CADTH Reimbursement Review
Treosulfan (Trecondyv)
Sponsor: Medexus Pharmaceuticals, Inc.
Therapeutic area: Conditioning treatment prior to stem cell transplant for acute myeloid leukemia or myelodysplastic syndromes
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Stakeholder Input
Clinical Review
Abbreviations
AE
adverse event
alloHSCT
allogeneic hematopoietic stem cell transplant
AML
acute myeloid leukemia
BM
bone marrow
BSA
body surface area
CI
confidence interval
CRFS
chronic GvHD-free and relapse or progression-free survival
CTTC
Cell Therapy Transplant Canada
DMC
data monitoring committee
EFS
event-free survival
FAS
full analysis set
GRADE
Grading of Recommendations, Assessment, Development, and Evaluation
GRFS
GvHD-free and relapse or progression-free survival
GvHD
graft versus host disease
HCT-CI
Hematopoietic Cell Transplantation-Specific Comorbidity Index
HR
hazard ratio
HRQoL
health-related quality of life
HSCT
hematopoietic stem cell transplant
HSOS
hepatic sinusoidal obstruction syndrome
IPSS-R
Revised International Prognostic Scoring System
LLSC
Leukemia and Lymphoma Society of Canada
MAC
myeloablative conditioning
MDS
myelodysplastic syndromes
MID
minimally important difference
MRD
matched related donor
MUD
matched unrelated donor
NRM
nonrelapse mortality
OH-CCO-CMHAC
Ontario Health (Cancer Care Ontario) Complex Malignant Hematology Advisory Committee
OS
overall survival
PB
peripheral blood
PPS
per-protocol set
RCT
randomized controlled trial
RIC
reduced-intensity conditioning
SAE
serious adverse event
TRM
transplant-related mortality
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Table 1: Background Information of Application Submitted for Review
Item | Description |
|---|---|
Drug product | Treosulfan (Trecondyv); 5 g/vial; IV infusion |
Sponsor | Medexus Pharmaceuticals, Inc. |
Indication | Treosulfan in combination with fludarabine as part of conditioning treatment before allogeneic hematopoietic stem cell transplantation in adult patients with acute myeloid leukemia or myelodysplastic syndromes at increased risk for standard conditioning therapies and in pediatric patients older than 1 year old with acute myeloid leukemia or myelodysplastic syndromes. |
Reimbursement request | Per sponsor request, this CADTH review focuses on the indication in adults. CADTH did not review the pediatric population at this time. |
Health Canada approval status | NOC |
Health Canada review pathway | Priority review |
NOC date | June 25, 2021 |
Recommended dose | Treosulfan 10 g/m2 BSA per day as a 2-hour IV infusion, given on 3 consecutive days (day –4, day –3, day –2) before stem cell infusion (day 0). The total treosulfan dose is 30 g/m2. Fludarabine 30 mg/m2 BSA per day as a 0.5-hour IV infusion, given on 5 consecutive days (day –6, day –5, day –4, day –3, day –2) before stem cell infusion (day 0). The total fludarabine dose is 150 mg/m2. Treosulfan should be administered before fludarabine on day –4, day –3, day –2 (FT10 regimen). |
BSA = body surface area; NOC = Notice of Compliance.
Introduction
Acute myeloid leukemia (AML) is a cancer of the blood and bone marrow (BM), characterized by an abnormal and occasionally poor proliferation of immature hematopoietic cells that infiltrate BM, blood, and other tissues. Genetic alterations in myeloid progenitor stem cells alter normal growth and the differentiation of myeloblasts.1 Approximately 40% of patients with AML younger than 60 years will be cured of their disease after treatment, whereas this estimate is 5% to 15% for those who are older than 60 years.1,2 The Canadian Cancer Society estimated that, as of 2018, about 19,310 people in Canada were living with leukemia (5-year prevalence).3 The most recent statistics from the Canadian Cancer Society report that 1,090 people in Canada were newly diagnosed with AML in 2016, and that 1,184 people in Canada died from AML in 2017.4 According to the clinical experts consulted by CADTH, it is estimated that, in Canada, 30% to 40% of patients with AML are not eligible for myeloablative conditioning (MAC);this is higher for patients with myelodysplastic syndromes (MDS), given that patients with MDS tend to be older. MDS are a type of cancer in which there is a lack of healthy blood cells and there are abnormal cells in the blood and/or BM. As a result, infections, anemia, or bleeding may occur.5,6 MDS will progress to AML in one-fourth to one-third of cases.5 The estimated overall age-adjusted incidence rate of MDS is 4.3 cases per 100,000 persons per year.7 According to a Canadian study conducted from January 1, 2011, to December 31, 2015, in the Calgary metropolitan area, the incidence rate of MDS was 2.60 per 100,000 person-years, corresponding to an age-standardized incidence of 3.69.8
Allogeneic hematopoietic stem cell transplant (alloHSCT) is currently the only known curative therapy for patients with AML and for high-risk patients with MDS.9-15 Conditioning therapy plays a central role in hematopoietic stem cell transplant (HSCT) by preparing or conditioning the patient’s body for the transplant.16-19 There are 3 common types of conditioning regimens: MAC, reduced-intensity conditioning (RIC), and nonmyeloablative. Patients who are not eligible for MAC regimens (e.g., older patients and those with comorbidities) usually receive an RIC regimen, such as busulfan in combination with fludarabine, to minimize treatment-related toxicity, nonrelapse mortality (NRM), and transplant-related mortality (TRM); however, the lower-dose intensity comes with a higher risk of relapse. A large proportion of patients with AML or MDS who undergo alloHSCT are at high risk of dying from either treatment-related toxicity or disease relapse. According to the clinical experts consulted by CADTH, the estimated survival probability is about 5% to 10% lower for patients who receive RIC regimens than for those who receive MAC regimens. There remains an unmet need for conditioning regimens that can reduce the risk of TRM without increasing the incidence of relapse, as conventional therapies can, ultimately improving survival rates and quality of life. In addition, the clinical experts consulted by CADTH stated that the limitation of alloHSCT is the increased risk of NRM, which can be from opportunistic infection, graft versus host disease (GvHD), or other complications; there is about a 15% to 20% chance of leukemia and/or MDS recurrence after alloHSCT.
The objective of CADTH’s Clinical Review Report is to assess and critically appraise the clinical evidence submitted by the sponsor on the beneficial and harmful effects of IV treosulfan (Trecondyv) at a dose of 10 g/m2 body surface area (BSA) per day in combination with IV fludarabine at a dose of 30 mg/m2 BSA per day as part of conditioning treatment administered before alloHSCT in adults with AML or MDS who are at increased risk with standard conditioning therapies. The focus will be on comparing treosulfan in combination with fludarabine to relevant comparators and identifying gaps in the current evidence.
Stakeholder Perspectives
The information in this section is a summary of input provided by the patient and clinician groups that responded to CADTH’s call for input and by clinical experts consulted by CADTH for the purpose of this review.
Patient Input
CADTH received 1 patient-group submission from the Leukemia and Lymphoma Society of Canada (LLSC). LLSC is a national organization with charitable status dedicated to finding a cure for blood cancers and to improve the quality of life of people affected by blood cancers and their families by funding life-enhancing research and providing educational resources, services, and support. LLSC conducted an online survey that had 108 respondents in July 2023. LLSC noted that the decision-making process for stem cell transplant has a significant impact on the mental health of patients and their families. According to the survey, 79% of respondents reported moderate to extreme levels of anxiety and 83% reported moderate to extreme levels of stress. Some of the factors often considered by respondents making decisions about the transplant are overall survival (OS); disease progression; quality of life; thoughts of dying; and posttransplant complications such as graft rejection, graft failure, infection, GvHD, and toxicity. LLSC emphasized that patients believed that knowing they would have access to conditioning therapy, with the potential for increased survival and fewer side effects, would have a significant positive impact on their mental health. When the respondents were asked about the impact of having a conditioning treatment that could reduce toxicity and minimize long-term effects, 62% reported that it would have an extremely positive impact on their anxiety, fear, and stress levels. There is an even more significant positive impact when there is a potential for a survival benefit; 82% of respondents indicated that a conditioning treatment that would improve their chances of survival would have an extremely positive impact on their outlook.
Clinician Input
Input From Clinical Experts Consulted by CADTH
The clinical experts consulted by CADTH stated that the limitation of alloHSCT is the increased risk of NRM, which can be from opportunistic infection, GvHD, or other complications; even after alloHSCT, the chance of a leukemia and/or MDS recurrence is about 15% to 20%. There remains an unmet need for improved conditioning regimens that can reduce the risk of TRM without increasing the incidence of relapse, as some conventional therapies do, ultimately improving survival rates and quality of life, according to feedback from the clinical experts consulted by CADTH. The clinical experts thought it would not be appropriate to recommend other conditioning regimens before considering treosulfan, as reserving an alternative treatment option that is potentially beneficial for a later line of therapy is not a reasonable way to optimize transplant outcomes. The clinical experts consulted by CADTH expect that treosulfan will cause a shift in the current treatment paradigm. They noted that a treosulfan plus fludarabine conditioning regimen is considered an RIC; therefore, patients for whom an RIC is indicated because of an increased risk for NRM (being older than 55 or 60 years or having multiple comorbidities, indicated by a Hematopoietic Cell Transplantation-Specific Comorbidity Index [HCT-CI] score above 3) would be best suited for conditioning treatment with treosulfan in combination with fludarabine. According to the clinical experts consulted by CADTH, OS, relapse-free survival, cumulative incidence of NRM, and cumulative incidence of relapse are mainly used to assess alloHSCT outcomes. Engraftment kinetics, GvHD incidence (acute and chronic), and the incidence of other infections, such as cytomegalovirus viremia, are used as additional end points. The clinical experts indicated that symptom-based assessments are rarely used to evaluate the efficacy or tolerability of specific transplant regimens. They stated that there are 2 occasions when treosulfan can be discontinued or changed to an alternative option: first, if the patient has active leukemia (blast count above 5%) or uncontrolled MDS (blast count above 10%), the transplant process itself will be not cleared to proceed; and second, if the medical circumstances of the patient indicate it, treosulfan can be switched to an alternative treatment. The clinical experts consulted by CADTH indicated that treosulfan in combination with fludarabine before alloHSCT will be used only in experienced allogeneic transplant centres.
Clinician Group Input
Two clinician groups provided input to the submission: Cell Therapy Transplant Canada (CTTC); and the Ontario Health (Cancer Care Ontario) Complex Malignant Hematology Advisory Committee (OH-CCO-CMHAC).
The clinical experts consulted by CADTH and both clinician groups agreed that allogeneic transplant is a potentially curative therapy for patients with AML or MDS, and the conditioning regimen of MAC or RIC depends on the patient’s age and comorbidity score. There are still limitations, such as NRM and GvHD, that can impair the outcome of the transplant. It was agreed that treosulfan in combination with fludarabine for alloHSCT will be used only in experienced allogeneic transplant centres.
Because treosulfan is part of the conditioning regimen, there is typically no response assessment and usually no need to consider discontinuation during administration, except in the case of hypersensitivity. The clinician groups noted that outcomes of transplants in patients who receive treosulfan-based conditioning will, however, be assessed using the standard outcome measures for alloHSCT.
Drug Program Input
Input was obtained from the drug programs that participate in the CADTH reimbursement review process. The following were identified as key factors that could potentially affect the implementation of a CADTH recommendation for treosulfan: relevant comparators, consideration for initiation of therapy, consideration for prescribing of therapy, generalizability, funding algorithm, care provision issues, and system and economic issues.
The clinical experts consulted by CADTH provided advice on the potential implementation issues raised by the drug programs. Refer to Table 4 for more details.
Clinical Evidence
Systematic Review
Description of Studies
A sponsor-submitted systematic review identified 1 study — the MC-FludT.14/L trial — which was a phase III, randomized, parallel-group, open-label, multicentre, international, group-sequential study conducted to compare the efficacy, noninferiority, and safety of treosulfan-based conditioning with a busulfan-based RIC regimen. The MC-FludT.14/L trial enrolled adults with AML or MDS who met the indication for alloHSCT and were considered ineligible for standard conditioning therapies (i.e., being 50 years or older and/or having an HCT-CI score above 2). The study had 2 groups: a treosulfan treatment group, and a busulfan treatment group. Eligible adults with AML or MDS (N = 570) were randomly assigned in a 1:1 ratio to either IV treosulfan (n = 280) administered at a dose of 10 g/m2 BSA once a day on day –4, day –3, and day –2, or IV busulfan (n = 290) administered at a dose of 0.8 mg/kg per day, administered every 6 hours on day –4 and day –3, followed by alloHSCT on day 0. These patients were recruited at 33 sites in 6 countries; there were no sites in Canada. The primary objective in the MC-FludT.14/L trial was to compare event-free survival (EFS) in the 2 years after alloHSCT between treosulfan plus fludarabine conditioning and busulfan plus fludarabine conditioning. The secondary objectives were to compare OS, the cumulative incidence of engraftment, the incidence of complete donor-type chimerism, the cumulative incidence of relapse and/or progression, NRM, and TRM. The cumulative incidence of acute and chronic GvHD and other safety end points were also assessed.
Most patients in the final analysis of the MC-FludT.14/L trial (database lock date: March 16, 2018) were male (60.8%), aged 50 years or older (94.9%), and had AML (63.9%). The diagnosis of AML was more common in the treosulfan group (184 of 268 patients [68.7%]) than in the treosulfan group (168 of 283 patients [59.4%]). Of the 199 patients with MDS, more had untreated MDS in the treosulfan group than in the busulfan group (50.0% versus 40.9%), and the mean blast count in BM was lower in the treosulfan group than in the busulfan group (5.83 versus 6.31).
Efficacy Results
Three confirmatory interim evaluations and 1 final analysis were planned. Patient recruitment into the trial was stopped after the second interim analysis (referred as the confirmatory interim analysis in this review), as the noninferiority of treosulfan-based conditioning was established. The data cut-off date was August 19, 2016, for the confirmatory interim analysis, and the database lock date was March 16, 2018, for the final analysis. This CADTH report primarily focused on the results from the final analysis, but did report the results for the primary outcome of EFS at the confirmatory interim analysis. In the final analysis, a total of 570 patients were randomized (280 in the treosulfan group and 290 in the busulfan group). These patients were recruited at 33 sites in 6 countries: Finland, France, Germany, Hungary, Italy, and Poland. This study had no sites in Canada.
Event-Free Survival
EFS was the primary end point in the MC-FludT.14/L trial. Generally, there were fewer EFS events in the treosulfan group than in the busulfan group. In the confirmatory interim analysis, 68 (30.9%) patients in the treosulfan group and 100 (41.7%) patients in the busulfan group experienced an event; in the final analysis, this increased to 97 (36.2%) patients in the treosulfan treatment group and 137 (48.4%) patients in the busulfan group. In the confirmatory interim analysis, the Kaplan-Meier estimate of EFS probability 24 months after HSCT was 64.0% (95% CI, 56.0% to 70.9%) in the treosulfan group and 50.4% (95% CI, 42.8% to 57.5%) in the busulfan group; in the final analysis, the estimate was 65.7% (95% CI, 59.5% to 71.2%) in the treosulfan group and 51.2% (95% CI, 45.0% to 57.0%) in the busulfan group. In the confirmatory interim analysis, the Kaplan-Meier estimate of EFS probability 36 months after HSCT was 59.5% (95% CI, 52.2% to 66.1%) in the treosulfan group and 49.7% (95% CI, 43.3% to 55.7%) in the busulfan group. The confirmatory interim analysis showed noninferiority in EFS for the treosulfan group compared to the busulfan group (hazard ratio [HR] = 0.65; 99.9702% CI, 0.36 to1.19; noninferiority P = 0.0000164; superiority P = 0.0051268; both noninferiority and superiority P values are compared against the prespecified 1-sided significance level of 0.000149). Findings from the per-protocol set (PPS) population were consistent with those from the full analysis set (FAS) population. Generally, subgroup analyses of EFS were consistent with the primary confirmatory interim analysis across all prespecified subgroups except for patients with MRD in risk group II (in confirmatory interim and final analyses) and MDS risk group I (only in the confirmatory interim analysis). The clinical experts consulted by CADTH confirmed that the overall subgroup results are as anticipated. They said they would not have expected treosulfan to have a differential treatment effect in patients with AML and those with MDS, as the 2 diseases have a similar disease biology.
Overall Survival
In the MC-FludT.14/L study, OS was a secondary end point. In the final analysis, including the postsurveillance evaluation, patients had been followed for a median of 29.7 months (range, 0.4 months to 52.1 months) in the treosulfan group and 29.4 months (range, 0.4 months to 54.3 months) in the busulfan group. At the time of the postsurveillance evaluation, 81 (30.2%) patients in the treosulfan group and 112 (39.6%) patients in the busulfan group had died (HR = 0.64; 95% CI, 0.48 to 0.87; nominal P = 0.0037). The median OS was not reached in either group. In the final analysis, the Kaplan-Meier estimate of OS probabilities decreased from 24 months to 36 months, from 72.7% (95% CI, 66.8% to 77.8%) to 66.8% (95% CI, 59.9% to 72.9%) in the treosulfan group and from 60.2% (95% CI, 54.0% to 65.8%) to 56.3% (95% CI, 49.6% to 62.6%) in the busulfan group. Generally, similar results were observed in the confirmatory interim analysis (database lock date: August 19, 2016).
Graft Failure
In the MC-FludT.14/L trial, graft failure was a secondary end point. In the final analysis, including the postsurveillance evaluation, there was a lower percentage of patients with graft failure (including primary and secondary) in the treosulfan group than in the busulfan group (0.4% versus 3.2%). No graft failure was reported during the postsurveillance period. Generally, similar results were observed in the confirmatory interim analysis.
Engraftment
In the MC-FludT.14/L trial, engraftment 28 days after HSCT was assessed as a secondary end point. In the final analysis, the conditional cumulative incidence of reconstitution of granulopoiesis 28 days after HSCT was 96.2% (95% CI, 93.4% to 99.1%) in the treosulfan group and 96.8% (95% CI, 94.6% to 99.1%) in the busulfan group, and the HR was 1.06 (95% CI, 0.91 to 1.24; nominal P = 0.4235). The conditional cumulative incidence of reconstitution of thrombopoiesis 28 days after HSCT was 94.7% (95% CI, 92.0% to 97.4%) in the treosulfan group and 97.8% (95% CI, 96.3% to 99.4%) in the busulfan group. The HR was 0.80 (95% CI, 0.68 to 0.93; nominal P = 0.0038) in favour of busulfan. Generally, similar results were observed in the confirmatory interim analysis.
Chimerism
In the MC-FludT.14/L trial, the incidence of complete donor-type chimerism 28 days after HSCT was assessed as a secondary end point. In the final analysis, the incidence of complete donor-type chimerism 28 days after HSCT was 93.2% (95% CI, 89.4% to 95.9%) in the treosulfan group and 83.3% (95% CI, 78.5% to 87.5%) in the busulfan group. The odds ratio was 2.81 (95% CI, 1.58 to 5.01; nominal P = 0.0159) in favour of treosulfan. Generally, similar results were observed in the confirmatory interim analysis.
Cumulative Incidence of Relapse or Progression
In the MC-FludT.14/L trial, the cumulative incidence of relapse or progression was assessed as a secondary end point. In the final analysis, a slightly lower proportion of patients in the treosulfan group experienced relapse and/or progression (61 [22.8%]) than in the busulfan group (72 [25.4%]). The cumulative incidence of relapse or progression 24 months after HSCT was 22.0% (95% CI, 16.9% to 27.1%) in the treosulfan group and 25.2% (95% CI, 20.0% to 30.3%) in the busulfan group. The HR was 0.82 (95% CI, 0.59 to 1.16; nominal P = 0.2631) in favour of treosulfan. Generally, similar results were observed in the confirmatory interim analysis.
GvHD-Free and Relapse or Progression-Free Survival
The incidence of GvHD-free and relapse or progression-free survival (GRFS) in the 2 years after HSCT was assessed as a secondary end point of the trial. In the final analysis, a lower proportion of patients in the treosulfan group than in the busulfan group experienced GvHD or relapse or progression (48.5% versus 59.7%). The Kaplan-Meier estimate of GRFS probability at 24 months was 50.3% (95% CI, 43.9% to 56.3%) in the treosulfan group and 37.1% (95% CI, 31.1% to 43.1%) in the busulfan group. The HR was 0.73 (95% CI, 0.57 to 0.92; nominal P = 0.0087) in favour of treosulfan. Generally, similar results were observed in the confirmatory interim analysis.
Chronic GvHD-Free and Relapse or Progression-Free Survival
The incidence of chronic GvHD-free and relapse or progression-free survival (CRFS) in the 2 years after HSCT was assessed as a secondary end point of the trial. In the final analysis, a lower proportion of patients experienced extensive chronic GvHD or relapse and/or progression in the treosulfan group than in the busulfan group (47.8% versus 59.4%). The Kaplan-Meier estimate of CRFS probability at 24 months was 51.4% (95% CI, 45.0% to 57.4%) in the treosulfan group and 37.2% (95% CI, 31.3% to 43.2%) in the busulfan group. The HR was 0.70 (95% CI, 0.55 to 0.88); nominal P = 0.0030) in favour of treosulfan. Generally, similar results were observed in the confirmatory interim analysis.
Nonrelapse Mortality
The cumulative incidence of NRM 24 months after HSCT was assessed as a secondary end point of the trial. In the final analysis, 35 (13.1%) patients in the treosulfan group and 56 (19.8%) patients in the busulfan group died without relapse or progression. The cumulative incidence of NRM 24 months after HSCT was 12.0% (95% CI, 8.0% to 15.9%) in the treosulfan group and 20.4% (95% CI, 15.5% to 25.2%) in the busulfan group. The HR was 0.63 (95% CI, 0.41 to 0.97; nominal P = 0.0343) in favour of treosulfan. Generally, similar results were observed in the confirmatory interim analysis.
Transplant-Related Mortality
The cumulative incidence of TRM 24 months after HSCT was assessed as a secondary end point of the trial. In the final analysis, 33 (12.3%) patients in the treosulfan group and 58 (20.5%) patients in the busulfan group died from a transplant-related cause. The cumulative incidence of TRM 24 months after HSCT was 12.8% (95% CI, 9.2% to 17.7%) in the treosulfan group and 24.1% (95% CI, 19.1% to 30.2%) in the busulfan group. The HR was 0.52 (95% CI, 0.34 to 0.82; nominal P = 0.0043) in favour of treosulfan. Generally, similar results were observed in the confirmatory interim analysis.
Health-Related Quality of Life
Health-related quality of life (HRQoL) was identified as important by patient groups and the clinical experts consulted by CADTH. HRQoL was not assessed in the MC-FludT.14/L trial.
Harms Results
The proportion of patients reporting at least 1 adverse event (AE) was a similar in the treosulfan and busulfan groups (92.6% versus 96.1%). The most common treatment-related adverse events occurring in at least 20% of patients in either treatment group included (treosulfan versus busulfan) edema limbs (22.6% versus 13.4%) and vomiting (21.9% versus 19.4%), which were reported more frequently in the treosulfan group than in the busulfan group, and oral mucositis (37.8% versus 47.7%), fever (34.4% versus 35.7%), nausea (33.0% versus 41.0%), and hypertension (14.1% versus 21.2%), which were reported less frequently in the treosulfan group than in the busulfan group. The proportion of patients reporting AES of grade 3 or higher was similar in the treosulfan and busulfan groups (54.8% versus 53.4%).
More patients in treosulfan group experienced at least 1 serious adverse event (SAE) than in the busulfan group (8.5% versus 7.1%). The most common SAEs occurring in at least 1% of patients in either treatment group included (treosulfan versus busulfan) sepsis (3.0% versus 1.8%), lung infection (2.2% versus 1.1%), and acute kidney injury sepsis (1.1% versus 0.4%), which were reported more frequently in the treosulfan group than in the busulfan group. None of the patients in the MC-FludT.14/L trial required a dose reduction or discontinuation due to drug-related toxicity. There were fewer deaths at 24 months in the treosulfan group than in the busulfan group (26.7% versus 37.8%), and fewer deaths in the postsurveillance period (30.0% versus 39.6%). Relapse or progression was the most frequently reported cause of death in the treosulfan group (12.6%), compared with 16.6% in the busulfan group, whereas transplant-related causes were the most frequently reported cause of death in the busulfan group (12.2%), compared with 20.5% in the busulfan group.
In the final analysis, the cumulative incidence of acute GvHD grade of III or IV at 100 days was 6.4% (95% CI, 3.4% to 9.3%) in the treosulfan group and 8.1% (95% CI, 4.9% to 11.3%) in the busulfan group. The cumulative incidence of chronic GvHD at 24 months was similar in the 2 treatment groups, at 61.7% (95% CI, 55.1% to 68.3%) in the treosulfan group and 60.3% (95% CI, 53.8% to 66.7%) in the busulfan group.
Critical Appraisal
The MC-FludT.14/L trial was a phase III, randomized, parallel-group, open-label, multicentre, international, group-sequential study conducted to compare the noninferiority, efficacy, and safety of treosulfan-based conditioning with a busulfan-based RIC regimen. An open-label trial can introduce detection and performance biases in the assessment of subjective outcomes reported by patients, such as AEs. Analyses of disease response outcomes (i.e., EFS, relapse and/or progression) were based on an independent data monitoring committee (DMC) to help mitigate the potential for detection and performance biases. The primary analysis of the study results was conducted in the PPS and FAS populations in the MC-FludT.14/L trial. The FAS includes all randomized patients from the safety analysis set with at least 1 documented efficacy parameter. Patients who were randomized but not eligible for the FAS may have had different characteristics and outcomes than those who were eligible. The extent and direction of potential selection bias cannot be determined because it is not clear whether patients who were excluded from the FAS were systematically different from those who were included.
The noninferiority of treosulfan compared to busulfan was demonstrated in the confirmatory interim analysis (database lock date: August 19, 2016), so the MC-FludT.14/L trial was stopped early for efficacy based on the DMC recommendation. The CADTH review team notes that the early stop of the trial may have led to an overestimation of the treatment effect, as the early stopping rule favours larger effect estimates. The study reported a 99.9702% CI for the HR of EFS in the confirmatory interim analysis; this interval is considered to be representative of the range of estimates that are reasonable to maintain trial integrity for the confirmatory interim analysis after the premature stop of the trial.
Of note, only the primary analysis of EFS in the confirmatory interim analysis was adjusted for multiplicity. The remaining end points (i.e., OS, graft failure, engraftment, chimerism, relapse or progression, and GvHD) in the confirmatory interim analysis and all end points in the final analysis were considered exploratory and, thus, not controlled for multiple comparisons. Although the subgroup analyses were prespecified, there is no evidence that the studies were powered to detect subgroups differences. HRQoL is considered a relevant outcome by patients with AML or MDS and the clinical experts consulted by CADTH; however, because there was no assessment for HRQoL in the MC-FludT.14/L trial, it is uncertain whether treatment with treosulfan would improve HRQoL in patients with AML or MDS.
The method used in the analysis of graft failure at 24 months (i.e., observed percentage) included death as a censoring event; it does not measure the probability of graft failure at 24 months, but instead measures the proportion of patients that had graft failure before a censoring event at 24 months. The reported estimates of complete chimerism at 28 days were based on empirical observation of the presence of chimerism at 28 days among patients alive at that time. The interpretation of this outcome should be considered carefully, as it does not measure the incidence of chimerism at 28 days in a meaningful population. The defined at-risk population does not consider censoring or death as a competing risk. The estimates could be interpreted as an approximation of cumulative incidence at 28 days, but 1 that is at risk of bias. However, the magnitude and direction of this bias is unclear.
The clinical experts consulted by CADTH confirmed that the eligibility criteria for the MC-FludT.14/L trial are in line with previous trials appropriate for the indication. Although patients who had undergone previous alloHSCT were excluded they may be considered eligible for treosulfan conditioning therapy in clinical practice. The MC-FludT.14/L trial defined a threshold for blast counts of less than 20% in the BM for MDS and an age cut-off for MAC of 50 years. According to the clinical experts consulted by CADTH, a 10% cut-off for pretransplant blast percentage and a MAC age criteria of 55 to 60 years is used in the case of MDS in some centres; this subgroup is expected to have an efficacy comparable to the overall findings. The MC-FludT.14/L trial only included patients with AML or MDS who were aged 18 to 70 years, yet patients outside of this age group are eligible to receive HSCT in clinical practice. Busulfan is a relevant comparator to treosulfan, per feedback from the clinical experts consulted by CADTH. TP53 and FLT3-ITD mutations are important prognostic factors in patients with AML or MDS, but were not investigated as subgroups. The clinical experts stated that patients with TP53 and FLT3-ITD mutations are at elevated risk of relapse even after HSCT. The CADTH review team noted that there may be uncertainty in the interpretation of the study results, as it is not known if the uncontrolled prognostic factors (i.e., TP53 and FLT3-ITD mutation status) were balanced between the treatment groups.
GRADE Summary of Findings and Certainty of the Evidence
For the pivotal MC-FludT.14/L trial identified in the sponsor’s systematic review, Grading of Recommendations, Assessment, Development and Evaluation (GRADE) was used to assess the certainty of the evidence for outcomes considered to be most relevant to CADTH’s expert committee deliberations, and a final certainty rating was determined as outlined by the GRADE Working Group.20,21 Following the GRADE approach, evidence from randomized controlled trials (RCTs) started as high-certainty evidence and could be rated down for concerns related to study limitations (which refers to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias.
The selection of outcomes for GRADE assessment was based on the sponsor’s Summary of Clinical Evidence, consultation with clinical experts, and input received from patient and clinician groups and public drug plans. The following list of outcomes was finalized in consultation with expert committee members: EFS, OS, GRFS, CRFS, graft failure, engraftment, complete chimerism, relapse or progression, NRM, TRM, and GvHD. No data were available for HRQoL.
When possible, certainty was rated in the context of the presence of an important (nontrivial) treatment effect; if this was not possible, certainty was rated in the context of the presence of any treatment effect (i.e., when the clinical importance is unclear). In all cases, the target of the certainty of evidence assessment was based on the point estimate and where it was located relative to the threshold for a clinically important effect (when a threshold was available) or to the null. The target of the certainty of evidence assessment was the presence or absence of a clinically important effect based on thresholds informed by the clinical experts consulted by CADTH for this review for EFS, OS, GRFS, CRFS, graft failure, engraftment, complete chimerism, relapse or progression, NRM, TRM, and GvHD.
Table 2: Summary of Findings for Treosulfan vs. Busulfan for Patients With AML or MDS
Outcome and follow-up | Patients (studies), N | Relative effect (95% CI) | Absolute effects | Certainty | What happens | ||
|---|---|---|---|---|---|---|---|
Busulfan | Treosulfan (95% CI) | Difference (95% CI) | |||||
Event-free survival (full analysis set) | |||||||
Probability of being alive and event-free at 24 months Follow-up (median):
| 460 (1 RCT) | NR | 50.4 per 100 | 64.0 per 100 (56.0 to 70.9 per 100) | 13.6 more per 100 (3.1 to 24.0 more per 100) | Lowa,b,c | Treosulfan may result in a clinically important higher probability of patients being alive and event-free at 24 months than busulfan |
Probability of being alive and event-free at 24 months Follow-up (median)
| 551 (1 RCT) | NR | 51.2 per 100 | 65.7 per 100 (59.5 to 71.2 per 100) | 14.5 more per 100 (6.1 to 22.9 more per 100) | Moderatea,d.e | Treosulfan likely results in a clinically important higher probability of patients being alive and event-free at 24 months than busulfan |
Probability of being alive and event-free at 36 months Follow-up (median)
| 551 (1 RCT) | NR | 49.7 per 100 | 59.5 per 100 (52.2 to 66.1 per 100) | 9.8 more per 100 (0.5 to 19.2 more per 100) | Lowa,b,e | Treosulfan may result in a clinically important higher probability of patients being alive and event-free at 36 months than busulfan |
Overall survival (full analysis set) | |||||||
Probability of being alive at 24 months Follow-up (median)
| 551 (1 RCT) | NR | 60.2 per 100 | 72.7 per 100 (66.8 to 77.8 per 100) | 12.5 more per 100 (4.4 to 20.7 more per 100) | Moderatea,e,f | Treosulfan likely results in a clinically important higher probability of patients being alive at 24 months than busulfan |
Probability of being alive at 36 months Follow-up (median)
| 551 (1 RCT) | NR | 56.3 per 100 | 66.8 (59.9 to 72.9 per 100) | 10.5 more per 100 (1.3 to 19.7 per 100) | Lowa,e,f | Treosulfan may result in a clinically important larger proportion of patients being alive at 36 months than busulfan |
Graft failure | |||||||
Observed percentage of patients with graft failure at 24 months Follow-up (median)
| 551 (1 RCT) | NR | 3.2 per 100 | 0.4 per 100 (0.0 to 2.1 per 100) | 2.8 fewer per 100 (0.6 fewer to 5.0 fewer) | Very lowe,g,h | The evidence is very uncertain about the effect of treosulfan on the percentage of patients with graft failure at 24 months compared with busulfan |
Engraftment | |||||||
Conditional cumulative incidence of reconstitution of granulopoiesis 28 days after HSCT Follow-up (median)
| 551 (1 RCT) | NR | 96.8 per 100 | 96.2 per 100 (93.4 to 99.1 per 100) | 1.3 fewer per 100 (4.7 fewer to 2.0 more per 100) | Lowa,e,i,j | Treosulfan may result in little to no clinically important difference in the conditional cumulative incidence of reconstitution of granulopoiesis 28 days after HSCT compared with busulfan |
Conditional cumulative incidence of reconstitution of thrombopoiesis (platelet count > 20 × 109/L) 28 days after HSCT Follow-up (median)
| 551 (1 RCT) | NR | 97.8 per 100 | 94.7 per 100 (92.0 per 100 to 97.4 per 100) | 2.8 fewer per 100 (6.4 fewer to 0.8 more per 100) | Lowa,e,i,j | Treosulfan may result in little to no clinically important difference in conditional cumulative incidence of reconstitution of thrombopoiesis (platelet count > 20 × 109/L) at 28 days after HSCT compared with busulfan |
Chimerism | |||||||
Incidence of complete chimerism at 28 days Follow-up (median)
| 551 (1 RCT) | NR | 83.3 per 100 | 93.2 per 100 (89.4 per 100 to 95.9 per 100) | 9.8 more per 100 (4.5 to 15.1 more per 100) | Very lowb,e,h | The evidence is very uncertain about the effect of treosulfan on the incidence of complete chimerism at 28 days compared with busulfan |
Relapse or progression | |||||||
Cumulative incidence of relapse or progression at 24 months Follow-up (median)
| 551 (1 RCT) | NR | 25.2 per 100 | 22.0 per 100 (16.9 to 27.1 per 100) | 3.2 fewer per 100 (10.4 fewer to 4.1 more per 100) | Lowa,b,e | Treosulfan may result in little to no clinically important difference in cumulative incidence of relapse or progression at 24 months compared with busulfan |
GvHD-free and relapse or progression-free survival | |||||||
Proportion of patients GvHD-free and relapse and/or progression-free at 24 months Follow-up (median)
| 551 (1 RCT) | NR | 37.1 per 100 | 50.3 per 100 (43.9 to 56.3 per 100) | 13.2 more per 100 (4.6 to 21.8 more per 100) | Lowa,b,e | Treosulfan may result in a clinically important larger proportion of patients being GvHD-free and relapse or progression-free at 24 months than busulfan |
Chronic GvHD-free and relapse or progression-free survival | |||||||
Proportion of patients being event-free and chronic GvHD-free at 24 months Follow-up (median)
| 551 (1 RCT) | NR | 37.2 per 100 | 51.4 per 100 (45.0 to 57.4 per 100) | 14.1 more per 100 (5.5 to 22.8 more per 100) | Moderatea,e,d | Treosulfan likely results in a clinically important larger proportion of patients being chronic GvHD-free and relapse or progression-free at 24 months than busulfan |
Nonrelapse mortality | |||||||
Cumulative incidence of nonrelapse mortality at 24 months Follow-up (median)
| 551 (1 RCT) | NR | 20.4 per 100 | 12.0 per 100 (8.0 per 100 to 15.9 per 100) | 8.4 fewer per 100 (2.2 to 14.7 fewer per 100) | Lowa,b,c | Treosulfan may result in a clinically important benefit on nonrelapse mortality at 24 months compared with busulfan |
Transplant-related mortality | |||||||
Probability of transplant-related mortality at 24 months Follow-up (median)
| 551 (1 RCT) | NR | 24.1 per 100 | 12.8 per 100 (9.2 per 100 to 17.7 per 100) | 11.3 fewer per 100 (4.4 to 18.2 fewer per 100) | Lowa,b,c | Treosulfan may result in a clinically important lower probability of transplant-related mortality at 24 months than busulfan |
HRQoL | |||||||
HRQoL by treatment | 551 (1 RCT) | No data available | No data available | No data available | No data available | NA | There is no evidence for the effect of treosulfan or busulfan on HRQoL |
Harms | |||||||
Cumulative incidence of acute GvHD of grade III or IV at 100 days Follow-up (median)
| 551 (1 RCT) | NR | 8.1 per 100 | 6.4 per 100 (3.4 to 9.3 per 100) | 1.8 fewer per 100 (6.1 fewer to 2.6 more per 100) | Moderatea,c,k | Treosulfan likely results in little to no clinically important difference in cumulative incidence of acute GvHD of grade III or IV at 100 days compared with busulfan |
Cumulative incidence of chronic GvHD at 24 months Follow-up (median)
| 551 (1 RCT) | NR | 60.3 per 100 | 61.7 per 100 (55.1 to 68.3 per 100) | 1.4 more per 100 (7.8 fewer to 10.7 more per 100) | Lowa,c,l | Treosulfan may result in little to no clinically important difference in cumulative incidence of chronic GvHD at 24 months compared to busulfan |
AML = acute myeloid leukemia; CI = confidence interval; GvHD = graft versus host disease; HRQ0L = health-related quality of life; HSCT = hematopoietic stem cell transplant; MDS = myelodysplastic syndrome; NA = not available; NR = not reported; RCT = randomized controlled trial; vs. = versus.
Note: Study limitations (which refer to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias were considered in the assessment of the certainty of the evidence. All serious concerns in these domains that led to the rating down of the level of certainty are documented in the table footnotes.
aRated down 1 level for serious risk of bias. The analysis used the full analysis set (FAS) rather than the intention-to-treat set. Patients who were randomized but not eligible for the FAS may have different characteristics and outcomes than those who were eligible, and thus may introduce bias.
bRated down 1 level for serious imprecision. There is no established minimally important difference (MID), but the clinical experts consulted by CADTH considered a 5% difference between groups to be a threshold of clinical importance. The point estimate and 1 side of the 95% CI for the between-group difference suggested a clinically important difference for treosulfan compared with busulfan, whereas the other side of the 95% CI suggested no clinically important difference between the 2 groups.
cIn the confirmatory interim analysis (database lock date: August 19, 2016), the null hypothesis was rejected for noninferiority, whereas the null hypothesis was not rejected for superiority in the primary analysis of EFS.
dImprecision was not rated down. There is no established MID, but the clinical experts consulted by CADTH considered a 5% difference between groups to be a threshold of clinical importance. The point estimate and the upper and lower bounds of the 95% CI for the between-group difference suggested a clinically important difference between the 2 groups.
eThe statistical testing for all end points in the final analysis (database lock date: March 16, 2018) of 551 patients in the FAS was not adjusted for multiplicity in the MC-FludT.14/L trial and should be considered supportive evidence.
fRated down 1 level for serious imprecision for OS at 36 months. There is no established MID, and the clinical experts consulted by CADTH considered 3% to be the threshold of important difference in the probability of patients who were alive at 24 and 36 months. The point estimate and the upper bound of the 95% CI for the between-group difference could suggest a clinical important difference between treosulfan and busulfan, whereas the lower bound of the 95% CI for the between-group difference suggests no clinically important difference between the 2 groups. Imprecision was not rated down for OS at 24 months; the point estimate and the upper and lower bounds of the 95% CI for the between-group difference suggest a clinically important difference between the 2 groups.
gRated down 1 level for serious imprecision. There is no established MID, but the clinical experts consulted by CADTH considered a 2% difference between groups in the cumulative incidence of graft failure at 24 months to be a threshold of clinical importance. The point estimate and the upper bound of the 95% CI for the between-group difference suggests a clinical important difference between treosulfan and busulfan, whereas the lower bound of the 95% CI suggests no clinically important difference between the 2 groups.
hRated down 2 levels for very serious risk of bias. The analysis used the FAS rather than the intention-to-treat set. Patients who were randomized but not eligible for the FAS may have different characteristics and outcomes than those who were eligible, which could introduce bias. In addition, the method used did not consider competing risk (i.e., death) and, thus, could have introduced bias.
iRated down 1 level for serious indirectness. The interpretation of the effect estimate is limited due to the lack of clarity in the interpretation of the outcome.
jImprecision was not rated down. There is no established MID, but the clinical experts consulted by CADTH considered a 10% difference between groups to be a threshold of clinical importance. The point estimate and the upper and lower bounds of the 95% CI for the between-group difference suggests no clinically important difference between the 2 groups.
kImprecision was not rated down. There is no established MID, and the clinical experts consulted by CADTH considered 10% to be the threshold of important difference in the cumulative incidence of acute GvHD of grade III- or V at 100 days. The point estimate and the upper and lower bounds of the 95% CI for the between-group difference suggests no clinically important difference between the 2 groups.
lRated down 1 level for very serious imprecision. There is no established MID, and the clinical experts consulted by CADTH considered 10% to be the threshold of important difference in the cumulative incidence of chronic GvHD at 24 months. The point estimate and lower bound of the 95% CI for the between-group difference suggests no clinically important difference between the groups; the upper bound of the 95% CI for the difference between groups suggests a clinically important harm of treosulfan.
Sources: MC-FludT.14/L Confirmatory Interim Analysis Clinical Study Report,22 MC-FludT.14/L Final Analysis Clinical Study Report.23 Details included in the table are from the sponsor’s Summary of Clinical Evidence.24
Long-Term Extension Studies
No long-term extension studies were identified for this review.
Indirect Comparisons
No indirect evidence was submitted for this review.
Studies Addressing Gaps in the Systematic Review Evidence
There were no results submitted by the sponsor for the retrospective study of patients with MDS who were ineligible to receive MAC conditioning therapy before alloHSCT that addressed the gap in the pivotal study resulting from the lack of Canadian sites.25
Conclusions
Patients and clinicians highlighted the need for effective treatments for AML and MDS that prolong life, control disease and symptoms, improve quality of life, and reduce side effects better than current treatments.
The phase III, open-label, multicentre, randomized, active-controlled, MC-FludT.14/L trial comparing treosulfan with busulfan (both in combination with fludarabine) as part of conditioning therapy demonstrated that treosulfan was noninferior to busulfan in terms of EFS, the primary outcome, in adults with AML or MDS who were not eligible for standard conditioning therapies. Superiority testing of treosulfan compared to busulfan did not show statistically significant results. However, there was a favourable trend toward improved EFS with treosulfan compared to busulfan, which, according to the clinical experts consulted by CADTH, was suggestive of a potentially clinically meaningful EFS benefit for treosulfan over busulfan. The OS data were considered immature, with an observed trend toward improved OS for treosulfan compared to busulfan. GRADE assessment of the MC-FludT.14/L trial suggested that treosulfan may result in a clinically important EFS and OS benefit compared with busulfan.
Compared with busulfan, treosulfan likely results in a clinically important benefit in CRFS at 24 months and little to no clinically important difference in the cumulative incidence of acute GvHD of grade III or VI at 100 days. Compared with busulfan, treosulfan may result in a clinically important benefits in GRFS, NRM, and TRM, and little to no clinically important benefits in relapse or progression, engraftment, and the cumulative incidence of chronic GvHD at 24 months. The evidence is very uncertain about the effect of treosulfan on graft failure and chimerism compared with busulfan. No new safety signals were identified in patients with AML or MDS. The clinical experts consulted by CADTH noted that, overall, the harms data for treosulfan and busulfan appear to be similar to the AEs observed in their own practices. The MC-FludT.14/L trial did not report HRQoL data.
Introduction
The objective of CADTH’s Clinical Review Report is to review and critically appraise the clinical evidence submitted by the sponsor on the beneficial and harmful effects of IV treosulfan 10 g/m2 BSA per day, in combination with IV fludarabine 30 mg/m2 BSA per day, as part of conditioning treatment before alloHSCT in adults with AML or MDS at elevated risk with standard conditioning therapies. The focus will be on comparing treosulfan in combination with fludarabine to relevant comparators and identifying gaps in the current evidence.
Disease Background
Content within this section has been informed by materials submitted by the sponsor and clinical expert input. The following has been summarized and validated by the CADTH review team.
