CADTH Reimbursement Review
Dostarlimab (Jemperli)
Sponsor: GlaxoSmithKline Inc.
Therapeutic area: Endometrial cancer
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Clinical Review
Abbreviations
AE
adverse event
BICR
blinded independent committee review
CI
confidence interval
CCO
Cancer Care Ontario
CCS
Canadian Cancer Society
CCSN
The Canadian Cancer Survivor Network
CSR
Clinical Study Report
DCR
disease control rate
dMMR
deficient mismatch repair
DoR
duration of response
ECOG PS
Eastern Cooperative Oncology Group Performance Status
EORTC QLQ-C30
European Organization for Research and Treatment of Cancer Core Quality of Life Questionnaire
EORTC QLQ-EN24
European Organization for Research and Treatment of Cancer Quality of Life Questionnaire Endometrial cancer module
FIGO
International Federation of Gynecological and Obstetrics
FA
final analysis
G-CSF
granulocyte colony-stimulating factor
GOC
The Society of Gynecologic Oncology of Canada
GRADE
Grading of Recommendations Assessment, Development and Evaluation
HR
hazard ratio
HRQoL
health-related quality of life
IHC
immunohistochemistry
IA
interim analysis
ITT
intention to treat
K-M
Kaplan-Meier
LSM
least squares mean
MID
minimal important difference
MMR
mismatch repair
MMRM
mixed model of repeated measures
pMMR
proficient mismatch repair
MSI-H
microsatellite instability-high
MSS
microsatellite stable
NR
not reported
ORR
objective response rate
OS
overall survival
PCR
polymerase chain reaction
PD
progressive disease
PFS
progression-free survival
QoL
quality of life
RCT
randomized controlled trial
RECIST v.1.1
Response Evaluation Criteria in Solid Tumours Version 1.1
SAE
serious adverse event
SD
standard deviation
SOC
standard of care
TEAE
treatment-emergent adverse event
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Table 1: Background Information of Application Submitted for Review
Item | Description |
|---|---|
Drug product | Dostarlimab (JEMPERLI), 500mg/10 mL (50 mg/mL), 500 mg every 3 weeks for 6 cycles followed by 1,000 mg every 6 weeks, solution for IV infusion |
Sponsor | GlaxoSmithKline Inc. |
Indication | Dostarlimab (JEMPERLI) is indicated in combination with carboplatin and paclitaxel for the treatment of adult patients with primary advanced or recurrent dMMR/MSI-H endometrial cancer who are candidates for systemic therapy. |
Reimbursement request | As per indication |
Health Canada approval status | NOC |
Health Canada review pathway | Priority review aligned to the Project Orbis pathway |
NOC date | November 15, 2023 |
Recommended dose | The recommended dose is dostarlimab 500 mg administered as an IV infusion over 30 minutes every 3 weeks for 6 doses in combination with carboplatin and paclitaxel followed by dostarlimab 1,000 mg every 6 weeks for all cycles thereafter. |
dMMR = deficient mismatch repair; MSI-H = microsatellite instability-high; NOC = Notice of Compliance.
Introduction
Uterine cancers are commonly endometrial carcinoma caused by development of malignant tumours in the cells of the uterus and can spread to other parts of the body.1 In Canada, an estimated 8,500 women will be diagnosed with uterine cancer in 2023, and 1,550 will die from it, with more than 95% of all uterine cancers being endometrial.1 Patients with endometrial cancer may present with abnormal vaginal bleeding, pelvic pain, back pain, feeling of a mass, or unintentional weight loss.2 Signs and symptoms of metastatic disease may include vaginal, bladder or rectal bleeding, abdominal or pelvic pain, lower abdominal or extremity swelling, shortness of breath, and chest or bone pain.3 Patients with endometrial cancer that is high-risk (serous adenocarcinoma, clear cell adenocarcinoma, grade 3 deeply invasive endometrioid carcinoma, pathologic stage III or IV disease of any histology) or recurrent (including disease localized to the vagina or pelvis, or metastatic disease) tend to have poor prognosis,4,5 such that treatment goals are palliative rather than curative.3 For most patients, primary advanced or recurrent endometrial cancer recurs within 3 years,6-9 with median overall survival (OS) of less than 3 years.10-13 Treatment of endometrial cancer is based on a patient’s stage, risk level at presentation, and previous treatments. Prognostic factors impacting local disease control and survival include site of recurrence, previous use of radiotherapy or chemotherapy, relapse-free interval, and histology.14 Approximately 25% of patients with endometrial cancer possess deficiencies in DNA repair mechanisms, resulting in 2 correlated phenotypes (deficient mismatch repair [dMMR] or microsatellite instability-high [MSI-H]).15-17 Frontline standard of care (SOC) treatment for advanced (stage III or IV) or recurrent endometrial cancer is doublet chemotherapy with carboplatin and paclitaxel.4,18,19 There is currently no standard of care for second-line or later treatments.20 Response rates in the setting of progression on or following treatment with platinum-containing regimens are poor.12,21,22 According to the clinical experts consulted by CADTH, treatment goals in the indicated population are aimed at prolonging life, delaying disease progression, and maintaining health-related quality of life (HRQoL).
The objective of CADTH’s Clinical Review Report is to review and critically appraise the clinical evidence submitted by the sponsor on the beneficial and harmful effects of dostarlimab 500 mg administered as an IV infusion every 3 weeks for 6 cycles in combination with carboplatin and paclitaxel (henceforth carboplatin-paclitaxel), followed by dostarlimab 1,000 mg every 6 weeks starting at cycle 7 for up to 3 years in the treatment of primary advanced or recurrent dMMR or MSI-H endometrial cancer in adult patients who are candidates for systemic therapy. Dostarlimab monotherapy was previously reviewed by CADTH.
Stakeholder Perspectives
The information in this section is a summary of input provided by the patient and clinician groups who responded to CADTH’s call for input and from clinical experts consulted by CADTH for the purpose of this review.
Patient Input
CADTH received 1 input from The Canadian Cancer Survivor Network (CCSN). CCSN conducted an online survey that also was reviewed and commented on by both the Colorectal Cancer Resource & Action Network and the Canadian Cancer Society (CCS). The survey respondents identified as female patients from Canada who had endometrial cancer but did not have experience with dostarlimab.
Survey respondents highlighted, lack of screening and early diagnosis, lack of help for after-care, lack of mental health support during treatment, limited local access to treatment and biopsy, and difficulty in driving to the clinic as some of the issues related to accessing health care. CCSN also highlighted that patients with advanced endometrial carcinoma have limited treatment options. Current treatments are associated with treatment-induced toxicities that compromise patients’ quality of life and fail to extend their longevity in a meaningful way. CCSN stated that caregivers also have a difficult experience while taking care of their patients.
Patients expect the following from a new treatment option, according to 5 survey respondents: the treatment should be easy to use, delay the onset of symptoms and/or recurrence, provide maintained quality of life, provide a cure or prolong life, reduce side effects, and provide an additional treatment option.
CCSN added that people with endometrial cancer are looking for another option that will provide them with a better quality of life and that patients are willing to experience some greater side effects if the treatment will extend survival for a longer period of time.
Clinician Input
Input From Clinical Experts Consulted by CADTH
The current SOC for patients with primary advanced or recurrent dMMR or MSI-H endometrial cancer is systemic therapy. According to the clinical experts consulted by CADTH, patients with primary advanced or recurrent dMMR or MSI-H endometrial cancer experience poor response rates to current treatments that are of short duration, and as such, require treatments that can prolong life, delay disease progression, and maintain HRQoL. The clinical experts consulted by CADTH expressed that dostarlimab has a mechanism of action that is distinct from chemotherapy and has the potential to address the underlying disease process among patients with dMMR or MSI-H endometrial cancer. They also said that dostarlimab, in combination with carboplatin and paclitaxel would be considered as first-line therapy for patients with advanced endometrial cancer who are chemotherapy naive and eligible for carboplatin and paclitaxel, and for patients with recurrent endometrial cancer who are chemotherapy naive or with more than 6 months since their last line of chemotherapy. The clinical experts consulted by CADTH highlighted that patients who are chemotherapy naive at diagnosis or with recurrent disease are at greatest need for long-term durable therapy and, therefore, most likely to respond to first-line treatment with dostarlimab plus chemotherapy. The clinical experts consulted by CADTH noted that patients who had adjuvant chemotherapy with carboplatin and paclitaxel would be eligible for single drug PD-1 inhibitors (pembrolizumab) or single drug chemotherapy for first-line recurrence and, more than likely, many physicians would continue to prescribe a single drug PD-1 inhibitor for these patients. Eligible patients would be diagnosed with primary endometrial cancer (via tissue biopsy). Further characterization of the cancer would include a companion diagnostic for mismatch repair (MMR) or microsatellite stable (MSS) status that is the SOC for endometrial cancer in Canada (via immunohistochemistry [IHC], next generation sequencing, or polymerase chain reaction [PCR]), and identification of the stage of the disease (either via imaging or clinical pathologic assessment). The clinical experts consulted by CADTH noted that eligible patients should be able to tolerate chemotherapy and PD-1 inhibitor and have an absence of significant exclusion criteria (e.g., severe endocrine disease, undergoing immunotherapy). According to the clinical experts consulted by CADTH, treatment response would be best assessed with survival, survival without progressive disease, performance status, disease symptoms, and HRQoL, such that treatment should be discontinued in the event of disease progression or intolerance to treatment. The clinical experts consulted by CADTH indicated that dostarlimab may be prescribed by gynecologic or medical oncologists who are familiar with managing immune-related side effects, in an inpatient or outpatient setting.
Clinician Group Input
Three clinician groups, the Society of Gynecologic Oncology of Canada (GOC) (based on 5 clinicians), the Canadian Clinician Group with expertise in treating women with advanced and recurrent endometrial cancer, coordinated by CCS (based on 10 clinicians), and Ontario Health – Cancer Care Ontario (CCO) Gynecology Cancer Drug Advisory Committee (based on 5 clinicians) provided input to this review.
The clinician groups agreed that patients’ unmet needs include improved overall and progression-free survival (PFS), durable disease control, sustained response to chemotherapy, and minimal adverse effects on quality of life (QoL). Moreover, Ontario Health – CCO identified the absence of molecular directed therapy as a treatment gap. The goals of treatment were reported as to prolong life, delay disease progression, reduce severity of symptoms, improve QoL, reduce burden on caregivers, maintain independence, and minimize toxicities.
The clinician groups stated that patients with primary advanced state or metastatic dMMR endometrial cancer are best suited for treatment with the dostarlimab combination. The clinician groups agreed that response to therapy would be evaluated based on patient symptoms and tumour assessment through imaging. GOC added that assessment of tumour markers, where applicable, would be another factor to evaluate response to therapy. The clinician groups noted that discontinuation of treatment would be based on disease progression, toxicity, intolerability, and patient preference.
Drug Program Input
Input was obtained from the drug programs that participate in the CADTH reimbursement review process. The following were identified as key factors that could potentially affect the implementation of a CADTH recommendation for dostarlimab: relevant comparators, considerations for initiation of therapy, considerations for discontinuation of therapy, considerations for prescribing of therapy, generalizability, funding algorithm, care provision issues, and system and economic issues.
The clinical experts consulted by CADTH provided advice on the potential implementation issues raised by the drug program. Refer to Table 4 for more details.
Clinical Evidence
Systematic Review
Description of Study
One phase III, multicentre, randomized, double-blind trial assessed the efficacy and safety of dostarlimab in combination with carboplatin and paclitaxel (hereafter referred to as carboplatin-paclitaxel) followed by dostarlimab monotherapy, compared with placebo in combination with carboplatin-paclitaxel followed by placebo. RUBY Part 1 is an ongoing trial that enrolled 118 patients aged 18 years or older with primary advanced (stage III or IV) or first recurrent dMMR or MSI-H endometrial cancer. The primary objectives of RUBY Part 1 were to evaluate PFS among patients with primary advanced or recurrent endometrial cancer (overall trial population) and patients with dMMR or MSI-H primary advanced or recurrent endometrial cancer (i.e., dMMR or MSI-H subpopulation), and OS among the overall population. OS assessment in the dMMR or MSI-H subpopulation was an additional analysis in RUBY Part 1. Secondary end points that were evaluated for the overall population and in the dMMR or MSI-H subpopulation included response outcomes, HRQoL (European Organization for Research and Treatment of Cancer Core Quality of Life Questionnaire [EORTC QLQ-C30] Global Health Status), and notable treatment-emergent adverse events (TEAEs) (immune-related adverse events, and infusion-related reactions). This review presents data from the RUBY trial Part 1 for patients in the dMMR or MSI-H subpopulation, which aligns with the Health Canada indication. The Clinical Study Report with a data cut-off of date of September 28, 2022 (first interim analysis), was the primary data source for the RUBY Part 1 trial. At this data cut-off, the median follow-up was |||| months in the dostarlimab plus carboplatin-paclitaxel group and |||| months in the placebo plus carboplatin-paclitaxel group. In addition, CADTH received updated data from the sponsor for OS and notable harms for the dMMR or MSI-H subpopulation from the RUBY Part 1 second interim analysis (data cut-off date of September 22, 2023; median follow-up was |||| months in the dostarlimab plus carboplatin-paclitaxel group and |||| months in the placebo plus carboplatin-paclitaxel group) which have been included in this review. At this time, the OS stopping boundary in the overall population was met and no further testing for OS is planned.
Patients with primary advanced or recurrent dMMR or MSI-H endometrial cancer in RUBY Part 1 were white (|||||) with a median age of |||| years (range, || || ||), Eastern Cooperative Oncology Group Performance Status (ECOG PS) of 0 (|||||), and endometrioid carcinoma (|||||). Nearly half of the enrolled patients had recurrent disease. The treatment groups were generally similar in medical history (histology and grade at diagnosis, International Federation of Gynecological and Obstetrics (FIGO) stage at initial diagnosis) and disease status (stage III, stage IV, recurrent disease). Approximately 14% of patients had received prior anticancer therapy and ||||| of patients had received prior anticancer surgical interventions for endometrial cancer. While ||||| of patients had received prior radiotherapy for endometrial cancer, fewer patients received external pelvic radiotherapy in the dostarlimab plus carboplatin-paclitaxel group compared with the placebo plus carboplatin-paclitaxel group (15.1% versus 20.0%, respectively).
Efficacy Results
Efficacy results were summarized for OS, PFS (investigator assessed), and the EORTC QLQ-C30 Global Health Status among patients in the dMMR or MSI-H subpopulation.
OS
At the interim analysis 2 data cut-off (September 22, 2023), median OS was not reached in the dostarlimab plus carboplatin-paclitaxel group, with 40% OS maturity. The 24-month OS probability (95% confidence interval [CI]) was 82.8% (|||| || ||||) and 57.5% (|||| || ||||) in the dostarlimab plus carboplatin-paclitaxel and placebo plus carboplatin-paclitaxel groups, respectively. The between-group difference (95% CI) was ||||| ||||| || |||||, favouring dostarlimab with carboplatin-paclitaxel. The 30-month OS probability (95% CI) was ||||| ||||| || ||||| and ||||| ||||| || ||||| in the dostarlimab plus carboplatin-paclitaxel and placebo plus carboplatin-paclitaxel groups, respectively. The between-group difference (95% CI) was ||||| ||||| || |||||, favouring dostarlimab with carboplatin-paclitaxel. The hazard ratio ([HR] [95% CI]) in the intention-to-treat (ITT) dMMR or MSI-H subpopulation was 0.32 (0.166 to 0.629; 1-sided P value = 0.0002) for dostarlimab plus carboplatin-paclitaxel versus placebo plus carboplatin-paclitaxel. This analysis was uncontrolled for multiplicity and considered supportive. No further testing for OS is planned, because the prespecified stopping boundary was met in the overall population at the second interim analysis.
PFS (Investigator Assessed)
At the interim analysis 1 data cut-off (September 28, 2022), median PFS based on investigator assessment was not reached in the dostarlimab plus carboplatin-paclitaxel group compared with 7.7 months in the placebo plus carboplatin-paclitaxel group with 56% PFS maturity in the dMMR or MSI-H subpopulation. The 12-month investigator-assessed PFS probability (95% CI) was 63.5% (|||| || ||||) and 24.4% (|||| || ||||) in the dostarlimab plus carboplatin-paclitaxel and placebo plus carboplatin-paclitaxel groups, respectively. The between-group difference was ||||| ||||| || |||||, favouring dostarlimab plus carboplatin-paclitaxel. The 24-month investigator-assessed PFS probability (95% CI) was 61.4% (46.3 to 73.4) and 15.7% (7.2 to 27.0) in the dostarlimab plus carboplatin-paclitaxel and placebo plus carboplatin-paclitaxel groups, respectively. The between-group difference was ||||| ||||| || |||||, favouring dostarlimab plus carboplatin-paclitaxel. The HR (95% CI) in the dMMR or MSI-H subpopulation was 0.28 (0.162 to 0.495; 1-sided P value < 0.0001) for dostarlimab plus carboplatin-paclitaxel versus placebo plus carboplatin-paclitaxel. Findings for PFS based on blinded independent central review (BICR) assessment were consistent with results for PFS based on investigator assessment. No further testing of PFS occurred, because the prespecified stopping boundary was met at the first interim analysis.
EORTC QLQ-C30
At the data cut-off of September 28, 2022, the least squares mean (LSM) change from baseline (95% CI) in the EORTC QLQ-C30 Global Health Status at day 1 of cycle 7 was ||| |||||| ||||| || |||| and |||| |||||| |||||| || ||||| in the dostarlimab plus carboplatin-paclitaxel and placebo plus carboplatin-paclitaxel groups, respectively (difference in LSM change from baseline = 9.4 points; 95% CI, ||| || |||||
P = 0.0125). The LSM change from baseline (95% CI) in the EORTC QLQ-C30 Global Health Status at day 1 of cycle 13 was ||| |||||| |||| || ||||| and |||| |||||| ||||| || |||| in the dostarlimab plus carboplatin-paclitaxel and placebo plus carboplatin-paclitaxel groups, respectively (difference in LSM change from baseline = ||| ||||||| ||| ||| |||| || ||||| | | ||||||). The analyses of EORTC QLQ-C30 were uncontrolled for multiplicity and considered supportive.
Harms Results
The analysis population for harms included all patients who received any amount of study drug, with patients grouped according to the treatment received. Safety data were from the interim safety analyses (data cut-off of September 28, 2022) and updated for notable harms (interim analysis 2 with data cut-off September 22, 2023).
All patients in the dMMR or MSI-H subpopulation experienced at least 1 TEAE. The most common TEAEs occurring in greater than 20% of patients in the dostarlimab plus carboplatin-paclitaxel or placebo plus carboplatin-paclitaxel groups, respectively, were alopecia (||| |||||| |||), fatigue (||| |||||| |||), nausea (||| |||||| |||), anemia (||| |||||| |||), peripheral neuropathy (||| |||||| |||), arthralgia (||| |||||| |||), diarrhea (||| |||||| |||), constipation (||| |||||| |||), myalgia (||| |||||| |||), hypomagnesemia (||| |||||| |||), vomiting (||| |||||| |||), rash (||| |||||| |||), dyspnea (||| |||||| |||), neutropenia (||| |||||| |||), abdominal pain (||| |||||| |||), peripheral sensory neuropathy (||| |||||| |||), decreased neutrophil count (||| |||||| |||), urinary tract infection (|| |||||| |||), hypertension (||| |||||| |||), and hypothyroidism (||| |||||| ||).
The number of patients in the dMMR or MSI-H subpopulation with at least 1 serious adverse event (SAE) was || ||||| patients in the dostarlimab plus carboplatin-paclitaxel group and || ||||| patients in the placebo plus carboplatin-paclitaxel group. SAEs occurring in at least 2% of patients in either the dostarlimab plus carboplatin-paclitaxel or placebo plus carboplatin-paclitaxel groups, respectively, were urinary tract infection (| |||||| ||||), anemia (| |||||| ||||), asthenia (| |||||| ||||), sepsis (|||| |||||| |), and pulmonary embolism (||||||| ||||). The number of patients with at least 1 TEAE of grade 3 or greater was || ||||| patients in the dostarlimab plus carboplatin-paclitaxel group and || ||||| patients in the placebo plus carboplatin-paclitaxel group. Grade 3 or greater TEAEs occurring in at least 10% of patients in either the dostarlimab plus carboplatin-paclitaxel or placebo plus carboplatin-paclitaxel group, respectively, were anemia (||| |||||| |||), neutropenia (||| |||||| |||), decreased neutrophil count (|| |||||| |||), and decreased white blood cell count (|| |||||| |||).
The number of patients in the dMMR or MSI-H subpopulation who discontinued study treatment due to an adverse event (AE) was ||| ||||||| patients in the dostarlimab plus carboplatin-paclitaxel group and || ||||||| patients in the placebo plus carboplatin-paclitaxel group. Withdrawals due to AEs in the dostarlimab plus carboplatin-paclitaxel group were due to (| |||||| ||||||| ||||) neurotoxicity, myelosuppression, drug hypersensitivity, infusion-related reaction, chronic kidney disease, rash maculo-papular, keratitis, muscular weakness, fatigue, and general physical health deterioration. Withdrawals due to AEs in the placebo plus carboplatin-paclitaxel group were due to peripheral neuropathy (| |||||||| ||||||) and thrombocytopenia (| |||||||| ||||||), cardiovascular accident (| ||||||| ||||||), infusion-related reaction (||||), increased amylase (||||), decreased platelet count (||||), peritonitis (||||), myelodysplastic syndrome (||||), and vaginal hemorrhage (||||). The number of deaths in the dMMR or MSI-H subpopulation were 7 (13.5%) patients in the dostarlimab plus carboplatin-paclitaxel group and 24 (36.9%) patients in the placebo plus carboplatin-paclitaxel group. Most deaths (||| patients and ||| patients) were due to disease progression in the dostarlimab plus carboplatin-paclitaxel and placebo plus carboplatin-paclitaxel group, respectively. ||| patients treated with dostarlimab plus carboplatin-paclitaxel experienced TEAEs leading to death (| ||||||| |||| || myelosuppression, and of hypovolemic shock).
Notable Harms
Immune-related AEs occurred in || ||||||| patients in the dostarlimab plus carboplatin-paclitaxel group and || ||||||| patients in the placebo plus carboplatin-paclitaxel group (between-group difference of ||| |||| ||| ||| || ||||). Infusion-related reactions occurred in || ||||||| patients in the dostarlimab plus carboplatin-paclitaxel group and || ||||||| patients in the placebo plus carboplatin-paclitaxel group (between-group difference of || |||| ||| |||| || ||||).
Critical Appraisal
Randomization using an interactive web response system was considered adequate for concealment of allocation sequence. MMR or MSI status was used to stratify randomization for the overall population of patients with primary advanced or recurrent endometrial cancer resulted in a between-groups imbalance in the number of patients with dMMR or MSI-H; however, sensitivity analyses for OS and investigator-assessed PFS showed results for randomization data were consistent with verified sources. Although a greater proportion of patients in the placebo plus carboplatin-paclitaxel group were older than 65 years, with ECOG PS of 0, and had prior external pelvic radiotherapy, imbalances did not systematically favour either treatment group and are likely compatible with chance. Nevertheless, prognostic balance requiring a large sample size was unlikely to have been fully achieved in RUBY Part 1 despite adequate randomization methods. Interim analyses were preplanned with adequately justified stopping boundaries to provide confidence that statistical significance of effects for PFS did not arise from type I error. There was a risk for magnitude of observed treatment effects to be overestimated,23-25 as neither median PFS nor median OS in the dostarlimab plus carboplatin-paclitaxel group had been reached at time of analysis and the information fraction for OS was notably small (40%). The small number of patients with dMMR or MSI-H and low number of events may render the observed effects to be unstable. Among patients in the dMMR or MSI-H subpopulation, OS and HRQoL were not included in the hierarchical testing strategy, increasing the risk of type I error. The potential for unblinding among patients who experienced an AE in the dostarlimab group at cycle 7 onwards (without carboplatin-paclitaxel) was neither evidenced in protocol deviations nor outcome measurement. While there were multiple protocol amendments for PFS based on investigator versus BICR assessments, sensitivity analyses demonstrated consistency in findings between both methods of assessment to reduce concerns of potential bias. Significant missing HRQoL data that were implicitly imputed through statistical analyses cannot provide confirmation that such missing data occurred at random, as assumed in the methods employed. The lack of sensitivity analyses to explore the impact of other imputation techniques (with assumptions for different missing data mechanisms) on treatment effect estimates resulted in a risk of bias from significant missing data that likely compromised randomization with an unknown direction of potential bias.
The population enrolled in RUBY Part 1 was representative of patients with primary advanced or recurrent dMMR or MSI-H endometrial cancer in clinical practice, according to the clinical experts consulted by CADTH. Further, the clinical experts noted that the timing of administering dostarlimab or placebo in combination with carboplatin and paclitaxel appeared to be aligned with the chemotherapy regimens in the current SOC, although a 3-year duration of therapy was not considered typical, since patients with primary advanced or recurrent dMMR or MSI-H have increased likelihood of disease recurrence over time. Further, radiographic evaluations to assess disease status were reported to be more frequent in RUBY than would be feasible in clinical practice (every 3 to 4 months). Doublet chemotherapy with carboplatin and paclitaxel were reported by the clinical experts consulted by CADTH to be the current SOC among patients with primary advanced disease and among patients with recurrent disease who are chemotherapy naive. Current treatments for patients with recurrent disease and prior chemotherapy include other options. Concomitant medications were reported by the clinical experts consulted by CADTH to be appropriate and aligned with clinical practice in Canada for systemic glucocorticoid use and granulocyte colony-stimulating factor (G-CSF) for clinicians who elect to use it in current practice. Subsequent treatment types, including pembrolizumab, hormonal therapy, and radiation therapy, among a greater proportion of patients in the placebo group, were aligned with higher rates of progressive disease in this group and the expectations of the clinical experts consulted by CADTH. As a result, OS reflects treatment with dostarlimab versus placebo (each with carboplatin and paclitaxel) in addition to subsequent treatments, such that survival results may be partially attributable to treatments administered after disease progression (rather than to the study treatment); nevertheless, the comparison is relevant because it is reflective of the intervention and comparator in clinical practice. OS and PFS were important outcomes to the clinical experts consulted by CADTH for clinical decision-making and were included in the RUBY trial. There is some evidence to suggest that a within-arm change in PFS is strongly correlated with a change in the OS in the same direction of effect, based on trials of first-line therapies among patients with primary advanced or recurrent endometrial cancer.26 However, evidence to support that a treatment effect on PFS will correspond to a treatment effect on OS was not identified. Longer follow-up would be useful to demonstrate whether a sustained survival benefit is observed. The clinical experts consulted by CADTH expressed that clinicians may opt to use practical tools (e.g., ECOG PS) over formal HRQoL evaluations to assess patients’ overall well-being.
GRADE Summary of Findings and Certainty of the Evidence
The selection of outcomes for a Grading of Recommendations Assessment, Development and Evaluation (GRADE) assessment was based on the sponsor’s Summary of Clinical Evidence, consultation with clinical experts, and input received from patient and clinician groups and public drug plans. The following list of outcomes was finalized in consultation with expert committee members: survival (OS, PFS based on investigator assessment), HRQoL (EORTC QLQ-C30 Global Health Status), and harms (immune-related AEs, and infusion-related reactions).
When possible, certainty was rated in the context of the presence of an important (nontrivial) treatment effect; if this was not possible, certainty was rated in the context of the presence of any treatment effect (i.e., the clinical importance is unclear). In all cases, the target of the certainty of evidence assessment was based on the point estimate and where it was located relative to the threshold for a clinically important effect (when a threshold was available) or to the null. The target of the certainty of evidence assessment was the presence or absence of a clinically important effect for probability of survival (OS and PFS), and harms (immune-related AEs, and infusion-related reactions) based on a threshold informed by the clinical experts consulted by CADTH for this review. The target of certainty of evidence assessment was the presence or absence of a clinically important effect for HRQoL (EORTC QLQ-C30 Global Health Status) based on a threshold identified in the literature.
Results of GRADE Assessments
Table 2 presents the GRADE summary of findings for dostarlimab plus carboplatin-paclitaxel versus placebo plus carboplatin-paclitaxel in adult patients with primary advanced or recurrent dMMR or MSI-H endometrial cancer.
Table 2: Summary of Findings for Dostarlimab in Combination With Carboplatin-Paclitaxel Versus Placebo in Combination With Carboplatin-Paclitaxel for Adult Patients With Primary Advanced or Recurrent dMMR or MSI-H Endometrial Cancer
Outcome and follow-up | Patients (studies), N | Relative effect (95% CI) | Absolute effects | Certainty | What happens | ||
|---|---|---|---|---|---|---|---|
Placebo + CAR-PAC | Dostarlimab + CAR-PAC | Difference | |||||
Survival | |||||||
Overall survival | |||||||
Probability of overall survival at 24 months Median follow-up: |||| months vs. |||| monthsa | 118 (1 RCT) | NR | 575 per 1,000 | 828 per 1,000 |||| || ||| ||| |||||| | ||| |||| ||| |||||||||| || ||| |||||b | Lowc | Dostarlimab plus CAR-PAC may result in a clinically important increase in the probability of overall survival at 24 months when compared with placebo plus CAR-PAC. |
Probability of overall survival at 30 months Median follow-up: |||| months vs. |||| monthsa | 118 (1 RCT) | NR | ||| ||| ||||| | ||| ||| |||||||||| || ||| ||| |||||| | ||| |||| ||| |||||||||| || ||| |||||b | Lowc | Dostarlimab plus CAR-PAC may result in a clinically important increase in the probability of overall survival at 30 months when compared with placebo plus CAR-PAC. |
Progression-free survival, investigator assessed | |||||||
Probability of progression-free survival at 12 months Median follow-up: |||| months vs. |||| monthsa | 118 (1 RCT) | NR | 244 per 1,000 | 635 per 1,000 |||| || ||| ||| |||||| | ||| |||| ||| |||||||||| || ||| |||||b | Moderated | Dostarlimab plus CAR-PAC likely results in a clinically important increase in the probability of PFS at 12 months when compared with placebo plus CAR-PAC. |
Probability of progression-free survival at 24 months Median follow-up: |||| months vs. |||| monthsa | 118 (1 RCT) | NR | 157 per 1,000 | 614 per 1,000 (463 to 734 per 1,000) | ||| |||| ||| |||||||||| || ||| |||||b | Moderated | Dostarlimab plus CAR-PAC likely results in a clinically important increase in the probability of PFS at 24 months when compared with placebo plus CAR-PAC. |
Health-related quality of life | |||||||
EORTC QLQ-C30 (0 [worst health-related quality of life] to 100 [best health-related quality of life]) | |||||||
Global Health Status, LSM change from baseline, points Follow-up: cycle 7, day 1 | 118 (1 RCT) | NR | |||| | ||| |||||| || |||| | 9.4 |||| || ||||| | Lowe | Dostarlimab plus CAR-PAC may result in little to no difference in EORTC QLQ-C30 Global Health Status at day 1 of cycle 7 when compared with placebo plus CAR-PAC. |
Global Health Status, LSM change from baseline, points Follow-up: cycle 13, day 1 | 118 (1 RCT) | NR | |||| | ||| ||||| || ||||| | ||| |||||| || ||||| | Very lowf | The evidence is very uncertain about the effect of dostarlimab plus CAR-PAC on EORTC QLQ-C30 Global Health Status at day 1 of cycle 13 when compared with placebo plus CAR-PAC. |
Harms | |||||||
Immune-related adverse events Follow-up: |||| months vs. |||| monthsa | ||| (1 RCT) | NR | ||| ||| ||||| | ||| ||| |||||||||| | ||| |||| ||| |||||||||| || ||| |||||b | Lowg | Dostarlimab plus CAR-PAC may result in an a clinically important increase in immune-related adverse events when compared with placebo plus CAR-PAC. |
Infusion-related reactions Follow-up: |||| months vs. |||| monthsa | ||| (1 RCT) | NR | ||| ||| ||||| | ||| ||| |||||||||| | || |||| ||| |||||||||| ||||| || ||| |||||b | Lowh | Dostarlimab plus CAR-PAC may result in little to no difference in infusion-related reactions when compared with placebo plus CAR-PAC. |
CAR-PAC = carboplatin-paclitaxel; CI = confidence interval; dMMR = deficient mismatch repair; EORTC QLQ-C30 = European Organization for Research and Treatment of Cancer Core Quality of Life Questionnaire; LSM = least squares mean; MID = minimal important difference; MSI-H = microsatellite instability-high; NR = not reported; RCT = randomized controlled trial; vs. = versus.
