CADTH Reimbursement Review
Cemiplimab (Libtayo)
Sponsor: Sanofi-Aventis Canada Inc.
Therapeutic area: Locally advanced or metastatic non–small cell lung cancer (first line)
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Clinical Review
Abbreviations
AE
adverse event
AESI
adverse events of special interest
ALT
alanine transaminase
CCSN
Canadian Cancer Survivor Network
CI
confidence interval
CR
complete response
CrI
credible interval
ECOG PS
Eastern Cooperative Oncology Group Performance Status
EORTC QLQ-C30
European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30
EORTC QLQ-LC13
European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire-Lung Cancer 13
FAS
full analysis set
GHS
global health status
GRADE
Grading of Recommendations Assessment, Development and Evaluation
HR
hazard ratio
HRQoL
health-related quality of life
IC
investigator choice
IDMC
independent data monitoring committee
IHC
immunohistochemistry
IRC
Independent Review Committee
ITC
indirect treatment comparison
LCC
Lung Cancer Canada
LHF
Lung Health Foundation
MAC
Medical Advisory Committee
NMA
network meta-analysis
NSCLC
non–small cell lung cancer
OH-CCO
Ontario Health-Cancer Care Ontario
OR
odds ratio
ORR
objective response rate
OS
overall survival
PBC
platinum-based chemotherapy
PFS
progression-free survival
PRISMA
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
PRO
patient-reported outcome
QoL
quality of life
RCT
randomized controlled trial
RECIST 1.1
Response Evaluation Criteria in Solid Tumours Version 1.1
SAE
serious adverse event
SD
standard deviation
SLR
systematic literature review
TEAE
treatment-emergent adverse event
TPS
Tumour Proportion Score
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Table 1: Background Information of Application Submitted for Review
Item | Description |
|---|---|
Drug product | Cemiplimab for injection (Libtayo), 350 mg/7 mL (50 mg/mL), single-use vial for IV infusion |
Sponsor | Sanofi-Aventis Canada Inc. |
Indication |
|
Reimbursement request | Per indication |
Health Canada approval status | Approved |
Health Canada review pathway | Standard |
NOC date | April 27, 2023 |
Recommended dose | 350 mg every 3 weeks administered as an IV infusion over 30 minutes |
NSCLC = non–small cell lung cancer; NOC = Notice of Compliance; PBC = platinum-based chemotherapy.
Introduction
Lung and bronchus cancer is the most commonly diagnosed cancer in Canada (excluding nonmelanoma skin cancers). In Canada in 2022, an estimated 30,000 people were diagnosed with lung and bronchus cancer, representing approximately 13% of all new cancer cases, and 20,700 people died from lung cancer, representing 24% of all cancer deaths that year. The risk factors include tobacco smoking, second-hand smoke, radon, asbestos, and other environmental exposures, which can lead to symptoms like cough, shortness of breath, and chest pain. Lung cancer is primarily divided into small cell lung cancer and non–small cell lung cancer (NSCLC), with NSCLC found in almost 80% of lung cancer cases. The prognosis largely depends on the stage at diagnosis, with half of all cases being diagnosed at stage IV. Advances in molecular testing and targeted therapies, especially for specific genetic mutations in NSCLC, along with the development of immune checkpoint inhibitors that target PD-1 and/or PD-L1, have significantly improved treatment outcomes. Diagnosis typically involves a combination of imaging tests, biopsies, and comprehensive biomarker testing.
The treatment of NSCLC varies based on disease stage, patient health, and tumour characteristics. Early-stage NSCLC (stage I, stage II, some stage IIIA) typically involves surgical resection, often in combination with chemotherapy and/or radiation. Advanced stages (IIIB or IIIC, IV) are treated with systemic therapies like immunotherapy, chemotherapy, or both, depending on factors like PD-L1 expression and the presence of specific genetic alterations. Platinum-based chemotherapy (PBC), once the mainstay, is now often combined with or replaced by targeted therapies and immunotherapies, especially for tumours without oncogenic alterations. In Canada, treatment strategies include targeted therapy for actionable genetic alterations, and immunotherapy and chemotherapy are used in various combinations based on PD-L1 expression and other factors.
The overarching goal in NSCLC management is to improve patient outcomes, which encompasses both extending overall survival (OS) and enhancing quality of life (QoL) by minimizing treatment-related toxicity. Although there have been improvements in outcomes due to the introduction of new systemic therapies, including targeted therapies and immunotherapies, not all patients benefit from these treatments. The heterogeneity of NSCLC, with its various subtypes and molecular profiles, means that some patients may not respond to available treatments or may develop a lack of response over time, leading to disease progression. The current mortality rate for NSCLC remains high, so there is a need for therapies that can offer a more durable response and ultimately improve survival rates. However, the toxicity associated with systemic therapies for NSCLC is a significant concern. Adverse effects can range from mild to severe and life-threatening. These side effects can impact a patient's QoL and may limit the ability to continue with the optimal treatment regimen. Therefore, there is a need for treatments that can maintain or improve efficacy while reducing the incidence and severity of side effects.
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of cemiplimab 350 mg every 3 weeks administered as an IV infusion in combination with PBC for the first-line treatment of adult patients with NSCLC whose tumours have no EGFR, ALK, or ROS1 aberrations and whose disease is:
locally advanced, and patients are not candidates for surgical resection or definitive chemoradiation, or
metastatic.
Cemiplimab has previously been reviewed by CADTH and has received a conditional positive reimbursement recommendation for:
the first-line treatment of adult patients with NSCLC expressing PD-L1 in at least 50% of tumour cells (Tumour Proportion Score [TPS] ≥ 50%), as determined by a validated test, with no EGFR, ALK, or ROS1 aberrations, who have locally advanced NSCLC who are not candidates for surgical resection or definitive chemoradiation, or metastatic NSCLC.
Cemiplimab has also been reviewed by CADTH and received conditional positive recommendations for other therapeutic areas, including cutaneous squamous cell carcinoma and basal cell carcinoma.
Stakeholder Perspectives
The information in this section is a summary of input provided by the patient and clinician groups that responded to CADTH’s call for input and from clinical experts consulted by CADTH for the purpose of this review.
Patient Input
Three patient groups provided input to CADTH: the Canadian Cancer Survivor Network (CCSN) (which reported responses from 9 patients, 1 caregiver), Lung Cancer Canada (LCC) (4 patients), and Lung Health Foundation (LHF) (15 patients, 1 caregiver). Input was gathered through surveys and discussions, focusing on experiences with lung cancer treatments, including cemiplimab. The disease significantly impacts the daily lives of patients and their families, causing physical and emotional strain. Key outcomes important to patients include symptom management, QoL, and delay in disease progression. The CCSN emphasized the challenges faced by patients and caregivers, including managing side effects and emotional burdens, with most patients reporting satisfactory access to existing treatments. LCC noted positive experiences with cemiplimab, particularly in symptom management and ease of use. The LHF reported on the significant impact of symptoms on patients' lives, the effectiveness of current treatments in symptom relief, and the desire for earlier biomarker testing. All groups underscored the need for treatments that effectively delay disease progression with minimal side effects.
Clinician Input
Input From Clinical Experts Consulted by CADTH
According to clinical experts consulted by CADTH, unmet needs for patients with NSCLC include improvement in survival and QoL and minimization of treatment toxicity. Cemiplimab, combined with PBC, is seen as an alternative to existing first-line therapies for patients with advanced or metastatic NSCLC without specific driver mutations and with varying PD-L1 expression levels. The experts noted that patients with a high disease burden receive the most benefit, and patients with significant comorbidities or poor performance status are least suitable for the drug. Response to treatment should be assessed clinically and radiologically, and should focus on tumour shrinkage and QoL. Discontinuation of treatment can be considered upon disease progression, unacceptable toxicity, or after 2 years of treatment. Treatment with cemiplimab is managed by a medical oncologist in outpatient settings.
Clinician Group Input
CADTH received input from 2 clinician groups: the LCC Medical Advisory Committee (LCC-MAC) and the Ontario Health-Cancer Care Ontario (OH-CCO) Lung Cancer Drug Advisory Committee. In total, 12 clinicians from the LCC-MAC and 3 clinicians from the OH-CCO Lung Cancer Drug Advisory Committee provided input to the submissions. The clinician groups agreed that the first line of treatment is chemotherapy and immunotherapy, or pembrolizumab alone for patients with a PD-L1 status greater than 50%. For patients not eligible for immunotherapy, platinum doublet chemotherapy remains an option. There was agreement among all clinicians that improvements in progression-free survival (PFS), OS, and QoL are treatment goals. The LCC-MAC noted that a benefit of cemiplimab is that it is administered as a flat dose of 350 mg; there is no weight-based option. This clinician group felt that this would provide significant advantages in delivering treatment closer to home for many patients with lung cancer because vial sharing would not be required. Both clinician groups agreed that in terms of place in therapy, cemiplimab in combination with PBC would be an alternative first-line treatment (i.e., combination pembrolizumab plus chemotherapy, and 2 cycles of platinum doublet plus ipilimumab and/or nivolumab).
The clinical experts consulted by CADTH noted that — in addition to patients with incurable NSCLC, patients with no EGFR, ALK, or ROS1 alterations, and those receiving first-line therapy — patients with any PD-L1 expression and an Eastern Cooperative Oncology Group Performance Status (ECOG PS) of 0 to 2 would meet the eligibility criteria. The LCC-MAC suggested that PD-L1 status should be determined to assess eligibility, and stated that patients in rural areas will benefit from cemiplimab because no vial sharing is required.
Clinical and radiological assessments were noted as the best ways to determine whether a patient is responding to the treatment, while disease progression, toxicity, patient preference, and certain adverse events (AEs) were noted as factors to be considered when deciding to discontinue treatment.
It was agreed that outpatient clinics under the supervision of a medical oncologist are the appropriate setting for treatment with cemiplimab in combination with platinum‐based chemotherapy. The LCC-MAC added that in many jurisdictions across Canada, particularly remote or rural communities, medical oncologists work in partnership with general practitioners in oncology to comanage patients.
Drug Program Input
The drug plans submitted questions concerning relevant comparators, the initiation of therapy, and discontinuation. The clinical experts provided insights into these questions. Specifically, on the topic of comparators, the clinical experts advised that cemiplimab plus PBC lacks direct evidence comparing it to other immunotherapies or combinations, making it difficult to definitively assess its relative effectiveness. On the topic of initiation of therapy, the clinical experts advised that patients with an ECOG PS of 2 can benefit from cemiplimab. On the topic of discontinuation, the clinical experts suggested alignment with other immunotherapy and chemotherapy combinations.
Clinical Evidence
Systematic Review
Description of Studies
One pivotal phase III, randomized controlled trial (RCT) was included in the systematic review: EMPOWER-Lung 3 (part 2). The EMPOWER-Lung 3 is a 2-part, phase III clinical trial comparing the efficacy and safety of cemiplimab in combination with PBC versus placebo plus PBC in patients with advanced NSCLC, regardless of PD-L1 expression levels. Part 2 of the study compared cemiplimab plus PBC to placebo plus PBC across different PD-L1 expression levels, and is the focus of this CADTH Clinical Review Report. EMPOWER-Lung 3 did not include sites in Canada and maintained separate protocols for part 1 and part 2. Part 1 was designed to evaluate the efficacy and safety of cemiplimab in the first-line treatment of patients with NSCLC and a PD-L1 expression level of less than 50%. Part 1 and part 2 are separate studies, with separate randomization schemes, inclusion criteria, and visit and/or event schedules; patients enrolled in part 1 did not contribute to the analyses in part 2, and vice versa. Two data cut-off dates were reported for the EMPOWER-Lung 3 trial (part 2): the first on June 14, 2021 (prespecified second interim analysis) after a median follow-up of 16.4 months, and the second on June 14, 2022 (prespecified final analysis) after approximately 28.4 months of follow-up. Because the efficacy boundary was crossed at the second interim analysis, no alpha was assigned to the prespecified final analysis for OS. The independent data monitoring committee (IDMC) recommended unblinding the study after the first data cut-off date, when statistical significance for OS was achieved. The primary objective of part 2 was to assess OS differences between the cemiplimab plus PBC and placebo plus PBC groups in the first-line treatment of patients with advanced NSCLC. Secondary objectives included PFS and objective response rate (ORR).
Patients were randomized in a 2:1 ratio to receive cemiplimab or placebo, stratified by histology and PD-L1 expression levels. Treatment continued for up to 108 weeks or until disease progression or unacceptable toxicity, with mandatory pemetrexed maintenance for nonsquamous histology. The study design instituted caps on enrolment based on PD-L1 expression and histology. Eligible participants were adults with advanced squamous or nonsquamous NSCLC who had received no prior systemic treatment for metastatic disease. Patients with certain genetic aberrations were excluded, as targeted therapies are the standard of care for those conditions. Enrolment was open to patients with adequately treated brain metastases, with controlled viral infections, and without significant autoimmune diseases. The main intervention was cemiplimab or placebo, administered intravenously in combination with PBC every 3 weeks for 4 cycles. The primary outcome, OS, was defined as the time from randomization to death from any cause. PFS, a key secondary outcome, was the time to disease progression or death, assessed by an Independent Review Committee (IRC) using Response Evaluation Criteria in Solid Tumours Version (RECIST) 1.1. ORR was the proportion of patients with a confirmed complete or partial response, reported as a key secondary outcome. The study also used the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 (EORTC QLQ-C30) and Quality of Life Questionnaire-Lung Cancer 13 (EORTC QLQ-LC13) questionnaires to measure health-related quality of life (HRQoL) as another secondary outcome.
Efficacy Results
At the secondary interim analysis (data cut-off date: June 14, 2021), cemiplimab plus PBC showed statistically significant improvements in OS, PFS, and ORR for patients with advanced NSCLC compared to placebo plus PBC (refer to Table 16). Results at the subsequent data cut-off date, June 14, 2022, including the final OS analyses, were consistent with the those seen at the previous data cut-off date. Because the efficacy boundary was crossed at the second interim analysis, no alpha was assigned to the final analysis.
At the June 14, 2022, data cut-off date, cemiplimab plus PBC showed improvements in OS and PFS for patients with advanced NSCLC compared to placebo plus PBC. Median OS was longer in the cemiplimab plus PBC group (21.1 months, with a 95% confidence interval [CI] of 15.9 to 23.5) versus the placebo plus PBC group (12.9 months, with a 95% CI of 10.6 to 15.7), with a stratified hazard ratio (HR) of 0.645 (95% CI, 0.507 to 0.820; P = 0.0003) in favour of cemiplimab plus PBC. Survival probabilities at 12 months and 24 months were 66.4% and 42.7%, respectively, in the cemiplimab plus PBC, and were 53.9% and 27.2%, respectively, in the placebo plus PBC group. Median PFS was longer in the cemiplimab plus PBC group (8.2 months, with a 95% CI of 6.4 to 9.0 months) than in the placebo plus PBC group (5.5 months, with a 95% CI of 4.3 to 6.2 months; P < 0.0001), with a stratified HR of 0.549 (95% CI, 0.441 to 0.683; P < 0.0001) in favour of cemiplimab plus PBC. PFS probabilities at 12 months and 24 months were 38.7% and 19.7%, respectively, in the cemiplimab plus PBC group and 16.1% and 3.6%, respectively, in the placebo plus PBC group. The ORR was higher in the cemiplimab plus PBC group (43.6%; 95% CI, 38.0% to 49.3%) versus the placebo plus PBC group (22.1%; 95% CI, 15.8% to 29.5%; P < 0.0001).
Harms Results
Safety results from the EMPOWER-Lung 3 trial (part 2) at the June 14, 2022, data cut-off date, indicated that, overall, the safety profile of the combination treatment appeared to be consistent with the known profiles of cemiplimab and PBC, as well as those of other PD-1 and/or PD-L1 targeting therapies used in combination with chemotherapy to treat patients with NSCLC. Similar proportions of patients in both treatment groups experienced AEs (96.5% in the cemiplimab plus PBC group and 94.8% in the placebo plus PBC group). The most frequent AEs (cemiplimab plus PBC versus placebo plus PBC) included anemia (45.8% versus 39.9%), alopecia (37.2% versus 43.8%), nausea (25.3% versus 16.3%), hyperglycemia (18.3% versus 11.8%), and increased alanine transaminase (ALT) levels (17.6% versus 15.0%). A total of 48.7% of patients in the cemiplimab plus PBC group and 32.7% of patients in the placebo plus PBC group experienced at least 1 treatment-emergent adverse event (TEAE) of at least grade 3. The most common TEAEs of at least grade 3 experienced by at least 2% of patients in the cemiplimab plus PBC group (cemiplimab plus PBC versus placebo plus PBC) included anemia (10.9% versus 6.5%), neutropenia (6.4% versus 5.9%), decreased white blood cell count (3.2% versus 2.0%), and thrombocytopenia (3.2% versus 1.3%). Numerically, a |||||| |||||||||| of serious adverse events (SAEs) were reported in the cemiplimab plus PBC group (|||||) than in the placebo plus PBC group (|||||), with |||||||||| ||||| of the most commonly reported SAE: ||||||||| (|||| in the cemiplimab plus PBC group, contrasted to |||| in the placebo plus PBC group), |||||| (|||| in the cemiplimab plus PBC group, contrasted to |||| in the placebo plus PBC group), ||||||| ||||||||||| (|||| in the cemiplimab plus PBC group, contrasted to |||| in the placebo plus PBC group), and death (8.7% in the cemiplimab plus PBC group, contrasted to 9.2% in the placebo plus PBC group). Adverse events of special interest (AESIs) were reported in |||| of patients in the cemiplimab plus PBC group and |||| in the placebo plus PBC group as of the June 14, 2022, data cut-off date. The most frequent AESI was ||||| | || |||||| |||||||||||||||| |||||||||, occurring in |||| of patients in the cemiplimab plus PBC group and |||| in the placebo plus PBC group. A total of ||| patients |||||| died due to a treatment-related TEAE in the cemiplimab plus PBC group and ||| patient |||||| died due to a treatment-related TEAE in the placebo plus PBC group.
Critical Appraisal
The EMPOWER-Lung 3 trial (part 2) was a double-blind, placebo-controlled, phase III RCT. The study's randomization was facilitated by an interactive web response system, stratified by histology and PD-L1 expression level. The study employed appropriate methods for time-to-event analysis, including the Kaplan-Meier method and Cox proportional hazards model.
Limitations of the EMPOWER-Lung 3 trial (part 2) included the fact that a higher percentage of subsequent anticancer therapies was received by patients in the placebo plus PBC group than in the cemiplimab plus PBC group, which may have introduced a confounding variable, potentially affecting OS results. Further, because the study was concluded at the secondary interim analysis, data between the interim analysis cut-off date of June 14, 2021, and the final analysis data cut-off date of June 14, 2022, were collected from an unblinded period of the study, potentially introducing biases in subjective outcomes, such as HRQoL and harms. In addition, the high rate of missing patient-reported outcomes (PROs) data over time, especially in the placebo group, makes interpretation of PROs a challenge, and the results remain inconclusive.
The clinical experts noted that the study's inclusion criteria and patient characteristics align with typical oncology trials and clinical practice in Canada, and they suggested that baseline demographic and tumour characteristics were generally consistent with the expected population of patients with NSCLC seen in their practices. A limitation to the generalizability of the findings was the trial's comparator (placebo plus PBC), which does not reflect current practice in Canada, where patients typically receive immunotherapy. No trial sites were located in Canada, so health care settings in Canada were not represented in the trial. The overall low rates of subsequent therapies in both groups reduces the generalizability of the results to practice in Canada. A further limitation is the study's early termination due to observed efficacy, restricting the collection of long-term safety and efficacy data.
GRADE Summary of Findings and Certainty of the Evidence
Methods for Assessing the Certainty of the Evidence
For the pivotal studies and RCTs identified in the sponsor’s systematic review, the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach was used to assess the certainty of the evidence for outcomes considered most relevant to inform CADTH’s expert committee deliberations, and a final certainty rating was determined as outlined by the GRADE Working Group.1,2
Following the GRADE approach, evidence from RCTs started as high-certainty evidence and could be rated down for concerns related to study limitations (which refer to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias.
When possible, certainty was rated in the context of the presence of an important (nontrivial) treatment effect; if this was not possible, certainty was rated in the context of the presence of any treatment effect (i.e., the clinical importance is unclear). In all cases, the target of the certainty of evidence assessment was based on the point estimate and where it was located relative to the threshold for a clinically important effect (when a threshold was available) or to the null. The target of the certainty of evidence assessment was the presence or absence of a clinically important effect on EORTC QLQ-C30 score, based on a threshold identified in the literature for this review. The target of the certainty of evidence assessment was the presence or absence of any (nonnull) effect for OS, PFS, ORR, and harms.
Results of GRADE Assessments
Table 2 presents the GRADE summary of findings for cemiplimab plus PBC and placebo plus PBC in patients with NSCLC.
Table 2: Summary of Findings for Cemiplimab Plus PBC Versus Placebo Plus PBC for Patients With Advanced NSCLC Whose Tumours Have No EGFR, ALK, or ROS1 Aberrations
Outcome and follow-up | Patients (studies), N | Relative effect | Absolute effects | Certainty | What happens | ||
|---|---|---|---|---|---|---|---|
Placebo + PBC | Cemiplimab + PBC | Difference | |||||
Overall survival | |||||||
OS Median follow-up: 28.42 months | 466 (1 RCT) | OS events (i.e., deaths) at data cut-off (June 14, 2022):
Median OS at data cut-off (June 14, 2022):
| Higha | Cemiplimab + PBC results in an increase in OS compared to PBC alone | |||
Progression-free survival | |||||||
PFS Median follow-up: 28.42 months | 466 (1 RCT) | PFS events (i.e., disease progression or death) at data cut-off (June 14, 2022):
Median PFS at last data cut-off (June 14, 2022):
| Higha | Cemiplimab + PBC results in an increase in PFS compared to PBC alone | |||
Response | |||||||
Objective response rate Follow-up: up to 108 weeks | 466 (1 RCT) | 2.82 (95% CI, 1.80 to 4.41) | 22.1 per 100 | 43.6 per 100 (95% CI, 38.0 to 49.3) | 21.51 more per 100 (95% CI, 12.96 to 30.07 more) | Highb | Cemiplimab + PBC results in an increase in the number of people achieving an objective response rate compared to PBC alone; the clinical importance of the increase is uncertain |
Health-Related Quality of Life | |||||||
EORTC QLQ-C30 GHS/QoL (range, 100 [best] to 0 [worst])c Follow-up: up to cycle 21 | 466 (1 RCT) | NA | |||| |||| |||||| | |||| |||| |||||| ||||| || ||||| | |||| |||| |||||| |||||| ||||| || |||| ||||| | Lowd | Cemiplimab + PBC may result in little to no clinically important difference in change in EORTC QLQ-C30 score, compared to PBC alone |
Harms | |||||||
Patients with any treatment-emergent adverse events of special interest Follow-up: on-treatment period | 466 (1 RCT) | NR | ||| ||| ||| | ||| ||| ||| | |||| |||||| || ||||| | Lowe | Cemiplimab + PBC may result in little to no difference in treatment-emergent adverse events of special interest, compared with PBC alone |
CI = confidence interval; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; GHS = global health status; NA = not applicable; NE = not estimated, NR = not reported; OS = overall survival; PBC = platinum-based chemotherapy; PFS = progression-free survival; QoL = quality of life; RCT = randomized controlled trial.
Note: Study limitations (which refer to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias were considered when assessing the certainty of the evidence. All serious concerns in these domains that led to the rating down of the level of certainty are documented in the table footnotes.
aIn the absence of available data for the between-group difference in event probabilities at clinically relevant time points, the judgment of imprecision was based on the 95% CI for the HR, using the null as the threshold. The clinical expert consulted by CADTH noted that the HR results are clinically meaningful. This observation is consistent with the decision by the trial data and safety monitoring board to terminate the study early due to demonstrated efficacy.
bNo published between-group minimal important difference was identified, and the clinical experts consulted by CADTH were unable to estimate a threshold for clinically important effects; therefore, the null was used. Not rated down for imprecision; a between-group difference larger than the null and a CI that excludes the null suggest benefit compared to PBC as judged by the CADTH review team.
cResults based on data collected for the secondary interim analysis, with a data cut-off date of June 14, 2021.
dRated down 2 levels for very serious risk of bias due to missing data. Data were available for less than 50% of patients after cycle 6 in the placebo + PBC group and after cycle 12 in the cemiplimab + PBC group. Not rated down for imprecision. Based on the literature, a 10-point change from the baseline in total score was clinically important; the point estimate and entire CI suggest little to no difference.
eRated down 2 levels for very serious concerns about imprecision due to the very small number of events.
Source: EMPOWER-Lung 3 (part 2) Clinical Study Report.3 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Long-Term Extension Studies
No long-term extension studies were submitted by the sponsor.
Indirect Comparisons
Description of Study
The indirect treatment comparison (ITC) submitted by the sponsor aimed to assess the comparative efficacy of cemiplimab plus PBC versus other Health Canada–approved therapies for the first-line treatment of patients who have locally advanced or metastatic NSCLC. Outcomes of interest included OS, PFS, ORR, and certain harms. A systematic literature review (SLR) was conducted, with searches updated until March 2022, to identify RCTs for inclusion in a network meta-analysis (NMA). The SLR focused on trials from 2010 onward. The review process included independent reviewers and a Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram documenting study selection. The feasibility of an NMA was assessed, considering the connectedness of the evidence, the similarity of comparators and the distribution of baseline characteristics. A Bayesian NMA was performed using both fixed-effects and random-effects models; the fixed-effects model was considered the default base case.
Efficacy Results
The SLR identified 11 relevant RCTs, with 5 unique RCTs included in the NMA for any PD-L1 expression and any histology. The evidence network allowed for comparisons of cemiplimab plus PBC with pembrolizumab plus PBC, nivolumab plus ipilimumab plus PBC, and investigator choice (IC) chemotherapy.
Cemiplimab plus PBC showed favourable OS (HR at 24 months = 0.66; 95% credible interval [CrI], 0.51 to 0.87), PFS (HR at 24 months = 0.61, 95% CrI, 0.48 to 0.78), and ORR (odds ratio [OR] = 2.76, 95% CrI = 1.79 to 4.37) compared to IC chemotherapy. This is consistent with the direct evidence established in the EMPOWER-Lung 3 trial (part 2). Comparisons with other immunotherapy combinations are much less robust and cannot inform on the efficacy of cemiplimab plus PBC relative to other immunotherapy combinations. Results for the indirect comparison of cemiplimab plus PBC with pembrolizumab plus PBC included an HR at 24 months for OS of 0.88 (95% CrI, 0.65 to 1.21), an HR at 24 months for PFS of 0.87 (95% CrI, 0.66 to 1.15), and an OR of 0.89 (95% CrI, 0.54 to 1.49) for ORR. Results for the indirect comparison of cemiplimab plus PBC with nivolumab plus ipilimumab plus PBC included an HR at 24 months for OS of 0.85 (95% CrI, 0.61 to 1.19), an HR at 24 months for PFS of 0.91 (95% CrI, 0.68 to 1.24), and an OR of 1.53 (95% CrI, 0.89 to 2.67) for ORR.
Harms Results
Due to the limited evidence base and small number of events, harms results are not reported.
Critical Appraisal
The sponsor-submitted ITC was performed through an SLR, which systematically identified all the trials in the network, according to prespecified criteria.
However, there was a lack of reporting on the result of the quality assessment, even though it was stated that the Cochrane risk-of-bias tool was used, and it is unknown how studies with a high risk of bias were handled, if applicable. Several limitations due to the sparse network might have contributed to high uncertainty in the results obtained. The small number of included studies in the network that used a Bayesian fixed-effects model mandated several untested assumptions, including the clinical homogeneity assumption. However, a significant concern is whether this assumption would have been held, given that there was significant heterogeneity across patient populations, highly varied subsequent therapies, differences in the levels of PD-L1 expression, histology, metastasis sites and status, chemotherapy, and maintenance therapy across the included studies.
Considering the limitations related to the sparse network and clinical heterogeneity across the included trials, it is not possible to conclude that the effects of cemiplimab plus PBC are similar to those of other immunotherapies used in combination with PBC on OS, PFS, and ORR. Considering the consistency of the direction of the indirect results for cemiplimab plus PBC versus placebo plus PBC in the ITC, with the direct and existing evidence in the form of the EMPOWER-Lung 3 trial (part 2), the indirect results can be considered supportive of the findings in the EMPOWER-Lung 3 trial (part 2).
Studies Addressing Gaps in the Evidence From the Systematic Review
No studies addressing gaps in the systematic review evidence were submitted by the sponsor.
Conclusions
Based on clinical data from the EMPOWER-Lung 3 study (part 2), cemiplimab plus PBC demonstrated a statistically significant benefit compared to placebo plus PBC in OS, PFS, and ORR for the treatment of patients with advanced NSCLC and no EGFR, ALK, or ROS1 aberrations, regardless of PD-L1 expression status. GRADE assessment suggests that there is high certainty that cemiplimab plus PBC will lead to better OS and PFS rates and a better ORR over a median follow-up period of 28.42 months. However, there is a low level of certainty that cemiplimab plus PBC results in little to no difference in HRQoL, measured by the EORTC QLQ-C30, compared to placebo plus PBC.
There is no notable increase in patients with treatment-emergent AESIs in the cemiplimab plus PBC group compared to the placebo plus PBC group. GRADE assessment of treatment-emergent AESIs suggests a low level of certainty that cemiplimab plus PBC results in little to no difference in harms of special interest compared to placebo plus PBC.
A sponsor-submitted ITC compared the efficacy of cemiplimab plus PBC with other Health Canada–approved treatments for first-line advanced or metastatic NSCLC, regardless of PD-L1 expression or histology. However, due to the small number of studies in the network, along with significant concerns related to clinical heterogeneity, no firm conclusions could be drawn about the efficacy and safety of cemiplimab plus PBC compared to pembrolizumab plus chemotherapy or nivolumab plus ipilimumab plus chemotherapy. Considering the consistency of the direction of the indirect results of cemiplimab plus PBC versus PBC in the ITC, with the direct and existing evidence in the form of the EMPOWER-Lung 3 trial (part 2), the indirect results can be considered supportive of the findings from the EMPOWER-Lung 3 trial (part 2).
Introduction
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of cemiplimab 350 mg every 3 weeks administered as an IV infusion in combination with PBC for the first-line treatment of adult patients with NSCLC whose tumours have no EGFR, ALK, or ROS1 aberrations and whose disease is:
locally advanced and patients are not candidates for surgical resection or definitive chemoradiation, or
metastatic.
Disease Background
The contents within this section have been informed by materials submitted by the sponsor and clinical expert input. The following have been summarized and validated by the CADTH review team.
Lung and bronchus cancer is the most frequently diagnosed cancer in Canada (excluding nonmelanoma skin cancers) and, in Canada, is the leading cause of cancer death.4 In Canada in 2022, an estimated 30,000 people were diagnosed with lung and bronchus cancer, representing approximately 13% of all new cancer cases, and 20,700 people died from lung cancer, representing 24% of all cancer deaths.5 In Canada, the overall 5-year net survival for lung cancer from 2015 to 2017 was estimated to be 19% for men and 26% for women.4 Based on 2022 Canadian estimates, on average, 82 people will be diagnosed and 57 people will die of lung and bronchus cancer every day.4 The risk of developing lung cancer increases with age. More than half of all newly diagnosed lung cancer cases occur in people aged 60 years or older.4 The most important risk factor for lung cancer is tobacco smoking, which is responsible for 72% of cases in Canada. Other known risk factors for lung cancer include second-hand smoke, radon, asbestos, occupational exposure to certain chemicals (such as arsenic), air pollution, positive family history, certain lung disease, radiation, weakened immune system, and beta carotene supplements in smokers.4 The most common signs and symptoms of lung cancer are cough, shortness of breath, chest pain, hemoptysis, wheezing, weight loss, fatigue, voice change, swollen lymph nodes, and difficulty swallowing.4
Lung cancers are histologically divided into small cell lung cancer, which accounts for almost 20% of cases, and NSCLC, which is found in almost 80% of cases.6 NSCLC is further categorized into 3 main subtypes: adenocarcinoma, which is the most diagnosed subtype; squamous cell carcinoma; and large cell carcinoma.6
Like most other cancers, lung cancers are classified as stage I, stage II, stage III, or stage 4, based on the extent of disease in the body at the time of diagnosis. This includes the size of the primary tumour and whether it has grown or spread into surrounding tissues or whether the cancer cells have spread to other parts of the body.7
The most important prognostic factor for lung cancer is the stage at diagnosis, although weight loss, performance status, sex, overall health, and genetic changes to the cancer cells are also important prognostic or predictive factors.8 Because the symptoms are often unnoticeable at early stages, most patients are being diagnosed at an advanced stage, resulting in a poor prognosis. Approximately half of all lung cancer cases in Canada are stage IV at diagnosis, at which point survival is extremely low.7 Median OS is poor in patients with metastatic NSCLC (stage IVA and stage IVB), ranging from 8 to 11 months; the 5-year net survival rate for patients with stage IV NSCLC is 5.2%.9 For patients with advanced NSCLC who are eligible for treatment, approximately 4% may die each week while waiting for therapy initiation.10
Several driver mutations have been identified in NSCLC. The most notable alterations are EGFR exon 19 deletion and exon 21 L858R mutation, ALK translocation, ROS1 rearrangement, and BRAF mutations. Tumours with these alterations are more common in never smokers (people who never smoked or who smoked fewer than 100 cigarettes in their lifetime), long time exsmokers (longer than 10 years), or light smokers (fewer than 15 pack-years). Characterizing tumours according to histological subtype and genetic composition has resulted in significant progress in the identification of response to certain drugs and personalized approaches in treating lung cancer.11 Targeted drugs that are active at these sites have led to a significant improvement in patient survival and QoL compared to conventional cytotoxic therapies. Clinical practice guidelines recommend routine testing for oncogenic drivers in NSCLC tumours to guide treatment strategies; consequently, molecular testing has become an essential part of managing NSCLC in clinical practice. Driver alterations affect a small proportion of patients with NSCLC.11 EGFR mutations are identified in about 10% to 30% of patients with nonsquamous NSCLC, while ALK and ROS1 rearrangements occur in about 2% to 5% and in about 1% to 4%, respectively, of nonsquamous NSCLC tumours. BRAF mutations are observed in 2% of patients with NSCLC.11
Immune checkpoint inhibitors have dramatically changed the landscape of NSCLC treatment, particularly in the metastatic setting, by targeting the PD-1 and/or PD-L1 immune checkpoint. PD-1 plays a vital role in inhibiting immune responses; the inhibition of PD-1 promotes an effective immune response against cancer cells. The expression of PD-L1 in malignant cells is also a biomarker for response to PD-1 and/or PD-L1 immune checkpoint inhibitors. PD-L1 immunohistochemistry (IHC), thus, is important in the selection of first-line therapy.11
Diagnosing lung cancer usually begins with a health history and physical exam, and typically includes a complete blood count, chest X-ray, CT scan, whole body PET scan, MRI, ultrasound, bone scan, biopsy, endoscopy, blood chemistry, sputum test, pulmonary function test, and heart function test.12 It is recommended that all targetable alterations in NSCLC be tested as part of a comprehensive panel at the time of diagnosis, and that comprehensive biomarker testing be performed upon development of resistance to targeted therapy.13
Standards of Therapy
Contents within this section have been informed by materials submitted by the sponsor and clinical expert input. The following have been summarized and validated by the CADTH review team.
The choice of treatment for NSCLC is determined primarily by the extent of disease, or disease stage, although patient-specific and tumour-specific factors should also be taken into consideration.14 Typically, patients with localized, early-stage (stage I or II), and resectable locally advanced NSCLC (some stage IIIA) are treated with surgical resection. In addition, adjuvant or neoadjuvant chemotherapy with or without radiation may be used with curative intent, depending on the stage of disease. Patients with advanced disease, including those with unresectable stage IIIB or IIIC NSCLC that have good perfomance status are eligible for concurrent or sequential chemotherapy and radiation and for consolidation treatment with durvalumab if there is no disease progression.14,15
For patients with unresectable locally advanced NSCLC (stage IIIB or IIIC) who are not candidates for definitive concurrent chemoradiation and for patients with metastatic NSCLC (stage IV) without actionable driver alterations, the primary treatment choice is systemic immunotherapy with or without chemotherapy, depending on PD-L1 expression status; surgery and radiation may still be used to palliate disease-related symptoms.14,16-18 Historically, chemotherapy was the only available systemic therapy option in this setting, and PBC regimens were considered the standard of care based on improvement in OS versus best supportive care.19 Platinum-based drugs (cisplatin or carboplatin) have been typically paired with cytotoxic drugs, such as vinorelbine, gemcitabine, pemetrexed, paclitaxel, and docetaxel.2 Although PBC has been shown to improve survival better than best supportive care, only 20% to 30% of patients have a response to therapy, with a median PFS of 3.5 to 5 months and a median OS of 8 to 12 months.20 Over the past decade, significant advances have been made in the treatment of advanced NSCLC due to an improved understanding and better detection of genomic alterations and biomarkers and the introduction of targeted therapies and immunotherapies.21 While chemotherapy remains an important component of systemic therapy for NSCLC, chemotherapy regimens alone have largely been replaced with molecularly targeted therapies and immunotherapy alone or in combination with chemotherapy. Anti–PD-1 and/or anti–PD-L1 antibodies as monotherapy or in combination with chemotherapy have now been adopted as standard first-line treatment options for patients with locally advanced NSCLC who are not candidates for surgical resection or definitive chemoradiation and for patients with metastatic NSCLC without oncogenic (e.g., EGFR, ALK, or ROS1) alterations.22
In Canada, patients whose disease has actionable driver alterations typically receive targeted therapy upfront, then combination chemotherapy for second-line treatment, and subsequently single-drug chemotherapy for third-line treatment if they maintain a good performance status.2 For patients with previously untreated locally advanced NSCLC (who are not candidates for surgical resection or definitive chemoradiation) and for patients with metastatic NSCLC without actionable oncogenic driver alterations whose tumours express PD-L1 in at least 50% of cells (as determined by a validated test), the current recommended first-line treatment options are typically pembrolizumab or cemiplimab monotherapy, although immunotherapy in combination with chemotherapy can still be an option.23 The clinical experts consulted by CADTH noted that in some cases, pembrolizumab plus chemotherapy would be considered for patients with high PD-L1-expression (PD-L1 ≥ 50%) NSCLC when disease burden is high and patients are young. Cemiplimab monotherapy is currently not funded for patients with high PD-L1 expression; however, it did receive a positive CADTH recommendation with conditions in June 2022, for the first-line treatment of patients with advanced NSCLC expressing PD-L1 (TPS ≥ 50%) and no actionable oncogenic driver alterations. For patients with any level of PD-L1 expression (including PD-L1 ≥ 50%), or if unknown, the current recommended treatment options are pembrolizumab plus PBC, nivolumab and/or ipilimumab plus abbreviated (2 cycles) PBC, or PBC if a the patient has a contraindication to immunotherapy.23
Drug Under Review
The key characteristics of cemiplimab and pembrolizumab are summarized in Table 3.
