CADTH Reimbursement Review
Cabozantinib (Cabometyx)
Sponsor: Ipsen Biopharmaceuticals Canada Inc.
Therapeutic area: Differentiated thyroid cancer
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Stakeholder Input
Clinical Review
Abbreviations
ACTH
adrenocorticotropic hormone
ALT
alanine aminotransferase
AST
aspartate aminotransferase
BSA
body surface area
BSC
best supportive care
CI
confidence interval
CNS
central nervous system
CR
complete response
CRO
Contract Research Organization
CSR
Clinical Study Report
CSS
Clinical Summary of Safety
CT
computed tomography
DNA
deoxyribonucleic acid
DOR
duration of response
ECG
electrocardiogram
ECOG
Eastern Cooperative Oncology Group
EORTC
European Organization for Research and Treatment of Cancer
EDC
electronic data capture
eGFR
estimated glomerular filtration rate
EMA
European Medicines Agency
ESC
Executive Safety Committee
ETM
event to monitor
FT4
free thyroxine
FTC
follicular thyroid cancer
GI
gastrointestinal
HCC
hepatocellular carcinoma
HR
hazard ratio
HRQoL
health-related quality of life
ICF
informed consent form
ICH
International Conference on Harmonisation
ICU
intensive care unit
IDMC
Independent Data Monitoring Committee
IEC
Independent Ethics Committee
INR
international normalized ratio
IP
investigational product
IRB
Institutional Review Board
IRT
interactive response technology
ITT
intent to treat
IxRS
interactive voice/web response system
LTFU
long-term follow-up
MRI
magnetic resonance imaging
MTC
medullary thyroid cancer
NDA
New Drug Application
OITT
overall response rate intent to treat
ORR
objective response rate
OS
overall survival
PD
progressive disease; disease progression
PFS
progression-free survival
PK
pharmacokinetic(s)
PM
product monograph
PR
partial response
PRES
posterior reversible encephalopathy syndrome
PROs
patient-reported outcomes
PS
performance status
PTC
papillary thyroid cancer
QD
once daily
QLQ-C30
Quality of Life Questionnaire-Core 30
QTcF
QT interval corrected for heart rate using Fridericia’s formula
RECIST
Response Evaluation Criteria in Solid Tumors version 1.1
SAE
serious adverse event
SAP
Statistical Analysis Plan
SD
standard deviation
TEAE
treatment-emergent adverse
TKI
tyrosine kinase inhibitor
TSH
thyroid-stimulating hormone
TTR
time to response
VAS
visual analogue scale
VEGF(R)
vascular endothelial growth factor (receptor)
VTE
venous and mixed/unspecified thrombotic event
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Item | Description |
|---|---|
Drug product | Cabozantinib (Cabometyx), tablets, 20 mg, 40 mg, 60 mg oral |
Indication | For the treatment of adult patients with locally advanced or metastatic differentiated thyroid carcinoma (DTC) that has progressed following prior VEGFR-targeted therapy and who are radioactive iodine-refractory or ineligible. |
Reimbursement request | As per indication |
Health Canada approval status | NOC |
Health Canada review pathway | Priority review |
NOC date | April 28, 2022 |
Sponsor | Ipsen Biopharmaceuticals Canada Inc. |
NOC = Notice of Compliance; VEGFR = vascular endothelial growth factor.
Introduction
Thyroid cancer is 1 of the most commonly diagnosed cancers in Canada and the world. It is considered the most common endocrine malignancy.1,2 In 2020, the incidence of thyroid cancer in Canada was estimated to be 23 per 100,000 patients, or about 8,600 new cases.3 Thyroid cancers arising from thyroid follicular cells include the differentiated thyroid cancer (DTC, which groups papillary thyroid cancer [PTC], follicular thyroid cancer [FTC], and Hurthle cell cancer), poorly differentiated thyroid cancer, and anaplastic thyroid cancer. Among all types of thyroid cancer, DTC is the most common, accounting for more than 95% of cases.4,5 Tumors that are localized and well-differentiated usually are curable with total thyroidectomy or lobectomy, followed by postoperative treatment with radioactive iodine (RAI) therapy – for patients at high risk of persistent disease or disease recurrence after total thyroidectomy. Up to 30% of patients with DTC may have recurrence of disease and 60% of these recurrences occur within the first decade after initial therapy. In patients with primary or secondary radioiodine-refractory thyroid carcinoma the prognosis becomes significantly poorer.6
Approximately 10% to 15% of thyroid cancer patients develop distant metastases.2,7,8 Prognosis for radioiodine resistant thyroid cancer with distant metastases is very poor, with an estimated median survival time of about 2.5 to 3.5 years.9 The overall mortality rates 5 and 10 years after diagnosis of distant metastases are 65% and 75%, respectively.2,8 Early diagnosis and early appropriate surgical treatment are considered to positively affect the prognosis of these patients.2,7,8
The objective of this report is to perform a systematic review of the beneficial and harmful effects of cabozantinib (Cabometyx) oral tablets, 20 mg, 40 mg, 60 mg for the treatment of adult patients with locally advanced or metastatic DTC that has progressed following prior VEGFR-targeted therapy and who are radioactive iodine-refractory (RAI-R) or ineligible.
Stakeholder Perspectives
The information in this section is a summary of input provided by the patient groups who responded to CADTH’s call for patient input and from clinical experts consulted by CADTH for the purpose of this review.
Patient Input
Two patient groups submitted 1 joint input for this review. Canadian Cancer Society (CCS) is the only national charity that supports all Canadians living with all cancers across the country through research, advocacy, and compassionate support activities. Thyroid Cancer Canada (TCC) is a national organization of thyroid cancer survivors dedicated to providing emotional support and information to those affected by the disease. The submission was based on results from a survey distributed by the 2 groups. Two patients responded to the survey, of which 1 had experience with cabozantinib. The patient groups noted that this type of thyroid cancer is rare.
The 2 patients said their ability to work, travel, exercise, conduct household chores, fulfill family obligations, and maintain positive mental health were impacted to a moderate degree by symptoms associated with DTC. Also, both patients indicated there are financial barriers related to treatment (e.g., loss of income, transportation costs). No specific details with respect to outcomes that are important to patients was provided in the input. Of note, patients reported experiencing adverse effects from their treatments such as nausea, vomiting, diarrhea, and fatigue.
Clinician Input
Input From Clinical Experts Consulted by CADTH
Clinical experts consulted by CADTH agreed that RAI-R DTC is a rare disease causing about 200 deaths per year in Canada. The clinical experts indicated that, as with most rare diseases, this raises issues about physician awareness and systemic barriers to access to therapy for patients. Although most patients respond to lenvatinib, all patients will eventually experience disease progression due to acquired drug resistance, per the clinical experts. The clinical experts reported that currently there are no funded and reliably effective treatments for these patients. The clinical experts indicated that treatment goals should be improving overall survival (OS), progression-free survival (PFS), and improve health-related quality of life (HRQoL) by controlling symptoms, minimizing adverse effects of treatments, and increasing work/life productivity. There is an unmet need, on which both clinical experts agree, that better treatments need to be available for patients who do not respond or progress after first-line therapy, and for those patients who have to discontinue due to side effects or multikinase inhibitor (MKI) resistance. The clinical experts noted that the ideal treatment should also have fewer harm effects.
Clinical experts agreed that cabozantinib would provide a second-line treatment option for patients progressing despite lenvatinib therapy. Experts also agreed that cabozantinib should not be used as first-line treatment but could be an alternative for patients who are intolerant of lenvatinib. As per the clinical experts, cabozantinib treatment can be associated with significant adverse events, so the main criteria for the timing and dosing of treatment would be based on clinical judgment considering patient factors such as tumour burden, age, comorbidities, and performance status. To monitor response, the clinical experts noted that patients should have baseline assessment and imaging and be assessed every 2 to 3 weeks to monitor for adverse effects and to modify drug dosing if necessary. Improved symptoms and a drop in serum thyroglobulin would be favourable signs of response early in treatment, per the clinical experts. The clinical experts indicated that in most patients, cabozantinib would be continued until there is unequivocal evidence of disease progression despite treatment or toxicity. The clinical experts suggested that patients should be under the care of a medical oncologist or endocrinologist experienced in TKI therapy for thyroid cancers. The clinical experts noted that, as RAI-R DTC is a rare condition, currently there is a small community of prescribers in Canada treating this disease. The clinical experts noted that indications for cabozantinib are growing, and a growing number of medical oncologists are becoming familiar with it.
Clinician Group Input
The Medical Advisory Panel of TCC with administrative support provided by the CCS provided input for this review. A total of 7 physicians (5 from Ontario, 1 from British Columbia, 1 from Alberta) were included and responded to the call for input.
In agreement with the clinical experts consulted by CADTH, the clinician group mentioned the lack of approved/funded options for patients with DTC who are radioactive iodine-refractory (or ineligible) and progress after VEGFR-targeted therapies. The clinician group believes that cabozantinib is expected to fill an urgent unmet need for patients who progress on prior therapy, since no other therapies are funded beyond lenvatinib as first line in Canada, cabozantinib would offer patients an option for therapy. The clinician group considers that the inclusion criteria for the COSMIC-311 trial define patient population best suited for cabozantinib treatment. In addition to the criteria listed in the COSMIC-311 trial, patients with progressing nonmeasurable disease, such as bone metastases, should not be excluded in the real-world clinical setting, this was also in alignment with the input from the clinical experts. To assess response to treatment, clinical assessment, tumour markers, and radiological imaging such as CT or MRI (CT/MRI) should generally be done every 3 to 4 months.
The group emphasized that radioiodine (RAI) refractory DTC is an extremely rare disease with significant unmet need and cabozantinib should be reviewed in this regard. They also acknowledge that surrogate end points in COSMIC-311 trial, i.e., ORR and PFS, as primary end points contribute to the uncertainty in the clinical benefit of cabozantinib.
Drug Program Input
The drug programs identified relevant implementation issues to be addressed through the CADTH’s reimbursement review process.
In terms of considerations for initiation of therapy, an implementation question was if patients who experience adverse effects with lenvatinib or sorafenib without progression should be eligible for treatment with cabozantinib. According to clinical experts consulted by CADTH, for most scenarios, the adverse effects of lenvatinib can be managed with dose modifications or use of adjunctive medications (e.g., for hypertension). However, there may be rare scenarios (e.g., true drug allergy, or hypertension requiring multiple antihypertensive drugs) where cabozantinib could be considered an alternative.
Based on the drug plans’ question about the considerations for renewal of therapy, the clinical experts mentioned that clinical assessment, tumour markers, and radiological imaging (CT/MRI) should be done every 3 to 4 months as assessment measures of treatment response. Similarly, when discussing what criteria for discontinuation of therapy should be used, the clinical experts mentioned how for some patients the drug may be discontinued due to intolerable adverse effects and difficulty in titrating cabozantinib doses. In most patients, cabozantinib would be continued until there is unequivocal evidence of disease progression despite treatment. Clinical experts also suggested that using cabozantinib in patients with ECOG PS of 2 and above would be not recommended due to the risk of adverse events.
Clinical Evidence
Pivotal Studies and Protocol Selected Studies
Description of Studies
One phase III clinical study was included in the systematic review. The COSMIC-311 is a randomized, double-blind, placebo-controlled trial, conducted in several centres across Europe, Asia, Latin America, US, and Canada to evaluate the efficacy and safety of cabozantinib 60 mg once daily versus placebo. The randomization was stratified by age (< 65 or ≥ 65 years) and previous use of lenvatinib. The population included patients with advanced or metastatic DTC previously treated with a vascular endothelial growth factor-tyrosine kinase inhibitor (VEGF-TKI) and who are RAI-resistant. The key end points objective response rate (ORR), PFS, OS, duration of response (DOR), and HRQoL were assessed in an initial cut-off date (August 19, 2020) with a total of 187 randomized patients (the intention-to-treat [ITT] and safety population) from which the first 100 randomized patients were obtained and assessed as a specific ITT population for the primary end points ORR and PFS (i.e., the overall response rate intention-to-treat [OITT] population). A second cut-offs date (February 8, 2021) with a total of 187 patients in the primary analysis subset and 258 patients in the full ITT population, provided longer follow-up assessments, including safety. Crossover to cabozantinib was permitted throughout the study for eligible patients who experienced radiographic disease progression per Response Evaluation Criteria in Solid Tumors version 1.1 (RECIST 1.1) by blinded independent radiology committee (BIRC). Patients in the COSMIC-311 had advanced or metastatic DTC with Eastern Cooperative Oncology Group (ECOG) performance status (PS) of 0 or 1, with a slight predominance of female patients, and an average age of 65 years.
Efficacy Results
For OS at the data cut-off date of August 19, 2020, with a median follow-up time of 6.24 months, the median OS was not reached (95% confidence interval, not estimable [NE] to NE) in either treatment group. The log-rank test for differences in the Kaplan–Meier (KM) curves for OS had a corresponding P value = 0.0879. For the cut-off date of February 8, 2021, with a median follow-up of 11.9 months, results of OS were overall consistent with the initial cut-off, with 34 deaths in the cabozantinib arm and 20 in the placebo arm (27% versus 32% respectively). Median OS was 19.4 (95% CI, 15.9 to NE) months in the cabozantinib group and was not reached (95% CI, NE to NE) in the placebo group. Of note, these results at a later data cut-off were assessed post hoc, following the primary analysis, and so, are considered supplemental to the primary analysis results.
PFS was a co-primary end point and adjusted for multiplicity. At the data cut-off of August 19, 2020; a total of 74 events were reported. The median time of follow-up was 6.24 months. The median PFS was not reached (96% CI, 5.7 to NE) in the cabozantinib arm compared with 1.9 months (1.8 to 3.6) in the placebo arm. The P value obtained from the log-rank stratified test was less than 0.0001. For the cut-off date of February 8, 2021, results of PFS were overall consistent. With a median follow-up time 11.9 months in the primary analysis population (n = 187), the median PFS was reached at 11.1 months (96% CI, 7.4 to 13.8) in the cabozantinib arm versus 1.9 months (1.8 to 3.8) in the placebo arm, with a P value obtained from the stratified log-rank test of less than 0.0001, below a critical P value used for testing of 0.00036.
ORR was a co-primary end point in the COSMIC-311 trial and adjusted for multiplicity. In the OITT population, at the cut-off date August 19, 2020, with median follow-up of 8.9 months, the ORR was 15% (99% CI, 5.8 to 29.3) in the cabozantinib group versus 0% (99% CI, 0 to 14.8) in the placebo group (P = 0.028, considered not significant at the prespecified critical value of 0.01). At the cut-off date of February 8, 2021, with a longer median follow-up time (11.9 months), the ORR was 15% (99% CI, 9.4 to 22.7) in the cabozantinib group versus 0% (99% CI, 0 to 5.8) in the placebo group (P = 0.0005).
HRQoL was assessed with the EQ-Index (a converted normalized measure of the EQ-5D-5L score for different countries) and EuroQoL Visual Analogue Scale (EQ-VAS). In both HRQoL measures, there was immaturity in the data and no evidence of different effects between arms of study through the length of the study at the end of week 65.
Harms Results
The most common adverse events (AEs) were more prevalent in the cabozantinib group as compared to placebo (166 [98%] vs 75 [85%] respectively) at the cut-off of February 8, 2021, and included diarrhea (62% versus 3.4% respectively), PPES (47% versus 1.1%), hypertension (32% vs 3.4%), decreased appetite (31% vs 13%), fatigue (29% versus 8%), nausea (28% versus 2.3%), increased liver enzymes (25% vs 2.3%), hypocalcemia (25% versus 3.4%), and decreased weight (22 versus 2.3%). There were no treatment-related deaths.
SAEs at the cut-off date of 8 February 2021 were also more common in the cabozantinib arm (66 patients [39%]) when compared to placebo (24 patients [27%]), and included diarrhea, pleural effusion, pneumonia, pulmonary embolism, and dyspnea. AEs of special interest also occurred more frequently in the cabozantinib group than in the placebo group, including severe diarrhea (7.6% versus 0% respectively), thromboembolism (10% versus 1.1%), hypertension (34% versus 3.4%), elevated liver enzymes (25% vs 2.3%), PPES (47% vs 1.1%), and hypocalcemia (25% versus 3.4%).
Table 2: Summary of Key Efficacy Results From COSMIC-311
Criteria | Cut-off date August 19, 2020 | Cut-off February 8, 2021 | ||
|---|---|---|---|---|
Cabozantinib (N = 125) | Placebo (N = 62) | Cabozantinib (N = 125) | Placebo (N = 62) | |
OS | ||||
Number of patients, N (%) | ||||
Censored | 108 (86) | 48 (77) | 91 (73) | 42 (68) |
Death | 17 (14) | 14 (23) | 34 (27) | 20 (32) |
Follow-up, median (months) | 6.24 | 11.9 | ||
Duration of OS (months) | ||||
Median (95% CI) | NE (NE, NE) | NE (NE, NE) | 19.4 (15.9, NE) | NE (NE, NE) |
Range | 0.07+, 15.74+ | 0.43+, 11.60+ | 0.39, 19.35 | 0.99+, 17.28+ |
P value (stratified log-rank test)a,b | 0.0879 | 0.277 | ||
Hazard ratio (95% CI; stratified)a,c | 0.54 (0.27, 1.11) | 0.74 (0.42, 1.28) | ||
PFS | ||||
Number of patients, N (%) | ||||
Censored | 94 (75) | 19 (31) | 69 (55) | 4 (6.5) |
Event | 31 (25) | 43 (69) | 56 (45) | 58 (94) |
Death | 6 (4.8) | 2 (3.2) | 9 (7.2) | 3 (4.8) |
Progressive disease | 25 (20) | 41 (66) | 47 (38) | 55 (89) |
Follow-up, median (months) | 6.24 | 11.9 | ||
Duration of PFS (months) | ||||
Median (96% CI) | NE (5.7, NE) | 1.9 (1.8, 3.6) | 11.1 (7.4, 13.8) | 1.9 (1.8, 3.8) |
Range | 0.03+, 15.67+ | 0.03+, 9.26+ | 0.03+, 16.76+ | 0.03+, 13.83+ |
P value (stratified by log-rank test)a,d | < 0.0001 | < 0.0001 | ||
Hazard ratio (96% CI; stratified)c | 0.22 (0.13, 0.36) | 0.22 (0.15, 0.32) | ||
ORR | ||||
N | 67 | 33 | 125 | 62 |
ORR (CR+PR), n (%) | 10 (15) | 0 (0) | 19 (15) | 0 |
99% CI | 5.8, 29.3 | 0, 14.8 | 9.4, 22.7 | 0.0, 5.8 |
Follow-up, median(months) | 8.85 | 11.9 | ||
Treatment difference (cabozantinib – placebo) (95% CI)e | 15 (3.7, 26.1) | 15 (8.9, 21.5) | ||
Observed unstratified Fisher exact test P valued | 0.0281 | 0.0005 | ||
For the cut-off August 19, 2021 results are from the ITT population except for the ORR, which is obtained from the OITT population, and for the cut-off February 8, 2021 results are from the primary analysis subset population.
ITT = intention to treat; KM = Kaplan–Meier; NE = not estimable; ORR = objective response rate; OS = overall survival; PFS = progression-free survival.
aStratification factors based on IxRS were receipt of prior lenvatinib (yes vs. no) and age at informed consent (≤ 65 years vs. > 65 years).
bP values were not controlled for multiplicity. P values for the later cut-off date of February 8, 2021 were considered as post-hoc analysis.
cEstimated using the Cox proportional-hazard model (adjusted for stratification factors if applicable). HR < 1 indicate results in favour of cabozantinib
dCut-off of the critical value for P was 0.00036 for PFS, and 0.01 for ORR.
eUsing asymptotic confidence limits based on large number theorem
Source: Clinical Study Report of Cabozantinib.10
Table 3: Summary of Harms From COSMIC-311, Safety Population, as of February 8, 2021 Data Cut-Off
Detail | Cabozantinib (N = 170) | Placebo (N = 88) |
|---|---|---|
Patients with ≥ 1 adverse event | ||
Any AE, n (%) | 166 (98) | 75 (85) |
SAE, n (%) | 66 (39) | 24 (27) |
WDAE (from study treatment), n (%) | 15 (8.8) | 0 |
Deaths, n (%) | 37 (22) | 13 (15) |
Notable harmsa | ||
Severe diarrhea (grade 3 or 4), n (%) | 13 (7.6) | 0 |
Thromboembolism (PE, DVT, pelvic venous, SVC), n (%) | 17 (10) | 1 (1.1) |
Hypertension, n (%) | 58 (34) | 3 (3.4) |
Hypertensive crisis, n (%) | 1 (0.6) | 0 |
Major hemorrhage/bleeding, n (%) | 4 (2.4) | 0 |
ALT increase, n (%) | 43 (25) | 2 (2.3) |
AST increase, n (%) | 42 (25) | 2 (2.3) |
Posterior reversible encephalopathy syndrome, n (%) | 1 (0.6) | 0 |
Palmar-plantar erythrodysesthesia syndrome, n (%) | 80 (47) | 1 (1.1) |
Hypocalcemia, n (%) | 42 (25) | 3 (3.4) |
QT prolongation, n (%) | 4 (2.4) | 1 (1.1) |
ALT = alanine aminotransferase; AST = aspartate transferase; DVT = deep venous thrombosis; SVC = superior vena cava syndrome; PE = pulmonary embolism.
aThose considered relevant based on clinicians and patient input as stated in the protocol of this CADTH review.