Note: Study limitations (which refer to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias were considered when assessing the certainty of the evidence. All serious concerns in these domains that led to the rating down of the level of certainty are documented in the table footnotes.
aFollow-up presented as dostarlimab + CAR-PAC vs. placebo + CAR-PAC.
bRisk difference (95%CI) was not included in the sponsor’s planned analyses; the absolute risk difference was requested by the CADTH review team for interpretation purposes.
cRated down 2 levels for very serious imprecision. The effect resulting from the second interim data cut is large (above the 5% to 10% threshold suggested by the clinical experts) and the sample size and number of events is very small, raising concern for prognostic imbalance and potential overestimation of the true effect. The number of OS events were 36 at 24 months and 38 at 30 months. OS in the dMMR or MSI-H subpopulation was not included in the statistical hierarchy.
dRated down 1 level for serious imprecision. The effect resulting from the first interim data cut is large (above the 10% to 15% threshold suggested by the clinical experts) and the sample size and number of events is small, raising concern for prognostic imbalance and potential overestimation of the true effect. The number of PFS events were 61 at 12 months and 66 at 24 months.
eRated down 1 level for serious study limitations. There is risk of bias due to missing outcome data. Rated down 1 level for serious imprecision. Based on a 10-point MID identified in the literature, the 95% CI included the possibility of little to no difference and clinically important benefit. This analysis was not adjusted for multiplicity and the results are considered to be supportive evidence.
fRated down 2 levels for very serious study limitations. There is risk of bias due to significant and imbalanced missing outcome data. Rated down 2 levels for very serious imprecision. Based on a 10-point MID identified in the literature, the 95% CI included the possibility of little to no difference and clinically important benefit. This analysis was not adjusted for multiplicity and the results are considered to be supportive evidence.
gRated down 2 levels for very serious imprecision. Effect estimate seems to be large based on a between-group difference of 5% identified as clinically important by the clinical experts consulted by CADTH, but the total sample size and number of events is low (n = 62).
hRated down 2 levels for very serious imprecision. Based on a 5% threshold suggested as clinically important by the clinical experts, the 95% CI for the difference between groups included the possibility of clinically important benefit and harm (increased adverse event).
Source: RUBY Clinical Study Report.27
Long-Term Extension Studies
No long-term extension studies were submitted in the systematic review evidence.
Indirect Comparisons
Description of Studies
No indirect treatment comparisons were submitted in the systematic review evidence.
Studies Addressing Gaps in the Evidence From the Systematic Review
No additional studies addressing important gaps in the systematic review evidence were identified.
Conclusions
Patients and clinicians identified a need for new treatments for primary advanced or recurrent dMMR or MSI-H endometrial cancer to delay onset of symptoms and prevent disease recurrence, while prolonging life and maintaining QoL, with reduced side effects. Evidence from a randomized phase III, double-blind trial (RUBY Part 1) in the subpopulation of 118 adult patients with primary advanced or recurrent dMMR or MSI-H endometrial cancer demonstrated that, compared with placebo plus carboplatin-paclitaxel, treatment with dostarlimab plus carboplatin-paclitaxel resulted in statistically significant improvements in PFS. The analysis of PFS met the trial’s predefined stopping boundary. Based on a CADTH review team appraisal, dostarlimab plus carboplatin-paclitaxel may result in a clinically important increase in OS at 24 months and 30 months (low certainty) and likely results in a clinically important increase in investigator-assessed PFS at 12 months and 24 months (moderate certainty) when compared with placebo plus carboplatin-paclitaxel. The estimated benefit appeared large, but certainty in its magnitude was reduced due to reliance on a study of small sample size with few events This was especially the case for OS, for which only a 40% information fraction had accrued. The stopping boundaries for statistical significance of PFS in the dMMR or MSI-H population and OS in the overall population were crossed at interim analysis 1 and interim analysis 2, respectively; therefore, no inferential analyses of PFS or OS will be performed for RUBY Part 1. The evidence demonstrated that dostarlimab plus carboplatin-paclitaxel may result in little to no difference in the EORTC QLQ-C30 Global Health Status at day 1 of cycle 7 (low certainty) when compared with placebo plus carboplatin-paclitaxel, but longer-term impact on HRQoL was uncertain. The safety profile with dostarlimab treatment appeared to be as expected, with similarity in the occurrence of AEs and SAEs compared to placebo. The evidence demonstrated that dostarlimab plus carboplatin-paclitaxel may result in a clinically important increase in immune-related AEs and little to no difference in infusion-related reactions (low certainty) when compared with placebo plus carboplatin-paclitaxel.
Introduction
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of dostarlimab 500 mg administered as an IV infusion every 3 weeks for 6 cycles in combination with carboplatin-paclitaxel followed by dostarlimab 1,000 mg every 6 weeks starting at cycle 7 for up to 3 years, in the treatment of primary advanced or recurrent dMMR or MSI-H endometrial cancer in adult patients who are candidates for systemic therapy.
Disease Background
Contents within this section have been informed by materials submitted by the sponsor and clinical expert input. The following have been summarized and validated by the CADTH review team.
Uterine cancer is caused by a malignant tumour that starts in the cells of the uterus and can spread to other parts of the body.1 Most uterine cancers are endometrial carcinoma, which starts from cells in the lining of the uterus (endometrium).1
Patients with endometrial cancer may present with abnormal vaginal bleeding, pelvic pain, back pain, feeling of a mass, or unintentional weight loss.28 Signs and symptoms of metastatic disease may include vaginal, bladder or rectal bleeding, abdominal pain, pelvic pain, lower abdominal or extremity swelling, anorexia, weight loss, shortness of breath, cough, chest pain, or bone pain.3
Risk factors for endometrial cancer include body mass index, hypertension, hyperinsulinemia, prolonged exposure to unopposed estrogen, endometrial hyperplasia, early menarche, late menopause, nulliparity, polycystic ovarian syndrome and genetic predisposition.1,11,28-31 More than 90% of endometrial cancer cases are sporadic, and 5% to10% are hereditary, which are mostly as part of the Lynch syndrome (hereditary nonpolyposis colorectal cancer syndrome).31
Diagnosis of endometrial cancer is based on histological evaluation of an endometrial biopsy, endometrial curettage, or hysterectomy specimen.5 Endometrial cancer is surgically staged according to the FIGO staging system, accounting for histological type, tumour pattern (e.g., tumour size of the extent of spread to lymph nodes or distant sites), and molecular classification (if performed).5 Generally, the higher the stage number, the more the cancer has spread.29 For patients with suspected metastatic disease, imaging of the chest, abdomen, and pelvis is necessary for staging. Additionally, biopsy confirms the diagnosis, and genomic analysis provides information about the molecular features of the tumour, and prognosis.3 DNA mismatch repair (MMR) is a process that maintains genomic stability.15 Defects in MMR result in MSI. MSI-H is a phenotype with a rapid accumulation of mutations which cause tumour development.15 PCR and IHC methods test MSI-H and dMMR statuses in solid tumours.15 Endometrial cancer has a high prevalence of MSI-H (25%) and dMMR (26%) rates.15
High-risk endometrial cancer includes patients with stage III or IV serous carcinoma, clear cell carcinoma, and carcinoma of any stage.5 Patients with endometrial cancer that is high-risk or recurrent (including disease localized to the vagina or pelvis, or metastatic disease) tend to have poor prognosis.5 Endometrial cancer is the most common gynecological cancer in high-income countries and the second most common gynecological cancer worldwide.32,33 The incidence and mortality rates of endometrial cancer are rising.20,31-34 An estimated 8,500 women in Canada will be diagnosed with, and 1,550 will die from, uterine cancer in 2023.1 More than 95% of all uterine cancers are endometrial.1 According to the American Cancer Society, endometrial cancer affects mainly women who are postmenopausal.34 The average age of women diagnosed with endometrial cancer is 60 years.34 Endometrial cancer is uncommon in women under the age of 45 years.34 Most patients with endometrial cancer are diagnosed with early-stage disease.20 The earlier uterine cancer is diagnosed, the better chance of 5 years of survival. For uterine cancer, 66.7% are diagnosed at the local stage. The 5-year relative survival for localized uterine cancer is 95%, for regional uterine cancer is 70%, and for distant disease is 18%.30 Around 10% to 15% of women diagnosed with endometrial cancer will experience a recurrence.7 The prognosis for recurrent endometrial cancer is poor, especially for the 50% of patients with endometrial cancer whose cancer presents with extrapelvic recurrence.35
Standards of Therapy
Contents within this section have been informed by materials submitted by the sponsor and clinical expert input. The following have been summarized and validated by the CADTH review team.
Current Treatment Paradigm
Treatment of endometrial cancer is based on a patient’s stage, risk level at presentation, and previous treatments.36 Surgery (e.g., total hysterectomy with bilateral salpingo-oophorectomy) to remove the uterus, cervix, fallopian tubes, and ovaries is the typical treatment approach for newly diagnosed patients with early-stage (stage I or II) endometrial cancer,20 with surgical staging performed concurrently through an assessment of the pelvic lymph node (sentinel lymph nodes, with or without para aortic lymphadenectomy, omentectomy), according to the clinical experts consulted by CADTH. The aim of surgery is to remove macroscopic tumours, examine for micrometastases, and determine the extent of disease and need for adjuvant therapy by surgical staging.20 For patients with advanced disease (stage III and IV), surgery should be considered when macroscopic resection is feasible with acceptable morbidity following preoperative staging. If surgery is not feasible, patients may instead require systemic treatment as a frontline option or radiation before surgery.30,37
Adjuvant therapy is considered postoperatively, depending on the patient’s risk of disease recurrence or progression.20 Surgical staging is used for prognostic stratification and identification of patients who may benefit from radiotherapy (e.g., external beam radiotherapy and vaginal brachytherapy) and/or adjuvant chemotherapy.20 Typically, patients with low-risk tumours undergo surgery alone, while those with high-risk tumours may benefit from adjuvant therapy to further reduce the risk of recurrence. There is no international consensus for patients with intermediate-risk tumours.38 Patient prognosis can also be assessed using molecular classification such as The Cancer Genome Atlas system, as specific molecular subgroups confer different levels of risk and treatment recommendations.37 In particular, a tumour with dMMR or MSI-H status may indicate the presence of Lynch syndrome, which would require further genetic testing and counselling for the patient, and is also a predictive biomarker for response to immunotherapy.39
At initial recurrence, prognostic factors that may impact local control and survival include the site of recurrence, previous use of radiotherapy or chemotherapy, relapse-free interval, and histology.14 For patients who are radiotherapy naive and present with locoregional recurrence, radiotherapy is often preferred. Patients presenting with locoregional recurrence who have received previous adjuvant radiotherapy can be considered for radical surgery like exenteration (complete surgical removal of bodily organs) only if complete tumour resection is feasible.37
The frontline SOC recommended in clinical practice guidelines is doublet chemotherapy with carboplatin-paclitaxel as first-line therapy for advanced (stage III or IV) or recurrent endometrial cancer.18,19,40 Although single drug chemotherapy may be considered in patients as first-line therapy, combination chemotherapy is favoured over single drug chemotherapy due to higher response rates.40 Long-term outcomes in primary advanced or recurrent endometrial cancer are poor, despite a 50% to 60% response rate to carboplatin-paclitaxel.12,41,42 Triplet combinations (e.g., cisplatin, doxorubicin, plus paclitaxel) and hormonal therapies may also be considered in some frontline settings.3 Triplet combinations have demonstrated similar efficacy but a less favourable toxicity profile.12 Hormone therapies such as megestrol, medroxyprogesterone, letrozole, and tamoxifen may be used for a small subset of patients with estrogen-receptor positive and/or progesterone-receptor positive and low grade histology, non–life-threatening disease, or patients with significant comorbidities that preclude the use of chemotherapy.18,19,40
Second-line or later treatments are considered for patients who do not respond or have subsequently progressed despite receiving frontline treatment. There is currently no SOC for this population.20 Response rates in the setting of progression on or following treatment with platinum-containing regimens are poor.12,21,22 In general, use of chemotherapy in this setting is limited by low response rates and baseline patient health, since it is associated with high rates of toxicity, including cytopenias and neuropathies, and substantial negative impacts on overall QoL.12,21,22 A subset of patients with endometrial cancer (approximately 25%) possess deficiencies in DNA repair mechanisms leading to 2 correlated phenotypes: dMMR or MSI-H.16,17,43 PD-1 inhibitors such as dostarlimab monotherapy and pembrolizumab monotherapy have emerged as novel and effective treatments for dMMR or MSI-H patients.44,45
Drug Under Review
Key characteristics of dostarlimab and other treatments available for patients with endometrial cancer are summarized in Table 3.
Dostarlimab is an PD-1 monoclonal antibody that binds with high affinity to the PD-1 receptor and effectively blocks interaction with PD-L1 and PD-L2, which results in restoring cytotoxic T-cell activity and freeing the T-cell to kill tumour cells. The recommended dosage for dostarlimab in combination with carboplatin-paclitaxel for the treatment of adult patients with advanced or recurrent dMMR or MSI-H endometrial cancer who are candidates for systemic therapy is 500 mg as an IV infusion over 30 minutes, every 3 weeks for 6 doses, followed by 1,000 mg monotherapy every 6 weeks, until progression of disease, or unacceptable toxicity, for up to 3 years. Notice of Compliance was received from Health Canada on November 15, 2023, for dostarlimab for IV injection in combination with carboplatin-paclitaxel for the treatment of adult patients with primary advanced or recurrent dMMR or MSI-H endometrial cancer who are candidates for systemic therapy.
Dostarlimab was previously approved by Health Canada as monotherapy for the treatment of adult patients with dMMR or MSI-H recurrent or advanced endometrial cancer that has progressed on or following prior treatment with a platinum-containing regimen; on September 2022, the pCODR Expert Review Committee (pERC) recommended that dostarlimab monotherapy not be reimbursed for this Health Canada indication.
Table 3: Key Characteristics of Dostarlimab, Carboplatin, and Paclitaxel
Characteristic | Dostarlimab | Carboplatin | Paclitaxel |
|---|---|---|---|
Mechanism of action | An anti- PD-1 monoclonal antibody that binds with high affinity to the PD-1 receptor and effectively blocks interaction with PD-L1 and PD-L2, restoring cytotoxic T-cell activity and freeing the T-cell to kill tumour cells. | A synthetic analogue of cisplatin. Like cisplatin, carboplatin interferes with DNA intrastrand and interstrand crosslinks in cells exposed to the drug. DNA reactivity has been correlated with cytotoxicity. | Antimicrotubule drug that promotes the assembly of microtubules from tubulin dimers and stabilizes microtubules by preventing depolymerization. |
Indicationa | Previously approved by Health Canada as monotherapy for the treatment of adult patients with dMMR or MSI-H recurrent or advanced endometrial cancer that has progressed on or following prior treatment with a platinum-containing regimen. Received Notice of Compliance from Health Canada in combination with carboplatin and paclitaxel for the treatment of adult patients with primary advanced or recurrent dMMR/ MSI-H endometrial cancer who are candidates for systemic therapy. | For the treatment of ovarian cancer of epithelial origin in the first-line therapy and in the second-line therapy, after other treatments have failed. | Ovarian carcinoma: First-line treatment in combination with other chemotherapeutic agents. Second-line treatment of metastatic carcinoma of the ovary after failure of standard therapy. Breast carcinoma: Adjuvant treatment of node-positive breast cancer administered sequentially to standard combination therapy. Second-line treatment of metastatic carcinoma of the breast after failure of standard therapy. Lung carcinoma: First-line treatment of advanced non–small cell lung cancer. Kaposi's sarcoma: Treatment of advanced, liposomal anthracycline-refractory AIDS-related Kaposi's Sarcoma. |
Route of administration | IV infusion | IV infusion | IV infusion |
Recommended dose | 500 mg every 3 weeks for 6 doses, followed by 1,000 mg every 6 weeks for all cycles thereafter. For the first 6 doses/cycles, dostarlimab should be administered before the chemotherapy (carboplatin and paclitaxel) when given on the same day. For cycle 7 and all cycles thereafter, dostarlimab is administered as monotherapy. | 400 mg/m2 as a single IV infusion over 15 to 60 minutes in previously untreated adults with normal renal function. Treatment should not be repeated until 4 weeks after the previous carboplatin course. | For metastatic carcinoma of the ovary: 175 mg/m2 over 3 hours in combination with cisplatin 75 mg/m2 every 3 weeks. In patients previously treated with chemotherapy, the recommended regimen is 175 mg/m2 intravenously over 3 hours every 3 weeks. For adjuvant treatment of node-positive breast cancer: 175 mg/m2 intravenously over 3 hours every 3 weeks for 4 courses sequentially to standard combination therapy. After failure of initial chemotherapy for metastatic disease or relapse within 6 months of adjuvant chemotherapy, a dose of 175 mg/m2 administered intravenously over 3 hours every 3 weeks has been shown to be effective. For non–small cell lung carcinoma: 175 mg/m2 intravenously over 3 hours every 3 weeks, followed by cisplatin. For AIDS-related Kaposi's Sarcoma: 135 mg/m2 intravenously over 3 hours with a 3-week interval between courses or 100 mg/m2 intravenously over 3 hours with a 2-week interval between courses (dose intensity of 45 g/m2/week to 50 g/m2/week). |
Serious adverse effects or safety issues | Immune-mediated adverse reactions such as pneumonitis, colitis, hepatitis, endocrinopathies (including adrenal insufficiency, hypophysitis, diabetes, thyroid disorders), nephritis, skin adverse reactions, myositis, myocarditis, encephalitis, demyelinating neuropathy (including Guillain Barré syndrome), sarcoidosis, transplant-related complications, infusion-related reactions. Monitor patients for immune-mediated adverse reactions and infusion-related reactions and modify treatment according to specified dosage modifications. | Highly toxic drug with a narrow therapeutic index, including serious and fatal infections following administration of live or live-attenuated vaccines, hypersensitivity reactions, bone marrow suppression, fatal veno-occlusive disease, fatal hemolytic anemia, fatal hemolytic-uremic syndrome, carcinogenesis and mutagenesis, cytotoxicity, risk of Tumour Lysis Syndrome, encephalopathy, and hemolytic-uremic syndrome. Monitor patients regularly for blood counts, renal and hepatic function tests, and signs and symptoms of vascular occlusion and thromboembolism. | Bone marrow suppression, severe cardiac conduction abnormalities, hypotension, hypertension, and hepatotoxicity in patients with hepatic impairment. Monitor patients regularly for blood counts, renal and hepatic function tests. Not to be used in patients with severe baseline neutropenia (< 1,500 cells/mm3) or AIDS-related Kaposi's Sarcoma with baseline or subsequent neutrophil counts of < 1,000 cells/mm3. |
dMMR = deficient mismatch repair; MSI-H = microsatellite instability-high.
aHealth Canada–approved indication.
Source: Product Monograph for dostarlimab,46 carboplatin,47 and paclitaxel.48
Stakeholder Perspectives
Patient Group Input
This section was prepared by the CADTH review team based on the input provided by patient groups. The full original patient input(s) received by CADTH have been included in the Stakeholder section of this report.
CADTH received 1 input from CCSN. CCSN is a national network of patients, families, community partners, funders, and sponsors who take action to promote SOC, and support cancer patients. CCSN conducted an online survey to gather data. The respondents of the survey identified as female patients from Canada, and none of them had experience with dostarlimab. The overall number of respondents was not reported.
Information on stage of endometrial cancer, was available for 4 survey respondents: 1 was stage 1b, and 1 each were stage 2, 3b, and 4a. The patients had received surgical therapy, chemotherapy, immunotherapy, hormonal therapy, and targeted therapy were the current treatments. Some of the adverse effects of current treatment reported were neuropathy, fatigue, change in sexual functioning, vaginal discomfort (dryness, itching, tightening, and burning), constipation, nausea, loss of stamina, bowel pain, and fluid retention.
From the point of view of some of the respondents, (1 patient per item that follows), lack of screening and early diagnosis, lack of help for after-care, lack of mental health support during treatment, limited local access to treatment and biopsy, and difficulty in driving to the clinic in winter are reported. CCSN also highlighted that patients with advanced endometrial carcinoma have limited treatment options. Current treatments are associated with treatment-induced toxicities that compromise patients’ QoL and fail to extend their life in a meaningful way. CCSN stated that caregivers also have a difficult experience while taking care of their patients.
Among 5 survey respondents, expectations for new treatments included: maintained QoL, delayed onset of symptoms and reduced recurrence, access to a new option of treatment, reduced side effects from current treatments, ease of use, prolong life, and provide a cure.
According to CCSN, on a scale of 1 to 10, with 1 being “no side effects” and 10 being “significant side effects,” among 5 respondents, there was wide variation in the side effect intensity considered as acceptable to extend survival by 2 months to 1 year. CCSN added that patients with endometrial cancer are looking for a therapy that will provide them with a better QoL and are willing to experience some greater side effects if the treatment will extend survival for a longer period of time. Having another option that could provide a more comfortable experience and allow them to lead a more normal life was reported as being important.
Clinician Input
Input From Clinical Experts Consulted by CADTH
All CADTH review teams include at least 1 clinical specialist with expertise regarding the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). The following input was provided by 2 clinical specialist(s) with expertise in the diagnosis and management of endometrial cancer.
Unmet Needs
The current SOC for patients with primary advanced dMMR or MSI-H endometrial cancer is surgery as applicable, followed by adjuvant chemotherapy with or without radiation, according to the clinical experts consulted by CADTH. The SOC chemotherapy regimen is platinum doublet with carboplatin and paclitaxel, based on the GOG 209 study,12 and without recommended maintenance therapy. The clinical experts consulted by CADTH indicated that patients with recurrent dMMR or MSI-H endometrial cancer can be treated with chemotherapy, immunotherapy, hormonal therapy, surgery, or radiation, depending on extent of disease and sites of recurrence; surgery or radiation may be considered for a single site of recurrence, whereas chemotherapy or hormonal therapy are preferred for extensive disease. The mainstay of treatment for recurrent endometrial cancer is chemotherapy or immunotherapy for the majority of patients, noting that hormonal therapy has demonstrated effectiveness in patients with low grade endometrioid endometrial cancer that is slow growing, according to the clinical experts consulted by CADTH. For patients who are chemotherapy naive, SOC for first-line treatment is platinum doublet chemotherapy with carboplatin and paclitaxel, as outlined by the clinical experts consulted by CADTH. If patients have experienced treatment failure with chemotherapy (carboplatin or paclitaxel), the clinical experts consulted by CADTH indicated that the SOC for patients with dMMR or MSI-H is a PD-1 inhibitor, such as pembrolizumab (funded) or dostarlimab (unfunded), and for patients with proficient mismatch repair (pMMR) or MSS, it is a combination of pembrolizumab and lenvatinib (funded). The clinical experts consulted by CADTH also reported second-line chemotherapy regimens to include doxorubicin, topotecan, paclitaxel, oxaliplatin, docetaxel, and bevacizumab. According to these experts, estimates of 7% to 20% for overall response rate and lower than median 6 months for duration of response have been evaluated in clinical trials for second-line chemotherapy regimens. Overall, according to the clinical experts consulted by CADTH, treatment goals are aimed at prolonging life, delaying disease progression, and maintaining HRQoL.
Place in Therapy
The clinical experts consulted by CADTH considered dostarlimab’s mechanism of action as distinct from chemotherapy and anticipated to address the underlying disease process among patients with dMMR, thereby causing a significant shift in the current treatment paradigm. According to the clinical experts consulted by CADTH, dostarlimab would be used as first-line therapy for patients with advanced endometrial cancer who are chemotherapy naive and eligible for carboplatin and paclitaxel, and for patients with recurrent endometrial cancer who are chemotherapy naive or with more than 6 months since their last line of chemotherapy. The clinical expert consulted by CADTH noted that patients who had adjuvant chemotherapy with carboplatin and paclitaxel, would be eligible for single drug PD-1 inhibitor (pembrolizumab) or single drug chemotherapy for first-line recurrence, and more than likely, many physicians would continue to prescribe a single drug PD-1 inhibitor for these patients. The clinical expert consulted by CADTH noted that that patients with advanced or recurrent dMMR or MSI-H endometrial cancer would be treated with dostarlimab in combination with carboplatin and paclitaxel for 6 cycles and then dostarlimab as maintenance therapy for 3 years, according to the clinical experts consulted by CADTH.
Patient Population
According to the clinical experts consulted by CADTH, patients who are chemotherapy naive at diagnosis or with recurrent disease are considered at greatest need for long-term durable therapy and therefore, most likely to respond to first-line treatment with dostarlimab plus chemotherapy. No data are available on early-stage (e.g., stage I or II) disease to inform treatment with dostarlimab, as noted by the clinical experts consulted by CADTH. The clinical experts consulted by CADTH indicated that eligible patients should be able to tolerate chemotherapy and PD-1 inhibitor and have an absence of significant exclusion criteria (e.g., severe endocrine disease, undergoing immunotherapy). Eligible patients would be diagnosed with primary endometrial cancer (via tissue biopsy) and include a companion diagnostic for MMR or MSS status that is the SOC for endometrial cancer in Canada (via immunohistochemistry, next generation sequencing or polymerase chain reaction), and further identified using stage of disease (either via imaging or clinical pathologic assessment), according to the clinical experts consulted by CADTH; however, patients with advanced disease who are unable to get a tissue diagnosis may represent a small subset of the endometrial cancer population and likely unsuitable for treatment due to advanced disease. The clinical experts consulted by CADTH indicated that while ECOG PS may help identify patients most likely to demonstrate a response to treatment, it has not been established as a direct prognostic factor.
Assessing the Response Treatment
The clinical experts consulted by CADTH reported that in clinical practice, patients are typically treated in 2-month to 3-month cycles or months, with intervals of 3 or 4 cycles or months to assess measurable disease (among patients with measurable disease considering that most adjuvant patients do not have measurable disease); such assessments of treatment were noted to occur less frequently than in clinical trials. According to the clinical experts consulted by CADTH, a clinically meaningful response to treatment that was unlikely to significantly vary between treating physicians included improved survival, PFS, a reduction in tumour size by 50%, and improvements in performance status, HRQoL (especially in activities of daily living), and disease symptoms.
Discontinuing Treatment
Disease progression (via clinical exam and imaging) and intolerance with treatment (i.e., AEs requiring dose interruptions or management with medications, allergic reactions) were key factors for discontinuing treatment with dostarlimab in combination with carboplatin and paclitaxel, according to the clinical experts consulted by CADTH.
Prescribing Considerations
The clinical experts consulted by CADTH indicated that dostarlimab may be prescribed by gynecologic or medical oncologists and emphasized the need for treating physicians to be familiar with immune-related side effects, particularly for management of commonly observed immune-related side effects, and to seek consultation with specialty care (e.g., gastrointestinal, medicine, ophthalmology, respirology, dermatology) as appropriate for immune-related side effects identified as severe, in an inpatient (e.g., community hospital) or outpatient (e.g., outpatient clinic) setting.
Clinician Group Input
This section was prepared by the CADTH review team based on the input provided by clinician groups. The full original clinician group input(s) received by CADTH have been included in the Stakeholder section of this report.
Three clinician groups: GOC (based on 5 clinicians), the Canadian Clinician Group with expertise in treating women with advanced and recurrent endometrial cancer, coordinated by CCS (based on 10 clinicians), and the Ontario Health – CCO Gynecology Cancer Drug Advisory Committee (5 author clinicians) provided input to this review.
According to the Ontario Health – CCO, current standard treatment for patients with primary advanced and recurrent advanced or metastatic endometrial cancer includes carboplatin plus paclitaxel. GOC stated that treatment for patients with advanced or metastatic endometrial cancer includes endocrine therapy with aromatase inhibitors and progestins, and cytotoxic chemotherapy. Ontario Health – CCO noted that for primary advanced cases, the SOC is chemotherapy (carboplatin/paclitaxel), but for recurrent cases, if the disease-free interval is greater than 6 months, patients would be retreated with carboplatin; and for dMMR, patients can be treated with single drug pembrolizumab after progression on platinum-based chemotherapy. The goals of treatment are reported as follows: prolong life, delay disease progression, reduce severity of symptoms, improve QoL, reduce burden on caregivers, maintain independence, and minimize toxicities.
The clinician groups agreed that patients’ unmet needs include improved overall and PFS, durable disease control, sustained response to chemotherapy, and minimal adverse effects on QoL. Moreover, Ontario Health – CCO identified the absence of molecular directed therapy as a treatment gap.
Regarding place in therapy, based on input from the clinician groups, dostarlimab combined with chemotherapy will address the disease process in a manner that is superior to the current treatment. Ontario Health – CCO added that, if patients with primary advanced endometrial cancer respond well to this treatment, it may be clinically indicated to interrupt treatment to have other modalities such as surgery or radiation. It is also reasonable for patients to have a treatment break if they have maintained a good response and then resume treatment before any disease progression occurred or if disease progression occurred during a break. The clinical expert consulted by CADTH highlighted that patients with dMMR or MSI-H endometrial cancer who were previously treated with adjuvant chemotherapy and then experienced recurrent disease (i.e., first-line recurrence) would be eligible for treatment with single drug PD-1 inhibitor or single drug chemotherapy, whereas patients who have not been treated with adjuvant chemotherapy will be eligible for chemotherapy (at first-line recurrence), followed by a single drug PD-1 inhibitor if they experience recurrent disease (i.e., second-line recurrence).
The clinician groups stated that patients with dMMR endometrial cancer are best suited for treatment with dostarlimab. Eligible patients would be diagnosed by biopsy and MMR immunohistochemistry screening. Ontario Health – CCO noted that both dMMR and pMMR will benefit from dostarlimab, although benefit may be greater for the dMMR or MSI-H population. GOC highlighted that patients who have poor performance status or notable comorbidities (including poorly controlled hypertension, uncontrolled autoimmune disease) would be least suitable for treatment with dostarlimab in combination with chemotherapy. The clinician groups agreed that response to therapy would be evaluated based on patient symptoms and tumour assessment through imaging. GOC added that assessment of tumour markers where applicable would be another factor to evaluate response to therapy. The clinician groups noted that discontinuation of treatment would be based on disease progression, toxicity, intolerability, and patient preference.
The clinical experts consulted by CADTH noted that outcomes used to determine response to treatment are OS, PFS, QoL, improvement of symptoms, and improvement in performance status.
The clinician groups stated that outpatient clinics in hospitals are appropriate setting for treatment, and GOC noted that a cancer centre by oncologists with expertise in systemic therapy for gynecologic cancers and managing immune-related adverse events is appropriate.
Drug Program Input
The drug programs provide input on each drug being reviewed through CADTH’s Reimbursement Review processes by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CADTH are summarized in Table 4.
Table 4: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Relevant comparators | |
The choice of comparator in RUBY Part 1 was carboplatin (AUC 5) + paclitaxel (175 mg/m2), which is aligned with the current standard of care in Canada in this setting. The main treatment choice is platinum-based chemotherapy in combination with a taxane. Other funded options can include single drug chemotherapy in cases of patient hypersensitivity or toxicity to platinum or taxane agents, as well as hormonal therapy in patients who are estrogen- and/or progesterone-receptor positive. | The clinical experts consulted by CADTH consider platinum doublet chemotherapy with carboplatin and paclitaxel to be the most appropriate comparator among patients with primary advanced (stages III and IV) endometrial cancer, since it is the current standard of care, and also applicable to patients with recurrent disease who are chemotherapy naive. Among patients with recurrent disease who have had prior chemotherapy, multiple treatment options are available, including a PD-1 inhibitor, doublet chemotherapy, singlet chemotherapy, or hormone therapy (for low grade cancers with limited disease). The clinical experts anticipated that clinicians would continue to prescribe a single drug PD-1 inhibitor for patients for first recurrence after prior chemotherapy. In the RUBY Part 1 trial in patients with dMMR or MSI-H disease, less than 10 patients in each treatment group received prior anticancer chemotherapy. |
Considerations for initiation of therapy | |
MSI/MMR testing and results are required to identify eligible patients. This testing is currently being done to identify patients in later lines of therapy but would not need to be done to identify eligibility for frontline use of dostarlimab. When should testing for MSI-H or dMMR take place in patients with endometrial cancer? | The clinical experts consulted by CADTH indicated that while there is variability across cancer centres regarding time frame for MMR-MSI testing (e.g., shortly upon diagnosis, after biopsy, after surgery), most patients are tested early during diagnosis and treatment as standard of care to identify markers in addition to MMR or MSI (e.g., Lynch syndrome). MSI/MMR testing is universally performed and funded, according to the clinical experts consulted by CADTH. |
Dostarlimab was combined with platinum-containing chemotherapy in RUBY Part 1.
|
|
Neoadjuvant/adjuvant systemic therapy was permitted in the trial, as long as 6 months had elapsed since the completion of treatment.
|
|
|
|
Considerations for discontinuation of therapy | |
|
|
Can pERC confirm the treatment duration for dostarlimab? The trial protocol appears to indicate treatment may be continued if there is clinical benefit. | The clinical experts consulted by CADTH agreed that there is currently insufficient evidence to guide a decision on prolonging treatment with dostarlimab beyond 3 years. It was noted that treatment with dostarlimab for 3 years was longer in duration than was employed in other studies (e.g., GY-018 trial). |
Considerations for prescribing of therapy | |
Cycles 1 to 6: dostarlimab 500 mg (flat dose) IV + platinum-containing chemotherapy every 21 days Cycle 7 onwards: dostarlimab 1,000 mg (flat dose) IV monotherapy every 42 days for up to 3 years total Is there evidence to support weight-based dosing to a maximum capped dose? | The RUBY trial employed a flat dose of 500 mg/m2 for up to six 3-week cycles, followed by 1,000 mg/m2 every 6 weeks, from cycle 7 onwards. For management of adverse events, dose delays or discontinuations were permitted according to specified dosage recommendations. Dose reductions were not permitted. The clinical experts consulted by CADTH were not aware of evidence to support weight-based dosing. |
Generalizability | |
Should patients with ECOG greater than 1 be eligible? | According to the clinical experts consulted by CADTH, patients with ECOG PS 0 to 2 would be considered eligible for treatment with dostarlimab in combination with carboplatin and paclitaxel if they were able to tolerate therapy. Patients with ECOG PS of greater than 2 would likely be unable to tolerate the combination of 2 chemotherapy drugs and immunotherapy. |
|
|
There is a time-limited need to allow patients currently on platinum-containing chemotherapy to add dostarlimab. What time frame is appropriate to add dostarlimab for patients on chemotherapy alone or who have recently completed chemotherapy? | The clinical experts consulted by CADTH considered patients who are already on chemotherapy to be able to add dostarlimab during the transition period (e.g., within 6 weeks of the patient’s last chemotherapy) but not for patients who have started chemotherapy more than 6 weeks ago. |
Funding algorithm | |
Pembrolizumab monotherapy is currently available in this setting for patients with unresectable or metastatic MSI-H or dMMR endometrial cancer whose tumours have progressed following prior therapy and who have no satisfactory alternative treatment options. | This is a comment from the drug plans to inform pERC deliberations. |
There is an anticipated submission to CADTH for pembrolizumab in the same setting based on the NRG-GY018 trial. Under what circumstances would dostarlimab be preferred over pembrolizumab? | Based on current approval and funding status, pembrolizumab monotherapy is indicated for the treatment of adult patients with unresectable or metastatic MSI-H or dMMR endometrial cancer whose tumours have progressed following prior therapy and who have no satisfactory alternative treatment options. The CADTH review team noted that it is not possible to comment on potential future comparators. |
Care provision issues | |
Dostarlimab vials are available as 500 mg strength, thus drug wastage is not expected if using a flat dose schedule. | This is a comment from the drug plans to inform pERC deliberations. |
Eligible patients will require earlier MMR-MSI testing than is currently required in this setting, as patients do not require testing for frontline therapy at this time (testing is done for later lines of therapy). | This is a comment from the drug plans to inform pERC deliberations. |
System and economic issues | |
Cost per cycle as well as duration of treatment of dostarlimab is anticipated to be significantly higher than currently funded chemotherapy comparators. | This is a comment from the drug plans to inform pERC deliberations. |
Pembrolizumab (available in the later line) has confidential pricing in place. | This is a comment from the drug plans to inform pERC deliberations. |
dMMR = deficient mismatch repair; ECOG PS = Eastern Cooperative Oncology Group Performance Status; MMR = mismatch repair; MSI = microsatellite instability; MSI-H = microsatellite instability-high; MSS = microsatellite stable; pMMR = proficient mismatch repair.
