
Drug Program Input
The drug programs identified issues related to relevant comparators and generalizability. For more information, refer to Table 4.
Clinical Evidence
Systematic Review
Description of Studies
Two open-label, single-arm clinical trials provided data on the efficacy and safety of avapritinib in adults with AdvSM. Eligible patients were aged 18 years or older with an adjudicated diagnosis of either ASM, SM-AHN, or MCL according to the WHO diagnostic criteria. The phase I EXPLORER study enrolled 86 patients, including 69 patients with AdvSM, who received avapritinib in either the dose escalation phase (part 1) or the extension phase (part 2). In the dose escalation phase, patients received avapritinib 30 mg to 400 mg daily and in the extension phase, the avapritinib starting dose was 300 mg or 200 mg daily. The phase II PATHFINDER study was ongoing at the time of this review and provided results for 62 patients at the first data cut-off date (the planned interim analysis), and for 105 patients at a second data cut-off date. Patients in the PATHFINDER study received an avapritinib starting dose of 200 mg daily. The key efficacy outcomes were overall response rate (ORR), OS, and change in patient-reported symptom severity, measured using the Advanced Systemic Mastocytosis Symptom Assessment Form (AdvSM-SAF) total symptom score (TSS).
The results presented are from the final data cut-off date of the EXPLORER study (January 19, 2023) as well as the first data cut-off date (June 23, 2020) and second data cut-off date (September 9, 2022) of the ongoing PATHFINDER study, which had a mean treatment duration of ████ ██████ ███ █ ██████ ███ ██████ ███ █ █████ ███ ████ ██████ ███ █ █████, respectively, in the safety population. The median OS follow-up duration was ████ ███████ ███ ██████ and 26.3 months in the EXPLORER study (in the final data cut-off) and the PATHFINDER study’s first and second data cut-offs, respectively.
The mean age of patients enrolled was 65.0 (standard deviation [SD] = 11.2) years and 67.5 (SD = 11.0) years in the EXPLORER and PATHFINDER studies, respectively, 41% and 45% of patients were female, respectively, and 59% and 55% of patients were male, respectively. In the EXPLORER and PATHFINDER studies, the most common AdvSM subtype was SM-AHN (70% and 69%, respectively), followed by MCL (19% and 16%, respectively), and ASM (12% and 15%, respectively). In the EXPLORER and PATHFINDER studies, most patients had an Eastern Cooperative Oncology Group Performance Status (ECOG PS) score of 0 or 1 (70% and 69%, respectively), with 20% and 23% of patients rated as having an ECOG PS score of 2, respectively, and 10% and 8% of patients rated as having a score of 3, respectively. In the EXPLORER study, 59% of patients had received prior antineoplastic therapy compared with 68% of patients in the PATHFINDER study (in the first data cut-off).
Efficacy Results
The ORR was the primary outcome in the PATHFINDER study and a secondary outcome in the EXPLORER study. Response was based on the centrally adjudicated modified International Working Group - Myeloproliferative Neoplasms Research and Treatment - European Competence Network on Mastocytosis (IWG-MRT-ECNM) criteria in the Response Assessment Committee–Response Evaluable (RAC-RE) population. In both studies, overall response was defined as patients with complete remission (CR), patients with complete remission with partial hematological recovery (CRh), patients with partial remission (PR), and patients with clinical improvement. The observed ORR was █████ ████ ██████████ ████████ █████ █████ ██ ██████ | | ███ in the EXPLORER study, 75.0% ███████ ███ █████ ██ ██████ | | ███ in the first data cut-off of the PATHFINDER study, and 74.1% (95% confidence interval [CI], 63.1% to 83.2%; N = 81) in the second data cut-off. According to the statistical analysis plans, the ORR was tested versus the 28% null value, which was the post hoc estimate of the ORR for midostaurin. In the EXPLORER study and in the first data cut-off of the PATHFINDER study, the P value was less than 0.0001 based on a 1-sided test.
OS was an exploratory outcome in the EXPLORER study and a secondary outcome in the PATHFINDER study, and was reported for the safety population. The median survival was not reached for either study, as ██ ██ ██ ██ ████████ ███████ were alive at the end of the EXPLORER study, and 84 of 105 (80.0%) patients were alive at the second data cut-off of the PATHFINDER study. In the EXPLORER study, the Kaplan-Meier estimates for the proportion of patients alive at | █████ ███ █████ ████ ███ █████ ██ ██████ ███ ██ █ █████ ███ █████ ████ ███ █████ ██ ██████. At the interim analysis of the PATHFINDER study, ██████ ██████ ███ █████ of patients were alive at 6 months, 12 months, and 18 months, respectively. As of the PATHFINDER study second data cut-off date, the Kaplan-Meier estimate for OS was 79.0% (95% CI, 70.8% to 87.3%) at 2 years.
The AdvSM-SAF TSS captures the severity of 8 symptoms (abdominal pain, nausea, vomiting, diarrhea, spots, itching, flushing, and fatigue) and is scored from 0 (no symptoms) to 80 points (worst imaginable), based on the average daily score over the prior week. Using anchor-based methods, the estimated within-person minimal important difference (MID) was 9 points to 14 points for the TSS.1 In the EXPLORER study, the AdvSM-SAF questionnaire was completed during part 2 only (safety population), with 40 (74%) patients reporting a baseline score. At baseline, the mean TSS was 19.1 (SD = 12.2) points, with a mean change from baseline of █████ ██████ ████ ██ █████ ██ █████ | | ███ at cycle 11, day 1.
In the PATHFINDER study, 56 of 62 (90%) patients reported a baseline AdvSM-SAF TSS at the first data cut-off date, and 91 of 105 (87%) patients reported a score at the second data cut-off date (safety population). For the first data cut-off, the baseline mean TSS was 18.3 (SD = 12.5) points (N = 56), with a mean change from baseline of –9.8 points (95% CI, –14.9 points to –4.6 points; N = 22) at cycle 11, day 1. For the second data cut-off, the baseline TSS was not reported and the mean change from baseline was –6.4 (SD = 9.7) points (N = 91) at cycle 11, day 1.
Among patients who met the overall response criteria, the median duration of response was ████ ██████ ████ ███ ████ ███████ ███ ██████████ in the EXPLORER study (N = 44). The median duration of response was not reached by the second data cut-off date of the PATHFINDER study (N = 60). At 24 months, █████ ████ ███ █████ ██ ██████ of responders in the EXPLORER study and 88.8% (95% CI, 80.4% to 97.3%) of responders in the PATHFINDER study had maintained the response. At 36 months, the proportion of patients was █████ ████ ███ █████ ██ ██████ and 84.6% (95% CI, 73.2% to 96.0%) in the EXPLORER and PATHFINDER trials, respectively. The median time to response was ███ ██████ ████ ███ ███ ██ █████ in the EXPLORER study, 2.0 months (95% CI, 0.3 months to 12.2 months) in the first data cut-off of the PATHFINDER study, and 2.2 months (95% CI, 0.3 months to 15.0 months) in the PATHFINDER study’s second data cut-off.
Progression-free survival (PFS) was an exploratory outcome in the EXPLORER study and a secondary outcome in the PATHFINDER study. In the EXPLORER study, the median PFS was 49.0 months (95% CI, 31.2 months to not estimable), and at 24 months the Kaplan-Meier PFS estimate was █████ ████ ███ █████ ██ ██████. The median PFS had not been reached in the ongoing PATHFINDER study, which reported a 24-month PFS survival estimate of 76.5% (95% CI, 66.9% to 86.0%) in the second data cut-off.
Harms Results
All patients in the EXPLORER and PATHFINDER trials reported at least 1 AE. The most common AEs were periorbital edema (69% and 41%), anemia (57% and 51%), diarrhea (49% and 31%), thrombocytopenia (41% and 43%), and peripheral edema (41% and 47%) in the EXPLORER and PATHFINDER studies (second data cut-off), respectively.
Serious adverse events (SAEs) were reported ███ and 51% of patients, and █████ and 23.8% of patients stopped treatment due to AEs in the EXPLORER and PATHFINDER studies (second data cut-off), respectively. In the EXPLORER study, the most common SAEs were ███████ ███████ █████████ ██████████ ████████ █████████ ████████████ ███████████ █████ ███████ █████████ ███ ███████. Limited information on specific AEs was available for the PATHFINDER study. █████ ████████ ██████ in the EXPLORER study and | ████████ ██████ in the PATHFINDER study (second data cut-off) died due to AEs.
Intracranial bleeding was identified as an AE of special interest by the sponsor and by the clinical experts who were consulted for this review. In the EXPLORER study ██ ████████ ███████ experienced intracranial bleeding. In the PATHFINDER study, 1 (1.6%) patient in the first data cut-off and 4 (3.7%) patients in the second data cut-off experienced intracranial bleeding.
Cognitive AEs were common and were reported by █████ and 27.6% of patients in the EXPLORER and PATHFINDER trials, respectively. These events included ██████ ███████████ █████████ █████████ ███████████ ██████ ████████ ██████████████ ███ ██████████.
Critical Appraisal
Both pivotal trials were open-label, single-arm studies, and thus provided no direct evidence on comparative efficacy or safety. The lack of controlled trials has implications for the overall strength and interpretability of the results. With single-arm studies, there is an increased risk of bias in the estimation of treatment effects due to the potential for confounding related to natural history and prognostic factors. Moreover, the extent of any selection bias is difficult to ascertain. The clinical experts emphasized that AdvSM is a heterogeneous disease, and prognosis varies substantially based on the disease subtype and other factors. The primary outcome (ORR) and other response-related outcomes were analyzed in a subset of patients enrolled in the studies, not in the entire population with AdvSM, which is another potential source of selection bias.
While the lack of a comparator group in the pivotal evidence limits the overall interpretation of the results, the feasibility of conducting a randomized controlled trial was low, given the rarity of AdvSM, and potential ethical issues were raised by the clinical experts consulted, due to the efficacy and safety of the available comparators.
The primary outcome was based on ORR according to the modified IWG-MRT-ECNM criteria. The clinical experts noted that response criteria used in clinical trials and in practice are evolving to best capture clinical benefit and to better define long-term outcomes, given the availability of targeted therapies. While the clinical experts consulted agreed that the International Working Group (IWG) criteria used in the trials was acceptable, there is no clear data to suggest which response criteria perform better in terms of predicting long-term outcomes like survival.
The pivotal trials were open-label, whereby the investigator and study participants were aware of their treatment status, potentially increasing the risk of detection bias and performance bias. As such, the open-label trial design limits the interpretability of the subjective study outcomes, such as AdvSM-SAF, and AEs, and may impact some components of the IWG-MRT-ECNM criteria. The AdvSM-SAF was further limited by the extent of missing data; ███ ███ ███ of patients were excluded from the analysis at baseline and due to attrition, ███ ███ ███ of patients had missing data at cycle 11 in the EXPLORER and PATHFINDER studies (in the first data cut-off), respectively. In the PATHFINDER study, the use of the last observation carried forward imputation method for patients with missing data also may have biased the findings.
Most of the time-to-event outcomes were considered immature, as the median OS was not met for either study, and the median PFS and duration of response were not met for the PATHFINDER trial. Additionally, comparative OS and PFS cannot be adequately assessed in a single-arm trial because all patients receive the same treatment. The FDA 2021 medical review report for Ayvakyt (avapritinib) oral (application number 212608) states that the effect of avapritinib on OS cannot be interpreted due to the single-arm, open-label design of the studies, which can return biased results.11
With regard to external validity, the results predominantly reflect patients with SM-AHN with an ECOG PS score of 0 or 1 and who had received prior systemic therapy for AdvSM. In Canada, SM-AHN is the most common type of AdvSM, which is consistent with the studies. However, clinical experts consulted noted that the proportion of patients with high ECOG PS scores was lower than expected in the trials. As a result, the study patients may have been less ill than patients who receive avapritinib in clinical practice. Both trials excluded patients with comorbidities such as seizure disorder, uncontrolled cardiovascular disease, and reduced renal and hepatic function, and those patients at higher risk of intracranial bleeding; thus, the safety and efficacy of avapritinib in these patients is unknown. Approximately three-quarters of patients in the EXPLORER study did not receive the Health Canada recommended starting dose, which may impact the generalizability of the findings to clinical practice, particularly for safety, as the sponsor identified dose-related toxicities.
GRADE Summary of Findings and Certainty of the Evidence
For pivotal studies identified in the sponsor’s systematic review, the Grading of Recommendations Assessment, Development and Evaluation (GRADE) tool was used to assess the certainty of the evidence for outcomes considered most relevant to inform the expert committee deliberations, and a final certainty rating was determined as outlined by the GRADE Working Group.12,13
Although GRADE guidance is not available for noncomparative studies, the review team assessed pivotal single-arm trials for study limitations (which refers to internal validity or risk of bias), inconsistency across studies, indirectness, the imprecision of effects, and publication bias to present these important considerations. Because the lack of a comparator arm does not allow for a conclusion to be drawn on the effect of the intervention versus any comparator, the certainty of evidence for single-arm trials started at very low certainty.
For the GRADE assessments, findings from the EXPLORER and PATHFINDER studies were considered together and summarized narratively per outcome because these studies were similar in population, interventions, design, and outcome measures.
The selection of outcomes for GRADE assessment was based on the Sponsor Summary of Clinical Evidence,14 consultation with clinical experts, and input received from patient and clinician groups and public drug plans.
Table 2: Summary of Findings for Avapritinib for Adults With AdvSM
Outcome and follow-up | Patients (EXPLORER and PATHFINDER studies), N | Effect | Certaintya | What happens |
|---|---|---|---|---|
Overall response: RAC-RE populationb | ||||
Proportion of patients with overall responsec (95% CI) Follow-up: 39.8 months or 10.2 monthsd | 89 (2 single-arm studies) | EXPLORER study
PATHFINDER study (first data cut-off)
| Very low | The evidence is very uncertain about the effect of avapritinib on overall response when compared with any comparator. |
OS: Safety populationb | ||||
Probability of being alive at 2 years (95% CI) Median OS follow-up: ████ ██ ████ monthsf | 174 (2 single-arm studies) | EXPLORER study
PATHFINDER study (second data cut-off)
| Very lowg | The evidence is very uncertain about the effect of avapritinib on the probability of being alive at 2 years when compared with any comparator. |
Probability of being alive at 4 years (95% CI) Median OS follow-up: ████ months | 69 (1 single-arm study) | EXPLORER study
| Very low | The evidence is very uncertain about the effect of avapritinib on the probability of being alive at 4 years when compared with any comparator. |
Patient-reported symptoms: Safety populationb | ||||
AdvSM-SAF TSS (0 [best] to 80 [worst]), within-group mean change from baseline (95% CI) Follow-up: Cycle 11, day 1 | 44 (2 single-arm studies) | EXPLORER study
PATHFINDER study (first data cut-off)
| Very lowh | The evidence is very uncertain about the effect of avapritinib on patient-reported symptoms (based on the AdvSM-SAF TSS) at 11 months when compared with any comparator. |
Duration of response: RAC-RE population with responseb | ||||
Probability of maintaining response at 2 years (95% CI) Follow-up: Not reported | 104 (2 single-arm studies) | EXPLORER study
PATHFINDER study (second data cut-off)
| Very low | The evidence is very uncertain about the effect of avapritinib on the duration of response when compared with any comparator. |
Time to response: RAC-RE population with responseb | ||||
Median time to response, months (range) Follow-up: Not reported | 104 (2 single-arm studies) | EXPLORER study
PATHFINDER study (second data cut-off)
| Very low | The evidence is very uncertain about the effect of avapritinib on the time to response when compared with any comparator. |
PFS: RAC-RE populationb | ||||
Probability of being alive without disease progression at 2 years (95% CI) Follow-up: ████ ██ ████ monthsi | 138 (2 single-arm studies) | EXPLORER study
PATHFINDER study (second data cut-off)
| Very low | The evidence is very uncertain about the effect of avapritinib on the probability of being alive without disease progression at 2 years when compared with any comparator. |
Notable harms: Safety populationb | ||||
Proportion of patients with SAEs Follow-up: Mean exposure duration of ████ ██ ████ monthsj | 191 (2 single-arm trials) | EXPLORER study
PATHFINDER study (second data cut-off)
| Very lowk | The evidence is very uncertain about the effect of avapritinib on SAEs when compared with any comparator. |
Proportion of patients with intracranial bleeding Follow-up: Mean exposure duration of ████ ██ ████ monthsj | 191 (2 single-arm trials) | EXPLORER study
PATHFINDER study (second data cut-off)
| Very lowk | The evidence is very uncertain about the effect of avapritinib on intracranial bleeding adverse events when compared with any comparator. |
Proportion of patients with cognitive adverse events Follow-up: Mean exposure duration of ████ ██ ████ monthsj | 191 (2 single-arm trials) | EXPLORER study
PATHFINDER study (second data cut-off)
| Very lowk | The evidence is very uncertain about the effect of avapritinib on cognitive adverse events when compared with any comparator. |
AdvSM = advanced systemic mastocytosis; AdvSM-SAF = Advanced Systemic Mastocytosis Symptom Assessment Form; CI = confidence interval; IWG-MRT-ECNM = International Working Group - Myeloproliferative Neoplasms Research and Treatment - European Competence Network on Mastocytosis; NR = not reported; ORR = overall response rate; OS = overall survival; PFS = progression-free survival; RAC-RE = Response Assessment Committee–Response Evaluable; SAE = serious adverse event; SM = systemic mastocytosis; TSS = total symptom score.
Note: All serious concerns with study limitations (which refers to internal validity or risk of bias), inconsistency across studies, indirectness, the imprecision of effects, and publication bias are documented in the Table 2 footnotes.
aIn the absence of a comparator group, conclusions about efficacy or safety relative to any comparator cannot be drawn and the certainty of evidence begins at very low. In addition, all outcomes were rated down 1 level for serious study limitations. The efficacy results are based on the small sample sizes of the EXPLORER and PATHFINDER studies and it is unclear if results would be replicable in a larger sample. All outcomes were rated down 1 level for indirectness as 70% or more of patients in the EXPLORER study did not receive the recommended avapritinib starting dose of 200 mg daily.
bThe RAC-RE population included all patients with AdvSM who received at least 1 dose of avapritinib, were deemed evaluable per modified IWG-MRT-ECNM criteria at baseline as assessed by a Study Steering Committee review, and had 1 of the following conditions: had 2 or more complete postbaseline bone marrow assessments and had been in the study for at least 6 cycles (6 × 28 days), or had an end-of-study visit. The safety population included all patients who received at least 1 dose of avapritinib. For efficacy outcomes in the EXPLORER study, the safety population only included patients with AdvSM (69 of 86 patients enrolled), but for adverse event outcomes, data from all patients were reported, including 17 patients with indolent or smouldering SM. Results from the EXPLORER study were based on patients who received any starting dose of avapritinib (30 mg to 400 mg daily); the PATHFINDER study first data cut-off included patients who had received a starting dose of 100 mg daily (2 patients) or 200 mg daily (60 patients), and the second data cut-off included patients who had received a starting dose of 200 mg daily (105 patients).
cOverall response was defined according to the modified IWG-MRT-ECNM criteria and included patients who experienced a best response of complete remission, complete remission with partial recovery of peripheral blood counts, partial remission, or clinical improvement.
dThe median follow-up was ████ months for the EXPLORER study and 10.2 months for the planned interim analysis of the PATHFINDER study.
eAs per the planned interim analysis of the PATHFINDER study, the ORR was tested at a 1-sided alpha of 0.00625; thus, the 98.75% CI was listed.
fMedian follow-up for survival was ████ months for the EXPLORER study and 26.3 months for the second data cut-off of the PATHFINDER study.
gRated down 1 level due to risk of bias, as the second data cut-off of the PATHFINDER study was not a preplanned interim analysis, according to the study protocol, and as such should be interpreted as supportive data.
hRated down 2 levels for risk of bias due to missing data and open-label design. Not all patients enrolled provided results at baseline (missing ███ ███ ███ of patients), with further attrition over time (███ ███ ███ of patients missing from the cycle 11 time point in the EXPLORER and PATHFINDER studies, respectively). The use of the last observation carried forward method in the PATHFINDER study may bias the results, given the magnitude of missing data at cycle 11. The open-label study design and patients’ and assessors’ knowledge of assigned treatment may lead to biased estimates of subjective outcomes.
iMedian follow-up was ████ months for the EXPLORER study and ████ months for the second data cut-off of the PATHFINDER study.
jMean avapritinib exposure duration was ████ months in the final data cut-off of the EXPLORER study, and ████ months in the second data cut-off of the PATHFINDER study.
kRated down 1 level because of risk of bias due to the open-label study design. Patients’ and assessors’ knowledge of assigned treatment may lead to biased estimates of subjective outcomes and harms. Due to the lack of a control group, the proportion of adverse events that is attributable to avapritinib versus the disease or other factors is unclear.
Sources: Final Clinical Study Report for the EXPLORER study,15 interim Clinical Study Report for the PATHFINDER study,16 PATHFINDER study clinical summary document,17 and the Sponsor Summary of Clinical Evidence.14 Additional data supplied by the sponsor (June 17, 2024).18
Long-Term Extension Studies
No long-term extension studies were submitted.
Indirect Comparisons
Description of Studies
The sponsor submitted 1 indirect treatment comparison and 1 observational comparison that evaluated the efficacy of avapritinib versus available treatments for patients with AdvSM. The indirect treatment comparison was based on a published matching-adjusted indirect comparison (MAIC) comparing avapritinib with midostaurin on OS, ORR, and CR. The individual patient-level data (IPD) observational comparison was based on inverse probability of treatment weighting (IPTW) methods comparing avapritinib with midostaurin, and with real-world best available therapy (BAT), on OS and the duration of treatment.
Efficacy Results
Overall Survival
In the MAIC of avapritinib (the pooled EXPLORER and PATHFINDER studies safety population) versus the pooled midostaurin cohort (the pooled D2201 and A2213 trials’ full analysis set), the OS hazard ratio (HR) was 0.42 (95% CI, 0.25 to 0.71), favouring avapritinib. Follow-up in the MAIC for OS was median 22.9 months and median 7.0 months in the EXPLORER and PATHFINDER studies for avapritinib, respectively; the follow-up duration was median 124 months and median 26 months in the A2213 and D2201 trials for midostaurin, respectively.
In the IPTW-weighted observational comparison of avapritinib first-line therapy (the PATHFINDER study safety population) versus BAT first-line therapy with follow-up of mean ████ ██████ ██████ ████ ████ ██████, respectively, the OS HR was ████ ████ ███ ████ ██ █████, favouring avapritinib first-line therapy.
In the IPTW-weighted observational comparison of avapritinib second-line or later-line therapy (the PATHFINDER study safety population) versus BAT second-line or later-line therapy with follow-up of mean ████ ██████ ██████ ████ ████ ██████, respectively, the OS HR was ████ ████ ███ ████ ██ █████, favouring avapritinib second-line or later-line therapy.
In the IPTW-weighted observational comparison of avapritinib first-line therapy (the PATHFINDER study safety population) versus in the midostaurin first-line therapy with follow-up of mean ████ ██████ ██████ ████ ████ ██████, the OS HR was ████ ████ ███ ████ ██ █████, favouring avapritinib first-line therapy.
Duration of Treatment
In the IPTW-weighted observational comparison of avapritinib first-line therapy (the PATHFINDER study safety population) versus BAT first-line therapy with follow-up of median ████ ██████ ██████ ██████ ███ ██████, respectively, the HR for the duration of treatment was ████ ████ ███ ████ ██ █████, favouring avapritinib first-line therapy.
In the IPTW-weighted observational comparison of avapritinib second-line or later-line therapy (the PATHFINDER study safety population) versus BAT second-line or later-line therapy with follow-up of median ████ ██████ ██████ ██████ ███ ██████, respectively, the HR for the duration of treatment was ████ ████ ███ ████ ██ █████, favouring avapritinib second-line or later-line therapy.
In the IPTW-weighted observational comparison of avapritinib first-line therapy (the PATHFINDER study safety population) versus in the midostaurin first-line therapy with follow-up of median ████ ██████ ██████ ██████ ████ ██████, the OS HR was ████ ████ ███ ████ ██ █████, favouring avapritinib first-line therapy.
Overall Response Rate
In the MAIC of avapritinib (the pooled EXPLORER and PATHFINDER studies RAC-RE population) versus the midostaurin cohort (the D2201 trial primary efficacy population), the odds ratio for ORR was 4.06 (95% CI, 3.09 to 5.33), favouring avapritinib.
Complete Remission
In the MAIC of avapritinib (the pooled EXPLORER and PATHFINDER studies RAC-RE population) versus midostaurin (the D2201 trial primary efficacy population), CR was attained by 10 of 79 (12.66%) patients and 1 of 89 (1.12%) patients, respectively, for an odds ratio of 9.56 (95% CI, 0.97 to 93.81), favouring avapritinib.
Harms Results
No comparative safety data were available in the indirect evidence.
Critical Appraisal
In the indirect treatment comparison (MAIC), methods for study selection were poorly reported. No information was provided on details of the literature search, study selection process, and data extraction. No information including rationale was provided for not assessing the quality of the included studies. Across the included cohorts, trial start dates were heterogenous and notably older in the midostaurin trials (2005 and 2008 for the A2213 and D2201 trials, respectively) than in the avapritinib trials (2016 and 2018 for the EXPLORER and PATHFINDER trials, respectively). The MAIC reported limited details regarding patients enrolled in the trials. Across the studies, differences were observed in the dosing of avapritinib (between the EXPLORER and PATHFINDER studies) and response evaluation (criteria across the 4 trials), and no information on time points used in evaluating response was provided for the trials. Prognostic factors associated with poor outcomes such as AdvSM subtypes of SM-AHN (particularly for type of myeloid neoplasm) and MCL, the KIT D816V variant allele frequency, and the type of gene mutation (e.g., SRSF2) were not included in the MAIC. The selection of prognostic factors used for matching was based on an arbitrary P value of less than 0.1 from exploratory subgroup analyses that contained the same data used for assessment, which is not consistent with recommended approaches in the National Institute for Health and Care Excellence (NICE) Decision Support Unit Technical Support Document 18.19 Information on patients who received prior systemic therapy in the midostaurin trials was not available. Patients in the avapritinib and midostaurin trials were matched on baseline imbalances that differed by outcome and by analysis populations. Similarities and differences between the populations of analyses were not detailed in the MAIC, making it challenging to determine the comparability of treatment groups and the interpretation of findings. Findings for OS and ORR after weighting resulted in reduced effective sample sizes to suggest incomplete overlap between the avapritinib and midostaurin populations and that results may be driven by a subset of the sample from the index trials that was not representative of the entire sample. The exclusion of data from the A2213 trial and the exploratory nature of the response analysis increase the potential for prognostic imbalance and the risk of type I error. In the MAIC, avapritinib 200 mg (the dose recommended by Health Canada for the indicated population) versus midostaurin was based on sensitivity analyses using the pooled the EXPLORER and PATHFINDER studies RAC-RE population. There is uncertainty in these results at least in part due to the small sample sizes in the avapritinib 200 mg cohort (44 patients and 42 patients for OS and ORR, respectively), which is reflected in the wide CI that crosses the null for survival and in findings that are driven by a reduced sample of the overall population.
No study protocol, statistical analysis protocol, or study report was provided for the observational comparison using IPTW analysis that was based on an updated data cut-off date of September 2022 for the PATHFINDER study. Information presented for the methods of the observational comparison were limited to the sponsor-provided observational comparison report and publication based on earlier analyses (data cut-off date of April 2021), where several inconsistencies and gaps in information were found. Four subgroup analyses that were specified in the sponsor-submitted observational comparison report were reported in the publication but did not match those reported in the updated analyses. Sensitivity analyses of OS described in the sponsor’s observational comparison report were not included in the submission. There were no sensitivity analyses reported to evaluate the potential impact of bias due to informative censoring on effect estimates in patients who were censored due to a new primary malignancy after the index date or due to avapritinib initiation in the BAT cohort. Patients in the avapritinib cohort were enrolled from March 2016 to March 2020 in the EXPLORER study and from November 2018 to June 2020 in the PATHFINDER study. Real-world patients with AdvSM who received BAT were enrolled from January 2009 to October 2021 and included as controls. Contextual information such as standards of care at a specified time point and across time was not directly captured. For patients in the external control group who received BAT as first-line therapy and then went on to receive avapritinib as second-line or later-line therapy either by enrolling in a trial (in the EXPLORER or PATHFINDER studies) or via compassionate program access, follow-up was censored at avapritinib initiation. No further information was detailed regarding how patients who received avapritinib in second-line therapy were included and/or analyzed in the observational comparison. Follow-up duration was not specified for patients included from the PATHFINDER study. The baseline period differed between the comparative cohorts (defined as the 8-week period up to the index date for avapritinib and the 12-week period up to the index date for BAT); no rationale was provided for the different time periods used to ascertain baseline characteristics. While AdvSM subtype was diagnosed based on the WHO criteria for all patients, the evaluation was confirmed by the RAC for the avapritinib cohort and based on local clinician assessment for the BAT cohort. There may be a greater risk of bias among patients who were diagnosed in the BAT cohort due to the retrospective nature of chart review and the lack of information on the assessors. Imbalances in covariates that were found to persist after IPTW weighting (including imbalances that increased for some covariates) for region, ECOG PS scores, anemia, thrombocytopenia, leukocyte counts, and serum tryptase concentrations. These imbalances suggested that there was a lack of sufficient overlap between the cohorts (i.e., the cohorts may have been meaningfully different). While findings for OS and duration of treatment were presented for both the safety and RAC-RE populations of analyses, imbalances in covariates differed for the safety and RAC-RE populations such that it was challenging to meaningfully assess how such differences may have translated to adjusted results (after IPTW weighting) and the comparability of the adjusted results between the analyzed populations. An analysis in the overall sample (avapritinib from the EXPLORER and PATHFINDER studies versus BAT from real-world patients regardless of lines of therapy) was not submitted by the sponsor for updated analyses (for the September 2022 data cut-off). Rather, 3 analyses with longer follow-up were submitted that appeared to be subgroup or post hoc analyses, given that the analysis comparing avapritinib with exclusively midostaurin was not prespecified in the sponsor’s observational comparison report or the publication. The small sample sizes, both overall and reduced for the avapritinib cohort compared to the BAT cohort, make it difficult to ensure prognostic matching was appropriate in the analyses. Median OS had not been reached in the avapritinib cohort in any line of therapy, indicating that OS data were immature. In the observational comparison, the avapritinib 200 mg dose was a subgroup analysis of the PATHFINDER study with small sample sizes. Variations in the timing of assessments and follow-up of patients who received BAT in the real-world setting may not fully match patients who received avapritinib in the EXPLORER and PATHFINDER trials; given the absence of information on follow-up duration (other than at least 3 months of follow-up in the BAT cohort) and this absence’s potential to create prognostic imbalance between the avapritinib and BAT cohorts, there is an unknown direction and magnitude of impact on the duration of treatment and survival. Several methods of imputations for missing data (e.g., ECOG PS score, serum tryptase) were at risk of underestimating disease severity among included patients, although the direction and magnitude of potential bias cannot be determined since the proportion of patients with missing data for the avapritinib cohort were not reported.
The findings from the indirect treatment comparison and observational comparison suggested a benefit of avapritinib (the point estimate and lower and upper bounds of the CIs suggested benefit) when indirectly compared to currently available treatments for ORR, the duration of treatment, and OS. Due to the substantial limitations identified in the analyses, there remains significant uncertainty in the magnitude of the benefit with avapritinib compared to currently available treatments. However, it appears unlikely that the benefit seen with avapritinib is solely explained by the noted limitations and sources of uncertainty of these comparisons. Therefore, while it is not possible to ascertain what the true effect is between the comparisons, it is likely to be in favour of avapritinib.
Studies Addressing Gaps in the Evidence From the Systematic Review
No studies addressing gaps were submitted by the sponsor.
Conclusions
Input from patient groups and clinicians highlighted that AdvSM is a rare, severe, and heterogeneous disease with poor prognosis. Patients have currently limited treatment options. It is estimated that the AdvSM incidence rate in Canada is 0.06 cases per 100,000 adults with presently no access to publicly funded targeted treatment options.
Two single-arm, open-label clinical trials (phase I of the EXPLORER study and the ongoing phase II PATHFINDER study) provided evidence of the efficacy and safety of avapritinib in adults with AdvSM. The studies showed that 75% of the patients who received avapritinib reported an adjudicated overall response, which the clinical experts consulted for this review considered to be clinically relevant and superior to currently available treatments. Due to the lack of a control group, the certainty of evidence was rated as very low, as the possibility of selection bias cannot be ruled out, particularly given the small sample size of the trials and the heterogeneity in patients with AdvSM.
Although OS and PFS were evaluated in the study, the single-arm design and the immaturity of the data limit the ability to attribute the study results to treatment with avapritinib. Patient-reported symptoms were identified as an important outcome but because of the noncomparative design, open-label study design, and high patient attrition rates in the trials, the effect of avapritinib on symptom severity remains inconclusive.
The safety data from the clinical trials were limited by the small sample size (a total of 191 patients) and treatment duration (a mean of ████ ██ ████ ██████). AEs, including SAEs, and AEs requiring dose reductions or discontinuation were common in the studies. However, due to the lack of a control group, the proportion of AEs that were attributable to avapritinib versus the disease or other factors is unclear. Intracranial bleeding and cognitive AEs were identified AEs of special interest for avapritinib. While the sponsor identified thrombocytopenia as a risk factor for intracranial bleeding and implemented patient selection and monitoring criteria to reduce the frequency of events, the risk of intracranial bleeding associated with avapritinib use in clinical practice is unclear.
The noncomparative design of the EXPLORER and PATHFINDER trials precludes the ability to assess the relative therapeutic benefit or safety of avapritinib in Canadian clinical practice. To address the evidence gap, the sponsor submitted indirect evidence on the comparative efficacy of avapritinib versus other treatments for AdvSM. The indirect evidence suggests that relative to midostaurin or a basket of treatments, avapritinib may be associated with improved response, duration of treatment, and OS. It appears unlikely that the benefit seen with avapritinib is solely explained by the limitations and sources of uncertainty that were identified in the comparative analyses. However, there was significant uncertainty in the magnitude of the comparative benefit with avapritinib due to substantial limitations, including heterogeneity in the data sources and patient characteristics, missing or unmeasured prognostic factors and effect modifiers, small sample sizes, few events, imbalanced follow-up times, the immaturity of survival data, and the exploratory nature of post hoc and subgroup analyses. Since there were no data on patient-reported outcomes or comparative safety in the indirect evidence, the relative effect of avapritinib versus currently available treatments on symptoms, health-related quality of life, or safety is unknown.
Introduction
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of avapritinib oral tablets in the treatment of adult patients with AdvSM, including those with ASM, SM-AHN, and MCL.
Disease Background
Content in this section has been informed by materials submitted by the sponsor and clinical expert input. The following has been summarized and validated by the CDA-AMC review team.
SM is a heterogenous group of rare disorders caused by a clonal, neoplastic proliferation of abnormal mast cells that accumulate typically in bone marrow and other extracutaneous tissues.1-3 Symptoms of SM are related to the release of mast cell mediators and mast cell tissue infiltration, which can vary widely from isolated symptoms to a constellation of symptoms, commonly including cutaneous involvement (e.g., skin flushing, pruritus, itching, hives, skin rash), wheezing and shortness of breath, dizziness, cardiovascular symptoms (e.g., rapid heart rate, chest pain, low blood pressure), gastrointestinal symptoms (e.g., diarrhea, nausea, vomiting, abdominal pain), fatigue, musculoskeletal symptoms (e.g., bone and/or muscle pain), and neuropsychiatric symptoms (e.g., headache, brain fog, cognitive dysfunction, anxiety, depression).4 Additionally, the symptoms of SM occur either spontaneously or in response to various triggers of mast cell activation (e.g., sunlight, heat, cold or sudden temperature changes, physical and emotional stress, food, alcohol consumption, insect stings, infections, drugs or medications, contrast dyes, surgery, other clinical procedures).4
The criteria for diagnosing SM per the WHO Classification2,6 and International Consensus Classification (ICC)6,20 requires the presence of either 1 major criterion and 1 minor criterion, or at least 3 of 4 minor criteria in the absence of the major criterion.3,6 The major criterion requires a biopsy to detect multifocal dense aggregates of mast cells in the bone marrow and/or other extracutaneous organs.6 The minor criteria include the presence of more than 25% of mast cells that are spindle-shaped or have atypical immature morphology in a bone marrow biopsy or in a section of other extracutaneous organs, mast cells in bone marrow, peripheral blood, or other extracutaneous organs expressing CD25, CD2, and/or CD30 markers in addition to mast cell markers, KIT D816V mutation, or another KIT mutation detected in bone marrow, peripheral blood, or other extracutaneous organs, and an elevated basal serum tryptase level that is persistently higher than 20 ng/mL.3,6 The clinical expert consulted for this review noted that due to the heterogenous clinical presentation and the lack of awareness of this disease among clinicians and pathologists, AdvSM may be underdiagnosed.
The WHO and ICC classify SM into distinct subtypes in order of increasing disease burden: indolent SM and bone marrow mastocytosis, smouldering SM, ASM, SM-AHN, and MCL.3-5 The classification system defines B-findings (indicative of high mast cell burden) and C-findings (indicative of SM induced organ damage) that are used to help establish the subtype of SM in addition to other histopathological findings such as the number of mast cells in the aspirate (for MCL) and the presence of an AHN (for SM-AHN). B-findings indicate a higher burden of SM, and include extensive bone marrow, spleen, or liver involvement without dysfunction.5 C-findings, commonly in patients with AdvSM, are defined by 1 or more signs of organ damage due to infiltration by neoplastic mast cells, including cytopenia(s) (i.e., an absolute neutrophil count < 1 × 109/L, a hemoglobin level < 10 g/dL, and/or a platelet count < 100 × 109/L due to bone marrow dysfunction), palpable splenomegaly with hypersplenism, skeletal involvement with large osteolysis (≥ 2 cm) with or without pathologic fractures, palpable hepatomegaly with impaired liver function and/or ascites and/or portal hypertension, and malabsorption with weight loss due to gastrointestinal mast cell infiltrates.4
AdvSM includes the disease variants of ASM, SM-AHN, and MCL.1 Diagnosis of ASM is based on meeting the general criteria for SM (but not for MCL or SM-AHN), and the presence of 1 or more C-findings.4 ASM is an uncommon but clinically severe form of SM.5 Diagnosis of SM-AHN is based on meeting the general criteria for SM and simultaneously meeting diagnostic criteria for another hematologic neoplasm according to WHO diagnostic criteria (most commonly myelodysplastic or myeloproliferative neoplasms, or an overlap of both diseases), with or without C-findings.4,5 In the ICC criteria, SM-AHN was revised to SM with an associated myeloid neoplasm (SM-AMN), given that AHNs of myeloid lineage are present in most patients (about 90%).3,4 Patients with SM-AHN comprised about 70% of patients with AdvSM in KIT inhibitor trials.4 The diagnosis of MCL is based on the presence of 20% or greater neoplastic mast cells on a bone marrow aspirate smear; MCL can present as a de novo disease or transform from ASM, SM-AHN, or indolent SM (in rare cases).4 MCL is the rarest and most aggressive subtype of SM.5
Several prognostic scoring tools have been developed for risk stratification of patients with SM.3 The Mayo Alliance Prognostic System and the Mutation-Adjusted Risk Score combine clinical variables and high molecular-risk mutations for risk stratification. The International Prognostic Scoring System for Mastocytosis is based on clinical variables only.4 The Global Prognostic Score for Mastocytosis is based on clinical variables that are prognostic for OS and PFS.4 Across the scoring systems, factors associated with poor prognosis among patients with AdvSM include age (≥ 60 years), tryptase level (≥ 125 ng/mL), leukocyte level (≥ 16 × 109/L), hemoglobin level (≤ 11 g/dL), platelet level (≤ 100 × 109/L), skin involvement, and the presence of high-risk mutations (i.e., SRSF2, ASXL1, and/or RUNX1).4
The prevalence rate of SM is estimated at 1 per 10,000 people of all ages.6 Based on estimates from the Danish incidence and German prevalence of adults with AdvSM, the estimated AdvSM incidence rate in Canada is 0.06 cases per 100,000 adults and the prevalence rate is 5.2 cases per million adults.7,8 Median OS has been estimated at 41 months for ASM,4,9 11 months to 42 months for SM-AHN depending on the type of AHN,4,10 and 2 months to 19.2 months for MCL.3,4
Standards of Therapy
Content in this section has been informed by materials submitted by the sponsor and clinical expert input. The following has been summarized and validated by the CDA-AMC review team.
According to the clinical experts consulted for this review, the primary goals of treatment for patients with AdvSM are to improve health-related quality of life, improve the ability to work and maintain independence, prevent life-threatening anaphylaxis, reverse or delay the progression of end organ damage, and prolong survival.
The 2024 NCCN guidelines recommend a stepwise treatment approach to managing symptoms from mast cell mediator release.4 Antihistamines, cromolyn sodium, leukotriene receptor antagonists, and corticosteroids may be used to control skin, gastrointestinal, neurologic, cardiovascular, and other symptoms.4 Omalizumab or venom immunotherapy is recommended to prevent life-threatening anaphylaxis.4 The clinical expert consulted for this review stated that anaphylaxis is far less common among patients with advanced disease compared to nonadvanced SM, so for the population under review, anaphylaxis is not a major driver of morbidity and mortality.
Cytoreduction is the principal treatment for AdvSM; it may improve quality of life, reverse or prevent organ damage, and prolong survival.4 In Canada, cytoreductive treatment options for AdvSM include midostaurin, cladribine, interferons (e.g., peginterferon alfa-2a), and imatinib. According to the NCCN guidelines, enrolment in a clinical trial or a KIT inhibitor, such as midostaurin or avapritinib, are recommended as first-line treatment for AdvSM.4 Midostaurin is an oral multikinase inhibitor that is approved for the treatment of AdvSM in Canada. In 2020, CADTH issued a negative recommendation for midostaurin, and currently it is not reimbursed by public drug plans in Canada. Due to its high costs and the lack of compassionate programs, the clinical experts consulted for this review indicated that midostaurin in largely inaccessible in Canada.
Cladribine is not approved by Health Canada for SM but is used off-label for all variants of AdvSM. It is recommended if rapid disease debulking is required, which may be needed when patients present very acutely at diagnosis.4 The clinical experts indicated that ORRs and the duration of response with cladribine are variable. Infectious complications and myelosuppression are significant and frequent AEs that limit the long-term use of this medication, especially in patients who are very frail, which the experts stated is common at disease presentation.4
Interferons (e.g., peginterferon alfa-2a) have been used off-label in Canada for patients with AdvSM. Based on NCCN guidelines, they may be considered for patients with ASM with very slowly progressive disease, patients with severe refractory bone issues that have not responded to other lines of treatment, and patients with SM-AHN (typically when the AHN component requires treatment).4 Interferons are not an appropriate treatment for patients who present acutely and require immediate disease control to prevent life-threatening organ failure as response rates and response times are variable and unreliable. In clinical practice, the clinical experts stated interferon is almost never the preferred or adequate front-line treatment for AdvSM.
Imatinib is approved by Health Canada for AdvSM in those without a KIT D816V mutation or with an unknown KIT mutational status. Since more than 90% of patients with SM have a KIT D816V mutation, imatinib has a very limited role in the treatment of AdvSM. Allogeneic hematopoietic stem cell transplant may also be considered for patients with AdvSM.4
Drug Under Review
Key characteristics of avapritinib are summarized in Table 3, with other treatments available for AdvSM.
Avapritinib is a type 1 kinase inhibitor that binds to the active conformation and inhibits a broad range of KIT and PDGFRA mutant kinases at clinically relevant concentrations, including KIT D816V mutants and PDGFRA D842 mutants as well as multiple KIT exon 11, 11/17, and 17 mutants, sparing activity on a range of other kinases, including VEGFR2. The constitutive activation of KIT and PDGFRA receptor tyrosine kinases have been implicated in the pathogenesis of several malignancies and rare hematologic diseases, including SM and AdvSM. KIT D816V mutations are observed in about 95% of AdvSM cases.
Avapritinib was approved by Health Canada for the treatment of adult patients with AdvSM. AdvSM includes patients with ASM, SM-AHN, and MCL. The reimbursement request aligns with the indication proposed to Health Canada. Avapritinib is available as 25 mg, 50 mg, 100 mg, and 200 mg oral tablets. The recommended dosage for avapritinib is 200 mg as an oral tablet once daily until disease progression or unacceptable toxicity. Treatment with avapritinib is not recommended in patients with a platelet count of less than 50 multiplied by 109/L.
The US FDA approved avapritinib for the treatment of adults with AdvSM, including patients with ASM, SM-AHN, and MCL, indolent SM, and unresectable or metastatic gastrointestinal stromal tumour harbouring a PDGFRA exon 18 mutation, including PDGFRA D842V mutations.21
The European Medicines Agency (EMA) authorized avapritinib as monotherapy for the treatment of adult patients with ASM, SM-AHN, or MCL, after at least 1 systemic therapy. Additionally, avapritinib was authorized by the EMA for the treatment of adult patients with indolent SM with moderate to severe symptoms inadequately controlled on symptomatic treatment.22 The EMA also authorized avapritinib for use in the European Union as monotherapy for the treatment of adult patients with unresectable or metastatic gastrointestinal stromal tumour harbouring the PDGFRA D842V mutation.
Table 3: Key Characteristics of Avapritinib, Midostaurin, Cladribine, Interferon, and Imatinib
Characteristic | Avapritinib | Midostaurin | Cladribine | Interferon | Imatinib |
|---|---|---|---|---|---|
Mechanism of action | A type 1 kinase inhibitor that binds to the active conformation and inhibits a broad range of KIT and PDGRFA mutant kinases at clinically relevant concentrations (e.g., KIT D816V mutants, PDGFRA D842 mutants, multiple KIT exon 11, 11/17, and 17 mutants), sparing activity on a range of other kinases, including VEGFR2. | A tyrosine kinase inhibitor that inhibits FLT3 and KIT kinase. Inhibition of FLT3 receptor signalling induces cell cycle arrest and apoptosis in leukemic cells expressing mutant receptors or overexpressing wild-type receptors. Also inhibits wild-type and KIT D816V mutants, resulting in inhibition of mast cell proliferation and survival, and histamine release. | A synthetic antineoplastic drug affecting purine metabolism that is cytotoxic to both actively dividing and quiescent lymphocytes and monocytes, inhibiting both DNA synthesis and repair. | Biosynthetic interferon alpha-2a or peginterferon alfa-2a bind to specific receptors on the cell surface, inhibiting viral replication in infected cells, inhibiting cell proliferation, and inducing immunomodulation. The clinical relevance of these in vitro activities is not known. | A protein tyrosine kinase inhibitor that inhibits receptor tyrosine kinases and the cellular events mediated by PDGFR receptors (PDGFRA and PDGFR-beta), the stem cell factor, and receptor (c-KIT). Also inhibits proliferation and induces apoptosis in gastrointestinal stromal tumour cells, which express an activating KIT mutation. |
Indicationa | For the treatment of adult patients with AdvSM. AdvSM includes patients with ASM, SM-AHN, and MCL. | For the treatment of adult patients with ASM, SM-AHN, or MCL. | Not approved; used off-label | Not approved; used off-label | Adults with aggressive subtypes of SM (ASM and SM-AHNMD) without the D816V c-KIT mutation. If c-KIT mutational status is not known or unavailable, treatment may be considered if there is no satisfactory response to other therapies. |
Route of administration | Oral tablet | Oral capsule | Subcutaneous injection or IV infusion | Subcutaneous injection | Oral tablet |
Recommended dosage | 200 mg once daily | 100 mg twice daily | 0.14 mg/kg per day from day 1 to day 5 of a 28-day course | 90 mcg weekly for 2 weeks followed by 180 mcg once weekly | 400 mg daily |
Serious adverse effects or safety issues | Intracranial hemorrhage, cognitive adverse events, fluid retention, thrombocytopenia, and photosensitivity reactions Not recommended for use in patients with a platelet count of less than 50 × 109/L. Monitor patients for intracranial hemorrhage and cognitive adverse events and modify treatment according to specified dosage modifications. | QTc interval prolongation, cardiac dysfunction, neutropenia and/or infections, interstitial lung disease, and pneumonitis Monitor patients for ANC levels, platelet count levels, hemoglobin levels, grade 3 or grade 4 nausea and/or vomiting, and grade 3 or grade 4 nonhematological malignancies, and modify treatment according to specified dosage modifications. | Bone marrow suppression, lymphopenia, serious or severe neurologic toxicity, and acute nephrotoxicity | Fatal or life-threatening neuropsychiatric, autoimmune, ischemic, and infectious disorders | Severe congestive heart failure and reduction in LVEF, rhabdomyolysis, severe hemorrhage, fluid retention, liver failure, and gastrointestinal perforation |
AdvSM = advanced systemic mastocytosis; ANC = absolute neutrophil count; ASM = aggressive systemic mastocytosis; LVEF = left ventricular ejection fraction; MCL = mast cell leukemia; QTc = corrected QT interval; SM = systemic mastocytosis; SM-AHN = systemic mastocytosis with an associated hematologic neoplasm; SM-AHNMD = systemic mastocytosis with an associated clonal hematologic non–mast cell disorder.
aHealth Canada–approved indication.
Sources: Product monograph for avapritinib,23 product monograph for midostaurin,24 product monograph for cladribine,25 product monograph for peginterferon alfa-2a,26 product monograph for imatinib,27 and Sponsor Summary of Clinical Evidence.14
Perspectives of Patients, Clinicians, and Drug Programs
Patient Group Input
This section was prepared by the CDA-AMC review team based on the input provided by patient groups. The full patient and clinician group submissions received by CDA-AMC are available in the consolidated patient and clinician group input document for this review on the project website.
CDA-AMC received 2 patient group submissions from Heal Canada and the LLSC. Heal Canada is a not-for-profit organization that aims to empower patients, provide patient education and awareness, improve health care outcomes, and advocate for equitable access to quality health care. LLSC is a national charitable organization dedicated to finding a cure and improving quality of life for people and their families affected by blood cancers through research, educational resources, services, and support.
Heal Canada conducted an online survey of patients living with blood cancer (from February to May 2024) and attempted to conduct interviews of patients with AdvSM via outreach to Mastocytosis Society Canada and The Mast Cell Disease Society. Since no patient with AdvSM was recruited and no patient was identified to have had experience with avapritinib, the patient group submission was based on the MCC patient registry data and its publications. According to the MCC patient registry publications, SM is a rare disease with complex and variable clinical presentation, an unpredictable onset of symptoms with varying triggers, and diagnosis difficulties such as delays or misdiagnosis. Patients with AdvSM (n = 13) reported a median time of 3 years between symptom onset and the diagnosis. Nearly one-half of the patients consulted 3 to 6 physicians while seeking a diagnosis and only 40% of patients recalled undergoing a bone marrow biopsy, which is included in SM diagnostic recommendations. Based on the MCC patient registry data, 5% to 10% of patients with SM are diagnosed with advanced disease. Among the 13 patients with AdvSM in the MCC patient registry, the most common moderately to severely bothersome symptoms were fatigue (85%), difficulty concentrating (85%), nausea (77%), abdominal pain (69%), difficulty sleeping (69%), nonabdominal pain (62%), anxiety (62%), vomiting (54%), itching (54%), and depression (54%). The MCC patient registry data reported that patients with AdvSM experienced impacts on activities of daily living (92%), feelings of worry (92%), and family and social activities (85%). Quality of life was moderately or extremely severely reduced for 64% of patients.
LLSC conducted 1-on-1 interviews with 3 patients with SM (1 patient each with AdvSM, indolent SM, and unknown SM subtype) and 1 caregiver whose father had AdvSM. One interviewed patient with ASM and a caregiver of a patient with ASM reported on their experience with avapritinib. Patients and the caregiver described SM as a rare disease with symptoms that vary in manifestation (skin irritation, abdominal pain, body aches, diarrhea) and severity (from mild to debilitating), which can impact accurate and timely diagnosis. One caregiver shared that their father’s symptoms, which were initially self-diagnosed as allergies, led to multiple referrals to dermatologists with no clear diagnosis, concluding with an official diagnosis of mastocytosis at aged 92 years. A patient highlighted their lengthy journey that involved various health care providers (i.e., a clinician at a walk-in clinic, a dermatologist, a naturopath, and a rare disease clinician) and diagnoses (i.e., celiac disease and allergy to corn), and treatment resulting in AEs, all of which concluded with a confirmation of cancer after 5 years.
According to the LLSC, patients commonly described symptoms they experienced related to skin issues (e.g., rashes, itching, flushing, hives), body pain (e.g., relentless pain in bones, joints, connective tissues, and/or muscles), sleep disturbances (e.g., problems falling or staying asleep due to symptoms), and fatigue, as highlighted by a patient who reported waking up in the night with hives and itching, which were often combined with pain. According to LLSC, the accumulation of mast cells containing histamine, which are released in response to triggers (e.g., allergic reactions to food or medication) places patients with SM at a greater risk of unexpected anaphylactic shock; as such, patients are sometimes advised to carry an EpiPen and may be prescribed daily antihistamines for prophylaxis. Additional symptoms reported by patients included itchy and dry eyes, fever, and brain fog. In addition to the variability and severity in symptoms, their unpredictability in the location of presentation (e.g., face, extremities), timing (e.g., sudden onset), and acuity (e.g., life-threatening anaphylaxis) significantly impacts patients’ activities of daily living, their ability to work, and their quality of life. Burden of care was expressed as a concern by both patients and caregivers due to limitations in daily activities imposed by the symptoms of SM.
LLSC expressed a significant unmet need for treatment options among patients with AdvSM; available treatments are limited in effectiveness and access, with intolerable adverse effects. LLSC reported that 1 patient’s experience with midostaurin included nausea, vomiting, and diarrhea, such that additional treatment with alternatives (e.g., antinausea medication, cannabis products) were needed to offset the debilitating adverse effects to maintain food intake. Patients also reported experiences with other treatments targeting their symptoms, including pain medication, compound creams, antihistamines, and UV light therapy. One caregiver shared that their father was able to access avapritinib through a clinical trial. Avapritinib was able to alleviate their father’s skin issues and intense itching to provide the father with better quality of life, according to the caregiver, who also reported the treatment regimen to be straightforward and easy for both the caregiver and their father. The caregiver reported that during treatment with avapritinib, their father experienced positive results with limited adverse effects, and survived 3 years after being diagnosed with AdvSM. One patient with AdvSM experienced severe adverse effects with imatinib (Gleevec) treatment (e.g., vomiting, hives) and cladribine chemotherapy (e.g., sweating, sleep disturbance, gastrointestinal problems, bone marrow toxicity) before treatment with avapritinib. Via compassionate care access, the patient was able to undergo treatment with avapritinib for 2 years at the time of the patient group submission, expressing immense gratitude for its life-changing impact in alleviating symptom burden and mental strain due to the disease, with no observable adverse effects.
There is a lack of accessible and effective treatments for patients with AdvSM in Canada. Patients seek better treatments that address the underlying disease, provide symptom relief, have tolerable side effects, allow the restoration of daily activities, and improve physical and mental well-being.
Clinician Input
Input From Clinical Experts Consulted by CDA-AMC
All CDA-AMC review teams include at least 1 clinical specialist with expertise regarding the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, providing guidance on the potential place in therapy). The following input was provided by 2 clinical specialists with expertise in the diagnosis and management of AdvSM.
Unmet Needs
The primary goals of treatment for patients with AdvSM are to improve health-related quality of life, improve the ability to work and maintain independence, prevent life-threatening anaphylaxis, reverse or delay progression of end organ damage, and prolong survival.
According to the clinical experts, there is a major treatment gap for patients with AdvSM in Canada. The off-label treatments currently available have low or unpredictable response rates, have a response of short duration, and may cause significant toxicity. The targeted therapy, midostaurin, is approved for the treatment of AdvSM in Canada but is not publicly funded and therefore is inaccessible. The clinical experts noted that internationally, KIT inhibitors are recommended by major guidelines as first-line treatment for patients with AdvSM.4 Most patients living in Canada with AdvSM do not have access to recommended first-line or second-line treatment, which represents a substantial care gap and equity issue; only patients who live near academic centres with the opportunity to participate in clinical trials or those with significant financial security may have access to recommended treatments.
Place in Therapy
The clinical experts stated that avapritinib would be used as first-line monotherapy in patients with AdvSM, except for patients who present very acutely and need rapid debulking with cladribine. In these cases, often a single cycle of cladribine could be offered for immediate disease control, followed by monotherapy with avapritinib. Avapritinib should not be used in patients with a platelet count of less than 50 multiplied by 109/L. A short course of midostaurin or cladribine may be used as initial cytoreduction to allow the platelet count to recover to greater than 50 multiplied by 109/L, then transition to avapritinib.
According to the clinical experts, avapritinib will be the second treatment approved to address the underlying disease process in patients with AdvSM and would cause a shift in the current treatment paradigm. The first drug approved that impacts the disease process, midostaurin, is currently inaccessible to patients in Canada.
Patient Population
As per the pivotal trials and the clinical expert input, patients most suitable for treatment with avapritinib include those who meet the WHO diagnostic criteria for AdvSM who are treatment-naive or who have received prior therapy for AdvSM. All subtypes of AdvSM (ASM, SM-AHN, and MCL) are predicted to benefit from avapritinib monotherapy, and the experts stated that in particular, patients with life-threatening organ damage and debilitating symptoms should be considered for treatment.
There is no companion diagnostic test needed other than the investigations outlined in the WHO diagnostic criteria, fifth edition. One expert indicated that there is some potential for the misclassification of patients with SM, such as those with indolent SM being classified as ASM. No other issues related to diagnosis or misdiagnosis were raised by the clinical experts. Patients with other mast cell disorders, such as mast cell activation syndrome, should not receive avapritinib.
Identifying which patients will have an optimal treatment response is not well defined and more research is needed in this area.
Assessing the Response Treatment
The clinical experts stated that the response criteria used in clinical trials continue to be frequently modified to best capture clinical benefit, better define long-term outcomes in the tyrosine kinase inhibitor era, and standardize response evaluation across clinical trials so that different drugs can be compared. Major response criteria that have been used in clinical trials and in clinical practice include the Valent criteria (plus its modified version), the Mayo criteria, the IMWG-MRT-ECNM criteria (plus its modified version), and more recently, the pure pathologic response criteria and the European Competence Network on Mastocytosis–American Initiative in Mast Cell Diseases criteria. The modified IWG-MRT-ECNM criteria used in the avapritinib trials are very specific and defining clinical responses to treatment can be complex due to the rigid criteria itself, drug adverse effects, and concomitant AHN, which makes it challenging to implement in a real-world setting. Many patients will have a partial response as per the aforementioned criteria but will have tremendous clinical improvement after starting treatment, which isn’t always captured by these response criteria. At this time, there are no clear data to suggest which response criteria perform better in terms of predicting long-term outcomes like survival.
According to the clinical experts consulted, the assessment of a clinically meaningful response requires the integration of patients’ goals of treatment with clinical and histopathological factors. From a clinical perspective, improvement in a patient symptom score is a critical part of the response assessment. Improvement in patients’ symptom scores often translates to improved quality of life and patient fitness. These, of course, are important factors for all patients but are additionally important if the goal is to improve fitness to proceed with an allogeneic hematopoietic stem cell transplant as patients with AdvSM can present with severe cachexia and poor performance status. This can limit the eligibility to proceed with an allogeneic stem cell transplant, which is the only curative treatment for AdvSM.
From a laboratory perspective, the normalization of complete blood counts and the reduction or absence of transfusion requirements not only improve patients’ quality of life but also liberates them and their caregivers from the time and financial burden of constantly needing to travel for count checks and transfusions. In those patients with liver involvement, the normalization of elevated liver enzymes, the reduction in liver size, and the reduction in the need for diuretics and/or therapeutic paracentesis have similar benefits on quality of life and reduced burden on the patient, caregivers, and health care system. Patients also commonly have splenomegaly and avapritinib can reduce spleen size, which is a key treatment target before an allogeneic hematopoietic stem cell transplant. The routine monitoring of basal serum tryptase levels is also an important surrogate for disease response.
From a histopathological perspective, a reduction in abnormal mast cell burden in bone marrow is a critical part of treatment response as well as treatment response to an AHN component such as improvement in blast count and the restoration of effective hematopoiesis. From a molecular perspective, the reduction in variant allele frequency of KIT variants is becoming an increasingly important marker for response to treatment, though 1 clinical expert stated that funding for this is not widely available in Canada.
Clinical and laboratory monitoring as summarized previously should be done at every visit, which is more frequent at the initiation of treatment. Outside of clinical trials, specific time points for the histopathological assessment of disease response are not well defined in the literature. Histopathological assessment should be done at 3 months after the initiation of avapritinib treatment and then can be considered every 3 months thereafter for the first 12 cycles of therapy and/or if there is evidence of loss of response or disease progression (e.g., worsening cytopenias or mastocytosis, increased peripheral blasts, increasing tryptase).
Discontinuing Treatment
As per the pivotal trials and input from the clinical experts, avapritinib should be discontinued in patients who are no longer getting clinical benefit from a symptom or quality of life perspective, in patients who experience intracranial bleeding, in patients with a platelet count lower than 50 multiplied by 109/L, in patients with persistent severe treatment-related AEs that cannot be managed with dose interruptions or dose reduction, in patients who are pregnant, or in patients where there is evidence of progressive disease of either the SM or AHN disease component.
Prescribing Considerations
Based on NCCN guidelines4 and clinical expert input, patients with AdvSM should be treated by medical teams with expertise in the diagnosis of, treatment of, and response assessment in AdvSM. For patients who live far from a centre, a shared care model with local partners should be considered.
Clinician Group Input
This section was prepared by the CDA-AMC review team based on the input provided by clinician groups. The full original clinician group input received by CDA-AMC is available on the CDA-AMC website.
Two clinician groups provided input for this review: Ontario Health (Cancer Care Ontario) Hematology Cancer Drug Advisory Committee (based on 2 clinicians) and the LLSC Clinician Network and Myeloproliferative Neoplasms Canada Clinician Group (based on 6 clinicians).
