CADTH Reimbursement Review
Olaparib (Lynparza)
Sponsor: AstraZeneca Canada Inc.
Therapeutic area: gBRCAm, HER2-negative, high-risk early breast cancer
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Stakeholder Input
Clinical Review
Abbreviations
AE
adverse event
AJCC
American Joint Committee on Cancer
BRCA
breast cancer susceptibility gene
CBCN
Canadian Breast Cancer Network
CI
confidence interval
CPS&EG
clinical and post-treatment pathologic stage and estrogen receptor status and histologic grade
CTCAE
Common Terminology Criteria for Adverse Events
DDFS
distant disease–free survival
DFS
disease-free survival
ECOG
Eastern Cooperative Oncology Group
EORTC
European Organisation for Research and Treatment of Cancer
ER
estrogen receptor
FACIT-F
Functional Assessment of Chronic Illness Therapy–Fatigue
FAS
full analysis set
gBRCA
germline BRCA
gBRCAm
germline BRCA mutation
HER2
human epidermal growth factor receptor 2
HR
hazard ratio
HR-positive
positive for expression of a hormone receptor
HRQoL
health-related quality of life
IDFS
invasive disease–free survival
ITC
indirect treatment comparison
ITT
intention-to-treat population
LS
least squares
MID
minimal important difference
MMRM
mixed-model for repeated measures
OH-CCO
Ontario Health (Cancer Care Ontario)
OS
overall survival
PARP
poly-(ADP-ribose) polymerase
PgR
progesterone receptor
POMS
Profile of Mood States
PRO
patient-reported outcome
QLQ-C30
Quality of Life Questionnaire Core 30
RCT
randomized controlled trial
SAE
serious adverse event
SD
standard deviation
SLR
systematic literature review
TNBC
triple-negative breast cancer
TRAE
treatment-related adverse event
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Item | Description |
|---|---|
Drug product | Olaparib (Lynparza) 100 mg and 150 mg, oral tablets |
Indication | For the adjuvant treatment of adult patients with deleterious or suspected deleterious gBRCA-mutated HER2-negative high-risk early breast cancer who have been treated with neoadjuvant or adjuvant chemotherapy. Patients must have confirmation of a germline BRCA mutation before olaparib treatment is initiated. |
Reimbursement request | As per indication |
Health Canada approval status | NOC/c |
Health Canada review pathway | Priority review |
NOC date | July 27, 2022 |
Sponsor | AstraZeneca Canada Inc. PIVINA Consulting Inc. |
BRCA = breast cancer susceptibility gene; gBRCA = germline BRCA; HER2 = human epidermal growth factor receptor 2; NOC = Notice of Compliance; NOC/c = Notice of Compliance with conditions.
Introduction
Breast cancer is the most commonly diagnosed cancer among women in Canada and the second most common cancer in men and women combined.1 In 2020, 27,700 women were diagnosed with breast cancer, representing about 25% of new cancer cases in Canada.1 Breast cancer is the second leading cause of cancer deaths among women, accounting for 14% of all cancer deaths.1 The 5-year net survival for breast cancer is more than 85% among women diagnosed before 85 years of age, after which it drops to about 73%.1 In men, the incidence of breast cancer is less than 1% per year, with 260 new cases diagnosed in 2021 in Canada.1 BRCA1 and BRCA2 are human breast cancer susceptibility genes (BRCAs) that produce proteins responsible for repairing damaged DNA and play an important role in maintaining the genetic stability of cells.2,3 A mutation in 1 or both BRCA genes reduces gene expression, which can lead to uncontrolled cell growth and is associated with an increased risk of cancer, including breast cancer.4-6
Hereditary, deleterious mutations account for 5% to 10% of all breast cancers, and 60% to 68% of these hereditary cancers occur in individuals with a germline BRCA (gBRCA) mutation (gBRCAm).4,7 In women harbouring a BRCA1 gene mutation, the estimated lifetime risk of developing breast cancer by the age of 80 years is 65% to 80%, and the 10-year actuarial risk of developing contralateral breast cancer is 25% to 31%.8,9 The estimated lifetime risk of developing breast cancer is approximately 76% among women with a BRCA2 mutation, while among men with BRCA1 or BRCA2 mutations, it ranges from 3% to 8%.8-10 BRCA mutations occur in women with all subtypes of breast cancer, but more commonly in those with early onset or a family history.9 Approximately 75% of patients with breast cancer who have a mutation in the BRCA1 gene are classified as having triple-negative breast cancer (TNBC).11-13 In contrast, patients with breast cancer carrying mutations in the BRCA2 gene are more likely to be positive for expression of a hormone receptor (HR-positive), and only approximately 20% have TNBC.13
Olaparib is a selective inhibitor of human poly-(ADP-ribose) polymerase (PARP) enzymes (PARP1, PARP2, and PARP3) involved in normal cellular functions, such as DNA transcription and DNA repair. Olaparib is approved by Health Canada for the adjuvant treatment of adult patients with a deleterious or suspected deleterious gBRCAm who have high-risk early breast cancer that is negative for human epidermal growth factor receptor 2 (HER2) and that has been treated with neoadjuvant or adjuvant chemotherapy.14 The recommended total daily dose of olaparib is 600 mg taken as 2 150 mg tablets twice daily for a total of 1 year or until disease recurrence or unacceptable toxicity, whichever occurs first. Olaparib is available as a 150 mg or 100 mg tablet.
Olaparib has been previously reviewed by CADTH for other indications, including as monotherapy for the maintenance treatment of adult patients with:
newly diagnosed advanced BRCA-mutated high-grade epithelial ovarian, fallopian tube, or primary peritoneal cancer who are in response (complete response or partial response) to first-line platinum-based chemotherapy, until disease progression or up to 2 years if no evidence of disease
platinum-sensitive relapsed BRCA-mutated epithelial ovarian, fallopian tube, or primary peritoneal cancer who are in response to platinum-based chemotherapy.15,16
The objective of this report is to perform a systematic review of the beneficial and harmful effects of olaparib 300 mg twice daily for the adjuvant treatment of adult patients with deleterious or suspected deleterious gBRCA-mutated, HER2-negative, high-risk early breast cancer who have been treated with neoadjuvant or adjuvant chemotherapy.
Stakeholder Perspectives
The information in this section is a summary of input provided by the patient groups who responded to CADTH’s call for patient and clinician input and from the clinical experts consulted by CADTH for the purpose of this review.
Patient Input
This section was prepared by CADTH staff based on the input provided by patient groups. The full original patient input(s) received by CADTH have been included in the stakeholder section at the end of this report.
Two patient groups, the Canadian Breast Cancer Network (CBCN) and Rethink Breast Cancer (Rethink) provided input for this review. CBCN is a national health charity aiming to ensure the best quality of care for all Canadians affected by breast cancer. The CBCN patient input was based on an online survey of 6 patients with gBRCA-mutated early breast cancer and a literature review of current studies and grey literature. Rethink is a Canadian charity with a focus on improving the experience and outcomes of patients with breast cancer. Rethink gathered information for this review from general observations and insights through various ongoing initiatives (including stories shared by patients, virtual support groups, working groups, and patient advisory boards), in-depth telephone interviews with 3 patients with a BRCA-mutated breast cancer who participated in the OlympiA study, as well as responses from people in the Rethink Instagram community with high-risk early breast cancer.
According to the patient input received, BRCA-mutated breast cancer is more likely to be detected in people at a young age. These young patients can face several age-specific issues such as fertility or family-planning challenges, diagnosis during pregnancy, childcare, impact on relationships, body image, dating and sexuality, feeling isolated from peers who do not have cancer, career hiatuses, and financial insecurity. The main factors influencing patients’ decisions about currently available treatment options included effectiveness of the treatment (i.e., how well the treatment could help stabilize disease and delay recurrence), prolonging life without sacrificing quality of life (i.e., how well the treatment could help the patient maintain a productive, active life with minimal disruption to daily routines), risk of side effects, and the cost and accessibility of treatments. The Rethink input revealed that patient respondents, especially those with stage III breast cancer, tended to endure side effects as well as their impacts on quality of life to achieve satisfactory effectiveness. In terms of experience with olaparib, none of the 3 patients from the Rethink group who had participated in the OlympiA study and did not experience a recurrence mentioned unendurable side effects.
Clinician Input
Input From Clinical Experts Consulted by CADTH
The clinical experts consulted by CADTH noted that current systemic treatment of patients with early breast cancer is based on the receptor status and pathological findings and does not consider the patient’s BRCA mutation status, as there is no treatment specific for mutation status. Therefore, there is a need for new therapeutic options to improve survival outcomes and increase the overall cure rate in this subgroup of patients. The clinical experts noted that patients who meet the inclusion criteria outlined in the OlympiA trial will be best suited for treatment with olaparib. According to the clinical experts, by improving survival and reducing disease recurrence, the patients who are cured will have a higher quality of life and longer life. The goal of treating BRCA-mutated early breast cancer is to eradicate disease and prevent metastatic spread, resulting in cure. It was further noted by the clinical experts that it remains unclear how to integrate olaparib within the current treatment paradigm with other drugs, such as capecitabine, pembrolizumab, abemaciclib, or a combination of drugs in the treatment of early breast cancer. The clinical experts consulted mentioned that companion diagnostic testing is perceived as a barrier, given that not all patients qualify for genetic testing based on provincial guidelines (i.e., patients who have a low likelihood of hereditary syndromes). The clinical experts indicated that current genetic testing guidelines vary by province, and BRCA mutations are underdiagnosed based on most provincial testing criteria. According to the clinical experts, toxicities and disease recurrence will be the main factors to consider when deciding to discontinue treatment with olaparib.
Clinician Group Input
The clinician group input was obtained from 2 clinician groups, including the Ontario Health (Cancer Care Ontario) (OH-CCO) Breast Cancer Drug Advisory Committee (1 clinician provided input) and a group of medical oncologists across Canada (4 clinicians provided input). Both clinician groups identified that the important goal of treatment for early breast cancer, including gBRCA-mutated early breast cancer, is to decrease the recurrence of cancer and improve survival. One potential barrier, which was mentioned by the OH-CCO Breast Cancer Drug Advisory Committee, is that the current guidelines for BRCA mutation testing are restrictive in terms of eligibility criteria; thus, many patients who carry a BRCA mutation may not receive the testing and thereby lose the opportunity to receive olaparib. Both clinician groups noted the reasons that may lead to the discontinuation of olaparib are recurrence or progression of disease, intolerant toxicity or severe side effects, and patient or physician preference.
Drug Program Input
Input was obtained from the drug programs that participate in the CADTH reimbursement review process. The following were identified as key factors that could potentially impact the implementation of a CADTH recommendation for olaparib:
considerations for the initiation of therapy
considerations for the discontinuation of therapy
considerations for prescribing therapy
care provision issues
generalizability.
The clinical experts consulted by CADTH provided advice on the potential implementation issues raised by the drug programs.
Clinical Evidence
Pivotal Studies and Protocol Selected Studies
Description of Studies
The OlympiA trial is an ongoing, phase III, randomized, multicentre, double-blind, placebo-controlled trial. The primary objective of the trial was to assess the efficacy and safety of olaparib versus placebo for the adjuvant treatment of patients with deleterious or suspicious deleterious germline BRCA1 or BRCA2 gene mutations, high-risk, HER2-negative early-stage breast cancer who had completed definitive local treatment and neoadjuvant or adjuvant chemotherapy. A total of 1,836 patients with breast cancer and gBRCA mutations were enrolled across 546 sites in 23 countries in North America (34 patients from Canada), South America, Europe, Asia Pacific, and South Africa. The primary efficacy end point was invasive disease–free survival (IDFS), and the key secondary efficacy end points were overall survival (OS) and distant disease–free survival (DDFS). Patient-reported outcomes (PROs) were assessed using the Functional Assessment of Chronic Illness Therapy–Fatigue (FACIT-F) questionnaire and the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 (EORTC QLQ-C30). Treatment with olaparib was given for up to 12 months, or until disease recurrence or unacceptable toxicity, whichever occurred first.
Overall, baseline characteristics were well balanced between treatment groups in the OlympiA trial. The mean age of patients was 43.3 years (standard deviation [SD] = 9.97 years), and about 68.7% of patients were between 30 and 49 years of age. Most patients were female (99.7%), premenopausal (61.3%), with an Eastern Cooperative Oncology Group (ECOG) Performance Status of 0 (88.7%), white (66.7%), and nonhispanic or Latino (88.1%). A total of 26.4% of patients received prior platinum therapy, and half of patients (50.1%) received neoadjuvant treatment. A total of 82.3% of the patients had TNBC, while 17.7% had HR-positive, HER2-negative breast cancer. Germline BRCA1 deleterious or suspected deleterious mutations were identified in 72.2% of patients, germline BRCA2 mutations in 27.1% of patients, and both germline BRCA1 and BRCA2 mutations in 0.4% of patients. The majority of patients with TNBC (60.3%) had a mutation in BRCA1, while the majority of patients with HR-positive, HER2-negative breast cancer (51.4%) had a mutation in BRCA2. A total of 36.1% of patients had clinical American Joint Committee on Cancer (AJCC) stage IIA, 21.0% had AJCC stage IIB, and 13.0% had AJCC stage IIIA.
Efficacy Results
Table 2 and Table 3 present a summary of key results from the OlympiA trial.
Overall Survival
At interim analysis 1 (March 27, 2020), the OS data were 7.9% mature. Deaths were reported in 59 patients (6.4%) in the olaparib group and 86 patients (9.4%) in the placebo group. The median OS was not estimable in either treatment arm and the stratified hazard ratio (HR) was 0.68 (99% confidence interval [CI], 0.44 to 1.05; P = 0.0236). At interim analysis 2 (July 12, 2021), the OS data were 10.0% mature. In the full analysis set (FAS), deaths were reported in 75 patients (8.1%) in the olaparib group and 109 patients (11.9%) in the placebo group. The median OS was not estimable, and the stratified HR was 0.68 (98.5% CI, 0.47 to 0.97; P = 0.0091) in favour of the olaparib group. The proportion of patients who remained alive at 4 years was 89.8% (95% CI, 87.2% to 91.9%) in the olaparib group and 86.4% (95% CI, 83.6% to 88.7%) in the placebo group (difference = 3.4%; 95% CI, −0.1% to 6.8%).17 The results of prespecified sensitivity and subgroup analyses were consistent with the primary analysis.
Table 2: Summary of Key Results From Pivotal Study
Characteristic | Olaparib (N = 921) | Placebo (N = 915) |
|---|---|---|
IDFS at interim analysis 1a | ||
Patients with events, n (%) | 106 (11.5) | 178 (19.5) |
Stratified HR (99.5% CIc) | 0.58 (0.41 to 0.82b) | |
Log-rank test P valued | 0.0000073 | Reference |
Median follow-upe (minimum, maximum), years | 2.3 (0 to 5.5) | 2.5 (0 to 5.5) |
Number of patients censored,f n (%) | 815 (88.5) | 737 (80.5) |
DDFS at interim analysis 1a | ||
Patients with events, n (%) | 89 (9.7) | 152 (16.6) |
Stratified HR (99.5% CIc) | 0.57 (0.39 to 0.83b) | |
Log-rank test: P valued | 0.0000257 | Reference |
Median follow-upe (minimum, maximum), years | 2.3 (0 to 5.5) | 2.5 (0 to 5.5) |
Number of patients censored,f n (%) | 832 (90.3) | 763 (83.4) |
OS at interim analysis 2g | ||
Patients with events, n (%) | 75 (8.1) | 109 (11.9) |
Stratified HR (98.5% CIc) | 0.68 (0.47 to 0.97b) | |
Log-rank test: P valued | 0.0091 | Reference |
Median follow-upe (minimum, maximum), years | 3.5 (0 to 6.8) | 3.6 (0 to 6.7) |
Number of patients censored,f n (%) | 846 (91.9) | 806 (88.1) |
FACIT-F | ||
Patients who had completed neoadjuvant chemotherapy | ||
At 6 months, nh | 371 | 356 |
LS mean (95% CI) | −1.5 (−2.2 to −0.7) | −0.2 (−1.0 to 0.6) |
LS mean differencei (95% CI) | −1.3 (−2.4 to −0.2) | |
P valuej | 0.024 | Reference |
At 12 months, nh | 371 | 356 |
LS mean (95% CI) | −1.5 (−2.4 to −0.6) | −0.0 (−0.9 to 0.9) |
LS mean differencei (95% CI) | −1.5 (−2.8 to −0.2) | |
P valuej | 0.025 | Reference |
Patients who had completed adjuvant chemotherapy | ||
At 6 months, nh | 375 | 403 |
LS mean (95% CI) | −0.7 (−1.4 to 0.1) | 0.6 (−0.1 to 1.3) |
LS mean differencei (95% CI) | −1.3 (−2.3 to −0.2) | |
P valuej | 0.017 | Reference |
At 12 months, nh | 375 | 403 |
LS mean (95% CI) | −0.8 (−1.6 to 0.0) | 0.5 (−0.3 to 1.2) |
LS mean differencei (95% CI) | −1.3 (−2.4 to 0.1) | |
P valuej | 0.027 | Reference |
Harms | ||
Patients with ≥ 1 AE, n (%) | 836 (91.8) | 758 (83.8) |
Patients with ≥ 1 TRAE, n (%) | 736 (80.8) | 480 (53.1) |
Patients with ≥ 1 AE of CTCAE grade ≥ 3, n (%) | 223 (24.5) | 102 (11.3) |
Patients who died due to AE, n (%) | 2 (2.7) | 4 (3.7) |
Patients with ≥ 1 SAE, n (%) | 79 (8.7) | 78 (8.6) |
Patients who discontinued study treatment due to AE, n (%) | 98 (10.8) | 42 (4.6) |
Patients with ≥ 1 AE leading to dose reduction, n (%) | 213 (23.4) | 33 (3.7) |
Patients with ≥ 1 AE leading to dose interruption, n (%) | 286 (31.4) | 99 (11.0) |
Notable harms, n (%) | ||
Myelodysplastic syndrome or acute myeloid leukemia | 2 (0.2) | 3 (0.3) |
Pneumonitis | 9 (1.0) | 12 (1.3) |
New primary cancer | 21 (2.3) | 36 (4.0) |
AE = adverse event; CI = confidence interval; CTCAE = Common Terminology Criteria for Adverse Events; DDFS = distant disease–free survival; FACIT-F = Functional Assessment of Chronic Illness Therapy–Fatigue; FAS = full analysis set; HER2 = human epidermal growth factor receptor 2; HR = hazard ratio; HR-positive = positive for expression of a hormone receptor; IDFS = invasive disease–free survival; KM = Kaplan-Meier; LS = least squares; MMRM = mixed-model for repeated measures; OS = overall survival; PRO = patient-reported outcome; SAE = serious adverse event; TRAE = treatment-related adverse event.
aData cut-off date: March 27, 2020.
bEstimate of the treatment HR was based on the stratified Cox proportional hazards model. The stratification factors were the same as those used in the stratified log-rank test. The CI for the HR was estimated using the profile likelihood approach.
cInferential, according to the alpha spending rules for the interim analysis.
dP value from a stratified log-rank test. Stratification was by chemotherapy type (adjuvant vs. neoadjuvant), hormone receptor status (HR-positive and HER2-negative vs. triple-negative breast cancer), and prior platinum therapy (yes vs. no). Stratification factors were based on the categories used in the randomization system and were chosen by the pooling strategy. Once the pooling strategy was applied, only the hormone receptor status stratification factor was selected.
eMedian clinical follow-up was calculated using the reverse censoring method.
fPatients who have not had a recorded event at the time of the analysis will be censored at the date of their last disease evaluation.
gData cut-off date: July 12, 2021.
hOnly patients with an evaluable baseline form were included.
IAdjusted LS mean changes, P values (2-sided), and 95% CIs were obtained from an MMRM analysis of the change from baseline. The model included treatment, time and treatment by time interaction, corresponding baseline score, and the baseline score by time interaction. The difference was the values for olaparib minus placebo.
jP value was not adjusted for multiple comparisons.
Sources: Clinical Study Reports for OlympiA.18,19
Table 3: Change From Baseline for EORTC QLQ-C30 Subscale Scores — PRO
Subscale measure | Patients who had completed neoadjuvant chemotherapy | Patients who had completed adjuvant chemotherapy | ||
|---|---|---|---|---|
Olaparib | Placebo | Olaparib | Placebo | |
EORTC QLQ-C30 global health status QoL | ||||
Baseline, n | ███ | ███ | ███ | ███ |
Mean (SD) | █ █ ██ ███████ | █ █ ██ ███████ | █ █ ██ ███████ | █ █ ██ ███████ |
At 6 months, n | ███ | ███ | ███ | ███ |
LS mean (95% CI) | █ █ ██ █ █ █ █ ██ █████ | █ ██ █ █ █ █ ██ █████ | █ █ ██ █ █ █ █ ██ █████ | █ ██ █ █ █ █ ██ █████ |
LS mean difference (95% CI) | █ █ ██ █ █ █ █ ██ █████ | █ █ ██ █ █ █ █ ██ ██████ | ||
P valuea | █████ | █████████ | █████ | █████████ |
At 12 months, n | ███ | ███ | ███ | ███ |
LS mean (95% CI) | █ ██ █ █ █ █ ██ █████ | █ ██ █ █ ███ █████ | █ ██ █ █ █ █ ██ █████ | █ ██ █ █ ███ █████ |
LS mean difference (95% CI) | █ █ ██ █ █ █ █ ██ █████ | █ █ ██ █ █ █ █ ██ ██████ | ||
P valuea | █████ | █████████ | █████ | █████████ |
At 18 months, n | ███ | ███ | ███ | ███ |
LS mean (95% CI) | █ ██ █ █ ███ █████ | █ ██ █ █ ███ █████ | █ ██ █ █ ███ █████ | █ ██ █ █ ███ █████ |
LS mean difference (95% CI) | █ █ ██ █ █ █ █ ██ █████ | █ █ ██ █ █ █ █ ██ █████ | ||
P valuea | █████ | █████████ | █████ | █████████ |
At 24 months, n | ███ | ███ | ███ | ███ |
LS mean (95% CI) | █ ██ █ █ █ █ ██ █████ | █ ██ █ █ ███ █████ | █ ██ █ █ ███ █████ | █ ██ █ █ ███ █████ |
LS mean difference (95% CI) | █ █ ██ █ █ █ █ ██ ██████ | █ █ ██ █ █ █ █ ██ █████ | ||
P valuea | █████ | █████████ | █████ | █████████ |
EORTC QLQ-C30 nausea and vomiting symptom scale | ||||
Baseline, n | 440 | 433 | 436 | 440 |
Mean (SD) | 3.2 (9.23) | 3.7 (10.82) | 3.1 (8.73) | 3.4 (9.92) |
At 6 months, n | 383 | 359 | 385 | 406 |
LS mean (95% CI) | 7.6 (6.2 to 9.0) | 1.6 (0.2 to 3.1) | 6.9 (5.5 to 8.2) | 1.6 (0.3 to 2.9) |
LS mean difference (95% CI) | 6.0 (4.0 to 8.0) | 5.3 (3.4 to 7.2) | ||
P valuea | █ █████ | █████████ | █ █████ | █████████ |
At 12 months, n | 383 | 359 | 385 | 406 |
LS mean (95% CI) | 7.3 (6.0 to 8.7) | 1.0 (–0.4 to 2.4) | 5.5 (4.2 to 6.7) | 1.0 (–0.2 to 2.1) |
LS mean difference (95% CI) | 6.3 (4.4 to 8.2) | 4.5 (2.8 to 6.2) | ||
P valuea | █ █████ | Reference | █ █████ | Reference |
At 18 months, n | 383 | 359 | 385 | 406 |
LS mean (95% CI) | 0.7 (–0.4 to 1.8) | 0.4 (–0.8 to 1.5) | 0.7 (–0.5 to 1.8) | 1.0 (–0.2 to 2.1) |
LS mean difference (95% CI) | 0.4 (–1.2 to 1.9) | –0.3 (–1.9 to 1.3) | ||
P valuea | █████ | Reference | █████ | Reference |
At 24 months, n | 383 | 359 | 385 | 406 |
LS mean (95% CI) | 1.3 (0.0 to 2.6) | –0.1 (–1.5 to 1.2) | –0.0 (–1.3 to 1.3) | 0.6 (–0.6 to 1.9) |
LS mean difference (95% CI) | 1.4 (–0.4 to 3.3) | –0.6 (–2.5 to 1.2) | ||
P valuea | █████ | Reference | █████ | Reference |
EORTC QLQ-C30 diarrhea symptom scale | ||||
Baseline, n | 438 | 431 | 435 | 440 |
Mean (SD) | 5.9 (15.79) | 6.1 (16.59) | 5.7 (14.61) | 5.9 (14.94) |
At 6 months, n | 380 | 357 | 384 | 406 |
LS mean (95% CI) | 1.6 (–0.0 to 3.3) | 1.3 (–0.4 to 3.0) | 0.0 (–1.7 to 1.8) | 1.7 (0.1 to 3.4) |
LS mean difference (95% CI) | 0.3 (–2.0 to 2.7) | –1.7 (–4.1 to 0.7) | ||
P valuea | █████ | Reference | █████ | Reference |
At 12 months, n | 380 | 357 | 384 | 406 |
LS mean (95% CI) | 4.0 (1.9 to 6.2) | 2.0 (–0.1 to 4.1) | 1.5 (–0.1 to 3.1) | 1.4 (–0.2 to 3.0) |
LS mean difference (95% CI) | 2.0 (–1.0 to 4.9) | 0.1 (–2.2 to 2.4) | ||
P valuea | █████ | Reference | █████ | Reference |
At 18 months, n | 380 | 357 | 384 | 406 |
LS mean (95% CI) | 2.7 (0.5 to 4.9) | 1.5 (–0.7 to 3.8) | –0.2 (–1.8 to 1.4) | –0.6 (–2.2 to 1.0) |
LS mean difference (95% CI) | 1.1 (–2.0 to 4.3) | 0.4 (–1.9 to 2.7) | ||
P valuea | █████ | Reference | █████ | Reference |
At 24 months, n | 380 | 357 | 384 | 406 |
LS mean (95% CI) | 1.3 (–1.0 to 3.5) | –0.5 (–2.9 to 1.8) | –1.6 (–3.2 to 0.1) | –0.6 (–2.2 to 1.1) |
LS mean difference (95% CI) | 1.8 (–1.5 to 5.0) | –1.0 (–3.4 to 1.4) | ||
P valuea | █████ | Reference | █████ | Reference |
CI = confidence interval; EORTC QLQ-30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; LS = least squares; MMRM = mixed-model for repeated measures; PRO = patient-reported outcome; QoL = quality of life; SD = standard deviation.
Note: Only patients with an evaluable baseline form were included.
Adjusted LS mean changes, P values (2-sided), and 95% CIs were obtained from an MMRM analysis of the change from baseline. The model included treatment, time and treatment by time interaction, corresponding baseline score, and the baseline score by time interaction. The difference was the values for olaparib minus placebo.
aP value was not adjusted for multiplicity.
Source: Clinical Study Report for OlympiA.18
Invasive Disease–Free Survival
At interim analysis 1 (March 27, 2020), 106 patients (11.5%) in the olaparib group and 178 patients (19.5%) in the placebo group had an IDFS event. The median IDFS was not estimable in either treatment arm, and the stratified HR for invasive disease recurrence or death was 0.58 (99.5% CI, 0.41 to 0.82; P = 0.0000073) in favour of the olaparib group. At interim analysis 2 (July 12, 2021), the stratified HR for invasive disease recurrence or death was 0.63 (95% CI, 0.50 to 0.78). The proportion of patients who remained invasive disease–free at 4 years was 82.7% (95% CI, 79.6% to 85.4%) in the olaparib group and 75.4% (95% CI, 72.2% to 78.3%) in the placebo group (difference = 7.3%; 95% CI, 3.0% to 11.5%).17 The results of prespecified sensitivity and subgroup analyses were consistent with the primary analysis.
Distant Disease–Free Survival
At interim analysis 1 (March 27, 2020), 89 patients (9.7%) in the olaparib group and 152 patients (16.6%) in the placebo group had a DDFS event. The median DDFS was not estimable in either treatment arm, and the stratified HR for distant disease recurrence or death was 0.57 (99.5% CI, 0.39 to 0.83; P = 0.0000257) in favour of the olaparib group. At interim analysis 2 (July 12, 2021), the stratified HR for distant disease recurrence or death was 0.61 (95% CI, 0.48 to 0.77). The proportion of patients who remained distant disease–free at 4 years was 86.5% (95% CI, 83.8% to 88.8%) in the olaparib group and 79.1% (95% CI, 76.0% to 81.8%) in the placebo group (difference = 7.4%; 95% CI, 3.6% to 11.3%).17 The results of prespecified sensitivity and subgroup analyses were consistent with the primary analysis.
Health-Related Quality of Life
Health-related quality of life (HRQoL) data were assessed only in the PRO analysis set using the FACIT-F or EORTC QLQ-C30 questionnaires. No strong conclusions could be drawn about the effect of olaparib compared with placebo on HRQoL due to an increased risk of type I error and a high risk of attrition bias.
Functional Assessment of Chronic Illness Therapy–Fatigue
No clinically meaningful differences were found between treatment groups in mean change in FACIT-F score at follow-up (less than the minimal important difference [MID] of 3 points). For the subgroup of patients who had previously received neoadjuvant chemotherapy (N = 727), the adjusted least squares (LS) mean difference for olaparib versus placebo was −1.3 (95% CI, −2.4 to −0.2; P = 0.024) at 6 months, and −1.5 (–2.8 to −0.2; P = 0.025) at 12 months. For the subgroup of patients who had previously received adjuvant chemotherapy (N = 778), the adjusted LS mean difference for olaparib versus placebo was −1.3 (95% CI, –2.3 to −0.2; P = 0.017) at 6 months and −1.3 (95% CI, –2.4 to 0.1; P = 0.027) at 12 months.
EORTC QLQ-C30
The adjusted LS mean difference for olaparib versus placebo in the global health status score was █ ███ █ █ █ █ ██ ██ █ █ ██ ██████) at 6 months, █ █ ██ █ █ █ █ ██ ██ █ █ ██ ███████ at 12 months, − █ ██ █ █ █ █ ██ ██ █ █ ██ ███████ at 18 months, and █ █ ██ █ █ █ █ ██ ██ █ █ █ ██ ███████ at 24 months. The adjusted LS mean difference between treatment groups in the nausea and vomiting symptom scale was 6.0 (95% CI, 4.0 to 8.0; P █ █████) at 6 months, 6.3 (95% CI, 4.4 to 8.2; █ ██████) at 12 months, 0.4 (95% CI, –1.2 to 1.9; █ ██████) at 18 months, and 1.4 (95% CI, –0.4 to 3.3; █ ███████ at 24 months. The adjusted LS mean difference between treatment groups in the diarrhea symptom scale was 0.3 (95% CI, –2.0 to 2.7; █ ███████ at 6 months, 2.0 (95% CI, –1.0 to 4.9; █ ██████) at 12 months, 1.1 (95% CI, –2.0 to 4.3; █ ██████) at 18 months, and 1.8 (95% CI, –1.5 to 5.0; █ ██████) at 24 months.
Patients Who Had Previously Received Adjuvant Chemotherapy
The adjusted LS mean difference for olaparib versus placebo in the global health status score was █ █ ██ █ █ █ █ ██ ██ █ █ █ ██ ███████ at 6 months, █ █ ██ █ █ █ █ ██ ██ █ █ █ ██ ███████ at 12 months, − █ ██ █ █ █ █ ██ ██ █ █ ██ ██████) at 18 months, and █ █ ██ █ █ █ █ ██ ██ █ █ ██ ███████ at 24 months. The adjusted LS mean difference between treatment groups in the nausea and vomiting symptom scale was 5.3 (95% CI, 3.4 to 7.2; █ ██████) at 6 months, 4.5 (95% CI, 2.8 to 6.2 █ ██ ██████ at 12 months, −0.3 (95% CI, –1.9 to 1.3; █ ██████) at 18 months, and −0.6 (95% CI, –2.5 to 1.2; █ ██████) at 24 months. The adjusted LS mean difference between treatment groups in the diarrhea symptom scale was −1.7 (95% CI, –4.1 to 0.7; █ ██████) at 6 months, 0.1 (95% CI, –2.2 to 2.4; █ ██████) at 12 months, 0.4 (95% CI, –1.9 to 2.7 █ ██ █████) at 18 months, and −1.0 (95% CI, –3.4 to 1.4; █ ██████) at 24 months.
Harms Results
A total of 836 patients (91.8%) in the olaparib group and 758 patients (83.8%) in the placebo group experienced at least 1 adverse event (AE). Common Terminology Criteria for Adverse Events (CTCAE) grade 3 to 5 AEs occurred in 24.5% of patients in the olaparib group and 11.3% of patients in the placebo group. A total of 736 patients (80.8%) in the olaparib group and 480 patients (53.1%) in the placebo group experienced at least 1 treatment-related adverse event (TRAE). The most common TRAEs occurring in the olaparib or placebo groups were anemia (20.6% and 1.7%, respectively), diarrhea (12.0% and 7.5%, respectively), decreased neutrophil count (14.9% and 4.6%, respectively), and decreased white blood cell count (14.1% and 4.5%, respectively). A total of 33 patients (33.6%) in the olaparib group and 6 patients (0.7%) in the placebo group experienced at least 1 serious TRAE. The majority of TRAEs were manageable with supportive care and/or dose modifications and consistent with the known safety profile of olaparib. There were 2 fatal AEs in the placebo group and 1 fatal AE in the olaparib group during the treatment period or within the 30-day follow-up period, as well as 2 fatal AEs in the placebo group and 1 fatal AE in the olaparib group 30 days after discontinuation.
The frequency of notable harms identified in the protocol was comparable between the treatment groups. The most commonly reported notable AE was new primary cancer (2.3% and 4.0% in the olaparib and placebo groups, respectively), followed by pneumonitis (1.0% and 1.3% in the olaparib and placebo groups, respectively), and myelodysplastic syndrome or acute myeloid leukemia (0.2% and 0.3% in the olaparib and placebo groups, respectively). No new safety concerns have been identified compared with previous trials in patients with metastatic breast cancer.
Critical Appraisal
The OlympiA trial used accepted methods for blinding, allocation concealment, and randomization with stratification. The demographic and baseline patient characteristics were generally balanced between the treatment groups, so randomization was successful. A relatively high proportion of patients prematurely discontinued the trial medication (25.6% and 20.4% in the olaparib and placebo groups, respectively); however, the clinical experts noted that this is reflective of clinical practice. Since the OlympiA trial is ongoing, the longer-term efficacy of adjuvant olaparib for IDFS, DDFS, and OS is unknown. Further, since all results are based on interim analyses, there is the potential that the benefit of olaparib relative to placebo is overestimated; however, the presence and extent of any overestimation is uncertain.20,21 All interim and subgroup analyses were prespecified in the statistical plan. Multiplicity adjustments for type I error were conducted for IDFS, DDFS, and OS according to a prespecified statistical hierarchy plan. The results were robust to a number of supportive and sensitivity analyses for the primary and key secondary outcomes. Subgroup analyses were prespecified in the OlympiA trial but may not have been powered to detect a treatment difference and there were no adjustments made for multiplicity. While improvement in quality of life was of primary importance to both patients and clinical experts, conclusions from the HRQoL assessment were limited, as no adjustments for multiplicity were made (so there is an increased risk of type I error). In addition, HRQoL was assessed using FACIT-F and EORTC QLQ-C30 questionnaires only in the PRO analysis set based on the evaluable baseline data; thus, there is a high risk of bias due to missing data, especially at later follow-up. There was a potential for unblinding of patients and investigators due to differences in the AE profile for olaparib relative to placebo. If unblinding were to occur, there would be a risk of performance and detection bias for self-reported quality of life and safety data; however, the direction and extent of any bias is uncertain.
The patient population in the OlympiA trial generally reflects patients in clinical practice in this setting. The majority of the study population was white and nonhispanic, and only 34 patients from Canada were recruited. However, the clinical experts consulted noted that although this may not be representative of the general breast cancer population, it is reflective of the population eligible for olaparib treatment, and the lack of representation of patients in Canada does not reduce the generalizability of results to Canadian clinical practice. To be enrolled in the OlympiA trial, patients were required to have completed at least 6 cycles of chemotherapy and all local therapies at least 2 weeks before randomization. The clinical experts consulted noted that olaparib would probably not be withheld if patients had previously received fewer than 6 cycles of chemotherapy for medical reasons. Patients with HR-positive, HER2-negative breast cancer were underrepresented in the OlympiA trial (17.7% with HR-positive, HER2-negative disease versus 82.3% with TNBC). The clinical experts consulted noted that these proportions are reflective of the group with hereditary breast cancer with BRCA mutations in clinical practice. Health Canada reviewers noted that due to the small number of patients with HR-positive, HER2-negative disease and lack of statistical power, the magnitude of the clinical benefit of olaparib in this subpopulation remains unclear.22 It was further indicated by the clinical experts that the criteria used in the OlympiA trial to determine a high risk of disease recurrence were reasonable, with the exception of a clinical and post-treatment pathologic stage and estrogen receptor (ER) status and histologic grade (CPS&EG) score of 3 or higher, which is not commonly used in clinical practice, although it is easily calculated. About 87.2% of patients in the OlympiA trial did not pass screening, most commonly because patients did not have a deleterious or suspected deleterious BRCA mutation in screening part 1. The clinician groups and clinical experts consulted agreed that companion diagnostic testing would be a challenge in Canada. They noted that current BRCA testing guidelines vary by province, and BRCA mutations are underdiagnosed based on most provincial testing criteria because current guidelines are restrictive in terms of eligibility criteria; thus, many patients who may carry a BRCA mutation may not receive the testing and thereby lose the opportunity to receive treatment with olaparib under current local or regional guidelines.
Indirect Comparisons
Description of Studies
To date, there have been no clinical trials directly comparing the efficacy of olaparib with other adjuvant treatments in patients diagnosed with HER2-negative, gBRCA-mutated, high-risk nonmetastatic breast cancer. The sponsor conducted a Bucher indirect treatment comparison (ITC) to address this gap.
The sponsor selected studies identified from a systematic literature review (SLR) to ensure that the population (or subpopulation), the control treatment, and the study design were aligned with those from the sponsor-conducted OlympiA trial.17 Relevant comparator interventions included adjuvant HER2-negative, high-risk breast cancer treatments publicly reimbursed in Canada. A feasibility assessment was then conducted to assess homogeneity between included studies and determine the appropriateness of inclusion in an ITC. The sponsor identified 1 randomized controlled trial (RCT), CIBOMA,19 that was feasible to be included in the ITC along with the sponsor-conducted OlympiA trial. The OlympiA trial was a phase III, double-blind RCT comparing olaparib with placebo in patients who were diagnosed with HER2-negative, gBRCA-mutated, high-risk early breast cancer and had received local treatment and neoadjuvant or adjuvant chemotherapy. The CIBOMA trial was a phase III, open-label RCT that compared capecitabine with observation in patients with TNBC who had been treated with neoadjuvant or adjuvant chemotherapy. Unlike the OlympiA trial, the CIBOMA trial did not require the participants to have confirmed gBRCA mutations. The median duration of follow-up was 2.5 years for the OlympiA trial and more than 7 years for the CIBOMA trial (interquartile range not reported).
The sponsor adopted the Bucher method to perform the ITC. The clinical end points included 3-year IDFS or disease-free survival (DFS) and OS. The risk of bias in the included studies was assessed independently by 2 reviewers using the checklist of the National Institute for Health and Care Excellence single technology appraisal user guide.23
Efficacy Results
The Bucher ITC compared olaparib versus capecitabine via the common comparator — placebo or observation — and estimated the HRs for IDFS or DFS and OS in patients with TNBC from the OlympiA and CIBOMA trials. No conclusions could be drawn about the efficacy of olaparib compared with capecitabine due to imprecision in the effect estimates (i.e., wide 95% CIs, including HR = 1).
No analysis of harms was reported in the sponsor-submitted ITC report.
Critical Appraisal
The SLR used to identify relevant studies was methodologically sound in terms of the sponsor using a comprehensive literature search strategy as well as performing study selection, data extraction, and risk-of-bias assessment in duplicate. However, it was unclear in the ITC report whether the feasibility assessment was carried out by a single or multiple assessors. Moreover, although the risk of bias in individual studies was assessed in the SLR, the assessment results were not incorporated and discussed in the ITC report. The sponsor conducted the ITC, based on the Bucher method,20 to estimate the relative treatment efficacy of olaparib against capecitabine. The Bucher method assumes that the trials included in the ITC should be sufficiently similar with respect to study population, study design, outcome measurements, and the distribution of treatment effect modifiers. The ITC has some limitations that reduce the CADTH team’s confidence in the effect estimates. There were notable differences across the 2 trials in the patient baseline demographics and disease characteristics (e.g., unknown BRCA mutation status in the CIBOMA trial) and trial design (e.g., double blind versus open label, outcome definitions) that might threaten the plausibility of the assumptions of the Bucher method. In addition, safety outcomes were not analyzed in the ITC report and no justification was provided, which precludes a balanced judgment of comparative benefits relative to comparative harms. Other outcomes that are important to patients, such as symptoms and HRQoL, were not investigated. Finally, the ITC was performed only in patients with TNBC, which only aligned with a part of the indication population specified in the sponsor’s application; therefore, the results may not be generalizable to all patients who meet the criteria in the reimbursement request.
Other Relevant Evidence
No other relevant evidence was submitted by the sponsor or identified from the literature.
Conclusions
Based on data from the OlympiA trial, olaparib demonstrated a clinically meaningful and statistically significant benefit compared with placebo in improving IDFS, DDFS, and OS in adult patients with HER2-negative, high-risk early breast cancer. The median IDFS, OS, and DDFS were not estimable in either treatment group because insufficient follow-up time had elapsed for these outcomes; thus, the longer-term efficacy of adjuvant olaparib is unknown. In addition, the estimates of the benefit of olaparib may be overestimated because the results are from interim analyses, although the presence and extent of any overestimation is uncertain. However, olaparib could help optimize adjuvant treatment in patients with BRCA-mutated early breast cancer to improve outcomes in terms of disease recurrence and survival, given its acceptable and manageable safety profile. The safety profile of olaparib was consistent with the known adverse effects profile of olaparib, and no new safety signals were identified. Strong conclusions could not be drawn related to the effect of olaparib on HRQoL due to the high risk of attrition bias and increased risk of type I error in the analyses of these outcomes. The evidence of olaparib was limited to 1 placebo-controlled pivotal trial, and no direct evidence of olaparib compared against other comparators was available for this review, most likely because the current systemic treatment of early breast cancer does not consider the patient’s BRCA mutation status. Uncertainties remain regarding the availability of BRCA mutation testing in Canada for clinical implementation in determining patient eligibility for olaparib treatment. No conclusions could be drawn from the ITC about the effect of olaparib relative to capecitabine on IDFS, DFS, or OS due to methodological limitations and imprecision in the effect estimates (wide 95% CIs, including HR = 1).
Introduction
Disease Background
Breast cancer is the most commonly diagnosed cancer among women in Canada, and the second most common cancer in men and women combined.1 In 2020, 27,700 women were diagnosed with breast cancer, representing about 25% of new cancer cases in Canada.1 Breast cancer is the second leading cause of cancer deaths among women, accounting for 14% of all cancer deaths.1 It is estimated that about 1 in 8 women in Canada (12%) will develop breast cancer during their lifetime, and about 38% of cases will be diagnosed in females aged 30 to 59 years.1 The 5-year net survival for breast cancer is more than 85% among women diagnosed before 85 years of age, after which it drops to about 73%.1 In men, the incidence of breast cancer is less than 1% per year, with 260 new cases diagnosed in 2021 in Canada.1 Breast cancer risk is influenced by several factors including age, family history, reproductive status (e.g., late menopause), birth control use, hormone exposures (e.g., estrogen), menopausal hormone therapy, inherited gene changes, race, and lifestyle factors, such as alcohol intake and physical inactivity.1,24 More than 90% of patients with breast cancer are diagnosed with early-stage disease, which is defined as not having spread beyond the breast tissue or that has spread to the axillary lymph nodes only. Early breast cancer includes ductal carcinoma in situ (stage 0) and stages I to IIIA but may also include invasive cancers within stages I to IIIC, excluding stage 0.1,25,26
Breast cancer susceptibility genes (BRCA1 and BRCA2) are human genes that produce proteins responsible for repairing damaged DNA through homologous recombination of DNA replication forks and double strand breaks, and play an important role in maintaining the genetic stability of cells.2,3 Germline mutations in 1 or both BRCA genes reduce gene expression, which can lead to uncontrolled cell growth and is associated with an increased risk of cancer, including breast cancer.4-6 Hereditary deleterious mutations contribute to 5% to 10% of all breast cancers, and 60% to 68% of these hereditary cancers occur in individuals with gBRCA mutations.4,7 The BRCA mutations occur in women with all subtypes of breast cancer, but more commonly in those with early onset or a family history of breast cancer.9 Approximately 2.5% of Ashkenazi Jewish women carry 1 of 3 founding mutations in the BRCA1 and BRCA2 genes, which are associated with a high lifetime risk of invasive breast cancer.27
Patients with breast cancer who inherit a harmful variant in the BRCA1 or BRCA2 genes have worse survival outcomes than those without BRCA mutations.28 In women harbouring a BRCA1 mutation, the estimated lifetime risk of developing breast cancer by the age of 80 years is 65% to 80%, and the 10-year actuarial risk of developing contralateral breast cancer is 25% to 31%.8,9 The estimated lifetime risk of developing breast cancer among women with a BRCA2 mutation is approximately 76%, while among men with BRCA1 or BRCA2 mutations, it ranges from 3% to 8%.8-10 Approximately 75% of patients with breast cancer who have a mutation in the BRCA1 gene are classified as having TNBC, which is distinguished by the absence of a hormone receptor (HR-negative), and no expression of HER2 (HER2-negative).11-13 More than 50% of patients with early-stage TNBC are bound to experience recurrence, of which 37% will die in the first 5 years after surgery.29 In contrast, patients with breast cancer carrying mutations in the BRCA2 gene are more likely to be positive for expression of the hormone receptor (HR-positive), and only approximately 20% have TNBC.13 Although many patients with HR-positive, HER2-negative disease will not experience recurrence or have distant recurrence with standard therapies alone, around 7% to 11% of patients with early breast cancer will experience a local recurrence during the first 5 years after treatment.30
The diagnosis of breast cancer is based on clinical examination in combination with imaging and is confirmed by pathological evaluation.9 Clinical examination includes bimanual palpation of the breasts and regional lymph nodes and assessment for distant metastases, while imaging includes bilateral mammography or ultrasound of the breast and regional lymph nodes. Pathological diagnosis should be based on a core needle biopsy. It also includes presence or absence of ductal carcinoma in situ, the histological type and grade, HER2 expression or HER2 gene amplification, and immunohistochemistry evaluation of progesterone receptor (PgR) or ER status.9 Genetic counselling and testing for a BRCA mutation are offered to patients with breast cancer in high-risk groups, including those with a strong family history of cancer, a diagnosis of breast cancer before the age of 50, and a recent or past history of ovarian or second breast cancer.9 Testing for gBRCA mutations involves blood or saliva tests.4 In addition, a small percentage of BRCA-related cancers contain purely somatic mutations that can be detected through direct analysis of the tumour tissue or circulating cell-free DNA.10
Standards of Therapy
The following section is based on input from the clinical experts and clinician groups consulted by CADTH for this review. The clinical experts and clinician groups consulted indicated that olaparib would be prescribed for the adjuvant treatment of adult patients with gBRCA-mutated, HER2-negative, high-risk early-stage breast cancer for 1 year after completion of adjuvant or neoadjuvant chemotherapy, and local therapy. Both the clinical experts and clinician groups agreed that the current systemic treatment for breast cancer does not consider the patient’s BRCA gene mutation status, as there is no treatment specific to mutation status. The clinical experts consulted indicated that, depending on the stage of the disease, most patients with high-risk early breast cancer start treatment with neoadjuvant therapy, such as chemotherapy (doxorubicin-cyclophosphamide plus paclitaxel [AC-T] or 5-fluorouracil-epirubicin-cyclophosphamide plus docetaxel [FEC-D]), followed by adjuvant therapy, depending on residual disease burden and tumour receptors (ER- or PgR-positive, or triple-negative). Both the clinical experts and clinician groups noted that clinicians currently use pembrolizumab therapy in combination with chemotherapy in the neoadjuvant setting followed by adjuvant pembrolizumab therapy for the treatment of patients with TNBC. They also noted that sometimes capecitabine can be used to treat patients with TNBC who have residual disease. The clinical experts consulted indicated that for the treatment of patients with HR-positive, HER2-negative breast cancer, clinicians currently use adjuvant endocrine therapy with or without abemaciclib, depending on whether patients meet monarchE trial criteria. The clinical experts highlighted that it remains unclear how adjuvant olaparib will be integrated into the treatment of HR-positive, HER2-negative breast cancer along with abemaciclib, as well as into the treatment of early TNBC along with pembrolizumab and capecitabine, as there are no clinical data to directly compare the efficacy and safety of these therapies for treating patients with a BRCA mutation. The clinical experts indicated the goal of therapy is to eradicate disease and prevent metastatic spread, resulting in cure.
Preferred treatment options outlined in the National Comprehensive Cancer Network,31 the St. Gallen International Consensus Guidelines,7 and the American Society of Clinical Oncology Hereditary Breast Cancer Guideline32 for patients with HER2-negative, early-stage (II or III) breast cancer with a high risk of recurrence and BRCA1 or BRCA2 mutations include olaparib or talazoparib therapy, irrespective of hormone receptor status.
Drug
Olaparib is a selective inhibitor of human PARP enzymes (PARP1, PARP2, and PARP3) involved in normal cellular functions, such as DNA transcription and DNA repair. It has been shown that olaparib blocks base excision repair by trapping PARP at the site of DNA damage, leading to the collapse of DNA replication forks and the accumulation of DNA double-stranded breaks. Thus, PARP inhibition has been identified as a targeted therapy that may exploit intrinsic defects in numerous cancer cells and has been reported to have selective cytotoxicity in breast cancer with mutations in the BRCA1 and/or BRCA2 genes.14
Olaparib underwent a priority review at Health Canada and obtained a Notice of Compliance with conditions on July 27, 2022, for the adjuvant treatment of adult patients with deleterious or suspected deleterious gBRCA-mutated, HER2-negative high-risk early breast cancer who have been treated with neoadjuvant or adjuvant chemotherapy. Patients must have confirmation of a gBRCAm before olaparib treatment is initiated.14 The sponsor’s requested reimbursement criteria for olaparib are aligned with the Health Canada–approved indication.33 Olaparib is the first and only PARP inhibitor approved for the adjuvant treatment of gBRCA-mutated high-risk stage breast cancer in Canada. Olaparib is available as a 100 mg or 150 mg tablet. The Health Canada–recommended total daily dose of olaparib is 600 mg, taken as 2 150 mg tablets twice daily for a total of 1 year or until disease recurrence or unacceptable toxicity, whichever occurs first.14 The recommended reduced total daily dose of olaparib for the management of AEs is 500 mg. If a further dose reduction is required, the recommended reduced total daily dose of olaparib is 400 mg.14 Patients with HR-positive breast cancer should continue concurrent treatment with endocrine therapy as per current clinical practice guidelines.14
Olaparib has been previously approved by Health Canada and reviewed by CADTH for use as monotherapy for the maintenance treatment of adult patients with newly diagnosed advanced BRCA-mutated high-grade epithelial ovarian, fallopian tube, or primary peritoneal cancer who are in response (complete response or partial response) to first-line platinum-based chemotherapy until disease progression or up to 2 years if there is no evidence of disease.16 Olaparib has been reviewed for use as monotherapy maintenance treatment of adult patients with platinum-sensitive relapsed BRCA-mutated epithelial ovarian, fallopian tube, or primary peritoneal cancer who are in response to platinum-based chemotherapy.34 Olaparib has also been reviewed for use as monotherapy for the treatment of adult patients with metastatic castration-resistant prostate cancer and deleterious or suspected deleterious germline and/or somatic mutations in the homologous recombination repair genes (BRCA1, BRCA2, and ATM) who have progressed following prior treatment with a new hormonal drug.35
Key characteristics of commonly used medical treatments for early breast cancer are presented in Table 4.
Table 4: Key Characteristics of Pharmacotherapies for Early-Stage Breast Cancer
Detail | Olaparib | Abemaciclib | Pembrolizumab | Capecitabinea |
|---|---|---|---|---|
Mechanism of action | Selective inhibitor of human PARP enzymes (PARP1, PARP2, and PARP3). It blocks base excision repair by trapping PARP enzymes at the site of DNA damage, leading to the collapse of DNA replication forks and the accumulation of DNA double-stranded breaks. | Selective and potent ATP-competitive inhibitor of CDK4 and CDK6 and blocking Rb protein phosphorylation, preventing cancer cell proliferation by arresting the cell cycle in the G1 phase, thereby suppressing DNA synthesis and inhibiting cancer cell growth. | High-affinity antibody against PD-1, which exerts dual ligand blockade of the PD-1 pathway, including PD-L1 and PD-L2, on antigen-presenting or tumour cells. By inhibiting the PD-1 receptor from binding to its ligands, pembrolizumab reactivates tumour-specific cytotoxic T lymphocytes in the tumour microenvironment. | Antimetabolite belonging to the fluoropyrimidine carbamate class. The cytotoxic effect of capecitabine is produced by inhibiting thymidylate formation, essential for DNA synthesis, and inhibiting RNA and protein synthesis. |
Indicationb | For the adjuvant treatment of adult patients with deleterious or suspected deleterious gBRCAm, HER2-negative high-risk early breast cancer who have been treated with neoadjuvant or adjuvant chemotherapy. Patients must have confirmation of a gBRCAm before olaparib treatment is initiated. | In combination with endocrine therapy for the adjuvant treatment of adult patients with HR-positive, HER2-negative, node-positive, early breast cancer at high risk of disease recurrence based on clinicopathological features and a Ki-67 score ≥ 20%. | For the treatment of adult patients with high-risk early-stage triple-negative breast cancer in combination with chemotherapy as neoadjuvant treatment, and then continued as monotherapy as adjuvant treatment after surgery. | For the treatment of advanced or metastatic breast cancer after failure of standard therapy (including a taxane unless therapy with a taxane is clinically contraindicated as monotherapy). In combination with docetaxel for advanced or metastatic breast cancer after failure of anthracycline-containing chemotherapy. |
Route of administration | Oral | Oral | IV | Oral |
Recommended dose | 600 mg, taken as two 150 mg tablets twice daily | In combination with ET, 150 mg twice daily | 200 mg IV fixed dose every 3 weeks | 1,250 mg/m2 administered twice daily for 14 days followed by a 7-day rest period |
Serious adverse effects or safety issues | Hematological toxicity: Anemia was the most common adverse reaction. Other reactions included MDS or AML as well as pneumonitis, venous thromboembolic events, and gastrointestinal disorders (nausea, vomiting, diarrhea) and fatigue or asthenia | Nonhematological toxicities, including interstitial lung disease or pneumonitis, diarrhea, increased aminotransferases, neutropenia, infections, venous thromboembolism, and second malignancy | Immune-mediated adverse reactions such as endocrinopathies nephritis and renal dysfunction, hepatitis, colitis, pneumonitis, severe skin reactions, thyroid disorders, type 1 diabetes mellitus, hypophysis, and adrenal insufficiency | Gastrointestinal disorders, thromboembolic events, hepatic failure, acute renal failure, immune-mediated adverse reactions such as angioedema, cutaneous lupus erythematosus, and toxic leukoencephalopathy |
AML = acute myeloid leukemia; ATP = adenosine triphosphate; BRCA = breast cancer susceptibility gene; CDK = cyclin-dependent kinase; ET = endocrine therapy; gBRCAm = germline BRCA mutation; HER2 = human epidermal growth factor receptor 2; HR-positive = positive for expression of a hormone receptor; MDS = myelodysplastic syndrome; PARP = poly-(ADP-ribose) polymerase; PD-1 = programmed cell death 1 protein; PD-L1 = programmed cell death 1 ligand 1; PD-L2 = programmed cell death 1 ligand 2; Rb = retinoblastoma; RNA = ribonucleic acid.
aCapecitabine may be used off-label for patients with triple-negative breast cancer.
bHealth Canada–approved indication.
Source: Product monographs for Lynparza14 Verzenio,36 Keytruda,37 and Xeloda.38
Stakeholder Perspectives
Patient Group Input
This section was prepared by CADTH staff based on the input provided by patient groups. The full original patient input(s) received by CADTH have been included in the stakeholder section at the end of this report.
Two patient groups, the CBCN and Rethink Breast Cancer (Rethink) provided input for this review. CBCN is a national health charity aiming to ensure the best quality of care for all Canadians affected by breast cancer. The CBCN patient input was based on an online survey (the CBCN’s 2017 Lived Experience Breast Cancer Patient Survey) of 6 patients with gBRCA-mutated early breast cancer, and a literature review of current studies and grey literature. Rethink is a Canadian charity with a focus on improving the experience and outcomes of patients with breast cancer. Rethink gathered information for this review from general observations and insights through various ongoing initiatives (including stories shared by patients, virtual support groups, working groups, and patient advisory boards), in-depth telephone interviews with 3 patients with a BRCA-mutated breast cancer who participated in the OlympiA study, as well as responses from people in the Rethink Instagram community with high-risk early breast cancer.
According to the patient input received from Rethink, BRCA-mutated breast cancer is more likely to be detected in people at a young age. These young patients can face several age-specific issues such as fertility or family-planning challenges, diagnosis during pregnancy, childcare, impact on relationships, body image, dating and sexuality, feeling isolated from peers who do not have cancer, career hiatuses, and financial insecurity. Moreover, they may suffer a physical and emotional toll, as being diagnosed with a BRCA-mutated breast cancer at a young age may require making treatment-related decisions such as double mastectomy, oophorectomy, hysterectomy, egg or embryo preservation, and even decisions such as possible genetic screening of embryos.
The survey conducted by CBCN identified several key factors influencing patient decision-making about currently available treatment options. These factors included effectiveness of the treatment (i.e., how well the treatment could help stabilize disease and delay recurrence), prolonging life without sacrificing quality of life (i.e., how well the treatment could help the patient maintain a productive, active life with minimal disruption to daily routines), risk of side effects, and the cost and accessibility of treatments. The Rethink input revealed that patient respondents, especially those with stage III breast cancer, tended to endure side effects as well as impacts on quality of life to achieve satisfactory effectiveness. In terms of experience with olaparib, none of the 3 patients from the Rethink group who had participated in the OlympiA study who had not had a recurrence mentioned unendurable side effects. Four of the 6 (66%) CBCN survey respondents with inherited BRCA mutations indicated they received chemotherapy and 2 (33%) received radiation therapy as part of their overall breast cancer treatment. None of the CBCN survey respondents reported having experience with olaparib treatment. Both patient groups expressed high interest in olaparib, as they had high hopes that it would bring benefits, from extension of progression-free disease to avoidance of metastasis.
Clinician Input
Input From the Clinical Experts Consulted by CADTH
All CADTH review teams include at least 1 clinical specialist with expertise regarding the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). The following input was provided by 2 clinical specialists with expertise in the diagnosis and management of breast cancer.
Unmet Needs
The clinical experts consulted by CADTH indicated that most patients with BRCA mutations have TNBC and, accordingly, different mechanisms of disease development due to their mutation status, which is not targeted by current treatment options. They also noted that not all patients respond to current treatments; therefore, there is a need for new therapeutic options to improve survival outcomes and increase the overall cure rate in patients with BRCA-mutated breast cancer.
Place in Therapy
The clinical experts agreed that current systemic treatment of breast cancer is based on the receptor status and pathological findings and considers the patient’s BRCA mutation status. According to the clinical experts, as the mechanism of action of olaparib is complementary, patients should still pursue appropriate neoadjuvant and adjuvant therapies as per their pathology and stage; however, olaparib would be an additional drug that would be recommended. The clinical experts indicated that olaparib would be used as adjuvant therapy for 1 year in patients with BRCA mutations who meet the OlympiA trial inclusion criteria, regardless of tolerance to prior therapies. The clinical experts agreed that it remains unclear how different drugs would be prioritized if tolerance became an issue to multiple drugs; it is likely that the drug most likely to cause toxicity will be stopped (i.e., in the case of severe hot flashes or vaginal dryness, endocrine therapy would be modified). They also highlighted that it remains unclear how to integrate olaparib into the current treatment paradigm with other drugs, such as capecitabine, pembrolizumab, abemaciclib, or a combination of drugs in the treatment of patients with breast cancer who have a BRCA mutation. The clinical experts consulted indicated that this is a change in practice for patients who carry the BRCA mutation and that a shift in the treatment paradigm would occur, as this is the new standard-of-care therapy in these patients.