The cemiplimab for injection, 350 mg/7 mL (50 mg/mL), single-use vial for IV infusion is indicated for use in combination with PBC for the first‐line treatment of adult patients with NSCLC whose tumours have no EGFR, ALK, or ROS1 aberrations and whose disease is locally advanced and patients are not candidates for surgical resection or definitive chemoradiation or whose disease is metastatic NSCLC. The sponsor’s reimbursement request is the same as the approved Health Canada indication. The Notice of Compliance date is September 10, 2021.
Cemiplimab has been previously reviewed by CADTH for the first-line treatment of adult patients with NSCLC expressing PD-L1 (TPS ≥ 50%), determined by a validated test, with no EGFR, ALK, or ROS1 aberrations, who have locally advanced NSCLC and are not candidates for surgical resection or definitive chemoradiation, and for patients who have metastatic NSCLC. The final recommendation was reimbursed with conditions and issued in June 2022. Cemiplimab has also been reviewed by CADTH and received conditional positive recommendations for other therapeutic areas, including cutaneous squamous cell carcinoma and basal cell carcinoma.
Cemiplimab is a recombinant human immunoglobulin G4 monoclonal antibody that binds to PD-1 and blocks its interaction with its ligands (PD-L1 and PD-L2), countering PD-1–mediated inhibition of the immune response, including the antitumour immune response. Its mechanism of action is based on the binding of PD-L1 and PD-L2 to PD-1 on T-cells, which inhibits T-cell proliferation and cytokine production.
Table 3: Key Characteristics of Cemiplimab and Pembrolizumab
Characteristic | Cemiplimab | Pembrolizumab |
|---|---|---|
Mechanism of action | Inhibits T-cell proliferation and cytokine production | Inhibits the PD-1 receptor from binding to its ligands, which reactivates tumour-specific cytotoxic T lymphocytes in the tumour microenvironment |
Indicationa | In combination with PBC for the first‐line treatment of adult patients with NSCLC whose tumours have no EGFR, ALK, or ROS1 aberrations and whose disease is locally advanced and who are not candidates for surgical resection or definitive chemoradiation, or for patients with metastatic NSCLC | For the first-line treatment of adult patients with metastatic NSCLC or stage III disease who are not candidates for surgical resection or definitive chemoradiation, and who express PD-L1 (Tumour Proportion Score ≥ 1%), determined by a validated test, but who have no EGFR or ALK genomic tumour aberrations For the treatment of adult patients with metastatic nonsquamous NSCLC, in combination with pemetrexed and PBC, who have no EGFR or ALK genomic tumour aberrations and who have received no prior systemic chemotherapy treatment for metastatic NSCLC For the treatment of adult patients with metastatic squamous NSCLC, in combination with carboplatin and either paclitaxel or nab-paclitaxel, who have received no prior systemic chemotherapy treatment for metastatic NSCLC |
Route of administration | IV | IV |
Recommended dose | 350 mg every 3 weeks, administered by IV infusion over 30 minutes | 200 mg every 3 weeks or 400 mg every 6 weeks, administered by IV infusion over 30 minutes |
Serious adverse effects or safety issues | Contraindicated in the case of hypersensitivity; should be administered under the supervision of health care practitioners experienced in the treatment of cancer Immune‐mediated adverse reactions, such as pneumonitis, colitis, hepatitis, endocrinopathies, thyroid disorders, hypophysitis, nephritis, skin reactions, meningitis, myositis, encephalomyelitis, and myocarditis Adrenal insufficiency and type 1 diabetes | Contraindicated in the case of hypersensitivity; should be administered under the supervision of physicians experienced in the treatment of cancer Immune-mediated adverse reactions, such as pneumonitis, colitis, hepatitis, endocrinopathies, thyroid disorders, hypophysitis, nephritis, skin reactions, uveitis, arthritis, myositis, encephalitis, sarcoidosis, myasthenic syndrome and/or myasthenia gravis, vasculitis, Guillain-Barré syndrome, hemolytic anemia, pancreatitis, myelitis, and hypoparathyroidism Adrenal insufficiency and type 1 diabetes |
Other | Inhibition of T-cell proliferation and cytokine production | Inhibits the PD-1 receptor from binding to its ligands, which reactivates tumour-specific cytotoxic T lymphocytes in the tumour microenvironment |
NSCLC = non–small cell lung cancer; PBC = platinum-based chemotherapy.
aHealth Canada–approved indication.
Sources: Cemiplimab product monograph, pembrolizumab product monograph.
Stakeholder Perspectives
Patient Group Input
This section was prepared by the CADTH review team based on the input provided by patient groups. The full original patient input(s) received by CADTH have been included in the Stakeholder section of this report.
CADTH received input from 3 patient groups: CCSN, LCC, and LHF.
CCSN is a national network of patients, families, community partners, funders, and sponsors who take action to promote standard of care and support patients with cancer. LCC is a national charity and a member of the Global Lung Cancer Coalition and the only organization focusing solely on lung cancer in Canada, focusing on increasing awareness, providing support to patients and caregivers, research, and advocate for access to the best practices. LHF is a charity foundation that provides support for patients with lung disease, their caregivers, and health care providers, and invests in lung research and advocates for improved policies in lung health.
CCSN conducted a survey and gathered information from 1 caregiver and 9 patients in Canada. Two of the patients had experience with cemiplimab. According to CCSN, at the time of diagnosis, most of the patients had metastatic-stage disease. Respondents reported that the most important aspects of their lives that they needed to get under control are survival, tumour, anxiety, emotions, weight loss, and shortness of breath. Current treatments for patients are radiation, surgical therapy, targeted therapy, immunotherapy, chemotherapy, and lenvatinib, or participation in clinical trials. In terms of accessibility of current treatments, most of the patients reported no issues; others reported limited availability, travel cost to have access, and long waiting time as issues.
CCSN stated that the issues a caregiver of a patient with lung cancer noted encountering are fatigue, management of side effects, emotional drain, anxiety and/or depression, hours spent in medical appointments, monetary concerns, absence from work, travel expenses, lifestyle changes, an inability to plan, anger, and feelings of helplessness. CCSN also reported that the caregiver rated the ability of current treatments to address the needs of lung cancer patients as good on a 4-point rating scale, ranging from excellent to very poor.
Symptoms that affect patients’ QoL were reported as fatigue, wheezing, chest pain, unexplained weight loss, loss of appetite, trouble swallowing, coughing up blood, persistent cough, trouble breathing, hoarseness, depression, and mood change. The patient respondents reported that the side effects of currently available treatments include fatigue, nausea, constipation, breathing problems, infection, pain, hair loss, bleeding, vomiting, and impaired sexual functioning. They also noted that rest, medication, meditation, exercise, and diet helped them to tolerate the side effects.
According to CCSN, respondents expected the new drug to improve QoL, delay symptom onset, stop disease progression, reduce side effects, and provide a new treatment option, ease of use, faster access, prolonged life, and a cure.
The 2 respondents who had experience with cemiplimab highlighted fatigue, anemia, hyperglycemia, diarrhea, nausea, and constipation as adverse effects. When asked whether they would recommend cemiplimab to other qualified patients, 1 of the 2 respondents rated the idea as a 5 on a scale of 1 to 5, and the other rated it a 3. In terms of comparison of cemiplimab with other therapies, most of the respondents found cemiplimab much better for symptom management, side effects, and ease of use, while others found it as little or no difference for disease progression.
LCC reported 4 patients who received cemiplimab, but only 2 of them were patients with lung cancer (1 from Canada and 1 from the UK), who were part of the clinical trial for cemiplimab. LCC highlighted delays in the diagnosis of lung cancer as a disease experience. This patient group noted that the flat-dosing option for cemiplimab fills an unmet need for those in rural or remote geographical regions because patients can receive treatment at a hospital close to home, which improves patient compliance and saves travel times. LCC noted that 1 patient experienced side effects, such nausea, a struggle with self-image after hair loss, and being unable to eat with chemotherapy, but not with cemiplimab. LCC stated that the desirable outcomes of treatment are manageable side effects, improved NSCLC symptoms and QoL, long-term remission, delayed disease progression, and improved survival. According to LCC, patients who received cemiplimab experienced positive results, with fewer disease symptoms, better QoL, and no or mild side effects, including itchy skin, fatigue, and mild joint pain.
LHF conducted a survey and collected information from 15 patients with lung cancer and 1 caregiver. None of them had experience with the drug under review. The respondents noted that their symptoms were shortness of breath (80%), fatigue (60%), depression (25%), cough (30%), difficulty fighting infection (21%), and chest tightness (14%). Weight loss, diminished appetite, low mood, and challenges with physical and emotional intimacy were also noted by a few respondents. Some respondents stated that these symptoms affected their daily life activities, as well as relationships with family and friends.
According to LHF, caregivers of patients with lung cancer are also affected in terms of ability to work and taking time off work to provide support to their patient, relationship, emotional well-being, and independence.
LHF stated that the treatments tried by the respondents included surgery, radiation, chemotherapy, targeted therapy, and immunotherapy. The medications tried included metoclopramide, memantine, cisplatin, docetaxel, gefitinib, entrectinib, alectinib, brigatinib, osimertinib, nivolumab, and ipilimumab. The benefits of currently available treatments are that they reduce cough, reduce shortness of breath, increase participation in daily activities, increase the ability to exercise, prolong life, delay disease progression, and reduce the severity of other disease-related symptoms. Some of the side effects reported by respondents were fatigue, nausea, vomiting, mood changes, diminished appetite, weight loss, hair loss, anemia, neuropathy, skin changes, and tissue scarring. Side effects from chemotherapy severely impact the patients’ QoL, ability to work and in some cases, the ability to perform activities of daily living. Regarding challenges with access to treatment, according to LHF, respondents struggled to navigate the health care system, and some were not clear where to go for information or support. Other issues are time spent to attend medical appointments, travel cost, and high cost of some medications.
The survey respondents stated that the key important treatment outcomes are delay of progression, minimal side effects, effectiveness, maintaining QoL, and more treatment options.
LHF noted that the majority of the respondents who went through biomarker testing indicated that they wished it had been done sooner. Depending on the stage of the cancer diagnosis, biomarker testing is not always an option at diagnosis.
Clinician Input
Input From Clinical Experts Consulted by CADTH
All CADTH review teams include at least 1 clinical specialist with expertise in the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). The following input was provided by 2 clinical specialists with expertise in the diagnosis and management of NSCLC.
Unmet Needs
The overarching goal in NSCLC management is to improve patient outcomes, which encompasses both extending OS and enhancing QoL by minimizing treatment-related toxicity. While there have been improvements in outcomes because of the introduction of new systemic therapies, including targeted therapies and immunotherapies, not all patients benefit from these treatments. The heterogeneity of NSCLC, with its various subtypes and molecular profiles, means that some patients may not respond to available treatments or may develop a lack of response over time, leading to disease progression. The current mortality rate for NSCLC remains high, so there is a need for therapies that can offer a more durable response and, ultimately, improve survival rates. In addition, the toxicity associated with systemic therapies for NSCLC is a significant concern. Adverse effects can range from mild to severe and life-threatening. These side effects can impact a patient's QoL and may limit the ability to continue with the optimal treatment regimen. Therefore, there is a need for treatments that can maintain or improve efficacy while reducing the incidence and severity of side effects.
Place in Therapy
Cemiplimab in combination with PBC would be an alternative to the current first-line treatments available, which include other PD-1 and/or PD-L1 inhibitors (such as pembrolizumab and nivolumab plus ipilimumab), often in combination with chemotherapy. The mechanism of action of cemiplimab is similar to these existing therapies, and it would likely be considered among the options for clinicians and patients deciding on a treatment strategy. Cemiplimab plus PBC may be a valuable addition to the treatment landscape, but it may not drastically change the current standard of care; rather, it would expand the options available to patients who are not suitable candidates for other treatments or who may not respond to existing therapies.
Patient Population
Based on the Health Canada indication, the patient population eligible for treatment with cemiplimab in combination with PBC can be characterized by several specific criteria. These include adult patients with advanced or metastatic NSCLC who have not previously received systemic therapy for their advanced disease. The patients must have tumours without known driver mutations, such as EGFR, ALK, or ROS1, as these genetic aberrations may respond differently to targeted therapies. Additionally, the tumours must be tested for PD-L1 expression, although there is no strict cut-off for PD-L1 positivity to be eligible for this treatment. According to the clinical experts, the prevalence of advanced or metastatic NSCLC is significant, as many patients present with or progress to this stage of the disease. Clinical trials in oncology tend to exclude patients with certain comorbidities or a poor performance status (e.g., ECOG PS > 1). However, the clinical experts expect that patients with an ECOG PS of 2 may also benefit from the treatment. The clinical experts suggest that patients with a range of PD-L1 expression levels could benefit from treatment with cemiplimab plus PBC. However, the greatest need for new treatments often lies with those who have a high disease burden and are unlikely to respond to other treatments due to tolerability, comorbidities, or other factors. Patients most likely to demonstrate a clinically meaningful response to treatment can sometimes be identified based on objective characteristics, such as PD-L1 expression level, tumour histology, or performance status. However, the identification of these patients in clinical practice requires comprehensive diagnostic work, including laboratory tests (such as PD-L1 immunohistochemistry) and assessments of performance status. Patients least suitable for treatment with cemiplimab plus PBC may include those with significant comorbidities that preclude the use of chemotherapy, those with a performance status too poor to tolerate treatment, and those with contraindications to the drugs involved.
Assessing the Response Treatment
The overall aim of treatment is to extend OS and improve QoL. Assessment of response is done through clinical assessment during follow-up visits and radiological imaging.
The clinical experts suggest that response to treatment should be assessed both clinically, with regular assessment by the treating physician, and radiologically, with imaging studies done on a 3-month internal. A positive treatment response would typically be stable disease or any degree of tumour shrinkage, indicating that the patient is deriving benefit from the treatment. The outcomes used to determine whether a patient is responding to treatment in clinical practice include a combination of radiological assessment, clinical examination, and consideration of PROs and symptoms. A clinically meaningful response to treatment would be 1 that extends survival, improves or maintains QoL, and/or results in tumour shrinkage or disease stabilization. The frequency of treatment response assessment should be individualized to the patient's clinical status, the specific treatment regimen, and the health care setting.
Discontinuing Treatment
The decision to discontinue cemiplimab plus PBC should be based on a comprehensive assessment of disease progression, unacceptable toxicity, patient preference, and overall treatment goals.
Prescribing Considerations
Treatment with cemiplimab plus PBC can be prescribed and managed in outpatient clinics under the supervision of a medical oncologist.
Clinician Group Input
This section was prepared by the CADTH review team based on the input provided by clinician groups. The full original clinician group inputs received by CADTH have been included in the Stakeholder section of this report.
CADTH received input from 2 clinician groups, LCC-MAC and the OH-CCO Lung Cancer Drug Advisory Committee. In total, 12 clinicians from LCC-MAC and 3 clinicians from the OH-CCO Lung Cancer Drug Advisory Committee provided input to the submissions. The clinician groups agreed that the first line of treatment is chemotherapy and immunotherapy, or pembrolizumab alone in patients with a PD-L1 status greater than 50%. For patients not eligible for immunotherapy, platinum doublet chemotherapy remains an option. There was agreement among all clinicians that improvements in PFS, OS, and QoL are treatment goals. LCC-MAC noted the benefits of cemiplimab having a flat dose of 350 mg, without a weight-based option. This clinician group felt that this would provide significant advantages in delivering treatment closer to home for many patients with lung cancer because vial sharing would not be required. Both clinician groups agreed that in terms of place in therapy, cemiplimab in combination with PBC would be an alternative first-line treatment (i.e., combination pembrolizumab plus chemotherapy, and 2 cycles of platinum doublet plus ipilimumab plus nivolumab).
Other than incurable NSCLC, first-line therapy, and no EGFR, ALK, or ROS1 alterations, the clinical expert consulted by CADTH noted that eligibility criteria should include any PD-L1 expression and an ECOG PS of 0 to 2; the LCC-MAC added determination of PD-L1 status, and stated that patients in rural areas will benefit more from cemiplimab because no vial sharing would be required.
Clinical and radiological assessments were noted as the best ways to determine whether a patient is responding to the treatment, while disease progression, toxicity, patient preference, and certain AEs were factors to be considered when deciding to discontinue treatment.
It was agreed that outpatient clinics under the supervision of a medical oncologist are the appropriate setting for treatment with cemiplimab in combination with platinum‐based chemotherapy. LCC-MAC added that in many jurisdictions across Canada, particularly in more remote or rural communities, medical oncologists work in partnership with general practitioners in oncology to comanage patients.
Drug Program Input
The drug programs provide input on each drug being reviewed through CADTH’s reimbursement review processes by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CADTH are summarized in Table 4.
Table 4: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Relevant comparators | |
The EMPOWER-Lung 3 trial compared cemiplimab plus PBC vs. PBC alone in patients with advanced NSCLC and no EGFR, ALK, or ROS1 driver mutations, irrespective of the PD-L1 status. More appropriate comparators include single-drug pembrolizumab (if PD-L1 expression is ≥ 50%); ipilimumab plus nivolumab plus chemotherapy; pembrolizumab plus pemetrexed plus platinum (nonsquamous only); and pembrolizumab plus nonpemetrexed platinum (squamous). How does cemiplimab plus chemotherapy compare to those immunotherapies ± chemotherapy regimens? | No direct evidence from clinical trials currently exists to compare cemiplimab plus PBC to other immunotherapies given as monotherapy or in combination with chemotherapy. Cross-trial comparisons are limited by the small sample size and short follow-up duration of the EMPOWER-Lung 3 study. Overall, the clinical experts consulted by CADTH anticipate that 2-year OS and PFS with cemiplimab plus PBC are likely comparable to other immunotherapies used in combination with chemotherapy. Furthermore, the clinical experts consulted by CADTH anticipate that the toxicity profile of cemiplimab plus chemotherapy will be similar to that of pembrolizumab plus chemotherapy. |
Considerations for initiation of therapy | |
The trial included never smokers, patients with treated brain metastases, and those with an ECOG PS of ≤ 1. Should cemiplimab plus chemotherapy be considered for patients with an ECOG PS of > 1? | Patients with an ECOG PS of 2 are likely to benefit from this treatment and should be considered. |
Are patients who have received previous adjuvant or neoadjuvant immunotherapy eligible for cemiplimab plus chemotherapy and, if so, is there a minimum disease-free interval that must be met? | Patients with NSCLC who have previously received adjuvant or neoadjuvant immunotherapy may be considered for subsequent treatment with cemiplimab in combination with chemotherapy. The optimal disease-free interval remains a subject of clinical judgment in the absence of robust evidence. The decision should be individualized, taking into account the duration and type of prior immunotherapy, the patient's disease course, and the potential benefits and risks of re-treatment with immunotherapy plus chemotherapy combinations. |
If a patient receives 108 weeks of cemiplimab and subsequently relapses, is there evidence to support re-treatment and, if so, would there be a maximum duration? | The clinical experts suggest aligning re-treatment eligibility for cemiplimab plus PBC with other reimbursed combinations of immunotherapy and chemotherapy combinations. |
Considerations for discontinuation of therapy | |
If a patient discontinues treatment before the completion of 108 weeks due to toxicity, but without relapse, could the patient restart and be treated to a maximum of 108 weeks? | Patients were allowed to resume therapy after the resolution of toxicity in the EMPOWER-Lung 3 trial (part 2). The clinical experts agreed that these trial criteria were applicable to clinical practice. |
Considerations for prescribing of therapy | |
Although CADTH had issued a positive recommendation, single-drug cemiplimab remains unfunded because a national agreement could not be reached. The CADTH assessment needs to account for the initiation of this regimen as a combination regimen. | Comment from the drug programs to inform pERC deliberations. |
Funding algorithm | |
Cemiplimab plus chemotherapy would be an alternative treatment option to existing immunotherapy ± chemotherapy regimens that are already funded. Under what conditions would cemiplimab plus chemotherapy be preferred over pembrolizumab ± chemotherapy, or over nivolumab plus ipilimumab plus chemotherapy? | Cemiplimab plus PBC may be a valuable addition to the treatment landscape, but it may not drastically change the current standard of care; rather, it could expand the options available to patients who are not suitable candidates for other treatments or who may not respond to existing therapies in the advanced setting. |
System and economic issues | |
In certain jurisdictions that do not fund drug wastage, cemiplimab may be a preferred option, given the flat dosing. The cost of cemiplimab plus chemotherapy should not exceed the drug program cost of existing funded immunotherapy plus chemotherapy regimens. | Comment from the drug programs to inform pERC deliberations. |
Confidential prices are in place for pembrolizumab and for ipilimumab plus nivolumab. | Comment from the drug programs to inform pERC deliberations. |
ECOG PS = Eastern Cooperative Oncology Group Performance Status; NSCLC = non–small cell lung cancer; PBC = platinum-based chemotherapy; pERC = CADTH pan-Canadian Oncology Drug Review Expert Review Committee.
Clinical Evidence
The objective of CADTH’s Clinical Review Report is to review and critically appraise the clinical evidence submitted by the sponsor on the beneficial and harmful effects of cemiplimab 350 mg every 3 weeks used in combination with PBC for the first-line treatment of patients with NSCLC whose tumours have no EGFR, ALK, or ROS1 aberrations; for patients who have locally advanced NSCLC and are not candidates for surgical resection or definitive chemoradiation; and for patients who have metastatic NSCLC. The focus will be placed on comparing cemiplimab with PBC to relevant comparators and identifying gaps in the current evidence.
A summary of the clinical evidence included by the sponsor in the review of cemiplimab with PBC is presented in 4 sections, with CADTH’s critical appraisal of the evidence included at the end of each section. The first section, the Systematic Review, includes pivotal studies and RCTs that were selected according to the sponsor’s systematic review protocol. CADTH’s assessment of the certainty of the evidence in this first section, using the GRADE approach, follows the critical appraisal of the evidence. The third section includes sponsor-submitted indirect evidence. The sponsor did not include long-term extension studies (second section) or additional studies addressing important gaps in the pivotal and RCT evidence (fourth section).
Included Studies
Clinical evidence from the following is included in the CADTH review and appraised:
1 pivotal RCT identified in the systematic review
1 ITC.
Systematic Review
The contents within this section have been informed by materials submitted by the sponsor. The following have been summarized and validated by the CADTH review team.
Description of Studies
Characteristics of the included study are summarized in Table 5.
Table 5: Details of the Study Included in the Systematic Review
Detail | EMPOWER-Lung 3 (part 2) |
|---|---|
Designs and populations | |
Study design | Double-blind, placebo-controlled, phase III RCT (part 2) |
Locations | 74 sites in 10 countries (China, Georgia, Greece, Malaysia, Poland, Romania, Russia, Thailand, Turkey, and Ukraine) |
Patient enrolment dates | Start date: May 31, 2019 (part 2) End date: Ongoing |
Randomized (N) | Total N = 466 n = 312 for cemiplimab + PBC n = 154 for placebo + PBC |
Inclusion criteriaa |
|
Exclusion criteria |
|
Drugs | |
Intervention | Cemiplimab 350 mg every 3 weeks + PBCb every 3 weeks for 4 cycles |
Comparator | Placebo every 3 weeks + PBCb every 3 weeks for 4 cycles |
Study duration | |
Screening phase | 28 days |
Treatment phase | 108 weeks |
Follow-up phase | 7 months |
Outcomes | |
Primary end point | OS at 2 prespecified interim analyses (i.e., at 146 events [50% of total OS events] and at 204 events [70% of total OS events]), and final OS analysis [291 events]) |
Secondary and exploratory end points | Key secondary:
Other secondary:
Exploratory:
|
Publication status | |
Publications | Gogishvili et al. (2022);24 Kalinka-Warzocha et al. (2022);25 Makharadze et al. (2021);26 Gogishvili et al. (2021);27 Gogishivili et al. (2019);28 Rizvi et al. (2018);29 ClinicalTrials.gov (NCT03409614);30 ICTRP (No. 12268960/EMPOWER-Lung 3); and EU Clinical Trials Register (EMPOWER-Lung 3 part 2); Makharadze et al. (2023);31 Makharadze et al. (2023);32 Makharadze et al. (2023);33 Kalinka et al. (2023);34 Gogishvili et al. (2022);35 Gandara et al. (2023);36 Baramidze et al. (2023).37 |
AE = adverse event; BOR = best overall response; CNS = central nervous system; DOR = duration of response; DLT = dose-limiting toxicity; ECOG PS = European Cooperative Oncology Group Performance Score; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; EORTC QLQ-LC13 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire-Lung Cancer 13; HBV = hepatitis B virus; HCV = hepatitis C virus; ICTRP = International Clinical Trials Registry; NSCLC = non–small cell lung cancer; ORR = objective response rate; OS = overall survival; PBC = platinum-based chemotherapy; PFS = progression-free survival; QoL = quality of life; RCT = randomized controlled trial; RECIST 1.1 = Response Evaluation Criteria in Solid Tumours Version 1.1; SAE = serious adverse event; TEAE = treatment-emergent adverse event.
aThe number of patients with squamous histology was capped at 50%. PD-L1 subgroups were also capped to ensure a homogenous representation of all PD-L1 levels. PD-L1 levels were capped as follows: at least 30% but no more than 40% of patients enrolled must have had tumours that express PD-L1 in ≥ 50% of tumour cells; enrolment of patients whose tumours express PD-L1 in < 1% of tumour cells was capped at 30%; and enrolment of patients with tumours that express PD-L1 in < 50% of tumour cells was capped at 70%.
bPlatinum doublet chemotherapy was investigator’s choice of histology-specific chemotherapy options, including paclitaxel plus carboplatin, paclitaxel plus cisplatin, pemetrexed plus carboplatin, and pemetrexed plus cisplatin. For patients with nonsquamous NSCLC for whom the investigator chose a pemetrexed-containing doublet, pemetrexed maintenance was mandatory.
cPFS and ORR were key secondary end points.
Sources: EMPOWER-Lung 3 (part 2) Clinical Study Report;3 Gogishvili et al. (2022).24 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
The EMPOWER-Lung 3 trial is a 2-part, global, double-blind, randomized, placebo-controlled, phase III trial investigating the first-line treatment of patients with locally advanced or metastatic, squamous, or nonsquamous NSCLC with any PD-L1 expression level. There were no sites in Canada. Part 1 of the trial compared the efficacy and safety of cemiplimab plus an abbreviated course of chemotherapy plus ipilimumab or cemiplimab plus PBC versus PBC in patients whose tumours express PD-L1 in less than 50% of tumour cells (measured using a PD-L1 IHC assay). Part 2 compared the efficacy and safety of cemiplimab plus PBC versus placebo plus PBC in patients, irrespective of PD-L1 expression level. Part 1 and part 2 are considered separate studies, with separate randomization schemes, inclusion criteria, and visit and/or event schedules. Patients enrolled in part 1 did not contribute to the analysis in part 2, and vice versa.
Only results from part 2 of the EMPOWER-Lung 3 trial are reported in this systematic review. Results are also reported for 2 data cut-off dates. The first data cut-off date, June 14, 2021, represents a median duration of follow-up of 16.4 months and corresponds with the prespecified second interim analysis, which was scheduled to occur when approximately 204 deaths (70% of total OS events) were observed. An IDMC reviewed the results based on a Lan-DeMets approach to the O’Brien-Flemming alpha-spending function and concluded that statistical significance was demonstrated for OS.24 The IDMC recommended that the study be unblinded, which was accepted by the sponsor, thereby concluding the study and designating these data as the primary analysis.24 The second data cut-off date, June 14, 2022, represents approximately 2 years of follow-up (median duration of 28.4 months) and includes the final protocol-specified OS results.31
The primary objective of part 2 was to compare OS in patients treated with cemiplimab plus PBC versus placebo plus PBC for the first-line treatment of advanced squamous or nonsquamous NSCLC, irrespective of PD-L1 expression level. The key secondary objective was to compare PFS and ORR for cemiplimab plus PBC versus placebo plus PBC in the same patient population. Part 2 of the trial included 3 periods — screening, treatment, and follow-up — as illustrated in Figure 1. Patients were randomly assigned in a 2:1 ratio by an interactive web response system to either cemiplimab 350 mg every 3 weeks or placebo every 3 weeks in combination with 4 cycles of PBC. Randomization was stratified by histology (nonsquamous versus squamous) and PD-L1 expression level (< 1% versus 1% to < 49% versus ≥ 50%). Patients with squamous NSCLC were capped at 50% of the total sample size. At least 30% but no more than 40% of enrolled patients had to have tumours that expressed PD-L1 in at least 50% of tumour cells. Enrolment of patients whose tumours expressed PD-L1 in less than 1% of tumour cells was capped at 30%, and those with PD-L1 in less than 50% of tumour cells was capped at 70%. This approach was adopted to mirror the natural distribution of PD-L1 expression levels historically seen in patients with NSCLC.
Patients were treated for a maximum of 108 weeks or until disease progression or unacceptable toxicity. Dose reductions of cemiplimab were not permitted. Pemetrexed maintenance therapy was mandatory for patients with nonsquamous histology who received a pemetrexed-containing regimen. After completion of the treatment period, patients entered the follow-up period and those in the cemiplimab treatment arm who experienced RECIST 1.138–defined progressive disease on anti–PD-L1 antibody therapy could continue treatment if the investigator judged the patient to be experiencing clinical benefit and if the patient had not completed the 108-week treatment period. Alternatively, patients in either study arm who progressed could opt to initiate a new anticancer treatment, another clinical trial, or best supportive care.
Figure 1: The EMPOWER-Lung 3 Study Design
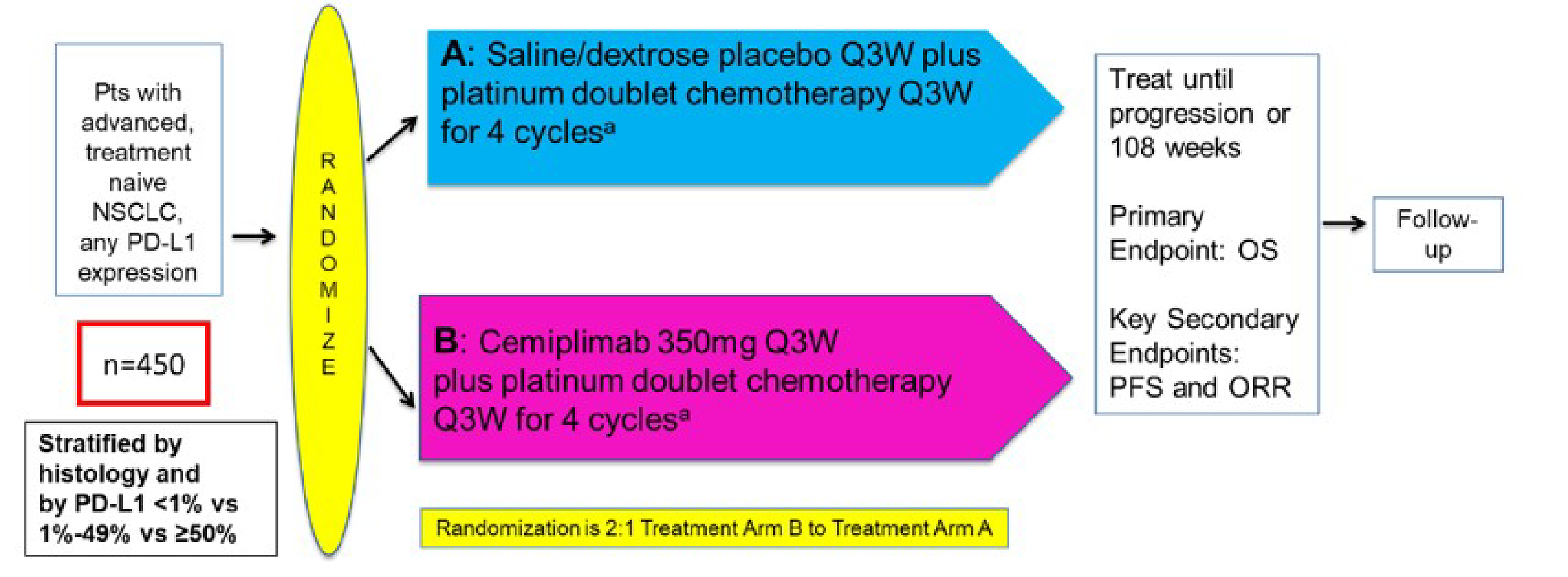
NSCLC = non–small cell lung cancer; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; Pts = patients; Q3W = every 3 weeks.
Note: The actual number of patients randomized to study treatment was 466.
Source: EMPOWER-Lung 3 (part 2) Clinical Study Report.3
Populations
Inclusion and Exclusion Criteria
Detailed key inclusion and exclusion criteria are provided in Table 5. Enrolled adults were diagnosed with cytologically or histologically documented squamous or nonsquamous advanced NSCLC and had received no prior systemic treatment for metastatic NSCLC. Patients who received adjuvant or neoadjuvant PBC and developed recurrent or metastatic disease more than 6 months after completing therapy were also eligible. Patients were eligible for enrolment irrespective of PD-L1 expression status, although enrolment was capped based on PD-L1 expression level, as previously described. To confirm patient eligibility, a central commercial laboratory was used to analyze EGFR, ALK, and ROS1 aberrations in tumour samples using an analytically validated IHC assay. Patients with EGFR, ALK, or ROS1 aberrations were excluded because the current standard of care is targeted therapy directed at the specific aberration. Patients with evidence of brain metastases at screening could be enrolled, provided that the metastases were adequately treated and patients had neurologically returned to baseline for at least 2 weeks before randomization. Similarly, patients with controlled hepatitis B virus, hepatitis C virus, or HIV infections could also be enrolled, and screening for these infections was not mandated. Patients with encephalitis, meningitis, or uncontrolled seizures in the year before enrolment, or with a history of interstitial lung disease or with active, noninfective pneumonitis or ongoing and/or recent evidence of significant autoimmune disease requiring systemic immunosuppressive therapy were excluded.
Interventions
The main study intervention was cemiplimab at a fixed dose of 350 mg or placebo (i.e., saline and/or dextrose solution) administered as a 30-minute IV infusion in combination with PBC given every 3 weeks for 4 cycles. When administered in combination with PBC, the chemotherapy drugs were infused first, followed by cemiplimab or placebo on the same day. Treatment continued for up to 108 weeks unless a patient experienced disease progression or unacceptable toxicity. Patients in the cemiplimab treatment arm who experienced progressive disease could continue treatment if the investigator judged the patient to be experiencing clinical benefit and if the patient had not completed the 108-week treatment period. Alternatively, patients in either study arm who progressed could opt to initiate a new anticancer treatment, another clinical trial, or best supportive care.
The choice of PBC was 1 of the regimens described in Table 6. The investigator could choose any of the 4 regimens, provided it was consistent with the local standard of care. The assignment of the PBC regimen was made before randomization. A treatment cycle was defined as 21 days (or 3 weeks).
Dose modifications of cemiplimab or placebo were not allowed in the study. Discontinuation was performed according to guidelines defined in the protocol. The criteria for restarting treatment included the resolution of toxicity to grade 0 to grade 1 or to baseline levels. The dose and schedule upon restarting remained the same. If the toxicity did not resolve within 84 days of the last infusion, permanent discontinuation would be considered, especially for any severe or life-threatening event.
Concomitant medications deemed necessary for a patient's welfare and not expected to affect the evaluation of cemiplimab could be administered at the investigator's discretion. Systemic corticosteroids, such as hydrocortisone, prednisone, prednisolone, and dexamethasone, were generally not recommended during the study, except in life-threatening emergencies or to treat immune-related AEs. However, physiologic replacement doses of systemic corticosteroids were allowed, even if they exceed 10 mg/day of prednisone equivalents. Short-term corticosteroid use was permissible for prophylaxis (e.g., contrast dye allergy) or to treat nonautoimmune conditions (e.g., delayed-type hypersensitivity reactions). Additionally, treatments for bone metastases, like bisphosphonates or denosumab, were permitted within the study. Pemetrexed maintenance therapy that followed local prescribing information and practice guidelines was also allowed.
Outcomes
A list of efficacy end points assessed in this Clinical Review Report is provided in Table 7, followed by descriptions of the outcome measures. Summarized end points are based on outcomes included in the sponsor’s Summary of Clinical Evidence, as well as any outcomes identified as important to this review by the clinical experts consulted by CADTH and stakeholder input from patient and clinician groups and public drug plans. Using the same considerations, the CADTH review team selected end points that were considered to be most relevant to inform CADTH’s expert committee deliberations and finalized this list of end points in consultation with members of the expert committee. All summarized efficacy end points were assessed using the GRADE approach. Select notable harms outcomes considered important to CADTH’s expert committee deliberations were also assessed using the GRADE approach.
Table 6: The EMPOWER-Lung 3 Trial (Part 2) — Platinum-Based Doublet Chemotherapy Regimens
Option | Chemotherapy regimen | Dosing frequency | Maintenance therapy |
|---|---|---|---|
1 | Paclitaxel 200 mg/m2 IV plus carboplatin AUC of 5 or 6 mg/mL per minute IV | Day 1 and every 21 days thereafter for 4 cycles Dose for carboplatin calculated using the Calvert formula | No maintenance therapy |
2 | Paclitaxel 200 mg/m2 IV plus cisplatin 75 mg/m2 IV | Day 1 and every 21 days thereafter for 4 cycles | |
3 | Pemetrexed 500 mg/m2 IV plus carboplatin AUC of 5 or 6 mg/mL per minute IV | Day 1 and every 21 days thereafter for 4 cycles Dose for carboplatin calculated using the Calvert formula | Mandatory pemetrexed maintenance 500 mg/m2 IV on day and 1 every 21 days thereafter; pemetrexed maintenance was administered according to local prescribing information and practice guidelines |
4 | Pemetrexed 500 mg/m2 IV plus cisplatin 75 mg/m2 IV | Day 1 and every 21 days thereafter for 4 cycles |
AUC = area under the curve.
Source: EMPOWER-Lung 3 (part 2) Clinical Study Report.3
Table 7: Outcomes Summarized From the Study Included in the GRADE Assessment
Outcome measure | Time point | EMPOWER-Lung 3 |
|---|---|---|
OS, Kaplan-Meier survival probability | 12 months | OS was the primary end pointa |
OS, Kaplan-Meier survival probability | 24 months | |
OS, Kaplan-Meier survival probability | 36 months | |
PFS, Kaplan-Meier survival probability | 24 monthsb | PFS was a key secondary end pointa |
Objective response rate | Up to 108 weeks | ORR was a key secondary end pointa |
EORTC QLQ-C30 | Up to 108 weeksc | Secondary end point |
Patients with any treatment-emergent adverse events of special interest | Up to 108 weeks | Safety outcome |
EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; GRADE = Grading of Recommendations Assessment, Development and Evaluation; OS = overall survival; PFS = progression-free survival.
aStatistical testing for these end points was adjusted for multiple comparisons (e.g., hierarchal testing).
bRadiographic tumour assessments were conducted every 9 weeks starting at week 9 during year 1 and then every 12 weeks starting at week 55 during year 2.
cMeasured at the beginning of each treatment cycle for the first 6 doses and then at the start of every 3 cycles and at the end of treatment, with the latest potential assessment 7 to 37 days after the last study treatment.
