CADTH Reimbursement Review
Darolutamide (Nubeqa)
Sponsor: Bayer Inc.
Therapeutic area: Metastatic castration-sensitive prostate cancer
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Stakeholder Input
Clinical Review
Abbreviations
ADT
androgen deprivation therapy
AE
adverse event
ALP
alkaline phosphatase
ARAT
androgen receptor-axis-targeted therapy
BPI-SF
Brief Pain Inventory (Short Form)
CCSN
Canadian Cancer Survivor Network
CI
confidence interval
CrI
credible interval
CRPC
castration-resistant prostate cancer
ECOG
Eastern Cooperative Oncology Group
eCRF
electronic case report form
ePRO
electronic patient-reported outcome
FAS
full analysis set
GnRH
gonadotropin-releasing hormone
GRADE
Grading of Recommendations, Assessment, Development and Evaluations
HR
hazard ratio
HRQoL
health-related quality of life
IF
inconsistency factor
ITC
indirect treatment comparison
KM
Kaplan-Meier
LHRH
luteinizing hormone-releasing hormone
mCRPC
metastatic castration-resistant prostate cancer
mCSPC
metastatic castration-sensitive prostate cancer
mHSPC
metastatic hormone-sensitive prostate cancer
MID
minimally important difference
NCCN-FACT FPSI-17
National Comprehensive Cancer Network prostate cancer symptom index 17 item questionnaire/Functional assessment of cancer therapy
NMA
network meta-analysis
NR
not reached
nsAA
nonsteroid antiandrogen
OS
overall survival
PFS
progression-free survival
PSA
prostate-specific antigen
RCT
randomized controlled trial
RECIST
Response Evaluation Criteria In Solid Tumors
rPFS
radiographic progression-free survival
SAE
serious adverse event
SAF
safety analysis set
SD
standard deviation
SLR
systematic literature review
SNA
standard nonsteroidal antiandrogen
SoC
standard of care
SSE
symptomatic skeletal event
SSE-FS
symptomatic skeletal event-free survival
TEAE
treatment-emergent adverse event
ULN
upper limit of normal
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Item | Description |
|---|---|
Drug product | Darolutamide (Nubeqa), 300 mg, tablet, for oral use |
Indication | The treatment of patients with metastatic castration-sensitive prostate cancer (mCSPC) in combination with docetaxel |
Reimbursement request | In combination with docetaxel for the treatment of metastatic castration-sensitive prostate cancer (mCSPC) in patients who are chemotherapy-eligible |
Health Canada approval status | Notice of Compliance |
Health Canada review pathway | Priority review, Project Orbis |
Notice of Compliance date | September 29, 2022 |
Sponsor | Bayer Inc. |
Introduction
Prostate cancer is the most common cancer and the third leading cause of death from cancer in men living in Canada.1 It is estimated that 24,600 men will be diagnosed with prostate cancer in 2022.1 Metastatic castration-sensitive prostate cancer (mCSPC) refers to cancer that responds to androgen deprivation therapy (ADT). Bone metastasis (84%) is common and often accompanied by bone pain.2 Disease-related skeletal complications such as pathological fracture and spinal cord compression can occur.3 Progression to metastatic castration-resistant prostate cancer (mCRPC), a disease state associated with morbidity, poor health-related quality of life (HRQoL), and poor prognosis, occurs despite standard of care (SoC) treatment. The median survival for mCSPC is approximately 5 years, with a large variability in survival among patients, according to the clinical experts consulted by CADTH.
Treatment intensification with docetaxel or androgen receptor-axis-targeted therapy (ARAT) (i.e., enzalutamide, apalutamide, or abiraterone plus prednisone) in addition to ADT is the current SoC in men with mCSPC and has been shown to improve survival and delay disease progression. Recently, “triplet therapy” with abiraterone and prednisone plus docetaxel and ADT is also observed in clinical practice in light of new clinical trial evidence.4 This triplet therapy is currently under review at CADTH for mCSPC. Treatment intensification is the SoC; however, there is currently no consensus on the optimal treatment intensification strategy for mCSPC. The choice of therapy, in general, depends on functional assessment, comorbidities, patient preference, drug toxicity profiles, and drug accessibility, as per the clinical experts.
Darolutamide is an ARAT that is indicated for the treatment of patients with mCSPC in combination with docetaxel. The product monograph recommends darolutamide 600 mg (2 tablets of 300 mg) to be given twice daily orally with food until disease progression or unacceptable toxicity. Patients receiving this drug should receive a gonadotropin-releasing hormone (GnRH) analogue concurrently or have had a bilateral orchiectomy.5 Darolutamide was previously reviewed by CADTH for the treatment of non-mCSPC.
The objective of this review is to perform a systematic review of the beneficial and harmful effects of darolutamide 300 mg oral tablet in combination with docetaxel for the treatment of patients with mCSPC who are chemotherapy-eligible.
Stakeholder Perspectives
The information in this section is a summary of input provided by the patient groups who responded to CADTH’s call for patient input, and from clinical experts consulted by CADTH for the purpose of this review.
Patient Input
Two patient groups, the Canadian Cancer Survivor Network (CCSN) and the Canadian Cancer Society, submitted patient group input for this review. The CCSN gathered data through an online survey with responses from 24 patients with prostate cancer (6 of whom were diagnosed with metastatic disease) and from 2 caregivers. The Canadian Cancer Society conducted surveys and interviews with 39 patients with mCSPC and with 2 caregivers. In both submissions, all patients were living in Canada and a total of 8 patients had experience with darolutamide.
The Canadian Cancer Society respondents indicated that symptoms associated with mCSPC had a moderate-to-severe negative impact on their ability to engage in sexual activity, work, exercise, and travel; fulfill family obligations; and maintain their mental health. Common side effects following currently available treatments by patients in both submissions included changes in libido and sexual function, hot flashes, fatigue, loss of muscle mass, incontinence, and weight gain. Five patients from the CCSN submission rated how their experience with darolutamide compared to other treatments, with 4 of these patients indicating that darolutamide was easier to use and better addressed disease progression, 3 patients stating that they experienced a reduction in side effects compared to current treatments, and 1 indicating that it was better able to control their symptoms. Adverse events (AEs) identified among respondents with experience with darolutamide were consistent with those of currently available treatments. Across both submissions, respondents reported that they would like to see future treatments that delay the onset of symptoms and the need for chemotherapy, have fewer side effects, improve survival, are easy to use, and allow them to maintain their HRQoL.
Clinician Input
Input From Clinical Experts Consulted by CADTH
The clinical experts noted that although there are currently 2 available treatment-intensification strategies using chemotherapy or ARAT that can improve long-term outcomes beyond ADT alone, they are not curative. There remains a compelling need to extend survival longer while improving and maintaining quality of life overall. The clinical experts expected triplet therapy with darolutamide plus docetaxel and ADT to be considered as a first-line treatment option for men with mCSPC who are eligible for cytotoxic chemotherapy. The clinical experts noted that a major shift in the prescribing pattern is unlikely in the absence of direct evidence between darolutamide triplet therapy versus ARAT plus ADT, the most common regimen currently prescribed in Canada.
The clinical experts noted that there is no consensus among clinicians in Canada on who should be offered triplet therapy, and that the decision usually involves a case-by-case discussion between the patient and the treating physician. The clinical experts agreed that triplet therapy with darolutamide, docetaxel, and ADT should be available to all men with mCSPC who are candidates for cytotoxic chemotherapy.
The clinical experts noted that treatment response is, in general, evaluated based on clinical status, radiologic response, and prostate-specific antigen (PSA) response, and that the frequency of assessment is highly variable in clinical practice. The clinical experts noted that treatment discontinuation is considered in patients who have unacceptably toxicities or disease progression (clinical, PSA, and/or radiologic progression). In addition, the clinical experts noted that rapid progression and the absence of ongoing clinical benefit may warrant the initiation of a subsequent line of therapy.
Clinician Group Input
Clinician group input was received from 7 groups: the BC Cancer Agency (12 clinicians); the Canadian Cancer Society (12 clinicians); genitourinary oncologists from the Maritime provinces (5 clinicians); the Allan Blair Cancer Centre (5 clinicians); the Ottawa Hospital Cancer Centre — Genitourinary Oncology Group (3 clinicians); the Ontario Health — Cancer Care Ontario Genitourinary Cancer Drug Advisory Committee (4 clinicians); and the Genitourinary Disease Site Group of the Cancer Centre of Southeastern Ontario (2 clinicians). The various submissions noted that current treatment goals are to reduce symptom burden, prolong survival, and delay disease progression. The clinician groups noted that current treatment for mCSPC includes either chemotherapy (docetaxel) or an ARAT (i.e., abiraterone acetate plus prednisone, enzalutamide, or apalutamide) in combination with ADT. The clinician groups noted that mCSPC is incurable and that many patients fail systemic treatment shortly after treatment initiation. The groups emphasized a significant unmet need for treatments that further improve survival, increase HRQoL, and increase duration of treatment response while providing less toxicity burden. In terms of place in therapy, the submissions stated that darolutamide would be used as a first-line treatment for mCSPC in combination with ADT and docetaxel in patients who are fit for chemotherapy. The submissions stated that response to treatment would be assessed using PSA response, radiographic response, and clinical assessment (i.e., worsening pain or symptoms). Treatment would typically be discontinued upon disease progression (PSA, radiological, or symptomatic progression) or unacceptable toxicities.
Drug Program Input
The drug plans noted interest in understanding the treatment eligibility of patients with regional lymph node metastases, Eastern Cooperative Oncology Group (ECOG) performance status greater than or equal to 2, prior ADT in the adjuvant setting, and recent initiation of ADT in the metastatic setting, as well as identifying the appropriate criteria for treatment discontinuation and switch in therapy.
The clinical experts noted that, to receive triplet therapy, patients should have hormone sensitivity at the onset of treatment. Therefore, eligible patients would include those who are naive to ADT or who had received ADT within 6 months of starting the intensification, or metastatic patients who had completed adjuvant ADT more than 1 year prior. Patients who develop nodal disease alone should also be considered for triplet therapy. The clinical experts noted that the requirement for ECOG performance status is less stringent in regular practice than the inclusion criteria of ECOG performance status greater than or equal to 2 in the ARASENS trial. Patients with a poor baseline performance status should not be necessarily excluded from treatment and their overall medical status should be thoroughly assessed, as per the clinical experts.
The clinical experts noted that patients who are unable to tolerate all 6 cycles of docetaxel should be allowed to continue darolutamide plus ADT and that it is reasonable for patients who are unable to tolerate darolutamide to switch to an alternative ARAT (i.e., abiraterone) plus docetaxel plus ADT. The clinical experts commented that it would be reasonable to align discontinuation criteria for darolutamide with other ARATs. The clinical experts noted that the treatment should be discontinued upon unacceptable toxicity or disease progression as determined by the composite of clinical, radiological, and PSA determinants.
The clinical experts commented that the addition of darolutamide to docetaxel plus ADT would be reasonable if done at the onset of treatment intensification before the completion of docetaxel cycles. They noted that a switch in treatment regimen in patients who have well-controlled disease on an established regimen is unlikely in clinical practice. It would be uncommon for a treating physician to consider switching from ARAT plus ADT to triplet therapy except in the early phase of treatment (i.e., within 3 months of ADT initiation).
Clinical Evidence
Pivotal Studies and Protocol-Selected Studies
Description of Studies
The CADTH systematic review identified 1 relevant study, ARASENS,6 which was a phase III, double-blind, randomized controlled trial (RCT) comparing darolutamide (600 mg twice daily) to placebo, in combination with docetaxel (75 mg/m2 via IV infusion every 21 days for 6 cycles) and ADT in patients with de novo or metachronous mCSPC (N = 1,306) in a first-line metastatic setting. Patients were randomized to the treatment arms on a 1:1 ratio and continued treatment until disease progression (symptomatic disease progression or a change of therapy) or unacceptable toxicity. The primary end point was overall survival (OS), and the secondary end points were time to castration-resistant prostate cancer (CRPC), time to initiation of subsequent systemic antineoplastic therapy, time to pain progression, time to first symptomatic skeletal event (SSE), and symptomatic skeletal event-free survival (SSE-FS).
In the final efficacy analysis (data cut-off on October 25, 2021), the median age of patients at baseline was 67.0 (range = 41 to 89) years. The majority of patients were white (52.0%) or Asian (36.4%), and had stage IV disease at initial diagnosis (87.6%), an ECOG performance status of 0 (71.1%), and bone metastases (82.8%) at baseline. Most patients did not receive prior local therapy and no patients had prior systemic antineoplastic therapy for prostate cancer other than ADTs.
Efficacy Results
The key efficacy results from the ARASENS trial are summarized in Table 2.
Overall Survival
In the final OS analysis (primary outcome), the median duration of follow-up in the darolutamide plus docetaxel and ADT arm, and placebo plus docetaxel and ADT arm, was 43.7 months and 42.4 months (standard deviation [SD] not reported in both), respectively. The median OS was not reached in the darolutamide plus docetaxel and ADT arm and was 48.9 (95% confidence interval [CI], 44.4 to not reached [NR]) months in the placebo plus docetaxel and ADT arm, which corresponded to a hazard ratio (HR) of 0.68 (95% CI, 0.57 to 0.80; P < 0.0001), in favour of darolutamide.
Time to CRPC
The median time to CRPC (secondary outcome) was not reached in the darolutamide plus docetaxel and ADT arm, and was 19.1 (95% CI, 16.5 to 21.8) months in the placebo plus docetaxel and ADT arm, with an HR of 0.36 (95% CI, 0.30 to 0.42; P < 0.0001) in favour of darolutamide.
Time to Initiation of Subsequent Systemic Antineoplastic Therapy
The median time to initiation of subsequent systemic antineoplastic therapy (secondary outcome) was not reached in the darolutamide plus docetaxel and ADT arm, and was 25.3 (95% CI, 23.1 to 28.8) months in the placebo plus docetaxel and ADT arm, with a HR of 0.39 (95% CI, 0.33 to 0.46; P < 0.0001), in favour of darolutamide.
Time to Pain Progression
The median time to pain progression (secondary outcome) was not reached in the darolutamide plus docetaxel and ADT arm, and was 27.5 (95% CI, 22.0 to 36.1) months in the placebo plus docetaxel and ADT arm, with a HR of 0.79 (95% CI, 0.66 to 0.95; P = 0.0058), in favour of darolutamide.
Health-Related Quality of Life
HRQoL (exploratory outcome) was measured using the National Comprehensive Cancer Network prostate cancer symptom index 17 item questionnaire/Functional assessment of cancer therapy (NCCN-FACT FPSI-17) questionnaire. The mean total score and subscale scores were similar between treatment arms at baseline and remained stable at most assessment time points until near the end of the treatment, when the scores trended toward deterioration in both arms. There was no notable difference in the mean change in score from baseline between treatment arms at most time points; however, the difference between treatments was not statistically tested.
Objective Response Rate
This outcome was not measured in the study.
Time to First SSE
The median time to first SSE (secondary outcome) was not reached in both treatment arms and the HR was 0.71 (95% CI, 0.54 to 0.94; P = 0.0081), in favour of darolutamide.
Symptomatic Skeletal Event-Free Survival
The median SSE-FS (secondary outcome) was 51.2 (95% CI, 47.2 to NR) months in the darolutamide plus docetaxel and ADT arm, and 39.7 (95% CI, 36.0 to 42.3) months in the placebo plus docetaxel and ADT arm, with a HR of 0.61 (95% CI, 0.52 to 0.72; P < 0.0001), in favour of darolutamide.
PSA Outcomes
The following analyses were exploratory and the difference between treatment arms was not adjusted for multiplicity.
The median time to PSA progression was not reached in the darolutamide plus docetaxel and ADT arm, and was 22.4 (95% CI, 22.1 to 27.6) months in the placebo plus docetaxel and ADT arm, with an HR of 0.26 (95% CI, 0.21 to 0.31).
The risk difference in absolute PSA response rate (the proportion of patients with PSA level below 0.2 ng/mL) between treatment arms was 25.0% (95% CI, 20.0% to 29.9%) at 6 months, and 34.2% (95% CI, 29.2% to 39.1%) at 12 months.
The relative 90% PSA response rate (proportion of patients with at least 90% PSA reduction) was numerically higher in the darolutamide plus docetaxel and ADT arm than the placebo plus docetaxel and ADT arm at 3, 6, and 12 months. Analyses of relative 50% and 30% PSA response rate showed similar findings.
Harms Results
The key harms results from the ARASENS trial are summarized in Table 2.
Table 2: Summary of Key Results From the Pivotal Study
Outcomes | ARASENS | |
|---|---|---|
Darolutamide + docetaxel + ADT (N = 651) | Placebo + docetaxel + ADT (N = 654) | |
Primary outcome: overall survival (FAS) | ||
Death event, n (%) | 229 (35.2) | 304 (46.5) |
Overall survival (month),a median (95% CI) | NR | 48.9 (44.4 to NR) |
Hazard ratiob (95% CI) | 0.68 (0.57 to 0.80) | |
P valuec | < 0.0001 | |
Secondary outcome: time to castration-resistant prostate cancer (FAS) | ||
CRPC event,d n (%) | 225 (34.6) | 391 (59.8) |
Time to CRPCa (month), median (95% CI) | NR | 19.1 (16.5 to 21.8) |
Hazard ratiob (95% CI) | 0.36 (0.30 to 0.42) | |
P valuec | < 0.0001 | |
Secondary outcome: time to initiation of subsequent systemic antineoplastic therapy (FAS) | ||
Initiation of subsequent systemic antineoplastic therapy event, n (%) | 219 (33.6) | 395 (60.4) |
Time to initiation of subsequent systemic antineoplastic therapy (month),a median (95% CI) | NR | 25.3 (23.1 to 28.8) |
Hazard ratiob (95% CI) | 0.39 (0.33 to 0.46) | |
P valuec | < 0.0001 | |
Secondary outcome: time to pain progression (FAS) | ||
Pain progression event, n (%) | 222 (34.1) | 248 (37.9) |
Time to pain progression (month),a median (95% CI) | NR (30.5 to NR) | 27.5 (22.0 to 36.1) |
Hazard ratiob (95% CI) | 0.79 (0.66 to 0.95) | |
P valuec | 0.0058 | |
Secondary outcome: time to first symptomatic skeletal event (FAS) | ||
Symptomatic skeletal event,d n (%) | 95 (14.6) | 108 (16.5) |
Time to first symptomatic skeletal event (month),a median (95% CI) | NR | NR |
Hazard ratiob (95% CI) | 0.71 (0.54 to 0.94) | |
P valuec | 0.0081 | |
Harms outcomes (SAF) | ||
Patient with ≥ 1 TEAE,e n (%) | 649 (99.5) | 643 (98.9) |
Patient with ≥ 1 serious TEAE,e n (%) | 292 (44.8) | 275 (42.3) |
Patient who discontinued darolutamide or placebo due to TEAE,e n (%) | 88 (13.5) | 69 (10.6) |
Patient who discontinued docetaxel due to TEAE,e n (%) | 52 (8.0) | 67 (10.3) |
Deaths, n (%) | 229 (35.1) | 304 (46.8) |
ADT = androgen deprivation therapy; CI = confidence interval; CRPC = castration-resistant prostate cancer; FAS = full analysis set; NR = not reached; SAF = safety analysis set; TEAE = treatment-emergent adverse event.
aBased on Kaplan-Meier estimates.
bThe hazard ratio and 95% CI were based on a Cox regression model, stratified by extent of disease (M1a vs. M1b vs. M1c) and alkaline phosphatase (< upper limit of normal vs. ≥ upper limit of normal).
cP value was derived from the 1-sided log-rank test, stratified by extent of disease (M1a vs. M1b vs. M1c) and alkaline phosphatase (< upper limit of normal vs. ≥ upper limit of normal).
dPatients with multiple events were only counted for the category in which the first event occurred.
eTEAEs were defined as any event(s) arising or worsening after the first dose of darolutamide or placebo, until 30 days after the last dose of darolutamide or placebo administration.
Data cut-off: October 25, 2021.
Source: ARASENS Clinical Study Report.7
Almost all patients reported at least 1 treatment-emergent adverse event (TEAE) in both treatment arms (99.5% of patients in the darolutamide plus docetaxel and ADT arm, and 99.8% of patients in the placebo plus docetaxel and ADT arm). There was no notable difference in the TEAEs between treatment arms, except for the incidence of decreased appetite of any grade and hypertension of grade 3 or higher, both of which were numerically higher in the darolutamide plus docetaxel and ADT arm than the placebo plus docetaxel and ADT arm (decreased appetite of any grade: 18.6% versus 13.1%; hypertension of grade 3 or higher: 6.6% versus 3.2%). At least 1 serious TEAE was reported in 44.8% of patients in the darolutamide plus docetaxel and ADT arm, and 42.3% of patients in the placebo plus docetaxel and ADT arm, with the most common serious TEAE in both arms being febrile neutropenia (6.1% and 6.0%, respectively).
The proportion of patients who discontinued darolutamide or placebo due to TEAE was 13.5% in the darolutamide plus docetaxel and ADT arm, and 10.6% in the placebo plus docetaxel and ADT arm, while the proportion of patients who discontinued docetaxel due to TEAE was 8.0% in the darolutamide plus docetaxel and ADT arm, and 10.3% in the placebo plus docetaxel and ADT arm. Death events were reported in 35.1% of patients in the darolutamide plus docetaxel and ADT arm, and 46.8% of patients in the placebo plus docetaxel and ADT arm. The majority of deaths were attributed to disease progression in both treatment arms.
Critical Appraisal
Appropriate methods of randomization were used in the study. Reporting bias in favour of the darolutamide arm might have been involved for subjective efficacy outcomes (i.e., time to pain progression, time to first SSE, SSE-FS, and HRQoL) as a result of unblinding by error, although the extent of bias was likely to be small given the small number of unblinded patients (|||||| in the darolutamide triplet arm, |||||| in the control arm). A high number of important protocol deviations (||||||) was reported, which, according to the sponsor, was due to the use of broad and conservative definitions for important deviations and was not expected to compromise study data. The sponsor noted that none of the important protocol deviations was considered to be major according to the old International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use (ICH E3) classification. The statistical analyses were generally well designed, with adequate sample size and power considerations and multiplicity adjustments for all secondary outcomes using a hierarchal gatekeeping approach. HRQoL, PSA outcomes, and subgroup analyses, however, were not adjusted for multiplicity and were considered exploratory due to increased risk of type I error. There is also uncertainty in the HRQoL outcomes due to high risk of bias in measurement of the outcome and large losses to follow-up. The clinical experts noted the duration of follow-up for OS (median approximately 3.5 years) was adequate for assessing the efficacy and safety of systemic treatments for mCSPC, although longer follow-up would increase certainty of the OS results.
In consultation with the clinical experts, the inclusion and exclusion criteria of the trial were generally reflective of the treatment eligibility criteria in clinical practice; however, the exclusion of patients with significant comorbidities (e.g., cardiovascular diseases) and poor performance status may limit the generalizability of study results because this patient population is commonly seen in clinical practice. ARATs were the most commonly used subsequent antineoplastic therapy in the darolutamide arm. However, the clinical experts noted that the use of a second-line ARAT is unlikely to be adopted in clinical practice because second- or later-line re-treatment with an alternate ARAT is not funded by most jurisdictions. While the comparator regimen, docetaxel plus ADT, is an appropriate and relevant comparator, it accounts for a small proportion of treatment regimens prescribed for chemotherapy-eligible patients with mCSPC in Canada. In the absence of direct evidence, the comparative efficacy between darolutamide plus docetaxel and ADT versus ARAT plus ADT, the most commonly prescribed treatment regimen for mCSPC, is unknown and represents a gap in evidence. The clinical experts considered the benefits of darolutamide plus docetaxel and ADT in survival and delaying disease progression to be clinically meaningful. The clinical relevance of the HRQoL outcome was uncertain considering the NCCN-FACT FPSI-17 instrument is not routinely administered in clinical practice, as noted by the clinical experts. Nevertheless, the instrument does capture common symptoms (e.g., pain, difficulty in urination) and treatment-related side effects (e.g., fatigue, weight gain, decreased sexual function), which are very relevant in the clinical assessment of these patients in practice, according to the clinical experts.
Indirect Comparisons
Description of Studies
As part of the development of a |||||| cost-effectiveness model for darolutamide in mCSPC, the sponsor conducted and submitted a network meta-analysis (NMA) that was used to inform these analyses. The sponsor-submitted indirect treatment comparison (ITC) first conducted a systematic literature review (SLR) to identify evidence for inclusion in a |||||| ITC. The relative efficacy of darolutamide plus ADT and docetaxel from the ARASENS trial was indirectly compared to alternative treatments for patients with mCSPC via |||||||||||||||||||||||||||||||||||| NMA. Comparators of interest for the sponsor-submitted NMA included abiraterone and prednisone, apalutamide, enzalutamide, and docetaxel, in combination with ADT. Outcomes of interest included OS, time to CRPC, and radiographic progression-free survival (rPFS).8
Two additional NMAs were identified in the CADTH literature search (Menges et al. [2022], Yanagisawa et al. [2022]).9,10 The objective of the published SLR and NMA by Menges et al. was to assess the clinical effectiveness regarding survival and HRQoL, safety, and benefit-harm balance of metastatic hormone-sensitive prostate cancer (mHSPC) treatments, including docetaxel, abiraterone, enzalutamide, apalutamide, darolutamide, and radiotherapy (alone or in combination with ADT) via frequentist, random-effects NMA. Outcomes of interest evaluated in the study included OS, progression-free survival (PFS), HRQoL, and AEs; however, results for PFS and HRQoL were not available for comparisons involving darolutamide, and AEs were not available because comparisons were only made to ADT monotherapy,9 and therefore were not of interest to this review.
The objective of the published SLR and NMA by Yanagisawa et al. was to analyze the benefit of triplet combination therapies with androgen receptor signalling inhibitors (abiraterone acetate, apalutamide, darolutamide, and enzalutamide) in combination with docetaxel and ADT, compared to available treatment regimens in patients with mHSPC via frequentist, random-effects NMA. Outcomes of interest included OS, PFS, and AEs; however, results for PFS were not available for comparisons involving darolutamide, and comparisons for AEs were only made to ADT monotherapy10 and therefore were not of interest to this review.
Efficacy Results
The sponsor-submitted NMA included a total of |||||| trials. In the |||||||||||||||||| NMA for OS, darolutamide plus ADT and docetaxel was favoured over ADT and docetaxel (||||||||||||||||||||||||||||||||||||) and ADT alone (||||||||||||||||||||||||||||||||||||); however, comparisons between darolutamide plus ADT and docetaxel and enzalutamide (||||||||||||||||||||||||||||||||||||), apalutamide (||||||||||||||||||||||||||||||||||||), and abiraterone acetate (||||||||||||||||||||||||||||||||||||) were affected by imprecision, precluding conclusions about comparative efficacy. For time to CRPC, darolutamide plus ADT and docetaxel was favoured over apalutamide and ADT (||||||||||||||||||||||||||||||||||||), abiraterone and ADT (||||||||||||||||||||||||||||||||||||), docetaxel and ADT (||||||||||||||||||||||||||||||||||||), and ADT alone (||||||||||||||||||||||||||||||||||||), but over the comparison to enzalutamide and ADT (||||||||||||||||||||||||||||||||||||) was imprecise, precluding conclusions about comparative efficacy. Results for sensitivity analyses using |||||||||||| models were consistent with the base-case analyses, although 95% credible intervals (CrIs) were wider.
The NMA by Menges et al. included a total of 10 studies. In the frequentist, random-effects NMA for OS, darolutamide plus ADT and docetaxel was favoured over ADT and docetaxel (HR, 0.68 [95% CI, 0.57 to 0.81]). The comparisons of darolutamide plus ADT and docetaxel to abiraterone acetate plus ADT and prednisone, enzalutamide and ADT, apalutamide and ADT, and apalutamide plus ADT and docetaxel were affected by imprecision, precluding conclusions.
The NMA by Yanagisawa et al. included a total of 8 studies. In the frequentist, random-effects NMA for OS, darolutamide plus ADT and docetaxel was favoured over ADT and docetaxel (HR, 0.68 [95% 0.56 to 0.82]), and ADT and abiraterone acetate (HR, 0.74 [95% CI, 0.55 to 0.99]). No analyses were conducted for other comparators of interest.
Harms Results
Harms results were only reported for the published NMAs, although most comparisons were only conducted versus ADT monotherapy. No harms results were reported in the sponsor-submitted NMA. Results of the NMA focusing on AEs conducted by Yanagisawa et al. also showed wide CIs for the comparison of darolutamide plus ADT and docetaxel to abiraterone and ADT (OR, 26.62 [95% CI, 7.46 to 94.99]), precluding conclusions.
Critical Appraisal
Appraisal points across the 3 NMAs were similar. The sponsor-submitted NMA and both published NMAs were informed by SLRs; however, no information was provided in the sponsor-submitted report on the methods of study selection or data extraction (i.e., duplicate reviewers), or whether a risk-of-bias assessment was conducted. Both published NMAs followed appropriate methods for identification, inclusion, and assessment of studies. Both published NMAs also conducted a quality assessment using the Cochrane risk-of-bias 2.0 tool;11 however, the results for the individual domains varied, despite authors reaching the same conclusion, that the studies were at a low risk of bias.
In general, treatments included in the NMAs were considered appropriate; however, there were some treatments, such as ADT monotherapy (included in all NMAs) and radiotherapy, which were not considered relevant comparators for this review. Additionally, the sponsor-submitted NMA did not consider the combination of abiraterone plus ADT and docetaxel, which was noted by the clinical experts consulted by CADTH as a relevant treatment option currently in Canada. Of note, the clinical experts reported that the combination has recently begun to be used by some clinicians in light of new clinical trial evidence4 and would not have been considered relevant at the time the NMA was conducted by the sponsor. The outcomes assessed across NMAs were also appropriate; however, important outcomes such as AEs and HRQoL were not considered in the sponsor’s NMA. While HRQoL and AEs were evaluated across the published NMAs, comparisons either did not include darolutamide plus ADT and docetaxel, or used ADT monotherapy as a reference, and were therefore not included in this report. Across NMAs, in most cases, comparisons were based on single trials and all evidence for comparisons to darolutamide plus ADT and docetaxel were indirect, increasing the uncertainty of the estimates of comparative efficacy. Additionally, results for OS were generally only in favour of darolutamide plus ADT and docetaxel over ADT and docetaxel alone and demonstrated wide 95% CIs, suggesting uncertainty and imprecision in the comparative efficacy estimates.
The main concern across the NMAs was the potential for heterogeneity across studies, which would result in violation of the underlying transitivity assumption, which introduces an unknown degree of bias into the results. In the sponsor-submitted NMA, potential effect modifiers were considered from results of the ARASENS subgroup analysis, but consultation with clinical experts or other empirical evidence was not reported. There were notable differences in study design (i.e., blinded versus open label) and baseline characteristics that could potentially result in changing relative treatment effects, and, although identified, these were not accounted for (i.e., PSA level and prostate cancer stage). Differences in prior treatment requirements, the time period during which the studies were undertaken, and follow-up duration were also evident across studies. Baseline characteristics were not available for all factors of interest across all studies. Although many baseline characteristics appeared similar across trials, other differences (e.g., study design, prior treatment, outcome definitions, length of follow-up, and time period during which the studies were undertaken) were not feasible to address. For Menges et al., the authors note that transitivity was assessed using epidemiological criteria and the presence of potential effect modifiers, along with considerations of clinical plausibility. No rationale or further discussion of the transitivity assessment is provided in the publication or supplementary material; therefore, it is difficult to conclude whether the transitivity assumption was met. Heterogeneity was assessed visually and by means of I2 values and was reported to be low for OS in the overall NMA. Some potentially important effect modifiers were reported in the study but were not adjusted for or discussed (e.g., use of prior therapy, Gleason score), and follow-up duration varied across studies. In the Yanagisawa et al. NMA, potential sources of heterogeneity were evaluated in the initial meta-analysis via Cochran’s Q test; however, results did not suggest any important heterogeneity and therefore it was not explored for the NMA. As a result, it was unclear if the transitivity assumption was met. Additionally, no consideration was given to treatment effect modifiers, and thus the impact of any potential effect modifiers remains unknown. The authors noted that the publications included in the NMA included different patient populations with regards to the proportions of patients with de novo disease and disease burden. As such, the findings of all NMAs, although supportive of the ARASENS trial, were highly uncertain due to the methodological limitations as well as wide CrIs/CIs.
Other Relevant Evidence
No long-term extension studies or other relevant studies were included in the sponsor’s submission to CADTH.
Conclusions
In the ARASENS trial, darolutamide in combination with docetaxel and ADT demonstrated a clinically meaningful improvement of OS compared with docetaxel plus ADT in patients with mCSPC. Analyses of secondary outcomes supported the efficacy of darolutamide plus docetaxel and ADT in delaying progression to mCRPC, the need for subsequent antineoplastic therapy, worsening of pain, and SSEs, compared to docetaxel plus ADT. Due to limitations in the statistical analysis, no definitive conclusions can be drawn from the exploratory PSA and HRQoL analyses. The exclusion of patients with significant comorbidities and impaired performance status and the use of a comparator regimen that has low utilization in Canada may limit the generalizability of study findings. Across the included NMAs, the findings for the comparative survival benefit observed with darolutamide plus ADT and docetaxel compared to ADT and docetaxel supported the findings of the ARASENS trial; however, the findings of these NMAs are associated with uncertainty due to probable violation of the underlying transitivity assumption. Comparisons to other drugs of interest were uncertain due to the aforementioned methodological limitations as well as wide CIs. The safety profile of darolutamide plus docetaxel and ADT was overall similar to that of docetaxel and ADT in the ARASENS trial, with no additional serious safety concern.
Introduction
Disease Background
Prostate cancer is the most common cancer (excluding non-melanoma skin cancers) and the third leading cause of death from cancer in men living in Canada.1 It is estimated that 24,600 men will be diagnosed with prostate cancer and that 4,600 deaths from prostate cancer will occur in Canada in 2022.1
Approximately 9% of prostate cancers are metastatic at diagnosis.12 mCSPC refers to metastatic prostate cancer that responds to ADT. The disease can occur de novo (newly diagnosed in the metastatic state) or present as metachronous disease (progressed from localized disease despite treatment). The most common sites of metastasis are bone (84%) and distant lymph nodes (11%).2 The clinical presentations of mCSPC patients are highly variable. Some patients are asymptomatic after receiving local therapy of curative intent in the non-metastatic stage and were identified to have metachronous disease upon routine follow-up, while others present symptomatically, with bone pain and lower urinary tract symptoms being the most common symptoms, according to the clinical experts consulted by CADTH. In patients with bone metastasis, disease-related skeletal complications including pathological fracture and spinal cord compression may occur.3
mCSPC is an incurable disease. Progression to mCRPC, a disease state that is no longer responsive to ADT, is associated with increased disease burden and/or worsening symptoms. According to the clinical experts, the median survival for mCSPC is approximately 5 years, with a large variability in survival among patients.
The diagnosis of mCSPC involves physical examination, digital rectal exam, PSA test, biopsy, and imaging (e.g., CT, MRI, and bone scan).13
Standards of Therapy
ADT, achieved either by surgical castration (orchiectomy), or pharmacologically with GnRH agonists or antagonists, has been the cornerstone therapy for mCSPC.14 Treatment intensification with the addition of docetaxel or ARAT (i.e., enzalutamide, apalutamide, or abiraterone plus prednisone) to ADT is the current SoC in men with mCSPC and has been shown to improve survival and slow disease progression compared to ADT alone.14,15 Recently, triplet therapy with ADT, docetaxel, and abiraterone plus prednisone is also observed in clinical practice in light of new clinical trial evidence,4 according to the clinical expert consulted by CADTH. This triplet therapy is currently under review at CADTH for mCSPC. Treatment intensification is the SoC; however, there is currently no consensus on the optimal treatment intensification strategy for mCSPC: the choice of therapy in general depends on functional assessment, comorbidities, patient preference, drug toxicity profiles, and drug accessibility, as per the clinical experts.
In select patients with a low-volume metastatic disease burden, ADT and external beam radiation therapy, directed toward the primary tumour(s) in the prostate, are considered.14,15
The key treatment goals of mCSPC include improving survival, delaying progression to mCRPC and the need for subsequent antineoplastic therapy, and improving symptoms and HRQoL, according to the clinical expert consulted by CADTH.
Drug
Darolutamide is an androgen receptor pathway inhibitor that antagonizes the androgen receptor by binding directly to receptor ligand binding domain, leading to competitive inhibition of androgen binding, nuclear translocation of androgen receptor, and androgen receptor-mediated transcription. The drug has been shown to inhibit prostate cancer cell proliferation and tumour growth in animal models.
Darolutamide has been previously reviewed by CADTH for the treatment of non-mCRPC. Darolutamide was granted a Health Canada Notice of Compliance for the indication of the treatment of patients with mCSPC in combination with docetaxel on September 29, 2022. The sponsor is seeking reimbursement of darolutamide in combination with docetaxel for the treatment of mCSPC in patients who are chemotherapy-eligible.
As per the product monograph, the anticipated recommended dose of darolutamide is 600 mg (2 tablets of 300 mg) twice daily orally with food until disease progression or unacceptable toxicity.5 It is recommended that patients receive a GnRH analogue concurrently or have had a bilateral orchiectomy.5
The key characteristics of treatments for mCSPC are summarized in Table 3.
Table 3: Key Characteristics of Darolutamide, Enzalutamide, Apalutamide, and Abiraterone
Characteristic | Darolutamide | Enzalutamide | Apalutamide | Abiraterone |
|---|---|---|---|---|
Mechanism of action | An ARAT that inhibits androgen binding to AR and therefore inhibits AR translocation and AR transcription | An ARAT that inhibits androgen binding to AR and therefore inhibits AR translocation and AR transcription | An ARAT that inhibits androgen binding to AR and therefore inhibits AR translocation and AR transcription | An ARAT that inhibits CYP17, an enzyme required for androgen biosynthesis in the prostate |
Indicationa |
|
|
|
|
Route of administration | Oral | Oral | Oral | Oral |
Recommended dose | 600 mg twice daily, in combination with docetaxel,e and concurrent GnRH or orchiectomy | 160 mg daily, with concurrent GnRH or orchiectomy | 240 mg once daily, with concurrent GnRH or orchiectomy | 1 g daily, with prednisone, with concurrent GnRH or orchiectomy |
Serious warnings and precautions | None |
| None |
|
ADT = androgen deprivation therapy; AR = androgen receptor; ARAT = androgen receptor-axis-targeted therapy; CV = cardiovascular; CYP17 = 17Alpha-hydroxylase/C17,20-lyase; GnRH = gonadotropin-releasing hormone; mCRPC = metastatic castration-resistant prostate cancer; mCSPC = metastatic castration-sensitive prostate cancer; nmCRPC = non-metastatic castration-resistant prostate cancer.
aHealth Canada–approved indication.
bThe drug has not been studied in patients with nmCRPC at low risk of developing metastases. The benefit and risk profile in these patients is unknown.
cIn patients who are: chemotherapy-naive with asymptomatic or mildly symptomatic disease after failure of ADT; have received docetaxel therapy.
dIn patients who are asymptomatic or mildly symptomatic after failure of ADT or who have received prior chemotherapy containing docetaxel after failure of ADT.
eThe first of 6 cycles of docetaxel should be administered within 6 weeks after the start of darolutamide treatment.
Source: Nubeqa Product Monograph,5 Xtandi Product Monograph,16 Erleada Product Monograph,17 and Zytiga Product Monograph.18
Stakeholder Perspectives
Patient Group Input
This section was prepared by CADTH staff based on the input provided by patient groups. The full original patient input(s) received by CADTH has been included in the stakeholder section at the end of this report.
Two patient groups, the CCSN and the Canadian Cancer Society, submitted patient group input for this review. The CCSN gathered data through an online survey with responses from 24 patients with prostate cancer (6 of whom were diagnosed with metastatic disease) and from 2 caregivers. The Canadian Cancer Society conducted surveys and interviews with 39 patients with mCSPC and with 2 caregivers. Demographic information was provided for the Canadian Cancer Society respondents, with the majority identifying as male (98%), white (95%), and 70 to 79 years of age (49%). In both submissions, all patients were from Canada and a total of 8 patients had experience with darolutamide.
The Canadian Cancer Society respondents indicated that symptoms associated with mCSPC had a moderate-to-severe negative impact on their ability to engage in sexual activity (76%), work (49%), exercise (44%), and travel (32%); fulfill family obligations (32%); and maintain their mental health (32%). Common side effects following currently available treatments by patients in both submissions included changes in libido and sexual function, hot flashes, fatigue, loss of muscle mass, incontinence, and weight gain. Patients who had experience with darolutamide reported also currently taking or having taken ADT monotherapy, enzalutamide plus ADT, docetaxel plus ADT, and abiraterone acetate with prednisone plus ADT. Five patients from the CCSN submission rated how their experience with darolutamide compared to other treatments, with 4 of these patients indicating that darolutamide was easier to use and better addressed disease progression, 3 patients stating that they experienced a reduction in side effects compared to current treatments, and 1 indicating that it was better able to control their symptoms. AEs identified among respondents with experience with darolutamide were consistent with those of currently available treatments. Across both submissions, respondents reported that they would like to see future treatments that delay the onset of symptoms, delay the need for chemotherapy, have fewer side effects, improve survival, are easy to use, and allow them to maintain their HRQoL.
Clinician Input
Input From Clinical Experts Consulted by CADTH
All CADTH review teams include at least 1 clinical specialist with expertise in the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). The following input was provided by 2 clinical specialists with expertise in the diagnosis and management of mCSPC.
Unmet Needs
The clinical experts noted that the goals of therapy for mCSPC include improving survival, delaying disease progression, reducing symptoms, and improving HRQoL. The clinical experts noted that although there are currently 2 available treatment intensification strategies using chemotherapy or ARAT that can improve long-term outcomes beyond ADT alone, these are not curative. There remains a compelling need to extend survival longer while improving and maintaining quality of life overall, as per the clinical experts.
Place in Therapy
The clinical experts expected triplet therapy with darolutamide, docetaxel, and ADT to be considered as a first-line treatment option for men with mCSPC who are eligible for cytotoxic chemotherapy. The clinical experts noted that ARAT plus ADT regimens account for the majority of treatment regimens prescribed for mCSPC in Canada, and in the absence of head-to-head evidence comparing darolutamide plus docetaxel and ADT triplet therapy versus ARAT plus ADT, a major shift in the prescribing pattern is unlikely. The clinical experts noted that in patients for whom treatment with docetaxel plus ADT is considered, the addition of darolutamide is supported by the ARASENS trial and will likely be favoured over docetaxel-plus-ADT–only regimen by clinicians.
Patient Population
The clinical experts noted that, among clinicians in Canada, there is no consensus on who should be offered triplet therapy, and that it usually involves a case-by-case discussion between the patient and the treating physician. A clinical expert noted that in their clinical practice, triplet therapy is considered in patients with aggressive disease who are lacking in competing causes of mortality and eligible for chemotherapy. The clinical experts agreed that triplet therapy with darolutamide, docetaxel, and ADT should be available to all men with mCSPC who are candidates for cytotoxic chemotherapy.
Assessing Response to Treatment
The clinical experts noted that the approach to assessing treatment response is highly heterogeneous in clinical practice and that it usually involves assessment of clinical status, radiologic response, and PSA response. The clinical experts also indicated that the frequency of assessment is highly variable in clinical practice. One clinical expert noted that, in their practice, clinical and PSA assessments are conducted every 3 months in the first year and every 6 months thereafter.
Discontinuing Treatment
The clinical experts noted that treatment discontinuation is considered in patients who have unacceptably toxicity or disease progression, which is generally determined based on a composite of clinical, PSA, and radiologic factors at the physician’s discretion in clinical practice. Most physicians consider progression in at least 2 of 3 parameters to be indicative of disease progression, according to the clinical experts. In addition, the clinical experts noted that rapid progression and the absence of ongoing clinical benefit may warrant the use of a subsequent line of therapy.
Prescribing Conditions
The clinical experts noted that darolutamide plus docetaxel and ADT should be prescribed by a medical oncologist.
Clinician Group Input
This section was prepared by CADTH staff based on the input provided by clinician groups. The full original clinician group input received by CADTH has been included in the stakeholder section at the end of this report.
Clinician group input was received from 7 groups: the BC Cancer Agency (12 clinicians); the Canadian Cancer Society (12 clinicians); genitourinary oncologists from the Maritime provinces (5 clinicians); the Allan Blair Cancer Centre (5 clinicians); the Ottawa Hospital Cancer Centre — Genitourinary Oncology Group (3 clinicians); the Ontario Health — Cancer Care Ontario Genitourinary Cancer Drug Advisory Committee (4 clinicians); and the Genitourinary Disease Site Group of the Cancer Centre of Southeastern Ontario (2 clinicians). The various submissions noted that current treatment goals are to reduce symptom burden, prolong survival, and delay disease progression. The clinician groups noted that current treatment for mCSPC includes either chemotherapy (docetaxel) or a second-generation androgen receptor inhibitor (i.e., abiraterone acetate plus prednisone, enzalutamide, or apalutamide) in combination with ADT. The clinician groups noted that mCSPC is incurable and that many patients fail systemic treatment shortly after treatment initiation. The groups emphasized a significant unmet need for treatments that further improve survival, increase HRQoL, and increase duration of treatment response while providing lower toxicity burden. In terms of place in therapy, the submissions stated that the darolutamide would be used as a first-line treatment for mCSPC in combination with ADT and docetaxel in patients who are fit for chemotherapy. The submissions stated that response to treatment would be assessed using PSA response, radiographic response, and clinical assessment (i.e., worsening pain or symptoms). Treatment would typically be discontinued upon disease progression (PSA, radiological, or symptomatic progression) or unacceptable toxicities.
Drug Program Input
The drug programs provide input on each drug being reviewed through CADTH’s reimbursement review processes by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CADTH are summarized in Table 4.
Table 4: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Relevant comparators | |
The comparator in the ARASENS trial is ADT + docetaxel. Other publicly funded comparators in this therapeutic space include apalutamide + ADT, enzalutamide +ADT, and abiraterone + prednisone + ADT. Patients receiving ARAT + ADT may have been sequentially treated with docetaxel. How does darolutamide + ADT + docetaxel compare with other publicly funded alternatives? | Addressed in the Clinical Review report |
There is currently a non-sponsored reimbursement review under way for abiraterone + prednisone + ADT + docetaxel for mCSPC PEACE-1 trial). How does darolutamide + ADT + docetaxel compare with abiraterone + prednisone + ADT + docetaxel? | Addressed in the Clinical Review report |
Initiation of therapy | |
Patients with regional lymph node metastases only were not eligible for the ARASENS trial. If darolutamide + ADT+ docetaxel is recommended for reimbursement, should patients with regional lymph node metastases only be excluded? | The clinical experts agreed that there is no compelling reason to exclude patients with regional lymph node metastases and that these patients could potentially benefit from darolutamide + ADT+ docetaxel in the long-term. |
ARASENS eligibility criteria included ECOG performance status of 0 to 1. Are the results of the trial generalizable to patients with an ECOG performance status ≥ 2? | The clinical experts agreed that the requirement for performance status in determining treatment eligibility is less stringent in clinical practice. One clinical expert also noted that while it is known that patients with a poor performance status will unlikely tolerate cytotoxic chemotherapy, some patients who initially present with ECOG performance status > 2 but experience profound and rapid clinical improvement after lead-in treatment with ADT may be candidates for darolutamide plus docetaxel and ADT. The clinical experts noted that patients with poor baseline performance status should not be necessarily excluded from treatment and that their overall medical status should be thoroughly assessed. |
Should patients who received ADT in the adjuvant setting and completed therapy more than 1 year prior (i.e., considered hormone sensitive) be eligible for darolutamide + ADT + docetaxel? | The clinical experts noted that to receive triplet therapy, patients should have hormone sensitivity at the onset of treatment; therefore, patients who received ADT in the adjuvant setting and completed therapy more than 1 year prior should be eligible for darolutamide + ADT + docetaxel. |
Are the ARASENS trial results consistent among patients with high-risk and low-risk disease? | Addressed in the Clinical Review report |
In the ARASENS trial, patients had to have started ADT (+/− first-generation antiandrogen), but not longer than 12 weeks before randomization. CADTH recommendations for apalutamide and enzalutamide + ADT for mCSPC specified that patients must not have had prior ADT in the metastatic setting or be within 6 months of initiating ADT in the metastatic setting. Should criteria for darolutamide + ADT+ docetaxel align? | The clinical experts agreed that it would be appropriate to use darolutamide + ADT + docetaxel in patients who are naive to ADT, or who had received ADT within 6 months of starting the intensification, because it is reasonable to expect that they have hormone sensitivity at the onset of treatment. |
Discontinuation of therapy | |
Should patients unable to tolerate 6 cycles of docetaxel be eligible to continue with darolutamide + ADT? | The clinical experts agreed that patients who are unable to tolerate docetaxel should be eligible to continue with darolutamide + ADT. |
Should patients unable to tolerate darolutamide be eligible to switch to an alternative ARAT + docetaxel + ADT provided all other criteria are met? | The clinical experts noted that it is unlikely that patients are unable to tolerate darolutamide; however, in case of intolerance to darolutamide, a switch to a different ARAT (i.e., abiraterone) + docetaxel + ADT is considered clinically appropriate. |
In the ARASENS trial, darolutamide continued until symptomatic disease progression or unacceptable toxicity. In the CADTH recommendations for enzalutamide and apalutamide + ADT for mCSPC, treatment was to be discontinued until disease progression or unacceptable toxicity. Should discontinuation criteria for darolutamide align with previous CADTH recommendations? | The clinical experts noted that disease progression is generally determined based on assessments of a combination of clinical, PSA, and radiologic factors in clinical practice. They agreed that symptoms should be factored into the assessment for treatment discontinuation but that worsening of symptoms may not always be present in patients in whom treatment discontinuation is indicated. Therefore, it may be reasonable to align discontinuation criteria for darolutamide with other ARATs. |
Generalizability | |
Should patients who recently initiated docetaxel + ADT for mCSPC be eligible to add on darolutamide? If so, what is the appropriate time frame? | The clinical experts noted that there is currently no clinical evidence to inform the addition of darolutamide in patients who recently initiated docetaxel + ADT. The clinical experts that the addition of darolutamide to docetaxel + ADT would be reasonable if done at the onset of treatment intensification before the completion of docetaxel cycles. |
Should patients receiving ARAT (apalutamide, enzalutamide or abiraterone + prednisone) + ADT for mCSPC be eligible to switch to darolutamide + ADT + docetaxel at the time of funding? | The clinical experts noted that there is currently no evidence to inform switching from an existing ARAT + ADT to darolutamide + ADT + docetaxel. The clinical experts noted that this is an unlikely clinical scenario because it is unusual in clinical practice to consider a switch in treatment regimen in patients who have well-controlled disease on an established regimen. They also noted that it would be uncommon for a treating physician to consider switching from ARAT plus ADT to triplet therapy, except in the early phase of treatment (i.e., within 3 months of ADT initiation). |
ADT = androgen deprivation therapy; ARAT = androgen receptor-axis-targeted therapy; ECOG = Eastern Cooperative Oncology Group; mCSPC = metastatic castration-sensitive prostate cancer; PSA = prostate-specific antigen.
Clinical Evidence
The clinical evidence included in the review of darolutamide is presented in 3 sections. The first section, the Systematic Review, includes pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those studies that were selected according to an a priori protocol. The second section includes indirect evidence from the sponsor and indirect evidence selected from the literature that met the selection criteria specified in the review. The third section includes additional relevant studies that were considered to address important gaps in the evidence included in the systematic review.
Systematic Review (Pivotal and Protocol-Selected Studies)
Objectives
To perform a systematic review of the beneficial and harmful effects of darolutamide 300 mg oral tablet in combination with docetaxel for the treatment of patients with mCSPC who are chemotherapy-eligible.
Methods
Studies selected for inclusion in the systematic review included pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those meeting the selection criteria presented in Table 5. Of note, the systematic review protocol presented below was established before the granting of a Notice of Compliance from Health Canada. Table 5 shows the outcomes included in the CADTH review protocol, which reflect outcomes considered to be important to patients, clinicians, and drug plans.
Table 5: Inclusion Criteria for the Systematic Review
Criteria | Description |
|---|---|
Patient population | Patients with metastatic castration-sensitive prostate cancer who are chemotherapy-eligible Subgroups:
|
Intervention | Darolutamide 600 mg twice daily orally + docetaxel + ADTa |
Comparators |
|
Outcomes | Efficacy outcomes:
Harms outcomes:
|
Study design | Published and unpublished phase III and IV RCTs |
ADT = androgen deprivation therapy; AE = adverse event; ECOG = Eastern Cooperative Oncology Group; HRQoL = health-related quality of life; ORR = objective response rate; OS = overall survival; PSA = prostate-specific antigen; RCT = randomized controlled trial; SAE = serious adverse event; WDAE = withdrawal due to adverse event.
aIn the input received by CADTH from patient groups, these outcomes were identified as being of particular importance to patients.
The literature search for clinical studies was performed by an information specialist using a peer-reviewed search strategy according to the PRESS Peer Review of Electronic Search Strategies checklist.19
Published literature was identified by searching the following bibliographic databases: MEDLINE All (1946–) via Ovid and Embase (1974–) via Ovid. All Ovid searches were run simultaneously as a multifile search. Duplicates were removed using Ovid deduplication for multifile searches, followed by manual deduplication in EndNote. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s Medical Subject Headings (MeSH), and keywords. The main search concept was Nubeqa (darolutamide). Clinical trials registries were also searched: the US National Institutes of Health’s clinicaltrials.gov, WHO’s International Clinical Trials Registry Platform (ICTRP) search portal, Health Canada’s Clinical Trials Database, and the European Union Clinical Trials Register.
No filters were applied to limit the retrieval by study type. Retrieval was not limited by publication date or by language. Conference abstracts were excluded from the search results. Refer to Appendix 1 for the detailed search strategies.
The initial search was completed on July 13, 2022. Regular alerts updated the search until the meeting of the CADTH pan-Canadian Oncology Drug Review Expert Committee (pERC) on November 9, 2022.
Grey literature (literature that is not commercially published) was identified by searching relevant websites from the Grey Matters: A Practical Tool For Searching Health-Related Grey Literature checklist.20 Included in this search were the websites of regulatory agencies (US FDA and European Medicines Agency). Google was used to search for additional internet-based materials. Refer to Appendix 1 for more information on the grey literature search strategy.
These searches were supplemented through contacts with appropriate experts. In addition, the sponsor of the drug was contacted for information regarding unpublished studies.
Two CADTH clinical reviewers independently selected studies for inclusion in the review based on titles and abstracts, according to the predetermined protocol. Full-text articles of all citations considered potentially relevant by at least 1 reviewer were acquired. Reviewers independently made the final selection of studies to be included in the review, and differences were resolved through discussion.
Findings From the Literature
One study submitted by the sponsor (the ARASENS trial)6 was eligible for inclusion in the systematic review (Figure 1). The included study is summarized in Table 6.
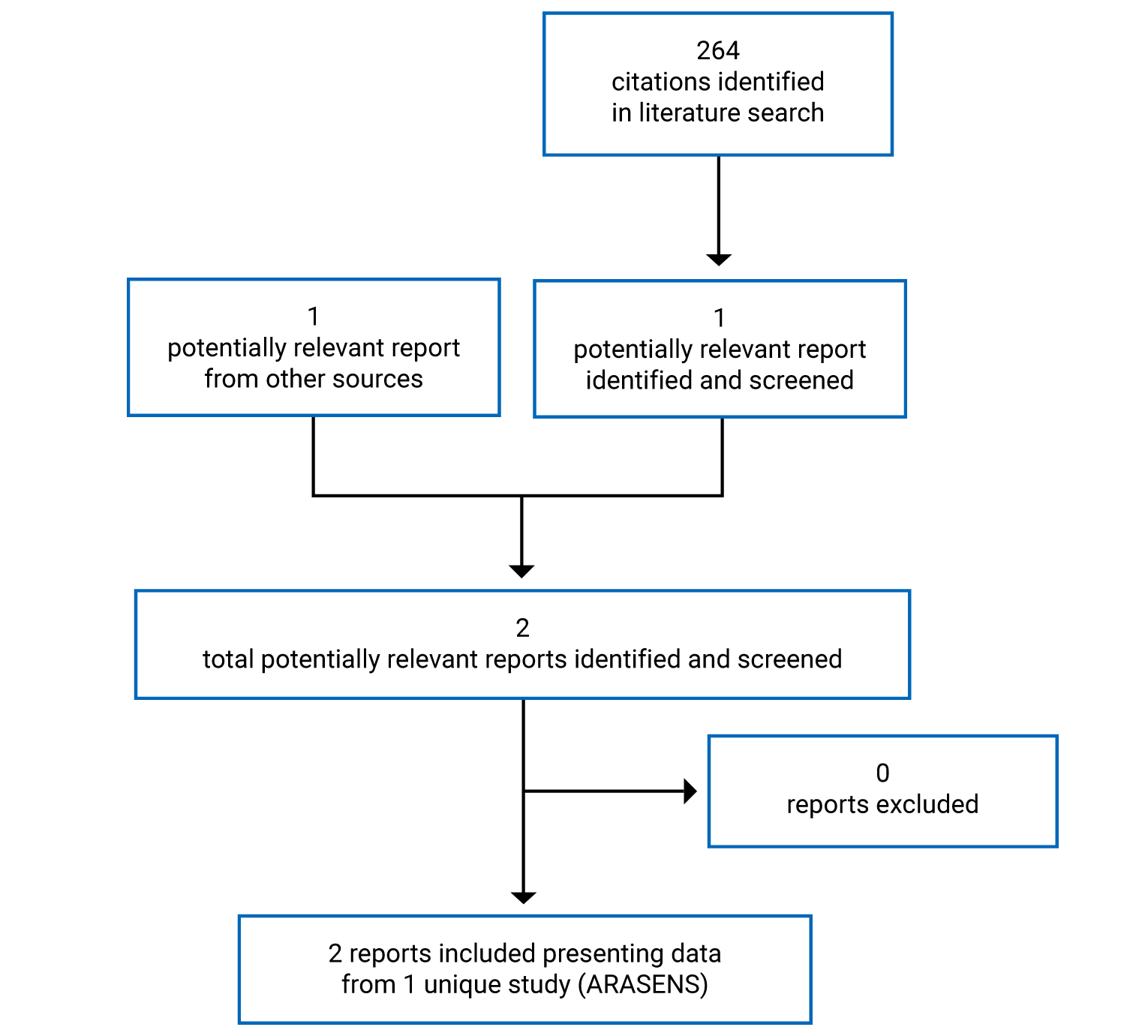
Table 6: Details of Included Studies
ARASENS trial | |
|---|---|
Design and population | |
Study design | Phase III, multicentre, double-blind RCT |
Locations | 301 sites in 23 countries or regions: Europe (115), Asia (106), North America (66 sites in total, including 5 in Canada), South America (9), Australia (5) |
Study duration | Start date: November 30, 2016 |
Data cut-off date | Primary analysis: October 25, 2021 |
Randomized (N) | 1,306 |
Inclusion criteria |
|
Exclusion criteria |
|
Drugs | |
Intervention | Darolutamide 600 mg twice daily (two 300 mg tablets) orally with food until symptomatic disease progression or unacceptable toxicity + docetaxel 75 mg/m2 via IV infusion every 21 days for 6 cycles (with or without prednisone or prednisolone)e + ADTf |
Comparator | Placebo twice daily orally with food until symptomatic disease progression or unacceptable toxicity + docetaxel 75 mg/m2 via IV infusion every 21 days for 6 cycles (with or without prednisone or prednisolone)e + ADTf |
Duration | |
Phase | |
Screening | Up to 28 days |
Treatment | Until disease progression (symptomatic progressive disease, change of antineoplastic therapy), or unacceptable toxicity |
Active follow-up | Up to 1 year |
Long-term (survival) follow-up | Until death or end of study |
Outcomes | |
Primary end point | Overall survival |
Secondary and exploratory end points | Secondary:
Exploratory:
|
Notes | |
Publications | Smith et al. (2022)6 |
ADT = androgen deprivation therapy; BPI-SF = Brief Pain Inventory (Short Form); CT = CT; ECOG = Eastern Cooperative Oncology Group; HRQoL = health-related quality of life; LHRH = luteinizing hormone-releasing hormone; NCCN-FACT FPSI-17 = National Comprehensive Cancer Network prostate cancer symptom index 17 item questionnaire/Functional assessment of cancer therapy; NYHA = New York Heart Association; PSA = prostate-specific antigen; RCT = randomized controlled trial.
aMetastatic disease was defined as either malignant lesions in bone scan or measurable lymph nodes above the aortic bifurcation or soft tissue/visceral lesions according to Response Evaluation Criteria In Solid Tumors (RECIST) v1.1. Patients with regional lymph node metastases only (N1, below the aortic bifurcation) were not eligible for the study. Only patients with non-regional lymph node metastases (M1a) and/or bone metastases (M1b) and/or other sites of metastases with or without bone disease (M1c) were eligible.
bSecond-generation androgen receptor inhibitors such as enzalutamide, apalutamide, darolutamide, and other investigational androgen receptor inhibitors.
cCytochrome P17 enzyme inhibitor such as abiraterone acetate or oral ketoconazole.
dUncontrolled hypertension was defined as a resting systolic blood pressure ≥ 160 mm Hg or diastolic BP ≥ 100 mm Hg despite medical management.
eDocetaxel could be administered in combination with prednisone/prednisolone at the discretion of the Investigator.
fAll patients received an ADT of the Investigator’s choice (LHRH agonist/antagonists or orchiectomy) because standard therapy started ≤ 12 weeks before randomization (if combined with a first-generation antiandrogen, such as bicalutamide, flutamide, nilutamide, or cyproterone acetate, it had to be stopped before randomization). For patients receiving LHRH agonists, treatment in combination with a first-generation antiandrogen for at least 4 weeks before randomization was recommended.
Source: ARASENS Clinical Study Report.7
Description of Studies
One study (ARASENS)6,7 met the inclusion criteria for the CADTH systematic review. The ARASENS trial was a phase III, multicentre, double-blind RCT that aimed to compare the efficacy and safety of darolutamide in addition to ADT and docetaxel versus placebo in addition to ADT and docetaxel in adult males with mCSPC (n = 1,306). The study was initiated on November 30, 2016, and final analysis is complete. Patients were enrolled at 301 sites in 23 countries, including 5 Canadian sites.
The ARASENS trial consisted of 4 phases: screening, treatment, active follow-up, and long-term (survival) follow-up. Following a screening phase of up to 28 days to assess study eligibility, eligible patients entered the double-blind treatment phase, in which they were randomized in a 1:1 ratio to receive darolutamide or placebo, in addition to ADT and docetaxel. Randomization was stratified by the extent of disease (non-regional lymph nodes metastases only, bone metastases with or without lymph node metastases, visceral metastases with or without lymph node metastases or with or without bone metastases), and alkaline phosphatase (ALP) level (ALP less than the upper limit of normal [ULN]; ALP greater or equal to the ULN) using the Interactive Voice/Web Response System. Patients received study treatments until symptomatic disease progression, unacceptable toxicity, or change of antineoplastic therapy, and they were subsequently monitored in the active follow-up phase for safety and select efficacy outcomes for up to 1 year. Survival continued to be assessed in the long term follow-up period.
This report presents the final efficacy analysis in the ARASENS trial at the data cut-off on October 25, 2021.
Populations
Inclusion and Exclusion Criteria
The key inclusion and exclusion criteria of the ARASENS trial are summarized in Table 6. The study enrolled adult males aged 18 years or older with metastatic prostate adenocarcinoma who started ADT (luteinizing hormone-releasing hormone [LHRH] agonist or antagonist, or orchiectomy) no longer than 12 weeks before randomization and had an ECOG performance status of 0 or 1. Patients were excluded if they had regional lymph node metastases only or had prior treatment with 1 of the following: second-generation androgen receptor inhibitors (e.g., enzalutamide, apalutamide, darolutamide); cytochrome P17 enzyme inhibitors (e.g., abiraterone), chemotherapy or immunotherapy for prostate cancer; or radiotherapy within 2 weeks before the study.
Baseline Characteristics
The baseline patient demographic, disease characteristics, and prior cancer therapy were generally balanced between treatment arms, as shown in Table 7. Overall, the study population had a median age of 67.0 (range, 41 to 89) years. Fifty-two percent of patients were white, and 36.4% were Asian. Most patients had stage IV disease (87.6%) and a Gleason score of 8 or higher (78.2%) at initial diagnosis. At study baseline, the majority of patients had an ECOG performance status of 0 (71.1%) and bone metastases with or without lymph node metastases (82.8%). In 55.5% of patients, the ALP level was above the ULN, and the serum testosterone was at castrate level (< 0.5 ng/mL). Most patients had no prior local therapy and had prior systemic antineoplastic therapy (98.1%), all of which were ADTs. Almost all patients entered the study with ADT (99.8%), while others initiated ADT at randomization. The majority of patients were treated with an LHRH agonist or antagonist only (97.3%).