Patient Population
The clinical experts consulted by CADTH agreed that patients who meet the inclusion criteria outlined in the OlympiA trial will be best suited for treatment with olaparib (i.e., patients who have a germline BRCA1 or BRCA2 pathogenic or likely pathogenic variant; have high-risk, HER2-negative primary breast cancer who have completed at least 6 cycles of neoadjuvant or adjuvant chemotherapy containing anthracyclines, taxanes, or both drugs; and completed all local therapy, including radiotherapy at least 2 weeks and not more than 12 weeks before trial entry). The clinical experts noted that adjuvant bisphosphonates in postmenopausal patients and endocrine therapy for HR-positive breast cancer are allowed; however, no chemotherapy is allowed after surgery in patients who received neoadjuvant chemotherapy. The clinical experts consulted mentioned that companion diagnostic testing would be a challenge, especially as clinicians would request BRCA mutation testing for patients who do not qualify for genetic testing based on provincial guidelines (i.e., patients who have a low likelihood of hereditary syndromes) but who meet the criteria for adjuvant olaparib in the presence of a BRCA mutation. The clinical experts indicated that current genetic testing guidelines vary by province, and BRCA mutations are underdiagnosed based on most provincial testing criteria. In addition, there are concerns that BRCA mutation testing may not happen fast enough; therefore, increased access to genetic testing and reduced turnaround times will likely be necessary.
Assessing Response to Treatment
The clinical experts consulted noted that since the current indication is for the adjuvant setting, treatment response cannot be assessed. They agreed that improved long-term survival is the important outcome at a population level. It was further noted by the clinical experts that by improving survival and reducing disease recurrence, patients who are cured will have a higher quality and quantity of life. The goal of therapy is to eradicate disease and prevent metastatic spread, resulting in cure.
Discontinuing Treatment
According to the clinical experts consulted, toxicity from treatment with olaparib and disease recurrence would be the main factors to consider when deciding to discontinue treatment with olaparib.
Prescribing Conditions
The clinical experts consulted agreed that olaparib should be prescribed in a standard outpatient medical oncology clinic (i.e., in a community hospital or tertiary setting) by medical oncologists and general practitioners in oncology who have medical oncology training. The clinical experts also noted that ideally, pharmacists with expertise in oncology drugs should be utilized; however, outpatient retail pharmacies will also be able to access and dispense this drug in certain jurisdictions, as it is an oral drug.
Clinician Group Input
This section was prepared by CADTH staff based on the input provided by clinician groups. The full original clinician group input received by CADTH has been included in the stakeholder section at the end of this report.
Clinician group input was obtained from 2 clinician groups, including the OH-CCO Breast Cancer Drug Advisory Committee (1 clinician provided input) and a group of medical oncologists across Canada (4 clinicians provided input). The medical oncologist group stated that no therapy other than surgical treatment has been adopted specifically for patients with BRCA mutation–associated tumours, which are often more aggressive. Both clinician groups identified that the important goal of treatment for early breast cancer, including gBRCA-mutated early breast cancer, is to decrease the recurrence of cancer and improve survival.
Both clinician groups agreed that patients must have confirmation of a gBRCA mutation before receiving olaparib. The medical oncologist group highlighted the increasing demand and workload for germline mutation testing. One potential barrier, which was mentioned by the OH-CCO Breast Cancer Drug Advisory Committee, is that the current guidelines for BRCA mutation testing are restrictive, so patients who may carry a BRCA mutation may not receive the testing and thereby lose the opportunity to receive olaparib. It was further noted by the clinician groups consulted that timely BRCA testing will be needed to ensure patients and clinicians have access to the results to initiate treatment with olaparib.
To assess treatment response, the OH-CCO Breast Cancer Drug Advisory Committee indicated that standard cancer care follow-up without diagnostic imaging will suffice unless patients show signs or symptoms suggestive of recurrent or progressive disease; in such cases, radiographic imaging or biopsy may be conducted. Both clinician groups pointed out several reasons that may lead to the discontinuation of olaparib, including recurrence or progression of disease, intolerant toxicity or severe side effects, and patient or physician preference.
Drug Program Input
The drug programs provide input on each drug reviewed through CADTH’s reimbursement review processes by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CADTH are summarized in Table 5.
Table 5: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Relevant comparators | |
No issues were identified, as OlympiA was a placebo-controlled trial. | No response required. For pERC consideration. |
Considerations for initiation of therapy | |
Disease diagnosis, scoring, or staging for eligibility: What are the criteria for defining “high risk” for eligibility (e.g., clinical or pathologic stage, receptor status, nuclear grade)? | Most clinicians would use the criteria used to define high-risk groups in the OlympiA trial:
According to the OlympiA trial, those with HER2-positive cancer would not be offered olaparib. |
Prior therapies required for eligibility: Is there a minimum number of chemotherapy cycles that should be completed for eligibility? | While at least 6 cycles of chemotherapy had to be used in the trial, in real practice, there might be situations where chemotherapy was stopped early (e.g., due to toxicity) and patients who had 4 to 5 cycles may still be offered olaparib. |
Considerations for discontinuation of therapy | |
Treatment interruptions: Should olaparib be restarted if there was a prolonged treatment break? | It depends on the reason. If the reason for the prolonged break is not a toxicity, it is reasonable to wait longer than 4 to 6 weeks. In practice, with other drugs, most clinicians do not restart treatment if a 2-month or longer break is needed in the adjuvant or neoadjuvant setting. |
Considerations for prescribing of therapy | |
Recommended dose is 600 mg daily, taken as 2 × 150 mg tablets twice daily. There are 100 mg tablets for dose reductions if needed. This is for 1 year or until disease recurrence, whichever occurs first. Oral tablet for administration. | No response required. For pERC consideration. |
Concerns related to combination usage: Would olaparib ever be prescribed in combination with capecitabine and/or pembrolizumab for TNBC? | There are reasonably convincing safety data on olaparib in combination with pembrolizumab for other disease sites, and fewer data on the safety of the combination of olaparib and capecitabine. However, there are no efficacy data for these combinations in early breast cancer. Given the lack of good options and significant mortality if metastases develop, it is possible that in some situations clinicians will prescribe olaparib in combination with other drugs, such as pembrolizumab. However, it is unlikely that olaparib will be combined with capecitabine, or capecitabine combined with pembrolizumab. |
Generalizability | |
Patients on active treatment with a time-limited opportunity to switch to the drug(s) under review: Is there a time-limited need to add olaparib for up to 1 year for any patients who otherwise meet the listing (reimbursement) criteria and who have not progressed on treated with neoadjuvant or adjuvant chemotherapy? | There may be situations where some high-risk patients will start treatment beyond the 12-week window used in the trial; these patients would include legacy patients. |
Care provision issues | |
Patients must have confirmation of a germline BRCA mutation before Olaparib treatment can start. | No response required. For pERC consideration. |
BRCA = breast cancer susceptibility gene; CPS&EG = clinical and post-treatment pathologic stage and estrogen receptor status and histologic grade; HER2 = human epidermal growth factor receptor 2; HR-positive = positive for expression of a hormone receptor; pCR = pathological complete response; pERC = CADTH pan-Canadian Oncology Drug Review Expert Review Committee; TNBC = triple-negative breast cancer.
Clinical Evidence
The clinical evidence included in the review of olaparib is presented in 3 sections. The first section, the systematic review, includes pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those studies that were selected according to an a priori protocol. The second section includes indirect evidence from the sponsor and indirect evidence selected from the literature that met the selection criteria specified in the review. The third section includes sponsor-submitted long-term extension studies and additional relevant studies that were considered to address important gaps in the evidence included in the systematic review.
Systematic Review (Pivotal and Protocol Selected Studies)
Objectives
To perform a systematic review of the beneficial and harmful effects of olaparib, 300 mg (2 × 150 mg tablets) twice daily for the adjuvant treatment of adult patients with deleterious or suspected deleterious gBRCA-mutated, HER2-negative, high-risk early breast cancer who have been treated with neoadjuvant or adjuvant chemotherapy.
Methods
Studies selected for inclusion in the systematic review include pivotal studies provided in the sponsor’s submission to CADTH and Health Canada as well as those meeting the selection criteria presented in Table 6. The outcomes included in the CADTH review protocol reflect outcomes considered to be important to patients, clinicians, and drug plans.
Table 6: Inclusion Criteria for the Systematic Review
Criteria | Description |
|---|---|
Population | Adult patients with deleterious or suspected deleterious gBRCA-mutated, HER2-negative, high-risk early breast cancer who have been treated with neoadjuvant or adjuvant chemotherapy. Subgroups of interest:
|
Intervention | Olaparib at 600 mg, taken as 2 × 150 mg tablets twice daily for 1 year or until disease recurrence or unacceptable toxicity, whichever occurs first. The 100 mg tablet is available for dose reduction. |
Comparator |
|
Outcomes | Efficacy outcomes:
Harms outcomes:
Notable harms and harms of special interest:
|
Study designs | Published and unpublished phase III and IV RCTs |
AML = acute myeloid leukemia; CPS&EG = clinical and post-treatment pathologic stage and estrogen receptor status and histologic grade; ET = endocrine treatment; gBRCA = germline breast cancer susceptibility gene; gBRCAm = germline BRCA mutation; HER2 = human epidermal growth factor receptor 2; HR-positive = positive for expression of a hormone receptor; HRQoL = health-related quality of life; MDS = myelodysplastic syndrome; RCT = randomized controlled trial; TNBC = triple-negative breast cancer.
aMay be used off-label for the treatment of patients with triple-negative breast cancer.
bNot funded in Canada; however, considered relevant by clinicians.
The literature search for clinical studies was performed by an information specialist using a peer-reviewed search strategy according to the PRESS Peer Review of Electronic Search Strategies checklist.39
Two CADTH clinical reviewers independently selected studies for inclusion in the review based on titles and abstracts, according to the predetermined protocol. Full-text articles of all citations considered potentially relevant by at least 1 reviewer were acquired. Reviewers independently made the final selection of studies to be included in the review, and differences were resolved through discussion.
Published literature was identified by searching the following bibliographic databases: MEDLINE All (1946–) through Ovid and Embase (1974–) through Ovid. All Ovid searches were run simultaneously as a multifile search. Duplicates were removed using Ovid deduplication for multifile searches followed by manual deduplication in Endnote. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were Lynparza (olaparib) and breast cancer. Clinical trials registries were searched: the US National Institutes of Health’s clinicaltrials.gov, the WHO’s International Clinical Trials Registry Platform (ICTRP) search portal, Health Canada’s Clinical Trials Database, and the European Union Clinical Trials Register.
CADTH-developed search filters were applied to limit retrieval to RCTs or controlled clinical trials. Retrieval was not limited by publication date or by language. Conference abstracts were excluded from the search results. See Appendix 1 for the detailed search strategies.
The initial search was completed on August 31, 2022. Regular alerts updated the search until the meeting of the CADTH pan-Canadian Oncology Drug Review Expert Committee (pERC) on January 11, 2023.
Grey literature (literature that is not commercially published) was identified by searching relevant websites from the Grey Matters: A Practical Tool For Searching Health-Related Grey Literature checklist.39 Included in this search were the websites of regulatory agencies (FDA and European Medicines Agency). Google was used to search for additional internet-based materials. See Appendix 1 for more information on the grey literature search strategy. A focused literature search for network meta-analyses dealing with olaparib or breast cancer was run in MEDLINE All (1946–) on August 26, 2022. No search limits were applied.
These searches were supplemented by reviewing bibliographies of key papers. In addition, the sponsor of the drug was contacted for information regarding unpublished studies.
Findings From the Literature
A total of 4 reports17-19,40 of 1 study were identified from the literature for inclusion in the systematic review (Figure 1). The included studies are summarized in Table 7. A list of excluded studies is presented in Appendix 2.
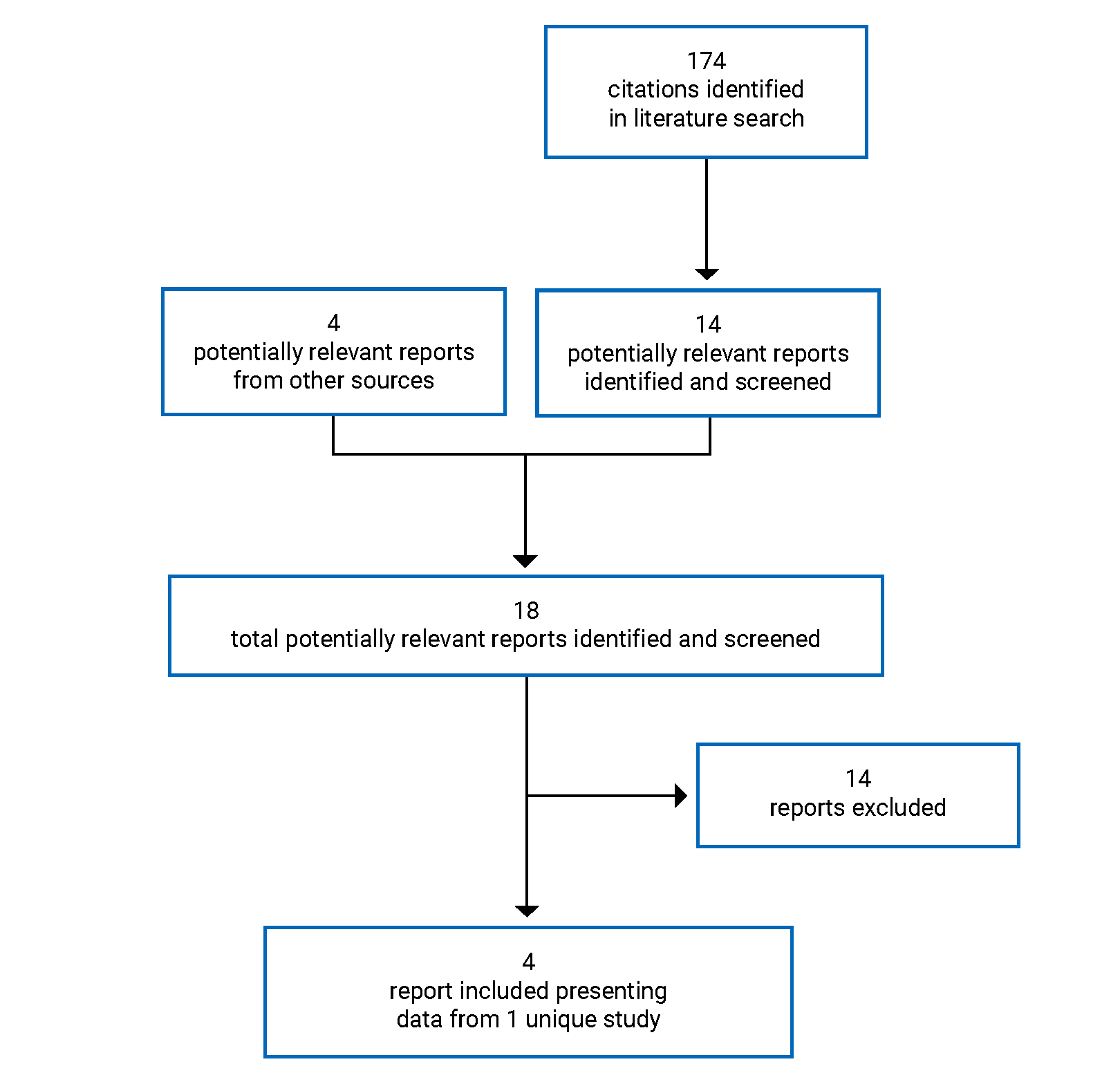
Table 7: Details of the OlympiA Study
Detail | OlympiA |
|---|---|
Designs and populations | |
Study design | Multicentre, randomized, double-blind, placebo-controlled, phase III trial |
Locations | Patients enrolled across 546 sites in 23 countries worldwide (comprising 211 sites in the US and 335 sites in the rest of the world) |
Patient enrolment dates | From April 22, 2014, to April 17, 2019 |
Data cut-off dates | The OlympiA trial is ongoing:
|
Randomized (N) | 1,836 patients |
Inclusion criteria | ≥ 18 years of age For patients who underwent initial surgery and received adjuvant chemotherapy:
For patients who underwent neoadjuvant chemotherapy followed by surgery:
Histologically confirmed nonmetastatic primary invasive adenocarcinoma of the breast that was 1 of the 2 following phenotypes:
Documented germline mutation in BRCA1 or BRCA2 that was predicted to be deleterious or suspected to be deleteriousc Completed adequate breast surgery Completed adequate axilla surgery defined as the following:
Completed at least 6 cycles of neoadjuvant or adjuvant chemotherapy containing anthracyclines, taxanes, or a combination of both Patients must have had adequate organ and bone marrow function measured within 28 days before randomization with no blood transfusions in the past 28 days before testing for organ and bone marrow function Serum or plasma creatinine ≤ 1.5 × ULN ECOG Performance Status of 0 or 1 Patient should be randomized to the study ideally within a maximum of 8 weeks after the completion of the last treatment, including surgery, chemotherapy, or radiation therapy, but in no case longer than 12 weeks |
Exclusion criteria |
|
Drugs | |
Intervention | Olaparib 300 mg tablets orally (2 × 150 mg tablets), twice daily |
Comparator(s) | Matching placebo tablets orally (2 tablets), twice daily |
Duration | |
Phase | |
Screening part 1 | Any time before, during, or after neoadjuvant or adjuvant chemotherapy or radiotherapyh |
Screening part 2 | Within 28 days before randomizationi |
Double blind | 12 months |
Safety follow-upj | 30 days after the last dose of study medication |
Efficacy follow-upk | Approximately 10 years |
Survival follow-upl | Until 10 years after the last patient was randomized |
Outcomes | |
Primary end point | IDFSm |
Secondary and exploratory end points | Secondary:
Exploratory:
Safety:
|
Notes | |
Publications | Tutt et al.40 Geyer et al.17 |
AE = adverse event; BGI = Beijing Genomics Institute; BRCA = breast cancer susceptibility gene; CPS&EG = clinical and post-treatment pathologic stage and estrogen receptor status and histologic grade; CTCAE = Common Terminology Criteria for Adverse Events; DCIS = ductal carcinoma in situ; DDFS = distant disease–free survival; ECG = electrocardiogram; ECOG = Eastern Cooperative Oncology Group; ER = estrogen receptor; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; FACIT-F = Functional Assessment of Chronic Illness Therapy–Fatigue; gBRCA = germline breast cancer susceptibility gene; gBRCA1 = germline BRCA1 gene; gBRCA2 = germline BRCA2 gene; gBRCAm = germline BRCA mutation; GI = gastrointestinal; HER2 = human epidermal growth factor receptor 2; IDFS = invasive disease–free survival; IHC = immunohistochemistry; ISH = in situ hybridization; OS = overall survival; PARP = poly-(ADP-ribose) polymerase; pCR = pathological complete response; PgR = progesterone receptor; pN0 = axillary node–negative; pN1 = axillary node–positive; pT2 = pathological tumour size > 2 cm; QoL = quality of life; RCT = randomized controlled trial; SAE = serious adverse event; TNBC = triple-negative breast cancer; ULN = upper limit of normal.
aDefined as IHC 0 or 1+ without ISH, or IHC 2+ and ISH nonamplified with ratio < 2.0 and, if reported, average HER2 copy number < 4 signals per cell, or ISH nonamplified with ratio < 2.0 and if reported, average HER2 copy number < 4 signals per cell (without IHC).
bIHC 0 or 1+ without ISH, or IHC 2+ and ISH nonamplified with ratio < 2.0 and, if reported, average HER2 copy number < 4 signals per cell, or ISH nonamplified with ratio < 2.0 and, if reported, average HER2 copy number < 4 signals per cell (without IHC).
cKnown or predicted to be detrimental or lead to a loss of function. Local gBRCA testing results, if available, were used for establishing eligibility.
dFor example, “variants of uncertain clinical significance” or “variant of unknown significance” or “variant, favour polymorphism,” or “benign polymorphism.”
eThere were 2 exceptions. The first was adequately treated nonmelanoma skin cancer, curatively treated in situ cancer of the cervix, DCIS, or stage I grade 1 endometrial carcinoma. The second was other solid tumours and lymphomas (without bone marrow involvement) diagnosed > 5 years before randomization and treated with no evidence of disease recurrence and for which no more than 1 line of chemotherapy was applied.
fThe required washout period before starting study treatment was 2 weeks.
gThe required washout period before starting study treatment was 5 weeks for enzalutamide or phenobarbital and 3 weeks for other drugs.
hOnly patients requiring a gBRCA status Myriad or BGI test before randomization.
IPatients with confirmed gBRCA status by Myriad or BGI, or if BRCA status was known before study entry.
jSafety follow-ups were implemented during the 1-year study treatment period and 30 days after its discontinuation.
kEfficacy follow-ups were implemented every 3 months during the first 2 years following end of treatment, and every 6 months for years 3, 4, and 5 and annually thereafter for approximately 10 years.
lUntil 10 years after the last patient was randomized.
mDefined as the time from randomization to date of first recurrence, where recurrence was defined as invasive locoregional, distant recurrence, contralateral invasive breast cancer, second primary nonbreast invasive malignancy, or death from any cause.
nDefined as the time from the date of randomization until death due to any cause.
oDefined as the time from randomization until documented evidence of the first distant recurrence of breast cancer or death from any cause.
Sources: Clinical Study Reports for OlympiA.18,19
Description of the OlympiA Trial
The OlympiA trial is an ongoing, phase III, randomized, multicentre, double-blind, placebo-controlled trial. The primary objective of the trial was to assess the efficacy and safety of olaparib versus placebo as adjuvant treatment in patients with deleterious or suspicious deleterious germline BRCA1 or BRCA2 mutations and high-risk HER2-negative early-stage breast cancer who had completed definitive local treatment and neoadjuvant or adjuvant chemotherapy. This was a collaborative study that was coordinated worldwide by Breast International Group in partnership with Frontier Science, NRG Oncology, and AstraZeneca. A total of 1,836 patients with breast cancer and gBRCA mutations were enrolled across 546 sites in 23 countries in North America (34 patients from Canada), South America, Europe, Asia Pacific, and South Africa. The primary efficacy end point was IDFS and the key secondary efficacy end points were OS and DDFS. PROs were assessed using the FACIT-F questionnaire and European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 (EORTC QLQ-C30). Treatment with olaparib was given for up to 12 months, or until disease recurrence or unacceptable toxicity, whichever occurred first.
In the OlympiA trial, the first superiority interim analysis was performed when 50% of the events required for the primary IDFS analysis (165 events) had been reached in the first 50% of recruited patients (900 patients). The second interim analysis was performed when 330 IDFS events had been reported. The first interim database lock was executed on March 27, 2020, and the first clinical database lock was executed on December 15, 2020. The second interim database lock was executed on July 12, 2021, and the second clinical database lock was executed on December 17, 2021. Both interim analyses were performed by the independent data-monitoring committee.
Randomization, Treatment Allocation, and Blinding
Interactive response technology was used to randomly assign patients using permuted blocks in a 1:1 ratio to either olaparib at a dose of 300 mg twice daily (N = 921) or matching placebo (N = 915). The last patient was randomized to study treatment on May 28, 2019. Randomization was stratified by:
hormone receptor status (ER or PgR), HER2-negative versus TNBC
prior neoadjuvant versus adjuvant chemotherapy
prior platinum use for breast cancer (yes versus no).
Ideally, patients should have been randomized in the OlympiA trial within a maximum of 8 weeks after the completion of their last treatment, including surgery, chemotherapy, or radiation therapy, but in no case longer than 12 weeks. Both patients and investigators were blinded to the study treatments administered during the trial. A schematic of the OlympiA trial is presented in Figure 2. An independent data-monitoring committee was responsible for reviewing the unblinded safety and efficacy analyses.
Study Phases
Screening Phase: In the OlympiA trial, there were 2 screening parts. Screening part 1 was performed at any time before, during, or after neoadjuvant or adjuvant chemotherapy. It was applied only to patients with unknown gBRCA status before enrolment in the trial and was conducted to determine if the patient was considered eligible for local or central Myriad testing for BRCA status. Once this phase was successfully completed and patients had the BRCA test results, they moved on to screening part 2. Screening part 2 was applied to patients with known gBRCA status, confirmed by Myriad or local testing, who had a deleterious or suspected deleterious mutation. These patients underwent screening assessments, including evaluation of eligibility criteria, baseline characteristics, and concomitant medications. Patients with known BRCA status were required to consent to participate in the OlympiA trial within 28 days before randomization.
Treatment Phase: The treatment phase started with the first dose of treatment following randomization (olaparib and placebo in the intervention and control groups, respectively). During the treatment phase, all patients had assessments every 2 weeks during the first month, every 4 weeks for the following 5 months, and every 3 months for the remaining 6 months of study treatment. The following assessments were performed during the onsite visits: physical examination, vital signs, hematology, radiological tests, and concomitant medications.
Safety Follow-Up: A follow-up visit was conducted 30 days after the last dose of olaparib or placebo. Patients who discontinued study treatment before completing week 52 were required to attend the study treatment discontinuation visit followed by the 30-day follow-up visit. The date of discontinuation, the reasons, and details of the specific cancer therapies were recorded.
Efficacy Follow-Up: Efficacy assessments were performed every 3 months for the first 2 years following end of treatment to assess disease recurrence and new cancers. During years 3, 4, and 5, patients were assessed every 6 months and then annually for approximately 10 years. Assessments for disease recurrence, new cancers, and OS were performed based on signs and symptoms, clinical assessment, mammograms, and/or MRI and vital signs.
Survival Follow-Up: After completion of approximately 10 years of efficacy follow-up assessment, patients will enter the annual survival follow-up phase, which will continue until 10 years after the last patient is randomized. If the patient met the primary end point (IDFS) due to a breast cancer–related distant recurrence, the patient entered the survival follow-up phase of the trial with annual assessments, which continued until 10 years after the last patient was randomized. If the IDFS end point was reached due to events other than distant recurrence, patients continued efficacy assessments until breast cancer–related distant recurrence or approximately 10 years after their randomization into the study. During this phase, no onsite clinical visits were required.
Protocol Amendments
Several modifications were made to the study protocol and after the start of patient recruitment that were documented in the Clinical Study Report. The amendments dated October 21, 2015, included the:
inclusion of patients with ER-positive and/or PgR-positive high-risk HER2-negative breast cancer
addition of hormone receptor status to the stratification factors
extension of the randomization window
inclusion of specific requirements and definitions for patients with HR-positive and HER2-negative cancer
collection of the family cancer detection
increase in the number of centres and number of randomized patients from 1,500 to 1,800.
The amendments dated July 27, 2018, included:
extension of study recruitment to 5 years
confirmation that the interim analysis would be triggered by events in the first 900 patients
inclusion of pneumonitis in the events occurring after 30-day follow-up period
addition of serious adverse events (SAEs) reports for all new primary cancers.
There were several modifications to the statistical analysis plan for the study that were documented in the statistical analysis plan amendments. The amendments dated April 9, 2015, included: addition of prior platinum therapy and HR status to the subgroup analyses; update time for interim analysis to a minimum of 165 IDFS events observed from the first 750 patients recruited; addition of formal statistical analyses for multiple end points for IDFS, OS, and DDFS; and addition of a description for the imputation for missing data. The amendments dated May 18, 2018, included: sample size was increased to 1,800 with 90% power, time for the primary analysis was changed to 330 IDFS events, time for the interim analysis was updated to a minimum of 165 IDFS events observed for the first 900 patients, censoring rules were added, a hierarchy of IDFS events was added, the baseline and demographic analyses were updated, the incidence of new cancers was updated, several sensitivity analyses were added, the method of subgroup analysis was expanded, and more detail was added to global interaction. Additional changes not specified in the statistical analysis plan amendment included the addition of a list of all protocol deviations related to COVID-19 and the exclusion of 2 patients who were stratified as patients with TNBC but whose disease was subsequently found to be HER2-positive or of unknown status.
Figure 2: Study Schema for the OlympiA Trial
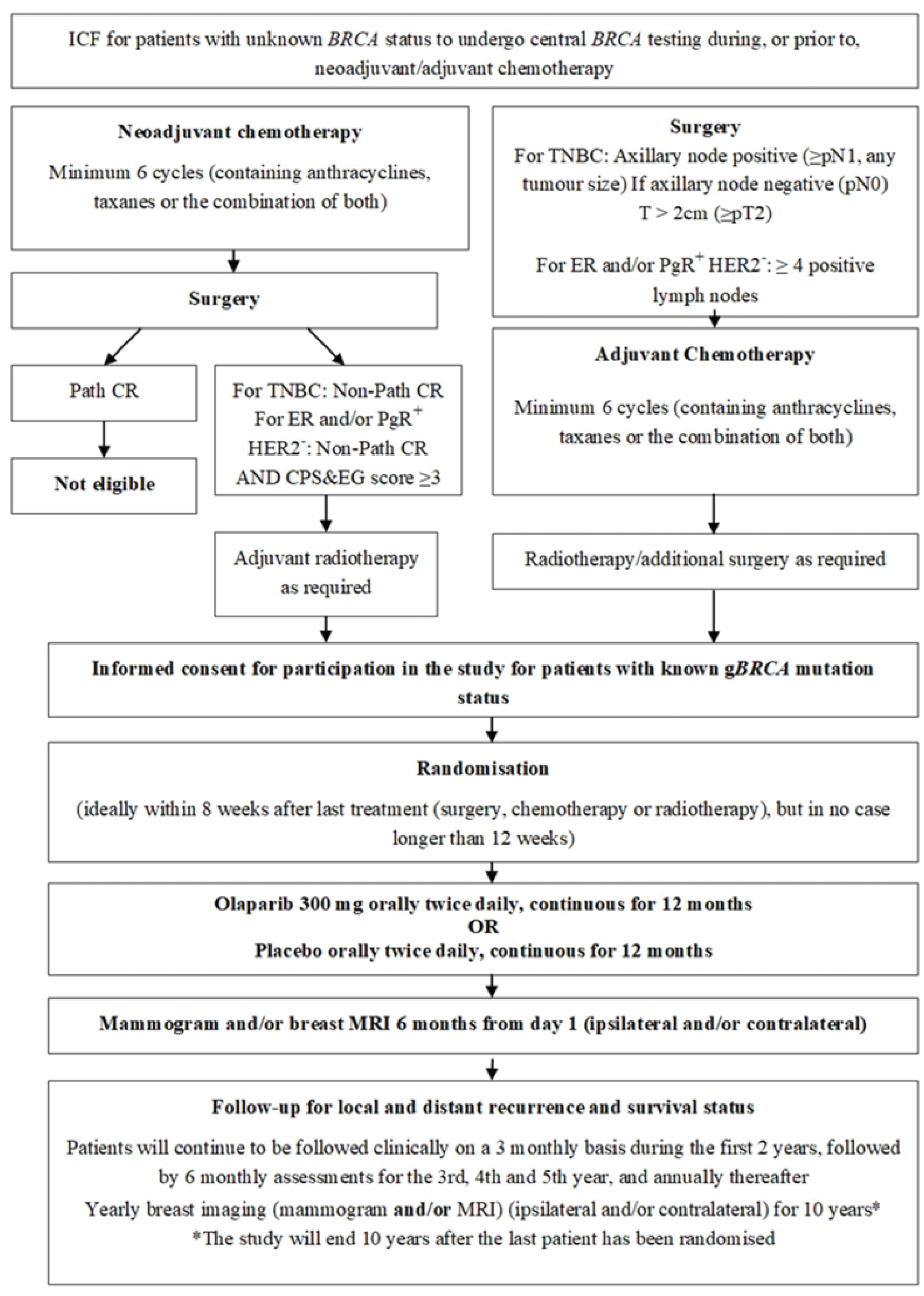
BRCA = breast cancer susceptibility gene; CPS&EG = clinical and post-treatment pathologic stage and estrogen receptor status and histologic grade; ER = estrogen receptor; gBRCA = germline BRCA; HER2 = human epidermal growth factor receptor 2; ICF = informed consent form; path CR = pathological complete resistance; PgR = progesterone receptor; pN0 = axillary node–negative; pN1 = axillary node–positive; pT2 = tumour > 2 cm; t = tumour; TNBC = triple-negative breast cancer.
Populations
Inclusion and Exclusion Criteria
The key inclusion and exclusion criteria applied to the OlympiA trial are summarized in Table 6. Briefly, patients eligible for enrolment in the OlympiA trial had a documented germline BRCA1 or BRCA2 pathogenic or likely pathogenic variant, and high-risk early-stage HER2-negative primary breast cancer after definitive local treatment and neoadjuvant or adjuvant chemotherapy. To be enrolled in the trial, patients had to have known BRCA status, which could be determined using local genetic testing or could be assessed as part of the study-entry procedure through central Myriad testing. Patients must have completed all local therapy and at least 6 cycles of neoadjuvant or adjuvant chemotherapy containing anthracyclines, taxanes, or both drugs. All patients had either TNBC or ER- and/or PgR-positive disease, HER2-negative breast cancer. Patients with TNBC who were treated with adjuvant chemotherapy were required to have axillary node–positive disease or axillary node–negative disease with an invasive primary tumour measuring at least 2 cm on pathological analysis. Those who were treated with neoadjuvant chemotherapy were required to have residual invasive breast cancer in the breast and/or resected lymph nodes. Patients who were treated with adjuvant chemotherapy for HR-positive, HER2-negative breast cancer were required to have at least 4 pathologically confirmed positive lymph nodes. Those who were treated with neoadjuvant chemotherapy were required to have residual invasive cancer in the breast and/or resected lymph nodes (i.e., did not achieve a pathological complete response) and a CPS&EG score of 3 or higher. Patients were excluded from the OlympiA trial if they had metastatic breast cancer, any previous treatment with a PARP inhibitor, secondary primary malignancy, or were concomitantly using strong or moderate CYP3A inhibitors or CYP3A inducers, as the required washout period before starting study treatment was 2 to 3 weeks. Patients who received systemic chemotherapy within 3 weeks before randomization or those who received adjuvant radiotherapy within 2 weeks before randomization were also excluded.
Baseline Characteristics
A summary of baseline characteristics is presented in Table 8 and Table 9. Baseline characteristics were well balanced between the treatment groups. The mean age of all randomized patients in the OlympiA trial was 43.3 years (SD = 9.97 years), and 68.7% of patients were between 30 and 49 years of age. Most patients were female (99.7%) and premenopausal (61.3%), had an ECOG Performance Status of 0 (88.7%), and were white (66.7%) or nonhispanic or Latino (88.1%). A total of 26.4% of patients received prior platinum therapy and half of patients (50.1%) received neoadjuvant treatment. Most patients underwent nonconservative surgery (74.7%) and received a regimen that included both anthracycline and taxane therapy (93.7%) as prior adjuvant or neoadjuvant chemotherapy.
A total of 82.3% of the patients had TNBC (HR-negative and HER2-negative), while 17.7% had HR-positive, HER2-negative breast cancer. Germline BRCA1 deleterious or suspected deleterious mutations were identified in 72.2% of patients, gBRCA2 mutations in 27.1% of patients, and both gBRCA1 and gBRCA2 mutations in 0.4% of patients. The majority of patients with TNBC (60.3%) had a mutation in BRCA1, while the majority of patients with HR-positive, HER2-negative breast cancer (51.4%) had a mutation in BRCA2. For patients for whom both local and central Myriad BRCA testing was available, the test results were concordant. Of 1,836 patients randomized in the OlympiA trial, 83.8% were confirmed to have a gBRCA mutation using the central Myriad test. A total of 36.1% of patients had clinical AJCC stage IIA, 21.0% had AJCC stage IIB, and 13.0% had AJCC stage IIIA breast cancer.
Table 8: Summary of Baseline Characteristics — FAS
Characteristic | Olaparib (N = 921) | Placebo (N = 915) |
|---|---|---|
Demographic characteristics | ||
Mean age, years (SD) | 43.0 (9.82) | 43.6 (10.12) |
Median age, years (Q1 to Q3) | 42.0 (22 to 77) | 43.0 (24 to 78) |
Age groups, n (%) | ||
< 30 years | 51 (5.5) | 59 (6.4) |
30 to 39 years | 333 (36.2) | 306 (33.4) |
40 to 49 years | 315 (34.2) | 308 (33.7) |
50 to 59 years | 166 (18.0) | 172 (18.8) |
60 to 69 years | 48 (5.2) | 66 (7.2) |
≥ 70 years | 8 (0.9) | 4 (0.4) |
Sex, n (%) | ||
Female | 919 (99.8) | 911 (99.6) |
Male | 2 (0.2) | 4 (0.4) |
Race,a n (%) | ||
White | 626 (68.0) | 599 (65.5) |
Asian | 259 (28.1) | 272 (29.7) |
Black or African American | 19 (2.1) | 29 (3.2) |
Native Hawaiian or other Pacific Islander | 1 (0.1) | 0 |
American Indian or Alaska Native | 3 (0.3) | 1 (0.1) |
Other | 3 (0.3) | 6 (0.7) |
Missing | 10 (1.1) | 8 (0.9) |
Ethnicity, n (%) | ||
Nonhispanic or Latino | 805 (87.4) | 812 (88.7) |
Hispanic or Latino | 31 (3.7) | 24 (2.6) |
Unknown | 82 (8.9) | 79 (8.6) |
Ashkenazi Jewish descent, n (%) | ||
Not Ashkenazi Jewisha | 880 (95.5) | 876 (95.7) |
Ashkenazi Jewish | 41 (4.5) | 36 (3.9) |
Missing | 0 | 3 (0.3) |
Geographic region, n (%) | ||
North America | 122 (13.2) | 132 (14.4) |
South America | 16 (1.7) | 12 (1.3) |
Europe | 481 (52.2) | 452 (49.4) |
Asia and South Africa | 302 (3.8) | 319 (34.9) |
Patient and disease characteristics | ||
█ █ ██ █ █ ██ █ █ █ █ ██ █████ | ||
█ █ ██ ████ | █ █ ██ ██████ | █ █ ██ ██████ |
█ █ █ █ ██ █ █ █ ██ ████ | █ █ ██ ██ ██ ████ | █ █ ██ ██ ██ ████ |
Menopausal status, n (%) | ||
Premenopausal | 572 (62.1) | 553 (60.4) |
Postmenopausal | 347 (37.7) | 358 (39.1) |
Male | 2 (0.2) | 4 (0.4) |
ECOG Performance Status, n (%) | ||
0 | 824 (89.5) | 804 (87.9) |
1 | 97 (10.5) | 111 (12.1) |
Hormone receptor status, n (%) | ||
TNBCb | 753 (81.8) | 758 (82.8) |
ER- and/or PgR-positive, HER2-negative | 168 (18.2) | 157 (17.2) |
Prior platinum, n (%) | ||
No | 674 (73.2) | 677 (74.0) |
Yes | 247 (26.8) | 238 (26.0) |
Prior chemotherapy, n (%) | ||
Adjuvant | 461 (50.1) | 455 (49.7) |
Neoadjuvant | 460 (49.9) | 160 (50.3) |
Prior chemotherapy by hormone receptor status, n (%) | ||
Adjuvant TNBC | 397 (43.1) | 390 (42.6) |
Adjuvant ER- and/or PgR-positive, HER2-negative | 64 (6.9) | 65 (7.1) |
Neoadjuvant TNBCb | 356 (38.7) | 368 (40.2) |
Neoadjuvant ER- and/or PgR-positive, HER2-negative | 104 (11.3) | 92 (10.1) |
Baseline gBRCAm status, n (%) | ||
BRCA1-mutated | 656 (71.2) | 669 (73.1) |
BRCA2-mutated | 260 (28.2) | 238 (26.0) |
BRCA1- and BRCA2-mutated | 2 (0.2) | 5 (0.5) |
No BRCA mutation | 2 (0.2) | 3 (0.3) |
Missing | 1 (0.1) | 0 |
Local BRCA status,c n (%) | ||
BRCA-mutated | 679 (73.7) | 680 (74.3) |
Non–BRCA-mutated | 1 (0.1) | 1 (0.1) |
No local results | 241 (26.2) | 234 (25.6) |
Central BRCA status,c n (%) | ||
BRCA-mutated | 777 (84.4) | 762 (83.3) |
Non–BRCA-mutated | 8 (0.9) | 5 (0.5) |
No mutation detected | 1 (0.1) | 4 (0.4) |
Inconclusive or unclassified | 4 (0.4) | 3 (0.3) |
No central results | 131 (14.2) | 141 (15.4) |
Prior neoadjuvant or adjuvant chemotherapy therapy for primary BC, n (%) | ||
Anthracycline and taxane regimen | 871 (94.6) | 849 (92.8) |
Anthracycline regimen (without taxane) | 7 (0.8) | 13 (1.4) |
Taxane regimen (without anthracycline) | 43 (4.7) | 52 (5.7) |
Missing | 0 | 1 (0.1) |
Prior hormone therapy,a n (%) | ||
Adjuvant | █ █████ | █ █████ |
Neoadjuvant | █ █████ | █ █████ |
Primary BC surgery before randomization, n (%) | 921 (100.0) | 913 (99.8) |
Nonconservative surgery | 698 (75.8) | 673 (73.6) |
Conservative surgery | 223 (24.2) | 240 (26.2) |
Unknownd | 0 | 2 (0.2) |
BC = breast cancer; BRCA = breast cancer susceptibility gene; BRCA1 = breast cancer susceptibility gene 1; BRCA2 = breast cancer susceptibility gene 2; DCIS = ductal carcinoma in situ; ECOG = Eastern Cooperative Oncology Group; eCRF = electronic case report form; ER = estrogen factor; FAS = full analysis set; gBRCAm = germline BRCA mutation; HER2 = human epidermal growth factor 2; NOS = not otherwise specified; PgR = progesterone factor; pN1 = axillary node–positive; Q1 = 25th percentile; Q3 = 75th percentile; SD = standard deviation; TNBC = triple-negative breast cancer.
aNot Ashkenazi Jewish could mean that the patient is Jewish but not Ashkenazi Jewish, not Jewish, or descent recorded as unknown.
bPost randomization, 2 patients (included as TNBC) were found not to have confirmed negative HER2 status. These patients were captured as important protocol deviations in the “No histologically confirmed nonmetastatic primary invasive adenocarcinoma of the breast” category.
cLocal BRCA results were only available for patients who knew their gBRCA mutation status before entry into the study. All randomized patients were required to have a central test. Myriad testing was not done in China. Beijing Genomics Institute (China) results were considered local results.
dPatient E106578 (placebo group) was reported to have had a right mastectomy (DCIS) in 2001 in the concomitant procedure in the eCRF and the patient received axillary lymph node dissection (pN1) before entering the OlympiA study. Patient E112449 (placebo group) was reported to have occult breast carcinoma on the histology report and no visible tumour in the breast per MRI; the patient received axillary lymph node dissection (pN1) before entering OlympiA study.
Sources: Clinical Study Reports for OlympiA.18,19
Table 9: Pathological Characteristics of Primary Breast Cancer — FAS
Characteristic | Olaparib (N = 921) | Placebo (N = 915) |
|---|---|---|
Bilateral invasive BC, n (%) | ||
███ | █ ██████ | █ ██████ |
██ | █ ██ ██████ | █ ██ ██████ |
██ █ █ █ █ ██ ██████ █ █ █ █ ██ ██ ██ ███ | ||
███ | █ ██ ██████ | █ ██ ██████ |
██ | █ ██████ | █ ██████ |
██ █ █ █ █ ██ ████ █ █ █ █ ██ █ █ █ █ █ ██ ███ | ||
██████ | █ ██ ██████ | █ ██ ██████ |
███████ | █ ██████ | █ ██████ |
█ █ █ █ ██ █ █ █ █ ██ ██ ████████ | █ █████ | █ ██████ |
███████ | █ █████ | █ █████ |
████████ | █ █████ | █ █████ |
██████ | █ █████ | █ █████ |
█████████ | █ ██████ | █ █████ |
██████████ | █ ██████ | █ █████ |
██ █ █ █ █ ██ █████████ | █ █████ | █ █████ |
██ █ █ █ █ ██ ███ | █ ██ ██████ | █ ██ ██████ |
█████████ | █ ██████ | █ ██████ |
█████ | █ ██████ | █ ██████ |
██ █ █ █ █ ██ █ █ █ █ ██ ██ █ █ █ █ ██ █████ █ █ █ █ █ ██ ███ | ||
██ | █ ██ ██████ | █ ██ ██████ |
███████ | █ ███████ | █ ██ ██████ |
██ █ █ █ █ ██ █ █ ██ █ █ █ █ █ ██ ███ | ||
██ | █ ██ ██████ | █ ██████ |
███ | █ ██ ██████ | █ ██ ██████ |
███ | █ ██ ██████ | █ ██ ██████ |
███████ | █ ██ ██████ | █ ██ ██████ |
██████ █ █ █ █ ██ █ █ █ █ ██ ██ █ █ █ █ ██ ██████████ | ||
██ | █ ██ █████ | █ ██ █████ |
AJCC = American Joint Committee on Cancer; BC = breast cancer; BRCA = breast cancer susceptibility gene; FAS = full analysis set; gBRCAm = germline BRCA mutation; ITT = intention to treat; NOS = not otherwise specified.
aMay be more than 1 type per patient.
Sources: Clinical Study Reports for OlympiA.18,19
Interventions
In the OlympiA trial, all eligible patients were randomized in a 1:1 ratio to receive 1 of 2 interventions: olaparib at a dose of 300 mg twice daily or matching placebo in a double-blind manner. The drugs were administered at the same time each morning and evening with an interval of about 12 hours with light food. The olaparib and placebo tablets were identical in packaging and labelling. Dose reduction was available with 100 mg tablets. If AEs occurred, such as moderate renal impairment, the initial daily dose of olaparib (600 mg) could be reduced to 500 mg or 400 mg. The daily dose of olaparib was reduced to 300 mg or 200 mg during concomitant administration of moderate or strong CYP3A inhibitors, respectively. After a dose reduction of olaparib, an increase to a higher dose was not permitted. Patients were not prescribed olaparib after the discontinuation of the study treatment.
Concomitant Medications
All concomitant medications were documented at each visit. Concomitant medications that were considered necessary for the patient’s welfare and that did not interfere with the study medication were allowed at the discretion of the investigator. Patients received adjuvant endocrine therapy per local policy or international guidelines. Bisphosphonates or denosumab were allowed during the study treatment and follow-up phases. Other antineoplastic medications were prohibited during study treatment and IDFS follow-up. Subsequent anticancer treatment was expected to be initiated after breast cancer recurrence. If it was necessary to initiate during the 1-year treatment phase, it was important that the study treatment be discontinued. If a patient developed nausea, vomiting, or diarrhea, these symptoms were recorded as AEs and appropriately treated. The use of natural or herbal products or other traditional remedies was discouraged.
Medications prohibited during the trial included: strong CYP3A inhibitors (e.g., itraconazole, clarithromycin), moderate CYP3A inhibitors (e.g., ciprofloxacin, erythromycin), strong CYP3A inducers (e.g., phenobarbital, rifampicin), moderate CYP3A inducers (bosentan, efavirenz, and modafinil), CYP3A4 substrates, CYP2B6 substrates (bupropion, efavirenz), OATP1B1 substrates, OCT2 substrates, OAT3 substrates (furosemide, methotrexate), and anticoagulant therapy.
Study Treatment Discontinuation
Patients had to be discontinued from the study treatment in the following circumstances:
patient decision: the patient was free at any time to discontinue study treatment, without prejudice to further clinical care
AE
completion of 1-year treatment period
the patient has a confirmed pregnancy during treatment
severe noncompliance with the clinical study protocol
locoregional breast cancer recurrence (ipsilateral invasive breast cancer recurrence, regional invasive breast cancer recurrence)
distant breast cancer recurrence
contralateral invasive breast cancer or new primary nonbreast invasive cancer
death
bone marrow findings consistent with myelodysplastic syndrome or acute myeloid leukemia
diagnosis of breast cancer recurrence or diagnosis of a secondary primary malignancy.
Patients were to be seen within at least 30 days of discontinuation of the study drug to collect and/or complete information on AEs.
Study Withdrawal
Patients withdrew from the study in the following circumstances:
voluntary withdrawal by the patient who was at any time free to discontinue their participation in the study without prejudice to further treatment
patient was enrolled incorrectly, for instance, the patient did not meet the required inclusion or exclusion criteria for the study; this option was applicable only to patients not randomized into the study (e.g., patients who did not pass screening and who were identified before randomization)
patient lost to follow-up
death.
Outcomes
A list of efficacy end points identified in the CADTH review protocol that were assessed in the clinical trials included in this review is provided in Table 10. These end points are further summarized subsequently. A detailed discussion and critical appraisal of the outcome measures is provided in Appendix 4.
The primary end point for the OlympiA trial was IDFS in the intention-to-treat (ITT) population. IDFS was defined per the Standardized Definitions for Efficacy End Points (STEEP) criteria41 as the time from randomization to date of first recurrence, where recurrence is defined as follows:
ipsilateral invasive breast tumour recurrence: invasive breast cancer involving the same breast parenchyma as the original primary
regional invasive breast cancer recurrence: invasive breast cancer in the axilla, regional lymph nodes, chest wall, and skin of the ipsilateral breast
distant recurrence, i.e., metastatic breast cancer that had either been biopsy-confirmed or radiologically diagnosed as recurrent invasive breast cancer
death attributable to any cause, including breast cancer, nonbreast cancer, or unknown cause
contralateral invasive breast cancer
new primary nonbreast invasive cancers (i.e., excluding new in situ carcinomas of any site). New primary nonbreast invasive cancers include hematologic cancers and myelodysplastic syndrome. Squamous or basal cell skin cancers were not counted as primary end point events.
Table 10: Summary of Outcomes of Interest Identified in the CADTH Review Protocol
Outcome measure | OlympiA trial |
|---|---|
Invasive disease–free survival | Primary |
Overall survival | Secondary |
Distant disease–free survival | Secondary |
Incidence of contralateral invasive breast cancer, contralateral noninvasive breast cancer, new primary ovarian cancer, new primary fallopian tube cancer, and new primary peritoneal cancer | Secondary |
Composite fatigue score (FACIT-F questionnaire) measured at 6 and 12 months after randomization | Secondary |
Patient-reported GI symptoms (nausea, vomiting, and diarrhea) at 6, 12, 18, and 24 months as measured by the EORTC QLQ-C30 scale | Secondary |
Composite fatigue score (FACIT-F) measured at 6, 12, 18, and 24 months after randomization | Secondary |
2-item global QoL score of the EORTC QLQ-C30 scale at 6, 12, 18, and 24 months | Secondary |
Different functional subscale scores as measured by the EORTC QLQ-C30 with particular interest in the emotional and physical subscales | Secondary |
EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; FACIT-F = Functional Assessment of Chronic Illness Therapy–Fatigue; GI = gastrointestinal; QoL = quality of life.
Sources: Clinical Study Reports for OlympiA.18,19
Locoregional recurrence of the disease (ipsilateral or regional invasive breast cancer) had to be confirmed by cytological or histological examination and appropriate imaging. Distant recurrence had to be diagnosed by radiological examination and/or histopathological assessment when the metastatic lesion is easily accessible for biopsy. Invasive contralateral breast cancer or invasive nonbreast secondary primary cancer was required to be confirmed by histopathological report.
The key secondary end points for the OlympiA trial were OS and DDFS in the ITT population. OS was defined as the time from the date of randomization to death due to any cause. Any patient not known to have died at the time of analysis was censored based on the last recorded date the patient was known to be alive.
DDFS was defined as the time from randomization to documented evidence of the first distant recurrence of breast cancer, including:
distant recurrence: metastatic disease breast cancer that was either biopsy-confirmed or radiologically diagnosed as recurrent invasive breast cancer
death attributable to any cause, including breast cancer, nonbreast cancer, or unknown cause
new primary nonbreast invasive cancer.
Evidence of distant recurrence had to be either biopsy-confirmed or radiologically diagnosed. New primary nonbreast invasive cancer had to be confirmed by histopathological report. The first site of distant recurrence was recorded and used in the analysis.
The incidence of contralateral invasive breast cancer, contralateral noninvasive breast cancer, new primary ovarian cancer, new primary fallopian tube cancer, and new primary peritoneal cancer were each considered separately in the ITT population. Evidence of new contralateral cancer and new ovarian, fallopian, or peritoneal cancers was confirmed by radiologic examination, with positive histology or cytology. Time to new contralateral cancer and new ovarian, fallopian, or peritoneal cancer was defined as the date of randomization to the date of the first occurrence of the event.
Patient-Reported Outcomes
The primary PRO was the composite fatigue score, which was assessed in the PRO dataset using the FACIT-F questionnaire and measured at 6 and 12 months after randomization. The secondary PRO outcomes included:
patient-reported gastrointestinal symptoms (nausea, vomiting, and diarrhea) at 6, 12, 18, and 24 months as measured by the EORTC QLQ-C30 scale
composite fatigue score (FACIT-F questionnaire) measured at 6, 12, 18, and 24 months after randomization
2-item global quality of life score of the EORTC QLQ-C30 scale at 6, 12, 18, and 24 months
different functional subscale scores as measured by the EORTC QLQ-C30 with particular interest in the emotional and physical subscales.
FACIT-F Questionnaire
The FACIT-F scale was originally developed for use in patients with cancer. It is a 13-item patient-reported scale of fatigue symptoms.42 Patients are asked to indicate to what extent each of the 13 items applies to them over the course of the previous 7 days. The response for each item is scored on a 5-point Likert scale from 0 (not at all) to 4 (very much). The total score of the FACIT-F scale is calculated by summing the scores of all 13 measurement items and ranges from 0 to 52, with a lower score indicating more fatigue.43,44
The FACIT-F is a generally valid and reliable scale for cancers, including breast cancer. Yellen et al.44 reported convergent–divergent validity (n = 50, including 12 patients with breast cancer with no staging information) through a strong correlation with the FACIT-F scale with the Profile of Mood States (POMS) fatigue scale (r = –0.83), the Piper Fatigue Scale (r = 0.61), and the POMS vigour scale (r = –0.77), indicating that the FACIT-F scale was significantly related to fatigue or anemia-relevant concepts (convergent validity) and was unrelated to concepts that were not assumed to be associated with fatigue or anemia (divergent validity) (if r > 0.35, or < –0.35, then significant at a significance level of 0.05). The FACIT-F scale was found to be strongly correlated with patient-rated ECOG Performance Status (r = –0.55).42 The FACIT-F scale was also able to discriminate patient membership classified by ECOG Performance Status (i.e., performance status of 0 versus 1 versus 2 or 3; P < 0.0001) under the assumption that a better performance status would be associated with higher quality of life scores.44 In terms of reliability, the FACIT-F scale demonstrated strong internal consistency (Cronbach alpha = 0.93 to 0.96), and a good test–retest reliability over a 3- to 7-day window (r = 0.90) in patients with cancer.42,44 No evidence of responsiveness to change was identified for the FACIT-F scale in patients with breast cancer.
Two studies estimated the MIDs for change in the FACIT-F scale in patients with cancer, including those with breast cancer.45,46 However, neither study provided details on the breast cancer stage. The estimates of the MID were reported as 3.0 points (no less than 2.7 points) using the anchor-based and distribution-based approaches, meaning 1 category change (better or worse) on 3 of the 13 items (23%) on the FACIT-F scale with no change in the other 10 items.45
EORTC QLQ C-30
The EORTC QLQ C-30 version 3.0 is 1 of the most-used PRO measures in oncology clinical trials. It is a multidimensional, cancer-specific, self-administered measure of HRQoL.47 Version 3.0 of the questionnaire is the most recent version and has been in use since December 1997.48 It is intended for use in the adult population only. The EORTC QLQ-C30 is composed of both multi-item scales and single-item measures. These include 5 functional scales (physical, role, cognitive, emotional, and social), 3 symptom scales (fatigue, pain, and nausea and vomiting), a global health status (HRQoL) scale, and 6 single items assessing additional symptoms commonly reported by patients with cancer (dyspnea, loss of appetite, insomnia, constipation, and diarrhea) as well as the perceived financial impact of the disease.47 The EORTC QLQ-C30 uses a 1-week recall period to assess functional status and symptoms. All scales and single-item measures are scored from 0 to 100. Most questions have 4 response options (“not at all,” “a little,” “quite a bit,” “very much”), with scores on these items ranging from 1 to 4. For the 2 items that form the global HRQoL scale, the response format is a 7-point Likert scale with anchors at 1 = “very poor” and 7 = “excellent.” Raw scores for each scale are computed as the average of the items that contribute to a particular scale. Each raw scale score is converted to a standardized score that ranges from 0 to 100 using a linear transformation, with a higher score reflecting better function on the function scales and better HRQoL, while a higher score in the symptom scale means a higher burden of symptoms and therefore a worse health state.49,50
The content validity was demonstrated by mapping the EORTC QLQ-C30 questionnaire with the WHO’s International Classification of Functioning framework based on the opinions of 21 experts.51 The discriminative validity of the psychosocial subscales of EORTC QLQ-C30 in patients with breast cancer (n = 150) was demonstrated through correlation with the ECOG Performance Status (Spearman rank correlation coefficient > 0.2).52 In terms of the interinstrument associations that occurred between the EORTC QLQ-C30 and POMS subscales (also known as convergent validity), the emotional function of the EORTC QLQ-C30 correlated very strongly with tension (Spearman rank correlation coefficient = 0.76), depression and dejection (Spearman rank correlation coefficient = 0.74) and the POMS total mood disturbance subscales (Spearman rank correlation coefficient = 0.74).52 A study investigated the inter-rater reliability among patients with metastatic breast cancer (n = 46). The median kappa coefficient for agreement across the 30 items in the EORTC QLQ-C30 was 0.86 (range, 0.48 to 1.00), and there was almost perfect agreement (kappa coefficient 0.8 to 1.00) for 19 items and “substantial agreement” (kappa coefficient, 0.61 to 0.80) for 6 items.
The estimates of the MID were evaluated in patients with advanced breast cancer (n = 723) using the anchor-based and distribution-based approaches and ranged from 5 to 14 points for within-group improvements and from −14 to −4 points for within-group deterioration, and from 4 to 11 points for between-group improvements and −18 to −4 points for between-group deterioration.53 Another study estimated the MIDs, using the anchor-based approach for any scale of the EORTC QLQ-C30 questionnaire, to be 10 points in patients with breast cancer (n = 246) and small-cell lung cancer (n = 111).54 Kawahara et al.55 indicated that the estimated MIDs in patients with metastatic breast cancer using the anchor-based approach ranged from 7 to 15 points for within-group improvements, −17 to −7 points for within-group deterioration, 5 to 11 points for between-group improvements, and –8 to −5 points for between-group deterioration.
Statistical Analysis
Sample Size Calculations
In the OlympiA trial, at least 330 IDFS events in the ITT population were required to achieve a 90% power at a 2-sided 5% significance level. Data on patients with high-risk breast cancer with gBRCA mutations are limited; therefore, some assumptions were made about the expected hazard rates in the study population to allow the estimation of the sample size. At the primary analysis, a true HR of 0.7 between the olaparib and placebo arms was chosen with a critical HR value of 0.805. It has been estimated that the 3-year incidence of IDFS is approximately 60% for patients without a complete pathological response who have previously received neoadjuvant therapy, and 77% for patients who have previously received adjuvant therapy. Therefore, assuming approximately 50% of patients will receive prior neoadjuvant therapy, the estimated overall 3-year IDFS rate for the total population is approximately 68%. Thus, the sponsor estimated that at least 1,800 patients needed to be enrolled, assuming a dropout rate of 8% for the first 12 months, and approximately 5 years to complete patient recruitment.
Analysis of Outcomes
Primary Outcome
IDFS was planned to be analyzed at the interim and primary IDFS analyses. The interim analysis was planned to be analyzed in both the ITT population with an estimated 254 events and in the supportive mature cohort population, which included the first 900 patients with 165 events anticipated. The inclusion of a mature cohort population at the interim analysis was intended to provide confidence that any observed treatment effect from the interim analysis in the ITT population is maintained with longer-term follow-up. Statistical significance was not required for the mature cohort population, and this analysis was considered supportive. Evidence of the superiority of IDFS could only be determined in the interim analysis if the results of both analyzed populations (ITT and mature cohort) show a sustained clinically relevant treatment effect. An independent data-monitoring committee evaluated both efficacy and safety data, and recommendations for the study were made based on the body of the evidence.