Source: EMPOWER-Lung 3 (part 2) Clinical Study Report.3 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Overall Survival
The primary outcome was OS, which was defined as the time from randomization to the date of death due to any cause. All deaths due to any cause occurring on or before the cut-off date in the full analysis set (FAS) were used in the OS analysis. A patient who was not known to have died or who was lost to follow-up at the time of the analysis cut-off date was censored at the last date that the patient was known to be alive. OS analyses at 12 months, 18 months, and 24 months provided the OS rate defined for the primary outcome at the designated time points. The clinical experts agreed with the position of the American Society of Clinical Oncology, that an 8% change in OS at 12 months can be considered clinically meaningful.39
Progression-Free Survival
Median time for PFS was a key secondary outcome assessed using the FAS population. PFS was defined as the time from randomization of a patient into the study to the date of the first documented progression of the disease or death due to any cause, whichever occurs first. Assessment of PFS employed RECIST 1.1.38 Progression of disease, according to RECIST 1.1, is characterized by at least a 20% increase in the sum of the diameters of target lesions, taking as reference the smallest on-study sum (this includes the baseline sum, if that is the smallest on study). In addition to the relative increase, there must also be an absolute increase of at least 5 mm. Furthermore, the appearance of 1 or more new lesions is also considered progression. The assessment of PFS is conducted by an IRC, which reviews imaging and clinical data to determine the time point of progression or death. For patients who did not have a documented date of disease progression or death at the time of the analysis, their data were censored at the last date they were known to be alive and without progression. The clinical experts consulted on this review did not identify a clinically meaningful threshold for the probability of PFS.
Objective Response Rate
ORR was a key secondary outcome, defined as the number of patients with a best overall response (best response recorded from the start of treatment until disease progression or recurrence, per RECIST 1.1) of a confirmed complete response (CR) or partial response divided by the number of patients in the FAS population. A CR is characterized by the disappearance of all target lesions, with no new lesions emerging, and the normalization of tumour marker levels, if applicable. A partial response is defined as at least a 30% decrease in the sum of the diameters of target lesions, taking as reference the baseline sum diameters, without the appearance of new lesions. Patients without baseline tumour assessment or with either unknown or missing best objective response were included in the denominator and were counted as nonresponders. The clinical experts consulted for this review did not identify a clinically meaningful threshold for ORR.
European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire
EORTC QLQ-C30 and the EORTC QLQ-LC13 are PRO measures designed to assess HRQoL in patients with cancer, with a specific focus on individuals with lung cancer. These were reported as other secondary outcomes. The EORTC QLQ-C30 is a cancer-specific instrument that includes 30 items organized into 5 functional scales (physical, role, emotional, cognitive, and social), 3 symptom scales (fatigue, nausea/vomiting, and pain), a global health status (GHS) scale, and 6 single items that assess additional symptoms (dyspnea, insomnia, appetite loss, constipation, diarrhea, and financial difficulties). The GHS and QoL scale (GHS/QoL) is measured on a 7-point scale, with anchors ranging from 1 (very poor) to 7 (excellent). The other items are scored on a 4-point scale, with response options ranging from 1 (not at all) to 4 (very much). EORTC QLQ-C30 scores are transformed to a score on a scale of 0 to 100, with higher scores on the functional scales and GHS/QoL indicating better functioning or QoL. Conversely, higher scores on the symptom scales indicate greater symptom severity. The EORTC QLQ-LC13 is a supplementary module used in conjunction with the EORTC QLQ-C30 for patients with lung cancer. It contains 13 items that assess lung cancer–associated symptoms and treatment-related side effects. The module includes a multiitem scale for dyspnea and single items for symptoms such as pain in the chest, arm, shoulder, or other body parts, as well as coughing, hemoptysis, sore mouth or tongue, dysphagia, peripheral neuropathy, and alopecia. As with EORTC QLQ-C30, higher scores on the EORTC QLQ-LC13 symptom scales indicate worse symptoms. Both the EORTC QLQ-C30 and EORTC QLQ-LC13 have been validated. They have demonstrated the ability to differentiate between subgroups of patients, supporting their construct validity. The instruments have also shown acceptable internal consistency, with Cronbach alpha values indicating reliable measurement of the constructs they are intended to assess. In terms of interpreting outcome data, a negative change from baseline in the symptom scales of these questionnaires indicates an improvement in symptoms, while a positive change indicates a deterioration. For the functional scales and GHS/QoL, a positive change from baseline indicates an improvement in functioning or QoL, and a negative change indicates a deterioration. A change of 10 points or more is considered to be a clinically meaningful difference in the context of these scales.40
Treatment-Emergent Adverse Events of Special Interest
As part of the safety analysis, AEs of special interest for this study included ||||| | || ||||||| |||||||||||||||| |||||||||| ||||| | || ||||||| ||||||||||||||||||||||||| |||||||||| ||||| | || ||||||| ||||||||||||||| |||| ||| ||||||||||||||| ||| || ||| ||||| || |||||||| |||||||||| ||||||| |||| |||||||||||||||||||| |||||||| |||||||||. The clinical experts consulted for this review did not identify a clinically meaningful threshold for ORR.
Table 8: Summary of Outcome Measures and Their Measurement Properties
Outcome measure | Type | Conclusions about measurement properties | MID |
|---|---|---|---|
EORTC QLQ-C30 | Cancer-specific self-reported measure of HRQoL. The 30-item questionnaire consists of 5 functional scales (physical, role, emotional, social, and cognitive), 9 symptom scales (fatigue, nausea/vomiting, pain, dyspnea, insomnia, appetite loss, constipation, diarrhea, and financial difficulties), and a GHS scale. A higher score for functional scales and for GHS represents better functioning ability or HRQoL. A higher score for symptom scales represents a worsening of symptoms.41 | For studies of patients with lung cancer. Validity: Moderate to strong correlations between the 5 EORTC QLQ-C30 functioning scales (r = 0.41 to 0.77); FACT-G and EORTC QLQ-C30 scales (r = 0.64 to 0.76);42 HADS with all EORTC QLQ-C30 functioning scales (r = 0.28 to 0.75); BPI scales with all EORTC QLQ-C30 scales except for nausea/vomiting (r = 0.20 to 0.72),43 supporting convergent validity. Known-groups approach: Able to differentiate across different measures of cancer severity: cancer stages (d = 0.49); ECOG PS (d = 0.65); and self-reported health status (d = 1.36).42 Reliability: Cronbach alpha ranging from 0.56 to 0.93, with 7 scales having acceptable internal consistency (alpha > 0.70).44 Responsiveness: No relevant studies identified. | For studies of patients with NSCLC. MID estimates for improvement (deterioration) using the ECOG PS and weight change, respectively, as anchors:
The EMPOWER-Lung 1 trial defined a clinically meaningful improvement in GHS score as a ≥ 10-point change.46 In the EMPOWER-Lung 3 trial, a decrease of 10 points or more and no subsequent observations with a decrease of less than 10 points from baseline was considered to be a definitive clinically meaningful deterioration for the GHS/QoL and functional scales. In a study of patients with lung cancer, an anchor-based approach is used in which patients who reported “a little” change on the SSQ had subsequent changes on a scale of the EORTC QLQ-C30 of 5 to 10 points.40 |
EORTC QLQ-LC13 | A tumour-specific questionnaire used to supplement the EORTC QLQ-C30 that contains 13 items related to lung cancer symptoms and treatment side effects, including a 3-item scale assessing dyspnea and 9 single items: pain in chest, pain in arm or shoulder, pain in other body parts, coughing, hemoptysis, sore mouth or tongue, dysphagia, peripheral neuropathy, and alopecia.41 Higher scores on the symptom scales indicate worse symptoms.41 | Validity: Good ability to differentiate between subgroups of patients, supporting construct validity; significantly higher scores for all pain items among patients with metastatic vs. local disease before treatment (P < 0.01). Changes in symptom measures over time were significantly associated with either chemotherapy (tingling in arms and legs and hair loss) or radiotherapy (difficulty swallowing) (P < 0.001).47 Reliability: Good internal consistency reliability for the dyspnea multiitem scale (alpha = 0.81).47 Responsiveness: No relevant studies identified. | No relevant studies identified. |
BPI = Brief Pain Inventory; ECOG PS = Eastern Cooperative Oncology Group Performance Status; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; EORTC QLQ-LC13 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire-Lung Cancer 13; FACT-G = Functional Assessment of Cancer Therapy-General; GHS = global health status; HADS = Hospital Anxiety and Depression Scale; HRQoL = health-related quality of life; MID = minimal important difference; NSCLC = non–small cell lung cancer; SSQ = Symptom Severity Questionnaire.
Statistical Analysis
A summary of the statistical analyses for the relevant efficacy outcomes is provided in Table 9.
Sample Size and Power Calculation
Based on historical data, it was assumed that the median OS would be 12 months for patients treated with PBC plus placebo, with an HR of |||| for the difference in OS between cemiplimab plus PBC and placebo plus PBC. Patients were to be randomized in a 2:1 ratio to the cemiplimab plus PBC group or the placebo plus PBC group. Under these assumptions, 291 deaths would yield approximately 93% power to detect a statistically significant difference in OS between groups, at a 2-sided type I error level of 0.05. Considering an enrolment period of || |||||| ||| |||||||| ||| ||||| ||| ||| ||||| | ||||||| || |||||||| ||| ||||| ||| ||||| | || || || |||||||| ||| ||||| |||||||||||, an approximate |||||||| ||||||||| |||||| ||| || ||||| |||||||||| || ||||||||||| ||| | ||| |||||| |||||||, the enrolment of approximately 450 randomized patients was needed to obtain 291 deaths for the final OS analysis. Further, based on these historical data, a median PFS of ||| |||||| was assumed for patients treated with PBC plus placebo, and an HR of |||||| in PFS between the cemiplimab plus PBC group and the placebo plus PBC group. With these assumptions and at a 2-sided 0.05 alpha level, the power for analysis of PFS was 90% or more if it was to be performed after 288 or more PFS events were observed.
Statistical Testing
For time-to-event outcomes (e.g., OS and PFS), the nonparametric Kaplan-Meier method was used to estimate the survival curves. The treatment difference in survival was assessed by the stratified log-rank test. A stratified Cox proportional hazards model with Ephron’s method of tie handling was used to assess the magnitude of the treatment difference (i.e., HR). The HR and its 95% CI from the stratified Cox model with a single treatment covariate was reported. The part-specific stratification factors at randomization (i.e., histology and PD-L1 expression level) were applied to both the stratified log-rank test and the stratified Cox model. Median OS and PFS, along with 95% CIs, are presented for each treatment arm using the Kaplan-Meier method.
ORR was analyzed using the Cochran-Mantel-Haenszel test, stratified by part-specific stratification factors at randomization, per the interactive web response system. ORR and the corresponding exact 95% CI were calculated using the Clopper-Pearson method for each treatment arm.
OS and PFS rates at a landmark (12 months, 18 months, 24 months, and other relevant time points), along with its 95% CI, were estimated using the Kaplan-Meier method for each treatment arm.
PRO data, measured by the EORTC QLQ-C30 and EORTC QLQ-LC13, were summarized descriptively and included patient disposition rates, patient completion rates, mean scores at each assessment, and change from baseline scores over time. Prespecified PRO analyses included overall change from baseline up to 32 months, estimated using a mixed-effects model for repeated measures, and the time to definitive clinically meaningful deterioration, analyzed using a stratified log-rank test and summarized using Kaplan-Meier estimation. Time to definitive clinically meaningful deterioration for the GHS/QoL scale was defined as the time from randomization to the first observation with at least a 10-point decrease and no subsequent observations with a decrease of less than 10 points from baseline or if patient dropout resulted in missing data.40 Time to definitive clinically meaningful deterioration for pain symptoms was defined as the time from randomization to the first observation with at least a 10-point increase from baseline and no subsequent observations with an increase of less than 10 points from baseline or if patient dropout resulted in missing data.40
To assess the relationship between baseline PD-L1 levels and clinical response, the primary and key secondary end points were evaluated by PD-L1 categories used for stratification: less than 1%, 1% to 49%, at least 50%.
Multiplicity Adjustment
The familywise type I error across the test of primary and key secondary outcomes and the repeated testing of OS in the 2 interim analyses and final analyses was controlled at a 2-sided 0.05 level. The multiplicity of OS, PFS, and ORR analyses was controlled at a 2-sided 0.05 level by the hierarchical testing approach and with an alpha-spending function, specifically the Lan-DeMets O'Brien-Fleming spending function, which controlled the familywise type I error rate across multiple interim analyses and the final analysis for OS. Specifically, the hierarchical testing approach was structured as follows: OS, PFS, and ORR. That is, the analysis of PFS was performed at a 2-sided 0.05 level only if analysis of OS was statistically significant, and the analysis of ORR was performed at a 2-sided 0.05 level only if analysis of PFS was statistically significant. The type I error for the 2 interim analyses of OS at approximately 146 (50%) and 204 (70%) events and final analysis of OS was controlled at a 2-sided 0.05 level, according to the Lan-DeMets O’Brien-Fleming alpha-spending function. The exact nominal P values needed to declare statistical significance at the time of these analyses for OS were to depend on the actual number of OS events at the time of the analyses. All other statistical comparisons were exploratory in nature and, therefore, not controlled for multiplicity; they should be interpreted accordingly.
Subgroup Analyses
Descriptive subgroup analyses were performed for the primary and key secondary outcomes to summarize the treatment effects across subpopulations. Forest plots were constructed. The prespecified subgroups were defined by the following baseline or screening factors:
age (< 65 versus ≥ 65)
race (white versus nonwhite)
sex (male versus female)
ethnicity (Hispanic or Latino versus other)
histology (squamous, nonsquamous)
PD-L1 expression levels for part 2 of the trial (< 1% versus 1% to 49% versus ≥ 50%)
ECOG PS (0 versus 1)
geographic region of enrolling site for part 2 of the trial (Europe, Asia)
brain metastasis (yes, no)
stage of disease (locally advanced, metastatic)
smoking history for part 2 of the trial (smokers, nonsmokers).
The subgroup analyses were considered exploratory in nature and were not adjusted for multiple comparisons. The clinical experts did not identify a need to include or assess results of the subgroups in this systematic review.
Analysis Populations
The analysis populations are defined in Table 10.
Table 9: Statistical Analysis of Efficacy End Points
End point | Statistical model | Adjustment factors | Handling of missing data | Sensitivity analyses |
|---|---|---|---|---|
EMPOWER-Lung 3 | ||||
OS |
| Randomization stratification factors | If a patient was not known to have died or was lost to follow-up, the patient was censored at the last date the patient was known to be alive | NA |
OS at 12, 18, and 24 months | Kaplan-Meier method with 95% CIs | NR | No data imputation | NA |
PFS |
| Randomization stratification factors | Censoring rules applied as follows: Patients were censored at their last evaluable tumour assessment if they had no documented tumour progression or death, or if they started new antitumour therapy without prior progression or death. Patients who withdrew consent before taking any study treatment or had no evaluable tumour assessments after randomization and did not die were censored at the date of randomization. | NA |
PFS at 12 months |
| NR | No data imputation | NA |
ORR |
| Randomization stratification factors | Patients deemed NE were considered not reaching CR/PR and considered nonresponders | NA |
QoL: EORTC QLQ-C30 and EORTC QLQ-LC13 |
| NR | Per the scoring manuals for each questionnaire | NA |
CI = confidence interval; CR = complete response; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; EORTC QLQ-LC13 = European Organisation for Research and Treatment of Cancer Quality of Life-Lung Cancer 13; GHS = global health status; NA = not applicable; NE = not evaluable; NR = not reported; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; PR = partial response; QoL = quality of life.
Sources: EMPOWER-Lung 3 (part 2) Clinical Study Report and Statistical Analysis Plan.3 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Table 10: Analysis Populations of the EMPOWER-Lung-3 Trial
Population | Definition | Application |
|---|---|---|
FAS N = 466 (100.0%) | Included all randomized patients and was the ITT population and was based on treatment allocation (as randomized) | All efficacy outcomes were analyzed using the FAS |
Safety analysis set SAF N = 465 (99.8%) | Included all randomized patients who received any study drug and was based on treatment received (as treated) | Treatment administration and all clinical safety variables were analyzed using the SAF |
PK population N = 295 (63.3%) | Included all randomized patients who received cemiplimab and who had at least 1 nonmissing cemiplimab concentration assay result after the first dose of cemiplimab up to end of the study | All PK outcomes were analyzed using the PK population |
ADA analysis set N = 273 (58.6%) | Included all treated patients who received any study drug and had at least 1 nonmissing postbaseline ADA assay result after the first dose of the study drug | All ADA immunogenicity outcomes were analyzed using the ADA analysis set |
ADA = antidrug antibodies; FAS = full analysis set; ITT = intention to treat; PK = pharmacokinetic; SAF = safety analysis set.
Source: EMPOWER-Lung 3 (part 2) Clinical Study Report and Statistical Analysis Plan.3 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Results
Patient Disposition
Patient disposition is summarized in Table 11. There was 1 (0.6%) patient in the placebo plus PBC group who was randomized but not treated. Of the 466 patients in the FAS, at the time of the June 14, 2021, data cut-off, 204 (65.4%) patients in the cemiplimab plus PBC group and 138 (89.6%) patients in the placebo plus PBC group had discontinued treatment. At the time of the June 14, 2022, data cut-off, 240 (76.9%) and 149 (96.8%) patients had discontinued treatment. The most common reason for treatment discontinuation in either group was disease progression (i.e., 160 [51.3%] patients in the cemiplimab plus PBC group and 105 [68.2%] patients in the placebo plus PBC group at the June 14, 2022, data cut-off date).
Table 11: The EMPOWER-Lung-3 Trial (Part 2) — Patient Disposition
Patient disposition | Data cut-off: June 14, 2021 | Data cut-off: June 14, 2022 | ||
|---|---|---|---|---|
Cemiplimab + PBC (N = 312) | Placebo + PBC (N = 154) | Cemiplimab + PBC (N = 312) | Placebo + PBC (N = 154) | |
Screened, N | 904 | |||
Reason for screening failure, N (%) | ||||
Adverse event | 1 (0.2) | |||
Does not meet inclusion or exclusion criteria | 297 (67.8) | |||
Withdrawal of consent | 46 (10.5) | |||
Lost to follow-up | 1 (0.2) | |||
Death | 16 (3.7) | |||
Other | 77 (17.6) | |||
Randomized, N (%) | 312 (100.0) | 154 (100.0) | 312 (100.0) | 154 (100.0) |
Randomized and not treated, N (%) | 0 (0) | 1 (0.6) | 0 (0) | 1 (0.6) |
Discontinued study, N (%) | ||| |||||| | ||| |||||| | ||| |||||| | ||| |||||| |
Reason for study discontinuation, N (%) | ||||
Adverse event | || | || | | ||||| | || |
Death | || |||||| | || |||||| | || |||||| | || |||||| |
Lost to follow-up | | ||||| | | ||||| | | ||||| | | ||||| |
Noncompliance with study drug(s) | | ||||| | || | | ||||| | || |
Patient decision | || ||||| | || |||||| | || ||||| | || |||||| |
Physician decision | | ||||| | | ||||| | | ||||| | | ||||| |
Disease progression | || |||||| | || |||||| | ||| |||||| | || |||||| |
Withdrawal of consent | || ||||| | | ||||| | || ||||| | | ||||| |
Other | | ||||| | || | | ||||| | || |
Discontinued treatment, N (%) | 204 (65.4) | 138 (89.6) | 240 (76.9) | 149 (96.8) |
Reason for treatment discontinuation, N (%) | ||||
Adverse events | 14 (4.5) | 4 (2.6) | 17 (5.4) | 6 (3.9) |
Death | 24 (7.7) | 10 (6.5) | 25 (8.0) | 10 (6.5) |
Lost to follow-up | 1 (0.3) | 3 (1.9) | 2 (0.6) | 3 (1.9) |
Noncompliance with study drug(s) | 1 (0.3) | 0 (0) | 2 (0.6) | 0 (0) |
Patient decision | 13 (4.2) | 17 (11.0) | 16 (5.1) | 17 (11.0) |
Physician decision | 4 (1.3) | 1 (0.6) | 5 (1.6) | 1 (0.6) |
Disease progression | 137 (43.9) | 100 (64.9) | 160 (51.3) | 105 (68.2) |
Withdrawal of consent | 8 (2.6) | 3 (1.9) | 9 (2.9) | 3 (1.9) |
Other | 2 (0.6) | 0 (0) | 4 (1.3) | 1 (0.6) |
FAS, N | 312 (100.0) | 154 (100.0) | 312 (100.0) | 154 (100.0) |
SAF, N | 312 (100.0) | 153 (99.4) | 312 (100.0) | 153 (99.4) |
FAS = full analysis set; PBC = platinum-based chemotherapy; SAF = safety analysis set.
Source: EMPOWER-Lung 3 (part 2) Clinical Study Report;3 EMPOWER-Lung 3 (part 2) final analysis Clinical Study Report.48 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Baseline Characteristics
Demographic and baseline tumour characteristics were largely similar in the 2 treatment groups in the EMPOWER-Lung 3 trial (part 2) and, according to the clinical experts consulted by CADTH, consistent with an expected population of patients with advanced NSCLC seen in clinical practice (Table 12). Patients were primarily white (405 [86.9%]) and male (391 [83.9%]), and more than half the patients were younger than 65 years, with median (range) age of 63.0 (25 to 84) years. Most patients were either current (248 [53.2%]) or past (151 [32.4%]) smokers, and 67 (14.4%) patients had never smoked. Overall, 266 [57.1%] patients presented with nonsquamous histology, whereas patients with squamous histology were capped, per protocol, at 50%. More patients (397 [85.2%]) had metastatic (stage IV) disease at screening than had locally advanced (69 [14.8%]; stage IIIB: || ||||||| or IIIC: || ||||||) disease. The distribution of PD-L1 expression levels was similar between the 2 groups, with a slightly higher percentage (175 [37.6%]) of patients’ tumours expressing PD-L1 levels from 1% to 49%, 139 (29.8%) patients’ tumours expressing PD-L1 levels of less than 1%, and 152 [32.6%] patients’ tumours expressing PD-L1 levels of at least 50%. Thirty-one (31 [6.7%]) patients had known and pretreated brain metastases.
Table 12: The EMPOWER-Lung-3 Trial (Part 2) — Summary of Baseline Characteristics (FAS)
Characteristic | EMPOWER-Lung-3 (part 2) | |
|---|---|---|
Cemiplimab + PBC (N = 312) | Placebo + PBC (N = 154) | |
Mean age (SD), years | |||| |||||| | |||| |||||| |
Median age (range), years | 63.0 (25 to 82) | 63.0 (34 to 84) |
Age groups, n (%) < 65 years ≥ 65 years | 184 (59.0) 128 (41.0) | 94 (61.0) 60 (39.0) |
Sex, n (%) Male Female | 268 (85.9) 44 (14.1) | 123 (79.9) 31 (20.1) |
Race, n (%) White Asian | 267 (85.6) 45 (14.4) | 138 (89.6) 16 (10.4) |
Ethnicity, n (%) Not Hispanic or Latino Not reported | 311 (99.7) 1 (0.3) | 149 (96.8) 5 (3.2) |
Geographic region, n (%) Europe Asia | 270 (86.5) 42 (13.5) | 138 (89.6) 16 (10.4) |
BMI (kg/m2) Mean (SD) Median (range) | 25.143 (5.0804) 24.750 (15.04 to 56.47) | 25.064 (4.6361) 24.475 (14.66 to 38.93) |
ECOG PS, n (%) 0 1 Missing | 51 (16.3) 259 (83.0) 2 (0.6) | 18 (11.7) 134 (87.0) 2 (1.3) |
Smoking status, n (%) Current smoker Past smoker Never smoked | 173 (55.4) 96 (30.8) 43 (13.8) | 75 (48.7) 55 (35.7) 24 (15.6) |
Histology and/or cytology, n (%) Squamous Nonsquamous Adenocarcinoma Large cell carcinoma Not otherwise specified | 133 (42.6) 179 (57.4) 168 (53.8) 2 (0.6) 9 (2.9) | 67 (43.5) 87 (56.5) 81 (52.6) 4 (2.6) 2 (1.3) |
Metastatic sites, n (%) | ||
Lung Liver Bone Adrenal Brain Lymph nodes intrathoracic Lymph nodes other | 255 (81.7) 49 (15.7) 59 (18.9) 66 (21.1) 24 (7.7) 235 (75.3) 82 (26.3) | 124 (80.5) 23 (14.9) 41 (26.6) 28 (18.2) 7 (4.5) 124 (80.5) 45 (29.2) |
Brain metastases, n (%) Yes No | 24 (7.7) 288 (92.3) | 7 (4.5) 147 (95.5) |
Mutation status, n (%) | ||
EGFR Wild-type Mutant | 312 (100.0) 0 (0) | 153 (99.4) 1 (0.6) |
ALK Translocation not present Translocation missing | 311 (99.7) 1 (0.3) | 154 (100.0) 0 (0.0) |
ROS1 Translocation not rearranged | 312 (100.0) | 154 (100.0) |
Cancer stage at screening, n (%) Stage IIIB Stage IIIC Stage IV | || |||||||| ||||| || |||||||| ||||| 267 (85.6) | || |||||||| ||||| || |||||||| ||||| 130 (84.4) |
Cancer stage at screening, n (%) Locally advanced Metastatic | 45 (14.4) 267 (85.6) | 24 (15.6) 130 (84.4) |
PD-L1 expression levels, n (%) < 1% 1% to 49% ≥ 50% | 95 (30.4) 114 (36.5) 103 (33.0) | 44 (28.6) 61 (39.6) 49 (31.8) |
Prior cancer-related therapy, n (%) Patients with any prior therapy Adjuvant therapy setting Other therapy setting | 55 (17.6) 5 (1.6) 1 (0.3) | 16 (10.4) 1 (0.6) 0 (0.0) |
BMI = body mass index; ECOG PS = European Cooperative Oncology Group Performance Status; FAS = full analysis set; PBC = platinum-based chemotherapy; SD = standard deviation.
Source: EMPOWER-Lung 3 (part 2) Clinical Study Report.3 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Exposure to Study Treatments
In the safety population, the median duration of exposure to cemiplimab plus PBC was longer than that to placebo plus PBC for both data cut-off dates (Table 13). More than ||| || |||||||| || |||||| ||||||||| ||||| |||| | ||| || | |||| ||||||||| || ||||| |||||||| ||||||||| ||||| || |||||| |||| ||||||||
Concomitant Medications and Cointerventions
Based on both data cut-off dates, almost all patients (||||| in the cemiplimab plus PBC group and |||| in the placebo plus PBC group) used at least 1 concomitant medication during the trial (Table 14). The classes of medications used most frequently (> 20% of patients) were generally similar between the treatment groups.
Table 13: The EMPOWER-Lung 3 Trial (Part 2) — Patient Exposure (SAF)
Exposure | Data cut-off: June 14, 2021 | Data cut-off: June 14, 2022 | ||
|---|---|---|---|---|
Cemiplimab + PBC (N = 312) | Placebo + PBC (N = 153) | Cemiplimab + PBC (N = 312) | Placebo + PBC (N = 153) | |
Duration in weeks, mean (SD) | 41.98 (25.500) | 28.31 (20.821) | 53.34 (38.314) | 29.98 (24.740) |
Duration, median (range), weeks | 38.45 (1.4 to 102.6) | 21.30 (0.6 to 95.0) | 38.75 (1.4 to 128.1) | 21.30 (0.6 to 115.1) |
Compliancea (≥ 80% to ≤ 100%) n (%) | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| |
NR = not reported; PBC = platinum-based chemotherapy; SAF = safety analysis set; SD = standard deviation.
aReported compliance is for cemiplimab (in the cemiplimab + PBC group) and for placebo (in the placebo + PBC group).
Sources: EMPOWER-Lung 3 (part 2) Clinical Study Report;3 EMPOWER-Lung 3 (part 2) final analysis Clinical Study Report.48 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Table 14: The EMPOWER-Lung 3 Trial (Part 2) — Concomitant Medication Use (SAF)
Medication | Data cut-off: June 14, 2021 | Data cut-off: June 14, 2022 | ||
|---|---|---|---|---|
Cemiplimab + PBC (N = 312) | Placebo + PBC (N = 153) | Cemiplimab + PBC (N = 312) | Placebo + PBC (N = 153) | |
Patients with ≥ 1 concomitant medication use, n (%) | ||| |||||| | ||| ||||||| | ||| |||||| | ||| ||||||| |
Most common medication classes used (> 20% of patients) | ||||
Systemic corticosteroids | ||| |||||| | ||| |||||| | ||| |||||| | ||| |||||| |
Antiemetics and antinauseants | |||| |||||| | |||| |||||| | |||| |||||| | ||||| |||||| |
Drugs for acid-related disorders | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| |
Systemic antihistamines | ||| |||||| | ||| |||||| | ||| |||||| | ||| |||||| |
Antianemic preparations | ||| |||||| | || |||||| | ||| |||||| | || |||||| |
Blood substitutes and perfusion solutions | |||| |||||| | ||| |||||| | |||| |||||| | ||| |||||| |
Anti-inflammatory and antirheumatic products | |||| |||||| | ||| |||||| | |||| |||||| | ||| |||||| |
Antithrombotic products | || |||||| | || |||||| | || |||||| | || |||||| |
Systemic antibacterials | || |||||| | || |||||| | || |||||| | || |||||| |
NR = not reported; PBC = platinum-based chemotherapy; SAF = safety analysis set.
Source: EMPOWER-Lung 3 (part 2) Clinical Study Report; EMPOWER-Lung 3 (part 2) final analysis Clinical Study Report.48
Subsequent Treatment
A smaller proportion of patients in the cemiplimab plus chemotherapy group received subsequent anticancer treatment after discontinuation of the study treatment (Table 15). At the first cut-off date of June 14, 2021, ||||| of patients in the cemiplimab plus PBC group (n = 312) and ||||| of patients in the placebo plus PBC group (n = 153) received subsequent therapy. By the second cut-off date of June 14, 2022, these percentages increased to ||||| and |||||, respectively. Radiotherapy was rarely used, with |||| ||| ||||||| |||||| in the cemiplimab plus PBC group at both data cut-off dates and |||| in the placebo group. Surgical interventions were also low, with |||| in each group at both time points. Systemic therapy was more common, with immunotherapy, chemotherapy, and other treatments being used. In the cemiplimab plus PBC group, the use of systemic therapy ||||||||| |||| ||||| || ||||| |||| ||| ||||, while in the placebo group, || |||| |||| ||||| || |||||. Notably, the use of chemotherapy as a subsequent therapy ||||||||| || ||| |||||||||| | ||| ||||| |||| |||| || |||||, and in the placebo group |||| |||| || |||||. Immunotherapy as a subsequent treatment ||||||||| || ||| ||||||| ||||| |||| |||| || |||||, while in the cemiplimab plus PBC group, || |||||||| |||||||||| |||||| ||||| || |||||. Other systemic therapies |||||||| |||||||||| || ||| |||||||||| | ||| ||||| ||||| || |||| |||| ||||||| ||| ||||||||| || ||| ||||||| ||||| |||| |||| || |||||
Table 15: Summary of Subsequent Treatment From the Study Included in the Systematic Review
Exposure | Data cut-off: June 14, 2021 | Data cut-off: June 14, 2022 | ||
|---|---|---|---|---|
Cemiplimab + PBC (N = 312) | Placebo + PBC (N = 153) | Cemiplimab + PBC (N = 312) | Placebo + PBC (N = 153) | |
Subsequent therapy, n (%) | || |||||| | || |||||| | || |||||| | || |||||| |
Radiotherapy, n (%) | | ||||| | | ||| | | ||||| | | ||| |
Surgery, n (%) | | ||||| | | ||||| | | ||||| | | ||||| |
Systemic therapy, n (%) Immunotherapy Chemotherapy Other | || |||||||| |||||||| ||| | || ||||||||| |||||||| || | || |||||||| |||||||| || | || ||||||||| ||||||||| || |
FAS = full analysis set; PBC = platinum-based chemotherapy.
Sources: EMPOWER-Lung 3 (part 2) Clinical Study Report;3 EMPOWER-Lung 3 (part 2) final analysis Clinical Study Report.48 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Efficacy
Summary of Efficacy Outcomes
The mean (standard deviation [SD]) duration of follow-up from randomization to the June 14, 2021, data cut-off date was 16.43 (3.584) months in the cemiplimab plus PBC group and 16.55 (3.509) months in the placebo plus PBC group. The median (range) duration of follow-up in the treatment groups was 16.34 (8.5 to 24.0) months and 16.69 (9.6 to 23.8) months, respectively. As of the June 21, 2021, data cut-off date, all (100%) patients had been followed for at least 6 months, and more than 87% of patients had been followed for at least 12 months.
The mean (SD) duration of follow-up from randomization to the June 14, 2022, data cut-off date was 28.42 (3.584) months in the cemiplimab plus PBC group and 28.54 (3.509) months in the placebo plus PBC group. The median (range) duration of follow-up in the cemiplimab plus PBC and placebo plus PBC groups was 28.34 (20.5 to 35.9) months and 28.68 (21.6 to 35.8) months, respectively. As of the June 14, 2022, data cut-off date, all (100%) patients had been followed for at least 18 months from the time of randomization and more than 87% of patients had been followed for at least 24 months.
A summary of the key efficacy outcomes is provided in Table 16.
Table 16: The EMPOWER-Lung-3 Trial — Key Efficacy Outcomes (FAS)
Outcome | Data cut-off: June 14, 2021 | Data cut-off: June 14, 2022 | ||
|---|---|---|---|---|
Cemiplimab + PBC (N = 312) | Placebo + PBC (N = 153) | Cemiplimab + PBC (N = 312) | Placebo + PBC (N = 153) | |
Overall survivala | ||||
Number of deaths, n (%) | 132 (42.3) | 82 (53.2) | 180 (57.7) | 111 (72.1) |
Number of censored patients, n (%) | 180 (57.7) | 72 (46.8) | 132 (42.3) | 43 (27.9) |
Median OS (95% CI), monthsb | 21.9 (15.5 to NE) | 13.0 (11.9 to 16.1) | 21.1 (15.9 to 23.5) | 12.9 (10.6 to 15.7) |
Stratified log-rank P valuec,d | 0.0140 | 0.0003 | ||
HR (95% CI)c,e | 0.706 (0.534 to 0.933) | 0.645 (0.507 to 0.820)f | ||
Estimated survival probability, % (95% CI)b | ||||
6 months | 85.0 (80.5 to 88.5) | 77.8 (70.2 to 83.6) | 85.0 (80.5 to 88.5) | 77.8 (70.2 to 83.6) |
12 months | 65.7 (59.9 to 70.9) | 56.1 (47.5 to 63.8) | 66.4 (60.8 to 71.5) | 53.9 (45.4 to 61.6) |
18 months | 50.6 (43.9 to 57.0) | 37.2 (27.8 to 46.6) | 53.7 (47.8 to 59.1) | 35.8 (28.0 to 43.7) |
24 months | NE (NE to NE) | NE (NE to NE) | 42.7 (36.9 to 48.4) | 27.2 (20.1 to 34.9) |
30 months | NR | NR | 33.1 (26.6 to 39.7) | 16.4 (9.1 to 25.6) |
36 months | NR | NR | NE (NE to NE) | NE (NE to NE) |
Progression-free survivala | ||||
Number of events, n (%) | 204 (65.4) | 122 (79.2) | 234 (75.0) | 133 (86.4) |
Progressive disease | 154 (49.4) | 94 (61.0) | 181 (58.0) | 101 (65.6) |
Deaths | 50 (16.0) | 28 (18.2) | 53 (17.0) | 32 (20.8) |
Number of censored patients, n (%) | 108 (34.6) | 32 (20.8) | 78 (25.0) | 21 (13.6) |
Median PFS (95% CI), monthsb | 8.2 (6.4 to 9.3) | 5.0 (4.3 to 6.2) | 8.2 (6.4 to 9.0) | 5.5 (4.3 to 6.2) |
Stratified log-rank P valuec,d | < 0.0001 | < 0.0001 | ||
HR (95% CI)c,e | 0.556 (0.442 to 0.699) | 0.549 (0.441 to 0.683)f | ||
Estimated event-free probability, % (95% CI)b | ||||
6 months | 66.1 (60.4 to 71.1) | 47.4 (39.0 to 55.3) | 65.8 (60.1 to 70.8) | 48.0 (39.7 to 55.8) |
12 months | 38.1 (32.4 to 43.8) | 16.4 (10.5 to 23.4) | 38.7 (33.1 to 44.3) | 16.1 (10.5 to 22.8) |
18 months | 22.4 (16.3 to 29.0) | 6.8 (2.4 to 14.2) | 27.4 (22.3 to 32.6) | 9.7 (5.4 to 15.5) |
24 months | NE (NE to NE) | NE (NE to NE) | 19.7 (15.1 to 24.6) | 3.6 (1.1 to 8.7) |
30 months | NR | NR | 18.7 (14.1 to 23.8) | 3.6 (1.1 to 8.7) |
36 months | NR | NR | NE (NE to NE) | NE (NE to NE) |
Objective response ratea | ||||
BOR, n (%) | ||||
CR | 8 (2.6) | 0 (0) | 13 (4.2) | 0 (0) |
PR | 127 (40.7) | 35 (22.7) | 123 (39.4) | 34 (22.1) |
Stable disease | 121 (38.8) | 74 (48.1) | 119 (38.1) | 75 (48.7) |
Non-CR and/or non-PD | 4 (1.3) | 1 (0.6) | 4 (1.3) | 1 (0.6) |
PD | 22 (7.1) | 24 (15.6) | 23 (7.4) | 24 (15.6) |
NE | 30 (9.6) | 20 (13.0) | 30 (9.6) | 20 (13.0) |
ORR, n (%) [95% CI]g | 135 (43.3) [37.7 to 49.0] | 35 (22.7) [16.4 to 30.2] | 136 (43.6) [38.0 to 49.3] | 34 (22.1) [15.8 to 29.5] |
Stratified CMH test P-valueh,i | < 0.0001 | < 0.0001f | ||
OR (95% CI)h,j | 2.682 (1.718 to 4.186) | 2.819 (1.801 to 4.413) | ||
EORTC QLQ-C30 (GHS/QoL) | ||||
Number of patients contributing to the analysis, n (%) | || | || | ||| | || |
Baseline, mean (95% CI) | |||| ||||| || ||||| | |||| ||||| || ||||| | |||| ||||| || ||||| | |||| ||||| || ||||| |
Least squares mean estimated overall change from baseline cycle 21 (MMRM) in the FAS (95% CI) | |||| ||||| || ||||| | |||||||||| || |||||| | || | || |
Mean change from baseline to cycle 21 date in the FAS (95% CI) | || | || | |||| |||| || ||||||| | |||| ||||| || |||||| |
Treatment group difference vs. control (95% CI) | |||| |||||| || ||||| | || | ||
P value | |||||| | || | ||
BOR = best overall response; CI = confidence interval; CMH = Cochran-Mantel-Haenszel; CR = complete response; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; FAS = full analysis set; GHS = global health status; HR = hazard ratio; MMRM = mixed models for repeated measures; NE = not evaluable; OR = odds ratio; ORR = objective response rate; OS = overall survival; PBC = platinum-based chemotherapy; PD = progressive disease; PFS = progression-free survival; PR = partial response.
aAdjusted for multiple testing at the June 14, 2021, data cut-off date.
bBased on the Kaplan-Meier method.
cStratified by histology (nonsquamous, squamous) and PD-L1 level (< 1%, 1% to 49%, and ≥ 50%). Significance threshold is set to 0.01631 using the O’Brien-Fleming alpha-spending function.
dTwo-sided P value.
eBased on stratified hazard model (cemiplimab plus PBC versus placebo plus PBC).
fNominal P value (not alpha adjusted).
gClopper-Pearson exact CI.
hStratified by histology (nonsquamous, squamous) and PD-L1 level (< 1%, 1% to 49%, and ≥ 50%).
iTwo-sided P value using stratified CMH test.
jBased on stratified CMH test (cemiplimab plus PBC versus placebo plus PBC).