Clinical Evidence
The objective of CADTH’s Clinical Review Report is to review and critically appraise the clinical evidence submitted by the sponsor on the beneficial and harmful effects of dostarlimab 500 mg administered intravenously every 3 weeks for 6 cycles in combination with carboplatin-paclitaxel, followed by dostarlimab 1,000 mg every 6 weeks for up to 3 years, in the treatment of primary advanced or recurrent dMMR or MSI-H endometrial cancer in adult patients who are candidates for systemic therapy. The focus will be placed on comparing dostarlimab in combination with carboplatin-paclitaxel to relevant comparators and identifying gaps in the current evidence.
A summary of the clinical evidence included by the sponsor in the review of dostarlimab in combination with carboplatin-paclitaxel is presented in 4 sections, with CADTH’s critical appraisal of the evidence included at the end of each section. The first section, the systematic review, includes pivotal studies and randomized controlled trials (RCTs) that were selected according to the sponsor’s systematic review protocol. CADTH’s assessment of the certainty of the evidence in this first section using the GRADE approach follows the critical appraisal of the evidence. The sponsor did not include long-term extension studies, indirect evidence, or additional studies addressing important gaps in the systematic review evidence.
Included Studies
Clinical evidence from the following are included in the CADTH review and appraised in this document:
1 pivotal phase III randomized trial identified in the systematic review.
Systematic Review
Contents within this section have been informed by materials submitted by the sponsor. The following have been summarized and validated by the CADTH review team.
Description of Study
Characteristics of the included study are summarized in Table 5.
The RUBY trial Part 1 is an ongoing multicentre, randomized, double-blind, phase III study of adult patients with primary advanced or recurrent endometrial cancer. RUBY Part 1 evaluated the efficacy and safety of dostarlimab plus carboplatin-paclitaxel followed by dostarlimab monotherapy, compared with placebo plus carboplatin-paclitaxel followed by placebo. RUBY Part 2 evaluates the efficacy and safety of treatment with dostarlimab plus carboplatin-paclitaxel, followed by dostarlimab plus niraparib, versus treatment with placebo plus carboplatin-paclitaxel, followed by placebo, in patients with recurrent or primary advanced (stage III or IV) endometrial cancer. Each part had a separate randomization, and analysis was performed separately for each part. Part 2 is not relevant to the indication under review and has not been summarized in this report.
The overall study design of the RUBY trial Part 1 is depicted in Figure 1. A total of 494 patients with primary advanced (stage III or IV) or recurrent endometrial cancer were enrolled from August 2019 to January 2021 across 164 sites in 20 countries, with 8 sites in Canada. Patients were randomized in a 1:1 ratio to each study group. The randomization was stratified by MMR-MSI status (dMMR or MSI-H or pMMR or MSS), prior external pelvic radiotherapy (yes or no), and disease status (recurrent, primary stage III, or primary stage IV). RUBY Part 1 included 118 patients (11 patients enrolled in Canada) with dMMR or MSI-H status. The dual primary objectives of RUBY Part 1 were to evaluate PFS based on investigator assessment in patients with primary advanced or recurrent endometrial cancer (i.e., overall population) and patients with dMMR or MSI-H primary advanced or recurrent endometrial cancer (i.e., dMMR or MSI-H subpopulation) and OS in the overall population. OS assessment in the dMMR or MSI-H subpopulation was an additional analysis in RUBY Part 1. Secondary objectives were assessed in the overall population and the dMMR or MSI-H subpopulation: PFS based on BICR assessment, DCR based on BICR and investigator assessment, objective response rate (ORR) based on BICR and investigator assessment, HRQoL, and safety and tolerability. This CADTH clinical report will present data from the RUBY Part 1 trial for patients in the dMMR or MSI-H population, which aligns with the Health Canada indication. The Clinical Study Report with a data cut-off of date of September 28, 2022 (first interim analysis) was the primary data source for RUBY Part 1. CADTH received updated data from the sponsor based on a second interim analysis (data cut-off date of September 22, 2023) of RUBY Part 1 for OS and notable harms for the dMMR or MSI-H subpopulation which have been included in this report.
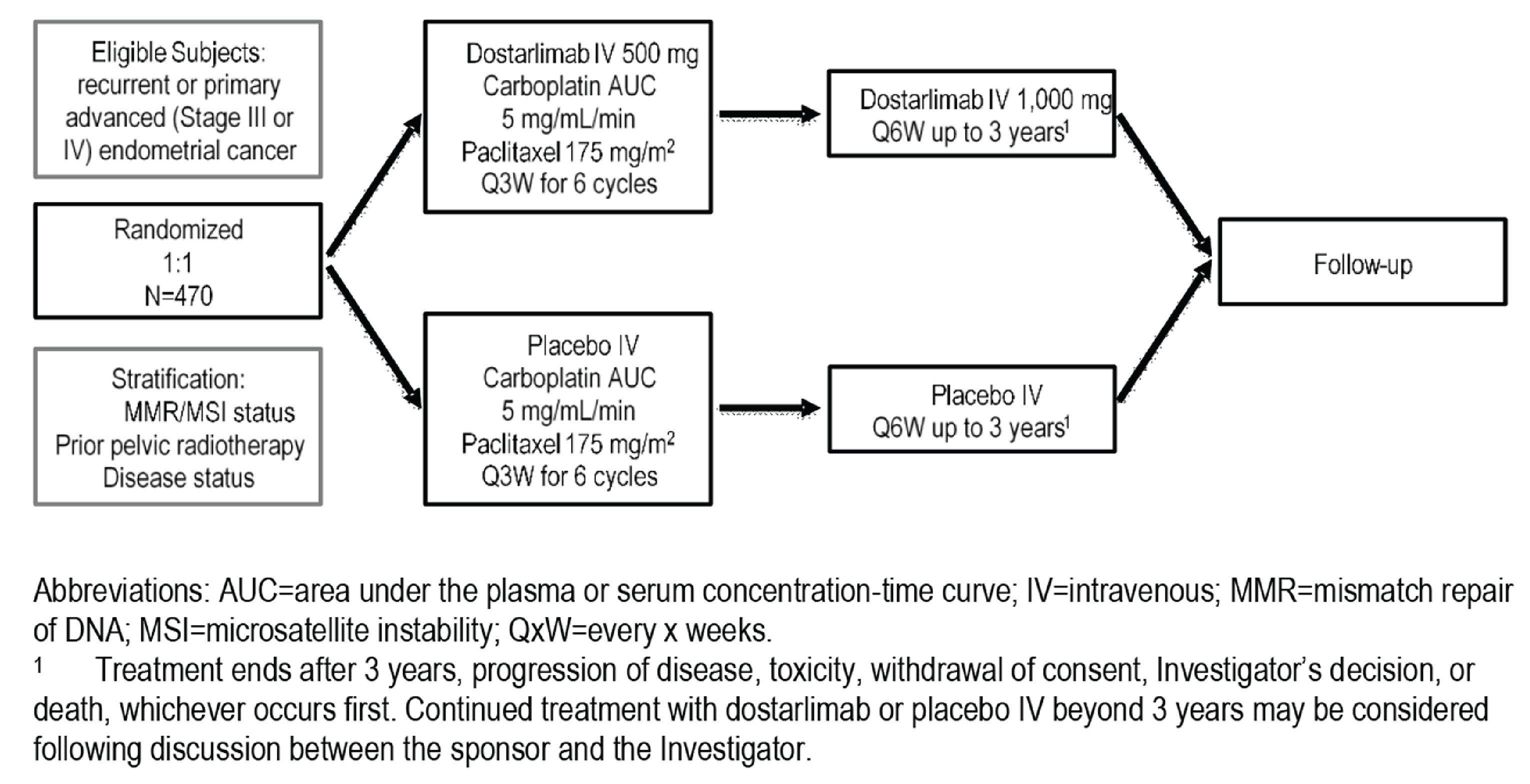
Table 5: Details of Study Included in the Systematic Review
Detail | RUBY Part 1 |
|---|---|
Designs and populations | |
Study design | Phase III, randomized, multicentre, double-blind study |
Locations | Patients enrolled across 164 sites in 20 countries (e.g., Canada [8 sites], European countries, UK, US) |
Patient enrolment dates | Start date: August 2019 End date: January 2021 |
Data cut-off date | September 28, 2022 (PFS, HRQoL, AEs); September 22, 2023 (OS and notable harms) |
Randomized (N) | N = 494, 118 of whom had dMMR or MSI-H status
|
Inclusion criteria | Adult females of ≥ 18 years of age. 1. Patient has histologically or cytologically proven endometrial cancer with advanced or recurrent disease. 2. Patient must provide adequate tumour tissue sample at screening for MMR-MSI status testing.a 3. Patient must have primary Stage III or Stage IV disease or first recurrent endometrial cancer with a low potential for cure by radiation therapy or surgery alone or in combination, and meet at least 1 of the following criteria: 3.1. Patient has primary Stage IIIA to IIIC1 disease with presence of evaluable or measurable disease per RECIST v1.1 based on investigator assessment. Lesions that are equivocal or can be representative of postoperative change should be biopsied and confirmed for the presence of tumour. 3.2.Patient has primary Stage IIIC1 disease with carcinosarcoma, clear cell, serous, or mixed histology (containing ≥ 10% carcinosarcoma, clear cell, or serous histology), regardless of presence of evaluable or measurable disease on imaging. 3.3. Patient has primary Stage IIIC2 or Stage IV disease, regardless of presence of evaluable or measurable disease. 3.4. Patient has first recurrent disease and is naive to systemic anticancer therapy. 3.5. Patient has received prior neoadjuvant/adjuvant systemic anticancer therapy and had a recurrence or progressive disease ≥ 6 months after completing treatment (first recurrence only). 4. Patient has an ECOG PS of 0 or 1. 5. Patient has adequate organ function.b 6. Patient must have a negative serum pregnancy test within 72 hours of the first dose of study medication, unless they are of nonchildbearing potential.c 7. Patients of childbearing potential must agree to use 2 adequate methods of contraception with their partners starting with the screening visit through 180 days after the last dose of study treatment.d |
Exclusion criteria | 1. Patient has received neoadjuvant or adjuvant systemic chemotherapy for primary stage III or IV disease and 1.1. has not had a recurrence or progressive disease before entering the study OR 1.2. has had a recurrence or progressive disease within 6 months of completing chemotherapy treatment before entering the study.e 2. Patient has had > 1 recurrence of endometrial cancer. 3. Patient has received prior therapy with an anti–programmed cell death-1, anti–programmed cell death-ligand 1, or anti–programmed cell death-ligand 2 drug. 4. Patient has received prior anticancer therapy (chemotherapy, targeted therapies, hormonal therapy, radiotherapy, or immunotherapy) within 21 days or < 5 times the half-life of the most recent therapy before Study Day 1, whichever is shorter.f 5. Patient has a concomitant malignancy, or patient has a prior nonendometrial invasive malignancy who has been disease-free for < 3 years or who received any active treatment in the past 3 years for that malignancy. Nonmelanoma skin cancer is allowed. 6. Patient has known uncontrolled central nervous system metastases, carcinomatosis meningitis, or both.g 7. Patient has a known history of HIV. 8. Patient has known active hepatitis B (e.g., hepatitis B surface antigen reactive) or hepatitis C (e.g., hepatitis C virus ribonucleic acid [qualitative] is detected). 9. Patient has an active autoimmune disease that has required systemic treatment in the past 2 years. Replacement therapy is not considered a form of systemic therapy (e.g., thyroid hormone or insulin). 10. Patient has a diagnosis of immunodeficiency or is receiving systemic steroid therapy or any other form of systemic immunosuppressive therapy within 7 days before the first dose of study treatment. 11. Patient has not recovered (i.e., to Grade ≤ 1 or to baseline) from cytotoxic therapy-induced adverse events.h 12. Patient has not recovered adequately from adverse events or complications from any major surgery before starting therapy. 13. Patient has a known hypersensitivity to carboplatin, paclitaxel, or dostarlimab components or excipients. 14. Patient is considered a poor medical risk due to a serious, uncontrolled medical disorder, nonmalignant systemic disease, or active infection requiring systemic therapy. |
Drugs | |
Intervention | Dostarlimab (Jemperli/TSR-042) for IV infusion over 30 minutes in combination with chemotherapy for the first 6 doses (carboplatin: area under the concentration–time curve, 5 mg per mL per minute and paclitaxel: 175 mg per m2 of body-surface area):
|
Comparator | Placebo for IV infusion over 30 minutes in combination with chemotherapy for the first 6 doses (carboplatin: area under the concentration–time curve, 5 mg per mL per minute and paclitaxel: 175 mg per m2 of body-surface area):
|
Study duration | |
Screening phase | In the 28 days before starting treatment |
Treatment phase | Up to 3 years or until progression, unacceptable toxicity, withdrawal of consent, investigator decision, or death |
Follow-up phase | Safety: 90 ± 7 days after treatment Survival assessment: Every 90 ± 14 days up to 4 years (ongoing) |
Outcomes | |
Dual primary end points |
|
Secondary end points |
|
Safety end points |
|
Exploratory end points | Biomarker analyses |
Publication status | |
Publications | Mirza et al. (2023) |
Trial registration | ClinicalTrials.gov Identifier: NCT03981796 |
BICR = blinded independent central review; DCR = disease control rate; dMMR = deficient mismatch repair; DoR = duration of response; ECOG = eastern cooperative oncology group; EORTC = European Organization for Research and Treatment of Cancer; MMR = mismatch repair; MSI = microsatellite instability; MSI-H = microsatellite instability-high; ORR = objective response rate; OS = overall survival; PD = progressive disease; PFS = progression-free survival; QLQ-C30 = core quality of life questionnaire; QLQ-EN24 = endometrial cancer module of the quality of life questionnaire; RECIST v.1.1 = Response Evaluation Criteria in Solid Tumours Version 1.1.
aThe quality of the tumour tissue sample must be confirmed by the central laboratory during screening. Patients should not be randomized without central laboratory confirmation.
bPatient has adequate organ function, defined as follows: 1) Absolute neutrophil count ≥ 1,500 cells/μL; 2) Platelets ≥ 100,000 cells/μL; 3) Hemoglobin ≥ 9 g/dL or ≥ 5.6 mmol/L; 4) Serum creatinine ≤ 1.5 × upper limit of normal (ULN) or calculated creatinine clearance ≥ 50 mL/min using the Cockcroft-Gault equation for patients with creatinine levels > 1.5 × institutional ULN; 5) Total bilirubin ≤ 1.5 × ULN and direct bilirubin ≤ 1 × ULN; 6) Aspartate aminotransferase and alanine aminotransferase ≤ 2.5 × ULN unless liver metastases are present, in which case they must be ≤ 5 × ULN; 6) International normalized ratio or prothrombin time (PT) ≤ 1.5 × ULN and activated partial thromboplastin time ≤ 1.5 × ULN. Patients receiving anticoagulant therapy must have a PT or partial thromboplastin within the therapeutic range of the intended use of anticoagulants.
cNonchildbearing potential is defined as follows: 1) Patient is ≥ 45 years of age and has not had menses for > 1 year. 2) A follicle-stimulating hormone value in the postmenopausal range upon screening evaluation if amenorrheic for < 2 years without a hysterectomy and oophorectomy. 3) Posthysterectomy, postbilateral oophorectomy, or posttubal ligation (Documented hysterectomy or oophorectomy must be confirmed with medical records of the actual procedure or confirmed by an ultrasound, MRI, or CT scan. Tubal ligation must be confirmed with medical records of the actual procedure; otherwise, the patient must fulfill the criteria in Inclusion Criterion 8. Information must be captured appropriately within the site’s source documents.).
dAbstinence is acceptable if this is the established and preferred contraception for the patient.
eLow-dose cisplatin given as a radiation sensitizer or hormonal therapies do not exclude patients from study participation.
fPalliative radiation therapy to a small field ≥ 1 week before Day 1 of study treatment may be allowed.
gPatients with previously treated brain metastases may participate provided they are stable (without evidence of PD by imaging [using the identical imaging modality for each assessment, either MRI or CT scan] for at least 4 weeks before the first dose of study treatment and any neurologic symptoms have returned to baseline), have no evidence of new or enlarging brain metastases, and have not been using steroids for at least 7 days before study treatment. Carcinomatous meningitis precludes a patient from study participation regardless of clinical stability.
hPatients with grade ≤ 2 neuropathy, grade ≤ 2 alopecia, or grade ≤ 2 fatigue are an exception to this criterion and may qualify for the study.
Source: RUBY Clinical Study Report.27 Details included in the table are from the sponsor’s Summary of Clinical Evidence.36
Populations
Inclusion and Exclusion Criteria
The key inclusion criteria were 18 years of age or older, with histologically or cytologically proven endometrial cancer with primary advanced (stage III or IV) or first recurrent disease, and a low potential for cure by radiation therapy or surgery alone or in combination. Patients also had to have an ECOG PS score of 0 or 1 and adequate organ function to be eligible for enrolment. The key exclusion criteria were having received neoadjuvant or adjuvant chemotherapy for primary stage III or IV disease without recurrence or progressive disease before first dose on the study, or with recurrence or progressive disease within 6 months of completing systemic anticancer therapy before first dose on study, having had more than 1 previous disease recurrence, and having had prior treatment with an anti–programmed cell death protein 1 or 2. Prior to randomization, tumour tissue samples were required for all patients to determine MMR or MSI status. Local MMR-MSI testing was used for enrolment when available (including IHC, PCR and next generation sequencing tests). Tumour tissue samples were submitted to the central laboratory for quality check during screening and before randomization.
Interventions
Patients were randomized to receive dostarlimab 500 mg or placebo as a 30-minute IV infusion in combination with carboplatin (area under the concentration–time curve of 5 mg/mL/minute) and paclitaxel (175 mg/m2 every 3 weeks for 6 cycles starting at cycle 1 day 1) for the first 6 cycles followed by dostarlimab 1,000 mg monotherapy or placebo IV every 6 weeks starting at cycle 7 day 1. Dostarlimab monotherapy or placebo was continued for up to 3 years or until progressive disease, unacceptable toxicity, withdrawal of consent, investigator’s decision, or death; continuation of treatment for longer than 3 years was considered following discussion with the sponsor and investigator. All patients were to be pretreated with corticosteroids, diphenhydramine, and H2 antagonists as indicated in the local product information, following administration of dostarlimab or placebo, and before administration of carboplatin and paclitaxel.
Dosing modifications for the management of specific immune-related AEs (for dostarlimab or placebo) and hematologic AEs (for carboplatin and paclitaxel) were prespecified. Notably, treatment must be withheld for study drug-related grade 3 or greater toxicities, and for specific immune-related AEs. Dose reductions of 1 or both of carboplatin and paclitaxel were permitted. Dose reductions for dostarlimab or placebo were not permitted. Doses of all 3 agents were to be interrupted or discontinued for toxicity related to the combination therapy. Patients whose treatment was interrupted were to resume study treatment within 3 weeks of a scheduled interruption, for a maximum of 6 weeks. Patients were permitted to discontinue either the dostarlimab or placebo, and continue on chemotherapy alone, or vice versa (i.e., discontinue chemotherapy and continue dostarlimab or placebo monotherapy). It is important to note that paclitaxel was not to be replaced by other taxanes (e.g., docetaxel, nab-paclitaxel) as the dostarlimab combination safety data are not available.27 Patients who discontinued treatment after a treatment interruption of more than 4 weeks should have had the end-of-treatment visit within 2 weeks of the decision to discontinue treatment or before initiation of alternate anticancer therapy, whichever occurred first.
Patients received rescue medications and/or supportive care for AEs experienced during treatment, including infusion-related reactions. Prophylactic cytokines (e.g., G-CSF) were permitted in cycles subsequent to cycle 1 according to American Society of Clinical Oncology (ASCO) guidelines.50 Concomitant medications that were prohibited during the screening and treatment phase of the study included treatments other than randomized study treatment (including systemic anticancer therapy, immunotherapy, chemotherapy, investigational drugs), surgery to treat the underlying disease, blood products or colony-stimulating factors (e.g., G-CSF, granulocyte-macrophage colony-stimulating factor, or recombinant erythropoietin) within 21 days before first dose of study drug, systemic glucocorticoids other than to manage symptoms of suspected immune-related AEs unless deemed necessary (e.g., acute asthma or chronic obstructive pulmonary disease) and based on investigator judgment, and live virus and bacterial vaccines. Patients could start subsequent treatments (e.g., follow-up anticancer therapy) once dostarlimab treatment was stopped (e.g., for disease progression or other reasons as described).
Outcomes
A list of efficacy end points assessed in this Clinical Review Report is provided in Table 6, followed by descriptions of the outcome measures. Summarized end points are based on outcomes included in the sponsor’s Summary of Clinical Evidence as well as any outcomes identified as important to this review according to the clinical expert(s) consulted by CADTH and stakeholder input from patient and clinician groups and public drug plans. Using the same considerations, the CADTH review team selected end points that were considered to be most relevant to inform CADTH’s expert committee deliberations and finalized this list of end points in consultation with members of the expert committee. All summarized efficacy end points were assessed using GRADE. Select notable harms outcomes considered important for informing CADTH’s expert committee deliberations were also assessed using GRADE.
Overall Survival
OS was defined as the time from randomization to death by any cause. According to the sponsor, following the end-of-treatment visit, survival status was collected by acceptable means including telephone contact. Patients not known to have died at the time of the analysis were censored on the last date when they were known to be alive.
Progression-Free Survival
PFS was defined as the time from randomization to the earliest date of radiographic assessment of progressive disease per Response Evaluation Criteria in Solid Tumours Version 1.1 (RECIST v.1.1)51 or death by any cause in the absence of progressive disease, whichever occurred first. For PFS by investigator assessment, censoring rules for PFS events were specified for the primary analysis and sensitivity analyses (refer to Appendix 1 Figure 7 and Figure 8).
Tumour imaging of the chest, abdomen, pelvis, and other affected sites, as clinically indicated, was performed by CT with contrast delivered IV and PO (or IV contrast if the patient was unable to tolerate both), or MRI if clinically appropriate (e.g., CT was contraindicated). The same imaging was to be used in a patient throughout the study. PET/CT was permitted according to RECIST v.1.1. guidelines as clinically indicated. Initial tumour imaging at screening was to be performed within 28 days before the first dose of study treatment. Radiographic evaluations to assess disease status were conducted every 6 weeks (± 7 days) until week 25, followed by every 9 weeks (± 7 days) until week 52. Subsequent tumour imaging was performed every 12 weeks (± 7 days) until radiographic progressive disease was documented by investigator assessment per RECIST v.1.1. This was followed by 1 additional imaging assessment 4 weeks to 6 weeks later, subsequent anticancer therapy was started consent for study participation was withdrawn, or the patient was lost to follow-up or death, or the study ended, whichever occurred first. Patients who discontinued treatment for other reasons were to have continued radiographic evaluations at the specified time intervals.
Health-Related Quality of Life
HRQoL was measured using the EORTC QLQ-C30 version 3. Assessments were done at each study visit (on treatment), the end-of-treatment visit, and at follow-up (after study treatment), and were to be collected before any procedure or intervention scheduled that day.
The EORTC QLQ-C30, version 3, is used to measure patient self-reported HRQoL. The tool incorporates 5 functional scales (physical, role, cognitive, emotional, and social), 3 symptom scales (fatigue, pain, and nausea and vomiting), a global health status/QoL scale (global health status, QoL), and 6 single items assessing additional symptoms commonly reported by cancer patients (dyspnea, appetite loss, insomnia, constipation, diarrhea, and financial difficulty).52 All items in any scale take the same range of values, with most items scored 1 to 4 with a range of 3 (except for items in the global health status/QoL, which are 7-point questions with a range of 6). Scores for each scale and single-item measure are averaged and transformed linearly to a score ranging from 0 to 100; a high score for a functional scale and for global health status/QoL represents a high/healthy level of functioning, whereas a high score for a symptom scale or item represents a high level of symptomatology or problems.53 A change of 10 points in the EORTC QLQ-C30 scale score and summary score is considered conventionally to be a minimal important difference (MID).54,55 No literature was identified that estimated MIDs specifically in patients with endometrial cancer.
Table 6: Outcomes Summarized From the Studies Included in the Systematic Review
Outcome measure | Time point | RUBY Part 1 |
|---|---|---|
Overall survival | Months 24, 30 | Primary efficacy end point (patients with primary advanced or recurrent endometrial cancer)a Additional analysis (patients with dMMR or MSI-H primary advanced or recurrent endometrial cancer)b |
Progression-free survival, investigator assessed | Months 12, 24 | Primary efficacy end pointa |
Progression-free survival, BICR assessed | Months 12, 24 | Secondary efficacy end point |
EORTC QLQ-C30 | Baseline to cycle 7 day 1 and baseline to cycle 13 day 1 | Secondary end point |
TEAEs (i.e., immune-related AEs, infusion-related reactions) | End of treatment (up to 3 years) | Secondary end point |
AE = adverse event; BICR = blinded independent central review; dMMR = deficient mismatch repair; EORTC QLQ-C30 = European Organization for Research and Treatment of Cancer Care Quality of life questionnaire; MSI-H = microsatellite instability-high; TEAE = treatment-emergent adverse event.
aStatistical testing for these end points was adjusted for multiple comparisons (e.g., hierarchical testing).
bOS in patients with dMMR or MSI-H primary advanced or recurrent endometrial cancer was conducted as a sensitivity analysis and was not adjusted for multiplicity.
Source: RUBY Clinical Study Report.27 Details included in the table are from the sponsor’s Summary of Clinical Evidence.36
Safety
Safety parameters in RUBY included TEAEs, SAEs (including grade ≥ 3 TEAEs), TEAEs leading to discontinuation, and TEAEs leading to death. TEAEs were defined as any AE or SAE that occurred on or after the start of treatment, through 90 days after the last dose of study treatment (or until the start of alternate anticancer therapy, whichever occurred earlier). No adverse events of special interest (an AE that is of scientific and medical concern specific to the study treatment) were identified (known to date) by the sponsor for dostarlimab. Two additional AE categories were prespecified based on a search list of preferred items and most recent MedDRA version by the sponsor (GlaxoSmithKline), using the prespecified GlaxoSmithKline terms of interest codes: a) immune-related AEs: any grade 2 or greater AEs, and b) infusion-related reactions: any drug component related AE which occurred on or within 1 day after drug component infusion.
Considerations that informed the selection of efficacy outcomes to be summarized in the report and assessed using GRADE include the following:
Survival outcomes that were identified as important by patients, clinician groups, and the clinical experts consulted by CADTH, included OS (at clinically relevant time points of 24 months and 30 months) and PFS (investigator and BICR assessed at 12 months and 24 months). OS and PFS were also key inputs in the sponsor’s pharmacoeconomic model.
The clinical experts consulted by CADTH did not identify treatment responses as most important for clinical decision-making, given the availability of OS and PFS outcome data. However, response outcomes are a relevant indicator for durable response to treatment. Therefore, while responses to treatment outcomes were not highlighted in the evidence appraisal, results for ORR, DCR, and DoR are summarized in Appendix 1 Table 17.
HRQoL was identified as important by patients, clinician groups, and the clinical experts consulted by CADTH; given the broad range of functioning and symptom subscales in the EORTC QLQ-C30, the CADTH review team focused on the global health status to encompass patients’ symptoms and overall well-being that were identified by stakeholders. Patients identified change in sexual functioning, which is part of the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire Endometrial cancer module (EORTC QLQ-EN24) instrument, as undesirable effects of current treatments. Therefore, specific symptom and functioning scales from the EORTC QLQ-EN24 were summarized in Appendix 1 Table 18.
Harms of treatment were identified as important by patients, input from clinician groups, and the clinical experts consulted by CADTH, highlighting immune-related AEs and infusion-related reactions as notable harms.
Statistical Analysis
Sample Size and Power Calculation
The sample size calculations for RUBY were driven by the primary efficacy end point of PFS by investigator assessment per RECIST v.1.1, using the following assumptions:
patients with primary advanced or recurrent endometrial cancer (all-comers): HR of 0.67, were assumed to be corresponding to an increase in median PFS from 10 months in group 2 (placebo plus carboplatin-paclitaxel followed by placebo) to 15 months in group 1 (dostarlimab plus carboplatin-paclitaxel followed by dostarlimab)
patients in the dMMR or MSI-H subpopulation: HR of 0.50, assumed to be corresponding to an increase in median PFS from 10 months in group 2 to 20 months in group 1
patient distribution by tumour MMR or MSI status: 25% with dMMR or MSI-H and 75% with pMMR or MSS
1:1 randomization
alpha = 0.02 (1-sided)
power = approximately 89% for testing of H1 (refer to Statistical Testing for details)
accrual over a period of 22 months
an annual dropout rate of 5%
exponential distribution of PFS.
Based on the assumptions for sample size calculations above, a group sequential log-rank test design with 2 analyses was planned: 1 interim analysis (IA) at approximately 84.6% information and 1 final analysis (FA), based on a Lan-DeMets (O’Brien-Fleming) alpha spending function,56 a total sample size of 470 patients was planned and approximately 118 patients were expected to be dMMR or MSI-H. To maintain the natural distribution of dMMR or MSI-H (25%) and pMMR or MSS (75%) patients in the overall endometrial cancer population in this study, the number of patients enrolled with dMMR or MSI-H or pMMR or MSS endometrial cancer was capped at approximately 120 or 350, respectively. In addition, the total number of patients with carcinosarcoma was capped at 50 (approximately 10%) to prevent overrepresentation of this patient population.
Statistical Testing
Multiplicity Control
Statistical analysis of OS and PFS in the RUBY Part 1 were controlled for type I error for multiple hypotheses and interim analyses using a graphical method.40 The family-wise type I error was controlled at 2.5% (1-sided alpha-allocation) for OS and PFS (including across interim analyses). The alpha level assigned to a subfamily was rolled over only if the hypotheses within the subfamily were all significant based on the weight for re-allocation presented on the dashed lines connecting subfamilies (refer to Figure 2). Within each subfamily, weights for re-allocation from each hypothesis to the other were represented on the solid lines connecting hypotheses (refer to Figure 2). Hypothesis testing for PFS in the overall population was only performed if the null hypothesis of PFS was rejected in dMMR or MSI-H. Hypothesis testing for OS in the overall population started at the time when the hypothesis testing for PFS was completed (i.e., no further hypothesis testing could be performed for PFS), or at re-allocated alpha level (2.5%) if both null hypotheses were rejected for H1 and H2; otherwise, OS was tested at initial alpha level (0.5%). All other end points were tested without multiplicity control.
To test hypothesis 1 (H1) (PFS in dMMR or MSI-H), 1 IA and 1 FA were planned. The IA was planned after approximately 77 events had occurred, with the FA being planned after 91 events had occurred. The boundary for declaring superiority of dostarlimab plus carboplatin-paclitaxel versus placebo plus carboplatin-paclitaxel was based on a Lan-DeMets (O’Brien-Fleming) alpha spending function (1-sided alpha = 0.02 as previously described).56 At the data cut-off of September 28, 2022, 66 PFS events were observed in the dMMR or MSI-H subpopulation, therefore the boundary for declaring superiority was adjusted to P = 0.00630.