To set boundaries, a 1-sided significance level (i.e., 2.5%) was to be split between the final and interim analyses using a bespoke spending function, where a fixed significance level was assigned at the interim analysis, and the remaining significance level at the final analysis, taking into account the correlation.56 A 2-sided significance level of 0.005 was assigned to the interim analysis, so a statistically significant result would need to be observed to declare superiority in the IDFS. A hierarchical testing strategy was utilized to control the overall type I error for multiple end points.57 If the primary IDFS end point was statistically significant (using the full 2.5% 1-sided alpha), then key secondary outcomes (DDFS and OS) were tested based on the weighted proportion of the significance level (1-sided 2% for DDFS and 1-sided 0.5% for OS). This testing procedure continued through each of the key secondary end points until the end point failed to reach statistical significance, after which subsequent key secondary end points were considered exploratory (Figure 3).
IDFS was analyzed using a log-rank test stratified by the stratification factors at randomization, and the corresponding P value was reported as the primary analysis result (Table 11). In addition, IDFS was analyzed using a stratified Cox proportional hazard model using the Efron approach for handling ties. The stratification factors were hormone receptor status (ER- and/or PgR-positive, HER2- negative versus TNBC), prior chemotherapy (neoadjuvant versus adjuvant chemotherapy), and prior platinum use for breast cancer (yes versus no). The difference between IDFS rates for each arm was reported with 95% CIs estimated by the profile likelihood approach. A Kaplan-Meier plot for IDFS was presented by treatment arms. The proportional hazards assumption was assessed by inspecting plots of complementary log-log (time) versus log (time), and formally testing using the Grambsch-Therneau test based on scaled Schoenfeld residuals from a Cox model including treatment group as a factor.
Figure 3: Multiplicity Strategy for the OlympiA Trial
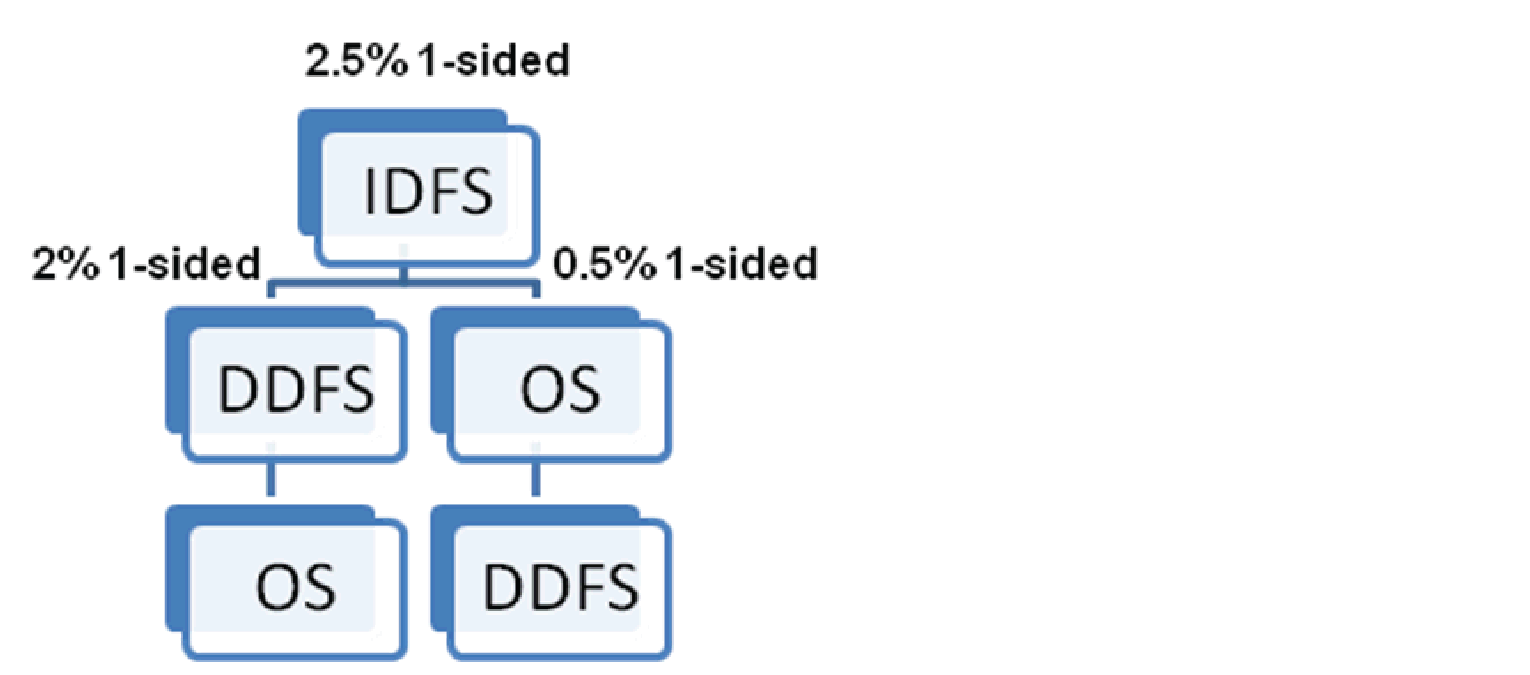
DDFS = distant disease–free survival; IDFS = invasive disease–free survival; OS = overall survival.
Source: Sponsor-submitted statistical analysis plan.58
Table 11: Statistical Analysis of Efficacy End Points
End point | Statistical model | Adjustment factors | Sensitivity analyses |
|---|---|---|---|
Invasive disease–free survival |
| Treatment group and stratification factors |
|
Overall survival |
| Treatment group and stratification factors |
|
Distant disease–free survival |
| Treatment group and stratification factors |
|
Incidence of contralateral invasive breast cancer, contralateral noninvasive breast cancer, new primary ovarian cancer, new primary fallopian tube cancer, and new primary peritoneal cancer | Fine-Gray competing risk analysis | Treatment group and stratification factors | NA |
Composite fatigue score (FACIT-F questionnaire) measured at 6 and 12 months after randomization | MMRM analysis | Time, treatment by time interaction, corresponding baseline score, and the baseline score by time interaction | NA |
Patient-reported GI symptoms (nausea, vomiting, and diarrhea) at6, 12, 18, and 24 months as measured by the EORTC QLQ-C30 scale | MMRM analysis | Time, treatment by time interaction, corresponding baseline score, and the baseline score by time interaction | NA |
Composite fatigue score (FACIT-F questionnaire) measured at 6, 12, 18, and 24 months after randomization | MMRM analysis | Time, treatment by time interaction, corresponding baseline score, and the baseline score by time interaction | NA |
2-item global QoL score of the EORTC QLQ-C30 scale at 6, 12, 18, and 24 months | MMRM analysis | Time, treatment by time interaction, corresponding baseline score, and the baseline score by time interaction | NA |
Different functional subscale scores as measured by the EORTC QLQ-C30 with particular interest in the emotional and physical subscales | MMRM analysis | Time, treatment by time interaction, corresponding baseline score, and the baseline score by time interaction | NA |
EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; FACIT-F = Functional Assessment of Chronic Illness Therapy–Fatigue; gBRCAm = germline BRCA mutation; MMRM = mixed-model for repeated measures; NA = not applicable; QoL = quality of life.
Sources: Clinical Study Reports for OlympiA18,19 and sponsor-submitted statistical analysis plan.58
IDFS was defined as the time from randomization to date of first recurrence. For confirmed local recurrence, the earliest date of diagnosis based on objective findings was used to determine the time to event for the analysis. For confirmed distant recurrence, the date of the earliest radiological or imaging examination or cytological or histological assessment was used to determine the time to event for the analysis. If 2 recurrence events (local and distant) were reported within 2 months of each other, then this was referred to as a simultaneous event and was considered as a single event, but the date of recurrence was the earliest date of the 2 events. If 2 recurrence events were reported more than 2 months apart, then these were treated as 2 separate recurrences and the earliest event and corresponding event date were used to derive the IDFS. If a patient died during the study with no documented disease recurrence or invasive contralateral breast cancer, or invasive nonbreast secondary primary cancer, then the date of death was used to derive the IDFS. Patients who did not have an IDFS event at the time of analysis were censored at the date of their last disease assessment. Patients were censored at 0.5 days after randomization under the following 3 circumstances:
patients who had an event before randomization
patients who were identified as inadvertent randomizations
patients who withdrew consent, received no treatment, and did not provide any follow-up data.
Sensitivity Analyses
The following sensitivity (exploratory) analyses were conducted for the primary end point:
A stratified Cox regression analysis, based on all randomized patients confirmed by a central Myriad test to have a gBRCAm, to compare against the primary IDFS analysis result if the analysis population differs from the ITT population.
Any patient mis-stratified in the randomization system was included in the primary analysis as stratified.
If the results of ER and PgR status from the local and central laboratories differed in more than 5% of randomized patients, then the same model as described previously was performed using the central laboratory results.
A “deviation bias” sensitivity analysis may be performed after excluding patients with important protocol deviations that may affect the efficacy of the trial therapy.
An unadjusted analysis was performed and compared with the primary results.
Subgroup Analyses
Subgroup analyses of IDFS in the ITT population were performed for the prespecified subgroups. Of the subgroups listed in the CADTH review protocol, the following were prespecified in the OlympiA trial:
BRCA mutation status: BRCA1, BRCA2, or both.
prior chemotherapy: neoadjuvant or adjuvant.
prior platinum therapy: yes or no.
hormone receptor status: ER- and/or PgR-positive and HER2-negative, or TNBC.
axillary nodal status: node-negative, or node-positive.
CPS&EG score: 2, 3, or 4 versus 5 or 6 (for the postneoadjuvant group only).
There was no multiplicity control for the subgroup analyses. As such, all subgroup analyses were exploratory in nature. Forest plots were created including the HRs and 95% CI and interaction P values for treatment-by-subgroup interactions.
Secondary Outcomes
Both key secondary outcomes, DDFS and OS, were analyzed in the ITT population. OS and DDFS were analyzed at the time of the IDFS analysis using the same methodology and model as for the IDFS analysis. Similar to IDFS, a bespoke spending function was applied to the OS and DDFS, where a fixed significance level was assigned to each analysis time point and to the remaining significance level assigned to the final analysis time point controlling the overall type I error. If the null hypothesis is rejected for DDFS and not for OS, then the following significance levels were recycled to OS from DDFS: IDFS, 99.5%; DDFS, 99.375%; and OS, 99%. If the null hypothesis is rejected for OS and not for DDFS, then the significant levels recycled to DDFS from OS were as follows: IDFS, 99.5%; DDFS, 99.375%; and OS, 99.0%.
For the analysis of OS, any patient not known to have died at the time of analysis was censored based on the last recorded date on which the patient was known to be alive. The final OS analysis will be conducted once the trial follow-up is complete.
For the analysis of DDFS, the date of the earliest radiological, cytological, or histological assessment was used to determine the time to event for the analysis. Patients without documented evidence of DDFS at the time of the analysis were censored at the date of their last clinical examination.
The incidence of contralateral invasive breast cancer, contralateral noninvasive breast cancer, new primary ovarian cancer, new primary fallopian tube cancer, and new primary peritoneal cancer was compared between groups using a Fine-Gray competing risk analysis, adjusted for stratification factors. Death was considered a competing risk for each end point. In addition, bilateral mastectomy after randomization was a competing risk for the contralateral breast cancer analyses, bilateral oophorectomy after randomization was considered a competing risk for the new primary ovarian cancers analysis, and removal of the fallopian tubes was considered a competing risk for the new primary fallopian tube cancer analysis.
Patient-Reported Outcomes
PROs were tested without adjustments for multiplicity and analyzed only in the PRO analysis set, which included patients who started treatment and provided evaluable data at baseline. The composite fatigue score (FACIT-F) measured at 6 and 12 months after randomization was compared between the 2 arms using a mixed-model for repeated measures (MMRM) analysis adjusted for time, treatment by time interaction, corresponding baseline score, and the baseline score by time interaction. Separate analyses were performed for patients who received neoadjuvant and adjuvant chemotherapy. To further assess the effect of olaparib on fatigue score over time, the composite fatigue score (FACIT-F questionnaire) measured at 6, 12, 18, and 24 months after randomization was analyzed using an MMRM model of all the postbaseline scores. Gastrointestinal symptoms, the 2-item global health status (quality of life) score measured at 3, 12, 18, and 24 months and the scores from the 5 multi-item EORTC QLQ-C30 functional scales were analyzed using the same MMRM model.
Missing PRO Data
If less than 50% of the subscale items were missing, the subscale score based on the nonmissing items was divided by the number of nonmissing items and multiplied by the total number of items on the subscale. If at least 50% of the items were missing, that subscale was treated as missing.
Harms
In the OlympiA trial, AEs were graded according to CTCAE version 4.03. Safety analyses were based on the safety population and included patients who had received at least 1 dose of the trial medication. All safety end points were reported using descriptive statistics. Separate summaries were provided for most notable safety end points, including myelodysplastic syndrome, acute myeloid leukemia, new primary cancers, and pneumonitis.
Analysis Populations
The FAS, also known as the ITT population (N = 1,836), consisted of all randomized patients (Table 12). The study was powered based on this population. Patients were analyzed according to their randomized group. Unless otherwise specified, all clinical efficacy end points were summarized and analyzed using the FAS.
The mature cohort (N = 900) included the first 900 randomized patients only. The analysis based on the mature cohort was regarded as supportive.
The PRO analysis set (N = 1,751) consisted of patients who consented to participate in the PRO assessment and who started treatment and provided evaluable FACIT-F or EORTC QLQ-C30 data at baseline. Baseline was defined as the last result on or before the first day of study treatment.
The safety analysis set or safety population (N = 1,815) consisted of all patients who received at least 1 dose of the randomized study drug.
Analysis set | Olaparib | Placebo | Overall |
|---|---|---|---|
Full analysis set, N | 921 | 915 | 1,836 |
Mature cohort, N | 449 | 451 | 900 |
Patient-reported outcome, N | 876 | 875 | 1,751 |
Safety, N | 911 | 904 | 1,815 |
Note: The mature cohort consists of the first 900 randomized patients.
Sources: Clinical Study Reports for OlympiA.18,19
Results
Patient Disposition
In the OlympiA trial, the first patient was randomized to study treatment on June 5, 2014, and the last patient was randomized on May 28, 2019. A total of 14,387 participants were screened; of these, 12,551 (87.2%) did not pass screening. The main reason for screening failures was not meeting eligibility criteria, predominantly because the patient did not have a deleterious or suspected deleterious BRCA mutation (95.0%) in screening part 1.
At interim analysis 1 (March 27, 2020), a total of 1,836 patients were successfully randomized (34 patients from Canada) in a 1:1 ratio to receive either olaparib (n = 921) or matching placebo (n = 915). A total of 294 patients (16.0%) discontinued from the study, 1,815 patients (98.9%) received study treatment, and 1,353 patients (73.7%) completed study treatment. A total of 423 patients (23.0%) discontinued study treatment, including 25.6% in the olaparib group and 20.4% in the placebo group (Table 36).
At interim analysis 2 (July 12, 2021), a total of 350 patients (19.1%) discontinued from the study, mainly due to death (18.0% and 20.1% in the olaparib and placebo groups, respectively), and patient decision (7.6% and 5.8% in the olaparib and placebo groups, respectively). A total of 1,815 patients received study medication, and 1,389 patients (75.7%) completed study treatment (Table 13). A total of 237 patients (25.7%) in the olaparib group and 189 patients (20.7%) in the placebo group discontinued study treatment. The most frequently reported reasons for discontinuation were AEs (10.6% and 4.7% in the olaparib and placebo groups, respectively), recurrence of disease (4.3% and 8.7% in the olaparib and placebo groups, respectively), and patient decision to stop study drug (6.4% and 3.3% in the olaparib and placebo groups, respectively).
Data on gBRCAm status for this study were obtained locally from medical records and/or a central Myriad laboratory. In terms of patient disposition, the subset of patients with confirmed Myriad gBRCAm status was similar to the overall study population (Table 38).
Table 13: Patient Disposition at Interim Analysis 2 — FAS
Characteristica | Olaparib | Placebo |
|---|---|---|
Screened, N | 14,387 | |
Randomized, N | 921 | 915 |
Patients ongoing study, n (%) | 755 (82.0) | 731 (79.9) |
Discontinued from study, n (%) | 166 (18.0) | 184 (20.1) |
Reason for discontinuation, n (%) | ||
Death | 75 (8.1) | 109 (11.9) |
Lost to follow-up | 18 (2.0) | 17 (1.9) |
Patient decision | 70 (7.6) | 53 (5.8) |
Other | 3 (0.3) | 5 (0.5) |
Treated, n (%) | 911 (98.9) | 904 (98.8) |
Receiving ongoing study treatment, n (%) | 0 | 0 |
Completed treatment, n (%) | 674 (73.2) | 715 (78.1) |
Discontinued study treatment,b n (%) | 237 (25.7) | 189 (20.7) |
Reason for treatment discontinuation, n (%) | ||
Adverse event | 98 (10.6) | 43 (4.7) |
Death | 1 (0.1) | 0 |
Recurrence of disease | 40 (4.3) | 80 (8.7) |
Lost to follow-up | 2 (0.2) | 1 (0.1) |
█ █ █ █ █ ██ ██ █ █ █ █ █ ██ ██ █ ██ █ █ █ ██ ████ | █ ██████ | █ ██████ |
█ █ █ █ █ ██ ██ █ █ █ █ █ ██ ██ █ █ █ █ ██ ██ █ █ █ █ ██ █ █ █ █ ██ ████ | █ ██████ | █ █████ |
█ █ █ █ █ ██ ██ █ █ █ █ █ ██ ███ █ █ █ █ ██ █ █ ██ █████ | █ ██████ | █ █████ |
Severe noncompliance | 0 | 5 (0.5) |
Other | 13 (1.4) | 20 (2.2) |
FAS = full analysis set.
aJuly 12, 2021, date cut-off.
bDoes not include patients who did not receive treatment.
Source: Clinical Study Reports for OlympiA.19
Patients Affected by the COVID-19 Pandemic
About █ ██ ███████ patients, including █████ in the olaparib group and █████ in the placebo group, had at least 1 visit affected by the COVID-19 pandemic. According to the sponsor, none of the protocol deviations related to the COVID-19 pandemic were considered significant and raised no concerns about the conduct of the study.
Exposure to Study Treatments
At interim analysis 1 (March 27, 2020), the median actual exposure to treatment was 350.0 days (range, 1 to 420) in the olaparib group, and 358.0 days (range, 2 to 404) in the placebo group (Table 38). The median treatment duration was 338.0 days (range, 1 to 420) in the olaparib group and 358.0 days (range, 2 to 404) in the placebo group.
At interim analysis 2 (July 12, 2021), the median intended duration of treatment exposure was 364.0 days (range, 1 to 492 days) in the olaparib group and 365.0 days (range, 2 to 414 days) in the placebo group (Table 14). The median actual exposure to treatment was similar for the olaparib and placebo groups (350.0 days (range, 1 to 420 days) and 359.0 days (range, 2 to 404 days), respectively) in the safety study population. The median actual treatment duration was 341.0 days (range, 1 to 420 days) in the olaparib group and 358.0 days (range, 2 to 404 days) in the placebo group.
A total of 228 patients (25.0%) in the olaparib group required a dose reduction compared with 47 patients (5.2%) in the placebo group, with AEs being the main reason for the dose reduction (24.4% and 3.9% in the olaparib and placebo groups, respectively) (Table 14). Dose interruptions lasting at least 3 days occurred in 405 patients (44.5%) in the olaparib group and 279 patients (30.9%) in the placebo group. The most frequently reported reasons for dose interruptions were AEs (36.2% and 14.2% in the olaparib and placebo groups, respectively), and surgery (24.8% and 26.3% in the olaparib and placebo groups, respectively). Treatment adherence was assessed based on the amount of study drug returned at the end of the treatment period.
Prior Therapy for Primary Breast Cancer
A total of 926 patients (50.4%) received antineoplastic therapy, including taxanes (49.6% and 49.1% in the olaparib and placebo groups, respectively), anthracyclines (47.7% and 46.2% in the olaparib and placebo groups, respectively), and nitrogen mustard analogues (48.0% and 47.2% in the olaparib and placebo groups, respectively). A total of 291 patients (89.5%) received prior and/or concurrent hormone therapy, including 86.9% of patients in the olaparib group and 92.4% in the placebo group. Most patients underwent a nonconservative breast surgery before randomization, including 755 patients (42.2%) who had previously received neoadjuvant chemotherapy, and 667 patients (36.3%) who had previously received adjuvant chemotherapy.
Table 14: Treatment Exposure at Interim Analysis 2 — Safety Population
Treatment exposurea | Olaparib (N = 911) | Placebo (N = 904) |
|---|---|---|
Total intended exposure (days)a | ||
Mean (SD) | 307.2 (115.02) | 323.1 (97.72) |
Median (minimum, maximum) | 364.0 (1, 492) | 365.0 (2, 414) |
Actual treatment exposure (days)b | ||
Mean (SD) | 295.0 (114.06) | 315.7 (97.77) |
Median (minimum, maximum) | 350.0 (1, 420) | 359.0 (2, 404) |
Number of days on 300 mg treatment twice dailyc | ||
Mean (SD) | 245.7 (142.00) | 307.0 (107.67) |
Median (minimum, maximum) | 341.0 (1, 420) | 358.0 (2, 404) |
Patients with a dose reduction, n (%) | 228 (25.0) | 47 (5.2) |
Reason for reduction, n (%) | ||
Adverse event | 222 (24.4) | 35 (3.9) |
Dosing error | 6 (0.7) | 10 (1.1) |
Administrative reasons | █ █████ | █ █████ |
Other | █ █████ | █ █████ |
Patients with a dose interruption, n (%) | 519 (57.0) | 405 (44.8) |
Patients with a dose interruption lasting at least 3 days, n (%) | 405 (44.5) | 279 (30.9) |
Reason for interruption, n (%) | ||
Adverse event | 330 (36.2) | 128 (14.2) |
Surgery | 226 (24.8) | 238 (26.3) |
Recurrence of disease | 38 (4.2) | 78 (8.6) |
Dosing error | 0 (0.0) | 3 (0.3) |
Administrative reasons | 21 (2.3) | 26 (2.9) |
Other | 6 (0.7) | 11 (1.2) |
Patients with dose interruption and reduction, n (%) | █ ██ ██████ | █ ██████ |
SD = standard deviation.
Note: July 12, 2021, data cut-off date.
Patients with partial treatment end dates were excluded.
Dose interruptions and reductions are based on investigator-initiated decisions; interruptions and reductions due to patient noncompliance are omitted.
aTotal intended exposure (days) = last dose date minus first dose date plus 1.
bActual treatment exposure (days) = intended exposure minus total duration of dose interruptions, where intended exposure was calculated as per previous footnote.
cNumber of days on 300 mg olaparib or placebo twice daily (actual exposure for the assigned starting dose).
Sources: Clinical Study Reports for OlympiA.18,19
Concomitant Therapy
Reported concomitant medication use was generally balanced between treatment arms. A total of 788 patients (85.6%) in the olaparib group and 762 patients (83.3%) in the placebo group received at least 1 concomitant medication initiated on or after the randomization date. The most commonly used classes of drugs were: propionic acid derivatives (18.3% and 18.6% in the olaparib and placebo groups, respectively), proton pump inhibitors (16.4% and 14.8% in the olaparib and placebo groups, respectively), propulsives (16.2% and 5.5% in the olaparib and placebo groups, respectively), antibacterials for systemic use (28.9% and 29.2% in the olaparib and placebo groups, respectively), paracetamol (20.8% and 20.5% in the olaparib and placebo groups, respectively), and ibuprofen (11.5% in both olaparib and placebo groups). A total of 5 patients (0.5%) in the olaparib group and 4 patients (0.4%) in the placebo group received disallowed concomitant medications, including antineoplastic drugs (0.4% and 0.2% in the olaparib and placebo groups, respectively), and radiotherapy (0.1% and 0.2% in the olaparib and placebo groups, respectively).
Subsequent Post-Event Therapy
In total, 258 patients (14.1%) received post-event treatments for breast cancer recurrence, new primary, contralateral invasive breast cancer malignancy, or nonprimary end point malignancies, including systemic therapy (10.9% and 17.3% in the olaparib and placebo groups, respectively), post-event radiotherapy (4.2% and 7.7% in the olaparib and placebo groups, respectively), and post-event surgery (5.8% and 8.6% in the olaparib and placebo groups, respectively). The most common subsequent systemic therapies received included platinum-containing regimens (4.7% and 8.4% in the olaparib and placebo groups, respectively), pyrimidine analogues (4.1% and 6.6% in the olaparib and placebo groups, respectively), taxanes (4.6% and 4.8% in the olaparib and placebo groups, respectively), and PARP inhibitors (4.7% and 5.2% in the olaparib and placebo groups, respectively).
Protocol Deviations
In total, 251 patients (13.7%) had at least 1 important protocol deviation, with similar frequencies across the treatment groups: 129 patients (14.0%) in the olaparib arm, and 122 patients (13.3%) in the placebo arm (Table 15). The most common protocol deviations included not fulfilling criteria for high-risk disease (2.7% and 1.5% in the olaparib and placebo arms, respectively), and no staging or insufficient staging as patients with metastatic breast cancer should have been excluded from the trial according to the exclusion criteria (7.3% in both olaparib and placebo arms). The important protocol deviations were identified and classified before database lock in a blinded manner.
Efficacy
Only those efficacy outcomes and analyses of subgroups identified in the review protocol are reported subsequently. See Appendix 3 for detailed efficacy data.
Overall Survival
At interim analysis 1 (March 27, 2020), the OS data were 7.9% mature. The median follow-up was 2.3 years in the olaparib group and 2.5 years in the placebo group (Table 16). In the FAS, median OS was not estimable, and the stratified HR was 0.68 (99% CI, 0.44 to 1.05; P = 0.0236). In the FAS, deaths were reported in 59 patients (6.4%) in the olaparib group and 86 patients (9.4%) in the placebo group. The proportion of patients who were alive at 3 years was 92.0% (95% CI, 89.6% to 93.9%) in the olaparib group and 88.3% (95% CI, 85.4% to 90.7%) in the placebo group. The Kaplan-Meier plot of OS for the FAS is presented in Figure 4.
Table 15: Protocol Deviations — FAS
Characteristic | Olaparib (N = 921) | Placebo (N = 915) |
|---|---|---|
Patients with at least 1 major protocol deviation, n (%) | █ ██ ██████ | █ ██ ██████ |
Patients with at least 1 major protocol deviation, triggering a sensitivity analysis, n (%) | █ ██████ | █ ██████ |
Not fulfilling criteria for high-risk disease | █ ██████ | █ ██████ |
No staging or insufficient staging | █ ██████ | █ ██████ |
Randomized but did not receive any study treatment | █ ██████ | █ ██████ |
Patients with at least 1 important GCP violation, n (%)a | █ ██████ | █ ██████ |
FAS = full analysis set; GCP = good clinical practice.
aThe same patient may have had more than 1 important protocol deviation.
Sources: Clinical Study Reports for OlympiA.18,19
At interim analysis 2 (July 12, 2021), the OS data were 10.0% mature. The median follow-up was 3.5 years in the olaparib group, and 3.6 years in the placebo group (Table 16). In the FAS, deaths were reported in 75 patients (8.1%) in the olaparib group and 109 patients (11.9%) in the placebo group. The median OS was not estimable, and the stratified HR was 0.68 (98.5% CI, 0.47 to 0.97; P = 0.0091) in favour of the olaparib group. The proportion of patients who were alive at 4 years was 89.8% (95% CI, 87.2% to 91.9%) in the olaparib group and 86.4% (95% CI, 83.6% to 88.7%) in the placebo group (difference = 3.4%; 95% CI, –0.1% to 6.8%).17 The Kaplan-Meier plot of IDFS for the FAS is presented in Figure 5. The sensitivity and subgroup analyses were consistent with the primary OS analysis (Table 45 and Table 46).
Table 16: Overall Survival — FAS
Characteristic | Interim analysis 1a | Interim analysis 2b | ||
|---|---|---|---|---|
Olaparib (N = 921) | Placebo (N = 915) | Olaparib (N = 921) | Placebo (N = 915) | |
Patients with events, n (%) | 59 (6.4) | 86 (9.4) | 75 (8.1) | 109 (11.9) |
Stratified HRc (99% CId) | 0.68 (0.44 to 1.05) | NA | ||
Stratified HRc (98.5% CId) | NA | 0.68 (0.47 to 0.97) | ||
95.0% CIe | 0.49 to 0.95 | 0.50 to 0.91 | ||
Log-rank P valuef | 0.0236 | 0.0091 | ||
Deaths deemed attributable to breast cancer, n (%) | 55 (6.0) | 82 (9.0) | 70 (7.6) | 103 (11.3) |
Median follow-up (minimum, maximum), years | 2.4 (0, 5.5) | 2.5 (0, 5.5) | 3.5 (0, 6.8) | 3.6 (0, 6.7) |
Number of patients censored,g n (%) | 862 (93.6) | 829 (90.6) | 846 (91.9) | 806 (88.1) |
Special cases censored at 0.5 daysh | 4 (0.4) | 7 (0.8) | 3 (0.3) | 6 (0.7) |
Inadvertent randomization | 1 (0.1) | 3 (0.3) | 0 (0) | 2 (0.2) |
Patient withdrew consent, not treated, not follow-up | 3 (0.3) | 4 (0.4) | 3 (0.3) | 4 (0.4) |
Event-free ratei (95% CI) at: | ||||
1 year | 98.1 (96.9 to 98.8) | 96.9 (95.5 to 97.9) | 98.0 (96.9 to 98.8) | 96.9 (95.5 to 97.9) |
2 years | 94.8 (93.0 to 96.2) | 92.3 (90.1 to 94.0) | 95.0 (93.3 to 96.2) | 92.8 (90.9 to 94.3) |
3 years | 92.0 (89.6 to 93.9) | 88.3 (85.4 to 90.7) | 92.8 (90.8 to 94.4) | 89.1 (86.7 to 91.0) |
4 years | NA | NA | 89.8 (87.2 to 91.9) | 86.4 (83.6 to 88.7) |
CI = confidence interval; ER = estrogen receptor; FAS = full analysis set; HER2 = human epidermal growth factor receptor 2; HR = hazard ratio; KM = Kaplan-Meier; NA = not applicable; OS = overall survival; PgR = progesterone receptor; TNBC = triple-negative breast cancer.
aData cut-off date: March 27, 2020.
bData cut-off date: July 12, 2021.
cEstimate of the treatment HR was based on the stratified Cox proportional hazards model. Stratification factors were the same as those used in the stratified log-rank test.
dInferential, according to the alpha spending rules for the interim analysis. The CI for the HR was estimated using the profile likelihood approach.
eExploratory, not inferential.
fP value from a stratified log-rank test. Stratification was by chemotherapy type (adjuvant vs. neoadjuvant), hormone receptor status (ER- and/or PgR-positive and HER2-negative vs. TNBC), and prior platinum therapy (yes vs. no). Stratification factors were based on the categories used in the randomization system and were chosen by the pooling strategy. Once the pooling strategy was applied, only the hormone receptor status stratification factor was selected. A 2-sided significance level of 0.01 was assigned to interim analysis 1. A 2-sided significance level of 0.015 was assigned to interim analysis 2.
gAny patient not known to have died at the time of analysis will be censored based on the last recorded date on which the patient was known to be alive.
hThese randomized patients will be counted in the FAS; however, they will be treated as being censored for the OS event just after randomization. Censoring these patients at day 0.5 will not affect the log-rank test; however, they will be counted in the total number on day 1 and in the KM plot. The reason for censoring at day 0.5 is to avoid ties with other patients censored on day 1.
IPercentage of patients (95% CI) alive from the KM estimates; the 95% CIs were calculated using the Greenwood formula.
Sources: Clinical Study Reports for OlympiA.18,19
Figure 4: Kaplan-Meier Estimates of OS at Interim Analysis 1 — FAS
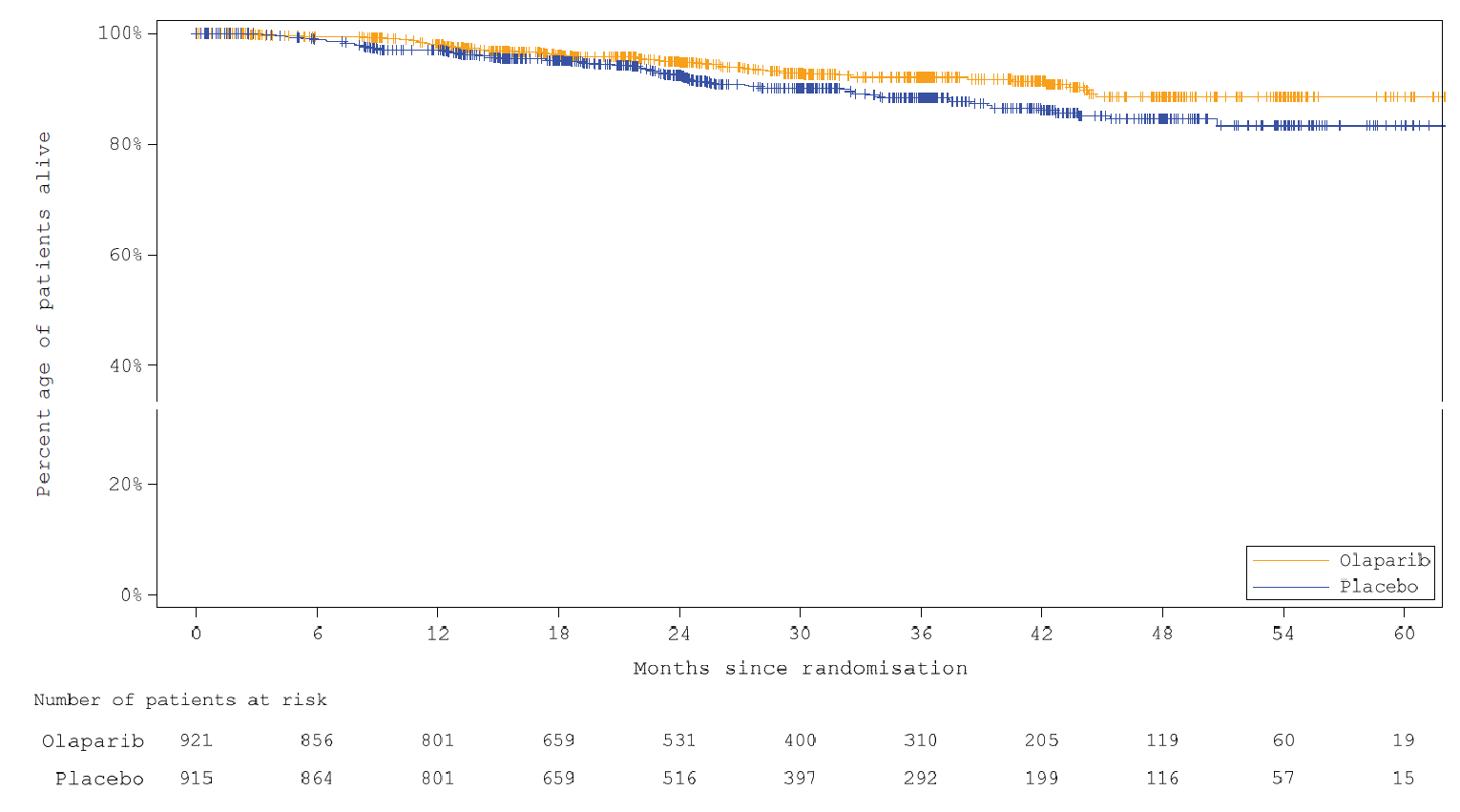
Data cut-off date: March 27, 2020.
OS = overall survival; FAS = full analysis set.
Source: Clinical Study Report for OlympiA.18
Figure 5: Kaplan-Meier Estimates of OS at Interim Analysis 2 — FAS
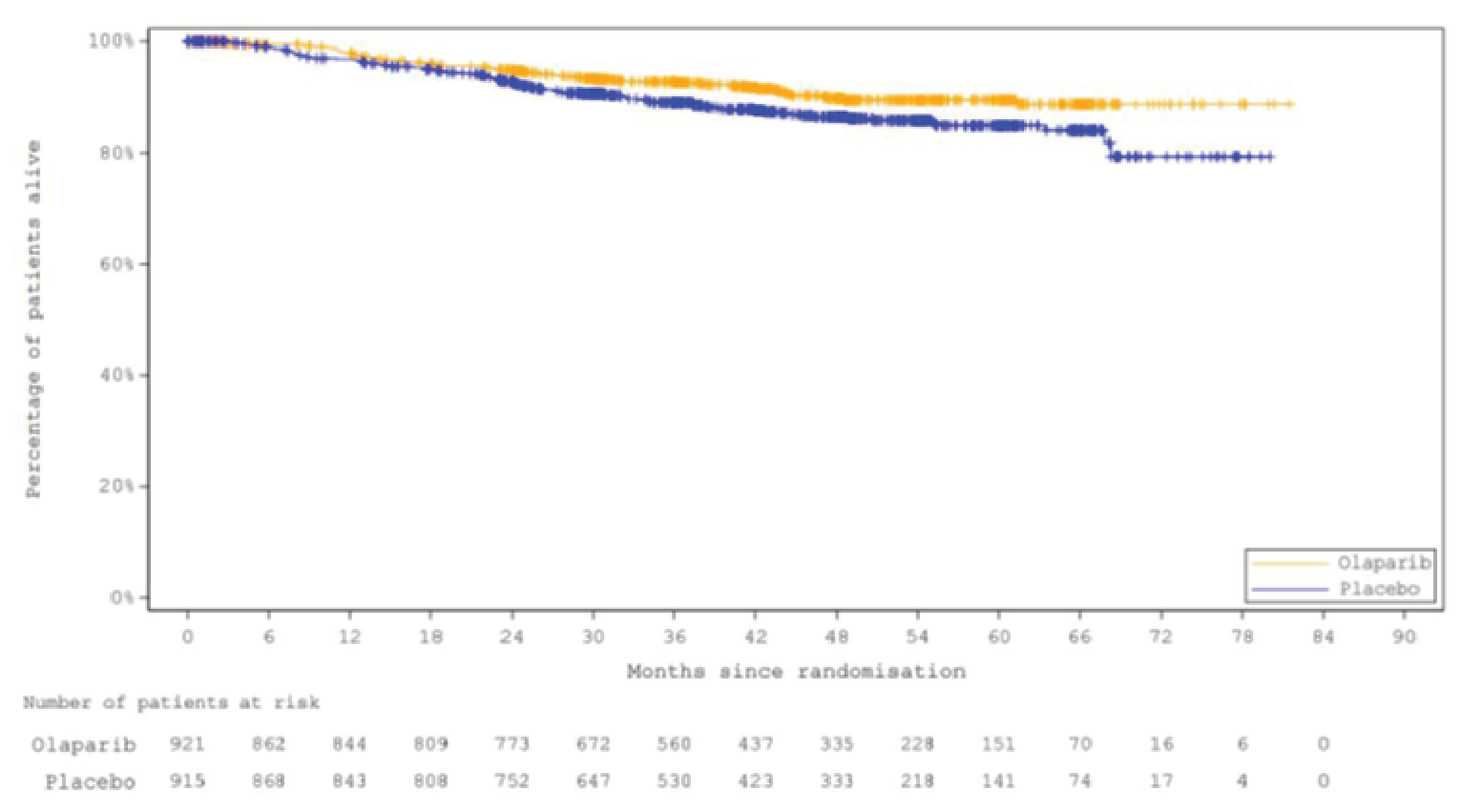
Note: July 12, 2021, data cut-off date.
OS = overall survival; FAS = full analysis set.
Source: Clinical Study Report for OlympiA.19
Invasive Disease–Free Survival
At interim analysis 1 (March 27, 2020), a total of 284 patients had an IDFS event (the data reached 15.5% maturity), including 106 patients (11.5%) in the olaparib group, and 178 patients (19.5%) in the placebo group. In the mature cohort that included the first 900 randomized patients, 65 patients (14.5%) in the olaparib group and 104 patients (23.1%) in the placebo group had an IDFS event (Table 40).
At interim analysis 2 (July 12, 2021), a total of 341 patients had an IDFS event (the data reached 18.6% maturity), including 134 patients (14.5%) in the olaparib group, and 207 patients (22.6%) in the placebo group. The most common type of event was a distant recurrence (Table 17).
Table 17: Summary of Type of First IDFS Event — FAS
Event | Interim analysis 1a | Interim analysis 2b | ||
|---|---|---|---|---|
Olaparib (N = 921) | Placebo (N = 915) | Olaparib (N = 921) | Placebo (N = 915) | |
IDFS events, n (%) | 106 (11.5) | 178 (19.5) | 134 (14.5) | 207 (22.6) |
Distant CNS recurrence, n (%) | 22 (2.4) | 36 (3.9) | 24 (2.6) | 38 (4.2) |
Distant recurrence (excluding CNS), n (%) | 50 (5.4) | 84 (9.2) | 64 (6.9) | 98 (10.7) |
Regional (ipsilateral) recurrence, n (%) | 6 (0.7) | 14 (1.5) | 9 (1.0) | 18 (2.0) |
Local (ipsilateral) recurrence, n (%) | 7 (0.8) | 11 (1.2) | 9 (1.0) | 12 (1.3) |
Contralateral invasive breast cancer | 8 (0.9) | 12 (1.3) | 15 (1.6) | 18 (2.0) |
New primary cancers | 11 (1.2) | 21 (2.3) | 11 (1.2) | 23 (2.5) |
New primary invasive nonbreast ovarian cancer | 2 (0.2) | 8 (0.9) | 2 (0.2) | 10 (1.1) |
New primary invasive nonbreast nonovarian cancer | 9 (1.0) | 13 (1.4) | 9 (1.0) | 13 (1.4) |
Death without a prior IDFS event | 2 (0.2) | 0 | 2 (0.2) | 0 |
CNS = central nervous system; FAS = full analysis et; IDFS = invasive disease–free survival.
aData cut-off date: March 27, 2020.
bData cut-off date: July 12, 2021.
Sources: Clinical Study Reports for OlympiA.18,19
Table 18: Invasive Disease–Free Survival — FAS
Characteristic | Interim analysis 1a | Interim analysis 2b | ||
|---|---|---|---|---|
Olaparib (N = 921) | Placebo (N = 915) | Olaparib (N = 921) | Placebo (N = 915) | |
Patients with events, n (%) | 106 (11.5) | 178 (19.5) | 134 (14.5) | 207 (22.6) |
Stratified HRc (99.5% CId) | 0.58 (0.41 to 0.82) | 0.63 (NR) | ||
95.0% CIe | 0.46 to 0.74 | (0.50 to 0.78) | ||
Log-rank test P valuef | 0.0000073 | Reference | NA | |
Median follow-upg (minimum, maximum), years | 2.3 (0, 5.5) | 2.5 (0, 5.5) | 3.5 (0, 6.7) | 3.6 (0, 6.6) |
Number of patients censored,h n (%) | 815 (88.5) | 737 (80.5) | 787 (85.5) | 708 (77.4) |
Special cases censored at 0.5 daysi | 5 (0.6) | 7 (0.9) | 4 (0.4) | 9 (1.0) |
Event before randomization | 2 (0.3) | 3 (0.4) | 2 (0.2) | 3 (0.3) |
Inadvertent randomization | 1 (0.1) | 2 (0.3) | 0 (0.0) | 2 (0.2) |
Patient withdrew consent, not treated, not followed up | 2 (0.3) | 2 (0.3) | 2 (0.2) | 4 (0.4) |
Event-free ratej (95% CI) at: | ||||
1 year | 93.3 (91.4 to 94.8) | 88.4 (86.1 to 90.4) | 93.4 (91.5 to 94.9) | 88.4 (86.1 to 90.3) |
2 years | 89.2 (86.8 to 91.3) | 81.5 (78.6 to 84.0) | 89.7 (87.4 to 91.6) | 81.4 (78.7 to 83.8) |
3 years | 85.9 (82.8 to 88.4) | 77.1 (73.7 to 80.1) | 86.1 (83.5 to 88.3) | 77.3 (74.3 to 80.0) |
4 years | NA | NA | 82.7 (79.6 to 85.4) | 75.4 (72.2 to 78.3) |
CI = confidence interval; ER = estrogen receptor; FAS = full analysis set; HER2 = human epidermal growth factor receptor 2; HR = hazard ratio; IDFS = invasive disease–free survival; KM = Kaplan-Meier; NA = not applicable, PgR = progesterone receptor; TNBC = triple-negative breast cancer.
aData cut-off date: March 27, 2020.
bData cut-off date: July 12, 2021.
cEstimate of the treatment HR was based on the stratified Cox proportional hazards model. Stratification factors were the same as those used in the stratified log-rank test. The CI for the HR was estimated using the profile likelihood approach.
dInferential, according to the alpha spending rules for the interim analysis.
eExploratory, not inferential.
fP value from a stratified log-rank test. Stratification was by chemotherapy type (adjuvant vs. neoadjuvant), hormone receptor status (ER- and/or PgR-positive and HER2-negative vs. TNBC), and prior platinum therapy (yes vs. no). Stratification factors were based on the categories used in the randomization system and were chosen by the pooling strategy. Once the pooling strategy was applied, only the hormone receptor status stratification factor was selected. A 2-sided significance level of 0.005 was assigned to IDFS at interim analysis 1.
gMedian clinical follow-up was calculated using the reverse censoring method.
hPatients who have not had a recorded IDFS event at the time of the analysis will be censored at the date of their last disease evaluation. Disease evaluation includes mammogram and/or breast MRI (MRI preferred for patients younger than 50 years), other radiological or other imaging or clinical examination (e.g., physical exam).
IThese randomized patients will be counted in the FAS; however, they will be treated as being censored for the IDFS event just after randomization. Censoring these patients at day 0.5 will not affect the log-rank test; however, they will be counted in the total number at risk and in the KM plot. The reason for censoring at day 0.5 is to avoid ties with other patients censored on day 1.
jPercentage (95% CI) of patients who were free from invasive disease from the KM estimates and the 95% CIs were calculated using the Greenwood formula.
The mature cohort includes the first 900 patients randomized.
Sources: Clinical Study Reports for OlympiA.18,19
At interim analysis 1 (March 27, 2020), the median follow-up was 2.3 years in the olaparib group and 2.5 years in the placebo group (Table 18), and the median IDFS was not estimable in either treatment arm. The stratified HR for invasive disease recurrence or death was 0.58 (99.5% CI, 0.41 to 0.82; P = 0.0000073) in favour of the olaparib group. The proportion of patients who remained invasive disease–free at 3 years was 85.9% (95% CI, 82.8% to 88.4%) in the olaparib group and 77.1% (95% CI, 73.7% to 800.12%) in the placebo group. The IDFS results in the FAS were consistent with the IDFS analysis performed using a mature cohort with a median follow-up of 3.5 years in both treatment groups (stratified HR = 0.61; 99.5% CI, 0.39 to 0.95) (Table 40). After reviewing the data for interim analysis 1, an independent data-monitoring committee concluded that the prespecified statistical threshold for the superiority of olaparib over placebo for IDFS was reached at a maturity of 15.5%; thus, this analysis constitutes the primary IDFS analysis for the OlympiA trial. The Kaplan-Meier plot of IDFS for the FAS is presented in Figure 6.
Subgroup Analyses
Primary end point subgroup analyses at interim analysis 1 are presented in Table 19. The treatment effects for all prespecified subgroups in the CADTH protocol were consistent with the main effect.
Figure 6: Kaplan-Meier Estimates of IDFS at Interim Analysis 1 — FAS
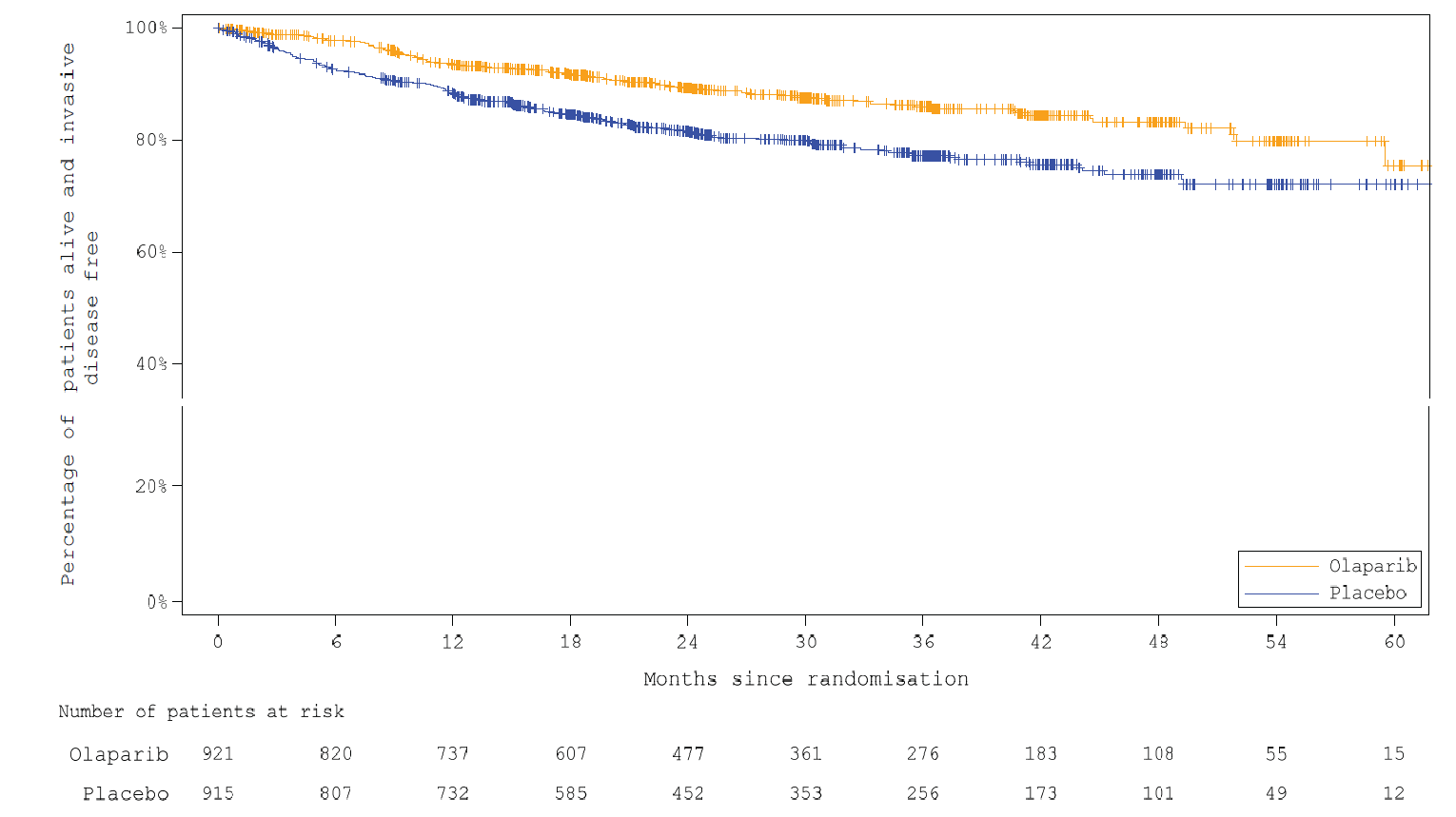
FAS = full analysis set; IDFS = invasive disease–free survival.
Note: March 27, 2020, data cut-off date.
Source: Clinical Study Reports for OlympiA.18
Table 19: Subgroup Analyses of IDFS at Interim Analysis 1 — FAS
Subgroupa | Olaparib Events, n (%) | Placebo Events, n (%) | HRb (95% CI) | Interaction P value |
|---|---|---|---|---|
Prior chemotherapy | ||||
Adjuvant | n = 461 36 (7.8) | n = 455 61 (13.4) | 0.60 (0.39 to 0.90) | 0.763 |
Neoadjuvant | n = 460 70 (15.2) | n = 460 117 (25.4) | 0.56 (0.41 to 0.75) | |
Prior platinum | ||||
Yes | n = 247 34 (13.8) | n = 239 43 (18.0) | 0.77 (0.49 to 1.21) | 0.144 |
No | n = 674 72 (10.7) | n = 676 135 (20.0) | 0.52 (0.39 to 0.69) | |
Hormone receptor status | ||||
HR-positivec and HER2-negative | n = 168 19 (11.3) | n = 157 25 (15.9) | 0.70 (0.38 to 1.27) | 0.509 |
TNBCd | n = 751 87 (11.6) | n = 758 153 (20.2) | 0.56 (0.43 to 0.73) | |
BRCA mutation type | ||||
BRCA1 | n = 552 69 (12.5) | n = 553 126 (22.8) | 0.52 (0.38 to 0.69) | 0.975 |
BRCA2 | n = 224 20 (8.9) | n = 206 37 (18.0) | 0.48 (0.27 to 0.82) | |
BRCA1 and BRCA2 | n = 1 0 (0.0) | n = 3 0 (0.0) | NA | |
Axillary nodal status | ||||
Node-negative | n = 203 13 (6.4) | n = 192 22 (11.5) | 0.61 (0.30 to 1.19) | 0.608 |
Node-positive | n = 174 15 (8.6) | n = 177 31 (17.5) | 0.48 (0.25 to 0.87) | |
CPS&EG score | ||||
CPS&EG score of 2, 3, or 4 | n = 398 55 (13.8) | n = 387 96 (24.8) | 0.51 (0.37 to 0.71) | 0.750 |
CPS&EG score of 5 or 6 | n = 22 11 (50.0) | n = 15 10 (66.7) | 0.44 (0.19 to 1.06) | |
BRCA = breast cancer susceptibility gene; CI = confidence interval; CPS&EG = clinical and post-treatment pathologic stage and estrogen receptor status and histologic grade; ER = estrogen receptor; FAS = full analysis set; HER2 = human epidermal growth factor receptor 2; HR = hazard ratio; HR-positive = positive for expression of a hormone receptor; IDFS = invasive disease–free survival; NA = not applicable; PgR = progesterone receptor; TNBC = triple-negative breast cancer.
aData cut-off date: March 27, 2020.
bThe Cox model included factors for treatment group, subgroup factor, and the treatment-by-subgroup interaction. All patients with nonmissing subgroup data were included in the model. The CI was calculated using a profile likelihood approach. These analyses are not inferential.
cHR-positive is defined as ER-positive and/or PgR-positive.
dTwo patients are excluded from the summary of the TNBC subset because they do not have confirmed HER2-negative status.
Source: Clinical Study Reports for OlympiA.18
Sensitivity Analyses
The sensitivity analyses for the primary IDFS end point at interim analysis 1 (Table 42), including patients with central pathology review data, unadjusted analysis, and interval censoring, as well as supportive analysis in patients with a Myriad-confirmed gBRCAm (Table 41), were consistent with the primary IDFS analysis.
At interim analysis 2 (July 12, 2021), the median follow-up was 3.5 years in the olaparib group and 3.6 years in the placebo group (Table 18). This was an exploratory analysis, as no alpha was reserved for IDFS since the superiority of olaparib over placebo for IDFS was demonstrated at interim analysis 1. The median IDFS was not estimable, and the stratified HR for invasive disease recurrence or death was 0.63 (95% CI, 0.50 to 0.78) in favour of the olaparib group. The proportion of patients who remained invasive disease–free at 4 years was 82.7% (95% CI, 79.6% to 85.4%) in the olaparib group and 75.4% (95% CI, 72.2% to 78.3%) in the placebo group (difference = 7.3%; 95% CI, 3.0% to 11.5%).17 The Kaplan-Meier plot of IDFS for the FAS is presented in Figure 7. The subgroup analyses across prespecified subgroups and sensitivity analyses were consistent with the primary IDFS analysis for interim analysis 2.
Figure 7: Kaplan-Meier Estimates of IDFS at Interim Analysis 2 — FAS
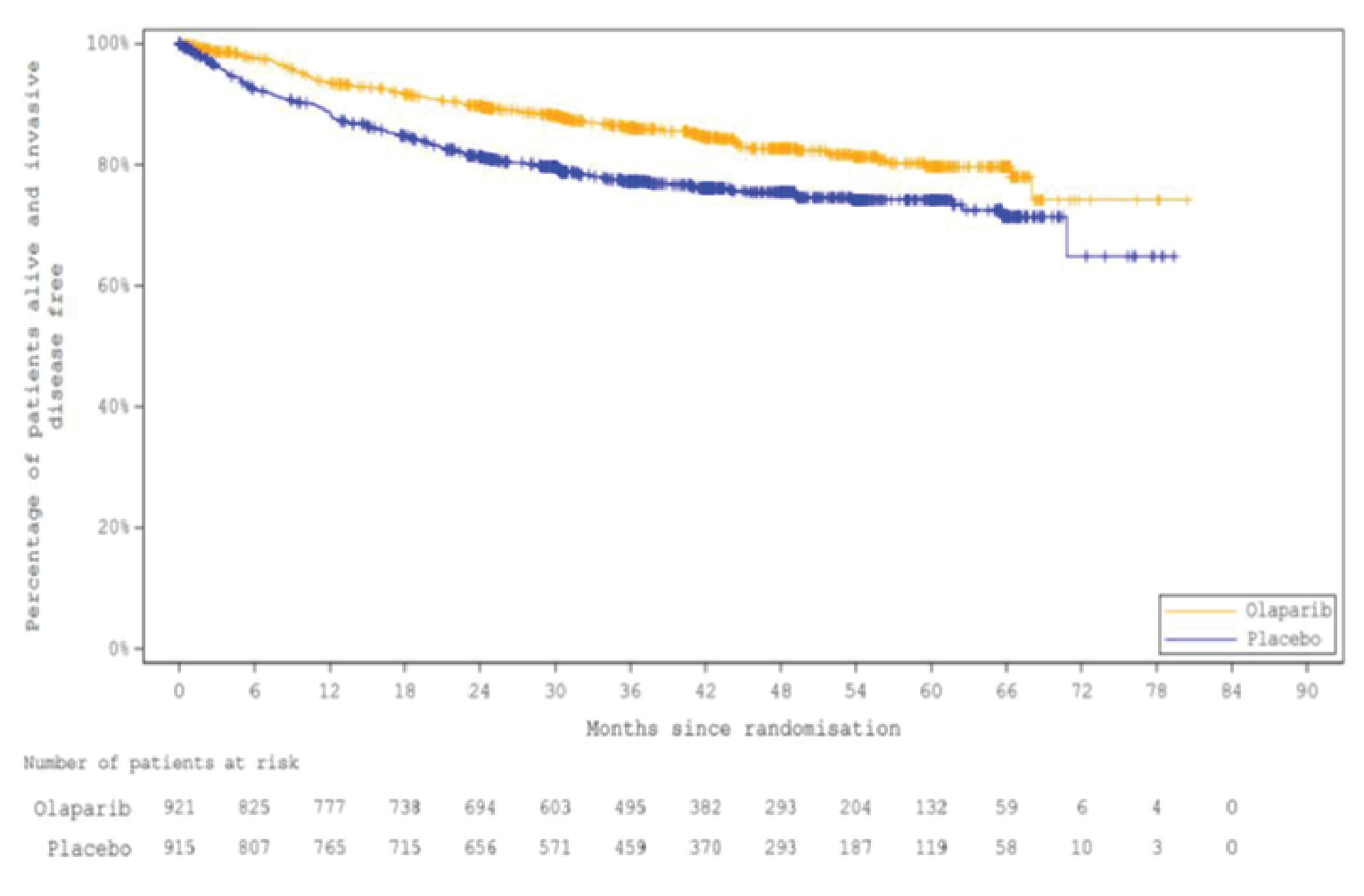
Note: July 12, 2021, data cut-off date.
IDFS = invasive disease–free survival; FAS = full analysis set.
Source: Clinical Study Reports for OlympiA.19
Distant Disease–Free Survival
At interim analysis 1 (March 27, 2020), the median follow-up was 2.3 years in the olaparib group and 2.5 years in the placebo group (Table 20). In the FAS, 89 patients (9.7%) in the olaparib group and 152 patients (16.6%) in the placebo group had a DDFS event. The median DDFS was not estimable in either arm, and the stratified HR for distant disease recurrence or death was 0.57 (99.5% CI, 0.39 to 0.83; P = 0.0000257) in favour of the olaparib group. The proportion of patients who remained distant disease–free at 3 years was 87.5% (95% CI, 84.6% to 89.9%) in the olaparib group and 80.4% (95% CI, 77.2% to 83.3%) in the placebo group. The Kaplan-Meier plot of DDFS for the FAS is presented in Figure 8.
