CADTH Reimbursement Review
Trastuzumab deruxtecan (Enhertu)
Sponsor: AstraZeneca Canada Inc.
Therapeutic area: Unresectable or metastatic HER2-low breast cancer
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Stakeholder Input
Clinical Review
Abbreviations
AE
adverse event
ASC
American Society of Clinical Oncology
BIC
blinded independent central review
BC
breast cancer
CAP
College of American Pathologists
CBCN
Canadian Breast Cancer Network
CDK
cyclin-dependent kinase
CI
confidence interval
CNS
central nervous system
DAC
Drug Advisory Committee
DOR
duration of response
ECOG PS
European Cooperative Oncology Group Performance Status
EORTC QLQ-BR23
European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire breast cancer module
EORTC QLQ-BR45
European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire updated breast cancer module
EORTC QLQ-C30
European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30
EQ-5D-5L
5-Level EQ-5D
EQ VAS
EQ-5D Visual Analogue Scale
ET
endocrine therapy
FASfull
analysis set
HRQoL
health-related quality of life
HR
hormone receptor
IHC
immunohistochemistry
ILD
interstitial lung disease
ISH
in situ hybridization
ITC
indirect treatment comparison
IXRS
interactive voice/web response system
KM
Kaplan-Meier
MAIC
matching adjusted indirect comparison
mBC
metastatic breast cancer
MID
minimally important difference
mRECIST 1.1
modified Response Evaluation Criteria for Solid Tumours Version 1.1
NCCN
National Comprehensive Cancer Network
NMA
network meta-analysis
OH-CCO
Ontario Health–Cancer Care Ontario
ORR
objective response rate
OS
overall survival
PFS
progression-free survival
RECIST
Response Evaluation Criteria for Solid Tumours
Rethink
Rethink Breast Cancer
RCT
randomized controlled trial
SAE
serious adverse event
SD
standard deviation
TPC
treatment of physician’s choice
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Table 1: Background Information of Application Submitted for Review
Item | Description |
|---|---|
Information on drug submitted for review | |
Drug product | Trastuzumab deruxtecan (Enhertu),100 mg, powder for solution for IV infusion |
Sponsor | AstraZeneca Canada Inc. |
Indication | For the treatment of adult patients with unresectable or metastatic HER2-low (IHC 1+ or IHC 2+/ISH−) breast cancer who have received at least 1 prior line of chemotherapy in the metastatic setting or developed disease recurrence during or within 6 months of completing adjuvant chemotherapy; patients with HR-positive breast cancer should have received at least 1 and be no longer considered for endocrine therapy |
Reimbursement request | As per indication |
Health Canada approval status | NOC |
Health Canada review pathway | Type A Project Orbis and Priority Review |
NOC date | January 6, 2023 |
Recommended dosage | 5.4 mg/kg given as IV once every 3 weeks |
HR = hormone receptor; IHC = immunohistochemistry; ISH = in situ hybridization; NOC = Notice of Compliance.
Introduction
Breast cancer (BC) is the most common cancer affecting females in Canada. In 2022, 28,600 new cases and 5,500 cancer-related deaths due to BC in Canada were projected in women. Biological testing is standard for determining standard treatment alongside disease staging. BC was historically classified as HER2-positive or HER2-negative based on the evidence or absence of HER2 amplification and/or overexpression and/or amplification based on immunohistochemistry (IHC) or by in situ hybridization (ISH) or fluorescence in situ hybridization. HER2-negative BC was defined as IHC 0, 1+ or 2+ with a negative ISH result.1,2 Now, IHC scores of 1+, or 2+ with a negative ISH result are defined as HER2-low BC. In Canada, prevalence estimates of HER2-low BC show that hormone receptor (HR)-positive disease is predominant (89%) compared to HR-negative disease (11%). Patients who have been historically classified as HER2-negative and HR-positive are recommended to receive first-line endocrine therapy (ET) in combination with a cyclin-dependant kinase (CDK) 4/6 inhibitor, upon progression; if refractory to ET, single-drug chemotherapy is recommended. In patients who have been historically classified as HER2-negative and HR-negative, the standard of care is sequential single-drug chemotherapy, with the addition of pembrolizumab depending on programmed death ligand 1 status.
The objective of CADTH’s Clinical Review Report is to review and critically appraise the clinical evidence submitted by the sponsor of the beneficial and harmful effects of trastuzumab deruxtecan (5.4 mg/kg IV every 3 weeks) for the treatment of unresectable or metastatic HER2-low (IHC 1+ or IHC 2+/ISH−) BC. The target population consists of adult patients who have received at least 1 prior line of chemotherapy in the metastatic setting or developed disease recurrence during or within 6 months of completing adjuvant chemotherapy. Patients with HR-positive BC should have also received at least 1 ET and no longer be considered for further ET.
Stakeholder Perspectives
The information in this section is a summary of input provided by the patient and clinician groups who responded to CADTH’s call for input and from clinical experts consulted by CADTH for the purpose of this review.
Patient Input
Input from 2 patient groups, Rethink Breast Cancer (Rethink) and the Canadian Breast Cancer Network (CBCN), were summarized for this CADTH review. Input from Rethink was based on meetings with BC patients and the results from an online survey of 78 patients with metastatic breast cancer (mBC) in Canada. Input received from the CBCN was obtained via online surveys that collected data from 50 patients who reported being metastatic HER2-negative before a reclassification of HER2-low. Both patient groups highlighted that disease symptom burden due to metastasis negatively affects patient quality of life noting that the disease restricts patient employment and career progress, their ability to care for children and dependents, and their ability to be social and meaningfully participate in their community. Both groups highlighted the importance of treatments that control disease progression (extend life) and manage cancer-related symptoms (improve quality of life).
Clinician Input
Input From Clinical Experts Consulted by CADTH
Two clinical experts with experience treating mBC highlighted the current unmet need for targeted therapies in the HER2-low population. The clinical experts agreed that standard outcome measures of treatment response, duration of response (DOR), survival statistics, toxicities, and quality of life measures are aligned with the outcomes used in current DESTINY-Breast04 clinical trial. The clinical experts suggested that trastuzumab deruxtecan be prescribed in a hospital setting or a specialty clinic that has the expertise and staffing to administer chemotherapy and monitor and manage treatment-related toxicities. An expert pathologist who was also consulted for the review indicated that, with increased awareness and adequate training, Canadian pathologists and oncologists will be able to correctly identify HER2-low patients.
Clinician Group Input
Input from 1 clinician group, the Ontario Health–Cancer Care Ontario (OH-CCO) Breast Cancer Drug Advisory Committee (DAC), was summarized for this review. The clinician group agreed broadly with the clinical experts consulted for this review; namely, the need for targeted treatments that patients can tolerate. The DAC also highlighted the need for access to interstitial lung disease (ILD) monitoring, a safety issue associated with the use of trastuzumab deruxtecan, and access to experts who can manage ILD in patients treated with trastuzumab deruxtecan.
Drug Program Input
The drug programs provide input on each drug being reviewed through CADTH’s reimbursement review processes by identifying issues that may affect their ability to implement a recommendation. The drug plans identified implementation issues related to relevant comparators, considerations for initiation, generalizability, funding algorithm, care provision, system issues, and economic considerations. The clinical experts consulted by CADTH for this review weighed evidence from the included study and other clinical considerations to provide responses to the drug plan’s implementation questions.
Clinical Evidence
Pivotal Studies and Randomized Controlled Trial Evidence
Description of Studies
DESTINY-Breast04 was a randomized, double-arm, phase III, open-label, multicentre trial to compare the safety and efficacy of trastuzumab deruxtecan versus the treatment of physician’s choice (TPC) in patients with HER2-low, unresectable, and/or mBC. A total of 557 patients were randomized in a 2:1 ratio to receive open-label treatment with trastuzumab deruxtecan or TPC. Randomization was stratified by HER2 IHC status of tissue samples assessed by a central laboratory (HER2 IHC 1+ versus HER2 IHC 2+/ISH−), number of prior lines of chemotherapy (1 versus 2), HR/CDK status (HR-positive mBC with prior CDK 4/6 inhibitor treatment versus HR-positive mBC without prior CDK 4/6 inhibitor treatment versus HR-negative mBC). The primary objective was to compare the progression-free survival (PFS) benefit of trastuzumab deruxtecan to that of TPC in a cohort of patients with HER2-low, HR-positive mBC, based on a blinded independent central review (BICR). Key secondary objectives were the PFS benefit of trastuzumab deruxtecan compared with TPC in all randomized patients regardless of hormone-receptor status (i.e., the full analysis set [FAS]) based on a BICR, the overall survival (OS) benefit of trastuzumab deruxtecan compared to TPC in patients with HER2-low, HR-positive mBC, and the OS benefit of trastuzumab deruxtecan compared to TPC in the FAS. The mean age in both cohorts of the FAS was 56.5 (standard deviation [SD] = 10.58 in the trastuzumab deruxtecan arm and 11.51 in the TPC arm). A small proportion of patients, 6.4% in the FAS trastuzumab deruxtecan arm and 4.3% in the FAS TPC arm, had baseline central nervous system (CNS) metastasis.
Efficacy Results
Overall Survival
In the HR-positive cohort, the median OS in the trastuzumab deruxtecan arm was 23.9 months (95% confidence interval [CI], 20.8 to 24.8) while in the TPC arm it was 17.5 months (95% CI, 15.2 to 22.4; P = 0.0028). The estimated hazard ratio comparing patients exposed to trastuzumab deruxtecan to patients on TPC was 0.64 (95% CI, 0.48 to 0.86).
In the FAS, the median OS in the trastuzumab deruxtecan arm was 23.4 months (95% CI, 20.0 to 24.8) while in the TPC arm it was 16.8 months (95% CI, 14.5 to 20.0; P value = 0.0010). The hazard ratio was 0.64 (95% CI, 0.49 to 0.84).
Health-Related Quality of Life
Health-related quality of life (HRQoL) results were available for the HR-positive cohort. According to the global health status parameter of the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 (EORTC QLQ-C30), both treatment arms remained stable throughout the study. The mean baseline global health status was 36.26 (SD = 21.842) in the trastuzumab deruxtecan arm and 37.89 (SD = 22.511) in the TPC arm. Mean change from baseline was |||| |||||||| in the trastuzumab deruxtecan arm and |||| |||||||| in the TPC arm.
According to the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire updated breast cancer module (EORTC QLQ-BR45) (European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire breast cancer module [EORTC QLQ-BR23]), the mean baseline breast symptoms scores were ||||| |||||||| in the trastuzumab deruxtecan arm and ||||| |||||||| in the TPC arm, and the mean changes from baseline were ||||| |||||||| and ||||| |||||||| in the trastuzumab deruxtecan and TPC arms, respectively.
According to the 5-Level EQ-5D (EQ-5D-5L) questionnaire, the mean baseline index scores were ||||| |||||||| in the trastuzumab deruxtecan arm and ||||| |||||||| in the TPC arm. Mean changes from baseline to end of treatment were |||||| |||||||| and |||||| |||||||| in the trastuzumab deruxtecan and TPC arms, respectively.
Progression-Free Survival
In the HR-positive cohort, the median PFS in the trastuzumab deruxtecan arm was 10.1 months (95% CI, 9.5 to 11.5) while in the TPC arm it was 5.4 months (95% CI, 4.4 to 7.1; P < 0.0001). The hazard ratio was 0.51 (95% CI, 0.40 to 0.64).
In the FAS, the median PFS in the trastuzumab deruxtecan arm was 9.9 months (95% CI, 9.0 to 11.3) while in the TPC arm it was 5.1 months (95% CI, 4.2 to 6.8; P < 0.0001). The hazard ratio was 0.50 (95% CI, 0.40 to 0.63).
Objective Response Rate
The objective response rate (ORR) of the 331 patients who received trastuzumab deruxtecan in the HR-positive cohort was 52.9% (95% CI, 47.3 to 58.4), 3.6% of whom experienced complete responses, while the 163 patients in the HR-positive cohort who received TPC had an ORR of 16.6% (95% CI, 11.2 to 23.2), 0.6% of whom experienced complete responses. In the FAS, the ORR of the 373 patients who received trastuzumab deruxtecan was 52.3% (95% CI, 47.1 to 57.4), 3.5% of whom experienced complete responses, while the 184 patients who received TPC had an ORR of 16.3% (95% CI, 11.3 to 22.5), 1.1% of whom experienced complete responses.
Duration of Response
In the 176 patients who received trastuzumab deruxtecan in the HR-positive cohort and recorded a complete or partial response, the median DOR was 10.7 months (95% CI, 8.5 to 13.7), compared to 27 patients in the TPC arm, with a median response of 6.8 months (95% CI, 6.5 to 9.9). In the FAS, the 196 patients in the trastuzumab deruxtecan arm who recorded a complete or partial response experienced a median DOR of 10.7 (95% CI, 8.5 to 13.2), compared to 30 patients in the TPC arm, with a median response of 6.8 months (95% CI, 6.0 to 9.9).
Harms Results
In total, 99.5% of patients in the trastuzumab deruxtecan arm and 98.3% of patients in the TPC arm reported at least 1 adverse event (AE). Serious adverse events (SAEs) of any grade were reported in 27.8% of patients in the trastuzumab deruxtecan arm and 25% of patients in the TPC arm. AEs leading to treatment discontinuation were reported in 16.2% of patients receiving trastuzumab deruxtecan and 8.1% in the TPC arm. Overall, 39.9% of patients in the trastuzumab deruxtecan arm and 51.2% of patients in the TPC arm had died by the January 11, 2022, data cut-off. The most common reasons leading to death in both arms were disease progression and AEs.
ILD and/or pneumonitis and left ventricular dysfunction were AEs of special interest and were more common in the trastuzumab deruxtecan arm (12.1% and 4.6%, respectively) compared to the TPC arm (0.6% and 0%, respectively).
Table 2: Summary of Key Results from Pivotal Studies and RCT Evidence
Result | Trastuzumab deruxtecan | Treatment of physician’s choice |
|---|---|---|
Overall survival, HR-positive cohorta | N = 331 | N = 163 |
Patients with event (death), n (%) | 126 (38.1) | 73 (44.8) |
Median overall survival, months (95% CI)b | 23.9 (20.8 to 24.8) | 17.5 (15.2 to 22.4) |
P valuec | 0.0028 | |
Hazard ratio (95% CI)d | 0.64 (0.48 to 0.86) | |
Overall survival, full analysis set | N = 373 | N = 184 |
Patients with event (death), n (%) | 149 (39.9) | 90 (48.9) |
Median overall survival, months (95% CI)b | 23.4 (20.0 to 24.8) | 16.8 (14.5 to 20.0) |
P valuec | 0.0010 | |
Hazard ratio (95% CI)d | 0.64 (0.49 to 0.84) | |
Health-related quality of life, HR-positive cohorte | N = 331 | N = 163 |
EORTC QLQ-C30 questionnaire | ||
Global health status/quality of life | ||
Mean at baseline (SD); n | 36.26 (21.842); 319 | 37.89 (22.511); 150 |
Mean change from baseline (SD); n | |||| ||||||||| ||| | |||| ||||||||| ||| |
Time to deterioration by ≥ 10 points, months (95% CI) | 11.4 (8.8 to 16.3) | 7.5 (5.9 to 9.5) |
Time to deterioration hazard ratio (95% CI) | 0.69 (0.52 to 0.92) | |
P valuef | 0.0096 | |
EORTC QLQ-BR45 (EORTC QLQ-BR23) questionnaire | ||
Breast symptoms | ||
Mean at baseline (SD); n | ||||| ||||||||| ||| | ||||| ||||||||| ||| |
Mean change from baseline (SD); n | ||||| ||||||||| ||| | ||||| ||||||||| ||| |
Time to deterioration by ≥ 10 points, median months (95% CI) | NE (24.7 to NE) | NE (NE to NE) |
Time to deterioration hazard ratio (95% CI) | 0.71 (0.50 to 1.01) | |
P valuef | 0.1008 | |
Arm symptoms | ||
Mean at baseline (SD); n | ||||| ||||||||| ||| | ||||| ||||||||| ||| |
Mean change from baseline (SD); n | ||||| ||||||||| ||| | |||| ||||||||| ||| |
Time to deterioration by ≥ 10 points, median months (95% CI) | 14.4 (11.9 to 23.0) | 8.7 (5.6 to NE) |
Time to deterioration hazard ratio (95% CI) | 0.62 (0.45 to 0.85) | |
P valuef | 0.0027 | |
EQ-5D-5L questionnaire | ||
Index | ||
Mean at baseline (SD); n | ||||| ||||||||| ||| | ||||| ||||||||| ||| |
Mean change from baseline (SD); n | |||||| ||||||||| ||| | |||||| ||||||||| ||| |
Visual Analogue Scale | ||
Mean at baseline (SD); n | |||| |||||||| ||| | |||| |||||||| ||| |
Mean change from baseline (SD); n | |||| |||||||| ||| | |||| |||||||| ||| |
Time to deterioration by ≥ 10 points, median months (95% CI) | 12.0 (9.9 to 15.2) | 6.8 (4.9 to 11.4) |
Time to deterioration hazard ratio (95% CI) | 0.73 (0.54 to 0.97) | |
P valuee | 0.0288 | |
Progression-free survival by BICR, HR-positive cohorta | N = 331 | N = 163 |
Patients with events, n (%) | 211 (63.7) | 110 (67.5) |
Median progression-free survival, months (95% CI)b | 10.1 (9.5 to 11.5) | 5.4 (4.4 to 7.1) |
P valueg | < 0.0001 | |
Hazard ratio (95% CI)d | 0.51 (0.40 to 0.64) | |
Progression-free survival based on BICR, full analysis set | N = 373 | N = 184 |
Patients with events, n (%) | 243 (65.1) | 127 (69.0) |
Median progression-free survival, months (95% CI)b | 9.9 (9.0 to 11.3) | 5.1 (4.2 to 6.8) |
P valueg | < 0.0001 | |
Hazard ratio (95% CI)d | 0.50 (0.40 to 0.63) | |
Confirmed objective response rate, HR-positive cohorta | N = 331 | N = 163 |
Based on BICR | ||
n (%) | 175 (52.9) | 27 (16.6) |
Response rate (95% CI)h | (47.3 to 58.4) | (11.2 to 23.2) |
P valuei | < 0.0001 | |
Confirmed objective response rate, full analysis set | N = 373 | N = 184 |
Based on BICR | ||
n (%) | 195 (52.3) | 30 (16.3) |
Response rate (95% CI)h | (47.1 to 57.4) | (11.3 to 22.5) |
P valuei | < 0.0001 | |
Duration of response, HR-positive cohorta | N = 331 | N = 163 |
Median duration of CR/PR (months) (95% CI)j | 10.7 (8.5 to 13.7) | 6.8 (6.5 to 9.9) |
Duration of response, full analysis set | N = 373 | N = 184 |
Median duration of CR/PR (months) (95% CI)j | 10.7 (8.5 to 13.2) | 6.8 (6.0 to 9.9) |
BICR = blinded independent central review; CDK = cyclin-dependent kinase; CI = confidence interval; CR = complete response; EORTC QLQ-BR23 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire breast cancer module; EORTC QLQ-BR45 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire updated breast cancer module; EORTC QLC-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; EQ-5D-5L = 5-Level EQ-5D; HR = hormone receptor; NE = not estimable; PR = partial response; RCT = randomized controlled trial; SD = standard deviation.
Note: Data cut-off: January 11, 2022.
aBased on HR-positive cohort: trastuzumab deruxtecan group N = 331 and treatment of physician’s choice group N = 163.
bMedian PFS or OS was from KM analysis. The CI for medians was computed using the Brookmeyer-Crowley method.
cTwo-sided P value from a stratified log-rank test, included in the hierarchical testing structure. The prespecified interim analysis efficacy stopping boundary was 0.00748 (information fraction 59.8%).
dHazard ratio and 95% CI from a stratified Cox proportional hazards model with stratification factors: HER2 status, number of prior lines of chemotherapy, and HR/CDK status as defined by an interactive web/voice response system.
eHRQoL data have been updated since publication of the DESTINY-Breast04 Clinical Study Report. Following a data check, an update was made to how the last assessment/deterioration was programmed. As such, these data are reflective of the time to definitive deterioration data.
fNot included in the hierarchical testing structure.
gTwo-sided P value from a stratified log-rank test, included in the hierarchical testing structure.
hBased on Clopper-Pearson method for single proportion and for the difference of 2 proportions with continuity correction.
iTwo-sided P value based on a Cochran-Mantel-Haenszel test adjusted for stratification factors: HER2 status, number of prior lines of chemotherapy, HR/CDK status as defined by an interactive web/voice response system. Not included in the hierarchical testing structure.
jMedian was from a Kaplan-Meier estimate. The CI for medians was computed using the Brookmeyer-Crowley method.
Source: DESTINY-Breast04 Clinical Study Report.3
Critical Appraisal
Patients in the DESTINY-Breast04 trial were randomized according to appropriately chosen stratification factors. Stratification was based on an interactive voice/web response system (IXRS) at the time of randomization, which differed from the electronic data capture, which corrected for mis-stratification at randomization. The overall number of patients who were mis-stratified with regard to HR status in the primary analysis was low and the impact on the conclusions of the trial was likely small. Primary and secondary end points were tested in a hierarchical sequence. OS analysis allowed for early stopping at the interim analysis. Early stopping rules preserve type I error rates of the OS significance test, but increase the possibility of overestimating the benefits. The open-label design may have resulted in an informative censoring mechanism in which certain patients exited the study before the first postbaseline tumour assessment. In the FAS analysis of PFS, 8.2% of patients in the TPC arm were censored due to the absence of a postbaseline tumour assessment, compared to only 0.8% in the trastuzumab deruxtecan arm. A post hoc sensitivity analysis was conducted to assess the impact of an alternative censoring strategy in which patients with no postbaseline tumour assessment are assumed to have not experienced a progression event until the end of the study. Results of this post hoc sensitivity analysis were consistent with those of the primary analysis.
The DESTINY-Breast04 study population was considered by the clinical experts consulted by CADTH to be representative and generalizable to the Canadian population. The investigated dose of trastuzumab deruxtecan was 5.4 mg/kg, IV, every 3 weeks, consistent with the expected Health Canada–approved dose. The clinical experts consulted for this report suggested that the basket of chemotherapies used for the TPC arm of the DESTINY-Breast04 study was appropriate and representative of Canadian practice.
Long-Term Extension Studies
No long-term extension studies were submitted as part of this review.
Indirect Comparisons
The sponsor provided a feasibility assessment for conducting an indirect treatment comparison (ITC) in the HR-negative population against the comparator sacituzumab govitecan. A network meta-analysis (NMA) was deemed infeasible due to the major differences in the clinical trial characteristics and small number of patients included. A matching adjusted indirect comparison (MAIC), while feasible, would likely produce biased and imprecise estimates due to the identified limitations.
Studies Addressing Gaps in the Pivotal and Randomized Controlled Trial Evidence
No studies addressing gaps were submitted as part of this review.
Conclusions
Evidence from the DESTINY-Breast04 trial showed statistically significant and clinically meaningful benefit in PFS and OS with trastuzumab deruxtecan 5.4 mg/kg every 3 weeks compared to TPC in patients with unresectable or metastatic HER2-low BC who have received at least 1 prior line of chemotherapy in the metastatic setting or who developed disease recurrence during or within 6 months of completing adjuvant chemotherapy. HRQoL was identified from patient input as a key end point important to patients. The evidence provided by the DESTINY-Breast04 study was not sufficient for drawing conclusions about HRQoL. An evidence gap remains for the relative efficacy comparison against sacituzumab govitecan in the HR-negative cohort of patients, although the cohort of patients for whom this comparison is relevant was small compared to the overall patient population. The clinical experts consulted for this review considered the safety profile of trastuzumab deruxtecan to be manageable and in line with their expectations.
Introduction
The objective of this report is to review and critically appraise the evidence submitted by the sponsor on the beneficial and harmful effects of trastuzumab deruxtecan, 100 mg, dosed at 5.4 mg/kg of body weight, administered by IV once every 3 weeks (21-day cycle) until disease progression or unacceptable toxicity.
Disease Background
The content of this section was informed by materials submitted by the sponsor and clinical expert input. The following have been summarized and validated by the CADTH review team.
BC is the most common cancer affecting females in Canada. In 2022, 28,600 new cases and 5,500 cancer-related deaths due to BC were projected in women according to the Canadian Cancer Statistics report.4 Among those assigned male at birth, 270 new cases and 55 cancer-related deaths were projected in the same year.4 Although BC is often detected at early stages (about 82% of cases in Canada are diagnosed at stage I and II5), 30% to 40% of patients diagnosed with early-stage and localized invasive disease progress to metastatic disease.6-9 Symptoms commonly associated with metastatic disease include pain, fatigue, cognitive difficulties, and insomnia. Metastatic disease imposes financial burdens and limitations on activities of daily life,10 and significantly affects patients’ quality of life.11
Biological marker testing (e.g., HER2 and HR status [i.e., progesterone receptor and estrogen receptor status, respectively]) is highly recommended at diagnosis in guidelines from the American Society of Clinical Oncology (ASCO) and College of American Pathologists (CAP) alongside disease staging, to facilitate treatment selection and disease management.12 Historically, BC was classified as either HER2-positive or HER2-negative based on the evidence for or absence of HER2 amplification and/or overexpression and/or amplification based on IHC, ISH, or fluorescence in situ hybridization. HER2-negative BC was defined as IHC 0, 1+, or IHC 2+ with a negative ISH result.1,2 Now, IHC scores of 1+ or 2+ with a negative ISH result are defined as HER2-low BC.
An estimated 80% to 85% of patients with BC are HER2-negative,1,2 of whom 50% are HER2-low.13,14 HER2-low distribution varies with HR-positive and HR-negative disease. In Canada, prevalence estimates of HER2-low BC show that HR-positive disease is predominant (89%) compared to HR-negative disease (11%).4,15 Among cancers previously classified as HER2-negative and HR-positive BC, about 65% can now be classified as HER2-low, whereas among those previously classified as HER2-negative and HR-negative, about 37% can be now be classified as HER2-low.15 Estimates from the Alberta Health Service Registry show that about ||||| of patients diagnosed with BC in Canada (excluding Quebec) are HER2-negative,16 of whom 80.8% would be considered HER2-negative and HR-positive and 19.2% HER2-negative and HR-negative.15 The OS of HER2-negative patients varies based on HR status. The median OS for stage IV HER2-negative, HR-positive disease is approximately 35 months and only about 9 months for patients with stage IV HER2-negative and HR-negative disease.17 Patient survival also appears to decrease significantly postprogression on first-line and second-line treatments; the median OS reported in this group of patients is only about 15 months and the PFS is about 4 months.18
Other diagnostic methods used for detecting BC include blood tests, tissue biopsies, genetic testing, and imaging techniques (bilateral diagnostic mammogram, bone scan and X-ray, PET and CT scans, or ultrasound).
Standards of Therapy
Contents within this section have been informed by materials submitted by the sponsor and clinical expert input. The following have been summarized and validated by the CADTH review team.
Metastatic BC remains an incurable disease. The main goal of treatment includes extending survival and delaying progression of disease with minimal toxicity, while maintaining or improving HRQoL.19,20 HER2-low has not been differentiated from tumours historically defined as HER2-negative; as such, patients with HER2-low tumours represent a subset of patients who would have historically been identified as HER2-negative, and current treatments align with those provided for patients with HER2-negative disease, which depends on the HR status of the tumour.
There are no Canada-specific guidelines for the treatment of BC. Oncologists in Canada typically follow guidance from international agencies, including the National Comprehensive Cancer Network (NCCN), ASCO, and the European Society of Medical Oncology. Guidelines for the management of HER2-negative mBC have been published by ASCO and NCCN for the US and by the European Society of Medical Oncology for Europe.21-25
Patients that have been historically classified as HER2-negative and HR-positive are recommended to receive first-line ET in combination with a CDK 4/6 inhibitor (palbociclib or ribociclib). Upon progression, and if the treating physician expects further benefit, additional lines of ET can be offered. If the treating physician does not expect further benefit from ET (i.e., refractory), single-drug chemotherapy is recommended.
In patients historically classified as HER2-negative and HR-negative the standard of care is sequential single-drug chemotherapy, with the addition of pembrolizumab, depending on programmed death ligand 1 status. Standard options used are taxanes, platinum drugs, capecitabine, gemcitabine, anthracyclines, eribulin, and vinorelbine. An optimal treatment sequence has not been determined, and the treatment sequence varies by jurisdiction in Canada.20 Recently, sacituzumab govitecan received a positive funding recommendation and has been approved for the treatment of adult patients with unresectable locally advanced or metastatic triple-negative BC who have received 2 or more prior therapies, with at least 1 for metastatic disease.20 However, sacituzumab govitecan is currently the subject of negotiations with the pan-Canadian Pharmaceutical Alliance and is not yet widely available.
Drug Under Review
Key characteristics of trastuzumab deruxtecan are summarized in Table 3, along with other treatments available for unresectable or metastatic HER2-low (IHC 1+ or IHC 2+/ISH−) BC.
Trastuzumab deruxtecan, dosed at 5.4 mg/kg of body weight, is administered by IV, once every 3 weeks (21-day cycle), until disease progression or unacceptable toxicity. The approved Health Canada indication is for the treatment of adult patients with unresectable or metastatic HER2-low (IHC 1+ or IHC 2+/ISH−) BC who have received at least 1 prior line of chemotherapy in the metastatic setting or developed disease recurrence during or within 6 months of completing adjuvant chemotherapy. Patients with HR-positive BC should have also received at least 1 prior line of ET and be no longer considered eligible for ET.
Trastuzumab deruxtecan is a HER2-targeted antibody-drug conjugate composed of a humanized anti-HER2 immunoglobin G1 monoclonal antibody and a topoisomerase I inhibitor conjugate. Trastuzumab deruxtecan binds to HER2 on tumour cells, undergoes internalization and intracellular linker cleavage by lysosomal enzymes that are upregulated in cancer cells, and inhibits the activity of topoisomerase I, thereby causing DNA damage and apoptotic cell death. Trastuzumab deruxtecan can cross the cellular membrane, killing neighbouring cells that may or may not express HER2 through a bystander effect.
Trastuzumab deruxtecan underwent a priority review via Project Orbis at Health Canada and received a Notice of Compliance on January 6, 2023. The sponsor’s reimbursement request aligns with the Health Canada indication.
Table 3: Key Characteristics of Trastuzumab Deruxtecan, Capecitabine, Eribulin, Gemcitabine, and Paclitaxel
Characteristic | Trastuzumab deruxtecan26 | Capecitabine27 | Eribulin28 | Gemcitabine29 | Paclitaxel30 |
|---|---|---|---|---|---|
Mechanism of action | An HER2-targeted antibody-drug conjugate composed of a linker and a topoisomerase I inhibitor; after binding to HER2 receptors on tumour cells, trastuzumab deruxtecan undergoes internalization and intracellular linker cleavage by lysosomal enzymes that are upregulated in cancer cells; upon release, the membrane-permeable topoisomerase I inhibitor causes DNA damage and apoptotic cell death | A tumour-activated antineoplastic antimetabolite in the novel fluoropyrimidine carbamate class; selectively activated to the cytotoxic moiety, 5-FU, by thymidine phosphorylase in tumours. 5-FU is further metabolized to 5-fluoro-2′-deoxyuridine monophosphate and 5-fluorouridine triphosphate, which cause cell injury by both DNA and RNA-derived mechanisms | A dynamics inhibitor of the growth phase of microtubules that does not affect the shortening phase; sequesters tubulin into nonproductive aggregates, exerting anticancer effects via a tubulin-based antimitotic mechanism leading to G2/M cell-cycle blockage, disruption of mitotic spindles, and, ultimately, apoptotic cell death after prolonged and irreversible mitotic blockage | A cell-cycle dependent oncolytic deoxycytidine analogue (difluoro-deoxycytidine) that is metabolized intracellularly to the active diphosphate and triphosphate nucleosides; the cytotoxic effects are exerted through dFdCDP-assisted incorporation of dFdCTP into DNA, resulting in inhibition of DNA synthesis and induction of apoptosis | An antimicrotubule drug that blocks cell replication in the late G2 and/or M phases of the cell cycle; it also produces unusual cytoskeletons characterized by discrete bundles or microtubules and the formation of abnormal spindle asters during mitosis |
Indicationa | For treatment of adults with unresectable or HER2-low (IHC 1+ or IHC 2+/ISH−) mBC who have received at least 1 prior line of chemotherapy in the metastatic setting or developed disease recurrence during or within 6 months of completing adjuvant chemotherapy; patients with HR-positive BC should have received at least 1 ET and be no longer eligible for ET | For treatment of advanced or mBC after failure of standard therapy, including a taxane unless therapy with a taxane is clinically contraindicated | For the treatment of patients with mBC who have previously received at least 2 chemotherapeutic regimens for the treatment of metastatic disease; prior therapy should have included an anthracycline and a taxane administered in either the adjuvant or metastatic setting | For treatment, in combination with paclitaxel, of patients with unresectable, locally recurrent, or mBC who have good performance status and have relapsed following adjuvant anthracycline-based chemotherapy | For second-line treatment of metastatic carcinoma of the breast after failure of standard therapy |
Route of administration | IV | Oral | IV | IV | IV |
Recommended dosage | 5.4 mg/kg, administered as an IV infusion once every 3 weeks (21-day cycle) until disease progression or unacceptable toxicity | 1,250 mg/m2 administered twice daily (morning and evening; equivalent to a total daily dose of 2,500 mg/m2) for 14 days followed by a 7-day rest period | 1.4 mg/m2 administered IV over 2 to 5 minutes on days 1 and 8 of a 21-day cycle | 175 mg/m2 on day 1 over approximately 3 hours as an IV infusion followed by a 30-minute, 1,250 mg/m2 infusion on days 1 and 8 of each 21-day cycle | 175 mg/m2 administered IV over 3 hours every 3 weeks |
Serious adverse effects or safety issues |
|
|
| Leucopenia, thrombocytopenia, and anemia, and acute shortness of breath |
|
Other | Do not replace trastuzumab deruxtecan with trastuzumab or trastuzumab emtansine | — | — | — | — |
5-fluorouracil 5-FU; BC = breast cancer; dFdCDP = difluoro-deoxycytidine metabolized intracellularly to active diphosphate; dFdCTP = difluoro-deoxycytidine metabolized intracellularly to active triphosphate; ET = endocrine therapy; IHC = immunohistochemistry; ISH = in situ hybridization; mBC = metastatic breast cancer.
aHealth Canada–approved indication.
Sources: Trastuzumab deruxtecan product monograph,26 capecitabine product monograph,27 eribulin product monograph,28 gemcitabine product monograph,29 and paclitaxel product monograph.30
Stakeholder Perspectives
Patient Group Input
This section was prepared by CADTH staff based on the input provided by patient groups. The full, original patient inputs received by CADTH have been included in the stakeholder section at the end of this report.
Input from 2 patient groups, Rethink and the CBCN, were summarized for this CADTH review. Rethink is a Canadian charity that educates, empowers, and advocates for system changes to improve the experience and outcomes of those with BC, focusing on historically underserved groups: people diagnosed at a younger age; those with mBC; and people systemically marginalized due to race, income, or other factors. The CBCN is a leading, patient-directed, national health charity committed to ensuring the best quality of care for all Canadians affected by BC through the promotion of information, education, and advocacy activities.
Input from Rethink was based on general observations and insights gathered through programming and meetings with BC patients and results from an online survey of 78 patients with mBC completed between September 2018 and April 2019, which documented the lived experience of patients and caregivers in Canada. Rethink also provided data from 2 patients in Canada and 1 patient living in the UK with HER2-low status receiving trastuzumab deruxtecan from a survey conducted in November 2022. Input received from the CBCN was obtained via online surveys (the CBCN’s 2017 Lived Experience Breast Cancer Patient Survey and the CBCN 2012 Metastatic Breast Cancer Patient and Caregiver Survey). No respondent in the CBCN survey had direct experience with trastuzumab deruxtecan. The CBCN collected survey data from 50 patients who reported being diagnosed with metastatic HER2-negative BC before the reclassification of HER2-negative into subgroups based on the presence of the HER2 gene, which includes HER2-low groups.
Both patient groups highlighted that disease symptom burden due to metastasis negatively affects patient quality of life. The Rethink group reported that younger patients with BC experience several challenges, experienced by younger patients with BC such as fertility or family-planning challenges, diagnosis during pregnancy, childcare, impact on relationships, body image, dating and sexuality, feeling isolated from peers who do not have cancer, career hiatuses, and financial insecurity. The CBCN group noted similar impacts of disease symptom and progression in mBC as the Rethink group, such as restrictions on patient employment and career, the ability to care for children and dependents, and the ability to be social and participate meaningfully in their community.
Regarding current treatment options available to patients with metastatic HER2-low disease who have progressed, the CBCN group noted that patients with metastatic HER2-low status have limited treatment line options as their disease progresses. Both groups generally expressed that patients diagnosed with mBC fear running out of treatment options (particularly patients with HER2-low metastatic disease, as there are limited lines of treatment), experience harsh side effects, and a have diminished quality of life. Rethink highlighted chemotherapy drugs such as eribulin, capecitabine, gemcitabine, nab-paclitaxel, and paclitaxel that are currently available to patients with HER2-low metastatic disease in Canada. Rethink noted that, although initial lines of therapy may provide a few months of PFS, survival decreases substantially with later lines of therapy.
Both groups emphasized the importance of treatments that control disease progression (extend life) and manage cancer-related symptoms (improve quality of life). Respondents in the CBCN survey noted that treatment effectiveness, the treatment’s ability to prolong life without sacrificing quality of life, side-effect management, cost, and treatment accessibility are important factors that influence their decisions when choosing treatments. Respondents in both groups expressed a willingness to tolerate toxicity-related effects and any impacts on their quality of life if the treatment could control their cancer.
Three respondents with HER2-low status interviewed by Rethink had experience with trastuzumab deruxtecan. The most common AEs noted by all 3 respondents were tiredness or fatigue and nausea. One of the 3 reported that “experiencing fatigue was worse than nausea.” Regarding stable disease or decrease in metastasis, both respondents interviewed in Canada reported stable disease or decreased metastasis following treatment with trastuzumab deruxtecan, while a third patient who lived in the UK and received trastuzumab deruxtecan via a clinical trial reported that they had stable disease for almost 1.5 years and had manageable side effects. The patient in the UK emphasized that fatigue and nausea were the most common events in the first couple of treatment cycles with trastuzumab deruxtecan. This patient also had sores and dry mouth, which eased off. The respondent reported experiencing a better quality of life, including freedom and the ability to work, while receiving trastuzumab deruxtecan.
Clinician Input
Input From Clinical Experts Consulted by CADTH
All CADTH review teams include at least 1 clinical specialist with expertise in the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). The following input was provided by 2 clinical specialists with expertise in the diagnosis and management of unresectable or mBC and 1 expert pathologist with experience in the diagnostic testing required for detections of HER2-low BC.
Unmet Needs
The clinical experts noted that, because no treatments are available for patients with HER2-low BC, these patients are treated as if they are HER2-negative. As such, there is an unmet need for treatments that target the HER2-low population. The expert explained that not all patients respond to available treatments and those that do respond will eventually progress. Patients who are HR-positive generally tolerate ETs; however, when they progress to chemotherapy, they experience increasing toxicities. The clinical experts noted that there is a need for therapies that are better tolerated by patients who progress in their disease.
Place in Therapy
The clinical experts suggested that trastuzumab deruxtecan would be used in alignment with the Health Canada indication and the design of the DESTINY-Breast04 trial. The clinical experts noted that most HR-positive patients would receive 1 to 2 lines of ET before receiving chemotherapy and then proceed to trastuzumab deruxtecan; however, if the treating physician anticipated that the patient would continue to benefit from ET, additional lines of ET could be offered. The clinical experts highlighted that the only time a patient with HR-positive BC would not receive ET in the first line is if the HR-positive signalling was low, mimicking an HR-negative status, or in a setting of visceral crisis. The clinical experts noted that, for patients with HR-negative disease, chemotherapy would be offered first, with trastuzumab deruxtecan offered as a second-line option. The clinical experts suggested that, for patients with HER2-low BC, trastuzumab deruxtecan may be preferred over sacituzumab govitecan in the second line, as the former is specifically targeted to the HER2 protein; however, there is no clear consensus on the sequencing of these drugs.
Patient Population
The clinical experts suggested that the patients most likely to benefit from treatment with trastuzumab deruxtecan would be those that meet the DESTINY-Breast04 study criteria. The clinical experts explained that patients suitable for treatment would be identified by the primary treating physician based on diagnosis, clinical examination (performance status), physician judgment about suitability of patient, and confirmation of clinical and/or radiographic disease progression after preceding lines of therapy. Given their advanced stage, an underdiagnosis is unlikely to occur. If it were to occur it would likely be a result of heterogeneity within tumours and receptor shift over time. The clinical experts noted that presymptomatic patients may undergo treatment to prevent cancer symptoms, or wait until they are more symptomatic to avoid treatment-related side effects but at the risk of fewer treatment options, adding that this is a clinical decision many patients and clinicians face in the real world. The clinical experts noted that there are no indicators that can be used to predict those most likely respond to trastuzumab deruxtecan; however, those who are HER2-negative (IHC 0) would not be expected to benefit.
Assessing the Response Treatment
The clinical experts reported that the outcomes used in the study were aligned with clinical practice. Responses are determined based on symptoms, laboratory markers, and radiographic scans, and tumour measurements, with scans usually performed at least every 3 months initially. Treatment is continued if the disease is either stable or responding radiographically according to Response Evaluation Criteria for Solid Tumours (RECIST) criteria. The clinical experts listed the following clinically meaningful responses:
improvement in OS and/or PFS, noting specifically at least a 2- to 3-month survival advantage
reduction in the frequency or severity of symptoms (e.g., pain, dyspnea)
improvement of organ function (bone, liver, lung)
stabilization and/or improvement of symptoms
maintenance or improvement of performance status
ability to maintain or increase activities of daily living
tumour radiographic response with either stabilization of disease or response by RECIST criteria.
Discontinuing Treatment
The clinical experts listed disease progression, intolerable toxicity (ILD in particular), organ function no longer meeting treatment parameters, and patient refusal as reasons for discontinuing treatment.
Prescribing Considerations
The clinical experts suggested that trastuzumab deruxtecan be prescribed in a hospital setting or a specialty clinic that has the expertise and staff to administer chemotherapy and monitor and manage treatment-related toxicities. Treatment should be prescribed only by certified medical oncologists or an associated team physicians with expertise in cancer therapies and toxicity management.
Additional Considerations
According to the clinical experts, the benefits seen in the DESTINY-Breast04 trial are meaningful and valuable, particularly because no other therapy has demonstrated this magnitude of survival benefit in the HER2-low patient population. Given the limited treatment options and poor prognosis in those with metastatic and advanced BC, this drug would have increased uptake. The clinical experts suggested that the documented benefits commensurate with patient values and the toxicities are predictable and manageable by medical oncologists.