AML is the most common form of acute leukemia in adults, representing approximately 24% of leukemia cases. AML is a cancer of the blood and BM. The BM makes blood stem cells (immature cells) that become mature blood cells over time, developing into either myeloid or lymphoid stem cells. In AML, the myeloid stem cells usually become immature blood cells called myeloblasts (or myeloid blasts) or leukemia cells (or blasts) that infiltrate BM, blood, and other tissues.26 Genetic alterations in myeloid progenitor stem cells alter normal growth and the differentiation of myeloblasts.1 When abnormal blood cells build up in the BM and blood, there is less room for healthy cells, which can lead to infection, anemia, or easy bleeding. Abnormal blood cells can also spread to other parts of the body (e.g., the brain and spinal cord, skin, and gums) or form a solid tumour known as myeloid sarcoma.26 Approximately 40% of patients with AML who are younger than 60 years will be cured of their disease after treatment; for those older than 60 years, this estimate is between 5% and 15%.1,2 In Canada, the 5-year net survival for patients with AML is 23%, and the median survival of older patients with AML is estimated to range from 5 to 10 months with current treatment options.1,4 The clinical experts consulted by CADTH remarked that, generally, the estimated survival probability for patients who are ineligible for high-intensity conditioning regimens (e.g., myeloablative) is around 5% to 10% lower than for patients who are eligible. This is because patients who receive an RIC may be older and have more comorbidities than patients who receive MAC, according to clinical experts consulted by CADTH. The Canadian Cancer Society estimated that, as of 2018, about 19,310 people in Canada were living with leukemia (5-year prevalence).3 The Canadian Cancer Society also reports that 1,090 people in Canada were newly diagnosed with AML in 2016 and that 1,184 died from AML in 2017.4 According to the clinical experts consulted by CADTH, it is estimated that the percentage of patients in Canada who are not eligible for MAC ranges from 30% to 40% for patients with AML; this is higher for patients with MDS, given that those patients tend to be older.
Although the exact cause of AML is unknown, there are factors known to contribute to an increased risk of diagnosis; in particular, risk increases with age and is higher among males. Additional known risk factors include smoking, prior anticancer treatments, the presence of certain genetic abnormalities (trisomy 21; Fanconi anemia; Bloom syndrome; familial mutations of CEBPA, DDX41, RUNX1), blood disorders (e.g., myelodysplasia and myeloproliferative disorders), exposure to chemicals (e.g., benzene, pesticides), and radiation. Signs and symptoms of AML are related to pancytopenia (i.e., anemia, neutropenia, and thrombocytopenia), including fatigue, pale skin, weakness, infections, and hemorrhagic findings such as gingival bleeding (i.e., bleeding gums), ecchymoses (i.e., bruises), epistaxis (i.e., bleeding from nose), and menorrhagia (i.e., heavy menstrual bleeding). Additionally, patients can experience bone pain, especially in the lower extremities.27 According to Alberta Health Services guidelines, the diagnosis of AML can be confirmed from the peripheral blood (PB), but all patients considered for therapy will need to undergo a BM aspiration and a biopsy. The threshold number of immature clonal cells, typically blasts, required to make the diagnosis of AML is at least 20% of total nucleated cells in the BM by morphology. Exceptions include AML with t(8;21), inv(16), t(16;16), or t(15;17), in which case the diagnosis of AML is made regardless of the percentage of BM blasts.28
MDS are a type of cancer in which there is a lack of healthy blood cells and there are abnormal cells in the blood and/or BM. As a result, infections, anemia, or bleeding may occur.5,6 Sometimes, MDS develop into AML. MDS will progress to AML in one-fourth to one-third of cases.5 The estimated overall age-adjusted incidence rate of MDS is 4.3 cases per 100,000 persons per year.7 According to a Canadian study conducted from January 1, 2011, to December 31, 2015, in the Calgary metropolitan area, the incidence rate of MDS was 2.60 per 100,000 person-years, corresponding to an age-standardized incidence of 3.in for Canada.8 The male-to-female ratio was 1.35, and the median age at diagnosis was 75 years. These data indicate that 1,295 new cases of MDS annually would be predicted in Canada.29 The etiology of MDS is only known in 15% of cases. Some of the risk factors for MDS are smoking, radiation, chemotherapy, chemical exposure, and advanced age, and incidence is higher among males.5,30-32 Signs and symptoms of MDS are related to anemia, neutropenia, and thrombocytopenia, such as fatigue, loss of appetite, dizziness, infections, gingivitis, bruising, and bleeding.26 The survival rate in patients with MDS ranges from a few weeks to many years. Median OS has been reported to range from 15 to 30 months, and the 5-year AML progression rate has been estimated to range from 25% to 35%. Higher-risk patients with MDS have a major risk of progression to AML and have short survival outcomes.5 The clinical experts consulted by CADTH estimated that approximately more than 40% of patients with MDS are not eligible for a MAC regimen. Diagnostic tests for MDS are complete blood count, blood smear, and BM examination. The diagnosis is established with BM aspiration and biopsy, and requires persistent cytopenia, a blast count of less than 20% in the PB and/or BM, and either characteristic cytogenetic and/or molecular features or a dysplastic morphology.5,33
Standards of Therapy
Content within this section has been informed by materials submitted by the sponsor and clinical expert input. The following has been summarized and validated by the CADTH review team.
Treatment with alloHSCT is currently the only known curative therapy for patients with AML and for high-risk patients with MDS.9-15 Conditioning therapy plays a central role in HSCT by preparing or conditioning the patient’s body for the transplant.16-19 There are 3 common types of conditioning regimens: MAC, RIC, and nonmyeloablative. MAC regimens are considered standard conditioning therapies, and include fractionated total body irradiation and high-dose busulfan as toxic components of stem cells. Commonly used chemotherapeutic drugs in conditioning regimens are cyclophosphamide, melphalan, and fludarabine. Other cytotoxic drugs, like cytarabine, etoposide, thiotepa, and nitrosourea, are sometimes administered in addition to prevent early relapse of the underlying malignancy.34 High-intensity MAC regimens are highly effective at reducing the relapse risk; however, they are associated with a significant risk of morbidity, treatment-related toxicity, and TRM, especially among patients with comorbid conditions and advanced age. RIC and nonmyeloablative regimens involve lower doses of chemotherapy than MAC to reduce treatment-related toxicity in high-risk patients (Figure 1). Currently, no consensus guidelines are available on the choice of optimal conditioning regimens, as this choice mainly depends on patient- related, disease-related, and donor-related factors, such as disease status (e.g., remission, refractory or relapsed disease), age, performance status, and comorbid conditions, all of which are important considerations when selecting the optimal conditioning regimen to improve survival and transplant and patient outcomes.35,36 The clinical experts consulted by CADTH indicated that for a conditioning regimen, MAC and RIC are the standard, depending on patient age and/or comorbidities.
Patients who are not eligible for MAC regimens (e.g., older patients and those with comorbidities) usually receive an RIC regimen, such as busulfan in combination with fludarabine, to minimize treatment-related toxicity, NRM, and TRM; but the lower-dose intensity comes with a higher risk of relapse. One meta-analysis reported that RIC regimens led to a nearly 1.6-fold increase in the risk of relapse across the entire cohort of patients compared with high-dose myeloablative regimens, regardless of disease type or status.9 As a result, a large proportion of patients with AML or MDS who undergo alloHSCT are at high risk of dying from either treatment-related toxicity or disease relapse. Based on expert opinion provided by the clinical experts consulted by CADTH, the survival probability of patients who receive RIC regimens is estimated to be around 5% to 10% lower than patients who receive MAC regimens. In addition, the clinical experts consulted by CADTH stated that a key limitation of alloHSCT is the increased risk of NRM, which can result from opportunistic infection, GvHD, or other complications, and there is still about a 15% to 20% chance of leukemia and/or MDS recurrence after alloHSCT. There remains an unmet need for conditioning regimens that can reduce the risk of TRM without increasing the incidence of relapse, as conventional therapies do, and that ultimately improve survival rates and quality of life.
In Canada, busulfan in combination with fludarabine is the most commonly used RIC, as melphalan is not indicated or recommended before HSCT in provincial treatment regimens for patients with AML.37-39 Furthermore, although it may be used off-label in rare cases as a conditioning drug before autologous HSCT, melphalan is not used in Canada before alloHSCT, per the experts in Canada consulted by the sponsor.
Figure 1: Provisional Algorithm Diagram
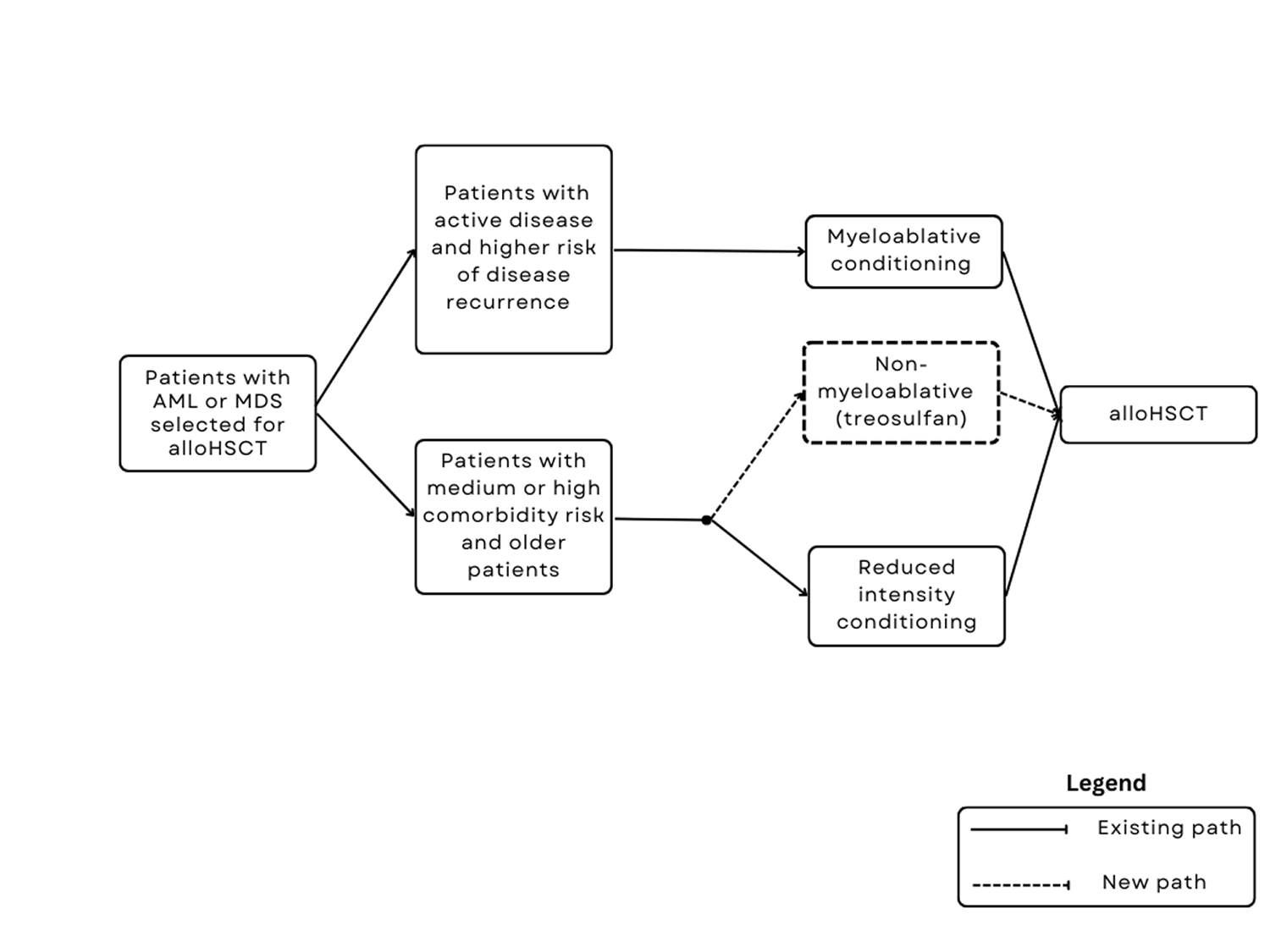
alloHSCT = allogeneic hematopoietic stem cell transplant; AML = acute myeloid leukemia; MDS = myelodysplastic syndrome.
Source: Submitted Clinical Evidence Summary.24
Drug Under Review
The key characteristics of treosulfan and busulfan as part of conditioning treatment before alloHSCT are summarized in Table 3.
The recommended regimen of treosulfan and its schedule of administration is as follows:
Treosulfan 10 g/m2 BSA per day as a 2-hour IV infusion, given on 3 consecutive days (day –4, day –3, day –2) before stem cell infusion (day 0). The total treosulfan dose is 30 g/m2.
Fludarabine 30 mg/m2 BSA per day as a 0.5-hour IV infusion, given on 5 consecutive days (day –6, day –5, day –4, day –3, day –2) before stem cell infusion (day 0). The total fludarabine dose is 150 mg/m2.
Treosulfan should be administered before fludarabine on day –4, day –3, and day –2 (FT10 regimen).
No dose adjustment is necessary for mild or moderate liver or renal impairment, but treosulfan is contraindicated in patients with severe impairment. IV treosulfan should be administered using a safe technique to avoid extravasation and should be supervised by a physician experienced in conditioning treatment followed by alloHSCT.
Treosulfan has not been previously reviewed by CADTH. The Notice of Compliance was issued on June 25, 2021.
Treosulfan is a prodrug that converts to epoxides, which affect DNA and result in stem-cell-depleting, immune-suppressive, and antineoplastic effects.
The sponsor’s reimbursement request to CADTH is for treosulfan in combination with fludarabine as part of conditioning treatment before alloHSCT in adults with AML or MDS who are at increased risk with standard conditioning therapies. Note that the sponsor’s reimbursement request differs from the approved Health Canada indication, in that pediatric patients are not included. The Health Canada indication is for treosulfan in combination with fludarabine as part of a conditioning treatment before alloHSCT in adults with AML or MDS who are at increased risk with standard conditioning therapies and in pediatric patients with AML or MDS who are older than 1 year. Per the sponsor’s request, this CADTH review focuses on the indication in adults. CADTH did not review the pediatric population.
Table 3: Key Characteristics of Treosulfan and Busulfan
Characteristic | Treosulfan | Busulfan |
|---|---|---|
Mechanism of action | Treosulfan converts to epoxides, which result in stem-cell-depleting, immune-suppressive, and antineoplastic effects | Busulfan is an alkylating drug that produces DNA cross-linking and chromosomal damage that can be lethal to rapidly dividing cells |
Indicationa | Indicated in combination with fludarabine as part of conditioning treatment before alloHSCT in adults with AML or MDS at increased risk with standard conditioning therapies and in pediatric patients with AML or MDS who are older than 1 year | Indicated for use in combination with other chemotherapeutic drugs and/or radiotherapy as a conditioning regimen before hematopoietic progenitor cell transplant, including acute lymphocytic leukemia, acute nonlymphocytic leukemia, AML, chronic myeloid leukemia, non-Hodgkin’s lymphoma, Hodgkin’s disease, multiple myeloma, and MDS |
Route of administration | IV | IV |
Recommended dose | 10 g/m2 BSA per day as a 2-hour IV infusion, given on 3 consecutive days (day –4, day –3, day –2) before stem cell infusion (day 0); the total treosulfan dose is 30 g/m2 | For MAC: IV busulfan 0.8 mg/kg administered with a central venous catheter as a 2-hour infusion every 6 hours for 4 consecutive days, for a total of 16 doses For RIC: There is no recommended RIC dose in the busulfan product monograph; according to the clinical experts consulted by CADTH, busulfan is administered as a 3.2 mg/kg IV infusion for 2 consecutive days; the total busulfan dose is 6.4 mg/kg |
Serious adverse effects or safety issues | Severe and prolonged myelosuppression; HSCT is required to prevent potentially fatal complications of prolonged myelosuppression | Contraindicated for patients who are sensitive, allergic, or intolerant of the drug or its vehicle Profound myelosuppression, including granulocytopenia, thrombocytopenia, and anemia |
alloHSCT = allogeneic hematopoietic stem cell transplant; AML = acute myeloid leukemia; BSA = body surface area; HSCT = hematopoietic stem cell transplant; MAC = myeloablative conditioning; MDS = myelodysplastic syndromes; RIC = reduced-intensity conditioning.
aHealth Canada–approved indication.
Source: Treosulfan product monograph, busulfan product monograph.
Stakeholder Perspectives
Patient Group Input
This section was prepared by the CADTH review team based on the input provided by patient groups. The full original patient input received by CADTH has been included in the Stakeholder section of this report.
CADTH received 1 patient group submission from LLSC. LLSC is a national charitable status organization dedicated to finding a cure for blood cancers and improving the quality of life of people affected by blood cancers and their families by funding life-enhancing research and providing educational resources, services, and support.
LLSC conducted an online survey in July 2023. The majority of the 108 respondents identified as a past or present patient with AML (61%) or a caregiver of a patient with AML (17%). About 16% of respondents identified as a past or present patient with MDS and 3% identified as a caregiver of a patient with MDS. LLSC stated that the survey asked for input from patients and caregivers who had experience with MDS or AML and who had received or considered receiving an alloHSCT. Among the respondents, 81% identified as alloHSCT recipients and 8% were considering an alloHSCT.
The most common age range for the patients with AML or MDS at the time of transplant was 56 to 64 years (30.93%), followed by 41 to 55 years (25.77%). About 3% of patients were younger than 18 years.
LLSC stated that the questions in this survey were not intended to measure the efficacy of the drug under review against currently available treatments; instead, the questions were aimed at highlighting the mental status of patients with MDS or AML and their families when they have to make a decision about a stem cell transplant. Moreover, the survey set out to explore how access to a pretransplant conditioning treatment with more potential benefits and fewer side effects affects patients’ decision-making and the level of mental burden.
LLSC noted the decision-making and preparation process for a stem cell transplant has a significant impact on the mental health of patients and their families. According to the survey, 79% of respondents reported moderate to extreme levels of anxiety and 83% reported moderate to extreme levels of stress.
Survey respondents hoped that a transplant would improve their odds of OS, improve their quality of life, and prevent disease progression. They also noted that the thought of losing time and becoming ineligible for alloHSCT, and posttransplant complications, such as graft rejection, graft failure, infection, GvHD, and toxicity, were factors they considered before deciding whether or not to undergo transplant.
LLSC noted that patients expressed that knowing they would have access to conditioning therapy with the potential for increased survival and fewer side effects had a significant positive impact on their mental health. When the respondents were asked how they would feel about a conditioning treatment that could reduce toxicity and minimize long-term effects, 62% replied that it would have an extremely positive impact on their anxiety, fear, and stress levels. The positive impact is even more significant when there is a potential for a survival benefit; 82% of respondents indicated that a conditioning treatment that could improve their chance of survival would have an extremely positive impact on their outlook.
Clinician Input
Input From Clinical Experts Consulted by CADTH
All CADTH review teams include at least 1 clinical specialist with expertise in the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). The following input was provided by 2 clinical specialists with expertise in the diagnosis and management of adults with AML or MDS.
Unmet Needs
According to the clinical experts consulted by CADTH, the current standard treatment for patients with AML or MDS for whom transplant is indicated is busulfan with fludarabine-based conditioning therapy followed by stem cell infusion from the donor and GvHD prophylaxis. The clinical experts consulted by CADTH noted that MAC and RIC conditioning regimens, which both involve busulfan, are the standard, depending on patient age and/or comorbidities. The clinical experts stated that AML and MDS are very similar in terms of treatment modality and treatment and management options, but there are some minor differences in terms of the management of AML and MDS, such as different risk systems.
According to the clinical experts consulted by CADTH, alloHSCT is known to be the only treatment that can modify the course of the disease and can achieve long-term cure. However, the clinical experts stated that the limitation of alloHSCT is the increased risk of NRM, which can result from opportunistic infection, GvHD, or other complications; there is still about a 15% to 20% chance of leukemia or MDS recurrence after alloHSCT.
Place in Therapy
The clinical experts consulted by CADTH indicated that the best way to optimize survival in patients receiving alloHSCT is to provide the best regimen for transplant using the best available donor in a timely manner before disease recurrence. The clinical experts stated that it would not be appropriate to recommend that patients try other conditioning regimens before considering treosulfan, as reserving a treatment that is potentially beneficial for later lines of therapy is not a reasonable way to optimize transplant outcomes. Accordingly, the clinical experts also indicated that reserving treosulfan for patients who experience intolerance to or failure of a first transplant is not a good approach. The clinical experts stressed that the best available treatment option, a conditioning regimen, GvHD prophylaxis, and the best-suited donor should be used. The clinical experts indicated that treosulfan conditioning provides a survival benefit without increasing the risk of relapse. They expect that treosulfan will cause a shift in the current treatment paradigm.
Patient Population
The clinical experts consulted by CADTH indicated that treosulfan with a fludarabine-based conditioning regimen is considered to be RIC; therefore, patients who meet the criteria for RIC, owing to increased risk of NRM because of age (older than 55 or 60 years) or a high level of comorbidities (such as HCT-CI score above 3), would be best suited for a conditioning treatment with treosulfan in combination with fludarabine. The clinical experts stated that there is evidence to support the superiority of treosulfan with fludarabine over the myeloablative regimen of a 4-day course of busulfan with fludarabine or cyclophosphamide in patients who are eligible for MAC without any age issue (younger than 60 years) or comorbidity issue (HCT-CI score below 3).40
The clinical experts consulted by CADTH stated that the current algorithm used to determine conditioning intensity, and therefore RIC or MAC, is mainly based on age and HCT-CI score, with some clinician discretion. The clinical experts indicated that disease risk is 1 more factor to be considered; in the case of the adverse-risk disease group, MAC is preferred over RIC. However, the clinical experts stated that age and HCT-CI score usually override the disease factor when determining conditioning regimen intensity. In clinical practice, though, there may be situations in which the determination of conditioning intensity can be a challenge.
Assessing the Response Treatment
According to the clinical experts consulted by CADTH, OS, relapse-free survival, the cumulative incidence of NRM, and the cumulative incidence of relapse are mainly used for alloHSCT outcome assessment. The clinical experts stated that engraftment kinetics, GvHD incidence (acute and chronic), and other infection rates (such as cytomegalovirus viremia incidence) are used as additional end points. They indicated that symptom-based assessments are rarely used to evaluate the efficacy or tolerability of specific transplant regimens.
Discontinuing Treatment
The clinical experts consulted by CADTH indicated that the decision about which conditioning treatment to use (e.g., treosulfan-based) is made before the patient is selected for transplant, and that they would not discontinue the treatment if a patient is selected for transplant. The clinical experts stated that there are 2 occasions when treosulfan can be discontinued or switched to an alternative treatment option: first, if a patient has active leukemia (blast count above 5%) or uncontrolled MDS (blast count above 10%), the transplant process will be not cleared to proceed; and second, if the medical circumstances of a patient indicate it, treosulfan can be switched to another treatment.
Prescribing Considerations
The clinical experts consulted by CADTH indicated that treosulfan in combination with fludarabine for alloHSCT should be used only in experienced allogeneic transplant centres.
Clinician Group Input
This section was prepared by the CADTH review team based on the input provided by clinician groups. The full original clinician group inputs received by CADTH have been included in the Stakeholder section of this report.
Two clinician groups provided input to the submission: CTTC and the OH-CCO-CMHAC.
CTTC is a member-led, national, multidisciplinary organization that provides leadership and promotes excellence in patient care, research, and education in the field of HSCT and cell therapy. CTTC advocates, nationally and internationally, for improvement in the outcomes and accessibility of cellular therapies and transplant for people in Canada.
The OH-CCO complex malignant hematology program provides oversight on planning, access, funding, and quality initiatives to support the delivery of stem cell transplant, immune effector cell therapies, and the treatment of acute leukemia in Ontario.
Both clinician groups noted that allogeneic transplant is a potentially curative therapy for patients with AML or MDS. Young and fit patients are eligible for MAC, whereas RIC is recommended for older patients and those with comorbidities. Despite the use of RIC for allogeneic transplants in older patients and/or in those with comorbidities, significant rates of NRM, TRM, and toxicity impair the outcomes of transplants. CTTC believes that, based on the data, treosulfan-based conditioning has myeloablative and antineoplastic effects and is associated with reduced NRM in adults. CTTC also stated that, based on available data, treosulfan-based conditioning is safe and effective in pediatric patients with hematological malignancies.
CTTC and OH-CCO-CMHAC agreed that compared to busulfan-based conditioning, treosulfan-based conditioning is associated with better survival and lower rates of TRM. OH-CCO-CMHAC added that improved overall and event-free survival, significantly lower rates of NRM, fewer graft failures, and lower rates of GvHD have been seen with treosulfan-based conditioning.25,41-48 CTTC believes there is sufficient evidence that treosulfan-based conditioning may bridge the gap in the need for alloHSCT more safely to older patients with AML or MDS.
OH-CCO-CMHAC and CTTC both commented that adults undergoing alloHSCT for AML or MDS who are ineligible for MAC on the basis of age and/or comorbidities would be best suited for treosulfan-based conditioning, whereas patients undergoing alloHSCT for AML or MDS who are eligible for MAC would be least suitable for treosulfan-based conditioning. OH-CCO-CMHAC also noted that in the Health Canada monograph, there are no specific details regarding age and/or comorbidity index score. Additionally, patients without a suitable matched related donor (MRD) or matched unrelated donor (MUD) and those who are eligible for haploidentical HSCT with ex vivo T-cell depletion might be excellent candidates.
CTTC believes that because treosulfan is given for a finite duration (3 days in total) as part of a conditioning treatment ahead of alloHSCT for patients with AML or MDS, there is typically no response assessment to the drug during this time. Both clinician groups noted that the outcomes of transplants in patients who receive treosulfan-based conditioning will, however, be assessed using the outcome measures standard in alloHSCT literature. According to CTTC, some of the important outcomes are OS (typically reported at 2 years), TRM (typically reported at 100 days and 2 years), relapse (typically reported at 2 years), relapse-free survival (typically reported at 2 years), the cumulative incidence of acute GvHD (typically reported at 100 days), the cumulative incidence of chronic GvHD (typically reported at 2 years), and GRFS (typically reported at 2 years). CTTC also added that for children and adolescents who undergo HSCT, in addition to the aforementioned standard outcome measures, the disease-specific outcomes defining cure (i.e., for hemoglobinopathies, the phenotype should be corrected by donor-derived erythropoiesis) are often used.
CTTC and OH-CCO-CMHAC both stated that because treosulfan is given for a finite duration (3 days in total) there is usually no need to consider discontinuation during the administration. The only instance in which treatment with treosulfan may be discontinued, and which is highly unlikely, is when a patient develops severe hypersensitivity and/or allergic reaction to the drug. Any toxicity issues related to the conditioning would be seen later in the course of the allogeneic transplant.
CTTC and OH-CCO-CMHAC both stated that treosulfan should only be prescribed for this indication by specialists working in a clinical setting associated with alloHSCT programs. In Canada, these are generally in cancer centres associated with tertiary care hospitals.
Drug Program Input
The drug programs provide input on each drug being reviewed through CADTH’s reimbursement review processes by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CADTH are summarized in Table 4.
Table 4: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Relevant comparators | |
The comparator to treosulfan is busulfan. Treosulfan and busulfan are both given in combination with fludarabine as part of a reduced-intensity conditioning regimen before alloHSCT. Busulfan is funded in all provinces. | Comment from the drug programs to inform pERC deliberations. |
Considerations for initiation of therapy | |
Eligibility for the trial included Karnofsky score ≥ 60%; AML in first or consecutive complete response (blast counts < 5% in bone marrow, according to the 2008 WHO revised classification; MDS (blast counts < 20% in the bone marrow, according to the 2008 revised classification); and indication for alloHSCT in a patient at increased risk for MAC based on being 50 years or older, having an HSCT-specific comorbidity index of > 2, or both. Are these criteria appropriate and/or applicable for selection in Canadian practice? What criteria should be used to define AML and MDS to identify eligible patients? | The clinical experts consulted by CADTH indicated that the eligibility criteria for the MC-FludT.14/L trial are generally appropriate for allogeneic transplant in patients with AML or MDS, except for the blast count in bone marrow < 20% for patients with MDS. A 10% cut-off for pretransplant blast percentage is used for patients with MDS in some centres. The clinical experts consulted by CADTH stated that it is reasonable to offer transplant to patients with a Karnofsky performance status of 60% or above. For MAC criteria, the clinical experts indicated that some centres use an age cut-off of 50 years, whereas some use 55 to 60 years. The clinical experts confirmed that the results of the MC-FludT.14/L trial can be generalized to a 10% cut-off for pretransplant blast percentage for MAC criteria in patients with MDS and patients aged 55 to 60 years. This is because blast percentage is only 1 factor considered when assessing MDS risk; other important factors include karyotype and molecular studies. The clinical experts stated that a cut-off based solely on blast count ignores the complexity and nuance of MDS as a disease. The clinical experts commented that biologic age by itself is an imperfect predictor of transplant outcome; thus, it is inappropriate to base the MAC vs. RIC decision on age alone. The clinical experts indicated that clinicians consider comorbidities, frailty, and performance status as well. |
Other criteria for eligibility in the trial were age from 18 to70 years, no significant organ dysfunction, and no active or noncontrolled infectious diseases. Should these criteria also apply? | The clinical experts indicated that other criteria for eligibility in the MC-FludT.14/L trial regarding age, organ dysfunction, and infectious diseases are common criteria for transplant. The clinical experts noted that these criteria should be met before transplant. |
The trial did not specify therapies before conditioning. Would standard of care per transplant centre be appropriate for prior therapies? | The clinical experts consulted by CADTH agreed to let each transplant centre decide the standard of care before transplant. The clinical experts noted that patients will be eligible for transplant using treosulfan in combination with fludarabine if they meet the criteria of a blast count < 5% for AML and a blast count < 20% (or 10%) for MDS before transplant. |
Should patients be eligible for a second transplant with busulfan after relapse and/or graft failure? Should patients be eligible for a second transplant with treosulfan after relapse and/or graft failure with busulfan conditioning? | The clinical experts consulted by CADTH indicated that patients will be eligible for a second transplant with busulfan after relapse and/or graft failure or a second transplant with treosulfan after relapse and/or graft failure with busulfan conditioning. The clinical experts suggested leaving it up to the treating transplant centre to decide on the appropriate conditioning regimen for a second transplant. |
Patients with previous alloHSCT were excluded from the MC-FludT.14/L trial. Should they be eligible? Patients with active and uncontrolled infectious disease were excluded from the trial. Should they be eligible? | The clinical experts consulted by CADTH felt that results from the MC-FludT.14/L trial can be generalized to patients who received a previous alloHSCT. The clinical experts stated that this group of patients is at higher risk of nonrelapse mortality and morbidity, so they would receive more benefit from treosulfan in combination with fludarabine, as treosulfan has good antileukemic efficacy with low toxicity, which is important for patients with a second transplant. The clinical experts noted that any patients with active and uncontrolled infection should be excluded from transplant. |
Considerations for prescribing of therapy | |
Fludarabine dosing is the same as in busulfan protocols. IV treosulfan is given at a dose of 10 mg/m2 on day –4, day –3, and day –2 before stem cell infusion (day 0). Busulfan is given in 2 doses before stem cell infusion. | Comment from the drug programs to inform pERC deliberations. |
If treosulfan is administered in the inpatient setting, the adoption may be dependent on the extent of drug coverage, given that inpatient drug costs fall outside of provincial drug plan budgets in some jurisdictions. | Comment from the drug programs to inform pERC deliberations. |
Generalizability | |
Busulfan is used in myeloablative conditioning regimens. Could treosulfan be considered an alternate in these regimens? | The clinical experts consulted by CADTH stated that younger patients who would be otherwise eligible for myeloablative conditioning but are worried about liver dysfunction may benefit from treosulfan 14 g/m2 per day (for a total dose of 42 g/m2). This is because the higher treosulfan dosing may have less specific liver toxicity than busulfan myeloablative dosing and a similar overall toxicity profile in terms of pancytopenia and mucosal toxicity. As these younger patients are a small group, the clinical experts are uncertain whether there is enough evidence for treosulfan to replace busulfan as the standard myeloablative conditioning. |
Funding algorithm (oncology only) | |
Treosulfan may replace busulfan in reduced-intensity conditioning regimens. | Comment from the drug programs to inform pERC deliberations. |
Care provision issues | |
The trial used a standard GvHD prophylaxis protocol of cyclosporine, methotrexate, and (if MUD) antithymocyte globulin. Would it be reasonable for centres to choose to follow this approach and/or use the institutional protocol for GvHD prophylaxis? | The clinical experts consulted by CADTH stated that there is heterogeneity from centre to centre in terms of GvHD prophylaxis strategies. For example, some centres may not use antithymocyte globulin. Therefore, the clinical experts suggested that it is best for the patient to receive GvHD prophylaxis strategies that the institution has experience with. |
System and economic issues | |
The manufacturer assumes a fairly low uptake for a drug that is becoming the new standard of care for reduced-intensity conditioning regimens. | Comment from the drug programs to inform pERC deliberations. |
Busulfan is generic. | Comment from the drug programs to inform pERC deliberations. |
alloHSCT = allogeneic hematopoietic stem cell transplant; AML = acute myeloid leukemia; GvHD = graft versus host disease; MAC = myeloablative conditioning; MDS = myelodysplastic syndrome; MUD = matched unrelated donor; pERC = CADTH pan-Canadian Oncology Review Expert Review Committee; vs. = versus.
Clinical Evidence
The objective of CADTH’s Clinical Review Report is to review and critically appraise the clinical evidence submitted by the sponsor on the beneficial and harmful effects of IV treosulfan 10 g/m2 BSA per day in combination with IV fludarabine 30 mg/m2 BSA per day as part of conditioning treatment before alloHSCT in adults with AML or MDS at elevated risk with standard conditioning therapies. The focus will be on comparing treosulfan in combination with fludarabine to relevant comparators and identifying gaps in the current evidence.
A summary of the clinical evidence included by the sponsor in the review of treosulfan in combination with fludarabine is presented in the Systematic Review section, with CADTH’s critical appraisal of the evidence presented at the end of the section. The Systematic Review section includes the pivotal studies and RCTs that were selected in accordance with the sponsor’s systematic review protocol. CADTH’s assessment of the certainty of the evidence using the GRADE approach follows the critical appraisal of the evidence.
Included Studies
Clinical evidence from the following study is included in the CADTH review and appraised in this document:
a pivotal phase III, multicentre, open-label, active treatment RCT (MC-FludT.14/L), which was identified in the systematic review.
Systematic Review
Content within this section has been informed by materials submitted by the sponsor. The following has been summarized and validated by the CADTH review team.
Description of Studies
Characteristics of the included study is summarized in Table 5.
Table 5: Details of the Study Included in the Systematic Review
Detail | MC-FludT.14/L |
|---|---|
Designs and populations | |
Study design | Open-label, multicentre, international, group-sequential, phase III RCT |
Locations | 33 sites across Finland, France, Germany, Hungary, Italy, and Poland |
Patient enrolment dates | Start date: November 24, 2008 End date: December 7, 2016 |
Randomized (N) | N: 570 Busulfan: 290 Treosulfan: 280 |
Inclusion criteria |
|
Exclusion criteria |
|
Drugs | |
Intervention |
|
Comparator(s) |
|
Study duration | |
Screening phase | NA |
Run-in phase | NA |
Treatment phase | Patients in the test group were treated on 3 consecutive days with treosulfan (day –4, day –3, day –2) with treosulfan, whereas patients in the reference group were treated on 2 consecutive days (day –4 and day –3) with busulfan |
Follow-up phase | Postsurveillance follow-up with respect to EFS, OS, relapse and/or progression, and NRM in patients who terminated the study alive 2 years after the transplant was conducted1 year after the last randomized patient underwent transplant |
Outcomes | |
Primary end point | EFS (in the 2 years after alloHSCT) |
Secondary and exploratory end points | Secondary:
Exploratory:
|
Publication status | |
Publications | |
alloHSCT = allogeneic hematopoietic stem cell transplant; AML = acute myeloid leukemia; CNS = central nervous system; CTC = Common Terminology Criteria; EFS = event-free survival; GvHD = graft versus host disease; HCT-CI = Hematopoietic Cell Transplantation-Specific Comorbidity Index; HLA = human leukocyte antigen; MAC = myeloablative conditioning; MDS = myelodysplastic syndromes; NA = not applicable; NRM = nonrelapse mortality; OS = overall survival; RCT = randomized controlled trial; TRM = transplant-related mortality.
aDonor selection is based on molecular high-resolution typing (4 digits) of class II alleles of the DRB1 and DQB1 gene loci and molecular (at least) low-resolution typing (2 digits) of class I alleles (i.e., antigens) of the HLA-A, HLA-B, and HLA-C gene loci. In case no class I or class II completely identical donor (10 out of 10 gene loci) can be identified, 1 antigen disparity (class I) and/or 1 allele disparity (class II) between patient and donor are acceptable. Conversely, disparity of 2 antigens (irrespective of the involved gene loci) cannot be accepted. These definitions for the required degree of histocompatibility apply to the selection of related and unrelated donors.
Source: MC-FludT.14/L Final Analysis Clinical Study Report.23 Details included in the table are from the sponsor’s Summary of Clinical Evidence.24
One pivotal trial (the MC-FludT.14/L trial) was included in the systematic review. The MC-FludT.14/L trial is a phase III, randomized, open-label, multicentre, international, group-sequential study conducted to compare the efficacy and safety of treosulfan-based conditioning therapy with a busulfan-based RIC regimen. This study enrolled adults with AML or MDS who met the indication criteria for alloHSCT and were considered ineligible for standard conditioning therapies (i.e., patients 50 years and older and/or those with an HCT-CI score > 2).
Patients were enrolled between November 24, 2008, and December 7, 2016. Three confirmatory interim evaluations and 1 final analysis were planned. Patient recruitment into the trial was stopped after the second interim analysis (referred to as the confirmatory interim analysis in this review), as the noninferiority of treosulfan-based conditioning was established. The data cut-off date was August 19, 2016, for the confirmatory interim analysis, and the database lock date was March 16, 2018, for the final analysis. This CADTH report primarily focused on the results from the final analysis, but did report the results for the primary outcome of EFS at the confirmatory interim analysis. In the final analysis, 570 patients were randomized (280 in the treosulfan group and 290 in the busulfan group). These patients were recruited from 33 sites in 6 countries: Finland, France, Germany, Hungary, Italy, and Poland. This study had no sites in Canada.
Eligible patients were followed for, at most, 2 years after transplant. In addition, the postsurveillance follow-up with respect to EFS, OS, relapse and/or progression, and NRM of patients who terminated the study alive 2 years after transplant was conducted 1 year after the last randomized patient underwent transplant, irrespective of any premature stop of the trial. The primary objective of the MC-FludT.14/L trial was to compare EFS in the 2 years after alloHSCT in patients who received treosulfan plus fludarabine conditioning and those who received busulfan plus fludarabine conditioning. Events for the primary outcome were defined as relapse and/or progression of disease, graft failure, or death (whichever occurred first). Treosulfan plus fludarabine conditioning was also compared to busulfan plus fludarabine conditioning in the secondary end points, including OS, the cumulative incidence of engraftment, the incidence of complete donor-type chimerism, the cumulative incidence of relapse and/or progression, NRM, and TRM. The cumulative incidence of acute and chronic GvHD and other safety end points was also assessed.
Eligible patients were randomly assigned to either IV treosulfan administered at a dose of 10 g/m2 BSA once a day on day –4, day –3, and day –2, or 4 infusions of IV busulfan at a dose of 0.8 mg/kg per day administered every 6 hours on day –4 and day –3, followed by alloHSCT on day 0. Patients in both treatment groups also received IV fludarabine at a dose of 30 mg/m2 BSA per day on day –6 to day –2 as part of the conditioning regimens. Treatment groups were assigned by computer-generated randomization in a 1:1 ratio using a permuted block technique, with stratification by donor type (MUD versus MRD), participating institution, and cytogenetic and/or molecular risk group (low risk and intermediate risk for patients with AML or very low, low, or intermediate Revised International Prognostic Scoring System [IPSS-R] risk for patients with MDS versus high risk for patients with AML and high or very high IPSS-R risk for patients with MDS).
Populations
Inclusion and Exclusion Criteria
Patients were eligible for the MC-FludT.14/L study if they were between 18 and 70 years of age, had AML or MDS that met the 2008 WHO (WHO) revised classification, met the indication criteria for alloHSCT but were considered ineligible for a MAC regimen because they were 50 years or older and/or had an HCT-CI score higher than 2. Eligibility also included a Karnofsky Performance Scale Index of 60% or higher, and the availability of a human leucocyte antigen (HLA)-identical sibling (MRD) or HLA-identical unrelated donor (MUD). Patients were excluded if they had substantial vital organ function impairment, had undergone previous alloHSCT, and had active and uncontrolled infectious diseases under treatment, including active viral liver infection.
Interventions
Patients were initially randomized in a 1:1 ratio to receive either treosulfan at a dose of 10 g/m2 per day administered as a 2-hour IV infusion once a day on day –4, day –3, and day –2, or 4 infusions of busulfan at a dose of 0.8 mg/kg per day administered as a 2-hour IV infusion at 6-hour intervals on day –4 and day –3, followed by alloHSCT on day 0. Patients in both treatment groups also received IV fludarabine at a dose of 30 mg/m2 daily for 5 days (day –6 to day –2) before and after the protocol modification. Prophylaxis for GvHD was standardized in both groups and based on ciclosporin from day –1 (5 mg/kg daily, concentration adapted) and short-course methotrexate (15 mg/m2 on day + 1 and 10 mg/m2 on day + 3 and day + 6). All MUD recipients received anti-T-lymphocyte immune globulin (either antithymocyte globulin at a dose of 10 mg/kg on day –4, day –3, and day –2; or thymoglobulin at a dose of 2·5 mg/kg on day –2 and day –1).
Protocol Amendments
In the MC-FludT.14/L trial, a total of 6 protocol amendments were reported. Protocol amendment 3, made January 25, 2013 followed recommendations of the responsible and independent DMC (dated February 20, 2012) after evaluation of the first planned interim analysis of protocol MC-FludT.14/L. Because increased infectious complications after treosulfan treatment were associated with an imbalanced dosing of the test and reference drug, it was recommended that the comparative trial be continued after implementation of an amendment.49 Accordingly, the dosing regimen of the test group was reduced from 3 doses of 14 g/m2 of treosulfan to 3 doses of 10 g/m2. In addition, the treatment regimen of the test group was changed so that administration of both the test and reference drugs was started the same day (day –4 before alloHSCT). Moreover, the follow-up period of transplanted patients was extended from 1 year to 2 years after transplant. Importantly, only patients who enrolled after the implementation of the amendment 3 were included in the confirmatory interim and final analyses; the 330 patients already recruited for the MC-FludT.14/L trial before its reactivation with amendment 3 were excluded. The rationale provided by the sponsor for this was that all patients previously randomized to the treatment regimen with 14 g/m2 of treosulfan do not provide information on the safety and efficacy of the newly developed regimen of 10 g/m2. In addition, all patients previously randomized to busulfan may not be representative of future randomized patients due to potential selection and performance bias.
Outcomes
A list of outcomes assessed in this Clinical Review Report is provided in Table 6, followed by descriptions of these measures. Summarized outcomes were identified from the sponsor’s Summary of Clinical Evidence and determined to be important to this review by the clinical experts consulted by CADTH and stakeholder input from patient and clinician groups and public drug plans. Using the same considerations, the CADTH review team selected end points that were considered to be most relevant to CADTH’s expert committee deliberations and finalized this list of end points in consultation with members of the expert committee. All summarized outcomes in Table 6 were assessed using GRADE.
Table 6: Outcomes Summarized From the Study Included in the Systematic Review
Outcome measure | Time point | MC-FludT.14/L |
|---|---|---|
EFS | ||
Kaplan-Meier estimate of EFS probability | 24 months | Primary |
36 months | Exploratory | |
OS | ||
Kaplan-Meier estimate of OS probability | 24 months | Secondary |
36 months | Exploratory | |
Graft failure | ||
Graft failure rate | 24 months | Secondary |
Engraftment | ||
Cumulative incidence of reconstitution of granulopoiesis | 28 days after HSCT | Secondary |
Cumulative incidence of reconstitution of thrombopoiesis > 20 × 109/L | ||
Chimerism | ||
Incidence of complete chimerism | 28 days after HSCT | Secondary |
Relapse or progression | ||
Cumulative incidence of relapse or progression | 24 months | Secondary |
Kaplan-Meier estimate of GvHD-free and relapse or progression-free survival probability | 24 months | Exploratory |
Kaplan-Meier estimate of chronic GvHD-free and relapse or progression-free survival probability | 24 months | |
Mortality | ||
Cumulative incidence of nonrelapse mortality | 24 months | Secondary |
Kaplan-Meier estimate of transplant-related mortality | 24 months | Secondary |
Health-related quality of life | NR | NR |
Safety outcomes | ||
Cumulative incidence of acute GvHD of grade III or IV | 100 days after HSCT | Secondary |
Cumulative incidence of chronic GvHD | 24 months |
EFS = event-free survival; GvHD = graft versus host disease; HCST = hematopoietic stem cell transplant; NR = not reported; OS = overall survival.
Note: Only the P value in the confirmatory interim analysis (data cut-off date: August 19, 2016) of EFS was adjusted for multiple comparison. P values for all other outcomes were not adjusted for multiplicity.
Sources: MC-FludT.14/L Confirmatory Interim Analysis Clinical Study Report22 and MC-FludT.14/L Final Analysis Clinical Study Report.23
Efficacy Outcomes
Event-Free Survival
The primary end point was EFS, which was defined by the interval between day 0 to the day of relapse of disease, graft failure, or death (whatever occurs first). EFS was considered to be an important outcome by patients and/or clinicians and provides the source for key inputs in the pharmacoeconomic model submitted to CADTH.
The definition of relapse or progression was based on the publications of Cheson et al. (2006)50 and Cheson et al. (2003),51 but additionally considered the following transplant-specific aspects.
Relapse in patients with AML:
A morphologic relapse involved the reappearance of leukemic blasts in PB or a blast count of at least 5% in BM after complete remission not attributable to any other cause (e.g., BM regeneration; if there were no blasts in PB and BM examination revealed 5% to 20% blasts, a repeat BM evaluation performed at least a week later was necessary to distinguish relapse from BM regeneration); the reappearance or development of cytologically proven extramedullary disease also indicated relapse.
A cytogenetic relapse involved the reappearance of a cytogenetic abnormality, which was to be confirmed by a repeated diagnostic analysis before the start of any therapeutic intervention and by an absolute decline of chimerism by at least 5%.