Table 20: Distant Disease–Free Survival — FAS
DDFS | Interim analysis 1a | Interim analysis 2b | ||
|---|---|---|---|---|
Olaparib (N = 921) | Placebo (N = 915) | Olaparib (N = 921) | Placebo (N = 915) | |
Patients with events, n (%) | 89 (9.7) | 152 (16.6) | 107 (11.6) | 172 (18.8) |
Stratified HR (99.5% CIc) | 0.57 (0.39 to 0.83)d | 0.61 (NR) | ||
95.0% CIe | 0.44 to 0.74 | 0.48 to 0.77 | ||
Log-rank test: P valuef | 0.0000257 | Reference | NA | |
Median follow-up (minimum, maximum), years | 2.3 (0, 5.5) | 2.5 (0, 5.5) | 3.5 (0, 6.7) | 3.5 (0, 6.6) |
Number of patients censored,g n (%) | 832 (90.3) | 763 (83.4) | 814 (88.4) | 743 (81.2) |
Special cases censored at 0.5 daysh | 5 (0.5) | 7 (0.8) | 4 (0.4) | 7 (0.8) |
Event before randomization | 1 (0.1) | 1 (0.1) | 1 (0.1) | 1 (0.1) |
Inadvertent randomization | 1 (0.1) | 2 (0.2) | 0 (0) | 2 (0.2) |
Patient withdrew consent, not treated, not followed up | 3 (0.3) | 4 (0.4) | 3 (0.3) | 4 (0.4) |
Event-free ratei (95% CI) at: | ||||
1 year | 94.3 (92.4 to 95.6) | 90.2 (88.1 to 92.0) | 94.4 (92.6 to 95.7) | 90.3 (88.2 to 92.1) |
2 years | 90.0 (87.6 to 92.0) | 83.9 (81.2 to 86.3) | 90.6 (88.4 to 92.4) | 84.0 (81.4 to 86.3) |
3 years | 87.5 (84.6 to 89.9) | 80.4 (77.2 to 83.3) | 88.0 (85.5 to 90.1) | 81.0 (78.1 to 83.5) |
4 years | NA | NA | 86.5 (83.8 to 88.8) | 79.1 (76.0 to 81.8) |
CI = confidence interval; DDFS = distant disease–free survival; ER = estrogen receptor; FAS = full analysis set; HER2 = human epidermal growth factor receptor 2; HR = hazard ratio; IDFS = invasive disease–free survival; KM = Kaplan-Meier; NA = not applicable; NR = not reported; PgR = progesterone receptor; TNBC = triple-negative breast cancer.
aData cut-off date: March 27, 2020.
bData cut-off date: July 12, 2021.
cInferential, according to the alpha spending rules for the interim analysis. The CI for the HR was estimated using the profile likelihood approach.
dEstimate of the treatment HR was based on the stratified Cox proportional hazards model. Stratification factors were the same as those used in the stratified log-rank test.
eExploratory, not inferential.
fP value from a stratified log-rank test. Stratification was by chemotherapy type (adjuvant vs. neoadjuvant), hormone receptor status (ER- and/or PgR-positive and HER2-negative vs. TNBC), and prior platinum therapy (yes vs. no). Stratification factors were based on the categories used in the randomization system and were chosen by the pooling strategy. Once the pooling strategy was applied, only the hormone receptor status stratification factor was selected. A 2-sided significance level of 0.005 was assigned to the interim analysis of DDFS.
gPatients who have not had a recorded DDFS event at the time of the analysis will be censored at the date of their last clinical evaluation (i.e., last physical exam or radiological evaluation).
hThese randomized patients will be counted in the FAS; however, they will be treated as being censored for the DDFS event just after randomization. Censoring these patients at day 0.5 will not affect the log-rank test, however, they will be counted in the total number at risk and in the KM plot.
IPercentage (95% CI) of patients who were distant disease–free from the KM estimates and the 95% CIs were calculated using the Greenwood formula.
Sources: Clinical Study Reports for OlympiA.18,19
Figure 8: Kaplan-Meier Estimates of DDFS at Interim Analysis 1 — FAS
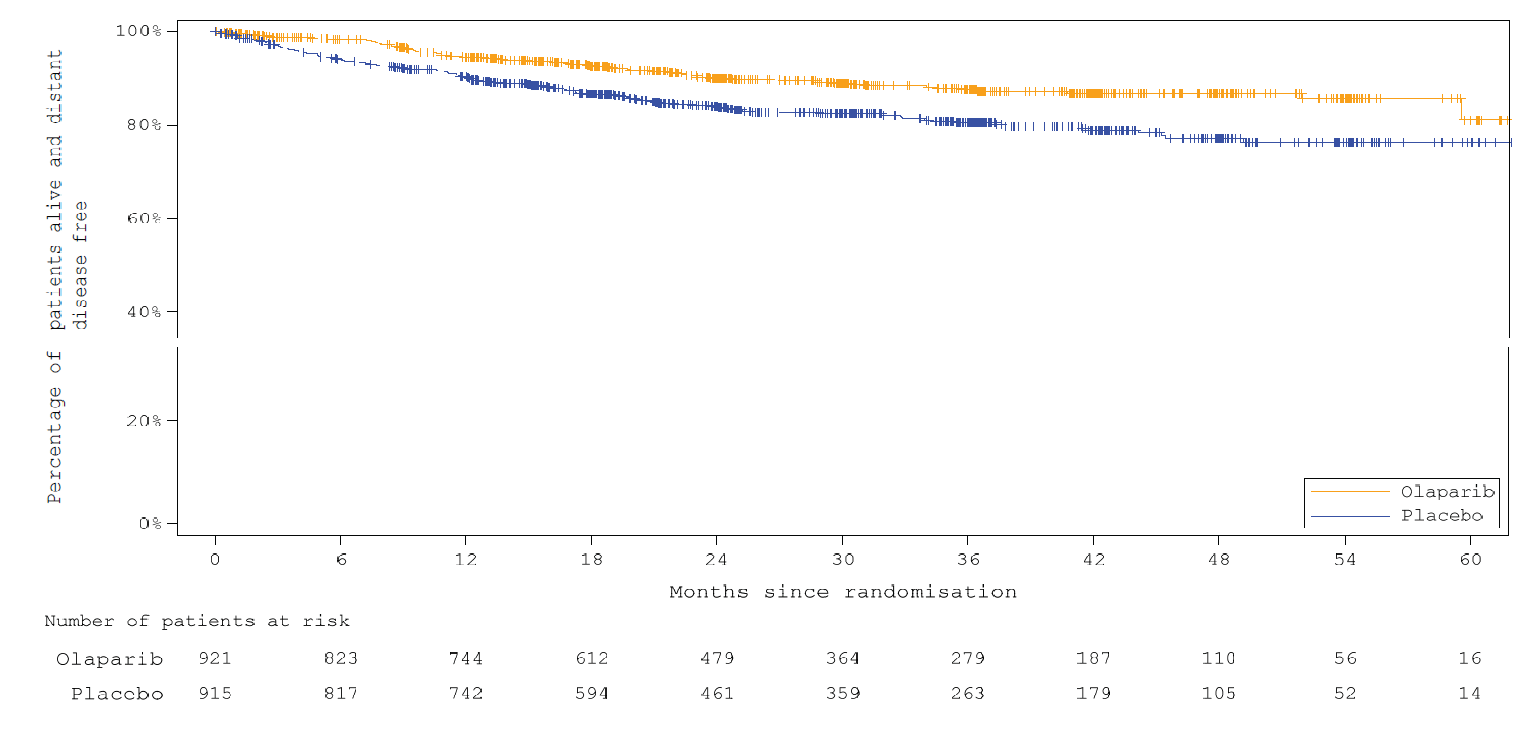
DDFS = distant disease–free survival; FAS = full analysis set.
Note: March 27, 2020, data cut-off date.
Source: Clinical Study Reports for OlympiA.18
Subgroup Analyses
Subgroup analyses for the DDFS end point for interim analysis 1 in the OlympiA trial are presented in Table 45. The treatment effects for all prespecified subgroups in the CADTH protocol were consistent with the main effect.
Sensitivity Analyses
The sensitivity analyses for the DDFS end point at interim analysis 1 (Table 43), including patients with central pathology review data, unadjusted analysis, and interval censoring, as well as the supportive analysis in patients with a Myriad-confirmed gBRCAm (Table 42), were consistent with the primary analysis of DDFS.
At interim analysis 2 (July 12, 2021), the median follow-up was 3.5 years in the olaparib group and 3.6 years in the placebo group (Table 20). This was an exploratory analysis, as no alpha was reserved for DDFS since the superiority of olaparib over placebo for DDFS had been demonstrated at interim analysis 1. In the FAS, 107 (11.6%) patients in the olaparib group and 172 patients (18.8%) in the placebo group had a DDFS event. The stratified HR for distant disease recurrence or death was 0.61 (95% CI, 0.48 to 0.77). The proportion of patients who remained distant disease–free at 4 years was 86.5% (95% CI, 83.8% to 88.8%) in the olaparib group and 79.1% (95% CI, 76.0% to 81.8%) in the placebo group (difference = 7.4%; 95% CI, 3.6% to 11.3%).17 The Kaplan-Meier plot of IDFS for the FAS is presented in Figure 9.
Figure 9: Kaplan-Meier Estimates of DDFS at Interim Analysis 2 — FAS
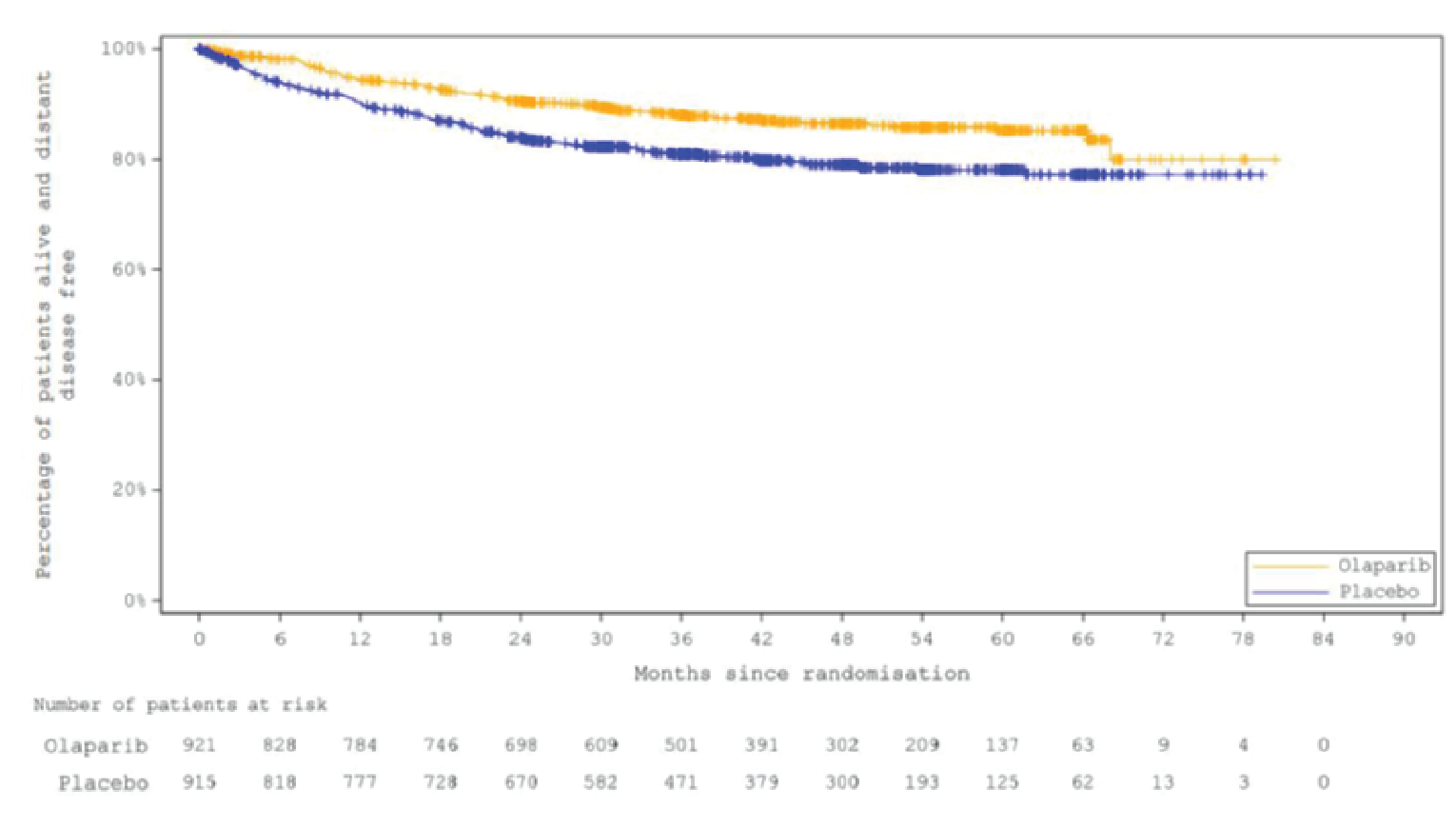
DDFS = distant disease–free survival; FAS = full analysis set.
Note: July 12, 2021, data cut-off date.
Source: Clinical Study Report for OlympiA.19
Health-Related Quality of Life
In the OlympiA trial, HRQoL data were assessed only in the PRO analysis set using the FACIT-F or EORTC QLQ-C30 questionnaires. The PRO set comprised patients who consented to participate in HRQoL assessment and started treatment, and the analyses were based only on a PRO subset with evaluable baseline data for FACIT-F or EORTC QLQ-C30. For both the FACIT-F and EORTC QLQ-C30 questionnaires, compliance rates were similar between treatment groups at baseline and follow-up in the placebo group compared with the olaparib group, and compliance diminished over time in both groups (to less than 70% after 24 months) (Table 21). Two separate analyses were conducted to compare differences between treatment groups at follow-up in FACIT-F and EORTC QLQ-C30 scores among patients who had previously received neoadjuvant versus those who had received postsurgical adjuvant chemotherapy, as the timing of chemotherapy can have a potential impact on the HRQoL outcome.
Table 21: Compliance Rates for HRQoL Questionnaires — PRO
Detail | Olaparib (N = 876) | Placebo (N = 875) |
|---|---|---|
Compliance ratea | ||
FACIT-F, (%) | ||
Baseline | ████ | ████ |
6 months | ████ | ████ |
12 months | ████ | ████ |
18 months | ████ | ████ |
24 months | ████ | ████ |
EORTC QLQ-C30, (%) | ||
Baseline | █████ | ████ |
6 months | ████ | ████ |
12 months | ████ | ████ |
18 months | ████ | ████ |
24 months | ████ | ████ |
EORTC QLQ-30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; FACIT-F = Functional Assessment of Chronic Illness Therapy–Fatigue questionnaire; HRQoL = health-related quality of life; PRO = patient-reported outcome.
aNumber of evaluable forms divided by the number of expected forms.
Source: Clinical Study Report for OlympiA.18
Functional Assessment of Chronic Illness Therapy–Fatigue
Using an MMRM analysis, no clinically meaningful differences were found between treatment groups in mean change in FACIT-F score at 6 and 12 months (less than the MID of 3 points45). For the subgroup of patients who had previously received neoadjuvant chemotherapy (N = 727), the adjusted LS mean difference for olaparib versus placebo was –1.3 (–2.4 to –0.2; P = 0.024) at 6 months and –1.5 (–2.8 to –0.2; P = 0.025) at 12 months. For the subgroup of patients who had previously received adjuvant chemotherapy (N = 780), the adjusted LS mean difference for olaparib versus placebo was –1.3 (–2.3 to –0.2; P = 0.017) at 6 months and –1.3 (–2.4 to 0.1; P = 0.027) at 12 months (Table 22, Figure 10, and Figure 11).
Table 22: Change in FACIT-F Score From Baseline at 6 and 12 Months — PRO
Characteristic | Olaparib | Placebo |
|---|---|---|
Patients who had completed neoadjuvant chemotherapy | ||
6 months, na | 371 | 356 |
LS mean (95% CI) | –1.5 (–2.2 to –0.7) | –0.2 (–1.0 to 0.6) |
LS mean differenceb | –1.3 (–2.4 to –0.2) | |
P valuec | 0.024 | Reference |
12 months, na | 371 | 356 |
LS mean (95% CI) | –1.5 (–2.4 to –0.6) | –0.0 (–0.9 to 0.9) |
LS mean differenceb | –1.5 (–2.8 to –0.2) | |
P valuec | 0.025 | Reference |
Patients who had completed adjuvant chemotherapy | ||
6 months, na | 375 | 403 |
LS mean (95% CI) | –0.7 (–1.4 to 0.1) | 0.6 (–0.1 to 1.3) |
LS mean differenceb | –1.3 (–2.3 to –0.2) | |
P valuec | 0.017 | Reference |
12 months, na | 375 | 403 |
LS mean (95% CI) | –0.8 (–1.6 to 0.0) | 0.5 (–0.3 to 1.2) |
LS mean differenceb | –1.3 (–2.4 to 0.1) | |
P valuec | 0.027 | Reference |
CI = confidence interval; FACIT-F = Functional Assessment of Chronic Illness Therapy–Fatigue; LS = least squares; MMRM = mixed-model for repeated measures; PRO = patient-reported outcome.
aOnly patients with an evaluable baseline form were included.
bThe adjusted LS mean changes, P values (2-sided), and 95% CIs were obtained from an MMRM analysis of the change from baseline. The model included treatment, time and treatment by time interaction, corresponding baseline score, and the baseline score by time interaction. The difference was the values for olaparib minus placebo.
CThe P value was not adjusted for multiplicity.
Source: Clinical Study Report for OlympiA.18
Figure 10: Change From Neoadjuvant Baseline for FACIT-F Score — PRO
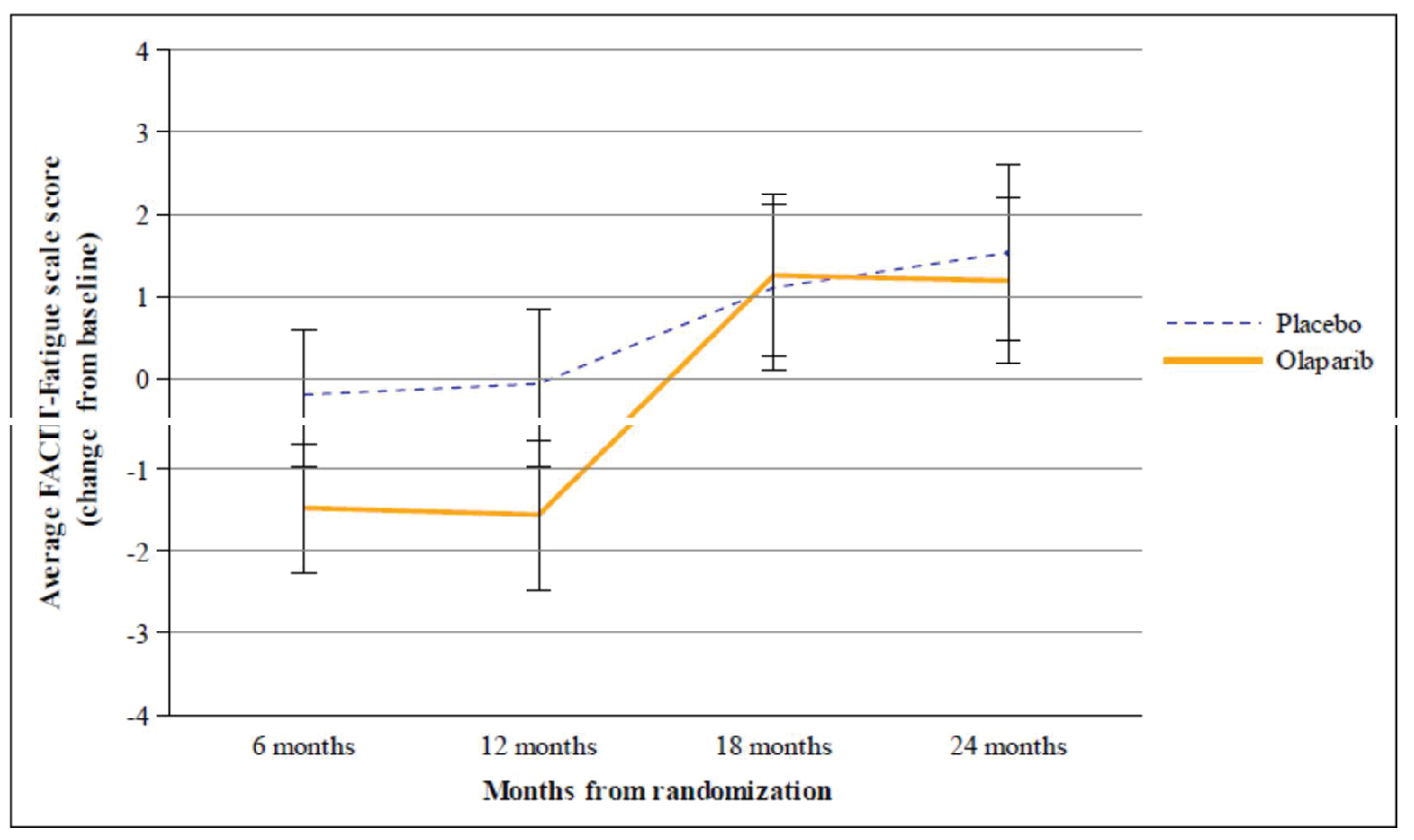
CI = confidence interval; FACIT-F = Functional Assessment of Chronic Illness Therapy–Fatigue questionnaire; LS = least squares; MMRM = mixed-model for repeated measures; PRO = patient-reported outcome.
Note: Adjusted LS mean changes and 95% CI are obtained from an MMRM analysis of the change from baseline. The model includes treatment, time and treatment by time interaction, corresponding baseline score, and the baseline score by time interaction.
Source: Clinical Study Report for OlympiA.18
Figure 11: Change From Adjuvant Baseline for FACIT-F Score — PRO
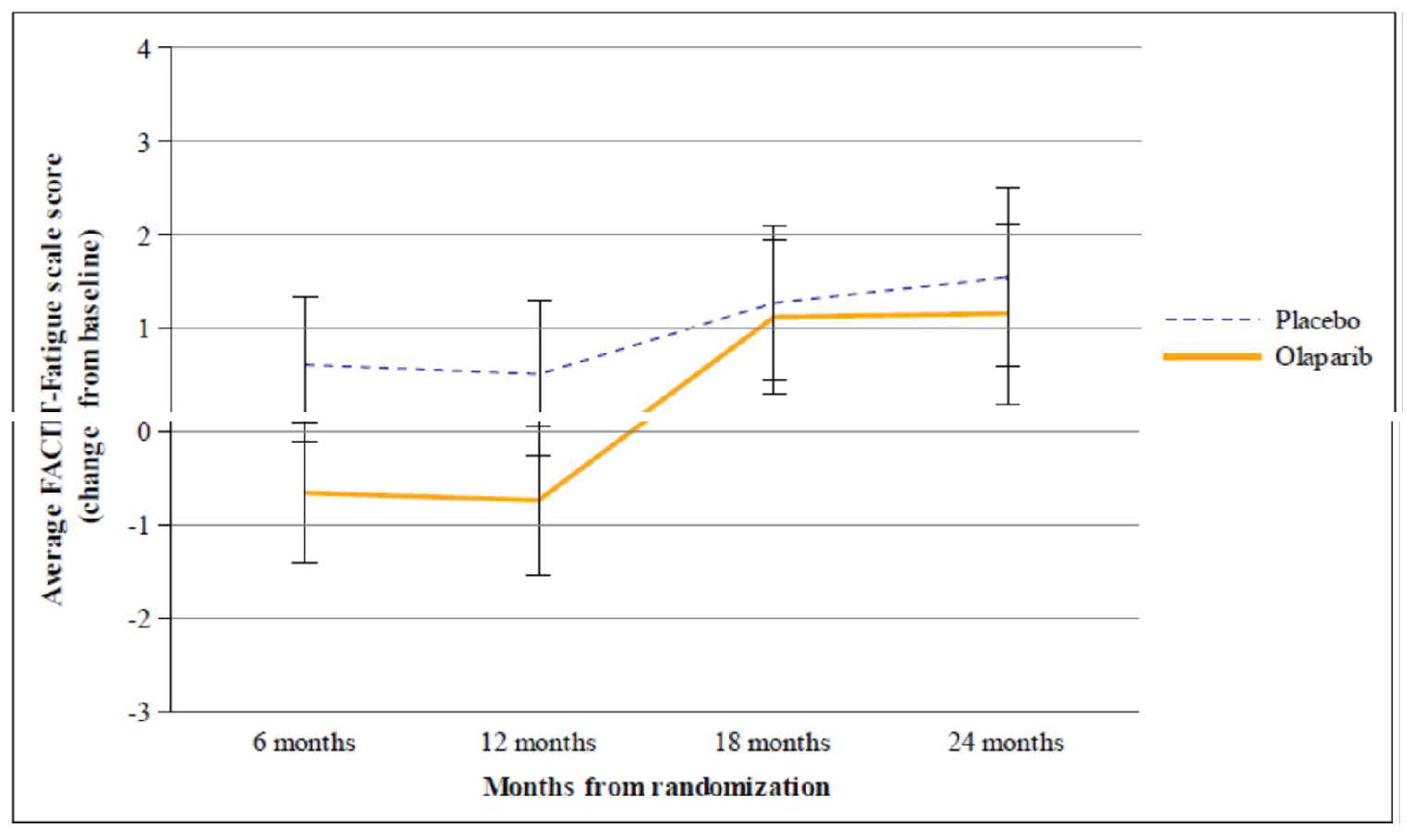
CI = confidence interval; FACIT-F = Functional Assessment of Chronic Illness Therapy–Fatigue questionnaire; LS = least squares; MMRM = mixed-model for repeated measures; PRO = patient-reported outcome.
Note: Adjusted LS mean changes and 95% CIs were obtained from an MMRM analysis of the change from baseline. The model includes treatment, time and treatment by time interaction, corresponding baseline score, and the baseline score by time interaction.
Source: Clinical Study Report for OlympiA.18
EORTC QLQ-C30
Patients Who Had Previously Received Neoadjuvant Chemotherapy: The adjusted LS mean difference for olaparib versus placebo in the global health status score was █ █ ██ █ █ █ █ ██ ██ █ █ ██ ███████ at 6 months, █ █ ██ █ █ █ █ ██ ██ █ █ ██ ██████) at 12 months, █ █ ██ █ █ █ █ ██ ██ █ █ ██ ██████) at 18 months, and █ █ ██ █ █ █ █ ██ ██ █ █ █ ██ ██████) at 24 months (Table 23). The adjusted LS mean difference between treatment groups in the nausea and vomiting symptom scale was 6.0 (95% CI, 4.0 to 8.0; █ ██ ██████ at 6 months, 6.3 (95% CI, 4.4 to 8.2 █ ██ █████) at 12 months, 0.4 (95% CI, –1.2 to 1.9; █ ██████) at 18 months, and 1.4 (95% CI, –0.4 to 3.3; █ ██████) at 24 months. The adjusted LS mean difference between treatment groups in the diarrhea symptom scale was 0.3 (95% CI, –2.0 to 2.7; █ ██████) at 6 months, 2.0 (95% CI, –1.0 to 4.9; █ ██████) at 12 months, 1.1 (95% CI, –2.0 to 4.3 █ ██ █████) at 18 months, and 1.8 (95% CI, –1.5 to 5.0; █ ██████) at 24 months.
Patients Who Had Previously Received Adjuvant Chemotherapy: The adjusted LS mean difference for olaparib versus placebo in the global health status score was █ █ ██ █ █ █ █ ██ ██ █ █ █ ██ ██████) at 6 months █ █ █ ██ █ █ █ █ ██ ██ █ █ █ ██ ███████ at 12 months, █ █ ██ █ █ █ █ ██ ██ █ █ ██ ███████ at 18 months, and █ █ ██ █ █ █ █ ██ ██ █ █ ██ ███████ at 24 months (Table 23). The adjusted LS mean difference between treatment groups in the nausea and vomiting symptom scale was 5.3 (95% CI, 3.4 to 7.2; █ ██ █████) at 6 months, 4.5 (95% CI, 2.8 to 6.2; █ ██ █████) at 12 months, –0.3 (95% CI, –1.9 to 1.3; █ ██████) at 18 months, and –0.6 (95% CI, –2.5 to 1.2; █ ███████ at 24 months. The adjusted LS mean difference between treatment groups in the diarrhea symptom scale was –1.7 (95% CI, –4.1 to 0.7; █ ███████ at 6 months, 0.1 (95% CI, –2.2 to 2.4; █ ███████ at 12 months, 0.4 (95% CI, –1.9 to 2.7; █ ██████) at 18 months, and –1.0 (95% CI, –3.4 to 1.4; █ ██████) at 24 months.
Incidence of Contralateral Breast Cancer and New Primary Ovarian, Fallopian Tube, and Peritoneal Cancer
The incidences of contralateral breast cancers (invasive and noninvasive), new primary ovarian cancer, and new primary invasive nonbreast nonovarian cancers in the olaparib and placebo groups are shown in Table 24. The competing risks analysis showed that the stratified HR for the incidence of contralateral invasive breast cancer was 0.97 (95% CI, 0.52 to 1.79; P = 0.900) (Table 24).
Table 23: Change From Baseline for EORTC QLQ-C30 Subscale Scores — PRO
Subscale measure | Patients who had completed neoadjuvant chemotherapy | Patients who had completed adjuvant chemotherapy | ||
|---|---|---|---|---|
Olaparib | Placebo | Olaparib | Placebo | |
EORTC QLQ-C30 global health status QoL | ||||
Baseline, n | ███ | ███ | ███ | ███ |
Mean (SD) | █ █ ██ ███████ | █ █ ██ ███████ | █ █ ██ ███████ | █ █ ██ ███████ |
6 months, n | ███ | ███ | ███ | ███ |
LS mean (95% CI) | █ █ ██ █ █ █ █ ██ █████ | █ ██ █ █ █ █ ██ █████ | █ █ ██ █ █ █ █ ██ █████ | █ ██ █ █ █ █ ██ █████ |
LS mean difference (95% CI) | █ █ ██ █ █ █ █ ██ █████ | █ █ ██ █ █ █ █ ██ ██████ | ||
P valuea | █████ | █████████ | █████ | █████████ |
12 months, | ███ | ███ | ███ | ███ |
LS mean (95% CI) | █ ██ █ █ █ █ ██ █████ | █ ██ █ █ ███ █████ | █ ██ █ █ █ █ ██ █████ | █ ██ █ █ ███ █████ |
LS mean difference (95% CI) | █ █ ██ █ █ █ █ ██ █████ | █ █ ██ █ █ █ █ ██ ██████ | ||
P valuea | █████ | █████████ | █████ | █████████ |
18 months, n | ███ | ███ | ███ | ███ |
LS mean (95% CI) | █ ██ █ █ ███ █████ | █ ██ █ █ ███ █████ | █ ██ █ █ ███ █████ | █ ██ █ █ ███ █████ |
LS mean difference (95% CI) | █ █ ██ █ █ █ █ ██ █████ | █ █ ██ █ █ █ █ ██ █████ | ||
P valuea | █████ | █████████ | █████ | █████████ |
24 months, n | ███ | ███ | ███ | ███ |
LS mean (95% CI) | █ ██ █ █ █ █ ██ █████ | █ ██ █ █ ███ █████ | █ ██ █ █ ███ █████ | █ ██ █ █ ███ █████ |
LS mean difference (95% CI) | █ █ ██ █ █ █ █ ██ ██████ | █ █ ██ █ █ █ █ ██ █████ | ||
P valuea | █████ | █████████ | █████ | █████████ |
EORTC QLQ-C30 nausea and vomiting symptom scale | ||||
Baseline, n | 440 | 433 | 436 | 440 |
Mean (SD) | 3.2 (9.23) | 3.7 (10.82) | 3.1 (8.73) | 3.4 (9.92) |
6 months, n | 383 | 359 | 385 | 406 |
LS mean (95% CI) | 7.6 (6.2 to 9.0) | 1.6 (0.2 to 3.1) | 6.9 (5.5 to 8.2) | 1.6 (0.3 to 2.9) |
LS mean difference (95% CI) | 6.0 (4.0 to 8.0) | 5.3 (3.4 to 7.2) | ||
P valuea | █ █████ | █████████ | █ █████ | █████████ |
12 months, n | 383 | 359 | 385 | 406 |
LS mean (95% CI) | 7.3 (6.0 to 8.7) | 1.0 (–0.4 to 2.4) | 5.5 (4.2 to 6.7) | 1.0 (–0.2 to 2.1) |
LS mean difference (95% CI) | 6.3 (4.4 to 8.2) | 4.5 (2.8 to 6.2) | ||
P valuea | █ █████ | █████████ | █ █████ | █████████ |
18 months, n | 383 | 359 | 385 | 406 |
LS mean (95% CI) | 0.7 (–0.4 to 1.8) | 0.4 (–0.8 to 1.5) | 0.7 (–0.5 to 1.8) | 1.0 (–0.2 to 2.1) |
LS mean difference (95% CI) | 0.4 (–1.2 to 1.9) | –0.3 (–1.9 to 1.3) | ||
P valuea | █████ | █████████ | █████ | █████████ |
24 months, n | 383 | 359 | 385 | 406 |
LS mean (95% CI) | 1.3 (0.0 to 2.6) | –0.1 (–1.5 to 1.2) | –0.0 (–1.3 to 1.3) | 0.6 (–0.6 to 1.9) |
LS mean difference (95% CI) | 1.4 (–0.4 to 3.3) | –0.6 (–2.5 to 1.2) | ||
P valuea | █████ | █████████ | █████ | █████████ |
EORTC QLQ-C30 diarrhea symptom scale | ||||
Baseline, n | 438 | 431 | 435 | 440 |
Mean (SD) | 5.9 (15.79) | 6.1 (16.59) | 5.7 (14.61) | 5.9 (14.94) |
6 months, n | 380 | 357 | 384 | 406 |
LS mean (95% CI) | 1.6 (–0.0 to 3.3) | 1.3 (–0.4 to 3.0) | 0.0 (–1.7 to 1.8) | 1.7 (0.1 to 3.4) |
LS mean difference (95% CI) | 0.3 (–2.0 to 2.7) | –1.7 (–4.1 to 0.7) | ||
P valuea | █████ | █████████ | █████ | █████████ |
12 months, n | 380 | 357 | 384 | 406 |
LS mean (95% CI) | 4.0 (1.9 to 6.2) | 2.0 (–0.1 to 4.1) | 1.5 (–0.1 to 3.1) | 1.4 (–0.2 to 3.0) |
LS mean difference (95% CI) | 2.0 (–1.0 to 4.9) | 0.1 (–2.2 to 2.4) | ||
P valuea | █████ | █████████ | █████ | █████████ |
18 months, n | 380 | 357 | 384 | 406 |
LS mean (95% CI) | 2.7 (0.5 to 4.9) | 1.5 (–0.7 to 3.8) | –0.2 (–1.8 to 1.4) | –0.6 (–2.2 to 1.0) |
LS mean difference (95% CI) | 1.1 (–2.0 to 4.3) | 0.4 (–1.9 to 2.7) | ||
P valuea | █████ | █████████ | █████ | █████████ |
24 months, n | 380 | 357 | 384 | 406 |
LS mean (95% CI) | 1.3 (–1.0 to 3.5) | –0.5 (–2.9 to 1.8) | –1.6 (–3.2 to 0.1) | –0.6 (–2.2 to 1.1) |
LS mean difference (95% CI) | 1.8 (–1.5 to 5.0) | –1.0 (–3.4 to 1.4) | ||
P valuea | █████ | █████████ | █████ | █████████ |
CI = confidence interval; EORTC QLQ-30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; LS = least squares; MMRM = mixed-model for repeated measures; PRO = patient-reported outcome; QoL = quality of life; SD = standard deviation.
Note: Only patients with an evaluable baseline form were included.
Adjusted LS mean changes, P values (2-sided), and 95% CIs were obtained from an MMRM analysis of the change from baseline. The model included treatment, time and treatment by time interaction, corresponding baseline score, and the baseline score by time interaction. The difference was the values for olaparib minus placebo.
aP value was not adjusted for multiplicity.
Source: Clinical Study Report for OlympiA.18
Table 24: Summary of Cancers Occurring Post Randomization at Interim Analysis 2 — FAS
Type of cancera | Olaparib ((N = 921) | Placebo (N = 915) |
|---|---|---|
Contralateral invasive breast cancer, n (%) | 20 (2.2) | 22 (2.4) |
Contralateral noninvasive breast cancer, n (%) | 2 (0.2) | 4 (0.4) |
New primary ovarian cancer,b n (%) | 2 (0.2)c | 10 (1.1) |
New primary ovarian cancer | █ █████ | █ █████ |
New primary fallopian tube cancer | █ █████ | █ █████ |
New primary peritoneal cancer | █ | █ |
New primary invasive nonbreast nonovarian cancers, n (%) | 10 (1.1) | 14 (1.5) |
FAS = full analysis set.
Note: Summary of cancers without considering competing risks.
aData cut-off date: July 12, 2021.
bIncludes new primary ovarian, fallopian, and peritoneal cancers, without considering competing risks.
cOne instance of ovarian cancer recurrence (patient E104618) was captured in the database.
Source: Clinical Study Report for OlympiA.19
Progression-Free Survival
Progression-free survival was not measured or reported in the OlympiA trial.
Time to Progression
Time to progression was not measured or reported in the OlympiA trial.
Breast Cancer Symptoms
Breast cancer symptoms were not measured or reported in the OlympiA trial.
Need for Surgery
Need for surgery was not measured or reported in the OlympiA trial.
Table 25: Contralateral Invasive Breast Cancer at Interim Analysis 2 — FAS
Detaila | Olaparib (N = 921) | Placebo (N = 915) |
|---|---|---|
███████ █ █ █ █ ██ ██ █ █ █ █ ██ █ █ █ █ ██ ██████ | ||
██ █ █ █ █ ██ █ █ ██ █ █ █ █ █ ██ ███ | █ ██████ | █ ██████ |
█ ██ ██ ████ █ █ █ █ ██ █ █ █ ██ █ █ ██ ███ | █ █ ██ █ █ █ █ ██ ██████ | |
█ ██████ | █████ | █████████ |
███ █ █ █ █ █ ██ ███ | ||
█ █ █ █ █ ██ █ █ █ ██ ██ █ █ █ █ █ ██ ██ ██ █████ | █ █████ | █ █████ |
█ █ █ ██ █ █ █ █ ██ ██████████████ | █ ███ | █ ███ |
█████ █ █ █ █ ██ █████████████ | █ ███ | █ █████ |
█ █ █ █ █ ██ ██ █ █ █ █ ██ ██ █ █ █ █ ██ ██ ███ █ █ █ █ ██ ██ ██████████ | █ █████ | █ █████ |
CI = confidence interval; ER = estrogen receptor; FAS = full analysis set; HER2 = human epidermal growth factor receptor 2; HR = hazard ratio; PgR = progesterone receptor; TNBC = triple-negative breast cancer.
aData cut-off date: July 12, 2021.
bEstimate of the treatment HR based on the cause-specific hazards from a stratified Cox proportional hazards model (accounting for competing risks); < 1 indicates a lower risk with olaparib arm compared with placebo arm. Stratification is by chemotherapy type (adjuvant vs. neoadjuvant), hormone receptor status (ER- and/or PgR-positive and HER2-negative vs. TNBC), and prior platinum therapy (yes vs. no). Stratifications was based on the categories used in the randomization system and are chosen by the pooling strategy.
cP value calculated from the Fine-Gray model adjusted for treatment group and stratification factors. The P value was not adjusted for multiplicity.
dThese randomized patients will be counted in the FAS; however, they will be treated as being censored for the contralateral invasive breast cancer event just after randomization. Censoring these patients at day 0.5 will not affect the log-rank test; however, they will be counted in the total number at risk and in the Kaplan-Meier plot. The reason for censoring at day 0.5 is to avoid ties with other patients censored on day 1.
Source: Clinical Study Report for OlympiA.19
Harms
Only those harms identified in the review protocol are reported subsequently.
Adverse Events
At interim analysis 2 (July 12, 2021), 836 patients (91.8%) in the olaparib group and 758 patients (83.8%) in the placebo group experienced at least 1 AE (Table 26). Common AEs, AEs with a CTCAE grade of 3 or higher, and the preferred term for the AE are summarized in Table 27. A total of 736 patients (80.8%) in the olaparib group and 480 patients (53.1%) in the placebo group experienced at least 1 TRAE (Table 28). The most common TRAEs occurring in the olaparib and placebo groups were anemia (20.6% and 1.7%, respectively), diarrhea (12.0% and 7.5%, respectively), decreased neutrophil count (14.9% and 4.6%, respectively), and decreased white blood cell count (14.1% and 4.5%, respectively). The majority of TRAEs were manageable with supportive care and/or dose modifications and consistent with the known safety profile for olaparib.
Table 26: Summary of Adverse Events — Safety Population
AE categorya | Olaparib (N = 911) | Placebo (N = 904) |
|---|---|---|
Patients with ≥ 1 AE, n (%) | 836 (91.8) | 758 (83.8) |
Patients with ≥ 1 TRAE,b n (%) | 736 (80.8) | 480 (53.1) |
Patients with ≥ 1 AE of CTCAE grade ≥ 3, n (%) | 223 (24.5) | 102 (11.3) |
Patients who died due to AE, n (%) | 1 (0.1) | 2 (0.2) |
Patients with ≥ 1 SAE (including fatal SAE), n (%) | 79 (8.7) | 78 (8.6) |
Patients who discontinued study treatment due to AEc n (%) | 98 (10.8) | 42 (4.6) |
Patients with ≥ 1 AE leading to dose reduction, n (%) | 213 (23.4) | 33 (3.7) |
Patients with ≥ 1 AE leading to dose interruption, n (%) | 286 (31.4) | 99 (11.0) |
AE = adverse event; CTCAE = Common Terminology Criteria for Adverse Events; SAE = serious adverse event; TRAE = treatment-related adverse event.
aPatients with multiple events in the same category were counted only once in that category; patients with events in more than 1 category were counted once in each of the categories.
bAs assessed by the investigator.
cIncludes AEs that led to a dose interruption or reduction and did not lead to the permanent discontinuation of the study treatment.
Source: Clinical Study Report for OlympiA.18
Table 27: Adverse Events Reported in at Least 5% of Patients in Either Treatment Arm — Safety Population
Preferred term | Olaparib (N = 911) | Placebo (N = 904) | ||
|---|---|---|---|---|
CTCAE grade, n (%) | ||||
Any CTCAE grade | CTCAE grade ≥ 3 | Any CTCAE grade | CTCAE grade ≥ 3 | |
Patients with any 1 frequent AE | 798 (87.6) | 223 (24.5) | 673 (74.4) | 102 (11.3) |
Nausea | 520 (57.1) | 7 (0.8) | 213 (23.6) | 0 (0) |
Fatigue | 367 (40.3) | 16 (1.8) | 248 (27.4) | 6 (0.7) |
Headache | 180 (19.8) | 2 (0.2) | 152 (16.8) | 1 (0.1) |
Diarrhea | 160 (17.6) | 3 (0.3) | 124 (13.7) | 3 (0.3) |
Vomiting | 206 (22.6) | 6 (0.7) | 74 (8.2) | 0 (0) |
Anemia | 215 (23.6) | 79 (8.7) | 35 (3.9) | 3 (0.3) |
Neutrophil count decrease | 147 (16.1) | 45 (4.9) | 59 (6.5) | 7 (0.8) |
Arthralgia | 89 (9.8) | 2 (0.2) | 115 (12.7) | 2 (0.2) |
White blood cell count decrease | 144 (15.8) | 27 (3.0) | 52 (5.8) | 3 (0.3) |
Decreased appetite | 119 (13.1) | 2 (0.2) | 53 (5.9) | 0 (0) |
Dizziness | 104 (11.4) | 1 (0.1) | 66 (7.3) | 1 (0.1) |
████████████ | █ ██████ | ██ | █ ██████ | ██ |
███ █ █ █ █ ██ ████ | █ ██████ | █ █████ | █ ██████ | █ █████ |
█ █ █ ██ █████ █ █ █ █ ██ █ █ █ ██ █████████ | █ ██████ | █ ███ | █ ██████ | █ █████ |
█████ | █ ██████ | ██ | █ ██████ | ██ |
█ ██ █████ | █ ██████ | █ ███ | █ ██████ | █ █████ |
█████████ | █ ██ ██████ | ██ | █ ██████ | ██ |
████ | █ ██████ | █ ███ | █ ██████ | █ █████ |
█ █ ██ ████ | █ ██████ | █ █████ | █ ██████ | █ █████ |
████████ | █ ██████ | █ █████ | █ ██████ | █ █████ |
█ █ █ ██ ██████████ | █ ██████ | ██ | █ ██████ | ██ |
██████████ | █ ██████ | ██ | █ ██████ | ██ |
███ █ █ █ █ ██ █ █ ██ ███████ | █ ██████ | █ █████ | █ ██████ | █ ███ |
███████ | █ ██████ | █ █████ | █ ██████ | █ ███ |
█████████ | █ ██████ | ██ | █ ██████ | ██ |
███████ | █ ██████ | █ █████ | █ ██████ | █ █████ |
███████████████ | █ ██████ | ██ | █ ██████ | ██ |
████ █ █ █ █ ██ █ █ █ ██ ████████ | █ ██████ | █ ██████ | █ ██████ | █ █████ |
AE = adverse event; CTCAE = Common Terminology Criteria for Adverse Events; NR = not reported.
Source: Clinical Study Report for OlympiA.18
Table 28: TRAEs Reported in More Than 1% of Patients in Either Treatment Arm — Safety Population
███ █ █ █ █ ██ ████ | ████ █ █ █ █ █ ██ ███ | ███ █ █ █ █ █ ██ ███ |
|---|---|---|
███ █ █ █ █ ██ ██████████ | █ ██ ██████ | █ ██ ██████ |
██████ | █ ██ ██████ | █ ██████ |
███ █ █ █ █ ██ ██████████ | █ ██████ | █ █████ |
███ █ █ █ █ ██ ██████████ | █ ██████ | █ █████ |
███ █ █ █ █ ██ ████ | █ ██████ | █ ██████ |
███ █ █ █ █ ██ █ █ ██ █████ | █ ██████ | █ ██████ |
████████████ | █ ██████ | █ ██████ |
████████ | █ ██ ██████ | █ ██████ |
█ ██ █████ | █ ██████ | █ ██████ |
█████████ | █ ██████ | █ ██████ |
██████████ █ █ █ █ ██ █ █ █ █ ██ ███████ | █ ██████ | █ █████ |
██████████ | █ ██████ | █ ██████ |
████████ | █ ██████ | █ █████ |
█ █ █ █ █ ██ ██████████ █ █ █ █ ██ █████████ | █ ██████ | █ ██████ |
███ █ █ █ █ ██ ██████████ █ █ █ █ ██ █████████ | █ ██████ | █ ██████ |
█ █ █ ██ ████ █ █ █ █ ██ █████████ | █ ██████ | █ ███ |
████ █ █ █ █ ██ █ █ █ ██ █████████ | █ ██████ | █ █████ |
████ █ █ █ █ ██ █ █ █ ██ █████████ | █ ██ ██████ | █ ██████ |
██ █ █ █ █ ██ █ █ █ ██ █████████ | █ ██████ | █ █████ |
█ █ █ ██ █ █ █ ██ █ █ ██ █ █ █ ██ █████████ | █ ██ ██████ | █ ██████ |
██████████ | █ ██████ | █ ██████ |
█ █ ██ ████ | █ ██████ | █ █████ |
███████ | █ ██████ | █ ██████ |
█████████ | █ ██████ | █ ██████ |
█████████ | █ ███████ | █ ██████ |
████████ | █ ███████ | █ ██████ |
████████ | █ ██████ | █ ██████ |
█████ | █ ██████ | █ ██████ |
███████ | █ ██████ | █ ██████ |
████████ | █ ██████ | █ ██████ |
TRAE = treatment-related adverse event.
Source: Clinical Study Report for OlympiA.18
Serious Adverse Events
At interim analysis 2 (July 12, 2021), 79 patients (8.7%) in the olaparib group and 78 patients (8.6%%) in the placebo group experienced at least 1 SAE (Table 29). No individual SAE occurred in more than 2% of patients. A total of 33 patients (3.6%) in the olaparib group and 6 patients (0.7%) in the placebo group experienced at least 1 serious TRAE.
Withdrawals Due to Adverse Events
At interim analysis 2 (July 12, 2021), withdrawal of study treatment due to AEs was required in 98 patients (10.8%) in the olaparib group and 42 patients (4.6%) in the placebo group. The most common reasons for discontinuation were nausea (2.2% and 0.3% in the olaparib and placebo groups, respectively), anemia (1.8% and 0% in the olaparib and placebo groups, respectively), fatigue (1.6% and 0.4% in the olaparib and placebo groups, respectively), and decreased neutrophil count (1.0% and 0.1% in the olaparib and placebo groups, respectively). A total of 84 patients (9.2%) in the olaparib group and 16 patients (1.8%) in the placebo group discontinued the study treatment due to TRAEs.
Dose Interruption and Reduction Due to Adverse Events
At interim analysis 2 (July 12, 2021), 286 patients (31.4%) in the olaparib group and 99 (11.0%) in the placebo group experienced at least 1 AE leading to dose interruption. The most common reasons for dose interruption were anemia (11.4% and 0.2% in the olaparib and placebo groups, respectively), decreased neutrophil count (5.9% and 0.7% in the olaparib and placebo groups, respectively), nausea (5.5% and 0.7% in the olaparib and placebo groups, respectively), and decreased white blood cell count (3.6% and 0.3% in the olaparib and placebo groups, respectively). A greater proportion of patients in the olaparib group experienced AEs leading to dose reduction compared with the placebo group (23.4% versus 3.7%, respectively). The most common reasons for dose reduction were █ █ █ █ ██ █ █ █ ██ ██ █████ in the olaparib and placebo groups, respectively, █ █ █ █ ██ █ █ █ ██ ██ █████ in the olaparib and placebo groups, respectively), ████ █ █ █ █ ██ █ █ █ ██ ███ █ █ █ █ ██ █ █ █ ██ ██ █████ in the olaparib and placebo groups, respectively), █ ██ █ █ █ █ █ ██ █ █ █ ██ ██ █████ in the olaparib and placebo groups, respectively). AEs leading to both dose interruption and reduction were reported in █ ██ ███████ patients in the olaparib group and █ ███████ in the placebo group.
Notable Harms
The frequencies of notable harms identified in the protocol were comparable between the treatment groups (Table 29). At interim analysis 2 (July 12, 2021), a new primary cancer (excluding myelodysplastic syndrome and acute myeloid leukemia) was the most commonly reported notable AEs (2.3% and 4.0% in the olaparib and placebo groups, respectively), followed by pneumonitis (1.0% and 1.3% in the olaparib and placebo groups, respectively), and myelodysplastic syndrome or acute myeloid leukemia (0.2% and 0.3% in the olaparib and placebo groups, respectively). No new safety concerns were identified compared with previous trials in patients with metastatic breast cancer.
Mortality
In total, at interim analysis 2 (July 12, 2021), there were 75 deaths (8.1%) in the olaparib group and 10 deaths (11.9%) in the placebo group (Table 30), including 2 fatal AEs in the olaparib group and 4 fatal AEs in the placebo group. There were 2 fatal AEs in the placebo group (acute myeloid leukemia, ovarian cancer) and 1 fatal AE in the olaparib group (cardiac arrest) during the treatment period or within the 30-day follow-up period. There were 2 fatal AEs in the placebo group (pancreatic carcinoma, leukemia) and 1 fatal AE in the olaparib group (acute myeloid leukemia) 30 days after discontinuation.
Table 29: SAEs Reported in More Than 0.3% of Patients in Either Treatment Arm and Notable Harms — Safety Population
Preferred term | Olaparib (N = 911) | Placebo (N = 904) |
|---|---|---|
Patients with ≥ 1 SAE, n (%) | 79 (8.7) | 78 (8.6) |
Anemia | █ ██████ | █ █████ |
Febrile neutropenia | █ █████ | █ ███ |
Pyrexia | █ █████ | █ █████ |
Device-related infection | █ █████ | █ █████ |
Mastitis | █ █████ | █ █████ |
Breast cancer | █ █████ | █ █████ |
Malignant melanoma | █ █████ | █ █████ |
Ovarian cancer | █ ███ | █ █████ |
Patients with ≥ 1 serious TRAE, n (%) | █ ██████ | █ █████ |
Anemia | █ ██████ | █ ███ |
Notable harms, n (%) | ||
Myelodysplastic syndrome or acute myeloid leukemia | 2 (0.2) | 3 (0.3) |
Pneumonitis | 9 (1.0) | 12 (1.3) |
New primary cancer | 21 (2.3) | 36 (4.0) |
Thrombocytopenia | NR | NR |
Fatigue or asthenia | NR | NR |
Hand-foot syndrome | NR | NR |
NR = not reported; SAE = serious adverse event; TRAE = treatment-related adverse event.
Source: Clinical Study Report for OlympiA18
Table 30: Deaths — Full Analysis Set
Category | Olaparib (N = 911) | Placebo (N = 904) |
|---|---|---|
Deaths, n (%) | 75 (8.1) | 109 (11.9) |
Primary cause of death, n (%) | ||
Breast cancer recurrence | 70 (93.3) | 103 (94.5) |
Adverse events | 2 (2.7) | 4 (3.7) |
Other | 3 (4.0) | 2 (1.8) |
Time to death from last dose, n (%) | ||
< 30 days | █ █████ | █ █████ |
> 30 days | █ ███████ | █ ██ ██████ |
Source: Clinical Study Report for OlympiA.18
Critical Appraisal
Internal Validity
The OlympiA trial used accepted methods for blinding, allocation concealment, and randomization with stratification. An interactive response methodology using a permuted block randomization scheme was used, and randomization with stratification was performed centrally, which typically has a low risk of bias. The baseline demographic and disease characteristics of patients were generally balanced between the treatment groups, so randomization was successful. Although the OlympiA trial was double-blinded and the investigators were blinded to treatment assignment, risk of bias cannot be ruled out. In the olaparib group, about 80.8% of patients experienced at least 1 AE, which may have made the investigators and patients aware of the treatment assignment. Knowledge of the assigned treatment could have led to bias in the reporting and measurement of subjective outcomes, including PROs (i.e., fatigue, HRQoL) and subjective AEs. However, the extent and direction of bias due to treatment knowledge is uncertain. Protocol deviations were reported in 13% to 14% of patients across the 2 treatment groups, and the proportion of protocol deviations was comparable between groups and identified before database lock in a blinded manner.
In the OlympiA trial, the primary (IDFS) and key secondary (OS and DDFS) outcomes were considered appropriate for the disease setting. The clinical experts consulted noted that the standardized STEEP criteria used to define IDFS and DDFS were appropriate, and IDFS and DDFS are considered early indicators of patients’ survival, especially in early breast cancer. According to the clinical experts consulted, improved survival is the most important outcome for both clinicians and patients and is sometimes difficult to achieve, especially in patients with TNBC, as the prognosis of palliative chemotherapy options in this population is quite poor. Based on the enrolled sample size, the study was powered to test its primary end point (based on the ITT population). Although patients with HR-positive, HER2-negative disease were included in the OlympiA trial following an early protocol amendment (October 21, 2015), the study design was not affected because hormone receptor status was used as a stratification factor. The statistical analysis methods appear to be acceptable. Both interim analyses were planned a priori. A hierarchical testing strategy to sequentially test the primary and secondary outcomes was used to reduce the risk of type I error across these analyses. Both interim analyses applied a bespoke spending function, which is deemed conservative in controlling type I error across the primary and 2 key secondary outcomes tested.
The analyses of primary and key secondary outcomes were conducted using the ITT population, which maintains randomization and minimizes the risk of bias by comparing groups with similar prognostic factors. Since the IDFS, DDFS, and OS results are from interim analyses, there is a risk that the effect of olaparib compared with placebo is overestimated; however, the existence and extent of any overestimation is questionable.20,21 The results were robust to a number of sensitivity analyses for the primary and key secondary outcomes, which were performed by:
including only patients with central pathology review data for HR status
using unadjusted analysis
using interval censoring.
Supportive analysis results for IDFS, DDFS, and OS based on all randomized patients with confirmed BRCA germline mutations were consistent with the primary analyses. Subgroup analyses by BRCA status, prior chemotherapy, prior platinum therapy, hormone receptor status, axillary nodal status, and CPS&EG score were prespecified in the OlympiA trial and considered exploratory. The analyses may not have been powered to detect a treatment difference and there were no adjustments made for multiplicity, and the results should be viewed as supportive evidence only for the overall effect of olaparib.
HRQoL was assessed using FACIT-F and EORTC QLQ-C30 only in the PRO analysis set based on the evaluable baseline data. Both the FACIT-F and EORTC QLQ-C30 are generally valid and reliable questionnaires for breast cancer; however, no evidence of responsiveness for these tools in patients with breast cancer was identified. The clinical experts consulted indicated that these tools are not commonly used in clinical practice but are used in multiple trials, allowing comparisons between different treatments. No strong conclusions could be drawn about the effect of olaparib compared with placebo on HRQoL due to an increased risk of type I error and a high risk of attrition bias, especially at longer follow-up. Approximately 20% of patients had missing data at follow-up for FACIT-F score (in the ITT population), and 20% to 35% for EORTC QLQ-C30 scores. Thus, there is a risk of bias, as patients who completed the questionnaires may be different than those who did not complete them (e.g., differences in treatment response, AEs). There is an increased risk of type I error due to the lack of adjustment for multiple comparisons. Some of the outcomes identified by CADTH as important to patients and clinicians were not measured or reported in the OlympiA trial (e.g., time to progression, breast cancer symptoms, need for surgery). Although HRQoL was measured, there were methodological issues that precluded any strong conclusions, so there remains a knowledge gap.
External Validity
The patient population in the OlympiA trial generally reflects patients in clinical practice in this setting. To be enrolled in the OlympiA trial, patients were required to have completed at least 6 cycles of chemotherapy and all local therapies at least 2 weeks before randomization. The clinical experts consulted noted that most patients with high-risk early breast cancer would get at least 6 cycles of chemotherapy; however, they mentioned that olaparib treatment would probably not be withheld if patients had previously received fewer than 6 cycles of chemotherapy for medical reasons. It was further indicated by the clinical experts that the criteria used in the OlympiA trial to determine high risk of disease recurrence were reasonable, with the exception of a CPS&EG score of 3 or higher, which is not commonly used in clinical practice, although it is easily calculated. Although olaparib is recommended for the adjuvant treatment of patients with high-risk early breast cancer, regardless of hormone receptor status, patients with HR-positive, HER2-negative breast cancer were underrepresented in the OlympiA trial (17.7% with HR-positive, HER2-negative disease versus 82.3% with TNBC). The clinical experts consulted by CADTH noted that these proportions are reflective of the group with hereditary BRCA-mutated breast cancer in clinical practice. The Health Canada reviewers noted that due to the small number of patients with HR-positive, HER2-negative disease and lack of statistical power, the magnitude of the clinical benefit of olaparib in this subpopulation remains unclear.22 The mean age of the patients was 43.3 years, and the number of patients with BRCA1 mutations was higher (71.1%) compared with those with BRCA2 mutations (27.1%). The clinical experts consulted noted that this is reflective of clinical practice, and that these patients represent a younger and generally healthy population with curative treatment intent. In addition, the majority of patients were white and nonhispanic, and only 34 patients from Canada were recruited. The clinical experts consulted noted that this is reflective of the population eligible for olaparib treatment, and the lack of representation of patients in Canada does not reduce the generalizability of the results to Canadian clinical practice. The use of placebo in the adjuvant setting was considered appropriate due to the lack of standard-of-care therapies for patients with BRCA mutations, as there is no evidence for the use of other drugs for the treatment of breast cancer, such as abemaciclib or pembrolizumab, in patients with BRCA mutations.
