CADTH Reimbursement Review
Sotorasib (Lumakras)
Sponsor: Amgen Canada Inc.
Therapeutic area: KRAS G12C-mutated, advanced non–small cell lung cancer
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Clinical Review
Abbreviations
AE
adverse event
ALP
alkaline phosphatase
ALT
alanine aminotransferase
AST
aspartate aminotransferase
BICR
blinded independent central review
BPI-SF
Brief Pain Inventory – Short Form
BSC
best supportive care
CCSN
Canadian Cancer Survivor Network
CI
confidence interval
CNS
central nervous system
CR
complete response
DCR
disease control rate
DOR
duration of response
ECOG PS
Eastern Cooperative Oncology Group Performance Status
EAP
expanded access program
EORTC QLQ-C30
European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30
EORTC QLQ-LC13
European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Lung Cancer Module
EQ VAS
EQ visual analogue scale
FACT-G
Functional Assessment of Cancer Therapy – General
GI
gastrointestinal
HR
hazard ratio
IPCW
inverse-probability-of-censoring weighting
LC DAC
Lung Cancer Drug Advisory Committee
LCC
Lung Cancer Canada
LHF
Lung Health Foundation
MAIC
matching-adjusted indirect comparison
MID
minimal important difference
MAIC
matching-adjusted indirect comparison
NE
not evaluable
NGS
next-generation sequencing
NOC/c
Notice of Compliance with conditions
NSCLC
non–small cell lung cancer
NSCLC-SAQ
Non–Small Cell Lung Cancer Symptom Assessment Questionnaire
OH-CCO
Ontario Health – Cancer Care Ontario
ORR
objective response rate
OS
overall survival
PD-1
programmed cell death 1
PD-L1
programmed death-ligand 1
PFS
progression-free survival
PGIC
patient global impression of change
PGIS
patient global impression of severity
PK
pharmacokinetic
PR
partial response
PRO
patient-reported outcome
PRO-CTCAE
Patient-Reported Outcomes version of the Common Terminology Criteria for Adverse Events
RCT
randomized controlled trial
RECIST 1.1
Response Evaluation Criteria in Solid Tumours Version 1.1
RPSFT
rank-preserving structural failure time
SAE
serious adverse event
SD
standard deviation
TEAE
treatment-emergent adverse event
TTR
time to response
ULN
upper limit of normal
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Item | Description |
|---|---|
Drug product | Sotorasib (Lumakras), 120 mg, oral tablet |
Indication | For the treatment of adult patients with KRAS G12C-mutated, locally advanced (not amenable to curative therapy) or metastatic NSCLC who have received at least 1 prior systemic therapy |
Reimbursement request | As per indication |
Health Canada approval status | NOC/c |
Health Canada review pathway | Advance consideration under NOC/c and Project Orbis |
NOC date | September 10, 2021 |
Sponsor | Amgen Canada Inc. |
NOC = Notice of Compliance; NOC/c = Notice of Compliance with conditions; NSCLC = non–small cell lung cancer.
Introduction
Lung cancer is 1 of the most diagnosed cancers, with non–small cell lung cancer (NSCLC) accounting for approximately 80% to 88% of all lung cancer diagnoses in Canada.1,2 In 2020, the incidence of NSCLC in Canada was estimated to be 60.5 per 100,000 persons.3 In 2021, an estimated 29,600 new cases of lung cancer and 21,150 deaths due to lung cancer were projected.4 Survival from lung cancer across all stages and histologies is poor, with a 5-year net survival rate of 22%.5 NSCLC often remains asymptomatic until the disease is in its advanced stages.6,7 When patients with NSCLC present with symptoms, these are usually nonspecific and difficult to attribute to lung cancer.7 Compared to other advanced cancers, advanced NSCLC is associated with a higher prevalence and intensity of symptoms, such as pain, dyspnea, cough, decreased appetite, weight loss, and depression, as well as lower health-related quality of life (HRQoL).8 Because early diagnosis of NSCLC is challenging,9 approximately two-thirds of patients have advanced or metastatic disease at diagnosis, at which point curative treatments are not possible.4,10 The median overall survival (OS) of patients with metastatic NSCLC (stages IVA and IVB) is poor, ranging from 8 months to 11 months; the 5-year OS ranges from 4% to 6%. The 5-year net survival rate for stage IV NSCLC is 5.2%.11
NSCLC often holds oncogenic driver mutations that lead to uncontrolled cell growth and proliferations.12 Of these, mutations within the RAS family account for more than 30% of all mutated oncogenes in NSCLC, causing approximately 1 million deaths worldwide annually.13 Within the RAS family, KRAS is the isoform most frequently altered in NSCLC. Approximately 1 in 4 patients with NSCLC harbour KRAS mutations.14 Patients with KRAS G12C-mutated NSCLC have a lower proportion of response to cytotoxic chemotherapy and decreased survival compared to the overall population of patients with NSCLC.15 The KRAS G12C subtype represents almost half of all KRAS mutations in NSCLC and is identified in approximately 13% of patients with NSCLC.16,17 Based on an estimation in the Health Canada Reviewers Report, the incidence of patients in Canada living with NSCLC and harbouring the KRAS G12C mutation is approximately 7.9 per 100,000 persons.18
Sotorasib is a highly selective inhibitor of KRAS G12C that suppresses the rapid growth of cancer cells. Sotorasib forms an irreversible, covalent bond with the unique cysteine of KRAS G12C, locking the protein in an inactive state that prevents downstream signalling without affecting wild-type KRAS. Sotorasib blocks KRAS signalling, inhibits cell growth, promotes apoptosis, and is associated with antitumour inflammatory responses and immunity in KRAS G12C tumour models. On September 10, 2021, sotorasib received a Notice of Compliance with conditions (NOC/c) from Health Canada for the treatment of adult patients with KRAS G12C-mutated, locally advanced (not amenable to curative therapy) or metastatic NSCLC who have received at least 1 prior systemic therapy. The Health Canada market authorization with conditions is pending the results of trials to verify the clinical benefit of sotorasib. Sotorasib underwent advance consideration under NOC/c, as well as Project Orbis, at Health Canada. Health Canada recommends that sotorasib be administered at a dose of 960 mg (8 × 120 mg tablets) orally once daily until disease progression or unacceptable toxicity. Up to 2 dose reductions are permitted in the case of adverse events (AEs).
The objective of this review is to evaluate the beneficial and harmful effects of sotorasib 960 mg (8 × 120 mg oral tablets) for the treatment of KRAS G12C-mutated, locally advanced (not amenable to curative therapy) or metastatic NSCLC in adult patients who have received at least 1 prior systemic therapy.
Stakeholder Perspectives
The information in this section is a summary of input provided by the patient groups who responded to CADTH’s call for patient input and from clinical experts consulted by CADTH for the purpose of this review.
Patient Input
The Lung Health Foundation (LHF) (formerly the Ontario Lung Association), Lung Cancer Canada (LCC) and the Canadian Cancer Survivor Network (CCSN) submitted joint input. A total of 5 people (4 patients and 1 caregiver) responded to telephone survey interviews conducted from August 2022 to September 2022. Of the 4 patients with lung cancer, 3 had experience with sotorasib; 1 patient with KRAS G12C-mutated lung cancer had no experience with sotorasib. All respondents were female. All respondents but 1 were from Canada (Nova Scotia, British Columbia, Quebec, and Ontario); the remaining respondent was from the US.
From the submitted input, 1 patient said they felt “rock bottom” when their lung cancer progressed on chemotherapy and radiation, leading them to be on oxygen, to acquire a debilitating cough as well as shortness of breath from eating or talking, and to require assistance to shower. Another patient detailed the mental and emotional side effects associated with multiple courses of immunotherapy and chemotherapy, such as depression, anxiety, panic attacks, and severe mood swings, which remained debilitating even during remission. The sole caregiver interviewed stated that it is mentally, physically, and financially challenging to care for a patient with lung cancer with comorbidities (e.g., preparing meals, making arrangements for transportation to medical appointments, managing daily responsibilities) and that they felt burned out without many sources of support. Three patients who had experience with sotorasib reported significant tumour reduction (i.e., ranging from a 50% to 65% reduction to no evidence of disease within 5 weeks to 1.5 years). They said they experienced mild side effects (e.g., fatigue, aches, and pains when walking for extended periods of time, a minor rash, diarrhea, shortness of breath, and increased liver enzymes) while on sotorasib. However, they said these side effects did not have much impact on their daily activities and/or quality of life. According to their input, these patients felt hopeful that they could plan for the future.
In terms of important key outcomes, 1 patient said they were most interested in obtaining a cure while maintaining a good quality of life. Respondents also expressed their hope for a treatment option with an oral route of administration that would be accessible from home, delay the onset of symptoms, prolong their life, and improve functionality and mobility, with fewer side effects. The caregiver expressed the importance of treatment that can be accessed from home, limiting the need to travel to infusion clinics. Lastly, it was pointed out in the survey that wait times for lung surgeries across Canada are unacceptable; patients and caregivers would like to treat the lung cancer in the early stages. The caregiver surveyed said that the wait time for the surgery was the most difficult aspect (or the most challenging adverse effect) of current treatment.
Clinician Input
Input From Clinical Experts Consulted by CADTH
According to the clinical experts, the treatment options for patients with KRAS G12C-mutated NSCLC who have progressed on standard therapy are limited. There is an unmet need in this patient population for an efficacious treatment associated with fewer AEs. According to the clinical experts consulted for this review, sotorasib would change the line of therapies for patients with KRAS G12C-mutated NSCLC. The clinical experts anticipated that sotorasib would be used following immunotherapy and platinum-doublet chemotherapy. Accordingly, docetaxel would then move to being either third-line or fourth-line therapy. The clinical experts noted that sotorasib would not be combined with other drugs at this time. They suggested that sotorasib be limited to patients with KRAS G12C-mutated NSCLC. Moreover, they noted that treatment with sotorasib would not be suitable for patients with an Eastern Cooperative Oncology Group Performance Status (ECOG PS) of 3 or 4, with severe organ dysfunction, or with untreated, symptomatic brain metastasis. The clinical experts did note that patients with untreated, asymptomatic brain lesions may be suitable for sotorasib; ideally, these patients should have their cases discussed at a multidisciplinary tumour board round at a centre with expertise in stereotactic radiosurgery. Based on input from the clinical experts, patients should undergo clinical and toxicity assessment per cycle (typically every 3 to 4 weeks) and imaging every 3 months to assess response to treatment in clinical practice. Based on input from the clinical experts, improved progression-free survival (PFS), improved OS, and maintenance or improvement in quality of life are considered meaningful responses to treatment in this population. The clinical experts suggested that treatment with sotorasib be discontinued under the following 3 scenarios: patient decision to stop treatment with sotorasib; unacceptable toxicity due to sotorasib; and disease progression without clinical benefits. The clinical experts agreed that patients with documented disease progression could continue sotorasib if they were deriving clinical benefit. They also noted that sotorasib may be prescribed by a medical oncologist in an outpatient oncology clinical setting.
Clinician Group Input
Clinician group input was provided by 2 groups: the Ontario Health – Cancer Care Ontario (OH-CCO) Lung Cancer Drug Advisory Committee (LC DAC), which provided input from 3 clinicians who had joint discussion through email; and LCC, which provided input based on a review of the literature and proceedings from recent conferences compiled by 26 clinicians. Both groups identified the following 3 goals of therapy: reducing tumour burden; improving symptoms; and prolonging life while upholding patients’ values and desires. Both groups also noted that all patients eventually progress on currently available treatment; thus, durability of response is also an important treatment goal. In addition, LCC added the need for treatment that is associated with reduced toxicity and resource utilization. Indeed, the OH-CCO LC DAC endorsed the advent of an oral anticancer treatment without the side effects and life impacts associated with chemotherapy to slow disease progress and improve length and quality of life. According to input from the OH-CCO LC DAC, sotorasib would be placed as a second- or third-line monotherapy for patients who have progressed on, or are unable to tolerate, platinum-based chemotherapy and immunotherapy (where appropriate) and possibly docetaxel. The OH-CCO LC DAC clinician group stated that sotorasib would not affect immunotherapy or platinum-doublet chemotherapy use; however, sotorasib may be preferred to docetaxel if it can demonstrate a meaningful improvement in survival or quality of life, given that docetaxel has a proven survival benefit compared to best supportive care (BSC) and other chemotherapy regimens (ifosfamide), albeit with an unfavourable side effect profile.
The input from LCC placed sotorasib as a second-line standard of care for patients with advanced KRAS G12C NSCLC and suggested that it be used as a single drug after at least 1 line of prior systemic treatment has not worked. According to both clinician groups, patients with KRAS G12C-mutated, advanced NSCLC (i.e., stage IV or recurrent) who had received prior therapy would be best suited for sotorasib. LCC added that it is uncertain whether patients with an ECOG PS of 3 or 4 would benefit from treatment with sotorasib. Both clinician groups noted that patients eligible for treatment with sotorasib should be identified by a validated molecular diagnostic test, preferably next-generation sequencing (NGS). Both clinician groups noted that improvement in symptoms, stability of disease, tumour shrinkage, radiographic reduction of disease site from baseline, and prolonged survival are indicative of a clinically meaningful response to treatment. The OH-CCO LC DAC added that the definition of a clinically meaningful improvement in frequency or severity of symptoms depends on patients and varies across physicians. Based on input from LCC, response to treatment should be determined by the treating physician based on CT imaging and assessed every 2 to 3 months, similarly to other oral tyrosine kinase inhibitors used in Canada.
Based on input from the clinician groups, discontinuing treatment with sotorasib should be considered in the event of loss of clinical benefit (as indicated by unequivocal disease progression, such as symptoms, polyprogression, and so on) or intolerable side effects. LCC noted that treatment with sotorasib may continue in patients with oligoprogression who are amenable to local therapy (radiation or surgery); who are newly diagnosed or have experienced progression of brain metastases and have been treated with brain radiation or surgery; and who have asymptomatic disease without overt progression on imaging associated with increased symptom burden. The OH-CCO LC DAC emphasized that a combination of clinical judgment, radiological interpretation, and clinically standardized scales, such as the Edmonton Symptom Assessment System, should be used to determine if a patient is benefiting from therapy. The OH-CCO-LC also noted that the Response Evaluation Criteria in Solid Tumours Version 1.1 (RECIST 1.1) and its derivatives are designed for clinical trials, not clinical practice, and should not be used to determine discontinuation of treatment. Both clinician groups agreed that outpatient clinics would be an appropriate treatment setting for sotorasib in addition to the hospital setting. Both groups stated that a medical oncologist, general practitioner in oncology under medical oncology supervision, or respirologist experienced in treating patients with lung cancers should be involved in diagnosing, treating, and monitoring patients on sotorasib.
Drug Program Input
Input was obtained from the drug programs that participate in the CADTH reimbursement review process. The following were identified as key factors that could potentially affect the implementation of a CADTH recommendation for sotorasib:
consideration for prescribing of therapy
care provision
systemic and economic issues.
Clinical Evidence
Pivotal Studies and Protocol-Selected Studies
Description of Studies
Two sponsor-conducted studies were included in this systematic review: the CodeBreaK 100 study (the pivotal trial) and the CodeBreaK 200 study.19-21
The CodeBreaK 100 study is an ongoing, multicentre, nonrandomized, open-label, single-group, phase I and II study. Phase I of the CodeBreaK 100 study was a first-in-human dose exploration (part 1) and dose expansion (part 2) study aimed at evaluating the safety, tolerability, pharmacokinetics (PKs), and pharmacodynamics of sotorasib in adult patients with KRAS G12C-mutated advanced NSCLC, colorectal cancer, and other solid tumours.19 Phase II of the CodeBreaK 100 study was designed to evaluate the efficacy and safety of sotorasib as monotherapy in adult patients with KRAS G12C-mutated advanced NSCLC, colorectal cancer, and other solid tumours.20 CADTH’s review of the CodeBreaK 100 study focused on the phase II efficacy and safety results in adult patients with KRAS G12C-mutated advanced NSCLC. Phase II of the CodeBreaK 100 study enrolled a total of 224 patients with KRAS G12C-mutated advanced solid tumours across 59 sites. Of the patients enrolled, 126 (56.3%) had NSCLC. Patients self-administered sotorasib 960 mg (8 × 120 mg tablets) orally once daily and continued treatment without interruption until disease progression, treatment intolerance, withdrawal of consent, or death. Tumour response was assessed through contrast-enhanced CT or MRI and assessed per RECIST 1.1 by blinded independent central review (BICR). Patients underwent a safety follow-up visit 30 days (± 7 days) after the last dose of sotorasib before any new anticancer treatment was started. Following safety follow-up visits, patients were followed long-term for health condition, disease status, and subsequent anticancer treatment every 12 weeks (± 2 weeks) for up to 3 years after the last patient was enrolled or until withdrawal of consent, loss to follow-up, or death, whichever occurred first. The study team was blinded to the efficacy data. The primary efficacy end point for phase II of the CodeBreaK 100 study was objective response rate (ORR), which was a composite of CR and partial response (PR). Response was assessed by BICR. Secondary efficacy end points included duration of response (DOR), disease control rate (DCR), time to response (TTR), PFS, OS, and the Non–Small Cell Lung Cancer Symptom Assessment Questionnaire (NSCLC-SAQ). Exploratory outcomes included changes in patient-reported, cancer-specific symptoms and HRQoL measures, including the European Organisation for Research and Treatment Quality of Life Questionnaire Core 30 (EORTC QLQ-C30) and its Lung Cancer Module (EORTC QLQ-LC13); the EQ-5D-5L and EQ visual analogue scale (EQ VAS); item GP5 (“I am bothered by side effects of treatment”) from the Functional Assessment of Cancer Therapy – General (FACT-G); the patient global impression of change (PGIC) and patient global impression of severity (PGIS) questionnaires; and the Patient-Reported Outcomes version of the Common Terminology Criteria for Adverse Events (PRO-CTCAE). The data cut-off date for the primary analysis of phase II was September 1, 2020, which was updated at the data cut-off date of March 15, 2022. The updated data cut-off date for OS at 2 years was September 9, 2022.
Patients enrolled in the CodeBreaK 100 study had a mean age of 62.9 years (standard deviation [SD] = 9.3 years). Most patients were aged 18 years to 64 years (53.2%) and white (81.7%); 81% were former smokers. Regarding disease characteristics, 61.9% and 98% of patients had stage IV disease at initial diagnosis and screening, respectively. At the time of screening, metastatic disease was identified in 96.8% of enrolled patients, with the most common site of metastasis found in the bone (48.4%). The most common histology type among enrolled patients was nonsquamous adenocarcinoma (95.2%). A total of 42.9%, 34.9%, and 22.2% of patients had received 1, 2, or 3 prior lines of anticancer therapy, respectively. The most common types of prior anticancer therapy were immunotherapy checkpoint inhibitors (92.1%) and chemotherapy (91.3%). A total of 81% of patients had received both platinum-based chemotherapy and anti–programmed cell death 1 (PD-1) or anti–programmed cell death-ligand 1 (PD-L1) immunotherapy.
The CodeBreaK 200 study is an ongoing, multicentre (148 sites across 22 countries), randomized (1:1), open-label, parallel-group, phase III study evaluating the efficacy of oral sotorasib (960 mg daily) (n = 171) versus IV docetaxel (75 mg/m2 every 3 weeks) (n = 174) in adult patients with KRAS G12C-mutated NSCLC who progressed after prior platinum-based chemotherapy and a checkpoint inhibitor. Randomization was stratified by the number of prior lines of therapy in advanced disease (1 versus 2 versus > 2), race (Asian versus non-Asian), and history of central nervous system (CNS) involvement (present or absent). Patients continued treatment without interruption until disease progression, treatment intolerance, withdrawal of consent, or death. Tumour response was assessed through contrast-enhanced CT or MRI and assessed per RECIST 1.1 by BICR every 6 weeks from cycle 1, day 1 until week 49, and then at 9-week intervals thereafter. A cycle was defined as 21 days in length (± 3 days), unless a delay was medically necessary. Patients randomized to the docetaxel treatment group who experienced disease progression, confirmed by radiological assessment after study initiation, were permitted to cross over to the sotorasib treatment group (n = 46). The primary end point of the CodeBreaK 200 study was PFS. Key secondary end points included OS, ORR, and HRQoL, as assessed by the EORTC QLQ-C30 and EORTC QLQ-LC13. Other secondary end points included DOR, TTR, and DCR. The data cut-off date of the primary analysis was August 2, 2022.
Patients randomized in the CodeBreaK 200 study had a mean age of 63.5 years (SD = 9.5 years). Most patients were aged 18 years to 64 years (53.9%), white (82.9%), and current or former smokers (96.2%). With regard to disease characteristics, metastatic disease was identified in 95.1% of randomized patients. The most common histology type among the randomized patients was nonsquamous (96.8%). A total of 42.9%, 40.9%, and 16.2% of patients received 1, 2, and 3 or more complete prior lines of therapy, respectively; 34.2% were on maintenance therapy. Between the 2 treatment groups, a greater proportion of patients were male in the sotorasib treatment group (63.7%) relative to the docetaxel treatment group (54.6%). Other imbalances in baseline characteristics between the sotorasib and docetaxel treatment groups were noted for the following: PD-L1 protein expression greater than or equal to 1% and less than 50% (sotorasib = 26.9%; docetaxel = 40.2%); ECOG PS score of 0 at cycle 1, day 1 (sotorasib = 38.6%; docetaxel = 33.9%); primary refractory to last prior line of therapy (sotorasib = 39.2%; docetaxel = 32.8%); and initial response with subsequent growth (sotorasib = 20.5%; docetaxel = 27.0%).
Baseline patient characteristics were generally similar between the CodeBreaK 100 study and the CodeBreaK 200 study.
Efficacy Results
A summary of key results for the CodeBreaK 100 study and the CodeBreaK 200 study is presented in Table 2. In the CodeBreaK 200 study, the Maurer-Bretz22 multiple testing procedure was used to control the study-level overall type I error rate below 1-sided 0.025 levels, starting with PFS. If all 3 hypotheses of PFS, ORR, and OS were sequentially rejected, then the end points of change from baseline over 12 weeks for the symptoms of dyspnea, cough, and pain, as measured by the EORTC QLQ-C30 and EORTC QLQ-LC13, would be tested using Holm’s procedure. The key secondary HRQoL outcomes assessed in the CodeBreaK 200 study were not statistically tested because the hierarchical testing was stopped at the non–statistically significant OS end point.
Overall Survival
In CodeBreaK 100, the proportion of observed deaths at the time of the primary data cut-off (September 1, 2020) was 38.1%. The median OS was 12.0 months (95% confidence interval [CI], 9.5 months to not evaluable [NE]). The probabilities of survival based on Kaplan-Meier (KM) estimates at 3 months, 6 months, 9 months, and 12 months were 89.5% (95% CI, 82.7% to 93.8%), 75.5% (95% CI, 66.8% to 82.2%), 63.4% (95% CI, 53.8% to 71.5%), and 51.6% (95% CI, 36.7% to 64.5%), respectively. Results for OS at the updated analysis with the data cut-off date of March 15, 2021, were generally consistent with the results from the primary data cut-off date, with median OS of 12.5 months (95% CI, 10.0 months to NE). The results for OS at 2 years, with the data cut-off date of September 9, 2022, were consistent with the results from the previous data cut-off dates, with median OS of 12.48 months (95% CI, 9.99 months to 19.29 months). The probabilities of survival based on KM estimates at 18 months and 24 months were 42.08% (95% CI, 32.97% to 50.90%) and 31.56% (95% CI, 23.15% to 40.29%), respectively.
In the CodeBreaK 200 study, the proportions of observed deaths at the time of data cut-off (August 2, 2022) were 63.7% and 54.0% in the sotorasib and docetaxel treatment arms, respectively. The CodeBreaK 200 study was not powered to detect a difference in OS. The median OS rates were 10.64 months (95% CI, 8.94 months to 13.96 months) in the sotorasib group and 11.3 months (95% CI, 9.00 months to 14.85 months) in the docetaxel group. The stratified hazard ratio (HR) for OS was 1.01 (95% CI, 0.77 to 1.33; P = 0.53) following treatment with sotorasib versus docetaxel. In total, 59 patients randomized to docetaxel crossed over to receive treatment with sotorasib; crossover occurred in 46 patients following disease progression (per protocol), while 13 patients received sotorasib as subsequent treatment upon disease progression. The results of the sensitivity analyses exploring the crossover effect on OS in the CodeBreaK 200 study were consistent with the main analysis. In the analyses based on patients who were per-protocol crossovers, the HRs for survival were 1.01 (95% CI, 0.66 to 1.49) in the rank-preserving structural failure time (RPSFT) analysis; 0.99 (95% CI, 0.73 to 1.34) in the inverse-probability-of-censoring weighting (IPCW) adjusted analysis; and 0.885 (95% CI, 0.17 to 1.33) in the 2-stage approach adjusted analysis. Sensitivity analysis of OS exploring the crossover effect among all 59 crossover patients using the 2-stage approach resulted in an HR for survival of 0.82 (95% CI, 0.14 to 1.33). KM plots of sensitivity analysis of OS exploring crossover effects are presented in Figure 20 for 46 patients who were per-protocol crossovers and in Figure 21 for all 59 patients who received sotorasib upon progression.
Progression-Free Survival
In the CodeBreaK 100 study, 56.9% of patients experienced progression or death due to any cause at the time of the September 2020 data cut-off. The median PFS was 6.7 months (95% CI, 4.9 months to 8.1 months). The probabilities of PFS at 3 months, 6 months, and 9 months were 67.5% (95% CI, 58.2% to 75.2%), 51.5% (95% CI, 41.9% to 60.4%), and 36.2% (95% CI, 26.7% to 45.8%), respectively. The sensitivity analysis for PFS using the investigator’s assessment was consistent with the results obtained by BICR. At the time of the March 2021 data cut-off, 70.2% of patients had experienced progression or death due to any cause. The median PFS rate was consistent with the earlier data cut-off (6.8 months; 95% CI, 5.1 months to 8.2 months).
Among patients in the CodeBreaK 200 study, disease progression or death on or before the data cut-off date was observed in 71.3% of patients in the sotorasib treatment group and 58.0% of patients in the docetaxel group. The median PFS was 5.62 months (95% CI, 4.27 months to 7.75 months) in the sotorasib group and 4.47 months (95% CI, 3.02 months to 5.68 months) in the docetaxel group at the time of data cut-off. The stratified HR for disease progression or death was 0.66 (95% CI, 0.51 to 0.86; P = 0.002) in favour of sotorasib versus docetaxel. The results of the sensitivity analyses for PFS using the investigator’s assessment were consistent with the results obtained by BICR.
Patient-Reported Outcomes
European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30: In the CodeBreaK 100 study, 98 patients (78%) completed the EORTC QLQ-C30 at baseline. The number of patients available to complete the measure diminished consistently with each cycle. At the end of treatment, 38 patients (43.2%) completed the assessment. Over time, scores for both global health status and physical functioning appeared to remain relatively stable. Change from baseline in global health status ranged from –5.33 (SD = 15.57) (cycle 11, n = 25) to + 1.37 (SD = 19.44) (cycle 5, n = 61). Change from baseline in physical functioning ranged from –8.57 (SD = 20.33) (cycle 13, n = 14) to + 6.67 (SD = 22.05) (cycle 7, n = 33).
In the CodeBreaK 200 study, the baseline EORTC QLQ-C30 — a key secondary outcome — was completed by 168 patients (98.2%) and 158 patients (90.8%) in the sotorasib and docetaxel treatment groups, respectively. Compliance rates for the questionnaire remained consistently high, above 90%. The number of patients available to complete the measure diminished consistently with each cycle. At cycle 5, day 1 (week 12), the EORTC QLQ-C30 was completed by 69 patients (39.7%) in the docetaxel treatment group and by 106 patients (62.0%) in the sotorasib treatment group. The differences between groups in least squares change from baseline to week 12 were 6.93 (95% CI, 3.66 to 10.19) for global health status and 8.78 (95% CI, 5.39 to 12.17) for physical functioning, favouring treatment with sotorasib (n = 106) relative to docetaxel (n = 69).
EQ-5D-5L and EQ VAS: In the CodeBreaK 100 study, results for the EQ-5D-5L remained relatively stable during the treatment period. At baseline (n = 86), most patients (68% to 94%) reported that they had no problems or slight problems with the dimensions of health assessed by the EQ-5D-5L. At the end of the treatment phase (n = 28; 22.2%), 42.9% and 21.4% of patients reported that they had no problems or slight problems, respectively. EQ VAS scores remained relatively stable during the treatment period. The mean EQ VAS score at baseline was 70.2 (SD = 17.5; n = 86), indicating that patients generally rated their health favourably (with a score of 100 indicating best health imaginable). Change in mean score from baseline over the treatment period ranged from –24.0 (SD = 32.8) in cycle 15 (n = 4) to 2.7 (SD = 18.6) in cycle 3 (n = 69); and 2.7 (SD = 16.6; cycle 7, n = 31). By the end of the treatment phase, the mean EQ VAS score was 61.5 (SD = 19.5; n = 28), which was associated with a mean change from baseline of –10.6 (SD = 19.3). The number of patients available to complete both the EQ-5D-5L and the EQ VAS dropped by more than 50% after cycle 6 in the CodeBreaK 100 study.
In the CodeBreaK 200 study, a baseline EQ-5D-5L was completed by 160 patients (93.6%) in the sotorasib treatment group and 138 patients (79.3%) in the docetaxel treatment group. The number of patients available to complete the measure diminished consistently with each cycle. At cycle 5, day 1, the EQ-5D-5L was completed by 105 patients (61.4%) in the sotorasib treatment group and 67 patients (38.5%) in the docetaxel treatment group. At baseline, most patients in both the sotorasib treatment group (64.4% to 93.2%) and docetaxel treatment group (69.6% to 90.6%) reported that they had no problems or slight problems with the dimensions of health assessed by the EQ-5D-5L. At cycle 5, day 1, 79.0% to 96.2% of patients in the sotorasib treatment group and 61.2% to 85.1% of patients in the docetaxel treatment group reported that they had no problems or slight problems. Between-group differences for the change from baseline on the EQ-5D-5L scales were not reported. Baseline EQ VAS — a secondary outcome — was completed by 166 patients (97.1%) and 154 patients (88.5%) in the sotorasib and docetaxel treatment groups, respectively. Compliance rates for this measure were consistently greater than 80%. The number of patients available to complete the measure diminished consistently with each cycle. At cycle 5, day 1, the EQ VAS was completed by 106 patients (62.0%) in the sotorasib group and 69 patients (39.7%) in the docetaxel group. At baseline, mean EQ VAS scores were 67.6 (SD = 19.9) and 68.3 (SD = 20.3) in the sotorasib and docetaxel treatment groups, respectively. At cycle 5, day 1, the mean EQ VAS score for patients in the sotorasib treatment group was 73.2 (SD = 18.6), which was associated with a mean change from baseline of 2.2 (SD = 15.5) for sotorasib. For patients in the docetaxel treatment group (n = 67), the mean EQ VAS score at cycle 5, day 1 was 67.7 (SD = 20.8), which was associated with a mean change from baseline of –5.8 (SD = 18.2). Between-group differences for change from baseline on the EQ VAS were not reported.
EORTC QLQ-C30 Symptom Scales: In the CodeBreaK 100 study, baseline EORTC QLQ-C30 symptom scales were completed by 94 patients (76.4%). The number of patients available to complete the measure diminished consistently with each cycle. After cycle 6, the number of patients available to complete assessments had dropped by more than 50%. From baseline (n = 94) to the end of the treatment phase of the study (n = 32), mean scores were sustained for diarrhea (no change) and dyspnea (mean change from baseline = 3.13 [SD = 39.1]). The symptom scores for fatigue, nausea and/or vomiting, and pain increased during the study period.
In the CodeBreaK 200 study, the dyspnea subscale was considered the most important, and was the only symptom-specific scale of the EORTC QLQ-C30 reported. At cycle 2, day 1, a total of 148 patients (86.5%) in the sotorasib treatment group and 112 patients (64.4%) in the docetaxel treatment group completed the dyspnea subscale. At cycle 5, day 1, the proportions of patients available to complete the dyspnea subscale of the EORTC QLQ-C30 were 61.4% and 38.5% in the sotorasib and docetaxel treatment groups, respectively. The difference between groups in the least squares change from baseline for dyspnea at week 12 was –10.09 (95% CI, –13.39 to–6.78), favouring treatment with sotorasib (n = 105) relative to docetaxel (n = 67).
EORTC QLQ-LC13 Symptom Scales: The 3 main symptoms of lung cancer are dyspnea, cough, and chest pain; thus, these were the focus of the assessment. In the CodeBreaK 100 study, the least squares mean scores were maintained or decreased over time for the EORTC QLQ-LC13 subscales of dyspnea, cough, and chest pain from baseline (n = 86) to the end of the treatment phase at cycle 17 (n = 28). The least squares mean changes from baseline ranged from –11.2 (95% CI, –16.2 to –6.1) in cycle 2 (n = 77) to –7.1 (95% CI, –13.2 to –1.1) in cycle 6 (n = 45) for cough; from –4.9 (95% CI, –10.3 to 0.4) in cycle 7 (n = 31) to –0.44 (95% CI, –5.12 to 4.24) in cycle 6 (n = 45) for chest pain; and from –3.4 (95% CI, –7.8 to 1.0) in cycle 4 (n = 58) to –0.14 (95% CI, –5.7 to 5.41) in cycle 9 (n = 25) for dyspnea. After cycle 6, the number of patients available to complete assessments had dropped by more than 50%.
In the CodeBreaK 200 study, the dyspnea, cough, and chest pain subscales of the EORTC QLQ-LC13 were completed at baseline by 166 patients (97.1%) and 154 patients (88.5%) in the sotorasib and docetaxel treatment groups, respectively. Compliance rates were consistently high, mostly above 90%. The numbers of patients who completed the EOTRC QLQ-LC13 at cycle 5, day 1 (week 12) in the sotorasib and docetaxel treatment groups were 106 (62.0%) and 69 (39.7%), respectively. The total number of patients available to provide assessments dropped by more than 50% at cycle 6, day 1. The odds of improved symptoms at week 12 favoured sotorasib relative to docetaxel for cough (odds ratio = 3.21; 95% CI, 1.55 to 6.65) and for dyspnea (odds ratio = 3.58; 95% CI, 1.98 to 6.46). The odds of improved chest pain at week 12 favoured sotorasib compared to docetaxel (odds ratio = 1.56; 95% CI, 0.82 to 2.96).
Objective Response Rate
In CodeBreaK 100, 1.6% of patients were documented as having CR on sotorasib, while 35.8% had PR to treatment at the time of the September 2020 data cut-off. The ORR (CR plus PR) was 37.4% (95% CI, 28.84% to 46.58%). The study achieved the predetermined threshold for a positive outcome (lower limit of the 95% CI for ORR > 23%). The mean time to objective response was 1.95 months (SD = 1.23 months). At the time of the March 2021 data cut-off, 3.2% of patients were documented as having CR, while 33.9% had PR. The ORR (CR plus PR) was consistent with the earlier data cut-off (37.1%; 95% CI, 28.60% to 46.23%). The mean time to objective response as observed at the updated analysis was 2.11 months (SD = 1.71 months).
In the CodeBreaK 200 study, the proportions of patients documented as having an objective response (CR or PR) to treatment at the time of data cut-off in the sotorasib and docetaxel groups were 28.1% (95% CI, 21.5 to 35.4) and 13.2% (95% CI, 8.6 to 19.2), respectively, resulting in a difference in proportion of 14.8% (95% CI, 6.4 to 23.1; P < 0.001) in favour of sotorasib. The odds of objective response were higher among patients randomized to the sotorasib group relative to those randomized to docetaxel (odds ratio = 2.6; 95% CI, 1.48 to 4.56; P < 0.001). The mean time to objective response as of the August 2, 2022, data cut-off date was 2.43 months (SD = 1.80 months) among patients in the sotorasib treatment group and 3.24 months (SD = 2.08 months) in the docetaxel treatment group. Of note, there was an imbalance across groups in the proportion of patients for whom response assessments were not done (5.8% and 24.1% of patients in the sotorasib and docetaxel groups, respectively). The sponsor clarified that the majority of patients who did not have ORR measured did not receive docetaxel because of withdrawal of consent or other reasons.
Duration of Response
In the CodeBreaK 100 study, a DOR of at least 3 months and of at least 6 months was documented in 76.1% and 50.0% of patients, respectively, at the primary data cut-off (September 1, 2020). The median DOR was 8.4 months (95% CI, 6.9 months to 8.4 months). The probabilities of response based on KM estimates at 3 months and 6 months were 89.9% (95% CI, 75.3% to 96.1%) and 76.2% (95% CI, 59.1 to 86.9), respectively. Results for DOR at the updated analysis with the data cut-off date of March 15, 2021, were consistent overall with the results from the primary data cut-off, with DORs of at least 3 months and 6 months documented in 82.6% and 60.9% of patients, respectively. The median DOR was 11.1 months (95% CI, 6.9 months to NE), and the probabilities of objective response based on KM estimates at 3 months and 6 months were 90.5% (95% CI, 76.7 to 96.3) and 70.8% (95% CI, 54.3 to 82.2), respectively. At 9 months and 12 months, the probabilities of objective response were 57.3% (95% CI, 40.4 to 71.0) and 48.2% (95% CI, 31.5 to 63.0), respectively.
In the CodeBreaK 200 study, the proportions of patients with DORs of at least 3 months and 6 months were not available to the CADTH review team. The median DORs based on BICR of disease response per RECIST v1.1 were 8.64 months (95% CI, 7.06 months to 17.97 months) and 6.80 months (4.27 months to 8.28 months) in the sotorasib and docetaxel treatment groups, respectively. No comparative effect estimate was provided.
Harms Results
Adverse Events
At the September 1, 2020, data cut-off date in the CodeBreaK 100 study, a total of 125 patients (99.2%) in the NSCLC cohort had AEs. Overall, 75 patients (59.5%) had grade 3 or worse AEs, and 21 patients (16.1%) had grade 4 or worse AEs. The 3 most common AEs reported were diarrhea (49.2%), nausea (29.4%), and fatigue (24.6%). AEs reported at the subsequent updated analysis with the data cut-off date of March 15, 2021, were consistent overall with those from the primary data analysis. At the time of the updated analysis, 125 patients (99.2%) reported at least 1 AE; among these, 77 patients (61.1%) had grade 3 or worse AEs and 24 patients (19.0%) had grade 4 or worse AEs. The 3 most common AEs reported at the time of the updated analysis were diarrhea (50.8%), nausea (31.0%), and fatigue (25.4%).
In the CodeBreaK 200 study, 98% of patients in both the sotorasib and docetaxel treatment groups reported at least 1 AE. The most common AEs reported in the sotorasib treatment group were diarrhea (41.4%), nausea (26.0%), and decreased appetite (23.1%). The most common AEs reported in the docetaxel treatment group were fatigue (29.8%), diarrhea (25.8%), and nausea (25.8%). Alopecia occurred in 3 patients (1.8%) in the sotorasib group and 35 patients (23.2%) in the docetaxel group. Grade 3 or worse AEs were reported by 121 patients (71.6%) in the sotorasib treatment group and 91 patients (60.3%) in the docetaxel treatment group. Grade 4 or worse AEs were reported in 48 patients (28.4%) and 35 patients (23.2%) in the sotorasib and docetaxel treatment groups, respectively. The most common grade 3 or worse AEs in the sotorasib treatment group were diarrhea (13.6%), NSCLC (10.1%), increased alanine aminotransferase (ALT) (8.3%), and increased aspartate aminotransferase (AST) (5.9%). In the docetaxel treatment group, the most common grade 3 or worse AEs were neutropenia (8.6%), anemia (6.6%), fatigue (6.0%), pneumonia (6.0%), and febrile neutropenia (5.3%).
Serious Adverse Events
In the CodeBreaK 100 study, a total of 63 patients (50%) in the NSCLC cohort had at least 1 serious adverse event (SAE) at the time of primary data analysis (September 1, 2020). The most frequently reported SAEs were pneumonia (7.1%), NSCLC (6.3%), and pleural effusion (4.8%). Of those reporting SAEs, 60 patients (47.6%) had a grade 3 or worse AE and 19 patients (15.1%) had a grade 4 or worse AE. SAEs at the time of the subsequent updated analysis with the March 15, 2021, cut-off date were documented in 69 patients (54.8%). The grades of SAEs at the time of the updated analysis were not available to the CADTH review team. The most frequently reported SAEs at the time of the updated analysis were pneumonia (7.1%), NSCLC (6.3%), and pleural effusion (4.0%).
In the CodeBreaK 200 study, SAEs were reported by 91 patients (53.8%) in the sotorasib treatment group and by 67 patients (44.4%) in the docetaxel treatment group. The most frequently reported SAE in the sotorasib treatment group was NSCLC (10.7%). The most frequently reported SAE in the docetaxel treatment group was pneumonia (6.6%).
Withdrawals Due to AEs
A total of 11 patients (8.7%) in the NSCLC cohort of the CodeBreaK 100 study discontinued treatment due to AEs at the time of primary data analysis (September 1, 2020) and subsequent updated analysis (March 15, 2022). The most common reasons for treatment discontinuation were drug-induced liver injury (2.4%), increased ALT (1.6%), increased AST (1.6%), and pneumonitis (1.6%) at the time of both the primary and updated analyses.
In the CodeBreaK 200 study, 28 patients (16.6%) and 24 patients (15.9%) in the sotorasib and docetaxel treatment groups, respectively, discontinued treatment due to AEs. Reasons for discontinuing treatment in the sotorasib treatment group included increased ALT (3.6%), NSCLC (3.0%), increased blood bilirubin (2.4%), increased AST (1.2%), asthenia (1.2%), and increased blood alkaline phosphatase (ALP) (1.2%). In the docetaxel treatment group, reasons for discontinuing treatment included fatigue (2.0%), NSCLC (1.3%), anemia (1.3%), febrile neutropenia (1.3%), pneumonitis (0.7%), and asthenia (0.7%).
Dose Modification Due to AEs
In the CodeBreaK 100 study, a total of 48 patients (38.1%) and 22 patients (17.5%) required dose modification of sotorasib due to AEs at the time of the primary data analysis (September 1, 2020) and the subsequent updated analysis (March 15, 2021), respectively. Reasons for dose modification were consistent at both data analysis points. The most common reasons for dose modification due to AE were diarrhea (8.7%), increased AST (8.7%), increased ALT (8.7%), and increased blood ALP (4.0%).
In the CodeBreaK 200 study, dose modifications due to AEs were required by 26 patients (15.4%) and 43 patients (28.5%) in the sotorasib and docetaxel treatment groups, respectively. The most frequently reported reason for dose modification in the sotorasib treatment group was diarrhea (8.3%), followed by increased ALT (3.6%), increased AST (1.8%), and increased blood ALP (0.6%). In the docetaxel treatment group, the most frequently reported reasons for dose modification were neutropenia (4.6%) and fatigue (4.0%), followed by asthenia (3.3%) and diarrhea (2.0%).
Dose Interruption
In the CodeBreaK 100 study, dose interruptions due to AEs were documented in 46 patients (36.5%) at the time of the March 15, 2021, data cut-off date.
In the CodeBreaK 200 study, dose interruptions due to AEs were reported in 85 patients (50.9%) in the sotorasib treatment group and in 42 patients (27.8%) in the docetaxel treatment group. The most frequently reported reasons for dose interruption in the sotorasib treatment group were diarrhea (15.4%), increased ALT (5.9%), increased AST (5.3%), nausea (4.7%), decreased appetite (3.0%), and fatigue (1.2%). In the docetaxel treatment group, dose interruptions were due to pneumonia (4.6%), fatigue (3.3%), and nausea (0.7%).
Mortality
At the time of the primary data analysis at the data cut-off of September 1, 2020, in the CodeBreaK 100 study, 18 patients (14.3%) had died due to an AE. At the time of the subsequent, updated analysis on March 15, 2021, 20 patients (15.9%) had died due to an AE. None of the deaths were considered attributable to treatment-related AEs.
In the CodeBreaK 200 study, fatal AEs were recorded in 37 patients (21.9%) in the sotorasib treatment group and in 18 patients (11.9%) in the docetaxel treatment group. Seventeen patients (10.1%) in the sotorasib treatment group and 5 patients (3.3%) in the docetaxel group experienced fatal AEs related to NSCLC disease progression.
Notable Harms
At the time of the CodeBreaK 100 primary data analysis on September 1, 2020, a total of 40 patients (31.7%) in the NSCLC cohort reported hepatotoxicity, with the most common documented as increased AST (21.4%), increased ALT (20.6%), and increased blood ALP (13.5%). Renal toxicity was reported in 21 patients (16.7%) in the NSCLC cohort, and included hyponatremia (5.6%) and hypoalbuminemia (3.2%), hyperkaliaemia (2.4%), hypocalcemia (2.4%), hypophosphatemia (1.6%), and increased blood creatine (0.8%). There were no documented cases of interstitial lung disease. Pneumonitis was reported in 3 patients (2.4%) in the NSCLC cohort. Peripheral neuropathy was reported in 1 patient (0.8%) in the NSCLC cohort. Lastly, gastrointestinal (GI) toxicity was reported in 93 patients (73.8%) in the NSCLC cohort, and included diarrhea (49.2%), nausea (29.4%), and vomiting (18.3%). Reported notable harms at the subsequent updated analysis with the data cut-off date of March 15, 2021, were consistent overall with those from the primary data analysis. At the updated data analysis on March 15, 2021, a total of 40 patients (31.7%) reported hepatoxicity, with the most common documented as increased AST (21.4%), increased ALT (20.6%), and increased blood ALP (13.5%). Renal toxicity was reported in 23 patients (18.3%) and included hyponatremia (7.1%), hypoalbuminemia (3.2%), increased blood creatine (0.8%), hyperkalemia (2.4%), hypocalcemia (3.2%), and hypophosphatemia (2.4%). There were no documented cases of interstitial lung disease at the time of the updated analysis. Pneumonitis was reported in 3 patients (2.4%) in the NSCLC cohort. Peripheral neuropathy was reported in 1 patient (0.8%) in the NSCLC cohort. The overall number of patients with GI toxicity was not reported at the time of the updated analysis. The following notable AEs related to GI toxicity were reported: diarrhea (50.8%), nausea (31.0%), vomiting (18.3%), constipation (19.0%), and abdominal pain (8.7%).
In the CodeBreaK 200 study, hepatoxicity AEs, including increased AST (10.7%), increased ALT (10.7%), increased blood ALP (7.7%), and increased gamma-glutamyltransferase (4.0%), were reported in the sotorasib treatment group, while in the docetaxel treatment group, 2% or less of patients reported hepatoxicity due to these reasons. Renal toxicity related to hyponatremia was reported in 8 patients (4.7%) in the sotorasib treatment group and in 4 patients (2.6%) in the docetaxel treatment group, while hypoalbuminemia was reported in 4 patients (2.4%) in the sotorasib treatment group and 8 patients (5.3%) in the docetaxel treatment group. Interstitial lung disease was reported in 1 patient in the sotorasib treatment group, and pneumonitis was reported in 3 patients (1.8%) in the sotorasib treatment group and 3 patients (2.0%) in the docetaxel treatment group. Peripheral neuropathy was documented in 1 patient (0.6%) in the sotorasib treatment group and in 16 patients (10.6%) in the docetaxel group. Notable GI toxicities reported in the sotorasib treatment group included diarrhea (41.4%), nausea (26.0%), vomiting (13.0%), constipation (13.0%), and abdominal pain (11.8%). Notable GI toxicities reported in the docetaxel treatment group included diarrhea (25.8%), nausea (24.5%), constipation (19.2%), and vomiting (9.9%).
Table 2: Summary of Key Results From CodeBreaK 100 and CodeBreaK 200 Studies
Outcomes | CodeBreaK 100 study, phase II (NSCLC cohort) | CodeBreaK 200 study | ||
|---|---|---|---|---|
Sotorasib 960 mg N = 126 | Sotorasib 960 mg N = 171 | Docetaxel 75 mg/m2 N = 174 | ||
Data cut-off date September 1, 2020 | Data cut-off date March 15, 2021 | Data cut-off date August 2, 2022 | ||
OS (CodeBreaK 100 safety analysis set; CodeBreaK 200 full analysis set) | ||||
n | 126 | 126 | 171 | 174 |
Events, n (%) | 48 (38.1) | 64 (50.8) | 109 (63.7) | 94 (54.0) |
Death due to any cause | 48 (38.1) | 64 (50.8) | 109 (63.7) | 94 (54.0) |
OS (KM), months | ||||
Median (95% CI) | 12.0 (9.5 to NE) | 12.5 (10.0 to NE) | 10.64 (8.94 to 13.96) | 11.30 (9.00 to 14.85) |
Median OS follow-up time, months | 9.3 (9.0 to 9.5) | 15.3 (15.2 to 15.7) | 17.71 (16.95 to 19.15) | 16.33 (16.07 to 17.08) |
KM estimates, survival % (95% CI) | ||||
At 3 months | 89.5 (82.7 to 93.8)a | 89.5 (82.7 to 93.8)a | NR | NR |
At 6 months | 75.5 (66.8 to 82.2)a | 75.5 (66.8 to 82.2)a | 72.01 (64.54 to 78.16)b | 67.53 (59.50 to 74.31)b |
At 9 months | 63.4 (53.8 to 71.5)a | 63.5 (54.3 to 71.4)a | NR | NR |
At 12 months | 51.6 (36.7 to 64.5)a | 51.3 (41.9 to 59.9)a | 45.96 (38.17 to 53.39) | 46.49 (38.34 to 54.24)b |
At 24 months | NRm | NRm | NE | 33.89 (25.24 to 42.73) |
Stratified analysisc | ||||
HR (95% CI)d | NA | NA | 1.01 (0.77 to 1.33) | |
P valuee | NA | NA | 0.53 | Reference |
PFS by RECIST 1.1 (full analysis set) | ||||
n | 123 | 124 | 171 | 174 |
Events, n (%) | 70 (56.9) | 87 (70.2) | 122 (71.3) | 101 (58.0) |
Progressive disease | 60 (48.8) | 74 (59.7) | 100 (58.5) | 68 (39.1) |
Death due to any cause | 10 (8.1) | 13 (10.5) | 22 (12.9) | 33 (19.0) |
PFS (KM), months | ||||
Median (95% CI) | 6.7 (4.9 to 8.1) | 6.8 (5.1 to 8.2) | 5.62 (4.27 to 7.75) | 4.47 (3.02 to 5.68) |
KM estimates, survival % (95% CI) | ||||
At 3 months | 67.5 (58.2 to 75.2)a | 67.8 (58.5 to 75.4)a | 71.73 (64.01 to 78.08)b | 59.42 (50.66 to 67.13)b |
At 6 months | 51.5 (41.9 to 60.4)a | 52.2 (42.6 to 60.9)a | 46.49 (38.27 to 54.30)b | 39.06 (30.22 to 47.79)b |
At 9 months | 36.2 (26.7 to 45.8)a | 37.5 (28.5 to 46.5)a | NR | NR |
At 12 months | 0.0 (NE to NE)a | 27.4 (19.2 to 36.1)a | 24.84 (17.90 to 32.38)b | 10.12 (4.68 to 18.02)b |
At 18 months | NR | NR | 13.52 (7.67 to 21.04)b | 7.59 (2.69 to 15.91)b |
Follow-up time (KM), months | ||||
Median (95% CI) | 8.3 (8.2 to 8.3) | 13.8 (13.7 to 13.8) | 15.24 (14.85 to 17.31) | 6.87 (5.42 to 12.52) |
Stratified hazardc | ||||
HR (95% CI)d | NA | NA | 0.66 (0.51 to 0.86) | |
P valuee,f | NA | NA | 0.002 | Reference |
ORR by RECIST 1.1 (full analysis set) | ||||
n | 123 | 124 | 171 | 174 |
Best overall response, n (%) | ||||
Complete response | 2 (1.6) | 4 (3.2) | 2 (1.2) | 0 (0) |
Partial response | 44 (35.8) | 42 (33.9) | 46 (26.9) | 23 (13.2) |
Not done | 2 (1.6) | 2 (1.6) | 10 (5.8) | 42 (24.1) |
ORR (CR plus PR) | ||||
Confirmed ORR, n (%) | 46 (37.4) | 46 (37.1) | 48 (28.1) | 23 (13.2) |
95% CIg | 28.84 to 46.58 | 28.60 to 46.23 | 21.5 to 35.4 | 8.6 to 19.2 |
P valuee | NA | NA | < 0.001 | Reference |
OR (95% CI)h | NA | NA | 2.6 (1.48 to 4.56) | |
Time to objective response, monthsi | ||||
Mean (SD) | 1.95 (1.23) | 2.11 (1.71) | 1.91 (1.32) | 3.3 (2.41) |
Median (minimum, maximum) | 1.35 (1.2 to 6.1) | 1.35 (1.2 to 10.1) | 1.41 (1.2 to 8.3) | 2.76 (1.3 to 11.3) |
DOR by RECIST 1.1 (full analysis set) | ||||
n | 123 | 124 | 171 | 174 |
Duration of objective response,j n (%) | ||||
≥ 3 months | 35 (76.1) | 38 (82.6) | NR | NR |
≥ 6 months | 23 (50.0) | 28 (60.9) | NR | NR |
≥ 9 months | 0 (0) | 20 (43.5) | NR | NR |
≥ 12 months | 0 (0) | 15 (32.6) | NR | NR |
Duration of response, months (KM) | ||||
Median (95% CI) | 8.4 (6.9, 8.4) | 11.1 (6.9 to NE) | 8.64 (7.06 to 17.97) | 6.80 (4.27 to 8.28) |
KM estimates (95% CI)k | ||||
At 3 months | 89.9 (75.3 to 96.1) | 90.5 (76.7 to 96.3) | NR | NR |
At 6 months | 76.2 (59.1 to 86.9) | 70.8 (54.3 to 82.2) | NR | NR |
At 9 months | 0 (NE to NE) | 57.3 (40.4 to 71.0) | NR | NR |
At 12 months | 0 (NE to NE) | 48.2 (31.5 to 63.0) | NR | NR |
Harms, n (%) (safety analysis set) | ||||
n | 126 | 126 | 169 | 151 |
AEs | 125 (99.2) | 125 (99.2) | 166 (98.2) | 148 (98.0) |
SAEs | 63 (50.0) | 69 (54.8) | 91 (53.8) | 67 (44.4) |
Treatment discontinuation due to AE | 11 (8.7) | 11 (8.7) | 28 (16.6) | 24 (15.9) |
Dose modification due to AE | 48 (38.1) | 22 (17.5) | 26 (15.4) | 43 (28.5) |
Dose interruption due to AE | NR | 46 (36.5%) | 86 (50.9) | 42 (27.8) |
Deaths | 18 (14.3) | 20 (15.9) | 37 (21.9) | 18 (11.9) |
Notable harms, n (%) (safety analysis set) | ||||
n | 126 | 126 | 169 | 151 |
Hepatoxicityl | 40 (31.7) | 40 (31.7) | NAm | NAm |
AST increased | 27 (21.4) | 27 (21.4) | 18 (10.7) | 1 (0.7) |
ALT increased | 26 (20.6) | 26 (20.6) | 18 (10.7) | 1 (0.7) |
Blood ALP increased | 17 (13.5) | 17 (13.5) | 13 (7.7) | 3 (2.0) |
Gamma-glutamyltransferase increased | 5 (4.0) | 5 (4.0) | 5 (3.0) | 2 (1.3) |
Renal toxicityl | 21 (16.7) | 23 (18.3) | NAm | NAm |
Hyponatremic | 7 (5.6) | 9 (7.1) | 8 (4.7) | 4 (2.6) |
Hypoalbuminemia | 4 (3.2) | 4 (3.2) | 4 (2.4) | 8 (5.3) |
Blood creatine increased | 1 (0.8) | 1 (0.8) | 5 (3.0) | 1 (0.7) |
Hyperkalemia | 3 (2.4) | 3 (2.4) | 5 (3.0) | 5 (3.3) |
Hypocalcemia | 3 (2.4) | 4 (3.2) | 6 (3.6) | 2 (1.3) |
Hypophosphatemia | 2 (1.6) | 3 (2.4) | 3 (1.8) | 1 (0.7) |
Interstitial lung diseasel | 0 (0) | 0 (0) | 1 (0.6) | 0 (0) |
Pneumonitisl | 3 (2.4) | 3 (2.4) | 3 (1.8) | 3 (2.0) |
Peripheral neuropathyl | 1 (0.8) | 1 (0.8) | 1 (0.6) | 16 (10.6) |
GI toxicityl | 93 (73.8) | NR | NR | NR |
Diarrhea | 62 (49.2) | 64 (50.8) | 70 (41.4) | 39 (25.8) |
Nausea | 37 (29.4) | 39 (31.0) | 44 (26.0) | 37 (24.5) |
Vomiting | 23 (18.3) | 23 (18.3) | 22 (13.0) | 15 (9.9) |
Constipation | 22 (17.5) | 24 (19.0) | 22 (13.0) | 29 (19.2) |
Abdominal pain | 11 (8.7) | 11 (8.7) | 20 (11.8) | 9 (6.0) |
AE = adverse event; ALP = alkaline phosphatase; ALT = alanine aminotransferase; AST = aspartate aminotransferase; CI = confidence interval; CNS = central nervous system; CR = complete response; DOR = duration of response; GI = gastrointestinal; HR = hazard ratio; KM = Kaplan-Meier; NA = not applicable; NE = not evaluable; NR = not reported; NSCLC = non–small cell lung cancer; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; PR = partial response; RECIST 1.1 = Response Evaluation Criteria in Solid Tumours Version 1.1; SAE = serious adverse event; SD = standard deviation; vs. = versus.
Notes: Randomization stratification factors are number of prior lines of therapy in advanced disease (1 vs. 2 vs. > 2), race (Asian vs. non-Asian), and history of CNS involvement (yes vs. no).
For patients who continued treatment postprogression or patients who crossed over from docetaxel to sotorasib, the first date of progression is used for PFS analysis; the patient’s response post–first progression or postcrossover is not used in the primary analyses to evaluate objective response or DOR.
The median OS at 2 years in the CodeBreaK 100 study with data cut-off September 9, 2022, was 12.48 (95% CI, 9.99 to 19.29). The probabilities of survival based on KM estimates at 18 months and 24 months were 42.08% (95% CI, 32.97 to 50.90%) and 31.56% (95% CI, 23.15 to 40.29%), respectively.
Survival status may include publicly available records (where permitted) searched by investigator after the patient ended the study.
a95% CIs are based on estimated variance for log-log transformation of the KM survival estimate.
bPFS and OS rates and 95% CIs were estimated using the method by Kalbfleisch and Prentice with log-log transformation.
cStratification factors: number of lines of therapy in advanced disease (1 vs. 2 vs. > 2), race (Asian vs. non-Asian), history of CNS involvement (yes vs. no).
dHR and 95% CI were estimated using a stratified Cox proportional hazard model. An HR of less than 1.0 represents a lower average death rate and longer OS for sotorasib relative to docetaxel. The P value was calculated using a stratified log-rank test.
eThe P value was adjusted for multiple comparison using the Maurer-Bertz multiple testing procedure. The PFS and ORR hypothesis was rejected before testing OS.
fThe P value was calculated using a stratified log-rank test.
gThe exact 95% CI was calculated using the Clopper-Pearson method.
hCalculated using the stratified Cochran-Mantel-Haenszel chi-square test.
ITime to response was calculated among confirmed responders’ best overall response of PR or CR.
jDOR was calculated among confirmed responders.
k95% CIs were based on estimated variance for log-log transformation of the KM survival estimate.
lFrequency greater than 0% in any treatment group.
mIn the CodeBreaK 200 study, hepatotoxicity of interest was reported using Standardised MedDRA Query for hepatic disorders (narrow). Hepatotoxicity of interest was reported in 7 patients (4.6%) in the docetaxel group and 41 patients (24.3%) in the sotorasib group. Renal toxicity of interest was reported using Standardized MedDRA Query (acute renal failure, chronic kidney disease). Renal toxicity of interest did not occur in the docetaxel group, but was reported for the sotorasib group in 10 patients (5.9%), including acute kidney injury and renal failure in 3 patients each.
Sources: Clinical Study Report for phase II of the CodeBreaK 100 study;20 Clinical Study Report for the CodeBreaK 200 study.21
Critical Appraisal
The single-group, open-label, nonrandomized design of the CodeBreaK 100 study makes interpretation of the efficacy and safety of sotorasib challenging. The lack of comparison with an active comparator, BSC, and/or placebo precludes the ability to draw causal inferences or assess the relative therapeutic benefits or safety of sotorasib. Interpretation of time‐to‐event end points, such as OS and PFS, is limited in single‐group studies; because all patients with KRAS G12C-mutated advanced NSCLC received the same treatment, the extent to which the observed survival is due to the natural history of the tumour, or the intervention remains unclear. The CodeBreaK 100 trial included no formal statistical significance or hypothesis testing and point estimates with 95% CIs were reported to estimate the magnitude of treatment effect. To mitigate the limitations associated with open-label studies, tumour response and disease progression outcomes were blinded to the study investigator and assessed by BICR. However, as noted by the FDA assessment of sotorasib, the analyses of PFS and OS are uninterpretable in the single-group study.23 The results for patient-reported outcomes (PROs) were inconclusive, given the noncomparative, open-label design of the trial and the substantial decline in the number of patients available to provide assessments over time. Due to the previously mentioned limitations, the ability to draw firm conclusions on the magnitude of clinical benefit and safety of sotorasib was limited. The results were found to be generalizable, overall, to the clinical setting by the clinical experts consulted by CADTH for the purpose of this review; however, the patients in the trial were judged to be younger and healthier (i.e., with lower ECOG PS scores) than those typically seen in practice. In addition, patients with active brain metastases, who may be considered for treatment in practice, were excluded.