Source: Clinical Study Report of Cabozantinib.10
Critical Appraisal
Overall, the COSMIC-311 trial is at low risk of bias. It was a double-blind randomized trial with adequate randomization, concealment allocation, masking, and assessment of outcomes. Some concerns of internal validity remain, such as the high number of patients who crossed over from the placebo to the intervention group, and the possibility of patients and researchers being aware of the intervention administered due to AEs more commonly observed in the cabozantinib arm (potential unblinding). Overall baseline characteristics were balanced. The authors performed an adequate adjustment for multiplicity on the 2 co-primary end points ORR and PFS. Other outcomes, including HRQoL, were not adjusted for multiple comparisons. Concerns on external validity included the exclusion of patients who had brain metastases or previous radiation therapy for bone metastases. Furthermore, the study estimations for OS had a relatively short period of follow-up (median of 11.9 months at the cut-off date of February 8, 2021) denoting immaturity of the data for this outcome. The interpretation of the OS data is also limited by the sample size and crossover of patients from placebo to open-label cabozantinib. There is a gap in the overall body of evidence since no comparative efficacy or harms data were available for comparators of interest in the Canadian clinical context, such as selpercatinib or larotrectinib.
Indirect Comparisons
No indirect treatment comparisons were included in this report.
Other Relevant Evidence
No other relevant evidence was included in this report.
Conclusions
Evidence from 1 randomized, double-blind, placebo-controlled trial suggests that cabozantinib prolongs PFS when compared with placebo among patients with progressive, radioiodine-refractory DTC previously treated with VEGFR-targeted therapy. There is uncertainty related to the efficacy of cabozantinib in other clinically important outcomes such as OS, mostly due to immature data, need for more follow-up time, and lack of control for multiple comparisons. There is uncertainty regarding the effect of cabozantinib on HRQoL because this outcome was not controlled for multiple comparisons. Overall, the population assessed in the evidence obtained is generalizable to the Canadian population, although some uncertainty remain in some groups such as patients with brain metastases and ECOG PS scores of 2 and above. There is lack of comparative evidence (direct or indirect) between cabozantinib and key active comparators applicable in the current Canadian clinical context, such as selpercatinib and larotrectinib. The safety profile in the population assessed was considered manageable and consistent with the known safety profile of cabozantinib.
Introduction
Disease Background
Thyroid cancer is 1 of the most commonly diagnosed cancers in Canada and the world. Although it embodies less than 1% of all human tumours, it is considered the most common endocrine malignancy and the fifth most common cancer among women.1,2 It was estimated that 8,200 new cases of thyroid cancer would be diagnosed in those living in Canada in 2019 and about 230 people would die from it.11 For 2020, the incidence of thyroid cancer in Canada was estimated to be 23 per 100,000 patients, or about 8,600 new cases.3
Thyroid cancer can originate from either thyroid follicular cells or parafollicular cells (c cells). Medullary thyroid cancer (MTC) originates from parafollicular cells, while thyroid cancers arising from follicular cells include the DTC, which groups PTC, FTC, and Hurthle cell cancer), poorly differentiated thyroid cancer, and anaplastic thyroid cancer. Among all types of thyroid cancer, DTC is the most common, accounting for more than 95% of cases.4,5
Tumors that are localized and well-differentiated usually are curable with total thyroidectomy or lobectomy, followed by postoperative treatment with RAI therapy – for patients at high risk of persistent disease or disease recurrence after total thyroidectomy. Up to 30% of patients with DTC may have recurrence of disease and 60% of these recurrences occur within the first decade after initial therapy. In patients with primary or secondary radioiodine-refractory thyroid carcinoma the prognosis becomes significantly poorer.6
Diagnosis is based on physical examination and history, neck ultrasound, and ultrasound guided fine-needle aspiration cytology. Levels of calcitonin are helpful to rule out MTC, especially with levels above 100 pg/mL.12 Mutations and translocations in the genes coding the mitogen-activated protein kinase cellular signalling pathway have been implicated in the genetic basis of most thyroid cancers. Some of these mutations include the point mutation in the BRAF gene leading to PTC and PTC-associated anaplastic thyroid cancer. In FTC, mutations in RAS proto-oncogene are most common (40% to 50%) and translocation in PAX8–peroxisome proliferator-activated receptor γ (PPARγ) has been identified in around 30% to 35% of FTC.5
Approximately 10% to 15% of thyroid cancer patients develop distant metastases.2,7,8 Prognosis for radioiodine resistant thyroid cancer with distant metastases is very poor, with an estimated median survival time of about 2.5 to 3.5 years.9 The overall estimates of mortality rates 5 years and 10 years after diagnosis of distant metastases are 65% and 75%, respectively.2,8 Early diagnosis and, if possible, early appropriate surgical treatment are considered to positively affect the prognosis of these patients.
Standards of Therapy
In patients with DTC, early diagnosis and surgical therapy with total thyroidectomy and resection of local and regional metastases followed by RAI therapy depending on recurrence risk assessment is the basis for initial treatment and possibility of cure.5 In rare cases of radioiodine-refractory tumours, additional options include strict suppression of thyroid-stimulating hormone (TSH) and external local radiotherapy.9 Some patients with metastatic disease without further options may need repeated radioactive iodine therapy as palliative treatment.
In Canada, 2 vascular endothelial growth factor receptor (VEGFR) TKI are approved and, according to clinical experts consulted by CADTH, are potentially available as first-line treatment in patients with RAI-resistant DTC (RAI-R-DTC): sorafenib and lenvatinib. However, in the Canadian context, only lenvatinib is currently reimbursed by public drug plans and in use for progressive metastatic radioiodine resistant thyroid cancer,13 while the use of sorafenib is limited to patients paying out-of-pocket or with private insurance coverage. These antineoplastic agents belong to the family of receptor tyrosine kinase (RTK) inhibitors that selectively inhibit the kinase activities of VEGFR1, VEGFR2, and VEGFR3, in addition to other proangiogenic and oncogenic pathway-related RTKs including rearranged during transcription (RET) mutations. Evidence from a single randomized controlled trial (RCT) showed that lenvatinib prolongs PFS compared to placebo.14 However, the effects on OS, HRQoL, and long-term cumulative toxicities remain unknown. Lenvatinib treatment is associated with frequent adverse effects that often necessitate dose reductions and sometimes discontinuation of treatment such as hypertension and its complications, cardiac failure, arterial thromboembolism, GI perforation, hepatotoxicity, hepatic failure, renal failure, and hemorrhage.13,14
Other options aimed at treating patients with RAI-R-DTC were recently approved in Canada including drugs that target RET mutations and tropomyosin receptor kinase (TRK) fusions, which are not rare in patients with RAI-R-DTC. These include larotrectinib and entrectinib, both orally-bioavailable, adenosine triphosphate (ATP)-competitive and highly selective TRK kinase inhibitors; and selpercatinib, a highly selective, ATP-competitive small-molecule inhibitor of the RET receptor. Of these, selpercatinib and larotrectinib (at the time of writing this report) have received a positive recommendation for reimbursement from CADTH; entrectinib is under review at CADTH at the time of writing this report.
The treatment goals In patients with DTC are aimed at curing, improving survival, delaying disease progression, and developing better HRQoL by controlling symptoms, minimizing adverse effects of treatments, and increasing work/life productivity.9
Drug
Cabozantinib (Cabometyx) is a multitargeted TKI that aims at the mesenchymal-epithelial transition (MET) and AXL gene pathways to inhibit tumour invasiveness while targeting VEGF tumour angiogenesis, hence, progression of cancer.15 Key characteristics of cabozantinib and other drugs used to treat RAI-R-DTC are summarized in Table 4.
Cabozantinib is administered orally at a dose of 60 mg daily, and it has a Health Canada–approved indication for the treatment of adult patients with locally advanced or metastatic DTC that has progressed following prior VEGFR-targeted therapy and who are RAI-refractory or ineligible. It is also indicated for renal cell carcinoma (in treatment-naive adults with advanced cancer with intermediate or poor risk and in patients who have received prior VEGF-targeted therapy), and hepatocellular carcinoma (patients who have been previously treated with sorafenib). Treatment with cabozantinib is administered under supervision of an oncologist and an interdisciplinary team that includes specialists in surgery, endocrinology, pathology, nuclear medicine, among other health professionals.
This is the first CADTH reimbursement review submission of cabozantinib with the submitted indication for the treatment of adult patients with locally advanced or metastatic DTC that has progressed following prior VEGFR-targeted therapy and who are radioactive iodine-refractory or ineligible. This indication received Notice of Compliance (NOC) from Health Canada on April 28, 2022. Cabozantinib has the same indication in the US and European Union. Cabozantinib has been previously reviewed by CADTH for the treatment of hepatocellular carcinoma and for the treatment of renal cell carcinoma (in both cases, it received a recommendation to be reimbursed with conditions).
Table 4: Key Characteristics of Cabozantinib, Selpercatinib, and Larotrectinib
Key characteristics | Cabozantinib | Selpercatinib | Larotrectinib |
|---|---|---|---|
Mechanism of Action | A small molecule that inhibits multiple RTKs implicated in tumour growth and angiogenesis, pathologic bone remodelling, drug resistance, and metastatic progression of cancer, with primary inhibition targets of VEGF receptors. | Small-molecule kinase inhibitor aimed at inhibiting the RET RTK. | TRK kinase inhibitor. It targets the TRK family of proteins inclusive of TRKA, TRKB, and TRKC that are encoded by NTRK1, NTRK2, and NTRK3 genes, respectively. |
Indicationa | DTC: for the treatment of adult patients with locally advanced or metastatic DTC that has progressed following prior VEGFR-targeted therapy and who are RAI-refractory or ineligible. RCC: for the treatment of advanced RCC In treatment-naive adults with intermediate or poor risk and in adult patients who have received prior VEGF-targeted therapy. In combination with nivolumab, is indicated for the first-line treatment of adult patients with advanced (not amenable to curative surgery or radiation therapy) or metastatic RCC. HCC: for the treatment of patients with HCC who have been previously treated with sorafenib. | Indicated as monotherapy for the treatment of:
RET fusion-positive DTC in adult patients with advanced or metastatic disease (not amenable to surgery or radioactive iodine therapy) following prior treatment with sorafenib and/or lenvatinib. | For the treatment of adult and pediatric patients with solid tumours that have a Neurotrophic Tyrosine Receptor Kinase (NTRK) gene fusion without a known acquired resistance mutation, are metastatic or where surgical resection is likely to result in severe morbidity and have no satisfactory treatment options. |
Route of Administration | Oral tablet 20 mg, 40 mg, 60 mg | Oral capsules 40 and 80 mg | Capsules 25 mg and 100 mg larotrectinib, and oral solution 20 mg/mL larotrectinib |
Recommended Dose | As a single drug, oral 60 mg once daily without food | < 50 kg: 120 mg twice daily ≥ 50 kg: 160 mg twice daily | Adults:100 mg taken orally, twice daily (total dose of 200 mg) until the patient is no longer clinically benefiting from therapy or until unacceptable toxicity occurs. Pediatrics: In patients 1 month to 18 years old is 100 mg/m2 taken orally, twice daily with a maximum of 100 mg per dose (maximum total dose of 200 mg) until the patient is no longer clinically benefiting from therapy or until unacceptable toxicity occurs |
Serious Adverse Effects or Safety Issues | Thromboembolism, hypertension, gastrointestinal perforation and fistulas, major bleeding, hepatotoxicity, posterior reversible encephalopathy syndrome. | Hemorrhage, hepatotoxicity, QTc prolongation, hypertension. | Hepatotoxicity, neurologic/psychiatric, constipation, diarrhea, dizziness, anemia, vomiting nausea, and pyrexia. |
DTC = differentiated thyroid carcinoma; CI = confidence interval; HCC = hepatocellular carcinoma; MTC = medullary thyroid cancer; NSCLC = non–small cell lung cancer; OR = odds ratio; RAI = radioactive iodine; RCC = renal cell carcinoma; RET = rearranged during transfection or ret proto-oncogene; RTK = receptor tyrosine kinases; TRK = Tropomyosin Receptor Kinase; VEGFR = vascular endothelial growth factor receptor.
aHealth Canada–approved indication
Source: Product monographs for selpercatinib,16 larotrectinib,17 and cabozantinib.15
Stakeholder Perspectives
Patient Group Input
This section was prepared by CADTH staff based on the input provided by patient groups. The full original patient input(s) received by CADTH have been included in the stakeholder section at the end of this report.
Two patient groups submitted 1 joint input for this review. The CCS is the only national charity that supports all those living in Canada, with all cancers across the country with donors and volunteers through research, advocacy, and compassionate support activities. TCC is a national organization of thyroid cancer survivors dedicated to providing emotional support and information to those affected by the disease. CCS disseminated a survey and a call for interview to patients through a thyroid cancer panel, Cancer Connection forums. Also, clinical investigators in the COSMIC-311 trial, the IPSEN Cares program, several thyroid organizations in Canada and internationally were reached in an effort to include more patients (including Thyroid Foundation of Canada, the American Thyroid Association, the Thyroid Cancer Survivors Association, Inc., Thyroid Federation International). Only 2 patients responded to the survey, of which 1 had experience with cabozantinib.
The 2 patients said their ability to work, travel, exercise, conduct household chores, fulfill family obligations, and maintain positive mental health were impacted to a moderate degree by symptoms associated with DTC. Also, both patients indicated there are financial barriers, such as loss of income due to absence from work and transportation costs (gas, parking fees, public transit fees, etc.) related with treatment. No specific response with respect to outcomes that are important to patients was provided. Of note, 1 patient who has previously tried lenvatinib and is currently taking cabozantinib said nausea and vomiting were worst while on lenvatinib and diarrhea was the worst while taking cabozantinib. The other patient who underwent surgery and chemotherapy said fatigue had the most significant impact.
Clinician Input
Input from Clinical Experts Consulted by CADTH
All CADTH review teams include at least 1 clinical specialist with expertise regarding the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol; assisting in the critical appraisal of clinical evidence; interpreting the clinical relevance of the results; and providing guidance on the potential place in therapy). The following input was provided by 2 clinical specialists with expertise in the diagnosis and management of advanced thyroid cancer.
Unmet Needs
The clinical experts reported that RAI-R DTC is a rare disease with about 200 deaths per year attributable in Canada. As with most rare disease, this raises issues about physician awareness and systemic barriers to access to therapy for patients, as per the clinical experts. The clinical experts noted that although most patients respond to lenvatinib therapy, all patients will eventually experience disease progression due to acquired drug resistance. The clinical experts indicated that other than access to agents targeting RET and NTRK fusions via special access programs for the small subset of patients eligible for these, currently there are no funded and reliably effective treatments for these patients. The clinical experts suggested that treatment goals should be improving OS, PFS, and improve HRQoL by controlling symptoms, minimizing adverse effects of treatments, and increasing work/life productivity. There is an unmet need, on which both clinical experts agree, that better treatments need to be available for patients who do not respond or progress after first-line therapy, and/or for those patients who have to discontinue due to side effects or MKI resistance. The clinical experts highlighted that an ideal treatment should also have fewer harmful effects.
Place in Therapy
The clinical experts noted that cabozantinib would provide a second-line treatment option for patients progressing despite lenvatinib therapy in Canada to optimize the quality and quantity of life for RAI-R DTC patients and, in the clinical experts’ opinion, would become the de facto second-line standard of care for these patients. Experts also agreed that cabozantinib should not be used as first-line treatment but could be an alternative for patients who are intolerant of lenvatinib. The clinical experts noted that, in patients with tumours with RET or NTRK fusions, the optimal sequencing of lenvatinib and cabozantinib with agents targeting RET and NTRK is unclear. Based on high tumour response and low toxicity rates the clinical experts thought that these targeted agents could be used earlier rather than later in the treatment sequence.
Patient Population
The clinical experts considered that patients demonstrating radiologically progressive disease on or after lenvatinib therapy should be considered for cabozantinib therapy. The clinical experts indicated that no companion diagnostics is required, and it is not possible to identify patients more likely to respond. The clinical experts noted that cabozantinib treatment can be associated with significant AEs, so the main criteria for the timing and dosing of treatment would be based on clinical judgment considering patient factors such as tumour burden, age, comorbidities, and PS.
Assessing Response to Treatment
Per the clinical experts, patients should have baseline assessment of symptoms, serum thyroglobulin, and cross-sectional imaging. Early in their treatment, patients are assessed every 2 to 3 weeks to monitor for adverse effects and to modify drug dosing, if necessary, per the clinical experts. The clinical experts noted that improved symptoms and a drop in serum thyroglobulin would be favourable signs of response early in treatment. The clinical experts reported that, typically, assessment of response occurs quarterly with repeat cross-sectional imaging. Per the clinical experts, most clinicians would consider evidence of tumour shrinkage or lack of growth on imaging as favourable. The clinical experts noted that in patients ascertained to be benefiting from cabozantinib without intolerable side effects, quarterly clinical assessments and imaging are reasonable; however, the intensity of assessment may vary slightly between clinicians and due to specific patient factors.
Discontinuing Treatment
According to clinical experts, for some patients it may be impossible to titrate cabozantinib to a tolerable dose, and the drug may be discontinued due to adverse effects. In most patients, cabozantinib would be continued until there is unequivocal evidence of disease progression despite treatment, per the clinical experts. The clinical experts noted that, occasionally, a patient may show progression in 1 or 2 areas without other signs of progressive disease and be offered stereotactic body radiation therapy (SBRT) to these areas plus continued drug therapy.
Prescribing Conditions
Clinical experts stated that under regular conditions all cabozantinib candidates will have been receiving lenvatinib under a clinician’s supervision. Therefore, most of these patients would already be under the care of a medical oncologist or endocrinologist experienced in TKI therapy for thyroid cancers. As RAI-R DTC is a rare condition, currently there is a small community of prescribers in Canada currently treating this disease, per the clinical experts consulted by CADTH. The clinical experts noted that the indications for cabozantinib are growing, and a growing number of medical oncologists are becoming familiar with it.
Additional Considerations
The clinical experts indicated that RAI-R DTC patients do appear to have lower clearance of TKIs than other cancer patients, so may be at higher risk for AEs, and awareness of this is important.
The clinical experts noted that, for most scenarios, the adverse effects of lenvatinib can be managed with dose modifications or use of adjunctive medications (e.g., for hypertension). There may be very uncommon scenarios (e.g., true drug allergy, or hypertension requiring multiple antihypertensive drugs) where the clinical experts would agree that cabozantinib should be considered as an alternative.
Clinician Group Input
This section was prepared by CADTH staff based on the input provided by clinician groups. The full original clinician group input(s) received by CADTH have been included in the stakeholder section at the end of this report.
A total of 7 physicians (5 from Ontario, 1 from British Columbia, 1 from Alberta), some of whom are members of the Medical Advisory Panel of TCC and some of whom were investigators of COSMIC-311 trial, contributed to the input submission with administrative support provided by the CCS. These physicians treat head and neck cancers, endocrine cancers, participate in clinical trials, conduct observational research, are involved in local, provincial, and national clinical guideline development, in addition to health technology assessment. They gathered information through clinical experience in treating thyroid cancer, a literature review, and a virtual discussion among experts.
Unmet Needs
The clinician group stated that there are currently no approved/funded options for patients with DTC who are radioactive iodine-refractory or ineligible and progress after VEGFR-targeted therapies. The group added that palliative treatment with doxorubicin is occasionally tried where appropriate and best supportive care is the only remaining regular option in this patient population group.
Place in Therapy
The clinician group believes that cabozantinib is expected to address an unmet need for patients who progress on prior therapy. The group said that since no other therapies are funded beyond lenvatinib as first line in Canada, cabozantinib would offer patients an option for second-line therapy.
Patient Population
The clinician group suggested that patients meeting the following criteria would be best suited for cabozantinib treatment: histologically or cytologically confirmed diagnosis of DTC; radiographic or symptomatic progression of disease on prior VEGFR-TKI; previously treated with or deemed ineligible for treatment with Iodine131 for DTC; and an ECOG PS of 0 or 1. According to the clinician group, patients with progressing nonmeasurable disease, such as bone metastases, should not be excluded in the real-world clinical setting.
Assessing Response to Treatment
The clinician group indicated the treatment response is assessed using clinical assessment, tumour markers, and radiological imaging (CT/MRI) generally done every 3 to 4 months.
Discontinuing Treatment
The physicians indicated that systemic therapy with cabozantinib would be stopped when 1 or more of the following situations are met: patient’s decision to stop, significant AEs, or disease progression.
Prescribing Conditions
Based on the clinician group input, a medical oncologist would prescribe cabozantinib and endocrinologists would manage some patients depending on geographical location. According to the physicians, patients can take cabozantinib at home.
Additional Considerations
The clinician group emphasized that RAI-refractory DTC is a rare disease with significant unmet need and cabozantinib should be reviewed in this regard.
Drug Program Input
The drug programs provide input on each drug being reviewed through CADTH’s reimbursement review processes by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CADTH are summarized in Table 5.