Clinician Group Input
This section was prepared by CADTH staff based on the input provided by clinician groups. The full original clinician group inputs received by CADTH are included in the stakeholder section at the end of this report.
Input from 1 clinician group, the OH-CCO DAC, was summarized for this review. The DAC provides timely evidence-based clinical and health system guidance on drug-related issues in support of OH-CCO’s mandate, including the Provincial Drug Reimbursement Programs and the Systemic Treatment Program. The DAC recognized needs not met by currently available treatments. The DAC pointed out that not all patients respond to available treatments, patients become refractory to current treatment options, and there are no available treatments to reverse the course of disease, creating a need for treatments that patients can better tolerate. The DAC anticipated that trastuzumab deruxtecan, if approved for public funding, could shift the currently used chemotherapy options to later lines of therapy for HER2-low patients. The DAC noted that there may be issues related to pathologic testing of specimens and identification of HER2-low status, adding that, although HER2 testing is routinely performed for all newly diagnosed BC patients, identification of the HER2-low subset of patients will require careful review by pathologists who are experts in BC. The group noted that treatment will likely be discontinued upon disease progression or treatment-related toxicity. The DAC also anticipated a need for access to ILD monitoring, a safety issue associated with the use of trastuzumab deruxtecan, and access to experts who can manage ILD for patients treated with trastuzumab deruxtecan. The DAC input generally aligns with that of the clinical experts consulted during the CADTH review.
Drug Program Input
Drug programs provide input on each drug being reviewed through CADTH’s reimbursement review processes by identifying issues that may affect their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CADTH are summarized in Table 4.
Table 4: Summary of Drug Plan Input and Clinical Expert Responses
Drug program implementation questions | Clinical experts response |
|---|---|
Relevant comparators | |
The DESTINY-Breast04 phase III study used physician’s choice of chemotherapy, including capecitabine, eribulin, gemcitabine, paclitaxel, or nab-paclitaxel, for the standard arm. In some provinces, nab-paclitaxel is restricted to use in patients who develop a severe hypersensitivity reaction to taxanes or have a contraindication to the premedications used with taxanes. Eribulin may be restricted to patients who have previously received both a taxane and an anthracycline. The rest of the comparators from the trial are funded in all provinces, but the choice of chemotherapy regimen for subsequent lines depends on what was used as a first-line treatment for mBC, and usually involves a drug with a different mechanism or from a different class of drugs than that used in the first-line setting. HER2-negative, HR-positive mBC:
HER2-negative, HR-negative mBC:
| For consideration by pERC. |
Considerations for initiation of therapy | |
For historical cases, does a HER2-low status need to be reconfirmed by pathology or can previously reported IHC and ISH scores be used to determine eligibility? | Previously reported IHC and ISH scores can be used to determine HER2-low eligibility. |
In the DESTINY-Breast04 study, all patients must have had a recent tumour tissue sample after the most recent treatment regimen or agree to undergo a tissue biopsy before randomization. Is a recent tumour tissue sample required in real-world practice to determine eligibility for public funding? | It is common for retesting to occur when a patient transitions to metastatic disease, and HER2 status can change throughout the course of disease. However, a requirement for recent testing or testing following each line of therapy, as was the case in the DESTINY-Breast04 study, is not aligned with clinical practice. |
In the DESTINY-Breast04 study, patients must have been treated with at least 1 and at most 2 prior lines of chemotherapy in the recurrent or metastatic setting; if recurrence occurred within 6 months of (neo)adjuvant chemotherapy, (neo)adjuvant therapy would count as 1 line of chemotherapy. Is there a maximum number of previous lines of chemotherapy to determine eligibility for public funding? If there is a maximum number of previous lines of chemotherapy, should patients on active treatment be allowed to switch to trastuzumab deruxtecan due to the potential time-limited opportunity? | If the patient can tolerate the treatment, access to trastuzumab deruxtecan should not be limited by a maximum number of previous lines of chemotherapy. Additionally, once trastuzumab deruxtecan becomes readily available it is unlikely that patients would receive extended lines of chemotherapy before receiving trastuzumab deruxtecan. Patients should not switch from a treatment that is working to receive trastuzumab deruxtecan; however, if clinicians are faced with a choice between switching or access to trastuzumab deruxtecan, clinicians may choose to switch their patients to prevent loss of access to trastuzumab deruxtecan. |
In the DESTINY-Breast04 study patients who were HR-positive were eligible if considered refractory to ET, defined as having progressed on at least 1 ET and determined by the investigator that they would no longer benefit from further treatment with ET. Should the same definition be used to determine eligibility for public funding for HR-positive patients, or should all reasonable ETs be used in addition to receiving at least 1 line of chemotherapy before considering trastuzumab deruxtecan? | The definition used in the DESTINY-Breast04 trial is appropriate. Patients who are HR-positive must receive at least 1 line of ET. In the second and following lines of therapy, clinician judgment should be used to determine whether the patient is refractory. |
Pembrolizumab in combination with chemotherapy recently received a conditional positive pERC recommendation for first-line treatment of metastatic triple-negative BC. Some of these patients may also be HER2-low, and therefore may also be eligible for trastuzumab deruxtecan. PAG would like confirmation on whether BC patients previously classified as triple-negative, but are also HER2-low would be eligible for trastuzumab deruxtecan following first-line treatment with pembrolizumab in combination with chemotherapy. | Patients classified as having triple-negative BC but who are truly HER2-low and have received first-line pembrolizumab in combination with chemotherapy should be eligible for second-line treatment with trastuzumab deruxtecan. |
Generalizability | |
In the DESTINY-Breast04 study, only patients with an ECOG PS of 0 or 1 were eligible. Should patients with an ECOG PS > 1 be considered eligible for public funding? | In clinical practice, there will likely be patients who are borderline ECOG PS 1 to 2 who will be considered by clinicians to be suitable for trastuzumab deruxtecan. |
Funding algorithm (oncology only) | |
Clarification may be required on eligibility for drugs previously recommended by pERC for metastatic triple-negative BC (e.g., pembrolizumab, sacituzumab govitecan) as some of these patients may now be classified as HER2-low, HR-negative instead of triple-negative. An updated algorithm for mBC would help clarify eligibility for all available treatments and sequences. | For consideration by pERC. |
Care provision issues | |
Trastuzumab deruxtecan is another look-alike, sound-alike member of the trastuzumab group (e.g., trastuzumab emtansine, trastuzumab). There is concern with operational issues to ensure all these drugs do not get inadvertently mixed up. Trastuzumab deruxtecan has a “black box” warning for potential medication errors related to this. The drug vials should be stored refrigerated and further diluted in D5W bags only (not normal saline). The drug should be administered only with an infusion set made of polyolefin or polybutadiene with a 0.2 µm or 0.22 µm in-line polyethersulfone or polysulfone filter. After reconstitution, trastuzumab deruxtecan vials must be used immediately; vial sharing is therefore likely not feasible. As vials are only available in 100 mg strength and the trastuzumab deruxtecan uses weight-based dosing, some drug wastage is anticipated. Given the potentially large patient population for this indication, the magnitude of drug wastage may be significant. Larger treatment centres may be able to mitigate some drug wastage by coordinating treatment appointments for patients at similar times and/or standardized days. | For consideration by pERC. |
System and economic issues | |
Due to the potentially large patient population, a substantial budget impact is anticipated. | For consideration by pERC. |
BC = breast cancer; CDK = cyclin-dependent kinase; D5W = dextrose 5% in water; ECOG PS = European Cooperative Oncology Group Performance Status; ET = endocrine therapy; HR = hormone receptor; IHC = immunohistochemistry; ISH = in situ hybridization; mBC = metastatic breast cancer; PAG = provincial advisory group; pERC = pan-Canadian Oncology Drug Review Expert Review Committee.
Clinical Evidence
The objective of CADTH’s Clinical Review Report is to review and critically appraise the clinical evidence submitted by the sponsor of beneficial and harmful effects of trastuzumab deruxtecan (5.4 mg/kg every 3 weeks) for the treatment of unresectable or metastatic HER2-low (IHC 1+ or IHC 2+/ISH−) BC. The target population consists of adult patients who have received at least 1 prior line of chemotherapy in the metastatic setting or developed disease recurrence during or within 6 months of completing adjuvant chemotherapy, patients with HR-positive BC should have also received at least 1 ET and no longer be considered for further ET. The focus will be placed on comparing trastuzumab deruxtecan to relevant comparators and identifying gaps in the current evidence.
A summary of the clinical evidence included by the sponsor in the review of trastuzumab deruxtecan is presented in 2 sections, and CADTH’s critical appraisal of the evidence is included after each section. The first section, the systematic review, includes pivotal studies and randomized controlled trials (RCTs) that were selected according to the sponsor’s systematic review protocol. The second section includes a summary of the indirect evidence from the sponsor.
Included Studies
Clinical evidence from the following are included in the CADTH review and appraised in this document:
One pivotal study (RCT evidence)
One feasibility assessment for conducting an ITC.
Pivotal Studies and Randomized Controlled Trial Evidence
Contents within this section have been informed by materials submitted by the sponsor. The following have been summarized and validated by the CADTH review team.
Description of Studies
Characteristics of the included studies are summarized in Table 5.
DESTINY-Breast04 was a randomized, double-arm, phase III, open-label, multicentre trial to compare the safety and efficacy of trastuzumab deruxtecan versus TPC in patients with HER2-low, unresectable and/or mBC. The trial was initially designed to include only patients with HR-positive, HER2-low BC; however, after initial review of the DESTINY-Breast04 protocol by the FDA, a cohort of HR-negative, HER2-low patients was added given the high unmet need in the population with triple-negative BC (inclusive of HER2-low patients). Enrolment of HR-negative patients was capped at approximately 60 out of 540 patients (11.1%) to mimic the estimated proportion of patients with HR-negative disease in the general HER2-low population.
The primary objective was to compare the PFS benefit of trastuzumab deruxtecan to that of TPC in a cohort of patients with HER2-low, HR-positive mBC, based on a BICR. Key secondary objectives were to compare the PFS benefit of trastuzumab deruxtecan to that of TPC in all randomized patients regardless of hormone-receptor status (i.e., the FAS) based on a BICR, to compare the OS benefit of trastuzumab deruxtecan to that of TPC in patients with HER2-low HR-positive mBC, and to compare the OS benefit of trastuzumab deruxtecan to that of TPC in the FAS.
Table 5: Details of Pivotal Studies and RCT Evidence Identified by the Sponsor
Study detail | DESTINY-Breast04 |
|---|---|
Designs and populations | |
Study design | Phase III, multicentre, randomized, double-arm, open-label, active-controlled study |
Locations | Patients were enrolled and treated at 161 study sites in the following countries: US (27 study sites), Japan (18), France (16), China (15), Italy (13), Spain (12), Greece (8), Portugal (8), Republic of Korea (8), Israel (6), Switzerland (6), Austria (4), Belgium (4), Russia (3), Sweden (3), Taiwan (3), UK (3), Canada (2), and Hungary (2). |
Patient enrolment dates | Start date: December 21, 2018 End date: December 31, 2021 |
Randomized (N) | Randomized (N) = 557 Trastuzumab deruxtecan group = 373 Chemotherapy TPC = 184 |
Inclusion criteria |
|
Exclusion criteria | Patients with any of the following were disqualified from entering the study:
|
Drugs | |
Intervention | Trastuzumab deruxtecan, 5.4 mg/kg, IV injection, every 3 weeks |
Comparator(s) | Patients in the TPC arm were assigned to 1 of the following 5 treatment options:
For patients randomized to TPC, dose, regimen, administration, and dose modification followed the label approved in the country of drug administration or the NCCN guidelines; dose regimens according to NCCN guidelines detailed previously |
Study duration | |
Screening phase | 28 days |
Open-label treatment | Until progressive disease according to mRECIST 1.1, clinical progression, unacceptable toxicity, treatment delay of at least 28 days, withdrawal of consent by patient, physician decision, or death, whichever occurred first |
Follow-up phase | Every 3 months (± 14 days) from the date of the 40-day (± 7 days) follow-up assessments until death, withdrawal of consent, loss to follow-up, or study termination, whichever occurred first |
Outcomes | |
Primary end point | PFS based on BICR, in patients with HR-positive mBC; PFS was defined as the time from the date of randomization to the earliest date of the first objective documentation of radiographic disease progression via BICR according to mRECIST 1.1 or death due to any cause |
Secondary and exploratory end points | Secondary The key secondary efficacy end points were:
Other secondary efficacy end points included the following, for both the HR-positive cohort and the full analysis set:
Exploratory The exploratory efficacy end points included the following, for both the HR-positive cohort and the full analysis set:
Other
|
Publication status | |
Publications | Modi et al. (2022)31 Ueno et al. (2022)32 |
ADC = antibody-drug conjugate; ASCO-CAP = American Society of Clinical Oncology–College of American Pathologists; BC = breast cancer; BICR = blinded independent central review; BOR = best overall response; CBR = clinical benefit rate; CDK = cyclin-dependent kinase; CR = complete response; DCR = disease control rate; DOR = duration of response; ECOG PS = Eastern Cooperative Oncology Group Performance Status; EORTC QLQ-BR23 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire breast cancer module; EORTC QLQ-BR45 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire modified breast cancer module; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; ET = endocrine therapy; HR = hormone receptor; IHC = immunohistochemistry; ILD = interstitial lung disease; ISH = in situ hybridization; mBC = metastatic breast cancer; mRECIST 1.1 = modified Response Evaluation Criteria in Solid Tumours Version 1.1; NCCN = National Comprehensive Cancer Network; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; PFS2 = progression-free survival on the next line of therapy; PR = partial response; PR = partial response; RCT = randomized controlled trial; TPC = treatment of physician’s choice; TTR = time to response; ULN = upper limit of normal.
Note: Details from the table have been taken from the sponsor’s Summary of Clinical Evidence.
Source: DESTINY-Breast04 Clinical Study Report.3
Following screening, adult patients were enrolled from December 21, 2018, to December 31, 2021, and treated at 161 study sites, 2 of which were in Canada. A total of 557 patients were randomized in a 2:1 ratio to receive open-label treatment with trastuzumab deruxtecan or TPC. Randomization was stratified by HER2 IHC status of tissue samples assessed by a central laboratory (HER2 IHC 1+ versus HER2 IHC 2+/ISH−), number of prior lines of chemotherapy (1 versus 2), HR/CDK status (HR-positive mBC with prior CDK 4/6 inhibitor treatment versus HR-positive mBC without prior CDK 4/6 inhibitor treatment versus HR-negative mBC). The data cut-off for analyses was January 11, 2022.
Populations
Inclusion and Exclusion Criteria
Adult patients (18 years and older) with pathologically documented unresectable or mBC and a history of low HER2 expression according to the 2018 HER2 testing guidelines established by ASCO and CAP were eligible for the trial. Patients were excluded if they had received prior treatment with any drug identified as a TPC comparator in a metastatic setting or had a known contraindication to the treatment.
Interventions
Trastuzumab Deruxtecan Arm
Patients received trastuzumab deruxtecan dosed at 5.4 mg/kg of body weight, administered by IV, every 3 weeks (21-day cycle).
The initial dose of trastuzumab deruxtecan was calculated based on the patient’s body weight at screening. Dose recalculation was allowed at any point during the treatment if a patient’s weight changed by at least 10%.
Treatment of Physician’s Choice Arm
Patients received 1 of the following chemotherapy treatments under TPC, according to local or NCCN guidelines:
Capecitabine: 1,000 mg/m2 to 1,250 mg/m2, orally, twice daily on days 1 to 14; cycled every 21 days
Eribulin: 1.4 mg/m2, IV, on days 1 and 8; cycled every 21 days
Gemcitabine:
Option 1: 800 mg/m2 to 1,200 mg/m2, IV, on days 1 and 8; cycled every 21 days
Option 2: 800 mg/m2 to 1,200 mg/m2, IV, on days 1, 8, and 15; cycled every 28 days
Paclitaxel:
Option 1: 175 mg/m2, IV, on day 1; cycled every 21 days
Option 2: 80 mg/m2, IV, on day 1 weekly
Nab-paclitaxel:
Option 1: 260 mg/m2, IV, cycled every 21 days
Option 2: 100 mg/m2 or 125 mg/m2, IV, on days 1, 8, and 15; cycled every 28 days.
Patients received trastuzumab deruxtecan or any chemotherapy treatment under the TPC arm, until disease progression, unacceptable toxicity, treatment delay of at least 28 days, withdrawal of consent, physician decision, or death, whichever occurred first.
Dose adjustments (interruptions or modifications, delay, and discontinuations) to manage drug-related toxicities of trastuzumab deruxtecan based on prespecified recommendations were outlined in the study protocol. Dose increases were not allowed for trastuzumab deruxtecan. Two dose reductions were allowed in the study (starting dose: 5.4 mg/kg; dose level 1: 4.4 mg/kg; and dose level 2: 3.2 mg/kg). Once a dose reduction due to toxicity was implemented for trastuzumab deruxtecan, all subsequent treatment cycles were administered at the lower dose, unless further dose reductions were required. A patient was permanently discontinued from the study drug if toxicity continued after 2 dose reductions. No dose re-escalations were allowed. Trastuzumab deruxtecan could be interrupted or delayed for up to 28 days from the planned date of administration. However, patients who required a dose delay of longer than 28 days were permanently discontinued from the study drug.
Dose adjustments for drugs under TPC were allowed and implemented in accordance with the local drug label guidelines in the country or in accordance with the NCCN guidelines for up to 28 days from the planned date of administration (49 days from the last infusion date). However, patients who required a dose delay longer than 28 days were permanently discontinued from the study drug and followed for survival.
Patients could withdraw from the trial for the following reasons: disease progression according to modified Response Evaluation Criteria in Solid Tumors Version 1.1 (mRECIST 1.1), clinical progression (definitive clinical signs of disease progression), AE, death, pregnancy, patient withdrew consent, patient lost to follow-up, protocol deviation reported, physician decision, and study termination by the sponsor or for other reason. Patients who discontinued study treatments were recommended to complete all protocol-specified withdrawal and follow-up procedures outlined in the study protocol.
Hematopoietic growth factors for prophylaxis or treatment were permitted at the investigator’s discretion (except within 1 week before screening), as well as prophylactic antiemetic drugs, bisphosphonates, or inhibitors of the receptor activator of nuclear factor kappa-beta ligand pathway.
Prohibited medications included other anticancer drugs such as chloroquine or hydroxychloroquine (if treatment with chloroquine or hydroxychloroquine was absolutely required for COVID-19, the study drug was required to be interrupted); radiotherapy (except for palliative radiation to known metastatic sites as long as it does not affect assessment of response or interrupt treatment for more than the maximum time specified in the dose-modification section); and chronic systemic (IV or oral) corticosteroids or other immunosuppressive medications (except drugs used to manage AEs).
Outcomes
A list of efficacy end points assessed in this clinical review report is provided in Table 6 and summarized in the following section. Included end points are based on those in the sponsor’s Summary of Clinical Evidence or identified as relevant according to clinical experts, clinician groups, or patient groups. Outcomes are presented in descending order of importance to patients, with the most important outcomes presented first.
The primary efficacy end point was PFS based on BICR, in patients with HR-positive BC. PFS was defined as the time from the date of randomization to the earliest date of the first objective documentation of radiographic disease progression via BICR according to mRECIST 1.1 or death due to any cause. Patients who were alive with no objective documentation of (radiographic) disease progression by the data cut-off date for PFS analysis were censored at the date of their last evaluable tumour assessment before the data cut-off. Patients were censored at the date of last evaluable tumour assessment if disease progression or death occurred after missing 2 or more consecutive scheduled tumour assessments or if they started a new anticancer therapy drug before progression or death.
The key secondary efficacy end points were:
PFS, based on BICR, in all randomized patients (i.e., HER2-low HR-positive and HR-negative cohorts)
OS in patients with HER2-low HR-positive mBC
OS in all randomized patients, regardless of HR status.
OS was defined as the time from the date of randomization to the date of death due to any cause. If a death was not reported for a patient before the data cut-off for the OS analysis, OS was censored at the last contact date at which the patient was known to be alive.
Tumour response was assessed using mRECIST 1.1. Progressive disease was defined as at least a 20% increase in the sum of the diameters of target lesions, taking as reference the smallest sum on study (this includes the baseline sum if that is the smallest on study); the sum must also demonstrate an absolute increase of at least 5 mm. A partial response was defined as at least a 30% decrease in the sum of the diameters of target lesions, taking as reference the baseline sum diameters. A complete response was defined as disappearance of all target lesions with a reduction of the short axis of any pathological lymph nodes to less than 10 mm. Stable disease was defined as neither sufficient shrinkage (compared to baseline) to qualify for partial response nor sufficient increase (taking as reference the smallest sum diameters while on study) to qualify for progressive disease.
AEs that began or worsened on or after the start of study treatment until 47 days after the last dose of study drug were captured. AEs were defined as any untoward medical occurrence and were coded according to the Medical Dictionary for Regulatory Activities version 23.033 and graded according to the National Cancer Institute Common Terminology Criteria for Adverse Events version 5.0.34
Table 6: Outcomes Summarized From Pivotal Studies and RCT Evidence Identified by the Sponsor
Outcome measure | Time point | DESTINY-Breast04 |
|---|---|---|
OS in patients with HER2-low HR-positive BC | Time from date of randomization to date of death due to any cause | Key secondary efficacy end point |
OS in all randomized patients | Time from date of randomization to date of death due to any cause | Key secondary efficacy end point |
OS based on BICR for HR-negative cohort | Time from date of randomization to date of death due to any cause | Exploratory efficacy end point |
EORTC QLQ-C30 | NA | Other: Health economic outcomes research end point |
EORTC QLQ-BR45 (EORTC QLQ-BR23) | NA | Other: Health economic outcomes research end point |
EQ-5D-5L | NA | Other: Health economic outcomes research end point |
PFS based on BICR in patients with HR-positive BC | Time from date of randomization to earliest date of documentation of radiographic disease progression via BICR according to RECIST 1.1 or death due to any cause | Primary efficacy end point |
PFS based on BICR in all randomized patients | Time from date of randomization to earliest date of documentation of radiographic disease progression via BICR according to RECIST 1.1 or death due to any cause | Key secondary efficacy end point |
PFS based on BICR for HR-negative cohort | Time from date of randomization to earliest date of documentation of radiographic disease progression via BICR according to RECIST 1.1 or death due to any cause | Exploratory efficacy end point |
PFS based on investigator assessment for the HR-positive cohort and FAS | Time from date of randomization to earliest date of documentation of radiographic disease progression via investigator assessment according to RECIST 1.1 or death due to any cause | Other secondary efficacy end point |
Confirmed ORR for the HR-positive cohort and FAS | NA | Other secondary efficacy end point |
Confirmed ORR based on BICR in HR-negative cohort | NA | Exploratory efficacy end point |
DOR for HR-positive cohort and FAS | Time from date of first documentation of objective response (confirmed CR or PR) to the date of the first documentation of disease progression or death, based on BICR and investigator assessment | Other secondary efficacy end point |
TEAE; TEAE associated with dose reduction, study drug interruption, discontinuation, or death; SAE; AESI | NA | Safety end point |
AESI = adverse event of special interest; BC = breast cancer; BICR = blinded independent central review; CR = complete response; DOR = duration of response; EORTC QLQ-BR23 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire breast cancer module; EORTC QLQ-BR45 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire updated breast cancer module; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; EQ-5D-5L = 5-Level EQ-5D; FAS = full analysis set; HR = hormone receptor; NA = not applicable; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; PR = partial response; RECIST 1.1 = Response Evaluation Criteria in Solid Tumours Version 1.1; SAE = serious adverse event; TEAE = treatment-emergent adverse event.
Source: DESTINY-Breast04 Clinical Study Report.3
Patient-reported outcomes were also reported in the trial and included the following measures: EORTC QLQ-C30 and its BC module (EORTC QLQ-BR45 [QLQ-BR23]), as well as EQ-5D-5L. The EORTC QLQ-C30 and QLQ-BR45 (EORTC QLQ-BR23) were administered before infusion on day 1 of cycle 1, every 2 cycles thereafter, and at the end-of-treatment visit. Patients were followed up at day 40 (± 7 days) and at the first of the long-term survival follow-up visit 3 months after, which was the last data collection point for the questionnaires.
The EORTC QLQ-C30 is a multidimensional, cancer-specific, self-administered measure of HRQoL consisting of 30 questions across 5 multi-item functional scales, 3 multi-item symptom scales, 6 single-item symptom scales, and a 2-item global HRQoL scale; each item is evaluated using 4- and 7-point Likert scales, raw scores for each scale are computed as the average of the items that contribute to a particular scale, and each raw scale score is converted to a standardized score that ranges from 0 to 100 using a linear transformation, with a higher score reflecting better function on the function scales, worse symptoms on the symptom scales, and better HRQoL on the global quality-of-life scale.35
The EORTC QLQ-BR23 consists of 23 questions related to quality of life, scored on a 4-point Likert scale (1 = not at all, 4 = very much). It is composed of questions citing the extent to which the patient has experienced symptoms or problems during the past week and during the past 4 weeks, separated into 4 functional scales (body image, sexual functioning, sexual enjoyment, future perspective), and 4 symptom scales (systemic therapy side effects, breast symptoms, arm symptoms, upset by hair loss). Time to definitive deterioration on the “breast symptoms” and “arm symptoms” subscales of the EORTC QLQ-BR45 were also assessed, with definitive deterioration defined as an increase (from baseline) of 10 points or more.36
The EQ-5D-5L is a generic, preference-based measure of HRQoL consisting of 5 domains: mobility, self-care, usual activities, pain/discomfort, and anxiety and/or depression; index scores range from 0 to 1, with 0 and 1 representing the health states “dead” and “perfect health,” respectively, while EQ-5D Visual Analogue Scale (EQ VAS) scores range from 0 to 100, with 0 and 100 representing “worst imaginable health” and ”best imaginable health,” respectively.37
Table 7: Summary of Outcome Measures and Their Measurement Properties
Outcome measure | Type | Conclusions about measurement properties | MID |
|---|---|---|---|
EORTC QLQ-C30 | A 30-item, patient-reported, cancer-specific, HRQoL questionnaire using 4- and 7-point Likert scales35 | Content validity: When mapping to the WHO’s ICF framework, 25 of the 30 items in the EORTC QLQ-C30 were endorsed by the experts.41 Discriminant validity: As represented by correlation with external parameters such as ECOG Performance Status (Spearman’s rank correlation values ranging from 0.02 to 0.56) in patients with mBC.42 Convergent validity: As represented by correlation with scores on the Profile of Mood States and Psychosocial Adjustment to Illness Scale, was also deemed to be acceptable (Spearman’s rank correlation values ranging from 0.02 to 0.76) in patients with mBC.42 Reliability: Interrater reliability: As represented by patient-observer agreement on the EORTC QLQ-C30 questionnaire, the median kappa coefficient for agreement across the 30 in the EORTC QLQ-C30 was 0.86, with a range of 0.48 to 1.00, in patients with mBC, representing substantial to near-perfect agreement for most items.43,44 Responsiveness: No literature was identified that assessed responsiveness in patients with BC. | For patients with advanced BC, MIDs for within-group changes ranged from 5 to 14 points for improvements and from −14 to −4 points for deterioration across the individual scales. For between-group differences, MIDs ranged from 4 to 11 points for improvements and from −18 to −4 points for deterioration across the individual scales.39 For patients with mBC, MIDs for within-group improvement varied from 7 to 15 and those for deterioration varied from −7 to −17. For between-group difference, MIDs varied from 5 to 11 for improvement and from −5 to –8 for deterioration across EORTC QLQ-C30 scales.40 |
EORTC QLQ-BR23 | A 45-item patient-reported, BC-specific, HRQoL questionnaire using 4-point Likert scales.36 | Content (face) validity: All the newly added 22 items of the EORTC QLQ-BR45 fulfilled at least 5 of the 8 prespecified inclusion criteria with a mean score greater than 1.5 in patients with BC.36 Reliability: Internal consistency reliability: All EORTC QLQ-BR45 subscales demonstrated acceptable internal consistency by exceeding the accepted Cronbach alpha threshold of > 0.70 in patients with BC.36 Responsiveness: No literature was identified that assessed responsiveness in patients with BC. | No literature was identified that estimated MIDs in patients with BC. |
EQ-5D-5L and EQ VAS | EQ-5D-5L index score: Generic, preference-based measure of HRQoL consisting of 5 domains: mobility, self-care, usual activities, pain/ discomfort, and anxiety/depression. Scores range from 0 to 1 with higher scores indicating better health status.37 EQ VAS: Generic, preference-based measure of HRQoL presented as a scale from 0 to 100 with 0 anchored as the worst possible health state and 100 as the best possible health state.37 | Validity: Construct validity was assessed using the known-group approach. Patients presenting evidence of disease and receiving chemotherapy and/or radiotherapy showed significantly lower mean utility index as compared to their counterparts both in the English and Chinese samples.45 Convergent validity: The EQ-5D-5L utility index and VAS were strongly correlated with the Functional Assessment of Cancer Therapy–Breast total score (Spearman’s correlation coefficient, r, ranging from 0.53 to 0.73) in patients with BC.45 Reliability: Test-retest reliability: The EQ-5D-5L index and EQ VAS demonstrated substantial to almost perfect agreement44 in English-speaking patients living with BC and no history of brain metastasis based on an ICC of 0.81 (95% CI, 0.73 to 0.87) and 0.83 (95% CI, 0.76 to 0.89), respectively.45 Responsiveness: Responsiveness was demonstrated in patients with BC following curative treatment; however, small changes in health were not recognized as being meaningful.46,47 | MID for the index score was estimated to range from 0.037 to 0.056 in the general Canadian population.38 An MID specific to patients with BC was not identified. MID for the EQ VAS was estimated to range from 7 to 12 in advanced cancer patients.48 |
BC = breast cancer; CI = confidence interval; ECOG PS = European Cooperative Oncology Group Performance Status; EORTC QLQ-BR23 = Organisation for Research and Treatment of Cancer Quality of Life Questionnaire breast cancer module; EORTC QLQ-BR45 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire updated breast cancer module; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; EQ-5D-5L = 5-Level EQ-5D; EQ VAS = EQ-5D Visual Analogue Scale; HRQoL = health-related quality of life; ICC = intraclass correlation coefficient; ICF = International Classification of Functioning, Disability and Health; mBC = metastatic breast cancer; MID = minimal important difference.
Neither the measurement properties nor the minimal important difference (MID) of these instruments have been specifically established in patients with HER2-low mBC. However, differences in the EQ-5D-5L index score of approximately 0.037 to 0.056 in the general Canadian population, differences of approximately 7 to 12 points in the EQ VAS among advanced cancer patients, and differences of approximately 4 to 18 points in EORTC QLQ-C30 individual items and scale scores among patients with mBC are typically considered significant.38-40 The MIDs for EORTC QLQ-BR23 individual items and scale scores are uncertain.
Statistical Analysis
Approximately 480 patients with HR-positive mBC were planned to be randomized (320 trastuzumab deruxtecan and 160 TPC). In addition, up to 60 patients with HR-negative mBC (approximately 40 trastuzumab deruxtecan and 20 TPC) were planned to be enrolled for exploratory purposes. A summary of the statistical analysis of efficacy end points is shown in Table 8.
For patients with HR-positive mBC, it was hypothesized that treatment with trastuzumab deruxtecan would result in a hazard ratio of 0.68 compared to TPC. This specified hazard ratio would correspond to a 47% improvement in hypothesized population median PFS from 4.2 months in the TPC arm to 6.2 months in the trastuzumab deruxtecan arm, if the PFS events are assumed to follow an exponential model. The final PFS analysis was to occur after approximately 318 PFS events had been documented in patients with HR-positive BC. If 318 PFS events occurred within the study, the study would have 90% power for a log-rank test to reject the null hypothesis of no difference in PFS distributions at an overall 2-sided significance level of 0.05, assuming a proportional hazards ratio of 0.68 and equal censoring distributions.49
Statistical analysis of efficacy outcomes in the DESTINY-Breast04 trial were controlled for type I error by using a hierarchical testing strategy. The primary efficacy end point and the key secondary efficacy end points were tested hierarchically to maintain the overall 2-sided type I error rate of 0.05 or less, in the following order:
PFS based on BICR in the HR-positive cohort
PFS based on BICR in the FAS
OS in the HR-positive cohort (up to 3 analyses)
OS in the FAS (up to 3 analyses).
The statistical testing for a key secondary end point was performed only when the analyses in the hierarchy above that end point demonstrated statistical significance.
Up to 3 analyses (2 interim analyses and a final analysis) of OS were planned:
Provided PFS was significant in both the HR-positive cohort and the FAS, the first interim analysis comparing the trastuzumab deruxtecan and TPC arms was planned at the time of the final analysis for PFS, at which point a total of 162 OS events (49% information fraction) in the HR-positive cohort were expected.
If the first OS interim analysis was not significant, a second interim analysis for OS was planned when approximately 233 OS events (70% information fraction) in the HR-positive cohort had been documented.
If the second OS interim analysis was not significant, a final analysis for OS was planned after approximately 333 OS events in the HR-positive cohort had been documented.
A 3-look Lan-DeMets alpha spending function with an O’Brien-Fleming–type stop boundary was used to construct the efficacy stopping boundaries with an overall 2-sided significance level of 0.05. To control for multiplicity the statical plan allowed for stopping boundaries derived separately for the HR-positive cohort and the FAS based on the actual number of OS events documented at the cut-off date, and the actual information fractions and the alpha already spent at the previous interim analyses (if the first testing of OS was not significant).
Table 8: Statistical Analysis of Efficacy End Points
End point | Statistical model | Adjustment factors | Sensitivity analyses | Censoring rules | Handling of missing data |
|---|---|---|---|---|---|
PFS based on BICR in patients with HR-positive mBC (primary) Position in statistical hierarchy = 1 | 2-sided log-rank test stratified by randomization factors; KM analysis with median PFS and 95% CIs calculated via the Brookmeyer-Crowley method; PFS rates at fixed time points from KM analysis with 2-sided CIs; hazard ratios and CIs calculated using a stratified Cox proportional hazards model with treatment arm as a model factor and stratification from IXRS as strata | Stratification factors: HER2 status, number of prior lines of chemotherapy, and HR/CDK status as defined by an interactive voice/web response system |
|
| Noninformative censoring |
PFS based on BICR in all randomized patients (key secondary) Position in statistical hierarchy = 2 | According to primary analysis | According to primary analysis | Supportive analysis: multiple Cox regression analysis with additional covariates ECOG PS (0, 1), lines of ET received in the metastatic setting (0, 1, 2, ≥ 3), history CNS metastases (yes, no), and age (< 65, ≥ 65 years old) | According to primary analysis of PFS a defined by the BICR | Noninformative censoring |
OS in patients with HR-positive BC (key secondary) Position in statistical hierarchy = 3 | According to primary analysis | According to primary analysis | Supportive analysis: multiple Cox regression analysis with additional covariates ECOG PS (0, 1), lines of ET received in the metastatic setting (0, 1, 2, ≥ 3), history CNS metastases (yes, no), and age (< 65, ≥ 65 years old) | At the last contact date at which the patient is known to be alive | Noninformative censoring |
OS in all randomized patients (key secondary) Position in statistical hierarchy = 4 | According to primary analysis | According to primary analysis | Supportive analysis: multiple Cox regression analysis with additional covariates ECOG PS (0, 1), lines of ET received in the metastatic setting (0, 1, 2, ≥ 3), history CNS metastases (yes, no), and age (< 65, ≥ 65 years old). | NA | NA |
PFS based on investigator assessment for the HR-positive cohort and FAS (other secondary) | According to primary analysis | According to primary analysis | NA | According to primary analysis of PFS as defined by the BICR | Noninformative censoring |
Confirmed ORR for the HR-positive cohort and FAS (other secondary) | ORRs and 2-sided 95% CIs calculated using the Clopper-Pearson method for single proportion and for the difference of 2 proportions with continuity correction 2-sided P value based on the Cochran-Mantel-Haenszel test adjusted for stratification factors | According to primary analysis | None | NA | NA |
DOR for HR-positive cohort and FAS (other secondary) | Median was from a KM estimate. CI for median was computed using the Brookmeyer-Crowley method | None | None | According to primary analysis of PFS as defined by the BICR | Noninformative censoring |
EORTC QLQ-C30 (other) | Descriptive and summary statistics | None | None | NA | Imputation according to EORTC QLQ-C30 manual |
EORTC QLQ-BR45 (EORTC QLQ-BR23) (other) | Descriptive and summary statistics | None | None | NA | Imputation according to EORTC QLQ-BR45 manual |
EQ-5D-5L (other) | Descriptive and summary statistics | None | None | NA | Imputation according to EQ-5D-5L manual |
BICR = blinded independent central review; CDK = cyclin-dependent kinase; CI = confidence interval; CNS = central nervous system; DOR = duration of response; ECOG PS = European Cooperative Oncology Group Performance Status; EORTC QLQ-BR23 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire breast cancer module; EORTC QLQ-BR45 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire updated breast cancer module; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; EQ-5D-5L = 5-Level EQ-5D; ET = endocrine therapy; FAS = full analysis set; HR = hormone receptor; KM = Kaplan-Meier; mBC = metastatic breast cancer; ORR = objective response rate; OS = overall survival; PFS = progression-free survival.
aThis censoring rule was used for sensitivity analysis.
Source: DESTINY-Breast04 Statistical Analysis Plan.49
Analysis Populations
Table 9 summarizes the analysis populations in the DESTINY-Breast04 trial. The HR-positive cohort included all HR-positive patients randomized into the study, while the FAS included all patients randomized into the study regardless of hormone status.
Table 9: Analysis Populations of DESTINY-Breast04
Population | Definition | Application |
|---|---|---|
HR-positive cohort | All HR-positive patients randomized into the study, including those who did not receive a dose of study treatment | Primary analysis set for all efficacy analysis of the HR-positive patients; patients analyzed according to treatments assigned at randomization |
Full analysis set | All patients randomized into the study, including those who did not receive a dose of study treatment | Primary analysis set for all efficacy analysis of all randomized patients; patients analyzed according to treatments assigned at randomization |
Safety analysis set | All randomized patients who received at least 1 dose of study treatment; patients summarized according to treatment actually received | Safety analyses is performed using the safety analysis set |
Per-protocol analysis set | All patients in the intention-to-treat analysis set who complied with the protocol sufficiently in exposure to study treatment, availability of tumour assessment, and absence of major protocol violations | Sensitivity analysis of primary efficacy end point is performed on the per-protocol analysis set |
HR = hormone receptor.
Note: Details from the table have been taken from the sponsor’s Summary of Clinical Evidence.
Source: DESTINY-Breast04 Clinical Study Report.3
Results
Patient Disposition
A summary of the patient disposition in the DESTINY-Breast04 trial is provided in Table 10. In the FAS |||| of patients randomized to TPC were randomized but not treated compared to |||| of patients in the trastuzumab deruxtecan group. The most common reason for discontinuation beyond disease progression was an AE, with 16.2% of patients in the FAS receiving trastuzumab deruxtecan discontinuing treatment compared to 8.1% of patients in the FAS TPC arm. At the time of data cut-off in the FAS, 15.6% of patients in the trastuzumab deruxtecan arm were receiving treatment compared with 1.7% of patients in the TPC arm.
Baseline Characteristics
Baseline characteristics are summarized in Table 11. Characteristics were well balanced between treatment groups in both the HR-positive cohort and the FAS, including the IXRS stratification factors of HER2-low status, HR/previous CDK 4/6 inhibitor, and number of prior lines of chemotherapy in the metastatic setting. The mean age in both cohorts of the FAS was 56.5 (SD = 10.58 in the trastuzumab deruxtecan arm and 11.51 in the TPC arm). A small proportion of patients had baseline CNS metastasis: 6.4% in the FAS trastuzumab deruxtecan arm and 4.3% in the FAS TPC arm. The proportion of patients who had received prior lines of chemotherapy in any setting differed slightly, with 24.9%, 47.2%, and 27.9% of patients in the FAS trastuzumab deruxtecan arm having received either 1, 2, or 3 prior lines of chemotherapy, respectively, while in the FAS TPC arm the proportions were 28.3%, 38.6%, and 32.6%.
Table 10: Summary of Patient Disposition from Pivotal Studies and RCT Evidence Submitted by the Sponsor
Patient disposition | HR-positive cohort | Full analysis set | ||||
|---|---|---|---|---|---|---|
Trastuzumab deruxtecan (N = 331) | TPC (N = 163) | Total (N = 494) | Trastuzumab deruxtecan (N = 373) | TPC (N = 184) | Total (N = 557) | |
Randomized, N | 331 | 163 | 494 | 373 | 184 | 557 |
Randomized but not treated, n (%) | | ||||| | || ||||| | || ||||| | 2 (0.5) | 12 (6.5) | 14 (2.5) |
Study duration (months)a | ||||||
Mean (SD) | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| |
Median (range) | |||| ||||| ||||| | |||| ||||| ||||| | |||| ||||| ||||| | |||| ||||| ||||| | |||| ||||| ||||| | |||| ||||| ||||| |
Treatment status, N (%)b | ||||||
Ongoing | || |||||| | | ||||| | || |||||| | 58 (15.6) | 3 (1.7) | 61 (11.2) |
Discontinued | ||| |||||| | ||| |||||| | ||| |||||| | 313 (84.4) | 169 (98.3) | 482 (88.8) |
Reason for discontinuation, N (%) | ||||||
Progressive disease according to 49 1.1 | ||| |||||| | ||| |||||| | ||| |||||| | 220 (59.3) | 130 (75.6) | 350 (64.5) |
Adverse event | || |||||| | || ||||| | || |||||| | 60 (16.2) | 14 (8.1) | 74 (13.6) |
Withdrawal by patient | || ||||| | || ||||| | || ||||| | 12 (3.2) | 11 (6.4) | 23 (4.2) |
Clinical progression per investigator | | ||||| | | ||||| | || ||||| | 10 (2.7) | 8 (4.7) | 18 (3.3) |
Death | | ||||| | | ||||| | | ||||| | 5 (1.3) | 2 (1.2) | 7 (1.3) |
Physician decision | | ||||| | | ||||| | | ||||| | 4 (1.1) | 3 (1.7) | 7 (1.3) |
Other | | ||||| | | ||||| | | ||||| | 2 (0.5) | 0 | 2 (0.4) |
Lost to follow-up | | ||||| | | ||||| | | ||||| | 0 | 1 (0.6) | 1 (0.2) |
Full analysis set, N | — | — | — | 373 (100.0) | 184 (100.0) | 557 (100.0) |
Safety analysis set, N | — | — | — | 371 (99.5) | 172 (93.5) | 543 (97.5) |
Per-protocol analysis set, N | — | — | — | 361 (96.8) | 164 (89.1) | 525 (94.3) |
Pharmacokinetic analysis set | — | — | — | 370 (99.2) | 0 | 370 (66.4) |
RECIST 1.1 = Response Evaluation Criteria in Solid Tumours Version 1.1; SD = standard deviation; TPC = treatment of physician’s choice.
aStudy duration for a patient (months) was defined as (date of last known alive minus date of randomization plus 1)/365.25 × 12.
bThe percentage was based on the safety analysis set.