In the CodeBreaK 200 study, patients were randomized centrally using interactive response technology, a method that is typically adequate for concealing allocation until treatment assignment. While the randomization stratification factors appear to be appropriate, several between-group imbalances at baseline suggest that prognostic balance may not have been achieved between groups. Of concern was the proportion of patients in the docetaxel treatment group who were randomized but not dosed (13.2%), namely due to refusal of treatment, and discontinued the study by way of withdrawal of consent (22.4%). As a result, unequal censoring between the sotorasib and docetaxel treatment groups was observed (e.g., a 10% difference in censoring between the groups for OS and a 13% difference in censoring for PFS), introducing uncertainty about treatment effects. In addition, a sizable proportion of patients in the docetaxel treatment group (24%) had an outcome of “not measured” in the ORR analysis. The sponsor clarified that the majority of patients who did not have ORR measured did not receive docetaxel because of withdrawal of consent or other reasons. The extent and direction of bias associated with the ORR analysis are uncertain. The risk of attrition bias cannot be ruled out due to the disproportionate loss of patients by way of self-withdrawal. There is added uncertainty for the PFS rates measured over the study period due to the limited number of patients at risk by month 12. To minimize the risk of bias in the measurement of the outcomes associated with the open-label design, patients’ responses to treatment were blinded to the study investigator, and tumour response was confirmed by radiologic evidence and done by BICR, as per RECIST 1.1. The sensitivity analyses of PFS and ORR demonstrated consistency between the BICR and the investigator’s assessment of tumour response, suggesting that the risk for bias in response outcomes from the open-label design is likely not substantial. Objective outcomes, like OS, are not prone to bias due to knowledge of the intervention.
The CodeBreaK 200 study assessed HRQoL and symptom burden — outcomes deemed important by patients and clinicians — as key secondary outcomes. However, the key secondary HRQoL outcomes were not statistically tested because the hierarchical testing was stopped at the non–statistically significant OS end point. Of note, due to protocol amendments that allowed for crossover and subsequent reduction in sample size, the CodeBreaK 200 study was not powered to detect a difference in OS. Furthermore, the open-label nature of the CodeBreaK 200 study increases the risk of bias in the measurement of the subjective HRQoL24,25 Missing baseline data and the low completion rates in both the sotorasib and docetaxel treatment groups add further uncertainty to the HRQoL and other symptom burden outcomes. Focusing on the docetaxel treatment group, after cycle 3, fewer than 50% of patients were available to provide assessment for the EORTC QLQ-C30, the subscales of the EORTC QLQ-LC13, and the EQ-5D-5L. Consequently, there would be no reliable assessment for the docetaxel treatment group for HRQoL and symptom burden measures. The HRQoL and symptom burden outcomes are at high risk of attrition bias because long-term survivors tend to be healthier patients. The analysis of efficacy results followed a defined statistical analysis plan, employed appropriate censoring criteria, and accounted for patient crossover from the docetaxel treatment group to the sotorasib treatment group. The sponsor conducted additional sensitivity analyses of OS that adjusted for the effect of crossover. The results of these analyses were consistent with the main analysis in that the CIs were too wide to draw any conclusions of certainty with respect to whether sotorasib or docetaxel was favoured for OS.
Indirect Comparisons
At the time of initial submission to CADTH in August 2022, data from the CodeBreaK 200 study were not available. In the absence of direct comparative data between sotorasib and docetaxel from the CodeBreaK 200 trial, the sponsor submitted a matching-adjusted indirect comparison (MAIC), which was used to inform the pharmacoeconomic model. The unanchored MAIC estimated the comparative OS and PFS between sotorasib and docetaxel in patients with locally advanced or metastatic NSCLC (stages IIB to IV) and confirmed KRAS mutation in the absence of direct comparative evidence from a randomized trial. The MAIC was based on individual patient data from the single-group, open-label index trial, the CodeBreaK 100 study, and from aggregate-level data from the docetaxel (75 mg/m2) plus placebo group of the double-blind, randomized SELECT-1 trial.26 In November 2022, this submission was temporarily suspended because the sponsor informed CADTH that the economic evaluation would be revised to include data from the CodeBreaK 200 study. In May 2023, the temporary suspension was lifted upon receipt of the revised economic model from the sponsor. After receiving data from the CodeBreaK 200 study, which provided direct comparative evidence between sotorasib and docetaxel, the CADTH review team determined that the MAIC no longer addressed any gap in the evidence; therefore, the submitted MAIC was not included in the clinical report.
Other Relevant Evidence
This section summarizes the partial results of the global expanded access program (EAP). Although this study did not meet the systematic review inclusion criteria, it provides supportive evidence for patients with an ECOG PS of 2, which was a patient group excluded from the CodeBreaK 100 study and the CodeBreaK 200 study. Furthermore, the clinical expert consulted by CADTH and the input received from clinician groups for this submission also expressed a desire to treat patients with ECOG PS 2. The input received from the clinician group, LCC, for this submission indicated that benefit in patients with ECOG PS 3 and 4 remains debatable. The CADTH review team summarized the study designs and data of the global EAP to provide supplemental evidence for decision-making.
The global EAP provided for compassionate use of sotorasib before local regulatory approval. Patients eligible for the EAP were aged 18 years to 99 years with an ECOG PS equal to or less than 2, and had pathologically documented, locally advanced and unresectable or metastatic, KRAS G12C-mutated NSCLC confirmed through molecular testing. Patients had to demonstrate that they had exhausted other standard of care options for locally advanced and unresectable or metastatic NSCLC, including platinum-based combination chemotherapy and PD-1 and/or PD-L1 immunotherapy (unless medically contraindicated). Patients were excluded from participating if they were participating in any ongoing clinical study of sotorasib; if they had mixed small cell lung cancer or mixed NSCLC histology, active brain metastases, active hepatitis B or hepatitis C virus, or current active malignancy other than NSCLC; and if they had previously enrolled in a prior sotorasib study. The primary end points included safety (such as treatment-emergent adverse events [TEAEs], AEs of interest, and SAEs). Key secondary end points included OS and treatment duration, with real-world PFS as the ad hoc end point. The sponsor-submitted abstract, poster, and presentation summarized the data from 2 global protocols under the EAP (Amgen studies 20190236 [Study 436] and 20190442 [Study 442]) that evaluated the safety and efficacy of sotorasib outside the registrational trial setting in patients with advanced KRAS G12C-mutated NSCLC in multiple countries (US, Spain, Argentina, Brazil, Israel, Saudi Arabia, and Taiwan) across 49 centres.27,28 Real-world PFS was estimated for Study 436 and defined as the time from the start of treatment to end of protocol due to disease progression or death, any death before new anticancer therapy, or end of commercial sotorasib, whichever occurred first.
A total of 147 patients received sotorasib 960 mg daily under EAP Study 436. The median number of prior lines of anticancer therapy reported by patients before receiving sotorasib was 2 (up to 8). At baseline, a total of 25.2% of patients had an ECOG PS of 2, and 32.7% of patients had brain metastases.
Efficacy Results
Real-world PFS was estimated for the 92 patients enrolled in Study 436 of the global EAP study.27 The median real-world PFS as of the data cut-off date of June 24, 2022, was 6.7 months (95% CI, 4.6 months to 8.3 months) with 60 events (65.2%). OS was estimated for 147 patients. The median OS as of the data cut-off date of November 8, 2022, was 9.5 months (95% CI, 8.6 months to 12.0 months). The median real-world PFS was comparable to the PFS efficacy results reported in the CodeBreaK 100 study and the CodeBreaK 200 study.
Harms Results
The global EAP study27 presented AEs as TEAEs; thus, these were not reported by the CADTH review team.
Critical Appraisal
The CADTH review team was unable to complete a robust critical appraisal of the internal and external validity of the study results. A key limitation to the global EAP study is its noncomparative design and lack of statistical testing, precluding causal conclusions. The study was open-label, and the method for ascertaining PFS or OS was not reported; therefore, the potential for and extent of any bias in the measurement of this outcome is unknown. Although the results were comparable to the PFS efficacy results reported in the CodeBreaK 100 and CodeBreaK 200 trials, the magnitude of the treatment effect for the real-world PFS should be interpreted with uncertainty in light of these limitations. The study did not report on outcomes other than PFS and OS that are important to patients, clinicians, and drug plans (e.g., HRQoL, symptoms, harms).
Conclusions
One nonrandomized, single-group, open-label, phase I and II study (the CodeBreaK 100 study) and 1 randomized, comparative, open-label, phase III study (the CodeBreaK 200 study) provided evidence for the efficacy and safety of sotorasib in adult patients with KRAS G12C-mutated, advanced NSCLC. In the CodeBreaK 100 study, the results for ORR and DOR were considered clinically meaningful in the target population by the clinical experts consulted by CADTH. There was uncertainty around the magnitude of the clinical benefit, given the limitations in the evidence from the noncomparative phase I and II clinical trial. The nonrandomized design of the CodeBreaK 100 study made interpreting the PFS and OS events attributable to sotorasib challenging because it is unclear whether the observations were due to natural history or the effect of treatment with sotorasib. In the CodeBreaK 200 study, treatment with sotorasib demonstrated a beneficial impact on PFS and ORR compared to docetaxel. Although the difference in median PFS of approximately 1 month was modest, the clinical experts consulted by CADTH felt that the PFS rates for sotorasib at 12 months appeared encouraging and clinically meaningful. The clinical experts agreed that the impact of sotorasib on objective response was clinically meaningful. There was uncertainty around the treatment effect observed in the CodeBreaK 200 study because a larger proportion of patients in the docetaxel treatment group versus the sotorasib group withdrew from the trial before receiving treatment and because of unequal censoring between the sotorasib and docetaxel treatment groups. The CIs associated with the treatment effect of sotorasib relative to docetaxel on OS in the CodeBreaK 200 study were too wide to determine if either treatment was favoured. The results for HRQoL and symptom severity were descriptive in nature and remained inconclusive due to diminishing numbers of patients available to complete the assessments over time. The clinical experts consulted by CADTH noted that the TEAEs observed with sotorasib could be adequately managed in clinical practice and that sotorasib appeared to have a favourable toxicity profile compared to docetaxel.
Introduction
Disease Background
Lung cancer is 1 of the most diagnosed cancers, and NSCLC accounts for 80% to 88% of all lung cancer diagnoses in Canada.1,2 In 2020, the incidence of NSCLC in Canada was estimated to be 60.5 per 100,000 persons.3 In 2021, an estimated 29,600 new cases of lung cancer and 21,150 deaths due to lung cancer were projected.4 Survival from lung cancer across all stages and histologies is poor, with a 5-year net survival rate of 22%.5 NSCLC often remains asymptomatic until the disease is in its advanced stages.6,7 Because early diagnosis is challenging,9 approximately two-thirds of patient have advanced disease at diagnosis, when curative treatments are not possible.4,10 Indeed, 20% of patients are diagnosed with locally advanced disease (stage III), and 50% are diagnosed with metastatic disease. Median OS is poor in patients with metastatic NSCLC (stages IVA and IVB), ranging from 8 months to 11 months; 5-year OS ranges from 4% to 6%. The 5-year net survival rate for stage IV NSCLC is 5.2%.11 Among patients with metastatic disease, the most common sites of metastases are brain, liver, and bone. Among those patients with advanced NSCLC who are eligible for treatment, approximately 4% may die each week while waiting for therapy initiation.29
NSCLC is classified according to histologic subtypes, with the most common being adenocarcinoma and squamous cell carcinoma. Squamous cell cancer is a subtype of NSCLC that usually starts in the cells that line the bronchi in the centre of the lungs, whereas the adenocarcinoma subtypes typically start in the glandular cells on the outer part of the lung. In addition, NSCLC often holds an oncogenic driver mutation that leads to uncontrolled cell growth and proliferation. Gene mutations discovered in NSCLC include anaplastic lymphoma kinase, epidermal growth factor receptor, ROS proto-oncogene 1, and RAS.12 Mutations within the RAS family account for more than 30% of all mutated oncogenes in NSCLC, causing approximately 1 million deaths worldwide annually.13 Approximately 1 in 4 patients with NSCLC harbour KRAS mutations.14 KRAS is the isoform most frequently altered in NSCLC. It is most commonly found in patients who smoke or have formerly smoked, in Western populations (versus Asian populations), and in patients with nonsquamous histology. Patients with KRAS G12C-mutated NSCLC have a lower proportion of response to cytotoxic chemotherapy and decreased survival compared to the overall population of patients with NSCLC.15 The KRAS G12C subtype represents almost half of all KRAS mutations in NSCLC and is identified in approximately 13% of patients with nonsquamous NSCLC.16,17 Based on an estimation in the Health Canada Reviewers Report, the incidence of patients living in Canada with NSCLC harbouring the KRAS G12C mutation was approximately 7.9 per 100,000 persons.18 The KRAS G12C mutation does not usually occur in the presence of other known driver mutations in NSCLC.30
When patients with NSCLC present with symptoms, these are usually nonspecific and difficult to attribute to lung cancer.7 The most common symptoms include fatigue, cough, chest, or shoulder pain, hemoptysis, weight loss, dyspnea, hoarseness, bone pain, and fever.7 Advanced NSCLC is associated with a higher prevalence and intensity of symptoms such as pain, dyspnea, cough, decreased appetite, weight loss, and depression, as well as lower HRQoL compared to other advanced cancers.8 When lung cancer is suspected, diagnostic procedures include imaging with CT, PET, and/or MRI scans, bronchoscopy with or without endobronchial ultrasound bronchoscopy, and tissue biopsy.31 Pathologic testing of biomarkers on lung biopsy specimens assists in determining treatment options and risk stratification.
Standards of Therapy
According to the clinical experts consulted by CADTH for this review, the goals of treatment in the noncurative setting are preserving or improving quality of life and extending quantity of life.
The current treatment algorithm for locally advanced (not amenable to curative treatment) or metastatic NSCLC without a driver mutation is first-line immunotherapy with or without platinum-doublet chemotherapy. Based on input from the clinical experts consulted by CADTH for this review, immunotherapy-based regimens are superior to chemotherapy alone. The clinical experts agreed that chemotherapy by itself would be considered as a treatment option only for patients who are ineligible for immunotherapy; therefore, sequencing chemotherapy followed by an immunotherapy would be extremely rare. The clinical experts noted that for patients who have progressed on immunotherapy and a platinum-doublet chemotherapy, standard therapy options are docetaxel or BSC. However, docetaxel has low response rates and is quite toxic. The clinical experts highlighted that while KRAS G12C-mutated lung adenocarcinomas do benefit from immunotherapy, patients who progress on immunotherapy have limited treatment options and limited life expectancy.
The clinical experts anticipated that sotorasib will be used to replace docetaxel (i.e., clinicians would first exhaust platinum-based chemotherapy and immunotherapy options before moving on to sotorasib). The clinical experts noted that there is insufficient evidence at this time to inform alternative sequencing (e.g., immunotherapy in the first line, sotorasib in the second line, followed by platinum-based chemotherapy or docetaxel).
Drug
Sotorasib is a highly selective inhibitor of KRAS G12C that suppresses the rapid proliferation of cancer cells. Sotorasib forms an irreversible, covalent bond with the unique cysteine of KRAS G12C, locking the protein in an inactive state that prevents downstream signalling without affecting wild-type KRAS. Sotorasib blocks KRAS signalling, inhibits cell growth, promotes apoptosis, and is associated with antitumour inflammatory responses and immunity in KRAS G12C tumour models.
On September 10, 2021, sotorasib received an NOC/c from Health Canada for the treatment of adult patients with KRAS G12C-mutated, locally advanced (not amenable to curative therapy) or metastatic NSCLC who have received at least 1 prior systemic therapy. The Health Canada market authorization with conditions is pending the results of trials to verify sotorasib’s clinical benefit. Sotorasib underwent advance consideration under NOC/c, as well as Project Orbis, at Health Canada. The sponsor’s reimbursement request is aligned with the Health Canada indication. Health Canada recommends that sotorasib be administered at a dose of 960 mg (8 × 120 mg tablets) orally once daily until disease progression or unacceptable toxicity. A maximum of 2 dose reductions are permitted in the case of AEs.
The product monograph for sotorasib documents the following common side effects: diarrhea, musculoskeletal pain, nausea, fatigue, hepatotoxicity, and cough. The product monograph also contains warmings for serious side effects, including hepatotoxicity and interstitial lung disease/pneumonitis.
Submission History
At the time of the initial submission to CADTH in August 2022, data from the CodeBreaK 200 study were not available. In the absence of a head-to-head comparison of sotorasib and docetaxel, the sponsor submitted an indirect treatment comparison in the form of an unanchored MAIC, which was used to inform the pharmacoeconomic model. The unanchored MAIC estimated the comparative OS and PFS between sotorasib and docetaxel in patients with locally advanced or metastatic NSCLC (stages IIB to IV) and confirmed KRAS mutation in the absence of direct comparative evidence from a randomized trial. The MAIC was based on individual patient data from the single-group, open-label index trial, the CodeBreaK 100 study, and aggregate-level data from the docetaxel 75 mg/m2 plus placebo group of the double-blind, randomized SELECT-1 trial.26 In November 2022, this submission was temporarily suspended because the sponsor informed CADTH that the economic evaluation would be revised to include data from the CodeBreaK 200 study. In May 2023, the temporary suspension was lifted upon receipt of the revised economic model from the sponsor. After receiving data from the CodeBreaK 200 study, which provided direct evidence comparing sotorasib and docetaxel, the CADTH review team determined that the MAIC no longer addressed any gap in the evidence, given that the CodeBreaK 200 study was a phase III, head-to-head, randomized controlled trial (RCT) comparing the efficacy and safety of sotorasib and docetaxel. Therefore, the MAIC was not included in the clinical report.
Stakeholder Perspectives
Patient Group Input
This section was prepared by CADTH staff based on the input provided by patient groups. The full original patient input received by CADTH is included in the stakeholder section at the end of this report.
The LHF (formerly the Ontario Lung Association), LCC, and the CCSN submitted joint input. The LHF is a registered charity that provides programs and services to patients and health care providers, invests in lung research, and advocates for improved policies in lung health. LCC, a member of the Global Lung Cancer Coalition, is a registered national charitable organization that serves as a resource for education, patient support, research, and advocacy, focusing exclusively on lung cancer. The CCSN is a national network of patients, families, friends, community partners, and sponsors who promote the best standard of care, patient support, survivorship, and quality of end-of-life care. A total of 5 people (4 patients and 1 caregiver) responded to a telephone survey interview from August to September 2022. Of the 4 patients with lung cancer, 3 had experience with sotorasib; 1 patient with KRAS G12C-positive lung cancer did not. All respondents were female. All but 1 were from Canada (Nova Scotia, British Columbia, Quebec, and Ontario); the remaining respondent was from the US.
From the submitted input, 1 patient said they felt “rock bottom” when their lung cancer progressed on chemotherapy and radiation, leading them to be on oxygen, to acquire a debilitating cough as well as shortness of breath from eating or talking, and to require assistance to shower. Another patient detailed the mental and emotional side effects associated with multiple courses of immunotherapy and chemotherapy, such as depression, anxiety, panic attacks, and severe mood swings, which remained debilitating even while in remission. The sole caregiver interviewed stated that it is mentally, physically, and financially challenging to take care of a patient with lung cancer with comorbidities (e.g., preparing meals, making arrangements for transportation to medical appointments, managing daily responsibilities) and that they feel burned out without many sources of support.
Three patients who had experience with sotorasib reported significant tumour reduction (i.e., ranging from a 50% to 65% reduction to no evidence of disease within 5 weeks to 1.5 years). They said they experienced mild side effects while on sotorasib, such as fatigue, aches, and pains when walking for extended periods of time, a small or minor rash, diarrhea, shortness of breath, and increased liver enzymes. However, they said these side effects did not have much impact on their daily activities or quality of life. According to the input, these patients felt hopeful again that they could plan for the future.
In terms of important key outcomes, 1 patient said they were most interested in obtaining a cure while maintaining a good quality of life. Respondents also expressed their hope for a treatment option with an oral route of administration that would be accessible from home, delay the onset of symptoms, prolong their life, and improve functionality and mobility, with fewer side effects. The caregiver expressed the importance of treatment that can be accessed from home, limiting the need to travel to infusion clinics. Lastly, it was pointed out in the survey that wait times for lung surgeries across Canada are unacceptable; patients and caregivers would like to treat the lung cancer in the early stages. The caregiver surveyed said that the wait time for the surgery was the most difficult aspect (or the most challenging adverse effect) of current treatment.
Clinician Input
Input From Clinical Experts Consulted by CADTH
All CADTH review teams include at least 1 clinical specialist with expertise regarding the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol; assisting in the critical appraisal of clinical evidence; interpreting the clinical relevance of the results; and providing guidance on the potential place in therapy). The following input was provided by 2 clinical specialists with expertise in the diagnosis and management of NSCLC.
Unmet Needs
According to the clinical experts, treatment options for patients with KRAS G12C-mutated NSCLC who have progressed on standard therapy are limited. The clinical experts noted that KRAS was once believed to be undruggable. A new class of drugs, including sotorasib, has provided targeted options for patients with KRAS G12C-mutated NSCLC. However, given that no publicly funded, targeted drugs are currently accessible, therapy options are limited to docetaxel, which is associated with high levels of toxicity. Therefore, there is an unmet need for an efficacious treatment associated with fewer AEs. The clinical experts were careful to note that lung cancer is a stigmatized disease due to its association with smoking. The availability of a targeted treatment in a population of patients who smoke or have smoked is unprecedented. The clinical experts also expressed a need for a targeted therapy that can be administered orally versus an IV drug that requires patients to travel to cancer centres. Finally, in this patient population with high rates of intracranial metastases, 1 clinical expert expressed the need for a treatment that would also be able to treat brain metastases.
Place in Therapy
According to the clinical experts consulted for this review, sotorasib would change the sequence of therapies for patients with KRAS G12C-mutated NSCLC. The clinical experts expect that sotorasib would be used following immunotherapy and platinum-doublet chemotherapy. The clinical experts noted that sotorasib is anticipated to displace docetaxel, but not platinum-based chemotherapy (i.e., clinicians would exhaust platinum-based chemotherapy and immunotherapy options before moving on to sotorasib). Accordingly, docetaxel would move to being a third- or fourth-line therapy. Based on feedback from the clinical experts consulted by CADTH for this review, there is insufficient evidence at this time to inform alternative sequencing (e.g., immunotherapy in first-line therapy and sotorasib in second-line therapy, followed by platinum-based chemotherapy or docetaxel), given that patients enrolled in the CodeBreaK 200 study were required to have progressed on a PD-1 or PD-L1 inhibitor and platinum-based chemotherapy; accordingly, there is no phase III evidence to support the use of sotorasib as second-line treatment after first-line, single-drug PD-1 or PD-L1 inhibitors. The clinical experts noted that sotorasib would not be combined with other drugs at this time.
Patient Population
Patients with KRAS G12C-mutated NSCLC are identified through NGS. According to the clinical experts, NGS is standard of care for adenocarcinomas of the lung, and any patient with nonsquamous histology has reflexive molecular testing performed to evaluate for any mutations.
The clinical experts suggested that sotorasib be limited to patients with KRAS G12C-mutated NSCLC. They stated that sotorasib should not be extended to other KRAS G12C-mutated NSCLC because the biology of the G12C mutation is distinct from those of other KRAS subtypes. Moreover, treatment with sotorasib is not suitable for patients with an ECOG PS of 3 or 4, with severe organ dysfunction, or with untreated, symptomatic brain metastasis. The clinical experts did note that patients with untreated, asymptomatic brain lesions may be suitable for treatment with sotorasib; ideally, these patients should have their cases discussed at a multidisciplinary tumour board round at a centre with expertise in stereotactic radiosurgery.
Assessing Response to Treatment
Based on input from the clinical experts, patients should undergo clinical and toxicity assessments per cycle (typically every 3 weeks to 4 weeks) and imaging approximately every 3 months to assess their response to treatment in clinical practice. Based on input from the clinical experts, improved PFS, improved OS, and maintenance or improvement in quality of life are considered meaningful responses to treatment in this population.
Discontinuing Treatment
Based on input from the clinical experts, treatment with sotorasib should be discontinued under the following 3 scenarios: patient decision to stop treatment with sotorasib; unacceptable toxicity due to sotorasib; and disease progression without clinical benefits. The clinical experts agreed that patients with documented disease progression could continue sotorasib if they were deriving clinical benefit.
Prescribing Conditions
The clinical experts suggested that sotorasib be prescribed by a medical oncologist in an outpatient oncology clinical setting.
Clinician Group Input
This section was prepared by CADTH staff based on the input provided by clinician groups. The full original clinician group input received by CADTH has been included in the stakeholder section at the end of this report.
Input was received from 2 clinician groups: the OH-CCO LC DAC and LCC. The OH-CCO LC DAC provides clinical and health system guidance on drug-related issues in support of CCO’s mandate, including the provincial drug reimbursement programs and the systemic treatment program. Input from the OH-CCO was provided by 3 clinicians who had joint discussions through email. LCC is a national charity that increases awareness on lung cancer, advocates for and educates patients with lung cancer and their families, and supports research on and access to the best care for lung cancer. Input from LCC was compiled by 26 clinicians and was based on a review of the literature and proceedings from recent conferences.
Both clinician groups identified the following goals of therapy: reducing tumour burden; improving symptoms; and prolonging life while upholding patients’ values and desires. Both clinician groups also noted that all patients eventually progress on currently available treatment; thus, durability of response is an important treatment goal. In addition, LCC added the need for treatment that is associated with reduced toxicity and resource utilization. Indeed, OH-CCO LC DAC endorsed the advent of an oral anticancer treatment without the side effects and life impacts associated with chemotherapy to slow disease progress and ideally improve length and quality of life. According to input from the OH-CCO LC DAC, sotorasib would be placed as second- or third-line monotherapy for patients who have progressed on or are unable to tolerate platinum-based chemotherapy and immunotherapy (where appropriate) and possibly docetaxel. The OH-CCO LC DAC clinician group stated that sotorasib would not affect the use of immunotherapy or platinum-doublet chemotherapy; however, sotorasib may be preferred to docetaxel if it can demonstrate a meaningful improvement in survival or quality of life, given that docetaxel has a proven survival benefit compared to BSC and other chemotherapy regimens (ifosfamide), albeit with an unfavourable side effect profile. Input from LCC places sotorasib as second-line standard of care for patients with advanced KRAS G12C-mutated NSCLC and suggests that sotorasib be used as a single drug after at least 1 line of prior systemic treatment has failed. Based on input from both clinician groups, patients with a KRAS G12C-mutated, advanced NSCLC (stage IV or recurrent) who received prior therapy would be best suited for sotorasib. The LCC added that it is uncertain whether patients with an ECOG PS of 3 or 4 would benefit from treatment with sotorasib. Both clinician groups noted that patients eligible for treatment with sotorasib should be identified by a validated molecular diagnostic test, preferably NGS. Both clinician groups noted that improvement in symptoms, stable disease, tumour shrinkage, radiographic reduction of disease site from baseline, and prolonged survival are indicative of a clinically meaningful response to treatment. The OH-CCO LC DAC added that the definition of a clinically meaningful improvement in frequency or severity of symptoms varies from 1 patient to another and across physicians. Based on input from LCC, response to treatment should be determined by the treating physician based on CT imaging and assessed every 2 months to 3 months, as is done in Canada when using other oral tyrosine kinase inhibitors. Based on input from the clinician groups, discontinuing treatment with sotorasib should be considered in the event of loss of clinical benefit (as indicated by unequivocal disease progression, including symptoms, polyprogression, and so on) or intolerable side effects. The LCC noted that treatment with sotorasib may continue in patients with oligoprogression who are amenable to local therapy (radiation or surgery); who are newly diagnosed or have experienced progression of brain metastases and have been treated with brain radiation or surgery; and who have asymptomatic disease (without overt progression on imaging associated with increased symptom burden). The OH-CCO LC DAC emphasized that a combination of clinical judgment, radiological interpretation, and clinically standardized scales, such as the Edmonton Symptom Assessment System, should be used to determine if a patient is benefiting from therapy. The OH-CCO-LC also noted that RECIST 1.1 and its derivatives are designed for clinical trials, not clinical practice, and should not be used to determine discontinuation of treatment. Both clinician groups agreed that outpatient clinics would be an appropriate treatment setting for sotorasib in addition to the hospital setting. Both groups stated that a medical oncologist, general practitioner in oncology under medical oncology supervision, or respirologist experienced in treating patients with lung cancers should be involved in diagnosing, treating, and monitoring patients on sotorasib.
Drug Program Input
The drug programs provide input on each drug being reviewed through CADTH’s reimbursement review processes by identifying issues that may affect their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CADTH are summarized in Table 3.
Table 3: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Considerations for prescribing of therapy | |
Sotorasib comes available in a bottle containing either 120 or 240 tablets or as blister cards containing 8 tablets in a carton containing 30 blister cards, for a total of 240 tablets. | Comment from the drug programs to inform pERC deliberations |
Recommended dosing, frequency, and dose intensity are as follows: 960 mg (8 × 120 mg tablet) orally once daily until disease progression or unacceptable toxicity. | Comment from the drug programs to inform pERC deliberations |
Sotorasib tablets are to be swallowed whole and taken with or without food. The tablets may not be chewed, crushed, or split. In cases where swallowing is difficult, tablets may be dispersed in 120 mL of noncarbonated, room temperature water without crushing. No other liquids may be used. Dispersed tablets must be consumed immediately. The container dispensing the dispersed tablets must be rinsed with an additional 120 mL water and drank immediately. If the mixture cannot be consumed immediately, stir the mixture again and consume within 2 hours of preparation. | Comment from the drug programs to inform pERC deliberations |
Avoid the coadministration of sotorasib with PPIs and H2 receptor antagonists. If needed, take sotorasib 4 hours before or 10 hours after the administration of a local antacid. | Comment from the drug programs to inform pERC deliberations |
Avoid the coadministration of sotorasib with strong CYP3A4 inducers because these may reduce the efficacy of sotorasib. | Comment from the drug programs to inform pERC deliberations |
Sotorasib is a moderate CYP3A4 inducer. If needed, increase CYP3A4 substrate dosage. | Comment from the drug programs to inform pERC deliberations |
Avoid the coadministration of sotorasib with P-gp substrates. If needed, decrease P-gp substrate dosage. | Comment from the drug programs to inform pERC deliberations |
Care provision | |
Sotorasib should be stored at 15°C to 30°C. | Comment from the drug programs to inform pERC deliberations |
Oral medications are funded through variable mechanisms across Canada, which may complicate access. | Comment from the drug programs to inform pERC deliberations |
The sponsor assumes that KRAS testing is already incorporated in the Canadian health care system. However, currently, KRAS testing is not performed routinely in all jurisdictions. | Comment from the drug programs to inform pERC deliberations |
Serious adverse events have been documented as occurring in 51% of patients (8% pneumonia, 5% musculoskeletal pain, 3% hepatotoxicity, 2% diarrhea). It is recommended that AST, ALT, and total bilirubin be monitored for hepatotoxicity, and the dose adjusted as needed. Grade 3 and 4 ILD/pneumonitis has been documented in 0.8% of patients; accordingly, patients should be monitored for dyspnea, cough, and fever. Where ILD/pneumonitis is suspected, treatment with sotorasib should be withheld. | Comment from the drug programs to inform pERC deliberations |
System and economic issues | |
Docetaxel is available as a generic. Accordingly, confidential pricing is likely in place. | Comment from the drug programs to inform pERC deliberations |
ALT = alanine aminotransferase; AST = aspartate aminotransferase; CYP3A4 = cytochrome P450 3A4 enzyme; ILD = interstitial lung disease; pERC = CADTH pan-Canadian Oncology Drug Review Expert Review Committee; P-gp = permeability glycoprotein; PPI = proton pump inhibitor.
Clinical Evidence
The clinical evidence included in the review of sotorasib is presented in 3 sections. The first section, the Systematic Review, includes pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those studies that were selected according to an a priori protocol. The second section would normally include indirect evidence from the sponsor and indirect evidence selected from the literature that met the selection criteria specified in the review; however, for this review, no relevant indirect evidence was identified. The third section includes an additional relevant study that was considered to address an important gap in the evidence included in the systematic review.
Systematic Review (Pivotal and Protocol-Selected Studies)
Objective
To perform a systematic review of the beneficial and harmful effects of sotorasib 960 mg (8 × 120 mg oral tablets) for the treatment of KRAS G12C-mutated, locally advanced (not amenable to curative therapy) or metastatic NSCLC in adult patients who have received at least 1 prior systemic therapy.
Methods
Studies selected for inclusion in the systematic review included pivotal studies provided in the sponsor’s submission to CADTH and Health Canada as well as those meeting the selection criteria presented in Table 4. Outcomes included in the CADTH review protocol reflect those considered important to patients, clinicians, and drug plans.
Table 4: Inclusion Criteria for the Systematic Review
Criteria | Description |
|---|---|
Population | Adult patients with KRAS G12C-mutated, locally advanced (not amenable to curative therapy) or metastatic NSCLC who have received at least 1 prior systemic therapy Subgroups:
|
Intervention | Sotorasib, 960 mg (8 × 120 mg oral tablets) once daily |
Comparator |
|
Outcomes | Efficacy outcomes:
Harms outcomes: AEs, SAEs, WDAEs, mortality, and notable harms or harms of special interest, including hepatotoxicity, renal toxicity, interstitial lung disease, pneumonitis, and GI toxicity |
Study designs | Published and unpublished phase III and IV RCTs |
AE = adverse event; DOR = duration of response; ECOG = Eastern Cooperative Oncology Group; GI = gastrointestinal; HRQoL = health-related quality of life; NSCLC = non–small cell lung cancer; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; RCT = randomized controlled trial; SAE = serious adverse event; WDAE = withdrawal due to adverse event.
The literature search for clinical studies was performed by an information specialist using a peer-reviewed search strategy according to the PRESS Peer Review of Electronic Search Strategies checklist.32
Published literature was identified by searching the following bibliographic databases: MEDLINE through Ovid and Embase through Ovid. All Ovid searches were run simultaneously as a multifile search. Duplicates were removed using Ovid deduplication for multifile searches followed by manual deduplication in Endnote. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. Search concepts were developed based on the elements of the Patients, Interventions, Comparisons, and Outcomes (PICO) framework and research questions. The main search concept was Lumakras or sotorasib. The following clinical trial registries were searched: the US National Institutes of Health’s clinicaltrials.gov, the WHO International Clinical Trials Registry Platform search portal, Health Canada’s Clinical Trials Database, and the European Union Clinical Trials Register.
No filters were applied to limit the retrieval by study type. Retrieval was not limited by publication date or by language. Conference abstracts were excluded from the search results. Refer to Appendix 1 for the detailed search strategies.
The initial search was completed on September 19, 2022. Regular alerts updated the search until the meeting of the CADTH pan-Canadian Oncology Drug Review Expert Committee on September 12 and 13, 2023.
Grey literature (literature that is not commercially published) was identified by searching relevant websites from CADTH’s Grey Matters: A Practical Tool For Searching Health-Related Grey Literature checklist.33 Included in this search were the websites of regulatory agencies (i.e., the FDA and European Medicines Agency). Google was used to search for additional internet-based materials. Refer to Appendix 1 for more information on the grey literature search strategy.
These searches were supplemented through contacts with appropriate experts. In addition, the sponsor was contacted for information regarding unpublished studies.
Two CADTH clinical reviewers independently selected studies for inclusion in the review based on titles and abstracts, according to the predetermined protocol. Full-text articles of all citations considered potentially relevant by at least 1 reviewer were acquired. Reviewers independently made the final selection of studies to be included in the review, and differences were resolved through discussion.
Findings From the Literature
A total of 2 studies were identified from the literature for inclusion in the systematic review (Figure 1). The included studies are summarized in Table 5. A list of excluded studies is presented in Appendix 2.
Table 5: Details of Included Studies
Category | CodeBreaK 100 study, phase II | CodeBreaK 200 study |
|---|---|---|
Designs and populations | ||
Study design | Multicentre, nonrandomized, single-group, open-label, phase I and II study | Multicentre, parallel-group, open-label, phase III RCT |
Locations | 59 sites across 11 countries: US, Canada, France, Belgium, Germany, Switzerland, Austria, Japan, South Korea, Australia, and Brazil | 148 sites across 22 countries in Europe, North America, Asia, Australia, and South America |
Patient enrolment dates | FPE: August 13, 2019 LPE: February 5, 2020 | FPE: June 4, 2020 LPE: April 26, 2021 |
Enrolled or randomized (N) | 224 patients enrolled:
| 345 patients randomized:
|
Inclusion criteria |
NSCLC-specific: For combination of sotorasib with pembrolizumab, all patients with NSCLC must be KRAS G12-mutated and have ≥ 1% TPS for PD-L1. Prior therapy with anti-PD-1 or anti-PD-L1 therapy was not required. |
|
Exclusion criteria |
|
|
Drugs | ||
Intervention | Sotorasib, 960 mg, orally once daily | Sotorasib, 960 mg, orally once daily |
Comparator(s) | None | Docetaxel, IV 75 mg/m2 every 3 weeks |
Duration | ||
Screening | 28 days | Up to 28 days |
Study | 3 years | Until discontinuation of IP followed by short-term, 30-day follow-up after last dose |
Follow-up | 12 weeks | Up to 5 years |
Outcomes | ||
Primary end point | Objective response (CR plus PR) | PFS |
Secondary and exploratory end points | Secondary:
Exploratory:
| Key Secondary:
Secondary:
Exploratory:
|
Data cut-off dates | ||
Primary analysis | September 1, 2020 | August 2, 2022 |
Interim analysis | December 1, 2020 | NR |
Updated analysis (1) | March 15, 2021 | NR |
Updated analysis (2) | September 9, 2022 | NR |
Notes | ||
Publicationsa | Skoulidis et al.34 | De Langen et al.35 |
AE = adverse event; ALK = anaplastic lymphoma kinase; ALT = alanine aminotransferase; ANC = absolute neutrophil count; AST = aspartate aminotransferase; AUC = area under the curve; BPI-SF = Brief Pain Inventory – Short Form; CHF = congestive heart failure; Cmax = maximum plasma concentration; CNS = central nervous system; CR = complete response; CRC = colorectal cancer; DCR = disease control rate; DOR = duration of response; ECOG PS = Eastern Cooperative Oncology Group Performance Status; EGFR = epidermal growth factor receptor; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; EORTC QLQ-LC13 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Lung Cancer Module; EQ VAS = EQ visual analogue scale; FACT-G = Functional Assessment of Cancer Therapy – General; FPE = first patient enrolled; GI = gastrointestinal; HRQoL = health-related quality of life; INR = international normalized ratio; IP = investigational product; LPE = last patient enrolled; MI = myocardial infarction; MDRD = Modification of Diet in Renal Disease; NR = not reported; NSCLC = non–small cell lung cancer; NSCLC-SAQ = Non–Small Cell Lung Cancer Symptom Assessment Questionnaire; OS = overall survival; PD-1 = programmed cell death 1; PD-L1 = programmed cell death 1 ligand 1; PFS = progression-free survival; PFS 2 = progression-free survival on next line of treatment; PGIC = patient global impression of change; PGIS = patient global impression of severity; PK = pharmacokinetic; PR = partial response; PRO-CTCAE = patient-reported outcome version of the Common Terminology Criteria for Adverse Events; PTT = partial thromboplastin time; QTc = correct heart rate interval; RCT = randomized controlled trial; RECIST 1.1 = Response Evaluation Criteria in Solid Tumours Version 1.1; ROS1 = ROS proto-oncogene 1 receptor tyrosine kinase; TPS = Tumour Proportion Score; TTR = time to response; ULN = upper limit of normal.
aThree additional reports were included: the Clinical Study Report for phase II of the CodeBreaK 100 study;20 Clinical Study Report for the CodeBreaK 200 study,21,36 and Health Canada Reviewers Report.18
Only inclusion and exclusion criteria applied to the indication population are reported. The list of exclusion criteria for the CodeBreaK 200 study represents key criteria and is not exhaustive.
Sources: Clinical Study Report for phase II of the CodeBreaK 100 study;20 Clinical Study Report for the CodeBreaK 200 study.21
Description of Studies
Two sponsor-conducted studies were included in this systematic review: the CodeBreaK 100 study and the CodeBreaK 200 study.
CodeBreaK 100 Study
The CodeBreaK 100 study was the pivotal study submitted by the sponsor. It is an ongoing, phase I and II multicentre, nonrandomized, open-label, single-group study.19,20 Phase I was a first-in-human dose exploration (part 1) and dose expansion (part 2) study aimed at evaluating the safety, tolerability, PKs, and pharmacodynamics of sotorasib in adult patients with KRAS G12C-mutated advanced NSCLC, colorectal cancer, and other solid tumours.19 Phase II was designed to evaluate the efficacy and safety of sotorasib as monotherapy in adult patients with KRAS G12C-mutated advanced NSCLC, colorectal cancer, and other solid tumours.20 A schematic of the CodeBreaK 100 study design is illustrated in Figure 2. CADTH’s review of the CodeBreaK 100 study focuses on the phase II efficacy and safety results in adult patients with KRAS G12C-mutated, advanced NSCLC.
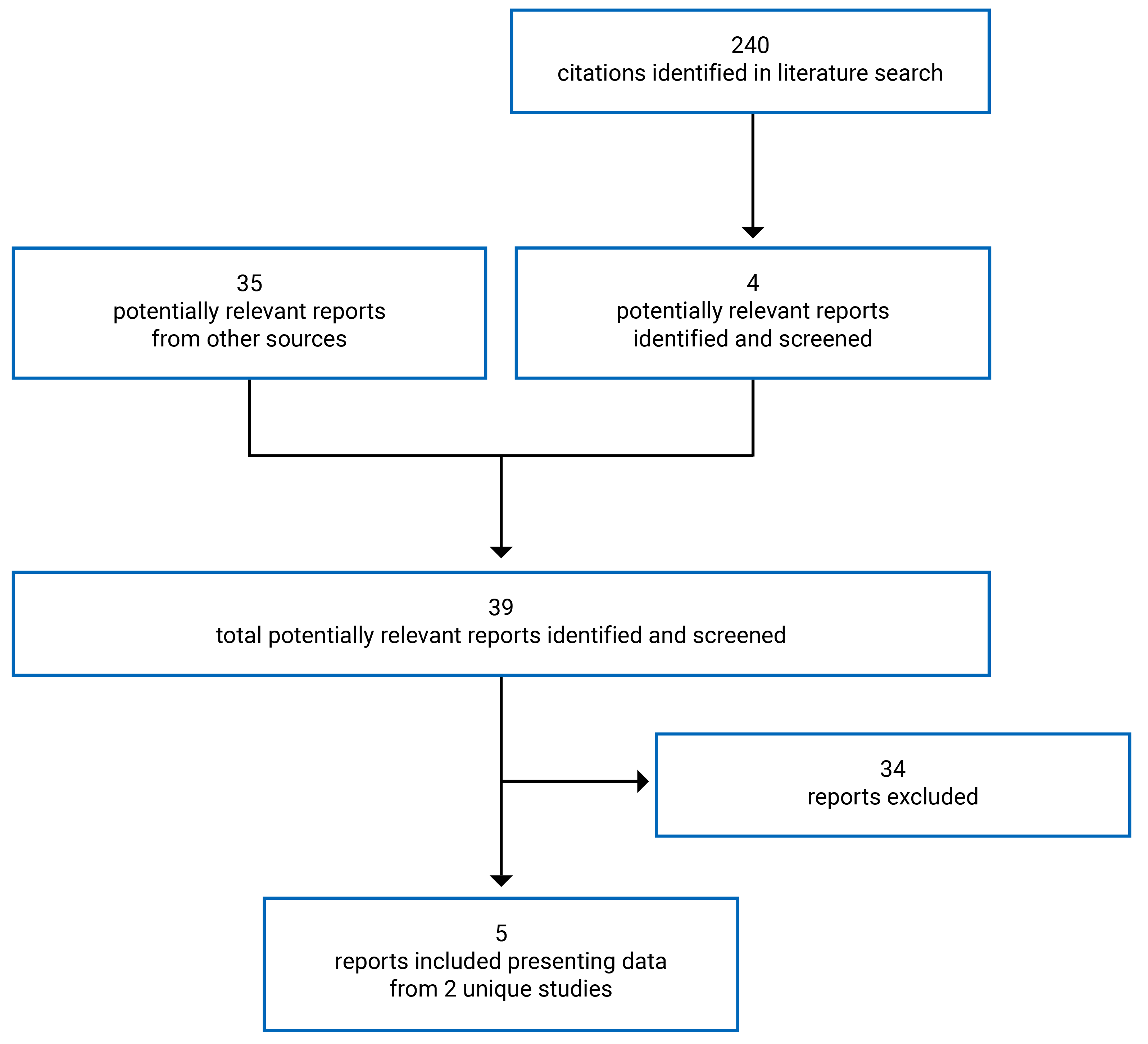
A total of 224 patients with KRAS G12C-mutated, advanced solid tumours were enrolled at 59 sites across 11 countries, including 8 patients (3.6%) across 2 sites in Canada. At enrolment, each patient received a unique study identification number, which was provided on all study documentation and used to identify the patient throughout the clinical study. The study identification number was assigned by an interactive response technology. Of the patients enrolled, 126 patients (56.3%) had NSCLC. Sotorasib was dispensed at the study centre by a qualified staff member. On study visit days, patients were required to take sotorasib at the study centre. At all other times, patients self-administered sotorasib at home. Patients self-administered sotorasib 960 mg (8 × 120 mg tablets) orally once daily and continued treatment without interruption until disease progression, treatment intolerance, withdrawal of consent, or death. Tumour response was assessed using contrast-enhanced CT or MRI and per RECIST 1.1 through BICR using an independent radiological central laboratory. Patients underwent safety follow-up visits 30 days (± 7 days) after the last dose of sotorasib or before any new anticancer treatment was started. Following safety follow-up visits, patients were followed long-term for health condition, disease status, and subsequent anticancer treatment every 12 weeks ( ± 2 weeks) for up to 3 years after the last patient was enrolled or until withdrawal of consent, loss to follow-up, or patient death, whichever occurred first. The study team was blinded to the efficacy data.
The primary efficacy end point for phase II of the CodeBreaK 100 study was ORR, which was a composite of CR and PR. Secondary efficacy end points included DOR, DCR, TTR, PFS, and OS. Exploratory outcomes included changes in cancer-specific symptoms and patient-reported HRQoL.
An independent data review team conducted interim safety reviews after 30, 50, 70, and 100 patients had been enrolled and treated with sotorasib for at least 21 days. The data cut-off date for the primary analysis was determined on the assumption that most responders would experience a response in the first 1.5 months to 3 months from the start of treatment. The data cut-off date for phase II was September 1, 2020. Interim and updated analyses were conducted on December 1, 2020, and March 15, 2021, respectively. The results of the primary and updated analysis of March 15, 2021, are presented in this review because the results from the December 1, 2020, analysis were consistent with both the primary and updated analyses. The updated data cut-off date for OS at 2 years was September 9, 2022, and is also presented.
Figure 2: Schematic of CodeBreaK 100 Study
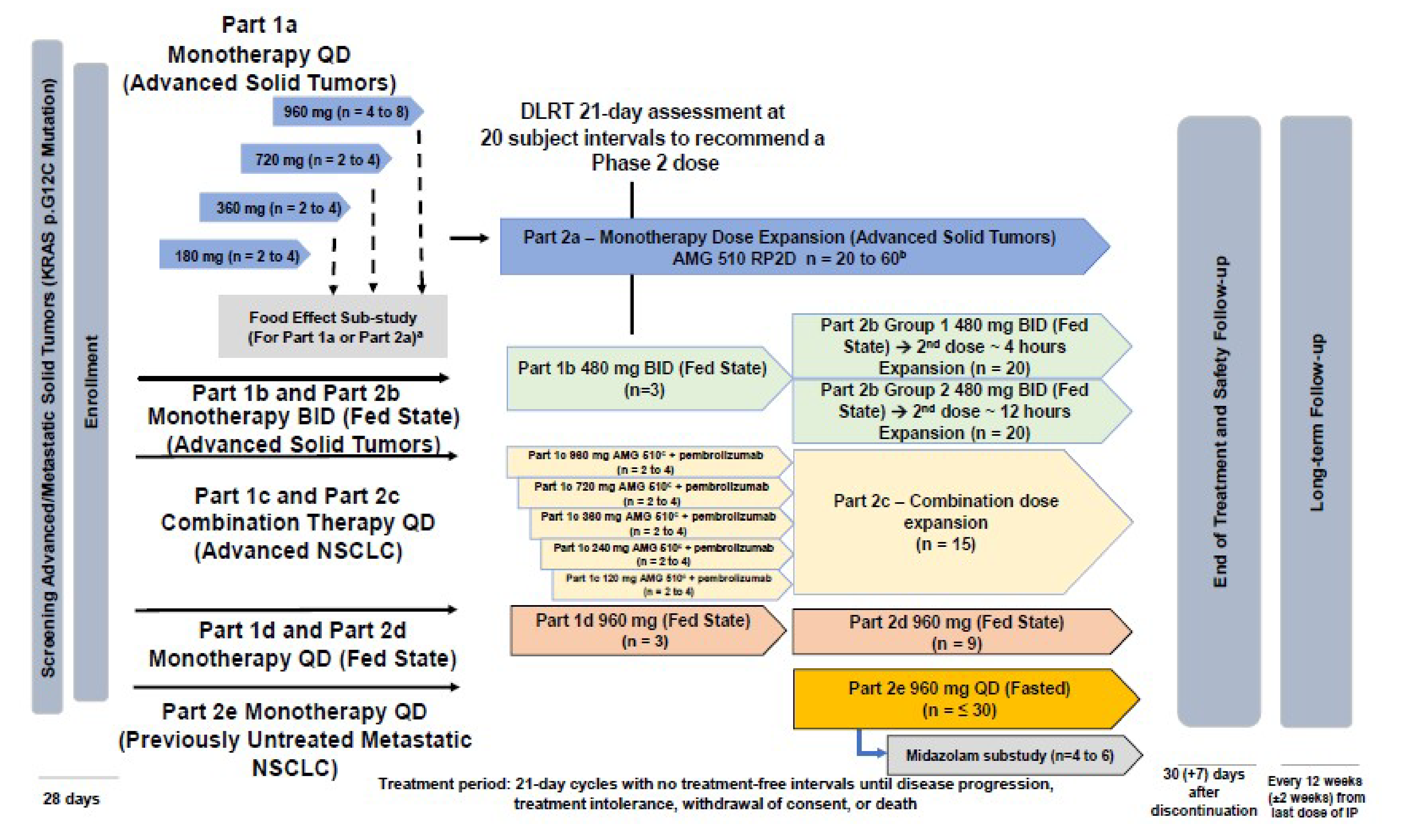
AMG 510 = sotorasib; BID = twice daily; DLRT = dose level review team; IP = investigational product; NSCLC = non–small cell lung cancer; QD = once daily; RP2D = recommended phase II dose.
Note: The DLRT was responsible for reviewing data in the dose expansion phase to confirm the RP2D and determine the benefit to risk ratio of proceeding to phase II of the study, according to the futility and efficacy thresholds described in the statistical analysis section.
Source: Clinical Study Report for phase II of the CodeBreaK 100 study.20
CodeBreaK 200 Study
The CodeBreaK 200 study is an ongoing, multicentre, randomized, open-label, parallel-group, phase III study evaluating the efficacy and safety of oral sotorasib versus IV docetaxel in adult patients with KRAS G12C-mutated NSCLC who progressed after prior platinum-based chemotherapy and a checkpoint inhibitor.21 A schematic of the CodeBreaK 200 study design is illustrated in Figure 3.
Figure 3: Schematic of CodeBreaK 200 Study
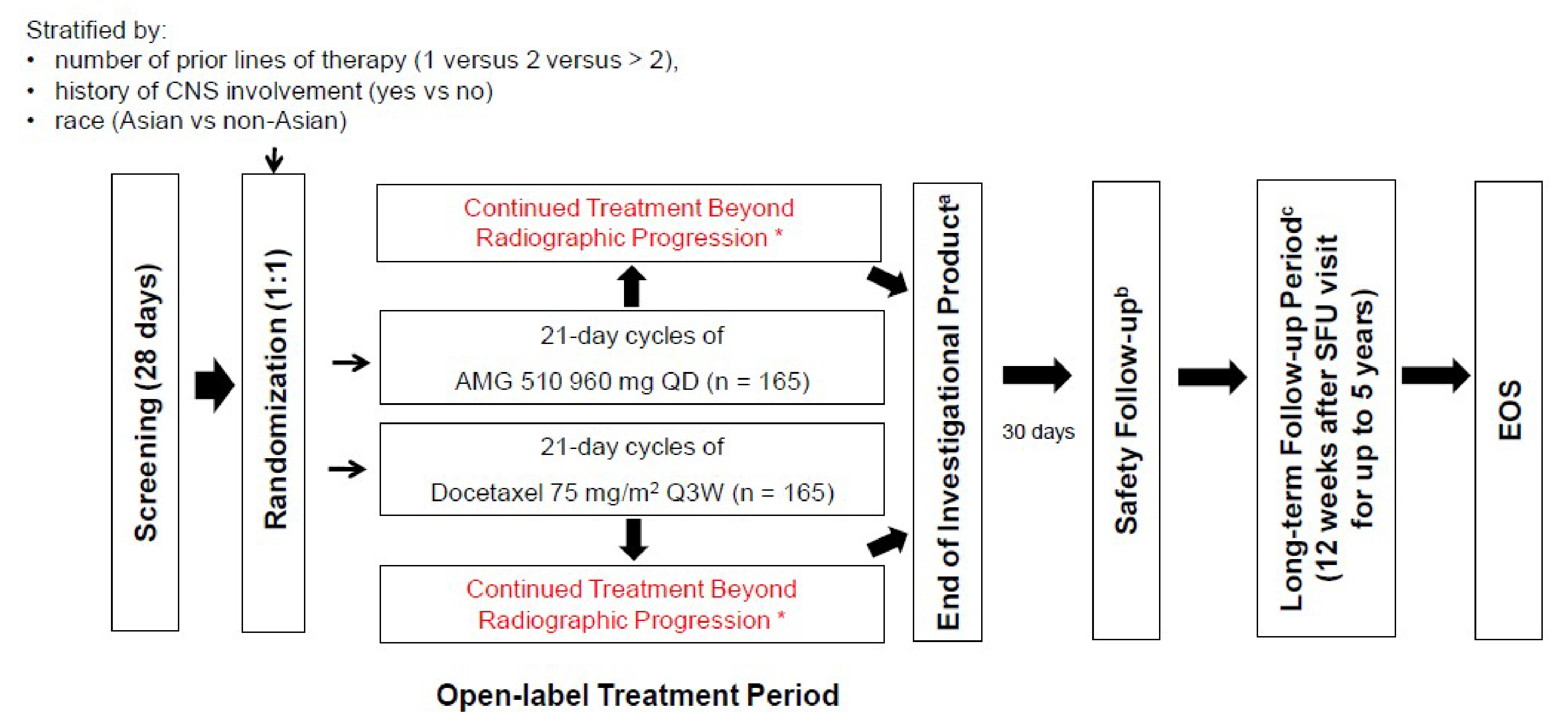
AMG 510 = sotorasib; CNS = central nervous system; EOS = end of study; Q3W = every 3 weeks; QD = once daily; vs. = versus.
a Treatment with investigational product continued until independent central confirmation of progression, intolerance of treatment, initiation of another anticancer
therapy, withdrawal of consent, or death. Patients who consented to treatment beyond progression or consented to cross over from docetaxel to sotorasib continued to
receive the investigational product after independent central confirmation of progression at the time of first progressive disease.
b Upon permanent discontinuation from the study treatment for any reason, a safety follow-up visit was performed 30 days (± 7 days) after the end of the last dosing
interval of the investigational product.
Source: Clinical Study Report for the CodeBreaK 200 study.21
A total of 345 patients with KRAS G12C-mutated, advanced solid tumours were enrolled at 148 sites across 22 countries, including 4 patients (1.16%) at 3 sites in Canada. Patients were randomized 1:1 to receive oral sotorasib 960 mg once daily (n = 171) or IV docetaxel 75 mg/m2 every 3 weeks (n = 174). Randomization was stratified by number of prior lines of therapy in advanced disease (1 versus 2 versus > 2), race (Asian versus non-Asian), and history of CNS involvement (present or absent). Each of the following were considered as 1 line of prior therapy: chemoradiation for locally advanced and unresectable disease, if progression occurred within 6 months of end of treatment; chemoradiation followed by planned systematic therapy, including checkpoint inhibitor, or vice versa without documented intervening progression, if progression occurred within 6 months of end of treatment; adjuvant therapy, if progression occurred within 6 months of end of treatment; and each new systematic anticancer regimen for progressive locally advanced and unresectable or metastatic disease. Maintenance therapy and chemotherapy regimen adjustments for intolerability were not considered new lines of therapy. At enrolment, each patient received a unique study identification number that was provided on all study documentation and used to identify the patient throughout the clinical study. The study identification number was assigned by an interactive response technology. The first day a patient received study medication was noted as cycle 1, day 1. Each treatment cycle was 21 (± 3) days. Patients continued treatment without interruption until disease progression, treatment intolerance, withdrawal of consent, or death. Tumour response was assessed using contrast-enhanced CT or MRI and per RECIST 1.1 using an independent radiological central laboratory. Patients randomized to the docetaxel treatment group who experienced radiologic disease progression according to RECIST 1.1 were given the opportunity to cross over into the sotorasib treatment group. Patients randomized to the sotorasib treatment group could continue study treatment following radiologic progression if they continued to demonstrate clinical benefit. Patients who consented to treatment beyond progression or to cross over from docetaxel to sotorasib continued to receive the investigational product after independent central confirmation of progression at the time of first progressive disease. Patients who discontinued treatment before RECIST 1.1 disease progression were followed with tumour assessment until independent central confirmation of progression, withdrawal of consent, or start of another anticancer therapy, then followed for subsequent anticancer therapy and survival.
The primary end point for the CodeBreaK 200 study was PFS as assessed by BICR per RECIST 1.1. Key secondary end points included OS, ORR, and cancer-specific HRQoL measures, while secondary outcomes included DCR, disease- and treatment-related symptoms, and other patient-reported HRQoL measures.
There were 2 planned PFS efficacy analyses. These were conducted when approximately 160 (interim) and 230 (primary) PFS events occurred. An interim analysis of OS was planned for superiority of sotorasib over docetaxel, either at the time when PFS achieved statistical significance or after 175 OS events were observed, whichever occurred later. The primary OS analysis was to occur when at least 198 OS events had been observed. The primary analysis of ORR was to be performed when PFS was claimed to be statistically significant and the last randomized patient had had the opportunity to have at least 12 weeks of follow-up. Patients will be followed for 5 years after the last patient is enrolled, or until withdrawal of consent, loss to follow-up, or death, whichever occurs first. The data cut-off date for the CodeBreaK 200 study was August 2, 2022, at which point the results from the planned primary analysis of PFS were analyzed.
Protocol Amendments
The protocol for the CodeBreaK 100 study was amended 6 times. The phase II portion of the CodeBreaK 100 study was added with amendment 2. The protocol-defined statistical analyses were amended twice. In amendment 3 (May 22, 2019), the sample size was adjusted based on a new benchmark rate (i.e., 23%) to exclude from the lower limit of the 95% CI for observed ORR; and the futility interim analysis was updated to allow for continuous monitoring using the Bayesian predictive probability method. In amendments 3 and 4, PROs were added. In amendment 5, the planned sample size was increased to 250 patients from 200 patients. In amendment 6, the frequency of tumour assessments was increased, and language was added to allow treatment with sotorasib to continue beyond disease progression in patients who continue to have clinical benefit, in the investigator’s opinion.
The protocol for the CodeBreaK 200 study was amended 4 times. In amendment 3 (February 15, 2021), after initiation of the study and per regulatory guidance, the initial planned enrolment of 650 patients (powered for the secondary end point of OS) was reduced to 330 patients (powered for the primary end point of PFS), and crossover from docetaxel to sotorasib was permitted following disease progression. The PFS interim analysis, planned at approximately 70% information fraction (by which time about 160 PFS events had been observed from both groups), was also incorporated at this time. Other amendments included administrative changes and clarifications.
Populations
Inclusion and Exclusion Criteria
The key inclusion and exclusion criteria for phase II of the CodeBreaK 100 study and for the CodeBreaK 200 study are summarized in Table 5. Briefly, patients eligible for inclusion in both studies were aged 18 years or older with advanced KRAS G12C-mutated solid tumours identified by molecular testing. For patients with NSCLC, KRAS G12C mutation was confirmed by central testing through therascreen KRAS Rapid Gast Quenching polymerase chain reaction from Qiagen before enrolment. For inclusion, patients must have had at least 1 prior line of anticancer therapy, progressed on the prior line of therapy, have measurable disease per RECIST 1.1 criteria, have an ECOG PS score of 1 or less, have a corrected heart rate interval of 470 msec or less, have the ability to take oral medications, and have adequate hematological, renal, hepatic, and coagulation laboratory assessments. Patients with active brain metastases from nonbrain tumours were excluded from the study. Of note, patients in the CodeBreaK 200 study must have progressed on immunotherapy and platinum-based chemotherapy, whereas patients in the CodeBreaK 100 study must have progressed after receiving anti-PD-1 or anti-PD-L1 immunotherapy, unless contraindicated, and/or platinum-based combination chemotherapy and targeted therapy, if actionable oncogenic driver mutations were identified (i.e., epidermal growth factor receptor, anaplastic lymphoma kinase, or ROS proto-oncogene 1).