In general, the clinician groups’ input was consistent with the input provided by the clinical experts consulted for this review. The clinician groups agreed that there is a significant treatment gap for patients with AdvSM in Canada, who have poor outcomes with high symptomatic burden and a need for reduced transfusions, improved treatment administration, and affordable therapies. Goals of treatment for patients with AdvSM include controlling the disease, improving health-related quality of life, preventing life-threatening anaphylaxis, reversing end organ damage, minimizing severe adverse effects, and prolonging survival.
The clinician groups agreed that patients with AdvSM should be managed by hematologists or medical teams with expertise in diagnosis, treatment, and response evaluation. Input from clinician groups indicated that standardized response criteria are evolving and may be used in conjunction with evaluations of clinical benefit, including patient-reported symptoms and health-related quality of life, laboratory measurements (e.g., complete blood count and tryptase levels, spleen volume), and histopathological measurements (e.g., bone marrow measurements of abnormal mast cell burden, blast count).
Neither Ontario Health (Cancer Care Ontario) nor the LLSC group of clinicians reported experience with avapritinib; however, they anticipated that avapritinib would be used as first-line monotherapy and eligible for use in any line of therapy among patients with AdvSM in Canada. Ontario Health (Cancer Care Ontario) indicated that patients with ASM would be best suited for treatment with avapritinib since the driver mutation is present in 95% of these patients. The group of clinicians anticipated that patients with all subtypes of AdvSM would benefit from avapritinib, particularly among those with life-threatening organ damage and debilitating symptoms. However, they acknowledged that identifying which patients would have an optimal response is unclear and requires further research. The clinician groups agreed that treatment with avapritinib should be discontinued among patients whose health-related quality of life is impacted by a lack of clinical benefit, a platelet count of less than 50 multiplied by 109/L, detectable disease progression, or significant adverse effects.
Drug Program Input
The drug programs provide input on each drug being reviewed through the reimbursement review processes of CDA-AMC by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CDA-AMC are summarized in Table 4.
Table 4: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Relevant comparators | |
Currently, there is no standard of care for AdvSM. Comparators may include cladribine, interferon, imatinib, and midostaurin. Although midostaurin has been approved by Health Canada for AdvSM, it received a do not reimburse recommendation from CADTH. How does the efficacy and safety of avapritinib compare to the aforementioned? | According to the clinical experts, cladribine is the most accessible therapy for AdvSM, and response rates are typically low and of short duration. Funding for interferon is limited and it is difficult to access this drug. Further, it is not an appropriate treatment for patients who present acutely and require immediate disease control to prevent life-threatening organ failure as it may take up to a year of treatment before the patient demonstrates any improvement with therapy. Imatinib is only appropriate for a small subset of patients with AdvSM who do not have the KIT D816V mutation or have an unknown KIT mutational status (< 10%), and midostaurin is largely unavailable in Canada. Thus, the experts indicated that there is a significant unmet need for effective therapies to treat patients with AdvSM. The experts anticipated that avapritinib will offer a better, more durable response and better tolerated treatment for patients in Canada. |
Generalizability | |
Should patients currently on other systemic therapies be switched to avapritinib? | The experts indicated that patients who are stable on an existing therapy would likely remain on that treatment, unless they were experiencing toxicity or showing signs of disease progression. |
AdvSM = advanced systemic mastocytosis.
Clinical Evidence
The objective of the CDA-AMC Clinical Review Report is to review and critically appraise the clinical evidence submitted by the sponsor on the beneficial and harmful effects of avapritinib oral tablets in the treatment of adult patients with AdvSM, including ASM, SM-AHN, and MCL. The focus will be placed on comparing avapritinib to relevant comparators and identifying gaps in the current evidence.
A summary of the clinical evidence included by the sponsor in the review of avapritinib is presented in 2 sections, with the CDA-AMC critical appraisal of the evidence included at the end of each section. The first section, the systematic review, includes pivotal studies and other studies that were selected according to the sponsor’s systematic review protocol. The CDA-AMC assessment of the certainty of the evidence in this first section using the GRADE approach follows the critical appraisal of the evidence. The second section includes indirect evidence from the sponsor. No long-term extension studies or studies addressing gaps in the evidence were submitted by the sponsor.
Included Studies
Clinical evidence from the following is included in the CDA-AMC review and appraised in this document:
2 pivotal studies identified in the systematic review
2 studies with indirect evidence (1 indirect treatment comparison, and 1 observational comparison).
Systematic Review
Content in this section has been informed by materials submitted by the sponsor. The following has been summarized and validated by the CDA-AMC review team.
Description of Studies
Characteristics of the included studies are summarized in Table 5.
Two single-arm, open-label studies met the inclusion criteria for the systematic review: EXPLORER and PATHFINDER studies.
The EXPLORER study was a phase I study to evaluate the safety, tolerability, pharmacokinetics, pharmacodynamics, and efficacy of avapritinib. Eligible patients were adults with AdvSM and relapsed or refractory myeloid malignancies. The EXPLORER study was completed in 2 parts.
Part 1 was a dose escalation study to determine the maximum tolerable dose and recommended phase II dosage. Part 1 used a 3 plus 3 design, with the first patients receiving avapritinib 30 mg daily, escalating to a maximum of 400 mg per day (N = 32). The primary outcomes were safety, maximum tolerable dose, and recommended phase II dosage.
Table 5: Details of Studies Included in the Systematic Review
Detail | EXPLORER study (BLU-285 to 2101) | PATHFINDER study (BLU-285 to 2202) |
|---|---|---|
Designs and populations | ||
Study design | Phase I, open-label study in 2 parts:
| Phase II, open-label study (ongoing) |
Locations | 2 centres in the UK and 9 centres in the US | 10 sites in the US, 1 site in Canada, 3 sites in Germany, 1 site in Italy, 1 site in Norway, 1 site in Poland, 1 site in Spain, and 1 site in the UK |
Key dates | Start date: March 10, 2016 First data cut-off date: May 27, 2020 Final data cut-off date: January 19, 2023 | Start date: November 21, 2018 First data cut-off date: June 23, 2020 Second data cut-off date: September 09, 2022 |
Randomized (N) | First and second data cut-offs: 86 patients (safety population, RAC adjudication)
Part 1: 32 patients Part 2: 54 patients
| First data cut-off: 62 patients (32 patients in cohort 1 and 30 patients in cohort 2)
Second data cut-off: 105 patients (81 patients in cohort 1 and 24 patients in cohort 2), excluding 2 patients who received avapritinib 100 mg as a starting dose
|
Key inclusion criteria |
|
|
Key exclusion criteria |
|
|
Drugs | ||
Intervention | Avapritinib orally once daily in 28-day cycles Part 1: Dose escalation with a starting dose of 30 mg, then 60 mg, 100 mg, 130 mg, 200 mg, 300 mg, and 400 mg daily Part 2: Starting doses were 300 mg daily in cohort 1 and 200 mg daily in cohort 2a | Avapritinib orally once daily and continuously for 28-day cycles Starting dose of 200 mg daily, or 100 mg daily for patients with platelet counts from 25 × 109/L to 50 × 109/L at baseline (protocol later modified to exclude patients with platelet count < 50 × 109/L) |
Comparator | No comparator (single-arm trial) | No comparator (single-arm trial) |
Study duration | ||
Screening phase | 56 days | 56 days |
Treatment phase | Enrolment period of up to 48 months; study completed when all patients were no longer receiving study drug | Interim analysis: When 32 patients were evaluable for response Final analysis: When 63 patients had had the opportunity for 10 cycles of treatment |
Follow-up phase | 14 days after last dose, with a safety follow-up at 30 days; survival follow-up was conducted every 3 months until death or study closure | Same as the EXPLORER study |
Outcomes | ||
Primary end point |
| Adjudicated ORR per modified IWG-MRT-ECNM criteriaa |
Secondary and exploratory end points | Secondary end points
Exploratory end points
| Key secondary end point
Secondary end points
Exploratory end point (both cohorts)
|
Publication status | ||
Publications | EXPLORER study interim Clinical Study Report28 EXPLORER study final Clinical Study Report15 DeAngelo et al. (2021)29 NCT0256198830 | PATHFINDER study interim Clinical Study Report16 PATHFINDER study clinical summary document17 Gotlib et al. (2021)31 NCT0358065532 |
AdvSM = advanced systemic mastocytosis; AdvSM-SAF = Advanced Systemic Mastocytosis Symptom Assessment Form; AHN = associated hematologic neoplasm; ALT = alanine aminotransferase; AML = acute myeloid leukemia; ASM = aggressive systemic mastocytosis; AST = aspartate aminotransferase; BM = bone marrow; ECOG PS = Eastern Cooperative Oncology Group Performance Status; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; ISM = indolent systemic mastocytosis; IWG-MRT-ECNM = International Working Group - Myeloproliferative Neoplasms Research and Treatment - European Competence Network on Mastocytosis; MC = mast cell; MCL = mast cell leukemia; ORR = overall response rate; PGI-S = Patient Global Impression–Severity; RAC = Response Assessment Committee; RAC-RE = Response Assessment Committee–Response Evaluable; SM-AHN = systemic mastocytosis with an associated hematologic neoplasm; SSM = smouldering systemic mastocytosis; ULN = upper limit of normal; VAF = variant allele frequency.
Note: C-findings include thrombocytopenia, anemia, and neutropenia due to BM involvement; splenomegaly with hypersplenism; and elevated AST and ALT, hypoalbuminemia, and ascites due to liver infiltration.
aBased on protocol amendment 7, patients subsequently enrolled in cohort 1 of the EXPLORER study received a starting dose of 200 mg daily.
bResponse-based outcomes were evaluated in the RAC-RE population.
cPatients from both cohorts from part 2 of the EXPLORER study.
Sources: Clinical Study Reports for the EXPLORER study,15,28 interim Clinical Study Report for the PATHFINDER study,16 clinical summary for the PATHFINDER study,17 and Sponsor Summary of Clinical Evidence.14 Additional data supplied by the sponsor (June 17, 2024).18
Part 2 of the EXPLORER study was an open-label extension to further evaluate the safety, tolerability, pharmacokinetics, and efficacy of avapritinib. For part 2, patients with a local diagnosis of AdvSM (N = 54) were enrolled and received an avapritinib starting dose of 300 mg daily. Protocol amendments were implemented during the EXPLORER study and with protocol amendment 6, a second cohort was added that enrolled patients who were evaluable according to the modified IWG-MRT-ECNM criteria (i.e., required to have at least 1 measurable C-finding attributable to SM, except for patients with a diagnosis of MCL). Patients in cohort 2 received a starting dose of 200 mg per day. Those who were not evaluable according to the modified IWG-MRT-ECNM criteria continued to be enrolled in cohort 1 and received a starting dose of 300 mg daily, until the implementation of protocol amendment 7, when the starting dose was reduced to 200 mg daily.
A total of 86 patients were enrolled from the US and UK, including 32 patients who entered part 1 and an additional 54 patients who entered part 2. No patients from part 1 continued into part 2 of the study. The first patient in the EXPLORER study was enrolled on March 10, 2016, an initial data cut-off was made on May 27, 2020, and a final data cut-off was made on January 19, 2023. In total, there were 4 data cut-off dates in support of regulatory requirements. In this report, data from the final data cut-off of January 19, 2023, have been summarized. The study schematic is shown in Figure 1. Outcome data from patients who received any dose of avapritinib (30 mg daily to 400 mg daily) were included in this report; however, the recommended starting dose is 200 mg daily according to the product monograph. Data from the avapritinib 200 mg subgroup (N = 21) have also been presented.
Figure 1: Study Schematic for the EXPLORER Study
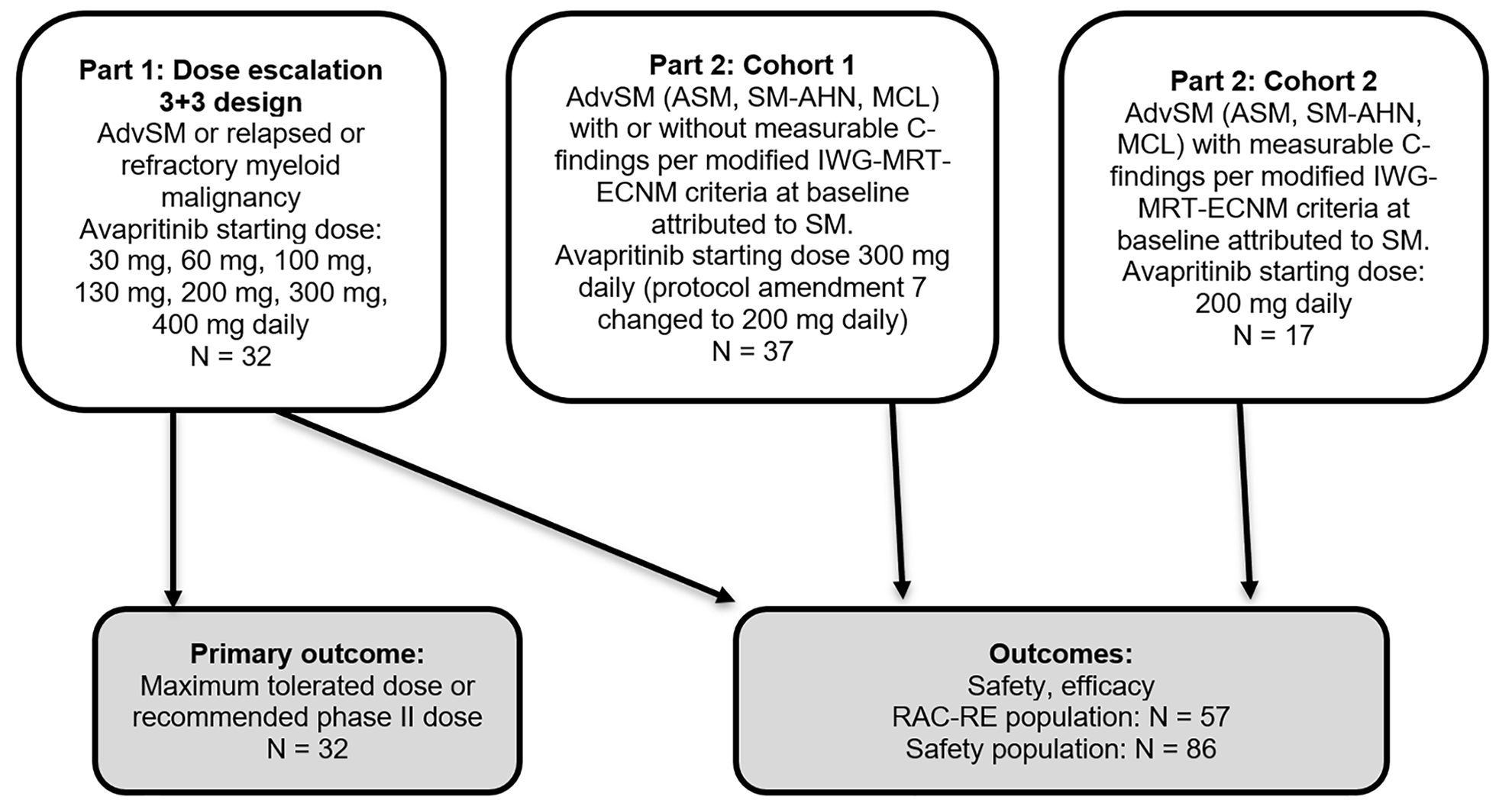
AdvSM = advanced systemic mastocytosis; ASM = aggressive systemic mastocytosis; IWG-MRT-ECNM = International Working Group - Myeloproliferative Neoplasms Research and Treatment - European Competence Network on Mastocytosis; MCL = mast cell leukemia; RAC-RE = Response Assessment Committee–Response Evaluable; SM = systemic mastocytosis; SM-AHN = systemic mastocytosis with an associated hematologic neoplasm.
Sources: Created by CDA-AMC based on data from the final Clinical Study Report for the EXPLORER study15 and additional data supplied by the sponsor (June 17, 2024).18
The PATHFINDER study is an ongoing, single-arm, phase II study (Figure 2). Adults with AdvSM (ASM, myeloid SM-AHN, or MCL) were enrolled in 2 cohorts based on the presence of evaluable AdvSM C-findings at baseline. The objective of the study is to determine the adjudicated ORR according to the modified IWG-MRT-ECNM criteria. The study was to continue until 63 patients had the opportunity to receive 10 cycles, with a planned interim analysis when 32 patients were evaluable for response. The study includes patients from Canada, the US, and Europe. The first patient was enrolled on November 21, 2018, with an initial data cut-off on June 23, 2020 (62 patients) and 3 other data cut-offs for outcome adjudication and publication purposes (April 2021, September 2022, and September 2023). This report has summarized the data from the June 23, 2020, data cut-off date (the first data cut-off and planned interim analysis, with 62 patients) and the September 9, 2022, data cut-off date — hereafter referred to as the second data cut-off (with 105 patients). According to the sponsor, the final Clinical Study Report is expected to be available in the first quarter of 2025.
Figure 2: Study Schematic for the PATHFINDER Study
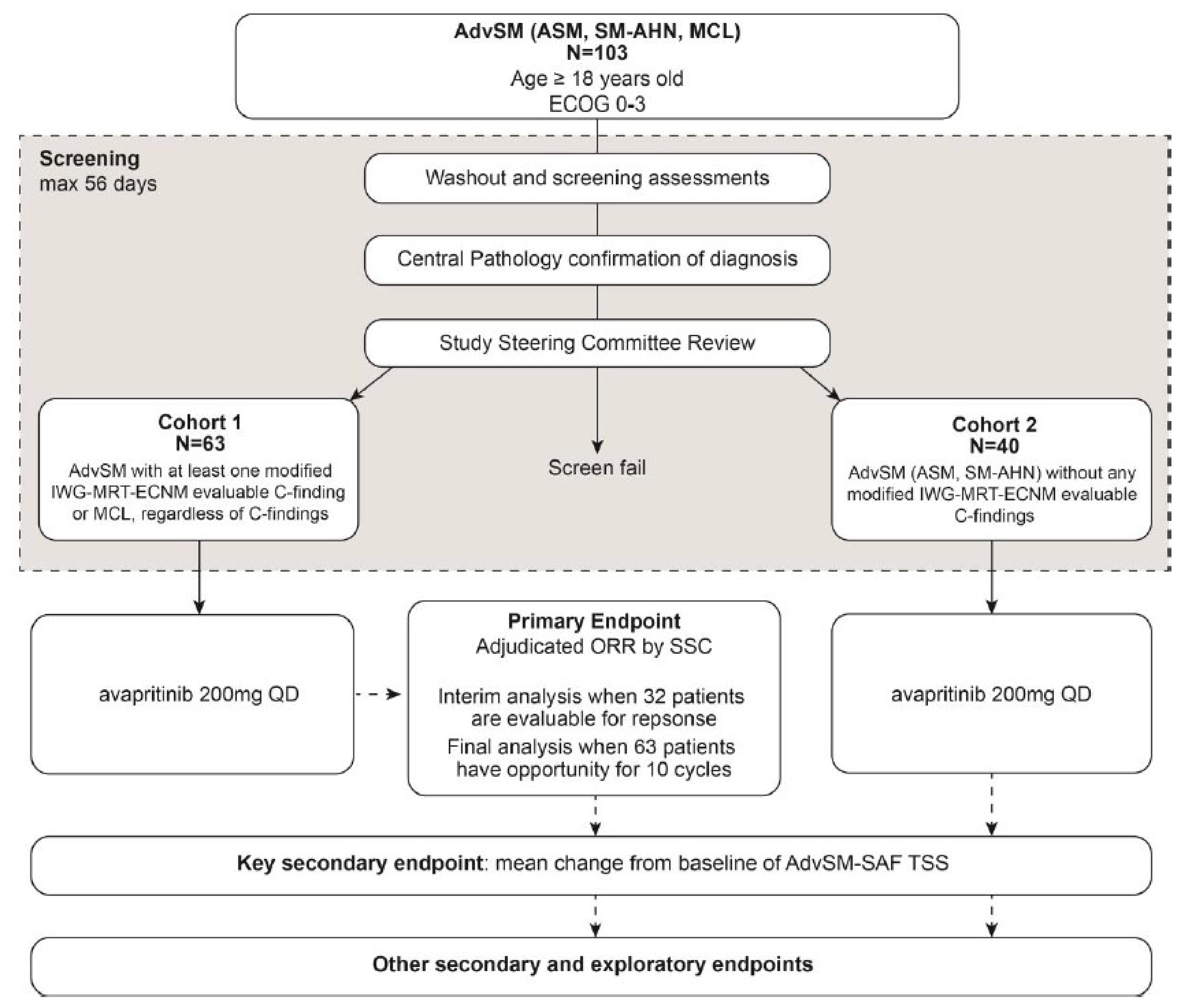
AdvSM = advanced systemic mastocytosis; AdvSM-SAF = Advanced Systemic Mastocytosis Symptom Assessment Form; ASM = aggressive systemic mastocytosis; CDA-AMC = Canada’s Drug Agency; ECOG = Eastern Cooperative Oncology Group; IWG-MRT-ECNM = International Working Group - Myeloproliferative Neoplasms Research and Treatment - European Competence Network on Mastocytosis; MCL = mast cell leukemia; ORR = overall response rate; QD = once a day; SM-AHN = systemic mastocytosis with an associated hematologic neoplasm; SSC = Study Steering Committee; TSS = total symptom score.
Note: The sponsor stated that this figure is based on the interim Clinical Study Report for the PATHFINDER study; 2 additional patients (to a total of 105) were enrolled after that cut-off and are accounted for in the clinical summary document for the PATHFINDER study. The CDA-AMC reviewer noted that the number of patients in cohort 1 and cohort 2 are inconsistent with the additional data supplied by the sponsor (June 17, 2024),18 which states 83 patients were included in cohort 1 and 24 patients were included in cohort.2.
Source: Interim Clinical Study Report for the PATHFINDER study.16
Populations
Inclusion and Exclusion Criteria
For the EXPLORER and PATHFINDER trials, eligible patients were aged 18 years or older and had 1 of the following diagnoses (based on WHO diagnostic criteria): ASM, SM-AHN, or MCL. For patients with SM-AHN, the hematologic neoplasm must have been myeloid or incidental indolent, low-grade, lymphoid AHNs (e.g., chronic lymphocytic leukemia) not requiring treatment. C-findings included thrombocytopenia, anemia, and neutropenia due to bone marrow involvement; splenomegaly with hypersplenism; elevated aspartate aminotransferase and alanine aminotransferase due to liver infiltration; hypoalbuminemia; and symptomatic ascites or pleural effusion requiring medical intervention.
In the EXPLORER study, patients with histologically or cytologically confirmed myeloid malignancy that was relapsed or refractory to standard treatments were eligible for enrolment to part 1, the dose escalation phase, but not part 2. In part 2, patients were eligible if they had a local diagnosis of AdvSM (whose subtypes are ASM, SM-AHN, or MCL), including those patients with or without measurable C-findings at baseline attributed to SM (according to the modified IWG-MRT-ECNM criteria). With protocol amendment 6, a second cohort was added that included modified IWG-MRT-ECNM–evaluable patients only (i.e., must have had at least 1 measurable C-finding per modified IWG-MRT-ECNM criteria at baseline, attributed to SM, unless the diagnosis was MCL, which did not require a C-finding).
Patients in the PATHFINDER study were required to have a bone marrow biopsy within 56 days of the first dose of avapritinib and be on stable doses of non-antineoplastic SM therapies and corticosteroids (as supportive care) for 14 days or more before screening. The PATHFINDER study enrolled adults with AdvSM into 2 cohorts.
Cohort 1 — This cohort consisted of patients with 1 or more modified IWG-MRT-ECNM criteria for evaluable disease (i.e., had severe and quantifiable organ damage [an evaluable C-finding] or had MCL [regardless of C-findings]) as confirmed by the Study Steering Committee.
Cohort 2 — This cohort consisted of patients who were not considered eligible for an adjudicated response and were confirmed centrally to have ASM or SM-AHN but were lacking an evaluable C-finding as determined by the Study Steering Committee.
The sponsor stated that patients were assessed by the Study Steering Committee throughout the study on whether they continued to meet the criteria for each cohort and could transition between cohorts, if their eligibility status changed.33
In the PATHFINDER study, enrolment of the SM-AHN subgroup was capped at approximately 70% of the planned 63-patient sample size of cohort 1 (i.e., a maximum of 45 patients), which the sponsor stated was to ensure that the study population reflects the general AdvSM patient population.
Patients were excluded from the EXPLORER and PATHFINDER studies if they had liver, renal, or hematological abnormalities (low platelet or neutrophil count), eosinophilia and positivity for the FIP1L1-PDGFRA fusion, a diagnosis of high-risk or very high-risk acute myeloid leukemia, myelodysplastic syndrome, or Philadelphia chromosome–positive malignancy. Patients were also excluded from the EXPLORER and PATHFINDER studies if they underwent antineoplastic therapy less than 14 days before bone marrow assessment or had radiotherapy or major surgical procedures less than 14 days before the first dose of the study drug.
Interventions
In both studies, open-label avapritinib treatment was administered orally once daily in the morning from day 1 to day 28 in 28-day cycles. Dosing was continuous with no intercycle rest periods. The drug was supplied as capsules in the EXPLORER study and as tablets in the PATHFINDER study.
In part 1 of the EXPLORER trial, the first patients were administered avapritinib 30 mg once daily and in subsequent cohorts, the dose increased to 60 mg, 100 mg, 130 mg, 200 mg, 300 mg, and 400 mg daily. Dose escalation proceeded at increments of up to 100% until 1 or more patients treated at a given dose had at least a grade 2 nonhematologic AE or a grade 4 hematologic AE and the AE (nonhematologic or hematologic) was not clearly attributable to a cause other than avapritinib, or the dose exceeded the highest dose determined to be safe in the EXPLORER study. Based on part 1, the recommended phase II dose was set as 300 mg daily, and patients enrolled in part 2 initially received this dose. According to the sponsor, further data revealed that most patients who started at the 300 mg dose reduced their dose to 200 mg daily, most often due to cytopenia, fluid retention, and/or gastrointestinal or cognitive AEs. The study protocol was amended to add a second cohort that included only modified IWG-MRT-ECNM–evaluable patients who received a starting dose of 200 mg daily. Nonevaluable patients continued to enrol in cohort 1 at 300 mg daily; however, with protocol amendment 7 (dated April 17, 2019), enrolment at 300 mg daily ended and all patients enrolled at 200 mg daily.
In the EXPLORER study, intrapatient dose modification was allowed for patients in part 1 to minimize the number of patients treated at potentially inactive doses. Patients who completed 2 or more cycles without experiencing a grade 3 or higher nonhematologic toxicity or a grade 4 hematologic toxicity could have their dose escalated (up to the maximum tolerated dose). Patients who experienced dose-limiting toxicity during cycle 1 of part 1 had avapritinib treatment interrupted until the AE resolved (defined as ≤ grade 1 or the patient’s baseline value), with platelet counts of at least 25 multiplied by 109/L and an absolute neutrophil count of at least 0.5 multiplied by 109/L. After resolution of the AE, patients could resume avapritinib with a reduction of 1 dose level, or at the previous dose with the sponsor’s approval. If the patients required a dose interruption of more than 3 weeks due to an AE that was considered related to avapritinib, the treatment was discontinued.
During part 2 of the EXPLORER study (and after the dose escalation phase of part 1), dose modifications and re-escalation were allowed. Specific criteria were outlined for patients who developed thrombocytopenia, cognitive adverse effects, or another toxicity, with stepwise dose reductions (≥ 200 mg to 100 mg, then 50 mg, and 25 mg) and with treatment stopped if the AE occurred at the 25 mg daily dose level. After resolution of the AE, stepwise re-escalation up to the starting dose was allowed, with each dose level administered for 1 cycle before moving to the next higher dose. Dose interruptions of up to 56 days were allowed, and any longer interruptions had to be approved by the medical monitor. The study drug was discontinued if the patient experienced intracranial bleeding of any grade.
In the PATHFINDER study, the avapritinib starting dose was 200 mg daily. To manage thrombocytopenia and bleeding risk, the starting dose was reduced to 100 mg daily for patients with platelet counts of between 25 multiplied by 109/L and 50 multiplied by 109/L at baseline (protocol amendment 3). Subsequently, based on protocol amendment 5, patients with platelet counts of less than 50 multiplied by 109/L at baseline were excluded from the enrolment. During the trial, dose reductions for thrombocytopenia or another toxicity were permitted, with patients first dropping to 100 mg daily, then 50 mg daily, and 25 mg daily. Patients on the 25 mg dose who required a dose reduction either had treatment interrupted or permanently discontinued. Doses could be interrupted for up to 56 days, but if nonhematologic avapritinib-related toxicity did not resolve to grade 2 or lower, or had not returned to baseline, then the sponsor’s medical monitor was contacted. Stepwise re-escalation from a reduced dose up to the initial starting dose was allowed, with each dose increase administered for 1 cycle before the next dose increase started. Dose escalation was allowed if the prior dose was well tolerated (e.g., no grade 3 or grade 4 AEs). After 8 weeks of treatment, the investigator was permitted to increase the dose to 300 mg daily (in the absence of toxicity) for suboptimal response. Suboptimal response was defined as no better than stable disease by day 1 of cycle 3 or later, according to the modified IWG-MRT-ECNM response criteria. If a patient experienced study drug-related intracranial bleeding of any grade, the study drug was permanently discontinued.
In the PATHFINDER study, palliative and supportive care for disease-related symptoms were permitted. This included histamine blockers, proton pump inhibitors, osteoclast inhibitors, leukotriene inhibitors, corticosteroids (not to exceed 20 mg of prednisone or an equivalent per day), cromolyn sodium or another mast cell stabilizer, and omalizumab. Antiemetics and hematopoietic growth factors could be used at the investigator’s discretion and in accordance with clinical guidelines. Similar criteria for concomitant medications were applied during the EXPLORER study.
Patients were prohibited from receiving strong CYP3A4 inhibitors, or strong or moderate CYP3A4 inducers, as well as any other antineoplastic treatments (excluding local radiotherapy to treat localized bone lesions) in both studies. Patients were withdrawn from the studies if they experienced study drug-related intracranial bleeding of any grade, pregnancy, death, confirmed SM progressive disease (4 weeks after initial documentation), confirmed AHN progressive disease requiring the initiation of other cytoreductive therapy, SM or AHN clinical progression (i.e., not meeting the modified IWG-MRT-EDNM criteria) requiring alternative cytoreductive treatment, the initiation of other cytoreductive therapy, the withdrawal of consent, or as the result of an investigator or sponsor decision. Patients may have been withdrawn due to AEs, nonadherence, protocol deviation, investigator decision, or loss to follow-up.
Outcomes
A list of efficacy end points assessed in this Clinical Review Report is provided in Table 6, followed by descriptions of the outcome measures. Summarized end points are based on outcomes included in the Sponsor Summary of Clinical Evidence as well as any outcomes identified as important to this review, according to the clinical experts consulted for this review and input received from patient and clinician groups and public drug plans. Using the same considerations, the review team selected end points that were considered the most relevant to inform the expert committee deliberations and finalized this list of end points in consultation with members of the expert committee. All summarized efficacy end points were assessed using GRADE. Select notable harms outcomes considered important for informing the expert committee deliberations were also assessed using GRADE.
Table 6: Outcomes Summarized From the Studies Included in the Systematic Review
Outcome measure | Time point | EXPLORER study | PATHFINDER study |
|---|---|---|---|
ORR (CR + CRh + PR + ClinI based on modified IWG-MRT-ECNM criteria) | On treatment | Secondary | Primarya |
OS | The time from the start of treatment to the date of death | Exploratory | Secondary |
Change from baseline in AdvSM-SAF TSS | Cycle 11, day 1 | Secondary | Key secondaryb |
Duration of response | The time from the first documented response to the date of the first documented progressive disease, loss of response, or death | Secondary | Secondary |
Time to response | The time from the start of treatment to the date of the first documented response | Exploratory | Secondary |
PFS | The time from the start of treatment to the date of the first documented progressive disease or death due to any cause | Exploratory | Secondary |
SAE | On treatment | Other | Other |
Intracranial bleed | On treatment | Other | Other |
Cognitive adverse events | On treatment | Other | Other |
AdvSM-SAF = Advanced Systemic Mastocytosis Symptom Assessment Form; ClinI = clinical improvement; CR = complete remission; CRh = complete remission with partial hematological recovery; IWG-MRT-ECNM = International Working Group - Myeloproliferative Neoplasms Research and Treatment - European Competence Network on Mastocytosis; ORR = overall response rate; OS = overall survival; PFS = progression-free survival; PR = partial remission; SAE = serious adverse event; TSS = total symptom score.
Note: One cycle is 28 days in length.
aThere was a planned interim analysis of ORR once 32 patients enrolled in cohort 1 in the PATHFINDER study were evaluable for response. The null hypothesis was to be rejected if the 1-sided P value was less than 0.00625, and then the interim analysis would be used to support a marketing application.
bAnalysis of AdvSM-SAF TSS at cycle 11, day 1, was a key secondary end point and analyzed in a sequential manner if the primary end point in the PATHFINDER study was met to control the studywise type I error rate.
Sources: Clinical Study Report for the EXPLORER study15 and interim Clinical Study Report for the PATHFINDER study.16
Based on input received, overall response rate, OS, duration of response, time to response, and patient-reported symptoms were identified as important outcomes. The clinical experts consulted for this review selected these end points based on their relevance to patients and their use in making treatment decisions. PFS was also considered relevant by the clinical experts and was used to inform the pharmacoeconomic analysis. While the patient input stated that adverse effects of treatment were a significant concern, SAEs, cognitive AEs, and intracranial bleeding were selected as the key harms for avapritinib due to their potential to cause substantial morbidity. The clinical experts discussed the heterogeneity among patients with AdvSM, and thus identified AdvSM subtype as subgroups of interest. Data for subgroups based on prior antineoplastic therapy were also included in the Clinical Review Report to inform the pharmacoeconomic analysis (specifically PFS). Based on input from the clinical experts, the GRADE assessment focused on the overall AdvSM population in the EXPLORER study regardless of the starting dose received, as the mean daily dose was similar to that of the PATHFINDER study, which used the Health Canada recommended starting dose of 200 mg daily.
At the request of the sponsor, data for the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 (EORTC QLQ-C30) global health score were added to Appendix 1 but were not evaluated using GRADE.
Overall Response
The primary end point for the PATHFINDER study, and a secondary end point for the EXPLORER study, was adjudicated ORR assessed by the modified IWG-MRT-ECNM criteria (Table 7), which the sponsor stated were modified from the original IWG-MRT-ECNM criteria in consultation with AdvSM experts, regulatory authorities, and authors who published the initial criteria, to address some issues and challenges that were noted in the EXPLORER trial.15 The key modification was to add a subcategory for patients with CRh. The modified criteria also allowed for a 4-week confirmation of progressive disease, rather than the 8-week time frame in the original criteria. Changes were also made to the criteria for patients with splenomegaly to remove criteria requiring the resolution of difficult to measure or subjective symptoms.15
Assessments of response were based on bone marrow biopsy and aspirate, serum tryptase, organomegaly on imaging and physical examination, and the assessment of ascites and pleural effusions, which were performed at baseline and repeated at cycle 3, cycle 5, cycle 7, cycle 11, and cycle 18, and then every 6 months thereafter (a bone marrow biopsy was not performed in cycle 5). Investigators were also asked for their subjective assessment if worsening in these findings was attributed to SM. Bone marrow samples, radiographs, and laboratory samples were evaluated centrally by independent specialists. The Response Assessment Committee (RAC) adjudicated response during response assessment meetings, held twice a year, using available data from all visits. The RAC reviewed central pathology assessments, tryptase levels, and imaging, together with local data to assess C-finding changes.
The ORR was defined as the proportion of patients in the RAC-RE population who had an adjudicated best response of CR, CRh, PR, or clinical improvement based on the modified IWG-MRT-ECNM criteria shown in Table 7. Patients meeting response criteria were confirmed 12 or more weeks after the initial response was documented.
Overall Survival
For both studies, OS was defined as the time from the start of treatment to the date of death. Patients who died before or on the data cut-off date were considered to have had an OS event. All patients who did not have a death record before or on the cut-off date were censored at the last date known alive. Survival follow-up occurred every 3 months until death or closure of the study by the sponsor.
Advanced Systemic Mastocytosis Symptom Assessment Form
The AdvSM-SAF is a patient-reported, 10-item symptom questionnaire that can be scored at the item level and domain level, and summed for a total daily score. It includes the severity of 8 symptoms over a 24-hour recall period (abdominal pain, nausea, vomiting, diarrhea, spots, itching, flushing, and fatigue) that were each scored on a numeric rating scale from 0 (indicating no symptoms) to 10 (indicating worst symptoms imaginable) and the frequency of vomiting and diarrhea using a discrete numerical value.34 At the domain level, a gastrointestinal symptom score comprised 4 items (abdominal pain, nausea, vomiting, and diarrhea; the daily domain score was 0 to 40) and a skin symptom score comprised 3 items (spots, itching, and flushing; the daily domain score was 0 to 30).34 The daily TSS was calculated by summing all items (excluding the frequency items) for a total score of 0 to 80.34
The change from baseline in the AdvSM-SAF TSS was a secondary end point in the EXPLORER study part 2 and a key secondary end point in the PATHFINDER study. Patients in both studies completed the AdvSM-SAF daily using an electronic diary from 7 days before the first dose of the study drug to cycle 12, day 28, in the EXPLORER study, and up to cycle 17, day 28, in the PATHFINDER study. The individual symptom, domain, or TSSs are determined by the 7-day average for the prior week, where at least 4 of the 7 days have a score available.
The sponsor developed the AdvSM-SAF to address the lack of patient-reported tools validated among patients with AdvSM. The sponsor designed the AdvSM-SAF using concept elicitation interviews with clinician experts and patients with AdvSM for evaluating symptoms in patients with AdvSM.34 Based on patients with AdvSM enrolled in cohort 1 (300 mg; n = 35) and cohort 2 (200 mg; planned n = 20) of the expansion phase of the EXPLORER study, 31 patients were included in the evaluation of the AdvSM-SAF using the reference measure of the EORTC QLQ-C30, the Patient Global Impression–Severity (PGI-S), and the ECOG PS.34 Patients had a mean age of 63.7 (SD = 10.3) years and consisted of 51.6% females and 48.4% males, and most had an ECOG PS score of 1 (35.5%), a KIT D816V mutation (87.1%), and a median tryptase level of 217.8 ng/mL (range, 12.8 ng/mL to 765.3 ng/mL).34 Construct validity evaluated using Spearman correlation coefficients indicated strong correlations for the TSS with the PGI-S (r = 0.614) and the EORTC QLQ-C30 on fatigue (r = 0.710), pain (r = 0.752), and nausea and vomiting (r = 0.811).34 Among patients with a baseline and at least 1 follow-up visit score, internal consistency reliability was met (Cronbach alpha > 0.7) for all AdvSM-SAF items and the TSS.34 Among patients with AdvSM-SAF scores at baseline who did not have a change in their ECOG PS score from baseline to day 18 of cycle 1, test-retest reliability between day 1 and day 8 of cycle 1 was met (intraclass correlation > 0.7) for all AdvSM-SAF items and the TSS.34 Change scores in the gastrointestinal symptom score were moderately to strongly correlated with change scores in the PGI-S, serum tryptase levels, and EORTC QLQ-C30 items and domains (r = 0.240 to 0.697).34 Change scores in the skin symptom score were moderately correlated with the change scores in ECOG PS, and the EORTC QLQ-C30 items of dyspnea, insomnia, and fatigue (r = 0.341 to 0.433).34 Change scores in the TSS were moderately to strongly correlated with change scores in the PGI-S, ECOG PS, and EORTC QLQ-C30 items and domains (r = 0.306 to 0.812).34 Using anchor-based methods, within-person MIDs were estimated as 6 to 9 for the gastrointestinal symptom score, 1 to 4 for the skin symptom score, and 9 to 14 for the TSS.34 Using distribution-based methods, between-group differences were estimated as 2 to 4 for the gastrointestinal symptom score, 2 to 3 for the skin symptom score, and 4 to 7 for the TSS.34
European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30
EORTC QLQ-C30 is a 30-item questionnaire that includes 5 functional domains (physical, cognitive, role, emotional, and social), 3 symptom scales (fatigue, nausea and vomiting, and pain), a global health status or quality of life scale, and 6 single items (dyspnea, insomnia, appetite loss, constipation, diarrhea, and financial difficulties). Each subscale and single item are evaluated on a standardized scale of 0 to 100; higher scores indicate better functioning (functional scales), better quality of life (the global health status scale), or poorer symptoms (symptom scales and single items). Patients completed the EORTC QLQ-C30 on day 1 of each cycle in the PATHFINDER study, and day 1 of cycle 1 to cycle 12 of part 2 of the EXPLORER study. The sponsor was not aware of a reported MID for the EORTC QLQ-C30 specifically in AdvSM but cited 2 publications of studies in other cancers. In patients with multiple myeloma, the estimated MID was 8 points to 12 points.35 A review of 21 studies in 9 different cancer types (brain, breast, colorectal, head or neck, lung, melanoma, ovarian, and prostate) reported that most anchor-based MID estimates ranged from 5 points to 10 points but varied by scale, improvement or deterioration, within or between comparisons, and by cancer type.36 The anchor-based MID for the within-group change in the global health status score ranged from 4 to 14 for improvement and −11 to −5 for deterioration.36
Duration of Response
For the EXPLORER and PATHFINDER trials, duration of response was defined as the time from the first documented overall response to the date of first documented progressive disease, loss of response, or death due to any cause, whichever occurred first. Responses were determined by modified IWG criteria. Patients who were still in response at the data cut-off date were censored at their last valid assessment. Patients without confirmed response were excluded from this analysis.
Time to Response
In both studies, time to response was defined as the time from the start of treatment to the time an overall response by modified IWG-MRT-ECNM criteria was first met. Patients without confirmed response were excluded from this analysis.
Progression-Free Survival
In the EXPLORER and PATHFINDER trials, PFS was defined as the time from the start of treatment to the date of first documented progressive disease or death due to any cause, whichever occurred first. For patients without an event, PFS was censored at the date of the last valid assessment that noted loss of response or better. Development of acute myeloid leukemia was considered disease progression. Progressive disease was confirmed 4 weeks after initial documentation as per the modified IWG-MRT-ECNM criteria.
Safety
The sponsor identified 2 AEs of special interest, cognitive effects and intracranial bleeding; AEs related to these events were aggregated. In both studies, cognitive effects consisted of 4 preferred terms: cognitive disorder, confusional state, encephalopathy, and memory impairment, and intracranial bleeding consisted of 3 preferred terms: cerebral hemorrhage, hemorrhage intracranial, and subdural hematoma.
Treatment-emergent AEs were defined as any AE occurring during or after administration of the first dose of avapritinib through to 30 days after the last dose, and any event considered study drug related regardless of the start date. It also included events present at baseline that worsened or subsequently were considered to be treatment-related by the investigator. Disease progression was not reported as an AE. SAEs were any event that was fatal or life-threatening, or led to inpatient hospitalization or prolongation of hospitalization, persistent or significant disability or incapacity, or a congenital anomaly or birth defect, or was an important medical event that jeopardized the patient and required intervention to prevent 1 of the SAEs described earlier. Intracranial bleeding was considered an SAE.
Table 7: Modified IWG-MRT-ECNM Consensus Response Criteria in Advanced Systemic Mastocytosis
Response | Criteria for response | |
|---|---|---|
CRa | Requires all 4 of the following criteria, and response duration must be ≥ 12 weeks:
| |
CRha | Requires that all criteria for CR be met and response duration must be ≥ 12 weeks; however, a patient may have residual cytopenias. The following minimum recovery of peripheral blood counts is required:
| |
PRa | Requires all 3 of the following criteria to be met, and response duration must be ≥ 12 weeks, in the absence of CR or CRh, and PD:
| |
ClinIa | Response duration must be ≥ 12 weeks Requires 1 or more of the nonhematologic and/or hematologic response criteria to be fulfilled in the absence of CR, CRh, PR, or PD. | |
Stable disease | Not meeting criteria for CR, CRh, PR, ClinI, or PD | |
PD | Requires at least 1 element from the following criteria to have been met (duration must be ≥ 4 weeks) | |
Baseline | Postbaseline | |
Any grade 2 nonhematologic organ damage |
| |
≥ grade 2 albumin |
| |
≥ grade 3 nonhematologic organ damage |
| |
≥ grade 2 transfusion-independent anemia or thrombocytopenia |
| |
Transfusion-dependent anemia or thrombocytopenia |
| |
≥ grade 3 neutropenia |
| |
Baseline spleen size of not palpable or < 5 cm |
| |
Splenomegaly ≥ 5 cm |
| |
LOR | Loss of a documented CR, CRh, PR, or ClinI that must be for ≥ 8 weeks. Downgrading of CR or CRh to PR or PR to ClinI is considered as such but is not considered a LOR unless ClinI is also lost for a minimum of 8 weeks. The baseline value for LOR is the pretreatment measurement(s) and not the nadir values during response. | |
ANC = absolute neutrophil count; BM = bone marrow; ClinI = clinical improvement; CR = complete remission; CRh = complete remission with partial hematological recovery; Hb = hemoglobin; IWG-MRT-ECNM = International Working Group - Myeloproliferative Neoplasms Research and Treatment - European Competence Network on Mastocytosis; LOR = loss of response; MC = mast cell; PD = progressive disease; PR = partial remission; PRBC = packed red blood cell; SM = systemic mastocytosis.
Note: Guidelines for assessing response are only disease-related grade 2 or higher organ damage is evaluable as a primary end point; response assessments of CR, CRh, PR, SD, PD, and LOR should only be applied to these grade 2 or higher organ damage findings in the context of trials; disease status at the time of patient removal from the study singularly relates to the updated status of initial grade 2 or higher organ damage finding(s); the exclusion of drug-related toxicity and/or other clinical issues (e.g., gastrointestinal tract bleeding in the case of worsening anemia and/or transfusion dependence) should be undertaken before assigning the designation PD or LOR in a patient with a worsening of baseline grade 2 or higher organ damage.
aResponses that are not maintained for a period of at least 12 weeks do not fulfill criteria for CR or CRh, PR, or ClinI; however, both maintained and unmaintained responses (< 12 weeks’ duration) should be recorded in the electronic case report form each time they are observed to measure the duration of response.
bOnly valid as a response criterion if the pretreatment serum tryptase level is 40 ng/mL or more (i.e., if pretreatment serum tryptase is < 40 ng/mL, it will not be considered as a criterion in the evaluation of response).
cBiopsy of organ(s) in addition to the BM to evaluate for SM-related organ damage may be considered.
dOnly valid as a response criterion if the pretreatment BM MCs are 5% or more (i.e., if pretreatment BM MCs are < 5%, BM MCs will not be considered as a criterion in the evaluation of response).
eThe preservation of at least 1 ClinI finding permits a patient to maintain the response of ClinI if 1 or more ClinI findings are lost but none meet criteria for PD. However, if 1 or more of the ClinI findings become PD, then the ClinI finding assignment is lost and the patient meets criteria for PD. The baseline value for evaluating PD is the pretreatment measurement(s). The PD findings must be considered related to the underlying disease and not to other clinical factors. Progression of an underlying chronic myeloid neoplasm to acute myeloid leukemia is also considered PD.
Source: Final Clinical Study Report for the EXPLORER study.15
Statistical Analysis
EXPLORER Study
The ORR was estimated using frequency, percentage, and 95% CI based on the exact binomial distribution (Clopper-Pearson) and Wald test P value (1-sided alpha = 0.025) in the RAC-RE population. Statistical testing was conducted versus the null value of 28%, which was based on the midostaurin registration trial (the D2201 study) response data that were calculated post hoc using the original IWG-MRT-ECNM criteria.37 An alternate response rate (defined as CR, CRh, and PR by modified IWG criteria) was statistically tested versus the null of 17% (Wald test P value, 1-sided alpha = 0.025). The 17% ORR was based on a US FDA post hoc assessment using the IWG criteria for CR plus PR for midostaurin.38 According to the statistical analysis plan, response rates using other criteria (e.g., CR + CRh) were reported descriptively with no statistical testing.
AdvSM-SAF data were collected during part 2 of the EXPLORER study. One-way analysis of a variance model was used to estimate the change from baseline in the all-AdvSM population that reported AdvSM-SAF data at baseline. A paired t test was performed at day 1 of cycle 3, cycle 7, and cycle 11 to explore whether the mean change was significantly different from 0. There was no imputation for missing data. Summary statistics for the change from baseline in the EORTC QLQ-C30 scores were reported, with no imputation for missing data.
Time-to-event analyses were estimated using Kaplan-Meier methods as per the PATHFINDER study. There was no control for multiplicity mentioned in the statistical analysis plan. No interim analysis was planned for this study.
PATHFINDER Study
The PATHFINDER study estimated the ORR using frequency, percentage, and 95% CI based on the exact binomial distribution (Clopper-Pearson) and Wald test P value in the RAC-RE population. Statistical testing for efficacy was conducted versus the assumed null value of 28%.37 There was 1 interim analysis planned once 32 patients enrolled in cohort 1 were evaluable for response. The null hypothesis was to be rejected if the 1-sided P value was less than 0.00625, and then the interim analysis would be used to support a marketing application. If the 1-sided P value was 0.00625 or more at the interim analysis, the final analysis would be used to support a marketing application. The final analysis of the primary efficacy end point is planned to occur after 63 patients (with the SM-AHN subgroup capped at approximately 70%) are enrolled in cohort 1 and have had the opportunity to receive avapritinib treatment for at least 10 cycles or discontinued treatment earlier. The final primary efficacy analysis in this ongoing study will be tested at a 1-sided alpha level of 0.02178.
Statistical testing was planned for the proportion of patients who attained a best response of CR plus CRh plus PR against a null of 17%, using similar statistical methods as for the primary end point. However, this end point was not part of the statistical testing hierarchy used to control the familywise type I error rate. Other response categories were reported descriptively with no statistical testing, based on methods similar to those of ORR.
The key secondary outcome was the change from baseline in the AdvSM-SAF TSS. The change in AdvSM-SAF TSS was calculated from baseline to cycle 11, day 1, for patients on treatment for more than 10 cycles. The last observation carried forward method was used for patients who ended treatment before completing 10 cycles. The mean change was calculated for all patients in the safety population and tested against the null hypothesis of greater than or equal to 0 in the mean change of the TSS. The null hypothesis was rejected if the 1-sided 1-sample t test P value was less than 0.025. To control the studywise type I error rate, testing for this key secondary end point was to proceed only if the null hypothesis for the primary objective was rejected. A sensitivity analysis was planned for the change from baseline to cycle 7, day 1, for patients on treatment for more than 6 cycles, using the same statistical methods.
Summary statistics for the change from baseline in the EORTC QLQ-C30 scores were reported, with no imputation for missing data.
Time-to-event analyses (i.e., PFS, OS, duration of response, and time to response) were conducted using the Kaplan-Meier method. Median survival with a 2-sided 95% CI was estimated, as well as event rates at specific time points (e.g., 3 months, 6 months, 9 months).
Sample Size and Power Calculation
The PATHFINDER study was estimated to have 93.5% power to detect a difference for the adjudicated ORR versus the null hypothesis ORR of 28%. The power calculations were based on a sample size of 63 patients in the modified IWG-MRT-ECNM–evaluable cohort (cohort 1), using the exact 1-sample binomial test and a 1-sided type I error rate of 0.025. A sample size of 63 patients was estimated to have greater than 90% power to test the key secondary outcome, the change from baseline in the AdvSM-SAF TSS. This was based on an assumed null hypothesis of a mean change in the TSS of 0 or higher versus the alternative hypothesis of a mean change in the TSS of less than or equal to –10 with avapritinib treatment, an SD of a mean change in TSS of 20, and a 1-sided type I error rate of 0.025, in all treated patients in cohort 1 and cohort 2.
In the EXPLORER study, an estimated 25 patients would be enrolled in the dose-escalating part 1 of the trial. In part 2, the study planned to enrol approximately 35 patients (including 15 patients with ASM, 15 patients with SM-AHN, and 5 patients with MCL) in cohort 1 with a starting dose of 300 mg per day, and 20 patients in cohort 2 (with a starting dose of 200 mg per day).
Subgroup Analyses
Both studies analyzed ORR for the subgroups of age (< 65 years or ≥ 65 years), sex (male or female), region (North America or Europe), baseline SRSF2, ASXL1, and RUNX1 genotype (positive or negative), prior treatment with midostaurin (yes or no), and prior antineoplastic therapy (yes or no). The PATHFINDER study also analyzed PFS and OS for subgroups based on baseline SRSF2, ASXL1, and RUNX1 genotype, and prior antineoplastic or midostaurin use. Results were also presented according to AdvSM subtype in both studies (ASM, SM-ADH, or MCL) and by avapritinib dose in the EXPLORER study.
Of the subgroup analyses planned, prior antineoplastic treatment and AdvSM subtype were subgroups of interest to this review, based on clinical expert input and on informing the pharmacoeconomic analysis.
Table 8: Statistical Analysis of Efficacy End Points for the EXPLORER and PATHFINDER Studies
End point | Statistical model | Adjustment factors | Handling of missing data | Sensitivity analyses |
|---|---|---|---|---|
EXPLORER and PATHFINDER studies | ||||
Overall response rate per modified IWG-MRT-ECNM (SSC adjudicated response in the RAC-RE population) | Frequency, percentage, and 95% CI (Clopper-Pearson method) with Wald test P value against null of 28% (1-sided alpha = 0.025) | None | No imputation was performed for missing data |
|
EXPLORER: Change from baseline in AdvSM-SAF TSS (part 2 patients only) | A 1-way analysis of variance model for change from baseline Mean values at cycle 3, day 1, at cycle 7, day, 1, and at cycle 11, day 1, were tested against a change of 0 using a paired t test | None | No imputation for missing data | None |
PATHFINDER: Change from baseline to cycle 11, day 1, in AdvSM-SAF TSS (in patients who completed 10 cycles) | A 1-way analysis of variance model for change from baseline Mean values were tested against a change of 0 using a paired t test | None | LOCF for patients who stopped treatment before completing 10 cycles | Change from baseline to cycle 7, day 1, in AdvSM-SAF (in patients who completed 6 cycles) |
OS, PFS, duration of response, time to response | Kaplan-Meier method | None | No imputation was performed for missing data | Clopper-Pearson binomial distribution for 95% CIs |
AdvSM-SAF = Advanced Systemic Mastocytosis Symptom Assessment Form; CI = confidence interval; IWG-MRT-ECNM = International Working Group - Myeloproliferative Neoplasms Research and Treatment - European Competence Network on Mastocytosis; LOCF = last observation carried forward; OS = overall survival; PFS = progression-free survival, RAC-RE = Response Assessment Committee–Response Evaluable; SSC = Study Steering Committee; TSS = total symptom score.
Sources: Final Clinical Study Report for the EXPLORER study and interim Clinical Study Report for the PATHFINDER study.15,16
Analysis Populations
The primary efficacy outcome (ORR) and other response-related end points in both studies were based on the RAC-RE population (Table 9). This included all patients who had received at least 1 dose of avapritinib and were evaluable according to the modified IWG-MRT-ECNM criteria, had either completed at least 2 postbaseline bone marrow assessments and had been in the study for at least 6 cycles, or had an end-of-study visit. OS, AdvSM-SAF, and safety outcomes were reported for the safety population, which included all patients who had received at least 1 dose of avapritinib. For the EXPLORER study, only patients with AdvSM were included in the efficacy analyses.
Table 9: Analysis Populations of the EXPLORER and PATHFINDER Studies
Study | Population | Definition | Application |
|---|---|---|---|
EXPLORER | Safety | All patients who received ≥ 1 dose of avapritinib Split into an AdvSM subpopulation and an ISM or SSM subpopulation Patients from part 1 and part 2 (both cohorts) were included. | Analyses of safety and efficacy end points that were not based on the modified IWG-MRT-ECNM response criteria Efficacy analyses from the EXPLORER study were based on the AdvSM subpopulation. |
RAC-RE | All patients who received ≥ 1 dose of avapritinib, were deemed evaluable per modified IWG-MRT-ECNM criteria at baseline as assessed by SSC review, and had 1 of the following conditions:
This included patients with a diagnosis of AdvSM from part 1 and part 2 (both cohorts) who met the aforementioned criteria. | Analyses of overall response and related end points (e.g., DOR, PFS) | |
PATHFINDER | Safety | All patients who received ≥ 1 dose of avapritinib (cohort 1 and cohort 2) | Analyses of safety and efficacy end points that were not based on the modified IWG-MRT-ECNM response criteria |
RAC-RE | All patients who received ≥ 1 dose of avapritinib, were deemed evaluable per modified IWG-MRT-ECNM criteria at baseline as assessed by SSC review, and had 1 of the following conditions:
This included patients from cohort 1 only. | Analyses of overall response and related end points (e.g., DOR, PFS) |
AdvSM = advanced systemic mastocytosis; DOR = duration of response; EOS = end of study, ISM = indolent systemic mastocytosis; IWG-MRT-ECNM = International Working Group - Myeloproliferative Neoplasms Research and Treatment - European Competence Network on Mastocytosis; PFS = progression-free survival; RAC-RE = Response Assessment Committee–Response Evaluable; SSC = Study Steering Committee; SSM = smouldering systemic mastocytosis.
Sources: Final Clinical Study Report for the EXPLORER study,15 interim Clinical Study Report for the PATHFINDER study,16 and Sponsor Summary of Clinical Evidence.14
Results
Patient Disposition
In total, 86 patients were treated with avapritinib in part 1 or part 2 of the EXPLORER study, including 69 patients with a diagnosis of AdvSM, and 57 patients who met the criteria for the RAC-RE population (part 1 = 18 patients; part 2 = 39 patients). A total of 21 patients received an avapritinib starting dose of 200 mg per day in either part 1 or part 2 of the trial. At the end of the EXPLORER study, all patients had stopped treatment with avapritinib. In the safety population, the most common reasons for discontinuing treatment were ███████ █████████ █████ ███ ██████ ██████████ ████ ███ ████████ ██ █████ ███ █████ ████████ ███████ ███████████ ████████ ███████ ██████ ████████ ██████████ ██ ███████ ██ ██████████████ ████████ █████ ███ (Table 10). Of the ██ patients who progressed during the study, ||████████ ████ progressed due to █████ ███████ ████████. Other reasons for progression were ███ ██ ██████████ ███████ ██████████████ ████████ ██ ██████████ ███ █ ███████ ████ ███ ██ ████ ████ ███████ ███ █████████████ ███████████████ █████████ ████ ███ █████████ ████████. The most common reasons for discontinuation from the study were ███████ ████████ ███████ ██ █████ ███████.
At the first data cut-off date in the PATHFINDER study, 62 patients were included in the analysis, of whom 32 patients from cohort 1 met the criteria for the RAC-RE population. In the safety population, 10 (16.1%) patients discontinued treatment and | ████████ ███████ had discontinued from the study. The most common reasons for stopping treatment were AEs (9.7%) and disease progression (4.8%). The reasons for stopping the study were death ██████ or AEs ██████ (Table 11).
At the second data cut-off date, a total of 105 patients had received avapritinib at a starting dose of 200 mg daily, and 81 patients were included in the RAC-RE population (cohort 1). In the safety population, 47 (44.8%) patients had stopped treatment, due mainly to AEs ████████ disease progression ███████ or sponsor decision ██████. A total of 34 (32.4%) patients discontinued the study because of █████ ████████ ██████████ ██ ███████ ██████ ██ █████ ███████ ██████.
The number of patients screened for inclusion in the trials was not reported in either study.
In both studies, the primary efficacy outcome was based on the RAC-RE population, which is a subset of the overall study population. The reasons for exclusion from the RAC-RE population are summarized in Table 12.
Table 10: EXPLORER Study Patient Disposition (Final Data Cut-Off at January 19, 2023)
Disposition category | RAC-RE population (N = 57)a | AdvSM population (N = 69) | Safety population 200 mg dose (N = 21) | Safety population (N = 86)b |
|---|---|---|---|---|
Discontinued from treatment | ██ █████ | ██ █████ | ██ █████ | ██ █████ | |
Continuing treatment | | ███ | | ███ | ██ | | ███ |
Discontinued from study | ██ █████ | ██ █████ | ██ █████ | ██ █████ | |
Reasons for discontinuation from treatment | ||||
███████ ████████ | ██ ██████ | ██ ██████ | | ██████ | ██ ██████ |
███████ ███████████ | ██ ██████ | ██ ██████ | | ██████ | ██ ██████ |
███ | | ██████ | | ██████ | | █████ | | █████ |
███████ ████████ | | ██████ | ██ ██████ | | ██████ | ██ ██████ |
████████ ███████ | | █████ | | █████ | | █████ | | █████ |
█████████████ █████ | | █████ | | █████ | | █████ | | █████ |
█████████████████ | | █████ | | █████ | | █████ | | █████ |
████ ██ █████████ | | █████ | | █████ | | █████ | | █████ |
Reason for discontinuation from study | ||||
███████ ████████ | ██ ██████ | ██ ██████ | | ██████ | ██ ██████ |
███████ ████████ | | ███ | | ███ | ██ | | ███ |
█████ | ██ ██████ | ██ ██████ | | ██████ | ██ ██████ |
████████ ███████ | | ██████ | | ██████ | | ██████ | ██ ██████ |
████ ██ █████████ | | █████ | | █████ | | ██████ | | █████ |
████████ ███████ ██████████ ███████ | | █████ | | █████ | ██ | | █████ |
██████████████ ████████ | | █████ | | █████ | | █████ | | █████ |
███ █ █████ ███████ █████████ ██████ █ ████████ ██████████ █████████ ████████████████████
a███ ██████ ██████████ ████████ ██ ████████ ████████ ██ ████ █ ███ ██ ████████ ████████ ██ ████ ██ ███ ███████████ ████████ ████ ███ █ ███ ██ ██ ██████████ ███ ██ ███ ██████████ ██ █ ███ ██ ███ ██████████
b███ ██████ ██████████ ████████ ██ ████████ ████████ ██ ████ █ ███ ██ ████████ ████████ ██ ████ ██ ███ ███████████ ████████ ████ ███ █ ███ ██ ███ ██████████ ███ ██ ███ ██████████ ██ █ ███ ██ ███ ███████████
c███ ███████ ███ ████████████ ██ █ █████████ █████████ ██████ ███ ████████ █████████ ███|
Sources: Final Clinical Study Report for the EXPLORER study15 and Sponsor Summary of Clinical Evidence.14 Additional data supplied by the sponsor (June 17, 2024).18
Table 11: PATHFINDER Study Patient Disposition
Category | First data cut-off date: June 23, 2020 All doses, n (%) | Second data cut-off date: September 9, 2022 200 mg dose, n (%) | ||
|---|---|---|---|---|
RAC-RE population (N = 32) | Safety population (N = 62)a | RAC-RE population (N = 81)b | Safety population (N = 105)b, c | |
Discontinued from treatment | | ██████ | 10 (16.1) | 31 (38.3) | 47 (44.8) |
Continuing on treatment | ██ ██████ | 52 (83.9) | 50 (61.7) | 58 (55.2) |
Discontinued from study | | ██████ | | ██████ | 25 (30.9) | 34 (32.4) |
Reasons for discontinuation of treatment | ||||
Disease progression | | █████ | 3 (4.8) | | █████ | | █████ |
AML | | █████ | 1 (1.6) | | █████ | | █████ |
Adverse event(s) | | ██████ | 6 (9.7) | ██ ██████ | ██ ██████ |
Death | ██ | ██ | ██ | ██ |
Withdrew consent | | █████ | 1 (1.6) | | █████ | | █████ |
Sponsor decision | ███ | ███ | | █████ | | █████ |
Administrative or other | ███ | ███ | | █████ | | █████ |
Reasons for discontinuation from study | ||||
Death | | ██████ | | █████ | ██ ██████ | ██ ██████ |
Disease progression | ██ | ██ | ██ | ██ |
Adverse event(s) | | ██████ | | █████ | ██ | ██ |
Loss to follow-up | ██ | ██ | ██ | ██ |
Withdrew consent | | █████ | | █████ | | █████ | | █████ |
Sponsor decision | | █████ | | █████ | ██ | ██ |
Administrative or other | | █████ | | █████ | | █████ | | █████ |
AML = acute myeloid leukemia; PPRE = pure pathologic response evaluable; RAC-RE = Response Assessment Committee–Response Evaluable.
aIncludes 32 patients from cohort 1 and 30 patients from cohort 2.
bExcludes 2 patients who received avapritinib at a starting dose of 100 mg daily.
cIncludes 81 patients from cohort 1 and 24 patients from cohort 2.