A molecular relapse (if and only if a cytogenetic marker was not detectable) involved a clinically relevant increase in molecular markers (proven by at least 2 documented evaluations) that had already been detected before patient inclusion and that required a therapeutic intervention (e.g., tapering or withdrawal of immunosuppression, donor lymphocyte infusions, cytotoxic or radiotherapeutic treatment).
Relapse or progression in patients with MDS involved:
an increase in blasts to greater than 5% in BM or PB (if the blast count is greater than 5% at study entry and the patient experienced “BM complete remission” after allogeneic transplant) not attributable to other causes (e.g., BM regeneration)
the reappearance of a cytogenetic abnormality (e.g., in case an MDS subtype without blasts in BM was included), which had to be confirmed by a repeated diagnostic analysis before the start of any therapeutic intervention and by an absolute decline of chimerism by at least 5%
at least 1 of the following —
a decline of at least 50% from the maximum response level (after engraftment) of neutrophils or platelets in the absence of other conditions and/or reasons (e.g., antiviral or antibiotic or GvHD therapy) and an absolute decline of chimerism by at least 5%
a reduction of blood hemoglobin concentration by at least 1.5 g/dL from the maximum response level or transfusion dependency after previous recovery in the absence of other conditions and/or reasons (e.g., concomitant antiviral or antibiotic or GvHD therapy or hemolysis due to ABO incompatibility) and an absolute decline of chimerism by at least 5%.
Graft failure was determined in PB samples scheduled on day 28, day 100, and months 6, 9, 12, 15, 18, 21, and 24, and defined as follows:
A primary graft failure has to be documented in case, on day 28 after transplant, a neutrophil count of no more than 0.5 × 109/L and a total white blood cell count of no more than 1 × 109/L is detected (without previously documented engraftment or relapse and/or persisting disease). In addition, a donor-type chimerism of less than 10% in the BM is required. As routinely done, a BM biopsy must be performed to confirm the diagnosis of primary graft failure.
A secondary graft failure has to be documented in case a sustained decline in neutrophil count of no more than 0.5 × 109/L and a total white blood cell count of no more than 1 × 109/L is analyzed in the PB (after initial engraftment, but in the absence of relapse or other conditions, like concomitant antiviral, antibiotic, or GvHD therapy, considered responsible for temporary decline of values). As routinely done, a BM biopsy must be performed to confirm the diagnosis of secondary graft failure.
The definition of graft failure applied to patients with AML and those with MDS.
Death from any cause was considered an event.
Overall Survival
OS is a secondary end point and was defined as the probability of survival, irrespective of disease status, at any point in time from any cause in the 2 years after transplant. OS was considered as an important outcome by patients and/or clinicians and provides the source for key inputs in the pharmacoeconomic model submitted to CADTH.
Graft Failure
Graft failure is a secondary end point and the definitions of primary and secondary graft failure in patients with AML or MDS are provided in the Event-Free Survival section.
Relapse or Progression
The definitions of relapse and/or progression in patients with AML or MDS are provided in the Event-Free Survival section. Relapse or progression is a secondary end point and was measured using the incidence of relapse or progression, which is defined as the probability of having a relapse or progression. Patients are considered to have experienced an event after a relapse and/or progression. Death without relapse and/or progression and graft failures are competing risks. Patients who are alive with no history of relapse or progression are censored at time of the last clinical examination of disease status. Relapse or progression were considered to be important outcomes by patients and clinicians. The cumulative incidence of relapse and/or progression at 24 months was selected to be summarized in the report and assessed using GRADE based on inputs from the clinical experts consulted by CADTH and considered to be an important outcome by clinician groups. The cumulative incidence of relapse or progression at 36 months was not selected, as failures of therapy (relapse or death) occur predominantly in the first year after transplant.30
GvHD-Free and Relapse and/or Progression-Free Survival
GRFS in the 2 years after transplant was measured from the end of HSCT (day 0) to the time the event was analyzed. The associated time span was defined as the interval from day 0 to acute GvHD of at least grade III, extensive chronic GvHD, relapse and/or progression, or death (whichever occurred first). The date of the event was either the documented date of GvHD or relapse and/or progression, or the date of death.
If a patient was alive and no acute or chronic GvHD of the grade and/or intensity previously specified and no relapse and/or progression was reported, the censoring date was assigned to the last date of examination of relapse status in the 24-month trial period (i.e., excluding postsurveillance evaluation). Patients without an event and without any information with regard to relapse and/or progression were censored at day 0.
Chronic GvHD-Free and Relapse or Progression-Free Survival
CRFS in the 2 years after transplant was measured from the end of HSCT (day 0) to the time the event was analyzed. The associated time span was defined as the interval from day 0 to extensive chronic GvHD, relapse or progression, or death (whichever occurred first). The date of the event was either the documented date of extensive chronic GvHD or relapse or progression, or the date of death.
If a patient was alive with no extensive chronic GvHD, and no relapse and/or progression was reported, the censoring date was assigned to the last date of examination of relapse status in the 24-month trial period (i.e., excluding postsurveillance evaluation). Patients without an event and without any information with regard to relapse or progression were censored at day 0.
Engraftment
Engraftment was defined as the first of 3 consecutive days for each of the following 4 criteria:
leucocyte count of greater than 1 × 109 /L
absolute neutrophil count of greater than 0.5 × 109 /L
platelet count of at least 20 × 109/L in the absence of platelet transfusion
platelet count of at least 50 × 109/L in the absence of platelet transfusion.
According to the sponsor, consecutive days is defined as 3 consecutive blood samples taken on different days. The cumulative incidence of engraftment after alloHSCT was determined 28 days after HSCT.
The date engraftment is reached is the documented date of engraftment. Death (regardless of cause) and relapse or progression until the date of primary graft failure or documentation of engraftment status (whichever occurred first) were competing events. If events occurred on the same day, they were considered to occur in the following order: engraftment, then relapse or progression, then death (i.e., if engraftment and relapse or progression occurred on the same day, engraftment is counted as the event). Patients alive without relapse or progression and without engraftment until the documented date of engraftment assessment were censored. The censoring date is the documented date of engraftment assessment or date of primary graft failure, whichever occurred first. Patients without a competing event and without any documented engraftment information (i.e., neutrophilic granulocytes or platelets missing) were censored at day 0. The date of occurrence of the competing event was the earliest time when relapse or progression had been observed or when death (regardless of cause) was documented.
Engraftments of neutrophilic granulocytes and platelets were selected to be summarized in the report and assessed using GRADE based on inputs from the clinical experts consulted by CADTH, as they are major transplant outcomes. According to the clinical experts consulted by CADTH, a delay in neutrophil engraftment (i.e., reconstitution of granulopoiesis) is associated with a major increase in infection risk, and a delay in reconstitution of thrombopoiesis is associated with a major increase in bleeding risk. In addition, the clinical experts indicated that neutrophil engraftment correlates very well with white blood cell count recovery (i.e., reconstitution of leukopoiesis). The clinical experts remarked that a platelet count of at least 20 × 109/L in the absence of a platelet transfusion is aligned with the threshold used in their clinical practices. Therefore, engraftment of leukocytes and engraftment of platelets (platelet count of ≥ 50 × 109/L in the absence of a platelet transfusion) were not selected.
Chimerism
Chimerism means that donor cells have durably engrafted in the recipient. Complete donor-type chimerism was defined as the detection of a donor-to-patient ratio of at least 95%. Chimerism analysis was performed on a BM sample of the recipient 28 days after HSCT. PB could also be used 100 days after HSCT. Chimerism at 28 days was selected to be summarized in the report and assessed using GRADE based on inputs from the clinical experts consulted by CADTH.
Nonrelapse Mortality
NRM was a secondary end point and defined as the probability of dying in the absence of persisting disease or the previous occurrence of relapse or progression. It was measured from day 0 to the day of death in patients with no previous disease recurrence or progression in the 2 years after transplant. NRM at 24 months was selected to be summarized in the report and assessed using GRADE based on inputs from the clinical experts consulted by CADTH and was considered to be an important outcome by clinician groups. NRM at 36 months was not selected, as failures of therapy (relapse or death) occur predominantly in the first year after transplant.42
Transplant-Related Mortality
The time span of TRM was defined as the interval from day 0 to death from a transplant-related cause in the 24-month trial period (i.e., excluding postsurveillance evaluation) (i.e., upon documentation of GvHD, cardiac toxicity, pulmonary toxicity, interstitial pneumonitis, hemorrhage, hepatic sinusoidal obstruction syndrome [HSOS], skin toxicity, Epstein-Barr virus proliferative disease, renal failure, gastrointestinal toxicity, rejection and/or poor graft function, central nervous system toxicity, multiple organ failure, infections [bacterial, viral, fungal, parasitic, unknown], or other HSCT-related causes). If a patient was alive or died from nontransplant-related causes, the censoring date was the time of last follow-up or the date of death, respectively. The cumulative incidence of TRM was evaluated in the 2 years after transplant.
Of note, NRM deaths are considered to be unrelated to a relapse, whereas TRM includes transplant-related deaths in patients with or without relapse. TRM was selected to be summarized in the report and assessed using GRADE based on inputs from the clinical experts consulted by CADTH and was considered to be an important outcome by clinician groups.
Health-Related Quality of Life
Patient groups identified HRQoL as an important outcome. The MC-FludT.14/L trial did not assess HRQoL in adults with AML or MDS at increased risk with standard conditioning therapies.
Harms
In the MC-FludT.14/L trial, the proportion of patients who experienced serious and nonserious AEs from 6 days before and 28 days after HSCT had their experiences recorded and reported using the National Cancer Institute Common Terminology Criteria for Adverse Events (version 4.03). All AEs were followed until resolved or stabilized, for a maximum of 100 days after transplant. AEs of special interest included acute and chronic GvHD.
Acute and Chronic GvHD
The cumulative incidence and the severity of acute and chronic GvHD were documented in both treatment groups. Acute (day 0 to day 100) and chronic (day 101 to the end of total follow-up, 1 year after transplant) GvHD were graded according to Glucksberg criteria and the modified Seattle criteria.52-54 The cumulative incidence of GvHD at 100 days and the cumulative incidence of chronic GvHD were considered to be important outcomes by patients and/or clinicians and provide the source for key inputs in the pharmacoeconomic model submitted to CADTH.
Statistical Analysis
An analysis of clinical end points in the MC-FludT.14/L trial is summarized in Table 7.
Sample Size and Power Calculation
The sample size was calculated on the basis of an assumed setting, in which treosulfan-based conditioning and the comparator (alternative hypothesis) are equally effective. With a noninferiority HR margin of 1.3, the power of the trial was chosen to be 80%. An experiment-wise 1-sided type I error significance alpha of 2.5% was chosen, accounting for 3 interim analyses and 1 final look, and was calculated using futility and efficacy boundaries. Therefore, the selection of a formal noninferiority margin for statistical decision-making was based on a combination of clinical judgment and statistical reasoning. Based on discussions with the clinical experts consulted by the sponsor, the largest increase in the risk of any disadvantage associated with treosulfan-based conditioning that one would be willing to accept was one-third of the risk of busulfan-based RIC, if it is in addition to the point estimates of the study-specific efficacy parameter and the main safety parameters are in favour of treosulfan. Thus, the noninferiority margin on the HR scale was fixed at θ0 = 1.3 (–log HR = –0.2624).
With the previously discussed considerations, a commitment to, at most, 481 events was given in the study protocol. It was intended that 10 patients per month would be accrued in the first 6 months, 15 patients per month would be accrued thereafter up to 24 months after start of the trial, and 25 patients would be accrued per month thereafter. Furthermore, sample size calculation took into account the fact that follow-up continued until 2 years after transplant and that a 12-month EFS rate of 68.5% with busulfan-based RIC was observed in a previously conducted trial. Under an assumed exponential distribution of the EFS times, the 24-month EFS rate with busulfan-based conditioning was expected to be roughly 46.9%. With these accrual and event rates in the busulfan group, the required number of events would have been reached with, at most, 930 patients qualifying for the FAS. The maximum expected study duration (accrual plus follow-up) to reach the required number of events was expected to occur approximately 64 months after the first patient was randomized. In particular, the expected duration was 40 months under the null hypothesis and 58 months under the alternative hypothesis of noninferiority. Assuming that roughly 3% of patients had to be excluded from the FAS, at most 960 patients would have been enrolled in this trial. Results of the second preplanned interim analysis (November 9, 2016) that assessed 460 evaluable patients randomly assigned to the latest protocol (modified on January 25, 2013) prompted the DMC to recommend stopping patient recruitment, because the primary trial objective had been met. At the time of the DMC recommendation, 570 patients had been randomized, and data collection continued for patients remaining on study.
Statistical Test or Model
The primary efficacy end point of the MC-FludT.14/L trial was EFS in the 2 years after transplant, measured from of the end of HSCT (day 0). For confirmatory interim analysis of noninferiority of treosulfan-based conditioning, a Cox proportional hazards regression model (stratified by centre), with donor type (MUD versus MRD), risk group (low risk and intermediate risk for AML or very low, low, or intermediate IPSS-R risk for MDS versus high risk for AML and high or very high IPSS-R risk for MDS), and treatment as factors was used to test for the efficacy of treatment on EFS. Each factor included in the model was used in the randomization procedure. An unadjusted Kaplan-Meier estimator was used to estimate the distribution of EFS for each treatment group.
Instead of presenting a 1-sided (1 – alpha) CI, a 2-sided (1 to 2 alpha) CI is provided to facilitate interpretation for the primary analysis of EFS in the confirmatory interim analysis (data cut-off date: August 19, 2016). An experiment-wise 1-sided type I error significance level of 0.025 was applied, as adjusted for the interim analysis. The primary analysis was based on the FAS. All other CIs were 2-sided, unless otherwise noted, and at a confidence coefficient of 1 – alpha = 0.95. P values (2-sided unless otherwise noted) for secondary end points are to be interpreted in an explorative manner.
Interim Analyses
The trial was planned as a group-sequential trial with 3 interim analyses. The first formal interim analysis was planned to be performed after 45 events or 220 patients to allow for a broad review of the benefits and risks of the dose reduction and change of the treatment regimen implemented with amendment 3 of the trial. Further interim analyses were planned after 137 and 239 events occurred, or after 460 and 700 patients were randomized. The final analysis was planned after 481 events or the inclusion of 930 patients.
The confirmatory interim analysis was performed after enrolment of 476 patients, 460 of whom qualified for the FAS. When reviewing the results of the confirmatory interim analysis, the DMC recommended that recruitment for this trial stop because the primary objective, proof of noninferiority of treosulfan compared to busulfan, had been achieved. As a result, the sponsor stopped recruitment to the trial after the confirmatory interim analysis, at which point 476 of 570 patients had been analyzed. A total of 168 events was considered in the confirmatory interim analysis, representing an information fraction of 34.9%, based on the 481 events planned for the final analysis foreseen in the prespecified study protocol if the trial was not stopped prematurely. The information fraction of 34.9% corresponds to an alpha level of 0.000149 in this interim analysis, according to the O`Brien-Fleming alpha-spending function.
The final analysis included 570 patients enrolled in the trial, 551 of whom qualified for the FAS. The final analysis was performed after all patients had been followed for at least 1 year and when the postsurveillance documentation had been performed for patients who finished the trial alive 2 years after HSCT. This report describes the results of the primary end point of EFS in the confirmatory interim analysis, as it was controlled for multiplicity, and the results for primary and secondary outcomes of the final analysis, as it included more patients and had a longer follow-up than the confirmatory interim analysis.
Multiple Testing Procedure
In the confirmatory interim analysis (data cut-off date: August 19, 2016), significance levels of the testing procedures were adjusted for multiple comparisons using a group-sequential approach and a hierarchical testing strategy. In the confirmatory interim analysis of 476 patients that included 168 events, the prespecified 1-sided significance level for the testing of noninferiority of EFS was calculated as 0.000149, derived by applying the protocol-defined event-driven O'Brien-Fleming type of group-sequential efficacy stopping boundary. An experiment-wise 1-sided type I error significance level of 0.025 was applied for the EFS analysis, as adjusted for interim analysis. In the final analysis (database lock date: March 16, 2018), statistical testing for all end points were not adjusted for multiple comparison. In the confirmatory interim analysis, according to the group-sequential study approach and a hierarchical test strategy, if significant noninferiority in the PPS can be shown, a sequential testing approach will be applied, starting with a test of the noninferiority within the FAS. In case of statistical significance, superiority within the FAS with respect to the primary study end point of EFS will be tested based on the points to consider in the switch between superiority and noninferiority.
Data Imputation Methods
All analyses and descriptive summaries were based on the observed data. Missing data were imputed unless otherwise specified.
Subgroup Analyses
The primary end point of EFS was evaluated in subgroups denoted by donor type (MUD versus MRD), risk group (low risk and intermediate risk for AML or very low, low, and intermediate IPSS-R risk for MDS versus high risk for AML and high or very high IPSS-R risk for MDS), combination of donor type and risk group, disease (AML versus MDS), age group (< 50 years versus ≥ 50 years), HCT-CI score (≤ 2 versus > 2), remission status in AML (first complete remission versus second or later complete remission), MDS status at trial entry (untreated versus treated), risk group in patients with AML, and risk group in patients with MDS. For each subgroup, the associated sample size, the number of events, the 24-month Kaplan-Meier estimates (12-month estimates for the interim analyses), the HR of treosulfan compared to busulfan, and the respective CI derived under an assumed Cox proportional hazards model with treatment as the only factor were included. In addition, statistical tests for the presence of a treatment-by-subgroup interaction were performed for the primary end point of EFS. If the associated P value was less than 0.1, this was reported as evidence of heterogeneity of the treatment effects across subgroups.
Sensitivity Analyses
To further evaluate the robustness of the results of the analysis of the primary end point of EFS, sensitivity analyses in the FAS were conducted. The key sensitivity analyses included:
a Cox regression model with treatment as the only factor
a Cox regression model with treatment as a factor and site as a strata variable
a Cox regression model with treatment and disease (AML or MDS) as factors
the inclusion of the disease (AML or MDS) as a factor.
Secondary Outcomes of the Studies
Overall Survival
Patients still alive had their event times censored at their last follow-up (within the 24-month trial period; i.e., excluding postsurveillance evaluation). Both 12-month and 24-month OS probabilities were estimated using the Kaplan-Meier estimator and associated 95% CIs. A test of difference of the treatment-specific Kaplan-Meier curves was conducted using the log-rank test. A stratified Cox regression model for treatment was fit, accounting for the stratification variables of centre and risk group (I versus II), conditional on a factor variable for donor type (MUD versus MRD). The 2-sided P values based on a Wald test of the estimated HR and CI are provided.
Graft Failure
The percentage of primary graft failure was estimated as the number of patients with primary graft failure at 24 months divided by the total number of patients receiving HSCT. The percentage of secondary graft failure was estimated as the number of patients with secondary graft failure at 24 months divided by the total number of patients whose neutrophilic granulocytes had engrafted after stem cell transplant or were never below the required level.
Engraftment (Granulocytes and Platelets)
A Fine-Gray model with the stratification factor of risk group, conditional on a factor variable for donor type (MUD versus MRD), was used to estimate the cause-specific HR of engraftment. For the comparison of treatment groups, a Pepe-Mori test was used to quantify the difference between the curves. Cumulative incidences were also estimated in subgroups of patients defined by donor type and age (< 50 years versus ≥ 50 years).
The conditional cumulative incidence for reconstitution of granulopoiesis and thrombopoiesis greater than 20 × 109/L were estimated using conditional probability functions. The cumulative incidence function for a given cause at a specified time is defined as the probability of failure due to that specific cause at or before the specified time. The conditional cumulative probability function for a given cause at a specified time is defined as the probability of failure due to that specific cause, given that no other cause led to failure before the specified time.
Chimerism
The incidence of complete donor-type chimerism (with exact 95% CI) at 28 days was estimated as the number of patients with complete chimerism divided by the total number of patients at risk. Patients were at risk, for the purpose of statistical analysis of chimerism, at 28 days if they had an examination at the day-28 visit or they had survived 29 days after alloHSCT. The analysis of complete donor-type chimerism at 28 days used a Cochran-Mantel-Haenszel test, stratified by donor type (MUD versus MRD) and risk group (I versus II). Missing values accounted as a no for the calculation of odds ratios.
Relapse or Progression
The event time to relapse or progression was defined as the elapsed time from day 0 to relapse or progression in the 24-month trial period (i.e., excluding postsurveillance evaluation). Patients alive with no history of relapse or progression or a competing event (i.e., death) were censored at the last date of examination of relapse status. The relapse or progression date was assigned to the earliest time that relapse or progression was observed. Patients without a competing event and without any documented date for examination of the relapse status were censored at day 0.
The probability of a relapse or progression event occurring in a healthy population was summarized using the cumulative incidence, and estimated under an assumed Fine-Gray model, stratified by risk group (I versus II) and conditional on a factor variable for donor type (MUD versus MRD). The HR, 95% CIs, and a 2-sided P value for testing treatment effect are presented under an assumed cause-specific proportional hazard. For additional exploratory analysis, cumulative incidence curves are also presented by donor type, risk group and combinations thereof, disease, age group, and HCT-CI score. These factors were judged to be potential prognostic factors.
GvHD-Free and Relapse or Progression-Free Survival
The 12-month and 24-month GRFS rates were estimated using a Kaplan-Meier curve, together with associated 95% CIs, and a log-rank test was used to quantify the difference between the curves. Additionally, a stratified Cox regression model for treatment was fit, accounting for the stratification variables of centre and risk group (I versus II), conditional on a factor variable for donor type (MUD versus MRD). The 2-sided P values based on a Wald test of the estimated HR and CI are provided.
Chronic GvHD-Free and Relapse or Progression-Free Survival
The 12-month and 24-month CRFS rates were estimated using a Kaplan-Meier curve, together with associated 95% CIs, and a log-rank test was used to quantify the difference between the curves. Additionally, a stratified Cox regression model for treatment was fit, accounting for the stratification variables of centre and risk group (I versus II), conditional on a factor variable for donor type (MUD versus MRD). The 2-sided P values based on a Wald test of the estimated HR and CI are provided.
Nonrelapse Mortality
The cumulative incidence curves of NRM were estimated in each treatment group. The statistical methods to be applied for statistical analysis match those already described for the analysis of relapse and/or progression.
Transplant-Related Mortality
The probability of TRM was estimated using a Kaplan-Meier curve. The 24-month survival probability was reported with the associated 95% CI.
A comparison of treatment-specific Kaplan-Meier curves was initially performed using the log-rank test. A stratified Cox regression model that included the stratification variables of centre and risk group (I versus II), conditional on a factor variable for donor type (MUD versus MRD), was used to estimate the HR across treatment groups.
Health-Related Quality of Life
The MC-FludT.14/L trial did not assess HRQoL in adults with AML or MDS at increased risk with standard conditioning therapies.
Table 7: Statistical Analysis of the Efficacy End Points of the MC-FludT.14/L Trial
End point | Statistical models and tests | Adjustment factors | Handling of missing data | Sensitivity analyses |
|---|---|---|---|---|
Event-free survival | Cox regression Kaplan-Meier | Donor type as a factor and risk group and centre as strata | NA | Cox regression models with different prognostic subgroups as factors or strata were performed as preplanned sensitivity analyses The prognostic subgroups are:
|
Overall survival | Cox regression Kaplan-Meier | Donor type as a factor and risk group and centre as strata | NA | Cox regression models with different prognostic subgroups as factors or strata were performed as preplanned sensitivity analyses The prognostic subgroup is disease |
Percentage of patients with graft failure | NA | NA | NA | NA |
Conditional cumulative incidence of engraftment | Fine-Gray regression | Donor type as a factor and risk group as a stratum | NA | NA |
Incidence of complete donor-type chimerism | Stratified Cochran-Mantel-Haenszel test | Donor type as a factor and risk group and centre as strata | NA | NA |
Cumulative incidence of relapse or progression | Fine-Gray regression | Donor type as a factor and risk group as a stratum | NA | Subgroup analysis:
|
GvHD-free survival and relapse or progression-free survival | Kaplan-Meier log-rank test Cox regression | Donor type as a factor and risk group and centre as strata | NA | NA |
Chronic GvHD-free and relapse or progression-free survival | ||||
Cumulative incidence of nonrelapse mortality | Fine-Gray regression | Donor type as a factor and risk group as a stratum | NA | Score of the most frequent HCT-CI categories as a factor Subgroup analysis:
|
Transplant-related mortality | Cox regression Kaplan-Meier log-rank test | Adjusted for donor type as a factor and risk group and centre as strata | NA | Score of the most frequent HCT-CI categories as a factor Subgroup analysis:
|
Cumulative incidence of acute GvHD | Fine-Gray regression | Donor type as a factor and risk group and centre as strata | NA | NA |
Cumulative incidence of chronic GvHD | Fine-Gray regression | NA | NA | NA |
GvHD = graft versus host disease; HCT-CI = Hemopoietic Stem Cell Transplantation-Specific Comorbidity Index; NA = not applicable.
Sources: MC-FludT.14/L Final Analysis Clinical Study Report23 and Beelen et al. (2022).48 Details included in the table are from the sponsor’s Summary of Clinical Evidence.24
Analysis Populations
A summary of analysis populations used in the MC-FludT.14/L trial is provided in Table 8.
The safety analysis set consists of all randomized patients who were treated at least 1 time with the study medication. All patients were analyzed in their group of actual treatment.
The FAS includes all randomized patients from the safety analysis set with at least 1 documented efficacy parameter. The patients in the FAS were analyzed in their initial group of randomization
The PPS comprised all patients from the FAS who met the following criteria:
all of the inclusion criteria and none of the exclusion criteria are fulfilled
correct allocation to treatment group
compliance with respect to the administration of the study medication; patients with a deviation of, at most, plus or minus 20% between the amount of actually-applied study medication and the amount of protocol-required study medication were considered to be compliant
administration of short-course methotrexate until day + 6, unless medical reasons for a deviation have been documented
administration of antithymocyte globulin in the case of MUD, unless medical reasons for a deviation have been documented
lack of any concomitant prophylactic and/or adjuvant donor lymphocyte infusion or cytotoxic therapy and/or radiotherapy after transplant, but the absence of relapse and/or disease progression.
Confirmatory statistical analysis of the primary end point of EFS was performed for the PPS and FAS populations. This review focused on results from the FAS. Refer to Appendix 1 for results from the PPS.
Table 8: Analysis Populations of the MC-FludT.14/L Trial
Population | Definition | Application |
|---|---|---|
Full analysis set | Included all randomized patients from the safety analysis set with at least 1 efficacy parameter documented after baseline | All efficacy analyses |
Safety analysis set | Included all randomized patients who were treated at least 1 time with the study medication | All safety analyses |
Per-protocol set | Included all patients from the full analysis set without any major protocol violations | Secondary efficacy end points |
Source: MC-FludT.14/L Final Analysis Clinical Study Report.23 Details included in the table are from the sponsor’s Summary of Clinical Evidence.24
Results
Patient Disposition
Patient disposition in the MC-FludT.14/L trial final analysis (database lock date: March 16, 2018) is summarized in Table 9. In the MC-FludT.14/L trial, 134 (47.9%) patients in the treosulfan group and 116 (40.0%) patients in the busulfan group completed the study treatments. Fewer patients in the treosulfan group than in the busulfan group discontinued the study treatment (31.8% versus 43.1%). Death was the predominant reason for premature study discontinuation. fewer patients in the treosulfan group than in the busulfan group had death as the reported reason for discontinuation (25.7% versus 36.9%). More patients in the treosulfan group than in the busulfan group were alive at the month 24 visit and had completed postsurveillance evaluation (41.4% versus 34.8%). The postsurveillance evaluation included 125 (44.6%) patients in the treosulfan group and 107 (36.9%) patients in the busulfan group.
Table 9: Summary of Patient Disposition From the Study Included in the Systematic Review
Patient disposition | MC-FludT.14/L (Database lock date: March 16, 2018) | |
|---|---|---|
Treosulfan N = 280 | Busulfan N = 290 | |
Screened, N | 280 | 290 |
Randomized, N (%) | 280 | 290 |
Discontinued before medication administration, N (%) | 10 (3.6) | 7 (2.4) |
Reason for discontinuation, n (%) | ||
Withdrawal of consent | 0 | 1 (0.3) |
Screening failurea | 10 (3.6) | 6 (2.1) |
Did not receive transplant but received medication | 2 (0.7) | 0 |
Completed study treatment, n (%) | 134 (47.9) | 116 (40.0) |
Discontinued from study, n (%) | 89 (31.8) | 125 (43.1) |
Reason for discontinuation from study, n (%) | ||
Withdrawal of consent | 2 (0.7) | 3 (1.0) |
Lost to follow-up | 0 | 7 (2.4) |
Death | 72 (25.7) | 107 (36.9) |
Screening failurea | 10 (3.6) | 6 (2.1) |
Not evaluable for efficacy due to not receiving transplantb | 2 (0.7) | 0 |
Site closure | 2 (0.7) | 2 (0.7) |
Disease progression | 1 (0.4) | 0 |
If patient terminated study alive at the month 24 visit, survival status at postsurveillance, n (%) | ||
Patients alive at the month 24 visit | 135 (48.2) | 117(40.3) |
Not applicablec | 10 (3.6) | 10 (3.4) |
Lost to follow-up | 0 | 1 (0.3) |
Patient alive | 116 (41.4) | 101 (34.8) |
Death | 9 (3.2) | 5 (1.7) |
Patients who completed the postsurveillance analysis | 125 (44.6) | 107 (36.9) |
Full analysis set, N | 268 | 283 |
Per-protocol set, N | 262 | 275 |
Safety analysis set, N | 270 | 283 |
aAfter randomization but before conditioning treatment, the investigator became aware of new information leading to patients no longer meeting the inclusion and/or exclusion criteria.
bCancellation of donor’s clearance after the start of conditioning treatment, so no transplant took place (1 patient); death occurred between randomization and HSCT (1 patient).
cPostsurveillance visit was not applicable for 20 patients (10 patients in each group) because the postsurveillance visit was at the 24-month visit ± 2 months. For 2 patients, postsurveillance was completed, although the month 24 visit was not done.
Source: MC-FludT.14/L Final Analysis Clinical Study Report.23 Details included in the table are from the sponsor’s Summary of Clinical Evidence.24
Major Protocol Deviations
Major protocol deviations in the MC-FludT.14/L trial final analysis (database lock date: March 16, 2018) are summarized in Table 10. Generally, major protocol deviations were slightly less common in the treosulfan group than in the busulfan group; 91 (32.5%) patients in the treosulfan group and 110 (37.9%) patients in the busulfan group had any major deviation. The most frequently reported major protocol deviation was procedure deviation, which affected a slightly lower proportion of patients in the treosulfan group than in the busulfan group (16.1% versus 18.6%).
Table 10: Frequency Distribution of Major Protocol Deviations (All Patients)
Major protocol deviation | MC-FludT.14/L (database lock date: March 16, 2018) | |
|---|---|---|
Treosulfan N = 280 | Busulfan N = 290 | |
Patients with any major deviation | 91 (32.5) | 110 (37.9) |
Procedure deviation | 45 (16.1) | 54 (18.6) |
Adherence to other relevant specifications of the protocol | 28 (10.0) | 24 (8.3) |
Randomization error | 15 (5.4) | 24 (8.3) |
Treatment deviation | 12 (4.3) | 20 (6.9) |
Time schedule deviation | 7 (2.5) | 4 (1.4) |
Inclusion and/or exclusion error at study entry | 1 (0.4) | 1 (0.3) |
Excluded concomitant medication | 1 (0.4) | 0 |
Source: MC-FludT.14/L Final Analysis Clinical Study Report.23
Baseline Characteristics
The baseline characteristics outlined in Table 11 are limited to those that are most relevant to this review or were felt to affect the outcomes or interpretation of the study results in the FAS.
In the MC-FludT.14/L trial final analysis (database lock date: March 16, 2018), the treosulfan and busulfan groups were generally similar in baseline characteristics. Most patients were male (60.8%), aged 50 years or older (94.9%), and had AML (63.9%). More patients in the treosulfan group than in the busulfan group were diagnosed with AML (184 [68.7%] versus 168 [59.4%]). Of the 199 patients with MDS, more patients in the treosulfan group than in the busulfan group had untreated MDS (50.0% versus 40.9%), and the mean blast count in BM was lower in the treosulfan group than in the busulfan group (5.83 versus 6.31).
Table 11: Summary of Baseline Characteristics From the Study Included in the Systematic Review (FAS)
Characteristic | MC-FludT.14/L (Database lock date: March 16, 2018) | |
|---|---|---|
Treosulfan N = 268 | Busulfan N = 283 | |
Age, years | ||
Mean (SD) | 59.3 (6.5) | 59.9 (6.0) |
Median (range) | 60.0 (37 to 70) | 60.0 (31 to 70) |
< 50 | 16 (6.0) | 12 (4.2) |
≥ 50 | 252 (94.0) | 271 (95.8) |
Sex, n (%) | ||
Male | 162 (60.4) | 173 (61.1) |
Female | 106 (39.6) | 110 (38.9) |
Weight, kg | ||
Mean (SD) | 80.9 (16.7) | 79.4 (17.7) |
Median (range) | 80.0(48.0 to 144.0) | 79.0 (46.0 to 141.9) |
Indications for alloHSCT | ||
AML, n (%) | 184 (68.7) | 168 (59.4) |
MDS, n (%) | 84 (31.3) | 115 (40.6) |
Disease status for AML, n (%) | ||
n | 184 | 168 |
CR1 | 159 (86.4) | 144 (85.7) |
> CR1 | 25 (13.6) | 24 (14.3) |
Blast count in bone marrow for AML | ||
n | 183 | 168 |
Mean (SD) | 1.95 (1.29) | 2.1 (1.53) |
Median (range) | 2.5 (0.0 to 5.0) | 2.5 (0.0 to 11.5) |
Disease status for MDS, n (%) | ||
n | 84 | 115 |
Untreated | 42 (50.0) | 47 (40.9) |
Treated | 42 (50.0) | 68 (59.1) |
Blast count in bone marrow for MDS | ||
n | 83 | 114 |
Mean (SD) | 5.83 (4.65) | 6.31 (4.79) |
Median (range) | 5.0 (0.0 to 19.0) | 5.0 (0.0 to 19.0) |
HCT-CI score at baseline, n (%) | ||
Patients with HCT-CI score > 2 | 156 (58.2) | 167 (59.0) |
Karnofsky Performance Scale score, n (%) | ||
60 | 4 (1.5) | 1 (0.4) |
70 | 9 (3.4) | 7 (2.5) |
80 | 64 (23.9) | 59 (20.8) |
90 | 94 (35.1) | 113 (39.9) |
100 | 97 (36.2) | 103 (36.4) |
Donor type, n (%) | ||
MRD | 62 (23.1) | 68 (24.0) |
MUD | 206 (76.9) | 215 (76.0) |
Concomitant illnesses (≥ 10% of either treatment group) | ||
Patients with concomitant illnesses | 220 (82.1) | 237 (83.7) |
Vascular disorders | 115 (42.9) | 118 (41.7) |
Metabolism and nutrition disorders | 63 (23.5) | 64 (22.6) |
Cardiac disorders | 47 (17.5) | 51 (18.0) |
Musculoskeletal and connective tissue disorders | 38 (14.2) | 34 (12.0) |
Respiratory, thoracic, and mediastinal disorders | 36 (13.4) | 31 (11.0) |
Infections and infestations | 33 (12.3) | 30 (10.6) |
Gastrointestinal disorders | 29 (10.8) | 33 (11.7) |
alloHSCT = allogeneic hematopoietic stem cell transplant; AML = acute myeloid leukemia; CR1 = first complete remission; FAS = full analysis set; HCT-CI = Hematopoietic Cell Transplantation-Specific Comorbidity Index; MDS = myelodysplastic syndromes; MRD = matched related donor; MUD = matched unrelated donor; SD = standard deviation.
Sources: MC-FludT.14/L Final Analysis Clinical Study Report23 and Beelen et al. (2022).48 Details included in the table are from the sponsor’s Summary of Clinical Evidence.24
Exposure to Study Treatments
In the MC-FludT.14/L trial at the final analysis (database lock date: March 16, 2018), 3 infusions of treosulfan, at a once-daily dose of 10 g/m2, were given on day –4, day –3, and day –2. The median absolute dose of treosulfan was 57.8 g (range, 19 g to 79 g), or 30.0 g/m2 (range, 9.8 g/m2 to 42.0 g/m2). In total, 8 infusions of busulfan were given, at a rate of 4 infusions per day on day –4 and day –3, each at a dose of 0.8 mg/kg. The median absolute dose of busulfan was 500.0 mg (range, 296 mg to 792 mg), or 6.4 mg/kg (range, 4.7 mg/kg to 9.5 mg/kg).
Table 12: Summary of Patient Exposure From the Study Included in the Systematic Review (Safety Analysis Set)
Exposure | MC-FludT.14/L (Database lock date: March 16, 2018) | |
|---|---|---|
Treosulfan N = 270 | Busulfan N = 283 | |
Total absolute dose of treosulfan | ||
Mean (SD) | 57.7 g(7.5 g) | 494.5 mg (97.7 mg) |
Median (range) | 57.8 g (19.0 g to 79.0 g) | 500.0 mg (296.0 mg to 792.0 mg) |
Total absolute dose per BSA (g/m2)/body weight (mg/kg) | ||
Mean (SD) | 29.7 g/m2 (2.1 g/m2) | 6.4 mg/kg (0.4 mg/kg) |
Median (range) | 30.0 g/m2 (9.8 g/m2 to 42.0 g/m2) | 6.4 mg/kg (4.7 to 9.5 mg/kg) |
Number of days with treatment | ||
Median (range) | 3.0 (1.0 to 3.0) | 2.0 (2.0 to 3.0) |
BSA = body surface area; SD = standard deviation.
Source: MC-FludT.14/L Final Analysis Clinical Study Report.23
Concomitant Medications and Cointerventions
The treatment schedule for concomitant therapies by treatment group in the MC-FludT.14/L trial final analysis (database lock date: March 16, 2018) is presented in Table 13. The patients were not allowed to participate in another experimental drug trial in the 4 weeks before day –6, per the protocol. For the prevention of seizures, either phenytoin or benzodiazepine was administered daily to all patients in the busulfan group between day –5 and day –2. Therefore, all (100%) patients in the busulfan group but no patients in the treosulfan group received phenytoin or benzodiazepine. Patients in both groups received IV fludarabine at a dose of 30 mg/m2 per day from day –6 to day –2. Due to the complexity of conditioning treatment, which included cytotoxic therapy, pretransplant and posttransplant immunosuppression, and other prophylactic treatments (to prevent infections and liver, renal, or central nervous system toxicity), relevant concomitant treatments were standardized and declared mandatory in both trial groups.
Table 13: Frequency of and Exposure to Concomitant Medication (Safety Analysis Set)
Concomitant medication | MC-FludT.14/L (Database lock date: March 16, 2018) | |
|---|---|---|
Treosulfan N = 270 | Busulfan N = 283 | |
Any medication, n (%) | 269 (99.6) | 283 (100.0) |
ATG | 208 (77.0) | 212 (74.9) |
Phenytoin or benzodiazepine | 0 | 283 (100.0) |
GvHD prophylaxis medication | 268 (99.3) | 283 (100.0) |
HSOS medication | 173 (64.1) | 178 (62.9) |
Mucositis medication | 96 (35.6) | 106 (37.5) |
Growth factors | 34 (12.6) | 39 (13.8) |
ATG = antithymocyte globulin; GvHD = graft versus host disease; HSOS = hepatic sinusoidal obstruction syndrome.
Source: MC-FludT.14/L Final Analysis Clinical Study Report.23
Subsequent Treatments
Subsequent treatments were standardized in the treatment groups and included ciclosporin, methotrexate, and calcium folinate. Data on the types and frequency of subsequent treatments was not reported in the MC-FludT.14/L trial final analysis (database lock date: March 16, 2018).
Efficacy
Findings for key efficacy outcomes in the FAS of the MC-FludT.14/L trial are summarized in Table 14 and Table 15. After the prespecified confirmatory interim analysis (data cut-off date: August 19, 2016), the noninferiority of treosulfan compared to busulfan had been formally demonstrated. This report describes the results of the primary end point of EFS in the confirmatory interim analysis, as it was inferentially tested, and the results of the final analysis, as it enrolled more patients and had a longer follow-up than the confirmatory interim analysis. Of note, 95% CIs and P values were not adjusted for multiplicity for outcomes in the final analysis or for the postsurveillance evaluation.
Event-Free Survival
Findings for the primary end point of EFS in the MC-FludT.14/L trial are summarized in Table 14. Patients with relapse of disease, graft failure, or death were censored in the analysis of EFS in both the confirmatory interim and final analyses.
In the confirmatory interim analysis (data cut-off date: August 19, 2016), the median duration of follow-up for EFS was 15.4 months (range, 3.2 months to 26.4 months) in the treosulfan group and 17.4 months (range 3.0 months to 26.3 months) in the busulfan group. Patients in the treosulfan group had fewer EFS events than those in the busulfan group; 68 patients (30.9%) in the treosulfan treatment group and 100 patients (41.7%) in the busulfan group experienced an event. The Kaplan-Meier estimate of EFS probability 24 months after HSCT was 64.0% (95% CI, 56.0% to 70.9%) in the treosulfan group and 50.4% (95% CI, 42.8% to 57.5%) in the busulfan group. The confirmatory interim analysis for EFS demonstrated the noninferiority of treosulfan compared to the busulfan group and a trend toward superiority (HR = 0.65; 99.9702% CI, 0.36 to 1.19; noninferiority P = 0.0000164; superiority P = 0.0051268; both noninferiority and superiority P values are compared against the prespecified 1-sided significance level of 0.000149). The Kaplan-Meier estimate of the EFS distribution in the final analysis population is depicted in Figure 2.
In the final analysis, including the postsurveillance evaluation (database lock date: March 16, 2018), the median duration of follow-up of EFS was 29.7 months (range, 3.0 months to 52.1 months) in the treosulfan group and 29.4 months (range, 3.0 months to 54.3 months) in the busulfan group. Patients in the treosulfan group had fewer EFS events than those in the busulfan group; 97 (36.2%) patients in the treosulfan treatment group and 137 (48.4%) patients in the busulfan group experienced an EFS event. The median EFS was not reached in the treosulfan group and was 33.0 months (95% CI, 14.7 months to not available) in the busulfan group. The Kaplan-Meier estimate of EFS probability 24 months after HSCT was 65.7% (95% CI, 59.5% to 71.2%) in the treosulfan group and 51.2% (95% CI, 45.0% to 57.0%) in the busulfan group. The Kaplan-Meier estimate of EFS probability 36 months after HSCT was 59.5% (95% CI, 52.2% to 66.1%) in the treosulfan group and 49.7% (95% CI, 43.3% to 55.7%) in the busulfan group. The HR in the final analysis was 0.216 (95% CI, 0.131 to 0.357; noninferiority: nominal P = 0.0000001 versus prespecified 1-sided significance level of 0.001262; superiority: nominal P = 0.0005787). The Kaplan-Meier estimate of the EFS distribution in the final analysis population is depicted in Figure 3.
In the confirmatory interim analysis (data cut-off date: August 19, 2016) and in the final analysis, including the postsurveillance evaluation (data cut-off: March 16, 2018), similar results were observed in the PPS population. Refer to Table 17 in Appendix 1 for detailed results from the PPS for both analyses.
In the confirmatory interim analysis (data cut-off date: August 19, 2016) and the final analysis, including the postsurveillance evaluation (data lock date: March 16, 2018), subgroup analyses of EFS were generally consistent with the primary confirmatory interim analysis across all prespecified subgroups, except for patients with MRD in risk group II and with MDS in risk group I, (the latter was only in the confirmatory interim analysis). Refer to Appendix 1 for detailed subgroup analyses data.
In the confirmatory interim analysis (data cut-off date: August 19, 2016), results for the preplanned sensitivity analyses of conditional Cox model estimates for different prognostic subgroups as factors were generally consistent with the results of the primary confirmatory interim analysis and showed HR values ranging from 0.56 (99.9702% CI, 0.24 to 1.31) to 0.95 (99.9702% CI, 0.33 to 2.70). In the final analysis, including the postsurveillance evaluation (database lock date: March 16, 2018), the results were generally consistent with the results of the primary final analysis and showed HR values ranging from 0.60 (95% CI, 0.38 to 0.97) to 0.93 (95% CI, 0.55 to 1.54).