Baseline Characteristics
Baseline demographics, disease characteristics, and prior treatments of patients enrolled in the CodeBreaK 100 study and the CodeBreaK 200 study are summarized in Table 6.
Patients enrolled in the CodeBreaK 100 study had a mean age of 62.9 years (SD = 9.3 years). Most patients were aged 18 years to 64 years (53.2%), white (81.7%), and current or former smokers (92.9%). In regard to disease characteristics, most patients were assessed as having stage IV disease at initial diagnosis (61.9%) and screening (96.0%). At the time of screening, metastatic disease was identified in 96.8% of enrolled patients, with the most common site of metastasis found in the bone (48.4%). The most common histology type among enrolled patients was nonsquamous adenocarcinoma (95.2%). A total of 42.9%, 34.9%, and 22.2% of patients received 1, 2, or 3 prior lines of anticancer therapy, respectively. The most common types of anticancer therapy were immunotherapy checkpoint inhibitors (92.1%) and chemotherapy (91.3%). A total of 81.0% of patients received both platinum-based chemotherapy and anti-PD-1 or anti-PD-L1 immunotherapy.
Patients enrolled in the CodeBreaK 200 study had a mean age of approximately 63 years (SD range, 9.1 to 9.9 years). Most patients were aged 18 years to 64 years (53.9%), white (82.9%), and current or former smokers (96.2%). In regard to disease characteristics, metastatic disease was identified in 95.1% of randomized patients. The most common histology type among the randomized patients was nonsquamous (96.8%). A total of 42.9%, 40.9%, and 16.2% of patients received 1, 2, or 3 or more complete prior lines of therapies, respectively; 34.2% were on maintenance therapy. Overall, 25.7% and 20.1% of patients had received prior treatment with platinum-based chemotherapy in the sotorasib and docetaxel treatment groups, respectively, while 7.6% and 5.7%, respectively, had received non–platinum-containing chemotherapy. Prior treatment with immunotherapy with platinum and alone was received by 37.4% and 25.1% of patients in the sotorasib group, respectively, and by 39.7% and 30.5% of patients in the docetaxel group, respectively. Liver, bone, and brain metastases were documented in 17.5%, 47.4%, and 33.9% of patients in the sotorasib treatment group, respectively, and in 20.1%, 39.7%, and 34.5% of patients in the docetaxel treatment group, respectively. Between the 2 treatment groups, a greater proportion of patients were male in the sotorasib treatment group (63.7%) relative to the docetaxel treatment group (54.6%). Other imbalances in baseline characteristics between the sotorasib and docetaxel treatment groups were noted: PD-L1 protein expression greater than or equal to 1% and less than 50% (sotorasib = 26.9%; docetaxel = 40.2%); ECOG PS of 0 at cycle 1, day 1 (sotorasib = 38.6%; docetaxel = 33.9%); primary refractory to last prior line of therapy (sotorasib = 39.2%; docetaxel = 32.8%); and initial response with subsequent growth (sotorasib = 20.5%; docetaxel = 27.0%).
Baseline patient characteristics were generally similar between the CodeBreaK 100 study and the CodeBreaK 200 study.
Interventions
Intervention
In both the CodeBreaK 100 study and the CodeBreaK 200 study, patients received 960 mg sotorasib (8 × 120 mg tablet) orally once daily in a fasted state (i.e., no food or liquid other than water 2 hours before to 1 hour after dosing). In the CodeBreaK 200 study, a cycle was defined as 21 days in length, unless a delay was medically necessary. Sotorasib was dispensed in clinic by a qualified staff member. Patients were instructed to take sotorasib at approximately the same time each day (± 2 hours) without interruption. Patients were instructed to skip a dose if 6 hours had passed from the scheduled time of dosing. A dose could be replaced if the patient had vomited within 15 minutes of dosing, and if all the tablets administered were accounted for and intact by visual inspection.
In the event of toxicity or AEs, up to 2 dose reductions (when sotorasib was given as monotherapy) were permitted. Patients were required to permanently discontinue sotorasib if they experienced an AE that required dose reductions to less than 240 mg of sotorasib as monotherapy.
Treatment with sotorasib was discontinued in the event of a toxicity that warranted stopping of treatment, in the opinion of the investigator. Patients were permanently discontinued from treatment with sotorasib in the event that:
AST or ALT was 3 times the upper limit of normal (ULN) and the international normalized ratio was 1.5 times the ULN in the presence of no important alternative causes for evaluated AST or ALT values.
AST or ALT was 3 times the ULN, and total bilirubin was 2 times the ULN, in the presence of no important alternative causes of elevated AST or ALT and/or total bilirubin values.
In the CodeBreaK 100 study and the CodeBreaK 200 study, treatment with sotorasib following disease progression was permitted in patients who continued to have clinical benefits from the therapy, based on investigator’s judgment, providing the following protocol-defined criteria were met:37
The patient provided a separate informed consent beyond disease progression.
There was no threat to vital organs or anatomic sites requiring urgent alternative medical intervention.
No other treatment discontinuation criteria were met.
There were no significant, unacceptable, or irreversible toxicities related to any dose of sotorasib or any treatment-related AEs (based on the Common Terminology Criteria for Adverse Events, grade 4) at the current dose at the time of progression.
There were no current signs or symptoms of clinical disease progression that decreased the ECOG PS to greater than 2.
The patient had disease progression in terms of small metastases or oligometastases, or the patient had disease progression and was a candidate for stereotactic body radiotherapy, palliative radiation, or surgery.
The patient was willing to undergo a biopsy of a progressing lesion. (If tumour biopsy was not clinically feasible or advisable, the patient could continue only upon agreement by the investigator and Amgen Inc. medical monitor.)
The Amgen Inc. medical monitor approved the continuation.
Palliative radiation and/or surgery for new, progressive, or symptomatic lesions was permitted, but sotorasib was required to be withheld during these treatments.
If the time between the patient’s initial progression scan and the restart of sotorasib was more than 4 weeks, the scan had to be repeated to serve as the new baseline.
Continued growth of tumour(s) on subsequent scans resulted in permanent discontinuation from sotorasib.
Table 6: Summary of Baseline Characteristics for Patients Enrolled in CodeBreaK 100 and CodeBreaK 200 Studies
Characteristics | CodeBreaK 100 study (N = 126) | CodeBreaK 200 study (N = 345) | |
|---|---|---|---|
Sotorasib 960 mg | Sotorasib 960 mg (n = 171) | Docetaxel 75 mg/m2 (n = 174) | |
Demographics (full analysis set) | |||
Sex, n (%) | |||
Male | 63 (50.0) | 109 (63.7) | 95 (54.6) |
Female | 63 (50.0) | 62 (36.3) | 79 (45.4) |
Age, years | |||
Mean (SD) | 62.9 (9.3) | 63.4 (9.9) | 63.6 (9.1) |
Age groups by years, n (%) | |||
18 to 64 | 67 (53.2) | 91 (53.2) | 95 (54.6) |
65 to 74 | 49 (38.9) | 58 (33.9) | 58 (33.3) |
75 to 84 | 10 (7.9) | 20 (11.7) | 20 (11.5) |
≥ 85 | 0 (0.0) | 2 (1.2) | 1 (0.6) |
Race, n (%) | |||
White | 103 (81.7) | 142 (83.0) | 144 (82.8) |
Asian | 19 (15.1) | 21 (12.3) | 22 (12.6) |
Black or African American | 2 (1.6) | 2 (1.2) | 0 (0) |
Native Hawaiian [wording from original source] or Other Pacific Islander | 0 (0) | 0 (0) | 0 (0) |
Multiple | 0 (0) | 1 (0.6) | 0 (0) |
Other | 2 (1.6) | 4 (2.3) | 7 (4.0) |
Unknown | NA | 1 (0.6) | 1 (0.6) |
Smoking history, n (%; safety analysis set) | |||
Never | 6 (4.8) | 5 (2.9) | 8 (4.6) |
Current | 15 (11.9) | 32 (18.7) | 35 (20.1) |
Former | 102 (81.0) | 134 (78.4) | 131 (75.3) |
Missing | 3 (2.4) | 0 (0) | 0 (0) |
Disease characteristics (safety analysis set for CodeBreaK 100 study; full analysis set for CodeBreaK 200 study) | |||
Stage at initial diagnosis, n (%) | |||
Stage I | 11 (8.7) | NR | NR |
Stage II | 14 (11.1) | NR | NR |
Stage III | 22 (17.5) | NR | NR |
Stage IV | 78 (61.9) | NR | NR |
Missing | 1 (0.8) | NR | NR |
Stage at screening, n (%) | |||
Stage III | 5 (4.0) | NR | NR |
Stage IV | 121 (96.0) | NR | NR |
Locally advanced and unresectable | NR | 9 (5.3) | 8 (4.6) |
Metastatic | NR | 162 (94.7) | 166 (95.4) |
Other | NR | 0 (0) | 0 (0) |
Unknown | NR | 0 (0) | 0 (0) |
Differentiation, n (%) | |||
Well-differentiated | 6 (4.8) | NR | NR |
Moderately differentiated | 15 (11.9) | NR | NR |
Poorly differentiated | 24 (19.0) | NR | NR |
Undifferentiated | 0 (0) | NR | NR |
Other | 0 (0) | NR | NR |
Unknown | 81 (64.3) | NR | NR |
PD-L1 protein expression, n (%) | |||
< 1% | 33 (26.2) | 57 (33.3) | 55 (31.6) |
≥ 1% and < 50% | 24 (19.0) | 46 (26.9) | 70 (40.2) |
≥ 50% | 35 (27.8) | 60 (35.1) | 40 (23.0) |
Unknown | 34 (27.0) | 8 (4.7) | 9 (5.2) |
Histology type, n (%) | |||
Squamous | 1 (0.8) | 1 (0.6) | 7 (4.0) |
Adenosquamous carcinoma | 0 (0) | NR | NR |
Squamous cell carcinoma | 1 (0.8) | NR | NR |
Nonsquamous | 125 (99.2) | 169 (98.8) | 165 (94.8) |
Adenocarcinoma | 120 (95.2) | NR | NR |
Mucinous | 8 (6.3) | NR | NR |
Large cell carcinoma | 3 (2.4) | NR | NR |
Bronchoalveolar carcinoma | 2 (1.6) | NR | NR |
Sarcomatoid | 0 (0) | NR | NR |
Undifferentiated | 0 (0) | NR | NR |
Other | 0 (0) | 1 (0.6) | 2 (1.1) |
Co-mutations, n (%) | |||
ALK | NR | 1 (0.6) | 0 (0) |
ATM | 1 (0.8) | NR | NR |
BRAF | 1 (0.8) | 1 (0.6) | 1 (0.6) |
CTNNB1 | 1 (0.8) | NR | NR |
EGFR | 3 (2.4) | 1 (0.6) | 0 (0) |
FBXW7 | 1 (0.8) | NR | NR |
GNAS | 2 (1.6) | NR | NR |
HER2 | NR | 0 (0) | 0 (0) |
KEAP1 | 1 (0.8) | 2 (1.2) | 1 (0.6) |
KIT | 1 (0.8) | NR | NR |
MET | 2 (1.6) | 1 (0.6) | 2 (1.1) |
MYC | 1 (0.8) | NR | NR |
NTRK | NR | 0 (0) | 0 (0) |
NRAS | NR | 0 (0) | 0 (0) |
PIK3CA | 2 (1.6) | 0 (0) | 0 (0) |
RB1 | 1 (0.8) | NR | NR |
RET | NR | 0 (0) | 0 (0) |
ROS1 | NR | 1 (0.6) | 0 (0) |
SMARCA4 | 1 (0.8) | NR | NR |
SMARCB1 | 1 (0.8) | NR | NR |
STK11 | 7 (5.6) | 4 (2.3) | 4 (2.3) |
TP53 | 13 (10.3) | 4 (2.3) | 6 (3.4) |
Metastatic, n (%) | |||
Yes | 122 (96.8) | 162 (94.7) | 166 (95.4) |
No | 4 (3.2) | 9 (5.3) | 8 (4.6) |
Number of body sites of metastatic disease, n (%) | |||
0 | 4 (3.2) | NR | NR |
1 | 51 (40.5) | NR | NR |
2 | 30 (23.8) | NR | NR |
3 | 24 (19.0) | NR | NR |
> 3 | 17 (13.5) | NR | NR |
History of CNS involvement | |||
Yes | NR | 58 (33.9) | 60 (34.5) |
No | NR | 113 (66.1) | 114 (65.5) |
Sites of selected metastasis, n (%) | |||
Liver | 26 (20.6) | 30 (17.5) | 35 (20.1) |
Brain | 26 (20.6) | 58 (33.9%) | 60 (34.5) |
Bone | 61 (48.4) | 81 (47.4) | 69 (39.7) |
Performance (safety analysis set for CodeBreaK 100 study; full analysis set for CodeBreaK 200 study) | |||
ECOG PS at screening,a n (%) | |||
0 | NR | 59 (34.5) | 59 (33.9) |
1 | NR | 112 (65.5) | 115 (66.1) |
2 | NR | NR | NR |
ECOG PS at cycle 1 day 1, n (%) | |||
0 | 38 (30.2) | 66 (38.6) | 46 (26.4) |
1 | 88 (69.8) | 100 (58.5) | 105 (60.3) |
2 | 0 (0) | 1 (0.6) | 1 (0.6) |
3 | NR | 0 (0) | 1 (0.6) |
Missing | NR | 4 (2.3) | 21 (12.1) |
Prior anticancer therapyb (safety analysis set) | |||
Prior lines of anticancer therapy, n (%) | |||
1 | 54 (42.9) | 171 (100) | 174 (100) |
2 | 44 (34.9) | 97 (56.7) | 100 (57.5) |
3 | 28 (22.2) | 29 (17.0) | 27 (15.5) |
≥ 4 | 0 (0) | 8 (4.7) | 9 (5.1) |
Maintenance | NR | 62 (36.3) | 56 (32.2) |
Other | NR | 2 (1.2) | 2 (1.1) |
Number of complete lines of therapy, n (%) | |||
1 | NR | 74 (43.3) | 74 (42.5) |
2 | NR | 68 (39.8) | 73 (42.0) |
> 2 | NR | 29 (17.0) | 27 (15.5) |
Number of advanced lines of therapy | |||
1 | NR | 77 (45.0) | 78 (44.8) |
2 | NR | 65 (38.0) | 69 (39.7) |
> 2 | NR | 29 (17.0) | 27 (15.5) |
Median number of prior lines | 2 | NR | NR |
Types of prior anticancer therapy,b n (%) | |||
Chemotherapy | 115 (91.3) | NR | NR |
Platinum-based chemotherapy | 113 (89.7) | 44 (25.7) | 35 (20.1) |
Non–platinum-containing regimen | NR | 13 (7.6) | 10 (5.7) |
Immunotherapy | 116 (92.1) | NR | NR |
Checkpoint inhibitors | 116 (92.1) | NR | NR |
Anti-PD-1 or anti-PD-L1 | 115 (91.3) | NR | NR |
With platinum | NR | 64 (37.4) | 69 (39.7) |
Alone | NR | 43 (25.1) | 53 (30.5) |
Platinum-based chemotherapy and anti-PD-1 or anti-PD-L1c | 102 (81.0) | NR | NR |
Hormonal therapy | 0 (0) | NR | NR |
Targeted biologics | 30 (23.8) | NR | NR |
Anti-VEGF biological therapy | 25 (19.8) | NR | NR |
Targeted small molecules | 9 (7.1) | NR | NR |
Other | 1 (0.8) | 7 (4.1) | 7 (4.0) |
Best response to last prior line of therapy, n (%)d | |||
Complete response | 1 (0.8) | NR | NR |
Partial response | 12 (9.5) | 35 (20.5) | 47 (27.0) |
Stable disease | 33 (26.2) | 50 (29.2) | 53 (30.5) |
Progressive disease | 48 (38.1) | NR | NR |
Unevaluable | 1 (0.8) | 10 (5.8) | 11 (6.3) |
Unknown/not applicable/not done | 27 (21.4) | NR | NR |
Missing | 4 (3.2) | NR | NR |
Primary refractory (progression on first scan) | NR | 67 (39.2) | 57 (32.8) |
Non-PD or non-CR | NR | 9 (5.3) | 6 (3.4) |
CNS = central nervous system; CR = complete response; ECOG PS = Eastern Cooperative Oncology Group Performance Status; EGFR = epidermal growth factor receptor; KEAP1 = Kelch-like ECH-associated protein 1; NR = not reported; PD-1 = programmed cell death 1; PD-L1 = programmed cell death 1 ligand 1; SD = standard deviation; VEGF = vascular endothelial growth factor.
Note: The data cut-off dates were September 1, 2020, and March 15, 2021, for the CodeBreaK 100 study and August 2, 2022, for the CodeBreaK 200 study.
aBaseline ECOG PS is measured at screening visit predose. Patients may satisfy the ECOG PS enrolment eligibility during the screening period, but subsequently have a baseline ECOG PS of 2 before the first dose.
bEach patient may have multiple prior therapies. Types of prior anticancer therapies were adjudicated and included therapies given in any treatment setting.
cPlatinum-based chemotherapy and anti-PD-1 or anti-PD-L1 could be in combination or across different lines.
dNumber of prior lines and best response on prior lines of therapy include therapies in metastatic disease and adjuvant therapy immediately before metastasis with progression occurring by or within 6 months of treatment ending.
Sources: Clinical Study Report for phase II of the CodeBreaK 100 study20 and Clinical Study Report for the CodeBreaK 200 study.21
Comparator
No comparator intervention was used in the CodeBreaK 100 study.
The comparator intervention in the CodeBreaK 200 study was docetaxel. Docetaxel was administered by IV at a dose of 75 mg/m2 every 3 weeks following the failure of prior platinum-based chemotherapy and immune checkpoint inhibitors. Docetaxel was infused in clinic by a qualified staff member over 1 hour. Additional administration time was allowed, as per local guidelines. Dose reduction of docetaxel was permitted, based on investigator opinion, in the event of select toxicities, including: grade 3 or higher related thrombocytopenia associated with bleeding; febrile neutropenia; neutrophils greater than 500 cells/mm3 for more than 1 week; grade 4 anemia; absolute neutrophil count of less than 1,500 cells/mm3; severe or cumulative cutaneous reactions; other grade 3 or 4 nonhematological toxicities; grade 3 or higher peripheral neuropathy; bilirubin greater than the ULN or — if AST and/or ALT is greater than 1.5 times the ULN, concomitant with ALP — greater than 2.5 times the ULN; grade 3 or greater AST or ALT elevation related to docetaxel for more than 2 weeks; concurrent AST or ALT greater than 3 times the ULN and total bilirubin greater than 2 times the ULN if related to docetaxel; and severe hypersensitivity. Patients could continue docetaxel after radiologic progression if the investigator believed they would continue to derive clinical benefit from treatment and if the criteria outlined earlier for continuing treatment with sotorasib after disease progression were met.
Crossover From Docetaxel to Sotorasib
Patients randomized to the docetaxel treatment group in the CodeBreaK 200 study who discontinued docetaxel due to disease progression were allowed to cross over to the sotorasib group at the discretion of the principal investigators. Treatment with sotorasib after crossover could not be initiated any earlier than 14 days after the last dose of docetaxel, regardless of time of disease progression. Patients who entered the long-term follow-up phase of the CodeBreaK 200 study were not permitted to cross over into the sotorasib treatment group if they received any systematic anticancer therapy other than docetaxel.
The CodeBreaK 200 study employed 2 crossover conditions. Crossover condition 1 required patients who permanently discontinued chemotherapy due to an AE, or for any reason other than progressive disease, to have had radiologic progression and undergo independent central confirmation of progression at the time of first progressive disease before crossover. Crossover after progressive disease was considered based on the following conditions:
Disease progression limited to CNS only must be treated before crossover.
Patients with symptomatic brain metastasis could not cross over.
There was no threat to vital organs or critical anatomic sites (e.g., CNS metastasis, respiratory failure due to tumour compression, spinal cord compression) requiring urgent alternative medical intervention.
Brain imaging (CT or MRI with contrast) was completed before initiating crossover therapy with sotorasib. If a brain scan was performed more than 28 days from the date of the first crossover dose of sotorasib, then the brain scan was repeated.
All inclusion criteria requirements were met on administration day 1 of crossover treatment with sotorasib.
No treatment discontinuation criteria were met.
No significant, unacceptable, or irreversible toxicities related to any dose of docetaxel or treatment-related AEs at the current dose at the time of progression were reported (with the exception of alopecia and nail discoloration). Additional nonsignificant toxicities were allowed, but had to be approved by the medical monitor before crossover.
No current signs or symptoms of clinical disease progression that have decreased the ECOG PS to greater than 2 were observed.
Palliative radiation and/or surgery for new, progressive, or symptomatic lesions was permitted before crossover, provided that treatment with sotorasib was withheld until after completion of these treatments and until 7 days after completion of radiation.
No other systemic anticancer directed therapeutic drugs were required during crossover.
Crossover condition 2 required consideration of immediate crossover for all patients who were randomized to receive docetaxel, should an early efficacy of the study be noted by the data monitoring committee.
Concomitant Treatment
In both the CodeBreaK 100 study and the CodeBreaK 200 study, patients were permitted to receive any concomitant medications or treatment deemed necessary by the investigator to provide adequate supportive care. Medications and supplements that were known to be strong inducers of cytochrome P450 3A4 enzyme (e.g., St. John’s wort), or that were known cytochrome P450 3A4 enzyme–sensitive substrates with a narrow therapeutic window, were not provided for 14 days before enrolment or during the study period unless approved by the principal investigator and the sponsor’s medical monitor. In the CodeBreaK 200 study, coadministration of sotorasib with proton pump inhibitor and H2 receptor antagonists was to be avoided; when this was not possible, then sotorasib was to be administered 4 hours before or 10 hours after a local antacid.
Outcomes
A list of efficacy end points identified in the CADTH review protocol that were assessed in the clinical trials included in this review is provided in Table 7. These end points are further summarized here. A detailed discussion and critical appraisal of the outcome measures is provided in Appendix 5.
Table 7: Summary of Outcomes of Interest Identified in the CADTH Review Protocol
Outcome measure | CodeBreaK 100 study, phase II (NSCLC cohort) | CodeBreaK 200 study |
|---|---|---|
OS | Secondary | Key secondary |
12-month OS | Secondary | NA |
PFS | Secondary | Primary |
6-month and 12-month PFS | Secondary | NA |
HRQoL | Exploratory | Key secondary |
EORTC QLQ-C30 and EORTC QLQ-LC13 | — | — |
NSCLC-SAQ | Exploratory | NA |
FACT-G item GP5 | Exploratory | Exploratory |
EQ-5D-5L | Exploratory | Secondary |
EQ VAS | Exploratory | Secondary |
Symptom burden | Exploratory | Secondary |
NSCLC-SAQ | — | — |
FACT-G | Exploratory | Exploratory |
Symptom-specific scales of the EORTC QLQ-C30 | Exploratory | Secondary |
Symptom-specific scales of the EORTC QLQ-LC13 | Exploratory | Secondary |
PRO-CTCAE | Exploratory | Exploratory |
PGIS and PGIC | Exploratory | Exploratory |
BPI-SF | NA | Exploratory |
Objective response (CR plus PR) | Primary | Key secondary |
DOR | Secondary | Secondary |
Incidence and severity of AE | Secondary | Secondary |
AE = adverse event; BPI-SF = Brief Pain Inventory – Short Form; CR = complete response; DOR = duration of response; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; EORTC QLQ-LC13 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Lung Cancer Module; EQ VAS = EQ visual analogue scale FACT-G = Functional Assessment of Cancer Therapy – General; HRQoL = health-related quality of life; NA = not assessed; NSCLC-SAQ = Non–Small Cell Lung Cancer Symptom Assessment Questionnaire; OS = overall survival; PFS = progression-free survival; PGIC = patient global impression of change; PGIS = patient global impression of severity; PR = partial response; PRO-CTCAE = patient-reported outcome version of the Common Terminology Criteria for Adverse Events.
Sources: Clinical Study Report for phase II of the CodeBreaK 100 study;20 Protocol and Clinical Study Report for the CodeBreaK 200 study.21,36
Overall Survival
OS was designated a secondary outcome measure in phase II of the CodeBreaK 100 study and a key secondary outcome in the CodeBreaK 200 trial. The outcome was defined as the time from the start of treatment (the CodeBreaK 100 study) or time of randomization (the CodeBreaK 200 study) until the event of death due to any cause. Patients were censored at the date on which they were last known to be alive. If the last known date alive was after the date that triggered the analysis (i.e., the data cut-off date), patients were censored at the analysis trigger date. In the CodeBreaK 200 study, OS was estimated regardless of the subsequent anticancer therapy (for patients who started new anticancer therapies during the trial) and regardless of crossover from the docetaxel to sotorasib group.
Progression-Free Survival
PFS was a secondary outcome measure in phase II of the CodeBreaK 100 study and was designated as the primary end point in the CodeBreaK 200 study. PFS was defined as the interval from the start of treatment (the CodeBreaK 100 study) or time of randomization (the CodeBreaK 200 study) to disease progression or death due to any cause, whichever came first. The censoring strategies used in the CodeBreaK 100 study and the CodeBreaK 200 study are described in Appendix 3. Patients who did not progress or die were censored at their last date of evaluable disease assessment (including those who started a new anticancer therapy before a PFS event). Progression was based on independent radiologic assessment by BICR of disease response per RECIST 1.1. Among patients who continued treatment postprogression or crossed over from docetaxel to sotorasib in the CodeBreaK 200 study, the first date of progression was used for analysis, and patients’ response to post–first progression or postcrossover were not used in the analysis of this end point.
Health-Related Quality of Life
In the CodeBreaK 100 study, the following HRQoL outcome measures were assessed as exploratory outcomes: EORTC QLQ-C30; EORTC QLQ-LC13; and the EQ-5D-5L and EQ VAS.
In the CodeBreaK 200 study, the EORTC QLQ-C30 subscales of physical functioning and global health status and the EORTC QLQ-LC13 subscales of dyspnea, cough, and chest pain were assessed as key secondary outcomes, while the EQ VAS portion of the EQ-5D-5L was assessed as a secondary outcome.
The EORTC QLQ-C30 is a self-reported, multidimensional, cancer-specific, self-administered questionnaire for evaluating HRQoL. The questionnaire consists of 30 questions, including 5 function scales (physical, role, cognitive, emotional, and social), 1 global health status/global quality of life scale, 3 symptom scales (fatigue, pain, nausea, and vomiting), and 6 single items that assess additional symptoms (dyspnea, appetite loss, sleep disturbance, constipation, and diarrhea) and financial impact.38 Scales and single items of the questionnaire range in score from 0 to 100, with higher scores on the functional and global health status/quality of life scales indicating higher levels of functioning and health status/quality of life, respectively. Higher scores on the symptom scales or items represent a greater presence of symptoms.38 The construct and convergent validity of the EORTC QLQ-C30 has been deemed good in a cohort of patients with NSCLC who are not amenable to curative or life-prolonging treatments.25 All items included in the scale except cognitive function and pain showed acceptable reliability.25,39 The CADTH review team did not identify an estimated minimal important difference (MID) for the EORTC QLQ-C30 among patients with NSCLC. Estimations of within-patient meaningful improvement and worsening on key scores that were used by the sponsor are summarized in Table 8.
Table 8: Meaningful Improvement and Worsening on Key Scales of the EORTC QLQ-C30
Scale | Improvement | Worsening |
|---|---|---|
Dyspnea | –3 | 6 |
Physical functioning | 5 (range, 5 to 9) | –4 (range, –4 to –6) |
Global health status/QoL | 4 (range, 4 to 9) | –4 (range, –4 to –6) |
EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; QoL = quality of life.
Sources: Cocks et al. (2012);40 Maringwa et al. (2011).41
The EORTC QLQ-LC13 is a responsive questionnaire specific to lung cancer that is supplementary to the EORTC QLQ-C30 and consists of 13 items addressing symptoms associated with lung cancer and its standard treatment. Symptoms mentioned in the EORTC QLQ-C30 include cough (1 question), hemoptysis (1 question), dyspnea (3 questions), and pain (3 questions); pain medication is also included (1 question). Treatment-related side effects mentioned include sore mouth or tongue (1 question), dysphagia (1 question), neuropathy (1 question), and alopecia (1 question). All items are scored on a 4-point categorical scale ranging from 1 (not at all) to 4 (very much), except for 1 pain-related item that has a dichotomous response category of yes or no. Scale and items scores are transformed on a scale ranging from 0 to 100, with higher scores representing increased symptom burden.42 The construct validity has been established between pain score and disease type and between ECOG PS and scores for dyspnea, coughing, and pain; correlation between spirometry results and dyspnea scores was found to be weak.42 The internal consistency estimated for the dyspnea scale has been confirmed to be acceptable (i.e., Cronbach alpha > 0.7), while the internal consistency for pain was found to be unacceptable when used alone, without the EORTC QLQ-C30 core questionnaire pain items.39 The CADTH review team did not identify an estimated MID for the EORTC QLQ-LC13 among patients with NSCLC.
The EQ-5D-5L is a generic, self-reported HRQoL outcome measure that may be applied to a variety of health conditions and treatments.43 Its first 2 components assesses 5 domains: mobility, self-care, usual activities, pain or discomfort, and anxiety or depression.43 Each domain has 5 levels: no problem; slight problems; moderate problems; severe problems; and extreme problems. The descriptive system classifies respondents (aged ≥ 12 years) based on the following 5 dimensions: mobility, self-care, usual activities, pain or discomfort, and anxiety or depression. The EQ-5D-5L has 5 possible levels for each domain, and respondents are asked to choose the level that reflects their health state for each of the 5 domains.43 The second component of the EQ-5D-5L is a 20 cm EQ-VAS that has end points labelled 0 and 100, with respective anchors of “worst imaginable health state” and “best imaginable health state.” Respondents are asked to rate their health by drawing a line from an anchor box to the point on the EQ-VAS that best represents their health on that day. The EQ-5D-5L index score is generated by applying a multiattribute utility function to the descriptive system.44 Different utility functions are available that reflect the preferences of specific populations (e.g., in the US or UK). Scores less than 0 represent health states that are valued by society as being worse than dead, while scores of 0 and 100 are assigned to the health states “dead” and “perfect health,” respectively. The measurement properties have not been assessed in patients with NSCLC. The CADTH review team did not identify an estimated MID for the EQ-5D-5L or EQ VAS among patients with NSCLC.
Symptom Burden
The following symptom burden scales were assessed as exploratory outcomes in both the CodeBreaK 100 study and the CodeBreaK 200 study:
FACT-G
PGIS and PGIC
PRO-CTCAE.
The CodeBreaK 100 study also assessed the NSCLC-SAQ and the symptom-specific scales of the EORTC QLQ-C30 and the EORTC QLQ LC13 as exploratory outcomes. The Brief Pain Inventory – Short Form (BPI-SF) was assessed as an exploratory outcome in the CodeBreaK 200 study.
The NSCLC-SAQ is a self-reported, symptom-based PRO instrument that consists of 7 scale items assessing 1 of 5 symptom concepts of NSCLC: cough, pain, dyspnea, fatigue, and appetite. The recall period is 1 week. Each of the 7 items is scored on a 5-point verbal rating scale from 0 to 4 (from “not at all” to “very severe” for 3 items assessing intensity and from “never” to “always” for 4 items assessing frequency). The total NSCLC-SAQ score is the sum of all 5 domain scores, ranging from 0 to 20. Higher scores are indicative of more severe symptomatology. Of note, if any domain score is missing, the total score is not calculated.45,46 The NSCLC-SAQ has been found to be valid: content validity was ensured during the developmental phase; convergent validity has been ensured using the National Comprehensive Cancer Network Functional Assessment of Cancer Therapy Lung Symptom Index 17-Item Version, EORTC QLQ-C30, EORTC QLQ-LC13, and the EQ-5D-5L (Spearman rank-order r = 0.3 to 0.5); and known-group validity has been ensured with other questionnaires [P < 0.0001 to 0.001]). It has also been found to be reliable (i.e., Cronbach alpha > 0.7 for internal consistency and interclass correlation coefficient > 0.7 for reliability, based on test-retest 1 week to 2 weeks apart) and responsive (to improvement over 18 weeks; P < 0.001).45,47,48 Improvement in symptoms is indicated by a decrease in total score of 3 to 5 points, which was identified using categories of correlated anchor variables (PGIS for lung cancer).48
FACT-G is a cancer-specific, preference-based HRQoL instrument that can be used across a variety of tumour types. FACT-G item GP5 asks patients to respond to the statement, “I am bothered by side effects of treatment” on a 5-point Likert scale from 0 (not at all) to 4 (very much).49 No validation information was identified by the CADTH review team. The MID for item GP5 is unknown.
The PGIS and PGIC are collected for the symptoms of cough, dyspnea, and chest pain to provide context for the interpretation of key lung cancer symptoms. Patients are asked to rate their experiences of any cough, chest pain, and shortness of breath in the preceding week as being none, mild, moderate, or severe. They are then asked to compare their current experience of cough, chest pain, and shortness of breath to their experiences of these at the beginning of the study and report whether they were now much better, a little better, about the same, a little worse, or much worse. The CADTH review team did not identify validation information or an estimated MID for the PGIS and PGIC among patients with NSCLC.
The PRO-CTCAE is a PRO measure designed to evaluate symptomatic toxicity in patients enrolled in clinical trials of cancer drugs.50 Based on the phase I dose exploration portion of the CodeBreaK 100 study, the following questions were selected for assessment in the CodeBreaK 100 study and the CodeBreaK 200 study: mouth sores (severity, interference), mouth cracking (severity), itchy skin (severity), numbness (severity, interference), pain (frequency, severity, interference), aching muscles (frequency, severity, interference), and aching joints (frequency, severity, and interference). Patients are asked to assess the frequency, severity, and/or interference of adverse effects. The recall period for the PRO-CTACE is the preceding 7 days. The CADTH review team did not identify validation information or an estimated MID for the PRO-CTCAE among patients with NSCLC.
The BPI-SF is a self-administered assessment tool used to measure the severity of pain and its impact of functioning.51 The BPI-SF consists of 9 questions targeting the occurrence of pain; areas of pain; rating of pain at its worst in the last 24 hours; rating of pain at its least in the last 24 hours; specifying the average pain level; specifying the current pain level; specifying the treatments or medications currently being taken; specifying the percentage of pain relief obtained from medications in the preceding 24 hours; and specifying how much the pain has interfered in several areas of life in the preceding 24 hours (i.e., general activity, mood, walking ability, normal work, relationships, sleep, and enjoyment of life). The BPI-SF was administered to patients in clinics to interpret changes in patient-reported symptoms of chest pain. The CADTH review team did not identify validation information or an estimated MID for the BPI-SF among patients with NSCLC.
Objective Response
Objective response was designated as the primary outcome measure in phase II of the CodeBreaK 100 study and was a key secondary end point in the CodeBreaK 200 study; it was reported as a rate. The ORR was defined as the proportion of patients with a best overall response of confirmed CR or confirmed PR as measured by CT or MRI scans and assessed by RECIST 1.1. Response was assessed by BICR.
Among patients who continued treatment postprogression or who crossed over from docetaxel to sotorasib in the CodeBreaK 200 study, the first date of progression was used for analysis; the patient’s response to post–first progression or postcrossover were not used in the analysis of this end point.
Duration of Response
The DOR was a secondary outcome in phase II of the CodeBreaK 100 study and in the CodeBreaK 200 study. DOR was defined as the time from first CR or PR to disease progression or death due to any cause. DOR was calculated only for those patients who had a confirmed best overall response of PR or CR.
Among patients who continued treatment postprogression or who crossed over from docetaxel to sotorasib in the CodeBreaK 200 study, the first dates of progression were used for analysis, and patients’ responses to post–first progression postcrossover were not used in the analysis of this end point.
Statistical Analysis
Sample Size Determination
In the CodeBreaK 100 study, sample size determination was based on the phase III REVEL clinical trial of ramucirumab plus docetaxel as second-line treatment, which demonstrated an ORR of 23% (95% CI, 20% to 26%),52,53 establishing the selected benchmark ORR to exclude as 23%. A sample size of 105 patients with NSCLC was determined to provide 90% probability that the lower limit of the ORR 95% CI exceeded the tumour-specific benchmark ORR of 23%.
In the CodeBreaK 200 study, sample size determination was based on the assumption that the true treatment effect HR for PFS was 0.65 for sotorasib versus docetaxel. With 230 PFS events at the time of the primary PFS analysis, there would be approximately 90% power to show a statistically significant difference between groups at a 0.025 1-sided significant level. It was estimated that, with 330 patients enrolled, approximately 19 months would be required to reach 230 PFS events, and 13 months would be required to reach 70% of the target PFS events (interim PFS analysis). This estimation was based on a median PFS of 5 months and 7.7 months for the docetaxel and sotorasib groups, respectively,54 with a 10% dropout rate.
Planned Analyses
Primary Analyses
In the CodeBreaK 100 study, the primary analysis for ORR was set to occur approximately 8.5 months after 105 patients with NSCLC were enrolled in phase II. The timing of the primary analysis was based on the assumption that response to treatment would be seen at the first or second scan. Patients with unconfirmed PR or CR were counted as responders for this analysis if they were still enrolled in the study at the time of data cut-off and had the potential for future confirmative scans.
In the CodeBreaK 200 study, the primary analysis for PFS was expected to occur at approximately 19 months, when 230 PFS events were observed. The primary analysis for OS was expected to occur when at least 198 OS events (approximately 60% maturity) were observed (approximately 3 months after the PFS primary analysis). The estimation was based on a median OS of 9 months for the docetaxel group and 12 months for the sotorasib group, for an HR of 0.75. Multiplicity was adjusted as necessary based on the O’Brien-Fleming–type alpha spending function. The primary analysis of ORR was performed when PFS was claimed to be statistically significant and the last randomized patient had had the opportunity to have at least 12 weeks of follow-up.
Final Analyses
The final analyses for both the CodeBreaK 100 study and the CodeBreaK 200 study are set to occur when the ends of the studies (last patient, last visit) have been reached. The purpose of the final analyses is to summarize the efficacy and safety after all patients have completed long-term follow-up. Patients will be followed for 3 years and 5 years in the CodeBreaK 100 study and the CodeBreaK 200 study, respectively. The final analysis will be based on BICR of disease response per RECIST 1.1.
Interim Analyses and Early Stopping
In the CodeBreaK 100 study, safety was assessed after approximately 30, 50, 70, and 100 patients had been treated with sotorasib for 21 days. There were no formal stopping rules for safety. Interim futility analyses were conducted in a continuous manner using Bayesian predictive probability.55 For patients with NSCLC, interim futility analysis began after approximately 25 patients had received at least 1 dose of sotorasib and had at least 7 weeks of response data starting from day 1. After the initial interim analysis, subsequent interim analyses were conducted after each set of 10 patients became evaluable for a tumour response. For the purposes of the futility analysis, patients with unconfirmed PR or CR were counted as responders if they were still in enrolled in the study at the time of data cut-off and if future confirmation scans were a possibility. The go criterion was considered to be met if the probability of the true ORR exceeded the benchmark set at probability (ORR > 0.23) greater than or equal to 80%. The futility analysis was based on site-assessed disease response per RECIST 1.1.
In the CodeBreaK 200 study, an interim analysis of PFS was planned when approximately 70% (160) of the target PFS events had been observed from both groups, or when the enrolment was completed and the last randomized patient had at least 6 weeks of follow-up, whichever occurred last. The monitoring boundary for early stopping for efficacy was based on an O’Brien-Fleming–type alpha spending function for multiplicity adjustment. If PFS achieved statistical significance at the interim analysis, an administrative interim summary for OS was set to be performed. An administrative interim summary of OS was performed at the PFS interim analysis, with approximately 107 OS events (approximately 32% maturity) observed. A nominal alpha of 0.01% was spent on this interim summary.
Multiplicity
In the CodeBreaK 200 study, the Maurer-Bretz22 multiple testing procedure among PFS, OS, and ORR was used to control the study-level, overall type I error rate below 1-sided 0.025 levels. The testing procedure is illustrated in Figure 4. Starting with PFS, if the null hypothesis of PFS (i.e., that PFS survival distribution of the sotorasib treatment group is the same as in the docetaxel group) was rejected, then ORR would be tested using a 1-sided alpha divided by 5 (0.005) level. If the ORR null hypothesis (i.e., that the odds ratio of the ORR between the sotorasib group and the docetaxel group is 1) failed to be rejected, then OS would be tested using a 1-sided 0.001 level at the time of PFS interim analysis, otherwise using 4 alpha divided by 5 (0.002) level. With the rejection of OS null hypothesis (i.e., that OS survival distribution of the sotorasib group is the same as for docetaxel group), ORR could be retested using the 1-sided full alpha (0.025) level.
If all 3 hypotheses of PFS, OS, and ORR are rejected, then the next 3 end points of change from baseline over 12 weeks for the symptoms of dyspnea, cough, and pain, as measured by the EORTC QLQ-C30 and EORTC QLQ-LC13, would be tested using Holm’s procedure (Figure 5). Hypotheses (i.e., that differences in the mean change from baseline over time to 12 weeks equal 0) would be rejected sequentially based on the smallest P value.
If the 6 hypotheses listed are rejected, the change from baseline over time to week 12 in physical functioning (i.e., EORTC QLQ-C30) and global health status (i.e., EORTC QLQ-C30) are then tested using Holm’s procedure (Figure 6). The hypotheses (i.e., that differences in mean change from baseline over time to 12 weeks equal 0) would be rejected sequentially based on the smallest P value.
Figure 4: Maurer-Bretz Multiple Testing Procedure for PFS, OS, and ORR in CodeBreaK 200 Study
ORR = objective response rate; OS = overall survival; PFS = progression-free survival.
Source: Protocol for the CodeBreaK 200 study.36
Figure 5: Holm’s Multiple Testing Procedure for Change Over Time in Dyspnea, Cough, and Pain in CodeBreaK 200 Study
dysp. = dyspnea.
Source: Protocol for the CodeBreaK 200 study.36
Figure 6: Holm’s Multiple Testing Procedure for Change Over Time in Physical Functioning and Global Health Status in CodeBreaK 200 Study
ghs = global health status; phys. = physical functioning.
Source: Protocol for the CodeBreaK 200 study.36
Statistical Methods
The statistical analyses of the efficacy end points in the CodeBreaK 100 study and the CodeBreaK 200 study are summarized in Table 9.
Overall Survival
The distribution of OS, including median, was estimated using the KM method (curves, quartiles) in both the CodeBreaK 100 study and the CodeBreaK 200 study. Also reported were the OS rates at selected time points. In the CodeBreaK 100 study, the 95% CI for the median and other percentiles was constructed using the Klein and Moeschberger method with log-log transformation.56 The 95% CI for the OS rate was estimated using the method by Kalbfleisch and Prentice with log-log transformation.57 In the CodeBreaK 200 study, OS was estimated using the KM method with the HR and 95% CI estimated using a Cox proportional hazards model stratified by the randomization stratification factors.
Additional analyses of OS that adjusted for the potential confounding effect of patients randomized to docetaxel who later cross over to receive sotorasib were conducted and included the RPSFT model,58 IPCW,59 and 2-stage approach.60 The RPSFT model provides a randomization-based estimate of the treatment effect, assumes a multiplicative effect of treatment on time to event, and allows reconstruction of the hypothetical docetaxel time to event, assuming that all patients initially randomized to docetaxel would not cross over to sotorasib. The IPCW method censors patients who cross over at the time of crossover (i.e., weight = 0 during the interval after crossover; therefore, dropped from the model), then up-weights similar patients who did not cross over; as a result, it adjusts for bias of informative censoring. The 2-stage approach adjusts for the crossover effect by estimating the relative treatment effect of OS that would have been observed in the docetaxel group in the absence of crossover, based on the adjusted survival time fitted. Both the 2-stage approach and IPCW method assume no unmeasured confounders.
Progression-Free Survival
In the CodeBreaK 100 study, PFS was analyzed using the same method as described previously for OS.
In the CodeBreaK 200 study, the primary efficacy outcome of PFS was estimated using the KM method. The HR and its 95% CI were estimated using a Cox proportional hazards model stratified by the randomization factors.
HRQoL and PRO Outcomes
Among the HRQoL outcomes assessed in the CodeBreaK 100 study, continuous variables (i.e., EORTC QLQ-C30, EORTC QLQ-LC13, NSCLC-SAQ, and EQ-5D-5L) were summarized by sample size, mean, and SD, median, 25th and 75th percentiles, and minimum and maximum. Categorical variables (i.e., PRO-CTCAE, GP5, EQ-5D-5L non-VAS items, PGIS, and PGIC) were summarized by sample size and percentage in each category. The percentages were based on the nonmissing categories.
In both the CodeBreaK 100 study and the CodeBreaK 200 study, changes from baseline to week 12 on the EORTC QLQ-C30 (dyspnea, physical functioning, and global health status) and EORTC-LC13 (dyspnea, cough, and chest pain) were analyzed using a restricted-maximum, likelihood-based, mixed-effects model for repeated measures under the assumption of missing at random. The model included time and baseline score as fixed effects and used an unstructured covariance structure. A stratified analysis of change from baseline was explored by adding the following baseline covariates: number of prior lines of therapy (1 versus > 1); race (Asian versus non-Asian); and brain metastasis (yes or no). Covariates with less than 5% of the whole population in 1 category were excluded.
The presentations for all other HRQoL and PRO measures were descriptive in nature.
Objective Response Rate
In the CodeBreaK 100 study, the primary efficacy outcome of objective response was summarized as a percentage, with a Clopper-Pearson exact 95% CI. Patients without a postbaseline tumour assessment were considered nonresponders.
In the CodeBreaK 200 study, the outcome of objective response was summarized as a percentage, with a Clopper-Pearson exact 95% CI. The inferential comparison for ORR was made using the Cochran-Mantel-Haenszel chi-square test controlling for the randomization stratification factors. An estimate of the common odds ratio was provided as a measure of the relative treatment effect.
Duration of Response
DOR was calculated only for those patients who had an overall response of PR or better. The distribution of DOR, including median and quartiles, was characterized using KM methods. The 95% CI for median and quartiles for DOR were constructed using the same methods described for OS. The rates for selected duration were reported and estimated using the methods described previously. Patients were censored following the same censoring strategy applied to PFS. KM curves were constructed only if at least 10 patients had PR or CR.
Table 9: Statistical Analysis of Efficacy End Points
End point | Statistical model | Adjustment factors | Sensitivity analyses |
|---|---|---|---|
CodeBreaK 100 study | |||
OS 12-month OS | Kaplan-Meier curves, quartiles, and rates | None | None |
PFS 6-month and 12-month PFS | Kaplan-Meier curves, quartiles, and rates | None |
|
ORR (CR plus PR) | Percentage, with Clopper-Pearson exact CI | None | Investigator assessment per RECIST 1.1 |
DOR | Kaplan-Meier quartiles and rates | None | Investigator assessment per RECIST 1.1 |
EORTC QLQ-C30 EOTRC QLQ-LC13 | MMRM under assumption of missing at random |
| None |
FACT-G item GP5 EQ-5D-5L and EQ VAS NSCLC-SAQ PRO-CTCAE PGIS and PGIC Symptom-specific scales of EORTC QLQ-C30 and EORTC QLQ-LC13 | Descriptive | None | None |
CodeBreaK 200 study | |||
OS |
|
| To adjust for crossover effect:
|
PFS | — | — | Based on different censoring rules |
ORR |
| — | NR |
EORTC QLQ-C30 EOTRC QLQ-LC13 |
| — | Multiple imputation approach with nonignorable missing pattern |
EQ-5D-5L and EQ VAS FACT-G PGIS PGIC PRO-CTCAE BPI-SF | Descriptive | NR | NR |
BPI-SF = Brief Pain Inventory – Short Form; CI = confidence interval; CNS = central nervous system; CR = complete response; DOR = duration of response; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; EORTC QLQ-LC13 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Lung Cancer Module; EQ VAS = EQ visual analogue scale; FACT-G = Functional Assessment of Cancer Therapy – General; GEE = generalized estimating equation; HR = hazard ratio; IPCW = inverse-probability-of-censoring weighting; MMRM = mixed-effects model for repeated measures; NR = not reported; NSCLC-SAQ = Non–Small Cell Lung Cancer Symptom Assessment Questionnaire; OR = odds ratio; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; PGIC = patient global impression of change; PGIS = patient global impression of severity; PR = partial response; PRO = patient-reported outcome; PRO-CTCAE = patient-reported outcome version of the Common Terminology Criteria for Adverse Events; RECIST 1.1 = Response Evaluation Criteria in Solid Tumours Version 1.1; RBEE = randomization-based estimate of treatment effect; RPSFT = rank-preserving structural failure time; vs. = versus.
Sources: Clinical Study Report for phase II of the CodeBreaK 100 study;20 Clinical Study Report for the CodeBreaK 100 study PRO data;61 Protocol for the CodeBreaK 200 study;36 Clinical Study Report for the CodeBreaK 200 study.21
Subgroup Analysis
For each of the primary end points and selected secondary end points, the following predefined subgroup analyses relevant to the CADTH protocol were performed in both the CodeBreaK 100 study and the CodeBreaK 200 study:
ECOG PS (0, 1)
tumour histology (squamous, nonsquamous)
number of prior lines of anticancer therapy (1, 2, > 2)
prior anti-PD1 or anti-PD-L1 therapy (yes, no)
prior platinum-based chemotherapy (yes, no)
prior platinum-based chemotherapy and prior anti–PD1 or anti-PD-L1 therapy (yes, no).
No formal hypothesis testing in the subgroups was performed.
Analysis Populations
Four populations were defined for the purpose of data analysis related to the CodeBreaK 100 study, and 5 populations were defined for the CodeBreaK 200 study. Definitions of the populations are summarized in Table 10.
Table 10: Summary of Analysis Populations
Population | Definition | Analysis evaluated |
|---|---|---|
CodeBreaK 100 study | ||
Full analysis set | All patients who received > 1 dose of sotorasib and had 1 or more measurable lesions at baseline, as assessed by BICR using RECIST 1.1 | Response-related end point in the primary and final analyses |
Safety analysis set | All patients who received at least 1 dose of sotorasib | Safety and OS in the primary and final analyses |
ORR analysis seta | All patients in the full analysis who were followed for at least 7 weeks starting from day 1 | Interim futility analysis and interim summary of ORR, DOR, and TTR |
PRO analysis set | All patients with a nonmissing baseline result and at least 1 nonmissing postbaseline result on any subscale on a HRQoL or PRO measure | HRQoL and PRO |
CodeBreaK 200 study | ||
Full analysis set (ITT) | All randomized patients, analyzed according to the treatment to which they were randomized | Primary and key secondary efficacy end points |
Safety analysis set | All patients in the full analysis set who received at least 1 dose of the investigational product; patients were analyzed according to actual treatment received | Safety analysis |
PP | Subset of the full analysis set, which includes patients who did not have important protocol deviations | Sensitivity analyses of PFS, OS, and ORR |
EORTC QLQ-C30 analysis set | All randomized patients with a nonmissing baseline result and at least 1 nonmissing postbaseline result on any EORTC QLQ-C30 subscale | EORTC QLQ-C30 |
EORTC QLQ-LC13 analysis set | All randomized patients with a nonmissing baseline result and at least 1 nonmissing postbaseline result on any EORTC QLQ-LC13 subscale | EORTC QLQ-LC13 |
PRO analysis set | All randomized patients with nonmissing baseline results and at least 1 nonmissing postbaseline result | EQ-5D-5L, PRO-CTCAE, FACT-G item GP5, PGIS, PGIC, BPI-SF |
BPI-SF = Brief Pain Inventory – Short Form; BICR = blinded independent central review; DOR = duration of response; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; EORTC QLQ-LC13 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Lung Cancer Module; FACT-G = Functional Assessment of Cancer Therapy – General; HRQoL = health-related quality of life; ITT = intention to treat; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; PGIC = patient global impression of change; PGIS = patient global impression of severity; PP = per protocol; PRO = patient-reported outcome; PRO-CTCAE = patient-reported outcome version of the Common Terminology Criteria for Adverse Events; RECIST 1.1 = Response Evaluation Criteria in Solid Tumours Version 1.1; TTR = time to response.
aPatients who stopped disease assessment before 7 weeks were included if the data cut-off date was at least 7 weeks after their first dose date.
Sources: Clinical Study Report for phase II of the CodeBreaK 100 study;20 Protocol for the CodeBreaK 200 study;36 Clinical Study Report for the CodeBreaK 200 study.21
Results
Patient Disposition
Patient disposition is summarized in Table 11.
Among the 126 patients who were enrolled and received treatment in the CodeBreaK 100 study, 70.6% discontinued treatment. The most common reason for treatment discontinuation was disease progression (55.6%), followed by AEs (8.7%). Of the 57 patients who discontinued from the study, death was cited as the main reason in 45.2%. A total of 123 patients were included in both the full analysis set and the ORR analysis set. By the time of the updated data cut-off date of March 15, 2021, 81.7% of patients had discontinued treatment. The most common reason for treatment discontinuation was disease progression (65.9%), followed by AEs (8.7%). Of the 75 patients who had discontinued from the study by the time of the updated analysis, death was the main reason for study discontinuation (50.0%).
In the CodeBreaK 200 study, approximately 44% of the 616 patients screened were not randomized into the study. The most common reason for this was the absence of documentation of KRAS G12C mutation confirmed by central testing before enrolment (23.6%), followed by having active brain metastases (22.5%), other reasons (9.6%), not having an ECOG PS of equal to or less than 1 (8.9%), and not having adequate hematological laboratory assessments (5.2%). In total, 171 patients and 174 patients were randomized to receive sotorasib 960 mg orally once daily or docetaxel infusion 75 mg/m2 every 3 weeks, respectively. Of those randomized, 1.2% of patients in the sotorasib treatment group and 13.2% of those in the docetaxel group were not dosed with an investigational product. Of the 23 patients who were not dosed in the docetaxel treatment group, 16 were not dosed on request of the patient. Of those who received at least 1 dose of the investigational product, 147 patients (86.5%) and 143 patients (82.2%) discontinued treatment in the sotorasib and docetaxel treatment groups, respectively. The most common reason for treatment discontinuation was disease progression (experienced by 60.2% of patients in the sotorasib treatment group and 54.6% of patients in the docetaxel treatment group). Of the 247 patients who discontinued from the study, 121 patients (70.8%) and 126 patients (72.4%) were from the sotorasib and docetaxel treatment groups, respectively. Death was cited as the main reason for study discontinuation in both the sotorasib treatment group (60.8%) and the docetaxel treatment group (48.9%). A greater proportion of patients in the docetaxel treatment group (22.4%) withdrew consent from study participation relative to the sotorasib treatment group (7.0%). At the time of the August 2, 2022, data cut-off date, the full analysis set included 171 and 174 patients in the sotorasib and docetaxel treatment groups, respectively.
During the CodeBreaK 200 study, 46 patients (26.4%) who had been randomized to the docetaxel treatment group crossed over to receive treatment with sotorasib following confirmed progressive disease; an additional 13 patients (7.5%) received sotorasib as a new anticancer therapy. The sponsor clarified that the 13 patients who crossed over outside of the protocol did not differ structurally from the per-protocol crossover patients. All 13 patients received sotorasib upon radiographic progression; however, for most patients, crossover was not available at the clinical site. For 1 patient, the investigator opted not to request crossover from the medical monitor and sought sotorasib administration outside of the clinical trial protocol. At the time of the August 2, 2022, data cut-off date, 12 crossover patients (26.1%) were continuing treatment with sotorasib, while 34 crossover patients (73.9%) had discontinued treatment with sotorasib. The most common reason for discontinuing treatment with sotorasib was disease progression (in 26 crossover patients [56.5%]). Radiographic and clinical disease progression was documented in 22 crossover patients (47.8%) and 4 crossover patients (8.7%), respectively. As of the data cut-off date, 25 crossover patients (54.3%) were continuing in the study, and 21 crossover patients (45.7%) had discontinued the study due to death (n = 17; 37%) or withdrawal of consent (n = 4; 8.7%).
Disposition | CodeBreaK 100 study, phase II (NSCLC cohort) | CodeBreaK 200 study | ||
|---|---|---|---|---|
Sotorasib 960 mg | Sotorasib 960 mg | Docetaxel 75 mg/m2 | ||
Data cut-off date September 1, 2020 | Data cut-off date March 15, 2021 | Data cut-off date August 2, 2022 | ||
Screened, N | NR | NR | 616 | |
Enrolled or randomized, N | 126 | 126 | 171 | 174 |
Randomized but not dosed, N (%) | NA | NA | 2 (1.2) | 23 (13.2) |
Reason for not dosed, N (%) | ||||
Adverse event | NA | NA | 1 (0.6) | 0 (0) |
Patient request | NA | NA | 1 (0.6) | 16 (9.2) |
Disease progression | NA | NA | 0 (0) | 1 (0.6) |
Lost to follow-up | NA | NA | 0 (0) | 1 (0.6) |
Othera | NA | NA | 0 (0) | 5 (2.9) |
Received at least 1 dose of treatment, N (%) | 126 (100) | 126 (100) | 169 (98.8) | 151 (86.8) |
Discontinued treatment, N (%) | 89 (70.6) | 103 (81.7) | 147 (86.0) | 143 (82.2) |
Reason for treatment discontinuation, N (%) | ||||
Disease progression | 70 (55.6) | 83 (65.9) | 103 (60.2) | 95 (54.6) |
Adverse event | 11 (8.7) | 11 (8.7) | 29 (17.0) | 25 (14.4) |
Patient request | 5 (4.0) | 5 (4.0) | 6 (3.5) | 10 (5.7) |
Death | 1 (0.8) | 2 (1.6) | 4 (2.3) | 6 (3.4) |
Noncompliance | 1 (0.8) | 1 (0.8) | 0 (0) | 0 (0) |
Requirement for alternative treatment | 1 (0.8) | 1 (0.8) | 1 (0.6) | 0 (0) |
Decision by sponsor | 0 (0) | 0 (0) | 1 (0.6) | 0 (0) |
Otherb | NR | NR | 3 (1.8) | 7 (4.0) |
Discontinued study, N (%) | 57 (45.2) | 75 (59.5) | 121 (70.8) | 126 (72.4) |
Death | 47 (37.3) | 63 (50.0) | 104 (60.8) | 85 (48.9) |
Withdrawal of consent from study | 10 (7.9) | 10 (7.9) | 12 (7.0) | 39 (22.4) |
Lost to follow-up | 0 (0) | 2 (1.6) | 5 (2.9) | 2 (1.1) |
FAS, N | 123 | NR | 171 (100) | 174 (100) |
ORR analysis set, N | 123 | NR | NA | NA |
Safety, N | 126 | NR | 169 (98.8) | 151 (86.8) |
PP | NA | NA | 159 (93) | 163 (93.7) |
FAS = full analysis set; NA = not applicable; NR = not reported; NSCLC = non–small cell lung cancer; ORR = objective response rate; PI = principal investigator; PP = per protocol.
aOther included patient refusal to participate in the study, PI decision, and withdrawal of consent.
bOther included investigator decision, no clinical benefit, withdrawal of consent, ineligibility to resume sotorasib, loss of clinical benefit.
Sources: Clinical Study Report for phase II of the CodeBreaK 100 study;20 Clinical Study Report for the CodeBreaK 200 study.21
Protocol Deviations
Protocol deviations during the CodeBreaK 100 study and the CodeBreaK 200 study are summarized in Table 12.
In the CodeBreaK 100 study, important protocol deviations were documented for 40.5% of patients. The most-cited deviations involved missing data (31.7%), comprising 22.2% related to missing key safety or laboratory samples and 9.5% related to missing screening assessments. In the CodeBreaK 200 study, important protocol deviations were documented in 67.3% and 49.4% of patients in the sotorasib and docetaxel treatment groups, respectively. The most-cited protocol deviations in the CodeBreaK 200 study were off-schedule procedures, which occurred in 36.8% and 27.6% of patients in the sotorasib and docetaxel treatment groups, respectively.