Source: DESTINY-Breast04 Clinical Study Report.3
Table 11: Summary of Baseline Characteristics of Pivotal Studies and RCT Evidence Submitted by the Sponsor
Characteristic | HR-positive cohort | Full analysis set | ||
|---|---|---|---|---|
Trastuzumab deruxtecan (N = 331) | TPC (N = 163) | Trastuzumab deruxtecan (N = 373) | TPC (N = 184) | |
Age (years), mean (SD) | 56.3 (10.57) | 56.3 (11.39) | 56.5 (10.58) | 56.5 (11.51) |
Female sex, n (%) | 329 (99.4) | 163 (100.0) | 371 (99.5) | 184 (100.0) |
Weight (kg), mean (SD) | |||| ||||||| | |||| ||||||| | |||| ||||||| | |||| ||||||| |
Body mass index (kg/m2), mean (SD) | |||| |||||| | |||| |||||| | |||| |||||| | |||| |||||| |
Patients from North America, n (%) | 54 (16.3) | 30 (18.4) | 60 (16.1) | 33 (17.9) |
Race, n (%) | ||||
White | 156 (47.1) | 78 (47.9) | 176 (47.2) | 91 (49.5) |
Black or African American | 7 (2.1) | 2 (1.2) | 7 (1.9) | 3 (1.6) |
Asian | 131 (39.6) | 66 (40.5) | 151 (40.5) | 72 (39.1) |
Native Hawaiian or Other Pacific Islander | 0 | 0 | 1 (0.3) | 0 |
Other | 37 (11.2) | 16 (9.8) | 38 (10.2) | 17 (9.2) |
Missing data | 0 | 1 (0.6) | 0 | 1 (0.5) |
Ethnicity, n (%) | ||||
Hispanic or Latino | 14 (4.2) | 5 (3.1) | 14 (3.8) | 7 (3.8) |
Non-Hispanic or Non-Latino | 267 (80.7) | 137 (84.0) | 308 (82.6) | 153 (83.2) |
Unknown | 9 (2.7) | 4 (2.5) | 9 (2.4) | 7 (3.8) |
Not applicable | 41 (12.4) | 17 (10.4) | 42 (11.3) | 17 (9.2) |
Stratification factor: HER2-low status from IXRS, n (%) | ||||
IHC 1+ | 193 (58.3) | 95 (58.3) | 215 (57.6) | 106 (57.6) |
IHC 2+ and ISH− | 138 (41.7) | 68 (41.7) | 158 (42.4) | 78 (42.4) |
Stratification factor: HR/CDK status from IXRS, n (%) | ||||
HR-positive with prior CDK 4/6 | 233 (70.4) | 115 (70.6) | 233 (62.5) | 115 (62.5) |
HR-positive without prior CDK 4/6 | 98 (29.6) | 48 (29.4) | 98 (26.3) | 48 (26.1) |
HR-negative | 0 | 0 | 42 (11.3) | 21 (11.4) |
HR status – derived, n (%)a | ||||
Positive | 328 (99.1) | 162 (99.4) | 333 (89.3) | 166 (90.2) |
Negative | 3 (0.9) | 1 (0.6) | 40 (10.7) | 18 (9.8) |
ECOG PS score, n (%) | ||||
0 | 187 (56.5) | 95 (58.3) | 200 (53.6) | 105 (57.1) |
1 | 144 (43.5) | 68 (41.7) | 173 (46.4) | 79 (42.9) |
Metastasis n (%) | ||||
Baseline CNS metastases | 18 (5.4) | 7 (4.3) | 24 (6.4) | 8 (4.3) |
Baseline liver metastases | 247 (74.6) | 116 (71.2) | 266 (71.3) | 123 (66.8) |
Baseline lung metastases | 98 (29.6) | 58 (35.6) | 120 (32.2) | 63 (34.2) |
Previous cancer therapy, n (%) | ||||
Targeted therapy | 259 (78.2) | 132 (81.0) | 279 (74.8) | 140 (76.1) |
CDK 4/6 inhibitor | 233 (70.4) | 115 (70.6) | 239 (64.1) | 119 (64.7) |
Immunotherapy | 10 (3.0) | 8 (4.9) | 20 (5.4) | 12 (6.5) |
Other | 128 (38.7) | 70 (42.9) | 140 (37.5) | 76 (41.3) |
ET | 330 (99.7) | 160 (98.2) | 347 (93.0) | 165 (89.7) |
Chemotherapy | 331 (100) | 162 (99.4) | 373 (100) | 183 (99.5) |
Stratification factor: number of prior lines of chemotherapy from IXRS | ||||
1 | 197 (59.5) | 96 (58.9) | 212 (56.8) | 103 (56.0) |
2 | 134 (40.5) | 67 (41.1) | 161 (43.2) | 81 (44.0) |
Number of prior lines of systemic therapy in metastatic setting, n (%) | ||||
1 | 23 (6.9) | 14 (8.6) | 39 (10.5) | 19 (10.3) |
2 | 85 (25.7) | 41 (25.2) | 100 (26.8) | 53 (28.8) |
≥ 3 | 223 (67.4) | 108 (66.3) | 234 (62.7) | 112 (60.9) |
Number of prior lines of chemotherapy in the metastatic setting, n (%) | ||||
0 | 1 (0.3) | 1 (0.6) | 1 (0.3) | 1 (0.5) |
1 | 203 (61.3) | 93 (57.1) | 221 (59.2) | 100 (54.3) |
2 | 124 (37.5) | 69 (42.3) | 145 (38.9) | 83 (45.1) |
≥ 3 | 3 (0.9) | 0 | 6 (1.6) | 0 |
Number of prior lines of chemotherapy in any setting, n (%) | ||||
0 | 0 | 1 (0.6) | 0 | 1 (0.5) |
1 | 89 (26.9) | 49 (30.1) | 93 (24.9) | 52 (28.3) |
2 | 155 (46.8) | 61 (37.4) | 176 (47.2) | 71 (38.6) |
≥ 3 | 87 (26.3) | 52 (31.9) | 104 (27.9) | 60 (32.6) |
CDK = cyclin-dependent kinase; CNS = central nervous system; ECOG = Eastern Cooperative Oncology Group Performance Status; EDC = electronic data capture; ET = endocrine therapy; IHC = immunohistochemistry; IXRS = interactive web/voice response system; ISH = in situ hybridization; TPC = treatment of physician’s choice.
aHR (based on factors from EDC): Positive = estrogen receptors negative and progesterone receptors positive; estrogen receptors positive and progesterone receptors negative; estrogen receptors positive and progesterone receptors positive; estrogen receptors positive and progesterone receptors indeterminate; estrogen receptors indeterminate and progesterone receptors positive. Negative = estrogen receptors negative and progesterone receptors negative. Indeterminate = estrogen receptors negative and progesterone receptors indeterminate; estrogen receptors indeterminate and progesterone receptors negative; estrogen receptors indeterminate and progesterone receptors indeterminate. Data presented here are based on EDC. Data from IXRS could not be modified. The derived data in EDC captured the correct status.
Sources: DESTINY-Breast04 Clinical Study Report3
Exposure to Study Treatments
Treatment exposure in the safety analysis set in the DESTINY-Breast04 study is summarized in Table 12. The mean treatment duration in the trastuzumab deruxtecan arm was ||| |||||| months while in the TPC arm it was ||| |||||| months. The mean relative dose intensity was ||||| |||||| in the trastuzumab deruxtecan arm and ranged from ||||| and |||||| across the individual chemotherapy regimens included in the TPC basket.
Table 13 summarizes the subsequent therapies received by patients in the DESTINY-Breast04 study in the FAS. In the trastuzumab deruxtecan arm, ||||| of patients received subsequent therapy with chemotherapy ||||||| representing the most common subsequent therapy. In the TPC arm, ||||| of patients received subsequent therapy with chemotherapy ||||||| representing the most common subsequent therapy.
Efficacy
Overall Survival
OS results in the HR-positive cohort are summarized in Table 14. The median OS values were 23.9 months (95% CI, 20.8 to 24.8) in the trastuzumab deruxtecan arm and 17.5 months (95% CI, 15.2 to 22.4; P = 0.0028) in the TPC arm. The estimated hazard ratio comparing patients exposed to trastuzumab deruxtecan to patients on TPC was 0.64 (95% CI, 0.48 to 0.86). The proportions of patients alive at 12 months were 80.7% (95% CI, 76.0% to 84.6%) in the trastuzumab deruxtecan arm and 69.6% (95% CI, 61.3% to 76.4%) in the TPC arm. The OS Kaplan-Meier curves for the HR-positive cohort are shown in Figure 1.
Table 12: Summary of Patient Exposure From the Safety Analysis Set in DESTINY-Breast04
Treatment exposure | Trastuzumab deruxtecan N = 371 | Physician’s choice of chemotherapy | |||||
|---|---|---|---|---|---|---|---|
Overall (N = 172) | Eribulin (N = 89) | Capecitabine (N = 36) | Nab-paclitaxel (N = 17) | Gemcitabine (N = 16) | Paclitaxel (N = 14) | ||
Treatment duration (months) | |||||||
Mean (SD) | ||| |||||| | ||| |||||| | ||| |||||| | ||| |||||| | ||| |||||| | ||| |||||| | ||| |||||| |
Median (range) | ||| ||||| ||||| | ||| ||||| | | ||| ||||| ||||| | ||| ||||| ||||| | ||| ||||| ||||| | ||| ||||| |||| | ||| ||||| |||| |
Patient-years of exposure | 283.55 | 63.59 | |||| ||||||| | | |||| ||||||| | | |||| ||||||| | | |||| ||||||| | | |||| ||||||| | |
Dose intensity (units per 3 weeks) | |||||||
Mean (SD) | |||| ||||||| | | |||| ||||||| | | |||| ||||||| | | |||| ||||||| | | |||| ||||||| | | |||| ||||||| | | |||| ||||||| | |
Median (range) | |||| ||||||| | | |||| ||||||| | | |||| ||||||| | | |||| ||||||| | | |||| ||||||| | | |||| ||||||| | | |||| ||||||| | |
Relative dose intensity (%) | |||||||
Mean (SD) | |||| |||||| | |||| ||||||| | | |||| ||||||| | | ||||| ||||||| | ||||| |||||| | ||||| |||||| | ||||| |||||| |
Median (range) | |||| ||||||| | | |||| ||||||| | | |||| ||||||| | | |||| ||||||| | | |||| ||||||| | | |||| ||||||| | | |||| ||||||| | |
SD = standard deviation.
Note: Units for drugs are mg/kg (transtuzumab deruxtecan), mg/m2 (capecitabine, gemcitabine, paclitaxel, nab-paclitaxel), and mg/m2 (eribulin, where 1.23 mg eribulin base = 1.4 mg eribulin mesylate). 1 month = 365.25/12 = 30.44 days. Treatment duration (months) = (date of last dose – date of first dose) + a cycle length (days)/30.44. Total patient-years of exposure = sum of treatment duration (days) of all patients (months)/12. Dose intensity (units/cycle length in weeks) = cumulative dose level (units)/(duration of treatment [days]/cycle length [days]). Relative dose intensity (%) = dose intensity/planned dose intensity × 100, where planned dose intensity (units/cycle lengths in weeks) = planned cumulative dose (units)/planned duration of exposure (days)/cycle length in day. Due to different cycle durations among the individual chemotherapy treatments, dose intensity and relative dose intensity are not presented for the overall chemotherapy arm.
Source: DESTINY-Breast04 Clinical Study Report.3
Table 13: Summary of Subsequent Treatment From Pivotal Studies and RCT Evidence Submitted by the Sponsor
Subjects receive any post-anticancer systemic treatment, n (%) | Full analysis set | ||
|---|---|---|---|
Trastuzumab deruxtecan (N = 373) | Treatment of physician’s choice (N = 184) | Total (N = 557) | |
Yes (class/subclass) | ||| |||||| | ||| |||||| | ||| |||||| |
Targeted therapy | || |||||| | || |||||| | ||| |||||| |
Cyclin-dependent kinase 4/6 inhibitor | || ||||| | || |||||| | || ||||| |
Immunotherapy | | ||||| | | ||||| | || ||||| |
No subclass specified | || |||||| | || |||||| | ||| |||||| |
Endocrine therapy | || |||||| | || |||||| | ||| |||||| |
Chemotherapy | ||| |||||| | ||| |||||| | ||| |||||| |
Supportive therapy | ||| |||||| | ||| |||||| | ||| |||||| |
Other | ||| |||||| | ||| |||||| | ||| |||||| |
Uncoded | ||| |||||| | ||| |||||| | ||| |||||| |
RCT = randomized controlled trial.
Note: Details from the table have been taken from the sponsor’s Summary of Clinical Evidence.
Source: DESTINY-Breast04 Clinical Study Report.3
Table 14: Analysis of Overall Survival in the HR-Positive Cohort
Parameter | Trastuzumab deruxtecan N = 331 | Treatment of physician’s choice N = 163 |
|---|---|---|
Patients with event (death), n (%) | 126 (38.1) | 73 (44.8) |
Patients with no event (censored), n (%) | 205 (61.9) | 90 (55.2) |
Alive | 183 (55.3) | 67 (41.1) |
Lost to follow-up | 5 (1.5) | 1 (0.6) |
Withdrawal by patient | 16 (4.8) | 22 (13.5) |
Other | 1 (0.3) | 0 |
Median overall survival, months (95% CI)a | 23.9 (20.8 to 24.8) | 17.5 (15.2 to 22.4) |
P valueb | 0.0028 | |
Hazard ratio (95% CI)c | 0.64 (0.48 to 0.86) | |
Percentage of patients alive over timed | ||
3 months (95% CI) | 97.0 (94.4 to 98.4) | 96.1 (91.5 to 98.2) |
6 months (95% CI) | 93.6 (90.3 to 95.8) | 89.2 (83.0 to 93.3) |
9 months (95% CI) | 87.4 (83.3 to 90.6) | 76.7 (68.9 to 82.8) |
12 months (95% CI) | 80.7 (76.0 to 84.6) | 69.6 (61.3 to 76.4) |
18 months (95% CI) | 63.5 (57.4 to 69.0) | 48.8 (39.5 to 57.5) |
24 months (95% CI) | 48.9 (40.9 to 56.5) | 37.4 (26.8 to 48.0) |
CDK = cyclin-dependent kinase; CI = confidence interval; HR = hormone receptor.
Note: Data cut-off: January 11, 2022.
aMedian OS was from Kaplan-Meier analysis. The CI for medians was computed using the Brookmeyer-Crowley method.
bTwo-sided P value from stratified log-rank test, included in the hierarchical testing structure. The prespecified interim analysis efficacy stopping boundary was 0.00748 (information fraction 59.8%).
cHazard ratio and 95% CI from a stratified Cox proportional hazards model with stratification factors: HER2 status, number of prior lines of chemotherapy, and HR/CDK status as defined by an interactive voice/web response system.
dEstimate and CI for OS rate at the specified time point were from Kaplan-Meier analysis.
Source: DESTINY-Breast04 Clinical Study Report.3
Figure 1: Kaplan-Meier Plot of Overall Survival by Treatment Arm in the Hormone Receptor–Positive Cohort
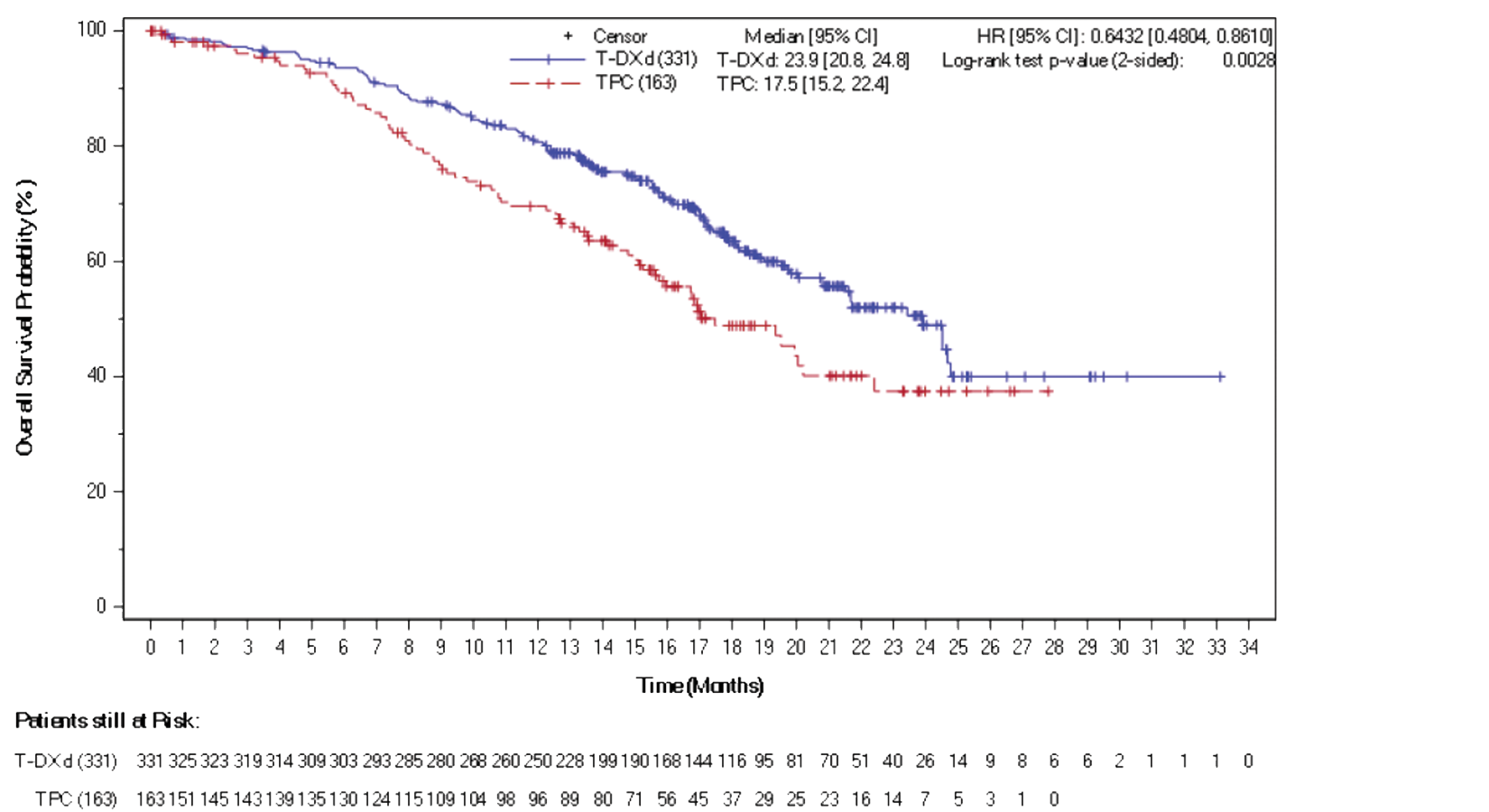
CI = confidence interval; HR = hazard ratio; T-DXd = trastuzumab deruxtecan; TPC = treatment of physician’s choice.
Note: Stratified Cox proportional hazards model for hazard ratio and stratified log-rank test for the P value. Prespecified interim analysis efficacy stopping boundary was 0.00748 (information fraction 59.8%).
Source: DESTINY-Breast04 Clinical Study Report3
OS results in the FAS are summarized in Table 15. The median OS in the trastuzumab deruxtecan arm was 23.4 months (95% CI, 20.0 to 24.8) while in the TPC arm it was 16.8 months (95% CI, 14.5 to 20.0; P value = 0.0010). The hazard ratio was 0.64 (95% CI, 0.49 to 0.84). The proportions of patients alive at 12 months were 78.8% (95% CI, 74.3% to 82.7%) in the trastuzumab deruxtecan arm and 66.5% (95% CI, 58.8% to 73.2%) in the TPC arm. The OS Kaplan-Meier curves for the FAS cohort are shown in Figure 2.
Table 15: Analysis of Overall Survival in the Full Analysis Set
Parameter | Trastuzumab deruxtecan N = 373 | Treatment of physician’s choice N = 184 |
|---|---|---|
Patients with event (death), n (%) | 149 (39.9) | 90 (48.9) |
Patients with no event (censored), n (%) | 224 (60.1) | 94 (51.1) |
Alive | 201 (53.9) | 70 (38.0) |
Lost to follow-up | 6 (1.6) | 1 (0.5) |
Withdrawal by patient | 16 (4.3) | 23 (12.5) |
Other | 1 (0.3) | 0 |
Median overall survival, months (95% CI)a | 23.4 (20.0 to 24.8) | 16.8 (14.5 to 20.0) |
Stratified log-rank P valueb | 0.0010 | |
Hazard ratio (95% CI)c | 0.64 (0.49 to 0.84) | |
Percentage of patients alive over timed | ||
3 months (95% CI) | 96.2 (93.7 to 97.8) | 95.3 (90.9 to 97.6) |
6 months (95% CI) | 92.4 (89.2 to 94.7) | 88.1 (82.2 to 92.2) |
9 months (95% CI) | 85.3 (81.3 to 88.5) | 74.0 (66.6 to 80.0) |
12 months (95% CI) | 78.8 (74.3 to 82.7) | 66.5 (58.8 to 73.2) |
18 months (95% CI) | 61.7 (55.9 to 66.9) | 45.9 (37.5 to 54.0) |
24 months (95% CI) | 48.1 (40.8 to 54.9) | 32.0 (21.9 to 42.4) |
CDK = cyclin-dependent kinase; CI = confidence interval; HR = hormone receptor.
Note: Data cut-off: January 11, 2022.
aMedian overall survival was from a Kaplan-Meier analysis. The CI for medians was computed using the Brookmeyer-Crowley method.
bTwo-sided P value from stratified log-rank test, included in the hierarchical testing structure. Prespecified interim analysis efficacy stopping boundary was 0.00748 (information fraction 59.8%).
cHazard ratio and 95% CI from a stratified Cox proportional hazards model with stratification factors: HER2 status, number of prior lines of chemotherapy, and HR/CDK status as defined by an interactive voice/web response system.
dEstimate and CI for overall survival at the specified time point were from a Kaplan-Meier analysis.
Source: DESTINY-Breast04 Clinical Study Report.3
Figure 2: Kaplan-Meier Plot of Overall Survival by Treatment Arm in the Full Analysis Set
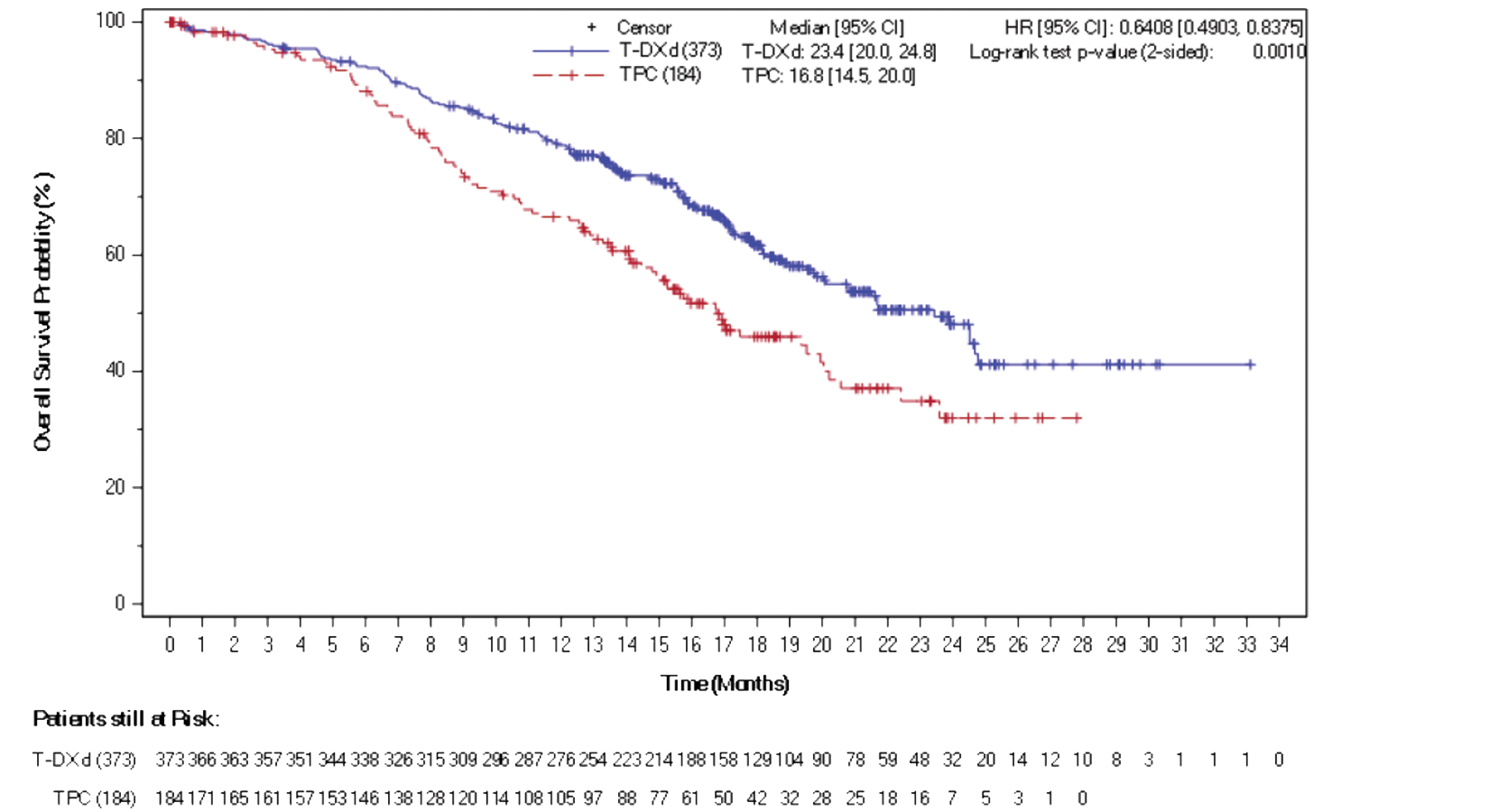
CI = confidence interval; HR = hazard ratio; T-DXd = trastuzumab deruxtecan; TPC = treatment of physician’s choice.
Note: Stratified Cox proportional hazards model for the hazard ratio and a stratified log-rank test for the P value. The prespecified interim analysis efficacy stopping boundary was 0.00748.
Source: DESTINY-Breast04 Clinical Study Report.3
Overall Survival in the HR-Negative Cohort (Exploratory End Point)
OS in the HR-negative cohort was an exploratory outcome; the reported results are from an electronic data capture, unlike the methodology used for the primary analysis. Using the electronic data capture, 40 patients in the trastuzumab deruxtecan arm were classified as HR-negative and 18 patients in the TPC arm were classified as HR-negative. The median OS values in the HR-negative cohort were 18.2 months (95% CI, 13.6 to not evaluable) in the trastuzumab deruxtecan group and 8.3 months (95% CI, 5.6 to 20.6) in the TPC group (hazard ratio = 0.48; 95% CI, 0.24 to 0.95).
Subgroup Analysis of Overall Survival in the HR-Positive Cohort
Prespecified subgroup analyses are summarized in Appendix 1, Table 28. Point estimates favoured trastuzumab deruxtecan in most subgroups, with the exception of patients with moderate renal impairment at baseline and those who had received 1 prior line of ET in the metastatic setting.
Health-Related Quality of Life
EORTC QLQ-C30 scores from the DESTINY-Breast04 study are summarized in Table 16, with the change from baseline across time points presented in Figure 3. According to the global health status parameter of the EORTC QLQ-C30, both treatment arms remained stable throughout the study. Mean baselines in global health status were 36.26 (SD = 21.842) in the trastuzumab deruxtecan arm and 37.89 (SD = 22.511) in the TPC arm. Mean changes from baseline were |||| |||||||| in the trastuzumab deruxtecan arm and |||| |||||||| in the TPC arm. The symptom scale with the greatest difference in mean change from baseline was nausea and vomiting, in favour of the TPC arm, with |||| |||||||| and ||||| |||||||| in the trastuzumab deruxtecan arm and TPC arm, respectively.
Table 16: EORTC QLQ-C30 Scores in DESTINY-Breast04 (Hormone Receptor–Positive Cohort)
Parameter | Trastuzumab deruxtecan N = 331 | Treatment of physician’s choice N = 163 |
|---|---|---|
Global health status | ||
Baseline | ||
n | 319 | 150 |
Mean (SD) | 36.26 (21.842) | 37.89 (22.511) |
Median (range) | ||||| ||||| |||||| | ||||| ||||| |||||| |
End of treatment | ||
n | ||| | ||| |
Mean (SD) | ||||| |||||||| | ||||| |||||||| |
Median (range) | ||||| ||||| |||||| | ||||| ||||| |||||| |
Change from baseline to end of treatment | ||
n | ||| | ||| |
Mean (SD) | |||| |||||||| | |||| |||||||| |
Median (range) | |||| ||||||| ||||| | |||| ||||||| ||||| |
Physical functioning | ||
Baseline | ||
n | ||| | ||| |
Mean (SD) | ||||| |||||||| | ||||| |||||||| |
Median (range) | ||||| ||||| |||||| | ||||| ||||| ||||| |
End of treatment | ||
n | ||| | ||| |
Mean (SD) | ||||| |||||||| | ||||| |||||||| |
Median (range) | ||||| ||||| |||||| | ||||| ||||| ||||| |
Change from baseline to end of treatment | ||
n | ||| | ||| |
Mean (SD) | |||| |||||||| | |||| |||||||| |
Median (range) | |||| ||||||| ||||| | |||| ||||||| ||||| |
Role functioning | ||
Baseline | ||
n | ||| | ||| |
Mean (SD) | ||||| |||||||| | ||||| |||||||| |
Median (range) | ||||| ||||| |||||| | ||||| ||||| |||||| |
End of treatment | ||
n | ||| | ||| |
Mean (SD) | ||||| |||||||| | ||||| |||||||| |
Median (range) | ||||| ||||| |||||| | ||||| ||||| |||||| |
Change from baseline to end of treatment | ||
n | ||| | ||| |
Mean (SD) | |||| |||||||| | ||||| |||||||| |
Median (range) | |||| |||||||| ||||| | |||| ||||||| ||||| |
Emotional functioning | ||
Baseline | ||
n | ||| | ||| |
Mean (SD) | ||||| |||||||| | ||||| |||||||| |
Median (range) | ||||| ||||| |||||| | ||||| ||||| |||||| |
End of treatment | ||
n | ||| | ||| |
Mean (SD) | ||||| |||||||| | ||||| |||||||| |
Median (range) | ||||| ||||| |||||| | ||||| ||||| |||||| |
Change from baseline to end of treatment | ||
n | ||| | ||| |
Mean (SD) | |||| |||||||| | |||| |||||||| |
Median (range) | |||| ||||||| ||||| | |||| ||||||| ||||| |
Cognitive functioning | ||
Baseline | ||
n | ||| | ||| |
Mean (SD) | ||||| |||||||| | ||||| |||||||| |
Median (range) | ||||| ||||| |||||| | ||||| ||||| ||||| |
End of treatment | ||
n | ||| | ||| |
Mean (SD) | ||||| |||||||| | ||||| |||||||| |
Median (range) | ||||| ||||| |||||| | ||||| ||||| |||||| |
Change from baseline to end of treatment | ||
n | ||| | ||| |
Mean (SD) | |||| |||||||| | |||| |||||||| |
Median (range) | |||| ||||||| ||||| | |||| ||||||| ||||| |
Social functioning | ||
Baseline | ||
n | ||| | ||| |
Mean (SD) | ||||| |||||||| | ||||| |||||||| |
Median (range) | ||||| ||||| |||||| | ||||| ||||| |||||| |
End of treatment | ||
n | ||| | ||| |
Mean (SD) | ||||| |||||||| | ||||| |||||||| |
Median (range) | ||||| ||||| |||||| | ||||| ||||| |||||| |
Change from baseline to end of treatment | ||
n | ||| | ||| |
Mean (SD) | |||| |||||||| | |||| |||||||| |
Median (range) | |||| ||||||| ||||| | |||| ||||||| |||||| |
Fatigue | ||
Baseline | ||
n | ||| | ||| |
Mean (SD) | ||||| |||||||| | ||||| |||||||| |
Median (range) | ||||| ||||| |||||| | ||||| ||||| |||||| |
End of treatment | ||
n | ||| | ||| |
Mean (SD) | ||||| |||||||| | ||||| |||||||| |
Median (range) | ||||| ||||| |||||| | ||||| ||||| |||||| |
Change from baseline to end of treatment | ||
n | ||| | ||| |
Mean (SD) | |||| |||||||| | |||| |||||||| |
Median (range) | |||| ||||||| ||||| | |||| ||||||| ||||| |
Nausea and vomiting | ||
Baseline | ||
n | ||| | ||| |
Mean (SD) | |||| |||||||| | |||| |||||||| |
Median (range) | |||| ||||| |||||| | |||| ||||| |||||| |
End of treatment | ||
n | ||| | ||| |
Mean (SD) | ||||| |||||||| | |||| |||||||| |
Median (range) | |||| ||||| |||||| | |||| ||||| |||||| |
Change from baseline to end of treatment | ||
n | ||| | ||| |
Mean (SD) | |||| |||||||| | ||||| |||||||| |
Median (range) | |||| ||||||| |||||| | |||| ||||||| ||||| |
Pain | ||
Baseline | ||
n | ||| | ||| |
Mean (SD) | ||||| |||||||| | ||||| |||||||| |
Median (range) | ||||| ||||| |||||| | ||||| ||||| |||||| |
End of treatment | ||
n | ||| | ||| |
Mean (SD) | ||||| |||||||| | ||||| |||||||| |
Median (range) | ||||| ||||| |||||| | ||||| ||||| |||||| |
Change from baseline to end of treatment | ||
n | ||| | ||| |
Mean (SD) | ||||| |||||||| | |||| |||||||| |
Median (range) | |||| |||||||| |||||| | |||| ||||||| ||||| |
EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; SD = standard deviation.
Note: Linear transformations were applied to global health status and all subscales of the EORTC QLQ-C30 such that a high score for the global health status represents a low quality of life (change of direction from raw score), a high score for a functional scale represents a low or unhealthy level of functioning, and a high score for a symptom scale or item represents a high level of symptomatology or problems.
Source: DESTINY-Breast04 Clinical Study Report.3
In the HR-positive cohort, the median times to a deterioration of 10 or more points in the global health status were 11.4 months (95% CI, 8.8 to 16.3) in the trastuzumab deruxtecan arm and 7.5 months (95% CI, 5.9 to 9.5) in the TPC arm. The hazard ratio was 0.69 (95% CI, 0.52 to 0.92).
Table 17 summarizes the EORTC QLQ-BR45 (QLQ-BR23) scores in the HR-positive cohort. The mean baseline breast symptoms score was ||||| |||||||| in the trastuzumab deruxtecan arm and ||||| |||||||| in the TPC arm, mean changes from baseline were ||||| |||||||| and ||||| |||||||| in the trastuzumab deruxtecan and TPC arms, respectively. The numbers of patients contributing to the change from baseline to end of treatment results for breast symptoms were ||| in the trastuzumab deruxtecan arm and ||| in the TPC arm.
In the HR-positive cohort, the median times to deterioration by 10 or more points according to the EORTC QLQ-BR45 (QLQ-BR23) breast symptoms were not evaluable (95% CI, 24.7 to not evaluable) in the trastuzumab deruxtecan arm and not evaluable (95% CI, not evaluable to not evaluable) in the TPC arm. The hazard ratio was 0.71 (95% CI, 0.50 to 1.01). For arm symptoms, median times to deterioration by 10 points or more were 14.4 months (95% CI, 11.9 to 23.0) in the trastuzumab deruxtecan arm and 8.7 months (95% CI, 5.6 to not evaluable). The hazard ratio was 0.62 (95% CI, 0.45 to 0.85).
Figure 3: Change From Baseline of EORTC QLQ-C30 — Global Health Status (HR-Positive Cohort)
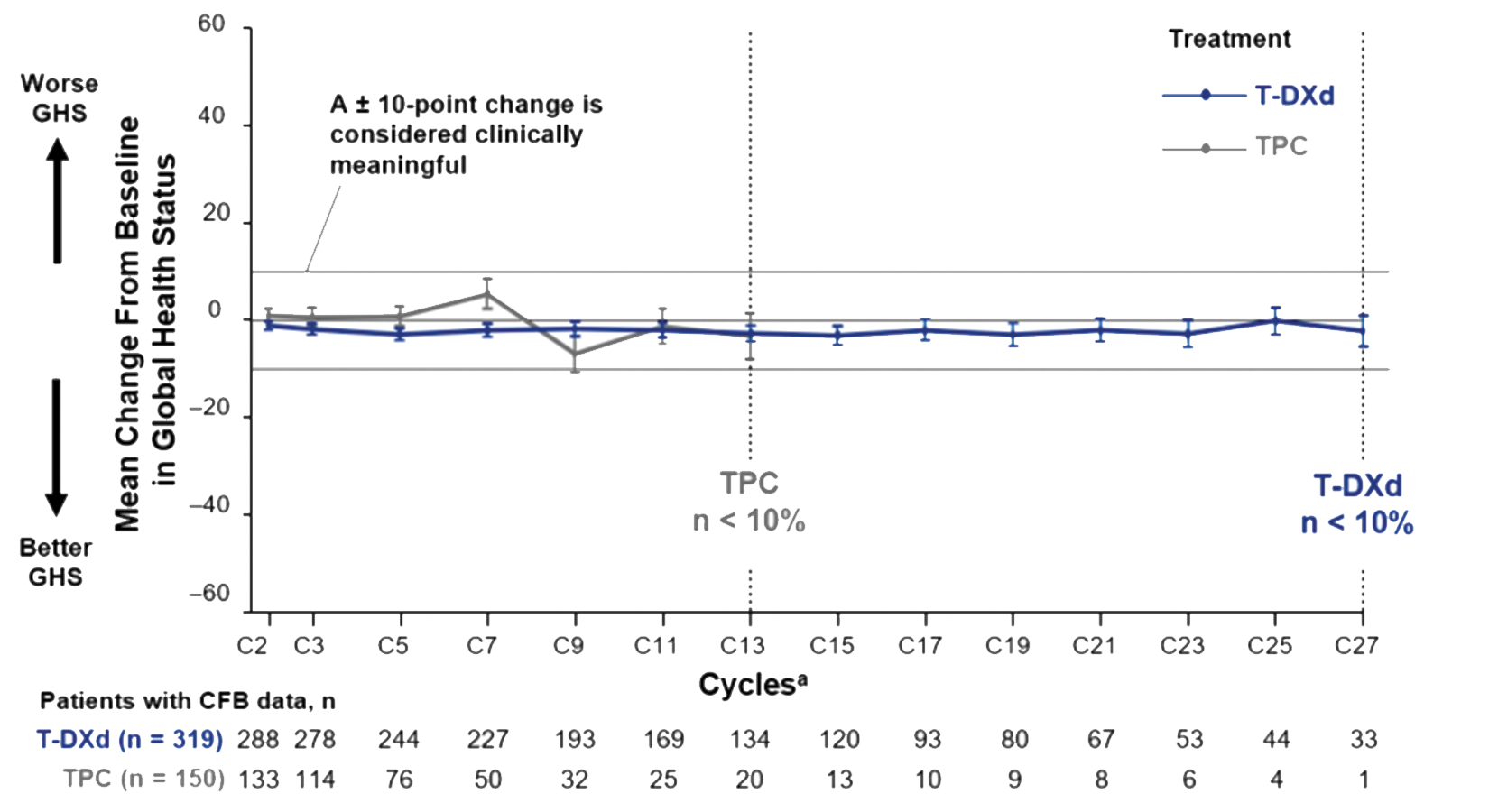
CFB = change from baseline; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; GHS = global health status; HR = hormone receptor; T-DXd = trastuzumab deruxtecan; TPC = physician’s choice of chemotherapy.
Note: Scores range from 0 to 100; a linear transformation was applied to the raw global health status score; thus, a higher score represents lower (“worse”) global health status (overall quality of life). T-DXd and TPC treatment arms are only comparable through cycle 13 (until the number of patients with available change from baseline data fell below 10% in the TPC arm). Data in the T-DXd treatment arm are interpretable through cycle 27 (until the number of patients with available change from baseline data fell below 10%).
a Assessment was conducted on day 1 of each cycle.
Source: Sponsor submission package.49
Table 17: EORTC QLQ-BR45 (EORTC QLQ-BR23) Scores in DESTINY-Breast04 (HR-Positive Cohort)
Parameter | Trastuzumab deruxtecan N = 331 | Treatment of physician’s choice N = 163 |
|---|---|---|
Breast symptoms | ||
Baseline | ||
n | ||| | ||| |
Mean (SD) | ||||| |||||||| | ||||| |||||||| |
Median (range) | |||| ||||| |||||| | |||| ||||| ||||| |
End of treatment | ||
n | ||| | ||| |
Mean (SD) | |||| |||||||| | ||||| |||||||| |
Median (range) | |||| ||||| ||||| | |||| ||||| ||||| |
Change from baseline to end of treatment | ||
n | ||| | ||| |
Mean (SD) | ||||| |||||||| | ||||| |||||||| |
Median (range) | |||| ||||||| ||||| | |||| ||||||| ||||| |
Arm symptoms | ||
Baseline | ||
n | ||| | ||| |
Mean (SD) | ||||| |||||||| | ||||| |||||||| |
Median (range) | ||||| ||||| |||||| | ||||| ||||| ||||| |
End of treatment | ||
n | ||| | ||| |
Mean (SD) | ||||| |||||||| | ||||| |||||||| |
Median (range) | ||||| ||||| |||||| | ||||| ||||| ||||| |
Change from baseline to end of treatment | ||
n | ||| | ||| |
Mean (SD) | ||||| |||||||| | |||| |||||||| |
Median (range) | |||| |||||||| ||||| | |||| ||||||| ||||| |
EORTC QLQ-BR23 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire breast cancer module; EORTC QLQ-BR45 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire updated breast cancer module; HR = hormone receptor; SD = standard deviation.
Note: Linear transformations are applied to all subscales of the EORTC QLQ-BR23 such that a high score for functional subscales represents a low/unhealthy level of functioning (change of direction from the raw score) and a high score for a symptom scale or item represents a high level of symptomatology/problems.