About 87.2% of the patients in the OlympiA trial did not pass screening, most commonly because they did not have a deleterious or suspected deleterious BRCA mutation in screening part 1. The clinical experts consulted noted that the number of screening failures in the trial seems reasonable. According to both clinical experts and the clinician groups consulted by CADTH, the companion diagnostic testing would be a challenge in Canada, as current BRCA testing guidelines vary by province and BRCA mutations are underdiagnosed based on most provincial testing criteria. The clinician group consulted noted that the current guidelines for BRCA mutation testing are restrictive in terms of eligibility criteria; thus, many patients who carry a BRCA mutation may not receive the testing and thereby lose the opportunity to receive olaparib. The clinical experts consulted indicated that clinicians will most likely request BRCA mutation testing for patients who do not qualify for genetic testing based on provincial guidelines but who meet the criteria for adjuvant olaparib in the presence of BRCA mutation. In this case, patients who want to access BRCA testing would need to consider private-pay options and must be willing to pay for it. It was further mentioned by the clinical experts that increased access to genetic testing will likely be necessary, as patients with BRCA-mutated breast cancer are the ones that derive benefit from olaparib, and it is important to ensure that all these individuals are captured. While olaparib has been approved by Health Canada for use as an adjuvant treatment in adult patients with HER2-negative, high-risk early breast cancer regardless of hormone receptor status, the magnitude of the clinical benefit of olaparib in patients with HR-positive, HER2-negative disease remains unclear due to the small proportion of these patients in the trial. According to the clinical experts, it is not clear how to integrate olaparib into the current treatment paradigm with other drugs, including capecitabine, pembrolizumab, and abemaciclib in the treatment of early breast cancer. They agreed that clinicians would likely prefer olaparib to capecitabine for the treatment of patients with TNBC who have residual disease; however, at the same time, they would likely prefer adjuvant abemaciclib with endocrine therapy to olaparib for the treatment of patients with HR-positive, HER2-negative breast cancer, and olaparib would be another option in the adjuvant setting if patients have a BRCA mutation. It was further noted by the clinical experts that there are no efficacy data to support the use of olaparib with other drugs in the treatment of early breast cancer.
The clinical experts did not identify any major concerns or discrepancies between the OlympiA trial and real-world settings in terms of treatment exposure and follow-up duration. A higher proportion of patients prematurely discontinued the trial medication due to AEs in the olaparib group (10.8%) compared with the placebo group (4.6%); however, the clinical experts noted that this is reflective of clinical practice. Dose modifications for olaparib were allowed in the OlympiA trial and outlined in the protocol. The clinical experts consulted indicated that dose adjustments for olaparib are expected in clinical practice in situations of toxicity.
Indirect Evidence
Objectives and Methods for the Summary of Indirect Evidence
The objective of this section is to summarize and critically appraise available indirect evidence comparing olaparib with other relevant treatments (identified in the protocol) in patients with HER2-negative, gBRCA-mutated, high-risk nonmetastatic breast cancer. A focused literature search for ITCs dealing with breast cancer was run in MEDLINE All (1946–) on August 31, 2022. No limits were applied to the search. Titles, abstracts, and full-text articles were screened for inclusion by 1 reviewer based on the population, intervention, comparator, and outcome criteria outlined in accordance with the protocol for the CADTH review. No published ITCs were found from the CADTH literature search comparing olaparib with comparators of interest based on the inclusion criteria in this Clinical Report.
Description of the Indirect Comparison
A single sponsor-submitted ITC report59 was provided as part of the submission and has been described and critically appraised in the sections that follow. The sponsor’s ITC report included 2 studies identified from an SLR conducted by the sponsor and submitted in a separate report.60 The 2 included studies compared olaparib with placebo18 and capecitabine with observation,61 respectively.
Methods of Sponsor-Submitted ITC
Objectives
The sponsor conducted an ITC to determine the efficacy of olaparib relative to other adjuvant breast cancer treatments reimbursed in Canada in patients diagnosed with HER2-negative, gBRCA-mutated, high-risk nonmetastatic breast cancer.
Study Selection Methods
Based on the prespecified eligibility criteria as outlined in Table 31, the sponsor conducted an SLR60 to identify studies investigating the efficacy and safety of several interventions, including olaparib, capecitabine, endocrine therapy, and immune-oncology drugs (i.e., atezolizumab, pembrolizumab) in patients diagnosed with nonmetastatic, primary invasive HER2-negative, gBRCA-mutated breast cancer. Systematic literature searches were done in electronic databases (i.e., Ovid Embase, Ovid MEDLINE, Ovid Evidence-Based Medicine Reviews), reference lists of eligible studies, conference proceedings, global health technology assessment bodies, additional relevant websites, and clinical trial registries. The literature search was last updated on January 11, 2023. The study screening and selection process was conducted by 2 independent reviewers. Any discrepancies were resolved by consensus between the 2 reviewers. Studies identified from the systematic literature search were first screened based on the title and abstract. Full-text screening was then carried out for studies selected from the title and abstract screening stage. Two independent reviewers extracted data and assessed the risk of bias in the included studies using the checklist from the National Institute for Health and Care Excellence single technology appraisal user guide.23 A third reviewer was involved to resolve any discrepancies during the risk-of-bias assessment.
From the evidence base created from the SLR described earlier, the sponsor further identified studies that were potentially eligible for an ITC based on a set of additional criteria listed in Table 31. To be eligible to be included in the ITC, the population (or subpopulation), the control treatment, and the study design of the study identified from the SLR had to be aligned with those from the sponsor-conducted OlympiA trial.18 Moreover, the intervention of the study had to be an adjuvant HER2-negative, high-risk breast cancer treatment publicly reimbursed in Canada. The studies that were potentially eligible for an ITC were further assessed for ITC feasibility, including whether the potentially eligible studies could be connected with the OlympiA trial in a network, whether the studies were similar enough to the OlympiA trial in terms of effects modifiers such as patient characteristics and methodological characteristics such as trial design, and whether the outcomes reported in the potentially eligible studies were similar to those from the OlympiA trial (e.g., outcome definition, time points). Only the studies that the sponsor considered sufficiently similar to the OlympiA trial were included.
After assessing a total of 13 RCTs identified in the SLR, 2 RCTs were included for feasibility assessment; of these, 1 RCT61 (referred to as the CIBOMA trial) that compared capecitabine with observation was eligible to be included in the ITC with the sponsor-conducted OlympiA trial. However, the population investigated in the CIBOMA trial was not fully aligned with the population (i.e., high-risk, gBRCAm) investigated in the OlympiA trial; in the CIBOMA trial, only the patients with TNBC were considered by the sponsor to be sufficiently similar to the TNBC subpopulation in the OlympiA trial. Therefore, in the ITC, the treatment effects of olaparib in the TNBC subpopulation and patients with TNBC who received neoadjuvant chemotherapy in the OlympiA trial were compared with the treatment effects of capecitabine in the TNBC population and high-risk TNBC subpopulation (i.e., patients with TNBC without a pathological complete response after neoadjuvant therapy) in the CIBOMA trial, respectively.
In terms of outcomes, the 3-year IDFS reported by the OlympiA trial and 3-year DFS reported by the CIBOMA trial were considered broadly comparable by the sponsor and were therefore analyzed as 3-year IDFS or DFS in the ITC. The OlympiA trial defined IDFS as “the time from randomisation until the date of first occurrence of 1 of the following events: ipsilateral invasive breast tumour, locoregional invasive disease, distant recurrence, contralateral invasive breast cancer, second primary invasive cancer, or death from any cause,” while DFS was measured from “the date of random assignment in the ITT population to locoregional or distant recurrence, second primary malignancy, or death date, whichever occurred first” in the CIBOMA trial.59 In addition to IDFS and DFS, OS, reported by both the OlympiA and CIBOMA trials, was also analyzed in the ITC. The OlympiA trial defined OS as the time from randomization to death by any cause.40 The sponsor indicated that the definition of OS was not reported by the CIBOMA trial. However, from the clinical trial registry of CIBOMA (NCT00130533), the CADTH review team identified the definition of OS as “death from any cause.”
Table 31: Study Selection Criteria and Methods for SLR and ITC
Characteristic | For SLR conducted by sponsor | For ITC submitted by sponsor |
|---|---|---|
Population | OlympiA included adult female and male patients (≥ 18 years) with germline BRCA mutations (BRCA1 and/or BRCA2) and nonmetastatic primary invasive HER2-negative adenocarcinoma of the breast, who had:
Inclusion criteria for the current SLR were adult female and male patients (≥ 18 years) with nonmetastatic primary invasive HER2-negative adenocarcinoma of the breast who are receiving treatment in the postsurgical adjuvant setting. Further, studies that randomized patients during the neoadjuvant period and studies with mixed HER2-negative and HER2-positive status were considered for inclusion. Studies where the HER2 status is not reported were excluded. | The population or the subpopulation of the study selected from SLR should be aligned with those from the OlympiA trial, including:
|
Intervention or comparators | The interventions of interest were restricted to the adjuvant setting for the following:
Interventions not of interest include:
| The intervention of the study identified from the SLR should be publicly reimbursed adjuvant HER2-negative, high-risk breast cancer treatments in Canada. The control arm in the study identified from the SLR should be aligned with the control arm in the OlympiA trial. |
Outcome | Studies reporting at least 1 outcome of interest (to include efficacy and safety outcomes reported in the OlympiA study), including: Efficacy:
Safety:
HRQoL:
| Same as for the SLR |
Study design | Prospective RCTs (phase II to IV) with active or placebo or best supportive care controls with no restriction on blinding. Systematic reviews and meta-analyses were excluded. | The study design should align with that of the OlympiA trial. |
Language | English language publications or non–English language publications with an English abstract | Same as for the SLR |
AE = adverse event; BRCA = breast cancer gene; CDK = cyclin-dependent kinase; DDFS = distant disease–free survival; DFS = disease-free survival; HER2 = human epidermal growth factor receptor 2; HR-positive = positive for expression of a hormone receptor; HRQoL = health-related quality of life; IDFS = invasive disease–free survival; ITC = indirect treatment comparison; NA = not applicable; OS = overall survival; PARP = poly-(ADP-ribose) polymerase; PRO = patient-reported outcome; RCT = randomized controlled trial; RECIST = Response Evaluation Criteria in Solid Tumors; RFS = relapse-free survival; SAE = serious adverse event; SLR = systematic literature review; TNBC = triple-negative breast cancer.
Sources: Sponsor ITC and SLR reports.59,60
The sponsor included the CIBOMA trial61 and the OlympiA trial18 in the ITC and compared olaparib with capecitabine via the common comparator versus placebo or observation. The network diagram was shown in Figure 12.
Figure 12: Schematic of the Indirect Treatment Comparison Methodology
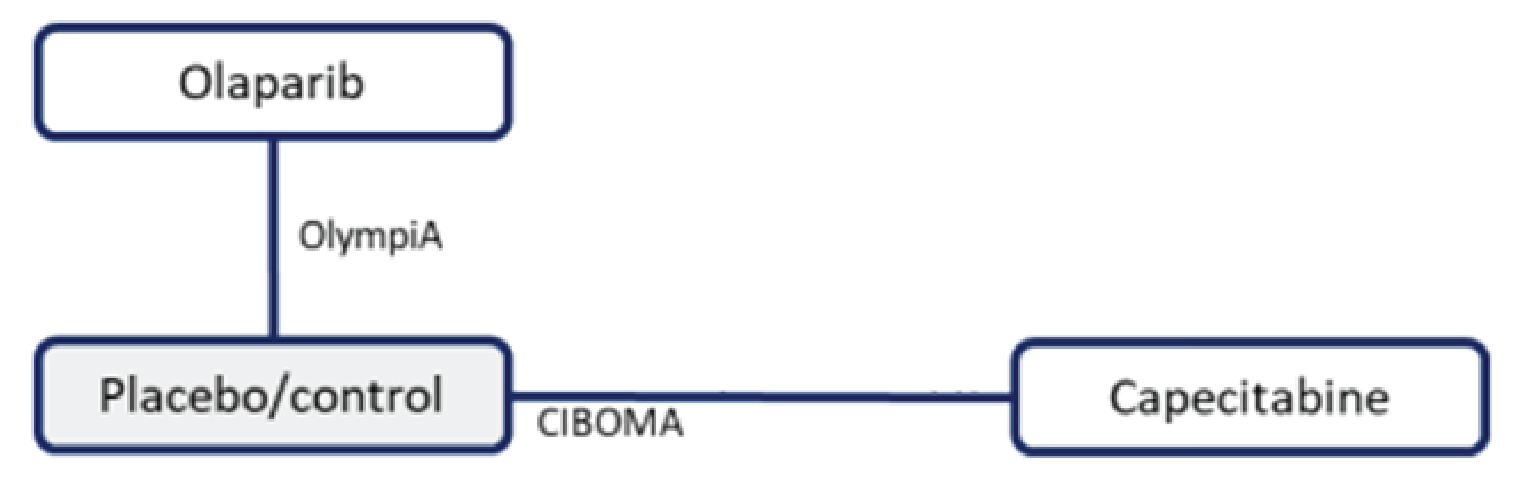
Source: Sponsor’s indirect treatment comparison.59
The sponsor adopted the Bucher method62 to perform the ITC. The Bucher method uses a common comparator arm between 2 trials to estimate the relative treatment efficacy between 2 drugs that have previously not been investigated in a head-to-head trial while maintaining randomization. This method assumes the treatment effects are homogenous between trials and that there is no between-trial variation of treatment effect modifiers or prognostic factors. According to the sponsor’s descriptions of the Bucher method,59 the variance for the indirect comparison was based on the sum of the variances for the direct comparisons.
Results of the Sponsor-Submitted ITC
Summary of Included Studies
A summary of the included trials in the sponsor-submitted ITC is provided in Table 32. The OlympiA trial was a phase III, double-blind RCT that compared olaparib with placebo, whereas the CIBOMA trial was a phase III, open-label RCT that compared capecitabine with observation. Although the sponsor-submitted ITC did not specify, the observation arm in the CIBOMA trial referred to “no intervention,” according to the information from the clinical trial registry of CIBOMA (NCT00130533). The comparator group in the OlympiA trial involved matching placebo tablets. The population investigated in the OlympiA trial comprised all patients with gBRCA-mutated breast cancer, while the gBRCAm status was not reported in the CIBOMA trial. The OlympiA trial included patients with HER2-negative breast cancer, including patients with TNBC, whereas all of the participants in the CIBOMA trial were diagnosed with TNBC. All of the patients in the OlympiA trial were considered to have high-risk breast cancer, as defined in Table 32. However, the CIBOMA trial included patients regardless of risk. In the ITC report, the sponsor defined patients in the CIBOMA trial with TNBC with no pathological response after neoadjuvant therapy as high-risk patients. The sponsor considered these patients comparable to the subgroup of patients who received neoadjuvant chemotherapy in the OlympiA trial.
Table 32: Summary of Included Trials in the Sponsor-Submitted ITC
Detail | OlympiA | CIBOMA |
|---|---|---|
Intervention | Olaparib 600 mg (two 150 mg tablets, twice per day) | 8 cycles of capecitabine 2,000 mg/m2 (1,000 mg/m2 twice per day) on days 1 to 14 every 3 weeks |
Comparator | Placebo (matching placebo tablets) | Observation (no intervention) |
Phase | █ █████ | █ █████ |
Number of patients at randomization | 1,836 | 876 |
Randomization | Patients were randomized to either olaparib (n = 921) or placebo (n = 915). Randomization was stratified by hormone receptor status (ER- and/or PgR-positive and HER2-negative vs. TNBC), by prior neoadjuvant vs. adjuvant chemotherapy, and prior platinum use for breast cancer (yes vs. no). | Patients were randomly assigned to capecitabine (n = 448) or observation (n = 428). Randomization was stratified according to basal status (yes vs. no), institution, number of axillary lymph nodes (0 vs. 1 to 3 vs. 4 or more), and type of adjuvant chemotherapy (anthracyclines plus taxanes vs. anthracyclines alone). |
Study duration | June 2014 through May 2019 | October 2006 through September 2011 |
Method of blinding | Double blind | Open label |
Follow-up, median years (IQR) | 2.5 (NR) |
|
Population | Patients with HER2-negative, gBRCA-mutated, high-risk primary breast cancer after definitive local treatment and neoadjuvant or adjuvant chemotherapy. | Patients with mixed-risk operable TNBC after neoadjuvant or adjuvant chemotherapy. Subgroup data were reported for high-risk patients. BRCA mutation status was unknown in this study. |
Inclusion criteria |
|
|
Definitions of high-risk breast cancer | All patients enrolled were classified as high risk. Patients who underwent neoadjuvant chemotherapy followed by surgery:
Patients who underwent adjuvant chemotherapy:
| NR by the trial conductors. The sponsor classified a subgroup of patients as high risk (15% of the total study population: observation, n = 61; capecitabine, n = 69), defined as patients with TNBC without pathological response after neoadjuvant therapy. The sponsor considered this subgroup to be comparable to the patients who received neoadjuvant chemotherapy in the OlympiA trial. |
Exclusion criteria | NR | NR |
BRCA1 = breast cancer gene 1; BRCA2 = breast cancer gene 2; CPS&EG = clinical and post-treatment pathologic stage and estrogen receptor status and histologic grade; ECOG PS = Eastern Cooperative Oncology Group Performance Status; ER = estrogen receptor; gBRCA = germline breast cancer gene; HER2 = human epidermal growth factor receptor 2; IHC = immunohistochemistry; IQR = interquartile range; ITC = indirect treatment comparison; NR = not reported; pCR = pathologic complete response; PgR = progesterone receptor; pT2 = pathological tumour size 2; TNBC = triple-negative breast cancer.
Sources: Sponsor’s ITC report59 and CIBOMA Clinical Study Report.61
Baseline patient characteristics for the 2 included studies are summarized in Table 33. The median age of the total and TNBC populations in the OlympiA trial was lower than the CIBOMA trial. The race profile in the OlympiA and CIBOMA trials was primarily white, but 28.9% of the total population in the OlympiA trial was Asian (30% of patients in the TNBC subpopulation were Asian), whereas the CIBOMA trial did not report the inclusion of Asian patients. All participants in the CIBOMA trial were patients diagnosed with TNBC. In the OlympiA trial, patients with TNBC accounted for 81.5% (751 out of 921) and 82.8% (758 out of 915) of the participants in the olaparib arm and the placebo arm, respectively. The rest of the patients in the OlympiA trial were diagnosed with either ER-positive or PgR-positive breast cancer. More than 70% of the patients with TNBC in the OlympiA trial received mastectomy for primary breast cancer, while only 45% of the patients with TNBC in the CIBOMA trial were treated with mastectomy. In terms of prior chemotherapy setting, just more than half of the patients with TNBC in the OlympiA trial underwent adjuvant treatments, whereas around 80% of the patients with TNBC in the CIBOMA trial received adjuvant treatments.
Table 33: Summary of Patient Baseline Characteristics
Characteristic | OlympiA, total population | OlympiA, TNBC subpopulation | CIBOMA, total population | |||
|---|---|---|---|---|---|---|
Olaparib (N = 921) | Placebo (N = 915) | Olaparib (N = 751) | Placebo (N = 758) | Capecitabine (N = 448) | Control (observation) (N = 428) | |
Median age, years (IQR) | 42 (36 to 49) | 43 (36 to 50) | 42 (36 to 49) | 36 (36 to 50) | 50 (20 to 79) | 49 (23 to 82) |
Race, n (%) | ||||||
White | 626 (68) | 599 (65.5) | 502 (66.8) | 490 (64.6) | 313 (69.9) | 309 (72.2) |
Asian | 259 (28.1) | 272 (29.7) | 220 (29.3) | 232 (30.6) | NR | NR |
Hispanic | NR | NR | NR | NR | 107 (23.9) | 97 (22.7) |
Black or African American | 19 (2.1) | 29 (3.2) | 13 (1.7) | 25 (3.3) | 16 (3.6) | 11 (2.6) |
Hormone receptor status, n (%) | ||||||
ER- or PgR-positive | 168 (18.2) | 157 (17.2) | — | — | — | — |
TNBC | 751 (81.5) | 758 (82.8) | 751 (100) | 758 (100) | 448 (100) | 428 (100) |
Menopausal status, n (%) | ||||||
Pre | 572/919 (62.2) | 553/911 (60.7) | 473/750 (63) | 457 (60.3) | 136 (30.4) | 140 (32.7) |
Post | 347/919 (37.8) | 358/911 (39.3) | 277/750 (36.9) | 301 (39.7) | 312 (69.6) | 288 (67.3) |
Surgery for primary breast cancer, n (%) | ||||||
Mastectomy | 698 (75.8) | 673 (73.6) | 553 (73.6) | 543 (71.6) | 205 (45.8) | 185 (43.2) |
Conservative surgery only | 223 (24.2) | 240 (26.2) | 198 (26.4) | 214 (28.2) | 237 (52.9) | 242 (56.5) |
Prior chemotherapy setting, n (%) | ||||||
Adjuvant | 461 (50.1) | 455 (49.7) | 397 (52.9) | 390 (51.5) | 353 (78.8) | 352 (82.2) |
Neoadjuvant | 460 (49.9) | 460 (50.3) | 354 (47.1) | 368 (48.5) | NR | NR |
Neoadjuvant ± adjuvant | 0 | 0 | 0 | 0 | 89 (19.9) | 75 (17.5) |
ER = estrogen receptor; ITC = indirect treatment comparison; IQR = interquartile range; NR = not reported; PgR = progesterone receptor; TNBC = triple-negative breast cancer.
Source: Sponsor ITC report.59
Efficacy Results of the Sponsor-Submitted ITC
The HRs for IDFS, DFS, and OS from the individual studies, along with the indirect estimates for olaparib versus capecitabine from the Bucher ITC, are presented in Table 34. No conclusions could be drawn for the effect of olaparib compared with capecitabine on IDFS, DFS, or OS due to imprecision in the effect estimates (i.e., wide CIs).
Table 34: Sponsor-Submitted ITC Results
Outcome | OlympiA | CIBOMA | ITC estimates: | ||
|---|---|---|---|---|---|
Population | Direct estimate: | Population | Direct estimate: | ||
IDFS or DFS | Patients with TNBC (82% in the OlympiA study population, all high-risk patients) | 0.62 (0.49 to 0.79) | Patients with TNBC (100% in the CIBOMA study population, mixed-risk patients) | 0.82 (0.63 to 1.06) | 0.76 (0.53 to 1.08) |
Patients with TNBC who received neoadjuvant chemotherapy | 0.63 (0.46 to 0.85) | Patients with TNBC without pCR after neoadjuvant therapy (high-risk patients) | 1.12 (0.64 to 1.97) | 0.56 (0.30 to 1.06) | |
OS | Patients with TNBC (82% in the OlympiA study population, all high-risk patients) | 0.64 (0.46 to 0.88) | Patients with TNBC (100% in the CIBOMA study population, mixed-risk patients) | 0.92 (0.66 to 1.28) | 0.70 (0.44 to 1.11) |
Patients with TNBC that received neoadjuvant chemotherapy | 0.63 (0.42 to 0.92) | Patients with TNBC without pCR after neoadjuvant therapy (high-risk patients) | — | — | |
CI = confidence interval; DFS = disease–free survival; HR = hazard ratio; IDFS = invasive disease–free survival; ITC = indirect treatment comparison; OS = overall survival; pCR = pathological complete response; TNBC = triple-negative breast cancer; vs. = versus.
Source: Sponsor’s ITC report.59
Critical Appraisal of Sponsor-Submitted ITC
Overall, the SLR used to identify potentially relevant studies for the ITC was methodologically sound in terms of the sponsor using a comprehensive literature search strategy; performing study selection, data extraction, and risk-of-bias assessment in duplicate; and providing a list of excluded studies and justifying the exclusions. However, it was unclear in the ITC report whether the feasibility assessment was carried out by a single or multiple assessors. Additionally, although the risk of bias in individual studies was assessed in the SLR, the assessment results were not incorporated and discussed in the ITC report.
The sponsor conducted the ITC based on the methodology described by Bucher et al.62 to estimate the relative treatment efficacy between olaparib and capecitabine through the common comparator, placebo (i.e., matching placebo tablets) or observation only (i.e., no intervention). The Bucher method assumes the trials included in the ITC should be sufficiently homogeneous with respect to study population, study design, outcome measurements, and the distribution of treatment effect modifiers. There were, however, some differences between the OlympiA trial and the CIBOMA trial in patient characteristics, trial methodology, and outcome definitions, which might increase the uncertainty of the ITC analysis. One of the most important differences was the gBRCAm status of the study population: the OlympiA trial required the participants to have BRCA1- or BRCA2-mutated breast cancer, whereas the gBRCAm status was unknown in the CIBOMA trial. Given that confirmation of gBRCAm is a prerequisite for the use of olaparib, according to the clinical experts consulted, heterogeneity in the mutation status between the OlympiA and CIBOMA trials might pose a substantial threat to the validity of the ITC analysis.
Moreover, by conducting a feasibility assessment, the sponsor determined that data from the CIBOMA trial did not allow an ITC in populations that were fully aligned with the OlympiA population. Patients with TNBC without pathological response after neoadjuvant therapy in the CIBOMA trial were considered by the sponsor as high-risk patients and “most closely aligned” with the high-risk TNBC subgroup in the OlympiA trial. However, the characteristics of the high-risk patients in the CIBOMA trial defined by the sponsor were not reported by the trial authors. As a result, we were unable to ascertain whether the characteristics of the high-risk patients in the CIBOMA trial were similar enough to those of the high-risk patients in the OlympiA trial to uphold the homogeneity assumption of the Bucher ITC.
Other notable differences between the 2 trials included the following:
The OlympiA trial was a double-blind RCT while the CIBOMA trial was an open-label RCT.
The median age of the total patients and the patients with TNBC in the OlympiA trial was lower than that in the CIBOMA trial.
The majority of the patients in the OlympiA trial (75% in the total population, 73% in the TNBC subpopulation) received mastectomy, while the largest proportion of patients in CIBOMA (54.7%) underwent conservative surgery only.
The OlympiA and CIBOMA trials used matching placebo tablets; no intervention was used in the control arms of either study.
The ITC estimates were too imprecise (i.e., wide 95% CIs, including HR = 1) to draw a conclusion about the comparative effect of olaparib versus capecitabine on IDFS, DFS, or OS. Safety outcomes were not analyzed in the ITC report, and no justification was provided, which precludes a balanced judgment of comparative benefits relative to comparative harms. Outcomes that are important to patients, such as HRQoL, were also not analyzed in this ITC. Finally, the ITC was performed only in patients with TNBC breast cancer, which only aligned with a part of the indication population specified in the sponsor’s application. As a result, the results of the ITC may not be generalizable to all patients with breast cancer who satisfy the criteria in the reimbursement request.
Other Relevant Evidence
No other relevant evidence was submitted by the sponsor or identified from the literature.
Discussion
Summary of Available Evidence
The CADTH systematic review included 1 pivotal trial (OlympiA) and 1 network meta-analysis submitted by the sponsor.
The OlympiA trial18,19 is an ongoing, phase III, randomized, multicentre, placebo-controlled, double-blind trial that aims to assess the efficacy and safety of olaparib at 300 mg twice daily versus matched placebo for the adjuvant treatment of adult patients with deleterious or suspected deleterious gBRCA-mutated, HER2-negative high-risk early breast cancer who have been treated with neoadjuvant or adjuvant chemotherapy. Patients must have had confirmation of a gBRCAm before olaparib treatment was initiated. The trial was initiated in April 2014 with 546 sites in 23 countries in North America (34 patients recruited in Canada), South America, Europe, Asia Pacific, and South Africa. In the OlympiA trial, 1,836 patients were randomized in a 1:1 ratio to receive either olaparib (N = 921) or placebo (N = 915). The patients had a mean age of 43.3 years (SD = 9.97 years). Most patients were female (99.7%), white (66.7%), nonhispanic or Latino (88.1%); 82.3% of patients had TNBC, half of patients received neoadjuvant treatment (50.1%), and 72.2% of patients had BRCA1 mutations. The primary outcome was IDFS and the key secondary outcomes were DDFS and OS. Other secondary outcomes in the trial that were important to the CADTH review included HRQoL assessed by the FACIT-F and EORTC QLQ-30 questionnaires. Harms and notable harms (identified in the CADTH systematic review protocol) were assessed.
The sponsor-submitted ITC59 evaluated the relative efficacy of olaparib against capecitabine in patients diagnosed with nonmetastatic TNBC. The ITC included 2 studies: the sponsor-conducted OlympiA trial18 comparing olaparib with placebo as well as the CIBOMA trial61 comparing capecitabine with observation. The ITC was performed using the Bucher method. The clinical end points used for ITC estimates included 3-year IDFS and DFS reported by the OlympiA trial and the CIBOMA trial, respectively, as well as OS reported by both trials. No comparative efficacy conclusions could be drawn for either outcome due to imprecision in the effect estimates (i.e., wide CIs). The ITC has some limitations that reduce the CADTH team’s confidence in the effect estimates. There were notable differences across the 2 trials in patient baseline demographic and disease characteristics (e.g., unknown BRCA mutation status in the CIBOMA trial) and trial design (e.g., double blind versus open label, outcome definitions) that might threaten the plausibility of the assumptions of the Bucher method. There were also notable limitations with respect to the external validity of the ITC results. The ITC was performed only in patients with TNBC breast cancer, which only aligned with a part of the indication population specified in the sponsor’s application.
Interpretation of Results
Efficacy
The OlympiA trial appeared to have appropriate methods for blinding, allocation concealment, randomization with stratification to minimize bias, and adequate power for the primary, and the type I error was adequately controlled and accounted for in the IDFS, OS, and DDFS analyses. Definitive conclusions could not be drawn for HRQoL data due to the lack of adjustment for multiplicity and a high risk of attrition bias. One other key limitation of the OlympiA trial was the limited clinical evidence on the benefit of olaparib relative to placebo in patients with HR-positive, HER2-negative early breast cancer, making it difficult to generalize the results to all patients with BRCA-mutated early breast cancer who may be treated in a Canadian setting. In addition, since the results are from interim analyses, there is a risk of overestimation of benefit, but the presence and extent of any estimation in uncertain.20,21
The superiority of olaparib over placebo was demonstrated at the first interim IDFS analysis with a median follow-up of 2.5 years and data maturity of 15.5% (stratified HR = 0.58; 99.5% CI, 0.41 to 0.82). This treatment benefit of olaparib was maintained at the second, exploratory analysis of IDFS with a median follow-up of 3.5 years and 98.9% of patients having completed or discontinued from the study treatment (stratified HR = 0.63; 95% CI, 0.50 to 0.78). The 4-year event-free rate was 82.7% (95% CI, 79.6% to 85.4%) in the olaparib group and 75.4% (95% CI, 72.2% to 78.3%) in the placebo group (difference = 7.3%; 95% CI, 3.0% to 11.5%).17 The median time to invasive disease recurrence or death was not estimable because insufficient follow-up time had elapsed for this outcome.
The superiority of olaparib over placebo was demonstrated at the first interim analysis of DDFS with a median follow-up of 2.5 years (stratified HR = 0.57; 99.5% CI, 0.39 to 0.83). This treatment benefit of olaparib was maintained at the second, exploratory analysis of DDFS with a median follow-up of 3.5 years (stratified HR = 0.61; 95% CI, 0.48 to 0.77). The 4-year event-free rate was 86.5% (95% CI, 83.8% to 88.8%) in the olaparib group and 79.1% (95% CI, 76.0% to 81.8%) in the placebo group (difference = 7.4%; 95% CI, 3.6% to 11.3%).17 The median time to distant disease recurrence or death was not estimable because insufficient follow-up time had elapsed for this outcome.
The superiority of olaparib over placebo was demonstrated at the second interim analysis of OS with a median follow-up of 3.5 years, and data maturity of 10% (stratified HR = 0.68; 98.5% CI, 0.47 to 0.97). The percentage of patients who were alive 4 years after randomization was 89.8% (95% CI, 87.2% to 91.9%) in the olaparib group and 86.4% (83.6% to 88.7%) in the placebo group (difference = 3.4%; 95% CI, –0.1% to 6.8%).17 The median time to death was not estimable because insufficient follow-up time had elapsed for this outcome.
According to the clinical experts consulted by CADTH, the between-group differences in the OS, IDFS, and DDFS end points were clinically meaningful. However, the long-term efficacy of adjuvant olaparib for IDFS, OS, and DDFS is unknown, as the OlympiA trial is ongoing. Several sensitivity analyses were conducted for IDFS, OS, and DDFS outcomes, such as by:
including only patients with central pathology review data for HR status
using unadjusted analysis
using interval censoring, and the results were consistent with the primary analyses.
Supportive analysis results for IDFS, DDFS, and OS based on all randomized patients with confirmed BRCA germline mutations were also consistent with the primary analyses. The subgroup analyses may not have been powered to detect a treatment difference; there were no adjustments made for multiplicity and the results should be viewed as supportive evidence only for the overall effect of olaparib.
The patient and clinician groups consulted by CADTH highlighted improvement in HRQoL as an important outcome and treatment goal for patients with early breast cancer. HRQoL was measured using the FACIT-F and EORTC QLQ-C30 questionnaires. Both are generally valid and reliable questionnaires for breast cancer. There were small mean differences between treatment groups in both FACIT-F total score and EORTC QLQ-C30 subscales at follow-up, and strong conclusions could not be drawn for these outcomes due to the high risk of attrition bias and increased risk of type I error.
One sponsor-submitted ITC was summarized for this review to supplement the assessment of olaparib compared with capecitabine for the adjuvant treatment of adult patients with high-risk, early-stage TNBC. No conclusions could be drawn from the ITC about the effect of olaparib relative to capecitabine on IDFS, DFS, or OS due to methodological limitations and imprecision in the effect estimates (wide 95% CIs).
Harms
Most patients (91.8% of patients in the olaparib group and 83.8% of patients in the placebo group) experienced at least 1 AE. Compared with the placebo group, a higher proportion of patients experienced AEs of grade 3 or higher (24.5% versus 11.3%), TRAEs (80.8% versus 53.1%), and treatment-emergent SAEs (3.6% versus 0.7%). The clinical experts consulted by CADTH noted that most AEs experienced on olaparib were predictable and clinically manageable. It was further noted by the clinical experts that treatment with olaparib generally revealed no new safety issues in the OlympiA trial and was consistent overall with its known safety profile in patients with advanced or metastatic breast cancer. According to the patient input received, patient respondents, especially those with stage III breast cancer, tended to endure side effects as well as their impacts on quality of life to achieve satisfactory effectiveness.
█ ██ █ █ ██ █ █ █ █ ██ █ █ █ ██ ███ █ █ █ █ █ ██ ██ ██ ██ █ █ █ █ █ ██ ██ █ █ █ █ ██ █ █ █ █ ██ █ █ ██ █ █ █ █ ██ █ █ █ █ ██ ██ ██ █ █ ██ ████████ █ █ █ █ ██ ██ █ █ █ █ ██ █ █ █ █ ██ ██ ██ █ █ ██ ████████ █ █ █ █ ██ ████ █ █ █ █ ██ ██ ██ █ █ ██ █ █ █ ██ █ █ ██ █ █ █ ██ ███ █ █ █ █ ██ █ █ █ █ ██ ██ ██ █ █ ██ ██ ██ █ █ ██ ██ ██ █ █ ██ ██████████████. A higher incidence of grade 3 or higher AEs was observed in the olaparib group compared with the placebo group, with the difference mainly driven by a higher incidence of anemia (8.7%), decrease in neutrophil count (4.9%), and fatigue (1.8%). The clinical experts consulted noted they would expect more AEs in the olaparib group compared with the placebo group, given that an additional treatment was added to the regimen. The majority of AEs and TRAEs were manageable with supportive care and/or dose modifications and consistent with the known safety profile for olaparib. According to the clinical experts consulted, the type and distribution of AEs observed in the OlympiA trial were expected and reflective of clinical practice. It was further noted by the clinical experts that the more prior treatments a patient has had, the more susceptible the patient may be to AEs, with less ability to tolerate them with each subsequent line of treatment.
The frequency of notable harms was comparable between the treatment groups. Similar to the metastatic setting, the notable AEs identified in the OlympiA trial included new primary cancer (2.3% and 4.0% in the olaparib and placebo groups, respectively), pneumonitis (1% and 1.3% in the olaparib and placebo groups, respectively), and myelodysplastic syndrome or acute myeloid leukemia (0.2% and 0.3% in the olaparib and placebo groups, respectively). However, the key long-term safety end point for myelodysplastic syndrome and acute myeloid leukemia will require longer follow-up for complete assessment. No new safety concerns were identified compared with previous trials conducted in patients with metastatic breast cancer. According to the clinical experts consulted by CADTH, it is not clear what proportion of the notable harms identified in the trial was attributable to prior treatment in neoadjuvant or adjuvant settings rather than treatment with olaparib. It was further noted by the clinical experts that myelodysplastic syndrome and acute myeloid leukemia are often related to anthracycline chemotherapy, radiation may increase the risk of subsequent cancer, and taxane-based chemotherapy may contribute to the development of pneumonitis.
The proportion of patients who discontinued treatment because of AEs and TRAEs was higher in the olaparib group compared with the placebo group (10.8% versus 4.6%, and 9.2% versus 1.8%, respectively). The most common reasons for treatment discontinuation were nausea, anemia, fatigue, and decreased neutrophil count. The proportion of patients who required dose reduction or interruption because of AEs was higher in the olaparib group compared with the placebo group (31.4% versus 11.0%, and 23.4% versus 3.7%, respectively). There were 2 fatal AEs in the placebo group (acute myeloid leukemia, ovarian cancer) and 1 fatal AE in the olaparib group (cardiac arrest) during the treatment period or within the 30-day follow-up period, as well 2 fatal AEs in the placebo group (pancreatic carcinoma, leukemia) and 1 fatal AE in the olaparib group (acute myeloid leukemia) 30 days after discontinuation. No specific patterns in etiology or a temporal relationship with treatment exposure have been reported for fatal AEs.
Conclusions
Based on data from the OlympiA trial, olaparib demonstrated a clinically meaningful and statistically significant benefit compared with placebo in improving IDFS, DDFS, and OS in adult patients with HER2-negative, high-risk early breast cancer. The median IDFS, OS, and DDFS were not estimable in either treatment group because insufficient follow-up time had elapsed for these outcomes; thus, the longer-term efficacy of adjuvant olaparib is unknown. In addition, the estimates of the benefit of olaparib may be overestimated because the results are from interim analyses, although the presence and extent of any overestimation is uncertain. However, olaparib could help optimize adjuvant treatment in patients with BRCA-mutated early breast cancer to improve outcomes in terms of disease recurrence and survival, given its acceptable and manageable safety profile. The safety profile of olaparib was consistent with the known adverse effects profile of olaparib, and no new safety signals were identified. Strong conclusions could not be drawn related to the effect of olaparib on HRQoL due to the high risk of attrition bias and increased risk of type I error in the analyses of these outcomes. The evidence of olaparib was limited to 1 placebo-controlled pivotal trial, and no direct evidence of olaparib compared with other comparators was available for this review, most likely because current systemic treatment of early breast cancer does not consider the patient’s BRCA mutation status. Uncertainties remain regarding the availability of BRCA mutation testing in Canada for clinical implementation in determining patient eligibility for olaparib treatment. No conclusions could be drawn from the ITC about the effect of olaparib relative to capecitabine on IDFS, DFS, or OS due to methodological limitations and imprecision in the effect estimates (wide 95% CIs, including HR = 1).
References
1.Canadian Cancer Statistics Advisory Committee, Canadian Cancer Society, Statistics Canada, Public Health Agency of Canada. Canadian Cancer Statistics 2021. Toronto (ON): Canadian Cancer Society; 2021: Accessed 2022 Aug 25.
2.O’Shaughnessy J, Brezden-Masley C, Cazzaniga M, et al. Prevalence of germline BRCA mutations in HER2-negative metastatic breast cancer: global results from the real-world, observational BREAKOUT study. Breast Cancer Res. 2020;22(1):114. PubMed
3.Tarsounas M, Sung P. The antitumorigenic roles of BRCA1-BARD1 in DNA repair and replication. Nat Rev Mol Cell Biol. 2020;21(5):284-299. PubMed
4.Carroll JC, Cremin C, Allanson J, et al. Hereditary breast and ovarian cancers. Can Fam Physician. 2008;54(12):1691-1692. PubMed
5.Godet I, Gilkes DM. BRCA1 and BRCA2 mutations and treatment strategies for breast cancer. Integr Cancer Sci Ther. 2017;4(1). PubMed
6.Tung NM, Boughey JC, Pierce LJ, et al. Management of Hereditary Breast Cancer: American Society of Clinical Oncology, American Society for Radiation Oncology, and Society of Surgical Oncology Guideline. J Clin Oncol. 2020;38(18):2080-2106. PubMed
7.Burstein HJ, Curigliano G, Loibl S, et al. Estimating the benefits of therapy for early-stage breast cancer: the St. Gallen International Consensus Guidelines for the primary therapy of early breast cancer 2019. Ann Oncol. 2019;30(10):1541-1557. PubMed
8.Paluch-Shimon S, Cardoso F, Sessa C, et al. Prevention and screening in BRCA mutation carriers and other breast/ovarian hereditary cancer syndromes: ESMO Clinical Practice Guidelines for cancer prevention and screening. Ann Oncol. 2016;27(suppl 5):v103-v110. PubMed
9.Cardoso F, Kyriakides S, Ohno S, et al. Early breast cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up†. Ann Oncol. 2019;30(8):1194-1220. PubMed
10.Tung NM, Garber JE. BRCA1/2 testing: therapeutic implications for breast cancer management. Br J Cancer. 2018;119(2):141-152. PubMed
11.Brouckaert O, Wildiers H, Floris G, Neven P. Update on triple-negative breast cancer: prognosis and management strategies. Int J Womens Health. 2012;4:511-520. PubMed
12.Zavitsanos PJ, Wazer DE, Hepel JT, Wang Y, Singh K, Leonard KL. BRCA1 Mutations Associated With Increased Risk of Brain Metastases in Breast Cancer: A 1: 2 Matched-pair Analysis. Am J Clin Oncol. 2018;41(12):1252-1256. PubMed
13.Mavaddat N, Barrowdale D, Andrulis IL, et al. Pathology of breast and ovarian cancers among BRCA1 and BRCA2 mutation carriers: results from the Consortium of Investigators of Modifiers of BRCA1/2 (CIMBA). Cancer Epidemiol Biomarkers Prev. 2012;21(1):134-147. PubMed
14.Lynparza (olaparib): 100 mg and 105 mg oral tablets [product monograph]. Mississauga (ON): AstraZeneca Canada Inc.; 2022 Aug 18.
15.pan-Canadian Oncology Drug Review Committee (pERC) final recommendation: olaparib (Lynparza) resubmission.
16.pan-Canadian Oncology Drug Review Committee (pERC) final recommendation: olaparib (Lynparza).
17.Geyer CE, Jr., Garber JE, Gelber RD, et al. Overall survival in the OlympiA phase III trial of adjuvant olaparib in patients with germline pathogenic variants in BRCA1/2 and high-risk, early breast cancer. Ann Oncol. 2022;33(12):1250-1268. PubMed
18.Clinical Study Report: D081CC00006 (BIG 6-13; NSABP B-55). A randomised, double-blind, parallel group, placebo-controlled multi-centre phase III study to assess the efficacy and safety of olaparib versus placebo as adjuvant treatment in patients with germline BRCA1/2 mutations and high risk HER2 negative primary breast cancer who have completed definitive local treatment and neoadjuvant or adjuvant chemotherapy [internal sponsor’s report]. Gaithersburg (MD): AstraZeneca; 2021 Sep 03.
19.Clinical Study Report: D081CC00006 (BIG 6-13; NSABP B-55) Addendum 1. A randomised, double-blind, parallel group, placebo-controlled multi-centre phase III study to assess the efficacy and safety of olaparib versus placebo as adjuvant treatment in patients with germline BRCA1/2 mutations and high risk HER2 negative primary breast cancer who have completed definitive local treatment and neoadjuvant or adjuvant chemotherapy: analysis of overall survival and safety update [internal sponsor’s report]. Gaithersburg (MD): AstraZeneca; 2022 May 05.
20.Bassler D, Briel M, Montori VM, et al. Stopping randomized trials early for benefit and estimation of treatment effects: systematic review and meta-regression analysis. JAMA. 2010;303(12):1180-1187. PubMed
21.Briel M, Bassler D, Wang AT, Guyatt GH, Montori VM. The dangers of stopping a trial too early. J Bone Joint Surg Am. 2012;94(Suppl 1):56-60. PubMed
22.Health Canada reviewer’s report: Lynparza (olaparib) [internal sponsor’s report]. In: Drug Reimbursement Review sponsor submission: Lynparza (olaparib), 100 mg, or 150 mg oral tablets. Mississauga (ON): AstraZeneca Canada Inc.; 2022 Jun 22.
23.Systematic reviews: CRD’s guidance for undertaking reviews in health care. York (UK): Centre for Reviews and Dissemination, University of York; 2009: Accessed 2022 Oct 27.
24.Shah-Manek B, Galanto JS, Nguyen H, Ignoffo R. Value Frameworks for the Patient-Provider Interaction: A Comparison of the ASCO Value Framework Versus NCCN Evidence Blocks in Determining Value in Oncology. J Manag Care Spec Pharm. 2017;23(6-a Suppl):S13-S20.
25.Harbeck N, Penault-Llorca F, Cortes J, et al. Breast cancer. Nat Rev Dis Primers. 2019;5(1):66. PubMed
26.Sawaki M, Shien T, Iwata H. TNM classification of malignant tumors (Breast Cancer Study Group). Jpn J Clin Oncol. 2019;49(3):228-231. PubMed
27.Warner E, Foulkes W, Goodwin P, et al. Prevalence and penetrance of BRCA1 and BRCA2 gene mutations in unselected Ashkenazi Jewish women with breast cancer. J Natl Cancer Inst. 1999;91(14):1241-1247. PubMed
28.Liu M, Xie F, Liu M, Zhang Y, Wang S. Association between BRCA mutational status and survival in patients with breast cancer: a systematic review and meta-analysis. Breast Cancer Res Treat. 2021;186(3):591-605. PubMed
29.Costa RLB, Gradishar WJ. Triple-Negative Breast Cancer: Current Practice and Future Directions. J Oncol Pract. 2017;13(5):301-303. PubMed
30.Aromatase inhibitors versus tamoxifen in premenopausal women with oestrogen receptor-positive early-stage breast cancer treated with ovarian suppression: a patient-level meta-analysis of 7030 women from four randomised trials. Lancet Oncol. 2022;23(3):382-392. PubMed
31.Ma K, Lu Y, Jiang S, Tang J, Li X, Zhang Y. The Relative Risk and Incidence of Immune Checkpoint Inhibitors Related Pneumonitis in Patients With Advanced Cancer: A Meta-Analysis. Front Pharmacol. 2018;9:1430. PubMed
32.Tung NM, Zakalik D, Somerfield MR. Adjuvant PARP Inhibitors in Patients With High-Risk Early-Stage HER2-Negative Breast Cancer and Germline BRCA Mutations: ASCO Hereditary Breast Cancer Guideline Rapid Recommendation Update. J Clin Oncol. 2021;39(26):2959-2961. PubMed
33.Drug Reimbursement Review sponsor submission: Lynparza (olaparib), 100 mg and 105 mg oral tablets [internal sponsor’s package]. Mississauga (ON): AstraZeneca Canada Inc.; 2022 Aug 18.
34.Remon J, Pardo N, Martinez-Marti A, et al. Immune-checkpoint inhibition in first-line treatment of advanced non-small cell lung cancer patients: Current status and future approaches. Lung Cancer. 2017;106:70-75. PubMed
35.pan-Canadian Oncology Drug Review Committee (pERC) final recommendation: olaparib (Lynparza).
36.Verzenio (abemaciclib): 50 mg, 100 mg, 150 mg, or 200 mg oral tablets [product monograph]. Toronto (ON): Eli Lilly Canada Inc.; 2022 Jan 10.
37.Keytruda (pembrolizumab): solution for infusion 100 mg/4 mL per vial, solution for infusion [product monograph]. Kirkland (QC): Merck Canada Inc.; 2022 Apr 5.
38.Xelodav(capecitabine): 150mg and 500 mg oral tablets [product monograph]. Mississauga (ON): Hoffmann-La Roche Limited.; 2022 April 4.
39.McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS Peer Review of Electronic Search Strategies: 2015 guideline statement. J Clin Epidemiol. 2016;75:40-46. PubMed
40.Tutt ANJ, Garber JE, Kaufman B, et al. Adjuvant Olaparib for Patients with BRCA1- or BRCA2-Mutated Breast Cancer. N Engl J Med. 2021;384(25):2394-2405. PubMed
41.Hudis CA, Barlow WE, Costantino JP, et al. Proposal for standardized definitions for efficacy end points in adjuvant breast cancer trials: the STEEP system. J Clin Oncol. 2007;25(15):2127-2132. PubMed
42.Butt Z, Lai JS, Rao D, Heinemann AW, Bill A, Cella D. Measurement of fatigue in cancer, stroke, and HIV using the Functional Assessment of Chronic Illness Therapy - Fatigue (FACIT-F) scale. J Psychosom Res. 2013;74(1):64-68. PubMed
43.Amarsheda S, Bhise AR. Systematic review of cancer-related fatigue instruments in breast cancer patients. Palliat Support Care. 2022;20(1):122-128. PubMed
44.Yellen SB, Cella DF, Webster K, Blendowski C, Kaplan E. Measuring fatigue and other anemia-related symptoms with the Functional Assessment of Cancer Therapy (FACT) measurement system. J Pain Symptom Manage. 1997;13(2):63-74. PubMed
45.Cella D, Eton DT, Lai JS, Peterman AH, Merkel DE. Combining anchor and distribution-based methods to derive minimal clinically important differences on the Functional Assessment of Cancer Therapy (FACT) anemia and fatigue scales. J Pain Symptom Manage. 2002;24(6):547-561. PubMed
46.Patrick DL, Gagnon DD, Zagari MJ, Mathijs R, Sweetenham J. Assessing the clinical significance of health-related quality of life (HrQOL) improvements in anaemic cancer patients receiving epoetin alfa. Eur J Cancer. 2003;39(3):335-345. PubMed
47.Aaronson NK, Ahmedzai S, Bergman B, et al. The European Organization for Research and Treatment of Cancer QLQ-C30: a quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst. 1993;85(5):365-376. PubMed
48.Bjordal K, de Graeff A, Fayers PM, et al. A 12 country field study of the EORTC QLQ-C30 (version 3.0) and the head and neck cancer specific module (EORTC QLQ-H&N35) in head and neck patients. EORTC Quality of Life Group. Eur J Cancer. 2000;36(14):1796-1807. PubMed
49.Nicklasson M, Bergman B. Validity, reliability and clinical relevance of EORTC QLQ-C30 and LC13 in patients with chest malignancies in a palliative setting. Qual Life Res. 2007;16(6):1019-1028. PubMed
50.Fayers P, Bottomley A. Quality of life research within the EORTC-the EORTC QLQ-C30. European Organisation for Research and Treatment of Cancer. Eur J Cancer. 2002;38(Suppl 4):S125-133. PubMed
51.Letellier ME, Dawes D, Mayo N. Content verification of the EORTC QLQ-C30/EORTC QLQ-BR23 with the International Classification of Functioning, Disability and Health. Qual Life Res. 2015;24(3):757-768. PubMed
52.McLachlan SA, Devins GM, Goodwin PJ. Validation of the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire (QLQ-C30) as a measure of psychosocial function in breast cancer patients. Eur J Cancer. 1998;34(4):510-517. PubMed
53.Musoro JZ, Coens C, Fiteni F, et al. Minimally Important Differences for interpreting EORTC QLQ-C30 scores in patients with advanced breast cancer. JNCI Cancer Spectr. 2019;3(3):pkz037. PubMed
54.Osoba D, Rodrigues G, Myles J, Zee B, Pater J. Interpreting the significance of changes in health-related quality-of-life scores. J Clin Oncol. 1998;16(1):139-144. PubMed
55.Kawahara T, Taira N, Shiroiwa T, et al. Minimal important differences of EORTC QLQ-C30 for metastatic breast cancer patients: Results from a randomized clinical trial. Qual Life Res. 2022;31(6):1829-1836. PubMed
56.Stone A. The application of bespoke spending functions in group-sequential designs and the effect of delayed treatment switching in survival trials. Pharm Stat. 2010;9(2):151-161. PubMed
57.Tan X, Chen BE, Sun J, Patel T, Ibrahim JG. A hierarchical testing approach for detecting safety signals in clinical trials. Stat Med. 2020;39(10):1541-1557. PubMed
58.Addeo A, Banna GL, Metro G, Di Maio M. Chemotherapy in Combination With Immune Checkpoint Inhibitors for the First-Line Treatment of Patients With Advanced Non-small Cell Lung Cancer: A Systematic Review and Literature-Based Meta-Analysis. Front Oncol. 2019;9:264. PubMed
59.Pharmacological therapies in non-metastatic, primary, invasive HER2-negative early breast cancer: indirect treatment comparison report for AstraZeneca Canada [internal sponsor’s report]. In: Drug Reimbursement Review sponsor submission: Lynparza (olaparib), 100 mg and 105 mg oral tablets. Mississauga (ON): AstraZeneca Canada Inc.; 2022 Aug 18.
60.Pharmacological therapies in non-metastatic, primary, invasive HER2-negative breast cancer: clinical systematic literature review report for AstraZeneca Canada [internal sponsor’s report]. In: Drug Reimbursement Review sponsor submission: Lynparza (olaparib), 100 mg and 105 mg oral tablets. Mississauga (ON): AstraZeneca Canada Inc.; 2022 July 26.
61.Lluch A, Barrios CH, Torrecillas L, et al. Phase III Trial of Adjuvant Capecitabine After Standard Neo-/Adjuvant Chemotherapy in Patients With Early Triple-Negative Breast Cancer (GEICAM/2003-11_CIBOMA/2004-01). J Clin Oncol. 2020;38(3):203-213. PubMed
62.Bucher HC, Guyatt GH, Griffith LE, Walter SD. The results of direct and indirect treatment comparisons in meta-analysis of randomized controlled trials. J Clin Epidemiol. 1997;50(6):683-691. PubMed
63.Fasching PA, Link T, Hauke J, et al. Neoadjuvant paclitaxel/olaparib in comparison to paclitaxel/carboplatinum in patients with HER2-negative breast cancer and homologous recombination deficiency (GeparOLA study). Ann Oncol. 2021;32(1):49-57. PubMed
64.Gelmon KA, Fasching PA, Couch FJ, et al. Clinical effectiveness of olaparib monotherapy in germline BRCA-mutated, HER2-negative metastatic breast cancer in a real-world setting: phase IIIb LUCY interim analysis. Eur J Cancer. 2021;152:68-77. PubMed
65.Hodgson D, Lai Z, Dearden S, et al. Analysis of mutation status and homologous recombination deficiency in tumors of patients with germline BRCA1 or BRCA2 mutations and metastatic breast cancer: OlympiAD. Ann Oncol. 2021;32(12):1582-1589. PubMed
66.Pusztai L, Yau C, Wolf DM, et al. Durvalumab with olaparib and paclitaxel for high-risk HER2-negative stage II/III breast cancer: Results from the adaptively randomized I-SPY2 trial. Cancer Cell. 2021;39(7):989-998.e985. PubMed
67.Domchek SM, Postel-Vinay S, Im SA, et al. Olaparib and durvalumab in patients with germline BRCA-mutated metastatic breast cancer (MEDIOLA): an open-label, multicentre, phase 1/2, basket study. Lancet Oncol. 2020;21(9):1155-1164. PubMed
68.Im SA, Xu B, Li W, et al. Olaparib monotherapy for Asian patients with a germline BRCA mutation and HER2-negative metastatic breast cancer: OlympiAD randomized trial subgroup analysis. Sci Rep. 2020;10(1):8753. PubMed
69.Armstrong AC, Clay V. Olaparib in germline-mutated metastatic breast cancer: implications of the OlympiAD trial. Fut Oncol. 2019;15(20):2327-2335. PubMed
70.Robson M, Ruddy KJ, Im SA, et al. Patient-reported outcomes in patients with a germline BRCA mutation and HER2-negative metastatic breast cancer receiving olaparib versus chemotherapy in the OlympiAD trial. Eur J Cancer. 2019;120:20-30. PubMed
71.Robson ME, Tung N, Conte P, et al. OlympiAD final overall survival and tolerability results: Olaparib versus chemotherapy treatment of physician’s choice in patients with a germline BRCA mutation and HER2-negative metastatic breast cancer. Ann Oncol. 2019;30(4):558-566. PubMed
72.Robson M, Im SA, Senkus E, et al. Olaparib for Metastatic Breast Cancer in Patients with a Germline BRCA Mutation. N Engl J Med. 2017;377(6):523-533. PubMed
73.Gelmon KA, Tischkowitz M, Mackay H, et al. Olaparib in patients with recurrent high-grade serous or poorly differentiated ovarian carcinoma or triple-negative breast cancer: a phase 2, multicentre, open-label, non-randomised study. Lancet Oncol. 2011;12(9):852-861. PubMed
74.Loap P, Loirat D, Berger F, et al. Combination of Olaparib with radiotherapy for triple-negative breast cancers: One-year toxicity report of the RADIOPARP Phase I trial. Int J Cancer. 2021;149(10):1828-1832. PubMed
75.Sang M, Meng L, Ma C, et al. Effect of AR antagonist combined with PARP1 inhibitor on sporadic triple-negative breast cancer bearing AR expression and methylation-mediated BRCA1 dysfunction. Biomed Pharmacother. 2019;111:169-177. PubMed
76.Matulonis UA, Wulf GM, Barry WT, et al. Phase I dose escalation study of the PI3kinase pathway inhibitor BKM120 and the oral poly (ADP ribose) polymerase (PARP) inhibitor olaparib for the treatment of high-grade serous ovarian and breast cancer. Ann Oncol. 2017;28(3):512-518. PubMed
77.Bundred N, Gardovskis J, Jaskiewicz J, et al. Evaluation of the pharmacodynamics and pharmacokinetics of the PARP inhibitor olaparib: a phase I multicentre trial in patients scheduled for elective breast cancer surgery. Invest New Drugs. 2013;31(4):949-958. PubMed
78.Groenvold M, Klee MC, Sprangers MA, Aaronson NK. Validation of the EORTC QLQ-C30 quality of life questionnaire through combined qualitative and quantitative assessment of patient-observer agreement. J Clin Epidemiol. 1997;50(4):441-450. PubMed
79.Ousmen A, Conroy T, Guillemin F, et al. Impact of the occurrence of a response shift on the determination of the minimal important difference in a health-related quality of life score over time. Health Qual Life Outcomes. 2016;14(1):167. PubMed
80.Littlewood TJ, Bajetta E, Nortier JW, Vercammen E, Rapoport B. Effects of epoetin alfa on hematologic parameters and quality of life in cancer patients receiving nonplatinum chemotherapy: results of a randomized, double-blind, placebo-controlled trial. J Clin Oncol. 2001;19(11):2865-2874. PubMed
Appendix 1: Literature Search Strategy
Note that this appendix has not been copy-edited.
Overview
Interface: Ovid
Databases:
MEDLINE All (1946–present)
Embase (1974–present)
Note: Subject headings and search fields have been customized for each database. Duplicates between databases were removed in Ovid.
Date of search: August 31, 2022
Alerts: Bi-weekly search updates until project completion
Search filters applied: RCTs or controlled clinical trials
Limits:
Publication date limit: none
Language limit: none
Conference abstracts: excluded
Syntax | Description |
|---|---|
/ | At the end of a phrase, searches the phrase as a subject heading |
MeSH | Medical Subject Heading |
* | Before a word, indicates that the marked subject heading is a primary topic; or, after a word, a truncation symbol (wildcard) to retrieve plurals or varying endings |
.ti | Title |
.ot | Original title |
.ab | Abstract |
.hw | Heading word; usually includes subject headings and controlled vocabulary |
.kf | Author keyword heading word (MEDLINE) |
.dq | Candidate term word (Embase) |
.pt | Publication type |
.rn | Registry number |
.nm | Name of substance word (MEDLINE) |
medall | Ovid database code: MEDLINE All, 1946 to present, updated daily |
oemezd | Ovid database code; Embase, 1974 to present, updated daily |
Multidatabase Strategy
(olaparib* or lynparza* or lyhnparza* or AZD-2281 or AZD2281 or AZD-221 or AZD221 or KU-0059436 or KU0059436 or KU-59436 or KU59436 or MK-7339 or MK7339 or NSC-747856 or NSC747856 or WOH1JD9AR8).ti,ab,kf,ot,hw,rn,nm.
exp breast neoplasms/
(((breast* or mamma or mammar* or lobular*) adj5 (cancer* or carcinoid* or carcinoma* or carcinogen* or adenocarcinoma* or adeno-carcinoma* or malignan* or neoplas* or sarcoma* or tumo?r* or mass* or triple-negative)) or mBC or m-BC or LABC or TNBC or mTNBC).ti,ab,kf,ot,hw.