Sources: Interim Clinical Study Report for the PATHFINDER study,16 the PATHFINDER study clinical summary document,17 and Sponsor Summary of Clinical Evidence.14 Additional data supplied by the sponsor (June 17, 2024).18
Table 12: Reasons for Exclusion From the RAC-RE Population (EXPLORER and PATHFINDER Studies)
Detail | EXPLORER study, all doses Final data cut-off: January 19, 2023 | PATHFINDER study, all doses First data cut-off: June 23, 2020 | PATHFINDER study, 200 mg dose Second data cut-off: September 9, 2022 |
|---|---|---|---|
██ | ██ | ██ | ██ |
███ ████ █████████ ████ ██ | ██ ██████ | ██ | ██ |
██ █████ █████████ ███████ ██ ████ | ██ ██████ | | ██ ██████ | ██ ██████ |
██ █████ ██████ ██ ██████ ███ ███ ██ ██ ██████████ | ██ | ██ ██████ | | █████ |
█████ █ ████████ ████████ █████████████ ███ █ ██████████ ████████ █████████████ ████ █████████ █████████ ████████████ ███ █ ███ ██ █████████████████████ █ █████████████ ███████ ████████████████████████ █████████ ████████ ███ █████████ ███ ████████ ██████████ ███████ ██
Source: Additional data supplied by the sponsor (July 15, 2024).33
Baseline Characteristics
The baseline characteristics outlined in Table 13, Table 15, and Table 16 are limited to those that are most relevant to this review or were felt to affect the outcomes or interpretation of the study results.
Table 13 shows the baseline characteristics of the different analysis populations in the EXPLORER study. In this trial, 69 of the 86 (80%) patients enrolled were adjudicated as having AdvSM, 14 (16%) patients had indolent SM, 2 (2%) patients had smouldering SM, and 1 (1%) patient had chronic myelomonocytic leukemia without SM. Patients with a diagnosis of nonadvanced SM or AdvSM were included in the safety population, which was used for the reporting of harms. Efficacy outcomes were based on patients with AdvSM in the RAC-RE population (i.e., response and PFS), and the all-AdvSM safety population (OS). Generally, the characteristics of the patients were similar across the different analysis populations. The mean age of patients in the all-AdvSM group was ████ █████ ███ █ █████, 41% of patients were female and 59% of patients were male. The most common AdvSM subtype was SM-AHN (70%), followed by MCL (19%) and ASM (12%). In total, 70% of patients had an ECOG PS score of 0 or 1, with 20% and 10% of patients rated as having a score of 2 or 3, respectively. Most patients had received prior antineoplastic therapy for SM (59%), including 33% of patients who had received prior midostaurin. Table 14 provides a summary of the number of prior lines of therapy for AdvSM.
Table 13: EXPLORER Study Baseline Characteristics (Final Data Cut-Off at January 19, 2023)
Characteristic | RAC-RE populationa (N = 57) | All-AdvSM populationa (N = 69) | Safety population 200 mg dose (N = 21) | Safety populationa (N = 86) |
|---|---|---|---|---|
Age (years), mean (SD) | ██████████ | ████ █████ | ██████████ | █████████ |
< 65 years, n (%) | ██ ██████ | ██ ██████ | ██ ██████ | ██ ██████ |
≥ 65 years, n (%) | ██ ██████ | ██ ██████ | ██ ██████ | ██ ██████ |
Female, n (%) | ██ ██████ | 28 (40.6) | | ██████ | ██ ██████ |
Male, n (%) | ██ ██████ | 41 (59.4) | ██ ██████ | ██ ██████ |
Race, n (%) | ||||
Asian | | █████ | | █████ | ██ | | █████ |
Black or African American | | █████ | | █████ | ██ | | █████ |
White | ██ ██████ | ██ ██████ | ██ ██████ | ██ ██████ |
Unknown | | █████ | | █████ | | █████ | | █████ |
Other | ██ | ██ | ██ | | █████ |
BMI (kg/m2), N | ██ | ██ | ██ | ██ |
Mean (SD) | ████ █████ | ████ █████ | ████ █████ | ████ █████ |
Disease diagnosis (central assessment) | ||||
AdvSM | ██ █████ | 69 (100) | ██ ██████ | ██ ██████ |
ASM | | █████ | 8 (11.6) | | █████ | | █████ |
SM-AHN | ██ ██████ | 48 (69.6) | ██ ██████ | ██ ██████ |
MCL | ██ ██████ | 13 (18.8) | | ██████ | ██ ██████ |
Otherb | ██ | ██ | ██ | ██ ███████ |
Baseline disease characteristics (local assessment) | ||||
Major and minor WHO dx criteria for SM | ||||
Major: multifocal dense infiltrations for MC | ██ ██████ | ██ ██████ | ██ ██████ | ██ ██████ |
Minor: > 25% MC atypical or spindle-shaped in biopsy, or immature or atypical in aspirate | ██ ██████ | ██ ██████ | ██ ██████ | ██ ██████ |
Minor: expression of CD markers CD2 and/or CD25 | ██ ██████ | ██ ██████ | ██ ██████ | ██ ██████ |
Minor: KIT mutation at codon 816 | ██ ██████ | ██ ██████ | ██ ██████ | ██ ██████ |
Minor: baseline serum tryptase > 20 ng/mL | ██ ██████ | ██ ██████ | ██ ██████ | ██ ██████ |
WHO dx criteria for SM subclassification | ||||
≥ 20% MCs in BM aspirate (MCL)c | ██ ██████ | ██ ██████ | | ██████ | ██ ██████ |
WHO B-findings (organ infiltration) | ||||
BMMC and serum tryptase, elevatedd | | ██████ | | ██████ | | ██████ | ██ ██████ |
Borderline myelodysplasiae | | █████ | | █████ | | █████ | | █████ |
Organomegaly (without impaired function)f | | ██████ | ██ ██████ | | ██████ | ██ ██████ |
WHO C-findings (organ damage) | ||||
Cytopeniasg | ██ ██████ | ██ ██████ | ██ ██████ | ██ ██████ |
Impaired liver functionh | ██ ██████ | ██ ██████ | | █████ | ██ ██████ |
Hypersplenismi | ██ ██████ | ██ ██████ | | ██████ | ██ ██████ |
Malabsorptionj | ██ ██████ | ██ ██████ | | ██████ | ██ ██████ |
Large osteolytic lesionsk | | █████ | | █████ | | ██████ | ██ ██████ |
Extracutaneous organ involvement, n (%) | ██ ██████ | ██ ██████ | | ██████ | ██ ██████ |
ECOG PS, n (%) | ||||
0 | ██ ██████ | ██ ██████ | | ██████ | ██ ██████ |
1 | ██ ██████ | ██ ██████ | | ██████ | ██ ██████ |
2 | ██ ██████ | ██ ██████ | | ██████ | ██ ██████ |
3 | | ██████ | | ██████ | | █████ | | █████ |
Corticosteroid use for SM, n (%) | ██ ██████ | ██ ██████ | ██ ██████ | ██ ██████ |
Prior therapy, n (%) | ||||
Antineoplastic | ██ ██████ | ██ ██████ | ██ ██████ | ██ ██████ |
Tyrosine kinase inhibitor | ██ ██████ | ██ ██████ | ██ ██████ | ██ ██████ |
Midostaurin | ██ ██████ | 23 (33.3) | ██ ██████ | ██ ██████ |
AdvSM = advanced systemic mastocytosis; ASM = aggressive systemic mastocytosis; BM = bone marrow; BMMC = bone marrow mast cell; BMI = body mass index; CMML = chronic myelomonocytic leukemia; dx = diagnosis; ECOG PS = Eastern Cooperative Oncology Group Performance Status; ISM = indolent systemic mastocytosis; MC = mast cell; MCL = mast cell leukemia; RAC-RE = Response Assessment Committee–Response Evaluable; SD = standard deviation; SM = systemic mastocytosis; SM-AHN = systemic mastocytosis with an associated hematologic neoplasm; SSM = smouldering systemic mastocytosis.
aRepresents combined data for patients with starting avapritinib doses of 30 mg, 60 mg, 100 mg, 130 mg, 200 mg, 300 mg, and 400 mg.
bThe safety population included 16 patients with ISM or SSM, and 1 patient with CMML (without SM) based on central committee adjudication.
cAt least 20% immature MCs in BM aspirate smears.
dMC infiltration in BM biopsy of more than 30% and serum tryptase of more than 200 ng/mL.
eSigns of dysplasia or myeloproliferation, in non–mast cell lineage(s), but insufficient criteria for a definitive diagnosis of a hematopoietic neoplasm, with normal or only slightly abnormal blood counts.
fOrganomegaly (without impaired organ function), including palpable hepatomegaly and/or palpable splenomegaly without hypersplenism and/or palpable lymphadenopathy (or on CT or ultrasound > 2 cm).
gCytopenia(s), including an absolute neutrophil count of less than 1.0 multiplied by 109/L, hemoglobin of less than 10 g/dL, or a platelet count of less than 100 multiplied by 109/L.
hHepatomegaly with impaired liver function — namely, elevated transaminases and/or bilirubin levels and/or hypoalbuminemia (with or without ascites or portal hypertension).
iPalpable splenomegaly with hypersplenism (e.g., as documented by thrombocytopenia — namely, platelet count < 100 × 109/L).
jMalabsorption with hypoalbuminemia and/or significant weight loss defined as more than 10% weight loss over the last 6 months.
kSkeletal involvement with large osteolytic lesions and/or pathologic fractures.
Sources: Final Clinical Study Report for the EXPLORER study15 and Sponsor Summary of Clinical Evidence.14
For the PATHFINDER study, the baseline characteristics for the RAC-RE and safety populations for the first data cut-off are shown in Table 15 and for the second data cut-off in Table 16. At the first data cut-off on June 23, 2020 (N = 62), the mean age of the safety population was 67.5 (SD = 11.0) years, 45% of patients were female, and 55% of patients were male. The highest proportion of patients were diagnosed with SM-AHN (69%), followed by MCL (16%) and ASM (15%). Most patients had an ECOG PS score of 0 or 1 (69%), with 23% and 8% of patients rated as having a score of 2 or 3, respectively. A total of 68% of patients had received prior antineoplastic therapy, including 55% of patients who had received prior midostaurin.
Table 14: EXPLORER Study Number of Prior Systemic Treatments for AdvSM (Final Data Cut-Off at January 19, 2023)
Prior lines of systemic therapy for AdvSM, n (%) | RAC-RE population (N = 57) | All-AdvSM population (N = 69) | Safety population 200 mg dose (N = 20) | Safety population (N = 86) |
|---|---|---|---|---|
No prior therapy | ██ ██████ | 28 (40.6) | | ██████ | ██ ██████ |
1 prior treatment | ██ ██████ | ██ ██████ | | ██████ | ██ ██████ |
2 prior treatments | ██ ██████ | ██ ██████ | | ██████ | ██ ██████ |
3 or more treatments | | █████ | | █████ | | █████ | | █████ |
AdvSM = advanced systemic mastocytosis; RAC-RE = Response Assessment Committee–Response Evaluable.
Source: Additional data supplied by the sponsor (July 15, 2024).33
As for the second PATHFINDER study data cut-off on September 9, 2022 (N = 105), the sponsor provided limited information on the characteristics of the patients analyzed, but based on the data available, the characteristics are generally similar to those of the initial data cut-off. In the safety population, the median age of patients was 68 years (range, 31 years to 88 years), with 42% female patients and 58% male patients. The proportion of patients with SM-AHN, ASM, and MCL was 66%, 20%, and 14%, respectively. The ECOG PS score was rated as 0 or 1 (74%), 2 (18%), and 3 (8%), and 64% of patients had received prior antineoplastic therapy (including midostaurin for 53% of patients). A summary of the number of prior lines of therapy for AdvSM is listed in Table 17.
Table 15: PATHFINDER Study Baseline Characteristics, All Doses (First Data Cut-Off at June 23, 2020)
Category | RAC-RE population (N = 32) | Safety population (N = 62) |
|---|---|---|
Age (years), mean (SD) | ████ ██████ | ████ ██████ |
< 65 years, n (%) | ██ ██████ | ██ ██████ |
≥ 65 years, n (%) | ██ ██████ | ██ ██████ |
Female, n (%) | 14 (43.8) | 28 (45.2) |
Male, n (%) | 18 (56.3) | 34 (54.8) |
Race, n (%) | ||
Asian | 0 | | █████ |
White | 32 (100.0) | ██ ██████ |
Unknown | 0 | | █████ |
Other | 0 | | █████ |
BMI (kg/m2), N | ██ | ██ |
Mean (SD) | ████ █████ | ████ █████ |
AdvSM subtype by SSC, n (%) | ||
ASM | 2 (6.3) | 9 (14.5) |
SM-AHN | 26 (81.3) | 43 (69.4) |
MCL | 4 (12.5) | 10 (16.1) |
Major and minor WHO dx criteria for SM by SSC | ||
Major: Multifocal dense infiltrations of MCs | ██ ██████ | ██ ██████ |
Minor | ||
> 25% MCs atypical or spindle-shaped in biopsy, or immature or atypical in aspirate | ██ ██████ | ██ ██████ |
Expression of CD markers CD2 and/or CD25 | ██ ██████ | ██ ██████ |
KIT mutation at codon 816 | ██ ██████ | ██ ██████ |
Baseline serum tryptase | ██ ███████ | ██ ███████ |
WHO dx criteria for AdvSM subclassifications by SSC | ||
MCL only (without C-finding)a | ██ | ██ |
Cytopenia(s)b | ██ ██████ | ██ ██████ |
Hepatomegaly with impaired liver functionc | | ██████ | ██ ██████ |
Palpable splenomegaly with hypersplenismd | | ██████ | | █████ |
Malabsorption with hypoalbuminemia and/or significant weight losse | | █████ | | ██████ |
Skeletal involvement with large osteolytic lesions with pathologic features | ██ | | █████ |
Life-threatening organ damage in other organ systems caused by local MC infiltration in tissues | ██ | | █████ |
Extracutaneous organ involvement, n (%) | ██ ██████ | ██ ██████ |
ECOG PS, n (%) | ||
0 | | ██████ | ██ ██████ |
1 | ██ ██████ | ██ ██████ |
2 | | ██████ | ██ ██████ |
3 | | ██████ | | █████ |
Corticosteroid use for SM, n (%) | ██ ██████ | ██ ██████ |
Prior therapy, n (%) | ||
Antineoplastic | 23 (71.9) | 42 (67.7) |
Tyrosine kinase inhibitor other than midostaurin | ██ ██████ | ██ ██████ |
Midostaurin | 17 (53.1) | 34 (54.8) |
AdvSM = advanced systemic mastocytosis; AHN = associated hematologic neoplasm; ASM = aggressive systemic mastocytosis; BMI = body mass index; CEL = chronic eosinophilic leukemia; CMML = chronic myelomonocytic leukemia; CRF = case report form; dx = diagnosis; ECOG PS = Eastern Cooperative Oncology Group Performance Status; ISM = indolent systemic mastocytosis; MC = mast cell; MCL = mast cell leukemia; MDS = myelodysplastic syndrome; MPN = myeloproliferative neoplasm; MPN-U = myeloproliferative neoplasm-unclassifiable; PPRE = pure pathologic response evaluable; RAC-RE = Response Assessment Committee–Response Evaluable; SD = standard deviation; SM = systemic mastocytosis; SM-AHN = systemic mastocytosis with an associated hematologic neoplasm; SSC = Study Steering Committee; SSM = smouldering systemic mastocytosis.
aNote that this refers to patients who had MCL and no C-finding.
bIncluding an absolute neutrophil count of less than 1.0 multiplied by 109/L, hemoglobin of less than 10 g/dL, or a platelet count of less than 100 multiplied by 109/L.
cThat is, elevated transaminase and/or bilirubin levels and/or hypoalbuminemia (with or without ascites or portal hypertension).
dFor example, as documented by thrombocytopenia (i.e., platelet count < 100 × 109/L).
eWeight loss defined as more than a 10% loss over the last 6 months.
Sources: Interim Clinical Study Report for the PATHFINDER study16 and Sponsor Summary of Clinical Evidence.14
Table 16: PATHFINDER Study Baseline Characteristics, Avapritinib 200 mg Dose (Second Data Cut-Off at September 9, 2022)
Characteristic | RAC-RE population (N = 81) | Safety population (N = 105) |
|---|---|---|
Age, median years (range) | 68 (31 to 88) | 68 (31 to 88) |
Female, n (%) | 29 (35.8) | 44 (41.9) |
Male, n (%) | 52 (64.2) | 61 (58.1) |
ECOG PS, n (%) | ||
0 | 17 (21.0) | 22 (21.0) |
1 | 42 (51.9) | 56 (53.3) |
2 | 15 (18.5) | 19 (18.1) |
3 | 7 (8.6) | 8 (7.6) |
AdvSM subtype, n (%) | ||
ASM | 13 (16.0) | 21 (20.0) |
SM-AHN | 53 (65.4) | 69 (65.7) |
MCL | 15 (18.5) | 15 (14.3) |
KIT D816V, n (%) | 71 (87.7) | 94 (89.5) |
KIT D816V VAF, median % (range) | 19.4 (0.0 to 46.7) | 15.0 (0.0 to 47.5) |
SRSF2, ASXL1 or RUNX1 mutation, n (%) | 39 (48.1) | 47 (44.8) |
BM mast cell burden, median % (range) | 50.0 (1.0 to 95.0) | 50.0 (1.0 to 95.0) |
Serum tryptase level, median ng/mL (range) | 312.0 (23.8 to 1,600.0) | 259.2 (23.8 to 1600.0) |
Spleen volume, median mL (range) | 944.1 (44.2 to 2,897.1) | 829.8 (44.2 to 2,897.1) |
Prior systemic therapy,a n (%) | 51 (63.0) | 67 (63.8) |
Midostaurin | 41 (50.6) | 56 (53.3) |
Cladribine | 8 (9.9) | 10 (9.5) |
Interferon alpha | 7 (8.6) | 10 (9.5) |
Hydroxyurea | 5 (6.2) | 5 (4.8) |
Imatinib | 5 (6.2) | 5 (4.8) |
Dasatinib | 4 (4.9) | 4 (3.8) |
Azacitidine | 3 (3.7) | 3 (2.9) |
Investigational antineoplastic drugs | 2 (2.5) | 2 (1.9) |
Peginterferon alfa | 1 (1.2) | 2 (1.9) |
Stem cells NOS | 1 (1.2) | 2 (1.9) |
Brentuximab vedotin | 0 | 1 (1.0) |
Decitabine | 1 (1.2) | 1 (1.0) |
Nilotinib | 1 (1.2) | 1 (1.0) |
Protein kinase inhibitors | 1 (1.2) | 1 (1.0) |
Purine analogues | 1 (1.2) | 1 (1.0) |
Radiotherapy | 0 | 1 (1.0) |
Thalidomide | 1 (1.2) | 1 (1.0) |
AdvSM = advanced systemic mastocytosis; ASM = aggressive systemic mastocytosis; BM = bone marrow; ECOG PS = Eastern Cooperative Oncology Group Performance Status; MCL = mast cell leukemia; NOS = not otherwise specified; RAC-RE = Response Assessment Committee–Response Evaluable; SM-AHN = systemic mastocytosis with an associated hematologic neoplasm; VAF = variant allele fraction.
aPrior therapies are coded using WHO Drug Dictionary B2 Enhanced, version March 2017.
Sources: Clinical summary document for the PATHFINDER study17 and Sponsor Summary of Clinical Evidence.14
Exposure to Study Treatments
Table 18 summarizes treatment exposure for the final data cut-off of the EXPLORER study (safety population) and includes data from part 1 (dose escalation) and part 2 (extension). In part 1 (N = 32), the avapritinib starting dose was less than 200 mg, 200 mg, 300 mg, and 400 mg daily for 15 patients, 4 patients, 6 patients, and 7 patients, respectively. In the total study population (N = 86), most patients received a starting dose of 300 mg (43 [50%] patients), with 21 (24%) patients starting with 200 mg daily, 15 (17%) patients starting with less than 200 mg per day (i.e., 30 mg, 60 mg, 100 mg, or 130 mg), and 7 (8%) patients starting with 400 mg daily. The distribution of patients who received an avapritinib starting dose of less than 200 mg, 200 mg, or greater than 200 mg was ████ ████ ███ ███ in the all-AdvSM population (total N = 69), and ████ ████ ███ ███ in the RAC-RE population (total N = 57), respectively.
Table 17: PATHFINDER Study Number of Prior Systemic Treatments for AdvSM (First and Second Data Cut-Offs)
Prior line of systemic therapy for AdvSM, n (%) | First data cut-off date: June 23, 2020 | Second data cut-off date: September 9, 2022 | ||
|---|---|---|---|---|
RAC-RE population (N = 32) | Safety population (N = 62) | RAC-RE population (N = 83) | Safety population (N = 107) | |
No prior therapy | 9 (28.1) | 20 (32.3) | 30 (36.1) | 38 (35.5) |
1 prior treatment | ██ ██████ | ██ ██████ | ██ ██████ | ██ ██████ |
2 prior treatments | | ██████ | ██ ██████ | ██ ██████ | ██ ██████ |
3 or more treatments | | ██████ | | ██████ | | ██████ | ██ █████ |
AdvSM = advanced systemic mastocytosis; RAC-RE = Response Assessment Committee–Response Evaluable.
Source: Additional data supplied by the sponsor (July 15, 2024).33
In the EXPLORER study, the mean duration of treatment was ████ ██████ ███ █ █████ with a mean daily dose of █████ ██ ███ █ █████ for the safety population. For the 69 patients with AdvSM, the mean treatment duration was ████ ██████ ███ █ █████, and in the RAC-RE population (N = 57), the mean treatment duration was ████ ██████ ███ █ █████.18 Dose reductions due to AEs were common and dose-related, with ████ ████ ███ ███ of patients in the safety population reducing their dose at least once in the less than 200 mg, 200 mg, and 300 mg starting dose groups, respectively. Most patients reported ██ █████ | dose interruption due to AEs (███ ██ ███), with no clear dose relationship.
In the PATHFINDER study first data cut-off (on June 23, 2020), the mean treatment duration was ███ ██████ ███ █ ████ in the RAC-RE population, and ███ ██████ ███ █ ████ in the safety population. The mean daily dose was █████ ██ ███ █ █████ (Table 19). ███ ██████ ██ ████████ had at least 1 dose reduction and ███ had a dose interruption due to AEs. As of the September 9, 2022, data cut-off date, among patients who received a 200 mg avapritinib starting dose, the mean treatment duration was ████ ██████ ███ █ █████ in the RAC-RE population and ████ ██████ ███ █ █████ in the safety population.18 The median average daily doses of avapritinib were █████ ██ ███████ ████ ██ ██████ in the subgroup of patients who were previously treated and █████ ██ ███████ ████ ██ ██████ in the subgroup of patients who were previously untreated.
During the EXPLORER (for the final data cut-off) and PATHFINDER (for the first data cut-off) studies, ███ ███ ███ of patients were receiving drugs for peptic ulcers, ███ ███ ███ were receiving antihistamines, ███ ███ ███ received diuretics, ███ ███ ███ received corticosteroids, and ███ ███ ███ received opioids, respectively (Table 20). Concomitant medications were not reported in the sponsor-provided clinical summary document for the second PATHFINDER study data cut-off. Neither study provided information on subsequent therapies received.
Table 18: EXPLORER Study Patient Exposure Based on Avapritinib Starting Dose (Safety Population — Data Cut-Off at January 19, 2023)
Parameter statistic | < 200 mg (N = 15) | 200 mg (N = 21) | 300 mg (N = 43) | All doses (N = 86) |
|---|---|---|---|---|
Duration of treatmenta (months) | ||||
Mean (SD) | ███ █████ | ███ █████ | ███ █████ | ████████ |
Median | ████ | ████ | ████ | ████ |
Minimum to maximum | ████ ████ | ████ ████ | ████ ████ | ████ ████ |
Cumulative doseb (mg) | ||||
Mean (SD) | ████████ | ████████ | ████████ | ████████ |
Median | ████████ | ███████ | ███████ | ███████ |
Minimum to maximum | ████ ████ | ████ ████ | ████████ | ████████ |
Average daily dosec (mg) | ||||
Mean (SD) | ███ █████ | ████ ████ | ████████ | ██ ██████ |
Median | ████ | █████ | █████ | █████ |
Minimum to maximum | ███ ███ | ███ ███ | ███ ███ | ███ ███ |
≥ 1 dose reductions due to AEs, n (%) | | ████ | ██ ████ | ██ ████ | ██ ████ |
≥ 1 dose interruptions due to AEs, n (%) | ██ ████ | ██ ████ | ██ ████ | ██ ████ |
AE = adverse event; SD = standard deviation.
aDuration of treatment is defined as ([treatment end date – treatment start date] + 1) ÷ 30.4375.
bCumulative dose is defined as the sum of all doses actually taken.
cAverage daily dose: Cumulative dose divided by the number of days actually dosed.
Sources: Final Clinical Study Report for the EXPLORER study15 and Sponsor Summary of Clinical Evidence.14
Table 19: PATHFINDER Study Patient Exposure Based on Avapritinib Starting Dose (Safety Population — First Data Cut-Off at June 23, 2020)
Parameter statistic | 200 mg dose (N = 60) | All doses (N = 62) |
|---|---|---|
Duration of treatment (months)a | ||
Mean (SD) | ███ █████ | ███ █████ |
Median (minimum to maximum) | ███ █████ █████ | ███ ████ █████ |
Cumulative dose (mg)b | ||
Mean (SD) | █████ ████████ | ████████████ |
Median (minimum to maximum) | ███ ████ ██████ | ███ ███ █████ |
Average daily dose (mg)c | ||
Mean (SD) | █████ ██████ | █████ ██████ |
Median (minimum to maximum) | ███ ████ ████ | ███ ████ ████ |
≥ 1 dose reductions due to AEs, n (%) | ██ ████ | ██ ████ |
≥ 1 dose interruptions due to AEs, n (%) | ██ ████ | ██ ████ |
AE = adverse event; SD = standard deviation.
aDefined as ([treatment end date – treatment start date] + 1) ÷ 30.4375.
bDefined as the sum of all doses actually taken.
cDefined as the cumulative dose divided by the number of days actually dosed.
Sources: Interim Clinical Study Report for the PATHFINDER study16 and Sponsor Summary of Clinical Evidence.14
Table 20: Concomitant Therapy (Safety Population)
Parameter statistic | EXPLORER study Final data cut-off date: January 19, 2023 N = 86 | PATHFINDER study First data cut-off date: June 23, 2020 N = 62 |
|---|---|---|
█████ ███ ████ █████████████ | ██ ██████ | ██ ██████ |
████████████ █ ████████ ██ | ██ ██████ | ██ ██████ |
████████████ █████████ | ██ ██████ | ██ ██████ |
███████████████ ███ ███████ | ██ ██████ | ██ ██████ |
███████ | ██ ██████ | ██ ██████ |
Sources: Final Clinical Study Report for the EXPLORER study15 and interim Clinical Study Report for the PATHFINDER study.16
Efficacy
Overall Response Rate
Table 21 provides a summary of the adjudicated best response according to the modified IWG-MRT-ECNM criteria in the RAC-RE population in both pivotal trials. The ORR was defined as patients with a best response of CR, CRh, PR, or clinical improvement, which was the primary outcome in the PATHFINDER study and a secondary outcome in the EXPLORER study. The observed ORR was similar in the final data cut-off of the EXPLORER study ██████ ████ ███ █████ ██ ███████ | | ███ as in the first data cut-off of the PATHFINDER study (75.0% ███████ ███ █████ ██ ███████ | | ███ and the second data cut-off at 74.1% (95% CI, 63.1% to 83.2%; N = 81).
According to the statistical analysis plans, the ORR was tested versus the 28% null value in all patients with AdvSM in the RAC-RE population who received any dose of avapritinib in part 1 or part 2 of the EXPLORER study (N = 57) and any dose of avapritinib in the preplanned interim analysis (i.e., first data cut-off) of the PATHFINDER study (N = 32). In both studies, the P value was less than 0.0001 based on a 1-sided test (alpha = 0.025 for EXPLORER; alpha = 0.00625 for PATHFINDER interim analysis).
CR was attained by █████, 0%, and 13.6% of patients in the EXPLORER and PATHFINDER studies’ first and second data cut-offs, respectively. Data for other response categories are shown in Table 21.
The ORR for the subgroup with ASM was ████, 100%, and 76.9% in the EXPLORER and PATHFINDER studies’ first and second data cut-offs, respectively (Table 41, Table 42, and Table 43 in Appendix 1). For patients with SM-AHN, the ORR was █████, 80.8%, and 75.5%, and for patients with MCL the ORR was █████, 25.0%, and 66.7% in the EXPLORER and PATHFINDER studies’ first and second data cut-offs, respectively. For patients with and without prior antineoplastic therapy, the ORR was █████ ██████ █████ in the EXPLORER study, 73.9% versus 77.8% in the PATHFINDER study’s first data cut-off, and 64.7% versus 90.0% in the PATHFINDER study’s second data cut-off, respectively (Appendix 1, Table 46).
Overall Survival
OS was an exploratory outcome in the EXPLORER study and a secondary outcome in the PATHFINDER study. The median survival was not reached for either study, as ██ ██ ██ ██ ████████ ███████ were alive at the end of the EXPLORER study, ██ ██ ██ ████████ ███████ were alive at the interim analysis of the PATHFINDER study, and 84 of 105 patients were alive at the PATHFINDER study’s second data cut-off (80.0%).
Table 21: Adjudicated Best Response by Modified IWG-MRT-ECNM Criteria (RAC-RE Population)
Response category, n (%) | EXPLORER study Final data cut-off date: January 19, 2023 | PATHFINDER study June 23, 2020 | PATHFINDER study Second data cut-off date: September 9, 2022 | |
|---|---|---|---|---|
All-AdvSMa (N = 57) | AdvSM (N = 17) | All-AdvSMa (N = 32) | AdvSM (N = 81) | |
Median follow-up, months (95% CI) | ██ █████ | ██ █████ | ██ █████ | ██ █████ |
Overall response: Primary efficacy end point | ||||
ORR (CR + CRh + PR + ClinI), n (%) | ██ █████ | ██ █████ | 24 (75.0) | 60 (74.1) |
95% CI | ██ █████ | █████ █ | (56.6 to 88.5) | (63.1 to 83.2) |
98.75% CI | ██ | ██ | █████ ████ | ██ |
P value | ███████ | ██ | < 0.0001c | ██ |
CR or PR | ||||
CR + CRh + PR, n (%) | ██ █████ | ██ ██████ | 16 (50.0) | ██ |
95% CI | ██ █████ | ██ █████ | ██ █████ | ██ |
98.75% CI | ██ | ██ | █████ ████ | ██ |
P value | ███████ | ██ | ███████ | ██ |
CR with full or partial recovery of peripheral blood counts | ||||
CR + CRh, n (%) | ██ ████ | | ██████ | 6 (18.8) | ██ |
95% CI | ███████ | █████ █ | █████ █████ | ██ |
Best response, n (%) | ||||
CR | ██ █████ | | ██████ | 0 | 11 (13.6) |
CRh | ██ █████ | | ██████ | 6 (18.8) | 11 (13.6) |
PR | ██ █████ | | ██████ | 10 (31.3) | 35 (43.2) |
ClinI | | █████ | ██ | 8 (25.0) | 3 (3.7) |
Stable disease | ██ █████ | | ██████ | 4 (12.5) | ██ |
Progressive disease | ██ | ██ | 1 (3.1) | ██ |
Not evaluable | | █████ | | █████ | 3 (9.4) | ██ |
AdvSM = advanced systemic mastocytosis; CI = confidence interval; ClinI = clinical improvement; CR = complete remission; CRh = complete remission with partial hematological recovery; IWG-MRT-ECNM = International Working Group - Myeloproliferative Neoplasms Research and Treatment - European Competence Network on Mastocytosis; ORR = overall response rate; PR = partial remission; RAC-RE = Response Assessment Committee–Response Evaluable.
aIncluded all starting doses of avapritinib (EXPLORER: 30 mg to 400 mg daily; PATHFINDER: 100 mg or 200 mg daily). In the EXPLORER study, the proportion of patients who received an avapritinib starting dose of less than 200 mg, 200 mg, or greater than 200 mg was 14%, 30%, and 56%, respectively, in the RAC-RE population. In the PATHFINDER study (first data cut-off), 1 (3%) patient received a starting dose of 100 mg; all other patients received avapritinib 200 mg.
bStatistical test on binomial proportion of ORR against a null hypothesis of 28%, 1-sided alpha of 0.025, Wald test P value, for the all-AdvSM patient population (any dose of avapritinib in part 1 and part 2).
cStatistical test on binomial proportion against a null of 28% was performed using a 1-sided alpha of 0.025. Null was rejected at the interim analysis as the 1-sided P value was less than 0.00625 (Wald test P value).
dStatistical test on binomial proportion of ORR against a null hypothesis of 17%, 1-sided alpha of 0.025, Wald test P value, for the all-AdvSM patient population (any dose of avapritinib). The P value was not controlled for multiple testing.
Sources: Final Clinical Study Report for the EXPLORER study,15 interim Clinical Study Report for the PATHFINDER study,16 the PATHFINDER study clinical summary document,17 and Sponsor Summary of Clinical Evidence.14 Additional data supplied by the sponsor (June 17, 2024).18
In the EXPLORER study, the Kaplan-Meier estimates for the proportion of patients alive at 12 months, 24 months, 36 months, 48 months, and 66 months were ██████ ██████ ██████ ██████ ███ █████, respectively (Table 22). At the interim analysis of the PATHFINDER study, ██████ ██████ ███ █████ of patients were alive at 6 months, 12 months, and 18 months, respectively. As of the second data cut-off date, the Kaplan-Meier estimate for OS was 79.0% (95% CI, 70.8% to 87.3%) at 24 months (200 mg dose group; N = 105).
The Kaplan-Meier OS curve for the EXPLORER and PATHFINDER studies (second data cut-off, 200 mg dose group) for the safety study population and AdvSM subtypes are shown in Figure 3 and Figure 4. Data for OS in subgroups with and without prior antineoplastic therapy are shown in Appendix 1, Table 47 and Figure 9. The OS estimates for the RAC-RE population (N = 57) were similar to those in the all-AdvSM population (N = 69) in the EXPLORER study, and in the 2 populations based on the first data cut-off of the PATHFINDER study (RAC-RE population, N = 32; all-AdvSM population, N = 62).
Table 22: EXPLORER and PATHFINDER Studies Overall Survival (Safety Population)
Overall survival | EXPLORER study January 19, 2023 | PATHFINDER study June 23, 2020 | PATHFINDER study Second data cut-off date: September 9, 2022 | |
|---|---|---|---|---|
All-AdvSMa (N = 69) | All-AdvSM 200 mg (N = 20) | All-AdvSMa (N = 62) | All-AdvSM 200 mg dose (N = 105) | |
Events, n (%) | ██ ██████ | | ██████ | | █████ | ██ ██████ |
Censored, n (%) | ██ ██████ | ██ ██████ | ██ ██████ | 84 (80.0) |
Median overall survival follow-up, months (95% CI) | ████ ██ | ████ ██ | ████ ██ | ████ ██ |
Kaplan-Meier estimates | ||||
Median overall survival, months (95% CI) | ██ ██████ | ████ ██ | ██ ████ █ | ██ |
████ ██████ █████████ ██████ █████████ ██████ █████████ ███ | ||||
3 months | ████████ | ███████ | ████ ██████ | ██ |
6 months | ████ ███ | ████ ███ | ████ ███ | ██ |
9 months | ████ ███ | ████ ███ | ████ ███ | ██ |
12 months | ████ ███ | ████ ███ | ████ ███ | ██ |
18 months | ████ ███ | ████ ███ | ████ ███ | ██ |
24 months | ████ ███ | ████ ███ | ██ | 79.0 (70.8 to 87.3) |
30 months | ████ ███ | ████ ███ | ██ | ██ |
36 months | ████ ███ | ████ ███ | ██ | ██ |
42 months | ████ ███ | ████ ███ | ██ | ██ |
48 months | ████ ███ | ████ ███ | ██ | ██ |
54 months | ████ ███ | ████ ███ | ██ | ██ |
60 months | ████ ███ | ██ | ██ | ██ |
66 months | ████ ███ | ██ | ██ | ██ |
72 months | ████ ███ | ██ | ██ | ██ |
AdvSM = advanced systemic mastocytosis; CI = confidence interval; NE = not estimable.
aIncluded all starting doses of avapritinib (EXPLORER: 30 mg to 400 mg daily; PATHFINDER: 100 mg or 200 mg daily). In the EXPLORER study, the proportion of patients who received an avapritinib starting dose of less than 200 mg, 200 mg, or greater than 200 mg was 13%, 29%, and 58%, respectively, in the all-AdvSM population. In the PATHFINDER study (in the first data cut-off), 2 (3%) patients received a starting dose of 100 mg; all other patients received avapritinib 200 mg.
Sources: Final Clinical Study Report for the EXPLORER study,15 interim Clinical Study Report for the PATHFINDER study,16 the PATHFINDER study clinical summary document,17 and Sponsor Summary of Clinical Evidence.14
Figure 3: EXPLORER Study Overall Survival, All Doses (Safety Population — Final Data Cut-Off at January 19, 2023) [Redacted]

AdvSM = advanced systemic mastocytosis; ASM = aggressive systemic mastocytosis; ISM/SSM = indolent systemic mastocytosis/smouldering systemic mastocytosis; MCL = mast cell leukemia; SM-AHN = systemic mastocytosis with an associated hematologic neoplasm.
Source: Final Clinical Study Report for the EXPLORER study.15
Figure 4: PATHFINDER Study Overall Survival, Avapritinib 200 mg Dose (Safety Population — Second Data Cut-Off at September 9, 2022)
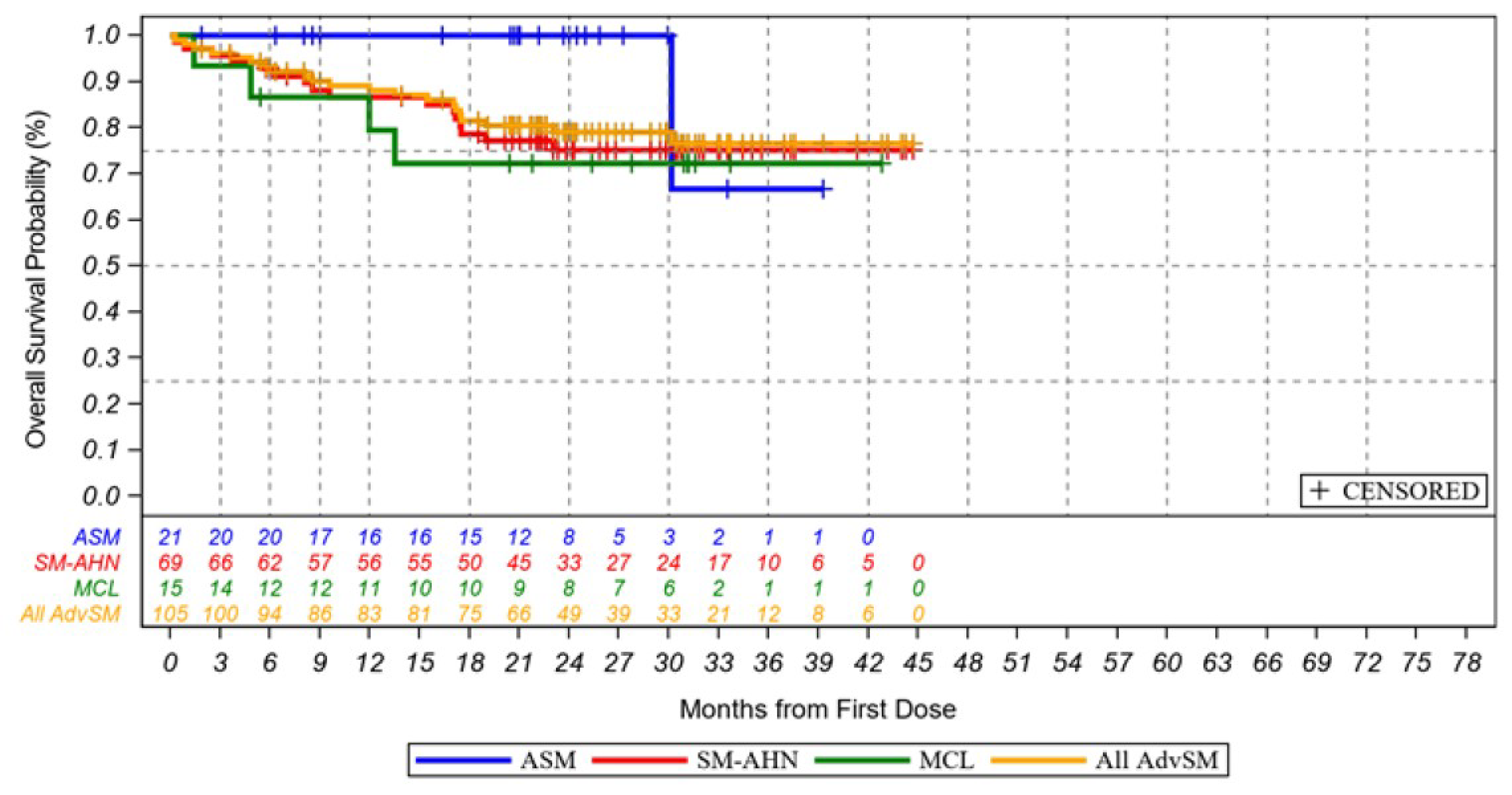
AdvSM = advanced systemic mastocytosis; ASM = aggressive systemic mastocytosis; MCL = mast cell leukemia; SM-AHN = systemic mastocytosis with an associated hematologic neoplasm.
Source: PATHFINDER study clinical summary document.17
Patient-Reported Outcomes
The AdvSM-SAF TSS captures the severity of 8 symptoms (abdominal pain, nausea, vomiting, diarrhea, spots, itching, flushing, and fatigue) and is scored from 0 (no symptoms) to 80 points (worst symptoms imaginable) based on the average daily score over the prior week. Using anchor-based methods, the estimated within-person MID was 9 points to 14 points for the TSS.1
In the EXPLORER study, the AdvSM-SAF questionnaire was completed during part 2 only. At baseline, ██ ██ ██ ████████ █████ enrolled in part 2 had reported an AdvSM-SAF TSS, which dropped to ██ ████████ █████ at cycle 11. At baseline, the mean TSS was 19.1 (SD = 12.2) points (N = 40), with a mean change from baseline of ████ ██████ ████ ███ █████ ██ █████ | | ███ on cycle 3, day 1, and █████ ██████ ████ ███ █████ ██ █████ | | ███ at cycle 11, day 1 (Table 23).
In the PATHFINDER study, 56 of 62 (90%) patients reported a baseline TSS at the first data cut-off, and 91 of 105 (87%) patients reported a score at the second data cut-off. At baseline, the mean TSS was 18.3 (SD = 12.5) points (N = 56) at the first data cut-off date, with a mean change from baseline of –7.1 (SD = 9.9) points (N = 51) at cycle 3, day 1, and –9.8 points (95% CI, –14.9 points to –4.6 points; N = 22) at cycle 11, day 1. For the second data cut-off, the baseline TSS was not reported. The mean change from baseline was –5.4 (SD = 9.1) points (N = 90) at cycle 3, day 1, and –6.4 (SD = 9.7) points (N = 91) at cycle 11, day 1.
Table 23: Change From Baseline in AdvSM-SAF TSS (Safety Population — Patients With AdvSM)
AdvSM-SAF TSS | EXPLORER study January 19, 2023 | PATHFINDER study June 23, 2020 | PATHFINDER study Second data cut-off date: September 9, 2022 |
|---|---|---|---|
All-AdvSMa (N = 54; part 2) | All-AdvSMa (N = 62) | AdvSM 200 mg (N = 105) | |
Baseline, n | ██ | 56 | 91 |
Mean (SD) | ████ ██████ | 18.3 (12.5) | NR |
Change from baseline to cycle 3, day 1, n | ██ | 51 | 90 |
Mean (SD) | ████ ██████ | –7.1 (9.9) | –5.4 (9.1) |
95% CI | ███████ █████ | ██ | NR |
P valueb | ██████| | ██ | < 0.0001c |
Change from baseline to cycle 7, day 1, n | ██ | ██ | | 85 |
Mean (SD) | ████ ██████ | ████ ██████ | –6.2 (10.0) |
95% CI | ███████ █████ | ████████ | NR |
P valueb | ██████ | ██████ | < 0.0001c |
Change from baseline to cycle 11, day 1, n | ██ | 22d | 91 |
Mean (SD) | █████ ██████ | –9.8 ██████ | –6.4 (9.7) |
95% CI | ███████ ███ | –14.9 to –4.6 | NR |
P valueb | ██████ | | < 0.001e | < 0.0001c |
Change from baseline to cycle 15, day 1, n | 89 | ||
Mean (SD) | ██ | ██ | –6.9 (10.3) |
P value | ██ | ██ | NR |
Change from baseline to cycle 18, day 1, n | 79 | ||
Mean (SD) | ██ | ██ | –7.4 (10.4) |
P value | ██ | ██ | NR |
AdvSM = advanced systemic mastocytosis; AdvSM-SAF = Advanced Systemic Mastocytosis Symptom Assessment Form; CI = confidence interval; GI = gastrointestinal; NR = not reported; SD = standard deviation; TSS = total symptom score.
aIncluded all starting doses of avapritinib (EXPLORER: 30 mg to 400 mg daily; PATHFINDER: 100 mg or 200 mg daily). The distribution of doses received was not reported for this outcome.
bTwo-sided P value of paired t test. The null hypothesis was that the mean change from baseline was 0.
cThe P value was not controlled for multiple testing.
dUnobserved patients were imputed using the last observation carried forward method.
eAnalysis of AdvSM-SAF TSS at cycle 11, day 1, was a key secondary end point in the PATHFINDER study and was analyzed in a sequential manner if the primary end point was met to control the studywise type I error rate.
Sources: Final Clinical Study Report for the EXPLORER study,15 interim Clinical Study Report for the PATHFINDER study,16 the PATHFINDER study clinical summary document,17 and Sponsor Summary of Clinical Evidence.14
Duration of Response
Duration of response was a secondary outcome in both studies.
In the EXPLORER study, the median estimated duration of response for all 44 patients with AdvSM who met the overall response criteria in the RAC-RE population was ████ ██████ ████ ███ ████ ███████ ███ ██████████. The proportions of patients with AdvSM who maintained their response were █████ at 12 months, ████ | at 24 months, and █████ at 36 months (Table 24). Among patients with AdvSM who received a 200 mg starting dose (N = 11), █████ ███ █████ maintained their response at 12 months and 24 months, respectively.
Among patients who attained an overall response in the PATHFINDER study, the median estimated duration of response had not been reached at either the first data cut-off date (June 23, 2020) or the second data cut-off date (September 9, 2022). No patients had an event at the first data cut-off date (N = 24), whereas | ███████ of 60 patients had an event at the second data cut-off date. In the second data cut-off, the Kaplan-Meier estimates of ongoing response among all responders were 94.6% at 12 months, 88.8% at 24 months, 84.6% at 36 months, and 70.5% at 42 months (Table 24).
Time to Response
Time to response was an exploratory outcome in the EXPLORER study and a secondary outcome in the PATHFINDER study.
The median time to response was ███ ██████ ████ ███ ███ ██ █████ in the EXPLORER study, 2.0 months (95% CI, 0.3 months to 12.2 months) in the first data cut-off of the PATHFINDER study, and 2.2 months (95% CI, 0.3 months to 15.0 months) in the second data cut-off of the PATHFINDER study (Table 25).
Table 24: Adjudicated Duration of Responses by Modified IWG-MRT-ECNM Criteria (RAC-RE Population — Responders)
Duration of response | EXPLORER study January 19, 2023 | PATHFINDER study June 23, 2020 | PATHFINDER study Second data cut-off date: September 9, 2022 | |
|---|---|---|---|---|
All-AdvSMa (N = 44) | All-AdvSM (N = 11) | All-AdvSMa (N = 24) | All-AdvSM 200 mg dose (N = 60) | |
Events, n (%) | ██ ██ | ██ ██ | ██ | | ██████ |
Censored, n (%) | ██ ██ | ██ ██ | ██ ██ | 52 (86.7) |
Kaplan-Meier estimates | ||||
Median duration of response, months (95% CI) | ██ ██ | ██ ██ | ██ ██ | NE (37.1 to NE) |
Response rate, % (95% CI) at time point | ||||
3 months | ██ ██ | ██ ██ | ██ ██ | ██ |
6 months | ██ ██ | ██ ██ | ██ ██ | ██ |
9 months | ██ ██ | ██ ██ | ██ ██ | ██ |
12 months | ██ ██ | ██ ██ | ██ ██ | 94.6 (88.6 to 100.0) |
18 months | ██ ██ | ██ ██ | ██ | ██ |
24 months | ██ ██ | ██ ██ | ██ | 88.8 (80.4 to 97.3) |
30 months | ██ ██ | ██ ██ | ██ | ██ |
36 months | ██ ██ | ██ | ██ | 84.6 (73.2 to 96.0) |
42 months | ██ ██ | ██ | ██ | 70.5 (43.5 to 97.4) |
48 months | ██ ██ | ██ | ██ | ██ |
54 months | ██ ██ | ██ | ██ | ██ |
60 months | █████ █ | ██ | ██ | ██ |
AdvSM = advanced systemic mastocytosis; CI = confidence interval; ClinI = clinical improvement; CR = complete remission; CRh = complete remission with partial hematological recovery; IWG-MRT-ECNM = International Working Group - Myeloproliferative Neoplasms Research and Treatment - European Competence Network on Mastocytosis; NE = not estimable; PR = partial remission; RAC-RE = Response Assessment Committee–Response Evaluable.
Note: Duration of response is defined as the time in months from the first documented response (CR, CRh, PR, or ClinI) to the date of the first documented progressive disease or loss of response or death due to any cause, whichever occurs first. Patients without confirmed response were excluded from this analysis. Patients who were still responding at the time of the data cut-off date were censored at their last valid assessment.
aAll starting doses of avapritinib (EXPLORER: 30 mg to 400 mg daily; PATHFINDER: 100 mg or 200 mg daily). The distribution of doses received was not reported for this outcome.
Sources: Final Clinical Study Report for the EXPLORER study,15 interim Clinical Study Report for the PATHFINDER study,16 the PATHFINDER study clinical summary document,17 and Sponsor Summary of Clinical Evidence.14
Table 25: Adjudicated Time to Response by Modified IWG-MRT-ECNM Criteria (RAC-RE Population — Responders)
End point statistic | EXPLORER study | PATHFINDER study | PATHFINDER study |
|---|---|---|---|
All-AdvSMa (N = 44) | All-AdvSMa (N = 24) | AdvSM 200 mg dose (N = 60) | |
Time to response (months) | |||
Mean (SD) | ███ █████ | 3.27 (2.782) | — |
Median (range) | ███ █████ █████ | 2.0 (0.3 to 12.2) | 2.2 (0.3 to 15.0) |
AdvSM = advanced systemic mastocytosis; ClinI = clinical improvement; CR = complete remission; CRh = complete remission with partial hematological recovery; IWG-MRT-ECNM = International Working Group - Myeloproliferative Neoplasms Research and Treatment - European Competence Network on Mastocytosis; PR = partial remission; RAC-RE = Response Assessment Committee–Response Evaluable; SD = standard deviation.
Note: Time to response is defined as the time in months from the start of treatment to the time that criteria for response (CR, CRh, PR, or ClinI) are first met. Patients without confirmed response were excluded from this analysis.
aAll starting doses of avapritinib (EXPLORER: 30 mg to 400 mg daily; PATHFINDER: 100 mg or 200 mg daily). The distribution of doses received was not reported for this outcome.
Sources: Final Clinical Study Report for the EXPLORER study,15 interim Clinical Study Report for the PATHFINDER study,16 the PATHFINDER study clinical summary document,17 and Sponsor Summary of Clinical Evidence.14
Progression-Free Survival
PFS was an exploratory outcome in the EXPLORER study and a secondary outcome in the PATHFINDER study (Table 26).
At the final data cut-off date of the EXPLORER study, ██ ██ ██ ████████ ███████ reported an event and ██ ████████ were censored. The median PFS was ████ ██████ ████ ██ █████ ███ ██████████ among patients in the RAC-RE population who received any dose of avapritinib. The estimated PFS rates at 12 months, 24 months, 36 months, and 66 months were ██████ ██████ ██████ ███ █████, respectively.
At the interim analysis of the PATHFINDER study, | ██ ██ ████████ ███████ in the RAC-RE population had an event and ██ patients were censored, and at the second data cut-off date, 20 of 81 (24.7%) patients had events and 61 patients were censored. The median PFS was not estimable at either time point. For the second data cut-off, the estimated PFS rates at 12 months, 24 months, and 36 months were 83.5%, 76.5%, and 73.4%, respectively.
PFS Kaplan-Meier survival curves for both studies are available in Appendix 1. PFS according to prior antineoplastic therapy is shown in Appendix 1, Table 48, for the PATHFINDER study.
Table 26: Adjudicated Progression-Free Survival by Modified IWG-MRT-ECNM Criteria (RAC-RE Population)
Progression-free survival | EXPLORER study January 19, 2023 | PATHFINDER study June 23, 2020 | PATHFINDER study Second data cut-off date: September 9, 2022 | |
|---|---|---|---|---|
All-AdvSMa (N = 57) | All-AdvSM 200 mg dose (N = 17) | All-AdvSMa (N = 32) | All-AdvSM 200 mg dose (N = 81) | |
Events, n (%) | ██ ██ | ██ ██ | ██ ██ | 20 (24.7) |
Censored, n (%) | ██ ██ | ██ ██ | ██ ██ | 61 (75.3) |
Median follow-up, months (95% CI) | ██ ██ | ██ ██ | ██ ██ | ███ █████ ████ |
Kaplan-Meier estimates | ||||
Median PFS, months (95% CI) | ██ ██ | ██ ██ | ██ ██ | NE (39.4 to NE) |
PFS rate, % (95% CI) at time point: | ||||
3 months | ██ ██ | ██ ██ | ██ ██ | ██ |
6 months | ██ ██ | ██ ██ | ██ ██ | ██ |
9 months | ██ ██ | ██ ██ | ██ ██ | ██ |
12 months | ██ ██ | ██ ██ | 79.0 ██ ██ | 83.5 (75.2 to 91.7) |
18 months | ██ ██ | ██ ██ | ██ | ██ |
24 months | ██ ██ | ██ ██ | ██ | 76.5 (66.9 to 86.0) |
30 months | ██ ██ | ██ ██ | ██ | ██ |
36 months | ██ ██ | ██ ██ | ██ | 73.4 (62.5 to 84.3) |
42 months | ██ ██ | ██ ██ | ██ | 62.9 (41.7 to 84.2) |
48 months | ██ ██ | ██ ██ | ██ | ██ |
54 months | ██ ██ | ██ ██ | ██ | ██ |
60 months | ██ ██ | ██ ██ | ██ | ██ |
66 months | ██ ██ | ██ ██ | ██ | ██ |
AdvSM = advanced systemic mastocytosis; ASM = aggressive systemic mastocytosis; CI = confidence interval; IWG-MRT-ECNM = International Working Group - Myeloproliferative Neoplasms Research and Treatment - European Competence Network on Mastocytosis; MCL = mast cell leukemia; NE = not estimable; PFS = progression free survival; RAC-RE = Response Assessment Committee–Response Evaluable; SM-AHN = systemic mastocytosis with an associated hematologic neoplasm.
aIncluded all starting doses of avapritinib (EXPLORER: 30 mg to 400 mg daily; PATHFINDER: 100 mg or 200 mg daily). In the EXPLORER study, the proportion of patients who received an avapritinib starting dose of less than 200 mg, 200 mg, or greater than 200 mg was 14%, 30%, and 56%, respectively, in the RAC-RE population. In the PATHFINDER study (the first data cut-off), 1 (3%) patient received a starting dose of 100 mg; all other patients received avapritinib 200 mg.
Sources: Final Clinical Study Report for the EXPLORER study,15 interim Clinical Study Report for the PATHFINDER study,16 and the PATHFINDER study clinical summary document.17
EORTC QLQ-C30 Global Health Score
Figure 12 and Figure 13 in Appendix 1 show the change from baseline over time for the EORTC QLQ-C30 global health status score. Both studies reported an increase in the mean global health score ranging from ████ ██████ ███ █ █████ ██ ████ ██████ ███ █ █████ at cycle 2, day 1 (N = 40), and cycle 12, day 1 (N = 21), respectively, of the EXPLORER study (final data cut-off date of January 19, 2023), and from 13.3 (SD = 24.3) points at cycle 2, day 1 (N = 80), 18.7 (SD = 28.0) points at cycle 11, day 1 (N = 62), and 20.9 (SD = 28.5) points at cycle 17, day 1 (N = 51), in the PATHFINDER study (second data cut-off date of September 9, 2022). At baseline, ██ ██ ██ ████████ ████) with AdvSM in the EXPLORER study provided EORTC QLQ-C30 results, with ███ ███ ███ of patients reporting data at cycle 2 and cycle 12, respectively. In the PATHFINDER study (second data cut-off), baseline data were available for 97 of 105 (92%) patients, 59% of patients at cycle 11 and 49% of patients at cycle 17.
Harms
Refer to Table 27 for harms data for the EXPLORER study final data cut-off, and the PATHFINDER study’s first and second interim data cut-offs, which had a mean treatment duration of ████ ██████ ███ █ ██████ ███ ██████ ███ █ █████ ███ ████ ██████ ███ █ █████, respectively.
Adverse Events
All patients in the EXPLORER and PATHFINDER studies reported at least 1 AE. The most commonly reported AEs in the EXPLORER and PATHFINDER studies (the second data cut-off) were periorbital edema (69% and 41%, respectively), anemia (57% and 51%, respectively), diarrhea (49% and 31%, respectively), thrombocytopenia (41% and 43%, respectively) and peripheral edema (41% and 47%, respectively).
In the EXPLORER study, ███ of patients experienced at least 1 AE that was at least grade 3 in severity, among which hematologic AEs were common, including ████████████████ ██████ ██████ █████ ███ ███████████ █████. Grade 3 or more severe AEs were reported by 68% of patients in the PATHFINDER study (in the first data cut-off). The most common events were anemia (16%), neutropenia ██████ █████████ ██████████ █████ ██████ ████████ █████ █████████ █████ and thrombocytopenia ████. For the second data cut-off, 83% of patients had experienced at least 1 grade 3 or higher event. ██████ ██████ ███████████ ██████ ███ ████████████████ █████ were reported most commonly.
Serious Adverse Events
SAEs were reported ████ ███ and 51% of patients in the EXPLORER study (in the final data cut-off) and the PATHFINDER study (in the first and second data cut-offs), respectively. In the EXPLORER study, the most common SAEs were ███████ ███████ █████████ ██████████ ████████ █████████ ████████████ ███████████ █████ ███████ █████████ ███ ███████. Limited data on specific SAEs were reported for the PATHFINDER study.
Withdrawals Due to Adverse Events
The proportion of patients who stopped treatment due to AEs was ██████ █████ and 23.8% in the EXPLORER study and in the first and second data cut-offs of the PATHFINDER study, respectively. ████████████ ███████████ █████████ █████████ ███████ ███ █████ ███████ ████████ were the most common reasons reported in the EXPLORER study. Limited information was available for the PATHFINDER study.
Mortality
█████ ████████ ██████ died due to AEs in the EXPLORER study. In the PATHFINDER study, 3 (4.8%) patients and ██ ████████ ██████ died due to AEs in the first and second data cut-offs. Table 27 provides a description of the cause of death.