Source: DESTINY-Breast04 Clinical Study Report.3
Table 18 summarizes the EQ-5D-5L index scores as well as the EQ VAS in the HR-positive cohort. The mean baseline index score was ||||| |||||||| in the trastuzumab deruxtecan arm and ||||| |||||||| in the TPC arm. Mean changes from baseline to end of treatment were |||||| |||||||| and |||||| |||||||| in the trastuzumab deruxtecan and TPC arms, respectively. The numbers of patients contributing to the change from baseline to end-of-treatment results for EQ-5D-5L index score were ||| in the trastuzumab deruxtecan arm and ||| in the TPC arm.
In the HR-positive cohort, the median times to deterioration by 10 or more points according to the EQ VAS were 12.0 months (95% CI, 9.9 to 15.2) in the trastuzumab deruxtecan arm and 6.8 months (95% CI, 4.9 to 11.4) in the TPC arm. The hazard ratio was 0.73 (95% CI, 0.54 to 0.97).
Progression-Free Survival
PFS results in the HR-positive cohort are summarized in Table 19. The median PFS in the trastuzumab deruxtecan arm was 10.1 months (95% CI, 9.5 to 11.5) while in the TPC arm it was 5.4 months (95% CI, 4.4 to 7.1; P < 0.0001). The hazard ratio was 0.51 (95% CI, 0.40 to 0.64). The proportions of patients in PFS at 12 months were ||||| |||||| || |||||| in the trastuzumab deruxtecan arm and ||||| |||||| || |||||| in the TPC arm. The PFS Kaplan-Meier curves for the HR-positive cohort are shown in Figure 4.
Table 18: EQ-5D-5L Scores in the DESTINY-Breast04 (Hormone Receptor–Positive Cohort)
Parameter | Trastuzumab deruxtecan N = 331 | Treatment of physician’s choice N = 163 |
|---|---|---|
EQ-5D-5L index score | ||
Baseline | ||
n | ||| | ||| |
Mean (SD) | ||||| |||||||| | ||||| |||||||| |
Median (range) | ||||| |||||||| |||||| | |||||| |||||||| |||||| |
End of treatment | ||
n | ||| | ||| |
Mean (SD) | ||||| |||||||| | ||||| |||||||| |
Median (range) | ||||| |||||||| |||||| | ||||| |||||||| |||||| |
Change from baseline to end of treatment | ||
n | ||| | ||| |
Mean (SD) | |||||| |||||||| | |||||| |||||||| |
Median (range) | ||||| |||||||| |||||| | |||||| |||||||| |||||| |
EQ VAS | ||
Baseline | ||
n | ||| | ||| |
Mean (SD) | |||| ||||||| | |||| ||||||| |
Median (range) | |||| ||| |||| | |||| ||| |||| |
End of treatment | ||
n | ||| | ||| |
Mean (SD) | |||| ||||||| | |||| ||||||| |
Median (range) | |||| ||| |||| | |||| ||| |||| |
Change from baseline to end of treatment | ||
n | ||| | ||| |
Mean (SD) | |||| ||||||| | |||| ||||||| |
Median (range) | |||| ||||| ||| | |||| ||||| ||| |
EQ-5D-5L = 5-Level EQ-5D; EQ VAS = EQ-5D Visual Analogue Scale; SD = standard deviation.
Note: The EQ-5D-5L is scored according to the UK Crosswalk Value Set. The health scale is measured on a 0-to-100 mm visual analogue scale.
Source: DESTINY-Breast04 Clinical Study Report.3
Table 19: Progression-Free Survival Based on BICR in the Hormone Receptor–Positive Cohort
Parameter | Trastuzumab deruxtecan N = 331 | Treatment of physician’s choice N = 163 |
|---|---|---|
Patients with events, n (%) | 211 (63.7) | 110 (67.5) |
Progressive disease | 180 (54.4) | 101 (62.0) |
Death | 31 (9.4) | 9 (5.5) |
Patients without event (censored), n (%) | 120 (36.3) | 53 (32.5) |
No baseline evaluable tumour assessment | 0 | 0 |
No postbaseline tumour assessment | 3 (0.9) | 14 (8.6) |
Event after missing 2 consecutive assessments | 28 (8.5) | 15 (9.2) |
Lost to follow-up | 0 | 1 (0.6) |
Withdrew consent | 4 (1.2) | 7 (4.3) |
Ongoing without event | 67 (20.2) | 8 (4.9) |
Adequate tumour assessment no longer available | 18 (5.4) | 8 (4.9) |
Median progression-free survival, months (95% CI)a | 10.1 (9.5, 11.5) | 5.4 (4.4, 7.1) |
P valueb | < 0.0001 | |
Hazard ratio (95% CI)c | 0.51 (0.40 to 0.64) | |
Percentage of patients alive and progression-free over timed | ||
3 months (95% CI) | |||| |||||| ||||| | |||| |||||| ||||| |
6 months (95% CI) | |||| |||||| ||||| | |||| |||||| ||||| |
9 months (95% CI) | |||| |||||| ||||| | |||| |||||| ||||| |
12 months (95% CI) | |||| |||||| ||||| | |||| |||||| ||||| |
18 months (95% CI) | |||| |||||| ||||| | |||| ||||| ||||| |
24 months (95% CI) | |||| |||||| ||||| | ||| ||||| ||||| |
BICR = blinded independent central review; CDK = cyclin-dependent kinase; CI = confidence interval; HR = hormone receptor.
Note: Data cut-off: January 11, 2022.
aMedian progression-free survival was from a Kaplan-Meier analysis. The CI for medians was computed using the Brookmeyer-Crowley method.
bTwo-sided P value from stratified log-rank test, included in the hierarchical testing structure.
cHazard ratio and 95% CI from stratified Cox proportional hazards model with stratification factors: HER2 status, number of prior lines of chemotherapy, and HR/CDK status as defined by the interactive voice/web response system.
dEstimate and CI for progression-free survival rate at the specified time point are from a Kaplan-Meier analysis.
Source: DESTINY-Breast04 Clinical Study Report.3
Sensitivity analyses conducted for PFS according to the BICR in the HR-positive cohort are summarized in Table 20. Each sensitivity analysis addressed the robustness to the assumptions of the primary analysis. These analyses included testing for a difference in PFS event times without stratification, treating progression that occurred within 2 missed consecutive assessments as events, not censoring at the time of new anticancer therapy, back-dating PFS that occurred within a missed assessment, and choosing an alternative censoring for randomized but not treated patients. The benefit in favour of trastuzumab deruxtecan was consistent in all sensitivity analyses.
Table 20: Sensitivity Analysis of Progression-Free Survival in a BICR of the HR-Positive Cohort
Type of analysis | Number (%) of patients with events | Median PFS (95% CI) montha | Hazard ratio (95% CI) |
|---|---|---|---|
Unstratified analysis | |||
Trastuzumab deruxtecan | 211 (63.7) | 10.1 (9.5, 11.5) | 0.51b (0.40 to 0.64) |
Treatment of physician’s choice | 110 (67.5) | 5.4 (4.4, 7.1) | Reference |
Not censoring for missing 2 consecutive assessments | |||
Trastuzumab deruxtecan | 239 (72.2) | 10.3 (9.5, 11.5) | 0.51c (0.41 to 0.64) |
TPC | 126 (77.3) | 5.8 (4.5 to 7.1) | Reference |
Censoring for new anticancer therapy d | |||
Trastuzumab deruxtecan | 175 (52.9) | 10.9 (9.6 to 13.8) | 0.44c (0.33 to 0.57) |
TPC | 84 (51.5) | 5.4 (4.3 to 6.9) | Reference |
Back-dating PFS e | |||
Trastuzumab deruxtecan | 239 (72.2) | 9.6 (8.3 to 10.5) | 0.50 (0.40 to 0.63) |
TPC | 126 (77.3) | 5.3 (4.0 to 6.2) | Reference |
Randomized-not-treated censoringf | |||
Trastuzumab deruxtecan | |||| |||| | |||| |||| | |||| |||||| ||||| |
TPC | |||| |||| | |||| |||| | Reference |
BICR = blinded independent central review; CDK = cyclin-dependent kinase; CI = confidence interval; HR = hormone receptor; PFS = progression-free survival.
aMedian PFS is from a Kaplan-Meier analysis. The CI for medians was computed using the Brookmeyer-Crowley method.
bUnstratified Cox regression analysis.
cHazard ratio and 95% CI from stratified Cox proportional hazards model using stratification factors: HER2 status, number of prior lines of chemotherapy, HR/CDK status, as defined by an interactive web/voice response system.
dPatients were censored at the last evaluable tumour assessment date before starting the new anticancer therapy.
eBackdated PFS event time in the case that PFS event occurred after missing 1 or more tumour assessments.
fPFS for randomized-not-treated early censored subjects was imputed by the following algorithm: if death date is not missing, the death is imputed as PFS event, with PFS = death date -randomization date + 1. Otherwise PFS = data cut-off date − randomization date + 1.
Source: DESTINY-Breast04 Clinical Study Report.3
Figure 4: Kaplan-Meier Plot of PFS Based on BICR in the Hormone Receptor–Positive Cohort by Treatment Arm
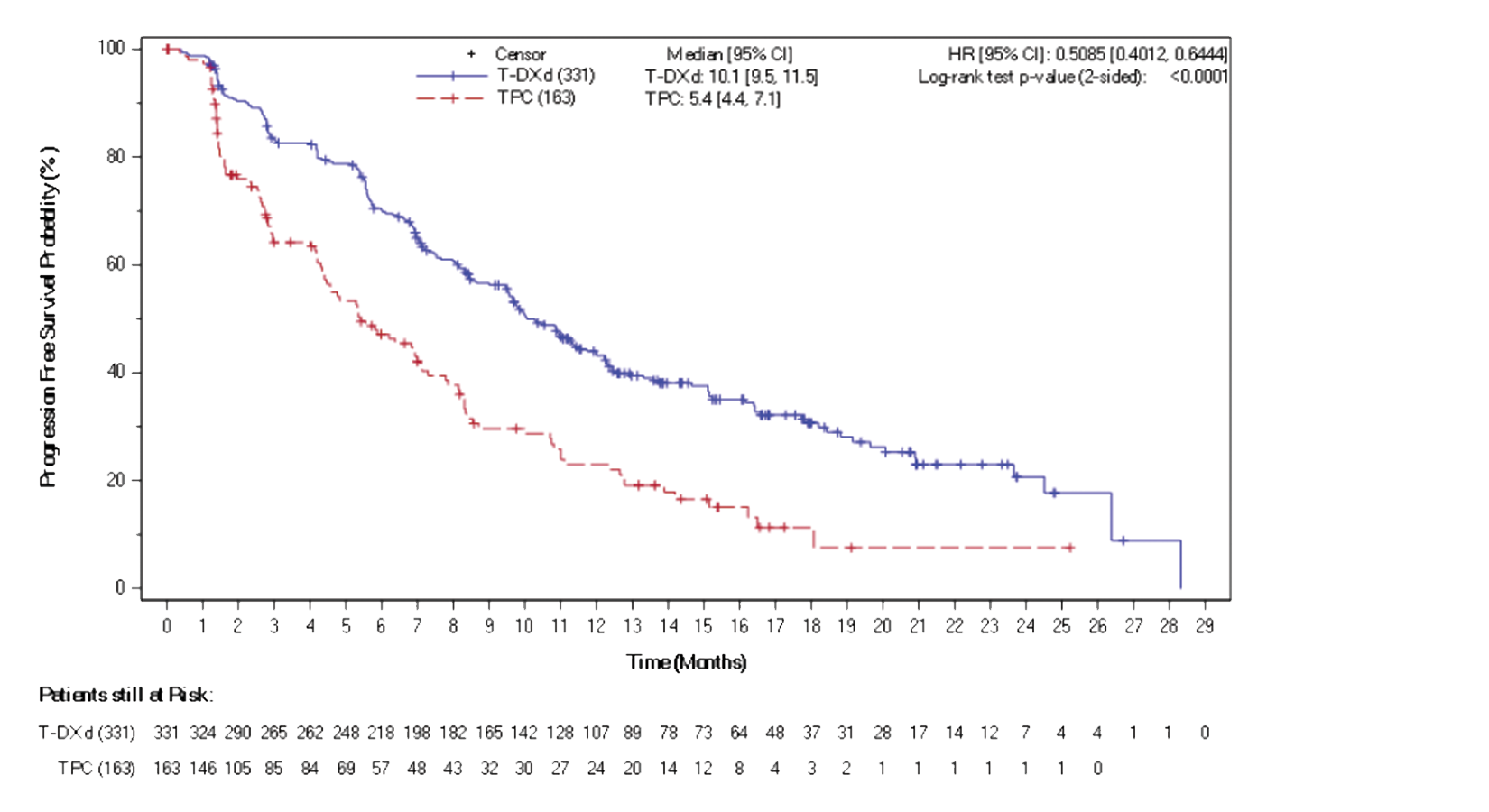
BICR = blinded independent central review; CI = confidence interval; HR = hazard ratio; PFS = progression-free survival; T-DXd = trastuzumab deruxtecan; TPC = treatment of physician’s choice.
Note: A stratified Cox proportional hazards model was used for the hazard ratio and a stratified log-rank test for the P value. Data cut-off: January 11, 2022.
Source: DESTINY-Breast04 Clinical Study Report.3
PFS results in the FAS are summarized in Table 21. The median PFS in the trastuzumab deruxtecan arm was 9.9 months (95% CI, 9.0 to 11.3) while in the TPC arm it was 5.1 months (95% CI, 4.2 to 6.8; P < 0.0001). The hazard ratio was 0.50 (95% CI, 0.40 to 0.63). The proportions of patients in PFS at 12 months were ||||| |||||| || |||||| in the trastuzumab deruxtecan arm ||| ||||| |||||| || |||||| in the TPC arm. The PFS Kaplan-Meier curves for the FAS are shown in Figure 5.
Table 21: Progression-Free Survival Based on BICR in the Full Analysis Set
Parameter | Trastuzumab deruxtecan N = 373 | Treatment of physician’s choice N = 184 |
|---|---|---|
Number (%) of patients with events | 243 (65.1) | 127 (69.0) |
Progressive disease | 208 (55.8) | 117 (63.6) |
Death | 35 (9.4) | 10 (5.4) |
Number (%) of patients without event (censored) | 130 (34.9) | 57 (31.0) |
No baseline evaluable tumour assessment | 0 | 0 |
No post-baseline tumour assessment | 3 (0.8) | 15 (8.2) |
Event after missing 2 consecutive assessments | 31 (8.3) | 17 (9.2) |
Lost to follow-up | 0 | 1 (0.5) |
Withdrew consent | 4 (1.1) | 7 (3.8) |
Ongoing without event | 69 (18.5) | 8 (4.3) |
Adequate tumour assessment no longer available | 23 (6.2) | 9 (4.9) |
Median progression-free survival (months) (95% CI)a | 9.9 (9.0 to 11.3) | 5.1 (4.2 to 6.8) |
P valueb | < 0.0001 | |
Hazard ratio (95% CI)c | 0.50 (0.40 to 0.63) | |
Percentage of patients alive and progression-free over timed | ||
3 months (95% CI) | |||| |||||| ||||| | |||| |||||| ||||| |
6 months (95% CI) | |||| |||||| ||||| | |||| |||||| ||||| |
9 months (95% CI) | |||| |||||| ||||| | |||| |||||| ||||| |
12 months (95% CI) | |||| |||||| ||||| | |||| |||||| ||||| |
18 months (95% CI) | |||| |||||| ||||| | |||| ||||| ||||| |
24 months (95% CI) | |||| |||||| ||||| | ||| ||||| ||||| |
BICR = blinded independent central review; CDK = cyclin-dependent kinase; CI = confidence interval; HR = hormone receptor.
Note: Data cut-off: January 11, 2022.
aMedian progression-free survival was from a Kaplan-Meier analysis. The CI for medians was computed using the Brookmeyer-Crowley method.
bTwo-sided P value from stratified log-rank test, included in the hierarchical testing structure.
cStratified Cox proportional hazards model with stratification factors: HER2 status, number of prior lines of chemotherapy, and HR/CDK status as defined by an interactive web/voice response system.
dEstimate and CI for progression-free survival rate at the specified time point are from a Kaplan-Meier analysis.
Source: DESTINY-Breast04 Clinical Study Report.3
Progression-Free Survival Subgroup Analyses
Subgroup analysis of PFS (based on strata from the IXRS) in the HR-positive cohort was consistent with the primary efficacy analysis, showing improvement in PFS in favour of the trastuzumab deruxtecan arm, regardless of IHC status, and prior chemotherapy or CDK 4/6 inhibitor use. The hazard ratios were |||| ||||| || ||||) for patients with an HER2 status of IHC 1+ and |||| ||||| || ||||| for patients with a HER2 status of IHC 2+/ISH−. The hazard ratios were |||| ||||| || ||||| for patients who had received 1 prior line of chemotherapy and |||| ||||| || ||||| for patients who had received 2 prior lines of chemotherapy. The hazard ratios were |||| ||||| || ||||| for patients who had received prior CDK 4/6 inhibitor therapy ||| |||| ||||| || ||||| for patients who had not received prior CDK 4/6 inhibitor therapy. A full summary of all subgroup analyses is provided in Appendix 1, Table 27.
Figure 5: Kaplan-Meier Plot of PFS Based on BICR by Treatment Arm in the Full Analysis Set
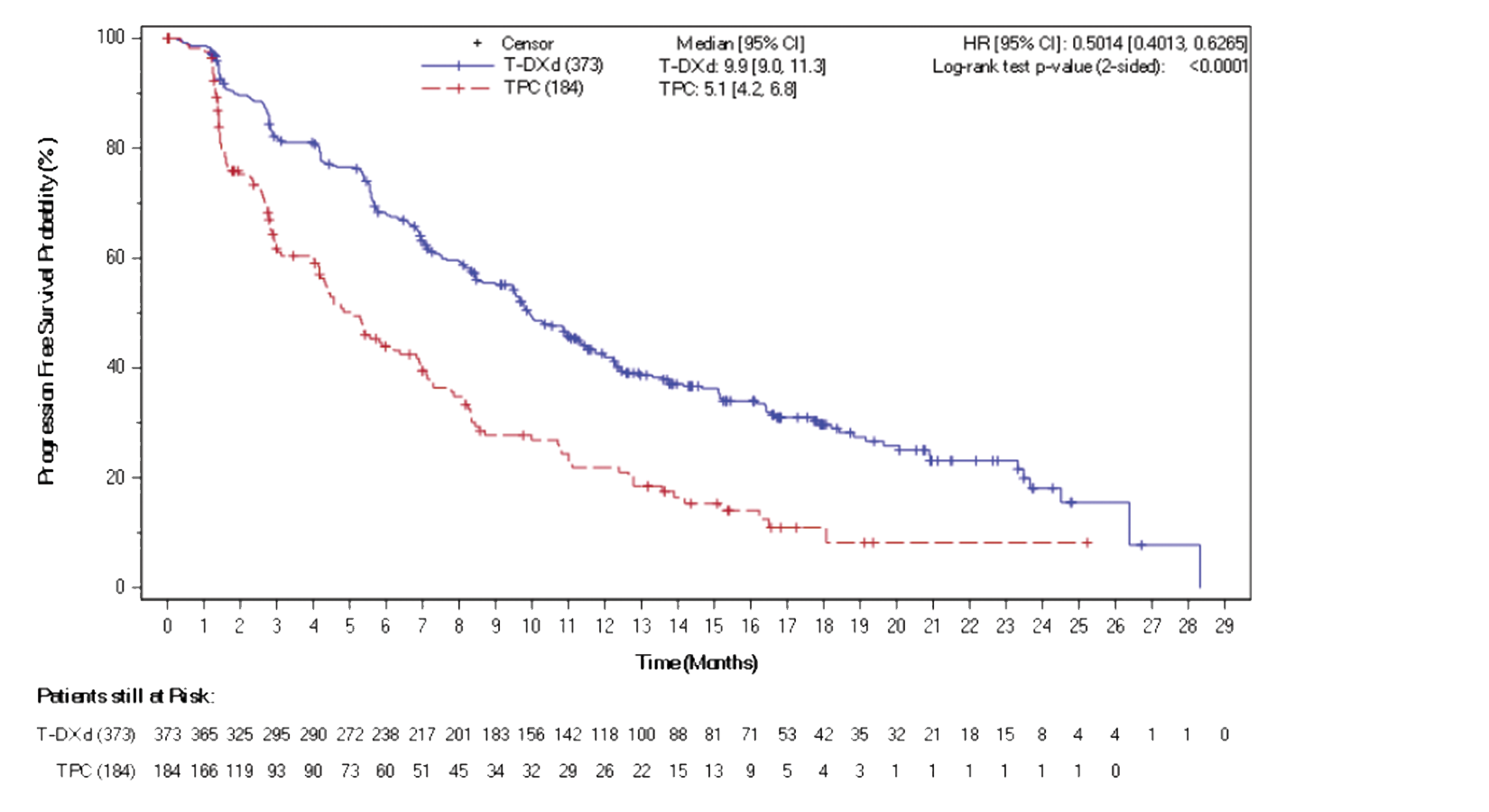
BICR = blinded independent central review; CI = confidence interval; HR = hazard ratio; PFS = progression-free survival; T-DXd = trastuzumab deruxtecan; TPC = treatment of physician’s choice.
Note: Stratified Cox proportional hazard model used for hazard ratio and stratified log-rank test for the P value. Data cut-off: January 11, 2022.
Source: DESTINY-Breast04 Clinical Study Report.3
Progression-Free Survival in the HR-Negative Cohort (Exploratory End Point)
PFS in the HR-negative cohort was an exploratory outcome; results are from an electronic data capture, unlike the methodology used for the primary analysis. Using the electronic data capture, 40 patients in the trastuzumab deruxtecan arm and 18 patients in the TPC arm were classified as HR-negative. Median PFS values in the HR-negative cohort were 8.5 months (95% CI, 4.3 to 11.7) in the trastuzumab deruxtecan group and 2.9 months (95% CI, 1.4 to 5.1) in the TPC group (hazard ratio = 0.48; 95% CI, 0.24 to 0.95).
Objective Response Rate
Table 22 summarizes the ORR based on BICR in both the HR-positive cohort and the FAS. The ORR of the 331 patients who received trastuzumab deruxtecan in the HR-positive cohort was 52.9% (95% CI, 47.3 to 58.4) while the 163 patients in the HR-positive cohort who received TPC had an ORR of 16.6% (95% CI, 11.2 to 23.2). In the FAS, the ORR of the 373 patients who received trastuzumab deruxtecan in the HR-positive cohort was 52.3% (95% CI, 47.1 to 57.4) while the 184 patients in the HR-positive cohort who received TPC had an ORR of 16.3% (95% CI, 11.3 to 22.5).
Table 22: Best Overall Response and Confirmed ORR Based on BICR in the HR-Positive Cohort and the Full Analysis Set
Parameter | HR-positive cohort | Full analysis set | ||||
|---|---|---|---|---|---|---|
Trastuzumab deruxtecan N = 331 | TPC N = 163 | Trastuzumab deruxtecan vs. TPC | Trastuzumab deruxtecan N = 373 | TPC N = 184 | Trastuzumab deruxtecan vs. TPC | |
Best overall response | ||||||
Based on BICR | ||||||
Complete response | 12 (3.6) | 1 (0.6) | 3.0 | 13 (3.5) | 2 (1.1) | 2.4 |
Partial response | 164 (49.5) | 26 (16.0) | 33.5 | 183 (49.1) | 28 (15.2) | 33.9 |
Stable disease | 115 (34.7) | 81 (49.7) | −15.0 | 129 (34.6) | 91 (49.5) | −14.9 |
Progressive disease | 26 (7.9) | 34 (20.9) | −13.0 | 31 (8.3) | 41 (22.3) | −14.0 |
Not evaluable | 14 (4.2) | 21 (12.9) | −8.7 | 17 (4.6) | 22 (12.0) | −7.4 |
Confirmed objective response rate (complete response + partial response) | ||||||
Based on BICR | ||||||
ORR, n (%) | 175 (52.9)a | 27 (16.6) | 36.3 | 195 (52.3)a | 30 (16.3) | 36.0 |
95% CIb | (47.3 to 58.4) | (11.2 to 23.2) | (28.0 to 44.6) | (47.1 to 57.4) | (11.3 to 22.5) | (28.2 to 43.7) |
P value (stratified analysis)c | < 0.0001 | < 0.0001 | ||||
BICR = blinded independent central review; CDK = cyclin-dependent kinase; CI = confidence interval; HR = hormone receptor; ORR = objective response rate: TPC = treatment of physician’s choice.
Note: Data cut-off: January 11, 2022.
aOne patient in the trastuzumab deruxtecan arm who had a confirmed best overall response of complete or partial response received a baseline scan after randomization but before the first dose and was therefore considered a nonresponder in the calculation of confirmed ORR.
bBased on the Clopper-Pearson method for single proportion and for the difference of 2 proportions with continuity correction.
cTwo-sided P value based on the Cochran-Mantel-Haenszel-test adjusted for stratification factors: HER2 status, number of prior lines of chemotherapy, HR/CDK status as defined by an interactive web/voice response system. P value not controlled for multiplicity.
Source: DESTINY-Breast04 Clinical Study Report.3
Modi et al. (2022)50 reports the results for the HR-negative cohort. This analysis used a more accurate electronic data capture method, differing from the methodology used for the primary analysis. In 40 patients from the HR-negative cohort who received trastuzumab deruxtecan, the ORR was 50.0% (95% CI, 33.8 to 66.2), 2.5% of whom had CRs, compared to 18 patients from the HR-negative cohort who received TPC, with an ORR of 16.7% (95% CI, 3.6 to 41.4), 5.6% of whom had CRs. Median times to response were 1.51 months in patients who received trastuzumab deruxtecan and 1.41 months in patients who received TPC.
Duration of Response
Duration of confirmed response based on the BICR is summarized in Table 23. In the 176 patients who received trastuzumab deruxtecan in the HR-positive cohort and recorded a complete or partial response, the median DOR was 10.7 months (95% CI, 8.5 to 13.7), compared to 27 patients in the TPC arm, with a median response of 6.8 months (95% CI, 6.5 to 9.9). In the FAS, 196 patients in the trastuzumab deruxtecan arm recorded a complete or partial response and the median DOR was 10.7 (95% CI, 8.5 to 13.2), compared to 30 patients in the TPC arm, with a median response of 6.8 months (95% CI, 6.0 to 9.9).
Table 23: Duration of Confirmed Response Based on BICR in the HR-Positive Cohort and the Full Analysis Set
Parameter | HR-positive cohort | Full analysis set | ||
|---|---|---|---|---|
Trastuzumab deruxtecan N = 331 | TPC N = 163 | Trastuzumab deruxtecan N = 373 | TPC N = 184 | |
Patients with complete or partial response | 176 | 27 | 196 | 30 |
Patients with events, n (%) | 100 (56.8) | 18 (66.7) | 113 (57.7) | 20 (66.7) |
Progressive disease | 87 (49.4) | 16 (59.3) | 99 (50.5) | 18 (60.0) |
Death | 13 (7.4) | 2 (7.4) | 14 (7.1) | 2 (6.7) |
Patients with no events (censored), n (%) | 76 (43.2) | 9 (33.3) | 83 (42.3) | 10 (33.3) |
Event after missing 2 consecutive assessments | 13 (7.4) | 2 (7.4) | 15 (7.7) | 3 (10.0) |
Lost to follow-up | 0 | 0 | 0 | 0 |
Withdrew consent | 3 (1.7) | 1 (3.7) | 3 (1.5) | 1 (3.3) |
Ongoing without event | 49 (27.8) | 4 (14.8) | 51 (26.0) | 4 (13.3) |
Adequate tumour assessment no longer available | 11 (6.3) | 2 (7.4) | 14 (7.1) | 2 (6.7) |
Median (95% CI)a duration of CR/PR (months) | 10.7 (8.5 to 13.7) | 6.8 (6.5 to 9.9) | 10.7 (8.5 to 13.2) | 6.8 (6.0 to 9.9) |
BICR = blinded independent central review; CI = confidence interval; CR = complete response; HR = hormone receptor; PR = partial response; TPC = treatment of physician’s choice.
Note: Duration of response was defined as the time from date of the first documentation of objective response (complete or partial response) to the date of the first documentation of disease progression based on BICR or death. Percentage was calculated using number of patients with complete or partial response. Data cut-off: January 11, 2022.
aMedian was from a Kaplan-Meier estimate. The CI for the medians was computed using the Brookmeyer-Crowley method.
Source: DESTINY-Breast04 Clinical Study Report.3
Harms
Harms data were reported for all patients who received at least 1 dose of study drug in the safety analysis set of the DESTINY-Breast04 trial. Table 24 presents detailed harms data from the DESTINYBreast-04 trial by the January 11, 2022, data cut-off.
Adverse Events
In total, 99.5% of patients in the trastuzumab deruxtecan arm and 98.3% of patients in the TPC arm reported 1 or more AEs by the January 11, 2022, data cut-off.
Serious Adverse Events
SAEs of any grade were reported in 27.8% of patients in the trastuzumab deruxtecan arm and 25% of patients in the TPC arm by the January 11, 2022, data cut-off.
Withdrawal Due to Adverse Events
AEs leading to treatment discontinuation were reported in 16.2% of patients receiving trastuzumab deruxtecan and 8.1% in the TPC arm by the January 11, 2022, data cut-off.
Mortality
Overall, 39.9% of patients in the trastuzumab deruxtecan arm and 51.2% of patients in the TPC arm had died by the January 11, 2022, data cut-off. The most common reasons leading to death in both arms were disease progression and AEs.
Notable Harms
AEs of special interest reported in the DESTINY-Breast04 trial by the January 11, 2022, data cut-off are presented in Table 24. ILD/pneumonitis and left ventricular dysfunction were more common in the trastuzumab deruxtecan arm (12.1% and 4.6%, respectively) compared to the TPC arm (0.6% and 0%, respectively).
Table 24: Summary of Harms in DESTINY-Breast04 — Safety Analysis Set
Adverse events | Trastuzumab deruxtecan (N = 371) | Treatment of physician’s choice (N = 172) |
|---|---|---|
Most common adverse events (more than 10% in either treatment arm), n (%) | ||
Any treatment-emergent adverse event | 369 (99.5) | 169 (98.3) |
Nausea | 282 (76.0) | 52 (30.2) |
Fatigue | 199 (53.6) | 83 (48.3) |
Vomiting | 150 (40.4) | 23 (13.4) |
Alopecia | 147 (39.6) | 57 (33.1) |
Anemia | 143 (38.5) | 47 (27.3) |
Neutropenia | 126 (34.0) | 90 (52.3) |
Constipation | 126 (34.0) | 38 (22.1) |
Increased transaminases | 120 (32.3) | 54 (31.4) |
Decreased appetite | 118 (31.8) | 33 (19.2) |
Diarrhea | 100 (27.0) | 38 (22.1) |
Musculoskeletal pain | 99 (26.7) | 45 (26.2) |
Thrombocytopenia | 95 (25.6) | 16 (9.3) |
Leukopenia | 89 (24.0) | 56 (32.6) |
Abdominal pain | 65 (17.5) | 23 (13.4) |
Decreased weight | 60 (16.2) | 14 (8.1) |
Headache | 55 (14.8) | 11 (6.4) |
Upper respiratory tract infection | 51 (13.7) | 9 (5.2) |
Stomatitis | 49 (13.2) | 19 (11.0) |
Pyrexia | 46 (12.4) | 22 (12.8) |
Interstitial lung disease | 45 (12.1) | 1 (0.6) |
Arthralgia | 43 (11.6) | 20 (11.6) |
Decreased blood potassium | 41 (11.1) | 13 (7.6) |
Epistaxis | 39 (10.5) | 2 (1.2) |
Dyspnea | 38 (10.2) | 16 (9.3) |
Peripheral sensory neuropathy | 18 (4.9) | 19 (11.0) |
Palmar-plantar erythrodysesthesia syndrome | 5 (1.3) | 24 (14.0) |
Serious adverse events (more than 1% in either treatment arm), n (%) | ||
Any serious treatment-emergent adverse event | 103 (27.8) | 43 (25.0) |
Interstitial lung disease | 16 (4.3) | 1 (0.6) |
Pneumonia | 7 (1.9) | 1 (0.6) |
Dyspnea | 5 (1.3) | 2 (1.2) |
Musculoskeletal pain | 5 (1.3) | 0 |
Sepsis | 5 (1.3) | 0 |
Febrile neutropenia | 4 (1.1) | 4 (2.3) |
Anemia | 4 (1.1) | 1 (0.6) |
Hypercalcemia | 4 (1.1) | 0 |
Nausea | 4 (1.1) | 0 |
Pyrexia | 4 (1.1) | 0 |
Vomiting | 4 (1.1) | 0 |
Fatigue | 3 (0.8) | 2 (1.2) |
Pleural effusion | 3 (0.8) | 2 (1.2) |
Neutropenia | 2 (0.5) | 4 (2.3) |
Disease progression | 2 (0.5) | 2 (1.2) |
Hepatic failure | 1 (0.3) | 2 (1.2) |
Hyponatremia | 1 (0.3) | 2 (1.2) |
Overdose | 0 | 5 (2.9) |
Medication error | 0 | 3 (1.7) |
Colitis | 0 | 2 (1.2) |
Femur fracture | 0 | 2 (1.2) |
Patients who stopped treatment due to adverse events, n (%) | ||
Patients who stopped | 60 (16.2) | 14 (8.1) |
Interstitial lung disease | 31 (8.4) | 0 |
Left ventricular dysfunction | 3 (0.8) | 0 |
Increased blood bilirubin | 2 (0.5) | 0 |
Dyspnea | 2 (0.5) | 0 |
Pleural effusion | 2 (0.5) | 0 |
Decreased blood potassium | | ||||| | | ||||| |
Colitis ischemic | | ||||| | | ||||| |
Disseminated intravascular coagulation | | ||||| | | ||||| |
Electrocardiogram QT prolongation | | ||||| | | ||||| |
Fatigue | | ||||| | | ||||| |
Febrile neutropenia | | ||||| | | ||||| |
Hepatic failure | | ||||| | | ||||| |
Left atrial enlargement | | ||||| | | ||||| |
Lymphopenia | | ||||| | | ||||| |
Nausea | | ||||| | | ||||| |
Pneumonia | | ||||| | | ||||| |
Staphylococcal bacteremia | | ||||| | | ||||| |
Stress cardiomyopathy | | ||||| | | ||||| |
Vomiting | | ||||| | | ||||| |
Weight decreased | | ||||| | | ||||| |
Peripheral sensory neuropathy | 0 | 4 (2.3) |
Abdominal pain | | ||||| | | ||||| |
Angina pectoris | | ||||| | | ||||| |
Breast pain | | ||||| | | ||||| |
Colitis | | ||||| | | ||||| |
Hemorrhoids | | ||||| | | ||||| |
Peripheral neuropathy | | ||||| | | ||||| |
Ocular hypertension | | ||||| | | ||||| |
Palmar-plantar erythrodysesthesia syndrome | | ||||| | | ||||| |
Polyneuropathy | | ||||| | | ||||| |
Pulmonary embolism | | ||||| | | ||||| |
Superior vena cava occlusion | | ||||| | | ||||| |
Deaths by primary cause, n (%) | ||
Any death | 148 (39.9) | 88 (51.2) |
Disease progression | 122 (32.9) | 79 (45.9) |
Adverse event | 10 (2.7) | 0 |
Other | 3 (0.8) | 3 (1.7) |
Cachexia due to cancer | | ||||| | | ||||| |
Clinical progression | | ||||| | | ||||| |
Disease progression (liver dysfunction) | | ||||| | | ||||| |
Disease worsening under study | | ||||| | | ||||| |
Respiratory arrest | | ||||| | | ||||| |
Respiratory failure due to pneumonitis, pulmonary embolus | | ||||| | | ||||| |
Unknown | | ||||| | | ||||| |
On-treatment deatha | 14 (3.8) | 8 (4.7) |
Disease progression | 4 (1.1) | 7 (4.1) |
Adverse event | 8 (2.2) | 0 |
Other | 1 (0.3) | 1 (0.6) |
Cachexia due to cancer | | ||||| | | ||||| |
Disease progression (liver dysfunction) | | ||||| | | ||||| |
Unknown | 1 (0.3) | 0 |
Adverse events of special interest, n (%) | ||
Interstitial lung disease/pneumonitis | 45 (12.1) | 1 (0.6) |
Left ventricular dysfunction | 17 (4.6) | 0 |
Note: Details from the table have been taken from the sponsor’s Summary of Clinical Evidence. Data cut-off: January 11, 2022.
aAn on-treatment death was defined as a death that occurred between the start of treatment and 47 days after the last dose.
Source: DESTINY-Breast04 Clinical Study Report.3
Critical Appraisal
Internal Validity
DESTINY-Breast04 was a phase III, multicentre, randomized, double-arm, open-label, active-controlled study. Patients were randomly assigned to receive either trastuzumab deruxtecan or TPC in a 2:1 ratio. Randomization was stratified according to HER2 status, number of prior lines of chemotherapy, and HR status and/or prior exposure to CDK 4/6 inhibitors was defined by an IXRS. The stratification factors were chosen appropriately and validated by clinical experts consulted by CADTH. However, stratification was based on an IXRS at the time of randomization, which differed from an electronic data capture that corrected for mis-stratification at randomization. The overall number of patients who were mis-stratified with regards to HR status in the primary analysis was low (63 HR-negative patients in the uncorrected analysis and 58 HR-negative patients in the corrected analysis), and prespecified PFS sensitivity analyses conducted in the HR-positive cohort suggested that stratification did not have a meaningful impact on that specific end point. Additional discrepancies between the IXRS stratification and the corrected electronic data capture were found in the prior lines of chemotherapy stratification factor. In the trastuzumab deruxtecan arm, 161 patients were recorded by the IXRS as having received 2 prior lines of chemotherapy compared to the corrected value of |||. In the TPC arm, 81 patients were recorded by the IXRS as having received 2 prior lines of chemotherapy compared to the corrected value of ||. The clinical experts consulted by CADTH confirmed that, in general, heavily pretreated patients have worse expected outcomes, and because the trastuzumab deruxtecan arm was less heavily pretreated than the IXRS stratification suggests, there may be a bias in favour of trastuzumab deruxtecan, although the magnitude is unknown.
The primary end point in the study was PFS based on BICR in the HR-positive cohort, with secondary end points (PFS based on BICR in the FAS and OS in both the HR-positive cohort and FAS) tested in a hierarchical sequence. The statistical analysis plan allowed for 2 interim analyses and 1 final analysis of OS. Stopping boundaries appear to be calculated appropriately to account for multiplicity; however, the OS analysis was stopped at the first interim analysis, with an information fraction of ||||| (a measure of the amount of information present at an interim analysis in relation to the total information available). Early stopping rules preserve type I error rates of the OS significance tests but increase the possibility that benefits are overestimated.51
Although the open-label design of the study may have biased the subjective HRQoL end points in favour of trastuzumab deruxtecan, the BICR and RECIST methodologies likely reduced the impact of this bias on the PFS end point. The open-label design may have resulted in an informative censoring mechanism in which certain patients exited the study before the first postbaseline tumour assessment. In the FAS analysis of PFS with |||| of patients in the TPC arm censored due to no postbaseline tumour assessment, compared to only |||| in the trastuzumab deruxtecan arm. A post hoc sensitivity analysis was conducted to assess the impact of an alternative censoring strategy in which patients with no postbaseline tumour assessment who were assumed to have not experienced a progression event until the end of the study. Results of this post hoc sensitivity analysis were consistent with those of the primary analysis but resulted in a smaller estimated hazard ratio || |||| |||| || |||||||||||| for PFS and |||| |||| || |||||| |||||| for OS in the FAS. The directions in change of the estimated hazard ratios in the sensitivity analysis were expected and provide a conservative estimate of the hazard ratio if the differences in censoring due to withdrawal were noninformative but driven solely by the treatment assignment. No provided sensitivity analyses explored the sensitivity of the results to violations of the noninformative censoring assumption.
No HER2-low BC-specific MID studies were identified for the HRQoL outcomes. However, the clinical experts consulted by CADTH suggested that it would be reasonable to assume MIDs validated in BC patients in general would apply to the HER2-low population. MIDs for EQ-5D-5L and the EORTC QLQ-C30 validated in cancer and mBC patients aided in the interpretation and generalizability of the HRQoL outcomes in the DESTINY-Breast04 trial, although these outcomes were exploratory and not adjusted for multiplicity. As no MID studies were identified for the EORTC QLQ-BR45 (EORTC QLQBR23), results are uncertain.
External Validity
The DESTINY-Breast04 study population was considered by the clinical experts consulted by CADTH to be representative and generalizable to the Canadian population. The investigated dose of trastuzumab deruxtecan was 5.4 mg/kg, IV, every 3 weeks, consistent with the expected Health Canada–approved dose. The clinical experts consulted suggested that the basket of chemotherapies used for the TPC arm of the DESTINY-Breast04 study was appropriate and representative of Canadian practice. They also suggested that it is reasonable to infer there are no meaningful differences in efficacy between the chemotherapy options for the patient population.
In the study, 30% of HR-positive patients had not received any prior treatment with CDK 4/6 inhibitors. This is not consistent with the Canadian population given that CDK 4/6 inhibitors are a standard first-line therapy for HR-positive patients, although the clinical experts did not expect this discrepancy would affect the generalizability of the study results.
Long-Term Extension Studies
No long-term extension studies were submitted by the sponsor
Indirect Evidence
Contents within this section have been informed by materials submitted by the sponsor. The following have been summarized and validated by the CADTH review team.
Objectives and Methods for the Summary of Indirect Evidence
Trastuzumab deruxtecan has been compared to TPC in patients with unresectable or metastatic HER2-low BC who have received at least 1 prior line of chemotherapy in the metastatic setting or developed disease recurrence during or within 6 months of completing adjuvant chemotherapy. However, TPC did not contain any treatments targeting HER2-low patients and the trial did not examine head-to-head evidence comparing trastuzumab deruxtecan with other relevant comparators for treatment of mBC in the HER2-low population. Sacituzumab govitecan has received a conditional positive recommendation from CADTH and is currently the subject of price negotiations for an indication of metastatic triple-negative BC. As such, sacituzumab govitecan would be considered a comparator of interest for HR-negative patients in the DESTINY-Breast04 trial.
Description of Indirect Comparison
The sponsor submitted a feasibility assessment for an NMA to assess the relative effectiveness of trastuzumab deruxtecan versus relevant comparators to support reimbursement in HER2-low unresectable BC and/or mBC populations.