Figure 2: Kaplan-Meier Estimates of EFS in the Confirmatory Interim Analysis (Data Cut-Off Date: August 19, 2016; FAS)
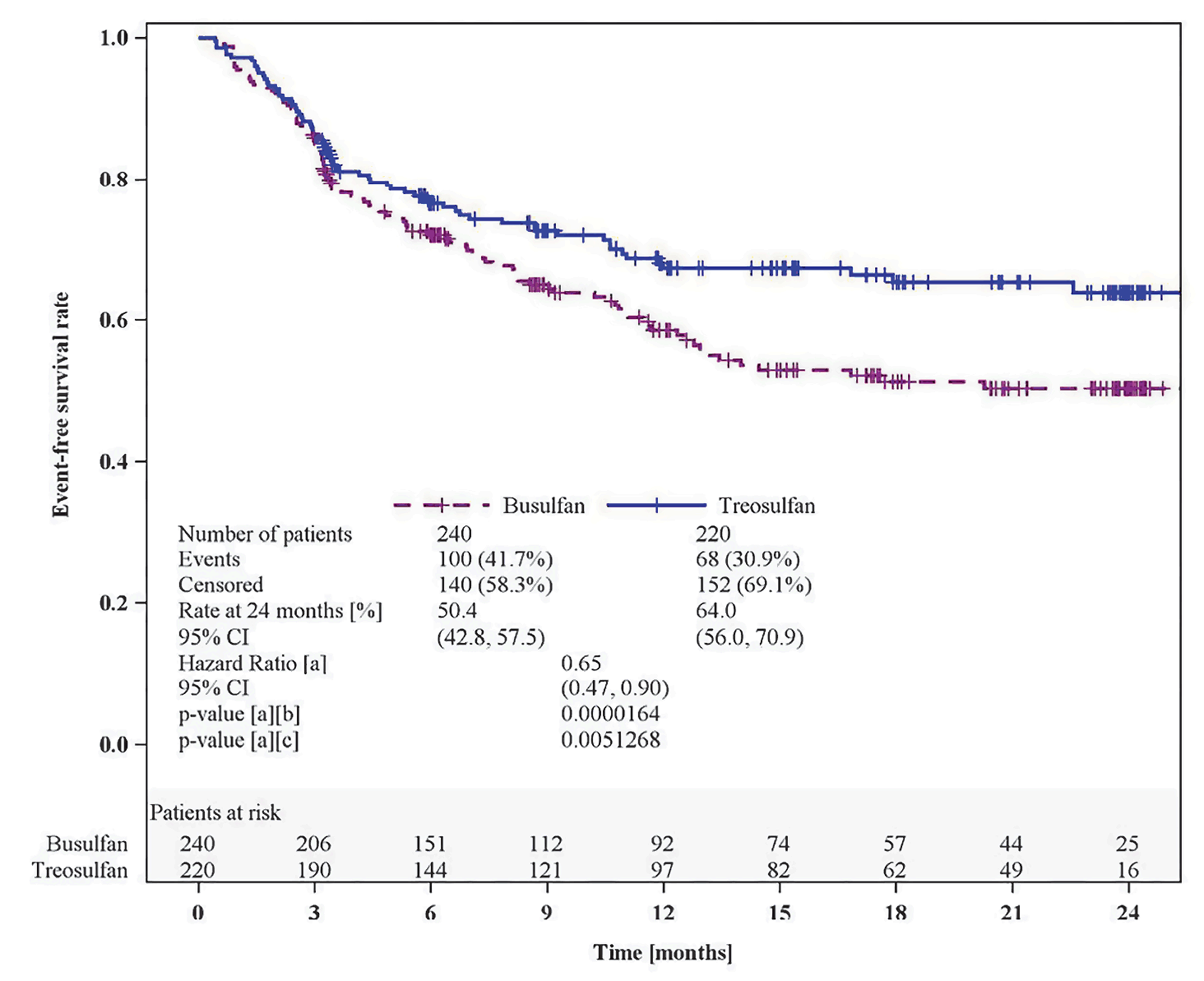
CI = confidence interval; EFS = event-free survival; FAS = full analysis set.
a Adjusted for donor type as a factor and risk group and centre as strata in a Cox regression.
b For testing the noninferiority of treosulfan compared to busulfan.
c For testing the superiority of treosulfan compared to busulfan.
Source: MC-FludT.14/L Confirmatory Interim Analysis Clinical Study Report.22
Figure 3: Kaplan-Meier Estimates of EFS in the Final Analysis (Database Lock Date: March 16, 2018; FAS)
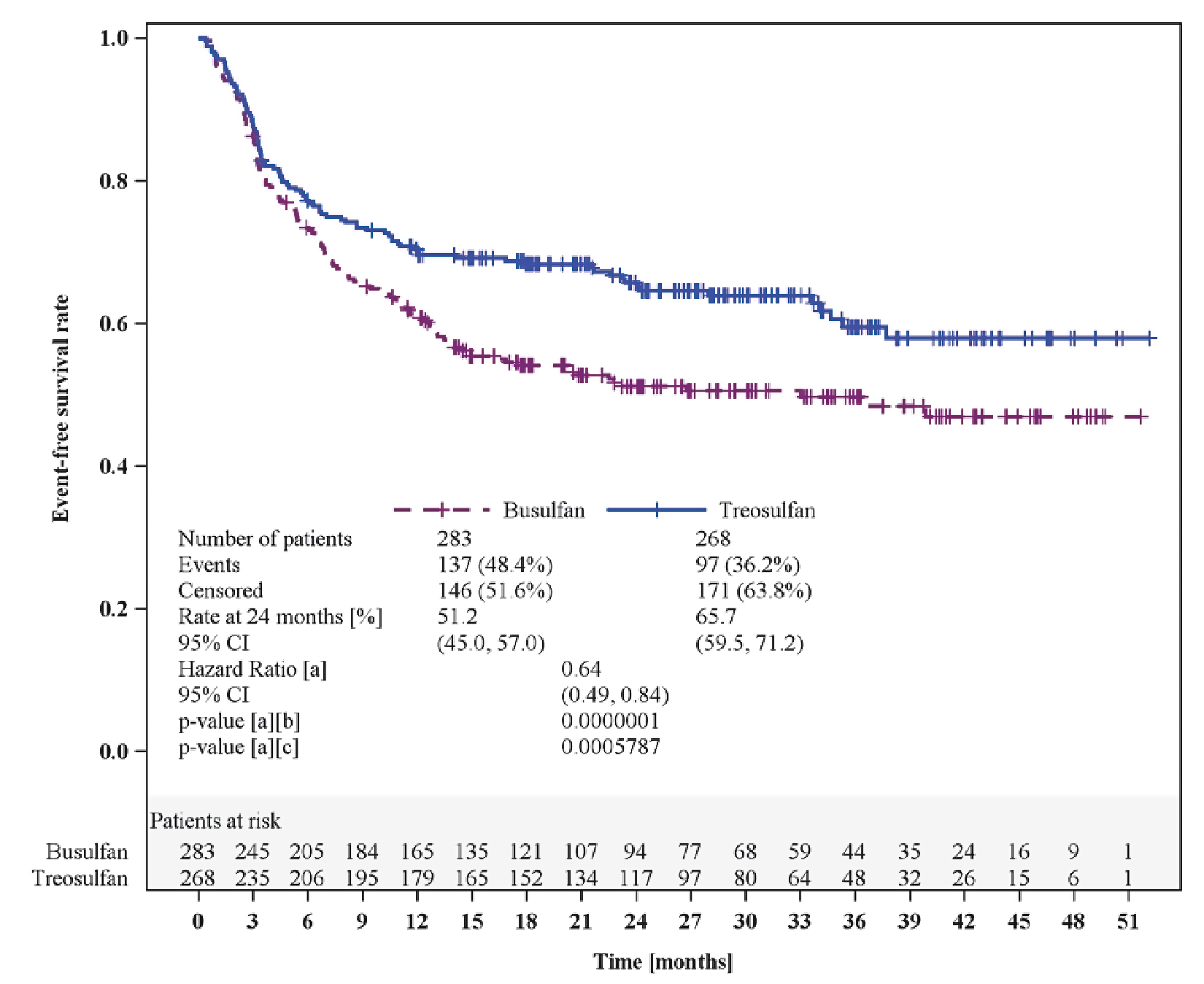
CI = confidence interval; EFS = event-free survival; FAS = full analysis set.
a Adjusted for donor type as a factor and risk group and centre as strata in a Cox regression.
b For testing the noninferiority of treosulfan compared to busulfan.
c For testing the superiority of treosulfan compared to busulfan.
Source: MC-FludT.14/L Final Analysis Clinical Study Report.23
Overall Survival
In the MC-FludT.14/L study, OS was a secondary end point. in the final analysis, including the postsurveillance evaluation (database lock date: March 16, 2018), patients had been followed for a median of 29.7 months (range, 0.4 months to 52.1 months) in the treosulfan group and 29.4 months (range, 0.4 months to 54.3 months) in the busulfan group (Figure 4). There were 81 (30.2%) patients in the treosulfan group and 112 (39.6%) patients in the busulfan group who had died by the postsurveillance evaluation (HR = 0.64; 95% CI, 0.48 to 0.87; nominal P = 0.0037). Median OS was not reached in either group. The Kaplan-Meier estimate of OS probabilities decreased from 72.7% (95% CI, 66.8% to 77.8%) to 66.8% (95% CI, 59.9 to 72.9) in the treosulfan group and from 60.2% (95% CI, 54.0% to 65.8%) to 56.3% (95% CI, 49.6% to 62.6%) in the busulfan group from 24 to 36 months. Generally, similar results were observed in the confirmatory interim analysis (data cut-off date: August 19, 2016). Refer to Table 18 in Appendix 1 for detailed results from the confirmatory interim analysis.
Figure 4: Kaplan-Meier Estimates of OS in the Final Analysis (Database Lock Date: March 16, 2018; FAS)
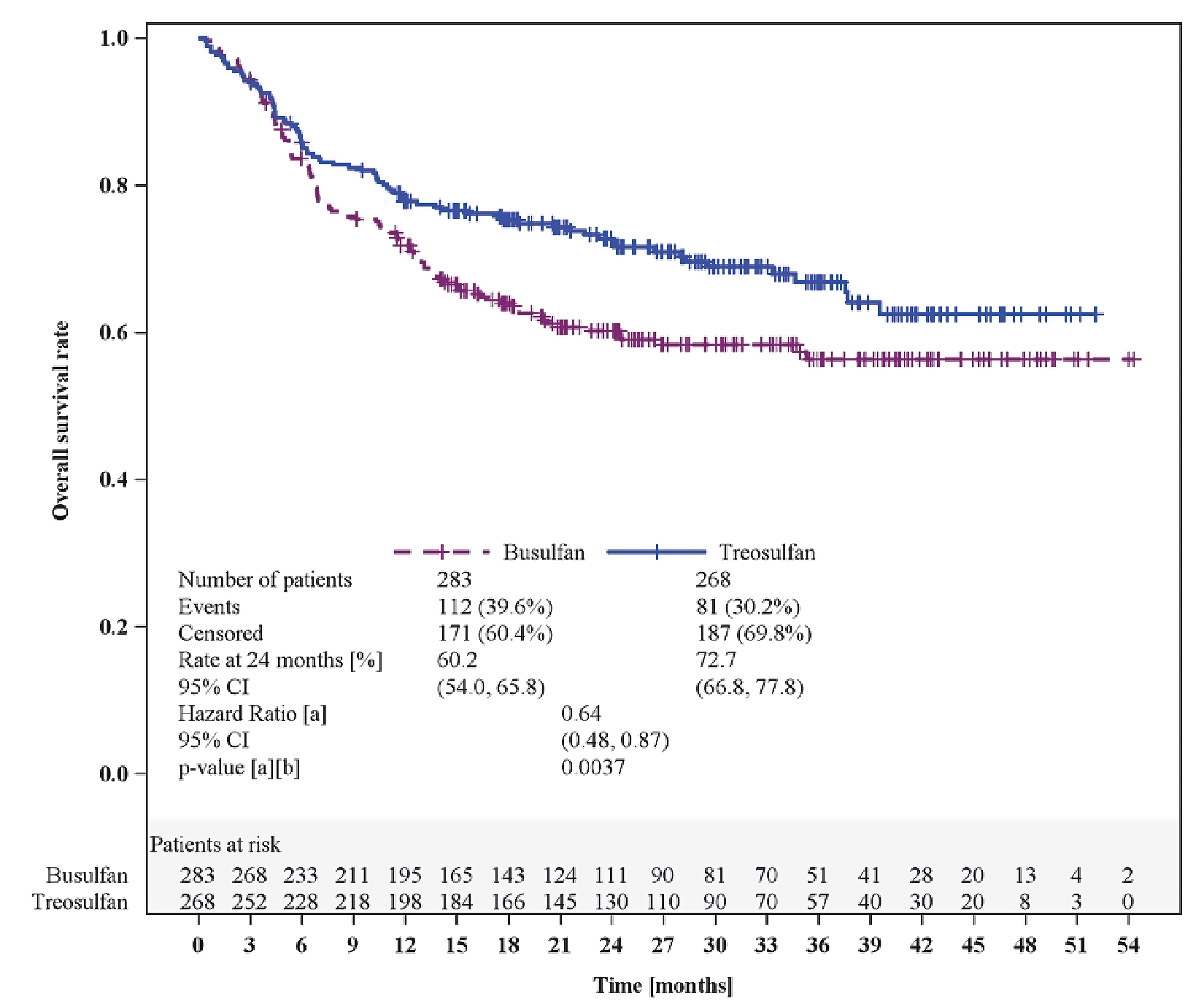
CI = confidence interval; FAS = full analysis set; OS = overall survival.
a Adjusted for donor type as a factor and risk group and centre as strata using the Cox regression model.
b For testing the noninferiority of treosulfan compared to busulfan.
c For testing the superiority of treosulfan compared to busulfan.
Source: MC-FludT.14/L Final Analysis Clinical Study Report.23
Graft Failure
Graft failure was a secondary end point in the final analysis, including the postsurveillance evaluation (database lock date: March 16, 2018). Patients in the treosulfan group had a lower percentage of graft failure (primary and secondary) than patients in the busulfan group (0.4% versus 3.2%). No event of graft failure was reported during the postsurveillance period. Generally, similar results were observed in the confirmatory interim analysis (data cut-off date: August 19, 2016). Refer to Table 18 in Appendix 1 for detailed results from the confirmatory interim analysis.
Engraftment
Engraftment 28 days after HSCT was assessed as a secondary end point in the final analysis (database lock date: March 16, 2018). The number of patients with reconstitution of granulopoiesis was similar in the 2 treatment groups; 263 (98.1%) patients in the treosulfan group and 279 (98.6%) patients in the busulfan group were with documented reconstitution of granulopoiesis. The conditional cumulative incidence of reconstitution of granulopoiesis 28 days after HSCT was 96.2% (95% CI, 93.4% to 99.1%) in the treosulfan group and 96.8% (95% CI, 94.6% to 99.1%) in the busulfan group. The cause-specific HR was 1.06 (95% CI, 0.91 to 1.24; nominal P = 0.4235) in favour of treosulfan.
In the same analysis, the number of patients with reconstitution of thrombopoiesis greater than 20 × 109/L was similar in the treosulfan and busulfan groups (97.0% versus 96.8%). The conditional cumulative incidence of reconstitution of thrombopoiesis 28 days after HSCT was 94.7% (95% CI, 92.0% to 97.4%) in the treosulfan group and 97.8% (95% CI, 96.3% to 99.4%) in the busulfan group. The cause-specific HR was 0.80 (95% CI, 0.68 to 0.93; nominal P = 0.0038) in favour of busulfan.
Generally, similar results were observed in the confirmatory interim analysis (data cut-off date: August 19, 2016). Refer to Table 18 in Appendix 1 for detailed results from the confirmatory interim analysis.
Chimerism
The observed incidence of complete donor-type chimerism 28 days after HSCT was assessed as a secondary end point in the final analysis (database lock date: March 16, 2018). At the day 28 visit, the incidence of complete donor-type chimerism was 93.2% (95% CI, 89.4% to 95.9%) in the treosulfan group and 83.3% (95% CI, 78.5% to 87.5%) in the busulfan group. The odds ratio was 2.8083 (95% CI, 1.58 to 5.01; nominal P = 0.0159) in favour of treosulfan. Generally, similar results were observed in the confirmatory interim analysis (data cut-off date: August 19, 2016). Refer to Table 18 in Appendix 1 for detailed results from the confirmatory interim analysis.
Relapse or Progression
Cumulative Incidence of Relapse or Progression
The cumulative incidence of relapse or progression was assessed as a secondary end point in the final analysis, including the postsurveillance evaluation (database lock date: March 16, 2018). A slightly lower proportion of patient in the treosulfan group than in the busulfan group reported relapse or progression; 61 (22.8%) patients in the treosulfan group and 72 (25.4%) patients in the busulfan group experienced relapse or progression. The cumulative incidence of relapse and/or progression 24 months after HSCT was 22.0% (95% CI, 16.9% to 27.1%) in the treosulfan group and 25.2% (95% CI, 20.0% to 30.3%) in the busulfan group. The cause-specific HR was 0.82 (95% CI, 0.59 to 1.16; nominal P = 0.2631) in favour of treosulfan. Generally, similar results were observed in the confirmatory interim analysis (data cut-off date: August 19, 2016). Refer to Table 18 in Appendix 1 for detailed results from the confirmatory interim analysis.
GvHD-Free and Relapse or Progression-Free Survival
The incidence of GRFS in 2 the years after HSCT was assessed as a secondary end point in the final analysis (database lock date: March 16, 2018). A lower proportion of patients in the treosulfan group than in the busulfan group experienced GvHD or relapse or progression (48.5% versus 59.7%). The Kaplan-Meier estimate of GRFS probability at 24 months was 50.3% (95% CI, 43.9% to 56.3%) in the treosulfan group and 37.1% (95% CI, 31.1% to 43.1%) in the busulfan group. The HR was 0.73 (95% CI, 0.57 to 0.92; nominal P = 0.0087) in favour of treosulfan. The Kaplan-Meier plot of GRFS in the final analysis is depicted in Figure 5. Generally, similar results were observed in the confirmatory interim analysis (data cut-off date: August 19, 2016). Refer to Table 18 in Appendix 1 for detailed results from the confirmatory interim analysis.
Figure 5: Kaplan-Meier Estimates of GRFS in the Final Analysis (Database Lock Date: March 16, 2018; FAS)
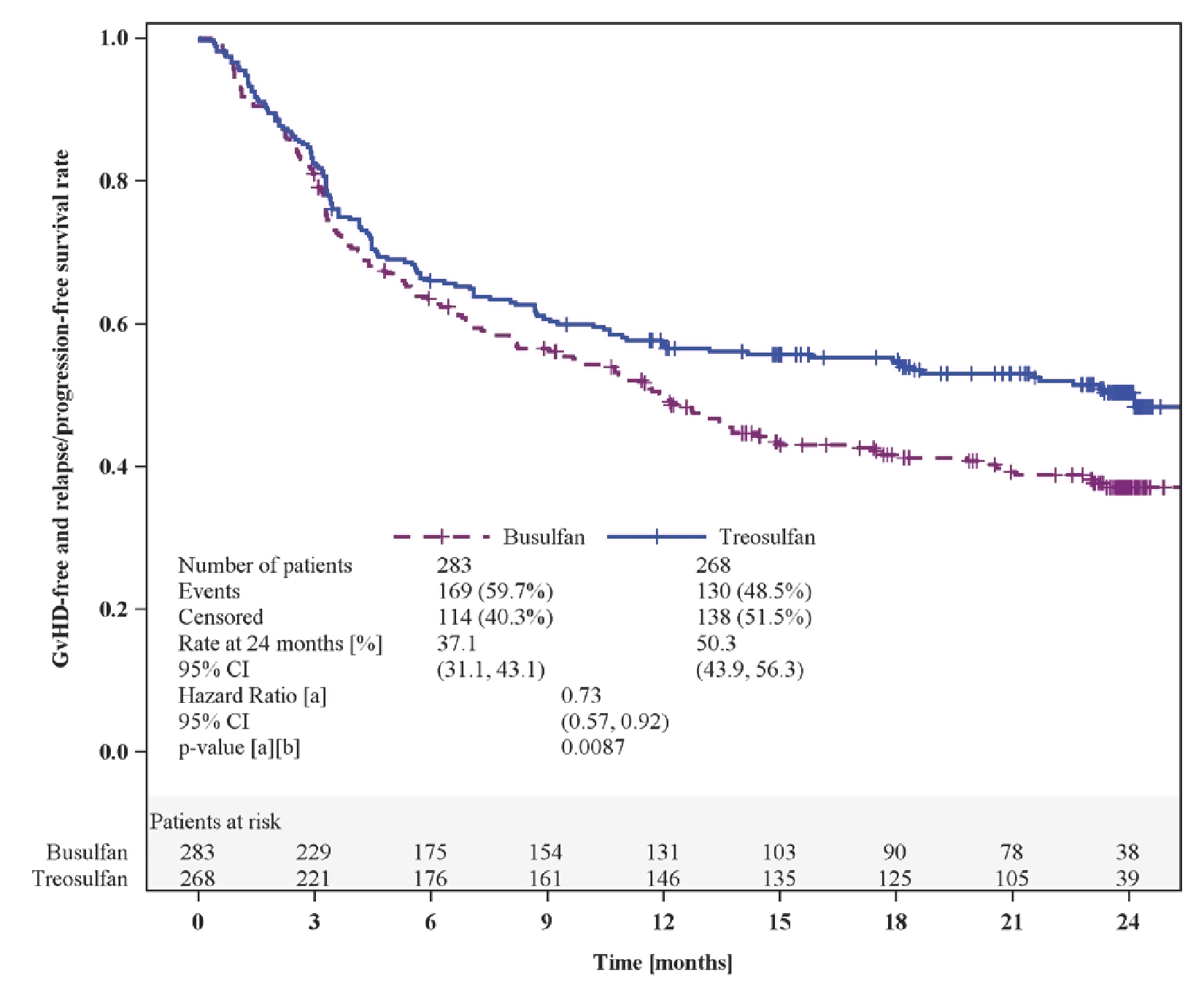
CI = confidence interval; FAS = full analysis set; GRFS = GvHD-free and relapse and/or progression-free survival; GvHD = graft versus host disease.
Note: GvHD-free survival is defined as no acute GvHD of at least grade III and no extensive chronic GvHD.
a Adjusted for donor type as a factor and risk group and centre as strata using the Cox regression model.
b For testing the difference between treosulfan and busulfan.
Source: MC-FludT.14/L Final Analysis Clinical Study Report.23
Chronic GvHD-Free and Relapse or Progression-Free Survival
The incidence of CRFS in the 2 years after HSCT was assessed as a secondary end point in the final analysis (database lock date: March 16, 2018). A lower proportion of patients in the treosulfan group than in the busulfan group experienced extensive chronic GvHD or relapse or progression; 128 (47.8%) patients in the treosulfan group and 168 (59.4%) patients in the busulfan group experienced relapse or progression. The Kaplan-Meier estimates of CRFS probability at 24 months were 51.4% (95% CI, 45.0% to 57.4%) in the treosulfan group and 37.2% (95% CI, 31.3% to 43.2%) in the busulfan group. The HR was 0.70 (95% CI, 0.55 to 0.88); nominal P = 0.0030) in favour of treosulfan. The Kaplan-Meier plot of CRFS in the final analysis is depicted in Figure 6. Generally, similar results were observed in the confirmatory interim analysis (data cut-off date: August 19, 2016). Refer to Table 18 in Appendix 1 for detailed results from the confirmatory interim analysis.
Figure 6: Kaplan-Meier Estimates of CRFS in the Final Analysis (Database Lock Date: March 16, 2018; FAS)
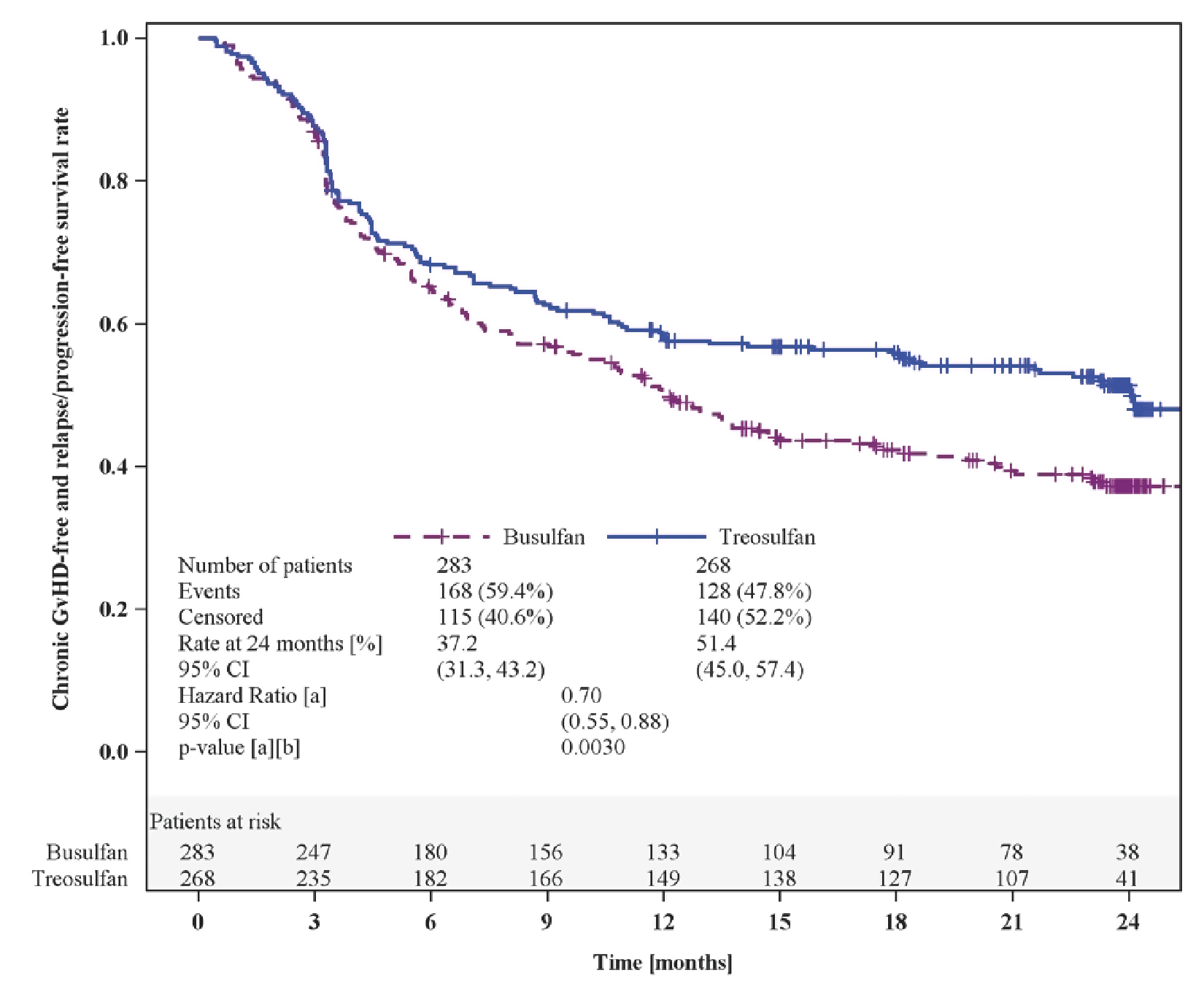
CI = confidence interval; CRFS = chronic GvHD-free and relapse and/or progression-free survival; GvHD = graft versus host disease.
Note: Chronic GvHD-free survival is defined as no extensive chronic GvHD.
a Adjusted for donor type as a factor and risk group and centre as strata using the Cox regression model.
b For testing the difference between treosulfan and busulfan.
Source: MC-FludT.14/L Final Analysis Clinical Study Report.23
Mortality
Nonrelapse Mortality
The cumulative incidence of NRM 24 months after HSCT was assessed as a secondary end point of the trial. In the final analysis, including the postsurveillance evaluation (database lock date: March 16, 2018), 35 (13.1%) patients in the treosulfan group and 56 (19.8%) patients in the busulfan group died without relapse and/or progression. The cumulative incidence of NRM 24 months after HSCT was 12.0% (95% CI, 8.0% to 15.9%) in the treosulfan group and 20.4% (95% CI, 15.5% to 25.2%) in the busulfan group. The cause-specific HR was 0.63 (95% CI, 0.41 to 0.97; nominal P = 0.0343) in favour of treosulfan. Generally, similar results were observed in the confirmatory interim analysis (data cut-off date: August 19, 2016). Refer to Table 18 in Appendix 1 for detailed results from the confirmatory interim analysis.
Transplant-Related Mortality
The cumulative incidence of TRM 24 months after HSCT was assessed as a secondary end point of the trial. In the final analysis (database lock date: March 16, 2018), 33 (12.3%) patients in the treosulfan group and 58 (20.5%) patients in the busulfan group died from a transplant-related cause. The cumulative incidence of TRM 24 months after HSCT was 12.8% (95% CI, 9.2% to 17.7%) in the treosulfan group and 24.1% (95% CI, 19.1% to 30.2%) in the busulfan group. The cause-specific HR was 0.52 (95% CI, 0.34 to 0.82; nominal P = 0.0043) in favour of treosulfan. Generally, similar results were observed in the confirmatory interim analysis (data cut-off date: August 19, 2016). Refer to Table 18 in Appendix 1 for detailed results from the confirmatory interim analysis.
Health-Related Quality of Life
HRQoL was identified as important by patient groups and the clinical experts consulted by CADTH. HRQoL was not assessed in the MC-FludT.14/L trial.
Table 14: Summary of Results for EFS, the Primary Outcome of the Study Included in the Systematic Review (FAS)
End points | MC-FludT.14/L confirmatory interim analysis (data cut-off date: August 19, 2016) | MC-FludT.14/L final analysis (database lock date: March 16, 2018) | ||
|---|---|---|---|---|
Treosulfan N = 220 | Busulfan N = 240 | Treosulfan N = 268 | Busulfan N = 283 | |
EFS | ||||
Median follow-up time,a months (range) | 15.4 (3.2 to 26.4) | 17.4 (3.0 to 26.3) | 29.7 (3.0 to 52.1) | 29.4 (3.0 to 54.3) |
Patients with event, n (%) | 68 (30.9) | 100 (41.7) | 97 (36.2) | 137 (48.4) |
Death | 23 (10.5) | 41 (17.1) | 35 (13.1) | 56 (19.8) |
Relapse or progression | 45 (20.5) | 51 (21.3) | 61 (22.8) | 72 (25.4) |
Primary graft failure | 0 | 1 (0.4) | 1 (0.4) | 1 (0.4) |
Secondary graft failure | 0 | 7 (2.9) | 0 | 8 (2.8) |
Median EFS, months (95% CI) | Not reached | Not reached | Not reached | 33.0 (14.7 to not reached) |
Estimates of probability of EFS at 24 months,b % (95% CI) | 64.0 (56.0 to 70.9) | 50.4 (42.8 to 57.5) | 65.7 (59.5 to 71.2) | 51.2 (45.0 to 57.0) |
Absolute difference in EFS probability between study groups at 24 months,b % (95% CI) | 13.6 (3.1 to 24.0) | 14.5 (6.1 to 22.9) | ||
Estimates of EFS probability at 36 months,b % (95% CI) | NA | NA | 59.5 (52.2 to 66.1) | 49.7 (43.3 to 55.7) |
Absolute difference in survival probability between study groups at 36 months,b % (95% CI) | NA | 9.8 (0.5 to 19.2) | ||
HR (99.9702% CI)c | 0.65 (0.36 to 1.19) | NA | ||
HR (95% CI)c | 0.65 (0.47 to 0.90) | 0.64 (0.49 to 0.84) | ||
P valuec | Noninferiority: 0.0000164d | Noninferiority: nominal P = 0.0000001 | ||
CI = confidence interval; EFS = event-free survival; HR = hazard ratio, NA = not applicable.
Note: Only the P value in the confirmatory interim analysis (data cut-off date: August 19, 2016) of EFS was adjusted for multiple comparison. P values for all other outcomes were not adjusted for multiplicity.
aBased on reverse Kaplan-Meier estimates for OS.
bBased on Kaplan-Meier estimates.
cAdjusted for donor type as a factor and risk group and centre as strata using the Cox regression model.
dThe nominal 1-sided significance level resulting from an O'Brien-Fleming type of group-sequential efficacy stopping boundary is 0.000149.
Sources: MC-FludT.14/L Confirmatory Interim Analysis Clinical Study Report,22 MC-FludT.14/L Final Analysis Clinical Study Report,23 and Beelen et al. (2022).48 Details included in the table are from the sponsor’s Summary of Clinical Evidence.24
Table 15: Summary of the Results of Secondary Outcomes From the Study Included in the Systematic Review (FAS)
End points | MC-FludT.14/L final analysis (data cut-off: March 16, 2018) | |
|---|---|---|
Treosulfan N = 268 | Busulfan N = 283 | |
OS | ||
Median follow-up time, months (range) | 29.7 (0.4 to 52.1) | 29.4 (0.4 to 54.3) |
Patients with event, n (%) | 81 (30.2) | 112 (39.6) |
Median OS, months (95% CI) | NA | NA |
Estimates of OS probability at 24 months,a % (95% CI) | 72.7 (66.8 to 77.8) | 60.2 (54.0 to 65.8) |
Absolute difference in survival probability between study groups at 24 months,a % (95% CI) | 12.5 (4.4 to 20.7) | |
Estimates of OS probability at 36 months,a % (95% CI) | 66.8 (59.9 to 72.9) | 56.3 (49.6 to 62.6) |
Absolute difference in survival probability between study groups at 36 months,a % (95% CI) | 10.5 (1.3to 19.7) | |
HR (95% CI) | 0.64 (0.48 to 0.87) | |
Nominal P valueb | 0.0037 | |
Graft failure | ||
Median follow-up time, months (range) | NA | NA |
Observed percentage of patients with graft failure (primary and secondary) at 24 months, % (95% CI) | 0.4 (0.0 to 2.1) | 3.2 (1.5 to 6.0) |
Difference between study groups, % (95% CI) | –2.8 (– 5.0 to –0.6) | |
Engraftment at day 28 | ||
Reconstitution of granulopoiesisc | ||
Median follow-up time, days (range) | 18 (7 to 42) | 19 (1 to 38) |
Patients with event, n (%) | 263 (98.1) | 279 (98.6) |
Patients without event (censored) or with competing event, n (%) | 5 (1.9) | 4 (1.4) |
Censored | 1 (0.4) | 1 (0.4) |
Deathd | 4 (1.5) | 2 (0.7) |
Relapse or progressiond | 0 | 1 (0.4) |
Conditional cumulative incidence at 28 days, n (95% CI) | 96.2 (93.4 to 99.1) | 96.8 (94.6 to 99.1) |
Absolute difference in cumulative incidence of reconstitution of granulopoiesis between study groups at 28 days, % (95% CI) | –1.3 (–4.7 to 2.0) | |
Cause-specific HRe (95% CI) | 1.06 (0.91 to 1.24) | |
Nominal P valuee | 0.4235 | |
Reconstitution of thrombopoiesisf | ||
Median follow-up time, days (range) | 13 (0 to 38) | 12 (0 to 32) |
Patients with event, n (%) | 260 (97.0) | 274 (96.8) |
Patients without event (censored) or with competing event, n (%) | 8 (3.0) | 9 (3.2) |
Censored | 3 (1.1) | 2 (0.7) |
Deathd | 5 (1.9) | 4 (1.4) |
Relapse or progressiond | 0 (0.0) | 3 (1.1) |
Conditional cumulative incidence at 28 days, n (95% CI) | 94.7 (92.0 to 97.4) | 97.8 (96.3 to 99.4) |
Absolute difference in cumulative incidence of reconstitution of thrombopoiesis between study groups at 28 days, % (95% CI) | –2.8 (–6.4 to 0.8) | |
Cause-specific HRe (95% CI) | 0.80 (0.68 to 0.93) | |
Nominal P valuee | 0.0038 | |
Chimerism | ||
Incidence of complete chimerism at day 28 visit, n (95% CI) | 93.2 (89.4 to 95.9) | 83.3 (78.5 to 87.5) |
Median follow-up time, days (95% CI) | NA | NA |
Absolute difference of incidence of chimerism between study groups at 28 days, % (95% CI) | 9.8 (4.5 to 15.1) | |
Odds ratiog (95% CI) | 2.81 (1.58 to 5.01) | |
Nominal P value h | 0.0159 | |
Relapse or progression | ||
Cumulative incidence of relapse or progression | ||
Median follow-up time, months (95% CI) | 26.3 (0.4 to 52.1) | 22.5 (0.4 to 51.6) |
Patients with event, n (%) | 61 (22.8) | 72 (25.4) |
Cumulative incidence of relapse or progression at 24 months, % (95% CI) | 22.0 (16.9 to 27.1) | 25.2 (20.0 to 30.3) |
Absolute difference of cumulative incidence of relapse or progression between study groups at 24 months, % (95% CI) | –3.2 (–10.4 to 4.1) | |
Cause-specific HR (95% CI) | 0.82 (0.59 to 1.16) | |
Nominal P value e | 0.263 | |
GRFS | ||
Patients with event, n (%) | 130 (48.5) | 169 (59.7) |
Median follow-up time, months (95% CI) | 23.7 (0.0 to 26.5) | 23.7 (0.4 to 54.3) |
Estimates of GvHD-free and relapse or progression-free survival probability at 24 months,a % (95% CI) | 50.3 (43.9 to 56.3) | 37.1 (31.1 to 43.1) |
Absolute difference in Kaplan-Meier GRFS probability between study groups at 24 months, % (95% CI) | 13.2 (4.6 to 22.8) | |
HR (95% CI)b | 0.73 (0.57 to 0.92) | |
Nominal P valueb | 0.0087 | |
CRFS | ||
Patients with event, n (%) | 128 (47.8) | 168 (59.4) |
Median follow-up time, months (95% CI) | 23.7 (0.4 to 26.5) | 23.7 (0.4 to 26.3) |
Estimates of CRFS probability at 24 months,a % (95% CI) | 51.4 (45.0 to 57.4) | 37.2 (31.3 to 43.2) |
Absolute difference in Kaplan-Meier CRFS probability between study groups at 24 months, % (95% CI) | 14.1 (5.5 to 22.8) | |
HR (95% CI)b | 0.70 (0.55 to 0.88) | |
Nominal P valueb | 0.0030 | |
NRM | ||
Patients with event, n (%) | 35 (13.1) | 56 (19.8) |
Median follow-up time, months (95% CI) | 24.3 (0.4 to 52.1) | 21.1 (0.4 to 54.3) |
Cumulative NRM incidence at 24 months, % (95% CI) | 12.0 (8.0 to 15.9) | 20.4 (15.5 to 25.2) |
Absolute difference in cumulative incidence of NRM between study groups at 24 months, % (95% CI) | –8.4 (–14.7 to –2.2) | |
Cause-specific HR (95% CI)e | 0.63 (0.41 to 0.97) | |
Nominal P valuee | 0.0343 | |
TRM | ||
Patients with event, % (95% CI) | 33 (12.3) | 58 (20.5) |
Median follow-up time, months (95% CI) | 23.6 (0.4 to 26.5) | 23.2 (0.4 to 26.3) |
Estimates of TRM probability at 24 months,a % (95% CI) | 12.8 (9.2 to 17.7) | 24.1 (19.1 to 30.2) |
Absolute difference in TRM between study groups at 24 months,a % (95% CI) | –11.3 (–18.2 to 2.6) | |
HR (95% CI)b | 0.52 (0.34 to 0.82) | |
Nominal P valueb | 0.0043 | |
CI = confidence interval; CRFS = chronic GvHD-free and relapse and/or progression-free survival; FAS = full analysis set; GRFS = GvHD-free and relapse and/or progression-free survival; GvHD = graft versus host disease; HR = hazard ratio; NA = not available; NRM = nonrelapse mortality; OS = overall survival; TRM = transplant-related mortality.
Note: P values for all outcomes were not adjusted for multiplicity in the final analysis (database lock date: March 16, 2018).
aBased on Kaplan-Meier estimates.
bAdjusted for donor type as a factor and risk group and centre as strata using the Cox regression model.
cReconstitution of granulopoiesis was documented on the first of 3 consecutive days, with a neutrophilic granulocyte count > 0.5 × 109/L in the peripheral blood.
dOnly if this event occurred first.
eAdjusted for donor type as a factor and risk group as stratum using the Fine-Gray model.
fReconstitution of thrombopoiesis was documented on the first of 3 consecutive days, with platelet count > 20 × 109/Lin the absence of platelet transfusion.
gAdjusted for donor type and risk group. Missing values were considered a no for odds ratio calculation.
hStratified Cochran-Mantel-Haenszel test adjusted for donor type and risk group.
Sources: MC-FludT.14/L Final Analysis Clinical Study Report23 and Beelen et al. (2022).48 Details included in the table are from the sponsor’s Summary of Clinical Evidence.24
Harms
Harms data in the MC-FludT.14/L trial final analysis (database lock date: March 16, 2018) are summarized in Table 16.
Adverse Events
At least 1 AE was reported in a similar proportion of patients in the treosulfan and busulfan groups (92.6% versus 96.1%). The most common treatment-related AE occurring in at least 20% of patients in either treatment group included (treosulfan versus busulfan) edema in the limbs (22.6% versus 13.4%) and vomiting (21.9% versus 19.4%), which were reported more frequently in the treosulfan group than in the busulfan group, and oral mucositis (37.8% versus 47.7%), fever (34.4% versus 35.7%), nausea (33.0% versus 41.0%), and hypertension (14.1% versus 21.2%), which were reported less frequently in the treosulfan group than in the busulfan group.
A similar proportion of patients in the treosulfan and busulfan groups reported grade 3 or higher AEs (54.8% versus 53.4%). The most common grade 3 or higher AEs occurring in at least 5% of patients in either treatment group included (treosulfan versus busulfan) infections and infestations (15.2% versus 9.2%), febrile neutropenia (14.8% versus 11.0%), and increased alanine aminotransferase (5.2% versus 3.2%), which were reported more frequently in the treosulfan group than in the busulfan group, and hypertension (7.8% versus 9.5%), oral mucositis (5.9% versus 7.4%), increased gamma-glutamyl transferase (4.4% versus 8.8%), and nausea (3.0% versus 6.0%), which were reported less frequently in the treosulfan group than in the busulfan group.
Serious Adverse Events
Overall, more patients in treosulfan group than the busulfan group experienced at least 1 SAE (8.5% versus 7.1%). The most common SAEs occurring in at least 1% of patients in either treatment group included (treosulfan versus busulfan) sepsis (3.0% versus 1.8%), lung infection (2.2% versus 1.1%), and acute kidney injury sepsis (1.1% versus 0.4%), which were reported more frequently in the treosulfan group than in the busulfan group.
Withdrawals Due to Adverse Events
None of the patients in the MC-FludT.14/L trial were deemed to require a dose reduction or to discontinue treatment due to drug-related toxicity.
Mortality
Overall, fewer patients had died in the treosulfan group than in the busulfan group (26.7% versus 37.8%) at 24 months. Relapse and/or progression was the most frequently reported cause of death in the treosulfan group (treosulfan versus busulfan) (12.6% versus 16.6%), whereas transplant-related causes were the most frequently reported cause of death in the busulfan group (12.2% versus 20.5%). Other common causes of death were infection (9.3% versus 14.1%) and GvHD (4.8% versus 7.4%), which were reported less frequently in the treosulfan group than in the busulfan group; renal failure was reported more frequently in the treosulfan group than in the busulfan group (1.9% versus 0.4%). In the postsurveillance analysis, overall, fewer patients died in the treosulfan group than in the busulfan group (30.0% versus 39.6%). The cause of death was not recorded during the postsurveillance period.
Notable Harms
In the final analysis, the cumulative incidence of acute GvHD of grade III or IV at 100 days was 6.4% (95% CI, 3.4% to 9.3%) in the treosulfan group and 8.1% (95% CI, 4.9% to 11.3%) in the busulfan group. The cumulative incidence of chronic GvHD at 24 months was similar in the 2 treatment groups, at 61.7% (95% CI, 55.1% to 68.3%) in the treosulfan group and 60.3% (95% CI, 53.8% to 66.7%) in the busulfan group. Grade III or IV mucositis, HSOS, seizures, and increased bilirubin were considered significant AEs. The cumulative incidence of grade III or IV mucositis was 5.9% (95% CI, 3.4% to 9.4%) in the treosulfan group and 7.4% (95% CI, 4.7% to 11.1%) in the busulfan group. One patient in the busulfan group reported HSOS, and 1 patient in the treosulfan group reported seizure. A slightly higher proportion of patients in the treosulfan group than in the busulfan group reported increased blood bilirubin (3.3% versus 2.8%).