Table 12: Protocol Deviations in CodeBreaK 100 and CodeBreaK 200 Studies
Protocol deviation | CodeBreaK 100 study, phase II (NSCLC cohort) | CodeBreaK 200 study | |
|---|---|---|---|
Sotorasib 960 mg (n = 126) | Sotorasib 960 mg (n = 171) | Docetaxel 75 mg/m2 (n = 174) | |
Patients with at least 1 important protocol deviation, N (%) | 51 (40.5) | 115 (67.3) | 86 (49.4) |
Total number of important deviationsa | 89 | 300 | 207 |
Total number of off-schedule procedures (other than TA or TC)a | NR | 166 | 92 |
Off-schedule procedure (other than TA or TC) | NR | 63 (36.8) | 48 (27.6) |
Out-of-window imaging assessments | NR | 35 (20.5) | 42 (24.1) |
Predose procedure(s) | NR | 40 (23.4) | 10 (5.7) |
Screening procedure(s) | NR | 4 (2.3) | 4 (2.3) |
Total number of missing data (other than TA or TC)a | 66 | 40 | 38 |
Types of missing data (other than TA or TC) | 40 (31.7) | 32 (18.7) | 28 (16.1) |
Missing key safety or laboratory samples | 28 (22.2) | 4 (2.3) | 7 (4.0) |
Missing screening assessments | 12 (9.5) | 4 (2.3) | 0 (0) |
Missing end-of-treatment or safety follow-up procedures | 6 (4.8) | 7 (4.1) | 6 (3.4) |
Missing imaging | 2 (1.6) | 7 (4.1) | 13 (7.5) |
Missing predose assessments | 2 (1.6) | 14 (8.2) | 6 (3.4) |
Missing key PK data | 1 (0.8) | 0 (0) | 0 (0) |
Total number of other treatment compliancea | NR | 36 | 24 |
Other treatment compliance | NR | 25 (14.6) | 15 (8.6) |
Treatment beyond progression eligibility | NR | 10 (5.8) | 4 (2.3) |
Dose compliance cannot be assessed | NR | 6 (3.5) | 1 (0.6) |
Incorrect stratification in IRT: prior lines of therapy | NR | 3 (1.8) | 4 (2.3) |
Crossover or treatment beyond progression | NR | 5 (2.9) | 1 (0.6) |
Incorrect stratification in IRT: CNS disease history | NR | 4 (2.3) | 0 (0) |
Patients not premedicated with oral corticosteroids before docetaxel administration | NR | 0 (0) | 4 (2.3) |
Crossover eligibility | NR | 0 (0) | 2 (1.1) |
Incorrect stratification in IRT: race | NR | 0 (0) | 1 (0.6) |
Total number of other deviations, including important GCPa | 10 | 27 | 23 |
Other violations of GCP | 10 (7.9) | 21 (12.3) | 17 (9.8) |
Total number of patients who entered the study even though entry criteria were not satisfieda | 4 | 15 | 16 |
Active brain metastases | 0 (0) | 2 (1.2) | 6 (3.4) |
Adequate hematologic laboratory assessments | 0 (0) | 3 (1.8) | 2 (1.1) |
QTc less than or equal to 470 msec in women and less than or equal to 450 msec in men | 0 (0) | 2 (1.2) | 3 (1.7) |
Prior therapies within 4 weeks of study day 1 | NA | 1 (0.6) | 2 (1.1) |
Had documentation of KRAS G12C mutation identified through central laboratory testing with the investigational Qiagen KRAS therascreen assay | 0 (0) | 2 (1.2) | 0 (0) |
Adequate platelet function | 0 (0) | 1 (0.6) | 1 (0.6) |
Cytochrome P450 34A–sensitive substrates | 0 (0) | 1 (0.6) | 1 (0.6) |
Use of antibiotics within 2 weeks of randomization | NA | 1 (0.6) | 0 (0) |
Mixed NSCLC | 0 (0) | 0 (0) | 1 (0.6) |
Informed consent | 2 (1.6) | 0 (0) | 0 (0) |
Hepatitis infection | 1 (0.8) | 1 (0.6) | 0 (0) |
Pathologically documented, locally advanced or metastatic malignancy with KRAS G12C mutation and history of prior treatment | 1 (0.8) | 0 (0) | 0 (0) |
Total number of patients who received the wrong treatment or incorrect dosea | 4 | 10 | 13 |
Total number of patients who developed withdrawal criteria but were not withdrawna | 3 | 3 | 1 |
Total number of patients receiving an excluded concomitant treatmenta | NR | 3 | 0 |
CNS = central nervous system; GCP = good clinical practice; IRT = interactive response technology; NR = not reported; NSCLC = non–small cell lung cancer; PK = pharmacokinetic; QTc = correct heart rate interval; TA = received the wrong treatment or incorrect dose; TC = other treatment adherence.
Notes: Deviation categories are not mutually exclusive. Multiple deviations within the same category are counted once per patient.
Data cut-off dates were September 1, 2020, for the CodeBreaK 100 study and August 2, 2022, for the CodeBreaK 200 study.
aEach occurrence is counted, including multiple events of the same important protocol deviation for a single patient.
Sources: Clinical Study Report for phase II of the CodeBreaK 100 study;20 Clinical Study Report for the CodeBreaK 200 study.21
Exposure to Study Treatments
Exposure to Investigational Product
Patients’ exposure to investigational products in the CodeBreaK 100 study and the CodeBreaK 200 study is summarized in Table 13.
In the CodeBreaK 100 study, the median treatment duration with sotorasib was 24.07 weeks (range, 1.0 week to 52.1 weeks) at a median dose intensity of 100% (range, 15.1% to 100%). The median number of doses per patient was 168 (range, 7 doses to 360 doses). At the time of the updated March 15, 2021, data cut-off date, the median treatment duration with sotorasib was 24.07 weeks (range, 1.0 week to 50.00 weeks) at a median dose intensity of 100% (range, 90.31% to 100%). The median number of doses per patient at the time of the updated data cut-off was 168 (range, 68.0 doses to 338.0 doses).
In the CodeBreaK 200 study, the median treatment duration with sotorasib was 19.86 weeks (range, 0.4 weeks to 101.3 weeks), administered over a median of 7.0 cycles (range, 1 cycle to 34 cycles) at a median relative dose intensity of 100% (range, 23.7% to 100%). Among patients randomized to receive sotorasib, 28 patients (16.4%) continued treatment with sotorasib after initial disease progression. In the docetaxel group, the median duration of treatment was 12 weeks (range, 3.0 weeks to 101.0 weeks) over a median of 4.0 cycles (range, 1 cycle to 33 cycles) at a median relative dose intensity of 94.8% (range, 48.9% to 105.6%).
Of the 46 patients randomized to docetaxel in the CodeBreaK 200 study who crossed over to the sotorasib treatment group, the median time from randomization to first administration of sotorasib after crossover was 5.83 months (range, 1.87 months to 13.63 months). The median treatment duration with sotorasib was 21.0 weeks (range, 2.6 weeks to 62.0 weeks) over 7.0 cycles (range, 1 cycle to 21 cycles) at a relative dose intensity of 97.07% (range, 36.8% to 100%).
Table 13: Exposure to Investigational Products in CodeBreaK 100 and CodeBreaK 200 Studies (Safety Analysis Set)
Exposure to sotorasib | CodeBreaK 100 study, phase II (NSCLC cohort) | CodeBreaK 200 study | ||
|---|---|---|---|---|
Sotorasib 960 mg (n = 126) | Sotorasib 960 mg (n = 169) | Docetaxel 75 mg/m2 (n = 151) | ||
Data cut-off date September 1, 2020 | Data cut-off date March 15, 2021 | Data cut-off date August 2, 2022 | ||
Number of cycles started | ||||
Mean (SD) | 8.0 (4.7) | 10.1 (7.5) | 10.8 (9.0) | 5.6 (5.6) |
Median (minimum, maximum) | 7.0 (1 to 18) | 7.5 (1 to 26) | 7.0 (1 to 34) | 4.0 (1 to 33) |
Number of doses per patient | ||||
Mean (SD) | 166.6 (102.9) | 210.2 (159.9) | NR | NR |
Median (minimum, maximum) | 168.0 (7 to 360) | 168.0 (68.0 to 338.0) | NR | NR |
Duration on treatment (weeks) | ||||
Mean (SD) | 25.12 (14.55) | 31.59 (23.12) | 32.3 (27.4) | 17.41 (17.47) |
Median (minimum, maximum) | 24.07 (1.0 to 52.1) | 24.07 (12.00 to 50.00) | 19.86 (0.4 to 101.3) | 12 (3.0 to 101.0) |
Patients with treatment duration, n (%) | ||||
< 3 months | 38 (30.2) | 38 (30.2) | NR | NR |
≥ 3 months | 88 (69.8) | 88 (69.8) | NR | NR |
≥ 6 months | 60 (47.6) | 60 (47.6) | NR | NR |
≥ 9 months | 36 (28.6) | 41 (32.5) | NR | NR |
≥ 12 months | 0 (0) | 31 (24.6) | NR | NR |
≥ 18 months | 0 (0) | 0 (0) | NR | NR |
Cumulative dose (mg) | ||||
Mean (SD) | 151,846.7 (98,084.4) | 189,073.3 (149,073.1) | 179,318.9 (160,878.4) | 370.71 (341.51) |
Median (minimum, maximum) | 134,220.0 (6,720 to 345,600) | 138,480.0 (6.720 to 504,000) | 116,160.0 (2,880 to 631,680) | 240.0 (74.2 to 2,062.2) |
Average dose delivered per administration, mga | ||||
Mean (SD) | 857.63 (190.89) | 854.12 (195.28) | 877.68 (163.25) | 70.35 (7.35) |
Median (minimum, maximum) | 960.0 (145.1 to 960) | 960.0 (866.94 to 960.00) | 960.0 (308.6 to 960.6) | 74.66 (41.9 to 79.2) |
Relative dose intensity, %b | ||||
Mean (SD) | 89.34 (19.88) | 88.91 (20.34) | 86.42 (21.05) | 90.35 (13.10) |
Median (minimum, maximum) | 100.0 (15.1 to 100) | 100.00 (90.31 to 100.00) | 100 (23.7 to 100) | 94.8 (48.9 to 105.6) |
IP = investigational product; NR = not reported; NSCLC = non–small cell lung cancer; SD = standard deviation.
aThe average dose delivered is the cumulative dose divided by the number of days on treatment.
bThe relative dose intensity is equal to the actual dose intensity divided by the planned dose intensity multiplied by 100, where actual (planned) dose intensity is the actual (planned) cumulative dose (in mg) divided by the actual (planned) duration of IP administration.
Sources: Clinical Study Report for phase II of the CodeBreaK 100 study;20 Clinical Study Report for the CodeBreaK 200 study.21
Concomitant Medications
The use of concomitant medications in the CodeBreaK 100 study and the CodeBreaK 200 study is summarized in Table 14.
All patients in the CodeBreaK 100 study reported treatment with a concomitant medication. The most used concomitant medication was paracetamol (44%), followed by ibuprofen (23.8%), pantoprazole (23.0%), and folic acid (22.2%).
In the CodeBreaK 200 study, the use of concomitant medications was reported in 100% and 98.7% of patients in the sotorasib and docetaxel treatment groups, respectively. The most common concomitant medication used in the sotorasib treatment group was paracetamol (45.0%), followed by viral vaccine (21.9%), loperamide hydrochloride (20.7%), and pantoprazole (20.1%). In the docetaxel treatment group, the most common concomitant medication used was paracetamol (42.4%), followed by viral vaccines (21.2%) and ondansetron (22.5%).
Table 14: Use of Concomitant Medication in CodeBreaK 100 and CodeBreaK 200 Studies (Safety Analysis Set)
Protocol deviation | CodeBreaK 100 study, phase II (NSCLC cohort) | CodeBreaK 200 study | |
|---|---|---|---|
Sotorasib 960 mg (n = 126) | Sotorasib 960 mg (n = 169) | Docetaxel 75 mg/m2 (n = 151) | |
Number of patients reporting use of concomitant medications, n (%) | 126 (100) | 169 (100) | 149 (98.7) |
Used by ≥ 15% patients in any treatment group, n (%) | |||
Paracetamol | 56 (44.4) | 76 (45.0) | 64 (42.4) |
Ibuprofen | 30 (23.8) | 24 (14.2) | 16 (10.6) |
Pantoprazole | 29 (23.0) | 34 (20.1) | 26 (17.2) |
Folic acid | 28 (22.2) | 22 (13.0) | 21 (13.9) |
Loperamide hydrochloride | 25 (19.8) | 35 (20.7) | 13 (8.6) |
Salbutamol | 25 (19.8) | 14 (8.3) | 13 (8.6) |
Oxycodone | 23 (18.3) | 32 (18.9) | 23 (15.2) |
Acetylsalicylic acid | 22 (17.5) | 19 (11.2) | 25 (16.6) |
Ondansetron | 22 (17.5) | 19 (11.2) | 34 (22.5) |
Prednisone | 21 (16.7) | 20 (11.8) | 17 (11.3) |
Dexamethasone | 20 (15.9) | 17 (10.1) | 22 (14.6) |
Colecalciferol | 19 (15.1) | 2 (1.2) | 2 (1.3) |
Gabapentin | 19 (15.1) | 13 (7.7) | 8 (5.3) |
Omeprazole | 19 (15.1) | 19 (11.2) | 24 (15.9) |
Fentanyl | 15 (11.9) | 22 (13.0) | 23 (15.2) |
Metoclopramide | 8 (6.3) | 20 (11.8) | 30 (19.9) |
Viral vaccine | NR | 37 (21.9) | 32 (21.2) |
Pegfilgrastim | NR | 0 (0) | 25 (16.6) |
NR = not reported; NSCLC = non–small cell lung cancer.
Note: The data cut-off dates were September 1, 2020, for the CodeBreaK 100 study and August 2, 2022, for the CodeBreaK 200 study.
Sources: Clinical Study Report for phase II of the CodeBreaK 100 study;20 Clinical Study Report for the CodeBreaK 200 study.21
New and Subsequent Therapy
A summary of new anticancer therapy used in the CodeBreaK 200 study is presented in Table 15. The per-protocol definition of the requirements to be eligible to receive a new anticancer therapy was not provided. The administration of new anticancer therapy before any per-protocol crossover was documented in 62 patients (36.3%) and 28 patients (16.1%) in the sotorasib and docetaxel treatment groups, respectively.
Table 15: Summary of New Anticancer Therapy in CodeBreaK 200 Study (Full Analysis Set)
Categories | Sotorasib 960 mg (n = 171) | Docetaxel 75 mg/m2 (n = 174) |
|---|---|---|
Time from randomization to start of first dose of sotorasib for crossover patients (months)a | ||
n | NA | 46 |
Mean (SD) | NA | 5.86 (3.02) |
Median (range) | NA | 5.83 (1.87 to 13.63) |
Number of patients with any new anticancer therapy use, n (%)b | 62 (36.3) | 28 (16.1) |
Time from randomization to start of first subsequent anticancer therapy (months)b | ||
n | 62 | 28 |
Mean (SD) | 6.77 (4.88) | 4.03 (2.47) |
Median (range) | 4.45 (0.46 to 18.20) | 3.32 (0.07 to 9.49) |
Anticancer regimens, n (%) | ||
Checkpoint inhibitor and platinum-containing drug | 5 (2.9) | 1 (0.6) |
Combined chemotherapy and radiation therapy with non–platinum-containing drug | 2 (1.2) | 0 (0) |
Combined chemotherapy and radiation therapy with platinum-containing drug | 1 (0.6) | 0 (0) |
Non–checkpoint inhibitor immunotherapy | 4 (2.3) | 0 (0) |
Non–platinum-containing chemotherapy | 22 (12.9) | 7 (4.0) |
Docetaxel | 7 (4.1) | 0 (0) |
Gemcitabine | 5 (2.9) | 1 (0.6) |
Paclitaxel | 2 (1.2) | 1 (0.6) |
Gemcitabine | 2 (1.2) | 0 (0) |
Taxol | 2 (1.2) | 0 (0) |
Taxotere | 2 (1.2) | 0 (0) |
Vinorelbine | 2 (1.2) | 0 (0) |
Other anticancer therapy | 21 (12.3) | 8 (4.6) |
Platinum-containing chemotherapy | 8 (4.7) | 2 (1.1) |
Single-drug checkpoint inhibitor | 9 (5.3) | 8 (4.6) |
Single-drug non–platinum-containing chemotherapy | 5 (2.9) | 3 (1.7) |
Single-drug platinum chemotherapy | 2 (1.2) | 1 (0.6) |
Targeted therapy | 6 (3.5) | 6 (3.4) |
NA = not applicable; SD = standard deviation.
Note: Data cut-off date August 2, 2022.
aSummarizes crossover patients per protocol flagged based on whether the patients randomized to docetaxel received at least 1 dose of sotorasib.
bSummarizes patients who received any new anticancer therapy. Patients who received both new anticancer therapy and crossover therapy were included only if anticancer therapy was received before crossover.
Source: Clinical Study Report for the CodeBreaK 200 study.21
A summary of subsequent anticancer therapy is presented in Table 16. The need for any subsequent anticancer therapy, including crossover therapy, was documented in 36.3% and 42.0% of patients in the sotorasib and docetaxel treatment groups, respectively. Among patients in the sotorasib group who required subsequent anticancer therapy, chemotherapy was the most frequently administered therapy (21.1%). In the docetaxel treatment group, KRAS G12C inhibitor was the most frequently administered subsequent anticancer therapy (33.95%).
Table 16: Summary of Subsequent Anticancer Therapy in CodeBreaK 200 Study (Full Analysis Set)
Categories | Sotorasib 960 mg (n = 171) | Docetaxel 75 mg/m2 (n = 174) |
|---|---|---|
Any subsequent anticancer therapy, including crossover therapy, n (%) | 62 (36.3) | 73 (42.0) |
Chemotherapy | 36 (21.1) | 21 (12.1) |
KRAS G12C inhibitor | 6 (3.5) | 59 (33.9) |
Immunotherapy | 16 (9.4) | 10 (5.7) |
Checkpoint inhibitor | 14 (8.2) | 10 (5.7) |
Other | 25 (14.6) | 18 (10.3) |
Note: The data cut-off date was August 2, 2022.
Source: Clinical Study Report for the CodeBreaK 200 study.21
Efficacy
Only those efficacy outcomes and analyses of subgroups identified in the review protocol are reported. Refer to Appendix 4 for detailed efficacy data.
Overall Survival
OS data for the CodeBreaK 100 study and the CodeBreaK 200 study are summarized in Table 17. A KM plot of median OS for patients with NSCLC in the CodeBreaK 100 study is illustrated in Figure 7 for the data cut-off date of March 15, 2021, and in Appendix 4 for the data cut-off date of September 1, 2020. The results for OS at 2 years in the CodeBreaK 100 study are summarized in Appendix 4. The KM plot of OS for patients in the CodeBreaK 200 study is illustrated in Figure 8.
In the CodeBreaK 100 study, the proportion of observed deaths at the time of primary data cut-off (September 1, 2020) was 38.1%. The median OS was 12.0 months (95% CI, 9.5 months to NE). The probabilities of survival based on KM estimates at 3 months, 6 months, 9 months, and 12 months were 89.5% (95% CI, 82.7% to 93.8%), 75.5% (95% CI, 66.8% to 82.2%), 63.4% (95% CI, 53.8% to 71.5%), and 51.6% (95% CI, 36.7% to 64.5%), respectively. Results for OS at the updated analysis with data cut-off date of March 15, 2021, were generally consistent with the results from the primary data cut-off date, with median OS of 12.5 months (95% CI, 10.0 months to NE). The results for OS at 2 years, with a data cut-off date of September 9, 2022, were consistent with the results from the previous data cut-off dates, with a median OS of 12.48 months (95% CI, 9.99 months to 19.29 months). The probabilities of survival based on KM estimates at 18 months and 24 months were 42.08% (95% CI, 32.97% to 50.90%) and 31.56% (95% CI, 23.15% to 40.29%), respectively.
In the CodeBreaK 200 study, the proportions of observed deaths at the time of data cut-off (August 2, 2022) were 63.7% and 54.0% in the sotorasib and docetaxel treatment groups, respectively. The median OS was 10.64 months (95% CI, 8.94 months to 13.96 months) in the sotorasib group and 11.3 months (95% CI, 9.00 months to 14.85 months) in the docetaxel group. The stratified HR for OS was 1.01 (95% CI, 0.77 to 1.33; P = 0.53) following treatment with sotorasib versus docetaxel. At the time of the analysis, 36.3% and 46.0% of patients in the sotorasib and docetaxel groups, respectively, were censored. The imbalance was accounted for mainly by more patients withdrawing consent in the docetaxel group (18.4%) than in the sotorasib group (4.7%).
Sensitivity Analysis
In total, 59 patients randomized to docetaxel crossed over to receive treatment with sotorasib; per-protocol crossover occurred in 46 patients following disease progression, while 13 patients received sotorasib as subsequent treatment following disease progression. The sensitivity analyses of OS exploring the crossover effect in the CodeBreaK 200 study led to results that were consistent with the main analysis. In the analyses based on patients who were per-protocol crossovers, the HRs for survival were 1.01 (95% CI, 0.66 to 1.49) in the RPSFT analysis, 0.99 (95% CI, 0.73 to 1.34) in the IPCW adjusted analysis, and 0.885 (95% CI, 0.17 to 1.33) in the 2-stage approach adjusted analysis. A sensitivity analysis of OS exploring the crossover effect among all 59 crossover patients using the 2-stage approach resulted in an HR for survival of 0.82 (95% CI, 0.14 to 1.33). KM plots of sensitivity analysis of OS exploring crossover effect are presented in Figure 20 for 46 patients who were per-protocol crossovers and in Figure 21 for all 59 patients who received sotorasib upon progression.
Progression-Free Survival
PFS data for the CodeBreaK 100 study and the CodeBreaK 200 study are summarized in Table 18. KM plots for median PFS for patients with NSCLC in the CodeBreaK 100 study and the CodeBreaK 200 study are illustrated in Figure 9 and Figure 10, respectively.
Table 17: OS by RECIST 1.1 Based on BICR in CodeBreaK 100 Study (Safety Analysis Set) and CodeBreaK 200 Study (Full Analysis Set)
OS | CodeBreaK 100 study, phase II (NSCLC cohort) | CodeBreaK 200 study | ||
|---|---|---|---|---|
Sotorasib 960 mg (n = 126) | Sotorasib 960 mg (n = 171) | Docetaxel 75 mg/m2 (n = 174) | ||
Data cut-off September 1, 2020 | Data cut-off March 15, 2021 | Data cut-off August 2, 2022 | ||
Events, n (%) | 48 (38.1) | 64 (50.8) | 109 (63.7) | 94 (54.0) |
Censored, n (%) | 78 (61.9) | 62 (49.2) | 62 (36.3) | 80 (46.0) |
Alive at last follow-up | 69 (54.8) | 51 (40.5) | 50 (29.2) | 48 (27.6) |
Withdrew consent | 9 (7.1) | 9 (7.1) | 8 (4.7) | 32 (18.4) |
Lost to follow-up | 0 (0) | 2 (1.6) | 4 (2.3) | 0 (0) |
OS (KM), months | ||||
Median (95% CI) | 12.0 (9.5 to NE) | 12.5 (10.0 to NE) | 10.64 (8.94 to 13.96) | 11.30 (9.00 to 14.85) |
KM estimates, survival % (95% CI) | ||||
At 3 months | 89.5 (82.7 to 93.8)a | 89.5 (82.7 to 93.8)a | NR | NR |
At 6 months | 75.5 (66.8 to 82.2)a | 75.5 (66.8 to 82.2)a | 72.01 (64.54 to 78.16)b | 67.53 (59.50 to 74.31)b |
At 9 months | 63.4 (53.8 to 71.5)a | 63.5 (54.3 to 71.4)a | NR | NR |
At 12 months | 51.6 (36.7 to 64.5)a | 51.3 (41.9 to 59.9)a | 45.96 (38.17 to 53.39) | 46.49 (38.34 to 54.24)b |
At 24 months | NRc | NRc | NE | 33.89 (25.24 to 42.73) |
Follow-up time for OS (KM), months | ||||
Median (95% CI) | 9.3 (9.0 to 9.5) | 15.3 (15.2 to 15.7) | 17.71 (16.95 to 19.15) | 16.33 (16.07 to 17.08) |
Stratified analysisd | ||||
HR (95% CI)e | NR | NR | 1.01 (0.766 to 1.331) | |
P valuef | NR | NR | 0.53g | Reference |
BICR = blinded independent central review; CI = confidence interval; CNS = central nervous system; HR = hazard ratio; KM = Kaplan-Meier; NE = not evaluable; NR = not reported; NSCLC = non–small cell lung cancer; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; RECIST 1.1 = Response Evaluation Criteria in Solid Tumours Version 1.1; vs. = versus.
Note: Survival status may include publicly available records (where permitted) searched by the investigator after patients ended the study.
a95% CIs are based on estimated variance for log-log transformation of the KM survival estimate.
bOS rates and 95% CIs were estimated using the method by Kalbfleisch and Prentice with log-log transformation.
cThe median OS at 2 years in the CodeBreaK 100 study with data cut-off September 9, 2002, was 12.48 months (95% CI, 9.99 months to 19.29 months). The probabilities of survival based on KM estimates at 18 months and 24 months were 42.08% (95% CI, 32.97% to 50.90%) and 31.56% (95% CI, 23.15% to 40.29%), respectively.
dStratification factors: number of lines of therapy in advanced disease (1 vs. 2 vs. > 2), race (Asian vs. non-Asian), history of CNS involvement (yes vs. no).
eThe HR and 95% CI were estimated using a stratified Cox proportional hazard model. An HR of less than 1.0 represents a lower average death rate and longer OS for sotorasib relative to docetaxel.
fThe P value was calculated using a stratified log-rank test.
gThe P value was adjusted for multiple comparison using the Maurer-Bertz multiple testing procedure. The PFS and ORR hypothesis was rejected before testing OS.
Sources: Clinical Study Report for phase II of the CodeBreaK 100 study;20 Clinical Study Report for the CodeBreaK 200 study.21
In the CodeBreaK 100 study, 56.9% of patients had experienced progression or death due to any cause by the time of the September 2020 data cut-off. The median PFS was 6.7 months (95% CI, 4.9 months to 8.1 months). The probabilities of PFS at 3 months, 6 months, and 9 months were 67.5% (95% CI, 58.2% to 75.2%), 51.5% (95% CI, 41.9% to 60.4%), and 36.2% (95% CI, 26.7% to 45.8%), respectively. The results of the sensitivity analysis for PFS using the investigator’s assessment were consistent with the results obtained by BICR. At the time of the March 2021 data cut-off, 70.2% of patients had experienced progression or death due to any cause. Median PFS was consistent with the earlier data cut-off (i.e., 6.8 months; 95% CI, 5.1 months to 8.2 months).
Figure 7: KM Plot of OS of NSCLC in CodeBreaK 100 Study at the Data Cut-Off Date of March 15, 2021 (Safety Analysis Set)
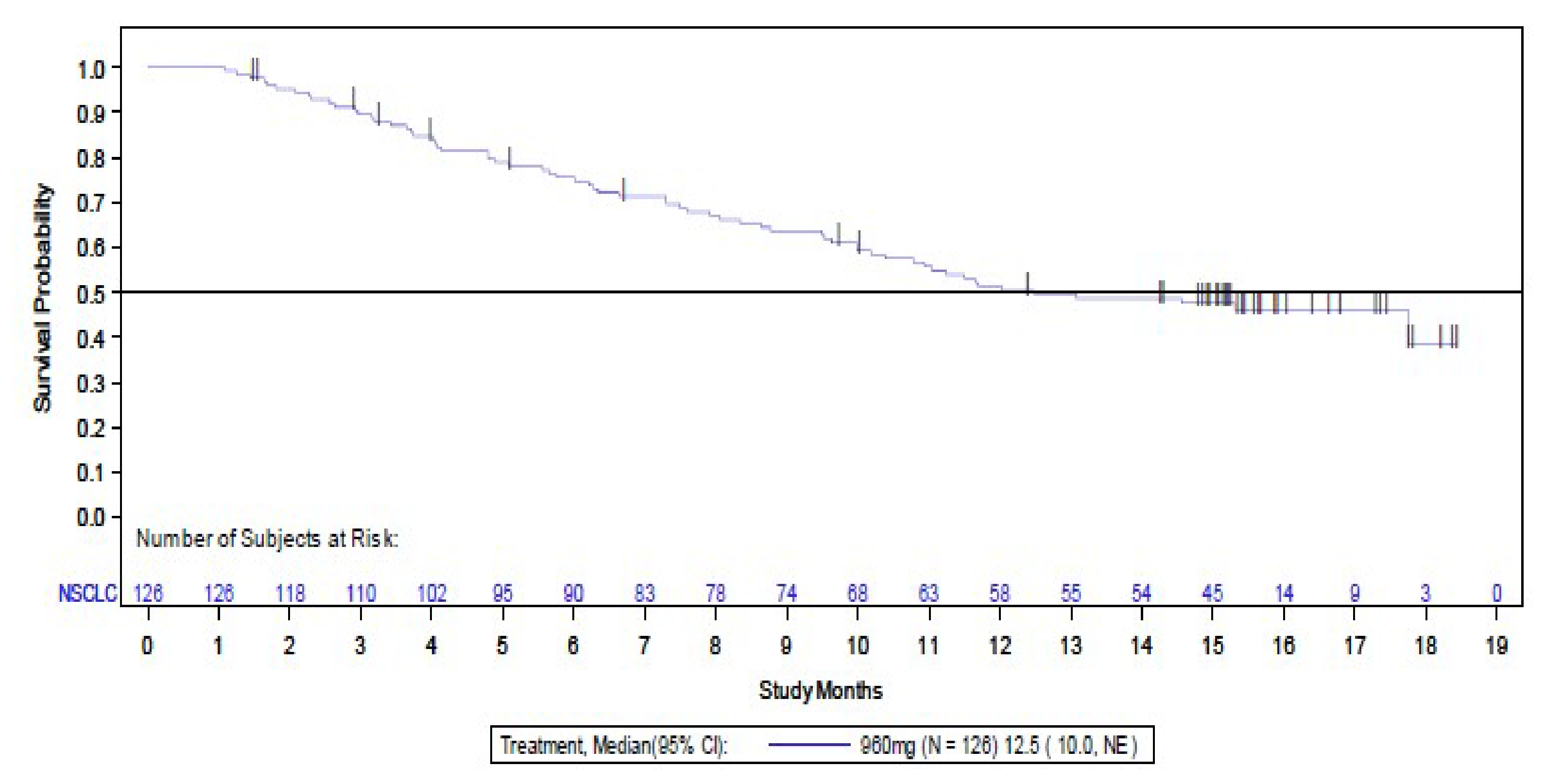
CI = confidence interval; KM = Kaplan-Meier; NE = not evaluable; NSCLC = non–small cell lung cancer; OS = overall survival.
Note: Death is considered an event.
Source: Clinical Study Report for phase II of the CodeBreaK 100 study.20
Figure 8: KM Plot of OS in CodeBreaK 200 Study at the Data Cut-Off Date of August 2, 2020 (Full Analysis Set)
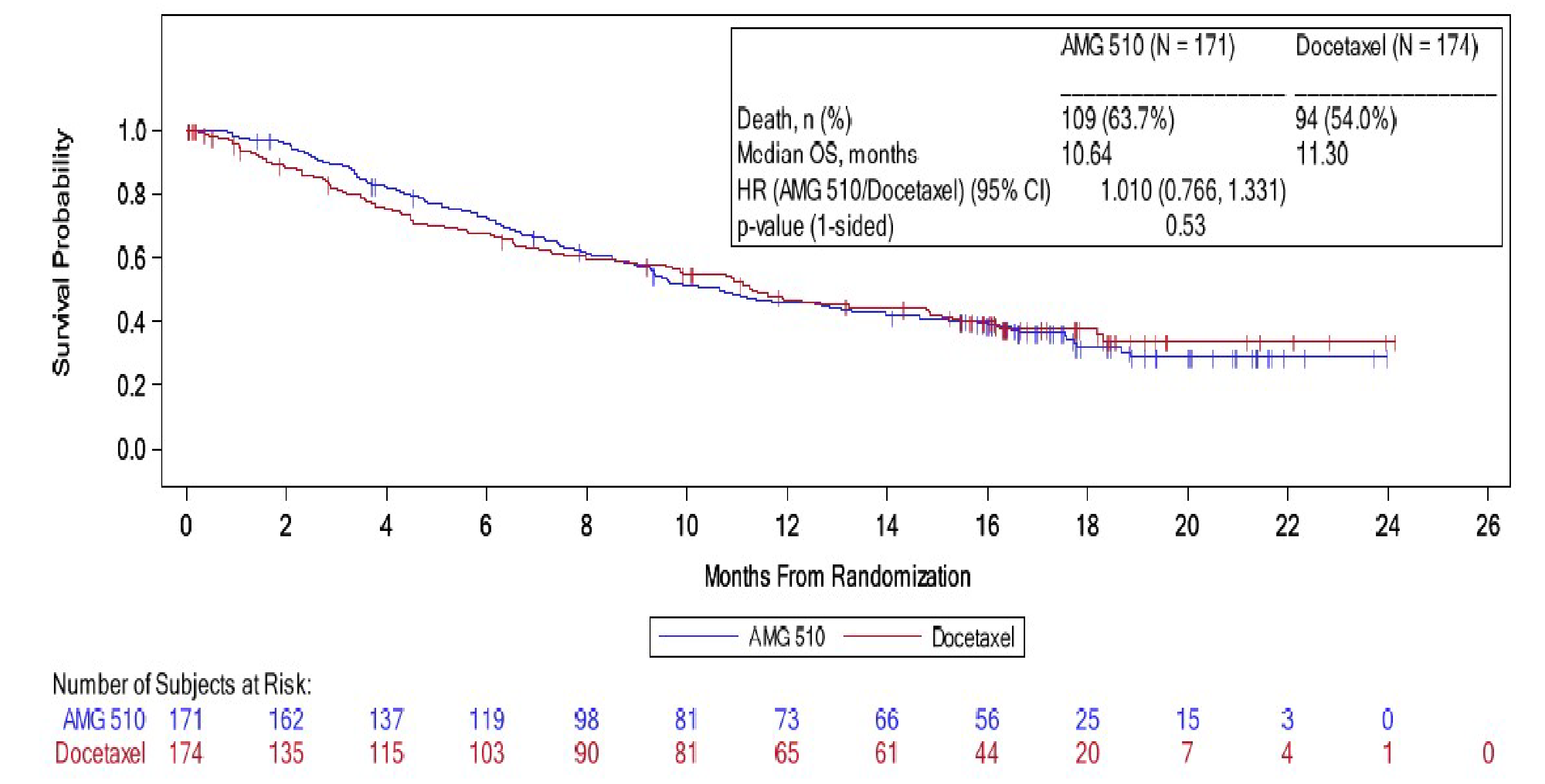
AMG 510 = sotorasib; CI = confidence interval; HR = hazard ratio; KM = Kaplan-Meier; OS = overall survival.
Source: Clinical Study Report for the CodeBreaK 200 study.21
Among patients in the CodeBreaK 200 study, disease progression or death on or before the data cut-off date was observed in 71.3% of patients in the sotorasib treatment group and 58.0% of patients in the docetaxel group. The median PFS was 5.62 months (95% CI, 4.27 months to 7.75 months) in the sotorasib group and 4.47 months (95% CI, 3.02 months to 5.68 months) in the docetaxel group at the time of data cut-off. The stratified HR for disease progression or death was 0.66 (95%, 0.51 to 0.86; P = 0.002) in favour of sotorasib versus docetaxel. At the time of the analysis, 28.7% and 42.0% of patients in the sotorasib and docetaxel groups, respectively, were censored. The imbalance was mainly accounted for by more patients without a baseline disease assessment in the docetaxel group (11.5%) compared with the sotorasib group (0.6%).
The results of the sensitivity analysis for PFS using the investigator’s assessment were consistent with the results obtained by BICR.
Table 18: PFS by RECIST 1.1 Based on BICR in CodeBreaK 100 and CodeBreaK 200 Studies (Full Analysis Set)
Progression-free survival | CodeBreaK 100 study, phase II (NSCLC cohort) | CodeBreaK 200 study | ||
|---|---|---|---|---|
Sotorasib 960 mg (n = 123) | Sotorasib 960 mg (n = 124) | Sotorasib 960 mg (n = 171) | docetaxel 75 mg/m2 (n = 174) | |
Data cut-off September 1, 2020 | Data cut-off March 15, 2021 | Data cut-off August 2, 2022 | ||
Events, n (%) | 70 (56.9) | 87 (70.2) | 122 (71.3) | 101 (58.0) |
Progressive disease | 60 (48.8) | 74 (59.7) | 100 (58.5) | 68 (39.1) |
Death due to any cause | 10 (8.1) | 13 (10.5) | 22 (12.9) | 33 (19.0) |
Censored, n (%) | 53 (43.1) | 37 (29.8) | 49 (28.7) | 73 (42.0) |
On study without disease progression | 40 (32.5) | 20 (16.1) | 15 (8.8) | 7 (4.0) |
Started new anticancer therapy | 6 (4.9) | 8 (6.5) | 24 (14.0) | 31 (17.8) |
Missed ≥ 1 consecutive assessment | 4 (3.3) | 5 (4.0) | 8 (4.7) | 11 (6.3) |
Withdrew consent | 3 (2.4) | 3 (2.4) | 1 (0.6) | 4 (2.3) |
No baseline disease assessment | 0 (0) | 0 (0) | 1 (0.6)a | 20 (11.5)a |
PFS (KM), months | ||||
Median (95% CI) | 6.7 (4.9 to 8.1) | 6.8 (5.1 to 8.2) | 5.62 (4.27 to 7.75) | 4.47 (3.02 to 5.68) |
KM estimates, PFS % (95% CI)b | ||||
At 3 months | 67.5 (58.2 to 75.2) | 67.8 (58.5 to 75.4) | NR | NR |
At 6 months | 51.5 (41.9 to 60.4) | 52.2 (42.6 to 60.9) | NR | NR |
At 9 months | 36.2 (26.7 to 45.8) | 37.5 (28.4 to 46.5) | NR | NR |
At 12 months | 0.0 (NE to NE) | 27.4 (19.2 to 36.1) | NR | NR |
PFS rate (95% CI), %c | ||||
3 months | NR | NR | 71.73 (64.01 to 78.08) | 59.42 (50.66 to 67.13) |
6 months | NR | NR | 46.49 (38.27 to 54.30) | 39.06 (30.22 to 47.79) |
12 months | NR | NR | 24.84 (17.90 to 32.38) | 10.12 (4.68 to 18.02) |
18 months | NR | NR | 13.52 (7.67 to 21.04) | 7.59 (2.69 to 15.91) |
PFS follow-up time (KM), months | ||||
Median (95% CI) | 8.3 (8.2 to 8.3) | 13.8 (13.7 to 13.8) | 15.24 (14.85 to 17.31) | 6.87 (5.42 to 12.52) |
Stratified hazardd | ||||
HR (95% CI)e | NR | NR | 0.66 (0.51 to 0.86) | |
P valuef,g | NR | NR | 0.002 | Reference |
BICR = blinded independent central review; CI = confidence interval; CNS = central nervous system; HR = hazard ratio; KM = Kaplan-Meier; NR = not reported; NSCLC = non–small cell lung cancer; PFS = progression-free survival; RECIST = Response Evaluation Criteria in Solid Tumours; vs. = versus.
Note: In the CodeBreaK 200 study, for patients who continued treatment postprogression or patients who crossed over from docetaxel to sotorasib, the first date of progression is used for PFS analysis.
aPatients who did not have any postbaseline tumour assessment per the investigator assessment were not reviewed by the BICR. These patients were considered as having no baseline in the BICR database and summarized accordingly in the table.
b95% CIs are based on estimated variance for log-log transformation of the KM survival estimate.
cEstimated using the method by Kalbfleisch and Prentice with log-log transformation.
dStratification factors: number of lines of therapy in advanced disease (1 vs. 2 vs. > 2), race (Asian vs. non-Asian), history of CNS involvement (yes vs. no).
eHR and 95% were estimated using a Cox proportional hazard model. An HR of less than 1.0 indicates a lower average event rate and a longer PFS for sotorasib relative to docetaxel.
fThe P value was calculated using a stratified log-rank test.
gThe P value was adjusted for multiple comparison using the Maurer-Bertz multiple testing procedure.
Sources: Clinical Study Report for phase II of the CodeBreaK 100 study;20 Clinical Study Report for the CodeBreaK 200 study.21
Figure 9: KM Plot of PFS of NSCLC in CodeBreaK 100 Study at Cut-Off Date of March 15, 2021 (Full Analysis Set)
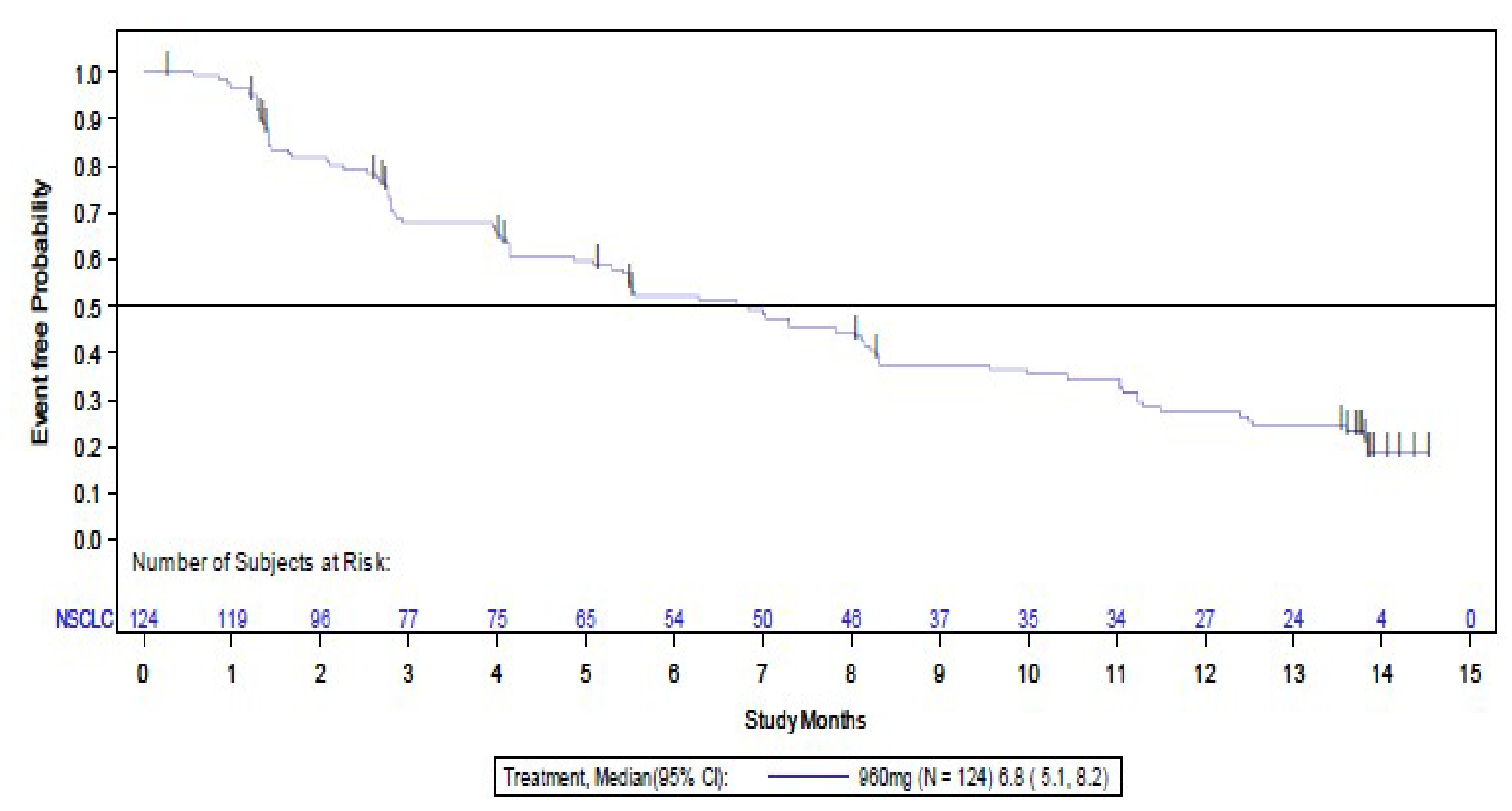
CI = confidence interval; KM = Kaplan-Meier; NSCLC = non–small cell lung cancer; PFS = progression-free survival.
Note: An event is radiological progression or death, whichever occurs first.
Source: Clinical Study Report for phase II of the CodeBreaK 100 study.20
Subgroup Analysis
Subgroup analyses of PFS among patients in the CodeBreaK 200 study at the time of the August 2, 2022, data cut-off are presented in Table 19. The findings for PFS for sotorasib versus docetaxel were generally consistent across the subgroups and consistent with the overall effect.
Figure 10: KM Plot of PFS of Sotorasib Versus Docetaxel in CodeBreaK 200 Study at Data Cut-Off Date of August 2, 2022 (Full Analysis Set)
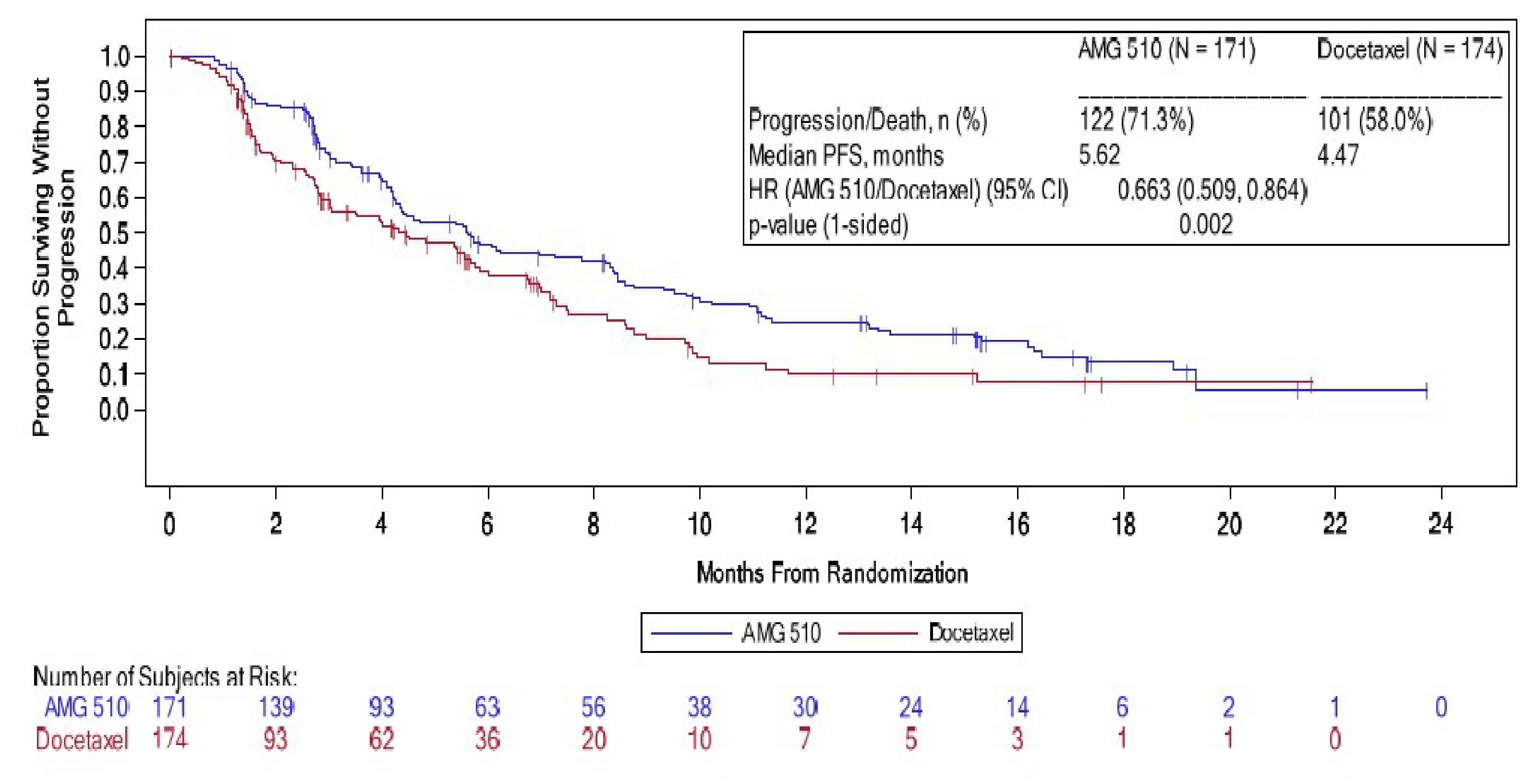
AMG 510 = sotorasib; CI = confidence interval; HR = hazard ratio; KM = Kaplan-Meier; PFS = progression-free survival.
Note: An event is radiological progression or death, whichever occurs first.
Source: Clinical Study Report for the CodeBreaK 200 study.21
Table 19: Subgroup Analysis of PFS by BICR in CodeBreaK 200 Study
Subgroup | Eventsa/patients (%) | Median PFS (95% CI),b months | Hazard ratio (95% CI)c | ||
|---|---|---|---|---|---|
Sotorasib | Docetaxel | Sotorasib | Docetaxel | ||
ECOG Performance Status at baseline | |||||
0 | 39/59 (66.1) | 31/59 (52.5) | 8.44 (5.72 to 11.24) | 6.74 (4.47 to 7.49) | 0.63 (0.38 to 1.05) |
1 | 83/112 (74.1) | 70/115 (60.9) | 4.37 (3.94 to 5.68) | 2.79 (1.94 to 5.39) | 0.61 (0.44 to 0.84) |
Histology | |||||
Squamous | 1/1 (100) | 6/7 (85.7) | NR | NR | NR |
Nonsquamous | 120/169 (71.0) | 93/165 (56.4) | 5.68 (4.34 to 8.21) | 4.83 (3.48 to 6.01) | 0.69 (0.53 to 0.91) |
Prior lines of anticancer therapy | |||||
1 | 52/77 (67.5) | 46/78 (59.0) | 4.17 (3.12 to 8.38) | 4.21 (2.73 to 5.55) | 0.70 (0.47 to 1.04) |
2 | 46/65 (70.8) | 40/69 (58.0) | 5.72 (4.47 to 9.53) | 4.83 (2.83 to 7.00) | 0.61 (0.40 to 0.92) |
> 2 | 24/29 (82.8) | 15/27 (55.6) | 4.70 (4.07 to 8.57) | 4.01 (1.45 to 8.97) | 0.74 (0.37 to 1.46) |
CI = confidence interval; CNS = central nervous system; ECOG = Eastern Cooperative Oncology Group; NR = not reported; PFS = progression-free survival; vs. = versus.
Note: Randomization stratification factors are number of prior lines of therapy in advanced disease (1 vs. 2 vs. > 2), race (Asian vs. non-Asian), and history of CNS involvement (yes vs. no). For subgroup analyses, a stratification factor is not used for the stratified analysis if the stratification factor is the subgroup of interest. If the number of patients in a subgroup level is less than 10 within any treatment group, then only the numbers of events and/or patients are displayed for that subgroup, not the inferential statistics. Data cut-off date August 2, 2022.
aEvents are disease progression and death.
bMedians were estimated using the Kaplan-Meier method; 95% CIs were estimated using the method by Klein and Moeschberger with log-log transformation.
cHazard ratios and 95% CIs were estimated using a stratified Cox proportional hazards model. A hazard ratio of less than 1.0 indicates a lower average death rate and a longer OS for sotorasib relative to docetaxel.
Source: Clinical Study Report for the CodeBreaK 200 study.21
Health-Related Quality of Life
In the CodeBreaK 200 study, hierarchical testing was stopped at the non–statistically significant OS end point. Accordingly, the reporting of key secondary HRQoL outcomes in the CodeBreaK 200 study is descriptive. All HRQoL and PRO data presented from the CodeBreaK 100 study and the CodeBreaK 200 study should be considered descriptive in nature.
European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30
In the CodeBreaK 100 study, 98 patients (78%) completed the EORTC QLQ-C30 at baseline. Compliance rates for the questionnaire were consistently high, above 90%. The number of patients available to complete the measure diminished over time. At the end of treatment, 38 patients (43.2%) completed the assessment. Least squares mean changes from baseline in EORTC QLQ-C30 global health status and physical function — the health scales deemed most important by patients — over time are illustrated in Figure 11 and Figure 12, respectively. Over time, scores for both global health status and physical functioning appeared to remain relatively stable. Changes from baseline in global health status ranged from –5.33 (SD = 15.57) in cycle 11 (n = 25) to + 1.37 (SD = 19.44) in cycle 5 (n = 61). Changes from baseline in physical functioning ranged from –8.57 (SD = 20.33) in cycle 13 (n = 14) to + 6.67 (SD = 22.05) in cycle 7 (n = 33).
In the CodeBreaK 200 study, the EORTC QLQ-C30 — a key secondary outcome — was completed at baseline by 168 patients (98.2%) and 158 patients (90.8%) in the sotorasib and docetaxel treatment groups, respectively. The number of patients available to complete the measure diminished with each cycle. At cycle 5, day 1 (week 12), the EORTC QLQ-C30 was completed by 69 patients (39.7%) in the docetaxel treatment group and 106 patients (62.0%) in the sotorasib treatment group. The least squares mean changes from baseline at week 12 for the EORTC QLQ-C30 global health status and physical functioning scales are illustrated in Figure 13. The differences between groups in least squares change from baseline to week 12 were 6.93 (95% CI, 3.66 to 10.19) for global health status and 8.78 (95% CI, 5.39 to 12.17) for physical functioning, favouring treatment with sotorasib (n = 106) relative to docetaxel (n = 69).
EQ-5D-5L and EQ VAS
A summary of the EQ-5D-5L results for the CodeBreaK 100 study is presented in Table 20. Patients’ results on the EQ-5D-5L remained relatively stable during the treatment period. At baseline (n = 86; 68.3%), most patients (68% to 94%) reported that they had no problems or slight problems with the dimensions of health assessed by the EQ-5D-5L. At the end of the treatment phase (n = 28; 22.2%), 42.9% and 21.4% of patients reported no problems or slight problems, respectively. The EQ VAS scores remained relatively stable during the treatment period. The mean EQ VAS score at baseline was 70.2 (SD = 17.5; n = 86), indicating that patients generally rated their health favourably (with a score of 100 indicating best health imaginable). Change in mean score from baseline over the treatment period ranged from –24.0 (SD = 32.8) in cycle 15 (n = 4) to 2.7 (SD = 18.6) in cycle 3 (n = 69) and 2.7 (SD = 16.6; cycle 7, n = 31). By the end of the treatment phase (n = 28), the mean EQ VAS score was 61.5 (SD = 19.5), which was associated with a mean change from baseline of –10.6 (SD = 19.3). For both the EQ-5D-5L and the EQ VAS, the number of patients available to complete assessments dropped by more than 50% after cycle 6 in the CodeBreaK 100 study.
In the CodeBreaK 200 study, a baseline EQ-5D-5L was completed by 160 patients (93.6%) in the sotorasib treatment group and 138 patients (79.3%) in the docetaxel treatment group. The number of patients available to complete the measure diminished consistently with each cycle. At cycle 5, day 1, the EQ-5D-5L was completed by 105 patients (61.4%) in the sotorasib treatment group and 67 patients (38.5%) in the docetaxel treatment group. A summary of the EQ-5D-5L scales in the CodeBreaK 200 study is presented in Table 21. At baseline, most patients in both the sotorasib (64.4% to 93.2%) and docetaxel (69.6% to 90.6%) treatment groups reported that they had no problems or slight problems with the dimensions of health assessed by the EQ-5D-5L. At cycle 5, day 1, 79.0% to 96.2% of patients in the sotorasib treatment group and 61.2% to 85.1% of patients in the docetaxel treatment group reported that they had no problems or slight problems. Between-group differences for change from baseline on the EQ-5D-5L scales were not reported. Baseline EQ VAS — a secondary outcome — was completed by 166 patients (97.1%) and 154 patients (88.5%) in the sotorasib and docetaxel treatments, respectively. Compliance rates for this measure were consistently greater than 80%. The number of patients available to complete the measure diminished consistently with each cycle. At cycle 5, day 1, the EQ VAS was completed by 106 patients (62.0%) in the sotorasib group and 69 patients (39.7%) in the docetaxel group. Changes in EQ VAS scores following treatment with sotorasib and docetaxel in the CodeBreaK 200 study are illustrated in Figure 14. At baseline, mean EQ VAS scores were 67.6 (SD = 19.9) and 68.3 (SD = 20.3) in the sotorasib and docetaxel treatment groups, respectively. At cycle 5, day 1, the mean EQ VAS score for patients in the sotorasib treatment group was 73.2 (SD = 18.6), which was associated with a mean change from baseline of 2.2 (SD = 15.5) for sotorasib. For patients in the docetaxel treatment group (n = 67), the mean EQ VAS score at cycle 5, day 1 was 67.7 (SD = 20.8), which was associated with a mean change from baseline of –5.8 (SD = 18.2). Between-group differences for change from baseline on the EQ VAS were not reported.
Figure 11: Least Squares Mean Change From Baseline in EORTC QLQ-C30 Global Health Status Over Time in CodeBreaK 100 Study (PRO Analysis Set)

EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; NSCLC = non–small cell lung cancer; PRO = patient-reported outcome.
Note: The data cut-off date was September 1, 2020.
Source: Clinical Study Report for CodeBreaK 100 study PRO data.61
Figure 12: Least Squares Mean Change From Baseline in EORTC QLQ-C30 Physical Functioning Over Time in CodeBreaK 100 Study (PRO Analysis Set)
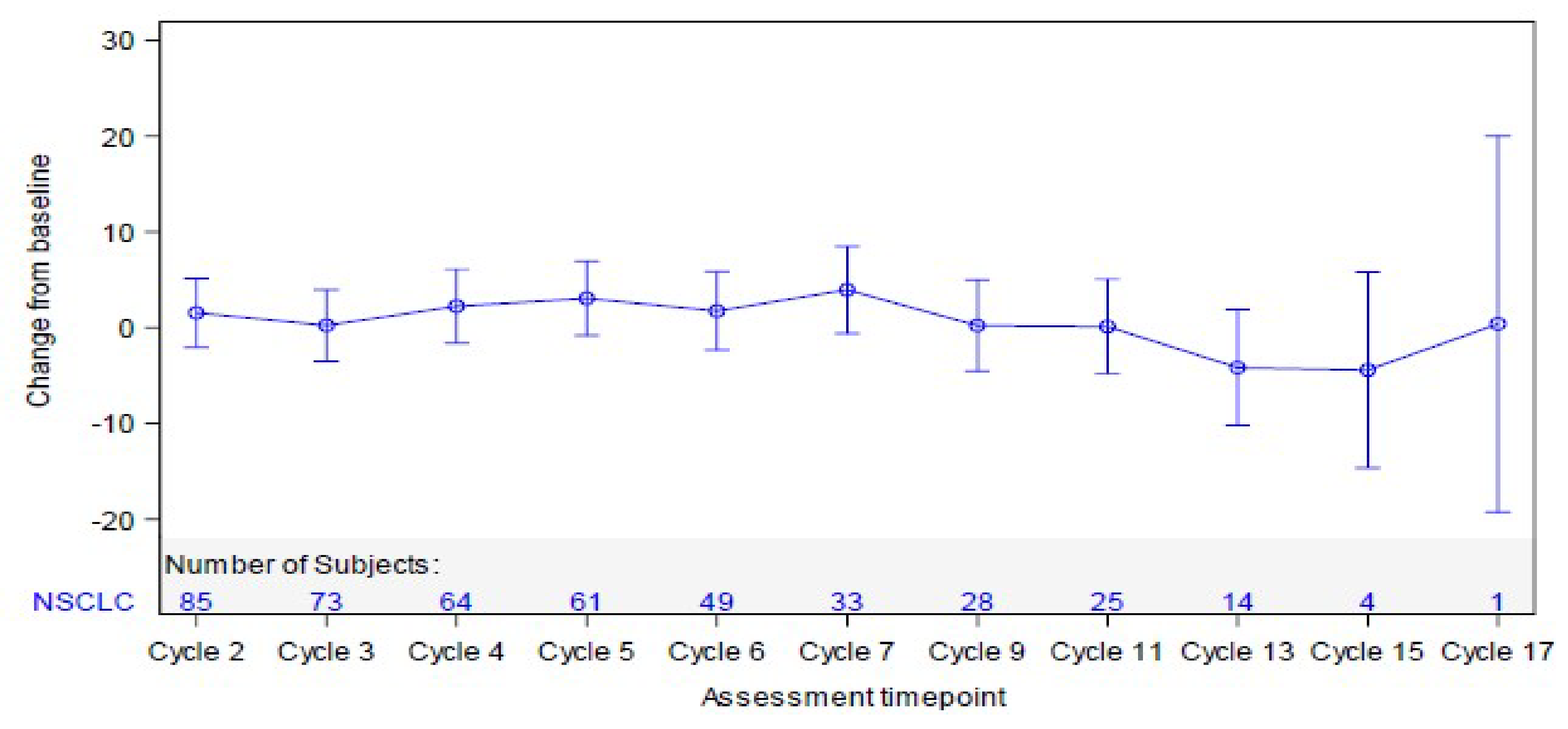
EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; NSCLC = non–small cell lung cancer; PRO = patient-reported outcome.
Note: The data cut-off date was September 1, 2020.