Table 25: Study Selection Criteria and Methods for ITC Feasibility Assessment Submitted by Sponsor
Characteristics | Indirect comparison feasibility |
|---|---|
Population | Primary: Adult (age ≥ 18 years) patients with HR+/HER2-negative, unresectable, and/or mBC Secondary: Adult (age ≥ 18 years) patients with triple-negative, unresectable, and/or mBC who have previously been treated in the metastatic setting or after disease recurrence within 6 months of (neo)adjuvant chemotherapy; studies that assess a mixed population shall be included if > 80% of the study population is the target population described here. |
Intervention | Any, with the exception of ETs |
Comparator | Any, with the exception of Ets |
Outcomes |
|
Study designs |
|
Publication characteristics | English (from 2011 onward) |
Exclusion criteria |
|
Databases searched |
|
Selection process |
|
Data extraction process |
|
Quality assessment |
|
BC = breast cancer; ECOG PS = European Cooperative Oncology Group Performance Status; ET = endocrine therapy; HR = hormone receptor; mBC = metastatic breast cancer; NICE = National Institute for Health and Care Excellence; RCT = randomized controlled trial.
Note: If it was unclear whether a study meets any criterion during the level 1 screening process, the study was progressed to full-text screening to confirm its inclusion in the review.
Source: Sponsor-submitted NMA feasibility assessment.52
ITC Design
Objectives
Table 26: Comparison of Treatment-Effect Modifiers Reported for Studies Included in the Networks
Trial | IHC status | Median age | Prior lines of (chemo)therapy in the advanced setting (%) | ECOG PS (%) | Location of tumours (%) | Race (%) | Brain metastases (%) |
|---|---|---|---|---|---|---|---|
DESTINY-Breast0450 | HER2-low | 59.3 | 1: 38.1 2: 35.7 ≥ 3: 26.2 | 0: 31 1: 69 | Liver: 45.2 Lung: 52.4 | White: 47.6 Asian: 47.6 | 14.3 |
ASCENT, 202253 | HER2-low | 55 | 2 to 3:71 > 3:29 | 0:46 1:54 | NR | White: 87 Asian: 5 | NR |
ASCENT, 202154 | Triple Negativea | 54 | 2 to 3: 71 > 3:29 | 0:46 1:54 | Lung: 46 Liver: 42 | White: 80 Asian: 4 | 0 |
ECOG PS = Eastern Cooperative Oncology Group Performance Status; IHC = immunohistochemistry; NR = not reported.
aThe full ASCENT trial was conducted in the metastatic triple negative indication. This includes both HER2-low and HER2-negative.
Source: Sponsor-submitted NMA feasibility assessment.52
Summary of the Sponsor-Conducted Feasibility Assessment
The sponsor conducted a systematic review to inform an ITC feasibility assessment to evaluate the relative effectiveness of trastuzumab deruxtecan against relevant comparators in the unresectable BC and/or metastatic HER2-low BC population. Of the 17 studies identified in the review, 1 study (ASCENT 2022) met the required criteria of Table 25. The ASCENT trial was a global, open-label, randomized trial that assessed the benefit of sacituzumab govitecan versus TPC (TPC therapies included capecitabine, eribulin, vinorelbine, or gemcitabine) in HER2 IHC 0 and HER2-low metastatic triple-negativAppen BC patients. PFS and OS were the outcomes of interest for this analysis. The HER2-low subgroup of interest for the ITC was defined post hoc, and analyses were exploratory within the ASCENT trial. The sponsor subdivided the HER2-low population to HR-positive/HER2-low and HR-negative/HER2-low to assess OS and PFS outcomes. For the HR-negative/HER2-low mBC patient population, sacituzumab govitecan was the only comparator identified that was connected to trastuzumab deruxtecan with TPC as a common comparator in the network. No relevant studies were identified for the HR-positive/HER2-low population.
Although a potential network was constructed between trastuzumab deruxtecan and sacituzumab govitecan, conducting an NMA was not considered feasible due to several limitations. In particular, the sponsor noted large differences in baseline characteristics across the 2 studies, particularly in ECOG PS, race, presence of brain metastases, and prior lines of treatment (Table 26). These variables were identified by the sponsor as potential effect modifiers based on a review of the literature and expert opinion, and may have resulted in biased estimates. The clinical experts consulted during the CADTH review agreed that the observed imbalances in baseline characteristics across the 2 studies would likely affect the treatment effect in the HER2-negative patient population. The sponsor’s conclusion that this NMA was infeasible was therefore considered appropriate.
The sponsor submitted a MAIC feasibility assessment to compare trastuzumab deruxtecan to sacituzumab govitecan in the HR-negative/HER2-low mBC population. The sponsor noted that HR-negative cohorts of both trials were considered relatively small and suggested this would result in unreliable results from a MAIC due to reductions in the effective sample size. In addition, detailed patient characteristics were not reported in the ASCENT 2021 publication nor were these details provided in the subsequent HER2-low subgroup analysis. The sponsor noted that key characteristics, such as tumour location, prior lines of treatment, and presence of brain metastases, which were shown to be critical treatment-effect modifiers, were not reported. The sponsor concluded that an attempt to match the DESTINY-Breast04 trial to the ASCENT 2022 trial population would have to assume that the characteristics from the previous ASCENT 2021 publication (full triple-negative BC population inclusive of IHC 0) do not change and remain as is in the ASCENT 2022 publication (HER2-low cohort). Although the rationale provided by the sponsor does not clearly make a MAIC infeasible in this setting, the CADTH review team agreed with the sponsor that a MAIC would likely produce biased and imprecise estimates due to the identified limitations. Results from the MAIC would therefore be unlikely to informative for a reimbursement decision.
Studies Addressing Gaps in the Pivotal and Randomized Controlled Trial Evidence
No additional studies addressing gaps in the evidence were submitted by the sponsor.
Discussion
Summary of Available Evidence
The pivotal trial submitted for this review, DESTINY-Breast04 (N = 557), is a phase III, randomized, open-label, active-controlled trial of trastuzumab deruxtecan compared to TPC in patients with HER2-low unresectable or mBC. The trial included an HR-positive cohort and a FAS cohort that included a small number of patients with HR-negative, HER2-low BC. The primary end point was PFS according to a BICR in the HR-positive cohort with key secondary end points including OS in the HR-positive cohort and both PFS and OS in the FAS. Patients in the DESTINY-Breast04 study had a mean age of 56.5 years and 54.8% had an ECOG PS of 0.
The sponsor also provided a feasibility assessment for conducting an ITC in the HR-negative population against the comparator sacituzumab govitecan. An ITC was deemed infeasible due to the major differences in the clinical trial characteristics and small number of patients included.
Interpretation of Trial Results
Efficacy
In the DESTINY-Breast04 study, trastuzumab deruxtecan showed a statistically significant benefit in the primary end point of PFS in the HR-positive cohort when compared to TPC. Similar benefits were observed in the FAS, which included HR-negative patients as well. This benefit was recognized by the clinical experts as a clinically meaningful difference for patients. An OS benefit in favour of trastuzumab deruxtecan was shown in the FAS, with median OS values of 23.4 months (95% CI, 20.0 to 24.8) in the trastuzumab deruxtecan arm and 16.8 months (95% CI, 14.5 to 20.0) in the TPC arm, (hazard ratio = 0.64, 95% CI, 0.49 to 0.84, P = 0.0010). Similar benefits were observed in the HR-positive cohort. With the acknowledgement that early stopping of interim OS analyses increases the possibility of overestimating the benefits, the clinical experts consulted by CADTH considered the OS benefits to be clinically meaningful (suggesting that about 2 treatment cycles is usually interpreted as clinically meaningful) for patients, even for the most conservative estimates, based on the 95% CI. Patient input emphasized the importance of access to treatments that control disease progression, extend life, and manage cancer-related symptoms.
The design of DESTINY-Breast04 intentionally enrolled a smaller number of patients with HR-negative disease to better reflect the true distribution of patients in clinical practice. While this increases the generalizability of the FAS results to the expected Canadian population, the consequence of the design is that the HR-negative subgroup results are exploratory. Although no conclusions can be drawn directly from the HR-negative cohort results, they appear to be similar to those of the primary analysis. The clinical experts suggested that it is reasonable to assume that trastuzumab deruxtecan would have a similar benefit regardless of HR status, given that trastuzumab deruxtecan does not target the HR.
HRQoL was identified by patients as a key outcome for consideration in the treatment of mBC. As the DESTINY-Breast04 trial was not powered to detect differences in HRQoL outcomes, conclusions cannot be drawn regarding the impact that trastuzumab deruxtecan will have on the HRQoL of patients. Descriptively, there did not appear to be a deterioration in HRQoL in patients who received trastuzumab deruxtecan as the MID for the EORTC QLQ-C30 and EQ VAS were not exceeded over time. No MIDs specific to mBC were identified for the EQ-5D-5L index scores or the EORTC QLQ-BR45 (EORTC QLQ-BR23), limiting the usefulness of even descriptive comments for those outcomes.
The potential for an ITC comparing trastuzumab deruxtecan against sacituzumab govitecan was discussed by the sponsor and ultimately deemed infeasible. Sacituzumab govitecan is a comparator of interest. Given that it is indicated for triple-negative BC following treatment with chemotherapy, a subset of those patients would be classified as HER2-low in the new testing paradigm, and this subset aligns with the HR-negative cohort in the DESTINY-Breast04 trial. Sacituzumab govitecan is currently the subject of price negotiations following a conditional positive recommendation from CADTH. Given the lack of comparative evidence, the relative efficacy of trastuzumab deruxtecan against sacituzumab govitecan is unknown; however, the clinical experts suggested that, if the patient is classified as HER2-low, the use of a targeted therapy may be preferred, although it was suggested that these drugs may be used sequentially in clinical practice.
Harms
In the DESTINY-Breast04, the safety profile of trastuzumab deruxtecan was comparable to that of TPC. AEs and SAEs occurred in roughly the same proportion of patients in both treatment arms. There was a higher occurrence of nausea and ILD in the trastuzumab deruxtecan arm, with ILD resulting in a higher proportion of patients stopping treatment; however, the clinical experts consulted considered these occurrences to be manageable. The trastuzumab family of drug products has a well-defined safety profile and is used in many BC indications. There does not appear to be any evidence of additional safety concerns for the unresectable or metastatic HER2-low BC population.
Other Considerations
The impact of HER2-low on the testing paradigm for mBC in Canada was discussed with clinical experts consulted by CADTH. A pathologist expert was also consulted. HER2-low (IHC 1+ or IHC 2+/ISH−) is a new classification within the BC landscape; however, it is defined using the established 2018 ASCO and CAP testing guidelines for HER2 testing. The pathology expert consulted by CADTH confirmed that existing samples for patients already tested can be re-read to determine HER2-low status, with no need for an additional biopsy. The clinical experts further highlighted that patients may also be retested for HER2 expression following disease progression from local to metastatic disease, as HER2 expression can drift throughout the course of disease.
The pathologist expert consulted noted that, depending on calibration, some assays used in Canada may detect a higher proportion of HER2-low compared with other assays. The pathologist expert also noted that there may be interobserver discordance and lack of reproducibility when differentiating 0 and 1+ to determine HER2 IHC status, as interpretation of these 2 categories has been less rigorous historically. However, the pathologist expert indicated that, with increased awareness and adequate training, Canadian pathologists and oncologists will be able to correctly identify HER2-low patients.
Conclusion
Evidence from the DESTINY-Breast04 trial showed statistically significant and clinically meaningful benefits in PFS and OS with trastuzumab deruxtecan 5.4 mg/kg every 3 weeks compared to TPC in patients with unresectable or metastatic HER2-low BC who have received at least 1 prior line of chemotherapy in the metastatic setting or developed disease recurrence during or within 6 months of completing adjuvant chemotherapy. HRQoL was identified in patient input as a key end point important to patients. The evidence provided by the DESTINY-Breast04 study was not sufficient to draw conclusions about the effect on HRQoL. There remains an evidence gap for the relative efficacy comparison against sacituzumab govitecan in the HR-negative cohort of patients, although the cohort of patients for whom this comparison is relevant is small compared to the overall patient population. The clinical experts consulted for this review described the safety profile of trastuzumab deruxtecan as manageable and in line with their expectations.
References
1.Mitri Z, Constantine T, O'Regan R. The HER2 Receptor in Breast Cancer: Pathophysiology, Clinical Use, and New Advances in Therapy. Chemother Res Pract. 2012;2012:743193. PubMed
2.Slamon DJ, Clark GM, Wong SG, Levin WJ, Ullrich A, McGuire WL. Human breast cancer: correlation of relapse and survival with amplification of the HER-2/neu oncogene. Science. 1987;235(4785):177-182. PubMed
3.Clinical Study Report: DS8201-A-U303. A Phase 3, Multicenter, Randomized, Open-label, Active-controlled Trial of Trastuzumab Deruxtecan (T-DXd), an Anti-HER2-antibody Drug Conjugate (ADC), versus Treatment of Physician’s Choice for HER2-low, Unresectable and/or Metastatic Breast Cancer Subjects [internal sponsor's report]. Basking Ridge (NJ): Daiichi Sankyo Inc.; 2022 May 3.
4.Brenner DR, Poirier A, Woods RR, et al. Projected estimates of cancer in Canada in 2022. CMAJ. 2022;194(17):E601-E607. PubMed
5.Public Health Agency of Canada. Breast cancer in Canada. 2021; https://www.canada.ca/en/public-health/services/publications/diseases-conditions/breast-cancer.html. Accessed 2023 Jan 19.
6.Redig AJ, McAllister SS. Breast cancer as a systemic disease: a view of metastasis. J Intern Med. 2013;274(2):113-126. PubMed
7.O'Shaughnessy J. Extending survival with chemotherapy in metastatic breast cancer. Oncologist. 2005;10 Suppl 3:20-29. PubMed
8.Visovsky C. Treatment Considerations for the Management of Patients With Hormone Receptor-Positive Metastatic Breast Cancer. J Adv Pract Oncol. 2014;5(5):321-330. PubMed
9.Hess KR, Esteva FJ. Effect of HER2 status on distant recurrence in early stage breast cancer. Breast Cancer Res Treat. 2013;137(2):449-455. PubMed
10.Irvin W, Jr., Muss HB, Mayer DK. Symptom management in metastatic breast cancer. Oncologist. 2011;16(9):1203-1214. PubMed
11.Mokhtari-Hessari P, Montazeri A. Health-related quality of life in breast cancer patients: review of reviews from 2008 to 2018. Health Qual Life Outcomes. 2020;18(1):338. PubMed
12.Wolff AC, Hammond MEH, Allison KH, et al. Human Epidermal Growth Factor Receptor 2 Testing in Breast Cancer: American Society of Clinical Oncology/College of American Pathologists Clinical Practice Guideline Focused Update. J Clin Oncol. 2018;36(20):2105-2122. PubMed
13.Tarantino P, Hamilton E, Tolaney SM, et al. HER2-Low Breast Cancer: Pathological and Clinical Landscape. J Clin Oncol. 2020;38(17):1951-1962. PubMed
14.Marchio C, Annaratone L, Marques A, Casorzo L, Berrino E, Sapino A. Evolving concepts in HER2 evaluation in breast cancer: Heterogeneity, HER2-low carcinomas and beyond. Semin Cancer Biol. 2021;72:123-135. PubMed
15.Schettini F, Chic N, Braso-Maristany F, et al. Clinical, pathological, and PAM50 gene expression features of HER2-low breast cancer. NPJ Breast Cancer. 2021;7(1):1. PubMed
16.Oncology Outcomes (2022). Real world evidence study to assess Treatment Patterns and Outcomes in HER2 Normal Metastatic or Recurrent Breast Cancer. Alberta, Canada. Unpublished.
17.Seung SJ, Traore AN, Pourmirza B, Fathers KE, Coombes M, Jerzak KJ. A population-based analysis of breast cancer incidence and survival by subtype in Ontario women. Curr Oncol. 2020;27(2):e191-e198. PubMed
18.Kaufman PA, Awada A, Twelves C, et al. Phase III open-label randomized study of eribulin mesylate versus capecitabine in patients with locally advanced or metastatic breast cancer previously treated with an anthracycline and a taxane. J Clin Oncol. 2015;33(6):594-601. PubMed
19.Smith I. Goals of Treatment for Patients with Metastatic Breast Cancer. Semin Oncol. 2006;33(Suppl 2):S2-5. PubMed
20.CADTH Reimbursement Review: Sacituzumab Govitecan (Trodelvy). Can J Health Technol. 2022;2(4). https://www.cadth.ca/sites/default/files/DRR/2022/PC0254-Trodelvy-CombinedReport.pdf. Accessed 2023 Jan 16.
21.Gennari A, Andre F, Barrios CH, et al. ESMO Clinical Practice Guideline for the diagnosis, staging and treatment of patients with metastatic breast cancer. Ann Oncol. 2021;32(12):1475-1495. PubMed
22.Moy B, Rumble RB, Carey LA, Chemotherapy and Targeted Therapy for H. E. R. Negative Metastatic Breast Cancer that is Either Endocrine-Pretreated or Hormone Receptor-Negative Expert Panel. Chemotherapy and Targeted Therapy for Human Epidermal Growth Factor Receptor 2-Negative Metastatic Breast Cancer That Is Either Endocrine-Pretreated or Hormone Receptor-Negative: ASCO Guideline Rapid Recommendation Update. J Clin Oncol. 2022;40(26):3088-3090. PubMed
23.Moy B, Rumble RB, Come SE, et al. Chemotherapy and Targeted Therapy for Patients With Human Epidermal Growth Factor Receptor 2-Negative Metastatic Breast Cancer That is Either Endocrine-Pretreated or Hormone Receptor-Negative: ASCO Guideline Update. J Clin Oncol. 2021;39(35):3938-3958. PubMed
24.Burstein HJ, Somerfield MR, Barton DL, et al. Endocrine Treatment and Targeted Therapy for Hormone Receptor-Positive, Human Epidermal Growth Factor Receptor 2-Negative Metastatic Breast Cancer: ASCO Guideline Update. J Clin Oncol. 2021;39(35):3959-3977. PubMed
25.NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines): Breast Cancer. Version 4.2022. Plymouth Meeting (PA): National Comprehensive Cancer Network; 2022 June 21: https://www.nccn.org/. Accessed 2023 Jan 12.
26.Enhertu (trastuzumab deruxtecan): powder for concentrate for infusion, 100 mg/vial, intravenous infusion [product monograph]. Mississauga (ON): AstraZeneca Canada Inc.; 2023 Jan 6: https://pdf.hres.ca/dpd_pm/00069043.PDF. Accessed 2023 Jan 18.
27.Capecitabine: tablets, 150 mg and 500 mg, oral [product monograph]. Boucherville (QC): JAMP Pharma Corporation; 2022: https://pdf.hres.ca/dpd_pm/00066694.PDF. Accessed 2023 Jan 18.
28.Halaven (eribulin mesylate): 0.5 mg/mL solution for injection [product monograph]. Mississauga (ON): Eisai Limited; 2017: https://pdf.hres.ca/dpd_pm/00040614.PDF. Accessed 2023 Jan 18.
29.Gemcitabine (as gemcitabine hydrochloride): 1 g and 2 g vial [product monograph]. Kirkland (QC): Accord Healthcare Inc.; 2021: https://pdf.hres.ca/dpd_pm/00062070.PDF. Accessed 2023 Jan 18.
30.Paclitaxel: 6 mg/mL sterile, for injection [product monograph]. Boucherville (QC): Sandoz Canada Inc.; 2021: https://pdf.hres.ca/dpd_pm/00063296.PDF. Accessed 2023 Jan 18.
31.Modi S, Jacot W, Yamashita T, et al. Trastuzumab Deruxtecan in Previously Treated HER2-Low Advanced Breast Cancer. N Engl J Med. 2022;387(1):9-20. PubMed
32.Ueno NT, Jacot W, Yamashita T, et al. 217O - Patient-reported outcomes (PROs) from DESTINY-Breast04, a randomized phase III study of trastuzumab deruxtecan (T-DXd) vs treatment of physician's choice (TPC) in patients (pts) with HER2-low metastatic breast cancer (MBC). Ann Oncol. 2022;33(suppl_7):S88-S121.
33.Medical Dictionary for Regulatory Activities (MedDRA) version 23.0. Geneva (CH): International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use; 2020: https://www.meddra.org. Accessed 2023 Jan 16.
34.Common Terminology Criteria for Adverse Events (CTCAE v5.0). Bethesda (MD): National Cancer Institute; 2017: https://ctep.cancer.gov/protocoldevelopment/electronic_applications/ctc.htm#ctc_50. Accessed 2023 Jan 16.
35.Aaronson NK, Ahmedzai S, Bergman B, et al. The European Organization for Research and Treatment of Cancer QLQ-C30: a quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst. 1993;85(5):365-376. PubMed
36.Bjelic-Radisic V, Cardoso F, Cameron D, et al. Corrigendum to An international update of the EORTC questionnaire for assessing quality of life in breast cancer patients: EORTC QLQ-BR45: Ann Oncol 2020; Volume 31, Issue 2, Pages 283-288. Ann Oncol. 2020;31(4):552. PubMed
37.Nakada T, Sugihara K, Jikoh T, Abe Y, Agatsuma T. The Latest Research and Development into the Antibody-Drug Conjugate, [fam-] Trastuzumab Deruxtecan (DS-8201a), for HER2 Cancer Therapy. Chem Pharm Bull (Tokyo). 2019;67(3):173-185. PubMed
38.McClure NS, Sayah FA, Xie F, Luo N, Johnson JA. Instrument-Defined Estimates of the Minimally Important Difference for EQ-5D-5L Index Scores. Value Health. 2017;20(4):644-650. PubMed
39.Musoro JZ, Coens C, Fiteni F, et al. Minimally Important Differences for Interpreting EORTC QLQ-C30 Scores in Patients With Advanced Breast Cancer. JNCI Cancer Spectr. 2019;3(3):pkz037. PubMed
40.Kawahara T, Taira N, Shiroiwa T, et al. Minimal important differences of EORTC QLQ-C30 for metastatic breast cancer patients: Results from a randomized clinical trial. Qual Life Res. 2022;31(6):1829-1836. PubMed
41.Letellier ME, Dawes D, Mayo N. Content verification of the EORTC QLQ-C30/EORTC QLQ-BR23 with the International Classification of Functioning, Disability and Health. Qual Life Res. 2015;24(3):757-768. PubMed
42.McLachlan SA, Devins GM, Goodwin PJ. Validation of the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire (QLQ-C30) as a measure of psychosocial function in breast cancer patients. Eur J Cancer. 1998;34(4):510-517. PubMed
43.Groenvold M, Klee MC, Sprangers MA, Aaronson NK. Validation of the EORTC QLQ-C30 quality of life questionnaire through combined qualitative and quantitative assessment of patient-observer agreement. J Clin Epidemiol. 1997;50(4):441-450. PubMed
44.Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. 1977;33(1):159-174. PubMed
45.Lee CF, Ng R, Luo N, et al. The English and Chinese versions of the five-level EuroQoL Group's five-dimension questionnaire (EQ-5D) were valid and reliable and provided comparable scores in Asian breast cancer patients. Support Care Cancer. 2013;21(1):201-209. PubMed
46.Kimman ML, Dirksen CD, Lambin P, Boersma LJ. Responsiveness of the EQ-5D in breast cancer patients in their first year after treatment. Health Qual Life Outcomes. 2009;7:11. PubMed
47.Conner-Spady B, Cumming C, Nabholtz JM, Jacobs P, Stewart D. Responsiveness of the EuroQol in breast cancer patients undergoing high dose chemotherapy. Qual Life Res. 2001;10(6):479-486. PubMed
48.Pickard AS, Neary MP, Cella D. Estimation of minimally important differences in EQ-5D utility and VAS scores in cancer. Health Qual Life Outcomes. 2007;5:70. PubMed
49.Drug Reimbursement Review sponsor submission: Enhertu (trastuzumab deruxtecan), powder for concentrate for infusion, 100 mg/vial, intravenous infusion [internal sponsor's package]. Mississauga (ON): AstraZeneca Canada Inc.; 2022 Dec 13.
50.Modi S, Jacot W, Yamashita T, et al. Trastuzumab Deruxtecan in Previously Treated HER2-Low Advanced Breast Cancer. N Engl J Med. 2022;387(1):9-20. PubMed
51.Mueller PS, Montori VM, Bassler D, Koenig BA, Guyatt GH. Ethical issues in stopping randomized trials early because of apparent benefit. Ann Intern Med. 2007;146(12):878-881. PubMed
52.A feasibility assessment of indirect treatment comparisons with T-DXd in HER2-low unresectable and/or metastatic breast cancer [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Enhertu (trastuzumab deruxtecan), powder for concentrate for infusion, 100 mg/vial, intravenous infusion. Mississauga (ON): AstraZeneca Canada Inc; 2022 Dec 13.
53.Hurvitz SA, Bardia A, Punie K, et al. 168P Sacituzumab govitecan (SG) efficacy in patients with metastatic triple-negative breast cancer (mTNBC) by HER2 immunohistochemistry (IHC) status: Findings from the phase III ASCENT study. Ann Oncol. 2022;33:S200-S201.
54.Bardia A, Hurvitz SA, Tolaney SM, et al. Sacituzumab Govitecan in Metastatic Triple-Negative Breast Cancer. N Engl J Med. 2021;384(16):1529-1541. PubMed
Appendix 1: Detailed Outcome Data
Note that this appendix has not been copy-edited.
Table 27: Subgroup Analysis of Progression-Free Survival Based on BICR, HR-Positive Cohort of Full Analysis Set
Subgroup | Number of patients with events | Median PFS (95% CI), monthsa | HR (95% CI)b Trastuzumab deruxtecan vs. TPC | ||
|---|---|---|---|---|---|
Trastuzumab deruxtecan | TPC | Trastuzumab deruxtecan | TPC | ||
HER2 status | |||||
HER2 IHC 1+ (n = 288) | 119/192 | 66/96 | 10.3 (8.6 to 12.3) | 5.3 (4.1 to 7.8) | 0.4771 (0.3512 to 0.6483) |
HER2 IHC2+/ISH− (n = 206) | 92/139 | 44/67 | 10.1 (8.2 to 12.2) | 5.9 (4.3 to 7.9) | 0.5529 (0.3833 to 0.7976) |
Number of prior lines of chemotherapy in metastatic setting – derived | |||||
1 (n = 296) | 129/203 | 63/93 | 10.9 (8.5 to 12.3) | 6.8 (4.5 to 8.2) | 0.5389 (0.3969 to 0.7317) |
≥ 2 (n = 196) | 81/127 | 47/69 | 9.9 (8.3 to 11.7) | 4.6 (2.8 to 6.2) | 0.4733 (0.3278 to 0.6835) |
Prior CDK 4/6 – based on baseline value from EDC | |||||
Yes (n = 348) | 149/233 | 74/115 | 10.0 (8.3 to 11.4) | 5.4 (4.0 to 7.8) | 0.5532 (0.4166 to 0.7347) |
No (n = 143) | 60/96 | 35/47 | 11.7 (9.5 to 17.7) | 5.9 (4.3 to 8.2) | 0.4211 (0.2750 to 0.6446) |
Age | |||||
< 65 (n = 380) | 170/260 | 79/120 | 9.8 (8.4 to 11.3) | 5.4 (4.1 to 7.8) | 0.5140 (0.3919 to 0.6742) |
≥ 65 (n = 114) | 41/71 | 31/43 | 12.0 (9.5 to 14.7) | 5.6 (4.3 to 10.8) | 0.4739 (0.2936 to 0.7650) |
< 75 (n = |||) | ||||||| | ||||||| | |||| ||||| ||||| | ||| ||||| |||| | |||||| |||||||| ||||||| |
Race | |||||
White (n = 234) | 100/156 | 43/78 | 10.0 (8.5 to 12.2) | 7.1 (4.0 to 10.0) | 0.6362 (0.4426 to 0.9146) |
Asian (n = 197) | 83/131 | 54/66 | 11.0 (8.4 to 13.8) | 4.8 (4.2 to 6.4) | 0.3952 (0.2782 to 0.5614) |
Other (n = 53) | 25/37 | 11/16 | 6.0 (5.4 to 10.5) | 7.0 (1.4 to 11.0) | 0.8331 (0.4096 to 1.6945) |
Region | |||||
Asia (n = 188) | 81/128 | 48/60 | 10.9 (8.4 to 14.7) | 5.3 (4.2 to 6.8) | 0.4054 (0.2814 to 0.5839) |
North America (n = 84) | 40/54 | 18/30 | 8.5 (6.3 to 11.3) | 4.5 (2.9 to 8.2) | 0.5421 (0.3035 to 0.9683) |
Europe + Israel (n = 222) | 90/149 | 44/73 | 10.8 (8.5 to 13.0) | 7.1 (3.0 to 10.7) | 0.6207 (0.4311 to 0.8936) |
Lines of prior ET received in the metastatic setting – derived | |||||
0 (n = ||) | ||||| | ||||| | |||| ||||| ||||| | ||| ||||| |||| | |||||| |||||||| ||||||| |
1 (n = |||) | |||||| | ||||| | ||| ||||| ||||| | ||| ||||| ||||| | |||||| |||||||| ||||||| |
2 (n = |||) | |||||| | ||||| | |||| |||||| ||||| | ||| ||||| |||| | |||||| |||||||| ||||||| |
≥ 3 (n = |||) | ||||| | ||||| | |||| |||||||||| | ||| ||||| ||||| | |||||| |||||||| ||||||| |
Best response to the last prior cancer systemic therapy | |||||
Partial response (n = ||) | ||||| | ||||| | |||| ||||| ||||| | ||| ||||| |||| | |||||| |||||||| ||||||| |
Stable disease (n = |||) | ||||| | ||||| | |||| ||||| ||||| | ||| ||||| ||||| | |||||| |||||||| ||||||| |
Progressive disease (n = |||) | ||||||| | ||||| | ||| ||||| ||||| | ||| ||||| |||| | |||||| |||||||| ||||||| |
Unknown (n = ||) | ||||| | ||||| | |||| ||||| ||||| | ||| ||||| ||| | |||||| |||||||| ||||||| |
Reported history of CNS metastases | |||||
Yes (n = ||) | ||||| | |||| | ||| |||||||||| | ||| ||||| ||||| | |||||| |||||||| ||||||| |
No (n = |||) | ||||||| | ||||||| | |||| ||||| ||||| | ||| ||||| |||| | |||||| |||||||| ||||||| |
Baseline CNS metastases | |||||
Yes (n = 25) | ||||| | ||| | ||| ||||| ||||| | ||| ||||| ||| | |||||| |||||||| ||||||| |
No (n = 469) | ||||||| | ||||||| | |||| ||||| ||||| | ||| ||||| |||| | |||||| |||||||| ||||||| |
Renal function at baseline | |||||
Normal function (n = |||) | ||||||| | ||||| | |||| |||||||||| | ||| ||||| |||| | |||||| |||||||| ||||||| |
Mild impairment (n = |||) | |||||| | ||||| | ||| ||||| ||||| | ||| ||||| |||| | |||||| |||||||| ||||||| |
Moderate impairment (n = ||) | ||||| | ||||| | |||| ||||| ||| | ||| ||||| ||| | |||||| |||||||| ||||||| |
Hepatic function at baseline | |||||
Normal function (n = |||) | |||||| | ||||| | |||| ||||| ||||| | ||| ||||| |||| | |||||| |||||||| ||||||| |
Mild impairment (n = |||) | ||||||| | ||||| | ||| ||||| ||||| | ||| ||||| |||| | |||||| |||||||| ||||||| |
Baseline visceral disease | |||||
Yes (n = 444) | 196/298 | 100/146 | 9.8 (8.5 to 11.1) | 5.8 (4.4 to 7.1) | 0.5424 (0.4248 to 0.6927) |
No (n = 50) | 15/33 | 10/17 | 17.9 (10.9 to 26.4) | 4.5 (1.6 to 12.4) | 0.2275 (0.0947 to 0.5469) |
ECOG PS | |||||
0 (n = 282) | 116/187 | 55/95 | 10.9 (9.5 to 13.0) | 7.0 (4.2 to 8.5) | 0.5582 (0.4028 to 0.7734) |
1 (n = 212) | 95/144 | 55/68 | 9.7 (7.3 to 11.5) | 4.6 (2.9 to 6.2) | 0.4544 (0.3234 to 0.6384) |
BICR = Blinded Independent Central Review; CDK4/6 = cyclin-dependent kinase 4 and 6; CI = confidence interval; CNS = central nervous system; ECOG PS = Eastern Cooperative Oncology Group Performance Status; EDC = Electronic Data Capture; ET = endocrine therapy; HR = hazard ratio; IHC = immunohistochemistry; ISH = in situ hybridization; NE = Not Estimable; PFS = progression-free survival; SAP = Statistical Analysis Plan; TPC = treatment of physician’s choice
Note: PFS is defined as the time from the date of randomization to the date of the first radiographic disease progression or death due to any cause, whichever comes first. Refer to SAP for the handling of censored cases. Subgroup analyses will be presented only if at least 10 PFS events in each group.
aMedian PFS is from Kaplan-Meier analysis. CI for median was computed using the Brookmeyer-Crowley method.
bHazard ratio is from unstratified Cox proportional hazards model with treatment as the only covariate.
Source: DESTINY-Breast04 Clinical Study Report.3
Table 28: Subgroup Analysis of Overall Survival, HR-Positive Cohort of Full Analysis Set
Subgroup | Number of patients with events | Median OS (95% CI), monthsa | Hazard ratio (95% CI)b Trastuzumab deruxtecan vs. TPC | |||
|---|---|---|---|---|---|---|
Trastuzumab deruxtecan | TPC | Trastuzumab deruxtecan | TPC | |||
HER2 status | ||||||
HER2 IHC 1+ (n = 288) | |||||| | ||||| | |||| |||||| ||| | |||| |||||| ||||| | |||||| |||||||| ||||||| | |
HER2 IHC2+/ISH− (n = 206) | |||||| | ||||| | |||| |||||| ||||| | |||| |||||| ||| | |||||| |||||||| ||||||| | |
Number of prior lines of chemotherapy in metastatic setting – derived | ||||||
1 (n = 296) | |||||| | ||||| | |||| |||||| ||| | |||| |||||| ||| | |||||| |||||||| ||||||| | |
≥ 2 (n = 196) | |||||| | ||||| | |||| |||||| ||| | |||| |||||| ||||| | |||||| |||||||| ||||||| | |
Prior CDK 4/6 – derived based on baseline value from EDC | ||||||
Yes (n = 348) | |||||| | |||||| | |||| |||||| ||||| | |||| |||||| ||||| | |||||| |||||||| ||||||| | |
No (n = 143) | ||||| | ||||| | || |||| ||| | |||| |||||| ||| | |||||| |||||||| ||||||| | |
Age | ||||||
< 65 (n = 380) | ||||||| | |||||| | |||| |||||| ||| | |||| |||||| ||||| | |||||| |||||||| ||||||| | |
≥ 65 (n = 114) | ||||| | ||||| | |||| |||||| ||| | |||| ||||| ||| | |||||| |||||||| ||||||| | |
< 75 (n = |||) | ||||||| | |||||| | |||| |||||| ||| | |||| |||||| ||||| | |||||| |||||||| ||||||| | |
Race | ||||||
White (n = 234) | |||||| | ||||| | |||| |||||| ||||| | |||| |||||| ||||| | |||||| |||||||| ||||||| | |
Asian (n = 197) | |||||| | ||||| | || |||||| ||| | |||| |||||| ||| | |||||| |||||||| ||||||| | |
Other (n = 53) | ||||| | |||| | |||| |||||| ||| | |||| ||||| ||| | |||||| |||||||| ||||||| | |
Region | ||||||
Asia (n = 188) | |||||| | ||||| | || |||||| ||| | |||| |||||| ||| | |||||| |||||||| ||||||| | |
North America (n = 84) | ||||| | ||||| | |||| |||||| ||||| | |||| ||||| ||||| | |||||| |||||||| ||||||| | |
Europe + Israel (n = 90) | |||||| | ||||| | |||| |||||| ||| | |||| |||||| ||| | |||||| |||||||| ||||||| | |
Lines of prior ET received in the metastatic setting – derived | ||||||
0 (n = ||) | |||| | |||| | || |||||| ||| | |||| ||||| ||| | |||||| |||||||| ||||||| | |
1 (n = |||) | |||||| | ||||| | |||| |||||| ||| | |||| |||||| ||| | |||||| |||||||| ||||||| | |
2 (n = |||) | |||||| | ||||| | |||| |||||| ||| | |||| |||||| ||||| | |||||| |||||||| ||||||| | |
≥ 3 (n = |||) | ||||| | ||||| | |||| |||||| ||| | |||| |||||| ||| | |||||| |||||||| ||||||| | |
Best response to the last prior cancer systemic therapy | ||||||
Partial Response (n = ||) | ||||| | ||||| | |||| |||||| ||| | |||| ||||| ||| | |||||| |||||||| ||||||| | |
Stable disease (n = |||) | ||||| | ||||| | |||| |||||| ||| | |||| |||||| ||||| | |||||| |||||||| ||||||| | |
Progressive Disease (n = |||) | |||||| | ||||| | |||| |||||| ||||| | |||| |||||| ||| | |||||| |||||||| ||||||| | |
Unknown (n = ||) | ||||| | |||| | || |||||| ||| | |||| |||||| ||| | |||||| |||||||| ||||||| | |
Reported history of CNS metastases | ||||||
Yes (n = ||) | ||||| | |||| | |||| |||||| ||||| | || ||||| ||| | |||||| |||||||| ||||||| | |
No (n = |||) | ||||||| | |||||| | |||| |||||| ||| | |||| |||||| ||||| | |||||| |||||||| ||||||| | |
Baseline CNS metastases | ||||||
Yes (n = 25) | ||||| | ||| | |||| |||||| ||||| | ||| ||||| ||| | |||||| |||||||| ||||||| | |
No (n = 469) | ||||||| | |||||| | |||| |||||| ||| | |||| |||||| ||||| | |||||| |||||||| ||||||| | |
Renal function at baseline | ||||||
Normal function (n = |||) | |||||| | ||||| | |||| |||||| ||||| | |||| |||||| ||| | |||||| |||||||| ||||||| | |
Mild impairment (n = |||) | |||||| | ||||| | || |||||| ||| | |||| |||||| ||| | |||||| |||||||| ||||||| | |
Moderate impairment (n = ||) | ||||| | |||| | |||| |||||| ||| | || |||||| ||| | |||||| |||||||| ||||||| | |
Hepatic function at baseline | ||||||
Normal function (n = |||) | |||||| | ||||| | |||| |||||| ||| | || |||||| ||| | |||||| |||||||| ||||||| | |
Mild impairment (n = |||) | |||||| | ||||| | |||| |||||| ||||| | |||| ||||| ||||| | |||||| |||||||| ||||||| | |
Baseline visceral disease | ||||||
Yes (n = 444) | ||||||| | |||||| | |||| |||||| ||||| | |||| |||||| ||||| | |||||| |||||||| ||||||| | |
No (n = 50) | |||| | |||| | || |||| ||| | |||| |||||| ||| | |||||| |||||||| ||||||| | |
ECOG PS | ||||||
0 (n = 282) | |||||| | ||||| | |||| |||||| ||| | |||| |||||| ||| | |||||| |||||||| ||||||| | |
1 (n = 212) | |||||| | ||||| | |||| |||||| ||||| | |||| |||||| ||||| | |||||| |||||||| ||||||| | |
BICR = Blinded Independent Central Review; CDK4/6 = cyclin-dependent kinase 4 and 6; CI = confidence interval; CNS = central nervous system; ECOG PS = Eastern Cooperative Oncology Group Performance Status; EDC = Electronic Data Capture; ET = endocrine therapy; HR = hazard ratio; IHC = immunohistochemistry; ISH = in situ hybridization; NE = not estimable; OS = overall survival; TPC = treatment of physician’s choice.
Note: OS is defined as the time from the date of randomization to the date of death due to any cause, whichever comes first. If there is no death reported for a patient before the data cut-off for OS analysis, OS will be censored at the last contact date at which the patient is known to be alive. Subgroup analyses will be presented only if at least 10 PFS events in each group.
aMedian OS is from Kaplan-Meier analysis. CI for median was computed using the Brookmeyer-Crowley method.
bHR is from unstratified Cox proportional hazards model with treatment as the only covariate.
Source: DESTINY-Breast04 Clinical Study Report.3
Pharmacoeconomic Review
Abbreviations
AE
adverse event
BIA
budget impact analysis
ET
endocrine therapy
HR
hormone receptor
HRQoL
health-related quality of life
ICER
incremental cost-effectiveness ratio
IHC
immunohistochemistry
ISH
in situ hybridization
OS
overall survival
PFS
progression-free survival
PSM
partitioned survival model
QALY
quality-adjusted life-year
TTD
time to treatment discontinuation
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Trastuzumab deruxtecan (Enhertu), powder for reconstitution for IV infusion |
Submitted price | Trastuzumab deruxtecan, 100 mg, vial: $2,440.00 |
Indication | For the treatment of adult patients with unresectable or metastatic HER2-low (IHC 1+ or IHC 2+/ISH−) breast cancer who have received at least 1 prior line of chemotherapy in the metastatic setting or developed disease recurrence during or within 6 months of completing adjuvant chemotherapy; patients with HR-positive breast cancer should have received at least 1 and be no longer considered for endocrine therapy. |
Health Canada approval status | NOC |
Health Canada review pathway | Priority review, Project ORBIS |
NOC date | January 6, 2023 |
Reimbursement request | As per indication |
Sponsor | AstraZeneca Canada |
Submission history | Indication: Treatment of adult patients with unresectable or metastatic HER2-positive breast cancer who have received at least 1 prior anti-HER2-based regimen either in the metastatic setting, or in the neoadjuvant or adjuvant setting and developed disease recurrence during or within 6 months of completing neoadjuvant or adjuvant therapy Recommendation date: September 28, 2022 Recommendation: Reimburse with clinical criteria and/or conditions |
IHC = immunohistochemistry; ISH = in situ hybridization; NOC = Notice of Compliance.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Partitioned survival model |
Target population | Patients with HER2-low (IHC 1+ or IHC 2+/ISH−) unresectable and/or metastatic breast cancer who have been treated with at least 1 prior line of chemotherapy in the metastatic setting or have developed disease recurrence during or within 6 months of completing adjuvant chemotherapy; patients with hormone receptor–positive breast cancer should have received at least 1, and be no longer considered eligible for, endocrine therapy |
Treatment | Trastuzumab deruxtecan |
Comparators | Standard of care (consisting of choice of eribulin, capecitabine, vinorelbine, gemcitabine, or paclitaxel) |
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs, life-years |
Time horizon | Lifetime (12 years) |
Key data source | DESTINY-Breast04 trial |
Submitted results | ICER = $210,047 per QALY gained (incremental cost = $132,945; incremental QALYs = 0.63) |
Key limitations |
|
CADTH reanalysis results |
|
AE = adverse event; ICER = incremental cost-effectiveness ratio; IHC = immunochemistry; ISH = in situ hybridization; PSM = partitioned survival model; QALY = quality-adjusted life-year.