Sources: EMPOWER-Lung 3 (part 2) Clinical Study Report; EMPOWER-Lung 3 (part 2) final analysis Clinical Study Report.48
At the secondary interim analysis (data cut-off date: June 14, 2021), cemiplimab plus PBC showed statistically significant improvements in OS, PFS, and ORR for patients with advanced NSCLC compared to placebo plus PBC (refer to Table 16). Results at the subsequent data cut-off date (June 14, 2022), including the final OS analyses, were consistent with the those seen at the previous data cut-off date.
The trial was stopped early, per the recommendation of the IDMC, because the prespecified OS efficacy criteria were met at the secondary interim analysis (data-cut-off date: June 14, 2021). Because the efficacy boundary was crossed at the second interim analysis, no alpha was assigned to the final analysis.
Overall Survival
As of the June 14, 2022, data cut-off date, there were 291 deaths. Median OS was greater in the cemiplimab plus PBC group (21.1 months; 95% CI, 15.9 to 23.5 months) than in the placebo plus PBC group (12.9 months; 95% CI, 10.6 to 15.7 months; P = 0.0003), corresponding to an HR of 0.645 (95% CI, 0.507 to 0.820), as detailed in Table 16. For patients in the cemiplimab plus PBC group, the estimated probability of surviving from baseline through 12 months was 66.4% (95% CI, 60.8% to 71.5%), through 18 months was 53.7% (95% CI, 47.8% to 59.1%), through 24 months was 42.7% (95% CI, 36.9% to 48.4%), and through 30 months was 33.1% (95% CI, 26.6% to 39.7%). For patients in the placebo plus PBC group, the corresponding proportions of patients for 12, 18, 24, and 30 months, respectively, were 53.9% (95% CI, 45.4% to 61.6%), 35.8% (95% CI, 28.0% to 43.7%), 27.2% (95% CI, 20.1% to 34.9%), and 16.4% (95% CI, 9.1% to 25.6%). For both treatment groups, the estimated survival probability at 36 months was not yet evaluable.
A subgroup analysis of patients with PD-L1 expression levels less than 1% (n = 139) showed that median OS was 12.8 months (95% CI, 9.6 to 15.6 months) in the cemiplimab plus PBC group and 14.2 months (95% CI, 9.1 to 18.0 months) in the placebo plus PBC group (HR, 0.939; 95% CI, 0.619 to 1.423). By comparison, patients with PD-L1 expression levels from 1% to 49% (n = 175) had a median OS of 23.2 months (95% CI, 18.1 to 27.2 months) in the cemiplimab plus PBC group and 12.0 months (95% CI, 8.3 to 15.7 months) in the placebo plus PBC group (HR, 0.496; 95% CI, 0.335 to 0.735), and patients with PD-L1 expression levels of at least 50% (n = 152) had a median OS of 23.5 months (95% CI, 17.9 months to not evaluable) in the cemiplimab plus PBC group and 14.4 months (95% CI, 9.3 to 19.5 months) in the placebo plus PBC group (HR, 0.559; 95% CI, 0.362 to 0.862).
Figure 2: The EMPOWER-Lung 3 Trial (Part 2) — Kaplan-Meier Curve of OS (FAS)
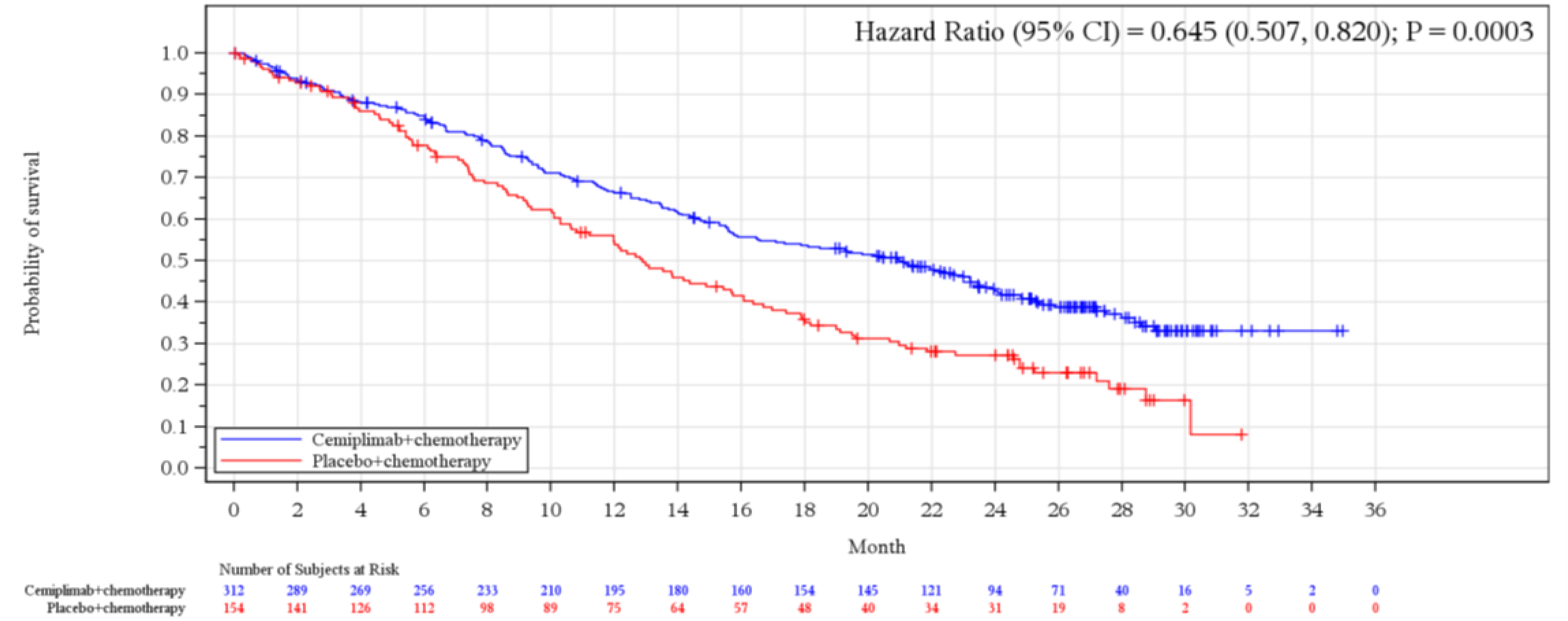
CI = confidence interval; FAS = full analysis set; OS = overall survival.
Note: Data cut-off date was June 14, 2022.
Sources: EMPOWER-Lung 3 (part 2) Clinical Study Report; EMPOWER-Lung 3 (part 2) final analysis Clinical Study Report.
Progression-Free Survival
At the January 14, 2022, data cut-off date, median PFS determined by IRC was greater in the cemiplimab plus PBC group than in the placebo plus PBC group (8.2 months [95% CI, 6.4 to 9.0 months] versus 5.5 months [95% CI, 4.3 to 6.2 months]; P < 0.0001), and the HR was 0.549 (95% CI, 0.441 to 0.683) (Table 16). For patients in the cemiplimab plus PBC group, the estimated event-free probability from baseline through 12 months was 38.7% (95% CI, 33.1% to 44.3%), through 18 months was 27.4% (95% CI, 22.3% to 32.6%), through 24 months was 19.7% (95% CI, 15.1% to 24.6%), and through 30 months was 18.7% (95% CI, 14.1% to 23.8%); it was not yet evaluable through 36 months. For patients in the placebo plus PBC group, the corresponding event-free probabilities for 12, 18, 24, and 30 months, respectively, were 16.1% (95% CI, 10.5% to 22.8%), 9.7% (95% CI, 5.4% to 15.5%), 3.6% (95% CI, 1.1% to 8.7%), and 3.6% (95% CI, 1.1% to 8.7%); it was not yet evaluable through 36 months.
Figure 3: The EMPOWER-Lung 3 Trial (Part 2) — Kaplan-Meier Plot of PFS (FAS)
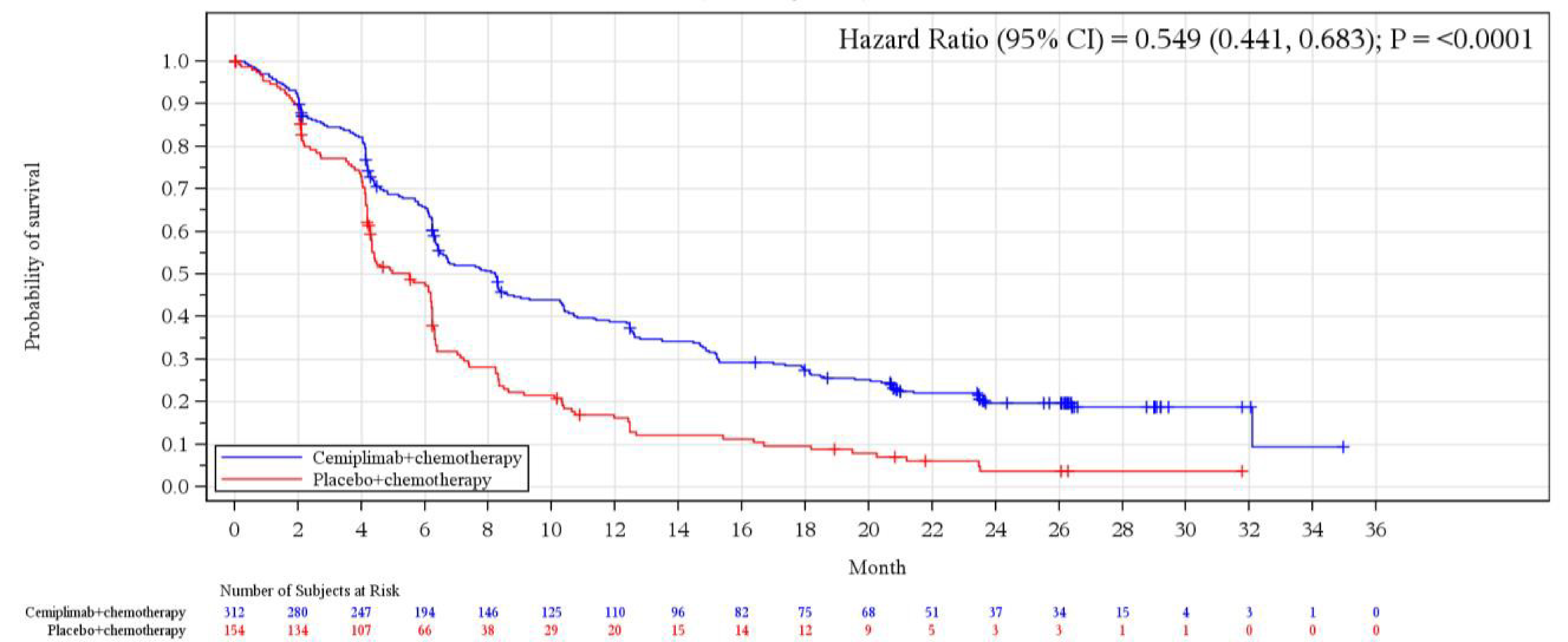
CI = confidence interval; FAS = full analysis set; PFS = progression-free survival.
Note: Data cut-off date was June 14, 2022.
Sources: EMPOWER-Lung 3 (part 2) Clinical Study Report; EMPOWER-Lung 3 (part 2) final analysis Clinical Study Report.48
Objective Response Rate
At the January 14, 2022, data cut-off date, the ORR determined by IRC remained greater in the cemiplimab plus PBC group (136/312 [43.6%]; 95% CI, 38.0% to 49.3%) than in the placebo plus PBC group (34/153 [22.1%]; 95% CI, 15.8% to 29.5%), as detailed in Table 16. The OR for the comparison of cemiplimab plus PBC to placebo plus PBC was 2.819 (95% CI, 1.801 to 4.414; 2-sided P < 0.0001). In the cemiplimab plus PBC group, among 136 responders, 123 of 312 (39.4%) patients experienced a partial response and 13 of 312 (4.2%) patients experienced a CR. In the placebo plus PBC group, among 34 responders, 34 of 153 (22.1%) patients experienced a PR and no patient experienced a CR. The ORR results consistently favoured the cemiplimab plus PBC group over the placebo plus PBC group in the predefined subgroups.
The median duration of response was 16.4 (95% CI, 13.1 to 18.9; range = 1.7 to 32.9) months for the cemiplimab plus PBC group and 7.3 (95% CI, 4.2 to 11.3; range = 1.8 to 29.6) months for the placebo plus PBC group.
Patient-Reported Outcomes
Baseline completion rates for EORTC QLQ-C30 and EORTC QLQ-LC13 scores were above 97% on all scales for both treatment groups. Postbaseline completion rates, adjusted for study attrition, were greater than 91% through cycle 21 for patients expected to complete the PRO assessments. Mean [SD] baseline scores for the GHS/QoL and functioning scales of the EORTC QLQ-C30 were similar for patients in the cemiplimab plus PBC group and those in the placebo plus PBC groups (GHS/QoL baseline scores, ||||||||| and |||||||||||, respectively).
At the June 14, 2021, data cut-off date, the following overall changes from baseline to cycle 21 in the GHS/QoL score of the EORTC QLQ-C30 questionnaire were observed in the cemiplimab plus PBC group (i.e., least squares mean change, ||||; 95% CI, |||| || ||||) and the placebo plus PBC group (least squares mean change: ||||| 95% CI, ||||| || ||||). The overall difference between treatment groups was |||| (95% CI, |||| || ||||; | | |||||).
Mean baseline symptom scores for the EORTC QLQ-LC13 were similar between the treatment groups. When comparing the cemiplimab plus PBC and placebo plus PBC groups, the descriptive changes from baseline for all symptom scales, per EORTC QLQ-LC13, were numerically similar.
No comparative results for PRO were available for the final analysis at the data cut-off date of June 14, 2022. When comparing cemiplimab plus PBC with placebo plus PBC in descriptive analyses, mean changes from baseline in GHS/QoL score and all functional scales, per EORTC QLQ-C30, were numerically similar.
Mean baseline scores for the 9 symptom scales and/or items on the EORTC QLQ-C30 questionnaire were similar for patients in the cemiplimab plus PBC and placebo plus PBC treatment groups. Similarly, when comparing EORTC QLQ-LC13 scores, mean changes from baseline on all symptom scales, per EORTC QLQ-LC13, were numerically similar in the 2 groups (refer to Figure 5 in Appendix 1).
For the EORTC QLQ-C30 and EORTC QLQ-LC13, the number of patients available to complete the questionnaires diminished with each cycle. After cycle 6, the number of patients providing assessments had dropped to less than 50% in the placebo plus PBC group. In the cemiplimab plus PBC group, after cycle 9 and cycle 12, less than 60% and less than 50% of patients, respectively, were available to provide assessments.
Harms
A summary of key harms in the EMPOWER-Lung 3 trial as of the June 14, 2021, and June 14, 2022, cut-off dates is provided in Table 17.
Table 17: The EMPOWER-Lung 3 Trial Summary of Key Harms (SAF)
Adverse events | Data cut-off: June 14, 2021 | Data cut-off: June 14, 2022 | ||
|---|---|---|---|---|
Cemiplimab + PBC (N = 312) | Placebo + PBC (N = 153) | Cemiplimab + PBC (N = 312) | Placebo + PBC (N = 153) | |
Most common AEs, n (%)a | ||||
Patients with ≥ 1 AE | 299 (95.8) | 144 (94.1) | 301 (96.5) | 145 (94.8) |
Anemia | 136 (43.6) | 61 (39.9) | 143 (45.8) | 61 (39.9) |
Alopecia | 115 (36.9) | 66 (43.1) | 116 (37.2) | 67 (43.8) |
Nausea | 78 (25.0) | 25 (16.3) | 79 (25.3) | 25 (16.3) |
Hyperglycemia | 55 (17.6) | 18 (11.8) | 57 (18.3) | 18 (11.8) |
Decreased appetite | 53 (17.0) | 18 (11.8) | 55 (17.6) | 19 (12.4) |
Increased ALT | 51 (16.3) | 22 (14.4) | 55 (17.6) | 23 (15.0) |
Arthralgia | 48 (15.4) | 20 (13.1) | 50 (16.0) | 20 (13.1) |
Neutropenia | 48 (15.4) | 19 (12.4) | 50 (16.0) | 19 (12.4) |
Increased AST | 46 (14.7) | 18 (11.8) | 50 (16.0) | 19 (12.4) |
Constipation | 43 (13.8) | 17 (11.1) | 44 (14.1) | 17 (11.1) |
Thrombocytopenia | 41 (13.1) | 19 (12.4) | 43 (13.8) | 19 (12.4) |
Dyspnea | 39 (12.5) | 10 (6.5) | 42 (13.5) | 10 (6.5) |
Asthenia | 38 (12.2) | 18 (11.8) | 42 (13.5) | 18 (11.8) |
Fatigue | 38 (12.2) | 11 (7.2) | 44 (14.1) | 12 (7.8) |
Vomiting | 38 (12.2) | 15 (9.8) | 39 (12.5) | 15 (9.8) |
Decreased weight | 35 (11.2) | 13 (8.5) | 39 (12.5) | 13 (8.5) |
Insomnia | 34 (10.9) | 11 (7.2) | 36 (11.5) | 11 (7.2) |
Diarrhea | 33 (10.6) | 10 (6.5) | 35 (11.2) | 10 (6.5) |
Hypoalbuminemia | 32 (10.3) | 9 (5.9) | 34 (10.9) | 10 (6.5) |
Serious adverse events, n (%)b | ||||
Patients with ≥ 1 SAE | || |||||| | || |||||| | || |||||| | || |||||| |
||||||||| | | ||||| | | ||||| | | ||||| | | ||||| |
|||||| | | ||||| | | ||||| | | ||||| | | ||||| |
||||||| ||||||||||| | | ||||| | | ||||| | | ||||| | | ||||| |
||||| | || ||||| | || ||||| | || ||||| | || ||||| |
Patients who stopped treatment due to AEs, n (%)c | ||||
Patients with ≥ 1 WDAE | 16 (5.1) | 4 (2.6) | 19 (6.1) | 7 (4.6) |
Increased ALT | 2 (0.6) | 0 (0.0) | 2 (0.6) | 1 (0.7) |
Anemia | 2 (0.6) | 0 (0.0) | 3 (1.0) | 0 (0.0) |
Deaths, n (%)d | ||||
Patients with any AE resulting in death | 19 (6.1) | 12 (7.8) | 27 (8.7) | 14 (9.2) |
Death | 5 (1.6) | 0 (0.0) | 9 (2.9) | 2 (1.3) |
Sudden death | 2 (0.6) | 0 (0.0) | 2 (0.6) | 0 (0.0) |
Pulmonary embolism | 1 (0.3) | 2 (1.3) | 4 (1.3) | 2 (1.3) |
Adverse events of special interest, n (%) | ||||
Patients with any treatment-emergent AESIe | || ||||| | | ||||| | || ||||| | | ||||| |
||||| | | ||||||||||||||||| ||||||||| ||||| | || ||||| | || ||||| | || ||||| | || ||||| |
||||| | | |||||||||| |||||||||||||||| ||||||||| | || ||||| | || ||| | || ||||| | || ||| |
||||| | | |||||||||||||||| ||| | || ||||| | || ||||| | || ||||| | || ||||| |
||||||||||||||| ||| || |||| ||||| || |||||||| ||||||||||| ||||||| |||| | ||||| |||||||||| | || ||| | || ||| | || ||| | || ||| |
AE = adverse event; AESI = adverse event of special interest; ALT = alanine aminotransferase; AST = aspartate aminotransferase; PBC = platinum-based chemotherapy; PI3-K = phosphatidylinositol 3-kinase; SAE = serious adverse event; SAF = safety analysis set; TE = treatment-emergent; WDAE = withdrawal due to adverse event.
aReported AEs are those of any grade that occurred in ≥ 10% of patients in either treatment group.
bReported SAEs are those that occurred in ≥ 2% of patients in either treatment group.
cReported WDAEs are those that occurred in > 1 patient in either treatment group.
dReported AEs leading to death are those that occurred in > 1 patient in either treatment group.
eBased on case report form collection criteria.
fNo patients receiving PI3-K inhibitors were enrolled in part 2 of the trial.
Source: EMPOWER-Lung 3 (part 2) Clinical Study Report;3 Gogishvili et al. (2022);24 EMPOWER-Lung 3 (part 2) final analysis Clinical Study Report.48
Safety Evaluation Plan
The primary objective of the clinical safety analysis was to detect safety signals and to assess the safety profile of cemiplimab in combination with PBC in comparison to PBC alone in patients with advanced squamous and nonsquamous NSCLC. The safety and tolerability of the treatment groups was evaluated in the SAF, which included all randomized patients who received at least 1 dose of any study drug (N = 465). The on-treatment period for the EMPOWER-Lung-3 trial is from the time of the first dose of the study drug up to 90 days after the last dose of the study drug, or to 1 day before patients receive another anticancer systemic therapy, or to the data cut-off date (i.e., either June 14, 2021, or June 14, 2022), whichever is earlier. All reported AEs are TEAEs unless otherwise noted. AEs are presented by incidence and by preferred term.
Overview of Safety
Adverse Events
The proportions of patients who experienced at least 1 AE were similar in the cemiplimab plus PBC group and the placebo plus PBC group for both data cut-off dates (i.e., 95.8% [299/312] versus 94.1% [144/153] for the June 14, 2021, data cut-off date and 96.5% [301/312] versus 94.8% [145/153] for the June 14, 2022 data cut-off date) (Table 17).
Similar proportions of patients in the cemiplimab plus PBC and placebo plus PBC treatment groups experienced infusion interruptions (1.6% [5/312] versus 2.0% [3/153]) or dose modifications (4.2% [13/312] versus 5.2% [8/153]), based on the June 14, 2022, data cut-off date. As dose reduction was not permitted for cemiplimab treatment, the dose modifications pertain to the chemotherapy components of the treatment regimens. TEAEs leading to dose delays occurred in 36.2% (113/312) of patients in the cemiplimab plus PBC group and 25.5% (39/153) of patients in the placebo plus PBC group, based on the June 14, 2022, data cut-off date. When adjusted for exposure, the TEAEs leading to dose delays were similar in the 2 treatment groups.
Based on the June 14, 2022, data cut-off date, the most frequently reported AEs of any grade by preferred term (experienced by ≥ 15% of patients in either treatment group) were (cemiplimab plus PBC versus placebo plus PBC) anemia (45.8% [143/312] versus 39.9% [61/153]), alopecia (37.2% [116/312] versus 43.8% [67/153]), nausea (25.3% [79/312] versus 16.3% [25/153]), hyperglycemia (18.3% [57/312] versus 11.8% [18/153]), decreased appetite (17.6% [55/312] versus 12.4% [19/153]), ALT increased (17.6% [55/312] versus 15.0% [23/153]), arthralgia (16.0% [50/312] versus 13.1% [20/153]), neutropenia (16.0% [50/312] versus 12.4% [19/153]), and AST increased (16.0% [50/312] versus 12.4% [19/153]). Similar results were reported for the June 14, 2021, data cut-off date.
Grade 3 and Greater AEs
As of June 2022, in the cemiplimab plus PBC group, TEAEs of grade 3, 4, or 5 were experienced by 48.7% of patients. Frequent (greater than 1%) AEs of grade 3, 4, or 5 included anemia (10.9%), neutropenia (6.4%), thrombocytopenia (3.2%), and leukopenia (1.9%). Metabolic and nutritional disorders, such as hyperglycaemia (1.9%), decreased appetite (1.3%), and hyponatremia (2.9%), were also reported. Other AEs of grade 3, 4, or 5 in this group were increased alanine aminotransferase (2.6%), fatigue (2.9%), pneumonia (2.9%), and dyspnea (2.6%).
In the placebo plus PBC group, TEAEs of grade 3, 4, or 5 occurred in 32.7% of patients. The most common events were anemia (6.5%), neutropenia (5.9%), thrombocytopenia (1.3%), and leukopenia (1.3%). Investigation-related AEs like increased alanine aminotransferase (2.0%) and increased aspartate aminotransferase (2.0%) were observed. Metabolic disturbances included hypokalemia (1.3%) and hyponatremia (1.3%). Other AEs of grade 3, 4, or 5 in the placebo group comprised pneumonia (3.3%), diarrhea (2.0%), and asthenia (1.3%).
Serious Adverse Events
The proportions of patients who experienced at least 1 SAE were ||||||| in the cemiplimab plus PBC group and the placebo plus PBC group for the June 14, 2021, data cut-off date (i.e., ||||| |||||||| || ||||| ||||||||| respectively) (Table 17). For the June 14, 2022, data cut-off date, the proportions of patients were ||||| |||||||| for the cemiplimab plus PBC group and ||||| |||||||| for the placebo plus PBC group. As of the June 2022, data cut-off date, the most frequent SAEs by preferred term (experienced by ≥ 2% of patients in either treatment group) included ||||||||| ||||| ||||||| || |||| ||||||||| |||||| ||||| |||||||| || |||| ||||||||| ||| ||||||| ||||||||||| ||||| ||||||| || |||| |||||||| in the cemiplimab plus PBC group vs placebo plus PBC anemia group, respectively.
Withdrawals Due to AEs
The proportions of patients who experienced at least 1 AE leading to discontinuation of the study treatment were (cemiplimab plus PBC versus placebo plus PBC) 5.1% (16/312) versus 2.6% (4/153) for the June 14, 2021, data cut-off date and 6.1% (19/312) versus 4.6% (7/153) for the June 14, 2022, data cut-off date. The most frequent AEs leading to study treatment discontinuation (experienced by > 1 patient each) were increased ALT and anemia (i.e., for both, 0.6% [2/312] of patients in the cemiplimab plus PBC group and 0% in the placebo plus PBC group) for the June 14, 2021, data cut-off date. For the June 14, 2022, data cut-off date, 0.6% (2/312) of patients in the cemiplimab plus PBC group and 0.7% (1/153) of patients in the placebo plus PBC group discontinued study treatment due to increased ALT, whereas 1.0% (3/312) of patients and 0% (0/153) of patients, respectively, discontinued study treatment due to anemia.
Deaths
As of the June 14, 2021, data cut-off date, 6.1% (19/312) of patients in the cemiplimab plus PBC group and 7.8% (12/153) of patients in the placebo plus PBC group experienced SAEs resulting in death, and for the June 14, 2022, data cut-off date, the proportions of patients were 8.7% (27/312) and 9.2% (14/153) in the 2 treatment groups, respectively (Table 17). The most common AEs resulting in death at the June 14, 2021, data cut-off date were reported to be (cemiplimab plus PBC versus placebo plus PBC) death (1.6% [5/312] versus 0% [0/153]), sudden death (0.6% [2/312] versus 0% [0/153]), and pulmonary embolism (0.3% [1/312] versus 1.3% [2/153]). At the June 14, 2022, data cut-off date, the most common AEs resulting in death were similar, and the proportions of patients, respectively, were 2.9% (9/312) versus 1.3% (2/153) for death, 0.6% (2/312) versus 0% (0/153) for sudden death, and 1.3% (4/312) versus 1.3% (2/153) for pulmonary embolism. In the cemiplimab plus PBC arm, |||| ||||||| of patients experienced treatment-related TEAEs resulting in death |||| || |||||| ||||||| |||||||| |||||| |||||||||||||| |||||||||| |||||| ||||||||||| ||| ||||||||||||, which was similar to the frequency of treatment-related deaths in the placebo plus PBC group ||||| ||||||| of patients).
Adverse Events of Special Interest
The AESIs reported in Table 17 are based on investigator assessment and used case report form collected criteria. The incidence of treatment-emergent AESIs based on the case report form collection criteria for the June 14, 2022, data cut-off date was |||| |||||||| in the cemiplimab plus PBC group and |||| ||||||| in the placebo plus PBC group. Overall, the incidence of AESIs was ||| in both treatment groups. The most frequent treatment-emergent AESIs was ||||| | | |||||||||||||||| ||||||||| which occurred in |||| ||||||| patients in the cemiplimab plus PBC group and |||| ||||||| patients in the placebo plus PBC group. Data from June 14, 2021, data cut-off date were similar.
Critical Appraisal
Internal Validity
The EMPOWER-Lung 3 study (part 2) is a double-blind, placebo-controlled, phase III RCT. The study used an interactive web response system for randomization, with stratification by histology and PD-L1 expression level. Allocation concealment methods were adequate. However, as the study was considered to have achieved its objective at the second interim analysis, corresponding to the June 14, 2021, data cut-off date, data for the study period subsequent to this date and until the data cut-off date of June 14, 2022, were unblinded, which potentially introduced biases in subjective outcomes such as HRQoL and harms. The study generally reports balanced baseline characteristics, which is indicative of effective randomization and reduces the risk of confounding. Treatment discontinuation events were mostly those captured by the end points. The primary end point of OS is objective and less prone to bias. The criteria for disease progression and tumour response are based on radiographic images and clinical assessment, with the potential for subjective interpretation. To mitigate this potential bias, a blinded IRC reviewed all available radiographic tumour assessments to determine tumour response based on RECIST 1.1 criteria. The study was powered to detect a difference in OS, with a sample size calculation based on historical data. The use of the Kaplan-Meier method, stratified log-rank test, and Cox proportional hazards model for time-to-event analysis is appropriate.
Several potential limitations can be observed in the EMPOWER-Lung 3 trial (part 2). First, the impact of subsequent anticancer therapies on OS introduces a confounding variable. The study documents indicate that a higher percentage of patients in the placebo plus PBC group than in the cemiplimab plus PBC group received subsequent therapies. This differential could potentially introduce a confounding effect on OS, as the survival results might be partially attributable to treatments administered after disease progression, rather than the study treatment itself. The magnitude and direction of this limitation is unclear; in general, patients receiving subsequent treatments are likely to have progressed and may not exhibit a favourable prognosis. Second, although high treatment compliance was reported, there were differences between the reported median and mean duration of exposure. Additionally, a substantial proportion of patients discontinued treatment early, predominantly due to disease progression, but also due to patient decision or AEs, particularly in the placebo group. This differential in treatment exposure could bias the efficacy results, likely in favour of cemiplimab plus PBC, as patients with longer exposure to the study treatment may have had more opportunity to derive benefit. Last, missing data on PROs present a challenge when evaluating the effect on HRQoL. With nearly half of the patients in the placebo plus PBC group failing to report PROs after cycle 6, the HRQoL results remain inconclusive.
External Validity
The clinical experts consulted by CADTH noted that the inclusion and exclusion criteria, as well as the baseline characteristics, were, overall, in line with other oncology trials and mostly representative of the patient population. However, there are a number of limitations that may affect the generalizability of the results. Included in these limitations is the fact that the trial only included patients with an ECOG PS of 1, limiting generalizability to other ECOG PSs, and the lack of sites in Canada, which may potentially lessen the generalizability of the results to clinical practice in Canada. The clinical experts consulted by CADTH noted that patients with an ECOG PS of 2 are likely to benefit from cemiplimab plus PBC and should be considered.
An important limitation of the study is the use of placebo plus PBC as the comparator, as opposed to another immunotherapy plus PBC. Currently in clinical practice in Canada, patients are offered immunotherapy rather than PBC alone. The clinical experts consulted by CADTH anticipate that the efficacy of cemiplimab plus PBC will be similar to that of other currently available immunotherapy plus chemotherapy combinations in this setting.
It is also worth noting that the number of patients who receive subsequent immunotherapy is, overall, considerably lower than expected in practice in Canada, according to the clinical experts consulted by CADTH. Although this could possibly limit the generalizability of the results, as OS could potentially have been longer in patients who discontinued due to disease progression, particularly in the placebo plus PBC group, the direction and magnitude of this potential bias remain unclear. Information from the sponsor’s submission suggests that the low numbers of patients receiving subsequent immunotherapy are likely due to immunotherapy not being approved, reimbursed, or readily available in the countries where the trial was conducted, and that in the cemiplimab plus PBC group, patients had already received on-study immunotherapy and re-treatment with immunotherapy is not recommended for patients who have progressed on first-line immunotherapy.
Finally, the trial was stopped early, per the recommendation of the IDMC, because the prespecified OS efficacy criteria were met at the secondary interim analysis (data-cut-off date: June 14, 2021,). This limits the availability of long-term evidence on the safety and efficacy of the intervention.
GRADE Summary of Findings and Certainty of the Evidence
Methods for Assessing the Certainty of the Evidence
For pivotal studies and RCTs identified in the sponsor’s systematic review, GRADE was used to assess the certainty of the evidence for outcomes considered most relevant to inform CADTH’s expert committee deliberations, and a final certainty rating was determined as outlined by the GRADE Working Group.1,2
High certainty: We are very confident that the true effect lies close to that of the estimate of the effect.
Moderate certainty: We are moderately confident in the effect estimate — The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. We use the word “likely” for evidence of moderate certainty (e.g., “X intervention likely results in Y outcome”).
Low certainty: Our confidence in the effect estimate is limited — The true effect may be substantially different from the estimate of the effect. We use the word “may” for evidence of low certainty (e.g., “X intervention may result in Y outcome”).
Very low certainty: We have very little confidence in the effect estimate — The true effect is likely to be substantially different from the estimate of effect. We describe evidence of very low certainty as “very uncertain.”
Following the GRADE approach, evidence from RCTs started as high-certainty evidence and could be rated down for concerns related to study limitations (which refers to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias.
When possible, certainty was rated in the context of the presence of an important (nontrivial) treatment effect; if this was not possible, certainty was rated in the context of the presence of any treatment effect (i.e., the clinical importance is unclear). In all cases, the target of the certainty of evidence assessment was based on the point estimate and where it was located relative to the threshold for a clinically important effect (when a threshold was available) or to the null.
Results of GRADE Assessments
Table 2 presents the GRADE summary of findings for cemiplimab plus PBC and placebo plus PBC.
Long-Term Extension Studies
No long-term extension studies were submitted.
Indirect Evidence
Contents within this section have been informed by materials submitted by the sponsor. The following have been summarized and validated by the CADTH review team.
Objectives for the Summary of Indirect Evidence
The comparative efficacy and safety of cemiplimab plus PBC was evaluated against PBC; however, head-to-head RCT evidence is lacking for comparisons with other treatments of interest.
The objective of this section was to obtain estimates of the comparative efficacy of cemiplimab in combination with chemotherapy versus other relevant interventions approved for the treatment of advanced or metastatic NSCLC among patients who have not received prior systemic therapy for their advanced and/or metastatic disease (i.e., first-line) by means of an NMA of RCTs identified from an SLR.
Description of Indirect Comparison(s)
The sponsor submitted 1 sponsor-initiated ITC. It is unclear if the sponsor conducted a search of the literature to identify any existing published ITCs. The ITC was informed by a SLR to identify eligible RCTs. The ITC was conducted through a Bayesian NMA framework. An SLR was performed to gather existing evidence on the efficacy of cemiplimab in combination with chemotherapy and relevant competing interventions for the treatment of patients with advanced or metastatic NSCLC, regardless of PD-L1 expression, who have not received prior systemic therapy for their advanced and/or metastatic disease (i.e., first-line).49 Database searches for the original SLR were executed in October 2019, with updates performed in May 2021 and March 2022. Predefined eligibility criteria guided the identification and selection of studies, as shown in Table 18. The target population included adult patients with advanced or metastatic (stage IIIB, IIIC, or IV) treatment-naive squamous or nonsquamous NSCLC with no known driver mutations (i.e., EGFR, ALK, ROS1) who were tested for PD-L1 (regardless of PD-L1 expression level).
Table 18: Study Selection Criteria and Methods for the ITC Submitted by the Sponsor
Criteria | Inclusion criteria | Exclusion criteria |
|---|---|---|
Population |
Subgroups of interest
|
|
Interventionsb |
|
|
Comparators |
| Interventions or comparators other than those explicitly listed in the PICOS |
Outcomesc | At least 1 of the following:
| Outcomes other than those explicitly listed in the PICOS |
Study designe | RCTs, phase II or III |
|
Publication characteristics |
|
|
Databases searched |
| |
Selection process | Two independent reviewers conducted abstract and full-text selection. Any discrepancies between reviewers were resolved through discussion, and a third reviewer was involved, if necessary. The process of study identification and selection was summarized with a PRISMA flow diagram. | |
Data extraction process | All data of interest were extracted from primary publications, whereas only additional data reported for relevant outcomes of interest or subgroups of interest were extracted from subsequent publications. Data extraction was conducted by 2 reviewers working independently. Any discrepancies between reviewers were resolved through discussion, and a third reviewer was involved, if necessary. Data were stored and managed in a Microsoft Excel workbook. Decision rules that were applied to the extracted data to generate the necessary dataset for the trials included in the feasibility assessment are outlined in the full NMA technical report.49 | |
Quality assessment | Two independent reviewers assessed the risk of bias of the included studies for which full-text publications were available. After reconciliation between the 2 investigators, a third investigator was included to reach consensus for any remaining discrepancies. The Cochrane Collaboration’s risk-of-bias tool was used to assess risk of bias in included clinical trials. | |
AE = adverse event; AJCC = American Joint Committee on Cancer; ASCO = American Society of Clinical Oncology; ECOG PS = Eastern Cooperative Oncology Group Performance Status; ELCC = European Lung Cancer Congress; ESMO = European Society for Medical Oncology; ITC = indirect treatment comparison; NSCLC = non–small cell lung cancer; PICOS = population, intervention, comparison, outcomes, and study design; PRISMA = Preferred Reporting Items for Systematic Reviews and Meta-Analyses; RCT = randomized control trial; SITC = Society for Immunotherapy of Cancer; WCLC = World Conference on Lung Cancer.
aPopulations consisting of mixed oncogene-positive and wild-type patients were included, assuming all other PICOS criteria were met.
bStudies that exclusively focused on comparisons of different doses, administration regimens, or treatment schedules were excluded.
cStudy selection was guided by the availability of efficacy and/or HRQoL data; however, AE data were extracted, where reported.
dRCTs reporting HRQoL outcomes were included in the SLR, but data will be extracted and synthesized as part of a separate HRQoL SLR, should another update be conducted in the future.
eLong-term follow-up RCTs and post hoc analyses of RCTs were included and crossover details were extracted; pooled analyses of RCTs were excluded, but crossover information was flagged during citation screening.
Source: Sponsor NMA technical report.49 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
ITC Design
Objectives
The objective of this ITC was to evaluate the comparative efficacy of cemiplimab plus PBC versus other Health Canada–approved interventions among patients with advanced or metastatic NSCLC with no known driver mutations (i.e., EGFR, ALK, ROS1) who have not received prior systemic therapy for their advanced and/or metastatic disease (i.e., first-line) with respect to OS, PFS, ORR, grade 3 to 5 all-cause AEs, grade 3 to 5 immune-mediated AEs, and discontinuations due to all-cause AEs.