Table 7: Summary of Baseline Characteristics (FAS)
Characteristic | ARASENS | |
|---|---|---|
Darolutamide + docetaxel + ADT (N = 651) | Placebo + docetaxel + ADT (N = 654) | |
Demographics | ||
Age, years | ||
Median (range) | 67.0 (41 to 89) | 67.0 (42 to 86) |
Race, n (%) | ||
White | 345 (53.0) | 333 (50.9) |
Black or African American | 26 (4.0) | 28 (4.3) |
Asian | 230 (35.3) | 245 (37.5) |
Other | 7 (1.1) | 2 (0.3) |
Not reported | 43 (6.6) | 46 (7.0) |
Disease characteristics | ||
Extent of metastatic disease,a,b n (%) | ||
M1a (non-regional lymph nodes metastases only) | 21 (3.2) | 22 (3.4) |
M1b (bone metastases with or without lymph node metastases) | 540 (82.9) | 541 (82.7) |
M1c (visceral metastases with or without lymph node metastases, or with or without bone metastases) | 90 (13.8) | 91 (13.9) |
ALP levelb (U/L), n (%) | ||
ALP < ULN | 290 (44.5) | 291 (44.5) |
ALP ≥ ULN | 361 (55.5) | 363 (55.5) |
Stage of prostate cancer at initial diagnosis (TNM classification),c n (%) | ||
Stage I | 12 (1.8) | 10 (1.5) |
Stage IIA | 18 (2.8) | 10 (1.5) |
Stage IIB | 15 (2.3) | 10 (1.5) |
Stage III | 36 (5.5) | 38 (5.8) |
Stage IV | 563 (86.5) | 580 (88.7) |
Stage IV, M0 | 5 (0.8) | 14 (2.1) |
Stage IV, M1 | 558 (85.7) | 566 (86.5) |
Missing | 7 (1.1) | 6 (0.9) |
Gleason score at initial diagnosis, n (%) | ||
< 8 | 122 (18.7) | 118 (18.0) |
≥ 8 | 505 (77.6) | 516 (78.9) |
Missing | 24 (3.7) | 20 (3.1) |
PSA level (ng/mL) | ||
n | 651 | 653 |
Mean (SD) | 248.47 (714.08) | 204.71 (742.54) |
ECOG performance status, n (%) | ||
0 | 466 (71.6) | 462 (70.6) |
1 | 185 (28.4) | 190 (29.1) |
Missing | 0 | 2 (0.3) |
Testosterone level, n (%) | ||
< 0.5 ng/mL | 339 (52.1) | 353 (54.0) |
≥ 0.5 ng/mL | 309 (47.5) | 296 (45.3) |
Missing | 3 (0.5) | 5 (0.8) |
Prior cancer therapy | ||
Prior local therapy, n (%) | ||
Prostatectomy | 44 (6.8) | 42 (6.4) |
Surgery | 31 (4.8) | 21 (3.2) |
Radiation | 28 (4.3) | 22 (3.4) |
Transurethral resection of the prostate | 8 (1.2) | 7 (1.1) |
Other | 4 (0.6) | 3 (0.5) |
Prior systemic antineoplastic therapy, n (%) | 640 (98.3) | 640 (97.9) |
Bicalutamide | 385 (59.1) | 397 (60.7) |
Leuprorelin | 259 (39.8) | 287 (43.9) |
Goserelin | 155 (23.8) | 164 (25.1) |
Degarelix | 126 (19.4) | 138 (21.1) |
Triptorelin | 88 (13.5) | 63 (9.6) |
Buserelin | 24 (3.7) | 12 (1.8) |
Flutamide | 11 (1.7) | 19 (2.9) |
Gonadorelin | 2 (0.3) | 1 (0.2) |
Histrelin | 0 (0.0) | 1 (0.2) |
ADT at study entry,d n (%) | 651 (100) | 652 (99.7) |
LHRH agonist or antagonist only | 635 (97.5) | 635 (97.1) |
Orchiectomy only | 11 (1.7) | 12 (1.8) |
LHRH agonist/antagonist and orchiectomy | 5 (0.8) | 5 (0.8) |
ADT = androgen deprivation therapy; ALP = alkaline phosphatase; ECOG = Eastern Cooperative Oncology Group; FAS = full analysis set; LHRH = luteinizing hormone-releasing hormone; PSA = prostate-specific antigen; SD = standard deviation; TNM = tumour, nodes, and metastases; ULN = upper limit of normal.
aThe extent of metastatic disease was determined using the TNM classification system.
bBased on data collected via Interactive Voice/Web Response System for randomization or stratification.
cAccording to the American Joint Committee on Cancer Staging Manual, 7th edition, stage IV could be M1 or M0 disease. In this analysis, the stage IV M0 group was defined as the time interval of > 3 months between initial diagnosis and initial diagnosis of metastases. The stage IV M1 group was defined as the time interval of ≤ 3 months between initial diagnosis and initial diagnosis of metastases.
dThis captures the proportion of patients who entered the study with ADT. Patients who initiated ADT at randomization were not captured here.
Data cut-off: October 25, 2021.
Source: ARASENS Clinical Study Report.7
Interventions
In the double-blind treatment period, patients were assigned to either darolutamide 600 mg (2 tablets of 300 mg) or a matching placebo, twice daily by mouth with food. All patients also received a background ADT (LHRH agonist or antagonists, or orchiectomy), which was initiated less than or equal to 12 weeks before randomization, and docetaxel 75 mg/m2 via IV infusion every 21 days for 6 cycles starting within 6 weeks after the initiation of darolutamide or placebo. Docetaxel was administered in combination with prednisone or prednisolone at the discretion of the investigators. The study treatments were given until symptomatic progressive disease, change of antineoplastic therapy, or unacceptable toxicity. When clinically significant toxicities were present, the dosing of darolutamide was delayed for a maximum of 28 consecutive days or reduced to 300 mg twice daily, and dose reduction of docetaxel to 60 mg/m2 was allowed. The darolutamide and placebo tablets were identical in appearance.
Initiation of the following medications was prohibited during the treatment period: radiopharmaceuticals, immunotherapy, cytotoxic chemotherapy (other than docetaxel), first- or second-generation antiandrogen (e.g., enzalutamide, apalutamide, bicalutamide, flutamide [other than darolutamide]), cytochrome P17 inhibitors (e.g., abiraterone, TAK-700), systemic ketoconazole as antineoplastic treatment for prostate cancer, and a switch from ADT to an LHRH agonist.
Concomitant use of analgesics (opioid and non-opioid), palliative radiation therapy or surgical intervention, bisphosphonate, and denosumab was allowed. Switching ADT to an LHRH antagonist, administering dexamethasone as a premedication for docetaxel infusion, and supportive care for docetaxel toxicity (e.g., granulocyte colony-stimulating factor) were permitted.
Outcomes
A list of efficacy end points identified in the CADTH review protocol that were assessed in the clinical trials included in this review is provided in Table 8. These end points are further summarized below. A detailed discussion and critical appraisal of these outcome measures is provided in Appendix 3.
Table 8: Summary of Outcomes of Interest Identified in the CADTH Review Protocol
Outcome measure | ARASENS | End points measured in ARASENS |
|---|---|---|
Overall survival | Primary | Overall survival |
Time to castration-resistant prostate cancer | Secondary | Time to castration-resistant prostate cancer |
Time to initiation of subsequent antineoplastic therapy | Secondary | Time to initiation of subsequent systemic antineoplastic therapy |
Time to pain progression | Secondary | Time to pain progression based on BPI-SF |
Health-related quality of life | Exploratory | Change from baseline in NCCN-FACT FPSI-17 scores |
Objective response rate | Not measured | Not measured |
Time to skeletal-related events | Secondary | Time to first symptomatic skeletal event Symptomatic skeletal event-free survival |
Time to PSA progression | Exploratory | Time to PSA progression |
PSA response rates | Exploratory | Absolute PSA response rate Relative PSA response rate |
Harms (AE, SAE, WDAE, mortality) | Secondary | AE, SAE, WDAE, deaths, laboratory safety assessment, vital signs, and electrocardiogram |
AE = adverse event; BPI-SF = Brief Pain Inventory (Short Form); NCCN-FACT FPSI-17 = National Comprehensive Cancer Network prostate cancer symptom index 17 item questionnaire/Functional assessment of cancer therapy; PSA = prostate-specific antigen; SAE = serious adverse event; WDAE = withdrawal due to adverse event.
Efficacy Outcomes
The primary efficacy end point of the ARASENS trial was OS, which was defined as the time from the date of randomization until death from any cause.
The secondary efficacy end points that were of interest to this review include time to CRPC, time to initiation of subsequent systemic antineoplastic therapy, time to pain progression, time to first SSE, and SSE-FS. These end points were defined as follows:
Time to CRPC, a composite end point of time to PSA progression, time to progression by soft-tissue lesions, or time to progression by bone lesions, was defined as the time from randomization to the time of the occurrence of 1 of the following events, whichever came first:
PSA progression, which was defined as a 25% or greater increase and an absolute increase of 2 ng/mL or more from the nadir in 2 consecutive assessments. This definition required serum testosterone at castrate levels of less than 0.50 ng/mL and a first assessment date at least 12 weeks from randomization.
Radiological progression by soft-tissue and visceral lesions, as per Response Evaluation Criteria In Solid Tumors (RECIST) v1.1.
Radiological progression by bone lesions, as per Prostate Cancer Clinical Trials Working Group 3.
Time to initiation of subsequent systemic antineoplastic therapy was defined as the time from randomization to initiation of the first subsequent systemic antineoplastic therapy.
Time to pain progression was defined as the time from randomization to the first date a patient experienced pain progression based on the Brief Pain Inventory (Short Form) (BPI-SF) questionnaire. Pain progression was defined as an increase of 2 or more points in the worst pain score from nadir (i.e., lowest at or after baseline) in 2 consecutive evaluations (and a worst pain score of 4 or above if patient was symptomatic), or initiation of short- or long-acting opioid use for pain.
The BPI-SF is a patient-reported generic questionnaire for pain intensity and impact. Each item is scored on an 11-point scale from 0 to 10, where 0 is no pain/no interference and 10 is the worst pain/complete interference.21 The validity, reliability, responsiveness, and minimally important difference (MID) estimate of the BPI-SF instrument have not been evaluated in patients with mCSPC. A MID estimate of 2 or more points or 30% change in pain intensity items from baseline was previously used in 2 studies in mCRPC patients.22,23 Detailed information on the scoring and validity of the BPI-SF instrument is provided in Appendix 3.
Time to first SSE was defined as the time from randomization to the first occurrence of an SSE. An SSE was defined as the occurrence of 1 of the following: external beam radiation therapy to relieve skeletal symptoms, new symptomatic pathologic bone fracture, occurrence of spinal cord compression, or tumour-related orthopedic surgical intervention.
SSE-FS was defined as the time from randomization to the first occurrence of an SSE or death from any cause.
The exploratory efficacy end points included HRQoL via NCCN-FACT FPSI-17, time to PSA progression, and absolute and relative PSA response rates. These end points were defined as follows:
NCCN-FACT FPSI-17 is a 17-item, cancer-specific questionnaire developed to assess symptoms and well-being among patients with advanced prostate cancer who are undergoing treatment.24 It consists of 4 main subscales that assess physical and emotional disease-related symptoms, treatment side effects, and function/well-being on a 5-point scale. Higher subscale scores and total scores indicate better outcomes on the aforementioned scales.25 The validity, reliability, responsiveness, and MID estimate of the NCCN-FACT FPSI-17 have not been evaluated in patients with mCSPC. A study in mCRPC patients identified the MID estimates to be 4 to 6 points for the total score; 2 to 3.5 points for the disease-related symptoms, physical subscale; 0.5 points for the disease-related symptoms, emotional subscale; 1 to 1.5 points for the treatment side effects subscale; and 0.5 to 1 points for the function and well-being subscale.25 Detailed information on the scoring and validity of the NCCN-FACT FPSI-17 instrument is provided in Appendix 3.
Time to PSA progression was defined as the time from the date of randomization to the date of first PSA progression with testosterone at castrate level of less than 0.5 ng/mL.
Absolute PSA response rate was defined as the number of patients with absolute PSA response divided by the total number of patients randomized, and was evaluated at 6 and 12 months. Absolute PSA response was defined as a postbaseline PSA level below 0.2 ng/mL in 2 consecutive evaluations.
Relative PSA response rate was defined as the number of patients with relative PSA response divided by the total number of patients randomized, and was evaluated at 3, 6, and 12 months. Relative 30% PSA response was defined as a postbaseline 30% or greater reduction of the PSA level compared to the baseline value in 2 consecutive evaluations. Relative 50% and 90% PSA response were defined in the same way.
The efficacy outcomes were assessed at baseline and then every 12 weeks until end of treatment in the treatment period. Outcomes related to SSE, pain, subsequent antineoplastic therapy, and survival continued to be assessed in the follow-up period.
Harms Outcomes
The harms outcomes included AEs, serious AEs, withdrawal due to AE, deaths, laboratory safety assessment, vital signs, and electrocardiogram. During the treatment period, these outcomes were assessed every 12 weeks until end of treatment. Study drug–related AEs and serious AEs were assessed every 12 weeks in the follow-up period.
Statistical Analysis
A summary of the statistical analyses of efficacy outcomes in the ARASENS trial is provided in Table 9.
Sample Size and Power Calculation
The sample size calculation was based on the primary end point of OS. The study required a sample size of 1,300 patients to achieve at least 509 death events to detect an HR of 0.75 with respect to OS at a 1-sided alpha of 0.025 with a power of 90% using a log-rank test, based on the following assumptions:
Fifty patients were enrolled per month.
There were exponential distributions of the OS event time.
Median time of OS in the control group was 60 months.
Dropout rate was 5%.
There was a 6-month enrolment ramp-up period.
Interim and Final Analyses
One interim analysis for futility and 1 final (primary) analysis were planned to occur after 153 and 509 death events, respectively. A 1-sided overall beta of 0.1 was used for the interim and final analyses. For the interim analysis, the prespecified futility boundary of an HR for darolutamide over placebo greater than or equal to 1.166 was calculated using an O’Brien-Fleming beta-spending function. The independent data monitoring committee reviewed the interim results and recommended the study to proceed as planned.
Multiplicity Adjustment
Multiplicity adjustment using a hierarchical gatekeeping approach was implemented within the final efficacy analysis. The primary end point of OS was first tested with a 1-sided alpha of 0.025 using a stratified log-rank test. If the null hypothesis of OS was rejected, the secondary efficacy end points were tested hierarchically using the same significance level as the primary end point in the following order:
Time to CRPC
Time to pain progression
SSE-FS
Time to first SSE
Time to initiation of subsequent systemic antineoplastic therapy
Handling of Missing Data
No imputation was performed to account for missing data in all efficacy end points (except for partial dates). Censoring rules were used to avoid excluding patients with missing or incomplete data from the analyses (Table 9).
Table 9: Statistical Analysis of Efficacy End Points
End point | Statistical model | Adjustment factors | Sensitivity analyses | Hierarchical testing sequence |
|---|---|---|---|---|
Overall survival |
|
|
| 1 |
Time to castration-resistant prostate cancer |
|
| Based on both central and local PSA data | 2 |
Time to initiation of subsequent systemic antineoplastic therapy |
|
| Not performed | 6 |
Time to pain progression based on BPI-SF |
|
|
| 3 |
NCCN-FACT FPSI-17 scores over time | Descriptive statistics | NA | Not performed | NA |
BPI-SF scores over time | Descriptive statistics | NA | Not performed | NA |
Time to first symptomatic skeletal event |
|
| Not performed | 5 |
Symptomatic skeletal event-free survival |
|
| Not performed | 4 |
Time to PSA progression |
| NA | Based on both central and local laboratory data | NA |
Absolute PSA response rate | Stratified CMH model to estimate risk difference and 95% CI |
| Not performed | NA |
Relative PSA response rate | Stratified CMH model to estimate risk difference and 95% CI |
| Not performed | NA |
ALP = alkaline phosphatase; BPI-SF = Brief Pain Inventory (Short Form); CI = confidence interval; CMH = Cochran-Mantel-Haenszel; eCRF = electronic case report form; ePRO = electronic patient-reported outcome; IxRS = Interactive Voice/Web Response System; KM = Kaplan-Meier; NA = not applicable; NCCN-FACT FPSI-17 = National Comprehensive Cancer Network prostate cancer symptom index 17 item questionnaire/Functional assessment of cancer therapy; PSA = prostate-specific antigen; SSE = symptomatic skeletal event.
aThis analysis was planned to occur only when there were more than 5% of patients with different values between IxRS and eCRF.
Source: ARASENS Statistical Analysis Plan.26
Statistical Analysis for Primary Efficacy End Point
In the primary analysis of OS, the difference in OS between treatment arms in the full analysis set (FAS) population was tested using a 1-sided log-rank test stratified by extent of disease (non-regional lymph nodes metastases only, bone metastases with or without lymph node metastases, or visceral metastases with or without lymph node metastases or with or without bone metastases) and ALP level (ALP less than the ULN or ALP greater than or equal to the ULN). The HR and the 95% CI were based on a Cox proportional hazards model, stratified by extent of disease and ALP level. Median (95% CI) OS was estimated using the Kaplan-Meier (KM) method. The KM estimates for median OS, and the corresponding 95% CI, along with the estimated OS probability at every 12 months, were presented.
Three prespecified sensitivity analysis were conducted to assess the impact of different stratification strategies, including an unstratified analysis (using unstratified log-rank test and Cox model), an electronic case report form (eCRF)–variables stratified analysis (using stratification factors collected from eCRF, as opposed to from the Interactive Voice/Web Response System used in the primary analysis), and a stratified analysis using extent of disease data collected from the central imaging review (as opposed to from local imaging review in the primary analysis). A post hoc sensitivity analysis by docetaxel cycles was also performed.
Prespecified subgroup analyses with respect to OS were conducted using an unstratified Cox proportional hazards model. Descriptive statistics and HR estimates with 95% CI were presented. The subgroups that were assessed in the trial and of interest to this review included ECOG performance status at baseline (0 versus 1), Gleason score (less than 8, greater than or equal to 8) at initial diagnosis, and extent of disease (non-regional lymph node metastases only, bone metastases with or without lymph node metastases, or visceral metastases with or without lymph node metastases or with or without bone metastases). No adjustment for type I error was involved and no statistical testing was performed for treatment-by-subgroup interaction in the subgroup analyses.
Statistical Analyses for Secondary Efficacy End Points
The secondary efficacy end points were analyzed in the FAS population. Time-to-event end points were analyzed using the same statistical approach as the primary analysis of OS.
A sensitivity analysis was conducted for the secondary end point of time to CRPC using both central and local PSA data (as supposed to central PSA data only in the primary analysis). For time to pain progression end point, a sensitivity analysis using data from both electronic patient-reported outcome (ePRO) device and paper questionnaire were used (as opposed to from ePRO only in the primary analysis). Three additional sensitivity analyses were performed for time to pain progression, which aimed to evaluate the impact of using different definitions of time to pain progression (i.e., an increase of 2 or more points in the “worst pain in 24 hours” from either (1) baseline, (2) nadir after completion of docetaxel, or (3) baseline after completion of docetaxel).
Statistical Analyses for Exploratory Efficacy End Points
Time to PSA progression was analyzed using descriptive statistics based on KM estimates and their 95% CI. A sensitivity analysis based on both central and local PSA data (as supposed to central PSA data only in the primary analysis) was performed. Absolute and relative PSA response rates were evaluated descriptively and a stratified Cochran-Mantel-Haenszel model was used to estimate the risk difference between treatment arms, and the 95% CI. Descriptive statistics were presented for NCCN-FACT FPSI-17 score at each assessment time and for change from baseline by treatment arm.
Safety Analyses
The safety analyses were performed in the safety analysis set (SAF) population and were summarized using descriptive statistics.
Analysis Populations
FAS: included all patients randomized in the study, and was analyzed by treatment assignment.
SAF: included all randomized patients who received at least 1 dose of darolutamide or placebo, except for cases with critical Good Clinical Practice violations. Patients were analyzed by the actual treatment received.
Results
Patient Disposition
A summary of patient disposition is shown in Table 10. Of 1,686 screened patients, 380 (22.5%) were screen failures, the majority of which was due to failure to meet eligibility criteria (18.3%). A total of 1,306 patients were randomized to darolutamide plus docetaxel and ADT arm (N = 651), and placebo plus docetaxel and ADT arm (N = 654); 1 patient was excluded from the FAS due to a Good Clinical Practice violation (darolutamide plus docetaxel and ADT group). As of the data cut-off on October 25, 2021, the proportion of patients who discontinued from study treatment was higher in the placebo plus docetaxel and ADT arm (80.4%) than the darolutamide plus docetaxel and ADT arm (54.1%), with the most common reasons being clinical disease progression (41.6% versus 19.5.%) and radiological disease progression (20.2% versus 12.9%).
Disposition | ARASENS | |
|---|---|---|
Darolutamide + docetaxel + ADT | Placebo + docetaxel + ADT | |
Screened, n | 1,686 | |
Randomized, n | 651 | 654 |
Treated, n (%) | 651 (100) | 651 (99.5) |
Discontinued study treatment, n (%) | 352 (54.1) | 526 (80.4) |
Clinical disease progression | 127 (19.5) | 272 (41.6) |
Radiological disease progression | 84 (12.9) | 132 (20.2) |
AE not associated with clinical disease progression | 48 (7.4) | 27 (4.1) |
Withdrawal by patients | 25 (3.8) | 35 (5.4) |
AE associated with clinical disease progression | 24 (3.7) | 26 (4.0) |
Non-compliance | 14 (2.2) | 12 (1.8) |
Additional primary malignancy | 11 (1.7) | 6 (0.9) |
Death | 8 (1.2) | 5 (0.8) |
Lost to follow-up | 4 (0.6) | 1 (0.2) |
Other | 3 (0.5) | 4 (0.6) |
Physician decision | 3 (0.5) | 6 (0.9) |
Protocol deviation | 1 (0.2) | 0 (0.0) |
FAS, n | 651 | 654 |
SAF, n | 652 | 650 |
ADT = androgen deprivation therapy; AE = adverse event; FAS = full analysis set; SAF = safety analysis set.
Note: In addition to the full analysis set and safety analysis set, the study also included a pharmacokinetics analysis set (PKS), which is not of interest to this review.
Data cut-off: October 25, 2021.
Source: ARASENS Clinical Study Report.7
Protocol Deviations
Important protocol deviations are summarized in Table 11. An important protocol deviation was reported in ||||||| of the study population, with the most common important deviation categories being procedure deviations (|||||||) and treatment deviations (|||||||). Procedure deviations were most frequently related to consent obtainment and study assessment (missed, incorrect, or incomplete procedures). Treatment deviations were most frequently related to incorrect dose, frequency, timing or method of drug delivery, and time frame between docetaxel administrations being less than 21 days. There was no imbalance in the important protocol deviations between treatment arms, with the exception that unblinding by error was notably more common in the placebo plus docetaxel and ADT arm (|||||||) than the darolutamide plus docetaxel and ADT arm (|||||||). Investigators were found to be unblinding patients to assist in determining the best subsequent treatment option. The sponsor indicated that the high number of protocol deviations was due to the use of a much broader and conservative approach in defining important protocol deviations than the definition by the International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use and was not expected to compromise the integrity of study data.
Table 11: Important Protocol Deviations (FAS)
Important protocol deviations | ARASENS | |
|---|---|---|
Darolutamide + docetaxel + ADT | Placebo + docetaxel + ADT | |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| |
||||||||||||||||||||||||||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| |
||||||||||||||||||||||||||||||||||||||||||| | ||
||||||||||||||||||||||||||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| |
||||||||||||||||||||||||||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| |
||||||||||||||||||||||||||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| |
||||||||||||||||||||||||||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| |
||||||||||||||||||||||||||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| |
||||||||||||||||||||||||||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| |
||||||||||||||||||||||||||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| |
||||||||||||||||||||||||||||||||||||||||||| | ||
||||||||||||||||||||||||||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| |
||||||||||||||||||||||||||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| |
||||||||||||||||||||||||||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| |
||||||||||||||||||||||||||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| |
||||||||||||||||||||||||||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| |
||||||||||||||||||||||||||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| |
||||||||||||||||||||||||||||||||||||||||||| | ||||||||||||||||||| | ||||||||||||||||||| |
ADT = androgen deprivation therapy; FAS = full analysis set; PSA = prostate-specific antigen.
aFrequency ≥ 10%.
Data cut-off: October 25, 2021.
Source: ARASENS Clinical Study Report.7
Exposure to Study Treatments
Exposure to study treatments is summarized in Table 12. In the darolutamide plus docetaxel and ADT arm, the median duration of darolutamide treatment was 41.0 (range = 0.1 to 56.5) months, while in the placebo plus docetaxel and ADT arm, the median duration of placebo treatment was 16.7 (range = 0.3 to 55.8) months. The median relative dose intensity was 100% in both arms (range = 32.1% to 100.1% in darolutamide plus docetaxel and ADT arm; range = 48.4% to 100.4% in placebo plus docetaxel and ADT arm).
The median duration of docetaxel treatment was 6 (range = 1 to 6) months in both treatment arms. The median relative dose intensity of docetaxel was 98.6% (range = 72.8% to 109.9%) in the darolutamide plus docetaxel and ADT arm, and 98.5% (range = 51.8% to 105.4%) in the placebo plus docetaxel and ADT arm.
All patients received ADT in the treatment period and most patients received a LHRH agonist or antagonist only, as summarized in Table 7.
Table 12: Study Treatment Exposure (SAF)
Exposure | ARASENS | |
|---|---|---|
Darolutamide + docetaxel + ADT (N = 652) | Placebo + docetaxel + ADT (N = 650) | |
Darolutamide or placebo | ||
Duration of exposurea (month) | ||
Mean (SD) | 31.9 (16.8) | 22.2 (15.3) |
Median (range) | 41.0 (0.1 to 56.5) | 16.7 (0.3 to 55.8) |
Relative dose intensityb (%) | ||
Mean (SD) | 97.2 (9.3) | 98.5 (6.1) |
Median (range) | 100 (32.1 to 100.1) | 100 (48.4 to 100.4) |
Docetaxel | ||
Total number of cycles | ||
Mean (SD) | 5.6 (1.1) | 5.7 (1.1) |
Median (range) | 6 (1 to 6) | 6 (1 to 6) |
Relative dose intensityb (%) | ||
Mean (SD) | 96.0 (6.3) | 95.8 (6.6) |
Median (range) | 98.6 (72.8 to 109.9) | 98.5 (51.8 to 105.4) |
ADT = androgen deprivation therapy; SAF = safety analysis set; SD = standard deviation.
aDuration of exposure = day of last dose of study drug – day of first dose of study drug + 1, divided by 30.44.
bRelative dose intensity refers to the percent of planned dose, which incorporates treatment interruptions and dose reductions in the calculation.
Data cut-off: October 25, 2021.
Source: ARASENS Clinical Study Report.7
Concomitant Medications
All patients in the darolutamide plus docetaxel and ADT arm, and 99.1% in the placebo plus docetaxel and ADT arm, had concomitant medications. The most frequently used concomitant medication was ophthalmologicals (96.2%; similar in both groups). Bone-disease medications and analgesics were used concomitantly with the study treatments in 25.4% and 71.5% of patients, respectively. Of the patients who used concomitant corticosteroids (91.3%), prednisolone and prednisone were used in 20.3% and 20.8% of patients, respectively, while on docetaxel. Overall, there was no notable difference in the use of the concomitant medications between treatment arms.
Efficacy
Only those efficacy outcomes and analyses of subgroups identified in the review protocol are reported below. Refer to Appendix 2 for detailed efficacy data. The results presented are based on the data cut-off on October 25, 2021, and represent the final efficacy analysis of the ARASENS trial.
Overall Survival
The primary end point of OS is summarized in Table 13. A KM plot of OS is shown in Figure 2.
Table 13: Overall Survival Outcomes (FAS)
Overall survival | ARASENS | |
|---|---|---|
Darolutamide + docetaxel + ADT (N = 651) | Placebo + docetaxel + ADT (N = 654) | |
Death event, n (%) | 229 (35.2) | 304 (46.5) |
Overall survival (months),a median (95% CI) | NR | 48.9 (44.4 to NR) |
Hazard ratiob (95% CI) | 0.68 (0.57 to 0.80) | |
P valuec | < 0.0001 | |
Follow-up time (months), median (range) | 43.7 (not reported) | 42.4 (not reported) |
Survival probability, % (95% CI) | ||
12 months | 94.9 (93.2 to 96.6) | 90.3 (88.0 to 92.5) |
24 months | 83.1 (80.2 to 86.0) | 76.8 (73.5 to 80.1) |
36 months | 72.3 (68.8 to 75.8) | 63.8 (60.1 to 67.6) |
48 months | 62.7 (58.7 to 66.7) | 50.4 (46.3 to 54.6) |
ADT = androgen deprivation therapy; CI = confidence interval; FAS = full analysis set; NR = not reached.
aBased on Kaplan-Meier estimates.
bThe hazard ratio and 95% CI were based on a Cox regression model, stratified by extent of disease (M1a vs. M1b vs. M1c) and alkaline phosphatase (< upper limit of normal vs. ≥ upper limit of normal).
cP value was derived from the 1-sided log-rank test, stratified by extent of disease (M1a vs. M1b vs. M1c) and alkaline phosphatase (< upper limit of normal vs. ≥ upper limit of normal); the significance threshold was set at a 1-sided alpha of 0.025.
Data cut-off: October 25, 2021.
Source: ARASENS Clinical Study Report.7
The OS analysis was based on a median duration of follow-up of 43.7 (range not reported) months in the darolutamide plus docetaxel and ADT arm, and 42.4 months (range not reported) in the placebo plus docetaxel and ADT arm, when a total of 533 death events occurred (229 events [35.2%] and 304 events [46.5%], in respective arms). The KM estimate for the median OS was not reached in the darolutamide plus docetaxel and ADT arm, and was 48.9 (95% CI, 44.4 to NR) months in the placebo plus docetaxel and ADT arm, with an HR of 0.68 (95% CI, 0.57 to 0.80; P < 0.0001), in favour of darolutamide.
Sensitivity Analyses of OS
Results of the 3 prespecified sensitivity analyses of OS using different stratification approaches (unstratified analysis, using stratification data from eCRF, and using extent-of-disease stratification data from the central imaging review) were consistent with the results of the primary OS analysis.
Figure 2: Kaplan-Meier Plot of Overall Survival (FAS)
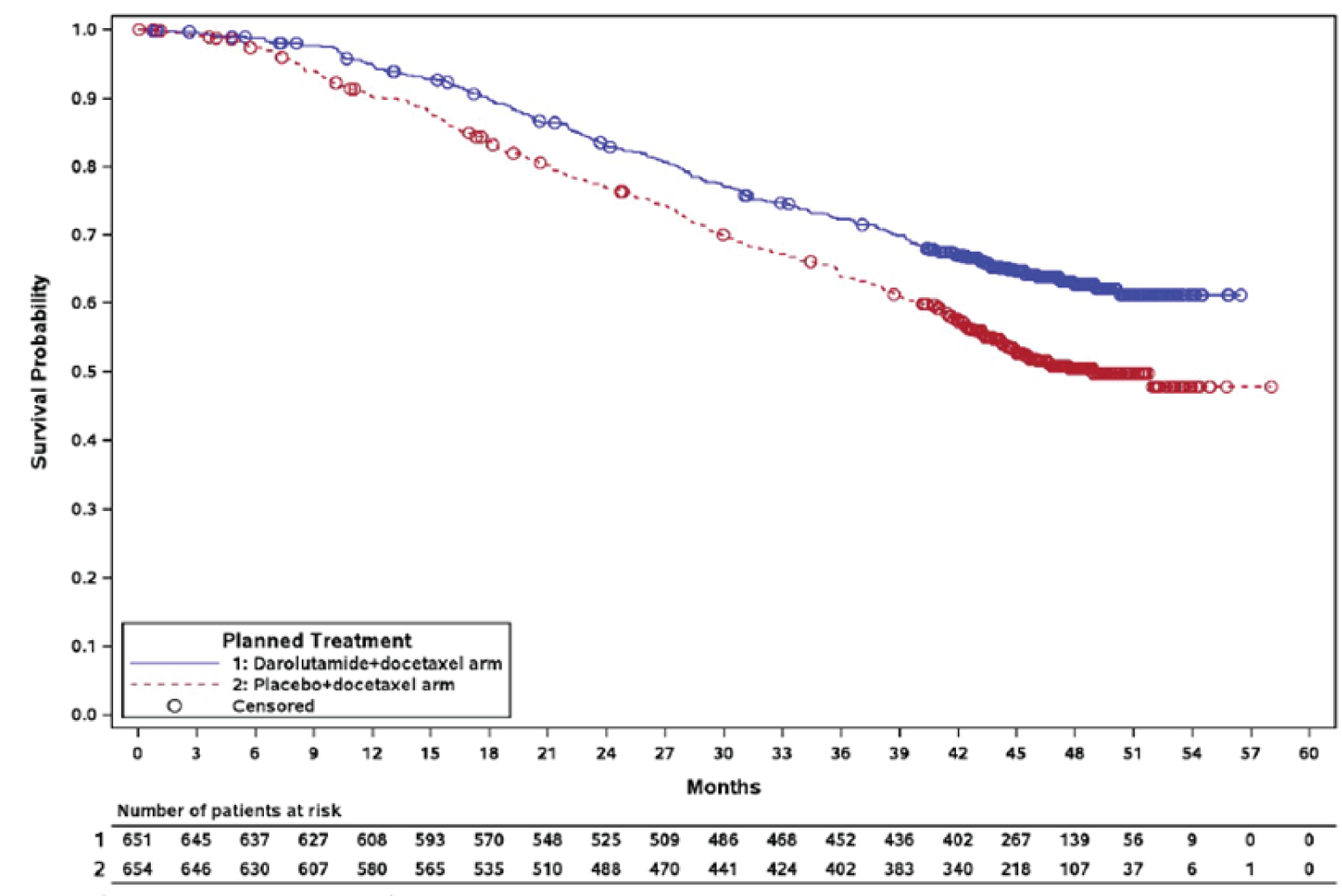
FAS = full analysis set.
Data cut-off: October 25, 2021.
Source: ARASENS Clinical Study Report.7
Table 14: Subgroup Analysis for OS (FAS)
Subgroup | ARASENS | ||
|---|---|---|---|
Darolutamide + docetaxel + ADT events per N | Placebo + docetaxel + ADT events per N | Hazard ratioa (95% CI) | |
ECOG performance status | |||
ECOG = 0 | 150/466 | 188/462 | 0.75 (0.61 to 0.93) |
ECOG = 1 | 79/185 | 115/190 | 0.58 (0.43 to 0.77) |
Gleason score | |||
< 8 | 33/122 | 44/118 | 0.65 (0.42 to 1.03) |
≥ 8 | 187/505 | 248/516 | 0.71 (0.59 to 0.86) |
Extent of metastatic diseaseb | |||
Non-regional lymph nodes metastases only | 5/23 | 5/16 | 0.65 (0.19 to 2.25) |
Bone metastases with or without lymph node metastases | 171/517 | 237/520 | 0.67 (0.55 to 0.81) |
Visceral metastases with or without lymph node metastases or with or without bone metastases | 53/111 | 62/118 | 0.79 (0.55 to 1.14) |
ADT = androgen deprivation therapy; CI = confidence interval; ECOG = Eastern Cooperative Oncology Group; FAS = full analysis set.
aThe hazard ratio and 95% CI were based on an unstratified Cox regression model.
bBased on electronic case report form...
Data cut-off: October 25, 2021.
Source: ARASENS Clinical Study Report.7
A post hoc sensitivity analysis by number of cycles of docetaxel received postbaseline was conducted. The treatment effect was consistent across all subgroups (6 cycles versus 5 and fewer cycles; 6 and 5 cycles versus 4 and fewer cycles).
Subgroup Analyses of OS
A summary of the planned subgroup analyses of OS that are of interest to this review is presented in Table 14. Across the subgroups of interest, results were consistent across groups.
Time to CRPC
An analysis of time to CRPC, a secondary end point, is summarized in Table 15. A KM plot of CRPC events is presented in Figure 3.
The proportion of patients with a CPRC event was 34.6% in the darolutamide plus docetaxel and ADT arm, and 59.8% in the placebo plus docetaxel and ADT arm. The majority of CRPC events were attributed to PSA progression in both arms. The median time to CRPC was not reached in the darolutamide plus docetaxel and ADT arm, and was 19.1 (95% CI, 16.5 to 21.8) months in the placebo plus docetaxel and ADT arm, with an HR of 0.36 (95% CI, 0.30 to 0.42; P < 0.0001), in favour of darolutamide. Results of the sensitivity analysis performed based on both central and local PSA data were consistent with the primary analysis of time to CRPC.
Outcome | ARASENS | |
|---|---|---|
Darolutamide + docetaxel + ADT (N = 651) | Placebo + docetaxel + ADT (N = 654) | |
CRPC event,a n (%) | 225 (34.6) | 391 (59.8) |
PSA progressionb | |||||||||||||||| | |||||||||||||||| |
Radiological progression by bone lesionsb | |||||||||||||||| | |||||||||||||||| |
Radiological progression by soft tissue and visceral lesionsc | |||||||||||||||| | |||||||||||||||| |
Time to CRPCd (months), median (95% CI) | NR | 19.1 (16.5 to 21.8) |
Hazard ratio (95% CI)e | 0.36 (0.30 to 0.42) | |
P valuef | < 0.0001 | |
ADT = androgen deprivation therapy; CI = confidence interval; CRPC = castration-resistant prostate cancer; FAS = full analysis set; NR = not reached; PSA = prostate-specific antigen.
aPatients with multiple events were only counted for the category in which the first event occurred.
bBased on the Prostate Cancer Clinical Trials Working Group 3 criteria.
cBased on Response Evaluation Criteria In Solid Tumors (RECIST) version 1.1 criteria.
dBased on Kaplan-Meier estimates.
eThe hazard ratio and 95% CI were based on a Cox regression model, stratified by extent of disease (M1a vs. M1b vs. M1c) and alkaline phosphatase (< upper limit of normal vs. ≥ upper limit of normal).
fP value was derived from the 1-sided log-rank test, stratified by extent of disease (M1a vs. M1b vs. M1c) and alkaline phosphatase (< upper limit of normal vs. ≥ upper limit of normal).
Data cut-off: October 25, 2021.
Source: ARASENS Clinical Study Report.7
Figure 3: Kaplan-Meier Plot of CRPC (FAS)
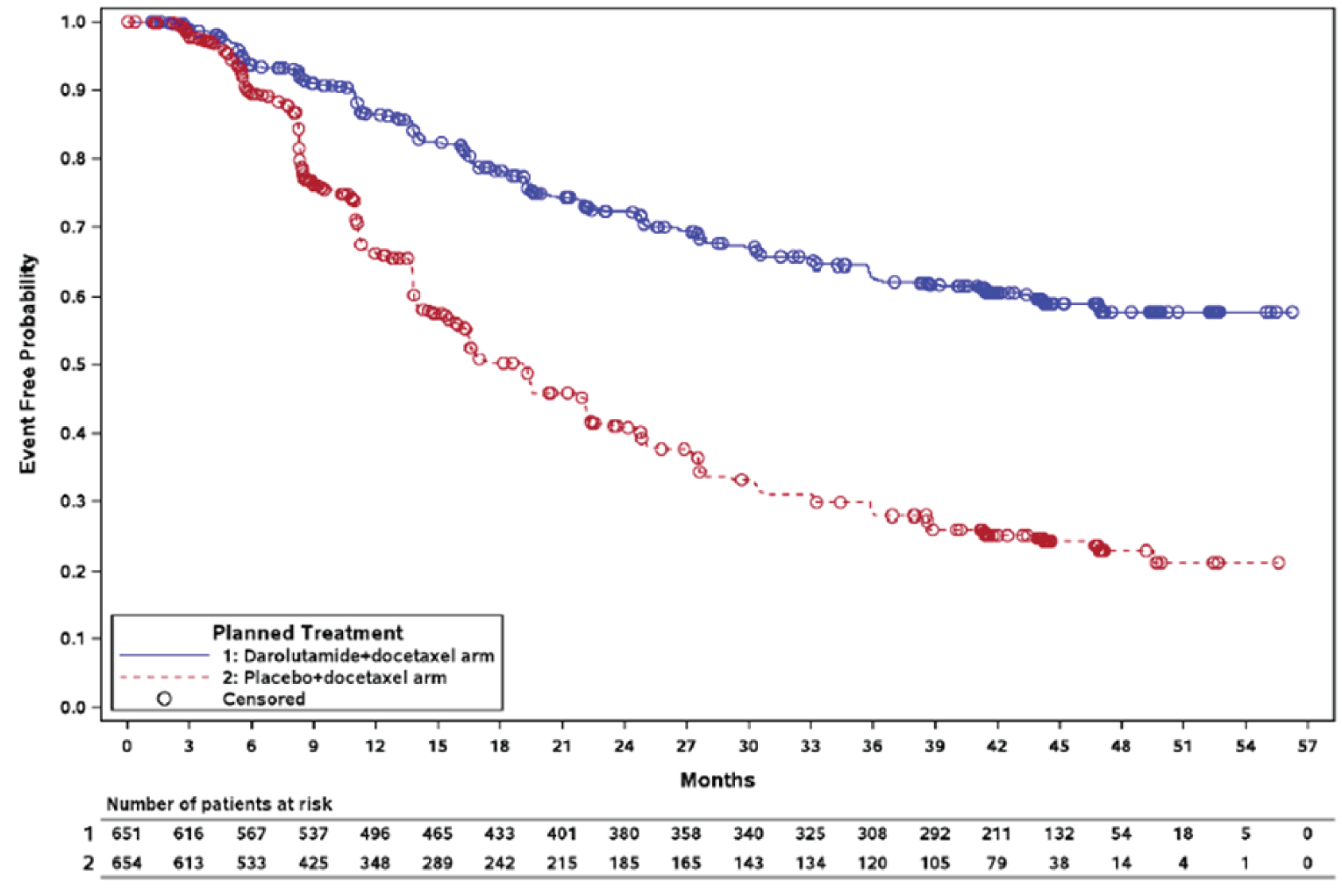
FAS = full analysis set.
Data cut-off: October 25, 2021.
Source: ARASENS Clinical Study Report.7
Time to Initiation of Subsequent Antineoplastic Therapy
An analysis of time to initiation of subsequent systemic antineoplastic therapy, a secondary end point, is summarized in Table 16. A KM plot of initiation of subsequent systemic antineoplastic therapy is presented in Figure 4.
Initiation of a new systemic antineoplastic therapy after discontinuation of study treatment occurred in 33.6% of patients in the darolutamide plus docetaxel and ADT arm, and 60.4% of patients in the placebo plus docetaxel and ADT arm. The median time to initiation of subsequent systemic antineoplastic therapy was not reached in the darolutamide plus docetaxel and ADT arm, and was 25.3 (95% CI, 23.1 to 28.8) months in the placebo plus docetaxel and ADT arm, with a HR of 0.39 (95% CI, 0.33 to 0.46; P < 0.0001), in favour of darolutamide. The most frequently used subsequent systemic antineoplastic therapies were abiraterone, enzalutamide, and cabazitaxel.
Table 16: Time to Initiation of Subsequent Systemic Antineoplastic Therapy (FAS)
Outcome | ARASENS | |
|---|---|---|
Darolutamide + docetaxel + ADT (N = 651) | Placebo + docetaxel + ADT (N = 654) | |
Initiation of subsequent systemic antineoplastic therapy event, n (%) | 219 (33.6) | 395 (60.4) |
Time to initiation of subsequent systemic antineoplastic therapy (months),a median (95% CI) | NR | 25.3 (23.1 to 28.8) |
Hazard ratiob (95% CI) | 0.39 (0.33 to 0.46) | |
P valuec | < 0.0001 | |
Most frequently used subsequent systemic antineoplastic therapy,d n (%) | ||
Abiraterone | 112 (17.2) | 232 (35.5) |
Enzalutamide | 48 (7.4) | 136 (20.8) |
Cabazitaxel | 57 (8.8) | 89 (13.6) |
Docetaxel | 46 (7.1) | 89 (13.6) |
Bicalutamide | 32 (4.9) | 54 (8.3) |
Carboplatin | 30 (4.6) | 31 (4.7) |
Radium Ra 223 dichloride | 19 (2.9) | 34 (5.2) |
Etoposide | 18 (2.8) | 9 (1.4) |
Cisplatin | 9 (1.4) | 13 (2.0) |
ADT = androgen deprivation therapy; CI = confidence interval; FAS = full analysis set; NR = not reached.
aBased on Kaplan-Meier estimates.
bThe hazard ratio and 95% CI were based on a Cox regression model, stratified by extent of disease (M1a vs. M1b vs. M1c) and alkaline phosphatase (< upper limit of normal vs. ≥ upper limit of normal).
cP value was derived from the 1-sided log-rank test, stratified by extent of disease (M1a vs. M1b vs. M1c) and alkaline phosphatase (< upper limit of normal vs. ≥ upper limit of normal).
dSubsequent systemic antineoplastic therapy used in ≥ 2% of patients are summarized.
Data cut-off: October 25, 2021.
Source: ARASENS Clinical Study Report.7
Time to Pain Progression
An analysis of time to pain progression, a secondary end point, is summarized in Table 17. A KM plot of pain progression is presented in Figure 5. Pain progression occurred in 34.1% of patients in the darolutamide plus docetaxel and ADT arm, and in 37.9% of patients in the placebo plus docetaxel and ADT arm. The median time to pain progression was not reached (95% CI, 30.5 months to NR) in the darolutamide plus docetaxel and ADT arm, and was 27.5 (95% CI, 22.0 to 36.1) months in the placebo plus docetaxel and ADT arm, with an HR of 0.79 (95% CI, 0.66 to 0.95; P = 0.0058), in favour of darolutamide. Results of the sensitivity analyses (3 using different definitions of time to pain progression and 1 based on both ePRO device and paper questionnaires) were consistent with the primary analysis.
Figure 4: Kaplan-Meier Plot of Initiation of Subsequent Antineoplastic Therapy (FAS)
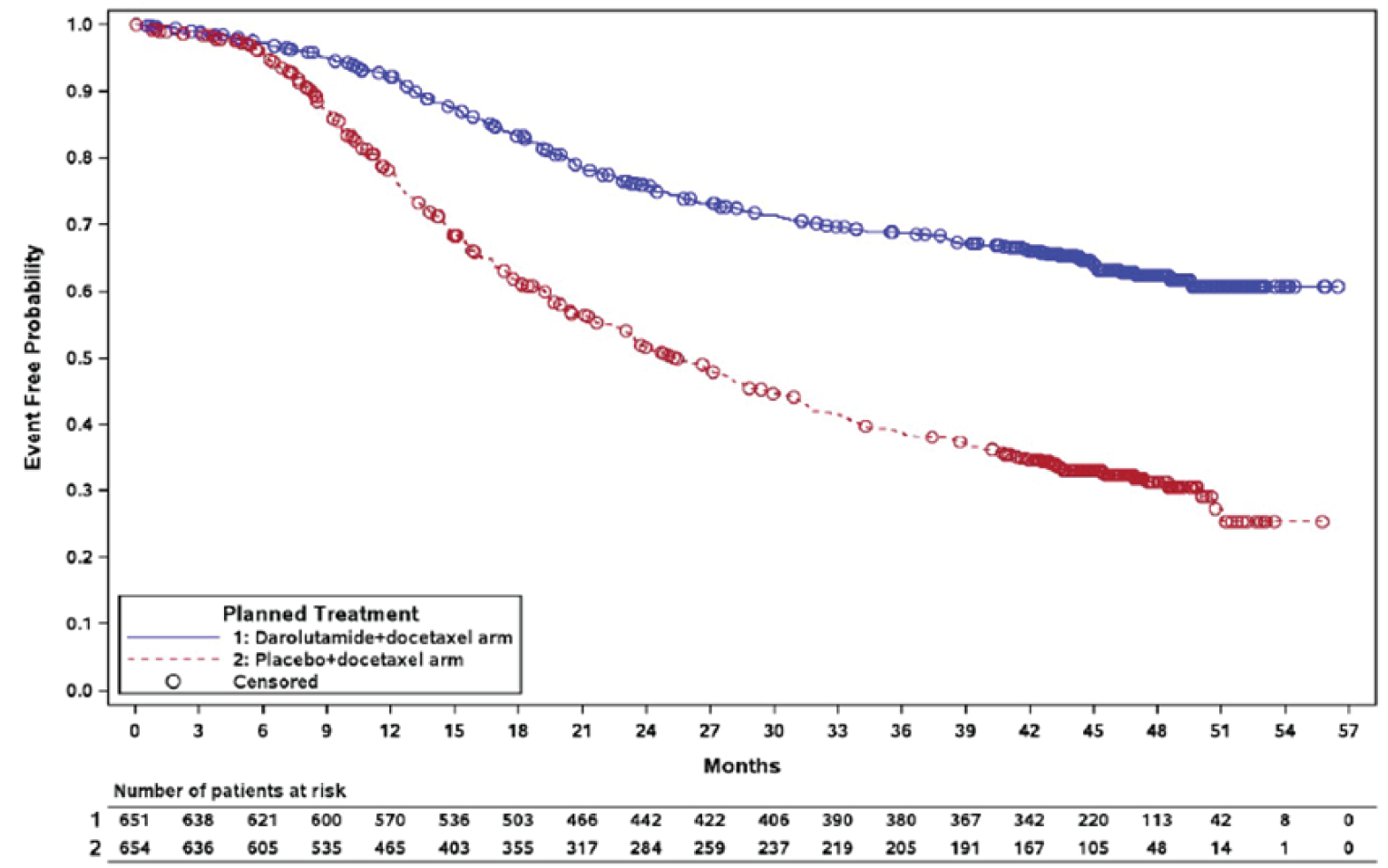
FAS = full analysis set.
Data cut-off: October 25, 2021.
Source: ARASENS Clinical Study Report.7
Table 17: Time to Pain Progression (FAS)
Outcome | ARASENS | |
|---|---|---|
Darolutamide + docetaxel + ADT (N = 651) | Placebo + docetaxel + ADT (N = 654) | |
Pain progression event, n (%) | 222 (34.1) | 248 (37.9) |
Time to pain progression (months),a median (95% CI) | NR (30.5 to NR) | 27.5 (22.0 to 36.1) |
Hazard ratiob (95% CI) | 0.79 (0.66 to 0.95) | |
P valuec | 0.0058 | |
ADT = androgen deprivation therapy; CI = confidence interval; FAS = full analysis set; NR = not reached.
aBased on Kaplan-Meier estimates.
bThe hazard ratio and 95% CI were based on a Cox regression model, stratified by extent of disease (M1a vs. M1b vs. M1c) and alkaline phosphatase (< upper limit of normal vs. ≥ upper limit of normal).
cP value was derived from the 1-sided log-rank test, stratified by extent of disease (M1a vs. M1b vs. M1c) and alkaline phosphatase (< upper limit of normal vs. ≥ upper limit of normal).
Data cut-off: October 25, 2021.
Source: ARASENS Clinical Study Report.7
Figure 5: Kaplan-Meier Plot of Pain Progression (FAS)
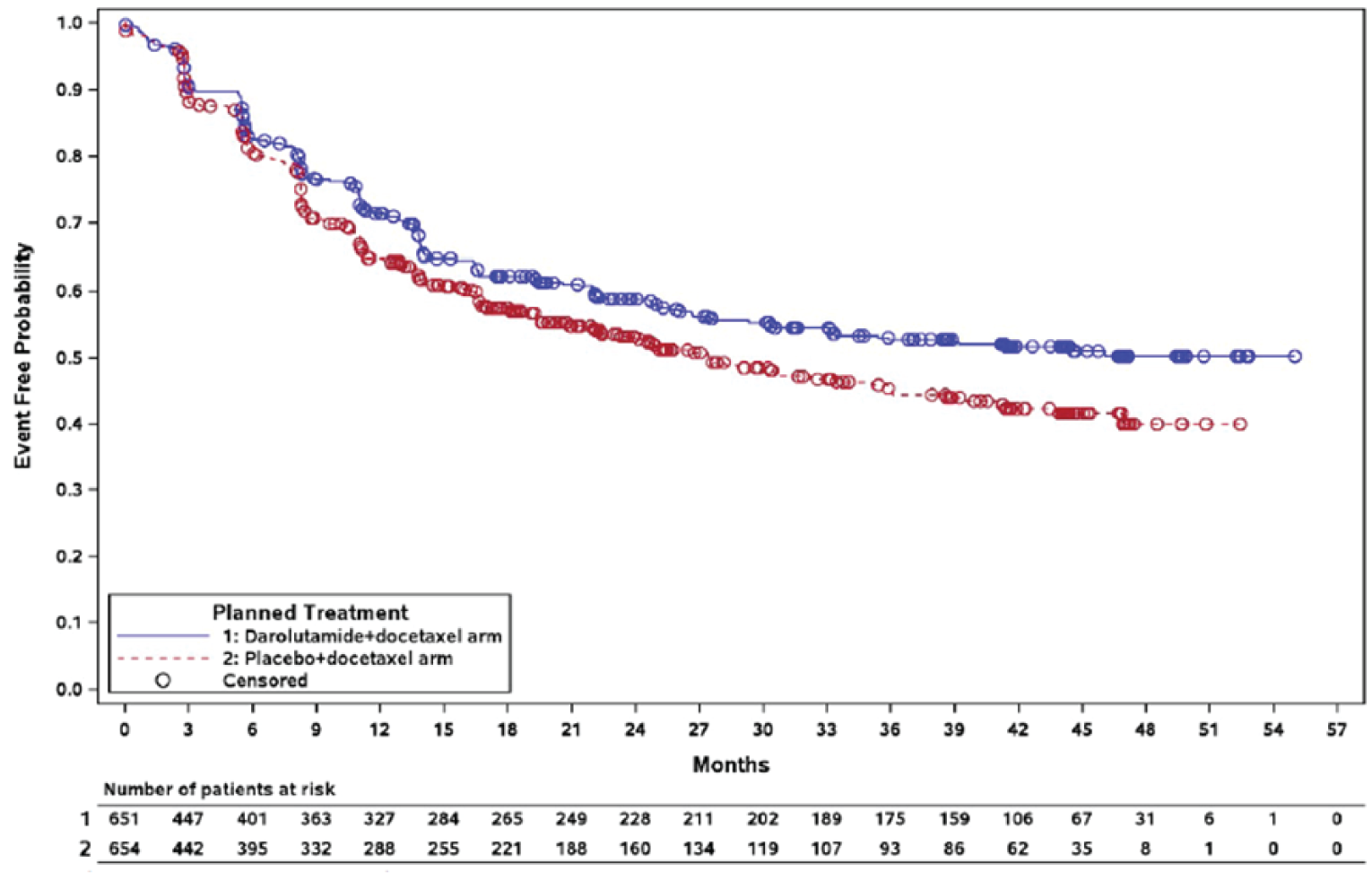
FAS = full analysis set.
Data cut-off: October 25, 2021.
Source: ARASENS Clinical Study Report.7
Health-Related Quality of Life
NCCN-FACT FPSI-17 questionnaire
HRQoL was an exploratory outcome; in the ARASENS trial, the NCCN-FACT FPSI-17 was used to approximate HRQoL. The mean total score and mean subscale scores (disease-related physical symptoms, disease-related emotional symptoms, treatment side effects, function, and well-being) over time are shown in Figure 6, Figure 11, Figure 12, Figure 13, and Figure 14, respectively.
The proportion of patients who completed the questionnaire in the FAS population was above 80% in both treatment arms at baseline. Other than week ||||||||||||||||, the proportion was above 50% up until week ||||||| in the darolutamide plus docetaxel and ADT arm, and up until week ||||||| in the placebo plus docetaxel and ADT arm.
The mean total score at baseline was ||||||||||||||||||||| in the darolutamide plus docetaxel and ADT arm, and ||||||||||||||||||||| in the placebo plus docetaxel and ADT arm. At the end of treatment, the mean change in score from baseline was ||||||||||||||||||||| in the darolutamide plus docetaxel and ADT arm, and ||||||||||||||||||||| in the placebo plus docetaxel and ADT arm.
Analyses of the subscales scores were consistent with the total score analysis, in which the mean baseline scores were similar between treatments arms. The mean score was stable at most time points but a decrease in score was observed near the end of treatment in both treatment arms. There was no notable difference in the mean change in score from baseline between treatment arms at most time points; however, this was not formally tested.
Objective Response Rate
This outcome was not measured in the study.
Time to Skeletal-Related Events
Analyses of time to first SSE and SSE-FS, which are secondary end points, are shown in Table 18.
Time to First SSE
The median time to first SSE was not reached in both treatment arms, with an HR of 0.71 (95% CI, 0.54 to 0.94; P = 0.0081), in favour of darolutamide. In both arms, most of the first SSE is attributed to the use of external beam radiation therapy to relieve skeletal symptoms. The KM plot of time to first SSE is shown in Figure 6.
Table 18: Time to First SSE and SSE-FS (FAS)
Outcome | ARASENS | |
|---|---|---|
Darolutamide + docetaxel + ADT (N = 651) | Placebo + docetaxel + ADT (N = 654) | |
Time to first SSE (months),a median (95% CI) | NR | NR |
Hazard ratiob (95% CI) | 0.71 (0.54 to 0.94) | |
P valuec | 0.0081 | |
SSE-FS (months),a median (95% CI) | 51.2 (47.2 to NR) | 39.7 (36.0 to 42.3) |
Hazard ratiob (95% CI) | 0.61 (0.52 to 0.72) | |
P valuec | < 0.0001 | |
SSE-FS event,d n (%) | 257 (39.5) | 329 (50.3) |
Death | 162 (24.9) | 221 (33.8) |
External beam radiation therapy | 60 (9.2) | 89 (13.6) |
New symptomatic pathologic bone fracture | 17 (2.6) | 8 (1.2) |
Spinal cord compression | 14 (2.2) | 9 (1.4) |
Tumour-related orthopedic surgical intervention | 4 (0.6) | 2 (0.3) |
ADT = androgen deprivation therapy; CI = confidence interval; FAS = full analysis set; NR = not reached; SSE = symptomatic skeletal event; SSE-FS = symptomatic skeletal even-free survival.
aBased on Kaplan-Meier estimates.
bThe hazard ratio and 95% CI were based on a Cox regression model, stratified by extent of disease (M1a vs. M1b vs. M1c) and alkaline phosphatase (< upper limit of normal vs. ≥ upper limit of normal).
cP value was derived from the 1-sided log-rank test, stratified by extent of disease (M1a vs. M1b vs. M1c) and alkaline phosphatase (< upper limit of normal vs. ≥ upper limit of normal).
dPatients with multiple events were only counted for the category in which the first event occurred.
Data cut-off: October 25, 2021.
Source: ARASENS Clinical Study Report.7
Figure 6: Kaplan-Meier Plot of Time to First SSE (FAS)
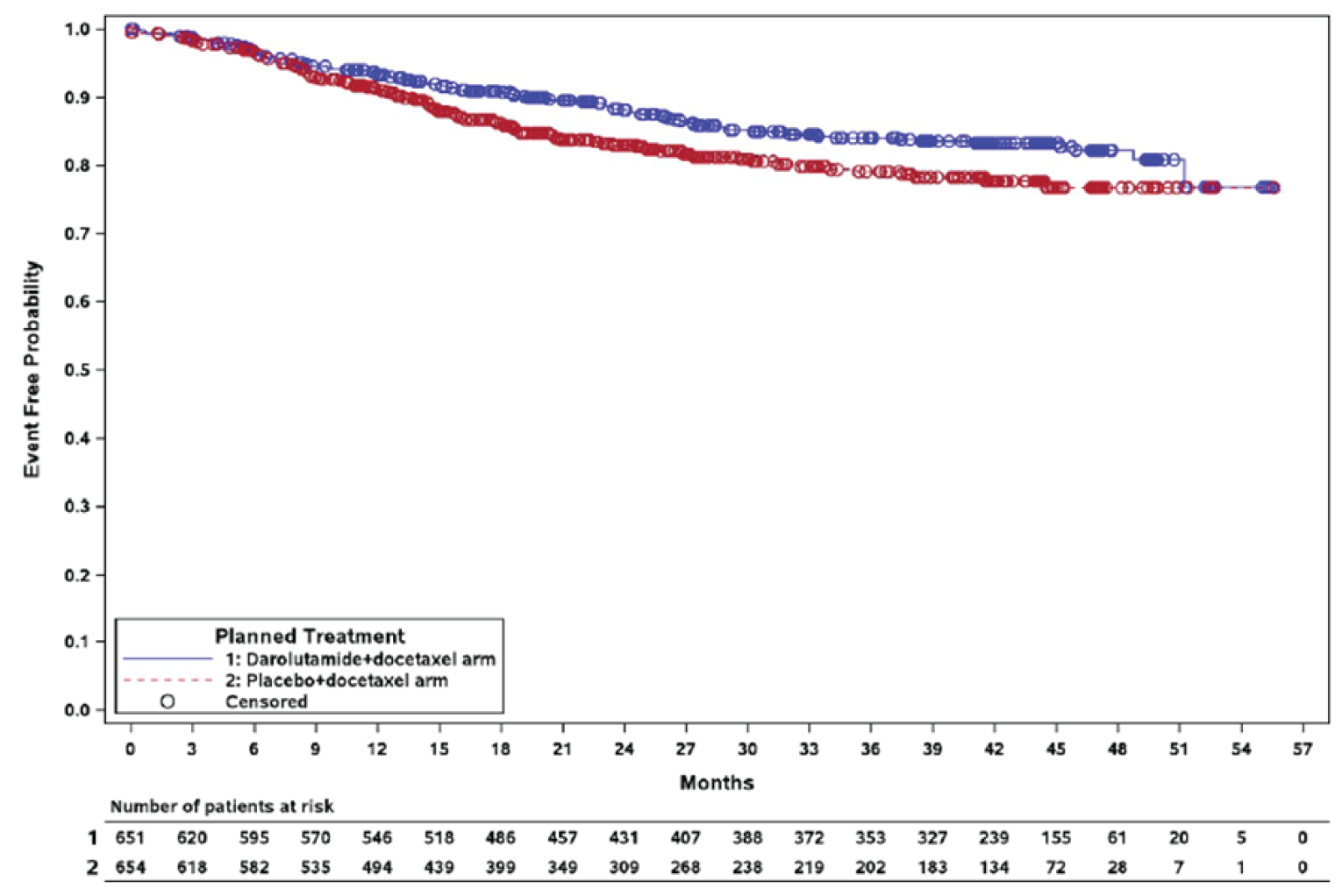
FAS = full analysis set; SSE = symptomatic skeletal event.
Data cut-off: October 25, 2021.
Source: ARASENS Clinical Study Report7
Symptomatic Skeletal Event-Free Survival
The median SSE-FS was 51.2 (95% CI, 47.2 to NR) months in the darolutamide plus docetaxel and ADT arm, and 39.7 (95% CI, 36.0 to 42.3) months in the placebo plus docetaxel and ADT arm, with an HR of 0.61 (95% CI, 0.52 to 0.72; P < 0.0001), in favour of darolutamide. The most common event in both treatment groups was death.
PSA Outcomes
Time to PSA progression and PSA response rate are exploratory end points and are summarized in Table 19.
Table 19: Time to PSA Progression and PSA Response Rates (FAS)
Outcome | Darolutamide + docetaxel + ADT (N = 651) | Placebo + docetaxel + ADT (N = 654) |
|---|---|---|
Time to PSA progression | ||
PSA progression event,a n (%) | 136 (20.9) | 310 (47.4) |
Time to PSA progression (months),b median (95% CI) | NR | 22.4 (22.1 to 27.6) |
Hazard ratioc (95% CI) | 0.26 (0.21 to 0.31) | |
P valued | < 0.0001 | |
Absolute PSA response rates | ||
Absolute PSA response rate,e 6 months (%) (95% CI) | 48.7 ||||||||||||||| | 23.9 ||||||||||||||| |
Rate differencef (%) (95% CI) | 25.0 ||||||||||||||| | |
P valued | < 0.0001 | |
Absolute PSA response,e 12 months (%) (95% CI) | 60.2 ||||||||||||||| | 26.1 ||||||||||||||| |
Rate differencef (%) (95% CI) | 34.2 ||||||||||||||| | |
P valued | < 0.0001 | |
Relative PSA response rates | ||
Relative 90% PSA response rate,g 3 months (%) (95% CI) | 67.6 ||||||||||||||| | 42.8 ||||||||||||||| |
Rate differencef (%) (95% CI) | 24.8 ||||||||||||||| | |
P valued | < 0.0001 | |
Relative 90% PSA response rate,g 6 months (%) (95% CI) | 82.0 ||||||||||||||| | 54.4 ||||||||||||||| |
Rate differencef (%) (95% CI) | 27.6 ||||||||||||||| | |
P valued | < 0.0001 | |
Relative 90% PSA response rate,g 12 months (%) (95% CI) | 84.3 ||||||||||||||| | 57.5 ||||||||||||||| |
Rate differencef (%) (95% CI) | 26.8 ||||||||||||||| | |
P valued | < 0.0001 | |
ADT = androgen deprivation therapy; CI = confidence interval; FAS = full analysis set; NR = not reached; PSA = prostate-specific antigen.
aBased on the Prostate Cancer Clinical Trials Working Group 3 criteria.
bBased on Kaplan-Meier estimates.
cThe hazard ratio and 95% CI were based on a Cox regression model, stratified by extent of disease (M1a vs. M1b vs. M1c) and alkaline phosphatase (< upper limit of normal vs. ≥ upper limit of normal).
dThe P value has not been controlled for type I error and was derived from the 1-sided log-rank test, stratified by extent of disease (M1a vs. M1b vs. M1c) and alkaline phosphatase (< upper limit of normal vs. ≥ upper limit of normal).
eAbsolute PSA response was defined as a postbaseline PSA level below 0.2 ng/mL in 2 consecutive evaluations.
fThe risk difference and 95% CI were based on Cochran-Mantel-Haenszel test comparing between treatment arm, stratified by extent of disease (M1a vs. M1b vs. M1c) and alkaline phosphatase (< upper limit of normal vs. ≥ upper limit of normal).
gRelative 90% PSA response was defined as a postbaseline 90% or greater reduction of the PSA level compared to the baseline in 2 consecutive evaluations.
Data cut-off: October 25, 2021.
Source: ARASENS Clinical Study Report.7
Time to PSA Progression
PSA progression occurred in 20.9% of patients in the darolutamide plus docetaxel and ADT arm, and 47.4% of patients in the placebo plus docetaxel and ADT arm. The median time to PSA progression was not reached in the darolutamide plus docetaxel and ADT arm, and was 22.4 (95% CI, 22.1 to 27.6) months in the placebo plus docetaxel and ADT arm, with an HR of 0.26 (95% CI, 0.21 to 0.31). Results of the sensitivity analysis based on central and local PSA data were consistent with the primary analysis.
PSA Response Rates
The absolute PSA response rate (the proportion of patients with PSA level below 0.2 ng/mL) was 48.7% at 6 months and 60.2% at 12 months in the darolutamide plus docetaxel and ADT arm, while in the placebo plus docetaxel and ADT arm, the rate was 23.9% at 6 months and 26.1% at 12 months. The risk difference between treatment arms was 25.0% ||||||||||||||||||||| at 6 months and 34.2% ||||||||||||||||||||| at 12 months.