Table 27: Summary of Harms Results From Studies Included in the Systematic Review (EXPLORER Study Final Data Cut-off, and PATHFINDER Study First and Second Data Cut-offs)
AE | EXPLORER study, all dosesa Final data cut-off: January 19, 2023 (N = 86) | PATHFINDER study, all dosesa First data cut-off: June 23, 2020 (N = 62) | PATHFINDER study, 200 mg dose Second data cut-off: September 9, 2022 (N = 105) |
|---|---|---|---|
Exposure duration, months, mean (SD) | ████ ██████ | ███ █████ | ████ ██████ |
Most common AEs, n (%)b | |||
Patients with at least 1 AE | ██ █████ | 62 (100.0) | 105 (100.0) |
Periorbital edema | ██ ██████ | ██ ██████ | 43 (41.0) |
Anemia | ██ ██████ | ██ ██████ | 54 (51.4) |
Diarrhea | ██ ██████ | 14 (22.6) | 33 (31.4) |
Nausea | ██ ██████ | 11 (17.7) | 25 (23.8) |
Fatigue | ██ ██████ | 9 (14.5) | 20 (19.0) |
Thrombocytopenia | ██ ██████ | ██ ██████ | 45 (42.9) |
Edema, peripheral | ██ ██████ | 31 (50.0) | 49 (46.7) |
Vomiting | ██ ██████ | 11 (17.7) | 21 (20.0) |
Arthralgia | ██ ██████ | | █████ | 18 (17.1) |
Hair colour changes | ██ ██████ | | █████ | 17 (16.2) |
Memory impairment | ██ ██████ | 3 (4.8) | NR |
Pruritus | ██ ██████ | | █████ | 14 (13.3) |
Decreased appetite | ██ ██████ | | █████ | NR |
Abdominal pain | ██ ██████ | | ██████ | 13 (12.4) |
Constipation | ██ ██████ | | █████ | 15 (14.3) |
Headache | ██ ██████ | | █████ | 14 (13.3) |
Hypokalemia | ██ ██████ | | █████ | 8 (7.6) |
Dizziness | ██ ██████ | | █████ | 10 (9.5) |
Dysgeusia | ██ ██████ | | ██████ | 18 (17.1) |
Neutropenia | ██ ██████ | | ██████ | 24 (22.9) |
SAEs occurring in ≥ 2 patients, n (%) | |||
Patients with at least 1 SAE | ██ ██████ | ██ ██████ | 53 (50.5) |
Anemia | | █████ | | █████ | ██ |
Pleural effusion | | █████ | ██ | ██ |
Pneumonia | | █████ | ██ | ██ |
Subdural hematoma | | █████ | 1 (1.6) | ██ |
Hemorrhage, intracranial | | █████ | ██ | ██ |
Acute myeloid leukemia | | █████ | | █████ | ██ |
Ascites | | █████ | | █████ | ██ |
Abdominal pain | | █████ | ██ | ██ |
Acute kidney injury | | █████ | ██ | ██ |
Pyrexia | | █████ | ██ | ██ |
Cholecystitis | | █████ | ██ | ██ |
Vomiting | | █████ | ██ | ██ |
Gastric hemorrhage | | █████ | ██ | ██ |
Gastrointestinal hemorrhage | | █████ | | █████ | ██ |
Upper gastrointestinal hemorrhage | | █████ | ██ | ██ |
Diverticulitis | | █████ | ██ | ██ |
Gastroenteritis | | █████ | ██ | ██ |
Large intestine perforation | | █████ | ██ | ██ |
Pancreatitis | | █████ | ██ | ██ |
Encephalopathy | | █████ | ██ | ██ |
Chronic kidney disease | | █████ | ██ | ██ |
Hypokalemia | | █████ | ██ | ██ |
Permanent treatment discontinuation due to AEs in ≥ 2 patients, n (%) | |||
Patients who stopped treatment | ██ ██████ | | ██████ | 25 (23.8) |
Intracranial hemorrhage | | █████ | ██ | ██ |
Cognitive disorder | | █████ | ██ | ██ |
Ascites | | █████ | ██ | ██ |
Acute myeloid leukemia | | █████ | | █████ | ██ |
Deaths, n (%) | |||
On-study deaths due to AEs | | █████ | 3 (4.8) | | █████ |
Description (each event reported in 1 patient only) | ██ ██████ | Disease progression Necrotizing fasciitis Hemorrhagic shock | ██ ██████ |
AEs of special interest, n (%) | |||
Intracranial bleeding | ██ ██████ | 1 (1.6) | 4 (3.7) |
Hemorrhage, intracranial | | █████ | ██ | ██ |
Subdural hematoma | | █████ | 1 (1.6) | ██ |
Cognitive effects | ██ ██████ | 7 (11.3) | 29 (27.6) |
Memory impairment | ██ ██████ | 3 (4.8) | ██ |
Cognitive disorder | ██ ██████ | 2 (3.2) | ██ |
Confusional state | ██ ██████ | 3 (4.8) | ██ |
Amnesia | | █████ | ██ | ██ |
Encephalopathy | | █████ | ██ | ██ |
Somnolence | | █████ | ██ | ██ |
AE = adverse event; NR = not reported; SAE = serious adverse event; SD = standard deviation.
aIn the EXPLORER study, 15%, 24%, and 58% of patients in the safety population received an avapritinib starting dose of less than 200 mg, 200 mg, or greater than 200 mg, respectively. In the PATHFINDER study (in the first data cut-off), 2 of 62 (3%) patients received a starting dose of 100 mg; all other patients received avapritinib 200 mg.
bAEs reported in 20% or more of patients in any study population.
Sources: Final Clinical Study Report for the EXPLORER study,15 interim Clinical Study Report for the PATHFINDER study,16 the PATHFINDER study clinical summary document,17 and Sponsor Summary of Clinical Evidence.14
Notable Harms
Intracranial bleeding was identified as an AE of special interest by the sponsor, and by the clinical experts who were consulted for this review. In the EXPLORER study ██ ████████ ███████ experienced intracranial bleeding. In the PATHFINDER study, 1 (1.6%) patient in the first data cut-off and 4 (3.7%) patients in the second data cut-off experienced intracranial bleeding.
Cognitive AEs were common and were reported by █████, 11.3%, and 27.6% of patients in the EXPLORER study and in the first and second data cut-offs of the PATHFINDER study, respectively. These events included ██████ ███████████ █████████ █████████ ███████████ ██████ ████████ ███████████████ ███ ██████████.
Critical Appraisal
Internal Validity
The sponsor submitted information on a completed phase I trial (with 86 patients) and an ongoing phase II trial (with 62 patients and 105 patients in the first and second data cut-offs, respectively). Both pivotal trials were open-label, single-arm studies, and thus provided no direct evidence on comparative efficacy or safety. The lack of controlled trials has implications for the overall strength and interpretability of the results. With single-arm studies, there is an increased risk of bias in the estimation of treatment effects due to the potential for confounding related to natural history and prognostic factors. Moreover, the extent of any selection bias is difficult to ascertain. The clinical experts emphasized that AdvSM is a heterogeneous disease, and prognosis varies substantially based on the disease subtype and other factors. In the trials, few patients had a diagnosis of ASM or MCL, which typically have the most and least favourable prognosis of the 3 subtypes, respectively. Most patients had a diagnosis of SM-AHN, which the clinical experts stated has a variable prognosis, depending largely on the type of concurrent hematologic neoplasm. The distribution of AdvSM subtypes has the potential to affect the results, but the extent of the impact is unknown. In addition, the Clinical Study Reports did not provide any information on the number of patients screened for inclusion in the trial or the reasons for exclusion, so there is no information on the pool of patients who were considered for enrolment. The primary outcome (ORR) and other response-related outcomes were analyzed in a subset of patients enrolled in the studies, not in the entire population with AdvSM. The RAC-RE population consisted of patients who, at baseline, were evaluable according to modified IWG-MRT-ECNM criteria and who met the follow-up requirements (≥ 2 complete postbaseline bone marrow assessments and had been in the study for ≥ 6 cycles, or had an end-of-study visit). The RAC-RE population consisted of 83%, 52%, and 77% of the overall AdvSM population enrolled in the EXPLORER study and in the first and second data cut-offs of the PATHFINDER study, respectively. Although the baseline characteristics of the RAC-RE population and the overall study population appeared to be similar, and the OS estimates were comparable in both populations, the analysis of a subpopulation for the response-related end points is another potential source of selection bias. It is unclear if patients who were evaluable based on the modified IWG-MRT-ECNM criteria (i.e., had 1 or more C-findings attributable to AdvSM) are prognostically similar to patients who did not meet these criteria.
While the lack of a comparator group in the pivotal evidence limits the overall interpretation of the results, the feasibility of conducting a randomized controlled trial was low, given the rarity of AdvSM, and potential ethical issues were raised by the clinical experts consulted due to the efficacy and safety of the available comparators.
The primary outcome was based on ORR according to the modified IWG-MRT-ECNM criteria. The clinical experts noted that response criteria used are evolving to best capture clinical benefit and to better define long-term outcomes, given the availability of targeted therapies. Major response criteria that have been used in clinical trials and in clinical practice include the Valent criteria (plus its modified version), the Mayo criteria, the IMWG-MRT-ECNM criteria (plus its modified version), and more recently, the pure pathologic response criteria and the European Competence Network on Mastocytosis–American Initiative in Mast Cell Diseases criteria. According to the clinical experts consulted, there are no clear data to suggest which response criteria perform better in terms of predicting long-term outcomes like survival. In the pivotal trials, overall response was defined as patients with CR, CRh, PR, and clinical improvement, which the clinical experts agreed were relevant measures. The FDA decision on avapritinib was based on patients with CR or PR, excluding those whose best response was clinical improvement. The clinical experts consulted, however, stated that clinical improvement, without a PR or CR, can have a profound impact on a patient’s quality of life and survival; thus, they advocated for using the broader definition of response.
The pivotal trials were open-label, whereby the investigator and the study participants were aware of their treatment status, potentially increasing the risk of detection bias and performance bias. As such, the open-label trial design limits the interpretability of the subjective study outcomes, such as AdvSM-SAF, and AEs. The sponsor noted that there is subjectivity in assessing some components of the modified IWG-MRT-ECNM criteria, specifically if the C-findings are attributable to SM or to some other cause. The sponsor attempted to mitigate the reporting bias by requiring response outcomes to be adjudicated by a central committee, using bone marrow samples, radiographs, and laboratory samples that were evaluated centrally by independent specialists. Sensitivity analyses were conducted for ORR using an algorithm and investigator-assessed response. In the EXPLORER study, the ORR was similar for the RAC (█████), algorithm (█████), and investigator assessment of overall response (█████) which were based on the modified IWG criteria, as well as the ORR based on the unmodified IWG-MRT-ECNM criteria (█████). However, greater variation was noted across assessment methods in the PATHFINDER study interim analysis (June 23, 2020), which reported an algorithm-assessed ORR of █████ (based on the unmodified IWG-MRT-ECNM criteria) and an investigator-assessed ORR of █████ (based on modified IWG-MRT-ECNM criteria). Both estimates were lower than the centrally assessed ORR (75.0%), which was based on the modified IWG-MRT-ECNM criteria. The sponsor attributed the lower scores to the differences in the criteria and to the investigator basing decisions on data from response assessment visits only versus all study visits for the RAC. It is possible that the methods used to assess response could bias the findings, but the magnitude of any reporting bias remains unclear.
The sponsor initially supplied results from 2 data cut-offs for the PATHFINDER study. Results from these data cut-off dates are the focus of this report. The first data cut-off date was the protocol-specified interim analysis (June 23, 2020) and according to the sponsor, the second data cut-off date (September 9, 2022) was performed to provide data to the Study Steering Committee for regular response adjudication and for publication. Two other adjudication data cut-offs were conducted, dated April 2021 and September 15, 2023. Later on during the review, in response to an additional information request from the review team, the sponsor provided limited information on the results of the September 15, 2023, data cut-off, which appeared to be supportive of the earlier results submitted by the sponsor. For a brief summary of the updated findings, refer to the Interpretation of Results section. The primary outcome was tested versus a historical null value (28%), which was based on the midostaurin registration trial data and was calculated post hoc using the original IWG-MRT-ECNM criteria.37 According to the study’s protocol, if at the interim analysis the primary outcome was statistically significant versus the 28% null value, these data would be used for marketing applications. Early assessment of study outcomes may be associated with inflated findings, and in this study, the interim analysis was conducted when 32 of the 62 patients were evaluable (information fraction = 51.6%). However, considering that subsequent data cut-off dates showed results similar to the interim data, some concerns regarding inflated results are allayed. The September 2022 and September 2023 data cut-offs provided data with a larger sample size and longer follow-up duration than the interim results, but since these were not based on preplanned interim analyses, these data should be interpreted as exploratory. Moreover, the P values reported for the September 2022 and September 2023 data cut-offs were not controlled for multiplicity; thus, there is an inflated familywise risk of type I error. There was no control of type I error in the EXPLORER study.
Patient input expressed how the symptoms of AdvSM may have a substantial impact on their quality of life. The clinical experts noted that changes in symptoms may not be captured in response criteria; consequently, an assessment of patient-reported symptoms was an important outcome in the clinical trials. The studies reported data for the AdvSM-SAF questionnaire, which the sponsor developed and evaluated using data from 31 patients from the EXPLORER study. Based on their analysis, the TSS showed good construct validity and reliability, and moderate responsiveness. The AdvSM-SAF results were not available for all patients, with data missing for ███ ███ ███ of patients at baseline, and for ███ ███ ███ of patients at cycle 11, for the EXPLORER and PATHFINDER studies (in the first data cut-off), respectively. There was no imputation for missing data in the EXPLORER study but in the PATHFINDER study, the last observation carried forward method was used to impute data for patients who stopped treatment before completing 10 cycles. Given the extent of missing data, this imputation method will overestimate the precision of the estimates, with 95% CIs that are too narrow relative to the amount of data actually observed. The AdvSM-SAF results may be biased due to the extent of missing data and the imputation methods used, limiting the interpretability of these data.
The trials reported Kaplan-Meier estimates for the time-to-event outcomes. OS, PFS, and time to response were exploratory end points in the EXPLORER study and secondary outcomes in the PATHFINDER study. The median OS was not met for either study, and the median PFS was not met for the PATHFINDER trial; thus, these data were considered immature. Additionally, comparative OS and PFS cannot be adequately assessed in a single-arm trial because all patients receive the same treatment. The FDA 2021 medical review report for Ayvakyt (avapritinib) oral (application number 212608) states that OS and patient-reported outcomes cannot be interpreted due to the absence of a preplanned comparator in the trials and the open-label design of the studies; therefore, according to the FDA report, the presentation of OS results had an exploratory purpose.11
According to the EXPLORER study’s statistical analysis plan, efficacy outcomes were based on patients who received any dose of avapritinib. Only 21 of 86 (24%) patients received the Health Canada recommended starting dose of 200 mg daily. One-half of the patients enrolled received a 300 mg per day starting dose, 17% of patients received less than 200 mg per day (i.e., 30 mg, 60 mg, 100 mg, or 130 mg), and 8% of patients started with 400 mg daily. The dose distribution was similar for the RAC-RE population (████ ███ ███ ███ received < 200 mg, 200 mg, and > 200 mg starting doses, respectively). Despite the different starting doses, the average mean daily dose was comparable in the 200 mg subgroup (█████ ██) to the overall safety population (█████ ██). The results reported for the 200 mg subgroup were generally consistent with those of the overall population but should be interpreted with caution considering the limited sample size (17 patients and 20 patients for ORR and OS, respectively). It is unclear how variation in starting doses received impacted the efficacy findings. However, according to the sponsor, some AEs were associated with higher starting doses. Based on the data from the EXPLORER trial, the dosing and patient enrolment criteria were modified for the PATHFINDER study to improve safety.
Overall, the sample size of the trials was limited, with a total of 86 patients, 69 patients, and 57 patients providing data on safety, OS, and response end points, respectively, in the EXPLORER trial. For the PATHFINDER study, 62 patients provided safety and OS data and 32 patients provided response data in the first data cut-off. A total of 105 patients provided safety data and 86 patients provided response data in the second data cut-off. The magnitude of the treatment effect estimates observed in a relatively small study sample may not be replicable in a larger study sample. Interpretation of the safety data should consider the limited sample size and the mean exposure duration (████ ██████ ███ ████ ██████ for the EXPLORER and PATHFINDER studies, respectively). Although results were reported for subgroups by AdvSM subtypes, the ASM and MCL subgroups were particularly small (4 patients to 15 patients, depending on the outcome and data cut-off); thus, the results should be interpreted with caution. Results for the subgroups with and without prior treatments for SM may be confounded due to differences between groups at baseline and should be interpreted as exploratory.
The sponsor-submitted materials for both studies lacked clarity for aspects of the trial methods, particularly the disposition of patients in the different cohorts and data cut-offs, and the statistical analysis of the results. Further, the data supplied for the PATHFINDER study’s second data cut-off were incomplete and based on a summary document rather than on a Clinical Study Report. Several errors and omissions were found in the Sponsor Summary of Clinical Evidence template that was received for this review.
External Validity
The studies enrolled similar patient populations of adults with a confirmed diagnosis of AdvSM according to the WHO diagnostic criteria. The EXPLORER study also enrolled 20% of patients with other forms of SM, who were not consistent with the indicated population. Patients with nonadvanced forms of SM contributed to the safety data but not for efficacy outcomes in the EXPLORER trial. The average age of patients enrolled was late 60s, and most patients had a diagnosis of SM-AHN and an ECOG PS score of 0 or 1. In Canada, SM-AHN is the most common type of AdvSM, which is consistent with the studies. The majority of study patients had received systemic treatments for AdvSM, including 33% to 53% of patients who had received midostaurin. This treatment pattern is not consistent with clinical practice, as midostaurin is largely unavailable to patients with AdvSM in Canada. However, the experts consulted for this review did not believe that prior exposure to midostaurin would significantly impact response to avapritinib. The clinical experts consulted noted that the proportion of patients with high ECOG PS scores was lower than expected; thus, the study patients may have been less ill than patients who receive avapritinib in clinical practice. The trials excluded patients with comorbidities such as seizure disorder, long QT syndrome, HIV or active viral hepatitis, clinically significant uncontrolled cardiovascular disease, and reduced renal or hepatic function. In addition, patients with a higher risk of intracranial bleeding were excluded; thus, the safety and efficacy of avapritinib in these patients is unknown.
As noted earlier, only one-quarter of patients in the EXPLORER study received the recommended starting dose of avapritinib (200 mg), with most patients receiving a higher-than-recommended initial dose. This may impact the generalizability of the findings to the real-world population, particularly for safety, as the sponsor identified dose-related toxicities.
The outcomes reported in the trial were identified as important in the patient input submitted. While the clinical experts expressed that the components of the response criteria used in the trial to evaluate treatment response (e.g., mast cell burden in bone marrow; hematologic values and tryptase levels; the need for transfusions, diuretics, or paracentesis; a reduction in liver or spleen size and improvement in liver function tests) were relevant and appropriate, they noted that the detailed and specific nature of the IWG response criteria can make it time-consuming to use in clinical practice. Patients’ perception of the severity of symptoms and their impact on quality of life was also identified as important in the patient input submitted. While patient-reported symptoms were assessed in the trials, these data had limited internal validity and, therefore, their external validity cannot be assessed.
GRADE Summary of Findings and Certainty of the Evidence
Methods for Assessing the Certainty of the Evidence
For pivotal studies identified in the sponsor’s systematic review, GRADE was used to assess the certainty of the evidence for outcomes considered most relevant to inform the CDA-AMC expert committee deliberations, and a final certainty rating was determined as outlined by the GRADE Working Group.12,13
“High certainty: We are very confident that the true effect lies close to that of the estimate of the effect.
Moderate certainty: We are moderately confident in the effect estimate — The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. We use the word ‘likely’ for evidence of moderate certainty (e.g., ‘X intervention likely results in Y outcome’).
Low certainty: Our confidence in the effect estimate is limited — The true effect may be substantially different from the estimate of the effect. We use the word ‘may’ for evidence of low certainty (e.g., ‘X intervention may result in Y outcome’).
Very low certainty: We have very little confidence in the effect estimate — The true effect is likely to be substantially different from the estimate of effect. We describe evidence of very low certainty as ‘very uncertain.’”
Although GRADE guidance is not available for noncomparative studies, the CDA-AMC review team assessed pivotal single-arm trials for study limitations (this refers to internal validity or risk of bias), inconsistency across studies, indirectness, the imprecision of effects, and publication bias to present these important considerations. Because the lack of a comparator arm does not allow for a conclusion to be drawn on the effect of the intervention versus any comparator, the certainty of evidence for single-arm trials started at very low certainty with no opportunity for rating up.
For the GRADE assessments, findings from the EXPLORER and PATHFINDER trials were considered together and summarized narratively per outcome because these studies were similar in population, interventions, design, and outcome measures.
Results of GRADE Assessments
Table 2 presents the GRADE summary of findings for avapritinib.
Indirect Evidence
Content in this section has been informed by materials submitted by the sponsor. The following has been summarized and validated by the CDA-AMC review team.
Objectives for the Summary of Indirect Evidence
The pivotal evidence for efficacy of avapritinib was based on single-arm trials (EXPLORER and PATHFINDER studies). In the absence of comparative evidence for avapritinib with currently available treatments for AdvSM, the sponsor submitted 1 indirect treatment comparison and 1 observational comparison to address this knowledge gap. This section provides a summary and appraisal of the indirect evidence submitted by the sponsor. The indirect treatment comparison and updated results of the observational comparison were used to inform the sponsor’s economic analyses.
Description of Indirect Treatment Comparison and Observational Comparison
The indirect treatment comparison was based on a published MAIC comparing avapritinib with midostaurin on OS, ORR, and CR. The IPD observational comparison was based on propensity scoring methods comparing avapritinib with midostaurin, and with real-world BAT, on OS and the duration of treatment. The objective of the sponsor-submitted analyses was to estimate the relative efficacy of avapritinib versus currently available treatments in Canada for patients with AdvSM. The objective of the indirect treatment comparison was to estimate the relative efficacy of avapritinib and midostaurin based on a published MAIC in patients with AdvSM.39 The objective of the IPD observational comparison (the BLU-285 to 2405 study; identification number NCT04695431) was to estimate the relative efficacy of avapritinib and real-world patients receiving BAT (including cladribine, imatinib, interferon, and midostaurin) for AdvSM, based on a published external cohort study40 and the sponsor’s observational comparison report41 with updated (unpublished) analyses.42-44
Analyses based on an initial data cut-off date of April 20, 2021, were conducted but not presented in this Clinical Review Report based on the sponsor’s identification of its limited relevance arising from the limited follow-up duration and the data not being submitted in the pharmacoeconomic model.
Study Selection Methods
Methods of identifying studies for inclusion in the indirect evidence are summarized in Table 28.
Indirect Treatment Comparison
A systematic literature review was conducted on January 22, 2021, to identify potential studies for inclusion in the MAIC. Of 3,001 potentially relevant records identified from database searches, 166 citations were relevant to the research question and 6 additional records were identified from conference searches, bibliographic searching, and Clinical Study Reports, for a total of 58 publications representing 31 studies included in the systematic literature review. Details of the literature search (e.g., databases, date parameters, search filters), study selection process (e.g., duplicate reviewers), and data extraction (e.g., single reviewer, duplicate extraction) were not reported. Assessment of study quality was not reported in the MAIC.
Observational Comparison
Methods used to screen and select studies for inclusion in the observational comparison were not reported.
Table 28: Study Selection Criteria and Methods for the Indirect Treatment Comparison and Observational Comparison
Criteria | Indirect treatment comparison | Observational comparison |
|---|---|---|
Population (study selection) | Adult patients with AdvSM, including ASM, SM-AHN, and MCL | Adult patients aged 18 years or older with AdvSM with documented subtype (ASM, SM-AHN, and MCL) |
Intervention | Study selection:
| Index cohort:
|
Comparator | Study selection:
| External control cohort:
|
Outcome | Including but not limited to:
Subgroups:
|
|
Study design (study selection) | RCTs, non-RCTs, single-arm trials, retrospective and prospective cohort studies, real-world evidence studies, bibliographies of systematic reviews and meta-analyses | Not reported |
Publication characteristics (study selection) | Published and unpublished studies | Not reported |
Exclusion criteria | Study selection:
| External control cohort:
|
Databases searched | Not reported | Not reported |
Selection process | Not reported | Not reported |
Data extraction process | Not reported | Not reported |
Quality assessment | Not reported | Not reported |
AdvSM = advanced systemic mastocytosis; AE = adverse event; AHN = associated hematologic neoplasm; ASM = aggressive systemic mastocytosis; BAT = best available therapy; CR = complete remission; MCL = mast cell leukemia; ORR = overall response rate; OS = overall survival; RCT = randomized controlled trial; SM = systemic mastocytosis; SM-AHN = systemic mastocytosis with associated hematologic neoplasm.
Sources: Pilkington et al.,39 Reiter et al.,40 the sponsor’s observational comparison report,41 and Sponsor Summary of Clinical Evidence.14
Analysis Methods
Analysis methods for the indirect treatment comparison and the observational comparison are summarized in Table 29.
Indirect Treatment Comparison
Four open-label, single-arm trials of patients with AdvSM were included in the MAIC evaluating avapritinib (EXPLORER and PATHFINDER studies) and midostaurin (the D2201 and A2213 trials). As described previously in the Systematic Review section (pivotal evidence), the EXPLORER study was a phase I trial that included a dose escalation stage to assess safety and tolerability (in part 1) and a dose expansion stage to evaluate efficacy (ORR as a secondary outcome and OS as an exploratory outcome) and safety (in part 2); the PATHFINDER study is an ongoing phase II trial that assessed adjudicated ORR per modified IWG-MRT-ECNM as the primary end point and OS as a secondary end point. The D2201 study (identification number NCT00782067) and the A2213 study (identification number NCT00233454) were phase II trials that assessed ORR as a primary end point; the D2201 trial assessed Study Steering Committee–adjudicated ORR per modified Valent criteria whereas the A2213 trial assessed investigator-adjudicated ORR per original Valent criteria. For the MAIC, OS (defined as the time from the start of study treatment to death due to any cause) was the primary end point based on consistency in definition across the included studies.
Since all identified studies in the MAIC were single-arm trials, precluding anchored indirect comparison techniques, an unanchored MAIC based on the methods described by Signorovitch et al.,45 Phillippo et al.,46 and NICE guidance19 was used to estimate the relative efficacy of avapritinib versus midostaurin on OS, ORR, and CR. Analyses were performed using R with the MAIC software package, and Kaplan-Meier plots were produced using the survminer software package.
Exploratory subgroup analyses were conducted to identify variables for matching used in the MAIC, harnessing pooled data for avapritinib (EXPLORER and PATHFINDER studies RAC-RE population) that were also reported in the midostaurin trials (the D2201 and A2213 trials’ primary efficacy population) for OS, ORR, and CR:
study (PATHFINDER or EXPLORER)
age (≥ median or > median in comparator population)
gender (female or male)
race (non-white or white) [from original source]
ECOG PS score (≥ 2 or ≤ 1)
prior systemic therapy (yes or no)
AdvSM subtype (ASM, MCL, or SM-AHN)
KIT D816V mutation status (D816V negative or D816V positive)
bone marrow mast cell burden (≥ median or > median in comparator population)
serum tryptase level (≥ median or > median in comparator population)
number of C-findings (0, 1, 2, or ≥ 3).
Patient characteristics were explored in univariate Cox proportional hazards models for OS and in univariate logistic regression models for ORR and CR; P values of less than 0.1 indicated the potential of a characteristic being a prognostic factor for the corresponding end point.
Sensitivity analyses in the MAIC are listed in Table 29.
Subgroup analyses of the primary end point of OS were not reported in the MAIC.
Observational Comparison
IPD were retrospectively collected using data from the EXPLORER and PATHFINDER trials for avapritinib and from the medical chart data of participating study sites for the BAT cohort. Data for the avapritinib cohort included patients enrolled in the EXPLORER study (from March 2016 to March 2020) and the PATHFINDER study (from November 2018 to June 2020) from study sites in Europe, the US, and Canada (1 site). Data for the BAT cohort included patients who received systemic treatment at study sites in Austria, Germany, Spain, the UK, and the US from January 2009 to October 2021. A later data cut-off date of September 9, 2022, for the avapritinib data was considered more relevant by the sponsor due to a longer follow-up. Additionally, the sponsor reported that as a result of consultations with the EMA, analyses for the observational comparison using IPTW were restricted to the PATHFINDER trial with a larger sample size where most patients received an avapritinib 200 mg dose, for inclusion in an integrated dataset for updated analyses.
The avapritinib cohort included patients enrolled in the PATHFINDER study with a confirmed AdvSM diagnosis of a known subtype, as determined by the RAC, and who initiated any dose of avapritinib. Patients in the BAT cohort were identified based on the inclusion and exclusion criteria of the avapritinib trials, and included adult patients aged 18 years or older who had a confirmed AdvSM diagnosis of a known subtype and had received at least 1 line of systemic therapy for AdvSM (refer to Table 29 for key inclusion criteria). The primary efficacy end point in the observational comparison was OS. In the avapritinib cohort, OS was defined as the time from the first dose of avapritinib to death due to any cause. In the BAT cohort, OS was defined as the time from the initiation of each eligible line of systemic treatment (first line of therapy, or a second line or later line of therapy) to death due to any cause. The secondary efficacy end point in the observational comparison was the duration of treatment, defined in the avapritinib cohort as the time from the first dose of avapritinib to the last dose of avapritinib and defined in the BAT cohort as the time from an eligible line of systemic treatment to discontinuation of the same line of treatment, for any reason. While duration of treatment was not included as an outcome in the pivotal evidence and the clinical experts consulted for this review did not identify this as an important outcome, time on treatment was used to inform the sponsor’s pharmacoeconomic model. The safety end point included AEs described for the BAT cohort (i.e., the occurrence of AEs that resulted in treatment modification or discontinuation, hospitalization, or death); since AEs for the avapritinib population were not reported, available information on AEs are not presented in the results.
Baseline covariates including prognostic factors and treatment effect modifiers were identified through published literature; key covariates that were used in adjusted comparative analyses were based on published literature, prognostic scores (e.g., Mutation-Adjusted Risk Score, International Prognostic Scoring System for Mastocytosis), and clinical input.40 Comparative analyses, adjusting for key baseline covariates, were conducted using a 2-step process to obtain an effect estimate:47 1) before reviewing or analyzing outcome data, stabilized IPTW weights were created and applied to balance the differences in key covariates between the avapritinib and BAT cohorts, and 2) an IPTW-weighted multivariable Cox proportional hazards model, with further adjustment for remaining imbalances in the distribution of key covariates in the weighted cohorts, was used to compare survival between the avapritinib and BAT cohorts. The IPTW approach used weights to create a “pseudopopulation” (an effective sample after IPTW weighting) in which the distribution of baseline covariates was approximately the same in each patient cohort under comparison, to mitigate potential confounding by measured baseline characteristics (Austin and Stuart).48 Imbalances in baseline characteristics between the avapritinib and BAT cohorts were first assessed using standardized differences. For each variable, a standardized difference greater than 10% was considered indicative of meaningful imbalance between the 2 cohorts (Austin and Stuart).48 To implement the IPTW approach, weights were created through propensity score modelling, where the propensity score was defined as the probability of receiving treatment (i.e., receiving treatment with avapritinib), conditional on an observed set of baseline covariates. All a priori specified key covariates, regardless of the magnitude of the standardized difference, were included in the propensity score model. Based on the propensity score, for each line of therapy included in the analysis, IPTW weights were calculated as the inverse of the conditional probability of being in the respective treatment group (i.e., avapritinib or BAT), conditional on the prespecified key covariates included in the model. To enhance precision in the effect estimates, the weight for each included line of therapy was stabilized by the marginal probability of being in the respective treatment group. Stabilized IPTW weights were calculated to include the marginal probability that the line of therapy was received as part of the avapritinib cohort and the marginal probability that the line of therapy was received as part of the external BAT cohort. To reduce variability, stabilized weights were truncated at the first and 99th percentiles.
Unadjusted OS was analyzed using the Kaplan-Meier method, with an unadjusted Cox proportional hazards model estimating HRs, with corresponding 95% CIs and P values. Unadjusted survival rates were obtained using the Nelson-Aalen estimator49,50 at 3 months, 6 months, 9 months, 12 months, 18 months, 24 months, 30 months, 36 months, 48 months, and 60 months; unadjusted OS estimates were obtained using the Kaplan-Meier method with a log-rank test. Robust variance estimation was estimated to account for the within-patient correlation of BAT cohort patients who contributed multiple lines of therapy as well as the application of weights. The proportional hazards assumption was evaluated using the Kolmogorov-type supremum tests,51 in which a P value of less than 0.05 suggested violation of the proportionality assumption. An adjusted Cox proportional hazards model provided the HR with a corresponding 95% CI and P value. Adjusted survival rates at 3 months, 6 months, 9 months, 12 months, 18 months, 24 months, 30 months, 36 months, 48 months, and 60 months were obtained using the Nelson-Aalen estimator,49,50 weighted by stabilized IPTW weights. Adjusted OS estimates up to each of these time points were obtained using the Kaplan-Meier method with a log-rank test, weighted by stabilized IPTW weights. A 2-sided P value less than 0.05 was considered statistically significant without a multiplicity adjustment. All data cleaning and analyses were conducted using SAS Enterprise Guide version 7.1 software and R version 3.6.3. Patients in the avapritinib cohort who were alive during the observation period were censored at the last date known to be alive. Patients in the BAT cohort who were alive during the observation period were censored at the date of last contact with the study site.
Descriptive analyses and IPTW were performed for baseline characteristics for each subgroup; an unadjusted comparison and the IPTW-weighted comparison with covariate adjustment were used for the OS primary end point analysis for subgroup analyses (refer to Table 29). Updated analyses were conducted comparing avapritinib as first-line therapy to BAT first-line therapy (excluding midostaurin), avapritinib as second-line or later-line therapy to BAT (including midostaurin) as second-line or later-line therapy, and avapritinib first-line therapy to midostaurin first-line therapy for the outcomes of OS and the duration of treatment.
The duration of treatment was described using Kaplan-Meier analysis and compared between the trial and external cohorts using a Cox proportional hazards model weighted by the stabilized weights as described for OS. If the treatment start date and end date were the same, it was assumed that the patient received 1 cycle of treatment with a treatment duration of 1 day. The median duration of treatment and adjusted HR with a corresponding 95% CI were reported. The proportion of patients with no treatment discontinuation was reported for 3 months, 6 months, 9 months, 12 months, and 18 months after the index date and the duration of treatment for up to each of these time points was compared between the 2 cohorts using a log-rank test weighted by the stabilized weights. Patients in the avapritinib cohort who had not ended treatment were censored at the date of the last dose or if missing, at the data cut-off date. Patients in the BAT cohort who had not discontinued a given line of therapy by the study end date were censored at the date of the last known treatment prescription or medication dose or if missing, at the date of the last recorded follow-up.
In the sponsor’s pharmacoeconomic model, cladribine, imatinib, and interferon were included in the BAT cohort for first-line and second-line treatments. Midostaurin was included in the BAT cohort for first-line (as a scenario) and second-line treatments.
Table 29: Indirect Treatment Comparison and Observational Comparison Analysis Methods
Methods | Indirect treatment comparison | Observational comparison |
|---|---|---|
Analysis methods | Unanchored MAIC | IPTW |
Comparators | Avapritinib vs. midostaurin |
|
Data sources | Data cut-off date of April 2020 Avapritinib
Midostaurin
| Updated analyses from data cut-off date of September 9, 2022 (OS) Avapritinib 200 mg
Real-world cohort
|
Population | Adult patients with AdvSM, including ASM, SM-AHN, and MCL | Adult patients 18 years or older with a confirmed AdvSM diagnosis of known subtype Avapritinib
BAT
|
Outcomes | Primary
Additional
| Primary
Secondary
Safety
|
Timing of end points (follow-up) | OS, months, median
Months, median (not by end point or analysis population)
| OS follow-up, months, mean
Duration of treatment (IPTW-weighted), months, median
|
Model estimation |
|
|
Variable identification approach | Matching variables (prognostic factors) used in the MAIC were identified using exploratory subgroup analyses: univariate Cox proportional hazards models for OS, and univariate logistic regression models for ORR and CR. | Prognostic factors and treatment effect modifiers were identified from literature and clinical input. |
Covariates included | OS
ORR, CR
| OS, duration of treatment
|
Criteria for selection of covariates | Based on patient characteristics reported in the avapritinib trials that were also reported in the midostaurin trials; factors with a P value < 0.1 (arbitrary) based on exploratory subgroup analyses for the corresponding end points were selected for matching The number of C-findings per patient (0, 1, 2, or ≥ 3) could not be used as a covariate due to the noncomparability of this factor across studies of avapritinib (patients in the EXPLORER and PATHFINDER studies could have a maximum of 5 C-findings) and midostaurin (patients in the D2201 and A2213 trials could have a maximum of 8 to 10 C-findings). | Based on key covariates available and harmonization of outcome definitions in the integrated dataset containing patient-level data. For each covariate, a standardized difference > 10% was considered indicative of meaningful imbalance between the 2 cohorts. Patients in the BAT cohort were excluded if they had missing data on a key adjustment covariate. |
Assessment of distribution or overlap in propensity score or patient weights | Effective sample size was evaluated to assess the impact of matching and adjusting on the sample size. | Distribution of weights and propensity score by treatment (avapritinib or BAT) in unadjusted weightings, with further adjustment for key covariates that remained unbalanced after weighting (2-sided P < 0.05 considered statistically significant without multiplicity adjustment). Robust variance estimation to account for within-patient correlation of BAT cohort patients who contributed multiple lines of therapy, as well as for application of weights |
Assessment of balance | Comparison of baseline characteristic summary statistics before and after matching and adjusting | Comparison of standardized mean differences before and after weighting to assess degree of covariate balance |
Sensitivity analyses | Primary population: Efficacy population (pooled RAC-RE population in the EXPLORER and PATHFINDER studies and pooled primary efficacy population in D2201 and A2213 trials)
| For OS
|
Subgroup analysis | None | For OS
|
1L = first-line; 2L+ = second-line or later-line; AdvSM = advanced systemic mastocytosis; AE = adverse event; ASM = aggressive systemic mastocytosis; BAT = best available therapy; CR = complete remission; ECOG PS = Eastern Cooperative Oncology Group Performance Status; HR = hazard ratio; IPTW = inverse probability of treatment weighting; IWG-MRT-ECNM = International Working Group - Myeloproliferative Neoplasms Research and Treatment - European Competence Network on Mastocytosis; MAIC = matching-adjusted indirect comparison; MCL = mast cell leukemia; ORR = overall response rate; OS = overall survival; RAC-RE = Response Assessment Committee–Response Evaluable; SM-AHN = systemic mastocytosis with associated hematologic neoplasm; vs. = versus.
Sources: Pilkington et al.,39 Reiter et al.,40 the sponsor’s observational comparison report,41 and Sponsor Summary of Clinical Evidence.14
Results of Indirect Treatment Comparison and Observational Comparison
Summary of Included Studies
Indirect Treatment Comparison
In the MAIC, differences were observed across the avapritinib trials (the RAC-RE populations of the EXPLORER study [N = 53] and the PATHFINDER study [N = 32]), and the midostaurin trials (the A2213 trial [N = 26] and the D2201 trial [N = 89]) for ECOG PS, prior therapy, AdvSM subtypes, serum tryptase level, and a KIT D816V mutation status. While most patients across all trials had a KIT D816V mutation, nearly all of the patients in the avapritinib trials were positive for the mutation status. More patients in the avapritinib trials had an ECOG PS score of 0 or 1 and SM-AHN compared to the midostaurin trials. More patients in the midostaurin trials had ASM and were without a KIT D816V mutation compared to those in the avapritinib trials. In the avapritinib trials, C-findings were more evenly distributed among the 4 categories (0, 1, 2, or ≥ 3), with most patients having 1 C-finding. In the midostaurin trials, most patients had 2 to 3 or more C-findings. The baseline characteristics of patients in the safety population of the avapritinib trials (EXPLORER: n = 69; PATHFINDER: N = 62) and the full analysis set of the midostaurin trials (the A2213 trial [N = 26] and the D2201 trial [N = 116]) were similar overall to those of patients in the RAC-RE population of the avapritinib trials and the primary analysis set of the midostaurin trials.
Table 30: Baseline Characteristics Before Matching for Avapritinib and Midostaurin in the Indirect Treatment Comparison
Characteristic | EXPLORER study: data cut-off April 2020 | PATHFINDER study; data cut-off April 2020 | A2213 study | D2201 study |
|---|---|---|---|---|
Treatment | Avapritinib | Avapritinib | Midostaurin | Midostaurin |
Population | RAC-RE (n = 53) | RAC-RE (n = 32) | PEP (n = 26) | PEP (n = 89) |
Age (years), median (range) | 65 (34 to 83) | 68 (37 to 85) | 64.5 (24 to 79) | 64 (25 to 82) |
Sex, n (%) | ||||
Male | 30 (57) | 18 (56) | 15 (58) | 57 (64) |
Female | 23 (43) | 14 (44) | 11 (42) | 32 (36) |
Race, n (%) | ||||
White | 47 (89) | 32 (100) | 21 (81)a | 86 (97) |
Other | 3 (6) | 0 (0) | NR | 2 (2) |
Unknown | 3 (6) | 0 (0) | NR | 1 (1) |
ECOG PS, n (%) | ||||
0 or 1 | 36 (68) | 21 (66) | 12 (46) | 57 (64) |
2 or 3 | 17 (32) | 11 (34) | 14 (54) | 32 (36) |
Prior therapy, n (%) | ||||
No | 21 (40) | 9 (28) | 5 (19) | 52 (58) |
Yes | 32 (60) | 23 (72) | 21 (81) | 37 (42) |
Subtype of AdvSM, n (%) | ||||
ASM | 3 (6) | 2 (6) | 3 (12) | 16 (18) |
SM-AHN | 37 (70) | 26 (81) | 17 (65) | 57 (64) |
MCL | 13 (25) | 4 (13) | 6 (23) | 16 (18) |
KIT D816V mutation status, n (%) | ||||
Positive | 51 (96) | 30 (94) | 19 (77) | 73 (87) |
Negative | 2 (4) | 2 (6) | 5 (19) | 10 (11) |
Other or unknown | 0 (0) | 0 (0) | 1 (4)b | 2 (2)c |
Bone marrow mast cell burden, %, median (range) | 50 (5 to 95) | 50 (10 to 95) | 50 (5 to 95) | 50 (8 to 98) |
Serum tryptase level, mcg/L, median (range) | 182.4 (21.2 to 765.3) | 293.0 (23.8 to 1,600.0) | 323 (22 to 1,255) | 236 (27 to 12,069) |
Number of C-findings per patient, n (%) | ||||
0 | 7 (13) | 6 (19) | 0 (0) | 0 (0) |
1 | 18 (34) | 12 (38) | 3 (12) | 31 (35) |
2 | 13 (25) | 8 (25) | 10 (38) | 20 (22) |
≥ 3 | 15 (28) | 6 (19) | 13 (50) | 38 (43) |
AdvSM = advanced systemic mastocytosis; ASM = aggressive systemic mastocytosis; ECOG PS = Eastern Cooperative Oncology Group Performance Status; MCL = mast cell leukemia; NR = not reported; PEP = primary efficacy population; RAC-RE = Response Assessment Committee–Response Evaluable; SM-AHN = systemic mastocytosis with associated hematologic neoplasm.
aThis number was calculated by subtracting the proportion of people classified as Caucasians in the D2201 trial from the pooled analysis of the D2201 and A2213 trials presented in the Australian Public Assessment Report.52
bThe patient was positive for the KIT S451C mutation.
cThe KIT D816V mutation status was unknown.
Sources: Reproduced with permission from Pilkington et al.39 Details included in Table 30 are from Sponsor Summary of Clinical Evidence.14
Observational Comparison
The baseline characteristics of the avapritinib cohort and the BAT cohort, regardless of lines of therapy, were reported for the April 1, 2021, data cut-off date only; the baseline characteristics of the 2 cohorts using updated analyses from the PATHFINDER study (September 9, 2022) were not included in the sponsor’s submission.
For the data cut-off date of September 9, 2022, patient characteristics in the PATHFINDER study safety population and the real-world BAT cohort before and after weighting for OS are summarized in Table 31 (avapritinib first-line therapy versus BAT first-line therapy, excluding midostaurin), Table 32 (avapritinib second-line or later-line therapy versus BAT [including midostaurin] second-line or later-line therapy), and Table 33 (avapritinib first-line therapy versus midostaurin first-line therapy). Patients in the avapritinib and BAT cohorts differed slightly in the proportion of imbalanced characteristics depending on outcome (OS and the duration of treatment) and population (safety and RAC-RE).
For OS, imbalances (standardized differences of greater than 10%) in the proportion of patients with avapritinib first-line therapy versus BAT first-line therapy (excluding midostaurin) were observed for age, sex, region, an ECOG PS score of 2 or higher, anemia, thrombocytopenia, AdvSM subtypes (SM-AHN, ASM, and MCL), a leukocyte count of 16 multiplied by 109/L or higher, a serum tryptase concentration of 125 ng/mL or higher, and 1 mutated gene within the SRSF2, ASXL1, and RUNX1 mutation panel. After weighting, imbalances remained for region (█████), an ECOG PS score of 2 or greater (█████), and thrombocytopenia (█████). The truncated stabilized weights for OS had a mean of ████ ███ █ █████ ██████ ████ ██ █████ for avapritinib first-line therapy (the PATHFINDER study safety population) versus BAT first-line therapy (excluding midostaurin).
For the duration of treatment, imbalances in the proportion of patients in the safety population with avapritinib first-line therapy versus BAT first-line therapy (excluding midostaurin) were similar to those for OS except for ECOG PS. After weighting, imbalances remained for region (█████) and thrombocytopenia (█████). Notably, standardized differences before versus after weighting increased to more than ███ for an ECOG PS score of 2 or greater (████ ██████ █████). For the duration of treatment, imbalances in covariates among patients in the RAC-RE population were similar overall to those of the safety population; however, imbalances that remained after weighting included age (█████), thrombocytopenia (█████), skin involvement (█████), and a serum tryptase concentration of 125 ng/mL or higher (█████). A greater imbalance after weighting was noted for region (█████ ██████ █████). The truncated stabilized weights for the duration of treatment had a mean of ████ ███ █ █████ ██████ ████ ██ █████ for avapritinib first-line therapy (the PATHFINDER study safety population) versus BAT first-line therapy (excluding midostaurin).
Table 31: Baseline Characteristics Before and After IPTW Weighting for Avapritinib 1L Therapy (PATHFINDER Study, Safety Population, Data Cut-Off at September 2022) and BAT 1L Therapy (Excluding Midostaurin) in the Observational Comparison — Overall Survival
Baseline characteristicsb | Unweighted sample | IPTW-weighted samplea | ||||
|---|---|---|---|---|---|---|
Avapritinibc | BATc | Standard difference,d % | Avapritinibc | BATc | Standard difference,d % | |
Number of unique patients | | | ██ | | | ██ | ██ | ██████ | ██████ | ██ |
Number of lines of therapy | | | ██ | | | ██ | ██ | ██████ | ██████ | ██ |
Demographic characteristics | ||||||
Age (years)e | || | || | ████| | || | || | ███ |
Mean (SD) | ███ ███ | ████ █ | || | ███ ███ | ███ ███ | || |
Median (range) | ██████ | ██████ | || | ██████ | ██████ | || |
Sex, n (%) | || | || | ████| | || | || | ███ |
Female | ██ ████ | ██ ████ | || | ██ █████ | ██ ████ | || |
Male | ██ ████ | ██ ████ | || | ██ █████ | ██ ████ | || |
Region, n (%) | || | || | ████ | || | || | ████| |
North America | ██ ██████ | ██ ██████ | || | ██ █████ | ██ ██████ | || |
Europe | ██ ██████ | ██ ██████ | || | ██ █████ | ██ ██████ | || |
Medical history | ||||||
ECOG PS score,g n (%) | ██ █████ | ██ █████ | || | ██ █████ | ██ ██████ | || |
Mean (SD) | ███ █████ | ███ █████ | || | ███ ████ | ███ █████ | || |
Median (range) | ██████ | ██████ | || | ██████ | ██████ | || |
ECOG PS category, n (%) | ||||||
0 | | ██████ | | ██████ | ███ | ██ █████ | ██ ██████ | ███ |
1 | ██ ██████ | ██ ██████ | ███ | ██ █████ | ██ ██████ | ███ |
≥ 2 | | ██████ | | ██████ | ████ | ██ █████ | ██ ██████ | ████| |
Anemia,h n (%) | ██ ██████ | ██ ██████ | ████ | ██ █████ | ██ ██████ | ███ |
Thrombocytopenia,i n (%) | | ██████ | ██ ██████ | ████ | ██ █████ | ██ ██████ | ████ |
Disease characteristics | ||||||
AdvSM subtype diagnosis,j n (%) | ||||||
SM-AHN | ██ ██████ | ██ ██████ | ████ | ██ █████ | ██ ██████ | ███ |
ASM | | ██████ | ██ ██████ | ████ | ██ █████ | ██ ██████ | ███ |
MCL | | █████ | | █████ | ████ | ██ █████ | ██ █████ | ███ |
Any skin involvement, n (%) | ██ ██████ | ██ ██████ | ███ | ██ █████ | ██ ██████ | ███ |
Leukocyte count, ≥ 16 × 109/L, n (%) | | ██████ | | ██████ | ████ | ██ █████ | ██ ██████ | ███ |
Serum tryptase,k ≥ 125 ng/mL, n (%) | ██ ██████ | ██ ██████ | ████ | ██ █████ | ██ ██████ | ███ |
SRSF2, ASXL1, and RUNX1 mutation panel | ||||||
Patients who were tested for at least 1 mutation, n (%) | ██ ██████ | ██ ██████ | || | ██ █████ | ██ ██████ | || |
Number of mutated genes within SRSF2, ASXL1, and RUNX1 panel, n (%) | ||||||
0 | ██ ██████ | ██ ██████ | || | ██ █████ | ██ ██████ | || |
1 | ██ ██████ | ██ ██████ | ████| | ██ █████ | ██ ██████ | ███ |
≥ 2 | | ██████ | | ██████ | ███ | ██ █████ | ██ ██████ | ███ |
Prior systemic therapy | ||||||
Patients with prior systemic therapy, n (%) | | █████ | | █████ | || | | █████ | | █████ | || |
1L = first-line; AdvSM = advanced systemic mastocytosis; ASM = aggressive systemic mastocytosis; BAT = best available therapy; ECOG PS = Eastern Cooperative Oncology Group Performance Status; IPTW = inverse probability of treatment weighting; MCL = mast cell leukemia; SD = standard deviation; SM-AHN = systemic mastocytosis with an associated hematologic neoplasm.
█████████ ████ ███████ █████████ ███ ████ ████ ███████ ████ ██ ██████ ██████ ███████████ ████ ████ ██ ██████ ████████████████ █████████ █████ ████ ████ ███ █ ██|████ █████ ████████ ████ ████████████ █████████ █████ ██ ███████|██ ██ ███████ █████ ████████ █████████████ ██ ███ █████ ██ ███████ ██████ ██ ███████ █████ ██████ ███ █████████████████ ██████ ██████ ██ █████ █████ ██ ████████ ███ █████ ██ █████ ████████ ██ ██████ ████████████ ██████████ ███████ ████ ██████ ██ ███ ███ ███ ████ ████████████ || ███ █████ ████ ███ ███ ████ ██ ██████████ ██ ███████████ ███ ███ ███████████ ██████ ██████ ████████ ████ ███ ████████ ███ ██████████ ████████ ███ ███ ████ ██ ██████████ ██ ████ ████████ ████ ██ ████████ ███████ ████████ ██ ███ █████ ████ ███ ███ ███ ██████████ ████████████ ██████ ██████ ██████████ ██████████ ████████ ████ ███ ███ ██████████ ████████████ ██████ █████ ██████████ ████████ █████ ██ ████████ ███ ████████ ██████ ███ ███████ ██ █ █████ ███████ ██ ██ ███ █████ ████ ███ ███ ███████████ ██████ ███ ███ ██ █████ ███████ ██ ██ ███ █████ ████ ███ ███ ███ ██████████ ████████████ ███████ ██████ █████████ ██████████ ███████████████ ████████ ███ ██████ ██ ██ ███████ ██ ███ █████ ████ ██████ ███ ████████ ███████ || ███ ██████ ██████████ ████ █████████ █████ █████████ ██████████ ██ ███ ████████ ██████████ █████████ ████ ███ ████████ ███ ██████████ ██████ ███ █████ ███ █████ ███ ██████████ ███████ ████ ██████████ ██ ████████ ████ █████████ ████ ██ █████ ██████ ███ ████ ██████ ██ █ ██████ █████ ███ █████ ████ ███ █████████ █████ ████████ ██████ ██ ███ ██████ █████████ █ █████ ██ ███ █████ ██ ███████ ████ ███████████ ██ ██ ██████████ ████████ ██ ███ ██████████ ███ ██████████ ████████████ ███████ || ███ ██████████ ██████████ ███ ████████████ ██████████ ███ ██████████ ██ ████████ ███ ████████ ██████████ ██ █████ ██ ███████████ ██████ ███ ███ ██████████ ████████████ ██████ ██ ███ ██████ ████████ █████████ ██ ████ ████████ ███ ██████ ████████ █████████ ███ ███ ██████ ████ ██ ███ ███████ ██ ███ ███████ ████████ ███████████ ███ ███████████ █████████ ████ █ ███████ ███ ████████████ ██████████ ███ ██████████ █████ ███ █████████ ████████ █████ ██ ███ ███ ██████████ ██████████ ██ ███████████ ███████ ███ ██ ███ ███ ██████████ ██████████ ██ ███ ██████████ ████████████ ███████ █████████████████ █████ | | ██████████ ███ ████ █████████ █ ████████████ ██████████ ███████ ████ ███ ███ ██████████ ██ ██████████ █████████ ███████ ███ ███ ████████ ███ ██████ ███ ██████ █████ ███ ████ ███████ ████ ██████ ██████ ███ ██████ ███ ██████ ███████ ████ ████████ ████ █████ ███████ ███████████ ██ █████████ █████████ ██████ █████ ███ ██████████ █████ ██ ████████ ██████ █████████ ███████ ██ █████████████ ████████ ██████████ ██ █████████ ████ ███ ████████████████████| ████ ███ ████ ██ █████ ███ █████████ ███ ███ ███ ██████████ ████████████ ███████ █████████ ███ ███ ██████████ █████ ███ █████████ ██ ███ █████ ████ ██ ███████████ █████ ██ ██████ || ████████████ ██████████ ███████ ████ █████| ███ ███ ███ ██████████ ████████████ ███████ ████ ██ ███ █████████ ██████ ████████ ██████ ███ ████ ██████ ██ █ ██████ █████ ███ █████ ████ ████ ███████████ ███ ███ █████ ██ ███████ ███ █████ ████████ ███ ██ ████ ██ █████ ██ ██████ ██████ ████ ██████ ██ | | █████ ██ █████████ ███ █████████ █████ ███████ ██ ███ █████ ████ ██ ███ ████ ██████ ███ █████████ ██ ██ ████ ██ ██████ ██ ███ █████████ █████ ███ ████████ ██████ ████ ███████ ███ ██████████ ███ █████████ █████████ ██ █████ █████ ███████ █████ ███████ █████ ███████ ███ ██████ █████ █████████ █████ ████████ █████ ████████ ███ ████████ ████████ ██ ███ ███████ ███████████ ████████ ██████ ██ █ ████ █████ ██████████ █████
| ███ ████ ███ ███████████ ██████ ███ ███ ███ ██████████ ████████████ ███████ ██████ ████████ ████████ ██████ ███ ██████████ ████ ████ ██ ██████| ███ ████ ███ ███████████ ██████ ███ ███ ███ ██████████ ████████████ ███████ ████████████████ ████████ ████████ ████████████████ ███ ████████ █████ ████ ████ ███ █ ██|███ || ███ █████ ███████ ███ ████████ ██ ███ ████ █████████ ██████████ █████ ██ ██ ██ ███ █████ █████ ███ ███ ███████████ ███████ ███ █████ ███████ █████████ ████████ ████ ███████████ ██ ███ ████████ ██████████ ██████████ || ████████████ ████ ███████ █████ ████████ ████ ███████ ██ ███ ██████ █████ ████████ █████ ██ ███ █████ ██ █████████
Source: Observational comparison with updated results for avapritinib 1L treatment vs. BAT 1L treatment, excluding midostaurin.18
For OS, standardized differences of greater than 10% in the proportion of patients with avapritinib as a second line or later line of therapy (the PATHFINDER study safety population) versus BAT as a second line or later line of therapy were observed for region, an ECOG PS score (1 and ≥ 2), anemia, thrombocytopenia, AdvSM subtypes (SM-AHN and MCL), a leukocyte count of 16 multiplied by 109/L or higher, a serum tryptase concentration of 125 ng/mL or higher, 1 mutated gene within the SRSF2, ASXL1, and RUNX1 mutation panel, and prior systemic therapy (tyrosine kinase inhibitor, cytotoxic, and biologic or other systemic therapy). After weighting, imbalances remained for region (█████), thrombocytopenia (█████), the SM-AHN subtype (█████), a leukocyte count of 16 multiplied by 109/L or higher (█████), and a serum tryptase concentration of 125 ng/mL or higher (█████). Imbalances that were not present before versus after weighting occurred for age (████ ██████ █████), an ECOG PS score of 0 (████ ██████ █████), and 2 prior lines of systemic therapy received (████ ██████ █████). For avapritinib second-line or later-line therapy (the PATHFINDER study safety population) versus BAT second-line or later-line therapy, truncated stabilized weights for OS had a mean of ████ ███ █ █████ ██████ ████ ██ █████.
For the duration of treatment, imbalances in the proportion of patients in the safety population with avapritinib second-line or later-line therapy (the PATHFINDER study safety population) versus BAT second-line or later-line therapy were similar to those for OS. After weighting, imbalances remained for region (█████), thrombocytopenia (█████), the SM-AHN subtype (█████), a leukocyte count of 16 multiplied by 109/L or higher (█████), and a serum tryptase concentration of 125 ng/mL or higher (█████). Notably, imbalances that were not present before versus after weighting occurred for age (████ ██████ █████) and ASM subtype (████ ██████ █████). For the duration of treatment, imbalances in covariates among patients in the RAC-RE population were similar overall to those of the safety population; however, imbalances that remained after weighting included region (█████), an ECOG PS score of 1 (█████), thrombocytopenia (█████), tyrosine kinase inhibitor therapy (█████), and cytotoxic therapy (█████). Imbalances that were not present before versus after weighting occurred for sex (█████ ██████ █████) and skin involvement (████ ██████ █████). For avapritinib second-line or later-line therapy (the PATHFINDER study safety population) versus BAT second-line or later-line therapy, truncated stabilized weights for the duration of treatment had a mean of ████ ███ █ █████ ██████ ████ ██ █████.