Study Selection Methods
The SLR applied a date restriction for studies published from 2010 onward to align with the premarket approval of the PD-L1 IHC 22C3 pharmDx assay by the FDA in 2015, which is essential for the PD-L1 testing of patients with NSCLC. Studies published before 2010 were manually excluded before study screening began. Database searches were conducted on March 22, 2022, of MEDLINE, Embase, and the Cochrane Central Register of Controlled Trials (CENTRAL). These searches were supplemented by conference proceedings accessed through the Northern Light database as of March 29, 2022, and included major oncology conferences such as the American Society of Clinical Oncology (ASCO), European Society for Medical Oncology (ESMO), World Conference on Lung Cancer (WCLC), European Lung Cancer Congress (ELCC), and Society for Immunotherapy of Cancer (SITC). Proceedings up to January 31, 2023, that were not yet indexed were hand-searched. Additional searches included the US National Institutes of Health Clinical Trial Registry and the bibliographies of recent systematic reviews and meta-analyses, as well as product monographs and drug labels up to January 6, 2023. The SLR process was conducted by 2 independent reviewers who performed abstract and full-text selection, data extraction, and risk-of-bias assessment. The study identification and selection process were documented using a PRISMA flow diagram, and the included and excluded publications were summarized in appendices. Decision rules that applied to the extracted data were outlined to create the dataset for the trials included in the feasibility assessment, with calculated values being clearly marked. No information existed regarding methods of handling disagreements between reviewers or any actions taken to address studies that were considered to have high-risk of bias (Table 18).
ITC Analysis Methods
A feasibility assessment was conducted to gauge the appropriateness of proceeding with an NMA.50,51 The feasibility assessment process included: a determination of whether the RCT evidence for the interventions of interest formed 1 connected network for the overall population and each outcome of interest, and an assessment of the distribution of trial characteristics across the network; an assessment of the similarity of common comparator treatments; an exploration of the distribution of baseline patient characteristics both within and between comparisons to identify factors that may bias indirect estimates (i.e., identify effect modifiers); an assessment of outcome availability, definitions, and the time points at which outcomes are reported; and an exploration of the observed treatment effects to assess variability in outcome reporting and the proportional hazards assumption. The feasibility assessment process aligned with ISPOR, National Institute for Health and Care Excellence (NICE), and PRISMA guidelines.52-54 Potentially important treatment effect modifiers were identified based on a brief review of subgroup results from key trials included in the clinical evidence base and from recently published relevant SLRs and NMAs,55-69 and included age, sex, race and/or region (Asian, non-Asian), ECOG PS, PD-L1 biomarker status, smoking status, histology, disease stage at baseline, brain metastases at baseline, and liver metastases at baseline. When results of the RCTs identified in the SLR formed a connected evidence network and were deemed to be sufficiently similar for the population of interest, they were synthesized by means of NMAs by outcome of interest. All analyses were performed in a Bayesian framework and involved a model with parameters, data and a likelihood distribution, and prior distributions.
Both fixed-effects and random-effects models (with vague and informative priors for the between-study heterogeneity parameter) were considered for each analysis for completeness. The deviance information criterion and an assessment of overall stability were used to guide the identification of the appropriate model (i.e., fixed-effects or random-effects). In general, the assumptions of random-effects models are preferred, as they are expected to be more plausible than fixed-effects models. However, based on the feasibility assessment, it was expected that only a limited evidence base would inform the analysis, and random-effects models with noninformative priors for the between-study heterogeneity were expected to lead to unstable estimates and, therefore, fixed-effects models were preferred for all analyses. For the random-effects models, 1 parameter for the between-study heterogeneity was used, assuming that the between-study heterogeneity was the same for each intervention relative to the overall reference treatment of choice. As a sensitivity analysis, random-effects models using informative priors for the between-trial variance were explored according to Turner et al. (2015).70 The intervention comparison type was pharmacological versus pharmacological and, according to outcome, the informative priors for between-study heterogeneity were OS (outcome type all-cause mortality log-normal [meanlog = −4.18; sdlog = 1.41]), PFS and response (outcome type cause-specific mortality and/or major morbidity event and/or composite mortality or morbidity log-normal [meanlog = −3.95; sdlog = 1.79]), and AEs (outcome type adverse events log-normal [meanlog = −2.10; sdlog = 1.58]).
The proportional hazards assumption was evaluated using the Grambsch-Therneau test,71 log-cumulative hazard plots, and Schoenfeld residual plots.72 Violations of the proportional hazards assumption led to the adoption of the 2-step multivariate NMA described by Cope et al. (2020)73 for OS and PFS analyses. This approach was preferred even when the proportional hazards assumption was not violated, allowing for a more comprehensive data integration. The first step involved fitting 7 survival distributions (Weibull, Gompertz, log-normal, log-logistic, exponential, gamma, and generalized gamma) to each trial arm. The second step synthesized these parameters using a multivariate NMA framework. The exponential distribution, with its constant hazard function, was the only 1 with constant HRs over time. The generalized gamma distribution's third parameter was fixed across all models, based on the combined arm-level data, and affected the NMA results if any comparators were excluded.
Sensitivity analyses were conducted using constant HRs, with the most mature data from peer-reviewed publications. Two additional sensitivity analyses were performed: 1 using the longest follow-up data available, and another excluding the KEYNOTE-021G trial.
For binary outcomes such as ORR and AEs, logistic regression models with noninformative priors were used to estimate relative treatment effects as ORs.
Model selection for both the 2-step NMA and constant HR NMA was guided by the deviance information criterion, balancing model fit and complexity. The best-fitting models were identified based on the Akaike information criterion, visual inspections, and plausibility of extrapolations.
Model parameters were estimated using Markov Chain Monte Carlo methods in Just Another Gibbs Sampler (JAGS) software, with analyses performed in R. The selection of the best-fitting model was based on a comprehensive assessment of the evidence and external constraints.
Table 19: ITC Analysis Methods
Methods | Description |
|---|---|
Analysis methods |
|
Priors | Both fixed-effects and random-effects models (with vague and informative priors for the between-study heterogeneity parameter) were considered for each analysis. It was not feasible to estimate the between-study heterogeneity parameter of a random-effects model because the evidence networks consisted of relatively few trials and, therefore, led to unstable estimates. Thus, fixed-effects models were preferred for all analyses. As a sensitivity analysis, random-effects models using informative priors for the between-trial variance were explored according to Turner et al.(2015).70 |
Assessment of model fit |
|
Assessment of consistency | Not applicable; no closed loops in any evidence networks |
Assessment of convergence | Convergence was assessed using Gelman-Rubin plots, trace plots, and density plots. |
Outcomes | OS, PFS, ORR, grade 3 to 5 all-cause AEs, grade 3 to 5 IMAEs, and DAEs |
Follow-up time points |
|
Construction of nodes |
|
Sensitivity analyses |
|
Methods for pairwise meta-analysis | Not applicable; due to network geometry, the pairwise analysis is the same as that of the NMA |
AE = adverse event; AIC = Akaike information criterion; DAE = discontinuation due to adverse event; HR = hazard ratio; IMAE = immune-mediated adverse event; ITC = indirect treatment comparison; NMA = network meta-analysis; ORR = objective response rate; OS = overall survival; PFS = progression-free survival.
Source: Sponsor NMA technical report.64 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Results of Sponsor-Submitted ITC
Summary of Included Studies
The systematic literature search identified 12,537 initial citations, which was reduced to 8,791 after removing duplicates. Further screening and the inclusion of grey literature and other sources resulted in 269 citations, representing 76 unique trials. Ultimately, 233 citations corresponding to 41 unique trials with results were included for further screening, of which 11 unique RCTs were relevant to the target populations and of which only 5 unique RCTs were included in the scenario for any PD-L1, any histology: EMPOWER-Lung 3 (part 2),24 KEYNOTE-021G,74 KEYNOTE-189,61 KEYNOTE-407,75 and CheckMate 9LA.62 Of these 5 multicenter RCTs, 4 were phase III trials and 1 was a phase II trial (KEYNOTE-021G). The design of these trials varied; 3 were double-blind and 2 (KEYNOTE-021G and CheckMate 9LA) were open-label. However, in the open-label trials, outcome assessors for response and PFS were blinded to treatment assignment. The KEYNOTE-021G phase II trial was distinct in that it had a smaller sample size and was conducted in only 2 countries (Taiwan and the US).
Inclusion criteria across the trials were generally consistent, with all trials requiring an ECOG PS of 0 to 1, measurable disease per RECIST 1.1, and a life expectancy of at least 3 months. The trials included patients with various stages of disease, with some trials including patients with stage IIIB to stage IV disease and others restricted to patients with stage IV or recurrent disease. The KEYNOTE trials were pooled to represent an any-histology population, reflecting the indication for pembrolizumab plus chemotherapy in both squamous and nonsquamous histologies. Biomarker status was also a consideration; patients harbouring EGFR or ALK mutations were excluded from all trials except KEYNOTE-407, which did not report mutation status. Additionally, only 1 trial (EMPOWER-Lung 3 [part 2]) tested for ROS1 mutation status and excluded patients who tested positive. The trials used different but concordant assays to determine PD-L1 expression levels, which were considered equivalent for analysis purposes.
The proportion of patients receiving subsequent immunotherapy after initial chemotherapy treatment varied considerably across trials, with implications for the interpretation of the NMA results, ranging from 9.3% (KEYNOTE-407) to 35.5% (CheckMate 9LA). Ethnic composition in the included trials showed the EMPOWER-Lung 3 and CheckMate 9LA trials as having a higher proportion of non–East Asian patients than the KEYNOTE series. The proportion of patients who were current nor former smokers varied between 75% in the KEYNOTE-021G trial and up to 93.2% in the KEYNOTE-407 trial. Median age was relatively similar across the included trials. Patients with an ECOG PS of 1 represented up to 84.3% of the study population in the EMPOWER-Lung 3 trial. In contrast, patients with an ECOG PS of 1 represented 56% of the study population in the KEYNOTE- 021G trial.
Various chemotherapies were pooled together into the same node under the assumption of equivalency. This pooling included combinations of cisplatin or carboplatin with paclitaxel or pemetrexed, as well as pembrolizumab with these chemotherapies. Additionally, pooling of pembrolizumab combination regimens, regardless of histology, was performed; this included pembrolizumab with carboplatin or cisplatin, combined with either paclitaxel or pemetrexed.
Maintenance therapy varied across trials, with some requiring pemetrexed maintenance for nonsquamous disease and others making it optional. An assumption was made that these differences would not significantly affect the analysis results.
Table 20: Assessment of Homogeneity for the ITC
Characteristics | Description and handling of potential effect modifiers |
|---|---|
Trial characteristics | |
Study design |
|
Trial eligibility criteria |
|
Biomarker status before enrolment |
|
Crossover |
|
Subsequent immunotherapy among patients initially treated with chemotherapy |
|
Treatment characteristics | |
Chemotherapy regimens |
|
Pembrolizumab combination regimens |
|
Pemetrexed maintenance therapy for patients with nonsquamous NSCLC (optional or required) |
|
Patient characteristics | |
Baseline characteristics |
|
Outcome availability, definitions, and time points | |
Efficacy outcome availability |
|
Efficacy outcome definitions |
|
Time points of efficacy outcomes |
|
Safety outcome availability |
|
Safety outcome definitions |
|
Time points of safety outcomes |
|
AE = adverse event; CTCAE = Common Terminology Criteria for Adverse Events; DAE = discontinuation due to adverse events; DCO = data cut-off; ECOG PS = Eastern Cooperative Oncology Group Performance Status; HR = hazard ratio; IC = investigator’s choice; IMAE = immune-mediated adverse event; IRC = Independent Review Committee; ITC = indirect treatment comparison; ITT = intention to treat; KM = Kaplan-Meier; NCCN = National Comprehensive Cancer Network; NMA = network meta-analysis; NSCLC = non–small cell lung cancer; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; RECIST 1.1 = Response Evaluation Criteria in Solid Tumours Version 1.1 ; SA = sensitivity analysis.
Source: Sponsor NMA technical report.64 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Results
Evidence Networks
Table 21: OS and PFS Evidence Networks for the Any PD-L1, Any Histology Scenario Based on Constant or Time-Varying HR NMA
Scenario | Overall survival | Progression-free survival | ||
|---|---|---|---|---|
Constant HR | Time-varying HR | Constant HR | Time-varying HR | |
||| |||||| ||| ||||||||| | ||| | ||| | ||| | ||| |
HR = hazard ratio; NMA = network meta-analysis; OS = overall survival; PFS = progression-free survival.
Source: Sponsor NMA technical report.64 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Table 22: ORR Evidence Networks for the Any PD-L1, Any Histology Scenario
Scenario | Objective response rate |
|---|---|
||| |||||| ||| ||||||||| | ||| |
ORR = objective response rate.
Source: Sponsor NMA technical report.64 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Overall Survival
Time-varying OS HR results from the fixed-effects NMA for cemiplimab plus chemotherapy versus competing interventions using the best-fitting (log-logistic) model are presented in Table 23. The estimated relative treatment effects were applied to a pooled reference modelled survival function (IC chemotherapy) to generate OS proportions over time for each intervention. Cemiplimab plus chemotherapy demonstrated OS results that did not exclude the null within the CrI versus pembrolizumab plus chemotherapy (3 months: || ||||| ||| ||| |||| || ||||; 36 months: || ||||| ||| ||| |||| || |||||) and nivolumab plus ipilimumab plus chemotherapy (3 months: || ||||| ||| ||| |||| || ||||; 36 months: || ||||| ||| ||| |||| || |||||). Cemiplimab plus chemotherapy demonstrated a favourable improvement in OS versus IC chemotherapy at all time points (3 months: || ||||| ||| ||| |||| || ||||; 36 months: || ||||| ||| ||| |||| || |||||).
Results from the fixed-effects sensitivity analysis using constant HRs were generally consistent with the base-case results described previously.64 Results from the corresponding random-effects model with informative priors produced point estimates consistent with the fixed-effects model,64 but the random-effects models resulted in 95% CrIs that were marginally wider than the fixed-effects results.
In patients with any PD-L1, any histology, OS NMA results were consistent between the base-case and the sensitivity analyses using the longest follow-up data from any source or excluding the KEYNOTE-021G trial.
Table 23: Estimated OS HRs Over Time for Cemiplimab Plus Chemotherapy Versus Competing Interventions Among Patients With Any PD-L1 Expression and Any Histology From the Fixed-Effects 2-Step NMA (Log-Logistic Model)
Cemiplimab + chemotherapy vs. | Time-varying HR (95% CrI) | |||||||
|---|---|---|---|---|---|---|---|---|
3 months | 6 months | 9 months | 12 months | 18 months | 24 months | 30 monthsa | 36 monthsb | |
Chemotherapy | ||||| ||||| ||||| | ||||| ||||| ||||| | ||||| ||||| ||||| | ||||| ||||| ||||| | ||||| ||||| ||||| | ||||| ||||| ||||| | ||||| ||||| ||||| | ||||| ||||| ||||| |
Pembrolizumab + chemotherapy | ||||| ||||| ||||| | ||||| ||||| ||||| | ||||| ||||| ||||| | ||||| ||||| ||||| | ||||| ||||| ||||| | ||||| ||||| ||||| | ||||| ||||| ||||| | ||||| ||||| ||||| |
Nivolumab + ipilimumab + chemotherapy | ||||| ||||| ||||| | ||||| ||||| ||||| | ||||| ||||| ||||| | ||||| ||||| ||||| | ||||| ||||| ||||| | ||||| ||||| ||||| | ||||| ||||| ||||| | ||||| ||||| ||||| |
CrI = credible interval; HR = hazard ratio; NMA = network meta-analysis; OS = overall survival; vs. = versus.
aThe time point past the shortest median follow-up of trials was included in a given comparison.
bEstimates were based on model extrapolations.
Source: Sponsor NMA technical report.64 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Progression-Free Survival
Time-varying PFS HR results from the fixed-effects NMA for cemiplimab plus chemotherapy versus competing interventions using the best-fitting (log-logistic) model are presented in Table 24. The estimated relative treatment effects were applied to a pooled reference modelled survival function (IC chemotherapy) to generate PFS proportions over time for each intervention. Cemiplimab plus chemotherapy demonstrated PFS results that included the null within the CrI versus pembrolizumab plus chemotherapy (3 months: || ||||| ||| ||| |||| || ||||; 36 months: || ||||| ||| ||| |||| || ||||) and nivolumab plus ipilimumab plus chemotherapy (3 months: || ||||| ||| ||| |||| || ||||; 36 months: || ||||| ||| ||| |||| || ||||). Cemiplimab plus chemotherapy demonstrated a favourable improvement in PFS versus IC chemotherapy at all time points (3 months: || ||||| ||| ||| |||| || ||||; 36 months: || ||||| ||| ||| |||| || ||||).
Results from the fixed-effects sensitivity analysis using constant HRs were generally consistent with the base-case results described previously.64 Results from the corresponding random-effects model with informative priors produced point estimates and 95% CrIs consistent with the fixed-effects model.64
In patients with any PD-L1, any histology, PFS NMA results were consistent between the base-case and the sensitivity analyses using the longest follow-up data from any source or excluding the KEYNOTE-021G trial.
Table 24: Estimated PFS HRs Over Time for Cemiplimab Plus Chemotherapy Versus Competing Interventions Among Patients With Any PD-L1 and Any Histology From the Fixed-Effects 2-Step NMA (Log-Logistic Model)
Cemiplimab + chemotherapy vs. | Time-varying HR (95% CrI) | |||||||
|---|---|---|---|---|---|---|---|---|
3 months | 6 months | 9 months | 12 months | 18 months | 24 months | 30 monthsa | 36 monthsb | |
Chemotherapy | ||||| ||||| ||||| | ||||| ||||| ||||| | ||||| ||||| ||||| | ||||| ||||| ||||| | ||||| ||||| ||||| | ||||| ||||| ||||| | ||||| ||||| ||||| | ||||| ||||| ||||| |
Pembrolizumab + chemotherapy | ||||| ||||| ||||| | ||||| ||||| ||||| | ||||| ||||| ||||| | ||||| ||||| ||||| | ||||| ||||| ||||| | ||||| ||||| ||||| | ||||| ||||| ||||| | ||||| ||||| ||||| |
Nivolumab + ipilimumab + chemotherapy | ||||| ||||| ||||| | ||||| ||||| ||||| | ||||| ||||| ||||| | ||||| ||||| ||||| | ||||| ||||| ||||| | ||||| ||||| ||||| | ||||| ||||| ||||| | ||||| ||||| ||||| |
CrI = credible interval; HR = hazard ratio; NMA = network meta-analysis; PFS = progression-free survival; vs. = versus.
aThe time point past the shortest median follow-up of trials was included in a given comparison.
bEstimates were based on model extrapolations.
Source: Sponsor NMA technical report.64 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Objective Response Rate
A fixed-effects NMA was performed as the base-case analysis to assess ORR for cemiplimab plus chemotherapy versus competing interventions among patients with any PD-L1 and any histology based on the evidence network in Table 22. The estimated ORs from the NMA for cemiplimab plus chemotherapy versus competing interventions are presented in Figure 4. Among patients with any PD-L1 and any histology, cemiplimab plus chemotherapy demonstrated comparable ORR results to pembrolizumab plus chemotherapy (|| ||||| ||| ||| |||| || ||||) and nivolumab plus ipilimumab plus chemotherapy (|| ||||| ||| ||| |||| || ||||). Cemiplimab plus chemotherapy was associated with a favourably greater odds of ORR than IC chemotherapy (|| ||||| ||| ||| |||| || ||||). Results from the corresponding random-effects model with informative priors produced point estimates and 95% CrIs consistent with the fixed-effects model (refer to the full report).64
Figure 4: ORs From Fixed-Effects NMA for ORR Among Patients With Any PD-L1, Any Histology
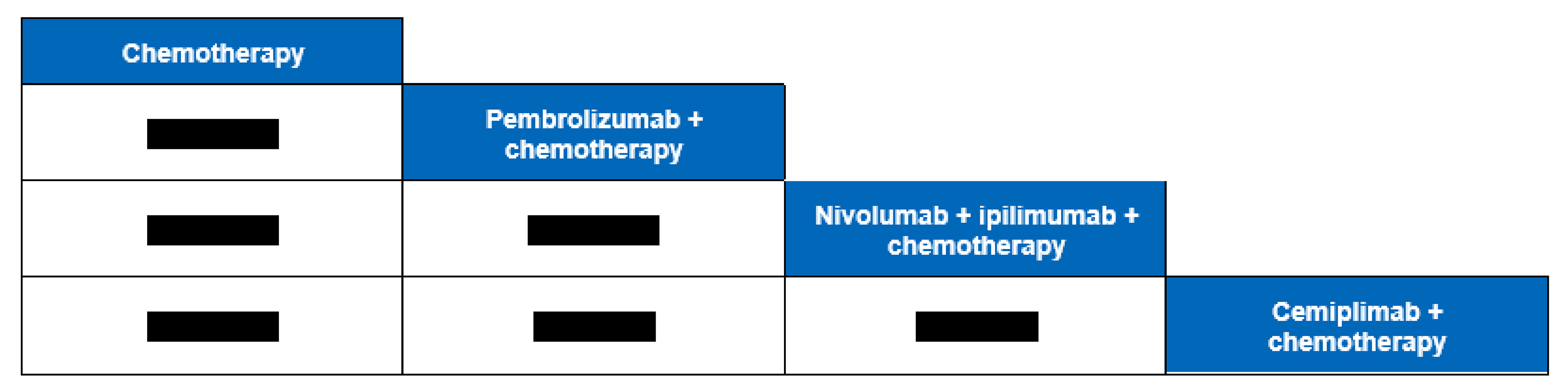
CrI = credible interval; DIC = deviance information criterion; NMA = network meta-analysis; OR = odds ratio; ORR = objective response rate.
Note: Each cell represents the comparison (OR and 95% CrI) of the row treatment versus the column treatment. DIC = 17.13; deviance = 9.12.
Source: Sponsor NMA technical report.64 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Critical Appraisal of Sponsor-Submitted ITC
The sponsor-submitted ITC was performed through an SLR, which systematically identified all the trials in the network, according to prespecified criteria.
However, there was a lack of reporting on the result of the quality assessment, even though it was stated that the Cochrane risk-of-bias tool was used, and it is unknown how studies with a high risk of bias were handled, if applicable.
The ITC reported on outcomes that were identified as important in the main body of the report. These included OS, PFS, and ORR. The ITC also reported on certain harms results. However, due to the limited evidence and events informing harms and the lack of applicability to the harms identified in the review as being of special interest, these have not been reported.
Several limitations due to the sparse network might have contributed to high uncertainty of the results obtained. The small number of included studies in the network with a Bayesian fixed-effects model mandated several untested assumptions, including the clinical homogeneity assumption. However, a significant concern is whether this assumption would have been held, given that there was significant heterogeneity across patient populations and interventions. Specifically, notable variations were noted across included studies in the proportion of patients receiving subsequent therapies, the proportion of patients with different levels of PD-L1 expression, tumour histology, metastasis sites, ECOG PS, chemotherapy regimens, maintenance therapy, and follow-up times. The combination between the observed clinical heterogeneity and sparse network substantially increases the uncertainty associated with the results.
Studies Addressing Gaps in the Systematic Review Evidence
No additional studies to address gaps within the systematic review evidence were submitted.
Discussion
Summary of Available Evidence
One pivotal phase III, RCT informed the systematic review: the EMPOWER-Lung 3 trial (part 2) was a phase III clinical trial comparing the efficacy and safety of cemiplimab plus PBC with placebo plus PBC in patients with advanced NSCLC, regardless of PD-L1 expression levels. The EMPOWER-Lung 3 trial (part 2) did not include sites in Canada. Two data cut-off dates are presented in this report for the EMPOWER-Lung 3 trial (part 2); the first was June 14, 2021, after a median follow-up of 16.4 months, and the second was June 14, 2022, after about a median follow-up of 28.4 months. The primary outcome was to assess OS, and key secondary outcomes included PFS and ORR. The trial met its primary end point by demonstrating a statistically significant prolongation of OS with cemiplimab plus PBC compared with placebo plus PBC at the secondary interim analysis, which had a data cut-off date of June 14, 2021. Median OS was longer in the cemiplimab plus PBC group than in the placebo plus PBC group (21.9 versus 13.0 months; HR = 0.706; 95% CI, 0.534 to 0.933; P = 0.0140) at the June 14, 2021, data cut-off date. Median OS results were maintained at the final analysis, which had a June 14, 2022, data cut-off date (21.1 versus 12.9 months; HR = 0.645; 95% CI, 0.507 to 0.820; P = 0.0003). The OS benefit provided by cemiplimab plus PBC was further corroborated by consistent and statistically significant improvements in multiplicity-adjusted key secondary end points (PFS and ORR).
Additionally, an ITC was conducted to compare the efficacy of cemiplimab plus PBC against other Health Canada–approved treatments for first-line advanced or metastatic NSCLC, regardless of PD-L1 expression or histology. This included an SLR and an NMA of RCTs from 2010 onward. The ITC found that cemiplimab plus PBC showed favourable OS, PFS, and ORR compared to chemotherapy, which is supportive of the results observed in the EMPOWER-Lung 3 trial (part 2). However, the results were less conclusive when compared to other immunotherapy combinations due to limitations related to sparse network and observable clinical heterogeneity across the included trials.
Interpretation of Results
Efficacy
The EMPOWER-Lung 3 trial provides pivotal data on the efficacy and safety of cemiplimab in combination with PBC for the first-line treatment of advanced NSCLC in patients without EGFR, ALK, or ROS1 aberrations. The trial met its primary end point, demonstrating a statistically significant improvement in OS for cemiplimab plus PBC compared to placebo plus PBC. Additionally, key secondary end points, such as PFS and ORR, were statistically significantly improved with the addition of cemiplimab. Certain limitations affect the internal validity and generalizability of the results. Specifically, imbalances in treatment exposure and subsequent therapy across study groups may limit the generalizability of the findings and bias the results; however, the magnitude and direction of this potential bias remains unclear. Overall, the GRADE assessment suggests that there is high certainty that cemiplimab plus PBC will lead to improved OS, PFS, and ORR compared to placebo plus PBC. Although these results were statistically significant, their interpretation and application to the general population in Canada is limited, as the trial's comparator (placebo plus PBC) does not reflect current practice in Canada, in which patients typically receive immunotherapy. The generalizability of the EMPOWER-Lung 3 trial results may be affected by several other factors. The study population was restricted to patients with an ECOG PS of 0 or 1, potentially excluding a subset of patients with poorer performance status who might also benefit from cemiplimab. Additionally, the trial did not include sites in Canada, which may limit the applicability of the findings to the health care context in Canada. Evidence regarding the long-term efficacy and safety of cemiplimab plus PBC is limited due to the early termination of the trial.
Comparison of cemiplimab to other members of the drug class, such as pembrolizumab and nivolumab, is based on indirect and uncertain evidence. The ITC found that cemiplimab plus PBC showed favourable OS, PFS, and ORR compared to chemotherapy, which is supportive of the results observed in the EMPOWER-Lung 2 trial (part 2). Considering the limitations related to sparse network and clinical heterogeneity across the included trials, it is not possible to conclude that cemiplimab plus PBC has an effect similar to other immunotherapies in combination with chemotherapies on OS, PFS, and ORR.
The EMPOWER-Lung 3 trial included PROs from the EORTC QLQ-C30 and QLQ-LC13 questionnaires. No clinically meaningful or statistically significant improvements in QoL or symptom control with cemiplimab plus PBC versus placebo were observed. A significant decline in the number of patients providing assessments over time makes interpretation of the PRO data challenging, and results remain inconclusive. HRQoL outcomes have been identified as being important to patients.
The clinical experts have highlighted the potential place of cemiplimab plus PBC as an alternative first-line treatment option for patients with advanced NSCLC without actionable driver alterations. Clinician group input supports the relevance of cemiplimab plus PBC in clinical practice.
Harms
Overall, the safety profile of cemiplimab plus PBC appeared consistent with the known profiles of cemiplimab and of chemotherapy, as well as profiles of other PD-1 and/or PD-L1 targeting therapies used in combination with chemotherapy to treat patients with NSCLC.81 Similar proportions of patients in both treatment groups experienced AEs and SAEs, and rates of infusion interruptions, dose modifications, and treatment discontinuations due to AEs were comparable. The most frequent AEs in both groups included anemia, alopecia, nausea, and increased ALT levels. Most TEAS were of grade 1 or grade 2. A total of 48.7% of patients in the cemiplimab plus PBC group and 32.7% of patients in the placebo plus PBC group experienced at least 1 TEAE of grade 3 or higher. Of these, anemia was reported by more patients in the cemiplimab plus PBC group than in the placebo plus PBC group (10.9% versus 6.5%), as were neutropenia (6.4% versus 5.9%), thrombocytopenia (3.2% versus 1.3%), and leukopenia (1.9% versus 1.3%). Metabolic and nutritional disorders were also noted, with hyperglycaemia affecting 1.9% of patients in the cemiplimab plus PBC group and 0.0% in the placebo plus PBC group. Hyponatremia was reported in 2.9% of patients in the cemiplimab plus PBC group and by 1.3% in the placebo plus PBC group. AESIs were reported in |||| of patients in the cemiplimab plus PBC group and |||| in the placebo plus PBC group as of the June 14, 2022, data cut-off date. The most frequent AESI was ||||| | || |||||| |||||||||||||||| |||||||||, occurring in |||| of patients in the cemiplimab plus PBC group and |||| in the placebo plus PBC group.
Conclusion
Based on clinical data from the EMPOWER-Lung 3 study (part 2), cemiplimab plus PBC demonstrated a statistically significant benefit compared to placebo plus PBC in OS, PFS, and ORR for the treatment of patients with advanced NSCLC and no EGFR, ALK, or ROS1 aberrations, regardless of PD-L1 expression status. GRADE assessment suggests that there is a high certainty that cemiplimab plus PBC will lead to a better OS, PFS, and ORR over a median follow-up period of 28.42 months. However, there is a low level of certainty that cemiplimab plus PBC results in little to no difference in HRQoL, measured by the EORTC QLQ-C30, compared to placebo plus PBC.
There is no notable increase in patients with treatment-emergent AESIs in the cemiplimab plus PBC group compared to the placebo plus PBC group. GRADE assessment of treatment-emergent AESIs suggests a low level of certainty that cemiplimab plus PBC results in little to no differences in harms of special interest compared to placebo plus PBC.
A sponsor-submitted ITC compared the efficacy of cemiplimab plus PBC against other Health Canada–approved treatments for the first-line treatment of patients with advanced or metastatic NSCLC, regardless of PD-L1 expression or histology. However, due to the small number of studies in the network, along with significant concerns related to clinical heterogeneity, no firm conclusions could be drawn about the efficacy and safety of cemiplimab plus PBC compared to pembrolizumab plus chemotherapy or nivolumab plus ipilimumab plus chemotherapy. Considering the consistency of the direction of the indirect results for cemiplimab plus PBC versus chemotherapy in the ITC, with the direct and existing evidence in the form of the EMPOWER-Lung 3 trial (part 2), the indirect results can be considered supportive of the findings in the EMPOWER-Lung 3 trial (part 2).
References
1.Balshem H, Helfand M, Schünemann HJ, et al. GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol. 2011;64(4):401-406. PubMed
2.Santesso N, Glenton C, Dahm P, et al. GRADE guidelines 26: informative statements to communicate the findings of systematic reviews of interventions. J Clin Epidemiol. 2020;119:126-135. PubMed
3.Clinical Study Report: R2810-ONC-16113. A two-part randomized, phase 3 study of combinations of cemiplimab (anti-PD-1 antibody) and platinum-based doublet chemotherapy in first-line treatment of patients with advancedor metastatic non-small cell lung cancer [internal sponsor's report]. Tarrytown (NY): Regeneron Pharmaceuticals, Inc; 2021.
4.Canadian Cancer Society. Lung and brochus cancer statistics. 2023; https://cancer.ca/en/cancer-information/cancer-types/lung/statistics. Accessed 2023 May 25.
5.Libtayo (cemiplimab): 50 mg/mL solution for infusion [product monograph]. Laval (QC): Sanofi-aventis Canada; 2023 Aug 15.
6.Zheng M. Classification and pathology of lung cancer. Surg Oncol Clin N Am. 2016;25(3):447-468. PubMed
7.Canadian Cancer Statistics Advisory Committee. Canadian Cancer Statistics: A 2020 special report on lung cancer. Toronto (ON): Canadian Cancer Society 2020.
8.Canadian Cancer Society. Prognosis and survival for lung cancer. 2020; https://cancer.ca/en/cancer-information/cancer-types/lung/prognosis-and-survival. Accessed 2023 May 25.
9.SEER*Stat Database: Incidence - SEER 21 regs limited-field research data + Hurricane Katrina impacted Louisiana cases, Nov 2018 sub (2000-2016) <Katrina/Rita population adjustment> - linked to county attributes - total U.S. 1969-2017 counties [sponsor provided reference]. Bethesda (MD): National Cancer Institute, Surveillance, Epidemiology, and End Results Program; 2018.
10.Stewart DJ, Maziak DE, Moore SM, et al. The need for speed in advanced non-small cell lung cancer: a population kinetics assessment. Cancer Med. 2021;10(24):9040-9046. PubMed
11.CADTH reimbursement recommendation: cemiplimab (Libtayo) for first-line treatment of adult patients with non–small cell lung cancer (NSCLC) expressing PD-L1 (Tumour Proportion Score [TPS] ≥ 50%), as determined by a validated test, with no EGFR, ALK, or ROS1 aberrations, who have locally advanced NSCLC who are not candidates for surgical resection or definitive chemoradiation, or metastatic NSCLC. Can J Health Technol. 2022;2(6). https://www.cadth.ca/sites/default/files/DRR/2022/PC0262%20Libtayo%20NSCLC%20%20%E2%80%93%20CADTH%20Final%20Rec.pdf. Accessed 2023 Nov 5.
12.Canadian Cancer Society. Diagnosis of lung cancer. 2020; https://cancer.ca/en/cancer-information/cancer-types/lung/diagnosis. Accessed 2023 May 25.
13.Ionescu DN, Stockley TL, Banerji S, et al. Consensus recommendations to optimize testing for new targetable alterations in non-small cell lung cancer. Curr Oncol. 2022;29(7):4981-4997. PubMed
14.NCCN clinical practice guidelines in oncology (NCCN guidelines): non-small cell lung cancer. Version 3.2023 Plymouth Meeting (PA): National Comprehensive Cancer Network; 2023 Apr 13.
15.Daly ME, Singh N, Ismaila N, et al. Management of stage III non-small-cell lung cancer: ASCO guideline. J Clin Oncol. 2022;40(12):1356-1384. PubMed
16.Singh N, Jaiyesimi IA, Ismaila N, et al. Therapy for stage IV non-small-cell lung cancer with driver alterations: ASCO living guideline, version 2023.1. J Clin Oncol. 2023;41(15):e42-e50. PubMed
17.Zhang M, Li G, Wang Y, et al. PD-L1 expression in lung cancer and its correlation with driver mutations: a meta-analysis. Sci Rep. 2017;7(1):10255. PubMed
18.Ernani V, Stinchcombe TE. Management of brain metastases in non-small-cell lung cancer. J Oncol Pract. 2019;15(11):563-570. PubMed
19.NSCLC Meta-Analyses Collaborative Group. Chemotherapy in addition to supportive care improves survival in advanced non-small-cell lung cancer: a systematic review and meta-analysis of individual patient data from 16 randomized controlled trials. J Clin Oncol. 2008;26(28):4617-4625. PubMed
20.Leighl NB. Treatment paradigms for patients with metastatic non-small-cell lung cancer: first-, second-, and third-line. Curr Oncol. 2012;19(Suppl 1):S52-58. PubMed
21.Arbour KC, Riely GJ. Systemic therapy for locally advanced and metastatic non-small cell lung cancer: a review. JAMA. 2019;322(8):764-774. PubMed
22.Health Canada clarimail: Libtayo (cemiplimab for injection) [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Libtayo (cemiplimab for injection) 350 mg every three (3) weeks as an intravenous (IV) infusion. Mississauga (ON): Sanofi Genzyme; 2021 Oct 13.
23.Sponsor's summary of clinical evidence [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Libtayo (cemiplimab for injection) 350 mg every three (3) weeks as an intravenous (IV) infusion. Mississauga (ON): Sanofi Genzyme; 2021 Oct 13.
24.Gogishvili M, Melkadze T, Makharadze T, et al. Cemiplimab plus chemotherapy versus chemotherapy alone in non-small cell lung cancer: a randomized, controlled, double-blind phase 3 trial. Nat Med. 2022;28(11):2374-2380. PubMed
25.Kalinka-Warzocha E, Gogishvili M, Makharadze T, et al. Cemiplimab with platinum-based chemotherapy (chemo) for first-line (1L) locally advanced non-small cell lung cancer (laNSCLC): EMPOWER-Lung 3 subgroup analysis. Ann Oncol. 2022;33(Supplement 7):S983-S984.
26.Makharadze T, Quek RG, Melkadze T, et al. 93P Patient-reported outcomes (PROs) with cemiplimab or placebo plus platinum-doublet chemotherapy (chemo) for first-line (1L) treatment of advanced non-small cell lung cancer (aNSCLC): EMPOWER-Lung 3 trial. Ann Oncol. 2021;32(Supplement 7):S1414.
27.Gogishvili M, Melkadze T, Makharadze T, et al. LBA51 EMPOWER-Lung 3: cemiplimab in combination with platinum doublet chemotherapy for first-line (1L) treatment of advanced non-small cell lung cancer (NSCLC). Ann Oncol. 2021;32(Supplement 5):S1328.
28.Gogishvili M, Mobashery N, Makharadze T, et al. P2.01-26 EMPOWER-Lung 3: phase 3 study of combinations of cemiplimab and chemotherapy in first-line treatment of advanced NSCLC. J Thorac Oncol. 2019;14(10 Supplement):S649.
29.Rizvi N, Lee S, Curtis P, Caldwell W, Gao B, Rietschel P. EMPOWER-Lung 3: a phase 3 study of cemiplimab, ipilimumab and chemotherapy in advanced NSCLC with PD-L1 <50%. J Thorac Oncol. 2018;13(10 Supplement):S931.
30.CADTH. Keytruda (pembrolizumab) for advanced non-small cell lung carcinoma (first-line) - details. https://www.cadth.ca/keytruda-advanced-non-small-cell-lung-carcinoma-first-line-details. Accessed 2023 May 25.
31.Makharadze T, Gogishvili M, Melkadze T, et al. Cemiplimab plus chemotherapy versus chemotherapy alone in advanced NSCLC: 2-year follow-up from the phase 3 EMPOWER-lung 3 part 2 trial. J Thorac Oncol. 2023;18(6):755-768. PubMed
32.Makharadze T, Quek RGW, Melkadze T, et al. Quality of life with cemiplimab plus chemotherapy for first-line treatment of advanced non-small cell lung cancer: patient-reported outcomes from phase 3 EMPOWER-Lung 3. Cancer. 2023;129(14):2256-2265. PubMed
33.Makharadze T, Gogishvili M, Melkadze T, et al. 50 - Cemiplimab plus chemotherapy versus chemotherapy alone in non-small cell lung cancer: longer follow-up results from the Phase 3 EMPOWER-Lung 3 tria. J Thorac Oncol. 2023;18:S38-S39.