Conclusions
Based on the CADTH Clinical Review of the DESTINY-Breast04 trial, trastuzumab deruxtecan was associated with a statistically and clinically significant progression-free survival (PFS) and overall survival (OS) benefit compared with standard of care in adult patients with HER2-low unresectable or metastatic breast cancer who had received at least 1 prior line of chemotherapy in the metastatic setting or developed disease recurrence during or within 6 months of completing adjuvant chemotherapy. Patients with a hormone receptor (HR)-positive status should have received at least 1 endocrine therapy (ET) and be no longer considered eligible for ET. The long-term clinical effectiveness of trastuzumab deruxtecan beyond the trial period (maximum follow-up of 33 months) is uncertain. Harms observed in the trial were aligned with clinician expectations and noted to be manageable. The impact of trastuzumab deruxtecan on health-related quality of life (HRQoL) was uncertain. An evidence gap remains regarding the relative efficacy and safety of trastuzumab deruxtecan in comparison with sacituzumab govitecan in the HR-negative cohort of patients.
CADTH identified several additional limitations with the economic analyses submitted by the sponsor. CADTH conducted a reanalysis that included changes to the time horizon, assumed that treatment duration was equal to PFS, changed the health-utility values from treatment-specific to health state–specific values incorporating adverse event (AE) disutilities, and changed the proportion of patients receiving subsequent treatments following trastuzumab deruxtecan to be equivalent to those on standard of care. Based on the CADTH reanalysis, treatment with trastuzumab deruxtecan was $168,104 more costly and yielded 0.55 more quality-adjusted life-years (QALYs), resulting in an incremental cost-effectiveness ratio (ICER) of $303,924 per QALY gained. The probability of trastuzumab deruxtecan being cost-effective at a willingness-to-pay threshold of $50,000 per QALY gained was 0%. A price reduction of at least 75% would be necessary to achieve an ICER of $50,000 per QALY gained.
The results remained robust across CADTH scenario analyses, including scenarios that considered the population stratified by HR status to account for an underlying survival difference in these 2 populations. Additional uncertainty remains in all reanalyses due to limitations with the partitioned survival model (PSM) approach that could not be addressed. A greater price reduction may be required to account for the remaining uncertainty.
Stakeholder Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, registered clinicians, and drug plans that participated in the CADTH review process.
Two patient groups provided input for this review: the Canadian Breast Cancer Network and Rethink Breast Cancer. Patient input was based on 2 online surveys focused on Canadian patients with metastatic breast cancer and one-on-one interviews focused on patients with HER2-low metastatic breast cancer. The input noted that treatment options for these patients include standard chemotherapy such as eribulin, capecitabine, gemcitabine, nab-paclitaxel, or paclitaxel. Patient feedback emphasized the desire to avoid the AEs caused by standard chemotherapy, although it was noted most patients seek extension of life, and some patients were willing to trade off toxicity to control disease progression. Patients also indicated that they would consider some side effects, including fatigue, nausea, depression, and others, to be acceptable for 6 months of extended progression-free disease, but this trade-off would not be acceptable if the side effect was pain. Other patients indicated that maintaining quality of life was paramount.
One clinician group, the Ontario Health–Cancer Care Ontario Breast Cancer Drug Advisory Committee, provided input for this review. Clinician input emphasized that treatment goals are not being met in the indicated population, and they noted issues with currently available treatments include a lack of response and refractory disease in some patients, as well as a lack of treatments that can be better tolerated. The clinician input indicated that the proposed place in therapy of trastuzumab deruxtecan would shift the currently used chemotherapy options to later lines. The clinician feedback raised concerns about the increased risk of pneumonitis with trastuzumab deruxtecan, indicating the need for a risk-benefit assessment for the treatment of patients with severe underlying lung disease, particularly underlying interstitial lung disease. It was noted that access to specialty services may be needed in the case of development of pneumonitis, and that there may be a need for monitoring with CT scans at a greater frequency than usual compared with standard of care. The clinician feedback also indicated that identification of the HER2-low subset will require careful review by pathologists who are experts in breast cancer.
Drug plan input considered whether patients who were treated with several lines of chemotherapy or ET would be eligible for treatment with trastuzumab deruxtecan. It was also noted that HER2 status would need to be reconfirmed by a pathologist and considered whether patients would need recent tumour tissue samples to determine HER2 status. The drug plan feedback indicated this population lies in a complex therapeutic space, with multiple lines of therapy and subpopulations. Clarification may therefore be required on patient eligibility for drug options available for metastatic triple-negative breast cancer, such as pembrolizumab and sacituzumab govitecan. Finally, the drug plans also anticipated a substantial budget impact due to the large patient population.
Several of these concerns were addressed in the sponsor’s model:
The sponsor’s submitted model accounted for quality of life and length of life by using QALYs as the primary outcome.
The comparators of interest in the model were aligned with those identified in physician input.
CADTH was unable to address the concern raised in stakeholder input regarding inclusion of all grades of pneumonitis and relevant pneumonitis management.
Economic Review
The current review is for trastuzumab deruxtecan (Enhertu) for the treatment of patients with unresectable and/or metastatic HER2-low (immunohistochemistry [IHC] 1+ or IHC 2+/in situ hybridization [ISH]−) breast cancer who have received at least 1 prior line of chemotherapy in the metastatic setting or have developed disease recurrence during or within 6 months of completing adjuvant chemotherapy. Patients with HR-positive breast cancer should be refractory to prior ET.1
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted a cost-utility analysis of trastuzumab deruxtecan compared with standard chemotherapy consisting of a basket of comparators.1 The modelled population comprised adult patients with unresectable and/or metastatic HER2-low (IHC 1+ or IHC 2+/ISH−) breast cancer who have been treated with at least 1 prior line of chemotherapy in the metastatic setting or have developed disease recurrence during or within 6 months of completing adjuvant chemotherapy. Furthermore, patients with HR-positive breast cancer were refractory to prior ET. The modelled population was aligned with the Health Canada–indicated population.2
The recommended dosage of trastuzumab deruxtecan is 5.4 mg/kg given as an IV infusion once every 3 weeks, until disease progression or unacceptable toxicity.2 Trastuzumab deruxtecan should be administered over an initial 90-minute period, which may be reduced to 30 minutes for subsequent doses. At the sponsor’s submitted price of $2,440.00 per 100 mg vial, the cost of trastuzumab deruxtecan per 21-day cycle is $9,574, or $165,949 annually if patients remain on treatment for a full year. Wastage was assumed for IV drugs (i.e., no vial sharing).
The sponsor assumed that standard of care would consist of a basket of standard chemotherapy options that included eribulin (51.1%), capecitabine (20.1%), vinorelbine (10.3%), gemcitabine (10.3%), and paclitaxel (8.2%). The 21-day-cycle costs for the standard of care was $1,824 or $31,616 annually. In addition, for patients with HR-negative, HER2-low metastatic breast cancer, sacituzumab govitecan was included as a comparator in a scenario analysis. The 21-day cost for sacituzumab govitecan was $11,424 or $195,397 annually.
The clinical outcomes of interest were QALYs and life-years. The economic analysis was undertaken over a lifetime (12-year) time horizon from the perspective of the Canadian public health care payer. Discounting (1.5% per year) was applied to both costs and outcomes.
Model Structure
The sponsor submitted a PSM with 3 health states: preprogression, postprogression and death (Figure 1).1 All patients entered the model in the preprogression health state, in which they received either trastuzumab deruxtecan or standard chemotherapy (modelled as a single basket of comparators), as defined by the PFS measure assessed in the DESTINY-Breast04 trial. During each cycle, patients either remained progression-free, transitioned to the progressive-disease state, or they progressed to death. The proportion of patients in the progressive-disease state was calculated by subtracting the proportion of patients alive and progression-free (based on the PFS curve) from the proportion of patients alive (based on the OS curve). Patients in the postprogression state could either remain in the same state or move to death. Death was modelled as an absorbing state. The sponsor further divided the progression-free state by treatment status (on or off treatment) as time to treatment discontinuation (TTD) was modelled independently of PFS. The model assumed a cycle length of 3 weeks.
Model Inputs
The baseline population characteristics and clinical efficacy parameters in the model were informed by the DESTINY-Breast04 trial, a randomized, open-label, active-controlled, phase III study designed to evaluate the efficacy of trastuzumab deruxtecan compared with standard of care in adult patients with HER2-low (IHC 1+ or IHC 2+/ISH−) unresectable and/or metastatic breast cancer who have been treated with at least 1 prior line of chemotherapy in the metastatic setting or have developed disease recurrence during or within 6 months of completing adjuvant chemotherapy, and, if HR-positive, patients had to be refractory to prior ET.3 The sponsor assumed that the DESTINY-Breast04 trial population (baseline characteristics: mean age = 56.5 years; 99.6% female; mean weight = 63.4 kg; mean body surface = 1.67 m2) and distribution of the basket of comparators used within the trial reflected the Canadian population.
Efficacy outcomes (OS, PFS, TTD) for trastuzumab deruxtecan and standard of care were based on the DESTINY-Breast04 trial (median follow-up of 15.3 months, and maximum follow-up observation of 33.1 months). Parametric survival modelling was used to extrapolate TTD, PFS, and OS data beyond the trial period, with survival distributions fitted separately to DESTINY-Breast04 trial data for each treatment arm. The base-case parametric functions were selected based on graphic inspection of fit, statistical goodness of fit, and clinical plausibility of long-term projections. The sponsor chose the gamma function to extrapolate PFS, OS, and TTD for trastuzumab deruxtecan and standard of care. Patients were censored at the last contact before data cut-off. As such, general population mortality was included in the model based on age- and gender-specific data from Canadian life tables, weighted to the gender distribution of patients in DESTINY-Breast04. For the comparison with sacituzumab govitecan, sacituzumab govitecan’s efficacy outcomes were assumed to be the same as trastuzumab deruxtecan’s outcomes. The sponsor determined that it was infeasible to conduct an indirect comparison to determine sacituzumab govitecan’s relative efficacy due to differences in patient populations, small sample sizes, and unavailable reporting of patient characteristics. Grade 3 or higher AEs that occurred at a frequency of more than 2% observed in the DESTINY-Breast04 trial were incorporated into the model with an associated cost. These were applied as a one-time cost decrement in the first cycle of the PFS state.
The submitted model incorporated treatment-specific health-state utility values for progression-free and progressive-disease health states, which were derived from the DESTINY-Breast04 trial. Utility decrements for AEs in the model were based on various sources in the literature. However, utility decrements due to AEs were not included in the sponsor’s base case because the sponsor assumed the effect of AEs on patients was already reflected in the treatment-specific utility values estimated from the DESTINY-Breast04 trial.
Costs in the model included the costs of drug acquisition, administration, AEs, subsequent treatments, treatment monitoring, and disease management. Drug-acquisition costs for comparators were obtained from the IQVIA Delta PA database, with the costs of therapy weighted by the proportion of patients who received each of the therapies in the DESTINY-Breast04 trial.4 Wastage was assumed for parental drugs (i.e., no vial sharing). Administration costs were obtained from the literature.5 AE costs were derived from the Ontario Case Costing Initiative and the literature for inpatient and ambulatory care, depending on the AE type.6
The sponsor assumed that patients would receive subsequent treatments following progression, with the following treatment options considered: eribulin, capecitabine, vinorelbine, gemcitabine, and paclitaxel. The sponsor assumed that the proportion of patients receiving each of the subsequent therapies would differ depending on the treatment received, based on data from the DESTINY-Breast04 trial. The proportion of patients receiving each subsequent treatment per treatment arm was also based on data from DESTINY-Breast04 trial and reweighted to match 1 of the 5 subsequent treatment options selected by the sponsor (i.e., eribulin, gemcitabine, vinorelbine, paclitaxel, and capecitabine). The sponsor’s assumption that the duration of subsequent treatment was 3 months was based on the EMBRACE trial.7 Subsequent treatment costs were obtained from the IQVIA DeltaPA database and administration costs were sourced from the literature.4
For treatment monitoring and disease-management costs, the sponsor assumed resource-utilization frequency to be the same among treatments considered in the submission. The frequencies of resource use were obtained from the literature and feedback from clinical experts consulted by the sponsor. Unit costs for physician visits were obtained from the Ontario Schedule of Benefits for Physician Services, while unit costs for laboratory tests were obtained from the Ontario Schedule of Benefits for Laboratory Services.8,9 End-of-life costs were derived from the literature and applied as one-off costs.10
Summary of Sponsor’s Economic Evaluation Results
All analyses were run probabilistically (1,000 iterations for the base-case and scenario analyses). The deterministic and probabilistic results were similar. The probabilistic findings are presented in the following section.
Base-Case Results
In the sponsor’s base-case analysis, treatment with trastuzumab deruxtecan was associated with incremental costs of $132,945 and a gain of 0.63 QALYs compared with standard of care over the lifetime (12-year) time horizon, resulting in an ICER of $210,047 per QALY gained (Table 3). The probability of trastuzumab deruxtecan being cost-effective at a willingness-to-pay threshold of $50,000 per QALY gained compared to standard of care was 0%. Approximately 51% of the incremental QALYs in the sponsor’s base case accrued after 33.1 months, the maximum follow-up of the DESTINY-Breast04 trial. The submitted analysis is based on the publicly available list prices of all treatments, other than trastuzumab deruxtecan, including subsequent therapies.
Table 3: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER vs. standard of care ($ per QALY) |
|---|---|---|---|---|---|
Standard of care | 54,731 | Reference | 1.37 | Reference | Reference |
Trastuzumab deruxtecan | 187,677 | 132,945 | 2.00 | 0.63 | 210,047 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Source: Sponsor’s pharmacoeconomic submission.1
Sensitivity and Scenario Analysis Results
The sponsor presented 2 key scenario analyses stratifying the population by HR status (Table 11). When considering the HR-positive population, the ICER was $259,557 per QALY gained in comparison with standard of care. When considering the HR-negative population, the model also included sacituzumab govitecan as a comparator, although it was dominated by trastuzumab deruxtecan based on an assumption of equal efficacy and greater costs for sacituzumab govitecan. This analysis produced a sequential ICER of $108,389 per QALY gained for trastuzumab deruxtecan in comparison with standard of care.
The sponsor also assessed the impact of altering several model parameters in probabilistic scenario analyses. When the TTD was assumed to be equal to PFS, the ICER increased to $265,492 per QALY gained. In addition, changes to the next optimistic and/or pessimistic OS distributions for trastuzumab deruxtecan showed OS was a major driver in this analysis, reducing the ICER to $123,374 when the next most optimistic OS distribution (log-logistic) was chosen and increasing the ICER to $277,121 per QALY gained when the next most pessimistic OS distribution (Weibull) was chosen.
CADTH Appraisal of the Sponsor’s Economic Evaluation
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the economic analysis:
The long-term comparative efficacy of trastuzumab deruxtecan with current standard of care was uncertain: The sponsor submitted a cost-utility analysis in which the long-term clinical efficacy of trastuzumab deruxtecan was based on the sponsor’s extrapolations of data for PFS and OS from the DESTINY-Breast04 trial (median follow-up of15.3 months; maximum follow-up of 33.1 months) to 12 years using parametric survival analysis. Although the PFS and OS curves from the trial were mature, 51% of QALYs derived from treatment with trastuzumab deruxtecan accrued after the maximum trial follow-up duration. The results of this cost-effectiveness analysis are sensitive to the sponsor’s extrapolation assumptions, reflecting the uncertainty in the long-term clinical efficacy of trastuzumab deruxtecan treatment. In addition, it is uncertain whether the subsequent treatments used in the DESTINY-Breast04 trial affected the magnitude of the OS benefit, given patients received a range of subsequent treatments that are not available as therapy options for this indication in Canada.
Upon validation of the sponsor’s chosen survival extrapolations, CADTH noted that the sponsor’s OS extrapolation resulted in 0.5% of patients surviving beyond a time horizon of 10 years in the trastuzumab deruxtecan arm. The proportion of patients alive at the 10-year time point was considered overestimated according to clinical experts consulted by CADTH during this review, as they expected no patients to survive beyond 10 years. This likely overestimated the survival benefit and incremental QALYs associated with trastuzumab deruxtecan.
The trastuzumab deruxtecan indication under review includes patients classified as either HR-positive or HR-negative. Clinical expert feedback obtained by CADTH noted each subpopulation has a different underlying survival rate. CADTH’s Guidelines for the Economic Evaluation of Health Technologies: Canada suggest stratified analyses when heterogeneity in the patient population may be present. However, upon inspection of the sponsor’s scenario analyses in which the population was stratified by HR status, CADTH noted concerns with estimates of survival gains from the analysis of HR-negative patients, as this subgroup presented with approximately twice as much benefit compared with the HR-positive population (0.98 life-years gained versus 0.55 life-years gained for HR-negative and HR-positive patients, respectively). The HR-negative population benefits were associated with high uncertainty in the CADTH Clinical Review given the HR-negative population had a small sample size (n = 58), with the analysis considered to be exploratory. Clinical experts consulted by CADTH for this review were uncertain why trastuzumab deruxtecan would provide a greater relative or absolute survival benefit in the HR-negative subgroup and described these results as highly uncertain.
CADTH addressed the limitation of the sponsor’s model overestimating survival beyond 10 years by restricting the time horizon to 10 years, which is aligned with CADTH economic evaluation guidelines, which suggest a time horizon long enough to capture all relevant differences in future costs and outcomes. CADTH could not address the limitation with the uncertainty of the long-term comparative efficacy with trastuzumab deruxtecan, as the sponsor’s model did not allow for a treatment-waning effect to be incorporated; however, CADTH conducted a scenario analysis with a 33-month time horizon to consider the cost-effectiveness of trastuzumab deruxtecan for the period for which there are observed data.
CADTH would usually stratify the base case by subgroups where important heterogeneity is present. However, given the limitations with the available evidence in the HR-negative subgroup, this approach was considered inappropriate. CADTH did conduct a scenario analysis with the population stratified by HR status, which addressed the uncertainty associated with the magnitude of benefit in the HR-negative population. In this scenario analysis, the relative effect of trastuzumab deruxtecan in the HR-negative population for OS was assumed to be the same as the relative effect observed in HR-positive patients in the DESTINY-Breast04 trial. Overall, the sponsor's base case was dominated by HR-positive patients; however, the clinical experts consulted by CADTH for this review anticipated that the relative effect observed in the HR-positive group would be applicable to HR-negative patients, although these subgroups would have a different underlying OS.
The modelling approach introduced uncertainty associated with proportion of patients in the progression-free, off-treatment health state: The sponsor submitted a PSM to assess the cost-effectiveness of trastuzumab deruxtecan in comparison with standard of care. The use of a PSM requires that trial outcomes used to model patient transitions within a PSM (i.e., PFS, OS and TTD) are assumed to be independent from each other (i.e., no explicit relationship between TTD and PFS was modelled), and independently extrapolated over a time horizon of 12 years using parametric survival analysis. Given TTD and PFS were assumed to be independent, differences in TTD and PFS curves indicated that a significant proportion of patients would remain progression-free but off treatment as the model time horizon increased (i.e., at 23 months, more than 50% of patients who were in the progression-free state were off treatment after initially being on trastuzumab deruxtecan). CADTH also noted that patients were spending a prolonged amount of time in the progression-free, off-treatment state. For example, after 45 months in the trastuzumab deruxtecan treatment group, between 1% and 2% of patients remained progression-free and off treatment for a period of 15 months, while less than 1% of patients remained progression-free and on treatment, suggesting that patients were staying progression-free but off treatment for a prolonged period, instead of experiencing disease progression or death. Clinical experts consulted by CADTH for this review advised that the most common causes for a patient to definitively stop treatment, besides disease progression, were severe AEs or patient preference. However, the proportion of patients expected in clinical practice to stop treatment for reasons other than disease progression and who remain untreated and progression-free was expected to be small and last for an average of 3 months. The sponsor’s approach therefore lacks face validity and biases the results in favour of trastuzumab deruxtecan, as patients continued to benefit by remaining progression-free while not incurring drug-acquisition costs, which are higher with trastuzumab deruxtecan.
CADTH addressed this limitation by assuming the TTD was equal to PFS using the functionality within the sponsor’s model.
The proportion of newly progressed patients over time lacked face validity: The PSM health states were populated with PFS and OS data obtained from the DESTINY-Breast04 trial and extrapolated independently over a time horizon of 12 years. Because the model does not explicitly account for the relationship between PFS and OS, or transition rates among distinct health states, after 17 months for trastuzumab deruxtecan and 11 months for standard of care, all progression events in the model were recorded as deaths (i.e., patients who are progression-free and experience a progression event after those time points may only experience death). When all new progression events were death, the number of newly progressed patients was reduced to 0, which consequently also reduced the subsequent treatments’ costs to 0, and the life-years and QALYs accrued in the progressed state to 0. The clinical experts consulted by CADTH for this review indicated that patients are expected to experience a similar likelihood of a disease progression event being death versus progressed disease over time and the model likely does not accurately reflect the disease pathway.
CADTH could not address this limitation associated with the model structure.
The sponsor assumed sacituzumab govitecan was equivalent to trastuzumab deruxtecan with regard to PFS and OS in the absence of available comparative evidence: Sacituzumab govitecan was considered a relevant comparator in patients with HR-negative, HER2-low metastatic breast cancer. The sponsor determined that it was unfeasible to conduct an indirect comparison to determine sacituzumab govitecan’s relative efficacy to trastuzumab deruxtecan due to differences in patient populations, small sample sizes, and unavailable reporting of patient characteristics. The CADTH Clinical Review team agreed that the major differences between the trials made a network meta-analysis infeasible, and while CADTH considers a matching adjusted indirect comparison to be feasible given the evidence available, it is uncertain whether the results would have provided reliable estimates for the relative efficacy of trastuzumab deruxtecan in comparison to sacituzumab govitecan. In the sponsor’s scenario considering sacituzumab govitecan in the HR-negative subpopulation, sacituzumab govitecan was dominated by trastuzumab deruxtecan, as both treatments were assumed to have the same QALY and life-year gains, and trastuzumab deruxtecan had a lower drug-acquisition and total costs. However, without any evidence on comparative effectiveness, no conclusions on the incremental cost-effectiveness can be drawn when comparing sacituzumab govitecan to trastuzumab deruxtecan.
CADTH could not address this limitation.
The use of treatment-specific health-utility values is inappropriate: The model submitted by the sponsor included health-utility values that were treatment-specific for the progression-free and postprogression health states. According to CADTH’s Guidelines for the Economic Evaluation of Health Technologies: Canada, the health-state utility scores should not be treatment-specific but differentiated by health state and/or event, with treatment efficacy captured via health-state occupancy and event occurrence driving the difference in observed QALYs. In addition, CADTH noted that the mean health-utility population norm available in Canada for that age group (0.84) was similar to the health-utility value obtained from the DESTINY-Breast04 trial for the postprogression disease state (0.83), and as such, appears to overestimate the HRQoL of patients with unresectable or metastatic HER2-low breast cancer whose disease had progressed.11 Studies in the literature report a significant reduction in mean utilities after disease progression (e.g., a reduction of 0.205 points in mean utility score, from a meta-regression that included 117 studies targeting metastatic breast cancer).12,13
Given the use of treatment-specific health-utility values, the sponsor did not include disutilities related to occurrence of AEs in its base-case analysis. This approach is not aligned with CADTH’s Guidelines for the Economic Evaluation of Health Technologies: Canada, which recommends adjustment of the utility for a specific health state by applying a disutility for an AE to allow the utility for the health state with an AE to be estimated.
CADTH addressed this limitation by using the same utility values by health state for both trastuzumab deruxtecan and standard of care. CADTH applied the values obtained for the standard-of-care arm in the DESTINY-Breast04 trial and incorporated AE-related disutilities based on AE rates.
In a scenario analysis, CADTH used the mean utility values obtained from a meta-regression adjusted by disease state (response and/or progression) identified in the literature.12
Estimates on the proportion of patients receiving subsequent treatments upon disease progression were not aligned with clinical expectations: The sponsor assumed that 74.5% of patients receiving trastuzumab deruxtecan and 80.3% of patients receiving standard of care would receive subsequent treatments. Clinician input obtained by CADTH for this review indicated that patients on trastuzumab deruxtecan would be expected to have a comparable, if not greater, likelihood of receiving subsequent therapy, given they would have more remaining treatment options for later lines of therapy. The sponsor’s approach resulted in lower estimated subsequent therapy costs with trastuzumab deruxtecan, biasing results in favour of trastuzumab deruxtecan.
CADTH addressed this limitation by changing the proportion of patients receiving subsequent therapies to 80.3% for both trastuzumab deruxtecan and standard of care.
Additionally, the following key assumptions were made by the sponsor and have been appraised by CADTH (Table 4).
Table 4: Key Assumptions of the Submitted Economic Evaluation (Not Noted as Limitations to the Submission)
Sponsor’s key assumption | CADTH comment |
|---|---|
Costs and disutilities related to grade 3+ AEs with an incidence of at least 2% in the trial DESTINY-Breast04 were included in the model. | Inappropriate. The sponsor selected an arbitrary threshold to capture the impact of treatment-related AEs rather than include the most clinically meaningful AEs in the model. CADTH’s Guidelines for the Economic Evaluation of Health Technologies: Canada recommend that all AEs that have a clinical or cost significance be included in the model. As noted in the CADTH Clinical Review and the clinician input received by CADTH for this review, pneumonitis (all grades) was more common among patients who received trastuzumab deruxtecan compared with standard of care. The inclusion of only grade 3 or higher AEs in the pharmacoeconomic model may underestimate the costs associated with pneumonitis, as additional visits to a health care provider and drug treatments may be required regardless of grade. |
Total management costs for AEs and disutilities related to AEs were applied only once during the first model cycle, estimated as the sum of the costs and disutilities of the AE incidence. | Uncertain. This approach does not allow for discounting of AE costs or utilities as all are applied in the first cycle and assumes that all AEs occur in the first cycle. |
The sponsor did not consider the potential for additional costs related to HER2 retesting, or staff training. | Uncertain. Consultations with clinical experts indicated that the differentiation between HER2-negative and HER2-low may not be always accurate as it previously had no clinical implications (i.e., patients classified as HER2-low had the same treatment options as if they were HER2-negative). The pathology expert consulted by CADTH confirmed that existing samples for patients already tested can be re-read to determine HER2-low status, with no need for an additional biopsy. However, there may be a need for appropriate staff training, including education about quality assurance programs with clinically validated standardized external controls for the immunochemistry test to differentiate between scores 0 (HER2-negative) and 1+ (HER2-low). |
The sponsor assumed that the treatment effect would not differ based on the line of therapy involved. | Unknown. Trastuzumab deruxtecan may be received in 2 different lines of therapy; however, CADTH could not assess the cost-effectiveness of trastuzumab deruxtecan based on the line of therapy in which it was received. |
AE = adverse event; QALY = quality-adjusted life-year.
CADTH Reanalyses of the Economic Evaluation
Base-Case Results
The CADTH base case was derived by making changes in model parameter values and assumptions, in consultation with clinical experts. Table 5 details each change made to derive the CADTH revised base case, which was conducted in a stepwise approach to highlight the impact of each change. A summary of results from the stepped reanalysis is presented in Table 6 and Table 10.
Table 5: CADTH Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
None | — | — |
Changes to derive the CADTH base case | ||
1. Model time horizon | 12 years | 10 years |
2. TTD | Patients who were progression-free were stratified into on treatment and off treatment, with the on-treatment proportion modelled using TTD (i.e., TTD and PFS curves were fitted independently) | Patients who were progression-free were assumed to be on treatment (TTD equal to PFS) |
3. Health-state utilities | Treatment-specific health-state utility values obtained from the DESTINY-Breast04 trial. AEs disutilities were not included in the analysis | Health state–specific utility values based on the standard-of-care values derived from the DESTINY-Breast04 trial. AEs disutilities were included |
4. Proportion of patients receiving subsequent treatments | 74.5% and 80.3% patients in the trastuzumab deruxtecan and standard-of-care arm received subsequent therapy, respectively | 80.3% for both trastuzumab deruxtecan and standard of care received subsequent therapy, respectively |
CADTH base case | 1 + 2 + 3 + 4 | |
AE = adverse event; PFS = progression-free survival; TTD = time to treatment discontinuation.
Results from the CADTH base-case reanalysis suggested that, compared to standard of care, trastuzumab deruxtecan was associated with higher costs ($229,735) and yielded more QALYs (0.55), resulting in an ICER of $303,924 per QALY gained (Table 6). The estimated ICER was higher than the sponsor's base case, driven primarily by the assumption that TTD was equal to PFS, and changing from treatment-specific utility values to health state–specific utilities only. In the CADTH base case, trastuzumab deruxtecan had a 0% probability of being cost-effective at a willingness-to-pay threshold of $50,000 per QALY gained.
Table 6: Summary of the Stepped Analysis of the CADTH Reanalysis Results
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($ per QALY) |
|---|---|---|---|---|
Sponsor’s base case (deterministic) | Standard of care | 54,734 | 1.36 | Reference |
Trastuzumab deruxtecan | 187,843 | 2.00 | 209,195 | |
CADTH reanalysis 1 | Standard of care | 54,727 | 1.36 | Reference |
Trastuzumab deruxtecan | 187,825 | 1.99 | 210,343 | |
CADTH reanalysis 2 | Standard of care | 61,576 | 1.36 | Reference |
Trastuzumab deruxtecan | 229,943 | 2.00 | 264,608 | |
CADTH reanalysis 3 | Standard of care | 54,734 | 1.35 | Reference |
Trastuzumab deruxtecan | 187,843 | 1.91 | 237,252 | |
CADTH reanalysis 4 | Standard of care | 54,734 | 1.36 | Reference |
Trastuzumab deruxtecan | 188,031 | 2.00 | 209,491 | |
CADTH base case (probabilistic) | Standard of care | 61,631 | 1.35 | Reference |
Trastuzumab deruxtecan | 229,735 | 1.90 | 303,924 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Scenario Analysis Results
CADTH undertook a price-reduction analyses for trastuzumab deruxtecan based on the sponsor’s base case and the CADTH base case (Table 7). This analysis demonstrated that a price reduction of 75% would be necessary for trastuzumab deruxtecan to achieve cost-effectiveness at a willingness-to-pay threshold of $50,000 per QALY gained when considering the CADTH base case.
Table 7: CADTH Price-Reduction Analyses
Analysis | ICERs for trastuzumab deruxtecan vs. standard of care ($ per QALY) | |
|---|---|---|
Price reduction | Sponsor base case | CADTH reanalysis |
No price reduction | 209,192 | 302,270 |
10% | 186,345 | 268,687 |
20% | 163,498 | 235,127 |
30% | 140,650 | 201,566 |
40% | 117,803 | 168,006 |
50% | 94,956 | 134,446 |
60% | 72,109 | 100,885 |
70% | 49,262 | 67,325 |
80% | 26,415 | 33,764 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
In addition, CADTH conducted a series of scenario analyses to determine the impact of alternative assumptions on the cost-effectiveness of trastuzumab deruxtecan:
Time horizon of 33 months (maximum observation time in DESTINY-Breast04 trial) to account for uncertainty with long-term OS.
Stratified analysis by HR status given different underlying survival expectations for these 2 populations. Due to the uncertainty associated with OS benefits in the HR-negative population, in this scenario analysis, CADTH applied the OS hazard ratio for trastuzumab deruxtecan versus standard of care from the HR-positive population in the DESTINY-Breast04 trial (hazard ratio = 0.64) to the HR-negative standard-of-care curve.
Use of health-state utilities obtained from the literature (0.7513 and 0.4523 for progression-free and progressed states, respectively), instead of the values used in the CADTH reanalysis (0.8261 and 0.7887 for progression-free and progressed states, respectively).
Results from these scenarios are presented in Table 13. CADTH considered a scenario analysis to explore the substantial uncertainty associated with OS benefits by reducing the time horizon of the analysis to 33 months. In the scenario analysis, the ICER increased substantially to $597,714 per QALY gained. A second scenario analysis using the HR-positive population hazard ratio to calculate the OS benefit of the HR-negative population resulted in an increased ICER of $401,855 per QALY gained due to the reduction of the incremental life-year benefit from 0.98 to 0.36 in comparison with the CADTH base-case analysis. The analysis of the HR-positive population resulted in an ICER of $262,433 per QALY gained. Finally, when the health-state utilities identified from the literature were used in the cost-utility model instead of the health utilities from the DESTINY-Breast04 trial, the ICER increased to $366,792 per QALY gained.
Issues for Consideration
Stakeholder input noted that storage of trastuzumab deruxtecan vials requires refrigeration and, after reconstitution, trastuzumab deruxtecan vials must be used immediately. Vial sharing is therefore unlikely to be feasible, leading to drug wastage. Drug wastage was accounted for in the sponsor and CADTH analyses.
Consultations with clinical experts indicated that the differentiation between HER2-negative and HER2-low previously might not always be accurate as it had no clinical implications (i.e., patients classified as HER2-low had the same treatment options as patients classified as HER2-negative). The pathology expert consulted by CADTH confirmed that existing samples for patients already tested can be re-read to determine HER2-low status, with no need for an additional biopsy. However, there may be a need for appropriate staff training, including education involving quality assurance programs with clinically validated standardized external controls to differentiate between scores of 0 (HER2-negative) and 1+ (HER2-low).
The sponsor based the drug-acquisition cost for sacituzumab govitecan on a prior CADTH submission. However, the recommendation for sacituzumab govitecan suggested a large price reduction for sacituzumab govitecan was required for sacituzumab govitecan to be cost-effective.14
Overall Conclusions
Based on the CADTH Clinical Review of the DESTINY-Breast04 trial, trastuzumab deruxtecan was associated with a statistically and clinically significant PFS and OS benefit in comparison with standard of care in adult patients with HER2-low unresectable or metastatic breast cancer who had received at least 1 prior line of chemotherapy in the metastatic setting or developed disease recurrence during or within 6 months of completing adjuvant chemotherapy. Furthermore, patients with HR-positive breast cancer should have received at least 1 ET and be no longer considered eligible for ET. The long-term clinical effectiveness of trastuzumab deruxtecan beyond the trial period (maximum follow-up of 33 months) is uncertain. Harms observed in the trial were aligned with clinician expectations and noted to be manageable. The impact of trastuzumab deruxtecan on HRQoL was uncertain, as the DESTINY-Breast04 trial was not powered to detect differences in HRQoL outcomes. An evidence gap remains for the relative efficacy and safety of trastuzumab deruxtecan in comparison with sacituzumab govitecan in the HR-negative cohort of patients.
CADTH identified several additional limitations with the economic analysis submitted by the sponsor. These key limitations included an OS extrapolation for trastuzumab deruxtecan lacking face validity beyond 10 years; issues with the model structure leading to an overestimate of patients who were progression-free and off treatment, as well as the lack of patients experiencing a progression event rather than death as the time horizon progressed, which was not aligned with clinical expectations; use of treatment-specific utility values; and inappropriate assumptions regarding the proportion of patients receiving subsequent therapy with trastuzumab deruxtecan in comparison with standard of care. CADTH conducted a reanalysis that changed the time horizon; assumed that TTD was equal to PFS; selected health-utility values that were health state–specific rather than treatment-specific and incorporated AE disutilities; and changed the proportion of patients receiving subsequent treatments following trastuzumab deruxtecan to be equivalent to that of standard of care. Based on the CADTH reanalysis, treatment with trastuzumab deruxtecan was $168,104 more costly and yielded 0.55 more QALYs compared with standard of care, resulting in an ICER of $303,924 per QALY gained. The probability of trastuzumab deruxtecan being cost-effective at a willingness-to-pay threshold of $50,000 per QALY gained was 0%. A price reduction of at least 75% would be necessary to achieve an ICER of $50,000 per QALY gained.
The results remained robust across CADTH scenario analyses. This included the scenario analysis that considered the population stratified by HR status to account for the underlying survival difference. However, the results from the HR-negative subgroup should be interpreted with caution, as the relative treatment effect with trastuzumab deruxtecan is uncertain in this subpopulation and CADTH’s reanalysis in this subpopulation relies on an assumption that the relative treatment effectiveness would be similar to that of the HR-positive population. Furthermore, a robust analysis comparing trastuzumab deruxtecan with sacituzumab govitecan in the HR-negative population could not be completed due to a lack of comparative clinical evidence. While analyses suggest sacituzumab govitecan is dominated by trastuzumab deruxtecan, this result is based on an assumption of equivalence and public list prices for sacituzumab govitecan. Finally, additional uncertainty remains in all reanalyses due to limitations with the PSM approach that could not be addressed. A greater price reduction therefore may be required to account for the remaining uncertainty.
References
1.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Enhertu (trastuzumab deruxtecan), powder for concentrate for infusion, 100 mg/vial, intravenous infusion. Mississauga (ON): AstraZeneca Canada Inc.; 2022 Dec 13.
2.Enhertu (trastuzumab deruxtecan): powder for concentrate for infusion, 100 mg/vial, intravenous infusion [product monograph]. Mississauga (ON): AstraZeneca Canada Inc.; 2023 Jan 6.
3.Modi S, Jacot W, Yamashita T, et al. Trastuzumab Deruxtecan in Previously Treated HER2-Low Advanced Breast Cancer. N Engl J Med. 2022;387(1):9-20. PubMed
4.DeltaPA. [Ottawa (ON)]: IQVIA; 2022: https://www.iqvia.com/. Accessed 2023 Jan 16.
5.Tam VC, Ko YJ, Mittmann N, et al. Cost-effectiveness of systemic therapies for metastatic pancreatic cancer. Curr Oncol. 2013;20(2):e90-e106. PubMed
6.Ontario Case Costing Initiative (OCCI). Toronto (ON): Ontario Health and Long-Term Care; 2017: https://data.ontario.ca/dataset/ontario-case-costing-initiative-occi. Accessed 2023 Jan 16.
7.Cortes J, O'Shaughnessy J, Loesch D, et al. Eribulin monotherapy versus treatment of physician's choice in patients with metastatic breast cancer (EMBRACE): a phase 3 open-label randomised study. Lancet. 2011;377(9769):914-923. PubMed
8.Schedule of benefits for physician services under the Health Insurance Act: effective October 1, 2021. Toronto (ON): Ontario Ministry of Health; 2022: https://www.health.gov.on.ca/en/pro/programs/ohip/sob/physserv/sob_master.pdf. Accessed 2023 Jan 16.
9.Schedule of benefits for laboratory services: effective July 1, 2020. Toronto (ON): Ontario Ministry of Health; 2020: https://www.health.gov.on.ca/en/pro/programs/ohip/sob/lab/lab_mn2020.pdf. Accessed 2023 Jan 16.
10.Beauchemin C, Letarte N, Mathurin K, Yelle L, Lachaine J. A global economic model to assess the cost-effectiveness of new treatments for advanced breast cancer in Canada. J Med Econ. 2016;19(6):619-629. PubMed
11.Yan J, Xie S, Johnson JA, et al. Canada population norms for the EQ-5D-5L. Eur J Health Econ. 2023. PubMed
12.Peasgood T, Ward SE, Brazier J. Health-state utility values in breast cancer. Expert Rev Pharmacoecon Outcomes Res. 2010;10(5):553-566. PubMed
13.Lloyd A, Nafees B, Narewska J, Dewilde S, Watkins J. Health state utilities for metastatic breast cancer. Br J Cancer. 2006;95(6):683-690. PubMed
14.CADTH reimbursement recommendation: Sacituzumab govitecan (Trodelvy). Can J Health Technol. 2022;2(2). https://www.cadth.ca/sites/default/files/DRR/2022/PC0254%20Trodelvy%20-%20CADTH%20Final%20Rec-meta.pdf. Accessed 2023 Mar 14.
15.Kawahara T, Taira N, Shiroiwa T, et al. Minimal important differences of EORTC QLQ-C30 for metastatic breast cancer patients: Results from a randomized clinical trial. Qual Life Res. 2022;31(6):1829-1836. PubMed
16.Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Enhertu (trastuzumab deruxtecan), powder for concentrate for infusion, 100 mg/vial, intravenous infusion. Mississauga (ON): AstraZeneca Canada Inc.; 2022 Dec 13.
Appendix 1: Cost-Comparison Table
Note that this appendix has not been copy-edited.
The comparators presented in the Table 8 have been deemed to be appropriate based on feedback from clinical expert(s). Comparators may be recommended (appropriate) practice or actual practice. Existing product listing agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 8: CADTH Cost-Comparison Table for HER2-Low Metastatic Breast Cancer
Treatment | Strength/concentration | Form | Price | Recommended dosage | Daily cost | Average 28-day cost |
|---|---|---|---|---|---|---|
Trastuzumab deruxtecan (Enhertu) | 100 mg | Vial for IV infusion | 2,440.0000a | 5.4 mg/kg once every 3 weeks | 464.76 | 13,013 |
Single-drug treatments | ||||||
Capecitabine (generic) | 150 mg 500 mg | Tablet | 0.4575 1.5250 | 1,250 mg/m2 twice daily for 14 days followed by 7-day rest period | 8.74 | 245 |
Eribulin (generic) | 1 mg/ 2mL | 2 mL vial for IV infusion | 422.0000 | 1.4 mg/m2 on days 1 and 8 of a 21-day cycle | 120.57 | 3,376 |
Gemcitabine (generic) | 1,000 mg 2000 mg | Lyophilized powder | 270.0000 540.0000 | 1,250 mg/m2 on day 1 and 8 of a 21-day cycle | 77.14 | 2,160 |
Paclitaxel (generic) | 6 mg/mL | 30 mg vial for IV infusion 96 mg vial for IV infusion 150 mg vial for IV infusion 300 mg vial for IV infusion | 300.0000 1,196.8000 1,870.0000 3,740.0000 | 175 mg/m2 on day 1 every 3 weeks for 4 cycles | 178.10 | 4,889 |
Vinorelbine (generic) | 10 mg/mL | 1 mL vial for injection 5 mL vial for injection | 80.0000 400.00000 | 30 mg/m2 weekly | 68.57 | 1,920 |
Monoclonal Antibody | ||||||
Sacituzumab govitecan | 180mg | Lyophilized powder | 1,478.0000b | 10 mg/kg on days 1 and 8 of continuous 21-day treatment cycle | 563.05 | 15,765 |
Note: All prices are from the DeltaPA database15 (accessed January 2023), unless otherwise indicated, and do not include dispensing fees.
Assumes mean patient weight of 63.4 kg and BSA = 1.671 m2 as per sponsor’s submission.
aSponsor submitted price.
bPrice obtained from CADTH’s review of sacituzumab govitecan.
CPrice per millilitre.
Appendix 2: Submission Quality
Note that this appendix has not been copy-edited.
Description | Yes/No | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | No | Concerns with generalizability of patient population, refer to CADTH appraisal |
Model has been adequately programmed and has sufficient face validity | No | Limitations identified with modelling of subsequent treatments and proportion of patients on progression-free and off-treatment health state, refer to CADTH appraisal for more details |
Model structure is adequate for decision problem | Yes | No comment |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | Yes | No comment |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | Yes | No comment |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | Yes | No comment |
Appendix 3: Additional Information on the Submitted Economic Evaluation
Note that this appendix has not been copy-edited.