Figure 2: Multiplicity Control Strategy for Comparisons Between Dostarlimab Plus Carboplatin-Paclitaxel Followed by Dostarlimab and Placebo Plus Carboplatin-Paclitaxel Followed by Placebo in RUBY Part 1
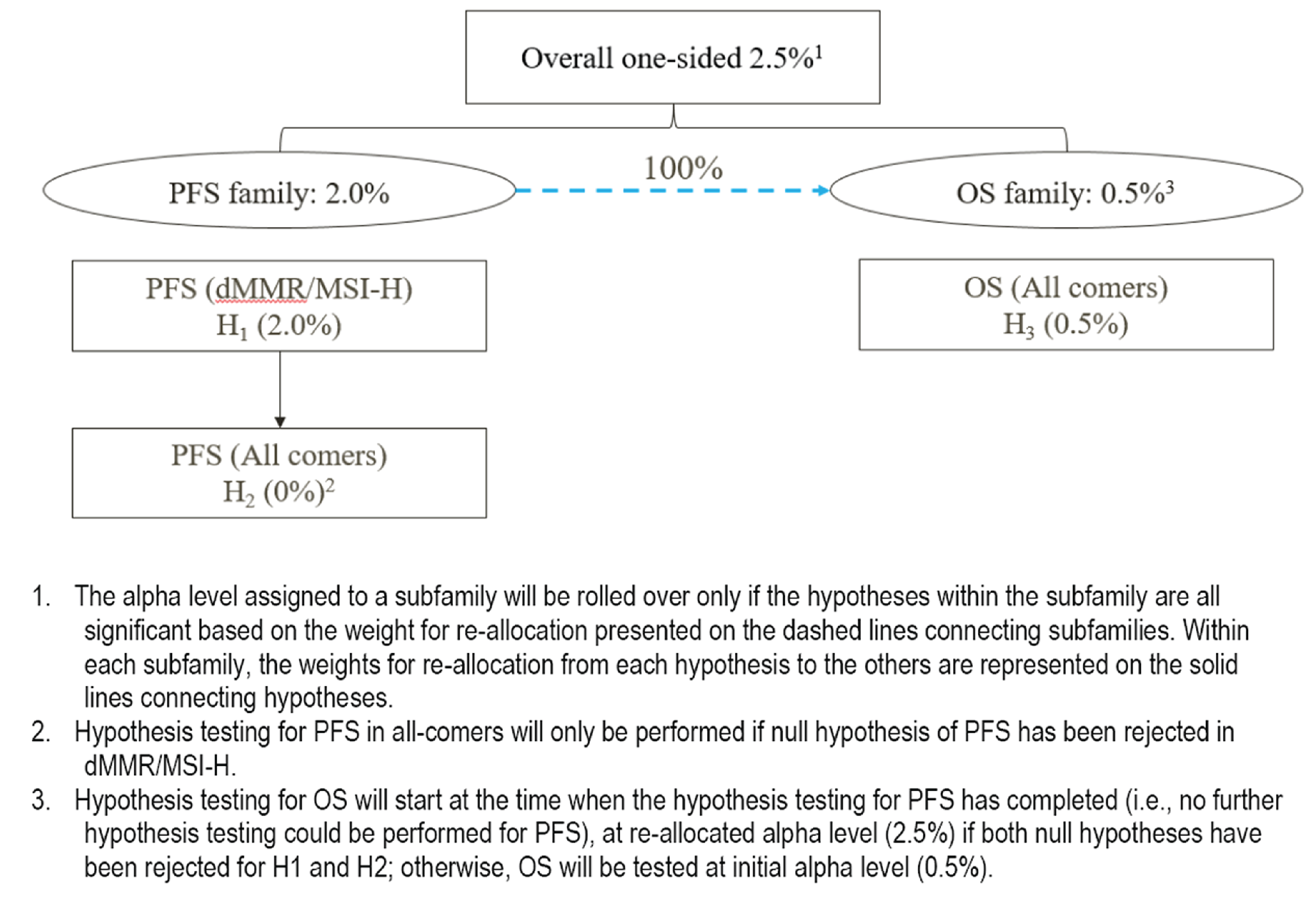
Source: RUBY Clinical Study Report.27
Primary End Points
OS was a primary end point for the ITT analysis set of the overall population. OS in the dMMR or MSI-H subpopulation was an additional analysis to the primary OS analysis. PFS based on investigator assessment was the primary efficacy end point analyzed in the dMMR or MSI-H subpopulation and the overall population.
The HR with 2-sided CI associated with significance level for hypothesis testing was estimated using a stratified Cox proportional hazards model of OS and PFS per the investigator’s assessment. For the dMMR or MSI-H subpopulation for PFS per investigator’s assessment, the 2 stratification factors entered for randomization (prior external pelvic radiotherapy and disease status) were used in the primary analysis. The distributions of OS and PFS per investigator’s assessment were estimated using the Kaplan-Meier
(K-M) method and compared using a stratified log-rank test at the significance level. Median OS and PFS for each treatment group was to be reported with 95% CIs based on the Brookmeyer-Crowley method. OS probabilities with 95% CIs were to be reported at months 12, 18, 24, and 30. PFS probabilities with 95% CIs were to be reported at months 6, 12, 18, and 24. CIs were computed using loglog within the LIFETEST procedure. Underlying assumptions of proportional hazards were checked based on a visual inspection of a survival curve fit to K-M data, inspection of log-cumulative hazard plots over time, and statistical goodness of fit based on relative Akaike and Bayesian information criterion values.57
Subgroup Analyses
Subgroup analyses for OS and PFS by investigator assessment were performed in the dMMR or MSI-H subpopulation using an unstratified Cox proportional hazards model reported as a HR for treatment with associated 95% CIs. The analyses were exploratory and intended to understand whether treatment effects were consistent across the subgroups. Forest plots were produced to graphically depict treatment effect estimates in the subgroups. No inferential statistics (P values) were produced. Survival estimates were provided using K-M curves and reported as medians with 95% CIs. Prespecified subgroups included the following:
age (< 65 years or ≥ 65 years)
race (White or Other)
region (North America or Europe or Western Europe or Eastern Europe)
histology (Endometrioid carcinoma or Other)
disease status at baseline (recurrent, primary Stage III, or primary Stage IV) according to the electronic case report form
MMR or MSI status (dMMR or MSI-H or pMMR or MSS or dMMR) according to the electronic case report form
prior external pelvic radiotherapy (yes or no) according to the electronic case report form
patients with “no disease” at baseline.
Sensitivity Analyses
Sensitivity analyses for PFS by investigator assessment were performed based on the overall population and the dMMR or MSI-H subpopulation to test the robustness of the primary PFS findings for various assumptions employed in the analyses (refer to Table 7).
Secondary End Points
PFS (BICR Assessed)
PFS based on BICR assessment employed the same statistical analyses as the primary analysis except that it was based on BICR assessment.
Health-Related Quality of Life
EORTC QLQ-C30 and EORTC QLQ-EN24
Descriptive statistics (mean, standard deviation [SD], median, first quartile, third quartile, and range) were used to summarize the observed values and changes from baseline HRQoL data at each scheduled assessment time point. For the global health status, functional scales and symptom scales of the EORTC QLQ-C30, and the symptoms scales of the EORTC QLQ-EN24, the scale score change from baseline was categorized as follows: improved (change from baseline ≥ 10), stable (–10 < change from baseline < 10), and worsened (change from baseline ≤ –10 or “patient was too ill” is answered as the reason for not completing the EORTC QLQ-C30 form at visit). The proportion of patients who have a response of improved, stable, or worsened, were calculated using the denominator of all patients with nonmissing corresponding EORTC QLQ-C30 scale scores at baseline and at each corresponding visit. A mixed-effects model for repeated measures (MMRM) was performed for the global health status/QoL scale, 2 symptom scales (fatigue, pain), and 1 functional scale (physical functioning) of the EORTC QLQ-C30 questionnaire to compare between-treatment difference adjusting for correlations across multiple time points within a patient and controlling for the baseline value. The adjustment factors for MMRM included fixed effects (treatment, analysis visit, and treatment-by-visit interaction) and a random effect (patient), with baseline value as a continuous covariate along with baseline-by-visit interaction. Adjusted mean difference and 95% CIs were presented to illustrate the effect of treatment. Analyses of EORTC QLQ-C30 and EORTC QLQ-EN24 were based on the dMMR or MSI-H subpopulation. Missing items were considered missing without imputation for single-item measures. For scales with multiple items, scores were calculated based on the available items if at least half of the items were available, but treated as missing if more than half of the items were missing. No imputation was conducted for the missing domain score nor for the missing scheduled assessment.
Safety
Descriptive statistics (number, percentage) were tabulated for each treatment group for TEAEs, SAEs, grade 3 or greater TEAEs, withdrawals due to AEs, AEs leading to study treatment discontinuations, AEs leading to deaths, immune-related TEAEs, and infusion-related reactions. An AE with missing onset and stop dates, or with the onset date missing and a stop date later than the first dose of either study treatment, were considered to be treatment emergent.
Analysis Populations
Analysis sets included in RUBY Part 1 for the dMMR or MSI-H subpopulation are summarized in Table 8.
Results
Patient Disposition
At the data cut-off of September 28, 2022, 494 patients were enrolled and randomized in RUBY Part 1 (refer to Table 9). The prespecified dMMR-MSI-H subpopulation was determined by the source-verified value of MMR-MSI status. This classification for the primary analysis was based on the “true” source-verified value entered by the site (collected in electronic case reporting forms) for dMMR or MSI-H status at the time of database lock, and not the site data entry for randomization purposes at the time of randomization. Therefore, the imbalance between groups in the dMMR or MSI-H subpopulation (53 patients for dostarlimab plus carboplatin-paclitaxel versus 65 patients for placebo plus carboplatin-paclitaxel) was due to mis-stratification of MMR and MSI data entered during randomization. Treatment discontinuations were commonly due to progressive disease according to RECIST v.1.1. criteria by investigator assessment in ||||| of patients and ||||| of patients, respectively. There was a greater proportion of patients who discontinued the study in the placebo plus carboplatin-paclitaxel group ||||||| compared with the dostarlimab plus carboplatin-paclitaxel group |||||||, which was mainly due to deaths (||||| |||||| |||||, respectively).
Table 7: Statistical Analysis of Efficacy End Points in RUBY Part 1
End point | Statistical model | Adjustment factors | Handling of missing data | Sensitivity analyses |
|---|---|---|---|---|
Overall survival |
| Stratified by the same stratification factors employed in randomization:
| Patients without documented death at time of final analysis were censored to the last date known to be alive. | The same as the primary analysis except MMR and MSI subsets are based on MMR or MSI classification entered for randomization instead of the source-verified MMR or MSI classification collected in the electronic case reporting form. |
Progression-free survival, investigator assessed |
| Stratified by the same stratification factors employed in randomization:
| Refer to censoring rules in Appendix 1 Figure 7 and Figure 8. |
|
EORTC QLQ-C30 | MMRM | Treatment, visit, and treatment-by-visit interaction as fixed effects, baseline as a continuous covariate along with baseline-by-visit interaction (fixed effects), and patient is a random effect. | Single-item measures: if the item was missing, the score S was set to missing (i.e., applying linear transformation to 0 to 100 to obtain the score S). Scales requiring multiple items: if at least half of the items from the scale were available, the score S was calculated based on available items. If more than half of the items from the scale were missing, the score S was set to missing (i.e., applying linear transformation to 0 to 100 to obtain the score S). | None |
BICR = blinded independent committee review; CI = confidence interval; EORTC QLQ-C30 = European organization for research and treatment of cancer core quality of life questionnaire; KM = Kaplan-Meier; MMR = mismatch repair; MMRM = mixed-effects model for repeated measures; MSI = microsatellite instability; NA = not applicable; RECIST v 1.1 = Response Evaluation Criteria in Solid Tumours Version 1.1.
Source: RUBY Clinical Study Protocol. Details included in the table are from the sponsor’s Summary of Clinical Evidence.
Table 8: Analysis Populations of RUBY Part 1
Study | Population | Definition | Application |
|---|---|---|---|
RUBY Part 1 | ITT | All patients analyzed according to randomized treatment | Efficacy analyses (PFS, OS, and HRQoL) |
SAS | Patients who received any amount of study drug were analyzed according to treatment received. | Safety analyses |
HRQoL = health-related quality of life; ITT = intention to treat; OS = overall survival; PFS = progression-free survival; SAS = safety analysis set.
Source: RUBY Clinical Study Protocol. Details included in the table are from the sponsor’s Summary of Clinical Evidence.36
Baseline Characteristics
Baseline characteristics of the RUBY Part 1 study among the patient subpopulation with primary advanced or recurrent dMMR or MSI-H are limited to those that are most relevant to this review or were felt to affect the outcomes or interpretation of the study results (refer to Table 10).
Most of the dMMR or MSI-H subpopulation were white (|||||), with a median age of ||| years (range, || || ||), ECOG PS of 0 (|||||), with endometrioid carcinoma histology at diagnosis (|||||). Nearly half of the enrolled patients had recurrent disease. The treatment groups were generally similar in medical history (histology and grade at diagnosis, FIGO stage at initial diagnosis) and disease status (stage III, stage IV, recurrent disease).
Approximately 14% of patients in the dMMR or MSI-H subpopulation received prior anticancer therapy that was balanced between dostarlimab plus carboplatin-paclitaxel and placebo plus carboplatin-paclitaxel (13.2% versus 15.4%, respectively). Most patients (|||||) had received prior anticancer surgical interventions for endometrial cancer. While ||||| of patients had received prior radiotherapy, fewer patients received external pelvic radiotherapy in the dostarlimab plus carboplatin-paclitaxel group compared with the placebo plus carboplatin-paclitaxel group (15.1% versus 20.0%, respectively).
Table 9: Summary of Patient Disposition in RUBY Part 1, dMMR or MSI-H Subpopulation
Patient disposition | RUBY Part 1 | |
|---|---|---|
Dostarlimab + CAR-PAC | Placebo + CAR-PAC | |
Screened, N | 607 | |
Reason for screening failure, n (%) | ||
Did not meet eligibility criteria | 88 (14.5) | |
Met eligibility criteria but not enrolled | 25 (4.1) | |
Reason for nonenrolment, n (%) | ||
Carcinosarcoma cap has previously been met | | ||||| | |
MSS cap has previously been met | | ||||| | |
Patient withdrew consent | || ||||| | |
Other | || ||||| | |
Randomizeda, N | 245 | 249 |
dMMR or MSI-H, n | 53 | 65 |
Discontinued study treatment, n (%)b | || ||||| | || ||||| |
Discontinued dostarlimab or placebo, n (%)b | || |||||| | || |||||| |
Reason for discontinuing dostarlimab or placebo, n (%)b | ||
AE | | |||||| | | |||||| |
Clinical progression | | ||||| | ||||| |
PD according to RECIST v 1.1 criteria per investigator assessment | || |||||| | || |||||| |
Risk to patient, as judged by investigator, sponsor, or both | | ||||| | | ||||| |
Withdrawal by patient | | ||||| | | ||||| |
Lost to follow-up | | ||||| | | ||||| |
Death from any cause | | ||||| | ||||| |
Other | | ||||| | | ||||| |
Reason for discontinuing paclitaxel, n (%)b | ||
AE | | ||||| | || |||||| |
Clinical progression | | ||||| | ||||| |
PD according to RECIST v 1.1 criteria per investigator assessment | | ||||| | | ||||| |
Risk to patient, as judged by investigator, sponsor, or both | | ||||| | ||||| |
Withdrawal by patient | ||||| | | ||||| |
Lost to follow-up | | ||||| | ||||| |
Patient has completed planned course | | ||||| | | ||||| |
Completed planned course | || |||||| | || |||||| |
Other | ||||| | | ||||| |
Reason for discontinuing carboplatin, n (%)b | ||
AE | | ||||| | | ||||| |
Clinical progression | | ||||| | ||||| |
PD according to RECIST v 1.1 criteria per investigator assessment | | ||||| | | ||||| |
Risk to patient, as judged by investigator, sponsor, or both | | ||||| | ||||| |
Withdrawal by patient | ||||| | | ||||| |
Lost to follow-up | | ||||| | ||||| |
Patient has completed planned course | | ||||| | | ||||| |
Completed planned course | || |||||| | || |||||| |
Other | ||||| | | ||||| |
Discontinued from study, n (%) | || |||||| | || |||||| |
Reason for discontinuation, n (%) | ||
Withdrawal of consent | | ||||| | | ||||| |
Lost to follow-up | | ||||| | | ||||| |
Other | | ||||| | | ||||| |
Death from any cause | | |||||| | || |||||| |
Main cause of death, n (%) | ||
Disease progression | | ||||| | || |||||| |
AE | | ||||| | ||||| |
Unknown | ||||| | | ||||| |
ITT, N | 53 | 65 |
Safety, N | || | 65 |
AE = adverse event; CAR-PAC = carboplatin-paclitaxel; dMMR = deficient mismatch repair; ITT = intention to treat; MSI-H = microsatellite instability-high; MSS = microsatellite stable; PD = progressive disease; RECIST v.1.1 = Response Evaluation Criteria in Solid Tumours Version 1.1; vs. = versus.
aThe overall randomized population included all patients with primary advanced or recurrent endometrial cancer, regardless of MMR or MSI status.
bThe number of patients who discontinued study treatment is reported in the safety analysis set (||| vs. 65 for dostarlimab + CAR-PAC vs. placebo + CAR-PAC, respectively). Percentages are based on the safety analysis set in the denominator.
Source: RUBY Clinical Study Report.27 Details included in the table are from the sponsor’s Summary of Clinical Evidence.36
Exposure to Study Treatments
Patient exposure to study treatments in the RUBY trial for the dMMR or MSI-H subpopulation at IA 1 is summarized in Table 11. The median (range) duration of treatment was 76.5 weeks (3.0 to 150.3) for dostarlimab plus carboplatin-paclitaxel and 31.9 weeks (3.0 to 153.0) for placebo plus carboplatin-paclitaxel. Accordingly, patients underwent a greater number of treatment cycles (median 15.5 cycles versus 8.0 cycles) with dostarlimab plus carboplatin-paclitaxel versus placebo plus carboplatin-paclitaxel, respectively.
Table 10: Summary of Baseline Characteristics in RUBY Part 1, dMMR or MSI-H Subpopulation — ITT Analysis Set
Characteristic | Dostarlimab + CAR-PAC N = 53 | Placebo + CAR-PAC N = 65 |
|---|---|---|
Age, years | ||
Mean (SD) | 63.5 ||||||| | 63.1 ||||||| |
Median (IQR) | 61.0 ||||| || ||||| | 66.0 ||||| || ||||| |
Range | 45 to 81 | 39 to 85 |
Age group, n (%) | ||
19 to 64 years | || |||||| | || |||||| |
≥ 65 years | 23 (43.4) | 35 (53.8) |
Race, n (%) | ||
White | 44 (83.0) | 56 (86.2) |
Black | 4 (7.5) | 6 (9.2) |
Asian | 2 (3.8) | 0 |
American Indian or Alaska Native | 0 | 1 (1.5) |
Native Hawaiian or other Pacific Islander | 1 (1.9) | 0 |
Unknown | 1 (1.9) | 1 (1.5) |
Not reported | 1 (1.9) | 1 (1.5) |
Weight, kg | ||
n | || | 65 |
Mean (SD) | ||||| ||||||| | ||||| ||||||| |
Median (IQR) | ||||| |||||| || |||||| | ||||| |||||| || ||||||| |
Range | |||| || ||||| | |||| || ||||| |
Body mass index, kg/m2 | ||
n | || | 65 |
Mean (SD) | 31.28 |||||| | 35.44 |||||| |
Median (IQR) | 30.55 |||||| || |||||| | 35.50 |||||| || |||||| |
Range | 20.1 to 54.4 | 17.9 to 58.1 |
ECOG PS, n (%)a | ||
n | || | 65 |
0 | 28 (53.8) | 39 (60.0) |
1 | 24 (46.2) | 26 (40.0) |
Histology at diagnosis, n (%) | ||
Carcinosarcoma | 4 (7.5) | 1 (1.5) |
Endometrioid carcinoma (adenocarcinoma or adenocarcinoma-variants) | 44 (83.0) | 56 (86.2) |
Mixed carcinoma with ≥ 10% carcinosarcoma, clear cell, or serous histology | 2 (3.8) | 4 (6.2) |
Serous adenocarcinoma | 1 (1.9) | 1 (1.5) |
Other | 2 (3.8) | 3 (4.6) |
Grade at diagnosis, n (%) | ||
Grade 1 | || |||||| | || |||||| |
Grade 2 | || |||||| | || |||||| |
Grade 3 | || |||||| | || |||||| |
Not assessable | | ||||| | | ||||| |
FIGO stage at initial diagnosis, n (%) | ||
I | 18 (34.0) | 22 (33.8) |
II | 3 (5.7) | 5 (7.7) |
III | 14 (26.4) | 20 (30.8) |
IV | 14 (26.4) | 15 (23.1) |
Unknown | 4 (7.5) | 3 (4.6) |
Disease statusb, n (%) | ||
Primary stage III | 10 (18.9) | 14 (21.5) |
Primary stage IV | 16 (30.2) | 19 (29.2) |
Recurrent | 27 (50.9) | 32 (49.2) |
Prior radiotherapyc for endometrial cancer, n (%) | ||
External pelvic | 8 (15.1) | 13 (20.0) |
Internal pelvic | | |||||| | || |||||| |
Other | | |||||| | | |||||| |
Prior anticancer therapy | ||
Prior anticancer therapy, n (%) | 7 (13.2) | 10 (15.4) |
Paclitaxel with carboplatin | 4 (7.5) | 6 (9.2) |
Carboplatin | | ||||| | | ||||| |
Cisplatin | | ||||| | | ||||| |
Paclitaxel | | ||||| | ||| |
Docetaxel | | ||||| | ||| |
Letrozole | ||| | | ||||| |
CAR-PAC = carboplatin-paclitaxel; dMMR = deficient mismatch repair; ECOG = Eastern Cooperative Oncology Group; FIGO = International Federation of Gynecology and Obstetrics; IQR = interquartile range; ITT = intent to treat; MSI-H = microsatellite instability-high; SD = standard deviation; vs. = versus.
aPercent is calculated using the denominator for patients with data (||| vs. 65).
bDisease status according to electronic case report form.
cPatients may be included in more than 1 category for prior radiotherapy for endometrial cancer.
Source: RUBY Clinical Study Report.27 Details included in the table are from the sponsor’s Summary of Clinical Evidence.36
At IA 1, the median duration of follow-up was 24.8 months (median |||| months for dostarlimab plus carboplatin-paclitaxel versus median |||| months for placebo plus carboplatin-paclitaxel). At IA 2, the median duration of follow-up was |||| months for dostarlimab plus carboplatin-paclitaxel versus |||| months for placebo plus carboplatin-paclitaxel.
Concomitant Medications
All patients in the dMMR or MSI-H subpopulation reported taking concomitant medications, which were numerically similar between treatment groups. The most common types of concomitant medications (used by ≥ 40% of patients) based on IA 1 are summarized in Table 12.
Table 11: Summary of Treatment Exposure in RUBY Part 1, dMMR or MSI-H Subpopulation — Safety Analysis Set
Exposure | RUBY Part 1 | |
|---|---|---|
Dostarlimab + CAR-PAC (N = 52) | Placebo + CAR-PAC (N = 65) | |
Overall duration of treatment (weeks) | ||
Mean (SD) | |||| |||||| | |||| |||||| |
Median (IQR) | 76.5 ||||| || |||||| | 31.9 ||||| || ||||| |
Range | 3.0 to 150.3 | 3.0 to 153.0 |
Overall duration of treatment (cycles) | ||
Mean (SD) | |||| ||||| | |||| ||||| |
Median (IQR) | 15.5 |||| || ||||| | 8.0 |||| || ||||| |
Range | 1 to 28 | 1 to 28 |
Duration of treatment interval, n (%) | ||
Week 1 to ≤ week 3 | | ||||| | | ||||| |
Week 4 to ≤ week 6 | | ||||| | |||| |
Week 7 to ≤ week 9 | |||| | | ||||| |
Week 10 to ≤ week 12 | | ||||| | | ||||| |
Week 13 to ≤ week 15 | | ||||| | |||| |
Week 16 to ≤ week 18 | | |||||| | | ||||| |
Week 19 to ≤ week 24 | | ||||| | || |||||| |
Week 25 to ≤ week 30 | | ||||| | | |||||| |
Week 31 to ≤ week 36 | | ||||| | | ||||| |
Week 37 to ≤ week 42 | |||| | | ||||| |
Week 43 to ≤ week 48 | | ||||| | | |||||| |
Week 49 to ≤ week 54 | | ||||| | | ||||| |
> Week 54 | || |||||| | || |||||| |
> Week 102 | || |||||| | | |||||| |
CAR-PAC = carboplatin-paclitaxel; dMMR = deficient mismatch repair; IQR = interquartile range; MSI-H = microsatellite instability-high; SD = standard deviation.
Source: RUBY Clinical Study Report.27 Details included in the table are from the sponsor’s Summary of Clinical Evidence.36
Subsequent Treatment
Subsequent treatments among patients in the dMMR or MSI-H subpopulation at IA 1 are summarized in Table 13. In RUBY Part 1, subsequent treatments included medications other than per-protocol study treatment, which started after the study treatment was discontinued. A total of 53 patients (15 treated with dostarlimab plus carboplatin-paclitaxel and 38 treated with placebo plus carboplatin-paclitaxel) received subsequent anticancer therapy in the dMMR or MSI-H subpopulation. Notably more patients in the placebo plus carboplatin-paclitaxel versus dostarlimab plus carboplatin-paclitaxel group received immunotherapy with pembrolizumab (30.8% versus 7.5%), hormonal therapy including letrozole (|||| |||||| ||||), and radiation therapy including radiotherapy (||||| |||||| ||||).
Table 12: Summary of Concomitant Medications in RUBY Part 1, dMMR or MSI-H Subpopulation — Safety Analysis Set
Concomitant medication | RUBY Part 1 | |
|---|---|---|
Dostarlimab + CAR-PAC (N = 52) | Placebo + CAR-PAC (N = 65) | |
Patients who received any concomitant medication, n (%) | || ||||||| | || ||||||| |
Concomitant medications used by ≥ 40% of patients in any group, n (%) | ||
Ondansetron | || |||||| | || |||||| |
Dexamethasone | || |||||| | || |||||| |
Paracetamol | || |||||| | || |||||| |
Famotidine | || |||||| | || |||||| |
Diphenhydramine | || |||||| | || |||||| |
CAR-PAC = carboplatin-paclitaxel; dMMR = deficient mismatch repair; MSI-H = microsatellite instability-high.
Source: RUBY Clinical Study Report.27 Details included in the table are from the sponsor’s Summary of Clinical Evidence.36
Table 13: Summary of Subsequent Treatment in RUBY Part 1, dMMR or MSI-H Subpopulation — ITT Analysis Set
Subsequent therapy | RUBY Part 1 | |
|---|---|---|
Dostarlimab + CAR-PAC (N = 53) | Placebo + CAR-PAC (N = 65) | |
Patients who received any subsequent therapy, n (%) | 15 (28.3) | 38 (58.5) |
Immunotherapy | 8 (15.1) | 25 (38.5) |
Dostarlimab | 0 | 3 (4.6) |
Pembrolizumab | 4 (7.5) | 20 (30.8) |
Pembrolizumab/Lenvatinib | 3 (5.7) | 2 (3.1) |
Pembrolizumab/Tamoxifen | 1 (1.9) | 0 |
Retifanlimab/Epacadostat | 1 (1.9) | 0 |
Chemotherapy | | |||||| | || |||||| |
Single chemotherapy | ||
Carboplatin | | ||||| | ||| |
Cisplatin | ||| | | ||||| |
Doxorubicin | | ||||| | | ||||| |
Epirubicin | | ||||| | ||| |
Gemcitabine | ||| | | ||||| |
Paclitaxel | | ||||| | ||| |
Pegylated liposomal doxorubicin | | ||||| | | ||||| |
Topotecan | ||| | | ||||| |
Combination chemotherapy | ||
Carboplatin/Vinorelbine | ||| | | ||||| |
Paclitaxel/Carboplatin | | ||||| | | ||||| |
Hormonal Therapy | | ||||| | | |||||| |
Everolimus | | ||||| | ||| |
Everolimus/Letrozole | | ||||| | ||| |
Letrozole | | ||||| | | ||||| |
Megestrol acetate | | ||||| | | ||||| |
Megestrol acetate/Tamoxifen | | ||||| | | ||||| |
Radiation Therapy | | ||||| | | |||||| |
Radiotherapy | | ||||| | | |||||| |
Stereotactic radiosurgery | | ||||| | ||| |
Other (Pemigatinib) | | ||||| | ||| |
CAR-PAC = carboplatin-paclitaxel; dMMR = deficient mismatch repair; MSI-H = microsatellite instability-high.
Source: RUBY Clinical Study Report.27 Details included in the table are from the sponsor’s Summary of Clinical Evidence.36
Efficacy
Findings for key efficacy outcomes in RUBY Part 1 for patients in the dMMR or MSI-H subpopulation are summarized in Table 14.
Overall Survival
At the data cut-off on September 22, 2023 (IA 2), median OS had not been reached in the dostarlimab plus carboplatin-paclitaxel group with 40% OS maturity (refer to Figure 3). The number of patients who died in the dostarlimab plus carboplatin-paclitaxel and placebo plus carboplatin-paclitaxel group were 12 (22.6%) patients and 35 (53.8%) patients, respectively. The number of patients who were censored was 41 (77.4%) and 30 (46.2%) in the dostarlimab plus carboplatin-paclitaxel and placebo plus carboplatin-paclitaxel groups, respectively. The 24-month OS probability (95% CI) was 82.8% ||||| || ||||| and 57.5% ||||| || ||||| in the dostarlimab plus carboplatin-paclitaxel and placebo plus carboplatin-paclitaxel group, respectively (difference = |||||| ||| ||| |||| || ||||). The 30-month OS probability (95% CI) was ||||| ||||| || ||||| and ||||| ||||| || ||||| in the dostarlimab plus carboplatin-paclitaxel and placebo plus carboplatin-paclitaxel groups, respectively (difference = |||||| ||| ||| |||| || ||||). The HR (95% CI) in the dMMR or MSI-H subpopulation was 0.32 (0.166 to 0.629; 1-sided P value = 0.0002) for dostarlimab plus carboplatin-paclitaxel versus placebo plus carboplatin-paclitaxel. OS findings from IA 2 were consistent with IA 1 (data cut-off of September 28, 2022) (refer to Appendix 1 Table 17); the sponsor noted that the stopping boundary for statistical significance of OS in the overall population was met at IA 2, and therefore, no further testing for OS will be conducted.
PFS (Investigator Assessed)
At data cut-off on September 28, 2022 (IA 1), median PFS based on investigator assessment was not reached in the dostarlimab plus carboplatin-paclitaxel group, compared with 7.7 months in the placebo plus carboplatin-paclitaxel group (refer to Figure 4) with 56% PFS maturity in the dMMR or MSI-H subpopulation. Among 19 of 53 (35.8%) patients in the dostarlimab plus carboplatin-paclitaxel group and 47 of 65 (72.3%) patients in the placebo plus carboplatin-paclitaxel group who had experienced an event, |||| ||||||| and || |||||||, respectively, were due to disease progression, and | |||||| and | ||||||, respectively, were due to deaths. The number of patients who were censored were 34 (64.2%) and 18 (27.7%) in the dostarlimab plus carboplatin-paclitaxel and placebo plus carboplatin-paclitaxel groups, respectively. The 12-month investigator-assessed PFS probability (95% CI) was 63.5% ||||| || ||||| and 24.4% ||||| || ||||| in the dostarlimab plus carboplatin-paclitaxel and placebo plus carboplatin-paclitaxel groups, respectively. The 24-month investigator-assessed PFS probability (95% CI) was 61.4% (46.3 to 73.4) and 15.7% (7.2 to 27.0) in the dostarlimab plus carboplatin-paclitaxel and placebo plus carboplatin-paclitaxel groups, respectively. The difference in investigator-assessed PFS probability (95% CI) was ||||| ||||| || ||||| at 12 months and ||||| ||||| || ||||| at 24 months, favouring dostarlimab plus carboplatin-paclitaxel. The HR (95% CI) in the dMMR or MSI-H subpopulation was 0.28 (0.162 to 0.495; 1-sided P value < 0.0001) for dostarlimab plus carboplatin-paclitaxel versus placebo plus carboplatin-paclitaxel. PFS was not analyzed at the second IA (data cut-off date of September 22, 2023), as statistical significance was achieved in the first IA.
Figure 3: Kaplan-Meier Curves of Overall Survival in RUBY Part 1, dMMR or MSI-H Subpopulation, Data Cut-off Date September 22, 2023 — ITT Analysis Set
![The Kaplan-Meier curves of OS in the dMMR or MSI-H population showed early crossover during treatment with separation at about 7 months after randomization between dostarlimab plus carboplatin-paclitaxel (blue), compared with placebo plus carboplatin-paclitaxel (red). Median OS was not reached after [redacted] months and [redacted] months of follow-up in the dostarlimab plus carboplatin-paclitaxel and placebo plus carboplatin-paclitaxel groups, respectively.](https://canjhealthtechnol.ca/index.php/cjht/article/download/PC0325r/version/939/2044/7795/PC0325CL-fig03.png)
dMMR = deficient mismatch repair; HR = hazard ratio; m = months; mOS = median overall survival; MSI-H = microsatellite instability-high; NE = not estimable; vs = versus.