Table 5: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Relevant comparators | |
Placebo was chosen as the comparator in the COSMIC-311 study due to the lack of available treatments in this population. | For pERC information. |
There are no standard comparators funded in Canada at this time. | For pERC information. |
Considerations for initiation of therapy | |
Should patients who experience adverse effects with lenvatinib or sorafenib without progression be eligible for treatment with cabozantinib? | For most scenarios, the adverse effects of lenvatinib can be managed with dose modifications or use of adjunctive medications (e.g., for hypertension). There may be very uncommon scenarios (e.g., true drug allergy, or hypertension requiring multiple antihypertensive drugs) where I would agree that cabozantinib should be considered as an alternative. |
Considerations for renewal of therapy | |
Patients in the COSMIC-311 trial were assessed every 8 weeks for 12 months, then every 12 weeks until clinical benefit no longer experienced or intolerable toxicity. In clinical practice what is the most appropriate frequency to determine treatment response? | Clinical assessment, tumour markers, and radiological imaging (CT/MRI) should be done every 3 to 4 months as assessment measures of treatment response. |
Considerations for discontinuation of therapy | |
In the trial, patients were able to continue cabozantinib as long as there was continued clinical benefit in the opinion of the investigator. What are the discontinuation criteria for cabozantinib? | For some patients it may be impossible to titrate cabozantinib to a tolerable dose, and drug may be discontinued due to adverse effects. In most patients, cabozantinib would be continued until there is unequivocal evidence of disease progression despite treatment. Occasionally, a patient may show progression in 1 or 2 anatomic areas without other signs of progressive disease and be offered SBRT to these areas plus continued drug therapy. |
Considerations for prescribing of therapy | |
The recommended dose is 60 mg once daily without food. Dose interruptions are recommended for CTCAE grade 3 or greater toxicities or intolerable grade 2 toxicities. Upon resolution the dose can be reduced to 40 mg daily then to 20 mg daily. | For pERC information. |
Generalizability | |
Can the trial results be generalized to patients with ECOG > 2? | Clinical experts considered that including patients with ECOG PS of 1 or 2 would be desirable, but ECOG PS above 2 would be inadvisable due to the risk of serious adverse events. |
Care provision issues | |
Cabometyx has potential for drug-drug, drug-food, and drug-herb interactions, requiring assessment and/or intervention. | For pERC information. |
CTCAE = common terminology criteria for adverse events; ECOG = Eastern Cooperative Oncology Group; pERC = pan-Canadian Oncology Drug Review Expert Review Committee.
Clinical Evidence
The clinical evidence included in the review of cabozantinib is presented in 3 sections. The first section, the Systematic Review, includes pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those studies that were selected according to an a priori protocol. The second section includes indirect evidence from the sponsor (if submitted) and indirect evidence selected from the literature that met the selection criteria specified in the review. The third section includes sponsor submitted long-term extension studies and additional relevant studies that were considered to address important gaps in the evidence included in the systematic review.
Systematic Review (Pivotal and Protocol Selected Studies)
Objectives
To perform a systematic review of the beneficial and harmful effects of cabozantinib (Cabometyx) oral tablets, 20 mg, 40 mg, 60 mg for the treatment of adult patients with locally advanced or metastatic DTC that has progressed following prior VEGFR-targeted therapy and who are RAI-R or ineligible.
Methods
Studies selected for inclusion in the systematic review included pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those meeting the selection criteria presented in Table 6. Outcomes included in the CADTH review protocol reflect outcomes considered to be important to patients, clinicians, and drug plans.
Table 6: Inclusion Criteria for the Systematic Review
Criteria | Description |
|---|---|
Patient population | Adult patients with locally advanced or metastatic DTC that has progressed following prior VEGFR-targeted therapy and who are radioactive iodine-refractory or ineligible. Subgroups:
|
Intervention | Cabozantinib (Cabometyx) 20 mg, 40 mg and 60 mg, oral tables. Dose: 60 mg once daily as a single drug. |
Comparators |
|
Outcomesa | Efficacy outcomes:
Harms outcomes:
|
Study design | Published and unpublished phase II, III, and IV RCTs. |
AE = adverse events; DoR = duration of response; DTC = differentiated thyroid cancer; ECOG = Eastern Cooperative Oncology Group; EQ-5D-5L = EuroQoL 5-dimension 5 level questionnaire; HRQoL = quality of life; ORR = overall response rate; OS = overall survival; RCT = randomized controlled trial; PFS = progression-free survival; SAE = serious adverse events; WDAE = withdrawal due to adverse events.
aThese outcomes were identified as being of particular importance to patients in the input received by CADTH from patient groups.
The literature search for clinical studies was performed by an information specialist using a peer-reviewed search strategy according to the PRESS Peer Review of Electronic Search Strategies checklist.
Published literature was identified by searching the following bibliographic databases: MEDLINE All (1946–) via Ovid and Embase (1974–) via Ovid. All Ovid searches were run simultaneously as a multifile search. Duplicates were removed using Ovid deduplication for multifile searches, followed by manual deduplication in Endnote. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Patient Headings), and keywords. The main search concepts were Cabometyx (cabozantinib) and DTC. Clinical trials registries were searched: the US National Institutes of Health’s clinicaltrials.gov, WHO’s International Clinical Trials Registry Platform (ICTRP) search portal, Health Canada’s Clinical Trials Database, and the European Union Clinical Trials Register.
No filters were applied to limit the retrieval by study type. Retrieval was not limited by publication date or by language. Conference abstracts were excluded from the search results. Refer to Appendix 1 for the detailed search strategies.
The initial search was completed on May 26, 2022. Regular alerts updated the search until the meeting of the CADTH pan-Canadian Oncology Drug Review Expert Committee (pERC) on September 14, 2022.
Grey literature (literature that is not commercially published) was identified by searching relevant websites from the Grey Matters: A Practical Tool for Searching Health-Related Grey Literature checklist. Included in this search were the websites of regulatory agencies (US FDA and European Medicines Agency). Google was used to search for additional internet-based materials. Refer to Appendix 1 for more information on the grey literature search strategy.
Two CADTH clinical reviewers independently selected studies for inclusion in the review based on titles and abstracts, according to the predetermined protocol. Full-text articles of all citations considered potentially relevant by at least 1 reviewer were acquired. Reviewers independently made the final selection of studies to be included in the review, and differences were resolved through discussion.
Findings from the Literature
A total of 1 study were identified from the literature for inclusion in the systematic review (Figure 1). The included studies are summarized in Table 7. A list of excluded studies is presented in Appendix 2.
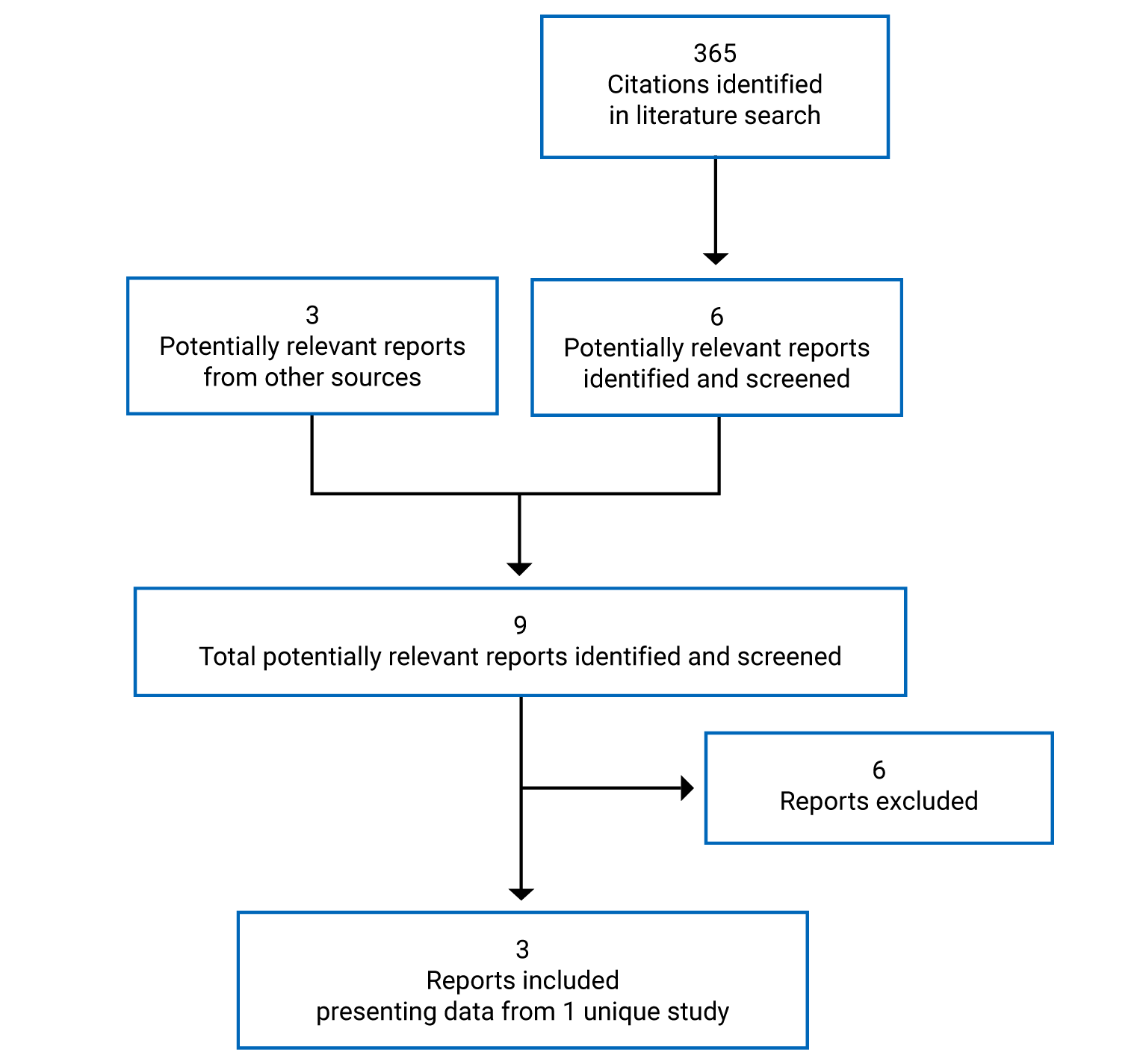
Table 7: Details of Included Studies
Criteria | COSMIC-311 |
|---|---|
Design and population | |
Study design | Phase III, randomized, double-blind, placebo-controlled trial |
Locations | Canada, US, Europe, Latin America, and Asia. |
Patient enrolment dates | First patient randomized: February 27, 2019 Data cut-off date 1: August 19, 2020 (minimum of 6 months of follow-up for the first 100 patients) Data cut-off date 2: February. 8, 2021 |
Randomized (N) | N = 187 as of the August 19, 2020 data cut-off N = 258 as of the Feb. 8, 2021 data cut-off |
Inclusion criteria |
|
Exclusion criteria |
|
Drugs | |
Intervention | Cabozantinib arm: Oral cabozantinib (60 mg) once daily |
Comparator(s) | Placebo arm: Oral cabozantinib-matched placebo once daily |
Duration | 6 months (first cut-off date) for final data collection for primary outcome measure; 20 months of study planned duration for PFS; estimated completion December 2022. |
Phase | |
Pretreatment period | Potential patients were screened to determine if they met the required eligibility criteria. Qualifying screening assessments were performed within 28 days before randomization unless otherwise specified. |
Double-blind treatment period | Patients who met all study eligibility criteria were randomized in a 2:1 ratio to receive either cabozantinib or cabozantinib-matched placebo, stratified by receipt of prior lenvatinib (yes vs no) and age at informed consent (≤ 65 years vs > 65 years). |
Crossover period | Patients were allowed to crossover to receive cabozantinib upon experiencing radiographic PD as determined by the investigator per RECIST 1.1 and confirmed by the BIRC. |
Follow-up | 6 months for the first data cut-off date. Patients received blinded study treatment or unblinded treatment with cabozantinib as long as they continued to experience clinical benefit in the opinion of the investigator or until there was unacceptable toxicity or the need for nonprotocol systemic anticancer treatment. Posttreatment Follow-Up visit occurred 30 ( + 14) days after the date of the decision to discontinue study treatment. |
Outcomes | |
Primary end point |
|
Secondary and exploratory end points | Secondary:
|
Notes | |
Publications | Brosse, et al. 202118 |
BIRC = blinded independent radiology committee; CT = CT; DB = double-blind; DNA = DNA; DTC = differentiated thyroid cancer; ECOG = Eastern Cooperative Oncology Group; EQ-5D-5L = EuroQoL Health questionnaire instrument; FTC = follicular thyroid cancer; MRI = MRI; OS = overall survival; ORR = objective response rate; PD = progressive disease; PD-1 = programmed cell death-1; PD-L1 = programmed cell death ligand 1; PFS = progression-free survival; PS = performance status; RCT = randomized controlled trial; RECIST = Response Evaluation Criteria in Solid Tumors criteria; TKI = tyrosine kinase inhibitor.
Source: CSR of Cabozantinib.10
Description of Studies
The COSMIC-311 study is an ongoing multicenter, phase III, double-blind, placebo-controlled study of oral cabozantinib (60 mg once daily) administered in patients with RAI-refractory, cytologically confirmed, DTC (papillary or follicular and its variants) that has progressed after prior VEFGR targeted therapy. Patients were randomized 2:1 to receive cabozantinib or matching placebo, respectively. Randomization was stratified by receipt of prior lenvatinib (yes vs no) and age at informed consent (≤ 65 years vs > 65 years).This study was conducted in 161 investigational sites among 25 different countries, including Canada, US, and countries in Asia, Latin America, and Europe.
The objective of the COSMIC-311 study was to evaluate the effect of cabozantinib compared with placebo on PFS and ORR in patients with RAI-refractory DTC who have progressed after prior VEGFR-targeted therapy. A first Clinical Study Report (CSR) presented the prespecified primary end point analysis of ORR on the first randomized 100 patients and an interim primary end point analysis of PFS on the 187 randomized patients as of August 19, 2020 (data cut-off; minimum of 6 months’ follow-up for the first 100 patients).
Potential patients were screened to determine if they met the required eligibility criteria. Patients who met all study eligibility criteria were randomized to receive either cabozantinib or cabozantinib-matched placebo. Patients in the placebo group were allowed to crossover to receive cabozantinib upon experiencing radiographic progressive disease (PD) as determined by the investigator per RECIST 1.1 and confirmed by the BIRC. Those patients who were ineligible or opted not to crossover to receive cabozantinib had study treatment discontinued and proceeded with posttreatment assessments. Patients received blinded study treatment or unblinded treatment with cabozantinib after radiographic PD per RECIST 1.1 as long as they continued to experience clinical benefit in the opinion of the investigator or until there was unacceptable toxicity or the need for nonprotocol systemic anticancer treatment (NPACT).
Populations
Inclusion and Exclusion Criteria
Patients must have had radiographic progression per RECIST version 1.1 during or following treatment with a VEGFR-TKI. Patients were also required to have an ECOG PS of 0 or 1, adequate organ and bone marrow function, and must have been receiving thyroxine replacement therapy with serum TSH.
Key exclusion criteria included previous treatment with selective BRAF inhibitors, concurrent treatment with oral anticoagulants or platelet inhibitors (excluding low-dose Aspirin and low-dose low-molecular-weight heparins), presence of untreated brain metastases, and uncontrolled, significant intercurrent illness.
Baseline Characteristics
Baseline demographic information, disease characteristics, and prior medications are described in Table 8 and Table 9. These tables report the main baseline characteristics for the ITT and OITT populations for the cut-off date of August 19, 2020.
Table 8: Summary of Baseline Characteristics
Characteristic | ITT population | OITT population | ||
|---|---|---|---|---|
Cabozantinib (N = 125) | Placebo (N = 62) | Cabozantinib (N = 67) | Placebo (N = 33) | |
Age (years), Median (range) | 65.0 (32, 85) | 66.0 (37, 81) | 62.0 (32, 82) | 63.0 (47, 81) |
Age category, n (%) | ||||
≥ 18 | 125 (100) | 62 (100) | 67 (100) | 33 (100) |
< 65 | 62 (50) | 29 (47) | 35 (52) | 17 (52) |
≥ 65 | 63 (50) | 33 (53) | 32 (48) | 16 (48) |
65 to < 75 | 48 (38) | 23 (37) | 26 (39) | 13 (39) |
75 to < 85 | 14 (11) | 10 (16) | 6 (9.0) | 3 (9.1) |
≥ 85 | 1 (0.8) | 0 | 0 | 0 |
Sex Male, n (%) | 57 (46) | 28 (45) | 32 (48) | 12 (36) |
Sex Female, n(%) | 68 (54) | 34 (55) | 35 (52) | 21 (64) |
Race, n (%)a | ||||
American Indian/Alaska Native | 3 (2.4) | 0 | 1 (1.5) | 0 |
Asian | 20 (16) | 14 (23) | 10 (15) | 9 (27) |
Black/African American | 1 (0.8) | 2 (3.2) | 1 (1.5) | 1 (3.0) |
Native Hawaiian/Other Pacific Islander | 0 | 0 | 0 | 0 |
White | 90 (72) | 41 (66) | 47 (70) | 20 (61) |
Multiple | 0 | 0 | 0 | 0 |
Other | 2 (1.6) | 1 (1.6) | 2 (3.0) | 0 |
Not Reported | 8 (6.4) | 4 (6.5) | 6 (9.0) | 3 (9.1) |
Missing | 1 (0.8) | 0 | 0 | 0 |
Geographic region, n (%) | ||||
Asia | 16 (13) | 13 (21) | 6 (9.0) | 8 (24) |
North America (US/Canada) | 13 (10) | 9 (15) | 8 (12) | 6 (18) |
Europe | 65 (52) | 32 (52) | 35 (52) | 14 (42) |
Rest of the world | 31 (25) | 8 (13) | 18 (27) | 5 (15) |
Age at informed consent, n (%) | ||||
≤ 65 years | 63 (50) | 30 (48) | 35 (52) | 17 (52) |
> 65 years | 62 (50) | 32 (52) | 32 (48) | 16 (48) |
ECOG PS, n (%) | ||||
0 | 59 (47) | 30 (48) | 33 (49) | 17 (52) |
1 | 66 (53) | 32 (52) | 34 (51) | 16 (48) |
Smoking history, n (%) | ||||
Current | 2 (1.6) | 2 (3.2) | 0 | 0 |
Former | 40 (32) | 19 (31) | 24 (36) | 9 (27) |
Never | 83 (66) | 41 (66) | 43 (64) | 24 (73) |
Weight (kg), median (range) | 69.50 (40.3, 117.0) | 64.80 (43.0, 135.5) | 69.80 (44.0, 117.0) | 68.15 (43.6, 135.5) |
BMI (kg/m2), median (range) | 24.94 (15.5, 43.5) | 23.69, (17.3, 46.3) | 26.51, (15.5, 43.5) | 24.96, (17.7, 46.3) |
BMI = body mass index; CRF = case report form; ECOG PS = Eastern Cooperative Oncology Group performance status; ITT = intent to treat; OITT = overall response rate intention to treat.
aMore than one category could be reported for each patient.