34.Kalinka E, Bondarenko I, Gogishvili M, et al. 114MO - First-line cemiplimab for locally advanced non-small cell lung cancer: updated subgroup analyses from EMPOWER-Lung 1 and EMPOWER-Lung 3. J Thorac Oncol. 2023;18:S106.
35.Gogishvili M, Melkadze T, Makharadze T, et al. EMPOWER-Lung 3: cemiplimab in combination with platinum doublet chemotherapy for first-line (1L) treatment of advanced non-small cell lung cancer (NSCLC). Ann Oncol. 2022;33:S1567-S1568.
36.Gandara DR, Gogishvili M, Sezer A, et al. Predictive utility of patient-reported outcomes for survival in 1st-line treated patients with a NSCLC in EMPOWER-Lung 1 and 3. World Conference on Lung Cancer; 2023; Singapore.
37.Baramidze A, Gessner C, Gogishvili M, et al. Cemiplimab-based treatment in advanced NSCLC with liver metastases: updated analysis from EMPOWER-Lung 1 and EMPOWER-Lung 3. World Conference on Lung Cancer; 2023; Singapore.
38.Eisenhauer EA, Therasse P, Bogaerts J, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer. 2009;45(2):228-247. PubMed
39.Ellis LM, Bernstein DS, Voest EE, et al. American Society of Clinical Oncology perspective: raising the bar for clinical trials by defining clinically meaningful outcomes. J Clin Oncol. 2014;32(12):1277-1280. PubMed
40.Osoba D, Rodrigues G, Myles J, Zee B, Pater J. Interpreting the significance of changes in health-related quality-of-life scores. J Clin Oncol. 1998;16(1):139-144. PubMed
41.Aaronson NK, Ahmedzai S, Bergman B, et al. The European Organization for Research and Treatment of Cancer QLQ-C30: a quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst. 1993;85(5):365-376. PubMed
42.Teckle P, Peacock S, McTaggart-Cowan H, et al. The ability of cancer-specific and generic preference-based instruments to discriminate across clinical and self-reported measures of cancer severities. Health Qual Life Outcomes. 2011;9:106. PubMed
43.Nicklasson M, Bergman B. Validity, reliability and clinical relevance of EORTC QLQ-C30 and LC13 in patients with chest malignancies in a palliative setting. Qual Life Res. 2007;16(6):1019-1028. PubMed
44.Ozturk A, Sarihan S, Ercan I, Karadag M. Evaluating quality of life and pulmonary function of long-term survivors of non-small cell lung cancer treated with radical or postoperative radiotherapy. Am J Clin Oncol. 2009;32(1):65-72. PubMed
45.Maringwa JT, Quinten C, King M, et al. Minimal important differences for interpreting health-related quality of life scores from the EORTC QLQ-C30 in lung cancer patients participating in randomized controlled trials. Support Care Cancer. 2011;19(11):1753-1760. PubMed
46.Drug Reimbursement Review sponsor submission: Libtayo (cemiplimab for injection) 350 mg every three (3) weeks as an intravenous (IV) infusion [internal sponsor's package]. Mississauga (ON): Sanofi Genzyme; 2021 Oct 13.
47.Bergman B, Aaronson NK, Ahmedzai S, Kaasa S, Sullivan M. The EORTC QLQ-LC13: a modular supplement to the EORTC Core Quality of Life Questionnaire (QLQ-C30) for use in lung cancer clinical trials. EORTC Study Group on Quality of Life. Eur J Cancer. 1994;30A(5):635-642. PubMed
48.Alimta (pemetrexed disodium for injection): 100 mg or 500 mg per vial [product monograph]. Toronto (ON): Eli Lilly Canada Inc; 2013 May 10.
49.Paclitaxel for Injection (paclitaxel): 6 mg/mL [product monograph]. Kirkland (QC): Pfizer Canada ULC; 2020 May 6.
50.Jansen JP, Naci H. Is network meta-analysis as valid as standard pairwise meta-analysis? It all depends on the distribution of effect modifiers. BMC Med. 2013;11:159. PubMed
51.Cope S, Zhang J, Saletan S, Smiechowski B, Jansen JP, Schmid P. A process for assessing the feasibility of a network meta-analysis: a case study of everolimus in combination with hormonal therapy versus chemotherapy for advanced breast cancer. BMC Med. 2014;12:93. PubMed
52.Hutton B, Salanti G, Caldwell DM, et al. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: checklist and explanations. Ann Intern Med. 2015;162(11):777-784. PubMed
53.Hoaglin DC, Hawkins N, Jansen JP, et al. Conducting indirect-treatment-comparison and network-meta-analysis studies: report of the ISPOR Task Force on indirect treatment comparisons good research practices: part 2. Value Health. 2011;14(4):429-437. PubMed
54.Dias S, Sutton AJ, Ades AE, Welton NJ. Evidence synthesis for decision making 2: a generalized linear modeling framework for pairwise and network meta-analysis of randomized controlled trials. Med Decis Making. 2013;33(5):607-617. PubMed
55.Mok TSK, Wu YL, Kudaba I, et al. Pembrolizumab versus chemotherapy for previously untreated, PD-L1-expressing, locally advanced or metastatic non-small-cell lung cancer (KEYNOTE-042): a randomised, open-label, controlled, phase 3 trial. Lancet. 2019;393(10183):1819-1830. PubMed
56.Reck M, Rodríguez-Abreu D, Robinson AG, et al. Pembrolizumab versus chemotherapy for PD-L1-positive non-small-cell lung cancer. N Engl J Med. 2016;375(19):1823-1833. PubMed
57.Reck M, Rodríguez-Abreu D, Robinson AG, et al. Updated analysis of KEYNOTE-024: pembrolizumab versus platinum-based chemotherapy for advanced non-small-cell lung cancer with PD-L1 tumor proportion score of 50% or greater. J Clin Oncol. 2019;37(7):537-546. PubMed
58.Spigel D, De Marinis F, Giaccone G, et al. IMpower110: Interim overall survival (OS) analysis of a phase III study of atezolizumab (atezo) vs platinum-based chemotherapy (chemo) as first-line (1L) treatment (tx) in PD-L1–selected NSCLC. Ann Oncol. 2019;30:v915.
59.Syrigos KN, Vansteenkiste J, Parikh P, et al. Prognostic and predictive factors in a randomized phase III trial comparing cisplatin-pemetrexed versus cisplatin-gemcitabine in advanced non-small-cell lung cancer. Ann Oncol. 2010;21(3):556-561. PubMed
60.Paz-Ares L, Ciuleanu TE, Yu X, et al. LBA3 Nivolumab (NIVO) + platinum-doublet chemotherapy (chemo) vs chemo as first-line (1L) treatment (tx) for advanced non-small cell lung cancer (aNSCLC): checkMate 227 - part 2 final analysis. Ann Oncol. 2019;30.
61.Gandhi L, Rodriguez-Abreu D, Gadgeel S, et al. Pembrolizumab plus chemotherapy in metastatic non-small-cell lung cancer. N Engl J Med. 2018;378(22):2078-2092. PubMed
62.Paz-Ares L, Ciuleanu TE, Cobo M, et al. First-line nivolumab plus ipilimumab combined with two cycles of chemotherapy in patients with non-small-cell lung cancer (CheckMate 9LA): an international, randomised, open-label, phase 3 trial. Lancet Oncol. 2021;22(2):198-211. PubMed
63.West H, McCleod M, Hussein M, et al. Atezolizumab in combination with carboplatin plus nab-paclitaxel chemotherapy compared with chemotherapy alone as first-line treatment for metastatic non-squamous non-small-cell lung cancer (IMpower130): a multicentre, randomised, open-label, phase 3 trial. Lancet Oncol. 2019;20(7):924-937. PubMed
64.Carter GC, Barrett AM, Kaye JA, Liepa AM, Winfree KB, John WJ. A comprehensive review of nongenetic prognostic and predictive factors influencing the heterogeneity of outcomes in advanced non-small-cell lung cancer. Cancer Manag Res. 2014;6:437. PubMed
65.Jiang P, Mao Z, Wang Q, et al. An indirect comparison between nivolumab+ ipilimumab+ two cycles of chemotherapy vs. pembrolizumab+ chemotherapy as first-line treatment for metastatic non-small cell lung cancer. Front Oncol. 2021;11. PubMed
66.Kawaguchi T, Takada M, Kubo A, et al. Performance status and smoking status are independent favorable prognostic factors for survival in non-small cell lung cancer: a comprehensive analysis of 26,957 patients with NSCLC. J Thorac Oncol. 2010;5(5):620-630. PubMed
67.Soo RA, Kawaguchi T, Loh M, et al. Differences in outcome and toxicity between Asian and Caucasian patients with lung cancer treated with systemic therapy. Future Oncol. 2012;8(4):451-462. PubMed
68.Kawaguchi T, Matsumura A, Fukai S, et al. Japanese ethnicity compared with Caucasian ethnicity and never-smoking status are independent favorable prognostic factors for overall survival in non-small cell lung cancer: a collaborative epidemiologic study of the National Hospital Organization Study Group for Lung Cancer (NHSGLC) in Japan and a Southern California Regional Cancer Registry databases. J Thorac Oncol. 2010;5(7):1001-1010. PubMed
69.Sezer A, Kilickap S, Gumus M, et al. EMPOWER-Lung 1: Phase III first-line (1L) cemiplimab monotherapy vs platinum-doublet chemotherapy (chemo) in advanced non-small cell lung cancer (NSCLC) with programmed cell death-ligand 1 (PD-L1) >=50%. Ann Oncol. 2020;31(Suppl 4):S1182-S1183.
70.Turner RM, Jackson D, Wei Y, Thompson SG, Higgins JP. Predictive distributions for between-study heterogeneity and simple methods for their application in Bayesian meta-analysis. Stat Med. 2015;34(6):984-998. PubMed
71.Grambsch PM, Therneau TM. Proportional hazards tests and diagnostics based on weighted residuals. Biometrika. 1994;81(3):515-526.
72.Schoenfeld D. Partial residuals for the proportional hazards regression model. Biometrika. 1982;69(1):239-241.
73.Cope S, Chan K, Jansen JP. Multivariate network meta‐analysis of survival function parameters. Res Synth Methods. 2020;11(3):443-456. PubMed
74.Langer CJ, Gadgeel SM, Borghaei H, et al. Carboplatin and pemetrexed with or without pembrolizumab for advanced, non-squamous non-small-cell lung cancer: a randomised, phase 2 cohort of the open-label KEYNOTE-021 study. Lancet Oncol. 2016;17(11):1497-1508. PubMed
75.Paz-Ares L, Luft A, Vicente D, et al. Pembrolizumab plus chemotherapy for squamous non-small-cell lung cancer. N Engl J Med. 2018;379(21):2040-2051. PubMed
76.Mao Z, Jiang P, Zhang Y, et al. First‐line immune‐based combination therapies for advanced non‐small cell lung cancer: a Bayesian network meta‐analysis. Cancer Med. 2021;10(24):9139-9155. PubMed
77.Peng TR, Lin HH, Tsai FP, Wu TW. Immune checkpoint inhibitors for first‐line treatment of advanced non‐small‐cell lung cancer: a systematic review and network meta‐analysis. Thorac Cancer. 2021;12(21):2873-2885. PubMed
78.Johnson DH, Fehrenbacher L, Novotny WF, et al. Randomized phase II trial comparing bevacizumab plus carboplatin and paclitaxel with carboplatin and paclitaxel alone in previously untreated locally advanced or metastatic non-small-cell lung cancer. J Clin Oncol. 2004;22(11):2184-2191. PubMed
79.Al-Saleh K, Quinton C, Ellis PM. Role of pemetrexed in advanced non-small-cell lung cancer: meta-analysis of randomized controlled trials, with histology subgroup analysis. Curr Oncol. 2012;19(1):e9-e15. PubMed
80.Xiao HQ, Tian RH, Zhang ZH, Du KQ, Ni YM. Efficacy of pemetrexed plus platinum doublet chemotherapy as first-line treatment for advanced nonsquamous non-small-cell-lung cancer: a systematic review and meta-analysis. Onco Targets Ther. 2016;9:1471-1476. PubMed
81.Health Canada reviewer's report: Libtayo (cemiplimab) [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Libtayo (cemiplimab for injection) 350 mg every three (3) weeks as an intravenous (IV) infusion. Mississauga (ON): Sanofi Genzyme; 2021 Oct 13.
Appendix 1: Detailed Baseline Data
Table 25: ITC Baseline Characteristics of Included Trials
Trial | Treatment | Pop. | N | Age, median | Male n (%) | Geographic region, n (%) | Smoking status, n (%) | ECOG performance status, n (%) | Histology, n (%) | Disease stage at baseline, n (%) | Brain mets. at baseline, n (%) | Liver mets. at baseline, n (%) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
East Asian | Non-East Asian | Current / Former smoker | Never smoker | 0 | 1 | Squa mous | Non-squa mous | IIIB | IIIC | IV | ||||||||
EMPOWER-Lung 3 Part 2 | Cemi + IC chemo | ITT, any PD-L1, any histology | 312 | 63.0 | 268 (85.9) | 45 (14.4) | 267 (85.6) | 269 (86.2)a | 43 (13.8) | 51 (16.3) | 259 (83.0) | 133 (42.6) | 179 (57.4) | 45 (14.4) | 267 (85.6) | 24 (7.7) | 49 (15.7) | |
IC chemo | 154 | 63.0 | 123 (79.9) | 16 (10.4) | 138 (89.6) | 130 (84.4)a | 24 (15.6) | 18 (11.7) | 134 (87.0) | 67 (43.5) | 87 (56.5) | 24 (15.6) | 130 (84.4) | 7 (4.5) | 23 (14.9) | |||
KEYNOTE- 021G (non.sq) | Pembro + pem + carb | ITT, any PD-L1, nonsq. | 60 | 62.5 | 22 (37.0) | 5 (8.0)b | 55 (92.0)b | 45 (75.0)c | 15 (25.0) | 24 (40.0) | 35 (58.0)d | -- | 60 (100)e | 1 (2.0) | -- | 59 (98.0) | 9 (15.0) | -- |
Carb + pem | 63 | 63.2 | 26 (41.0) | 5 (8.0)b | 58 (92.0)b | 54 (86.0)c | 9 (14.0) | 29 (46.0) | 34 (54.0) | -- | 63 (100)e | 2 (3.0)f | -- | 60 (95.0) | 6 (10.0) | -- | ||
KEYNOTE- 189 (non- sq.) | Pembro + IC chemo | ITT, any PD-L1. nonsq. | 410 | 65.0 | 254 (62.0) | 4 (1.0) | 406 (99.0) | 362 (88.3)c | 48 (11.7) | 186 (45.4) | 221 (53.9) | -- | 410 (100)e | -- | -- | 410 (100)e | 73 (17.8) | 66 (16.1) |
IC chemo | 206 | 63.5 | 109 (52.9) | 6 (2.9) | 200 (97.1) | 181 (87.9)c | 25 (12.1) | 80 (38.8) | 125 (60.7) | -- | 206 (100)e | -- | -- | 206 (100)e | 35 (17.0) | 49 (23.8) | ||
KEYNOTE- 407 (sq.) | Pembro + IC chemo | ITT, any PD-L1, sq. | 278 | 65.0 | 220 (79.1) | 54 (19.4) | 224 (80.6) | 256 (92.1)c | 22 (7.9) | 73 (26.3) | 205 (73.7) | 272 (97.8)f | -- | -- | -- | 278 (100)e | 20 (7.2) | -- |
IC chemo | 281 | 65.0 | 235 (83.6) | 52 (18.5) | 229 (81.5) | 262 (93.2)c | 19 (6.8) | 90 (32.0) | 191 (68.0) | 274 (97.5)f | -- | -- | -- | 281 (100)e | 24 (8.5) | -- | ||
KEYNOTE pooled weighted averages by treatment arm | Pembro + chemo | Any PD- L1, any histology | -- | 64.8 | (66.3) | (8.4) | (91.6) | (88.7) | (11.7) | (38.1) | (61.9) | (36.4) | (63.6)g | -- | -- | (99.9) | (13.6) | (16.1) |
Chemo | -- | 64.2 | (67.3) | (11.5) | (88.5) | (90.4) | (9.6) | (36.2) | (63.8) | (49.8) | (50.1)g | -- | -- | (99.5) | (11.8) | (23.8) | ||
CheckMate 9LA | Nivo + ipi + IC chemo | ITT, any PD-L1, any histology | 361 | 65.0 | 252 (69.8) | 30 (8.3)b | 331 (91.7)b | 315 (87.0) | 46 (13.0) | 113 (31.0) | 247 (68.0) | 113 (31.0) | 248 (69.0) | -- | -- | 330 (91.0)h | 51 (14.0)h | 68 (19.0) |
IC chemo | 358 | 65.0 | 252 (70.4) | 30 (8.4)b | 328 (91.6)b | 306 (86.0) | 52 (14.0) | 112 (31.0) | 245 (68.0) | 111 (31.0) | 247 (69.0) | -- | -- | 338 (94.0)h | 50 (14.0)h | 86 (24.0) | ||
Notes: Baseline characteristics for pembrolizumab + chemotherapy are based on values per trial (grey cells) as well as the weighted average of each characteristic for KEYNOTE-021G, KEYNOTE-189, and KEYNOTE-407 (white cells), with comparisons made to EMPOWER-Lung 3 Part 2and CheckMate 9LA based on the weighted average. a) Calculated as the sum of current and former smoking status; b) Patients were broadly classified as Asian, White, or Black race; c) Reported as current/former smoking status; d) One patient in the pembro + chemo arm had an ECOG of 2—this patient did not receive study treatment; e) Assumed based on trial eligibility criteria; f) 2.2% of patients in the Pembro + IC chemo arm and 2.5% of patients in the IC chemo arm were of adenosquamous histology; although squamous histology was a criterion for entry, patients whose tumours were of any histology were eligible if there was a squamous component in the specimen; g) KEYNOTE-189 adopted a 2:1 randomization scheme, resulting in a higher proportion of patients with nonsquamous histology in the pembrolizumab + chemotherapy arm relative to the chemotherapy arm in the pooled KEYNOTE node; h) Calculated. Abbreviations: Carb, carboplatin; Cemi, cemiplimab; Chemo, platinum-based chemotherapy; ECOG, Eastern Oncology Cooperative Group; IC, investigator’s choice; Ipi, ipilimumab; ITT, intention to treat; mets., metastases; Nivo, nivolumab; Non- sq, Nonsquamous; Pem, pemetrexed; Pembro, pembrolizumab; Pop, population; Sq, squamous.
Note: This table has not been copy-edited.
Source: Sponsor NMA technical report.64 Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Figure 5: Longitudinal Plots of the EORTC QLQ-C30 — Observed Mean (FAS) GHS/QoL
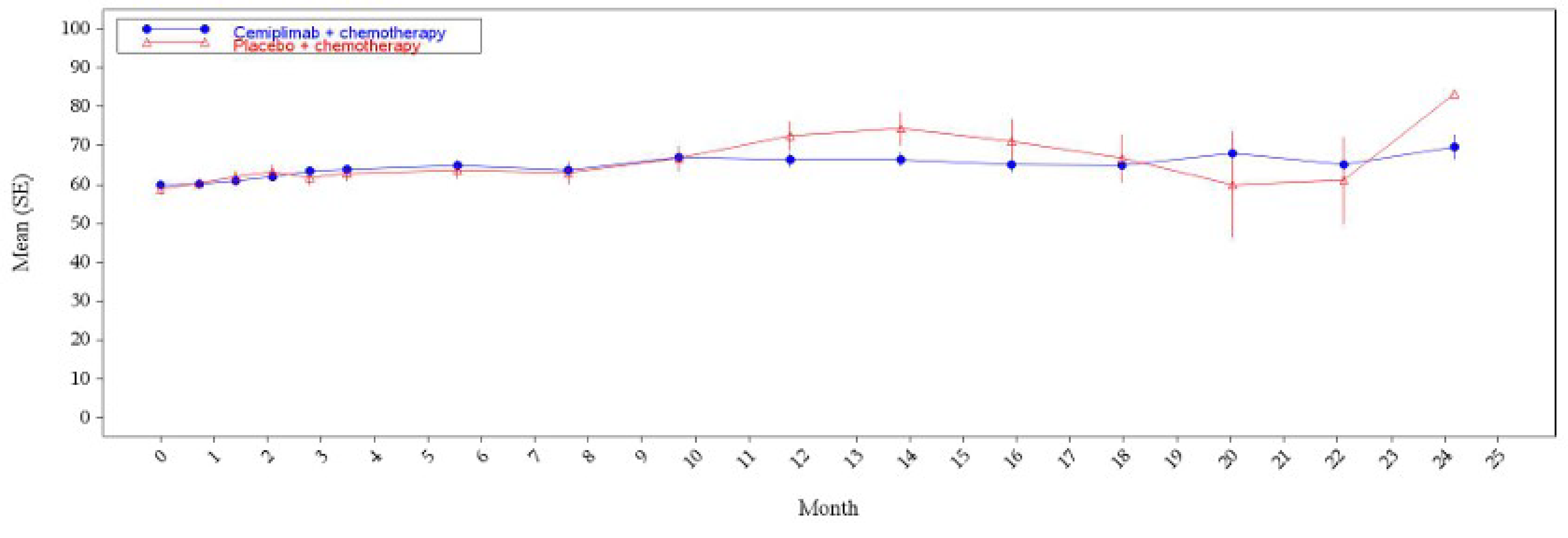
FAS = full analysis set; GHS = Global Health Status; QoL = quality of life.
Note: This figure has not been copy-edited.
Source: Study EMPOWER-Lung 3 Part 2 Clinical Study Report.58
Pharmacoeconomic Review
Abbreviations
AE
adverse event
BIA
budget impact analysis
EORTC QLQ-C30
European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30
HR
hazard ratio
HRQoL
health-related quality of life
ICER
incremental cost-effectiveness ratio
NMA
network meta-analysis
NSCLC
non–small cell lung cancer
PBC
platinum-based chemotherapy
PFS
progression-free survival
PSM
partitioned survival model
QALY
quality-adjusted life-year
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Cemiplimab (Libtayo), 350 mg sterile solution for infusion (IV) |
Indication | In combination with platinum-based chemotherapy for the first-line treatment of adult patients with NSCLC whose tumours have no EGFR, ALK, or ROS1 aberrations,
|
Health Canada approval status | NOC |
Health Canada review pathway | Standard review |
NOC date | April 27, 2023 |
Reimbursement request | As per indication |
Sponsor | Sanofi-Aventis Canada Inc. |
Submission history | Previously reviewed: Yes Indication: For the first-line treatment of adult patients with NSCLC expressing PD-L1 in ≥ 50% of tumour cells (Tumour Proportion Score [TPS] ≥ 50%), as determined by a validated test, with no EGFR, ALK or ROS1 aberrations, who have locally advanced NSCLC who are not candidates for surgical resection or definitive chemoradiation, or metastatic NSCLC Recommendation date: June 2, 2022 Recommendation: Reimburse with clinical criteria and/or conditions Indication: For the treatment of patients with locally advanced or metastatic basal cell carcinoma previously treated with a hedgehog pathway inhibitor Recommendation date: March 4, 2022 Recommendation: Reimburse with clinical criteria and/or conditions Indication: For the treatment of adult patients with metastatic or locally advanced cutaneous squamous cell carcinoma who are not candidates for curative surgery or curative radiation Recommendation date: January 22, 2020 Recommendation: Reimburse with clinical criteria and/or conditions |
NOC = Notice of Compliance; NSCLC = non–small cell lung cancer.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Partitioned survival model |
Target population | First-line treatment of adult patients with NSCLC whose tumours have no EGFR, ALK, or ROS1 aberrations, who have
|
Treatment | Cemiplimab in combination with PBC |
Dose regimen | 350 mg every 3 weeks, until progression or unacceptable toxicity |
Submitted price | Cemiplimab 350 mg: $8,200 per viala |
Submitted treatment costs | Cemiplimab + PBC = $183,025 per patient annually, if patients remain on treatment for a full year |
Comparators |
|
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs, LYs |
Time horizon | Lifetime (30 years) |
Key data sources | Phase III EMPOWER-Lung 3 trial for the efficacy of cemiplimab + PBC and PBC alone Sponsor-submitted NMA, including the EMPOWER-Lung 3, CheckMate 9LA, KEYNOTE-189, KEYNOTE 407, and KEYNOTE-021G trials, for the efficacy of the other comparators |
Submitted results | The ICER for cemiplimab + PBC vs. PBC alone was $97,502 per QALY gained (incremental costs = $111,501; incremental QALYs = 1.14). The other comparators were dominated (i.e., higher costs and lower QALYs). |
Key limitations |
|
CADTH reanalysis results |
|
ICER = incremental cost-effectiveness ratio; LY = life-year; NMA = Network meta-analysis; NSCLC = non–small cell lung cancer; PBC = platinum-based chemotherapy; QALY = quality-adjusted life-year; WTP = willingness to pay.
aThe sponsor has confirmed that the 250 mg vial is being discontinued in Canada.
Conclusions
The CADTH clinical review of the EMPOWER-Lung 3 trial found that cemiplimab (Libtayo) plus platinum-based chemotherapy (PBC) demonstrated a statistically significant benefit over placebo plus PBC (PBC alone) in overall survival (OS), progression-free survival (PFS), and objective response rate for the treatment of patients with advanced non–small cell lung cancer (NSCLC), no EGFR, ALK, or ROS1 aberrations, regardless of PD-L1 expression status. There was no clinically meaningful improvement in health-related quality of life (HRQoL) with cemiplimab plus PBC versus PBC alone, or in the risk of adverse events (AEs) of special interest. The sponsor-submitted network meta-analysis (NMA) attempted to provide indirect evidence comparing cemiplimab plus PBC to other immunotherapies. However, due to several limitations of the sponsor-submitted NMA, in particular concerns with clinical heterogeneity, no firm conclusions could be drawn on the efficacy and safety of cemiplimab plus PBC compared with pembrolizumab plus PBC or with nivolumab plus ipilimumab plus PBC.
According to clinical expert feedback and current practice in Canada, immunotherapies are the most relevant comparators for this patient population. However, the sponsor-submitted NMA did not provide sufficient evidence that cemiplimab plus PBC is clinically different than pembrolizumab plus PBC or than nivolumab plus ipilimumab plus PBC. Evidence from the EMPOWER-Lung 3 trial for cemiplimab plus PBC versus PBC alone may not reflect patients receiving PBC alone in Canada and, as such, may overestimate the OS benefit of cemiplimab plus PBC, given the lower proportion of patients in the PBC-alone arm who received subsequent therapy.
CADTH identified several limitations of the sponsor’s economic submission that could be addressed: aligning the long-term survival of patients on PBC alone with more plausible estimates, given the low rate of subsequent therapy in the trial; using a direct head-to-head comparison from the EMPOWER-Lung 3 trial to model the comparative efficacy of cemiplimab plus PBC with PBC alone; assuming equal efficacy of all immunotherapies used in first-line treatment; applying weight-based dosing for pembrolizumab and nivolumab; and aligning the proportion of patients receiving subsequent therapy costs with that in the EMPOWER-Lung 3 trial.
There is no robust clinical evidence to justify a price premium for cemiplimab plus PBC over the least costly immunotherapy available in first-line treatment. In the CADTH base case, cemiplimab plus PBC is dominated by pembrolizumab plus PBC, when equal efficacy across immunotherapies is assumed. At the listed prices, a minimum price reduction of 20% for cemiplimab is required for cemiplimab plus PBC to be similar to pembrolizumab plus PBC in terms of total costs.
For the small numbers of patients for whom PBC alone is a relevant comparator, CADTH’s base case was aligned with the sponsor’s results: cemiplimab plus PBC is associated with higher costs, increased QALYs, and is not cost-effective at a $50,000 per quality-adjusted life-year (QALY) willingness-to-pay (WTP) threshold (it would require a price reduction of 71%). However, there is remaining uncertainty concerning the generalizability of OS rates for the PBC-alone arm from the EMPOWER-Lung 3 trial.
Outstanding uncertainty remains regarding the model structure (limited to capture the benefits of subsequent therapies), the confidential discounts negotiated by public plans, and the cost-effectiveness of cemiplimab plus PBC versus pembrolizumab monotherapy (excluded from the sponsor’s submission). Given the remaining uncertainty, further price reductions may be sought.
Stakeholder Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, registered clinicians, and drug plans that participated in the CADTH review process, and specifically, information that pertains to the economic submission.
Patient input was received from the Canadian Cancer Survivor Network, Lung Cancer Canada, and the Lung Health Foundation (formerly known as The Ontario Lung Association), which collected perspectives from caregivers and patients with lung cancer through online surveys, questionnaires, and interviews. Patients with lung cancer reported shortness of breath, fatigue, depression, cough, a weakened immune system, and chest tightness. Caregivers also experienced disruptions to daily life and the ability to work because they were providing care. Current treatments for patients are surgery, radiation, chemotherapy, targeted therapy, and immunotherapy (pembrolizumab). Treatment goals included stopping or delaying disease progression, inducing long-term remission, reducing AEs related to treatment, improving lung cancer symptoms, and improving quality of life. Among the 4 patients who had experience with cemiplimab, mild AEs were noted, such as fatigue, mild joint pain, anemia, hyperglycemia, diarrhea, nausea, and constipation. These patients also noted that cemiplimab did not eliminate all lung cancer symptoms.
Clinician input was received from Lung Cancer Canada and Ontario Health-Cancer Care Ontario. The clinician input noted that current treatments for patients with lung cancer include pembrolizumab plus PBC, nivolumab plus ipilimumab plus PBC, pembrolizumab monotherapy for patients with PD-L1 expression in at least 50% of tumour cells, and PBC alone (pemetrexed or paclitaxel in combination with cisplatin or carboplatin). Furthermore, cemiplimab plus PBC would be an alternative first-line option to these regimens. The clinicians noted that clinically meaningful treatment goals included tumour shrinkage, improvement of symptoms and quality of life, and prolongation of survival. A clinically meaningful treatment response would be measured with a clinical assessment of symptoms or imaging (CT scans or X-rays) every 6 to 12 weeks. Treatment should be continued until disease progression, intolerable AEs, or completion of the treatment course (36 cycles over 108 weeks). The clinician input also noted that cemiplimab has the potential to facilitate access to care in remote areas because there is no need for vial sharing to reduce drug wastage (as is currently done at large infusion centres).
The drug plans highlighted relevant comparators: pembrolizumab monotherapy (if PD-L1 expression is ≥ 50%), pembrolizumab plus pemetrexed plus platinum (for nonsquamous NSCLC only), pembrolizumab plus nonpemetrexed plus platinum (for squamous NSCLC) and ipilimumab plus nivolumab plus PBC. The plans also suggested considerations for the initiation, prescribing, and discontinuation of therapy. They also noted that certain jurisdictions, which do not fund drug wastage, may prefer cemiplimab because of its flat dosing.
Several of these concerns were addressed in the sponsor’s model:
treatment goals of OS and PFS, and vial sharing.
In addition, CADTH addressed some of these concerns, as follows:
CADTH adopted weight-based dosing for pembrolizumab and nivolumab in the pharmacoeconomic and budget impact analysis (BIA), in accordance with the most common clinical practice and as confirmed by the drug plans.
CADTH was unable to address the following concerns raised from stakeholder input:
The cost-effectiveness of cemiplimab plus PBC versus pembrolizumab monotherapy as the comparator was excluded from the sponsor’s submission.
Economic Review
The current review is for cemiplimab (Libtayo) plus PBC for the first-line treatment of adult patients with NSCLC whose tumours have no EGFR, ALK, or ROS1 aberrations and whose disease is locally advanced but who are not candidates for surgical resection or definitive chemoradiation, or for patients with metastatic NSCLC.
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted a cost-utility analysis of cemiplimab plus PBC versus pembrolizumab plus PBC, nivolumab plus ipilimumab plus PBC, and PBC alone. The model population included patients with NSCLC whose tumours have no EGFR, ALK, or ROS1 aberrations and whose disease is locally advanced but who are not candidates for surgical resection or definitive chemoradiation, or for patients with metastatic NSCLC. It is aligned with the Health Canada–indicated population and reimbursement request.
Cemiplimab is available in 350 mg vials. The recommended dosage of cemiplimab is 350 mg administered intravenously every 3 weeks until progression or unacceptable toxicity. At the submitted price of $8,200 per vial, the annual cost of cemiplimab is $142,621, and in combination with PBC is $183,025 if patients remain on treatment for a full year, as calculated by the sponsor. For pembrolizumab, the sponsor adopted a fixed dosing of 200 mg every 3 weeks, resulting in an annual cost of $153,057 (for approximately 17 cycles) and, when combined with PBC in $194,673 per year. For the combination of nivolumab plus ipilimumab, the sponsor adopted fixed dosing of 360 mg every 3 weeks for nivolumab and 1 mg/kg every 6 weeks for ipilimumab. At this dosing, the annual costs are $122,445 for nivolumab, $101,066 for ipilimumab, and in combination with PBC, $265,127. A 2-year stopping rule was applied for all immunotherapies. The average annual cost of PBC alone was $42,261, which was calculated as the weighted average of 4 different combinations: pemetrexed plus cisplatin, pemetrexed plus carboplatin, paclitaxel plus cisplatin, and paclitaxel plus carboplatin. Pemetrexed maintenance treatment was given until progression, except when administered in combination with nivolumab plus ipilimumab, in which case the treatment duration was 2 months. The sponsor assumed full doses (i.e., no relative dose intensity adjustments were made) and no vial sharing, except for pembrolizumab and nivolumab, for which vial sharing was assumed.
The model used a 1-month cycle length and simulated life-years, QALYs, and costs for each treatment over a lifetime time horizon (30 years). The base-case analysis was undertaken from the perspective of Canada’s publicly funded health care system. Discounting (1.5% per annum) was applied to both costs and outcomes.
Model Structure
The sponsor submitted a partitioned survival model (PSM) with 3 mutually exclusive health states: preprogression, postprogression, and death (Appendix 3, Figure 1). All patients began in the preprogression health state and were assumed to be stable or responding to therapy. The proportion of preprogression patients and the proportion of patients alive at each time point were estimated independently, using PFS and OS curves, respectively. The proportion of patients in the postprogression health state was calculated as the difference between the proportion of living patients (estimated from the OS curve) and the proportion of preprogression patients (estimated from the PFS curve). In the preprogression state, time on treatment was specific to each treatment arm and was assumed to continue for as long as patients remained progression-free (i.e., assumed to be equal to PFS). In the postprogression health state, time on treatment and monitoring were assumed to vary, depending on the subsequent therapy (8 cycles for immunotherapy, 4 cycles for chemotherapy, and dependent on which first-line therapy patients received). For the remaining time in the postprogression health state, patients were assumed to be receiving disease management. Before entering the death state, all patients incurred a one-time cost for end-of-life care.
Model Inputs
The baseline patient characteristics in the sponsor’s model were aligned with the population in the EMPOWER-Lung 3 trial (R2810-ONC-16113), a phase III trial consisting of patients 18 years and older with NSCLC and no EGFR, ALK, or ROS1 aberrations who have stage IIIb or stage IIIc cancer and who are not candidates for surgical resection or definitive chemoradiation or who have stage IV cancer and who have received no prior systemic therapy for advanced NSCLC (mean age, ||||| years; mean weight, ||||| kg; 83.9% male).1
Key inputs used to inform the clinical efficacy of PBC alone (i.e., OS and PFS) were derived from the EMPOWER-Lung 3 trial, which had a maximum follow-up of approximately 2.5 years (data cut-off date of June 2022).1 All clinical outcomes were extrapolated beyond the trial duration by fitting parametric survival curves to the PBC-alone trial data. The sponsor selected a log-logistic distribution for both the PFS and OS curves. Model selection was based on statistical fit (Akaike information criterion, Bayesian information criterion, deviance information criterion), clinical plausibility, internal validation against the PBC arm of the EMPOWER-Lung 3 trial, and external validation against the KEYNOTE-407 and KEYNOTE-189 trials.2,3 The model was adjusted for the crossing over of PFS and OS curves (i.e., PFS could not be greater than OS), and OS was capped using the general population mortality rates.
Clinical efficacy for cemiplimab plus PBC, pembrolizumab plus PBC, and nivolumab plus ipilimumab plus PBC was incorporated into the model using a hazard ratio (HR) approach, applied to the PFS and OS curves of the PBC-alone arm. The HRs were derived from a sponsor-conducted NMA anchored by the PBC-alone arms of each trial (including the EMPOWER-Lung 3, KEYNOTE-189, KEYNOTE-407, KEYNOTE-021G, and CheckMate 9LA trials).4 The sponsor adopted a 2-step multivariate approach and derived time-varying HRs for PFS and OS for each intervention because of a violation of the proportional hazards assumption.
The preprogression (|||||) and postprogression (|||||) health utility for patients with advanced NSCLC was derived from the EMPOWER-Lung 3 trial.1 In the trial, patient-reported data on HRQoL was measured using the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 (EORTC QLQ-C30) instrument. The sponsor used an algorithm described by Longworth et al. (2014) to map the EORTC QLQ-C30 scores to EQ-5D-5L utility values using Canadian tariffs.5,6 The model also incorporated a one-time utility decrement for AEs in all treatment arms, which were obtained from published literature.7,8 The analysis included all AEs of grade 3 or higher that occurred in at least 5% of patients in any treatment arm of the trials (EMPOWER-Lung 3, KEYNOTE-189, KEYNOTE-407, and CheckMate 9LA trials).1-3,9
The submitted model included costs associated with drug acquisition, treatment administration, monitoring, disease management, AEs, and terminal care. Drug-acquisition costs were obtained from the IQVIA DeltaPA database and published literature.10-12 A 2-year stopping rule, or disease progression, was applied for all immunotherapies (cemiplimab, pembrolizumab, nivolumab, and ipilimumab). The duration of paclitaxel plus cisplatin and of paclitaxel plus carboplatin was assumed to be 3 months when PBC was used alone or in combination with pembrolizumab or cemiplimab, and assumed to be 2 months when combined with nivolumab plus ipilimumab. The proportion of patients receiving different chemotherapy components varied across first-line treatment arms (Table 10 in Appendix 3). Subsequent treatments after disease progression included second-line treatment with immunotherapy (pembrolizumab, nivolumab, and atezolizumab) and/or chemotherapy (docetaxel, paclitaxel, and pemetrexed). The distribution of subsequent treatments was obtained from the EMPOWER-Lung 3 trial, and the mean treatment duration was obtained from the study by Insinga et al. (2021) (Table 11, Appendix 3).1,13 Treatment administration costs with IV infusions were obtained from the Ontario Schedule of Benefits.14 Monitoring costs accrued while patients remained on first-line treatment. Disease-management costs accrued monthly to all patients alive, regardless of whether they were on or off treatment. Both monitoring and disease-management costs were obtained from the Ontario schedules for physician fees and for laboratory services.14,15 AE and terminal-care costs were applied as one-time costs at the beginning of the first cycle and upon death, respectively. AE and terminal-care costs were obtained from the Ontario schedule of physician services and published literature respectively.14,16
Summary of Sponsor’s Economic Evaluation Results
All analyses were run probabilistically (5,000 iterations), and the deterministic and probabilistic results were similar. The probabilistic findings are presented here. Additional results from the sponsor’s submitted economic evaluation base case are presented in Appendix 3.