The relative 90% PSA response rate (the proportion of patients with at least 90% PSA level reduction compared to baseline) was 67.6% at 3 months, 82.0% at 6 months, and 84.3% at 12 months in the darolutamide plus docetaxel and ADT arm, while in the placebo plus docetaxel and ADT arm, the rate was 42.8%, 54.4%, and 57.5% in the placebo plus docetaxel and ADT arm. The risk difference between treatment arms was 24.8% ||||||||||||||||||||| at 3 months, 27.6% ||||||||||||||||||||| at 6 months, and 26.8% ||||||||||||||||||||| at 12 months. Analyses of relative 30% and 50% response rates were consistent with the result of the relative 90% response rate analysis, in which there was a numerically higher proportion of PSA responders in the darolutamide plus docetaxel and ADT arm than the placebo plus docetaxel and ADT arm.
The relative 90% PSA response rate (the proportion of patients with at least 90% PSA level reduction compared to baseline) was 67.6% at 3 months, 82.0% at 6 months, and 84.3% at 12 months in the darolutamide plus docetaxel and ADT arm, while in the placebo plus docetaxel and ADT arm, the rate was 42.8%, 54.4%, and 57.5% in the placebo plus docetaxel and ADT arm. The risk difference between treatment arms was 24.8% ||||||||||||||||||||| at 3 months, 27.6% ||||||||||||||||||||| at 6 months, and 26.8% ||||||||||||||||||||| at 12 months. Analyses of relative 30% and 50% response rates were consistent with the result of the relative 90% response rate analysis, in which there was a numerically higher proportion of PSA responders in the darolutamide plus docetaxel and ADT arm than the placebo plus docetaxel and ADT arm.
Harms
Only those harms identified in the review protocol are reported here. Refer to Table 20 for detailed harms data.
Adverse Events
Almost all patients in the study reported at least 1 TEAE (99.5% in the darolutamide plus docetaxel and ADT arm; 98.9% in the placebo plus docetaxel and ADT arm). There is generally no notable difference in the incidence of all TEAEs between treatment arms, except that a numerically higher incidence of decreased appetite was observed in the darolutamide plus docetaxel and ADT arm (18.6%) compared to the placebo plus docetaxel and ADT arm (13.1%). The most common TEAEs in both treatment arms were alopecia (40.5% in the darolutamide plus docetaxel and ADT arm versus 40.6% in the placebo plus docetaxel and ADT arm), fatigue (33.1% versus 32.9%), and anemia (27.8% versus 25.1%).
Table 20: Summary of Harms (SAF)
Harms | ARASENS | |
|---|---|---|
Darolutamide + docetaxel + ADT (N = 652) | Placebo + docetaxel + ADT (N = 650) | |
Patients with ≥ 1 TEAEa | ||
n (%) | 649 (99.5) | 643 (98.9) |
Most common events,b n (%) | ||
Alopecia | 264 (40.5) | 264 (40.6) |
Fatigue | 216 (33.1) | 214 (32.9) |
Anemia | 181 (27.8) | 163 (25.1) |
Arthralgia | 178 (27.3) | 174 (26.8) |
Peripheral edema | 173 (26.5) | 169 (26.0) |
Neutrophil count decreased | 170 (26.1) | 155 (23.8) |
Diarrhea | 167 (25.6) | 156 (24.0) |
White blood cell count decreased | 155 (23.8) | 143 (22.0) |
Constipation | 147 (22.5) | 130 (20.0) |
Hot flush | 124 (19.0) | 122 (18.8) |
Back pain | 123 (18.9) | 123 (18.9) |
Decreased appetite | 121 (18.6) | 85 (13.1) |
Weight increased | 116 (17.8) | 102 (15.7) |
Nausea | 115 (17.6) | 133 (20.5) |
ALT increased | 102 (15.6) | 84 (12.9) |
Pain in extremity | 98 (15.0) | 78 (12.0) |
Patients with ≥ 1 grade 3 or higher TEAEa | ||
n (%) | 458 (70.2) | 439 (67.5) |
Most common events,c n (%) | ||
Neutrophil count decreased | 151 (23.2) | 140 (21.5) |
White blood cell count decreased | 110 (16.9) | 97 (14.9) |
Neutropenia | 56 (8.6) | 68 (10.5) |
Febrile neutropenia | 51 (7.8) | 48 (7.4) |
Hypertension | 42 (6.4) | 21 (3.2) |
Anemia | 31 (4.8) | 33 (5.1) |
Hyperglycemia | 18 (2.8) | 24 (3.7) |
Patients with ≥ 1 serious TEAEa | ||
n (%) | 292 (44.8) | 275 (42.3) |
Most common events,d n (%) | ||
Febrile neutropenia | 40 (6.1) | 39 (6.0) |
Neutrophil count decreased | 18 (2.8) | 10 (1.5) |
Pneumonia | 16 (2.5) | 21 (3.2) |
Neutropenia | 12 (1.8) | 14 (2.2) |
Pyrexia | 9 (1.4) | 15 (2.3) |
Patients who discontinued study treatment due to TEAEa | ||
n (%) | 88 (13.5) | 69 (10.6) |
Most common eventse, n (%) | ||
AST increased | 6 (0.9) | 2 (0.3) |
ALT increased | 5 (0.8) | 1 (0.2) |
COVID-19 pneumonia | 4 (0.6) | 1 (0.2) |
Bone pain | 2 (0.3) | 9 (1.4) |
Deaths | ||
n (%) | 229 (35.1) | 304 (46.8) |
Cause of death, n (%) | ||
Progressive disease | 170 (26.1) | 234 (36.0) |
Unknown | 22 (3.4) | 26 (4.0) |
AE not associated with clinical disease progression | 22 (3.4) | 16 (2.5) |
Other | 13 (2.0) | 19 (2.9) |
AE associated with clinical disease progression | 2 (0.3) | 9 (1.4) |
ADT = androgen deprivation therapy; AE = adverse event; ALT = alanine aminotransaminase; AST = aspartate aminotransferase; SAF = safety analysis set; TEAE = treatment-emergent adverse event.
aTEAEs were defined as any event(s) arising or worsening after the first dose of darolutamide or placebo until 30 days after the last dose of darolutamide or placebo administration.
bFrequency ≥ 15%.
cFrequency ≥ 3%.
dFrequency ≥ 2%.
eReported in ≥ 4 patients.
Data cut-off: October 25, 2021.
Source: ARASENS Clinical Study Report.7
At least 1 grade 3 or higher TEAE was reported in 70.2% of patients in the darolutamide plus docetaxel and ADT arm and in 67.5% in the placebo plus docetaxel and ADT arm. The most common TEAEs of grade 3 or higher (at least 10% of patients in either arm) were decreased white blood cell count (16.9% in the darolutamide plus docetaxel and ADT arm versus 14.9% in the placebo plus docetaxel and ADT arm), and neutropenia (8.6% versus 10.5%). The incidence of hypertension was numerically higher in the darolutamide plus docetaxel and ADT arm (6.4%) than the placebo plus docetaxel and ADT arm (3.2%).
Serious Adverse Events
At least 1 serious TEAE was reported in 44.8% of patients in the darolutamide plus docetaxel and ADT arm, and 42.3% of patients in the placebo plus docetaxel and ADT arm, with the most common serious TEAE in both arms being febrile neutropenia (6.1% in the darolutamide plus docetaxel and ADT arm, and 6.0% in the placebo plus docetaxel and ADT arm).
Withdrawals Due to AEs
Study treatment discontinuation due to TEAE was reported in 13.5% of patients in the darolutamide plus docetaxel and ADT arm, and 10.6% in the placebo plus docetaxel and ADT arm. The most common TEAEs that led to treatment discontinuation in the darolutamide plus docetaxel and ADT arm were increased aspartate aminotransferase level (0.9%) and increased alanine aminotransaminase level (0.6%).
Mortality
Death events were reported for 35.1% of patients in the darolutamide plus docetaxel and ADT arm, and 46.8% of patients in the placebo plus docetaxel and ADT arm. The majority of deaths in both arms were attributed to progressive disease (26.1% in the darolutamide plus docetaxel and ADT arm, and 36.0% in the placebo plus docetaxel and ADT arm). No specific TEAE was identified to account for the majority of deaths in either arm.
Critical Appraisal
Internal Validity
The ARASENS trial was a phase III, double-blind RCT. The methods of randomization, which involved stratification by extent of metastatic disease and ALP level, and Interactive Voice/Web Response System for concealment of the randomized assignment, were appropriate. The baseline characteristics of patients were generally balanced between treatment arms, suggesting randomization was adequate. A higher proportion of patients was unblinded by error during the study in the placebo plus docetaxel and ADT arm (|||||||) than the darolutamide plus docetaxel and ADT arm (|||||||), suggesting some inconsistencies in the implementation of blinding between treatment arms. Investigators were found to be unblinding patients to assist in determining the best subsequent treatment option. Bias in the measurement of the outcome in favour of darolutamide may result for subjective efficacy outcomes, including time to pain progression, time to first SSE, SSE-FS, and HRQoL. There is also a risk of bias in favour of the placebo group for harms outcomes (i.e., more frequent reporting of known harms in the darolutamide group). However, the extent of bias was likely to be small given the small number of unblinded patients. Reporting of objective outcomes—including OS, time to CRPC, time to initiation of subsequent systemic antineoplastic therapy, and PSA outcomes—would not be affected by unblinding.
A high number of important protocol deviations were reported in the study population (|||||||), which was mainly attributed to procedure deviations (|||||||) and treatment deviations (|||||||). Important protocol deviations were most frequently related to consent obtainment, study assessment (missed, incorrect, or incomplete procedures), incorrect dosing or method of drug delivery, and time frame between docetaxel administrations being too short. The sponsor indicated that the high number of protocol deviations was due to the use of a much broader and conservative approach in defining important protocol deviation than the definition by the ICH E3 classification and was not expected to compromise the integrity of study data. The sponsor noted that none of the important protocol deviations was considered to be major according to the old ICH E3 classification.
The statistical analyses were generally well designed. The efficacy analysis was conducted in the full analysis set, in which all randomized patients were included and analyzed by treatment assignment. The results correspond to the final efficacy analysis, which was conducted as planned a priori based on the number of death events occurred. A hierarchical gatekeeping approach was appropriately used to account for multiplicity in all secondary efficacy end points. No formal hypothesis testing was conducted for all exploratory efficacy end points (time to PSA progression, PSA response rates, HRQoL), and the statistical testing for PSA progression and response rates were associated with an increased risk of type I error due to the lack of control for multiplicity. For the prespecified OS subgroup analysis, there was a lack of sample size consideration, control for multiplicity, and treatment-by subgroup interaction analysis, which renders the findings exploratory. With respect to the Cox proportional hazards model for time-to-event analyses, visual inspection of the KM plots indicates that there do not appear to be any major violations of the proportional hazards assumption.
A higher proportion of patients discontinued treatment in the placebo plus docetaxel and ADT arm (80.4%) than the darolutamide plus docetaxel and ADT arm (54.1%). The most common reasons for treatment discontinuation were clinical disease progression (41.6% in the placebo plus docetaxel and ADT arm, and 19.5% in the darolutamide plus docetaxel and ADT arm) and radiologic disease progression (20.2% and 12.9%, respectively), while treatment discontinuation due to all other causes was balanced between treatment arms. There was no concern with the censoring rules.
A large amount of missing data was noted for the NCCN-FACT FPSI-17 questionnaire, which was used to approximate HRQoL by the sponsor. The completion rate declined to less than 50% after week ||||||| in the darolutamide plus docetaxel and ADT arm, and after week ||||||| in the placebo plus docetaxel and ADT arm. No data imputation was involved. There is a high risk of bias in measurement of the outcome from patients who remained in the trial, affecting the interpretability of HRQoL trends over time. The direction of the potential bias is difficult to predict. It should also be noted that the instrument has not been validated in patients with mCSPC, and most items in the questionnaire were measuring symptoms. As such, it is uncertain if the instrument can adequately capture HRQoL of the study population.
Time to pain progression was assessed based on the BPI-SF questionnaire and an MID estimate of 2 points was used to define pain progression. It should be noted that evidence for validity, reliability, and responsiveness of the BPI-SF instrument was not available for mCSPC and that most available evidence was for mCRPC. An MID for mCSPC has not yet been established. In consultation with the clinical experts, the MID estimate of 2 points used by the sponsor for defining time to pain progression was considered reasonable, although patients’ perspective on this is unknown.
External Validity
According to the clinical experts consulted by CADTH, the inclusion and exclusion criteria of the trial were reflective of the selection criteria for chemotherapy-eligible patients with mCSPC in clinical practice, except that the requirement for ECOG performance status is less stringent in clinical practice. The clinical experts noted that patients with significant comorbidities (e.g., cardiovascular diseases) and impaired performance status were excluded from the trial, limiting the generalizability of study results in this patient population commonly seen in clinical practice. With regard to baseline characteristics, the clinical experts noted that the study population had a younger median age and that there were more patients who identified as Asian, who had an ECOG performance status of 0, and who had de novo metastatic disease, compared to the general patient population in Canada. However, the clinical experts did not expect any of these differences to significantly affect the applicability of study findings in clinical practice.
The dosing of darolutamide, docetaxel, and ADT was consistent with the product monograph and clinical practice. Darolutamide was administered until disease progression (symptomatic disease progression or change in antineoplastic therapy) or unacceptable toxicity. The clinical experts noted that the treatment discontinuation criteria align with clinical practice where clinical presentation, radiographic findings, and PSA levels are factored into response evaluation and the decision to discontinue treatment. A limitation to note is that in the darolutamide plus docetaxel and ADT arm, ARATs were the most commonly prescribed subsequent antineoplastic therapy. This does not align with the clinical experts’ expectation, considering second- or later-line re-treatment with an alternate ARAT is currently not funded by most jurisdictions. The clinical experts noted that cabazitaxel, radium-223 chloride, and poly-(ADP-ribose)-polymerase inhibitors are used instead as subsequent therapies in most cases.
It should also be noted that ARAT (enzalutamide, apalutamide, or abiraterone plus prednisone) plus ADT accounts for the majority of systemic treatments currently prescribed for mCSPC in Canada according to the clinical experts. The clinical experts noted that docetaxel plus ADT was the SoC at the time the trial was designed; however, with new clinical evidence for ARAT plus ADT available in recent years, ARAT plus ADT became the most commonly prescribed regimen (and therefore the most relevant comparator). The generalizability of study results is therefore uncertain given that the use of docetaxel plus ADT is limited in the current practice. The absence of head-to-head evidence between darolutamide plus docetaxel and ADT versus ARAT plus ADT represents an evidence gap in mCSPC.
The trial included many outcomes that were indicated to be important in the clinician and patient input. The clinical experts noted that, from clinicians’ perspective, end points related to survival and disease progression (OS, time to mCRPC, and time to initiation of subsequent antineoplastic therapy) were the most important when evaluating treatment efficacy. Outcomes related to symptoms, SSE, PSA level, and HRQoL are important but generally serve as supporting evidence to inform treatment decisions, as per the clinical experts. The clinical experts agreed that the benefits of darolutamide plus docetaxel and ADT in survival and delaying disease progression were clinically meaningful. Of note, the clinical experts commented that the median time to mCRPC in the comparator arm (19.1 months) is shorter than anticipated (approximately 24 months) based on their clinical experience; as such, it is uncertain if the observed magnitude of benefit of darolutamide plus docetaxel and ADT will translate in clinical practice.
Objective response rate, an outcome of interest in the CADTH protocol, was not measured in the trial, although it was not a concern as per the clinical experts. The clinical experts commented that objective response rate is a RECIST criteria-based end point, and that it cannot be applied to the assessment of bone metastasis, which accounts for the majority of metastasis in mCSPC, due to the biology of the disease. The clinical experts noted that time to CRPC was a more appropriate end point for disease progression in the context of prostate cancer.
The clinical relevance of NCCN-FACT FPSI-17 instrument is uncertain, considering it is not routinely administered in clinical practice, according to the clinical experts. Nevertheless, the instrument does capture common symptoms (e.g., pain, difficulty in urination) and treatment-related side effects (e.g., fatigue, weight gain, decreased sexual function) indicated in the patient input, which are very relevant in the clinical assessment of patients with mCSPC in practice, as per the clinical experts.
Indirect Evidence
Objectives and Methods for the Summary of Indirect Evidence
As part of the development of a ||||||| cost-effectiveness model for darolutamide in mCSPC, the sponsor conducted and submitted an NMA that was used to inform these analyses, in the absence of direct evidence. The objective of this section is to summarize and critically appraise the methods and findings of the sponsor-submitted ITC on the relative efficacy of darolutamide and ADT in combination with docetaxel, which was indirectly compared to alternative treatments for patients with mCSPC.8
In addition to the sponsor-submitted ITC, a focused literature search for ITCs dealing with darolutamide and mCSPC was run in MEDLINE All (1946–) on July 13, 2022. No limits were applied. A total of 50 citations were identified and 8 full-text articles were retrieved for scrutiny. Two publications met the inclusion criteria for this review.9,10
Description of Indirect Comparisons
The sponsor-submitted ITC first conducted an SLR to identify evidence for inclusion in a ||||||| ITC. The relative efficacy of darolutamide plus ADT and docetaxel from the ARASENS trial was indirectly compared to alternative treatments for patients with mCSPC via ||||||| NMA. Comparators of interest for the sponsor-submitted NMA included ADTs, abiraterone and prednisone, apalutamide, enzalutamide, and docetaxel. Outcomes of interest included OS, time to CRPC, and rPFS.8
Two additional NMAs were identified in the CADTH literature search (Menges et al. [2022] and Yanagisawa et al. [2022]).9,10
The objective of the published SLR and NMA by Menges et al. was to assess the clinical effectiveness regarding survival and HRQoL, safety, and benefit-harm balance of mHSPC treatments, including docetaxel, abiraterone, enzalutamide, apalutamide, darolutamide, and radiotherapy (alone or in combination with ADT).9
The objective of the published SLR and NMA by Yanagisawa et al. was to analyze the benefit of triplet combination therapies with androgen receptor signalling inhibitors (abiraterone acetate, apalutamide, darolutamide, and enzalutamide) in combination with docetaxel and ADT, compared to available treatment regimens in patients with mHSPC.10
The populations, interventions, comparators, and designs of studies included in the sponsor-submitted NMA and the published NMAs are summarized in Table 21. Further details and results of these NMAs are provided subsequently.
Table 21: Study Selection Criteria and Methods for SLRs From ITCs
PICOS | Sponsor-submitted NMA | Menges et al. NMA | Yanagisawa et al. NMA |
|---|---|---|---|
Population | Adult patients (age ≥ 18 years) with mCSPC | Adult men with mHSPC newly diagnosed (either as de novo or at progression after prior local therapy) | Patients with mHSPC |
Interventions |
| ADT + docetaxel (75 mg/m2 body surface area, administered IV every 3 weeks for 6 cycles) in combination with prednisone 10 mg/day during 6 cycles, followed by ADT alone | ARSI + docetaxel + ADT |
Comparators |
|
| Currently available systemic treatment strategies (not further specified) |
Outcomes |
|
|
|
Study design |
| RCTs, including multiarm, multistage designs | RCTs |
Publication characteristics |
|
|
|
Exclusion criteria |
|
|
|
ADT = androgen deprivation therapy; AE = adverse event; ARSI = androgen receptor signalling inhibitor; CR = complete response; CRPC = castration-resistant prostate cancer; EBRT = external beam radiation therapy; HRQoL = health-related quality of life; ITC = indirect treatment comparison; LHRH = luteinizing hormone-releasing hormone; mHSPC = metastatic hormone-sensitive prostate cancer; mCSPC = metastatic castration-sensitive prostate cancer; NMA = network meta-analysis; ORR = objective response rate; OS = overall survival; nsAA = non-steroid antiandrogen; PFS = progression-free survival; PICO = Population, Intervention, Comparison, Outcomes; PR = partial response; PSA = prostate-specific antigen; RCT = randomized controlled trial; RoB = risk of bias; rPFS = radiographic progression-free survival; SLR = systematic literature review; SNA = nonsteroidal antiandrogen.
Source: Sponsor-submitted NMA,8 Menges et al. (2022),9 Yanagisawa et al. (2022).10
Methods of Sponsor-Submitted NMA
Objectives
The objective of the sponsor-submitted NMA was to inform the ||||||| cost-effectiveness model for darolutamide in mCSPC by indirectly comparing darolutamide and ADT in combination with docetaxel to alternative treatments ||||||||||||||, as well as to Canadian comparators of interest ||||||||||||||||||||.
Study Selection Methods
The sponsor-submitted NMA was informed by an SLR. Methods for identification of citations were limited to database searches of MEDLINE® In-Process (using Pubmed.com), Embase+ and MEDLINE (using Embase.com), and the Cochrane Library. The date of the search was not reported. No information on screening or data extraction methods, or methods for assessing risk of bias of the trials included in the SLR, were provided.
|||||||| Evidence Base
The SLR informing the sponsor-submitted NMA was originally conducted to inform the |||||||| NMA. There were |||||||| studies identified from the SLR as potentially relevant for inclusion in the |||||||| NMA. Minimal information on the selection of studies from the SLR for evaluation in the NMA were provided and appeared based solely on treatments evaluated in the trials identified by the SLR. Trials including docetaxel were grouped separately from those in which docetaxel was not included (other treatments for mCSPC including anti-androgens, radiotherapy, castration). In total, |||||||| trials were excluded from the |||||||| NMA based on treatment type. Reason for exclusion of these studies was provided and included irrelevancy of comparators ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||, or lack of comparator specification ||||||||||||||||||||||||.
Canadian Evidence Base
|||||||||||||||||||||||| some treatments that were not relevant to the Canadian market ||||||||||||||||||||||||||||||||||||||||:
Enzalutamide and ADT with docetaxel: Studies evaluating enzalutamide with docetaxel and ADT (subgroups of the ENZAMET trial) were removed from consideration for the Canadian NMA as enzalutamide and ADT with docetaxel is not indicated, reimbursed, or commonly used in Canada, per the sponsor’s report.
Abiraterone and ADT with docetaxel: The regimen of abiraterone and ADT with docetaxel (subanalysis of the PEACE-1 trial) is not indicated, reimbursed, or commonly used in Canadian clinical practice; and was therefore not considered an appropriate comparator. Additionally, the sponsor noted methodological limitations of the PEACE-1 trial that precluded its inclusion in the Canadian NMA.
Standard nonsteroidal antiandrogens (SNAs): SNAs include bicalutamide, nilutamide, and flutamide. SNAs no longer represent the SoC in mCSPC since the availability of docetaxel and the androgen receptor-axis-targeted class of therapies. Current Canadian and international mCSPC guidelines do not recommend the use of SNAs in mCSPC and were not considered as appropriate comparators of interest for the NMA.
As such, the treatments of interest for the Canadian submission included the following:
Darolutamide plus ADT and docetaxel
Enzalutamide and ADT
Apalutamide and ADT
Abiraterone and prednisone with ADT
Docetaxel and ADT
The sponsor also considered ADT monotherapy as a relevant comparator for the Canadian submission; however, results from this comparison were not reported in this review because it was not considered an appropriate comparator since it was not included in the CADTH systematic review protocol (Table 5).
In total, |||||||| additional studies were excluded ||||||||||||||||||||||||. A summary of studies identified for inclusion in the |||||||| NMA is depicted in Figure 7.
Although the ENZAMET study was a key trial of interest for enzalutamide, SNA was the main comparator in this study. The ENZAMET trial also included a subgroup of patients who received the concurrent combination of enzalutamide and ADT with docetaxel; however, this evaluation was not prespecified. The ENZAMET trial was excluded from this analysis because it does not provide evidence relative to other relevant treatments for Canada. To explore the implications of excluding this trial from the NMA, a comparison between the enzalutamide arms from the ENZAMET trial and the ARCHES trial was conducted. The ARCHES trial, the pivotal study of enzalutamide, included ADT as a comparator. ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. The resulting HR (95% CI) was |||||||||||||||||||||||| for the ARCHES trial versus the ENZAMET trial, favouring the ARCHES trial. As such, it was deemed conservative to exclude the ENZAMET trial, ||||||||||||||||||||||||||||||||||||||||||||||||||||||||.
Figure 7: Flowchart of Studies Identified for Inclusion in the NMA (Redacted)

Note that this figure has been redacted.
The end points of interest for the Canadian NMA were stricter than that of the SLR (Table 21) and included OS, time to CRPC, and rPFS. Time to CRPC was defined according to the ARASENS trial as the time from randomization to occurrence of the following events: PSA progression, radiological progression by bone lesions, or radiological progression by soft-tissue and visceral lesions, whichever occurred first. The sponsor considered time to CRPC as a more conservative definition of disease progression than rPFS because it has a closer representation of clinical practice, since clinical decisions in mCSPC are driven by disease progression through radiographic and biochemical means. Thus, time to CRPC was the preferred end point to model disease progression in the base-case NMA, and rPFS was included as a sensitivity analysis.
ITC Analysis Methods
In addition to the treatments evaluated and considered for the Canadian evidence base noted previously, an assessment of the heterogeneity of the eligible trials was conducted based on evaluation of trial design, the patient population, inclusion and exclusion criteria, and visual analysis of baseline characteristics, including age, ECOG performance status, Gleason score, PSA levels, and prostate cancer stage. No studies were excluded based on the heterogeneity assessment. An exploratory analysis of the individual patient data from the ARASENS trial was conducted to identify potential treatment effect modifiers.
The NMA was carried out using a ||||||||||||||||||||||||. All outcomes in the NMA were time-to-event outcomes (OS, time to CRPC, and rPFS). For these analyses, the reported HR and associated variance estimates (standard error or 95% CI) were used to derive the input data for the analysis. Additionally, the log HR and the standard error were also required from each study, and where these data were not reported, sufficient data to calculate these measures were required. ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. Both fixed and random-effects models were considered for the analysis of all outcomes, and model comparison methods were used to compare the goodness-of-fit. The preferred model was selected based on clinical plausibility of the estimated relative treatment effects and deviance information criterion, and/or the total residual deviance. For all outcomes, |||||||||||||||||||||||||||||||| were chosen as the base case based on the ||||||||||||||||.
Relative treatment effects were estimated using Markov chain Monte Carlo methods. A first series of iterations was discarded as “burn-in,” and the inferences were based on additional iterations using 3 chains with different starting values and checking convergence using the Brooks-Gelman-Rubin statistic and plots of posterior density.28 The number of burn-in iterations discarded was not specified. If there was evidence that the Markov chain Monte Carlo had not converged, the number of burn-in iterations was increased. Once convergence had been achieved, further samples were generated from the posterior distribution to estimate treatment effects and 95% CrIs. Autocorrelation was assessed using autocorrelation plots to determine whether samples within each chain were highly correlated, and a suitable thinning interval was applied if needed to ensure that the chain mixed well and was representative of the posterior distribution.
In line with visual assessment of heterogeneity, statistical heterogeneity was evaluated based on the I2 statistic derived from direct head-to-head meta-analysis of those treatment comparisons in each network that were reported by more than 1 study.
For all outcomes analyzed, inconsistency was assessed via “node-splitting” using the van Valkenhoef et al. method when closed loops were present.29 Direct and indirect estimates along with CIs for each split treatment comparison were compared. Inconsistency was also presented as an inconsistency factor (IF) with an associated 95% CI. If the relative treatment effect was a ratio measure (e.g., OR HR), then the IF is the ratio of the direct and indirect estimates of the relative treatment effect such that if the 2 estimates are perfectly consistent then IF = 1.
Sensitivity Analysis
Sensitivity analyses were conducted on the choice of prior distribution by comparing 3 alternative prior distributions, which were non-informative and in line with those specified in the National Institute for Health and Clinical Excellence Decision Support Unit Technical Support Document 2 (NICE DSU TSD 2), to allow the posterior distribution to be primarily driven by the data.30 The following prior distributions for the between-trials SD were assessed:
Unif(0, 3): A uniform distribution indicating that any value of the between-trial SD between 0 and 3 is equally probable.
Unif(0, 5): A uniform distribution indicating that any value of the between-trial SD between 0 and 5 is equally probable.
Unif(0, 10): A uniform distribution indicating that any value of the between-trial SD between 0 and 10 is equally probable.
Radiographic PFS was not an outcome in the ARASENS trial. Additionally, time to CRPC was a composite of PSA progression and metastatic progression, while rPFS measures metastatic progression but not PSA. As such, rPFS was only included as a sensitivity analysis for modelling disease progression.
Results of Sponsor-Submitted NMA
Summary of Included Studies
A summary of potential sources of heterogeneity from the ||||| eligible studies is provided in Table 22. Each stage of the STAMPEDE trial was considered 1 study for a total of ||||| studies. No studies were excluded based on substantial heterogeneity. The studies were published between 2013 and 2020. Most studies were phase III (n = 6), 3 were open-label, and 4 were double-blind RCTs. Most studies had placebo/best SoC as comparator (n = 4), while 3 had active and placebo-controlled comparators. The median duration of follow-up varied across studies, ranging from 191 weeks to 364.5 weeks.
The definition of the population in each trial varied across the studies. The ARASENS, ARCHES, and CHAARTED trials defined the population as mHSPC, while the TITAN and LATITUDE trials describe the trial population as metastatic CSPC, although these definitions are generally used interchangeably. The GETUG-AFU 15 study included patients with non-castrate metastatic prostate cancer, and the STAMPEDE trial defined their trial population as patients with prostate cancer.
Baseline characteristics were visually assessed. Due to absence of data, it was not possible to assess the similarity of these baseline characteristics for all studies. Age, ECOG performance status, and Gleason score were generally similar across studies. All studies had a greater proportion of patients with ECOG performance status of 0. Per the sponsor’s analysis, of the studies that report ECOG, none was a clear outlier. There were notable differences in PSA levels in each study, ranging from just over 0 ng/mL to 100 ng/mL, and 1 study not reporting PSA level. Finally, prostate cancer stage was only reported in 4 studies, with the ARASENS trial differing from the 3 other studies that reported stage. Most patients in the ARASENS trial were T4, while most patients in the other studies were T3. The sponsor considered that T4 patients have a worse relative effect compared to T3 patients, and therefore the estimate using all patients for the ARASENS trial would be conservative. A notable difference across the trials was the presence and type of prior treatments; several trials did not report the proportion of patients having received specific prior treatments. Treatment with chemotherapy was also considered as an effect modifier that could have invalidated the transitivity assumption, as eligibility for chemotherapy is based on considerations including patient preference, age, performance status, and the presence of comorbidities. Outcomes of interest were not defined in the same way across all trials; therefore, in some cases, proxies needed to be used (e.g., failure-free survival in place of time to CRPC in some trials).
Table 22: Study Design and Other Characteristics Included in Heterogeneity Assessment
Study (publication year) | Sample size | Design | Comparator | Median follow-wp (weeks) | Age (years) | ECOG performance status | Prior therapy |
|---|---|---|---|---|---|---|---|
ARASENS (2021) | 1,305 | Phase III, DB, RCT | Docetaxel + ADT | 189.9 | ≥ 18 | 0 to 1 | Mostly untreated: ADT (LHRH agonist/antagonist or orchiectomy) with or without first-generation antiandrogen, but no longer than 12 weeks before randomization. |
ARCHES (2019) | 1,150 | Phase III, DB, RCT | Active and PBO/BSC | 193.8 | Adult | 0 to 1 | Some: Prior ADT and up to 6 cycles of prior docetaxel chemotherapy were permitted. |
CHAARTED (2015) | 790 | Phase III, open-label RCT | Active controlled | 233.3 | ≥ 18 | 0 to 1 | Some: Prior adjuvant ADT was allowed for under 24 months. Chemotherapy was also allowed. |
GETUG-AFU 15 (2013) | 385 | Phase III, open-label RCT | PBO/BSC | 364.5 | ≥ 18 | 0 to 2 | Some: Previous chemotherapy or ADT, or both, were allowed when treatment was discontinued 12 months before study. |
LATITUDE (2017) | 1,199 | Phase III, DB, RCT | PBO/BSC | 225 | ≥ 18 | NR | Mostly untreated: Patients were excluded if they had received previous chemotherapy, radiation therapy, or surgery for metastatic prostate cancer except for 3 months or less of ADT. |
STAMPEDE (2016 to 2019) | 2,962 | Phase II/III, open-label RCT | Active and PBO/BSC | 339.8 | 0 to 120 | 0 to 2 | Some: 12 months maximum length on ADT and 1 year of no ADT required before beginning the trial. Radiotherapy and surgery allowed. Systemic therapy not allowed. |
TITAN (2019) | 1,052 | Phase III, DB, RCT | PBO/BSC | 191.2 | ≥ 18 | 0 to 2 | Some: Previous docetaxel use (up to 6 cycles), ADT, 1 course of radiation or surgical therapy and other localized therapies. |
ADT = androgen deprivation therapy; BSC = best standard of care; DB = double-blind; ECOG = Eastern Cooperative Oncology Group; LHRH = luteinizing hormone-releasing hormone; NR = not reported; PBO = placebo; RCT = randomized controlled trial.
Source: Sponsor-Submitted NMA.8
Results of Sponsor-Submitted NMA
The network of evidence (Figure 8) for outcomes of interest including OS, time to CRPC, and rPFS were informed by the same set of studies. In total, ||||| studies comprising 6 treatment regimens were included in the analyses. Each stage of STAMPEDE was included as a separate study in the network.
The ||||||||||||| model was selected as the base case for OS, and time to CRPC based on the |||||||||||||||. Results of the |||||||||||||||||||| model comparing darolutamide plus ADT and docetaxel to relevant comparators for all end points is summarized in Table 23.
Figure 8: Sponsor-Submitted NMA Network Diagram
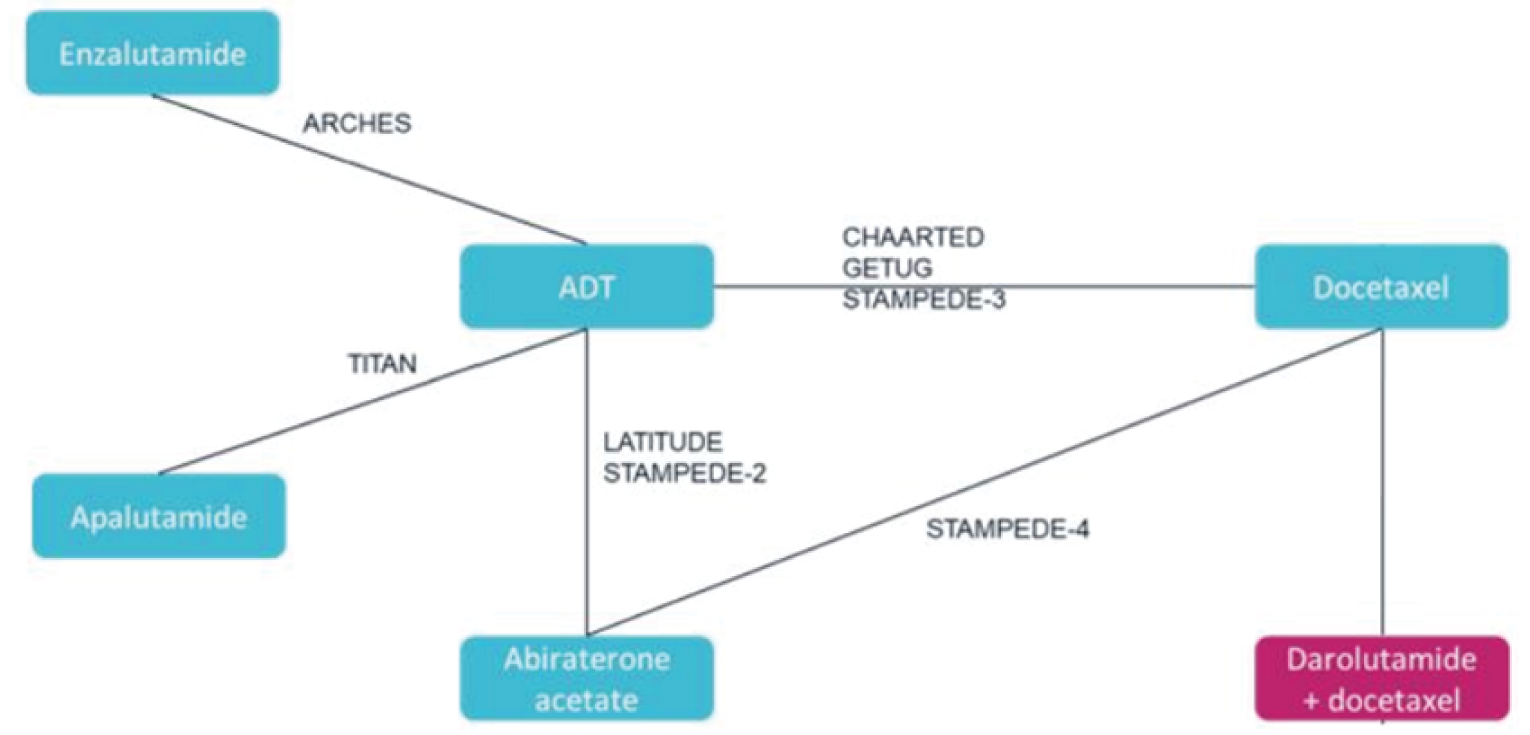
ADT = androgen deprivation therapy.
Each stage of the STAMPEDE trial was included as a separate study.
Source: Sponsor-submitted NMA.8
Table 23: ||||||||||||||||||||||||| Model for Relative Effect of Darolutamide Plus ADT and Docetaxel Compared to All Treatments for OS, Time to CRPC, and rPFS
Darolutamide + ADT + docetaxel vs. | ||||||||||||||||| (Base case) | ||
|---|---|---|---|
OS HR (95% CrI) | Time to CRPC HR (95% CrI) | rPFSa HR (95% CrI) | |
Enzalutamide + ADT | ||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| |
Apalutamide + ADT | ||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| |
Abiraterone acetate + ADT | ||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| |
ADT + Docetaxel | ||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| |
ADT = androgen deprivation therapy; CrI = credible interval; CRPC = castration-resistant prostate cancer; HR = hazard ratio; OS = overall survival; rPFS = radiographic progression-free survival.
aThe analysis of rPFS was considered a sensitivity analysis for modelling disease progression.
Source: Sponsor-Submitted NMA8
Overall Survival
For OS, darolutamide plus ADT and docetaxel was favoured over docetaxel and ADT (|||||||||||||||||||||||||||||||||||). There was insufficient evidence to show a difference between darolutamide plus ADT and docetaxel and enzalutamide, apalutamide, or abiraterone acetate, and the 95% CrIs were wide.
Inconsistency assessments between direct and indirect evidence for OS showed some differences (Figure 16). However, 95% CIs overlapped, and therefore no statistically significant differences were found. Inconsistency could not be tested specifically for comparisons to darolutamide plus ADT and docetaxel because these were informed only by indirect evidence. For all pairwise comparisons informed by at least 2 studies, the I2 statistic was |||||.
Time to CRPC
For time to CRPC, darolutamide plus ADT and docetaxel was favoured over most treatments in the network, including apalutamide and ADT (|||||||||||||||||||||||||||||||||||), abiraterone and ADT (|||||||||||||||||||||||||||||||||||), and docetaxel and ADT (||||||||||||||||||||||||||||||||||), although the evidence was insufficient to show a difference compared to enzalutamide and ADT (||||||||||||||||||||||||||||||||||||) as the 95% CrIs were wide.
Inconsistency assessments for time to CRPC showed little differences between direct and indirect estimates (Figure 17). Inconsistency could not be tested specifically for comparisons with darolutamide plus ADT and docetaxel, because these were informed only by indirect evidence. The I2 statistic was reported to be ||||||||||||||||||||||||||||||||||| for all pairwise comparisons informed by at least 2 studies except for |||||||||||||||||||||||||||||||||||.
Radiographic PFS
As a sensitivity analysis, for rPFS, darolutamide plus ADT and docetaxel was favoured over all other treatments in the network with HRs of ||||||||||||||||||||||||||||||||||| compared to docetaxel and ADT, ||||||||||||||||||||||||||||||||||| compared to apalutamide and ADT, ||||||||||||||||||||||||||||||||||| compared to abiraterone and ADT, and ||||||||||||||||||||||||||||||||||| compared to enzalutamide and ADT.
Inconsistency assessments for rPFS showed few differences between direct and indirect estimates (Figure 18). The I2 statistic indicated that the variance due to heterogeneity across studies was reported to be ||||||||||||||||||||||||||||||||||| for all pairwise comparisons informed by at least 2 studies except for |||||||||||||||||||||||||||||||||||.
Additional sensitivity analyses for OS, time to CRPC, and rPFS using ||||||||||||||||||||||||| are summarized in Table 24. Results for sensitivity analyses were consistent with the base-case analyses, although 95% CrIs were wider.
Table 24: ||||||||||||||||| Model for Relative Effect of Darolutamide Plus ADT and Docetaxel Compared to All Treatments for OS, Time to CRPC, and rPFS
Darolutamide + ADT + docetaxel vs. | HR (95% CrI) | ||
|---|---|---|---|
||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| | |
OS | |||
Enzalutamide + ADT | ||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| |
Apalutamide + ADT | ||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| |
Abiraterone acetate + ADT | ||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| |
Docetaxel + ADT | ||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| |
Time to CRPC | |||
Enzalutamide + ADT | ||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| |
Apalutamide + ADT | ||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| |
Abiraterone acetate + ADT | ||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| |
Docetaxel + ADT | ||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| |
rPFSa | |||
Enzalutamide + ADT | ||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| |
Apalutamide + ADT | ||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| |
Abiraterone acetate + ADT | ||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| |
Docetaxel + ADT | ||||||||||||||||| | ||||||||||||||||| | ||||||||||||||||| |
ADT = androgen deprivation therapy; CrI = credible interval; CRPC = castration-resistant prostate cancer; HR = hazard ratio; OS = overall survival; rPFS = radiographic progression-free survival.
aThe analysis of rPFS was considered a sensitivity analysis for modelling disease progression.
Source: Sponsor-submitted NMA.8
Critical Appraisal of Sponsor-Submitted NMA
The sponsor-submitted NMA was informed by a ||||||||| SLR that included planned searches of multiple databases; other sources were not searched, but it is unclear whether this would have resulted in relevant studies being missed. Inclusion of studies was based on prespecified PICOS criteria; however, no information was provided on the methods of study selection or data extraction (e.g., duplicate reviewers), or conduct and results of a risk-of-bias assessment. As a result, there is a potential risk for bias and/or error in the SLR; however, the extent of this risk cannot be quantified. CADTH was unable to assess the quality of clinical studies included in the NMA, although, given that only phase III RCTs were included, the risk of bias of the trials was not expected to be high for objective outcomes.
There was no mention of an a priori protocol to inform the SLR and resulting NMA, and therefore it is unclear if the criteria for inclusion in the Canada-specific NMA were prespecified. Regardless, Canadian NMA criteria were more restrictive than for the ||||||||| SLR, and were based on appropriate Canadian comparators, including ADTs, abiraterone and prednisone, apalutamide, enzalutamide, and docetaxel. The combination of abiraterone plus ADT and docetaxel was considered a comparator of interest for this review by the clinical experts consulted by CADTH as well as the drug plans, but was not included in the sponsor’s analysis. Of note, the clinical experts reported that the combination has recently begun to be used by some clinicians in light of new clinical trial evidence4 and would not have been considered relevant at the time the NMA was conducted. As such, the comparative efficacy of darolutamide plus ADT and docetaxel and abiraterone plus ADT and docetaxel remains unknown.
The sponsor conducted a feasibility assessment to evaluate potential areas of heterogeneity based on study design and baseline characteristics, including age, ECOG performance status, Gleason score, PSA levels, and prostate cancer stage. No formal search for potential treatment effect modifiers was conducted; instead, the sponsor evaluated subgroups from the ARASENS trial, which were not powered to detect differences across subgroups. Overall, the sponsor did not exclude any studies based on heterogeneity, and although some heterogeneity was noted by the sponsor, it did not consider any baseline characteristics to be treatment-effect modifiers. The CADTH team and the clinical expert consulted by CADTH noted that important factors were considered; however, there remained notable differences in the baseline characteristics that could potentially result in changing relative treatment effects, including differences in PSA level, and prostate cancer stage. Additionally, there were differences in study design characteristics, including in blinding, in which 3 were open label and 4 were double blind. Open-label studies are more susceptible to bias, which could influence treatment effects. Differences in prior treatment requirements; a wide time span between trials (2013 to 2020), during which SoC may have changed; some differences in outcome definitions across the trials; and differences in follow-up duration were also evident. Although differences in study design are not feasible to address, there remains increased potential that the underlying transitivity assumption of the NMA has been violated.
In most cases, comparisons for almost all competing interventions were based on single trials, although 1 closed loop was formed between the connection of ADT, docetaxel and ADT, and abiraterone acetate (the LATITUDE, STAMPEDE-2, STAMPEDE-3, GETUG-AFU 15, CHAARTED, and STAMPEDE-4 studies) for which consistency between direct and indirect evidence was assessed. Direct and indirect evidence were not entirely consistent for OS. Statistical heterogeneity varied based on I2 ||||||||| across outcome comparisons) and in general, there were few studies informing these comparisons; thus, they are subject to substantial bias and difficult to interpret. Comparisons to darolutamide plus ADT and docetaxel were informed entirely by indirect evidence, and therefore are associated with increased uncertainty.
Base-case analyses were conducted using |||||||||||||| models based on the ||||||||||||||, which was considered appropriate. However, |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||. This assumption was derived from the ARASENS subgroup analysis, but the ARASENS trial was not powered to draw conclusions across subgroups. It does not appear that these assumptions were corroborated by other empirical evidence or expert opinion; thus, it is uncertain if |||||||||||||||||||||||||||| models were truly most appropriate. Regardless, sensitivity analyses using |||||||||||||||||||||| models with varying alternative prior distribution were conducted, for which results were consistent with the base case, although point estimates were associated with wide CrIs, highlighting the uncertainty in the results.
Outcomes included in the NMA were relevant to the treatment of mCSPC, focusing mainly on OS. In the sponsor-submitted NMA, time to CRPC was considered a proxy for modelling disease progression over rPFS because it has a closer representation of clinical practice, according to the sponsor. This assumption was also considered appropriate by the clinical experts consulted by CADTH. No outcomes related to HRQoL or safety were evaluated; thus, the impact of darolutamide plus ADT and docetaxel compared to other relevant treatments on HRQoL and safety remains unknown.
In the |||||||||||||| analysis comparing darolutamide plus ADT and docetaxel to other therapies available in Canada, the sponsor considered darolutamide plus ADT and docetaxel the most efficacious treatment versus comparators of interest for OS and time to CRPC. While point estimates trended in the direction favouring darolutamide plus ADT and docetaxel, the 95% CrIs were wide, often crossing the threshold of no effect, particularly for the main outcome of OS, thereby increasing the uncertainty in the comparative effect estimates. Results for sensitivity analyses using |||||||||||||| models were consistent with the ||||||||||||||, although 95% CrIs were even wider, suggesting increased uncertainty.
Methods of NMA by Menges et al. (2022)9
Objectives
This NMA aimed to comprehensively assess the clinical effectiveness regarding survival and HRQoL, as well as the safety and benefit-harm balance of combinations of docetaxel, ARATs, and radiotherapy with ADT compared to ADT alone in patients with mHSPC.
As previously noted, comparisons to ADT monotherapy are not of interest to this review because ADT monotherapy was not considered an appropriate comparator in the CADTH systematic review protocol (Table 5). As such, results for comparisons to ADT monotherapy were not reported in this review.
Study Selection Methods
A protocol for the systematic review for the NMA was registered on PROSPERO (CRD42020171129). Three databases (MEDLINE, EMBASE, and Cochrane Central Register of Controlled Trials [CENTRAL]) and ClinicalTrials.gov were searched for records of studies published up until February 25, 2020, with an update on March 1, 2022, for studies or updated results published between January 2020 and March 1, 2022. Relevant conference proceedings (American Society of Clinical Oncology [ASCO], American Urological Association [AUA], European Society for Medical Oncology [ESMO], European Association of Urology [EAU], AUA from 2016 to 2020, and APCCC from 2017 and 2019) were searched for publications between January 2016 and April 2020. Reference lists of recently published SLRs were also screened, although no date range for the year of publication was defined. Only RCTs, including multiarm, multistage RCTs, were considered for inclusion in the SLR. The full screening, eligibility assessment, data extraction, and risk-of-bias assessment was performed in duplicate by 3 reviewers and during the search update; this process was performed by 1 reviewer and the data and risk-of-bias assessment were verified by a second reviewer (studies including darolutamide were included at the stage of the update search). The risk of bias in the studies was assessed by reviewers using the Cochrane risk-of-bias 2.0 tool;11 the information from the bias assessment was presented alongside the results. Appraisal using the Grading of Recommendations, Assessment, Development and Evaluations (GRADE) approach was undertaken to assess the certainty of evidence for direct, indirect, and NMA effect estimates, and was presented alongside the results.31
Eligible studies included men with newly diagnosed mHSPC who had not previously received systemic treatment for prostate cancer. Studies including patients pretreated with ADT alone in or combination with non-steroid antiandrogen (nsAA) for no longer than 24 months and at least 12 months before enrolment, or for less than 6 months before enrolment, were considered eligible. Patients with non-metastatic prostate cancer or with receipt of chemotherapy before enrolment were not considered eligible.
The following interventions were eligible for inclusion: ADT and docetaxel (75 mg/m2 body surface area IV every 3 weeks for 6 cycles) in combination with prednisone 10 mg/day during 6 cycles, followed by ADT alone; ADT and abiraterone acetate (1,000 mg/day orally) in combination with prednisone 5 mg/day until disease progression; ADT and enzalutamide (160 mg/day orally) until disease progression; ADT and apalutamide (240 mg/day orally) until disease progression; ADT and darolutamide (1,200 mg/day orally) until disease progression; and ADT and radiotherapy (external beam radiation therapy to the prostate with unspecified dose and frequency), followed by ADT alone. Any concurrent or per-protocol immediate sequential combination of these treatments was also considered eligible. Comparators of interest included ADT alone or in combination with placebo (various administrations or orchiectomy); and ADT plus nsAA alone or in combination with placebo (various administrations including orchiectomy).
Outcomes included OS, PFS, HRQoL, and AEs. The PFS and HRQoL analysis did not include any studies that studied darolutamide and the network was not provided; therefore, the results for PFS and HRQoL are not discussed in this report. The AE analysis included darolutamide, but it was only compared to ADT in the analysis; thus, it was not included in this report.9 A quantitative benefit-harm assessment was also conducted; however, this was not considered an outcome of interest for this review and is therefore not discussed.
Analysis Methods
The list of eligible interventions and comparators included specific dosages and administration routes; therefore, individual studies with the same intervention and comparator arms were pooled and their effect estimates analyzed with an NMA to obtain pooled results at the intervention level. Effect estimates obtained from this analysis informed the direct estimates in the subsequent pairwise analysis and NMA.9
Of note, studies using ADT and nsAA therapy as a comparator arm (the ENZAMET and NCT02058706 trials) were not excluded from the main analysis but were combined with the ADT-only comparator in their group (which included the ARCHES trial using ADT alone as a comparator) and assumed to be equivalent. Authors noted that this was in line with existing evidence from systematic reviews and with approaches taken in other analysis groups. In addition, correlation matrices based on the overlap in patient accrual in different time periods assuming a constant variance were estimated for arms C and G in the STAMPEDE trial due to the multiarm, multistage design, and were used to estimate the overall NMA model; this assumed no relevant variation across different treatments or time periods.9
A frequentist, random-effects pairwise meta-analysis and NMA was conducted using study-level aggregate data. The frequentist framework was chosen for the meta-analysis based on the limited number of included studies and a recommendation by Langan et al.32 Random-effects models were selected because the authors assumed there would be important study-level variation.9
Transitivity was assessed according to epidemiological criteria based on the presence of potential effect modifiers and clinical plausibility. Heterogeneity was assessed visually and using the I2 statistic. Direct estimates, indirect estimates, and the results from the NMA were assessed individually for certainty of evidence using the GRADE criteria and extension for network meta-analysis. The presence of inconsistency between direct and indirect estimates was evaluated using IFs (HR from direct evidence divided by HR from indirect evidence, with a variance equal to the sum of direct and indirect variances). Potential publication bias was considered by the authors as the likelihood that a trial would have been conducted but not published, and using a comparison-based funnel plot with ADT plus docetaxel and darolutamide as a reference.9
Preplanned subgroup analyses were conducted for 4 patient groups, which were selected based on published clinical guidelines and conversations with clinical exports: high and low volume (defined as visceral metastases or 4 or more bone lesions with 1 or more outside of the vertebral bodies and pelvis, per the CHAARTED trial); de novo mHSPC or mHSPC progressing after prior local therapy; low or high risk (defined as at least 2 of Gleason score ≥ 8 and/or ≥ 3 lesions on bone scan and/or presence of measurable visceral lesions, per the LATITUDE trial); and high or reduced ECOG score (0 and ≥ 1).9 All comparisons were made versus ADT alone and are therefore not reported.
In addition, several sensitivity analyses were performed to explore the influences of uncertainties relating to the evidence itself, including the exclusion of evidence from the LATITUDE trial due to high-risk de novo mHSPC population, the ENZAMET and NCT02058706 trials due to uncertainties regarding patient populations and ADT and nsAA as comparator, the GETUG-AFU 15 and CHAARTED trials due to likely incomplete recording of AEs suggested by substantially lower AE rates compared to other studies, and the ARASENS trial due to effect estimates being estimated only indirectly through NMA.9
Results of NMA by Menges et al.9
Summary of Included Studies
From the SLR, a total of 10 trials were eligible for analysis representing data from 11,557 patients, which informed the NMA. The STAMPEDE trial arms C, G, and H were reported as distinct trials based on their different interventions, resulting in a total of 12 studies.
Study and participant characteristics of included RCTs were summarized in a supplementary appendix. The authors noted several key differences between the studies in study design and baseline characteristics. The majority of included RCTs were open label (n = 8), with the remaining 4 trials double blinded. The 3 arms of the STAMPEDE trial were all multiarm, multistage design. In terms of interventions, 3 RCTs each investigated ADT plus docetaxel and ADT and enzalutamide, 2 RCTs each investigated ADT plus abiraterone acetate and ADT plus radiotherapy, and 1 RCT each investigated ADT plus apalutamide, and ADT plus docetaxel and darolutamide. All RCTs were found to be at low risk of bias, although the authors noted some uncertainty regarding overproportioned censoring in the ADT plus enzalutamide group and inconsistencies in reporting censoring and death events in 1 study. Follow-up times for OS ranged from 34 to 83 months.
Mean age was similar across all included RCTs, ranging from 63 to 70 years, with 6 RCTs reporting age ranges greater than 12 years. Race and other demographic characteristics were not reported. Across included studies, the proportion of patients with prior local therapy ranged from 0% to 42%, the proportion with de novo mHSPC ranged from 63% to 100% (not reported in 2 RCTs), 55% to 98% had a Gleason score between 8 and 10, and the proportion of patients with high-volume disease ranged from 41% to 82% (not reported in 1 RCT). The proportion of patients with an ECOG performance status greater than or equal to 1 ranged across RCT arms from 1% to 56%. The proportion of patients with visceral metastases was all under 20%.
Results
The network diagram for the NMA is presented in Figure 9. A total of 21 distinct intervention plus comparator combinations were evaluated for the primary outcome of OS. Performance characteristics for the models were not presented.
Overall Survival
Results of the NMA for OS for comparisons involving darolutamide are summarized in Table 25. For OS, darolutamide plus ADT and docetaxel was favoured over ADT and docetaxel (HR, 0.68 [95% CI, 0.57 to 0.81]). There was no difference in terms of OS between darolutamide plus ADT and docetaxel and other comparators consisting of abiraterone acetate plus ADT and prednisone, enzalutamide and ADT, apalutamide and ADT, and apalutamide plus ADT and docetaxel.
The GRADE assessments conducted on the direct and indirect estimates reported either “low” or “very low” ratings for all but 2 of the estimates of interest from the NMA; studies with a “low” or “very low” score were downgraded due to imprecision in the estimate.
Figure 9: Network Diagram for OS (Menges et al. [2022])
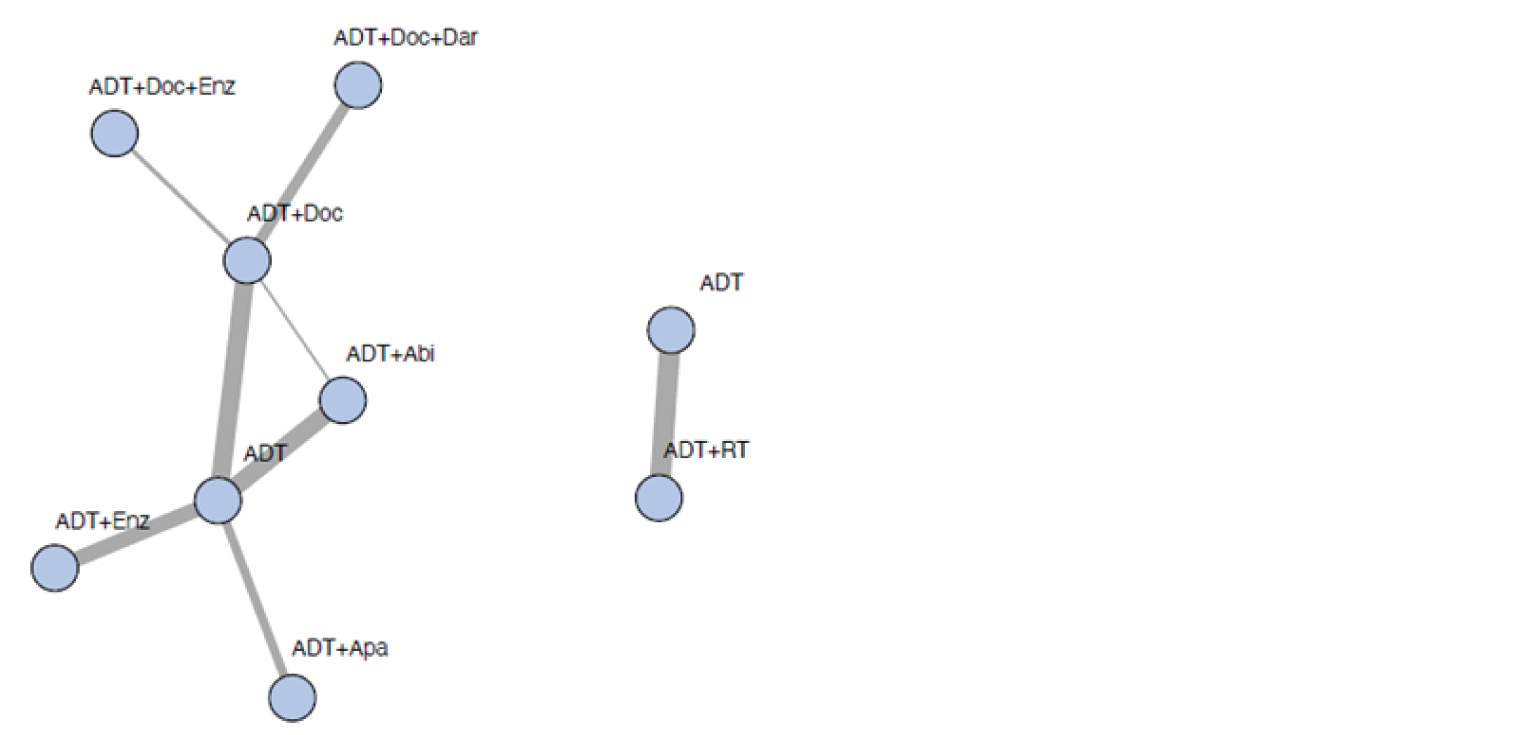
Abi = abiraterone; ADT = androgen deprivation therapy; Apa = apalutamide; Dar = darolutamide; Doc = docetaxel; Enz = enzalutamide; RT = radiotherapy.
Thickness represents the number of supporting studies (scale not defined in publication).
Source: Menges et al. (2022).9
Table 25: Findings and GRADE Assessment of Direct, Indirect, and NMA Evidence on OS (Menges et al.)
Darolutamide + ADT + docetaxel vs. | HR (95% CI) | |||||
|---|---|---|---|---|---|---|
Direct estimatea | GRADE rating | Indirect estimate | GRADE rating | NMA estimate | GRADE rating | |
ADT + docetaxel | 0.68 (0.57 to 0.81) | High | — | — | 0.68 (0.57 to 0.81) | High |
ADT + abiraterone acetate | — | — | 0.80 (0.63 to 1.01) | Low | 0.80 (0.63 to 1.01) | Low |
ADT + enzalutamide | — | — | 0.86 (0.66 to 1.13) | Very low | 0.86 (0.66 to 1.13) | Very low |
ADT + apalutamide | — | — | 0.80 (0.60 to 1.06) | Low | 0.80 (0.66 to 1.06) | Low |
ADT + docetaxel + enzalutamide | — | — | 0.76 (0.50 to 1.14) | Very low | 0.76 (0.50 to 1.14) | Very low |
ADT = androgen deprivation therapy; CI = confidence interval; HR = hazard ratio; GRADE = Grading of Recommendations, Assessment, Development and Evaluations; NMA = network meta-analysis.
aDirect estimates for individual treatments were informed by pairwise meta-analysis (results not shown).
Source: Menges et al. (2022).9
Critical Appraisal of NMA by Menges et al. (2022)
The NMA by Menges et al. was informed by an SLR in 2020 that included a comprehensive search comprising multiple databases and several cancer-focused conference proceedings, as well as searching for potential clinical trials in progress but not yet published. In addition, an update of the SLR was conducted on March 1, 2022, to include emerging therapies. Methods of screening, data extraction, and quality assessment were outlined and considered appropriate. A risk-of-bias assessment of the included studies was conducted per the Cochrane risk-of-bias 2.0 tool,11 in which the authors considered all studies to have a low risk of bias for the main outcome of OS. The population, interventions, and outcomes of the NMA were also considered relevant to Canadian clinical practice. Funding for this study was obtained from the Swiss Medical Board and was not supported by the sponsor.
The authors note that transitivity was assessed using epidemiological criteria and the presence of potential effect modifiers, along with considerations of clinical plausibility. It is not clear how these effect modifiers were identified. Some potentially important effect modifiers were reported in the study but were not adjusted for nor discussed. Follow-up duration was noted but was not considered an effect modifier, or considered in the analyses. Given the outcome of OS and the use of HRs that rely on the assumption that a patient has survived to that point, this could have implications for the results, because studies with longer follow-up may have captured more robust results. Other potentially important factors would be the use of prior therapy, which may have an impact on treatment effects, because 2 studies permitted prior docetaxel and 1 permitted early use of docetaxel in the trial itself. Additionally, Gleason score, which may represent a treatment-effect modifier, ranged from 55% to 98% across studies for scores of 8 to 10 representing high-grade cancer; thus, differences by cancer grade may have varied but were not explored. As a result, it is likely that the underlying transitivity assumption of the NMA was violated.
Heterogeneity was assessed visually and by means of I2 values. No information on the visual heterogeneity assessment was provided. Although minimal given the limited number of studies per comparison, there was evidence of moderate statistical heterogeneity in the comparison of the ENZAMET and NCT02058706 trials (I2 = 33%). A sensitivity analysis was conducted excluding these 2 studies, which led to some changes in the overall results, although this did not impact the comparisons involving darolutamide. Reported heterogeneity in the overall NMA was low (I2 = 0.0%) for OS. However, given the small number of studies, the I2 value presented is prone to bias.
The authors conducted a frequentist, random-effects, pairwise meta-analysis and NMA. No information on model selection and fit was provided, and therefore it remains uncertain whether this choice was appropriate. However, given the evidence base, random-effects models were likely appropriate to allow for the possibility of heterogeneity between studies. No scenario analyses were conducted for different models. The authors used the GRADE criteria to assign certainty ratings to the direct and indirect estimates of the NMA results. In comparisons involving darolutamide, certainty of NMA estimates was often considered to be low or very low, suggesting that the comparative effects derived from the NMA are likely to be quite different than the true effects.
Only the end point of OS contained complete information for inclusion in this review. In general, comparisons were associated with wide 95% CIs, suggesting imprecision and uncertainty in the results. Sensitivity and subgroup analyses, while conducted and generally in line with the primary analysis, were only comparing treatments to ADT monotherapy. While PFS, HRQoL, and AEs were assessed as part of the objectives of this review, PFS and HRQoL did not include data for darolutamide plus ADT and docetaxel. Results for AEs were only reported in aggregate, by grade, and were only compared to a reference treatment of ADT; thus, they were not considered relevant to this review.
Methods of NMA by Yanagisawa et al. (2022)10
Objectives
The objective of the NMA by Yanagisawa et al. (2022) was to analyze the oncologic outcomes of combination therapy with androgen receptor signalling inhibitors plus docetaxel and ADT and to compare their efficacy to currently available treatments.
As previously noted, comparisons to ADT monotherapy are not of interest to this review because ADT monotherapy was not considered an appropriate comparator in the CADTH systematic review protocol (Table 5). As such, results for comparisons to ADT monotherapy were not reported in this review.
Study Selection Methods
The systematic review was conducted according to an a priori protocol that was registered on the PROspective Multicentre Study to Identify Diagnostic Key PERfOrmance Indicators in Upper GI Endoscopy (PROSPERO) (CRD42022298107). In April 2022, a literature search was performed in PubMed, Web of Science, and Scopus databases to identify publications investigating the oncologic outcomes of systemic therapy for mHSPC. Abstracts for relevant conference proceedings (ASCO and ESMO) were also searched. No restrictions to the search were placed on publication year or language. In addition, manual searches of the reference lists from relevant articles, as well as those from all papers ultimately included in the analysis, were performed to identify additional studies of interest. Only RCTs were considered for inclusion. Studies that did not include original patient data, review articles, letters, editorial comments, replies from authors, case reports, and articles not written in English were excluded. In cases where studies contained duplicate cohorts, the highest-quality or most recent publication was selected for inclusion.
Initial screening was performed by 2 authors based on titles and abstracts, and then potentially relevant studies were subject to a full-text review. Data were extracted independently by 2 authors. Study risk of bias was assessed independently by 2 authors using the Cochrane risk-of-bias 2.0 tool.11 Results of the assessment were reported alongside the other results in the study. At all stages of screening and extraction, disagreements or discrepancies were resolved by consensus with coauthors.
Eligible studies included those that enrolled patients with mHSPC who were treated with triplet combination therapy using an androgen receptor signalling inhibitor plus docetaxel and ADT compared to patients treated with other currently available, systemic treatment strategies. No further information on eligible interventions or comparators was provided.