Source: CSR of Cabozantinib.10
Table 9: Summary of Baseline Disease History and Previous Therapy – COSMIC-311
Characteristic | ITT population | OITT population | ||
|---|---|---|---|---|
Cabozantinib (N = 125) | Placebo (N = 62) | Cabozantinib (N = 67) | Placebo (N = 33) | |
Disease history | ||||
Diagnosis of DTC by histology or cytology, n (%) | 125 (100) | 62 (100) | 67 (100) | 33 (100) |
DTC subtypes (per CRF), n (%)a,b | ||||
Papillary thyroid carcinoma | 67 (54) | 35 (56) | 39 (58) | 20 (61) |
Follicular thyroid carcinoma | 62 (50) | 28 (45) | 30 (45) | 13 (39) |
Time to randomization since initial histological/cytological diagnosis of DTC (n) | 125 | 61 | 67 | 32 |
Median years (range) | 7.63 (0.1, 33.0) | 8.08 (1.0, 29.5) | 7.83 (2.0, 26.8) | 6.20 (1.0, 29.5) |
Metastatic disease (per CRF), n (%) | 117 (94) | 60 (97) | 63 (94) | 32 (97) |
Measurable disease per investigator, n (%) | 125 (100) | 62 (100) | 67 (100) | 33 (100) |
Measurable disease per BIRC, n (%) | 119 (95) | 60 (97) | 62 (93) | 31 (94) |
Extent of baseline disease per tumour assessment, per BIRC, n (%) | ||||
Bone | 40 (32) | 14 (23) | 20 (30) | 10 (30) |
Important visceral sites | 92 (74) | 43 (69) | 51 (76) | 25 (76) |
Lung | 86 (69) | 41 (66) | 48 (72) | 24 (73) |
Liver | 20 (16) | 8 (13) | 11 (16) | 7 (21) |
All other sitesc | 94 (75) | 52 (84) | 52 (78) | 26 (79) |
Lymph noded | 80 (64) | 46 (74) | 46 (69) | 21 (64) |
Pleural cavity | 17 (14) | 17 (27) | 5 (7.5) | 9 (27) |
Number of target lesions per BIRC, n (%) | ||||
1 | 68 (54) | 30 (48) | 37 (55) | 20 (61) |
2 | 34 (27) | 22 (35) | 16 (24) | 4 (12) |
≥ 3 | 17 (14) | 8 (13) | 9 (13) | 7 (21) |
Prior radioiodine therapy | ||||
Refractory to RAI therapy for DTC, n (%) | 121 (97) | 62 (100) | 65 (97) | 33 (100) |
Ineligible for RAI therapy for DTC, n (%)a | 5 (4.0) | 0 | 3 (4.5) | 0 |
Received prior RAI therapy for DTC, n (%)c | 113 (90) | 61 (98) | 60 (90) | 33 (100) |
Median (range) time from end of last prior RAI therapy to randomization, months | 48.2 (3, 204) | 43.8 (2, 225) | 49.0 (4, 152) | 39.8 (2, 225) |
Prior nonradiation anticancer therapy | ||||
Therapy type for DTC, n (%)a | ||||
Systemic | 123 (98) | 60 (97) | 66 (99) | 32 (97) |
Local | 11 (8.8) | 8 (13) | 8 (12) | 5 (15) |
Unknown | 6 (4.8) | 2 (3.2) | 4 (6.0) | 1 (3.0) |
Other | 1 (0.8) | 1 (1.6) | 1 (1.5) | 1 (3.0) |
Number of prior VEGFR-TKI drugs per patient, n (%) | ||||
0 | 0 | 1 (1.6)c | 0 | 0 |
1 | 91 (73) | 47 (76) | 46 (69) | 24 (73) |
≥ 2 | 34 (27) | 14 (23) | 21 (31) | 9 (27) |
Median (range) | 1.0 (1, 2) | 1.0 (0, 2) | 1.0 (1, 2) | 1.0 (1, 2) |
Number of prior PD-1/PD-L1 agents per patient, n (%) | ||||
0 | 119 (95) | 58 (94) | 63 (94) | 30 (91) |
1 | 6 (4.8) | 4 (6.5) | 4 (6.0) | 3 (9.1) |
≥ 2 | 0 | 0 | 0 | 0 |
Median (range) | 0 (0, 1) | 0 (0, 1) | 0 (0, 1) | 0 (0, 1) |
Received prior sorafenib for DTC, n (%) | 77 (62) | 35 (56)c | 45 (67) | 20 (61) |
Received prior lenvatinib for DTC, n (%) | 79 (63) | 39 (63) | 41 (61) | 21 (64) |
Received prior sorafenib and lenvatinib, n (%) | 31 (24.8) | 13 (21.0) | 19 (28.4) | 8 (24.2) |
Progression on most recent prior VEGFR-TKI therapy for DTC, n (%) | 97 (78) | 46 (74) | 55 (82) | 24 (73) |
Median (range) time on most recent prior VEGFR-TKI therapy for DTC, months | 18.20 (0.2, 94.9) | 14.88 (0.9, 81.8) | 13.83 (0.2, 94.9) | 14.65 (2.2, 73.6) |
Median (range) time from end of most recent prior VEGFR-TKI therapy to randomization, months | 1.51 (0.4, 47.3) | 1.84 (0.5, 58.0) | 1.51 (0.4, 32.9) | 1.97 (0.5, 58.0) |
Progression while receiving sorafenib or lenvatinib for DTC at any time, n (%) | 111 (89) | 51 (82) | 61 (91) | 27 (82) |
Median (range) duration of prior sorafenib, months | 11.60 (0.2, 90.8) | 14.72 (2.4, 61.5) | 10.97 (0.2, 90.8) | 14.80 (2.4, 48.4) |
Total duration of treatment on prior sorafenib (months) for DTC, n (%) | ||||
< 1 month | 2 (1.6) | 0 | 2 (3.0) | 0 |
≥ 1 to < 3 months | 5 (4.0) | 3 (4.8) | 2 (3.0) | 3 (9.1) |
≥ 3 to < 6 months | 14 (11) | 2 (3.2) | 12 (18) | 2 (6.1) |
≥ 6 months | 56 (45) | 30 (48) | 29 (43) | 15 (45) |
Median (range) duration of prior lenvatinib for DTC, months | 18.73 (1.0, 94.9) | 16.23 (0.9, 81.8) | 13.90 | 14.00 |
Total duration of treatment on prior lenvatinib (months) for DTC, n (%) | ||||
< 1 month | 2 (1.6) | 1 (1.6) | 1 (1.5) | 0 |
≥ 1 to < 3 months | 2 (1.6) | 2 (3.2) | 1 (1.5) | 2 (6.1) |
≥ 3 to < 6 months | 6 (4.8) | 6 (9.7) | 3 (4.5) | 5 (15) |
≥ 6 months | 69 (55) | 30 (48) | 36 (54) | 14 (42) |
Reason for stopping most recent prior nonradiation anticancer drug for DTC, n (%) | ||||
Progression | 107 (86) | 48 (77) | 59 (88) | 25 (76) |
Toxicity | 12 (9.6) | 10 (16) | 6 (9.0) | 7 (21) |
Completion | 4 (3.2) | 4 (6.5) | 1 (1.5) | 1 (3.0) |
Other | 2 (1.6) | 0 | 1 (1.5) | 0 |
Prior radiation therapy for DTC | ||||
Incidence of prior radiation therapy by indication, n (%) | ||||
DTC | 67 (54) | 30 (48) | 36 (54) | 18 (55) |
Other | 1 (0.8) | 1 (1.6) | 1 (1.5) | 0 |
Number of prior radiation therapies for DTC per patient, n (%) | ||||
1 | 32 (26) | 14 (23) | 15 (22) | 9 (27) |
2 | 16 (13) | 9 (15) | 11 (16) | 4 (12) |
≥ 3 | 19 (15) | 7 (11) | 10 (15) | 5 (15) |
Median (range)e | 2.0 (1, 11) | 2.0 (1, 8) | 2.0 (1, 11) | 1.5 (1, 8) |
BIRC = blinded independent radiology committee; CRF = case report form; CT = CT; DTC = differentiated thyroid cancer; ITT = intent to treat; MRI = MRI; OITT = overall response rate intention to treat.
aPatients may be counted in more than one category.
bFive patients (4 in the cabozantinib arm and 1 in the placebo arm) in the ITT population were noted as having both papillary and follicular histologic subtypes.
cAll other sites shown are those with ≥ 25% incidence in either arm.
dLymph nodes are considered as one organ and only counted once.
eOnly patients who received prior radiation therapy for DTC were included.
Source: CSR of Cabozantinib.10
The median age was similar in the evaluated populations (from 62 to 65 years), as well as the distribution of sex, race/ethnic groups, and most patients were from Europe centres, with only 10% to 18% from US and Canada.
The ECOG status of 0 or 1 was equally distributed among the populations – i.e., half of patients having an ECOG PS of 0 and the other half an ECOG PS of 1. A similar distribution was observed with the type of DTC (papillary and FTC).
More than 94% of patients had metastatic disease at entry into the study in all groups. Most patients (from 69% to 76%) had 1 prior VEGFR-TKI drug and about 1 in 4 had 2 or more. Between 61% and 64% received prior lenvatinib for the treatment of DTC (Table 9).
Interventions
Cabozantinib was administered orally as 60 mg tablets, once daily at bedtime. The control group received a matched-administration placebo with similar and undistinguishable characteristics at the same schedule. Two dose reductions, in decrements of 20 mg cabozantinib or matched placebo, were permitted to manage or prevent worsening of an AE or toxicity. Patients continued blinded study treatment as long as they continued to experience clinical benefit, in the opinion of the investigator, or until unacceptable toxicity, the need for nonprotocol subsequent systemic anticancer therapy, or other reasons for treatment discontinuation. Study treatment assignment was unknown to the patients, investigators, study centres, the sponsor, and any contract research organization affiliated with the study.
For the crossover phase, upon authorization from the sponsor, the investigator could unblind individual patients with BIRC-confirmed radiographic PD via the interactive response technology (IRT) system. Patients without BIRC-confirmed radiographic PD were not unblinded and either discontinued blinded study treatment or continued to receive blinded study treatment and assessments.
For the primary analysis of ORR and interim analysis of PFS, limited sponsor personnel were unblinded for the purposes of data analysis and submission to regulatory agencies.
Allowed concomitant therapies included antiemetics and antidiarrheal medications, granulocyte colony-stimulating factors (G-CSF or GM-CSF), bisphosphonates, transfusions, hormone replacement, and anticoagulation. During the study, some therapies were not allowed, including NPACT (e.g., chemotherapy, immunotherapy, radionuclides, drugs, or herbal products used expressly for treating DTC) and erythropoietic agents. Local anticancer treatment including palliative radiation, ablation, embolization, or surgery with impact on tumour lesions was not to be performed until radiographic progression per RECIST 1.1 had been established.
Outcomes
In Table 10, the primary and key secondary end points evaluated in the COSMIC-311 trial and assessed based on the protocol of this review are presented.
The co-primary efficacy end points in the COSMIC-311 trial included:
PFS per Response Evaluation Criteria in Solid Tumors (RECIST) 1.1 by BIRC
ORR per RECIST 1.1 by BIRC
Additional secondary end points in the COSMIC-311 trial included:
OS
duration of objective tumour response
safety and tolerability
PK of cabozantinib
relationship of baseline and postbaseline changes in biomarkers
change in mobility, self-care, usual activities, pain/discomfort, anxiety/depression, and global health as assessed by the EuroQoL Health questionnaire instrument (EQ-5D-5L).
Radiographic tumour assessments included CT or MRI scans and bone scans, at screening and every 8 weeks (± 7 days) after randomization during the first 12 months on study, then every 12 weeks (± 14 days) thereafter.
A detailed discussion and critical appraisal of the outcome measures is provided in Appendix 4.
Table 10: Summary of Outcomes of Interest Identified in the CADTH Review Protocol
Outcome measure | COSMIC-311 study |
|---|---|
Overall Survival | Key secondary end point |
Progression-Free Survival | Co-primary efficacy end point |
Objective Response Rate | Co-primary efficacy end point |
Duration of Response | Key secondary end point |
HRQoL – EQ-5D-5L | Key secondary end point |
EQ-5D-5L = EuroQoL questionnaire; HRQoL = health-related quality of life.
Source: CSR of Cabozantinib.10
The ORR was assessed in the first 100 randomly assigned patients (i.e., the ORR intention-to-treat [OITT] population) and PFS in all randomly assigned patients (the intention-to-treat [ITT] population), both based on evaluations by BIRC. The ORR was defined as the proportion of patients with a best overall response of confirmed complete response (CR) or confirmed partial response (PR) per RECIST 1.1 after a minimum 6-month follow-up in the OITT population.
The duration of PFS was defined as time from randomization to the earlier of either PD per BIRC per RECIST 1.1 or death from any cause. The primary analysis of PFS was event-driven and was planned to be conducted after at least 193 events had been observed. Primary analysis of PFS included radiographic progression events as determined by BIRC per RECIST 1.1 and deaths. Clinical deterioration or radiographic progression determined by the investigator were not to be considered as events for the primary analysis. The recorded date of radiographic progression was the date of the tumour assessment visit at which progression was declared. General censoring rules for the primary analysis of PFS were as follows:
Patients who received systemic NPACT, or local NPACT for disease under study, nonprotocol radiation therapy for disease under study (other than to bone), or surgery to resect tumour lesions before experiencing an event were right censored at the date of the last adequate tumour assessment (ATA).
Patients who had not experienced an event (and were not otherwise censored) at the time of data cut-off were right censored on the date of their last tumour assessment after randomization that was on or before the data cut-off.
Patients who missed 2 or more ATAs followed by an event (progression or death) were right censored on the date of their most recent ATA before the missing assessments.
Duration of OS was defined as the time from randomization to death due to any cause. For patients who were alive at the time of data cut-off but were permanently lost to follow-up, duration of OS was right censored at the date the patient was last known to be alive. Those who withdrew consent from survival follow-up and were alive were right censored at the date the patient withdrew consent from survival follow-up. Patients alive on or after the data cut-off or those who died after the data cut-off were right censored at the date of data cut-off.
DOR was defined as the time from the first documentation of objective response by BIRC or by the investigator (subsequently confirmed at a visit at least 28 days later) to disease progression or death due to any cause.
HRQoL was evaluated by the EQ-5D-5L questionnaire, and then converted into a single index (EQ-Index) value normalized across different countries where the index is validated. For EQ-Index and EQ-VAS, descriptive statistics for change from baseline at each time were calculated. The minimal important differences (MID) for these questionnaires in cancer patients were considered as 0.06 to 0.08 for EQ-5D Index, and 7 for EQ-VAS based on previous estimations.19 In addition, the effect size for change from baseline was calculated as mean of change in score/pooled SD for baseline scores. An effect size ≥ 0.3 was considered potentially clinically meaningful.20,21
EQ-5D-5L measure of health status questionnaires were applied every 4 weeks through week 25, then every 8 weeks, irrespective of whether study treatment was given, reduced, interrupted, or discontinued, until the later of investigator-assessed radiographic disease progression per RECIST 1.1 that was confirmed by BIRC or the date of the decision to permanently discontinue study treatment.
Statistical Analysis
Analysis of End Points
The ORR for patients on cabozantinib was compared to those on placebo using the Fisher’s exact test at the 2-sided Alpha = 0.01 level of significance. Analysis using the Cochran-Mantel-Haenszel (CMH) method to adjust for stratification factors per IRT was also conducted. Point estimates of ORR, the difference in ORR between the 2 treatment arms, and associated CIs were provided. The odds ratio and its CIs were also provided. The 2-sided 95% and 99% CIs were calculated using exact methods except for the difference in ORR between the 2 treatment arms and for the odds ratio which used asymptotic confidence limits.
The PFS for patients on cabozantinib was compared to those on placebo using the stratified log-rank test with a 2-sided, 0.04 or 0.05 level of significance. The significance level was determined by the fallback testing procedure used to control for the overall type I error rate (see details regarding multiple testing below).The median duration of PFS and the associated 96% or 95% CI for each treatment arm were estimated using the KM method. The stratified hazard ratio (HR) and its 96% or 95% CI were estimated using a Cox proportional-hazard model with treatment group as the independent variable and stratified by the same randomization stratification factors used for the log-rank test.
The median duration of OS and the associated 95% CI for each treatment arm were estimated using the KM method. The unstratified and stratified HR and their 95% CI were estimated using a Cox proportional-hazard model with treatment group as the independent variable. The stratification factors were the same as those used to stratify the randomization. Log-rank P values were calculated and presented for descriptive purposes; formal inferences were not drawn. Analysis of the additional end point OS was descriptive and noninferential as OS was not a controlled end point for the study.
Duration of objective response was computed only among patients who experienced an objective response (CR or PR) and was analyzed by the KM method. Dates of progression and censoring were determined as described for the primary end point analysis of PFS.
HRQoL was evaluated within each treatment arm with descriptive statistics (number of observations, mean and standard deviation) as assessed by the EQ-5D-5L questionnaire. The mean change from baseline at each time point and the corresponding 95% CI and P value from 1-sample t-test; effect size for change from baseline within arm (as mean of change in score/pooled standard deviation for baseline scores); and shift in the severity scale since baseline were calculated. The EQ-5D-5L was converted into a single index (EQ-Index) value normalized across different countries where the index is validated. For EQ-Index and EQ-VAS, descriptive statistics for change from baseline at each time were calculated.
Harms were evaluated using the safety and O-Safety populations. No formal statistical comparisons were made between treatment arms.
Power and Sample Size
The study was designed to provide adequate power for the multiple primary end points of ORR and PFS. It was estimated that 100 patients would be adequate to evaluate the multiple primary end point of ORR alone, and 300 patients would be needed to evaluate the multiple primary end point of PFS. Thus, to allow an earlier evaluation of ORR, this study employed a trial within a trial design. The primary analysis of ORR was limited to the first 100 patients randomized to the study and defined as the OITT population.
For ORR, 100 patients provided a 2-sided 0.01 test of difference in proportions with greater than 90% power to reject the null hypothesis of no difference in ORR, assuming a true ORR of 2% in the placebo arm and 35% in the cabozantinib arm (a 33 percentage point difference), a pooled variance estimate, and a 2:1 allocation ratio.
For the primary analysis of PFS, assuming exponential distribution, proportional hazards, and a 2:1 treatment allocation ratio (cabozantinib: placebo), 193 events would be required to provide 90% power to detect an HR of 0.61 using the log-rank test and a 2-sided significance level of 0.04. This corresponds to a 36% reduction in the risk of progression or death, or a 64% improvement in median PFS from 5.5 months to 9.0 months.
Sensitivity Analysis
A sensitivity analysis of the ORR based on tumour assessments per RECIST 1.1 per investigator was planned to compare it to the assessment by BIRC (both in the OITT population). ORR and supportive analyses per BIRC and per investigator were also performed for the ITT population using the same analysis methods as for the OITT population.
For OS, sensitivity analysis was conducted censoring for receipt of any subsequent anticancer therapy in the ITT population. An exploratory OS analysis for the ITT population was also planned, adjusting for crossover of placebo patients to cabozantinib as a time-dependent covariate.
A sensitivity analysis of PFS on the ITT population, by the investigator as compared to the BIRC, was also performed to evaluate the influence of the assessor of radiographic progression based upon RECIST 1.1. Additional sensitivity and supplementary analyses of PFS were performed to define additional clinical outcomes as events and also evaluate the impact of informative censoring. Analyses of PFS per RECIST 1.1 by BIRC and by investigator on the OITT population were also conducted.
Subgroup Analysis
Exploratory analyses of PFS, ORR, and OS were conducted to evaluate the effect on subgroups defined by baseline characteristics, and these included age category (≤ 65 years, > 65 years),sex, race, region, ECOG PS at baseline, receipt of prior lenvatinib or sorafenib, prior VEGFR-TKI anticancer therapy, RAI, histology (Papillary, Follicular), and type of metastases.
Multiplicity Adjustments
Inflation of type I error associated with 2 multiple primary end points was controlled by a modified Bonferroni procedure. ORR was tested at the 2-sided 1% Alpha significance level, and PFS was tested at the 2-sided 4% Alpha significance level. Additionally, the fallback method for alpha allocation was implemented:
If the null hypothesis was rejected for ORR, its alpha allocation of 1% would be passed to PFS, which would then be tested at the 5% level.
If the null hypothesis was not to be rejected for ORR, PFS would be tested at its original alpha allocation of 4%.
Inflation of type I error arising from multiple analyses of PFS was to be controlled by a Lan-DeMets O’Brien alpha spending function, using the actual information fraction at the interim analysis. The multiplicity issue resulting from analysis of 2 multiple primary efficacy end point (ORR and PFS), was addressed by applying a modified Bonferroni procedure (dividing the alpha between the multiple primary end points).
Analysis Populations
The number of patients evaluated in each population is presented in Table 11. The definitions of these populations assessed are as follows:
ITT Population
The ITT population consisted of all randomized patients regardless of whether any study treatment or the correct study treatment was received.
Overall Response Rate Intention-to-Treat (OITT) Population
The OITT population consisted of the first 100 patients randomized, regardless of whether any study treatment or the correct study treatment was received.
Safety Population
The safety population included all randomized patients who received any amount of study treatment (either cabozantinib or cabozantinib-matched placebo). Analyses based on the safety population were performed according to the actual treatment received.
Overall Response Rate Safety (O-Safety) Population
The O-Safety population consisted of patients included in the OITT population receiving any amount of study treatment (either cabozantinib or cabozantinib-matched placebo).
Table 11: Analysis Populations, COSMIC-311 Study, Cut-Off August 19, 2020
Population | Cabozantinib, N | Placebo, N |
|---|---|---|
ITT populationa | 125 | 62 |
OITT populationa,b | 67 | 33 |
Safety populationc | 125 | 62 |
O-Safety populationd | 67 | 33 |
Placebo crossover patientse | N/A | 19 |
Pharmacokinetic populationf | 107 | 54 |
BIRC = blinded independent radiology committee; ITT = intent to treat; O-Safety = overall response rate safety population; OITT = overall response rate intent to treat; PD = disease progression; PK = pharmacokinetic; RECIST = Response Evaluation Criteria in Solid Tumors.
aIncludes all randomized patients in the respective population (ITT or OITT).
bOITT population consisted of the first 100 patients who were randomized to receive study treatment.
cSafety population comprised all patients who received any amount of study treatment.
dO-Safety population comprised all patients in the OITT population who received any amount of study treatment.
ePlacebo crossover patients consisted of eligible patients in the ITT population who were randomized to placebo then crossed over to receive cabozantinib upon experiencing BIRC-confirmed radiographic PD per RECIST 1.1.
fThe PK population consisted of all patients with available PK data.
Source: CSR of Cabozantinib.10
Results
Patient Disposition
The COSMIC-311 trial screened a total of 227 patients using the described inclusion criteria. Of these, 40 patients (17.6%) failed the eligibility criteria, as depicted in Table 12. The most common reasons for failure to screening were known brain metastases, other histologically confirmed diagnosis, and significant clinical disorders.