Source: Clinical Study Report for CodeBreaK 100 study PRO data.61
Figure 13: Least Squares Mean Change From Baseline for EORTC QLQ-C30 Scales in CodeBreaK 200 Study — MMRM (EORTC QLQ-C30 Analysis Set)
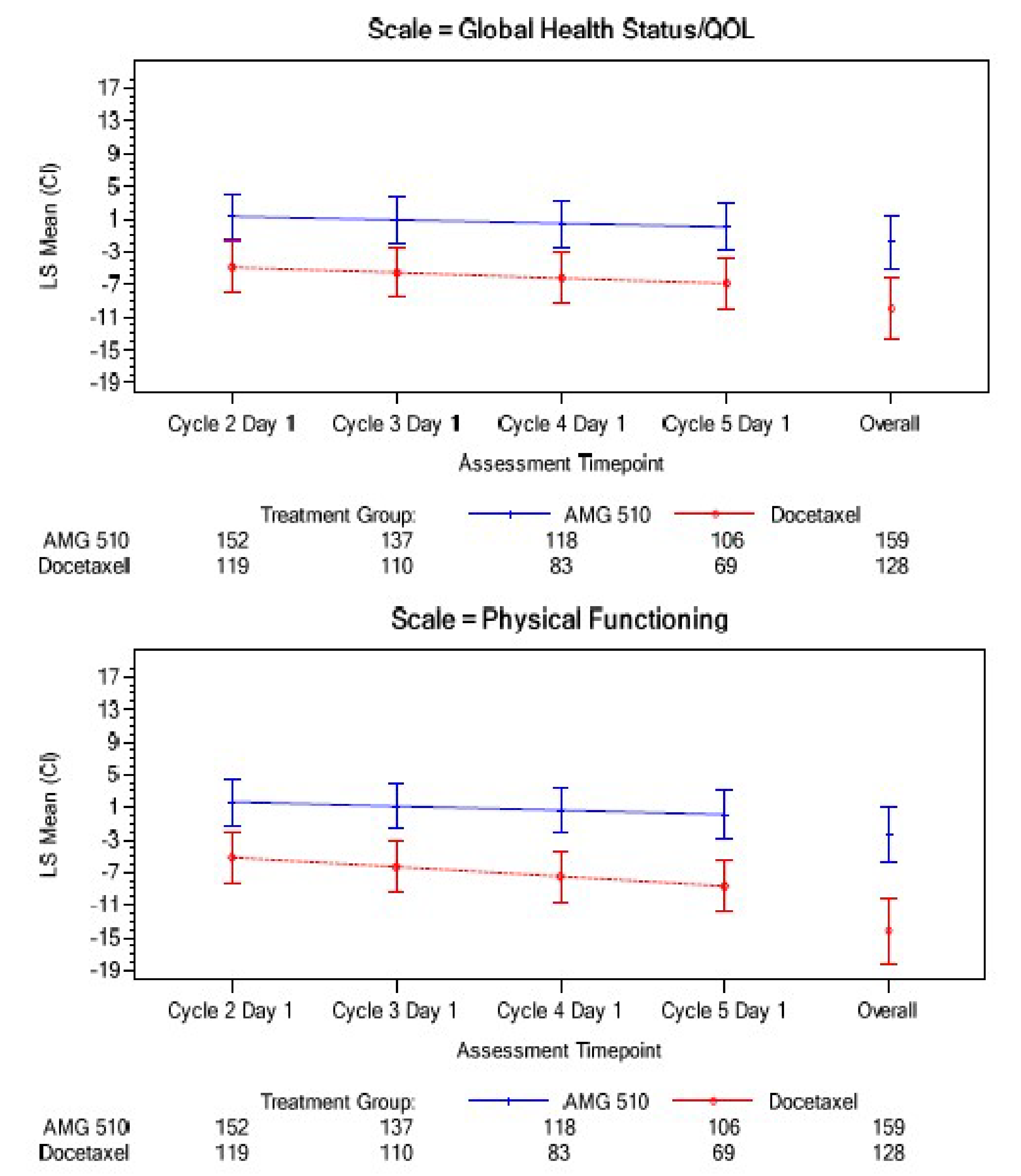
AMG 510 = sotorasib; CI = confidence interval; CNS = central nervous system; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; LS = least squares; MMRM = mixed-effects model for repeated measures; QOL = quality of life; vs. = versus.
Notes: The data cut-off date was August 2, 2022.
MMRM is based on change from baseline up to cycle 5, day 1 (week 12) as the dependent variable; intercept, time, baseline score, treatment, treatment-by-time interaction, and randomization stratification factors as fixed effects; and patient intercept and slope of time for the change from baseline as random effects. Overall represents all postbaseline visits, including visits beyond cycle 5, day 1, excluding follow-up visits. Randomization stratification factors: number of prior lines of therapy in advanced disease (1 vs. 2 vs. > 2), race (Asian vs. non-Asian), and history of CNS involvement (yes vs. No).
Source: Clinical Study Report for the CodeBreaK 200 study.21
Table 20: Summary of EQ-5D-5L in CodeBreaK 100 Study (PRO Analysis Set)
EQ-5D-5L responses | CodeBreaK 100 study, phase II (NSCLC cohort) Sotorasib 960 mg EQ-5D-5L scales | ||||
|---|---|---|---|---|---|
Mobility | Self-care | Usual activities | Pain or discomfort | Anxiety or depression | |
Baseline, n (%) | |||||
n | 86 | 86 | 86 | 86 | 86 |
No problems | 49 (57.0) | 73 (84.9) | 43 (50.0) | 33 (38.4) | 53 (61.6) |
Slight problems | 18 (20.9) | 8 (9.3) | 30 (34.9) | 25 (29.1) | 22 (25.6) |
Moderate problems | 14 (16.3) | 5 (5.8) | 9 (10.5) | 17 (19.8) | 7 (8.1) |
Severe problems | 5 (5.8) | 0 (0) | 1 (1.2) | 9 (10.5) | 4 (4.7) |
Unable to perform | 0 (0) | 0 (0) | 3 (3.5) | 2 (2.3) | 0 (0) |
End of treatment,a n (%) | |||||
n | 28 | 28 | 28 | 28 | 28 |
No problems | 12 (42.9) | 18 (64.3) | 6 (21.4) | 5 (17.9) | 14 (50.0) |
Slight problems | 6 (21.4) | 6 (21.4) | 12 (42.9) | 9 (32.1) | 9 (32.1) |
Moderate problems | 6 (21.4) | 1 (3.6) | 7 (25.0) | 9 (32.1) | 3 (10.7) |
Severe problems | 4 (14.3) | 3 (10.7) | 3 (10.7) | 4 (14.3) | 2 (7.1) |
Unable to perform | 0 (0) | 0 (0) | 0 (0) | 1 (3.6) | 0 (0) |
NSCLC = non–small cell lung cancer; PRO = patient-reported outcome.
Note: The data cut-off date was September 1, 2020.
aEnd of treatment was defined as the last assessment for the protocol-specified treatment phase of the study for an individual patient.
Source: Clinical Study Report of PRO data for the CodeBreaK 100 study.61
Table 21: Summary of EQ-5D-5L Dimensions in CodeBreaK 200 Study (EQ-5D-5L Analysis Set)
EQ-5D-5L responses | EQ-5D-5L dimensions | ||||
|---|---|---|---|---|---|
Mobility | Self-care | Usual activities | Pain or discomfort | Anxiety or depression | |
Baseline, n (%) | |||||
Sotorasib | |||||
n | 160 | 160 | 160 | 160 | 160 |
No problem | 79 (49.4) | 127 (79.4) | 77 (48.1) | 48 (30.0) | 82 (51.3) |
Slight problem | 41 (25.6) | 22 (13.8) | 45 (28.1) | 55 (34.4) | 49 (30.6) |
Moderate problem | 32 (20.0) | 8 (5.0) | 26 (16.3) | 42 (26.3) | 21 (13.1) |
Severe problem | 8 (5.0) | 3 (1.9) | 8 (5.0) | 15 (9.4) | 7 (4.4) |
Extreme problem | 0 (0) | 0 (0) | 4 (2.5) | 0 (0) | 1 (0.6) |
Docetaxel | |||||
n | 138 | 138 | 138 | 138 | 138 |
No problem | 61 (44.2) | 104 (75.4) | 52 (37.7) | 55 (39.9) | 67 (48.6) |
Slight problem | 35 (25.4) | 21 (15.2) | 51 (37.0) | 41 (29.7) | 44 (31.9) |
Moderate problem | 29 (21.0) | 8 (5.8) | 22 (15.9) | 31 (22.5) | 21 (15.2) |
Severe problem | 13 (9.4) | 4 (2.9) | 10 (7.2) | 9 (6.5) | 5 (3.6) |
Extreme problem | 0 (0) | 1 (0.7) | 3 (2.2) | 2 (1.4) | 1 (0.7) |
Cycle 15, day 1, n (%) | |||||
Sotorasib | |||||
n | 52 | 52 | 52 | 52 | 52 |
No problem | 28 (53.8) | 45 (86.5) | 33 (63.5) | 27 (51.9) | 42 (80.8) |
Slight problem | 18 (34.6) | 7 (13.5) | 16 (30.8) | 17 (32.7) | 8 (15.4) |
Moderate problem | 6 (11.5) | 0 (0) | 3 (5.8) | 8 (15.4) | 2 (3.8) |
Severe problem | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Extreme problem | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Docetaxel | |||||
n | 10 | 10 | 10 | 10 | 10 |
No problem | 7 (70.0) | 10 (100) | 7 (70.0) | 6 (60.0) | 6 (60.0) |
Slight problem | 1 (10.0) | 0 (0) | 1 (10.0) | 1 (10.0) | 3 (30.0) |
Moderate problem | 0 (0) | 0 (0) | 1 (10.0) | 3 (30.0) | 1 (10.0) |
Severe problem | 2 (20.0) | 0 (0) | 1 (10.0) | 0 (0) | 0 (0) |
Extreme problem | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
Note: The data cut-off date was August 2, 2022.
Source: Clinical Study Report for the CodeBreaK 200 study.21
Figure 14: Cumulative Distribution Function Plot of Change From Baseline for EQ VAS Score in CodeBreaK 200 Study (EQ-5D-5L Analysis Set)

AMG 510 = sotorasib; EQ VAS = EQ visual analogue scale.
Notes: The data cut-off date was August 2, 2022. Only visits on cycle 1, day 1, cycle 3, day 1, cycle 4, day 1, and cycle 5, day 1 are included in the analysis.
Source: Clinical Study Report for the CodeBreaK 200 study.21
Symptom Burden
EORTC QLQ-C30 Symptom Scales
A summary of the EORTC QLQ-C30 symptom scores from the CodeBreaK 100 study is presented in Table 22. The symptoms presented in the table were those deemed most important to patients. Baseline EORTC QLQ-C30 symptom scores were completed by 94 patients (76.4%). The number of patients available to complete the measure diminished consistency with each cycle. After cycle 6, the number of patients available to complete assessments had dropped by more than 50%. From baseline (n = 94) to the end of the treatment phase of the study (n = 32), mean scores were sustained for diarrhea (no change) and dyspnea (mean change from baseline = 3.13 [SD = 39.1]). The symptom scores for fatigue, nausea or vomiting, and pain increased during the study period.
In the CodeBreaK 200 study, the dyspnea subscale was considered the most important of all symptom subscales, and was the only symptom-specific subscale of the EORTC QLQ-C30 reported. The least squares mean change from baseline to week 12 in each group for the dyspnea composite scale of the EORTC QLQ-C30 is illustrated in Figure 15. At cycle 2, day 1, a total of 148 patients (86.5%) in the sotorasib treatment group and 112 patients (64.4%) in the docetaxel treatment group completed the dyspnea subscale. At cycle 5, day 1, the proportions of patients available to complete the dyspnea subscale of the EORTC QLQ-C30 were 61.4% and 38.5% in the sotorasib and docetaxel treatment groups, respectively. The difference between groups in least squares change from baseline for dyspnea at week 12 was –10.09 (95% CI, –13.39 to –6.78), favouring treatment with sotorasib (n = 105) relative to docetaxel (n = 67).
Table 22: Summary of EORTC QLQ-C30 Symptom Scales in CodeBreaK 100 Study (PRO Analysis Set)
Scores | CodeBreaK 100 study, phase II (NSCLC cohort) Sotorasib 960 mg EORTC QLQ-C30 symptom scale scores | ||||
|---|---|---|---|---|---|
Fatigue | Nausea or vomiting | Pain | Dyspnea | Diarrhea | |
Baseline | |||||
n | 94 | 94 | 94 | 94 | 94 |
Mean (SD) | 38.3 (23.1) | 7.3 (13.3) | 29.3 (28.6) | 40.1 (28.8) | 6.7 (14.3) |
End of treatmenta | |||||
n | 32 | 32 | 32 | 32 | 32 |
Mean (SD) | 49.0 (29.7) | 14.6 (19.3) | 48.4 (31.2) | 38.5 (30.7) | 6.25 (13.2) |
Change from baseline to end of treatmenta | |||||
Mean (SD) | 9.0 (26.1) | 4.7 (25.5) | 12.5 (25.4) | 3.13 (39.1) | 0.0 (20.7) |
EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; NSCLC = non–small cell lung cancer; PRO = patient-reported outcome; SD = standard deviation.
Note: The data cut-off date was September 1, 2020.
aEnd of treatment was defined as the last assessment for the protocol-specified treatment phase of the study for an individual patient.
Source: Clinical Study Report of PRO data for the CodeBreaK 100 study.61
Figure 15: Least Squares Mean Change From Baseline to Week 12 in EORTC QLQ-C30 Symptoms of Dyspnea in CodeBreaK 200 Study (EORTC QLQ-C30 Analysis Set)
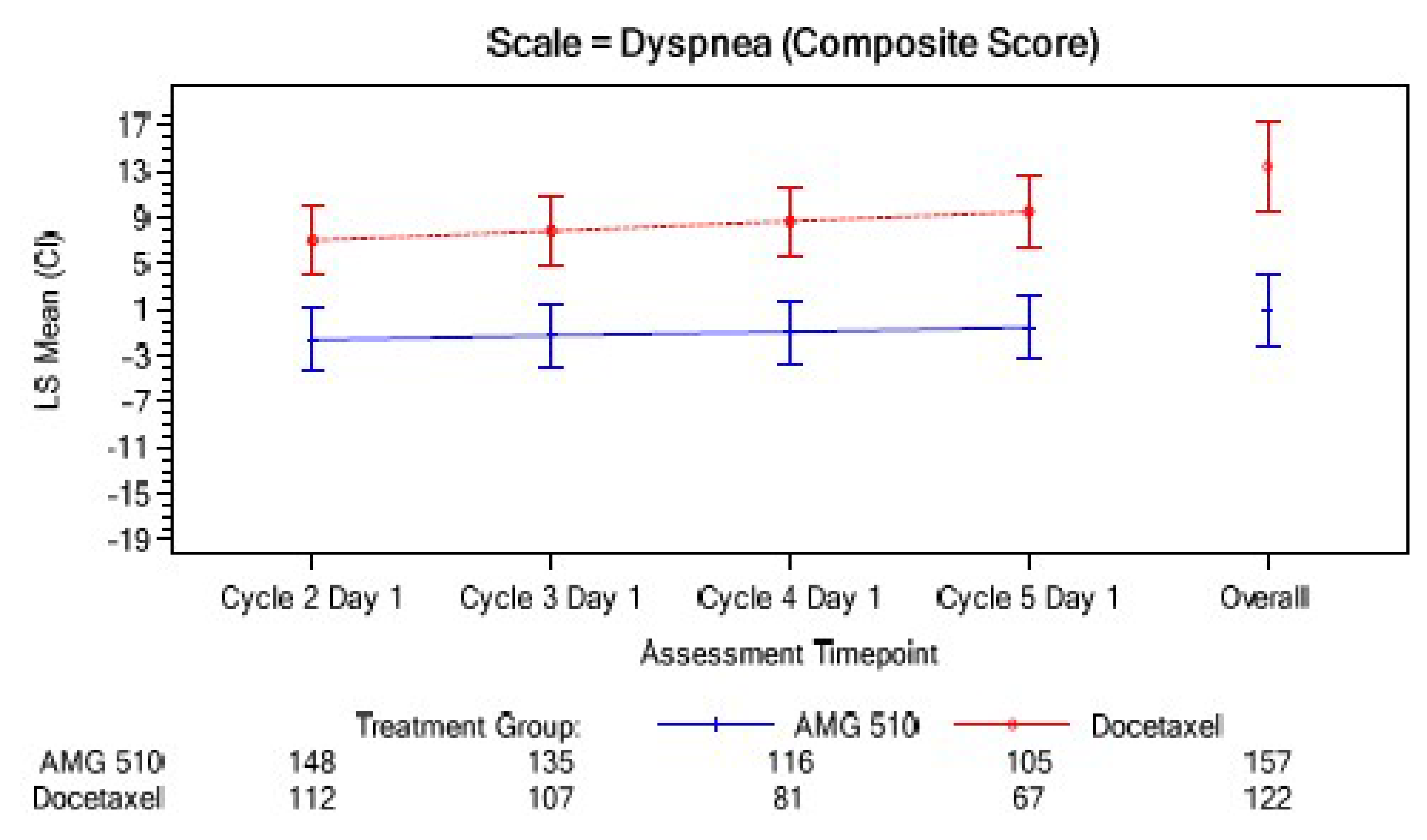
AMG 510 = sotorasib; CI = confidence interval; CNS = central nervous system; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; LS = least squares; MMRM = mixed-effects model for repeated measures; vs. = versus.
Notes: The data cut-off date was August 2, 2022.
MMRM is based on change from baseline to cycle 5, day 1 (week 12) as the dependent variable; intercept, time, baseline score, treatment, treatment-by-time interaction, and randomization stratification factors as fixed effects; and patient intercept and slope of time for the change from baseline as random effects. Overall represents all postbaseline visits, including visits beyond cycle 5, day 1, excluding follow-up visits. Randomization stratification factors: number of prior lines of therapy in advanced disease (1 vs. 2 vs. > 2), race (Asian vs. non-Asian), and history of CNS involvement (yes vs. no).
Source: Clinical Study Report for the CodeBreaK 200 study.21
EORTC QLQ-LC13 Symptom Scales
The 3 main symptoms of lung cancer are dyspnea, cough, and chest pain; thus, these were the focus of the assessment. Least squares mean changes from baseline for the EORTC QLQ-LC13 subscales for dyspnea, cough, and chest pain from the CodeBreaK 100 study are illustrated in Figure 16. The EORTC QLQ-LC13 was completed by 90 patients (71.4%) at baseline and by 36 patients (40.9%) at the end of the treatment phase. After cycle 6, the total number of patients available to complete assessments had dropped by more than 50%. Least squares mean scores were maintained or decreased over time for the EORTC QLQ-LC13 subscales of dyspnea, cough, and chest pain from baseline (n = 86) to the end of the treatment phase. The least squares mean changes ranged from –11.2 (95% CI, –16.2 to –6.1) in cycle 2 (n = 77) to –7.1 (95% CI, –13.2 to –1.1) in cycle 6 (n = 45) for cough; from –4.9 (95% CI, –10.3 to 0.4) in cycle 7 (n = 31) to –0.44 (95% CI, –5.12 to 4.24) in cycle 6 (n = 45) for chest pain; and from –3.4 (95% CI, –7.8 to 1.0) in cycle 4 (n = 58) to –0.14 (95% CI, –5.7 to 5.41) in cycle 9 (n = 25) for dyspnea.
Figure 16: Least Squares Mean Change From Baseline in EORTC QLQ-LC13 Symptoms of Dyspnea, Cough, and Chest Pain in CodeBreaK 100 Study (PRO Analysis Set)
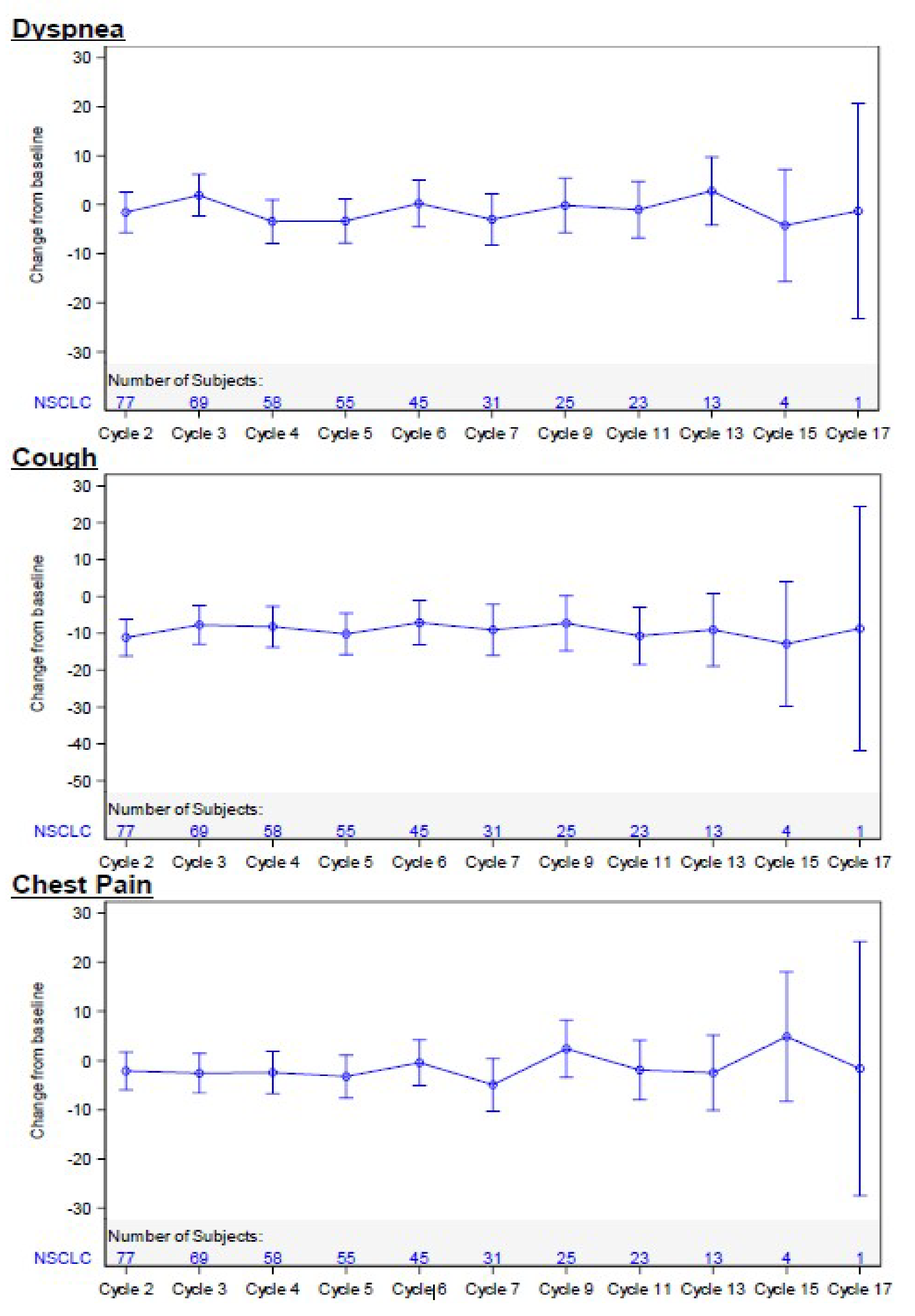
CI = confidence interval; EORTC QLQ-LC13 – European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Lung Cancer Module; NSCLC = non–small cell lung cancer; PRO = patient reported outcome.
Note: Data cut-off date September 1, 2020, for the CodeBreaK 100 study.
Source: Clinical Study Report of PRO data for the CodeBreaK 100 study.61
In the CodeBreaK 200 study, the dyspnea, cough, and chest pain subscales of the EORTC QLQ-LC13 were completed at baseline by 166 patients (97.1%) and 154 patients (88.5%) in the sotorasib and docetaxel treatment groups, respectively. Compliance rates were consistently high, mostly above 90%. The numbers of patients who completed the EORTC QLQ-LC13 at cycle 5, day 1 (week 12) in the sotorasib and docetaxel treatment groups were 106 (62.0%) and 69 (39.7%), respectively. The total number of patients available to provide assessments dropped by more than 50% at cycle 6 day 1. The odds of improved symptoms at week 12 (cycle 5, day 1) are presented in Table 23. The odds of improved symptoms at week 12 favoured sotorasib relative to docetaxel for cough (odds ratio = 3.21; 95% CI, 1.55 to 6.65) and dyspnea (odds ratio = 3.58; 95% CI, 1.98 to 6.46). The odds ratio of improved chest pain at week 12 was 1.56 (95% CI, 0.82 to 2.96) for sotorasib compared to docetaxel.
Patient Global Impression of Severity
In the CodeBreaK 100 study, no patient completed the PGIS questionnaire from baseline through to cycle 3. Given that the PGIS analysis set required patients to have a baseline value, the analysis for PGIS was not completed.
In the CodeBreaK 200 study, baseline PGIS was completed by 140 patients (81.9%) in the sotorasib treatment group and 107 patients (61.5%) in the docetaxel treatment group. At cycle 5, day 1, the proportions of patients who completed the PGIS were 62.0% in the sotorasib treatment group and 39.7% in the docetaxel treatment group. The proportions of patients in the sotorasib treatment group reporting none, mild, moderate, and severe baseline symptoms on the PGIS for cough were 35.0%, 47.9%, 14.3%, and 2.9%, respectively; for chest pain, these proportions were 50.7%, 32.1%, 15.7%, and 1.4%, respectively; for dyspnea, the proportions were 27.1%, 52.9%, 15.7%, and 4.3%, respectively. At cycle 5, day 1, the proportions of patients receiving sotorasib who reported no, mild, moderate, and severe symptoms for cough were 50.5%, 38.1%, 9.5%, and 1.9%, respectively; for chest pain, the proportions were 74.3%, 20.0%, 2.9%, and 2.9%, respectively; and for dyspnea, the proportions were 35.2%, 51.4%, 10.5%, and 2.9%, respectively. The proportions of patients in the docetaxel treatment group reporting no, mild, moderate, and severe symptoms at baseline for cough were 32.7%, 44.9%, 15.0%, and 7.5%, respectively; for chest pain, 62.6%, 26.2%, 11.2%, and 0.0%, respectively; and for dyspnea, 27.1%, 46.7%, 20.6%, and 5.6%, respectively. By cycle 5, day 1, the proportions of patients receiving docetaxel who reported no, mild, moderate, and severe symptoms for cough were 35.8%, 38.8%, 16.4%, and 9.0%, respectively; for chest pain, the proportions were 68.7%, 20.9%, 10.4%, and 0.0%, respectively; and for dyspnea, 17.9%, 47.8%, 25.4%, and 9.0%, respectively. Differences between groups were not reported at any time point.
Patient Global Impression of Change
In the CodeBreaK 100 study, 1 patient completed the PGIC from baseline to cycle 4. From cycles 6 (n = 17) to 13 (n = 21), 90% to 100% of patients rated their cough, chest pain, and shortness of breath on the PGIC as “about the same,” “a little better,” or “much better.” At the end of the treatment phase (n = 18), 77.8% to 88.9% of patients rated their symptoms on the PGIC as “about the same,” “a little better,” or “much better.” The number of patients available to complete assessments for the PGIC scale was low overall, with the largest number being assessed at cycle 11 (n = 32).
In the CodeBreaK 200 study, 137 patients (80.1%) in the sotorasib treatment group and 109 patients (62.6%) in the docetaxel group completed the PGIC at cycle 3, day 1. The proportions of patients who completed the PGIC at cycle 5 day were 106 (62.0%) and 69 (39.7%) in the sotorasib and docetaxel treatment groups, respectively. At cycle 3, day 1, approximately half the patients who received treatment with sotorasib reported on the PGIC that their symptoms were about the same relative to baseline for cough (48.2%), chest pain (46.7%), and dyspnea (46.7%). By cycle 5, day 1, more than half the patients in the sotorasib group reported that their symptoms were a little or much better for cough (59.4%), chest pain (56.6%), and dyspnea (60.3%). For patients who received docetaxel, at cycle 3, day 1, more than half reported that their symptoms were just about the same relative to baseline for cough (55.0%), chest pain (57.8%), and dyspnea (52.3%). By cycle 5, day 1, less than half of the patients who received docetaxel maintained that their symptoms were about the same for cough (43.5%), chest pain (44.9%), and dyspnea (49.3%). Differences between groups were not reported at any time point.
Table 23: Change From Baseline on EORTC QLQ-LC13 Symptom Scales in CodeBreaK 200 Study (GEE; EORTC QLQ-LC13 Analysis Set)
Symptom scale | Sotorasib | Docetaxel | Odds ratio (95% CI)a,b | ||
|---|---|---|---|---|---|
n | Improved n (%) | n | Improved n (%) | ||
Dyspnea | |||||
Cycle 2, day 1 | 148 | 56 (37.8) | 112 | 33 (29.5) | 1.99 (1.28 to 3.10) |
Cycle 3, day 1 | 135 | 51 (37.8) | 107 | 35 (32.7) | 2.18 (1.35 to 3.52) |
Cycle 4, day 1 | 116 | 50 (43.1) | 81 | 25 (30.9) | 2.72 (1.65 to 4.48) |
Cycle 5, day 1 | 105 | 52 (49.5) | 67 | 18 (26.9) | 3.58 (1.98 to 6.48) |
Overallc | 157 | NR | 122 | NR | 4.43 (1.73 to 11.36) |
Cough | |||||
Cycle 2, day 1 | 148 | 41 (27.7) | 112 | 20 (17.9) | 2.03 (1.21 to 3.42) |
Cycle 3, day 1 | 135 | 41 (30.4) | 107 | 20 (18.7) | 1.83 (1.05 to 3.19) |
Cycle 4, day 1 | 116 | 38 (32.8) | 81 | 20 (24.7) | 2.89 (1.55 to 5.37) |
Cycle 5, day 1 | 105 | 39 (37.1) | 67 | 16 (23.9) | 3.21 (1.55 to 6.65) |
Overallc | 157 | NR | 122 | NR | 3.58 (2.19 to 5.85) |
Chest pain | |||||
Cycle 2, day 1 | 148 | 35 (23.6) | 112 | 17 (15.2) | 1.0 (0.59 to 1.70) |
Cycle 3, day 1 | 135 | 31 (23.0) | 107 | 20 (18.7) | 1.30 (0.74 to 2.27) |
Cycle 4, day 1 | 116 | 32 (27.6) | 81 | 14 (17.3) | 1.93 (1.02 to 3.63) |
Cycle 5, day 1 | 105 | 27 (25.7) | 67 | 7 (10.4) | 1.56 (0.82 to 2.96) |
Overallc | 157 | NR | 122 | NR | 1.04 (0.42 to 2.55) |
CI = confidence interval; EORTC QLQ-LC13 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Lung Cancer Module; GEE = generalized estimating equation; NR = not reported.
Note: The data cut-off date was August 2, 2022.
aOdds ratios and 95% CIs were estimated using a GEE model based on change from baseline as the dependent variable and intercept, time, baseline score, treatment, treatment-by-time interaction, and randomization stratification factors as fixed effects. All postbaseline visits are considered, excluding follow-up visits.
bAn odds ratio greater than 1.0 indicates higher improvement in symptom scale for sotorasib relative to docetaxel.
cOverall represents all postbaseline visits, including visits beyond cycle 5, day 1, excluding follow-up visits.
Source: Clinical Study Report for the CodeBreaK 200 study.21
PROs Version of the Common Terminology Criteria For Adverse Events
In the CodeBreaK 100 study, the number of patients providing baseline PRO-CTCAE assessments ranged from 69 patients (54.8%) for aching joints to 73 patients (57.9%) for aching muscles and 88 patients (69.8%) for numbness, itchy skin, mouth cracking, and mouth or throat sores. The numbers of patients completing end-of-treatment phase PRO-CTCAE assessments were 6 patients (4.8%) for mouth or throat sores, 12 patients (9.5%) for numbness, 16 patients (12.7%) for aching muscles, 19 patients (15.1%) for aching joints, and 23 patients (18.3%) for pain. At baseline, most patients had no symptoms of mouth or throat sores (90%), mouth cracking (89%), itchy skin (73%), or numbness (58%), while symptom severity of pain, aching muscles, and aching joints was mild or moderate in 75%, 83%, and 84% of patients, respectively, and reported to be severe in 23%, 13%, and 9% of patients, respectively. For all symptoms, an increase from grade 0 to grade 3 in the Common Terminology Criteria for Adverse Events at any point postbaseline occurred in no more than 1 patient. A shift of symptoms from grade 1 to 2 at baseline to grade 3 or 4 at any point postbaseline occurred in fewer than 20% of patients.
At baseline, symptom interference with daily activities (i.e., mouth or throat sores, numbness, pain, aching muscles, and aching joints) was rated as:
“not at all” or “a little bit” in 58% to 78% of patients
“somewhat” in 14% to 27% of patients
“quite a bit” in 5% to 14% of patients
“very much” in 0% to 5% of patients.
Symptom interference with daily activities remained similar during treatment. At the end-of-visit assessment, symptoms of pain, aching muscles, and aching joints were reported to interfere with daily activities “quite a bit” in 35%, 25%, and 26% of patients, respectively.
Symptom frequency remained relatively stable during the treatment period. Between baseline and cycle 13 (13 patients evaluated), fewer than 28% of patients reported experiencing symptoms “frequently” or “almost constantly.”
In the CodeBreaK 200 study, the number of patients available to provide baseline PRO-CTCAE assessments of symptom severity in the sotorasib treatment group ranged from 75 patients (43.9%) for aching muscles to 147 patients (86.0%) for mouth or throat sores, mouth cracking, itchy skin, and numbness. At baseline, most patients had no symptoms of mouth or throat scores (89.8%), mouth cracking (91.8%), itchy skin (76.2%), or numbness (65.3%), while symptoms severity of pain, aching muscles, and aching joints were mild or moderate in 73.6%, 89.4%, and 81.9% of patients, respectively; these were reported to be severe in 19.5%, 9.3%, and 11.7% of patients, respectively. By week 12, the number of patients available in the sotorasib group to provide assessments ranged from 61 patients (35.7%) to 101 patients (59.1%). At week 12, most patients had no symptoms of mouth or throat scores (91.1%), mouth cracking (95.0%), itchy skin (66.3%), or numbness (62.4%), while the severity of pain, aching muscle symptoms, and aching joint symptoms was mild or moderate in 73.6%, 90.2%, and 80.3% of patients, respectively; these were reported to be severe in 10.5%, 4.9%, and 6.1% of patients, respectively. In the docetaxel treatment group, the number of patients available to provide baseline PRO-CTCAE assessments ranged from 51 patients (29.3%) for aching muscles to 112 patients (64.4%) for mouth or throat sores, mouth cracking, itchy skin, and numbness. At baseline, most patients had no symptoms of mouth or throat scores (92.9%), mouth cracking (93.8%), itchy skin (72.3%), or numbness (67.9%), while the severity of pain, aching muscle symptoms, and aching joint symptoms was mild or moderate in 73.8%, 76.5%, and 72.1% of patients, respectively; these symptoms were reported to be severe in 16.3%, 15.7%, and 16.4% of patients, respectively. By week 12, the number of patients available to provide assessments ranged from 26 patients (14.9%) to 60 patients (24.5%). At week 12, most patients had no symptoms of mouth or throat scores (91.1%), mouth cracking (95.0%), itchy skin (66.3%), or numbness (62.4%), while the severity of pain, aching muscle symptoms, and aching joint symptoms was mild or moderate in 73.6%, 90.2%, and 80.3% of patients, respectively; these were reported to be severe in 10.5%, 4.9%, and 6.1% of patients, respectively.
The number of patients available to provide PRO-CTCAE assessments of symptom interference ranged from 15 patients (8.8%) to 111 patients (64.9%) in the sotorasib treatment group and from 8 patients (4.6%) to 76 patients (43.7%) in the docetaxel group at baseline. Symptom inference with daily activities at baseline in the sotorasib treatment group was rated as “not at all” or “a little bit” in 59.4% to 100% of patients; as “somewhat” in 5.8% to 24% of patients; as “quite a bit” in 6.7% to 16.2% of patients; and as “very much” in 1.3% to 6.5% of patients. In the docetaxel group, symptom inference with daily activities at baseline was rated as “not at all” or “a little bit” in 60.5% to 88.9% of patients; as “somewhat” in 5.6% to 22.9% of patients; as “quite a bit” in 5.6% to 19.7% of patients; and as “very much” in 3.9% to 7.1% of patients. Symptom interference with daily activities remained similar during treatment in both groups.
Symptom frequency remained relatively stable during the treatment period. In patients randomized to receive sotorasib, “frequently” or “almost constantly” experiencing pain, aching muscles, and aching joints was reported by 33.3%, 9.5%, and 11.6% of patients, respectively, at baseline (n = 147). By cycle 5, day 1 (n = 101), 18.8%, 3.0%, and 5.0% of patients in the sotorasib treatment group reported “frequently” or “almost constantly” experiencing pain, aching muscles, and aching joints, respectively. In patients randomized to receive docetaxel, “frequently” or “almost constantly” experiencing pain, aching muscles, and aching joints was reported by 27.7%, 7.2%, and 14.3% of patients, respectively, at baseline (n = 112). By cycle 5, day 1 (n = 60), 23.3%, 10.0%, and 11.6% of patients in the docetaxel treatment group reported “frequently” or “almost constantly” experiencing pain, aching muscles, and aching joints, respectively.
Non–Small Cell Lung Cancer Symptom Assessment Questionnaire
A summary of baseline and end-of-treatment scores for the NSCLC-SAQ symptom scales in the CodeBreaK 100 study are presented in Table 24. A baseline NSCLC-SAQ was completed by 84 patients (66.7%), while 27 patients (21.4%) completed end-of-treatment NSCLC-SAQ assessments. The total mean NSCLC-SAQ score at baseline was 6.7 (SD = 3.7), with symptom scores ranging from 1.0 for cough (SD = 0.9; n = 84) to 1.8 for dyspnea (SD = 1.2; n = 84). At the end of the treatment phase, mean scores appeared to be numerically sustained compared to baseline scores. The end-of-treatment total mean score was 7.9 (SD = 3.7; n = 27), and symptom scores ranged from 1.0 for cough (SD = 0.9; n = 27) to 1.9 for fatigue (SD = 1.1; n = 27). Total mean change from baseline to end of treatment was 0.6 (SD = 4.2), with change in mean symptom scores ranging from –0.2 for cough (SD = 1.0) to 0.6 for pain (SD = 0.4). After cycle 6, the number of patients available to complete assessments had dropped by more than 50%.
Table 24: Summary of NSCLC-SAQ Symptom Scales in CodeBreaK 100 Study (NSCLC-SAQ Analysis Set)
Scores | CodeBreaK 100 study, phase II (NSCLC cohort) Sotorasib 960 mg Symptom scale scores | |||||
|---|---|---|---|---|---|---|
Total score | Cough | Pain | Dyspnea | Fatigue | Appetite | |
Baseline | ||||||
n | 84 | 84 | 84 | 84 | 84 | 84 |
Mean (SD) | 6.7 (3.7) | 1.0 (0.9) | 1.2 (1.1) | 1.8 (1.2) | 1.7 (1.0) | 1.1 (1.3) |
End of treatmenta | ||||||
n | 27 | 27 | 27 | 27 | 27 | 27 |
Mean (SD) | 7.9 (3.7) | 1.0 (0.9) | 1.5 (1.1) | 1.9 (1.1) | 1.9 (1.1) | 1.6 (1.4) |
Change from baseline to end of treatmenta | ||||||
Mean (SD) | 0.6 (4.2) | –0.2 (1.0) | 0.4 (1.1) | –0.1 (1.2) | 0.1 (1.0) | 0.3 (1.8) |
NSCLC = non–small cell lung cancer; NSCLC-SAQ = Non–Small Cell Lung Cancer Symptom Assessment Questionnaire; SD = standard deviation.
Note: The data cut-off date was September 1, 2020.
aEnd of treatment was defined as the last assessment for the protocol-specified treatment phase of the study for an individual patient.
Source: Clinical Study Report of PRO data for the CodeBreaK 100 study.61 (The NSCLC-SAQ was not assessed in the CodeBreaK 200 study.)
FACT-G Item GP5
Baseline and end-of-treatment results for item GP5 on the FACT-5 for the CodeBreaK 100 study and the CodeBreaK 200 study are presented in Table 25.
In the CodeBreaK 100 study, a total of 92 patients (73.0%) completed baseline assessments for item GP5 on the FACT-5. The number of patients who completed item GP5 on the FACT-5 at the end of the treatment phase was 32 (25.4%). The number of patients available to complete assessments had dropped by more than 50% after cycle 6. Overall, 87% of patients reported that they were “not at all” or “a little bit” bothered by the side effects of their treatment at baseline. Patients’ reports of being bothered by side effects remained similar up to cycle 13, with about 21% to 46% reporting some degree of being bothered. Between cycles 2 and 17, fewer than 8% of patients reported being bothered by side effects of treatment “quite a bit;” 0% said they were bothered “very much.” The proportions of patients who were “quite bothered” or “very much bothered” by the side effects of treatment were 3.3% at baseline and 15.6% at the end of treatment.
Stacked bar charts showing responses to item GP5 on the FACT-5 for patients in the sotorasib and docetaxel treatment groups of the CodeBreaK 200 study are illustrated in Figure 17. Item GP5 was completed by 146 patients (85.4%) and 112 patients (64.4%) in the sotorasib and docetaxel treatment groups at baseline, respectively. The proportions of patients who completed assessments at cycle 5, day 1 were 59.1% and 34.5% in the sotorasib and docetaxel treatment groups, respectively. Overall, 89.7% of patients in the sotorasib treatment group and 93.8% of patients in the docetaxel treatment group reported that they were “not at all” or “a little bit” bothered by the side effects of their treatment at baseline. Over the course of treatment, patients randomized to receive sotorasib were less severely bothered by side effects compared to those who received docetaxel. By week 12, the proportions of patients in the sotorasib and docetaxel groups reporting that they were “not at all” or “a little bit” bothered by the side effects of their treatment were 86.2% and 61.7%, respectively.
Table 25: Summary of FACT-G Item GP5 in CodeBreaK 100 and CodeBreaK 200 Studies (FACT-G Analysis Set)
GP5 response | CodeBreaK 100 study, phase II (NSCLC cohort) | CodeBreaK 200 study | |
|---|---|---|---|
Sotorasib 960 mg | Sotorasib 960 mg | Docetaxel 75 mg/m2 | |
I am bothered by side effects of treatment… | |||
Baseline | |||
n | 92 | 146 | 112 |
Not at all | 65 (70.7) | 113 (77.4) | 91 (81.3) |
A little bit | 15 (16.3) | 18 (12.3) | 14 (12.5) |
Somewhat | 9 (9.8) | 9 (6.2) | 4 (3.6) |
Quite a bit | 2 (2.2) | 6 (4.1) | 1 (0.9) |
Very much | 1 (1.1) | 0 (0) | 2 (1.8) |
Cycle 15, day 1 | |||
n | 4 | 49 | 10 |
Not at all | 4 (100) | 32 (65.3) | 4 (40.0) |
A little bit | 0 (0) | 16 (32.7) | 3 (30.0) |
Somewhat | 0 (0) | 1 (2.0) | 2 (20.0) |
Quite a bit | 0 (0) | 0 (0) | 0 (0) |
Very much | 0 (0) | 0 (0) | 1 (10.0) |
FACT-G = Functional Assessment of Cancer Therapy Tool – General; NSCLC = non–small cell lung cancer.
Note: The data cut-off dates were September 1, 2020, for the CodeBreaK 100 study and August 2, 2022, for the CodeBreaK 200 study.
Sources: Clinical Study Report for phase II of the CodeBreaK 100 study;20 Clinical Study Report for the CodeBreaK 200 study.21
Figure 17: Stacked Bar Chart for FACT-G Item GP5 in CodeBreaK 200 Study (FACT-G Item GP5 Analysis Set)
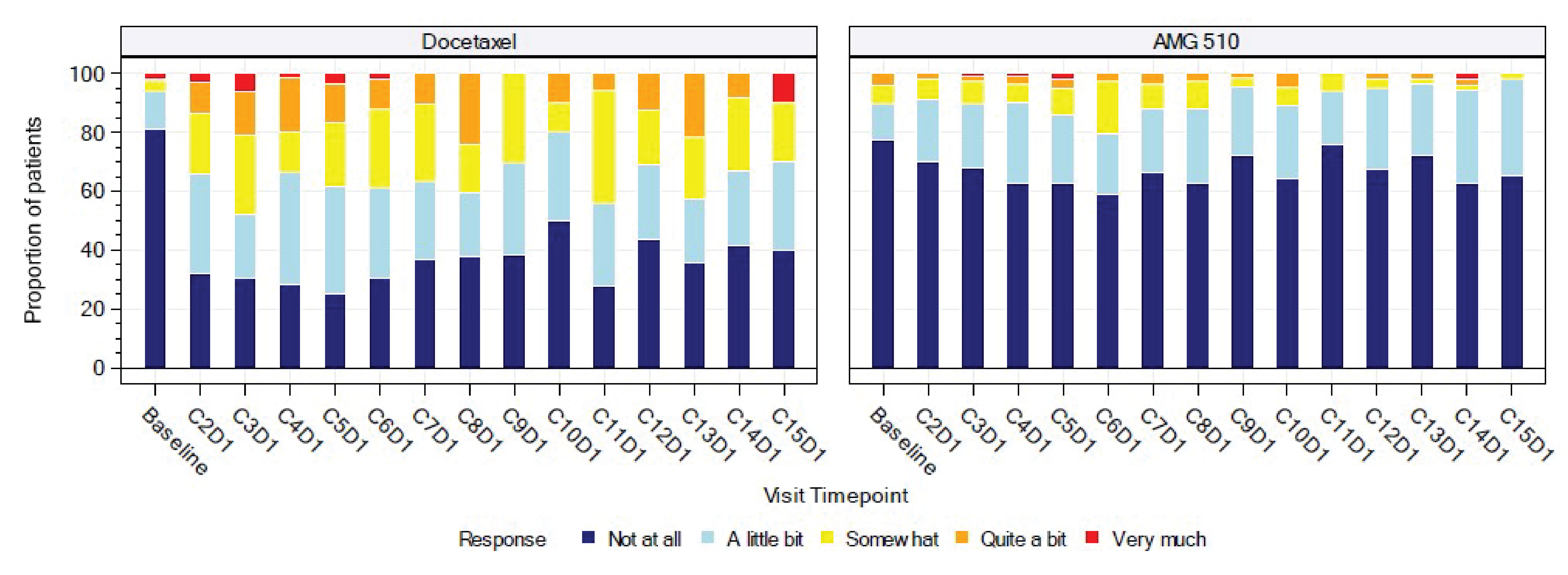
AMG 510 = sotorasib; C = cycle number; D = day number; FACT-G = Functional Assessment of Cancer Therapy Tool – General.
Note: The data cut-off date was August 2, 2022.
Source: Clinical Study Report for the CodeBreaK 200 study.21
Brief Pain Inventory – Short Form
The BPI-SF was not assessed in the CodeBreaK 100 study.
BPI-SF scores in the CodeBreaK 200 study are summarized in Table 26. Baseline BPI-SF scores were provided by 157 patients (91.8%) in the sotorasib treatment group and 122 patients (70.1%) in the docetaxel group. At baseline, the mean BPI-SF scores of pain at its worst were 3.5 (SD = 2.7) in the sotorasib group and 3.0 (SD = 2.8) in the docetaxel group. By cycle 5, day 1, BPI-SF scores remained stable for 49.5% patients in the sotorasib group and 61.2% of patients in the docetaxel group. Improvements in BPI-SF scores were reported in 28.6% and 19.9% of patients, and worsening scores were reported in 21.9% and 20.9% of patients, in the sotorasib and docetaxel groups, respectively. The number of patients available to complete assessment dropped by more than 50% by cycle 6 day 1. Differences between groups were not reported at any time point.
Table 26: BPI-SF (BPI Analysis Set) in CodeBreaK 200 Study
BPI-SF: Pain at its worst | Sotorasib 960 mg | Docetaxel 75 mg/m2 |
|---|---|---|
Baseline | ||
n | 157 | 122 |
Mean (SD) | 3.5 (2.7) | 3.0 (2.8) |
Cycle 5, day 1 | ||
n | 105 | 67 |
Mean (SD) | 2.7 (2.7) | 2.5 (2.8) |
Change from baseline | ||
Mean (SD) | –0.3 (2.8) | 0.3 (2.6) |
Direction of change, n (%) | ||
Improveda | 30 (28.6) | 12 (17.9) |
Stableb | 52 (49.5) | 41 (61.2) |
Worseningc | 23 (21.9) | 14 (20.9) |
BPI = Brief Pain Inventory; BPI-SF = Brief Pain Inventory – Short Form; SD = standard deviation.
Note: The data cut-off date was August 2, 2022.
aTwo or more lower than baseline.
bBetween 1 lower and 1 higher than baseline.
cTwo or more higher than baseline.
Source: Clinical Study Report for the CodeBreaK 200 study.21
Table 27: Objective Response to Treatment by RECIST 1.1 Based on BICR in CodeBreaK 100 and CodeBreaK 200 Studies (Analysis Set)
Objective response | CodeBreaK 100 study, phase II (NSCLC cohort) | CodeBreaK 200 study | ||
|---|---|---|---|---|
Sotorasib 960 mg (n = 123) | Sotorasib 960 mg (n = 124) | Sotorasib 960 mg (n = 171) | Docetaxel 75 mg/m2 (n = 174) | |
Data cut-off September 1, 2020 | Data cut-off March 15, 2021 | Data cut-off August 2, 2022 | ||
Best overall response, n (%) | ||||
Complete response | 2 (1.6) | 4 (3.2) | 2 (1.2) | 0 (0) |
Partial response | 44 (35.8) | 42 (33.9) | 46 (26.9) | 23 (13.2) |
Stable disease | 53 (43.1) | 54 (43.5) | 93 (54.4) | 82 (47.1) |
Progressive disease | 20 (16.3) | 20 (16.1) | 17 (9.9) | 24 (13.8) |
Noncomplete response/ nonprogressive disease | NR | NR | 2 (1.2) | 1 (0.6) |
Not evaluable | 2 (1.6) | 2 (1.6) | 1 (0.6) | 2 (1.1) |
Not done | 2 (1.6) | 2 (1.6) | 10 (5.8)a | 42 (24.1)a |
ORR (CR plus PR) | ||||
Confirmed ORR, n (%) | 46 (37.4) | 46 (37.1) | 48 (28.1) | 23 (13.2) |
95% CIb | 28.84 to 46.58 | 28.60 to 46.23 | 21.5 to 35.4 | 8.6 to 19.2 |
P valuec | NA | NR | < 0.001 | Reference |
OR (95% CI)c | NA | NA | 2.6 (1.48 to 4.56) | |
Difference in proportion of objective response (95% CI)c | NA | NA | 14.8 (6.4 to 23.1) | |
P value (1-sided)d | NA | NA | < 0.001 | Reference |
Time to objective response, monthse | ||||
n | 46 | 46 | 47 | 25 |
Mean (SD) | 1.95 (1.23) | 2.11 (1.71) | 2.43 (1.80) | 3.24 (2.08) |
Median (minimum, maximum) | 1.35 (1.2 to 6.1) | 1.35 (1.2 to 10.1) | 1.48 (1.2 to 11.0) | 2.76 (1.3 to 9.4) |
BICR = blinded independent central review; CI = confidence interval; CNS = central nervous system; CR = complete response; NA = not applicable; NR = not reported; NSCLC = non–small cell lung cancer; OR = odds ratio; ORR = objective response rate; PR = partial response; RECIST 1.1 = Response Evaluation Criteria in Solid Tumours Version 1.1; SD = standard deviation; vs. = versus.
Notes: Randomization stratification factors are number of prior lines of therapy in advanced disease (1 vs. 2 vs. > 2), race (Asian vs. non-Asian), and history of CNS involvement (yes vs. no).
For patients who continued treatment postprogression or crossed over from docetaxel to sotorasib, the first date of progression is used for progression-free survival analysis, and the patient’s response post–first progression or postcrossover is not used in the primary analyses to evaluate objective response and duration of response.
a“Not done” includes patients who were randomized but did not receive any tumour assessment before the end of the study or before starting new anticancer therapy. Patients who did not have any postbaseline tumour assessment were considered as having no baseline and summarized accordingly in the table.
bThe exact 95% CIs were calculated using the Clopper-Pearson method.
cThe P values were adjusted for multiple comparison using the Maurer-Bertz multiple testing procedure.
dCalculated using the stratified Cochran-Mantel-Haenszel chi-square test.
eTime to response was calculated among confirmed responders’ best overall response of PR or CR.
Sources: Clinical Study Report for phase II of the CodeBreaK 100 study;20 Clinical Study Report for the CodeBreaK 200 study.21
Objective Response Rate
ORR data are summarized in Table 27.
Among patients in the phase II portion of the CodeBreaK 100 study, 1.6% were documented as having CR to sotorasib, while 35.8% had PR to treatment at the time of the September 2020 data cut-off. The ORR (CR plus PR) was 37.4% (95% CI, 28.84% to 46.58%). The study achieved the predetermined threshold for a positive outcome (i.e., lower limit of the 95% CI for ORR > 23%). The mean time to objective response was 1.95 months (SD = 1.23 months). At the time of the March 2021 data cut-off, 3.2% of patients were documented as having CR, while 33.9% had PR. The ORR (CR plus PR) was consistent with that of the earlier data cut-off (37.1%; 95% CI, 28.60% to 46.23%). The mean time to objective response as observed at the updated analysis was 2.11 months (SD = 1.71 months).
Among patients in the CodeBreaK 200 study, the proportions of patients documented as having an objective response (CR or PR) to treatment at the time of data cut-off in the sotorasib and docetaxel groups were 28.1% (95% CI, 21.5% to 35.4%) and 13.2% (95% CI, 8.6% to 19.2%), respectively, resulting in a difference in proportion of 14.8% (95% CI, 6.4% to 23.1%; P < 0.001) in favour of sotorasib. The odds of objective response were higher among patients randomized to the sotorasib group relative to those randomized to docetaxel (odds ratio = 2.6; 95% CI, 1.48 to 4.56; P < 0.001). The mean times to objective response as of the August 2, 2022, data cut-off date were 2.43 months (SD = 1.80 months) among patients in the sotorasib treatment group and 3.24 months (SD = 2.08 months) in the docetaxel treatment group. Of note, there was an imbalance across groups in the proportion of patients for whom response assessments were not done (5.8% and 24.1% of patients in the sotorasib and docetaxel groups, respectively).
Subgroup Analysis
Subgroup analyses of ORR in the CodeBreaK 100 study are presented in Table 28. The results for all subgroups were generally consistent with the main effect.
Duration of Response
DOR data are summarized in Table 29. A KM plot of median DOR for patients with NSCLC in phase II of the CodeBreaK 100 study is illustrated in Figure 18, while the swimmer’s plot is presented in Appendix 4.
Table 28: Subgroup Analysis of Objective Response in CodeBreaK 100 Study by Central Review (Full Analysis Set)
Subgroup | CodeBreaK 100 study, phase II (NSCLC cohort) (N = 123) Sotorasib 960 mg | |||
|---|---|---|---|---|
September 1, 2020, data cut-off date | March 15, 2021, data cut-off date | |||
n | Objective response rate, % (95% CI)a | n | Objective response rate, % (95% CI)a | |
ECOG Performance Status at baseline | ||||
0 | 37 | 43.2 (27.1 to 60.5) | 37 | 43.2 (27.1 to 60.5) |
1 | 86 | 34.9 (24.9 to 45.9) | 87 | 34.5 (24.6 to 45.4) |
Histology | ||||
Squamous | 1 | 0 (0.0 to 97.5) | 1 | 0 (0.0 to 97.5) |
Nonsquamous | 122 | 37.7 (29.1 to 46.9) | 123 | 37.4 (28.8 to 46.6) |
Prior lines of anticancer therapy | ||||
1 | 53 | 41.5 (28.1 to 55.9) | 53 | 39.6 (26.5 to 54.0)) |
2 | 43 | 32.6 (19.1 to 48.5) | 43 | 32.6 (19.1 to 48.5) |
> 2 | 27 | 37.0 (19.4 to 57.6) | 28 | 39.3 (21.5 to 59.4) |
Prior anti-PD-1 or anti-PD-L1 | ||||
Yes | 112 | 36.6 (27.7 to 46.2) | 113 | 36.3 (27.4 to 45.9) |
No | 11 | 45.5 (16.7 to 76.6) | 11 | 45.5 (16.7 to 76.6) |
Prior platinum-based chemotherapy | ||||
Yes | 110 | 33.6 (24.9 to 43.3) | 111 | 33.3 (24.7 to 42.9) |
No | 13 | 69.2 (38.6 to 90.9) | 13 | 69.2 (38.6 to 90.9) |
Prior platinum-based chemotherapy and prior anti-PD-1 or anti-PD-L1 | ||||
Yes | 99 | 32.3 (23.3 to 42.5) | 100 | 32.0 (23.0 to 42.1) |
No | 24 | 58.3 (36.6 to 77.9) | 24 | 58.3 (36.6 to 77.9) |
CI = confidence interval; CR = complete response; ECOG = Eastern Cooperative Oncology Group; NSCLC = non–small cell lung cancer; PD-1 = programmed cell death 1; PD-L1 = programmed cell death-ligand 1; PR = partial response.
aEvents are confirmed responders (PR or CR). Exact CIs were calculated using the Clopper-Pearson method.
Source: Clinical Study Report for phase II of the CodeBreaK 100 study.20
Among patients in the phase II portion of the CodeBreaK 100 study, at the time of the September 2020 data cut-off, DORs of at least 3 months and at least 6 months were documented in 76.1% and 50.0% of patients, respectively. The median DOR was 8.4 months (95% CI, 6.9 months to 8.4 months). The probabilities of objective response based on KM estimates at 3 months and 6 months were 89.9% (95% CI, 75.3% to 96.1%) and 76.2% (95% CI, 59.1% to 86.9%), respectively. At the time of the March 2021 data cut-off, DORs of at least 3 months and at least 6 months were documented in 82.6% and 60.9% of patients, respectively. The median DOR was 11.1 months (95% CI, 6.9 months to NE). The probabilities of objective response based on KM estimates at 3 months and 6 months were consistent with those of the earlier data cut-off (90.5% [95% CI, 76.7% to 96.3%] and 70.8% [95% CI, 54.3% to 82.2%], respectively). At 9 months and 12 months, the probabilities of objective response were 57.3% (95% CI, 40.4% to 71.0%) and 48.2% (95% CI, 31.5% to 63.0%), respectively.
Among patients in the CodeBreaK 200 study, the proportions with DORs of at least 3 months and 6 months were not available to the CADTH review team. The median DORs were 8.64 months (95% CI, 7.06 months to 17.97 months) and 6.80 months (4.27 months to 8.28 months) in the sotorasib and docetaxel treatment groups, respectively. No comparative effect estimate was provided.
Table 29: Duration of Objective Response by RECIST 1.1 Based on BICR (Full Analysis Set)
Duration of response | CodeBreaK 100 study, phase II (NSCLC cohort) | CodeBreaK 200 study | ||
|---|---|---|---|---|
Sotorasib 960 mg (n = 123) | Sotorasib 960 mg (n = 124) | Sotorasib 960 mg (n = 171) | docetaxel 75 mg/m2 (n = 174) | |
Data cut-off September 1, 2020 | Data cut-off March 15, 2021 | Data cut-off unknown August 2, 2022 | ||
Duration of objective response,a n (%) | ||||
≥ 3 months | 35 (76.1) | 38 (82.6) | NR | NR |
≥ 6 months | 23 (50.0) | 28 (60.9) | NR | NR |
≥ 9 months | 0 (0) | 20 (43.5) | NR | NR |
≥ 12 months | 0 (0) | 15 (32.6) | NR | NR |
Censored, n (%) | 32 (69.6) | 24 (52.2) | 21 (43.8) | 9 (39.1) |
On study without disease progression | 28 (60.9) | 17 (37.0) | NR | NR |
Started new anticancer therapy | 3 (6.5) | 5 (10.9) | NR | NR |
Withdrew consent | 1 (2.2) | 1 (2.2) | NR | NR |
Duration of response, months (KM) | ||||
Median (95% CI) | 8.4 (6.9 to 8.4) | 11.1 (6.9 to NE) | 8.64 (7.06 to 17.97) | 6.80 (4.27 to 8.28) |
KM estimates, probability of objective response (95% CI)b | ||||
At 3 months | 89.9 (75.3 to 96.1) | 90.5 (76.7 to 96.3) | NR | NR |
At 6 months | 76.2 (59.1 to 86.9) | 70.8 (54.3 to 82.2) | NR | NR |
At 9 months | 0 (NE to NE) | 57.3 (40.4 to 71.0) | NR | NR |
At 12 months | 0 (NE to NE) | 48.2 (31.5 to 63.0) | NR | NR |
Follow-up time (KM), months | ||||
Median (95% CI) | 6.9 (5.6 to 7.0) | 12.4 (11.1 to 12.6) | NR | NR |
BICR = blinded independent central review; CI = confidence interval; CNS = central nervous system; KM = Kaplan-Meier; NE = not evaluable; NR = not reported; NSCLC = non–small cell lung cancer; RECIST 1.1 = Response Evaluation Criteria in Solid Tumours Version 1.1; vs. = versus.
Notes: Randomization stratification factors are number of prior lines of therapy in advanced disease (1 vs. 2 vs. > 2), race (Asian vs. non-Asian), and history of CNS involvement (yes vs. no).
For patients who continued treatment postprogression or who crossed over from docetaxel to sotorasib, the first date of progression is used for progression-free survival analysis, and the patient’s response post–first progression or postcrossover is not used in the primary analyses to evaluate objective response and duration of response.
aDuration of response was calculated among confirmed responders.
b95% CIs were based on estimated variance for log-log transformation of the KM survival estimate.