Outcomes included in the review consisted of OS, PFS, or AEs. Analysis of PFS in the NMA did not include any results from the ARASENS trial; thus, the results for PFS are not discussed in this report. Results for AEs from the NMA were presented by grade and by preferred term, although analyses were only conducted for comparisons to ADT, which was not a relevant comparator and therefore is not discussed in this review.
Analysis Methods
Following the SLR, an initial fixed-effects pairwise meta-analysis was conducted to analyze the relationships between combination therapy and PFS and OS using the HRs from included trials. Results for this meta-analysis are not summarized in this review.
Network diagrams were utilized to illustrate the connectivity of the treatment networks in terms of OS, PFS, and AEs. For OS and PFS outcomes, a frequentist NMA using random effects was performed for direct and indirect treatment comparisons. No justification was provided for either the choice of meta-analysis model or the choice of NMA model for outcomes. Contrast-level data from individual studies were used, including HRs and SD or 95% CIs. Results for OS were presented for each unique intervention against ADT alone, ADT and docetaxel, and ADT plus docetaxel and abiraterone. The relative effects were presented as HRs and 95% CIs. Subgroup analyses for PFS and OS included high- versus low-volume disease and de novo versus metachronous metastasis. Heterogeneity for the NMA was assessed using Cochrane’s Q statistic when more than 1 trial was available for comparisons. I2 statistics were not reported for the NMAs, despite being prespecified.
Sensitivity analyses were conducted for patients with de novo/metachronous metastasis, and tumour burden due to differences in patient populations. It was unclear if this sensitivity analysis was prespecified.
Results of NMA by Yanagisawa et al. (2022)10
Summary of Included Studies
After title, abstract, and full-text screening, a total of 17 publications representing 11 RCTs and 7,679 patients were included in the meta-analysis and NMAs. Trials included in the analysis were the ARASENS, ARCHES, CHAARTED, ENZAMET, GETUG-AFU15, LATITUDE, PEACE-1, STAMPEDE (arms G, C, and G; and B, C, and E), and TITAN trials. Due to duplicate cohorts, only arms C versus G from the STAMPEDE trial were included in the primary analysis for OS, while arms B, C, E, and G were included from prior publications for the subgroup analyses. Patients treated with androgen receptor signalling inhibitor plus ADT and docetaxel in the PEACE-1, ARCHES, ENZAMET, and TITAN trials were extracted from their subgroup analyses. Only the abiraterone acetate and ADT arm from the LATITUDE trial was included, because none of the patients in the study received docetaxel.
Characteristics of all studies were reported descriptively; they consisted of dosages, ages, proportions with de novo disease, disease volume, the number of patients treated with docetaxel, HRs for all outcomes and for post-hoc subgroups, and the length of the follow-up period. Information on study designs of the included studies was not reported. Risk-of-bias assessments indicated that the majority of included RCTs had a high risk of bias in terms of outcome assessment and the blinding of participants and personnel. Follow-up time, representing another potential source of heterogeneity for outcome assessment, ranged from 34 to 83.9 months.
The interventions represented in these RCTs were abiraterone acetate and SoC (with or without radiotherapy), abiraterone acetate and ADT, apalutamide and ADT, docetaxel and ADT, darolutamide plus ADT and docetaxel, and enzalutamide and ADT. The comparator arms represented by these studies were SoC (with or without radiotherapy), placebo plus docetaxel and ADT, placebo and ADT, nsAA and ADT, docetaxel and ADT, and ADT alone.
Median age was similar across all arms of studies, ranging from 63 to 70 years. The proportion of patients with de novo disease ranged from 66% to 100%, and the proportion with high- and low-volume disease ranged from 47% to 82% and 18% to 53%, respectively. Out of 11 RCTs, 6 reported on de novo metastasis, 5 reported on prior local treatment, and 5 reported on docetaxel use during the trial.
Results
The network diagram for the NMA assessing OS is presented in Figure 10. A total of 7 individual interventions were analyzed in the NMA for OS. No performance measures were reported for the model fit and results were not adjusted for any effect modifiers.
Figure 10: Network Diagram for OS NMA (Yanagisawa et al. [2022])
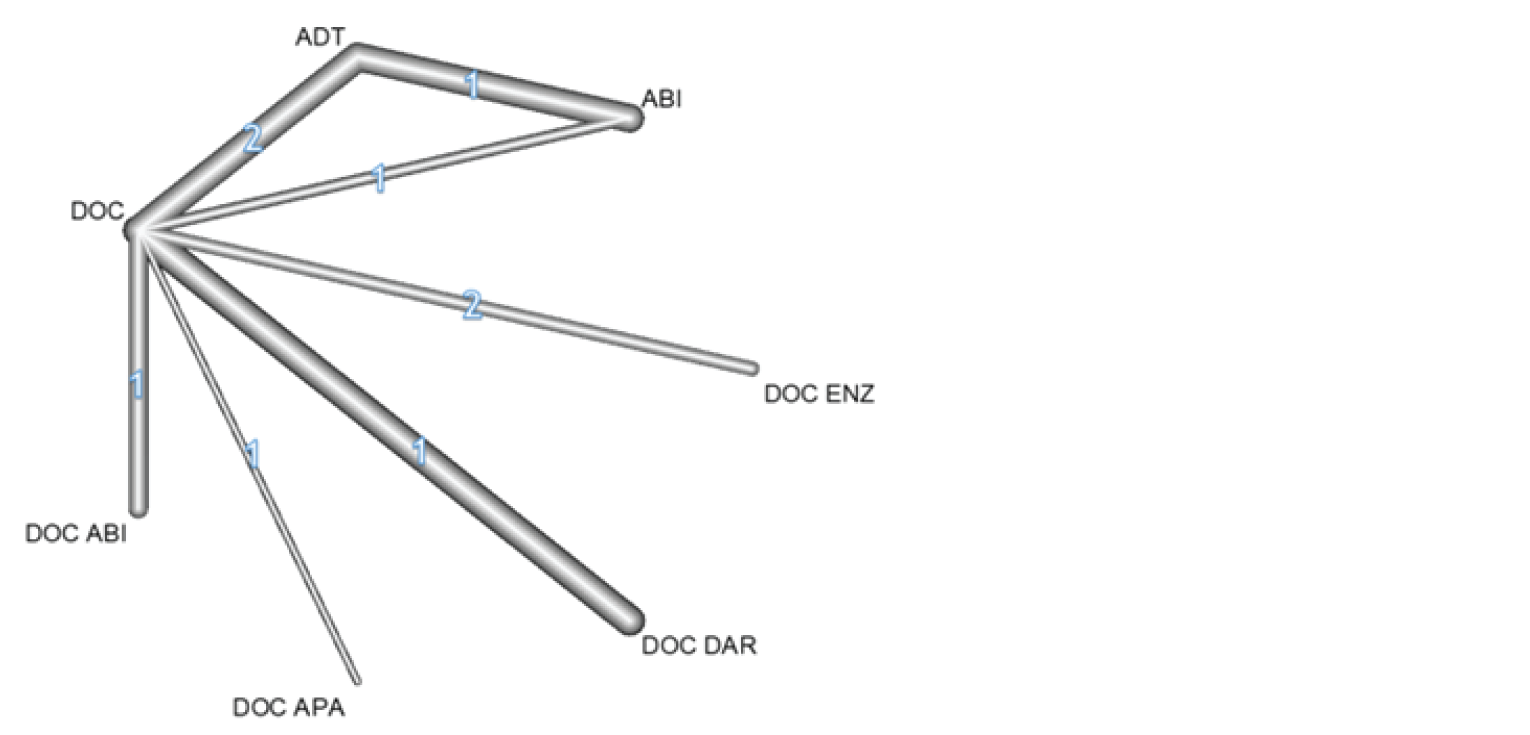
ABI = abiraterone; ADT = androgen deprivation therapy; APA = apalutamide; DAR = darolutamide; DOC = docetaxel; ENZ = enzalutamide; NMA = network meta-analysis; OS = overall survival.
Source: Yanagisawa et al. (2022).10
Overall Survival
Table 26 demonstrates the full results of the NMA for OS for darolutamide from the primary analysis, including all patients, as well as from the subgroup analysis of de novo metastatic patients and metachronous patients, against the comparators of ADT and docetaxel, and ADT and abiraterone acetate.
For OS, darolutamide plus ADT and docetaxel was favoured over ADT and docetaxel (0.68 [0.56 to 0.82]) and ADT and abiraterone acetate (HR, 0.74 [95% CI, 0.55 to 0.99]). Among the subgroup of studies reporting on de novo patients, darolutamide plus ADT and docetaxel was favoured over ADT and docetaxel (HR, 0.71 [95% CI, 0.55 to 0.92]). There was no difference in OS between darolutamide plus ADT and docetaxel versus ADT and docetaxel.
Table 26: OS NMA Results (Yanagisawa et al. [2022])
Analysis group | Darolutamide + docetaxel + ADT vs. (HR [95% CI]) | |
|---|---|---|
ADT + docetaxel | Abiraterone + ADT | |
All patients | 0.68 (0.56 to 0.82) | 0.74 (0.55 to 0.99) |
De novo patients | 0.71 (0.55 to 0.92) | 0.87 (0.59 to 1.28) |
Metachronous patients | 0.60 (0.35 to 1.05) | — |
ADT = androgen deprivation therapy; CI = confidence interval; HR = hazard ratio; NMA = network meta-analysis; OS = overall survival.
Source: Yanagisawa et al. (2022).10
Results for subgroup analysis in patients with high- or low-volume disease were not available for darolutamide.
Adverse Events
No network diagram was available for the NMA of AEs. For comparators of interest for the analysis of AEs, darolutamide plus ADT and docetaxel was only compared to abiraterone and ADT for the AE of febrile neutropenia, when darolutamide plus ADT and docetaxel was associated with greater odds of febrile neutropenia (OR, 26.62 [95% CI, 7.46 to 94.99]).
Critical Appraisal of NMA by Yanagisawa et al. (2022)10
The ITC conducted by Yanagisawa et al. was informed by an adequately conducted SLR that included planned searches of multiple databases, and conference proceedings. Screening was conducted based on standard methods, with studies selected independently in duplicate. A risk-of-bias assessment of the included studies was conducted, per the Cochrane risk-of-bias 2.0 tool,11 in which, overall, the authors considered all included studies to be at a low risk of bias due to the prospective, randomized design. However, the authors also judged there to be a high risk of bias for outcome assessment blinding (detection bias) and participant or personnel blinding (performance bias). No adjustments or sensitivity analyses, excluding studies with these biases, were undertaken. Some authors mentioned competing conflicts of interest for this study; however, funding for this study was not related to the sponsor.
Networks were constructed based on the available studies; however, it was unclear which studies were informing comparisons based on the network structure, and whether direct or indirect evidence was assessed. One closed loop was formed in the network for OS; however, no assessment of consistency was conducted. For the NMA, potential sources of heterogeneity were only evaluated statistically using Cochrane’s Q test; however, results of the heterogeneity assessment were not reported. Heterogeneity of comparisons was also evaluated in the initial meta-analysis via Cochrane’s Q test, although results did not suggest any important heterogeneity (P = 0.5). Given that no significant heterogeneity was observed, it was not explored for the NMA. As a result, it was unclear if the transitivity assumption was met, because no assessment of clinical heterogeneity via study design or baseline characteristics was conducted. Additionally, no consideration was given to treatment-effect modifiers, and thus the impact of any potential effect modifiers remains unknown. The authors noted that the publications included in the NMA included different patient populations with regards to proportions of patients with de novo disease and disease burden. As a result, the authors conducted sensitivity analyses that excluded studies based on population; however, they noted that the results must be interpreted with caution due to the limited sample sizes, thus decreasing statistical power. Given the relative lack of attention to potential effect modifiers, it is likely that the transitivity assumption underlying the NMA was violated.
The NMA was conducted using a frequentist, random-effects model. No model-fit statistics or justification for model choice was provided, and therefore it remains unclear if random-effects models were the most appropriate choice. However, given the potential for increased, unexplored heterogeneity across studies, random-effects models were likely the most appropriate. No scenario analyses were conducted for different models. All OS estimates were informed by contrast-level data, which was considered appropriate given the time-to-event–related outcomes. This method also allows for preservation of randomization across comparisons. For AEs, arm-level data were used, which, given that the method of reporting of AEs in clinical trials was also considered appropriate, however, does not preserve randomization across comparisons. Additionally, for the STAMPEDE trial, only certain arms were included in the analysis, and therefore randomization throughout the NMA was not preserved for these comparisons.
Overall survival and AEs were analyzed in this NMA. The intervention of interest to this review, darolutamide plus ADT and docetaxel, was only compared to ADT and docetaxel, and to abiraterone plus ADT and docetaxel. The network diagram for this analysis also included comparators of enzalutamide and apalutamide, for which no comparative results were displayed; thus, comparative efficacy remains unknown for this analysis. In all cases, darolutamide plus ADT and docetaxel was favoured; however, this was generally associated with wide 95% CIs, suggesting imprecision and uncertainty in the estimates, although the reason for this was unexplored and remains unknown.
Summary
In total, 3 NMAs were eligible for inclusion in this review, 1 which was commissioned and submitted by the sponsor, and 2 of which were published NMAs. The sponsor-submitted NMA included a systematic review with unclear methodology and used a |||||||||||||| approach to evaluate the relative clinical efficacy of darolutamide plus ADT and docetaxel compared to enzalutamide and ADT, apalutamide and ADT, abiraterone plus prednisone and ADT, and docetaxel and ADT in adult patients with mHSPC. In the published NMAs by Menges et al. and Yanagisawa et al., SLRs were also conducted before evaluation using a frequentist approach in both cases. In the study by Menges et al., the authors aimed to assess the survival, HRQoL, and safety of mHSPC treatments including docetaxel, abiraterone, enzalutamide, apalutamide, darolutamide in combination with ADT. In the study by Yanagisawa et al. the authors aimed to analyze the survival and safety benefits of abiraterone acetate, apalutamide, darolutamide, and enzalutamide in combination with docetaxel and ADT, compared to other treatments in patients with mHSPC.
The evidence included across NMAs was generally similar and evaluated mostly the same treatments. There were ||||||||, 10, and 8 studies (combining STAMPEDE trials) included in the NMAs by the sponsor, Menges et al., and Yanagisawa et al., respectively. All NMAs included the ARASENS, ARCHES, CHAARTED, LATITUDE, TITAN, and STAMPEDE trials, although different arms of the STAMPEDE trial were included across NMAs. The GETUG-AFU15 study was included in both the sponsor-submitted NMA and Menges et al. The ENZAMET study was included in both published NMAs. The PEACE-1 trial was only included in the NMA by Yanagisawa et al. and the HORRAD and NCT02058706 trials were only included in Menges et al. The NCT02058706 study was included in the sponsor’s SLR but not included in the NMA based on the treatments included (enzalutamide and ADT versus bicalutamide and ADT). The HORRAD trial evaluated radiotherapy and ADT versus ADT alone, and therefore was not of interest to the other NMAs. Other reasons for differences in included studies across NMAs were unknown.
Both published NMAs conducted a risk-of-bias assessment using the same tool from Cochrane (Figure 19 and Figure 2). As previously noted, similar studies were included across NMAs. Although the authors of both papers concluded that the included studies in their NMAs were at low risk of bias, the results for the individual domains varied. Menges et al. considered there to be a low risk of bias in all domains for all studies. Conversely, Yanagisawa et al. noted that there was a high risk of bias in blinding of participants and outcome assessment (performance and detection biases). No risk of assessment was conducted for the sponsor-submitted NMA, which included similar studies; therefore, the risk of bias remains uncertain and open to interpretation.
The sponsor-submitted NMA reported on outcomes of OS, time to CRPC, and rPFS. Conversely, comparative efficacy results reported for darolutamide plus ADT and docetaxel were only available for OS from the published NMAs. The sponsor-submitted NMA used a |||||||||||||||||||||||||||| framework. Results of the sponsor-submitted NMA for the end point of OS reported that darolutamide plus ADT and docetaxel was favoured over ADT and docetaxel, while comparisons to enzalutamide, apalutamide, and abiraterone combinations were inconclusive due to wide CIs. For time to CRPC and rPFS, darolutamide plus ADT and docetaxel was generally favoured over all other treatment combinations. In contrast to the sponsor-submitted NMA, the 2 published NMAs used a frequentist, random-effects framework for their analyses. For the end point of OS, results were consistent for the NMA conducted by Menges et al. with darolutamide plus ADT and docetaxel favoured only over ADT and docetaxel; however, compared to enzalutamide, apalutamide, and abiraterone combinations, the evidence was inconclusive due to wide CIs. For Yanagisawa et al., comparative results for OS of darolutamide plus ADT and docetaxel were limited to ADT and docetaxel, and abiraterone and ADT, in which darolutamide plus ADT and docetaxel was favoured over both combinations.
A common critical appraisal among the NMAs was the choice of model fit, in which the sponsor-submitted NMA conducted |||||||||||||| analyses and the published NMAs conducted random-effects NMAs. Only the sponsor-submitted NMA reported model-fit statistics, while published NMAs did not; thus, it was unclear if the proper model was selected for these analyses, although given the potential for heterogeneity, the models chosen were likely appropriate. There were generally some differences noted across populations in each NMA regarding baseline disease characteristics that may have affected the results, including prostate cancer stage, PSA level, disease volume, and prior treatment; however, these were not explored. Overall, none of the NMAs considered there to be significant heterogeneity across studies; however, given the wide 95% CrIs and 95% CIs, it was believed that there was unaccounted-for heterogeneity within the analyses, in addition to the limited number of studies per comparison and the small sample sizes.
Other Relevant Evidence
No long-term extension studies or other relevant studies were included in the sponsor’s submission to CADTH.
Discussion
Summary of Available Evidence
This report summarizes the evidence for darolutamide in combination with docetaxel and ADT in the treatment of mCSPC based on 1 phase III RCT and 3 NMAs.
One trial was included in the CADTH systematic review. The ARASENS trial was a phase III, double-blind RCT that aimed to demonstrate superiority of darolutamide plus docetaxel and ADT compared to placebo plus docetaxel and ADT in patients with mCSPC (N = 1,306) in the first-line, metastatic setting. The primary end point was OS; secondary end points included time to CRPC, time to initiation of subsequent systemic antineoplastic therapy, time to pain progression, time to first SSE, and SSE-FS. In the final efficacy analysis (data cut-off on October 25, 2021), the median age was 67.0 (range = 41 to 89) years. The majority of patients were white (52.0%) or Asian (36.4%) and had stage IV disease at initial diagnosis (87.6%), ECOG performance status of 0 (71.1%), and bone metastases (82.8%) at baseline. Most patients did not receive prior local therapy and no patients had prior systemic antineoplastic therapy for prostate cancer other than ADTs.
In total, 3 NMAs were eligible for inclusion in this review. One was commissioned and submitted by the sponsor and evaluated the comparative efficacy of darolutamide plus ADT and docetaxel compared to enzalutamide and ADT, apalutamide and ADT, abiraterone plus prednisone and ADT, and docetaxel and ADT on OS, time to CRPC, and rPFS in adult patients with mHSPC. Two were published NMAs that evaluated comparative OS for darolutamide plus ADT and docetaxel compared to other available treatment regimens in patients with mHSPC.
Interpretation of Results
Efficacy
In the pivotal, phase III ARASENS trial, the primary end point of OS was met in the final efficacy analysis, supporting the superiority of darolutamide plus docetaxel and ADT compared to placebo plus docetaxel and ADT in patients with mCSPC. OS was an outcome noted by patients and clinicians to be highly important. The clinical experts consulted by CADTH considered the magnitude of OS benefit of darolutamide plus docetaxel and ADT combination to be clinically meaningful. It should be noted that the distribution of subsequent antineoplastic therapy used in the darolutamide plus docetaxel and ADT arm did not align with clinical practice as per the clinical experts, which may introduce uncertainties into the generalizability of OS results. It is unclear whether a different distribution of subsequent treatments that is more reflective of Canadian clinical practice would have resulted in different effect estimates. Subgroup analyses by baseline ECOG performance status, Gleason score, and extent of metastatic disease were performed; however, no conclusion can be drawn due to the exploratory nature, lack of control for multiplicity, and the risk of confounding in the absence of randomization in the comparisons.
In addition to improving OS, delaying disease progression to CRPC and the need for a subsequent line of therapy are important goals of treatment for mCSPC because mCRPC is associated with morbidity, poor HRQoL, and poor prognosis, according to the clinical experts. The magnitude of benefits observed for secondary end points of time to CRPC and time to initiation of subsequent systemic antineoplastic therapy was considered clinically meaningful by the clinical experts. It should be noted that the median time to CPRC in the placebo group was lower than anticipated by the clinical experts based on their clinical experience; as such, it is uncertain if the observed magnitude of benefit of darolutamide plus docetaxel and ADT will translate in clinical practice.
Results of the time to pain progression, time to first SSE, and SSE-FS analyses were in favour of the darolutamide plus docetaxel and ADT arm, supporting the efficacy of this combination in delaying pain progression and SSE, which are events noted to be burdensome by patients. Of note, unblinding occurred by error in some patients during the study (||||||| in the darolutamide plus docetaxel and ADT arm, and ||||||| in the control arm), which could potentially introduce reporting bias in favour of darolutamide (i.e., toward an inflated efficacy of darolutamide plus docetaxel and ADT) in these subjective efficacy outcomes, although the impact is likely to be small given that the number of unblinded patients was small.
HRQoL, measured using the NCCN-FACT FPSI-17 questionnaire, was an exploratory outcome of interest to patients and clinicians. The mean total and subscale scores were stable at most time points and trending toward deterioration by the end of treatment in both treatment arms. There was with no notable difference in the mean change in score from baseline between treatment arms, in general, based on the sponsor-identified MID estimate of 3 points; however, no statistical testing was conducted for the difference between treatment arms, which precludes conclusion on the effect of darolutamide on HRQoL outcomes when used in combination with docetaxel and ADT. Further, this outcome is subject to a high risk of bias resulting from unblinding by error and a large amount of missing data. The instrument is also not routinely administered in clinical practice and has not been validated in patients with mCSPC, and most items in the questionnaire are measuring symptoms, although the sponsor has used the tool to assess HRQoL. Overall, no definitive conclusion can be drawn about the effect of the darolutamide plus docetaxel and ADT combination on HRQoL based on available data.
Per the clinical experts, the biochemical factor PSA is assessed along with radiologic and clinical factors to inform treatment-response evaluations in patients with mCSPC. Results of the exploratory PSA analyses suggested that darolutamide plus docetaxel and ADT was associated with a delay in time to PSA progression and numerically higher PSA response rates compared to docetaxel and ADT; however, these results were not controlled for multiplicity and, therefore, were subject to an increased risk of false-positive findings.
Although the study results were generally in favour of darolutamide, it should be noted that there was a high number of important protocol deviations in the study, many of which pertain to missed study assessments, incorrect or incomplete assessment procedure, and incorrect dosing or method of drug delivery. These deviations could potentially compromise the completeness and reliability of study data, although none of the important protocol deviations was considered major, as per the sponsor. Further, the generalizability of the study results is limited by the exclusion of patients with significant comorbidities (e.g., cardiovascular diseases) and impaired performance status commonly seen in clinical practice and the fact that the comparator regimen, docetaxel and ADT, only accounts for a small proportion of systemic treatments prescribed for mCSPC. In the absence of direct evidence, the comparative efficacy between darolutamide plus docetaxel and ADT versus ARAT plus ADT, which is the most commonly prescribed regimen in Canada, according to the clinical experts, is unknown and represents a gap in evidence.
As part of the development of a ||||||| cost-effectiveness model for darolutamide in mCSPC, the sponsor conducted and submitted an NMA that was used to inform these analyses. The sponsor-submitted NMA aimed to indirectly compare darolutamide plus ADT and docetaxel from the ARASENS trial to alternative treatments for patients with mCSPC. Across NMAs, results for all end points were associated with wide 95% CrIs and 95% CIs, which failed to demonstrate differences across comparisons and resulted in uncertainty and loss of precision in estimates, precluding comparative efficacy conclusions for darolutamide plus ADT and docetaxel. Additionally, all comparisons of darolutamide plus ADT and docetaxel were informed by indirect evidence, resulting in greater uncertainty. The sponsor-submitted NMA reported that darolutamide plus ADT and docetaxel was favoured over ADT and docetaxel for OS benefit. Two published NMAs were also included, which also reported that darolutamide plus ADT and docetaxel was favoured over ADT and docetaxel despite differences in included studies and analysis methods. However, the sponsor-submitted NMA and the Menges et al. and Yanagisawa et al. NMAs demonstrated wide CIs that precluded conclusions for comparisons between darolutamide plus ADT and docetaxel and other androgen receptor signalling inhibitors, including abiraterone, apalutamide, or enzalutamide. Results from the ARASENS trial demonstrated improved survival over ADT and docetaxel; thus, the reviewed indirect evidence did not provide any additional comparative effectiveness insight regarding OS. One published NMA also demonstrated improved survival with darolutamide plus ADT and docetaxel over abiraterone and ADT. Time to CRPC and rPFS were also evaluated in the sponsor-submitted NMA, for which darolutamide plus ADT and docetaxel was favoured over all treatments except enzalutamide and ADT for the outcome of time to CRPC.
Harms
Overall, the safety profile of darolutamide plus docetaxel and ADT arm was similar to that of the placebo plus docetaxel and ADT arm in the ARASENS trial, with a similar incidence of TEAEs, treatment discontinuations due to TEAE, and deaths due to AE between treatment arms. Almost all patients experienced at least 1 TEAE in both treatment arms, with the most frequently reported TEAEs (in at least 25% of patients in either arm) being alopecia, fatigue, anemia, arthralgia, peripheral edema, decreased neutrophil count, and diarrhea, all of which are common AEs of docetaxel. Although decreased appetite (any grade) and hypertension of grade 3 or higher were more common AEs in the darolutamide plus docetaxel and ADT arm, they are known AEs of ARATs and are manageable in clinical practice, according to the clinical experts. Based on the safety findings in the ARASENS trial, it is unlikely that darolutamide plus docetaxel and ADT can fulfill the need for new treatments with reduced toxicity burden expressed by patient and clinician groups. In the NMA by Yanagisawa et al., darolutamide plus ADT and docetaxel was only compared to abiraterone and ADT for the AE of febrile neutropenia. Although darolutamide plus ADT and docetaxel was associated with greater odds of experiencing febrile neutropenia, the results were highly uncertain, given the wide 95% CIs.
Conclusions
In the ARASENS trial, darolutamide in combination with docetaxel and ADT demonstrated a clinically meaningful improvement of OS compared to docetaxel plus ADT in patients with mCSPC. Analyses of secondary outcomes supported the efficacy of darolutamide plus docetaxel and ADT in delaying progression to mCRPC, the need for subsequent antineoplastic therapy, worsening of pain, and SSEs compared to docetaxel plus ADT. Due to limitations in the statistical analysis, no definitive conclusions can be drawn from the exploratory PSA and HRQoL analyses. The exclusion of patients with significant comorbidities and impaired performance status and the use of a comparator regimen that has low utilization in Canada may limit the generalizability of study findings. Across the included NMAs, the findings for the comparative survival benefit observed with darolutamide plus ADT and docetaxel compared to ADT and docetaxel supported the findings of the ARASENS trial; however, the findings of these NMAs are associated with uncertainty due to probable violation of the underlying transitivity assumption. Comparisons to other drugs of interest were uncertain due to the aforementioned methodological limitations as well as wide CIs. The safety profile of darolutamide plus docetaxel and ADT was overall similar to that of docetaxel and ADT in the ARASENS trial, with no additional serious safety concern.
References
1.Prostate Cancer Statistics. Canadian Cancer Society; 2022: https://cancer.ca/en/cancer-information/cancer-types/prostate/statistics. Accessed 2022 Aug 16.
2.Gandaglia G, Abdollah F, Schiffmann J, et al. Distribution of metastatic sites in patients with prostate cancer: A population-based analysis. Prostate. 2014;74(2):210-216. PubMed
3.Overview of systemic treatment for advanced, recurrent and metastatic castration-sensitive prostate cancer and local treatment for patients with metastatic disease. UpToDate; 2022: https://www.uptodate.com/contents/overview-of-systemic-treatment-for-advanced-recurrent-and-metastatic-castration-sensitive-prostate-cancer-and-local-treatment-for-patients-with-metastatic-disease. Accessed 2022 Jul 04.
4.Fizazi K, Foulon S, Carles J, et al. Abiraterone plus prednisone added to androgen deprivation therapy and docetaxel in de novo metastatic castration-sensitive prostate cancer (PEACE-1): a multicentre, open-label, randomised, phase 3 study with a 2 x 2 factorial design. Lancet. 2022;399(10336):1695-1707. PubMed
5.Nubeqa (darolutamide): 300mg, oral tablets [product monograph]. Mississauga (ON): Bayer Inc; 2022 May 12.
6.Smith MR, Hussain M, Saad F, et al. Darolutamide and Survival in Metastatic, Hormone-Sensitive Prostate Cancer. N Engl J Med. 2022;386(12):1132-1142. PubMed
7.Clinical Study Report: ARASENS. A randomized, double–blind, placebo–controlled Phase III study of darolutamide (ODM–201) versus placebo in addition to standard androgen deprivation therapy and docetaxel in patients with metastatic hormone–sensitive prostate cance [internal sponsor's report]. Whippany (NJ): Bayer Inc; 2022 Feb 15.
8.Darolutamide for metastatic castration-sensitive prostate cancer. Network-meta analysis for public payer submissions in Canada. In: Drug Reimbursement Review sponsor submission: Nubeqa, 300 mg, Oral tablet. Mississauga (ON): Bayer Inc.; 2022 May 12.
9.Menges D, Yebyo HG, Sivec-Muniz S, et al. Treatments for Metastatic Hormone-sensitive Prostate Cancer: Systematic Review, Network Meta-analysis, and Benefit-harm assessment. Eur Urol Oncol. 2022;19:19. PubMed
10.Yanagisawa T, Rajwa P, Thibault C, et al. Androgen Receptor Signaling Inhibitors in Addition to Docetaxel with Androgen Deprivation Therapy for Metastatic Hormone-sensitive Prostate Cancer: A Systematic Review and Meta-analysis. Eur Urol. 2022;19:19. PubMed
11.Sterne JAC, Savović J, Page MJ, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366:l4898. PubMed
12.Canadian Cancer Statistics: A 2018 Special Report on Cancer Incidence by Stage. Canadian Cancer Society; 2018: https://cdn.cancer.ca/-/media/files/research/cancer-statistics/2018-statistics/canadian-cancer-statistics-2018-en.pdf. Accessed 2022 Aug 16.
13.Diagnosis of Prostate Cancer. Canadian Cancer Society; 2021: https://cancer.ca/en/cancer-information/cancer-types/prostate/diagnosis. Accessed 2022 Aug 16.
14.So AI, Chi KN, Danielson B, et al. Canadian Urological Association-Canadian Urologic Oncology Group guideline on metastatic castration-naive and castration-sensitive prostate cancer. Can Urol Assoc J. 2020;14(2):17-23. PubMed
15.NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) Prostate Cancer Version 4.0. National Comprehensive Cancer Network; 2022: https://www.nccn.org/professionals/physician_gls/pdf/prostate.pdf. Accessed 2022 Aug 16.
16.Xtandi (enzalutamide): 40mg, oral capsules [product monograph]. 2022: https://pdf.hres.ca/dpd_pm/00064474.PDF. Accessed 2022 Jul 30.
17.Erleada (apalutamide): 60mg, oral tablet [product monograph]. 2022: https://pdf.hres.ca/dpd_pm/00066114.PDF. Accessed 2022 Jul 30.
18.Zytiga (abiraterone acetate): 250mg uncoated oral tablet, 500mg film-coated oral tablet [product monograph]. 2018: https://pdf.hres.ca/dpd_pm/00044223.PDF. Accessed 2022 Jul 30.
19.McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS Peer Review of Electronic Search Strategies: 2015 Guideline Statement. J Clin Epidemiol. 2016;75:40-46. PubMed
20.Grey matters: a practical tool for searching health-related grey literature. Ottawa (ON): CADTH; 2019: https://www.cadth.ca/grey-matters. Accessed 2022 Jul 4.
21.Cleeland C, Ryan K. Pain assessment: global use of the Brief Pain Inventory. Annals, academy of medicine, Singapore. 1994. PubMed
22.Logothetis CJ, Basch E, Molina A, et al. Effect of abiraterone acetate and prednisone compared with placebo and prednisone on pain control and skeletal-related events in patients with metastatic castration-resistant prostate cancer: exploratory analysis of data from the COU-AA-301 randomised trial. Lancet Oncol. 2012;13(12):1210-1217. PubMed
23.Kuppen MCP, Westgeest HM, van den Eertwegh AJM, et al. Health-related Quality of Life and Pain in a Real-world Castration-resistant Prostate Cancer Population: Results From the PRO-CAPRI Study in the Netherlands. Clin Genitourin Cancer. 2020;18(3):e233-e253. PubMed
24.Victorson DE, Beaumont JL, Rosenbloom SK, Shevrin D, Cella D. Efficient assessment of the most important symptoms in advanced prostate cancer: the NCCN/FACT‐P Symptom Index. Psycho‐Oncology. 2011;20(9):977-983. PubMed
25.Beaumont JL, Butt Z, Li R, Cella D. Meaningful differences and validity for the NCCN/FACT‐P Symptom Index: An analysis of the ALSYMPCA data. Cancer. 2019;125(11):1877-1885. PubMed
26.Statistical Analysis Plan: ARASENS. A randomized, double–blind, placebo–controlled Phase III study of darolutamide (ODM–201) versus placebo in addition to standard androgen deprivation therapy and docetaxel in patients with metastatic hormone–sensitive prostate cance [internal sponsor's report]. 2021 Nov 11.
27.Guyot P, Ades AE, Ouwens MJNM, Welton NJ. Enhanced secondary analysis of survival data: reconstructing the data from published Kaplan-Meier survival curves. BMC Med Res Methodol. 2012;12(1):9. PubMed
28.Brooks SP, Gelman A. General Methods for Monitoring Convergence of Iterative Simulations. Journal of Computational and Graphical Statistics. 1998;7(4):434-455.
29.van Valkenhoef G, Dias S, Ades AE, Welton NJ. Automated generation of node-splitting models for assessment of inconsistency in network meta-analysis. Research Synthesis Methods. 2016;7(1):80-93. PubMed
30.Dias S WN, Sutton AJ, et al. NICE DSU Technical Support Document 2: A Generalised Linear Modelling Framework for Pairwise and Network Meta-Analysis of Randomised Controlled Trials [Internet]. London: National Institute for Health and Care Excellence (NICE). 2014: https://www.ncbi.nlm.nih.gov/books/NBK310366/.
31.Brignardello-Petersen R, Izcovich A, Rochwerg B, et al. GRADE approach to drawing conclusions from a network meta-analysis using a partially contextualised framework. BMJ. 2020;371:m3907. PubMed
32.Langan D, Higgins JPT, Jackson D, et al. A comparison of heterogeneity variance estimators in simulated random-effects meta-analyses. Res Synth Methods. 2019;10(1):83-98. PubMed
33.Robinson DW, Zhao N, Dawkins F, Qi M, Revicki D. Pain questionnaire performance in advanced prostate cancer: comparative results from two international clinical trials. Qual Life Res. 2013;22(10):2777-2786. PubMed
34.Gater A, Abetz-Webb L, Battersby C, et al. Pain in castration-resistant prostate cancer with bone metastases: a qualitative study. Health and quality of life outcomes. 2011;9(1):1-11. PubMed
35.Skaltsa K, Longworth L, Ivanescu C, Phung D, Holmstrom S. Mapping the FACT-P to the preference-based EQ-5D questionnaire in metastatic castration-resistant prostate cancer. Value Health. 2014;17(2):238-244. PubMed
36.Cleeland CS. The brief pain inventory user guide. Houston, TX: The University of Texas MD Anderson Cancer Center. 2009:1-11.
37.Fizazi K, De Bono J, Flechon A, et al. Randomised phase II study of siltuximab (CNTO 328), an anti-IL-6 monoclonal antibody, in combination with mitoxantrone/prednisone versus mitoxantrone/prednisone alone in metastatic castration-resistant prostate cancer. Eur J Cancer. 2012;48(1):85-93. PubMed
38.Chu FM, Picus J, Fracasso PM, Dreicer R, Lang Z, Foster B. A phase 1, multicenter, open-label study of the safety of two dose levels of a human monoclonal antibody to human αv integrins, intetumumab, in combination with docetaxel and prednisone in patients with castrate-resistant metastatic prostate cancer. Invest New Drugs. 2011;29(4):674-679. PubMed
39.Clark MJ, Harris N, Griebsch I, Kaschinski D, Copley-Merriman C. Patient-reported outcome labeling claims and measurement approach for metastatic castration-resistant prostate cancer treatments in the United States and European Union. Health Qual Life Outcomes. 2014;12:104. PubMed
40.FACIT. National Comprehensive Cancer Network/Functional Assessment of Cancer Therapy Prostate Cancer Symptom Index - 17 Item Version. 2021: https://www.facit.org/measures/NFPSI-17. Accessed July 27 2022.
41.Hoskin P, Sartor O, O'Sullivan JM, et al. Efficacy and safety of radium-223 dichloride in patients with castration-resistant prostate cancer and symptomatic bone metastases, with or without previous docetaxel use: a prespecified subgroup analysis from the randomised, double-blind, phase 3 ALSYMPCA trial. The Lancet Oncology. 2014;15(12):1397-1406. PubMed
Appendix 1: Literature Search Strategy
Note that this appendix has not been copy-edited.
Clinical Literature Search
Overview
Interface: Ovid
Databases:
MEDLINE All (1946 to present)
Embase (1974 to present)
Note: Subject headings and search fields have been customized for each database. Duplicates between databases were removed in Ovid.
Date of search: July 13, 2022
Alerts: Weekly search updates until project completion
Search filters applied: No filters were applied to limit the retrieval by study type.
Limits:
Publication date limit: none
Language limit: none
Conference abstracts: excluded
Syntax | Description |
|---|---|
/ | At the end of a phrase, searches the phrase as a subject heading |
MeSH | Medical Subject Heading |
exp | Explode a subject heading |
* | Before a word, indicates that the marked subject heading is a primary topic; or, after a word, a truncation symbol (wildcard) to retrieve plurals or varying endings |
# | Truncation symbol for one character |
adj# | Requires terms to be adjacent to each other within # number of words (in any order) |
.ti | Title |
.ot | Original title |
.ab | Abstract |
.hw | Heading word; usually includes subject headings and controlled vocabulary |
.kf | Keyword heading word |
.dq | Candidate term word (Embase) |
.pt | Publication type |
.rn | Registry number |
.nm | Name of substance word (MEDLINE) |
medall | Ovid database code: MEDLINE All, 1946 to present, updated daily |
oemezd | Ovid database code; Embase, 1974 to present, updated daily |
Multi-Database Strategy
(darolutamide* or nubeqa* or darramamide* or bay-1841788 or bay1841788 or odm-201 or odm201 or orm-16497 or orm16497 or orm-16555 or orm16555 or X05U0N2RCO).ti,ab,kf,ot,hw,nm,rn.
1 use medall
*darolutamide/ or (darolutamide* or nubeqa* or darramamide* or bay-1841788 or bay1841788 or odm-201 or odm201 or orm-16497 or orm16497 or orm-16555 or orm16555).ti,ab,kf,dq.
3 use oemezd
4 not (conference review or conference abstract).pt.
2 or 5
remove duplicates from 6
Clinical Trials Registries
ClinicalTrials.gov
Produced by the US National Library of Medicine. Targeted search used to capture registered clinical trials.
Search: Nubeqa (darolutamide); metastatic castration sensitive prostate cancer (mCSPC)
WHO ICTRP
International Clinical Trials Registry Platform, produced by WHO. Targeted search used to capture registered clinical trials.
Search: Nubeqa (darolutamide); metastatic castration sensitive prostate cancer (mCSPC)
Health Canada’s Clinical Trials Database
Produced by Health Canada. Targeted search used to capture registered clinical trials.
Search: Nubeqa (darolutamide); metastatic castration sensitive prostate cancer (mCSPC)
EU Clinical Trials Register
European Union Clinical Trials Register, produced by the European Union. Targeted search used to capture registered clinical trials.
Search: Nubeqa (darolutamide); metastatic castration sensitive prostate cancer (mCSPC)
Grey Literature
Search dates: July 4, 2022 to July 13, 2022
Keywords: Nubeqa (darolutamide); metastatic castration sensitive prostate cancer (mCSPC)
Limits: Publication years: None
Updated: Search updated prior to the completion of stakeholder feedback period
Relevant websites from the following sections of the CADTH grey literature checklist Grey Matters: A Practical Tool for Searching Health-Related Grey Literature were searched:
Health Technology Assessment Agencies
Health Economics
Clinical Practice Guidelines
Drug and Device Regulatory Approvals
Advisories and Warnings
Drug Class Reviews
Clinical Trials Registries
Databases (free)
Internet Search
Open Access Journals
The complete search archive of sites consulted for this report is available on request.
Appendix 2: Detailed Outcome Data
Note that this appendix has not been copy-edited.
Figure 11: NCCN-FACT FPSI-17 Questionnaire — Total Score (Redacted)

Note that this figure has been redacted.
Figure 12: NCCN-FACT FPSI-17 Questionnaire — Disease-Related Symptom Subscale — Physical Score (Redacted)

Note that this figure has been redacted.
Figure 13: NCCN-FACT FPSI-17 Questionnaire — Disease-Related Symptoms Subscale — Emotional Score (Redacted)

Note that this figure has been redacted.
Figure 14: NCCN-FACT FPSI-17 Questionnaire — Treatment Side Effects Subscale Score (Redacted)

Note that this figure has been redacted.
Figure 15: NCCN-FACT FPSI-17 Questionnaire — Function and Well-Being Subscale Score (Redacted)

Note that this figure has been redacted.
Figure 16: Assessment of Inconsistency Based on Node-Splitting for OS (Redacted)

Note that this figure has been redacted.
Figure 17: Assessment of Inconsistency Based on Node-Splitting for Time to CRPC (Redacted)

Note that this figure has been redacted.
Figure 18: Assessment of Inconsistency Based on Node-Splitting for rPFS (Redacted)

Note that this figure has been redacted.
Figure 19: Risk of Bias in Studies Regarding Overall Survival (Menges et al. [2022])
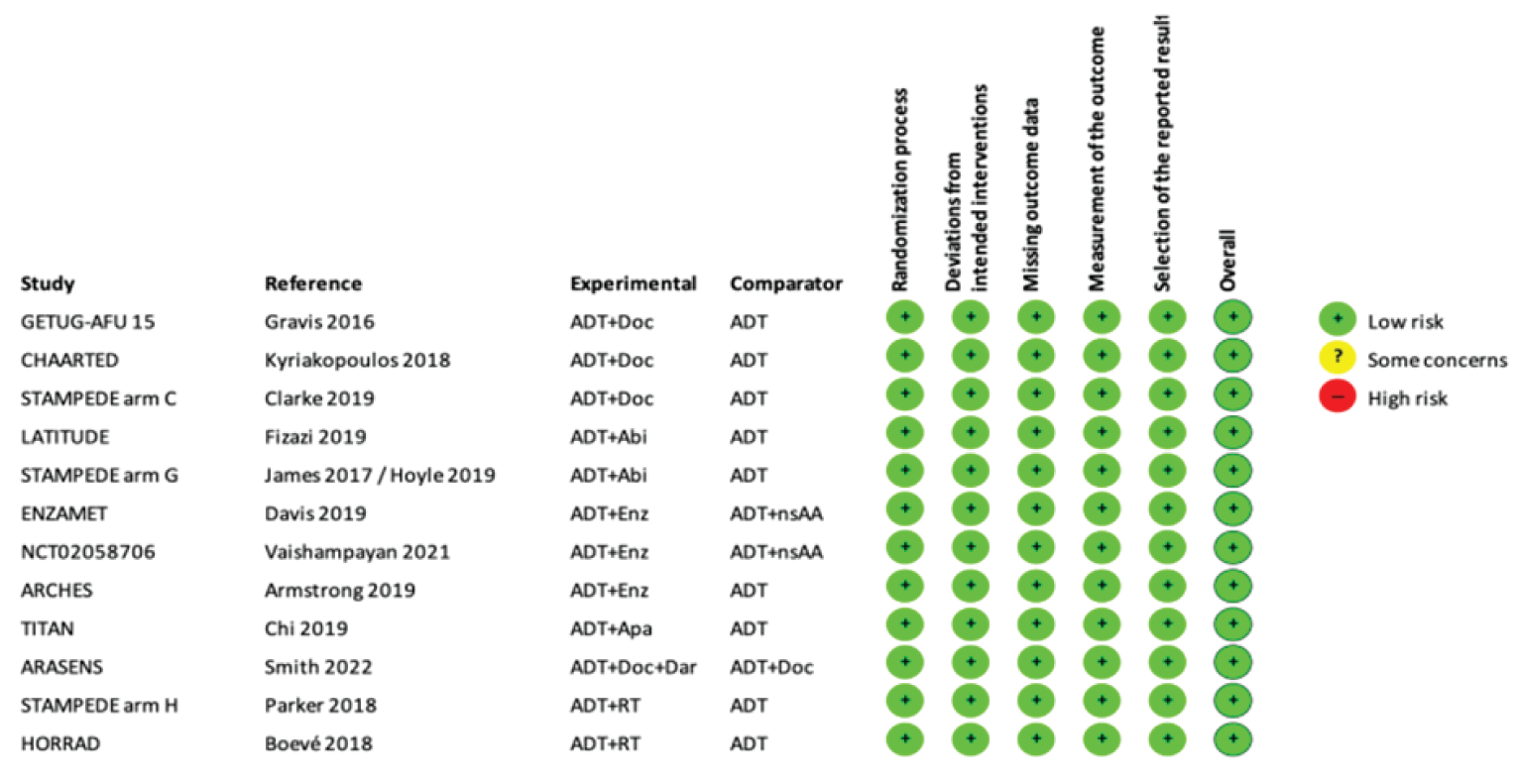
Source: Menges et al. (2022).9
Figure 20: Risk of Bias Assessment of the Included RCTs (Yanagisawa et al. [2022])
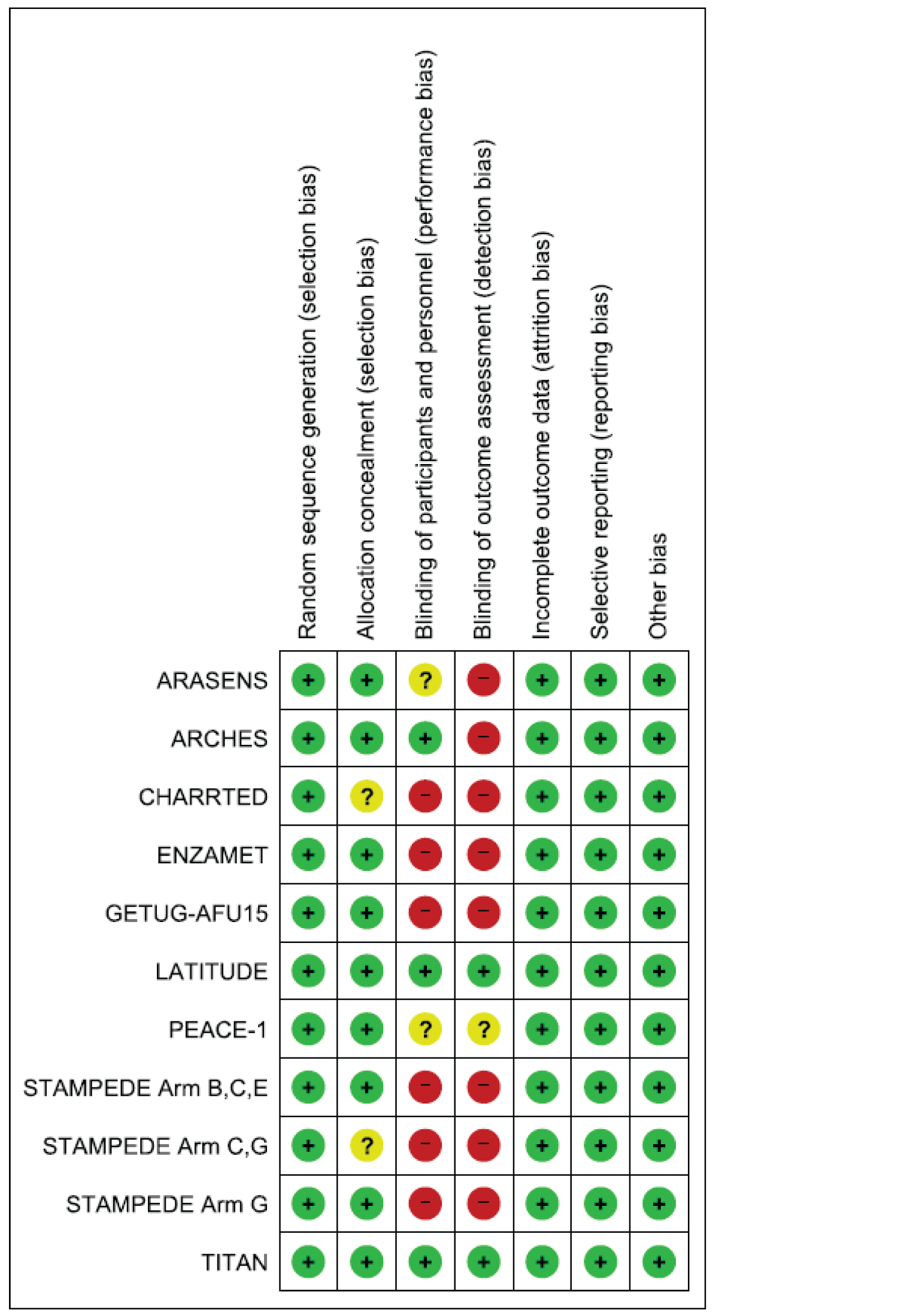
Source: Yanagisawa et al. (2022).10
Appendix 3: Description and Appraisal of Outcome Measures
Note that this appendix has not been copy-edited.
Aim
To describe the following outcome measures and review their measurement properties (validity, reliability, responsiveness to change, and MID):
Brief Pain Inventory - Short Form (BPI-SF)
National Comprehensive Cancer Network/ Functional Assessment of Cancer Therapy-Prostate Symptom Index - 17 (NCCN-FACT FPSI-17)
Findings
Table 28: Summary of Outcome Measures and Their Measurement Properties
Outcome measure | Type | Conclusions about measurement properties | MID |
|---|---|---|---|
Brief Pain Inventory -Short Form | Patient-reported generic questionnaire for pain intensity and impact. Each item is scored on an 11-point scale from 0 to 10, where 0 is no pain/no interference and 10 is the worst pain/complete interference.21 A composite of the 4 pain items (a mean severity score) can be presented and pain interference is typically scored as the mean of the 7 interference items.21 | Validity: Strong correlations between worst pain and average pain items (r = 0.79) and between the worst pain item and the PPI (r = 0.52).33 Support for content validity via in-depth interviews for worst pain item in a study of patients with mCRPC and bone metastases.34 Reliability: Good internal consistency reliability in study of mCRPC patients with alpha ≥ 0.89 and good internal consistency reliability with ICC values ≥ 0.73.33 Responsiveness: Not assessed in indicated population. | Not assessed in indicated population. |
National Comprehensive Cancer Network/ Functional Assessment of Cancer Therapy-Prostate Symptom Index - 17 | A 17-item, cancer-specific questionnaire developed to examine symptoms and function/well-being among people undergoing treatment for advanced prostate cancer.24 Has 4 main subscales that assess: physical and emotional disease-related symptoms, treatment side effects, and function/well-being. Each item is ranked on a 5-point scale with higher scores indicating lesser symptoms and better function/well-being.25 Total score range is 0 to 156.35 | Validity: Construct validity supported by ability to discriminate between levels of ECOG performance status and ALP scores in mCRPC patients.25 Reliability: Good internal consistency reliability in a study of mCRPC patients with alpha ≥ 0.67 for all scales except TSE.25 Responsiveness: Most scales responsive to change in ECOG performance status, presence of a skeletal event, and PSA response in a trial of mCRPC patients.25 | Not assessed in indicated population. For mCRPC patients: Total score: 4 to 6 points DRS-P: 2 to 3.5 points DRS-E: 0.5 points TSE: 1 to 1.5 points F/WB: 0.5 to 1 points.25 |
ALP = alkaline phosphatase; BPI-SF = Brief Pain Inventory - Short Form; DRS-P = disease-related symptoms–physical subscale; DRS-E = disease-related symptoms–emotional subscale; ECOG = Eastern Cooperative Oncology Group F/WB = Function/Well-Being subscale; HRQoL = health-related quality of life; mCRPC = metastatic castration-resistant prostate cancer; MID = minimal important difference; PSA = prostate-specific antigen; PPI = Present Pain Intensity (PPI) component of the McGill Pain Questionnaire; TSE: Treatment Side Effects subscale.
Brief Pain Inventory — Short Form (BPI-SF)
Description and Scoring
The BPI is a patient-reported pain questionnaire designed and validated to assess cancer pain,36 and was used in the ARASENS trial to measure time to pain progression. It is used to assess the intensity of pain experienced, as well as the degree to which this pain interferes with function.21 The BPI is available as a long and short version, the latter of which has a 24-hour recall period for both worst pain and least pain items.33 It consists of a diagram of a human body onto which the location of pain is recorded.36 There is a section for reporting use of analgesics and the relief these provide. Pain measurement is divided into 2 categories: intensity and interference with function. The intensity category consists of 4 items: pain now, average pain, worst pain, and least pain. The interference with function category is divided into 7 items: general activity, mood, walking ability, normal work, relations with other persons, sleep, and enjoyment of life. Each item is scored on an 11-point scale from 0 to 10, where 0 is no pain or no interference and 10 is the worst pain or complete interference. With respect to the pain interference category, a mean can be reported if a minimum of 4 of the 7 items are assessed. There is no total score for the BPI-SF. A composite of the 4 pain items (a mean severity score) can be presented and pain interference is typically scored as the mean of the 7 interference items.36
Validity and Reliability
Robinson et al. examined data from 2 trials evaluating siltuximab37 (n = 93) or intetumumab in combination with docetaxel38 (n = 131) among patients with mCRPC.33 Results demonstrated good construct validity with strong Pearson correlations between the BPI-SF worst pain and average pain items (r = 0.79; P <0.006) as well as between the BPI-SF worst pain item and the Present Pain Intensity (PPI) component of the McGill Pain Questionnaire (r = 0.52; P < 0.006).33 A moderate correlation was found between the BPI-SF worst pain item and the FACT-P total score (r = −0.42; P < 0.006).33
Gater et al. conducted in-depth interviews with 17 patients (aged 53 to 86 years) with mCRPC and bone metastases to assess the content validity of the BPI-SF average pain and worst pain items.34 Results indicated that patients understood the worst pain item but had some difficulty in determining their average pain. A total of 11 patients based their average pain on the value between their worst pain and least pain while 6 patients based their average pain value on the level of pain that they experienced most of the time. Recall periods for average pain varied between participants (e.g., since beginning treatment or in the last week). Therefore, evidence supports the content validity of the worst pain item as a measure of pain intensity for use in this patient population and notes limitations in patients’ interpretation of the average pain item.34,39
Robinson et al. also examined the reliability of the BPI-SF pain intensity scale (4 items).33 Internal consistency reliability was evaluated using Cronbach’s alpha which was reported as good to excellent, with values of 0.89 and 0.93 for each trial, respectively. Test-retest reliability was evaluated using intraclass correlation coefficient (ICC) among a cohort of patients in each trial who completed the questionnaire at 2 initial visits and were clinically stable between visits (with a mean (SD) of 12 (7) days between visits). Results found good internal consistency reliability for the BPI-SF pain intensity scale with ICC values of 0.73 and 0.91 for each trial, respectively.33
Responsiveness
Responsiveness of the instrument was not assessed in the indicated patient population.
MID
An MID was not assessed in the indicated patient population. An MID estimate of 2 or more points or 30% change in pain intensity items from baseline was previously used in studies in mCRPC patients.22,23
National Comprehensive Cancer Network/Functional Assessment of Cancer Therapy-Prostate Symptom Index 17 (NCCN-FACT FPSI-17).
Description and Scoring
The NCCN-FACT FPSI-17 is a cancer-specific questionnaire developed to examine the symptoms and function/well-being among people undergoing treatment for advanced prostate cancer,24 and was used in the ARASENS trial to approximate HRQoL. Developed in consultation with medical experts (n = 66) and patients (n = 74) in 2010, the instrument includes a 17-item index that produces a total score and is also divided into 4 main subscales that assess disease-related symptoms: Disease-Related Symptoms–Physical (DRS-P), Disease-Related Symptoms–Emotional (DRS-E), Treatment Side Effects (TSE), and Function/Well-Being (F/WB). Each item is ranked on a 5-point scale ranging from 0 (not at all) to 4 (very much).40 Higher subscale and total scores indicate lesser symptoms and better function/well-being.25
Validity and Reliability
Beaumont et al., used data from the ALSYMPCA trial41 among mCRPC patients to assess the construct validity of the instrument using the known groups approach.25 All baseline sources significantly differed among groups based on ECOG performance status, except for the DRS-E subscale. Also, all baseline scores, except for the NFPSI–DRS-E, significantly differed between total ALP scores (< 220 U/L versus ≥ 220 U/L), providing support for construct validity of the instrument in this patient population.41
Cronbach’s alpha was used to estimate the internal consistency reliability of the instrument, with good reliability for the total score (alpha = 0.80) as well as the F/WB (alpha = 0.78) and DRS-P (alpha = 0.67) subscales.25 The TSE subscale had poor internal consistency reliability (alpha = 0.47) likely due to the diverse set of common AEs that comprise the subscale.25
Responsiveness
The instrument’s total score and all subscale scores were shown to be responsive to change in ECOG performance status in the aforementioned study.25 Effect sizes for those who worsened were ≥ 0.50 for the instrument’s total score and all subscale scores except for the DRS-E subscale which had a small effects size of 0.12. The instrument was also responsive to the presence of a skeletal-related event during treatment the with effect sizes ≥ 0.54 for all scales except for the DRS-E subscale. The instrument was responsive to patients who did not experience a PSA response before the end of treatment with effect sizes ranging from 0.36 to 0.47 for all scales except for the DRS-E. Effect sizes for PSA responders improved by a similar magnitude for all scales except for TSE subscale.25
MID
Both distribution- and anchor-based methods were used to determine an MID for the instrument based on trial data among mCRPC patients.25 Results indicated an MID of 4 to 6 points for the total score, 2 to 3.5 points for the DRS-P, 0.5 points for the DRS-E, 1 to 1.5 points for TSE, and 0.5 to 1 point for the F/WB subscales.25
Pharmacoeconomic Review
Abbreviations
ADT
androgen deprivation therapy
AE
adverse event
ARAT
androgen receptor-axis-targeted therapy
HR
hazard ratio
ICER
incremental cost-effectiveness ratio
ITC
indirect treatment comparison
mCRPC
metastatic castration-resistant prostate cancer
mCSPC
metastatic castration-sensitive prostate cancer
NMA
network meta-analysis
OS
overall survival
PFS
progression-free survival
QALY
quality-adjusted life-year
ToT
time on treatment
TTCROD
time to castration resistance or death
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Darolutamide (Nubeqa), tablets |
Submitted price | Darolutamide, 300 mg tablet: $28.34 |
Indication | For the treatment of patients with metastatic castration-sensitive prostate cancer (mCSPC) in combination with docetaxel |
Health Canada approval status | NOC |
Health Canada review pathway | Priority review, Project Orbis |
NOC date | October 4, 2022 |
Reimbursement request | For the treatment of patients with mCSPC in combination with docetaxel in patients who are chemotherapy-eligible |
Sponsor | Bayer Inc. |
Submission history | Previously reviewed: Yes Indication: Non-metastatic castration-resistant prostate cancer Recommendation date: April 22, 2020 Recommendation: Reimburse with clinical criteria and/or conditions |
mCSPC = metastatic castration-sensitive prostate cancer; NOC = Notice of Compliance.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Partitioned survival model |
Target population | Patients with mCSPC eligible for chemotherapy, which is aligned with the reimbursement request |
Treatments | Darolutamide + docetaxel + ADT |
Comparators | Docetaxel + ADT Abiraterone and prednisone + ADT Apalutamide + ADT Enzalutamide + ADT ADT alone (degarelix, leuprorelin, goserelin, or triptorelin) |
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs, LYs |
Time horizon | Lifetime (25 years) |
Key data source |
|
Submitted results |
|
Key limitations |
|
CADTH reanalysis results |
|
ADT = androgen deprivation therapy; AE = adverse event; ARAT = androgen receptor-axis-targeted therapy; ICER = incremental cost-effectiveness ratio; LY = life-year; mCSPC = metastatic castration-sensitive prostate cancer; NMA = network meta-analysis; OS = overall survival; QALY = quality-adjusted life-year; RCT = randomized controlled trial.
Conclusions
The CADTH Clinical Review concluded that darolutamide plus docetaxel and androgen deprivation therapy (ADT) demonstrated clinically meaningful improvement of overall survival (OS) compared to docetaxel and ADT in patients with metastatic castration-sensitive prostate cancer (mCSPC) in the ARASENS trial. Analyses of secondary outcomes supported the efficacy of darolutamide plus docetaxel and ADT in delaying progression to metastatic castration-resistant prostate cancer (mCRPC), the need for subsequent antineoplastic therapy, worsening of pain, and symptomatic skeletal events compared to docetaxel and ADT. Regarding the sponsor-submitted indirect treatment comparison (ITC), the CADTH Clinical Review noted that, for OS, there was insufficient evidence to show a difference between darolutamide plus docetaxel and ADT and either abiraterone and ADT, apalutamide and ADT, and enzalutamide and ADT. For time to mCRPC, darolutamide plus docetaxel and ADT was favoured over all treatments except enzalutamide and ADT. The reviewers noted the potential for biases related to heterogeneity in study design, prior treatment requirements, and follow-up duration across included studies. The clinical review noted that there remains increased potential that the underlying transitivity assumption of the network meta-analysis (NMA) has been violated.
CADTH undertook reanalyses to the sponsor’s economic evaluation; these included using a gamma extrapolation for the OS results and updating costs for docetaxel.
The results of the CADTH reanalysis were in line with those submitted by the sponsor: darolutamide plus docetaxel and ADT is not a cost-effective treatment for mCSPC at a willingness-to-pay threshold of $50,000 per quality-adjusted life-year (QALY). Based on the CADTH sequential analysis, darolutamide plus docetaxel and ADT is more costly and more effective than abiraterone and ADT (incremental costs: $121,237; incremental QALYs: 0.77), resulting in an ICER of $156,172 per QALY. A price reduction of 58% would be required for darolutamide in order for the treatment regimen (i.e., darolutamide plus docetaxel and ADT) to be cost-effective compared to abiraterone and ADT at a $50,000-per-QALY threshold. The sponsor’s OS extrapolations were uncertain and resulted in overestimates of survival according to clinical experts, who indicated that a Weibull extrapolation might also be appropriate. CADTH conducted a scenario analysis in which a Weibull extrapolation was used for OS, which resulted in an incremental cost-effectiveness ratio (ICER) of $180,113 per QALY compared to abiraterone and ADT.
Results of the CADTH base case and scenario analyses are uncertain given the results of the NMA, which found no statistical difference in OS for darolutamide plus docetaxel and ADT compared to abiraterone, apalutamide, or enzalutamide and ADT. The results were imprecise, and the 95% credible intervals were wide. This imprecision was evident in the sponsor’s base-case model, which predicted incremental QALYs ranging from –1.4 to 3.3 for the comparison of darolutamide plus docetaxel and ADT to abiraterone and ADT across different probabilistic iterations. The CADTH base case predicts an incremental LY gain of 0.80 for darolutamide plus docetaxel and ADT compared to abiraterone and ADT, despite the lack of strong conclusions that can be drawn from the results of the NMA. Furthermore, in the CADTH base case, 72% of the incremental QALYs gained for darolutamide plus docetaxel and ADT compared to abiraterone and ADT were obtained after the maximum follow-up in the ARASENS trial. The results of the model are dependent on a survival benefit for darolutamide plus docetaxel and ADT being realized relative to comparators, which is uncertain given the aforementioned limitations. The scenario analysis in which no differences in OS were assumed between darolutamide plus docetaxel and ADT and comparators resulted in an ICER of $520,548 per QALY compared to abiraterone and ADT and a price reduction of 75% for darolutamide. This scenario highlights the impact of OS assumptions on the ICER and resulting price reduction required to achieve cost-effectiveness at a $50,000-per-QALY threshold.
Stakeholder Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, registered clinicians, and drug plans that participated in the CADTH review process.
Patient input was received from 2 groups: the Canadian Cancer Society and the Canadian Cancer Survivor Network. The Canadian Cancer Society conducted surveys and interviews of 39 patients and 2 caregivers. The Canadian Cancer Survivor Network conducted online surveys with 24 patients and 2 caregivers. All survey respondents lived in Canada. Patients reported previous experience with hormone therapy, radiation, antiandrogens, surgery, and chemotherapy. The most common side effects of currently available therapy that had a significant impact on daily life were sexual dysfunctions, hot flashes, and fatigue. Patient expectations for a new therapy were for it to result in improved quality of life (reduced side effects) and delayed symptom onset. Six of the patients surveyed had current experience with darolutamide, and 1 was interviewed in detail. Side effects with darolutamide included sexual dysfunction, fatigue, weight gain, and loss of muscle mass, among others. Most patients with experience on darolutamide reported improved outcomes in terms of prostate-specific antigen and quality of life, and stated that the benefits of the treatment outweigh the side effects.
CADTH received 7 registered clinician input submissions for this review, which consisted of clinician groups from Southeastern Ontario; BC Cancer; the Canadian Cancer Society; Ontario Health; the Maritime provinces; Regina, Saskatchewan; and The Ottawa Hospital. The baseline therapy for all patients with mCSPC is ADT, with clinical trial evidence showing a benefit for the addition of docetaxel, or an androgen receptor-axis-targeted therapy (ARAT), namely, abiraterone, enzalutamide, and apalutamide. Although the standard care a decade ago was ADT alone, clinicians currently treat patients with ADT in addition to docetaxel, or in addition to an ARAT, with some clinicians advocating for the use of “triplet therapy” (ARAT plus docetaxel and ADT). Darolutamide would fall into this category of triplet therapy in that it would be given, first-line, in combination with docetaxel and ADT. The goals of treatment are to improve and extend disease control for as long as possible, improve and extend quality of life, and extend OS.