The study randomized a total of 187 patients to receive in a 2:1 ratio (ITT population) cabozantinib or placebo. A total of 125 patients were assigned to receive cabozantinib arm and 62 placebo. After the August 19, 2020 cut-off date, patients continued to enrol in the study and receive blinded study treatment. At the interim analysis, enrolment stopped due to improvement in PFS, as assessed by the investigators, and the last patient was randomized on February 8, 2021, with a total of 258 patients (170 patients in the cabozantinib arm and 88 patients in the placebo arm). Sites remained blinded through the efficacy analyses and were ultimately unblinded and provided with individual treatment assignments on April 16, 2021 to enable potential crossover. Patients continue to be followed for efficacy and safety.
The proportion of patients who discontinued blinded study treatment were overall similar between arms of the study. Only 1 patient from the cabozantinib group transitioned to an open-label intervention, while 21 (34%) in the placebo group made the transition and crossed over to an open-label treatment.
The first 100 patients randomized to receive study treatment comprised the OITT population and included 67 patients in the cabozantinib arm and 33 in the placebo arm. As of the data cut-off date, 45% of patients in the cabozantinib arm and 73% of patients in the placebo arm had discontinued blinded study treatment, mostly related to transitioning to open-label treatment.
Table 12: Patient Disposition, COSMIC-311, Cut-Off Date August 19, 2020
Criteria | Cabozantinib | Placebo |
|---|---|---|
Screened, N | 227 | |
Screen failures, n (%) | 40 (17.6) | |
Randomized, n (%)a | 125 (100) | 62 (100) |
Discontinued blinded study treatment, n (%) | 36 (29) | 36 (58) |
Reason for discontinuation, n (%) | ||
Adverse events | 8 (6.4) | 1 (1.6) |
Progressive disease | 13 (10) | 8 (13) |
Transition to Open-Labelb | 1 (0.8) | 21 (34) |
Clinical deterioration | 10 (8.0) | 6 (9.7) |
Withdrawal by patient | 2 (1.6) | 0 |
Lack of clinical benefit | 1 (0.8) | 0 |
Lost to follow-up | 1 (0.8) | 0 |
ITT, Na | 125 (100) | 62 (100) |
Safety, N | 125 (100) | 62 (100) |
OITTc | ||
Randomized n (%) | 67 (100) | 33 (100) |
Discontinued blinded study treatment, n (%) | 30 (45) | 24 (73) |
Reason for discontinuation, n (%) | ||
Adverse events | 6 (9.0) | 1 (3.0) |
Progressive disease | 12 (18) | 7 (21) |
Transition to Open-Label | 1 (1.5) | 12 (36) |
Clinical deterioration | 8 (12) | 4 (12) |
Withdrawal by patient | 1 (1.5) | 0 |
Lack of clinical benefit | 1 (1.5) | 0 |
Lost to follow-up | 1 (1.5) | 0 |
BIRC = blinded independent radiology committee; ITT = intention to treat; OITT = Overall Response Rate ITT population; PP = per protocol.
aIn this study, safety and ITT populations were considered the same.
bTransition to open-label study treatment required patients to have BIRC-confirmed progressive disease.
cOITT population consisted of the first 100 patients who were randomized to receive study treatment for primary analysis.
Source: CSR of Cabozantinib.10
Exposure to Study Treatments
The median duration of exposure (including dose interruptions) was 4.4 months in the cabozantinib only arm and 2.3 months in the placebo arm. Treatment exposure and dose interruptions are presented in Table 18, in the Harms section The median daily dose was 42 mg cabozantinib and 60 mg placebo; the corresponding median dose intensities were 70.0% and 100%, respectively. There were 117 patients still receiving blinded treatment at the time of the data cut-off date of August 19, 2020; 89 patients were still on cabozantinib and 28 were still on placebo.
Concomitant medications were administered in a balanced fashion between treatment arms, except for loperamide (antidiarrheal), amlodipine, urea, calcium, paracetamol (acetaminophen), and clobetasol, which had a at least 10% higher incidence in the cabozantinib only arm compared with the placebo arm by decreasing frequency.
A total of 12 patients (9.6%) in the cabozantinib only arm and 3 patients (4.8%) in the placebo arm had their dose interrupted due to patient noncompliance for reasons other than an AE.
Efficacy
Only those efficacy outcomes and analyses of subgroups identified in the review protocol are reported below. Refer to Appendix 3 for detailed efficacy data.
Survival Outcomes
Overall Survival
At the data cut-off date of August 19, 2020 (with a median follow-up time of 6.24 months), there were 17 deaths in the cabozantinib arm and 14 in the placebo arm (14% versus 23% respectively, refer to Table 13). Median OS was not reached (95% CI, NE to NE) in either treatment group with OS estimates of 85% in the cabozantinib group versus 73% in the placebo group at 6 months (Figure 2).
Table 13: Survival outcomes in COSMIC-311, per BIRC, ITT population, Cut-Off Date August 19, 2020
Criteria | Cabozantinib (N = 125) | Placebo (N = 62) |
|---|---|---|
OS | ||
Number of patients, N (%) | ||
Censored | 108 (86) | 48 (77) |
Death | 17 (14) | 14 (23) |
Follow-up, median (months) | 6.24 | |
Duration of OS (months)a | ||
Median (95% CI) | NE (NE, NE) | NE (NE, NE) |
25th percentile | NE | 5.4 |
75th percentile | NE | NE |
Range | 0.07+, 15.74+ | 0.43+, 11.60+ |
P value (stratified log-rank test)b,c | 0.0879 | |
Hazard ratio (95% CI; stratified)b,d | 0.54 (0.27, 1.11) | |
K-M landmark estimates (% of patients event-free) at: | ||
3 months | 96.5 | 86.6 |
6 months | 84.8 | 73.4 |
9 months | 77.0 | 70.2 |
12 months | 77.0 | NEe |
PFS | ||
Number of patients, N (%) | ||
Censored | 94 (75) | 19 (31) |
Event | 31 (25) | 43 (69) |
Death | 6 (4.8) | 2 (3.2) |
Progressive disease | 25 (20) | 41 (66) |
Follow-up, median (months) | 6.24 | |
Duration of PFS (months) | ||
Median (96% CI) | NE (5.7, NE) | 1.9 (1.8, 3.6) |
25th percentile, 75th percentilea | 4.4, NE | 1.6, 5.4 |
Range | 0.03+, 15.67+ | 0.03+, 9.26+ |
P value (stratified by log-rank test)b,e | < 0.0001 | |
Hazard ratio (96% CI; stratified)b,d | 0.22 (0.13, 0.36) | |
K-M estimates (% of patients event-free) | ||
3 months | 88.2 | 42.4 |
6 months | 56.9 | 16.9 |
9 months | 54.3 | 6.3 |
12 months | 54.3 | NEf |
ITT = intention to treat; KM = Kaplan–Meier; NE = not estimable; OS= overall survival; PFS = progression-free survival.
+indicates a censored observation.
aPercentiles were based on KM estimates.
bStratification factors based on IxRS were receipt of prior lenvatinib (yes vs no) and age at informed consent (≤ 65 years vs > 65 years).
cP value has not been adjusted for multiple comparators.
dEstimated using the Cox proportional-hazard model (adjusted for stratification factors if applicable). HR < 1 indicate results in favour of cabozantinib.
eCut-off of the critical value for P was 0.00036.
fMaximum duration of OS in the placebo arm for the ITT population was 11.60 months and 9.26 months for PFS at the data cut-off date.
Source: CSR of Cabozantinib.10
Figure 2: Kaplan–Meier Plot of OS, Cut-Off August 19, 2020, ITT Population
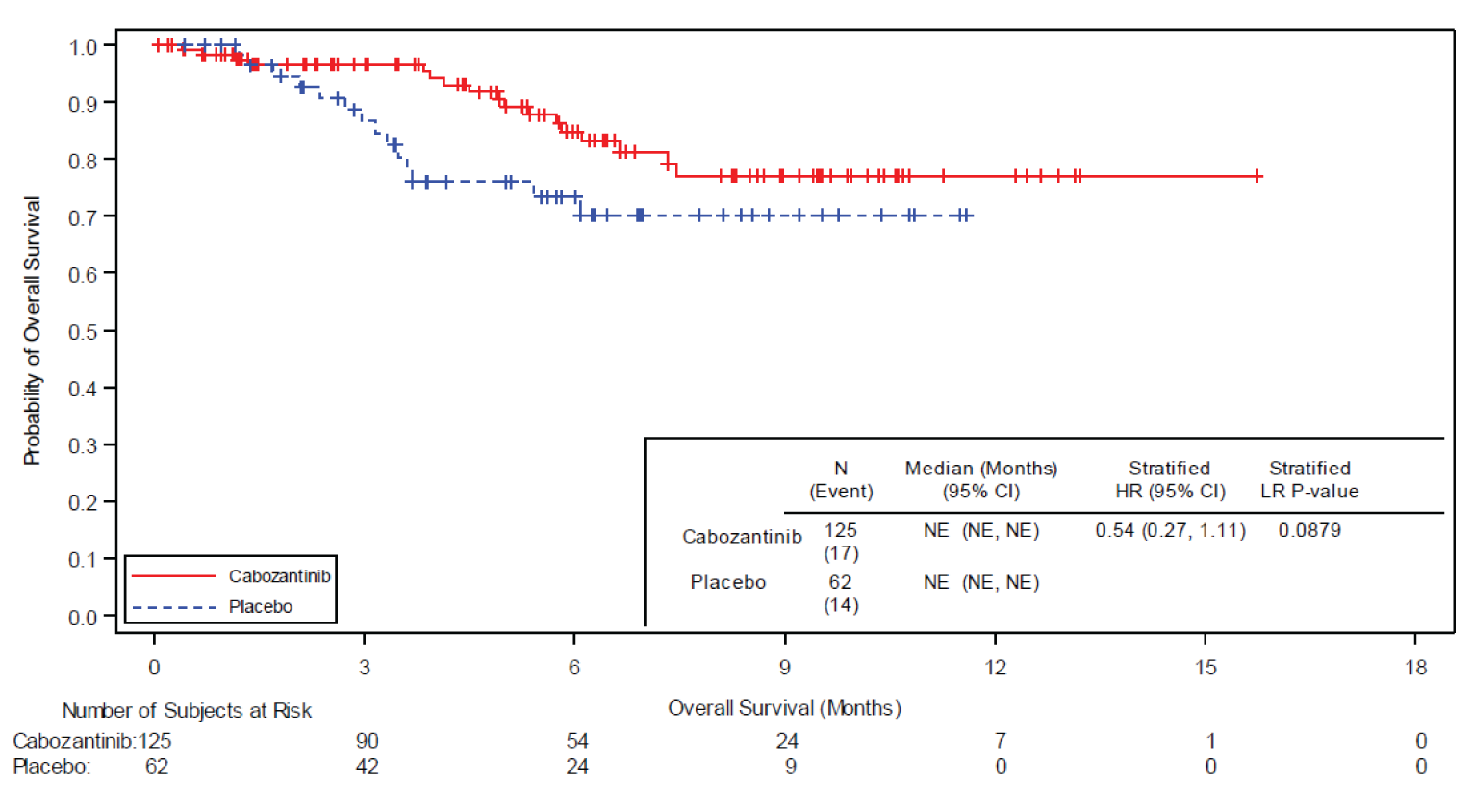
CI = confidence; HR = hazard ratio, ITT = intention to treat; IxRS = interactive voice/web response system; LR = log-rank test, NE = not estimable.
+ Indicates censored observation
Stratification factors (per IxRS) comprise receipt of prior lenvatinib (yes vs no) and age at informed consent (≤ 65 years vs > 65 years).
Source: CSR of Cabozantinib.10
The log-rank test for differences in the KM curves for OS had a corresponding P value = 0.0879. The estimated Cox Proportional Hazards (PH) HR was 0·54 (95% CI, 0.27 to 1·11); of note, this end point and corresponding Cox PH HR and P values were not controlled for multiplicity, hence cannot be used to support inference for this outcome without risk for increased type I error.
The number of patients who used subsequent systemic anticancer therapy was 3 (2%) of 125 in the cabozantinib group and 4 (6%) of 62 in the placebo group; this does not include the 19 patients (31%) in the placebo group who crossed over to open-label cabozantinib.
For the cut-off date of February 8, 2021, with a median follow-up of 11.9 months, results of OS were overall consistent (Table 14, Figure 3), with 34 deaths in the cabozantinib arm and 20 in the placebo arm (27% versus 32% respectively). Median OS was 19.4 (95% CI, 15.9 to NE) months in the cabozantinib group and was not reached (95% CI, NE to NE) in the placebo group. In this cut-off date, the log-rank test for OS had a corresponding P value = 0.0277, and the Cox PH model estimated the HR = 0.74 (95% CI, 0.42 to 1.28). Of note, these results should be interpreted as supplemental evidence as they are based on data from a cut-off date following the primary analysis.
Table 14: Survival outcomes in COSMIC-311, Cut-Off February 8, 2021
Criteria | Primary analysis subset (N = 187) | Full ITT Population (N = 258) | ||
|---|---|---|---|---|
Cabozantinib (N = 125) | Placebo (N = 62) | Cabozantinib (N = 170) | Placebo (N = 88) | |
OS | ||||
Number of patients, n (%) | ||||
Censored | 91 (73) | 42 (68) | 133 (78) | 67 (76) |
Death | 34 (27) | 20 (32) | 37 (22) | 21 (24) |
Follow-up, median (months) | 11.9 | 10.1 | ||
Duration of OS (months)a | ||||
Median (95% CI) | 19.4 (15.9, NE) | NE (NE, NE) | 19.4 (15.9, NE) | NE (NE, NE) |
25th percentile | 10.5 | 5.4 | 10.5 | 6.1 |
75th percentile | 19.4 | NE | 19.4 | NE |
Range | 0.39, 19.35 | 0.99+, 17.28+ | 0.20+, 19.35 | 0.23+, 17.28+ |
P value (stratified log-rank test)b,c | 0.277 | 0.3260 | ||
Hazard ratio (95% CI; stratified)b,d | 0.74 (0.42, 1.28) | 0.76 (0.45, 1.31) | ||
K-M landmark estimates (% of patients event-free) at: | ||||
3 months | 96.0 | 88.5 | 96.4 | 89.7 |
6 months | 86.9 | 73.8 | 86.6 | 76.5 |
9 months | 80.0 | 70.4 | 79.7 | 73.0 |
12 months | 72.0 | 65.3 | 71.7 | 67.7 |
18 months | 55.8 | NE | 55.6 | NEe |
PFS | ||||
Number of patients, N (%) | ||||
Censored | 69 (55) | 4 (6.5) | 108 (64) | 19 (22) |
Event | 56 (45) | 58 (94) | 62 (36) | 69 (78) |
Death | 9 (7.2) | 3 (4.8) | 12 (7.1) | 4 (4.5) |
Progressive disease | 47 (38) | 55 (89) | 50 (29) | 65 (74) |
Follow-up, median (months) | 11.9 | 10.1 | ||
Duration of PFS (months) | ||||
Median (96% CI) | 11.1 (7.4, 13.8) | 1.9 (1.8, 3.8) | 11.0 (7.4, 13.8) | 1.9 (1.9, 3.7) |
25th percentile, 75th percentilea | 5.1, 16.6 | 1.7, 5.5 | 4.7, 16.6 | 1.8, 5.5 |
Range | 0.03+, 16.76+ | 0.03+, 13.83+ | 0.03+, 16.76+ | 0.03+, 13.83+ |
P value (stratified by log-rank test)b,c | < 0.0001 | < 0.0001 | ||
Hazard ratio (96% CI; stratified)b,d | 0.22 (0.15, 0.32) | 0.22 (0.15, 0.31) | ||
K-M estimates (% of patients event-free) | ||||
3 months | 89.0 | 45.9 | 89.1 | 46.8 |
6 months | 64.7 | 20.8 | 63.7 | 19.5 |
9 months | 54.9 | 13.2 | 54.0 | 12.4 |
12 months | 46.3 | 1.9 | 45.6 | 1.8 |
ITT = intention to treat; KM = Kaplan–Meier; NE = not estimable; OS = overall survival; PFS = progression-free survival.
+indicates a censored observation.
aPercentiles were based on KM estimates.
bStratification factors based on IxRS were receipt of prior lenvatinib (yes vs no) and age at informed consent (≤ 65 years vs > 65 years).
cThis is a supplementary analysis at a later cut-off date and not meant for primary analysis.
dEstimated using the Cox proportional-hazard model (adjusted for stratification factors if applicable). HR < 1 indicate results in favour of cabozantinib.
eMaximum duration of OS in the placebo arm for the full ITT population was 17.28 months at the data cut-off date.
Source: Addendum 1, CSR of Cabozantinib.10
Figure 3: Kaplan–Meier Plot of OS, Cut-Off February 8, 2021, ITT population (Primary Analysis Subset, N = 187)
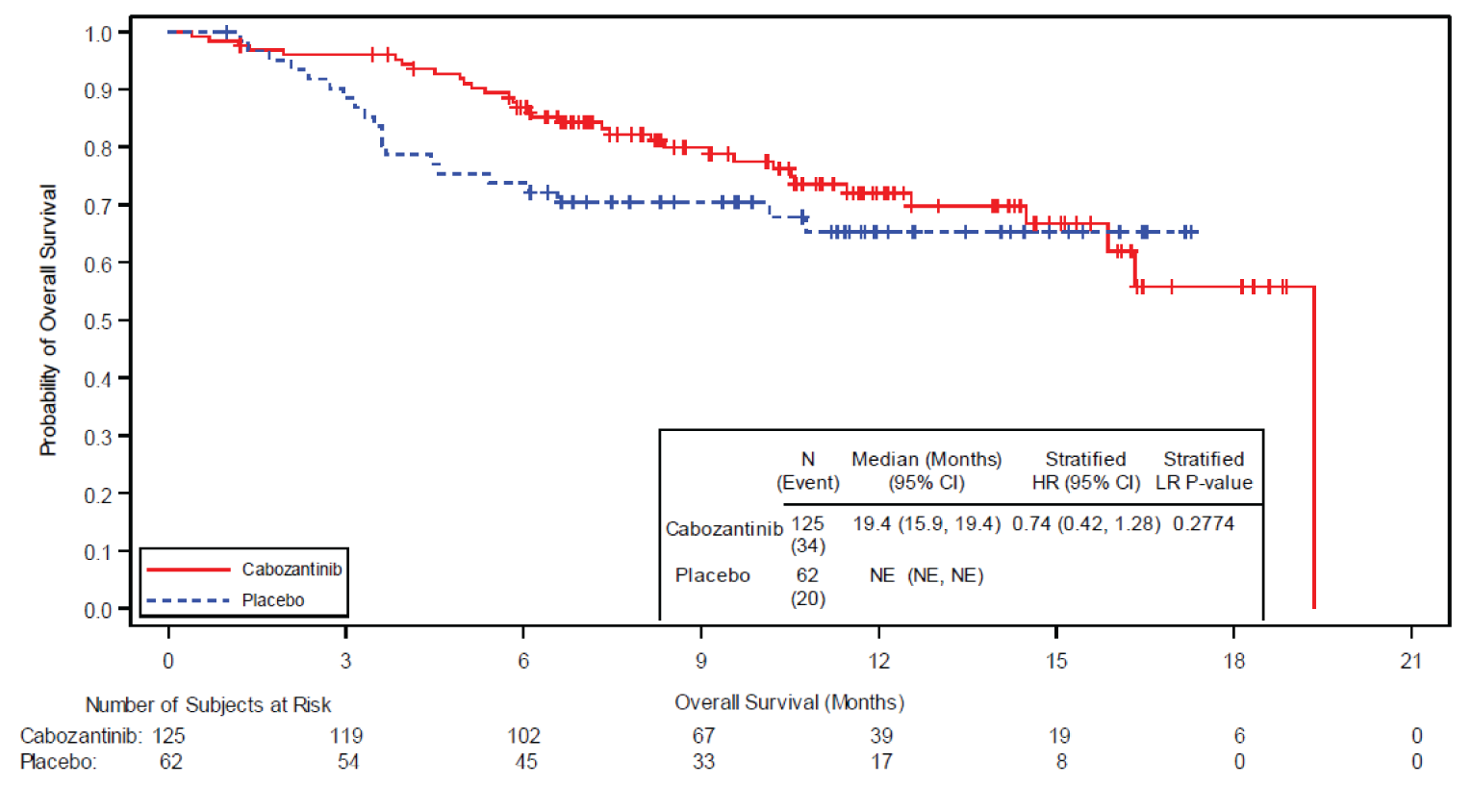
CI = confidence; HR = hazard ratio; ITT = intent to treat; IxRS = interactive voice/web response system; LR = log-rank test, NE = not estimable; OS = overall survival.
+Indicates censored observation
Stratification factors (per IxRS) comprise receipt of prior lenvatinib (yes vs no) and age at informed consent (≤ 65 years vs > 65 years).
The upper limit of the 95% CI for median OS should be interpreted as NE.
The last remaining patient in the cabozantinib arm had an event leading the survival probability to 0% as no patient remained at risk anymore.