Table 16: Summary of Harms Results From the Study Included in the Systematic Review (Safety Analysis Set)
Adverse events | Treosulfan N = 270 | Busulfan N = 283 |
|---|---|---|
Most common AEs (≥ 20% of either treatment group), n (%) | ||
Patients with ≥ 1 adverse event | 250 (92.6) | 272 (96.1) |
Oral mucositis | 102 (37.8) | 135 (47.7) |
Fever | 93 (34.4) | 101 (35.7) |
Nausea | 89 (33.0) | 116 (41.0) |
Edema in the limbs | 61 (22.6) | 38 (13.4) |
Vomiting | 59 (21.9) | 55 (19.4) |
Hypertension | 38 (14.1) | 60 (21.2) |
Most common grade 3 or higher AEs (≥ 5% of either treatment group), n (%) | ||
Patients with ≥ 1 grade 3 or higher AE | 148 (54.8) | 151 (53.4) |
Infections and infestations | 41 (15.2) | 26 (9.2) |
Febrile neutropenia | 40 (14.8) | 31 (11.0) |
Hypertension | 21 (7.8) | 27 (9.5) |
Oral mucositis | 16 (5.9) | 21 (7.4) |
Increased alanine aminotransferase | 14 (5.2) | 9 (3.2) |
Increased gamma-glutamyl transferase | 12 (4.4) | 25 (8.8) |
Nausea | 8 (3.0) | 17 (6.0) |
SAEs (≥ 1% of either treatment group), n (%) | ||
Patients with ≥ 1 SAE | 23 (8.5) | 20 (7.1) |
Sepsis | 8 (3.0) | 5 (1.8) |
Lung infection | 6 (2.2) | 3 (1.1) |
Acute kidney injury | 3 (1.1) | 1 (0.4) |
Patients who stopped treatment due to AEs, n (%) | ||
Patients who stopped | 0 (0.0) | 0 (0.0) |
Deaths, n (%) | ||
Patients who had died at 24 months, n (%) | 72 (26.7) | 107 (37.8) |
Cause of death, n (%) | ||
Relapse and/or progression | 34 (12.6) | 47 (16.6) |
Transplant-relateda | 33 (12.2) | 58 (20.5) |
Infection | 25 (9.3) | 40 (14.1) |
GvHD | 13 (4.8) | 21 (7.4) |
Renal failure | 5 (1.9) | 1 (0.4) |
Multiple organ failure | 6 (2.2) | 6 (2.1) |
Cardiac toxicity | 1 (0.4) | 5 (1.8) |
Secondary malignancy | 1 (0.4) | 1 (0.4) |
Unknown | 1 (0.4) | 1 (0.4) |
Other | 3 (1.1) | 0 (0.0) |
AEs of special interest, % (95% CI; full analysis set) | Treosulfan N = 268 | Busulfan N = 283 |
Cumulative incidence of acute GvHD of grade III or IV at 100 daysb | 6.4 (3.4 to 9.3) | 8.1 (4.9 to 11.3) |
Median follow-up time, days (range) | 100 (0.0 to 100) | 100 (10.0 to 100) |
Absolute risk difference in cumulative incidence acute GvHD of grade III or IV between study groups at 100 days,b % (95% CI) | –1.8 (–6.1 to 2.6) | |
Cumulative incidence of chronic GvHD at 24 monthsb | 61.7 (55.1 to 68.3) | 60.3 (53.8 to 66.7) |
Median follow-up time, months (range) | 23.6 (3.3 to 26.5) | 20.5 (3.3 to 26.3) |
Absolute risk difference in cumulative incidence of chronic GvHD between study groups at 24 months,b % (95% CI) | 1.4 (–7.8 to 10.7) | |
Cumulative incidence of grade III or IV mucositis,b % (95% CI) | 5.9 (3.4 to 9.4) | 7.4 (4.7 to 11.1) |
Incidence of HSOS,b % (95% CI) | 0.0 (0.0 to 1.4) | 0.4 (0.0 to 2.0) |
Incidence of seizures,b % (95% CI) | 0.4 (0.0 to 2.0) | 0.0 (0.0 to 1.3) |
Incidence of increased blood bilirubin, %b (95% CI) | 3.3 (1.5 to 6.2) | 2.8 (1.2 to 5.5) |
AE = adverse event; CI = confidence interval; GvHD = graft versus host disease; HSOS = hepatic sinusoidal obstruction syndrome; SAE = serious adverse event.
aEvents occurred in ≥ 1% of either treatment group.
bBased on empirical incidence.
Sources: MC-FludT.14/L Final Analysis Clinical Study Report23 and Beelen et al. (2022).48 Details included in the table are from the sponsor’s Summary of Clinical Evidence.24
Critical Appraisal
Internal Validity
The MC-FludT.14/L trial was a phase III, randomized, parallel-group, open-label, multicentre, international, group-sequential study conducted to compare noninferiority, efficacy, and safety between treosulfan-based conditioning therapy and a busulfan-based RIC regimen. Eligible patients were assigned in a 1:1 ratio to a treatment group with a computer-generated randomization schedule, which involved a permuted block technique with stratification by donor type, study centre, cytogenetic and/or molecular risk group for AML, and IPSS-R for MDS. Imbalances in baseline characteristics between the treosulfan and busulfan treatment groups were noted for the following factors: AML and MDS. According to the clinical experts consulted by CADTH, it is unlikely that those imbalances would influence treatment response. Other baseline characteristics were generally balanced between the treatment groups, which indicated that the randomization was successful.
An open-label trial can introduce detection and performance biases in the assessment of subjective outcomes reported by patients, such as AEs. Analyses of disease response outcomes (i.e., EFS, relapse and/or progression) were based on an independent DMC to help mitigate the potential for detection and performance biases.
Patients in the treosulfan group had a median of 3 days of exposure, whereas patients in the busulfan group had a median of 2 days of exposure. The observed duration on treatment was aligned with the recommended dose and schedule of administration in the treosulfan product monograph and the busulfan dose for RIC used in clinical practice. With regard to concomitant medications, all patients in the busulfan group but no patients in the treosulfan group received phenytoin or benzodiazepine. According to the clinical experts consulted by CADTH, busulfan would increase the risk of seizure, so patients in the busulfan group received phenytoin or benzodiazepine as prophylaxis. The clinical experts consulted by CADTH felt that this imbalance in concomitant medication between groups was unlikely to lead to differential treatment effects.
The method used in the analysis of graft failure at 24 months (i.e., observed percentage) included death as a censoring event. It did not measure the probability of graft failure at 24 months, but instead measured the proportion of patients who had graft failure before a censoring event at 24 months. The reported estimates of complete chimerism at 28 days were based on empirical observation of the presence of chimerism at 28 days in patients alive at that time. The interpretation of this outcome should be considered carefully, as it does not measure the incidence of chimerism at 28 days in a meaningful population. The defined at-risk population does not consider censoring or death as a competing risk. The estimates could be interpreted as an approximation of the cumulative incidence at 28 days, although 1 that is at risk of bias. However, the magnitude and direction of this bias is unclear.
The primary analysis of the study results was conducted in the PPS and FAS populations of the MC-FludT.14/L trial. The FAS included all randomized patients who were treated at least once with the study medication and who had at least 1 documented efficacy parameter. Patients who were randomized but not eligible for the FAS may have different characteristics and outcomes than those who were eligible. The extent and direction of a potential selection bias cannot be determined because it is not clear whether patients who were excluded from the FAS were systemically different from those who were included.
For the analysis of the primary end point of EFS, a group-sequential and hierarchical testing strategy was employed to adjust for multiple comparisons across multiple time points, thereby controlling the type I error of the primary hypothesis. Although the primary end point of EFS was adjusted for multiplicity in the confirmatory interim analysis, secondary end points in the confirmatory interim analysis and all end points in the final analysis were considered to be exploratory and, thus, not controlled for multiple comparisons. The noninferiority of treosulfan compared to busulfan was demonstrated in the confirmatory interim analysis, so, based on a DMC recommendation, the MC-FludT.14/L trial was stopped early for efficacy. The CADTH review team noted that the early stop of the trial may have led to an overestimation of the treatment effect, as the early stopping rule favours larger effect estimates.55 The study reported a 99.9702% CI for the HR of EFS in the confirmatory interim analysis; this interval is considered to be representative of the range of estimates that is required to reasonably maintain trial integrity for the confirmatory interim analysis due to the premature stop of the trial. Although the subgroup analyses were prespecified, the MC-FludT.14/L trial was not designed to formally assess comparative treatment effects in subgroups. The analyses across multiple time points were based on a DMC recommendation, which was considered by the CADTH review team to be an appropriate way to maintain trial integrity with the interim analyses.
HRQoL is considered to be a relevant outcome by patients with AML or MDS and the clinical experts consulted by CADTH. However, there was no assessment of HRQoL in the MC-FludT.14/L trial and, therefore, the impact of treosulfan conditioning therapy on HRQoL remains unknown.
External Validity
The clinical experts consulted by CADTH confirmed that the eligibility criteria of the MC-FludT.14/L trial are in line with previous trials and appropriate for the indication. Patients who had undergone previous alloHSCT were excluded; however, the clinical experts consulted by CADTH agreed that those patients may be considered eligible for treosulfan conditioning therapy in clinical practice. According to the clinical experts consulted by CADTH, treosulfan has good antileukemic efficacy and low toxicity, which is important for patients undergoing a second transplant. Although the MC-FludT.14/L trial did not include patients who received haploidentical HSCT, which is received by about 20% to 30% of patients, according to the clinical experts, the reported efficacy of the treosulfan conditioning therapy may be generalizable to this patient population. The MC-FludT.14/L trial defined a threshold of blast counts of less than 20% in the BM of patients with MDS and an age cut-off for MAC of at least 50 years. According to the clinical experts consulted by CADTH, a 10% cut-off for pretransplant blast percentage in patients with MDS and a MAC age criteria of 55 to 60 years is used in some centres in clinical practice. The clinical experts consulted by CADTH felt that the results of the MC-FludT.14/L trial can be generalized to patients in clinical practice, despite the aforementioned variations. The MC-FludT.14/L trial included patients with AML or MDS who were aged 18 to 70 years, yet patients older than 70 years are eligible to receive HSCT in clinical practice. The clinical experts consulted by CADTH confirmed that the results of the MC-FludT.14/L trial can be generalized to patients older than 70 years. The MC-FludT.14/L trial did not report ethnicity information for included patients; the clinical experts consulted by CADTH commented that, usually, the patient population in clinical practice is more diverse than the population of patients in clinical trials, but agreed that ethnicity was unlikely to influence treatment effect.
The MC-FludT.14/L trial used busulfan conditioning therapy as the treatment for the comparator group. The clinical experts consulted by CADTH commented that busulfan is a relevant comparator and currently considered a standard therapy for patients with AML or MDS in their clinical practice who are ineligible for a MAC regimen due to older age and/or comorbidities. TP53 and FLT3-ITD mutations are important prognostic factors in patients with AML or MDS that were not investigated as subgroups. The clinical experts stated that patients with TP53 and FLT3-ITD mutations are at increased risk of relapse, even after HSCT. Outcomes for patients with an FLT3-ITD mutation can be improved using a posttransplant FLT3-ITD inhibitor. The clinical experts estimated that there are about 5% of patients with the TP53 mutation and 30% of patients with the FLT3-ITD mutation in their clinical practice. The CADTH review team noted that there may be uncertainty in the interpretation of the study results, as it is not known if these uncontrolled prognostic factors (i.e., TP53 and FLT3-ITD mutation status) were balanced in the 2 treatment groups.
GRADE Summary of Findings and Certainty of the Evidence
Methods for Assessing the Certainty of the Evidence
For the pivotal MC-FludT.14/L trial identified in the sponsor’s systematic review, GRADE was used to assess the certainty of the evidence for outcomes considered to be most relevant to CADTH’s expert committee deliberations, and a final certainty rating was determined as outlined by the GRADE Working Group:20,21
High certainty: We are very confident that the true effect lies close to that of the estimate of the effect.
Moderate certainty: We are moderately confident in the effect estimate. The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. We use the word likely for evidence of moderate certainty (e.g., X intervention likely results in Y outcome).
Low certainty: Our confidence in the effect estimate is limited. The true effect may be substantially different from the estimate of the effect. We use the word may for evidence of low certainty (e.g., X intervention may result in Y outcome).
Very low certainty: We have very little confidence in the effect estimate. The true effect is likely to be substantially different from the estimate of effect. We describe evidence of very low certainty as very uncertain.
Following the GRADE approach, evidence from RCTs started as high-certainty evidence and could be rated down for concerns related to study limitations (which refers to internal validity or risk of bias), inconsistency across studies, indirectness, imprecision of effects, and publication bias.
When possible, certainty was rated in the context of the presence of an important (nontrivial) treatment effect; if this was not possible, certainty was rated in the context of the presence of any treatment effect (i.e., the clinical importance is unclear). In all cases, the target of the certainty of evidence assessment was based on the point estimate and where it was located relative to the threshold for a clinically important effect (when a threshold was available) or relative to the null. The target of the certainty of evidence assessment was the presence or absence of a clinically important effect, based on thresholds informed by the clinical experts consulted by CADTH for this review, for EFS, OS, GRFS, CRFS, graft failure, engraftment, complete chimerism, relapse and/or progression, NRM, TRM, and GvHD.
Results of GRADE Assessments
Table 2 presents the GRADE summary of findings for treosulfan and busulfan.
Long-Term Extension Studies
No long-term extension studies were identified for this review.
Indirect Evidence
No indirect evidence was submitted for this review.
Studies Addressing Gaps in the Systematic Review Evidence
No results for the retrospective study of patients with MDS who were ineligible to receive MAC conditioning therapy before alloHSCT were submitted by the sponsor to address the gap in the pivotal study caused by a lack of Canadian sites.25
Discussion
Summary of Available Evidence
A sponsor-submitted systematic review identified 1 study. MC-FludT.14/L was a phase III, randomized, parallel-group, open-label, multicentre, international, group-sequential study that compared the efficacy, noninferiority, and safety of treosulfan-based conditioning with a busulfan-based RIC regimen. The MC-FludT.14/L trial enrolled adults with AML or MDS who met the indication criteria for alloHSCT and were considered ineligible for standard conditioning therapies (i.e., age ≥ 50 years and/or a HCT-CI score > 2). The study had 2 treatment groups: treosulfan in combination with fludarabine and busulfan in combination with fludarabine. Eligible adults with AML or MDS (N = 570) were randomly assigned in a 1:1 ratio to either IV treosulfan (n = 280) at a dose of 10 g/m2 BSA, administered once a day on day –4, day –3, and day –2, or IV busulfan (n = 290) at a dose of 0.8 mg/kg per day, administered every 6 hours on day –4 and day –3, followed by alloHSCT on day 0. Both groups received IV fludarabine at a dose of 30 mg/m2 per day, administered from day –6 to day –2. Patients were recruited at 33 sites in 6 countries, although there were no sites in Canada. The primary objective in the MC-FludT.14/L trial was to compare treosulfan plus fludarabine conditioning with busulfan plus fludarabine conditioning for EFS in the 2 years after patients underwent alloHSCT. The secondary objectives were the comparative evaluation of OS, cumulative incidence of engraftment, incidence of complete donor-type chimerism, cumulative incidence of relapse and/or progression, NRM, and TRM. The cumulative incidence of acute and chronic GvHD and other safety end points were also assessed.
Most patients in the MC-FludT.14/L trial final analysis (database lock date: March 16, 2018) were male (60.8%), aged 50 years or older (94.9%), and had AML (63.9%). More patients in the treosulfan group than in the busulfan group were diagnosed with AML, at 184 (68.7%) patients in the treosulfan group and 168 (59.4%) patients in the busulfan group. Of the 199 patients with MDS, more patients in the treosulfan group than in the busulfan group were diagnosed with untreated MDS (50.0% versus 40.9%), and the mean blast count in BM was lower in the treosulfan group than in the busulfan group (5.83 versus 6.31).
Interpretation of Results
Efficacy
Treosulfan plus fludarabine is indicated for use as part of a conditioning treatment before alloHSCT in adults with AML or MDS who are not eligible for MAC due to their age and/or the presence of comorbidities. The pivotal MC-FludT.14/L trial compared the efficacy and safety of treosulfan-based conditioning with a busulfan-based RIC regimen. Donor type, participating institution, and cytogenetic and/or molecular risk group were used as stratification factors in the randomization of treatment.
Outcomes in the final analysis (database lock date March 16, 2018) and secondary outcomes in the confirmatory interim analysis (data cut-off date August 19, 2016) were not adjusted for multiplicity in testing; therefore, they should be interpreted as supportive evidence for assessments of certainty in the effect estimates.
As the aim of treatment for patients with AML or MDS is curative, survival was considered by patients, the clinical experts consulted by CADTH, and clinicians to be an important outcome. Prevention of or delayed disease progression, NRM, and TRM were also identified as being important to patients and clinicians. As such, the survival outcomes for EFS, OS, GRFS, and CRFS, which were captured in the MC-FludT.14/L trial, are relevant to stakeholders.
Based on results from the MC-FludT.14/L trial, treosulfan demonstrated noninferiority in the primary end point of EFS compared with busulfan in patients with AML or MDS (HR = 0.65; 99.9702% CI, 0.36 to1.19; P = 0.0000164). The totality of the efficacy results presented suggest that treosulfan may result in a clinically important higher proportion of patients being alive and event-free at 24 months than busulfan. Even though, based on stringent superiority testing, the P value did not formally meet the prespecified significance level (superiority P = 0.0051268; compared against the prespecified 1-sided significance level of 0.000149), there was a clear separation between the curves observed in the Kaplan-Meier plots of EFS in the confirmatory interim and the final analyses. The clinical experts consulted by CADTH commented that there was an observed trend toward EFS benefit with treosulfan, with the potential to translate into OS benefit, because relapse after transplant most often leads to death. Generally, subgroup analyses were consistent with the primary analysis of EFS, except for patients with MDS in risk group I and with MRD in risk group II. The clinical experts do not anticipate that treosulfan will have a differential treatment effect in patients with AML and MDS, as the 2 diseases have a similar disease biology. The MC-FludT.14/L was not designed to assess comparative treatment effects in subgroups. The small number of patients and events in the subgroups may have resulted in the inconsistent results observed in some subgroups.
The OS data were considered immature at the time of the confirmatory interim and final analyses (median follow-up ranged from 15.4 months to 29.7 months) and were based on a low number of events (event rate ranged from 23.6% to 39.6%). According to the clinical experts consulted by CADTH, a difference in OS is very difficult to achieve in a clinical trial. There was a clear separation of the curves observed in the Kaplan-Meier plots of OS in the confirmatory interim and final analyses, and the clinical experts consulted by CADTH commented that there was an observed trend toward OS benefit with treosulfan. Treosulfan likely results in a clinically important higher proportion of patients being alive at 24 months, and may result in an OS benefit at 36 months. However, longer-term survival data are required to confirm the treatment effect of treosulfan conditioning therapy on OS compared with busulfan conditioning treatment.
With regard to other end points, generally, the totality of efficacy results presented suggest that, compared with busulfan, treosulfan likely results in a clinically important benefit on CRFS, may result in a clinically important benefit on GRFS, NRM, and TRM, results in little to no clinically important benefit on engraftment and relapse and/or progression, and results in an uncertain effect on chimerism and graft failure. The clinical experts consulted by CADTH stated that they would expect the graft failure rate to be low, in general, as it is an uncommon event after HSCT in clinical practice. The clinical experts consulted by CADTH acknowledged that chimerism assessed in BM samples is more accurate than that assessed in PB samples. However, they noted that chimerism assessment in BM would cost more than that in PB, and said they would use PB rather than BM to avoid adding to the financial burden on patients. In general, the clinical experts would reserve chimerism assessment for patients who have reached engraftment.
HRQoL was identified as an important outcome by patients and the clinical experts consulted by CADTH, but was not assessed in the MC-FludT.14/L trial. The clinical experts consulted by CADTH indicated that they would expect HRQoL for patients in the treosulfan group to improve, as they anticipated that treosulfan would have less toxicity than busulfan, allowing patients in the treosulfan group to recover faster from their conditioning-related toxicity.
The MC-FludT.14/L trial considered patients to be ineligible for MAC due to age and the inability to meet a threshold of blast counts of less than 20% in the BM for MDS. These criteria are similar to but not entirely reflective of the thresholds used in clinical practice. According to clinical experts consulted by CADTH, blast percentage is only 1 factor used to assess MDS risk; other important factors include karyotype and molecular studies. The clinical experts stated that a cut-off based solely on blast count would ignore the complexity and nuance of MDS as a disease, and that biologic age by itself would be an imperfect predictor of transplant outcome; thus, it would be inappropriate to determine whether to use MAC or RIC based on age alone. Patients aged 18 to 70 years were eligible for the MC-FludT.14/L trial; however, the clinical experts consulted by CADTH commented that patients older than 70 years could receive HSCT and, thus, were potential candidates for treosulfan in their clinical practices. Moreover, the MC-FludT.14/L trial excluded patients who had undergone previous alloHSCT but who were considered eligible for treosulfan-based conditioning therapy, according to the clinical experts consulted by CADTH. The clinical experts remarked that these patients tend to have worse transplant-related outcomes (i.e., NRM) than patients who underwent frontline transplant. In addition, there was no study site in Canada in the MC-FludT.14/L trial, which may compromise the generalizability of the study results to clinical practice in Canada.
Harms
Generally, no new safety signals were identified in the MC-FludT.14/L trial in patients with AML or MDS. Slightly more patients in the treosulfan group than in the busulfan group experienced at least 1 SAE and grade 3 to 4 AEs. According to the clinical experts consulted by CADTH, AEs that occur more often in the treosulfan group (i.e., vomiting, edema, and increased alanine aminotransferase) are not clinically critical and can be well managed by the treating clinician. Given that treosulfan is an alkylating drug, the clinical experts do not expect that treosulfan will reduce short-term toxicity; rather, they expect that the toxicity profile of treosulfan will be similar to that of busulfan. The toxicity profiles of treosulfan and busulfan observed in the trial were similar to what the clinical experts observe in their clinical practices. A higher proportion of patients in the treosulfan group than in the busulfan group reported grade 3 or higher infections and febrile neutropenia, which are reversible and can be easily treated with an IV antibiotic, according to the clinical experts. Organ toxicity and risk of relapse are considered to be more clinically relevant, per feedback from the clinical experts. Overall, though, patients in the treosulfan group reported an elevated rate of AEs, such as acute kidney injury, increased alanine aminotransferase, and lung infection, and reported death caused by renal failure. The clinical experts indicated that the differences observed between treatment groups are not clinically meaningful. AEs of special interest included GvHD, grade III or IV mucositis, HSOS, and increased blood bilirubin. Grade III or IV mucositis was less commonly reported in the treosulfan group than in the busulfan group. A slightly higher proportion of patients in the treosulfan group than in the busulfan group reported increased blood bilirubin. One patient in the busulfan group reported HSOS and 1 patient in the treosulfan group reported seizure. The clinical experts commented that grade III or IV mucositis is reversible and does not cause any long-term sequalae, whereas HSOS is fatal. Other significant fatal AEs that should be included are diffuse alveolar hemorrhage, idiopathic pulmonary syndrome, and acute respiratory distress syndrome, per feedback from the clinical experts consulted by CADTH. There were no data available for diffuse alveolar hemorrhage, idiopathic pulmonary syndrome, or acute respiratory distress syndrome in the MC-FludT.14/L trial. The clinical experts stated that GvHD is an outcome that they would monitor to check for any unexpected events in clinical practice, but they would not expect there to be significant differences in GvHD incidence between the 2 conditioning protocols in general.
Conclusion
Patients and clinicians highlighted the need for new effective treatments for patients with AML or MDS that prolong life, control disease and symptoms, improve quality of life, and reduce side effects better than current treatments.
One phase III, open-label, multicentre, randomized, active-controlled trial (MC-FludT.14/L), comparing treosulfan in combination with fludarabine with busulfan in combination with fludarabine as part of conditioning therapy, demonstrated that treosulfan was noninferior to busulfan in terms of EFS, the primary outcome, in adults with AML or MDS who were not eligible for standard conditioning therapies. Superiority testing of treosulfan compared to busulfan did not show statistically significant results. However, there was a favourable trend toward improved EFS with treosulfan, which, according to the clinical experts consulted by CADTH, was suggestive of a potentially clinically meaningful EFS benefit with treosulfan. The OS data were considered immature, but had an observed trend toward improved OS with treosulfan compared to busulfan. GRADE assessment of data from the MC-FludT.14/L trial suggested that treosulfan may result in a clinically important EFS and OS benefit compared with busulfan.
Compared with busulfan, treosulfan likely results in a clinically important benefit in CRFS at 24 months and little to no clinically important difference in the cumulative incidence of acute GvHD of grade III or VI at 100 days. Compared with busulfan, treosulfan may result in clinically important benefits in GRFS, NRM, and TRM, and little to no clinically important benefits in relapse or progression, engraftment, and the cumulative incidence of chronic GvHD at 24 months. The evidence is very uncertain about the effect of treosulfan on graft failure and chimerism compared with busulfan. No new safety signals were identified in patients with AML or MDS. The clinical experts consulted by CADTH noted that, overall, the harms data for treosulfan and for busulfan appeared to be similar to the AEs observed in their own practices. The MC-FludT.14/L trial did not report any HRQoL data.
References
1.Döhner H, Weisdorf DJ, Bloomfield CD. Acute myeloid leukemia. N Engl J Med. 2015;373(12):1136-1152. PubMed
2.Eisfeld AK, Kohlschmidt J, Mrózek K, et al. Mutation patterns identify adult patients with de novo acute myeloid leukemia aged 60 years or older who respond favorably to standard chemotherapy: An analysis of Alliance studies. Leukemia. 2018;32(6):1338-1348. PubMed
3.Canadian Cancer Statistics Advisory in collaboration with the Canadian Cancer Society, Statistics Canada, Public Health Agency of Canada. Canadian Cancer Statistics: A 2022 special report on cancer prevalence [accessed by sponsor]. 2022.
4.Canadian Cancer Society. Leukemia statistics [accessed by sponsor]. 2022; https://cancer.ca/en/cancer-information/cancer-types/leukemia/statistics. Accessed May 1, 2023.
5.Fenaux P, Haase D, Santini V, et al. Myelodysplastic syndromes: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up†☆. Ann Oncol. 2021;32(2):142-156. PubMed
6.National Cancer Institute. MDS [accessed by sponsor]. 2023: https://www.cancer.gov/publications/dictionaries/cancer-terms/def/mds. Accessed October 11, 2023.
7.Leukemia and Lymphoma Society. Updated Data on Blood Cancers - Facts 2020 - 2021 [accessed by sponsor]. 2021; https://www.lls.org/sites/default/files/2021-08/PS80%20FactsBook_2020_2021_FINAL.pdf. Accessed March, 2023.
8.Slack J, Nguyen L, Naugler C, Rashid-Kolvear F. Incidence of myelodysplastic syndromes in a major Canadian metropolitan area. J Appl Lab Med. 2018;3(3):378-383. PubMed
9.Abdul Wahid SF, Ismail NA, Mohd-Idris MR, et al. Comparison of reduced-intensity and myeloablative conditioning regimens for allogeneic hematopoietic stem cell transplantation in patients with acute myeloid leukemia and acute lymphoblastic leukemia: A meta-analysis. Stem Cells Dev. 2014;23(21):2535-2552. PubMed
10.Aoudjhane M, Labopin M, Gorin NC, et al. Comparative outcome of reduced intensity and myeloablative conditioning regimen in HLA identical sibling allogeneic haematopoietic stem cell transplantation for patients older than 50 years of age with acute myeloblastic leukaemia: A retrospective survey from the Acute Leukemia Working Party (ALWP) of the European group for Blood and Marrow Transplantation (EBMT). Leukemia. 2005;19(12):2304-2312. PubMed
11.Luger SM, Ringden O, Zhang MJ, et al. Similar outcomes using myeloablative vs reduced-intensity allogeneic transplant preparative regimens for AML or MDS. Bone Marrow Transplant. 2012;47(2):203-211. PubMed
12.Marks DI, Wang T, Perez WS, et al. The outcome of full-intensity and reduced-intensity conditioning matched sibling or unrelated donor transplantation in adults with Philadelphia chromosome-negative acute lymphoblastic leukemia in first and second complete remission. Blood. 2010;116(3):366-374. PubMed
13.Martino R, Iacobelli S, Brand R, et al. Retrospective comparison of reduced-intensity conditioning and conventional high-dose conditioning for allogeneic hematopoietic stem cell transplantation using HLA-identical sibling donors in myelodysplastic syndromes. Blood. 2006;108(3):836-846. PubMed
14.Mohty M, Labopin M, Volin L, et al. Reduced-intensity versus conventional myeloablative conditioning allogeneic stem cell transplantation for patients with acute lymphoblastic leukemia: A retrospective study from the European Group for Blood and Marrow Transplantation. Blood. 2010;116(22):4439-4443. PubMed
15.Ringden O, Labopin M, Ehninger G, et al. Reduced intensity conditioning compared with myeloablative conditioning using unrelated donor transplants in patients with acute myeloid leukemia. J Clin Oncol. 2009;27(27):4570-4577. PubMed
16.del Campo L, Leon NG, Palacios DC, Lagana C, Tagarro D. Abdominal complications following hematopoietic stem cell transplantation. Radiographics. 2014;34(2):396-412. PubMed
17.Gyurkocza B, Sandmaier BM. Conditioning regimens for hematopoietic cell transplantation: One size does not fit all. Blood. 2014;124(3):344-353. PubMed
18.McCune JS, Bemer MJ. Pharmacokinetics, pharmacodynamics and pharmacogenomics of immunosuppressants in allogeneic haematopoietic cell transplantation: Part I. Clin Pharmacokinet. 2016;55(5):525-550. PubMed
19.Troy JD, Atallah E, Geyer JT, Saber W. Myelodysplastic syndromes in the United States: An update for clinicians. Ann Med. 2014;46(5):283-289. PubMed
20.Balshem H, Helfand M, Schünemann HJ, et al. GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol. 2011;64(4):401-406. PubMed
21.Santesso N, Glenton C, Dahm P, et al. GRADE guidelines 26: informative statements to communicate the findings of systematic reviews of interventions. J Clin Epidemiol. 2020;119:126-135. PubMed
22.Clinical Study Report: Clinical phase III trial to compare Treosulfan-based conditioning therapy with Busulfan-based reduced-intensity conditioning (RIC) prior to allogeneic haematopoietic stem cell transplantation in patients with AML or MDS considered ineligible to standard conditioning regimens-Confirmatory interim analysis [internal sponsor's report]. Toronto (ON): Medexus Pharmaceuticals Inc.; 2017 September 15.
23.Clinical Study Report: Clinical Phase III trial to compare treosulfan-based conditioning therapy with busulfan-based reduced intensity conditioning (RIC) prior to allogeneic haematopoietic stem cell transplantation in patients with AML or MDS considered ineligible to standard conditioning regimens - Final analysis including post-surveillance [internal sponsor's report]. Toronto (ON): Medexus Pharmaceuticals Inc.; 2018 July 18.
24.Treosulfan (Trecondyv) for Conditioning Therapy Prior to Allogeneic Hematopoietic Stem Cell Transplantation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Treosulfan (Trecondyv), 5g/vial, intravenous infusion. Toronto (ON): Medexus Pharmaceuticals Inc.; 2023.
25.Pasic I, Remberger M, Chen C, et al. O18 - Excellent transplant outcomes with fludarabine-treosulfan (FT) reduced-toxicity conditioning (RTC) in combination with dualt-cell depletion (TCD) in myeloablative conditioning (MAC)-ineligible patients with myelodysplastic syndrome (MDS) [accessed by sponsor]. Leuk Res. 2023;128(Supplement):107131. https://www.sciencedirect.com/science/article/abs/pii/S0145212623001273.
26.National Cancer Institute. Myelodysplastic Syndromes Treatment (PDQ) - Health Professional Version [accessed by sponsor]. 2022; https://www.cancer.gov/types/myeloproliferative/hp/myelodysplastic-treatment-pdq. Accessed March, 2023.
27.UpToDate. Clinical manifestations, pathologic features, and diagnosis of acute myeloid leukemia [accessed by sponsor]. 2023: https://www.uptodate.com/contents/clinical-manifestations-pathologic-features-and-diagnosis-of-acute-myeloid-leukemia. Accessed 2023, Sep 7.
28.Alberta Health Services. Clinical Practice Guideline LYHE-006 version 6 - Acute Myeloid Leukemia [accessed by sponsor]. 2019.
29.CADTH Reimbursement Review - Luspatercept (Reblozyl) [accessed by sponsor]. Can J Health Technol. 2022;2(2). https://www.cadth.ca/sites/default/files/DRR/2022/SR0670-Reblozyl-combinedReport.pdf.
30.Du Y, Fryzek J, Sekeres MA, Taioli E. Smoking and alcohol intake as risk factors for myelodysplastic syndromes (MDS). Leuk Res. 2010;34(1):1-5. PubMed
31.Poynter JN, Richardson M, Roesler M, et al. Chemical exposures and risk of acute myeloid leukemia and myelodysplastic syndromes in a population-based study. Int J Cancer. 2017;140(1):23-33. PubMed
32.Strom SS, Gu Y, Gruschkus SK, Pierce SA, Estey EH. Risk factors of myelodysplastic syndromes: A case-control study. Leukemia. 2005;19(11):1912-1918. PubMed
33.UpToDate. Clinical manifestations, diagnosis, and classification of myelodysplastic syndromes (MDS) [accessed by sponsor]. 2023; https://www.uptodate.com/contents/clinical-manifestations-diagnosis-and-classification-of-myelodysplastic-syndromes-mds. Accessed April 18, 2023.
34.Health Canada reviewer's report: Trecondyv (treosulfan) [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: trosulfan, 5g/vial, intravenous infusion. Ottawa (ON): Medexus Inc; 2021.
35.The EBMT Handbook: Hematopoietic Stem Cell Transplantation and Cellular Therapies [accessed by sponsor]. In: Carreras E, Dufour C, Mohty M, Kröger N, eds. Cham (CH): Springer - Copyright 2019, The Editor(s) (if applicable)and The Author(s). 2019.
36.Barba P, Burns LJ, Litzow MR, et al. Success of an international learning health care system in hematopoietic cell transplantation: The American Society of Blood and Marrow Transplantation Clinical Case Forum. Biol Blood Marrow Transplant. 2016;22(3):564-570. PubMed
37.Apotex, Inc. Product Monograph: MELPHALAN FOR INJECTION - Melphalan (as hydrochloride) [accessed by sponsor]. 2017.
38.B. C. Cancer Drug Manual. DRUG NAME: Melphalan [accessed by sponsor]. 2021; http://www.bccancer.bc.ca/drug-database-site/Drug%20Index/Melphalan%20monograph.pdf. Accessed 2023 May 3.
39.Cancer Care Ontario. Melphalan [accessed by sponsor]. 2019; https://www.cancercareontario.ca/en/drugformulary/drugs/monograph/43801. Accessed May 3, 2023.
40.Beelen DW, Iacobelli S, Koster L, et al. Comparison of a new reduced toxicity myeloablative treosulfan and fludarabine preparative regimen with myeloablative busulfan or melphalan in combination with fludarabine in older patients with acute myeloid leukemia or myelodysplastic syndromes: A retrospective matched pair analysis of patients from a prospective randomized trial and the European Blood and Marrow Transplantation Society Registry. Blood. 2019;134(Supplement_1):3326-3326. 10.1182/blood-2019-127108. Accessed 2023 Nov 7.
41.Danylesko I, Shimoni A, Nagler A. Treosulfan-based conditioning before hematopoietic SCT: More than a BU look-alike. Bone Marrow Transplant. 2012;47(1):5-14. PubMed
42.Ruutu T, Volin L, Beelen DW, et al. Reduced-toxicity conditioning with treosulfan and fludarabine in allogeneic hematopoietic stem cell transplantation for myelodysplastic syndromes: Final results of an international prospective phase II trial. Haematologica. 2011;96(9):1344-1350. PubMed
43.Gyurkocza B, Gutman J, Nemecek ER, et al. Treosulfan, fludarabine, and 2-Gy total body irradiation followed by allogeneic hematopoietic cell transplantation in patients with myelodysplastic syndrome and acute myeloid leukemia. Biol Blood Marrow Transplant. 2014;20(4):549-555. PubMed
44.Remberger M, Törlen J, Serafi IE, et al. Toxicological effects of fludarabine and treosulfan conditioning before allogeneic stem-cell transplantation. Int J Hematol. 2017;106(4):471-475. PubMed
45.Deeg HJ, Stevens EA, Salit RB, et al. Transplant conditioning with treosulfan/fludarabine with or without total body irradiation: A randomized phase II trial in patients with myelodysplastic syndrome and acute myeloid leukemia. Biol Blood Marrow Transplant. 2018;24(5):956-963. PubMed
46.Shimoni A, Robin M, Iacobelli S, et al. Allogeneic hematopoietic cell transplantation in patients with myelodysplastic syndrome using treosulfan based compared to other reduced-intensity or myeloablative conditioning regimens. A report of the chronic malignancies working party of the EBMT. Br J Haematol. 2021;195(3):417-428. PubMed
47.Beelen DW, Trenschel R, Stelljes M, et al. Treosulfan or busulfan plus fludarabine as conditioning treatment before allogeneic haemopoietic stem cell transplantation for older patients with acute myeloid leukaemia or myelodysplastic syndrome (MC-FludT.14/L): A randomised, non-inferiority, phase 3 trial. Lancet Haematol. 2020;7(1):e28-e39. PubMed
48.Beelen DW, Stelljes M, Remenyi P, et al. Treosulfan compared with reduced-intensity busulfan improves allogeneic hematopoietic cell transplantation outcomes of older acute myeloid leukemia and myelodysplastic syndrome patients: Final analysis of a prospective randomized trial. Am J Hematol. 2022;97(8):1023-1034. PubMed
49.Clinical Study Protocol: MC-FludT.14/L. Clinical phase III trial to compare Treosulfan-based conditioning therapy with Busulfan-based reduced-intensity conditioning (RIC) prior to allogeneic haematopoietic stem cell transplantation in patients with AML or MDS considered ineligible to standard conditioning regimens [internal sponsor's report]. Toronto (ON): Medexus Pharmaceuticals Inc.; 2016 December 02.
50.Cheson BD, Bennett JM, Kopecky KJ, et al. Revised recommendations of the International Working Group for Diagnosis, Standardization of Response Criteria, Treatment Outcomes, and Reporting Standards for Therapeutic Trials in Acute Myeloid Leukemia. J Clin Oncol. 2003;21(24):4642-4649. PubMed
51.Cheson BD, Greenberg PL, Bennett JM, et al. Clinical application and proposal for modification of the International Working Group (IWG) response criteria in myelodysplasia. Blood. 2006;108(2):419-425. PubMed
52.Shulman HM, Sullivan KM, Weiden PL, et al. Chronic graft-versus-host syndrome in man. A long-term clinicopathologic study of 20 Seattle patients. Am J Med. 1980;69(2):204-217. PubMed
53.Glucksberg H, Storb R, Fefer A, et al. Clinical manifestations of graft-versus-host disease in human recipients of marrow from HL-A-matched sibling donors. Transplantation. 1974;18(4):295-304. PubMed
54.Przepiorka D, Weisdorf D, Martin P, et al. 1994 Consensus Conference on Acute GVHD Grading. Bone Marrow Transplant. 1995;15(6):825-828. PubMed
55.Bassler D, Montori VM, Briel M, Glasziou P, Guyatt G. Early stopping of randomized clinical trials for overt efficacy is problematic. J Clin Epidemiol. 2008;61(3):241-246. PubMed
Appendix 1: Detailed Outcome Data
Note that this appendix has not been copy-edited.
Table 17: Summary of EFS Results From the Study Included in the Systematic Review (PPS)
End points | MC-FludT.14/L Confirmatory Interim Analysis (Data cut-off date: August 19, 2016) | MC-FludT.14/L Final Analysis (Database lock date: March 16, 2018) | ||
|---|---|---|---|---|
Treosulfan N = 215 | Busulfan N = 234 | Treosulfan N = 262 | Busulfan N = 275 | |
Event-free survival | ||||
Median follow-up timea, months (range) | 15.4 (3.2 to 26.4) | 17.4 (3.0 to 26.3) | 29.7 (3.0 to 52.1) | 29.4 (3.9 to 54.3) |
Patients with event, n (%) | 67 (31.2) | 97 (41.5) | 96 (36.6) | 134 (48.7) |
Death | 22 (10.2) | 38 (16.2) | 34 (13.0) | 53 (19.3) |
Relapse and/or Progression | 45 (20.9) | 51 (21.8) | 61 (23.3) | 72 (26.2) |
Primary Graft Failure | 0 | 1 (0.4) | 1 (0.4) | 1 (0.4) |
Secondary Graft Failure | 0 | 7 (3.0) | 0 | 8 (2.9) |
Median EFS, months (95% CI) | ||||
Kaplan-Meier estimates EFS probability at 24 months, % (95% CI) | 63.5 (55.4 to 70.5) | 51.1 (43.4 to 58.2) | 65.3 (59.0 to 70.9) | 51.1 (44.8 to 57.0) |
Kaplan-Meier estimates EFS probability at 36 months, % (95% CI) | NA | NA | 58.9 (51.5, 65.6) | 49.6 (43.1 to 55.7) |
HR (95% CI) | 0.67 (0.48 to 0.93) | 0.64 (0.48 to 0.84) | ||
HR (99.9702% CI) | 0.67 (0.37 to 1.23) | NA | ||
P value | Noninferiority: 0.0000424b | Noninferiority: nominal P = 0.0000001c | ||
CI = confidence interval; EFS = event-free survival; HR = hazard ratio, NA = not applicable; PPS = per protocol set.
aBased on reverse Kaplan-Meier estimates for overall survival.
bThe nominal 1-sided significance level resulting from an O'Brien-Fleming type of group-sequential efficacy stopping boundary is 0.000149.
cAdjusted for donor-type as factor, and risk group and centre as strata using Cox regression model.
Note: Only the P value in the confirmatory interim analysis (Data cut-off date: August 19, 2016) of EFS was adjusted for multiple comparison. P values for all other outcomes were not adjusted for multiplicity.
Source: MC-FludT.14/L Confirmatory Interim Analysis Clinical Study Report,22 MC-FludT.14/L Final Analysis Clinical Study Report,23 and Beelen (2022).48 Details included in the table are from the sponsor’s Summary of Clinical Evidence.24
Table 18: Summary of Key Efficacy Results in the Confirmatory Interim Analysis (FAS)
End points | MC-FludT.14/L Confirmatory Interim Analysis (Data cut-off date: August 19, 2016) | |
|---|---|---|
Treosulfan N = 220 | Busulfan N = 240 | |
Overall survival | ||
Median follow-up time, months (range) | 15.4 (3.2 to 26.4) | 17.4 (3.0 to 26.3) |
Patients with event, n (%) | 52 (23.6) | 82 (34.2) |
Kaplan-Meier estimates overall survival probability at 24 months, % (95% CI) | 71.3 (63.6 to 77.6) | 56.4 (48.4 to 63.6) |
HR (95% CI)a | 0.61 (0.42 to 0.88) | |
Nominal P value | 0.0082a | |
Graft failure | ||
Primary | ||
Number of patients contributing to the analysis, n | 220 | 240 |
Rate of primary graft failure, n (%) | 0 | 1 (0.4) |
Secondary | ||
Number of patients contributing to the analysis, n | 217 | 236 |
Secondary graft failure, n (%) | 0 | 7 (3.0) |
Engraftment at day 28 | ||
Reconstitution of granulopoiesisb | ||
Patients with event, n (%) | 217 (98.6) | 236 (98.3) |
Cumulative incidence at 28 days, n (95% CI) | 96.8 (93.5 to 100.0) | 96.2 (94.1 to 98.3) |
HR (95% CI)c | 1.09 (0.92 to 1.28) | |
Nominal P value | 0.3378c | |
Reconstitution of leukopoiesisd | ||
Patients with event, n (%) | 217 (98.6) | 237 (98.8) |
Cumulative incidence at 28 days, n (95% CI) | 99.5 (96.8 to 100.0) | 96.7 (94.3 to 99.0) |
HR (95% CI)c | 1.14 (0.97 to 1.34) | |
Nominal P value | 0.1225c | |
Reconstitution of thrombopoiesise | ||
Patients with event, n (%) | 215 (97.7) | 232 (96.7) |
Cumulative incidence at 28 days, n (95% CI) | 96.8 (94.2 to 99.3) | 97.9 (96.2 to 99.6) |
HR (95% CI)c | 0.86 (0.73 to 1.02) | |
Nominal P value | 0.0772c | |
Chimerism | ||
Number of patients contributing to the analysis, n | 215 | 239 |
Patients with complete chimerism, n (%) | 201 (93.5) | 196 (82.0) |
Incidence of complete chimerism at 28 days, n (95% CI) | 93.5 (89.3 to 96.4) | 82.0 (76.5 to 86.7) |
Odds ratio (95% CI)f | 3.21 (1.69 to 6.09) | |
Nominal P value | 0.0080g | |
Relapse or progression | ||
Cumulative incidence of relapse or progression | ||
Patients with event, n (%) | 45 (20.5) | 51 (21.3) |
Cumulative incidence of relapse or progression at 24 months, % (95% CI) | 24.6 (17.8 to 31.3) | 23.3 (17.6 to 29.0) |
HR (95% CI) | 0.87 (0.59 to 1.30) | |
Nominal P value | 0.5017a | |
GvHD-free and relapse or progression-free survival | ||
Patients with event, n (%) | 93 (42.3) | 128 (53.3) |
Kaplan-Meier estimates of GvHD-free and relapse or progression-free survival probability at 24 months, % (95% CI) | 51.4 (43.4 to 58.8) | 38.4 (31.3 to 45.5) |
HR (95% CI)a | 0.72 (0.54 to 0.95) | |
Nominal P value | 0.0224a | |
Chronic GvHD-free and relapse or progression-free survival | ||
Patients with event, n (%) | 90 (40.9%) | 125 (52.1%) |
Kaplan-Meier estimates of chronic GvHD-free and relapse or progression-free survival probability at 24 months, % (95% CI) | 52.3 (44.2, 59.7) | 38.5 (31.3, 45.6) |
HR (95% CI)a | 0.69 (0.52, 0.92) | |
Nominal P value | 0.0108a | |
Nonrelapse mortality | ||
Patients with event, n (%) | 23 (10.5%) | 41 (17.1%) |
Cumulative nonrelapse mortality incidence at 24 months, % (95% CI) | 11.4 (7.0 to 15.9) | 22.6 (16.2 to 28.9) |
HR (95% CI)c | 0.60 (0.36 to 1.01) | |
Nominal P value | 0.0530c | |
Transplant-related mortality | ||
Patients with event, % (95% CI) | 23 (10.5) | 45 (18.8) |
Kaplan-Meier estimates of transplant-related mortality probability at 24 months, % (95% CI) | 12.1 (8.1 to 17.7) | 28.2 (21.4 to 36.5) |
HR (95% CI)a | 0.54 (0.32 to 0.91) | |
Nominal P value | 0.0201a | |
CI = confidence interval; FAS = full analysis set; GvHD = graft versus host disease; HR = hazard ratio.
aAdjusted for donor type as factor, and risk group and centre as strata using Cox regression model.
bReconstitution of granulopoiesis was documented on the first of 3 consecutive days with absolute neutrophilic granulocyte count > 0.5 × 109/L in the peripheral blood.
cAdjusted for donor type as factor and risk group as stratum using Fine and Gray model.
dReconstitution of leukopoiesis was documented on the first of 3 consecutive days with total white blood cell count > 1 × 109/L in the peripheral blood.
eReconstitution of thrombopoiesis was documented on the first of 3 consecutive days with platelets > 20 × 109/L, in the absence of platelet transfusion.
fAdjusted for donor type and risk group. Missing values accounted as 'No' for odds ratio calculation.
gStratified Cochran-Mantel-Haenszel test adjusted for donor type and risk group.