Drug plan input for this review was interested in whether patients unable to tolerate 6 cycles of docetaxel should be eligible to continue with darolutamide and ADT, or whether patients unable to tolerate darolutamide would be eligible to switch another ARAT plus docetaxel and ADT. Plans wondered whether patients who recently initiated docetaxel and ADT for mCSPC would be eligible to add on darolutamide, or whether patients currently receiving an ARAT and ADT would switch to darolutamide plus docetaxel and ADT at the time of funding. Plans noted the presence of confidential, negotiated prices for comparators.
Several of these concerns were addressed in the sponsor’s model:
The sponsor included various comparators in their model, such as abiraterone, apalutamide, docetaxel, and enzalutamide in combination with ADT, along with ADT alone.
CADTH was unable to address the following concerns raised from stakeholder input:
Sexual dysfunction, noted to be 1 of the more common side effects of therapy, was not included as an adverse event in the sponsor’s model.
CADTH reanalyses are based on publicly available prices and do not incorporate the presence of confidential, negotiated prices.
Economic Review
The current review is for darolutamide (Nubeqa) in combination with docetaxel for patients with mCSPC.
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted a cost-utility analysis of darolutamide in combination with docetaxel compared to docetaxel, abiraterone and prednisone, apalutamide, enzalutamide, or ADT alone. All other treatments were also given alongside ADT. The modelled population consisted of patients with mCSPC eligible for chemotherapy, which is aligned with the eligibility criteria for the ARASENS clinical trial.1 The Health Canada indication states that darolutamide is indicated for “the treatment of patients with mCSPC in combination with docetaxel” without the explicit stipulation that patients must be eligible for chemotherapy;2 the reimbursement request represents patients with mCSPC who are chemotherapy-eligible, which is aligned with the clinical trial.1,3
Darolutamide is available in 300 mg oral tablets. The recommended dose is 600 mg twice daily, equivalent to a total daily dose of 1,200 mg.3 The dose may be reduced to 300 mg twice daily in the case of serious adverse events (AEs).3 Darolutamide is given in combination with docetaxel and ADT. Docetaxel has a recommended dose of 75 mg/m2 every 3 weeks for a maximum of 6 cycles and is given in combination with dexamethasone. ADT is included as a basket treatment received by all patients and consists of the following drugs, weighted by market share: degarelix, 12.6%; leuprorelin, 54.0%; goserelin, 31.9%; triptorelin, 1.5%. Market shares were obtained from IQVIA public claims data.3,4 The cost for darolutamide is $28.34 per tablet, leading to a 28-day cost of $3,175.3
The comparators for this analysis have been previously stated. The 28-day drug costs for the comparators used in the sponsor’s model are as follows: docetaxel, $97; abiraterone and prednisone, $872; apalutamide, $3,175; and enzalutamide, $3,270.1 All patients receive ADT; the 28-day costs for ADT are $417 in the first cycle and $356 in the second cycle due to degarelix requiring a higher loading dose.3
The clinical outcomes of interest were QALYs and life-years over a lifetime horizon of 25 years. Discounting (1.5% per annum) was applied to both costs and outcomes and a cycle length of 4 weeks was used. The base-case perspective was that of the Canadian publicly funded health care payer.
Model Structure
The sponsor submitted a partitioned survival model consisting of 3 mutually exclusive health states, mCSPC (i.e., progression-free), mCRPC (i.e., postprogression), and death. All patients entered the model in the progression-free state and received darolutamide plus docetaxel and ADT or a comparator. The proportion of patients in the progression-free state was defined by the progression-free survival (PFS) curves for the darolutamide plus docetaxel and ADT, and docetaxel and ADT treatments received in the ARASENS trial.1 Since the ARASENS trial did not capture radiographic PFS directly, progression was modelled using the secondary end point, time to castration resistance or death (TTCROD). TTCROD is a composite end point defined by any prostate-specific antigen progression, radiographic progression by soft-tissue or visceral lesions or radiographic progression by bone lesions, or death. The proportion of patients in the postprogression health state was equal to the difference between the OS and the PFS (defined by TTCROD) curves from the ARASENS trial. For comparators, the effect of treatment on OS and PFS was expressed in the model in terms of hazard ratios (HRs) based on an ITC. Patients in the postprogression state can receive subsequent line therapy. Patients transitioning into the death state remained there until the end of the model time horizon. A figure of the sponsor’s model structure is available in Appendix 3 (Figure 1).
Model Inputs
The target population of the economic evaluation was based on the ARASENS clinical trial, a phase III, double-blind, randomized controlled trial comparing darolutamide in combination with docetaxel and ADT to docetaxel and ADT.1 The mean age of the population was 66.8 years, mean weight was 77.5 kg, mean body surface area was 1.8 m2, and 100% of patients were male.1
For the comparison of darolutamide plus docetaxel and ADT and docetaxel and ADT, PFS, OS, and time on treatment (ToT) Kaplan-Meier data were derived directly from the ARASENS trial. Parametric extrapolations were performed to extrapolate the Kaplan-Meier data out to the model time horizon of 25 years. Curves were fitted independently for PFS (based on TTCROD), OS, and ToT, though the same extrapolations were chosen for both treatments. The sponsor’s base case extrapolations for PFS, OS, and ToT were the log-normal, log-logistic, and Gompertz extrapolations, respectively.
In the absence of direct comparative evidence to other comparators not included in the ARASENS trial, comparative effectiveness data were derived from a sponsor-commissioned ITC.5 |||||||||| studies, including the ARASENS trial, were identified as being relevant to the decision problem, and were included in an NMA.5 The NMA was used to generate HRs, which were applied to the parametric extrapolations for darolutamide plus docetaxel and ADT to generate comparator-specific survival curves. The OS HRs for the comparison of darolutamide plus docetaxel and ADT to other comparators ranged from |||||||||| (95% CI, |||||||||||||||||||| for ADT alone to |||||||||| 95% CI, |||||||||||||||||||| for both apalutamide and ADT and abiraterone and ADT (95% CI, |||||||||||||||||||| , favouring darolutamide plus docetaxel and ADT. The results were not significant (i.e., confidence interval includes the null) for abiraterone and ADT, apalutamide and ADT, and enzalutamide and ADT. The sponsor presented HRs for PFS according to TTCROD (base case) and radiographic PFS (scenario analysis); the HRs for the base case ranged from |||||||||| (95% CI, |||||||||||||||||||| for ADT alone to |||||||||| (95% CI, |||||||||||||||||||| for enzalutamide and ADT. ToT was assumed not to exceed PFS.
Regarding safety outcomes, the model considered grade 3+ AEs that occurred for at least 5% of patients for any of the treatments; these consisted of increased alanine aminotransferase, decreased neutrophil count, decreased white blood cell count, febrile neutropenia, hypertension, hypokalemia, and neutropenia.
The ARASENS trial collected health-related quality of life data from patients through various questionnaires but not via a generic, preference-based HRQoL measure such as the EQ-5D. Thus, EQ-5D utility data were collected from various sources in the literature. For the preprogression health state, a utility value of 0.847 was used based on the enzalutamide clinical trial ARCHES.6 The utility values for the first line of postprogression treatment in the mCRPC health state (0.782), and end-of-life (0.543) health states were obtained from the ARCHES trial using EQ-5D-5L measurements that applied Canadian tariffs.7 Finally, a value of 0.663 was used for second- and third-line mCRPC health states based on the mean of these 2 values. Disutilities, derived from various published sources, were included for all AEs except increased alanine aminotransferase and hypokalemia.3
The economic model included costs related to drugs (acquisition, administration, background ADT, and subsequent therapy), monitoring, AE management, and terminal care. The drug acquisition costs of darolutamide and comparators have been previously stated, as well as those for ADT. Costs for subsequent treatments were considered (e.g., abiraterone, enzalutamide, docetaxel, radium-223, cabazitaxel), with subsequent treatment breakdown obtained from patients in the ARASENS trial.8 However, these data were adjusted to account for the fact that some jurisdictions do not allow ARAT use in subsequent lines post-ARAT therapy for mCSPC. As such, enzalutamide was assumed not to be used after darolutamide and abiraterone use was reduced by 43% as its use post-ARAT therapy is only available in Ontario, Prince Edward Island, and New Brunswick. The subsequent treatment distribution for darolutamide plus docetaxel and ADT was assumed to apply to the other ARAT treatments, while the distribution for the docetaxel and ADT arm was assumed to apply to ADT alone.3 In addition to acquisition costs, an administration cost of $300 was included per administration of infusion therapies (e.g., docetaxel).9 Vial sharing was assumed to occur in the base case for docetaxel. Costs of AEs were applied as a one-off cost based on a weighted average of all AEs experienced in a given treatment. Regarding medical resource use, the following direct medical costs have been included in the model: cost of outpatient treatment (e.g., visits to urologist and/or oncologist, laboratory examinations, and emergency treatment); cost of drug therapies and concomitant medications, if applicable; administration costs; monitoring costs; hospitalization costs; and all follow-up treatment costs and costs for nursing care, with costs obtained from various published sources.3,10,11 Lastly, a one-off terminal care cost of $6,626 was applied when a patient dies, to reflect the costs of terminal care in the last 3 months of life.12
Summary of Sponsor’s Economic Evaluation Results
All analyses were run probabilistically (5,000 iterations for the base-case and scenario analyses). The deterministic and probabilistic results were similar. The probabilistic findings are presented below.
Base-Case Results
In the sponsor’s base case, darolutamide plus docetaxel and ADT was associated with an estimated cost of $219,925 and 5.78 QALYs over a lifetime horizon. In a sequential analysis, darolutamide plus docetaxel and ADT was associated with an ICER of $113,782 compared to abiraterone and ADT (incremental cost: $118,972, incremental QALYs: 1.05). Both apalutamide and enzalutamide were extendedly dominated in the sponsor’s base case, resulting in higher ICERs than the next most costly treatment. In the sponsor’s sequential analysis, darolutamide plus docetaxel and ADT had a 1% probability of being cost-effective at a willingness-to-pay threshold of $50,000 per QALY. In the sponsor’s base case, 79% of the incremental QALYs gained for darolutamide plus docetaxel and ADT compared to abiraterone and ADT were obtained after the maximum follow-up in the ARASENS trial (approximately 5 years). Additional results from the sponsor’s base case are available in Appendix 3.
Table 3: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total costs ($) | Total LYs | Total QALYs | Sequential ICER ($ per QALY) |
|---|---|---|---|---|
ADT alone | 76,950 | 4.20 | 3.15 | Reference |
Docetaxel + ADT | 93,593 | 5.80 | 4.40 | 13,382 |
Abiraterone + ADT | 100,954 | 6.00 | 4.73 | 22,010 |
Darolutamide + docetaxel + ADT | 219,925 | 7.07 | 5.78 | 113,782 |
ADT = androgen deprivation therapy; ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year.
Note: The submitted analyses are based on the publicly available prices of comparators and may not reflect confidential, negotiated prices. Only treatments on the cost-effectiveness frontier are reported in this table; apalutamide + ADT and enzalutamide + ADT were extendedly dominated by abiraterone + ADT and darolutamide + docetaxel + ADT.
Source: Sponsor’s pharmacoeconomic submission.3
Sensitivity and Scenario Analysis Results
The sponsor conducted several scenario analyses involving alternative time horizons, discount rates, subsequent treatment distribution based directly on the ARASENS trial, half-cycle correction, optimistic/pessimistic survival extrapolations, utilities, drug wastage, and PFS HRs based on radiographic PFS. The scenarios involving a discount rate of 5%, and shorter survival extrapolation resulted in the largest changes in the ICERs for darolutamide plus docetaxel and ADT compared to abiraterone, about $144,000 per QALY in both. Results from other scenarios had minimal impact on the overall results.
CADTH Appraisal of the Sponsor’s Economic Evaluation
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the economic analysis:
OS extrapolations are overestimated compared to general Canadian estimates. The sponsor’s base case used a log-logistic extrapolation for OS, which resulted in unrealistic OS estimates for patients receiving darolutamide plus docetaxel and ADT. The log-logistic extrapolation predicted that after 30 years, 5% of patients will still be alive, and after 40 years, 3% of patients will still be alive, with an average age of 107 years. For patients receiving docetaxel, the log-logistic extrapolation predicted that after 40 years, 2% of patients would still be alive. This is much higher than estimates of life expectancy in the general population in Canada, in which less than 1% of males are expected to still be alive at age 102.13 To address this issue, the sponsor adjusted the modelled OS to match the maximum age and sex-matched Canadian general population-based mortality hazard. This adjustment implies that the sponsor’s chosen extrapolation is inaccurate after a certain point — in the sponsor’s model, this occurs after 18.3 years. The adjustment increases the uncertainty in the analysis because it arbitrarily assumes a higher mortality for some patients that is not reflective of the chosen extrapolation, suggesting that the chosen extrapolation is flawed and unrepresentative of the data it is intended to model. Moreover, the adjustment also suggests that after 18.3 years, darolutamide plus docetaxel and ADT has “cured” the disease, such that patients with mCSPC experience the same mortality hazard as the general population. Finally, 5% of patients on darolutamide plus docetaxel and ADT and 3% of patients on docetaxel and ADT were still alive after 25 years (with an average age of 92), which was deemed unreasonable, according to clinical experts.
CADTH solicited clinician feedback to help determine the most appropriate OS curves. The feedback indicated that the sponsor’s chosen extrapolations were overestimated and emphasized that after 20 years, few patients would remain alive. Clinicians indicated that the gamma and Weibull extrapolations were more reflective of clinical expectations for this disease area. Clinicians agreed that the gamma extrapolation was most representative of clinical expectations.
As part of the base case, in consultation with clinical experts, CADTH selected a gamma extrapolation for both darolutamide plus docetaxel and ADT and docetaxel and ADT. These extrapolations resulted in less than 1% of patients remaining alive after 25 years. The Weibull extrapolation was tested in a scenario analysis.
There is uncertainty regarding clinical effects from the ITC. To inform the comparisons between darolutamide plus docetaxel and ADT and the other comparators abiraterone and ADT, apalutamide and ADT, and enzalutamide and ADT, the sponsor performed an ITC and NMA.1 As noted in the CADTH Clinical Review, results of this analysis indicated that there was insufficient evidence to show a difference between darolutamide plus docetaxel and ADT and these comparators for OS. The results were imprecise, as seen in the 95% credible intervals being wide. This imprecision was evident in the sponsor’s base-case model, which predicted incremental QALYs ranging from –1.4 to 3.3 for the comparison of darolutamide plus docetaxel and ADT to abiraterone and ADT across different probabilistic iterations. The clinical review also highlighted the lack of information regarding data extraction and risk of bias assessment, which results in a potential risk of bias and/or error in the systematic literature review that could not be quantified. Regarding heterogeneity, the clinical review stated that, while the heterogeneity assessment was reasonable and important factors were considered, there remained notable differences in the baseline characteristics that could potentially result in changing relative treatment effects that were not accounted for, including prostate-specific antigen level and prostate cancer stage. There were also differences in blinding, prior treatment requirements, and follow-up duration across included studies, and there remains increased potential that the underlying transitivity assumption of the NMA has been violated.
CADTH was unable to address this limitation due to a lack of evidence. As part of a scenario analysis, CADTH assumed no difference in OS between darolutamide plus docetaxel and ADT and abiraterone and ADT, apalutamide and ADT, and enzalutamide and ADT. This scenario analysis may be considered conservative.
Docetaxel costs are underestimated in the sponsor’s analysis. In their economic analysis, the sponsor used a cost per mg of docetaxel of $0.54 based on a published economic evaluation.14 However, the original pricing source could not be located and the cost of $0.54 per mg could not be verified. Because this value is substantially different than pricing data obtained from the IQVIA DeltaPA database,15 CADTH updated the cost of docetaxel based on the IQVIA database.
As part of the base case, CADTH updated the cost of docetaxel according to the unit costs summarized in the CADTH cost table (Table 8).
Subsequent therapy in the ARASENS trial does not align with expected clinical practice. In the sponsor’s model, costs of treatments for additional lines of therapy were added as a lump sum upon patients leaving the initial mCSPC health state. To estimate the costs of subsequent therapy, the proportions of subsequent treatment use postprogression in the ARASENS trial were used.8 In this trial, patients received various therapies following darolutamide plus docetaxel and ADT, including abiraterone, enzalutamide, docetaxel, radium-223, and cabazitaxel. The sponsor performed an adjustment to the subsequent therapy proportions whereby enzalutamide use was not assumed and abiraterone use was reduced by 43% based on the assumption that only patients in Ontario, Prince Edward Island, and New Brunswick could receive this therapy subsequent to an ARAT (darolutamide). These assumptions align partially with clinician feedback, which indicated that subsequent ARAT use in patients already having progressed on an ARAT is uncommon in Canada and unlikely to occur. However, in the ARASENS trial, patients did receive the ARATs enzalutamide (15.2%) and abiraterone (35.6%) post-darolutamide, which may have resulted in additional benefits to PFS and/or OS that were not considered or adjusted for. By excluding the costs of enzalutamide and 43% of the costs of abiraterone, the sponsor has artificially reduced the costs associated with the darolutamide plus docetaxel and ADT treatment while still maintaining any residual effectiveness. This potentially biases the results in favour of darolutamide plus docetaxel and ADT compared to docetaxel and ADT because patients are able to receive an ARAT post-docetaxel therapy.
The sponsor’s model provided an option to use the proportions of subsequent therapy observed directly in the ARASENS trial without an adjustment. This option was explored in a scenario analysis.
All relevant AEs were not included. The sponsor’s model included grade 3 or 4 AEs observed in the ARASENS trial, consisting of increased alanine aminotransferase, decreased neutrophil count, decreased white blood cell count, febrile neutropenia, hypertension, hypokalemia, and neutropenia.8 However, the patient input noted several other side effects of currently available therapies that have significant impact on daily life, including sexual dysfunctions, hot flashes, and fatigue. In addition, the clinical expert noted that enzalutamide, in particular, may be associated with neurocognitive toxicities such as dysgeusia, decreased concentration focus, and exacerbation of pre-existing depression or anxiety, all of which can affect quality of life in this population. These AEs were not included in the sponsor’s model, and their costs and quality-of-life impacts were not considered.
CADTH was unable to address this limitation due to a lack of data on the prevalence of AEs.
Treatment waning was not considered. The sponsor used HRs derived from the NMA and applied them to OS and PFS data from the ARASENS trial for the entirety of the model. This implicitly assumes that treatment effects observed in the NMA will be maintained throughout the model, up to 25 years, which is unreasonable given that the median follow-up of included studies ranged from 3.7 to 7.0 years. Without long-term data to substantiate this assumption, the survival benefits of darolutamide plus docetaxel and ADT are likely overestimated relative to comparators.
CADTH was unable to address this limitation due to a lack of long-term data. In scenario analyses, CADTH tested the impact of applying a full treatment waning effect (i.e., no further additional OS or PFS benefits) for darolutamide after 5 years.
Additional limitations were identified but were not considered to be key limitations. There were some small discrepancies between the costs for apalutamide and enzalutamide used by the sponsor and those listed in the Ontario Exceptional Access Program Formulary. However, the discrepancies were slight and did not affect the conclusions of the economic evaluation or the comparators on the efficiency frontier. Furthermore, dexamethasone is required to be given alongside docetaxel; the cost of dexamethasone was not included by the sponsor.
Additionally, the following key assumptions were made by the sponsor and have been appraised by CADTH (refer to Table 4).
CADTH Reanalyses of the Economic Evaluation
Base-Case Results
CADTH undertook reanalyses that addressed limitations within the model, as summarized in Table 5. The CADTH base case was derived by making changes in model parameters and assumptions, in consultation with clinical experts. All CADTH probabilistic reanalyses were based on 5,000 iterations.
CADTH undertook a stepped analysis, incorporating each changed proposed in Table 5 to the sponsor’s base case to highlight the impact of each change. A summary is presented in Table 6, while the full stepwise analysis is presented in Appendix 4 (Table 11). Disaggregated results of the CADTH base case are also presented in Appendix 4. In the CADTH base case, 72% of the incremental QALYs gained for darolutamide + docetaxel and ADT compared to abiraterone and ADT were obtained after the maximum follow-up in the ARASENS trial (approximately 5 years).
Scenario Analysis Results
CADTH undertook price-reduction analyses based on the sponsor’s and CADTH’s base case. The CADTH base case suggested that a price reduction of 58% would be required to achieve cost-effectiveness of darolutamide + docetaxel and ADT relative to abiraterone and ADT at a $50,000-per-QALY threshold (Table 7).
Table 4: Key Assumptions of the Submitted Economic Evaluation (Not Noted as Limitations to the Submission)
Sponsor’s key assumption | CADTH comment |
|---|---|
TTCROD is assumed to be equivalent to PFS. | Appropriate, according to the clinical expert consulted by CADTH, who stated that TTCROD is more comprehensive and clinically meaningful in this disease setting than PFS. In clinical practice, the decision of whether or not to start a specific treatment for mCRPC is based on a number of factors, including PSA, scanning, and clinical symptoms. A scenario analysis was performed in which PFS was defined by rPFS. |
Quality of life decreases with increasing lines of therapy. | Appropriate, according to clinical experts consulted by CADTH. |
A 1-time QALY decrement was applied at the beginning of the model horizon to account for all disutilities due to AEs. | Not appropriate, as this does not allow for discounting. However, this is unlikely to affect the results due to the relatively small disutilities applied. |
AE = adverse event; mCRPC = metastatic castration-resistant prostate cancer; PFS = progression-free survival; PSA = prostate-specific antigen; QALY = quality-adjusted life-year; rPFS = radiographic progression-free survival; TTCROD = time to castration resistance or death.
Table 5: CADTH Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Changes to derive the CADTH base case | ||
1. OS extrapolations | Log-logistic | Gamma |
2. Docetaxel costs | $0.54 / mg | $6.19 per mg ($990 per 160 mg) |
CADTH base case | — | Reanalysis 1 + 2 |
OS = overall survival.
Table 6: Summary of the CADTH Reanalysis Results
Drug | Total costs | Total QALYs | ICER vs. ADT ($ per QALY) | Sequential ICER ($ per QALY) |
|---|---|---|---|---|
Sponsor base case | ||||
ADT alone | 76,950 | 3.15 | Reference | Reference |
Docetaxel + ADT | 93,593 | 4.40 | 13,382 | 13,382 |
Abiraterone + ADT | 100,954 | 4.73 | 15,210 | 22,010 |
Darolutamide + docetaxel + ADT | 219,925 | 5.78 | 54,493 | 113,782 |
CADTH base case | ||||
ADT alone | 76,289 | 2.92 | Reference | Reference |
Abiraterone + ADT | 99,142 | 4.18 | 18,231 | 18,231 |
Darolutamide + docetaxel + ADT | 220,379 | 4.95 | 70,987 | 156,172 |
ADT = androgen deprivation therapy; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Note: Only products on the efficiency frontier are presented in this table. In the sponsor’s and CADTH’s base case, enzalutamide + ADT and apalutamide + ADT were dominated. In the CADTH base case only, docetaxel + ADT was also dominated. Full results are available in Appendix 4.
Table 7: CADTH Price Reduction Analyses
Analysis | ICERs for darolutamide + docetaxel + ADT vs. abiraterone + ADT | |
|---|---|---|
Price reduction | Sponsor base case | CADTH reanalysis |
No price reduction | 113,782 | 156,172 |
10% | 100,260 | 137,712 |
20% | 86,738 | 119,251 |
30% | 73,215 | 100,790 |
40% | 59,693 | 82,329 |
50% | 46,171 | 63,869 |
60% | 32,648 | 45,408 |
70% | 19,126 | 26,947 |
80% | 5,603 | 8,486 |
90% | Dominant | Dominant |
ADT = androgen deprivation therapy; ICER = incremental cost-effectiveness ratio.
CADTH undertook several scenario analyses to determine the impact of alternative assumptions on the cost-effectiveness of darolutamide plus docetaxel and ADT in the base case, which are outlined as follows:
Weibull extrapolations of the OS data from the ARASENS trial were used for darolutamide plus docetaxel and ADT, and docetaxel and ADT.
Proportions of subsequent therapy observed in the ARASENS trial were used directly without an adjustment.
In the sponsor-submitted NMA, PFS was defined by radiographic progression-free survival rather than time to CRPC.
In alignment with the results of the NMA, CADTH assumed no difference in OS between darolutamide plus docetaxel and ADT and abiraterone and ADT, apalutamide and ADT, and enzalutamide and ADT.
Full treatment waning was considered after 5 years.
The scenario analysis involving a Weibull extrapolation resulted in an ICER of $180,113 per QALY, indicating that results are sensitive to the choice of OS extrapolation. The scenario involving treatment waning at 5 years resulted in an ICER of $269,855 for darolutamide plus docetaxel and ADT compared to abiraterone and ADT, with an associated price reduction of 70% to ensure cost-effectiveness at a $50,000-per-QALY threshold. The scenario in which no OS benefit was assumed resulted in an ICER of $520,548 compared to abiraterone and ADT and a price reduction of 75% for darolutamide. Other scenarios tested did not meaningfully affect the results.
Issues for Consideration
Abiraterone plus docetaxel and ADT, while not a Health Canada–approved comparator, may become a relevant triplet therapy comparator soon, according to clinical experts. This comparator was not included in the sponsor-submitted NMA and, as such, the cost-effectiveness of darolutamide plus docetaxel and ADT compared to abiraterone plus docetaxel and ADT is unknown.
Overall Conclusions
The CADTH Clinical Review concluded that darolutamide plus docetaxel and ADT demonstrated clinically meaningful improvement of OS compared to docetaxel and ADT in patients with mCSPC in the ARASENS trial. Analyses of secondary outcomes supported the efficacy of darolutamide plus docetaxel and ADT in delaying progression to mCRPC, the need for subsequent antineoplastic therapy, worsening of pain, and symptomatic skeletal events compared to docetaxel and ADT. Regarding the sponsor-submitted ITC, the CADTH Clinical Review noted that, for OS, there was insufficient evidence to show a difference between darolutamide plus docetaxel and ADT and either abiraterone and ADT, apalutamide and ADT, or enzalutamide and ADT. For time to CRPC, darolutamide plus docetaxel and ADT was favoured over all treatments except enzalutamide and ADT. The reviewers noted the potential for biases related to heterogeneity in study design, prior treatment requirements, and follow-up duration across included studies. The CADTH Clinical Review noted that there remains increased potential that the underlying transitivity assumption of the NMA has been violated.
CADTH undertook reanalyses to the sponsor’s economic evaluation, which included using a gamma extrapolation for the OS results and updating costs for docetaxel.
The results of the CADTH reanalysis were in line with those submitted by the sponsor: darolutamide plus docetaxel and ADT is not a cost-effective treatment for mCSPC at a willingness-to-pay threshold of $50,000 per QALY. Based on the CADTH sequential analysis, darolutamide plus docetaxel and ADT is more costly and more effective than abiraterone and ADT (incremental costs $121,237; incremental QALYs: 0.77), resulting in an ICER of $156,172 per QALY. A price reduction of 58% would be required for darolutamide for the treatment regimen (i.e., darolutamide plus docetaxel and ADT) to be cost-effective compared to abiraterone and ADT at a $50,000-per-QALY threshold. The sponsor’s OS extrapolations were uncertain and resulted in overestimates of survival, according to clinical experts, who indicated that a Weibull extrapolation might also be appropriate. CADTH conducted a scenario analysis in which a Weibull extrapolation was used for OS; this resulted in an ICER of $180,113 per QALY compared to abiraterone and ADT.
Results of the CADTH base case and scenario analyses are uncertain given the results of the NMA, which found no statistical difference in OS for darolutamide plus docetaxel and ADT compared to abiraterone, apalutamide, or enzalutamide and ADT. The results were imprecise, and the 95% credible intervals were wide. This imprecision was evident in the sponsor’s base-case model, which predicted incremental QALYs ranging from –1.4 to 3.3 for the comparison of darolutamide plus docetaxel and ADT to abiraterone and ADT across different probabilistic iterations. The CADTH base case predicts an incremental life-years gain of 0.80 for darolutamide plus docetaxel and ADT compared to abiraterone and ADT, despite the lack of strong conclusions that can be drawn from the results of the NMA. Furthermore, in the CADTH base case, 72% of the incremental QALYs gained for darolutamide plus docetaxel and ADT compared to abiraterone and ADT were obtained after the maximum follow-up in the ARASENS trial. The results of the model are dependent on a survival benefit for darolutamide plus docetaxel and ADT being realized relative to comparators, which is uncertain given the aforementioned limitations. The scenario analysis in which no differences in OS were assumed between darolutamide plus docetaxel and ADT and comparators resulted in an ICER of $520,548 per QALY compared to abiraterone and ADT and a price reduction of 75% for darolutamide. This scenario highlights the impact of OS assumptions on the ICER and the resulting price reduction required to achieve cost-effectiveness at a $50,000-per-QALY threshold.
References
1.Smith M, Hussain M, Saad F, et al. Darolutamide and survival in metastatic, hormone-sensitive prostate cancer. N Engl J Med. 2022;386(12):1132-1142. PubMed
2.Nubeqa (darolutamide): 300mg, oral tablets [product monograph]. Mississauga (ON): Bayer Inc; 2022 May 12.
3.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Nubeqa (darolutamide), 300 mg tablets for the treatment of patients with metastatic castration-sensitive prostate cancer (mCSPC). Mississauga (ON): Bayer Inc; 2022 Jun 15.
4.PharmaStat. Ottawa (ON): IQVIA; 2022: https://www.iqvia.com/. Accessed 2022 Sep 25.
5.Darolutamide for metastatic castration-sensitive prostate cancer. Network-meta analysis for public payer submissions in Canada [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Nubeqa (darolutamide), 300 mg tablets for the treatment of patients with metastatic castration-sensitive prostate cancer (mCSPC). Mississauga (ON): Bayer Inc; 2022 Jun 15.
6.Armstrong A, Szmulewitz R, Petrylak D, al. e. Arches: a randomized, phase III study of androgen deprivation therapy with enzalutamide or placebo in men with metastatic hormone-sensitive prostate cancer. J Clin Oncol. 2019;37(32):2974-2986. PubMed
7.Saad F, Chilelli A, Hui B, al. e. Cost-effectiveness of enzalutamide versus apalutamide versus androgen deprivation therapy alone for the treatment of metastatic castration-sensitive prostate cancer in Canada. J Med Econ. 2022;25(1):583-590. PubMed
8.Clinical Study Report: ARASENS. A randomized, double–blind, placebo–controlled Phase III study of darolutamide (ODM–201) versus placebo in addition to standard androgen deprivation therapy and docetaxel in patients with metastatic hormone–sensitive prostate cance [internal sponsor's report]. Whippany (NJ): Bayer Inc; 2022 Feb 15.
9.Ng R, Hasan B, Mittmann N, al. e. Economic analysis of NCIC CTG JBR.10: a randomized trial of adjuvant vinorelbine plus cisplatin compared with observation in early stage non-small-cell lung cancer--a report of the Working Group on Economic Analysis, and the Lung Disease Site Group, National Cancer Institute of Canada Clinical Trials Group. J Clin Oncol. 2007;25(16):2256-2261. PubMed
10.Schedule of benefits for physician services under the Health Insurance Act: effective October 1, 2021. Toronto (ON): Ontario Ministry of Health; 2022: https://www.health.gov.on.ca/en/pro/programs/ohip/sob/physserv/sob_master.pdf. Accessed 2022 Aug 26.
11.Schedule of benefits for laboratory services: effective July 1, 2020. Toronto (ON): Ontario Ministry of Health; 2020: https://www.health.gov.on.ca/en/pro/programs/ohip/sob/lab/lab_mn2020.pdf. Accessed 2022 Aug 26.
12.de Oliveira C, Pataky R, Bremner K, al. e. Phase-specific and lifetime costs of cancer care in Ontario, Canada. BMC Cancer. 2016;16(1):809. PubMed
13.Table: 13-10-0114-01: Life expectancy and other elements of the life table, Canada, all provinces except Prince Edward Island. Ottawa (ON): Statistics Canada; 2022: https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310011401. Accessed 2022 Aug 26.
14.Beca J, Majeed H, Chan K, Hotte S, Loblaw A, Hoch J. Cost-effectiveness of docetaxel in high-volume hormone-sensitive metastatic prostate cancer. Can Urol Assoc J. 2019;13(12):396-403. PubMed
15.DeltaPA. Ottawa (ON): IQVIA; 2022: https://www.iqvia.com/. Accessed 2022 Sep 6.
16.Docetaxel: 10 mg/ mL as 20 mg/2 mL, 80 mg/8mL, 160 mg/16mL for injection [product monograph]. Boucherville (QC): Sandoz Canada Inc; 2020 Nov 17: https://pdf.hres.ca/dpd_pm/00058887.PDF. Accessed 2022 Sep 6.
17.Apo-abiraterone (abiraterone acetate): 250 mg and 500 mg, film-coated tablets [product monograph]. Toronto (ON): Apotex Inc; 2021 Apr 1: https://pdf.hres.ca/dpd_pm/00060444.PDF. Accessed 2022 Sep 6.
18.Xtandi (enzalutamide): 40 mg capsules [product monograph]. Markham (ON): Astellas Pharma Canada, Inc; 2022 Jan 24: https://pdf.hres.ca/dpd_pm/00064474.PDF. Accessed 2022 Sep 9.
19.Erleada (apalutamide): 60 mg oral tablets [product monograph]. Toronto (ON): Janssen Inc; 2022 May 31: https://pdf.hres.ca/dpd_pm/00066114.PDF. Accessed 2022 Sep 9.
20.Firmagon (degarelix): 120 mg, 80 mg per vial for injection [product monograph]. North York (ON): Ferring Phamaceuticals; 2016 Mar 18: https://pdf.hres.ca/dpd_pm/00034229.PDF. Accessed 2022 Sep 6.
21.Zoladex (goserelin depot): 3.6 mg [product monograph]. Mississauga (ON): AstraZeneca Canada Inc; 2017 Dec 21: https://pdf.hres.ca/dpd_pm/00042728.PDF.
22.Lupron (leuprolide acetate): 5 mg/mL sterile solution subcutaneous injection; Lupron Depot (leuprolide acetate for depot suspension): 3.75 mg/syringe (1-Month slow release), 7.5 mg/syringe (1-Month slow release), 11.25 mg/syringe (3-Month slow release), 22.5 mg/syringe (3-Month slow release), 30 mg/syringe (4-Month slow release), pre-filled dual-chamber syringe containing sterile lyophilized microspheres intramuscular injection [product monograph]. St-Laurent (QC): AbbVie Corporation; 2021 Nov 18: https://pdf.hres.ca/dpd_pm/00063626.PDF. Accessed 2022 Sep 6.
23.Trelstar (triptorelin): 3.75 mg per vial (1 month sustained-release formulation), 11.25 mg per vial (3 month sustained-release formulation), 22.5 mg per vial (6 month sustained-release formulation), intramuscular injection [product monograph]. Montreal (QC): Knight Therapeutics Inc; 2022 Sep 8: https://pdf.hres.ca/dpd_pm/00067340.PDF. Accessed 2022 Sep 6.
24.Nova Scotia Drug Formulary. Halifax (NS): Nova Scotia Department of Health; 2022. Accessed 2022 Sep 25.
25.Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Nubeqa (darolutamide), 300 mg tablets for the treatment of patients with metastatic castration-sensitive prostate cancer (mCSPC). Mississauga (ON): Bayer Inc; 2022 Jun 15.
26.Statistics Canada. Population projections for Canada, provinces and territories. 2015; https://www150.statcan.gc.ca/n1/pub/91-520-x/2010001/t147-eng.pdf. Accessed 2022 Sep 25.
27.Robles C, A M. Female population. Ottawa (ON): Statistics Canada; 2011: https://www150.statcan.gc.ca/n1/pub/89-503-x/2010001/article/11475-eng.htm. Accessed 2022 Sep 25.
28.Canadian Cancer Society. Prostate cancer statistics. 2022; https://cancer.ca/en/cancer-information/cancer-types/prostate/statistics. Accessed 2022 Sep 25.
29.Canadian Cancer Statistics Advisory Committee. Canadian cancer statistics. Toronto (ON): Canadian Cancer Society; 2021: https://cdn.cancer.ca/-/media/files/research/cancer-statistics/2021-statistics/2021-pdf-en-final.pdf. Accessed 2022 Sep 25.
30.Francini E, Gray KP, Xie W, et al. Time of metastatic disease presentation and volume of disease are prognostic for metastatic hormone sensitive prostate cancer (mHSPC). Prostate. 2018;78(12):889-895. PubMed
Appendix 1: Cost Comparison Table
Note that this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical experts. Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and, as such, the table may not represent the actual costs to public drug plans.
Table 8: CADTH Cost Comparison Table for Darolutamide Plus Docetaxel and ADT for the Treatment of Metastatic Castration-Sensitive Prostate Cancer (mCSPC)
Treatment | Strength / concentration | Form | Price ($) | Recommended dosage | Daily cost ($) | 28-day cost ($) | |
|---|---|---|---|---|---|---|---|
Darolutamide (Nubeqa) | 300mg | Tab | 28.3440 | 600 mg twice daily2 | 113.38 | 3,175 | |
Docetaxel (Generic) | 20 mg/mL 80 mg/4.0 mL 160 mg/8.0 mL | 1 mL Vial 4 mL Vial 8 mL Vial | 249.0000a 497.0000a 990.0000a | 75 mg/m2 as a 1-hour IV fusion every 3 weeks for 6 cyclesb,16 | 47.14 | 1,320 | |
Dexamethasone (Generic) | 0.5 mg 4 mg | Tab | 0.1564 0.6112 | 8 mg 3 times prior to docetaxel infusion16 | 0.17 | 5 | |
ADT | — | 9.10 to 15.10 | 255 to 423 | ||||
DDOC + ADT | 169.79 to 175.79 | 4,755 to 4,923 | |||||
Antiandrogen | |||||||
Abiraterone Acetate (Zytiga) | 250 mg 500 mg | Tab | 7.6563c 15.3125c | 1,000 mg daily17 | 30.63 | 858 | |
Prednisone (Generic) | 5 mg 50 mg | Tab | 0.0220 0.1735 | 5 mg daily17 | 0.02 | 1 | |
ADT | — | 9.10 to 15.10 | 255 to 423 | ||||
AAP + ADT | 39.75 to 45.75 | 1,114 to 1,282 | |||||
Abiraterone Acetate (Zytiga) | 250 mg 500 mg | Tab | 7.6563c 15.3125c | 1,000 mg daily17 | 30.63 | 858 | |
Docetaxel (Generic) | 20 mg/mL 80 mg/4.0 mL 160 mg/8.0 mL | 1 mL Vial 4 mL Vial 8 mL Vial | 249.0000a 497.0000a 990.0000a | 75 mg/m2 as a 1-hour IV fusion every 3 weeks for 6 cyclesb,16 | 47.14 | 1,320 | |
Dexamethasone (Generic) | 0.5 mg 4 mg | Tab | 0.1564 0.6112 | 8 mg 3 times prior to docetaxel infusion16 | 0.17 | 5 | |
Prednisone (Generic) | 5 mg 50 mg | Tab | 0.0220 0.1735 | 5 mg daily17 | 0.02 | 1 | |
ADT | — | 9.10 to 15.10 | 255 to 423 | ||||
AAP + DOC + ADT | 87.06 to 93.06 | 2,439 to 2, 607 | |||||
Enzalutamide (Xtandi) | 40 mg | Cap | 29.1954 | 160 mg daily18 | 116.78 | 3,270 | |
ADT | — | 9.10 to 15.10 | 255 to 423 | ||||
ENZ + ADT | 125.88 to 131.88 | 3,525 to 3,693 | |||||
Androgen synthesis inhibitor | |||||||
Apalutamide (Erleada) | 60 mg | Tab | 30.1250 | 240 mg daily19 | 120.50 | 3,374 | |
ADT | — | 9.10 to 15.10 | 255 to 423 | ||||
APA + ADT | 129.60 to 135.60 | 3,629 to 3,797 | |||||
Antineoplastic drug | |||||||
Docetaxel (Generic) | 20 mg/mL 80 mg/4.0 mL 160 mg/8.0 mL | 1 mL Vial 4 mL Vial 8 mL Vial | 249.0000a 497.0000a 990.0000a | 75 mg/m2 as a 1-hour IV fusion every 3 weeks for 6 cyclesb,16 | 47.14 | 1,320 | |
Dexamethasone (Generic) | 0.5 mg 4 mg | Tab | 0.1564 0.6112 | 8 mg 3 times prior to docetaxel infusion16 | 0.17 | 5 | |
ADT | — | 9.10 to 15.10 | 255 to 423 | ||||
DOC + ADT | 56.41 to 62.41 | 1,580 to 1,748 | |||||
ADT | |||||||
Degarelix (Firmagon) | 80 mg | Inj | 274.1760 | Initial dose: 240mg given as 2 SC injections of 120mg Maintenance: monthly administration of 80mg as 1 SC injection20 | Year 1: 10.30 Subsequent: 9.79 | Year 1: 742 Subsequent: 274 | |
120 mg | Inj | 370.9440 | |||||
Goserelin (Zoladex) | 3.6 mg 10.8 mg | Inj | 422.6778 1,204.7322 | 3.6mg SC injection every 28 days 10.8mg SC injection every 13 weeks21 | 15.10 13.24 | 423 371 | |
Leuprorelin / Leuprolide (Lupron) | 3.75 mg 7.5 mg 11.25 mg 22.5 mg 30 mg | Inj | 370.6000 387.9700 1,104.3000 1,071.0000 1,428.0000 | 7.5 mg monthly; 22.5 mg every 3 months; 30 mg every 4 months22 | 11.74 to 13.86 | 329 to 388 | |
Triptorelin (Trelstar) | 3.75 mg 11.25 mg 22.5 mg | Inj | 346.3100 1,038.9700 1,659.9000 | 3.75 mg monthly; 11.25 every 3 months; 22.5 mg every 6 months23 | 9.10 to 12.37 | 255 to 346 | |
AAP + ADT = abiraterone acetate plus prednisone in combination with androgen deprivation therapy; ADT = androgen deprivation therapy; APA + ADT = apalutamide in combination with androgen deprivation therapy; AAP + DOC + ADT = abiraterone acetate plus prednisone plus docetaxel in combination with androgen deprivation therapy; Cap = capsule; DDOC + ADT = darolutamide plus docetaxel in combination with androgen deprivation therapy; DOC + ADT = docetaxel in combination with androgen deprivation therapy; ENZ + ADT = enzalutamide in combination with androgen deprivation therapy; Inj = injection; Nas = nasal; PK = pack; SC = subcutaneous; Tab = tablet.
Note: All prices are from the Ontario Drug Benefit Formulary or Ontario Exceptional Access Program (accessed July 2022) unless otherwise indicated, and do not include dispensing fees.
aWholesale price reported by IQVIA DeltaPA, July 2022.15
bDocetaxel costs based on an average body surface area assumed to be equal to 1.8m2 from sponsor submission.3
cPrice reported by Nova Scotia Drug Formulary, accessed September 2022.24
Appendix 2: Submission Quality
Note that this appendix has not been copy-edited.
Description | Yes/No | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing. | Yes | No comment. |
Model has been adequately programmed and has sufficient face validity. | Yes | No comment. |
Model structure is adequate for decision problem. | Yes | No comment. |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis). | Yes | No comment. |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem. | Yes | No comment. |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details). | Yes | No comment. |
Appendix 3: Additional Information on the Submitted Economic Evaluation
Note that this appendix has not been copy-edited.
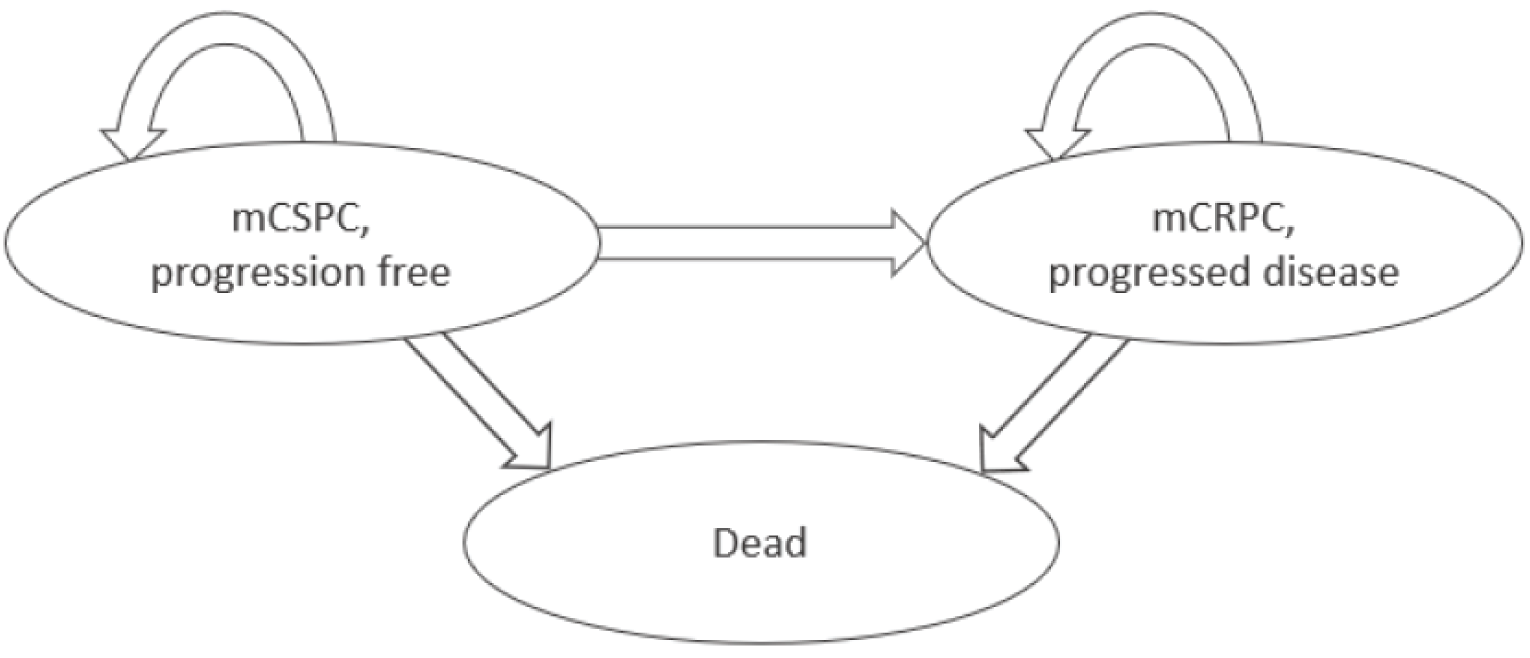
mCRPC = metastatic castration-resistant prostate cancer; mCSPC = metastatic castration-sensitive prostate cancer.
Source: Sponsor’s pharmacoeconomic submission.3
Detailed Results of the Sponsor’s Base Case
Table 10: Disaggregated Results of the Sponsor’s Base Case
Parameter | Darolutamide + docetaxel | Docetaxel | Abiraterone | Apalutamide | Enzalutamide | ADT alone |
|---|---|---|---|---|---|---|
Discounted LYs | ||||||
Total | 7.07 | 5.80 | 6.00 | 6.01 | 5.95 | 4.20 |
Progression-free LYs | 5.82 | 2.31 | 3.93 | 4.05 | 4.79 | 1.37 |
Postprogression LYs | 1.25 | 3.49 | 2.07 | 1.96 | 1.16 | 2.83 |
Discounted QALYs | ||||||
Total | 5.78 | 4.40 | 4.73 | 4.76 | 4.85 | 3.15 |
Progression-free QALYs | 4.92 | 1.96 | 3.33 | 3.42 | 4.05 | 1.16 |
Postprogression QALYs | 0.86 | 2.44 | 1.40 | 1.34 | 0.80 | 2.00 |
Disutilities due to AEs | –0.0015 | –0.0014 | –0.0009 | –0.0004 | –0.0001 | –0.0003 |
Discounted costs ($) | ||||||
Total | 219,925 | 93,593 | 100,954 | 174,980 | 193,997 | 76,950 |
Primary drug acquisition | 141,138 | 409 | 29,480 | 109,397 | 129,787 | 0 |
Administration of primary drug | 1,746 | 1,694 | 0 | 0 | 0 | 0 |
ADT background and administration | 35,747 | 29,351 | 30,330 | 30,406 | 30,097 | 21,260 |
Subsequent therapy | 18,251 | 41,777 | 22,644 | 19,235 | 18,888 | 42,483 |
Monitoring – preprogression | 11,852 | 5,063 | 6,661 | 6,873 | 8,133 | 2,315 |
Monitoring – postprogression | 2,375 | 6,611 | 3,914 | 3,713 | 2,195 | 5,364 |
AE costs | 4,386 | 4,104 | 3,343 | 776 | 308 | 724 |
Terminal care | 4,431 | 4,584 | 4,583 | 4,580 | 4,589 | 4,804 |
Pairwise ICER of darolutamide + docetaxel vs. comparator ($/QALY) | NA | 91,542 | 113,782 | 44,127 | 27,934 | 54,493 |
ADT = androgen deprivation therapy; AE = adverse event; ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year.
Appendix 4: Additional Details on the CADTH Reanalyses and Sensitivity Analyses of the Economic Evaluation
Note that this appendix has not been copy-edited.
Detailed Results of CADTH Base Case
Table 11: Summary of the Stepped Analysis of the CADTH Reanalysis Results
Stepped analysis | Drug | Total costs ($) | Total LYs | Total QALYs | Sequential ICER ($/QALY) |
|---|---|---|---|---|---|
Sponsor’s base case (deterministic) | ADT alone | 76,759 | 4.18 | 3.14 | Reference |
Docetaxel + ADT | 93,566 | 5.80 | 4.39 | 13,428 | |
Abiraterone + ADT | 100,652 | 5.96 | 4.71 | 22,381 | |
Apalutamide + ADT | 174,132 | 5.96 | 4.73 | Extendedly dominated | |
Enzalutamide + ADT | 191,989 | 5.89 | 4.83 | Extendedly dominated | |
Darolutamide + docetaxel + ADT | 219,381 | 7.07 | 5.79 | 109,861 | |
CADTH reanalysis 1 (deterministic) – OS extrapolations | ADT alone | 74,556 | 3.86 | 2.92 | Reference |
Docetaxel + ADT | 86,708 | 4.78 | 3.71 | 15,504 | |
Abiraterone + ADT | 95,672 | 5.17 | 4.15 | 20,035 | |
Apalutamide + ADT | 169,158 | 5.17 | 4.16 | Extendedly dominated | |
Enzalutamide + ADT | 187,469 | 5.12 | 4.21 | Extendedly dominated | |
Darolutamide + docetaxel + ADT | 212,837 | 6.00 | 4.95 | 146,941 | |
CADTH reanalysis 2 (deterministic) – docetaxel costs | ADT alone | 78,564 | 4.18 | 3.14 | Reference |
Docetaxel + ADT | 99,638 | 5.80 | 4.39 | Extendedly dominated | |
Abiraterone + ADT | 103,761 | 5.96 | 4.71 | 16,067 | |
Apalutamide + ADT | 176,628 | 5.96 | 4.73 | Extendedly dominated | |
Enzalutamide + ADT | 194,433 | 5.89 | 4.83 | Extendedly dominated | |
Darolutamide + docetaxel + ADT | 226,172 | 7.07 | 5.79 | 113,268 | |
CADTH base case – reanalysis 1 + 2 (deterministic) | ADT alone | 76,361 | 3.86 | 2.92 | Reference |
Docetaxel + ADT | 92,780 | 4.78 | 3.71 | Extendedly dominated | |
Abiraterone + ADT | 98,822 | 5.17 | 4.15 | 18,243 | |
Apalutamide + ADT | 171,693 | 5.17 | 4.16 | Extendedly dominated | |
Enzalutamide + ADT | 189,984 | 5.12 | 4.21 | Extendedly dominated | |
Darolutamide + docetaxel + ADT | 219,736 | 6.00 | 4.95 | 151,643 | |
CADTH base case – reanalysis 1 + 2 (probabilistic) | ADT alone | 76,289 | 3.86 | 2.92 | Reference |
Docetaxel + ADT | 92,666 | 4.79 | 3.71 | Extendedly dominated | |
Abiraterone + ADT | 99,142 | 5.20 | 4.18 | 18,231 | |
Apalutamide + ADT | 172,662 | 5.21 | 4.19 | Extendedly dominated | |
Enzalutamide + ADT | 192,038 | 5.17 | 4.25 | Extendedly dominated | |
Darolutamide + docetaxel + ADT | 220,379 | 6.00 | 4.95 | 156,172 |
ADT = androgen deprivation therapy; ICER = incremental cost-effectiveness ratio; LY = life-year; OS = overall survival; QALY = quality-adjusted life-year.
Table 12: Disaggregated Summary of CADTH’s Economic Evaluation Results
Parameter | Darolutamide + docetaxel | Docetaxel | Abiraterone | Apalutamide | Enzalutamide | ADT alone |
|---|---|---|---|---|---|---|
Discounted LYs | ||||||
Total | 6.00 | 4.79 | 5.20 | 5.21 | 5.17 | 3.86 |
Progression-free LYs | 5.14 | 2.31 | 3.75 | 3.82 | 4.32 | 1.37 |
Postprogression LYs | 0.86 | 2.48 | 1.46 | 1.39 | 0.85 | 2.49 |
Discounted QALYs | ||||||
Total | 4.95 | 3.71 | 4.18 | 4.19 | 4.25 | 2.92 |
Progression-free QALYs | 4.36 | 1.95 | 3.18 | 3.24 | 3.66 | 1.16 |
Postprogression QALYs | 0.59 | 1.75 | 1.00 | 0.96 | 0.58 | 1.76 |
Disutilities due to AEs | –0.0015 | –0.0014 | –0.0009 | –0.0004 | –0.0001 | –0.0003 |
Discounted costs ($) | ||||||
Total | 220,379 | 92,666 | 99,142 | 172,662 | 192,038 | 76,289 |
Primary drug acquisition | 145,700 | 4,714 | 29,487 | 109,587 | 130,072 | 0 |
Administration of primary drug | 1,761 | 1,708 | 0 | 0 | 0 | 0 |
ADT background and administration | 30,318 | 24,212 | 26,307 | 26,356 | 26,124 | 19,514 |
Subsequent therapy | 21,542 | 43,403 | 26,161 | 22,091 | 21,852 | 44,179 |
Monitoring – preprogression | 10,388 | 5,073 | 6,351 | 6,483 | 7,344 | 2,315 |
Monitoring – postprogression | 1,626 | 4,687 | 2,758 | 2,638 | 1,604 | 4,715 |
AE costs | 4,389 | 4,102 | 3,348 | 777 | 309 | 724 |
Terminal care | 4,655 | 4,765 | 4,730 | 4,729 | 4,733 | 4,841 |
Pairwise ICER of darolutamide + docetaxel vs. comparator ($/QALY) | NA | 102,577 | 156,172 | 63,044 | 40,235 | 70,987 |
ADT = androgen deprivation therapy; AE = adverse event; ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year.
Scenario Analyses
Table 13: Summary of Scenario Analyses Conducted on CADTH Base Case
Stepped analysis | Drug | Total costs ($) | Total LYs | Total QALYs | Sequential ICER ($/QALY) |
|---|---|---|---|---|---|
CADTH scenario analysis 1 – Weibull OS extrapolations | ADT alone | 75,827 | 3.76 | 2.86 | Reference |
Docetaxel + ADT | 91,066 | 4.54 | 3.54 | Extendedly dominated | |
Abiraterone + ADT | 97,632 | 4.96 | 3.98 | 19,474 | |
Apalutamide + ADT | 170,403 | 4.96 | 4.00 | Extendedly dominated | |
Enzalutamide + ADT | 189,794 | 4.91 | 4.04 | Extendedly dominated | |
Darolutamide + docetaxel + ADT | 217,426 | 5.64 | 4.65 | 180,113 | |
CADTH scenario analysis 2 – no adjustment to subsequent treatment patterns | ADT alone | 76,419 | 3.86 | 2.93 | Reference |
Docetaxel + ADT | 92,799 | 4.79 | 3.71 | Extendedly dominated | |
Abiraterone + ADT | 102,349 | 5.20 | 4.17 | 20,836 | |
Apalutamide + ADT | 180,013 | 5.21 | 4.19 | Extendedly dominated | |
Enzalutamide + ADT | 199,148 | 5.15 | 4.22 | Extendedly dominated | |
Darolutamide + docetaxel + ADT | 227,921 | 6.01 | 4.96 | 158,908 | |
CADTH scenario analysis 3 – progression based on rPFS | ADT alone | 76,037 | 3.86 | 2.96 | Reference |
Docetaxel + ADT | 92,760 | 4.79 | 3.71 | Extendedly dominated | |
Abiraterone + ADT | 98,692 | 5.20 | 4.16 | 18,883 | |
Apalutamide + ADT | 159,924 | 5.21 | 4.10 | Extendedly dominated | |
Enzalutamide + ADT | 177,955 | 5.17 | 4.17 | Extendedly dominated | |
Darolutamide + docetaxel + ADT | 219,895 | 6.00 | 4.94 | 156,076 | |
CADTH scenario analysis 4 – no OS differencea | ADT alone | 76,361 | 3.86 | 2.92 | Reference |
Docetaxel + ADT | 92,780 | 4.78 | 3.71 | Extendedly dominated | |
Abiraterone + ADT | 104,331 | 6.00 | 4.73 | 15,480 | |
Apalutamide + ADT | 177,241 | 6.00 | 4.75 | Extendedly dominated | |
Enzalutamide + ADT | 195,788 | 6.00 | 4.87 | Extendedly dominated | |
Darolutamide + docetaxel + ADT | 219,736 | 6.00 | 4.95 | 520,548b | |
CADTH scenario analysis 5 – treatment waning after 5 years | ADT alone | 76,517 | 3.86 | 2.93 | Reference |
Docetaxel + ADT | 93,037 | 4.79 | 3.71 | Extendedly dominated | |
Abiraterone + ADT | 100,984 | 5.53 | 4.52 | 15,350 | |
Apalutamide + ADT | 174,486 | 5.53 | 4.54 | Extendedly dominated | |
Enzalutamide + ADT | 194,042 | 5.50 | 4.56 | Extendedly dominated | |
Darolutamide + docetaxel + ADT | 220,378 | 6.01 | 4.96 | 269,855c |
ADT = androgen deprivation therapy; ICER = incremental cost-effectiveness ratio; LY = life-year; OS = overall survival; QALY = quality-adjusted life-year; rPFS = radiographic progression-free survival.
aDue to the nature of the scenario analysis (i.e., equivalent survival) this scenario was performed deterministically.
bA price reduction of 75% would be required in this scenario for darolutamide to be cost-effective at a $50,000 per QALY threshold.
cA price reduction of 70% would be required in this scenario for darolutamide to be cost-effective at a $50,000 per QALY threshold.
Appendix 5: Submitted Budget Impact Analysis and CADTH Appraisal
Note that this appendix has not been copy-edited.
Table 14: Summary of Key Take-Aways
Key take-aways of the budget impact analysis |
|---|
|
ADT = androgen deprivation therapy.
Summary of Sponsor’s Budget Impact Analysis
The submitted budget impact analysis (BIA) assessed the expected budgetary impact resulting from reimbursing darolutamide plus docetaxel and ADT for the treatment of patients with metastatic castration-sensitive prostate cancer (mCSPC). The BIA was conducted from the perspective of the Canadian public drug plans over a 3-year time horizon and used an epidemiologic approach. The sponsor’s pan-Canadian estimates reflect the aggregated results from provincial budgets (excluding Quebec), as well as the Non-Insured Health Benefits Program. The analysis was performed using jurisdiction-specific values by summing up individual provincial results to obtain consolidated results.25 The key inputs to the BIA are documented in Table 15.
The sponsor’s submission considered a reference scenario, in which patients received other ARAT therapies in combination with ADTs, including: abiraterone plus prednisone, apalutamide, docetaxel, enzalutamide, and ADT monotherapy.25 The submission additionally considered a new drug scenario in which darolutamide was reimbursed.
The following key assumptions were made by the sponsor:
The sponsor assumed a body surface area (BSA) of 1.8m2 to determine the appropriate dosing to be administered for docetaxel, as the therapy is BSA dependent.
The sponsor assumed that of all mCSPC patients, 57.5% have de novo disease and 42.5% have metachronous disease.
The sponsor assumed the reimbursement of darolutamide will have no impact of the market share of patients treated with ADT monotherapy.
Table 15: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as year 1 / year 2 / year 3 if appropriate) |
|---|---|
Target population | |
Base population | 30.6 million26 |
Proportion males | 49.6%27 |
Prostate cancer incidence | |
Proportion with mCSPC | 8.6%29 |
Proportion of mCSPC that is de novo | |
Proportion of de novo patients that initiate treatment | 92.2%a |
Proportion of patients that are chemotherapy-eligible | 80.7%a |
Proportion of patients publicly funded by provincial drug plans | 86%a |
Number of patients eligible for drug under review, Year 1 / Year 2 / Year 3 | 1,739 / 1,756 / 1,774 |
Market uptake (3 years) | |
Uptake (reference scenario) Abiraterone + prednisone + ADT Apalutamide + ADT Docetaxel + ADT Enzalutamide + ADT ADT monotherapy | 10.1% / 9.8% / 9.4% 38.0% / 38.2% / 38.5% 8.0% / 9.0% / 10.0% 32.9% / 33.0% / 33.1% 11.0% / 10.0% / 9.0% |
Uptake (new drug scenario) Darolutamide + docetaxel + ADT Abiraterone + prednisone + ADT Apalutamide + ADT Docetaxel + ADT Enzalutamide + ADT ADT monotherapy | 11.0% / 19.0% / 22.0% 9.7% / 8.8% / 8.4% 35.2% / 32.2% / 31.9% 2.0% / 1.0% / 0.0% 31.0% / 29.0% / 28.7% 11.0% / 10.0% / 9.0% |
Cost of treatment (per patient) | |
Cost of treatment over a 28-day cycle | |
ARATs and chemotherapy Darolutamide Abiraterone Apalutamide Docetaxel Enzalutamide Prednisone | $3,715 $858 $3,715 $97 $3,270 $1 |
ADTs Degarelix (initial) Degarelix (subsequent dosing) Goserelin Leuprorelin Triptorelin | $742 $274 $423 $367 $346 |
ADT = androgen deprivation therapy; ARAT = Androgen receptor-axis-targeted therapies; mCSPC = metastatic castration-sensitive prostate cancer.
aSponsor assumption.
Summary of the Sponsor’s BIA Results
The sponsor’s base case reported that the reimbursement of darolutamide for the treatment of patients with mCSPC would lead to an incremental budget impact of $4,518,028 in Year 1, $10,801,853 in Year 2, and $19,229,469 in Year 3. The total 3-year incremental cost was $34,549,349. Based on the model assumptions, the introduction of darolutamide would not expand the overall combination treated population and the new treatment would gradually replace the docetaxel plus ADT regimen.25
CADTH Appraisal of the Sponsor’s BIA
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
ADT costs for combination therapies not properly incorporated: The sponsor’s submitted BIA did not distinguish between ADT costs as a monotherapy and ADT costs as a background therapy for individuals receiving darolutamide plus docetaxel, abiraterone plus prednisone, apalutamide, docetaxel, and enzalutamide. The sponsor did not account for the market share of each treatment when determining ADT costs as a background therapy. Additionally, to determine the combined cost of ADT in the BIA, the sponsor used the ToT of ADT alone, overlooking that when used in combination with other therapies, ADT will be used for the duration of the combination therapy. Therefore, the yearly total costs for each treatment regimen were underestimated and the ADT total costs were overestimated.
To address this limitation, CADTH corrected the sponsor’s base case by including ADT as a background therapy cost to the yearly costs of darolutamide plus docetaxel, abiraterone plus prednisone, apalutamide, docetaxel monotherapy, and enzalutamide.
Underestimated drug cost for regimen under review: The sponsor used a cost per mg of docetaxel of $0.54 based on a published economic evaluation.14 However, the original pricing source could not be located and the cost of $0.54 per mg could not be verified. As this value is substantially different than pricing data obtained from the IQVIA DeltaPA database,15 CADTH updated the cost of docetaxel based on the IQVIA database. As docetaxel is used in the docetaxel plus ADT and darolutamide plus docetaxel and ADT treatment regimens, this alternative source underestimated their total costs.
To address this limitation, CADTH updated the cost of docetaxel according to the unit costs summarized in the CADTH cost table (Table 8).
Underestimated market uptake: The sponsor’s submitted BIA indicated that triplet therapy of darolutamide plus ADT and docetaxel would result in a Year 3 market share of 22%. The clinical experts consulted by CADTH did not agree with this market share assumption by the sponsor, and instead indicated the sponsor likely underestimated darolutamide plus ADT and docetaxel uptake. The experts felt the sponsor’s estimate that this therapy would capture 11% and 19% of the market share in Year 1 and Year 2 was reasonable, but they indicated that triplet therapy’s market share would likely continue to grow to 30% by Year 3.
To address this limitation, CADTH undertook a reanalysis with a Year 3 market share of 30% for darolutamide plus ADT and docetaxel.
Additional limitations were identified but were not considered to be key limitations. According to both the docetaxel product monograph and clinical experts consulted by CADTH, a preregimen of dexamethasone is required prior to docetaxel infusion and was not included in the sponsor’s submission. Due to the minimal ($5) annual costs of dexamethasone, the inclusion of the costs in the BIA did not significantly impact the results.
The results of the CADTH stepwise reanalysis are presented in summary format in Table 17 and a more detailed breakdown is presented in Table 18. Applying these changes resulted in a 3-year budget impact of $39,714,970.
CADTH also conducted a scenario analysis to explore the potential impact should the price reduction, based on the cost-effectiveness analysis of darolutamide, be achieved. In this scenario analysis the budget impact led to cost savings. This was driven by the fact that more than half the total uptake of darolutamide is from the highest priced comparators (i.e., apalutamide and enzalutamide); and with darolutamide’s price reduction, its cost falls below the treatment costs of those comparators (using their publicly available list price).