Source: CSR of Cabozantinib.10
Progression-Free Survival
PFS was a co-primary efficacy end point in the COSMIC-311 trial conducted in the ITT as a prespecified interim analysis and included radiographic progression events as determined by the BIRC per RECIST 1.1 or death due to any cause. At the data cut-off of August 19, 2020; a total of 74 events were reported (Table 13). The median time of follow-up through the data cut-off date was 6.24 months in the ITT population. The primary PFS was tested at the observed 38.3% information fraction using a critical P value of 0.00036 and a Lan-DeMets O’Brien alpha spending function at the original alpha level of 4% as the null hypothesis for ORR was not rejected.
A lower proportion of patients in the cabozantinib arm experienced disease progression compared with that in the placebo arm (20% vs 66%, respectively). A similar percentage of deaths occurred in each arm (4.8% vs 3.2%, respectively). Median PFS was not reached (96% CI, 5.7 to NE) in the cabozantinib arm compared with 1.9 months (1.8 to 3.6) in the placebo arm. The P value obtained from the log-rank stratified test was < 0.0001, supporting a difference in PFS between the cabozantinib and placebo arms. The HR from the Cox PH model was 0.22 (96% CI, 0.13 to 0.36). PFS assessed by investigator were generally consistent with outcomes by BIRC. Also, the PFS was maintained across predefined subgroups.
For the cut-off date of February 8, 2021 results of PFS were overall consistent (Table 14). With a median follow-up time11.9 months in the primary analysis population (N = 187), a lower proportion of patients in the cabozantinib arm experience disease progression compared to the placebo arm (45% versus 94% respectively). The median PFS reached at 11.1 months (96% CI, 7.4 to 13.8) in the cabozantinib arm vs 1.9 months (1.8 to 3.8) in the placebo arm. The HR obtained from the Cox PH was 0.22 (96% CI, 0.15 to 0.32) as shown in Figure 4. The P value obtained from the log-rank stratified test was less than 0.0001.
Response Outcomes
Objective Response Rate
ORR was a co-primary end point in the COSMIC-311 trial. In the OITT population, at the cut-off date August 19. 2020 and median follow-up of 5.8 months, the ORR by BIRC was 15% (99% CI, 5.8 to 29.3) in the cabozantinib group versus 0% (0 to 14.8) in the placebo group (P = 0.028, Table 15); this difference was considered nonstatistically significant based on that the observed P value was higher than the critical P value of 0·01 specified by the studies multiple testing procedure. Ten patients (15%) of 67 had confirmed partial responses by BIRC in the cabozantinib group, and there were no confirmed responses among 33 patients in the placebo group.
Figure 4: Kaplan–Meier Plot of PFS, RECIST 311, Cut-Off August 19, 2020, ITT Population, Determined by BIRC
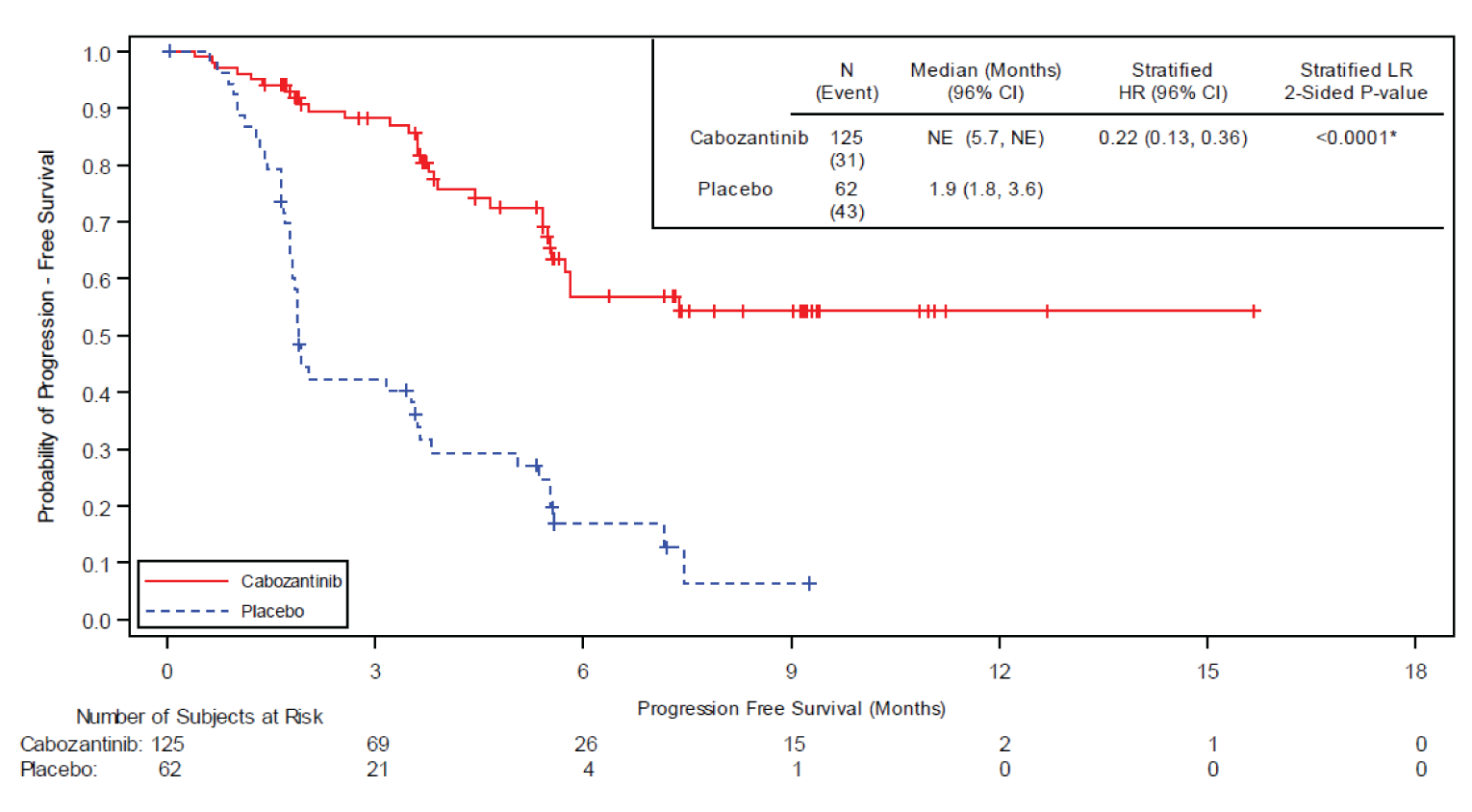
BIRC = blinded independent radiology committee; CI = confidence interval; HR = hazard ratio; ITT = intention to treat; IxRS = interactive voice/web response system; LR = log-rank test; NE = not estimable.
+ indicates a censored observation
Stratification factors (per IxRS) comprise receipt of prior lenvatinib (yes vs no) and age at informed consent (≤ 65 years vs > 65 years).
Source: CSR of Cabozantinib.10
Figure 5: Kaplan–Meier Plot of PFS per BIRC, Cut-Off February 8, 2021 (Primary Analysis Subset, N = 187)
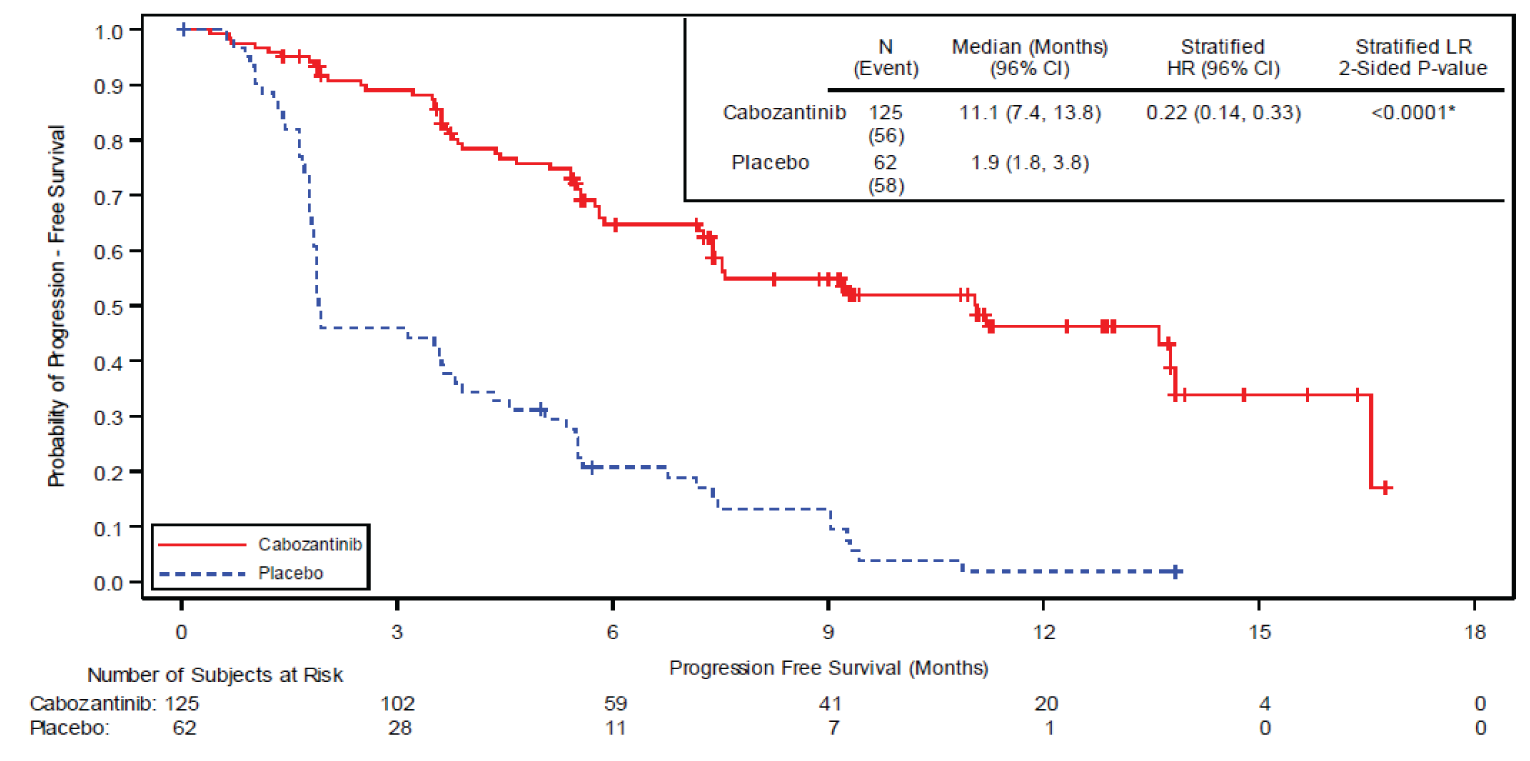
BIRC = blinded independent radiology committee; CI = confidence interval; HR = hazard ratio; ITT = intent to treat; IxRS = interactive voice/web response system; LR = log-rank test.
+ = indicates value from censored observation.
Stratification factors (per IxRS) comprise receipt of prior lenvatinib (yes vs no) and age at informed consent (≤ 65 years vs > 65 years).
Source: CSR of Cabozantinib.10
At the cut-off date of 8 February 2021 results were similar but with a longer median follow-up time (11.9 months). The ORR by BIRC was 15% (99% CI, 9.4 to 22.7) in the cabozantinib group versus 0% (0 to 5.8) in the placebo group (P = 0.0005, Table 16). In the same cut-off, 18 patients (14.4%) of 125 had confirmed partial responses by BIRC in the cabozantinib group, and there were no confirmed responses among 62 patients in the placebo group.
Duration of Response
Median DOR in the cabozantinib group had not been reached at the data cut-off of August 19,2020. The Kaplan–Meier estimate of median DOR per BIRC was NE (range 1.94 to 7.33 months) in the cabozantinib arm. Per investigator, objective responses were reported in 14 patients in the cabozantinib arm and none in the placebo arm, and the median DOR (range) was also NE (1.77 to 11.99 months) in the cabozantinib arm. For the cut-off date of February 8, 2021, the Kaplan–Meier estimate of median (range) DOR per BIRC was 10.2 (1.87+ to 12.85+) months in the cabozantinib arm. No objective responses were reported in the placebo arm.
Table 15: ORR, COSMIC-311, per RECIST 1.1, OITT population, Cut-Off August 19, 2020, Determined by BIRC
Criteria | Cabozantinib (N = 67) | Placebo (N = 33) |
|---|---|---|
ORR (CR+PR), N (%) | 10 (15) | 0 (0) |
99% CI | 5.8, 29.3 | 0, 14.8 |
Follow-up, median (months) | 8.85 | |
Treatment difference (cabozantinib – placebo) (99% CI)a | 15 (3.7, 26.1) | |
Observed stratified CMH test P value per IxRSb | 0.0220 | |
Observed unstratified Fisher exact test P valuec,d | 0.0281 | |
Best overall responsec | ||
Confirmed CR, N (%) | 0 (0) | 0 (0) |
Confirmed PR, N (%) | 10 (15) | 0 (0) |
Stable disease, N (%) | 46 (69) | 14 (42) |
CR = complete response; PR = partial response; SD = stable disease.
aUsing asymptotic confidence limits based on large number theorem.
bStratification factors (per IxRS) comprise receipt of prior lenvatinib (yes vs. no) and age at informed consent (≤ 65 years vs. > 65 years). This P value was obtained from a test conducting a sensitivity analysis and it is not the P value used for inference.
cP value from a test used for the primary end point compared to a critical value of 0.01 to control for multiple comparisons.
dBest overall response was assessed based on RECIST 1.1 criteria and was calculated based on patients in the OITT population.
BIRC = blinded independent radiology committee; CI = confidence interval; CMH = Cochran Mantel-Haenszel; OITT = overall response rate intention to treat; ORR = objective response rate; IxRS = interactive voice/web response system; RECIST = Response Evaluation Criteria in Solid Tumors.
Source: CSR of Cabozantinib.10
Table 16: ORR, COSMIC-311, per BIRC, Cut-Off February 8, 2021
Criteria | Primary analysis subset (N = 187) | Full ITT population (N = 258) | ||
|---|---|---|---|---|
Cabozantinib (N = 125) | Placebo (N = 62) | Cabozantinib (N = 170) | Placebo (N = 88) | |
ORR (CR+PR), n (%) | 19 (15) | 0 | 19 (11) | 0 |
99% CI | 9.4, 22.7 | 0.0, 5.8 | 6.9, 16.9 | 0.0, 4.1 |
Follow-up, median(months) | 11.9 | 10.1 | ||
Treatment difference (cabozantinib – placebo) (95% CI)a | 15 (8.9, 21.5) | 11 (6.4, 15.9) | ||
Observed stratified CMH test P value per IxRSb,c | 0.001 | 0.0009 | ||
Observed unstratified Fisher exact test P valuec | 0.0005 | 0.0003 | ||
Best overall responsec | ||||
Confirmed CR, n (%) | 1 (0.8) | 0 | 1 (0.6) | 0 |
Confirmed PR, n (%) | 18 (14.4) | 0 | 18 (10.6) | 0 |
Stable disease, n (%) | 87 (69.6) | 26 (41.9) | 117 (68.8) | 34 (38.6) |
BIRC = blinded independent radiology committee; CI = confidence interval; CMH = Cochran Mantel-Haenszel; OITT = overall response rate intention to treat; ORR = objective response rate; IxRS = interactive voice/web response system; RECIST = Response Evaluation Criteria in Solid Tumors.
aUsing asymptotic confidence limits based on large number theorem.
bStratification factors (per IxRS) comprise receipt of prior lenvatinib (yes vs no) and age at informed consent (≤ 65 years vs > 65 years).
cP values for a post-hoc analysis (later cut-off date) not to be used for inferential interpretation.
dBest overall response was assessed based on RECIST 1.1 criteria and was calculated based on patients in the OITT population.
Source: CSR of Cabozantinib.10
Health-Related Quality of Life
EuroQoL 5 Dimension 5 Level (EQ-5D-5L)
Patients completed a baseline questionnaire, and postbaseline assessments were collected every 4 weeks until week 25 followed by every 8 weeks. EQ-5D-5L scores are summarized by 5 functional and symptom dimensions (mobility, self-care, usual activities, pain/discomfort, anxiety/depression) each split into 5 increasing severity levels from 1 (no problem) to 5 (extreme problem). The MID for these questionnaires in cancer patients were previously established as 0.06 to 0.08 for EQ-5D Index, and 7 for EQ-VAS.19 In addition, the effect size for change from baseline was calculated as mean of change in score/pooled SD for baseline scores. An effect size ≥ 0.3 was considered potentially clinically meaningful. Patients were followed up until the end of the study at week 65.
EQ-Index
The EQ-5D-5L was converted into a single index value normalized across 10 countries in which the index has been validated. EQ-Index values ranges from 0 (dead) to 1 (full health), i.e., a higher index score indicates better health. At baseline, mean EQ-Index scores were 0.751 in the cabozantinib arm and 0.729 in the placebo arm. All treatment differences in mean change from baseline EQ-Index values were < 0.06 through W33D1 (MID = 0.06 to 0.08). Beyond this time point there were fewer than 5 patients in the placebo arm (Table 17).
EuroQoL Visual Analogue Scale
The EQ-VAS employs a 20-cm vertical thermometer to rate an individual’s current HRQoL state. In turn, the EQ-VAS representation was converted to a 1-dimensional EQ-VAS score from 0 (worst health) to 100 (best health). At baseline, mean EQ-VAS scores for the ITT population were 69.4 in the cabozantinib arm and 67.8 in the placebo arm. All treatment differences in mean change from baseline EQ-VAS values were < 7 through week 33 (MID = 7). Beyond this time point, there were fewer than 5 patients in the placebo arm.
Harms
Only those harms identified in the review protocol are reported below. The treatment exposures and interruptions in the safety population are presented in Table 18. AEs are presented in Table 19 for the latest cut-off date (February 8, 2021).
Table 17: EQ-VAS and EQ-Index Scores, COSMIC-311, Cut-Off August 19, 2020 a
Detail | Cabozantinib (N = 125) | Placebo (N = 62) |
|---|---|---|
EQ-Indexb | ||
n | 106 | 53 |
LS mean (SE) | –0.047 (0.018) | –0.038 (0.022) |
Difference in Mean Changec (pooled SD) | –0.009 (0.158) | |
Effect sized | –0.058 | |
P valuec | 0.679 | |
EQ-VASb | ||
n | 108 | 53 |
LS mean (SE) | –3.041 (1.674) | –2.672 (2.107) |
Difference in Mean Changec (pooled SD) | –0.3689 (15.376) | |
Effect sized | –0.024 | |
P valuec | 0.851 | |
ITT = intent to treat; LS Mean = least squares means; SD = standard deviation; SE = standard error; VAS = visual analogue scale.
aChange from Baseline, Repeated-Measures Analysis (ITT Population, Countries in Which Index Is Validated [Index]; ITT Population [VAS]).
bA higher score indicates better HRQoL.
cDerived from the prespecified repeated-measures mixed-effects model analysis of covariance. Predictors (fixed effects) were baseline scores, treatment, visit, and randomization strata. Individual patient nested within the planned treatment arm was the random effect. No adjustment was made for multiple comparisons.
dEffect size = (mean of change in score)/(pooled SD for both groups for baseline values). Effect size differences ≥ 0.3 were regarded as likely to be clinically relevant
Source: CSR of Cabozantinib.10
Table 18: Treatment Exposure and Dose Interruptions, Safety Population, COSMIC-311, Cut-Off August 19, 2020
Detail | Cabozantinib (N = 125) | Placebo (N = 62) |
|---|---|---|
Duration of exposure (including dose interruptions) in monthsa | ||
Mean (SD) | 5.03 (3.520) | 3.49 (2.544) |
Median (range) | 4.44 (0.0, 15.7) | 2.33 (0.3, 11.6) |
Average daily dose of cabozantinib/matched placebo (mg/day)b | ||
Mean (SD) | 41.83 (13.461) | 54.13 (10.856) |
Median (range) | 42.01 (9.5, 60.0) | 60.00 (18.4, 68.3)c |
Percent dose intensity of cabozantinib/matched placebo (%)c | ||
Mean (SD) | 69.71 (22.435) | 90.22 (18.094) |
Median (range) | 70.02 (15.8, 100.0) | 100.00 (30.6, 113.8) |
Duration of exposure (excluding dose interruptions) (months)d | ||
Mean (SD) | 4.21 (3.180) | 3.26 (2.595) |
Median (range) | 3.75 (0.0, 13.5) | 2.17 (0.3, 11.6) |
Patients with any dose interruption, n (%) | 90 (72) | 17 (27) |
Duration (days) of dose interruptions per patient, mean (SD)e | 29.9 (27.36) | 21.0 (14.85) |
Duration (days) of dose interruptions per patient, median (range)e | 23.0 (1, 172) | 16.0 (4, 63) |
aDuration of exposure = (date of decision to discontinue study treatment – date of first dose + 1)/30.4375. For patients still on study, the data cut-off date was used to calculate the exposure.
bAverage daily dose of cabozantinib (placebo) = total doses received (mg)/duration of exposure (days).
cPercent dose intensity of cabozantinib (placebo) = 100 × (average daily dose mg/day)/(60 mg/day).
dDuration of treatment = (date of decision to discontinue study treatment – date of first dose – total duration of dose interruptions + 1)/30.4375
eDuration of each dose interruption = interruption stop date – interruption start date + 1; n = number of patients who had dose holds due to an AE.