Table 32: Baseline Characteristics Before and After IPTW Weighting for Avapritinib 2L+ Therapy (PATHFINDER Study, Safety Population, Data Cut-Off at September 2022) and BAT 2L+ Therapy in the Observational Comparison — Overall Survival
Baseline characteristicsb | Unweighted sample | IPTW-weighted samplea | ||||
|---|---|---|---|---|---|---|
Avapritinibc | BATc | Standard difference,d % | Avapritinibc | BATc | Standard difference,d % | |
Number of unique patients | | | ██ | | | ██ | — | ███████ | ███████ | — |
Number of lines of therapy | | | ██ | | | ███ | — | ███████ | ███████ | — |
Demographic characteristics | ||||||
Age, yearse | ██ | ██ | ███ | ██ | ██ | ████| |
Mean (SD) | ██████ | ██████ | ██ | ██████ | ██████ | ██ |
Median (range) | ██████ | ██████ | ██ | ██████ | ██████ | ██ |
Sex, n (%) | ██ | ██ | ███ | ██ | ██ | ███ |
Female | ██ ████ | ██ █████ | ██ | ██ █████ | ██ █████ | ██ |
Male | ██ ████ | ██ █████ | ██ | ██ █████ | ██ █████ | ██ |
Region, n (%) | ██ | ██ | ████ | ██ | ██ | ████| |
North America | ██ ████ | | █████ | ██ | ██ █████ | ██ █████ | ██ |
Europe | ██ ████ | ██ █████ | ██ | ██ █████ | ██ █████ | ██ |
Medical history | ||||||
ECOG PS score,g n (%) | ██████ | ██████ | ██ | ██ █████ | ██ █████ | ██ |
Mean (SD) | ███ ███ | ██████ | ██ | ███ ████ | ███ ████ | ██ |
Median (range) | ██████ | ██████ | ██ | ██████ | ██████ | ██ |
ECOG PS category, n (%) | ||||||
0 | ██ ████ | ██ █████ | ███ | ██ █████ | ██ █████ | ████| |
1 | ██ ████ | ██ █████ | ████ | ██ █████ | ██ █████ | ███ |
≥ 2 | ██ ████ | ██ █████ | ████ | ██ █████ | ██ █████ | ███ |
Anemia,h n (%) | ██ ████ | ██ █████ | ████ | ██ █████ | ██ █████ | ███ |
Thrombocytopenia,i n (%) | ██ ████ | ██ █████ | ████ | ██ █████ | ██ █████ | ████| |
Disease characteristics | ||||||
AdvSM subtype diagnosis,j n (%) | ||||||
SM-AHN | ██ ████ | ██ █████ | ████ | ██ █████ | ██ █████ | ████ |
ASM | ██ ████ | ██ █████ | ███ | ██ █████ | ██ █████ | ███ |
MCL | ██ ████ | ██ █████ | ████ | ██ █████ | ██ █████ | ███ |
Any skin involvement, n (%) | ██ ████ | ██ █████ | ███ | ██ █████ | ██ █████ | ███ |
Leukocyte count, ≥ 16 × 109/L, n (%) | | ██████ | ██ █████ | ████ | ██ █████ | ██ █████ | ████ |
Serum tryptase,k ≥ 125 ng/mL, n (%) | ██ ████ | ██ █████ | ████| | ██ █████ | ██ █████ | ████ |
SRSF2, ASXL1, and RUNX1 mutation panel | ||||||
Patients who were tested for at least 1 mutation, n (%) | ██████ | ██ █████ | ██ | ██ ███ | ██ █████ | ██ |
Number of mutated genes within SRSF2, ASXL1, and RUNX1 mutation panel, n (%) | ||||||
0 | ██ ████ | ██ █████ | ██ | ██ █████ | ██ █████ | ██ |
1 | ██ ████ | ██ █████ | ████| | ██ █████ | ██ █████ | ███ |
≥ 2 | ██ ████ | ██ █████ | ███ | ██ █████ | ██ █████ | ███ |
Prior systemic therapy | ||||||
Patients with prior systemic therapy, n (%) | ██████ | ██████ | ██ | ██████ | ██████ | ██ |
Number of prior lines of systemic therapy received | ||||||
Mean (SD) | ███ ███ | ███ ████ | ██ | ███ ████ | ███ ████ | ██ |
Median (range) | ██████ | ███ ███ | ██ | ██████ | ██████ | ██ |
0, n (%) | | █████ | | █████ | ██ | ██ █████ | ██ █████ | ██ |
1, n (%) | ██ ████ | ██ █████ | ██ | ██ █████ | ██ █████ | ██ |
2, n (%) | ██ ████ | ██ █████ | ███ | ██ █████ | ██ █████ | ████| |
≥ 3, n (%) | | ██████ | ██ █████ | ███ | ██ █████ | ██ █████ | ███ |
Prior treatments received | ||||||
Drug-level information,l N | ██ | ██ | ██ | ██ | ██ | ██ |
Tyrosine kinase inhibitor therapy, n (%) | ██ ████ | ██ █████ | █████ | ██ █████ | ██ █████ | ███ |
Midostaurin | ██ ████ | ██ █████ | ██ | ██ █████ | ██ █████ | ██ |
Imatinib | | █████ | ██ █████ | ██ | ██ █████ | ██ █████ | ██ |
Cytotoxic therapy, n (%) | ██ ████ | ██ █████ | ████ | ██ █████ | ██ █████ | ███ |
Cladribine | ██ ████ | ██ █████ | ██ | █ ██████ | ██ █████ | ██ |
Hydroxyurea | | █████ | ██ █████ | || | ██ █████ | ██ █████ | ██ |
Biologic or other systemic therapy,m n (%) | ██ ████ | ██ █████ | ████ | ██ █████ | ██ █████ | ███ |
Interferon alpha | ██ ███ | ██ █████ | ██ | ██ █████ | ██ █████ | ██ |
Pegylated interferon | | █████ | | █████ | ██ | ██ █████ | ██ █████ | ██ |
2L+ = second-line or later-line; AdvSM = advanced systemic mastocytosis; ASM = aggressive systemic mastocytosis; BAT = best available therapy; ECOG PS = Eastern Cooperative Oncology Group Performance Status; IPTW = inverse probability of treatment weighting; MCL = mast cell leukemia; SD = standard deviation; SM-AHN = systemic mastocytosis with an associated hematologic neoplasm.
██████████ ████ ███████ █████████ ███ ████ ████ ███████ ████ ██ ██████ ██████ ███████████ ████ ████ ██ ██████ ████████████████ █████████ █████ ████ ████ ███ █ ██|████ █████ ████████ ████ ████████████ █████████ █████ ██ ███████|██ ██ ███████ █████ ████████ █████████████ ██ ███ █████ ██ ███████ ██████ ██ ███████ █████ ██████ ███ █████████████████ ██████ ██████ ██ █████ █████ ██ ████████ ███ █████ ██ █████ ████████ ██ ██████ ████████████ ██████████ ███████ ████ ██████ ██ ███ ███ ███ ████ ████████████ || ███ █████ ████ ███ ███ ████ ██ ██████████ ██ ███████████ ███ ███ ███████████ ██████ ██████ ████████ ████ ███ ██████████ ███████ ███ ███ ████ ██ ██████████ ██ ████ ████████ ████ ██ ████████ ███████ ████████ ██ ███ █████ ████ ███ ███ ███ ██████ ██████ ██████████ ██████████ ████████ ████ ███ ███ ██████ █████ ██████████ ████████ █████ ██ ████████ ███ ████████ ██████ ███ ███████ ██ █ █████ ███████ ██ ██ ███ █████ ████ ███ ███ ███████████ ██████ ███ ███ ██ █████ ███████ ██ ██ ███ █████ ████ ███ ███ ███ ███████ ██████ █████████ ██████████ ███████████████ ████████ ███ ██████ ██ ██ ███████ ██ ███ █████ ████ ██████ ███ ████████ ███████ || ███ ██████ ██████████ ████ █████████ █████ █████████ ██████████ ██ ███ ████████ ██████████ █████████ ████ ███ ██████████ █████ ███ █████ ███ █████ ███ ██████████ ███████ ████ ██████████ ██ ████████ ████ █████████ ████ █████ ██████ ███ ████ ██████ ██ █ ██████ █████ ███ █████ ████ ███ █████████ █████ ████████ ██████ ██ ███ ██████ █████████ █ █████ ██ ███ █████ ██ ███████ ████ ███████████ ██ ██ ██████████ ████████ ██ ███ ██████████ ███ ███████ || ███ ██████████ ██████████ ███ ████████████ ██████████ ███ ██████████ ██ ████████ ███ ████████ ██████████ ██ █████ ██ ███████████ ██████ ███ ███ ██████ ██ ███ ██████ ████████ █████████ ██ ████ ████████ ███ ██████ ████████ █████████ ███ ███ ██████ ████ ██ ███ ███████ ██ ███ ███████ ████████ ███████████ ███ ███████████ █████████ ████ █ ███████ ███ ████████████ ██████████ ███ ██████████ █████ ███ █████████ ████████ █████ || ███ ███ ██████████ ██████████ ██ ███████████ ███████ ███ || ███ ███ ██████████ ██████████ ██ ███ ███████ ████████ █████ ██ || █████ || ███████ ██ ████ ██████ ████ ██ █ ███████████ ██ █████ ████ █████ █ ██████ ██| ████ ||| ███████ ██ ██ ██████ ███ ██████ ███ ██████ ███████ ████ ████████ ████ █████ ███████ ███████████ ██ █████████ █████████ ██████ █████ ███ ██████████ █████ ██ ████████ ██████ █████████ ███████ ██ █████████████ ████████ ██████████ ██ █████████ ████ ███ ██████████████████ || ████ ███ ████ ██ █████ ███ █████████ ███ ███ ███ ███████ █████████ ███ ███ ██████████ █████ ███ █████████ ██ ███ █████ ████ ██ ███████████ █████ ██ ██████ || ████████████ ██████████ ███████ ████ █████| ███ ███ ███ ███████ ████ ██ ███ █████████ ██████ ████████ ██████ ███ ████ ██████ ██ █ ██████ █████ ███ █████ ████ ████ ███████████ ███ ███ █████ ██ ███████ ███ █████ ████████ ███ ██ ████ ██ █████ ██ ██████ ██████ ████ ██████ ██ | | █████ ██ █████████ ███ █████████ █████ ███████ ██ ███ █████ ████ ██ ███ ████ ██████ ███ █████████ ██ ██ ████ ██ ██████ ██ ███ █████████ █████ ███ ████████ ██████ ████ ███████ ███ ██████████ ███ █████████ █████████ ██ █████ █████ ███████ █████ ███████ █████ ███████ ███ ██████ █████ █████████ █████ ████████ █████ ████████ ███ ████████ ████████ ██ ███ ███████ ███████████ ████████ ██████ ██ █ ████ █████ ██████████ █████ || ███ ████ ███ ███████████ ██████ ███ ███ ███ ███████ ██████ ████████ ████████ ██████ ███ ██████████ ████ ████ ██ █████ || ███ ████ ███ ███████████ ██████ ███ ███ ███ ███████ ████████████████ ████████ ████████ ████████████████ ███ ████████ █████ ████ ████ ███ █ ██|███ || ███ █████ ███████ ███ ████████ ██ ███ ████ █████████ ██████████ █████ ██ ██ ██ ███ █████ █████ ███ ███ ███████████ ███████ ███ █████ ███████ █████████ ████████ ████ ███████████ ██ ███ ████████ ██████████ ██████████ || ████████████ ████ ███████ █████ ████████ ████ ███████ ██ ███ ██████ █████ ████████ ███████ ████ ██ █████ ██ ███ ███████| ███ ██████████ ██ ████████ ██ ███ ███ ██████ ███ ████████ █████ ███████████ █████████ ███ ████████ █████ ████████ ████ ███ █████ █████ ██████ ████████████ ████████████ ████ ████████ ████████ ██ █ ██ █████ ██ █████████ █████ ████ █████████ █████ ███████████ ███ █████████ ███ █████ █████████████| █████ ████████ ███████ ████████ ████████ ███ ███████████ ██ ████████████
Source: Observational comparison with updated results for avapritinib 2L+ therapy vs. BAT 2L+ therapy.43
For OS, imbalances in the proportion of patients with avapritinib first-line therapy (the PATHFINDER study safety population) versus midostaurin first-line therapy were observed for sex, region, the ECOG PS score (0, 1, or ≥ 2), anemia, thrombocytopenia, AdvSM subtypes (SM-AHN and ASM), skin involvement, a leukocyte count of 16 multiplied by 109/L or higher, and 1 mutated gene within the SRSF2, ASXL1, and RUNX1 mutation panel (Table 33). After weighting, imbalances remained for an ECOG PS score of 1 (█████) and 2 or greater (█████), anemia (█████), a leukocyte count of 16 multiplied by 109/L or higher (█████), and 1 mutated gene within the SRSF2, ASXL1, and RUNX1 mutation panel (█████). Imbalances that were present before but increased after weighting occurred for region (█████ ██████ █████), skin involvement (█████ ██████ █████), and 1 mutated gene within the SRSF2, ASXL1, and RUNX1 mutation panel (█████ ██████ █████).
For the duration of treatment comparing avapritinib first-line therapy (the PATHFINDER study safety population) versus midostaurin first-line therapy, imbalances in covariates were identical to those of OS.
For avapritinib first-line therapy (the PATHFINDER study safety population) versus midostaurin first-line therapy, truncated stabilized weights for both OS and the duration of treatment had a mean of ████ ███ █ █████ ██████ ████ ██ █████.
Table 33: Baseline Characteristics Before and After IPTW Weighting for Avapritinib 1L Therapy (PATHFINDER Study, Safety Population, Data Cut-Off at September 2022) and Midostaurin 1L Therapy in the Observational Comparison — Overall Survival
Baseline characteristicsb | Unweighted sample | IPTW-weighted samplea | ||||
|---|---|---|---|---|---|---|
Avapritinibc | Midostaurinc | Standard difference,d % | Avapritinibc | Midostaurinc | Standard difference,d % | |
Number of unique patients | | | ██ | | | ██ | — | ██████ ██ | ███████ | — |
Number of lines of therapy | | | ██ | | | ██ | — | ███████ | ███████ | — |
Demographic characteristics | ||||||
Age (years)e | ██ | ██ | ███ | ██ | ██ | ███ |
Mean (SD) | ███████ | ███████ | ██ | ███████ | ███████ | ██ |
Median (range) | ███████ | ███████ | ██ | ███████ | ███████ | ██ |
Sex, n (%) | ██ | ██ | ████ | ██ | ██ | ███ |
Female | ██ ████ | ██ ████ | ██ | ██ ████ | ██ ████ | ██ |
Male | ██ ████ | ██ ████ | ██ | ██ ████ | ██ ████ | ██ |
Region, n (%) | ██ | ██ | ████| | ██ | ██ | ████ |
North America | ██ ████ | ██ ████ | ██ | ██ ████ | ██ ████ | ██ |
Europe | ██ ████ | ██ ████ | ██ | ██ ████ | ██ ████ | ██ |
Medical history | ||||||
ECOG PS score,g n (%) | ██ █████ | ███████ | ██ | ██ █████ | ██ █████ | ██ |
Mean (SD) | ███ ████ | ███ ████ | ██ | ███ ████ | ███ ████ | ██ |
Median (range) | ███████ | ███████ | ██ | ███████ | ███████ | ██ |
ECOG PS category, n (%) | ||||||
0 | | ██████ | ██ █████ | ████ | ██ █████ | ██ █████ | ███ |
1 | ██ █████ | ██ █████ | ████ | ██ █████ | ██ █████ | ████| |
≥ 2 | | ██████ | ██ █████ | ████ | ██ █████ | ██ █████ | ████| |
Anemia,h n (%) | ██ █████ | ██ █████ | ████ | ██ █████ | ██ █████ | ████| |
Thrombocytopenia,i n (%) | | ██████ | ██ █████ | ████ | ██ █████ | ██ █████ | ███ |
Disease characteristics | ||||||
AdvSM subtype diagnosis,j n (%) | ||||||
SM-AHN | ██ █████ | ██ █████ | ████ | ██ █████ | ██ █████ | ███ |
ASM | | ██████ | ██ █████ | ████ | ██ █████ | ██ █████ | ███ |
MCL | | █████ | | █████ | ███ | ██ ████ | ██ ████ | ███ |
Any skin involvement, n (%) | ██ █████ | ██ █████ | ████ | ██ █████ | ██ █████ | ████ |
Leukocyte count, ≥ 16 × 109/L, n (%) | | ██████ | ██ █████ | ████ | ██ █████ | ██ █████ | ████ |
Serum tryptase,k ≥ 125 ng/mL, n (%) | ██ █████ | ██ █████ | ███ | ██ █████ | ██ █████ | ███ |
SRSF2, ASXL1, and RUNX1 mutation panel | ||||||
Patients who were tested for at least 1 mutation, n (%) | ██ █████ | ██ ████ | — | ██ █████ | ██ █████ | — |
Number of mutated genes within SRSF2, ASXL1, and RUNX1 panel, n (%) | ||||||
0 | ██ █████ | ██ █████ | ██ | ██ █████ | ██ █████ | ██ |
1 | ██ █████ | ██ █████ | ████ | ██ █████ | ██ █████ | ████| |
≥ 2 | | ██████ | | ██████ | ███ | ██ █████ | ██ █████ | ███ |
Prior systemic therapy | ||||||
Patients with prior systemic therapy, n (%) | | █████ | | █████ | — | | █████ | | █████ | — |
1L = first-line; AdvSM = advanced systemic mastocytosis; ASM = aggressive systemic mastocytosis; BAT = best available therapy; ECOG PS = Eastern Cooperative Oncology Group Performance Status; IPTW = inverse probability of treatment weighting; MCL = mast cell leukemia; SD = standard deviation; SM-AHN = systemic mastocytosis with an associated hematologic neoplasm.
██████████ ████ ███████ █████████ ███ ████ ████ ████ ██████ ██████ ███████████ █ ██ ██████ ████████████████ █████████ █████ █ ███ █ ██|████ █████ ████████ ████ ████████████ █████████ █████ ██ ███████|██ ██ ███████ █████ ████████ █████████████ ██ ███ █████ ██ ███████ ██████ ██ ███████ █████ ██████ ███ █████|█████|█████ ██████ ██████ ██ █████ █████ ██ ████████ ███ █████ ███ ██ ████████ ██████ ██████████ ██████████ ████████ ██ █████ ████████ ████████ ██ ██████ ████████████ ██████████ ███████ ████ ██████ ██ ███ ███ ███ ████ ████████████ || ███ █████ ████ ███ ███ ████ ██ ██████████ ██ ███████████ ███ ███ ███████████ ██████ ██████ ████████ ████ ███ ██████████ ███████ ███ ███ ████ ██ ██████████ ██ ███████████ ██████ ████████ ██ ███ █████ ████ ███ ███ ███████████ ██████ ██████ ██████████ ██████████ ███ ████████ ██████ ███ ███████ ██ █ █████ ███████ ██ ██ ███ █████ ████ ███ ███ ███████████ ██████ ███ ███ ██ █████ ███████ ██ ██ ███ █████ ████ ███ ███ ███████████ ███████ ██████ █████████ ██████████ ███████████████ ████████ ███ ██████ ██ ██ ███████ ██ ███ █████ ████ ██████ ███ ████████ ████████| ███ ██████ ██████████ ████ ███ ██████████ █████ ███ █████ ███ █████ ███ ██████████ ███████ ████ ██████████ ██ ████████ ████ █████████ ████ █████ ██████ ███ ████ ██████ ██ █ ██████ █████ ███ █████ █████ █ █████ ██ ██ ████████ ████ ████████ ██ ███ ███████████ ███████ || ███ ██████████ ██████████ ███ ████████████ ██████████ ███ ██████████ ██ ████████ ███ ████████ ██████████ ██ █████ ██ ███████████ ██████ ██████ ███████████ ██████ ██ ███ ██████ ████████ █████████ ██ ████ ████████ ███ ██████ ████████ █████████ ███ ███ ██████ ████ ██ ███ ███████ ██ ███ ███████ ████████ ███████████ ███ ███████████ █████████ ████ █ ███████ ███ ████████████ ██████████ ███ ██████████ █████ ███ █████████ ████████ █████ || ███ ███ ██████████ ██████████ ██ ███████████ ███████ ███ || ███ ███ ██████████ ██████████ ██ ███████████ ███████ ████████ █████ ██ || █████ || ███████ ██ ████ ██████ ████ ██ █ ███████████ ██ █████ ████ █████ █ ██████ ██| ████ ||| ███████ ██ ██ ██████ ███ ██████ ███ ██████ ███████ ████ ████████ ████ █████ ███████ ███████████ ██ █████████ █████████ █████ ███ ██████████ █████ ██ ████████ ██████ █████████ ███████ ██ █████████████ ████████ ██████████ ██ █████████ ████ ███ ████████████████████| ████ ███ ████ ██ █████ ███ █████████ ███ ███ ███████████ ███████ █████████ ███ ███ ██████████ █████ ███ █████████ ██ ███ █████ ████ ██ ███████████ █████ ██ ██████ || ████████████ ██████████ ███████ ████ █████| ███ ███ ███████████ ███████ ████ ███ █████████ ██████ ████████ ██████ ███ ████ ██████ ██ █ ██████ █████ ███ █████ ████ ████ ███████████ ███ ███ █████ ██ ███████ ███ █████ ████████ ███ ██ ████ █████ ██ ██████ ██████ ████ ██████ ██ | | █████ ██ █████████ ███ █████████ █████ ███████ ██ ███ █████ ████ ██ ███ ████ ██████ ███ █████████ ██ ██ ████ ██████ ██ ███ █████████ █████ ███ ████████ ██████ ████ ███████ ███ ██████████ ███ █████████ █████████ ██ █████ █████ ███████ █████ ███████ █████ ███████ ███ ██████ █████ █████████ █████ ████████ █████ ████████ ███ ████████ ████████ ██ ███ ███████ ███████████ ████████ ██████ ██ █ ████ █████ ██████████ █████ || ███ ████ ███ ███████
Source: Observational comparison with updated results for avapritinib 1L therapy vs. midostaurin 1L therapy.42
Results
For the indirect treatment comparison, results for avapritinib versus midostaurin were presented for OS, ORR, and CR. For the observational comparison, results for OS from the updated analyses (data cut-off date of September 9, 2022) were presented separately for comparisons of avapritinib first-line therapy versus BAT first-line therapy (excluding midostaurin), avapritinib second-line or later-line therapy versus BAT second-line or later-line therapy, and avapritinib first-line therapy versus midostaurin first-line therapy. Sensitivity analyses comparing results for the PATHFINDER study RAC-RE population were consistent overall with the findings for the PATHFINDER study safety population.
Overall Survival
Indirect Treatment Comparison
In the indirect treatment comparison, OS estimates for the MAICs ranged from an HR of 0.37 (95% CI, 0.19 to 0.73) to an HR of 0.59 (95% CI, 0.27 to 1.32), favouring avapritinib (Table 34). The HR of OS for the MAIC was 0.44 (95% CI, 0.25 to 0.76) based on an effective sample size of 68.1 comparing avapritinib (pooled EXPLORER and PATHFINDER studies RAC-RE population, n = 85) versus midostaurin (the D2201 trial primary efficacy population, n = 115), favouring avapritinib. The HR of OS for the MAIC was 0.42 (95% CI, 0.25 to 0.71) based on an effective sample size of 108.8 comparing the avapritinib cohort (pooled EXPLORER and PATHFINDER studies safety population, n = 131) versus the pooled midostaurin cohort (the pooled D2201 and A2213 trials’ full analysis set, n = 142), favouring avapritinib (Table 34). Results from the sensitivity analyses comparing the full trial populations (the safety population for avapritinib and the full analysis population for midostaurin) were consistent overall with findings from the primary analysis (the RAC-RE population for avapritinib and the primary efficacy population for midostaurin).
Table 34: Indirect Treatment Comparison — Overall Survival for Avapritinib Versus Midostaurin
Avapritinib population | Midostaurin population | Matching variables | ESS | Naive ITC, HR (95% CI) | MAIC, HR (95% CI) |
|---|---|---|---|---|---|
Pooled PATHFINDER and EXPLORER studies (RAC-RE), N = 85 | Pooled D2201 and A2213 trials’ PEP, | Age, AdvSM subtype, race | 68.1 | 0.54 (0.32 to 0.92) | 0.44 (0.25 to 0.76) |
Pooled PATHFINDER and EXPLORER studies (safety), N = 131 | Pooled D2201 and A2213 trials’ FAS, | Age, AdvSM subtype, race | 108.8 | 0.52 (0.32 to 0.85) | 0.42 (0.25 to 0.71) |
PATHFINDER study (RAC-RE), N = 32 | Pooled D2201 and A2213 trials’ PEP, | Age, AdvSM subtype | 25.2 | 0.51 (0.18 to 1.45) | 0.51 (0.17 to 1.57) |
Pooled PATHFINDER and EXPLORER studies (RAC-RE, prior therapya), N = 55 | Pooled D2201 and A2213 trials’ PEP, | Age, AdvSM subtype, race | 39.3 | 0.50 (0.26 to 0.96) | 0.39 (0.19 to 0.80) |
Pooled PATHFINDER and EXPLORER studies (RAC-RE, midostaurin-naiveb), N = 51 | Pooled D2201 and A2213 trials’ PEP, | Age, AdvSM subtype, race | 44.9 | 0.43 (0.22 to 0.84) | 0.37 (0.19 to 0.73) |
Pooled PATHFINDER and EXPLORER studies (RAC-RE, 200 mgc), N = 44 | Pooled D2201 and A2213 trials’ PEP, | Age, AdvSM subtype | 32.8 | 0.67 (0.31 to 1.42) | 0.59 (0.27 to 1.32) |
AdvSM = advanced systemic mastocytosis; CI = confidence interval; ESS = effective sample size; FAS = full analysis set; HR = hazard ratio; ITC = indirect treatment comparison; MAIC = matching-adjusted indirect comparison; MCL = mast cell leukemia; PEP = primary efficacy population; RAC-RE = Response Assessment Committee–Response Evaluable.
Note: Results were from the data cut-off date of April 2020.
aPatients who had prior systemic therapy.
bPatients with no prior midostaurin treatment.
cPatients who received a 200 mg starting dose.
Source: Reproduced with permission from Pilkington et al.39
Figure 5: Kaplan-Meier Plot of Overall Survival for Avapritinib (Pooled RAC-RE Population) Versus Midostaurin (Pooled Primary Efficacy Population) in the Indirect Treatment Comparison
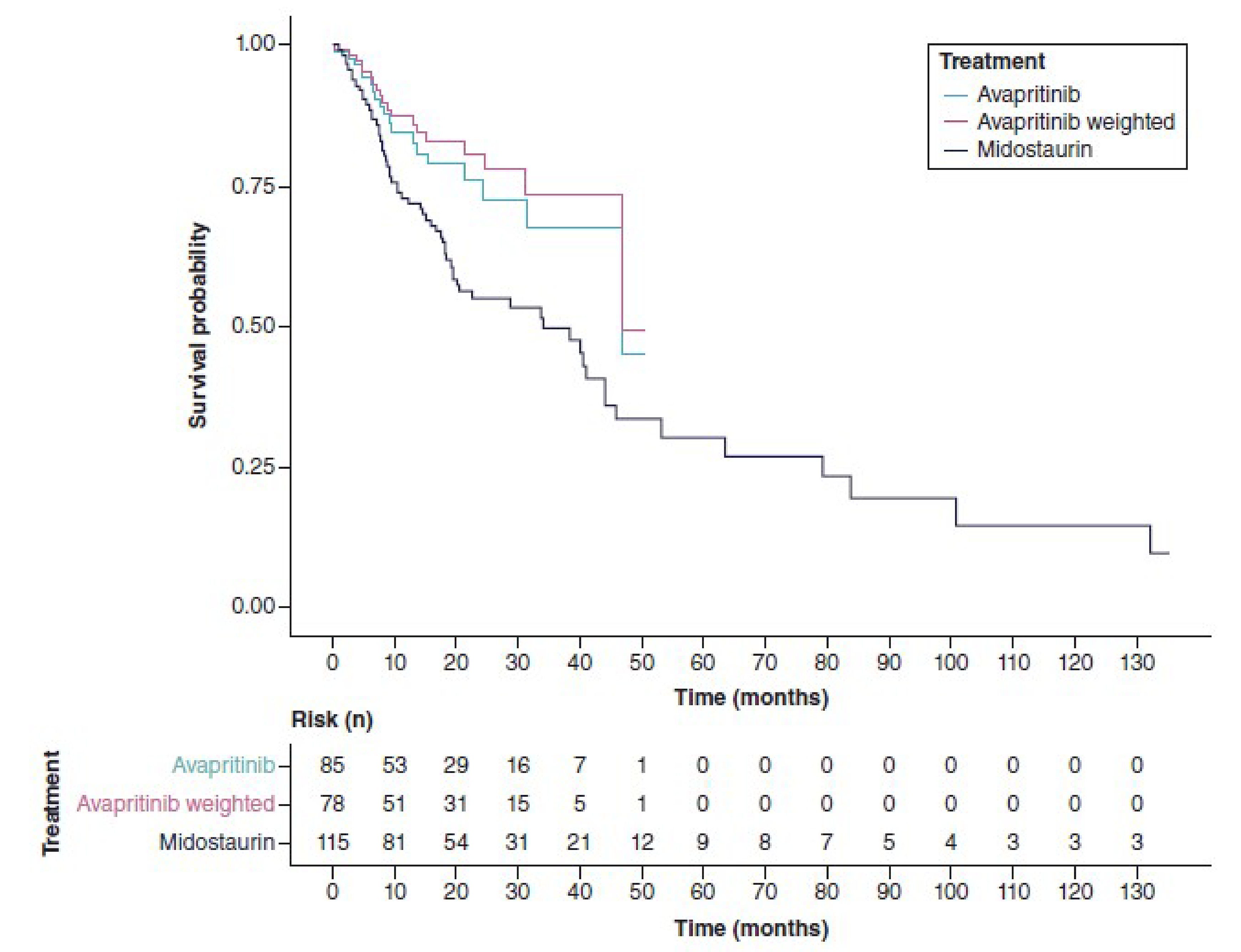
RAC-RE = Response Assessment Committee–Response Evaluable.
Note: Results were from the data cut-off date of April 2020.
Source: Reproduced with permission from Pilkington et al.39
Observational Comparison
The IPTW-weighted comparison of avapritinib first-line therapy versus BAT first-line therapy was based on follow-up of median ████ ██████ in the avapritinib first-line therapy cohort and median ████ ██████ in the BAT first-line therapy (excluding midostaurin) cohort. Deaths occurred in | ███████ patients in the avapritinib first-line therapy cohort and ██ ███████ patients in the BAT first-line therapy (excluding midostaurin) cohort. Median (95% CI) OS had not been reached ████ ███ ███ █████████ ██ ███ ██████████ in the avapritinib first-line therapy cohort and was median ████ ██████ ████ ███ ████ ██████ ██ ████ ███████ in the BAT first-line therapy (excluding midostaurin) cohort, favouring avapritinib first-line therapy (an HR of █████ ███ ███ ████ ██ █████ █ █████ █ ██████ (Table 35).
The IPTW-weighted comparison of avapritinib second-line or later-line therapy versus BAT second-line or later-line therapy was based on follow-up of median ████ ██████ in the avapritinib second-line or later-line therapy cohort and ████ ██████ in the BAT second-line or later-line therapy cohort. Deaths occurred in ██ ███████ patients in the avapritinib second-line or later-line therapy cohort and ██ ███████ patients in the BAT second-line or later-line therapy cohort. Median (95% CI) OS had not been reached ████ ███ ████ ██████ ██ ███ ██████████ in the avapritinib second-line or later-line therapy cohort and was median ████ ██████ ████ ███ ████ ██████ ██ ████ ███████ in the BAT second-line or later-line therapy cohort, favouring avapritinib second-line or later-line therapy (an HR of █████ ███ ███ ████ ██ █████ █ █████ █ ██████ (Table 35).
Table 35: Summary of Overall Survival for Avapritinib (PATHFINDER Study, Data Cut-Off at September 2022) Versus Best Available Therapy in the Observational Comparison
Outcome and analysis | Avapritinib 1L therapy vs. BAT 1L therapy, excluding midostaurin | Avapritinib 2L+ therapy vs. BAT 2L+ therapy | ||||
|---|---|---|---|---|---|---|
N | HR (95% CI) | P value | N | HR (95% CI) | P value | |
Overall survival, safety population | ||||||
Unweighted | ██ ███ | ████ ███ █ | ████ | ██ ███ | ███ █ | ████ |
IPTW-weighteda | ██ ███ | ████ ███ ██ | ████ | ██ ███ | ███ █ | ████ |
Overall survival, RAC-RE population | ||||||
Unweighted | ██ ███ | ████ ███ █ | ████ | ██ ███ | ███ █ | ████ |
IPTW-weighteda | ██ ███ | ███ ████ ██ | ████ | ██ ███ | ███ █ | ████ |
1L = first-line; 2L+ = second-line or later-line; BAT = best available therapy; CI = confidence interval; HR = hazard ratio; IPTW = inverse probability of treatment weighting; RAC-RE = Response Assessment Committee–Response Evaluable; vs. = versus.
█████████████ ███ ████████████ ███████ █████ ███████ ████████ ███ ██████████ ████ █ ████████████ ██████████ ██ ███████ ████ ███ █████ ██████████ █████ █ ██████ ██████ ██████████ █████████ █████████ ██ ██ ████ █████████████ ███ ██ ███ █ ██████
Source: Observational comparison with updated results for avapritinib 1L therapy vs. BAT 1L therapy excluding midostaurin18 and updated results for avapritinib 2L+ therapy vs. BAT 2L+ therapy.43
The IPTW-weighted comparison of avapritinib first-line therapy versus midostaurin first-line therapy was based on follow-up of median ████ ██████ in the avapritinib first-line therapy cohort and median ████ ██████ in the midostaurin first-line therapy cohort. Deaths occurred in | ███████ patients in the avapritinib first-line therapy cohort and ██ █████ patients in the midostaurin first-line therapy cohort. Median (95% CI) OS had not been reached ████ ███ ███ █████████ ██ ███ ██████████ in the avapritinib first-line therapy cohort and was median ████ ██████ ████ ███ ████ ██████ ██ ████ ███████ in the midostaurin first-line therapy cohort, favouring avapritinib first-line therapy (an HR of █████ ███ ███ ████ ██ █████ █ █████ █ █████) (Table 36).
Table 36: Summary of Overall Survival for Avapritinib 1L Therapy (PATHFINDER Study, Data Cut-Off at September 2022) Versus Midostaurin 1L Therapy in the Observational Comparison
Outcome and analysis | N | Avapritinib 1L therapy vs. midostaurin 1L therapy HR (95% CI) | P value |
|---|---|---|---|
Overall survival, safety population | |||
Unweighted | ██ ██ ██ | ████ █████ ██ █████ | █████ |
IPTW-weighteda | ██ ██ ██ | ████ █████ ██ █████ | █████ |
Overall survival, RAC-RE population | |||
Unweighted | █████ ██ | ████ █████ ██ █████ | █████ |
IPTW-weighteda | ██ ███ ██ | ████ █████ ██ █████ | | █████ |
1L = first-line; CI = confidence interval; HR = hazard ratio; IPTW = inverse probability of treatment weighting; RAC-RE = Response Assessment Committee–Response Evaluable; vs. = versus.
█████████████ ███ ████████████ ███████ █████ ███████ ████████ ███ ██████████ ████ █ ████████████ ██████████ ██ ███████ ████ ███ █████ ██████████ █████ █ ██████ ██████ ██████████ █████████ █████████ ██ ██ ████ █████████████ ███ ██ ███ █ ██████
Source: Observational comparison with updated results for avapritinib 1L therapy vs. midostaurin 1L therapy.42
Duration of Treatment
Results for the duration of treatment are summarized in Table 37 and Table 38. Duration of treatment was not evaluated in the indirect treatment comparison.
In the IPTW-weighted comparison in the PATHFINDER study safety population, the median (95% CI) duration of treatment was median ████ ██████ ████ ███ ████ ██████ ██ ███ ██████████ in the avapritinib first-line therapy cohort and was median ███ ██████ ████ ███ ███ ██████ ██ ███ ███████ in the BAT first-line therapy (excluding midostaurin) cohort, favouring avapritinib first-line therapy (an HR of █████ ███ ███ ████ ██ █████ | | █████). The IPTW-weighted comparison in the PATHFINDER study RAC-RE population was median ████ ██████ ████ ███ ████ ██████ ██ ███ ██████████ in the avapritinib first-line therapy cohort and median ███ ██████ ████ ███ ███ ██████ ██ ███ ███████ in the BAT first-line therapy (excluding midostaurin) cohort, favouring avapritinib first-line therapy (an HR of █████ ███ ███ ████ ██ █████ | | █████).
In the IPTW-weighted comparison in the PATHFINDER study safety population, the median (95% CI) duration of treatment was median ████ ██████ ████ ███ ████ ██████ ██ ███ ██████████ in the avapritinib second-line or later-line therapy cohort and was median ███ ██████ ████ ███ ███ ██████ ██ ███ ███████ in the BAT second-line or later-line therapy cohort, favouring avapritinib second-line or later-line therapy (an HR of █████ ███ ███ ████ ██ █████ | | █████). The IPTW-weighted comparison in the PATHFINDER study RAC-RE population with the median duration of treatment not reached ████ ███ ████ ██████ ██ ███ ██████████ in the avapritinib second-line or later-line therapy cohort and was median ███ ██████ ████ ███ ███ ██████ ██ ███ ███████ in the BAT second-line or later-line therapy cohort, favouring avapritinib second-line or later-line therapy (an HR of █████ ███ ███ ████ ██ █████ | | █████).
Table 37: Summary of Duration of Treatment for Avapritinib (PATHFINDER Study, Data Cut-Off at September 2022) Versus Best Available Therapy in the Observational Comparison
Outcome and analysis | Avapritinib 1L therapy vs. BAT 1L therapy, excluding midostaurin | Avapritinib 2L+ therapy vs. BAT 2L+ therapy | ||||
|---|---|---|---|---|---|---|
N | HR (95% CI) | P value | N | HR (95% CI) | P value | |
Duration of treatment, safety population | ||||||
Unweighted | █████ | ████ █████ █ | █████ | ██ ███ | ████ █ | | █████ |
IPTW-weighteda | █ █ ██ | ████ █████ █ | █████ | ██ ███ | ████ █ | | █████ |
Duration of treatment, RAC-RE population | ||||||
Unweighted | ██ ██ | ████ █████ █ | █████ | ██ ███ | ████ █ | | █████ |
IPTW-weighteda | ██ ██ | ████ █████ █ | █████ | ██ ███ | ████ █ | | █████ |
1L = first-line; 2L+ = second-line or later-line; BAT = best available therapy; CI = confidence interval; HR = hazard ratio; IPTW = inverse probability of treatment weighting; RAC-RE = Response Assessment Committee–Response Evaluable; vs. = versus.
█████████████ ███ ████████████ ███████ █████ ███████ ████████ ███ ██████████ ████ █ ████████████ ██████████ ██ ███████ ████ ███ █████ ██████████ █████ █ ██████ ██████ ██████████ █████████ █████████ ██ ██ ████ █████████████ ███ ██ ███ █ ██████
Source: Observational comparison with updated results for avapritinib 1L therapy vs. BAT 1L therapy excluding midostaurin18 and updated results for avapritinib 2L+ therapy vs. BAT 2L+ therapy.43
In the IPTW-weighted comparison in the PATHFINDER study safety population, the median (95% CI) duration of treatment was median ████ ██████ ████ ███ ████ ██████ ██ ████ ███████ in the avapritinib first-line therapy cohort and was median ████ ██████ ████ ███ ███ ██████ ██ ████ ███████ in the midostaurin first-line therapy cohort, favouring avapritinib first-line therapy (an HR of █████ ███ ███ ████ ██ █████ █ █████ █ ██████. The IPTW-weighted comparison in the PATHFINDER study RAC-RE population was median ████ ██████ ████ ███ ████ ██████ ██ ████ ███████ in the avapritinib first-line therapy cohort and was median ████ ██████ ████ ███ ███ ██████ ██ ████ ███████ in the midostaurin first-line therapy cohort, favouring avapritinib first-line therapy (an HR of █████ ███ ███ ████ ██ █████ | | ██████.
Table 38: Summary of Duration of Treatment for Avapritinib 1L Therapy (PATHFINDER Study, Data Cut-Off at September 2022) Versus Midostaurin 1L Therapy in the Observational Comparison
Outcome and analysis | N | Avapritinib 1L therapy vs. midostaurin 1L therapy HR (95% CI) | P value |
|---|---|---|---|
Duration of treatment, safety population | |||
Unweighted | ██ ███ ██ | ████ █████ ██ █████ | | █████ |
IPTW-weighteda | ██ ███ ██ | ████ █████ ██ █████ | █████ |
Duration of treatment, RAC-RE population | |||
Unweighted | ██ ███ ██ | ████ █████ ██ █████ | | █████ |
IPTW-weighteda | ██ ███ ██ | ████ █████ ██ █████ | | █████ |
1L = first-line; CI = confidence interval; HR = hazard ratio; IPTW = inverse probability of treatment weighting; RAC-RE = Response Assessment Committee–Response Evaluable; vs. = versus.
█████████████ ███ ████████████ ███████ █████ ███████ ████████ ███ ██████████ ████ █ ████████████ ██████████ ██ ███████ ████ ███ █████ ██████████ █████ █ ██████ ██████ ██████████ █████████ █████████ ██ ██ ████ █████████████ ███ ██ ███ █ ██████
Source: Observational comparison with updated results for avapritinib 1L therapy vs. midostaurin 1L therapy.42
Overall Response Rate
Results for ORR in the indirect treatment comparison are summarized in Table 39. ORR was not evaluated in the observational comparison.
The avapritinib trials evaluated response based on modified IWG-MRT-ECNM criteria while the midostaurin trials used the original Valent criteria per the investigator (the A2213 trial) and the modified Valent criteria per the adjudication committee (the D2201 trial). Due to the differences in criteria used to analyze response, a post hoc analysis of the D2201 trial data using the IWG-MRT-ECNM criteria was conducted to inform an indirect comparison between the EXPLORER, PATHFINDER, and the D2201 trials.
ORRs per IWG-MRT-ECNM criteria were numerically higher across all avapritinib RAC-RE populations for adjusted analyses (range, 61.52% to 69.50%) compared to the midostaurin primary efficacy population (35.96%). In the indirect treatment comparison, ORRs for the MAICs ranged from an odds ratio of 2.85 (95% CI, 1.96 to 4.15) to an odds ratio of 4.06 (95% CI, 3.09 to 5.33), favouring avapritinib (Table 39). The ORR comparing avapritinib (pooled EXPLORER and PATHFINDER studies RAC-RE population, n = 79) versus midostaurin (the D2201 trial primary efficacy population, n = 89) was an odds ratio of 4.06 (95% CI, 3.09 to 5.33) for the MAIC, favouring avapritinib. Results for ORRs from the sensitivity analyses of subsets of patients in the avapritinib population (PATHFINDER study-only data [n = 31], with prior systemic therapy [n = 53], who had not previously received midostaurin [n = 46], and who received avapritinib 200 mg dose [n = 42]) were consistent overall with findings from the primary analysis (the avapritinib pooled RAC-RE population compared with the midostaurin primary efficacy population).
Table 39: Indirect Treatment Comparison — Overall Response Rate for Avapritinib Versus Midostaurin
Avapritinib population | Avapritinib ORR (%) | Midostaurin population | Midostaurin ORR (%) | Matching variables | ESS | Naive ITC, OR (95% CI) | MAIC, OR (95% CI) |
|---|---|---|---|---|---|---|---|
Pooled PATHFINDER and EXPLORER studies (RAC-RE), N = 79 | 69.62 | D2201 trial PEP, | 35.96 | Age, AdvSM subtype, race, ECOG PS, KIT D816V mutation status, bone marrow mast cell burden | 53.9 | 4.08 (2.14 to 7.79) | 4.06 (3.09 to 5.33) |
PATHFINDER study (RAC-RE), N = 31 | 64.52 | D2201 trial PEP, | 35.96 | Age, AdvSM subtype, race, ECOG PS, KIT D816V mutation status, bone marrow mast cell burden | 23.3 | 3.24 (1.38 to 7.61) | 3.78 (2.31 to 6.19) |
Pooled PATHFINDER and EXPLORER studies (RAC-RE, prior therapya), N = 53 | 66.04 | D2201 trial PEP, | 35.95 | Age, AdvSM subtype, race, ECOG PS, KIT D816V mutation status, bone marrow mast cell burden | 40.0 | 3.46 (1.70 to 7.08) | 4.04 (2.96 to 5.52) |
Pooled PATHFINDER and EXPLORER studies (RAC-RE, midostaurin-naiveb), N = 46 | 76.09 | D2201 trial PEP, | 35.96 | Age, AdvSM subtype, race, ECOG PS, KIT D816V mutation status, bone marrow mast cell burden | 30.5 | 5.67 (2.54 to 12.66) | 3.83 (2.25 to 6.53) |
Pooled PATHFINDER and EXPLORER studies (RAC-RE, 200 mgc), N = 42 | 57.14 | D2201 trial PEP, | 35.96 | Age, AdvSM subtype, race, ECOG PS, KIT D816V mutation status, bone marrow mast cell burden | 28.8 | 2.37 (1.12 to 5.02) | 2.85 (1.96 to 4.15) |
AdvSM = advanced systemic mastocytosis; CI = confidence interval; ECOG PS = Eastern Cooperative Oncology Group Performance Status; ESS = effective sample size; ITC = indirect treatment comparison; MAIC = matching-adjusted indirect comparison; OR = odds ratio; ORR = overall response rate; PEP = primary efficacy population; RAC-RE = Response Assessment Committee–Response Evaluable.
Note: Results were from the data cut-off date of April 2020.
aPatients who had prior systemic therapy.
bPatients with no prior midostaurin treatment.
cPatients who received a 200 mg starting dose.
Source: Reproduced with permission from Pilkington et al.39
The proportion of patients who attained CR per IWG-MRT-ECNM criteria was numerically higher across all avapritinib populations for adjusted analyses (range, 9.80% to 12.34%) compared to the midostaurin primary efficacy population (1.12%). In the indirect treatment comparison comparing avapritinib (pooled EXPLORER and PATHFINDER studies RAC-RE population, n = 79) versus midostaurin (the D2201 trial primary efficacy population, n = 89), CR was attained by 10 (12.66%) patients and 1 (1.12%) patient, respectively, for an odds ratio of 9.56 (95% CI, 0.97 to 93.81) in the MAIC, favouring avapritinib (Table 40). Results from the sensitivity analyses comparing data for subsets of patients in the pooled RAC-RE population of the avapritinib group (with prior therapy, who had not previously received midostaurin) were consistent overall with findings from the primary analysis (avapritinib pooled RAC-RE population compared with midostaurin primary efficacy population).
Table 40: Indirect Treatment Comparison — Complete Remission for Avapritinib Versus Midostaurin
Avapritinib population | Avapritinib CR (%) | Midostaurin population | Midostaurin CR (%) | Matching variables | ESS | Naive ITC, OR (95% CI) | MAIC, OR (95% CI) |
|---|---|---|---|---|---|---|---|
Pooled PATHFINDER and EXPLORER studies (RAC-RE), N = 79 | 12.66 | D2201 trial PEP, | 1.12 | Age, AdvSM subtype, race, ECOG PS, KIT D816V mutation status, bone marrow mast cell burden | 53.9 | 12.75 (1.59 to 102.05) | 9.56 (0.97 to 93.81) |
Pooled PATHFINDER and EXPLORER studies (RAC-RE, prior therapya), N = 53 | 13.21 | D2201 trial PEP, | 1.12 | Age, AdvSM subtype, race, ECOG PS, KIT D816V mutation status, bone marrow mast cell burden | 40.0 | 13.39 (1.60 to 112.17) | 10.44 (0.96 to 113.57) |
Pooled PATHFINDER and EXPLORER studies (RAC-RE, midostaurin-naiveb), N = 46 | 17.39 | D2201 trial PEP, | 1.12 | Age, AdvSM subtype, race, ECOG PS, KIT D816V mutation status, bone marrow mast cell burden | 30.5 | 18.53 (2.24 to 153.33) | 12.39 (1.14 to 134.58) |
AdvSM = advanced systemic mastocytosis; CI = confidence interval; CR = complete remission; ECOG PS = Eastern Cooperative Oncology Group Performance Status; ESS = effective sample sizes; ITC = indirect treatment comparison; MAIC = matching-adjusted indirect comparison; OR = odds ratio; PEP = primary efficacy population; RAC-RE = Response Assessment Committee–Response Evaluable.
Note: Results were from the data cut-off of April 2020.
aPatients who had prior systemic therapy.
bPatients with no prior midostaurin treatment.
Source: Reproduced with permission from Pilkington et al.39
Critical Appraisal of Indirect Evidence
Indirect Treatment Comparison
In the indirect treatment comparison (MAIC), methods for study selection were poorly reported. No information was provided on details of the literature search (e.g., databases, date parameters, search filters), study selection process (e.g., duplicate reviewers), or data extraction (e.g., single reviewer, duplicate extraction). No information including rationale was provided for not assessing the quality of the included studies. Due to the lack of a common comparator, an unanchored MAIC was used to include single-arm, open-label trials comparing avapritinib (EXPLORER and PATHFINDER studies) versus midostaurin (the A2213 and D2201 trials). Based on some key differences between the 2 trials both for avapritinib and for midostaurin, the appropriateness of combining the trials for each cohort was unclear and no rationale or evaluation was provided by the sponsor. Across the included cohorts, trial start dates were heterogenous and notably older in the midostaurin trials (2005 and 2008 for the A2213 and D2201 trials, respectively) than in the avapritinib trials (2016 and 2018 for the EXPLORER and PATHFINDER studies, respectively). The MAIC reported limited details regarding patients enrolled in the trials. Patients were enrolled from Europe, the US, and Canada (1 site) in the PATHFINDER trial of avapritinib whereas the midostaurin trials enrolled patients mainly from Europe and the US. Across the studies, differences were observed in dosing of avapritinib (between the EXPLORER and PATHFINDER studies) and response evaluation (criteria across the 4 trials), and no information on time points used in evaluating response was provided for the trials. The MAIC method assumes that all sources of heterogeneity between studies can be explained by imbalances in prognostic and effect-modifying factors, which is generally an unreasonable assumption to have been met per the NICE Decision Support Unit Technical Support Document 18.19 The clinical experts identified prognostic factors associated with poor outcomes to include AdvSM subtypes of SM-AHN (particularly for the type of myeloid neoplasm) and MCL, the KIT D816V variant allele frequency, and the type of gene mutation (e.g., SRSF2). Among these, the MAIC included AdvSM subtypes (ASM, SM-AHN, and MCL) without distinguishing the malignancy of AHN, and the presence or absence of a KIT D816V mutation without specifying allele frequency. The selection of prognostic factors used for matching was based on an arbitrary P value of less than 0.1 from exploratory subgroup analyses that contained the same data used for assessment, which is not consistent with recommended approaches in the NICE Decision Support Unit Technical Support Document 18.19 Information on patients who received prior systemic therapy in the midostaurin trials was not available; as such, the subgroup analyses of patients on avapritinib who received prior systemic therapy were compared to the midostaurin population in which patients with and without prior systemic therapy were assumed to be similar. Since prior systemic therapy was not further categorized or specified according to the type of treatment received before study enrolment, the proportion of patients with specific prior therapies was unknown. Median follow-up times differed between patients on avapritinib and midostaurin, with the potential to bias the comparative OS estimates. Median OS follow-up time for the avapritinib trials was 22.9 months and 7.0 months for the EXPLORER and PATHFINDER studies, respectively. Median follow-up time was 124 months and 26 months in the A2113 trial and the D2201 trial, respectively. The magnitude and direction of this potential bias is unclear.
Patients in the avapritinib and midostaurin trials were matched on baseline imbalances that differed by outcome and by analysis populations. For OS, age, AdvSM subtype, and race were included in matching across all analysis populations, but with race excluded for 2 analyses, likely due to the population comprised mostly of patients who were white (the PATHFINDER study RAC-RE population versus the pooled D2201 and A2213 trials’ primary efficacy population, and the pooled the EXPLORER and PATHFINDER studies RAC-RE population with avapritinib 200 mg starting dose versus the pooled D2201 and A2213 trials’ primary efficacy population). For both ORR and CR, age, the AdvSM subtype, race, ECOG PS score, prior systemic therapy, serum tryptase level, and the KIT D816V mutation status were included in matching. Due to the evolving definition of C-findings, patients in the trials differed in the number of C-findings, with a maximum of 5 for both the EXPLORER and PATHFINDER trials and a maximum of 8 and 10 for the D2201 trial and the A2213 trial, respectively. As such, C-findings were not formally included as a prognostic factor for matching in the MAIC. In the MAIC, OS was analyzed in the full trial population (the RAC-RE population in the avapritinib trials versus the primary efficacy population in the midostaurin trials) and in the safety population (the safety population in the avapritinib trials versus the full analysis set in the D2201 trial) and ORR was analyzed in the full trial population. While the safety population (those patients who had received at least 1 dose of avapritinib) may be most applicable for survival estimates and the RAC-RE population may be most applicable for response analyses, a clear distinction of the similarities and differences between the populations of analyses were not detailed in the MAIC, making it challenging to determine the comparability of treatment groups and the interpretation of findings.
Findings for OS across the analysis populations ranged from an HR of 0.37 to 0.67. After weighting, the effective sample size compared to the original sample size was reduced to suggest an incomplete overlap between the avapritinib and midostaurin populations. Estimates of OS for the efficacy populations were based on effective sample sizes that ranged from 72% to 88% compared to the index trials. Findings for OS in the MAIC were not evaluated according to the AdvSM subtypes in either sensitivity or subgroup analyses, which limits the interpretation of findings given the differential survival estimates of patients with ASM, SM-AHN, and MCL. It should be acknowledged that while such estimates may be useful for patients and clinicians, the small number of patients with contributing data per subtype would likely result in findings with an increased uncertainty due to wide CIs. Results for OS comparing avapritinib versus midostaurin in the efficacy population (the pooled RAC-RE population [n = 85] versus the pooled primary efficacy population [n = 115]; HR = 0.44 [95% CI, 0.25 to 0.76]) were similar to those of the full trial population (the pooled safety population [n = 131] versus the pooled full analysis set [n = 142]; HR = 0.42 [95% CI, 0.25 to 0.71]). These survival estimates were noted by the experts to be reasonable and aligned with observations in clinical practice.
Patients in the avapritinib trials were evaluated for treatment response using the modified IWG-MRT-ECNM criteria based on steering committee adjudication, whereas patients in the A2213 trial were evaluated using the original Valent criteria based on investigator assessment and patients in the D2201 trial were evaluated using the modified Valent criteria based on steering committee adjudication. ORR and CR were evaluated in the MAIC according to the IWG-MRT-ECNM criteria, relying on a post hoc exploratory analysis of the D2201 trial for midostaurin. The exclusion of data from the A2213 trial and the exploratory nature of the response analysis increases the potential for prognostic imbalance and the risk of type I error. There was high uncertainty in the results for the CR rate in the MAIC due to so few patients attaining CR (12.7% versus 1.1% of patients in the avapritinib versus midostaurin groups, respectively). Estimates of response were based on low effective sample sizes (these ranged from 66% to 76% for both ORR and CR), indicating that findings drawn from a subset of the sample from the index trials may not be fully representative of the overall population of patients with AdvSM. Overall response was estimated at 69.5% versus 36.0% for avapritinib versus midostaurin, respectively (pooled odds ratio = 4.06 [95% CI, 3.09 to 5.33]). The clinical experts expressed that midostaurin may be more efficacious than other available treatments based on observations in clinical practice. The experts agreed that avapritinib is expected to confer a greater clinical benefit compared to that of midostaurin; however, the magnitude of that benefit is unclear given the lack of head-to-head evidence. The experts noted that subsets of patients who may attain optimal treatment response is neither well defined nor available in the literature. Overall, the experts highlighted that the response evaluation is complex, continuously evolving, and lacking empiric evidence predicting long-term outcomes such as survival.
In the MAIC, avapritinib 200 mg (the dose recommended by Health Canada for the indicated population) versus midostaurin were based on sensitivity analyses using the pooled the EXPLORER and PATHFINDER studies RAC-RE population. While patients in the EXPLORER study received various doses of avapritinib starting at 300 mg, nearly all patients in the PATHFINDER study received a starting dose of 200 mg. The avapritinib 200 mg starting dose was estimated to reduce the risk of death in the weighted population by ███ (HR = 0.59 [95% CI, 0.27 to 1.32]). Response in the weighted population was estimated at an odds ratio of 2.85 (95% CI, 1.96 to 4.15). There is uncertainty in these results at least in part due to the small sample sizes in the avapritinib 200 mg cohort (44 patients and 42 patients for OS and ORR, respectively), which is reflected in the wide CI that crosses the null for survival and in findings that are driven by a reduced sample of the overall population. No analyses were conducted for avapritinib 200 mg in the safety population, which is a larger sample size and the analysis population most relevant for OS. Since midostaurin was approved in Canada in 2017 but subsequently not recommended for reimbursement by CADTH in 2020, patients in Canada have very limited or no access to the drug. As such, midostaurin is not an applicable treatment comparator for most patients with AdvSM in Canada in any line of therapy, according to the clinical experts consulted for this review.
Observational Comparison
No study protocol, statistical analysis protocol, or study report was provided for the observational comparison using IPTW analysis that was based on an updated data cut-off date of September 2022 for the PATHFINDER trial. Information presented for the methods of the observational comparison were limited to the sponsor-provided observational comparison report41 and publication,40 which conducted analyses using an earlier data cut-off date of April 2021. As such, the review team found several inconsistencies and gaps in information between these sources and the updated analyses included in the sponsor’s submission, in addition to methods (e.g., statistical analyses employed) that were not explicitly detailed. Four subgroup analyses that were specified in the observational comparison report were identified in the publication. However, the inclusion and exclusion of midostaurin in the updated analyses only (i.e., second-line or later-line therapy patients who started avapritinib at 200 mg in the PATHFINDER study-only versus second-line or later-line therapy patients who received BAT, using the PATHFINDER study safety population and RAC-RE population, respectively) were neither prespecified in the observational comparison report nor presented in the publication. Prespecified subgroup analyses comparing avapritinib at a dose of 200 mg or lower were not included in the sponsor’s submission. The sponsor confirmed that no sensitivity analyses were conducted for the updated analyses.53 There were no sensitivity analyses reported to evaluate the potential impact of bias due to informative censoring on effect estimates in patients who were censored due to a new primary malignancy after the index date or due to avapritinib initiation in the BAT cohort. Of 2 sensitivity analyses of OS described in the observational comparison report, 1 sensitivity analysis (i.e., the impact of excluding patients with missing ECOG PS scores) matched that reported in the publication, but the remaining sensitivity analysis described in the observational comparison report (i.e., comparative analyses for OS that were repeated with additional covariates that had a prevalence of 10% or higher in both cohorts and a standardized difference greater than 10%) was misaligned with the publication (i.e., the index year of treatment was included as a covariate in the Cox model to assess the impact of trends over time in AdvSM care).
Patients in the avapritinib cohort were enrolled from March 2016 to April 2021 in EXPLORER and PATHFINDER studies, respectively. Real-world patients with AdvSM who received BAT were enrolled from January 2009 to October 2021 and included as controls. While the integrated dataset for comparative analyses aimed to maximize comparability between the cohorts based on available patient-level data across sources, contextual information such as standards of care at a specified time point and across time was not directly captured. For patients in the external control group who received BAT as first-line therapy and then went on to receive avapritinib as second-line or later-line therapy either by enrolling in a trial (in the EXPLORER or PATHFINDER studies), or obtaining it via compassionate program access, follow-up was censored at avapritinib initiation. No further information was detailed regarding how patients who received avapritinib in second-line therapy were included and/or analyzed in the observational comparison. According to the observational comparison report, patients in the BAT cohort had to have an index date of at least 3 months before the start of data collection to ensure at least 3 months of follow-up; however, follow-up duration was not specified for patients included from the PATHFINDER trial.
Baseline characteristics that were included for the avapritinib and BAT cohorts were values closest to the index date (the initiation date of avapritinib in the PATHFINDER study and the date of BAT therapy received among real-world patients). The baseline period differed between the comparative cohorts (defined as the 8-week period up to the index date for avapritinib and the 12-week period up to the index date for BAT); no rationale was provided for the different time periods used to ascertain baseline characteristics. IPTW uses weights based on propensity scores to create a sample where the distribution of measured baseline covariates is independent of the treatment assigned. Since propensity scores are estimated from what is measured, it is important that all covariates considered to be potential confounders be included. While important patient demographics and disease characteristics appear to have been included as prognostic factors and treatment effect modifiers, how the covariates were measured is critical to ensuring comparability between cohorts. While AdvSM subtype was diagnosed based on the WHO criteria for all patients, the evaluation was confirmed by the RAC for the avapritinib cohort and based on local clinician assessment for the BAT cohort. Although both the avapritinib and BAT cohorts were open-label (i.e., patients and assessors have knowledge of treatments received), there may be a greater risk of bias among patients who were diagnosed in the BAT cohort due to the retrospective nature of chart review and the lack of information on the assessors.
Before weighting in the observational comparison, there were several imbalances in baseline characteristics between the avapritinib and BAT cohorts including age, sex, region, ECOG PS scores, anemia, thrombocytopenia, AdvSM subtypes, leukocyte counts, serum tryptase concentrations, and number of mutated genes within the SRSF2, ASXL1, and RUNX1 mutation panel. The number of prior lines of therapy was an additional covariate included in the analyses comparing avapritinib to BAT in second-line or later-line therapy. While the imbalanced covariates appeared to be similar across outcomes (the duration of treatment and OS), the distributions of covariates and proportions differed slightly. Nevertheless, imbalances in covariates were found to persist after IPTW weighting (among them, imbalances that increased for some covariates), for region, ECOG PS scores, anemia, thrombocytopenia, leukocyte counts, and serum tryptase concentrations, to suggest that there was a lack of sufficient overlap between the cohorts (i.e., the cohorts may be meaningfully different).
The observational IPTW comparison reported on both the safety and RAC-RE populations of the PATHFINDER study patients receiving avapritinib 200 mg versus real-world patients receiving a basket of therapies. While findings for OS and duration of treatment were presented for both populations of analyses, imbalances in covariates differed for the safety and RAC-RE populations such that it was challenging to meaningfully assess how these differences may have translated to adjusted results (after IPTW weighting) and what the comparability of the adjusted results was between the analyzed populations. No details comparing the analyzed populations were provided in the observational comparison report, publication, or updated analyses.
The observational comparison using IPTW methods included the overall sample (avapritinib from the EXPLORER and PATHFINDER studies versus BAT from real-world patients regardless of line of therapy) in the original analyses (April 2021 data cut-off). An analysis in the overall sample was not submitted by the sponsor for updated analyses (September 2022 data cut-off); rather, 3 analyses with longer follow-up were submitted that appeared to be subgroup or post hoc analyses, given that the analysis comparing avapritinib with exclusively midostaurin was not prespecified in the observational comparison report or the publication. OS was estimated at an HR of ████ ████ ███ ████ ██ █████ for avapritinib versus BAT first-line therapy (excluding midostaurin), an HR of ████ ████ ███ ████ ██ █████ for avapritinib versus midostaurin first-line therapy, and an HR of ████ ████ ███ ████ ██ █████ for avapritinib versus BAT second-line or later-line therapy. The small sample sizes, both overall and reduced for the avapritinib cohort compared to the BAT cohort, make it difficult to ensure prognostic matching was appropriate in the analyses. Median OS had not been reached in the avapritinib cohort in any line of therapy, indicating that OS data were immature. According to the clinical experts consulted for this review, the differentiation of outcomes by line(s) of therapy is not applicable to patients in Canada who have very few treatment options. The clinical experts also weighed in, stating that an MID could not be estimated for survival given the disease rarity and limited heterogenous treatments to date with variable response rates, response durability, and AE profiles. According to the clinical experts consulted, the survival of patients with AdvSM is based on historical estimates that predate the era of tyrosine kinase inhibitor therapy. While the clinical experts anticipated that avapritinib is likely superior to currently available therapies, they indicated that the magnitude of OS estimates for avapritinib relative to BAT appeared to be overly optimistic.
In the observational comparison, the avapritinib 200 mg dose was a subgroup analysis of the PATHFINDER trial with small sample sizes in the safety population for OS (fewer than 40 patients in first-line therapy and 67 patients in second-line or later-line therapy) and in the RAC-RE population for duration of treatment (31 patients in first-line therapy and 47 patients in second-line or later-line therapy). The clinical experts expressed that dose modifications for avapritinib, such as among patients receiving different doses in the EXPLORER trial, are reasonable and in line with how avapritinib would be used in clinical practice (e.g., dose reductions for intolerance or AEs).