Base-Case Results
In the sponsor’s base-case analysis (Table 3), PBC alone and cemiplimab plus PBC remained on the cost-effectiveness efficiency frontier. Cemiplimab plus PBC was associated with higher costs (incremental cost = $111,501) and higher QALYs (incremental gain = 1.15) than PBC alone, resulting in a sequential incremental cost-effectiveness ratio (ICER) of $97,502 per QALY gained. There is a 0% probability of cemiplimab plus PBC being cost-effective at a WTP threshold of $50,000 per QALY. The majority of the incremental QALYs (77%) associated with cemiplimab plus PBC were accrued beyond the trial duration (approximately 30 months) and were based on the sponsor’s extrapolations of the trial data. Furthermore, more than half the QALYs were accrued in the postprogression health state (Table 12 in Appendix 3).
The results were driven by the drug-acquisition costs. In the preprogression health state, the incremental costs for cemiplimab plus PBC ($135,306 versus PBC alone) were only partly offset by reduced costs in the postprogression health state (incremental savings = $28,182 versus PBC alone). The submitted model predicted that 8.4% and 3.0% of patients would be alive in the cemiplimab plus PBC and PBC alone groups at the 10-year time horizon, respectively.
Table 3: Summary of the Sponsor’s Economic Evaluation Results (Probabilistic)
Drug | Total costs | Total QALYs | Sequential ICER ($ per QALY gained) |
|---|---|---|---|
PBC alone | $94,559 | 1.61 | Reference |
Cemiplimab plus PBC | $206,060 | 2.76 | $97,502 |
Dominated treatments | |||
Pembrolizumab plus PBC | $218,924 | 2.50 | Dominated by cemiplimab plus PBC |
Nivolumab plus ipilimumab plus PBC | $247,517 | 2.35 | Dominated by cemiplimab plus PBC |
ICER = incremental cost-effectiveness ratio; PBC = platinum-based chemotherapy; QALY = quality-adjusted life-year.
Source: Sponsor’s pharmacoeconomic submission.17
Sensitivity and Scenario Analyses Results
The sponsor conducted several scenario and 1-way sensitivity analyses to test alternative assumptions and parameter values. These included alternative utility values for the progression-free and progressed states, lower and upper bounds of the credible intervals around the parametric distributions of PFS and OS for cemiplimab plus PBC and PBC alone, alternative disease-management costs, the use of constant HRs, shorter time horizons (i.e., 10 and 20 years), alternative discounting rates (i.e., 0%, 3%), the inclusion of gemcitabine in first-line PBC, the assumption of vial sharing, the adoption of an alternative extrapolation of the OS curve (generalized gamma), and the adoption of a societal perspective. The sponsor’s base case was most influenced by assumptions related to the time horizon and alternative extrapolation assumptions for OS. When the OS curve for PBC alone was extrapolated using a generalized gamma distribution, the ICER increased to $117,477.
The sponsor conducted a scenario analysis from a societal perspective that included additional costs associated with productivity loss. In this analysis, the ICER per QALY gained was $106,147 versus PBC alone, which is similar to the sponsor’s base case using a health care payer perspective.
CADTH Appraisal of the Sponsor’s Economic Evaluation
CADTH identified several key limitations of the sponsor’s analysis that have notable implications for the economic analysis:
The trial data for PBC alone do not reflect current clinical practice, leading to uncertainty about the relative benefit of cemiplimab plus PBC. Current practice emphasizes the use of immunotherapy along with PBC. Furthermore, the clinical experts consulted by CADTH noted that a lower proportion of patients in the PBC-alone arm of the EMPOWER-Lung 3 trial received subsequent therapy (22%) than what is observed in Canadian clinical practice (30% or more). This is problematic because it may be underestimating OS with PBC alone and, consequently, overestimating the relative benefits of cemiplimab plus PBC. The magnitude of this overestimation is uncertain; however, it may not be as relevant for decision-making, as PBC alone is no longer the most relevant comparator in this clinical area. Most patients (approximately 95%) are expected to be treated with immunotherapy in the first line.
In the scenario analysis, CADTH explored an alternative value for the constant HR for OS in an attempt to address the potential overestimation of the relative effect of cemiplimab plus PBC.
The long-term extrapolation of survival for PBC alone lacks face validity: The sponsor modelled PFS and OS for the PBC-alone arm based on long-term extrapolations of data from the EMPOWER-Lung 3 trial.1 Due to the fact that a lower proportion of patients in the PBC-alone arm of the EMPOWER-Lung 3 trial received subsequent therapy (described in the first limitation), the extrapolation of OS for PBC alone seemed overestimated for an undertreated population (8% and 3% of patients were estimated to be alive at 5 and 10 years, respectively). The clinical experts assessed the plausibility of the extrapolation at various time points generated by alternative extrapolation curves and deemed that a 0% survival rate at 10 years is more plausible and aligned with their clinical expectations, due to the low rate of subsequent therapy after PBC alone in the EMPOWER-Lung 3 trial.
The CADTH reanalysis used the generalized gamma distribution to extrapolate OS for PBC alone (sponsor’s second best fit), based on clinical plausibility.
The comparative efficacy of cemiplimab plus PBC versus other immunotherapies is uncertain: The relative efficacy of cemiplimab plus PBC (and the other immunotherapy arms) was incorporated into the model, using an HR approach applied to the PFS and OS curves of the PBC-alone arm (extrapolated from the EMPOWER-Lung 3 trial data). In the absence of head-to-head comparisons of cemiplimab plus PBC with pembrolizumab plus PBC and nivolumab plus ipilimumab plus PBC, the sponsor estimated their comparative efficacy using an NMA (with PBC alone connecting the network of trials).4 CADTH’s clinical review noted several limitations with the sponsor-submitted NMA, particularly concerning clinical heterogeneity. Moreover, the NMA results did not provide evidence of any significant difference in OS or PFS between cemiplimab plus PBC and the other immunotherapy options (i.e., all HR credible intervals crossed the null value of 1). Hence, no conclusions could be firmly drawn about their comparative efficacy and safety. Additionally, the clinical experts consulted by CADTH during this review noted no biological plausibility to suggest that treatment with cemiplimab plus PBC is expected to have benefits superior to other immunotherapy combinations. Given the sponsor’s modelling choice and the limitations of the evidence from the NMA, the data from the EMPOWER-Lung 3 trial seem to remain the best source of relative efficacy versus PBC alone, with the caveat that it may be overestimated due to the low rates of subsequent therapy after PBC alone (described previously). The proportional hazards assumption did not seem to be violated in the trial data.
The CADTH reanalysis adopted a constant HR approach to model the comparative efficacy of cemiplimab plus PBC versus PBC alone (using the PFS and OS HRs derived from the EMPOWER-Lung 3 trial) and assumed the same relative efficacy (in PFS and OS) for all immunotherapy arms versus PBC alone (i.e., the same HRs were used for cemiplimab plus PBC). CADTH noted that the reanalysis might be overestimating the relative benefit of all immunotherapy arms equally (versus PBC alone) due to the potential overestimation of incremental benefits observed in the trial.
In the scenario analysis, CADTH explored an alternative value for the constant HR for OS in an attempt to address the potential overestimation of the relative effect of cemiplimab plus PBC. Also, CADTH explored the impact of adopting time-varying HRs to model the comparative efficacy of cemiplimab plus PBC versus PBC alone, using the sponsor’s NMA estimates when assuming equal efficacy across immunotherapy arms.
The treatment costs of pembrolizumab and nivolumab are overestimated: The sponsor adopted fixed dosing of 200 mg every 3 weeks and 360 mg every 3 weeks to estimate the treatment costs of pembrolizumab and nivolumab, respectively. However, the public drug plans and clinical experts noted that weight-based dosing (2 mg/kg up to a cap of 200 mg every 3 weeks) is commonly implemented across jurisdictions. Similarly, the recommended dosage of nivolumab is also weight-based (4.5 mg/kg up to a cap of 360 mg every 3 weeks) in the Cancer Care Ontario Drug Formulary.18 Based on the average weight of the modelled population, the sponsor has overestimated the doses and treatment costs of pembrolizumab and nivolumab comparators, which results in an underestimation of the incremental costs of cemiplimab plus PBC versus other immunotherapies.
In the reanalysis, CADTH assumed weight-based dosing to estimate drug costs for pembrolizumab and nivolumab.
In the scenario analysis, CADTH maintained the sponsor’s assumption of fixed dosing for pembrolizumab and nivolumab.
Pembrolizumab monotherapy is excluded, but it is a relevant comparator for a subset of the indicated population: The sponsor excluded pembrolizumab monotherapy from the analysis, noting that it is a treatment option for only a subset of the Health Canada–indicated population (i.e., patients whose tumours express PD-L1 in ≥ 50% of tumour cells). However, the clinical experts consulted for this review noted that cemiplimab plus PBC may be used to treat these patients, even if pembrolizumab monotherapy is available. Because pembrolizumab monotherapy was not included in the analysis, its cost-effectiveness versus cemiplimab plus PBC is unknown.
CADTH could not address this limitation.
The sponsor’s approach to modelling subsequent therapy is problematic: In the submitted pharmacoeconomic model, the cost of subsequent therapy incurred to all patients in the postprogression health state (refer to Table 11 in Appendix 3). However, the proportion of patients treated after progression in the trial is much lower (||||| in the PBC-alone arm, ||||| in the cemiplimab plus PBC arm). Although this affects all immunotherapy arms in the model, the sponsor’s approach is problematic because subsequent therapy after PBC alone is more costly (e.g., immunotherapy) than subsequent therapy after any immunotherapy (e.g., chemotherapy), disproportionately inflating the cost of the PBC-alone arm and underestimating the incremental costs of immunotherapies versus PBC alone.
In the reanalysis, the proportion of patients receiving subsequent therapy after disease progression was aligned with the proportion in the EMPOWER-Lung 3 trial.
The sustained relative treatment effect is uncertain: The sponsor’s extrapolations assumed that the relative PFS and OS benefit of cemiplimab plus PBC versus PBC alone is sustained indefinitely. Given the short-term nature of clinical trial data, in circumstances in which either treatment will be delivered for a time horizon longer than the trial duration, or that treatment is assumed to have a continued effect on event rates after delivery, assumptions related to the continuation of the long-term treatment effect must be considered carefully, per CADTH and National Institute for Health and Care Excellence (NICE) guidelines.19
CADTH conducted a scenario analysis to explore the impact of a waning treatment effect of cemiplimab plus PBC versus PBC alone, beginning at the end of trial follow-up (2 years) and continuing for the next 5 years, using the embedded options in the sponsor’s pharmacoeconomic model.
The model structure has important limitations for the decision problem. The sponsor used a PSM to estimate costs and outcomes associated with the treatment of NSCLC. Although PSMs are routinely used in economic evaluations, this approach is not suitable when patients can achieve a response on subsequent lines of therapy. In the postprogression health state, the model accounts for the costs of subsequent therapies over a lifetime time horizon, but has limited flexibility to capture changes to clinical outcomes (i.e., response). The clinical experts consulted by CADTH noted that patients can achieve a response in later lines of therapy and may experience survival improvements, especially with PBC alone, if they receive a higher rate of subsequent therapy with immunotherapy, as occurs in current clinical practice. Therefore, the magnitude of the benefit in the extrapolated period was inaccurately estimated.
CADTH was unable to address this limitation within the submitted model structure.
Additionally, the following key assumptions were made by the sponsor and have been appraised by CADTH (refer to Table 4).
Table 4: Key Assumptions of the Submitted Economic Evaluation (Not Noted as Limitations to the Submission)
Sponsor’s key assumption | CADTH comment |
|---|---|
The sponsor used mapping techniques to estimate health state utilities. | Uncertain. Health utilities were collected using the EORTC questionnaire, which does not collect patient preferences. Instead, mapping techniques were used to estimate health utility from patient-reported quality of life. The limitations of mapping techniques have been well described in published literature; one of them is the inaccurate characterization of uncertainty around the mean health utility estimates.20 It was also noted that the mapped utility values for the preprogression and postprogression health states were very similar. CADTH explored the impact of changing utilities and found that if the difference in utilities between health states is expected to be bigger (i.e., if postprogression utilities are lower) the ICERs may be even higher than estimated. |
The risk of adverse events between immunotherapies is different. | Uncertain. The risk of adverse events for each immunotherapy was obtained from individual trials, and no matching-adjusted analysis was performed to correct for imbalances in patient demographics. CADTH noted that the proportion of patients who have an adverse event was highest with pembrolizumab (52%) and lowest with cemiplimab (23%). However, these results are susceptible to confounding because of the influence of unmeasured and unadjusted confounders. CADTH found that excluding adverse events has a negligible impact on the cost-effectiveness results. |
The proportion of patients receiving different chemotherapy components with first-line treatments was obtained from the EMPOWER-Lung 3 trial. | The proportion of patients receiving different chemotherapy components with first-line treatments lacks face validity (refer to Appendix 3, Table 10). According to the Canadian Cancer Society, approximately 75% of NSCLCs are nonsquamous,21 and patients are prescribed cisplatin plus pemetrexed or carboplatin plus pemetrexed in current clinical practice. However, less than half of the patients (45%) are administered these regimens in combination with immunotherapy in the sponsor’s submission. CADTH also noted that the proportion of patients receiving different chemotherapy components did not add up to 100% in the PBC-alone arm. CADTH tested the impact of aligning the proportion of patients receiving different chemotherapy components with feedback from clinical experts, ensuring the percentages added up to 100%, and found that the alternative assumptions had minimal impact on the cost-effectiveness results. |
EORTC = European Organisation for Research and Treatment of Cancer; ICER = incremental cost-effectiveness ratio; NSCLC = non–small cell lung cancer; PBC = platinum-based chemotherapy.
CADTH Reanalyses of the Economic Evaluation
Base-Case Results
Several limitations of the sponsor’s submission could not be adequately addressed (i.e., the lack of head-to-head comparative clinical data with other immunotherapy, uncertainty regarding long-term clinical effectiveness, and the lack of a treatment effect from subsequent treatments within the model structure design).
The CADTH reanalysis addressed several limitations of the economic model. The CADTH base case was derived by applying the following changes: using an alternate parametric survival model to extrapolate OS for patients in the PBC-alone arm; modelling the comparative efficacy of cemiplimab plus PBC versus PBC alone using the EMPOWER-Lung 3 trial; assuming equal efficacy of all immunotherapies used in first-line treatment; applying weight-based dosing for pembrolizumab and nivolumab; and aligning the proportion of patients receiving subsequent therapy with the trial.
Table 5 details each change made to derive the CADTH revised base case, which was conducted using a stepwise approach to highlight the impact of each change. The summary of results from the reanalysis is presented in Table 6.
Table 5: CADTH Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Changes to derive the CADTH base case | ||
1. OS extrapolation for PBC alone | Log-logistic | Generalized gamma |
2. Comparative efficacy of cemiplimab plus PBC vs. PBC alone | Time-varying HRs obtained from the sponsor-submitted NMA | Constant HRs obtained from the EMPOWER-Lung 3 trial for the cemiplimab plus PBC arm PFS HR = 0.549 OS HR = 0.645 |
3. Comparative efficacy of cemiplimab, pembrolizumab, and nivolumab plus ipilimumab | Time-varying HRs obtained from the sponsor-submitted NMA | The same HRs applied to the cemiplimab plus PBC were used across all immunotherapy arms PFS HR = 0.549 OS HR = 0.645 |
4. Comparator dosing | Fixed dosing Pembrolizumab: 200 mg every 3 weeks Nivolumab: 360 mg every 3 weeks | Weight-based dosing Pembrolizumab: 2 mg/kg up to a cap of 200 mg every 3 weeks Nivolumab: 4.5 mg/kg up to a cap of 360 mg every 3 weeks |
5. Proportion of patients receiving subsequent therapy | 100% in all arms Refer to Table 11 in Appendix 3, | PBC alone: ||||| Immunotherapy arms: ||||| Aligned with the EMPOWER-Lung 3 trial |
CADTH base case | — | Reanalysis 1 + 2 + 3 + 4 + 5 |
HR = hazard ratio; NMA = network meta-analysis; OS = overall survival; PBC = platinum-based PBC; PFS = progression-free survival.
In the CADTH base case, cemiplimab plus PBC was associated with estimated total costs of $194,203 and total QALYs of 2.03, versus total costs of $63,829 and total QALYs of 1.28 for PBC alone. Cemiplimab plus PBC resulted in higher costs ($194,203 versus $166,127) than pembrolizumab plus PBC and equal QALYs (2.05 versus 2.05). The probability of cemiplimab being cost-effective at a WTP threshold of $50,000 was 0%. The results of CADTH’s base case are presented in Table 6, the stepped analysis in Table 13, and the disaggregated summary in Table 14. These results showed that the cost-effectiveness of cemiplimab plus PBC was highly sensitive to the parametric survival model used to extrapolate OS for PBC alone, comparative efficacy across immunotherapy arms, and dosing assumptions for the immunotherapy drugs. The proportion of incremental QALYs associated with cemiplimab plus PBC accrued beyond the maximum follow-up of the trial (approximately 30 months) decreased from 77% to 66%. Furthermore, the proportion of QALYs accrued in the postprogression health state decreased from 54% to 38%. Additionally, applying weight-based dosing with vial sharing for pembrolizumab significantly decreased the treatment cost of pembrolizumab plus PBC.
Table 6: Summary of the CADTH Base-Case Results, Probabilistic
Drug | Total costs ($) | Total LYs | Total QALYs | Sequential ICER ($ per QALY) |
|---|---|---|---|---|
Sponsor base case (probabilistic) | ||||
PBC alone | 94,559 | 1.97 | 1.61 | Reference |
Cemiplimab plus PBC | 206,060 | 3.36 | 2.76 | 97,502 |
Dominated treatments | ||||
Pembrolizumab plus PBC | 218,924 | 3.05 | 2.50 | Dominated by cemiplimab plus PBC |
Nivolumab plus ipilimumab plus PBC | 247,517 | 2.86 | 2.35 | Dominated by cemiplimab plus PBC |
CADTH base case (probabilistic) | ||||
PBC alone | 63,829 | 1.56 | 1.28 | Reference |
Pembrolizumab plus PBC | 166,127 | 2.49 | 2.05 | 132,739 |
Nivolumab plus ipilimumab plus PBC | 249,793 | 2.50 | 2.06 | 7,828,171 |
Dominated treatments | ||||
Cemiplimab plus PBC | 194,203 | 2.49 | 2.05 | Dominated by pembrolizumab plus PBC |
ICER = incremental cost-effectiveness ratio; LY = life-year; PBC = platinum-based chemotherapy; QALY = quality-adjusted life-years.
Scenario Analysis Results
A price reduction analysis based on the CADTH’s base case indicated that at a WTP threshold of $50,000 per QALY gained, cemiplimab plus PBC would require a 71% price reduction (from $8,200 to $2,378 per 21-day course) to be considered cost-effective versus PBC alone (Table 7). Up to a 20% price reduction, cemiplimab plus PBC continues to be dominated by pembrolizumab plus PBC.
Table 7: CADTH Price Reduction Analyses, Probabilistic
Price reduction | Unit drug cost | Sequential ICERs for cemiplimab + PBC | |
|---|---|---|---|
Sponsor base case | CADTH base case | ||
No price reduction | $8,200 | $97,502 vs. PBC | Dominated by pembrolizumab plus PBC |
10% | $7,380 | $85,549 vs. PBC | Dominated by pembrolizumab plus PBC |
20% | $6,560 | $74,141 vs. PBC | Dominated by pembrolizumab plus PBC |
30% | $5,740 | $62,732 vs. PBC | $118,750 vs. PBC |
40% | $4,920 | $51,324 vs. PBC | $101,894 vs. PBC |
50% | $4,100 | $39,916 vs. PBC | $85,038 vs. PBC |
60% | $3,280 | $28,507 vs. PBC | $68,182 vs. PBC |
70% | $2,460 | $17,099 vs. PBC | $51,326 vs. PBC |
80% | $2,394 | $5,691 vs. PBC | $34,471 vs. PBC |
90% | $1,640 | Dominant | $17,615 vs PBC |
ICER = incremental cost-effectiveness ratio; LY = life-year; PBC = platinum-based chemotherapy; ICER = incremental cost-effectiveness ratio.
Additionally, CADTH conducted scenario analyses using the CADTH base case to determine the impact of alternative assumptions on the cost-effectiveness of cemiplimab plus PBC (Table 15). These scenarios analyses explored the impact of the following model parameters and assumptions on the ICER: adopting time-varying HRs and assuming equal efficacy of immunotherapies, assuming an alternative value of HR to address overestimation of relative effectiveness in OS versus PBC alone, adopting fixed dosing for pembrolizumab and nivolumab, and assuming a treatment waning effect beginning at the end of trial follow-up and continuing for the next 5 years. The results were similar to the CADTH’s base case (i.e., cemiplimab plus PBC continued to be dominated by pembrolizumab plus PBC), except when assuming fixed dosing for pembrolizumab and nivolumab. The cost-effectiveness estimates for cemiplimab plus PBC were highly sensitive to the dosing strategy adopted for pembrolizumab and nivolumab. When fixed dosing was adopted (i.e., maximum dosing was assumed), cemiplimab plus PBC was on the cost-effectiveness frontier and the ICER was $171,113 per QALY gained compared to PBC alone.
Issues for Consideration
CADTH noted that the negotiation process with the pan-Canadian Pharmaceutical Alliance (pCPA) for cemiplimab monotherapy concluded on July 28, 2023, without agreement. It was recommended for the first-line treatment of adult patients with NSCLC expressing PD-L1 in at least 50% of tumour cells (Tumour Proportion Score ≥ 50%), determined by a validated test, and no EGFR, ALK, or ROS1 aberrations who have locally advanced NSCLC and who are not candidates for surgical resection or definitive chemoradiation, or for patients with metastatic NSCLC. These patients constitute part of the reimbursement patient population for the combination of cemiplimab plus PBC.
The modelled prices of all other comparators (e.g., pembrolizumab, nivolumab, other chemotherapy drugs) are based on publicly accessible list prices and do not reflect existing confidential pricing that has been negotiated by public plans. When existing confidential discounts are considered, greater price reductions than those referenced in this report may be required to achieve cost-effectiveness.
Overall Conclusions
The CADTH clinical review of the EMPOWER-Lung 3 trial showed that cemiplimab plus PBC demonstrated a statistically significant benefit versus placebo plus PBC for OS, PFS, and objective response rate for the treatment of patients with advanced NSCLC and no EGFR, ALK, or ROS1 aberrations, regardless of PD-L1 expression status. There was no clinically meaningful improvement in HRQoL versus PBC alone, or in the risk of AEs of special interest. The sponsor-submitted NMA attempted to provide indirect evidence comparing cemiplimab plus PBC to other immunotherapies. However, due to several limitations of the sponsor-submitted NMA, in particular concerns with clinical heterogeneity, no firm conclusions could be drawn about the efficacy and safety of cemiplimab plus PBC compared with pembrolizumab plus PBC and nivolumab plus ipilimumab plus PBC.
According to clinical expert feedback and current practice in Canada, immunotherapies are the most relevant comparators for this patient population. However, the sponsor-submitted NMA did not provide sufficient evidence that cemiplimab plus PBC is clinically different than pembrolizumab plus PBC or than nivolumab plus ipilimumab plus PBC. Evidence from the EMPOWER-Lung 3 trial for cemiplimab plus PBC versus PBC alone may not reflect patients receiving PBC alone in Canada and, as such, may overestimate the OS benefit of cemiplimab plus PBC, given the lower proportion of patients in the PBC-alone arm who received subsequent therapy.
The sponsor submitted a pharmacoeconomic model based on PFS and OS extrapolations of the PBC-alone arm of the EMPOWER-Lung 3 trial, and the relative efficacy of all immunotherapies was incorporated using an HR approach derived from the sponsor-submitted NMA. CADTH identified several limitations of the sponsor’s economic submission that could be addressed: aligning the long-term survival of patients treated with PBC alone with more plausible estimates, given the low rate of subsequent therapy in the trial; using a direct head-to-head comparison from the EMPOWER-Lung 3 trial to model the comparative efficacy of cemiplimab plus PBC versus PBC alone; assuming equal efficacy across all immunotherapies used in first-line treatment; applying weight-based dosing for pembrolizumab and nivolumab; and aligning the proportion of patients incurring subsequent therapy costs with the EMPOWER-Lung 3 trial.
There is no robust clinical evidence to justify a price premium for cemiplimab plus PBC over the least costly immunotherapy available in first-line treatment. In the CADTH base case, cemiplimab plus PBC is dominated by pembrolizumab plus PBC when equal efficacy across immunotherapies is assumed. At the listed prices, a minimum price reduction of 20% for cemiplimab is required for cemiplimab plus PBC to be similar to pembrolizumab plus PBC in terms of total costs.
For the small number of patients for whom PBC alone is a relevant comparator, CADTH’s base case was aligned with the sponsor’s results: cemiplimab plus PBC is associated with higher costs, increased QALYs, and is not cost-effective at a $50,000 per QALY WTP threshold (it would require a price reduction of 71%, from $8,200 to $2,378 per 21-day course). However, there is remaining uncertainty concerning the generalizability of the OS rate for the PBC-alone arm in the EMPOWER-Lung 3 trial.
The CADTH base-case results were driven by alternative extrapolations for OS in the PBC-alone treatment arm, comparative efficacy across immunotherapy arms, dosing assumptions for the other immunotherapies (weight-base versus fixed dosing), and the proportion of patients receiving subsequent therapy.
Outstanding uncertainty remains regarding the model structure (limited to capture the benefits of subsequent therapies), the confidential discounts negotiated by public plans, and the cost-effectiveness of cemiplimab plus PBC versus pembrolizumab monotherapy (excluded from the sponsor’s submission). Given the remaining uncertainty, further price reductions may be sought.
References
1.Clinical Study Report: R2810-ONC-16113. A two-part randomized, phase 3 study of combinations of cemiplimab (anti-PD-1 antibody) and platinum-based doublet chemotherapy in first-line treatment of patients with advancedor metastatic non-small cell lung cancer [internal sponsor's report]. Tarrytown (NY): Regeneron Pharmaceuticals, Inc; 2021.
2.Garassino MC, Gadgeel S, Speranza G, et al. Pembrolizumab plus pemetrexed and platinum in nonsquamous non–small-cell lung cancer: 5-year outcomes from the phase 3 KEYNOTE-189 study. J Clin Oncol. 2023:JCO. 22.01989.
3.Novello S, Kowalski DM, Luft A, et al. Pembrolizumab plus chemotherapy in squamous non-small-cell lung cancer: 5-Year update of the phase III KEYNOTE-407 study. J Clin Oncol. 2023(JCO2201990):1-8.
4.Network meta-analysis of clinical trials supporting cemiplimab in combination with chemotherapy in advanced or metastatic non-small cell lung cancer [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Libtayo (cemiplimab) 50 mg/mL solution for infusion. Laval (QC): Sanofi-aventis Canada; 2023 Sep 27.
5.Longworth L, Yang Y, Young T, et al. Use of generic and condition-specific measures of health-related quality of life in NICE decision-making: a systematic review, statistical modelling and survey. Health Technol Assess. 2014. PubMed
6.van Hout BA, Shaw JW. Mapping EQ-5D-3L to EQ-5D-5L. Value Health. 2021;24(9):1285-1293. PubMed
7.Wehler M, Storm M, Kowal S, Campbell C, Boscoe A. A health state utility model estimating the impact of ivosidenib on quality of life in patients with relapsed/refractory acute myeloid leukemia. EHA Library. 2018.
8.Nafees B, Stafford M, Gavriel S, Bhalla S, Watkins J. Health state utilities for non small cell lung cancer. Health Qual Life Outcomes. 2008;6(1):1-15. PubMed
9.Paz-Ares L, Ciuleanu TE, Cobo M, et al. First-line nivolumab plus ipilimumab combined with two cycles of chemotherapy in patients with non-small-cell lung cancer (CheckMate 9LA): an international, randomised, open-label, phase 3 trial. Lancet Oncol. 2021;22(2):198-211. PubMed
10.DeltaPA. Ottawa (ON): IQVIA; 2023: https://www.iqvia.com/. Accessed 2023 Nov 1.
11.Libtayo (cemiplimab): 50 mg/mL solution for infusion [product monograph]. Laval (QC): Sanofi-aventis Canada; 2023 Aug 15.
12.CADTH. Keytruda (pembrolizumab) for advanced non-small cell lung carcinoma (first-line) - details. https://www.cadth.ca/keytruda-advanced-non-small-cell-lung-carcinoma-first-line-details. Accessed 2023 May 25.
13.Insinga RP, Feliciano JL, Qiao N, Vandormael K, Zhang Y. Cost-effectiveness of pembrolizumab + chemotherapy versus chemotherapy and pembrolizumab monotherapy in first line treatment of NSCLC in the US - updated analyses with additional trial follow-up. J Med Econ. 2021;24(1):792-805. PubMed
14.Schedule of benefits for physician services under the Health Insurance Act: (June 29, 2023 (effective July 23, 2023)). Toronto (ON): Ontario Ministry of Health; 2023: https://www.health.gov.on.ca/en/pro/programs/ohip/sob/physserv/sob_master.pdf. Accessed by sponsor, no date provided.
15.Schedule of benefits for laboratory services: effective July 1, 2020. Toronto (ON): Ontario Ministry of Health; 2020: http://www.health.gov.on.ca/en/pro/programs/ohip/sob/lab/lab_mn2020.pdf. Accessed by sponsor, no date provided.
16.Walker H, Anderson M, Farahati F, et al. Resource use and costs of end-of-life/palliative care: Ontario adult cancer patients dying during 2002 and 2003. J Palliat Care. 2011;27(2):79-88. PubMed
17.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Libtayo (cemiplimab) 50 mg/mL solution for infusion. Laval (QC): Sanofi-aventis Canada; 2023 Sep 27.
18.Cancer Care Ontario. Funded evidence-informed regimens. 2023; https://www.cancercareontario.ca/en/drugformulary/regimens. Accessed 2023 Nov 1.
19.Coyle D, Haines A, Lee K. Extrapolating clinical evidence within economic evaluations. Can J Health Technol. 2023;3(5). PubMed
20.Longworth L, Rowen D. Mapping to obtain EQ-5D utility values for use in NICE health technology assessments. Value Health. 2013;16(1):202-210. PubMed
21.Canadian Cancer Statistics. A 2020 special report on lung cancer. Toronto (ON): Canadian Cancer Society; 2020: https://cdn.cancer.ca/-/media/files/cancer-information/resources/publications/2020-canadian-cancer-statistics-special-report/2020-canadian-cancer-statistics-special-report-en.pdf. Accessed 2023 Nov 1.
22.CADTH reimbursement review: pembrolizumab (Keytruda) for advanced endometrial cancer. Can J Health Technol. 2023;3(4). https://www.cadth.ca/sites/default/files/DRR/2023/PC0280-Keytruda_combined.pdf. Accessed 2023 Nov 1.
23.CADTH reimbursement review: nivolumab (Opdivo) in combination with ipilimumab (Yervoy) for malignant pleural mesothelioma. Can J Health Technol. 2021;1(9). https://www.cadth.ca/sites/default/files/DRR/2021/PC0229-Opdivo-Yervoy-combined.pdf. Accessed 2023 Nov 1.
24.Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Libtayo (cemiplimab) 50 mg/mL solution for infusion. Laval (QC): Sanofi-aventis Canada; 2023 Sep 27.
25.Antonia SJ, Villegas A, Daniel D, et al. Durvalumab after chemoradiotherapy in stage III non-small-cell lung cancer. N Engl J Med. 2017;377(20):1919-1929. PubMed
26.Brenner DR, Poirier A, Woods RR, et al. Projected estimates of cancer in Canada in 2022. CMAJ. 2022;194(17):E601-e607. PubMed
27.pan-Canadian Oncology Drug Review (pCODR) final clinical guidance report for durvalumab (Imfinzi) for non-small cell lung cancer. Ottawa (ON): CADTH; 2019: https://www.cadth.ca/sites/default/files/pcodr/Reviews2019/10131DurvalumabNSCLC_fnCGR_NOREDACT_Post_03May2019_final.pdf. Accessed 2023 Jul 25.
28.CADTH reimbursement review: nivolumab (Opdivo) for non–small cell lung cancer. Can J Health Technol. 2023; 3(4). https://www.cadth.ca/sites/default/files/DRR/2023/PC0303-Opdivo-NSCLC.pdf. Accessed 2023 Aug 15.
29.Canadian Partnership Against Cancer. Distribution of cases by stage at diagnosis for non-small cell lung cancer – 2013 diagnosis year. https://www.systemperformance.ca/disease-sites/lung/stage-distribution/. Accessed 2020 December 8.
30.Aacr Project GENIE Consortium. AACR Project GENIE: powering precision medicine through an international consortium. Cancer Discov. 2017;7(8):818-831. PubMed
31.Felip E, Altorki N, Zhou C, et al. Adjuvant atezolizumab after adjuvant chemotherapy in resected stage IB-IIIA non-small-cell lung cancer (IMpower010): a randomised, multicentre, open-label, phase 3 trial. Lancet. 2021;398(10308):1344-1357. PubMed
32.Hwang DM, Albaqer T, Santiago RC, et al. Prevalence and heterogeneity of PD-L1 expression by 22C3 assay in routine population-based and reflexive clinical testing in lung cancer. J Thorac Oncol. 2021;16(9):1490-1500. PubMed
33.Libtayo – cancer du poumon non à petites cellules Montreal (QC): INESSS; 2022: https://www.inesss.qc.ca/fileadmin/doc/INESSS/Inscription_medicaments/Avis_au_ministre/Novembre_2022/Libtayo_CPNPC_2022_10.pdf. Accessed 2023 Jun 20.
34.Statistics Canada. Table: 17-10-0005-01. Population estimates on July 1st, by age and sex. https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1710000501. Accessed 2023 Jun 20.
35.Statistics Canada. Table: 13-10-0747-01. Number of new cases and age-standardized rates of primary cancer, by cancer type and sex. https://www150.statcan.gc.ca/t1/tbl1/en/cv.action?pid=1310074701. Accessed 2023 May 11.
36.Mok TSK, Wu YL, Kudaba I, et al. Pembrolizumab versus chemotherapy for previously untreated, PD-L1-expressing, locally advanced or metastatic non-small-cell lung cancer (KEYNOTE-042): a randomised, open-label, controlled, phase 3 trial. Lancet. 2019;393(10183):1819-1830. PubMed
37.Gandhi L, Rodríguez-Abreu D, Gadgeel S, et al. Pembrolizumab plus chemotherapy in metastatic non-small-cell lung cancer. N Engl J Med. 2018;378(22):2078-2092. PubMed
38.Sezer A, Kilickap S, Gümüş M, et al. Cemiplimab monotherapy for first-line treatment of advanced non-small-cell lung cancer with PD-L1 of at least 50%: a multicentre, open-label, global, phase 3, randomised, controlled trial. Lancet. 2021;397(10274):592-604. PubMed
39.Reck M, Rodríguez-Abreu D, Robinson AG, et al. Pembrolizumab versus chemotherapy for PD-L1-positive non-small-cell lung cancer. N Engl J Med. 2016;375(19):1823-1833. PubMed
Appendix 1: Cost Comparison Table
Note this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from the clinical expert(s) and drug plan. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 8: CADTH Cost Comparison for NSCLC
Treatment | Strength | Form | Price ($) | Recommended dosage | Average daily cost ($) | Average 21-day course ($) |
|---|---|---|---|---|---|---|
Cemi + PBC | ||||||
Cemiplimab (Cemi) (Libtayo) | 50 mg/mL IV infusion | 7 mL Viala | 8,200.0000b | 350 mg on Day 1 every 3 weeks for a total of 34 cycles or 24 months | 390.48 | 8,200 |
CISPPEME + Cemi (CISPPEME for a total of 4 cycles)b | 431.19 | 9,055 | ||||
CRBPPEME + Cemi (carboplatin dose: AUC 5; CRBPPEME for a total of 4 cycles)b | 458.81 | 9,635 | ||||
CISPPACL + Cemi (paclitaxel dose: 200 mg /m2; CISPPACL for a total of 4 cycles)b | 616.43 | 12,945 | ||||
CRBPPACL + Cemi (paclitaxel dose: 200 mg /m2; carboplatin dose: 750 mg; CRBPPACL for a total of 4 cycles)b | 654.05 | 13,735 | ||||
PEME (MNT) (until disease progression)b | 21.43 | 450 | ||||
Platinum-based PBC (PBC alone) | ||||||
Pemetrexed (PEME) (generic) | 100 mg vial 500 mg vial | 10 mg/mL IV solution | 50.0000 250.0000 | 500 mg /m2 on Day 1 every 3 weeks | 21.43 | 450 |
Paclitaxel (PACL) (generic) | 30 mg vial 96 mg vial 150 mg vial 300 mg vial | 6 mg/mL IV solution | 300.0000 1,196.8000 1,870.0000 3,740.0000 | 175 to 200 mg /m2 on Day 1 every 3 weeks | 192.38 to 206.67 | 4,040 to 4,340 |
Cisplatin (CIS) (generic) | 50 mg vial 100 mg vial | 1 mg/mL IV solution | 135.0000 270.0000 | 75 mg /m2 on Day 1 every 3 weeks | 19.29 | 405 |
Carboplatin (CRB) (generic) | 50 mg vial 150 mg vial 450 mg vial 600 mg vial | 10 mg/mL IV solution | 70.0000 210.0000 600.0000 775.0000 | AUC 5 to 6 on Day 1 every 3 weeks | 46.90 to 56.90 | 985 to 1,195 |
CISPPEME (CISPPEME for a total of 3 cycles) | 40.71 | 855 | ||||
CRBPPEME (carboplatin dose: AUC 5; CRBPPEME for a total of 3 cycles) | 68.33 | 1,435 | ||||
CISPPACL (paclitaxel dose: 200 mg /m2; CISPPACL for a total of 3 cycles) | 225.95 | 4,745 | ||||
CRBPPACL (paclitaxel dose: 200 mg /m2; carboplatin dose: AUC 6; CRBPPACL for a total of 4 to 6 cycles) | 263.57 | 5,535 | ||||
PEME (MNT) (until disease progression) | 21.43 | 450 | ||||
Immunotherapy + PBC | ||||||
Pembro + PBC | ||||||
Pembrolizumab (Pembro) (Keytruda) | 100 mg vial | 100 mg / 4 mL IV solution | 4,400.0000c | 2 mg/kg (max 200 mg) on Day 1 every 3 weeksd | 314.29 | 6,600 |
Pembro (MNT) (for a total of 34 cycles or 24 months) | 314.29 | 6,600 | ||||
CISPPEME + Pembro (CISPPEME for a total of 4 to 6 cycles) | 355.00 | 7,455 | ||||
CRBPPEME + Pembro (carboplatin dose: AUC 5; CRBPPEME for a total of 4 to 6 cycles) | 382.62 | 8,035 | ||||
CRBPPACL + Pembro (paclitaxel dose: 200 mg /m2; carboplatin dose: AUC 6; CRBPPACL for a total of 4 to 6 cycles) | 577.86 | 12,135 | ||||
PEME (MNT) (until disease progression) | 21.43 | 450 | ||||
Nivo + Ipi + PBC | ||||||
Nivolumab (Nivo) | 40 mg vial 100 mg vial | 10 mg/mL IV solution | 782.2200e 1,955.5600e | 4.5 mg/kg (max 360 mg) on Day 1 every 3 weeks | 314.29 | 6,600 |
Ipilimumab (Ipi) | 50 mg vial | 5 mg/mL IV solution | 5,800.0000e | Cycle 1: 1 mg/kg on Day 1 every 3 weeks Cycle 2: No dose Maintenance cycles: 1 mg/kg on Day 1 every 6 weeks | Cycle 1: 552.38 Cycle 2: 0 Maintenance cycles: 276.19 | Cycle 1: 11,600 Cycle 2: 0 Maintenance cycles: 5,800 |
CISPPEME+Nivo+Ipi (CISPPEME for a total of 2 cycles) | Cycle 1: 907.38 Cycle 2: 355.00 | Cycle 1: 19,055 Cycle 2: 7,455 | ||||
CRBPPEME+Nivo+Ipi (carboplatin dose: AUC 5; CRBPPEME for a total of 2 cycles) | Cycle 1: 935.00 Cycle 2: 382.62 | Cycle 1: 19,635 Cycle 2: 8,035 | ||||
CRBPPACL+Nivo+Ipi (paclitaxel dose: 200 mg /m2; carboplatin dose: AUC 6; CRBPPACL for a total of 2 cycles) | Cycle 1: 1,130.24 Cycle 2: 577.86 | Cycle 1: 23,735 Cycle 2: 12,135 | ||||
Nivo+Ipi (MNT) (ipilimumab maintenance dose; for a total of 32 cycles or 22 months followed by Cycle 1 and Cycle 2) | Maintenance cycles: 590.48 | Maintenance cycles: 12,400 | ||||
AUC = area under the curve; Cemi = cemiplimab; CISP = cisplatin; CRB = carboplatin; Ipi = ipilimumab; MNT = monotherapy; Nivo = nivolumab; PACL = paclitaxel; PBC = platinum-based chemotherapy; Pembro = pembrolizumab; PEME = pemetrexed
Note: All prices are from IQVIA drug price database (accessed November 2023), unless otherwise indicated, and do not include dispensing fees. Dosing is based on Cancer Care Ontario Drug Formulary,18 unless otherwise indicated. For treatments using weight-based dosing, CADTH assumed 75 kg or 1.8 m2. The dose for carboplatin is estimated based on target AUC, adjusted for glomerular filtration rate, 125 mL/min. Drug wastage is included, expect for pembrolizumab and nivolumab.
aThe sponsor confirmed that the 250 mg vial is being discontinued in Canada.
bSponsor’s pharmacoeconomic submission.17
cCADTH review of pembrolizumab.22
dDespite a fixed dosing in the product monograph, Cancer Care Ontario Drug Formulary18 references a weight-based dosing (confirmed by clinical experts and drug plans feedback as the current practice across jurisdictions) and does not include wastage.
eCADTH review of nivolumab.23
Appendix 2: Submission Quality
Note this appendix has not been copy-edited.