CADTH Reanalyses of the BIA
Table 16: CADTH Revisions to the Submitted Budget Impact Analysis
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
1. Treatment cost | 28-day cost of docetaxel: $96.5214 | 28-day cost of docetaxel: $1,320.0015 |
2. Comparator costs | 28-day cost of apalutamide: $3,174.53 28-day cost of leuprorelin: $366.52 | 28-day cost of apalutamide: $3,374.00 28-day cost of leuprorelin: $387.97 |
Corrected sponsor’s base case | 1+2 | |
Changes to derive the CADTH base case | ||
1. ADT in combination therapies | ADT monotherapy and background therapy costs combined. | ADT background therapy costs included in all regimens. |
2. Market share | New Drug Scenario: DDOC + ADT: 11.0% / 19.0% / 22.0% AAP + ADT: 9.7% / 8.8% / 8.4% APA + ADT: 35.2% / 32.2% / 31.9% DOC + ADT: 2.0% / 1.0% / 0.0% ENZ + ADT: 31.0% / 29.0% / 28.7% ADT alone: 11.0% / 10.0% / 9.0% | New Drug Scenario: DDOC + ADT: 11.0% / 19.0% / 30.0% AAP + ADT: 9.7% / 8.8% / 6.4% APA + ADT: 35.2% / 32.2% / 29.9% DOC + ADT: 2.0% / 1.0% / 0.0% ENZ + ADT: 31.0% / 29.0% / 26.7% ADT alone: 11.0% / 10.0% / 7.0% |
CADTH base case | Reanalysis 1 + 2 | |
AAP + DOC + ADT = abiraterone acetate plus prednisone plus docetaxel in combination with androgen deprivation therapy; APA + ADT = apalutamide in combination with androgen deprivation therapy; DDOC + ADT = darolutamide plus docetaxel in combination with androgen deprivation therapy; DOC + ADT = docetaxel in combination with androgen deprivation therapy; ENZ + ADT = enzalutamide in combination with androgen deprivation therapy.
Table 17: Summary of the CADTH Reanalyses of the Budget Impact Analysis
Stepped analysis | Three-year total |
|---|---|
Submitted base case | $34,549,349 |
Corrected base case | $35,962,005 |
CADTH reanalysis 1 | $37,246,820 |
CADTH reanalysis 2 | $39,146,826 |
CADTH base case | $39,714,970 |
Table 18: Detailed Breakdown of the CADTH Reanalyses of the Budget Impact Analysis
Stepped analysis | Scenario | Year 0 (current situation) | Year 1 | Year 2 | Year 3 | Three-year total |
|---|---|---|---|---|---|---|
Submitted base case | Reference | $61,725,785 | $116,973,488 | $163,003,104 | $167,668,783 | $447,645,375 |
New drug | $61,725,785 | $121,491,516 | $173,804,957 | $186,898,251 | $482,194,725 | |
Budget impact | $0 | $4,518,028 | $10,801,853 | $19,229,469 | $34,549,349 | |
Corrected base case | Reference | $64,325,070 | $121,436,873 | $168,822,602 | $173,660,414 | $463,919,889 |
New drug | $64,325,070 | $126,290,612 | $180,243,776 | $193,347,505 | $499,881,894 | |
Budget impact | $0 | $4,853,740 | $11,421,174 | $19,687,092 | $35,962,005 | |
CADTH base case | Reference | $63,915,278 | $126,667,146 | $179,776,633 | $184,962,058 | $491,405,837 |
New drug | $63,915,278 | $131,875,649 | $192,198,902 | $207,046,255 | $531,120,807 | |
Budget impact | $0 | $5,208,502 | $12,422,270 | $22,084,198 | $39,714,970 | |
CADTH scenario analysis: 58% price reduction | Reference | $63,915,278 | $126,667,146 | $179,776,633 | $184,962,058 | $491,405,837 |
New drug | $63,915,278 | $127,265,564 | $179,558,288 | $181,625,317 | $488,449,169 | |
Budget impact | $0 | $598,417 | –$218,344 | –$3,336,741 | –$2,956,668 |
Stakeholder Input
Patient Input
Canadian Cancer Survivor Network
About the Canadian Cancer Survivor Network
The Canadian Cancer Survivor Network (CCSN) is a national network of patients, families, survivors, friends, community partners, funders, and sponsors who have come together to take action to promote the very best standard of care, whether it be it be early diagnosis, timely treatment and follow-up care, support for cancer patients, or issues related to survivorship or quality of end-of-life care. https://survivornet.ca/
Information Gathering
The Canadian Cancer Survivor Network utilized SurveyMonkey to create and collect all data for the survey on Darolutamide. We then utilized our newsletter as well as our social media platforms to disseminate the survey to collect responses. The survey was open from April 27, 2022, to May 30, 2022, to obtain responses. All respondents to the survey are from Canada. Out of the 26 respondents, 24 are patients and two are caregivers. Out of the 26 respondents, 24 are male and two are female. When the survey data was analyzed, it was clear that seven of the twenty-six patients (7 of 26) had experience with Darolutamide and seventeen of twenty-six patients (17 of 26) do not have experience with Darolutamide.
Disease Experience
When asked how their cancer was diagnosed, the 26 patients answered as follows:
Contrast-enhanced computed tomography (CT): 4
Magnetic resonance imaging (MRI): 4
Reporting of symptoms and/or discomforts: 1
Rectal exam: 15
Blood work: 19
Biopsy: 25
A combination of any of the above: 3
Does not apply: 0
Other: 5 (1 Biopsy was used twice, 3 Bone Scan, 1 Direct family members diagnosed with the disease)
When asked what stage of prostate cancer they had been diagnosed with, the following responses were received from five of the patients who have had experience with Darolutamide:
Middle Stage (2 or 3): 3
Late Stage (4) or metastatic: 4
Current treatments that were identified include:
Surgery: 3
Radiation therapy: 4
Chemotherapy (i.e. docetaxel, cabazitaxel): 1
Clinical Trial: 1
Hormone Therapy (ADT): 5
Antiandrogens (i.e. abiraterone, enzaltamide, apalutamide, darolutamide): 4
Other: 1 (1 Aberaterone and Dexamethazone)
Five patients who have experience with Darolutamide are also using, or have used, the following to treat their disease:
Docetaxel + androgen deprivation therapy (ADT): 2
Abiraterone acetate with prednisone (AAP) + ADT: 1
Enzalutamide + ADT: 1
ADT monotherapy: 1
Three patients were taking:
Lupron and Darolutamide
Darolutamide, 1 Lupron
Leuprolide inject every 3 months
When asked how many treatments they had been on prior to Darolutamide, three patients had been on one treatment and two patients had been on three or more treatments.
Experiences With Currently Available Treatments
Patients who did not have any experience with Darolutamide were at these stages:
High PSA test monitoring: 1
Late Stage (metastatic): 6
Three patients are post prostatectomy, one is four years, another is 20 years, and the last did not provide a date. One patient is NED for 11 years. One patient has slowly rising PSA. Two patients are prostate cancer survivors, one for 23 years and the other did not provide a date.
With the use of currently available treatments, patients reported that the following symptoms affected their quality of life and day-to-day living:
Weight gain: 4
Fatigue: 9
Loss of appetite: 1
Diarrhea: 1
Constipation: 1
Shortness of breath: 2
Dizziness: 2
Depression: 2
Anxiety: 1
Loss of muscle mass: 4
Loss of bone mass: 2
Hot flashes: 5
Urinary incontinence: 4
Erectile Dysfunction (ED): 12
Other: 1 (1 “Due to radiation therapy my bladder had to be removed in 2016 so I have an ileostomy.”)
When asked if they have had issues accessing any current therapy, 13 of the patients responded as follows:
Limited availability in my community: 2
Travel costs associated with accessing therapy/treatment: 1
I haven’t had any issues accessing therapy: 9
Two were not on therapy at this stage
Other: 1 (1 “Enzalutamide is delivered to me monthly free of charge. Also take Lupron.”)
When asked if any needs in their current therapy are not yet being met, seven patients said no, five were not on therapy, and one patient responded that, “Fatigue is a problem.”
When asked if they would like to share anything, patients shared the following about their cancer journey:
“The cure with radiation therapy has prolonged problems with damage to my colon and my bladder which was removed. It has caused a great deal of pain, bleeding, and depression. The positive is I would otherwise have died.”
“I had an open radical prostatectomy 23 years ago with external beam radiation twenty years later, followed by ADT for one year.”
“Impressed and grateful how enzalutamide is controlling my PSA (after 8 years) to near negligible levels.”
“I have run out of treatments for my castration resistant prostate cancer and the feeling of just waiting for the disease to progress is depressing.”
“I wish I had been offered SBRT by my radiation doctor when I requested it and his aggressive instance on standard 35 sessions of prostrate bed radiation.”
Improved Outcomes
When asked about the following issues that they would hope to see a new drug address to manage their disease:
Maintain quality of life: 11
Delay onset of symptoms: 5
Delay need for chemotherapy: 7
Access to a new option for treatment: 4
Reduce side effects from current medications or treatments: 4
Ease of use: 5
One patient hoped to, “Remove the need to lower my testosterone, improve sexual drive.”
When asked what side effects or symptoms they would expect on a new drug:
“If the new drug suppresses testosterone, then I would expect continuing feminimation of my body.”
None hopefully! 4
Fatigue: 2
Patients were then asked to rate adverse effects as either being acceptable or not acceptable:
Fatigue: Acceptable 7, Not Acceptable 5
Bone Fracture: Acceptable 0, Not Acceptable 12
Rash: Acceptable 5, Not Acceptable 7
Falls: Acceptable 0, Not Acceptable 12
Weight loss: Acceptable 7, Not Acceptable 3
Develop breasts or have tenderness: Acceptable 5, Not Acceptable 7
Feelings of depression (worsened after taking medication): Acceptable 1, Not Acceptable 11
Feelings of anxiety (worsened after taking medication): Acceptable 1, Not Acceptable 11
Hypertension: Acceptable 1, Not Acceptable 10
Vasodilatation and flushing: Acceptable 1, Not Acceptable 11
Cardiac Disorder: Acceptable 0, Not Acceptable 12
Diabetes and hyperglycemia: Acceptable 2, Not Acceptable 10
Cerebral ischemia: Acceptable 0, Not Acceptable 11
Seizure: Acceptable 0, Not Acceptable 12
Patients were asked to describe how much of an improvement would be needed from the new drug to make it better than the current treatment:
“Elimination of ED.”
“I do not require drugs except for antibiotics for monthly kidney infection.”
“60% improvement.”
“Less fatigue.”
“I am only on Goserelin to suppress testosterone production. I need more hope!”
“Anything to keep PSA down.”
Experience With Drug Under Review
When asked if they had any issues accessing their therapy, patients responded as follows:
Supplies or issues with administration: 1
I haven’t had any issues accessing therapy: 4
One patient stated, “Negative doctors who simply tell me that I only have 1-2 years of life left and that none of the drugs will work on me.”
Patients were asked if there were any current needs not being met yet, the respondents answered as follows:
“Support from others in my same situation and doctors who are not condescending and downright jerks.”
“Follow up with Bayer and/or other Nubeqa experts on side effects of med. Efficacy of Nubeqa to control PSA or is it other drugs? Potential reduction in drug costs for the med.”)
Patients were asked which centre they were prescribed Darolutamide, five patients responded as follows:
“Cross Cancer Institute, also the drug name that was used was Bicalutamide.”
“My urologist.”
“Southern Alberta Institute of Urology as part of the Darol study.”
“UHN Princes Margaret hospital.” (2)
When asked how long they have been taking Darolutamide, the patients responded as follows:
0-1 month: 1
6-12 months: 1
12-18 months: 1
18 months or longer: 2
The patients were then asked if they had stopped taking Darolutamide at any time, one patient responded with yes and four patients responded with no.
For the patient who did stop taking Darolutamide, they stated it was because, “Bicalutamide gave me a significant heart attack 2 days after I started taking it.”
Patients reported the following side effects when taking Darolutamide:
Weight gain: 4
Fatigue: 5
Abdominal cramping: 1
Shortness of breath: 2
Dizziness: 1
Depression: 2
Anxiety: 1
Loss of muscle mass: 5
Loss of bone mass: 1
Hot flashes: 5
Urinary incontinence: 1
Infertility: 2
Erectile dysfunction (ED): 5
One patient shared that they had a loss of energy and motivation and another patient stated that it had changed their life.
Patients reported the following adverse effects caused by taking Darolutamide:
Fatigue: 3
Rash: 1
Falls: 1
Develop breasts or have tenderness: 2
Feelings of depression (worsened after taking medication): 1
Feelings of anxiety (worsened after taking medication): 2
Vasodilatation and flushing: 1
Cardiac Disorder: 1
None: 1
Patients reported the following:
“Heart Attack from Bicalutamide in 2 days. Enzalutamide took 6 months to almost give me a second heart attack. Enzaluatmide also destroyed the muscles in my feet.”
“Cardiac bypass surgery 2021 not caused by Darolutamide.”
“Mild anemia but not sure if caused by Darolutimide or Lupron...has been present since started on first ADT sept 2020.”
When asked about which adverse effects of Darolutamide are acceptable or not acceptable:
Fatigue: Acceptable 4, Not Acceptable 1
Bone Fracture: Acceptable 0, Not Acceptable 4
Rash: Acceptable 2, Not Acceptable 3
Falls: Acceptable 0, Not Acceptable 4
Weight loss: Acceptable 4, Not Acceptable 0
Develop breasts or have tenderness: Acceptable 2, Not Acceptable 2
Feelings of depression (worsened after taking medication): Acceptable 1, Not Acceptable 3
Feelings of anxiety (worsened after taking medication): Acceptable 1, Not Acceptable 3
Hypertension: Acceptable 2, Not Acceptable 2
Vasodilatation and flushing: Acceptable 1, Not Acceptable 3
Cardiac Disorder: Acceptable 1, Not Acceptable 3
Diabetes and hyperglycemia: Acceptable 1, Not Acceptable 3
Cerebral ischemia: Acceptable 1, Not Acceptable 3
Seizure: Acceptable 1, Not Acceptable 3
Other: Acceptable 1, Not Acceptable 0
Patients were asked to rate if the following issues were better with Darolutamide with a yes or no answer:
Better able to control symptoms: Yes 1, No 4
Reduction in side effects from current medications or treatments: Yes 3, No 2
Ease of use: Yes 4, No 1
Disease progression: Yes 4, No 1
Other: Yes 1, No 0
Patients were asked to describe, in their own words, the positive and negative effects of Darolutamide:
“Bicalutamide destroys muscle function including the heart.”
“Addition of darolutamide controls my PSA with manageable side effects.”
“While on ADT PSA doubling time shortened to less than 6 months. Within 2 months of starting darolutamide, PSA dropped to undetectable where it has remained for approximately 18 months. Minimal change in ADT side effects.”
“Positive is that if I am indeed castrate resistant. This med keeps me in control mode for time being 0.33 latest PSA side affects may or may not be compounded by addition of darolutimide to my lupron--hard to distinguish which one is doing what I guess cost of drug is a negative but I am fortunate to have it paid for by private insurance company although it has impacted my premiums despite daily exercise I have gained weight in stomach and groin area along with mild gain in breasts”
“KEEPING ME ALIVE!”
Patients were then asked if they believe that the benefits of darolutamide outweigh the side effects, these were their responses:
“Yes. I have experienced very few side effects and none that had a significant impact on quality of life.”
“Absolutely. No new side effects other than increased fatigue and some recurrent vertigo.”
“If the darolutimide is definitively and primarily responsible for the disease control I have at the moment it outweighs the major side affects of weight gain, hot flashes and anemia I currently have.”
One patient stated that they do not believe that the benefits of Darolutamide outweigh the side effects and one patient stated that they do believe the benefits outweigh the side effects.
The patients were also asked about what challenges, if any, they have faced in dealing with the side effects of darolutamide:
“Heart problems and muscle destruction.”
“No challenges that are specific to darolutamide.”
“Minimal increase in ADT side effects which are manageable.”
“Anemia produces shortness of breath and fatigue making exercise a little more challenging. My immune system seems to be impacted with lower WBC and lymphocyte numbers..higher risk of infections?”
Patients were asked about their expectations for their long-term health and well-being as a result of taking darolutamide:
“I do not expect to take Darolutamide (Bicalutamide) again.”
“My PSA is currently at a low level but gradually rising. I know current therapy may not be effective for long. But I have had a good life for almost 20 years after diagnosis.”
“I am expecting progression free status will be increased from the average of 18 months to closer to 48 or even 60 months.”
“Once again if darolutimide is successful in controlling my disease and prolonging my life I am willing to tolerate the current identifiable side affects. I am worried though about long term impact on other major organs and overall health that have not as yet become evident.”
When asked if there was anything else that they would like to share about their cancer journey, they responded:
“I have many complaints about my cancer journey, but it would take several pages to list them all. Basically, it sucks to always being told that you are dying.”
“With a Gleason 8 (4+4) I have been very fortunate. My active participation in a local prostate cancer support group has been helpful and rewarding.”
“Navigation of the medical system and pharmaceutical systems continues to be difficult and costly because of interprovincial variations in health care. Patients deserve to be able to access treatments no matter the province or territory they reside in.”
“I am still a young individual and reasonably fit despite this 3-year battle that was negatively impacted by an unsuccessful HIFU procedure in April 2019 which I am not sure if it resulted in my having advanced prostate cancer. I would love being able to answer that question since my genetic testing reveals no gene mutation for this cancer.”
From a caregiver perspective, the following were issues that they encounter as a caregiver for someone with prostate cancer:
Fatigue
Emotional Drain
Anxiety/Worrying
Caregivers were also asked how caring for someone with prostate cancer has affected their daily routine or lifestyle:
“It is tiresome and sometimes frustrating as they get impatient and are moody and tired all the time.”
“Worry a lot.”
The caregivers were also asked what the most challenging adverse effects related to their loved one and their current therapy or treatment are:
“Fatigue mostly. But this leads to inability to bathe, shave by themselves, lots of sleep, depression.”
“Fatigue, lack of will to live.”
Companion Diagnostic Test
Not applicable.
Anything Else?
CCSN is well aware of the limitations of this submission given the small number of respondents and with only seven patients on Darolutamide.
Conflict of Interest Declaration — Canadian Cancer Survivor Network
To maintain the objectivity and credibility of the CADTH reimbursement review process, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This Patient Group Conflict of Interest Declaration is required for participation. Declarations made do not negate or preclude the use of the patient group input. CADTH may contact your group with further questions, as needed.
Did you receive help from outside your patient group to complete this submission?
No.
Did you receive help from outside your patient group to collect or analyze data used in this submission?
No.
List any companies or organizations that have provided your group with financial payment over the past 2 years AND who may have direct or indirect interest in the drug under review.
Table 1: Financial Disclosures for the Canadian Cancer Survivor Network
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Jansen-2021 | — | — | X | — |
Jansen-2022 | — | — | X | — |
Amgen-2022 | — | X | — | — |
Bayer-2022 | — | X | — | — |
Canadian Cancer Society
About the Canadian Cancer Society
Website Link: https://cancer.ca/en
Our purpose: To unite and inspire all Canadians to take control of cancer.
Our mission: In trusted partnership with donors and volunteers, we improve the lives of all those affected by cancer through world-class research, transformative advocacy and compassionate support.
We set ourselves apart from other cancer charities by taking a comprehensive approach against cancer. We are also the only national charity that supports all Canadians living with all cancers across the country.
We shared our survey and interview opportunity with patients with mCSPC and their caregivers through our Cancer Connection forums, patient panels, through various support groups and prostate cancer treating clinicians who agreed to share it with their patients.
Information Gathering
The Canadian Cancer Society gathered perspectives through survey and interview responses from patients with metastatic castration-sensitive prostate cancer (mCSPC) and their caregivers. Thirty-nine survey responses were gathered from patients with mCSPC and two were gathered from caregivers through the survey. Of the 41 patients/caregivers who engaged with us, one had direct experience with darolutamide and completed both the survey and an interview. The data was gathered within the time frame of June 13, 2022 – June 30, 2022.
To maintain anonymity, the individual that completed the interview will be referred to as Patient A for the purposes of this report.
Demographic Information
Demographic information collected from the survey is displayed below. Please note that not all survey options that were offered are shown within the Figures as they are limited to the options respondents actually selected. Percentages represented in Figures are rounded up to the nearest whole number.
What province or territory do you reside in?
Perspectives from nine of the 13 provinces and territories were captured. The majority of responders resided in Ontario (34%) and British Columbia (29%). The other 37% resided in Alberta, Manitoba, New Brunswick, Newfoundland and Labrador, Nova Scotia, Prince Edward Island and Quebec. Patient A resided in Ontario.
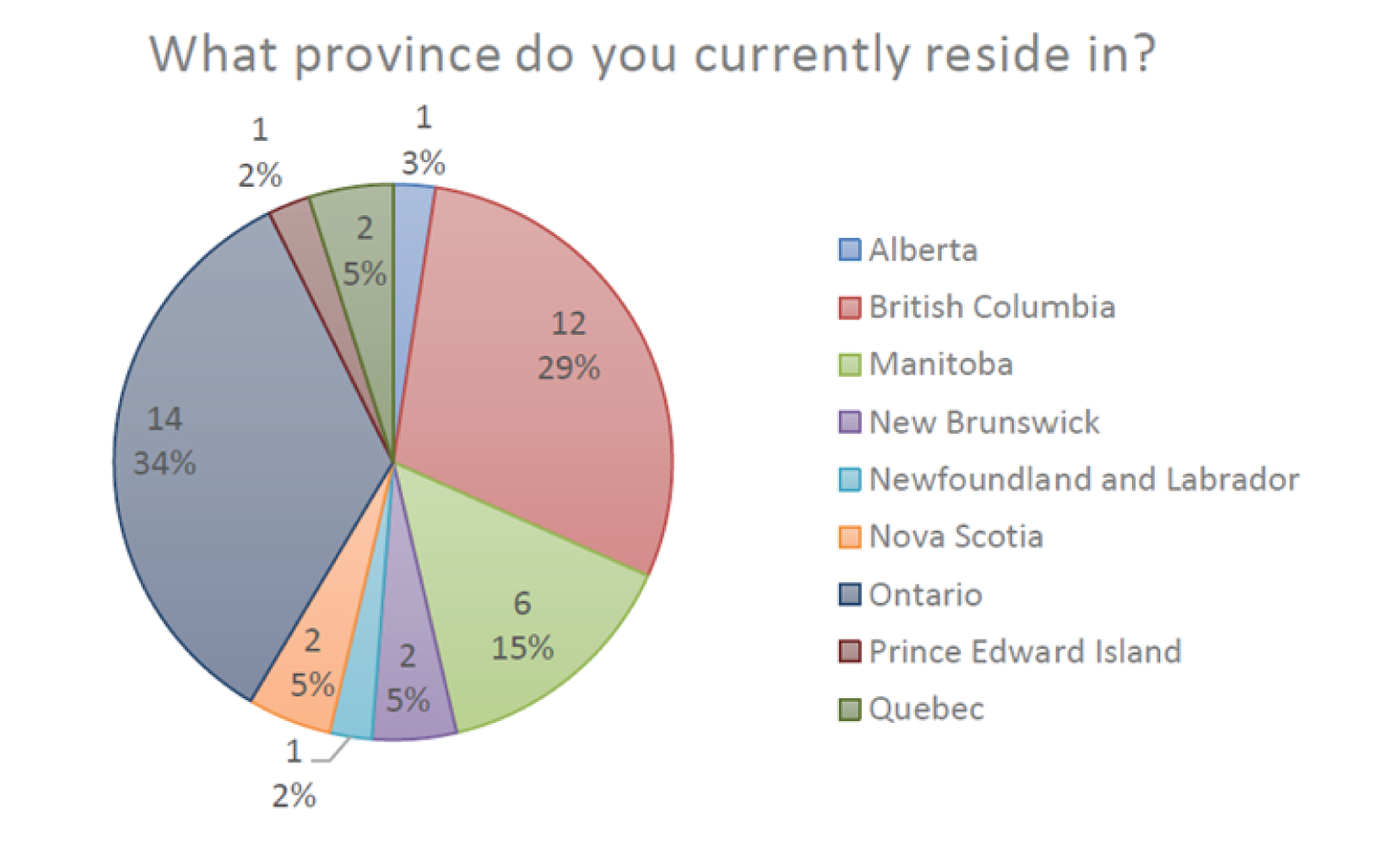
How old are you?
The majority of responders were between the ages of 70 – 79 years of age (49%), 37% are between 60 – 69, and those between the ages of 50-59 and 80 years and older maintained 7% of the distribution each. Patient A was between 60 – 69 years of age.

What gender do you identify with?
For inclusivity, responders had six options available to identify their gender including man, women, non-binary or third gender, two-spirit, prefer not to say, and prefer to self-describe with an open field. All responders identify as a man, including Patient A, with one of the caregivers indicating the patient they care for identifies as a women.
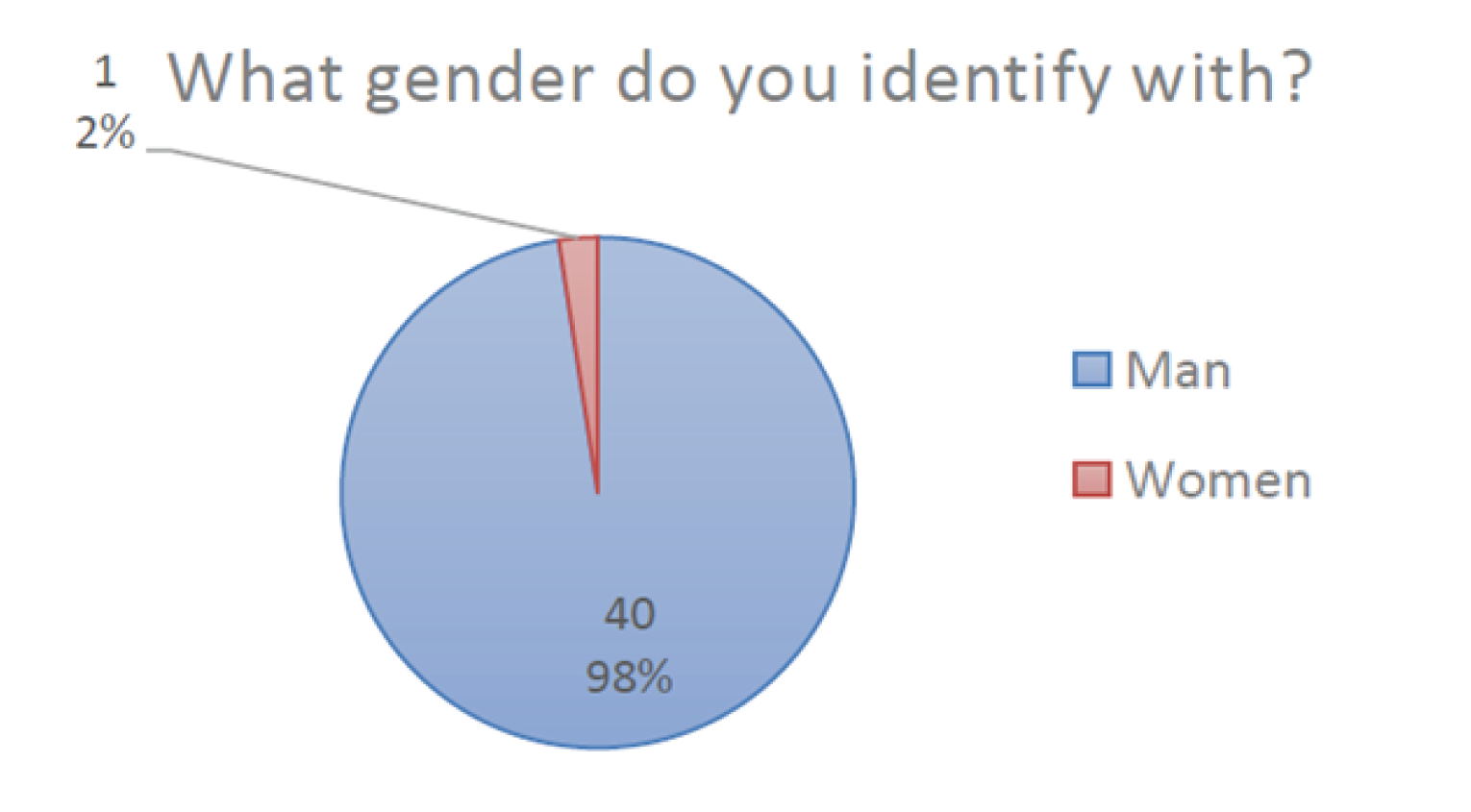
What is your racial or ethnic background?
For inclusivity, responders had 16 options including a self identify option and could select all racial or ethnic backgrounds that applied to them. Thirty-nine responders (95%) identified as white, one identified as Japanese (2.5%), and one (2.5%) self identifies as Sami (indigenous) and Irish. Patient A identified as white.
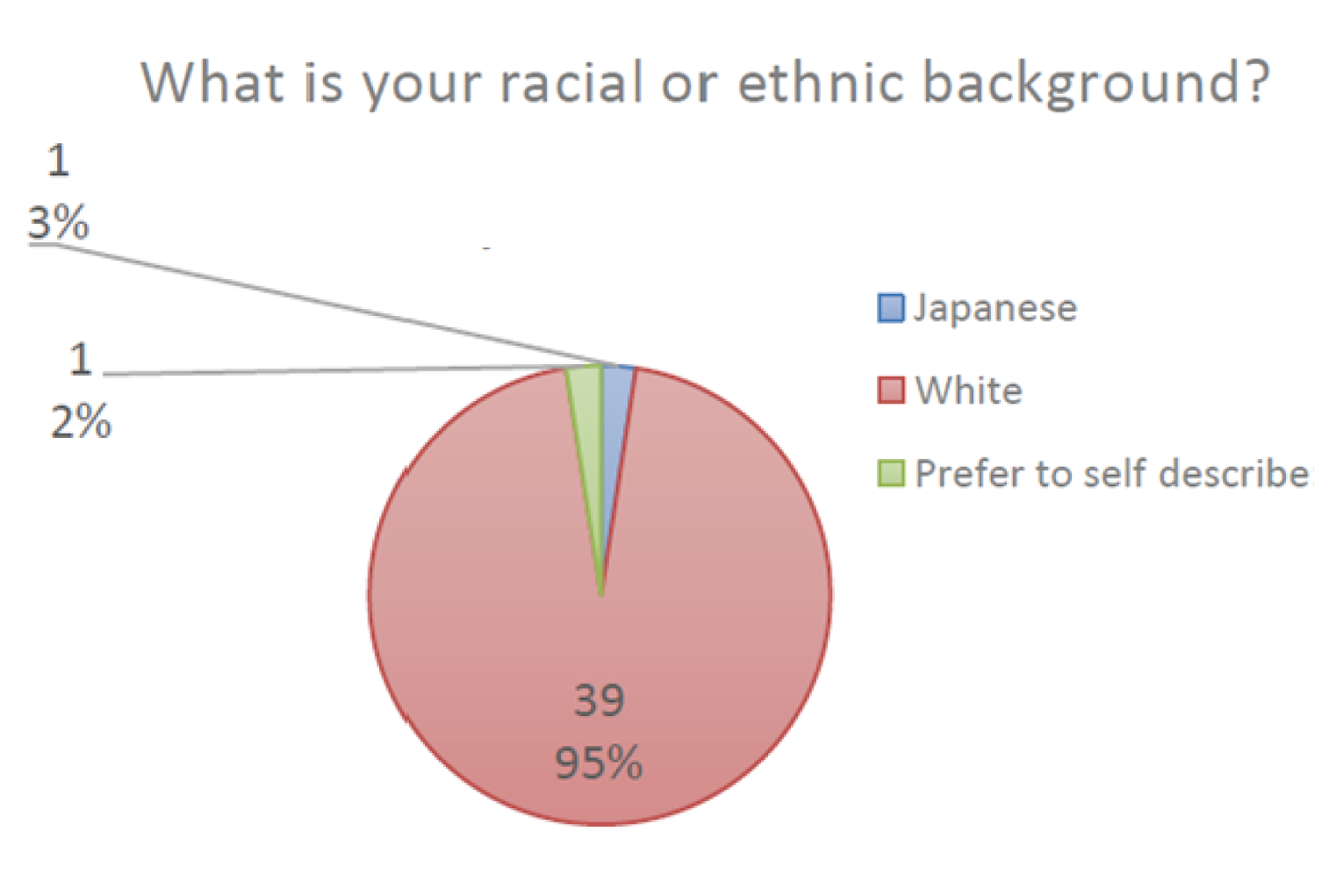
What is your household income before taxes?
For the 75% of respondents who answered this question, the majority indicated their household income before taxes was $120,000 or more (27%). The next highest majority indicated their household income is $20,000 – $39,999 per year (15%). The remainder of respondents were spread relatively evenly across the remaining options. Patient A indicated his annual household income before taxes is over $120,000 per year.
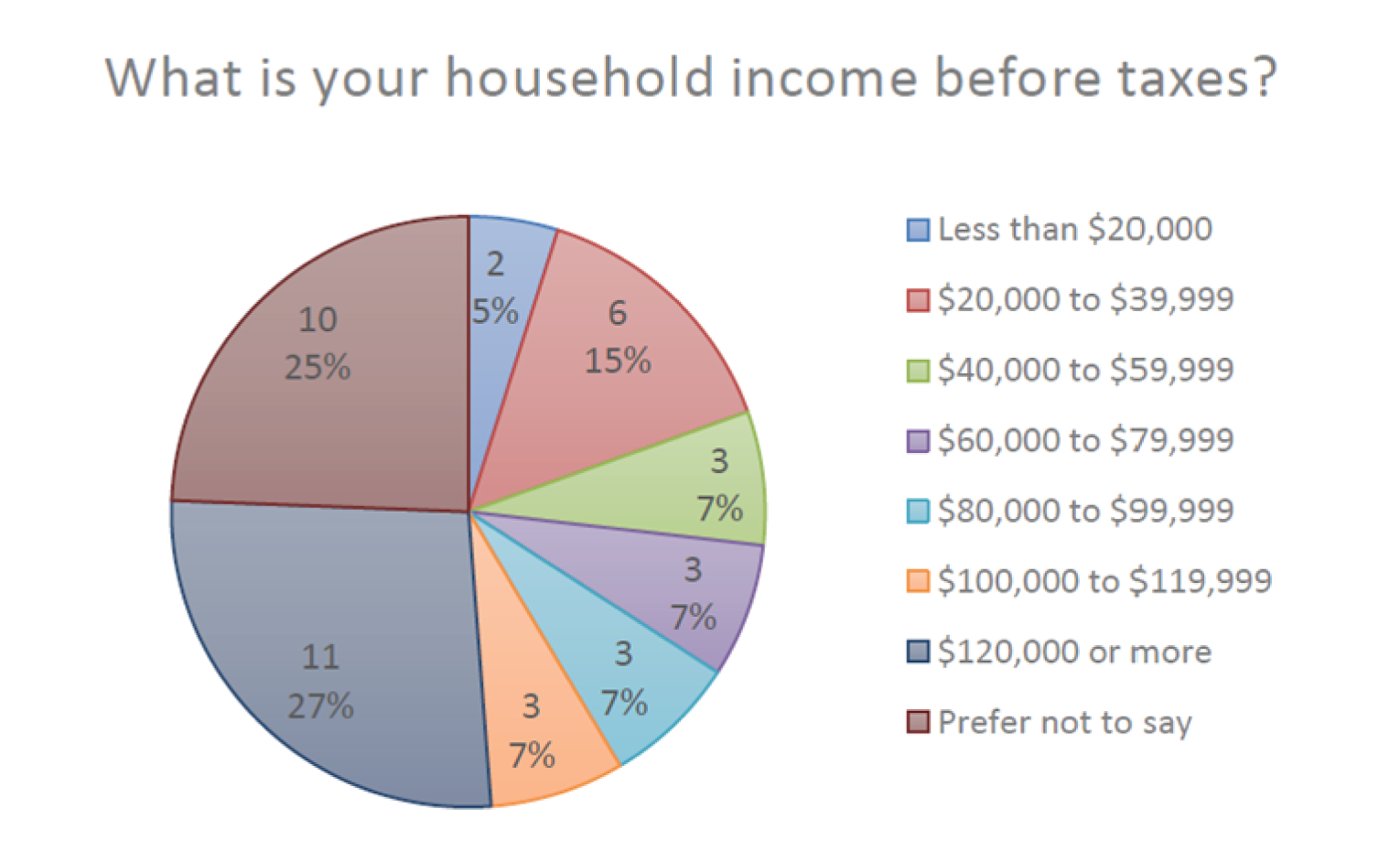
Disease Experience
How much of an impact do symptoms associated with metastatic castration-sensitive prostate cancer have on your day-to-day activities and quality of life? (Select all that apply).
The ability to engage in sexual activity scored highest as a quality of life impacting activity where patients experienced a negative impact, with 31 (76%) responses falling into the moderate to significant impact range. The second greatest impact was seen in the ability to work with 20 (49%) responses landing in the moderate to significant impact range. The ability to exercise was the next most impacted activity with 18 responses falling in the moderate to significant impact range (44%). Other impacted activities of note include the ability to travel, fulfill family obligations and maintain mental health with 32% of responses falling into the moderate to significant impact range each. For further detail, please refer to Table 2 and Figure 6.
There were 148 responses overall which fell in the moderate to significant impact range across the 41 participants. Thirty-six percent of the total responses landed in the moderate to significant impact range, indicating there were significant impacts to patients quality of life due to symptoms associated with their cancer and associated treatments.
One patient stated, “My life has been destroyed by the ADT drug degarelix and I have applied for MAID because of this and this alone.” This underscores the significant impact ADT can have on patients' quality of life.
Patient A
Patient A indicated he experienced a small impact in his ability to work, travel, conduct household chores, fulfill family obligations, spend time with family and friends, concentrate, fulfill practical needs and maintain mental health. He experiences a moderate impact in his ability to exercise and a significant impact in his ability to engage in sexual activity.
Specify any other areas of your life that have been impacted and how significant the impact is:
“Sleep because of the pain.”
“It led to a change in my career.”
“Changements physiques ie diminution génitale et gain de poids et de grosseur au niveau des seins et du ventre.” – Translation: “Physical changes i.e. genital size decrease, weight gain and lumpiness in the breast and belly.”
“The biggest impact is the hot flashes that wake me up 3-4 times a night”.
“My life has been destroyed by the ADT drug degarelix and i have applied for MAID because of this and this alone.”
“Chronic constipation, fat deposits in my body.”
“Ability to get a full night's sleep - moderate impact.”
“Caused my neuropathy to have increased pain in my hands and feet.”
“I can't tell whether it is the cancer which has had impact on my life or my age or medication.”
“Small impact to sleep quantity and quality.”
“Severe sexual impact, much lower energy level, lack stamina.”
“Broken hip—maybe due to cancer in pelvic area, neuropathy in my feet – significant impact. Medications– sleepiness, weight gain, mobility.”
“Socializing has been significantly effected also.”
“Family impact and [my] worry for [my] wife is huge.”
Table 2: Impact on Quality of Life
Task | Small impact | Moderate impact | Significant impact | I’m not sure | Not applicable or No impact |
|---|---|---|---|---|---|
Ability to work | 13 (32%) | 14 (34%) | 6 (15%) | 1 (2%) | 7 (17%) |
Ability to travel | 17 (41%) | 7 (17%) | 6 (15%) | 2 (5%) | 9 (22%) |
Ability to exercise | 17 (41%) | 9 (22%) | 9 (22%) | 1 (2%) | 5 (12%) |
Ability to conduct household chores | 19 (46%) | 8 (20%) | 4 (10%) | 0 (0%) | 10 (24%) |
Ability to fulfill family obligations | 16 (39%) | 9 (22%) | 4 (10%) | 0 (0%) | 12 (29%) |
Ability to spend time with family and friends | 20 (49%) | 9 (22%) | 1 (2%) | 0 (0%) | 11 (27%) |
Ability to concentrate | 18 (44%) | 7 (17%) | 5 (12%) | 2 (5%) | 9 (22%) |
Ability to fulfill practical needs (dressing, bathing, preparing meals) | 20 (49%) | 6 (15%) | 0 (0%) | 0 (0%) | 15 (36%) |
Ability to maintain positive mental health | 22 (54%) | 10 (24%) | 3 (7%) | 0 (0%) | 6 (15%) |
Ability to engage in sexual activity | 2 (5%) | 1 (2%) | 30 (73%) | 1 (2%) | 7 (17%) |
Note: Percentages have been rounded
Figure 6: Activities Most Impacted by mCSPC
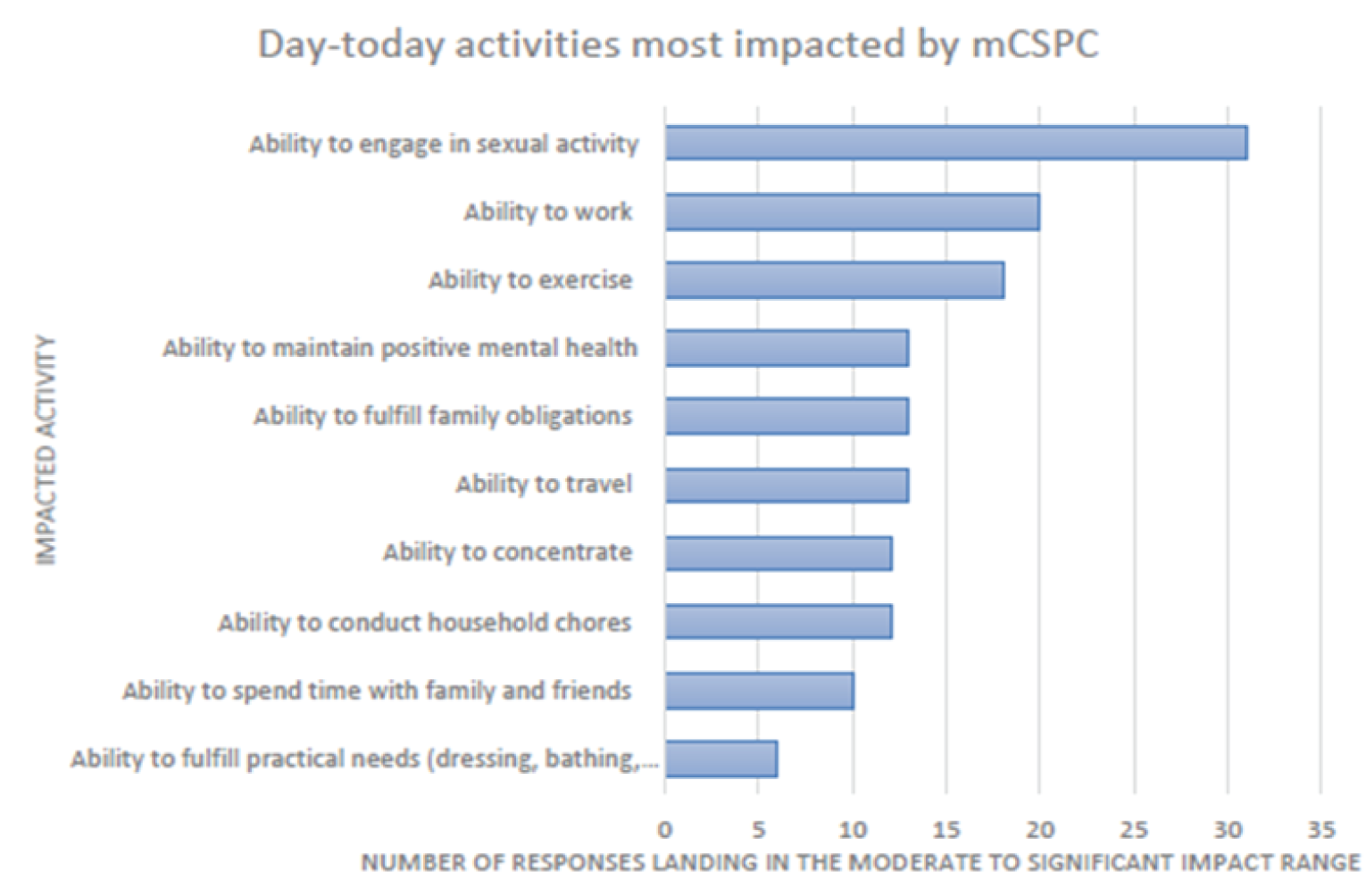
Note: There were a total of 41 responses for each impacted activity.
Experiences With Currently Available Treatments
What is the greatest financial barrier related to your treatment(s)?
Respondents had nine potential financial barriers to choose from and selected the one greatest financial barrier they are facing from the list. They also had an open field option if their greatest financial barrier was not present in the list.
Slightly under half of patients experienced a financial barrier related to their treatment. The greatest financial barriers, making up 10% of the distribution each, were drug costs and transportation costs. Other financial barriers identified included complementary medicines as recommended by the patients healthcare team (vitamins, supplements etc.), psychosocial support, loss of income due to absence from work and lodging and accommodations during treatment.
Three patients selected the “other” option. The first indicated they are not facing a great financial barrier, however, there are significant expenses. The second commented that their cancer drugs have been covered to date in Manitoba. The third indicated they have received no support, but did not clarify which financial barrier this comment was in relation to.
Patient A
Patient A indicated that drug costs were his greatest financial barrier. In order to access darolutamide, Patient A purchased additional private health insurance as part of his group plan, which approved coverage for NUBEQA. Patient A indicated his insurance premium increased after this request was approved by $800 - $900 per year. Patient A stated “I would be dipping into my savings to deal with this if I didn’t have private health insurance. If you don’t have the funds to do this, you would be in a very bad place. I would have found the means to stay alive, but if you didn’t have access [to the funds], I don’t know what you could do.”
When asked if he has concerns about his ability to access darolutamide in the future, Patient A stated “There may be a lifetime threshold on this particular drug, so that’s always the elephant in the room – at what point could that impact my decision making?”.
In addition, Patient A identified a potential barrier in accessing treatment related to the ability for your preferred pharmacy to dispense a drug. Patient A indicated there was uncertainty if his hospital/cancer centre pharmacy would dispense the drug or if Bayshore would need to dispense it. When Patient A was approved for coverage for darolutmide by his insurance company, his cancer centre pharmacy was not on their list of approved suppliers. There were several calls between his cancer centre pharmacy and his insurance company as they were legally able to dispense the drug and it would have been preferable for Patient A to get his prescription at that pharmacy, however, he was told he would only be able to obtain this prescription from Bayshore due to an agreement between the insurance company and that pharmacy. Patient A stated “If you get coverage, there are conditions on who can dispense it for you. I spent a month sorting that out.” Based on Patient A’s statement, it may be difficult for individuals living far away from a pharmacy on their private insurers approved list to access darolutamide.
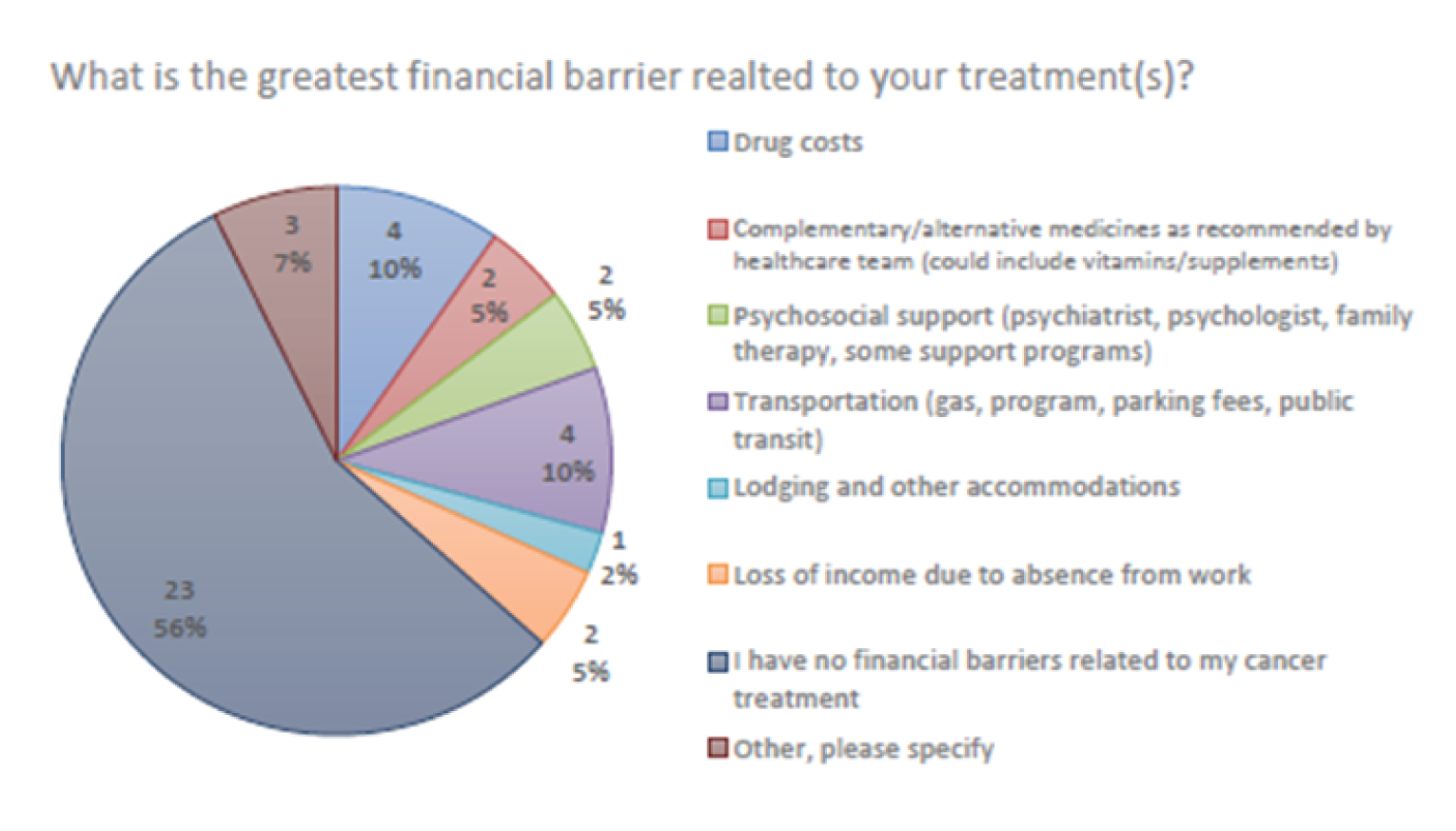
How many lines of treatment have you undergone?
A description of what a line of treatment entails was provided. The majority of patients indicated they had undergone 3 or more lines of therapy (56%) or two lines of therapy (29%). Three patients underwent one line of therapy, and three were unsure.
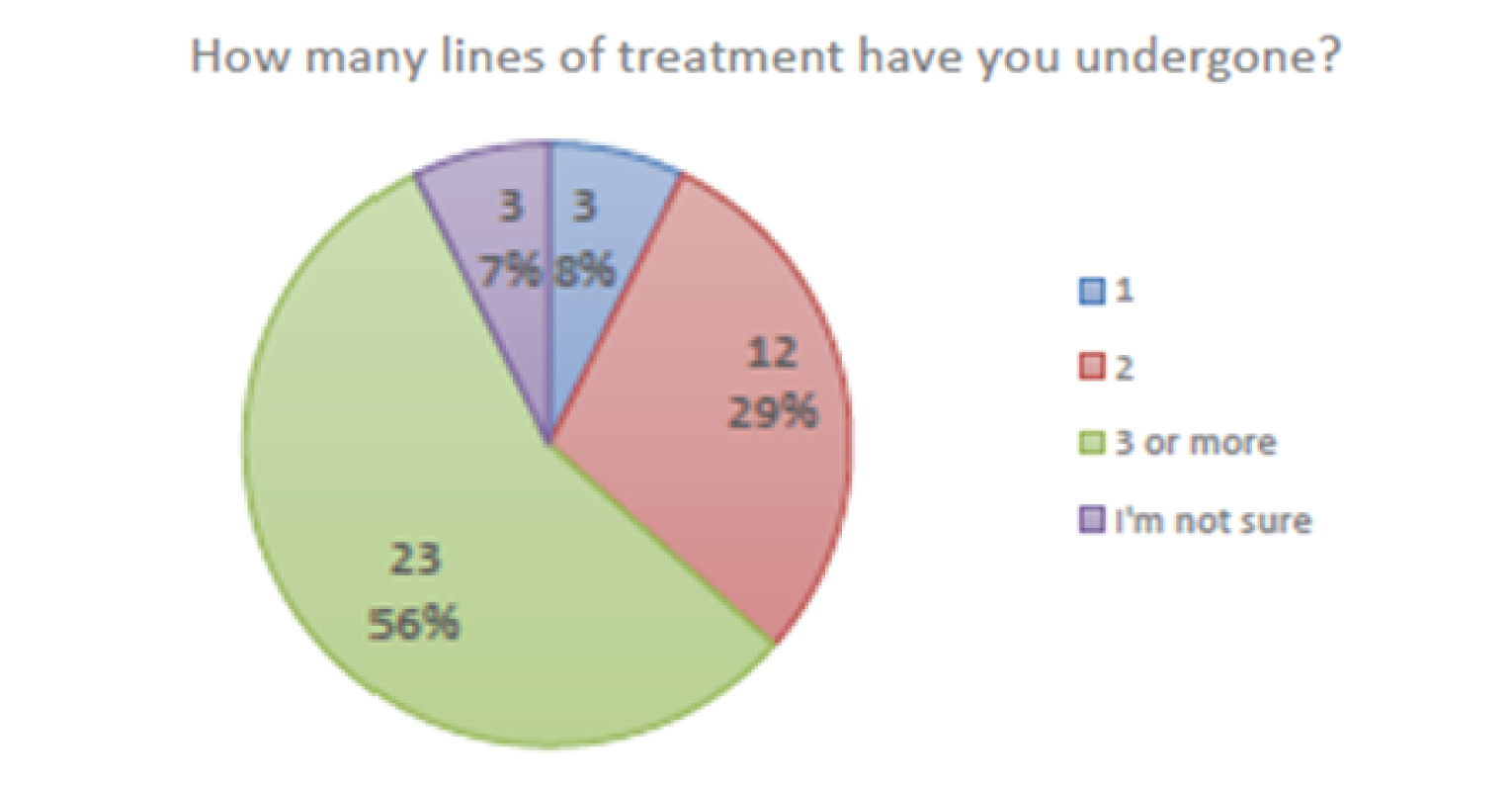
Since your diagnosis of prostate cancer, which treatments have you tried?
Respondents were able to select from 11 treatment types as well as indicate if their cancer has not been treated, if they are unsure, or provide additional information through an open field. Respondents were able to select all treatments that applied to them.
The majority of patients (80%) had tried luteinizing hormone-releasing hormone agonists at some point in their treatment journey. The next most common treatments tried were external beam radiation (73%), anti-androgen drugs (58%) and surgery (46%). Six patients had selected “other”. The comments shared when a patient selected “other” is below.
Patient comments on medications they had tried in relation to their cancer treatment:
“Prolia”
“Pregabalin, gabapentin”
“The ADT drug is what has destroyed my life.”
“High dose transdermal estradiol following the PATCH arm of the STAMPEDE trial in the UK.”
Patient A
Patient A is living with mCSPC with cancer that has spread to his lymph nodes and possibly his sacrum. He was genetically tested and was negative for BRCA. In 2019 he had a Gleason score of 7 with a PSA in the 8-9 range. Patient A tried HIFU to treat his prostate cancer which brought his PSA down to 4.2 in December 2019. Unfortunately, this procedure led to sepsis due to a catheter complication and the treatment was overall ineffective at eliminating his cancer. In January 2020, his PSA climbed to 6.2 and he began to take leuprolide in September 2020. Patient A and his physician also opted for radiation, which was deferred several times due to COVID-19. His physician initiated 40 sessions of radiation in April 2021 along with darolutamide (NUBEQA). In the summer of 2021, he also received a TURP. He accessed NUBEQA through permission from the Tumour Board.
If applicable, please specify which drugs or therapies you are currently using to treat your cancer.
Twenty-six patients provided a response to this question. This question was asked to provide further context into the common treatment combinations this group was using and the treatment side effects patients were experiencing (referenced in Q5). Some patients provided the brand of medication, while others offered the generic title.
Patient A
Patient A is currently taking darolutamide and leuprolide. Patient A is not taking docetaxel, but indicated he may in the future.
How much of an impact do the following cancer treatment side effects have on your daily life?
Figure 11 depicts the side effects that were ranked as moderate or severe with regard to how the side effect impacts the life of individual within this group. This question was asked to identify which treatment side effects had the most significant negative impacts on patients overall, and therefore indicate what side effects would be the most ideal to avoid or prevent worsening in new treatments and current treatments. For context, refer to Table 2 to review what treatments these patients are currently using and Figure 9 for information on what treatments this group has tried overall in the past or currently.
The most significant impacts on patients day-to-day lives were due to changes in libido and sexual function with 33 respondents (over 80%), rating it as having a severe impact and one respondent rating it as having a moderate impact. The second most impactful side effect in this group were hot flushes, with 68% of participants indicating it was either moderately or severely impacting their lives. Patient A commented “I see you address hot flashes as if they are but a side effect. In our opinion, they contribute a great deal to our well being.” Fatigue and loss of muscle mass where the next most impactful side effects with 68% and 46% of patients indicating the impacts were moderate or severe.
Of the 1353 responses across the 41 patients, 352 landed in the small impact category (26%), 170 fell into the moderate impact category (12.5%), and 143 landed in the severe category (10.5%). In addition, 125 responses fell into the “I’m not sure” category (9%) and 563 fell into the not applicable/no impact category (42%).
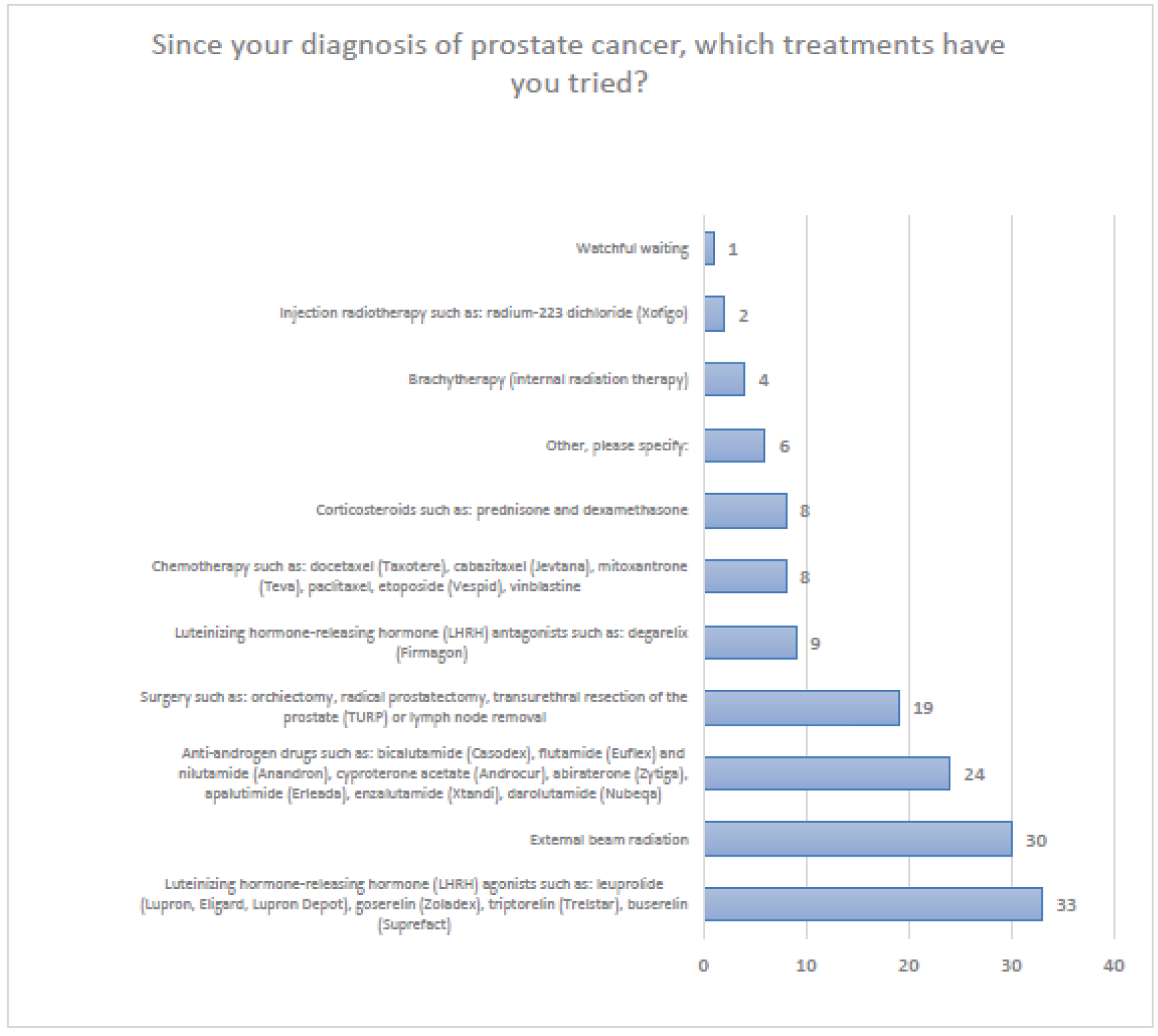
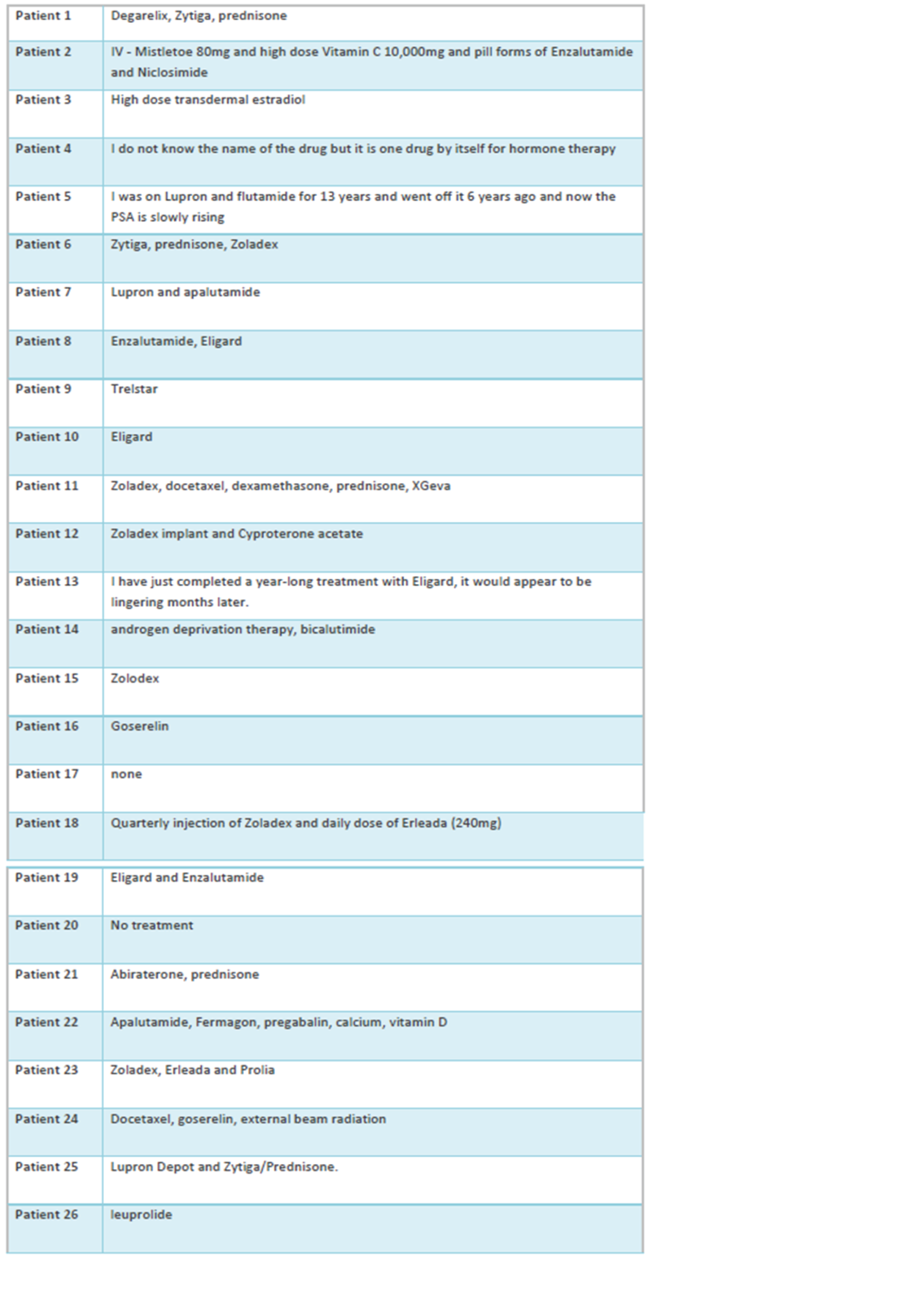
Patients provided several comments on the impact of their side effects below including the cost of complementary therapies that help with side effects, the impacts on self image and additional side effects that were not listed.
“[I] always feels better after IV injections of Vitamin C and Mistletoe, but I have to pay for it [at] 2800.00 dollars a month.”
“There isn’t enough space to write them [all the side effects] down. Degarelix has poisoned my body.”
“I am embarrassed by what has happened to my physical appearance and the chronic pain I must endure.”
“Mild anemia, impacts shortness of breath and lower immunity.”
“I've had head pressure leading to headaches for well over a year.”
“Night sweats, sleep issues.”
“I have flu like symptoms for about 24 hours after zoladex injection.”
“Diarrhea causes inflammation of the anus.”
Patient A
Patient A indicated that he experienced significant impacts due to loss of muscle mass, hot flushes and changes to libido and sexual function. He experienced moderate impacts due to fatigue, peripheral neuropathy, weight changes and mouth, tongue and throat problems such as sores and pain when swallowing. He experienced small impacts in various areas such as loss of bone density, hair loss, mild anemia, memory loss, heart disease, frequent infections, concentration and focus, pain, blood pressure changes, slow or difficulty breathing, incontinence or urgency to urinate, headaches and blurred vision. Patient A indicated that many of these side effects are related to his past treatments and leuprolide. He indicated he can not say for certain if any of these side effects were directly caused by darolutamide, but he hasn’t noticed any major changes in his side effect profile since taking darolutamide.
Patient A indicated that hot flashes are the most bothersome for him as he is still working and it has interrupted presentations he has conducted. Patient A indicated “this is a permanent constant side effect I have been dealing with prior to taking darolutamide.”