Detailed Results of the Sponsor’s Base Case
Table 10: Disaggregated Summary of CADTH’s Economic Evaluation Results
Parameter | Trastuzumab deruxtecan | Standard of care | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 2.39 | 1.70 | 0.69 |
By health state | |||
Preprogression | 1.12 | 0.62 | 0.51 |
Postprogression | 1.27 | 1.09 | 0.18 |
Discounted QALYs | |||
Total | 2.00 | 1.36 | 0.63 |
By health state | |||
Preprogression | 0.94 | 0.51 | 0.44 |
Postprogression | 1.05 | 0.86 | 0.20 |
Discounted costs ($) | |||
Total | $187,677 | $54,731 | $132,945 |
Acquisition | $145,270 | $13,337 | $131,933 |
Administration | $1,745 | $1,505 | $240 |
Subsequent treatment | $2,420 | $3,288 | -$869 |
Resource use | $6,579 | $4,416 | -$110 |
Adverse event–related | $593 | $703 | $2,163 |
End of life | $31,070 | $31,483 | -$413 |
ICER ($ per QALY) | 210,047 | ||
ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year.
Source: Sponsor’s pharmacoeconomic submission.1
Table 11: Summary of the Sponsor’s Scenario Analysis Results (Deterministic Analysis) Stratified by Hormone Receptor Status
Drug | Total costs ($) | Incremental costs ($) | Total LYs | Incremental LYs | Total QALYs | Incremental QALYs | ICER vs. standard of care ($ per QALY) |
|---|---|---|---|---|---|---|---|
HR-negative | |||||||
Standard of care | 48,216 | Reference | 1.05 | Reference | 0.85 | Reference | Reference |
Trastuzumab deruxtecan | 142,067 | 93,852 | 2.03 | 0.98 | 1.70 | 0.85 | 110,254 |
Sacituzumab govitecan | 174,175 | 32,108 | 2.03 | 0.00 | 1.70 | 0.00 | Dominated |
HR-positive | |||||||
Standard of care | 55,732 | Reference | 1.85 | Reference | 1.48 | Ref. | Reference |
Trastuzumab deruxtecan | 194,291 | 138,559 | 2.40 | 0.55 | 2.01 | 0.53 | 259,557 |
ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year.
Source: Sponsor’s pharmacoeconomic submission.1
Appendix 4: Additional Details on the CADTH Reanalyses and Sensitivity Analyses of the Economic Evaluation
Note that this appendix has not been copy-edited.
Detailed Results of CADTH Base Case
Table 12: Disaggregated Summary of CADTH’s Economic Evaluation Results
Parameter | Trastuzumab deruxtecan | Standard of care | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 2.39 | 1.70 | 0.68 |
By health state | |||
Preprogression | 1.12 | 0.62 | 0.51 |
Postprogression | 1.26 | 1.09 | 0.18 |
Discounted QALYs | |||
Total | 1.90 | 1.35 | 0.55 |
By health state | |||
Preprogression | 0.93 | 0.51 | 0.42 |
Postprogression | 0.99 | 0.86 | 0.14 |
Discounted costs ($) | |||
Total | 229,735 | 61,631 | 168,104 |
Acquisition | 186,828 | 19,547 | 167,281 |
Administration | 2,187 | 2,206 | −19 |
Subsequent treatment | 2,608 | 3,288 | −680 |
Resource use | 6,566 | 4,415 | 2,151 |
Adverse event–related | 593 | 703 | −110 |
End of life | 30,953 | 31,472 | −519 |
ICER ($per QALY) | 303,924 | ||
AE = adverse event; ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year.
Scenario Analyses
Stepped analysis | Comparator | Total costs ($) | Total QALYs | ICER ($ per QALY) |
|---|---|---|---|---|
CADTH’s base case (full population) | Standard of care | 61,569 | 1.35 | Reference |
Trastuzumab deruxtecan | 230,012 | 1.90 | 302,270 | |
CADTH scenario 1: Time horizon set to maximum follow-up of trial (33 months) | Standard of care | 55,196 | 1.18 | Reference |
Trastuzumab deruxtecan | 206,680 | 1.43 | 598,752 | |
CADTH scenario 2a: Use of HR-positive hazard ratio to model trastuzumab deruxtecan’s OS for HR-negative subgroup (HR = 0.64) | Standard of care | 53,025 | 0.84 | Reference |
Trastuzumab deruxtecan | 170,559 | 1.15 | 386,576 | |
Sacituzumab govitecan | 230,591 | 1.15 | Dominated by trastuzumab deruxtecan | |
CADTH scenario 2b: Use of hazard ratio to model trastuzumab deruxtecan’s OS for HR-positive subgroup (HR = 0.64) | Standard of care | 63,107 | 1.47 | Reference |
Trastuzumab deruxtecan | 215,909 | 2.05 | 261,690 | |
CADTH scenario 3: Health state utilities from literature | Standard of care | 61,631 | 0.94 | Ref. |
Trastuzumab deruxtecan | 229,735 | 1.40 | 368,418 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Appendix 5: Submitted Budget Impact Analysis and CADTH Appraisal
Note that this appendix has not been copy-edited.
Table 14: Summary of Key Take-Aways
Key take-aways of the budget impact analysis |
|---|
|
Summary of Sponsor’s Budget Impact Analysis
The sponsor submitted a budget impact analysis (BIA) estimating the budget impact of introducing trastuzumab deruxtecan as a treatment of adult patients with unresectable and/or metastatic HER2-low (IHC 1+ or IHC 2+/ISH−) breast cancer who have been treated with at least 1 prior line of chemotherapy in the metastatic setting or have developed disease recurrence during or within 6 months of completing adjuvant chemotherapy; patients with HR-positive breast cancer should have received at least 1 and be no longer considered eligible for ET.16 The analytic framework, which used a top-down epidemiology-based approach, leveraged data from multiple sources in the literature and assumptions based on clinical expert input to determine the estimated population size (Figure 2). The sponsor stratified the patient population by HR status. Patients with HR-positive unresectable and/or metastatic HER2-low breast cancer could receive trastuzumab deruxtecan as third- and fourth-line treatment, and the relevant comparator was assumed to be chemotherapy, modelled as a basket of therapeutic options. Alternatively, patients with HR-negative unresectable and/or metastatic HER2-low breast cancer would be eligible to receive trastuzumab deruxtecan as second- and third-line treatment, and the relevant comparators were assumed to be chemotherapy, similarly modelled as a basket of therapies, and sacituzumab govitecan. The sponsor compared a reference scenario where trastuzumab deruxtecan was not reimbursed, with a new drug scenario, where trastuzumab deruxtecan was funded, as per the Health Canada indication. The sponsor noted that the BIA model estimated newly diagnosed and newly recurrent metastatic breast cancer patients who would become eligible to receive trastuzumab deruxtecan. Existing patients were assumed to be captured by the sponsor’s patient support/free drug program and were accounted for as such in the BIA.
The BIA base case was undertaken from a publicly funded drug plan perspective considering only drug costs over a 3-year time horizon. Additional health care costs were considered in a scenario analysis from the health care payers perspective that included AE, administration, and high-resolution CT scans costs. Drug costs considered included that of initial line treatment and subsequent treatment regimens used among patients who progressed. trastuzumab deruxtecan costs were calculated by multiplying the recommended dosage (5.4 mg/kg) by an average patient weight of 63.4 kg, resulting in the need for 4 vials of 100 mg per patient. The sponsor assumed vials would not be shared among patients. Furthermore, treatment costs accounted for the duration of those treatments, which was observed during the DESTINY-Breast04 trial. The sponsor used PFS and OS curves from the DESTINY-Breast04 trial to determine disease progression and death. The sponsor assumed that 74.5% and 80.3% of patients initially receiving trastuzumab deruxtecan and standard of care, respectively, would receive subsequent treatment based on data from DESTINY-Breast04 trial (median follow-up of approximately 18 months). The proportion of patients receiving each subsequent treatment per treatment were based on data from the DESTINY-Breast04 trial and reweighted to match subsequent treatments options selected by the sponsor based on their relevance to the Canadian setting. The sponsor also assumed a delay of 1 cycle between treatment and subsequent treatments. Key inputs to the BIA are documented in Table 15.
Table 15: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as Year 1 / Year 2 / Year 3 if appropriate) | |
|---|---|---|
HR-positive | HR-negative | |
Target Population | ||
Number of mBC, HER2-negative patientsa | 4,930 | |
Proportion of patients by HR status | 80.8% | 19.2% |
Proportion of patients HER2-low | 65.4% | 36.5% |
Proportion of patients who received first-line treatment | ||||% | 80.0% |
Proportion of patients who received second-line treatment | ||||% | NAf |
Proportion of patients who received third-line treatment | ||||% | NAf |
Proportion of patients who received treatment with prior necessary therapy to be eligible at first treatment opportunityb,c | ||||%e | 80.0%f |
Proportion of patients who received treatment with prior necessary therapy to be eligible at second treatment opportunityb,d | ||||%e | 70.0%f |
Number of patients eligible for drug under review | 1,090 / 1,103 / 1,115 | 389 / 394 / 398 |
Market uptake (3 years) | ||
Uptake (reference scenario) | ||
Standard of care | 100% / 100% / 100% | 50% / 85% / 85% |
Sacituzumab govitecan | NA / NA / NA | 50% / 15% / 15% |
Uptake (new drug scenario) | ||
Trastuzumab deruxtecan | ||% / ||% / ||% | ||% / ||% / ||% |
Standard of care | ||% / ||% / ||% | ||% / ||% / ||% |
Sacituzumab govitecan | || / || / || | ||% / ||% / ||% |
Cost of treatment (per patient per 28-day cycle) | ||
Trastuzumab deruxtecan | $13,058 | |
Standard of care | $2,530 | |
Sacituzumab govitecan | $15,819 | |
HR = hormone receptor; NA = not applicable; mBC = metastatic breast cancer.
aFor simplicity, CADTH did not describe the steps to calculate the number of mBC, HER2 negative patients. In the sponsor’s model, this included the identification of patients as having mBC at time of diagnosis, patients with a late relapse to mBC and an early relapse to mBC.
bNecessary therapy for eligibility was defined as having received prior chemotherapy and ET for the HR-positive cohort, and prior chemotherapy for the HR-negative cohort.
cThe first treatment opportunity was third line for patients who were HR-positive, and second-line for patients who were HR-negative.
dThe second treatment opportunity was fourth line for patients who were HR-positive, and third line for patients who were HR-negative.
eAmong these patients, the sponsor assumed that 90% would be eligible to receive additional therapy.
fFor the epidemiological approach of HR-negative patients, the sponsor combined the proportion patients who received a second-line treatment with the proportion of patients who received a treatment with prior necessary therapy to be eligible at first treatment opportunity into 1 proportion of patients eligible (80%). The same approach was used for patients receiving third-line treatment and patients with prior necessary therapy to be eligible at second treatment opportunity, resulting in a proportion of 70%.
Source: Sponsor’s BIA submission.16
Figure 2: Sponsor’s Estimation of the Size of the Eligible Population
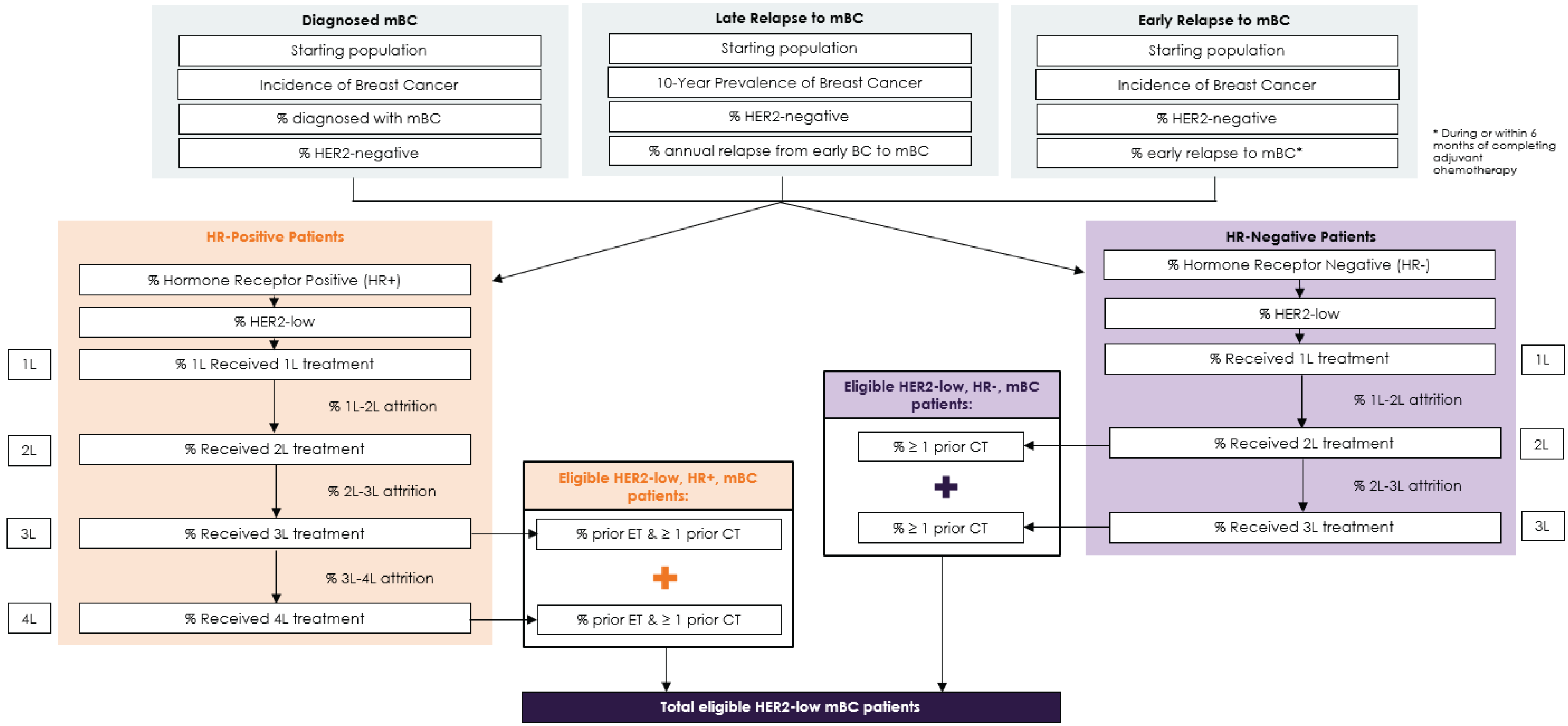
Source: Sponsor’s BIA submission.16
Summary of the Sponsor’s BIA Results
In the sponsor’s base case from the drug plan perspective, the estimated budget impact of funding trastuzumab deruxtecan for the indication under review was $44,746,512, $73,135,484, $77,114,047 for Year 1, 2, and 3, respectively. The 3-year total was $194,996,043.
In the scenario analysis from the health care payer perspective, the estimated budget impact of funding trastuzumab deruxtecan was $44,867,390, $73,327,246, $77,276,555 for Year 1, 2, and 3, respectively. The 3-year total was $195,471,191.
CADTH Appraisal of the Sponsor’s BIA
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
The proportions of HR-positive patients who previously received chemotherapy and were refractory to prior ET were underestimated: To be eligible for trastuzumab deruxtecan in the third or fourth line of therapy, patients who were HR-positive had to have had received treatment with chemotherapy and been refractory to ET from prior lines of therapy. The sponsor assumed that the proportions of patients who received second-line chemotherapy and were refractory to prior ET and patients who received third-line chemotherapy and were refractory to prior ET was ||% and ||%, respectively, based on data obtained via chart audit, analyzing data from ||| patients. The chart audit provided by the sponsor does not have enough detail for CADTH to evaluate the generalizability of the results, or the methodology used to calculate these proportions. Thus, CADTH could not evaluate the validity of sponsor’s estimates. According to clinical experts consulted by CADTH for this review, these estimates might underestimate the expected proportion of patients who received the appropriate prior treatments and who would be eligible for trastuzumab deruxtecan in the third- or fourth-line setting. ET is recommended and used as first-line treatment with a cyclin-dependent kinase inhibitor in Canada, and chemotherapy is often used in the subsequent line of therapy. The clinical experts consulted by CADTH noted that they would expect 60% to 80% and 90% of patients who are HR-positive to meet the prior treatment eligibility criteria in the third and fourth lines, respectively. The sponsor’s estimate may have underestimated the eligible population size, although CADTH acknowledges that the proportion of patients eligible for third- and fourth-line trastuzumab deruxtecan may vary due to jurisdictional differences in second-line ET funding across Canada.
CADTH changed the proportion of patients who were HR-positive who received second-line chemotherapy and were refractory to prior ET to 60%, and proportion of patients who received a third-line chemotherapy (i.e., eligible in third line) and were refractory to prior ET to 90% (i.e., eligible in the fourth line).
CADTH also addressed the uncertainty around the proportion of patients who received second-line chemotherapy and were refractory to prior ET by presenting a scenario analysis where the proportion was changed to 80%.
Estimates on the proportion of patients receiving subsequent treatments upon disease progression were not aligned with clinical expectations: The sponsor assumed that ||||% receiving trastuzumab deruxtecan and ||||% of patients receiving standard of care would receive subsequent treatments. Clinician input obtained by CADTH for this review indicated that patients on trastuzumab deruxtecan would be expected to have the same likelihood of receiving subsequent therapy, if not more likely to, given they would have more remaining treatment options for later lines of therapy. The sponsor’s approach resulted in lower estimated subsequent therapy costs for subsequent treatment following trastuzumab deruxtecan, biasing results in favour of trastuzumab deruxtecan.
CADTH addressed this limitation by changing the proportion of patients receiving subsequent therapies to ||||% for both trastuzumab deruxtecan and standard of care.
The market uptake for trastuzumab deruxtecan in the HR-negative subpopulation is uncertain: In their base case, the sponsor estimated that ||% of HR-negative patients would be prescribed trastuzumab deruxtecan in the first year and increasing to ||% in the second and third year. According to the clinical experts consulted by CADTH for this review, there is considerable uncertainty regarding final uptake percentages in this subgroup, given the uncertainty associated with the comparative clinical effectiveness of SG and trastuzumab deruxtecan for the treatment of HER2-low HR-negative patients. Although the comparative efficacy of trastuzumab deruxtecan against SG is unknown, the clinical experts consulted by CADTH for this review suggested that if the patient is classified as HER2-low the use of a targeted therapy may be preferred over a therapy intended for HER2-negative patients.
CADTH performed 2 scenario analyses to explore the uncertainty in the market uptake in the HR-negative population, guided by input from clinical experts consulted by CADTH for this review. In the first scenario, the market uptake rates were equally distributed among treatments (33.3%). In the second scenario, the market uptake rates were doubled for trastuzumab deruxtecan from the base case estimate (58% in the first year, and 64% in the second and third year) to represent a scenario where trastuzumab deruxtecan would be used as treatment of choice in this subgroup instead of SG.
Additional limitations were identified but were not considered to be key limitations. These limitations include:
Non-Insured Health Benefit (NIHB) population was not submitted although standard-of-care treatment includes drugs funded by NIHB: Standard of care treatments include drugs funded by NIHB. Therefore, the NIHB population should have been submitted to demonstrate the expected budget impact introduced by funding the drug under review within that context.
Potential use of SG and trastuzumab deruxtecan sequentially in patients who are HR-negative, HER2-low: Clinical experts consulted by CADTH for this review indicated that trastuzumab deruxtecan and SG could be used sequentially in clinical practice in patients who are HR-negative, and who would have originally been classified HER2-negative now reclassified as HER2-low. Although, at the moment, there is no evidence to support the use of the 2 therapies sequentially, it could be a potential scenario as research evolves. In this case, the cost of trastuzumab deruxtecan would be in addition to the cost of SG, instead of trastuzumab deruxtecan only displacing SG.
CADTH Reanalyses of the BIA
CADTH’s base case revised the proportion of HR-positive patients who received chemotherapy and ET in prior lines of therapy and eligible for trastuzumab deruxtecan, and the proportion of patients receiving subsequent treatments in the trastuzumab deruxtecan arm.
Table 16: CADTH Revisions to the Submitted Budget Impact Analysis
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
None | — | — |
Changes to derive the CADTH base case | ||
1. Proportions of HR-positive patients who received chemotherapy and ET in prior lines of therapy and eligible for trastuzumab deruxtecan | After first 2 lines of therapy: ||% After first 3 lines of therapy: ||% | After first 2 lines of therapy: 60% After first 3 lines of therapy: 90% |
2. Proportion of patients receiving subsequent treatments | ||||% and ||||% for patients receiving trastuzumab deruxtecan and standard of care, respectively | ||||% for both trastuzumab deruxtecan and standard of care received subsequent therapy, respectively |
CADTH base case | 1 + 2 | |
The results of the CADTH stepwise reanalysis is presented in summary format in Table 17 and a more detailed breakdown is presented in Table 18. Based on CADTH’s base case, the expected budget impact for funding trastuzumab deruxtecan is expected to be $48,554,076 in Year 1, $79,502,778 in Year 2, and $83,912,162 in Year 3, for a 3-year budget impact of $211,969,016. From the health care payer perspective, the estimated budget impact of funding trastuzumab deruxtecan was $48,711,139, $79,763,181, $84,149,672 for Year 1, 2, and 3, respectively, for a 3-year total of $212,623,992.
Table 17: Summary of the CADTH Reanalyses of the Budget Impact Analysis
Stepped analysis | Three-year total ($) |
|---|---|
Submitted base case | 194,996,043 |
CADTH reanalysis 1 | 211,874,985 |
CADTH reanalysis 2 | 195,082,761 |
CADTH base case | 211,969,016 |
CADTH also conducted additional scenario analyses to address remaining uncertainty, using the CADTH base case. The scenarios conducted were:
Revising the proportion of HR-positive patients who received a second line of chemotherapy and were refractory to prior ET to 80%.
Setting the market uptake to be equally distributed among all treatment options for HR-negative patients.
Setting the market uptake for trastuzumab deruxtecan in HR-negative patients to 54% in the first year and 64% in the second and third year.
Price reduction of trastuzumab deruxtecan was 75% (aligned with the price reduction from the economic evaluation appraisal).
Results of CADTH’s scenario analyses demonstrate that the estimated budget impact is sensitive to the changes in the proportion of patients receiving necessary prior therapy. In addition, a treatment price reduction of 75% would result in considerable decrease in the budget impact from the drug plan perspective.
Table 18: Detailed Breakdown of the CADTH Reanalyses of the Budget Impact Analysis
Stepped analysis | Scenario | Year 0 (current situation) | Year 1 | Year 2 | Year 3 | Three-year total |
|---|---|---|---|---|---|---|
Submitted base case | Reference | $16,262,927 | $28,074,702 | $40,370,333 | $46,061,135 | $114,506,170 |
New drug | $16,262,927 | $72,821,214 | $113,505,817 | $123,175,182 | $309,502,213 | |
Budget impact | $0 | $44,746,512 | $73,135,484 | $77,114,047 | $194,996,043 | |
CADTH base case | Reference | $16,927,521 | $28,903,158 | $41,213,289 | $46,914,636 | $117,031,082 |
New drug | $16,927,521 | $77,457,233 | $120,716,067 | $130,826,798 | $329,000,098 | |
Budget impact | $0 | $48,554,076 | $79,502,778 | $83,912,162 | $211,969,016 | |
CADTH scenario analysis 1: Proportion of HR-positive patients receiving necessary prior therapy changed to 80% | Reference | $17,193,453 | $29,233,657 | $41,547,945 | $47,253,130 | $118,034,732 |
New drug | $17,193,453 | $79,307,214 | $123,595,391 | $133,882,770 | $336,785,376 | |
Budget impact | $0 | $50,073,557 | $82,047,447 | $86,629,640 | $218,750,644 | |
CADTH scenario analysis 2: Market uptake equally distributed for HR-negative cohort | Reference | $16,927,521 | $28,903,158 | $41,213,289 | $46,914,636 | $117,031,082 |
New drug | $16,927,521 | $79,441,758 | $117,550,182 | $123,951,929 | $320,943,870 | |
Budget impact | $0 | $50,538,601 | $76,336,893 | $77,037,294 | $203,912,788 | |
CADTH scenario analysis 3: Market uptake for trastuzumab deruxtecan changed to 54%, 64%, and 64% in year 1, 2, and 3, respectively, in the HR-negative cohort | Reference | $16,927,521 | $28,903,158 | $41,213,289 | $46,914,636 | $117,031,082 |
New drug | $16,927,521 | $79,744,949 | $121,830,858 | $130,556,581 | $332,132,388 | |
Budget impact | $0 | $50,841,791 | $80,617,569 | $83,641,945 | $215,101,306 | |
CADTH scenario analysis 4: 75% price reduction | Reference | $16,927,521 | $28,903,158 | $41,213,289 | $46,914,636 | $117,031,082 |
New drug | $16,927,521 | $31,510,639 | $45,709,567 | $50,957,296 | $128,177,503 | |
Budget impact | $0 | $2,607,482 | $4,496,278 | $4,042,661 | $11,146,421 |
Stakeholder Input
Patient Input
Rethink Breast Cancer
About Rethink Breast Cancer
Rethink Breast Cancer is a Canadian charity known for making positive change. Rethink educates, empowers and advocates for system changes to improve the experience and outcomes of those with breast cancer, focusing on historically underserved groups: people diagnosed at a younger age, those with metastatic breast cancer and people systemically marginalized due to race, income or other factors. We foster spaces to connect, listen, empower and rethink breast cancer, together. Rethink’s strategic priorities and organizational direction are guided by the unique, unmet needs identified by breast cancer patients and their families.
Programs and Activities
Rethink Breast Cancer builds community, bringing patients with all stages of breast cancer together through our private and public social spaces, as well as in-person events
Rethink runs patient retreats and facilitates peer-support
Rethink creates and runs education forums and conferences
Rethink creates support and education tools, resources and content
Rethink funds and supports breast cancer research
You can find out more by visiting:
Rethink Breast Cancer Instagram
Information Gathering
For over 20 years, Rethink has been working closely with breast cancer patients in Canada. We learn from and listen to the community to understand their values, priorities and pain points to help drive change and system improvements. We learn from the 40 individuals that we work extremely closely with as key patient advisors; the 100 patients that share their stories on our blog; the 500 patients that participate in our virtual support groups; the 1,600 members of our private peer-support network; the 30,000 people that have joined our Instagram community; and the 150,000 individuals reached each month through that channel. We listen, learn, and engage in all these spaces.
Rethink Breast Cancer has several important patient advisory boards and working groups that offer experience-focused insights on issues related to those affected by and concerned about breast cancer, including:
Metastatic Breast Cancer Advisory Board
Early Breast Cancer Advisory Board
Equity, Diversity and Inclusion working group
Rethink also benefits from regular knowledge exchange with our Scientific Advisory Committee, which includes some of the leading clinician scientists in Canada who treat breast cancer.
For this submission, we have drawn on our general observations and insights gathered through programming and meetings with breast cancer patients as described above. We have also drawn on the results from an online survey with 78 metastatic breast cancer patients conducted by Rethink Breast Cancer to document the lived experience of patients and caregivers.
Patients completed the survey between September 2018 and April 2019.
In addition, we drew on recent in-depth one-on-one interviews in November 2022 with three Canadians who have HER2-low metastatic breast cancer: ||||| who is currently being treated with Enhertu through a clinical trial, |||||| who is currently paying out of pocket for Enhertu, and ||||||||| who is HER2-low and having had progression in January after three years on endocrine therapy and a CDK 4/6 inhibitor, hopes Enhertu will be an option in the future. We also interviewed |||||, a woman living in the United Kingdom whose access to Enhertu came through a clinical trial.
Please read testimonials from ||||| and ||||| in Appendix B.
Disease Experience
Most people in the Rethink community are diagnosed at a younger age. When young people get breast cancer it may be more aggressive, which can lead to tougher treatments. In addition, those diagnosed in their 20s, 30s and early 40s face age-specific issues such as fertility or family-planning challenges, diagnosis during pregnancy, childcare, impact on relationships, body image, dating and sexuality, feeling isolated from peers who don’t have cancer, career hiatuses, and financial insecurity. The physical and emotional toll that a breast cancer diagnosis and treatment takes on a young person’s life is devastating and traumatic.
In terms of a metastatic diagnosis, processing the reality of a life-limiting diagnosis is extremely difficult, especially for the young patients in our community and the emotional impacts on quality of life cannot be understated. Moreover, many develop brain metastasis, which is difficult to treat and has a heavy symptom burden with both physical impacts and often changes in mood, personality and thinking. These cognitive and psychosocial challenges negatively impact both the patients and their caregivers who often take on an overwhelming number of responsibilities. Other symptoms of metastatic breast cancer depend on the sites of the metastasis and include fatigue, shortness of breath for lung metastasis, pain and bone fractures for bone mets, as well as nausea, headache and of course challenges doing normal daily activity. Rethink’s MBC Advisory Board strongly believes in the benefit of metastatic patients accessing palliative/supportive care services early to help address these symptoms.
The HER2-low metastatic breast cancer patients we interviewed shared the different ways their metastatic diagnosis has impacted their day-to-day life:
||||||| is 54 years, married and stepmother to two young adult children.
Before her metastatic diagnosis, ||||||| was a marathon runner, socially active and worked full time and was a part-time university student. It was always a life dream of hers to get a university degree and just before her early breast cancer diagnosis, she had enrolled as a part-time student in disabilities studies. She was loving it so much that she set her sights on a master’s degree. ||||||| and her husband used to love going out for dinners and socializing with friends, but she now finds socializing more difficult because sometimes just focusing during the conversations is too draining. She walks to stay as active as she can but is no longer running. And due to the fatigue from treatments for her metastatic breast cancer, ||||||| had to stop working. For her, that has been “A big, big, big change. I feel like the psychology of it is…I feel very isolated sometimes at home during the day. I really miss the social component of work.” Unfortunately, fatigue from treatment made it too difficult to concentrate and focus on her university course work and paused her studies in 2021. In 2022, she had to accept the reality that she would not be able to resume her studies and made the difficult decision to formally withdraw from her program.
|||||| is 47 and has been married to her high-school sweetheart for 20 years.
|||||| is an only child, and she is primary caregiver to her parents who are in their mid-eighties with health problems.
|||||| had returned to work after a medical leave for treatment of her early breast cancer. She was ramping up slowly and had just started working full-time hours again, when she found out she was metastatic. She left her job because “It's like my full-time job became being a patient….your life just stops as you know it.” For ||||||, the diagnosis brought on “depression and anxiety… just this feeling of dread and anxiety, but I just hid from…from everyone. I would always just try to kind of put on this brave face.” A big part of how a metastatic diagnosis has impacted |||||| feeling guilty about things and being a burden on people.” She discussed feeling guilt about causing her husband too much worry and stress and talked at length about the worries she has for her aging parents. As an only child and primary (sole) caregiver to her parents, |||||| says, “I just felt like it was too much to tell them…after the first diagnosis, they were, you know, just totally shocked and it was just tears every time I would talk to my mom. And this went on and on and then December, the second diagnosis. I mean, I had to tell them because I was having this big surgery, but I couldn't…I couldn't then say ‘Oh, and by the way it's also spread to my bones.’”
Like |||||||, |||||| talked a lot about the physical and emotional isolation of her illness. She is home alone much of the time, which is a change from her lifestyle before her metastatic diagnosis when she worked and enjoyed dinners out and travelling with her husband and their friends. She would love to get a dog as a companion, but her worries and uncertainties about her future are roadblocks to getting a puppy. There’s an emotional component to her isolation too caused both by the disappointment in not being able to do things she used to do as well as the gap in understanding she experiences from non-cancer peers and friends who just don’t understand the reality of her diagnosis. “It was our 20th anniversary, and it would have been great to travel back to somewhere we’d enjoyed before but there was so much going on and like I said, you know, I had like full brain radiation just a month before so not being able to, not be able to plan things like that. I have friends that are you know, they plan all their travel like a year or more out and they're like, ‘oh, you know, do you want to sign up for Hawaii? Hawaii 2023? Hawaii 2024? You should go to Italy in May. We should do all this.’ Like yes, I would love that but when…. I don’t know.”
||||||||, age 51, is from Brazil and lived and worked in the US before meeting her Canadian husband and settling down in Vancouver. They have one daughter who is 8 and three big dogs. Prior to her breast cancer diagnosis, ||||||||| had an accomplished career in a leadership role as a professional engineer.||||||||| has ||||||| ||| ||||||| ||||||||| ||||||||| |||||||||| |||||||||| |||||||||| |||||||| || ||||||||||| || ||||||| ||| ||| and carried a lot of responsibility in her successful 21-year career. It’s been a huge shift to go from a high-powered career to being an MBC patient, but |||||||| applies some of her skill set to research and decision making around her treatment options. Her career plans had previously shifted a couple years earlier with the birth of her daughter, who they discovered was having some developmental delays, which eventually led to a diagnosis of autism.
|||||||| was diagnosed de novo metastatic breast cancer in December 2018. Her tumours were ER+PR+HER2- and her treatments were letrozole and Ibrance (palbociclib) then anastrozole combined and Ibrance (BC Cancer considers this to have been one line of treatment; letrozole and anastrozole are both aromatase inhibitors, and although side effects can be a bit different, they are considered equivalent). In 2020, she found out via a new biopsy she was HER2-low.
In January 2022, |||||||| had progression and needed to decide what to do post Ibrance. She had been following Enhertu results and explored accessing it through a clinical trial - specifically the Destiny Breast-04 and Destiny Breast-06 trials – but she did not meet qualifications. In the meantime, she qualified for the FINER study – a trial aiming to find out if cancer will remain under control for longer in patients given ipatasertib and fulvestrant, compared to fulvestrant on its own – which she joined.
In recent weeks, |||||||| has been presenting some new symptoms and had another CT scan and ultrasound – she’s currently waiting for the results. When they discussed the possibility of progression, her oncologist mentioned Enhertu as a future possible treatment.
|||||||| continues to actively follow the MBC research space, considering what could be her next treatment when and if she needs it – and as a person living with HER2-low MBC she is eagerly awaiting the availability of Enhertu. She said, “It’s been quite tough, trying to plan to help my daughter, but she is my motivation to try to survive.”
||||| is 57 years old and lives in London, England. ||||||| ||| ||||||| |||||| ||| ||||| || |||||||| – she was at her healthiest when she was diagnosed with primary (early stage) breast cancer at age 42. She was later diagnosed with secondary (metastatic) breast cancer in 2014 at age 49.
When ||||| was initially diagnosed with MBC her daily life wasn’t too affected – she was working full time and her mental and physical fitness levels were manageable and doable despite the side- effects of different treatments. “I guess exercise and my job has always kept me in good stead,” she shared. However, in recent years, she’s noticed that her energy levels have dropped, as well as her cognitive skills. And, due to all the hospital appointments, she is unable to work like she used to.
Her greatest concern is running out of treatment options and her body weakening. She shared, “Death never used to scare me, but seeing my mother at the end of her life earlier this year has made me question my own. Dying in pain and discomfort frightens me, and of course, the thought of leaving my family.”
Experiences With Currently Available Treatments
For metastatic HER2-low patients who have progressed, remaining options are standard chemotherapy such as eribulin, capecitabine, gemcitabine, nab paclitaxel or paclitaxel. These treatments are given sequentially usually with diminishing responses with each line of therapy. Although initial lines of therapy may provide a few months of progression free survival, this decreases substantially with later lines. These chemotherapies are what metastatic breast cancer patients dread as their remaining options.
|||||| is a Canadian metastatic breast cancer patient that Rethink has worked with and engaged over many years. |||||| was diagnosed with metastatic breast cancer 13 years ago and she has survived for so long by going to great lengths to avoid what she refers to as “the crappy weekly IV chemos.” She did this by accessing targeted treatments through clinical trials both in Boston and Toronto, going to great lengths including extensively researching options, advocating for herself, relocating her family when necessary and paying out of pocket for treatments. Why? Because, as |||||| who is now on eribulin says, “On weekly IV chemo, your normal life pretty much ends. It requires two visits per week for either blood work or for the chemo. The rest of the week is managing side effects of nausea, fatigue, pain, worsening neuropathy. And that’s with me being in the cohort of people who ‘tolerates well.’”
|||||| talked about the rapid decline she’s seen in the metastatic community once patients progress to having only standard chemotherapies as remaining options. She shared, “While your tumour is responding to endocrine therapy, you tend to be able to remain longer on the treatment and stable. Then when it starts to progress, and you need to go into chemo because you don't have anything else, it's just faster, you know, and things go down so quickly.”
Both of the Canadian patients we interviewed who are HER2-low and currently in treatment with Enhertu |||||||| ||||) both went to great lengths to avoid standard chemotherapy, which would have been their next treatment option.
Improved Outcomes
Each individual patient brings their own personal values and goals to their discussions with their oncology team. Communication and trust in their team is essential. It’s important that patients have a clear understanding of trade-offs and are well prepared for common side-effects of a given treatment.
In our experience, working closely with many young metastatic breast cancer patients, we find most are willing to trade toxicity to control their cancer. In other words, they will choose to endure additional side-effects and impacts on quality of life from the toxicity of a stronger therapy to ensure they are doing everything they can to stabilize their disease. As X stated, “Weighing the benefits of a treatment versus side-effects is a personal choice. Quality of life is paramount, but I would encourage patients to always try a drug.”
In our interviews with metastatic HER2-low patients—both those who have been able to access Enhertu, and those who have not but hope the treatment will be available before they progress and have to face IV chemotherapies—the primary improvement they seek is to extend their life.
Specifically, beyond what is expected with the current publicly-funded IV chemotherapy available and with a better quality of life. They also know a later-line therapy is likely not as easy to tolerate at their first-line MBC treatment was, but are anticipating better quality of life than on a weekly IV standard chemotherapy as noted in the previous section. The patients receiving Enhertu said they experience tiredness/fatigue, but both said it was manageable.
Experience With Drug Under Review
Rethink conducted in-depth interviews with HER2-low metastatic breast cancer patients who have experience with the drug under review.
||||| lives in Toronto and is paying out of pocket to access Enhertu for her HER2-low breast cancer.
||||| was diagnosed with early breast cancer in 2015 at age 40. She was diagnosed with MBC in September 2017 with a recurrence to her other breast and some mets in her bones. Her first line MBC treatment was letrizole and Ibrance (palbociclib). She experienced some bone progression in 2018 and began Verzenio (abemaciclib), and again in June 2021 and began capecitabine.
Three years after her MBC diagnosis, she experienced some brain mets and had radiation to the brain and moved onto the chemotherapy (IV taxol) in December 2021. In September 2022, a scan showed progression in her abdomen and that her ureter was being compressed. She had another surgery and knew she needed to change treatment again since the taxol was no longer working. She explored the option of a clinical trial and was excited to qualify; however, it was unblinded and after getting the standard therapy arm, she made a last-minute decision to withdraw from the trial. She went back to her medical oncologist to discuss options and learned her one option was just another standard of care chemotherapy blend. Her concern was that if there was further progression, then it might be trickier to manage; it might mean another surgery if there’s more progression to her abdomen and risk of further complications. She asked about Enhertu and was especially interested in hearing that those with brain metastasis were responding, saying “Since I have had four separate treatments for brain metastasis since last December, it just felt like a much better option right now than to wait and try to access it later and risk further progression on a new standard care chemo.” ||||| and her husband have made some adjustments to “make it work” and pay for Enhertu.
When asked, ||||| says she is “Feeling great and received amazing news last week. My latest scans came back stable. Enhertu is working.”
She is happy with her decision so far saying, “I don't have any of the, you know, some of the symptoms could be like you know, breathing issues and this type of thing. I've had none of that, basically, I just feel a little bit tired that evening and then I'm fine. So, I've had no complications; it's just been smooth sailing. ||||| also talked about how the thought of a break from the weekly IV treatments, which made it very difficult to support her parents needs such as getting them to their medical appointments, factored into her decision. She said, “The fact that the treatment is like once every three weeks instead of every week is great. I'm feel like I'm not there all the time. I mean I'm at hospital visits and doctor's visits but, you know, for other people! So, I've been feeling fine, like I have no issues with nausea. I mean, you know the long list of possible things that can happen once you've started; none of that has happened.”
||||| lives in Toronto and is accessing Enhertu through the clinical trial DB-06.
||||| was diagnosed with stage 2b early breast cancer in December 2017 and did 8 rounds of ATC chemo and her lymph nodes were clear, so she did not have radiation. She was on tamoxifen for a while before switching to an aromatase inhibitor. Near the end of 2019, X had a local recurrence to her lymph nodes that also led to the discovery of a single metastasis in her liver. She received her official diagnosis of metastatic breast cancer in March 2020, just as the world was shutting down. In the metastatic setting, she’s been treated with fulvestrant and Ibrance (palbociclib) (because she had already received letrozole). She had liver ablation to address the lone liver met and the metastasis on her lymph nodes was surgically removed so she spent some time with no evidence of disease (NED) before progressing in April 2022. For the most part, she tolerated her first-line MBC treatments quite well, but she was plagued with neutropenia and fatigue and the disease has certainly impacted her day-to- day life.
||||| was the one to ask about and proactively express interest in clinical trial opportunities.
She joined a Facebook group for Enhertu to learn more about what she might expect during the trial and saw some posts from people who were struggling with the side-effects but says “I didn't let that sway me.” She admits that “I was quite worried that this might be very severe and change my quality of life quite a bit. A lot of people really struggle with the nausea it seems like on this drug and some people are saying that they're in bed for like a week after treatments. Thankfully, I'm not in that category.” ||||| shared how she worked through these concerns and weighed the potential risks and benefits of her options. She said she talked a lot to the clinical trial coordinator and got answers and felt reassured. For her, she was actually more worried about the side effects from the control arm capecitabine than these potential side effects of Enhertu, saying “Xeloda would have been my drug had I not got on the trial drug. And I know people tolerate that very well but I'm a huge walker and walking is a big part of my mental health and my dog. I still walk every day, hiking in the summer as much as I can. And the thought of hand and foot syndrome scared me more to be honest. I thought if I lost my ability to walk because my feet were all blistered up that would hit me a lot harder than some nausea and fatigue. So, I guess between the two I was less scared for Enhertu.”