Source: MC-FludT.14/L Confirmatory Interim Analysis Clinical Study Report.22 Details included in the table are from the sponsor’s Summary of Clinical Evidence.24
Figure 7: Forest Plot for EFS by Prognostic Factors With 24-Month Event Rates in the Confirmatory Interim Analysis (Data Cut-Off Date: August 19, 2016; FAS)
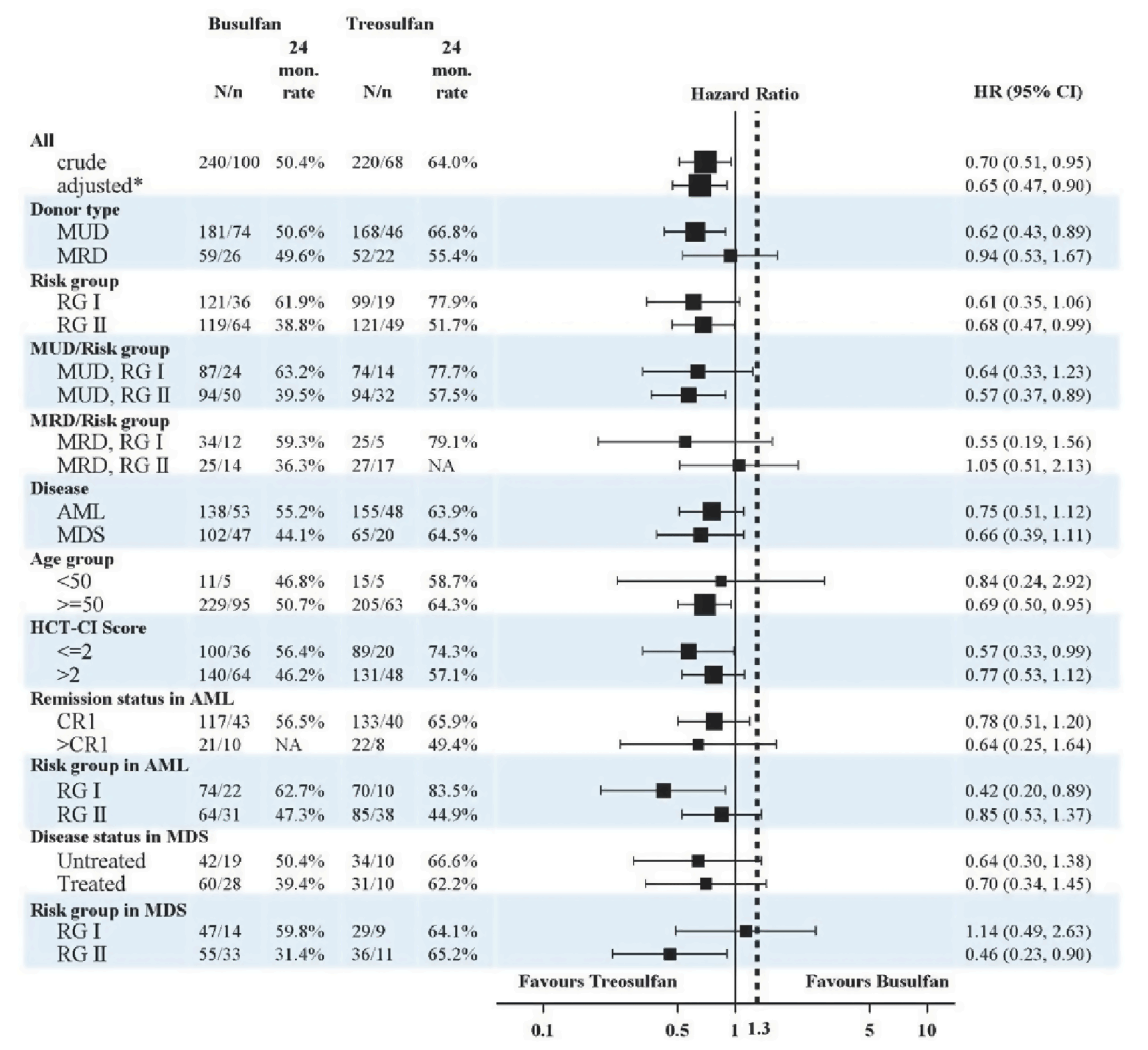
AML = acute myeloid leukemia; CI = confidence interval; CR = complete remission; EFS = event-free survival; FAS = full analysis set; HCT-CT = Hematopoietic Cell Transplantation-Specific Comorbidity Index; HR = hazard ratio; MDS = myelodysplastic syndrome; MRD = matched related donor; MUD = matched unrelated donor; N = number of patients; n = total number of events; RG = risk group.
Note: Asterisk denotes being adjusted for donor type as factor, and risk group and centre as strata using Cox regression model.
Source: MC-FludT.14/L Confirmatory Interim Analysis Clinical Study Report.22
Figure 8: Forest Plot for EFS by Prognostic Factors With 24-Month Event Rates in the Final Analysis (Database Lock Date: March 16, 2018; FAS)
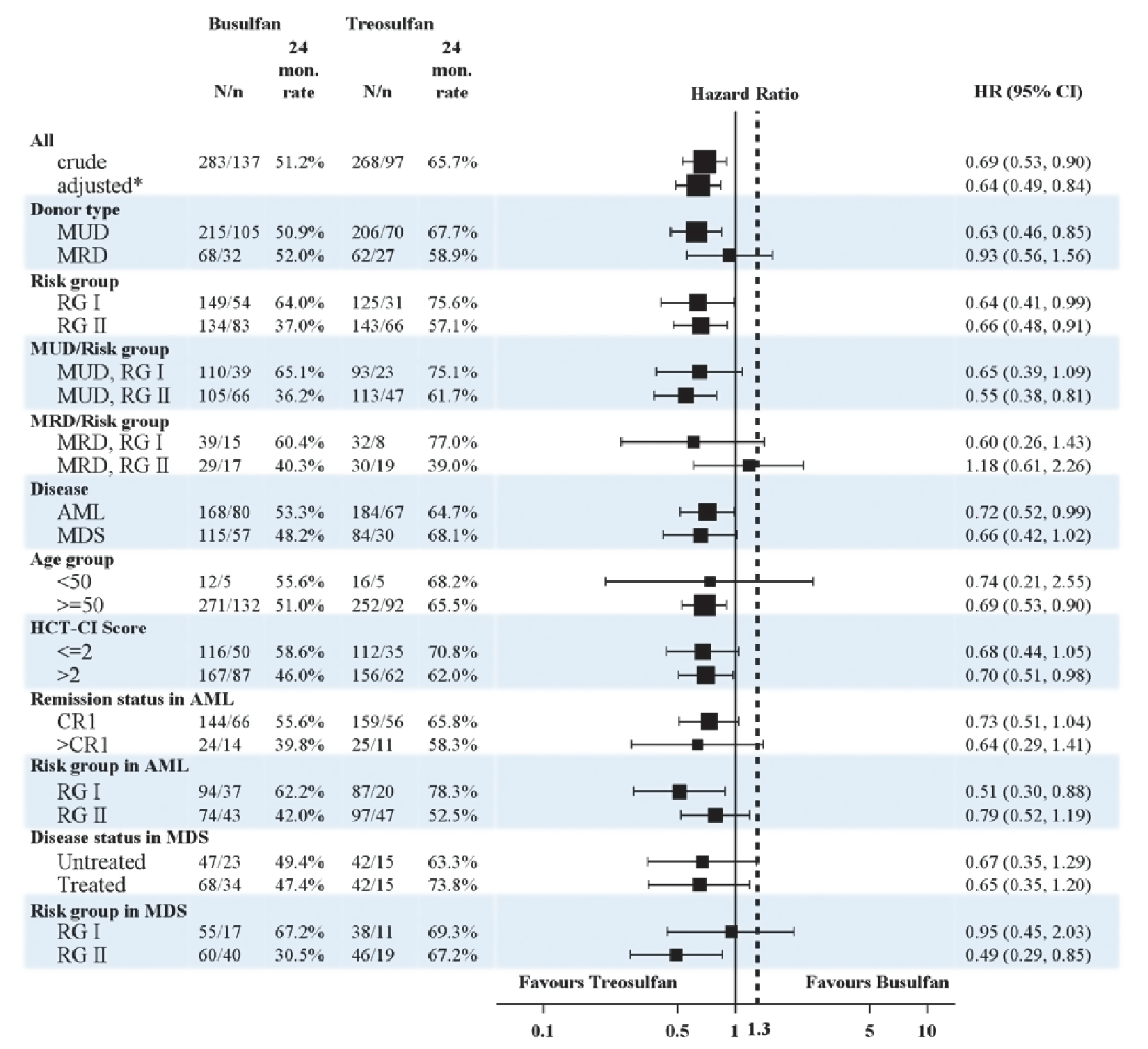
AML = acute myeloid leukemia; CI = confidence interval; CR = complete remission; EFS = event-free survival; FAS = full analysis set; HCT-CT = Hematopoietic Cell Transplantation-Specific Comorbidity Index; HR = hazard ratio; MDS = myelodysplastic syndrome; MRD = matched related donor; MUD = matched unrelated donor; N = number of patients; n = total number of events; RG = risk group.
Note: Asterisk denotes being adjusted for donor type as factor, and risk group and centre as strata using Cox regression model.
Source: MC-FludT.14/L Final Analysis Clinical Study Report.23
Pharmacoeconomic Review
Abbreviations
AE
adverse event
alloHSCT
allogenic hematopoietic stem cell transplant
AML
acute myeloid leukemia
BIA
budget impact analysis
BSA
body surface area
EFS
event-free survival
GRADE
Grading of Recommendations, Assessment, Development, and Evaluation
GvHD
graft versus host disease
LY
life-year
MDS
myelodysplastic syndromes
OS
overall survival
PSM
partitioned survival model
QALY
quality-adjusted life-year
RPGf
relapse, progression, or graft failure
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Treosulfan (Trecondyv), 5 g vial, lyophilized powder for IV infusion |
Submitted price | Treosulfan: $693.00 per 5 g vial |
Indication | Treosulfan in combination with fludarabine as part of conditioning treatment before alloHSCT in adult patients with AML or MDS at increased risk for standard conditioning therapies and in pediatric patients older than 1 year old with AML or MDS |
Health Canada approval status | NOC |
Health Canada review pathway | Priority review |
NOC date | June 25, 2021 |
Reimbursement request | Per indication for adultsa |
Sponsor | Medexus Pharmaceuticals, Inc. |
Submission history | Previously reviewed: No |
alloHSCT = allogenic hematopoietic stem cell transplant; AML = acute myeloid leukemia; MDS = myelodysplastic syndromes; NOC = Notice of Compliance.
aPer sponsor request, this CADTH review focuses on the indication in adults. CADTH did not review the pediatric population at this time.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Partitioned survival model |
Target population | Adults with AML or MDS at increased risk for standard conditioning therapies before alloHSCT |
Treatment | Treosulfan in combination with fludarabine |
Comparator | Busulfan in combination with fludarabine |
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs, LYs |
Time horizon | Lifetime (40 years) |
Key data source | MC-FludT.14/L trial |
Submitted results | Treosulfan dominates busulfan (incremental costs = $60,808; incremental QALYs = 0.83) |
Key limitations |
|
CADTH reanalysis results |
|
alloHSCT = allogenic hematopoietic stem cell transplant; AML = acute myeloid leukemia; EFS = event-free survival; GRADE = Grading of Recommendations, Assessment, Development, and Evaluation; LY = life-year; MDS = myelodysplastic syndromes; OS = overall survival; QALY = quality-adjusted life-year.
Conclusions
Evidence from the MC-FludT.14/L trial suggests that treosulfan in combination with fludarabine may result in a clinically important benefit in event-free survival (EFS) and overall survival (OS) compared with busulfan in combination with fludarabine. However, the CADTH clinical review noted that based on the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) assessment, there is low to moderate certainty associated with the potential benefit of treosulfan in combination with fludarabine for these 2 outcomes due to a serious risk of bias and imprecision.
Using the sponsor’s base case, treosulfan in combination with fludarabine is cost saving ($60,808 over the lifetime time horizon) and associated with a 0.83 incremental gain in quality-adjusted life-years (QALYs) and a 1.14 incremental gain in life-years (LYs) compared to busulfan in combination with fludarabine. These results are dependent on the predicted clinical benefit of treosulfan, which leads to cost offsets in the relapse and/or progression health state and comprises subsequent treatment costs (including the need for a second allogenic hematopoietic stem cell transplant [alloHSCT]) and costs associated with inpatient hospital stays (average of 4.6 days per month), platelet and red blood cell transfusions (average of 2.3 transfusions per month each), and other routine monitoring and procedures. The cost for the regimen of treosulfan in combination with fludarabine is $10,621, assuming a patient weight of 75 kg and a body surface area [BSA] of 1.9 m2); under the same assumptions, the cost for the regimen of busulfan in combination with fludarabine is $5,145. This results in an additional cost of $5,476 for the treosulfan regimen. Given that the cost of the conditioning regimen only occurs 1 time, the additional drug-acquisition cost of treosulfan is offset with only a small improvement in EFS in the sponsor’s model.
CADTH noted several limitations that add uncertainty to these results, including the low to moderate certainty in the clinical efficacy of treosulfan and the structural assumptions inherent in the model structure. However, CADTH was unable to use the sponsor’s economic model to derive a more reliable estimate of the cost-effectiveness of treosulfan in combination with fludarabine. The sponsor’s model used survival extrapolations for EFS and OS, which produced the most conservative estimate of the clinical benefits of treosulfan from among the available options, and the results were robust with regard to changes in the other parameters identified as potential limitations. However, the predicted clinical benefit of treosulfan remains uncertain, given that 74% of the predicted LY gains for treosulfan were accrued beyond the trial period, for which there is no clinical evidence.
Stakeholder Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, registered clinicians, and drug plans that participated in the CADTH review process.
Patient input was received from the Leukemia and Lymphoma Society of Canada, which collected input, using an online survey, from 108 respondents who were patients with lived experience with acute myeloid leukemia (AML) or myelodysplastic syndromes (MDS) and who had undergone or who were considering undergoing an alloHSCT and their caregivers. Patients and caregivers reported anxiety with regard to the decision to undergo alloHSCT. Patients also indicated that they typically were not provided the option of conditioning therapy; however, knowing that there may be an option that potentially improves survival and has fewer side effects had a positive impact on mental health.
Clinician input was received from Cell Therapy Transplant Canada and the Ontario Health (Cancer Care Ontario) Complex Malignant Hematology Advisory Committee. Clinician input indicated that treosulfan meets a clinical need for an alternative conditioning therapy for patients who require reduced-intensity conditioning that is associated with better outcomes (e.g., fewer toxicities and improved survival). Clinician input noted that, despite the age limit of 70 years applied in the phase III trial, eligibility for conditioning treatment with treosulfan should not have an upper age limit. There are 2 dosing regimens for treosulfan (30 g/m2 and 42 g/m2), and clinician input noted that although only the 30 g/m2 dose was assessed in the pivotal trial, the higher-dose regimen should be considered as an option, based on patient age and fitness.
Drug plan input raised questions about the eligibility of conditioning treatment with treosulfan and about whether the trial criteria used to determine if patients were considered at increased risk for myeloablative conditioning (including the age restriction applied in the trial) were applicable in Canadian practice. Additional questions were raised about the use of treosulfan for patients receiving a second transplant after relapse and/or graft failure, and the input noted that patients who had undergone previous alloHSCT were excluded from the trial. With regard to place in therapy, drug plan input noted that treosulfan is becoming the new standard of care for patient needing reduced-intensity conditioning regimens, so may have high uptake in Canada. It was also noted that busulfan is used in myeloablative conditioning regimens, and the question of whether treosulfan would be considered an alternate to these regimens was raised. With regard to budget impact, if treosulfan is administered in the inpatient setting, drug costs may fall outside of provincial drug plan oncology budgets in some jurisdictions.
Several of these concerns were addressed in the sponsor’s model:
The sponsor-submitted model accounted for treatment-related adverse events (AEs) and survival outcomes.
CADTH was unable to address the following concern raised in stakeholder input:
The use of treosulfan in myeloablative conditioning regimens was not considered.
Economic Review
The current review is for treosulfan in combination with fludarabine for the treatment of adults with AML or MDS at increased risk for standard conditioning therapies before alloHSCT.1
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted a cost-utility analysis comparing costs and outcomes for treosulfan and busulfan, both in combination with fludarabine. The model population comprised adults with AML or MDS at increased risk with standard conditioning therapies before alloHSCT. The modelled population was aligned with part of the Health Canada indication and the sponsor’s reimbursement request. The Health Canada indication also includes pediatric patients with AML or MDS older than 1 year; however, this review and the reimbursement request is focused on the adult population.
Treosulfan is administered intravenously, as a 2-hour infusion given on 3 consecutive days (day –4, day –3, day –2) before stem cell infusion (day 0). The recommended dose of treosulfan is 10 g/m2 per BSA per day on 3 consecutive days, in combination with fludarabine (30 mg/m2), given on 5 consecutive days.2 The total treosulfan dose is 30 g/m2, and the total fludarabine dose is 150 mg/m2. Treosulfan is provided in 5 g vials, at a submitted price of $693.00 per vial. The total regimen cost of treosulfan is $8,316.00, based on an average patient BSA of 1.9 m2. When used in combination with fludarabine, the total regimen cost is $9,651.29, which accounts for drug wastage for treosulfan but not fludarabine. For the base case, the sponsor considered busulfan in combination with fludarabine as the only relevant comparator. Busulfan is administered at a dose of 0.8 mg/kg per day, given every 6 hours for 2 consecutive days (day –3 and day –4) before stem cell infusion. The sponsor’s calculated total regimen cost for busulfan used in combination with fludarabine is $3,900.09.
The model used a 28-day cycle length and simulated costs, LYs, and QALYs for each treatment regimen over a lifetime time horizon (40 years) from the perspective of Canada’s publicly funded health care system. Costs and QALYs were discounted at a rate of 1.5% per annum, and a half-cycle correction was applied.
Model Structure
The sponsor submitted a partitioned survival model (PSM) with the following health states: alloHSCT recovery and/or remission (i.e., event-free); relapse, progression, or graft failure (RPGf); and death (Figure 1). All patients entered the model in the event-free state and could remain event-free or transition to the RPGf or death health states each cycle. Patients in the RPGf state would remain in that state or transition to the death state. The proportion of patients who were event-free, who had experienced RPGf, or were dead at any time was derived from survival curves for OS and EFS fitted to data from the MC-FludT.14/L trial. A cure point (i.e., the point at which a patient who has not entered the RPGf state is assumed to be functionally cured and no longer at risk of relapse after alloHSCT) was used to adjust OS and EFS curves.
Model Inputs
The baseline population characteristics used to inform the model were based on the MC-FludT.14/L trial. The mean age, weight, and BSA applied in the model was 59.6 years, 80.2 kg, and 1.9 m2, respectively. The modelled population was assumed to be 60.8% male; 63.9% of patients were assumed to have AML and the remaining 36.1% were assumed to have MDS.1
Clinical efficacy for both treosulfan and busulfan in combination with fludarabine was informed by the MC-FludT.14/L trial (data cut-off: August 2018). The MC-FludT.14/L trial had a median duration of follow-up of 29.7 months (range, 3 to 52 months) for the treosulfan group. PSM was used to extrapolate EFS and OS over the entire model time horizon. The sponsor assessed parametric distributions using mixture-cure model and nonmixture-cure model approaches to account for the point in time when patients were assumed to be functionally cured in the model. In the submitted model, OS was extrapolated using the nonmixture-cure model Weibull distribution for both the treosulfan and busulfan model arms. The submitted model assessed the log-normal nonmixture-cure model for EFS for both treatments. The submitted model also had the functionality to evaluate costs and outcomes for patients with AML and patients with MDS separately, including fitting distributions to survival data from the trial for the subpopulations independently.
The sponsor assumed that patients would be considered cured if they remained alive and event-free 5 years after alloHSCT. At the 5-year cure point, patients who remained event-free and alive were assumed to revert to the general population mortality rate adjusted by a standardized mortality ratio. The ratio in the submitted base-case analysis was estimated from a cohort of patients who had undergone HSCT for the treatment of multiple types of malignancies.3
Quality of life data were not collected in the MC-FludT.14/L trial. Published sources of health state utility values were identified through a systematic literature review by the sponsor and a review of prior AML and MDS technology appraisals. Health state utility values for the alloHSCT recovery and/or remission health state were derived from the study by Grulke et al. (2012)4 and mapped using an algorithm described in a report by Proskorovsky et al. (2014)5 for patients with multiple myeloma. The alloHSCT recovery and/or remission health state captured changes in quality of life over time by applying different health state utility values for short-term alloHSCT recovery (up to 6 months and 7 to 12 months) and long-term alloHSCT recovery (years 2, 3, and 4+). Health state utility values for the RPGf health state were based on a prior National Institute for Health Care Excellence (NICE) review(technology appraisal guidance reference TA399).6 The same utility values were applied for patients with AML and those with MDS. In the submitted model, the health state utility values were adjusted by patient characteristic, based on general population utility values (i.e., the health state utilities were adjusted for patient age over time).7
The submitted model included costs associated with drug acquisition, alloHSCT, medical resource use, AEs, subsequent treatments, and end of life. Health state costs accounted for remission monitoring tests (estimated using Ontario’s schedule of benefits),8,9 short-term recovery costs,10 and assumptions around the number of monitoring tests per cycle over time. Postprogression health state costs included specialist consultations, hospitalization costs per cycle (assuming 4.6 days in hospital per month), transfusions (assuming 2.3 red blood cell and 2.3 platelet transfusions per month), and monitoring costs. A 1-time cost of $97,831 at the time of death was applied, obtained from a health administrative data costing study conducted using Ontario records.11
In addition to extensive chronic graft versus host disease (GvHD) and stage III or IV acute GvHD, the model included all treatment-related grade 3 or higher AEs with an incidence of 1% or more from the MC-FludT.14/L trial. The cost per event for chronic GvHD and acute GvHD were obtained from a prior cost-utility analysis conducted by Furzer et al. (2020).12 Costs associated with other AEs were obtained from the Ontario Case Costing tool, from the Patient Cost Estimator, or from the Alberta Interactive Health Data Application.13-15 Costs and utilities associated with AEs were estimated using mean durations and applied over multiple cycles, assuming a constant rate of incidence over time. The submitted model applied disutilities associated with AEs sourced from published literature and key opinion leader assumptions.
The model included subsequent pharmacological treatments incurred when a patient experienced progressive or relapsed disease after the alloHSCT, and treatment costs were separated between early (< 12 months) and late (> 12 months) relapse and/or progression. For patients who experienced early relapse or progression (up to 12 months after alloHSCT), subsequent therapies included azacitidine (10% of patients), palliative chemotherapy (20% of patients), and combination treatment with venetoclax and azacitidine (70% of patients). Patients who experienced relapse or disease progression after 12 months were assumed to have been treated with fludarabine, cytarabine, a granulocyte colony stimulating factor and idarubicin (21% of patients), a combination of venetoclax and azacitidine (49% of patients), or to have undergone a second alloHSCT (30% of patients). Of patients assumed to have undergone a second alloHSCT, 50% received conditioning therapy with busulfan and 50% with treosulfan. Costs were applied per cycle based on the distribution of subsequent therapies and the number of treatment cycles informed by Canadian expert opinion. Only costs related to subsequent therapies were captured in the submitted model; costs related to postprogression survival benefits based on the treatment received were not.
Summary of Sponsor’s Economic Evaluation Results
All analyses were run probabilistically (5,000 iterations for the base-case and scenario analyses). The deterministic and probabilistic results were similar. The probabilistic findings are presented here.
Base-Case Results
In the sponsor’s base-case analysis, conditioning with treosulfan in combination with fludarabine was the dominant strategy, when compared with busulfan in combination with fludarabine; cost savings were estimated to be $60,808 and the gain in QALYs was estimated to be 0.83. The probability of treosulfan in combination with fludarabine being the dominant strategy was 72%. In 23% of the probabilistic iterations, treosulfan in combination with fludarabine was more costly and more effective, and in 5%, it was less costly and less effective. Approximately 71% of the incremental QALYs in the sponsor’s base case were accrued beyond 1,586 days, which was the maximum survival data follow-up in the MC-FludT.14/L trial that informed the submitted economic evaluation.
Table 3: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER vs. reference ($/QALY) |
|---|---|---|---|---|---|
Treosulfan plus fludarabine | 415,015 | Reference | 7.32 | Reference | Reference |
Busulfan plus fludarabine | 475,824 | 60,808 | 6.50 | –0.83 | Dominated |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; vs. = versus.
Note: The submitted analysis is based on publicly available prices of the comparator treatments.
Source: Sponsor’s pharmacoeconomic submission.1
Sensitivity and Scenario Analysis Results
The sponsor conducted several scenario and sensitivity analyses to test alternative parameter values and assumptions. These included alternative utility mapping, alternative assumptions around disutilities, multiple time horizons, and modelling patients with AML and MDS separately. The sponsor’s base case was most influenced in the analysis of patients with MDS alone, where the incremental cost-effectiveness ratio was $5,637 per QALY gained, which was driven by higher costs associated with treosulfan in combination with fludarabine (i.e., treosulfan in combination with fludarabine was not cost saving). The sponsor did not assess scenarios related to alternative extrapolations of EFS or alternative assumptions around health state resource use and valuation.
The sponsor conducted a scenario analysis from a societal perspective. This analysis included additional costs associated with a patient’s productivity loss. In this analysis, relative to busulfan in combination with fludarabine, treosulfan in combination with fludarabine was the dominant strategy. This result was the same as for the sponsor’s base case that used a health care payer perspective.
CADTH Appraisal of the Sponsor’s Economic Evaluation
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the economic analysis:
The clinical efficacy of treosulfan compared with busulfan, both in combination with fludarabine, is uncertain. The model submitted by the sponsor estimated a survival benefit of 1.14 LYs for patients treated with treosulfan in combination with fludarabine, which was driven by patients remaining event-free longer than those treated with busulfan in combination with fludarabine. The majority (74%) of LYs were accrued in the extrapolated time period for treosulfan in combination with fludarabine. The CADTH clinical review reported that the available evidence shows that treosulfan in combination with fludarabine may result in a clinically important benefit for EFS and OS, compared with busulfan in combination with fludarabine. However, these findings were noted to be associated with low to moderate certainty, according to the GRADE assessment, due primarily to limitations of the trial that led to a serious risk of bias and imprecision. As a result, there is uncertainty about the benefit associated with treosulfan in comparison with busulfan. CADTH noted that the majority of cost savings associated with treosulfan were driven by the gains in EFS and OS predicted in the sponsor’s submission.
CADTH noted that the selected extrapolations of EFS and OS used in the sponsor’s base-case analysis may ultimately overestimate OS and EFS in the extrapolated period; however, the magnitude of benefit predicted was conservative, compared to the predicted survival gains from other possible extrapolations available for use in the sponsor’s submitted model.
The model structure was inappropriate for the decision problem. The sponsor used a PSM to estimate costs and outcomes associated with conditioning with treosulfan in combination with fludarabine before alloHSCT. Although PSMs are routinely used in economic evaluations, this approach is not suitable when patients can achieve a response on subsequent lines of therapy. In the RPGf health state, the model accounts for the costs of subsequent therapies over a lifetime time horizon, but does not capture clinical outcomes (i.e., improvements in survival or quality of life). The clinical experts consulted by CADTH agreed that patients who experience early relapse are unlikely to experience substantial clinical benefit, but indicated that a proportion of patients who relapse after 12 months may experience improvements in length and quality of life. This was noted to be particularly true of patients who undergo a second alloHSCT. Therefore, the magnitude of benefit in the extrapolated period may have been inaccurately estimated, as the model did not allow for the possibility of future improvements in OS or quality of life.
CADTH was unable to address this limitation within the submitted model.
Poor modelling practices were employed. The sponsor’s submitted model included numerous IFERROR statements, which led to situations in which the parameter value is overwritten with an alternative value without alerting the user to the automated overwriting. The systematic use of IFERROR statements makes thorough auditing of the sponsor’s model impractical, and it remains unclear whether the model is running inappropriately by overriding errors.
CADTH was unable to address this limitation and noted that a thorough validation of the sponsor’s model was not possible.
Drug cost for busulfan may be outdated. CADTH was unable to verify the sponsor’s drug cost for busulfan (i.e., $160.30 per 10 mL vial). CADTH obtained drug prices from DeltaPA from January 2017 (the year the vials became available) to October 2023, and found that, over that time frame, the cost per 10 mL vial was $355.00.
CADTH conducted a scenario analysis that revised the cost per vial of busulfan. CADTH noted that this change increases the predicted cost savings of treosulfan in the sponsor’s base-case analysis, given the higher cost of the comparator.
Additionally, the key assumptions listed in Table 4 were made by the sponsor and have been appraised by CADTH.
Table 4: Key Assumptions of the Submitted Economic Evaluation (Not Noted as Limitations to the Submission)
Sponsor’s key assumption | CADTH comment |
|---|---|
The sponsor assumed that patients who remained in the alloHSCT recovery and/or remission health state at 5 years were considered cured. | Acceptable. The clinical experts consulted by CADTH agreed that patients could be considered cured 5 years after transplant because the majority of relapses happen 2 years after transplant. |
A standardized mortality ratio of 2.3 was applied to patients who were considered cured (i.e., remained progression-free at 5 years). | Acceptable. The clinical experts consulted by CADTH agreed that alloHSCT recipients remain at elevated risk of late mortality for 10 or more years after transplant, compared with the general population. |
AML and MDS efficacy data were pooled in the sponsor’s base-case analysis. | Uncertain. Typically, subgroup analyses should be conducted separately, and the cost-effectiveness in the full Health Canada indication should be based on the weighted subgroup results using Canadian prevalence data. The clinical experts consulted by CADTH for this review indicated that there is heterogeneity in AML and MDS outcomes, but noted that the effect of treatment with treosulfan, in comparison with busulfan, was not expected to be different for patients with AML than for those with MDS.16,17 The results of the model are not sensitive to this assumption. |
Health state resource use for the RPGf health state was based on expert opinion, and included costs associated with hospitalization, blood and platelet transfusions, and other monitoring. | Uncertain. There is patient and jurisdictional variability in resource use after relapse or progression. Additionally, it is likely that many costs captured in the RPGf health state are also being captured in end-of-life costs, which include many of the same costs incurred in the 12 months before death (as described in the subsequent key assumption). |
The inclusion of end-of-life costs likely resulted in a double counting of costs in the 12 months before death. | End-of-life costs were estimated with a phase-based costing method, using Ontario’s health administrative data, and included costs associated with cancer-specific treatment, OHIP claims, outpatient prescription drugs, inpatient hospitalizations, and emergency department visits, among other costs. These costs likely included some of the health state and adverse event costs that were already captured in the submitted model. However, the results of the model were not sensitive to assumptions around end-of-life costs. |
The utilities for adverse events applied in the model are uncertain. | Uncertain. The sponsor obtained utility estimates from the literature (including past technology appraisals) that were estimated in various patient populations that had differences in disease, jurisdiction and/or place of residence, and age. Although this is generally considered inappropriate, the results of the model were not sensitive to assumptions around adverse event–related disutilities. |
Donor lymphocyte infusion was excluded as part of subsequent therapies considered in the model. | Uncertain. The clinical experts consulted by CADTH agreed that in Canadian clinical practice, donor lymphocyte infusion is used along with azacitidine for patients who have experienced relapse after alloHSCT. The costs and benefits of donor lymphocyte infusion are not captured in the model, and it is uncertain how this may impact the results of the model. |
The proportion of patients receiving subsequent therapies is assumed to be the same for patients with AML and those with MDS. | Not acceptable. The clinical experts consulted by CADTH indicated that the subsequent therapies used for patients with AML are not typically the same as those used for patients with and MDS. Notably, they agreed that combination treatment with venetoclax and azacitidine is not used for patients with MDS. The results of the model are not sensitive to changes in subsequent therapy distributions. |
alloHSCT = allogenic hematopoietic stem cell transplant; AML = acute myeloid leukemia; MDS = myelodysplastic syndromes; OHIP = Ontario Health Insurance Plan; RPGf = relapse, progression, or graft failure.
CADTH Reanalyses of the Economic Evaluation
Base-Case Results
Given the limitations CADTH identified in the sponsor’s economic submission, CADTH was unable to derive estimates of the cost-effectiveness of treosulfan in combination with fludarabine that are more reliable than those estimated from the sponsor’s base case. When reviewing the sponsor’s base-case results, there was a 23% chance that treosulfan in combination with fludarabine would be more costly and more effective than busulfan in combination with fludarabine (i.e., a positive incremental cost-effectiveness ratio), and a 5% chance that treosulfan in combination with fludarabine would be associated with fewer QALYs than busulfan in combination with fludarabine. The remaining iterations showed treosulfan to be dominant over busulfan. The results of the sponsor’s model were robust with regard to changes in the costs of AEs, the use of alternative utility values, and the time point at which patients were assumed to be cured.
The sponsor’s base-case analysis predicted that treatment with treosulfan in combination with fludarabine is expected to save $60,808 over the lifetime time horizon. In the sponsor’s base-case analysis, the majority of cost savings predicted were related to reduced health state medical costs for the RPGf health state. Costs included for the RPGf health state were based on expert opinion solicited by the sponsor, and included subsequent treatment costs (including for the proportion of patients who undergo a second alloHSCT) and costs associated with inpatient hospital stays (4.6 days per month), platelet and red blood cell transfusions (2.3 transfusions per month each), and other routine monitoring and procedures.
Uncertainty remains with regard to the magnitude of benefit of treosulfan in comparison with busulfan for EFS and OS. Should treosulfan be considered noninferior to busulfan for these outcomes, rather than superior, there is insufficient evidence to support a price premium for treosulfan.
Scenario Analysis Results
CADTH conducted 2 scenario analyses to determine the impact of alternative assumptions on the cost-effectiveness of treosulfan in combination with fludarabine:
1 in which the price of a busulfan 10 mL vial was revised
1 in which the higher dose of treosulfan (14 g/m2) was considered.
The results of the scenario analysis using the revised cost of busulfan in the sponsor’s economic model are the same: treosulfan in combination with fludarabine dominates busulfan in combination with fludarabine (incremental cost savings = $74,376; incremental QALY gain = 0.92, deterministically).
The scenario that considered the higher dose of treosulfan (14 g/m2) showed that the results of the sponsor’s model are the same (i.e., treosulfan in combination with fludarabine dominates busulfan in combination with fludarabine). The estimated cost savings in this scenario are $69,199, which is slightly lower than that estimated using the 10 g/m2 dose.
Issues for Consideration
Clinical expert input received by CADTH indicated that there is an alternative dosing regimen for treosulfan in combination with fludarabine: 14 g/m2 given on 3 consecutive days (day –4 to day –2) before stem cell infusion. This regimen is not currently being reviewed by CADTH and, thus, was not considered in the submitted economic evidence because it was not assessed in the pivotal trial that informed the model. Using the higher-dose regimen in clinical practice would result in higher drug costs, which would influence the cost-effectiveness and budgetary impact of reimbursing treosulfan in combination with fludarabine. The estimated course cost per patient would be $12,474 for the higher dose of treosulfan, compared to $8,316 for the 10 g/m2 dose regimen. CADTH considered the higher dosing regimen as a scenario analysis. The predicted cost savings in this scenario declined slightly (by $2,100), given that conditioning is a 1-time therapy. CADTH noted that in this scenario, the clinical efficacy informing the model is based on the 10 g/m2 regimen.
The clinical experts consulted by CADTH agreed that there is reason to consider that treosulfan in combination with fludarabine has the potential to benefit patients who are eligible for myeloablative conditioning before alloHSCT and those with diseases other than AML and MDS (such as lymphoma, myelofibrosis, and other rarer conditions). Given that treosulfan does not have an indication for these uses, they have not been considered in CADTH’s review, and the cost-effectiveness and budgetary impact of its use in these settings is unknown.
Overall Conclusions
Evidence from the MC-FludT.14/L trial suggests that treosulfan in combination with fludarabine may result in a clinically important benefit in EFS and OS, compared with busulfan in combination with fludarabine. However, the CADTH clinical review noted that, based on the GRADE assessment, there is low to moderate certainty associated with the potential benefit of treosulfan in combination with fludarabine for these 2 outcomes due to a serious risk of bias and imprecision.
Using the sponsor’s base case, treosulfan in combination with fludarabine is cost saving ($60,808 over the lifetime time horizon) and associated with a gain of 0.83 incremental QALYs and 1.14 incremental LYs, compared to busulfan in combination with fludarabine. These results are dependent on the predicted clinical benefit of treosulfan, which led to cost offsets in the relapse and/or progression health state and comprises subsequent treatment costs (including the need for a second alloHSCT) and costs associated with inpatient hospital stays (average of 4.6 days per month), platelet and red blood cell transfusions (average of 2.3 transfusions per month each), and other routine monitoring and procedures. The cost of a regimen of treosulfan in combination with fludarabine is $10,621, assuming a patient weight of 75 kg and a BSA of 1.9 m2; under the same assumptions, the cost for the regimen of busulfan in combination with fludarabine is $5,145. This results in an additional cost of $5,476 for the treosulfan regimen. Given that the cost of the conditioning regimen only occurs 1 time, the additional drug-acquisition cost of treosulfan is offset with only a small improvement in EFS in the sponsor’s model.
CADTH noted several limitations that add uncertainty to these results, including the low to moderate certainty in the clinical efficacy of treosulfan and the structural assumptions inherent in the model structure. However, CADTH was unable to use the sponsor’s economic model to derive a more reliable estimate of the cost-effectiveness of treosulfan in combination with fludarabine. The sponsor’s model used survival extrapolations for EFS and OS, which produced the most conservative estimate of the clinical benefits for treosulfan from among the available options, and the results were robust with regard to changes in the other parameters identified as potential limitations. However, the predicted clinical benefit of treosulfan remains uncertain, given that 74% of the predicted gains in LYs for treosulfan were accrued beyond the trial period, for which there is no clinical evidence.
References
1.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Treosulfan, 10 g/m2 for infusion. Toronto (ON): Medexus Pharmaceuticals, Inc; 2023 Jul 12.
2.Medexus, Inc. Product Monograph Including Patient Medication Information: TRECONDYV (treosulfan for injection) [accessed by sponsor]. 2021; https://pdf.hres.ca/dpd_pm/00061950.PDF.
3.Martin PJ, Counts GW, Jr., Appelbaum FR, et al. Life expectancy in patients surviving more than 5 years after hematopoietic cell transplantation. J Clin Oncol. 2010;28(6):1011-1016. PubMed
4.Grulke N, Albani C, Bailer H. Quality of life in patients before and after haematopoietic stem cell transplantation measured with the European Organization for Research and Treatment of Cancer (EORTC) Quality of Life Core Questionnaire QLQ-C30. Bone Marrow Transplant. 2012;47(4):473-482. PubMed
5.Proskorovsky I, Lewis P, Williams CD, et al. Mapping EORTC QLQ-C30 and QLQ-MY20 to EQ-5D in patients with multiple myeloma. Health Qual Life Outcomes. 2014;12:35. PubMed
6.National Institute for Health Care Excellence. TA399: Azacitidine for treating acute myeloid leukaemia with more than 30% bone marrow blasts [accessed by sponsor]. 2016; https://www.nice.org.uk/guidance/ta399.
7.Guertin JR, Feeny D, Tarride JE. Age- and sex-specific Canadian utility norms, based on the 2013-2014 Canadian Community Health Survey. CMAJ. 2018;190(6):E155-E161. PubMed
8.Ministry of Health, Ministry of Long Term Care. Schedule of Benefits of Laboratory Services (Effective July 1, 2020) [accessed by sponsor]. 2020; http://www.health.gov.on.ca/en/pro/programs/ohip/sob/lab/lab_mn2020.pdf. Accessed May, 2023.
9.Ministry of Health, Ministry of Long Term Care. Schedule of Benefits: Physician Services Under the Health Insurance Act (Effective April 1, 2023) [accessed by sponsor]. 2023; https://www.health.gov.on.ca/en/pro/programs/ohip/sob/. Accessed May, 2023.
10.Couban S, Dranitsaris G, Andreou P, et al. Clinical and economic analysis of allogeneic peripheral blood progenitor cell transplants: A Canadian perspective. Bone Marrow Transplant. 1998;22(12):1199-1205. PubMed
11.de Oliveira C, Pataky R, Bremner KE, et al. Phase-specific and lifetime costs of cancer care in Ontario, Canada. BMC Cancer. 2016;16(1):809. PubMed
12.Furzer J, Gupta S, Nathan PC, et al. Cost-effectiveness of tisagenlecleucel vs standard care in high-risk relapsed pediatric acute lymphoblastic leukemia in Canada. JAMA Oncol. 2020;6(3):393-401. PubMed
13.Ontario's Health Data Branch Web Portal. Ontario Case Costing Analysis Tool [accessed by sponsor]. 2023; https://data.ontario.ca/en/dataset/ontario-case-costing-initiative-occi. Accessed April, 2023.
14.Alberta Health Interactive Health Data Team. Hospital Inpatient Care Case Costs - CMG/Plex [accessed by sponsor]. 2015; https://open.alberta.ca/opendata/hospital-inpatient-care-case-costs-cmgplex.
15.Canadian Institute for Health Information. Patient Cost Estimator [accessed by sponsor]. 2020; https://www.cihi.ca/en/patient-cost-estimator. Accessed October, 2020.
16.Bhatia S, Francisco L, Carter A, et al. Late mortality after allogeneic hematopoietic cell transplantation and functional status of long-term survivors: Report from the Bone Marrow Transplant Survivor Study. Blood. 2007;110(10):3784-3792. PubMed
17.Wingard JR, Majhail NS, Brazauskas R, et al. Long-term survival and late deaths after allogeneic hematopoietic cell transplantation. J Clin Oncol. 2011;29(16):2230-2239. PubMed
18.DeltaPA. [Ottawa (ON)]: IQVIA; 2023: https://www.iqvia.com/. Accessed 2023 Aug 30.
19.Statistics Canada. Projected population, by projection scenario, age and sex, as of July 1 (x 1,000); Table: 17-10-0057-01. Projection scenario M3: medium-growth [accessed by sponsor]. 2022; https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1710000501. Accessed April, 2023.
20.Canadian Cancer Society. Canadian Cancer Statistics: A 2022 special report on cancer prevalence [accessed by sponsor]. 2022; https://cancer.ca/Canadian-Cancer-Statistics-2022-EN. Accessed May 2, 2023.
21.Leukemia & Lymphoma Society of Canada. Blood Cancer in Canada Facts & Stats 2016 [accessed by sponsor]. 2016; https://www.llscanada.org/sites/default/files/National/CANADA/Pdf/InfoBooklets/Blood_Cancer_in_Canada_Facts_%26_Stats_2016.pdf. Accessed April 18, 2023.
22.CADTH Reimbursement Review: Luspatercept (Reblozyl) [accessed by sponsor]. Can J Health Technol. 2022;2(2). https://canjhealthtechnol.ca/index.php/cjht/article/view/sr0670r.
23.Cell Therapy Transplant Canada. Annual Report 2020/2021 [accessed by sponsor]. 2021; https://cdn.ymaws.com/www.cttcanada.org/resource/resmgr/2021/CTTC_2021_Annual_Report.pdf. Accessed March, 2023.
24.Khalil MMI, Lipton JH, Atenafu EG, et al. Impact of comorbidities constituting the hematopoietic cell transplant (HCT)-comorbidity index on the outcome of patients undergoing allogeneic HCT for acute myeloid leukemia. Eur J Haematol. 2018;100(2):198-205. PubMed
25.Fleurence RL, Hollenbeak CS. Rates and probabilities in economic modelling: Transformation, translation and appropriate application. Pharmacoeconomics. 2007;25(1):3-6. PubMed
Appendix 1: Cost Comparison Table
Note that this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical experts and CADTH-participating drug plans. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 5: CADTH Cost Comparison Table for Conditioning Treatment Prior to AlloHSCT
Treatment | Strength or concentration | Form | Price ($) | Recommended dosage | Course cost ($) |
|---|---|---|---|---|---|
Treosulfan (Trecondyv) | 5 g/mL | 5 g vial | 693.0000a | 10 g/m2 given on 3 consecutive days (days −4 to −2) before stem cell infusion | 8,316.00 |
Fludarabine (Fludara) | 25 mg/mL | 2 mL vial | 230.5000 | 30 mg/m2 given 5 consecutive days (days −6 to −2) before stem cell infusion | 2,305.00 |
Treosulfan in combination with fludarabine | 10,621.00 | ||||
Busulfan | 6 mg/mL | 10 mL vial | 355.0000 | 0.8 mg/kg given every 6 hours for 2 consecutive days (days −3 and −4) before stem cell infusion | 2,840.00 |
Fludarabine (Fludara) | 25 mg/mL | 2 mL vial | 230.5000 | 30 mg/m2 given 5 consecutive days (days −6 to −2) before stem cell infusion | 2,305.00 |
Busulfan in combination with fludarabine | 5,145.00 | ||||
AlloHSCT = allogenic hematopoietic stem cell transplant; BSA = body surface area.
Notes: Assumes mean patient weight of 75 kg and BSA of 1.9 m2. Daily and cycle costs assume wastage of excess medication. All prices are from the DeltaPA database (accessed August 2023), and do not include dispensing fees.18
aSponsor’s submitted price.1
Appendix 2: Submission Quality
Note that this appendix has not been copy-edited.