Sources: Clinical Study Report for phase II of the CodeBreaK 100 study;20 Clinical Study Report for the CodeBreaK 200 study.21
Figure 18: KM Plot of DOR in CodeBreaK 100 Study at the Data Cut-Off Date of March 15, 2021 (Full Analysis Set)
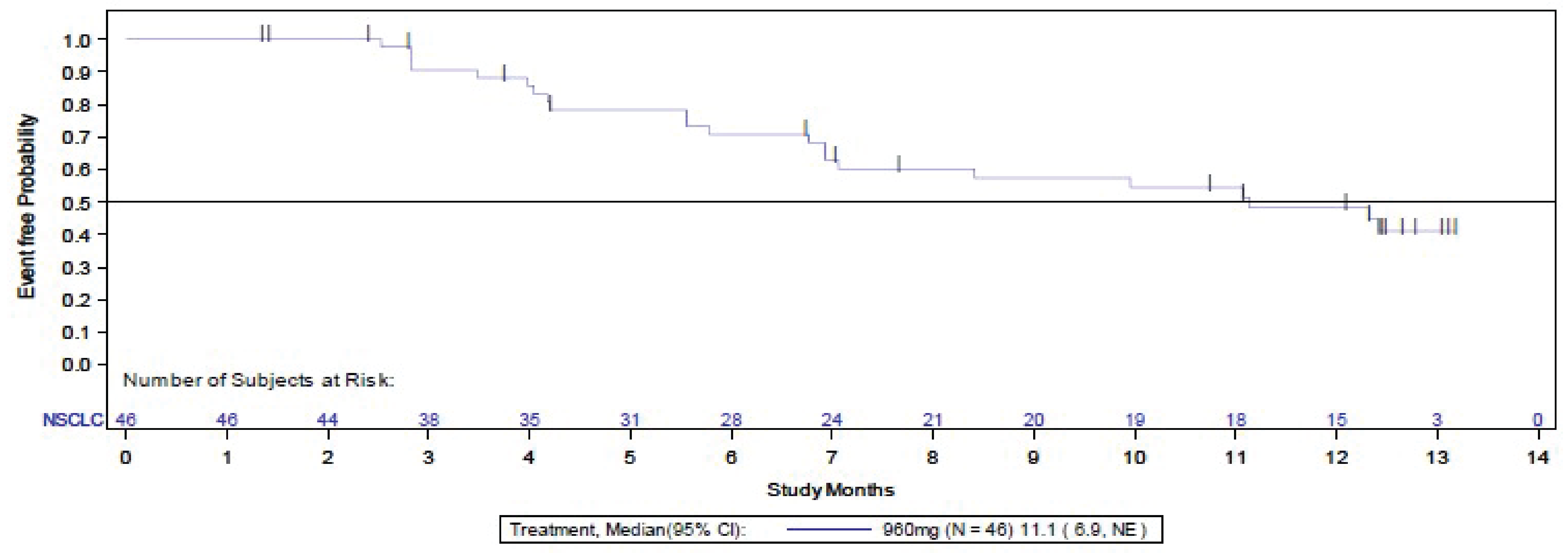
CI = confidence interval; DOR = duration of response; KM = Kaplan-Meier; NSCLC = non–small cell lung cancer; NE = not evaluable.
Note: An event is radiological progression or death, whichever occurs after confirming complete response or partial response.
Source: Clinical Study Report for phase II of the CodeBreaK 100 study.20
Harms
Only those harms identified in the review protocol are reported here.
Harms data for phase II of the CodeBreaK 100 study and for the CodeBreaK 200 study are presented in Table 30.
Adverse Events
In the CodeBreaK 100 study, a total of 125 patients (99.2%) in the NSCLC cohort had at least 1 AE. Overall, 75 patients (59.5%) had grade 3 or worse AEs, and 21 patients (16.1%) had grade 4 or worse AEs. The most common AEs reported were diarrhea (49.2%), nausea (29.4%), and fatigue (24.6%).
In the CodeBreaK 200 study, 98% of patients in both the sotorasib and docetaxel treatment groups reported at least 1 AE. The most common AEs reported in the sotorasib treatment group were diarrhea (41.4%), nausea (26.0%), and decreased appetite (23.1%). The most common AEs reported in the docetaxel treatment group were fatigue (29.8%), diarrhea (25.8%), and nausea (25.8%). Alopecia occurred in 3 patients (1.8%) in the sotorasib group and in 35 patients (23.2%) in the docetaxel group. Grade 3 or worse AEs were reported by 121 patients (71.6%) in the sotorasib treatment group and by 91 patients (60.3%) in the docetaxel treatment group. Grade 4 or worse AEs were reported in 48 patients (28.4%) and 35 patients (23.2%) in the sotorasib and docetaxel treatment groups, respectively. The most common grade 3 or worse AEs in the sotorasib treatment group were diarrhea (13.6%), NSCLC (10.1%), increased ALT (8.3%), and increased AST (5.9%). In the docetaxel treatment group, the most common grade 3 or worse AEs were neutropenia (8.6%), anemia (6.6%), fatigue (6.0%), pneumonia (6.0%), and febrile neutropenia (5.3%).
Serious Adverse Events
In the CodeBreaK 100 study, 63 patients (50%) in the NSCLC cohort had at least 1 SAE. The most frequently reported SAEs were pneumonia (7.1%), NSCLC (6.3%), and pleural effusion (4.0%). Of those reporting SAEs, 60 patients (47.6%) had a grade 3 or worse AE, and 19 patients (15.1%) had a grade 4 or worse AE.
In the CodeBreaK 200 study, SAEs were reported by 91 patients (53.8%) in the sotorasib treatment group and by 67 patients (44.4%) in the docetaxel treatment group. The most frequently reported SAEs in the sotorasib treatment group were NSCLC (10.7%) and diarrhea (3.0%). The most frequently reported SAEs in the docetaxel treatment group were pneumonia (6.6%), febrile neutropenia (4.6%), NSCLC, and anemia (3.3% each).
Withdrawals Due to AEs
In the CodeBreaK 100 study, a total of 11 patients (8.7%) in the NSCLC cohort discontinued treatment due to an AE. The most common reasons were drug-induced liver injury (2.4%), increased ALT and/or increased AST (1.6%), and pneumonitis (1.6%).
In the CodeBreaK 200 study, 28 patients (16.6%) and 24 patients (15.9%) discontinued treatment due to an AE in the sotorasib and docetaxel treatment groups, respectively. Reasons for discontinuing treatment in the sotorasib treatment group included increased ALT (3.6%), NSCLC (3.0%), increased blood bilirubin (2.4%), increased AST (1.2%), asthenia (1.2%), and increased blood ALP (1.2%). In the docetaxel treatment group, reasons for discontinuing treatment included fatigue (2.0%), NSCLC (1.3%), anemia (1.3%), febrile neutropenia (1.3%), pneumonitis (0.7%), and asthenia (0.7%).
Dose Modifications
In the CodeBreaK 100 study, a total of 48 patients (38.1%) in the NSCLC cohort required dose modification due to AEs. The most common reasons for dose modification included diarrhea (8.7%), increased AST (8.7%), increased ALT (8.7%), and increased blood ALP (4.0%).
In the CodeBreaK 200 study, dose modification due to AEs was required by 26 patients (15.4%) and 43 patients (28.5%) in the sotorasib and docetaxel treatment groups, respectively. The most frequently reported reasons for dose modification in the sotorasib treatment group were diarrhea (8.3%), followed by increased ALT (3.6%), increased AST (1.8%), and increased blood ALP (0.6%). In the docetaxel treatment group, the most frequently reported reasons for dose modification were neutropenia (4.6%) and fatigue (4.0%), followed by asthenia (3.3%) and diarrhea (2.0%).
Dose Interruptions
In the CodeBreaK 100 study, dose interruptions due to AEs were documented in 46 patients (36.5%) at the time of the March 15, 2021, data cut-off date in the CodeBreaK 200 study. Dose interruptions due to AEs were reported in 85 patients (50.9%) in the sotorasib treatment group and in 42 patients (27.8%) in the docetaxel treatment group. The most frequently reported reasons for dose interruption in the sotorasib treatment group were diarrhea (15.4%), increased ALT (5.9%), increased AST (5.3%), nausea (4.7%), decreased appetite (3.0%), and fatigue (1.2%). In the docetaxel treatment group, dose interruptions were due to pneumonia (4.6%), fatigue (3.3%), and nausea (0.7%).
Table 30: Summary of Harms (Safety Analysis Set)
Harms | CodeBreaK 100 study, phase II (NSCLC cohort) | CodeBreaK 200 study | ||
|---|---|---|---|---|
Sotorasib 960 mg (n = 126) | Sotorasib (n = 169) | Docetaxel (n = 151) | ||
Data cut-off date September 1, 2020 | Data cut-off date March 15, 2021 | Data cut-off date August 2, 2022 | ||
Patients with ≥ 1 AE | ||||
n (%) | 125 (99.2) | 125 (99.2) | 166 (98.2) | 148 (98.0) |
Most common events,a n (%) | ||||
Diarrhea | 62 (49.2) | 64 (50.8) | 70 (41.4) | 39 (25.8) |
Nausea | 37 (29.4) | 39 (31.0) | 44 (26.0) | 37 (24.5) |
Fatigue | 31 (24.6) | 32 (25.4) | 27 (16.0) | 45 (29.8) |
AST increased | 27 (21.4) | 27 (21.4) | 18 (10.7) | 1 (0.7) |
ALT increased | 26 (20.6) | 26 (20.6) | 18 (10.7) | 1 (0.7) |
Dyspnea | 24 (19.0) | 24 (19.0) | 32 (18.9) | 27 (17.9) |
Vomiting | 23 (18.3) | 23 (18.3) | 22 (13.0) | 15 (9.9) |
Constipation | 22 (17.5) | 24 (19.0) | 22 (13.0) | 29 (19.2) |
Back pain | 20 (15.9) | 21 (16.7) | 23 (13.6) | 16 (10.6) |
Arthralgia | 16 (12.7) | 27 (21.4) | 26 (15.4) | 21 (13.9) |
Cough | 16 (12.7) | 19 (15.1) | 22 (13.0) | 25 (16.6) |
Decreased appetite | 15 (11.9) | 16 (12.7) | 39 (23.1) | 29 (19.2) |
Anemia | 14 (11.1) | 18 (14.3) | 29 (17.2) | 35 (23.2) |
Alopecia | 2 (1.6) | 2 (1.6) | 3 (1.8) | 35 (23.2) |
TEAEs by grade, n (%) | ||||
Grade ≥ 2 | 110 (87.3) | 112 (88.9) | 152 (89.9) | 136 (90.1) |
Grade ≥ 3 | 75 (59.5) | 77 (61.1) | 121 (71.6) | 91 (60.3) |
Grade ≥ 4 | 21 (16.7) | 24 (19.0) | 48 (28.4) | 35 (23.2) |
Most common grade ≥ 3 TEAEs,b n (%) | ||||
Pneumonia | 9 (7.1) | 9 (7.1) | 1 (0.6) | 9 (6.0) |
AST increased | 9 (7.1) | 9 (7.1) | 10 (5.9) | 0 (0) |
ALT increased | 9 (7.1) | 9 (7.1) | 14 (8.3) | 0 (0) |
NSCLC | 8 (6.3) | 8 (6.3) | 17 (10.1) | 5 (3.3) |
Diarrhea | 7 (5.6) | 7 (5.6) | 23 (13.6) | 4 (2.6) |
Pleural effusion | 7 (5.6) | 9 (7.1) | 3 (1.8) | 3 (2.0) |
Dyspnea | 6 (4.8) | 8 (6.3) | 8 (4.7) | 5 (3.3) |
Anemia | NR | 1 (0.8) | 8 (4.7) | 10 (6.6) |
Fatigue | 2 (1.6) | 3 (2.4) | 4 (2.4) | 9 (6.0) |
Neutropenia | 1 (0.8) | 1 (0.8) | 0 (0) | 13 (8.6) |
Febrile neutropenia | NR | NR | 0 (0) | 8 (5.3) |
Patients with ≥ 1 SAE, n (%) | ||||
n (%) | 63 (50.0) | 69 (54.8) | 91 (53.8) | 67 (44.4) |
Most common events,c n (%) | ||||
Pneumonia | 9 (7.1) | 9 (7.1) | 1 (0.6) | 10 (6.6) |
NSCLC | 8 (6.3) | 8 (6.3) | 18 (10.7) | 5 (3.3) |
Pleural effusion | 6 (4.8) | 5 (4.0) | 2 (1.2) | 2 (1.3) |
Diarrhea | 2 (1.6) | 2 (1.6) | 5 (3.0) | 2 (1.3) |
Febrile neutropenia | NR | NR | 0 (0) | 7 (4.6) |
Anemia | NR | 1 (0.8) | 1 (0.6) | 5 (3.3) |
Treatment-emergent SAEs by grade, n (%) | ||||
Grade > 2 | 63 (50.0) | NR | NR | NR |
Grade ≥ 3 | 60 (47.6) | NR | NR | NR |
Grade ≥ 4 | 19 (15.1) | NR | NR | NR |
Fatal | 18 (14.3) | NR | NR | NR |
Most common grade > 3 treatment-emergent SAEs,c n (%) | ||||
Pneumonia | 9 (7.1) | 9 (7.1) | NR | NR |
NSCLC | 8 (6.3) | 8 (6.3) | NR | NR |
Pleural effusion | 5 (4.0) | 5 (4.0) | NR | NR |
Patients who stopped treatment due to AEs, n (%) | ||||
n (%) | 11 (8.7) | 11 (8.7) | 28 (16.6) | 24 (15.9) |
Most common events,c n (%) | ||||
ALT increased | 2 (1.6) | 2 (1.6) | 6 (3.6) | 0 (0) |
Patients requiring dose reduction due to AEs, n (%) | ||||
n (%) | 48 (38.1) | 22 (17.5) | 26 (15.4) | 43 (28.5) |
Most common events,b n (%) | ||||
Diarrhea | 11 (8.7) | 11 (8.7) | 14 (8.3) | 3 (2.0) |
AST increased | 11 (8.7) | 11 (8.7) | 3 (1.8) | 0 (0) |
ALT increased | 11 (8.7) | 11 (8.7) | 6 (3.6) | 0 (0) |
Patients requiring dose interruption due to AEs, n (%) | ||||
n (%) | NR | 46 (36.5) | 86 (50.9) | 42 (27.8) |
Most common events,b n (%) | ||||
Diarrhea | NR | NR | 26 (15.4) | 0 (0) |
ALT increased | NR | NR | 10 (5.9) | 0 (0) |
AST increased | NR | NR | 9 (5.3) | 0 (0) |
Deaths due to AEs, n (%) | ||||
n (%) | 18 (14.3) | 20 (15.9) | 37 (21.9) | 18 (11.9) |
Fatal AEs,d n (%) | ||||
NSCLC | 7 (5.6) | 7 (5.6) | 17 (10.1) | 5 (3.3) |
Lung neoplasm, malignant | 2 (1.6) | NR | 2 (1.2) | 0 |
Pancreatic carcinoma, metastatic | 0 (0) | NR | NR | NR |
Adenocarcinoma | 1 (0.8) | NR | 1 (0.6) | 0 (0) |
Respiratory failure | 1 (0.8) | NR | 0 (0) | 2 (1.3) |
Hypovolemic shock | 1 (0.8) | NR | NR | NR |
Cardiac arrest | 1 (0.8) | NR | 1 (0.6) | 1 (0.7) |
Cardiac failure | 1 (0.8) | NR | NR | NR |
Gastric ulcer | 1 (0.8) | NR | NR | NR |
Systemic inflammatory response syndrome | 1 (0.8) | NR | NR | NR |
Treatment-related fatal adverse events | 0 (0) | NR | 1 (0.6) | 2 (1.3) |
Notable harms, n (%) | ||||
Hepatotoxicityd | 40 (31.7) | 40 (31.7) | NAe | NAe |
AST increased | 27 (21.4) | 27 (21.4) | 18 (10.7) | 1 (0.7) |
ALT increased | 26 (20.6) | 27 (21.4) | 18 (10.7) | 1 (0.7) |
Blood alkaline phosphatase | 17 (13.5) | 17 (13.5) | 13 (7.7) | 3 (2.0) |
Gamma-glutamyltransferase increased | 5 (4.0) | 5 (4.0) | 5 (3.0) | 2 (1.3) |
Renal toxicityd | 21 (16.7) | 23 (18.3) | NAe | NAe |
Hyponatremic | 7 (5.6) | 9 (7.1) | 8 (4.7) | 4 (2.6) |
Hypoalbuminemia | 4 (3.2) | 4 (3.2) | 4 (2.4) | 8 (5.3) |
Blood creatine increased | 1 (0.8) | 1 (0.8) | 4 (2.4) | 2 (1.3) |
Hyperkalemia | 3 (2.4) | 3 (2.4) | 5 (3.0) | 5 (3.3) |
Hypocalcemia | 3 (2.4) | 4 (3.2) | 6 (3.6) | 2 (1.3) |
Hypophosphatemia | 2 (1.6) | 3 (2.4) | 3 (1.8) | 1 (0.7) |
Interstitial lung diseased | 0 (0) | 0 (0) | 1 (0.6) | 0 (0) |
Pneumonitisd | 3 (2.4) | 3 (2.4) | 3 (1.8) | 3 (2.0) |
Peripheral neuropathyd | 1 (0.8) | 1 (0.8) | 1 (0.6) | 16 (10.6) |
GI toxicityd | 93 (73.8) | NR | NR | NR |
Diarrhea | 62 (49.2) | 64 (50.8) | 70 (41.4) | 39 (25.8) |
Nausea | 37 (29.4) | 39 (31.0) | 44 (26.0) | 37 (24.5) |
Vomiting | 23 (18.3) | 23 (18.3) | 22 (13.0) | 15 (9.9) |
Constipation | 22 (17.5) | 24 (19.0) | 22 (13.0) | 29 (19.2) |
Abdominal pain | 11 (8.7) | 11 (8.7) | 20 (11.8) | 9 (6.0) |
AE = adverse event; ALT = alanine aminotransferase; AST = aspartate aminotransferase; GI = gastrointestinal; NA = not applicable; NR = not reported; NSCLC = non–small cell lung cancer; SAE = serious adverse event; TEAE = treatment-emergent adverse event.
aFrequency greater than 15% in any treatment group.
bFrequency greater than 5% in any treatment group.
cFrequency greater than or equal to 5 patients in any treatment group.
dFrequency greater than 0 patients in any treatment group.
eIn the CodeBreaK 200 study, hepatotoxicities of interest were reported using Standardised MedDRA Queries for hepatic disorders (narrow). Hepatotoxicities of interest were reported in 7 patients (4.6%) in the docetaxel group and 41 patients (24.3%) in the sotorasib group. Renal toxicities of interest were reported using Standardised MedDRA Query for acute renal failure or chronic kidney disease. Renal toxicities of interest were not reported for the docetaxel group, but were reported for the sotorasib group in 10 patients (5.9%), including acute kidney injury and renal failure in 3 patients each.
Sources: Clinical Study Report for phase II of the CodeBreaK 100 study;20 Clinical Study Report for the CodeBreaK 200 study.21
Mortality
In the CodeBreaK 100 study, 18 patients (14.3%) died due to an AE. None of the deaths were considered treatment-related.
In the CodeBreaK 200 study, fatal AEs were recorded in 37 patients (21.9%) in the sotorasib treatment group and in 18 patients (11.9%) in the docetaxel treatment group. Seventeen patients (10.1%) in the sotorasib treatment group and 5 patients (3.3%) in the docetaxel group experienced fatal AEs related to NSCLC disease progression.
In the CodeBreaK 200 study, hepatoxicity AEs, including increased AST (10.7%), increased ALT (10.7%), increased blood ALP (7.7%), and increased gamma-glutamyltransferase (3.0%), were reported in the sotorasib treatment group; in the docetaxel treatment group, 2% or less of patients experienced hepatoxicity AEs. Renal toxicity related to hyponatremia was reported in 8 patients (4.7%) in the sotorasib treatment group and in 4 patients (2.6%) in the docetaxel treatment group, while hypoalbuminemia was reported in 4 patients (2.4%) in the sotorasib treatment group and in 8 patients (5.3%) in the docetaxel treatment group. Interstitial lung disease was reported in 1 patient in the sotorasib treatment group. Pneumonitis was reported in 3 patients (1.8%) in the sotorasib treatment group and in 3 patients (2.0%) in the docetaxel treatment group. Peripheral neuropathy was documented in 1 patient (0.6%) in the sotorasib treatment group and in 16 patients (10.6%) in the docetaxel group. Notable GI toxicities reported in the sotorasib treatment group included diarrhea (41.4%), nausea (26.0%), vomiting (13.0%), constipation (13.0%), and abdominal pain (11.8%). Notable GI toxicities reported in the docetaxel treatment group included diarrhea (25.8%), nausea (24.5%), constipation (19.2%), and vomiting (9.9%).
Notable Harms
In the CodeBreaK 100 study, the most common hepatotoxicity AEs reported were increased AST (21.4%), increased ALT (20.6%), and increased blood ALP (13.5%). Renal toxicity was reported in 21 patients (16.7%) in the NSCLC cohort, with hyponatremia (5.6%) and hypoalbuminemia (3.2%) being the most commonly reported renal toxicity AEs. There were no documented cases of interstitial lung disease. Pneumonitis was reported in 3 patients (2.4%) in the NSCLC cohort. Peripheral neuropathy was reported in 1 patient (0.8%) in the NSCLC cohort. Lastly, GI toxicity was reported in 93 patients (73.8%) in the NSCLC cohort, with diarrhea (49.2%), nausea (29.4%), and vomiting (18.3%) being the most common.
Critical Appraisal
Internal Validity
CodeBreaK 100 Study
The single-group, open-label, nonrandomized study design of the CodeBreaK 100 study makes interpretation of the efficacy and safety of sotorasib challenging. The lack of comparison with an active comparator, BSC, and/or placebo precludes causal inferences and the ability to assess the relative therapeutic benefits or safety of sotorasib.
The ability to interpret time‐to‐event end points, such as OS or PFS, is limited in single‐group studies. While ORR may be directly attributable to the drug effect, the nonrandomized design makes interpreting PFS and OS events attributable to sotorasib challenging because all patients with KRAS G12C-mutated, locally advanced (not amenable to curative therapy) or metastatic NSCLC receive the same treatment. The extent to which the observed survival is due to the natural history of the tumour (which can be variable) or the intervention remains unclear.62 The open-label nature of the CodeBreaK 100 study increases the risk of bias in the measurement of the subjective outcomes, such as ORR, PFS, HRQoL, other PROs, and subjective harms.24,25 This has the potential to bias the efficacy outcomes in favour of sotorasib if the assessor (investigator or patient) believes the study drug is likely to provide a benefit. To mitigate the limitations associated with open-label studies, response outcomes were blinded to the study investigator and performed by BICR; as such, these outcomes (e.g., ORR, PFS) are probably at lower risk of bias. The sensitivity analysis of ORR demonstrated consistency between the BICR and the investigator’s assessment of tumour response, suggesting that the potential for bias in the measurement of response outcomes from the open-label design is likely not substantial. The risk of selection bias cannot be ruled out, given the lack of transparency regarding the selection and timing of enrolment of patients into the trial.
The CodeBreaK 100 efficacy end points were well-described and employed appropriate censoring criteria. However, no formal hypothesis testing was performed. Point estimates with 95% CIs were reported to estimate the magnitude of the treatment effect. Given that analyses were not adjusted for important baseline and prognostic characteristics, confounding cannot be ruled out. The low number of patients available to complete PRO outcomes leaves these measures at high risk of attrition bias. The ability to assess trends is limited by the substantial decline in the number of patients available to provide assessment over time (after cycle 6, fewer than half of the original patients were still available for completion) and by the tendency of long-term survivors to be the healthier patients. Given that the trial was noncomparative, the impact of sotorasib on PROs in relation to other therapies is unknown.
Several subgroup analyses were performed to examine the consistency of the treatment effect observed for the efficacy end points. Although the subgroups were prespecified, strong conclusions could not be drawn, due to the lack of sample size consideration.
CodeBreaK 200 Study
The CodeBreaK 200 study is an open-label, active comparator RCT. Patients were randomized centrally using interactive response technology, which is typically adequate for concealing allocation until treatment assignment. While the randomization stratification factors appear appropriate, several between-group imbalances at baseline suggest that the randomization procedure may not have been sufficient to achieve prognostic balance. Imbalances in baseline characteristics between the sotorasib and docetaxel treatment groups were noted in the following factors: male sex, PD-L1 protein expression (> 1% and < 50% versus ≥ 50%), and primary refractory to last prior line of therapy. According to the clinical experts consulted by CADTH for the purpose of this review, it is unknown if these imbalances could influence treatment response. However, the clinical experts noted that factors that are typically relevant for prognosis, including the presence of brain and liver metastases, were well balanced.
Of concern was the sizable proportion of patients randomized to receive docetaxel who were not dosed (13.2%), mostly due to refusal of treatment, and who discontinued the study by way of withdrawal of consent (22.4%). As a result, unequal censoring between the sotorasib and docetaxel treatment groups was observed (e.g., a 10% difference in censoring between the groups for OS and a 13% difference in censoring for PFS), introducing uncertainty about treatment effects; however, the extent and direction of any bias cannot be determined because it is not clear whether these patients were systematically different from those who continued in the trial. Additionally, a sizable proportion of patients in the docetaxel treatment group (24%) had an outcome of “not measured” in the ORR analysis. The sponsor clarified that the majority of patients who did not have ORR measured did not receive docetaxel because of withdrawal of consent or other reasons. The sponsor further noted that the higher percentage of patients withdrawing consent in the docetaxel group may be due to the open-label nature of the study and a lack of patients preferring docetaxel. Based on input from the clinician group, fewer than half the patients who receive platinum-doublet therapy are subsequently treated with docetaxel out of a desire to avoid potential side effects associated with IV drugs. The extent and direction of bias associated with the ORR analysis is uncertain.
There is added uncertainty in the PFS rates measured over the study period due to the limited number of patients at risk by month 12. Of note, due to protocol amendments that allowed for crossover and the subsequent reduction in sample size, the CodeBreaK 200 study was not powered to detect a difference in OS. There is additional uncertainty in the HR of OS because it is not clear whether the proportional hazard assumption was plausible based on visual inspection of the KM plot, which showed that the 2 curves crossed multiple times. The risk of attrition bias cannot be ruled out due to the disproportionate loss of patients by way of self-withdrawal. The extent and direction of any potential selection bias cannot be determined because it is not clear whether patients who self-withdrew were systematically different from those who continued in the trial.
The primary end point of the CodeBreaK 200 study was PFS. To minimize the risk of bias in the measurement of the outcomes associated with the open-label design, patients’ responses to treatment were blinded to the study investigator, and tumour response was confirmed by radiologic evidence and based on BICR as per RECIST 1.1. Similarly, ORR — a key secondary outcome in the CodeBreaK 200 study that is also prone to risk of measurement bias in open-label studies — was also based on BICR as per RECIST 1.1. The sensitivity analysis of PFS and ORR demonstrated consistency between the BICR and the investigator’s assessment of tumour response, suggesting that the potential for bias in response outcomes from the open-label design is likely not substantial. Objective outcomes, like OS, are not prone to bias due to knowledge of the intervention. Of note, according to the Health Canada Reviewer Report, there is insufficient evidence to ascertain whether PFS is a valid surrogate for OS in advanced NSCLC.18
The CodeBreaK 200 study assessed HRQoL and symptom burden — outcomes deemed important by both patients and clinicians — as key secondary outcomes. However, the key secondary HRQoL outcomes were not inferentially tested because the hierarchical testing was stopped at the non–statistically significant OS end point. Furthermore, changes from baseline at various time points and between-group comparisons were not reported for certain measures (e.g., PRO-CTCAE), limiting the comparative efficacy conclusions. The open-label nature of the CodeBreaK 200 study increases the risk of bias in the measurement of subjective outcomes, such as HRQoL, patient-reported symptom burden, and subjective harms.24,25 This has the potential to bias results and outcomes if the assessor (investigator or patient) believes the study drug is likely to provide a benefit. Adding further uncertainty to the HRQoL and other symptom burden outcomes were some missing baseline data and a decreasing number of patients available to complete the measures in both the sotorasib and docetaxel treatment groups. Focusing on the docetaxel treatment group, after cycle 3, fewer than half of the original patients were available to provide assessments for the EORTC QLQ-C30, the subscales of the EORTC QLQ-LC13, and the EQ-5D-5L. Consequently, there can be no reliable assessment for the docetaxel treatment group for HRQoL and symptom burden measures. The HRQoL and symptom burden outcomes are at high risk of attrition bias because the long-term survivors tend to be the healthier patients.
The analysis of efficacy results followed a defined statistical analysis plan and employed appropriate censoring criteria. Furthermore, secondary efficacy end points (i.e., ORR and OS) were addressed using the multiplicity hierarchical testing procedure, which controlled for type I error. The sponsor conducted additional analyses of OS that adjusted for the effect of crossover using RPSFT, RPSFT and IPCW, and the 2-stage approach. The results of these analyses were consistent with the main analysis in that the CIs were too wide to draw any conclusions with certainty as to whether sotorasib or docetaxel was favoured for OS. Moreover, the administration of subsequent treatments remains a source of uncertainty in the OS results. As with the main analysis, the 95% CIs indicate that either treatment could be favoured, precluding the ability to conclude that sotorasib is superior to docetaxel for OS. Notably, these analyses are associated with strong assumptions that may not be plausible.63 Accordingly, the OS results are uncertain, given the numerous limitations.
Subgroup analyses were performed for PFS to examine the consistency of the observed treatment effect. Although the subgroups were prespecified, strong conclusions could not be drawn due to the lack of sample size consideration and the absence of statistical testing for interaction effects.
External Validity
Overall, the clinical experts consulted by CADTH for this review agreed that the results of the CodeBreaK 100 study and the CodeBreaK 200 study were applicable to the patients seen in the Canadian clinical practice setting. However, they noted some differences between the study population and the patients typically seen in clinical practice. Of note, given the large proportion of screen failures and uncertainty with regards to the reasons, there is a potential that the patients evaluated for the CodeBreaK 200 study were not representative of all patients of the indication population.
Population
The clinical experts highlighted 2 notable differences in disease characteristics between the trial population and the population with NSCLC in Canada. First, the study populations in the CodeBreaK 100 study and the CodeBreaK 200 study were younger than what is typically observed in clinical practice. According to the clinical experts, the average age of patients seen in the clinical setting is 70 years or older, whereas the mean age of patients in the CodeBreaK 100 study and the CodeBreaK 200 study ranged from 62.9 years (SD = 9.3 years) to 63.6 years (SD = 9.1 years). Second, the clinical experts explained that the exclusion of patients with active brain metastases led to the creation of study populations that had lower rates of brain metastases than what is typically seen in clinical practice. According to clinical expert input, the lifetime risk of brain metastasis in patients with KRAS G12C is approximately 40%. The clinical experts noted that in clinical practice, patients with KRAS mutations often have symptomatic brain metastases and an ECOG PS greater than 2. Patients with active brain metastases were not included in either the CodeBreaK 100 study or the CodeBreaK 200 study, but the clinical experts agreed that they would treat patients with treated or stable asymptomatic CNS metastases.64 Similarly, while patients with an ECOG PS of 2 or higher were not included in the study, the clinical experts agreed that they would treat patients with sotorasib who have an ECOG PS of 2.
Prior Interventions
The clinical experts noted that the percentages of patients who had received 3 prior lines of therapy in the CodeBreaK 100 study (22.2%) and the CodeBreaK 200 study (15.5% to 17.0%) appeared high compared to Canadian clinical practice, in which patient numbers tend to drop off significantly with higher lines of therapy. The patient populations in both the CodeBreaK 100 study and the CodeBreaK 200 study were considered to be reflective of the patient population in the clinical setting in that they have exhausted all available treatment options.
Comparator
The clinical experts agreed that docetaxel was an appropriate comparator to sotorasib in the CodeBreaK 200 study. They noted that the docetaxel group appeared to experience better responses to treatment compared to what is typically seen in clinical practice.
Outcomes
According to the clinical experts, ORR and PFS are clinically meaningful end points for patients with advanced NSCLC who have progressed on or after prior lines of therapies. Tumour response outcomes are especially important in this patient population because of the accompanying delay in the worsening of symptoms and the slower decline in ECOG PS.
Companion Diagnostics
The clinical experts noted that co-mutations alongside KRAS may predict patients’ responses to immunotherapy. For example, the clinical experts stated that patients with STK11 mutations (5.6% of patients in the CodeBreaK 100 study) and KEAP1 mutations (0.8% of patients in the CodeBreaK 100 study) tend not to respond well to immunotherapy, but those with TP53 mutations (10.3% of patients in the CodeBreaK 100 study) do. However, due to the small proportion of patients with these mutations in the trial, no conclusion can be drawn as to whether the effects of sotorasib differed according to the presence of these mutations.
Indirect Evidence
The CADTH review team determined that the sponsor-submitted MAIC comparing sotorasib versus docetaxel did not address any gap in the evidence because the CodeBreaK 200 study was a phase III, head-to-head RCT comparing the efficacy and safety of sotorasib and docetaxel. Therefore, the MAIC was not included in the clinical report.
Other Relevant Evidence
This section includes 1 additional relevant study that was included in the sponsor’s submission to CADTH. Results from the global EAP data were summarized. Although this study did not meet the systematic review inclusion criteria, it provides supportive evidence for patients with an ECOG PS of 2, which was a patient group excluded from the CodeBreaK 100 study and the CodeBreaK 200 study. Furthermore, the clinical expert consulted by CADTH and the input received from clinician groups to this submission also expressed a desire to treat patients with an ECOG PS of 2. The input from LCC to this submission indicated that benefits for patients with ECOG PS 3 and 4 remain debatable. The CADTH review team summarized the study designs and data of the global EAP to provide supplemental evidence for decision-making.
Global EAP
A global EAP provided compassionate use of sotorasib before local regulatory approval. Patients eligible for the EAP were aged 18 years to 99 years with an ECOG PS equal to or less than 2, and had pathologically documented, locally advanced and unresectable or metastatic KRAS G12C-mutated NSCLC confirmed through molecular testing. Patients were required to demonstrate that they had exhausted other standard of care options for locally advanced and unresectable or metastatic NSCLC disease, including platinum-based combination chemotherapy and PD-1 or PD-L1 immunotherapy (unless medically contraindicated). Patients participating in any ongoing clinical study of sotorasib who had mixed small cell lung cancer or mixed NSCLC histology, active brain metastases, active hepatitis B or C virus, or any current active malignancy other than NSCLC were excluded from participating, as were those who were enrolled in prior sotorasib studies. The primary end points included safety (such as TEAEs, AEs of interest, and SAEs). Key secondary end points included OS and treatment duration, with real-world PFS as the ad hoc end point. The sponsor-submitted abstract, poster, and presentation summarized the data from 2 global protocols under the EAP: Amgen Study 20190236 (Study 436) and Amgen Study 20190442 (Study 442), which evaluated the safety and efficacy of sotorasib 960 mg daily outside the registrational trial setting in patients with advanced KRAS G12C-mutated NSCLC in multiple countries (US, Italy, Spain Argentina, Brazil, Israel, Saudi Arabia and Taiwan) at 49 centres.27,28 Real-world PFS was estimated for Study 436 and was defined as time from start of treatment to end of protocol due to disease progression or death, any death before new anticancer therapy, or end of commercial sotorasib, whichever occurred first.
Baseline Characteristics
A total of 147 patients received sotorasib 960 mg in Study 436. The median number of prior lines of anticancer therapy reported by patients before receiving sotorasib was 2 (up to 8). At baseline, a total of 25.2% of patients had an ECOG PS of 2, and 32.7% had brain metastases. The median age of patients was 66 years (range, 39 years to 87 years) (Table 31).
Table 31: Baseline Characteristics (Expanded Access Program Study 436)
Characteristic | Study 436 | |
|---|---|---|
Data cut-off June 24, 2022 N = 92 | Data cut-off November 8, 2022 N = 147a | |
Age, years, median (range) | 67.5 (46 to 87) | 66 (39 to 87) |
Sex, male, n (%) | 39 (42.4) | 69 (46.9) |
Race, white, n (%) | 87 (94.6) | NR |
Smoking status, n (%) | ||
Never | 6 (6.5) | 13 (8.8) |
Current | 11 (12.0) | 23 (15.6) |
Former | 75 (81.5) | 111 (75.5) |
ECOG PS, n (%) | ||
0 | 12 (13.0) | 110 (74.8) |
1 | 56 (60.9) | |
2 | 24 (26.1) | 37 (25.2) |
Number of prior lines of therapy, median (range)b | 2 (0 to 7) | 2 (0 to 8) |
Type of prior anticancer therapy, n (%) | ||
Platinum-based chemotherapy | 88 (95.7) | NR |
Anti-PD-1 or anti-PD-L1 therapy | 84 (91.3) | NR |
Anti-VEGF biological therapy | 18 (19.6) | NR |
KRAS G12C inhibitor | 4 (4.3) | 4 (2.7) |
History of brain or CNS metastases | 35 (38.0) | 48 (32.7) |
History of liver metastases | 17 (18.5) | NR |
History of bone metastases | 39 (42.4) | NR |
Prior lines of anticancer therapy,c n (%) | ||
1 | NR | 56 (38.1) |
2 | NR | 47 (32.0) |
≥ 3 | NR | 42 (28.6) |
PD-L1 expression, n (%) | ||
< 1% | NR | 48 (32.7) |
≥ 1% and < 50% | NR | 53 (36.1) |
≥ 50% | NR | 35 (23.8) |
Missing | NR | 9 (6.1) |
Unknown | NR | 2 (1.4) |
CNS = central nervous system; ECOG PS = Eastern Cooperative Oncology Group Performance Status; NR = not reported; PD-1 = programmed cell death 1; PD-L1 = programmed cell death 1 ligand 1; VEGF = vascular endothelial growth factor.
aA total of 148 patients were enrolled: 54 patients (36.5%) from the US, 38 patients (25.7%) from Israel, 20 patients (13.5%) from Brazil, 19 patients (12.8%) from Taiwan, 15 patients (10.1%) from Argentina, and 2 patients (1.4%) from Saudi Arabia. Sotorasib was not given to 1 patient (0.7%), based on their request.
bPatients could be enrolled if standard of care therapies were contraindicated.
cPrior lines of anticancer therapy in advanced setting.
Sources: Awad et al. (2022);27 Novello et al. (2023).28
Table 32: Partial Efficacy Results From Expanded Access Program Study 436
Efficacy results | Study 436 |
|---|---|
rwPFS | |
N | 92a |
Median rwPFS, months (95% CI) | 6.7 (4.6 to 8.3) |
Events, n (%) | 60 (65.2) |
OS | |
N | 147c |
Median OS, months (95% CI) | 9.5 (8.6 to 12.0) |
Deaths, n (%) | 76 (51.7) |
CI = confidence interval; OS = overall survival; rwPFS = real-world progression-free survival.
aAmong the 30 out of 92 patients (33%) who switched to commercial sotorasib, 25 patients initiated treatment with commercial sotorasib within 1 to 2 days after the end of protocol sotorasib; 3 patients started commercial sotorasib 4 days, 5 days, and 17 days after the end of protocol sotorasib; 2 patients discontinued protocol sotorasib due to an AE, but initiated commercial sotorasib 34 days and 99 days later. Data cut-off date: June 24, 2022.
bThe median durations of treatments were 5.8 months (95% CI, 2.3 months to 11.7 months) in patients with ECOG PS 0, and 6.2 months (95% CI, 3.4 to 9.1 months) in patients with ECOG PS 1.
cThe data cut-off date was November 8, 2022.
Sources: Awad et al. (2022);27 Novello et al. (2023).28
Results
The median real-world PFS for the 92 patients and the median OS for the 147 patients enrolled in Study 436 are summarized in Table 32. The median real-world PFS was 6.7 months (95% CI, 4.6 months to 8.3 months), with 60 (65.2%) events. The median OS was 9.5 months (95% CI, 8.6 months to 12.0 months), with 76 deaths (51.7%).
Harms
The global EAP study27 presented AEs as TEAEs; thus, these are not reported by the CADTH review team.
Critical Appraisal
Lacking the details of the study methodology, the CADTH review team was unable to complete a robust critical appraisal of the internal and external validity of the study. A key limitation to the global EAP study is the noncomparative design and lack of statistical testing. In the absence of a randomized comparator, causal conclusions regarding the relationship between sotorasib treatment and PFS or OS cannot be drawn.65 The study is open-label; the risk of bias in the assessment of PFS is uncertain because the person or group responsible for the outcome assessment was not reported (i.e., unblinded investigator or independent review committee). Although the results were comparable to the PFS efficacy results reported in the CodeBreaK 100 study and the CodeBreaK 200 study, the magnitude of the treatment effect for real-world PFS should be interpreted with uncertainty in light of the aforementioned limitations. The sotorasib dosage used in the study was aligned with the product monograph, and patients with ECOG PS of 0 to 2 were permitted to participate; a result, there is limited evidence for patients with ECOG 2, who were not included in the sponsor-conducted trials. The study did not report on outcomes other than PFS and OS (e.g., HRQoL, symptoms, harms) that are important to patients, clinicians, and drug plans.
Discussion
Summary of Available Evidence
Two sponsor-conducted studies were included in the clinical review: the CodeBreaK 100 study and the CodeBreaK 200 study.
The CodeBreaK 100 study is an ongoing, multicentre, nonrandomized, open-label, single-group, phase I and II study. The CADTH review focused only on the subset of patients with KRAS G12C-mutated, advanced NSCLC who were enrolled in phase II of the CodeBreaK 100 study, which was designed to evaluate the efficacy and safety of sotorasib as monotherapy. Patients self-administered sotorasib 960 mg (8 × 120 mg tablets) orally once daily and continued treatment without interruption until disease progression, treatment intolerance, withdrawal of consent, or death. Tumour response was assessed through contrast-enhanced CT or MRI and per RECIST 1.1 by an independent radiological central laboratory. The primary efficacy end point was ORR, which was a composite of CR and PR. Secondary efficacy end points included DOR, PFS, and OS. Exploratory outcomes included changes in patient-reported, cancer-specific symptoms, and HRQoL.
Among the 126 patients enrolled in the CodeBreaK 100 study, most were aged 18 years to 64 years (53.2%), had advanced local or metastatic disease (stage IV) at initial diagnosis (61.9%) and screening (96%), and had been treated with 1 or 2 lines of prior therapies (77.8%).
The single-group, open-label, nonrandomized design of the CodeBreaK 100 study makes interpretation of the efficacy and safety results challenging. The lack of comparison with an active comparator, BSC, and/or placebo precludes the ability to assess the relative therapeutic benefits or safety of sotorasib or to draw causal inferences. Due to the open-label design, subjective outcomes like HRQoL, other PROs, and subjective harms are at risk of bias. Further, the results for HRQoL and other PROs are at risk of attrition bias. The patient population was younger and healthier (i.e., with a lower ECOG PS) compared with patients typically seen in Canadian clinical practice, and those with active CNS metastases were excluded. The results were otherwise found to be generalizable to the clinical setting by the clinical experts consulted by CADTH for the purpose of this review.
The CodeBreaK 200 study is an ongoing, multicentre, open-label, randomized, phase III study evaluating the efficacy and safety of oral sotorasib (960 mg once daily) to IV docetaxel (75 mg/m2 every 3 weeks) in adult patients with KRAS G12C-mutated NSCLC who progressed after prior platinum-based chemotherapy and checkpoint inhibitor therapy. A total of 169 patients and 151 patients were randomized to receive sotorasib or docetaxel, respectively. The primary end point of the CodeBreaK 200 study was PFS. After study initiation, crossover from docetaxel to sotorasib was permitted following disease progression. Secondary end points included ORR, OS, HRQoL, and symptom burden.
As with the CodeBreaK 100 study, the patient population in the CodeBreaK 200 study was younger and healthier (i.e., lower ECOG PS) than patients typically seen in Canadian clinical practice. Between the 2 treatment groups, a greater proportion of males (63.7%) were in the sotorasib group relative to the docetaxel group (54.6%). Other imbalances in baseline characteristics between the sotorasib and docetaxel treatment groups were noted for PD-L1 protein expression (≥ 1% and < 50% versus ≥ 50%) and primary refractory to last prior line of therapy. Although the clinical experts consulted by CADTH for the purpose of this review were uncertain if these imbalances could influence treatment response, these imbalances may indicate that prognostic balance was not achieved through the randomization procedure. The assessment of response outcomes was performed using BICR, reducing the risk of bias in outcome assessment. However, the trial was not powered for OS. There was uncertainty around the treatment effect observed in the CodeBreaK 200 study because a larger proportion of patients in the docetaxel treatment group versus the sotorasib group withdrew from the trial before receiving treatment and because of unequal censoring between the sotorasib and docetaxel treatment groups.
In addition, the results of a global EAP study (n = 147) were summarized; this was a real-world study that provided evidence for patients with an ECOG PS of 2 and were excluded from the sponsor-conducted trials. However, due to limitations in the reporting of the EAP study, the CADTH team was unable to complete a robust appraisal of the internal and external validity of its results. Moreover, due to the lack of a randomized comparator, no causal conclusions can be drawn from this study.
Interpretation of Results
Efficacy
In the CodeBreaK 100 study, at the time of the primary analysis (September 1, 2020), approximately one-third of enrolled patients had experienced an objective response, demonstrating that sotorasib has antitumour activity in some patients. The results observed at the updated data cut-off date (March 15, 2021) were consistent with those observed at the primary data cut-off date. When compared to docetaxel in the CodeBreaK 200 study, a greater proportion of patients randomized to sotorasib experienced objective responses and had longer median PFS. However, 24% of patients in the docetaxel treatment group did not have an ORR outcome documented, mainly due to withdrawing consent before treatment start; this introduces uncertainty into the ORR results. The sponsor noted that the higher proportion of patients withdrawing consent in the docetaxel group may be due to the open-label nature of the study and the lack of preference for docetaxel among patients. The effect estimate for OS in the CodeBreaK 200 study was too imprecise to draw any conclusion as to the effect of sotorasib relative to docetaxel because the 95% CIs included the possibility that either treatment could be favoured. Input from patient advocacy groups, registered clinicians, and clinical experts consulted by CADTH highlighted HRQoL as an important outcome and treatment goal for patients. However, given the open-label design of the trial and the substantial decline in the number of patients available to provide assessments over time, the HRQoL results are inconclusive.
The single-group, open-label, nonrandomized study design of the CodeBreaK 100 study made interpretation of the efficacy and safety results of sotorasib challenging. In the CodeBreaK 200 study, PFS results were at risk of bias due to between-study group imbalances in the proportions of patients who withdrew from the study. The direction of this potential bias is uncertain. While the absolute benefit in median PFS between sotorasib and docetaxel was modest (about 1 month), the clinical experts felt that the absolute PFS benefit observed with sotorasib at 1 year (24.84% with sotorasib compared to 10.12% with docetaxel) appeared encouraging and clinically meaningful. However, a substantial proportion of patients were censored at baseline in the docetaxel groups (11.5%), and it is not possible to know whether these patients were systematically different from those who continued in the trial.
The primary efficacy outcomes assessed in the CodeBreaK 100 study and the CodeBreaK 200 study were objective response and PFS, respectively. With regard to objective response, ORR is not a validated surrogate for survival in the present target setting. The FDA guidance document Clinical Trial End points for the Approval of Non–Small Cell Lung Cancer Drugs and Biologics states, “Treatment effects on ORR have not been demonstrated to reliably predict corresponding effects on survival in NSCLC.” With regard to PFS, the European Medicines Agency recommends that when PFS is the primary end point, OS should be the secondary end point. This was the case in the CodeBreaK 200 study.66
Both the CodeBreaK 100 study and the CodeBreaK 200 study assessed HRQoL and symptoms burden, which were considered important outcomes to patients. In the CodeBreaK 100 study, HRQoL measures were at risk of bias due to the lack of comparative evidence, open-label design, and missing data. In CodeBreaK 200, conclusions about the effect of sotorasib on HRQoL outcomes relative to docetaxel could not be drawn due to the open-label and descriptive nature of the study and the diminishing number of patients available for assessment over time. The clinical experts noted that HRQoL for patients on docetaxel tends to diminish as treatment duration increases, with resulting dose-limiting toxicities. The clinical experts anticipated that sotorasib would be better tolerated by patients and would have fewer detrimental effects on HRQoL compared to chemotherapy.
The global EAP study, which included patients with ECOG PS of 2, demonstrated real-world PFS comparable to the CodeBreaK 100 study and the CodeBreaK 200 study for sotorasib. However, the CADTH review team was unable to draw any definitive conclusions, given the noncomparative study design.
Harms
The most-reported TEAEs among patients who received sotorasib in the CodeBreaK 100 study and the CodeBreaK 200 study included diarrhea, nausea, and fatigue. In the CodeBreaK 100 study, about half of the patients with KRAS G12C-mutated, locally advanced or metastatic NSCLC experienced SAEs; the most frequently reported SAEs were pneumonia, pleural effusion, and back pain. In the CodeBreaK 200 study, grade 3 or higher TEAEs were driven by AST or ALT increases and diarrhea, which the clinical experts anticipated could be well-managed by the treating clinician and through patient education. From the review of notable harms, it appeared that toxicities from sotorasib were mostly seen as increases in AST, ALT, blood ALP, and renal toxicity.
Given that the median duration of treatment in the sotorasib group was close to twice as long as that in the docetaxel group, the safety comparison between the study groups across all cycles may be biased against the sotorasib group. The sotorasib group had a higher proportion of patients remaining on study treatment as well as longer exposure to the study treatment compared with the docetaxel group; therefore, patients in the sotorasib group were more likely than the docetaxel group to report AEs during the treatment phase.
The clinical experts consulted by CADTH agreed with the registered clinicians providing input to this submission that the TEAEs observed with sotorasib could be adequately managed in clinical practice and that sotorasib appears to have a favourable toxicity profile compared with currently available docetaxel therapy. This was reflective of patients’ experience with sotorasib as reported in the patient input, which indicated that overall, patients had little challenge dealing with side effects of sotorasib.
The product monograph for sotorasib documents the following common side effects: diarrhea, musculoskeletal pain, nausea, fatigue, hepatotoxicity, and cough. The product monograph also contains warmings for serious side effects, including hepatotoxicity and interstitial lung disease/pneumonitis.
Conclusions
One nonrandomized, single-group, open-label, phase I and II study (the CodeBreaK 100 study) and 1 randomized, comparative, open-label, phase III study (the CodeBreaK 200 study) provided evidence for the efficacy and safety of sotorasib in adult patients with KRAS G12C-mutated, advanced NSCLC. In the CodeBreaK 100 study, the results for ORR and DOR were considered clinically meaningful in the target population by the clinical experts consulted by CADTH. There was uncertainty around the magnitude of the clinical benefit, given the limitations in the evidence from the noncomparative phase I and II clinical trial. The nonrandomized design of the CodeBreaK 100 study made interpreting the PFS and OS events attributable to sotorasib challenging because it is unclear whether the observations were due to natural history or the effect of treatment with sotorasib. In the CodeBreaK 200 study, treatment with sotorasib demonstrated a beneficial impact on PFS and ORR compared to docetaxel. Although the difference in median PFS of approximately 1 month was modest, the clinical experts consulted by CADTH felt that the PFS rates for sotorasib at 12 months appeared encouraging and clinically meaningful. The clinical experts agreed that the impact of sotorasib on objective response was clinically meaningful. There was uncertainty around the treatment effect observed in the CodeBreaK 200 study because a larger proportion of patients in the docetaxel treatment group versus the sotorasib group withdrew from the trial before receiving treatment and because of unequal censoring between the sotorasib and docetaxel treatment groups. The CIs associated with the treatment effect of sotorasib relative to docetaxel on OS in the CodeBreaK 200 study were too wide to determine if either treatment was favoured. The results for HRQoL and symptom severity were descriptive in nature and remained inconclusive due to diminishing numbers of patients available to complete the assessments over time. The clinical experts consulted by CADTH noted that the TEAEs observed with sotorasib could be adequately managed in clinical practice and that sotorasib appeared to have a favourable toxicity profile compared to docetaxel.
References
1.Canadian Cancer Statistics Advisory Committee. Canadian Cancer Statistics: A 2020 special report on lung cancer. Toronto (ON): Canadian Cancer Society; 2020: https://cdn.cancer.ca/-/media/files/cancer-information/resources/publications/2020-canadian-cancer-statistics-special-report/2020-canadian-cancer-statistics-special-report-en.pdf. Accessed 2022 Mar 23.
2.Dela Cruz CS, Tanoue LT, Matthay RA. Lung cancer: epidemiology, etiology, and prevention. Clin Chest Med. 2011;32(4):605-644. PubMed
3.Epiphany Partners Inc. EpicOncologyTM Cancer Epidemiology Service. [2020]; http://time4epi.com/. Accessed by the sponsor 2020 Feb 21 as referenced in the Health Canada Reviewers Report.
4.Canadian Cancer Statistics Advisory Committee. Canadian Cancer Statistics 2021. Toronto (ON): Canadian Cancer Society; 2021: https://cancer.ca/en/research/cancer-statistics/canadian-cancer-statistics. Accessed 2022 Sep 1.
5.Canadian Cancer Society. Survival statistics for non-small cell lung cancer. 2020; https://cancer.ca/en/cancer-information/cancer-types/lung/prognosis-and-survival/non-small-cell-lung-cancer-survival-statistics. Accessed 2022 Apr 21.
6.Detterbeck FC, Boffa DJ, Kim AW, Tanoue LT. The Eighth Edition Lung Cancer Stage Classification. Chest. 2017;151(1):193-203.
7.Birring SS, Peake MD. Symptoms and the early diagnosis of lung cancer. Thorax. 2005;60(4):268-269. PubMed
8.Barbera L, Seow H, Howell D, et al. Symptom burden and performance status in a population-based cohort of ambulatory cancer patients. Cancer. 2010;116(24):5767-5776. PubMed
9.Bradley SH, Kennedy MPT, Neal RD. Recognising Lung Cancer in Primary Care. Adv Ther. 2019;36(1):19-30. PubMed
10.Vinod SK, Wai E, Alexander C, Tyldesley S, Murray N. Stage III non-small-cell lung cancer: population-based patterns of treatment in British Columbia, Canada. J Thorac Oncol. 2012;7(7):1155-1163. PubMed
11.U.S. Department of Health and Human Services, National Institutes of Health, National Cancer Institute, Surveillance, Epidemiology, and End Results Program. SEER*Stat Database: Incidence - SEER 21 Regs Limited-Field Research Data + Hurricane Katrina Impacted Louisiana Cases, Nov 2018 Sub (2000-2016) <Katrina/Rita Population Adjustment> - Linked To County Attributes - Total U.S. 1969-2017 Counties, National Cancer Institute, DCCPS, Surveillance Research Program, released April 2019, based on the November 2018 submission. 2019; https://seer.cancer.gov/. Accessed by the sponsor 2020 Feb 10.
12.Lee T, Lee B, Choi YL, Han J, Ahn MJ, Um SW. Non-small Cell Lung Cancer with Concomitant EGFR, KRAS, and ALK Mutation: Clinicopathologic Features of 12 Cases. J Pathol Transl Med. 2016;50(3):197-203. PubMed
13.Cox AD, Fesik SW, Kimmelman AC, Luo J, Der CJ. Drugging the undruggable RAS: Mission possible? Nat Rev Drug Discov. 2014;13(11):828-851. PubMed
14.Dana-Farber Cancer Institute. Targeted drug achieves 43% response rate in KRAS-mutated lung cancer. 2022; https://www.dana-farber.org/newsroom/news-releases/2022/targeted-drug-achieves-43--response-rate-in-kras-mutated-lung-cancer/. Accessed 2022 Nov 17.
15.Barlesi F, Mazieres J, Merlio JP, et al. Routine molecular profiling of patients with advanced non-small-cell lung cancer: results of a 1-year nationwide programme of the French Cooperative Thoracic Intergroup (IFCT). Lancet. 2016;387(10026):1415-1426. PubMed
16.Arbour KC, Jordan E, Kim HR, et al. Effects of Co-occurring Genomic Alterations on Outcomes in Patients with KRAS-Mutant Non-Small Cell Lung Cancer. Clin Cancer Res. 2018;24(2):334-340. PubMed
17.Amgen Data on file [AACR GENIE]. In: Drug Reimbursement Review sponsor submission: Lumakras (sotorasib), 120 mg oral tablets. Mississauga (ON): Amgen Canada Inc.; 2022 Aug 19.
18.Health Canada reviewer's report: Lumakras (sotorasib) [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Lumakras (sotorasib), 120 mg oral tablets. Mississauga (ON): Amgen Canada Inc.; 2021 Sep 8.
19.Clinical Study Report: 20170543 (Phase-1 Portion). A Phase 1/2, Open-label Study Evaluating the Safety, Tolerability, Pharmacokinetics, Pharmacodynamics, and Efficacy of AMG 510 Monotherapy in Subjects With Advanced Solid Tumors With KRAS p.G12C Mutation and AMG 510 Combination Therapy in Subjects With Advanced NSCLC With KRAS p.G12C Mutation (CodeBreak 100) [internal sponsor's report]. Thousand Oaks (CA): Amgen Inc.; 2020 Nov 10.
20.Clinical Study Report: 20170543 Phase 2 Portion. A Phase 1/2, Open-label Study Evaluating the Safety, Tolerability, Pharmacokinetics, Pharmacodynamics, and Efficacy of AMG 510 Monotherapy in Subjects With Advanced Solid Tumors With KRAS p.G12C Mutation and AMG 510 Combination Therapy in Subjects With Advanced NSCLC With KRAS p.G12C Mutation (CodeBreak 100) [internal sponsor's report]. Thousand Oaks (CA): Amgen Inc.; 2020 Nov 10.
21.Clinical Study Report: 20190009. A phase 3 multicenter, randomized, open label, active controlled, study of AMG 510 versus docetaxel for the treatment of previously treated locally advanced and unresectable or metastatic NSCLC subjects With mutated KRAS p.G12C [internal sponsor's report]. Thousand Oaks (CA): Amgen Inc.; 2022 Nov 2.
22.Maurer W, Bretz F. Multiple testing in group sequential trials using graphical approaches. Stat Biopharm Res. 2013;5(4):311-320.
23.Nakajima EC, Drezner N, Li X, et al. FDA Approval Summary: Sotorasib for KRAS G12C-Mutated Metastatic NSCLC. Clin Cancer Res. 2022;28(8):1482-1486. PubMed
24.Swan JS, Lennes IT, Stump NN, et al. A Patient-Centered Utility Index for Non-Small Cell Lung Cancer in the United States. MDM Policy Pract. 2018;3(2):2381468318801565. PubMed
25.Nicklasson M, Bergman B. Validity, reliability and clinical relevance of EORTC QLQ-C30 and LC13 in patients with chest malignancies in a palliative setting. Qual Life Res. 2007;16(6):1019-1028. PubMed
26.Janne PA, van den Heuvel MM, Barlesi F, et al. Selumetinib Plus Docetaxel Compared With Docetaxel Alone and Progression-Free Survival in Patients With KRAS-Mutant Advanced Non-Small Cell Lung Cancer: The SELECT-1 Randomized Clinical Trial. JAMA. 2017;317(18):1844-1853. PubMed
27.Awad M, Pelizzari G, Stevenson JP, et al. 989P - Sotorasib in advanced KRAS p.G12C-mutated non-small cell lung cancer (NSCLC): Safety and efficacy data from the global expanded access program (EAP). Ann Oncol. 2022;33(suppl_7):S448-S554.
28.Novello S, Maimon N, Stevenson JP, et al. 7MO Sotorasib in KRAS G12C-mutated advanced non-small cell lung cancer (aNSCLC): Overall survival (OS) data from global expanded access program (EAP Study-436). J Thorac Oncol. 2023;18(4 suppl):S40-S41.
29.Stewart DJ, Maziak DE, Moore SM, et al. The need for speed in advanced non-small cell lung cancer: A population kinetics assessment. Cancer Med. 2021;10(24):9040-9046. PubMed
30.Zhuang X, Zhao C, Li J, et al. Clinical features and therapeutic options in non-small cell lung cancer patients with concomitant mutations of EGFR, ALK, ROS1, KRAS or BRAF. Cancer Med. 2019;8(6):2858-2866. PubMed
31.BC Cancer. Lung. 2019; http://www.bccancer.bc.ca/health-professionals/clinical-resources/cancer-management-manual/lung/lung. Accessed 2021 Jun 3.
32.McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS Peer Review of Electronic Search Strategies: 2015 guideline statement. J Clin Epidemiol. 2016;75:40-46. PubMed
33.Grey matters: a practical tool for searching health-related grey literature. Ottawa (ON): CADTH; 2019: https://greymatters.cadth.ca/. Accessed 2022 Sep 8.
34.Skoulidis F, Li BT, Dy GK, et al. Sotorasib for Lung Cancers with KRAS p.G12C Mutation. N Engl J Med. 2021;384(25):2371-2381. PubMed
35.de Langen AJ, Johnson ML, Mazieres J, et al. Sotorasib versus docetaxel for previously treated non-small-cell lung cancer with KRAS(G12C) mutation: a randomised, open-label, phase 3 trial. Lancet. 2023;401(10378):733-746. PubMed
36.Protocol 20190009: A Phase 3 Multicenter, Randomized, Open Label, Active-controlled, Study of AMG 510 Versus Docetaxel for the Treatment of Previously Treated Locally Advanced and Unresectable or Metastatic NSCLC Subjects With Mutated KRAS p.G12C [internal sponsor's report]. Thousand Oaks (CA): Amgen Inc.; 2022 Jan 6.