((breast* or mamma or mammar* or lobular*) adj5 (human epidermal growth factor receptor* adj5 negative*)).ti,ab,kf,ot,hw.
((breast* or mamma or mammar* or lobular*) adj5 (BRCA* or gBRCAm* or HER2- or HER2-neg* or HER2neg*)).ti,ab,kf,ot,hw.
or/2-5
1 and 6
7 use medall
*olaparib/
(olaparib* or lynparza* or lyhnparza* or AZD-2281 or AZD2281 or AZD-221 or AZD221 or KU-0059436 or KU0059436 or KU-59436 or KU59436 or MK-7339 or MK7339 or NSC-747856 or NSC747856 or WOH1JD9AR8).ti,ab,kf,dq.
or/9-10
exp breast tumor/
(((breast* or mamma or mammar* or lobular*) adj5 (cancer* or carcinoid* or carcinoma* or carcinogen* or adenocarcinoma* or adeno-carcinoma* or malignan* or neoplas* or sarcoma* or tumo?r* or mass* or triple-negative)) or mBC or m-BC or LABC or TNBC or mTNBC).ti,ab,kf,dq.
((breast* or mamma or mammar* or lobular*) adj5 (human epidermal growth factor receptor* adj5 negative*)).ti,ab,kf,dq.
((breast* or mamma or mammar* or lobular*) adj5 (BRCA* or gBRCAm* or HER2- or HER2-neg* or HER2neg*)).ti,ab,kf,dq.
or/12-15
11 and 16
17 use oemezd
18 not (conference abstract or conference review).pt.
8 or 19
(Randomized Controlled Trial or Controlled Clinical Trial or Pragmatic Clinical Trial or Equivalence Trial or Clinical Trial, Phase III).pt.
Randomized Controlled Trial/
exp Randomized Controlled Trials as Topic/
“Randomized Controlled Trial (topic)”/
Controlled Clinical Trial/
exp Controlled Clinical Trials as Topic/
“Controlled Clinical Trial (topic)”/
Randomization/
Random Allocation/
Double-Blind Method/
Double Blind Procedure/
Double-Blind Studies/
Single-Blind Method/
Single Blind Procedure/
Single-Blind Studies/
Placebos/
Placebo/
Control Groups/
Control Group/
(random* or sham or placebo*).ti,ab,hw,kf.
((singl* or doubl*) adj (blind* or dumm* or mask*)).ti,ab,hw,kf.
((tripl* or trebl*) adj (blind* or dumm* or mask*)).ti,ab,hw,kf.
(control* adj3 (study or studies or trial* or group*)).ti,ab,kf.
(Nonrandom* or nonrandom* or nonrandom* or quasi-random* or quasirandom*).ti,ab,hw,kf.
allocated.ti,ab,hw.
((open label or open-label) adj5 (study or studies or trial*)).ti,ab,hw,kf.
((equivalence or superiority or noninferiority or noninferiority) adj3 (study or studies or trial*)).ti,ab,hw,kf.
(pragmatic study or pragmatic studies).ti,ab,hw,kf.
((pragmatic or practical) adj3 trial*).ti,ab,hw,kf.
((quasiexperimental or quasi-experimental) adj3 (study or studies or trial*)).ti,ab,hw,kf.
(phase adj3 (III or “3”) adj3 (study or studies or trial*)).ti,hw,kf.
or/21-51
20 and 52
remove duplicates from 53
Clinical Trials Registries
ClinicalTrials.gov
Produced by the US National Library of Medicine. Targeted search used to capture registered clinical trials.
[Search -- olaparib OR lynparza OR lyhnparza OR AZD-2281 OR AZD2281 OR AZD-221 OR AZD221 OR KU-0059436 OR KU0059436 OR KU-59436 OR KU59436 OR MK-7339 OR MK7339 OR NSC-747856 OR NSC747856 Breast Cancer]
WHO ICTRP
International Clinical Trials Registry Platform, produced by the WHO. Targeted search used to capture registered clinical trials.
[Search terms -- (olaparib* OR lynparza* OR lyhnparza* OR AZD-2281 OR AZD2281 OR AZD-221 OR AZD221 OR KU-0059436 OR KU0059436 OR KU-59436 OR KU59436 OR MK-7339 OR MK7339 OR NSC-747856 OR NSC747856 OR WOH1JD9AR8) AND breast cancer]
Health Canada’s Clinical Trials Database
Produced by Health Canada. Targeted search used to capture registered clinical trials.
[Search terms -- olaparib and early breast cancer]
EU Clinical Trials Register
European Union Clinical Trials Register, produced by the European Union. Targeted search used to capture registered clinical trials.
[Search terms -- (olaparib OR lynparza OR lyhnparza) AND breast cancer]
Grey Literature
Search dates: August 19, 2022 – August 31, 2022
Keywords: [Provide terms used in grey literature search]
Limits: Publication years: 2017-present for guidelines, no date limits for other sections
Relevant websites from the following sections of the CADTH grey literature checklist Grey Matters: A Practical Tool for Searching Health-Related Grey Literature were searched:
Health Technology Assessment Agencies
Health Economics
Clinical Practice Guidelines
Drug and Device Regulatory Approvals
Advisories and Warnings
Drug Class Reviews
Clinical Trials Registries
Databases (free)
Internet Search
Appendix 2: Excluded Studies
Note that this appendix has not been copy-edited.
Reference | Reason for Exclusion |
|---|---|
Fasching et al.63 | Not relevant population |
Gelmon et al.64 | |
Hodgson et al.65 | |
Pusztai et al.66 | |
Domchek et al.67 | |
Im et al.68 | |
Armstrong et al.69 | |
Robson et al.70 | |
Robson et al.71 | |
Robson et al.72 | |
Gelmon et al.73 | |
Loap et al.74 | Not relevant study design |
Sang et al.75 | |
Matulonis et al.76 | |
Bundred et al.77 | Not relevant outcome |
Appendix 3: Detailed Outcome Data
Note that this appendix has not been copy-edited.
Table 37: Patient Disposition by Interim Analysis 1 — FAS
Characteristic | At interim analysis 1 | |
|---|---|---|
Olaparib | Placebo | |
Screened, N | 14,387 | |
Randomized, N | 921 | 915 |
Patients ongoing study, n (%) | 782 (84.9) | 760 (83.1) |
Discontinued from study, n (%) | 139 (15.1) | 155 (16.9) |
Reason for discontinuation, n (%) | ||
Death | 59 (6.4) | 86 9.4) |
Lost to follow-up | 12 (1.3) | 15 1.6) |
Patient decision | 65 (7.1) | 49 (5.4) |
Other | 3 (0.3) | 5 (0.5) |
Treated, n (%) | 911 (98.9) | 904 (98.8) |
Patients ongoing study treatment, n (%) | 19 (2.1) | 20 (2.2) |
Completed treatment, n (%) | 656 (71.2) | 697 (76.2) |
Discontinued study treatment,a n (%) | 236 (25.6) | 187 (20.4) |
Reason for treatment discontinuation, n (%) | ||
Adverse event | 97 (10.5) | 41 (4.5) |
Death | 1 (0.1) | 0 |
Recurrence of disease | 40 (4.3) | 80 (8.7) |
Lost to follow-up | 2 (0.2) | 1 (0.1) |
Patient decision to stop study drug | █ ██████ | █ ██████ |
Patient decision to provide survival status only | █ ██████ | █ █████ |
Patient decision to withdraw from study | █ ██████ | █ █████ |
Severe noncompliance | 0 | 5 (0.5) |
Other | 12 (1.3) | 18 (2.0) |
FAS = full analysis set.
aDoes not include patients who did not receive treatment.
Source: Clinical Study Report for OlympiA.19
Table 38: Patient Disposition in Myriad gBRCAm Patients
Detaila | Olaparib | Placebo |
|---|---|---|
█████ █ █ █ █ ██ █ | ███ | ███ |
██ █ █ █ █ ██ █ █ █ █ █ ██ █ █ █ █ █ ██ ███ | █ ██ ██████ | █ ██ ██████ |
██████ █ █ █ █ ██ █ █ ██ █ █ █ █ █ ██ ███ | █ ██ ██████ | █ ██ ██████ |
█ █ █ █ ██ ██ ███████████ █ █ █ █ █ ██ ███ | ||
█████ | █ ██████ | █ ██ ██████ |
█ █ █ ██ ██████████ | █ ██████ | █ ██████ |
█ █ █ █ █ ██ ████████ | █ ██████ | █ ██████ |
█████ | █ █████ | █ █████ |
██ █ █ █ █ █ ██ ███ | █ ██ ██████ | █ ██ ██████ |
███ █ █ █ █ ██ ████ █ █ █ █ █ ██ ███ | █ ██ ██████ | █ ██ ██████ |
█ ██ ██ ██ █ █ █ █ ██ ████ █ █ █ █ █ ██ ███ | ||
█ █ █ █ █ ██ █████ | █ █████ | █ |
█████ | █ █████ | █ █████ |
█ █ █ █ █ ██ ██████ | █ █████ | █ █████ |
████ █ █ █ █ █ ██ ████████ | █ | █ █████ |
█ █ █ █ ██ ██████████████ | █ █████ | █ █████ |
██████ █ █ █ █ ██ █ █ █ ██ █████ █ █ █ █ █ ██ ███ | █ ██ ██████ | █ ██ ██████ |
█ █ █ █ ██ ██ ████ █ █ █ █ ██ ██████████ █ █ █ █ █ ██ ███ | ||
█ █ █ █ █ ██ █████ | █ ███████ | █ ██████ |
█████ | █ █████ | █ |
████ █ █ █ █ █ ██ ████████ | █ ██████ | █ ██████ |
█ █ █ ██ ██████████ | █ █████ | █ █████ |
█ █ █ █ █ ██ ██ █ █ █ █ █ ██ ██ █ ██ █ █ █ ██ ████ | █ ██████ | █ ██████ |
█ █ █ █ █ ██ ██ █ █ █ █ █ ██ ██ █ █ █ █ ██ ██ █ █ █ █ ██ █ █ █ █ ██ ████ | █ █████ | █ █████ |
█ █ █ █ █ ██ ██ █ █ █ █ █ ██ ███ █ █ █ █ ██ █ █ ██ █████ | █ ██████ | █ █████ |
█ █ █ █ ██ ██████████████ | █ | █ █████ |
█████ | █ ██████ | █ ████████ |
gBRCAm = germline BRCA mutation.
aDoes not include patients who did not receive treatment.
Source: Clinical Study Report for OlympiA.19
Table 39: Treatment Exposure at Interim Analysis 1: Safety Population
Treatment exposure | Interim analysis 1a | |
|---|---|---|
Olaparib (N = 911) | Placebo (N = 904) | |
Total intended exposure (days)a | ||
Mean (SD) | 306.5 (114.80) | 322.4 (97.54) |
Median (minimum, maximum) | 364.0 (1 to 492) | 364.0 (2 to 414) |
Actual treatment exposure (days)b | ||
Mean (SD) | 294.4 (113.90) | 315.1 (97.59) |
Median (minimum, maximum) | 350.0 (1 to 420) | 358.0 (2 to 404) |
Number of days on 300 mg treatment twice dailyc | ||
Mean (SD) | 245.2 (141.68) | 306.3 (107.51) |
Median (minimum, maximum) | 338.0 (1 to 420) | 358.0 (2 to 404) |
SD = standard deviation.
aData cut-off date: March 27, 2020.
aTotal intended exposure (days) = (last dose date − first dose date + 1).
bActual treatment exposure (days) = intended exposure − total duration of dose interruptions, where intended exposure was calculated as above.
cNumber of days on 300 mg olaparib/placebo twice daily (actual exposure for the assigned starting dose).
Patients with partial treatment end dates were excluded.
Source: Clinical Study Report for OlympiA.18
███ █ █ █ █ ██ ████████ | ██ █ █ █ █ ██ ██ ██ ████ | ████ █ █ █ █ █ ██ ████ |
|---|---|---|
█ █ █ ██ ██ █ █ █ █ ██ ██ █ █ █ █ ██ ██████ | ||
█ █ ██ ████ | █ █ █ ██ ████████ | █ █ █ ██ ███████ |
█ █ █ █ ██ █ █ █ ██ ████ | █ █ █ █ ██ ██ █████ | █ █ █ █ ██ ██ █████ |
█ █ █ █ ██ ███ █ █ █ █ ██ ██ █ █ █ █ ██ ██████ | ||
█ █ ██ ████ | █ █ █ ██ ████████ | █ █ █ ██ ███████ |
█ █ █ █ ██ █ █ █ ██ ████ | █ █ █ █ ██ ██ █████ | █ █ █ █ ██ ██ █████ |
█ █ █ █ █ ██ ██ █ █ ██ ██ ███ ████ █ █ █ █ ██ █ █ █ ██ █████ | ||
█ █ ██ ████ | █ █ █ ██ ████████ | █ █ █ ██ ████████ |
█ █ █ █ ██ █ █ █ ██ ████ | █ █ █ █ ██ ██ █████ | █ █ █ █ ██ ██ █████ |
█ █ ██ █ █ █ █ █ ██ █ █ ██ █ █ ██ ██ ██████
SD = standard deviation.
Source: Clinical Study Report for OlympiA.18
Table 41: Invasive Disease–Free Survival in Mature Cohort, Interim Analysis 1
IDFSa | Olaparib (N = 449) | Placebo (N = 451) |
|---|---|---|
Patients with events, n (%) | 65 (14.5) | 104 (23.1) |
Stratified HRb (99.5% CId) | 0.61 (0.39 to 0.95) | |
95.0% CIc | 0.45 to 0.83 | |
Log-rank test P valued | 0.0018 | Reference |
Median follow-upe (minimum, maximum), years | 3.5 (0 to 5.5) | 3.5 (0 to 5.5) |
Event-free rateg (95% CI) at: | ||
1 year | 93.7 (90.9 to 95.7) | 88.0 (84.6 to 90.8) |
2 years | 89.6 (86.2 to 82.2) | 81.9 (77.9 to 85.2) |
3 years | 86.1 (82.2 to 89.1) | 77.5 (73.2 to 81.2) |
4 years | NA | NA |
CI = confidence interval; FAS = full analysis set; HR = hazard ratio; IDFS = invasive disease–free survival; KM = Kaplan-Meier.
aData cut-off date: March 27, 2020.
bEstimate of the treatment HR was based on the stratified Cox proportional hazards model. Stratification factors were the same as those used in the stratified log-rank test. The CI for the HR was estimated using the profile likelihood approach.
cInferential, according to the alpha spending rules for the interim analysis.
dExploratory, not inferential. P value was not adjusted for multiplicity.
eP value from a stratified log-rank test. Stratification was by chemotherapy type (adjuvant vs. neoadjuvant), hormone receptor status (ER- and/or PgR-positive and HER2-negative vs. TNBC), and prior platinum therapy (yes vs. no). Stratification factors were based on the categories used in the randomization system and were chosen by the pooling strategy. Once the pooling strategy was applied, only the hormone receptor status stratification factor was selected. P value was not adjusted for multiplicity.
fMedian clinical follow-up was calculated using the reverse censoring method.
gPercentage of patients were from the KM estimates and the 95% CIs were calculated using Greenwood’s formula.
The mature cohort included 169 IDFS events that occurred in the first 900 randomized patients.
Source: Clinical Study Reports for OlympiA.18
Table 42: Supportive Analysis of IDFS, DDFS, and OS in Confirmed Myriad gBRCAm Patients
Analysisa | Olaparib | Placebo |
|---|---|---|
IDFS in confirmed Myriad gBRCAm patients | ||
Patients with events, n (%) | 89 (11.5) | 163 (21.4) |
HRb (95% CI) | 0.51 (0.39 to 0.66) | |
█ █ █ █ ██ ██ █ █ █ █ ██ █████ █ █ █ █ ██ █ █ █ ██ █ █ █ ██ █████ | █ ███ ██ █████ | █ ███ ██ █████ |
███ █ █ █ █ ██ █ █ █ ██ █ █ ██ ██ ████ | ||
█ ████ | █ █ ██ █ █ █ █ ██ ██████ | █ █ ██ █ █ █ █ ██ ██████ |
█ █████ | █ █ ██ █ █ █ █ ██ ██████ | █ █ ██ █ █ █ █ ██ ██████ |
█ █████ | █ █ ██ █ █ █ █ ██ ██████ | █ █ ██ █ █ █ █ ██ ██████ |
DDFS in confirmed Myriad gBRCAm patients | ||
Patients with events, n (%) | 74 (9.5) | 138 (18.1) |
HRb (95% CI) | 0.50 (0.38 to 0.67) | |
█ █ █ █ ██ ██ █ █ █ █ ██ █████ █ █ █ █ ██ █ █ █ ██ █ █ █ ██ █████ | █ ███ ██ █████ | █ ███ ██ █████ |
███ █ █ █ █ ██ █ █ █ ██ █ █ ██ ██ ████ | ||
█ ████ | █ █ ██ █ █ █ █ ██ ██████ | █ █ ██ █ █ █ █ ██ ██████ |
█ █████ | █ █ ██ █ █ █ █ ██ ██████ | █ █ ██ █ █ █ █ ██ ██████ |
█ █████ | █ █ ██ █ █ █ █ ██ ██████ | █ █ ██ █ █ █ █ ██ ██████ |
OS in confirmed Myriad gBRCAm patients | ||
Patients with events, n (%) | 47 (6.0) | 79 (10.4) |
HRb (95% CI) | 0.58 (0.40 to 0.82) | |
█ █ █ █ ██ ██ █ █ █ █ ██ █████ █ █ █ █ ██ █ █ █ ██ █ █ █ ██ █████ | █ ███ ██ █████ | █ ███ ██ █████ |
███ █ █ █ █ ██ █ █ █ ██ █ █ ██ ██ ████ | ||
█ ████ | █ █ ██ █ █ █ █ ██ ██████ | █ █ ██ █ █ █ █ ██ ██████ |
█ █████ | █ █ ██ █ █ █ █ ██ ██████ | █ █ ██ █ █ █ █ ██ ██████ |
█ █████ | █ █ ██ █ █ █ █ ██ ██████ | █ █ ██ █ █ █ █ ██ ██████ |
BRCA = breast cancer susceptibility gene; CI = confidence interval; DDFS = distant disease–free survival; FAS = full analysis set; gBRCAm = germline BRCA mutation; HR = hazard ratio; IDFS = invasive disease–free survival; OS = overall survival.
aData cut-off date: March 27, 2020.
bEstimate of the treatment HR was based on the stratified Cox proportional hazards model, < 1 indicates a lower risk with olaparib compared with placebo arm. Stratification factors were the same as those used in the analysis of IDFS, DDFS, or OS in the FAS. The 95% CI for the HR was estimated using the profile likelihood approach.
cMedian clinical follow-up was calculated using the reverse censoring method.
dPercentage of patients were from the KM estimates and the 95% CIs were calculated using Greenwood’s formula.
Source: Clinical Study Reports for OlympiA.18
Table 43: Sensitivity Analysis of IDFS at Interim Analysis 1 — FAS
Analysisa | Olaparib | Placebo |
|---|---|---|
Patients with central pathology review datab | ||
Patients with events, n (%) | 86 (11.7) | 151 (21.0) |
HRc (95% CI) | 0.54 (0.41 to 0.70) | |
Unadjustedd analysis | ||
Patients with events, n (%) | 106 (11.5) | 178 (19.5) |
HRc (95% CI) | 0.58 (0.46 to 0.74) | |
Interval censoringe | ||
Patients with events, n (%) | 106 (11.5) | 178 (19.5) |
HRc (95% CIf) | 0.58 (0.46 to 0.74) | |
IDFS = invasive disease–free survival; HR = hazard ratio; CI = confidence interval.
Note: Percentages are of the number of patients in the population subgroup in question. Mis-stratification sensitivity analysis was not triggered as ≤ 5% of randomized patients were incorrectly stratified (i.e., randomization system data did not match baseline data). Sensitivity analysis excluding patients with important protocol deviations that may affect the efficacy of the study therapy (did not have the intended disease or indication; did not receive any randomized therapy) was not triggered as ≤ 10% of patients in either treatment group had important protocol deviations.
aData cut-off date: March 27, 2020.
bIncludes patients who had both central and local hormone receptor status results. Central pathology review data were not available for China. Stratification factors for hormone receptor status was according to the central pathology review.
cEstimate of the treatment HR was based on the stratified Cox proportional hazards model. The 95% CI for the HR was estimated using the profile likelihood approach.
dEstimate of the treatment HR was based on the unstratified Cox proportional hazards model.
eFor patients experiencing an event, and without follow-up according to the CSP (defined as more than 18 months between the event and the last visit), the interval from the last date at which the patient was known to be free of invasive disease to the date of recurrence or death, was used.
fThe 95% Wald CI for the HR. P value was not adjusted for multiplicity.
Source: Clinical Study Report for OlympiA.18
Table 44: Sensitivity Analysis of DDFS at Interim Analysis 1 — FAS
Analysisa | Olaparib | Placebo |
|---|---|---|
██ █ █ █ █ ██ █ █ ██ █ █ █ █ █ ██ ███ █ █ █ █ ██ █ █ █ █ ██ █████ | ||
██ █ █ █ █ ██ █ █ ██ █ █ █ █ █ █ ██ ███ | █ ██████ | █ ██ ██████ |
█ ██ █ █ ██ ███ | █ █ ██ █ █ █ █ ██ ██████ | |
█████ █ █ █ █ ██ ████████ | ||
██ █ █ █ █ ██ █ █ ██ █ █ █ █ █ █ ██ ███ | █ ██████ | 152 (16.6) |
█ ██ █ █ ██ ███ | █ █ ██ █ █ █ █ ██ ██████ | |
BGI = Beijing Genomics Institute; CI = confidence interval; DDFS = distant disease–free survival; HR = hazard ratio.
aData cut-off date: March 27, 2020.
bExcludes patients with only a local or BGI result. Myriad data were not available for China. Percentages are of the number of patients in the population subgroup in question.
cIncludes patients who have both central and local HR status results. Central pathology review data were not available for China.
dEstimate of the treatment HR based on the Cox proportional hazards model. Stratification factors for prior platinum therapy and chemotherapy are the same as those used in the analysis of DDFS, stratification factor for hormone receptor status is according to the central pathology review. The 95% CI for the HR was estimated using the profile likelihood approach.
eAn unstratified Cox model fitted.
Source: Clinical Study Reports for OlympiA.18
Table 45: Subgroup Analyses of DDFS at Interim Analysis 1 — FAS
Subgroupa | Olaparib Events, n (%) | Placebo Events, n (%) | HRb (95% CI) | Interaction Pe value |
|---|---|---|---|---|
█ █ █ ██ ████████████ | ||||
████████ | █ ██████ | █ ███████ | █ █ ██ █ █ █ █ ██ ██████ | 0.753 |
███████████ | █ ███████ | █ ██ ██████ | █ █ ██ █ █ █ █ ██ ██████ | |
█ █ █ ██ ████████ | ||||
███ | █ ███████ | █ ███████ | █ █ ██ █ █ █ █ ██ ██████ | 0.128 |
██ | █ ██████ | █ ██ ██████ | █ █ ██ █ █ █ █ ██ ██████ | |
█ ███████ | ||||
██████████████████████████ | █ ███████ | █ ███████ | █ █ ██ █ █ █ █ ██ ██████ | 0.551 |
█████ | █ ██████ | █ ██ ██████ | █ █ ██ █ █ █ █ ██ ██████ | |
█ █ ██ ██ █ █ █ █ ██ ████ | ||||
█████ | █ ███████ | █ ███████ | █ █ ██ █ █ █ █ ██ ██████ | 0.704 |
█████ | █ ██████ | █ ██ ██████ | █ █ ██ █ █ █ █ ██ ██████ | |
███████ | █ █████ | █ █████ | ██ | |
██ █ █ █ █ ██ █ █ █ ██ ██████ | ||||
█ █ ██ ████████ | █ █████ | █ ██████ | █ █ ██ █ █ █ █ ██ ██████ | 0.629 |
█ █ ██ ████████ | █ ██████ | █ ███████ | █ █ ██ █ █ █ █ ██ ██████ | |
█ █ █ █ ██ █████ | ||||
█ █ █ █ ██ █ █ █ █ ██ ██ ██ ██ ██ | █ ███████ | █ ███████ | █ █ ██ █ █ █ █ ██ ██████ | 0.702 |
█ █ █ █ ██ █ █ █ █ ██ ██ ██ ██ | █ ███████ | █ ███████ | █ █ ██ █ █ █ █ ██ ██████ | |
BRCA = breast cancer susceptibility gene; CI = confidence interval; CPS&EG = clinical stage (CS), estrogen receptor status (E), nuclear grade (G), and post-treatment pathologic stage (PS) – a disease scoring system; ER = estrogen receptor; HER2 = human epidermal growth factor receptor 2; HR = hazard ratio; HR-positive = positive for expression of a hormone receptor; NA = not applicable; PgR = progesterone receptor.
aData cut-off date: March 27, 2020.
bThe Cox model included factors for treatment group, subgroup factor, and the treatment-by-subgroup interaction. All patients with nonmissing subgroup data were included in the model. The CI was calculated using a profile likelihood approach. These analyses are not inferential.
cHR-positive is defined as ER-positive and/or PgR-positive.
dTwo patients are excluded from the summary of the TNBC subset because they do not have confirmed negative HER2 status.
eP value was not adjusted for multiplicity.
Source: Clinical Study Report for OlympiA.18
Table 46: Sensitivity Analysis of OS — FAS
Analysisa | Olaparib | Placebo |
|---|---|---|
Patients with central pathology review datac | ||
Patients with events, n (%) | 59 (8.0) | 91 (12.6) |
HRd (95% CI) | 0.62 (0.44 to 0.85) | |
█ █ █ █ ██ █ █ █ █ ██ ██████ █ █ █ █ █ ██ ██ █ █ █ ██ █ █ █ █ █ █ ██ ███ | █ ██████ | █ ███████ |
Unadjustede analysis | ||
Patients with events, n (%) | 75 (8.1) | 109 (11.9) |
HRd (95% CI) | 0.68 (0.50 to 0.91) | |
█ █ █ █ ██ █ █ █ █ ██ ██████ █ █ █ █ █ ██ ██ █ █ █ ██ █ █ █ █ █ █ ██ ███ | █ ██████ | █ ██ ██████ |
BGI = Beijing Genomics Institute; CI = confidence interval; HR = hazard ratio; OS = overall survival.
aData cut-off date: July 12, 2021.
bExcludes patients with only a local or BGI result. Myriad data were not available for China. Percentages are of the number of patients in the population subgroup in question.
cIncludes patients who have both central and local HR status results. Central pathology review data were not available for China.
dEstimate of the treatment HR based on the Cox proportional hazards model. Stratification factors for prior platinum therapy and chemotherapy are the same as those used in the analysis of DDFS, stratification factor for hormone receptor status is according to the central pathology review. The 95% CI for the HR was estimated using the profile likelihood approach.
eAn unstratified fitted Cox model.
Source: Clinical Study Report for OlympiA.19
Table 47: Subgroup Analyses of OS at Interim Analysis 2 — FAS
Subgroupa | Olaparib Events, n (%) | Placebo Events, n (%) | HRb (95% CI) | Interaction P valuee |
|---|---|---|---|---|
Prior chemotherapy | ||||
Adjuvant | 22 (4.8) | 28 (6.2) | 0.78 (0.44 to 1.36) | 0.543 |
Neoadjuvant | 53 (11.5) | 81 (17.6) | 0.64 (0.45 to 0.90) | |
Prior platinum | ||||
Yes | 27 (10.9) | 29 (12.2) | 0.88 (0.52 to 1.49) | 0.236 |
No | 48 (7.1) | 80 (11.8) | 0.60 (0.42 to 0.85) | |
HR status | ||||
HR-positivec/HER2-negative | 16 (9.5) | 17 (10.8) | 0.90 (0.45 to 1.78) | 0.381 |
TNBCd | 59 (7.9) | 92 (12.1) | 0.64 (0.46 to 0.88) | |
BRCA mutation type | ||||
BRCA1 | 49 (8.5) | 75 (12.8) | 0.64 (0.45 to 0.92) | 0.845 |
BRCA2 | 16 (6.8) | 28 (13.0) | 0.52 (0.27 to 0.95) | |
BRCA1 and BRCA2 | 0 (0.0) | 0 (0.0) | NA | |
Axillary nodal status | ||||
Node-negative | █ █████ | █ █████ | █ █ ██ █ █ █ █ ██ ██████ | █████ |
Node-positive | █ ██████ | █ ██████ | █ █ ██ █ █ █ █ ██ ██████ | |
CPS&EG score | ||||
CPS&EG score of 2, 3, or 4 | █ ██████ | █ ███████ | █ █ ██ █ █ █ █ ██ ██████ | █████ |
CPS&EG score of 5 or 6 | █ ███████ | █ ███████ | █ █ ██ █ █ █ █ ██ ██████ | |
BRCA = breast cancer susceptibility gene; CI = confidence interval; CPS&EG = clinical stage (CS), estrogen receptor status (E), nuclear grade (G), and post-treatment pathologic stage (PS) – a disease scoring system; ER = estrogen receptor; HER2 = human epidermal growth factor receptor 2; HR = hazard ratio; HR-positive = positive for expression of a hormone receptor; NA = not applicable; PgR = progesterone receptor.
aData cut-off date: July 12, 2021.
bThe Cox model included factors for treatment group, subgroup factor, and the treatment-by-subgroup interaction. All patients with nonmissing subgroup data were included in the model. The CI was calculated using a profile likelihood approach. These analyses are not inferential, as 95% CI was not adjusted for multiplicity.
cHR-positive is defined as ER-positive and/or PgR-positive.
dTwo patients are excluded from the summary of the TNBC subset because they do not have confirmed negative HER2 status.
eP value was not adjusted for multiplicity.
Source: Clinical Study Report for OlympiA.19
Appendix 4: Description and Appraisal of Outcome Measures
Note that this appendix has not been copy-edited.
Aim
To describe the following outcome measures and review their measurement properties (validity, reliability, responsiveness to change, and MID):
EORTC QLQ-C30
The 13-item FACIT-F scale
Table 48: Summary of Outcome Measures and Their Measurement Properties
Outcome measure | Type | Conclusions about measurement properties | MID |
|---|---|---|---|
EORTC QLQ-C30 | The EORTC QLQ-C30 is a 30-item, patient-reported, cancer-specific, HRQoL questionnaire.47 The core questionnaire consists of 5 functional scales (physical, role, cognitive, emotional, and social), 3 symptom scales (fatigue, pain, and nausea and vomiting), a global health status/HRQoL scale, and 6 single items assessing additional symptoms commonly reported by patients with cancer (dyspnea, loss of appetite, insomnia, constipation and diarrhea) as well as the perceived financial impact of the disease.47 Patients complete the questionnaire based on a 1-week recall period by rating on a 4-point Likert-type scale (1 = not at all; 2 = a little; 3 = quite a bit; 4 = very much) or a 7-point Likert-type scale (1 = very poor; 7 = excellent). Raw scores for each scale are computed as the average of the items that contribute to a particular scale. Scale sum scores are transformed such that a high score on the functional scales represents a high or healthy level of functioning, a high score on the symptom scales represents a high level of symptomatology, and a high score on the global health status/HRQoL scale represents a high HRQoL.50 | Validity: Content validity: When mapping to the WHO’s International Classification of Functioning framework, 25 of the 30 items in the EORTC QLQ-C30 were endorsed by the experts.51 Good discriminative validity of the global health/quality of life and social function subscales of the EORTC QLQ-C30 in patients subgroups defined by the clinical parameters of ECOG Performance Status, pain, suffering, fatigue, chemotherapy, and sleep disturbance was demonstrated. All Spearman rank correlation coefficients > 0.2, which was considered statistically significant (P < 0.01).52 Convergent validity was demonstrated through correlation of EORTC QLQ-C30 with the POMS. The emotional function of the EORTC QLQ-C30 correlated very strongly with tension (Spearman rank correlation coefficient = 0.76), depression/dejection (Spearman rank correlation coefficient = 0.74) and the total mood disturbance subscales (Spearman rank correlation coefficient = 0.74) (A correlation of 0.2 was considered significant [P < 0.01]) of the POMS.52 Reliability: Inter-rater reliability using patient (46 patients with metastatic breast cancer)-observer (1 observer) agreement on the EORTC QLQ-C30 questionnaire showed that the median kappa coefficient for agreement across the 30 items in the EORTC QLQ-C30 was 0.86 (range: 0.48 to 1.00), and there was almost perfect agreement (kappa coefficient 0.8 to 1.00) for 19 items and “substantial agreement” (kappa coefficient: 0.61 to 0.80) for 6 items.78 Responsiveness: No evidence that assessed responsiveness in patients with breast cancer was identified. | One study estimated that MIDs for within-group changes ranged from 5 to 14 points for improvements and from −14 to −4 points for deterioration across the individual scales in patients with advanced breast cancer. For between-group differences, estimated MIDs ranged from 4 to 11 points for improvements and from −18 to −4 points for deterioration across the individual scales in patients with advanced breast cancer.53 Another study estimated MIDs for within-group improvement that varied from 7 to 15 and those for deterioration that varied from −17 to −7 in patients with metastatic breast cancer. The estimated MIDs for between-group improvement varied from 5 to 11 and those for deterioration varied from −8 to −5 across EORTC QLQ-C30 scales in patients with metastatic breast cancer.55 |
13-item FACIT-F scale | The FACIT-F scale is a patient-reported, fatigue-specific, quality of life questionnaire which consists of 13 measurement items and was first designed to assess self-reported fatigue associated with anemia in patients with cancer, such as breast cancer, lung cancer, and colorectal cancer.44 Patients are asked to respond to each of the 13 measurement items based on the prior 7 days. The response for each measurement item is scored on a 5-point Likert scale from 0 (not at all) to 4 (very much). The total score of the FACIT-F scale is calculated by summing the scores of all 13 measurement items and ranges from 0 to 52 with a lower score indicating more fatigue.43,44 | Validity: Convergent–divergent validity was demonstrated through a strong correlation of the FACIT-F scale with the POMS fatigue scale (r = −0.83), the PFS (coefficient = 0.61), and the POMS vigour scale (r = −0.77) in patients with cancer, including those with breast cancer.44 Discriminant validity: the FACIT-F subscale successfully discriminated hemoglobin group membership by differentiating the patients with low hemoglobin level (< 11 g/dL) from those with high hemoglobin level (> 13 g/dL) (P = 0.04), and was also able to discriminate patient membership classified by ECOG Performance Status rating (i.e., performance status rating 0 vs. 1 vs. 2 or 3) in patients with cancer44 Reliability: One study showed that the FACIT-F scale had strong internal consistency on the initial administration and the test–retest administration over a 3- to 7-day window (Cronbach alpha = 0.93 and 0.96, respectively) and good test–retest reliability (r = 0.90) in patients with cancer.44 Another study also found that the FACIT-F scale had strong internal consistency (Cronbach alpha = 0.96) in patients with cancer.42 Responsiveness: No evidence of responsiveness was identified for the FACIT-F scale in patients with breast cancer. | Cella et al.45 estimated that the MID on the FACIT-F scale was 3.0 in patients with cancer, including breast cancer. Patrick et al.46 estimated that the MID on the FACIT-F scale as 4.24 in patients with cancer who are anemic, including patients with breast cancer. |
ECOG = Eastern Cooperative Oncology Group; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; FACIT-F = Functional Assessment of Chronic Illness Therapy–Fatigue scale; MID = minimal important difference; PFS = Piper Fatigue Scale; POMS = Profile of Mood States; QoL = quality of life.
Findings
The European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30
Description and Scoring
The EORTC QLQ-C30 is a multidimensional, cancer-specific, self-administered measure of HRQoL.47
The EORTC QLQ-C30 is composed of both multi-item scales and single-item measures. These include 5 functional scales (physical, role, cognitive, emotional, and social), 3 symptom scales (fatigue, pain, and nausea and vomiting), a global health status (HRQoL) scale, and 6 single items assessing additional symptoms commonly reported by patients with cancer (dyspnea, loss of appetite, insomnia, constipation, and diarrhea) as well as the perceived financial impact of the disease.47 Version 3.0 of the questionnaire is the most recent version and has been in use since December of 1997.48
The EORTC QLQ-C30 uses a 1-week recall period to assess functional status and symptoms. All scales and single-item measures are scored from 0 to 100. Most questions have 4 response options (“not at all,” “a little,” “quite a bit,” “very much”), with scores on these items ranging from 1 to 4. For the 2 items that form the global HRQoL scale, the response format is a 7-point Likert-type scale with anchors at 1 = “very poor” and 7 = “excellent.” Raw scores for each scale are computed as the average of the items that contribute to a particular scale. Scale sum scores are transformed such that a high score on the functional scales represents a high or healthy level of functioning, a high score on the symptom scales represents a high level of symptomatology, and a high score on the global health status scale represents a high HRQoL.50
According to the EORTC QLQ-C30 scoring algorithm, if there are missing items for a scale (i.e., the patient did not provide a response), the score for the scale can still be computed if there are responses for at least half of the items. The values for missing items are interpolated with the average of the respondent-completed items.50
Assessment of Validity, Reliability, and Responsiveness
One study51 assessed the content validity of the EORTC QLQ-C30 based on the opinions of 21 experts. When mapping to the WHO’s International Classification of Functioning framework, 25 of the 30 items in the EORTC QLQ-C30 were endorsed by the experts: 15 items mapping to impairment of body function, 7 mapping to activity limitations/participation restrictions, and 1 item mapping to both components. There were only 2 items of the EORTC QLQ-C30 that mapped content outside of functioning: Item 29 mapping to perceived health and item 30 mapping to global quality of health. The authors stated that the fact that most items from the EORTC QLQ-C30 can be linked to the International Classification of Functioning framework means that the instrument’s content reflects functioning, which is a key component of HRQoL.51
A study investigated the inter-rater reliability using patient (46 patients with metastatic breast cancer)-observer (1 observer) agreement on the EORTC QLQ-C30 questionnaire.78 The median kappa coefficient for agreement across the 30 items in the EORTC QLQ-C30 was 0.86 (range: 0.48 to 1.00), and there was almost perfect agreement (kappa coefficient 0.8 to 1.00) for 19 items and “substantial agreement” (kappa coefficient: 0.61 to 0.80) for 6 items.78
Another study52 investigated the discriminative and convergent validity of the psychosocial subscales of EORTC QLQ-C30 in 150 patients with breast cancer With a sample size of 150, Spearman rank correlation coefficients above 0.20 were considered statistically significant (P < 0.01).52 The study strongly supported the discriminative validity of the global health/quality of life and social function subscales of the EORTC QLQ-C30 in patients subgroups defined by the clinical parameters of ECOG Performance Status, pain, suffering, fatigue, chemotherapy, and sleep disturbance (All Spearman rank correlation coefficients > 0.2).52 In terms of interinstrument associations occurred between the EORTC QLQ-C30 and the POMS subscales (also known as convergent validity), the emotional function of the EORTC QLQ-C30 correlated very strongly with tension (Spearman rank correlation coefficient = 0.76), depression/dejection (Spearman rank correlation coefficient = 0.74) and the POMS total mood disturbance subscales (Spearman rank correlation coefficient = 0.74).52
Minimal Important Difference
One study from 199854 conducted in patients with breast cancer (N = 246) and small-cell lung cancer (N = 111), estimated that a change in score on any scale of the EORTC QLQ-C30 of 10 points would be clinically significant. This estimate was based on an anchor-based approach to estimate the MID in which patients who reported “a little” change (for better or worse) on the Patientive significance questionnaire (SSQ) had corresponding changes on a function or symptom scale of the EORTC QLQ-C30 of approximately 5 to 10 points. Patients who reported a “moderate” change had corresponding changes in the EORTC QLQ-C30 of about 10 to 20 points, and those who reported “very much” change had corresponding changes in the EORTC QLQ-C30 of more than 20 points.54
A more recent study from 201953 aimed to estimate the MID for the EORTC QLQ-C30 in patients with advanced breast cancer (N = 723). This study used anchor-based and distribution-based approaches, utilizing performance status and selected AEs as the anchor variables. Estimated MIDs for within-group changes ranged from 5 to 14 points for improvements and from −14 to −4 points for deterioration across the individual scales. For between-group differences, MIDs ranged from 4 to 11 points for improvements and from −18 to −4 points for deterioration across the individual scales.53
Kawahara and colleagues55 analyzed a dataset of 154 patients with metastatic breast cancer using anchors obtained from patients (transition items) and clinicians (performance status). MIDs were estimated in 8 of 15 scales of EORTC QLQ-C30. Estimated MIDs for within-group improvement varied from 7 to 15 points and those for deterioration varied from −17 to −7 points. Estimated MIDs for between-group improvement varied from 5 to 11 points and those for deterioration varied from −8 to −5 points across EORTC QLQ-C30 scales.55
In addition, a study from 201679 aimed to investigate the effect of response shift on MID over time for the EORTC QLQ- C30 in patients with breast cancer or suspicious breast cancer. A total of 381 patients recruited from 4 hospitals and care centres participated in this study, with a mean age of 58.4 years (SD = 11 years). This study used an anchor-based approach utilizing deterioration and improvement as the anchor variables. The minimal of estimated MID at 6 months (ranging from 0.5 to 10 points) was smaller in case of deterioration for EORTC QLQ-C30 compared to 3 months (ranging from 5 to 26 points). With regards to improvement, the estimated MID at 6 months (ranging from 0.8 to 7) was similar to the estimated MID at 3 months (ranging from 0.3 to 10 points).79
The 13-Item Functional Assessment of Chronic Illness Therapy–Fatigue Scale
Description and Scoring
The FACIT-F scale consists of 13 measurement items and was first designed to assess self-reported fatigue associated with anemia in patients with cancer, such as breast cancer, lung cancer, and colorectal cancer.44 Patients are asked to respond to each of the 13 measurement items based on the prior 7 days. The response for each measurement item is scored on a 5-point Likert scale from 0 (not at all) to 4 (very much). The total score of the FACIT-F scale is calculated by summing the scores of all 13 measurement items and ranges from 0 to 52 with a lower score indicating more fatigue.43,44
Assessment of Validity, Reliability, and Responsiveness
Yellen et al.44 reported convergent–divergent validity, discriminant validity, and reliability in 50 patients with cancer [median age = 56 years (range: 19 to 83); 54% female; 12 were diagnosed with breast cancer with no staging information]. In terms of convergent–divergent validity, the FACIT-F scale had a strong correlation with the POMS fatigue scale (r = −0.83), the Piper Fatigue Scale (r = 0.61), and the POMS vigour scale (coefficient = −0.77), indicating that the FACIT-F scale was significantly related to fatigue or anemia-relevant concepts (convergent validity) and was unrelated to concepts which were not assumed to be associated with fatigue or anemia (divergent validity) (If r > 0.35 or < −0.35, then significant at P = 0.05).44 In terms of discriminant validity, the FACIT-F scale successfully discriminated hemoglobin group membership in patients with cancer by differentiating the patients with low hemoglobin level (< 11 g/dL) from those with high hemoglobin level (> 13 g/dL) (P = 0.04).44 The FACIT-F scale was also able to discriminate patient membership classified by ECOG Performance Status rating (i.e., performance status rating 0 versus 1 versus 2/3) (P < 0.000) under the assumption that better performance status would be associated with higher quality of life scores.44 In terms of reliability, the FACIT-F scale showed strong internal consistency on the initial administration and the test-retest administration over a 3- to 7-day window (Cronbach alpha = 0.93 and 0.95, respectively) and demonstrated a good test-retest reliability (r = 0.90) in patients with cancer.44
Another study42 involved 297 patients with cancer (mean age = 58.1 years (SD = 13.5); 35.7% were female; 34% of patients had breast cancer, including 50% of patients with early breast cancer).42 The FACIT-F scale was found to be strongly correlated with patient-rated ECOG Performance Status rating (r = −0.55; P = 0.001). In terms of reliability, the FACIT-F scale showed strong internal consistency (Cronbach alpha = 0.96).42
Minimal Important Difference
Cella et al.45 estimated the MID for change in the FACIT-F scale in patients with cancer (59.8% were female; 17.6% of patients had breast cancer) using the anchor-based and distribution-based approaches. Among 2,583 patients with cancer, 455 were patients with breast cancer. However, the disease stage of the patients with breast cancer was not specified.45 The authors estimated that the MID for the FACIT-F scale was 3.0 (no less than 2.7), meaning 1 category change (better or worse) on 3 of the 13 items on the FACIT-F scale with no change in the other 10 items.
Patrick et al.46 estimated that the MID for the FACIT-F scale was 4.24 by analyzing hemoglobin and HRQoL data from a multinational, double-blind, placebo-controlled, randomized trial80 conducted in 375 patients with cancer who were anemic who received nonplatinum chemotherapy for nonmyeloid malignancies (age = 18.7 to 88.6 years; 66.9% were female; 46.4% of patients had breast cancer, 59% of whom were having stage III or IV breast cancer).80
Pharmacoeconomic Review
Abbreviations
AE
adverse event
BRCA
breast cancer susceptibility gene
gBRCA
germline breast cancer susceptibility gene
gBRCAm
germline breast cancer susceptibility gene–mutated
HER2
human epidermal growth factor receptor 2
HR-positive
positive for expression of a hormone receptor
ICER
incremental cost-effectiveness ratio
IDFS
invasive disease–free survival
ITC
indirect treatment comparison
ITT
intention to treat
mBC
metastatic breast cancer
non-mBC
nonmetastatic breast cancer
OS
overall survival
QALY
quality-adjusted life-year
TNBC
triple-negative breast cancer
TP
transition probability
WTP
willingness to pay
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Olaparib (Lynparza), oral tablets |
Submitted price | Olaparib, 100 mg and 150 mg: $66.62 per tablet |
Indication | Adjuvant treatment of adult patients with deleterious or suspected deleterious BRCAm, HER2-negative, high-risk early breast cancer who have been treated with neoadjuvant or adjuvant chemotherapy. Patients must have confirmation of a germline BRCA mutation before olaparib treatment is initiated. |
Health Canada approval status | Notice of Compliance with conditions |
Health Canada review pathway | Priority |
NOC date | July 27, 2022 |
Reimbursement request | As per indication |
Sponsor | AstraZeneca Canada Inc. |
Submission history | Previously reviewed: Yes Ovarian cancer, second line (2016): Indication: As monotherapy maintenance treatment of adult patients with platinum-sensitive, relapsed BRCA-mutated epithelial ovarian, fallopian tube, or primary peritoneal cancer who are in response to platinum-based chemotherapy. Recommendation: Do not reimburse. Ovarian cancer, second line (2017) (resubmission): Indication: As monotherapy maintenance treatment of adult patients with platinum-sensitive relapsed BRCA-mutated epithelial ovarian, fallopian tube, or primary peritoneal cancer who are in response to platinum-based chemotherapy. Recommendation: Reimburse with clinical criteria and/or conditions. Newly diagnosed ovarian cancer (2019): Indication: As monotherapy for the maintenance treatment of adult patients with newly diagnosed advanced BRCA-mutated high-grade epithelial ovarian, fallopian tube, or primary peritoneal cancer who are in response (complete response or partial response) to first-line platinum-based chemotherapy until disease progression or up to 2 years if no evidence of disease. Patients must have confirmation of a BRCA mutation (identified by either germline or tumour testing) before olaparib treatment is initiated. Recommendation: Reimburse with clinical criteria and/or conditions. Metastatic castration-resistant prostate cancer (2021): Indication: As monotherapy for the treatment of adult patients with metastatic castration-resistant prostate cancer and deleterious or suspected deleterious germline and/or somatic mutations in the homologous recombination repair BRCA1 and BRCA2 genes or ATM gene who have progressed following prior treatment with a new hormonal drug. Recommendation: Reimburse with clinical criteria and/or conditions. |
BRCA = breast cancer susceptibility gene; gBRCAm = germline BRCA–mutated; HER2 = human epidermal growth factor receptor 2.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Semi-Markov model |
Target population(s) | Adult patients (aged ≥ 18 years) with gBRCAm, HER2-negative, high-risk early breast cancer who have received prior adjuvant or neoadjuvant chemotherapy; target population included both patients with HER2-negative, HR-positive breast cancer and patients with TNBC. |
Treatment | Olaparib; patients with HER2-negative, HR-positive disease may also receive adjuvant endocrine therapy. |
Comparators | Watch and wait; patients with HER2-negative, HR-positive disease may also receive adjuvant endocrine therapy. Capecitabine was considered in scenario analyses for patients with TNBC. |
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs, LYs |
Time horizon | Lifetime (57 years) |
Key data source | OlympiA trial |
Submitted results | ICER = $45,237 per QALY (incremental costs = $74,206 and incremental QALYs = 1.64) |
Key limitations |
|
CADTH reanalysis results |
|
BRCA = breast cancer susceptibility gene; gBRCA = germline BRCA; gBRCAm = germline BRCA–mutated; HER2 = human epidermal growth factor receptor 2; HR-positive = hormone receptor–positive; ICER = incremental cost-effectiveness ratio; IDFS = invasive disease–free survival; ITC = indirect treatment comparison, ITT = intention to treat; LY = life-year; OS = overall survival; QALY = quality-adjusted life-year; TNBC = triple-negative breast cancer; WTP = willingness to pay.
Conclusions
The CADTH Clinical Review concluded that based on data from the OlympiA trial, adjuvant olaparib demonstrated a clinically meaningful and statistically significant benefit versus placebo for the treatment of germline breast cancer susceptibility gene (gBRCA)–mutated (gBRCAm), human epidermal growth factor receptor 2 (HER2)–negative, high-risk early breast cancer for invasive disease–free survival (IDFS) and overall survival (OS). However, the median IDFS and OS were not estimable due to insufficient follow-up time and the long-term efficacy of adjuvant olaparib is unknown. Further, since all results are based on interim analyses, there is the potential that the benefit of olaparib relative to placebo is overestimated; however, the presence and extent of any overestimation is uncertain. There remains uncertainty in the benefit of adjuvant olaparib in patients with HER2-negative, hormone receptor–positive (HR-positive) disease due to the small patient population in the OlympiA trial (HR-positive represented 17.7% of the population). In the absence of direct comparative evidence, the CADTH Clinical Review team noted that given the estimates in the submitted indirect treatment comparison (ITC), no conclusions could be drawn about the comparative efficacy of adjuvant olaparib versus capecitabine for patients with triple-negative breast cancer (TNBC) with regard to IDFS, disease-free survival, or OS based on the submitted ITC due to methodological limitations and imprecision in the effect estimates.
As a result of the heterogeneity in hormone receptor status in the trial and the differences in underlying survival and cure assumptions for the TNBC subgroup versus the HER2-negative, HR-positive subgroup, CADTH assessed the TNBC subgroup and the HER2-negative, HR-positive subgroup separately and utilized subgroup-specific data to inform IDFS.
The CADTH reanalysis resulted in an incremental cost-effectiveness ratio (ICER) of $43,599 per quality-adjusted life-year (QALY) (incremental costs = $74,660; incremental QALYs = 1.71) for adjuvant olaparib compared with watch and wait for the TNBC subgroup population, and an ICER of $157,407 per QALY (incremental costs = $84,098; incremental QALYs = 0.53) for the HER2-negative, HR-positive subgroup. While no price reduction is required for adjuvant olaparib in the TNBC population, a price reduction of 67% is required for adjuvant olaparib to be cost-effective compared with watch and wait in the HER2-negative, HR-positive subgroup at a willingness-to-pay (WTP) threshold of $50,000 per QALY. When considering the combined target population (calculated using a weighted average between the TNBC subgroup versus the HER2-negative, HR-positive subgroup informed by the proportion of patients present in the OlympiA trial), a price reduction of approximately 3% would be required. However, given the uncertainty in the efficacy data, further price reductions may be necessary to ensure the cost-effectiveness of adjuvant olaparib. This is especially true when considering the HER2-negative, HR-positive subgroup, as there were limitations in the data for that subgroup due to a small sample size within the OlympiA trial.
There remains uncertainty in the long term treatment effect of adjuvant olaparib for the treatment of patients with gBRCAm, HER2-negative, high-risk early breast cancer. Furthermore, the treatment landscape for gBRCAm, HER2-negative, high-risk early breast cancer is changing, as CADTH recently recommended abemaciclib and pembrolizumab (reimburse with conditions) for the treatment of patients with HER2-negative, HR-positive breast cancer and TNBC, respectively. The cost-effectiveness of adjuvant olaparib compared with these treatments is unknown.
Stakeholder Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, registered clinicians, and drug plans that participated in the CADTH review process.
Two patient groups, the Canadian Breast Cancer Network and Rethink Breast Cancer (Rethink), provided input for this submission. Patient input was gathered from a Canadian Breast Cancer Network online survey (including input from 6 Canadian patients identifying as being diagnosed with gBRCAm, HER2-negative, high-risk early breast cancer), whereas Rethink obtained patient input through programming and meetings with patients with breast cancer plus 3 in-depth telephone interviews and responses from members of the Rethink Instagram community with high-risk early breast cancer. All patients reported that reducing the risk of cancer recurrence and improving quality of life were the top 2 most important factors when making treatment decisions. The 3 patients interviewed by telephone by Rethink had experience with olaparib from the OlympiA study and reported improved IDFS, distant disease–free survival, and OS. None of these patients mentioned any consequential or noticeable adverse events (AEs) while on olaparib. Both patient groups expressed interest in olaparib for the treatment of patients with gBRCAm. Registered clinician input was received from 2 clinician groups, including the Ontario Health Breast Cancer Drug Advisory Committee and a group of medical oncologists across Canada. The clinicians noted that the early breast cancer treatment strategy depends on the subtype of breast cancer and the prognostic and predictive factors of the tumour and patient characteristics. For TNBC, the new standard of care for stage II and III disease is chemotherapy with paclitaxel, carboplatin, doxorubicin, and cyclophosphamide, plus pembrolizumab during the treatment and continued as monotherapy after surgery. However, pembrolizumab is not yet funded in Canada. The clinicians agreed that patients must have confirmation of a gBRCA mutation before receiving olaparib; however, the clinicians noted that current guidelines for BRCA mutation testing are restrictive regarding eligibility criteria. Furthermore, both clinician groups noted several reasons that may result in treatment discontinuation with olaparib, including recurrence or progression of disease, intolerant toxicity, severe side effects, and patient or physician preferences.
Feedback from the drug plans noted that clarification on the criteria for defining “high risk” for eligibility is required. The drug plans inquired about the feasibility of initiating olaparib treatment for patients who are not high risk but otherwise meet the olaparib treatment criteria and who have not progressed. The plans further highlighted the need for a gBRCA mutation to be confirmed before starting olaparib treatment.
Several of these concerns were addressed in the sponsor’s model:
disease-free survival and health state utilities capturing breast cancer symptoms and quality of life were included
AEs associated with olaparib adjuvant therapy were included
BRCA testing costs were considered in a scenario analysis.
CADTH was unable to address the following concerns raised from stakeholder input:
cost-effectiveness of olaparib compared with other potentially relevant comparators beyond watch and wait and capecitabine in TNBC (e.g., abemaciclib, pembrolizumab).
Economic Review
The current review is for olaparib (Lynparza) for the adjuvant treatment of early-stage high-risk, HER2-negative, gBRCAm breast cancer.
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted a cost-utility analysis to assess the cost-effectiveness of olaparib against watch and wait as an adjuvant treatment for patients with early-stage high-risk, HER2-negative, gBRCAm breast cancer. This model population aligned with the OlympiA trial population and Health Canada indication.1 Two predefined subgroups of interest based on hormone receptor status, TNBC versus HER2-negative, HR-positive, were explored as scenario analyses. In scenario analyses for the TNBC subpopulation only, capecitabine was considered as a comparator.
Olaparib is available as 150 mg and 100 mg oral tablets.1 The recommended dose of olaparib is 600 mg, taken as 2 150 mg tablets twice daily. For adjuvant treatment of HER2-negative, gBRCAm, high-risk early breast cancer, it is recommended that patients be treated for 1 year or until disease recurrence or toxicity, whichever occurs first.2 The submitted price of olaparib is $66.62 per tablet or $7,461.14 per 28-day cycle.1 The comparator for this analysis was watch and wait, based on the placebo arm of the OlympiA trial.1 All patients with HER2-negative/HR+ disease could also receive adjuvant endocrine therapy regardless of which treatment arm they were in until disease recurrence or death or for a fixed maximum duration (5 years in the base case).1
Outcomes of the model included QALYs and life-years over a lifetime horizon of 57 years. Discounting (1.5% per annum) was applied for both costs and outcomes and a cycle length of 1 month (30.4 days) was used with a half-cycle correction applied.1
Model Structure
The sponsor submitted a semi-Markov model consisting of 5 health states: IDFS, nonmetastatic breast cancer (non-mBC), early onset metastatic breast cancer (mBC), late onset mBC, and death (Figure 1). The separation of mBC into “early” and “late” was done to reflect the assumption that the risk of death after metastatic cancer differed based on the timing of recurrence as patients with early recurrence tend to have more aggressive disease that is less responsive to subsequent treatment than patients who experience late recurrence. The time point determining early versus late recurrence was set as 24 months in the base case. All health states were tunnel states; therefore, patients could only progress through health states via a predetermined sequence. Patients entered the model in the IDFS health state and could then transition into either the non-mBC, early mBC, late mBC, or death health states. Patients in the non-mBC health state could transition to the early onset mBC, late onset mBC, or death health states, whereas those in the early or late onset mBC could only transition to death.
Model Inputs
The target population was based on the intention-to-treat (ITT) population of the OlympiA trial (mean age = 43.3 years; mean weight = 68.7 kg; body surface area = 1.72 m2), which enrolled adult patients with gBRCAm, HER2-negative, high-risk early breast cancer who had received prior adjuvant or neoadjuvant chemotherapy.3 The sponsor’s base case included all patients regardless of hormone receptor status.
The clinical efficacy parameters were derived from the ITT patient population from the OlympiA trial (date of second data cut-off was July 12, 2021), OlympiAD (a trial designed to compare the efficacy and safety of olaparib versus the efficacy and safety of standard therapy (i.e., chemotherapy with a single drug chosen by a physician) for patients with HER2-negative mBC and a gBRCA mutation), or general-population mortality with adjustments.1,3-5 Parametric survival modelling was used to estimate health state transition probabilities (TPs) from the observed survival data from the OlympiA and OlympiAD trials to extrapolate TPs to the entire model time horizon. Selections of parametric survival models for the various TPs used in the sponsor’s base case were based on clinical plausibility, visual inspection, and statistical fit to the trial’s Kaplan-Meier data.1 The same survival distribution was selected for both included interventions for each treatment pathway, when applicable, based on recommendations from National Institute for Health and Care Excellence Decision Support Unit technical support document 14.6
The log-normal curve was selected in the sponsor’s base case to inform the TPs from IDFS (TP1 and TP2) based on the ITT population of the OlympiA trial. Adjustments of the hazard rates for long-term risk of IDFS were made where the risk of long-term recurrence was assumed to be zero after 5 years.1 Furthermore, it was assumed that the conditional probability of non-distant recurrence was the same across treatment arms due to the lack of evidence that olaparib treatment affected the type of recurrence event experienced. Annualized general-population mortality rates from Statistics Canada for females aged 43 to 100 years were used to inform the TPs from IDFS to death (TP3).7 A standardized mortality ratio from Mai et al. was used to adjust the general-population mortality rates to capture the increased mortality risks for patients with gBRCA mutations.8 TPs for the non-mBC to mBC (TP4) and non-mBC to death (TP5) pathways were also informed by ITT data from the OlympiA trial, where the log-normal curve and exponential parametric models were selected for TP4 and TP5, respectively. In both cases, pooled data from the olaparib and placebo arms in the OlympiA trial were used due to low patient numbers. As such, the same TPs were applied to both interventions assessed in the model.1 The TPs from early onset mBC to death (TP6) were based on the time from distant metastatic recurrence to death data from the OlympiA trial. The exponential survival curve was selected. It was assumed that patients receiving olaparib and placebo would have different risks of death, as the clinical experts consulted by the sponsor noted that patients with an early distant recurrence after olaparib are likely to have more aggressive disease and less likely to respond to subsequent treatment, thus enriching the placebo arm with more responsive patients.1 Lastly, the TP from late onset mBC to death (TP7) was modelled using data from 2 studies that reported the OS of patients with gBRCA mutations in a first-line mBC setting based on the following therapies received: single-drug chemotherapy4,5 and cyclin-dependent kinase 4 and 6 (CDK4/6) inhibitor plus endocrine therapy.9 Treatment survival probabilities for patients on single-drug chemotherapy and CKD4/6 were modelled independently using parametric survival models and were then combined as a weighted average using case weights reflective of subsequent treatments and then further weighted by TNBC and HER2-negative, HR-positive subgroup distributions. It was assumed that 100% of the patients in the TNBC subgroup were treated with single-drug chemotherapy in line with the 2022 National Comprehensive Cancer Network guidelines and clinical expert feedback received by the sponsor.1 For the HER2-negative, HR-positive subgroup, it was assumed, based on Canadian clinical expert feedback, that 10% of patients in this subgroup had single-drug chemotherapy and the remaining 90% would receive a CDK4/6 inhibitor plus endocrine therapy. The same case mix of treatment was applied regardless of the initial treatment for early breast cancer specified in the model.