Source: From sponsor in response to additional data request.58
Table 14: Summary of Key Efficacy Results in RUBY Part 1, dMMR or MSI-H Subpopulation — ITT Analysis Set
Outcome measure | Dostarlimab + CAR-PAC N = 53 | Placebo + CAR-PAC N = 65 |
|---|---|---|
Overall survivala | ||
Data cut-off date | September 22, 2023 | |
Median follow-up duration,b months (range) | ||||| ||||| || |||||| | ||||| ||||| || |||||| |
Number of patients contributing to the analysis, n (%) | 53 | 65 |
OS events, n (%) | 12 (22.6) | 35 (53.8) |
Censored, n (%) | 41 (77.4) | 30 (46.2) |
Median OS, months (95% CI)c | Not reached | 31.4 (20.3 to NE) |
K-M estimates of OS probability, % (95% CI) | ||
Month 12 | |||| |||| | |||| |||| |
Month 18 | |||| |||| | |||| |||| |
Month 24 | 82.8 ||||| || ||||| | 57.5 ||||| || ||||| |
Month 24, absolute difference (95% CI)d | |||| |||||| || ||||| | Reference |
Month 30 | |||| ||||| || ||||| | |||| ||||| || ||||| |
Month 30, absolute difference (95% CI)d | |||| |||||| || ||||| | Reference |
HR (95% CI)e | 0.32 (0.166 to 0.629) | Reference |
P valuef | 0.0002g | Reference |
Progression-free survival (investigator assessed) | ||
Data cut-off date | September 28, 2022 | |
Median follow-up duration,b months (range) | ||||| |||||| || |||||| | ||||| |||||| || |||||| |
Number of patients contributing to the analysis, n (%) | 53 | 65 |
PFS events, n (%) | 19 (35.8) | 47 (72.3) |
Disease progression, n (%) | || |||||| | || |||||| |
Death, n (%) | | ||||| | | ||||| |
Censored, n (%) | 34 (64.2) | 18 (27.7) |
Median PFS, months (95% CI)c | Not reached (11.8 to not reached) | 7.7 (5.6 to 9.7) |
K-M estimates of PFS probability, % (95% CI)d | ||
Month 6 | |||| ||||| || ||||| | |||| ||||| || ||||| |
Month 12 | 63.5 ||||| || ||||| | 24.4 ||||| || ||||| |
Month 12, absolute difference (95% CI)d | |||||||||| || ||||| | Reference |
Month 18 | |||| ||||| || ||||| | |||| |||| || ||||| |
Month 24 | 61.4 (46.3 to 73.4) | 15.7 (7.2 to 27.0) |
Month 24, absolute difference (95% CI)d | |||| |||||| || ||||| | Reference |
HR (95% CI)e | 0.28 (0.162 to 0.495) | Reference |
P valuef | < 0.0001 | Reference |
BICR = blinded independent committee review; CAR-PAC = carboplatin-paclitaxel; CI = confidence interval; dMMR = deficient mismatch repair; HR = hazard ratio; ITT = intention to treat; KM = Kaplan-Meier; MSI-H = microsatellite instability-high; NE = not estimable; OS = overall survival; PFS = progression-free survival.
aOS in the dMMR or MSI-H subpopulation was not adjusted for multiplicity. OS was a dual primary end point for patients with primary advanced or recurrent endometrial cancer (overall population), and a prespecified sensitivity analysis for OS was conducted in the dMMR or MSI-H subpopulation.
bDuration of follow-up was defined as the time from randomization to cut-off date.
c95% CI generated using the method of Brookmeyer and Crowley (1982).
dRisk difference (95%CI) generated using the method of Austin (2010) was not included in the sponsor’s planned analyses; the absolute risk difference was requested by the CADTH review team for interpretation purposes.
eBased on the Stratified Cox regression model.
f1-sided P value based on the Stratified log-rank test.
gP value has not been adjusted for multiplicity.
Source: RUBY Clinical Study Report.27 Details included in the table were additional data provided from the sponsor.58
Figure 4: Kaplan-Meier Curves of Investigator-Assessed Progression-Free Survival in RUBY Part 1, dMMR or MSI-H Subpopulation, Data Cut-off Date September 28, 2022 — ITT Analysis Set
![The Kaplan-Meier curves of investigator-assessed PFS in the dMMR or MSI-H subpopulation showed early crossover during treatment, with separation at about 5 months after randomization between dostarlimab + carboplatin-paclitaxel compared with placebo + carboplatin-paclitaxel. Median PFS was not reached after [redacted] months and [redacted] months of follow-up in the dostarlimab + carboplatin-paclitaxel and placebo + carboplatin-paclitaxel groups, respectively.](https://canjhealthtechnol.ca/index.php/cjht/article/download/PC0325r/version/939/2044/7805/PC0325CL-fig04.png)
dMMR = deficient mismatch repair; MSI-H = microsatellite instability-high.
Source: RUBY Clinical Study Report.27
Subgroup Analyses
The HRs (95% CI) for primary investigator-assessed PFS in the dMMR-MSI-H subpopulation generally favoured treatment with dostarlimab plus carboplatin-paclitaxel compared with placebo plus carboplatin-paclitaxel (refer to Figure 5). There seemed to be some inconsistency in effects across subgroups by disease stage, though it is unclear if this may be the result of small sample size for some of the groups.
Figure 5: Forest Plot of Investigator-Assessed Progression-Free Survival and 95% Confidence Intervals by Subgroup in RUBY Part 1, dMMR or MSI-H Subpopulation, Data Cut-off Date September 28, 2022 — ITT Analysis Set
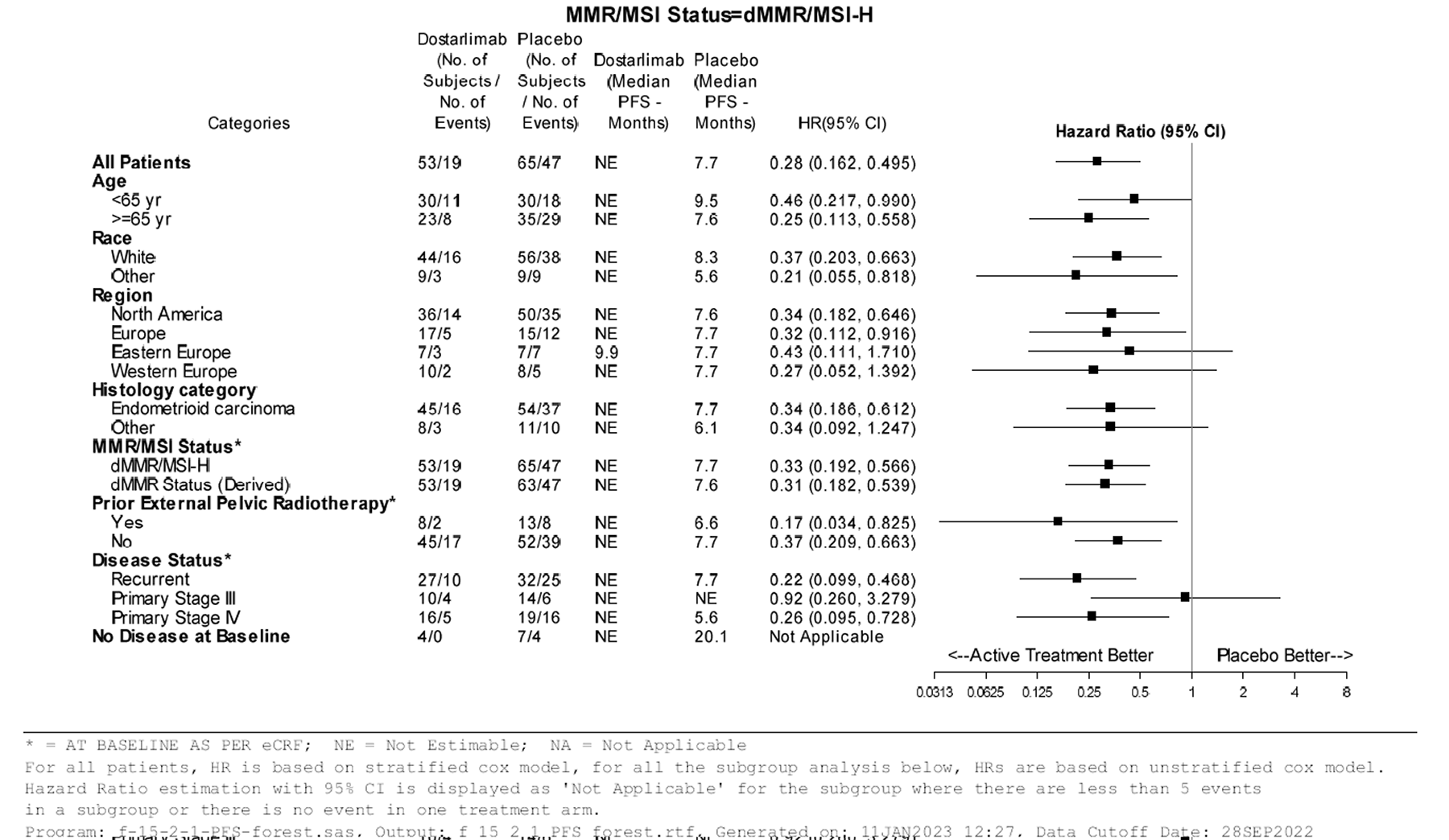
dMMR = deficient mismatch repair; MSI-H = microsatellite instability-high.
Source: RUBY Clinical Study Report.27
Sensitivity Analyses
Sensitivity analyses for investigator-assessed PFS among patients in the dMMR or MSI-H subpopulation based on the value entered at randomization (HR = ||||; 95% CI, |||| || ||||) were consistent with the primary analysis based on source-verified value for investigator-assessed PFS. Similarly, sensitivity analyses for PFS based on BICR assessment (HR = 0.29; 95% CI, 0.16 to 0.54) were consistent with PFS based on investigator assessment. All other sensitivity analyses for investigator-assessed PFS were consistent with the primary analysis.
Health-Related Quality of Life
EORTC QLQ-C30
At the time of data cut-off on September 28, 2022, the overall LSM change from baseline (from cycle 2 day 1 to end of treatment) (95% CI) in the EORTC QLQ-C30 Global Health Status was ||| |||||| ||||| || |||| in the dostarlimab plus carboplatin-paclitaxel group compared with |||| |||||| ||||| || ||||| in the placebo plus carboplatin-paclitaxel group (difference in LSM change from baseline = ||| ||||||| |||||| ||| || ||||| | | ||||||) (refer to Table 15). The LSM change from baseline (95% CI) in the EORTC QLQ-C30 Global Health Status at day 1 of cycle 7 was ||| |||||| ||||| || |||| and |||| |||||| |||||| || ||||| in the dostarlimab plus carboplatin-paclitaxel and placebo plus carboplatin-paclitaxel groups, respectively (difference in LSM change from baseline = 9.4 points; 95% CI, ||| || ||||; P = 0.0125). The LSM change from baseline (95% CI) in the EORTC QLQ-C30 Global Health Status at day 1 of cycle 13 was ||| |||||| |||| || ||||| and |||| |||||| ||||| || |||| in the dostarlimab plus carboplatin-paclitaxel and placebo plus carboplatin-paclitaxel groups, respectively (difference in LSM change from baseline = ||| ||||||| ||| ||| |||| || ||||| | | ||||||). The plot of mean change from baseline (95% CIs) in the EORTC QLQ-C30 Global Health Status for dostarlimab plus carboplatin-paclitaxel compared with placebo plus carboplatin-paclitaxel at all study visits is depicted in Figure 6.
Figure 6: Plot of Change from Baseline and Confidence Interval in EORTC QLQ-C30 Global Health Status in RUBY Part 1, dMMR or MSI-H Subpopulation, Data Cut-off Date September 28, 2022 — ITT Analysis Set
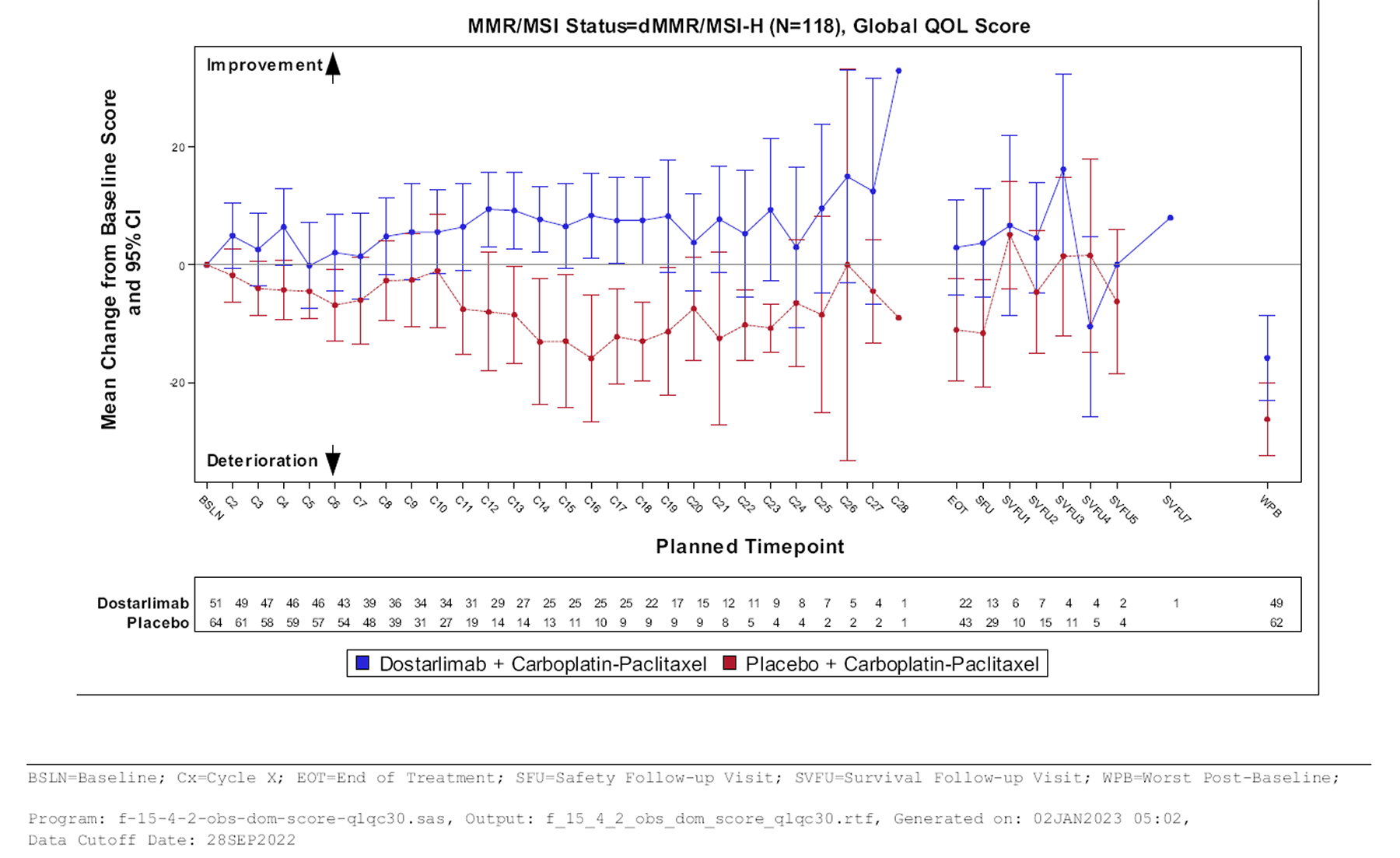
dMMR = deficient mismatch repair; MSI-H = microsatellite instability-high.
Source: RUBY Clinical Study Report.27
Table 15: Summary of EORTC QLQ-C30 Global Health Status Results in RUBY Part 1, dMMR or MSI-H Subpopulation — ITT Analysis Set
Outcome measure | Dostarlimab + CAR-PAC N = 53 | Placebo + CAR-PAC N = 65 |
|---|---|---|
Data cut-off date | September 28, 2022 | |
Median follow-upa duration, months (range) | ||||| |||||| || |||||| | ||||| |||||| || |||||| |
Baseline | ||
Number of patients contributing to the analysis, nb | || | || |
Mean (SD) | |||| ||||||| | |||| ||||||| |
Change from baseline, cycle 2 day 1 to end of treatment | ||
Number of patients contributing to the analysis, nb | || | || |
LSM (95% CI)c | ||| ||||| || |||| | |||| ||||| || ||||| |
Difference, LSM (95% CI)c | ||| |||| || ||||| | Reference |
P valuec | ||||||d | Reference |
Change from baseline at cycle 7 day 1 | ||
Number of patients contributing to the analysis, nb | || | || |
LSM (95% CI)c | ||| ||||| || |||| | |||| |||||| || ||||| |
Difference, LSM (95% CI)c | 9.4 |||| || ||||| | Reference |
P valuec | 0.0125d | Reference |
Change from baseline at cycle 13 day 1 | ||
Number of patients contributing to the analysis, nb | || | || |
LSM (95% CI)c | ||| |||| || ||||| | |||| ||||| || |||| |
Difference, LSM (95% CI)c | ||| ||||| || ||||| | Reference |
P valuec | ||||||d | Reference |
CAR-PAC = carboplatin-paclitaxel; CI = confidence interval; EORTC QLQ-C30 = European Organization for Research and Treatment of Cancer Core Quality of Life Questionnaire; LSM = least squares mean; SD = standard deviation; SE = standard error.
aDuration of follow-up was defined as the time from randomization to cut-off date.
bNumber of patients with nonmissing HRQoL value at specified visit.
cAdjusted means, 95% CI and P values are from a mixed model for repeated measures with treatment, visit, and treatment-by-visit interaction as fixed effects, baseline as a continuous covariate along with baseline-by-visit interaction (fixed effects), and patient as a random effect.
dP value has not been adjusted for multiplicity.
Source: RUBY Clinical Study Report.27 Details included in the table are from the sponsor’s Summary of Clinical Evidence.36
Harms
Harms data for RUBY Part 1 among patients with primary advanced or recurrent endometrial cancer in the dMMR or MSI-H subpopulation is summarized in Table 16. Harms data were reported for IA 1 (data cut-off of September 28, 2022) with updated data for notable harms from IA 2 (data cut-off September 22, 2023).
Adverse Events
All patients in the dMMR or MSI-H subpopulation experienced at least 1 TEAE. The most common TEAEs occurring in greater than 20% of patients in the dostarlimab plus carboplatin-paclitaxel or placebo plus carboplatin-paclitaxel groups, respectively, were alopecia (||| |||||| |||), fatigue (||| |||||| |||), nausea (||| |||||| |||), anemia (||| |||||| |||), peripheral neuropathy (||| |||||| |||), arthralgia (||| |||||| |||), diarrhea (||| |||||| |||), constipation (||| |||||| |||), myalgia (||| |||||| |||), hypomagnesemia (||| |||||| |||), vomiting (||| |||||| |||), rash (||| |||||| |||), dyspnea (||| |||||| |||), neutropenia (||| |||||| |||), abdominal pain (||| |||||| |||), peripheral sensory neuropathy (||| |||||| |||), decreased neutrophil count (||| |||||| |||), urinary tract infection (|| |||||| |||), hypertension (||| |||||| |||), and hypothyroidism (||| |||||| ||).
Serious Adverse Events
The number of patients in the dMMR or MSI-H subpopulation with at least 1 SAE was || ||||| patients in the dostarlimab plus carboplatin-paclitaxel group and || ||||| patients in the placebo plus carboplatin-paclitaxel group. The most common SAEs occurring in at least 2% of patients in either the dostarlimab plus carboplatin-paclitaxel or placebo plus carboplatin-paclitaxel groups, respectively, were urinary tract infection (| |||||| ||||), anemia (| |||||| ||||), asthenia (| |||||| ||||), sepsis (|||| |||||| |), and pulmonary embolism (| |||||| ||||). The number of patients with at least 1 TEAE of grade 3 or greater was || ||||| patients in the dostarlimab plus carboplatin-paclitaxel group and || ||||| patients in the placebo plus carboplatin-paclitaxel group. The most common Grade 3 or greater TEAEs occurring in at least 10% of patients in either the dostarlimab plus carboplatin-paclitaxel or placebo plus carboplatin-paclitaxel groups, respectively, were anemia (||| |||||| |||), neutropenia (||| |||||| |||), decreased neutrophil count (|| |||||| |||), and decreased white blood cell count (|| |||||| |||).
Withdrawals Due to Adverse Events
The number of patients in the dMMR or MSI-H subpopulation who discontinued study treatment due to an AE was | ||||||| patients in the dostarlimab plus carboplatin-paclitaxel group and || ||||||| patients in the placebo plus carboplatin-paclitaxel group. Withdrawals due to AEs in the dostarlimab plus carboplatin-paclitaxel group were due to (| |||||| ||||||| ||||) neurotoxicity, myelosuppression, drug hypersensitivity, infusion-related reaction, chronic kidney disease, rash maculo-papular, keratitis, muscular weakness, fatigue, and general physical health deterioration. Withdrawals due to AEs in the placebo plus carboplatin-paclitaxel group were due to peripheral neuropathy (||||| and thrombocytopenia (||||), cardiovascular accident (| ||||||| ||||||), infusion-related reaction (||||), increased amylase (||||), decreased platelet count (||||), peritonitis (||||), myelodysplastic syndrome (||||), and vaginal hemorrhage (||||).
Mortality
The number of deaths in the dMMR or MSI-H subpopulation were 7 (13.5%) patients in the dostarlimab plus carboplatin-paclitaxel group and 24 (36.9%) patients in the placebo plus carboplatin-paclitaxel group. Most deaths (||| patients and ||| patients) were due to disease progression in the dostarlimab plus carboplatin-paclitaxel and placebo plus carboplatin-paclitaxel groups, respectively. ||| patients treated with dostarlimab plus carboplatin-paclitaxel experienced TEAEs leading to death (| ||||||| |||| || myelosuppression, and of hypovolemic shock). No patient treated with placebo plus carboplatin-paclitaxel experienced TEAEs leading to death.
Notable Harms
Immune-Related Adverse Events
In RUBY Part 1 in the dMMR or MSI-H subpopulation, || ||||||| patients in the dostarlimab plus carboplatin-paclitaxel group and || ||||||| patients in the placebo plus carboplatin-paclitaxel group experienced an immune-related AE (difference = |||| ||| ||| || || ||).
Infusion-Related Reactions
The number of patients in the dostarlimab plus carboplatin-paclitaxel and placebo plus carboplatin-paclitaxel group, respectively, who experienced an infusion-related reaction were || ||||||| and || ||||||| (difference = ||| ||| ||| ||| || ||).
Table 16: Summary of Harms Results in RUBY Part 1, dMMR or MSI-H Subpopulation — Safety Analysis Set
Outcome measure | Dostarlimab + CAR-PAC N = 52 | Placebo + CAR-PAC N = 65 |
|---|---|---|
Data cut-off date | September 28, 2022 | |
Most common adverse events, n (%) | ||
Number of patients contributing to analysis, n | || | 65 |
Patients with ≥ 1 TEAE | || (100) | 65 (100) |
TEAEs in > 20% of patients in any group, n (%) | ||
Alopecia | || |||||| | || |||||| |
Fatigue | || |||||| | || |||||| |
Nausea | || |||||| | || |||||| |
Anemia | || |||||| | || |||||| |
Peripheral neuropathy | || |||||| | || |||||| |
Arthralgia | || |||||| | || |||||| |
Diarrhea | || |||||| | || |||||| |
Constipation | || |||||| | || |||||| |
Myalgia | || |||||| | || |||||| |
Hypomagnesemia | || |||||| | || |||||| |
Vomiting | || |||||| | || |||||| |
Rash | || |||||| | || |||||| |
Dyspnea | | |||||| | || |||||| |
Neutropenia | || |||||| | || |||||| |
Abdominal pain | | |||||| | || |||||| |
Peripheral sensory neuropathy | || |||||| | || |||||| |
Neutrophil count decreased | | ||||| | || |||||| |
Urinary tract infection | | ||||| | || |||||| |
Hypertension | || |||||| | | |||||| |
Hypothyroidism | || |||||| | | ||||| |
Serious adverse events, n (%) | ||
Number of patients contributing to analysis, n | ||| | 65 |
Patients with ≥ 1 SAE, n (%) | || |||||| | || |||||| |
Patients with grade ≥ 3 TEAE, n (%) | || |||||| | || |||||| |
Grade ≥ 3 TEAE in ≥ 10% of patients in any group, n (%) | ||
Anemia | | |||||| | || |||||| |
Neutropenia | | |||||| | | |||||| |
Neutrophil count decreased | | ||||| | || |||||| |
White blood cell count decreased | | ||||| | | |||||| |
Withdrawals due to adverse events, n (%) | ||
Number of patients contributing to analysis, n | ||| | ||| |
Patients who stopped study treatment, n (%) | | |||||| | || |||||| |
Withdrawals due to AEs in ≥ 2% patients in any group, n (%) | ||
Neuropathy peripheral | ||| | | ||||| |
Thrombocytopenia | ||| | | ||||| |
Deaths, n (%) | ||
Number of patients contributing to analysis, n | ||| | 65 |
Patients who died, n (%) | 7 (13.5) | 24 (36.9) |
Primary reason of death, n (%) | ||
Disease progression | | ||||| | || |||||| |
Unknown | ||| | | ||||| |
Adverse event | | ||||| | ||| |
Myelosuppression | | ||||| | ||| |
Hypovolemic shock | | ||||| | ||| |
Notable harms, n (%) | ||
Number of patients contributing to analysis, n | ||| | 65 |
Immune-related adverse event, n (%) | || |||||| | || |||||| |
Immune-related adverse event, risk difference (95% CI)a | || |||| || ||| | Reference |
Hypersensitivity, n (%) | || |||||| | || |||||| |
Infusion-related reaction | || |||||| | || |||||| |
Infusion-related reaction, risk difference (95% CI)a | |||||| || ||| | Reference |
CAR-PAC = carboplatin-paclitaxel; CI = confidence interval; dMMR = deficient mismatch repair; MSI-H = microsatellite instability-high; SAE = serious adverse event; TEAE = treatment-emergent adverse event.
aRisk difference (95%CI) was not included in the sponsor’s planned analyses; the absolute risk difference was requested by the CADTH review team for interpretation purposes.
Source: RUBY Clinical Study Report.27 Details included in the table are from the Summary of Clinical Evidence36 and additional data from the sponsor.58
Critical Appraisal
Internal Validity
Randomization was conducted using an interactive web response system, which is considered adequate to conceal the allocation sequence. MMR or MSI status was used to stratify randomization for the overall population of patients with primary advanced or recurrent endometrial cancer, ensuring that randomization was upheld in the dMMR or MSI-H subpopulation. However, initial MMR or MSI status was based on data entered at randomization from investigators. Based on verified data according to patients’ electronic case reporting forms, there was an imbalance in the number of patients with dMMR or MSI-H between dostarlimab plus carboplatin-paclitaxel versus placebo plus carboplatin-paclitaxel (53 versus 65, respectively). However, the risk of MMR or MSI misclassification to impact prognostic balance of groups was mitigated based on sensitivity analyses for primary end points (OS and investigator-assessed PFS), showing that results for randomization data were consistent with verified sources. There was a higher proportion of patients older than 65 years, with ECOG PS of 0, and having had prior external pelvic radiotherapy in the placebo plus carboplatin-paclitaxel group. These imbalances, which were not systematically favouring either intervention group, are likely to be compatible with chance. However, prognostic balance requires a large sample size, and therefore is unlikely to have been fully achieved in RUBY Part 1 despite adequate randomization methods.
Interim analyses for RUBY Part 1 were preplanned with adequately justified stopping boundaries, which provides confidence that the statistical significance of PFS in the dMMR or MSI-H subpopulation is not a result of type I error. However, there is a risk that the magnitude of observed treatment effects is overestimated,23-25 given that neither median PFS nor median OS in the dostarlimab plus carboplatin-paclitaxel group had been reached at the time of analysis and the information fraction for OS was notably small (40%). There was a small number of patients with dMMR or MSI-H (combined sample size of treatment groups) and a low number of events (approximately 60 for PFS at the first IA and 40 for OS at the second IA for the time points of interest) which may render the observed effects unstable. Among patients in the dMMR or MSI-H subpopulation, OS and HRQoL were not included in the hierarchical testing strategy, increasing the risk of type I error for these end points. Despite the absence of results for inspection and/or validation of the proportional hazards assumptions, visual inspection of the K-M curves for PFS and OS appear to indicate a clear separation (at approximately 5 months and 7 months, respectively), after which there appeared to be sustained proportionality throughout study treatment.
The sponsor noted that participants, study personnel, and the investigator were blinded to the study treatment from the time of randomization until the database lock. There was a risk for unblinding among patients who experienced an AE that is expected to be related to the study drug (in the dostarlimab group) during study treatment, particularly at cycle 7 and onwards when chemotherapy (carboplatin-paclitaxel) was not administered in either treatment group. However, there is no evidence of deviations from the intended interventions nor of bias in measurement of the outcomes as a result of potential unblinding. The primary end point, PFS, was revised from investigator to BICR (protocol amendment 1) and reverted to investigator (protocol amendment 4). The criteria for disease progression are based on radiographic images and clinical assessment, with the potential for subjective interpretation. However, findings from sensitivity analyses for PFS based on BICR assessment were consistent with investigator assessment, therefore the concern for potential bias is low.
Disease-related HRQoL was measured in RUBY Part 1 using the EORTC QLQ-C3052,59,60 that is widely employed by oncology clinical trials for various cancers and supplemented with the EORTC QLQ-EN2461-63 to capture symptoms specific to endometrial cancer. MIDs were based on values identified in the literature for EORTC QLQ-C3054,55 and extrapolated to apply to the EORTC QLQ-EN24 in the absence of an MID identified for patients with endometrial cancer. Outcome data for EORTC QLQ-C30 in the dostarlimab and placebo groups, respectively, were available for 39 (73%) and 48 (74%) patients at cycle 7; after cycle 8, the number of patients available to provide assessments had dropped to fewer than 70% and 50%, respectively, and fewer than 50% and 30%, respectively, after cycle 12. Though missing data were imputed implicitly using the MMRM model, it is not possible to confirm that the missing data occurred at random (as assumed in MMRM). Additionally, there was a lack of sensitivity analyses to explore the impact of other imputation techniques assuming different missing data mechanisms on treatment effect estimates, resulting in risk of bias due to significant missing data that is likely to have compromised randomization. The direction of the potential bias cannot be predicted.
External Validity
The population enrolled in RUBY Part 1 were representative of patients with primary advanced or recurrent dMMR or MSI-H endometrial cancer in clinical practice, according to the clinical experts consulted by CADTH. While patients with ECOG PS of 2 were excluded from the RUBY trial, the clinical experts considered these patients to be eligible for treatment with dostarlimab with chemotherapy.
The timing of administering dostarlimab or placebo in combination with carboplatin and paclitaxel appears to be aligned with the chemotherapy regimens in the current SOC, according to the clinical experts consulted by CADTH. Treatment duration was up to 3 years in RUBY if patients did not experience disease progression, unacceptable toxicity, or death. The clinical experts consulted by CADTH indicated that it is not typical for patients to be treated for such a lengthy duration, given that the cohort of patients with primary advanced or recurrent dMMR or MSI-H have increased likelihood of disease recurrence over time. Radiographic evaluations to assess disease status were reported by the clinical experts consulted by CADTH to be more frequent in the RUBY trial (every 6 weeks to week 25 followed by every 9 weeks to week 52) than would be feasible in clinical practice (every 3 to 4 months).
The comparator in RUBY Part 1 was placebo combined with carboplatin and paclitaxel. Doublet chemotherapy with carboplatin and paclitaxel was reported by the clinical experts consulted by CADTH to be the current SOC among patients with primary advanced disease and among patients with recurrent disease who are chemotherapy naive. The clinical expert consulted by CADTH noted that patients who had adjuvant chemotherapy with carboplatin and paclitaxel would be eligible for single drug PD-1 inhibitors (e.g., pembrolizumab) or single drug chemotherapy for first-line recurrence, and more than likely, many physicians would continue to prescribe a single drug PD-1 inhibitor for these patients. Patients without adjuvant chemotherapy who experience disease recurrence following treatment would be eligible for chemotherapy as first-line recurrence, followed by eligibility for treatment with pembrolizumab monotherapy as second-line recurrence. In the RUBY Part 1 trial in patients with dMMR or MSI-H disease, less than 10 patients in each treatment group received prior anticancer chemotherapy. Therefore, it is unclear whether dostarlimab plus carboplatin-paclitaxel followed by dostarlimab is most applicable to patients who experience first recurrence after adjuvant chemotherapy.
Concomitant medications were permitted in RUBY Part 1, including G-CSF and systemic glucocorticoids for the management of AEs during the study. While the use of systemic glucocorticoids is aligned with clinical practice in Canada, the clinical experts reported that side effects necessitating G-CSF are more common for highly chemo-sensitive myelosuppressive regimens in solid tumours or germ cell tumours. Nevertheless, the clinical experts consulted by CADTH considered it reasonable for clinicians to continue G-CSF as per their current practice, among those electing this option rather than reducing or delaying study drug dose.
The types of subsequent treatments, including the greater proportion of patients with subsequent treatments in the placebo group were aligned with expectations in clinical practice, according to the clinical experts consulted by CADTH for pembrolizumab (8% versus 31%), hormonal therapy (|| |||||| |||), and radiation therapy (|| |||||| |||) for the dostarlimab versus placebo group, respectively, given the higher rates of progressive disease among these patients. As a result, the assessment of OS is a reflection of treatment with dostarlimab versus placebo (each with carboplatin and paclitaxel) in addition to subsequent treatments. Therefore, survival results might be partially attributable to treatments administered after disease progression rather than the study treatment itself. This is a relevant comparison, however, as it is reflective of how the intervention and comparator would be used in practice.