Source: CSR of Cabozantinib.10
Adverse Events
For the cut-off August 19, 2020, AEs (all grades) that led to study treatment discontinuation in the cabozantinib arm were fatigue (2 patients); stomatitis, liver function test increased, and pain (all reported in 1 patient); hypercalcemia, hypertension, and renal impairment arthralgia; cardio-respiratory arrest; diarrhea; large intestine perforation, and myalgia (all in 1 patient). Dose reductions to manage adverse events were required by 70 (56%) of 125 patients in the cabozantinib group and 3 (5%) of 62 in the placebo group, and 28 (22%) of 125 and 1 (2%) of 62 patients required a second dose reduction, respectively. The most common AEs resulting in dose reduction of cabozantinib included palmar-plantar erythrodysesthesia (PPES; 24 [19%] of 125), diarrhea (13 [10%]), and fatigue (9 [7%]). In the placebo group, AEs resulting in dose reduction included fatigue, dyspnea, dysphagia, and pruritus (one [2%] of 62 for each).
For the cut-off date of February 8, 2021 (Table 19), the most common AEs in the cabozantinib group were diarrhea, PPES, hypertension, decreased appetite, fatigue, nausea, increased liver enzymes, hypocalcemia, and decreased weight. In the placebo arm, the most frequent (≥ 20% incidence) AEs reported were diarrhea, PPES, fatigue, nausea, and decreased appetite.
Table 19: Summary of Harms, Safety Population, COSMIC-311, Cut-Off February 8, 2021
Detail | Cabozantinib (N = 170) | Placebo (N = 88) |
|---|---|---|
Patients with ≥ 1 adverse event | ||
Any AE, n (%) | 166 (98) | 75 (85) |
Most common AEs, n (%)a | ||
Diarrhea | 105 (62) | 3 (3.4) |
Palmar-plantar erythrodysesthesia syndrome | 80 (47) | 1 (1.1) |
Hypertension | 54 (32) | 3 (3.4) |
Decreased appetite | 53 (31) | 11 (13) |
Fatigue | 49 (29) | 7 (8.0) |
Nausea | 48 (28) | 2 (2.3) |
Alanine aminotransferase increased | 43 (25) | 2 (2.3) |
Aspartate aminotransferase increased | 42 (25) | 2 (2.3) |
Hypocalcemia | 42 (25) | 3 (3.4) |
Weight decreased | 37 (22) | 2 (2.3) |
Vomiting | 31 (18) | 7 (8.0) |
Stomatitis | 30 (18) | 2 (2.3) |
Asthenia | 29 (17) | 12 (14) |
Mucosal inflammation | 29 (17) | 0 |
Hypomagnesaemia | 28 (16) | 3 (3.4) |
Proteinuria | 27 (16) | 2 (2.3) |
Dyspnea | 23 (14) | 16 (18) |
Anemia | 21 (12) | 10 (11) |
Constipation | 21 (12) | 6 (6.8) |
Dysgeusia | 21 (12) | 0 |
Dysphonia | 20 (12) | 0 |
Arthralgia | 18 (11) | 7 (8.0) |
Headache | 18 (11) | 4 (4.5) |
Hypokalemia | 17 (10) | 1 (1.1) |
Cough | 16 (9.4) | 17 (19) |
Patients with ≥ 1 SAE | ||
Any SAE, n (%) | 66 (39) | 24 (27) |
Most common SAE, n (%)b | ||
Diarrhea | 5 (2.9) | 0 |
Pleural effusion | 5 (2.9) | 3 (3.4) |
Pneumonia | 4 (2.4) | 1 (1.1) |
Pulmonary embolism | 4 (2.4) | 0 |
Dyspnea | 1 (0.6) | 5 (5.7) |
Grade 3 or 4 AE | 106 (62) | 25 (28) |
Grade 4 AE | 11 (6.5) | 2 (2.3) |
Grade 5 AE | 14 (8.2) | 7 (8.0) |
Patients who stopped treatment due to AEs | ||
AE leading to treatment discontinuation | 15 (8.8) | 0 |
Deaths | ||
Deaths (as of the February 8, 2021 cut-off date), n (%)c | 37 (22) | 13 (15) |
≤ 30 days after last dose of study treatment | 14 (8.2) | 14 (8.2) |
> 30 days after last dose of study treatment | 23 (14) | 6 (6.8) |
Notable harmsd | ||
Severe diarrhea (grade 3 or 4), n (%) | 13 (7.6) | 0 |
Thromboembolism (PE, DVT, pelvic venous, SVC), n (%) | 17 (10) | 1 (1.1) |
Hypertension, n (%) | 58 (34) | 3 (3.4) |
Hypertensive crisis, n (%) | 1 (0.6) | 0 |
Major hemorrhage/bleeding, n (%) | 4 (2.4) | 0 |
ALT increase, n (%) | 43 (25) | 2 (2.3) |
AST increase, n (%) | 42 (25) | 2 (2.3) |
Posterior reversible encephalopathy syndrome, n (%) | 1 (0.6) | 0 |
Palmar-plantar erythrodysesthesia syndrome, n (%) | 80 (47) | 1 (1.1) |
Hypocalcemia, n (%) | 42 (25) | 3 (3.4) |
QT prolongation, n (%) | 4 (2.4) | 1 (1.1) |
ALT = alanine aminotransferase; AST = aspartate transferase; DVT = deep venous thrombosis; SVC = superior vena cava syndrome; PE = pulmonary embolism.
aFrequency > 10%.
bFrequency > 2%.
cNine additional patients in the placebo crossover arm died as of the data cut-off date and are excluded from the total number of deaths in the placebo arm in the safety population.
dThose considered relevant based on clinicians and patient input as stated in the protocol of this CADTH review.
Source: CSR of Cabozantinib.10
At the same cut-off date, a total of 15 patients (8.8%) in the cabozantinib only arm and none in the placebo arm had AEs that led to discontinuation of study treatment. These events occurring in at least 2 patients in the cabozantinib only arm were fatigue (3 patients [1.8%]) and diarrhea (2 patients [1.2%]). Compared with data through the first cut-off date, there were 9 additional patients with 14 additional events that led to study treatment discontinuation in the cabozantinib only arm through the second cut-off: Abdominal pain, diarrhea, diverticular perforation, fatigue, neutrophil count decreased, polyneuropathy, posterior reversible encephalopathy syndrome (PRES), proteinuria, stress cardiomyopathy, thrombocytopenia, urinary retention, weight decreased, respiratory failure due to an aspiration pneumonia, and myelodysplastic syndrome (1 patient each).
Also, at this same cut-off date of February 8, 2021, a total of 40 patients who were randomized to placebo crossed over to receive cabozantinib upon experiencing BIRC-confirmed radiographic disease progression. The overall incidence of AEs in the placebo crossover arm was 93%.
Serious Adverse Events
SAEs were more common in the cabozantinib group (except for pleural effusion), although overall SAEs were not highly frequent. At the cut-off date of February 8, 2021, diarrhea, pleural effusion, pneumonia, pulmonary embolism, and dyspnea were among the most common SAEs reported.
Mortality
The number of deaths as of the cut-off date of February 8, 2021 was greater in the cabozantinib group (37 patients of 170 [22%]) as compared to the placebo group (13 out of 88 patients [15%])
Notable Harms
AEs of special interest occurred more frequently in the cabozantinib group than in the placebo group, including severe diarrhea (7.6% versus 0% respectively), thromboembolism (10% versus 1.1% respectively), hypertension (34% versus 3.4% respectively), elevated liver enzymes (25% versus 2.3% respectively), PPES (47% versus 1.1% respectively), and hypocalcemia (25% versus 3.4% respectively).
Critical Appraisal
Internal Validity
The COSMIC-311 study is a randomized, double-blind, placebo-controlled trial evaluating the efficacy and safety of cabozantinib in patients with advanced or metastatic RAI-refractory DTC who were previously treated with a VEGFR-targeted therapy. The study had an appropriate (block) randomization process, accomplished by a clinical research organization who maintained an unmasked team independent from the study, and used a live randomization schedule through a secured server, which ensured an adequate allocation concealment. The interactive voice–web response system ensured patients, investigators, site staff, and the study sponsor remained masked to treatment assignment at the outset of the study.
However, blinding of the assigned intervention could have been compromised during follow-up due to imbalance in AEs, more commonly observed in the cabozantinib arm, especially when patients experienced diarrhea, PPES, liver enzymes elevated, stomatitis, and vomiting. This situation can lead to increased risk of bias due to deviations from the intended intervention, possibly reflected in the number of patients who crossed over from placebo to the intervention arm.
Overall, baseline variables were balanced between study arms in the ITT and OITT populations with only small differences that are compatible with chance and do not seem to lead to a risk of bias in this domain.
The interpretation of the OS data is limited by the short duration of follow-up, sample size, and crossover of patients from placebo to open-label cabozantinib. Although there were a sizable number of patients who crossed over from placebo to open-label treatment (a total of 40 patients at the data cut-off of February 8, 2021), authors kept the random assignment as much as possible by adhering to the ITT analysis, which is considered a conservative measure to analyze the effect of assignment to the intervention and, in case of any effect, it would underestimate the observed effect of cabozantinib.
Considering the issue of the number of crossover patients, the sponsor submitted 3 further analyses for the pharmacoeconomic evaluation to adjust for crossover patients from the placebo to the intervention group to assess an effect estimate of survival (not presented in this CADTH clinical report). These analyses consisted of 3 adjustment methods: the Rank-Preserving Structural Failure Time (RPSFT), the 2-stage method, and the Inverse Probability of Censoring Weights (IPCW). All 3 methods use strong assumptions, such as the ‘common treatment effect’ for the RPSFT, the assumption of ‘no time-dependent confounding’ between the time of disease progression and the time of treatment switch for the 2-stage method, or ‘no unmeasured confounders’ in the IPCW. The assumptions for these analyses generally will result in a conservative, underestimate of the treatment effect for cabozantinib.22 When assessing the estimates of the placebo arm adjusted for crossover, the results in OS were consistent with the base-case analysis without adjustments in any of the 3 methods used.
The authors performed an adequate adjustment for multiplicity on the 2 co-primary end points ORR and PFS. Overall, sensitivity analyses were consistent with the base-case analysis and subgroup analyses did not show any effect based on the evaluated subgroups, although these were potentially underpowered and not controlled for multiple comparisons. Similarly, protocol deviations were in small numbers and did not show an imbalance between arms. In terms of concomitant interventions, there was an imbalance in some treatments, although these are likely related to the presence of AEs (for example, loperamide, an antidiarrheal medication, was more commonly administered in the cabozantinib group). This has implications in the possibility of patients and personnel being aware to the assigned intervention as mentioned above. HRQoL end points were assessed without accounting for multiplicity adjustments, also the data had fewer numbers of patients as the study progressed, a common limitation in HRQoL end points.
External Validity
The COSMIC-311 trial population consisted of adult patients with locally advanced or metastatic DTC who have progressed despite treatment with VEGFR-TKI therapy and are RAI-resistant or ineligible. According to input from clinical experts consulted by CADTH, the distribution of patients’ baseline characteristics (demographics, disease characteristics, and previous treatments) overall reflect the current clinical practice they usually observe when treating patients with DTC. However, some concerns of applicability could exist in a subgroup of patients with an ECOG of 2, 3, or more, as well as those with brain metastases. In the same venue, some therapies of frequent use in clinical practice in patients with DTC were not allowed during the COSMIC-311 trial – for example, chemotherapy, immunotherapy, radionuclides, erythropoietic agents, and local anticancer treatment including palliative radiation, ablation, embolization, or surgery with impact on tumour lesions were not allowed in the COSMIC-311 study.
The COSMIC-311 trial was placebo-controlled; therefore, it does not provide evidence regarding the comparative efficacy or harms of cabozantinib compared to other treatments currently used in Canada to treat patients with progressive, radioiodine-refractory DTC previously treated with VEGFR-targeted therapy (e.g., selpercatinib, larotrectinib).
Patients in the COSMIC-311 trial were heavily pretreated, and most of them had progressed on sorafenib or lenvatinib when they entered the study, with approximately 60% receiving lenvatinib. Since in Canada lenvatinib is the only approved and funded treatment for patients with DTC, the applicability focus of this review is on patients previously treated with lenvatinib. In this regard, the evidence does not suggest a subgroup effect based on the previous administration of lenvatinib versus sorafenib or both. Although this was only assessed in the primary end points (PFS and ORR), and some of the subgroups had relatively small patient numbers, there are no suggestions of modifying effects from the administration of lenvatinib or sorafenib, or from any other prespecified subgroup variable. The clinical experts consulted by CADTH noted that, a subset (24.8% of patients in the cabozantinib arm) were previously treated with sorafenib and lenvatinib. The clinical experts noted that these patients may be less treatment sensitive; therefore, this may underestimate cabozantinib efficacy compared to patients living in Canada who would have only previously failed with lenvatinib.
The immaturity of the data adds some uncertainty on the applicability of effect estimates; this was due to early completion of the primary analysis at the planned interim analysis in the first cut-off date of August 19, 2020. Even with additional time of follow-up (with a median follow-up time of 11.9 months for OS and PFS) at a later cut-off date analysis on February 8, 2021, there is immaturity of the OS and PFS when considering longer times of observation in a condition with an estimated median survival time of about 2.5 to 3.5 years.9
Indirect Evidence
A focused literature search for indirect treatment comparisons dealing with DTC was run in MEDLINE All (1946-) on May 25, 2022. No limits were applied to the search. No indirect treatment comparisons were submitted by the sponsor or detected by the CADTH team according to the prespecified criteria and hence not included in this report.
Other Relevant Evidence
This section includes submitted long-term extension studies and additional relevant studies included in the sponsor’s submission to CADTH that were considered to address important gaps in the evidence included in the systematic review. No other relevant literature was included in this report.
Discussion
Summary of Available Evidence
One phase III clinical trial was included in this report. The COSMIC-311 trial is an ongoing randomized, double-blind, placebo-controlled trial, conducted in several centres across Europe, Asia, Latin America, US, and Canada to evaluate the efficacy and safety of cabozantinib 60 mg once daily versus placebo. The patient population in the study consists of patients with advanced or metastatic DTC previously treated with a VEFGR-TKI and who are RAI-resistant. The 2:1 randomization to cabozantinib or placebo, respectively, was stratified by age (< 65 or ≥ 65 years) and previous use of lenvatinib (yes/no). Crossover to cabozantinib was permitted throughout the study for eligible patients who experienced radiographic disease progression per RECIST 1.1. by BIRC. Results from a prespecified interim analysis with an initial cut-off date analysis (August 19, 2020) was described with key end points of ORR, PFS, OS, DOR, and HRQoL. At this first analysis, the COSMIC-311 trial had randomized a total of 187 patients (the ITT and safety population), and the first 100 randomized patients were assessed as a specific ITT population for the primary end points ORR and PFS per RECIST 1.1 by BIRC (i.e., the OITT population). A second analysis was conducted with a cut-off date (February 8. 2021) and included a total of 187 patients in the primary analysis subset and 258 patients in the full ITT population, integrating longer follow-up assessments, including safety.
Patients in the COSMIC-311 trial had advanced or metastatic DTC with ECOG PS status of 0 or 1, with a slight predominance of female patients, and an average age of 65 years. The study is overall at low risk of bias, although some issues of internal and external validity remain, such as the high number of patients who crossed over from the placebo to the intervention group, the possibility of patients and researchers being aware of the intervention administered (unblinding), and the exclusion of patients who had brain metastases or previous radiation therapy for bone metastases. Furthermore, the study estimations for OS had a relatively short period of follow-up (median of 11.9 months at the cut-off date of February 8, 2021).
Interpretation of Results
Efficacy
The patient groups, clinical experts, and the clinician groups that provided input for this review highlighted that RAI-R DTC is rare and associated with a poor prognosis. The COSMIC-311 trial evaluated efficacy outcomes, including OS, PFS, ORR, and DOR, as well as HRQoL, that were deemed important for this CADTH review for decision-making in the Canadian clinical landscape also based on input from clinicians, patient groups, and drug programs.
OS was considered a critical outcome for decision-making. However, there was immaturity in the OS data, and results from the COSMIC-311 trial did not find evidence of a difference in OS between arms of study, either at the initial cut-off date of August 19, 2020 or at a later cut-off on February 8, 2021. With a median follow-up time of 11.9 months, the median OS in the placebo group was not reached while in the cabozantinib group it reached 19.4 months.
PFS was a co-primary end point considered important by the team of experts and assessed in the COSMIC-311 with multiplicity adjustments. At interim analysis (August 19, 2020), the PFS end point was met in the ITT population, with cabozantinib showing significant improvement over placebo. Results from the data cut-off of February 8. 2021 showed consistent results. Clinical experts consulted by CADTH considered this result for PFS clinically meaningful for patients and clinicians.
ORR was also a primary end point and adjusted for multiplicity in the COSMIC-311 trial. At the first cut-off date, the comparison of ORR in the OITT population did not meet the prespecified significance level. At the cut-off date February 8, 2021, results for ORR were consistent with those from the primary analysis.
HRQoL was assessed with the EQ-Index (a converted normalized measure of the EQ 5D 5L score for different countries) and EQ-VAS. In both there was immaturity in the data and no evidence of different effects between arms of study through the length of the study at the end of week 65. The same occurred when evaluating this end point with the VAS.
One key gap in the evidence is the lack of direct or indirect comparisons between cabozantinib and key comparators applicable in the Canadian context and identified in the protocol of this CADTH review (i.e., selpercatinib and larotrectinib).
Harms
Adverse effects of treatments are important to patients with DTC, per the patient group that provided input on this review. Both, at the initial cut-off date of August 19. 2020 and at the cut-off date of February 8, 2021, the most common AEs were more prevalent in the cabozantinib group as compared to placebo, and included diarrhea, PPES, hypertension, decreased appetite, fatigue, nausea, increased liver enzymes, hypocalcemia, and decreased weight. The 2 patients with DTC that were interviewed by the patient group that submitted input for this review indicated that experiencing fatigue and diarrhea had significant impacts on their daily life. There were no treatment-related deaths in the COSMIC-311 trial.
SAEs at the cut-off date of February 8, 2021 were also more common in the cabozantinib arm (66 patients [39%]) when compared to placebo (24 patients [27%]), and included diarrhea, pleural effusion, pneumonia, pulmonary embolism, and dyspnea. AEs of special interest also occurred more frequently in the cabozantinib group than in the placebo group, including severe diarrhea (7.6% vs 0% respectively), thromboembolism (10% versus 1.1%), hypertension (34% vs 3.4%), elevated liver enzymes (25% versus 2.3%), PPES (47% versus 1.1%), and hypocalcemia (25% versus 3.4%).
According to the clinical experts consulted by CADTH, these AEs frequencies are expected in this population. These AEs and SAEs are expected to be manageable and overall tolerated by patients. This aligned with the input from 1 patient who had experience with cabozantinib who provided input for this review through a survey conducted by patient groups, as they indicated that they felt the side effects of cabozantinib they experienced were tolerable.
Conclusions
Evidence from 1 randomized, double-blind, placebo-controlled trial suggests that cabozantinib prolongs PFS when compared with placebo among patients with progressive, radioiodine-refractory DTC previously treated with VEGFR-targeted therapy. There is uncertainty related to the efficacy of cabozantinib in other clinically important outcomes such as OS, mostly due to immature data, need for more follow-up time, and lack of control for multiple comparisons. There is uncertainty regarding the effect of cabozantinib on HRQoL because this outcome was not controlled for multiple comparisons. Overall, the population assessed in the evidence obtained is generalizable to the Canadian population, although some uncertainty remain in some groups such as patients with brain metastases and ECOG PS scores of 2 and above. There is lack of comparative evidence (direct or indirect) between cabozantinib and key active comparators applicable in the current Canadian clinical context, such as selpercatinib and larotrectinib. The safety profile in the population assessed was considered manageable and consistent with the known safety profile of cabozantinib.
References
1.Pacini F, Castagna MG, Brilli L, Pentheroudakis G, Esmo Guidelines Working Group. Thyroid cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2010;21 Suppl 5:v214-219. PubMed
2.Filetti S, Durante C, Hartl D, et al. Thyroid cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2019;30(12):1856-1883. PubMed
3.Brenner DR, Weir HK, Demers AA, et al. Projected estimates of cancer in Canada in 2020. CMAJ. 2020;192(9):E199-E205. PubMed
4.Cabanillas ME, McFadden DG, Durante C. Thyroid cancer. Lancet. 2016;388(10061):2783-2795. PubMed
5.Lee K, Anastasopoulou C, Chandran C, Cassaro S. Thyroid cancer. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021: https://www.ncbi.nlm.nih.gov/pubmed/29083690. Accessed 2022 Jul 22.