A summary of the extrapolation curves used in the sponsor’s base-case analysis can be found in Table 10. All TPs to death had to be at least as high as the general-population mortality data informed by Statistics Canada.10 In the TNBC subgroup analysis, a scenario analysis was conducted that included capecitabine as a comparator. Capecitabine efficacy was informed by the sponsor-summited ITC comparing the efficacy of olaparib with capecitabine, with data for capecitabine informed by the CIBOMA trial.
The AE rates for both olaparib and watch and wait were informed by the OlympiA trial and were modelled as a one-off cost in the first cycle based on incidence, duration, and the cost or disutility of each event.1 Only serious AEs of grade 3 or higher that occurred in at least 1% of patients in either treatment arm were included in the analysis.1
Health state utility values in the model were informed by published literature.11,12 The 5-level EQ-5D utility values from Torres et al. were used to inform the IDFS (0.87) and non-mBC (0.78) health states, while a Swiss study in breast cancer using the EQ-5D was used to inform the mBC health states (0.685).11,12 AE disutilities were also informed by published literature13,14 and adjusted by the duration of the AE, as reported in the OlympiA trial.1
In the sponsor’s base case, the costs included were drug acquisition costs, subsequent treatment costs, administration costs, and health state and disease management costs. The drug acquisition costs were taken from DeltaPA.15 Patients on adjuvant olaparib were modelled to complete up to 1 year of treatment with discontinuation rates informed by the OlympiA trial.1 Patients with HER2-negative, HR-positive disease were allowed to continue concurrent endocrine therapy until disease recurrence, death, or for a maximum of 5 years. The cost of watch and wait was assumed to be $0.1 Subsequent treatment costs were included in the model and applied as one-off costs upon progression into the respective health states. Unit costs for subsequent non-drug treatments were informed by the Ontario Schedule of Benefits.16 Administration costs for oral therapies were assumed to be $0, while IV administration costs were informed by published literature.17 Health state and disease management costs reflected outpatient visits, hospitalizations, general practitioner visits, oncology visits, CT scans, and mammograms. The unit costs for these resources were informed by the Ontario Schedule of Benefits and Ontario Case Costing Initiative, and the frequencies were informed by a Canadian real-world evidence study on patients with early-stage gBRCAm, HER2-negative, high-risk breast cancer supplied by the sponsor.16,18,19 In the sponsor’s base case, a cancer-related end-of-life cost was included in the model as a one-off cost applied to patients entering the death state from the non-mBC or mBC state, as it was assumed that death events from IDFS included non-cancer events.1,20 Lastly, costs associated with AEs were sourced from the Ontario Case Costing Initiative and published literature.18,21 All costs were expressed as 2021 Canadian dollars.
Summary of Sponsor’s Economic Evaluation Results
All analyses were run probabilistically (1,500 iterations). Submitted deterministic analyses were aligned with the probabilistic results. The probabilistic findings are presented subsequently.
Base-Case Results
The results of the sponsor’s probabilistic base-case analysis demonstrated that adjuvant olaparib was associated with an additional 1.64 QALYs at an additional cost of $74,206. Therefore, the ICER of adjuvant olaparib was $45,237 per QALY gained compared with watch and wait in the ITT population of the OlympiA trial. Based on the deterministic results, the majority (94%) of the incremental QALYs for olaparib were found to be accrued during the extrapolation period (i.e., after the 4 years of observed OlympiA trial data).
Table 3: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER vs. watch and wait ($/QALY) |
|---|---|---|---|---|---|
Watch and wait | 50,002 | Reference | 17.70 | Reference | Reference |
Olaparib | 124,208 | 74,206 | 19.34 | 1.64 | 45,237 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Source: Sponsor’s pharmacoeconomic submission.1
Additional results from the sponsor’s submitted economic evaluation base case are presented in Appendix 3.
Sensitivity and Scenario Analysis Results
The sponsor conducted several scenario analyses pertaining to different time horizons, discounting, perspectives, time points for determining early versus late recurrence, inclusion of wastage or costs of testing for BRCA1 and BRCA2, time points at which patients are no longer at risk of recurrence, health state utilities, and extrapolations informing the TPs. Results from the scenario analyses showed the ICER was most sensitive to changes in discounting. The results were also sensitive to assuming a 180-month time point for when patients are no longer at risk of recurrence (ICER increase of approximately 11% to $50,078) and selecting different distributions to inform the TP1 and TP2 transitions; that is, the selection of the generalized gamma distribution increased the ICER to $49,228 (approximately 9%), whereas selection of the Weibull distribution increased the ICER to $45,697 (approximately 1%).
The sponsor further conducted scenario analyses for the TNBC subgroup versus the HER2-negative, HR-positive subgroup separately. ICERs of $44,826 (incremental cost = $74,759; incremental QALYs = 1.67) and $58,528 (incremental costs = $77,341; incremental QALYs = 1.32) were associated with the TNBC subgroup and HER2-negative, HR-positive subgroup, respectively. Results from the TNBC subgroup analysis were aligned with the base case (i.e., ITT population from OlympiA), whereas fewer incremental QALYs were observed with the HER2-negative, HR-positive subgroup analysis due to the difference in cure assumption applied.
For the TNBC subgroup, capecitabine was included as a comparator in 2 scenario analyses. The first scenario used a hazard ratio of 0.82 from the overall mixed-group population from the CIBOMA trial for capecitabine versus placebo that resulted in an ICER of $90,325 (incremental costs = $76,643; incremental QALYs = 0.85). The second scenario utilized a hazard ratio of 1.12 from the high-risk subpopulation of the CIBOMA trial that resulted in an ICER of $30,630 (incremental costs = $71,459; incremental QALYs = 2.32).
CADTH Appraisal of the Sponsor’s Economic Evaluation
CADTH identified several key limitations to the sponsor’s analysis that have notable implications for the economic analysis:
The long-term efficacy of adjuvant olaparib treatment is unknown. The treatment efficacy data in the model were primarily informed by the randomized, double-blind, placebo-controlled OlympiA trial. By the second data cut-off (July 12, 2021), IDFS and OS had reached a data maturity of approximately 18.6% and 10%, respectively. As OS data from the trial was considered immature, the sponsor submitted a semi-Markov model using the TPs derived from parametric models fitted to the ITT population from the OlympiA trial for IDFS, non-mBC, and early mBC, where OS gains in the model were driven by differences in IDFS and timing of metastatic recurrence. Therefore, the sponsor’s model assumed that by remaining disease-free, the probability of death is lower and patients live longer. However, according to the clinical experts consulted by CADTH and the CADTH Clinical Review, although the trial findings on IDFS and OS for olaparib appeared to be statistically superior and clinically meaningful in comparison with watch and wait, the long-term impact of olaparib adjuvant therapy remains uncertain. Further, since all results are based on interim analyses, there is the potential that the benefit of olaparib relative to placebo is overestimated; however, the presence and extent of any overestimation is uncertain. Therefore, while a benefit with olaparib was deemed plausible, the magnitude of such a benefit is uncertain in the absence of more robust long-term evidence.
CADTH was unable to address this issue due to limitations in data availability. The impact of this limitation on the cost-effectiveness of olaparib is uncertain.
The inclusion of all patients regardless of hormone receptor status to inform the sponsor’s base-case analysis was inappropriate. The efficacy of olaparib in the sponsor’s base case was primarily informed by the ITT population of the phase III, double-blinded, randomized OlympiA trial, which enrolled adult patients with gBRCAm, HER2-negative, high-risk early breast cancer regardless of hormone receptor status. The sponsor noted that the ITT population was selected for the sponsor’s base case, as the patients with HER2-negative, HR-positive disease in the OlympiA trial were shown to present similar survival over a 5-year period due to the trial inclusion criteria identifying high-risk patients with HER2-negative, HR-positive disease who had disease progression and survival similar to that of patients with TNBC. However, the clinical expert feedback obtained by CADTH indicated that patients with HER2-negative, HR-positive breast cancer versus patients with TNBC have different rates of recurrence over time in clinical practice and there are differences in the cure assumptions for each. Specifically, patients with TNBC typically have higher rates of recurrence within the first 3 to 4 years and, after 5 years, patients can be considered cured. In comparison, patients with HER2-negative, HR-positive disease are at continued risk of recurrence over time, with risk of recurrence typically occurring at a more constant rate. Both the sponsor and feedback from clinical experts consulted by CADTH noted that the ITT patient population from the OlympiA trial primarily consisted of patients with TNBC (82.3% versus 17.7% for HER2-negative, HR-positive).
Given the expected survival differences between the 2 subgroups, the sponsor’s base case was therefore misaligned with CADTH guidelines, which indicate subgroups with differences in efficacy, natural history, or other key care pathway assumptions should be assessed separately to account for heterogeneity.22 The sponsor conducted scenario analyses for the TNBC subgroup and HER2-negative, HR-positive subgroup. For the TNBC subgroup analysis, only TNBC subgroup data were utilized to inform efficacy. ITT data were used as a proxy for the HER2-negative, HR-positive subgroup analysis despite the availability of data specific to patients with HER2-negative, HR-positive disease. Justification for the latter was not provided by the sponsor. Although the sponsor utilized different cure assumptions for the scenario analyses (i.e., patients with TNBC were assumed to be cured after 5 years while there was no cure assumption applied for the patients with HER2-negative, HR-positive disease), it remains inappropriate to assume the ITT data are generalizable to the HER2-negative, HR-positive subgroup, as a majority of the ITT efficacy is informed by patients with TNBC. However, as noted in the CADTH Clinical Report, analysis on the HER2-negative, HR-positive subgroup is associated with uncertainty, as the analyses of the trial data were limited by the small number of patients. Therefore, the cost-effectiveness of olaparib for patients with HER2-negative, HR-positive disease remains uncertain.
Separate analyses for the TNBC subgroup versus the HER2-negative, HR-positive subgroup were conducted for the CADTH base-case analysis using the sponsor-provided setting option where subgroup-specific data were used to inform treatment efficacy with regard to IDFS. However, limitations in the study data (e.g., population size, selection criteria) could not be addressed; thus, this analysis is associated with some uncertainty.
The comparative efficacy of adjuvant olaparib versus capecitabine is uncertain. For the sponsor-submitted scenario analysis of the TNBC subgroup, capecitabine was included as a comparator due to its off-label use. The relative efficacy of capecitabine in comparison with olaparib was informed by a sponsor-submitted ITC using data from the CIBOMA trial. Two hazard ratio values were produced, 1 for the overall mixed-group population from the CIBOMA trial and another using the high-risk subpopulation from CIBOMA. However, as noted in the CADTH Clinical Report, there were uncertainties in the ITC and no conclusion could be drawn about the comparative effect of adjuvant olaparib versus capecitabine on IDFS or OS among patients with TNBC due to notable differences between the baseline demographics and disease characteristics of the patients in the 2 trials (e.g., unknown BRCA mutation status in the CIMBOA trial) and methodological limitations in the sponsor-submitted ITC. In the sponsor-submitted scenario analyses, the ICERs varied depending on which hazard ratio was used, with significant impacts observed on the incremental QALYs associated with olaparib in comparison with capecitabine (i.e., incremental QALYs of 0.85 for the overall mixed-group population versus 2.32 for the high-risk subpopulation). As appraised by the CADTH Clinical Review team, the hazard ratio estimates of the overall mixed-group population and the high-risk subpopulation from the CIBOMA trial were inconclusive. Thus, the cost-effectiveness of olaparib in comparison with capecitabine is highly uncertain.
CADTH was unable to resolve this issue. The impact of this limitation on the cost-effectiveness of olaparib is unknown.
The model structure does not accurately capture the disease pathway with a nonmetastatic recurrence. In the sponsor-submitted economic model, it was assumed that patients would transition through the model via tunnel health states and therefore patients who progressed from the disease-free survival state could not transition back. However, this assumption is not fully aligned with the disease pathway, as the clinical expert feedback received by CADTH noted that non-mBC is treated with curative intent. Although these patients may be at a higher risk of developing metastatic disease, they would be considered disease-free if successful. The submitted pharmacoeconomic model did not reflect the curative intent of treating non-mBC.
CADTH could not address this limitation due to a lack of flexibility in the submitted model. The impact of this limitation is unlikely to have a significant impact on the cost-effectiveness of olaparib.
Subsequent treatment use may not be aligned with Canadian clinical practice. Subsequent treatment in the sponsor’s base case for patients who experienced recurrence after adjuvant olaparib or watch and wait was dependent on whether they experienced a nonmetastatic or metastatic recurrence. For metastatic recurrence, the subsequent treatment was further dependent on the time of recurrence since the start of adjuvant therapy. The proportion of patients receiving either surgery and/or radiotherapy was based on the OlympiA trial data, whereas the proportion of patients who would receive each type of treatment was based on the clinician input received by the sponsor. Based on the clinical expert feedback obtained by CADTH, it was noted that paclitaxel may also be used in the nonmetastatic setting in approximately 30% to 35% of patients with TNBC. However, the clinical expert feedback obtained by CADTH indicated that the choice of any chemotherapeutic drug would depend on how soon the patient’s cancer recurred after their original exposure, as clinicians are unlikely to re-expose patients experiencing a recurrence to a drug they had been previously and recently treated with, as it is likely the patient's disease is resistant to it.
Furthermore, the clinical expert feedback received by CADTH noted that significantly fewer patients would receive surgery in the metastatic setting as a subsequent treatment option than the ~██% specified by the sponsor. Lastly, olaparib would be considered in the metastatic setting for patients with BRCA mutation–positive disease who had not previously received olaparib.
CADTH conducted a scenario analysis assuming the following: that 30% of patients with TNBC receive paclitaxel in the nonmetastatic setting (with patients proportionally captured from the available therapies indicated in the sponsor’s base case, i.e., carboplatin, capecitabine, and doxorubicin) and that 10% of patients receive surgery in the metastatic setting. CADTH was unable to address the limitation regarding subsequent treatment options based on a patient’s original exposure due to the lack of data availability and limitations in the model structure.
Additionally, the following key assumptions were made by the sponsor and have been appraised by CADTH (Table 4).
CADTH Reanalyses of the Economic Evaluation
Base-Case Results
The CADTH base case was derived by making changes in model parameter values and assumptions, in consultation with the clinical experts. These changes, summarized in Table 5, involved conducting analyses for the TNBC subgroup versus the HER2-negative, HR-positive subgroup independently, while using the subgroup data provided by the sponsor to inform the efficacy data for IDFS.
Table 4: Key Assumptions of the Submitted Economic Evaluation (Not Noted as Limitations to the Submission)
Sponsor’s key assumption | CADTH comment |
|---|---|
Patients are on olaparib adjuvant therapy for 1 year (or until disease recurrence or unaccepted toxicity). | Reasonable. Aligned with the product monograph and confirmed by the clinical expert feedback obtained by CADTH. |
General-population mortality with adjustments to account for higher mortality rates among patients with breast cancer to inform transitions from IDFS to death. | Reasonable. Confirmed by the clinical expert feedback obtained by CADTH. |
The proportion of events leading to distant or non-distant recurrence would remain constant over time. | Reasonable. Confirmed by the clinical expert feedback obtained by CADTH. |
Patients with gBRCAm HER2-negative disease are at a relatively high and immediate risk of developing metastatic breast cancer or death after a locoregional event. | Reasonable. The clinical expert feedback obtained by CADTH noted this would be especially true for patients with TNBC. |
Risk of death after metastatic cancer is different based on timing (i.e., 2 years) of recurrence, as those with early recurrence have more aggressive disease that is less likely to respond to subsequent treatment. | Reasonable. The clinical expert feedback received by CADTH stated that early recurrence generally indicates a more aggressive biology. The feedback further noted that although more reflective of the TNBC subgroup, HER2-negative, HR-positive disease that has recurred within 2 to 3 years is more aggressive than disease that recurs at 5 years. Of note, selections of different time points for determining early vs. late metastatic recurrence (e.g., 12 months or 36 months) had minimal impact on the cost-effectiveness of olaparib. |
Utility values informed by Canadian study Torres et al.12 and Swiss study Lidgren et al.11 | Reasonable but uncertain. The clinical expert feedback obtained by CADTH confirmed that the utility values informed by Torres et al. and Lidgren et al. were likely reflective of patients in Canada and their experience. However, it was noted that patients with metastatic disease may experience a decrease in utility values with time and that there may be discrepancies in social and supportive care in Switzerland in comparison to Canada. It is unclear how this would impact the cost-effectiveness of olaparib. |
AEs associated with subsequent treatment were not considered in the analysis, as post-recurrence AEs would impact both of the primary interventions considered in the model. | Reasonable. The clinical expert feedback obtained by CADTH noted this was a reasonable simplifying assumption. Of note, the clinicians mentioned that patients pretreated more heavily are typically more susceptible to AEs with each subsequent line of treatment and less likely to tolerate them well. It is unclear how this would impact the cost-effectiveness of olaparib, as this varies by patient and how heavily pretreated they are as they move through lines of therapy. |
AE treatment costs were mostly informed by the OCCI. | Inappropriate. In the sponsor’s base-case analysis, AE treatment costs were informed by the OCCI. The clinical expert feedback obtained by CADTH noted that the AEs included in the model would largely be treated in the outpatient setting; therefore, OCCI inpatient costs would be inappropriate to inform the cost of an AE event. However, given that the impact of AEs within the economic model applies to only a single cycle, this is unlikely to have a large impact on the overall results. |
AE = adverse event; gBRCAm = germline BRCA–mutated; HER2 = human epidermal growth factor receptor 2; HR-positive = hormone receptor–positive; IDFS = invasive disease–free survival; OCCI = Ontario Case Costing Initiative; TNBC = triple-negative breast cancer.
Table 5: CADTH Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Changes to derive CADTH base case 1 | ||
Population and source of efficacy data informing IDFS | Trial ITT population and data | Independent subgroup analyses (i.e., patients with TNBC and patients with HR-positive, HER2-negative breast cancer) of subgroup data with relevant cure assumption (5 years for TNBC, none for HER2-negative, HR-positive) |
HER2 = human epidermal growth factor receptor 2; HR-positive = hormone receptor–positive; IDFS = invasive disease–free survival; ITT = intention to treat; TNBC = triple-negative breast cancer.
In the CADTH base case for the TNBC subgroup population, olaparib was associated with estimated total costs and QALYs of $120,637 and 19.42 compared with total costs and QALYs of $45,977 and 17.71 for patients on watch and wait. Therefore, the ICER for olaparib compared with watch and wait was $43,599 per QALY (incremental costs = $74,660; incremental QALYs = 1.71) and the probability of cost-effectiveness at a $50,000 per-QALY WTP threshold was 63%. When examining the HER2-negative, HR-positive subgroup, olaparib was associated with estimated total costs and QALYs of $190,259 and 14.04 compared with total costs and QALYs of $106,161 and 13.50 for patients on watch and wait. Therefore, the ICER for olaparib compared with watch and wait was $157,407 per QALY (incremental costs = $84,098; incremental QALYs = 0.53) and the probability of cost-effectiveness at a $50,000 per-QALY WTP threshold was 51%. However, as noted in the CADTH Clinical Report, the analysis of the HER2-negative, HR-positive subgroup was limited by the small number of patients; therefore, the cost-effectiveness results of adjuvant olaparib for patients with HER2-negative, HR-positive disease remain associated with significant uncertainty.
Based on the deterministic results, the majority (94% and 87% for the TNBC and HR-positive subgroups, respectively) of the incremental QALYs for olaparib were found to be accrued during the extrapolation period (i.e., after the 4 years of observed OlympiA trial data).
Table 6: Summary of the Stepped Analysis of the CADTH Reanalysis Results
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALYs) |
|---|---|---|---|---|
Sponsor’s base case | Watch and wait | 50,002 | 17.70 | Reference |
Olaparib | 124,208 | 19.34 | 45,237 | |
CADTH base case (patients with TNBC; analysis 1) | Watch and wait | 45,977 | 17.71 | Reference |
Olaparib | 120,637 | 19.42 | 43,599 | |
CADTH base case (patients with HR-positive disease; analysis 1) | Watch and wait | 106,161 | 13.50 | Reference |
Olaparib | 190,259 | 14.04 | 157,407 |
HR-positive = hormone receptor–positive; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; TNBC = triple-negative breast cancer.
Scenario Analysis Results
Two scenarios were conducted on each of the CADTH base-case analyses to investigate the impact of subsequent treatment use that is more aligned with Canadian clinical practice, and the inclusion of costs for BRCA mutation testing. The results of the scenario analyses are presented in Appendix 4. The analyses examining the impact of different subsequent treatment distributions resulted in ICERs of $44,114 and $145,018 per QALY for olaparib compared with watch and wait for the TNBC subgroup versus the HER2-negative, HR-positive subgroup, respectively. For the scenarios that included costs for gBRCA mutation testing that were based on the number needed to identify a case approach (i.e., it was assumed that 6.6 patients would need to be tested to identify 1 patient with gBRCAm and that the unit cost of BRCA testing was $322.1023), ICERs of $45,216 and $154,328 per QALY were obtained for olaparib compared with watch and wait for the TNBC subgroup versus the HER2-negative, HR-positive subgroup, respectively. These results are associated with uncertainty, as significant changes in the prevalence of gBRCA in patients may impact the cost-effectiveness results.
CADTH also undertook price reduction analyses based on the CADTH base case. These analyses demonstrated that no price reduction is required for olaparib to achieve cost-effectiveness when considering the TNBC population. Comparatively, a price reduction of 67% is required for olaparib to be cost-effective compared with watch and wait in the HER2-negative, HR-positive subgroup (Table 7). When considering the entire ITT population (calculated using the weighted average between the TNBC subgroup versus the HER2-negative, HR-positive subgroup informed by the proportion of patients present in the OlympiA trial), a price reduction of approximately 3% would be required to achieve cost-effectiveness at a WTP threshold of $50,000 per QALY.
Table 7: CADTH Price Reduction Analyses
Price reduction analysis | ICERs for olaparib vs. watch and wait | |||
|---|---|---|---|---|
Sponsor base case | CADTH reanalysis: | CADTH reanalysis: | CADTH reanalysis: weighted averagea ($) | |
No price reduction | 45,370 | 44,097 | 145,016 | 50,983 |
10% | 40,433 | 39,360 | 130,763 | 45,597 |
20% | 35,496 | 34,623 | 116,511 | 40,211 |
30% | 30,560 | 29,886 | 102,258 | 34,825 |
40% | 25,623 | 25,149 | 88,005 | 29,438 |
50% | 20,686 | 20,412 | 73,753 | 24,052 |
60% | 15,750 | 15,675 | 59,500 | 18,666 |
70% | 10,813 | 10,939 | 45,248 | 13,280 |
80% | 5,876 | 6,202 | 30,995 | 7,893 |
90% | 939 | 1,465 | 16,742 | 2,507 |
100% | Dominant | Dominant | 2,490 | Dominant |
HER2 = human epidermal growth factor receptor 2; HR-positive = hormone receptor–positive; ICER = incremental cost-effectiveness ratio; TNBC = triple-negative breast cancer.
Note: The price reduction analyses were conducted deterministically.
aThe CADTH reanalysis weighted average was calculated using an 82.3% and 17.7% distribution of TNBC vs. HER2-negative, HR-positive disease as informed by the OlympiA trial.
Issues for Consideration
The treatment paradigm in patients with gBRCAm, HER2-negative, high-risk early breast cancer is quickly shifting. In particular, abemaciclib recently received a reimburse with conditions recommendation from CADTH for the adjuvant treatment of adult patients with HR-positive, HER2-negative early breast cancer at a high risk of disease recurrence based on clinicopathological features and a Ki-67 score of 20% or higher.15 Additionally, pembrolizumab received a reimburse with conditions recommendation from CADTH for the treatment of adult patients with early-stage TNBC in combination with chemotherapy as neoadjuvant treatment, and then continued as monotherapy as adjuvant treatment after surgery.24 Neither abemaciclib nor pembrolizumab was compared with olaparib in the sponsor’s economic model.
The clinical expert feedback obtained by CADTH noted there may be an increase in BRCA mutation testing with the availability of olaparib, as a confirmed gBRCA mutation is required to initiate olaparib treatment. In the scenario where BRCA testing was included, it was assumed that 6.6 patients would need to be tested to identify 1 patient with gBRCAm in the OlympiA ITT population. The unit cost of BRCA testing was $322.10.23 Note that these cost assumptions for gBRCA mutation testing are associated with uncertainty, as they were dependent on the prevalence of gBRCA in patients with TNBC and HER2-negative, HR-positive disease based on Winter et al.25 Changes to the prevalence rate may have a significant impact on the cost-effectiveness of adjuvant olaparib. From these scenarios, the inclusion of BRCA mutation tests based on the sponsor-provided assumptions had minimal impact on the ICERs in both the TNBC subgroup and the HER2-negative, HR-positive subgroup.
Overall Conclusions
The CADTH Clinical Review concluded that based on data from the OlympiA trial, adjuvant olaparib demonstrated a clinically meaningful and statistically significant benefit versus placebo for the treatment of gBRCAm, HER2-negative, high-risk early breast cancer for IDFS and OS. However, the median IDFS and OS were not estimable due to insufficient follow-up time, and the long-term efficacy of adjuvant olaparib is unknown. Further, since all results are based on interim analyses, there is the potential that the benefit of olaparib relative to placebo is overestimated; however, the presence and extent of any overestimation is uncertain. There remains uncertainty in the benefit of adjuvant olaparib in patients with HER2-negative, HR-positive disease due to the small patient population in the OlympiA trial (HR-positive represented 17.7% of the population). In the absence of direct comparative evidence, the CADTH Clinical Review team noted that given the estimates in the submitted ITC, no conclusions could be drawn about the comparative efficacy of adjuvant olaparib versus capecitabine for patients with TNBC with regard to IDFS, disease-free survival, or OS based on the submitted ITC due to methodological limitations and imprecision in the effect estimates.
Given the heterogeneity in patient hormone receptor status in the OlympiA trial and the differences in survival outcomes for the TNBC subgroup versus the HER2-negative, HR-positive subgroup, CADTH conducted separate analyses for the TNBC subgroup versus the HER2-negative, HR-positive subgroup and utilized subgroup-specific data to inform efficacy when available (i.e., to inform IDFS).
In the CADTH reanalyses, for the TNBC subgroup, the ICER was $43,599 per QALY (incremental costs = $74,660; incremental QALYs = 1.71) for olaparib compared with watch and wait; for the HER2-negative, HR-positive subgroup, the ICER was $157,407 per QALY (incremental costs = $84,098; incremental QALYs = 0.53). While no price reduction may be required in the TNBC population, a price reduction of 67% is required for adjuvant olaparib to be cost-effective compared with watch and wait in the HER2-negative, HR-positive subgroup at a WTP threshold of $50,000 per QALY. When considering the entire ITT population (calculated using the weighted average between the TNBC subgroup versus the HER2-negative, HR-positive subgroup informed by the proportion of patients present in the OlympiA trial), a price reduction of approximately 3% would be required to achieve cost-effectiveness at a WTP threshold of $50,000 per QALY. However, given the uncertainty in the efficacy data, further price reductions may be necessary to ensure the cost-effectiveness of adjuvant olaparib. This is especially true when considering the HER2-negative, HR-positive subgroup, as there were limitations in that subgroup data due to a small sample size within the OlympiA trial.
There remains uncertainty in the long term treatment effect of adjuvant olaparib for the treatment of patients with gBRCAm, HER2-negative, high-risk early breast cancer. The treatment landscape for gBRCAm, HER2-negative, high-risk early breast cancer is changing, as abemaciclib and pembrolizumab recently received reimburse with conditions recommendations from CADTH for the treatment of patients with HER2-negative, HR-positive breast cancer and TNBC, respectively. As such, the cost-effectiveness of adjuvant olaparib compared with these treatments is unknown. Finally, the clinical experts consulted by CADTH noted there may be an increase in BRCA mutation testing in Canada because of the introduction of adjuvant olaparib, given the requirement for the presence of a confirmed gBRCA mutation before initiation of olaparib treatment. While BRCA mutation testing was included in a scenario analysis and resulted in limited impact on the cost-effectiveness of olaparib, there remains uncertainty in the number of new tests needed to identify patients eligible for olaparib, which affects the level of certainty in the results of this scenario analysis.
References
1.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Lynparza (olaparib), 100 mg and 105 mg oral tablets. Mississauga (ON): AstraZeneca Canada Inc.; 2022 Aug 18.
2.Lynparza (olaparib): 100 mg and 105 mg oral tablets [product monograph]. Mississauga (ON): AstraZeneca Canada Inc.; 2022 Aug 18.
3.Clinical Study Report: D081CC00006 (BIG 6-13; NSABP B-55). A randomised, double-blind, parallel group, placebo-controlled multi-centre phase III study to assess the efficacy and safety of olaparib versus placebo as adjuvant treatment in patients with germline BRCA1/2 mutations and high risk HER2 negative primary breast cancer who have completed definitive local treatment and neoadjuvant or adjuvant chemotherapy [internal sponsor's report]. Gaithersburg (MD): AstraZeneca; 2021 Sep 03.
4.Robson M, Ruddy KJ, Im SA, et al. Patient-reported outcomes in patients with a germline BRCA mutation and HER2-negative metastatic breast cancer receiving olaparib versus chemotherapy in the OlympiAD trial. Eur J Cancer. 2019;120:20-30. PubMed
5.Robson ME, Tung N, Conte P, et al. OlympiAD final overall survival and tolerability results: Olaparib versus chemotherapy treatment of physician's choice in patients with a germline BRCA mutation and HER2-negative metastatic breast cancer. Ann Oncol. 2019;30(4):558-566. PubMed
6.Latimer NR. Survival analysis for economic evaluations alongside clinical trials--extrapolation with patient-level data: inconsistencies, limitations, and a practical guide. Med Decis Making. 2013;33(6):743-754. PubMed
7.Life Tables, Canada, Provinces and Territories 1980/1982 to 2018/2020 (three-year estimates), and 1980 to 2020 (single-year estimates). Ottawa (ON): Statistics Canada; 2022: https://www150.statcan.gc.ca/n1/pub/84-537-x/84-537-x2021001-eng.htm. Accessed 2022 Oct 11.
8.Mai PL, Chatterjee N, Hartge P, et al. Potential excess mortality in BRCA1/2 mutation carriers beyond breast, ovarian, prostate, and pancreatic cancers, and melanoma. PLoS One. 2009;4(3):e4812. PubMed
9.Collins JM, Nordstrom BL, McLaurin KK, et al. A Real-World Evidence Study of CDK4/6 Inhibitor Treatment Patterns and Outcomes in Metastatic Breast Cancer by Germline BRCA Mutation Status. Oncol Ther. 2021;9(2):575-589. PubMed
10.Table: 13-10-0114-01. Life expectancy and other elements of the life table, Canada, all provinces except Prince Edward Island. Ottawa (ON): Statistics Canada; 2022: https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310011401. Accessed 2022 Sep 28.
11.Lidgren M, Wilking N, Jönsson B, Rehnberg C. Health related quality of life in different states of breast cancer. Qual Life Res. 2007;16(6):1073-1081. PubMed
12.Torres S, Bayoumi A, Trudeau M, et al. Abstract P4-12-11: Eq-5d-5l utility scores for patients with breast cancer. Cancer Res. 2022;82(4_Supplement):P4-12-11.
13.Nafees B, Stafford M, Gavriel S, Bhalla S, Watkins J. Health state utilities for non small cell lung cancer. Health Qual Life Outcomes. 2008;6:84. PubMed
14.Lloyd A, Nafees B, Narewska J, Dewilde S, Watkins J. Health state utilities for metastatic breast cancer. Br J Cancer. 2006;95(6):683-690. PubMed
15.DeltaPA. Ottawa (ON): IQVIA; 2022: https://www.iqvia.com/. Accessed 2022 Sep 28.
16.Schedule of benefits for physician services under the Health Insurance Act: effective July 1, 2022. Toronto (ON): Ontario Ministry of Health; 2022: https://www.health.gov.on.ca/en/pro/programs/ohip/sob/physserv/sob_master.pdf. Accessed 2022 Oct 06.
17.Tam VC, Ko YJ, Mittmann N, et al. Cost-effectiveness of systemic therapies for metastatic pancreatic cancer. Curr Oncol. 2013;20(2):e90-e106. PubMed
18.Ontario Case Costing Initiative (OCCI). Toronto (ON): Ontario Health and Long-Term Care; 2017: https://data.ontario.ca/dataset/ontario-case-costing-initiative-occi. Accessed 2022 Oct 06.
19.Real world evidence study to assess incidence, treatment patterns, clinical outcomes, and healthcare resource utilization in early stage, gBRCAm, high-risk, HER2 negative breast cancer (HR+/HER2- BC and TNBC) in Alberta Canada. In: Drug Reimbursement Review sponsor submission: Lynparza (olaparib), 100 mg and 105 mg oral tablets [internal sponsor's package]. Mississauga (ON): AstraZeneca Canada Inc.; 2022 Aug 18.
20.de Oliveira C, Pataky R, Bremner KE, et al. Phase-specific and lifetime costs of cancer care in Ontario, Canada. BMC Cancer. 2016;16(1):809. PubMed
21.Beauchemin C, Letarte N, Mathurin K, Yelle L, Lachaine J. A global economic model to assess the cost-effectiveness of new treatments for advanced breast cancer in Canada. J Med Econ. 2016;19(6):619-629. PubMed
22.Guidelines for the economic evaluation of health technologies: Canada. 4th ed. Ottawa (ON): CADTH; 2017: https://www.cadth.ca/guidelines-economic-evaluation-health-technologies-canada-4th-edition. Accessed 2022 Sep 01.
23.BRCAinBC. Paid Testing Options. 2022; https://www.BRCAinbc.ca/private-testing-options/. Accessed 2022 Oct 21.
24.pan-Canadian Oncology Drug Review Committee (pERC) final recommendation: pembrolizumab (Keytruda). Can J Health Technol. 2022;2(9). 10.51731/cjht.2022.448. Accessed 2022 Oct 18.
25.Winter C, Nilsson MP, Olsson E, et al. Targeted sequencing of BRCA1 and BRCA2 across a large unselected breast cancer cohort suggests that one-third of mutations are somatic. Ann Oncol. 2016;27(8):1532-1538. PubMed
26.Ontario Ministry of Health, Ontario Ministry of Long-Term Care. Ontario drug benefit formulary/comparative drug index. 2022; https://www.formulary.health.gov.on.ca/formulary/. Accessed 2022 Sep 28.
27.pan-Canadian Oncology Drug Review Committee (pERC) final recommendation: abemaciclib (Verzenio). Can J Health Technol. 2022;2(10). 10.51731/cjht.2022.475. Accessed 2022 Oct 18.
28.Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Lynparza (olaparib), 100 mg and 105 mg oral tablets. Mississauga (ON): AstraZeneca Canada Inc.; 2022 Aug 18.
29.Lluch A, Barrios CH, Torrecillas L, et al. Phase III trial of adjuvant capecitabine after standard neo-/adjuvant chemotherapy in patients with early triple-negative breast cancer (GEICAM/2003-11_CIBOMA/2004-01). J Clin Oncol. 2020;38(3):203-213. PubMed
Appendix 1: Cost Comparison Table
Note that this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical expert(s) and drug plans. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 8: CADTH Cost Comparison Table for the Adjuvant Treatment of HER2-Negative, Early Breast Cancer With Confirmed gBRCA Mutation
Treatment | Strength | Form | Price ($) | Recommended dosage | Average daily cost ($) | Average 28-day cycle cost ($) |
|---|---|---|---|---|---|---|
Olaparib (Lynparza) | 150 mg | Tablet | 66.6173a | 300 mg, | 266.47 | 7,461 |
Capecitabine monotherapy | ||||||
Capecitabine (Generic) | 150 mg 500 mg | Tablet | 0.4575b 1.5250b | 1,250 mg/m2, twice daily (2 × 150 mg, b.i.d.; 4 × 500 mg, bid) | 14.03 | 196c |
Endocrine therapy | ||||||
Anastrozole (Generic) | 1 mg | Tablet | 0.9522b | 1 mg, daily | 0.95 | 27 |
Letrozole (Generic) | 2.5 mg | Tablet | 1.3780b | 2.5 mg, daily | 1.38 | 39 |
Tamoxifen (Generic) | 10 mg 20 mg | Tablet | 0.1750b 0.3500b | 20 mg daily in single or divided doses to 40 mg daily in divided doses | 0.35 to 0.70 | 10 to 20 |
Abemaciclibd + endocrine therapy | ||||||
Abemaciclib (Verzenio) | 150 mg | Tablet | 98.4714e | 150 mg, twice daily | 196.94 | 5,514 |
+ Anastrozole | 197.90 | 5,541 | ||||
+ Letrozole | 198.32 | 5,553 | ||||
+ Tamoxifen (20 mg daily) | 197.29 | 5,524 | ||||
+ Tamoxifen (40 mg daily) | 197.64 | 5,534 | ||||
Pembrolizumab (adjuvant)f | ||||||
Pembrolizumab (Keytruda) | 100 mg/4mL | IV Infusion | 4,400.0000e | 200 mg every 3 weeks or 400 mg, every 6 weeks. | 419.05 | 11,733 |
b.i.d. = 2 times a day; HER2 = human epidermal growth factor receptor 2; HR-positive = hormone receptor–positive; TNBC = triple-negative breast cancer.
Prices do not include dispensing fees or markups. Costs assume a body weight of 75 kg or a body surface area of 1.8 m2 and include wastage of unused medication in vials.
aSponsor’s submitted price.1
bOntario Drug Benefit Formulary list price (accessed September 2022)26
cCapecitabine is only given for a single 14-Day regimen.
dAbemaciclib restricted to the HR-positive, HER2-negative subgroup.
ePrice obtained from prior CADTH reviews: pembrolizumab,24 abemaciclib.27
fPembrolizumab restricted to the TNBC subgroup.
Appendix 2: Submission Quality
Note that this appendix has not been copy-edited.
Description | Yes/No | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | Yes | No comment. |
Model has been adequately programmed and has sufficient face validity | Yes | No comment. |
Model structure is adequate for decision problem | No | Refer to CADTH critical appraisal. |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | No | CADTH identified errors relating to how data were incorporated into the model. An example is the toggle located on the < Settings > sheet that failed to allow users to accurately toggle between different selections for the utility source. |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | Yes | No comment. |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | No | CADTH identified discrepancies in the inputs reported between the sponsor’s economic model/ report, and source. For example, in the sponsor’s economic report, it was noted that the cost of leukopenia was informed by “Beauchemin et al. Assumed same as neutropenia” while the model only reported the leukopenia cost was “Assumed the same as neutropenia.” Furthermore, the sponsor-submitted model clarified that CMG code used to inform the neutropenia cost was 633 which is associated with agranulocytosis that has a reported 2018 cost of $6,984, which when inflated does not align with the sponsor used $7,180.99. |
Appendix 3: Additional Information on the Submitted Economic Evaluation
Note that this appendix has not been copy-edited.
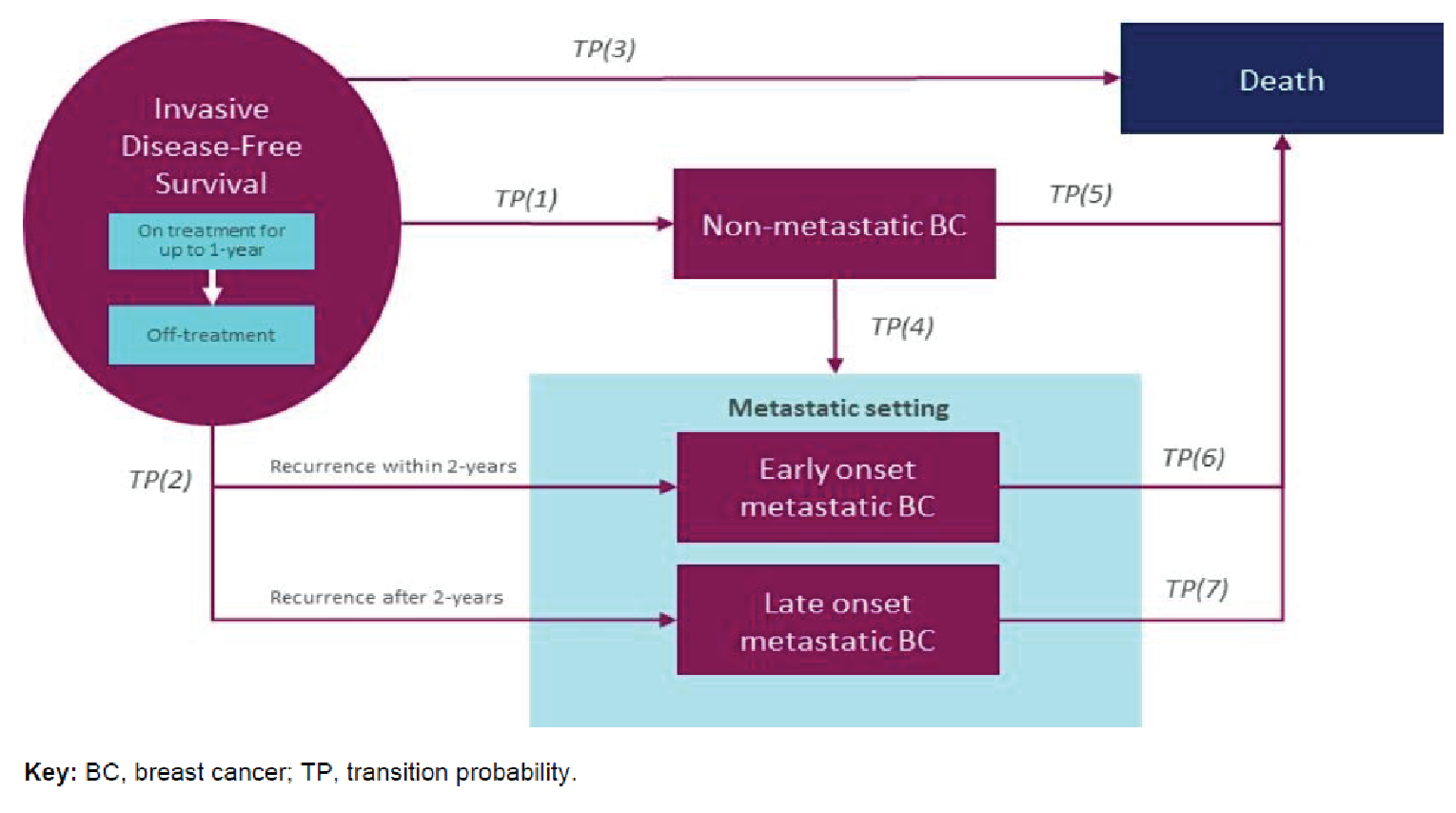
Table 10: Parametric Selections for Transition Probabilities in the Sponsor’s Base Case
Parameter | Parametric distribution selected | Source |
|---|---|---|
TP1 and TP2: IDFS to Disease Recurrence | Log-normal | OlympiA |
TP3: IDFS to Death | General-population mortality + standard mortality rate (based on gBRCAm) | Canadian life tables/ Mai et al., 20098 |
TP4: Non-mBC to mBC | Log-normal | OlympiA, pooled data from both treatments were used due to the low number of events |
TP5: Non-mBC to death | Exponential / Background mortality | OlympiA / Canadian life tables + SMR applied |
TP6: Early onset mBC to deatha | Exponential | OlympiA |
TP7: Late onset mBC to deathb | Log-normal | OlympiAD |
gBRCA = germline BRCA–mutated; IDFS = invasive disease–free survival; mBC = metastatic breast cancer; SMR = standardized mortality ratio; TP = transition probability.
aPatients progressing to mBC within 2 years of initiation with adjuvant therapy.
bPatients progression to mBC after 2 years of initiation with adjuvant therapy.
Source: Sponsor’s pharmacoeconomic submission.1
Detailed Results of the Sponsor’s Base Case
Table 11: Disaggregated Summary of Sponsor’s Economic Evaluation Results
Parameter | Olaparib | Watch and Wait | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 24.37 | 22.33 | 2.04 |
IDFS | 23.86 | 21.53 | 2.33 |
Non-mBC | 0.23 | 0.34 | −0.11 |
Early onset mBC | 0.08 | 0.22 | −0.14 |
Late onset mBC | 0.19 | 0.23 | −0.03 |
Discounted QALYs | |||
Total | 19.34 | 17.70 | 1.64 |
IDFS | 18.98 | 17.14 | 1.85 |
Non-mBC | 0.18 | 0.26 | −0.08 |
Early onset mBC | 0.05 | 0.15 | −0.10 |
Late onset mBC | 0.13 | 0.15 | −0.02 |
AEs | 0.00 | 0.00 | 0.00 |
Discounted costs ($) | |||
IDFS | |||
Treatment acquisition costs | $80,595.71 | $0.00 | $80,595.71 |
Treatment administration costs | $0.00 | $0.00 | $0.00 |
Monitoring costs | $39.55 | $0.00 | $39.55 |
Endocrine therapy costs | $201.11 | $185.89 | $15.22 |
Disease management costs: Y1 | $6,949.20 | $6,676.64 | $272.56 |
Disease management costs: Y2 to 5 | $14,034.63 | $12,806.55 | $1,228.08 |
Disease management costs: Y5+ | $1,255.61 | $1,127.12 | $128.49 |
Testing costs | $0.00 | $0.00 | $0.00 |
AE costs | $1,154.18 | $110.22 | $1,043.96 |
Non-mBC | |||
Treatment acquisition costs | $179.42 | $257.54 | -$78.12 |
Surgery costs | $12.20 | $17.36 | -$5.16 |
Treatment admin and monitoring costs | $30.30 | $43.41 | -$13.12 |
Disease management costs | $1,680.50 | $2,464.49 | -$783.99 |
Early onset mBC | |||
Treatment acquisition costs | $2,250.19 | $3,967.69 | -$1,717.50 |
Surgery costs | $23.82 | $45.20 | -$21.38 |
Treatment admin and monitoring costs | $207.71 | $351.50 | -$143.79 |
Disease management costs | $821.94 | $2,308.03 | -$1,486.08 |
Late onset mBC | |||
Treatment acquisition costs | $2,836.44 | $3,338.69 | -$502.25 |
Surgery costs | $31.28 | $36.72 | -$5.45 |
Treatment admin and monitoring costs | $246.63 | $290.45 | -$43.82 |
Disease management costs | $1,998.12 | $2,352.96 | -$354.83 |
Death | |||
Terminal care costs | $9,659.88 | $13,621.53 | -$3,961.66 |
ICER ($/QALY) | $45,237 | ||
AE = adverse event; ICER = incremental cost-effectiveness ratio; IDFS = invasive disease–free survival; LY = life-year; mBC = metastatic breast cancer; QALY = quality-adjusted life-year.
Source: Sponsor’s pharmacoeconomic submission.1
Appendix 4: Additional Details on the CADTH Reanalyses and Sensitivity Analyses of the Economic Evaluation
Note that this appendix has not been copy-edited.
Detailed Results of CADTH Base Case
Table 12: Disaggregated Summary of CADTH’s Economic Evaluation Results (TNBC Population)
Parameter | Olaparib | Watch and wait | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 24.49 | 22.36 | 2.14 |
IDFS | 24.02 | 21.60 | 2.42 |
Non-mBC | 0.23 | 0.33 | −0.10 |
Early onset mBC | 0.08 | 0.23 | −0.15 |
Late onset mBC | 0.16 | 0.20 | −0.03 |
Discounted QALYs | |||
Total | 19.42 | 17.71 | 1.71 |
IDFS | 19.08 | 17.17 | 1.91 |
Non-mBC | 0.18 | 0.25 | −0.08 |
Early onset mBC | 0.05 | 0.15 | −0.10 |
Late onset mBC | 0.11 | 0.13 | −0.02 |
AEs | 0.00 | 0.00 | 0.00 |
Discounted costs ($) | |||
IDFS | |||
Treatment acquisition costs | $80,199.30 | $0.00 | $80,199.30 |
Treatment administration costs | $0.00 | $0.00 | $0.00 |
Monitoring costs | $39.35 | $0.00 | $39.35 |
Endocrine therapy costs | $0.00 | $0.00 | $0.00 |
Disease management costs: Y1 | $6,950.72 | $6,668.02 | $282.70 |
Disease management costs: Y2 to 5 | $14,107.15 | $12,843.13 | $1,264.02 |
Disease management costs: Y5+ | $1,266.32 | $1,132.73 | $133.59 |
Testing costs | $0.00 | $0.00 | $0.00 |
AE costs | $1,153.39 | $108.96 | $1,044.43 |
Non-mBC | |||
Treatment acquisition costs | $201.06 | $291.94 | -$90.88 |
Surgery costs | $11.84 | $17.20 | -$5.36 |
Treatment admin and monitoring costs | $34.62 | $50.21 | -$15.59 |
Disease management costs | $1,675.59 | $2,396.21 | -$720.61 |
Early onset mBC | |||
Treatment acquisition costs | $1,141.06 | $2,098.36 | -$957.30 |
Surgery costs | $23.87 | $45.37 | -$21.50 |
Treatment admin and monitoring costs | $240.54 | $407.91 | -$167.38 |
Disease management costs | $827.96 | $2,327.52 | -$1,499.56 |
Late onset mBC | |||
Treatment acquisition costs | $1,403.52 | $1,700.02 | -$296.51 |
Surgery costs | $29.53 | $35.59 | -$6.06 |
Treatment admin and monitoring costs | $266.39 | $322.22 | -$55.83 |
Disease management costs | $1,692.81 | $2,041.98 | -$349.17 |
Death | |||
Terminal care costs | $9,371.54 | $13,489.93 | -$4,118.39 |
ICER ($/QALY) | $43,599 | ||
AE = adverse event; ICER = incremental cost-effectiveness ratio; IDFS = invasive disease–free survival; LY = life-year; mBC = metastatic breast cancer; QALY = quality-adjusted life-year.
Table 13: Disaggregated Summary of CADTH’s Economic Evaluation Results (HR-Positive Population)
Parameter | Olaparib | Watch and wait | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 17.64 | 17.00 | 0.63 |
IDFS | 15.49 | 14.85 | 0.64 |
Non-mBC | 0.71 | 0.71 | 0.00 |
Early onset mBC | 0.08 | 0.21 | −0.13 |
Late onset mBC | 1.36 | 1.23 | 0.13 |
Discounted QALYs | |||
Total | 14.04 | 13.50 | 0.53 |
IDFS | 12.60 | 12.06 | 0.55 |
Non-mBC | 0.51 | 0.52 | 0.00 |
Early onset mBC | 0.05 | 0.14 | −0.09 |
Late onset mBC | 0.87 | 0.79 | 0.08 |
AEs | 0.00 | 0.00 | 0.00 |
Discounted costs ($) | |||
IDFS | |||
Treatment acquisition costs | $82,168.73 | $0.00 | $82,168.73 |
Treatment administration costs | $0.00 | $0.00 | $0.00 |
Monitoring costs | $40.32 | $0.00 | $40.32 |
Endocrine therapy costs | $1,097.85 | $1,028.87 | $68.98 |
Disease management costs: Y1 | $7,033.07 | $6,833.30 | $199.78 |
Disease management costs: Y2 to 5 | $13,866.29 | $12,838.47 | $1,027.82 |
Disease management costs: Y5+ | $721.81 | $698.46 | $23.35 |
Testing costs | $0.00 | $0.00 | $0.00 |
AE costs | $1,155.36 | $110.42 | $1,044.94 |
Non-mBC | |||
Treatment acquisition costs | $164.78 | $162.12 | $2.66 |
Surgery costs | $37.24 | $37.12 | $0.12 |
Treatment admin and monitoring costs | $17.46 | $17.03 | $0.43 |
Disease management costs | $5,109.42 | $5,110.52 | -$1.10 |
Early onset mBC | |||
Treatment acquisition costs | $4,904.58 | $8,043.45 | -$3,138.87 |
Surgery costs | $22.99 | $41.94 | -$18.95 |
Treatment admin and monitoring costs | $96.38 | $158.04 | -$61.66 |
Disease management costs | $794.62 | $2,142.08 | -$1,347.46 |
Late onset mBC | |||
Treatment acquisition costs | $29,454.19 | $26,551.04 | $2,903.14 |
Surgery costs | $147.67 | $132.70 | $14.97 |
Treatment admin and monitoring costs | $566.14 | $507.50 | $58.64 |
Disease management costs | $13,987.47 | $12,635.96 | $1,351.51 |
Death | |||
Terminal care costs | $28,873.01 | $29,112.12 | -$239.11 |
ICER ($/QALY) | $157,407 | ||
AE = adverse event, ICER = incremental cost-effectiveness ratio, IDFS = invasive disease–free survival, LY = life-year, mBC = metastatic breast cancer, QALY = quality-adjusted life-year.
Scenario Analyses
Table 14: Summary of CADTH’s Economic Evaluation Results — Scenario Analyses
Scenario analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALY) |
|---|---|---|---|---|
TNBC subgroup | ||||
CADTH base case | Watch and Wait | $45,930 | 17.62 | Ref. |
Olaparib | $120,590 | 19.31 | $44,097 | |
Scenario Analysis 1: Adjusted Subsequent Therapies (i.e., 10% surgery in the mBC setting, include 30% paclitaxel use in the non-mBC setting) | Watch and Wait | $45,839 | 17.62 | Ref. |
Olaparib | $120,527 | 19.31 | $44,114 | |
Scenario Analysis 2: Include BRCA mutation testing costs | Watch and Wait | $45,930 | 17.62 | Ref. |
Olaparib | $122,484 | 19.31 | $45,216 | |
HR-positive subgroup | ||||
CADTH base case* | Watch and Wait | $131,159 | 13.52 | Ref. |
Olaparib | $214,763 | 14.10 | $145,016 | |
Scenario Analysis 1: Adjusted Subsequent Therapies (i.e., 10% surgery in the mBC setting) | Watch and Wait | $131,097 | 13.52 | Ref. |
Olaparib | $214,702 | 14.10 | $145,018 | |
Scenario Analysis 2: Include BRCA mutation testing costs | Watch and Wait | $131,159 | 13.52 | Ref. |
Olaparib | $220,132 | 14.10 | $154,328 | |
BRCA = breast cancer susceptibility gene, ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; RDI = relative dose intensity.
Note all analyses presented in this table were conducted deterministically.
Appendix 5: Submitted Budget Impact Analysis and CADTH Appraisal
Note that this appendix has not been copy-edited.
Table 15: Summary of Key Takeaways
Key takeaways of the budget impact analysis |
|---|
|
Summary of Sponsor’s Budget Impact Analysis
The submitted budget impact analysis (BIA) evaluated the introduction of olaparib for the adjuvant treatment of early HER2-negative breast cancer. The population for this BIA was restricted to adult patients with deleterious or suspected deleterious gBRCA mutation, HER2-negative status who have received neo or adjuvant chemotherapy. Estimates were generated from the perspective of individual drug plans participating in the CADTH process and the results were aggregated into pan-Canadian totals over a 3-year time horizon. An epidemiological approach was used to estimate the eligible population size for each participating plan. Key inputs to the BIA are documented in Table 16.
In the reference scenario, the sponsor assumed that olaparib would not be funded to treat the specified indication for the target population. Patients in the HR-positive, HER2-negative subgroup were eligible to receive Best-Supportive Care (BSC), whereas those in the TNBC could receive BSC or Capecitabine. BSC was defined as watch and wait following neo or adjuvant chemotherapy. In the new drug scenario, it was assumed that olaparib would displace market share from both treatments available in the reference scenario. Lastly, it was assumed that endocrine therapy was made available to patients in both scenarios. However, it was excluded from the BIA as olaparib is not meant to serve as a substitute for endocrine therapy.
In recognition of the genetic testing requirement to initiate olaparib treatment, the sponsor reported a second BIA which examined the impact of expanded access to genetic testing. The reference scenario for this secondary BIA was assumed to represent current testing standards. The sponsor assumed ~█% of patients undergoing neo or adjuvant chemotherapy would be eligible and undergo gBRCAm testing at present. Meanwhile, the new scenario represented an expansion of testing eligibility. The sponsor assumed that ~█%, ~█%, and ~█% of the same patients would receive gBRCAm testing in years 1 to 3.
Key assumptions:
In defining the target population, the sponsor assumed that approximately 7% of patients who receive (neo)adjuvant chemotherapy will be gBRCAm-positive.25
In the primary BIA, the sponsor assumed that olaparib coverage will be accompanied by a decision to expand access to genetic testing.
In the primary BIA, the sponsor assumed a 100% detection rate for gBRCA mutations. In other words, any patient with a gBRCA mutation who is tested will be detected.
In the base case of the primary BIA, the sponsor assumed that olaparib’s market share in years 1 to 3 would be ~█%, ~█%, and ~█%. Optimistic and pessimistic scenarios were considered where these values were subject to an adjustment of ± 25%.
In the base case of the primary BIA, costs were calculated without consideration of mark-up and dispensation fees. This was addressed in separate scenario analyses. Dosing followed the guidance specified in the respective product monographs. Duration on each treatment was assumed to be the median value form the OlympiA28 (olaparib: 11.1 months) and CIBOMA29 (capecitabine: 5.5 months) trials.
Table 16: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as year 1 / year 2 / year 3 if appropriate) |
|---|---|
Target population | |
Pan-Canadian population (excluding Quebec) | 24,028,895 |
Annual incidence of breast cancer | 21,369 (0.09%) |
Cases at stages I to III at diagnosis | 20,233 (95%) |
Stage I to III cases that are HER2-negative | 15,792 (78%) |
HER2-negative patients receiving surgery | 15,174 (96%) |
Receiving (neo)adjuvant chemotherapy | 12,553 (83%) |
gBRCAm-positive | 933 (7%) |
Considered to be high risk | 579 (62%) |
Eligible for public coverage | 365 (63%) |
Growth rate | 376 (1.4%) |
Patient identification | Year 1 / year 2 / year 3 |
Number of patients eligible for drug under reviewa | 209.5 / 251.2 / 274.4 |
gBRCAm testing parameters | |
Testing rate (current) | ███% / ███% / ███% |
Testing rate (proposed) | ███% / ███% / ███% |
Detection rate | 100% |
Market uptake (3 years) | |
Uptake (reference scenario) Olaparib Best supportive care Capecitabine | 0% / 0% / 0% ███% / ███% / ███% ███% / ███% / ███% |
Uptake (new drug scenario) Olaparib Best supportive care Capecitabine | ███% / ███% / ███% ███% / ███% / ███% ███% / ███% / ███% |
Cost of treatment (per patient) | |
Cost of treatment over: 1 year | |
Olaparib | $90,067 |
Best supportive care | $0.00 |
Capecitabine | $1,196 |
HER2-negative = Human Epidermal Growth Factor Receptor 2 – negative biomarker status; gBRCAm = germline BRCA mutation.
aEligible patients identified after consideration of proposed gBRCAm testing and detection rates
Summary of the Sponsor’s BIA Results
In the base case of the primary BIA, the net-budget impact of olaparib was estimated to be $11,305,410 in year 1, $15,812,426 in year 2, and $17,274,463 in year 3. The 3-year net-budget impact of olaparib was $44,392,299, Table 17. The budget impact specific to the TNBC and HR-positive, HER2-negative subgroups was not estimated in the sponsor BIA. The impact of distinct assumptions were explored through the use of scenario analyses. First, optimistic (+ 25%) and pessimistic (−25%) adjustments were made to the market share assumption. This yielded a 3-year net-budget impact of $55,490,374 (optimistic) and $33,294,224 (pessimistic). Second, increased (+ 10%) and decreased (−10%) incidence of breast cancer returned a 3-year net-budget impact of $48,831,529 (+ 10%) and $39,953,069. Lastly, the inclusion of mark-up and dispensation fees resulted in a 3-year net-budget impact of $46,563,537.