37.Amgen Inc. EudraCT 2020-005279-11. 20190442: A Multicenter, Open-label, Single-arm, Expanded-Access Protocol of AMG 510 (Sotorasib) for the Treatment of Subjects in Select European Countries with Previously Treated Locally Advanced and Unresectable or Metastatic Non-small Cell Lung Cancer with KRAS p.G12C Mutation. Amsterdam (NL): European Medicines Agency; 2020: https://www.clinicaltrialsregister.eu/ctr-search/search?query=2020-005279-11. Accessed 2022 Sep 29.
38.Zheng X, Luo J, Liu W, Ashby CR, Jr., Chen ZS, Lin L. Sotorasib: a treatment for non-small cell lung cancer with the KRAS G12C mutation. Drugs Today (Barc). 2022;58(4):175-185. PubMed
39.Reeve BB, Wyrwich KW, Wu AW, et al. ISOQOL recommends minimum standards for patient-reported outcome measures used in patient-centered outcomes and comparative effectiveness research. Qual Life Res. 2013;22(8):1889-1905. PubMed
40.Koller M, Musoro JZ, Tomaszewski K, et al. Minimally important differences of EORTC QLQ-C30 scales in patients with lung cancer or malignant pleural mesothelioma - Interpretation guidance derived from two randomized EORTC trials. Lung Cancer. 2022;167:65-72. PubMed
41.Maringwa JT, Quinten C, King M, et al. Minimal important differences for interpreting health-related quality of life scores from the EORTC QLQ-C30 in lung cancer patients participating in randomized controlled trials. Support Care Cancer. 2011;19(11):1753-1760. PubMed
42.Bergman B, Aaronson NK, Ahmedzai S, Kaasa S, Sullivan M. The EORTC QLQ-LC13: a modular supplement to the EORTC Core Quality of Life Questionnaire (QLQ-C30) for use in lung cancer clinical trials. EORTC Study Group on Quality of Life. Eur J Cancer. 1994;30a(5):635-642. PubMed
43.Brooks R. The EuroQol Group after 25 years. New York (NY): Springer; 2013.
44.Sinnott PL, Joyce VR, Barnett P. Preference measurement in economic analysis. Guidebook [sponsor reference]. Menlo Park (CA): VA Palo Alto, Health Economics Resource Center; 2007.
45.Bushnell DM, Atkinson TM, McCarrier KP, Liepa AM, DeBusk KP, Coons SJ. Non-Small Cell Lung Cancer Symptom Assessment Questionnaire: Psychometric Performance and Regulatory Qualification of a Novel Patient-Reported Symptom Measure. Curr Ther Res Clin Exp. 2021;95:100642. PubMed
46.DDT COA #000009: Non-Small Cell Lung Cancer Symptom Assessment Questionnaire (NSCLC-SAQ). Silver Spring (MD): U.S. Food & Drug Administration, Drug Development Tool Clinical Outcome Assessment (COA) Qualification Program; 2017: https://www.fda.gov/drugs/clinical-outcome-assessment-coa-qualification-program/ddt-coa-000009-non-small-cell-lung-cancer-symptom-assessment-questionnaire-nsclc-saq. Accessed 2023 May 18.
47.McCarrier KP, Atkinson TM, DeBusk KP, Liepa AM, Scanlon M, Coons SJ. Qualitative Development and Content Validity of the Non-small Cell Lung Cancer Symptom Assessment Questionnaire (NSCLC-SAQ), A Patient-reported Outcome Instrument. Clin Ther. 2016;38(4):794-810. PubMed
48.Williams P, Burke T, Norquist JM, et al. Non-Small Cell Lung Cancer Symptom Assessment Questionnaire (NSCLC-SAQ): Measurement Properties and Estimated Clinically Meaningful Thresholds From a Phase 3 Study. JTO Clin Res Rep. 2022;3(4):100298. PubMed
49.FACIT. FACT-G: Functional Assessment of Cancer Therapy - General. 2021; https://www.facit.org/measures/FACT-G. Accessed 2022 Sep 21.
50.U.S. Department of Health and Human Services, National Institutes of Health, National Cancer Institute. PRO-CTCAE: Overview. 2023; https://healthcaredelivery.cancer.gov/pro-ctcae/overview.html. Accessed 2022 Nov 21.
51.MD Anderson Cancer Centre. The Brief Pain Inventory. [2021]; https://www.mdanderson.org/research/departments-labs-institutes/departments-divisions/symptom-research/symptom-assessment-tools/brief-pain-inventory.html. Accessed 2021 Nov 21.
52.Garon EB, Ciuleanu T-E, Arrieta O, et al. Ramucirumab plus docetaxel versus placebo plus docetaxel for second-line treatment of stage IV non-small-cell lung cancer after disease progression on platinum-based therapy (REVEL): a multicenter, double-blind, randomized phase 3 trial. Lancet. 2014;384(9944):665-673. PubMed
53.Cyramza (ramucirumab) [package insert; sponsor reference]. Indianapolis (IN): Eli Lilly and Company; 2014.
54.Charpidou A, Vathiotis I, Gkiozos I, Syrigos K. Exceptional antitumor responses beyond immune checkpoint inhibition in non-small cell lung cancer patients: insights into optimal therapy sequencing. J Thorac Dis. 2019;11(3):E25-E31. PubMed
55.Lee JJ, Liu DD. A predictive probability design for phase II cancer clinical trials. Clin Trials. 2008;5(2):93-106. PubMed
56.Klein JP, Moeschberger ML. Survival Analysis: Techniques for Censored and Truncated Data. New York (NY): Springer-Verlag; 1997.
57.Kalbfleisch JD, Prentice RL. The Statistical Analysis of Failure Time Data. New York (NY): John Wiley & Sons; 1980.
58.Robins JM, Tsiatis AA. Correcting for non-compliance in randomized trials using rank preserving structural failure time models. Communications in Statistics - Theory and Methods. 1991;20(8):2609-2631.
59.Robins JM. Information recovery and bias adjustment in proportional hazards regression analysis of randomized trials using surrogate markers. Proceedings of the Biopharmaceutical Section, American Statistical Association. 1993:24-33.
60.Latimer NR, Abrams KR, Lambert PC, et al. Adjusting survival time estimates to account for treatment switching in randomized controlled trials--an economic evaluation context: methods, limitations, and recommendations. Med Decis Making. 2014;34(3):387-402. PubMed
61.Clinical Study Report: 20170543 (PRO Data). A Phase 1/2, Open-label Study Evaluating the Safety, Tolerability, Pharmacokinetics, Pharmacodynamics, and Efficacy of AMG 510 Monotherapy in Subjects With Advanced Solid Tumors With KRAS p.G12C Mutation and AMG 510 Combination Therapy in Subjects With Advanced NSCLC With KRAS p.G12C Mutation (CodeBreak 100) [internal sponsor's report]. Thousand Oaks (CA): Amgen Inc.; 2020 Nov 12.
62.Guidance for Industry: Clinical Trial Endpoints for the Approval of Cancer Drugs and Biologics. Silver Spring (MD): U.S. Food and Drug Administration (FDA); 2018: https://www.fda.gov/downloads/Drugs/Guidances/ucm071590.pdf. Accessed 2019 Sep 10.
63.Latimer NR, Abrams KR. NICE DSU Technical Support Document 16: Adjusting Survival Time Estimates in the Presence of Treatment Switching. (NICE Decision Support Unit Technical Support Documents). London (GB): National Institute for Health and Care Excellence (NICE); 2014: https://pubmed.ncbi.nlm.nih.gov/27466662/. Accessed 2021 Jun 16.
64.Lamberti G, Aizer A, Ricciuti B, et al. Incidence of Brain Metastases and Preliminary Evidence of Intracranial Activity With Sotorasib in Patients With KRAS(G12C)-Mutant Non-Small-Cell Lung Cancer. JCO Precis Oncol. 2023;7:e2200621. PubMed
65.Evans SR. Clinical trial structures. J Exp Stroke Transl Med. 2010;3(1):8-18. PubMed
66.Committee for Medicinal Products for Human Use (CHMP). Guideline on the clinical evaluation of anticancer medicinal products. London (GB): European Medicines Agency; 2019: https://www.ema.europa.eu/en/documents/scientific-guideline/draft-guideline-evaluation-anticancer-medicinal-products-man-revision-6_en.pdf. Accessed 2021 Apr 26.
67.Amgen. Lumakras®/Lumykras® (sotorasib) demonstrates superior progression-free survival over docetaxel in first positive phase 3 trial of a KRAS G12C inhibitor in non-small cell lung cancer. 2022; https://www.amgen.com/newsroom/press-releases/2022/09/lumakraslumykras-sotorasib-demonstrates-superior-progressionfree-survival-over-docetaxel-in-first-positive-phase-3-trial-of-a-kras-g12c-inhibitor-in-nonsmall-cell-lung-cancer. Accessed 2022 Oct 20.
68.Amgen. NCT04667234: A Multicenter, Open-label, Single-arm, Expanded Access Protocol of Sotorasib for the Treatment of Subjects With Previously Treated Locally Advanced Unresectable/Metastatic NSCLC With KRAS p.G12C Mutation. ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2023: https://classic.clinicaltrials.gov/ct2/show/NCT04667234. Accessed 2023 May 18.
69.Myers K, Barrett A, Leach C, et al. P52.01 Understanding Treatment Preferences of Patients With KRAS p.G12C[LC1] [MK2] – Mutated Advanced Non-Small Cell Lung Cancer. J Thorac Oncol. 2021;16(10 Suppl):S1121-S1122.
70.Dy GK, Govindan Ramaswamy, Velcheti V, et al. Abstract CT008: Long-term outcomes with sotorasib, including genomic profiles, in pre-treated KRAS p.G12C mutated NSCLC: 2-year analysis of CodeBreaK100. Cancer Res. 2022 82(12 suppl):CT008.
71.Dozier A, Fitzpatrick V, Liu D, Hull J, Varrieur T, McGuire L. P390 - Nursing experience with patients receiving sotorasib for KRAS G12C-mutated solid tumors: follow-up from the phase 1/2 CodeBreaK 100 study [conference poster]. The Oncology Nursing Society’s Signature Conference; 2022 Apr 27-May 1; Anaheim (CA). https://ons.confex.com/ons/2022/meetingapp.cgi/Paper/11993. Accessed 2023 May 18.
72.Fakih M, O’Neil B, Price TJ, et al. Phase 1 study evaluating the safety, tolerability, pharmacokinetics (PK), and efficacy of AMG 510, a novel small molecule KRASG12C inhibitor, in advanced solid tumors. J Clin Oncol. 2019;37(15 suppl):3003-3003.
73.Govindan R, Fakih MG, Price TJ, et al. Phase I study of AMG 510, a novel molecule targeting KRAS G12C mutant solid tumours. Ann Oncol. 2019;30(Suppl 5):v163-v164.
74.Govindan R, Fakih MG, Price TJ, et al. P2.15-C Phase 1 trial evaluating safety, efficacy, and PK of AMG 510, a novel KRASG12C inhibitor, in non-small cell lung cancer. J Thorac Oncol. 2019;14(11 Suppl 2):S1191-S1192.
75.Govindan R, Fakih MG, Price TJ, et al. OA01.06 Safety, Efficacy, and Pharmacokinetics (PK) of AMG 510, a Novel KRASG12C Inhibitor in Patients with Non-Small Cell Lung Cancer (NSCLC). J Thorac Oncol. 2019;14(11 Suppl 1):S1125-S1126.
76.Govindan R, Fakih M, Price T, et al. OA02.02 Phase 1 Study of Safety, Tolerability, PK and Efficacy of AMG 510, a Novel KRASG12C Inhibitor, Evaluated in NSCLC. J Thorac Oncol. 2019;14(10 Suppl):S208.
77.Heinzl S. Pretreated NSCLC. Sotorasib is also effective in non-small cell lung cancer with KRAS-G12C mutation. [German]. Arzneimitteltherapie. 2021;39(10):368-369.
78.Hong DS, Bang YJ, Barlesi F, et al. 1257O Durability of clinical benefit and biomarkers in patients (pts) with advanced non-small cell lung cancer (NSCLC) treated with AMG 510 (sotorasib). Ann Oncol. 2020;31(Suppl 4):S812.
79.Hong DS, Fakih MG, Strickler JH, et al. KRAS(G12C) Inhibition with Sotorasib in Advanced Solid Tumors. N Engl J Med. 2020;383(13):1207-1217. PubMed
80.Hong DS, Stickler JH, Fakih M, et al. Trial in progress: A phase 1b study of sotorasib, a specific and irreversible KRASG12C inhibitor, as monotherapy in non-small cell lung cancer (NSCLC) with brain metastasis and in combination with other anticancer therapies in advanced solid tumors (CodeBreaK 101). J Clin Oncol. 2021;39(15_suppl):TPS2669-TPS2669.
81.Intergroupe Francophone de Cancerologie Thoracique. NCT0527304: Assessment and Follow-up of Patients With KRAS G12C-mutated Metastatic Non-Small Cell Lung Cancer Who Received Sotorasib as Part of the French Early Access Program (ATU). ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2022: https://classic.clinicaltrials.gov/ct2/show/NCT05273047. Accessed 2023 May 18.
82.Johnson ML, De Langen J, Waterhouse DM, et al. LBA10 - Sotorasib versus docetaxel for previously treated non-small cell lung cancer with KRAS G12C mutation: CodeBreaK 200 phase III study. Ann Oncol. 2022;33(suppl_7):S808-S869.
83.Li B, Skoulidis F, Falchook G, et al. PS01.07 CodeBreaK 100: Registrational Phase 2 Trial of Sotorasib in KRAS p.G12C Mutated Non-Small Cell Lung Cancer. J Thorac Oncol. 2021;16(3 Suppl):S61. PubMed
84.Li BT, Velcheti V, Price TJ, et al. Largest evaluation of acquired resistance to sotorasib in KRAS p.G12C-mutated non-small cell lung cancer (NSCLC) and colorectal cancer (CRC): plasma biomarker analysis of CodeBreaK100. J Clin Oncol. 2022;40(16_suppl):102-102.
85.LoRusso PM, Sebolt-Leopold JS. One Step at a Time - Clinical Evidence That KRAS Is Indeed Druggable. N Engl J Med. 2020;383(13):1277-1278. PubMed
86.Metzger L. How effective and safe is sotorasib in non-small-cell lung cancer?. [German]. Tumor Diagnostik und Therapie. 2022;43(5):303-304.
87.Metzger L. How effective and safe is sotorasib for non-small cell lung cancer?. [German]. Pneumologie. 2021;75(12):922-923.
88.Ramalingam SS, Skoulidis F, Govindan R, et al. P52.03 Efficacy of sotorasib in KRAS p.G12C-mutated NSCLC with stable brain metastases: a post-hoc analysis of CodeBreaK 100. J Thorac Oncol. 2021;16(10 suppl):S1123.
89.Rosen N. Finally, Effective Inhibitors of Mutant KRAS. N Engl J Med. 2021;384(25):2447-2449. PubMed
90.Skoulidis F, Schuler M, Wolf J, et al. MA14.03 Genomic profiles and potential determinants of response and resistance in KRAS p.G12C-mutated NSCLC treated with sotorasib. J Thorac Oncol. 2021;16(10 suppl):S929-S930.
91.Skoulidis F, Li BT, Govindan R, et al. Overall survival and exploratory subgroup analyses from the phase 2 CodeBreaK 100 trial evaluating sotorasib in pretreated KRAS p.G12C mutated non-small cell lung cancer. J Clin Oncol. 2021;39(15 suppl):9003.
92.SWOG Cancer Research Network. NCT04625647: Phase II Study of AMG 510 in Participants With Previously Treated Stage IV or Recurrent KRAS G12C Mutated Non-Squamous Non-Small Cell Lung Cancer (ECOG-ACRIN LUNG-MAP SUB-STUDY). ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2022: https://classic.clinicaltrials.gov/ct2/show/NCT04625647. Accessed 2023 May 18.
93.Spira AI, Wilson FH, Shapiro G, et al. Patient-reported outcomes (PRO) from the phase 2 CodeBreaK 100 trial evaluating sotorasib in KRAS p.G12C mutated non-small cell lung cancer (NSCLC). J Clin Oncol. 2021;39(15_suppl):9057-9057.
94.Vestre Viken Hospital Trust. NCT05311709: Sotorasib in Advanced KRASG12C-mutated Non-small Cell Lung Cancer Patients With Comorbidities (SOLUCOM). ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine: https://classic.clinicaltrials.gov/ct2/show/NCT05311709. Accessed 2023 May 18.
95.Table 14-4.3.1. Summary of overall survival at 2 years. Additional data submitted by sponsor as a companion to Clinical Study Report: 20170543 Phase 2 Portion. A Phase 1/2, Open-label Study Evaluating the Safety, Tolerability, Pharmacokinetics, Pharmacodynamics, and Efficacy of AMG 510 Monotherapy in Subjects With Advanced Solid Tumors With KRAS p.G12C Mutation and AMG 510 Combination Therapy in Subjects With Advanced NSCLC With KRAS p.G12C Mutation (CodeBreak 100) [internal additional sponsor's information]. Thousand Oaks (CA): Amgen Inc.; 2023 Jul 6.
96.EORTC QLQ-C30 Scoring Manual. 3rd ed. Brussels (BE): EORTC; 2001: https://www.eortc.org/app/uploads/sites/2/2018/02/SCmanual.pdf. Accessed 2023 May 18.
97.Aaronson NK, Ahmedzai S, Bergman B, et al. The European Organization for Research and Treatment of Cancer QLQ-C30: a quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst. 1993;85(5):365-376. PubMed
98.Cohen J. A power primer. Psychol Bull. 1992;112(1):155-159. PubMed
99.van Reenen M, Janssen B, Stolk E, et al. EQ-5D-5L User Guide. Version 3.0. Rotterdam (NL): EuroQol Research Foundation; 2019: https://euroqol.org/publications/user-guides/. Accessed 2023 May 18.
100.Pickard AS, Neary MP, Cella D. Estimation of minimally important differences in EQ-5D utility and VAS scores in cancer. Health Qual Life Outcomes. 2007;5:70. PubMed
101.Cleeland CS, Ryan KM. Pain assessment: global use of the Brief Pain Inventory. Ann Acad Med Singap. 1994;23(2):129-138. PubMed
Appendix 1: Literature Search Strategy
Note that this appendix has not been copy-edited.
Clinical Literature Search
Overview
Interface: Ovid
Databases:
MEDLINE All (1946-present)
Embase (1974-present)
Note: Subject headings and search fields have been customized for each database. Duplicates between databases were removed in Ovid.
Date of search: September 19, 2022
Alerts: Bi-weekly search updates until project completion
Search filters applied: No filters were applied to limit the retrieval by study type.
Limits:
Conference abstracts: excluded.
Syntax | Description |
|---|---|
/ | At the end of a phrase, searches the phrase as a subject heading |
* | Before a word, indicates that the marked subject heading is a primary topic; or, after a word, a truncation symbol (wildcard) to retrieve plurals or varying endings |
.ti | Title |
.ot | Original title |
.ab | Abstract |
.hw | Heading word; usually includes subject headings and controlled vocabulary |
.kf | Keyword heading word |
.dq | Candidate term word (Embase) |
.pt | Publication type |
.rn | Registry number |
.nm | Name of substance word (MEDLINE) |
medall | Ovid database code: MEDLINE All, 1946 to present, updated daily |
oemezd | Ovid database code; Embase, 1974 to present, updated daily |
Multidatabase Strategy
(Lumakras* or Lumykras* or sotorasib* or AMG510 or AMG 510 or 2B2VM6UC8G).ti,ab,kf,ot,hw,rn,nm.
1 use medall
*sotorasib/
(Lumakras* or Lumykras* or sotorasib* or AMG510 or AMG 510).ti,ab,kf,dq.
3 or 4
5 not (conference review or conference abstract).pt.
6 use oemezd
2 or 7
remove duplicates from 8
Clinical Trials Registries
ClinicalTrials.gov
Produced by the US National Library of Medicine. Targeted search used to capture registered clinical trials.
[Search -- lumakras OR lumykras OR sotorasib OR amg510 OR “amg 510”]
WHO International Clinical Trials Registry Platform
International Clinical Trials Registry Platform, produced by WHO. Targeted search used to capture registered clinical trials.
[Search terms -- lumakras OR lumykras OR sotorasib OR amg510 OR “amg 510”]
Health Canada’s Clinical Trials Database
Produced by Health Canada. Targeted search used to capture registered clinical trials.
[Search terms -- lumakras, lumykras, sotorasib, AMG510, AMG 510]
EU Clinical Trials Register
European Union Clinical Trials Register, produced by the European Union. Targeted search used to capture registered clinical trials.
[Search terms -- lumakras OR lumykras OR sotorasib OR amg510 OR “amg 510”]
Grey Literature
Search dates: September 8, 2022 – September 15, 2022
Keywords: lumakras, lumykras, sotorasib, AMG510, AMG 510, KRAS, KRASG12C, non small cell lung cancer, NSCLC
Limits: None
Updated: No updates
Relevant websites from the following sections of the CADTH grey literature checklist Grey Matters: A Practical Tool for Searching Health-Related Grey Literature were searched:
Health Technology Assessment Agencies
Health Economics
Clinical Practice Guidelines
Drug and Device Regulatory Approvals
Advisories and Warnings
Drug Class Reviews
Clinical Trials Registries
Databases (free)
Internet Search
Appendix 2: Excluded Studies
Note that this appendix has not been copy-edited.
Reference | Reason for exclusion |
|---|---|
Amgen67 | Press release |
Amgen68 | Not RCT |
Amgen37 | Not RCT |
Bauml et al. 202169 | No added information |
Dy et al. 202270 | No added information |
Dozier et al. 202271 | No added information |
Fakih et al. 201972 | No added information |
Govindan et al. 201973 | No added information |
Govindan et al. 201974 | No added information |
Govindan et al.75 | No added information |
Govindan et al.76 | No added information |
Heinzl et al. 202177 | Editorial article |
Hong et al. 202078 | No added information |
Hong et al. 202079 | Not relevant study design |
Hong et al. 202180 | No added information |
Intergroupe Francophone de Cancerologie Thoracique81 | Not RCT |
Johnson et al.82 | Abstract |
Li et al. 202183 | No added information |
Li et al. 202284 | No added information |
LoRusso et al. 202085 | Editorial article |
Metzger et al. 202286 | Editorial article |
Metzger et al. 202187 | Editorial article |
Myers et al. 202169 | No added information |
Ramalingam et al. 202188 | No added information |
Rosen et al. 202189 | Editorial article |
Skoulidis et al. 202134 | Duplicate study |
Skoulidis et al. 202190 | No added information |
Skoulidis et al. 202191 | No added information |
Southwest Oncology Group92 | Not relevant study design |
Spira et al. 202193 | No added information |
Vestre Viken Hospital Trust94 | Not RCT |
RCT = randomized controlled trial.
Appendix 3: Censoring Rules
Note that this appendix has not been copy-edited.
Table 35: Censoring Rules Applied in CodeBreaK 100 and CodeBreaK 200 Studies for PFS and DOR
Situation up to DCO or EOS | Date of event or censor | Outcome |
|---|---|---|
No evaluable postbaseline tumour assessment per BICR, no death recorded | First dose of IP | Censor |
Progressive disease per BICR | First detection of progressive disease per BICR | Event |
Progressive disease per BICR, but no death recorded | Date of death | Event |
Start of new anticancer therapy before progressive disease per BICR or death | Date of last evaluable assessment per BICR before or on start of new anticancer therapy | Censor |
No progressive disease BICR, no death recorded, no start of new anticancer therapy | Date of last evaluable assessment per BICR | Censor |
Death or progressive disease per BICR immediately after consecutively missed more than 1 tumour assessment | Date of last evaluable assessment per BICT with documented nonprogression before missing assessment(s) a | Censor |
BICR = blinded independent central review; DCO = data cut-off; EOS = end of study; IP = investigational product.
aSupersedes the previous rules that result in PFS event at date of progressive disease or death.
Appendix 4: Detailed Outcome Data
Note that this appendix has not been copy-edited.
Figure 19: KM Plot of OS of NSCLC in CodeBreaK 100 Study at the Data Cut-Off Date of September 1, 2020 (Safety Analysis Set)
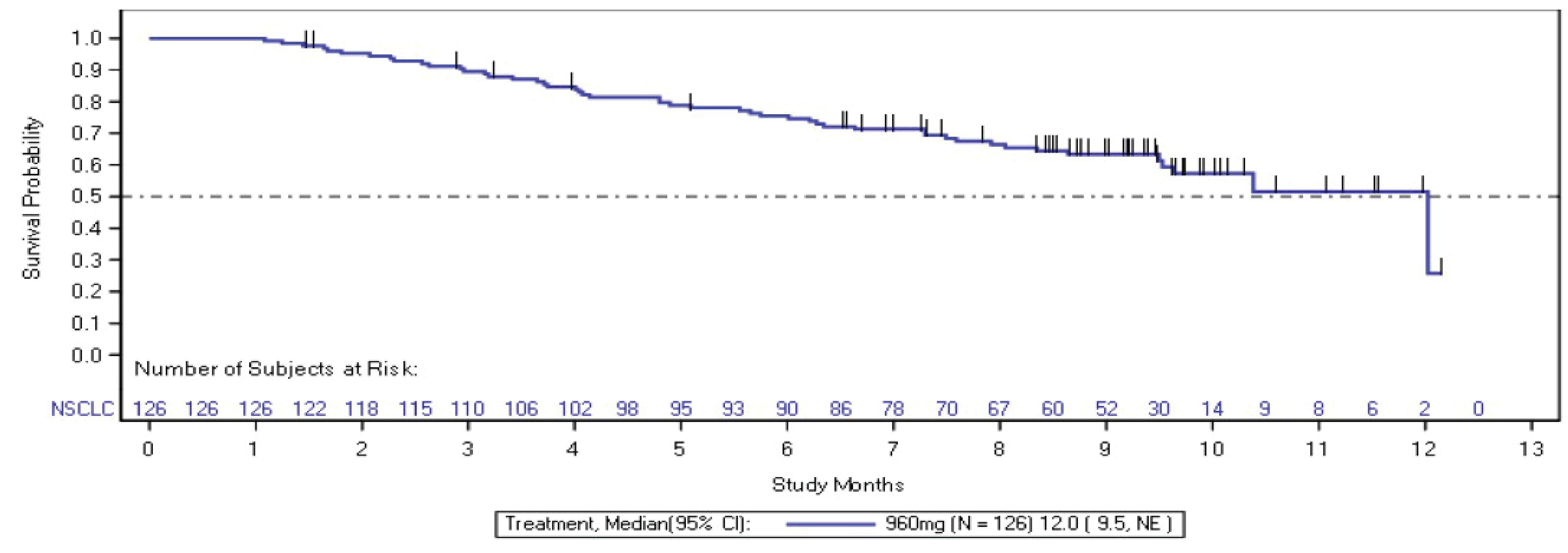
NE = not evaluable; NSCLC = non–small cell lung cancer.
Notes: Death is an event.
The data cut-off date was September 1, 2020, for the CodeBreaK 100 study.
Source: Clinical Study Report for phase II of the CodeBreaK 100 study.20
Figure 20: KM Plots of OS Per-Protocol Crossover Sensitivity Analysis Using the 2-Stage Method Approach (Full Analysis Set)
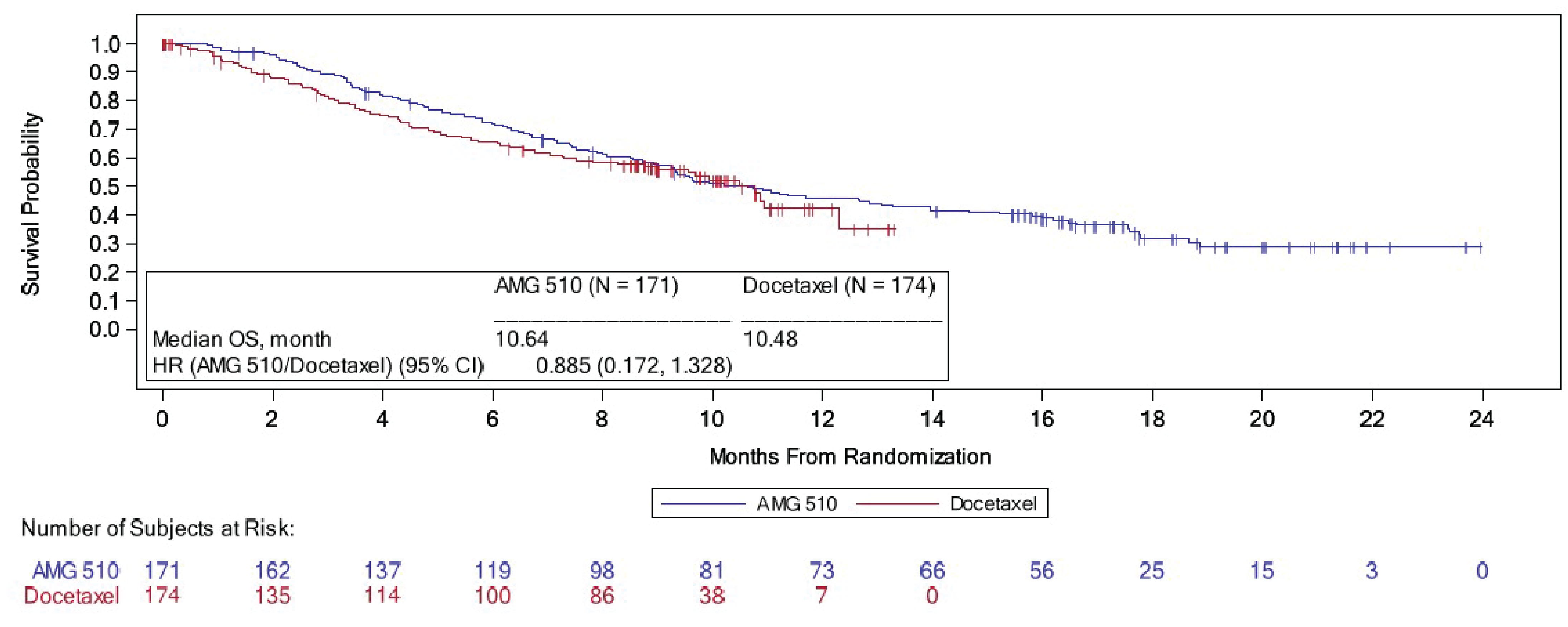
AMG 510 = sotorasib; CI = confidence interval; HR = hazard ratio; KM = Kaplan-Meier; OS = overall survival.
Note: The data cut-off date was August 2, 2022.
Source: Clinical Study Report for the CodeBreaK 200 study21
Figure 21: KM Plots of OS Crossover Sensitivity Analysis Using the 2-Stage Method Approach, Including Patients Who Received Commercial or EAP Sotorasib
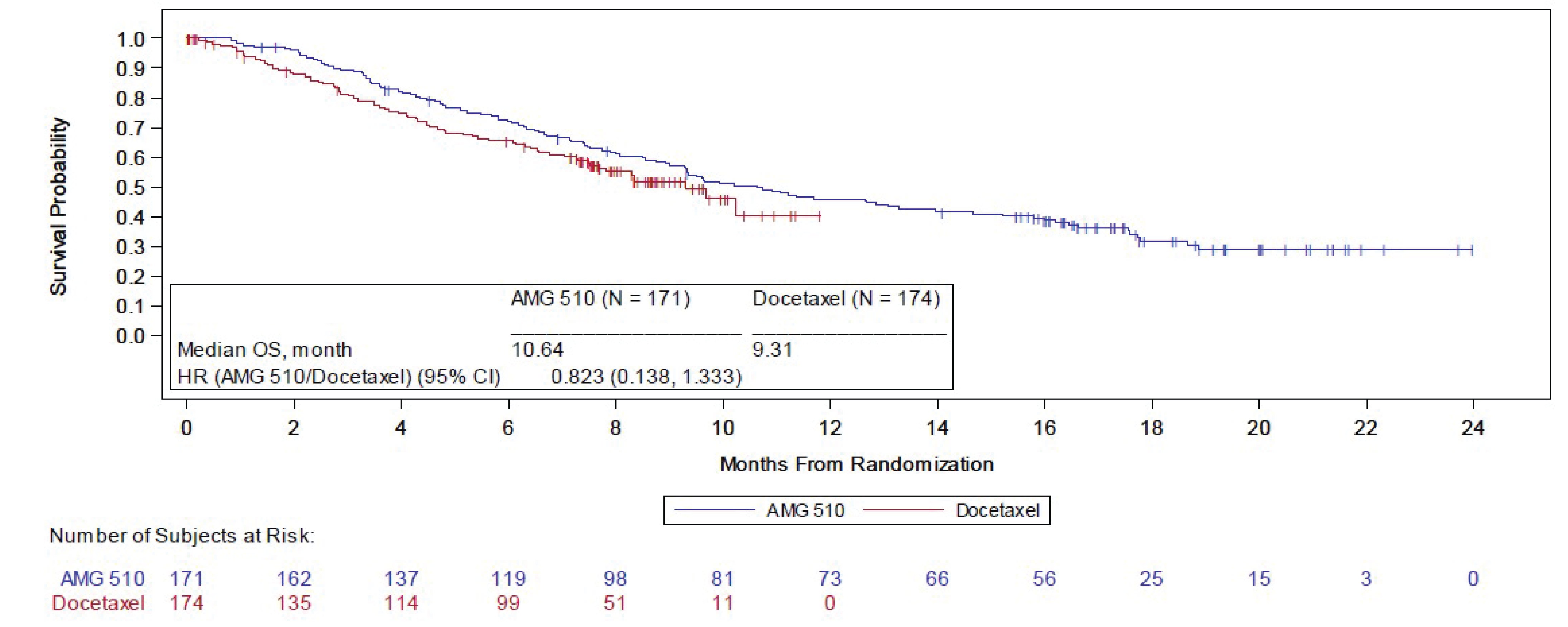
AMG 510 = sotorasib; CI = confidence interval; EAP = early access program; HR = hazard ratio; KM = Kaplan-Meier; OS = overall survival.
Note: The data cut-off date was August 2, 2022.
Source: Additional information submitted by the sponsor on May 9, 2023.21
Table 36: OS at 2 Years by RECIST 1.1 Criteria Based on BICR in CodeBreaK 100 Study at the Data Cut-Off Date of September 9, 2022 (Safety Analysis Set)
OS | CodeBreaK 100 study phase II NSCLC |
|---|---|
Sotorasib 960 mg (n = 126) | |
Events, n (%) | 91 (72.2) |
Censored, n (%) | 35 (27.8) |
Alive at last follow-up | 18 (14.3) |
Withdrew consent | 13 (10.3) |
Lost to follow-up | 4 (3.2) |
OS (KM), months | |
Median (95% CI) | 12.48 (9.99 to 19.29) |
KM estimates, survival % (95% CI)a | |
At 3 months | 89.54 (82.66 to 93.79) |
At 6 months | 75.47 (66.82 to 82.16) |
At 9 months | 63.55 (54.26 to 71.45) |
At 12 months | 51.27 (41.91 to 59.87) |
At 18 months | 42.08 (32.97 to 50.90) |
At 24 months | 31.56 (23.15 to 40.29) |
Follow-up time for OSb (KM), months | |
Median (95% CI) | 32.69 (32.23 to 33.15) |
BICR = blinded independent central review; CI = confidence interval; CNS = central nervous system; HR = hazard ratio; KM = Kaplan-Meier; NE = not evaluable; NR = not reported; NSCLC = non–small cell lung cancer; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; RECIST = Response Evaluation Criteria in Solid Tumours; SD = standard deviation; vs. = versus.
a95% CIs are based on estimated variance for log-log transformation of the KM survival estimate.
bFollow-up time is summarized by reversing the status indicator for censored and events.
cStratification factors: Number of lines of therapy in advanced disease (1 vs. 2 vs. > 2), race (Asian vs. non-Asian), history of CNS involvement (yes vs. no).
Note: Survival status may include publicly available records (where permitted) searched by investigator after patient ended the study.
Source: Additional sponsor-submitted data.95
Figure 22: KM Plot of PFS of NSCLC in CodeBreaK 100 Study at the Data Cut-Off Date of September 1, 2020 (Full Analysis Set)
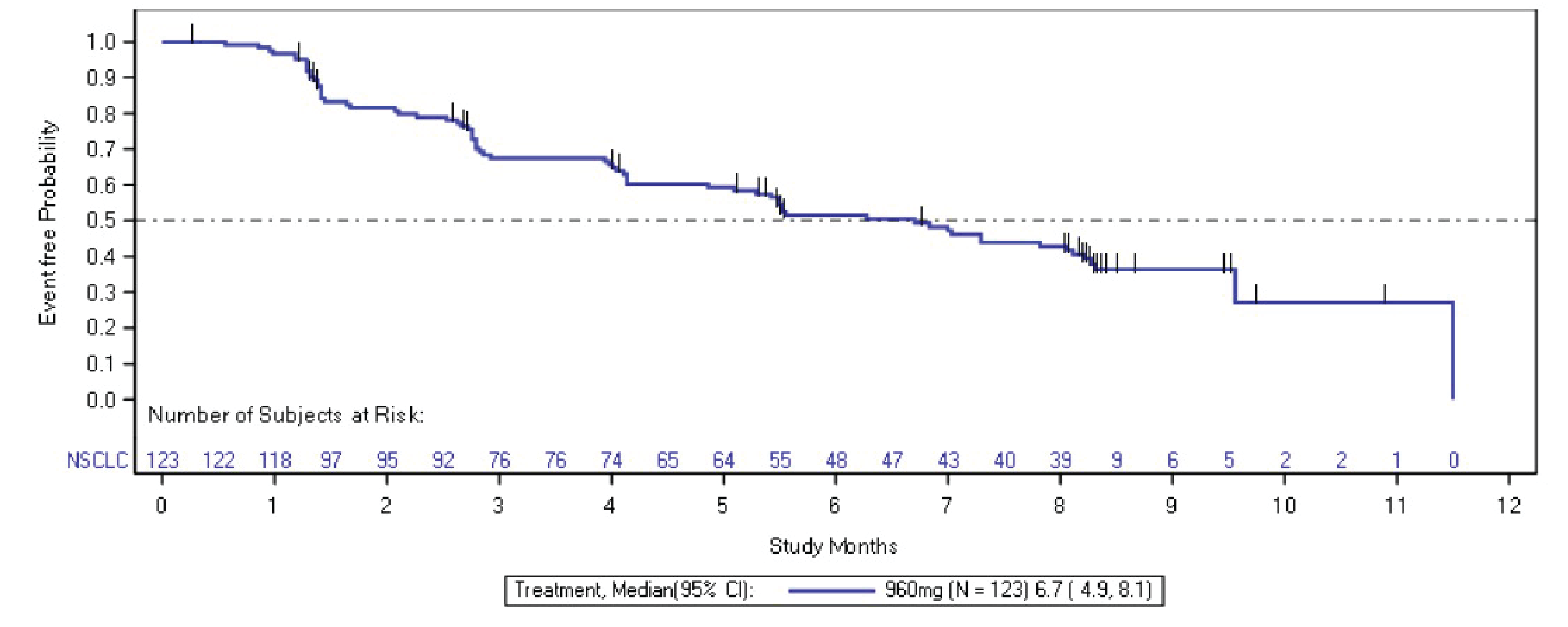
CI = confidence interval; KM = Kaplan-Meier; NE = not evaluable; NSCLC = non–small cell lung cancer; PFS = progression-free survival.
Note: An event is radiological progression or death, whichever occurs first.
Note: The data cut-off date was September 1, 2020 for the CodeBreaK 100 study.
Source: Clinical Study Report for phase II of the CodeBreaK 100 study.20
Figure 23: KM Plot of DOR of NSCLC Responders in CodeBreaK 100 Study at the Data Cut-Off Date of September 1, 2020 (Full Analysis Set)
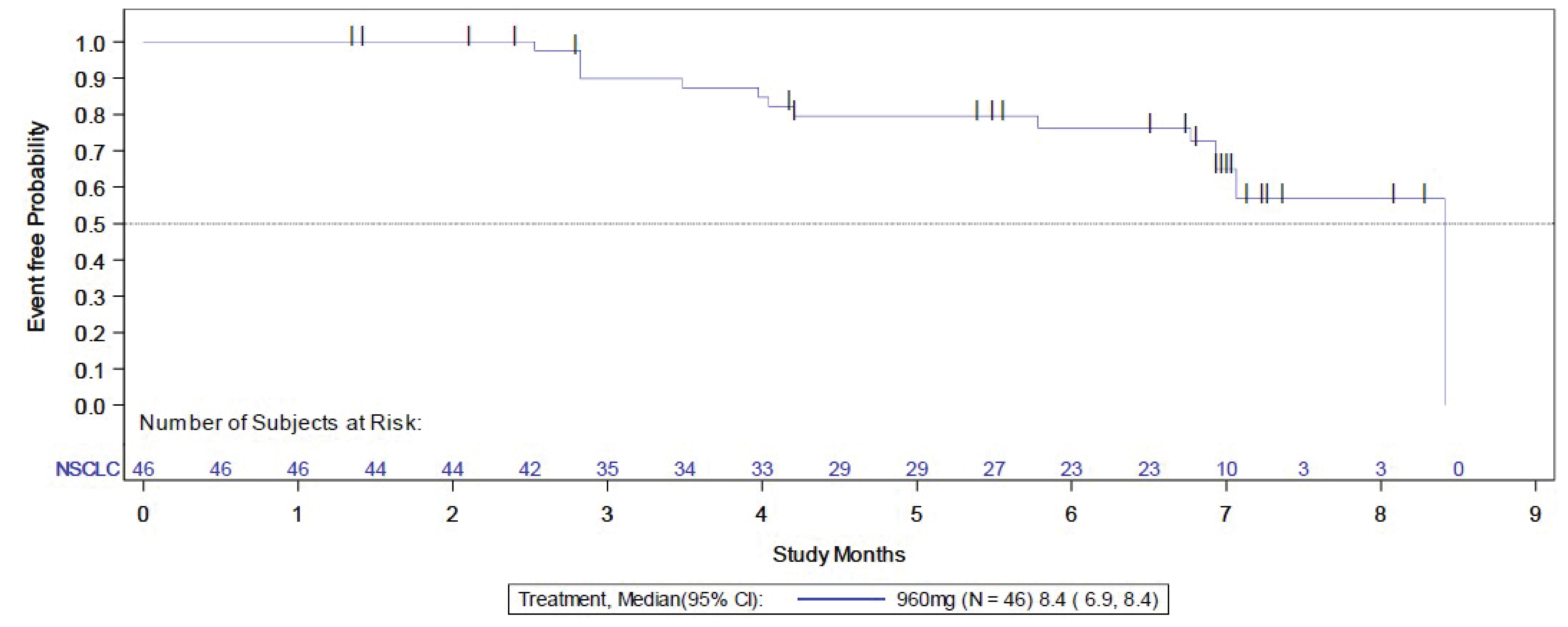
CI = confident interval; DOR = duration of response; KM = Kaplan- Meier; NSCLC = non–small cell lung cancer; NE = not evaluable.
Notes: An event is radiological progression or death, whichever occurs after confirming complete response or partial response.
The data cut-off date was September 1, 2020, for the CodeBreaK 100 study.
Source: Clinical Study Report for phase II of the CodeBreaK 100 study.20
Appendix 5: Description and Appraisal of Outcome Measures
Note that this appendix has not been copy-edited.
Aim
To describe the following PRO measures and review their measurement properties (validity, reliability, responsiveness to change, and MID):
EORTC QLQ-C30 and EORTC QLQ-LC13
NSCLC-SAQ
FACT-G
EQ-5D-5L and EQ VAS
BPI-SF.
Findings
Table 37: Summary of Outcome Measures and Their Measurement Properties
Outcome measure | Type | Conclusions about measurement properties | MID |
|---|---|---|---|
EORTC QLQ-C30 | A multidimensional, cancer-specific, self-administered questionnaire for evaluating HRQoL. Consists of 4 scales (30 questions):
Most questions have 4 response options (“not at all” [1], “a little” [2], “quite a bit” [3], “very much” [4]). The global quality of life scale is a 7-point Likert-type, with anchors between 1 (very poor) and 7 (excellent). Raw scores from each scale are converted to a 0 to 100 scale using a linear transformation, with a higher score reflecting better function on the function scale, higher symptom burden on the symptom scales, and better quality of life on global health status/QoL scale. Recall period is 1 week.96 | Nicklasson, et al.25 conducted a validation study with 112 Swedish patients diagnosed with lung cancer or pleural mesothelioma, including 85 (76%) patients with NSCLC not amenable to curative or life-prolonging treatment. Aaronson, et al.,97 tested measurement properties in 305 patients with nonresectable lung cancer (of 287 patients with reported histologic types, 63.1% had NSCLC) undergoing either radiotherapy or chemotherapy from 13 countries including Canada. Validity: Construct validity has been demonstrated with WHO PS (P < 0.0001) and a standard 6-minute walk test,25 as well as ECOG PS, weight loss, and WHO toxicity scales pre- and treatment (P < 0.001 to P < 0.05)97 for the majority of EORTC QLQ-C30 domains. Convergent validity has been established between EORTC QLQ-C30 emotional function and HADS anxiety scale (r = −0.75, P < 0.0001), as well as EORTC QLQ-C30 pain symptom and BPI intensity (r = 0.72, P < 0.0001), BPI interference (r = 0.68, P < 0.0001) scales.25 Reliability: All items in the multi-item scales except for cognitive function and pain (not measured) as well as global health scale showed acceptable reliability coefficient (alpha > 0.7).25,39 Also, all multi-item scales except for role function and global health scales demonstrated acceptable reliability coefficient (alpha > 0.7)39 both pre-treatment and during treatment periods.97 Responsiveness Between-group differences (improved vs. deteriorated based on ECOG PS) over 28 days between pretreatment and on-treatment periods showed statistically significant differences in physical (P < 0.001), role (P < 0.001), fatigue (P < 0.01), nausea and vomiting (P < 0.05), and global quality of life (P < 0.01) scales. No such difference was found in patients whose ECOG PS remained unchanged.97 | For patients with lung cancer or malignant pleural mesothelioma using anchor-based and distribution-based approaches:40 Within-group and between-group estimates (improvement, deterioration)
Distribution-based estimates (0.5 SD = SEM):
|
EORTC QLQ-LC13 | A self-reported, lung cancer-specific, supplementary questionnaire to EORTC QLQ-C30 with 13 items addressing symptoms associated with lung cancer and its standard treatment.
All items are scored on a 4-point categorical scale ranging from 1 (not at all) to 4 (very much), except for the 1 item on pain medication, which has dichotomous response categories (no or yes). All scale and item scores are linearly transformed to a 0 to 100 scale, with higher scores representing increased symptom burden.42 | Bergman, et al.42 tested measurement properties with 883 patients with nonresectable lung cancer (NSCLC: 62%) receiving either chemotherapy or radiotherapy from 17 countries (patients in Canada: n = 115). Nicklasson, et al.25 also measured properties in the same patient population as mentioned previously. Validity: Construct validity has been established between pain score and disease type (P < 0.001). Also, based on ECOG PS, construct validity was confirmed in dyspnea, coughing, and pain (P < 0.001) scores.42 Correlation between spirometry result and dyspnea score was found to be weak (r = 0.24). BPI intensity score and EORTC QLQ-LC13 pain score were found to be modestly correlated (r > 0.4).25 Reliability: Reliability coefficient (Cronbach alpha) range for dyspnea scores was 0.81 to 0.83. Reliability estimate for dyspnea scale has been confirmed to be acceptable,39 i.e., alpha = 0.76 in another study.25 However, internal consistency was found to be unacceptable39 for pain scores (alpha = 0.53 to 0.54) when EORTC QLQ-LC13 was used alone without EORTC QLQ-C30 core questionnaire pain items.42 Responsiveness: Dyspnea, coughing, and pain scores improved significantly over time between pre-treatment and on-treatment period (P < 0.001 for all except for extrathoracic pain which showed P < 0.05). Responsiveness of chest pain (P < 0.01), dyspnea (P < 0.001) and coughing (P < 0.001) to change in ECOG PS was also noted.42 | Unknown in patients with NSCLC |
NSCLC-SAQ | A self-reported, symptom-based PRO instrument to assess 5 symptom concepts of NSCLC (cough, pain, dyspnea, fatigue, appetite). Respondents respond to each of the 7 items using a 5-point verbal rating scale from 0 to 4 (from “not at all” to “very severe” for 3 items assessing intensity and from “never” to “always” for 4 items assessing frequency). For 2 pain items, worse response is selected; and for 2 fatigue items, mean is calculated to create single domain scores. A total score is sum of all 5 domain scores and ranges from 0 to 20. Higher scores indicate more severe symptomatology. If any domain score is missing, total score is not calculated. The recall period is 1 week. Both paper and electronic formats are available.45,46 Potential ceiling effects were observed in pain45,48 and appetite48 domains. Recommended target population:46
| An observational cross-sectional study45 and KEYNOTE-598 phase III clinical trial48 support measurement properties. The study population (n = 152) in the observational study45 reflects the recommended target population, whereas KEYNOTE-598 (n = 560) study population was restricted to stage IV NSCLC with PD-L1 TPS ≥ 50%.48 Limitations of studies include patients enrolled are only from the US45,47,48 and of ECOG PS 0 to 1.48 Validity: Content validity has been ensured during the developmental stage by having directly incorporated patient input (through concept elicitation interviews [n = 51] and cognitive interviews [n = 20]) and the advisory panel input, along with the literature reviews on peer-reviewed qualitative research in NSCLC and previously published NSCLC-targeted PRO instruments.47 Convergent validity has been proved as hypothesized that items in NSCLC-SAQ and FLSI-17 would be strongly correlated (r > 0.5)98 and NSCLC-SAQ total score would be most highly correlated with FLSI-17 DRS-P score (r > 0.8).45 Similarly, moderate (r = 0.3 to 0.5) to strong (r > 0.5) correlations98 have been observed between items, domains, and total scores of EORTC QLQ-C30, EORTC QLQ-LC13, EQ-5D-5L, and PGIS-LC.48 As for known-groups validity using PGIS, self-reported health status, and ECOG PS, NSCLC-SAQ total score differentiated health state categories (P < 0.001).45 Similarly, known-group validity using PGIS-LC, EORTC QLQ-C30 GHS/QoL, and ECOG PS was confirmed (P < 0.0001) by other study.48 Reliability: Internal consistency reliability (Cronbach alpha) for 7 items (0.78) and 5 domains (0.72) was acceptable (> 0.7).39,45 Another study confirmed acceptable level39 of internal consistency at baseline (0.74) and at Week 18 (0.78).48 Test-retest reliability (ICC) measured in stable patients 1 week apart (0.87)45 and 3 weeks apart (0.79)48 was also demonstrated. Responsiveness: Responsiveness of total score was supported by longitudinal differences in change from baseline to week 18 among PGIS-LC improvement groups (P < 0.001). Results were inconclusive for detecting worsening health status due to a small number of patients who had deteriorated.48 | Within-person change estimates using anchor-based (PGIS-LC) and distribution-based methods:48
|
FACT-G (GP5) | A cancer-specific, preference-based HRQoL instrument with 5-point Likert-type scale that can be applied to a variety of tumour types. Item GP5 notes, “I am bothered by side effects of treatment,” rated from 0 (not at all) to 4 (very much).49 | No validation information has been found for the single item GP5. | Unknown for single item GP5 |
EQ-5D-5L and EQ VAS | A generic, preference-based HRQoL questionnaire consisting of 2 parts. The descriptive system comprises of 5 dimensions (mobility, self-care, usual activities, pain/discomfort and anxiety/depression) with 5 increasing levels of severity (no problems [1], slight problems [2], moderate problems [3], severe problems [4] and unable to perform/extreme problems [5]). A unique health state profile can be generated as a 5-digit code, e.g., 21143 and/or converted to a single index score based on societal (countries/regions) preference weights. Index scores range from less than 0 (negative values represent worse than dead, which is represented by 0) to 1 (perfect health), with higher scores representing higher health utility. EQ VAS records respondent’s self-rated health on a scale of 0 (“the worst health you can imagine”) to 100 (“the best health you can imagine”) on that day.99 | Measurement properties have not been assessed in patients with NSCLC | EQ VAS For patients in lung cancer using anchor-based (FACT-G and ECOG PS) and distribution-based methods:100
Health utility index: Has not been estimated with 5L version. |
Brief Pain Inventory – Short Form | Patient-reported generic questionnaire for pain intensity and impact. Each item is scored on an 11-point scale from 0 to 10, where 0 is no pain/no interference and 10 is the worst pain/complete interference.101 | Measurement properties have not been assessed in patients with NSCLC. | Not assessed in indicated population. |
BPI = Brief Pain Inventory; BPI-SF = Brief Pain Inventory – Short Form; DRS-P = Disease-Related Symptoms-Physical; ECOG PS = Eastern Cooperative Oncology Group Performance Status; FACT-G = Functional Assessment of Cancer Therapy – General; FLSI-17 = National Comprehensive Cancer Network/Functional Assessment of Cancer Therapy Lung Symptom Index – 17 Item Version; GHS/QoL = global health status/Quality of Life scale; HRQoL = health-related quality of life; MID = minimal important difference; NA = not available; NSCLC = non–small cell lung cancer; NSCLC-SAQ = Non–Small Cell Lung Cancer Symptom Assessment Questionnaire; PD-L1 = programmed death-ligand 1; PGIS-LC = patient global impression of severity-lung cancer symptoms; PRO = patient-reported outcome; EORTC QLQ-C30 = Quality of Life Questionnaire Core 30; EORTC QLQ-LC13 = Quality of Life Questionnaire Lung Cancer Module; QoL = quality of life; SD = standard deviation; SEM = standard error of mean; TPS = tumour proportion score; EQ VAS = EQ visual analogue scale.
aNo prior chemotherapy for stage IIIB or IV NSCLC or not having received adjuvant chemotherapy for NSCLC within 6 months of study enrolment.
bReceived chemotherapy within 6 months and recovered from any prior treatment-related toxicities/adverse events to CTCAE v4.03 grade 1 or better.
Pharmacoeconomic Review
Abbreviations
AE
adverse event
BIA
budget impact analysis
CI
confidence interval
HR
hazard ratio
HRQoL
health-related quality of life
ICER
incremental cost-effectiveness ratio
LY
life-year
NSCLC
non–small cell lung cancer
OS
overall survival
PF
progression-free
PFS
progression-free survival
PP
postprogression
PSM
partitioned survival model
QALY
quality-adjusted life-year
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Sotorasib (Lumakras), oral tablets |
Submitted price | Sotorasib, 120 mg: $48.24 per tablet |
Indication | Treatment of adult patients with KRAS G12C-mutated, locally advanced (not amenable to curative therapy) or metastatic NSCLC who have received at least 1 prior systemic therapy |
Health Canada approval status | NOC/c |
Health Canada review pathway | Advance consideration under NOC/c and project Orbis |
NOC date | Sep 10, 2021 |
Reimbursement request | As per indication |
Sponsor | Amgen Canada Inc. |
Submission history | Previously reviewed: No |
NOC = Notice of Compliance; NOC/c = Notice of Compliance with conditions; NSCLC = non–small cell lung cancer.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis PSM |
Target population | Adult patients with KRAS G12C-mutated, locally advanced (not amenable to curative therapy) or metastatic NSCLC who have received at least 1 prior systemic therapy |
Treatment | Sotorasib monotherapy |
Comparator | Docetaxel monotherapy |
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs, LYs |
Time horizon | Lifetime (20 years) |
Key data sources | CodeBreaK 200 trial |
Submitted results | ICER = $261,528 per QALY gained (incremental costs = $96,112; incremental QALYs = 0.37) |
Key limitations |
|
CADTH reanalysis results |
|
AE = adverse event; CI = confidence interval; HR = hazard ratio; ICER = incremental cost-effectiveness ratio; LY = life-year; NSCLC = non–small cell lung cancer; OS = overall survival; PFS = progression-free survival; PSM = partitioned survival model; QALY = quality-adjusted life-year.
Conclusions
Estimates of relative efficacy were obtained from the direct comparison of sotorasib and docetaxel in the phase III CodeBreaK 200 trial. In the CodeBreaK 200 trial, treatment with sotorasib demonstrated a statistically significant impact on progression-free survival (PFS) compared to docetaxel. However, the confidence interval (CI) associated with the effect of sotorasib relative to docetaxel on overall survival (OS) in the CodeBreaK 200 trial was too wide to draw any conclusions with certainty. The results of the sensitivity analyses, conducted to account for treatment crossover in the trial, were consistent with those of the main analysis for OS, with the 95% CIs for all analyses including the possibility that either treatment could be favoured. Both OS and PFS were key parameters used in the economic evaluation.
CADTH attempted to address some of the key limitations of the sponsor’s economic submission. These changes involved the use of the OS hazard ratio (HR) CI, derived using the 2-stage approach; the use of health state utilities and the inclusion of disutility associated with adverse events (AEs) and drug administration; corrections to the partitioned survival model (PSM) calculations; and the inclusion of all relevant health care costs. In the CADTH base case, sotorasib was more effective (incremental quality-adjusted life-years [QALYs] = 0.32) and associated with greater total costs (incremental costs = $97,139) than docetaxel. This resulted in an incremental cost-effectiveness ratio (ICER) of $308,262 per QALY gained. Incremental QALYs were largely driven by an assumed mortality benefit associated with sotorasib (i.e., an additional 0.335 life-years [LYs] for patients receiving sotorasib relative to docetaxel), using the HR for OS from the CodeBreaK 200 trial adjusted for crossover using the 2-stage method.
Because the probabilistic output was not considered clinically valid, the CADTH base case was conducted deterministically. As a result, it could not fully explore the impact of the uncertainty in the evidence associated with both PFS and OS. Based on the CADTH base-case analysis, an 80% price reduction is required for sotorasib to be considered cost-effective at a threshold of $50,000 per QALY gained; this requires the HR for OS associated with sotorasib to be no larger than 0.823. If the HR for OS for sotorasib versus docetaxel trended closer toward 1, then greater price reductions would be required.
Finally, the sponsor assumes that sotorasib will displace docetaxel only in the second-line setting and beyond. The cost-effectiveness of sotorasib compared with other therapies used in this setting, such as doublet-platinum chemotherapy, is unknown.
Stakeholder Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, registered clinicians, and drug plans that participated in the CADTH review process.
Patient input for this review was obtained as a joint submission from the Lung Health Foundation, Lung Cancer Canada, and the Canadian Cancer Survivor Network. Patient perspectives were collected through an online survey and in a series of telephone interviews. A total of 5 people (4 patients and 1 caregiver) responded to a telephone survey interview from August to September 2022. Of the 4 patients with lung cancer, 3 had experience with sotorasib; 1 patient with KRAS G12C subtype lung cancer did not. All respondents were female. All but 1 were from Canada; the remaining respondent was from the US. A consensus among the interview participants with sotorasib experience was that the treatment led to improvements in PFS and OS. Only 2 patients experienced side effects on sotorasib treatment, and these were well managed. Lastly, the submission noted that sotorasib was much more tolerable than other interventions, such as chemotherapy; this was reflected through relative improvements in quality of life.
Registered clinician input was received from Lung Cancer Canada’s clinician group and the Ontario Health Cancer Care Ontario Drug Advisory Committee. Consensus among both groups was that the goal of the care pathway was to improve symptoms and prolong life. First-line treatment usually involves a form of systemic therapy (i.e., immunotherapy or platinum-based doublet chemotherapy). Following progression, second-line treatment would include the use of a taxane-based intervention, such as docetaxel. However, the Ontario Health Cancer Care Ontario Drug Advisory Committee noted that many patients have a strong preference to avoid IV drugs that have potentially toxic side effects. As a result, it was noted that many patients do not receive any systemic or taxane-based therapies. In the event of progression on second-line therapy, a patient may receive further systemic therapy. When no further systemic therapy is available, patients will receive best supportive care. Both submissions indicated that sotorasib would be viewed as a new line of therapy to consider alongside existing alternatives. Within the care pathway, sotorasib should be considered following the failure of first-line, platinum-based chemotherapy and immunotherapy.
No drug plan input was received for this review.
Several of these concerns were addressed in the sponsor’s model:
Resource use captured the IV administration of docetaxel.
The model incorporated evidence from the CodeBreaK 200 trial, which involved the direct comparison of sotorasib and docetaxel.
CADTH was able to address the following concerns raised in the stakeholder input:
the impact of the different modes of treatment administration (IV versus oral) on health-related quality of life (HRQoL)
the incorporation of the frequency and impact of AEs from both medications into estimates of costs and effects
Economic Review
The current review is for sotorasib (Lumakras) for the treatment of adult patients with KRAS G12C-mutated, locally advanced (not amenable to curative therapy) or metastatic non–small cell lung cancer (NSCLC) who have received at least 1 prior systemic therapy.
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted an economic evaluation comparing sotorasib against docetaxel.1 The population considered by the model included adults with KRAS G12C-mutated, locally advanced (not amenable to curative therapy) or metastatic NSCLC who have received at least 1 prior systemic therapy. This target population was aligned with the population indicated within the Health Canada Notice of Compliance and the sponsor’s reimbursement request.