According to Reiter et al., follow-up duration and response evaluations for patients in the BAT cohort did not follow the schedule of assessments typical in clinical trial settings.40 Variations in the timing of assessments and follow-up of patients who received BAT in the real-world setting may not fully match patients who received avapritinib in the EXPLORER and PATHFINDER studies; given the absence of information on follow-up duration (other than at least 3 months of follow-up in the BAT cohort) and its potential to create prognostic imbalance between the avapritinib and BAT cohorts, there is an unknown direction and magnitude of impact on the duration of treatment and survival.
Several methods of imputations for missing data were at risk of underestimating disease severity among included patients. Missing data for comorbidities and lab assessment values were categorized as negative or absent to allow all patients to be included in the analyses. For lines of therapy where patients had no ECOG PS scores recorded, the Karnofsky score closest to the index date in the same period (if available) was converted to an ECOG PS score. Observations without an ECOG PS or Karnofsky score recorded any time before 3 months after the index date were excluded from analysis for OS ███████ █████ ███ █████ for avapritinib first-line therapy versus BAT first-line therapy [excluding midostaurin], avapritinib second-line or later-line therapy versus BAT second-line or later-line therapy, and avapritinib first-line therapy versus midostaurin first-line therapy, respectively) and the duration of treatment (██████ █████ ███ █████ for avapritinib first-line therapy versus BAT first-line therapy [excluding midostaurin], avapritinib second-line or later-line therapy versus BAT second-line or later-line therapy, and avapritinib first-line therapy versus midostaurin first-line therapy, respectively).53 Observations with missing serum tryptase were imputed as not having a value of 125 ng/mL or greater for OS (██████ ██████ ███ █████ for avapritinib first-line therapy versus BAT first-line therapy [excluding midostaurin], avapritinib second-line or later-line therapy versus BAT second-line or later-line therapy, and avapritinib first-line therapy versus midostaurin first-line therapy, respectively) and the duration of treatment (██████ ██████ ███ █████ for avapritinib first-line therapy versus BAT first-line therapy [excluding midostaurin], avapritinib second-line or later-line therapy versus BAT second-line or later-line therapy, and avapritinib first-line therapy versus midostaurin first-line therapy, respectively).53 Given that patients’ ECOG PS scores and serum tryptase levels were key covariates used in the IPTW weighting, such nonconservative assumptions may bias findings, although the direction and magnitude cannot be determined since the proportion of patients with missing data for the avapritinib cohort was not reported.
The findings from the indirect treatment comparison and observational comparison suggested a benefit of avapritinib (the point estimate and lower and upper bounds of the CIs suggested benefit) when indirectly compared to currently available treatments for ORR, duration of treatment, and OS. Due to the substantial limitations identified in the analyses, there remains significant uncertainty in the magnitude of the benefit with avapritinib compared to currently available treatments. However, it appears unlikely that the benefit seen with avapritinib is solely explained by the noted limitations and sources of uncertainty of these comparisons. Therefore, while it is not possible to ascertain what the true effect is between the comparisons, it is likely to be in favour of avapritinib.
Discussion
Summary of Available Evidence
The systematic review included 2 open-label, single-arm clinical trials that provided data on the efficacy and safety of avapritinib in adults with AdvSM. The EXPLORER study enrolled 86 patients, including 69 patients with AdvSM, who received avapritinib 30 mg to 400 mg daily in the dose escalation period (part 1) or the extension period (part 2) of this phase I study. The PATHFINDER study was ongoing at the time of this review and provided results for 62 patients at the first data cut-off (the planned interim analysis), and for 105 patients at a second data cut-off. The key efficacy outcomes were ORR, OS, and change from baseline in the AdvSM-SAF TSS.
The mean age of patients enrolled was 65.0 (SD = 11.2) years and 67.5 (SD = 11.0) years in the EXPLORER and PATHFINDER studies, respectively; 41% and 45% of patients were female, respectively, and 59% and 55% were male, respectively. In the EXPLORER and PATHFINDER studies, the most common AdvSM subtype was SM-AHN (70% and 69%, respectively) followed by MCL (19% and 16%, respectively) and ASM (12% and 15%, respectively). In the EXPLORER and PATHFINDER trials, most patients had an ECOG PS score of 0 or 1 (70% and 69%, respectively), with 20% and 23% of patients rated as having an ECOG PS score of 2, respectively, and 10% and 8% of patients rated as having a score of 3, respectively. In the EXPLORER study, 59% of patients had received prior antineoplastic therapy compared with 68% of patients in the PATHFINDER trial (in the first data cut-off).
The sponsor also submitted indirect evidence from an unanchored MAIC that compared first-line therapy with avapritinib with midostaurin, using data from phase II, open-label, single-arm trials to estimate OS, ORR, and CR. The observational comparison submitted used IPTW methods to compare avapritinib to a basket of available treatments (including midostaurin, cladribine, imatinib, and interferon alpha) in different lines of therapy. The analyses were based on interim data from the PATHFINDER study and an external cohort study that used medical chart data from the US and Europe. The outcomes reported were duration of treatment and OS.
Interpretation of Results
Efficacy
The available evidence on the efficacy of avapritinib in adults with AdvSM is based on 2 single-arm, open-label clinical trials. As noted in the GRADE assessment, conclusions about efficacy relative to any comparator cannot be drawn from single-arm studies; thus, the certainty of evidence is rated as “very low.” The possibility of selection bias cannot be ruled out, particularly given the small sample size of the trials and the heterogeneity in patients with AdvSM. The clinical experts commented that prognosis varies substantially across and within AdvSM subtypes, with patients with MCL generally showing the worst outcomes; for those with SM-AHN, the type of hematologic neoplasm has a significant impact on the patient’s clinical course. The lack of a control group in the pivotal evidence limits the overall interpretation of the results. However, the feasibility of conducting a randomized controlled trial is low, given the rarity of AdvSM. The clinical experts consulted for this review also raised ethical concerns for a controlled trial, considering the efficacy and safety issues with the available comparators.
The clinical experts identified ORR as a key outcome and in the avapritinib trials, response was assessed using the modified IWG-MRT-ECNM criteria. The ORR results from the EXPLORER study and the interim data from the PATHFINDER study were generally consistent, with approximately 75% of patients showing an overall response. According to the clinical experts consulted, the response rate observed was clinically important; based on their clinical experience, they anticipated that response rates with avapritinib would be greater compared to other currently available treatments. The ORR was tested versus a 28% null value and found to be statistically significantly different in the EXPLORER study and at the first data cut-off of the PATHFINDER study (i.e., the planned interim analysis). The null value was based on a post hoc calculation of ORR using data from the single-arm midostaurin registration trial (the D2201 study). This comparison may not be appropriate, as it is uncertain if the estimated 28% midostaurin response rate can be applied to the patients enrolled in the EXPLORER and PATHFINDER studies. It is unclear if patients enrolled in the avapritinib and midostaurin trials were prognostically similar and if treatment effect modifiers were distributed equally. Further, the clinical experts noted that the criteria used to assess response continues to evolve, and there are no clear data to suggest which response criteria perform better in terms of predicting long-term outcomes like survival.
In the pivotal trials, most of the patients (approximately 70%) had a diagnosis of SM-AHN; thus, results largely reflect this patient group, which is relevant as this is the most common subtype of AdvSM. The available subgroup data suggest that patients with any subtype of AdvSM may respond to avapritinib; however, these data should be interpreted cautiously given the small number of patients in each group. For example, only 29 patients with ASM and 28 patients with MCL were included in total. The ORR in both studies was numerically higher in the subgroup of patients with no prior treatment exposure versus those who had received systemic therapies, but these data are difficult to interpret given the small sample size and possible confounding.
The median OS had not been reached in either study; thus, the survival data were considered immature. Given the lack of a control group, the limited number of survival events, and the availability of interim data only for the PATHFINDER study, the impact of avapritinib on OS is unclear.
In the EXPLORER study, the median PFS was 49.0 months (95% CI, 31.2 months to not estimable), and the median duration of response was ████ ██████ ████ ██ █████ ███ ██████████. Based on the interim data from the first and second data cut-off dates of the PATHFINDER study, the median PFS and duration of response had not been reached. The median time to response was ███ to 2.2 months in the studies. The clinical experts consulted considered PFS and durability of responses to be favourable to avapritinib compared to currently available therapy; however, based on the GRADE assessment, the certainty of evidence remains very low.
The PATHFINDER study was ongoing at the time of this review and the sponsor initially supplied data for the planned interim analysis (June 2020) as well as 1 other data cut-off (September 2022). Results from these data cut-off dates are the focus of this report. Later during the review, in response to an additional information request from the review team, the sponsor submitted limited data on the results for a more recent data cut-off of September 15, 2023.33,54 This data cut-off included 105 patients in the safety population and 81 patients in the RAC-RE population who had received a 200 mg avapritinib starting dose. The median follow-up duration was ██ ██████. The results of this data cut-off were similar to those described previously, with an ORR of █████ ████ ██ █████ ██ ██████ and a median time to response of 2.2 months (range, 0.3 months to ████ months). The median OS was not reached (Appendix 1, Figure 10), whereas the median PFS was ████ ██████ ████ ██ █████ ███ ██████████ (Appendix 1, Figure 11). The sponsor noted that this is not the final data cut-off and the final Clinical Study Report is expected in the first quarter of 2025. While these data are also interim, they appear to be supportive of the earlier results submitted by the sponsor.
Both the patient group input and clinician input reflected on the severity of symptoms that patients with AdvSM may experience and the impact on patients’ quality of life. The AdvSM-SAF questionnaire was developed by the sponsor to address the need for a SM-specific measure of symptom severity. The TSS includes 8 common symptoms in patients and is scored from 0 (no symptoms) to 80 (severe symptoms), averaged over the past week. The psychometric properties of the questionnaire were assessed using data from 31 patients in the EXPLORER study, and the sponsor reported a within-person MID of 9 points to 14 points for the TSS.34 The results at day 1, cycle 11, were more favourable (a mean change from baseline █████ ██████ ████ ███ █████ ██ █████ for the EXPLORER study and –9.8 points [95% CI, –14.9 points to –4.6 points] for the PATHFINDER study first data cut-off); however, the results were limited by the extent of missing data. Moreover, in the PATHFINDER study, the use of last observation carried forward imputation for missing data may also bias the findings. At this time point (which was a key secondary end point in the PATHFINDER study), data were available for 22 of 40 patients for the EXPLORER study and 22 of 56 patients for the PATHFINDER study (in the first data cut-off). Also, not all patients provided AdvSM-SAF scores, with ███ ███ ███ of the patients enrolled in the EXPLORER and PATHFINDER studies being excluded from the analyses at baseline. The data reported at cycle 11 for the second data cut-off of the PATHFINDER study were more complete (they excluded ███ of patients who did not report baseline results); however, the change from the baseline point estimate at –6.4 (SD = 9.7) points did not exceed the MID. Considering the issues with missing data and the lack of a comparator group, the impact of avapritinib on patient-reported symptoms is unclear.
Data for the EORTC QLQ-C30 were included at the request of the sponsor but were not assessed in GRADE as they were not identified as 1 of the most important outcomes to guide treatment selection in clinical practice. Descriptive results for the change from baseline over time in the global health status score are available in Appendix 1. The EORTC QLQ-C30 questionnaire includes 30 items with functional, symptom, and global health scales, each scored from 0 to 100, with higher scores indicating better function and global health, or worse symptoms. The sponsor reported MID values of 8 to 12 in patients with multiple myeloma,35 or 5 to 10 in 9 different cancers.36 For the global health status score specifically, the anchor-based MID estimates for the within-group change ranged from 4 to 14 for improvement and −11 to −5 for deterioration.36 The results in the avapritinib studies suggest an improvement in global health status, with a mean increase of ████ ██████ ███ █ █████ and 18.7 (SD = 28.0) points at cycle 11, day 1, in the EXPLORER study (the final data cut-off) and the PATHFINDER study (the second data cut-off), respectively. However, the results were limited by the extent of missing data with ███ of patients missing at day 1, cycle 11, in the EXPLORER study and 41% of patients missing in the PATHFINDER study.
In the absence of comparative evidence from a randomized trial, the sponsor submitted indirect evidence from an MAIC and from IPTW analyses comparing avapritinib to currently available treatments. There were substantial limitations in the indirect evidence to warrant cautious interpretation of the results. Comparators and outcomes of interest varied according to the sources of data, method of analysis, populations analyzed, and outcome evaluation. Disease knowledge and management have evolved over time such that there may be differences in AdvSM disease classification for both the midostaurin trials (with patients enrolled from 2005 to 2011 for the A2113 trial and from 2008 to 2017 for the D2201 trial) and the BAT cohort (with patients enrolled from 2009 to 2021) compared to patients in the avapritinib trials (enrolled from 2016 to 2020). There were regional differences between cohorts, which may impact access to treatments and standards of care. Since most patients in the avapritinib trials were equally distributed between sites in North America and Europe, it is unclear how comparable these patients were to the BAT cohort, who were mostly enrolled from sites in Europe. Based on the detected differences (in included studies, comparators, and outcomes), there was uncertainty in the comparability of the midostaurin and BAT cohorts that were used to evaluate efficacy (ORR, the duration of treatment, and OS) when compared indirectly with avapritinib for patients with AdvSM.
Both the MAIC and the observational comparison compared avapritinib to midostaurin for OS. Findings for OS estimated an HR of 0.44 (95% CI, 0.25 to 0.76) in the MAIC, an HR of 0.54 (95% CI, ████ to 0.95) in the MAIC with C-findings included as a matching variable, and an HR of ████ ████ ███ ████ ██ █████ in the observational IPTW comparison of both treatments as first-line therapy. Such wide-ranging differences in estimates may reflect a complex interlink of within-cohort (between-trial) and between-cohort (between-comparator) differences, including but not limited to the year of patient enrolment, standards of care for patients outside Canada, patients enrolled in trials as compared with patients in real-world settings, eligibility criteria for enrolment, patients excluded from the sample population or analysis, missing data, imbalanced follow-up duration, small sample sizes (particularly for the avapritinib 200 mg dose recommended by Health Canada), few events, and immature data. OS in both the indirect treatment comparison and the observational comparison were not evaluated according to AdvSM subtype. AdvSM subtypes were included in baseline characteristics that were used for matching (MAIC) and IPTW weighting (observational comparison); small sample sizes in this rare disease likely precluded sensitivity or subgroup analyses. Given the known differences in survival for AdvSM subtypes based on the natural history of the disease, there is uncertainty in the applicability of OS findings for subsets of patients. ORR and CR were assessed in the MAIC using the original IWG-MRT-ECNM criteria, which required a post hoc analysis of data in the D2201 trial of midostaurin that had evaluated response based on the modified Valent criteria. While the components are relatively comparable between the modified Valent criteria and the IWG-MRT-ECNM criteria, according to the clinical experts consulted for this review, there was a possibility that the CR rate in the MAIC may have been underestimated when compared to the pivotal evidence, given that patients with a partial hematologic recovery were treated as having PR versus a CRh using the original IWG-MRT-ECNM criteria versus the modified IWG-MRT-ECNM criteria, respectively.
Important gaps were identified in the indirect evidence for patients with AdvSM treated with avapritinib versus currently available treatments. Across the indirect evidence, prognostic factors identified as important by the experts (i.e., the type of malignancy within SM-AHN, the percentage of KIT D816V variant allele frequency, and the type of gene mutation in the SRSF2, ASXL1, and RUNX1 panel) were not included in baseline disease characteristics. The duration of follow-up was notably shorter in the BAT cohort compared to the avapritinib cohort for the duration of treatment. Baseline characteristics and results in the observational comparison were presented by line of therapy rather than for the total comparative sample regardless of line of therapy, which may be more generalizable to patients in Canada who have limited treatment options in any line of therapy. The duration of response (EXPLORER and PATHFINDER studies and the D2201 trials), the time to response (EXPLORER, PATHFINDER, and the D2201 trials), PFS (EXPLORER and PATHFINDER studies and the D2201 trials), and safety (AEs) (EXPLORER and PATHFINDER studies) were captured in individual trials; however, these outcomes were not included in the MAIC or the observational comparison. AEs in the avapritinib population were not reported in the MAIC and were available for the BAT cohort only in the observational comparison. In addition to the duration of treatment response and measures of survival, patient-reported outcomes (e.g., AdvSM-SAF, health-related quality of life) were an important outcome measure to patients and clinicians that was not captured by the relative treatment effect of avapritinib versus available therapies.
Despite the limitations identified in the indirect treatment comparison and observational comparison, overall, the findings suggested a benefit of avapritinib when indirectly compared to currently available treatments for ORR, duration of treatment, and OS, which is unlikely to be solely explained by the noted limitations and sources of uncertainty of these comparisons. However, there remains significant uncertainty in the magnitude of the benefit with avapritinib compared to currently available treatments due to the substantial limitations identified in the analyses. While it is not possible to ascertain what the true effect is between the comparisons, it is likely to be in favour of avapritinib.
The clinical experts highlighted that AdvSM is a rare, heterogeneous, and unpredictable disease for which no standard of care has been established. Given the nature of the disease, limited access to and/or affordability of treatments aimed at the indicated population, and treatments used off-label, patients with AdvSM in Canada have few treatment options that are effective with tolerable adverse effect profiles. While midostaurin is limited in access to patients with AdvSM in Canada due to the lack of universal funding by public drug plans and its prohibitive cost, other treatments have limited roles as highlighted by the clinical experts (e.g., imatinib is approved by Health Canada for patients with AdvSM without the KIT D816V mutation or with an unknown KIT mutation status; there is off-label use of cladribine and interferons, which have variable response rates and durability).
Harms
All patients in the pivotal trials experienced at least 1 AE, of which periorbital edema, anemia, diarrhea, nausea, fatigue, thrombocytopenia, and peripheral edema were most commonly reported. SAEs were also common, with ███ and 51% of patients reporting an event in the EXPLORER and PATHFINDER studies (in the second data cut-off), respectively. In both studies, a similar percentage of patients permanently stopped treatment due to AEs (███), and ███ ██████ ██ ████████ had 1 or more dose reductions due to AEs.
The frequency of intracranial bleeding was numerically higher in the EXPLORER study ███████ than in the PATHFINDER study (3.7%). Based on the results of an internal safety analysis, the sponsor identified severe thrombocytopenia (platelet count < 50 × 109/L) as the primary risk factor for intracranial bleeding. The protocol for the PATHFINDER study was amended to reduce the risk of bleeding; this included having a lower starting dose for patients with platelet counts of between 25 multiplied by 109/L and 50 multiplied by 109/L and later excluding the enrolment of patients with platelet counts less than 50 multiplied by 109/L. To mitigate the risk of intracranial bleeding in clinical practice, avapritinib is not recommended for patients with a platelet count of less than 50 multiplied by 109/L.23 The product monograph also recommends frequently monitoring platelet counts, interrupting treatment if thrombocytopenia occurs, and stopping therapy if the patient experiences intracranial bleeding.23
Cognitive AEs were commonly reported in both clinical trials, with 28% to ███ of patients reporting these AEs. The product monograph has recommendations for dose reductions, interruptions, or discontinuation, depending on the severity of the cognitive adverse effects.23
The available safety data from the clinical trials were limited by the small sample size of patients (a total of 191 patients) who were exposed for a mean of ████ ██ ████ ██████. As in all clinical trials, the trials enrolled a select patient population, and thus the frequency of AEs reported may not reflect the risk in clinical practice. The studies excluded patients with comorbidities such as uncontrolled cardiovascular disease, seizure disorder, and those with a history of cerebrovascular accident or intracranial bleeding; thus, the safety in these patients is unclear. As there was no control group, it is not possible to determine what proportion of AEs are attributable to avapritinib versus the disease or other factors. The indirect evidence submitted by the sponsor did not address safety outcomes. Since there are no direct or indirect comparative harms data in patients with AdvSM, the safety of avapritinib relative to any comparator is unknown. The clinical experts consulted by the review team anticipated that avapritinib would offer a more tolerable treatment for patients compared to currently available off-label therapy options.
Conclusions
Input from patient groups and clinicians highlighted that AdvSM is a rare, severe, and heterogeneous disease with a poor prognosis. Patients have currently limited treatment options. It is estimated that the AdvSM incidence rate in Canada is 0.06 cases per 100,000 adults with currently no access to publicly funded targeted treatment options.
Two single-arm, open-label clinical trials (the phase I EXPLORER study and the ongoing phase II PATHFINDER study) provided evidence of the efficacy and safety of avapritinib in adults with AdvSM. The studies showed that 75% of the patients who received avapritinib reported an adjudicated overall response, which the clinical experts consulted for this review considered to be clinically relevant and superior to currently available treatments. Due to the lack of a control group, the certainty of evidence was rated as very low, as the possibility of selection bias cannot be ruled out, particularly given the small sample size of the trials and the heterogeneity in patients with AdvSM.
Although OS and PFS were evaluated in the study, the single-arm design and immaturity of the data limit the ability to attribute the study results to treatment with avapritinib. Patient-reported symptoms were identified as an important outcome, but because of the noncomparative design, open-label study design, and high patient attrition rates in the trials, the effect of avapritinib on symptom severity remains inconclusive.
The safety data from the clinical trials were limited by the small sample size (a total of 191 patients) and treatment duration (a mean of ████ ██ ████ ██████). AEs, including SAEs, and AEs requiring dose reductions or discontinuation were common in the studies. However, due to the lack of a control group, the proportion of AEs that are attributable to avapritinib versus the disease or other factors is unclear. Intracranial bleeding and cognitive AEs were identified as AEs of special interest for avapritinib. While the sponsor identified thrombocytopenia as a risk factor for intracranial bleeding and implemented patient selection and monitoring criteria to reduce the frequency of events, the risk of intracranial bleeding associated with avapritinib use in clinical practice is unclear.
The noncomparative design of the EXPLORER and PATHFINDER studies precludes the ability to assess the relative therapeutic benefit or safety of avapritinib in Canadian clinical practice. To address the evidence gap, the sponsor submitted indirect evidence on the comparative efficacy of avapritinib versus other treatments for AdvSM. The indirect evidence suggests that relative to midostaurin or a basket of treatments, avapritinib may be associated with improved response, duration of treatment, and OS. It appears unlikely that the benefit seen with avapritinib is solely explained by the limitations and sources of uncertainty that were identified in the comparative analyses. However, there was significant uncertainty in the magnitude of the comparative benefit with avapritinib due to substantial limitations, including heterogeneity in the data sources and patient characteristics, missing or unmeasured prognostic factors and effect modifiers, small sample sizes, few events, imbalanced follow-up times, the immaturity of survival data, and the exploratory nature of post hoc and subgroup analyses. Since there were no data on patient-reported outcomes or comparative safety in the indirect evidence, the relative effect of avapritinib versus currently available treatments on symptoms, health-related quality of life, or safety is unknown.
References
1.Gotlib J. Advanced systemic mastocytosis: Management and prognosis. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2024: http://www.uptodate.com. Accessed 2024 May 28.
2.Khoury JD, Solary E, Abla O, et al. The 5th edition of the World Health Organization classification of haematolymphoid tumours: myeloid and histiocytic/dendritic neoplasms. Leukemia. 2022;36(7):1703-1719.
3.Pardanani A. Systemic mastocytosis in adults: 2023 update on diagnosis, risk stratification and management. Am J Hematol. 2023;98(7):1097-1116. PubMed
4.Gerds AT, Gotlib J, Abdelmessieh P, et al. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®). Systemic Mastocytosis. National Comprehensive Cancer Network; 2024 Apr 2024: https://www.nccn.org/professionals/physician_gls/pdf/mastocytosis.pdf.
5.Akin C, Gotlib J. Systemic mastocytosis: determining the subtype of disease. In: Post TW, ed. UpToDate. UpToDate ed. Waltham (MA): UpToDate; 2024: http://www.uptodate.com. Accessed 2024 May 28.
6.Castells MC, Akin C. Mastocytosis (cutaneous and systemic) in adults: epidemiology, pathogenesis, clinical manifestations, and diagnosis. In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2024: http://www.uptodate.com. Accessed 2024 May 28.
7.Cohen SS, Skovbo S, Vestergaard H, et al. Epidemiology of systemic mastocytosis in Denmark. Br J Haematol. 2014;166(4):521-528. PubMed
8.Schwaab J, Cabral do OHN, Naumann N, et al. Importance of adequate diagnostic workup for correct diagnosis of advanced systemic mastocytosis. J Allergy Clin Immunol Pract. 2020;8(9):3121-3127 e3121. PubMed
9.Lim KH, Tefferi A, Lasho TL, et al. Systemic mastocytosis in 342 consecutive adults: survival studies and prognostic factors. Blood. 2009;113(23):5727-5736. PubMed
10.Tefferi A, Shah S, Reichard KK, Hanson CA, Pardanani A. Smoldering mastocytosis: Survival comparisons with indolent and aggressive mastocytosis. Am J Hematol. 2018;94(1). PubMed
11.Center for Drug Evaluation Research. Medical review(s). Ayvakit (avapritinib) oral. Company: Blueprint Medicines Corporation. Application No.212608. Approval date: 06/16/2021 (FDA approval package). Silver Spring (MD): U.S. Food and Drug Administration (FDA); 2021 Jun 16: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2022/212608Orig1s006.pdf. Accessed 2024 Jul 10.
12.Balshem H, Helfand M, Schünemann HJ, et al. GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol. 2011;64(4):401-406. PubMed
13.Santesso N, Glenton C, Dahm P, et al. GRADE guidelines 26: informative statements to communicate the findings of systematic reviews of interventions. J Clin Epidemiol. 2020;119:126-135. PubMed
14.Sponsor Summary of Clinical Evidence [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: avapritinib 25 mg, 50 mg, 100 mg, and 200 mg tablet, oral. Toronto (ON): Medison Pharma Canada Inc; 2024 Apr.
15.Clinical Study Report: BLU-285-2101, EXPLORER. A phase 1 study of BLU-285 in patients with advanced systemic mastocytosis (ADVSM) and relapsed or refractory myeloid malignancies (data cut-off: 19Jan2023) [internal sponsor's report]. Cambridge (MA): Blueprint Medicines Corporation; 2024 Dec 12.
16.Clinical Study Report: BLU-285-2202, PATHFINDER, interim. An open-label, single-arm, phase 2 study to evaluate efficacy and safety of avapritinib (BLU-285), a selective kit mutation-targeted tyrosine kinase inhibitor, in patients with advanced systemic mastocytosis (data cut-off: 23June2020) [internal sponsor's report]. Cambridge (MA): Blueprint Medicines Corporation; 2020 Dec 7.
17.(PATHFINDER) Study to Evaluate Efficacy and Safety of Avapritinib (BLU-285), A Selective KIT Mutation-targeted Tyrosine Kinase Inhibitor, in Patients With Advanced Systemic Mastocytosis. Clinical summary of avapritinib use in patients with and without prior systemic therapy at a starting dose of 200 mg. (data cut-off:09Sept2022) [internal sponsor's report]. Cambridge (MA): BluePrint Medicines Corporation; 2024 Jan 30: PATH Report 2.
18.Medison Canada response to June 10, 2024 CADTH request for additional information regarding Avapritinib CADTH review [internal additional sponsor's information]. Toronto (ON): Medison Canada; 2024 Jun 17.
19.Phillippo DM, Ades AE, Dias S, Palmer S, Abrams KR, Welton NJ. NICE DSU TSD 18: methods for population-adjusted indirect comparisons in submissions to NICE. Bristol (GB): Nice Decision Support Unit; 2016: https://research-information.bris.ac.uk/ws/portalfiles/portal/94868463/Population_adjustment_TSD_FINAL.pdf. Accessed 2024 Feb 28.
20.Arber DA, Orazi A, Hasserjian RP, et al. International consensus classification of myeloid neoplasms and acute leukemias: integrating morphologic, clinical, and genomic data. Blood. 2022;140(11):1200-1228. PubMed
21.Blueprint Medicines Corporation. Prescribing information: Ayvakit (avapritinib) oral. Silver Spring (MD): U.S. Food and Drug Administration; 2023 May: https://www.accessdata.fda.gov/drugsatfda_docs/label/2023/212608s013lbl.pdf. Accessed 2024 May 22.
22.Product information: Ayvakyt (avapritinib). (European public assessment report). Amsterdam (Netherlands): European Medicines Agency; 2023 July 24: https://www.ema.europa.eu/en/documents/product-information/ayvakyt-epar-product-information_en.pdf. Accessed 2024 May 24.
23.Ayvakit (avapritinib): 25 mg, 50 mg, 100 mg, 200 mg tablet, oral [product monograph]. Toronto (ON): Medison Pharma Canada Inc; 2024 Sep 18.
24.Rydapt (midostaurin): 25 mg, oral capsule [product monograph]. Montreal (QC): Novartis Pharmaceuticals Canada Inc.; 2023 Mar 31: https://pdf.hres.ca/dpd_pm/00070168.PDF. Accessed 2024 May 24.
25.cladribine: 1 mg/mL, solution for intravenous injection [product monograph]. Richmond Hill (ON): Fresenius Kabi Canada Ltd.; 2015 Jun 9: https://pdf.hres.ca/dpd_pm/00030832.PDF. Accessed 2024 May 24.
26.Pegasys (peginterferon alfa-2a injection): 180 mcg/0.5 mL prefilled syringe, 180 mcg/1 mL single-use vial, and 180 mcg/0.5 mL ProClick Autoinjector [product monograph]. Mississauga (ON): Accelera Pharma Canada Inc.; 2024 Feb 1: https://pdf.hres.ca/dpd_pm/00074540.PDF. Accessed 2024 May 24.
27.GLEEVEC (imatinib mesylate), 100 mg and 400 mg oral tablets [product monograph]. Dorval (QC): Novartis Pharmaceuticals Canada Inc; 2022 Aug 31: https://pdf.hres.ca/dpd_pm/00067276.PDF. Accessed 2024 Jun 5.
28.Clinical Study Report: BLU-285-2101, EXPLORER, interim. A phase 1 study of BLU-285 in patients with advanced systemic mastocytosis (ADVSM) and relapsed or refractory myeloid malignancies (data cut-off: May 27, 2020) [internal sponsor's report]. . Cambridge (MA): Blueprint Medicines Corporation; 2020 Nov 25.
29.DeAngelo DJ, Radia DH, George TI, et al. Safety and efficacy of avapritinib in advanced systemic mastocytosis: the phase 1 EXPLORER trial. Nat Med. 2021;27(12):2183-2191. PubMed
30.Blueprint Medicines. NCT02561988: (EXPLORER) Study of BLU-285 in Patients With Advanced Systemic Mastocytosis (AdvSM) and Relapsed or Refractory Myeloid Malignancies. ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2023 Mar 17: https://clinicaltrials.gov/study/NCT02561988. Accessed 2024 Jan 31.
31.Gotlib J, Reiter A, Radia DH, et al. Efficacy and safety of avapritinib in advanced systemic mastocytosis: interim analysis of the phase 2 PATHFINDER trial. Nat Med. 2021;27(12):2192-2199. PubMed
32.Blueprint Medicines. NCT03580655: (PATHFINDER) Study to Evaluate Efficacy and Safety of Avapritinib (BLU-285), A Selective KIT Mutation-targeted Tyrosine Kinase Inhibitor, in Patients With Advanced Systemic Mastocytosis ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2023 Aug 2: https://clinicaltrials.gov/study/NCT03580655. Accessed 2024 Jan 31.
33.Medison Canada response to July 9, 2024 CDA-AMC additional information request regarding review of Avapritinib [internal additional sponsor's information]. Toronto (ON): Medison Pharma Canada Inc.; 2024 Jul 15.
34.Taylor F, Li X, Yip C, et al. Psychometric evaluation of the Advanced Systemic Mastocytosis Symptom Assessment Form (AdvSM-SAF). Leuk Res. 2021;108:106606. PubMed
35.Kvam AK, Fayers PM, Wisloff F. Responsiveness and minimal important score differences in quality-of-life questionnaires: a comparison of the EORTC QLQ-C30 cancer-specific questionnaire to the generic utility questionnaires EQ-5D and 15D in patients with multiple myeloma. Eur J Haematol. 2011;87(4):330-337. PubMed
36.Musoro JZ, Coens C, Sprangers MAG, et al. Minimally important differences for interpreting EORTC QLQ-C30 change scores over time: A synthesis across 21 clinical trials involving nine different cancer types. Eur J Cancer. 2023;188:171-182. PubMed
37.Committee for Medicinal Products for Human Use. Assessment report: Rydapt (midostaurin). (European public assessment report). London (GB): European Medicines Agency; 2017 Jul 20: https://www.ema.europa.eu/en/documents/assessment-report/rydapt-epar-public-assessment-report_en.pdf. Accessed 2024 May 22.
38.Novartis Pharmaceuticals Corporation. Prescribing information: Rydapt (midostaurin) oral. Silver Spring (MD): U.S. Food and Drug Administration; 2017 May: https://www.accessdata.fda.gov/drugsatfda_docs/label/2017/207997s000lbl.pdf. Accessed 2024 May 22.
39.Pilkington H, Smith S, Roskell N, Iannazzo S. Indirect treatment comparisons of avapritinib versus midostaurin for patients with advanced systemic mastocytosis. Future Oncol. 2022;18(13):1583-1594. PubMed
40.Reiter A, Gotlib J, Álvarez-Twose I, et al. Efficacy of avapritinib versus best available therapy in the treatment of advanced systemic mastocytosis. Leukemia. 2022;36(8):2108-2120. PubMed
41.Indirect Treatment Comparison between Avapritinib from Single-Arm Clinical Trials and Best Available Therapy in Real-world Use for Patients with Advanced Systemic Mastocytosis [internal sponsor's report]. Cambridge (MA): Blueprint Medicines Corporation; 2021 Dec 15.
42.Updated ECS results (PATHFINDER cut-off 09Sept2022): 1L avapritinib versus 1L midostaurin [internal sponsor's report]. Cambridge (MA): Blueprint Medicines Corporation; 2024.
43.Updated ECS results (PATHFINDER cut-off 09Sept2022): 2L+ avapritinib versus 2L+ BAT [internal sponsor's report]. Cambridge (MA): Blueprint Medicines Corporation; 2024.
44.Medison Pharma Canada Inc. response to May 13, 2024 CADTH request for additional information regarding avapritinib CADTH review: ECS Updated analysis for avapritinib 1L versus BAT 1L (excluding modostaurin) aggregate data [internal additional sponsor's information]. Toronto (ON): Medison Pharma Canada Inc; 2024 May 16.
45.Signorovitch JE, Sikirica V, Erder MH, et al. Matching-adjusted indirect comparisons: a new tool for timely comparative effectiveness research. Value Health. 2012;15(6):940-947. PubMed
46.Phillippo DM, Ades AE, Dias S, Palmer S, Abrams KR, Welton NJ. Methods for Population-Adjusted Indirect Comparisons in Health Technology Appraisal. Med Decis Making. 2018;38(2):200-211. PubMed
47.Funk MJ, Westreich D, Wiesen C, Stürmer T, Brookhart MA, Davidian M. Doubly Robust Estimation of Causal Effects. Am J Epidemiol. 2011;173(7):761-767. PubMed
48.Austin PC, Stuart EA. Moving towards best practice when using inverse probability of treatment weighting (IPTW) using the propensity score to estimate causal treatment effects in observational studies. Stat Med. 2015;34(28):3661-3679. PubMed
49.Aalen O. Nonparametric Inference for a Family of Counting Processes. Ann Stat. 1978;6(4):701-726.
50.Nelson W. Hazard Plotting for Incomplete Failure Data. J Qual Technol. 1969;1:27-52.
51.Lin DY, Wei LJ, Ying Z. Checking the Cox model with cumulative sums of martingale-based residuals. Biometrika. 1993;80(3):557-572.
52.Australian Public Assessment Report for Rydapt (midostaurin). Woden (AUS): Therapeutic Goods Administration (Australian Government Department of Health); 2019 Jan 03: https://www.tga.gov.au/resources/auspar/auspar-midostaurin. Accessed date unknown.
53.Medison Canada response to June 19, 2024 CDA-AMC additional information request regarding review of Avapritinib [internal additional sponsor's information]. Toronto (ON): Medison Pharma Canada Inc.; 2024 Jun 25.
54.(PATHFINDER) Study to Evaluate Efficacy and Safety of Avapritinib (BLU-285), A Selective KIT Mutation-targeted Tyrosine Kinase Inhibitor, in Patients With Advanced Systemic Mastocytosis. Clinical summary of avapritinib use in patients with and without prior systemic therapy at a starting dose of 200 mg. (data cut-off: 15 Sept 2023) [internal sponsor's report]. Cambridge (MA): BluePrint Medicines Corporation; 2024 May 13: PATH Report 3.
Appendix 1: Detailed Outcome Data
Please note that this appendix has not been copy-edited.
Progression-Free Survival
Figure 6: EXPLORER Study Progression-Free Survival, All Doses (RAC-RE Population — Final Data Cut-Off at January 19, 2023) [Redacted]

AdvSM = advanced systemic mastocytosis; ASM = aggressive systemic mastocytosis; MCL = mast cell leukemia; RAC-RE = Response Assessment Committee–Response Evaluable; SM-AHN = systemic mastocytosis with an associated hematologic neoplasm.
Source: Final Clinical Study Report for the EXPLORER study.15
Figure 7: PATHFINDER Study Progression-Free Survival, 200 mg Avapritinib (RAC-RE Population — First Data Cut-Off at June 23, 2020) [Redacted]

ASM = aggressive systemic mastocytosis; MCL = mast cell leukemia; RAC-RE = Response Assessment Committee–Response Evaluable; SM-AHN = systemic mastocytosis with an associated hematologic neoplasm.
Source: Interim Clinical Study Report for the PATHFINDER study.16
Figure 8: PATHFINDER Study Progression-Free Survival, 200 mg Avapritinib (RAC-RE Population — Second Data Cut-Off at September 9, 2022)
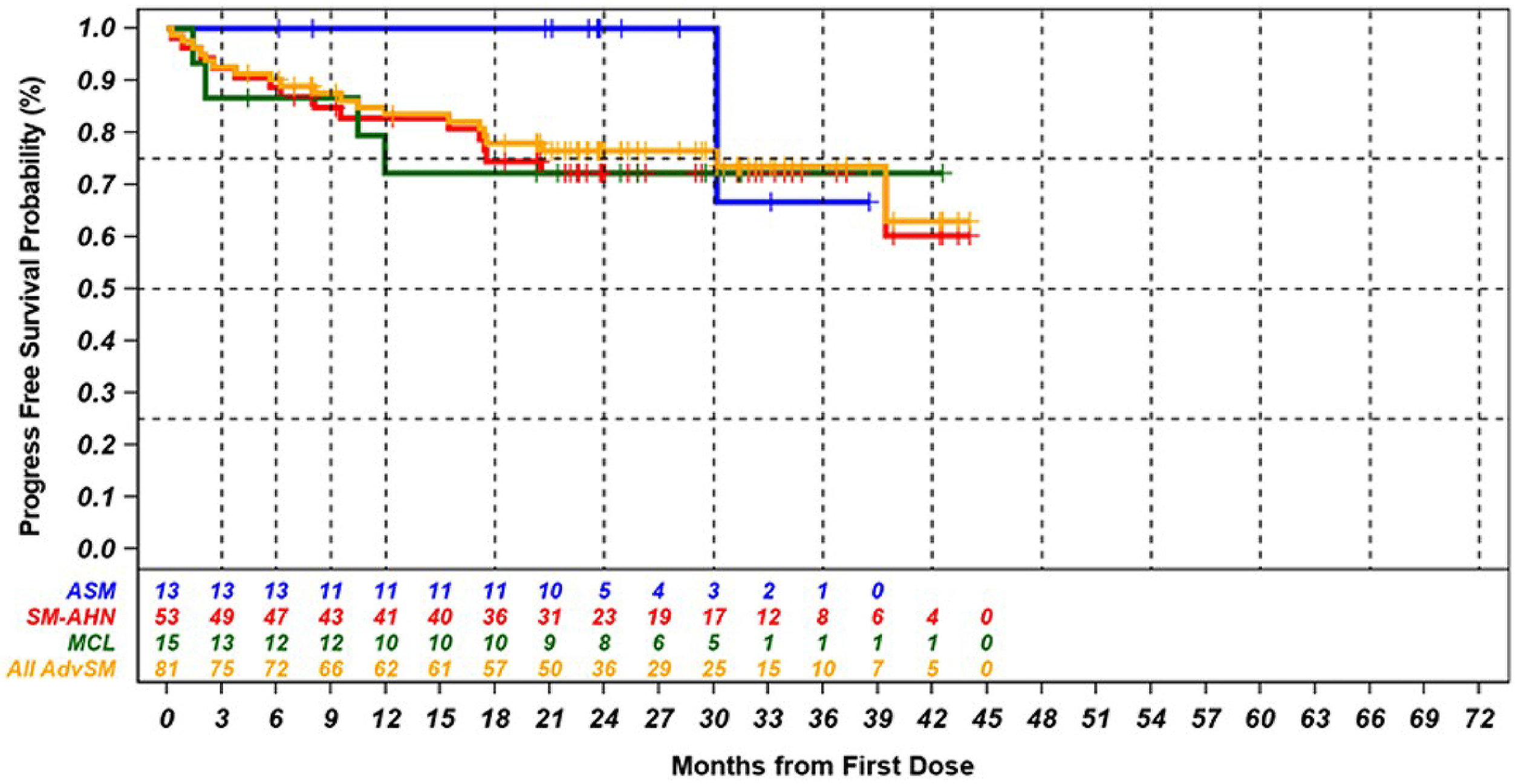
AdvSM = advanced systemic mastocytosis; ASM = aggressive systemic mastocytosis; MCL = mast cell leukemia; RAC-RE = Response Assessment Committee–Response Evaluable; SM-AHN = systemic mastocytosis with an associated hematologic neoplasm.
Source: PATHFINDER study clinical summary document.17
Subgroup Data by AdvSM Subtype
Overall Response
Table 41: EXPLORER Study Adjudicated Best Response by Modified IWG-MRT-ECNM Criteria, All Doses (RAC-RE Population — Final Data Cut-Off at January 19, 2023)
Response category, n (%) | ASMa (N = 4) | SM-AHNa (N = 40) | MCLa (N = 13) | All-AdvSMa (N = 57) |
|---|---|---|---|---|
Primary efficacy end point | ||||
ORR (CR + CRh + PR + ClinI), n (%) | | █████ | ██ █████ | ██ █████ | ██ █████ |
95% CI | ██████ ██ | ██████ | ██████ ██ | ██████ ██ |
P value | ██ | ██ | ██ | ███████ |
Other response categories | ||||
CR + CRh + PR rate, n (%) | | █████ | ██████ | | ██████ | ██ ██████ |
95% CI | ██████ ██ | ██████ | ██████ ███ | ██████ ███ |
P value | ██ | ██ | ██ | ███████ |
CR + CRh, n (%) | | ██████ | ██████ | | ██████ | ██ ██████ |
95% CI | ██████ █ | ██████ | ██████ ██ | ██████ ██ |
Best response, n (%) | ||||
CR | | ██████ | | ██████ | | ██████ | ██ ██████ |
CRh | | ██████ | | ██████ | | █████ | ██ ██████ |
PR | | ██████ | ███████ | | ██████ | ██ ██████ |
ClinI | ██ | ██ | | ██████ | | █████ |
Stable disease | ██ | ███████ | | ██████ | ██ ██████ |
Progressive disease | ██ | ██ | ██ | ██ |
Not evaluable | ██ | | █████ | ██ | | █████ |
AdvSM = advanced systemic mastocytosis; ASM = aggressive systemic mastocytosis; CI = confidence interval; ClinI = clinical improvement; CR = complete remission; CRh = complete remission with partial hematological recovery; IWG-MRT-ECNM = International Working Group - Myeloproliferative Neoplasms Research and Treatment - European Competence Network on Mastocytosis; MCL = mast cell leukemia; ORR = overall response rate; PR = partial remission; RAC-RE = Response Assessment Committee–Response Evaluable; SM-AHN = systemic mastocytosis with an associated hematologic neoplasm.
█████ ████ ██████ ██████████ ████████ ████ ███ ████████ ████ ████████ ███████████ █████ ██ ████ ███ ████ ████ ████ ████ ███ ███ █████
a████████ ███ █████ ██ █████████████
b███████████ ████ ██ ████████ ██████████ ██ ███ ███████ █ ████ ██████████ ██ ████ ███ █████ ████████ ████ ████ ████████ ███ ███ ███ █████ ███████ ██████████ ████ ████ ██ ███████████ ██ ████ █ ███ ████ ███
c███████████ ████ ██ ████████ ██████████ ██ ███ ███████ █ ████ ██████████ ██ ████ ███ █████ ████████ ████ ████ ████████ ███ ███ ███ █████ ███████ ██████████ ████ ████ ██ █████████████ █ █████ ███ ███ ██████████ ███ ████████ █████████
Sources: Final Clinical Study Report for the EXPLORER study15 and Sponsor Summary of Clinical Evidence.14
Table 42: PATHFINDER Study Adjudicated Best Response by Modified IWG-MRT-ECNM Criteria, All Doses (RAC-RE Population — First Data Cut-Off at June 23, 2020)
Response category, n (%) | ASM (N = 2) | SM-AHN (N = 26) | MCL (N = 4) | All-AdvSM (N = 32) |
|---|---|---|---|---|
Primary efficacy end point | ||||
ORR (CR + CRh + PR + ClinI), n (%) | 2 (100.0) | 21 (80.8) | 1 (25.0) | 24 (75.0) |
95% CI | (15.8 to 100.0) | (60.6 to 93.4) | (0.6 to 80.6) | (56.6, 88.5) |
P value | — | — | — | < 0.0001a |
Other response categories | ||||
CR + CRh + PR rate, n (%) | 2 (100.0) | 13 (50.0) | 1 (25.0) | 16 (50.0) |
95% CI | ██████ █ | ██████ █ | █████ ██ | ████ ███ |
P value | — | — | — | < 0.0001b |
CR + CRh, n (%) | 1 (50.0) | 5 (19.2) | 0 | 6 (18.8) |
95% CI | ███ █████ | █████ █ | ██ | ████ █████ |
Best response, n (%) | ||||
CR | 0 | 0 | 0 | 0 |
CRh | 1 (50.0) | 5 (19.2) | 0 | 6 (18.8) |
PR | 1 (50.0) | 8 (30.8) | 1 (25.0) | 10 (31.3) |
ClinI | 0 | 8 (30.8) | 0 | 8 (25.0) |
Stable disease | 0 | 2 (7.7) | 2 (50.0) | 4 (12.5) |
Progressive disease | 0 | 0 | 1 (25.0) | 1 (3.1) |
Not evaluable | 0 | 3 (11.5) | 0 | 3 (9.4) |
AdvSM = advanced systemic mastocytosis; ASM = aggressive systemic mastocytosis; CI = confidence interval; ClinI = clinical improvement; CR = complete remission; CRh = complete remission with partial hematological recovery; IWG-MRT-ECNM = International Working Group - Myeloproliferative Neoplasms Research and Treatment - European Competence Network on Mastocytosis; MCL = mast cell leukemia; ORR = overall response rate; PR = partial remission; RAC-RE = Response Assessment Committee–Response Evaluable; SM-AHN = systemic mastocytosis with an associated hematologic neoplasm.
aStatistical test on binomial proportion against a null of 28% was performed using 1-sided alpha = 0.025. Null was rejected at the interim analysis as the 1-sided P value was less than 0.00625 (Wald test P value).
bStatistical test on binomial proportion against a null of 17% was performed using 1-sided alpha = 0.025 (Wald test P value). P value was not controlled for multiple testing.
Sources: Interim Clinical Study Report for the PATHFINDER study16 and Sponsor Summary of Clinical Evidence.14
Table 43: PATHFINDER Study Adjudicated Best Response by Modified IWG-MRT-ECNM Criteria, Avapritinib 200 mg Dose (RAC-RE Population — Second Data Cut-Off at September 9, 2022)
Response category, n (%) | ASM (N = 13) | SM-AHN (N = 53) | MCL (N = 15) | All-AdvSM (N = 81) |
|---|---|---|---|---|
Primary efficacy end point | ||||
ORR (CR + CRh + PR + ClinI), n (%) | 10 (76.9) | 40 (75.5) | 10 (66.7) | 60 (74.1) |
95% CI | (46.2 to 95.0) | (61.7 to 86.2) | (38.4 to 88.2) | (63.1 to 83.2) |
Best response | ||||
CR | 0 | 8 (15.1) | 3 (20.0) | 11 (13.6) |
CRh | 2 (15.4) | 9 (17.0) | 0 | 11 (13.6) |
PR | 8 (61.5) | 20 (37.7) | 7 (46.7) | 35 (43.2) |
ClinI | 0 | 3 (5.7) | 0 | 3 (3.7) |
AdvSM = advanced systemic mastocytosis; ASM = aggressive systemic mastocytosis; CI = confidence interval; ClinI = clinical improvement; CR = complete remission; CRh = complete remission with partial hematological recovery; IWG-MRT-ECNM = International Working Group - Myeloproliferative Neoplasms Research and Treatment - European Competence Network on Mastocytosis; MCL = mast cell leukemia; ORR = overall response rate; PR = partial remission; RAC-RE = Response Assessment Committee–Response Evaluable; SM-AHN = systemic mastocytosis with an associated hematologic neoplasm.
Sources: PATHFINDER study clinical summary document17 and Sponsor Summary of Clinical Evidence.14
Overall Survival
Table 44: EXPLORER Study Overall Survival, All Doses (Safety Population — Final Data Cut-Off at January 19, 2023)
Overall survival | ASM (N = 8) | SM-AHN (N = 48) | MCL (N = 13) | All-AdvSM (N = 69) |
|---|---|---|---|---|
Events, n (%) | ██ | ██ ██████ | | ██████ | ██ ██████ |
Censored, n (%) | | █████ | ██ ██████ | ██ ██████ | ██ ██████ |
Median OS follow-up, months (95% CI) | ████ ███ | ████ ███ | ███████ | ████ ███ |
Kaplan-Meier estimates | ||||
Median OS, months (95% CI) | ██ ███ ███ | ████ ███ | ██ ███ ███ | ██ █████ |
OS rate, % (95% CI) at time point | ||||
3 months | ███ █████ | ███ █████ | ███ █████ | ███ █████ |
6 months | ███ █████ | ███ █████ | ███ █████ | ███ █████ |
9 months | ███ █████ | ███ █████ | ███ █████ | ███ █████ |
12 months | ███ █████ | ███ █████ | ███ █████ | ███ █████ |
18 months | ███ █████ | ███ █████ | ███ █████ | ███ █████ |
24 months | ███ █████ | ███ █████ | ███ █████ | ███ █████ |
30 months | ███ █████ | ███ █████ | ███ █████ | ███ █████ |
36 months | ███ █████ | ███ █████ | ███ █████ | ███ █████ |
42 months | ███ █████ | ███ █████ | ███ █████ | ███ █████ |
48 months | ███ █████ | ███ █████ | ███ █████ | ███ █████ |
54 months | ███ █████ | ███ █████ | ███ █████ | ███ █████ |
60 months | ███ █████ | ███ █████ | ███ █████ | ███ █████ |
66 months | ███ █████ | ███ █████ | ███ █████ | ███ █████ |
72 months | ███ █████ | ███ █████ | ███ █████ | ███ █████ |
AdvSM = advanced systemic mastocytosis; ASM = aggressive systemic mastocytosis; CI = confidence interval; MCL = mast cell leukemia; NE = not estimable; SM-AHN = systemic mastocytosis with an associated hematologic neoplasm.
Sources: Final Clinical Study Report for the EXPLORER study15 and Sponsor Summary of Clinical Evidence.14
Table 45: PATHFINDER Study Overall Survival, All Doses (Safety Population — First Data Cut-Off at June 23, 2020)
Overall survival | ASM (N = 9) | SM-AHN (N = 43) | MCL (N = 10) | All-AdvSM (N = 62) |
|---|---|---|---|---|
Events, n (%) | ██ | | █████ | | ██████ | | █████ |
Censored, n (%) | | ███████ | ██ ██████ | | ██████ | ██ ██████ |
Median OS follow-up, months (95% CI) | ███ ████ █ | ███ ███ ██ | ███ ████ ██ | ███ ████ █ |
Kaplan-Meier estimates | ||||
Median OS, months (95% CI) | ██ ████ ███ | ██ ████ ███ | ██ ████ ███ | ██ ████ ███ |
OS rate, % (95% CI) at time point | ||||
3 months | █████ █████ | ████ ████ | █████████ | ████ ████ |
6 months | █████ ██████ | ████ ████ | ████ ████ | ████ ███ |
9 months | █████ ██████ | ████ ███ | ████ ████ | ████ ███ |
12 months | █████ ████ | ████ ████ | ████ █████ | ████ ███ |
18 months | ██ | ████ ████ | ██ | ████ ████ |
AdvSM = advanced systemic mastocytosis; ASM = aggressive systemic mastocytosis; CI = confidence interval; MCL = mast cell leukemia; NE = not estimable; SM-AHN = systemic mastocytosis with an associated hematologic neoplasm.
Sources: Interim Clinical Study Report for the PATHFINDER study16 and Sponsor Summary of Clinical Evidence.14
Subgroup Data by Prior Antineoplastic Therapy
Overall Response
Table 46: Adjudicated Best Response by Modified IWG-MRT-ECNM Criteria in Patients With AdvSM by Treatment With Prior Antineoplastic Therapy (RAC-RE Population)
Response category, n (%) | EXPLORER study all-AdvSM Final data cut-off date: January 19, 2023 Prior antineoplastic therapy | PATHFINDER study all-AdvSM First data cut-off date: June 23, 2020 Prior antineoplastic therapy | PATHFINDER study AdvSM 200 mg Second data cut-off date: September 9, 2022 Prior antineoplastic therapy | |||
|---|---|---|---|---|---|---|
Yes (N = 35) | No (N = 22) | Yes (N = 23) | No (N = 9) | Yes (N = 51) | No (N = 30) | |
ORR (CR + CRh + PR + CI), n (%) | ██ ████ | ██ █████ | 17 (73.9) | 7 (77.8) | 33 (64.7) | 27 (90.0) |
95% CI | ██████ | ███ ███ | (51.6 to 89.8) | (40.0 to 97.2) | (50.1 to 77.6) | (73.5, 97.9) |
CR + CRh + PR rate, n (%) | ██ ████ | ██ █████ | 10 (43.5) | 6 (66.7) | ██ | ██ |
95% CI | ██████ | ██████ █ | ████ | ██████ | ██ | ██ |
Best response | ||||||
CR | | █████ | | ██████ | 0 | 0 | 5 (9.8) | 6 (20.0) |
CRh | | █████ | | ██████ | 3 (13.0) | 3 (33.3) | 5 (9.8) | 6 (20.0) |
PR | ██ ███ | | ██████ | 7 (30.4) | 3 (33.3) | 20 (39.2) | 15 (50.0) |
ClinI | | █████ | | █████ | 7 (30.4) | 1 (11.1) | 3 (5.9) | 0 |
Stable disease | | █████ | | ██████ | 2 (8.7) | 2 (22.2) | ██ | ██ |
PD | ██ | ██ | 1 (4.3) | 0 | ██ | ██ |
Not evaluable | | █████ | ██ | 3 (13.0) | 0 | ██ | ██ |
AdvSM = advanced systemic mastocytosis; CI = confidence interval; ClinI = clinical improvement; CR = complete remission; CRh = complete remission with partial hematological recovery; IWG-MRT-ECNM = International Working Group - Myeloproliferative Neoplasms Research and Treatment - European Competence Network on Mastocytosis; ORR = overall response rate; PD = progressive disease; PR = partial remission; RAC-RE = Response Assessment Committee–Response Evaluable.
Sources: Final Clinical Study Report for the EXPLORER study,15 interim Clinical Study Report for the PATHFINDER study,16 PATHFINDER study clinical summary document,17 and Sponsor Summary of Clinical Evidence.14
Overall Survival
Table 47: Overall Survival in Patients With AdvSM by Prior Antineoplastic Therapy, All Doses (Safety Population)
Overall survival | EXPLORER study all-AdvSM Final data cut-off date: January 19, 2023 Prior antineoplastic therapy | PATHFINDER study all-AdvSM First data cut-off date: June 23, 2020 Prior antineoplastic therapy | ||
|---|---|---|---|---|
Yes (N = 41) | No (N = 28) | Yes (N = 42) | No (N = 20) | |
Events, n (%) | ██ ██████ | ██ ██████ | | █████ | | █████ |
Censored, n (%) | ██ ██████ | ██ ██████ | ██ ██████ | ██ ██████ |
Kaplan-Meier estimates | ||||
Median OS, months (95% CI) | ██ ████ ███ | ███ ███ ███ | ██ ████ ███ | ██ ████ ███ |
OS rate, % (95% CI) at time point | ||||
6 months | ██████████ | ███████████ | ██ ██ █████ | ███ ██ ████ |
12 months | ██ ████ ███ | ████ ██ ████ | ██ ██ █████ | ██ ██ █████ |
18 months | ██ ███ ████ | ████ ██ ████ | ██ | ██ ███ ████ |
24 months | ██ ███ ███ | ██ ██ █████ | ██ | ██ |
36 months | ██ ███ ████ | ██ ███ ████ | ██ | ██ |
48 months | ██ ████████ | ██ ███ ███ | ██ | ██ |
60 months | ██ ███ ████ | ██ ███ ████ | ██ | ██ |
72 months | ██ ███ ████ | ██ | ██ | ██ |
AdvSM = advanced systemic mastocytosis; CI = confidence interval.
Source: Final Clinical Study Report for the EXPLORER study15 and interim Clinical Study Report for the PATHFINDER study.16
Figure 9: PATHFINDER Study Overall Survival by Prior Systemic Therapy, Avapritinib 200 mg Dose (Safety Population — Second Data Cut-Off at September 9, 2022)
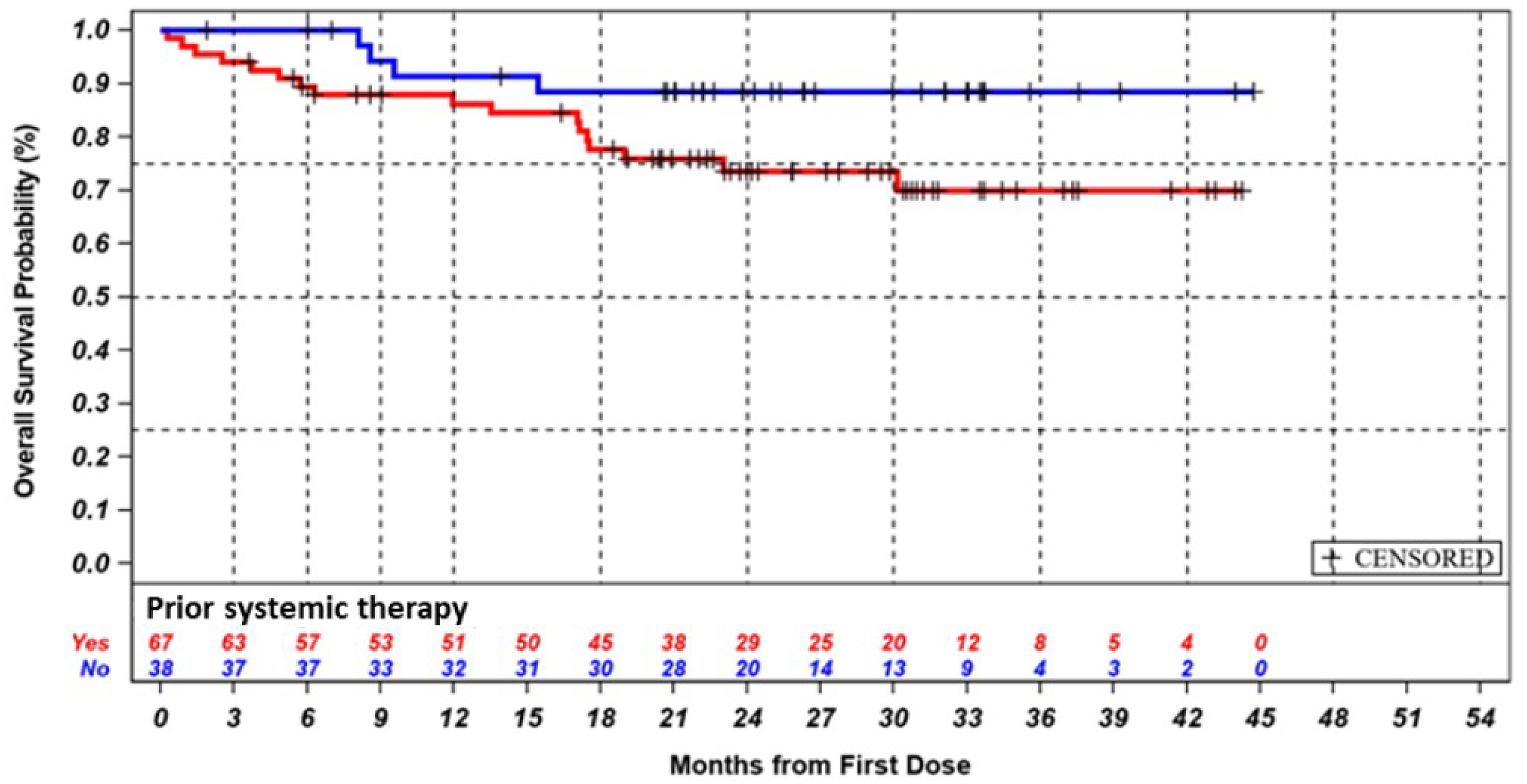
Note: Patients were grouped according to prior antineoplastic therapy (yes or no) without further subdivision according to prior midostaurin use.
Source: PATHFINDER study clinical summary document.17
Progression-Free Survival
PFS by prior antineoplastic therapy was not reported in the EXPLORER study.