What improvements would you like to see in new treatments that are not achieved in currently available treatments? For example: effectiveness for relieving certain symptoms or side effects, affordability, ease of use etc.
Overall, this group of patients with metastatic castration sensitive prostate cancer expressed that they would like to see a reduction in side effects in treatment offerings. Side effects noted include hot flashes, sexual function, lymphedema, fatigue, infection risk, constipation, weight gain, fear of increased risk of Alzheimer’s disease, bone density loss, neuropathy, anemia, incontinence, muscle weakness and muscle fatigue. In addition, some individuals expressed an interest in naturopathic treatment access such as IV injections of vitamin C and mistletoe. Two patients indicated an interest in access to surgical procedures such as liposuction to control weight gain and castration as an alternative to ADT. Some patients also expressed they are interested in the potential utility of transdermal estradiol to manage side effects. Lastly, longer term efficacy and survival was mentioned as an improvement that a patients would like to see.
Patient A
Patient A indicated he would like to see medications for prostate cancer that provide a reduction in hot flashes, lesser impact on muscle mass (however this side effect has stabilized for him), lesser impacts on sexual function, and better lipids control. Patient A underscored he would also like to see an increase in life expectancy and further indicated he would like to have the ability to survive another 20 years.
Select direct comments from survey responders on what they would like to see in new treatments:
“To have IV injections of Vitamin C and Mistletoe a part of Standard of Care while doing the drug treatments. It decreases the side affects of the cancer drugs I take!”
“More patients starting on any of drugs mentioned here need to be referred to the ADT Educational Program, free here in Canada and endorsed by the Canadian Urological Association. Taken before the side effects set in, it is by far the best thing I know of for helping patients deal with the side effects of all those drugs. [Refer to: www.LIFEonADT.com]”
“Traitements au niveau des problèmes d’érections sexuelles. Les traitements actuels sont soient trop invasifs ou ne fonctionnent pas du tout.” Translation: Treatments for sexual erection problems. Current treatments are either too invasive or don't work at all.
“My main problem at this point is the lack of sleep from the hot flashes due to the hormone therapy.”
“Less hot flashes and less fatigue.”
“I wonder why castration is not offered. After years of the expensive drugs and the side effects and damage of the drugs, I would have chosen the option of castration from the beginning.”
“[Access to] liposuction and constipation control.”
“I would like to see the government approve the use of immunotherapy and some naturopathic treatments.”
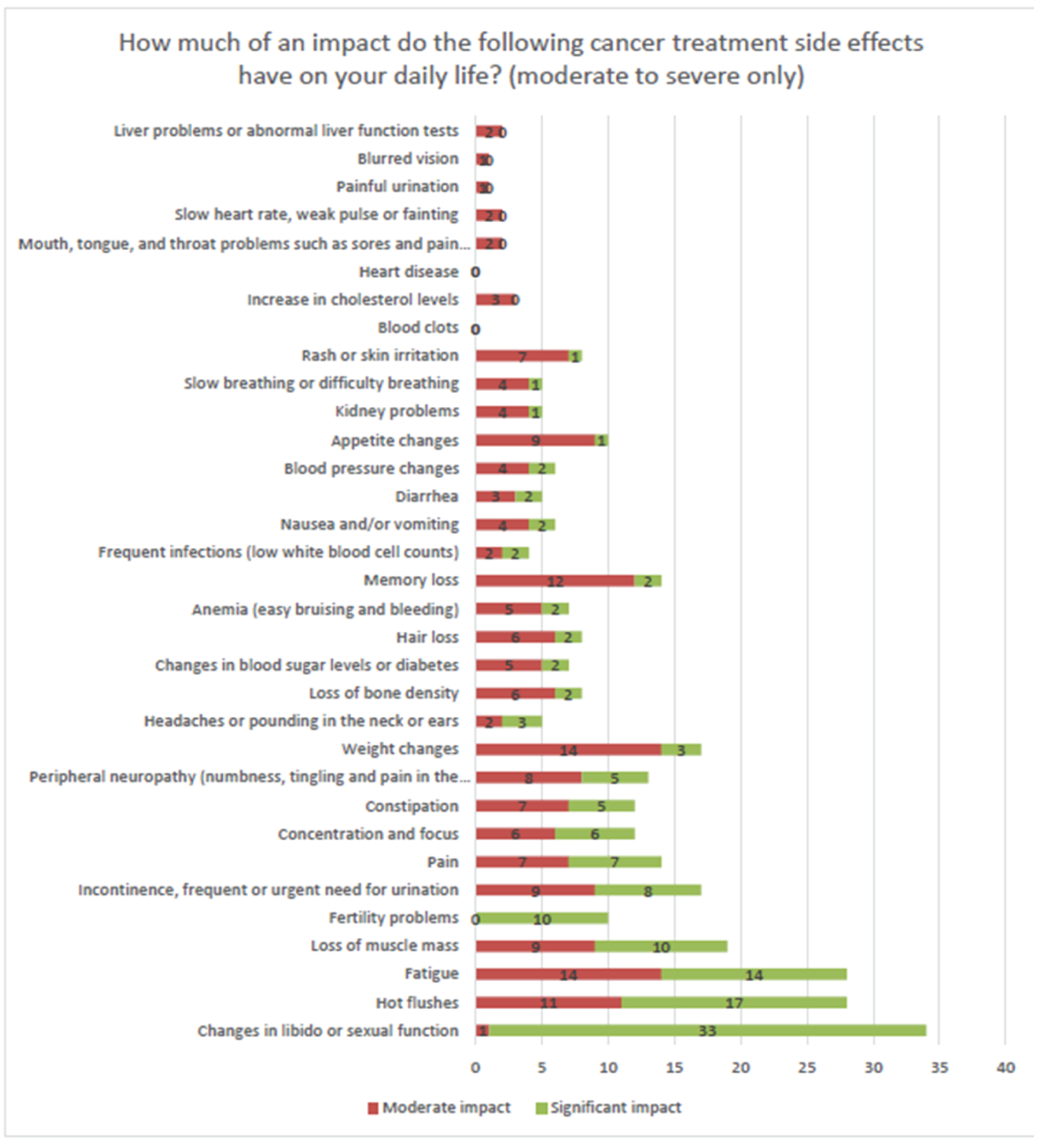
“Use of oestrogen patch to reduce side effects associated with loss of oestrogen rather than due directly to the reduced testosterone, such as sexual/libido, hot flashes, bone density loss, etc.”
“Better/greater use of transdermal estradiol for bone mineral loss prevention. This would also go towards alleviating night sweats as well, goes to quality of life issues.”
“My largest problem would be weight gain. I went from 190 lbs to 215 lbs over a year with Eligard. It's been a struggle to cut even a couple of pounds off four months after completing the treatment. My age, 74, may be attributing to that.”
“[Make treatments] affordable, clarity on the impact of neuropathy.”
“Compulsory PSA tests annually over 55 years, health care funding PSMA diagnostic tests.”
“Longer term efficacy.”
“Manage hot flashes better [and] reduce potential for anemia.”
“For almost 7 years I endured severe incontinence, that is up to 15 pads/day. The annual cost to me was around $1000 or more per year. I did claim these costs on my income tax but it had no impact on my getting any reimbursement. Also my lymphedema in the legs was very severe for many years and I have had one serious infection that needed to be treated in hospital.”
“Les bouffées de chaleur sont nombreuses, quotidiennes et durent depuis 13 mois. La libido est nulle depuis le début des traitements en bas 2021.” Translation: Hot flashes are numerous, daily, and have lasted for 13 months. Libido has been nil since starting treatments in early 2021."
“Easing hot flushes.”
“[Improving] muscle weakness & muscle fatigue.”
“Hot flashes need to be addressed and not glossed over. Is there medication?”
Improved Outcomes and Experience With Drug Under Review
This section of this report will be focused on Patient A. Patient A answered a series of questions about his experience with darolutamide in the form of a survey and engaged in a more in depth interview.
At the time of the interview, Patient A had been taking NUBEQA for approximately 14 months along with leuprolide. He is not currently taking docetaxel, but this is a future possibility. As of June 2022, his PSA is now 0.35 and was as low as 0.18 in December 2021. Patient A believes the TURP, radiation and darolutamide could have all contributed to his PSA score decreasing to different degrees but he can’t say for certain which had the greatest impact. Patient A stated “My quality of life has improved on the NUBEQA but I can’t attribute 100 percent of that to NUBEQA.” He indicated leuprolide alone was not sufficient in treating his cancer. Patient A will be undergoing tests in July to find out if the cancer has further spread, but has indicated he has been doing well since taking darolutamide and that overall he found it very tolerable. In addition, Patient A stated “If I could have avoided the radiation or TURP, I would have”.
With regard to Patient A’s cancer experience, he stated “The overall feeling – you’ve got to start with the mind as it has a big role to play in assessing symptoms and side effects and separating aging from side effects. I wish I had some intervention after reoccurrence. I was in uncharted waters. I was in a dark place when I was diagnosed with a recurrence. As soon as I started seeing improvements, that I was responding well, I was disappointed I might be becoming castrate resistant, the whole mindset improved again when I saw how well I responded to radiation and NUBEQA.”
When asked about his level of activity before and after taking NUBEQA, patient A indicated “The pandemic interrupted a lot of activities so it’s hard to measure my level of activity before and after NUBEQA.” As the pandemic has begin to alleviate, Patient A has noticed an improvement in his activity level and lifestyle. He is active and likes to golf and spend time outdoors and continues to work in an office environment.
What are the side effects that you have experienced with darolutamide (NUBEQA)? Please rate them on a scale of 1 to 5. 1 is "completely intolerable" and 5 is "very tolerable".
Side effect tolerability was explored to find out if the side effects associated with darolutamide allowed patients to live an acceptable quality of life. Patient A was provided with a list of common and uncommon side effects associated with darolutamide. He did not experience the following possible side effects as a result of darolutamide: rash, fertility issues, chest pain or tightness, painful or difficult urination, sore throat, fever or chills, cough with or without mucus, nausea, diarrhea, headache, blood in the urine, blurred vision, dizziness, nervousness, fast heart rate, slow heart rate/weak pulse, fainting, kidney problems, liver problems, blood clot in the lung or lung infections.
Since taking darolutamide, Patient A indicated he is uncertain if any of the side effects commonly associated with darolutamide that he experienced (refert to Figure 11) were caused by the drug or if they were caused by other treatments such as leuprolide or TURP. Patient A rated all side effects he experienced that could be related to darolutamide in the tolerable to very tolerable range with the exception of arm, leg, hand or foot pain which he provided a neutral rating. Patient A indicated that with regard to slowed or troubled breathing, he noticed he had experienced shortness of breath climbing a mountain with friends, but he is fine doing his other usual activities such as walking a golf course. The shortness of breath was tolerable for him and did not prevent him from continuing his activity, however, it slowed him down. He is unsure if this side effect is related to darolutamide, but based on the side effects associated with it, it is possible.
In addition, Patient A indicated he gained about 5 pounds around the stomach and breast area since he started darolutamide, however, this could have been related to inactivity due to quarantining due to the COVID-19 pandemic.
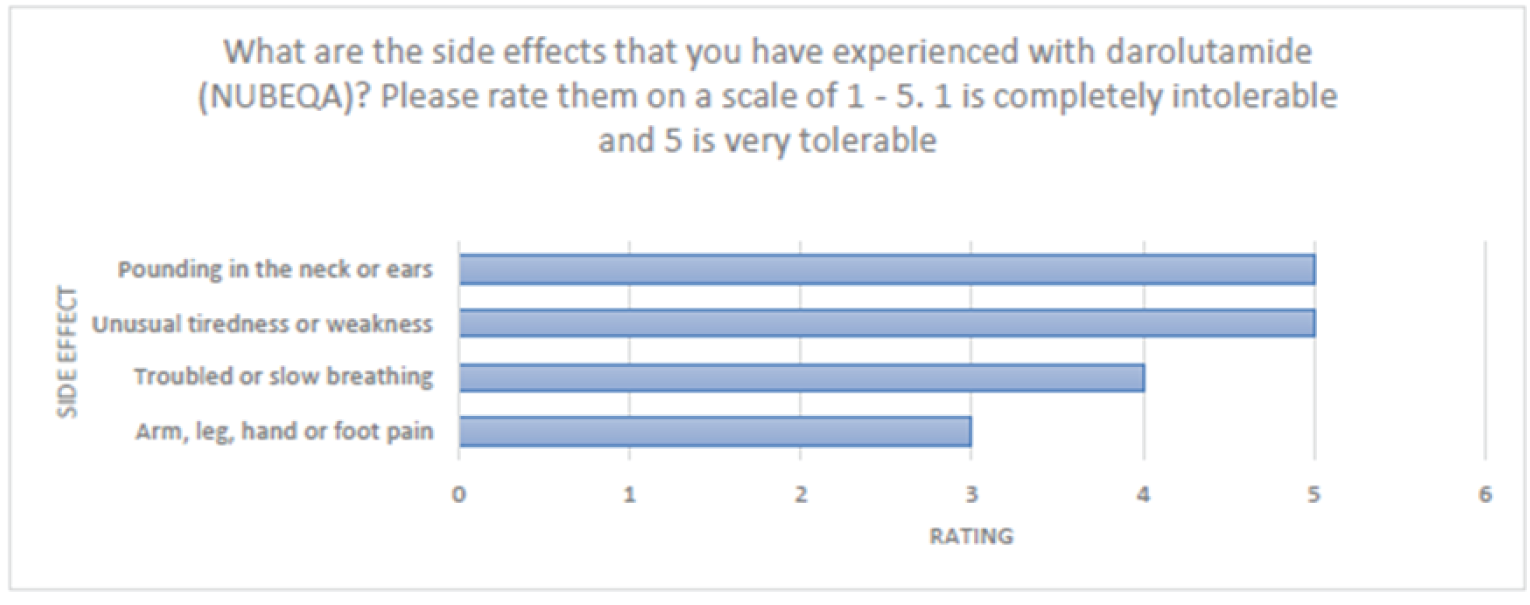
How much do you agree or disagree with the following statements about darolutamide (NUBEQA)?
Patient A was asked to rate statements about darolutamide on a scale of strongly disagree to strongly agree. Overall, the patient strongly felt the side effects were tolerable, strongly agreed that they would choose to take darolutamide again considering the side effects, strongly agreed darolutamide pills allowed him to spend less time in the clinic, and strongly agreed that he would recommend this treatment to others with mCSPC. Patient A agreed that darolutamide has been effective at controlling his cancer and that the pill form was easy to use.
Patient A provided some additional comments in relation to ease of use for darolutamide. Patient A stated “I wish it [darolutamide] could be dosed the same way as Lupron. It’s challenging to remember to take it. I would rather an at home injection. I had to call Bayer because I took my dose in the morning and I wasn’t sure if I forgot to take it. I accidently took too much. They told me that when they had done their trials they dosed double that amount and I should be okay.” He went on to indicate that if a patient were to pay out of pocket that “every pill is worth a fortune”, so it wouldn’t be ideal to accidently take your dose twice. However, overall, he found the pills easy to use.
When asked how valuable it was for him to be able to access darolutamide at home rather than in a clinic, Patient A stated “If you could take medications at home, it would be a lot easier. If I could do an injection at home of Lupron, I would do my PSA, and if it stayed the same, there would be no reason to see the doctor and we could talk over the phone. Anything that can be taken at home eliminates the need to go into the centre [for treatment].”
Table 3: Patients’ Level of Agreement on Statements Related to Darolutamide (NUBEQA)
Statements | Patient response |
|---|---|
Overall the side effects of darolutamide (NUBEQA) were tolerable | Strongly agree |
Considering the side effects I experienced so far, I would still choose to take darolutamide (NUBEQA) | Strongly agree |
Darolutamide (NUBEQA) has been effective at controlling my cancer | Agree |
Darolutamide (NUBEQA) pills allowed me to spend less time in the clinic receiving treatment compared to other treatments I’ve tried in the past | Strongly agree |
Darolutamide (NUBEQA) pills were easy to use | Agree |
I would recommend this treatment to others with metastatic castration sensitive prostate cancer | Strongly agree |
Anything Else?
Patient A
Please provide any further comments you would like CADTH and INESSS to consider when they are deciding if they should recommend darolutamide (NUBEQA) be covered by provincial drug plans for people with metastatic castration sensitive prostate cancer in Canada.
To answer this question in the survey, Patient A stated:
“I am not sure if there is a way to change darolutimide to a weekly or monthly inject as opposed to the twice daily pills totalling 1200mgs.” He also indicated that if there was a way to make darolutamide work without the need for leuprolide, he believes it would eliminate many of the side effects he is experiencing.
In addition, as part of the interview, Patient A made the following statement: “Accessing new medications is very important if it’s the key to my survivability and fighting the disease. If this [darolutamide] stops working, anything that’s new and recommended I would want to try. It is extremely important to me to access new medications if my current treatment stops working. I am lucky I purchased this private insurance, so I don’t have to use my retirement funds to survive. There is fear of wasting your family’s money in case a treatment doesn’t work.” Further, Patient A stated “I’m a believer NUBEQA is in part responsible for keeping my PSA at these low levels where [further] intervention is not required at this time”.
Is there anything else you want CADTH/INESSS to know about your cancer experience that you haven’t had the opportunity to express?
Patient A indicated that the “world of specialty cancer drugs is outside the scope of the general practitioner that is supposed to deal with the side effects. The oncologists and urologists are too busy to handle the load of symptoms and side effects patients experience, and the general practitioners are not up to speed. My general practitioner has only had one patient on Lupron in his entire career”. He further stated, “I had no direct follow up to see how I am doing on these drugs”. This was an area he would like to see improved in cancer care.
Further, he noticed a gap in his ability to access dietitians familiar with oncology drugs, such as darolutamide and leuprolide. He indicated it is important they understand how these drugs can impact your vitamin levels, minerals and how you can improve certain side effects with the correct diet and supplementation.
Overall, the sentiments expressed across responses include:
Patients with mCSPC’s quality of life is strongly impacted by their cancer and treatments, limiting their ability to engage in several day-to-day tasks. When asked how they would rate the impact on various daily activities, thirty-six percent of responses landed in the moderate to significant impact range.
Nearly 50% of patients experienced a financial barrier in accessing treatment. The most common barriers included drug costs and transportation costs. Take home cancer drugs, such as darolutamide, may alleviate some transportation costs as patients do not need to travel to the clinic to take them. Seventy-three percent of patients indicated their ability to travel was impacted by some degree due to their cancer. Depending on a patients distance to the clinic, take home cancer drugs may reduce that burden.
The most significant side-effects impacting patients day-to-day lives were due to changes in libido and sexual function, hot flushes, fatigue and loss of muscle mass among several others. Across the 41 patients, over 33 side effects were identified indicating that current treatments for mCSPC can inflict a wide range of life impacting symptoms.
Patients would like to see improvements in future prostate cancer treatments to reduce side effect profiles, increase efficacy and therefore their lifespan, attain better access to naturopathic medicines, complimentary medicines that treat side effects and alternative surgical procedures such as castration.
Patient A indicated his PSA went from 6.2 in 2020 to 0.35 as of June 2022. Leuprolide was ineffective alone when he began taking it in 2020, which led to radiation, darolutamide and a TURP in 2021. He is currently on darolutamide and leuprolide alone and his PSA is currently under control with no need for further intervention at this time. Patient A believes darolutamide is in part responsible for his low PSA.
Patient A indicates the side effects he experienced after taking darolutamide were tolerable, with the exception of peripheral neuropathy, however he can’t be certain this side effect is due to darolutamide. Patient A believes the majority of bothersome side effects are related to leuprolide.
Patient A believes darolutamide has been effective at controlling his cancer, reduced his time in the clinic, was easy to use and indicated he would strongly recommend this drug for others with mCSPC. In addition, he underscored the importance of being able to access new cancer drugs when previous drugs stop working and the importance of affordability so patients do not need to create a financial burden for their families.
Additional Figure
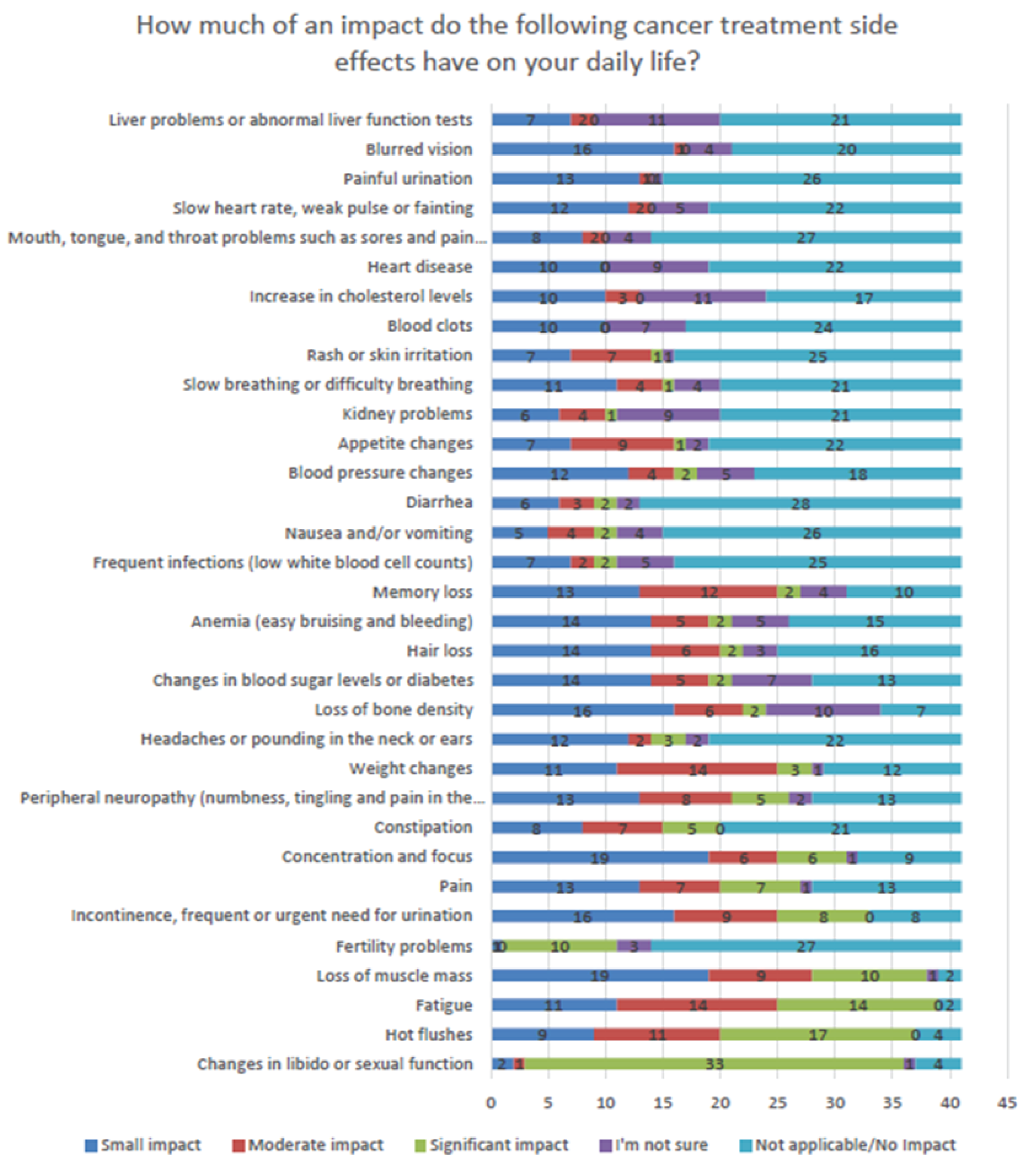
Conflict of Interest Declaration — Canadian Cancer Society
Did you receive help from outside your patient group to complete this submission?
No.
Did you receive help from outside your patient group to collect or analyze data used in this submission?
No.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review.
Table 4: Conflict of Interest Declaration for the Canadian Cancer Society
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Bayer | — | — | X | — |
Please let us know if you need information related to funding from other pharma companies that provide funds to CCS. To the best of our knowledge, this is the only COI. There was an additional 55K in 2019 that falls out of the two-year period.
Clinician Input
BC Cancer GU Medical Oncologists Group
About the BC Cancer GU Medical Oncologists Group
British Columbia Cancer Agency is part of the Provincial Health Service Authority and provides care for cancer patient across British Columbia. In each BC Cancer centre, there are medical oncologists subspecialized in treating patients with genito-urinary tumors. The medical oncologists listed in this group are all specialized in treating GU tumors.
Information Gathering
Review of the literature, data from previous applications in the same patients population from the BC Cancer pharmacy registry.
Current Treatments and Treatment Goals
Prostate cancer (PCa) is the most commonly diagnosed malignancy in Canada accounting for 1 in 5 (20%) of all newly diagnosed cancers.1 The prevalence of prostate cancer patients in Canada is 103,8402 of whom 4% have metastatic castrate sensitive prosate cancer - mCSPC (approximately 4,154 patients). Most of these patients (40-50%) have recurrent mCSPC while only 10% of newly diagnosed prostate cancer patients present with de novo mCSPC.3,4
mCSPC patients have a poorer prognosis than patients diagnosed with non metastatic prostate adenocarcinoma with an estimated median overall survival (mOS) of only about 32 months when treated with LHRH analogues or antagonist (LHRHa).5 Therefore, the goals of care in this population of patients is to improve OS, delay progression to castrate resistant prostate cancer and control the symptoms related to their metastatic disease without interfering with their quality of life. Traditional first line therapy for advanced PCa, including locally advanced and metastatic prostate cancer, includes androgen deprivation therapy (ADT) either through surgical or medical castration (LHRHa). The survival of patients with mCSPC is affected by several factors including: Gleason score, location of the metastatic disease, tumor burden.5-6
In the past 5 years the treatment landscape of mCSPC patients has significantly changes with the addition of either chemotherapy (docetaxel) or new generation androgen receptor pathway inhibitors (ARPI) to the LHRHa. The data supporting these additional drugs are summarized as following:
Docetaxel
High volume mCSPC disease in the CHAARTED clinical trial was defined by the presence of one of the following criteria: a. presence of visceral metastases or; b. presence of 4 or more bone lesions, with at least 1 outside the spine or the pelvis. The median overall survival (OS) of patients with high volume mCSPC is about 36 months with LHRHa alone. The addition of docetaxel chemotherapy to LHRHa has demonstrated to significantly increase median overall survival (mOS) of patients with high volume mCSPC. In the CHAARTED clinical trial, the mOS 17 months longer with the addition of early docetaxel to ADT than with ADT alone (49.2 months vs. 32.2 months; hazard ratio for death, 0.60; 95% CI, 0.45 to 0.81; P<0.001).5 These results were confirmed by an updated analysis with a longer follow up of 53.7 months.7
Apalutamide
Apalutamide is an oral next-generation androgen receptor inhibitor. The randomized phase III clinical trial TITAN demonstrated that the addition of the ARPI apalutamide to LHRHa provides clear clinical benefit in patients with mCSPC. The primary outcomes of the study were OS and rPFS as assessed by investigator. The trial met its primary outcomes and demonstrated a statistically significant improvement in rPFS in the apalutamide plus ADT group after a median follow-up time of 22.7 months. The percentage of patients with radiographic progression–free survival at 24 months was 68.2% in the apalutamide group and 47.5% in the placebo group (HR 0.48; 95% confidence interval [CI], 0.39 to 0.60; P<0.001), for a 52% lower risk of radiographic progression or death in the apalutamide group. The effect of apalutamide on radiographic progression–free survival was consistently favorable across the subgroups analyzed, including previous docetaxel use and both high and low disease volume. The first interim analysis for overall survival occurred after 200 deaths were observed (83 in the apalutamide group and 117 in the placebo group). The overall survival percentage at 24 months was 82.4% in the apalutamide group and 73.5% in the placebo group (hazard ratio for death, 0.67; 95% CI, 0.51 to 0.89; P = 0.005), and there was a 33% lower risk of death in the apalutamide group. The treatment effect on OS consistently favored apalutamide over placebo, with no significant difference in the effect of apalutamide according to disease volume. Apalutamide + ADT presented a manageable toxicity profile, with no difference in quality of life between apalutamide + ADT and placebo + ADT treatment arms.
Analysis of change from baseline in the FACT-P score with the use of a mixed effect repeated measures model showed that health- related quality of life was maintained with apalutamide, with no substantial between-group difference.8
Enzalutamide
Enzalutamide is an oral, next-generation androgen receptor inhibitor. The ENZAMET trial (a multi-centre, phase III, open-label study) compared enzalutamide + ADT vs. a first generation non-steroidal antiandrogen (NSAA) + ADT, in patients with mCSPC.9 The ENZAMET study demonstrated that treatment with enzalutamide + ADT provides significant clinical benefit through statistically significant and clinically meaningful improvements in PFS and OS.9 In addition, the ARCHES study demonstrated that treatment with enzalutamide + ADT provides clear clinical benefit through statistically significant improvement in radiographic progression free survival (rPFS). Enzalutamide also led to a significant delay in symptomatic skeletal events. Enzalutamide + ADT has a manageable toxicity profile, and adverse events between the enzalutamide and placebo groups were similar.
In ENZAMET 44.6% of patients had early use of docetaxel (enzalutamide = 45.1% and NSAA = 44.1%), and 42.8% in the enzalutamide group and 42.1% in the NSAA group had at least one dose of docetaxel after randomization. Approximately one-third of the patients received six cycles of docetaxel (enzalutamide = 27.9% and NSAA = 32.3%). At the time of the OS analysis, the median follow-up was 34.4 months. Treatment with enzalutamide was associated with a significant improvement in OS compared to the NSAA group (HR = 0.67; 95% CI, 0.52 to 0.86; P = 0.002). The survival rate at three years was 80% (N = 94) in the enzalutamide group and 72% (N = 130) in the NSAA group.
The subgroup analysis showed no significant differences among the pre-specified subgroups based on age, ECOG performance status, Gleason score at initial diagnosis, volume of disease, planned early use of docetaxel, and ACE-27 scores. Treatment with enzalutamide was associated with a significant improvement in clinical PFS compared to the NSAA group (HR = 0.40; 95% CI = 0.33 to 0.49; P < 0.001). The effect of enzalutamide on clinical PFS remained significant after adjusting for multiple testing. The median PSA PFS was not reached for the enzalutamide group. Treatment with enzalutamide was associated with a significant improvement in PSA PFS compared to the NSAA group (HR = 0.39; 95% CI, 0.33 to 0.47; P < 0.001). Kaplan-Meier curves for clinical and PSA PFS are shown in Figure 14.
There was no difference in Patient-Reported Outcomes between arms. The side effect profile was consistent with the previous experience with enzalutamide in the metastatic castration resistant setting, and broadly comparable between arms. The incidence and severity of AEs were broadly similar between groups.
The recent updated OS data confirmed the benefit of the addition of enzalutamide to LHRHa with a longer follow-up (median follow-up of 68 months). The hazard rate for death was 30% lower among all those assigned enzalutamide versus control (p<0.0001). Outcomes by volume status as well as the subgroups of interest with M1 high or low volume disease at diagnosis selected for concurrent docetaxel are shown in Table 5 below.10
Table 5: Updated Results of ENZAMET Trial
Results | Enzalutamide | NSAA | |||
|---|---|---|---|---|---|
Deaths/Total | 5 yrs OS % | Deaths/Total | 5 yrs OS % | HR (95% CI) | |
All participants | 208/563 | 67 | 268/562 | 57 | 0.70 (0.58 to 0.84) |
Concurrent docetaxel | |||||
No | 100/310 | 72 | 145/312 | 58 | 0.60 (0.47 to 0.78) |
Yes | 108/253 | 61 | 123/250 | 56 | 0.82 (0.63 to 1.06) |
Volume of Disease (Vol) | |||||
Low | 59/262 | 80 | 97/261 | 66 | 0.54 (0.39 to 0.74) |
High | 149/301 | 55 | 171/301 | 49 | 0.79 (0 .63 to 0.98) |
Vol by docetaxel | |||||
Low Vol, docetaxel no | 41/189 | 81 | 70/190 | 66 | 0.51 (0.35 to 0.75) |
Low Vol, docetaxel yes | 18/73 | 78 | 27/71 | 67 | 0.61 (0.33 to 1.10) |
High Vol, docetaxel no | 59/121 | 57 | 75/122 | 47 | 0.69 (0.49 to 0.97) |
High Vol, docetaxel yes | 90/180 | 54 | 96/179 | 51 | 0.87 (0.66 to 1.17) |
M1 at diagnosis | |||||
All M1, docetaxel yes | 79/181 | 60 | 96/181 | 52 | 0.73 (0.55 to 0.99) |
Low Vol, docetaxel yes | 14/48 | 73 | 21/44 | 57 | 0.57 (0.29 to 1.12) |
High Vol, docetaxel yes | 65/133 | 55 | 75/137 | 51 | 0.79 (0.57 to 1.10) |
Abiraterone + Prednisone
Abiraterone acetate (abiraterone) is an oral inhibitor of the cytochrome P-450c17, a critical enzyme involved in the androgen biosynthesis. The combination of abiraterone plus prednisone and LHRHa has been shown to significantly improve mOS of patients with high risk mCSPC in the phase III LATITUDE clinical trial. High risk patients had to present at least two of the three following high-risk factors associated with poor prognosis: a. Gleason score of 8 or more; b. At least three bone lesions; c. presence of measurable visceral metastasis. The control group patients were treated with LHRHa+ dual placebo. The two primary end points were OS and rPFS. After a median follow-up of 30.4 months at a planned interim analysis (after 406 patients had died), the mOS was significantly longer in the abiraterone group than in the placebo group (not reached vs. 34.7 months) (hazard ratio for death, 0.62; 95% confidence interval [CI], 0.51 to 0.76; P<0.001). The median length of radiographic progression-free survival was 33.0 months in the abiraterone group and 14.8 months in the placebo group (hazard ratio for disease progression or death, 0.47; 95% CI, 0.39 to 0.55; P<0.001).6 Quality of life of mCSPC on abiraterone was improved as demonstrated by a patient-reported outcomes analysis published after the first analysis.11
Abiraterone + Prednisone and Docetaxel
PEACE-1 was an open-label, randomised, phase 3 study with a 2 × 2 factorial design that enrolled patients with de novo mCSPC to be randomized to standard of care (LHRHa alone or with docetaxel), LHRHa plus radiotherapy, LHRHa plus abiraterone and prednisone or LHRHa plus radiotherapy plus abiraterone. The coprimary endpoints were rPFS and OS. Abiraterone efficacy was first assessed in the overall population and then in the population who received ADT with docetaxel as standard of care.
Median follow-up was 3·5 years for rPFS and 4·4 years for OS. Adjusted Cox regression modelling revealed no interaction between abiraterone and radiotherapy, enabling the pooled analysis of abiraterone efficacy. In the overall population, patients assigned to receive abiraterone (n=583) had longer rPFS (hazard ratio [HR] 0·54, 99·9% CI 0·41–0·71; p<0·0001) and OS (0·82, 95·1% CI 0·69–0·98; p=0·030) than patients who did not receive abiraterone (n=589). In the ADT with docetaxel population (n=355 in both with abiraterone and without abiraterone groups), the HRs were consistent (rPFS 0·50, 99·9% CI 0·34–0·71; p<0·0001; OS 0·75, 95·1% CI 0·59–0·95; p=0·017). Addition of abiraterone to ADT plus docetaxel did not increase the rates of neutropenia, febrile neutropenia, fatigue, or neuropathy compared with ADT plus docetaxel alone.12
Comparison of Treatment Options
There are no head-to-head comparison clinical trials demonstrating that targeting androgen receptor pathways is better than using docetaxel chemotherapy in mCSPC patients. OS prolongation has been the primary endpoint of all the above mentioned clinical trials that have led to Health Canada and FDA approval of these drug in mCSPC patients.
Treatment Gaps (Unmet Needs)
Considering the treatment goals, please describe goals (needs) that are not being met by currently available treatments.
Curative strategies for mCSPC patients are still not available. Despite the huge improvement in mCSPC clinical outcomes, progression to castration resistance inevitably occurs and patients die for their metastatic CRPC. Several data confirmed that the use of a secondary ARPI after progression on an ARPI is either inactive or has very limited efficacy.13 Therefore, treatment intensification and/ or patients selection for more intensified / personalized therapy is needed to prolong the life expectancy, delay castrate resistance progression and maintain quality of life of these patients.
None of the current treatment options are perfect for mCSPC patients and do affect their daily life. ARPI have the disadvantage of taking daily oral medications continuously for a long period of time, being therefore exposed to chronic side effects and potential drug to drug interaction (DDI). On the other hand, patients treated with docetaxel have a shorter course of active treatment (only 6 cycles of chemotherapy) but have more severe acute side effects.
Place in Therapy
How would the drug under review fit into the current treatment paradigm?
Darolutamide is a new generation AR inhibitor that has shown to significantly improve OS in patients with non metastatic prostate cancer.14 Its mechanism of action is very similar to apalutamide and enzalutamide (it binds to the ligand binding domain of the AR and inhibits its transcriptional activity and nuclear translocation) but its chemical structure and metabolism is different than apalutamide and enzalutamide. This difference accounts for the narrower DDI profile of darolutamide compared with apalutamide and enzalutamide and lower blood–brain barrier penetration.
In this review we support the use of darolutamide in combination with docetaxel and LHRHa for first line therapy in patients with mCSPC. The triplet combination with docetaxel AND an ARPI would represent an additional treatment option for first line therapy in patients with de novo or recurrent mCSPC.
The data supporting this triplet derives from the ARASENS clinical trial15 and are summarized below:
Clinical trial design: This international, randomized, double-blind, placebo-controlled trial enrolled patients with pathologically confirmed prostate adenocarcinoma, ECOG PS 0-1, with evidence of metastases detected on bone scanning, contrast-enhanced computed tomography (CT), or magnetic resonance imaging (MRI). Eligible patients had to be candidates for androgen-deprivation therapy and docetaxel, in the investigator’s judgment. Patients were randomly assigned in a 1:1 ratio to receive either darolutamide or placebo. Randomization was stratified according to the metastasis stage in the tumor–node–metastasis system (non-regional lymph-node metastases only [M1a], bone metastases with or without lymph-node metastases [M1b], or visceral metastases with or without lymph-node or bone metastases [M1c]) and according to whether the alkaline phosphatase level was below or at or above the upper limit of the normal range.
Treatments in ARASENS:
LHRH agonists or antagonists (LHRHa): All the patients received androgen-deprivation therapy (LHRH agonist or antagonist) or underwent orchiectomy within 12 weeks before randomization.
Docetaxel: All the patients received docetaxel that was administered intra-venously at the standard dose of 75 mg per square meter of body-surface area on day 1 and every 21 days for six cycles within 6 weeks after randomization.
Darolutamide or placebo: Darolutamide or placebo was administered orally at a dose of 600 mg [two 300-mg tablets] twice daily with food). Patients continued to receive darolutamide or placebo until symptomatic disease progression, a change in antineoplastic therapy, unacceptable toxic effects, patient or physician decision, death, or nonadherence.
Primary endpoint: Overall survival defined as the time from randomization until death from any cause.
Secondary end points: Time to castration-resistant prostate cancer, time to pain progression, symptomatic skeletal event–free survival, time to a first symptomatic skeletal event, time to initiation of subsequent systemic antineoplastic therapy, time to worsening of disease-related physical symptoms, time to initiation of opioid treatment for 7 or more consecutive days, and safety.
Statistical Analysis: Approximately 1300 patients were required to observe approximately 509 deaths, allowing for a 5% dropout rate, which provided the trial with 90% power to detect a 25% decrease in the risk of death in the darolutamide group versus the placebo group, at a two-sided alpha level of 0.05. The secondary end points were tested with a hierarchical gatekeeping procedure in the order described above only if the primary end point and each preceding secondary end point in the hierarchy were statistically significant. If the primary end point or a secondary end point did not reach significance, the hierarchical procedure was stopped, and subsequent analyses were considered to be exploratory. All the patients had metastatic disease at baseline; 79.5% had bone metastases (metastasis stage M1b) and 17.5% had visceral metastases (metastasis stage M1c). Most patients (86.1%) had disease that was metastatic at the time of the initial diagnosis.
Results: Between November 2016 and June 2018, a total of 1306 patients underwent randomization. A total of 651 patients were assigned to receive darolutamide and 655 patients were assigned to receive placebo, both in combination with androgen-deprivation therapy and docetaxel. Of these patients, 1305 patients (651 in the darolutamide group and 654 in the placebo group) were included in the full analysis set, and 1302 patients (652 in the darolutamide group and 650 in the placebo group) were included in the safety analysis set. Demographic and baseline characteristics were well balanced in the two groups. The median follow-up for overall survival was 43.7 months in the darolutamide group and 42.4 months in the placebo group.
Primary Endpoint: OS
The primary analysis of overall survival was performed after 533 patients had died (229 patients in the darolutamide group and 304 patients in the placebo group). The risk of death was 32.5% lower in the darolutamide group than in the placebo group (hazard ratio, 0.68; 95% confidence interval [CI], 0.57 to 0.80; P<0.001) (Figure 14).
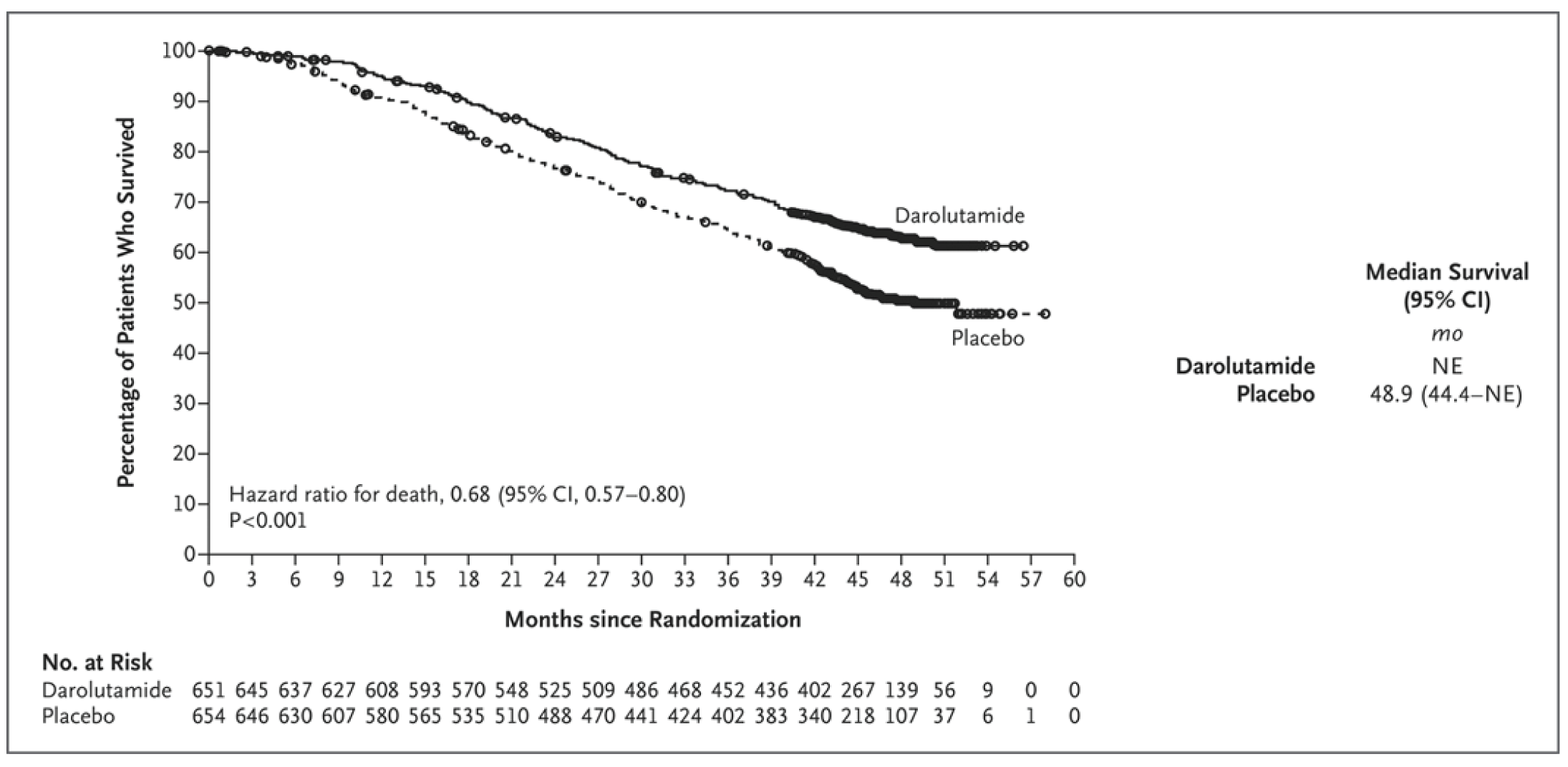
Kaplan−Meier estimates of overall survival are shown. For the analysis of overall survival, data were censored as of the last known date the patients were alive. One patient who was randomly assigned to the placebo group but received darolutamide was included in the placebo group in the full analysis set. CI denotes confidence interval, and NE not estimable
A significant improvement in overall survival was observed despite a high percentage of patients who received subsequent life-prolonging systemic therapies, primarily different androgen-receptor pathway inhibitors, among those who entered follow-up in the placebo group (374 of 495 patients [75.6%]). The overall survival at 4 years was 62.7% (95% CI, 58.7 to 66.7) in the darolutamide group and 50.4% (95% CI, 46.3 to 54.6) in the placebo group. The treatment effect of darolutamide with respect to overall survival was favorable across most subgroups (Figure 15).
Figure 15: Overall Survival in Prespecified Subgroups (Full Analysis Set, Unstratified)
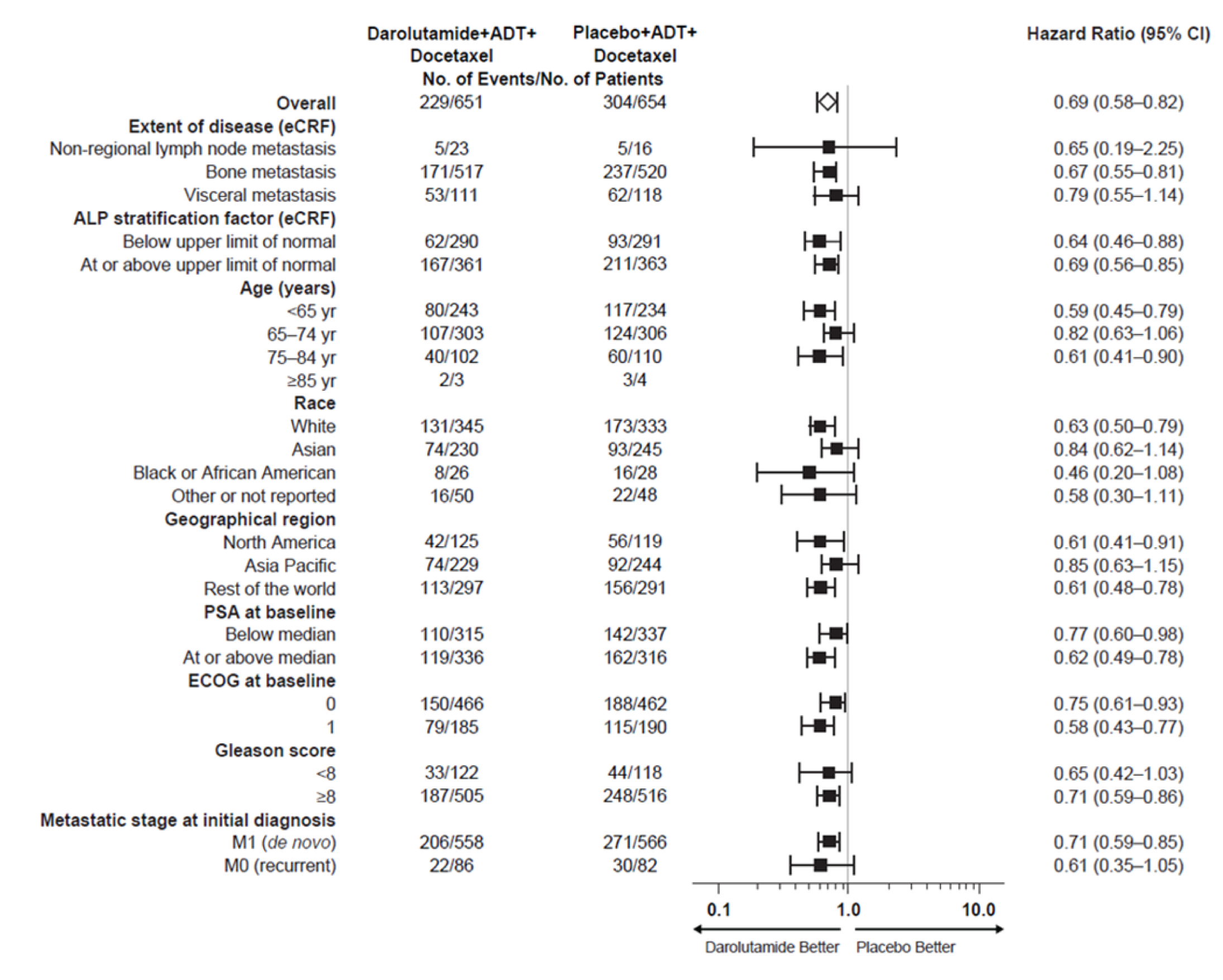
The “rest of the world” geographic region predominantly comprised European countries (Belgium, Bulgaria, Czech Republic, Finland, France, Germany, Italy, Netherlands, Poland, Russian Federation, Spain, Sweden, United Kingdom, Israel, Brazil, Mexico, Australia). ALP denotes alkaline phosphatase; CI denotes confidence interval; ECOG denotes Eastern Cooperative Oncology Group erformance status; eCRF denotes electronic case report form; NE denotes not estimable; and PSA denotes prostate-specific antigen.
Secondary Endpoints
Darolutamide was associated with significantly greater benefits than placebo for the first five secondary efficacy end points tested hierarchically (Table 6 and Figure 16). The time to development of castration-resistant disease was significantly longer in the darolutamide group (hazard ratio, 0.36; 95% CI, 0.30 to 0.42; P<0.001). The time to pain progression was also significantly longer in the darolutamide group (hazard ratio, 0.79; 95% CI, 0.66 to 0.95; P=0.01), as were symptomatic skeletal event–free survival (hazard ratio, 0.61; 95% CI, 0.52 to 0.72; P<0.001) and the time to a first symptomatic skeletal event (hazard ratio, 0.71; 95% CI, 0.54 to 0.94; P=0.02). The time to the initiation of subsequent systemic antineoplastic therapy was significantly longer in the darolutamide group (hazard ratio, 0.39; 95% CI, 0.33 to 0.46; P<0.001).
Table 6: Secondary Efficacy End Points (Full Analysis Set)
End Point | Darolutamide–ADT–Docetaxel | Placebo–ADT–Docetaxel | Hazard Ratio | P Value | ||
|---|---|---|---|---|---|---|
Median | Patients with Event | Median | Patients with Event | |||
mo | no. (%) | mo | no. (%) | |||
Time to castration-resistant prostate cancer | NR | 225 (35) | 19.1 | 391 (60) | 0.36 (0.30–0.42) | <0.001 |
Time to pain progression | NR | 222 (34) | 27.5 | 248 (38) | 0.79 (0.66–0.95) | 0.01 |
Symptomatic skeletal event–free survival | 51.2 | 257 (40) | 39.7 | 329 (50) | 0.61 (0.52–0.72) | <0.001 |
Time to first symptomatic skeletal event | NR | 95 (15) | NR | 108 (17) | 0.71 (0.54–0.94) | 0.02 |
Time to initiation of subsequent systemic antineoplastic therapy | NR | 219 (34) | 25.3 | 395 (60) | 0.39 (0.33–0.46) | <0.001 |
Time to worsening of disease-related physical symptoms | 19.3 | 351 (54) | 19.4 | 308 (47) | 1.04 (0.89–1.22) | 0.59 |
Time to initiation of opioid use for ≥7 consecutive days | NR | 92 (14) | NR | 117 (18) | 0.69 (0.52–0.91) | NA |
NR = not reached.
†One patient who was randomly assigned to the placebo group but received darolutamide was included in the placebo group in the full analysis set. Darolutamide and Survival in Metastatic, Hormone-Sensitive Prostate Cancer | NEJM
Figure 16: Analyses of Secondary End Points (Full Analysis Set)
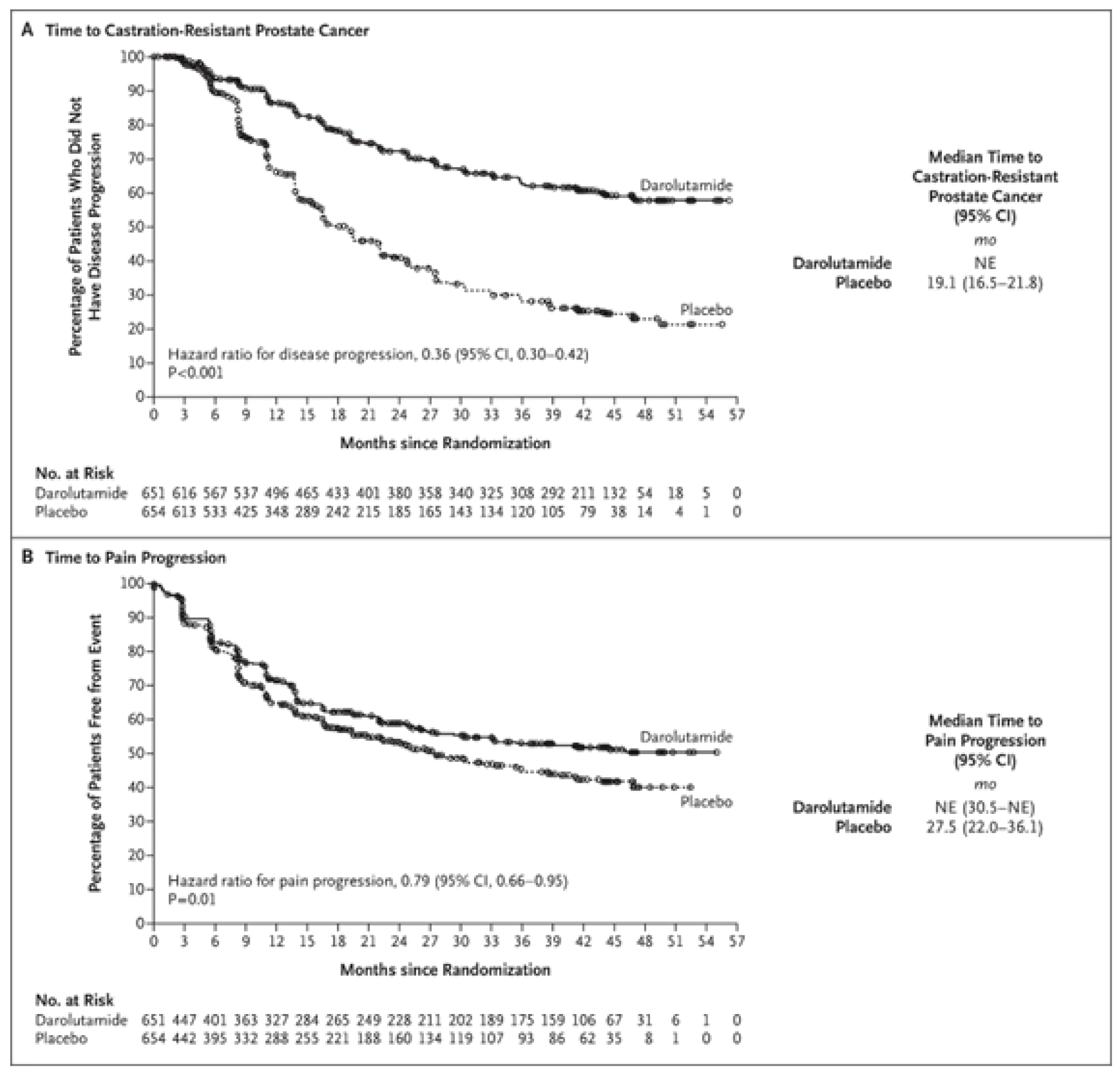
Panel A shows the time to castration-resistant prostate cancer, and Panel B shows the time to pain progression. The Kaplan−Meier method was used to estimate the time to events; data were censored at the date of the patients’ last assessment for that end point. One patient who was randomly assigned to the placebo group but received darolutamide was included in the placebo group in the full analysis set.
Safety
The incidences of adverse events of any grade, grade 3 to 5 adverse events, and serious adverse events were similar in the two groups (Table 7). The incidences of the most common adverse events (in ≥10% of the patients), many of which are known toxic effects related to docetaxel therapy, were highest in both groups during the period when the patients received both docetaxel and either darolutamide or placebo, and these effects progressively decreased thereafter, with grade 3 or 4 adverse events in 66.1% of the patients in the darolutamide group and 63.5% of those in the placebo group; neutropenia was the most common grade 3 or 4 event (in 33.7% and 34.2%, respectively).
Event | Darolutamide–ADT–Docetaxel | Placebo–ADT–Docetaxel |
|---|---|---|
Number of Patients (%) | ||
Any adverse event | 649 (99.5) | 643 (98.9) |
Worst grade | ||
Grade 1 | 28 (4.3) | 35 (5.4) |
Grade 2 | 162 (24.8) | 169 (26.0) |
Grade 3 | 248 (38.0) | 232 (35.7) |
Grade 4 | 183 (28.1) | 181 (27.8) |
Grade 5 | 27 (4.1) | 26 (4.0) |
Serious adverse event | 292 (44.8) | 275 (42.3) |
Adverse event leading to permanent discontinuation of trial agent | ||
Darolutamide or placebo | 88 (13.5) | 69 (10.6) |
Docetaxel | 52 (8.0) | 67 (10.3) |
Selected grade 3 or 4 adverse events† | ||
Neutropenia† | 220 (33.7) | 222 (34.2) |
Febrile neutropenia | 51 (7.8) | 48 (7.4) |
Hypertension | 42 (6.4) | 21 (3.2) |
Anemia | 31 (4.8) | 33 (5.1) |
Pneumonia | 21 (3.2) | 20 (3.1) |
Hyperglycemia | 18 (2.8) | 24 (3.7) |
†Darolutamide and Survival in Metastatic, Hormone-Sensitive Prostate Cancer | NEJM
Serious adverse events occurred in 44.8% of the patients in the darolutamide group and in 42.3% of those in the placebo group. The frequency of death due to adverse events was low and similar in the two groups (27 of 652 patients in the darolutamide group [4.1%] and 26 of 650 patients in the placebo group [4.0%]). Few patients discontinued darolutamide or placebo as a result of adverse events (13.5% of the patients in the darolutamide group and 10.6% of those in the placebo group). The most frequently reported adverse events were alopecia (in 40.5% of the patients in the darolutamide group and 40.6% of the patients in the placebo group), neutropenia (in 39.3% and 38.8%, respectively), fatigue (in 33.1% and 32.9%), and anemia (in 27.8% and 25.1%).
Certain adverse events are of special interest for patients receiving androgen-receptor pathway inhibitors. These events include fatigue, falls, fractures, mental impairment, rash, hypertension, and cardiovascular events. In this trial, the incidences of these events of interest were similar (with no more than a 2 percentage-point difference) in the two groups, with the exception of rash (in 16.6% of the patients in the darolutamide group and 13.5% of those in the placebo group) and hypertension (in 13.7% and 9.2%, respectively). Among the most frequently reported adverse events of interest, the incidences of vasodilation and flushing (in 20.4% of the patients in the darolutamide group and 21.7% of those in the placebo group) and diabetes mellitus and hyperglycemia (in 15.2% and 14.3%) were also similar in the two groups.
Which patients would be best suited for treatment with the drug under review? Which patients would be least suitable for treatment with the drug under review?
All patients with mCSPC fit enough to receive docetaxel should be considered for the triplet combination of darolutamdie+docetaxel+LHRHa.
In the ARASENS study, in fact, the eligible patients were not selected or stratified according to high or low volume or high or low risk disease. Locations of metastases (M1a, M1b or M1c) according to the TNM staging system was used for stratification of the patients. All patients treated with the triplet had a benefit in terms of OS as showed by the forest plot in Figure 15 (patients with exclusive bone metastases and patients presenting visceral metastases equally benefitted from the addition of darolutamide to docetaxel). The M1a group was very small; however also in these patients darolutamide addition demonstrated to prolong the OS.15
What outcomes are used to determine whether a patient is responding to treatment in clinical practice? How often should treatment response be assessed?
The primary outcome of the ARASENS study was OS and this is in line with the practice changing registration clinical trials which led to the approval of docetaxel, apalutamide, enzalutamide and abiraterone+prednisone in mCSPC patients.5,6,8,9,15
The addition of darolutamide to docetaxel and LHRHa significantly prolongs OS and rPFS. Moreover, there was a longer control of the cancer-related symptoms, a higher percentage of objective responses and of PSA responses.
PSA is a high-fidelity marker to evaluate treatment response and development of castrate resistant disease. Imaging tests could be used if castrate resistance progression is clinically suspected and/or at regular interval.
What factors should be considered when deciding to discontinue treatment with the drug under review?
In our clinical practice, the response is usually assessed by PSA and clinical assessment. Radiographic tests (CT scans or MRI) are usually used at the time of castration resistant prostate cancer or if progression is clinically suspected. Indeed, it is extremely rare to have progression to CRPC without a rising PSA.
The treatment with doralutamide should be started in conjunction with docetaxel and continued after docetaxel completion (6 cycles) until there is clear evidence of cancer progression. This is usually assessed by using the PCWG3 criteria for castration resistance. In the rare situations of castration resistance without PSA rising, the decision is made on the base of radiographic findings of cancer progression.
What settings are appropriate for treatment with [drug under review]? Is a specialist required to diagnose, treat, and monitor patients who might receive [drug under review]?
Treatment with doralutamide in combination with docetaxel should be administered by medical oncologists in chemotherapy specialized setting. Darolutamide maintenance therapy also requires specialized physicians (medical oncologists, uro-oncologists, radiation oncologists) for the management of the cancer and eventually manage the drug side effects.
Additional Information
The addition of darolutamide to docetaxel and LHRHa significantly prolongs OS in patients with mCSPC comparted to LHRHa+docetaxel which represented the only standard of care control arm at the time the study was designed. There is no data comparing the triplet therapy with darolutamide + docetaxel and LHRHa vs darolutamide + LHRHa or another ARPI (apalutamide, enzalutamide or abiraterone acetate +prednisone) +LHRHa which constitute optional standard of care in the same mCSPC patients population. By retrospective review of the literature of the clinical trials conducted in mCSPC and with all the limitations of cross-trials comparison, accounting for the heterogeneous patients population, there are no data suggesting that docetaxel is inferior to ARPI.
Another clinical trial (PEACE-1)12 has also demonstrated advantage in OS with the addition of ARPI (abiraterone+prednisone) to docetaxel+LHRHa compared to docetaxel+LHRHa, further highlighting the efficacy of treatment intensification for mCSPC patients.
References
Brenner DR, et al. Projected estimates of cancer in Canada in 2022. CMAJ May 02, 2022 194 (17) E601-E607
Canadian Cancer Society’s Advisory Committee on Cancer Statistics. Canadian Cancer Statistics 2017. Toronto, ON: Canadian Cancer Society; 2017. Available at: cancer.ca/Canadian-Cancer- Statistics-2017-EN.pdf
Amling, C.L., et al., Defining prostate specific antigen progression after radical prostatectomy: what is the most appropriate cut point? J Urol, 2001. 165(4): p. 1146-51.
Lee, W.R.et al. Increasing prostate-specific antigen profile following definitive radiation therapy for localized prostate cancer: clinical observations. J Clin Oncol, 1997. 15(1): p. 230-8.
Sweeney CJ et al. Chemohormonal Therapy in Metastatic Hormone-Sensitive Prostate Cancer. N Engl J Med. 2015 Aug 20;373(8):737-46.
Fizazi , K. et al. Abiraterone plus Prednisone in Metastatic, Castration-Sensitive Prostate Cancer. N Engl J Med. 2017 Jul 27;377(4):352-360.
Kyriakopoulos CE, et al. Chemohormonal Therapy in Metastatic Hormone-Sensitive Prostate Cancer: Long-Term Survival Analysis of the Randomized Phase III E3805 CHAARTED Trial. J Clin Oncol. 2018 Apr 10;36(11):1080-1087. doi: 10.1200/JCO.2017.75.3657. Epub 2018 Jan 31.
Chi, K, et al. Apalutamide for Metastatic, Castration-Sensitive Prostate Cancer. N Engl J Med. 2019 Jul 4;381(1):13-24.
Davis ID et al. Enzalutamide with Standard First-Line Therapy in Metastatic Prostate Cancer. N Engl J Med. 2019 Jul 11;381(2):121-131.
Davis ID et al. Updated overall survival outcomes in ENZAMET (ANZUP 1304), an international, cooperative group trial of enzalutamide in metastatic hormone-sensitive prostate cancer (mHSPC). Journal of Clinical Oncology 2022 40:17_suppl, LBA5004-LBA5004
Chi KN, et al. Patient-reported outcomes following abiraterone acetate plus prednisone added to androgen deprivation therapy in patients with newly diagnosed metastatic castration-naive prostate cancer (LATITUDE): an international, randomised phase 3 trial. Lancet Oncol. 2018 Feb;19(2):194-206.
Fizazi, K., et al. Abiraterone plus prednisone added to androgen deprivation therapy and docetaxel in de novo metastatic castration-sensitive prostate cancer (PEACE-1): a multicentre, open-label, randomised, phase 3 study with a 2 × 2 factorial design. Lancet. 2022 Apr 30;399(10336):1695-1707.
Khalaf DJ, et al. Optimal sequencing of enzalutamide and abiraterone acetate plus prednisone in metastatic castration-resistant prostate cancer: a multicentre, randomised, open-label, phase 2, crossover trial. Lancet Oncol. 2019 Dec;20(12):1730-1739. doi: 10.1016/S1470-2045(19)30688-6. Epub 2019 Nov 11.
Fizazi,K. et al. Darolutamide in Nonmetastatic, Castration-Resistant Prostate Cancer. N Engl J Med 2019; 380:1235-1246
Smith MR, et al., Darolutamide and Survival in Metastatic, Hormone-Sensitive Prostate Cancer. N Engl J Med. 2022 Mar 24;386(12):1132-1142.