Key outcomes for clinical decision-making included OS and PFS as highlighted by the clinical experts consulted by CADTH and were included in the RUBY trial. Importantly, the experts emphasized the value of PFS at 12 months to evaluate effects on disease progression that tends to occur early in treatment, and at 24 months to assess sustained treatment effects, with added value for assessing treatment response among patients lacking measurable disease who were enrolled (e.g., patients with stage III endometrial cancer without measurable disease). Data for PFS were only available from an early IA; however, the stopping boundary was met, and the sponsor confirmed that no further PFS analyses are planned. The sponsor provided a published study26 providing level 2 (suggestive) evidence64 for PFS as a surrogate for OS in the setting of first-line therapies for primary advanced or recurrent endometrial cancer. The study included 15 RCTs and showed that a within-arm change in PFS was strongly correlated with a change in OS in the same direction based on data from trials of first-line therapies among patients with primary advanced or recurrent endometrial cancer.26 Level 1 evidence64 (the most ideal) to show that the treatment effect on PFS would correspond to the treatment effect on OS, was not available.
Formal HRQoL evaluations such as the EORTC QLQ-C30 and EORTC QLQ-EN24 were reported by the clinical experts consulted by CADTH to not be routinely undertaken in clinical practice; rather, clinicians may use more practical tools (e.g., ECOG PS) to assess the overall well-being of patients during clinic visits in addition to spontaneous reporting by patients.
GRADE Summary of Findings and Certainty of the Evidence
Methods for Assessing the Certainty of the Evidence
For pivotal studies and RCTs identified in the sponsor’s systematic review, GRADE was used to assess the certainty of the evidence for outcomes considered most relevant to inform CADTH’s expert committee deliberations, and a final certainty rating was determined as outlined by the GRADE Working Group:65,66
High certainty: We are very confident that the true effect lies close to that of the estimate of the effect.
Moderate certainty: We are moderately confident in the effect estimate — The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. We use the word “likely” for evidence of moderate certainty (e.g., “X intervention likely results in Y outcome”).
Low certainty: Our confidence in the effect estimate is limited — The true effect may be substantially different from the estimate of the effect. We use the word “may” for evidence of low certainty (e.g., “X intervention may result in Y outcome”).
Very low certainty: We have very little confidence in the effect estimate — The true effect is likely to be substantially different from the estimate of effect. We describe evidence of very low certainty as “very uncertain.”
Following the GRADE approach, evidence from RCTs started as high-certainty evidence and could be rated down for concerns related to study limitations (which refers to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias.
When possible, certainty was rated in the context of the presence of an important (nontrivial) treatment effect; if this was not possible, certainty was rated in the context of the presence of any treatment effect (i.e., the clinical importance is unclear). In all cases, the target of the certainty of evidence assessment was based on the point estimate and where it was located relative to the threshold for a clinically important effect (when a threshold was available) or to the null. The target of the certainty of evidence assessment was the presence or absence of a clinically important effect for probability of survival (OS, and PFS), and harms (immune-related AEs, and infusion-related reactions) based on a threshold informed by the clinical experts consulted by CADTH for this review. The target of certainty of evidence assessment was the presence or absence of a clinically important effect for HRQoL (EORTC QLQ-C30 Global Health Status) based on a MID threshold identified in the literature.
Results of GRADE Assessments
Table 2 presents the GRADE summary of findings for dostarlimab plus carboplatin-paclitaxel versus placebo plus carboplatin-paclitaxel in adult patients with primary advanced or recurrent dMMR or MSI-H endometrial cancer.
Long-Term Extension Studies
Contents within this section have been informed by materials submitted by the sponsor. The following have been summarized and validated by the CADTH review team.
No long-term extension studies were submitted in the systematic review evidence.
Indirect Comparisons
Contents within this section have been informed by materials submitted by the sponsor. The following have been summarized and validated by the CADTH review team.
No indirect treatment comparisons were submitted in the systematic review evidence.
Studies Addressing Gaps in the Evidence From the Systematic Review
Contents within this section have been informed by materials submitted by the sponsor. The following have been summarized and validated by the CADTH review team.
No additional studies addressing important gaps in the systematic review evidence were identified.
Discussion
Summary of Available Evidence
One phase III, multicentre, double-blind, randomized trial (RUBY Part 1) assessed the efficacy and safety of dostarlimab plus carboplatin-paclitaxel compared with placebo plus carboplatin-paclitaxel. RUBY Part 1 enrolled 118 adult patients (11 patients in Canada) with primary advanced (stage III or IV) or recurrent dMMR or MSI-H endometrial cancer. The primary objectives of RUBY Part 1 were to evaluate investigator-assessed PFS (in the overall population and in the dMMR or MSI-H subpopulation) and OS in the overall population. Secondary objectives included response outcomes, BICR-assessed PFS, HRQoL (EORTC QLQ-C30), and safety.
In RUBY Part 1, most patients were white (|||||) with a median age of || years, with ECOG PS of 0 (|||||), and endometrioid carcinoma (|||||). Nearly half of the enrolled patients had recurrent disease. There was an imbalanced sample size between groups (53 patients versus 65 patients in the dostarlimab plus carboplatin-paclitaxel versus placebo plus carboplatin-paclitaxel group, respectively) due to mis-stratification of MMR or MSI status at randomization. The treatment groups were similar in medical history (histology and grade at diagnosis, FIGO stage at initial diagnosis) and disease status (stage III, stage IV, recurrent disease). Across both study groups, approximately 14% of patients had received prior anticancer therapy and ||||| of patients had received prior anticancer surgical interventions for endometrial cancer. While ||||| of patients had received prior radiotherapy for endometrial cancer across both study groups, fewer patients received external pelvic radiotherapy in the dostarlimab plus carboplatin-paclitaxel group compared with the placebo plus carboplatin-paclitaxel group (15.1% versus 20.0%, respectively).
Interpretation of Results
Efficacy
Patients with endometrial cancer identified a need for new treatments to delay onset of symptoms and prevent disease recurrence, while prolonging life and maintaining QoL, with reduced side effects. Clinicians also identified a need for prolonged survival among patients with primary advanced or recurrent dMMR or MSI-H endometrial cancer. For the dMMR or MSI-H subpopulation, the RUBY Part 1 trial included PFS as a primary end point, OS as an additional analysis, and HRQoL as a secondary end point, which aligned with stakeholder inputs.
The clinical experts consulted by CADTH agreed that a PFS benefit of 10% to 15% would be considered clinically meaningful. Based on this threshold, results of the RUBY trial suggested that, compared with placebo plus cisplatin-paclitaxel, treatment with dostarlimab plus cisplatin-paclitaxel likely results in clinically important improvements in PFS at 12 and 24 months with median PFS not reached versus 7.7 months. The analysis of PFS was statistically significant and met the trial’s predefined stopping boundary. The absolute between-group differences in PFS probability at relevant time points appeared large. However, certainty in the magnitude of the estimated effects was reduced because they were based on an IA with few events, in a trial subset of small sample size (n = 118) from which prognostic balance cannot be assured. As a result, there is a risk that the observed effects may be overestimated. The clinical experts consulted by CADTH noted that patients with primary advanced or recurrent dMMR or MSI-H endometrial cancer represent about 25% of patients with endometrial cancer, explaining the small size of the subgroup.
There is a lack of robust evidence to suggest that PFS can accurately predict and quantify the treatment effect on OS in this drug class. However, the sponsor submitted evidence to suggest that PFS and OS are strongly correlated in the population, independent of the treatment effect. OS was included as a supportive additional analysis (uncontrolled for multiplicity) but is the key clinical outcome of interest. The clinical experts consulted by CADTH suggested that an OS benefit of 5% to 10% would be considered clinically meaningful. Similar to the analysis of PFS, the between-group differences in OS probability at 24 and 30 months appeared large. However, the certainty in this finding was reduced due to small sample size and because the analysis was early, based on a small (40%) information fraction, resulting in a risk of overestimation of benefit. Duration of treatment was shorter among patients treated with placebo (median 32 weeks) compared with dostarlimab (median 77 weeks), and more patients in the former group received subsequent treatments including pembrolizumab, hormonal therapy, and radiation therapy. However, while survival results may be partially attributable to disease progression after administration of subsequent treatments rather than on-study treatments, OS is reflective of how the intervention and comparator would be used in practice. According to the sponsor, the predefined stopping boundary for OS in the overall population was met at IA2. Longer-term data may be useful to inform the durability and magnitude of the observed early OS benefit with dostarlimab.
While HRQoL was not reported to be formally assessed in clinical practice, the clinical experts highlighted the importance of evaluating patients’ symptoms and management of their disease, and tolerance to therapy. Patients identified changes in sexual functioning as undesirable side effects of current treatment (none had experience with dostarlimab). The clinical experts speculated that the observed benefit of reduced disease progression with dostarlimab could potentially translate to positive impacts on HRQoL, noting that dostarlimab as an add-on to chemotherapy would not be expected to have a substantial effect on quality of life in the short term. Evidence from the RUBY trial showed that dostarlimab plus carboplatin-paclitaxel may result in little to no difference in HRQoL at day 1 of cycle 7 compared to placebo plus carboplatin-paclitaxel (low certainty evidence). The between-group difference approached the MID of 10 points, but this finding was affected by imprecision (potential for little to no important difference and clinically important benefit) and risk of bias due to missing outcome data. Due to similar concerns, the effect of dostarlimab on HRQoL at later time points (cycle 13) was inconclusive, as less than 50% and 30% of patients were available to provide assessments in the dostarlimab and placebo groups, respectively (very low certainty evidence). The clinical experts consulted by CADTH noted that genitourinary and psychosexual issues should not be minimized among patients who experience bothersome symptoms (e.g., tingling, numbness, muscular pain, and hair loss) that may arise from their endometrial cancer, surgical treatment, and/or chemotherapy regimen. The EORTC QLQ-EN24 symptoms scale (sexual/vaginal problems) and functioning (sexual interest, activity, and enjoyment) demonstrated results that were consistent with the EORTC QLQ-C30 Global Health Status, but were highly variable (wide SDs) and similarly affected by large losses to follow-up. Over the long-term, the clinical experts speculated that quality of life could be improved for patients based on the initial gains in delaying progression and prolonging survival.
According to the clinical experts consulted by CADTH, platinum doublet chemotherapy with carboplatin and paclitaxel is the current SOC among patients with ovarian cancer with advanced disease (stage III and IV) and recurrent disease without prior chemotherapy, and, therefore, an appropriate comparator in the RUBY Part 1 trial.
Harms
Although none had experience with dostarlimab based on input for the current review, patients expressed reduced side effects as important for evaluating new treatments for endometrial cancer, with willingness to tolerate side effects to achieve extended survival. In the RUBY Part 1 trial, the safety profile of dostarlimab plus carboplatin-paclitaxel showed similar proportions in the patients with TEAEs, SAEs, discontinuations due to AEs, and deaths, except for immune-related AEs, which occurred at higher frequency among patients treated with dostarlimab plus carboplatin-paclitaxel. All patients in the dMMR or MSI-H population experienced TEAEs, most commonly alopecia, fatigue, nausea, anemia, peripheral neuropathy, arthralgia, and diarrhea. Among patients treated with dostarlimab plus carboplatin-paclitaxel who experienced fatal TEAEs, ||| were due to disease progression, ||| was due to myelosuppression, and ||| was due to hypovolemic shock. Among patients treated with placebo plus carboplatin-paclitaxel, ||| fatal TEAEs were due to disease progression and ||| were from unknown cause(s). The product monograph for dostarlimab in combination with carboplatin-paclitaxel highlighted immune-related AEs (including but not limited to immune-mediated pneumonitis, colitis, hepatitis, endocrinopathies, nephritis, and skin adverse reactions) and infusion-related reactions (including hypersensitivity) which occurred in RUBY. Based on evidence of low certainty, more patients who received dostarlimab plus carboplatin-paclitaxel compared with placebo plus carboplatin-paclitaxel, may experience a clinically important degree of increased immune-related AEs (||| |||| |||| ||| ||| || ||| |||||) and little to no difference in the occurrence of infusion-related reactions (||| patients and ||| patients in the dostarlimab plus carboplatin-paclitaxel and placebo plus carboplatin-paclitaxel group, respectively).
Overall, the clinical experts consulted by CADTH felt that the observed AEs in the RUBY trial were reasonably expected with immunotherapy; specifically, nearly all patients were expected to have toxicity with commonly prescribed carboplatin and paclitaxel, including the addition of AEs (e.g., immune-related) from dostarlimab, which are known (based on safety of dostarlimab monotherapy)31 and manageable.
Conclusion
Patients and clinicians identified a need for new treatments for primary advanced or recurrent dMMR or MSI-H endometrial cancer to delay onset of symptoms and prevent disease recurrence, while prolonging life and maintaining quality of life, with reduced side effects. Evidence from a randomized phase III, double-blind trial (RUBY Part 1) in the subpopulation of 118 adult patients with primary advanced or recurrent dMMR or MSI-H endometrial cancer demonstrated that, compared with placebo plus carboplatin-paclitaxel, treatment with dostarlimab plus carboplatin-paclitaxel resulted in statistically significant improvements in PFS. The analysis of PFS met the trial’s predefined stopping boundary. Based on CADTH review team appraisal, dostarlimab plus carboplatin-paclitaxel may result in a clinically important increase in OS at 24 months and 30 months (low certainty) and likely results in a clinically important increase in investigator-assessed PFS at 12 months and 24 months (moderate certainty) when compared with placebo plus carboplatin-paclitaxel. The estimated benefit appeared large, but certainty in its magnitude was reduced due to reliance on a study of small sample size with few events This was especially the case for OS, for which only 40% information fraction had accrued. The stopping boundaries for statistical significance of PFS in the dMMR or MSI-H population and OS in the overall population were crossed at IA 1 and IA 2, respectively; therefore, no further inferential analyses of PFS or OS will be performed for RUBY Part 1. The evidence demonstrated that dostarlimab plus carboplatin-paclitaxel may result in little to no difference in the EORTC QLQ-C30 Global Health Status at day 1 of cycle 7 (low certainty) when compared with placebo plus carboplatin-paclitaxel, but longer-term impact on HRQoL was uncertain. The safety profile with dostarlimab treatment appeared to be as expected, with similarity in the occurrence of AEs and SAEs compared to placebo. The evidence demonstrated that dostarlimab plus carboplatin-paclitaxel may result in a clinically important increase in immune-related AEs and little to no difference in infusion-related reactions (low certainty) when compared with placebo plus carboplatin-paclitaxel.
References
1.Canadian Cancer Society. What is uterine cancer? 2024: https://cancer.ca/en/cancer-information/cancer-types/uterine/what-is-uterine-cancer. Accessed 2024 Jan 02.
2.American Cancer Society. Signs and symptoms of endometrial cancer. https://www.cancer.org/cancer/endometrial-cancer/detection-diagnosis-staging/signs-and-symptoms.html. Accessed September 9, 2020. 2019.
3.Campos S, Cohn D. Initial treatment of metastatic endometrial cancer. UpToDate. Waltham (MA): UpToDate; 2023: http://www.uptodate.com. Accessed 2024 Jan 02.
4.Fleming G, DiSilvestro PA. Adjuvant treatment of high-risk endometrial cancers. UpToDate. Waltham (MA): UpToDate; 2023: http://www.uptodate.com. Accessed 2024 Jan 15.
5.Plaxe S, Mundt A. Overview of resectable endometrial carcinoma UpToDate. Waltham (MA): UpToDate; 2023: http://www.uptodate.com. Accessed 2024 Jan 02.
6.de Boer SM, Powell ME, Mileshkin L, et al. Adjuvant chemoradiotherapy versus radiotherapy alone in women with high-risk endometrial cancer (PORTEC-3): patterns of recurrence and post-hoc survival analysis of a randomised phase 3 trial. Lancet Oncol. 2019;20(9):1273-1285. PubMed
7.Huijgens AN, Mertens HJ. Factors predicting recurrent endometrial cancer. Facts Views Vis Obgyn. 2013;5(3):179-186. PubMed
8.National Comprehensive Cancer Network. Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Uterine Neoplasms. V. 2. 2023: https://www.nccn.org/guidelines/guidelines-detail?category=1&id=1473. Accessed 2023 May.
9.Randall ME, Filiaci VL, Muss H, et al. Randomized phase III trial of whole-abdominal irradiation versus doxorubicin and cisplatin chemotherapy in advanced endometrial carcinoma: a Gynecologic Oncology Group Study. J Clin Oncol. 2006;24(1):36-44. PubMed
10.Coleman. Treatment Patterns and Outcomes Among Patients with Advanced or Recurrent Endometrial Cancer Initiating First-Line Therapy in the United States. Draft manuscript for Value in Health. 2023.
11.Makker V, Green AK, Wenham RM, Mutch D, Davidson B, Miller DS. New therapies for advanced, recurrent, and metastatic endometrial cancers. Gynecologic oncology research and practice. 2017;4:19. PubMed
12.Miller DS, Filiaci VL, Mannel RS, et al. Carboplatin and paclitaxel for advanced endometrial cancer: final overall survival and adverse event analysis of a phase III trial (NRG Oncology/GOG0209). J Clin Oncol. 2020;38(33):3841-3850. PubMed
13.Nomura H, Aoki D, Takahashi F, et al. Randomized phase II study comparing docetaxel plus cisplatin, docetaxel plus carboplatin, and paclitaxel plus carboplatin in patients with advanced or recurrent endometrial carcinoma: a Japanese Gynecologic Oncology Group study (JGOG2041). Ann Oncol. 2011;22(3):636-642. PubMed
14.Rauh-Hain JA, Del Carmen MG. Treatment for advanced and recurrent endometrial carcinoma: combined modalities. Oncologist. 2010;15(8):852-861. PubMed
15.Lorenzi M, Amonkar M, Zhang J, Mehta S, Liaw K-L. Epidemiology of Microsatellite Instability High (MSI-H) and Deficient Mismatch Repair (dMMR) in Solid Tumors: A Structured Literature Review. J Oncol. 2020;2020:1807929.
16.Luna C, Balcacer P, Castillo P, Huang M, Alessandrino F. Endometrial cancer from early to advanced-stage disease: an update for radiologists. Abdom Radiol. 2021;46(11):5325-5336. PubMed
17.Morice P, Leary A, Creutzberg C, Abu-Rustum N, Darai E. Endometrial cancer. Lancet. 2016;387(10023):1094-1108. PubMed
18.Alberta Health Services. Clinical Practice Guidelines GYNE-002 Version 5. 2015: https://www.albertahealthservices.ca/assets/info/hp/cancer/if-hp-cancer-guide-gyne002-endometrial.pdf. Accessed 2023 Jul 17.
19.B.C. Cancer Agency. Endometrium. 2023: http://www.bccancer.bc.ca/health-professionals/clinical-resources/cancer-management-manual/gynecology/endometrium#Management-Endometrium. Accessed 17 July 2023.
20.Brooks RA, Fleming GF, Lastra RR, et al. Current recommendations and recent progress in endometrial cancer. CA Cancer J Clin. 2019;69(4):258-279. PubMed
21.Pectasides D, Xiros N, Papaxoinis G, et al. Carboplatin and paclitaxel in advanced or metastatic endometrial cancer. Gynecol Oncol. 2008;109(2):250-254. PubMed
22.Rose PG, Ali S, Moslemi-Kebria M, Simpkins F. Paclitaxel, Carboplatin, and Bevacizumab in Advanced and Recurrent Endometrial Carcinoma. Int J Gynecol Cancer. 2017;27(3):452-458. PubMed
23.Bassler D, Briel M, Montori VM, et al. Stopping Randomized Trials Early for Benefit and Estimation of Treatment Effects: Systematic Review and Meta-regression Analysis. JAMA. 2010;303(12):1180-1187. PubMed
24.Ciolino JD, Kaizer AM, Bonner LB. Guidance on interim analysis methods in clinical trials. J Clin Transl Sci. 2023;7(1):e124. PubMed
25.Liu S, Garrison SR. Overestimation of benefit when clinical trials stop early: a simulation study. Trials. 2022;23(1):747. PubMed
26.Garside J, Shen Q, Westermayer B, et al. Association Between Intermediate End Points, Progression-Free Survival, and Overall Survival in First-Line Advanced or Recurrent Endometrial Cancer. Clin Ther.
27.Clinical Study Report: 213361. A Phase 3, Randomized, Double-blind, Multicenter Study of Dostarlimab (TSR-042) plus Carboplatin-paclitaxel versus Placebo plus Carboplatin-paclitaxel in Patients with Recurrent or Primary Advanced Endometrial Cancer (RUBY) [internal sponsor's report]. Mississauga (ON): GlaxoSmithKline Inc.; 2023 Mar 07.
28.American Cancer Society. Endometrial Cancer Stages. 2019: https://www.cancer.org/cancer/types/endometrial-cancer/detection-diagnosis-staging/staging.html. Accessed 2024 Jan 02.
29.Canadian Cancer Society. Stages of uterine cancer. 2024: https://cancer.ca/en/cancer-information/cancer-types/uterine/staging. Accessed 2024 Jan 02.
30.National Cancer Institute. Cancer Stat Facts: Uterine Cancer. 2022; https://seer.cancer.gov/statfacts/html/corp.html. Accessed 2023 Feb.
31.Oaknin A, Gilbert L, Tinker AV, et al. Safety and antitumor activity of dostarlimab in patients with advanced or recurrent DNA mismatch repair deficient/microsatellite instability-high (dMMR/MSI-H) or proficient/stable (MMRp/MSS) endometrial cancer: interim results from GARNET-a phase I, single-arm study. J Immunother Cancer. 2022;10(1). PubMed
32.Global Cancer Observatory. Cancer factsheet (GLOBOCAN 2020): Corpus uteri. . 2020; https://gco.iarc.fr/today/data/factsheets/cancers/24-Corpus-uteri-fact-sheet.pdf. Accessed 2021 Jun 1.
33.Global Cancer Observatory. Cancer today online analysis (GLOBOCAN 2020): Estimated age-standardized incidence rates (World) in 2020, World, High income, females, all ages. 2020; https://gco.iarc.fr/today/online-analysis-multi-bars?v=2020&mode=cancer&mode_population=countries&population=900&populations=900_986&key=asr&sex=2&cancer=39&type=0&statistic=5&prevalence=0&population_group=0&ages_group%5B%5D=0&ages_group%5B%5D=17&nb_items=10&group_cancer=1&include_nmsc=0&include_nmsc_other=1&type_multiple=%257B%2522inc%2522%253Atrue%252C%2522mort%2522%253Afalse%252C%2522prev%2522%253Afalse%257D&orientation=horizontal&type_sort=0&type_nb_items=%257B%2522top%2522%253Atrue%252C%2522bottom%2522%253Afalse%257D#collapse-group-1-0-4. Accessed 2022 May 23.
34.American Cancer Society. Key Statistics for Endometrial Cancer 2019. 2019; https://www.cancer.org/cancer/endometrial-cancer/about/key-statistics.html#:~:text=Endometrial%20cancer%20affects%20mainly%20post,under%20the%20age%20of%2045 Accessed 2022 Oct 11.
35.Connor EV, Rose PG. Management Strategies for Recurrent Endometrial Cancer. Expert Rev Anticancer Ther. 2018;18(9):873-885. PubMed
36.Jemperli (Dostarlimab) In the Treatment of Primary Advanced or Recurrent Endometrial Cancer [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Jemperli (dostarlimab), 50mg/mL intravenous infusion. Mississauga (ON): GlaxoSmithKline Inc.; 2023.
37.Concin N, Matias-Guiu X, Vergote I, et al. ESGO/ESTRO/ESP guidelines for the management of patients with endometrial carcinoma. Int J Gynecol Cancer. 2021;31(1):12-39. PubMed
38.Rütten H, Verhoef C, van Weelden WJ, et al. Recurrent Endometrial Cancer: Local and Systemic Treatment Options. Cancers (Basel). 2021;13(24). PubMed
39.Fountzilas E, Kotoula V, Pentheroudakis G, et al. Prognostic implications of mismatch repair deficiency in patients with nonmetastatic colorectal and endometrial cancer. ESMO open. 2019;4(2):e000474. PubMed
40.Maurer W, Bretz F. Memory and other properties of multiple test procedures generated by entangled graphs. Stat Med. 2013;32(10):1739-1753. PubMed
41.Bae-Jump VL, Sill M, Gehrig PA, et al. A randomized phase II/III study of paclitaxel/carboplatin/metformin versus paclitaxel/carboplatin/placebo as initial therapy for measurable stage III or IVA, stage IVB, or recurrent endometrial cancer: An NRG Oncology/GOG study. Gynecol Oncol. 2020;159:7.
42.Miller D, Filiaci V, Fleming G, et al. Late breaking abstract 1: Randomized phase III noninferiority trial of first line chemotherapy for metastatic or recurrent endometrial carcinoma: A Gynecologic Oncology Group study. Gynecol Oncol. 2012;125(3):771-773.
43.Lorenzi M, Amonkar M, Zhang J, Mehta S, Kl L. Epidemiology of microsatellite instability high (MSI-H) and deficient mismatch repair (dMMR) in solid tumors: a structured literature review. J Oncol. 2020;10.1155/2020/1807929.
44.Product Monograph Including Patient Medication Information: Jemperli. 2023. https://pdf.hres.ca/dpd_pm/00069388.PDF. Accessed August 23, 2023.
45.Gsk. Data on File: A retrospective cohort study of outcomes in advanced endometrial cancer [sponsor supplied reference]. 2023.
46.Jemperli (dostralimab): 50mg/mL intravenous infusion [product monograph]. Mississauga (ON): GlaxoSmithKline Inc.; 2023 Nov 16.
47.PrCARBOplatin Injection BP. Solution for injection, 10mg of carbopltin / mL intravenous injection [product monograph]. Kirkland (QC): Accord Healthcare Inc.; 2022 Dec 19: https://pdf.hres.ca/dpd_pm/00068833.PDF.
48.Taxol (paclitaxel): 6mg/mL injection [product monograph]. Montreal (QC): Bristol-Myers Squibb Canada; 2010 https://pdf.hres.ca/dpd_pm/00009873.PDF.
49.Alberta Health Services. Clinical Practice Guideline Gyne-002 Version 5. 2015. 2015; https://www.albertahealthservices.ca/assets/info/hp/cancer/if-hp-cancer-guide-gyne002-endometrial.pdf.
50.Smith TJ, Khatcheressian J, Lyman GH, et al. 2006 update of recommendations for the use of white blood cell growth factors: an evidence-based clinical practice guideline. J Clin Oncol. 2006;24(19):3187-3205. PubMed
51.Eisenhauer EA, Therasse P, Bogaerts J, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer. 2009;45(2):228-247. PubMed
52.Aaronson NK, Ahmedzai S, Bergman B, et al. The European Organization for Research and Treatment of Cancer QLQ-C30: a quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst. 1993;85(5):365-376. PubMed
53.Proskorovsky I, Lewis P, Williams CD, et al. Mapping EORTC QLQ-C30 and QLQ-MY20 to EQ-5D in patients with multiple myeloma. Health Qual Life Outcomes. 2014;12:35. PubMed
54.de Vet HC, Terwee CB, Knol DL, Bouter LM. When to use agreement versus reliability measures. J Clin Epidemiol. 2006;59(10):1033-1039. PubMed
55.Osoba D, Rodrigues G, Myles J, Zee B, Pater J. Interpreting the significance of changes in health-related quality-of-life scores. J Clin Oncol. 1998;16(1):139-144. PubMed
56.Lan KKG, DeMets DL. Discrete Sequential Boundaries for Clinical Trials. Biometrika. 1983;70(3):659-663.
57.Pharmacoeconomic report: Jemperli (Dostarlimab) In the Treatment of Primary Advanced or Recurrent Endometrial Cancer [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Jemperli (dostarlimab), 50mg/mL intravenous infusion. Mississauga (ON): GlaxoSmithKline Inc.; 2023. Mississauga (ON): GlaxoSmithKline Inc.; 2023.
58.GlaxoSmithKline response to additional information regarding Jemperli (dostarlimab) CADTH review [internal sponsor's report]. Mississauga (ON): GlaxoSmithKline Inc.; 2024 Jan 12.
59.Bjordal K, de Graeff A, Fayers PM, et al. A 12 country field study of the EORTC QLQ-C30 (version 3.0) and the head and neck cancer specific module (EORTC QLQ-H&N35) in head and neck patients. EORTC Quality of Life Group. Eur J Cancer. 2000;36(14):1796-1807. PubMed
60.Gundy CM, Aaronson NK. Effects of mode of administration (MOA) on the measurement properties of the EORTC QLQ-C30: a randomized study. Health Qual Life Outcomes. 2010;8:35. PubMed
61.Gallardo-Rincón D, Toledo-Leyva A, Bahena-González A, et al. Validation of the QLQ-EN24 instrument for the assessment of health-related quality of life for women with endometrial cancer in México. Arch Gynecol Obstet. 2021;304(3):773-782. PubMed
62.Greimel E, Nordin A, Lanceley A, et al. Psychometric validation of the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire-Endometrial Cancer Module (EORTC QLQ-EN24). Eur J Cancer. 2011;47(2):183-190. PubMed
63.Stukan M, Zalewski K, Mardas M, et al. Independent psychometric validation of European Organization for Research and Treatment of Cancer Quality of Life Questionnaire-Endometrial Cancer Module (EORTC QLQ-EN24). Eur J Cancer Care (Engl). 2018;27(1). PubMed
64.European Network for Health Technology Assessment. EUnetHTA 21 - Individual Practical Guideline Document D4.4 - Outcomes (Endpoints). EUnetHTA; 2023 Jan 25: https://www.eunethta.eu/wp-content/uploads/2023/01/EUnetHTA-21-D4.4-practical-guideline-on-Endpoints-v1.0.pdf. Accessed 2024 Jan 24.
65.Balshem H, Helfand M, Schünemann HJ, et al. GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol. 2011;64(4):401-406. PubMed
66.Santesso N, Glenton C, Dahm P, et al. GRADE guidelines 26: informative statements to communicate the findings of systematic reviews of interventions. J Clin Epidemiol. 2020;119:126-135. PubMed
Appendix 1: Additional Information
Note that this appendix has not been copy-edited.
Figure 7: Censoring Rules for Primary and Sensitivity Analyses of PFS, Part A
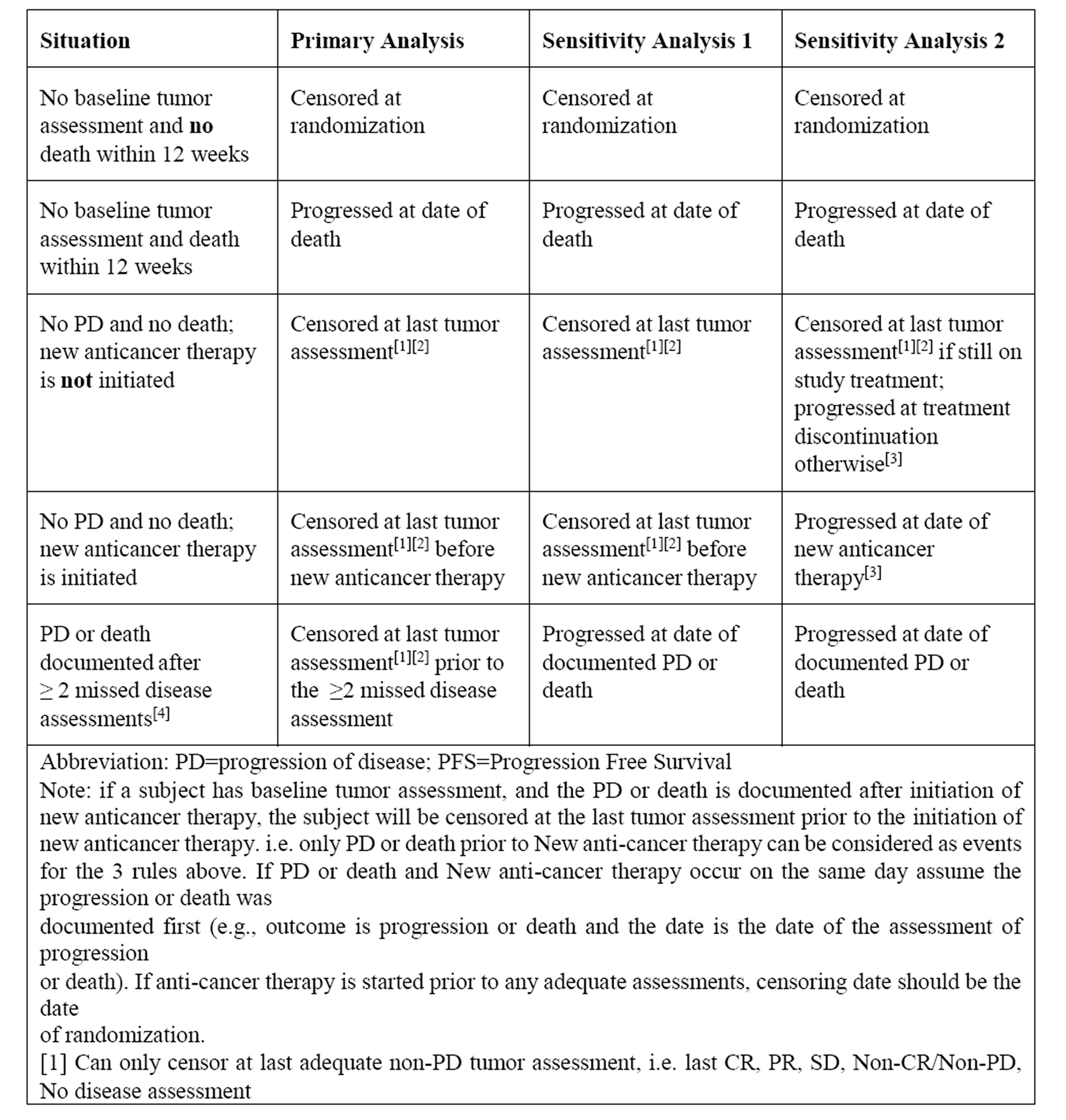
Source: RUBY Statistical Analysis Plan.