Table 48: PATHFINDER Study Adjudicated Progression-Free Survival by Modified IWG-MRT-ECNM Criteria in Patients With AdvSM per Treatment With Prior Antineoplastic Therapy, All Doses (RAC-RE Population)
Progression-free survival | PATHFINDER study all-AdvSM Prior antineoplastic therapy | PATHFINDER Study AdvSM 200 mg Prior antineoplastic therapy | ||
|---|---|---|---|---|
Yes (N = 23) | No (N = 9) | Yes (N = 51) | No (N = 30) | |
Events, n (%) | | ██████ | ██ | 16 (31.4) | 4 (13.3) |
Censored, n (%) | ██ ██████ | | ███████ | 35 (68.6) | 26 (86.7) |
Kaplan-Meier estimates | ||||
Median PFS, months (95% CI) | ██ ████ ███ | ██ ████ ███ | NE (30.2 to NE) | 39.4 (39.4 to NE) |
PFS rate, % (95%CI) at time point | ||||
6 months | ████ █████ | █████████ | — | — |
12 months | ████ █████ | ██ █████ | 77.9 (66.3 to 89.5) | 93.0 (83.6 to 100.0) |
24 months | ██ | ██ | 68.8 (55.5 to 82.0) | 89.4 (78.1 to 100.0) |
36 months | ██ | ██ | 64.2 (49.1 to 79.3) | 89.4 (78.1 to 100.0) |
48 months | ██ | ██ | 64.2 (49.1 to 79.3) | 44.7 (0.0 to 100.0) |
AdvSM = advanced systemic mastocytosis; CI = continued improvement; IWG-MRT-ECNM = International Working Group - Myeloproliferative Neoplasms Research and Treatment - European Competence Network on Mastocytosis; PFS = progression free survival; PR = partial remission; RAC-RE = Response Assessment Committee–Response Evaluable.
Sources: Interim Clinical Study Report for the PATHFINDER study,16 PATHFINDER study clinical summary document,17 and Sponsor Summary of Clinical Evidence.14
Additional Data Supplied by the Sponsor on July 15, 2024
Figure 10: PATHFINDER Study Overall Survival, Avapritinib 200 mg Dose (Safety Population — Additional Data Cut-Off at September 15, 2023) [Redacted]

AdvSM = advanced systemic mastocytosis; ASM = aggressive systemic mastocytosis; ISM/SSM = indolent/smouldering systemic mastocytosis MCL = mast cell leukemia; SM-AHN = systemic mastocytosis with an associated hematologic neoplasm.
Source: Additional data supplied by the sponsor (July 15, 2024).33
Figure 11: PATHFINDER Study Progression-Free Survival, 200 mg Avapritinib Dose (RAC-RE Population — Additional Data Cut-Off at September 15, 2023) [Redacted]

AdvSM = advanced systemic mastocytosis; ASM = aggressive systemic mastocytosis; ISM/SSM = indolent/smouldering systemic mastocytosis MCL = mast cell leukemia; SM-AHN = systemic mastocytosis with an associated hematologic neoplasm.
Source: Additional data supplied by the sponsor (July 15, 2024).33
EORTC QLQ-C30 Change From Baseline for the Global Health Score
Figure 12: EXPLORER Study Change From Baseline in EORTC QLQ-C30 Global Health Score in Patients With AdvSM (Safety Population — Final Data Cut-Off at January 19, 2023) [Redacted]

AdvSM = advanced systemic mastocytosis; C = cycle; D1 = day 1; EORTC QLQ-C30 = EORTC Core Quality of Life questionnaire; MAX = maximum; MIN = minimum; Q1 = Quartile 1; Q3 = Quartile 3; SAF = symptom assessment form; STD = standard deviation.
Note: Boxes represent the median and interquartile range. Diamonds represent the mean. Whiskers represent the 10th and 90th percentiles. Dots show data points outside percentiles.
Source: Final Clinical Study Report for the EXPLORER study.15
Figure 13: PATHFINDER Study Change From Baseline in EORTC QLQ-C30 Global Health Score in Patients With AdvSM (Safety Population, Avapritinib 200 mg Dose — Second Data Cut-Off at September 9, 2022)
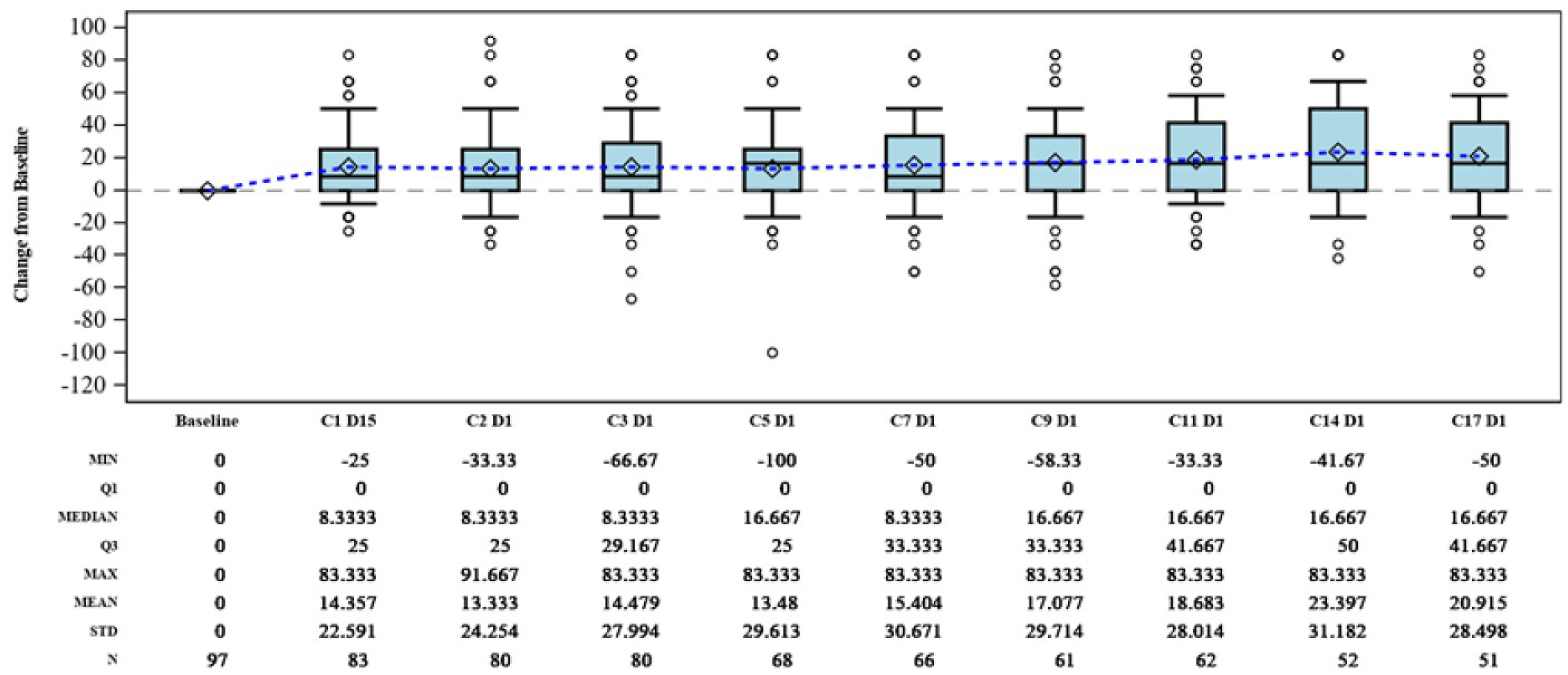
AdvSM = advanced systemic mastocytosis; C = cycle; D = day; EORTC QLQ-C30 = EORTC Core Quality of Life questionnaire; MAX = maximum; MIN = minimum; Q1 = Quartile 1; Q3 = Quartile 3; SAF = symptom assessment form; STD = standard deviation.
Note: Boxes represent the median and interquartile range. Diamonds represent the mean. Whiskers represent the 10th and 90th percentiles. Dots show data points outside percentiles.
Source: PATHFINDER study clinical summary document.17
Pharmacoeconomic_Review
Abbreviations
1L
first-line
2L+
second-line or later-line
AdvSM
advanced systemic mastocytosis
AE
adverse event
allo-HSCT
allogeneic hematopoietic stem cell transplant
AML
acute myeloid leukemia
ASM
aggressive systemic mastocytosis
BAT
best available therapy
BIA
budget impact analysis
CDA-AMC
Canada’s Drug Agency
CIHI
Canadian Institute for Health Information
CUA
cost-utility analysis
EORTC QLQ-30
European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30
HSCT
hematopoietic stem cell transplant
ICER
incremental cost-effectiveness ratio
IPTW
inverse probability of treatment weighting
KM
Kaplan-Meier
LLSC
Leukemia & Lymphoma Society of Canada
MCL
mast cell leukemia
NIHB
Non-Insured Health Benefits
OS
overall survival
PFS
progression-free survival
QALY
quality-adjusted life-year
RAC-RE
Response Assessment Committee–Response Evaluable
SC
subcutaneous
SM-AHN
systemic mastocytosis with an associated hematologic neoplasm
ToT
time on treatment
WTP
willingness to pay
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Avapritinib, 25 mg, 50 mg, 100 mg, and 200 mg oral tablets |
Indication | Proposed: For the treatment of adult patients with AdvSM. AdvSM includes patients with ASM, hematologic SM-AHN, and MCL. |
Health Canada approval status | NOC |
Health Canada review pathway | Standard |
NOC date | September 18, 2024 |
Reimbursement request | As per indication |
Sponsor | Medison Pharma Canada Inc. |
Submission history | No |
AdvSM = advanced systemic mastocytosis; ASM = aggressive systemic mastocytosis; MCL = mast cell leukemia; NOC = Notice of Compliance; SM-AHN = systemic mastocytosis with an associated hematologic neoplasm.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Partitioned survival model |
Target population | Adult patients with AdvSM, which includes patients with ASM, hematologic SM-AHN, and MCL, in 1L and 2L+ therapy |
Treatment | Avapritinib |
Dosage regimen | 200 mg once daily until progression or unacceptable toxicity |
Submitted price | Avapritinib: $1,343.36 per 25 mg, 50 mg, 100 mg, or 200 mg oral tablet |
Submitted treatment cost | Avapritinib: $37,614.08 per 28-day cycle ($490,362.40 annually) |
Comparators |
|
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs, LYs |
Time horizon | Lifetime (1L therapy population = 34 years; 2L+ therapy population = 28 years) |
Key data sources | IPTW-weighted analysis in which the effectiveness of avapritinib was informed by the PATHFINDER trial (an open-label, single-arm, phase II clinical trial) and the effectiveness of BAT was informed by the BLU-285 to 2405 study (an external control study of patients in the real world treated with BAT) |
Submitted results |
|
Key limitations |
|
CDA-AMC reanalysis results |
|
1L = first-line; 2L+ = second-line or later-line; AdvSM = advanced systemic mastocytosis; AML = acute myeloid leukemia; ASM = aggressive systemic mastocytosis; BAT = best available therapy; CDA-AMC = Canada’s Drug Agency; ICER = incremental cost-effectiveness ratio; IPTW = inverse probability of treatment weighting; KM = Kaplan-Meier; LY = life-year; MCL = mast cell leukemia; OS = overall survival; PFS = progression-free survival; QALY = quality-adjusted life-year; SM-AHN = systemic mastocytosis with an associated hematologic neoplasm; ToT = time on treatment; WTP = willingness to pay.
Note: 1L BAT comprises cladribine, peginterferon alfa-2a, and imatinib. 2L+ BAT comprises cladribine, peginterferon alfa-2a, imatinib, and midostaurin. When not specified, the term “BAT” encompasses both 1L and 2L+ BAT.
Conclusions
Based on the Clinical Review by Canada’s Drug Agency (CDA-AMC), avapritinib may be associated with improved overall survival (OS) relative to a basket of treatments. However, there was significant uncertainty in the magnitude of the findings due to substantial limitations, including heterogeneity in the data sources and patient characteristics, missing or unmeasured prognostic factors and effect modifiers, small sample sizes, few events, a lack of follow-up information, the immaturity of survival data, and the exploratory nature of post hoc and subgroup analyses. Since there were no data on patient-reported outcomes or comparative safety in the indirect evidence, the relative effect of avapritinib versus currently available treatments on symptoms, health-related quality of life, or safety is unknown.
The results of the alternative analyses by CDA-AMC remain highly uncertain and prone to bias, of which the direction and magnitude are both unknown due to limitations with the evidence and the analytical approach used by the sponsor. Consistent with the sponsor’s analyses, avapritinib was more costly and more effective than best available therapy (BAT) in both the first-line (1L) and second-line or later-line (2L+) therapy populations in the CDA-AMC alternative analysis. Results were driven by drug acquisition costs as they accounted for more than 90% of incremental costs in both populations. Moreover, the majority of the incremental benefit gained by avapritinib occurred in the period of the model that was extrapolated beyond the observation period of the PATHFINDER trial (78% in the 1L therapy population and 64% in the 2L+ therapy population, per the CDA-AMC alternative analysis).
The predicted life-years and quality-adjusted life-years (QALYs) produced in the CDA-AMC alternative analyses were broadly similar to those in the sponsor’s base case, and both analyses are subject to the same critical limitations in the clinical evidence. That clinical evidence suggests that avapritinib may produce an improvement in OS compared to BAT, but that the magnitude of the improvement could not be estimated rigorously. The results of the economic analysis were highly influenced by differences in time spent in the progression-free state. Time in this state was informed by clinical evidence that was highly uncertain, with a magnitude of difference that also could not be estimated rigorously. In both the CDA-AMC alternative reanalysis and the sponsor’s base case, a price reduction was needed to achieve cost-effectiveness at a willingness-to-pay (WTP) threshold of $50,000 per QALY gained. In the CDA-AMC alternative analysis, this price reduction was 87%; however, this estimate is also subject to the limitations of the underlying clinical evidence and the methods used within the sponsor’s model. Given the very high degree of uncertainty, further price reduction may be warranted.
Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, clinician groups, and drug plans that participated in the CDA-AMC review process.
Patient group input was collected from 2 groups: The Leukemia & Lymphoma Society of Canada (LLSC) and Heal Canada. Input from LLSC was informed by 3 patient interviews (1 patient had advanced systemic mastocytosis [AdvSM] and experience with avapritinib, 1 patient had an unspecified subtype of systemic mastocytosis, and 1 patient had indolent systemic mastocytosis) and 1 caregiver interview (the patient had AdvSM and experience with avapritinib). Input from Heal Canada was informed by the literature summarizing symptoms, impact on quality of life, current treatment options, and the efficacy of avapritinib. Patients interviewed by LLSC described the disease impact of mastocytosis, which included debilitating pain disrupting quality of life and impeding their ability to participate in the activities of daily living, sleep deprivation, fatigue, fever, brain fog, an enlarged liver, an enlarged spleen, low platelet levels, unexpected anaphylactic shock reactions, and skin symptoms such as spots, rashes, itching, and hives. LLSC input noted that patients struggle with the fear and concern of becoming a burden to their families or loved ones, while caregivers find themselves having to assume additional responsibilities to provide essential care and support for the patient. LLSC input noted that current treatment options are presently inaccessible without special or compassionate access programs, which are not always available. Input noted that patients who do not have effective treatment options available often receive no treatment at all and rely on alternative therapeutic options or over-the-counter treatment options to try to alleviate symptoms. Patients expressed a need for accessible treatment options that are efficacious, with limited toxicities, and that enable them to uphold a satisfactory quality of life. One patient and 1 caregiver had experience with avapritinib and described how avapritinib provided symptom alleviation, had minimal side effects, if any, and improved quality of life.
Clinician group input was received from the LLSC Clinician Network and Myeloproliferative Neoplasm Canada Clinician Group and the Ontario Health (Cancer Care Ontario) Hematology Cancer Drug Advisory Committee. Clinician input noted that current treatment options are limited and include cytoreductive therapies (e.g., midostaurin, cladribine, interferons [such as peginterferon alfa-2a], imatinib, cytarabine, azacitidine, hydroxyurea, and fludarabine) plus mast cell stabilizers or inhibitors of release (e.g., antihistamines). Group input stated that international guidelines and expert consensus recommend enrolment in a clinical trial or a KIT inhibitor (e.g., midostaurin, avapritinib) in the 1L therapy setting for AdvSM as well as cladribine when rapid debulking is required. Input commented that access to midostaurin is limited as it is not reimbursed by public plans across Canada and there are currently no compassionate access programs. It was further noted that cladribine and interferons have historically been used off-label in Canada, but interferons are generally not an adequate 1L therapy treatment option for AdvSM. It was also noted that imatinib has a very limited role in the treatment of AdvSM. Clinician group input noted that avapritinib would be used as 1L monotherapy.
Drug plan input commented that there is no standard of care in the indicated population but that comparators may include cladribine, interferon, imatinib, and midostaurin, the latter of which is Health Canada–indicated but received a negative recommendation from CADTH. Drug plans inquired about the relative efficacy and safety of avapritinib versus the relevant comparators as the submitted clinical trial evidence did not include the aforementioned comparators. Additionally, drug plans asked whether patients currently on other systemic therapies should be switched to avapritinib if avapritinib becomes publicly reimbursed.
Several of these concerns were addressed in the sponsor’s model:
The sponsor modelled comparative efficacy for OS based on a sponsor-conducted indirect treatment comparison.
In addition, CDA-AMC addressed some of these concerns as follows:
CDA-AMC removed midostaurin from the sponsor’s calculation of treatment costs in the 2L+ therapy population.
CDA-AMC was unable to address the following concerns raised from input relevant to the economic review:
CDA-AMC was unable to consider caregiver burden as the sponsor’s model structure did not permit the inclusion of caregiver costs or quality of life.
CDA-AMC was unable to consider comparative progression-free survival (PFS) and safety owing to a lack of clinical data.
Economic Review
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted a cost-utility analysis (CUA) assessing avapritinib compared with a weighted basket of treatments comprising cladribine, peginterferon alfa-2a, imatinib, and midostaurin (in the 2L+ therapy setting only) for adult patients with AdvSM, which includes patients with aggressive systemic mastocytosis (ASM), systemic mastocytosis with an associated hematologic neoplasm (SM-AHN), and mast cell leukemia (MCL).1 The modelled population was aligned with the safety population from the PATHFINDER clinical trial and Health Canada–indicated population.
Avapritinib is available as 25 mg, 50 mg, 100 mg, and 200 mg oral tablets. The recommended dosage of avapritinib is 200 mg orally once daily until progression or unacceptable toxicity.2 At a sponsor-submitted price of $1,343.36 per 25 mg, 50 mg, 100 mg, or 200 mg tablet, the cost per 28-day cycle is $37,614.08 or $490,326 annually.1 Drug wastage was assumed in the sponsor’s base case.
The sponsor assumed a dose of 0.14 mg/kg on day 1 to day 5 of a 28-day course for cladribine and a dose of 90 mcg weekly for 2 weeks followed by 180 mcg weekly for peginterferon alfa-2a.1 Dosing for imatinib and midostaurin was retrieved from the respective product monographs.3,4 The cost per 28-day cycle for peginterferon alfa-2a, imatinib, and midostaurin was $1,678.80, $538.28, and $38,668.00, respectively. Cladribine costs were applied as a one-off cost for both treatment costs ($13,350.75) and administration costs ($6,468.84) as the sponsor assumed a treatment length of 3 cycles and a patient body weight of 71.13 kg based on the mean weight from the PATHFINDER trial. The sponsor assumed an administration cost of $40.39 for each dose of peginterferon alfa-2a. Costs per cycle were weighted by their respective market shares in the 1L and 2L+ therapy populations. In the 1L therapy population, cladribine, peginterferon alfa-2a, and imatinib (hereafter referred to as 1L BAT) were weighted according to the distribution of their relative use among patients, which was assumed to be 52.8%, 42.2%, and 5%, respectively. In the 2L+ therapy population, cladribine, peginterferon alfa-2a, imatinib, and midostaurin (hereafter referred to as 2L+ BAT) were weighted according to the distribution of their relative use among patients, which was assumed to be 27.19%, 21.74%, 5%, and 46.07% respectively. When not specified, the term “BAT” encompasses both 1L and 2L+ BAT. Relative use for BAT was based on clinician feedback elicited by the sponsor, on the composition used in a previous CDA-AMC submission for AdvSM, and on data from the Blueprint Real-World External Control Study (hereafter referred to as the BLU-285 to 2405 study).5-7
The economic analysis was undertaken using a lifetime horizon (1L therapy population = 34 years; 2L+ therapy population = 28 years) from the perspective of the publicly funded health care payer. Costs, life-years, and QALYs were discounted at an annual rate of 1.5%.1
Model Structure
The sponsor submitted a partitioned survival model with 3 health states: progression-free, progressive disease, and death, whereby transitions between health states occurred on a monthly cycle length of 30.4 days (Appendix 3, Figure 1).1 All patients entered the model in the progression-free health state, where they received either avapritinib, cladribine, peginterferon alfa-2a, imatinib, or midostaurin (in the 2L+ therapy population only), with state occupancy defined by PFS. During each cycle, patients either remained progression-free, transitioned to the progressive disease state, or progressed to death. Death was modelled as an absorbing state. The proportion of patients in the progressive disease state was calculated by subtracting the proportion of patients alive and progression-free (based on the PFS curve) from the proportion of patients alive (based on the OS curve). Patients in the progressive disease state could either remain in the same state or transition to the death state.
The sponsor’s base case considered a subgroup of patients who had received an allogeneic hematopoietic stem cell transplant (allo-HSCT) and modelled this subgroup using a Markov model. The proportion of the cohort eligible to receive allo-HSCT was subtracted from the total progression-free cohort and started the simulation in the pre–allo-HSCT health state. Patients remain in the pre–Allo-HSCT health state for 6 months. At 6 months, patients transitioned to the post–allo-HSCT health state or progressed to death. The probability of death in the post–allo-HSCT health state was estimated based on the OS curve in patients receiving allo-HSCT.
Model Inputs
Baseline patient characteristics in the model reflected the PATHFINDER trial safety population for the 1L therapy population (median age = ████ years; proportion male = ███%; average weight = ███ kg) and the 2L+ therapy population (median age = ███ years; proportion male = ███%; average weight = ███ kg). The sponsor assumed that in the 1L therapy population, ███%, ███%, and ███% of patients have ASM, SM-AHN, and MCL, respectively, with ███%, ███%, and ███% of patients having the same, respectively, in the 2L+ therapy population based on the PATHFINDER trial safety population. CDA-AMC observed differences between the patient characteristics reflected in the submitted CUA and the CDA-AMC Clinical Review report. CDA-AMC does not expect these differences to have a meaningful impact on the cost-effectiveness results (refer to Table 5).
Clinical efficacy inputs for OS and time on treatment (ToT) in the model were derived from the sponsor-conducted inverse probability of treatment weighting (IPTW)-weighted analysis, whereby the effectiveness of avapritinib was informed by the PATHFINDER trial safety set population (with a data cut-off of September 9, 2022), and the effectiveness of BAT was informed by the BLU-285 to 2405 study, an external control study of patients in the real-world treated with BAT. Kaplan-Meier (KM) estimates of OS and ToT from the trial period were used to fit parametric survival curves to extrapolate the treatment effect beyond the observed data (approximately 3.7 years for avapritinib and 12 years for BAT) and over the entire model time horizon (1L therapy population = 34 years; 2L+ therapy population = 28 years). Several parametric survival functions were fitted to the KM data to determine the best-fitting distribution based on diagnostic plots, goodness-of-fit statistics, visual inspection, and clinical validity. The sponsor’s chosen parametric survival distributions for OS in the 1L therapy population were Weibull for avapritinib and log-logistic for 1L BAT. In the 2L+ therapy population, the sponsor’s chosen parametric survival distributions for OS were exponential for avapritinib and Weibull for 2L+ BAT. For ToT in the 1L therapy population, the sponsor’s chosen parametric survival distributions were exponential for avapritinib and Gompertz for 1L BAT. In the 2L+ therapy population, the sponsor’s chosen parametric survival distributions for ToT were exponential for avapritinib and Weibull for 2L+ BAT.
The sponsor assumed that PFS for avapritinib was equal to the Response Assessment Committee–Response Evaluable (RAC-RE) population from the PATHFINDER trial. The sponsor’s chosen parametric survival distributions for avapritinib PFS in the 1L therapy population and 2L+ therapy population were log-logistic and exponential, respectively. The sponsor assumed that PFS was equal to ToT for BAT in the 1L and 2L+ therapy populations.
Health state utility values in the progression-free health state were derived from European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 (EORTC QLQ-C30) data collected in the PATHFINDER trial RAC-RE population and mapped to EQ-5D-3L based on an algorithm published by Young et al.8 Progressive disease utility values were sourced from 4 acute myeloid leukemia (AML) publications that were then aggregated and calibrated to the progression-free health state values based a ratio.9-12 Utility values for the allo-HSCT cohort were obtained from Grulke et al.13 The sponsor further adjusted all health state utility values by age and gender based on a regression algorithm by Ara and Brazier.14 The model incorporated utility decrements for the impact of adverse events (AEs), which were sourced from the literature.15-18
The sponsor’s base case included costs related to drug acquisition and administration, disease management, AE management, allo-HSCT, and terminal care. Drug acquisition costs were sourced from IQVIA, the Ontario Drug Benefit Formulary, and the Ontario Exceptional Access Program Formulary.19-21 The subcutaneous (SC) administration cost for peginterferon alfa-2a was equated to 15 minutes of nurse time; the hourly wage was retrieved from the Government of Canada Job Bank.22 The IV administration cost for cladribine was sourced from a publication by Tam et al.23 Cladribine’s administration schedule was sourced from Lübke et al. and the sponsor assumed an administration time of 2 hours, applied as a one-off cost.24 Disease management costs were sourced from the Ontario Schedule of Benefits: Physician Services Under the Health Insurance Act (February 19, 2024 (effective September 25, 2023)), Canadian Institute for Health Information (CIHI) cost estimator, Government of Canada Job Bank, Ontario Schedule of Benefits For Laboratory Services: July 5, 2023 (Effective July 24, 2023), and published literature.22,25-28 Resource use was estimated based on Pardanani (2016)29 and validated by clinical experts via a sponsor-conducted survey.6 AE management costs were sourced from the CIHI patient cost estimator.26 AE incidence rates were sourced from the PATHFINDER trial for avapritinib and the European Medicines Agency for midostaurin,30 and Barete et al. for cladribine.31 The AE incidence rates for cladribine were used as a proxy for all other BAT treatments (excluding midostaurin). The incidence of AEs for 2L+ BAT were calculated by taking the weighted average of the AEs in midostaurin and the AEs in 1L BAT. A one-off hematopoietic stem cell transplant cost (HSCT) ($119,703.60) was derived by the sponsor and assumed to include a pre-HSCT conditioning cost, hospitalization costs, and medical oncologist follow-up costs with cost inputs sourced from the Ontario Schedule of Benefits: Physician Services and CIHI cost estimator.25,26 A one-time terminal care cost ($90,940.63) was included, encompassing expenses related to the final 12 months of life based on a study by de Oliveira et al. (2016).32 Unit costs were obtained from relevant Canadian sources and inflated to 2024 Canadian dollars where applicable.
Summary of Sponsor’s Economic Evaluation Results
All analyses were run probabilistically (3,000 iterations). The deterministic and probabilistic results were similar but probabilistic results were higher. The probabilistic findings are presented as follows. Additional results from the sponsor’s submitted economic evaluation base case are presented in Appendix 3. The sponsor submitted 2 subgroup analyses (on the 1L therapy population and 2L+ therapy population) to reflect the overall indicated population.
Base-Case Results
Among patients in the 1L therapy population, avapritinib was more costly (incremental costs = $2,012,744) and more effective (incremental QALYs = 5.19) than 1L BAT, resulting in an incremental cost-effectiveness ratio (ICER) of $387,771 per QALY gained over a lifetime horizon (Table 3). In the sponsor’s analysis, avapritinib had a 0% probability of being cost-effective at a WTP threshold of $50,000 per QALY gained. Results were driven by the drug acquisition costs of avapritinib (incremental drug acquisition costs = $1,914,077), which represented 95% of total incremental costs. Approximately 80% of the incremental QALYs were estimated through extrapolation (i.e., after the first 44 cycles for which there were observed data from the PATHFINDER trial safety population).
Table 3: Summary of the Sponsor’s Economic Evaluation Results — 1L Therapy Population
Drug | Total costs ($) | Incremental costs ($) | Total LYs | Incremental LYs | Total QALYs | Incremental QALYs | ICER vs. 1L BAT ($/QALY) |
|---|---|---|---|---|---|---|---|
1L BAT | 283,450 | Reference | 3.00 | Reference | 1.74 | Reference | Reference |
Avapritinib | 2,296,194 | 2,012,744 | 10.56 | 7.55 | 6.93 | 5.19 | 387,771 |
1L = first-line; BAT = best available therapy; ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year; vs. = versus.
Note: 1L BAT comprises cladribine, peginterferon alfa-2a, and imatinib.
Source: Sponsor’s pharmacoeconomic submission.1
Among patients in the 2L+ therapy population, avapritinib was more costly (incremental costs = $865,841) and more effective (incremental QALY = 1.77) than 2L+ BAT, resulting in an ICER of $488,109 per QALY gained (Table 4). In the sponsor’s analysis, avapritinib had a 0% probability of being cost-effective at a WTP threshold of $50,000 per QALY gained. Results were driven by the drug acquisition costs of avapritinib (incremental drug acquisition costs = $941,275), which represented more than 100% of total incremental costs. This result occurred due to the sponsor’s assumption that only patients who have progressed visit the emergency department and intensive care unit; since a higher proportion of patients progressed on 2L+ BAT, they accrued higher disease management costs (incremental disease management costs = –$81,746). Approximately 64% of the incremental QALYs were estimated through extrapolation (i.e., after the first 44 cycles for which there were observed data from the PATHFINDER trial safety population).
Table 4: Summary of the Sponsor’s Economic Evaluation Results — 2L+ Therapy Population
Drug | Total costs ($) | Incremental costs ($) | Total LYs | Incremental LYs | Total QALYs | Incremental QALYs | ICER vs. 2L+ BAT ($/QALY) |
|---|---|---|---|---|---|---|---|
2L+ BAT | 583,286 | Reference | 3.41 | Reference | 1.86 | Reference | Reference |
Avapritinib | 1,449,128 | 865,841 | 5.76 | 2.35 | 3.64 | 1.77 | 488,109 |
2L+ = second-line or later-line; BAT = best available therapy; ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year; vs. = versus.
Note: 2L+ BAT comprises cladribine, peginterferon alfa-2a, imatinib, and midostaurin.
Source: Sponsor’s pharmacoeconomic submission.1
Sensitivity and Scenario Analysis Results
The sponsor conducted various scenario analyses for both the 1L and 2L+ therapy populations encompassing considerations such as adopting alternative discount rates and utility values, excluding the allo-HSCT population, and applying an OS hazard ratio to the avapritinib PFS curve to derive the PFS curve for BAT. Base-case results remained robust across most analyses apart from the latter scenario, which increased the ICER to $399,756 in the 1L therapy population and $511,781 in the 2L+ therapy population.
No scenario analysis was conducted using a perspective other than that of the health care payer.
Appraisal of the Sponsor’s Economic Evaluation by CDA-AMC
CDA-AMC identified several key limitations to the sponsor’s analysis that have notable implications for the economic analysis.
The comparative efficacy (OS and PFS) of avapritinib versus BAT is highly uncertain and produces results that lack face validity: In the absence of direct head-to-head evidence, clinical efficacy inputs for OS were derived from the sponsor-conducted IPTW-weighted analysis, whereby the effectiveness of avapritinib was informed by the PATHFINDER trial safety set population (with a data cut-off of September 9, 2022), and the effectiveness of BAT was informed by the BLU-285 to 2405 study, an external control study of patients in the real-world treated with BAT. As noted in the Clinical Review report, avapritinib may be associated with improved response, duration of treatment, and OS. However, there was significant uncertainty in the magnitude of the findings due to substantial limitations, including heterogeneity in the data sources and patient characteristics, missing or unmeasured prognostic factors and effect modifiers, small sample sizes, few events, a lack of follow-up information, the immaturity of survival data, and the exploratory nature of post hoc and subgroup analyses.
Adding to the uncertainty, the sponsor included midostaurin in the weighted basket of treatments for 2L+ BAT. Clinical expert input received by CDA-AMC noted that the use of midostaurin in Canada is rare as it is not reimbursed by public drug plans for AdvSM, there are no compassionate access programs currently available for patients, and the drug acquisition cost is prohibitive. Clinical expert input highlighted that the efficacy of midostaurin compared to that of the other treatments included in the weighted basket (i.e., cladribine, peginterferon alfa-2a, and imatinib) is meaningfully different as patients typically have better outcomes with midostaurin. Additionally, a notable proportion of patients in the 2L+ therapy population had prior use of midostaurin and use of midostaurin was markedly higher for the avapritinib cohort in comparison to the 2L+ BAT cohort (in the IPTW-weighted category, avapritinib = 62.2% and 2L+ BAT = 46.9%; in the IPTW-unweighted category, avapritinib = 83.6% and 2L+ BAT = 37.3%).33 By including midostaurin in the 2L+ BAT weighted basket of treatments, and due to the high proportion of patients having previously been treated with midostaurin, the resulting basket is not representative of Canadian clinical practice and thus the comparative efficacy of avapritinib and BAT in the 2L+ therapy population within Canada is unknown.
Additional interrelated issues were identified related to the face validity and uncertainty associated with the sponsor’s clinical efficacy evidence. They are outlined as follows. First, the use of 2 different populations produced results that lacked face validity. As mentioned previously, OS was derived from the IPTW-weighted analysis, informed by the PATHFINDER trial safety set population. However, PFS was not informed by any comparative evidence and PFS for avapritinib used clinical trial data directly from the PATHFINDER trial RAC-RE clinical trial population without any adjustments. There are numerous issues associated with the sponsor’s approach. Based on the KM data informing the 1L therapy population avapritinib cohort, PFS exceeds OS (Appendix 3, Figure 2), and it is clinically implausible for more patients to be at risk of progression than alive. Additionally, as stated in the Clinical Review report, although PFS was evaluated in the PATHFINDER trial, the study’s single-arm design and the immaturity of the data limited the ability to attribute the study results to treatment with avapritinib. Further, the sponsor’s model predicts that in the 1L therapy population, 37.5% of the patients who received avapritinib will be progression-free at 10 years. Clinical expert input noted that while it is likely that a subset of patients will attain a sustained and durable response, it is also possible for all patients to have progressed disease at 10 years; thus, PFS, as estimated by the sponsor, may be overestimated.
Second, the sponsor assumed PFS was to equal ToT for the BAT cohort as this approach was preferred by clinical experts consulted by the sponsor over the alternative approach, which estimated PFS for BAT by applying the OS hazard ratio, derived from the network meta-analysis, and assuming proportional hazards. Clinical expert feedback elicited by CDA-AMC for this review noted that assuming BAT is administered until progression is unreasonable as cladribine is a fixed duration treatment; thus, patients will stop treatment at a select point in time (per Lübke et al.,24 the median number of treatment cycles is 3 28-day cycles [range, 1 cycle to 8 cycles]), irrespective of whether their disease has progressed. As a result, the 2 outcomes should not be equated.
Third, clinical expert input commented that OS estimates for avapritinib relative to 1L BAT in the 1L therapy population were higher than expected. Clinical experts commented that based on the available clinical trial evidence, it is reasonable to assume that avapritinib would have at least double the median OS of BAT. Clinical expert input noted that the median OS for BAT is approximately 26 months, aligned with the sponsor’s chosen extrapolation for 1L BAT. However, based on the sponsor’s chosen extrapolation for avapritinib (Weibull), median OS occurs at approximately 138 months, which is about 5 times higher than median OS for BAT. As noted in the Clinical Review report, median OS had not been reached in the avapritinib cohort in any line of therapy, indicating that OS data were likely immature. Given the immaturity of the data and the proportion of the incremental benefit gained in the extrapolated period (80% and 64% of the incremental QALYs in the 1L and 2L+ therapy populations, respectively), the sponsor’s extrapolations are highly uncertain and influential. Additionally, the sponsor’s chosen extrapolation for OS in the 1L therapy population predicts that 22% of patients will remain alive at aged 90 years, a result that lacks face validity. CDA-AMC notes that in the 1L therapy population, all of the extrapolated OS curves are higher than those of general population mortality over the entire modelled time horizon.
Fourth, the chosen OS and PFS extrapolations for BAT resulted in patients in the 2L+ therapy population attaining better quality-adjusted survival outcomes than those in the 1L therapy population (1.86 QALYs versus 1.74 QALYs, respectively). Clinical expert input elicited by CDA-AMC noted that while in Canada there is no notable differences in survival between the 1L and 2L+ therapy populations, generally the risk of death increases as the number of lines of therapy received increases. The modelling of BAT in the sponsor’s submitted economic evaluation does not follow this pattern and thus lacks face validity.
CDA-AMC noted discrepancies between the KM estimates used in the submitted pharmacoeconomic model versus those reported in the submitted indirect evidence.1,33,34 While the discrepancies were less than 1.1% different between the values used in the CUA and the submitted indirect evidence, they favoured avapritinib.
The limitations associated with the comparative efficacy (OS and PFS) of avapritinib versus BAT could not be addressed through reanalysis.
Given the limitations of the data, CDA-AMC could not conduct a rigorous base case. CDA-AMC conducted an alternative analysis to illustrate the impact of the uncertainty associated with the underlying evidence. In the 1L therapy population, CDA-AMC chose the most conservative parametric extrapolation for avapritinib’s OS curve (Gamma). CDA-AMC notes that 20.8% of the avapritinib cohort is still alive at age 90 years, meaning that this analysis still lacks face validity. Additionally, as PFS is not supported by direct or indirect comparative evidence, CDA-AMC chose a more conservative parametric extrapolation for avapritinib’s PFS curve (Weibull) in the 1L therapy population. This extrapolation results in a lower proportion of patients (23.5%) being progression-free at 10 years than was observed in the sponsor’s base case (37.5%). An alternative curve was not selected for the 2L+ therapy population, as the sponsor’s base case had already selected the most conservative parametric distribution.
Comparator treatment costs are uncertain: Treatment costs for BAT were calculated using a weighted basket approach. In the 2L+ therapy population, cladribine, peginterferon alfa-2a, imatinib, and midostaurin were weighted according to the distribution of their relative use among patients in the 2L+ therapy population data from the BLU-285 to 2405 study, and the remaining treatments were redistributed based on the same proportions from the 1L therapy population.1,7 The sponsor estimated midostaurin was used in 46.07% of 2L+ therapy patients with AdvSM in Canada. Per CDA-AMC drug reimbursement review procedures,35 midostaurin should not have been considered a comparator in base-case analyses as it is not reimbursed by public drug plans for AdvSM, there are no compassionate access programs currently available to patients, and midostaurin received a negative reimbursement recommendation from CADTH in 2020.36 Clinical expert input highlighted that midostaurin is not a relevant treatment comparator for patients with AdvSM in Canada, in any line of therapy, as virtually no patients have access to it. The inclusion of midostaurin introduces a bias that increases the overall cost of the 2L+ BAT basket as it has a notably higher per cycle cost than the other treatments included in 2L+ BAT (cladribine, peginterferon alfa-2a, and imatinib).
Additionally, the sponsor assumed that cladribine was administered as a dose of 0.14 mg/kg per day on day 1 to day 5 of a 28-day cycle. As cladribine is used off-label for AdvSM, clinical expert input noted that the recommended dosage may vary by jurisdiction. Based on a publication by Lübke et al.,24 the sponsor assumed that cladribine is administered for 3 cycles.1 CDA-AMC notes that Lübke et al. found that cladribine was administered between a range of 1 cycle and 8 cycles.24 Clinical expert input noted that cladribine may be administered for 1 cycle to 9 cycles. As such, assuming that the treatment duration of cladribine is fixed may underestimate or overestimate treatment costs. Furthermore, the sponsor assumed that cladribine was administered through IV infusion. Clinical experts consulted by CDA-AMC commented that cladribine may be administered subcutaneously or by IV infusion. Notably, based on publicly listed prices,37 a vial for IV infusion costs less than a vial for SC injection (IV = $890.05; SC = $939.01), which contrasts with the sponsor’s base-case assumption that IV infusion treatments are associated with higher drug administration costs (IV = $215.63; SC = $40.39).1
Clinical expert input emphasized that the availability of peginterferon alfa-2a varies across jurisdictions. Input noted that peginterferon alfa-2a is not considered a front-line therapy by most international experts and is appropriate only in specific scenarios (e.g., for those with slowly progressive disease). Due to the variability in access to peginterferon alfa-2a and it not being considered a front-line treatment option by many clinicians, the use of peginterferon alfa-2a may be lower in clinical practice than estimated by the sponsor (1L therapy population = 42.2%; 2L+ therapy population = 21.74%). As the sponsor used a weighted basket approach to model BAT, any uncertainties in the estimates of relative use directly affect the uncertainty of the treatment cost calculations.
In CDA-AMC reanalysis, midostaurin was assumed to have a 0% market share in the 2L+ therapy population. CDA-AMC notes that this assumption only impacts treatment costs; as a weighted basket was used to model efficacy, midostaurin is still included in the sponsor’s estimates of OS and ToT.
CDA-AMC was unable to address the uncertainty associated with cladribine treatment costs and the relative use of peginterferon alfa-2a but notes the limitations likely have a minimal impact on the cost-effectiveness of avapritinib.
The impact of avapritinib on patient quality of life is highly uncertain: The sponsor derived health state utility values for the progression-free health state from EORTC QLQ-C30 data collected in the PATHFINDER trial RAC-RE population. EORTC QLQ-C30 data were then mapped to EQ-5D-3L based on an algorithm published by Young et al.8 The sponsor stated that due to the lack of data on patients with progressive disease in the PATHFINDER trial, to derive the utility values for the progressive disease health state, the sponsor sourced utility values from 4 AML publications that were then aggregated and calibrated to the progression-free health state values based a ratio.9-12 This approach raises several concerns. First, the sourced utility values were from a different disease area, which affects their generalizability to AdvSM. Second, the utility values sourced from the AML literature lack face validity as 3 of 4 progression-free utility values either exceed or are close to the average quality of life reported by the typical person in Canada (0.863).1,38 Third, the difference between the progression-free utility values and the progressive disease utility values ranges from 0.01 to 0.515.9-12 This variation implies that there is both a negligible difference and a substantial difference in the quality of life between patients who are progression-free and those whose disease has progressed. Clinical expert input noted that while AdvSM is a heterogeneous disease, patients with progressed disease have a poorer quality of life than those who are progression-free. Fourth, based on a publication by Peasgood and Brazier (2015), utility values should not be pooled if the data are not valuing the same clinical health states.39 The utility values pooled by the sponsor are not informed by the same clinical health states.1 For example, the utility values pooled for the progression-free health state are defined as “Complete Remission” by Stein et al.,9 “Long-term follow-up > 1 year” by Joshi et al.,12 “No relapse” by Leunis et al.,10 and “Newly diagnosed (currently on first-line AML therapy)” by Mamolo et al.11 As such, it was inappropriate for the sponsor to pool the utility values. As noted by Peasgood and Brazier, “Pooling [health state utility values] (HSUVs) is problematic because of the fact that different valuation methods and different preference-based measures (PBMs) can generate different values on exactly the same clinical health state.”39 Furthermore, CDA-AMC notes that the literature-derived AML utility values were from the US, UK, and Netherlands, and used a variety of utility tariffs; as such, it is unclear whether the sourced utility values are generalizable to the Canadian population.
CDA-AMC notes that the sponsor assumed a standard error of 10% for the progressive disease and allo-HSCT utility values. Assuming a standard error for utility values does not allow for decision uncertainty to be accurately characterized and thus impacts the range of QALYs estimated in probabilistic analyses.
CDA-AMC was unable to address this limitation in reanalyses owing to a lack of alternative data.
The sponsor’s model had additional issues and lacked transparency: During the review process, there were numerous issues identified that were not prioritized given the magnitude and severity of the other issues identified. For example, the comparative safety of avapritinib versus BAT is unknown and the probabilities of AEs in the pharmacoeconomic model were based on naive comparisons, without adjustment or accounting for differences in patient characteristics; the model did not consider the most clinically meaningful AEs (i.e., intracranial bleeding); utility decrements and AE costs may not have been adequately considered; the heterogeneity of the AdvSM population may not have been fully captured; the decision to cap the predicted OS curves by the general population mortality risk was problematic as the 2 parameters are not interchangeable; the use of a weighted basket to model comparator efficacy may not have been appropriate; subsequent therapies were not explicitly modelled; dose reductions and dose interruptions were not considered; and decision uncertainty was not accurately characterized.
Additionally, the sponsor’s submitted model included numerous IFERROR statements, which lead to situations where the parameter value is overwritten with an alternative value without alerting the user to the automatized overwriting. The systematic use of IFERROR statements makes thorough auditing of the sponsor’s model impractical, as it remains unclear whether the model is running inappropriately by overriding errors.
CDA-AMC was unable to address this limitation and notes that a thorough validation of the sponsor’s model was not possible.
Additionally, the following key assumptions were made by the sponsor and have been appraised by CDA-AMC (refer to Table 5).
Table 5: Key Assumptions of the Submitted Economic Evaluation (Not Noted as Limitations to the Submission)
Sponsor’s key assumption | CDA-AMC comment |
|---|---|
Baseline patient characteristics in the model reflected the PATHFINDER trial safety population. | CDA-AMC notes that baseline characteristics in the submitted CUA — specifically, median age — did not align with the submitted clinical evidence and those characteristics reported in the Clinical Review report.1,33,34 CDA-AMC does not expect these differences to have a meaningful impact on the cost-effectiveness results as the differences were minor (e.g., median age of 1L population in CUA = 66.55 years; median age of 1L therapy population in the submitted clinical evidence and the Clinical Review report = 67.0 years). |
The sponsor submitted separate analyses for the 1L therapy population and the 2L+ therapy population. | Uncertain. Clinical expert input noted that the 1L and 2L+ therapy populations in Canada are not considerably different and there is no discrete difference between treatment options among the 2 populations. Due to the model structure and lack of available data, CDA-AMC was unable to consider the populations together. |
Only patients who have progressed disease will use an emergency department and/or intensive care unit and be hospitalized. | Uncertain. Clinical expert input noted that while patients who have progressed disease have a different quality of life than those who are progression-free, as the patient population is heterogenous, use of the emergency department and intensive care unit once patients have progressed will vary widely. Input commented that patients may use home care instead of inpatient care. |
1L = first-line; 2L+ = second-line or later-line; CDA-AMC = Canada’s Drug Agency; CUA = cost-utility analysis.
CDA-AMC Reanalyses of the Economic Evaluation
CDA-AMC Reanalysis
A robust CDA-AMC base case could not be determined as the clinical evidence was highly uncertain and lacked face validity. CDA-AMC undertook reanalyses for the 1L and 2L+ therapy populations, as outlined in Table 6 and Table 7, respectively, adopting different OS and PFS parametric distributions for avapritinib in the 1L therapy population and removing midostaurin from 2L+ BAT treatment costs. The CDA-AMC reanalyses were derived by making changes in model parameter values and assumptions, in consultation with clinical experts.
Table 6: CDA-AMC Revisions to the Submitted Economic Evaluation — 1L Therapy Population
Stepped analysis | Sponsor’s value or assumption | CDA-AMC value or assumption |
|---|---|---|
Changes to derive the CDA-AMC reanalysis | ||
1. Avapritinib OS parametric distribution | Weibull | Gamma |
2. Avapritinib PFS parametric distribution | Log-logistic | Weibull |
CDA-AMC alternative analysis | ― | Reanalysis 1 + 2 |
1L = first-line; CDA-AMC = Canada’s Drug Agency; OS = overall survival; PFS = progression-free survival.
Table 7: CDA-AMC Revisions to the Submitted Economic Evaluation — 2L+ Therapy Population
Stepped analysis | Sponsor’s value or assumption | CDA-AMC value or assumption |
|---|---|---|
Changes to derive the CDA-AMC reanalysis | ||
1. Relative use of comparators | Cladribine = 27.19% Peginterferon alfa-2a = 21.74% Imatinib = 5.00% Midostaurin = 46.07% | Aligned with 1L therapy population relative use estimates Cladribine = 52.80% Peginterferon alfa-2a = 42.20% Imatinib = 5.00% Midostaurin = 0.00% |
CDA-AMC alternative analysis | ― | Reanalysis 1 |
1L = first-line; 2L+ = second-line or later-line; CDA-AMC = Canada’s Drug Agency.
The stepwise results of the CDA-AMC reanalyses for the 1L and 2L+ therapy populations can be found in Table 8 and Table 9, respectively. Disaggregated results from the CDA-AMC reanalyses are presented in Appendix 4.
Table 8: Summary of the Stepped Analysis of the CDA-AMC Reanalysis Results — 1L Therapy Population
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALY) |
|---|---|---|---|---|
Sponsor’s base case | 1L BAT | 333,588 | 2.12 | Reference |
Avapritinib | 2,393,938 | 7.91 | 355,809 | |
CDA-AMC reanalysis 1 | 1L BAT | 333,500 | 2.12 | Reference |
Avapritinib | 2,371,032 | 7.75 | 362,409 | |
CDA-AMC reanalysis 2 | 1L BAT | 333,588 | 2.12 | Reference |
Avapritinib | 2,518,689 | 7.54 | 403,429 | |
CDA-AMC alternative analysis (reanalysis 1 + 2) | 1L BAT | 333,500 | 2.12 | Reference |
Avapritinib | 2,495,606 | 7.37 | 411,978 | |
CDA-AMC alternative analysis (reanalysis 1 + 2) (probabilistic) | 1L BAT | 283,782 | 1.74 | Reference |
Avapritinib | 2,289,049 | 6.34 | 435,876 |
1L = first-line; BAT = best available therapy; CDA-AMC = Canada’s Drug Agency; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Note: The CDA-AMC reanalysis is based on publicly available prices of the comparator treatments. The results of all steps are presented deterministically unless otherwise indicated, while the cumulative CDA-AMC alternative analysis is always presented both deterministically and probabilistically. 1L BAT comprises cladribine, peginterferon alfa-2a, and imatinib.
Results from the probabilistic analysis of the CDA-AMC reanalysis for the 1L therapy population found that avapritinib was more costly (incremental costs = $2,005,267) and more effective (incremental QALYs = 4.60) than 1L BAT, resulting in an ICER of $435,876 per QALY gained. Avapritinib had a 0% probability of being cost-effective at a WTP threshold of $50,000 per QALY gained. Consistent with the sponsor’s base case, results were driven by the drug acquisition costs of avapritinib (incremental drug acquisition costs = $1,867,653), which represent 93.1% of total incremental costs. Approximately 78% of the incremental QALYs were estimated through extrapolation (i.e., after the first 44 cycles for which there were observed data from the PATHFINDER trial safety population).
Results from the probabilistic analysis of the CDA-AMC reanalysis for the 2L+ therapy population found that avapritinib was more costly (incremental costs = $1,172,109) and more effective (incremental QALYs = 1.78) than 2L+ BAT, resulting in an ICER of $660,217 per QALY gained over a lifetime horizon. Avapritinib had a 0% probability of being cost-effective at a WTP threshold of $50,000 per QALY gained. Consistent with the sponsor’s base case, results were driven by the drug acquisition costs of avapritinib (incremental drug acquisition costs = $1,241,209), which represent more than 100% of total incremental costs as a higher proportion of patients progressed on 2L+ BAT and thus accrued higher disease management costs (incremental disease management costs = –$71,209). As no changes were made to the clinical efficacy or safety inputs, approximately 64% of the incremental QALYs were estimated through extrapolation, consistent with the sponsor’s base case.
Table 9: Summary of the Stepped Analysis of the CDA-AMC Reanalysis Results — 2L+ Therapy Population
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALY) |
|---|---|---|---|---|
Sponsor’s base case | 2L+ BAT | 546,968 | 1.80 | Reference |
Avapritinib | 1,402,393 | 3.71 | 449,988 | |
CDA-AMC alternative analysis (reanalysis 1) | 2L+ BAT | 281,753 | 1.80 | Reference |
Avapritinib | 1,414,624 | 3.71 | 595,130 | |
CDA-AMC alternative analysis (reanalysis 1) (probabilistic) | 2L+ BAT | 288,252 | 1.86 | Reference |
Avapritinib | 1,460,361 | 3.64 | 660,217 |
2L+ = second-line or later-line; BAT = best available therapy; CDA-AMC = Canada’s Drug Agency; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Note: The CDA-AMC reanalysis is based on publicly available prices of the comparator treatments. The results of all steps are presented deterministically unless otherwise indicated, while the cumulative CDA-AMC alternative analysis is always presented both deterministically and probabilistically. 2L+ BAT comprises cladribine, peginterferon alfa-2a, imatinib, and midostaurin.
Scenario Analysis Results
CDA-AMC undertook price reduction analyses based on the CDA-AMC alternative analyses for the 1L and 2L+ therapy populations (Table 10). These analyses suggest that a price reduction of 87% would be required for avapritinib to be considered cost-effective at a WTP threshold of $50,000 per QALY gained. However, given the limitations identified with the submitted model that could not be addressed through reanalysis, the price reduction is highly uncertain.
Table 10: CDA-AMC Price Reduction Analyses
Analysis | Unit drug cost ($) | 1L therapy population: ICERs for avapritinib vs. 1L BAT | 2L+ therapy population: ICERs for avapritinib vs. 2L+ BAT | ||
|---|---|---|---|---|---|
Price reduction | $ | Sponsor base case | CDA-AMC alternative analysis | Sponsor base case | CDA-AMC alternative analysis |
No price reduction | 1,343 | $387,771 | $435,876 | $488,109 | $660,217 |
10% | 1,209 | $348,005 | $391,512 | $417,852 | $590,019 |
20% | 1,075 | $308,240 | $347,149 | $347,595 | $519,820 |
30% | 940 | $268,474 | $302,786 | $277,338 | $449,621 |
40% | 806 | $228,708 | $258,422 | $207,081 | $379,422 |
50% | 672 | $188,942 | $214,059 | $136,824 | $309,223 |
60% | 537 | $149,176 | $169,695 | $66,567 | $239,024 |
70% | 403 | $109,411 | $125,332 | Dominant | $168,825 |
80% | 269 | $69,645 | $80,969 | Dominant | $98,627 |
90% | 134 | $29,879 | $36,605 | Dominant | $28,428 |
1L = first-line; 2L+ = second-line or later-line; BAT = best available therapy; CDA-AMC = Canada’s Drug Agency; ICER = incremental cost-effectiveness ratio; vs. = versus.
Note: 1L BAT comprises cladribine, peginterferon alfa-2a, and imatinib. 2L+ BAT comprises cladribine, peginterferon alfa-2a, imatinib, and midostaurin.
Issues for Consideration
Midostaurin was previously reviewed by CADTH for AdvSM and received a do not reimburse recommendation.40 The cost-effectiveness results of the economic evaluation may not be directly comparable to those in the current review, owing to differences in model structure, clinical effectiveness parameters, health state utility values, and cost inputs.
The sponsor is requesting that avapritinib be reimbursed for AdvSM. However, clinical expert input indicated that it is possible that avapritinib will be used off-label for indolent systemic mastocytosis. The potential for off-label use of avapritinib may be associated with considerable costs to the drug plans.
Overall Conclusions
Based on the CDA-AMC Clinical Review, avapritinib may be associated with improved OS relative to a basket of treatments. However, there was significant uncertainty in the magnitude of the findings due to substantial limitations, including heterogeneity in the data sources and patient characteristics, missing or unmeasured prognostic factors and effect modifiers, small sample sizes, few events, a lack of follow-up information, the immaturity of survival data, and the exploratory nature of post hoc and subgroup analyses. Since there were no data on patient-reported outcomes or comparative safety in the indirect evidence, the relative effect of avapritinib versus currently available treatments on symptoms, health-related quality of life, or safety is unknown.
The comparative efficacy (OS and PFS) of avapritinib relative to BAT is highly uncertain and lacks face validity, precluding CDA-AMC from conducting a rigorous base case. The degree of uncertainty is driven by limitations associated with the sponsor’s IPTW-weighted analysis, used in the absence of direct head-to-head evidence for OS and ToT; PFS not being informed by comparative data; the inclusion of midostaurin in the 2L+ BAT basket, resulting in the comparative efficacy being unknown in the 2L+ therapy population; OS exceeding PFS in the 1L therapy population, which is clinically implausible; OS in the 1L therapy population predicting patients living longer than the general population in Canada; and the sponsor’s results predicting that patients receiving BAT in the 2L+ therapy population attain better quality-adjusted survival outcomes than patients receiving BAT in the 1L therapy population. Additionally, numerous issues were identified that were not prioritized, given the magnitude of uncertainty associated with the clinical evidence. In consultation with clinical experts, CDA-AMC concluded that the sponsor’s economic evaluation included clinical efficacy inputs that lacked face validity and produced results that were likely implausible.
In consultation with clinical experts, CDA-AMC conducted alternative analyses in the 1L and 2L+ therapy populations to illustrate the impact of the uncertainty associated with the underlying evidence. In the 1L therapy population, CDA-AMC adopted more conservative OS and PFS parametric distributions for avapritinib. In the 2L+ therapy population, CDA-AMC removed midostaurin from the calculation of 2L+ BAT treatment costs. Consistent with the sponsor’s analyses, in the CDA-AMC alternative analyses, avapritinib was more costly and more effective than BAT in both the 1L and 2L+ therapy populations. In the 1L therapy population, CDA-AMC reanalyses produced an ICER of $435,876 per QALY gained over a lifetime horizon (incremental costs = $2,005,267; incremental QALYs = 4.60). In the 2L+ therapy population, CDA-AMC reanalyses produced an ICER of $660,217 per QALY gained over a lifetime horizon (incremental costs = $1,172,109; incremental QALYs = 1.78). Results were driven by drug acquisition costs as they accounted for more than 90% of incremental costs in both populations. Moreover, the majority of the incremental benefit gained by avapritinib occurred in the extrapolated portion of the model (78% in the 1L therapy population and 64% in the 2L+ therapy population).
In the CDA-AMC alternative analyses, avapritinib had a 0% probability of being cost-effective at a WTP threshold of $50,000 per QALY gained. Thus, the CDA-AMC alternative reanalyses suggest a price reduction of 87% would be required for avapritinib to be considered cost-effective at a WTP threshold of $50,000 per QALY gained. However, as the CDA-AMC alternative analyses are unable to adequately address the limitations associated with the comparative clinical data, the results of the CDA-AMC’s alternative analyses remain highly uncertain and prone to bias, of which the direction and magnitude are both unknown. Thus, the cost-effectiveness of avapritinib relative to BAT in both the 1L and 2L+ therapy populations is highly uncertain. A larger price reduction may be warranted given the high level of uncertainty around comparative efficacy and cost-effectiveness.
References
1.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Ayvakit (avapritinib), film-coated tablets, 25 mg, 50 mg, 100 mg and 200 mg, oral. Toronto (ON): Medison Pharma Canada Inc; 2024 Apr 19.
2.Ayvakyt (avapritinib): tablets, 25 mg, 50 mg, 100 mg and 200 mg, oral [product monograph]. Toronto (ON): Medison Pharma Canada Inc; 2024 Sep 18.
3.Novartis Pharmaceuticals Canada Inc. RYDAPT Product Monograph. https://www.novartis.com/ca-en. Accessed 2024 Mar 8.
4.Novartis Pharmaceuticals Canada Inc. Imatinib Product Monograph. 2022 [sponsor submitted reference].
5.European Medicines Agency. AYVAKYT (avapritinib) summary of product characteristics. 2021: https://www.ema.europa.eu/en/documents/product-information/ayvakyt-epar-product-information_en.pdf. [sponsor submitted reference].
6.Eversana. Avapritinib for the treatment of adult patients with Advanced Systemic Mastocytosis: Canadian Physician Interview Report. (2024). Generated: February 2024. [sponsor submitted reference].
7.Updated ECS results (PATHFINDER cut-off 09Sept2022). Cambridge (MA): Blueprint Medicines; 2024.
8.Young TA, Mukuria C, Rowen D, Brazier JE, Longworth L. Mapping functions in health-related quality of life: mapping from two cancer-specific health-related quality-of-life instruments to EQ-5D-3L. Med Decis Making. 2015;35(7):912-926. PubMed
9.Stein EM, Yang M, Guerin A, et al. Assessing utility values for treatment-related health states of acute myeloid leukemia in the United States. Health Qual Life Outcomes. 2018;16(1):193. PubMed
10.Leunis A, Redekop WK, Uyl-de Groot CA, Lowenberg B. Impaired health-related quality of life in acute myeloid leukemia survivors: a single-center study. Eur J Haematol. 2014;93(3):198-206. PubMed
11.Mamolo CM, Cappelleri JC, Hoang CJ, et al. A real-world, cross-sectional, community survey of symptoms and health-related quality of life of adults with acute myeloid leukemia. Future Oncol. 2019;15(16):1895-1909. PubMed
12.Joshi N, Hensen M, Patel S, Xu W, Lasch K, Stolk E. Health State Utilities for Acute Myeloid Leukaemia: A Time Trade-off Study. Pharmacoeconomics. 2019;37(1):85-92. PubMed
13.Grulke N, Albani C, Bailer H. Quality of life in patients before and after haematopoietic stem cell transplantation measured with the European Organization for Research and Treatment of Cancer (EORTC) Quality of Life Core Questionnaire QLQ-C30. Bone Marrow Transplant. 2012;47(4):473-482. PubMed
14.Ara R, Brazier JE. Populating an economic model with health state utility values: moving toward better practice. Value Health. 2010;13(5):509-518. PubMed
15.National Institute for Health Care Excellence. Lenalidomide with rituximab for previously treated follicular lymphoma [TA627]. 2020 [sponsor submitted reference].
16.Sullivan PW, Slejko JF, Sculpher MJ, Ghushchyan V. Catalogue of EQ-5D scores for the United Kingdom. Med Decis Making. 2011;31(6):800-804. PubMed
17.National Institute for Health Care Excellence. Idelalisib for Treating Follicular Lymphoma Refractory to 2 Treatments [TA604]. 2018 [sponsor submitted reference].
18.Shabaruddin FH, Chen L-C, Elliott RA, Payne K. A Systematic Review of Utility Values for Chemotherapy-Related Adverse Events. PharmacoEconomics. 2013;31(4):277-288. PubMed
19.Iqvia Solutions Canada Inc. Cladribine Cost. 2024. [sponsor submitted reference].
20.Ontario Drug Benefit Formulary. Imatinib Mesylate. 2023; https://www.formulary.health.gov.on.ca/formulary/results.xhtml?q=imatinib&type=1, 2024 Feb 15.