Description | Yes or No | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | No | Refer to the CADTH appraisal section “Pembrolizumab monotherapy is excluded but it is a relevant comparator for a subset of the indicated population.” |
Model has been adequately programmed and has sufficient face validity | No | Refer to the CADTH appraisal section “The trial data for PBC alone does not reflect clinical practice and its long-term extrapolation lacks face validity.” The OS and PFS curve extrapolations were derived using hard-coded shape and scale parameters, which made it difficult to validate the source of OS and PFS data. |
Model structure is adequate for decision problem | No | The PSM further introduces structural assumptions about the relationship between PFS and OS (i.e., nonmutually exclusive curves), which is potentially problematic since they are likely dependent outcomes. PSMs are not suitable to capture changes in response on subsequent lines of therapy, as this model structure only accounts for the costs of subsequent therapies in the progressed state but has limited flexibility to capture their clinical benefits. |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | Yes | No comment |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | Yes | No comment |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | Yes | No comment |
Appendix 3: Additional Information on the Submitted Economic Evaluation
Note this appendix has not been copy-edited.
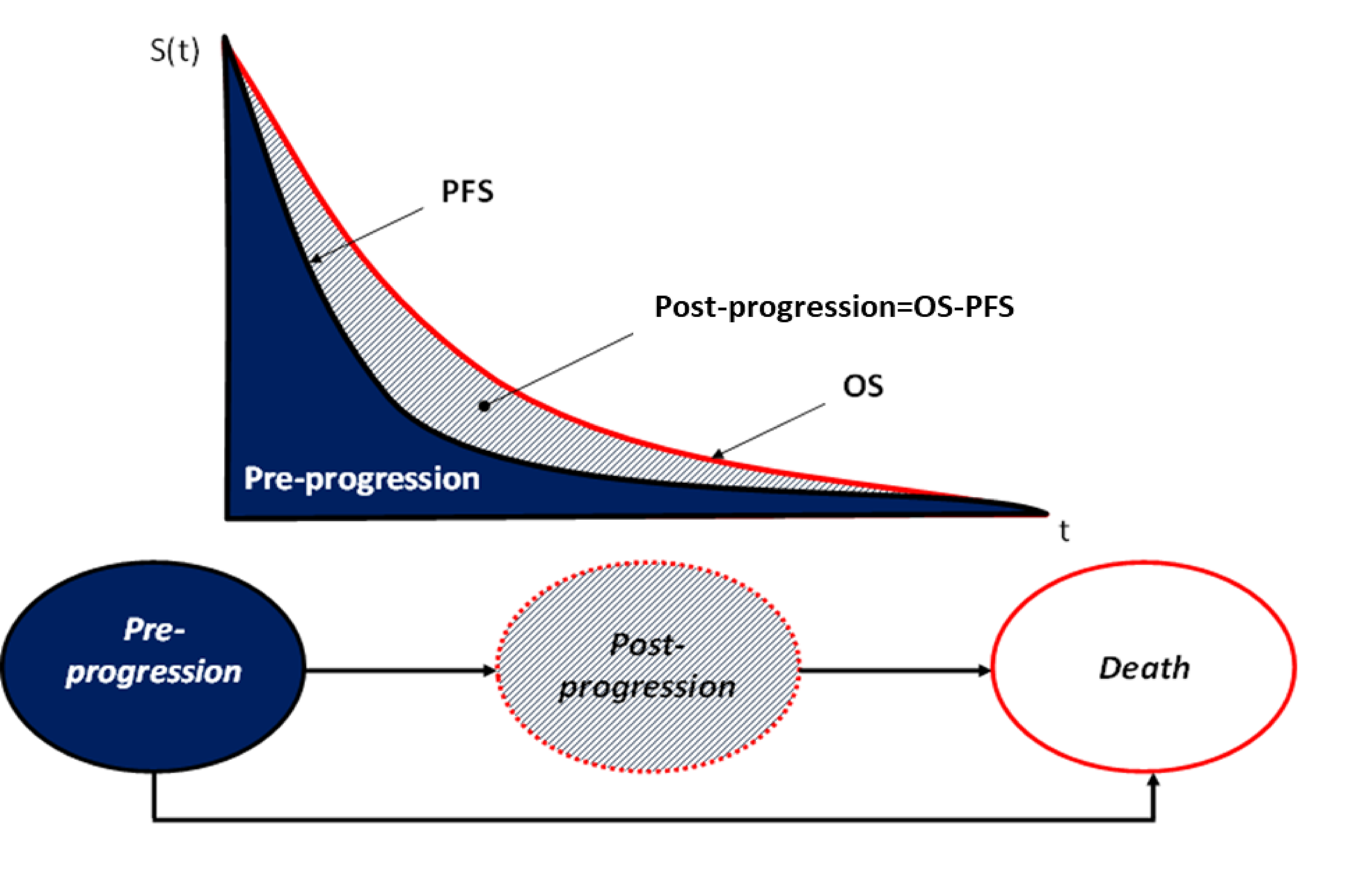
Table 10: Distribution of Patients Across First-Line PBC Components
First-line drug options | PBC | Pembro + PBC | Nivo + Ipi + PBC | Cemi + PBC |
|---|---|---|---|---|
Cemi | — | — | — | |||| |
Pembro | — | 100% | — | — |
Nivo | — | — | 100% | — |
Ipi | — | — | 100% | — |
Paclitaxel + Cisplatin | || | 0% | 0% | ||| |
Paclitaxel + Carboplatin | ||| | 55% | 55% | ||| |
Pemetrexed + Cisplatin | ||| | 8% | 8% | || |
Pemetrexed + Carboplatin | ||| | 37% | 37% | ||| |
Cemi = cemiplimab; Nivo = nivolumab; PBC = platinum-based chemotherapy; Pembro = pembrolizumab; Ipi = ipilimumab
Source: Sponsor’s pharmacoeconomic submission.17
Table 11: Distribution of Patients Across Subsequent Therapies After Progression
Postprogression drug options | PBC | Pembro + PBC | Nivo + Ipi + PBC | Cemi + PBC |
|---|---|---|---|---|
Pembro | || | || | || | || |
Nivo | ||| | || | || | || |
Atezolizumab | ||| | || | || | || |
Docetaxel | ||| | ||| | ||| | ||| |
Carboplatin | || | || | || | || |
Cisplatin | || | || | || | || |
Gemcitabine | || | || | || | || |
Paclitaxel | || | || | || | || |
Pemetrexed | || | ||| | ||| | ||| |
Total | 100% | 100% | 100% | 100% |
Cemi = cemiplimab; Nivo = nivolumab; PBC = platinum-based chemotherapy; Pembro = pembrolizumab; Ipi = ipilimumab
Source: Sponsor’s pharmacoeconomic submission.17
Detailed Results of the Sponsor’s Base Case
Table 12: Disaggregated Summary of Sponsor’s Economic Evaluation Results
Parameter | PBC | Pembro + PBC | Nivo + Ipi + PBC | Cemi + PBC |
|---|---|---|---|---|
Discounted LYs | ||||
Progression-free survival time (in months) | 8.20 | 17.39 | 15.39 | 19.07 |
Postprogression survival time (in months) | 16.82 | 21.99 | 21.54 | 24.96 |
Total life-years gained | 2.09 | 3.28 | 3.08 | 3.67 |
Discounted life-years gained | 1.97 | 3.05 | 2.86 | 3.36 |
Discounted QALYs | ||||
Discounted QALYs; preprogression | 0.56 | 1.16 | 1.02 | 1.25 |
Discounted QALYs; progressive disease | 1.05 | 1.35 | 1.33 | 1.50 |
Discounted QALYs lost due to adverse events | 0.00 | 0.00 | 0.00 | 0.00 |
Total discounted QALYs gained | 1.61 | 2.50 | 2.35 | 2.76 |
Discounted costs ($) | ||||
Discounted drug-acquisition and admin cost; preprogression | $11,928.35 | $160,998.88 | $190,263.46 | $147,351.04 |
Discounted drug-acquisition and admin cost; progressive disease | $37,444.36 | $9,376.31 | $9,421.07 | $9,238.06 |
Discounted total drug monitoring cost | $191.18 | $397.97 | $233.79 | $431.27 |
Discounted disease-management cost; preprogression | $2,060.57 | $4,261.51 | $3,758.03 | $4,614.63 |
Discounted disease-management cost; progressive disease | $5,936.17 | $7,597.12 | $7,468.51 | $8,472.85 |
Discounted disease-management cost; terminal care | $36,986.07 | $36,246.85 | $36,358.35 | $35,931.58 |
Discounted adverse event costs | $12.56 | $45.39 | $13.42 | $20.43 |
Discounted societal costs (excluding societal costs relating to treatment administration, which are captured as part of treatment administration) | $0.00 | $0.00 | $0.00 | $0.00 |
Total discounted costs | $94,559.26 | $218,924.03 | $247,516.62 | $206,059.86 |
Cemi = cemiplimab; LY = life-year; Nivo = nivolumab; PBC = platinum-based chemotherapy; Pembro = pembrolizumab; QALY = quality-adjusted life-year; Ipi = ipilimumab
Source: Sponsor’s pharmacoeconomic submission.17
Appendix 4: Additional Details on the CADTH Reanalyses and Sensitivity Analyses of the Economic Evaluation
Note this appendix has not been copy-edited.
Detailed Results of CADTH Base Case
Table 13: Summary of the Stepped Analysis of the CADTH Base-Case Results
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER vs. Reference ($ per QALY gained) | Sequential ICER ($ per QALY gained) |
|---|---|---|---|---|---|
Sponsor base case, deterministic | PBC alone | 94,501 | 1.61 | Reference | Reference |
Cemi plus PBC | 205,817 | 2.72 | 99,779 | 99,779 | |
Dominated treatments | |||||
Pembro plus PBC | 218,753 | 2.49 | 141,632 | Dominated by Cemi plus PBC | |
Nivo plus ipi plus PBC | 247,270 | 2.32 | 213,103 | Dominated by Cemi plus PBC | |
1. OS extrapolation for PBC alone: from log-logistic to generalized gamma | PBC alone | 94,574 | 1.27 | Reference | Reference |
Cemi plus PBC | 203,849 | 2.16 | 122,735 | 122,735 | |
Dominated treatments | |||||
Pembro plus PBC | 216,691 | 1.94 | 181,540 | Dominated by Cemi plus PBC | |
Nivo plus ipi plus PBC | 245,368 | 1.78 | 298,231 | Dominated by Cemi plus PBC | |
2. Comparative efficacy of cemi plus PBC vs. PBC alone: from time-varying HRs (NMA) to constant HRs (EMPOWER-Lung 3 trial) | PBC alone | 94,501 | 1.61 | Reference | Reference |
Cemi plus PBC | 206,171 | 2.97 | 82,127 | 82,127 | |
Pembro plus PBC | 219,963 | 3.03 | 88,191 | 219,284 | |
Dominated treatments | |||||
Nivo plus ipi plus PBC | 243,888 | 2.57 | 155,220 | Dominated by Cemi plus PBC | |
3. Comparative efficacy of all immunotherapies vs. PBC alone: same HRs as cemi plus PBC (EMPOWER-Lung 3 trial) | PBC alone | 94,501 | 1.61 | Reference | Reference |
Cemi plus PBC | 206,476 | 3.00 | 80,506 | 82,760 | |
Dominated treatments | |||||
Pembro + PBC | 216,284 | 3.00 | 87,687 | Dominated by Cemi + PBC | |
Nivo + ipi + PBC | 270,509 | 3.00 | 126,490 | Dominated by Cemi + PBC | |
4. Weight-based dosing for pembro, nivo and ipi | PBC alone | 93,172 | 1.61 | Reference | Reference |
Pembro + PBC | 179,430 | 2.49 | 98,323 | 98,323 | |
Cemi + PBC | 205,817 | 2.72 | 100,970 | 110,713 | |
Dominated treatments | |||||
Nivo + ipi + PBC | 238,349 | 2.32 | 202,512 | Dominated by Pembro + PBC | |
5. % patients receiving subsequent therapy aligned with the EMPOWER-Lung 3 trial | PBC | 65,360 | 1.61 | Reference | Reference |
Cemi + PBC | 198,067 | 2.72 | 118,953 | 118,953 | |
Dominated treatments | |||||
Pembro + PBC | 210,876 | 2.49 | 165,871 | Dominated by Cem + PBC | |
Nivo + ipi + PBC | 239,357 | 2.32 | 242,715 | Dominated by Cemi + PBC | |
CADTH base case, deterministic Changes 1 + 2 + 3 + 4 + 5 | PBC alone | 63,841 | 1.27 | Reference | Reference |
Pembro + PBC | 166,063 | 2.03 | 135,010 | 135,010 | |
Dominated treatments | |||||
Cemi + PBC | 194,058 | 2.03 | 171,517 | Dominated by Pembro + PBC | |
Nivo + ipi + PBC | 248,993 | 2.03 | 243,687 | Dominated by Pembro + PBC | |
CADTH base case, probabilistic Changes 1 + 2 + 3 + 4 + 5 | PBC alone | 63,829 | 1.28 | Reference | Reference |
Pembro + PBC | 166,127 | 2.05 | 132,739 | 132,739 | |
Nivo + ipi + PBC | 249,793 | 2.06 | 169,328 | 7,828,171 | |
Dominated treatments | |||||
Cemi + PBC | 194,203 | 2.05 | 238,001 | Dominated by Pembro + PBC |
Cemi = cemiplimab; Ipi = ipilimumab; Nivo = nivolumab; PBC = platinum-based chemotherapy; Pembro = pembrolizumab; vs. = versus.
Table 14: Disaggregated Summary of CADTH’s Economic Evaluation Results, Probabilistic
Parameter | PBC | Pembro + PBC | Nivo + Ipi + PBC | Cemi + PBC |
|---|---|---|---|---|
Discounted LYs | ||||
Progression-free survival time (in months) | 8.16 | 19.24 | 19.41 | 19.25 |
Postprogression survival time (in months) | 11.03 | 12.02 | 11.99 | 11.97 |
Total life-years gained | 1.60 | 2.61 | 2.62 | 2.60 |
Total life-years gained (discounted) | 1.56 | 2.49 | 2.50 | 2.49 |
Discounted QALYs | ||||
Discounted QALYs; preprogression | 0.56 | 1.27 | 1.28 | 1.27 |
Discounted QALYs; progressive disease | 0.72 | 0.78 | 0.78 | 0.78 |
Discounted QALYs lost due to adverse events | 0.00 | 0.00 | 0.00 | 0.00 |
Total discounted QALYs | 1.28 | 2.05 | 2.06 | 2.05 |
Discounted costs ($) | ||||
Discounted drug-acquisition and admin cost; preprogression | $11,921 | $118,269 | $202,106 | $146,346 |
Discounted drug-acquisition and admin cost; progressive disease | $8,314 | $1,588 | $1,587 | $1,587 |
Discounted total drug monitoring cost | $191 | $438 | $261 | $438 |
Discounted disease-management cost; preprogression | $2,048 | $4,665 | $4,728 | $4,691 |
Discounted disease-management cost; progressive disease | $4,048 | $4,378 | $4,360 | $4,376 |
Discounted disease-management cost; terminal care | $37,294 | $36,744 | $36,738 | $36,745 |
Discounted adverse event costs | $13 | $45 | $13 | $20 |
Discounted societal costs (excluding societal costs relating to treatment administration, which are captured as part of treatment administration) | $0 | $0 | $0 | $0 |
Total discounted costs | $63,829 | $166,127 | $249,793 | $194,203 |
Cemi = cemiplimab; ICER = incremental cost-effectiveness ratio; LY = life-year; Nivo = nivolumab; PBC = platinum-based chemotherapy; Pembro = pembrolizumab; QALY = quality-adjusted life-year.
Scenario Analyses
Table 15: Scenario Analysis (Deterministic)
Stepped analysis | Comparator | Total costs ($) | Total QALYs | Sequential ICER ($ per QALY gained) |
|---|---|---|---|---|
CADTH’s base case, deterministic | PBC alone | 63,841 | 1.27 | Reference |
Pembro + PBC | 166,063 | 2.03 | 135,010 | |
Dominated treatments | ||||
Cemi + PBC | 194,058 | 2.03 | Dominated by Pembro + PBC | |
Nivo + ipi + PBC | 248,993 | 2.03 | Dominated by Pembro + PBC | |
CADTH scenario 1: assuming equal efficacy of immunotherapies by adopting the sponsor’s time-varying HRs for cemi+ PBC in all immunotherapy arms | PBC alone | 63,841 | 1.27 | Reference |
Pembro | 167,314 | 2.16 | 116,487 | |
Dominated treatments | ||||
Cemi + PBC | 195,621 | 2.16 | Dominated by Pembro + PBC | |
Nivo + ipi + PBC | 251,714 | 2.16 | Dominated by Pembro + PBC | |
CADTH scenario 2: Adopting alternative value of constant OS HR (reducing incremental efficacy by 50%) | PBC alone | 63,841 | 1.27 | Reference |
Pembro + PBC | 163,330 | 1.57 | 335,951 | |
Dominated treatments | ||||
Cemi + PBC | 191,325 | 1.57 | Dominated by Pembro + PBC | |
Nivo + ipi + PBC | 246,957.76 | 1.57 | Dominated by Pembro + PBC | |
CADTH scenario 3: Adopting fixed dosing for pembro and nivo | PBC alone | 64,148 | 1.27 | Reference |
Cemi + PBC | 194,058 | 2.03 | 171,113 | |
Dominated treatments | ||||
Pembro + PBC | 203,866 | 2.03 | Dominated by cemi + PBC | |
Nivo + ipi + PBC | 258,938 | 2.03 | Dominated by cemi + PBC | |
CADTH scenario 4: Waning effect starting from the end of trial follow-up over 5 years | PBC alone | 63,841 | 1.27 | Reference |
Pembro + PBC | 164,144 | 1.80 | 187,749 | |
Dominated treatments | ||||
Cemi + PBC | 192,138 | 1.81 | Dominated by Pembro + PBC | |
Nivo + ipi + PBC | 248,265 | 1.81 | Dominated by Pembro + PBC |
Cemi = cemiplimab; ICER = incremental cost-effectiveness ratio; Nivo = nivolumab; PBC = platinum-based chemotherapy; Pembro = pembrolizumab; QALY = quality-adjusted life-year.
Note: All analyses were conducted deterministically.
Appendix 5: Submitted BIA and CADTH Appraisal
Note this appendix has not been copy-edited.
Table 16: Summary of Key Take-Aways
Key Takeaways of the BIA |
|---|
|
Summary of Sponsor’s Budget Impact Analysis
The submitted budget impact analysis (BIA) assessed the expected budgetary impact of reimbursing cemiplimab + PBC for the first-line treatment of adult patients with NSCLC whose tumours have no EGFR, ALK or ROS1 aberrations and is locally advanced where patients are not candidates for surgical resection or definitive chemoradiation, or metastatic NSCLC.24 The BIA was undertaken from the perspective of the Canadian public drug plans at base year (2024) and over a 3-year time horizon (2025 to 2027). The sponsor’s pan-Canadian estimates reflected the aggregated results from provincial budgets (excluding Quebec). Key inputs to the BIA are documented in Table 17.
The sponsor estimated the number of eligible patients for cemiplimab + PBC using an epidemiologic approach with data obtained from Canadian Cancer Statistics, published literature and the sponsor’s clinical experts.21,25-35 The sponsor adopted age-standardized incidence rates of lung cancer and narrowed the population to those with stage III or IV NSCLC without driver mutations. The sponsor restricted market size to those who have unresectable cancer and are eligible for PBC. The sponsor assumed that 43% of eligible patients would receive first-line treatment for advanced/metastatic cancer. The sponsor also included patients with recurrent NSCLC after 6 months in estimating the eligible population size.
Comparators included pembrolizumab + PBC, nivolumab + ipilimumab + PBC, cemiplimab monotherapy, pembrolizumab monotherapy and PBC alone. Drug dosages were obtained from published literature, clinical trials (EMPOWER-Lung 1/3, KEYNOTE-189/407/024 and CheckMate 9LA) and Cancer Care Ontario Drug Formulary.1,2,36 Drug-acquisition unit costs were obtained from the IQVIA Delta PA database and published literature.10,11 Drug costs were inclusive of drug wastage. The treatment duration was assumed to be the same as the median duration reported in clinical trials for cemiplimab, nivolumab, ipilimumab and PBC; and the mean treatment duration for pembrolizumab.1,9,37-39 The sponsor assumed that cemiplimab + PBC captured majority of its market share from pembrolizumab + PBC (89.4%).
Table 17: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as year 1 / year 2 / year 3 if appropriate) |
|---|---|
Target Population | |
Lung cancer incidence | 0.0544% / 0.0535% / 0.0525% |
Percentage with NSCLC | 89.0% |
Percentage of NSCLC by stage | |
Stage II | 8.9% |
Stage IIIa | 13.7% |
Stage IIIb/c | 5.7% |
Stage IV | 48.4% |
Percentage without driver mutation | 74.5% |
Percentage with unresectable cancer by stage | |
Stage IV | 100.0% |
Stage IIIa | 70.0% |
Stage IIIb/c | 90.0% |
Percentage with resectable cancer by stage | |
Stage II | 50.0% |
Stage IIIa | 30.0% |
Percentage ineligible for platinum-based chemoradiation and durvalumab | 50.0% |
Percentage eligible for platinum-based chemoradiation and durvalumab | 50.0% |
Percentage treated with platinum-based chemoradiation and durvalumab | 100.0% |
Percentage treated with PBC and atezolizumab | 100.0% |
Percentage with recurrence by PDL status | |
Any PD-L1 status | 44.1% |
PD-L1 ≥ 50% | 17.0% |
PD-L1 < 50% | 27.0% |
Percentage with PD-L1 ≥ 50% | 33.1% |
Percentage with PD-L1 < 50% | 66.9% |
Percentage with recurrence after 6 months from the last treatment dose | |
platinum-based chemoradiation and durvalumab | 70.0% |
PBC and atezolizumab | 90.0% |
Percentage treated for first-line advanced/metastatic treatment | 43.0% |
Number of patients eligible for drug under review (incidence) | |
Stage IV (unresectable) | 2,355 / 2,344 / 2,333 |
Stage IIIb/c (unresectable, ineligible for platinum-based chemoradiation and durvalumab) | 125 / 124 / 124 |
Number of patients eligible for drug under review (prevalence) | |
Stage IIIb/c (unresectable, eligible for and treated with platinum-based chemoradiation and durvalumab, recurrence for any PD-L1 status and after 6 months of last treatment dose) | 39 / 39 / 38 |
Stage IIIa (unresectable, eligible for and treated with platinum-based chemoradiation and durvalumab, recurrence for any PD-L1 status and after 6 months of last treatment dose) | 72 / 72 / 72 |
Stage IIIa (resectable, PD-L1 ≥ 50%, treated with PBC and atezolizumab, recurrence for PD-L1 ≥ 50% and after 6 months of last treatment dose) | 10 / 10 / 10 |
Stage IIIa (resectable, PD-L1 < 50% and recurrence for PD-L1 ≥ 50%) | 36 / 36 / 36 |
Stage II (resectable, PD-L1 ≥ 50%, treated with PBC and atezolizumab, recurrence for PD-L1 ≥ 50% and after 6 months of last treatment dose) | 11 / 11 / 11 |
Stage II (resectable, PD-L1 < 50% and recurrence for PD-L1 < 50%) | 39 / 39 / 39 |
Number of patients eligible for the drug under review | 2,687 / 2,675 / 2,663 |
Market Uptake (3 years) | |
Uptake (reference scenario) | |
Pembro + PBC | ||||| | |||| | ||||||||| | ||||||||| | |||| | |||||||| | |||| ||||||||||| | |
Nivo + ipi + PBC | ||||| | ||||| |
PBC alone | ||||| | ||||| |
Cemi monotherapy | ||||| | ||||| |
Pembro monotherapy | ||||| | ||||| |
Uptake (new drug scenario) | |
Cemi + PBC | 2.0% / 4.0% / 6.0% |
Pembro + PBC | ||||| | ||||| | |||||||| | ||| ||||||||| | ||||| ||||||||| | |||| | |
Nivo + ipilimumab + PBC | |||||||||| | ||||| | ||||| |
PBC alone | |||||||||| | ||||| | ||||| |
Cemi monotherapy | |||||||||| | ||||| | ||||| |
Pembro monotherapy | |||||||||| | ||||| | ||||| |
Distribution of platinum-based PBC regimens | |
Cemi | |
Paclitaxel and carboplatin | ||||| |
Paclitaxel and cisplatin | ||||| |
Pemetrexed and carboplatin | ||||| |
Pemetrexed and cisplatin | ||||| |
Pembro (nonsquamous) | |
Pemetrexed and carboplatin | 80.0% |
Pemetrexed and cisplatin | 20.0% |
Pembro (squamous) | |
Paclitaxel and carboplatin | 100.0% |
Nivo and ipi | |
Pemetrexed and carboplatin | 64.0% |
Pemetrexed and cisplatin | 16.0% |
Paclitaxel and carboplatin | 20.0% |
Platinum-based PBC | |
Paclitaxel and carboplatin | ||||| |
Paclitaxel and cisplatin | ||||| |
Pemetrexed and carboplatin | ||||| |
Pemetrexed and cisplatin | ||||| |
Cost of treatment (per patient, per treatment duration) | |
Cemi + PBC (median ||| months) | $||||||| |
Pembro + PBC (mean 7.4 months for nonsquamous, mean 6.3 months for squamous) | $103,637 |
Nivo + ipi+ PBC (median 6.1 months for nivolumab + ipilimumab) | $127,808 |
Cemi monotherapy (median 6.3 months) | $74,825 |
Pembro monotherapy (median 7.0 months) | $89,222 |
PBC alone (median ||| months) | $|||||| |
Cemi = cemiplimab; Nivo = nivolumab; NSCLC = non–small cell lung cancer; PBC = platinum-based chemotherapy; Pembro = pembrolizumab; Ipi = ipilimumab
aCost of pembrolizumab is weighted by histology, assuming 80.0% of NSCLC is nonsquamous and 20.0% is squamous.
Summary of the Sponsor’s BIA Results
The 3-year budget impact of introducing cemiplimab + PBC for the first-line treatment of adult patients with NSCLC whose tumours have no EGFR, ALK or ROS1 aberrations and is locally advanced where patients are not candidates for surgical resection or definitive chemoradiation, or metastatic NSCLC would be $ 4,018,181 (Year 1: $678,767; Year 2: $1,343,398; Year 3: $1,996,016).
CADTH Appraisal of the Sponsor’s BIA
CADTH identified several key limitations to the sponsor’s analysis that have notable implications for the results of the BIA:
Inconsistent approach to model treatment duration: The sponsor’s approach to modelling treatment duration adopted mean estimates for pembrolizumab + PBC and medians to estimate the treatment duration for other comparators (refer to Table 17). This is problematic because the median treatment duration does not represent the average duration of treatment exposure and underestimates treatment costs. The mean treatment duration for cemiplimab + PBC was longer than 1 year (approximately 53 weeks) in the EMPOWER-Lung 3 trial, which indicates that some patients who initiated immunotherapy with cemiplimab continued treatment in the subsequent year. Similarly, the product monographs for pembrolizumab and nivolumab note a maximum treatment duration of 2 years. Since the sponsor did not include prevalent patients in estimating the number of eligible patients after year 1, the sponsor’s submitted BIA model lacks the flexibility to adopt treatment durations longer than a year.
In reanalysis, CADTH updated treatment costs to reflect the mean treatment duration in the pharmacoeconomic model. CADTH obtained modelled treatment costs from the CADTH base case for the CUA. CADTH used cumulative 3-year costs to model treatment costs for incident (new) patients starting treatment in year 1, cumulative 2-year costs for patients starting treatment in year 2 and 1-year costs for patients starting treatment in year 3. Additionally, the costs extracted from the CUA model address any issues with weight-based dosing of pembrolizumab and nivolumab, with vial sharing, and align distribution of PBC components and subsequent therapies across treatment arms with the clinical trial. The budget estimates for each year are not precise to the annual costs as they reflect the cumulative costs of each patient within the BIA time horizon, however, the 3-year budget impact is not impacted by this modelling choice.
The dosing of pembrolizumab and nivolumab does not reflect clinical practice: The sponsor adopted fixed dosing for pembrolizumab and nivolumab, with no vial sharing, which lacks face validity. In current clinical practice, patients are administered weight-based dosing and vial sharing often occurs to avoid drug wastage. As such, the average administered dose and treatment cost of pembrolizumab and nivolumab have been overestimated in the sponsor’s model.
In the reanalysis described above, the extracted treatment costs from the CUA model already addressed issues with weight-based dosing of pembrolizumab and nivolumab, with vial sharing.
Since the sponsor excluded pembrolizumab and cemiplimab monotherapies from the CUA, the treatment duration of monotherapies was not changed. This has no impact on the incremental budget impact, only on the yearly budget estimates. Cemiplimab + PBC was not assumed to displace patients treated with monotherapies.
The market share of cemiplimab and pembrolizumab monotherapy may be overestimated: As the negotiation process for cemiplimab monotherapy did not reach an agreement with the pCPA, cemiplimab is not covered by public health care payers and should not have a market share in the BIA. Moreover, the clinical experts noted that the market share of pembrolizumab monotherapy may also be overestimated and is expected to be a maximum of 30% within this patient population.
In reanalysis, CADTH assumed the market share of cemiplimab monotherapy was 0%, decreased the market share of pembrolizumab to 30% and re-distributed the excess market share of patients in monotherapy to pembrolizumab + PBC.
The proportion of patients with a driver mutation is uncertain: The clinical experts consulted by CADTH noted the sponsor’s assumed proportion of patients without driver mutation (74.5%) was underestimated and should be closer to 80% (approx. 20% with a driver mutation).
In scenario analysis, the proportion of patients without driver mutation was assumed to be 80%.
CADTH Reanalyses of the BIA
CADTH revised the sponsor’s base case by adopting treatment costs from the CADTH base case of the CUA (which reflected mean treatment duration and weight-based dosing for pembrolizumab and nivolumab) and adjusting the market shares for cemiplimab and pembrolizumab monotherapy.
Table 18: CADTH Revisions to the Submitted BIA
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Changes to derive the CADTH base case | ||
1. Treatment costs of cemi + PBC, pembro + PBC, nivo + ipi + PBC and PBC alone | Inconsistent treatment duration estimates and fixed dosing Cemi + PBC (median ||| months): $||||||| Pembro + PBC (mean 7.4 months for nonsquamous, mean 6.3 months for squamous): $103,637 Nivo + ipi + PBC (median 6.1 months): $127,808 PBC alone (median ||| months): $|||||| | Aligned with the pharmacoeconomic model (CADTH base case for CUA) Cumulative treatment costs: 3-year, 2-year, 1-year Cemi + PBC: $145,389, $144,846, $111,100 Pembro + PBC: $117,092, $116,550, $89,875 Nivo + ipi + PBC: $203,681, $203,681, $154,947 PBC alone: $19,346, $18,394, $15,572 |
2. Market share (year 1, year 2, year 3) in the reference scenario | Pembro + PBC: |||| |||| ||| Cemi monotherapy: ||| ||| || Pembro monotherapy: |||| |||| ||| | Pembro + PBC: 59%, 59%, 59% Cemi monotherapy:0%, 0%, 0% Pembro monotherapy: 30%, 30%, 30% |
CADTH base case | Reanalysis 1 + 2 | |
Cemi = cemiplimab; CUA – cost-utility analysis; Ipi = ipilimumab Nivo = nivolumab; PBC = platinum-based chemotherapy; Pembro = pembrolizumab.
The results of the CADTH stepwise reanalysis are presented in summary format in Table 19 and a more detailed breakdown is presented in Table 20. The CADTH base case suggests that reimbursing cemiplimab + PBC in the target population would be associated with an incremental cost of $1,029,683 in year 1, $2,015,034 in year 2, and $2,235,088 in year 3, with a 3-year budgetary impact of $5,279,805.
Table 19: Summary of the CADTH Reanalyses of the BIA
Stepped analysis | Three-year total |
|---|---|
Submitted base case | $4,018,181 |
CADTH reanalysis 1 | $5,279,805 |
CADTH reanalysis 2 | $4,018,181 |
CADTH base case | $5,279,805 |
BIA = budget impact analysis
CADTH also conducted additional scenario analyses to address remaining uncertainty, using the CADTH base case. Results are provided in Table 20.
Assuming 80% of patients without driver mutation.
Assuming cemiplimab + PBC captures all its market share from pembrolizumab + PBC.
Assuming fixed-based dosing for pembrolizumab + PBC (200 mg every 3 weeks) and nivolumab + PBC (360 mg every 3 weeks).
Assuming a price reduction of 20%, at which price the treatment cost of all immunotherapies are relatively similar at listed prices (cemiplimab = $6,560.00, pembrolizumab = $6,411.68, nivolumab = $6,411.66).
Results of CADTH’s scenario analyses demonstrate that the budget impact is sensitive to assumptions of which immunotherapies are going to be displaced by cemiplimab + PBC. At a 20% price reduction, cemiplimab + PBC is estimated to reduce the 3-year total budgetary impact by approximately $2,085,269 because it assumes some displacement of nivolumab + ipilimumab + PBC. This is due to the assumption of equal efficacy across immunotherapies (adopted in the CUA) but the fact that the combination of nivolumab + ipilimumab + PBC has higher cumulative 3-year costs ($203,681) than cemiplimab + PBC ($145,389). If cemiplimab + PBC is assumed to only displace pembrolizumab + PBC, the 3-year total budgetary impact is still estimated to have an incremental cost of $7,939,386.
Table 20: Detailed Breakdown of the CADTH Reanalyses of the BIA
Stepped analysis | Scenario | Year 0 (current situation) | Year 1 | Year 2 | Year 3 | Three-year total |
|---|---|---|---|---|---|---|
Submitted base case | Reference | $250,548,353 | $250,267,892 | $249,830,610 | $249,287,657 | $749,386,159 |
New drug | $250,548,353 | $250,946,659 | $251,174,008 | $251,283,673 | $753,404,340 | |
Budget impact | $0 | $678,767 | $1,343,398 | $1,996,016 | $4,018,181 | |
CADTH base case | Reference | $256,115,407 | $289,881,067 | $288,717,674 | $238,552,118 | $817,150,859 |
New drug | $256,115,407 | $290,910,750 | $290,732,708 | $240,787,206 | $822,430,664 | |
Budget impact | $0 | $1,029,683 | $2,015,034 | $2,235,088 | $5,279,805 | |
CADTH scenario analysis 1: assuming cemi + PBC captures all its market share from pembro + PBC | Reference | $256,115,407 | $289,881,067 | $288,717,674 | $238,552,118 | $817,150,859 |
New drug | $256,115,407 | $291,401,796 | $291,745,235 | $241,943,213 | $825,090,244 | |
Budget impact | $0 | $1,520,730 | $3,027,561 | $3,391,095 | $7,939,386 | |
CADTH scenario analysis 2: assuming 80% of patients without driver mutation | Reference | $275,023,255 | $311,281,682 | $310,032,402 | $256,163,348 | $877,477,432 |
New drug | $275,023,255 | $312,387,382 | $312,196,196 | $258,563,443 | $883,147,022 | |
Budget impact | $0 | $1,105,700 | $2,163,795 | $2,400,095 | $5,669,590 | |
CADTH scenario analysis 3: assuming fixed dosing for pembro + PBC and Nivo + PBC | Reference | $256,115,407 | $351,584,677 | $350,267,767 | $284,740,525 | $986,592,970 |
New drug | $256,115,407 | $350,722,408 | $348,525,343 | $282,761,859 | $982,009,610 | |
Budget impact | $0 | -$862,269 | -$1,742,425 | -$1,978,666 | -$4,583,360 | |
CADTH scenario analysis 4: 20% price reduction | Reference | $256,115,407 | $289,881,067 | $288,717,674 | $238,552,118 | $817,150,859 |
New drug | $256,115,407 | $289,502,018 | $287,928,126 | $237,635,446 | $815,065,590 | |
Budget impact | $0 | -$379,049 | -$789,548 | -$916,672 | -$2,085,269 |
BIA = budget impact analysis; Cemi = cemiplimab; Nivo = nivolumab; Pembro = pembrolizumab
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for noncommercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.