Figure 8: Censoring Rules for Primary and Sensitivity Analyses of PFS, Part B
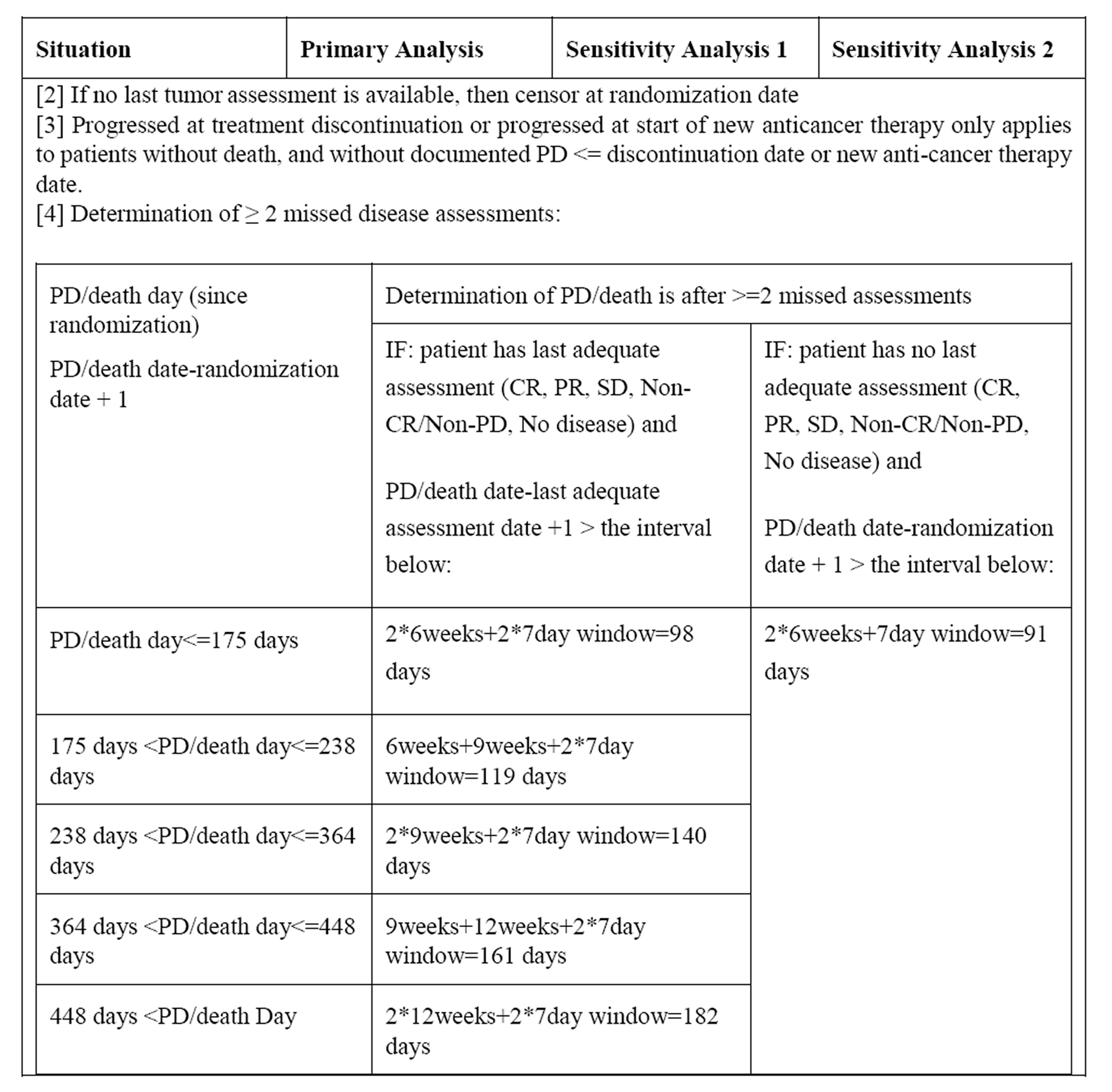
Source: RUBY Statistical Analysis Plan.
Table 17: Summary of Additional Efficacy Results From RUBY Part 1, dMMR or MSI-H Subpopulation — ITT Analysis Set
Outcome measure | Dostarlimab + CAR-PAC N = 53 | Placebo + CAR-PAC N = 65 |
|---|---|---|
Data cut-off date | September 28, 2022 | |
Median follow-upa duration, months (range) | ||||| |||||| || |||||| | ||||| |||||| || |||||| |
Overall survivalb | ||
Number of patients contributing to the analysis, n (%) | 53 | 65 |
OS events, n (%) | 7 (13.2) | 24 (36.9) |
Censored, n (%) | 46 (86.8) | 41 (63.1) |
Median OS, months (95% CI)c | Not reached | Not reached |
K-M estimates of OS probability, % (95% CI) | ||
Month 12 | 90.1 ||||| || ||||| | 79.6 ||||| || ||||| |
Month 18 | |||| ||||| || ||||| | |||| ||||| || ||||| |
Month 24 | 83.3 (66.8 to 92.0) | 58.7 (43.4 to 71.2) |
Month 24, absolute difference (95% CI)d | |||| |||||| || ||||| | Reference |
Month 30 | |||| ||||| || ||||| | |||| ||||| || ||||| |
Month 30, absolute difference (95% CI)d | |||| |||||| || ||||| | Reference |
HR (95% CI)e | 0.30 (0.127 to 0.699) | Reference |
P valuef | 0.0016g | Reference |
Progression-free survival (BICR assessed) | ||
Number of patients contributing to the analysis, n (%) | 53 | 65 |
PFS events, n (%) | ||| (30.2) | || (56.9) |
Disease progression, n (%) | || |||||| | || |||||| |
Death, n (%) | | ||||| | | ||||| |
Censored, n (%) | || |||||| | || |||||| |
Median PFS, months (95% CI)c | Not reached (not reached) | 9.5 (7.0 to 11.7) |
K-M estimates of PFS, % (95% CI) | ||
Month 6 | |||| ||||| || ||||| | |||| ||||| || ||||| |
Month 12 | 70.8 ||||| || ||||| | 36.2 ||||| || ||||| |
Month 12, absolute difference (95% CI)d | |||||||||| || ||||| | Reference |
Month 18 | |||| ||||| || ||||| | |||| ||||| || ||||| |
Month 24 | 66.3 ||||| || ||||| | 26.0 ||||| || ||||| |
Month 24, absolute difference (95% CI)d | |||||||||| || ||||| | Reference |
HR (95% CI)e | 0.29 (0.158 to 0.543) | Reference |
P valuef | < 0.0001g | Reference |
Disease control rate (BICR assessed) | ||
Number of patients contributing to the analysis, n (%) | 53 | 65 |
Best overall response, n (%) | ||
Complete response | || |||||| | | |||||| |
Partial response | || |||||| | || |||||| |
Stable disease | | ||||| | || |||||| |
Non-CR/non-PD | | ||||| | | ||||| |
No disease | | ||||| | | ||||| |
Progressive disease | | ||||| | | ||||| |
Not evaluable | | ||||| | | ||||| |
DCR, n (%) | || |||||| | || |||||| |
95% CIg | |||| || |||| | |||| || |||| |
Objective response rate (BICR assessed) | ||
Number of patients contributing to the analysis, n (%)h | 48 | 60 |
Best overall response, n (%) | ||
Complete response | 11 (22.9) | 8 (13.3) |
Partial response | 26 (54.2) | 30 (50.0) |
Stable disease | | ||||| | || |||||| |
Non-CR/non-PD | | ||||| | | ||||| |
Progressive disease | | ||||| | | ||||| |
Not evaluable | | ||||| | | ||||| |
ORR, n (%)i | 37 (77.1) | 38 (63.3) |
95% CIg | 62.7 to 88.0 | 49.9 to 75.4 |
Duration of response (BICR assessed) | ||
Number of patients contributing to the analysis, n (%) | 37 | 38 |
Duration of response, events, n (%) | ||
Disease progression | || |||||| | || |||||| |
Death | | ||||| | ||| |
Censored, n (%) | || |||||| | || |||||| |
KM estimates of DoR probability, % (95% CI) | ||
Month 6 | |||| ||||| || ||||| | |||| ||||| || ||||| |
Month 12 | |||| ||||| || ||||| | |||| ||||| || ||||| |
Month 18 | |||| ||||| || ||||| | |||| |||| || ||||| |
Month 24 | |||| ||||| || ||||| | |||| |||| || ||||| |
BICR = blinded independent committee review; CAR-PAC = carboplatin-paclitaxel; CI = confidence interval; CR = complete response; DCR = disease control rate; DoR = duration of response; ITT = intention to treat; K-M = Kaplan-Meier; ORR = objective response rate; OS = overall survival; PD = progressive disease.
aDuration of follow-up was defined as the time from randomization to cut-off date.
bOS in the dMMR or MSI-H population was not a primary end point in RUBY and therefore not adjusted for multiplicity. OS was a dual primary end point for patients with primary advanced or recurrent endometrial cancer (overall population), and a prespecified sensitivity analysis for OS was conducted in the dMMR or MSI-H subpopulation.
c95% CI generated using the method of Brookmeyer and Crowley (1982).
dRisk difference (95%CI) was not included in the sponsor’s planned analyses; data for absolute risk difference was requested by the CADTH review team for interpretation purposes.
eBased on Stratified Cox regression model.
f1-sided P value based on Stratified log-rank test.
gExact 2-sided 95% CI for the binomial proportion.
hNumber of patients with target lesion or nontarget lesion at baseline.
iDenominator is number of patients with target lesion at baseline.
Source: RUBY Clinical Study Report.27 Details included in the table are from the sponsor’s Summary of Clinical Evidence.36
PFS (BICR Assessed)
PFS by BICR assessment per RECIST v.1.1 was analyzed as a sensitivity analysis for the primary analysis of PFS per investigator assessment (refer to Table 17).
DCR
DCR, based on BICR assessment, was defined as the proportion of patients who achieved a best overall response of complete response, partial response, or stable disease per RECIST v.1.1. Assessments were as described for PFS. Proportions (number and percentage) of patients with best overall response of complete response, partial response, stable disease, noncomplete response or nonprogressive disease, or no disease according to RECIST v.1.1 were summarized for the treatment groups with exact 95% CIs. Analysis of DCR based on BICR assessment was performed for the dMMR or MSI-H subpopulation (refer to Table 17), and separately for the following cohorts within the dMMR or MSI-H subpopulation: a) patients with target lesion or nontarget lesion at baseline, and b) patients with target lesion at baseline.
ORR
ORR, based on BICR assessment, was defined as the time from first documentation of complete response or partial response per RECIST v.1.1. Assessments were as described for PFS. Proportions (number and percentage) of patients with ORR were presented by treatment group with exact 95% CIs. Analysis of ORR based on BICR assessment was performed separately for 2 cohorts within the dMMR or MSI-H subpopulation: a) patients with target lesion or nontarget lesion at baseline, and b) patients with target lesion at baseline (refer to Table 17).
Table 18: Summary of EORTC QLQ-EN24 Results in RUBY Part 1, dMMR or MSI-H Subpopulation – ITT Analysis Set
Outcome measure | Dostarlimab + CAR-PAC N = 53 | Placebo + CAR-PAC N = 65 |
|---|---|---|
Data cut-off date | September 28, 2022 | |
Median follow-upa duration, months (range) | ||||| |||||| || |||||| | ||||| |||||| || |||||| |
EORTC QLQ-EN24 | ||
Sexual interest score | ||
Baseline | ||
Number of patients contributing to the analysis, n | || | || |
Mean (SD) | ||| ||||||| | |||| ||||||| |
Change from baseline at cycle 7 day 1 | ||
Number of patients contributing to the analysis, n | 36 | 44 |
Mean (SD) | | ||||||| | |||| ||||||| |
Change from baseline at cycle 13 day 1 | ||
Number of patients contributing to the analysis, n | ||| | ||| |
Mean (SD) | ||| ||||||| | |||| ||||||| |
Sexual activity score | ||
Baseline | ||
Number of patients contributing to the analysis, n | ||| | ||| |
Mean (SD) | ||| ||||||| | ||| |||||| |
Change from baseline at cycle 7 day 1 | ||
Number of patients contributing to the analysis, n | 35 | 42 |
Mean (SD) | ||| ||||||| | ||| ||||||| |
Change from baseline at cycle 13 day 1 | ||
Number of patients contributing to the analysis, n | ||| | ||| |
Mean (SD) | ||| ||||||| | | ||| |
Sexual enjoyment score | ||
Baseline | ||
Number of patients contributing to the analysis, n | ||| | ||| |
Mean (SD) | |||| ||||||| | |||| ||||||| |
Change from baseline at cycle 7 day 1 | ||
Number of patients contributing to the analysis, n | ||| | ||| |
Mean (SD) | ||||| ||||||| | |||| ||||||| |
Change from baseline at cycle 13 day 1 | ||
Number of patients contributing to the analysis, n | ||| | ||| |
Mean (SD) | ||||| ||||||| | |||| |||| |
Sexual/vaginal problems score | ||
Baseline | ||
Number of patients contributing to the analysis, n | ||| | ||| |
Mean (SD) | |||| ||||||| | |||| ||||||| |
Change from baseline at cycle 7 day 1 | ||
Number of patients contributing to the analysis, n | ||| | ||| |
Mean (SD) | ||| ||||||| | |||| ||||||| |
Change from baseline at cycle 13 day 1 | ||
Number of patients contributing to the analysis, n | ||| | ||| |
Mean (SD) | | ||||||| | ||||| |||| |
CAR-PAC = carboplatin-paclitaxel; EORTC QLQ-EN24 = European Organization for Research and Treatment of Cancer Quality of Life Questionnaire Endometrial cancer module; NA = not assessed; SD = standard deviation.
aDuration of follow-up was defined as the time from randomization to cut-off date.
Source: RUBY Clinical Study Report.27
EORTC QLQ-EN24
The EORTC QLQ-EN24 is an endometrial cancer–specific module which supplements the EORTC QLQ-C30, and therefore should always be employed in conjunction with the EORTC QLQ-C30 (rather than on its own). It includes 5 symptom scales/items (lymphoedema, urological symptoms, gastrointestinal symptoms, poor body image, and sexual/vaginal problems), 5 individual symptom items (pain in back and pelvis, tingling/numbness, muscular pain, hair loss, and taste change), and 3 functional scales (sexual interest, sexual activity, and sexual enjoyment) which was reported by visit for each dose level or cohort, as appropriate. The scoring approach for the EORTC QLQ-EN24 is identical to the symptoms scales/single items of the EORTC QLQ-C30, with all items being scored 1 to 4 with a range of 3, whereby all scales and single-item measures range in score from 0 to 100 (a high score for functional items represents a high level of functioning, whereas a high score for the symptom scales and single items represent a high level of symptomatology or problems. An evaluation of the psychometric properties of the EORTC QLQ-EN24 module demonstrated it to be a reliable and valid instrument for evaluating the quality of life in endometrial cancer clinical trials and differentiating between clinical groups.62 A change of 10 points in the EORTC QLQ-EN24 scale score is considered conventionally as a MID.54,55 No literature was identified that estimated MIDs specifically in patients with endometrial cancer. EORTC QLQ-EN24 assessments were done at each study visit and follow-up assessment, and were to be collected before any procedure or intervention scheduled that day.
Pharmacoeconomic Review
Abbreviations
AE
adverse events
BSA
body surface area
dMMR
deficient mismatch repair
ICER
incremental cost-effectiveness ratio
LY
life-year
MSI-H
microsatellite instability-high
OS
overall survival
PD
progressed disease
PFD
progression-free disease
PFS
progression-free survival
PSM
partitioned survival model
QALY
quality-adjusted life-year
TTD
time to treatment discontinuation
WTP
willingness to pay
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Dostarlimab (Jemperli), solution for infusion |
Submitted price | Dostarlimab, 50 mg/mL, solution for infusion: $10,031.08 per 10 mL vial |
Indication | In combination with carboplatin and paclitaxel for the treatment of adult patients with primary advanced or recurrent mismatch repair deficient/microsatellite instability-high endometrial cancer who are candidates for systemic therapy. |
Health Canada approval status | NOC |
Health Canada review pathway | Priority review |
NOC date | November 15, 2023 |
Reimbursement request | As per indication |
Sponsor | GlaxoSmithKline Inc. |
Submission history | Previously reviewed: Yes Indication: monotherapy for the treatment of adult patients with mismatch repair deficient or microsatellite instability-high recurrent or advanced endometrial cancer that has progressed on or following prior treatment with a platinum containing regimen. Recommendation date: August 24, 2022 Recommendation: Do not reimburse |
NOC = Notice of Compliance.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-Utility Analysis PSM |
Target population | Adult patients with primary advanced (stage III or stage IV) or recurrent dMMR or MSI-H endometrial cancer |
Treatment | Dostarlimab plus carboplatin-paclitaxel |
Comparator | Carboplatin-paclitaxel |
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs, LYs |
Time horizon | Lifetime (approximately 37 years) |
Key data source | RUBY Part 1 trial |
Submitted results | ICER = $46,383 per QALY gained (incremental Costs = $275,343; incremental QALYs = 5.94) |
Key limitations |
|
CADTH reanalysis results |
|
ICER = incremental cost-effectiveness ratio; LY = life-year; OS = overall survival; PFS = progression-free survival; PSM = partitioned survival model; QALY = quality-adjusted life-year; dMMR = deficient mismatch repair; MSI-H = microsatellite instability-high.
Conclusions
The CADTH clinical review found that treatment with dostarlimab plus carboplatin-paclitaxel produces a clinically meaningful benefit in terms of overall survival (OS) and progression-free survival (PFS) relative to placebo plus carboplatin-paclitaxel. However, there was uncertainty in the magnitude of the estimated benefit due to the reliance on an interim analysis in a small sample size with few events. Both PFS and OS were key parameters in the economic evaluation, which affected estimates of state membership, and by extension the expected costs and QALYs for each arm of the decision model.
CADTH identified additional limitations within the submitted economic evaluation, including: unrealistic predictions of long-term survival (PFS and OS), and the improper characterization of uncertainty.
In the CADTH base case, dostarlimab plus carboplatin-paclitaxel was more costly (incremental costs: $285,186) and more effective (incremental QALYs: 5.453) than carboplatin-paclitaxel alone. The ICER for dostarlimab plus carboplatin-paclitaxel relative to carboplatin-paclitaxel was estimated to be $52,296 per QALY gained. A 4.3% price reduction would be required for dostarlimab plus carboplatin-paclitaxel to be considered cost-effective at a $50,000 per QALY threshold. The CADTH results were similar to those of the sponsor’s base case. The vast majority of incremental survival from the model was estimated through extrapolation beyond the period of the observed evidence. Because of the uncertainty around long-term OS and PFS, a greater price reduction may be warranted.
Stakeholder Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, registered clinicians, and drug plans that participated in the CADTH review process.
Patient input for this review was obtained from the Canadian Cancer Survivor Network. Information was collected from patients in Canada using an online survey between October 26, 2023, and November 8, 2023. Respondents to the survey reported experience with current treatment options including radiation, surgical therapy, targeted therapy, hormonal therapy, immunotherapy, and chemotherapy. Patients expressed a desire for treatments that improved survival or quality of life, even if that meant a higher risk of side effects. None of the respondents to the survey reported experience with the drug under review.
Registered clinician input was received from 3 groups: The Ontario Health Gynecology Cancer Drug Advisory Committee, the Canadian Clinician Group coordinated by the Canadian Cancer Society, and the Society of Gynecologic Oncology of Canada. Consensus among all submissions were treatment goals that included prolonged life, delayed disease progression, a reduction in symptom severity, and improved quality of life. The current standard of care is chemotherapy for primary advanced endometrial cancer or recurrent patients with a disease-free interval greater than 6 months. Some recurrent patients may receive pembrolizumab after progression on platinum-based chemotherapy. Each submission expected that the drug under review would be added to standard of care chemotherapy as first-line treatment with the expectation that this will lead to a meaningful reduction in recurrence or death.
Drug plan input sought clarification on the dosing strategy, patient eligibility for re-treatment, and dostarlimab’s place in therapy. Concerns were raised about the need for earlier biomarker testing, which is not required for first-line therapy. In addition, drug plans anticipated higher treatment acquisition costs compared to currently available treatment options.
Several of these concerns were addressed in the sponsor’s model:
The relative cost-effectiveness dostarlimab plus carboplatin-paclitaxel was estimated against the current standard of care (carboplatin-paclitaxel).
CADTH was unable to address the following concerns raised from stakeholder input:
The impact of conducting biomarker testing before inform eligibility for first-line treatment options.
Economic Review
The current review is for dostarlimab (Jemperli) for adult patients with primary advanced (stage III or stage IV) or recurrent deficient mismatch repair (dMMR) or microsatellite instability-high (MSI-H) endometrial cancer.
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted an economic evaluation of dostarlimab plus carboplatin-paclitaxel compared to carboplatin-paclitaxel for the treatment of adult patients with primary advanced (stage III or stage IV) or recurrent dMMR or MSI-H endometrial cancer.1 This target population was aligned with the proposed Health Canada indication and the reimbursement request.
Dostarlimab is available as a solution for infusion, at a concentration of 50 mg/mL and a cost of $10,031 per 10 mL vial. The recommended dose for dostarlimab is 500 mg every 3 weeks in combination with carboplatin-paclitaxel for 6 cycles, followed by 1,000 mg of dostarlimab monotherapy every 6 weeks. At the submitted price, dostarlimab will cost $10,031 every 21-days. Discontinuation criteria include disease progression, unacceptable toxicity, or a maximum treatment duration of 3 years.
The regimen carboplatin-paclitaxel is composed of 2 separate treatments. Carboplatin is available as a solution for infusion at a concentration of 10 mg/mL in vial sizes of 5 mL ($70), 15 mL ($210), 45 mL ($600), or 60 mL ($775). As per the Cancer Care Ontario regimen monograph, carboplatin should be administrated at an area under the concentration curve of 4 to 6 mg per mL per minute.2 Calculation of the recommended dose should incorporate the direct relationship between glomerular filtration rate and carboplatin clearance.2 A patient aged |||| years with a body surface area (BSA) of ||||| m2 would receive a calculated dose of |||||| mg when administered with an area under the concentration curve of 5 mg per mL per minute.1 Paclitaxel is available as a solution for infusion at a concentration of 6 mg/mL in vial sizes of 5 mL ($300) or 50 mL ($3,740). At a recommended dose of 175 mg/m2 for paclitaxel, a patient with a BSA of ||||| m2 would receive a calculated dose of |||||| mg.1,2 The 21-day cycle cost of the carboplatin-paclitaxel regimen with and without concomitant dostarlimab would be $14,231 (dostarlimab plus carboplatin-paclitaxel) and $4,200 (carboplatin-paclitaxel), respectively. Carboplatin-paclitaxel was the only comparator included in the analysis, based on a deviation request submitted by the sponsor and accepted by CADTH.
Modelled outcomes included life-years (LYs) and quality-adjusted life-years (QALYs). Costs were estimated from the perspective of the Canadian public health care payer. Model outputs were generated over a lifetime horizon of approximately 37 years, with a cycle length of 1 week (7 days). Costs and outcomes were discounted at 1.5%.1
Model Structure
The costs and effects for each alternative were estimated using a partitioned survival model (PSM).1 This model structure tracked patients across 3 mutually exclusive health states: progression-free disease (PFD), progressed disease (PD), and death. State membership was estimated using an “area under the curve” approach from 2 independent survival curves (PFS; OS). A third survival curve, time to treatment discontinuation (TTD), was used to determine the proportion of patients in the PFD state no longer on treatment. This allowed the model to incorporate the possibility of treatment withdrawal before progression.1
Model Inputs
Costs and effects were estimated using a homogeneous baseline population. All data summarizing baseline characteristics of the cohort were obtained from the RUBY Part 1 trial.3,4 This was a randomized phase III trial that involved the direct comparison of dostarlimab added to carboplatin-paclitaxel compared with placebo plus carboplatin-paclitaxel.3,4 Baseline characteristics of interest included age (mean = |||| years), sex (100% Female), BSA (mean = ||||| m2), and weight (mean = ||||| kg).1,3,4
The model relied on time-to-event data from the RUBY Part 1 trial to estimate the treatment-specific survival functions needed to estimate state membership.1 Parametric and flexible spline models were fit for 3 events: progression (PFS), death (OS), and treatment discontinuation (TTD). The sponsor fitted treatment-independent and treatment-dependent models using the exponential, log-logistic, log-normal, Weibull, Gompertz, gamma, and generalized gamma distributions.1 In addition, the sponsor fit time-to-progression data using flexible spline models using the hazards, normal, and spline distributions up to 3 knots.1 Selection of the base case configuration was informed by visual inspection of the available Kaplan-Mier curve, assessment of model fit statistics, inspection of log-cumulative hazard plots, and clinical plausibility. This resulted in the base case assumption that OS and TTD would follow the treatment-independent log-logistic and Weibull distributions. To obtain the OS curve for dostarlimab plus carboplatin-paclitaxel, the unstratified hazard ratio (0.32) was applied to the carboplatin-paclitaxel specific OS values. For PFS, it was assumed both arms would follow independently fitted 1-knot flexible spline models using the odds distribution.1
To ensure that the risk of death in the cohort would not fall below that expected for the general population, the predicted values for the OS curve were capped by the general population mortality risk. This was achieved using age and female-specific mortality risks estimated from Canadian Life Tables published by Statistics Canada.1,5 Similarly, the sponsor assumed that the predicted values for PFS and TTD could not exceed the predicted OS value at each time point in the model time horizon.1 For TTD, it was assumed that 100% of patients would discontinue treatment after 156 weeks (dostarlimab maintenance therapy) or 18 weeks (carboplatin-paclitaxel).1
In addition to tracking the proportion of the cohort in each health state, the model also tracked the occurrence of adverse events (AE). The specific AEs included in the model were: anemia, neutropenia, hypertension, hypokalemia, pulmonary embolism, and a decrease in lymphocyte count, neutrophil count, or white blood cell count. The treatment-specific risk of each AE was obtained from the RUBY Part 1 trial. It was assumed patients were only at risk of an AE in the first cycle on treatment.
Health-related quality of life was reflected by the combination of health state utilities and AE-specific disutilities. The health state utility values were obtained from the indirect measurement of patient preferences in the RUBY Part 1 trial using the EQ-5D questionnaire. Mean health state utilities of |||| (PF State, 95% CI: |||||||||) and |||| (PD State, 95% CI: |||||||||) were obtained by applying tariffs that corresponded to the preferences of the population in Canada.1,6 In the base case, the sponsor adjusted the EQ-5D health state utilities by age and sex. This involved multiplying the EQ-5D health state utilities by age- and sex-specific decrements estimated from general population utilities obtained from the Health Utilities Index Mark 3 (HUI3). Values for AE-specific disutilities were sourced from prior technology appraisals and published literature.1,7-12
The submission considered the costs associated with the acquisition, administration, and monitoring of first-line therapy, as well as those associated with the management of AEs, subsequent therapy, and end-of-life care. Treatment acquisition costs were calculated from the price per-units consumed based on the recommended dosage for each alternative considered in the model. The price of dostarlimab represented the sponsor’s submitted price, while all other drug prices were obtained from the IQVIA DeltaPA database. Eligible second-line treatments included: carboplatin-paclitaxel, paclitaxel, doxorubicin, gemcitabine, pembrolizumab, letrozole, and radiotherapy. Acquisition costs for these treatments were weighted by the percent of patients that initiated each therapy following first-line discontinuation in the RUBY Part 1 trial.1 Treatment administration costs were applied for any treatment that required IV administration, and included infusion, chair time, the per-visit physician billing fee, as well as pharmacy and nursing workload. Treatment monitoring costs reflected resource utilization associated with indication-specific disease pathway management procedures published by Cancer Care Ontario.1,13 Costs associated with outpatient consultation, imaging, laboratory testing, and physician or nurse visits were obtained from the Ontario Schedule of Benefits for Physician or Laboratory Services.1,14,15
Summary of Sponsor’s Economic Evaluation Results
The costs and QALYs of each alternative were generated using a Monte Carlo simulation of 1,000 iterations. Results from the probabilistic base case were aligned with those generated deterministically and are summarized in the following.
Base Case Results
The submitted analysis was based on the publicly available prices of the comparator treatments. Results from the base case of the submitted economic evaluation are presented in Table 3. The incremental costs and QALYs for dostarlimab plus carboplatin-paclitaxel relative to carboplatin-paclitaxel monotherapy were $275,343 and 5.94, respectively. 93% of incremental LY were generated through extrapolation beyond the observed period of the RUBY trial. This corresponded to an ICER of $46,383 for dostarlimab plus carboplatin-paclitaxel relative to carboplatin-paclitaxel monotherapy. At a willingness-to-pay (WTP) threshold of $50,000 per QALY, dostarlimab plus carboplatin-paclitaxel had a 68% probability of cost-effectiveness.
Table 3: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER ($/QALY) |
|---|---|---|---|---|---|
CAR-PAC | $87,442 | Reference | 3.77 | Reference | Reference |
Dostarlimab plus CAR-PAC | $362,785 | $275,343 | 9.70 | 5.94 | $46,383 |
CAR-PAC = carboplatin and paclitaxel; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Source: Sponsor’s pharmacoeconomic submission.1
Sensitivity and Scenario Analysis Results
In addition to the submitted base case, the sponsor conducted 12 independent scenario analyses. None of the scenario analyses affected the conclusion regarding the relative cost-effectiveness of dostarlimab plus carboplatin-paclitaxel. In addition, no scenario analysis was conducted using a perspective other than the health care payer.
CADTH Appraisal of the Sponsor’s Economic Evaluation
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the economic analysis:
Estimates of relative treatment efficacy are uncertain: The submitted economic evaluation estimated the cost-effectiveness of dostarlimab plus carboplatin-paclitaxel relative to carboplatin-paclitaxel alone. The CADTH clinical review of the direct comparison of the 2 treatments from the RUBY Part 1 trial concluded that dostarlimab plus carboplatin-paclitaxel may lead to improvements in OS and PFS compared to placebo plus carboplatin-paclitaxel. Due to the interim analysis, small sample size and few events for both outcomes, the magnitude of the benefit for dostarlimab plus carboplatin-paclitaxel is subject to uncertainty. Given that OS and PFS are key parameters to the economic model, the uncertainty in relative effect estimates is a meaningful source of uncertainty for the expected costs and QALYs considered in the economic evaluation.
Predicted survival probabilities produced unrealistic long-term results: In the submitted base case, the sponsor assumed that OS would follow a treatment-independent parametric survival model using a log-logistic distribution. For PFS, it was assumed both treatment strategies would follow independently fitted 1-knot flexible spline models using the odds distribution. Clinical experts consulted by CADTH suggested this configuration produced an overly optimistic long-term survival benefit for dostarlimab plus carboplatin-paclitaxel with regards to both outcomes. Experts suggested that less optimistic long-term survival benefits were more appropriate and realistic.
CADTH modified the economic evaluation to generate alternative estimates of long-term survival that were more consistent with clinical expert expectations. For OS, predicted values were estimated using a treatment-dependent parametric survival model using an exponential distribution. For PFS, predicted values were estimated using a treatment-dependent parametric survival model using a Weibull distribution.
Improper characterization of decision uncertainty: Consistent with CADTH guidelines, the sponsor’s base case used a Monte Carlo simulation to characterize parameter uncertainty. However, the mechanism by which state membership is determined in a PSM limits the usefulness of this approach.16 This is attributed to the fact that survival probabilities (PFS and OS) are predicted independently over the specified time horizon. As a result, there is a risk that some simulation trials represent situations where TTD or PFS exceed OS — which is clinically implausible. One way to avoid this problem would be to generate estimates of state occupancy using a Markov chain. In the context of a PSM, 1 would need to resample the trial data using bootstrapping to produce a series of correlated survival curves for OS, PFS, and TTD. While this may resolve concerns relating to the accuracy of predicted values in the within-trial period, limitations for the extrapolated portion of the time horizon will continue to persist.16
CADTH was unable to address this limitation. The probabilistic results were preserved in the CADTH base case to capture the uncertainty in the remaining model parameters.
CADTH Reanalyses of the Economic Evaluation
Base Case Results
The CADTH base case was derived by making changes in model parameter values and assumptions, in consultation with clinical experts. A summary of each of the changes applied to the economic evaluation is presented in Table 4. Each independent change was applied in the sequence detailed in the table to arrive at the CADTH base case. Consistent with the sponsor’s base case, the costs and effects for each alternative treatment strategy were generated from a Monte Carlo simulation of 1,000 iterations.
Table 4: CADTH Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
None | — | — |
Changes to derive the CADTH base case | ||
| OS: Independent parametric survival model, using a log-logistic distribution. PFS: Treatment-independent 1-knot flexible spline model using the odds distribution | OS: dependent parametric survival model, assuming an exponential distribution. PFS: treatment-dependent parametric survival model, using a Weibull distribution. |
CADTH base case | 1 | |
OS = overall survival; PFS = progression-free survival.