Because ||||| is part of the trial, she has scans every six weeks. Her last scan showed that all her mets are stable or had decreased. She said, “Being stable is what you hope for with MBC. If there is regression in some spots or they decrease in size, that’s a bonus.”
||||| also shared that what will come after Enhertu is a bigger worry. She said, “Holidays are coming up now. Like I certainly don't have a feeling that this is going to be my last Christmas….and I'm living fairly well on this medication although the fatigue is worse and I do have more nausea. But I believe my next treatment would be taxol and I had taxol when I had early-stage breast cancer. And with that came bone pain and I remember having to take, you know, at least for a couple of days after, having to take narcotics. And all these things are a part of my life now, knowing that that's my next line, now I'm a lot more aware like “Okay, this is probably not my last Christmas but is this going to be the last Christmas that I have the energy to do all the decorating, to do all the baking and, you know, to do all that kind of stuff.”
|||| lives in London, England and her access to Enhertu came through a clinical trial.
|||| was first diagnosed with primary (early-stage) breast cancer in 2007 at the age of 42. She was later diagnosed with metastatic breast cancer in 2014 at age 49. Her status changed and hormone therapy wasn’t working. She said, “It was really tough because I was rapidly going through treatment lines.” She was already HER2-low and at that time, there weren’t any targeted drugs available, and her oncologist knew little about this subtype.
|||| accessed Enhertu as part of a clinical trial and was stable for almost 1.5 years. She says, “For me the side effects are manageable. I had some fatigue and nausea in the first couple of cycles but those eased off. My mouth was sore and dry, but again, I managed to work through that…Enhertu gave me more freedom. I was able to still work whilst on Enhertu and that meant a lot to me.”
Companion Diagnostic Test
Nothing to report on this topic.
Anything Else?
A diagnosis of metastatic breast cancer is accompanied by a fear of running out of options. This is especially true for those with HER2-low metastatic breast cancer, as available lines of treatment have been limited – and patients are only left with weekly IV chemo treatment, and face harsh side- effects and a greatly diminished quality of life. The ability to now identify patients that are HER2-low and provide them with an effective and targeted treatment option is significant, and we hope that patients will be able to access this treatment without uncertainty or delay.
We ask a few more minutes of your time to read profiles of two metastatic HER2-low breast cancer patients, |||||||||||| which are included below.
Conflict of Interest Declaration — Rethink Breast Cancer
To maintain the objectivity and credibility of the CADTH reimbursement review process, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This Patient Group Conflict of Interest Declaration is required for participation. Declarations made do not negate or preclude the use of the patient group input. CADTH may contact your group with further questions, as needed.
Did you receive help from outside your patient group to complete this submission? If yes, please detail the help and who provided it.
No.
Did you receive help from outside your patient group to collect or analyze data used in this submission? If yes, please detail the help and who provided it.
No.
List any companies or organizations that have provided your group with financial payment over the past 2 years AND who may have direct or indirect interest in the drug under review.
Table 1: Financial Disclosures for Rethink Breast Cancer
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
AstraZeneca 2022 | — | — | — | X |
AstraZeneca 2021 | — | — | — | X |
Daiichi Sankyo 2022 | — | — | X | — |
Testimonials of the Unmet Need
|||||| 47 years old Living with MBC
Paying for Enhertu out-of-pocket
When you are diagnosed with stage-4 metastatic breast cancer, your life as you know it stops. Completely.
I’m ||||||. I’m 47 years old and live in Toronto with my husband. We recently celebrated our 20th wedding anniversary – we were high school sweethearts who still live in the home we purchased together after university. After university, I ended up working at Princess Margaret Hospital doing administrative work in cancer research. When I turned 40, I was diagnosed with breast cancer for the first time. It was stage 2b and I had a single mastectomy. Almost two years later to the day, in a routine mammogram, they found a lump in my other breast. With the staging, they then found the cancer was in my bones. September 2017 was when my metastatic breast cancer (MBC) journey began.
I think it’s important to share my reality of living with MBC to explain why Enhertu has been so important for me, and why accessing this drug is so important to people who need it. I was completely shocked to be diagnosed with MBC, as many of us are. I was still reeling from my initial diagnosis. I had just returned back to work full-time in July. I stopped that job when I was diagnosed and got a new one full-time job that I didn’t choose: being an MBC patient. It means days of not just researching things, but also making really hard decisions and facing the realities of this diagnosis each and every day.
I have struggled with sharing my MBC diagnosis with my loved ones, because I feel guilty about being a burden on people. Of course, my husband and some close friends know, but there are a lot of people in my life that don’t, including my parents. They knew I was diagnosed a second time, but not that it was MBC. I just felt like it was too much to tell them, knowing how hard my first diagnosis was on them. I know they would be so devastated to learn about the MBC diagnosis. I worry it would cause them further health issues with the stress and weight of knowing. At the same time, I feel so guilty for not telling them.
To some people around me, including my parents, there was a while where I looked like I was fine, because MBC can be an invisible disease depending on treatment. But, behind the scenes, I have dealt with depression and anxiety. I didn’t have any pain from the cancer, I felt well, so it was easier to hide my difficult reality. That changed last December when I had progression and had to start taking IV chemo. It became less invisible, but still, I hid it as I could.
This year in particular, being an only child has been really difficult as my parents continue to get older. They are in their mid-eighties and have had several health problems this year. I’m the only one navigating these challenges with them, while I’m also navigating my own MBC diagnosis. My parents rely on me for everything. They can’t go to medical appointments on their own. I’m their contact for all their doctors. My oncologist has cautioned me that there needs to be some kind of plan because I’m faced with this diagnosis and if something happened to me, then what will happen to them? I hyperventilate when I think of that because I don’t know. This weighs on me a lot. There’s been times where I’ve had to cancel my own appointments, like with my psychiatrist last week, because my dad was in the ER. I feel like I put myself on the backburner all the time to make sure I’m limiting how much I’m burdening people around me.
In September 2022, a CT scan showed progression in my abdomen, and we had to come up with a new treatment plan. I had been on Taxol since December 2021. One option was another standard-of-care chemo, Eribulin, but we were worried about starting a different type of chemo because if there was further progression, it would be trickier to manage and may mean surgery, or further complications. I also knew that chemo likely meant side effects. Exploring all options, it was at that point when I was introduced to Enhertu and learned how amazing the results had been for some, including those with brain metastases like me.
As someone navigating MBC, there is so much I would do, so many lengths I would go to, to get more time. I considered going to the U.S. for this treatment when we considered options for accessing Enhertu. We decided to pay for it out of pocket here at home, which is a sacrifice I’m grateful we are able to make for now, and so I started it at the end of October 2022. Paying out of pocket for this treatment is almost like a Hail Mary situation. I’ve tried all different kinds of treatments. I’m kind of down the line here. Now is the time for me to do this. This is a ground- breaking treatment. I’m thankful that we’re making it work, and I wish it was more accessible for people like me who need it, because I know this isn’t a possibility for everyone.
I have felt great on Enhertu so far, with no side effects other than feeling a bit tired the evening after my infusion. I can confidently say my quality of life has improved. The fact that this treatment is once every 3 weeks instead of every week is great because I have more time to do other things in my life. It’s nice to have more time to myself. To be with my husband. To spend time with my parents.
On top of feeling great, I also received amazing news last week. My latest scans came back stable. Enhertu is working.
Enhertu has given me a sense of hope. I have a lot of hope that this is going to improve things for me. Looking at the studies, there is so much potential. If I were instead on a weekly chemo infusion with all the side effects of chemo, my quality of life would drastically diminish. Enhertu is giving me the potential gift of time. The stakes are high when you are living with an MBC diagnosis. To have more time is something that perhaps someone who isn’t going through MBC wouldn’t realize the importance of. But I can tell you, it is extremely important. People living with metastatic breast cancer need more time, and Enhertu can give some of us that.
|||||||||| 54 years old Living with MBC
Accessing Enhertu in a clinical trial
Not only is Enhertu tolerable, but it’s working. It’s keeping me well, giving me a better quality of life. When I’m doing well, I’m a better person and a better partner.
My name is ||||||||||. I’m 54 years old and live in Toronto, Ontario. I’m married and have 2 stepchildren. I used to be a marathon runner. I was active. My husband and I would love to go out for dinners and see friends. This all changed when I was diagnosed with early-stage breast cancer, and then again with stage-4 metastatic breast cancer.
I was diagnosed the first time in 2017. Two and a half years later, I was diagnosed with MBC, in March of 2020 during the height of the COVID-19 pandemic.
When I had further progression in April 2022, my main motivation and goal was to keep fighting this disease. I had to advocate for myself to be able to access Enhertu for HER2-low metastatic breast cancer through a clinical trial. I asked my oncologist about clinical trials when we were figuring out a new treatment plan.
The reality of living with metastatic breast cancer for me is that I feel very isolated sometimes from the life I once had. I can’t work, and I really miss the social component of that. I have things that I can do, but sometimes I know I just can’t. Sometimes I’m just too tired.
Even with the fatigue, I think I still have a bit of healthy denial because I’m still relatively well considering my diagnosis. Plus, I had a year of No Evidence of Disease, so while I knew there would be progression at some point, I still felt like it was far enough away that I could push it out of my mind, although it still consumes my day, every day. I’m certainly not at a point where I don’t think several times a day that I have metastatic breast cancer.
And, even though I’m tired now on Enhertu, that is a manageable side effect for me. Xeloda would have been my treatment if I had not gotten into the clinical trial. I know people can tolerate that well, but walking and hiking is a huge part of my mental health care. I walk my dog every day, and hike in the summer as much as I can. The thought of a side effect like hand and foot syndrome scared me more than any associated side effects with Enhertu. If I lost my ability to walk because my feet were blistered, that would hit me a lot harder than some nausea and fatigue.
So, between the two, I was less scared of Enhertu. And while I do experience fatigue on Enhertu, I can still walk, and that makes me happy.
Because I'm part of the trial, I have scans every six weeks. My last scan showed that all my mets are stable or had decreased. Being stable is what you hope for with MBC. If there is regression in some spots or they decrease in size, that’s a bonus. After four treatments, I’ve already seen some of my spots become a few millimeters smaller, which is huge. My spots had a 20% decrease in size. Not only is Enhertu tolerable, but it’s working. It’s working better than what my next option would be. The longer that my disease is stable, the better off it is for my life expectancy, and I don’t have side effects. For me, Enhertu is keeping me out of the hospital and it’s keeping me well, giving me a better quality of life. When I’m doing well, I’m a better person and a better partner.
If the drug works even for a short period of time, it’s huge in our lives. If you look at another 6 months when you have an MBC diagnosis is huge. The more drugs you have access to, the better it is because not everything works for everyone, and when they do work really well, it can be so transformative.
The impact that hope can have on a person living with MBC is huge. As someone living with HER2-low metastatic breast cancer, Enhertu gives me that. When I’m on a drug that is working, I can live with hope. I can live less fearfully. I can have fun and make great memories, for at least one more year.
I hope Enhertu becomes more accessible, outside of a clinical trial, to the people like me who are HER2-low and need more time and more options to live a longer life, have stability and have a good quality of life because our lives matter.
Canadian Breast Cancer Network
About the Canadian Breast Cancer Network
The Canadian Breast Cancer Network (CBCN) is a leading, patient-directed, national health charity committed to ensuring the best quality of care for all Canadians affected by breast cancer through the promotion of information, education, and advocacy activities. Visit CBCN’s website here.
Information Gathering
CBCN’s 2017 Lived Experience Breast Cancer Patient Survey: Information for this submission was collected via CBCN’s 2017 Lived Experience Breast Cancer Patient Survey (2017 Survey). An online survey was distributed in English and French to patients living with breast cancer. No patients surveyed had direct experience with the treatment under review. Survey questions comprised of a combination of scoring options, and free form commentary. Patients were contacted through the membership databases of CBCN and other patient organizations.
In this submission, CBCN specifically utilizes the data provided by 50 patients from the 2017 Survey who identified as being diagnosed with metastatic human epidermal growth factor receptor 2 (HER2) - negative breast cancer and refers to this subgroup when discussing the 2017 Survey. This survey was done before the re-classification of HER2-negative into subgroups based on the presence of the HER2 gene, of which the HER2-low group is a part of.
The majority of these respondents were from Ontario (20), while 10 did not disclose their province of residence. The rest of the respondents were from British Columbia (5), Quebec (4), Manitoba (3), Saskatchewan (3), Alberta (2), Newfoundland and Labrador (1), and Nova Scotia (1). The language of the survey discussed sex of either male or female. Of the 50 respondents, 40 identified as female, and 10 did not identify their sex. The sexual orientation of heterosexual was reported by 36 respondents, homosexual by 3 respondents, and 11 did not identify their sexual orientation.
English was the first language for 36 respondents, while 3 identified French as their first language. German was the first language for one respondent, while 10 participants did not disclose their first language. Most of the respondents were first diagnosed with metastatic breast cancer when they were between the ages of 40 and 49 (17) or between the ages of 50 and 59 (14). 9 participants were between the ages of 60-69 at the time of diagnosis, and 7 were between the age of 30-39. Two participants were between the age of 70-79 at the age of diagnosis, and one respondent was below the age of 30. 32 participants reported that they were in a relationship, 8 reported that they were single and 10 did not disclose their relationship status. 70% of the respondents had children at the time of their diagnosis.
Respondents reported having a child or children that were between the ages of 2 and 5 (2), 6 and 12 (7), 13 and 19 (8) and 20 and older (26) at the time of diagnosis.
CBCN’s 2012 Metastatic Breast Cancer Patient and Caregiver Survey Report: Information for this submission was also gotten from CBCN’s 2012 Metastatic Breast Cancer Patient and Caregiver Survey Report (2012 Survey). This was an online survey conducted in collaboration with ReThink Breast Cancer which was distributed to patients living with mBC and their caregivers. No patients surveyed had experience with the treatment under review. Survey questions comprised of a combination of scoring options and free form commentary. Patients were contacted through the membership databases of CBCN and other patient organizations. 71 patients and 16 caregivers participated in the survey.
Printed sources: A review was conducted of current studies and grey literature to identify issues and experiences that are commonly shared among many women living with breast cancer.
Disease Experience
Metastatic breast cancer is the spread of cancerous cell growth to areas of the body other than where the cancer first formed. It commonly spreads to the bones, but can include the lungs, liver, brain and skin. In our 2017 Survey, the majority of metastatic HER2- negative breast cancer patients experienced metastases to their bones and liver: 84% reported metastases to their bones, while 38% reported metastases to their liver. Metastatic HER2-negative breast cancer patients in our 2017 Survey also experienced metastases to their lungs (28% of patients) and brain (10% of patients). 16% of the metastatic HER2-negative patients also reported experiencing metastases to body parts other than the bones, brain, liver and lungs.
The HER2 gene creates HER2 proteins which control the growth of breast cells and also help to repair breast cells, however, an overexpression of the HER2 protein causes an uncontrollable reproduction of breast cells1. Current clinical guidelines classify breast cancer as either HER2-positive (overexpression of the HER2 gene) or HER2-negative, where approximately 15-20% of breast cancers are HER2-positive, meaning that about 80-85% are HER2-negative2. Individuals diagnosed with HER2-negative breast cancer have a poorer prognosis than those diagnosed with HER2-positive breast cancer3.
The expression of the HER2 gene in breast cancer is classified by Immuno Histo Chemistry (IHC) scores, ranging from 0 to 3+, where 3+ is considered HER2-positive. Current therapies and current classification of breast cancer treat tumors with an IHC scores other than 3+ as HER2-negative. However, patients currently classified as HER2-negative might still be found to have some expression of the HER2 gene. Therefore, patients with IHC scores of 1+ or 2+ without gene amplification can be reclassified as HER2-low, rather than HER2-negative4. Many individuals fall into this new category, with approximately 50-55% of breast cancers falling under the HER2-low classification5.
The Physical Impact of Metastatic Breast Cancer
The symptoms, progression, and experience of mBC varies by patient, but many effects of metastatic breast cancer represent a significant or debilitating impact on their quality of life (QOL). In our 2012 Survey, patients were asked what impact cancer-related symptoms had on their quality of life.
54% of patients reported that fatigue resulted in a significant or debilitating impact, and 40% reported some or moderate impact.
39% of patients reported that insomnia resulted in a significant or debilitating impact, and 46% reported some or moderate impact.
37% of patients reported that pain resulted in a significant or debilitating impact, and 44% reported some or moderate impact.
The Social Impact of Metastatic Breast Cancer
The impact of this disease touches all aspects of a patient’s life, restricting an individual’s employment and career, ability to care for children and dependents, and their ability to be social and meaningfully participate in their community.
When asked in the 2012 Survey what kind of impact living with metastatic breast cancer has had on their quality of life:
Among those who were employed, 71% of patients identified significant restrictions to their ability to work
Among those with children or dependents, 21% identified significant restrictions and 53% reported some or moderate restrictions to their caregiving responsibilities
49% of patients identified significant restrictions and 38% identified some or moderate restrictions to their ability to exercise
42% of patients identified significant restrictions and 42% identified some or moderate restrictions to their ability to pursue hobbies and personal interests
41% of patients identified significant restrictions and 41% identified some or moderate restrictions to their ability to participate in social events and activities
22% of patients identified significant restrictions and 52% identified some or moderate restrictions to their ability to spend time with loved ones
Other experiences identified by patients included: guilt, the feeling of being a burden on caregivers, fear of death, poor body image, not knowing what functionality will be lost, fear of the impact of cancer and the loss of a parent on children, not knowing what will happen to children, the loss of support of loved ones, as well as marital stress/loss of fidelity and affection from husband.
Experiences With Currently Available Treatments
The Goals of Current Therapy
As with all treatment for metastatic breast cancer, the goal of treatment for metastatic HER2-low breast cancer, is to control disease progression (extending life) and to manage cancer-related symptoms (extending or stabilizing quality of life). Treatment options for mBC and their effectiveness vary among type of cancer, location of cancer, and how symptoms are experienced. Most cases of advanced disease will progress, and symptoms will worsen. Patients with a diagnosis of metastatic breast cancer understand the limitations of current treatment options and seek to live their remaining months and years with the best possible quality of life that they can achieve.
Generally, HER2-negative treatments involved a combination of targeted therapies and chemotherapy. Among the metastatic HER2- negative breast cancer patients in our 2017 Survey, 64% had undergone surgery, 64% had received radiation therapy, 52% had received chemotherapy and 74% reported receiving hormone therapy.
Since some patients in the group still have some expression of the HER2-gene, just at lower level, there is a need for treatments that target this gene. By reclassifying patients with IHC scores of 1+ and 2+ without gene amplification as HER2-low, patients can benefit from therapies that target the HER2 genes found in their tumors. Prior research shows that patients with HER2-negative breast cancer do not derive the same benefits from anti-HER2 therapies in the same way that patients with HER2-postive breast cancer benefit from them6. Therefore, patients who have HER2-low breast cancer represent those with a significant and targeted need as therapies for HER2-negative and HER2-positive breast cancer does not fully meet their needs. Additionally, when patients with metastatic HER2-low breast cancer have limited treatment line options as their disease progresses.
Key Factors for Decision-Making Around Treatment
Patients in our 2017 Survey discussed the importance of the following factors in influencing their decision-making around treatments:
Effectiveness of the treatment – how well the treatment stabilized their disease and delayed progression of their disease.
Prolonging life without sacrificing quality of life – being able to maintain productive, active lives with minimal disruption to daily routines.
Side effect management – minimizing risk while stabilizing their disease.
Cost and accessibility of treatments – affordability and ease of accessing treatments.
Treatment efficacy: Treatment effectiveness was ranked as the most important factor in treatment decision making by 68% of the 2017 Survey respondents. Respondents also talked about the importance of progression-free survival (PFS) in treatment decision making. PFS of less than 3 months was rated as important by 14% of patients and very important by 44% of patients. PFS of 3 to 5 months was rated as important by 20% of patients and very important by 50% of patients. PFS of 6 months or more was rated as important by 12% of patients and very important by 76% of patients. When asked about OS, 6% and 84% of metastatic HER2-negative breast cancer patients indicated that it was important and very important, respectively, when considering treatment options.
mBC patients with all types and subtypes of breast cancer in our 2017 Survey also spoke on the importance of treatment effectiveness in their decision-making anecdotally:
“The most important factors for me are progression free survival and quality of life.” – mBC patient respondent
“Anything to prolong my survival and maintain quality of life.” – mBC patient respondent
“Survival is of upmost importance to me.” – mBC patient respondent
Quality of life: Quality of life was routinely cited by patients as an important factor in making treatment decisions. In our 2017 Survey, quality of life was rated as important by 28% of metastatic HER2-negative patients and very important by 56% of metastatic HER2-negative patients. Further, patients reported on the importance of minimal side effects, mobility, and productivity when making decisions regarding treatment options.
In our 2017 Survey, minimal side effects were rated as important by 36% of patients and very important by 24% patients. Productivity was rated as important by 52% of patients, somewhat important by 26% of patients, and very important by 8% patients. Mobility was rated as important by 52% of patients and very important by 30% patients.
This concern was shared among all mBC respondents in our 2017 Survey:
“Quality of life over quantity.” – mBC patient respondent
“Making sure I have some quality of life so I can [spend] as much time with my kids and family[.] I don't want them to watch me suffer” – mBC patient respondent
“Trying to balance the most effective treatment regime with the least impact on my day to day living/quality of life. Maintaining a certain level of independence is important to me.” – mBC patient respondent
Patient willingness to tolerate treatment side effects: In our 2012 Metastatic Patient and Caregiver Survey, the responses to what level of side effects and how much impact on one’s quality of life would be worth extending progression-free disease by six months was shown to be determined at the personal level.
When asked to rate how much impact different symptoms of cancer and cancer treatment would be considered tolerable, almost two-thirds of patients indicated that when it comes to fatigue, nausea, depression, problems with concentration, memory loss, diarrhea and insomnia, some or a moderate impact on one’s quality of life would be considered acceptable, and approximately one quarter of patients indicated that a strong or debilitating impact would be considered acceptable. Regarding pain, 70% of patients indicated that some or a moderate impact on one’s quality of life would be considered acceptable, and 27% of patients indicated that a strong or debilitating impact would be considered acceptable.
2017 Survey respondents also reported on what were acceptable symptoms in exchange for 6 months or less of benefits from breast cancer treatment:
Pain was rated as not acceptable by 30% of patients, somewhat acceptable by 48%, and very acceptable by 12%.
Nausea was rated as not acceptable by 24% of patients, somewhat acceptable by 54%, and very acceptable by 10%.
Insomnia was rated as not acceptable by 22% of patients, somewhat acceptable by 60% of patients and very acceptable by 6% of patients.
Fatigue was rated as not acceptable by 6% of patients, somewhat acceptable by 48% of patients and very acceptable by 34% of patients.
Depression was rated as not acceptable by 34% of patients, somewhat acceptable by 48% of patients and very acceptable by 6% of patients.
Lack of concentration was rated as not acceptable by 10% of patients, somewhat acceptable by 64% of patients and very acceptable by 14% of patients.
Memory loss was rated as not acceptable by 20% of patients, somewhat acceptable by 58% of patients and very acceptable by 12% of patients.
Diarrhea was rated as not acceptable by 28% of patients, somewhat acceptable by 52% of patients and very acceptable by 8% of patients.
Vomiting was rated as not acceptable by 46% of patients, somewhat acceptable by 30% of patients and very acceptable by 8% of patients.
Hair loss was rated as not acceptable by 12% of patients, somewhat acceptable by 40% of patients, and very acceptable by 34% of patients.
The willingness to tolerate side effects was also reflected anecdotally:
“Definitely the balance of quality-of-life vs side effects with the [effectiveness].” – mBC patient respondent
“Mom so just want to live – high tolerance for SE as long as management options provided.” – mBC patient respondent
The financial burden of treating and managing breast cancer: The financial burden associated with living with metastatic breast cancer extends far beyond any loss of income during a temporary or permanent absence from employment. In addition to the loss of income during illness, metastatic breast cancer patients can incur substantial costs associated with treatment and disease management7. Research on the financial impact of breast cancer on patients identified the following:
80% of breast cancer patients report a financial impact due to their illness
44% of patients have used their savings, and 27% have taken on debt to cover costs
These findings were consistent with the responses in our 2012 Survey:
Nearly one-third of patients indicated that the cost of medication, the cost of alternative treatments (i.e. massage, physiotherapy, etc.) to manage symptoms and side effects, and the time required to travel to treatment had a significant or debilitating impact on their quality of life.
24% of patients indicated that the costs associated with travel had a significant or debilitating impact on their quality of life, and 41% of patients indicated that it had some or moderate impact on their quality of life.
In our 2017 Survey, patients reported that their diagnosis had some (28%) or a very large (42%) impact on their finances, while 12% reported their diagnosis hasn’t impacted their finances.
In addition, patients indicated that the time required to travel to treatment had a significant impact (26%) or some impact (40%) on quality of life. Cost to travel to treatment had a significant impact of the quality of life of 12% of patients, and some impact for 42%. The cost of prescription medications was indicated as having a significant impact on quality of life by 14% of respondents, and some impact by 44%. Cost of other treatments (i.e. massage, physiotherapy, etc.) had a significant impact on QOL for 26%, and some impact for 34% of respondents. Cost of devices had a significant impact on QOL for 4% of patients, and some impact for 24% of respondents.
The financial impacts of a metastatic breast cancer diagnosed was also reiterated anecdotally by respondents in our 2017 Survey:
“Always a concern as you never know if the next drug will be covered or how long it takes to get approval from private coverage. Many times it delays treatment and this weighs on one's mind.” – mBC patient respondent
“If my community did not raise the money for my [treatment] I would likely not be here today. When I contacted every group or charity NOONE offered financial assistance for treatment.” – mBC patient respondent
“Many of the next step treatments are very expensive [and not covered by government programs] and it is a HUGE struggle to get [coverage]. […] When dealing with an incurable disease the last thing you want to have to do is spend time on a letter writing campaign to argue about whether or not you should receive the drugs [recommended by your physician]. At about $1500.00 a week, I don't know many who can afford that.” – mBC patient respondent
“I wanted to try [immunotherapy], but it is [$]7500.00 every 3 weeks not covered by private insurance, now will probably have to go on chemo again, and the last ones were very hard on me causing toxicity and having to get blood transfusions.” – mBC patient respondent
“Just because I am not in the lowest income bracket does not mean I don't need assistance. I am excluded from all programs I have tried to access.” – mBC patient respondent
Other financial barriers that metastatic breast cancer patients mentioned include not qualifying for insurance at work, inability to change employers due to loss of insurance, and the prohibitive cost of new treatment options.
Patient Access to Local Resources and Supports During Treatment
When living with cancer, many patients experience significant barriers and challenges around availability of health care services and quality childcare in their community. In response to the 2012 Survey questions about the availability of supports such as childcare, transportation and alternative treatments in their community:
Among patients with children or other dependents, 53% indicated that there is minimal or no access to appropriate care for their loved ones when they are experiencing debilitating symptoms related to their cancer, and 40% identified barriers to accessing quality care during cancer treatment.
Among survey respondents who had children at the time of their diagnosis, 24% reported that finding appropriate care for their children/dependents when experiencing side effects of cancer treatments was not accessible, while 46% indicated it was somewhat accessible. Appropriate care for their children/dependents during cancer treatment was not accessible for 29%, while 44% found it somewhat accessible.
Among all metastatic HER2-negative breast cancer patients from our 2017 Survey, 14% indicated that finding transportation to appointments was not accessible, and 20% indicated that it was somewhat accessible. Mental health supports were somewhat accessible for 52% of respondents, and 10% indicated that it was not accessible. Cancer treatment in or close to respondents’ community was somewhat accessible for 38%, and not accessible for 4%. Symptom management options in or close to their community was not accessible for 16% of respondents, and 42% indicated that it was somewhat accessible
Patient Willingness to Tolerate Risk
When asked in the 2012 Survey about their willingness to tolerate risk with a new treatment:
34% of respondents were willing to accept serious risk with treatment if it would control the disease
45% of respondents were willing to accept some risk with treatment
21% of respondents were very concerned and felt less comfortable with serious risks with treatment
Need for Personal Choice
The open-ended questions and the key informant interviews showed that it is imperative that women with metastatic breast cancer have access to, and the option of what drugs they take. Most patients are well aware of the adverse effects of treatment up front, and they want to make a personal choice that works for them. Metastatic breast cancer patients expressed the need for personal choice and autonomy in our 2012 Survey as well as in the 2017 Survey:
“I think patients (ESPECIALLY young patients) should be given more decision making power in terms of access to radical treatments to control disease. […] With two small [children] I am determined to access any treatment that can extend my life and I hate struggling with doctors for this access.” – 2012 Survey
“I believe that I would prefer to tolerate severe restrictions in the quality of my life, if it meant that I would be able to have a longer period without progression.” – 2012 Survey
“It would be nice to have more choices and more information about them. I was lucky to get on a clinical trial perhaps because my oncologist was a research oncologist and involved in many. While I knew friend and acquaintances that had Stage IV BC and never informed of clinical trials, and sadly several did not survive the disease.” – 2017 Survey mBC patient respondent
“I am frustrated that ALL the treatment choices aren't given to me... I am told what I am taking next with no option or discussion on other options. My oncologist has assured me there are many treatments available, but have never shared which, so I have to turn to Facebook groups for guidance.” – 2017 Survey mBC patient respondent
“I wish my doctor would present me with options.” – 2017 Survey mBC HER2-positive breast cancer respondent “Accessibility to new drugs- not limiting choices.” – 2017 Survey mBC patient respondent
“Complete access to drug treatment choices and trials.” – 2017 Survey mBC patient respondent
Improved Outcomes
For mBC patients, extension of progression-free survival (PFS) is of critical concern. Like any other treatment for metastatic breast cancer, patients have an expectation that trastuzumab deruxtecan (Enhertu) will extend their PFS with good quality of life when first-line therapies stop working.
DESTINY-Breast048 is a phase III, global, multicenter, clinical trial exploring the efficacy and safety of trastuzumab deruxtecan (T-DXd) versus the Treatment of Physicians Choice (TPC) among individuals with metastatic or unresectable HER2-low breast cancer who were previously treated with 1 or 2 lines of chemotherapy in metastatic setting. The TPC included capecitabine, erbulin, gamcitabine, paclitaxel, and nab-paclitaxel. A total of 557 breast cancer patients from North America, Europe, and Asia were randomized into one of two groups at a 2:1 ratio. Patients were stratified by their HR status, HER2 IHC status, number of rounds of chemotherapy, and prior use of CDK-4/6 inhibitors. Patients were either given trastuzumab deruxtecan every 3 weeks (n=373), or TPC (n=184).
Median treatment duration for T-DXd was 8.2 months compared to 3.5 months within the TPC control group. The primary endpoint for the study was PFS for HR-positive patients; the secondary endpoint in the study was PFS and OS in patients with both HR-positive and HR-negative breast cancers. For patients with HR-positive, HER2-low metastatic breast cancer, median PFS was 10.1 months for the T- DXd group and 5.4 months for those in the TPC group. Among all patients, median PFS was 9.9 months in the T-Dxd group and 5.1 months in the TPC group. Median OS for the HR-positive, HER2-low group was 23.9 months for the T-Dxd group compared to 17.5 months for the TPC group. Among all patients, median OS for the T-Dxd group was 23.4 months and for the TPC group, it was 16.8 months.
Adverse Effects
Incidence of adverse events was similar in both the trastuzumab deruxtecan group and TPC group. The rate of adverse events (AEs) that were of grade 3 of higher was lower in the T-DXd group (53% vs 67% in TPC). Serious adverse effects occurred in 28% of patients receiving trastuzumab deruxtecan and in 25% of patients receiving TPC. Two AEs occurred more frequently amount patients that received trastuzumab deruxtecan compared to those who received TPC: left ventricular dysfunction (4.6% in the T-Dxd group versus 0% in the TPC group) and interstitial lung disease (ILD)/pneumonitis (12.1% in the T-Dxd group versus 0.6% in the TPC group). In the trastuzumab deruxtecan arm, the median time to onset of ILD was 129 days (ranging from 26 days to 710 days). While most of the cases of ILD were grade 1 or 2 (10%), 3 patients died who received T-Dxd from it.
A total of 4% of patients in the T-DXd arm experienced treatment-emergent adverse effects associated with death, compared to 3% in the TPC arm.
Overall, DESTINY-Breast04 showed that trastuzumab deruxtecan is tolerable and has a manageable toxicity profile.
Impact of Treatment Options to Patients
By delaying the progression of the disease, trastuzumab deruxtecan can relieve cancer-related symptoms, and improve a patient’s quality of life. Analyzed data from the DESTINY-Breast04 clinical trial showed a statistically significant improvement in PFS and OS with the treatment of trastuzumab deruxtecan compared to TPC. Results from this study show strong support for trastuzumab deruxtecan to be used as a targeted treatment for HER2-low patients. When living with no or with minimal cancer-related symptoms, and with minimal side effects from treatment, patients are able to reduce the impact of cancer on their ability to care for children and dependents, continue with their employment and earn income, spend time with loved ones and participate in their life in a meaningful way by engaging in social activities, travelling, maintaining friendships, and pursuing personal interests.
Value to Patients
The value to patients of extending the time that their cancer is progression-free cannot be overestimated. Patients living with metastatic breast cancer are aware that their advanced disease will progress with worsening symptoms until death, and embrace opportunities to try new treatments, even if benefits may be as little as a six-month extension of progression-free disease. It is also very important for patients to have good quality of life when receiving treatment for metastatic disease. Patients that we speak to on a regular basis acknowledge the importance to have the energy to attend their children’s activities and to spend time with family and friends.
Experience With Drug Under Review
Given that this treatment is not widely accessible in Canada, CBCN was unfortunately unable to connect with, and interview, breast cancer patients with experience on the treatment.
Companion Diagnostic Test
Not applicable.
Anything Else?
Not applicable.
References
Susan G. Komen, Treatments for Metastatic Breast Cancer. Accessed December 12, 2022. https://www.komen.org/breast-cancer/treatment/by- diagnosis/metastatic/
Canadian Breast Cancer Network, Subtypes of Breast Cancer. Accessed December 21, 2022. https://cbcn.ca/en/subtypes_of_breast_cancer
BMC, Landscape of HER2-low metastatic breast cancer (MBC): results from the Austrian AGMT_MBC-Registry. Accessed December 21, 2022. https://breast-cancer-research.biomedcentral.com/articles/10.1186/s13058-021-01492-x
BMC, Landscape of HER2-low metastatic breast cancer (MBC): results from the Austrian AGMT_MBC-Registry. Accessed December 21, 2022. https://breast-cancer-research.biomedcentral.com/articles/10.1186/s13058-021-01492-x
BMC, Landscape of HER2-low metastatic breast cancer (MBC): results from the Austrian AGMT_MBC-Registry. Accessed December 21, 2022. https://breast-cancer-research.biomedcentral.com/articles/10.1186/s13058-021-01492-x
BMC, Landscape of HER2-low metastatic breast cancer (MBC): results from the Austrian AGMT_MBC-Registry. Accessed December 21, 2022. https://breast-cancer-research.biomedcentral.com/articles/10.1186/s13058-021-01492-x
Dunbrack, J.(2010). Breast Cancer: Economic Impact and Labour Force Re-entry. Canadian Breast Cancer Network.
ASCO Daily News. (2022). DESTINY-Breast04 Establishes Trastuzumab Deruxtecan As a New Standard of Care for HER2-Low Metastatic Breast Cancer. https://dailynews.ascopubs.org/do/destiny-breast04-establishes-trastuzumab-deruxtecan-new-standard-care-her2-low
Conflict of Interest Declaration — Canadian Breast Cancer Network
To maintain the objectivity and credibility of the CADTH reimbursement review process, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This Patient Group Conflict of Interest Declaration is required for participation. Declarations made do not negate or preclude the use of the patient group input. CADTH may contact your group with further questions, as needed.
Did you receive help from outside your patient group to complete this submission? If yes, please detail the help and who provided it.
This submission was put together independently by the Canadian Breast Cancer Network, as was the compilation of information and data for the writing of this submission.
Did you receive help from outside your patient group to collect or analyze data used in this submission? If yes, please detail the help and who provided it.
CBCN did connect with the manufacturer, AstraZeneca, to access relevant clinical data for this submission and to try to connect with patients who had experience with the drug in the submission.
List any companies or organizations that have provided your group with financial payment over the past 2 years AND who may have direct or indirect interest in the drug under review.
Table 2: Financial Disclosures for the Canadian Breast Cancer Network
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
AstraZeneca | — | — | — | X |
The Canadian Breast Cancer Network is committed to adhering to the Code of Conduct Governing Corporate Funding
Clinician Input
Ontario Health-Cancer Care Ontario Breast Cancer Drug Advisory Committee
About the Ontario Health-Cancer Care Ontario Breast Cancer Drug Advisory Committee
OH-CCO’s Drug Advisory Committees provide timely evidence-based clinical and health system guidance on drug-related issues in support of CCO’s mandate, including the Provincial Drug Reimbursement Programs (PDRP) and the Systemic Treatment Program.
Information Gathering
The information was jointly discussed via email.
Current Treatments and Treatment Goals
Patients in DESTINY-BREAST04 has ER-positive (ER+) or ER-negative (ER-) HER2-low disease. Patients with ER+ or ER- disease have to have had one line of chemotherapy for their metastatic disease or had disease recurrence within 6 months of completion of adjuvant chemotherapy. Patients with ER+ disease have to have had one line of endocrine therapy.
The study randomized patients to either trastuzumab deruxtecan (T-Dxd) or chemotherapy of physician’s choice. The majority of patients in the ER-positive cohort had received CDK4/6 inhibitors before going on the study. The majority of patients had at least 3 lines of therapy for their metastatic disease. Therefore the use of chemotherapy or study drug does reflect the current practice in Ontario.
Metastatic breast cancer is incurable. The median survival in the physician’s choice group was 16.8 months, thus better treatment is needed. Additional important goals would be safety and quality of life.
Treatment Gaps (Unmet Needs)
Considering the treatment goals, please describe goals (needs) that are not being met by currently available treatments.
Metastatic breast cancer is incurable. The median survival in the physician’s choice group was 16.8 months, thus better treatment is needed. In this study, T-Dxd median survival was 23.4 months, a significant improvement over the controlled arm.
Specific treatment goals:
Not all patients respond to available treatments
Patients become refractory to current treatment options
No treatments are available to reverse the course of disease
Treatments are needed that are better tolerated
Place in Therapy
How would the drug under review fit into the current treatment paradigm?
Patients with ER+ disease were randomized after first-line endocrine-based therapy in the metastatic setting if they have relapsed within 6 months of adjuvant chemo. If ER+ patients relapsed >6 months after adjuvant chemo, they must also have received one line of chemotherapy in the metastatic setting.
Patients with ER- disease were randomized after at least one line of therapy for their metastatic disease or if they relapsed within 6 months of adjuvant chemo.
In the study, 90% of patients had at least 2 lines of prior therapy for their metastatic disease.
The study treatment (T-Dxd) will be used similarly – i.e., after at least one line of prior therapy in the metastatic setting. It would shift the currently used chemotherapy options to later lines of therapy.
Which patients would be best suited for treatment with the drug under review? Which patients would be least suitable for treatment with the drug under review?
Similar improvement (hazard ratios) were observed in the ER+ and ER- patients. Patients with stable brain metastases were eligible for the study drug.
T-Dxd has a unique toxicity – interstitial lung disease (ILD). It was observed in 12% of patients on the study drug and three patients had fatal toxicity. Frequent monitoring with CT scans of the chest are required at greater frequency than usual standard of care. The Breast DAC supports using the trial’s inclusion and exclusion criteria.
The Breast DAC wishes to flag that there may be issues related to pathologic testing of specimens and identification of HER2-low status. Although HER2 testing is routine for all newly diagnosed breast cancer patients, the identification of the HER2-low subset will require careful review by pathologists who are experts in breast cancers. The DAC suggests consultation with pathology experts during the review of this drug.
What outcomes are used to determine whether a patient is responding to treatment in clinical practice? How often should treatment response be assessed?
In the study, radiologic assessment of the disease was performed every 6 weeks. Assessment of cardiac function was assessed every 4 cycles. The 6-week interval was indicated to monitor the development of interstitial lung disease.
What factors should be considered when deciding to discontinue treatment with the drug under review?
Discontinue of treatment is usually related to disease progression or treatment-related toxicities.
What settings are appropriate for treatment with [drug under review]? Is a specialist required to diagnose, treat, and monitor patients who might receive [drug under review]?
Pathology expertise in the correct identification of HER2-low patients.
Access to monitoring of ILD and access to experts for the management of ILD are required.
Additional Information
Zhang H, Katerji H, Turner BM, Hicks DG. HER2-Low Breast Cancers. Am J Clin Pathol. 2022;157(3):328-336. doi:10.1093/ajcp/aqab117
Conflict of Interest Declarations for Ontario Health-Cancer Care Ontario Breast Cancer Drug Advisory Committee
To maintain the objectivity and credibility of the CADTH drug review programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This conflict of interest declaration is required for participation. Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please see the Procedures for CADTH Drug Reimbursement Reviews (section 6.3) for further details.
Did you receive help from outside your clinician group to complete this submission? If yes, please detail the help and who provided it.
Yes. Ontario Health provided secretariat functions to the DAC.
Did you receive help from outside your clinician group to collect or analyze any information used in this submission? If yes, please detail the help and who provided it.
No.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review.
Declaration for Clinician 1
Name: Dr. Andrea Eisen
Position: Lead, OH-CCO Breast Cancer Drug Advisory Committee
Date: 14-12-2022
Table 3: COI Declaration for Ontario Health-Cancer Care Ontario Breast DAC — Clinician 1
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to $50,000 | In Excess of $50,000 |
|---|---|---|---|---|
No COI | — | — | — | — |
Declaration for Clinician 2
Name: Dr. Phillip Blanchette
Position: Member, OH-CCO Breast Cancer Drug Advisory Committee
Date: 10-12-2022
Table 4: COI Declaration for Ontario Health-Cancer Care Ontario Breast DAC — Clinician 2
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to $50,000 | In Excess of $50,000 |
|---|---|---|---|---|
No COI | — | — | — | — |
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
Redactions: Confidential information in this document may be redacted at the request of the sponsor in accordance with the CADTH Drug Reimbursement Review Confidentiality Guidelines
Stakeholder Input: The views expressed in each submission are those of the submitting organization or individual; not necessarily the views of CADTH or of other organizations. As such, they are independent of CADTH and do not necessarily represent or reflect the view of CADTH. No endorsement by CADTH is intended or should be inferred. By filing with CADTH, the submitting organization or individual agrees to the full disclosure of the information. CADTH does not edit the content of the submissions.
CADTH does use reasonable care to prevent disclosure of personal information in posted material; however, it is ultimately the submitter’s responsibility to ensure no identifying personal information or personal health information is included in the submission. The name of the submitting organization or individual and all conflict of interest information are included in the submission; however, the name of the author, including the name of an individual patient or caregiver submitting the patient input, are not posted.
Accessibility: CADTH is committed to treating people with disabilities in a way that respects their dignity and independence, supports them in accessing material in a timely manner, and provides a robust feedback process to support continuous improvement. All materials prepared by CADTH are available in an accessible format. Where materials provided to CADTH by a submitting organization or individual are not available in an accessible format, CADTH will provide a summary document upon request. More details on CADTH’s accessibility policies can be found here.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.