Description | Yes or no | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing. | Yes | No comment. |
Model has been adequately programmed and has sufficient face validity. | No | CADTH identified programming errors in the submitted model. For example, the calculation of newly progressed patients estimated that there would be more newly progressed patients than patients in the RPGf health state during early model cycles, which did not meet face validity. |
Model structure is adequate for decision problem. | No | Refer to limitation: The model structure was inappropriate for the decision problem. |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis). | No | Refer to limitation: Poor modelling practices were employed. |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem. | Yes | No comment. |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details). | Yes | No comment. |
RPGf = relapse, progression, or graft failure.
Appendix 3: Additional Information on the Submitted Economic Evaluation
Note that this appendix has not been copy-edited.
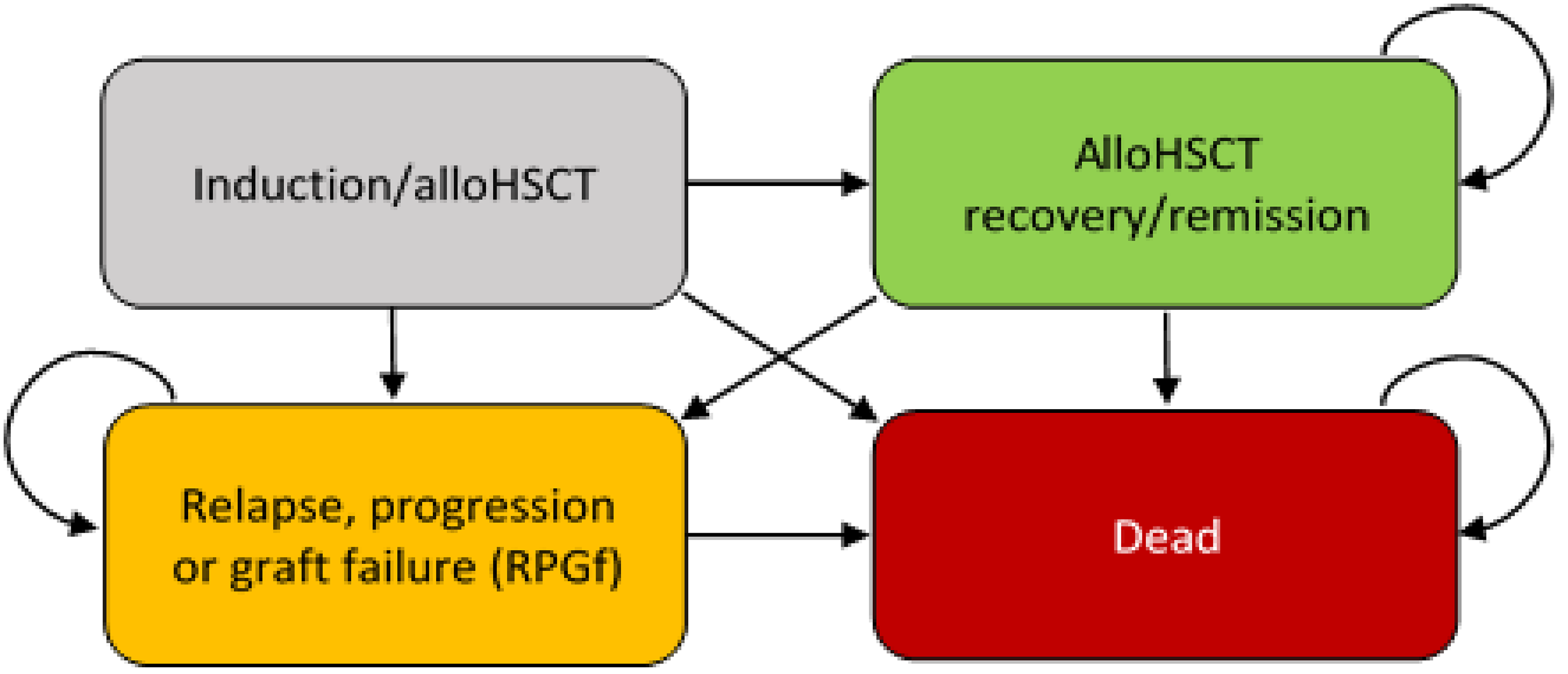
alloHSCT = allogenic hematopoietic stem cell transplant; RPGf = relapse, progression, or graft failure.
Source: Sponsor’s pharmacoeconomic submission.1
Detailed Results of the Sponsor’s Base Case
Table 7: Disaggregated Summary of the Sponsor’s Economic Evaluation Results (Probabilistic)
Parameter | Treosulfan and fludarabine | Busulfan and fludarabine | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 11.07 | 9.94 | 1.14 |
Discounted QALYs | |||
Total | 7.32 | 6.50 | 0.82 |
By health state or data source | |||
Event-free survival | 7.07 | 5.97 | 1.10 |
Relapse or progression: AML | 0.16 | 0.34 | –0.18 |
Relapse or progression: MDS | 0.09 | 0.19 | –0.10 |
Dead | 0.00 | 0.00 | 0.00 |
Discounted costs ($) | |||
Total | 415,015.46 | 475,823.81 | –60,808.35 |
Conditioning and alloHSCT costs | 223,796.76 | 218,102.05 | 5,694.71 |
Health state costs | 180,620.94 | 244,522.68 | –63,901.74 |
Adverse event costs | 10,597.76 | 13,199.08 | –2,601.32 |
ICER ($/QALY) | Dominant (i.e., results in lower costs and more QALYs) | ||
alloHSCT = allogenic hematopoietic stem cell transplant; AML = acute myeloid leukemia; ICER = incremental cost-effectiveness ratio; LY = life-year; MDS = myelodysplastic syndromes; QALY = quality-adjusted life-year.
Appendix 4: Submitted BIA and CADTH Appraisal
Note that this appendix has not been copy-edited.
Table 8: Summary of Key Take-Aways
Key take-aways of the BIA |
|---|
|
Summary of Sponsor’s BIA
The sponsor submitted a budget impact analysis (BIA) estimating the incremental budget impact of reimbursing treosulfan in combination with fludarabine as conditioning therapy before alloHSCT in adult patients with AML or MDS at increased risk for standard conditioning therapies. The analysis was undertaken using an epidemiologic approach from the perspective of the CADTH-participating Canadian public drug plans over a 3-year time horizon (2024 to 2026). Beginning with an estimate of the population in Canada (excluding Quebec) aged between 18 years and 75 years,19 the sponsor narrowed the population using estimates of prevalent leukemia cases,20 the proportion of leukemia patients expected to have AML;21 and prevalent MDS cases were estimated using the prevalence rate from the CADTH review report for luspatercept.22 The sponsor then applied the proportion of AML and MDS patients expected to undergo alloHSCT,23 and the proportion of those patients who would require reduced-intensity conditioning.24 Key inputs to the BIA are documented in Table 9.
The sponsor’s BIA included the following key assumptions:
All eligible patients were assumed to be publicly covered given that treatments are administered in the hospital.
The proportion of MDS patients expected to undergo alloHSCT was assumed to be one-third of the probability of the AML probability based on the number of transplants reported in the Cell Therapy Transplant Canada annual 2020 to 2021 report.23
Subsequent therapies are not included in the analysis.
Table 9: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as year 1 / year 2 / year 3 if appropriate) |
|---|---|
Target population | |
Population in Canada (excluding Quebec) aged 18 to 75 years | 22,944,800 / 23,253,000 / 23,556,600 |
Number of leukemia cases (2018) | 19,310 |
Proportion of leukemia cases that are AML | 24% |
Prevalence of MDS | 0.071%22 |
Annual probability of alloHSCT for prevalent AML cases | |
Annual probability of alloHSCT for prevalent MDS cases | 1.53%23 |
Proportion of alloHSCT on RIC regimen | 32%24 |
Eligible for public coverage | 100% |
Number of patients eligible for drug under review | 136 / 138 / 140 |
Market uptake (3 years) | |
Uptake (reference scenario) Busulfan and fludarabine | 100% / 100% / 100% |
Uptake (new drug scenario) Treosulfan and fludarabine Busulfan and fludarabine | 5% / 10% / 15% 95% / 90% / 85% |
Cost of treatment (per patient) | |
Cost of treatment over treatment course Treosulfan and fludarabine Busulfan and fludarabine | $10,621 $4,870 |
alloHSCT = allogenic hematopoietic stem cell transplant; AML = acute myeloid leukemia; MDS = myelodysplastic syndromes; RIC = reduced-intensity conditioning.
Summary of the Sponsor’s BIA Results
The sponsor estimated the net budget impact of funding treosulfan in combination with fludarabine as conditioning therapy before alloHSCT in adult patients with AML or MDS at increased risk for standard conditioning therapies to be $39,228 in year 1, $79,511 in year 2, and $120,823 in year 3, for a 3-year total budget impact of $239,562. A scenario analysis that included administration costs resulted in a lower 3-year budget impact ($181,071) due to the fewer number of doses of treosulfan compared to busulfan for the full course of treatment.
CADTH Appraisal of the Sponsor’s BIA
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
The market uptake of treosulfan in combination with fludarabine is underestimated. The sponsor’s submitted BIA indicated that treosulfan in combination with fludarabine would have a market uptake of 5% in year 1, 10% in year 2, and 15% in year 3 based on internal sponsor predictions. However, clinical experts consulted by CADTH for this review noted that if treosulfan in combination with fludarabine becomes publicly funded, the uptake in the indicated population is expected to be faster and more comprehensive than predicted by the sponsor, given the unmet needs in this disease area. They indicated that the majority of clinicians are likely to switch to treosulfan in combination with busulfan given their interpretation of the clinical evidence and potential benefits for their patients. This was also supported by drug plan input which indicated treosulfan is becoming the standard of care.
To address this limitation, CADTH undertook a reanalysis by revising the market shares for treosulfan in the new drug scenario to 40% in year 1, 60% in year 2, and 80% in year 3.
The number of patients with AML undergoing alloHSCT is underestimated. The sponsor estimated that 174 patients with AML will undergo alloHSCT in the base year of the budget impact model, based on the sponsor’s narrowing of the population which included an estimate of the annual probability of patients with AML undergoing alloHSCT of 4.53%. The sponsor’s estimate was based on the Cell Therapy Transplant Canada annual 2020 to 2021 report23 which reports numbers of alloHSCTs performed at participating centres by year. Clinical experts consulted by CADTH agreed that this number seems to underestimate the annual number of alloHSCT in patients with AML in CADTH-participating jurisdictions. Clinical experts consulted by CADTH estimated that approximately 30% of newly diagnosed patients with AML would eventually receive an alloHSCT. They also indicated that over time there are increasing numbers of alloHSCT being performed (e.g., due to increasing age limits for transplant). Clinical experts consulted by CADTH estimated that there may be 2 times as many alloHSCT performed per year in CADTH-participating jurisdictions in patients with AML than estimated by the sponsor.
CADTH conducted a scenario analysis exploring the budgetary impact, assuming that the probability of alloHSCT in patients with AML is 8.83%, to align with the expectations of the clinical experts consulted by CADTH. CADTH notes that this change also impacts the annual probability of alloHSCT in prevalent MDS patients, as it is assumed to be one-third of the probability applied to patients with AML.
CADTH Reanalyses of the BIA
CADTH revised the sponsor’s submitted analysis by adjusting the market share for treosulfan in combination with fludarabine to reflect the expectations of clinical experts consulted by CADTH. The changes applied to derive the CADTH base case are described in Table 10.
Table 10: CADTH Revisions to the Submitted Budget Impact Analysis
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
1. Price of busulfan | $160.30 per 10 mL vial | $355.00 per 10 mL vial |
Changes to derive the CADTH base case | ||
1. Market uptake | Year 1: 5% Year 2: 10% Year 3: 15% | Year 1: 40% Year 2: 60% Year 3: 80% |
CADTH base case | 1 | |
The results of the CADTH reanalysis are presented in summary format in Table 11 and a more detailed breakdown is presented in Table 12. The CADTH reanalysis suggests that reimbursing treosulfan in combination with fludarabine would be associated with an incremental cost of $143,839 in year 1, $218,657 in year 2, and $295,349 in year 3, for a 3-year budgetary impact of $657,845.
Table 11: Summary of the CADTH Reanalyses of the BIA
Stepped analysis | Three-year total |
|---|---|
Submitted base case | $239,562 |
Submitted base case, corrected | $109,801 |
CADTH base case | $657,845 |
BIA = budget impact analysis.
CADTH conducted an additional scenario analysis to address remaining uncertainty regarding the annual number of patients with AML expected to receive an alloHSCT using CADTH’s base-case analysis. CADTH’s scenario analysis assumed that the probability of alloHSCT for patients with AML is 8.83% (i.e., twice the prevalence as assumed in the sponsor’s base-case analysis, which estimated that there are 215 alloHSCT in patients with AML per year).
Results are provided in Table 12. This scenario analysis demonstrates that the budget impact is sensitive to changes in the patient population, with an estimated budget impact that is 97% greater than the CADTH base case, with a 3-year budgetary impact of $1,294,510.
Table 12: Detailed Breakdown of the CADTH Reanalyses of the BIA
Stepped analysis | Scenario | Year 0 (current situation) | Year 1 | Year 2 | Year 3 | Three-year total |
|---|---|---|---|---|---|---|
Submitted base case, corrected | Reference | $1,074,690 | $1,089,298 | $1,103,930 | $1,118,343 | $3,311,572 |
New drug | $1,074,690 | $1,107,278 | $1,140,373 | $1,173,721 | $3,421,372 | |
Budget impact | $0 | $17,980 | $36,443 | $55,378 | $109,801 | |
CADTH base case | Reference | $1,074,690 | $1,089,298 | $1,103,930 | $1,118,343 | $3,311,572 |
New drug | $1,074,690 | $1,233,137 | $1,322,587 | $1,413,692 | $3,969,417 | |
Budget impact | $0 | $143,839 | $218,657 | $295,349 | $657,845 | |
CADTH sensitivity analysis: number of alloHSCT for patients with AML | Reference | $2,114,778 | $2,143,524 | $2,172,316 | $2,200,679 | $6,516,519 |
New drug | $2,114,778 | $2,426,571 | $2,602,590 | $2,781,868 | $7,811,029 | |
Budget impact | $0 | $283,047 | $430,274 | $581,189 | $1,294,510 |
alloHSCT = allogenic hematopoietic stem cell transplant; AML = acute myeloid leukemia; BIA = budget impact analysis.
Stakeholder Input
Patient Input
The Leukemia & Lymphoma Society of Canada
About The Leukemia & Lymphoma Society of Canada
The Leukemia & Lymphoma Society of Canada — bloodcancers.ca
LLSC is a national charitable status organization dedicated to finding a cure for blood cancers and its ability to improve the quality of life of people affected by blood cancers and their families by funding life-enhancing research and providing educational resources, services, and support. The Leukemia and Lymphoma Society of Canada is the largest charitable organization in Canada dedicated to blood cancer, our focus includes:
Funding research from bench to bedside.
Rethinking how a person navigates their blood cancer experience
Providing targeted blood cancer information
Offering tools for psychological and emotional support
Empowering Canadians to take charge of their blood cancer experience through practical support and advocacy
Information Gathering
One online survey was created through SurveyMonkey. Information was gathered in July 2023. The survey was developed and distributed by LLSC, in English only. The survey was distributed through various social media channels and directly by email.
The survey asked for input from patients and caregivers who have lived experience with MDS or AML and have received or are considering receiving an allogeneic hematopoietic stem cell transplant (alloHSCT).
108 respondents qualified for this participated in this survey. The majority of respondents indicated that they were the AML patient and the caregiver for AML patient. The demographic breakdown is listed in the chart below.
Figure 1: Patients and Caregivers Who Have Lived Experience With MDS or AML and Have Received or Are Considering Receiving an alloHSCT
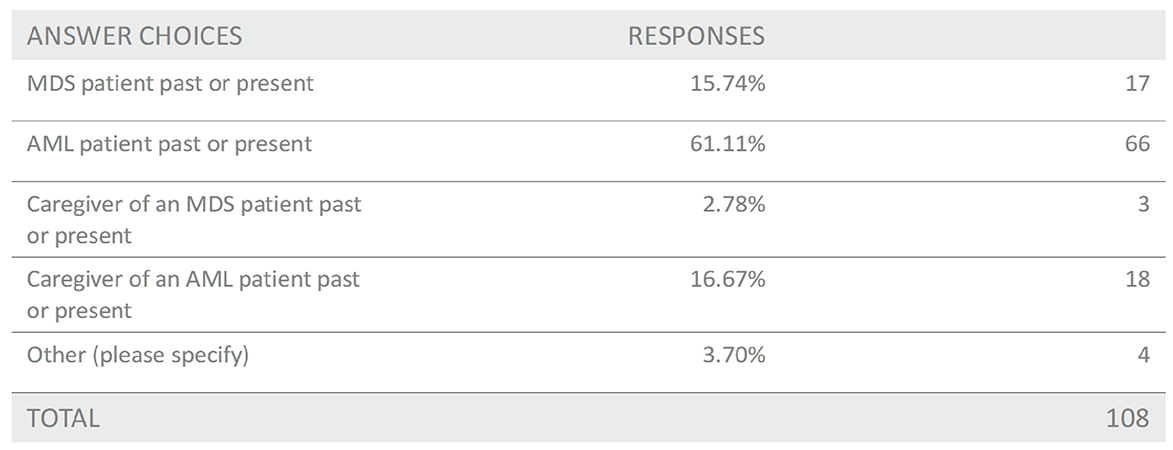
This is a breakdown of the ages of the AML and MDS patients at the time of alloHSCT.
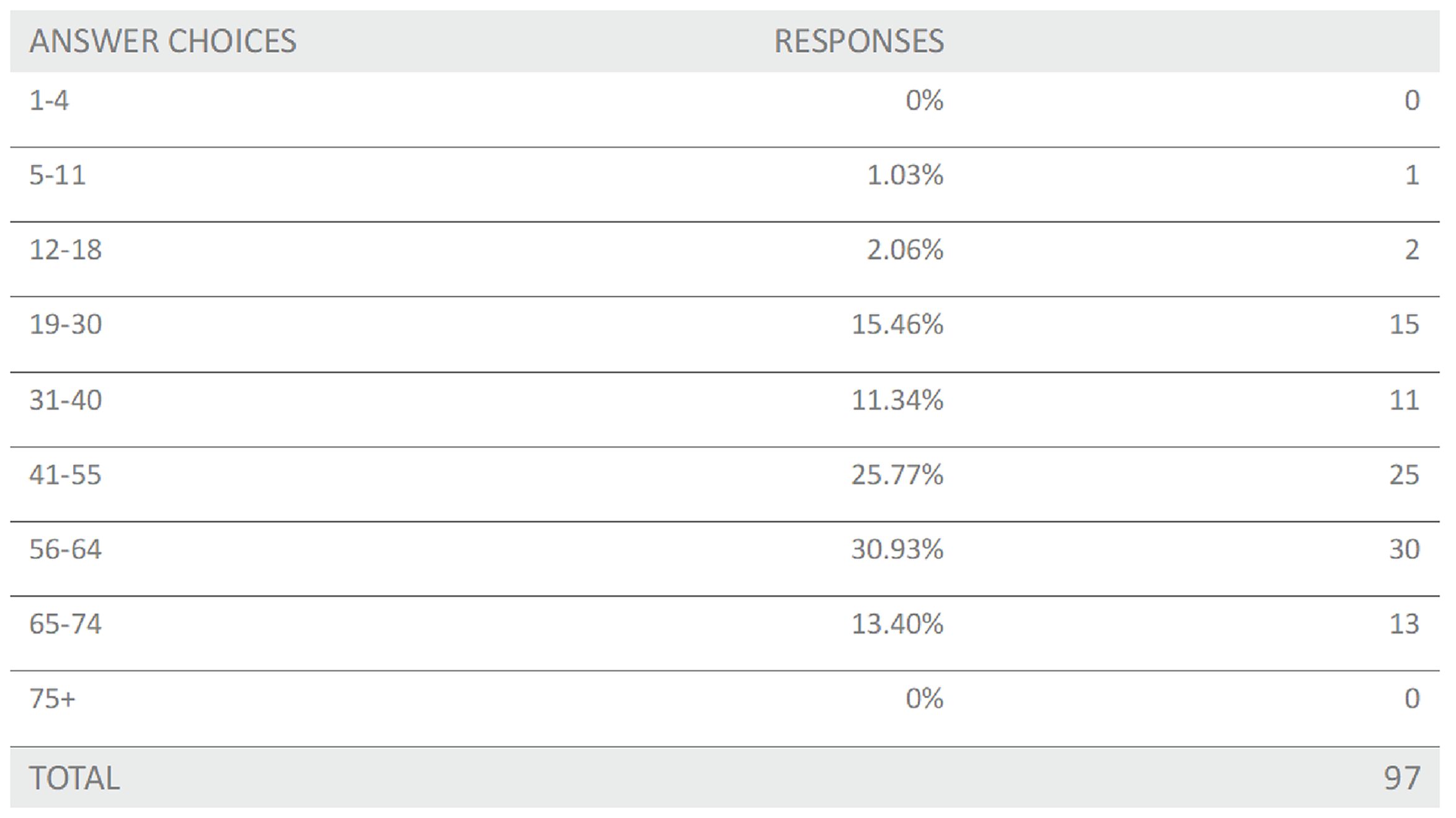
Most of the survey respondents were considering or have had an alloHSCT.
Figure 3: Were You or the Person You Care for a Recipient of an alloHSCT or Are Considering an alloHSCT in the Near Future?
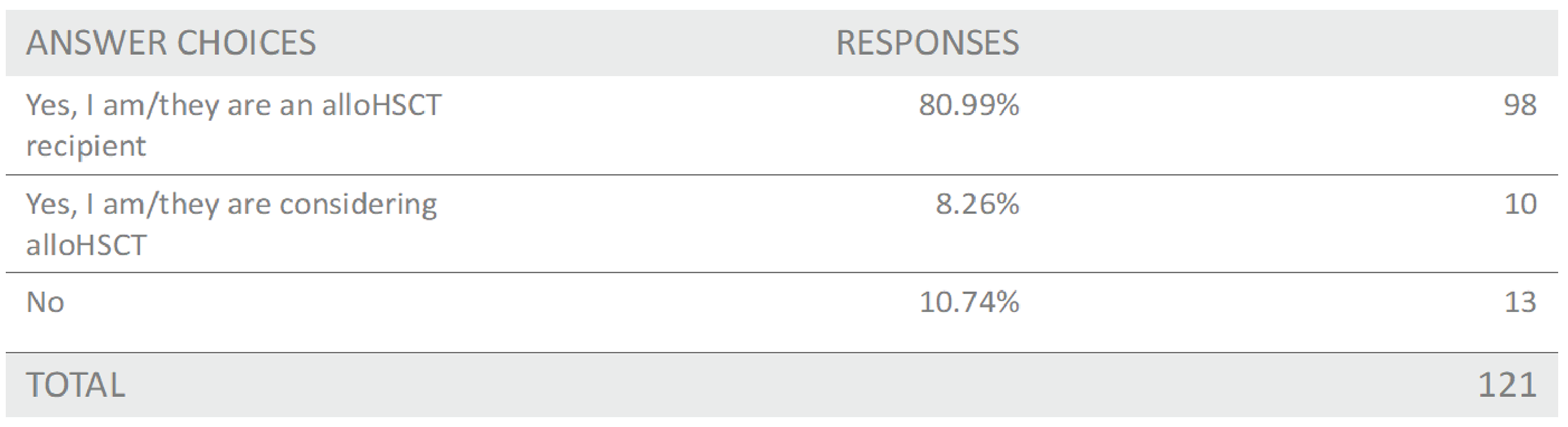
The questions respondents were asked in this survey were not intended to measure the efficacy of this treatment against currently available treatments. We recognize that when patients receive conditioning treatment in preparation for alloHSCT, they are usually not offered other options as they are generally prescribed whichever conditioning treatment is used as the standard of care at the cancer centre they are being treated at.
The questions in this survey were aimed at highlighting the mindset and mental status of MDS and AML patients and their families when they are forced to make the life-or-death decision of whether or not to go through with the stem cell transplant process. We wanted to bring attention to the mental burden, anxiety, stress, fear, and concern that patients and their families go through during this difficult time and ask, if you could have access to a pre-transplant conditioning treatment that offered potential benefits such as reduced toxicity, fewer adverse events, lower rates of Graft vs Host Disease and other post-transplant complications, shorter hospital stays post-transplant and lower readmission rates to hospital, and ultimately, significantly increase your odds of survivorship what would that mean to you and your loved ones? Would this affect your decision? Would this help to ease your mental burden? We know that positive mental outlook can play a large part in improving patient outcomes.
The respondent answers speak to the values and concerns of MDS and AML patients and their families when they are considering treatment options throughout their cancer experience. They speak to the very real fears and real-life impact that illness and unpredictable treatment outcomes can cause families to experience when a loved one or they themselves are going through the alloHSCT process. These issues are not limited to their physical health but include themes regarding effects on their well-being as a whole, considering their emotional and mental health as well.
Disease Experience and Experience With Current Treatments
The decision to undergo an alloHSCT and the experience of an alloHSCT can be a stressful time for patients and their families. alloHSCT still carries a high risk of failure and relapse. Those living with MDS are faced with, according to patients “impossible choices”. Those with MDS have an even more difficult decision. 10 – 35% of those living with MDS will progress to AML. For those at high risk, the chance of progression is as high as 40%. At first glance those odds may appear small, however if progression does happen, there is no way of predicting if the patient will still qualify for a HSCT.
As expected, the decision making, preparation process in deciding to undergo a stem cell transplant has significant impact on the mental health of patients and their families.
Figure 4: What Was Your Level of Anxiety During the Decision-Making/Preparation Process for alloHSCT?
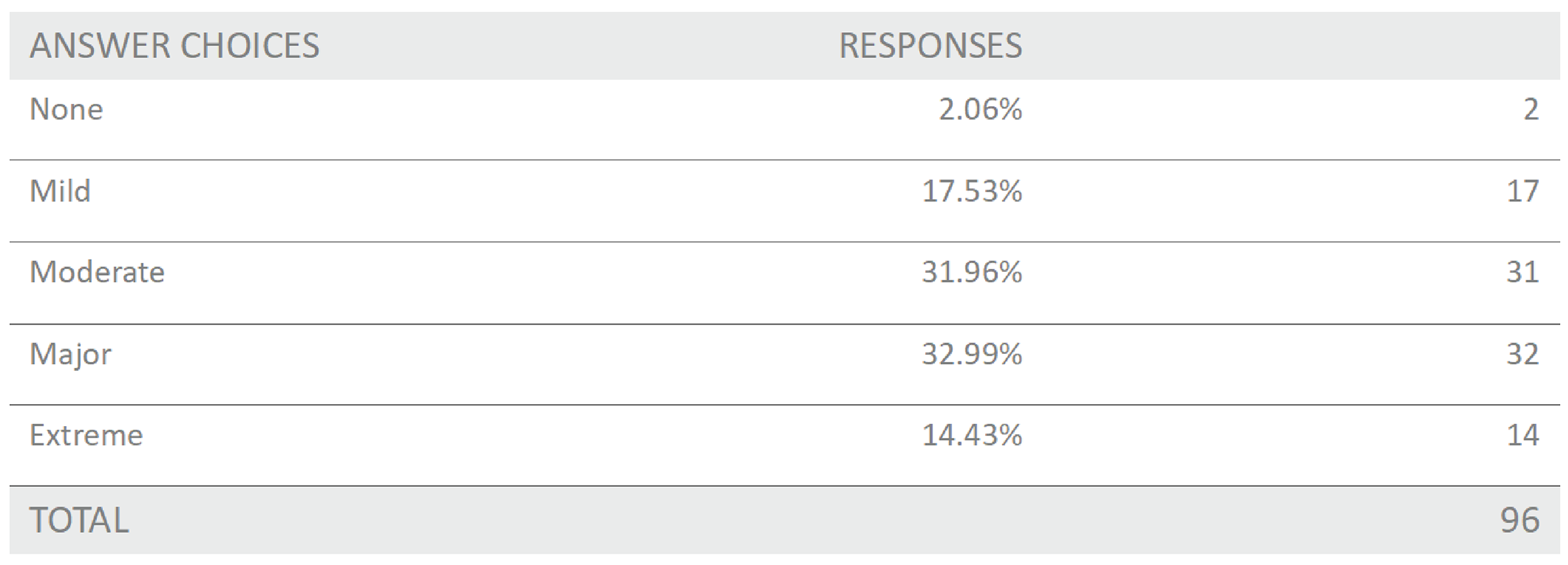
Figure 5: What Was Your Level of Stress During the Decision-Making/Preparation Process for alloHSCT?
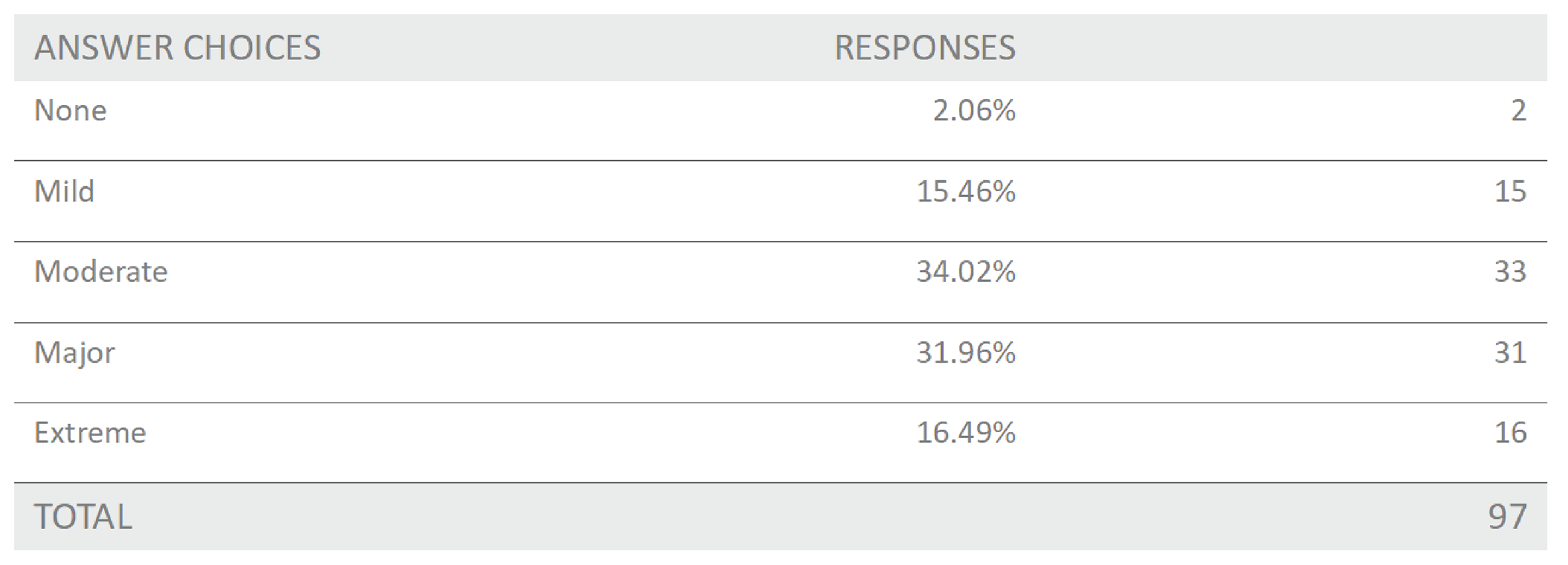
79.4% of respondents reported moderate to extreme and 47.4% of respondents reported major to extreme anxiety associated with the decision or preparation process for an alloHSCT. Similar levels of stress were also reported. The written comments reflected the difficulty of the decision.
“It's very daunting to discuss the potential lethal complications of an allo-hsct.”
“Panic attack on Day 0.”
“I have never been so scared in all my life. There was and still is a good chance I will not survive this treatment. The thought of dying really scares me, as did the procedure when they told me about it. I want to live and have lots of plans and things to do.”
Despite the risk of failure, hope for survival drove patient decisions to undergo an alloHSCT.
Increased odds of survival, hope in gaining quality of life and prevention of disease progression were the top three contributors to patients’ decisions to undergo an alloHSCT.
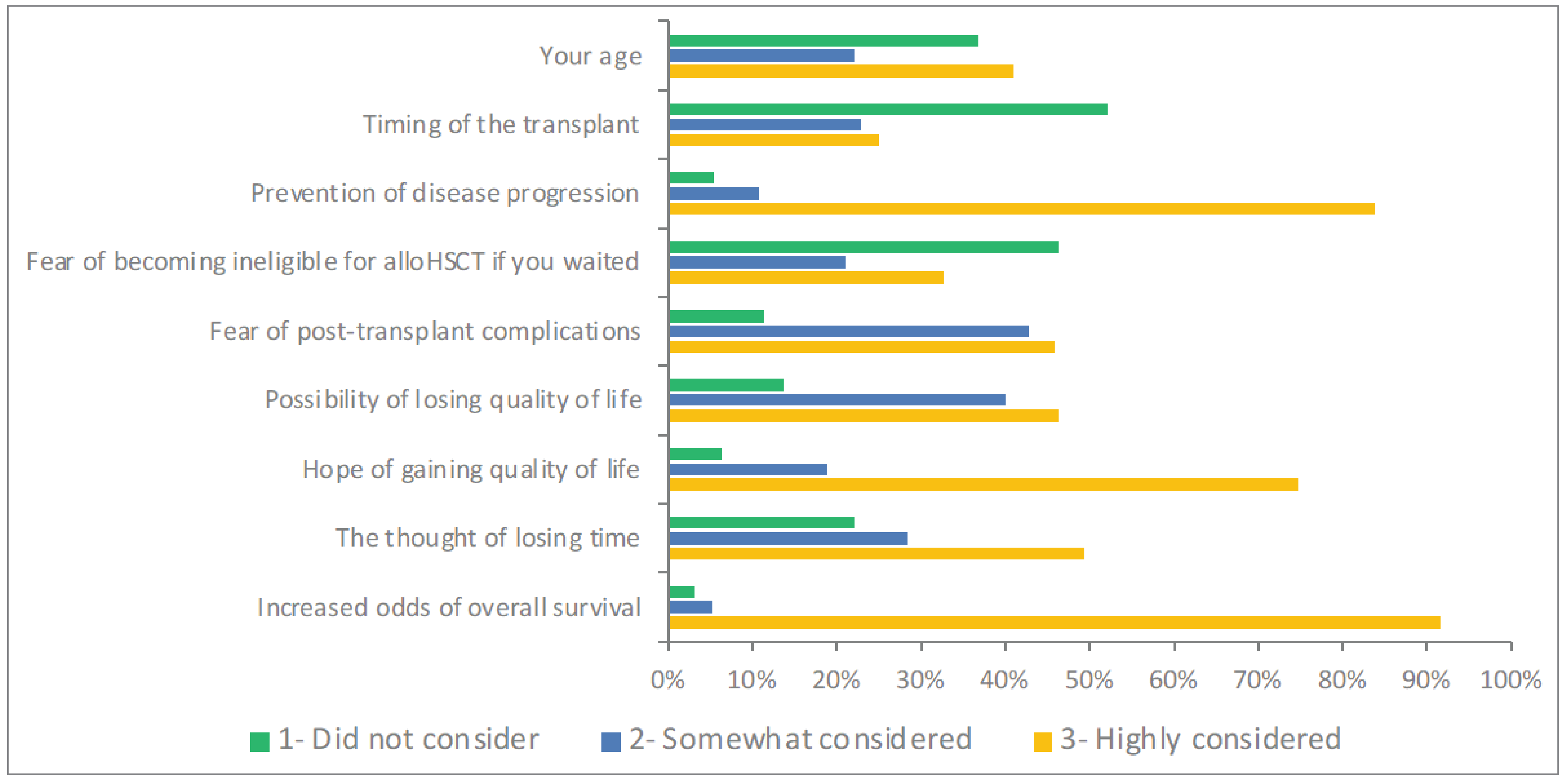
“Number one factor - I wasn’t ready to die and knew that would happen within a certain time frame as my dad had MDS and only treatment for him at the time was regular blood transfusions and he passed within “time frame” doctor told me I would pass if didn’t have transplant and I was already getting regular blood transfusions alongside my chemo.”
“I was very young with a husband and 2 small children. I wanted to be around to watch my children grow up! After extensive reading and consultation with several doctors I understood that if the transplant worked, it would be the best chance for long term survival. I knew I was flipping a coin but decided to take the chance.”
In addition to survival, graft-rejection and graft failure, factors highly related to success and survival were top two concerns for patients and their families. There were closely followed by toxicities, Graft versus Host Disease and infections as the concerns that families were most concerned about when undergoing an allHSCT.
Figure 7: In Addition to Survival in General, What Post-Transplant Were You Most Concerned About When Considering alloHSCT?
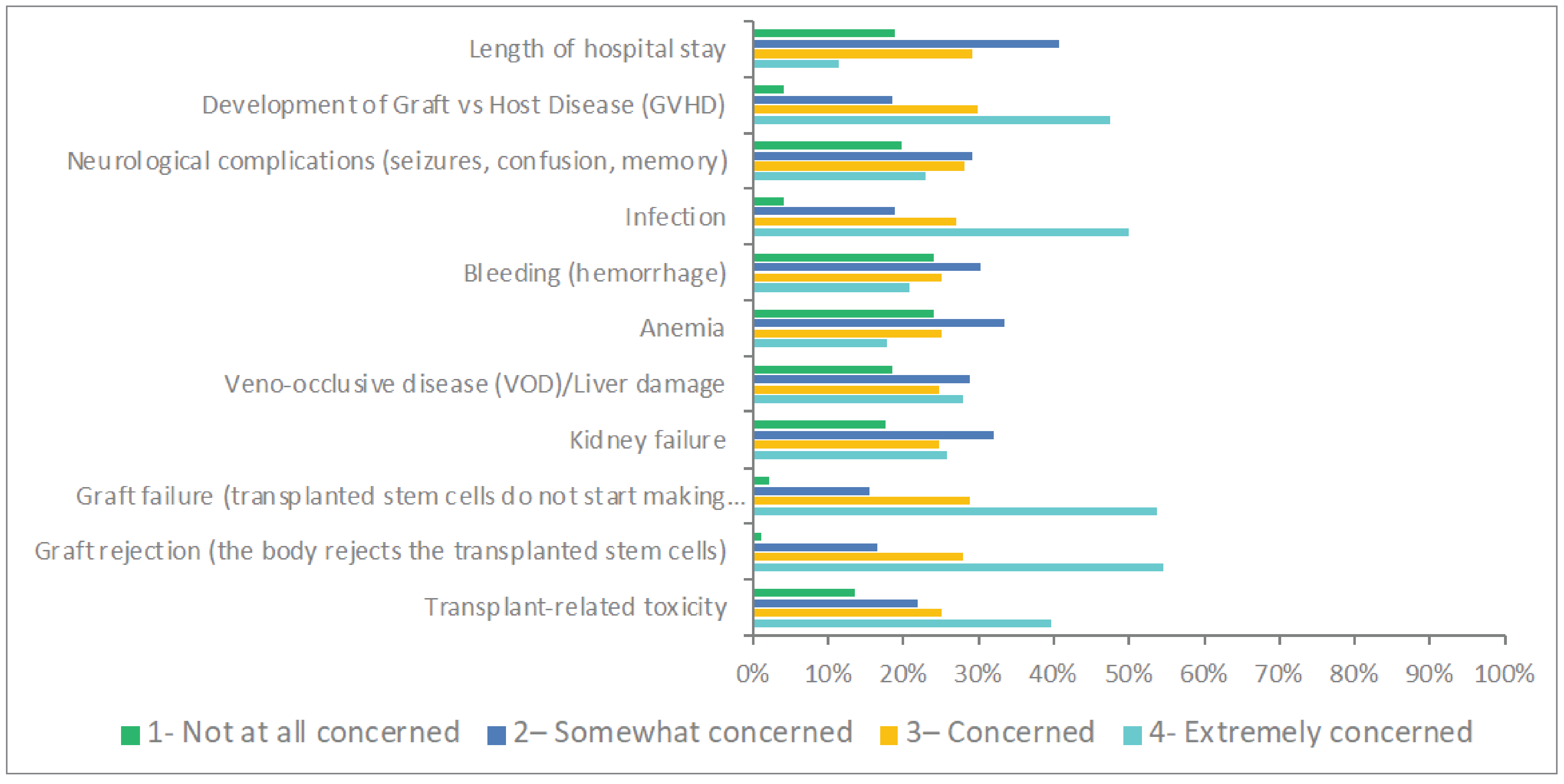
The risk of not surviving and the complications significantly negatively impact patient’s mental health.
“Our odds were 4% surviving the first 24 hours and that scared us the most.”
Treosulfan offers an option that can significantly improve survival and lower complications.
As mentioned above, patients do not have a choice of conditioning treatments. However, knowing that there is a potential and a chance for increased survivorship and less side effects, had significant positive impact on patient mental health.
When asked if there was a conditioning treatment that could reduce toxicity and minimize long term affects, 62% of respondents said that it would have an extremely positive impact on their anxiety, fear and stress. There is an even more significant positive impact when there is a potential for a survival benefit. 82% of respondents indicated that a conditioning treatment that could give them improved chances of survivorship had an extremely positive impact on their anxiety, fear and stress.
Figure 8: If There Was a Conditioning Treatment You Could Take Before alloHSCT That Could Reduce Toxicity and Minimize Long-Term Affects, How Would That Impact Your Levels of Anxiety/Fear/Stress Before Transplant?
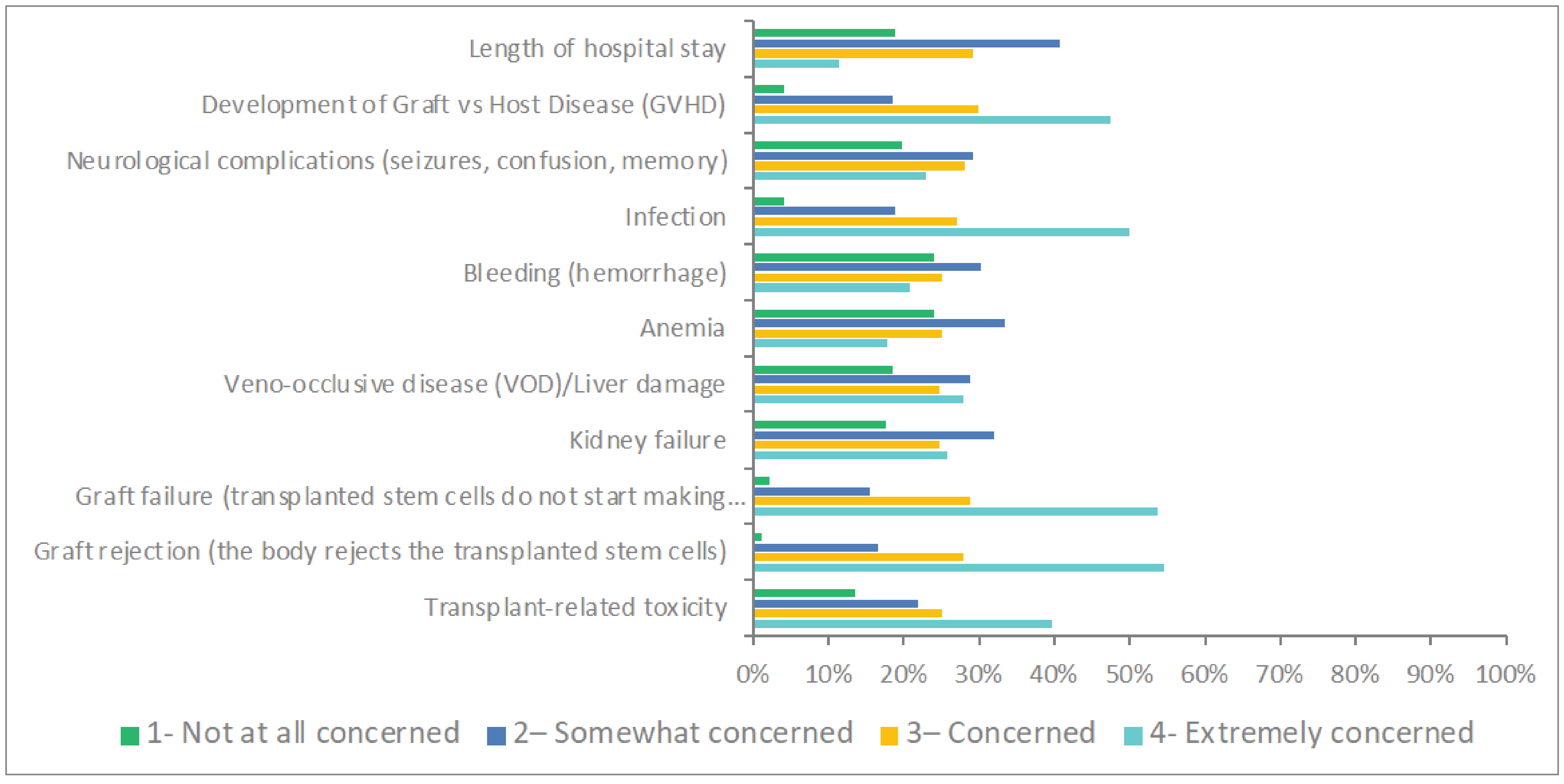
“Anything positive that could assist with treatment and long term affects of treatment would have helped overall facing the unknown and reducing stress or anxiety. You do not know what you will face until it happens. When you don't have many choices, you do what you have to do. There is plenty of worries, any reduction in those worries is beneficial.”