Results from the CADTH base case are presented in Table 5. As with the sponsor’s base case, the results were generated using publicly available prices of comparator treatments.
The expected costs and QALYs for dostarlimab plus carboplatin-paclitaxel were $365,195 and 8.65. Relative to carboplatin-paclitaxel, dostarlimab plus carboplatin-paclitaxel was more costly (incremental costs: $285,186) and more effective (incremental QALYs: 5.45) and the ICER was $52,296. The difference between the sponsor’s base case and CADTH’s was due to changes in the estimated QALYs for both treatments, as costs in the CADTH base case were similar to those of the sponsor’s base case. Similarly to the sponsor’s base case, 92% of incremental LY were generated through extrapolation beyond the observed period of the RUBY trial. At a WTP threshold of $50,000 per QALY gained, dostarlimab plus carboplatin-paclitaxel had a 38.7% probability of being cost-effective. Additional details summarizing the CADTH base case are presented in Appendix 4.
Table 5: Summary of the Stepped Analysis of the CADTH Reanalysis Results
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALY) |
|---|---|---|---|---|
Sponsor’s base case | CAR-PAC | 87,442 | 3.77 | Reference |
Dostarlimab plus CAR-PAC | 362,785 | 9.70 | 46,383 | |
CADTH Base Case (reanalysis 1) | CAR-PAC | 80,009 | 3.19 | Reference |
Dostarlimab plus CAR-PAC | 365,195 | 8.65 | 52,296 |
CAR-PAC = carboplatin and paclitaxel; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Scenario Analysis Results
A series of scenario analyses were conducted to explore the impact of incremental reductions on the acquisition cost of dostarlimab plus carboplatin-paclitaxel, and are presented in Table 6. Using the sponsor’s base case, no price reduction is required to obtain an ICER below a WTP threshold of $50,000 per QALY gained. However, from the CADTH base case, a 4.3% price reduction was required for dostarlimab plus carboplatin-paclitaxel to be considered cost-effective at the WTP threshold of $50,000 per QALY gained. Given the identified limitations, particularly concerning the characterization of uncertainty in a PSM, a greater price reduction may be necessary.
Table 6: CADTH Price Reduction Analyses
Analysis | ICERs for dostarlimab plus CAR-PAC vs. CAR-PAC ($/QALY) | |
|---|---|---|
Price reduction | Sponsor base case | CADTH reanalysis |
No price reduction | 46,383 | 52,296 |
4.3% | 44,315 | 50,000 |
10% | 41,510 | 46,990 |
20% | 36,636 | 41,684 |
30% | 31,762 | 36,379 |
40% | 26,888 | 31,074 |
50% | 22,014 | 25,768 |
60% | 17,140 | 20,463 |
70% | 12,226 | 15,157 |
80% | 7,392 | 9,852 |
90% | 2,518 | 4,546 |
100% | Dominates | Dominates |
CAR-PAC = carboplatin and paclitaxel; ICER = incremental cost-effectiveness ratio; NA = not applicable; vs. = versus.
Overall Conclusions
The CADTH clinical review found that treatment with dostarlimab plus carboplatin-paclitaxel produces a clinically meaningful benefit in terms of OS and PFS relative to placebo plus carboplatin-paclitaxel. However, the magnitude of this benefit is uncertain due to the interim analysis, and a small sample size with few events. Both PFS and OS were key parameters in the economic evaluation which affected estimates of state membership, and by extension the expected costs and QALYs for each arm of the decision model.
CADTH identified additional limitations within the submitted economic evaluation. These included: unrealistic predictions of long-term survival (PFS and OS), and the improper characterization of decision uncertainty. CADTH attempted to resolve some of these limitations through reanalysis. This involved using less optimistic predictions of long-term PFS and OS in the CADTH base case.
In the CADTH base case, dostarlimab plus carboplatin-paclitaxel was more costly (incremental costs: $285,186) and more effective (incremental QALYs: 5.45) than carboplatin-paclitaxel alone. The ICER for dostarlimab plus carboplatin-paclitaxel relative to carboplatin-paclitaxel was estimated to be $52,296 per QALY gained. The increase in this ICER from the sponsor’s base case can be attributed to the changes in the distributions used to predict PFS and OS. As a result, patients spent less time in the progression-free and progressed health states. A 4.3% price reduction may be required for dostarlimab plus carboplatin-paclitaxel to be considered cost-effective at a $50,000 per QALY threshold. The CADTH results were similar to those of the sponsor’s base case. The vast majority of incremental survival from the model was estimated through extrapolation beyond the period of the observed evidence. Because of the uncertainty around long-term OS and PFS, a greater price reduction may be warranted.
References
1.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Jemperli (dostarlimab) 500 mg/10 mL vial solution for infusion. MIssissauga (ON): GlaxoSmithKline; 2023 Oct 18.
2.Cancer Care Ontario. Drug Formulary- CRBPPACL [sponsor supplied reference]. 2021: https://www.cancercareontario.ca/en/drugformulary/regimens/monograph/45326. Accessed July 23 2023.
3.Mirza MR, Chase DM, Slomovitz BM, et al. Dostarlimab for Primary Advanced or Recurrent Endometrial Cancer. N Engl J Med. 2023;388(23):2145-2158. PubMed
4.Gsk. RUBY CSR. Data cutoff 28 September 2022 [sponsor supplied reference]. 2023.
5.Table: 13-10-0114-01. Life expectancy and other elements of the life table, Canada, all provinces except Prince Edward Island. Ottawa (ON): Statistics Canada; 2022: https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310011401. Accessed 2023 Nov 15.
6.Xie F, Pullenayegum E, Gaebel K, et al. A Time Trade-off-derived Value Set of the EQ-5D-5L for Canada. Med Care. 2016;54(1):98-105. PubMed
7.Swinburn P, Lloyd A, Nathan P, et al. Elicitation of health state utilities in metastatic renal cell carcinoma. Curr Med Res Opin. 2010;26(5):1091-1096. PubMed
8.Nafees B, Stafford M, Gavriel S, et al. Health state utilities for non small cell lung cancer. Health Qual Life Outcomes. 2008;6:84. PubMed
9.National Institute for Health Care Excellence. Niraparib for maintenance treatment of advanced ovarian, fallopian tube and peritoneal cancer after response to firstline platinum-based chemotherapy [TA673] [sponsor supplied reference]. Vol 20232021: https://www.nice.org.uk/guidance/ta673/history.
10.National Institute for Health Care Excellence. Necitumumab for untreated advanced or metastatic squamous non-small-cell lung cancer [TA411] [sponsor supplied reference]. 2016: https://www.nice.org.uk/guidance/ta411.
11.National Institute for Health Care Excellence. Niraparib for maintenance treatment of relapsed, platinum-sensitive ovarian, fallopian tube and peritoneal cancer [TA528]. [sponsor supplied reference]https://www.nice.org.uk/guidance/TA528. 2018.
12.Hannouf MB, Sehgal C, Cao JQ, et al. Cost-effectiveness of adding cetuximab to platinum-based chemotherapy for first-line treatment of recurrent or metastatic head and neck cancer. PLoS One. 2012;7(6):e38557. PubMed
13.Cancer Care Ontario. Endometrial Cancer Diagnosis Pathway Map [sponsor supplied reference]. 2021: https://www.cancercareontario.ca/sites/ccocancercare/files/assets/EndometrialCancerDiagnosisPathwayMap.pdf. Accessed July 29 2023.
14.Schedule of benefits for laboratory services: effective July 1, 2020. Toronto (ON): Ontario Ministry of Health; 2020: http://www.health.gov.on.ca/en/pro/programs/ohip/sob/lab/lab_mn2020.pdf. Accessed 2024 Jan 5.
15.Schedule of benefits for physician services under the Health Insurance Act: (June 29, 2023 (effective July 23, 2023)). Toronto (ON): Ontario Ministry of Health; 2023: https://www.health.gov.on.ca/en/pro/programs/ohip/sob/physserv/sob_master.pdf. Accessed 2024 Jan 5.
16.Woods B, Sideris E, Palmer S, Latimer N, Soares M. Partitioned survival analysis for decision modelling in health care: a critical review. (NICE DSU Technical Support Document 19). Sheffield (UK): Decision Support Unit, ScHARR, University of Sheffield; 2017: http://nicedsu.org.uk/wp-content/uploads/2017/06/Partitioned-Survival-Analysis-final-report.pdf. Accessed 2023 Nov 22.
17.DeltaPA. [Ottawa (ON)]: IQVIA; 2023: https://www.iqvia.com/. Accessed 2024 Jan 4.
18.Cancer Care Ontario. Drug Formulary - ANAS [sponsor supplied reference]. 2021: https://www.cancercareontario.ca/en/drugformulary/regimens/monograph/44526. Accessed November 15, 2023.
19.Cancer Care Ontario. Drug Formulary - TMXF [sponsor supplied reference]. 2022: https://www.cancercareontario.ca/en/drugformulary/regimens/monograph/46961. Accessed January 3, 2024.
20.Cancer Care Ontario. Drug Formulary - CISPDOXO [sponsor supplied reference]. 2019. https://www.cancercareontario.ca/en/drugformulary/regimens/monograph/45761. Accessed January 3, 2024.
21.Cancer Care Ontario. Drug Formulary - DOXO [sponsor supplied reference]. 2023. https://www.cancercareontario.ca/en/drugformulary/regimens/monograph/45206. Accessed January 3, 2024.
22.Cancer Care Ontario. Drug Formulary - EXEM [sponsor supplied reference]. 2020. https://www.cancercareontario.ca/en/drugformulary/regimens/monograph/44731. Accessed January 3, 2024.
23.Cancer Care Ontario. Drug Formulary - MEDR [sponsor supplied reference]. 2017. https://www.cancercareontario.ca/en/drugformulary/regimens/monograph/48176. Accessed January 3, 2024.
24.Cancer Care Ontario. Drug Formulary - MEGE [sponsor supplied reference]. 2019. https://www.cancercareontario.ca/en/drugformulary/regimens/monograph/48171. Accessed January 3, 2024.
25.Cancer Care Ontario. Drug Formulary- CRBPNPAC [sponsor supplied reference]. 2021: https://www.cancercareontario.ca/en/drugformulary/regimens/monograph/68401. Accessed July 29 2023.
26.Cancer Care Ontario. Drug Formulary - CRBPDOCE [sponsor supplied reference]. 2021. https://www.cancercareontario.ca/en/drugformulary/regimens/monograph/48181. Accessed January 3, 2024.
27.Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Jemperli (dostarlimab) 500 mg/10 mL vial solution for infusion. MIssissauga (ON): GlaxoSmithKline; 2023 Oct 18.
28.Brenner DR, Poirier A, Woods RR, et al. Projected estimates of cancer in Canada in 2022. CMAJ. 2022;194(17):E601-e607. PubMed
29.Cancer Care Ontario. Ontario Cancer Statistics [sponsor supplied reference]. 2022: https://www.cancercareontario.ca/en/data-research/view-data/statistical-reports/ontario-cancer-statistics-2022. Accessed July 20 2023.
30.Canadian Cancer Society. Cancerous tumours of the uterus [sponsor supplied reference]. 2021; https://www.cancer.ca/en/cancer-information/cancer-type/uterine/uterine-cancer/cancerous-tumours/?region=bc.
31.Canadian Cancer Society. Canadian Cancer Statistics: A 2018 special report on cancer incidence by stage [sponsor supplied reference]. 2018: https://cdn.cancer.ca/-/media/files/research/cancer-statistics/2018-statistics/canadian-cancer-statistics-2018-en.pdf.
32.Huijgens AN, Mertens HJ. Factors predicting recurrent endometrial cancer. Facts Views Vis Obgyn. 2013;5(3):179-186. PubMed
33.Lorenzi M, Amonkar M, Zhang J, et al. Epidemiology of microsatellite instability high (MSI-H) and deficient mismatch repair (dMMR) in solid tumors: a structured literature review. J Oncol. 2020; https://onlinelibrary.wiley.com/doi/10.1155/2020/1807929.
Appendix 1: Cost Comparison Table
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical expert(s). Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 7: CADTH Cost Comparison Table for Primary Advanced or Recurrent dMMR or MSI-H Endometrial Cancer
Treatment | Strength / concentration | Form | Price ($) | Recommended dosage | Daily cost | 21-Day Cost |
|---|---|---|---|---|---|---|
Dostarlimab (Jemperli) | 50 mg/mL | 10 mL vial for IV Infusion | 10,031.0800 | Loading: 500 mg every 3 weeks for 6, 21-day cycles. Maintenance: 1,000 mg every 6 weeks thereafter. | 477.67 | 10,031 |
Carboplatin (Generic) | 10 mg/mL | 5 mL vial 15 mL vial 45 mL vial 60 mL vial | 70.0000a 210.0000a 599.9985a 775.0020a | AUC 4 to 6 on day 1 for 6, 21-day cycles.b | 28.57 | 600 |
Paclitaxel (Generic) | 6 mg/mL | 5 mL vial 50 mL vial | 300.0000a 3,740.0000a | 175 mg/m2 on day 1 for 6, 21-day cycles. | 171.43 | 3,600 |
dostarlimab plus CAR-PAC: Loading Period | 677.67 | 14,231 | ||||
dostarlimab plus CAR-PAC: Maintenance Period | 477.67 | 10,031 | ||||
Platinum-based Chemotherapies | ||||||
Carboplatin-Paclitaxel | ||||||
Carboplatin (Generic) | 10 mg/mL | 5 mL vial 15 mL vial 45 mL vial 60 mL vial | 70.0000a 210.0000a 599.9985a 775.0020a | AUC 4 to 6 on day 1 for 6, 21-day cycles.b,c | 28.57 | 600 |
Paclitaxel | 6 mg/mL | 5 mL vial 50 mL vial | 300.0000a 3,740.0000a | 175 mg/m2 on day 1 for 6, 21-day cycles.c | 171.43 | 3,600 |
Carboplatin-Paclitaxel | 191.98 | 4,200 | ||||
Carboplatin-Docetaxel | ||||||
Carboplatin (Generic) | 10 mg/mL | 5 mL vial 15 mL vial 45 mL vial 60 mL vial | 70.0000a 210.0000a 599.9985a 775.0020a | AUC 4 to 6 on day 1 for 6, 21-day cycles.b,c | 28.57 | 600 |
Docetaxel | 10 mg/mL 20 mg/mL | 8 mL vial 16 mL vial 4 mL vial 8 mL vial | 970.2000a 1,850.0000a 497.0000a 990.0000a | 75 mg/m2 on day 1 for 6, 21-day cycles.c | 47.14 | 990 |
Carboplatin-Docetaxel | 75.71 | 1,590 | ||||
Cisplatin-Doxorubicin | ||||||
Cisplatin | 1 mg/mL | 10 mL vial 50 mL vial 100 mL vial | 135.0000a 270.0000a 646.0000a | 50 mg/m2 on day 1 for 8, 21-day cycles.c | 30.76 | 646 |
Doxorubicin | 2 mg/mL | 5 mL vial 25 mL vial | 50.0000a 255.0000a | 50 to 60 mg/m2 on day 1 for 7, 21-day cycles.c | 24.29 to 29.05 | 510 to 610 |
Cisplatin-Doxorubicin | 55.05 to 59.81 | 1,156 to 1,256 | ||||
Single-Drug Chemotherapies | ||||||
Carboplatin | 10 mg/mL | 5 mL vial 15 mL vial 45 mL vial 60 mL vial | 70.0000a 210.0000a 599.9985a 775.0020a | AUC 4 to 6 on day 1 for 6, 21-day cycles.b,c | 28.57 | 600 |
Cisplatin | 1 mg/mL | 50 mL vial 100 mL vial | 135.0000a 270.0000a | 50 to 75 mg/m2 on day 1 for 6, 21-day cycles.c | 30.76 to 43.62 | 646 to 916 |
Doxorubicin | 2 mg/mL | 5 mL vial 25 mL vial | 50.0000a 255.0000a | 50 to 60 mg/m2 on day 1 for 6, 21-day cycles.c | 24.29 to 29.05 | 510 to 610 |
Paclitaxel | 6 mg/mL | 5 mL vial 50 mL vial | 300.0000a 3,740.0000a | 175 mg/m2 on day 1 for 6, 21-day cycles.c | 171.43 | 3,600 |
Hormone Therapies | ||||||
Anastrozole | 1 mg | Tablet | 0.9522 | 1 mg dailyc | 0.95 | 20 |
Exemestane (Aromasin) | 25 mg | Tablet | 5.9490 | 25 mg dailyc | 5.95 | 125 |
Exemestane (Generic) | 25 mg | Tablet | 1.3263 | 25 mg dailyc | 1.32 | 28 |
Medroxyprogesterone (generic) | 2.5mg 5 mg 10 mg 100 mg | Tablet | 0.1183 0.2365 0.1670 1.2057 | 400 to 600 mg dailyc | 4.82 to 7.23 | 101 to 152 |
Megestrol | 40 mg 160 mg | Tablet | 1.3340 5.8151 | 160 to 320 mg daily.c | 5.82 to 11.63 | 122 to 244 |
Tamoxifen (generic) | 10 mg 20 mg | Tablet | 0.1750 0.3500 | 20 mg twice dailyc | 0.70 | 15 |
Tamoxifen (Nolvadex) | 20 mg | Tablet | 0.3910 | 20 mg twice dailyc | 0.78 | 16 |
dMMR = deficient mismatch repair; MSI-H = microsatellite instability-high; CAR-PAC = carboplatin and paclitaxel.
Note: All prices are from the Ontario Drug Benefit Formulary (accessed November 2023), unless otherwise indicated, and do not include dispensing fees. Where relevant, a body mass index of ||||| m2 was used to calculate required dose.
aPrices reflect IQVIA Delta PA wholesale list prices (accessed January 2024).17
bCarboplatin dose based on adjusted AUC target of 4 to 6 using the Calvert formula.
cCancer Care Ontario Regimen Monographs: Carboplatin-Paclitaxel (CRBPPACL); Cisplatin-Doxorubicin (CISPDOXO); Carboplatin-Paclitaxel (CRBPNPAC); doxorubicin (DOXO); anastrozole (ANAS); exemestane (EXEM); medroxyprogesterone (MEDR); megestrol (MEGE); tamoxifen (TMXF).2,18-26
Note that this table has not been copy-edited.
Appendix 2: Submission Quality
Note that this appendix has not been copy-edited.
Description | Yes/No | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | Yes | No comment. |
Model has been adequately programmed and has sufficient face validity | Yes | No comment. |
Model structure is adequate for decision problem | Yes | No comment. |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | No | See limitations regarding the characterization of parameter uncertainty. |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | No | See limitations regarding the characterization of parameter uncertainty. |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | Yes | No comment. |
Appendix 3: Additional Information on the Submitted Economic Evaluation
Note that this appendix has not been copy-edited.
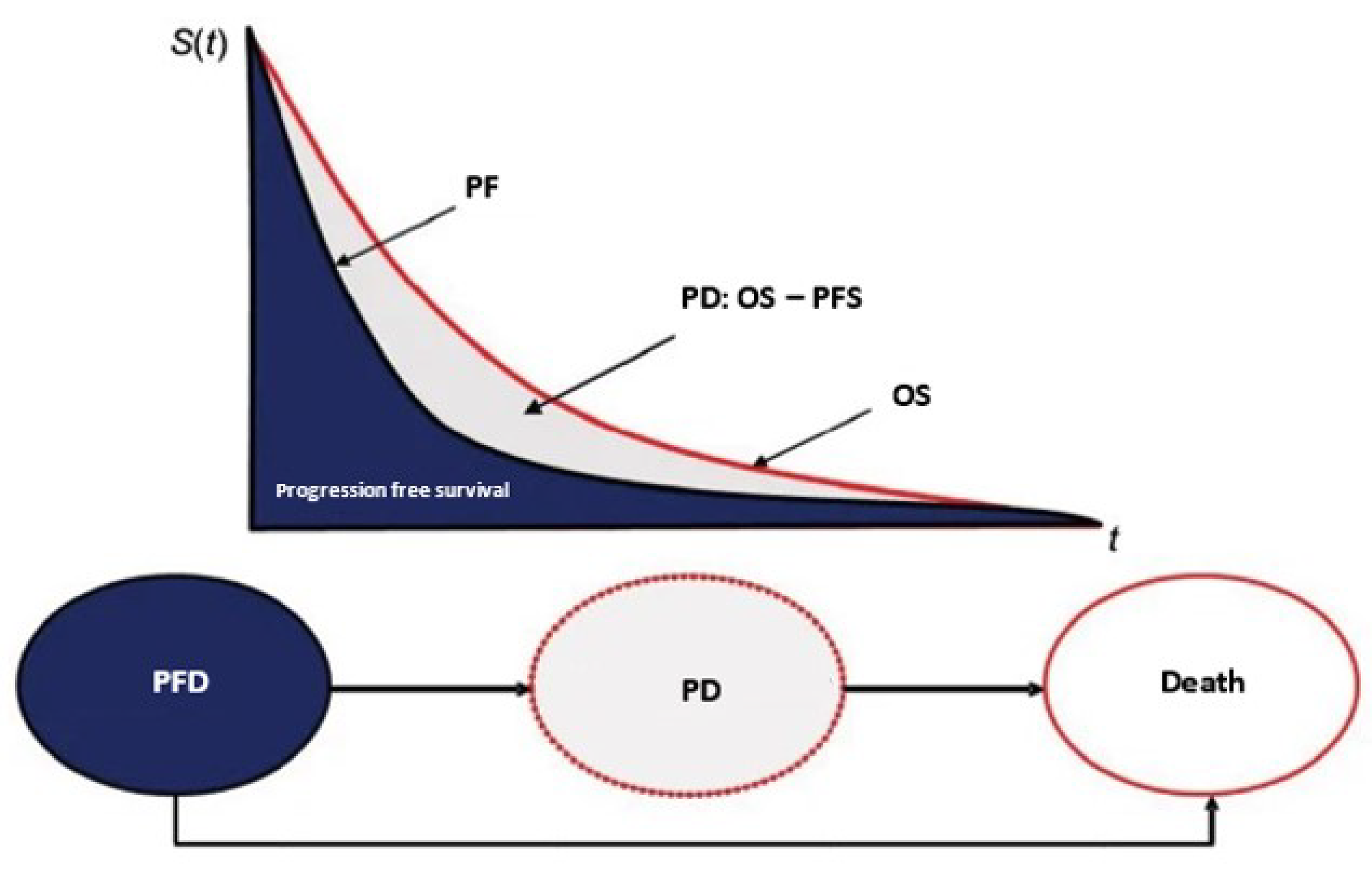
OS = Overall Survival; PD = Progressed Disease; PF = Progression Free; PFD = Progression-Free Disease; PFS = Progression-Free Survival.
Source: Sponsor’s pharmacoeconomic submission.1
Appendix 4: Additional Details on the CADTH Reanalyses and Sensitivity Analyses of the Economic Evaluation
Note that this appendix has not been copy-edited.
Detailed Results of CADTH Base Case
The CADTH base case reflects a series of modifications made to the sponsor’s submission to address some of the identified limitations with the economic evaluation. The specific changes that were applied are detailed in Table 4, and the results obtained from each revision are presented in Table 5. Disaggregated results from the CADTH base case are presented in Table 9.
Table 9: Disaggregated Summary of CADTH’s Economic Evaluation Results
Parameter | Dostarlimab plus CAR-PAC | CAR-PAC | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 11.57 | 4.08 | 7.49 |
By health state | |||
Progression Free | 3.23 | 1.01 | 2.22 |
Progressed Disease | 8.33 | 3.07 | 5.27 |
Discounted QALYs | |||
Total | 8.65 | 3.19 | 5.45 |
By health state | |||
Progression Free | 2.65 | 0.83 | 1.82 |
Progressed Disease | 6.00 | 2.36 | 3.64 |
Discounted costs ($) | |||
Total | 365,195 | 80,009 | 285,186 |
Acquisition | 305,108 | 21,202 | 283,906 |
Administration | 4,913 | 2,201 | 2,712 |
Health State Costs | 41,742 | 34,403 | 7,339 |
Subsequent Treatment | 13,019 | 21,776 | −8,757 |
Adverse Events | 413 | 428 | −15 |
ICER ($/QALY) | 52,296 | ||
CAR-PAC = carboplatin and paclitaxel; ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year.
Appendix 5: Submitted BIA and CADTH Appraisal
Note that this appendix has not been copy-edited.
Table 10: Summary of Key Take-Aways
Key Take-Aways of the BIA |
|---|
|
Summary of Sponsor’s BIA
The submitted budget impact analysis (BIA) evaluated the introduction of dostarlimab plus carboplatin-paclitaxel for the treatment of patients with primary advanced or recurrent dMMR or MSI-H endometrial cancer. Estimates were generated from the perspective of pCODR-participating drug plans (all but Quebec) and the results were aggregated into pan-Canadian totals over a three-year time horizon. An epidemiologic approach was used to estimate the eligible population size for the analysis (Figure 2).27 Key inputs to the BIA are in Table 11.
In the reference scenario, it was assumed that patients eligible for treatment would receive the carboplatin-paclitaxel regimen, which is the current standard of care. In the new drug scenario, it was assumed the dostarlimab plus carboplatin-paclitaxel would displace market share from the carboplatin-paclitaxel regimen.27
Key assumptions:
Province-specific incidence rates of uterine cancer were assumed to be 41.5 cases per 100,000 people.27,28 It was also assumed that the incidence of uterine cancer would increase by 1.2% each year.27,29
Estimates regarding the total population with endometrial cancer and by stage were assumed to follow estimates from the Canadian Cancer Society.27,30,31
It was assumed the risk of recurrence reflected the stage-classification in an analysis of time-to-recurrence data published in 2013.27,32
The sponsor assumed ||||% of patients with primary advanced or recurrent endometrial cancer will receive first-line therapy, and ||||% of those patients will be treated with platinum-based chemotherapy.
It was assumed all patients would be screened for dMMR or MSI-H in the new drug scenario. In addition, the sponsor assumed a prevalence rate of 26.0%.27,33
Given that all treatments are administered in a hospital setting, the sponsor assumed that 100% of patients will be eligible for public coverage.27
Figure 2: Sponsor’s Estimation of the Size of the Eligible Population [Redacted]

dMMR = mismatch repair deficient; EC = endometrial cancer; MSI-H: high microsatellite instability; PBCT = platinum-based chemotherapy; 1L = first-line.
Source: Sponsor’s pharmacoeconomic submission.27
Table 11: Summary of Key Model Parameters
Parameter | Sponsor’s estimate |
|---|---|
Target population | |
Total Female Population | 15,622,487 |
Annual Population Growth Rate | 1.7% |
Annual Incidence of Uterine Cancer | 41.5 cases per 100,000 |
Annual % Change in Incidence of Uterine Cancer | 1.2% |
Proportion with Endometrial Cancer | 95.0% |
% Stage I | 74.6% |
% Stage II | 6.2% |
% Primary Advanced Stage III | 12.0% |
% Primary Advanced Stage IV | 7.2% |
Lifetime incidence of Recurrence Stage I | 6.5% |
Lifetime incidence of Recurrence Stage II | 20.0% |
% Receiving First-Line Therapy | ||||% |
% Receiving Platinum-Based Chemotherapy | ||||% |
% Tested for dMMR or MSI-H | 100% |
% with dMMR or MSI-H | 26% |
% Age < 65 Years | 51% |
% Age ≥ 65 Years | 49% |
% Eligible for Coverage | 100% |
Number of patients eligible for drug under review (year 1 / year 2 / year 3) | 257 / 264 / 272 |
Market Uptake (3 years) | |
Uptake (reference scenario) | |
carboplatin-paclitaxel | 100% / 100% / 100% |
Uptake (new drug scenario) | |
dostarlimab plus carboplatin-paclitaxel | ||% / ||% / ||% |
carboplatin-paclitaxel | ||% / ||% / ||% |
Cost of treatment (per patient) | |
Cost of treatment over: 1 Year | |
dostarlimaba plus carboplatin-paclitaxel | $199,669.14 (Year 1), $174,469.14 (Year 2+) |
carboplatin-paclitaxel | $25,200 |
dMMR = mismatch repair deficient; MSI-H = microsatellite instability-high.
aDostarlimab costs calculated for a patient with the following characteristics: Age = |||||, Weight = ||||| ||, Body Surface Area = |||| ||, Creatinine Clearance Rate = ||||, and GFR = ||||||
Summary of the Sponsor’s BIA Results
In the base case, the net budget impact of dostarlimab plus carboplatin-paclitaxel was estimated to be $16,171,317 in Year 1, $38,589,126 in Year 2, and $56,606,768 in Year 3. The three-year net budget impact of dostarlimab plus carboplatin-paclitaxel was $111,367,211.
CADTH Appraisal of the Sponsor’s BIA
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
Assumptions used to estimate market size: In the submitted BIA, an epidemiological approach was used to estimate the eligible population size. To identify the number of patients eligible for treatment, the sponsor assumed that ||||% with primary advanced (Stage III or Stage IV) or recurrent (Stage I or Stage II) endometrial cancer will receive first-line therapy. Clinical experts consulted by CADTH suggested that this value may be overestimated. Patients with stage I cancer represented more than 70% of the population at this step of the analysis (See Figure 2). However, clinical experts consulted by CADTH suggested that only a small proportion of stage I patients would receive first-line therapy. Therefore, the size of the population eligible for dostarlimab and the corresponding budget impact may have been overestimated.
In the CADTH base case, it was assumed that 50% of patients with primary advanced or recurrent endometrial cancer will receive first-line therapy.
CADTH Reanalyses of the BIA
Table 12: CADTH Revisions to the Submitted BIA
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
None | — | — |
Changes to derive the CADTH base case | ||
1. Market Size: Proportion of patients with primary advanced or recurrent endometrial cancer that will receive first-line therapy. | ||||% | 50% |
CADTH base case | 1 | |
BIA = budget impact analysis.
The results of the CADTH step-wise reanalysis are presented in summary format in Table 13 and a more detailed breakdown is presented in Table 14. All CADTH reanalyses were based on publicly available prices of the comparator treatments. In the CADTH base case, the three-year net budget impact of dostarlimab plus carboplatin-paclitaxel was estimated to be $80,890,158. This decrease illustrates how the budget impact is sensitive to the proportion of patients with primary advanced or recurrent endometrial cancer who are eligible for first-line treatment.
In addition to the CADTH base case, a scenario analysis was conducted to explore how the budget impact would be affected by the price reduction identified in the economic evaluation. Assuming a 4.3% price reduction, the three-year net budget impact of dostarlimab was estimated to be $76,727,627.
Table 13: Summary of the CADTH Reanalyses of the BIA
Stepped analysis | Three-year total |
|---|---|
Submitted base case | $111,367,211 |
CADTH base case (reanalysis 1) | $80,890,158 |
BIA = budget impact analysis.
Table 14: Detailed Breakdown of the CADTH Reanalyses of the BIA
Stepped analysis | Scenario | Year 0 (current situation) | Year 1 | Year 2 | Year 3 | Three-year total |
|---|---|---|---|---|---|---|
Submitted base case | Reference | 12,761,437 | 17,390,774 | 18,003,201 | 18,522,107 | 53,916,082 |
New drug | 12,761,437 | 33,562,091 | 56,592,327 | 75,128,875 | 165,283,293 | |
Budget impact | 0 | 16,171,317 | 38,589,126 | 56,606,768 | 111,367,211 | |
CADTH base case | Reference | 9,263,798 | 12,627,317 | 13,075,810 | 13,456,346 | 39,159,473 |
New drug | 9,263,798 | 24,370,096 | 41,102,967 | 54,576,568 | 120,049,631 | |
Budget impact | 0 | 11,742,779 | 28,027,157 | 41,120,222 | 80,890,158 | |
CADTH scenario analysis: 4.3% price reduction | Reference | 9,263,798 | 12,627,317 | 13,075,810 | 13,456,346 | 39,159,473 |
New drug | 9,263,798 | 23,752,020 | 39,638,457 | 52,496,622 | 115,887,100 | |
Budget impact | 0 | 11,124,703 | 26,562,647 | 39,040,277 | 76,727,627 |
BIA = budget impact analysis.
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
Redactions: Confidential information in this document may be redacted at the request of the sponsor in accordance with the CADTH Drug Reimbursement Review Confidentiality Guidelines
Stakeholder Input: The views expressed in each submission are those of the submitting organization or individual; not necessarily the views of CADTH or of other organizations. As such, they are independent of CADTH and do not necessarily represent or reflect the view of CADTH. No endorsement by CADTH is intended or should be inferred. By filing with CADTH, the submitting organization or individual agrees to the full disclosure of the information. CADTH does not edit the content of the submissions.
CADTH does use reasonable care to prevent disclosure of personal information in posted material; however, it is ultimately the submitter’s responsibility to ensure no identifying personal information or personal health information is included in the submission. The name of the submitting organization or individual and all conflict of interest information are included in the submission; however, the name of the author, including the name of an individual patient or caregiver submitting the patient input, are not posted.
Accessibility: CADTH is committed to treating people with disabilities in a way that respects their dignity and independence, supports them in accessing material in a timely manner, and provides a robust feedback process to support continuous improvement. All materials prepared by CADTH are available in an accessible format. Where materials provided to CADTH by a submitting organization or individual are not available in an accessible format, CADTH will provide a summary document upon request. More details on CADTH’s accessibility policies can be found here.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.