Sotorasib is available as 120 mg tablets and should be administered orally. The recommended dose is 960 mg (8 × 120 mg tablets) once daily until disease progression or unacceptable toxicity.2 The submitted price of sotorasib was $11,577.60 for a package of 240 tablets, or $48.24 per tablet.1 In contrast, docetaxel is a solution available in single-dose vials of 160 mg (10 mg/mL) or 80 mg
(10 mg/mL).3 The sponsor included a recommended dosage of 75 mg/m2 administered through IV infusion every 21 days. The 21-day cycle cost of docetaxel was $994, assuming vial wastage using 2 single 80 mg vials. Given that docetaxel is administered through IV, the sponsor adjusted for wastage by assuming no vial-sharing for any IV based therapies.1
Effects in the model were estimated as QALYs and LYs.1 Costs and effects were estimated from the perspective of the publicly funded health care payer over a 20-year time horizon.4 As per CADTH guidelines, a 1.5% discount rate was applied to both costs and QALYs in the base case.1
Model Structure
The costs and effects of each treatment option were estimated using a PSM. This model structure relied on 2 independent survival curves: PFS and OS to track patients across 3 distinct health states: progression-free (PF), postprogression (PP), and death (Appendix 3). State membership was determined using an area-under-the-curve approach. The proportion of patients in the PP state was calculated as the difference between the OS and PFS curves. A third survival curve was used to determine the proportion of patients in the PFS state no longer on treatment. This time-to-treatment discontinuation curve allowed the model to incorporate the possibility of treatment withdrawal before progression and to capture the impact of drug use on costs.1
Model Inputs
For each treatment, costs and effects were estimated using a homogeneous baseline population. Characteristics of interest included baseline age, sex, height (cm), and weight (kg). Baseline height and weight were used to inform the administration of docetaxel.1 All data summarizing patient characteristics for this model were obtained from the CodeBreaK 200 trial.5 This was a randomized phase III trial that involved the direct comparison of sotorasib with docetaxel in the treatment of patients with previously treated, KRAS G12C-mutated, locally advanced and unresectable or metastatic NSCLC.1,5-7
The model required comparative efficacy data related to 3 distinct outcomes: PFS, OS, and the probability of remaining on treatment. All estimates were obtained from the direct comparison of sotorasib and docetaxel from the CodeBreaK 200 trial.1,5-7
For PFS, parametric survival curves were fitted to the time-to-progression data from the CodeBreaK 200 trial.1,5-7 Each model sought to estimate the relationship between treatment (sotorasib and docetaxel) and investigator-assessed PFS. As per CADTH guidelines, models were fitted using the exponential, log-logistic, log-normal, Weibull, Gompertz, gamma, and generalized gamma distributions.8 Following an assessment of model fit statistics, the log-logistic distribution was selected for the sponsor’s base case.1
For OS, parametric survival curves were fitted to the time-to-death data for the sotorasib arm of the CodeBreaK 200 trial. As per CADTH guidelines, models were fitted using the exponential, log-logistic, log-normal, Weibull, Gompertz, gamma, and generalized gamma distributions. Fitted models that explored the relationships between treatment arms and OS were not considered in the base case because the CodeBreaK 200 trial permitted crossover from docetaxel to sotorasib. In the context of the economic evaluation, this feature of the trial would have biased the OS results in favour of docetaxel. In response, OS data for docetaxel were generated by applying an HR to the selected parametric OS curve for sotorasib. This HR was estimated using a 2-stage method for crossover adjustment, following guidance published by the National Institute for Health and Care Excellence Decision Support Unit.1,9 The purpose of this 2-stage approach was to generate counterfactual survival times for each patient in the docetaxel arm who switched to sotorasib following progression in the trial.1,9 The HROS for sotorasib relative to docetaxel following crossover adjustment was estimated to be 0.823 (95% CI, 0.14 to 1.33). This result suggested a much stronger OS benefit compared to the unadjusted HROS (1.01; 95% CI, 0.77 to 1.33) estimated using the intention-to-treat data from the CodeBreaK 200 trial.1 Furthermore, the adjusted HROS was considered appropriate because it aligned with the predicted HROS (0.823; 95% CI, 0.690 to 0.982) from an analysis that combined evidence from several NSCLC trials to leverage the correlation between PFS and OS.1,10 While the adjusted HROS was assumed in the submitted base case, an additional scenario was considered that used the jointly fitted intention-to-treat data from the CodeBreaK 200 trial.1
The extrapolated OS curves considered in the model were capped by general population mortality risk. The latter was obtained using age- and gender-specific mortality risks estimated from the Canadian life tables published by Statistics Canada.11 The intent of this logical procedure was to ensure that the extrapolated hazard rates would not fall below the hazard rates expected for the general population.1 Separately, the sponsor also assumed that 11.2% of patients who experienced progression would transition to the death state rather than to the progressed state.
CodeBreaK 200 data were also used to estimate the probabilities of remaining on treatment for 3 distinct time periods. Treatment-specific estimates were generated for less than 1 month, 1 month to 12 months, and more than 12 months. These period-specific estimates were subsequently applied to the proportion of the cohort that occupied the PF state to determine the proportion of patients on treatment at a given cycle. However, the methods used to estimate the probability of remaining on treatment were not reported.1
In addition to tracking the proportion of the population in each health state, the model also tracked the occurrence of AEs. The specific AEs included in the model were restricted to grade 3 or 4 and included decreased neutrophils, diarrhea, dyspnea, fatigue, increased alanine aminotransferase, increase aspartate aminotransferase, neutropenia, pleural effusion, and pneumonia. The duration of each AE was not specified. The probabilities of each AE occurring while on sotorasib and docetaxel were sourced from the CodeBreaK 200 safety analysis set.1,6 In the base case, the sponsor assumed that the AE risks would follow the treatment-related AE incidence, and a scenario analysis considered the use of treatment-emergent AEs.1
Data relating to HRQoL were obtained from the CodeBreaK 200 trial, using separate analyses for each treatment. Preferences were elicited indirectly through the administration of the 5-Level EQ-5D. The survey was administered before any clinical assessments and treatment initiation. Repeated administration of the survey occurred at the beginning of each 3-week cycle for the first 7 cycles, and every 6 weeks thereafter until treatment discontinuation.1 Survey responses were converted to EQ-5D utilities using the value set from the Canadian population.12
Two approaches were used to estimate utility values for the economic evaluation. In the base case, a time-to-death approach was used in which the indirect preference data were grouped according to the amount of time between completing the survey and the patient’s death. The amount of time before death was classified into 4 groups: more than 6 months, 3 months to 6 months, 1 month to 3 months, and the last month.1 In the health state scenario, EQ-5D health state utilities were estimated for the PF and PP states. Additional utility decrements were available for each AE. In a separate scenario analysis, these decrements were applied any time a patient experienced an AE. It was assumed that the mean duration of an AE disutility was 4 weeks.1 Lastly, the model also included the ability to apply a utility decrement associated with the IV administration of docetaxel, obtained from Lewis 2010.13 However, this decrement was not considered in the sponsor’s base case.
Costs in the model were determined from the treatment costs (acquisition, administration, and monitoring) and changes in health service utilization over the time horizon. In the PF state, patients were assumed to be on either sotorasib or docetaxel. Following treatment discontinuation and transition to the PP state, patients were assumed to receive 1 line of subsequent therapy. For those who began with sotorasib, it was assumed that 60% would receive best supportive care (i.e., no additional costs), 30% would receive docetaxel chemotherapy, and 10% would receive platinum-doublet chemotherapy (pemetrexed plus cisplatin). Meanwhile, patients who began docetaxel were assumed to be eligible to receive best supportive care (90%) and platinum-doublet chemotherapy (10%). All treatment costs were based on list prices specified by the sponsor (sotorasib) or wholesale sources (docetaxel, pemetrexed, and cisplatin).14 Dosing for doublet chemotherapy followed the regimens specified by Cancer Care Ontario (i.e., CISPPEME)15 and BC Cancer (i.e., LUAJPP).16
Given that sotorasib is administered orally, a treatment administration cost was not considered. For docetaxel and the subsequent therapies, treatment administration costs included IV administration and the operation of outpatient clinics. It was assumed that vial-sharing would not be considered. Administration costs for IV therapies were calculated for each outpatient visit and incorporated the hourly rate for nurse monitoring time, pharmacist time, and chair time.17-20 The time to administer docetaxel was assumed to be 120 minutes, while that for platinum-doublet chemotherapy was assumed to be 1 hour.1,19
Treatment monitoring costs included outpatient oncology visits as well any imaging or testing procedures needed to monitor disease progression or AEs. The frequency of each event for each treatment and health state was obtained by reviewing a technology appraisal produced and published in 2015 by another jurisdiction and revisiting data inputs from that appraisal in consultation with clinical experts in Canada to determine health care resource use in Canada.21 However, in the base case, the sponsor assumed that the monitoring costs would be restricted to those involving the treatment of AEs. Costs for physician and laboratory services were obtained from the respective Ontario schedule of benefits.22,23 Lastly, costs relating to the specified AEs were obtained from the Ontario Case Costing Initiative.24
Summary of Sponsor’s Economic Evaluation Results
For the base case and each scenario analysis, the sponsor conducted a Monte Carlo simulation of 2,000 iterations.1 The results of the probabilistic simulation were aligned with those generated deterministically. This was expected from the approach used to characterize uncertainty with a PSM. Results from the probabilistic base case are summarized in this section.
Base-Case Results
The submitted analysis was based on the publicly available prices of the comparator treatments. Results from the base case of the submitted economic evaluation are presented in Table 3.
Sotorasib was estimated to be more effective (1.28 QALYs versus 0.91 QALYs) and more expensive ($112,313 versus $16,200) than docetaxel. At a threshold of $50,000 per QALY, sotorasib had an ICER of $261,528 and was not expected to be cost-effective. Additional results from the probabilistic base case are presented in Appendix 3.
Despite a 20-year time horizon, most of the costs and benefits were generated in the first 2 years of the model. In the deterministic base case, more than 75% of the sotorasib cohort occupied the death state 2 years after model entry. In contrast, more than 82% of the docetaxel cohort occupied the death state after the same amount of time.
Table 3: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER vs. docetaxel ($/QALY) |
|---|---|---|---|---|---|
Docetaxel | 16,200 | Reference | 0.91 | Reference | Reference |
Sotorasib | 112,313 | 96,112 | 1.28 | 0.37 | 261,528 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; vs. = versus.
Source: Sponsor’s pharmacoeconomic submission.1
Sensitivity and Scenario Analysis Results
In addition to the base case, the sponsor considered 51 scenario analyses. As per CADTH guidelines, the sponsor included distinct scenarios to consider discount rates of 0% and 3%. While each scenario had a slight impact on the estimated costs and effects, the findings remained higher than $50,000 per QALY, with the ICER varying between a minimum of $ 200,732 and a maximum of $408,263 per QALY gained.
CADTH Appraisal of the Sponsor’s Economic Evaluation
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the economic analysis.
Incorrect parameterization of relative efficacy for docetaxel OS: In the CodeBreaK 200 trial, some patients who received docetaxel switched to sotorasib after progression. To avoid biased estimates of OS that would favour docetaxel, the sponsor generated an OS curve for docetaxel by applying an HROS (adjusted to account for docetaxel crossover) to the parametric OS curve for sotorasib. One estimate of relative treatment efficacy was estimated using a 2-stage method for crossover adjustment, following guidance published by the National Institute for Health and Care Excellence Decision Support Unit. While the estimated HROS of 0.823 (95% CI, 0.14 to 1.33) was lower than that obtained from the intention-to-treat analysis, it was not the input that was considered in the economic model. Instead, the model relied on a predicted HROS of 0.823 (95% CI, 0.692 to 0.982), which combined evidence from several NSCLC trials.1,10 Although the point estimate used (0.823) aligned with the HR derived from the 2-stage method, a narrower CI was used. This was problematic for 2 reasons. First, the input that was used in the economic model did not reflect a direct comparison of sotorasib and docetaxel, as in the CodeBreaK 200 trial. The method relied on external evidence to estimate the relationship between progression and OS; however, it was unclear what group of patients informed the analysis. Moreover, the methodology was not adequately described. Second, the input had a narrower CI (0.692 to 0.982) that was much more favourable to sotorasib compared to the CI resulting from the crossover-adjusted HROS (0.14 to 1.33). This parameterization was incorrect because it prevented the economic evaluation from considering the impact of the uncertainty in HROS in a manner consistent with the best-available evidence. Finally, CADTH notes that 2 additional sensitivity analyses were conducted to analyze the impact of crossover. These included the rank-preserving structural failure time model and inverse probability of censoring weighting. Both analyses resulted in higher HRs of 0.99 (95% CI, 0.733 to 1.337) and 1.01 (95% CI, 0.663 to 1.492), respectively.
CADTH modified the economic evaluation to consider the 2-stage OS with the accompanying CI (i.e., HR = 0.823; 95% CI, 0.14 to 1.33). In addition, a separate scenario analysis was conducted that assumed no survival benefit (i.e., HROS = 1).
Validity of utility estimation: The sponsor’s base case assumed that time to death is the only factor that influences utility outside of treatment-related side effects. Three concerns were identified with this approach. First, the assumption is inconsistent with the sponsor’s submitted evidence. Data from the CodeBreaK 100 trial revealed that PP utilities were lower than when patients were PF. Second, given the relationship between progression and mortality risk, time-to-death utilities may be capturing the impact of progression over time rather than the HRQoL associated with the patient’s health status. Third, the methods used to arrive at the time intervals used for these utilities were not reported. The use of time-dependent health state utilities in an economic evaluation is not inappropriate; however, the methods and justifications must be described clearly and implemented in an appropriate manner.
Separately, the sponsor’s base case did not consider the effects of AEs or differences in modes of treatment administration on HRQoL. Both factors were identified as important elements in the clinician and patient feedback solicited by CADTH for this review.
The CADTH base case used utilities that were specific to each health state rather than time to death. In addition, utility decrements were considered for the mode of treatment administration and the occurrence of AEs.
Inclusion of relevant costs: The sponsor’s base case excluded the disease management costs associated with both treatments. This is inconsistent with CADTH guidelines, which require the incorporation of all relevant costs, including those relating to disease management. Disease management costs, such as oncology visits and monitoring tests, are important to the present decision problem. For example, due to differences in treatment toxicity, sotorasib may be associated with lower disease management costs than docetaxel. CADTH noted that the sponsor assumed that PP costs would be higher for patients for whom docetaxel fails versus those for whom sotorasib fails. For example, it was assumed those who progress on docetaxel would incur palliative care monitoring costs, whereas patients on sotorasib would never incur these costs. Specific details as to why this assumption was made were not provided. However, the clinical experts consulted by CADTH noted that PP costs will likely differ between these 2 groups.
The exclusion of disease management costs was corrected in the CADTH base case.
Failure to characterize decision uncertainty: Consistent with CADTH guidelines, the sponsor’s base case used a Monte Carlo simulation to characterize the uncertainty of relevant input parameters. However, the absence of a structural relationship between these parameters in the PSM model structure limits the usefulness of this approach.25 This is because the survival probabilities for each event (survival and progression) are predicted independently over the specified time horizon.25 This would lead to instances where PFS exceeds OS, which is clinically implausible. To fully address this problem, 1 would need to produce a series of correlated survival curves for OS and PFS — for example, by fitting parametric models to bootstrapped individual patient data. While this may resolve concerns relating to the within-trial period, limitations for the extrapolated period will persist.25
CADTH could not address this limitation. However, the probabilistic output was not used to inform the CADTH base case, given the uncertainties associated with the results.
Model transparency degraded by unnecessary complexity: The sponsor’s specification of 51 scenarios resulted in the degradation of the model’s transparency. While the process and sequence of steps for a PSM are relatively simple, the introduction of each scenario required the specification of distinct logical pathways for each assumption. The way in which this logic is implemented can have meaningful effects on the risk of error in an economic evaluation. This was a significant concern in the supplied spreadsheet, in which many independent formulas covering the same functionality were identified in multiple locations. Given that many of the scenarios were not relevant to assessments of structural uncertainty, their incorporation may have served only to introduce errors in the spreadsheet’s programming that could not be identified in this review. In 1 instance, the sponsor implemented a single HR value as 4 independent random parameters. This independence meant that the HR could vary from 0.7 until month 5, and then jump to 1.7. Given the clinical implausibility of this approach, it was deemed this was likely an error. Finally, CADTH notes that some model settings reverted to a default value after the completion of the probabilistic simulation. This required additional efforts by CADTH to verify that the desired modifications had been implemented.
The extent to which the sponsor’s results were affected by calculation or programming errors could not be determined. In the probabilistic analysis, CADTH removed the ability for the HR for OS to be randomly sampled multiple times at different time points.
Calculation of state membership: The structural assumption of a PSM is that membership of mutually exclusive health states must be determined from non–mutually exclusive survival curves.25 Unlike a Markov model, which can combine inputs from a variety of sources, a PSM is more restrictive. Estimates of state membership must be determined using survival probabilities so that the OS curve can be partitioned into distinct components for each health state.
In each cycle of the sponsor’s model, membership in the progressed state was calculated as 1 minus the difference between the membership in the PF and death states. The more appropriate formula for calculating membership in the PP state is S(t)OS – S(t)PFS. This is the difference in survival probabilities between the OS and PFS curves at time t.
The sponsor performed several modifications to the extrapolated PFS and OS curves that yielded inputs that were not necessary for a PSM. First, both sets of survival probabilities were converted from a continuous to a discrete period. This would have been an appropriate modification had state membership been determined using the Markov method. Both survival probabilities were modified further to determine the proportion of patients alive or PF at the beginning of each cycle. This transformation was unnecessary in a PSM, given that state membership is determined using survival probabilities.
The sponsor assumed that 11% of patients transitioning from the PF state would move to the death state rather than the progressed state. This assumption is inconsistent with the requirement that transitions be informed exclusively through an area-under-the-curve approach. In addition, the OS curves were modified to ensure the values were capped by the general population mortality risk. Capping the OS curve by the general population mortality risk would have been more appropriate if state membership had been calculated using transition probabilities for a Markov structure.
CADTH changed the formula used to calculate membership in the PP state to be PP state = S(t)OS – S(t)PFS. The assumption that 11% of patients transitioning from PFS would move to death rather than the progressed state was removed. The inputs used to determine state membership were modified to ensure these represented the unmodified survival probabilities extrapolated over the model’s time horizon.
CADTH notes that removing the 11% of patients who transitioned to death from PFS had a very minor impact on results. The remaining changes had no impact on the results, but ensured the calculations were conducted consistently with a PSM structure.
Additionally, the following key assumptions were made by the sponsor and have been appraised by CADTH (refer to Table 4).
Table 4: Key Assumptions of the Submitted Economic Evaluation (not Noted as Limitations to the Submission)
Sponsor’s key assumption | CADTH comment |
|---|---|
No costs related to KRAS testing. | Appropriate. Clinical expert opinion noted that KRAS testing is part of routine management. Therefore, if sotorasib was funded, there would not be additional KRAS testing because this cost would have been incurred before the decision to administer sotorasib. |
Patients enrolled in the CodeBreaK 200 trial were assumed to be representative of patients in Canada. | Uncertain. Clinical experts noted that patients in the CodeBreaK 200 trial were younger than those typically seen in clinical practice, who trend toward 70 years and older. Likewise, the experts noted that the trial excludes patients with an ECOG PS > 1 as well as those with active brain metastases, yet both groups represent patient populations that the clinical experts would treat with sotorasib. |
ECOG PS = Eastern Cooperative Oncology Group Performance Status; PFS = progression-free survival.
CADTH Reanalyses of the Economic Evaluation
Base-Case Results
The CADTH base case was derived by making changes in model parameter values and assumptions in consultation with clinical experts. A summary of the changes applied to the submitted economic evaluation is presented in Table 5. Each change was applied incrementally to arrive at the CADTH base case. Due to the limitations associated with the evidence base and model structure, the CADTH base case was restricted to results generated from the deterministic simulation of the revised model.
Results from the reanalysis of the sponsor’s economic evaluation are presented in Table 6. As with the sponsor’s base case, the reanalysis was based on publicly available prices of the comparator treatments. In the CADTH base case, sotorasib was more effective (1.29 QALYs versus 0.97 QALYs) and more costly ($130,506 versus $33,367) than docetaxel. With an ICER of $308,262, sotorasib is not expected to be cost-effective at a threshold of $50,000 per QALY. The CADTH base case was conducted deterministically because the probabilistic output produced erroneous results, with many simulations estimating that patients receiving docetaxel experience a life expectancy of more than 5 years.
Table 5: CADTH Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
None | — | — |
Changes to derive the CADTH base case | ||
1. Exclusion of costs relevant to the decision problem | Excluded disease management costs | Included disease management costs |
2. Utility estimation | Utilities estimated using a time-to-death approach | Utilities estimated for each health state (progression-free, progressed, death) |
Exclusion of utility decrement for IV vs. oral administration | Inclusion of utility decrement for IV vs. oral administration | |
Exclusion of utility decrement for adverse events | Inclusion of utility decrement for adverse events | |
3. HROS parameter uncertainty | HROS = 0.823 (95% CI, 0.692 to 0.982) HROS would be randomly resampled at 4 time points | HROS = 0.823 (95% CI, 0.17 to 1.33) HROS would be sampled only once per simulation |
4. Calculation of state membership | 11.2% of patients transitioning from the PF state would transition to the death state instead of the progressed state. | Removed. In a partitioned survival model, state membership is determined by survival curves. |
PFS and OS survival probabilities were converted from a continuous to a discrete time scale. | Removed. State membership was determined using unmodified survival probabilities. | |
OS was capped by the general population mortality risk. | Removed. State membership was determined using unmodified survival probabilities. | |
The postprogression state membership calculation was 1 – progression-free – death. | State membership was determined using correct formula: S(t)OS – S(t)PFS. | |
CADTH base case | Corrections plus reanalyses 1 to 4 | |
HR = hazard ratio; OS = overall survival; PFS = progression-free survival; vs. = versus.
Table 6: Summary of the Stepped Analysis of the CADTH Reanalysis Results
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALY) |
|---|---|---|---|---|
Sponsor’s base case (probabilistic) | Docetaxel | 16,200 | 0.913 | Reference |
Sotorasib | 112,313 | 1.281 | 261,528 | |
CADTH revision 1: Disease management costs (deterministic) | Docetaxel | 25,971 | 0.905 | Reference |
Sotorasib | 123,319 | 1.267 | 268,597 | |
CADTH revision 2: Utility estimation (deterministic) | Docetaxel | 18,334 | 0.971 | Reference |
Sotorasib | 113,620 | 1.287 | 302,383 | |
CADTH revision 3: HROS using the 2-stage method (deterministic) | Docetaxel | 18,946 | 0.90 | Reference |
Sotorasib | 114,229 | 1.267 | 262,896 | |
CADTH revision 4: State membership (deterministic) | Docetaxel | 18,140 | 0.905 | Reference |
Sotorasib | 113,259 | 1.267 | 262,446 | |
CADTH base case: Revisions 1 to 4 (deterministic) | Docetaxel | 33,367 | 0.97 | Reference |
Sotorasib | 130,506 | 1.29 | 308,262 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Scenario Analysis Results
A series of scenario analyses were conducted to explore the impact of incremental reductions on the acquisition cost of sotorasib and are presented in Table 7. In the sponsor’s base case, a 76% price reduction was required to achieve an ICER equal to or less than the CADTH threshold of $50,000 per QALY gained. However, an 80% price reduction was required to generate an ICER equal to or less than the threshold of $50,000 per QALY gained in the CADTH base case. An even greater price reduction may be necessary, given that neither base case fully characterized the effect of parameter uncertainty on the decision.
A scenario analysis was conducted to present the results from the probabilistic evaluation of the CADTH base case. The expected costs, LYs, and QALYs were generated from a Monte Carlo simulation of 5,000 iterations. In this analysis, sotorasib was more expensive ($130,153 versus $33,862) and more effective (1.30 QALYs versus 1.21 QALYs) relative to docetaxel. The probabilistic output showed that some probabilistic iterations created an implausible condition where patients would survive on docetaxel for more than 5 years, on average. Given the uncertainty and lack of validity, the probabilistic results were not used to inform the CADTH base-case conclusions.
Finally, CADTH conducted an additional scenario analysis to explore the cost-effectiveness of sotorasib versus docetaxel if there was no difference in survival between the 2 by assuming an HR of 1. This HR is in line with sensitivity analyses conducted to account for crossover using the inverse probability of censoring weighting and rank-preserving structural failure time model methods. In this analysis, the ICER for sotorasib versus docetaxel increased to $1,732,373 per QALY gained. Although incremental costs remained similar to those in the CADTH base case, incremental QALYs decreased to 0.05.
Table 7: CADTH Price Reduction Analyses
Analysis | ICERs for sotorasib vs. docetaxel ($/QALY) | |
|---|---|---|
Price reduction | Sponsor’s base case | CADTH reanalysis |
No price reduction | 262,924 | 308,262 |
10% | 234,551 | 275,629 |
20% | 206,179 | 242,996 |
30% | 177,807 | 210,364 |
40% | 149,434 | 177,731 |
50% | 121,062 | 145,098 |
60% | 92,690 | 112,466 |
70% | 64,317 | 79,833 |
76% | 47,294 | 60,254 |
80% | 35,945 | 47,200 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; vs. = versus.
Note: Bold text indicates the price reduction at which sotorasib is cost-effective at a threshold of $50,000 per QALY.
Overall Conclusions
Estimates of relative efficacy were obtained from the direct comparison of sotorasib and docetaxel in the phase III CodeBreaK 200 trial. In the CodeBreaK 200 trial, treatment with sotorasib demonstrated a statistically significant impact on PFS compared to docetaxel. The CI associated with the effect of sotorasib relative to docetaxel on OS in the CodeBreaK 200 trial was too wide to draw any conclusions with certainty. The results of the sensitivity analyses to account for treatment crossover in the trial were consistent with the main analysis of OS, with the 95% CIs for all analyses including the possibility that either treatment could be favoured. Both OS and PFS were key parameters in the economic evaluation, given that these were used to generate estimates of state membership over the model time horizon.
CADTH attempted to address some of the key limitations of the sponsor’s economic submission. These changes involved the use of health state utilities and the inclusion of disutility associated with AEs and drug administration; corrections to the calculation of state membership; and the inclusion of all relevant health care costs. In the CADTH base case, sotorasib was more effective (incremental QALYs = 0.32) and more expensive (incremental costs = $95,079) than docetaxel. This resulted in an ICER of $308,262 per QALY gained. Incremental QALYs were largely driven by an assumed mortality benefit associated with sotorasib (i.e., an additional 0.335 LYs for patients receiving sotorasib relative to docetaxel) using the HR for OS from the CodeBreaK 200 trial, adjusted for crossover using the 2-stage method.
Because the probabilistic results were not considered clinically valid, the CADTH base case was conducted deterministically. As a result, the CADTH base case could not fully explore the impact of the uncertainty in the evidence associated with both PFS and OS. Based on the CADTH base-case analysis, an 80% price reduction is required for sotorasib to be considered cost-effective at a threshold of $50,000 per QALY gained; this requires the HR for OS associated with sotorasib to be no larger than 0.823. If the HR for OS for sotorasib versus docetaxel trended closer to 1, higher price reductions would be required. CADTH notes that, of the 3 methods presented to adjust for crossover in the Clinical Study Report, the other 2 methods (the inverse probability of censoring weighting and rank-preserving structural failure time model) resulted in higher HRs (1.010 and 0.990, respectively). CADTH conducted a scenario analysis that assumed no survival benefit associated with sotorasib; this increased the ICER relative to docetaxel to $1,732,373 per QALY gained.
Finally, the sponsor assumes that sotorasib will displace docetaxel only in the second-line setting and beyond. The cost-effectiveness of sotorasib compared with other therapies used in this setting, such as doublet-platinum chemotherapy, is unknown.
References
1.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Lumakras (sotorasib), 120 mg oral tablets. Mississauga (ON): Amgen Canada Inc.; 2023 May 9.
2.Lumakras (sotorasib): 120 mg oral tablets [product monograph]. Mississauga (ON): Amgen Canada Inc.; 2021 Sep 9.
3.Cancer Care Ontario. Drug Formulary DOCE Regimen for Lung - Non-Small Cell, Palliative Intent. 2022; https://www.cancercareontario.ca/en/drugformulary/regimens/monograph/45841. Accessed 2022 Oct 18.
4.Clinical Study Report: 20170543 Phase 2 Portion. A Phase 1/2, Open-label Study Evaluating the Safety, Tolerability, Pharmacokinetics, Pharmacodynamics, and Efficacy of AMG 510 Monotherapy in Subjects With Advanced Solid Tumors With KRAS p.G12C Mutation and AMG 510 Combination Therapy in Subjects With Advanced NSCLC With KRAS p.G12C Mutation (CodeBreak 100) [internal sponsor's report]. Thousand Oaks (CA): Amgen Inc.; 2020 Nov 10.
5.de Langen AJ, Johnson ML, Mazieres J, et al. Sotorasib versus docetaxel for previously treated non-small-cell lung cancer with KRAS(G12C) mutation: a randomised, open-label, phase 3 trial. Lancet. 2023;401(10378):733-746. PubMed
6.Amgen data on file. CodeBreaK 200 Phase 3 NSCLC Cohort Safety Analysis Set, AUG 02, 2022 Data Cutoff. In: Drug Reimbursement Review sponsor submission: Lumakras (sotorasib), 120 mg oral tablets. Mississauga (ON): Amgen Canada Inc.; 2023 May 9.
7.Amgen. NCT04303780: A Phase 3 Multicenter, Randomized, Open Label, Active-controlled, Study of AMG 510 Versus Docetaxel for the Treatment of Previously Treated Locally Advanced and Unresectable or Metastatic NSCLC Subjects With Mutated KRAS p.G12C. ClinicalTrials.gov. Bethesda (MD): U.S. National Library of Medicine; 2020: https://classic.clinicaltrials.gov/ct2/show/NCT04303780?term=NCT04303780. Accessed 2022 Oct 3.
8.Guidelines for the economic evaluation of health technologies: Canada. 4th ed. Ottawa (ON): CADTH; 2017: https://www.cadth.ca/guidelines-economic-evaluation-health-technologies-canada-4th-edition. Accessed 2022 Oct 3.
9.Latimer NR, Abrams KR. NICE DSU Technical Support Document 16: Adjusting Survival Time Estimates in the Presence of Treatment Switching. (NICE Decision Support Unit Technical Support Documents). London (GB): National Institute for Health and Care Excellence (NICE); 2014: https://pubmed.ncbi.nlm.nih.gov/27466662/. Accessed 2022 Oct 3.
10.Amzal B. Surrogate Endpoints Under Attack: Is It Still Worth Performing Surrogacy Validation? Lessons from NSCLC [conference presentation]. ISPOR US; 2022 May 15-18; Washington (DC). 2022: https://www.ispor.org/docs/default-source/intl2022/ispor-us-2022issue-panel-223billy-amzalchoosing-the-right-analytical-method-is-critical.pdf. Accessed 2023 Jan 30.
11.Table: 13-10-0114-01. Life expectancy and other elements of the life table, Canada, all provinces except Prince Edward Island. Ottawa (ON): Statistics Canada; 2022: https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310011401. Accessed 2022 Oct 3.
12.Xie F, Pullenayegum E, Gaebel K, et al. A Time Trade-off-derived Value Set of the EQ-5D-5L for Canada. Med Care. 2016;54(1):98-105. PubMed
13.Lewis G, Peake M, Aultman R, et al. Cost-effectiveness of erlotinib versus docetaxel for second-line treatment of advanced non-small-cell lung cancer in the United Kingdom. J Int Med Res. 2010;38(1):9-21. PubMed
14.DeltaPA. [Ottawa (ON)]: IQVIA; 2022: https://www.iqvia.com/. Accessed 2022 Nov 16.
15.Cancer Care Ontario. Drug Formulary CISPPEME Regimen for Lung - Non-Small Cell, Palliative Intent. 2021; https://www.cancercareontario.ca/en/drugformulary/regimens/monograph/46001. Accessed 2022 Oct 18.
16.BC Cancer Protocol Summary for Adjuvant CISplatin and Pemetrexed Following Resection of Non-Small Cell Lung Cancer (LUAJPP). Vancouver (BC): BC Cancer; 2022: http://www.bccancer.bc.ca/chemotherapy-protocols-site/Documents/Lung/LUAJPP_Protocol.pdf. Accessed 2022 Oct 18.
17.Government of Canada. Pharmacist in Canada. Job Bank 2022; https://www.jobbank.gc.ca/marketreport/wages-occupation/18196/ca. Accessed 2022 Aug 16.
18.Government of Canada. Independent Practice - Registered Nurse in Canada. Job Bank 2022; https://www.jobbank.gc.ca/marketreport/wages-occupation/696/ca. Accessed 2022 Aug 16.
19.Ondhia U, Conter HJ, Owen S, et al. Cost-effectiveness of second-line atezolizumab in Canada for advanced non-small cell lung cancer (NSCLC). J Med Econ. 2019;22(7):625-637. PubMed
20.Pettigrew M, Kavan P, Surprenant L, Lim HJ. Comparative net cost impact of the utilization of panitumumab versus cetuximab for the treatment of patients with metastatic colorectal cancer in Canada. J Med Econ. 2016;19(2):135-147. PubMed
21.National Institute for Health and Care Excellence. Nintedanib for previously treated locally advanced, metastatic, or locally recurrent non‑small‑cell lung cancer. (Technology appraisal guidance TA347) 2015; https://www.nice.org.uk/guidance/ta347. Accessed 2023 Jul 5.
22.Schedule of benefits for physician services under the Health Insurance Act: effective October 1, 2021. Toronto (ON): Ontario Ministry of Health; 2022: https://www.health.gov.on.ca/en/pro/programs/ohip/sob/physserv/sob_master.pdf. Accessed 2022 Oct 3.
23.Schedule of benefits for laboratory services: effective July 1, 2020. Toronto (ON): Ontario Ministry of Health; 2020: http://www.health.gov.on.ca/en/pro/programs/ohip/sob/lab/lab_mn2020.pdf. Accessed 2022 Oct 3.
24.Ontario Case Costing Initiative (OCCI). Toronto (ON): Ontario Health and Long-Term Care; 2017: https://data.ontario.ca/dataset/ontario-case-costing-initiative-occi. Accessed 2022 Oct 3.
25.Woods B, Sideris E, Palmer S, Latimer N, Soares M. Partitioned survival analysis for decision modelling in health care: a critical review. (NICE DSU Technical Support Document 19). Sheffield (UK): Decision Support Unit, ScHARR, University of Sheffield; 2017: https://www.sheffield.ac.uk/nice-dsu/tsds/partitioned-survival-analysis. Accessed 2022 Oct 3.
26.Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Lumakras (sotorasib), 120 mg oral tablets. Mississauga (ON): Amgen Canada Inc.; 2022 Aug 19.
27.Alignment among public formularies in Canada, Part 2: Oncology Medicines. Ottawa (ON): Patented Medicine Prices Review Board; 2021: https://www.canada.ca/content/dam/pmprb-cepmb/documents/npduis/analytical-studies/formularies/PMPRB-P2-Formularies-en.pdf. Accessed 2023 Aug 9.
28.Dinh T, Sutherland G. Understanding the gap: a pan-Canadian analysis of prescription drug insurance coverage. Ottawa (ON): The Conference Board of Canada; 2017: https://www.conferenceboard.ca/e-library/abstract.aspx?did=9326. Accessed 2023 Aug 9.
Appendix 1: Cost Comparison Table
Note that this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical expert(s) and drug plans. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 8: CADTH Cost Comparison Table for Treatment of Adult Patients with KRAS
G12C-Mutated, Locally Advanced or Metastatic NSCLC
Treatment | Strength | Form | Price ($) | Recommended dosage | Daily cost | 28-day cost |
|---|---|---|---|---|---|---|
Sotorasib (Lumakras) | 120mg | Tablet | 48.2400a | 960mg once daily | $385.92 | $10,806 |
Docetaxel monotherapy | ||||||
Docetaxel (generic) | 80 mg/4 mL | Injected Solution | 497.0000b 990.0000b | 75mg/m2 to 100mg/m2 every 21 days | $47.33 to $70.81 | $1,325 to $1,983 |
160 mg/8 mL | ||||||
Platinum chemotherapy (regimen: CISPEME) | ||||||
Cisplatin (generic) | 50 mg/50 mL | Injected Solution | 135.0000b 270.0000b | 75mg/m2 every 21 days | $19.29 | $540 |
100 mg/100 mL | ||||||
Pemetrexed (generic) | 25mg/mL | 4mL in 4mL Vial 20mL in 20mL Vial 34mL in 34mL Vial 40mL in 40mL Vial | 429.0000b 2,145.0000b 3,646.5000b 4,290.0000b | 500mg/m2 every 21 days | $183.86 | $5,148 |
Cisplatin + pemetrexed | $203.15 | $5,688 | ||||
NSCLC = non–small cell lung cancer.
Note: Prices do not include dispensing fees or markups. Costs assume a body weight of 75kg or a body surface area of 1.8m2 and include wastage of unused medication in vials.
aSponsor’s submitted price.1
bIQVIA Delta Price Advisor wholesale price. Accessed November 2022. Docetaxel (Generic) price of $124.25 per mL (4mL vial) or $123.75 (8mL vial); Cisplatin (Generic) price of $2.7000 per mL; Pemetrexed (Generic) price of $107.25 per mL.14
Appendix 2: Submission Quality
Note that this appendix has not been copy-edited.
Description | Yes or no | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | Yes | No comment. |
Model has been adequately programmed and has sufficient face validity | No | Refer to limitations: Concerns Regarding Model Structure, Unnecessary Complexity Degraded Model Transparency. |
Model structure is adequate for decision problem | No | Refer to limitation: Concerns Regarding Model Structure |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | Yes | No comment. |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | No | Parameter uncertainty was assessed using Monte Carlo simulation. However, the various limitations of the model severely restricted its usefulness for the characterization of uncertainty. Structural uncertainty was explored through the specification of distinct structural assumptions. However, many of the structural assumptions were unnecessary. Refer to limitation: Inclusion of Unnecessary Scenarios. |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | Yes | No comment. |
Appendix 3: Additional Information on the Submitted Economic Evaluation
Note that this appendix has not been copy-edited.
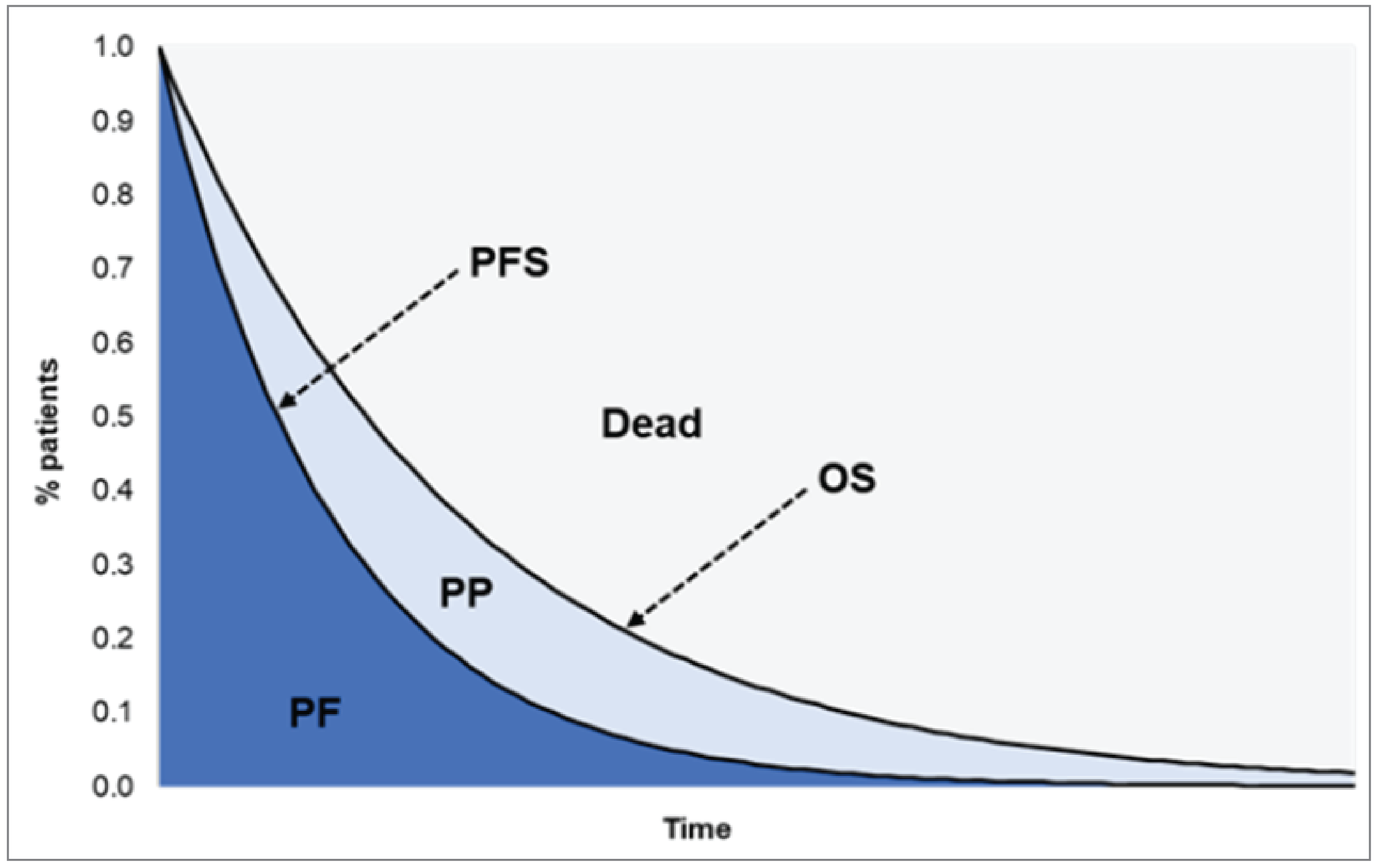
OS = overall survival; PF = progression-free, PFS = progression-free survival; PP = postprogression.
Source: Sponsor’s pharmacoeconomic submission.1
Detailed Results of the Sponsor’s Base Case
Table 10: Disaggregated Summary of Sponsor’s Economic Evaluation Results
Parameter | Sotorasib | Docetaxel | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 1.619 | 1.279 | 0.340 |
By health state | |||
Progression-free | 0.737 | 0.472 | 0.265 |
Postprogression | 0.882 | 0.807 | 0.075 |
Discounted QALYs | |||
Total | 1.281 | 0.913 | 0.368 |
By health statea | |||
Progression-free | NA | NA | NA |
Postprogression | NA | NA | NA |
Discounted costs ($) | |||
Total | 112,312.77 | 16,200.49 | 96,112.28 |
Acquisition | 103,132.18 | 5,738.03 | 97,394.16 |
Administration | 0.00 | 994.43 | –994.43 |
Concomitant Treatment | 0.00 | 0.00 | 0.00 |
Monitoring: Preprogression | 0.00 | 0.00 | 0.00 |
Monitoring: Postprogression | 0.00 | 0.00 | 0.00 |
Subsequent treatment | 360.69 | 193.97 | 166.71 |
Terminal care | 8,661.20 | 8,712.27 | –51.06 |
AEs | 158.69 | 561.70 | –403.10 |
ICER ($/QALY) | 261,528 | ||
AE = adverse event; ICER = incremental cost-effectiveness ratio; LY = life-year; NA = not available; QALY = quality-adjusted life-year.
aSponsor’s base case used the time-to-death method, which prevented the calculation of QALYs by health state.
Source: Sponsor’s pharmacoeconomic submission.1
Appendix 4: Additional Details on the CADTH Reanalyses and Sensitivity Analyses of the Economic Evaluation
Note that this appendix has not been copy-edited.
Detailed Results of CADTH Base Case
Table 11: Disaggregated Summary of CADTH’s Economic Evaluation Results
Parameter | Sotorasib | Docetaxel | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 1.602 | 1.266 | 0.335 |
By health state | |||
Progression-free | 0.735 | 0.470 | 0.265 |
Postprogression | 0.867 | 0.796 | 0.071 |
Discounted QALYs | |||
Total | 1.287 | 0.971 | 0.315 |
By health state | |||
Progression-free | 0.612 | 0.364 | 0.247 |
Postprogression | 0.675 | 0.618 | 0.057 |
Decrement due to AEs | –0.0008 | –0.0014 | 0.0006 |
Decrement due to administration mode | 0.0000 | –0.0097 | 0.0097 |
Discounted costs ($) | |||
Total | 130,506 | 33,367 | 97,139 |
Acquisition | 102,831 | 5,711 | 97,121 |
Administration | 0 | 989 | –989 |
Concomitant Treatment | 0 | 0 | 0 |
Monitoring: Preprogression | 4,380 | 2,800 | 1,580 |
Monitoring: Postprogression | 5,894 | 5,414 | 479 |
Subsequent treatment | 0 | 0 | 0 |
Terminal care | 17,243 | 17,342 | –99 |
AEs | 159 | 1,111 | –953 |
ICER ($/QALY) | 308,262 | ||
AE = adverse event; ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year.
Scenario Analyses
Table 12: Summary of CADTH Scenario Analysis (Probabilistic Base Case)
Drug | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER vs. docetaxel ($/QALY) |
|---|---|---|---|---|---|
Docetaxel | 33,862 | Reference | 1.21 | Reference | Reference |
Sotorasib | 130,153 | 96,291 | 1.30 | 0.09 | 1,032,243 |
ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year; vs. = versus.
Table 13: Summary of CADTH Scenario Analysis (No OS Survival Benefit HR = 1)
Drug | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER vs. docetaxel ($/QALY) |
|---|---|---|---|---|---|
Docetaxel | 35,549 | Reference | 1.232 | Reference | Reference |
sotorasib | 130,506 | 94,957 | 1.287 | 0.05 | 1,732,373 |
HR = hazard ratio; ICER = incremental cost-effectiveness ratio; OS = overall survival; QALY = quality-adjusted life-year; vs. = versus.
Appendix 5: Submitted Budget Impact Analysis and CADTH Appraisal
Note that this appendix has not been copy-edited.
Table 14: Summary of Key Take-Aways
Key take-aways of the budget impact analysis |
|---|
|
Summary of Sponsor’s Budget Impact Analysis
The submitted budget impact analysis (BIA) evaluated the introduction of sotorasib for the treatment of NSCLC. The population for this BIA was restricted to adult patients with locally advanced (not amenable to curative therapy) or metastatic NSCLC who carry a KRAS G12C mutation. In addition, patients must have received at least 1 prior systemic therapy. Estimates were generated from the perspective of drug plans (except Quebec) participating in the CADTH pan-Canadian Oncology Review Expert Review Committee, and the results were aggregated into pan-Canadian totals over a 3-year time horizon. An epidemiological approach was used to estimate the eligible population size for the analysis. Key inputs to the BIA are documented in Table 15.
In the reference scenario, it was assumed 100% of patients would receive taxane chemotherapy (docetaxel) as second-line therapy. In the new drug scenario, it was assumed that sotorasib would displace market share from the therapies available in the reference scenario.
Key assumptions:
All patients who initiate treatment will complete the treatment in the same model year.
The epidemiological approach to derive the relevant population size is reported in Figure 2.
In the reference scenario, 100% of patients who are eligible to receive second-line therapy are treated with docetaxel.
Figure 2: Sponsor’s Estimation of the Size of the Eligible Population
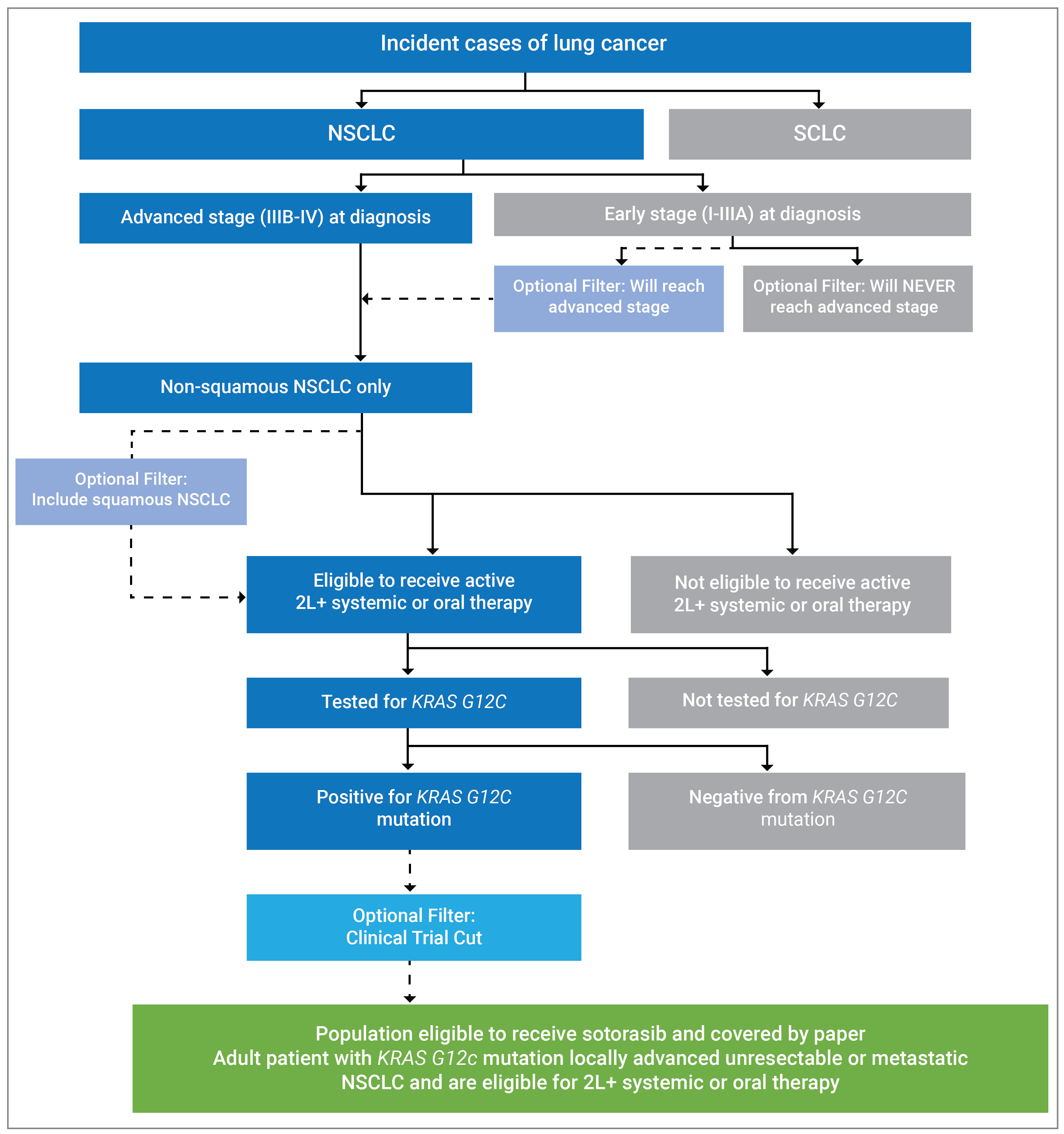
2L+ = second line or later; NSCLC = non–small cell lung cancer; SCLC = small cell lung cancer.
Source: Sponsor’s pharmacoeconomic submission.1
Table 15: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as year 1 / year 2 / year 3 if appropriate) | ||
|---|---|---|---|
Target population | |||
Pan-Canadian population (excluding Quebec) | 29,661,801 | ||
Annual incidence of lung cancer | 17,702 (0.06%) | ||
NSCLC | 15,567 (87.9%) | ||
Advanced stage (IIIB-IV) at diagnosis | 9,203 (59.12%) | ||
Nonsquamous NSCLC | 6,534 (71.0%) | ||
Eligible for 2L+ systemic therapy | 3,234 (49.5%) | ||
Tested for KRAS G12C mutation | 2,588 (80.0%) | ||
Positive for KRAS G12C mutation | 339 (13.1%) | ||
Eligible for sotorasib | 339 (100%) | ||
Eligible for public coverage | 271 (80.0%) | ||
Patient identification | Year 1 | Year 2 | Year 3 |
Number of patients eligible for drug under review | 278 | 286 | 294 |
Market uptake (3 years) | |||
Uptake (reference scenario) | |||
docetaxel | 100% | 100% | 100% |
Uptake (new drug scenario) | |||
sotorasib | 50% | 60% | 70% |
docetaxel | 50% | 40% | 30% |
Cost of treatment (per patient) | |||
Cost of treatment over: 1 year | |||
Sotorasib (average treatment duration: 6.8 months) | $79,875.79 | ||
Docetaxel (average treatment duration: 2.8 months) | $4,033.98 | ||
2L+ = second line or later; NSCLC = non–small cell lung cancer.
Source: Sponsor’s pharmacoeconomic submission.1
Summary of the Sponsor’s BIA Results
In the base case, the net-budget impact of sotorasib was estimated to be $10,556,790 in year 1, $13,008,834 in year 2, and $15,589,204 in year 3. The 3-year net-budget impact of sotorasib was $39,154,828.
CADTH Appraisal of the Sponsor’s BIA
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
Overestimation of docetaxel market share: Consistent with the economic evaluation, docetaxel was specified as the primary comparator intervention to sotorasib. However, the market share for docetaxel in the reference and new drug scenarios may have been overestimated. In the reference scenario, the sponsor assumed that every patient that proceeded to second-line therapy would receive docetaxel. CADTH’s clinical experts raised concerns with this assumption. Second-line docetaxel eligibility will be determined by the proportion of patients who experience treatment failure with first-line platinum-doublet chemotherapy. Those who experience failure of first-line immunotherapy may receive platinum-doublet chemotherapy before being considered for docetaxel. Therefore, the BIA overestimates the proportion of patients receiving docetaxel as some patients would receive a platinum-doublet chemo for their second-line treatment and not proceed onto docetaxel thereafter. The experts noted that sotorasib would likely only displace docetaxel given the evidence base.
Based on clinical expert opinion it was noted that roughly 70% of patients eligible for second-line therapy would receive docetaxel at some point in the treatment pathway. In the CADTH base case the market size of the population eligible for sotorasib was reduced by 30%. This reflected 30% of patients would not receive docetaxel and would therefore not be considered for sotorasib. CADTH notes if sotorasib would displace therapies other than docetaxel then the current BIA is not programmed to consider this.
Speed of market share uptake: Given docetaxel’s toxicity and route of administration, CADTH’s clinical experts expected sotorasib would displace docetaxel’s market share at a faster rate than what was assumed in the sponsor’s base case.
In the new drug scenario, it was assumed that sotorasib would obtain a market share of 60% from docetaxel in Years 1 increasing to 70% in years 2 to 3.
Coverage rates by province: The sponsor’s analysis assumed a flat rate of public coverage of 80% across all jurisdictions. On average, the public coverage rate for oncology drugs administered at home is expected to around 80% across Canada. However, a more accurate estimate would look at coverage rates by province and age. As the sponsor’s BIA provided an option to implement age and provincial specific estimates CADTH used this functionality to provide a more accurate estimate. In British Columbia, Alberta, Saskatchewan, Manitoba and noninsured health benefit, 100% public coverage was assumed.27 For other jurisdictions age specific coverage rates were taken from the Understanding the Gap report looking at percentage enrolment in public plans.28
In the CADTH base case the following public coverage rates were assumed:
Between 25 and 65 years of age (24% of patients): 100% (British Columbia, Alberta, Saskatchewan, Manitoba, NIHB), 11% (Ontario), 9% (New Brunswick), 10% (Nova Scotia), 17% (Prince Edward Island), 12% (Newfoundland).
Aged 65 years and older (76% of patients): 100% (British Columbia, Alberta, Saskatchewan, Manitoba, Ontario, Prince Edward Island, NIHB), 41% (New Brunswick), 65% (Nova Scotia), 50% (Newfoundland).
Overestimation of patients eligible for second-line therapy: consultation with clinical experts revealed that the number of patients who are eligible for second-line or later therapy may have been overestimated. Two issues were raised which led to this conclusion. First, while many patients may receive first-line therapy many may not survive long-enough to receive second-line therapy. Second, some patients may reject second-line therapy to avoid the risk of side effects from drugs like docetaxel.
This limitation was not addressed by CADTH. While the estimated value may have been overestimated, the risk of bias was considered low by the Clinical Experts.
Underestimation of KRAS testing: clinical experts consulted by CADTH agreed with the sponsor’s assumption that broad panel biomarker testing, including KRAS, through next-generation sequencing was the standard diagnostic procedure for NSCLC across all provinces. Further alignment was identified with the assumption that such testing reflected the current clinical standard of care. Despite this consensus, CADTH’s clinical experts raised concerns that the sponsor’s assumed testing rate of 80% may be too low. In the BIA, the sponsor justified this assumption by citing evidence that 10% to 20% of patients with nonsquamous NSCLC would not have sufficient biopsy sample at diagnosis to submit for tissue-based next-generation sequencing testing.
This limitation was not addressed by CADTH. As a scenario analysis, a 100% testing uptake was assumed.
CADTH Reanalyses of the BIA
Table 16: CADTH Revisions to the Submitted BIA
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Correctionsa to sponsor’s base case | ||
None | — | — |
Changes to derive the CADTH base case | ||
1. Estimation of market share | Assumed 100% of patients receive docetaxel and in year 1 sotorasib would displace 50% of docetaxel use, in year 2 60% would be displaced and finally 70% would be displaced in year 3. | Assumed only 70% of patients receive docetaxel and in year 1 sotorasib would displace 60% of docetaxel use, in year 2 70% would be displaced and finally 70% would be displaced in year 3. It was assumed 30% do not receive docetaxel and these therapies would not be displaced by sotorasib. |
2. Coverage rates by province | 80% (all provinces + NIHB). | 25 to 65 Years Old: 100% (British Columbia, Alberta, Saskatchewan, Manitoba, NIHB), 11% (Ontario), 9% (New Brunswick), 10% (Nova Scotia), 17% (Prince Edward Island), 12% (Newfoundland) 65+: 100% (British Columbia, Alberta, Saskatchewan, Manitoba, Ontario, Prince Edward Island, NIHB), 41% (New Brunswick), 65% (Nova Scotia), 50% (Newfoundland) |
CADTH base case | Reanalysis 1 + 2 | |
BIA = budget impact analysis; NIHB = noninsured health benefit.
aCorrections are minor errors (e.g., transcription errors between report and model, misapplication of distributions or SEs in probabilistic analyses) that are not identified as limitations.
The results of the CADTH stepwise reanalyses are presented in summary format in Table 17 and a more detailed breakdown is presented in Table 18. All CADTH reanalyses were based on publicly available prices of the comparator treatments. In the CADTH base case, the budget impact of sotorasib was estimated to be $32,198,481 over the 3-year period. This decrease is attributable to the assumption that fewer patients receive docetaxel than what was proposed in the sponsor’s base case.
A scenario analysis was considered to explore how the budget impact would be affected by the price reduction identified in the economic evaluation. Assuming an 80% price reduction, the 3-year budget impact of sotorasib was estimated to be $5,069,601. An additional scenario analysis was conducted to determine the impact of a 100% testing uptake. This likely represents the upper limit of the potential budget impact as noted testing uptake is unlikely to reach 100%. In this scenario the 3-year budget impact increases to $40,248,101 over 3 years.
Table 17: Summary of the CADTH Reanalyses of the BIA
Stepped analysis | Three-year total |
|---|---|
Submitted base case | $39,154,828 |
CADTH reanalysis 1 | $30,404,028 |
CADTH reanalysis 2 | $41,475,764 |
CADTH base case | $32,198,481 |
BIA = budget impact analysis.
Table 18: Detailed Breakdown of the CADTH Reanalyses of the BIA
Stepped analysis | Scenario | Year 0 (current situation) | Year 1 | Year 2 | Year 3 | Three-year total |
|---|---|---|---|---|---|---|
Submitted base case | Reference | $1,093,900 | $1,123,019 | $1,153,221 | $1,184,544 | $3,460,785 |
New drug | $1,093,900 | $11,679,809 | $14,162,055 | $16,773,749 | $42,615,613 | |
Budget impact | $0 | $10,556,790 | $13,008,834 | $15,589,749 | $39,154,828 | |
CADTH base case | Reference | $804,185 | $828,987 | $854,696 | $881,343 | $2,565,026 |
New drug | $804,185 | $10,180,327 | $12,102,922 | $12,480,258 | $34,763,507 | |
Budget impact | $0 | $9,351,339 | $11,248,227 | $11,598,915 | $32,198,481 | |
CADTH scenario: 80% price reduction | Reference | $804,185 | $828,987 | $854,696 | $881,343 | $2,565,026 |
New drug | $804,185 | $2,301,341 | $2,625,711 | $2,707,574 | $7,634,626 | |
Budget impact | $0 | $1,472,354 | $1,771,016 | $1,826,231 | $5,069,601 | |
CADTH scenario: 100% testing uptake | Reference | $1,005,231 | $1,036,234 | $1,068,369 | $1,101,678 | $3,206,282 |
New drug | $1,005,231 | $12,725,408 | $15,128,653 | $15,600,322 | $43,454,383 | |
Budget impact | $0 | $11,689,174 | $14,060,283 | $14,498,644 | $40,248,101 |
BIA = budget impact analysis.
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.