“Complete and thorough explanations keeping in mind people diagnosed are in shock and not always hearing or understanding what is going on and what is required. Time and patience with the patient so they fully understand what the road ahead will/could be, even an unwanted outcome, it is better knowing all possible outcomes and what is required every step of the way.”
“Having another party to speak to about what was going on afterward might have helped to ally some fears and concerns.”
“Don’t push the procedure if it’s not going to happen. It was pushed so hardcore that I thought if I didn’t get it I was going to die”
Figure 9: If There Was a Conditioning Treatment You Could Take That Could Increase Your Survivorship Odds after alloHSCT by, How Would That Impact Your Outlook and Decision-Making Going Into the Transplant Process?
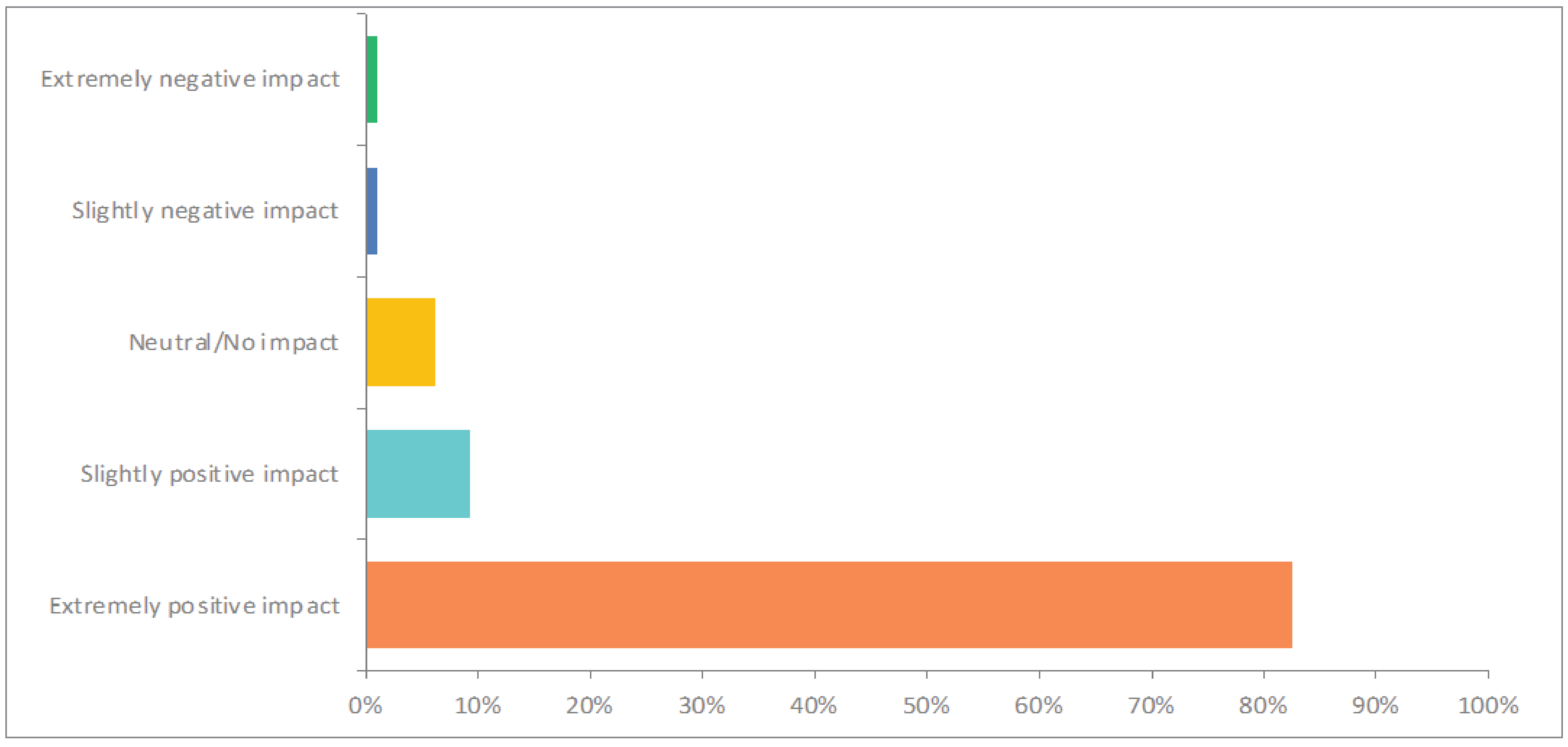
Improved Outcomes and Experience With Drug Under Review
An AML or MDS diagnosis brings considerable stress and anxiety to families. As one respondent said, “Being diagnosed with AML was the worst day of my life.” The decision to undergo a stem cell transplant carries an additional mental burden. The risk of dying and complications weigh heavily in the decision to undergo the procedure. Treosulfan is an option that can address both issues. It is the standard of care for MDS at Princess Margaret Hospital for MDS patients. They found that it is better tolerated than busulfan and reduced length of stay in hospital and readmission rates. Both these factors offset the additional cost of treosulfan over busulfan. Importantly though, they were able to demonstrate significant improvement of OS with treosulfan.
LLSC encourages CADTH to consider the ethical considerations of treatment. Our healthcare system has an ethical responsibility to equitably offer superior, less toxic treatment options if they exist and to make them accessible for patients and their families. This is especially significant for the pediatric population where we need to offer options with reduced toxicities to help minimize long term and lifelong side effects.
Some centres are able to get access, but MDS and AML are not postal code diseases. All Canadians of all ages, deserve equitable access to treatment and an equal chance at survivorship.
Companion Diagnostic Test
Not applicable.
Conflict of Interest Declaration — The Leukemia & Lymphoma Society of Canada
To maintain the objectivity and credibility of the CADTH reimbursement review process, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This Patient Group Conflict of Interest Declaration is required for participation. Declarations made do not negate or preclude the use of the patient group input. CADTH may contact your group with further questions, as needed.
Did you receive help from outside your patient group to complete this submission?
No.
Did you receive help from outside your patient group to collect or analyze data used in this submission?
No.
List any companies or organizations that have provided your group with financial payment over the past 2 years AND who may have direct or indirect interest in the drug under review.
Table 1: Financial Disclosures for The Leukemia & Lymphoma Society of Canada
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
No COI | — | — | — | — |
Clinician Input
Ontario Health Cancer Care Ontario Complex Malignant Hematology Advisory Committee
About Ontario Health Cancer Care Ontario Complex Malignant Hematology Advisory Committee
The Ontario Health (Cancer Care Ontario) Complex Malignant Hematology Program provides oversight on the planning, access, funding, and quality initiatives to support the delivery of stem cell transplant (SCT), immune effector cell therapies (IEC) and treatment of acute leukemia in Ontario. The Program works with physicians and health care administration from across Ontario to advise on the Program’s operations and initiatives, this includes the provision of feedback on emerging therapy options and implementation of these therapies.
Information Gathering
Information was gathered via videoconferencing and email.
Current Treatments and Treatment Goals
Allogeneic transplant is a key potentially curative therapy for patients with AML or MDS, which represent the commonest indications for this type of transplant. This treatment can be potentially very toxic, short and long term, and may result in significant morbidity and mortality even if the underlying disease is cured. AML and MDS are seen with increased frequency in older adults. Young, fit patients are eligible for myeloablative conditioning, but this type of conditioning is too risky in older adults or those with comorbidities. Thus, these types of patients are often prescribed less intensive conditioning, termed reduced intensity conditioning (RIC). Despite the use of RIC, which is associated with lower non-relapse mortality (NRM) compared with myeloablative conditioning, older or more comorbid adults still have significant rates of NRM and other toxicities which result in poor outcomes.
Treatment Gaps (Unmet Needs)
Considering the treatment goals, please describe goals (needs) that are not being met by currently available treatments.
Despite the use of RIC conditioning for allogeneic transplants in older and/or comorbid adults, there is still a significant rate of NRM and toxicity that impairs the outcome of the transplant. Rates of NRM may be as high as 50%. Busulfan based conditioning may also result in liver toxicity and seizures.
Place in Therapy
How would the drug under review fit into the current treatment paradigm?
In clinical development, treosulfan has pharmacological benefits compared to busulfan in terms of its mechanism of action which appears to be associated with a lower risk of liver toxicities and seizures.
In the pivotal phase III study, the use of treosulfan-based conditioning in patients with MDS and AML who could not receive myeloablative conditioning resulted in an improved overall and event-free survival, and significantly lower rates of NRM compared with busulfan-based conditioning. There were also fewer graft failures seen with treosulfan-based conditioning.
We are also aware of a retrospective case-control matched study done in Canada, which also showed a reduction in transplant-related mortality (TRM) and improvement in overall survival, relapse-free survival and lower rates of graft-versus-host disease in those patients who were given a treosulfan-based conditioning protocol Pasic, I., Mats R., et al. Excellent transplant outcomes with fludarabine-treosulfan (FT) reduced-toxicity conditioning (RTC) in combination with dual T-cell depletion (TCD) in myeloablative conditioning (MAC)-ineligible patients with myelodysplastic syndrome (MDS). Leuk Res 128: 107131 (2023). DOI: 10.1016/j.leukres.2023.107131).
Allogeneic transplants are typically a single episode of treatment; thus, the vast majority of patients would have not had allogeneic transplants previously.
Which patients would be best suited for treatment with the drug under review? Which patients would be least suitable for treatment with the drug under review?
Eligibility criteria would be best aligned with the pivotal phase III study. Best suited patients would be those with AML or MDS who are ineligible for myeloablative conditioning based on age and/or comorbidities. The study had an upper age limit of 70 years but in clinical practice those over 70 would be considered for potential allogeneic stem cell transplant using RIC protocol. Thus, there should be no upper age exclusion. In the Health Canada monograph, there are no specific details regarding age and/or comorbidity index score. Least suitable would be those patients who are eligible for myeloablative conditioning.
What outcomes are used to determine whether a patient is responding to treatment in clinical practice? How often should treatment response be assessed?
Standard outcomes in measuring response/survival in MDS or AML. GVHD is also measured using standard scoring systems.
What factors should be considered when deciding to discontinue treatment with the drug under review?
As treosulfan is given for 3 days during conditioning, there is no need usually to consider discontinuation during the course of administration. Theoretically perhaps only for a significant infusion reaction or hypersensitivity, which would be rare. Any toxicity issues that may be related to the conditioning would be seen later in the course of the allogeneic transplant.
What settings are appropriate for treatment with [drug under review]? Is a specialist required to diagnose, treat, and monitor patients who might receive [drug under review]?
This would be given in specialized centers performing allogeneic transplants.
Additional Information
Treosulfan has been reviewed for the same indication in the UK. They gave it a positive review, and they also found it to be cost-effective based on the submitted list price to the UK: https://www.nice.org.uk/guidance/ta640/chapter/3-Committee-discussion.
Conflict of Interest Declarations — Ontario Health Cancer Care Ontario Complex Malignant Hematology Advisory Committee
To maintain the objectivity and credibility of the CADTH drug review programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This conflict of interest declaration is required for participation. Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please refer to the Procedures for CADTH Drug Reimbursement Reviews (section 6.3) for further details.
Did you receive help from outside your clinician group to complete this submission? If yes, please detail the help and who provided it.
OH-CCO provided secretariat function to the group.
Did you receive help from outside your clinician group to collect or analyze any information used in this submission?
No.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review. Please note that this is required for each clinician who contributed to the input.
Declaration for Clinician 1
Name: Dr. Tom Kouroukis
Position: Lead, Ontario Health (CCO) Hematology Cancer Drug Advisory Committee
Date: 27-07-2023
Table 2: COI Declaration for Ontario Health (CCO) Complex Malignant Hematology Advisory Committee — Clinician 1
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
No COI | — | — | — | — |
Declaration for Clinician 2
Name: Dr. Chris Bredeson
Position: Lead, Ontario Health (CCO) Complex Malignant Hematology Advisory Committee
Date: 27-07-2023
Table 3: COI Declaration for Ontario Health (CCO) Complex Malignant Hematology Advisory Committee — Clinician 2
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
No COI | — | — | — | — |
Cell Therapy Transplant Canada
About Cell Therapy Transplant Canada
Cell Therapy Transplant Canada (CTTC; www.cttcanada.org) is a member-led, national, multidisciplinary organization providing leadership and promoting excellence in patient care, research, and education in the field of hematopoietic stem cell transplant and cell therapy. CTTC advocates, nationally and internationally, for improving the outcomes and accessibility of cellular therapies and transplantation for Canadians. Representation in CTTC includes physicians, nursing, laboratory and allied health professionals, along with an active family and caregiver group.
Information Gathering
Information was gathered through literature review, discussion and approved by two CTTC committees – the CTTC Board of Directors, and the CTTC standing committee of program directors, with representation from all 22 allogeneic stem cell transplant programs across Canada. This report was approved by both committees.
Current Treatments and Treatment Goals
Allogeneic hematopoietic cell transplantation (HCT) represents the only curative option for many patients with hematological malignancies. Acute myeloid leukemia (AML) and myelodysplastic syndrome (MDS) represent the two most common indications for allogeneic HCT in adults, with 67.5% of all transplants being offered for these conditions combined.1 Of all patients transplanted for AML or MDS, 46.1% receive myeloablative conditioning (MAC), while 53.9% of patients are ineligible for MAC based on advanced age or high hematopoietic cell transplant comorbidity index (HCT-CI) and receive reduced-intensity conditioning (RIC)1,2 The most commonly used RIC regimens involve total body irradiation (TBI) combined with chemotherapy (43%), fludarabine-melphalan (37%) and fludarabine-busulfan (18%).1 The use of RIC in older and comorbid patients is associated with lower non-relapse mortality (NRM) and better transplant outcomes overall.
For children and adolescents, it is of particular importance to reduce transplant-associated toxicities, in particular long-term toxicities, as patients have decades to live. With contemporary regimens more that 70% of children with cancer will develop at least one chronic physical health condition, 42% of which will develop a severe, life-threatening or disabling condition or die from a chronic condition.3 For children and adolescents with acute AML/MDS, myeloablative regimens are recommended to maximize the anti-leukemic effect.4 The majority of current standard of care conditioning regimens for children with AML/MDS are myeloablative, busulfan-based protocols. To reduce toxicities and to allow patients that are too sick to tolerate a busulfan-based regimen or who receive a second HSCT, treosulfan-based regimens have been successfully used in children. Given the favorable toxicity profile while maintaining myeloablative and immune suppressive properties, the use of treosulfan may be preferable to reduce pulmonary or neurocognitive toxicities, as examples, and to minimize non-relapse mortality (NRM).5,6
Treosulfan has a long track record of use in conditioning regimens for children and adolescents with non-malignant diseases These patients may be young at the time of transplant (e.g. severe combined immunodeficiency) or have comorbidities related to their disease and its treatment (e.g. thalassemia with chronic transfusions). Typically, TBI is avoided altogether for such conditions, and busulfan toxicities may be considered unacceptable due to neurotoxicity, sinusoidal obstruction syndrome and gonadal toxicity, as examples. Again, minimizing treatment-related mortality (TRM) is highly desirable- especially for non-malignant conditions and to reduce late complications of therapy such as infertility.7-9
References
Bolon YT, Atshan R, Allbee-Johnson M, Estrada-Merly N, Lee SJ. Current use and outcome of hematopoietic stem cell transplantation: CIBMTR summary slides, 2022.
Bacigalupo, A. et al. Defining the Intensity of Conditioning Regimens: Working Definitions. Biol Blood Marrow Tr 15, 1628–1633 (2009).
Oeffinger, KC et al. Chronic health conditions in adult survivors of childhood cancer. N Engl J Med, 2006 Oct 12;355(15):1572-82)
K. Tarlock et al. Hematopoietic Cell Transplantation in the Treatment of Pediatric Acute Myelogenous Leukemia and Myelodysplastic Syndromes: Guidelines from the American Society of Transplantation and Cellular Therapy. Transplant Cell Ther. 2022 Sep;28(9):530-545.doi: 10.1016/j.jtct.2022.06.005. Epub 2022 Jun 16
Nemecek ER, Hilger RA, Adams A, et al. Treosulfan, fludarabine, and low-dose total body irradiation for children and young adults with acute myeloid leukemia or myelodysplastic syndrome undergoing allogeneic hematopoietic cell transplantation: prospective phase II trial of the Pediatric Blood and Marrow Transplant Consortium. Biol Blood Marrow Transplant. 24, 1651-1656 (2018).
Boztug, Sykora KW, Slatter M, et al. European Society for Blood and Marrow Transplantation analysis of treosulfan conditioning before hematopoietic stem cell transplantation in children and adolescents with hematologic malignancies. Pediatr Blood Cancer 63, 139-48 (2016).
Slatter M, Gennery A. Treosulfan-based conditioning for inborn errors of immunity. Ther Adv Hematol 12, 20406207211013985 (2021).
Slatter M, Rao K, Hamid IJA, et al. Treosulfan and fludarabine conditioning for hematopoietic stem cell transplantation in children with primary immunodeficiency: UK experience. Biol Blood Marrow Transplant 24, 529-536 (2018).
Bernardo ME, Piras E, Vacca A, et al. Allogeneic hematopoietic stem cell transplantation in thalassemia major: results of a reduced-toxicity conditioning regimen based on the use of treosulfan.
Treatment Gaps (Unmet Needs)
Considering the treatment goals, please describe goals (needs) that are not being met by currently available treatments.
A recent study done on behalf of the Center for International Blood and Marrow Transplant Research (CIBMTR) reported that the number and proportion of allogeneic HCT performed in adults >70 increased rapidly in the past decade, with patients >70 representing only 0.1% of transplants in 2000 compared to 3.85% of transplants in 2013.1 AML and MDS represented the two most common indications for allogeneic HCT in this group, accounting for 76% of all transplants.1 Despite the use of RIC, allotransplantation of older individuals remains associated with unacceptably high rates of TRM. In a recent large single-center Canadian study of 332 patients with hematological malignancies, of whom 69% had AML or MDS, TRM was reported to significantly increase with patient age, with 2-y TRM of 25% among patients 60-65, 36% for patients 65-70 and 52% for individuals >70.2 This suggests that over half of patients >70 are lost due to transplant-related complications. In another Canadian study of 159 patients transplanted for high-risk AML or MDS, TRM at 2-y was reported to be as high as 38% for individuals age >55.3 Therefore, there remains a large gap in the need to deliver allogeneic HCT more safely to older patients with AML or MDS.
As treosulfan-based conditioning prior to allogeneic transplantation has been shown to have myeloablative, and antineoplastic effects associated with reduced NRM in adults, Kalwak et al. conducted a prospective phase II study to evaluated treosulfan based conditioning in pediatric patients with hematological malignancies. Sixty-five children with ALL (35.4%), AML (44.6%), MDS (15.4%), or juvenile myelomonocytic leukemia (4.6%) received treosulfan intravenously at a dose of 10 g/m2/day (7.7%), 12 g/m2/day (35.4%), or 14 g/m2/day (56.9%) in combination with fludarabine and thiotepa. At 36 months, NRM was only 3.1%, while a relapse incidence of 21.7%. The data confirmed that treosulfan based conditioning is safe and effective in pediatric patients with hematological malignancies.4,5 Based on these and other clinical data, the European Commission recently approved treosulfan for conditioning in pediatric patients older than 1 month with malignant diseases.6
In non-malignant conditions, the use of treosulfan in an effort to minimize TRM in patients is considered standard in many European countries due to the best published results with its use.7-9 For some non-malignant conditions, the comparatively favourable side effect profile of treosulfan makes the use of this drug preferable to busulfan to minimize acute and long-term toxicities of therapy.8,10
References
Muffly, L. et al. Increasing use of allogeneic hematopoietic cell transplantation in patients aged 70 years and older in the United States. Blood 130, 1156–1164 (2017).
Al-Shaibani, E. et al. Impact of age on hospitalization and outcomes post allogeneic hematopoietic cell transplantation outcome, a single center experience. Ann Hematol 102, 917–926 (2023).
Alanazi, W. et al. Post-Transplant Cyclophosphamide Combined with Anti-Thymocyte Globulin as Graft-versus-Host Disease Prophylaxis for Allogeneic Hematopoietic Cell Transplantation in High-Risk Acute Myeloid Leukemia and Myelodysplastic Syndrome. Acta Haematol-basel 144, 66–73 (2021).
Kalwak K, Mielcarek M, Patrick K, et al. Treosulfan-fludarabine-thiotepa-based conditioning treatment before allogeneic hematopoietic stem cell transplantation for pediatric patients with hematological malignancies. Bone Marrow Transplant. Oct;55(10):1996-2007 (2020).
Boztug, Sykora KW, Slatter M, et al. European Society for Blood and Marrow Transplantation analysis of treosulfan conditioning before hematopoietic stem cell transplantation in children and adolescents with hematologic malignancies. Pediatr Blood Cancer 63, 139-48 (2016).
European Medicines Agency. Union register of medicinal products marketing authorisation. Decision number (2019)4858 of 20 Jun 2019. 2019. https://ec.europa.eu/health/documents/community-register/html/h1351.htm
Slatter M, Gennery A. Treosulfan-based conditioning for inborn errors of immunity. Ther Adv Hematol 12, 20406207211013985 (2021).
Slatter M, Rao K, Hamid IJA, et al. Treosulfan and fludarabine conditioning for hematopoietic stem cell transplantation in children with primary immunodeficiency: UK experience. Biol Blood Marrow Transplant 24, 529-536 (2018).
Bernardo ME, Piras E, Vacca A, et al. Allogeneic hematopoietic stem cell transplantation in thalassemia major: results of a reduced-toxicity conditioning regimen based on the use of treosulfan.
Faraci M, Diesch T, Labopin M, et al. Gonadal function after busulfan compared with treosulfan in children and adolescents undergoing allogeneic hematopoietic stem cell transplant. Biol Blood Marrow Transplant 25, 1786-1791 (2019).
Place in Therapy
How would the drug under review fit into the current treatment paradigm?
Treosulfan has emerged as an alternative to busulfan as part of RIC chemotherapy in allotransplantation of patients with MDS or AML ineligible for MAC. Compared to busulfan-based conditioning, treosulfan-based conditioning is associated with improved survival and lower TRM in this group of patients.
In contrast to busulfan, which is a direct alkylating agent, treosulfan is a pro-drug which requires pH- and temperature-dependent non-enzymatic activation which occurs under physiologic conditions.1 While its myelosuppressive properties are similar to busulfan, it is more immunosuppressive than busulfan due to its more potent lymphodepleting activity and reduced activation of pro-inflammatory cytokines such as IL-2.1 Reports suggest that treosulfan is associated with lower risk of liver toxicity, sinusoidal obstruction syndrome/veno-occlusive disease (SOS/VOD), pneumonitis, hemorrhagic cystitis and seizures compared to busulfan.1
A number of early-phase studies support the use of treosulfan in conditioning of patients with AML or MDS. A study of 45 patients transplanted for MDS using fludarabine-treosulfan (FT) conditioning reported excellent 2-y overall survival (OS) of 71% and low 2-y TRM of 17%.2 Another study of 96 patients transplanted for AML or MDS using FT in combination with total body irradiation (TBI), reported 2-y OS of 73% and TRM of 8%.3 In a study of 118 patients with hematological malignancies and non-malignant disorders, of whom 42% had AML or MDS, allotransplantation with FT conditioning was associated with a very low rate of TRM of 11.9% at 1-y.4 SOS/VOD was reported in only one individual and hemorrhagic cystitis in two patients.4 In a randomized controlled trial (RCT) comparing conditioning with FT alone and FT in combination with TBI in a cohort of 100 patients with AML or MDS, the 1-y OS was 80% in the TBI arm vs. 69% in the non-TBI arm (not significant) and the 1-y TRM was only 9% in both arms.5 The largest retrospective study of treosulfan-based conditioning was published recently on behalf of the European Society for Blood and Marrow Transplantation (EBMT), where the outcome of 367 patients with MDS transplanted using FT was compared to outcomes of 687 patients with MDS transplanted using other standard RIC regimens and 668 patients transplanted using MAC.6 In multivariate analysis, using standard RIC as the reference, FT was associated with similar rate of TRM (hazard ratio [HR] 0.88, 95% confidence interval [CI]: 0.67-1.15), while MAC was associated with increased risk of TRM (HR 1.44, 95% CI: 1.15-1.80). Furthermore, FT was associated with lower rate of relapse (HR 0.55, 95% CI: 0.42-0.73) and improved OS (HR 0.72, 95% CI: 0.59-0.88), compared to reference. Together, these findings suggested that FT was able to deliver similar anti-disease intensity as MAC, while retaining similar level of toxicity as RIC, translating into improved patient outcomes overall.
The strongest evidence supporting conditioning with treosulfan comes from a well-designed phase III RCT which compared transplant outcomes between patients who received conditioning with FT to those who received conditioning with fludarabine-busulfan (FB) in a cohort of individuals with MDS and AML ineligible for MAC on the basis of age >50, HCT-CI>2, or both.7,8 Of the enrolled patients, 283 patients received FB and 268 received FT. The groups were well-matched with respect to major baseline characteristics. The primary outcome measure was event-free survival (EFS). At 3-y, EFS was 59.5% for patients who received FT compared to 49.7% for those who received FB (P=0.0000001 for testing non-inferiority of treosulfan compared to busulfan, P=0.0005787 for testing superiority of treosulfan compared to busulfan). Similarly, 3-y OS was 66.8% for patients who received FT compared to 56.3% for those who received FB (P=0.037). The FT and FB groups had similar rates of relapse at 3-y: 25.9% vs 26.0% (P=0.2631). TRM at 3-y was lower among patients who received FT compared to those who received FB: 14.2% vs. 21.0% (P=0.0343). Taken together, these data demonstrate that FT-based conditioning is associated with lower TRM and improved EFS and OS in AML and MDS patients who are ineligible for MAC on the basis of age and/or comorbidities.
A recently published Canadian study.9 compared transplant outcomes among MDS patients who received FT to a propensity-score matched cohort who received conditioning with fludarabine, busulfan and 200-cGy of total body irradiation (FB2T200). The groups were well matched with respect to most baseline and transplant characteristics. Patients who received FT had superior 1-y OS, relapse-free survival (RFS), graft-vs-host disease- and relapse-free survival (GRFS), and transplant related mortality compared to those who received FB2T200: 83.2% vs 53.2% (P = 0.003), 76.1% vs 42.7% (P = 0.005), 72.4% vs 37.9% (P = 0.003) and 8.6% vs 33.0% (P = 0.01).
Taken together, the described phase III RCT as well as the multiple retrospective studies, including the recent Canadian study, suggest that treosulfan-based conditioning is associated with lower TRM and improved transplant outcomes overall among AML and MDS patients who are ineligible for MAC on the basis of age and/or comorbidities. As such, CTTC believes that there is sufficient evidence that treosulfan-based conditioning may bridge the above-described gap in the need to deliver allogeneic HCT more safely to older patients with AML or MDS.
There are two common treosulfan dosing regimens. The so-called ‘low dose treosulfan’ is given at 10 g/m2 daily for three days (total dose 30 g/m2), while the ‘high dose treosulfan’ is given at 14 g/m2 daily for three days (total dose 42 g/m2). Both dosing regimens have been used with success in the early-phase studies described above.2-6 The phase III RCT7-8 used only the lower dose (30 g/m2). In the recently published Canadian study, both 30 g/m2 and 42 g/m2 were used, with the choice of dosing based on patient age and fitness. Both doses were well tolerated, including fit subjects age ≥70 who tolerated 42 g/m2 with no difficulties.
In children and adolescents, treosulfan is already widely used in most Canadian HCT centres [Dr. Schultz, Dr. Cuvelier, Dr. Wall and Dr. Guilcher, personal communication10]. Its use in patients with AML/MDS is often considered for very young children, children and adolescents with comorbidities, patients who require a second HCT and as standard of care in children with various non-malignant blood disorders.10-16 With decades of experience in Europe, treosulfan is considered a standard component of many pediatric conditioning regimens in European nations. As is often the case in pediatric HCT, most data are limited to Phase 2 clinical trials, case series and registry-based analysis due to the smaller number of transplants in children and adolescents compared to adults.
References
Danylesko, I., Shimoni, A. & Nagler, A. Treosulfan-based conditioning before hematopoietic SCT: more than a BU look-alike. Bone Marrow Transpl 47, 5–14 (2012).
Ruutu, T. et al. Reduced-toxicity conditioning with treosulfan and fludarabine in allogeneic hematopoietic stem cell transplantation for myelodysplastic syndromes: final results of an international prospective phase II trial. Haematologica 96, 1344–1350 (2011).
Gyurkocza, B. et al. Treosulfan, Fludarabine, and 2-Gy Total Body Irradiation Followed by Allogeneic Hematopoietic Cell Transplantation in Patients with Myelodysplastic Syndrome and Acute Myeloid Leukemia. Biol Blood Marrow Tr 20, 549–555 (2014).
Remberger, M. et al. Toxicological effects of fludarabine and treosulfan conditioning before allogeneic stem-cell transplantation. Int J Hematol 106, 471–475 (2017).
Deeg, H. J. et al. Transplant Conditioning with Treosulfan/Fludarabine with or without Total Body Irradiation: A Randomized Phase II Trial in Patients with Myelodysplastic Syndrome and Acute Myeloid Leukemia. Biol Blood Marrow Tr 24, 956–963 (2018).
Shimoni, A. et al. Allogeneic hematopoietic cell transplantation in patients with myelodysplastic syndrome using treosulfan based compared to other reduced‐intensity or myeloablative conditioning regimens. A report of the chronic malignancies working party of the EBMT. Brit J Haematol 195, 417–428 (2021).
Beelen, D. W. et al. Treosulfan or busulfan plus fludarabine as conditioning treatment before allogeneic haemopoietic stem cell transplantation for older patients with acute myeloid leukaemia or myelodysplastic syndrome (MC-FludT.14/L): a randomised, non-inferiority, phase 3 trial. Lancet Haematol 7, e28–e39 (2020).
Beelen, D. W. et al. Treosulfan compared with reduced‐intensity busulfan improves allogeneic hematopoietic cell transplantation outcomes of older acute myeloid leukemia and myelodysplastic syndrome patients: Final analysis of a prospective randomized trial. Am J Hematol 97, 1023–1034 (2022).
Pasic, I. et al. O18 Excellent transplant outcomes with fludarabine-treosulfan (FT) reduced-toxicity conditioning (RTC) in combination with dual T-cell depletion (TCD) in myeloablative conditioning (MAC)-ineligible patients with myelodysplastic syndrome (MDS). Leuk. Res. 128, 107131 (2023).
Ali et al., Effect of different conditioning regimens on survival and engraftment for children with hemophagocytic lymphohistiocytosis undergoing allogeneic hematopoeitic stem cell transplantation: A single institution experience. Pediatr Blood Cancer 2020 Sep;67(9).
Peters C, Dalle JH, Locatelli F, et al. Total body irradiation or chemotherapy conditioning in childhood ALL: a multinational, randomized, noninferiority phase III study. J Clin Oncol 39, 295-307 (2021).
Peters C, Poetschger U, Dalle JH, et al. Relapse is the most common treatment failure post-HSCT in children with ALL below 4 years of age given a chemo-based conditioning regimen. Results from the prospective multinational forum-trial. Blood 140, 897-899 (2022).
Boztug, Sykora KW, Slatter M, et al. European Society for Blood and Marrow Transplantation analysis of treosulfan conditioning before hematopoietic stem cell transplantation in children and adolescents with hematologic malignancies. Pediatr Blood Cancer 63, 139-48 (2016).
Slatter M, Gennery A. Treosulfan-based conditioning for inborn errors of immunity. Ther Adv Hematol 12, 20406207211013985 (2021).
Slatter M, Rao K, Hamid IJA, et al. Treosulfan and fludarabine conditioning for hematopoietic stem cell transplantation in children with primary immunodeficiency: UK experience. Biol Blood Marrow Transplant 24, 529-536 (2018).
Bernardo ME, Piras E, Vacca A, et al. Allogeneic hematopoietic stem cell transplantation in thalassemia major: results of a reduced-toxicity conditioning regimen based on the use of treosulfan.
Which patients would be best suited for treatment with the drug under review? Which patients would be least suitable for treatment with the drug under review?
Adult patients undergoing allogeneic HCT for AML or MDS who are ineligible for MAC on the basis of age and/or comorbidities would be best suited to receive treosulfan-based conditioning, as per the inclusion criteria of the described phase III RCT.1,2 Both dosing regimens (30 g/m2 and 42 g/m2) should be permitted with the choice of dosing being based on patient age and fitness. Patients undergoing allogeneic HCT for AML or MDS who are eligible for MAC would be least suitable to receive treosulfan-based conditioning, as they were excluded from the phase III RCT.1,2
Children with acute leukemia/MDS under the age of 4 years, children and adolescents with comorbidities and those with non-malignant indications for HCT (e.g. thalassemia, inborn errors of immunity) would be best suited.3-8 Additionally, patients without a suitable matched-related or unrelated donor and who are eligible for haploidentical HCT with ex vivo T cell depletion might be excellent candidates.9-10 Children and adolescents with acute lymphoblastic leukemia who can tolerate myeloablative TBI-dosing would be least suitable.3,5
References
Beelen, D. W. et al. Treosulfan or busulfan plus fludarabine as conditioning treatment before allogeneic haemopoietic stem cell transplantation for older patients with acute myeloid leukaemia or myelodysplastic syndrome (MC-FludT.14/L): a randomised, non-inferiority, phase 3 trial. Lancet Haematol 7, e28–e39 (2020).
Beelen, D. W. et al. Treosulfan compared with reduced‐intensity busulfan improves allogeneic hematopoietic cell transplantation outcomes of older acute myeloid leukemia and myelodysplastic syndrome patients: Final analysis of a prospective randomized trial. Am J Hematol 97, 1023–1034 (2022).
Peters C, Dalle JH, Locatelli F, et al. Total body irradiation or chemotherapy conditioning in childhood ALL: a multinational, randomized, noninferiority phase III study. J Clin Oncol 39, 295-307 (2021).
Peters C, Poetschger U, Dalle JH, et al. Relapse is the most common treatment failure post-HSCT in children with ALL below 4 years of age given a chemo-based conditioning regimen. Results from the prospective multinational forum-trial. Blood 140, 897-899 (2022).
Boztug, Sykora KW, Slatter M, et al. European Society for Blood and Marrow Transplantation analysis of treosulfan conditioning before hematopoietic stem cell transplantation in children and adolescents with hematologic malignancies. Pediatr Blood Cancer 63, 139-48 (2016).
Slatter M, Gennery A. Treosulfan-based conditioning for inborn errors of immunity. Ther Adv Hematol 12, 20406207211013985 (2021).
Slatter M, Rao K, Hamid IJA, et al. Treosulfan and fludarabine conditioning for hematopoietic stem cell transplantation in children with primary immunodeficiency: UK experience. Biol Blood Marrow Transplant 24, 529-536 (2018).
Bernardo ME, Piras E, Vacca A, et al. Allogeneic hematopoietic stem cell transplantation in thalassemia major: results of a reduced-toxicity conditioning regimen based on the use of treosulfan.
Shah RM, Elfeky R, Nademi Z, et al. T-cell receptor αβ and CD19 cell-depleted haploidentical and mismatched hematopoietic stem cell transplantation in primary immune deficiency. J Allergy Clin Immunology 141, 1417-1426 (2018).
Foell J, Kleinschmidt K, Jakob M, Troeger A, Corbacioglu S. Alternative donor: αβ/CD19 T-cell-depleted haploidentical hematopoietic stem cell transplantation for sickle cell disease. Hematol Oncol Stem Cell Ther 13, 98-105 (2020).
What outcomes are used to determine whether a patient is responding to treatment in clinical practice? How often should treatment response be assessed?
Since treosulfan is given for a finite duration (e.g. 3 days in total) as part of conditioning ahead of allogeneic HCT for AML or MDS, there is typically no response assessment to the drug during this time. Outcomes of transplants with treosulfan-based conditioning will, however, be assessed (and compared to other forms of conditioning) using the standard outcome measures in allogeneic HCT literature including: OS (typically reported at 2-y), TRM (typically reported at 100-d and 2-y), relapse (typically reported at 2-y), RFS (typically reported at 2-y), cumulative incidence of acute GVHD (typically reported at 100-d), cumulative incidence of chronic GVHD (typically reported at 2-y) and GRFS (typically reported at 2-y).1,2
For children and adolescents who undergo HCT, in addition to the aforementioned standard outcome measures, disease-specific outcomes defining cure are often used. For example, in inborn errors of immunity, the cell line(s) affected by the genetic disorder should be replaced in sufficient number and function such that normal immune function is achieved. Similarly, for hemoglobinopathies, the phenotype should be corrected by donor-derived erythropoiesis. International and institutional standards exist.3-5
References
Park, S.-S. et al. Graft-versus-Host Disease–Free, Relapse-Free Survival after Allogeneic Stem Cell Transplantation for Myelodysplastic Syndrome. Biol. Blood Marrow Transplant. 25, 63–72 (2019).
Salas, M. Q. et al. Improving Safety and Outcomes After Allogeneic Hematopoietic Cell Transplantation: A Single-Center Experience. Transplant Cell Ther 28, 265.e1-265.e9 (2022).
Shenoy S, Angelucci E, Arnold SD, et al. Current results and future research priorities in late effects after hematopoietic stem cell transplantation for children with sickle cell disease and thalassemia: a consensus statement from the Second Pediatric Blood and Marrow Transplant Consortium International Conference on Late Effects after Pediatric Hematopoietic Stem Cell Transplantation. Biol Blood Marrow Transplant 23, 552-561 (2017).
Kharfan-Dabaja MA, Kumar A, Ayala E, et al. Standardizing definitions of hematopoietic recovery, graft rejection, graft failure, poor graft function, and donor chimerism in allogeneic hematopoietic cell transplantation: a report on behalf of the American Society for Transplantation and Cellular Therapy. Transplant Cell Ther 27, 642-649 (2021).
Dietz AC, Duncan CN, Alter BP, et al. The Second Pediatric Blood and Marrow Transplant Consortium International Conference on Late Effects after Pediatric Hematopoietic Stem Cell Transplantation: defining the unique late effects of children undergoing hematopoietic cell transplantation for immune deficiencies, inherited marrow failure disorders, and hemoglobinopathies. Biol Blood Marrow Transplant 23, 24-29 (2017).
What factors should be considered when deciding to discontinue treatment with the drug under review?
Please refer to previous response. Since treosulfan is given for a finite duration (e.g. 3 days in total) as part of conditioning ahead of allogeneic HCT for AML or MDS, there is typically no response assessment to the drug during this time. Therefore, it is highly unlikely that the drug would be discontinued during this time. Furthermore, since treosulfan is a chemotherapeutic agent, most adverse effects (AE) will take place days after the administration of the drug has already taken place; it is therefore unlikely that the treatment with treosulfan would be discontinued due to AEs. The only, highly unlikely instance, where treatment with treosulfan may be discontinued would be if a patient developed severe hypersensitivity/allergic reaction to the drug.
What settings are appropriate for treatment with treosulfan? Is a specialist required to diagnose, treat, and monitor patients who might receive treosulfan?
This therapy should only be prescribed for this indication by specialists working in a clinical setting associated with allogeneic HCT programs. In general, these are in cancer centers associated with tertiary care hospitals in Canada.
Additional Information
The availability of a Health Canada approved and provincially funded treosulfan-based conditioning for MAC-ineligible patients with AML or MDS would be an important step forward for our community. There is a significant unmet need in transplantation of this patient group, with existing busulfan-based therapies being associated with higher rates of toxicity and inferior transplant outcomes overall. The completion of a randomized control trial for this indication was a large step forward for our community and our patients. Many of us have experience using treosulfan-based conditioning in transplantation of AML and MDS patients, and real-world effectiveness appears similar to that in the clinical trial, with very low rates of toxicity. We feel strongly that this therapy should be readily available for our patients.
Conflict of Interest Declarations — Cell Therapy Transplant Canada
To maintain the objectivity and credibility of the CADTH drug review programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This conflict of interest declaration is required for participation. Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please refer to the Procedures for CADTH Drug Reimbursement Reviews (section 6.3) for further details.
Did you receive help from outside your clinician group to complete this submission?
No help from outside the clinician group was obtained.
Did you receive help from outside your clinician group to collect or analyze any information used in this submission?
No help from outside the clinician group was obtained.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review. Please note that this is required for each clinician who contributed to the input.
Declaration for Clinician 1
Name: Ivan Pasic
Position: Staff Physician, Princess Margaret Cancer Centre; Assistant Professor, University of Toronto
Date: 07-07-2023
Table 4: COI Declaration for Cell Therapy Transplant Canada — Clinician 1
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Medexus Pharmaceuticals | — | X | — | — |
Jazz Pharmaceuticals | — | X | — | — |
Declaration for Clinician 2
Name: Greg Guilcher
Position: Paediatric Oncologist, Alberta Children’s Hospital, Associate Professor, University of Calgary
Date: 10-07-2023
Table 5: COI Declaration for Cell Therapy Transplant Canada — Clinician 2
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
No COI | — | — | — | — |
Declaration for Clinician 3
Name: Jonas Mattsson
Position: Director, Messner Allogeneic Transplant Program, Princess Margaret Cancer Centre; Professor of Medicine, University of Toronto
Date: 12-07-2023
Table 6: COI Declaration for Cell Therapy Transplant Canada — Clinician 3
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Sanofi Canada | X | — | — | — |
Takeda Canada Inc. | X | — | — | — |
Jazz Pharmaceuticals Canada Inc. | X | — | — | — |
Medexus Pharmaceuticals Inc. | X | — | — | — |
Declaration for Clinician 4
Name: Kirk R Schultz
Position: Pediatric Haematologist Oncologist, BC Children’s Hospital; Professor of Pediatrics, University of British Columbia
Date: 13-07-2023
Table 7: COI Declaration for Cell Therapy Transplant Canada — Clinician 4
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
No COI | — | — | — | — |
Declaration for Clinician 5
Name: Christopher Bredeson
Position: Head, Malignant Hematology, Transplant and Cellular Therapy, The Ottawa Hospital; Professor, University of Ottawa
Date: 24-07-2023
Table 8: COI Declaration for Cell Therapy Transplant Canada — Clinician 5
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Kite/Gilead | X | — | — | — |
Novartis | X | — | — | — |
Allogene | — | X | — | — |
Declaration for Clinician 6
Name: Kevin Song
Position: Medical Director, Leukemia/BMT Program of British Columbia, University of British Columbia
Date: 24-07-2023
Table 9: COI Declaration for Cell Therapy Transplant Canada — Clinician 6
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Sanofi Canada | X | — | — | — |
Janssen | — | X | — | — |
Amgen | X | — | — | — |
Jazz Pharmaceuticals Canada Inc. | X | — | — | — |
Gilead Sciences Canada | X | — | — | — |
Declaration for Clinician 7
Name: Victor Lewis
Position: Director of Oncology and Blood and Marrow Transplant, Alberta Children’s Hospital Calgary
Date: 24-07-2023
Table 10: COI Declaration for Cell Therapy Transplant Canada — Clinician 7
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
No COI | — | — | — | — |
Declaration for Clinician 8
Name: Genevieve Gallagher
Position: Medical director, Programme de transplantation de cellules hématopoïétiques et de thérapie cellulaire du CHU de Québec — Université Laval
Date: 24-07-2023
Table 11: COI Declaration for Cell Therapy Transplant Canada — Clinician 8
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
No COI | — | — | — | — |
Declaration for Clinician 9
Name: Imran Ahmad
Position: Hematologist, Cellular Therapy & Transplantation Program Director, HMR, Université de Montréal
Date: 25-07-2023
Table 12: COI Declaration for Cell Therapy Transplant Canada — Clinician 9
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Novartis | — | X | — | — |
Medexus Pharma | X | — | — | — |
Abbvie | X | — | — | — |
Declaration for Clinician 10
Name: Wilson Lam
Position: Staff Physician, Hans Messner Allogeneic Blood and Marrow Transplant Program, Princess Margaret Cancer Centre; Assistant Professor, University of Toronto
Date: 25-07-2023
Table 13: COI Declaration for Cell Therapy Transplant Canada — Clinician 10
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
No COI | — | — | — | — |
Declaration for Clinician 11
Name: Joerg Krueger
Position: Staff Physician, The Hospital for Sick Children, Associate Professor, University of Toronto
Date: 28-Jul-2023
Table 14: COI Declaration for Cell Therapy Transplant Canada — Clinician 11
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Medexus | X | — | — | — |
Vertex | X | — | — | — |
Kite/Gilead | X | — | — | — |
Novartis | X | — | — | — |
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
Redactions: Confidential information in this document may be redacted at the request of the sponsor in accordance with the CADTH Drug Reimbursement Review Confidentiality Guidelines
Stakeholder Input: The views expressed in each submission are those of the submitting organization or individual; not necessarily the views of CADTH or of other organizations. As such, they are independent of CADTH and do not necessarily represent or reflect the view of CADTH. No endorsement by CADTH is intended or should be inferred. By filing with CADTH, the submitting organization or individual agrees to the full disclosure of the information. CADTH does not edit the content of the submissions.
CADTH does use reasonable care to prevent disclosure of personal information in posted material; however, it is ultimately the submitter’s responsibility to ensure no identifying personal information or personal health information is included in the submission. The name of the submitting organization or individual and all conflict of interest information are included in the submission; however, the name of the author, including the name of an individual patient or caregiver submitting the patient input, are not posted.
Accessibility: CADTH is committed to treating people with disabilities in a way that respects their dignity and independence, supports them in accessing material in a timely manner, and provides a robust feedback process to support continuous improvement. All materials prepared by CADTH are available in an accessible format. Where materials provided to CADTH by a submitting organization or individual are not available in an accessible format, CADTH will provide a summary document upon request. More details on CADTH’s accessibility policies can be found here.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.