21.Ontario Drug Benefit: Exceptional Access Program. Exceptional Access Program. https://www.ontario.ca/page/exceptional-access-program-product-prices. Accessed 2024 Mar 9.
22.Government of Canada. Wages for Registered nurses and registered psychiatric nurses. 2024: https://www.jobbank.gc.ca/wagereport/occupation/993. [sponsor submitted reference].
23.Tam VC, Ko YJ, Mittmann N, et al. Cost-effectiveness of systemic therapies for metastatic pancreatic cancer. Curr Oncol. 2013;20(2):e90-e106. PubMed
24.Lübke J, Schwaab J, Naumann N, et al. Superior Efficacy of Midostaurin Over Cladribine in Advanced Systemic Mastocytosis: A Registry-Based Analysis. J Clin Oncol. 2022;40(16):1783-1794. PubMed
25.Government of Ontario. Schedule of Benefits. (2024) Physician Services Under the Health Insurance Act (February 19, 2024 (effective September 25, 2023)); https://www.ontario.ca/files/2024-03/moh-ohip-schedule-of-benefits-2024-03-28.pdf. Accessed: 2024 Apr 4.
26.Patient Cost Estimator. 2022. https://www.cihi.ca/en/patient-cost-estimator. Accessed 2024 Jan.
27.Government of Ontario. Schedule of Benefits for Laboratory Services. (2023) July 5, 2023 (Effective July 24, 2023): https://www.ontario.ca/files/2024-01/moh-ohip-schedule-of-benefits-laboratory-services-2024-01-24.pdf. Accessed: 2024 Apr 5.
28.Evans J, Kobewka D, Thavorn K, D’Egidio G, Rosenberg E, Kyeremanteng K. The impact of reducing intensive care unit length of stay on hospital costs: evidence from a tertiary care hospital in Canada. Can J Anaesth. 2018;65(6):627-635. PubMed
29.Pardanani A. Systemic mastocytosis in adults: 2017 update on diagnosis, risk stratification and management. Am J Hematol. 2016;91(11):1146-1159. PubMed
30.European Medicine Agency. Rydapt - Product Information. https://www.ema.europa.eu/en/documents/product-information/rydapt-epar-product-information_en.pdf. Accessed 2024 Jan.
31.Barete S, Lortholary O, Damaj G, et al. Long-term efficacy and safety of cladribine (2-CdA) in adult patients with mastocytosis. Blood. 2015;126(8):1009-1016; quiz 1050. PubMed
32.de Oliveira C, Pataky R, Bremner KE, et al. Phase-specific and lifetime costs of cancer care in Ontario, Canada. BMC Cancer. 2016;16(1):809. PubMed
33.Updated ECS results (PATHFINDER cut-off 09Sept2022): 2L+ avapritinib versus 2L+ BAT [internal sponsor's report]. Cambridge (MA): Blueprint Medicines Corporation; 2024.
34.Medison Pharma Canada Inc. response to May 13, 2024 CADTH request for additional information regarding avapritinib CADTH review: ECS Updated analysis for avapritinib 1L versus BAT 1L (excluding modostaurin) aggregate data [internal additional sponsor's information]. Toronto (ON): Medison Pharma Canada Inc; 2024 May 16.
35.CADTH. CADTH Drug Reimbursement Review Procedures. https://www.cda-amc.ca/sites/default/files/Drug_Review_Process/CADTH%20Drug%20Reimbursement%20Review%20Procedures.pdf. Accessed 2024 Jul 2.
36.CADTH. Midostaurin (Rydapt) Systemic Mastocytosis - pERC Final Recommendation. 2020 [sponsor submitted reference].
37.Ontario Ministry of Health, Ontario Ministry of Long-Term Care. Ontario drug benefit formulary/comparative drug index. 2024; https://www.formulary.health.gov.on.ca/formulary/. Accessed 2024 May 3.
38.Guertin JR, Feeny D, Tarride J-E. Age- and sex-specific Canadian utility norms, based on the 2013–2014 Canadian Community Health Survey. CMAJ. 2018;190(6):E155. PubMed
39.Peasgood T, Brazier J. Is Meta-Analysis for Utility Values Appropriate Given the Potential Impact Different Elicitation Methods Have on Values? Pharmacoeconomics. 2015;33(11):1101-1105. PubMed
40.CADTH. Rydapt Final Economic Guidance Report. 2024 Apr 4 2020 [sponsor submitted reference].
41.Exceptional Access Program (EAP). Toronto (ON): Ontario Ministry of Health; Ontario Ministry of Long-Term Care; 2024: http://www.health.gov.on.ca/en/pro/programs/drugs/odbf/odbf_except_access.aspx. Accessed 2024 May 3.
42.Helbig G, Koclęga A, Gaweł WB, et al. The Efficacy of Cladribine (2-CdA) in Advanced Systemic Mastocytosis. Indian J Hematol Blood Transfus. 2020;36(4):661-666. PubMed
43.Buonomo A, Nucera E, Criscuolo M. Treatment of Indolent and Advanced Systemic Mastocytosis. Mediterr J Hematol Infect Dis. 2022;14(1):e2022040. PubMed
44.British Columbia Cancer Agency. Protocol Summary for Peginterferon Alfa-2a Therapy of Chronic Myeloid Neoplasms and Hypereosinophilic Syndrome. 2021 [sponsor submitted reference].
45.Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Ayvakit (avapritinib), film-coated tablets, 25 mg, 50 mg, 100 mg and 200 mg, oral. Toronto (ON): Medison Pharma Canada Inc; 2024 Apr 19.
46.Ontario Drug Benefit Formulary. Imatinib Cost. 2024: https://www.formulary.health.gov.on.ca/formulary/results.xhtml?q=imatinib&type=1. [sponsor submitted reference].
47.Statistics Canada. Population estimates on July 1st, by age and sex. 2024 [sponsor submitted reference].
48.Government of Canada. First National and Inuit Health Branch: Non-Insured Health Benefits Program Annual Report 2021/2022. 2023: https://www.sac-isc.gc.ca/eng/1683039690813/1683039973755. [sponsor submitted reference].
49.Cohen SS, Skovbo S, Vestergaard H, et al. Epidemiology of systemic mastocytosis in Denmark. Br J Haematol. 2014;166(4):521-528. PubMed
50.Schwaab J, Cabral do OHN, Naumann N, et al. Importance of adequate diagnostic workup for correct diagnosis of advanced systemic mastocytosis. J Allergy Clin Immunol Pract. 2020;8(9):3121-3127.e1. PubMed
51.Gotlib J, Kluin-Nelemans HC, George TI, et al. Efficacy and safety of midostaurin in advanced systemic mastocytosis. N Engl J Med. 2016;374(26):2530-2541. PubMed
52.Eversana Canada Inc. Avapritinib Canadian Physician Questionnaire and Interview Report. 2024. [sponsor submitted reference].
53.pCodr. Midostaurin (Rydapt) for Systemic Mastocytosis: Final Economic Guidance Report. . 2020: https://www.cadth.ca/sites/default/files/pcodr/Reviews2020/10193MidostaurinSM_fnEGR_NOREDACT-ABBREV_Post02Apr2020_final.pdf. [sponsor submitted reference].
54.Medison Pharma Canada Inc. response to June 6, 2024 CADTH request for additional information regarding avapritinib CADTH review. Toronto (ON): Medison Pharma Canada Inc; 2024 May 16.
55.Gotlib J, Reiter A, Radia DH, et al. Efficacy and safety of avapritinib in advanced systemic mastocytosis: interim analysis of the phase 2 PATHFINDER trial. Nature Medicine. 2021;27(12):2192-2199. PubMed
Appendix 1: Cost Comparison Table
Table 11: CDA-AMC Cost Comparison Table for the Treatment of Adult Patients With Advanced Systemic Mastocytosis
Treatment | Strength/ concentration | Form | Price ($) | Recommended dosage | Daily cost ($) | 28-day cost ($) |
|---|---|---|---|---|---|---|
Avapritinib | 25 mg 50 mg 100 mg 200 mg | Tablet | 1,343.3600a 1,343.3600a 1,343.3600a 1,343.3600a | 200 mg once daily | 1,343.36 | 37,614 |
Tyrosine kinase inhibitors | ||||||
Imatinib (generic) | 100 mg 400 mg | Tablet | 5.2079 20.8314 | Patients without the D816V c-KIT mutation or with an unknown mutational status and not responding to other therapies: 400 mg daily Patients with associated eosinophilia: initial dose of 100 mg daily which may be increased up to 400 mg daily | 5.21 to 20.83 | 146 to 583 |
Midostaurin (Rydapt) | 25 mg | Capsule | 172.6250 | 100 mg twice daily | 1,381.00 | 38,668 |
Other drugs | ||||||
Cladribine (generic) | 1 mg/mL 1 mg/mL | 10 mL vial for IV infusion 10 mL vial for SC injection | 890.0500b 939.0100b | 0.14 mg/kg/day by IV infusion or SC for 5 consecutive days (1 cycle). Cycles are repeated at 4- to 12-week intervals for 1 to 9 cyclesc | 158.94 to 167.68 | 4,450 to 4,695 |
Peginterferon alfa-2a (Pegasys) | 180 mcg/0.5 mL | Prefilled syringe | 419.7000d | 90 mcg weekly for 2 weeks, then 180 mcg weeklye | 59.96 | 1,679 |
CDA-AMC = Canada’s Drug Agency; SC = subcutaneous.
Note: All prices are from the Ontario Drug Benefit Formulary (accessed May 2024),37 unless otherwise indicated, and do not include dispensing fees. For dosing that depends on weight, a patient weight of 70 kg was assumed.
The comparators presented in this table have been deemed to be appropriate based on feedback from clinical expert(s). Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
aSponsor-submitted cost.
bPrice retrieved from IQVIA DeltaPA (June 2024).41
cRecommended dosing per the clinical expert consulted by CDA-AMC. Daily dose is aligned with published literature.42,43
dPrice retrieved from Ontario Drug Benefit Exceptional Access Program (May 2024).41
eRecommended dose sourced from BC Cancer.44
Note: This table has not been copy-edited.
Appendix 2: Submission Quality
Please note that this appendix has not been copy-edited.
Description | Yes or no | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | No | Midostaurin is not a relevant comparator in Canda and should not have been included in the sponsor’s estimates of efficacy, safety, and costs in the 2L+ therapy population. |
Model has been adequately programmed and has sufficient face validity | No | As outlined in the Appraisal of the Sponsor’s Economic Evaluation by CDA-AMC, the model does not have sufficient face validity. Additionally, the model includes numerous IFERROR statements. The systematic use of IFERROR statements makes thorough auditing of the sponsor’s model impractical, as it remains unclear whether the model is running inappropriately by overriding errors. |
Model structure is adequate for decision problem | Yes | No comment. |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | No | As outlined in the Appraisal of the Sponsor’s Economic Evaluation by CDA-AMC, CDA-AMC noted discrepancies between the KM estimates used in the submitted pharmacoeconomic model vs. those reported in the submitted indirect evidence. |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | No | The use of a partitioned survival model prevents the ability to characterize all relevant sources of parameter uncertainty. Additionally, the sponsor assumed a 10% standard error for utility values which does not allow for decision uncertainty to be accurately characterized. |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | No | Information regarding the sponsor’s IPTW-weighted analysis was sparse and not transparent. |
CDA-AMC = Canada’s Drug Agency.
Appendix 3: Additional Information on the Submitted Economic Evaluation
Please note that this appendix has not been copy-edited.
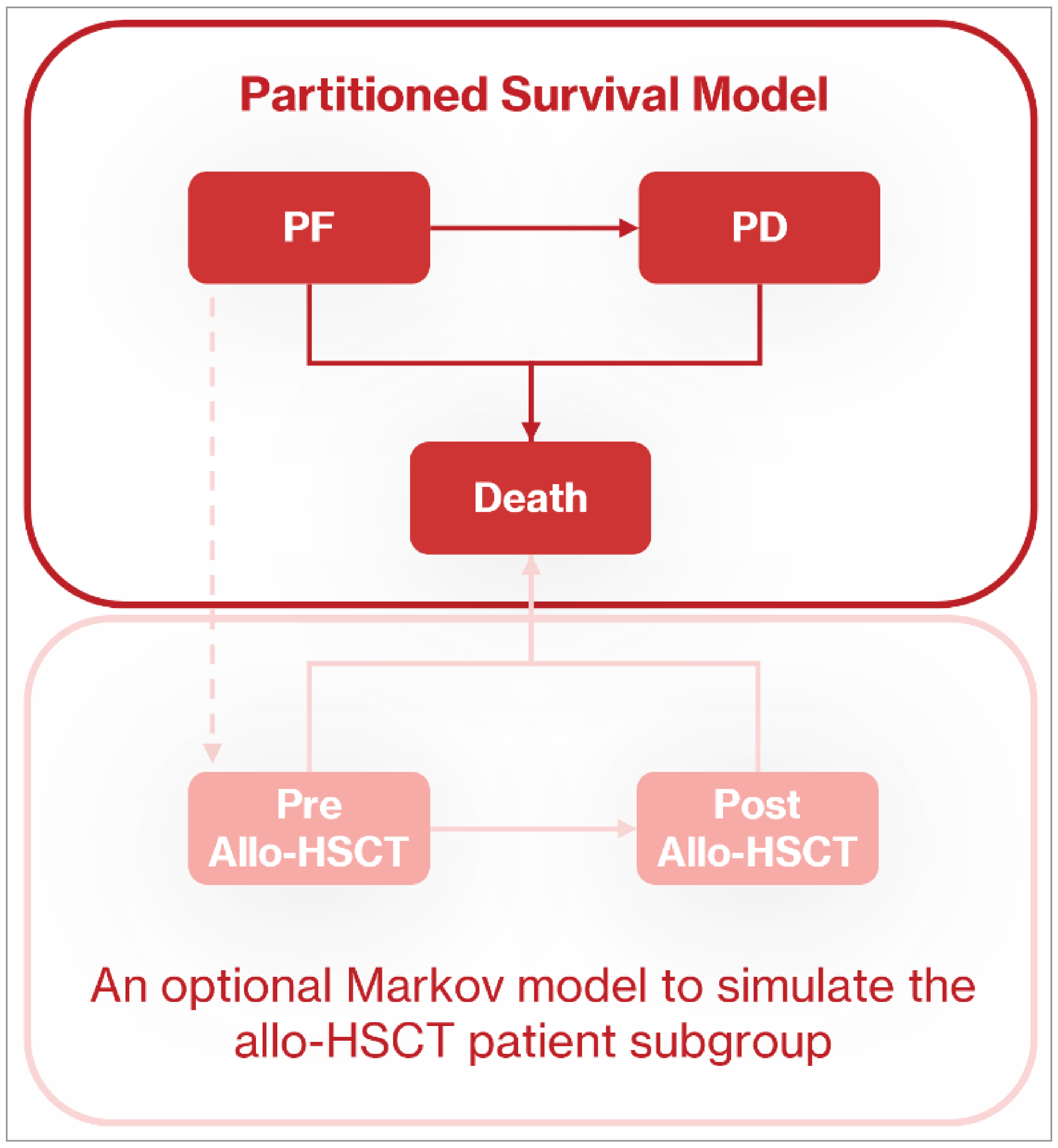
PF = progression-free; PD = progressive disease; allo-HSCT = allogeneic hematopoietic stem cell transplant.
Source: Sponsor’s pharmacoeconomic submission.1
Detailed Results of the Sponsor’s Base Case
Table 13: Disaggregated Summary of the Sponsor’s Economic Evaluation Results — 1L Therapy Population
Parameter | Avapritinib | 1L BAT |
|---|---|---|
Discounted LYs | ||
Total | 10.556 | 3.001 |
PF | 7.299 | 0.650 |
PD | 3.192 | 2.351 |
Pre-HSCT | 0.005 | 0.000 |
Post-HSCT | 0.060 | 0.000 |
Discounted QALYs | ||
Total | 6.932 | 1.742 |
PF | 5.167 | 0.470 |
PD | 1.719 | 1.272 |
Pre-HSCT | 0.003 | 0.000 |
Post-HSCT | 0.043 | 0.000 |
Discounted costs ($) | ||
Total | 2,296,194 | 283,450 |
Drug acquisition | 1,926,758 | 12,681 |
Drug administration | 0 | 4,045 |
Disease management | 276,244 | 176,686 |
Allo-HSCT | 1,052 | 0 |
Adverse events | 15,391 | 2,732 |
End of life | 76,749 | 87,306 |
1L = first-line; allo-HSCT = allogeneic hematopoietic stem cell transplant; BAT = best available therapy; HSCT = hematopoietic stem cell transplant; LY = life-year; PD = progressed disease; PF = progression-free; QALY = quality-adjusted life-year.
Source: Sponsor’s pharmacoeconomic submission.1
Figure 2: Avapritinib Outcomes — 1L Therapy Population
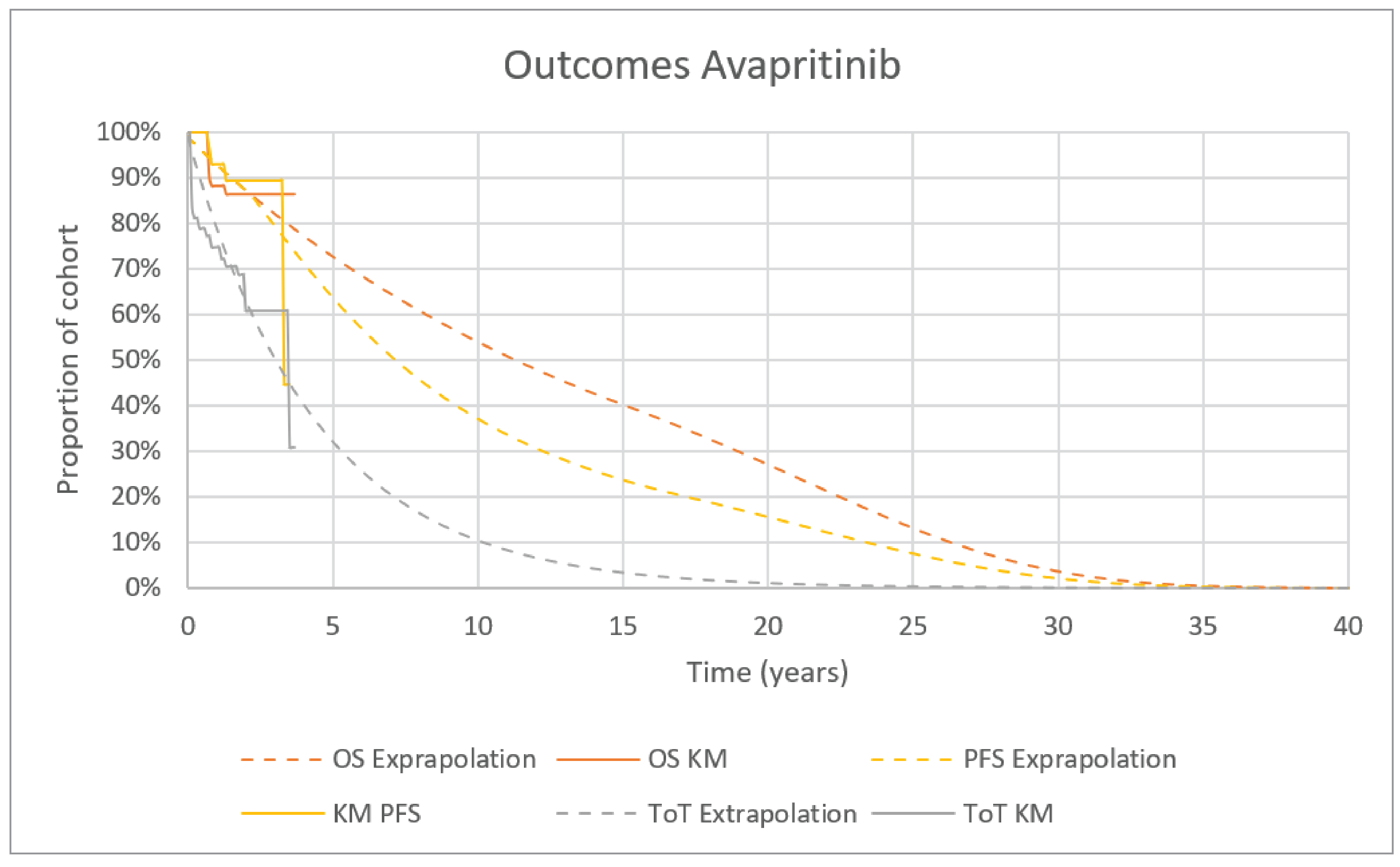
Source: Sponsor’s pharmacoeconomic submission.1
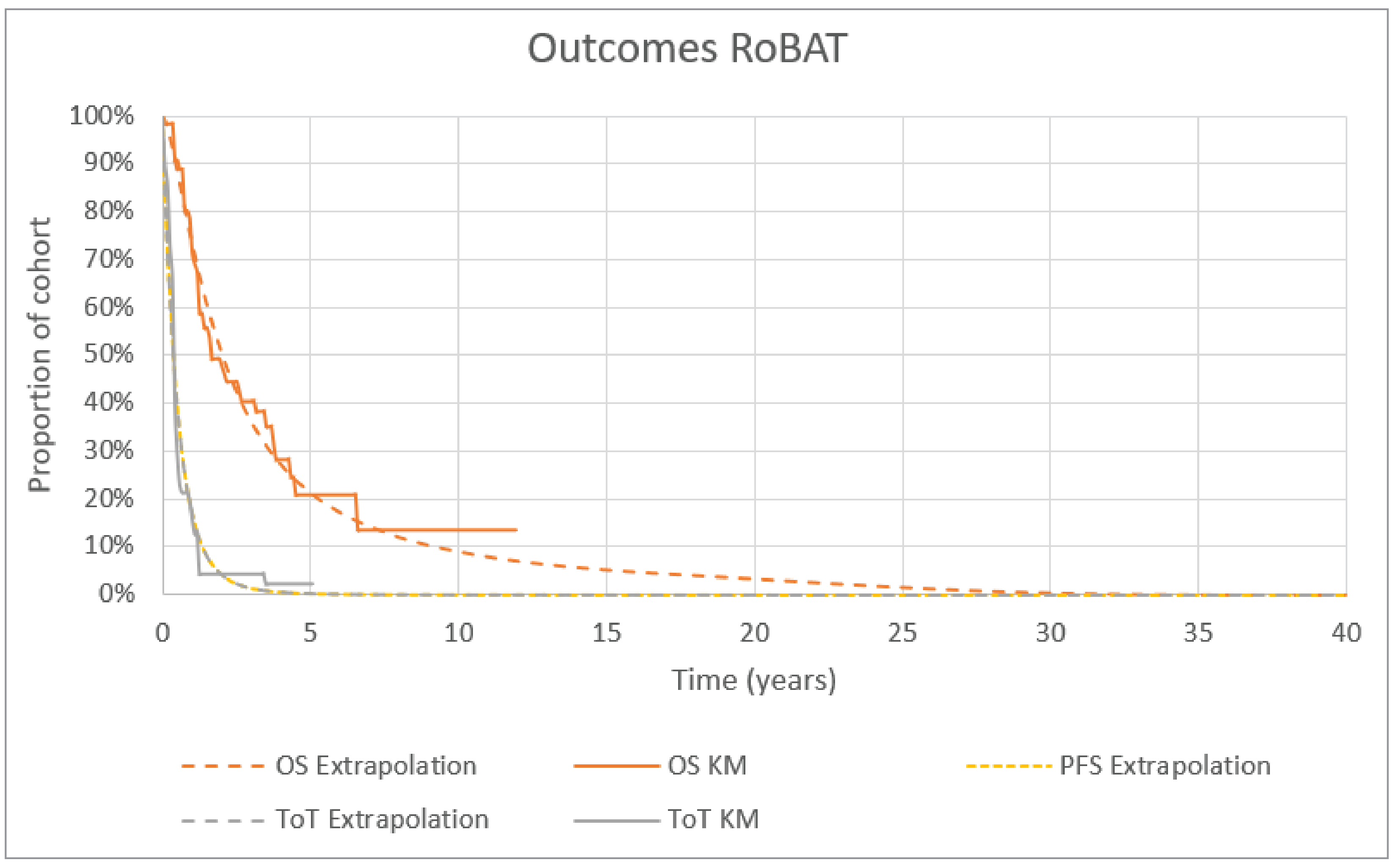
Table 14: Disaggregated Summary of the Sponsor’s Economic Evaluation Results — 2L+ Therapy Population
Parameter | Avapritinib | BAT |
|---|---|---|
Discounted LYs | ||
Total | 5.762 | 3.411 |
PF | 4.852 | 1.249 |
PD | 0.859 | 2.156 |
pre-HSCT | 0.004 | 0.000 |
post-HSCT | 0.047 | 0.005 |
Discounted QALYs | ||
Total | 3.637 | 1.863 |
PF | 3.190 | 0.825 |
PD | 0.411 | 1.034 |
pre-HSCT | 0.002 | 0.000 |
post-HSCT | 0.034 | 0.004 |
Discounted costs ($) | ||
Total | 1,449,128 | 583,286 |
Drug acquisition | 1,260,754 | 319,480 |
Drug administration | 0 | 2,179 |
Disease management | 81,036 | 162,782 |
Allo-HSCT | 799 | 90 |
Adverse events | 23,296 | 12,319 |
End of life | 83,243 | 86,437 |
2L+ = second-line or later-line; allo-HSCT = allogeneic hematopoietic stem cell transplant; BAT = best available therapy; HSCT = hematopoietic stem cell transplant; LY = life-year; PD = progressed disease; PF = progression-free; QALY = quality-adjusted life-year.
Source: Sponsor’s pharmacoeconomic submission.1
Figure 4: Avapritinib Outcomes — 2L+ Therapy Population
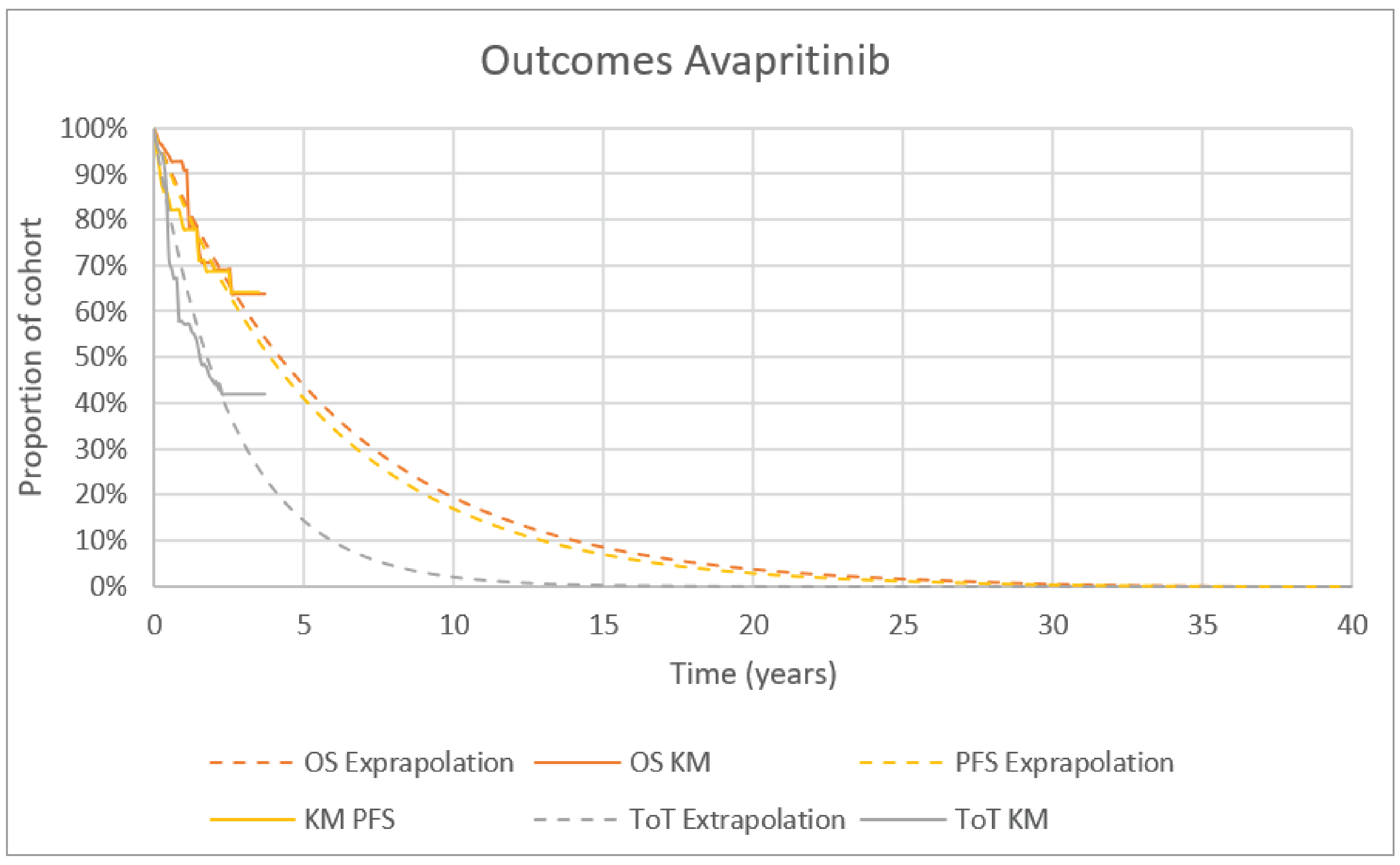
Source: Sponsor’s pharmacoeconomic submission.1
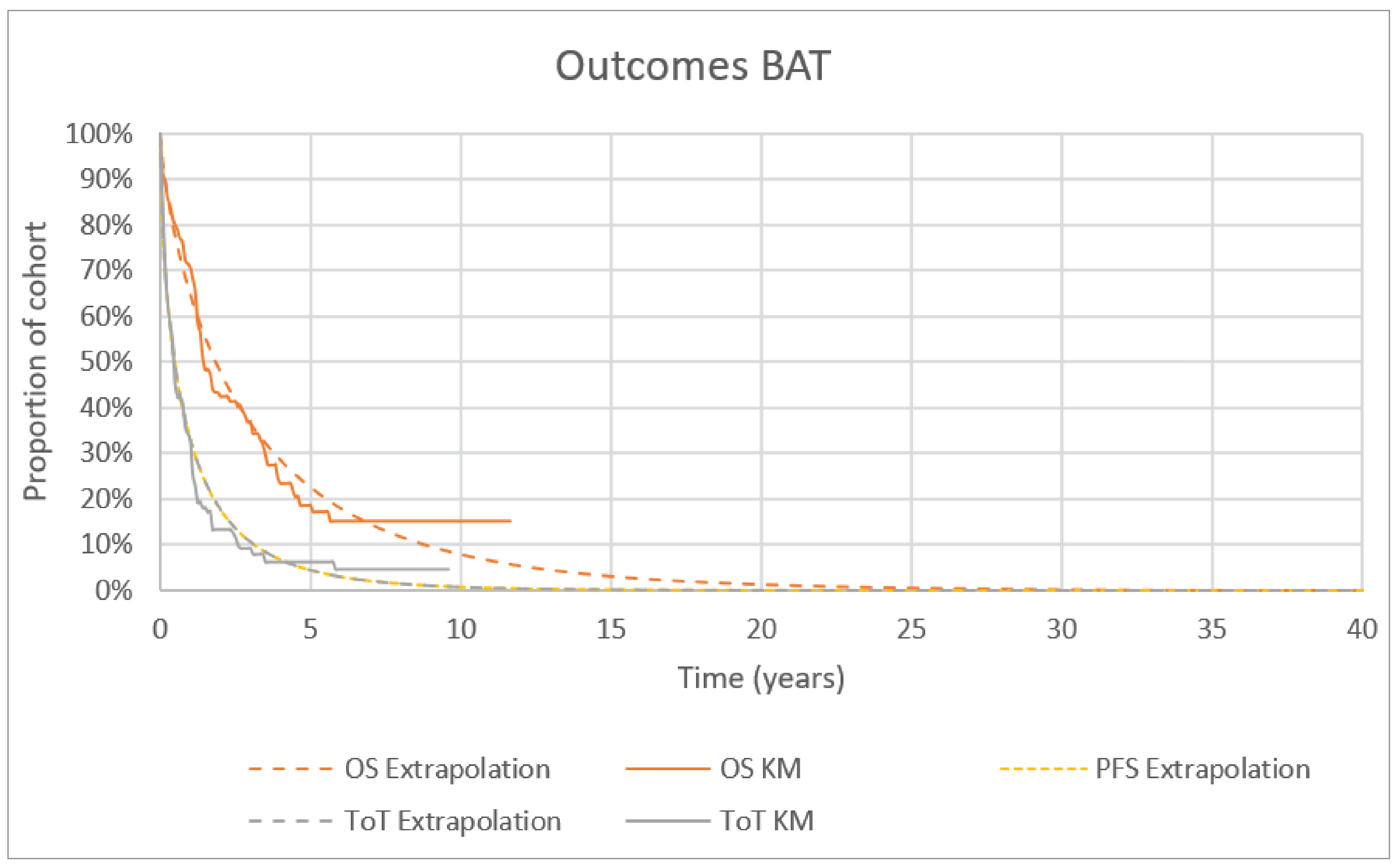
Appendix 4: Additional Details on the CDA-AMC Reanalyses and Sensitivity Analyses of the Economic Evaluation
Please note that this appendix has not been copy-edited.
Detailed Results of CDA-AMC Alternative Analysis
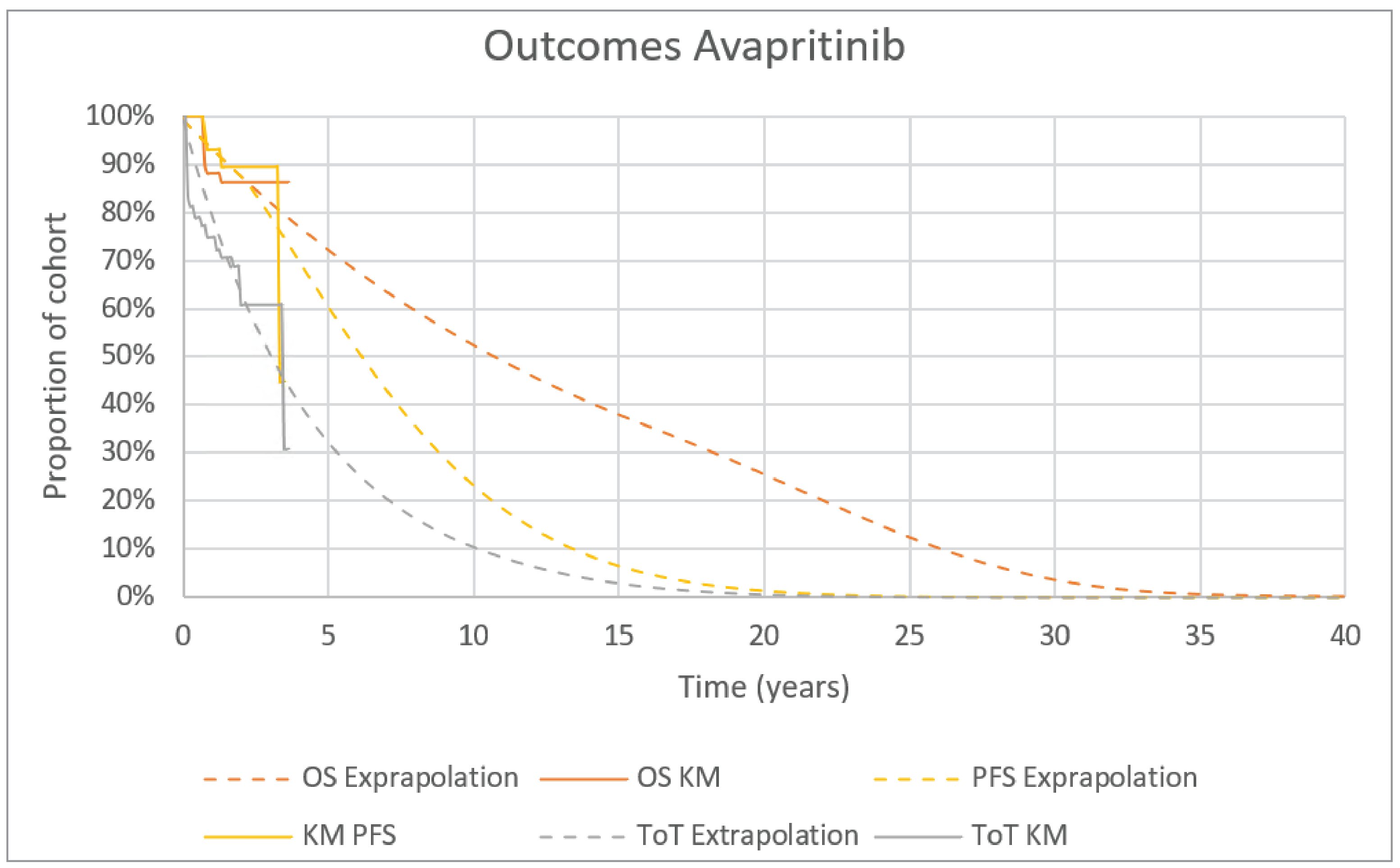
Table 15: Disaggregated Summary of CDA-AMC Alternative Analysis Results — 1L Therapy Population
Parameter | Avapritinib | BAT |
|---|---|---|
Discounted LYs | ||
Total | 9.868 | 3.008 |
PF | 5.912 | 0.653 |
PD | 3.891 | 2.355 |
Pre-HSCT | 0.005 | 0.000 |
Post-HSCT | 0.060 | 0.000 |
Discounted QALYs | ||
Total | 6.344 | 1.743 |
PF | 4.212 | 0.471 |
PD | 2.086 | 1.272 |
Pre-HSCT | 0.003 | 0.000 |
Post-HSCT | 0.042 | 0.000 |
Discounted costs ($) | ||
Total | 2,289,049 | 283,782 |
Drug acquisition | 1,880,320 | 12,668 |
Drug administration | 0 | 4,033 |
Disease management | 314,943 | 177,402 |
Allo-HSCT | 1,053 | 0 |
Adverse events | 15,029 | 2,752 |
End of life | 77,704 | 86,928 |
1L = first-line; allo-HSCT = allogeneic hematopoietic stem cell transplant; BAT = best available therapy; CDA-AMC = Canada’s Drug Agency; HSCT = hematopoietic stem cell transplant; LY = life-year; PD = progressed disease; PF = progression-free; QALY = quality-adjusted life-year.
Table 16: Disaggregated Summary of CDA-AMC Alternative Analysis Results — 2L+ Therapy Population
Parameter | Avapritinib | BAT |
|---|---|---|
Discounted LYs | ||
Total | 5.769 | 3.419 |
PF | 4.841 | 1.249 |
PD | 0.877 | 2.170 |
Pre-HSCT | 0.004 | 0.000 |
Post-HSCT | 0.047 | 0.000 |
Discounted QALYs | ||
Total | 3.640 | 1.865 |
PF | 3.183 | 0.824 |
PD | 0.420 | 1.041 |
Pre-HSCT | 0.002 | 0.000 |
Post-HSCT | 0.034 | 0.000 |
Discounted costs ($) | ||
Total | 1,460,361 | 288,252 |
Drug acquisition | 1,259,883 | 18,674 |
Drug administration | 0 | 4,463 |
Disease management | 93,012 | 164,222 |
Allo-HSCT | 798 | 0 |
Adverse events | 23,338 | 14,376 |
End of life | 83,330 | 86,517 |
2L+ = second-line or later-line; allo-HSCT = allogeneic hematopoietic stem cell transplant; BAT = best available therapy; CDA-AMC = Canada’s Drug Agency; HSCT = hematopoietic stem cell transplant; LY = life-year; PD = progressed disease; PF = progression-free; QALY = quality-adjusted life-year.
Appendix 5: Submitted Budget Impact Analysis and CDA-AMC Appraisal
Please note that this appendix has not been copy-edited.
Table 17: Summary of Key Take-Aways
Key take-aways of the BIA |
|---|
|
BIA = budget impact analysis; CDA-AMC = Canada’s Drug Agency; NIHB = Non-Insured Health Benefits.
Summary of Sponsor’s Budget Impact Analysis
In the submitted budget impact analysis (BIA), the sponsor assessed the introduction of avapritinib for the treatment of AdvSM including patients with ASM, SM-AHN, and MCL.45 The BIA was undertaken from the perspective of a Canadian public payer over a 3-year time horizon (2026 to 2028) using an epidemiological approach (Figure 7). The sponsor compared a reference scenario in which patients received either cladribine, interferon, imatinib, or midostaurin (2L+ therapy population only) to a new drug scenario in which avapritinib was reimbursed. The sponsor’s submission only considered annual drug acquisition costs which were obtained from IQVIA and ODB.19,21,46 Data informing key parameters of the model were obtained from various sources including Statistics Canada,47 the Government of Canada,48 published literature and protocols,24,44,49,50 the PATHFINDER trial,51 a previous CDA-AMC review,40 clinical expert feedback,6 the sponsor’s internal forecast estimates and market research, and assumption. Key inputs to the BIA are documented in Table 18.
Key assumptions included:
The incidence of AdvSM, sourced from a retrospective Danish study evaluating the incidence from 1997 to 2010, was reflective of the incidence of AdvSM in Canada.49
The prevalence of AdvSM, sourced from a retrospective German study evaluating the prevalence of AdvSM who were referred, diagnosed, and treated at a single German centre from 2009 to 2018, was reflective of the current number of patients with AdvSM in Canada.50
Incident patients were considered newly diagnosed and assumed to be eligible for first-line treatment. Prevalent patients were assumed to be on second-line therapy or beyond.
The annual cost of cladribine was calculated assuming patients would be treated with 3 cycles per year.
Midostaurin was only considered a comparator in the 2L+ therapy setting with a 5% market share given its limited reimbursement across Canada.
Figure 7: Sponsor’s Estimation of the Size of the Eligible Population
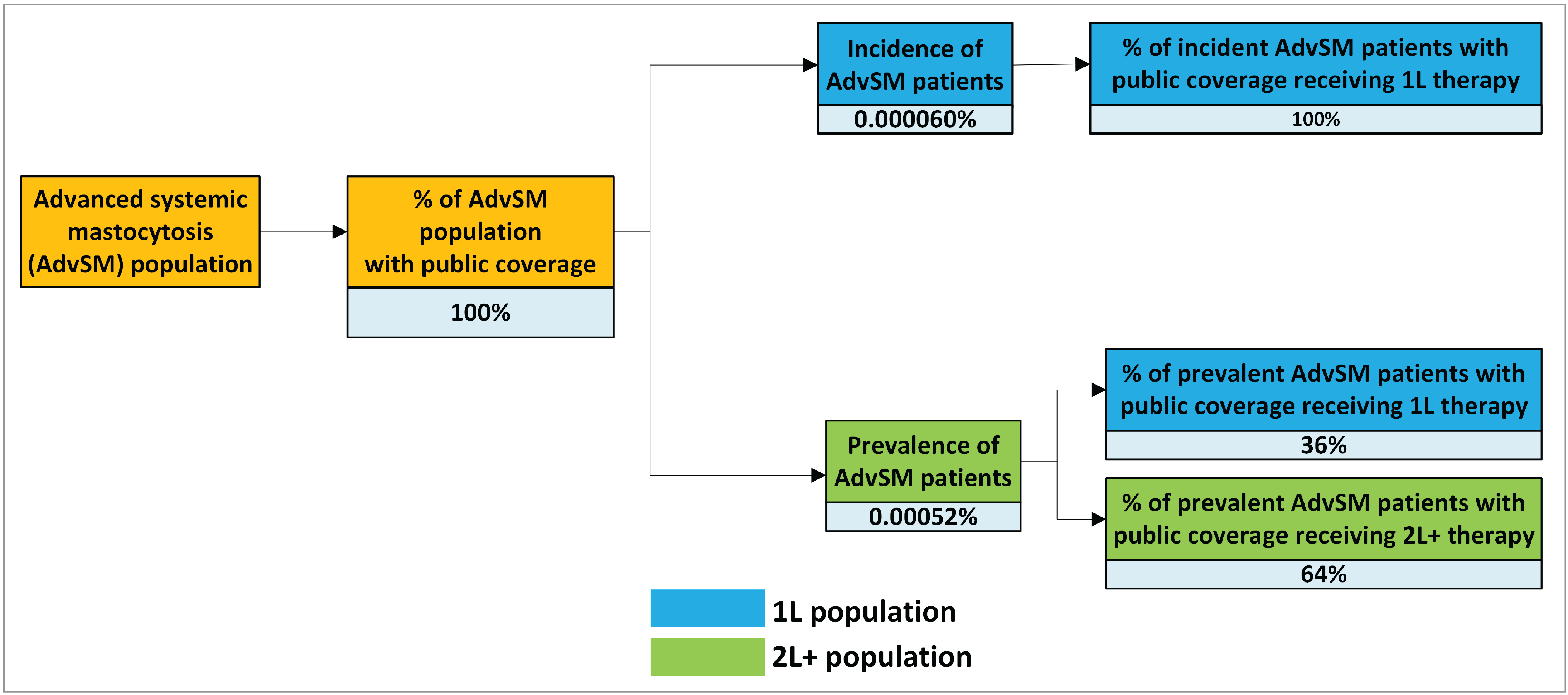
Source: Sponsor’s pharmacoeconomic submission.45
Table 18: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as year 1/year 2/year 3 if appropriate) | |
|---|---|---|
Target population | ||
Proportion of AdvSM population with public coveragea | 100% | |
Incidence of AdvSM49 | 0.0000006% | |
Prevalence of AdvSM50 | 0.0000052% | |
Proportion of patients with prevalent AdvSM receiving 2L+ therapy51 | 64% | |
Number of patients eligible for drug under review | 161 / 164 / 168 | |
Market uptake (3 years) | ||
Uptake (reference scenario) Cladribine Imatinib Midostaurin Peginterferon alfa-2a | 1L therapy population 52.8% / 52.8% / 52.8% 5.0% / 5.0% / 5.0% 0.0% / 0.0% / 0.0% 42.2% / 42.2% / 42.2% | 2L+ therapy population 50.0% / 50.0% / 50.0% 5.0% / 5.0% / 5.0% 5.0% / 5.0% / 5.0% 40.0% / 40.0% / 40.0% |
Uptake (new drug scenario) Avapritinib Cladribine Imatinib Midostaurin Peginterferon alfa-2a | 1L therapy population 50.0% / 75.0% / 85.0% 25.0% / 11.1% / 5.6% 5.0% / 5.0% / 5.0% 0.0% / 0.0% / 0.0% 20.0% / 8.9% / 4.4% | 2L+ therapy population 50.0% / 75.0% / 85.0% 23.7% / 10.5% / 5.3% 5.0% / 5.0% / 5.0% 2.4% / 1.1% / 0.5% 18.9% / 8.4% / 4.2% |
Cost of treatment (per patient, per year) | ||
Avapritinib Cladribine Imatinib Peginterferon alfa-2a | $490,362 $13,351 $21,824 $7,603 | |
1L = first-line; 2L+ = second-line or later-line; AdvSM = advanced systemic mastocytosis.
aBased on sponsor assumption.
Summary of the Sponsor’s BIA Results
The sponsor estimated that the 3-year budget impact of reimbursing avapritinib for the treatment of adult patients with AdvSM including ASM, SM-AHN, and MCL to be $158,848,851 (year 1: $36,968,860; year 2: $56,549,098; year 3: $65,330,893).
CDA-AMC Appraisal of the Sponsor’s BIA
CDA-AMC identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
Misalignment of model inputs between the sponsor-submitted CUA and BIA, overestimating drug acquisition costs: CDA-AMC noted that several model inputs and assumptions in the BIA were not aligned with the CUA submitted by the sponsor. First, in the BIA, the sponsor estimated the market shares in the 2L+ therapy population based on the previous CDA-AMC review for midostaurin and clinical expert input.52,53 CDA-AMC requested additional information from the sponsor to understand why the sponsor used different market shares in the CUA and BIA,54 The sponsor clarified that the estimates were informed by different sources. The discrepancy in the market shares (CUA = 46.07%; BIA = 5.00%) highlights the uncertainty in the sponsor’s estimates. As noted in the Appraisal of the Sponsor’s Economic Evaluation by CDA-AMC, midostaurin is not currently reimbursed by public drug plans for AdvSM, there are no compassionate access programs currently available, and clinical expert input highlighted that midostaurin is not an applicable treatment comparator for patients with AdvSM in Canada, in any line of therapy, given its limited access and prohibitive cost. Including midostaurin inflated comparator drug acquisition costs and underestimated the budget impact of reimbursing avapritinib.
Second, the sponsor assumed that no patients discontinued treatment during the 3-year BIA time horizon. However, in the CUA, treatment duration is modelled by ToT curves derived from the sponsor-conducted IPTW-weighted analysis whereby ToT for avapritinib was informed by the PATHFINDER trial safety set population, and the ToT for BAT was informed by the BLU-285 to 2405 study, an external control study of patients in the real-world treated with BAT. The assumption that no patients discontinue does not align with the sponsor’s CUA. The median ToT, per the sponsor’s selected extrapolations in the CUA, are approximately 37 and 22 months for avapritinib in the 1L and 2L+ therapy populations, respectively, and 4 months and 6 months for BAT in the 1L and 2L+ therapy populations, respectively. Critically, the sponsor’s assumption in the BIA does not align with the observed clinical data or clinical practice as patients discontinue treatment for many reasons, including but not limited to AEs, toxicity, progression, and death. Apart from cladribine which the sponsor has assumed is administered for 3 28-day cycles, the sponsor’s assumption that no patients discontinue treatment substantially overestimates drug acquisition costs. Annual treatment costs for cladribine are aligned between the CUA and BIA. The sponsor’s submitted model structure does not permit treatment durations and thus annual treatment costs to differ between the 1L and 2L+ therapy populations.
In the CDA-AMC BIA base case, the reference case market shares for the 2L+ therapy population were aligned with the reanalysis by CDA-AMC of the sponsor’s submitted economic evaluation for the 2L+ therapy population. As detailed in the Appraisal of the Sponsor’s Submitted Economic Evaluation by CDA-AMC, there remains uncertainty in the market share attributed to peginterferon alfa-2a.
To align treatment durations in the CUA and BIA, treatment costs for avapritinib, peginterferon alfa-2a, and imatinib were obtained from the CDA-AMC deterministic reanalyses of the 1L therapy population. To derive each annual treatment acquisition cost, the time horizon in the CUA was set equal to 1 year and the market share for the relevant comparator was set to equal to 100%. Midostaurin costs were assumed to be $0 as no market share is attributed to the treatment. Due to the submitted model structure, the CDA-AMC reanalysis does not accurately reflect the decline in total annual treatment costs over time due to a smaller proportion of incident patients remaining on treatment. For example, in the CUA, costs attributed to the 1L therapy population receiving avapritinib in years 1, 2, and 3 are $441,947.86, $345,925.08, and $272,198.91, respectively. Given this, and the magnitude of avapritinib treatment costs relative to BAT, the budget impact estimated by CDA-AMC remains overestimated. Moreover, the CDA-AMC BIA reanalysis assumes the treatment duration, as estimated by the 1L therapy population, applies to the 2L+ therapy population and thus, per the CUA, likely overestimates treatment costs among the 2L+ therapy population.
The eligible population size is uncertain: The sponsor used an epidemiologic approach to estimate both the number of incident patients and the number of prevalent patients eligible for avapritinib. To estimate the number of incident patients, the sponsor assumed the overall incidence of AdvSM to be 0.06 cases per 100,000 persons based on a retrospective Danish study.49 The sponsor estimated the prevalence rate of 5.2 cases per 1,000,000 based on a German study by Shwaab et al.50 Clinical expert input noted that while the sponsor’s estimated incidence and prevalence rates are informed by the best available published literature, the incidence rate may be an underestimate. Clinical expert input commented that both the incidence and prevalence of AdvSM are expected to increase with time. The sponsor’s model structure assumes the incidence and prevalent rate of AdvSM remain constant over time.
The sponsor assumed incident patients were newly diagnosed and eligible for 1L therapy. Prevalent patients were defined as those currently receiving 1L therapy, and those assumed to be on 2L+ therapy. Of the prevalent patients, the sponsor assumed 64% were on 2L+ therapy based on baseline date from the PATHFINDER trial.55 Clinical expert input noted that the sponsor’s estimate is likely biased toward US and European experience where patients have access to multiple lines of therapies that are not easily accessible in Canada (i.e., midostaurin), and therefore, without tolerable and effective treatments or access to clinical trials, many patients do not survive front-line therapy and thus not alive to be eligible for 2L+ treatment. Input suggested an estimate of 30% to 40% to be more reflective of Canadian practice.
The sponsor’s epidemiologic approach estimated that 161, 164, and 168 patients will be eligible for avapritinib in years 1, 2, and 3, respectively. Clinical expert input noted that the number of eligible patients across Canada may be between 200 and 250 patients and may increase with educational efforts on how to diagnose systematic mastocytosis and with new widespread availability of next-generation sequencing that contains KIT exon 17 coverage.
CDA-AMC was unable to address uncertainty in the incidence and prevalence rate of AdvSM. CDA-AMC explored uncertainty in the proportion of patients receiving 2L+ therapy in scenario analyses.
The Non-Insured Health Benefits (NIHB) program population was inappropriately calculated: The NIHB does not reimburse IV oncology medications. Instead, NIHB clients requiring treatment with IV oncology medications are funded by the province or territory within which the NIHB client resides and should therefore be counted as clients of that jurisdiction for the purposes of modelling the budget impact of reimbursing avapritinib. Additionally, the provinces of Saskatchewan and Alberta fund all oncology products for patients residing within their borders, including those who would otherwise be reimbursed by the NIHB, as does Ontario for patients aged younger than 25 years or 65 years and older. NIHB clients of the appropriate ages who are living within the borders of these 3 jurisdictions should therefore be considered clients of the provincial plan for the purposes of modelling the budget impact of reimbursing avapritinib.
CDA-AMC did not adjust for this limitation in reanalysis. The impact on pan-Canadian model results is expected to be minimal.
The market uptake of avapritinib is uncertain: The sponsor’s submitted base case assumed that 50%, 75%, and 85% of eligible patients would receive avapritinib in year 1, year 2, and year 3, respectively, based on the sponsor’s internal forecast estimates and market research. Clinical expert input received by CDA-AMC for this review suggests that the sponsor’s estimates may underestimate the uptake of avapritinib as clinicians are waiting for access to a targeted therapy. Input suggested that uptake may be 75%, 85%, and 95% year 1, year 2, and year 3, respectively.
CDA-AMC explored uncertainty in the uptake of avapritinib in scenario analyses.
Additional limitations were identified, but were not considered to be key limitations. These limitations include:
Cladribine treatment costs are uncertain: As detailed in the Appraisal of the Sponsor’s Submitted Economic Evaluation by CDA-AMC, cladribine treatment costs are uncertain owing to variation in the recommended dosage, treatment duration, and mode of administration.
CDA-AMC was unable to address this limitation, but notes cladribine treatment costs likely have a minimal impact on the overall budget impact due to the comparably high cost of avapritinib.
The relative use of peginterferon alfa-2a is uncertain: As detailed in the Appraisal of the Sponsor’s Submitted Economic Evaluation by CDA-AMC, clinical expert input emphasized that the availability of peginterferon alfa-2a varies across jurisdictions and that it is not considered a front-line therapy by most line by most international experts. In the BIA, the sponsor assumed peginterferon alfa-2a held the same market share across all jurisdictions.
CDA-AMC was unable to address this limitation in reanalyses.
CDA-AMC Reanalyses of the BIA
CDA-AMC revised the sponsor’s base case by aligning the market shares for the 2L+ therapy population with the CDA-AMC alternative reanalysis of the sponsor’s submitted CUA and deriving treatment acquisition costs from the CDA-AMC alternative reanalysis of the sponsor’s submitted CUA for the 1L therapy population (assuming $0 drug acquisition costs for midostaurin).
Table 19: CDA-AMC Revisions to the Submitted Budget Impact Analysis
Stepped analysis | Sponsor’s value or assumption | CDA-AMC value or assumption |
|---|---|---|
Changes to derive the CDA-AMC base case | ||
1. Market shares in 2L+ therapy population | Cladribine = 50.0% Peginterferon alfa-2a = 40.0% Imatinib = 5.0% Midostaurin = 5.0% | Aligned with CDA-AMC CUA reanalysis. Cladribine = 52.80% Peginterferon alfa-2a = 42.20% Imatinib = 5.00% Midostaurin = 0.00% |
2. Drug acquisition costs | Avapritinib = $490,326.40 Peginterferon alfa-2a = $21,824.40 Imatinib = $7,603.46 Midostaurin = $504,065.00 | Avapritinib = $441,947.86 Peginterferon alfa-2a = $9,397.50 Imatinib = $3,707.80 Midostaurin = $0 |
CDA-AMC BIA base case | Reanalysis 1 + 2 | |
2L+ = second-line or later-line; CDA-AMC = Canada’s Drug Agency; CUA = cost-utility analysis.
The results of the CDA-AMC stepwise reanalysis are presented in summary format in Table 20 and a more detailed breakdown is presented in Table 21. In the CDA-AMC BIA base case, the 3-year budget impact of reimbursing avapritinib for the treatment of adult patients with AdvSM including ASM, SM-AHN, and MCL to be $149,033,058 (year 1: $34,684,252; year 2: $53,054,704; year 3: $61,294,102).
Table 20: Summary of the CDA-AMC Reanalyses of the Budget Impact Analysis
Stepped analysis | 3-year total ($) |
|---|---|
Submitted base case | 158,848,851 |
CDA-AMC reanalysis 1: market shares in 2L+ therapy population | 163,875,091 |
CDA-AMC reanalysis 2: drug acquisition costs | 149,152,900 |
CDA-AMC BIA base case | 149,033,058 |
2L+ = second-line or later-line; CDA-AMC = Canada’s Drug Agency.
Note: The CDA-AMC reanalyses are based on publicly available prices of the comparator treatments.
CDA-AMC conducted the following scenario analyses to address remaining uncertainty, using the CDA-AMC BIA base case (results are provided in Table 21:
Assuming that the uptake of avapritinib is 75%, 85%, and 95% year 1, year 2, and year 3, respectively.
Assuming the proportion of prevalent patients receiving 2L+ therapy is 30%. This assumption implies that a proportion of prevalent patients (34%) do not receive any treatment.
Assuming that the price of avapritinib is reduced by 87% (the CDA-AMC estimated price reduction from the CUA).
Table 21: Detailed Breakdown of the CDA-AMC Reanalyses of the BIA
Stepped analysis | Scenario | Year 0 (current situation) ($) | Year 1 ($) | Year 2 ($) | Year 3 ($) | 3-year total ($) |
|---|---|---|---|---|---|---|
Submitted base case | Reference | 4,806,981 | 4,904,237 | 5,001,492 | 5,098,748 | 15,004,477 |
New drug | 4,806,981 | 41,873,097 | 61,550,590 | 70,429,641 | 173,853,328 | |
Budget impact | 0 | 36,968,860 | 56,549,098 | 65,330,893 | 158,848,851 | |
CDA-AMC BIA base case | Reference | 1,769,694 | 1,805,378 | 1,841,062 | 1,876,746 | 5,523,187 |
New drug | 1,769,694 | 36,489,630 | 54,895,767 | 63,170,848 | 154,556,245 | |
Budget impact | 0 | 34,684,252 | 53,054,704 | 61,294,102 | 149,033,058 | |
CDA-AMC scenario analysis 1: higher uptake | Reference | 1,769,694 | 1,805,378 | 1,841,062 | 1,876,746 | 5,523,187 |
New drug | 1,769,694 | 46,308,323 | 58,901,439 | 67,254,717 | 172,464,478 | |
Budget impact | 0 | 44,502,945 | 57,060,377 | 65,377,970 | 166,941,292 | |
CDA-AMC scenario analysis 2: 30% of 2L+ therapy prevalent patients receive treatment | Reference | 1,237,482 | 1,262,355 | 1,287,227 | 1,312,100 | 3,861,682 |
New drug | 1,237,482 | 25,514,246 | 38,381,829 | 44,164,984 | 108,061,059 | |
Budget impact | 0 | 24,251,891 | 37,094,602 | 42,852,884 | 104,199,376 | |
CDA-AMC scenario analysis 3: 87% price reduction | Reference | 1,769,694 | 1,805,378 | 1,841,062 | 1,876,746 | 5,523,187 |
New drug | 1,769,694 | 5,501,341 | 7,494,585 | 8,408,262 | 21,404,188 | |
Budget impact | 0 | 3,695,963 | 5,653,523 | 6,531,515 | 15,881,001 |
2L+ = second-line or later-line; CDA-AMC = Canada’s Drug Agency.
Note: The CDA-AMC reanalyses are based on publicly available prices of the comparator treatments.
ISSN: 2563-6596
Canada’s Drug Agency (CDA-AMC) is a pan-Canadian health organization. Created and funded by Canada’s federal, provincial, and territorial governments, we’re responsible for driving better coordination, alignment, and public value within Canada’s drug and health technology landscape. We provide Canada’s health system leaders with independent evidence and advice so they can make informed drug, health technology, and health system decisions, and we collaborate with national and international partners to enhance our collective impact.
Disclaimer: CDA-AMC has taken care to ensure that the information in this document was accurate, complete, and up to date when it was published, but does not make any guarantee to that effect. Your use of this information is subject to this disclaimer and the Terms of Use at cda-amc.ca.
The information in this document is made available for informational and educational purposes only and should not be used as a substitute for professional medical advice, the application of clinical judgment in respect of the care of a particular patient, or other professional judgments in any decision-making process. You assume full responsibility for the use of the information and rely on it at your own risk.
CDA-AMC does not endorse any information, drugs, therapies, treatments, products, processes, or services. The views and opinions of third parties published in this document do not necessarily reflect those of CDA-AMC. The copyright and other intellectual property rights in this document are owned by the Canadian Agency for Drugs and Technologies in Health (operating as CDA-AMC) and its licensors.
Questions or requests for information about this report can be directed to Requests@CDA-AMC.ca.