In the secondary BIA, the net-budget impact of expanding access to genetic testing was estimated to be $832,352 in year 1, $1,266,688 in year 2, and $1,499,322 in year 3. The 3-year net-budget impact of expanded genetic testing was $3,598,362. No scenario analyses were considered for this secondary BIA.
Table 17: Detailed Breakdown of the BIA
Stepped analysis | Scenario | Year 0 (current situation) | Year 1 | Year 2 | Year 3 | Three-year total |
|---|---|---|---|---|---|---|
Submitted base case | Reference | $18,859 | $30,063 | $36,041 | $39,373 | $105,477 |
New drug | $18,859 | $11,335,473 | $15,848,467 | $17,313,836 | $44,497,776 | |
Budget impact | $0 | $11,305,410 | $15,812,426 | $17,274,463 | $44,392,299 |
CADTH Appraisal of the Sponsor’s BIA
CADTH identified the following key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
Generalizability of the estimates used to identify the population with gBRCA mutations. In defining the target population, the sponsor assumed that approximately 7% of patients who received (neo)adjuvant chemotherapy will be gBRCAm-positive. This estimate was calculated as a weighted average of the gBRCAm prevalence in the TNBC (17%) and HR-positive, HER2-negative (6%) subgroups. These 2 inputs were calculated from data reported in a supplemental Table from Winter et al.,25 which included a sample of Swedish patients. It is uncertain if these inputs are generalizable to the Canadian population, however, the clinical experts consulted by CADTH for this review noted that in the absence of literature specific to the Canadian population, the estimate used by the sponsor was not unreasonable.
No change made to the sponsor’s base case.
Uncertainty in current and anticipated gBRCAm testing rates. The sponsor’s BIA submission specified 2 distinct sets of assumptions relating to gBRCAm testing rates to reflect current standards (“current”) and a proposed expansion of testing due to the availability of olaparib (“proposed”). Under current standards, ~█% of patients were assumed to undergo gBRCA testing, while the proposed expansion considered testing rates of ~█%, ~█%, and ~█% in years 1 to 3. Both values were based on internal estimates derived from clinical expert input obtained by the sponsor. The sponsor’s primary budget impact model only considered the sponsor’s “proposed” testing rates. While drug plan input indicated an expansion of access to testing was likely with the availability of olaparib, clinical expert input obtained by CADTH noted that both the current and proposed testing rates were likely overestimated as they did not align with current and anticipated clinical practice. There is therefore uncertainty in the size of the estimated target population. The sponsor’s assumptions likely resulted in the overestimation of olaparib’s budget impact; however, more robust estimates of the current and anticipated testing rates could not be obtained.
No change made to the sponsor’s base case.
Concerns with market share assumptions. Two issues were identified with the anticipated uptake of olaparib. Under the assumption that the only other drug available would be capecitabine for certain patients with TNBC, the anticipated uptake of olaparib was assumed to be ~█% in year 1 and rising to ~█% in years 2 and 3. This was thought to be underestimated by the clinical experts consulted by CADTH, who indicated olaparib would be prescribed to nearly all patients should there be no other available therapies for early high-risk, HER2-negative breast cancer. CADTH notes that increases in the anticipated market uptake of olaparib in the sponsor’s submitted analyses results in significant changes to the 3-year budget impact.
Additionally, both abemaciclib27 and pembrolizumab24 have recently received positive listing recommendations from pERC. The listing of either product will result in new comparators which will compete with olaparib for market share. While the exclusion of these alternatives was appropriate for this submission, their potential availability may have a significant effect on the budget impact of olaparib.
No change made to the sponsor’s base case.
CADTH Reanalyses of the BIA
In the absence of more reliable estimates to inform the key parameters associated with uncertainty, the sponsor’s submitted base case was maintained. CADTH expects that the budget impact of olaparib will change with the availability of new information. Such changes may be most pronounced as a result of Canadian-specific gBRCAm prevalence estimates, testing rates reflective of current standards, and the availability of abemaciclib and pembrolizumab for the treatment of HER2-negative early breast cancer.
Stakeholder Input
Patient Input
Canadian Breast Cancer Network
About the Canadian Breast Cancer Network
The Canadian Breast Cancer Network (CBCN) is a leading, patient-directed, national health charity committed to ensuring the best quality of care for all Canadians affected by breast cancer through the promotion of information, education, and advocacy activities. www.cbcn.ca
As a member of the Canadian Cancer Action Network, the Canadian Breast Cancer Network is committed to adhering to the Code of Conduct Governing Corporate Funding.
Information Gathering
Information for this submission was collected via: CBCN’s 2017 Lived Experience Breast Cancer Patient Survey
An online survey was distributed in English and French to patients living with breast cancer. No patients surveyed had direct experience with the treatment under review. Survey questions comprised of a combination of scoring options and free form commentary. Patients were contacted through the membership databases of CBCN and other patient organizations.
Patient Respondents Profile
In this submission, CBCN specifically utilizes the data provided by the 6 patients from the survey who identified as being diagnosed with germline BRCA-mutated (gBRCAm), human epidermal growth factor receptor 2 (HER2)-negative high risk early breast cancer.
The majority of these respondents were from Ontario (2) and Manitoba (2). The rest of the respondents were from Alberta (1), All participants identified as female. All participants identified English as their first language. Most participants identified themselves as Caucasian, and two specified Jewish ancestry.
Most of the respondents were first diagnosed with breast cancer when they were between the ages of 40 and 49 (5). 1 participant was diagnosed when they were between 30-39 years old.
5 participants reported that they were in a relationship, 1 did not disclose their relationship status. All of the respondents had children at the time of their diagnosis. At the time of their diagnosis, participants reported having a child or children that were between the ages of 0-1 (2), 2-5 (1),6 -12 (4), and 13-19 (1).
Printed sources: A review was conducted of current studies and grey literature to identify issues and experiences that are commonly shared among many women living with breast cancer.
Disease Experience
Approximately 3-5% of patients with breast cancer carry germline BRCA1 or BRCA2 pathogenic mutations. These variants are more likely to be detected in patients with a strong family history of breast cancer, who are younger, have breast and ovarian cancer, or are from ethnic groups associated with founder origin mutations. These patients often present with high tumour grades, face greater CNS metastases risk, and more contralateral or ipsilateral disease resulting in more aggressive cancers overall. BRCA-mutations are also associated with an increased risk of cancer. BRCA mutation carriers have a sixty-nine percent risk of developing cancer versus the 12.4 percent cancer risk in the general population. While the lifetime risk of breast cancer is about 12% for women overall, for women with BRCA mutations, it’s 72%.
Patients with a BRCA1 pathogenic variant have a particular predisposition to breast cancer that is triple negative (i.e., negative for human epidermal growth factor receptor 2 [HER2] and estrogen and progesterone receptors). Whereas estrogen-receptor–positive tumors often develop in patients with a BRCA2 pathogenic variant. Germline testing for such variants in Canada is currently performed selectively in patients with breast cancer. Until now, systemic therapy for patients with early-stage breast cancer has not differed on the basis of the presence of an underlying germline BRCA1 and/or BRCA2 mutation.
High risk patients with a BRCA1/2 germline mutation often present at a young age. BRCA1/2 mutation carriers face more aggressive surgical interventions for therapeutic and risk reducing purposes due to their high risk of developing breast cancer.
Selecting the best surgical approach for these patients requires consideration of several factors, including patient’s genetic risk, their family history, previous breast cancer biology, as well as patient’s own preferences.
Women who have a mutation in BRCA1 or BRCA2 and are treated with breast-conserving therapy not only face a high risk of local recurrence, but also a high risk of developing breast cancer in the other breast as well. Studies reveal that recurrence of breast cancer occurs in 20-30 percent of patients with HER2 negative, germline BRCA mutations.
The Goals of Current Therapy
The goals of treatment for patients with germline, BRCA1 or BRCA 2 mutations are eradicating disease and preserving normal breast tissue. This is typically achieved through a combination of surgical and radiation therapy. Often double mastectomy is recommended for all patients with these mutations.
In our 2017 survey, respondents indicated treatments they received. Sixty-six percent of respondents with inherited BRCA mutations, indicated that they had received chemotherapy and 33% received radiation therapy.
Since many breast cancer patients do not meet common germline BRCA testing criteria, these patients may miss the opportunity to benefit from systemic targeted treatment, such as PARP inhibition. Provincial eligibility criteria for genetic testing varies greatly across Canada and currently testing for both high-risk and other breast cancer patients is not routinely implemented.
Key Factors for Decision-Making Around Treatment
Early-stage, germline BRCA, HER2-negtive breast cancer patients in our 2017 Survey discussed the importance of the following factors in influencing their decision-making around treatments:
Effectiveness of the treatment – how well the treatment stabilized their disease and delayed recurrence of their disease.
Prolonging life without sacrificing quality of life – being able to maintain productive, active lives with minimal disruption to daily routines.
Side effect management – minimizing risk while stabilizing their disease.
Cost and accessibility of treatments – affordability and ease of accessing treatments.
Treatment efficacy: One hundred percent of early-stage, germline BRCA carrier patients ranked reducing the risk of cancer recurrence as the most important factor when making decisions about treatment. Additionally, respondents talked about the importance of treatment efficacy in decision-making. Fifty percent ranked it as very important, and 50 percent stated it was important.
Patients also spoke on the importance of treatment effectiveness in their decision-making anecdotally:
“I don’t want to have to go through this again. That’s the most important to me.” — Patient respondent
“Originally my treatments were not presented as options. I would have liked to know I had a choice beforehand.” — Patient respondent
“Life expectancy and survival are the most important for me.” — Patient respondent
Quality of life: Quality of life was routinely cited by patients as an important factor in making treatment decisions. In our 2017 Survey, quality of life was rated as important by 34% of germline BRCA mutated, HER2 negative patients and very important by 66% of germline BRCA mutated, HER2 negative patients. More specifically, patients reported on the importance of minimal side effects, mobility, and productivity when making decisions regarding treatment options. Among germline BRCA, HER2 negative patients in our 2017 Survey:
Minimal side effects were rated as important by 50% of patients and somewhat important by 16% patients.
Productivity was rated as very important by 16% of patients, and somewhat important by 33% of patients,
Mobility was rated as important by 33% of patients and very important by 16% patients.
These concerns were shared among the respondents in our 2017 Survey:
“I wanted to know the success rates for the treatment type, and to have the ability to talk to other patients using the same treatment and their experiences.” — Patient respondent
The financial burden of treating and managing breast cancer: The financial burden associated with living with breast cancer extends far beyond any loss of income during a temporary or permanent absence from employment. In addition to the loss of income during illness, breast cancer patients can incur substantial costs associated with treatment and disease management. Research on the financial impact of breast cancer on patients identified the following (Janet Dunbrack, Breast Cancer: Economic Impact and Labour Force Re-entry. Canadian Breast Cancer Network, 2010).
80% of breast cancer patients report a financial impact due to their illness
44% of patients have used their savings, and 27% have taken on debt to cover costs.
Improved Outcomes
For germline, BRCA mutated, HER2-negative patients, reducing the risk of recurrence is of key concern. Patients have an expectation that Olaparib (Lynparza) will reduce the rate of life-threatening recurrence and cancer spread. As the phase 3 OlympiA trial demonstrated olaparib elicited a statistically significant and clinically meaningful improvement in invasive disease-free survival (iDFS) vs placebo, reducing the risk of invasive recurrences, new cancers, or death by 42%. Furthermore, Patients treated with olaparib also achieved a benefit in overall survival (OS) compared with placebo, with a 32% reduced risk of death.
Additional findings from the study showed 3-year invasive disease-free survival of 85.9% and 77.1% in the olaparib and place the group receiving standard therapies followed by placebo. Three-year DDFS rates were 87.5% and 80.4% in the olaparib and placebo groups, respectively.
The OlympiA trial showed that 1 year of adjuvant olaparib can meaningfully reduce recurrence risk and prevent progression to metastatic disease among patients with high-risk early breast cancer and germline BRCA1 or BRCA2 pathogenic or likely pathogenic variants, with high adherence rates and primarily a low-grade toxicity profile. Patients with these variants are increasingly identified in patients with early breast cancer as a result of greater acceptance of the influence of germline BRCA1 or BRCA2 pathogenic or likely pathogenic variant status on treatment choices.
Adverse Effects
Regarding safety, the most common any-grade adverse effects (AEs) in the olaparib arm were nausea (57%), fatigue (42%), anemia (24%), vomiting (23%), headache (20%), diarrhea (18%), leukopenia (17%), neutropenia (16%), decreased appetite (13%), dysgeusia (12%), dizziness (11%) and stomatitis (10%). Approximately 10% of patients in the olaparib arm discontinued treatment due to AEs. The most common grade 3 or higher AEs included anemia (9%), neutropenia (5%), leukopenia (3%) and fatigue (1.8%).
Overall, OlympiA shows that olaparib is tolerable and has a manageable toxicity profile.
Impact of Treatment Options to Patients
By significantly improving disease-free survival, overall survival and reducing the risk of recurrence olaparib can relieve cancer-related symptoms and improve a patient’s quality of life. Results from the OlympiA trial are important because they show that adding parp inhibition to surgical, chemotherapy and radiation significantly benefits patients with early-stage disease
Results from this study show strong support for olaparib to become a practice-changing therapy for patients with germline, BRCA mutated breast cancers who currently do not have many therapeutic options available to them that significantly reduces their risk of recurrence and management of highly aggressive disease.
When living with no or with minimal cancer-related symptoms, and with minimal side effects from treatment, patients are able to reduce the impact of cancer on their ability to care for children and dependents, continue with their employment and earn income, spend time with loved ones and participate in their life in a meaningful way by engaging in social activities, travelling, maintaining friendships, and pursuing personal interests.
Value to Patients
The value to patients of extending the time that their cancer is recurrence-free cannot be overestimated. Patients living with breast cancer are aware that their advanced disease will progress with worsening symptoms until death, and embrace opportunities to try new treatments, even if benefits may be as little as a six-month extension of progression-free disease. It is also very important for patients to have good quality of life when receiving treatment for metastatic disease. Patients that we speak to on a regular basis acknowledge the importance to have the energy to attend their children’s activities and to spend time with family and friends.
Patients understand that olaparib was approved as treatment for people with HER2-negative, early-stage, BRCA mutated breast cancer in the U.S. Japan and in Europe. They are aware that there has been a reluctance to accept similar adjuvant therapies in Canada. The breast cancer patient community has expressed general concern that adjuvant treatments that have been accepted internationally as standard of care for early-stage breast cancer and having demonstrated value and clinical benefit for patients are not publicly accessible in Canada in the adjuvant setting.
Experience With Drug Under Review
Unfortunately, CBCN was unable to connect with patients with direct experience on this treatment, due to its limited availability in Canada.
Companion Diagnostic Test
Not applicable.
Anything Else?
Not applicable.
Conflict of Interest Declarations — Canadian Breast Cancer Network
Did you receive help from outside your patient group to complete this submission?
CBCN did connect with the manufacturer, AstraZeneca, to identify clinicians that could connect us with patients with experience on the treatment.
All other research, interviews and outreach to patients was conducted independently by the Canadian Breast Cancer Network, as was the compilation of information and data for the writing of this submission.
As a member of the Canadian Cancer Action Network, the Canadian Breast Cancer Network is committed to adhering to the Code of Conduct Governing Corporate Funding.
Did you receive help from outside your patient group to collect or analyze data used in this submission?
No. The Canadian Breast Cancer Network compiled and wrote this submission independently.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review.
Table 1: Financial Disclosures for the Canadian Breast Cancer Network
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Astra Zeneca | — | — | X | — |
Rethink Breast Cancer
About Rethink Breast Cancer
Rethink Breast Cancer (Rethink) is a Canadian charity known for making positive change. Rethink educates, empowers and advocates for system changes to improve the experience and outcomes of those with breast cancer, focusing on historically underserved groups: people diagnosed at a younger age, those with metastatic breast cancer and people systemically marginalized due to race, income or other factors. We foster spaces to connect, listen, empower and rethink breast cancer, together. Rethink’s strategic priorities and organizational direction are guided by the unique, unmet needs identified by breast cancer patients and their families.
Programs and Activities
Rethink Breast Cancer builds community, bringing patients with various stages of breast cancer together through our private and public social spaces as well as in-person events
Rethink runs patient retreats and facilitates peer-support
Rethink creates and runs education forums and conferences
Rethink creates support and education tools, resources and content
Rethink funds and supports breast cancer research
You can find out more by visiting Rethink Breast Cancer Instagram and the Rethink Breast Cancer Website
Information Gathering
For over two decades, Rethink has been working closely with breast cancer patients in Canada with a focus on those diagnosed in their 20s, 30s and early 40s. We learn from and listen to the community to understand their values, priorities and pain points to help drive change and system improvements. Each year, we learn from the patients we serve, survey and collaborate with. We learn from the 40 individuals that we work extremely closely with as key patient advisors; the 100 patients that share their stories on our blog; the 500 patients that participate in our virtual support groups; the 1,600 members of our private peer-support network; the 30,000 people that have joined our Instagram community; and the 150,000 individuals reached each month through the reach of that channel. We listen, learn, engage and have conversations in all these spaces.
Rethink Breast Cancer has several important patient advisory boards and working groups that offer experience-focused insights on issues related to those affected by and concerned about breast cancer, including:
Metastatic Breast Cancer Advisory Board
Early Breast Cancer Advisory Board
Equity, Diversity and Inclusion working group
Triple Negative Breast Cancer working group (all stages)
For this submission, we have drawn on our general observations and insights gathered through programming and meetings with breast cancer patients as described above. Rethink has a lot of experience supporting and working with young breast cancer patients with hereditary breast cancer as it is more likely to be diagnosed at a younger age. In 2015, Rethink made a documentary film called High Risk featuring women with BRCA mutated breast cancer and those at a higher risk for getting breast cancer and over the years, many people with a BRCA mutation have written about their experience for our blog and for our resources.
To further inform this input, Rethink conducted in-depth telephone interviews in August 2022 with three patients with a BRCA mutation who participated in the OLYMPIA study. All were diagnosed with Stage 3 breast cancer at least 6 years ago and have not had a recurrence. We also gathered responses from people in our Instagram community with high-risk early breast cancer in order to identify more general treatment goals and values of those with early breast cancer who have a high risk of it returning.
Disease Experience
Most people participating in Rethink support and education programming are diagnosed at a younger age. They face age-specific issues such as fertility or family-planning challenges, diagnosis during pregnancy, childcare, impact on relationships, body image, dating and sexuality, feeling isolated from peers who don’t have cancer, career hiatuses, and financial insecurity. When young people get breast cancer it may be more aggressive, which can lead to tougher treatments and confronting mortality at a young age. The physical and emotional toll that a breast cancer diagnosis and treatment take on a young person’s life is devastating and traumatic. Being diagnosed with a BRCA mutation can involve making even more treatment decisions, including double mastectomy, oophorectomy, hysterectomy, egg or embryo preservation and even decisions like possibly genetic screening of embryos. Often there is a time pressure to make these important decisions. One patient shared her experience on our blog:
“After learning that I was a BRCA1 carrier (in my 20s), I decided almost instantly that I wanted to involve genetic screening as a part of my future family planning. I was diagnosed with stage 3 triple negative breast cancer, at the age of 30, and just a day before my scheduled preventative double mastectomy. It is incredibly overwhelming to receive a cancer diagnosis and try to make many important decisions quickly. Two weeks following my double mastectomy I began IVF. It felt as though my partner and I were rushed into family planning overnight! I struggled with the fertility treatment as it was so soon after my double mastectomy and I was still healing and accepting the cancer diagnosis.”
When it comes to a high-risk diagnosis, it’s less about controlling an “aspect” of the illness and more a deep desire for their treatment to work well enough that they do not have a recurrence. Moreover, being diagnosed with an inherited mutation in your BRCA1 or BRCA2 genes can also come with extra concern about family members. A patient participated in the OlympiA study and in her recent interview, she told us:
“I am hoping to persuade everybody to get on board to do as much as they can for families like mine where all the siblings testing positive for BRCA2. Two of us have had breast cancer, myself and my sister, and all of the kids from my siblings who have been tested are also positive. Our dear auntie and her daughter died of breast cancer. In 2019 my niece was 34 years old and was diagnosed with cancer and had an 18-month-old and 4-year-old at the time.
“I phoned everyone in my family and said is there something that you feel is important? I canvassed my family, and the hope is just that there’s not many families like us. I’m hoping that other families get a break. It’s supposed to be only half, 50% positive 50% negative. This would be too scary for a lot of people. They’d be so scared all the time in their life. We’ve had success, we have survivors in our family, so I think that helps us. But you can’t help as an adult to be freaked out about the kids in your family. I’ve got 7 nephews and 2 nieces, and they have 6 kids. I worry about them.”
Experiences With Currently Available Treatments
The treatment of HER2-negative breast cancer depends on HR status and there are different treatment options for different subtypes of HER2-negative breast cancer. HER2-negative breast cancer that’s HR-positive can be treated with hormone therapies like tamoxifen, fulvestrant or aromatase inhibitors that help stop the cancer from recurring. Most of the young patients in the Rethink community are on these treatments for up to ten years. It’s very difficult for them both physically and psychologically to be thrown into premature menopause; however, they work with their cancer care teams and seek peer support to help tolerate and cope with the symptoms because they know it prevents recurrence. Breast cancer that’s triple-negative won’t respond to some of the treatments used for HER2-negative, HR-positive breast cancer. This includes hormone therapy and many targeted therapies. These cancers are treated with chemotherapy and recent data recommends the addition of pembrolizumab to chemotherapy.
Patients on the OlympiA trial were treated with these standard therapies (without pembrolizumab as it was before that data). The addition of olaparib improved invasive disease- free survival, distant disease-free survival and overall survival. Therefore, olaparib should be used in addition to standard therapies not as a replacement.
Improved Outcomes
Each individual patient brings their own personal values and goals to their discussions with their oncology team. Communication and trust in their team is essential.
In our experience working closely with many young high risk breast cancer patients, we find most, especially those with Stage 3 are willing to trade toxicity for confidence in knowing they’ve “thrown everything they could” at the cancer. In other words, they will choose to endure more treatments and additional side-effects and impacts on quality of life from the toxicity of a stronger therapy to ensure they are doing everything they can to treat what they know is an aggressive form of breast cancer. This is reflected in the responses to questions we posed on August 16, 2022, to patients in the Rethink Instagram community who have a stage two or stage three breast cancer diagnosis with a high risk of recurrence.
New treatments that reduce risk of recurrence and improve survival for high-risk early breast cancer patients matter to them because:
“I want to live a long and healthy life without the added stress of recurrence and metastasis”
“Improved outcomes, peace of mind and hope are some reasons this matters.”
“Fear of recurrence takes a toll on our mental health.”
“It can prolong my chances of survival, lessen my cancer anxiety and improve my lifestyle”
“TNBC has no maintenance treatment! So scary just waiting for the possibility of a recurrence.”
“No one wants to fight this again; I want to watch my kids grow and live a long life with my husband.”
“I never imagined I might not be able to retire from my career. I want to live.”
“I have children 12, 14, 16. I want to see them grow up.”
“It means I was able to eradicate residual low level and undetectable cancer cells”
“It gives me hope that there I have more life to live.”
“I feel like this answer is obvious. So, we can LIVE.”
“So, I can dream of having grey hair and wrinkles. I can hope to outlive my parents.”
“Having a brand-new baby with a stage 3 TNBC diagnosis is the main reason it matters”
“Diagnosed in 2021 with stage 2B lymph node involvement. I have 2 small kids. I can’t die.”
“My children”
Experience With Drug Under Review
Rethink conducted interviews with three patients who participated in the OlympiA study. All were diagnosed with Stage 3 breast cancer 6 or more years ago and have not had a recurrence.
Patient 1
Patient 1 was diagnosed in August of 2015 at age 57 with stage 3 estrogen and progesterone receptor positive, HER2 negative breast cancer and she carries the BRCA2 mutation.
“When I was diagnosed, it kind of sent me into a place where I always thought I’d be. I think somewhere in my mind, I understood that the chances were very good that I’d get breast cancer at some point in my life, because my mother had died of it, her sister died of it, their mother died of it, and her brother died of a cancer we don’t know, and maybe even before that. It seemed like a fact of life to me almost. We knew this was coming. So, when I was diagnosed with stage 3 breast cancer and found out I was BRCA2+, I was able to approach it quite practically.”
“Because I have BRCA2, I opted for a bilateral mastectomy, and when I heard of all the options, I knew there would be no surgery for reconstruction. No more mutilation of any kind. It changed my perspective and how I viewed my body. My body was a battleground for a while, and it was time to shut the war down and give it a bit more peace and quiet. That’s also what Olaparib did for me.”
“I was lucky to have accessed Olaparib through a clinical trial, which I heard about through my oncologist. I chose to enter the trial because I thought at least something was being done to help people in the future in my situation to have better treatment – this was my motivation. It felt amazing to have a sense of someone being behind me, having my back somehow.”
“Once I got out of treatment and spoke to others who have had a similar experience, I realized how traumatizing it all is, it’s almost hard to believe it’s over, and it’s really hard to let go of it and move on. Every little ache and pain, you worry about it, wondering if it’s the cancer returning. That’s how hyper-sensitive we get. It’s shattering because we all go on thinking, “I’ll see you tomorrow,” but we can’t say that with absolute certainty. A diagnosis like this really brings home how fragile we are, and when you’re really fragile, it would be a comfort to know that there’s something that can help you, like Olaparib.”
“Treatments like Olaparib are ones that people can rely on and give the potential for hope. It’s a very strange feeling to sit here and say I don’t know what I’m going to be doing next year, and no one does, but when you’re in a situation where you’ve been through things like cancer, you really don’t. It’s everything to have that bit of peace and comfort and understanding that things could be worked out when you have a diagnosis like this. So, it was everything for me to have access to Olaparib. It changed everything.”
“Physically, Olaparib was the only treatment I tried that didn’t give me any consequential or noticeable adverse effects. I tried Tamoxifen and others, and I could not tolerate it, most notably the body pain that was heightened and intensified while on them. My body just said no to them. And, on a personal level, Olaparib and this clinical trial put everything into context for me. Maybe this would be helpful to someone somewhere. I was struck many times from my mother’s and aunt’s experience firsthand, seeing the experiences they had which were so very different than my own.”
“There’s only one time that I cried throughout my whole treatment. I was in bed at night, I caught a glimpse of myself in my mirror, I was bald, I looked yellow and green, and I started to cry. I cried because I thought of how it would break my dad’s heart to see me like this, because, of course, he went through all this with my mother. I was reminded of this when I learned I was able to do the trial, because now I’m doing something that maybe can help. I’m seeing today how treatments have advanced since my mother’s time. If my diagnosis had been in my mother’s time, I probably wouldn’t have lived. Breast cancer is a part of our family in a sense and I’m glad that I was able to participate in something that maybe would change future paths.”
“I’ve been radically altered, externally and internally, from this whole experience – radically altered. Having that with you, knowing that there’s so much uncertainty and that we can’t predict, but also knowing there is something that could reduce the possibilities of recurrence, that is everything you would have at that point. That could be ALL you have at that point. The only hope. It would be essential, physically and emotionally. Having this bit, this glimmer of direction in the directionless world of high-risk cancer, could be all someone might have. And people in this position deserve to have access to it.”
Patient 2
Patient 2 was diagnosed with Stage 3 breast cancer and has the BRCA2 genetic mutation.
“I probably had a little cry when they told me the news, but I’ve been pretty stoic about moving forward. Don’t look at the big picture, just look at the next month and the road sort of thing. That’s sort of how I got through the whole thing. It’s a very emotional experience, you feel like you’re dying.”
“I made a conscious decision in everything that I did to try and extend my life and come out with the most positive outcome that I could. I feel like I’ve been very fortunate with everything that I’ve done, that I’ve been cancer free ever since. My cancer went from being stage 1 to, over the course of 2 months, stage 3, growing very rapidly, that was very scary. Anything you can do to try and get past this disease is important. That’s why I made the decision to be a part of the trial, 1) because I want to live and b) anything I can do to help another human being to not have to go through this or help them come out the other side of it, I’m more than willing to do.”
Patient 3
Marilyn was diagnosed in 2016 at age 62 with stage 3 estrogen and progesterone receptor positive, HER2 negative breast cancer and she carries the BRCA2 mutation.
“Unfortunately, my auntie D and her daughter both died of breast cancer. That’s from my dad’s side, that gene. That was my dad’s sister. My poor niece with her young kids, it was frightening as hell.
“Thank Gosh, in our branch of the family, we’ve had huge, good luck that we’re all ok after the cancer so far.”
“Of course, you have side effects from chemo. It’s not a walk in the park. But I can manage them or figure something out to inhibit them. As a family, we try our best to respect our health and pay attention to the things that we’re not allowed to do, like alcohol and stuff like that. We behave ourselves and remind each other that we have to behave and don’t do things that could potentially assist cancer.”
“My sister was pushing up against (stage) 4, and she is more analytical, so she told me recently, you feel like your cancer wasn’t as serious as mine, but it was. I’m way more positive. She’s more serious, she has anxiety and depression. I know the cancer doesn’t give a rat’s ass if you’re positive or not, but I think it’s so important to not worry yourself into a worse situation. I don’t want to project anything onto other people.”
“Better outcomes are this incredible quest in breast cancer, finding out how much longevity people can have, that’s important.”
Companion Diagnostic Test
It will be important for BRCA testing to be done as soon as possible after diagnosis to identify patients that will be eligible for Lynparza. Efforts are underway to expedite and expand testing in Canada since it affects treatment recommendations for several cancers.
Anything Else?
We’d like to emphasize that although most HER2-negative early breast cancers now have good outcomes, currently, for those in Canada with high-risk breast cancers and BRCA mutations the risk of recurrence is still very high with significant potential to become metastatic, which is almost universally incurable and drastically shortens the patient’s lifespan. So, as we ponder “anything else,” we think about the people we know with metastatic breast cancer and their loved ones. We know their cancer stories and we know, at least partly, the personal life stories too. We see their family pictures on Facebook and Instagram. We know what they have at stake. We know the feeling we get when we see their updates, living scan to scan posting about their stability, or their heartbreak over progression. And we think of those we’ve lost. Too, too many over the years. Their families will never be the same. For the BCRA positive, high risk breast cancer patients in our network, facing mortality at a young age, they want what all cancer patients want—care that will lead to the best possible outcomes, including reducing their future breast cancer risk. They want to do whatever they can to avoid metastasis. They want to survive, and eventually thrive.
Patients in Canada with a BRCA mutation have been waiting a long time for Lynparza. It’s exciting that the benefit is for both estrogen receptor positive and estrogen receptor negative patients with either a BRCA 1 or BRCA 2 mutation. Seeing the OlympiA results and knowing that people with high-risk breast cancer and a BRCA mutation could improve survival with no major impact on their quality of life is huge progress and a truly exciting advancement.
Conflict of Interest Declarations — Rethink Breast Cancer
To maintain the objectivity and credibility of the CADTH reimbursement review process, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This Patient Group Conflict of Interest Declaration is required for participation. Declarations made do not negate or preclude the use of the patient group input. CADTH may contact your group with further questions, as needed.
Did you receive help from outside your patient group to complete this submission?
No.
Did you receive help from outside your patient group to collect or analyze data used in this submission
No.
List any companies or organizations that have provided your group with financial payment over the past 2 years AND who may have direct or indirect interest in the drug under review.
Table 2: Financial Disclosures for Rethink Breast Cancer
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Astra Zeneca 2022 | — | — | — | X |
Astra Zeneca 2021 | — | — | — | X |
Clinician Input
Ontario Health Cancer Care Ontario Breast Cancer Drug Advisory Committee
About the Ontario Health Cancer Care Ontario Breast Cancer Drug Advisory Committee
OH-CCO’s Drug Advisory Committees provide timely evidence-based clinical and health system guidance on drug-related issues in support of CCO’s mandate, including the Provincial Drug Reimbursement Programs (PDRP) and the Systemic Treatment Program.
Information Gathering
The information was jointly discussed via email.
Current Treatments and Treatment Goals
The OlympiA clinical trial investigating the use of Olaparib in patients with BRCA1/2 mutated breast cancer demonstrated a 3-year invasive disease–free survival (IDFS) was 85.9% in the olaparib group and 77.1% in the placebo group (HR=0.58; 99.5% CI, 0.41 to 0.82; P<0.001). An updated presentation at the European Society of Medical Oncology (ESMO) Annual Meeting also showed a 3-year overall survival (OS) was 92.8% in the olaparib group versus 89.1% in the placebo group (HR=0.68; 95%CI, 0.47 to 0.97; P<0.015). Adjuvant olaparib significantly improved both IDFS and OS and is an important new therapy for patients with early-stage high risk HER2-negative breast cancer associated with a germline BRCA1/2 mutation.
Treatment Gaps (Unmet Needs)
Considering the treatment goals, please describe goals (needs) that are not being met by currently available treatments.
BRCA mutated breast cancer often impacts younger patients and carries as aggressive disease biology. Novel agents to improve survival outcomes are warranted. The use of Olaparib; an oral targeted therapy — a poly (ADP-ribose) polymerase (PARP) inhibitor exploits the biologic vulnerability of these specific cancers to optimize treatment. Olaparib is associated with manageable side effects including risk of fatigue, nausea, vomiting, diarrhea, and myelosuppression.
Place in Therapy
How would the drug under review fit into the current treatment paradigm?
Adjuvant Olaparib would be used in high-risk early stage, HER-2 negative breast cancers associated with a germline BRCA1 and BRCA2 mutation and would be given for one year after the completion of standard adjuvant or neoadjuvant chemotherapy and local therapy. This is an adjuvant treatment which would add to existing therapy. Olaparib and other PARP inhibitors are not currently funded for treatment in the advanced disease setting in Ontario.
We acknowledge that there will be uncertainty for choosing an optimal adjuvant therapy for patients with residual disease following neoadjuvant chemotherapy for triple negative breast cancer. Currently, adjuvant Capecitabine (CREATE-X) and Pembrolizumab (KEYNOTE-522) have also shown survival benefits for patients with triple negative breast cancer. However, we do not have any clinical data to compare the effectiveness of these adjuvant therapies as compared with Olaparib for patients with a germline BRCA1 and BRCA2 mutations. Additionally, among patients with high-risk early-stage hormone receptor positive, HER-2 negative breast cancer, there is also data for adjuvant Abemaciclib in combination with endocrine therapy (monarchE) and we similarly do not have comparative effectiveness data with respect to adjuvant Olaparib for patients with a germline BRCA1 and BRCA2 mutations. Given the uncertainty, we recommend an informed discussion between the clinician and patient to decide on adjuvant treatment(s) based on updated and available efficacy and safety data as well as patient preference.
Which patients would be best suited for treatment with the drug under review? Which patients would be least suitable for treatment with the drug under review?
Patients should be diagnosed with early-stage HER-2 negative breast cancer (Stage II-III) or have residual disease post neoadjuvant chemotherapy. For triple negative breast cancer patients: adjuvant patients must be ≥pT2 or ≥pN1 and for patients who received neoadjuvant chemotherapy must have had residual disease in the breast or lymph node (non-pCR). For hormone receptor positive patients, adjuvant patients must have ≥ 4 positive lymph nodes and for patient receiving neoadjuvant chemotherapy must have residual disease in the breast or lymph node (non pCR) and CPS+EG score ≥3. The CPS+EG scoring system estimates relapse probability on the basis of clinical and pathological stage (CPS) and estrogen-receptor status and histologic grade (EG); scores range from 0 to 6, with higher scores indicating worse prognosis. Patient are required to have a germline pathogenic or likely pathogenic mutation for eligibility for adjuvant olaparib. BRCA testing is available through medical genetics services across the province for patient with meeting eligibility criteria based on their cancer diagnosis and family history. Unfortunately, the current testing guidelines are restrictive and many patients who may carry a BRCA1 and BRCA2 mutation may not be identified and have the opportunity to benefit from adjuvant Olaparib. If we adopt a more universal testing strategy for all new breast cancer diagnoses, resources for genetic testing would need to be increased to accommodate for higher testing volumes. Timely BRCA1 and BRCA2 testing will be needed to ensure patients and clinicians have access to results to start to adjuvant Olaparib.
What outcomes are used to determine whether a patient is responding to treatment in clinical practice? How often should treatment response be assessed?
Patients will require standard cancer care follow-up. As this is an adjuvant treatment, no diagnostic imaging is required to assess response. Patients with signs or symptoms suggestive of recurrent or progressive disease may have radiographic imaging or biopsy as recommended by their health care provider. Adjuvant Olaparib will be given over a period of 1-year.
What factors should be considered when deciding to discontinue treatment with the drug under review?
Adjuvant Olapraib is given for 1-year. Treatment could be discontinued if there was recurrence or progression of disease, toxicity, severe side effects of patient or physician preference.
What settings are appropriate for treatment with [drug under review]? Is a specialist required to diagnose, treat, and monitor patients who might receive [drug under review]?
The treatment should be provided in specialized medical oncology clinics.
References
Tutt et al. Adjuvant Olaparib for Patients with BRCA1- or BRCA2-Mutated Breast Cancer. N Engl J Med 2021;384:2394-405.DOI: 10.1056/NEJMoa2105215
Tutt et al. Pre-specified event driven analysis of overall survival (OS) in the OlympiA phase III trial of adjuvant olaparib in germline BRCA1/2 mutation associated breast cancer. European Society of Clinical Oncology (ESMO) Annual Meeting. 2022; Ann Oncol. DOI: https://doi.org/10.1016/j.annonc.2022.03.008.
Conflict of Interest Declarations — Ontario Health Cancer Care Ontario Breast Cancer Drug Advisory Committee
To maintain the objectivity and credibility of the CADTH drug review programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This conflict of interest declaration is required for participation. Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please refer to the Procedures for CADTH Drug Reimbursement Reviews (section 6.3) for further details.
Did you receive help from outside your clinician group to complete this submission?
Yes. Ontario Health provided secretariat functions to the DAC.
Did you receive help from outside your clinician group to collect or analyze any information used in this submission?
No.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review. Please note that this is required for each clinician who contributed to the input — please add more tables as needed (copy and paste). It is preferred for all declarations to be included in a single document.
Declaration for Clinician 1
Name: Dr. Phillip Blanchette
Position: Member, Breast Cancer Drug Advisory Committee
Date: August 24, 2022
Table 3: COI Declarations for Ontario Health Cancer Care Ontario Breast Cancer Drug Advisory Committee — Clinician 1
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
No COI | — | — | — | — |
Medical Oncologists From British Columbia, Ontario, and Nova Scotia
About Medical Oncologists From British Columbia, Ontario, and Nova Scotia
The group is an interested group of medical oncologists at academic centres across Canada who are involved in clinical care, research, cancer guidelines and education. They have come together through their interest in providing patients with optimal up to date care.
Information Gathering
Information has been gathered from peer reviewed manuscripts, international guidelines, and clinical experience.
Current Treatments and Treatment Goals
The majority of oncology care in Canada is provided through academic and regional cancer centres who use peer reviewed guidelines which are international, provincial and national as the basis for treatment recommendations. The goal of adjuvant and neoadjuvant therapy in early breast cancer is to decrease recurrence of cancer and improve survival. Treatment of early breast cancer is provided by a multidisciplinary team which includes surgical, medical and radiation oncologists as well as nurses, pharmacists, physiotherapists, psychologists, hereditary cancer specialists, fertility experts and other health care providers. The treatment strategy depends on the subtype of the breast cancer and both prognostic as well as predictive factors in the tumour as well as characteristics of the patient including age, comorbidities, preference, prior therapies and now germline mutations. The cancer is considered to be high risk, intermediate risk or low risk depending on the biological factors of the cancer and on the extent of disease which includes the size of the tumour and the involvement of lymph nodes. More recently a binary division of high risk versus low risk has been used in some clinical trials.
Broadly speaking low risk cancers are low grade, estrogen/progesterone receptor positive and small, usually not involving lymph nodes. Intermediate risk cancers may be the same or intermediate grade and may involve lymph nodes. High risk cancers are usually higher grade, may be HER2 positive, may be either estrogen negative, estrogen low or estrogen positive with high grade, and may also be larger and/or involving lymph nodes. When neoadjuvant therapy is given, not achieving a pathological complete response is associated with a higher risk of relapse and is considered higher risk. It has been difficult to have experts agree on assigning absolute risk of relapse for these groups but generally quantifying it into numbers a low-risk cancer would have less than a 10% chance of relapse at 10 years while high risk would have a 15% risk of systemic relapse at 10 years.
Currently estrogen receptor positive cancers that are either node negative or have one to three nodes positive are eligible for an Oncotype recurrence score in Canada and are treated with endocrine therapy alone if the score is low and only have the addition of chemotherapy if the score is high or if they are node positive and premenopausal. Abemaciclib is a CDK4/6 inhibitor which is available on a compassionate basis for those persons with a high-risk lymph node positive endocrine positive cancer that has a Ki67 of greater than 20%. Other agents used in endocrine receptor positive cancers are all funded by our provincial governments.
For HER2 positive cancers, chemotherapy and anti HER2 therapy is recommended for all but the smallest cancers or in persons who are elderly with significant comorbidities. Stages II and III HER2 positive cancers are treated in the neoadjuvant setting and according to international guidelines should receive dual anti HER2 therapy with chemotherapy. In Canada, except for Quebec, pertuzumab is not funded and must be obtained from private insurance and therefore there is unequal access to this internationally approved therapy. Post neoadjuvant therapy with T-DM1 is approved for those persons who do not achieve a pathological complete response (pCR) as this was shown to improve outcomes. Standard chemotherapy with trastuzumab is given in the adjuvant setting. Although international guidelines recommend the addition of pertuzumab for node positive patients this is not approved.
For triple negative cancers (TNBC) the new standard of care for Stage II and III is chemotherapy with paclitaxel, carboplatin, doxorubicin, and cyclophosphamide with pembrolizumab during the treatment and continued as monotherapy after surgery. The Pembrolizumab is not yet funded in Canada but there is currently an access program and as this is a very aggressive subtype of breast cancer with devastating outcomes if it relapses, oncologists and patients are awaiting full funding. For patients who do not achieve a pCR, capecitabine for 8 cycles is generally recommended and is funded. In the adjuvant setting for Stage I, treatment with chemotherapy alone is standard.
All of the recommended treatments have been shown to decrease recurrence of disease and improve outcomes in early breast cancer. This has been shown in clinical trials and geographic, real-world data supports this. Although there are symptoms associated with adjuvant therapy most patients do well and there is an abundance of literature providing options for improving symptom control and enhancing adherence. Quality of life studies support current treatments.
Surgery may be mastectomy or partial mastectomy with clear guidelines for sampling the axilla. Radiation is given according to international guidelines to decrease recurrence with new shorter techniques now becoming more common.
THE GOAL OF TREATMENT OF EARLY BREAST CANCER IS TO IMPROVE SURVIVAL.
Treatment Gaps (Unmet Needs)
Considering the treatment goals, please describe goals (needs) that are not being met by currently available treatments.
The identification of germline mutations in cancers has provided information about these tumours both in terms of etiology and also behaviour. About 5 – 10% of breast cancers have a germline mutation. This number may increase as more persons are tested. BRCA1 and 2 were described 30 years ago and are the most common mutations seen in breast cancer. Over 75% of BRCA 1 associated tumours are estrogen negative, with the others either estrogen low, which is now associated with outcomes similar to TNBC, or estrogen high. In contrast about 75% of BRCA2 tumours are estrogen positive with the remaining being TNBC. Although HER2 overexpressing tumours are seen they are not commonly associated with BRCA mutations. Most mutations of BRCA are germline although somatic mutations are seen and behave in a similar fashion.
Studies have been contradictory in terms of the outcomes of these tumours. A number of large retrospective studies suggested that tumours with BRCA mutations had a worse outcome. A UK study suggested that outcomes were not worse, but this study has been criticized as having relatively short follow up. What is known and is not controversial is that the tumours appear to be more aggressive, with higher grade, more nodal involvement, occur in younger persons (age being a factor associated with a higher risk of recurrence) and other high-risk features such as large size and high Ki67. Studies in recurrent disease suggest shorter survival. Recent studies of CDK4/6 inhibitors show shorter progression free survival and responses to these agents. As well, there is the increased risk of other malignancies. Studies of platinum agents in the advanced setting have suggested improved responses, but this was not seen in the early setting where platinum in the neoadjuvant setting were not superior to other traditional chemotherapy in reaching pCR. Also, BRCA associated tumours without a pCR continue to have poor outcomes. Some neoadjuvant studies have reported a more chemo sensitive tumour type with a higher rate of pCR but this has not been associated with improved outcomes in some studies.
Thus, BRCA mutation associated tumours represent a group of cancers that are both more aggressive in nature and have not been treated with specific therapies. In fact, other than surgery no therapy has been used specifically for this group despite their high-risk features. BRCA mutation should be considered a unique and important target.
Guidelines for assessing germline mutations have been evolving but many places in Canada still lag behind due to outdated programs, lack of funding, and lack of staff to provide timely results.
Place in Therapy
How would the drug under review fit into the current treatment paradigm?
This agent would be a novel addition to our treatments for early breast cancer for persons with BRCA mutations and early breast cancer. This is the first of its kind for early disease. As this cancer occurs in young women often with aggressive breast cancer it is very exciting and important, particularly with a survival advantage. This would cause a shift in our current paradigm and would be used in the adjuvant setting after chemotherapy. It would not be reserved for persons intolerant to other therapies. Persons with endocrine sensitive tumours would receive endocrine therapy as was done in the OlympiA trial. Bone modifying agents would be used as recommended.
Patients with high-risk cancer would be treated with standard therapies that are already in use as was done in the OlympiA trial where >99% of patients on the Olaparib arm received our standard high-risk Anthracycline / Taxane based regimen. They would be identified usually during their neo or adjuvant therapy as having a germline BRCA mutation, although some may have already been identified. This would require blood or sputum testing, or rarely tumour testing for a BRCA mutation. The duration of neoadjuvant therapy often is ideal for getting the testing done and results available.
Patients with TNBC would usually be treated with neoadjuvant therapy and if they did not achieve a pCR would be candidates. Patients with ER low or endocrine sensitive cancers and high-risk disease would be treated often in the neoadjuvant setting and those without a pCR would be candidates for Olaparib. This would be discussed with them by their oncologist.
Patients with Stages II or III TNBC who receive adjuvant therapy would also be candidates for treatment with Olaparib after their adjuvant therapy and testing results. Patients with high-risk endocrine low or sensitive tumours being treated with chemotherapy would need to be identified and this is more challenging as many of our guidelines for testing are currently restricted to those with family histories. These testing guidelines need to be revised to allow persons who may be candidate for Olaparib treatment to be tested and this is being discussed.
The role of other therapies in the adjuvant setting in conjunction with Olaparib will be assessed on an individual basis by the oncologist and will be modified as new data emerges. A trial of pembrolizumab with Olaparib in early TNBC is being initiated to assess this and the KEYNOTE 522 is being analyzed to see the number and outcomes of persons on that trial with BRCA mutations. The two drugs can be given together and are effective in the advanced setting but there is not data from OlympiA with the combination.
Capecitabine is often given to TNBC in Canada if there is not a pCR. In the advanced setting study OLYMPIAD, Olaparib was more effective than capecitabine and as a targeted agent with an OS impact is likely preferred, but this will be up to the oncologist. Likewise, the MONARCHe study in hormone positive high-risk cancer gave abemaciclib and there is no data from OlympiA of this combination. As the abemaciclib and Olaparib would likely be poorly tolerated if given together, as the Olaparib has OS advantage and is specific to this population, as there is data in the advanced setting of less good outcomes with CDK4/6 in BRCA mutated cancers, and as the abemaciclib could be used after the year, it is recommended to give Olaparib but again, there is no direct comparative data and it will be individualized.
It should be recommended that persons who have BRCA mutated breast cancers receive Olaparib after neo or adjuvant chemotherapy as there is a survival benefit and good tolerance. This should be after surgery and radiation as per the trial.
Which patients would be best suited for treatment with the drug under review? Which patients would be least suitable for treatment with the drug under review?
Patients as per the Health Canada recommendation. “For the adjuvant therapy of adult patients with deleterious or suspected deleterious germline BRCA-mutated (gBRCAm), human epidermal growth factor receptor 2 (HER2) negative, high risk early breast cancer who have been treated with neoadjuvant or adjuvant chemotherapy. Patients must have confirmation of a germline BRCA mutation.
Patients with a low-risk cancer such as a small node negative tumour or persons who achieve a pCR with neoadjuvant therapy would not be candidates as per the OlympiA trial. As well, persons with significant comorbidities or with an expected survival of < 3 months should not be treated but they would not have chemotherapy in the neo or adjuvant setting.
This is targeted therapy and therefore both BRCA 1 and 2 and endocrine sensitive and estrogen negative cancers should be included. The target is the BRCA mutation. The study did not show heterogeneity. The survival benefit was for all patients. Due to the initial slow approval from FDA for the inclusion of BRCA 2 and endocrine sensitive the numbers of persons in those groups were smaller causing greater confidence intervals but the impact of Olaparib is clearly seen.
Patients will be identified by their oncologists, either medical or surgical, and sent for testing. Our hereditary cancer programs are being expanded to deal with increasing loads due to the need for assessing germline mutations in a number of cancers, not just breast cancer. As the identification of a germline mutation affects treatment recommendation, oncologists are now instituting testing on their own with genetic counselling often reserved for those persons with mutations and this will accelerate testing, decrease the burden on our hereditary programs, integrate hereditary testing and discussion as part of the assessment of risk for appropriate new breast cancer patients, and hopefully lead to less discrimination and more universal testing.
The companion diagnostic is a BRCA test which can be done by panel testing or by individual gene testing, but most commonly by panel testing in 2022. The number of genes on the panels varies by what is being assessed and by the test used. A number of commercial tests as well as service/academic tests exist. This is testing that is already in place but will be expanded and possibly modified. There is very little risk of a false negative or positive. There are missense mutations or variants of unknown significance, but all laboratories have the ability to adjudicate or send these results for adjudication to determine if they are true pathological mutations. Only pathological mutations would be eligible for treatment.
Patients with BRCA mutations and high-risk early breast cancer are most likely to respond and benefit.
What outcomes are used to determine whether a patient is responding to treatment in clinical practice? How often should treatment response be assessed?
The OlympiA study showed an improvement in invasive disease-free survival (85.9 vs 77.1%), distant disease free survival (87.5 vs 80.4%) and overall survival (92.0 vs 88.3%) for olaparib compared to placebo, respectively. All these are very important for our patients with early breast cancer. These are the outcomes that would be used.
As well, a very comprehensive quality of life (QoL) study that was part of the OlympiA study and has been presented by Dr Patricia Ganz showed good tolerance of the drug and no lasting QoL impact. By 18 and 24 months the two groups were equal. Prior to that there were some symptoms associated with the administration of olparib but the difference was not clinically significant.
Improved survival with no major impact on QoL is a major gain and is not seen with many of our adjuvant studies. Many studies of endocrine therapies that are now standard of care did not see this improvement in survival. Our goal is to cure early breast cancer and the addition of Olaparib appears to do that. BRCA mutation associated breast cancers often occur in young persons, so this translates into many additional years of good quality productive life.
No new toxicities have been seen with Olaparib administration and as one gets more familiar with the drug it becomes easier to avoid many of the gastrointestinal symptoms in patients, most of which are short lived regardless. There were concerns about long term toxicity and in particular MDS and leukemia but these have not been seen as of now. Longer follow up is necessary. Of reassurance is that Olaparib is used in a number of tumour types and MDS and leukemia have not been common in other tumour types. Persons with ovarian cancer and extensive prior carboplatin appear to be at greatest risk, so early breast cancer with a maximum of 4 to 6 cycles of carboplatin are likely at a lower risk but this will be followed on the long-term follow-up of OlympiA.
What factors should be considered when deciding to discontinue treatment with the drug under review?
The main reasons to discontinue would be disease recurrence. The Olaparib is given for a year, and it is rare for the cancer to recur in that year but if it did then this would be a strong reason to discontinue. Other reasons would be toxicity. No new toxicities were seen with the OlympiA trial. The GI toxicities particularly nausea can be usually alleviated with antinauseants and usually is only seen with the first cycle. The headache which is reported is usually mild. The main toxicity which may lead to discontinuation is anemia which may occur but is usually mild to moderate. If more severe and requiring frequent transfusions it may be a reason to stop but this is rare.
The age of the persons in the trial was young with a median of 42. It is well known that younger age is associated with more depression and anxiety in breast cancer. When a person is on a trial, does not know if they are on the drug or placebo and does not know if the experimental agent will be effective, it is easier to stop the drug so the discontinuation rate in the study may not reflect what will happen in practice. As clinicians are more familiar with the drug and as patients with high-risk cancer are informed of the survival benefit, the number who stop early will likely be lower than in the study. As well in Canada we tend to be very proactive in dealing with the psychological and social aspects of a diagnosis of breast cancer in the young, bringing in other health care providers where needed and supporting our young patients. which also improves compliance.
What settings are appropriate for treatment with [drug under review]? Is a specialist required to diagnose, treat, and monitor patients who might receive [drug under review]?
All these patients will be getting treated at cancer centres or hospital cancer units under the supervision of a medical oncologist with specialty in treating cancer patients and breast cancer patients. As well, the pharmacists in these units have specialization.
Additional Information
This is a very exciting advance with a new effective agent against a target that is associated with a high-risk breast cancer. This is important as well, as the population Is generally young with potential for long lives with their families and in their productive years. We want to decrease their risk of recurrence and Olaparib appears to be effective for many persons with this disease. Patients with BRCA1 or BRCA2 early breast cancers who fit the criteria and have received chemotherapy in the adjuvant or neoadjuvant setting will benefit from access to adjuvant Olaparib.
Conflict of Interest Declarations — Medical Oncologists From British Columbia, Ontario, Nova Scotia
To maintain the objectivity and credibility of the CADTH drug review programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This conflict of interest declaration is required for participation. Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please refer to the Procedures for CADTH Drug Reimbursement Reviews (section 6.3) for further details.
Did you receive help from outside your clinician group to complete this submission?
No outside help was used.
Did you receive help from outside your clinician group to collect or analyze any information used in this submission?
We did not receive any outside help.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review. Please note that this is required for each clinician who contributed to the input.
Declaration for Clinician 1
Name: Dr Sandeep Sehdev
Position: MD FRCPC, Assistant Professor, U of Ottawa. Medical Oncologist, The Ottawa Hospital Cancer Centre
Date: August 25, 2022
Table 4: COI Declarations for Medical Oncologists From BC, Ontario, Nova Scotia — Clinician 1
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
AstraZeneca | — | X | — | — |
Declaration for Clinician 2
Name: Daniel Rayson
Position: Medical Oncologist, QEII HSC, Halifax NS
Date: August 25, 2022
Table 5: COI Declarations for Medical Oncologists From BC, Ontario, Nova Scotia — Clinician 2
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Pfizer | — | X | — | — |
Astra Zeneca | — | X | — | — |
Merck | X | — | — | — |
Novartis | X | — | — | — |
Seagen | X | — | — | — |
Gilead | — | — | — | — |
Declaration for Clinician 3
Name: Stephen Chia
Position: Professor of Medicine, UBC,Medical Oncologist, BC Cancer
Date: August 25, 2022
Table 6: COI Declarations for Medical Oncologists From BC, Ontario, Nova Scotia — Clinician 3
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
AstraZeneca | X | — | — | — |
Pfizer | — | X | — | — |
Novartis | — | X | — | — |
Lilly | X | — | — | — |
Gilead | X | — | — | — |
Amgen | X | — | — | — |
Merck | X | — | — | — |
Exact Sciences | X | — | — | — |
Declaration for Clinician 4
Name: Tamara Shenkier
Position: Clinical Professor, UBC, Medical Oncologist, BC Cancer
Date: August 25, 2022
Table 7: COI Declarations for Medical Oncologists From BC, Ontario, Nova Scotia — Clinician 4
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
No COI | — | — | — | — |
Declaration for Clinician 5
Name: Karen A Gelmon
Position: Professor of Medicine, UBC, Medical Oncologist, BC Cancer
Date: August 25, 2022
Table 8: COI Declarations for Medical Oncologists From BC, Ontario, Nova Scotia — Clinician 5
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Astra Zeneca | — | X | — | — |
Pfizer | — | X | — | — |
Novartis | — | X | — | — |
Lilly | X | X | — | — |
Seagan | X | X | — | — |
Gilead | X | X | — | — |
Merck | X | — | — | — |
Ayala | X | — | — | — |
Knight Pharmaceuticals | X | — | — | — |
Declaration for Clinician 6
Name: Zahi Mitri
Position: Faculty, Medical Oncology – BC Cancer Center, Vancouver
Date: August 25, 2022
Table 9: COI Declarations for Medical Oncologists From BC, Ontario, Nova Scotia — Clinician 6
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
AstraZeneca | X | — | — | — |
Gilead Sciences | X | — | — | — |
Daiichi Sankyo | X | — | — | — |
Declaration for Clinician 7
Name: Caroline Lohrisch
Date: August 26, 2022
Table 10: COI Declarations for Medical Oncologists From BC, Ontario, Nova Scotia — Clinician 7
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Novartis | X | — | — | — |
Pfizer | X | — | — | — |
Veracyte | X | X | — | — |
Declaration for Clinician 8
Name: Nathalie Levasseur
Position: Clinical Assistant Professor, UBC, medical oncologist, BC Cancer
Date: August 26, 2022
Table 11: COI Declarations for Medical Oncologists From BC, Ontario, Nova Scotia — Clinician 8
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
AstraZeneca | X | — | — | — |
Gilead | X | — | — | — |
Knight Pharmaceuticals | X | — | — | — |
Lilly | X | — | — | — |
Merck | X | — | — | — |
Novartis | X | — | — | — |
Pfizer | X | — | — | — |
Roche | X | — | — | — |
Seagen | X | — | — | — |
Declaration for Clinician 9
Name: Dr. Alison Weppler
Position: Medical Oncologist (BC Cancer – Vancouver)
Date: August 26, 2022
Table 12: COI Declarations for Medical Oncologists From BC, Ontario, Nova Scotia — Clinician 9
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Bristol Myers Squibb | X | — | — | — |
Merck | X | — | — | — |
Pfizer | X | — | — | — |
Medison Pharma | X | — | — | — |
Declaration for Clinician 10
Name: Aalok Kumar
Position: Medical Oncologist
Date: August 26, 2022
Table 13: COI Declarations for Medical Oncologists From BC, Ontario, Nova Scotia — Clinician 10
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
AZ | X | — | — | — |
GSK | X | — | — | — |
Pfizer | X | — | — | — |
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
Redactions: Confidential information in this document may be redacted at the request of the sponsor in accordance with the CADTH Drug Reimbursement Review Confidentiality Guidelines
Stakeholder Input: The views expressed in each submission are those of the submitting organization or individual; not necessarily the views of CADTH or of other organizations. As such, they are independent of CADTH and do not necessarily represent or reflect the view of CADTH. No endorsement by CADTH is intended or should be inferred. By filing with CADTH, the submitting organization or individual agrees to the full disclosure of the information. CADTH does not edit the content of the submissions.
CADTH does use reasonable care to prevent disclosure of personal information in posted material; however, it is ultimately the submitter’s responsibility to ensure no identifying personal information or personal health information is included in the submission. The name of the submitting organization or individual and all conflict of interest information are included in the submission; however, the name of the author, including the name of an individual patient or caregiver submitting the patient input, are not posted.
Accessibility: CADTH is committed to treating people with disabilities in a way that respects their dignity and independence, supports them in accessing material in a timely manner, and provides a robust feedback process to support continuous improvement. All materials prepared by CADTH are available in an accessible format. Where materials provided to CADTH by a submitting organization or individual are not available in an accessible format, CADTH will provide a summary document upon request. More details on CADTH’s accessibility policies can be found here.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.