Conflict of Interest Declarations — BC Cancer GU Medical Oncologists Group
To maintain the objectivity and credibility of the CADTH drug review programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This conflict of interest declaration is required for participation. Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please refer to the Procedures for CADTH Drug Reimbursement Reviews (section 6.3) for further details.
Did you receive help from outside your clinician group to complete this submission?
No help received.
Did you receive help from outside your clinician group to collect or analyze any information used in this submission?
No help received.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review. Please note that this is required for each clinician who contributed to the input — please add more tables as needed (copy and paste). It is preferred for all declarations to be included in a single document.
Declaration for Clinician 1
Name: Lucia Nappi
Position: Medical Oncologist, BC Cancer - Vancouver Centre
Date: 02-05-2022
Table 8: COI Declaration for BC Cancer GU Medical Oncologists Group — Clinician 1
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to 50,000 | In excess of $50,000 |
|---|---|---|---|---|
Bayer | X | — | — | — |
Ipsen | — | — | — | X |
Astra Zeneca | X | — | — | — |
Pfizer | X | — | — | — |
Merck | X | — | — | — |
Janssen | — | — | — | X |
EMD Serono | — | — | — | X |
Declaration for Clinician 2
Name: Krista Noonan
Position: Chair GU Systemic BC
Date: 21-06-2022
Table 9: COI Declaration for BC Cancer GU Medical Oncologists Group — Clinician 2
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to 50,000 | In excess of $50,000 |
|---|---|---|---|---|
AstraZeneca | X | — | — | — |
Astellas | X | — | — | — |
Bayer | X | — | — | — |
EMD | X | — | — | — |
Serono | X | — | — | — |
Merck | X | — | — | — |
Pfizer | X | — | — | — |
Declaration for Clinician 3
Name: Jenny Ko
Position: Medical Oncologist, Head of Department – BC Cancer- Abbotsford Centre
Date: 22/06/2022
Table 10: COI Declaration for BC Cancer GU Medical Oncologists Group — Clinician 3
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to 50,000 | In excess of $50,000 |
|---|---|---|---|---|
Merck | X | — | — | — |
BMS | X | — | — | — |
Astellas | X | — | — | — |
Bayer | — | — | — | X |
Janssen | — | — | — | X |
AstraZeneca | X | — | — | — |
Pfizer | X | — | — | — |
Declaration for Clinician 4
Name: Maryam Soleimani
Position: Medical Oncology, BC Cancer- Vancouver Centre
Date: 21-06-2022
Table 11: COI Declaration for BC Cancer GU Medical Oncologists Group — Clinician 4
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to 50,000 | In excess of $50,000 |
|---|---|---|---|---|
Bayer | X | — | X | — |
Ipsen | X | — | — | — |
Pfizer | X | — | — | — |
AbbVie | — | — | X | — |
Astellas | — | — | X | — |
Declaration for Clinician 5
Name: Bernhard Eigl
Position: Medical Oncologist, BC Cancer –Vancouver Centre
Date: 26-06-2022
Table 12: COI Declaration for BC Cancer GU Medical Oncologists Group — Clinician 5
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to 50,000 | In excess of $50,000 |
|---|---|---|---|---|
Janssen | X | — | — | — |
AstraZeneca | X | — | — | — |
Merck | X | — | — | — |
Zomanex | X | — | — | — |
Roche | X | — | — | — |
Astellas | X | — | — | — |
Pfizer | X | — | — | — |
Paladin | X | — | — | — |
EMD Serono | X | — | — | — |
Seagen | X | — | — | — |
Bayer | X | — | — | — |
Sanofi | X | — | — | — |
Tokai | X | — | — | — |
Bristol-Myers Squibb | X | — | — | — |
Lilly/ImClone | X | — | — | — |
Declaration for Clinician 6
Name: Susan Ellard
Position: Medical Oncologist, BC Cancer –Kelowna Centre
Date: 26-06-2022
Table 13: COI Declaration for BC Cancer GU Medical Oncologists Group — Clinician 6
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to 50,000 | In excess of $50,000 |
|---|---|---|---|---|
No COI | — | — | — | — |
Declaration for Clinician 7
Name: Adam Fundytus
Position: Medical Oncologist
Date: 21-06-2022
Table 14: COI Declaration for BC Cancer GU Medical Oncologists Group — Clinician 7
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to 50,000 | In excess of $50,000 |
|---|---|---|---|---|
No COI | — | — | — | — |
Declaration for Clinician 8
Name: Bruce Keith
Position: Medical Oncologist, BC Cancer –Abbotsford Centre
Date: 26-06-2022
Table 15: COI Declaration for BC Cancer GU Medical Oncologists Group — Clinician 8
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to 50,000 | In excess of $50,000 |
|---|---|---|---|---|
No COI | — | — | — | — |
Declaration for Clinician 9
Name: Daygen Finch
Position: Medical Oncologist, BC Cancer - Kewlona Centre
Date: 28-06-2022
Table 16: COI Declaration for BC Cancer GU Medical Oncologists Group — Clinician 9
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to 50,000 | In excess of $50,000 |
|---|---|---|---|---|
Bayer | X | — | — | — |
Declaration for Clinician 10
Name: Joanna Vergidis
Position: Medical Oncologist, Head of Department, BC Cancer-Victoria Centre
Date: June 28, 2022
Table 17: COI Declaration for BC Cancer GU Medical Oncologists Group — Clinician 10
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to 50,000 | In excess of $50,000 |
|---|---|---|---|---|
No COI | — | — | — | — |
Declaration for Clinician 11
Name: Sunil Parimi
Position: Medical Oncologist, BC Cancer-Victoria Centre
Date: June 28, 2022
Table 18: COI Declaration for BC Cancer GU Medical Oncologists Group — Clinician 11
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to 50,000 | In excess of $50,000 |
|---|---|---|---|---|
Astellas | X | — | — | — |
Janssen | X | — | — | — |
Astra Zeneca | X | — | — | — |
Merck | X | — | — | — |
Bristol-Myers Squibb | X | — | — | — |
Bayer | X | — | — | — |
Declaration for Clinician 12
Name: Jean-Michel Lavoie
Position: Medical Oncologist, BC Cancer - Surrey
Date: 28-06-2022
Table 19: COI Declaration for BC Cancer GU Medical Oncologists Group — Clinician 12
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to 50,000 | In excess of $50,000 |
|---|---|---|---|---|
Bayer | X | — | — | — |
Pfizer | X | — | — | — |
EMD Serono | X | — | — | — |
TerSera | X | — | — | — |
Canadian GU Medical Oncologists With Special Interest in the Care of Men With Metastatic Prostate Cancer, Coordinating the Submission With the Canadian Cancer Society
About the Clinician Group
Website Link for Canadian Cancer Society: https://cancer.ca/en
Our purpose: To unite and inspire all Canadians to take control of cancer. Our mission: In trusted partnership with donors and volunteers, we improve the lives of all those affected by cancer through world-class research, transformative advocacy and compassionate support. We set ourselves apart from other cancer charities by taking a comprehensive approach against cancer. We are also the only national charity that supports all Canadians living with all cancers across the country.
The Canadian Cancer Society sourced several Canadian GU medical oncologists with a special interest in the care of people with metastatic prostate cancer for this submission.
Information Gathering
The initial version of the submission was drafted by U. Emmenegger and the Canadian Cancer Society and circulated to a select group of Canadian thought leaders in the care of advanced prostate cancer for input. The final version of the submission integrated all feedback before obtaining approval for submission by all participants.
Current Treatments and Treatment Goals
While localized prostate cancer is a highly curable condition, metastatic prostate cancer remains incurable to date and is the main reason for the death of around 4,500 Canadian men annually. Around 10% of Canadian men dying from prostate cancer have metastases at the time of diagnoses, whereas 90% develop metastases following unsuccessful curative treatment attempts for localized prostate cancer. Most men with metastatic prostate cancer die within less than five years.
The therapeutic foundation for metastatic prostate cancer is androgen deprivation therapy (ADT). Since 2014, several studies have shown that (i) the success of the first line of treatment for metastatic prostate cancer is a strong predictor of eventual outcome, and that (ii) the following treatments prolong the life of patients with metastatic castration-sensitive prostate cancer (mCSPC) by more than one year on average when added to ADT:
Docetaxel chemotherapy: typically reserved for chemotherapy-fit patients with high metastatic tumor burden;
Second-generation androgen receptor signaling inhibitors (ARSi) such as (in alphabetical order) abiraterone, apalutamide, and enzalutamide: utilized for patients with low to high tumor burden;
Radiation therapy to the prostate: reserved for patients with low metastatic tumor burden.
Although guidelines (e.g., Canadian Urological Association - Canadian Urologic Oncology Group guideline) strongly support the use of these additional therapies, access to some of these treatments is not universal across Canada, and real-world evidence suggests that many patients are still treated with ADT alone.
Despite contemporary therapies, almost all men eventually progress. Utilization of subsequent follow-up lines of therapy is poor. Therefore, treatment intensification with both chemotherapy and ARSi at the same time is likely to ensure that more patients are able to benefit from each of these proven life prolonging treatments.
More intense first line therapy with ADT and combination partners not only prolong the life of patients with mCSPC, but also result in more robust and frequent tumor responses (e.g., PSA responses), symptom control, and maintenance of qualify of life as well as independence. Individual patients and their oncologists aim for choosing the treatment option with the best chances to prolong life as well as delay prostate cancer progression (including the appearance of symptoms) and with the lowest risk of incurring treatment-related side effects.
Despite these recent advances in the treatment of mCSPC patients invariably will progress to the fatal stage of prostate cancer (i.e., metastatic castration-resistant prostate cancer, mCRPC). Established treatments for mCRPC include chemotherapy and ARSi amongst others. However, the benefit achieved with these agents at the mCRPC stage is inferior to using them for mCSPC.
Treatment Gaps (Unmet Needs)
Considering the treatment goals, please describe goals (needs) that are not being met by currently available treatments.
While the administration of double combination therapy (e.g., ADT + ARSi) was a long-awaited step forward in the treatment of mCSPC, many patients progress to the ultimately fatal stage of mCRPC within two to three years of starting double therapy. There is a lack of validated predictive markers of poor outcome despite double therapy. Furthermore, at the mCRPC stage patients might be less fit regarding tolerating certain treatments such as chemotherapy.
Compared to the current treatment paradigm of double therapy (most commonly under the form of ADT + ARSi), the upfront use of triple therapy for mCSPC as successfully studied in the ARASENS study (i.e., combination of ADT + docetaxel + darolutamide) addresses a number of medical needs:
Triple therapy:
prolongs survival (hazard ratio [95% confidence interval] 0.68 [0.57-0.80], p<0.0001);
prolongs time to mCRPC (0.36 [0.30-0.42], p<0.0001);
prolongs time to worsening pain (0.79 [0.66-0.95], p=0.0116); and
prolongs the time to starting the subsequent line of antineoplastic therapy (0.39 [0.33-0.46], p <0.0001).
Triple therapy is very well tolerated and is not associated with a noticeable increase in the frequency or severity of side effects when compared to ADT + docetaxel double therapy (i.e., there appear to be no interactions between docetaxel and darolutamide).
More patients might be deemed suitable for docetaxel chemotherapy when used at the early mCSPC stage compared to later mCRPC, when patients are older, may be more frail, and might have more co-morbidities.
The ARASENS study results are in line with another form of triple therapy, i.e., ADT + docetaxel + abiraterone (as per PEACE-1 study). Unfortunately, abiraterone is not universally available for patients with mCSPC across Canada. Moreover, accounting for differences between abiraterone and darolutamide, having multiple treatment choices facilitates precision treatment planning tailored to individual patients.
Place in Therapy
How would the drug under review fit into the current treatment paradigm?
The upfront combination of ADT + darolutamide + docetaxel is efficacious (as outlined above [4.1]) and well tolerated. The superior outcome of patients undergoing darolutamide-based triple therapy compared to ADT + docetaxel (i.e., ARASENS control arm) can be explained by the simultaneous targeting of androgen-sensitive and androgen-insensitive tumor clones by ADT/darolutamide and docetaxel, respectively. This is a treatment option in patients who are chemotherapy-fit, who are assessed by clinicians to be in need of chemotherapy, yet this triple therapy will improve outcomes over just docetaxel + ADT despite similar tolerability to ADT + docetaxel.
Which patients would be best suited for treatment with the drug under review? Which patients would be least suitable for treatment with the drug under review?
In ARASENS, subjects eligible for darolutamide-based triple therapy were patients with mCSPC who “had to be candidates for androgen-deprivation therapy and docetaxel, in the investigator’s judgment”. Subgroup analyses did not reveal patient or disease characteristics predicting response to triple therapy or lack thereof. Hence, in real-world practice most oncologists would consider darolutamide-based triple therapy in patients suitable for ADT + docetaxel, notably patients with clinical characteristics of poor prognosis such as high metastatic tumor burden and de novo metastatic presentation.
What outcomes are used to determine whether a patient is responding to treatment in clinical practice? How often should treatment response be assessed?
The therapeutic monitoring of patients with mCSPC comprises blood analyses (notably PSA testing), imaging (typically every 3 to 6 months), and the assessment for symptoms associated with response/progression (e.g., skeletal pain; at least every 3 months, initially more frequently) and treatment-related side effects (at least every 3 months, initially more frequently). Patients undergoing successful darolutamide-based triple therapy are expected to achieve a PSA decline of at least 50% within the first six months and should not develop cancer-related worsening of pain for the first two to three years on treatment. For the average triple therapy patient, it will take more than 3 years before there is a need to change antineoplastic therapy because of the development of symptomatic mCRPC amongst others.
What factors should be considered when deciding to discontinue treatment with the drug under review?
When it comes to decisions with respect to discontinuing mCSPC treatment and considering the next line of antineoplastic therapy typically three dimensions are considered (ranked in order of importance):
Intolerance to the drug or (new) cancer symptoms, usually happening after PSA and radiological progression;
signs of radiological progression; and
PSA progression (most commonly the first sign of progression).
Patients progressing in at least two dimensions are considered for a treatment change. However, the appearance of symptoms or marked radiological changes alone might suffice as arguments for changing therapy.
What settings are appropriate for treatment with darolutamide? Is a specialist required to diagnose, treat, and monitor patients who might receive darolutamide?
ADT and ARSi treatment are initiated and monitored by prostate cancer specialists across the medical spectrum (i.e., medical oncologists, urological oncologist, radiation oncologists). However, docetaxel chemotherapy administration is exclusively supervised by a medical oncologist in most constituencies across Canada. As such, medical oncologists would be considered the gate keepers for triple therapy, at least during the first 4.5 months of docetaxel administration.
Additional Information
Not applicable.
Conflict of Interest Declarations
To maintain the objectivity and credibility of the CADTH drug review programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This conflict of interest declaration is required for participation. Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please refer to the Procedures for CADTH Drug Reimbursement Reviews (section 6.3) for further details.
Did you receive help from outside your clinician group to complete this submission?
Not applicable.
Did you receive help from outside your clinician group to collect or analyze any information used in this submission?
Not applicable.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review. Please note that this is required for each clinician who contributed to the input — please add more tables as needed (copy and paste). It is preferred for all declarations to be included in a single document.
Declaration for Clinician 1
Name: Urban Emmenegger
Position: Staff Medical Oncologist, Odette Cancer Centre, Toronto, ON
Date: 10-07-2022
Table 20: COI Declaration for GU Medical Oncologist — Clinician 1
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to 50,000 | In excess of $50,000 |
|---|---|---|---|---|
Amgen | — | X | — | — |
Astellas | — | — | X | — |
AstraZeneca | — | — | X | — |
Bayer | — | — | X | — |
Ferring | X | — | — | — |
Janssen | — | X | — | — |
Knight | X | — | — | |
Merck | — | X | — | — |
Novartis (including Endocyte and Advanced Accelerator Applications) | — | X | — | — |
Pfizer | X | — | — | — |
Point Biopharma | X | — | — | — |
Roche-Genentech | X | — | — | — |
Declaration for Clinician 2
Name: Jay Detsky
Position: Staff Physician, Radiation Oncologist, Odette Cancer Centre
Date: 13-07-2022
Table 21: COI Declaration for GU Medical Oncologist — Clinician 2
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to 50,000 | In excess of $50,000 |
|---|---|---|---|---|
Verity | X | — | — | — |
Abbvie | X | — | — | — |
Declaration for Clinician 3
Name: Dr Hans Chung
Position: Radiation Oncologist, Sunnybrook Odette Cancer Centre
Date: 15-07-2022
Table 22: COI Declaration for GU Medical Oncologist — Clinician 3
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to 50,000 | In excess of $50,000 |
|---|---|---|---|---|
No COI | — | — | — | — |
Declaration for Clinician 4
Name: Dr Stanley Liu
Position: Clinician-Scientist, Sunnybrook Research Institute; Radiation Oncologist, Odette Cancer Centre, Sunnybrook Health Sciences Centre
Date: 12-07-2022
Table 23: COI Declaration for GU Medical Oncologist — Clinician 4
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to 50,000 | In excess of $50,000 |
|---|---|---|---|---|
No COI | — | — | — | — |
Declaration for Clinician 5
Name: Steven Yip
Position: Medical Oncologist
Date: 07-07-2222
Table 24: COI Declaration for GU Medical Oncologist — Clinician 5
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to 50,000 | In excess of $50,000 |
|---|---|---|---|---|
Janssen | — | — | — | Fellowship grant |
Merck | advisory board/consultant | — | — | — |
Bayer | — | — | — | Fellowship grant |
AstraZeneca | — | — | — | ESCR |
Pfizer | Sponsorship, advisory board/consultant | — | — | |
Novartis | advisory board/consultant | — | — | — |
BMS | advisory board/consultant | — | — | — |
Hoffman-La Roche | advisory board/consultant | — | — | — |
EMD Serono | advisory board/consultant | — | — | — |
Declaration for Clinician 6
Name: Di (Maria) Jiang
Position: Medical oncologist
Date: 07-Jul-2022
Table 25: COI Declaration for GU Medical Oncologist — Clinician 6
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to 50,000 | In excess of $50,000 |
|---|---|---|---|---|
Janssen Oncology | X | — | — | — |
Ipsen | X | — | — | — |
Bayer | X | — | — | — |
EMD Serono Canada | X | — | — | — |
Amgen | X | — | — | — |
McKesson Canada | X | — | — | — |
Declaration for Clinician 7
Name: Dr Rachel Glicksman
Position: Radiation Oncologist, Princess Margaret Cancer Centre, University Health Network; Assistant Professor, Department of Radiation Oncology, University of Toronto
Date: 22-06-2022
Table 26: COI Declaration for GU Medical Oncologist — Clinician 7
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to 50,000 | In excess of $50,000 |
|---|---|---|---|---|
Bayer | X | — | — | — |
Declaration for Clinician 8
Name: Christopher Wallis
Position: Urologic Oncologist; Assistant Professor
Date: 06-21-2022
Table 27: COI Declaration for GU Medical Oncologist — Clinician 8
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to 50,000 | In excess of $50,000 |
|---|---|---|---|---|
Janssen Oncology | — | — | X | — |
SESEN Bio | — | — | X | — |
Precision Point Specialty LLC | X | — | — | |
Bayer | X | — | — | — |
EMD Serono | X | — | — | — |
Haymarket Media | X | — | — | — |
Healing and Cancer Foundation | X | — | — | — |
Knight Therapeutics | X | — | — | — |
TerSera Canada | X | — | — | — |
Tolmar Pharmaceuticals | X | — | — | — |
Declaration for Clinician 9
Name: Paul Toren
Position: Professeur agregé, Université Laval, Uro-Oncologue, Hôtel-Dieu de Québec; Chercheur, Centre de recherche de CHU de Québec-Université Laval
Date: 5-6-2022
Table 28: COI Declaration for GU Medical Oncologist — Clinician 9
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to 50,000 | In excess of $50,000 |
|---|---|---|---|---|
Knight Pharmaceuticals | X | — | — | — |
Bayer | X | — | — | — |
TerSera | X | — | — | — |
Abbvie | X | — | — | — |
Tolmar | X | — | — | — |
AstraZeneca | — | — | — | Institutional Research Funding |
Declaration for Clinician 10
Name: Bobby Shayegan
Position: MD, FRCSC, Associate Professor and Head of Division of Urology, McMaster University
Date: 11-07-2022
Table 29: COI Declaration for GU Medical Oncologist — Clinician 10
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to 50,000 | In excess of $50,000 |
|---|---|---|---|---|
Bayer | — | X | — | — |
Janssen | — | X | — | — |
Astellas | — | X | — | — |
Declaration for Clinician 11
Name: Lucia Nappi
Position: Medical Oncologist, BC Cancer - Vancouver Centre
Date: 28-06-2022
Table 30: COI Declaration for GU Medical Oncologist — Clinician 11
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to 50,000 | In excess of $50,000 |
|---|---|---|---|---|
Bayer | X | — | — | — |
Ipsen | X | — | — | — |
Astra Zeneca | X | — | — | — |
Pfizer | X | — | — | — |
Merck | X | — | — | — |
Declaration for Clinician 12
Name: Chia-Lin Tseng
Position: Radiation Oncologist
Date: 13-July-2022
Table 31: COI Declaration for GU Medical Oncologist — Clinician 12
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to 50,000 | In excess of $50,000 |
|---|---|---|---|---|
Elekta | X | — | — | — |
Ontario Health (Cancer Care Ontario) Genitourinary Cancer Drug Advisory Committee
About the Ontario Health (Cancer Care Ontario) Genitourinary Cancer Drug Advisory Committee
OH-CCO’s Drug Advisory Committees provide timely evidence-based clinical and health system guidance on drug-related issues in support of CCO’s mandate, including the Provincial Drug Reimbursement Programs (PDRP) and the Systemic Treatment Program.
Information Gathering
Information was jointly discussed at a DAC meeting.
Current Treatments and Treatment Goals
Standard treatment for patients with metastatic, hormone-sensitive prostate cancer includes the addition of either docetaxel or an androgen-receptor pathway inhibitor to androgen-deprivation therapy. In two randomized, phase 3 trials involving such patients, overall survival was longer among those who received docetaxel plus androgen-deprivation therapy than among those who received androgen-deprivation therapy alone. Subsequent randomized, phase 3 trials have shown that the addition of an androgen-receptor pathway inhibitor (abiraterone, enzalutamide, or apalutamide) to androgen-deprivation therapy has greater clinical benefit than the use of androgen-deprivation therapy alone.
Treatments goals for this drug would be prolonged life and delayed disease progression.
Treatment Gaps (Unmet Needs)
Considering the treatment goals, please describe goals (needs) that are not being met by currently available treatments.
Better treatment options are needed. The drug under review would be more beneficial than current available regimens.
Place in Therapy
How would the drug under review fit into the current treatment paradigm?
Darolutamide would be first-line for mCSPC.
Which patients would be best suited for treatment with the drug under review? Which patients would be least suitable for treatment with the drug under review?
Patients best suited with be patients with mCSPC that are fit to receive chemotherapy.
What outcomes are used to determine whether a patient is responding to treatment in clinical practice? How often should treatment response be assessed?
As per standard of care assessment including clinician and/or lab and/or imaging.
What factors should be considered when deciding to discontinue treatment with the drug under review?
Clinical progression or intolerability of darolutamide.
What settings are appropriate for treatment with [drug under review]? Is a specialist required to diagnose, treat, and monitor patients who might receive [drug under review]?
Hospital (outpatient clinic) for darolutamide. A specialist with expertise in prostate cancer is required.
Additional Information
Not applicable.
Conflict of Interest Declarations — Ontario Health (Cancer Care Ontario) Genitourinary Cancer Drug Advisory Committee
To maintain the objectivity and credibility of the CADTH drug review programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This conflict of interest declaration is required for participation. Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please refer to the Procedures for CADTH Drug Reimbursement Reviews (section 6.3) for further details.
Did you receive help from outside your clinician group to complete this submission? If yes, please detail the help and who provided it.
Yes, Ontario Health provided secretariat function to the DAC.
Did you receive help from outside your clinician group to collect or analyze any information used in this submission?
No.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review. Please note that this is required for each clinician who contributed to the input — please add more tables as needed (copy and paste). It is preferred for all declarations to be included in a single document.
Declaration for Clinician 1
Name: Dr. Girish Kulkarni
Position: Ontario Health (CCO) Genitourinary Cancer Drug Advisory Committee Lead
Date: 16-06-2022
Table 32: COI Declaration for Ontario Health (CCO) Genitourinary Cancer DAC — Clinician 1
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to 50,000 | In excess of $50,000 |
|---|---|---|---|---|
No COI | — | — | — | — |
Declaration for Clinician 2
Name: Dr. Christina Canil
Position: Medical oncologist
Date: 16-06-2022
Table 33: COI Declaration for Ontario Health (CCO) Genitourinary Cancer DAC — Clinician 2
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to 50,000 | In excess of $50,000 |
|---|---|---|---|---|
Bayer | X | — | — | — |
Declaration for Clinician 3
Name: Dr. Aly-Khan Lalani
Position: Medical oncologist
Date: 16-06-2022
Table 34: COI Declaration for Ontario Health (CCO) Genitourinary Cancer DAC — Clinician 3
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to 50,000 | In excess of $50,000 |
|---|---|---|---|---|
Bayer | X | — | — | — |
Declaration for Clinician 4
Name: Dr. Chris Morash
Position: Medical oncologist
Date: 16-06-2022
Table 35: COI Declaration for Ontario Health (CCO) Genitourinary Cancer DAC — Clinician 4
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to 50,000 | In excess of $50,000 |
|---|---|---|---|---|
No COI | — | — | — | — |
GU Oncologists of the Maritime Provinces
About GU Oncologists of the Maritime Provinces
We are a group of genitourinary oncology specialists, representing urology, radiation oncology and medical oncology perspectives, practicing in major centres in the Maritime provinces (Halifax, NS and Saint John, NB).
Information Gathering
Targeted literature review, including recent clinical practice guidelines.
Current Treatments and Treatment Goals
Metastatic prostate cancer is an incurable disease, associated with significant morbidity. Systemic therapy is the main modality of treatment for patients with this disease, with androgen deprivation therapy (ADT) being the key initial treatment. The majority of patients will initially respond to ADT in the metastatic castration sensitive prostate cancer (mCSPC) setting, but all patients eventually progress and develop castration resistant disease.
Systemic therapy for mCSPC is primarily given with the goal of prolonging overall survival, however it also is given with the purpose of reducing symptom burden (e.g., pain from bone metastases), preventing complications of progressive disease (pain crises, pathological fracture due to bone metastases, neurological compromise from spinal cord compression), and maintaining quality of life.
Several phase III clinical trials have demonstrated that treatment intensification with an additional form of systemic therapy combined with ADT significantly improves overall survival compared to ADT alone, in addition to a number of other outcomes (such as time to pain progression, time to castration resistance, and patient reported outcomes). These additional treatments include either six cycles of docetaxel chemotherapy, or an oral androgen receptor axis targeting agent (ARAT) such as abiraterone acetate, enzalutamide, or apalutamide. All of these options are available in Canada, and are recommended in several clinical practice guidelines, including the Canadian Urological Association (CUA) guidelines (So et al., 2020). In practice, most clinicians favour a “doublet” ADT plus ARAT option over docetaxel + ADT due to the ARATs having excellent clinical activity and tolerance; however, certain high risk patient populations may be offered docetaxel over an ARAT. None of the combination therapies have been compared in prospective clinical trials, so the choice of agent to combine with ADT generally depends on patient factors (comorbidities, potential contraindications, patient preference), clinician preference/comfort, and accessibility.
Despite the availability of highly effective treatments for mCSPC, all patients eventually succumb to their disease. Further, a subset of patients with poor prognostic disease factors derive less benefit and limited survival, even with treatment intensification with an ADT doublet with an ARAT or docetaxel.
Recent data from phase III randomized control trials have demonstrated the benefit of a “triplet therapy” strategy involving the combination of ADT, docetaxel, and an ARAT in mCSPC. This includes the ARASENS trial, involving darolutamide (currently under review, see below for details), and the PEACE-1 trial, with abiraterone acetate. The combination of ADT, docetaxel, and abiraterone is potentially accessible currently, as abiraterone is available for the treatment of mCSPC, as is docetaxel.
Treatment Gaps (Unmet Needs)
Considering the treatment goals, please describe goals (needs) that are not being met by currently available treatments.
With the current standard “doublet” therapies involving ADT plus either docetaxel or an ARAT outlined above, a small proportion of patients will fail to respond altogether. Another subset of patients will initially respond but develop progressive disease after a short interval. All patients eventually will progress on doublet therapy.
Identifying patients at risk for a poor response to doublet therapy is not well defined. However, some clinical factors that can potentially predict for aggressive disease biology include a high burden of disease (including visceral metastases), high grade disease, de novo presentation with metastatic disease, short interval from primary tumour treatment to development of metastatic disease, and younger patient age.
Treatments to improve outcomes in patients with poor prognostic factors and high-risk disease are warranted. Additionally, highly motivated and fit patients may desire a more aggressive treatment to improve their chances of prolonging disease control and survival. Triplet therapy with ADT, docetaxel and an ARAT is a further intensified treatment strategy that has been shown in the ARASENS and PEACE-1 trials to improve outcomes, including survival, including in patients with higher risk disease. While the triplet combination of ADT, docetaxel and abiraterone may be an option for such treatment intensification, abiraterone may not be a suitable choice for some patients due to the potential for hypertension, liver toxicity, and the need for prolonged co-administration of prednisone with abiraterone. Having an alternative ARAT to pair with ADT and docetaxel, particularly one that is well tolerated and easily administered, is critical to offering this strategy to all patients who may be eligible and derive benefit.
Place in Therapy
How would the drug under review fit into the current treatment paradigm?
Darolutamide in this application would be utilized as a first-line treatment for mCSPC in combination with ADT and docetaxel. This approach was shown in the phase III ARASENS randomized control trial to significantly improve overall survival compared to ADT, docetaxel, and placebo. Other key secondary endpoints were also improved with the darolutamide combination, including time to pain progression, time to symptomatic skeletal related event, and time to castration resistance. Of note, about 75% of patients in the control arm received an ARAT as subsequent therapy, indicating that early introduction of darolutamide was key in driving the observed survival benefit. The addition of darolutamide to ADT and docetaxel was also well tolerated, with little difference in toxicity rates between the two arms in the trial.
The results of this trial and the PEACE-1 trial both demonstrated superiority of triplet therapy over ADT plus docetaxel. These results argue for triplet therapy to be used over ADT plus docetaxel as first-line therapy for mCSPC, which represents a paradigm shift. It is unknown whether triplet therapy is superior to ADT plus ARAT doublet combinations, however. In the current context, darolutamide is a well-tolerated option to utilize in a triplet strategy.
It would not be appropriate for patients to try an alternative treatment prior to proceeding with darolutamide in combination with ADT and docetaxel. This treatment strategy should be implemented early, shortly after initiation of ADT, as was done in the ARASENS clinical trial. This treatment also should not be reserved for patients with intolerance or contraindication to other therapies, as the evidence supporting use of this drug is in treatment-naïve patients who have not trialed other therapies.
Which patients would be best suited for treatment with the drug under review? Which patients would be least suitable for treatment with the drug under review?
The ARASENS trial included patients with metastatic CSPC, who were treatment-naïve, ECOG performance status 0-1, eligible for both ADT and docetaxel, with treatment initiated within 12 weeks of starting ADT. The overall survival improvement appeared to be consistent across all subgroups, regardless of age, ECOG performance status, race, stage at diagnosis, whether visceral metastases were present or not, and Gleason score. Therefore, the trial data would suggest that patients who meet the eligibility criteria for the trial should be candidates to receive darolutamide in combination with docetaxel and ADT.
In practice, likely only a subset of these patients will receive triplet therapy with darolutamide, as some patients who meet the above criteria may have favourable prognostic factors, and may be offered ADT plus an ARAT alone. Further, some patients may prefer to avoid docetaxel chemotherapy due to potential toxicities or convenience. The decision to proceed with a triplet combination versus ADT plus an ARAT will therefore hinge on multiple factors and require a detailed discussion between the patient and their oncology specialist.
What outcomes are used to determine whether a patient is responding to treatment in clinical practice? How often should treatment response be assessed?
Outcomes used to determine whether a patient is responding to therapy in practice include biochemical/PSA response, biochemical control (usually assessed every 3 months), radiographic response, and clinical response. A clinical response can be identified by reported improvement in patient symptoms (i.e. pain from bone metastases, urinary symptoms, fatigue). However, in patients without disease-related symptoms, this may not be apparent. A clinically meaningful response would range from any reduction or prolonged stability of PSA values or tumour volume on imaging.
What factors should be considered when deciding to discontinue treatment with the drug under review?
Treatment would typically be discontinued upon disease progression (usually indicated by a combination of a rising PSA, radiographic progression and/or clinical progression).
Toxicities are also a possible reason for discontinuation, in scenarios where dose reduction of darolutamide or other supportive care measures are ineffective. This would include persistent grade 2 toxicities adversely affecting quality of life, and/or grade 3 or 4 toxicities.
What settings are appropriate for treatment with [drug under review]? Is a specialist required to diagnose, treat, and monitor patients who might receive [drug under review]?
Darolutamide, as an oral agent, would be administered on an outpatient basis. It would be appropriate to be prescribed by specialist in genitourinary oncology (urologists, radiation oncologists, medical oncologists) in any outpatient setting. Of note, docetaxel chemotherapy, when administered in combination with darolutamide, would be prescribed by a medical oncologist and administered in an appropriate hospital or infusion clinic setting.
Additional Information
Darolutamide has fewer drug interactions than other drugs in its class. We expect this to simplify concerns when initiating the agent and limiting morbidity from either drug interactions or modifying effective pharmaceutical management for other comorbidities.
Conflict of Interest Declarations — GU Oncologists of the Maritime Provinces
To maintain the objectivity and credibility of the CADTH drug review programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This conflict of interest declaration is required for participation. Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please refer to the Procedures for CADTH Drug Reimbursement Reviews (section 6.3) for further details.
Did you receive help from outside your clinician group to complete this submission?
No.
Did you receive help from outside your clinician group to collect or analyze any information used in this submission?
No.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review. Please note that this is required for each clinician who contributed to the input — please add more tables as needed (copy and paste). It is preferred for all declarations to be included in a single document.
Declaration for Clinician 1
Name: Myuran Thana
Position: Medical Oncologist, QEII Health Sciences Centre, Halifax NS
Date: 11-07-2022
Table 36: COI Declaration for GU Oncologists of the Maritime Provinces — Clinician 1
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to 50,000 | In excess of $50,000 |
|---|---|---|---|---|
Advanced Accelerator Applications/Novartis | X | — | — | — |
AstraZeneca | X | — | — | — |
Bayer | X | — | — | — |
BMS | X | — | — | — |
Ipsen | X | — | — | — |
Merck | X | — | — | — |
Pfizer | X | — | — | — |
Declaration for Clinician 2
Name: Samantha Gray
Position: Medical Oncologist, Saint John Regional Hospital, Saint John NB
Date: 11-07-2022
Table 37: COI Declaration for GU Oncologists of the Maritime Provinces — Clinician 2
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to 50,000 | In excess of $50,000 |
|---|---|---|---|---|
Bayer | X | — | — | — |
BMS | X | — | — | — |
Essai | X | — | — | — |
Ipsen | X | — | — | — |
Merck | X | — | — | — |
Declaration for Clinician 3
Name: Michael Kucharczyk
Position: Radiation Oncologist, QEII Health Sciences Centre, Halifax NS
Date: 07-11-2022
Table 38: COI Declaration for GU Oncologists of the Maritime Provinces — Clinician 3
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to 50,000 | In excess of $50,000 |
|---|---|---|---|---|
AbbVie | X | — | — | — |
Bayer | X | — | — | — |
Ferring | X | — | — | — |
Jannsen | X | — | — | — |
McKesson | X | — | — | — |
Palette Life Sciences | X | — | — | — |
TerSera | X | — | — | — |
Verity | X | — | — | — |
Declaration for Clinician 4
Name: Dr. Robyn Macfarlane
Position: Medical Oncologist, QEII Health Sciences Centre, Halifax NS
Date: 11-07-2022
Table 39: COI Declaration for GU Oncologists of the Maritime Provinces — Clinician 4
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to 50,000 | In excess of $50,000 |
|---|---|---|---|---|
Merck | X | — | — | — |
Ipsen | — | X | — | — |
Bayer | X | — | — | — |
Sanofi | X | — | — | — |
Janssen | X | — | — | — |
Astellas | X | — | — | — |
Declaration for Clinician 5
Name: Ricardo Rendon
Position: Urologist, QEII Health Sciences Centre, Halifax NS
Date: 11-07-2022
Table 40: COI Declaration for GU Oncologists of the Maritime Provinces — Clinician 5
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to 50,000 | In excess of $50,000 |
|---|---|---|---|---|
Abbvie | X | — | — | — |
Amgen | X | — | — | — |
Astellas | X | — | — | — |
AstraZeneca | X | — | — | — |
Bayer | X | — | — | — |
Janssen | X | — | — | — |
Ferring | X | — | — | — |
McKesson | X | — | — | — |
Sanofi | X | — | — | — |
Allan Blair Cancer Centre
About the Allan Blair Cancer Centre
We are a group of GU oncologists from Allan Blair Cancer Centre in Regina, Saskatchewan
Information Gathering
The results of ARASENS trial were published in NEJM and our GU group has had a discussion about the favorable patients beefits for OS using triple therapy with Darolutamide plus docetaxel and ADT
Current Treatments and Treatment Goals
The landscape for mcspc has rapidly evolved. It has changed from the use of Docetaxel with ADT to using more ARATS and ADT and most recently to intensify with triple therapy(CHAARTED, STAMPEDE, LATITUDE,TITAN, ARCHES, PEACE1, ARASENS). The use of triple therapy targets the tumor heterogeneity in mcspc by targeting androgen dependent and androgen independent pathways earlier in the disease.
Treatment Gaps (Unmet Needs)
Considering the treatment goals, please describe goals (needs) that are not being met by currently available treatments.
The landscape for mcspc has rapidly evolved. It has changed from the use of Docetaxel with ADT to using more ARATS and ADT and most recently to intensify with triple therapy(CHAARTED, STAMPEDE, LATITUDE,TITAN, ARCHES, PEACE1, ARASENS). The use of triple therapy targets the tumor heterogeneity in mcspc by targeting androgen dependent and androgen independent pathways earlier in the disease
Place in Therapy
How would the drug under review fit into the current treatment paradigm?
The drug under review Darolutamide will be used in combination with other treatments like docetaxel and ADT. There is a shift in treatment paradigm because the triple therapy improves the OS by 32.5%
Which patients would be best suited for treatment with the drug under review? Which patients would be least suitable for treatment with the drug under review?
Patients with high burden (TNM CLASSIFICATION m1b, m1c) all comers mcspc.
What outcomes are used to determine whether a patient is responding to treatment in clinical practice? How often should treatment response be assessed?
Biochemical and radiographic response.
What factors should be considered when deciding to discontinue treatment with the drug under review?
Additional unexpected toxicities beyond the drug monograph.
What settings are appropriate for treatment with [drug under review]? Is a specialist required to diagnose, treat, and monitor patients who might receive [drug under review]?
Cancer centre setting or infusion clinics for docetaxel.
Additional Information
Not applicable.
Conflict of Interest Declarations — Allan Blair Cancer Centre
To maintain the objectivity and credibility of the CADTH drug review programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This conflict of interest declaration is required for participation. Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please refer to the Procedures for CADTH Drug Reimbursement Reviews (section 6.3) for further details.
Did you receive help from outside your clinician group to complete this submission?
Not applicable.
Did you receive help from outside your clinician group to collect or analyze any information used in this submission?
Not applicable.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review. Please note that this is required for each clinician who contributed to the input — please add more tables as needed (copy and paste). It is preferred for all declarations to be included in a single document.
Declaration for Clinician 1
Name: Dr. Osama Souied
Position: Medical oncologist
Date: 17-06-2022
Table 41: COI Declaration for Allan Blair Cancer Centre — Clinician 1
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to 50,000 | In excess of $50,000 |
|---|---|---|---|---|
Bayer | X | — | — | — |
Pfizer | X | — | — | — |
Ispen | X | — | — | — |
Janssen | X | — | — | — |
Declaration for Clinician 2
Name: Dr. Asim Amjad
Position: Radiation Oncologist
Date: 17-June -2022
Table 42: COI Declaration for Allan Blair Cancer Centre — Clinician 2
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to 50,000 | In excess of $50,000 |
|---|---|---|---|---|
No COI | — | — | — | — |
Declaration for Clinician 3
Name: Dr. Kimberly Hagel
Position: Medical Oncologist
Date: June 17, 2022
Table 43: COI Declaration for Allan Blair Cancer Centre — Clinician 3
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to 50,000 | In excess of $50,000 |
|---|---|---|---|---|
Bayer | X | — | — | — |
Astellas | X | — | — | — |
Declaration for Clinician 4
Name: Dr. Muhammad Salim
Position: Medical Oncologist
Date: 17-06-2022
Table 44: COI Declaration for Allan Blair Cancer Centre — Clinician 4
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to 50,000 | In excess of $50,000 |
|---|---|---|---|---|
No COI | — | — | — | — |
Declaration for Clinician 5
Name: Dr. Habib Khan
Position: Medical Oncologist
Date: 17-06-2022
Table 45: COI Declaration for Allan Blair Cancer Centre — Clinician 5
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to 50,000 | In excess of $50,000 |
|---|---|---|---|---|
No COI | — | — | — | — |
The Ottawa Hospital Cancer Centre – Genitourinary Oncology Group
About the Ottawa Hospital Cancer Centre – Genitourinary Oncology Group
We are a multidisciplinary group of expert oncologist clinicians (Medical Oncologist, Radiation Oncologist, Urologic Oncologist) whose practices significantly involves caring for patients with metastatic castration sensitive prostate cancer (mCSPC). We exist within a larger group of oncologists caring for prostate cancer patients – 3 more urologist oncologists, 4 more medical oncologists, 6 more radiation oncologists. We practice at The Ottawa Hospital and The Ottawa Hospital Cancer Centre, and conduct research at the Ottawa Hospital Research Institute. We each practice within a larger group of clinicians at The Ottawa Hospital to manage advanced prostate cancer for the entire Champlain LHIN (referral region of 1.6 million people). The vision of The Ottawa Hospital is “To provide each patient with the world-class care, exceptional service and compassion we would want for our loved ones”. The mission includes that The Ottawa Hospital “develops, shares and applies new knowledge and technology in the delivery of patient care through world-leading research programs in partnership with the Ottawa Hospital Research Institute (OHRI)”, such as use of darolutamide in prostate cancer treatment.
https://www.ottawahospital.on.ca/
Information Gathering
We have gathered information from the ARASENS clinical trial, including the review of the clinical trial data presented at the Genitourinary American Society of Clinical Oncology 2022 Meeting, including the ARASENS publication in the New England Journal of Medicine.
We have considered other published data for comparable agents in the treatment of mCSPC such as abiraterone acetate, apalutamide, enzalutamide, and docetaxel. These data include the LATITUDE, TITAN, ARCHES, STAMPEDE, and CHAARTED randomized clinical trials that have compared outcomes from androgen deprivation therapy (ADT) alone versus ADT + intensification agent. We have discussed these trials at continuing medical education events throughout the years.
We have conducted a network meta-analysis of randomized trials and published to consider the additional benefit of darolutamide + docetaxel + ADT above and beyond other standards of care, published recently (in press, attached to this submission). https://euoncology.europeanurology.com/article/S2588-9311(22)00092-X/fulltext
We have considered multiple individual patient cases of mCSPC discussed at our genitourinary multidisciplinary case rounds which occurs each Monday at The Ottawa Hospital and considered areas of unmet need for these cases. We have considered feedback given to us from individual patients that we have seen in clinic.
We have considered expert opinion amongst peers in the country, including Dr. Ong chairing a national debate at The 17th Annual Genitourinary Medical Oncologists of Canada meeting in Charlottetown, Prince Edward Island on June 24, 2022 about the value of ‘doublet’ therapy (ADT + AR-targeted agent) versus ‘triplet’ therapy (ADT + docetaxel chemotherapy + AR-targeted agent, which is the intervention in the ARASENS trial) (agenda of GUMOC conference attached).
Current Treatments and Treatment Goals
Metastatic castration sensitive prostate cancer (mCSPC) is an incurable condition in which prostate cancer has spread to other organs, and commonly involving lymph nodes, bones, lungs, or liver. Because this condition cannot be cured with radiation therapy or surgery, and sometimes has developed in-spite of radiation therapy or surgery, the treatment goals are to improve and extend disease control for as long as possible, improve and extend quality of life, and improve and extend disease control the overall survival of patients.
The ‘old’ paradigm (i.e., circa 2014) for mCSPC treatment was to give androgen deprivation therapy (ADT) alone and only add additional medical treatments when prostate cancer became resistant. However multiple reported clinical trials since then have proven that the addition of active systemic treatments up-front (i.e. at the time of ADT) improve all metrics of disease control, including biochemical response (prostate specific antigen, PSA), radiographic response (bone scans, CT scans), symptom control, time to subsequent treatments, time to subsequent radiation, and most importantly, overall survival of patients. In fact, substantial gains in median overall survival have been reported for both chemotherapy with docetaxel given up to 6 cycles, and also for all the AR-pathway inhibitors (ARPIs: abiraterone acetate, apalutamide, enzalutamide, and now darolutamide).
As the multiple randomized trials have been consistent in the significant improvements in survival and major disease control endpoints (PSA, radiographic control of disease, symptoms related to disease including pain and quality of life) for all of the ARPIs added to ADT as well as docetaxel when added to ADT, more recent data and discussion have focused on who to give ARPIs + ADT only, and who to give ‘triplet therapy’ with docetaxel + ARPI + ADT stratifying by the following factors: 1) ‘de-novo’ (i.e. newly diagnosed) metastatic prostate cancer versus ‘recurrent’ prostate cancer (i.e. after prior local treatment). 2) ‘high-volume’ vs. ‘low-volume’ burden of bone metastases 3) visceral metastases vs. non-visceral metastases 4) good performance status / low-comorbid patients vs. poor performance status / higher-comorbid patients.
Treatment goals also include reduction in treatment-related toxicities, and relevant ones are avoidance of ‘neurocognitive toxicities’ of certain ARPIs such as enzalutamide and apalutamide, avoidance of cardiac/cardiovascular toxicities seen with abiraterone acetate with prednisone, and avoidance of drug-drug interactions that do occur with many ARPIs.
In addition to systemic therapy goals, one more goal of effective local control of the primary prostate cancer has been met by data sets showing that radiotherapy to the prostate at the time of ADT seems to improve overall survival of patients and local control of prostate cancer primary.
An ideal treatment would:
have the longest control of disease
have the longest survival benefit
have the longest improvement in quality of life
cost the least amount of money
be suitable for patients both with comorbidities and with no-comorbidities
have the least additional burden of toxicities (and therefore less monitoring for toxicities)
from a mechanistic point of view would address the multiple alternative pathways for cancer progression/proliferation that are not driven by androgen-receptor (AR).
Treatment Gaps (Unmet Needs)
Considering the treatment goals, please describe goals (needs) that are not being met by currently available treatments.
Unfortunately, there remain many unmet needs of metastatic hormone-sensitive prostate cancer:
The disease state remains incurable.
Many patients fail systemic treatment shortly after treatment initiation.
In particular patients with high disease burden (high-volume bone metastases, visceral metastases, poor histological category (Gleason 8-10)) have short survival despite treatment (i.e. <3 years)
Treatments are needed that further increase time to treatment failure, increase survival, increase QOL, and increase longevity of ADT + ARPI response.
Treatments that provide less toxicity burden: less requirement for monitoring for toxicities, less drug-drug interactions, less neurocognitive syndrome, less cardiac toxicities, less seizure risk, less fall-risk.
Current ‘rescue’ treatments are also not ideal once patients have failed ARPIs + ADT. In this state (‘metastatic castration-resistance prostate cancer (mCRPC)), the mainstay of treatment is docetaxel chemotherapy, and the survival benefit of docetaxel is very modest and toxicity burden is high in this state.
Place in Therapy
How would the drug under review fit into the current treatment paradigm?
The drug under review is darolutamide with docetaxel, as used in the ARASENS randomized clinical trial, in addition to standard ADT.
In the current treatment paradigm for mCSPC, a patient can be treated by one of three scenarios:
ADT alone
ADT + ARPI (such as abiraterone acetate + prednisone, or enzalutamide, or apalutamide)
ADT + docetaxel
Many patients nowadays are being offered and treated with ADT + ARPIs due to good tolerance of treatment and very similar survival outcomes as those treated with ADT + docetaxel.
In this drug under review, it would add a fourth category of ‘triplet’ therapy: ADT + docetaxel + ARPI (darolutamide).
This new category could be considered as a potential standard of care for anyone receiving taxane therapy for mCSPC (i.e. replacing category #3), and could also be an option and alternative for any patient receiving ADT + ARPI and who is fit and eligible for docetaxel chemotherapy.
While there were other clinical trials that did support the use of triplet therapy with abiraterone acetate or enzalutamide or apalutamide, all only had a subset of patients who were docetaxel treated – ARASENS represents a data set that is more robust for patients who were fit and eligible for docetaxel chemotherapy in the mCSPC setting.
There are several reasons to choose to have ‘triplet’ therapy with darolutamide + docetaxel + ADT:
Darolutamide has improved and favourable tolerance compared to other ARPIs, including reduced drug-drug interactions in comparison to enzalutamide or apalutamide, especially in the elderly age category.
Darolutamide has less brain/CNS penetration – therefore less falls, less fracture risk, less neurocognitive syndrome, less seizure risk compared to other ARPIs such as enzalutamide and apalutamide.
Darolutamide has theoretical advantages in that certain AR-mutations as resistance mechanisms are targeted by this drug.
There is a significant improvement in survival and disease-control outcomes with the addition of darolutamide to docetaxel + ADT.
In network meta-analyses, the survival outcomes of darolutamide + docetaxel + ADT are similar to if not potentially better than ARPI + ADT. Certainly on a patient-by-patient basis, therefore the triplet therapy needs to be considered because docetaxel administered later in the course of disease has a very modest benefit and given early in the disease may confer a larger margin of benefit.
In summary, access to darolutamide + docetaxel in the mCSPC setting is a standard worth considering on a patient-by-patient basis.
Which patients would be best suited for treatment with the drug under review? Which patients would be least suitable for treatment with the drug under review?
The patients best suited to benefit from the drug under review are:
Metastatic hormone-sensitive prostate cancer patients who are deemed by a medical oncologist to potentially benefit from docetaxel chemotherapy in addition to ADT. These are complex decisions that require weighing many factors including patient preference, patient fitness / comorbidities, disease burden and symptoms, availability of alternatives and multidisciplinary care, all of which should be discussed and considered by a medical oncologist.
What outcomes are used to determine whether a patient is responding to treatment in clinical practice? How often should treatment response be assessed?
The following are used to determine response to treatment:
PSA response. This biomarker is the earliest objective readout and in trials correlates highly with prognosis and disease outcome.
Radiographic response (CT, bone scan) – usually conducted at baseline, PSA nadir, and PSA progression, if not more frequently.
Quality of life scores (e.g., ESAS) – at least in Ontario is conducted every visit.
Tolerance and compliance of drugs – reviewed by nurses administering drugs and reviewing for clinical visits.
Pain scores – reviewed as part of ESAS scores.
Survival outcomes of patients – available for audit of clinical practice.
What factors should be considered when deciding to discontinue treatment with the drug under review?
The following factors are important in determining when to discontinue therapy:
Disease-related symptoms for the patient
Radiographic patterns of response or progression (CT or bone scan or other imaging modalities)
Biochemical patterns of response or progression (PSA)
Tolerance / Toxicity related to the drug.
Usually persistent grade 2 (‘moderate’) or grade 3-4 (‘severe’) drug toxicities lead to treatment interruption, modification, or discontinuation.
5.5 What settings are appropriate for treatment with [drug under review]? Is a specialist required to diagnose, treat, and monitor patients who might receive [drug under review]?
Any prostate cancer specialist will be able to prescribe darolutamide.
However, docetaxel will need to be prescribed by an oncologist comfortable with its dosing and management, typically a medical oncologist, and typically in coordination with a specialty pharmacy / chemotherapy treatment unit for chemotherapy prescription and delivery.
Additional Information
None.
Conflict of Interest Declarations — The Ottawa Hospital Cancer Centre – Genitourinary Oncology Group
To maintain the objectivity and credibility of the CADTH drug review programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This conflict of interest declaration is required for participation. Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please refer to the Procedures for CADTH Drug Reimbursement Reviews (section 6.3) for further details.
Did you receive help from outside your clinician group to complete this submission?
No, we did not receive help.
Did you receive help from outside your clinician group to collect or analyze any information used in this submission?
No, we did not receive help.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review. Please note that this is required for each clinician who contributed to the input — please add more tables as needed (copy and paste). It is preferred for all declarations to be included in a single document.
Declaration for Clinician 1
Name: Dr. Michael Ong
Position: Medical Oncologist, The Ottawa Hospital
Date: 10-Jul-2022
Table 46: COI Declaration for The Ottawa Hospital Cancer Centre – Genitourinary Oncology Group — Clinician 1
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to 50,000 | In excess of $50,000 |
|---|---|---|---|---|
Bayer | — | X | — | — |
Jannsen | — | X | — | — |
Astellas | X | — | — | — |
AstraZeneca | X | — | — | — |
Declaration for Clinician 2
Name: Dr. Shawn Malone
Position: Radiation Oncologist, The Ottawa Hospital
Date: 10-Jul-2022
Table 47: COI Declaration for The Ottawa Hospital Cancer Centre – Genitourinary Oncology Group — Clinician 2
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to 50,000 | In excess of $50,000 |
|---|---|---|---|---|
Janssen | — | X | — | — |
Astellas | — | X | — | — |
TerSera | X | — | — | — |
AstraZeneca | X | — | — | — |
Amgen | X | — | — | — |
Sanofi | X | — | — | — |
Abbvie | X | — | — | — |
Knight Therapeutics | X | — | — | — |
Bayer | — | X | — | — |
Declaration for Clinician 3
Name: Dr. Ilias Cagiannos
Position: Urologist Oncologist, The Ottawa Hospital
Date: 10-Jul-2022
Table 48: COI Declaration for The Ottawa Hospital Cancer Centre – Genitourinary Oncology Group — Clinician 3
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to 50,000 | In excess of $50,000 |
|---|---|---|---|---|
Bayer | — | X | — | — |
Abbvie | — | X | — | — |
Janssen | X | — | — | — |
Ferring | X | — | — | — |
Genitourinary Disease Site Group of the Cancer Centre of Southeastern Ontario
About the Genitourinary Disease Site Group of the Cancer Centre of Southeastern Ontario
We are a multidisciplinary group of physicians specializing in the management of genitourinary malignancies including prostate cancer and work through the Cancer Centre of Southeastern Ontario. We are also active in clinical trials involving advanced prostate cancer through both the Centre for Applied Urological Research as well as the Cancer Centre of Southeastern Ontario.
Information Gathering
The information gathered for this submission is an accumulation of our clinical experience in this disease space as well as our research and clinical trial expertise as academic physicians with expertise in this disease space.
Current Treatments and Treatment Goals
Prior to 2015, the standard of care for treatment of men with metatastic castration sensitive prostate cancer was simply ablating a patient’s testosterone with androgen deprivation therapy (ADT). Then, in 2015 the CHAARTED study showed an improvement in overall survival from a median of 47 months in those receiving ADT to 57 months in those who received docetaxel chemotherapy in combination with ADT with the bulk of the benefit being in patients with high volume disease. At that point docetaxel in combination with ADT became the standard of care for patients with high volume metastatic castration sensitive prostate cancer. Subsequent to this, 3 different hormonal drugs (abiraterone, enzalutamide and apalutamide) were shown in randomized controlled trials to also improve overall survival for men with metastatic castration sensitive prostate cancer when given in combination with ADT compared to ADT alone. All of these drugs have similar mechanisms of action by targeting activation of the androgen receptor which drives prostate cancer growth. These 3 hormonal drugs as such are referred to as androgen receptor pathway inhibitors (ARPIs) or androgen receptor-axis-targeted therapies (ARATs). These three drugs have never been compared against each other in a head to head randomized controlled trial in this disease space, but the magnitude of benefit compared to ADT alone in their pivotal phase III studies is roughly the same. In the LATITUDE study, abiraterone reduced risk of death by 34% compared to ADT alone. In the ENZAMET study, enzalutamide reduced risk of death by 33% compared to ADT alone. In the TITAN study, apalutamide reduced risk of death by 35% compared to ADT alone.
Therefore, the current treatment paradigm was to treat patients with metastatic castration sensitive prostate cancer with either an ARAT or docetaxel. The decisions of which of these drugs to use in any individual patient was not based on any overall survival analysis in a head to head trial. Up until the ARASENS trial, no phase III trial had yet compared any ARAT against another ARAT or against docetaxel to assess for superiority in overall survival. Although some of the trials had contained patients who had received docetaxel either concurrently with or immediately preceding treatment with an ARAT. However, this was not done in a randomized fashion and largely done at investigator discretion, so no real conclusions can be drawn from this data.
At this point in time, standard of care would be treatment of men with metastatic castration sensitive prostate cancer with either docetaxel or an ARAT. All of these drugs provide a survival advantage compared to ADT alone. In addition, there is quality of life literature from the pivotal phase III studies to show at least maintenance in quality of life over time, with some studies showing improvement in quality of life compared with treatment by ADT alone. However, the fact remains that this is a non-curable disease and over half of men will succumb to their disease within the next 5 years depending on their initial volume of disease at time of presentation. However, 5 years is still a long enough period of time that we want to be extremely cognizant of treatment toxicities.
As such, our goals in this patient population is to continue to improve survival in this non-curable disease while at that same time maintaining or improving quality of life and minimizing treatment related adverse events in a patient population that is still going to live several years.
Treatment Gaps (Unmet Needs)
Considering the treatment goals, please describe goals (needs) that are not being met by currently available treatments.
In 2022, metastatic castration sensitive prostate cancer is still a non-curable, lethal disease. The prostate cancer will eventually develop resistance to all currently available treatments options over time. Current goals are to continue to extend survival while at the same time maintaining quality of life through prevention of disease progression and avoidance of toxicities of treatment.
Place in Therapy
How would the drug under review fit into the current treatment paradigm?
The mechanism of action of darolutamide is similar to currently available ARATs available in this disease space. However, darolutamide would be given in combination with docetaxel chemotherarpy, which is one of the current 1st line standard of care therapies for this disease. Docetaxel has a distinctly different mechanism of action from the ARATs as it is cytotoxic chemotherapy that works as a microtubule disassembly inhibitor. In the ARASENS study, the addition of darolutamide to docetaxel substantially improved overall survival and reduced the risk of death by 32% when compared to docetaxel by itself. This is a drug that would be used as a first line therapy in combination with docetaxel, which is an already approved 1st line standard of care therapy for men with metastatic castration resistant prostate cancer. Because it is a drug that is being added to a current standard of care therapy, it would not be reserved for patients who are intolerant of other therapies. In patients for whom the decision has been made to move forward with docetaxel chemotherapy (a current 1st line standard of care), these patients would also be given darolutamide as the ARASENS data unequivocally shows us that it improves survival by 32% in this patient population with a very minimal side effect profile compared to docetaxel by itself. We do not believe it would be appropriate to recommend patients try other treatment before initiating treatment with docetaxel and darolutamide in combination. Darolutamide adds very little in terms of toxicity to patients already on a docetaxel regimen based on the ARASENS data. So if the concern is the added toxicity from darolutamide, there is very little. If the concern is that there are other medications that may work better, there are no other phase III studies specifically examining the combination of docetaxel with another drug in a randomized control fashion showing a survival advantage. There is one other study, the PEACE-1 study which did show that the combination of abiraterone to “standard of care” improved overall survival. In that study, the standard of care arm changed throughout the course of the study. So 273 patients received ADT alone as the standard of care, 592 patients had the option of receiving docetaxel in combination with ADT at the investigator’s discretion and 308 patients received docetaxel and ADT as the study mandated standard of care. The addition of abiraterone did improve overall survival by 18% compared to standard of care. This effect seemed to be even higher in those patients who received docetaxel and ADT as the standard of care where the addition of abiraterone reduced risk of death by 25%. Currently, there is also a separate application under review with CADTH to have abiraterone approved for use in combination with docetaxel in men with metastatic castration sensitive prostate cancer.
Which patients would be best suited for treatment with the drug under review? Which patients would be least suitable for treatment with the drug under review?
All patients with newly diagnosed metastatic castration sensitive prostate cancer are in need of intervention with medical therapy. We have effective medical therapies to treat this non-curable lethal disease. There is already a decision clinicians make daily on whether to give docetaxel or an ARAT in the 1st line setting for patients with newly diagnosed metastatic castration sensitive prostate cancer. That decision is based on numerous factors including disease volume, location of disease, PSA level, patient co-morbidities and patient performance status. This is largely based on physician judgement of these factors. The decision to use darolutamide would be dependent on the outcome of that first decision. In patients, in whom a decision is made to use docetaxel, then we now have unequivocal proof from the ARASENS trial that the addition of darolutamide to docetaxel will improve survival in these men by 32% when compared to docetaxel itself with very limited additional toxicity. Therefore, in all men in whom a decision has been made to give docetaxel, should also be given darolutamide. There are not usually any issues related to diagnosis. Although the PSA test is used as part of the diagnostic process, it is not a companion diagnostic test per se. There is no companion diagnostic test required. It is unlikely that men will be misdiagnosed in clinical practice. Subset analysis from the ARASENS trial showed that all subgroups of men analyzed benefited from the addition of darolutamide to docetaxel. So, we would expect most men receiving docetaxel to benefit from the addition of darolutamide.
What outcomes are used to determine whether a patient is responding to treatment in clinical practice? How often should treatment response be assessed?
The outcomes used in clinical trials are the same outcomes used in clinical practice to determine either response or progression on treatment. These outcomes include biochemical parameters (namely response in PSA values), as well as ensuring there is no signs of radiographic progression or clinical progression (worsening pain or worsening performance status). The most clinically meaningful response is the prolongation in overall survival which was strongly shown in the ARASENS trial. In addition, the trial also showed a 21% improvement in the time to pain progression, 29% improvement in the time to first symptomatic skeletal related event. Our current practice of following patients with metastatic castration sensitive prostate cancer on ARAT treatment, is a repeat clinical and biochemical evaluations at baseline, 6 weeks, 12 weeks and then every 12 weeks thereafter. Repeat radiographic exams are done at baseline and then yearly as well on demand if there are signs of biochemical progression on repeat laboratory. This is roughly the same as what was done in the trial and consistent with current clinical practice in this space of disease.
What factors should be considered when deciding to discontinue treatment with the drug under review?
Factors that should be considered when decided to discontinue treatment should be unequivocal signs of progression as assessed from repeat clinical, biochemical and radiographic exams. The safety profile of darolutamide is well established with very few attributable toxicities over placebo. However, unacceptable toxicity as determined by patient and provider would be a rare reason for discontinuation as well.
What settings are appropriate for treatment with [drug under review]? Is a specialist required to diagnose, treat, and monitor patients who might receive [drug under review]?
This is a drug that is already currently used for other indications in prostate cancer by medical oncologists, radiation oncologists and urologists in both community and academic outpatient settings.
Additional Information
Not applicable.
Conflict of Interest Declarations — Genitourinary Disease Site Group of the Cancer Centre of Southeastern Ontario
To maintain the objectivity and credibility of the CADTH drug review programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This conflict of interest declaration is required for participation. Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please refer to the Procedures for CADTH Drug Reimbursement Reviews (section 6.3) for further details.
Did you receive help from outside your clinician group to complete this submission?
No.
Did you receive help from outside your clinician group to collect or analyze any information used in this submission?
No.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review. Please note that this is required for each clinician who contributed to the input — please add more tables as needed (copy and paste). It is preferred for all declarations to be included in a single document.
Declaration for Clinician 1
Name: Jason Izard
Position: Urologist, Associate Professor, Dept of Urology, Dept of Oncology, Queen’s University
Date: 10-07-2022
Table 49: COI Declaration for Genitourinary Disease Site Group of the Cancer Centre of Southeastern Ontario — Clinician 1
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to 50,000 | In excess of $50,000 |
|---|---|---|---|---|
Janssen | — | X | — | — |
Bayer | — | X | — | — |
Astellas | X | — | — | — |
Tolmar | X | — | — | — |
Abbvie | — | X | — | — |
Knight | X | — | — | — |
Merck | X | — | — | — |
Declaration for Clinician 2
Name: Francisco E. Vera Badillo
Position: Medical Oncologist, Associate Professor, Queen’s University and Kingston Health Sciences Center
Date: 10-07-2022
Table 50: COI Declaration for Genitourinary Disease Site Group of the Cancer Centre of Southeastern Ontario — Clinician 2
Company | $0 to $5,000 | $5,001 to $10,000 | $10,001 to 50,000 | In excess of $50,000 |
|---|---|---|---|---|
AZ | X | — | — | — |
Bayer | X | — | — | — |
Janssen | X | — | — | — |
Pfizer | X | — | — | — |
Merck | X | — | — | — |
AAA | X | — | — | — |
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
Redactions: Confidential information in this document may be redacted at the request of the sponsor in accordance with the CADTH Drug Reimbursement Review Confidentiality Guidelines
Stakeholder Input: The views expressed in each submission are those of the submitting organization or individual; not necessarily the views of CADTH or of other organizations. As such, they are independent of CADTH and do not necessarily represent or reflect the view of CADTH. No endorsement by CADTH is intended or should be inferred. By filing with CADTH, the submitting organization or individual agrees to the full disclosure of the information. CADTH does not edit the content of the submissions.
CADTH does use reasonable care to prevent disclosure of personal information in posted material; however, it is ultimately the submitter’s responsibility to ensure no identifying personal information or personal health information is included in the submission. The name of the submitting organization or individual and all conflict of interest information are included in the submission; however, the name of the author, including the name of an individual patient or caregiver submitting the patient input, are not posted.
Accessibility: CADTH is committed to treating people with disabilities in a way that respects their dignity and independence, supports them in accessing material in a timely manner, and provides a robust feedback process to support continuous improvement. All materials prepared by CADTH are available in an accessible format. Where materials provided to CADTH by a submitting organization or individual are not available in an accessible format, CADTH will provide a summary document upon request. More details on CADTH’s accessibility policies can be found here.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.