6.Haugen BR, Alexander EK, Bible KC, et al. 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid. 2016;26(1):1-133. PubMed
7.Robbins RJ, Wan Q, Grewal RK, et al. Real-time prognosis for metastatic thyroid carcinoma based on 2-[18F]fluoro-2-deoxy-D-glucose-positron emission tomography scanning. J Clin Endocrinol Metab. 2006;91(2):498-505. PubMed
8.Ruegemer JJ, Hay ID, Bergstralh EJ, Ryan JJ, Offord KP, Gorman CA. Distant metastases in differentiated thyroid carcinoma: a multivariate analysis of prognostic variables. J Clin Endocrinol Metab. 1988;67(3):501-508. PubMed
9.Schmidbauer B, Menhart K, Hellwig D, Grosse J. Differentiated thyroid cancer-treatment: state of the art. Int J Mol Sci. 2017;18(6). PubMed
10.Clinical Study Report: XL184-311. A phase III, randomized, double-blind, placebo-controlled study of cabozantinib (XL184) in subjects with radioiodine-refractory differentiated thyroid cancer who have progressed after prior VEGFR-targeted therapy [internal sponsor's report]. Alameda (CA): Exelixis, Inc; 2021 Apr 30.
11.Thyroid cancer. Ottawa (ON): Public Health Agency of Canada (PHAC); 2017: https://www.canada.ca/en/public-health/services/chronic-diseases/cancer/thyroid-cancer.html. Accessed 2022 Jul 07.
12.Viola D, Elisei R. Management of Medullary Thyroid Cancer. Endocrinol Metab Clin North Am. 2019;48(1):285-301. PubMed
13.Lenvima (lenvatinib as lenvatinib mesylate): 4 mg and 10 mg oral capsules [product monograph]. Mississauga (ON): Eisai Limited; 2021 Jul 22: https://pdf.hres.ca/dpd_pm/00062284.PDF. Accessed 2022 Jul 22.
14.Schlumberger M, Tahara M, Wirth LJ, et al. Lenvatinib versus placebo in radioiodine-refractory thyroid cancer. N Engl J Med. 2015;372(7):621-630. PubMed
15.Cabometyx (cabozantinib as cabozantinib (S)-malate): 20 mg, 40 mg, and 60 mg oral tablets [product monograph]. Mississauga (ON): Ipsen Biopharmaceuticals Canada, Inc.; 2022 Apr 27.
16.Retevmo (selpercatinib): 40 mg and 80 mg oral capsules [product monograph]. Toronto (ON): Eli Lilly Canada Inc.; 2022 Apr 19: https://pdf.hres.ca/dpd_pm/00065504.PDF. Accessed 2022 Jul 7.
17.Vitrakvi (larotrectinib as larotrectinib sulfate): 25 mg and 100 mg oral capsules; Vitrakvi (larotrectinib as larotrectinib sulfate): 20 mg/mL oral solution [product monograph]. Mississauga (ON): Bayer Inc.; 2022 Jan 24: https://pdf.hres.ca/dpd_pm/00064510.PDF. Accessed 2022 Jul 22.
18.Brose MS, Robinson B, Sherman SI, et al. Cabozantinib for radioiodine-refractory differentiated thyroid cancer (COSMIC-311): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2021;22(8):1126-1138. PubMed
19.Pickard AS, Neary MP, Cella D. Estimation of minimally important differences in EQ-5D utility and VAS scores in cancer. Health Qual Life Outcomes. 2007;5:70. PubMed
20.Sloan JA, Cella D, Hays RD. Clinical significance of patient-reported questionnaire data: another step toward consensus. J Clin Epidemiol. 2005;58(12):1217-1219. PubMed
21.Yost KJ, Eton DT. Combining distribution- and anchor-based approaches to determine minimally important differences: the FACIT experience. Eval Health Prof. 2005;28(2):172-191. PubMed
22.Watkins C, Huang X, Latimer N, Tang Y, Wright EJ. Adjusting overall survival for treatment switches: commonly used methods and practical application. Pharm Stat. 2013;12(6):348-357. PubMed
23.Cohen J. A power primer. Psychol Bull. 1992;112(1):155-159. PubMed
24.Zeng X, Sui M, Liu B, et al. Measurement Properties of the EQ-5D-5L and EQ-5D-3L in Six Commonly Diagnosed Cancers. Patient. 2021;14(2):209-222. PubMed
25.Lubitz CC, De Gregorio L, Fingeret AL, et al. Measurement and Variation in Estimation of Quality of Life Effects of Patients Undergoing Treatment for Papillary Thyroid Carcinoma. Thyroid. 2017;27(2):197-206. PubMed
26.Norman GR, Sloan JA, Wyrwich KW. Interpretation of changes in health-related quality of life: the remarkable universality of half a standard deviation. Med Care. 2003;41(5):582-592. PubMed
27.Jin X, McClure NS, Le CY, et al. Minimally Important Differeces for EQ-5D instruments: a systematic review of estimates in published literature. Poster presented at: 2019 Canadian Agency for Drugs and Technologies in Health Symposium. Edmonton (AB): CADTH; 2019 Apr 14 - 16.
28.van Reenen M, Janssen B, Stolk E, et al. EQ-5D-5L User Guide. Rotterdam (NL): EuroQol Research Foundation; 2019: https://euroqol.org/publications/user-guides. Accessed 2022 Jun 20.
29.McClure NS, Sayah FA, Xie F, Luo N, Johnson JA. Instrument-Defined Estimates of the Minimally Important Difference for EQ-5D-5L Index Scores. Value Health. 2017;20(4):644-650. PubMed
30.Herdman M, Gudex C, Lloyd A, et al. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual Life Res. 2011;20(10):1727-1736. PubMed
31.Alberta Population Norms for EQ-5D-5L. Edmonton (AB): Alberta PROMs & EQ-5D Research & Support Unit (APERSU); 2018: https://apersu.ca/wp-content/uploads/2020/10/Alberta-Norms-Report_APERSU-1.pdf. Accessed 2022 Jun 20.
32.Gallop K, Kerr C, Simmons S, McIver B, Cohen EE. A qualitative evaluation of the validity of published health utilities and generic health utility measures for capturing health-related quality of life (HRQL) impact of differentiated thyroid cancer (DTC) at different treatment phases. Qual Life Res. 2015;24(2):325-338. PubMed
Appendix 1: Literature Search Strategy
Note that this appendix has not been copy-edited.
Clinical Literature Search
Overview
Interface: Ovid
Databases:
MEDLINE All (1946-present)
Embase (1974-present)
Note: Patient headings and search fields have been customized for each database. Duplicates between databases were removed in Ovid.
Date of search: May 26, 2022
Alerts: Bi-weekly search updates until project completion
Search filters applied: No filters were applied to limit the retrieval by study type.
Limits:
Publication date limit: none
Language limit: none
Conference abstracts: excluded
Table 20: Clinical Literature Search Syntax Guide
Syntax | Description |
|---|---|
/ | At the end of a phrase, searches the phrase as a patient heading |
MeSH | Medical Patient Heading |
* | Before a word, indicates that the marked patient heading is a primary topic; or, after a word, a truncation symbol (wildcard) to retrieve plurals or varying endings |
.ti | Title |
.ot | Original title |
.ab | Abstract |
.hw | Heading word; usually includes patient headings and controlled vocabulary |
.kf | Author keyword heading word (MEDLINE) |
.dq | Candidate term word (Embase) |
.pt | Publication type |
.rn | Registry number |
.nm | Name of substance word (MEDLINE) |
medall | Ovid database code: MEDLINE All, 1946 to present, updated daily |
oemezd | Ovid database code; Embase, 1974 to present, updated daily |
Multidatabase Strategy
(cabometyx* or cometriq* or kabometics* or cabozanix* or cabozantinib* or XL 184 or XL184 or BMS 907351 or BMS907351 or 1C39JW444G or DR7ST46X58).ti,ab,kf,ot,hw,rn,nm.
exp Thyroid Neoplasms/ or Carcinoma, Papillary/ or exp Adenocarcinoma, Follicular/
Thyroid Gland/ and exp Neoplasms/
Thyroidectomy/
((thyroid* or thyreoid* or papillary* or follicular* or Hurthle or oxyphil*) adj5 (cancer* or neoplas* or carcinoma* or tumor* or tumour* or adenoma* or adenocarcinoma* or oncolog* or macrocarcinoma* or microcarcinoma* or malignan* or metastat*)).ti,ab,kf.
((differentiat* or follicular* or papillary*) adj5 (thyroid* or thyreoid*)).ti,ab,kf.
thyroidectom*.ti,ab,kf.
or/2-7
1 and 8
9 use medall
*cabozantinib/
(cabometyx* or cometriq* or kabometics* or cabozanix* or cabozantinib* or XL 184 or XL184 or BMS 907351 or BMS907351).ti,ab,kf,dq.
or/11-12
exp thyroid tumor/ or exp papillary carcinoma/ or exp follicular carcinoma/
exp thyroid gland/ and exp neoplasm/
thyroidectomy/
((thyroid* or thyreoid* or papillary* or follicular* or Hurthle or oxyphil*) adj5 (cancer* or neoplas* or carcinoma* or tumor* or tumour* or adenoma* or adenocarcinoma* or oncolog* or macrocarcinoma* or microcarcinoma* or malignan* or metastat*)).ti,ab,kf,dq.
((differentiat* or follicular* or papillary*) adj5 (thyroid* or thyreoid*)).ti,ab,kf,dq.
thyroidectom*.ti,ab,kf,dq.
or/14-19
13 and 20
21 use oemezd
22 not conference abstract.pt.
10 or 23
remove duplicates from 24
Clinical Trials Registries
ClinicalTrials.gov
Produced by the US National Library of Medicine. Targeted search used to capture registered clinical trials.
[Search -- Studies with results | Cabometyx OR Cometriq OR Kabometics OR cabozantinib OR XL-184 OR XL184 OR BMS 907351 OR BMS907351 | Thyroid cancer]
WHO International Clinical Trials Registry Platform
ICTRP, produced by WHO. Targeted search used to capture registered clinical trials.
[Search terms -- (Cabometyx OR Cometriq OR Kabometics OR cabozantinib OR XL-184 OR XL184 OR BMS-907351 OR BMS907351) AND thyroid]
Health Canada’s Clinical Trials Database
Produced by Health Canada. Targeted search used to capture registered clinical trials.
[Search terms -- cabozantinib]
EU Clinical Trials Register
European Union Clinical Trials Register, produced by the European Union. Targeted search used to capture registered clinical trials.
[Search terms -- cabozantinib AND differentiated]
Grey Literature
Search dates: May 13, 2022 – May 26, 2022
Keywords: [Cabometyx OR Cometriq OR Kabometics OR cabozantinib OR thyroid cancer OR differentiated OR DTC]
Limits: Publication years: 1996-present
Updated: Search updated prior to the completion of stakeholder feedback period
Relevant websites from the following sections of the CADTH grey literature checklist Grey Matters: A Practical Tool for Searching Health-Related Grey Literature were searched:
Health Technology Assessment Agencies
Health Economics
Clinical Practice Guidelines
Drug and Device Regulatory Approvals
Advisories and Warnings
Drug Class Reviews
Clinical Trials Registries
Databases (free)
Internet Search.
Appendix 2: Excluded Studies
Note that this appendix has not been copy-edited.
Reference | Reason for exclusion |
|---|---|
Brose MS, Robinson B, Sherman SI, et al. Cabozantinib for radioiodine-refractory differentiated thyroid cancer (COSMIC-311): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2021;22(8):1126-1138. | Duplicate publication |
Cabanillas ME, Brose MS, Holland J, Ferguson KC, Sherman SI. A phase I study of cabozantinib (XL184) in patients with differentiated thyroid cancer. Thyroid. 2014;24(10):1508-1514. | Study design |
Cabanillas ME, de Souza JA, Geyer S, et al. Cabozantinib As Salvage Therapy for Patients With Tyrosine Kinase Inhibitor-Refractory Differentiated Thyroid Cancer: Results of a Multicenter Phase II International Thyroid Oncology Group Trial. J Clin Oncol. 2017;35(29):3315-3321. | Study design |
Kish JK, Chatterjee D, Wan Y, Yu HT, Liassou D, Feinberg BA. Lenvatinib and Subsequent Therapy for Radioactive Iodine-Refractory Differentiated Thyroid Cancer: A Real-World Study of Clinical Effectiveness in the United States. Adv Ther. 2020;37(6):2841-2852. | Study population, intervention |
Klein Hesselink EN, Steenvoorden D, Kapiteijn E, et al. Therapy of endocrine disease: response and toxicity of small-molecule tyrosine kinase inhibitors in patients with thyroid carcinoma: a systematic review and meta-analysis. Eur. 2015;172(5):R215-225. | Review article |
Oba T, Chino T, Soma A, et al. Comparative efficacy and safety of tyrosine kinase inhibitors for thyroid cancer: a systematic review and meta-analysis. Endocr J. 2020;67(12):1215-1226. | Review article |
Appendix 3: Detailed Outcome Data
Note that this appendix has not been copy-edited.
Figure 6: Kaplan-Meier Plot of OS, Cut-Off February 8, 2021 (Full ITT Population, N = 258)
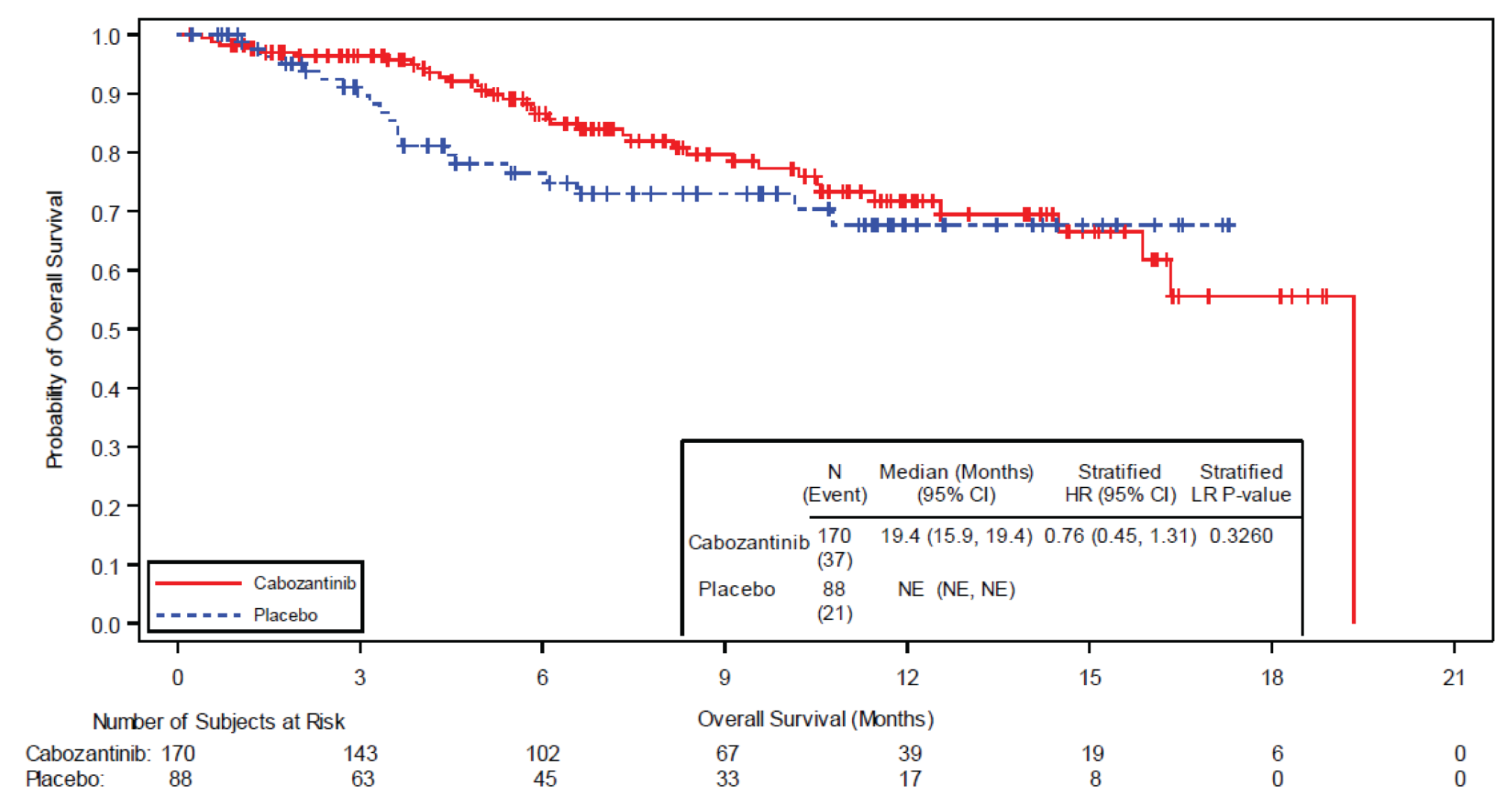
CI = confidence; HR = hazard ratio; ITT = intent to treat; IxRS = interactive voice/web response system; LR = log-rank test, NE = not estimable; OS = overall survival.
+Indicates censored observation.
Stratification factors (per IxRS) comprise receipt of prior lenvatinib (yes vs no) and age at informed consent (≤ 65 years vs>65 years).
The upper limit of the 95% CI for median OS should be interpreted as NE.
The last remaining patient in the cabozantinib arm had an event leading the survival probability to 0% as no patient remained at risk anymore.
Source: CSR of Cabozantinib.10
Figure 7: Kaplan-Meier Plot of PFS per BIRC, Cut-Off February 8, 2021 (Full ITT, N = 258)
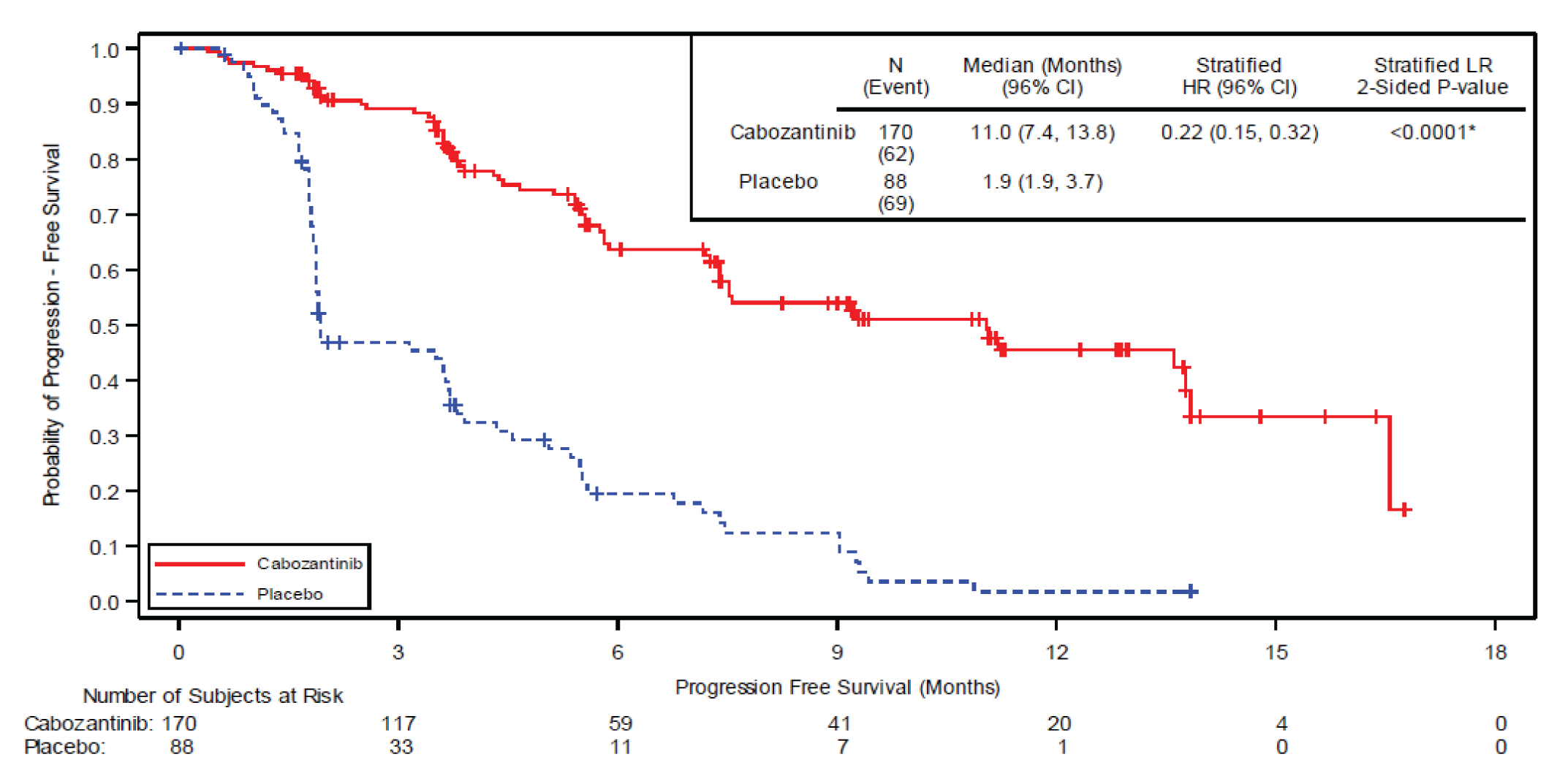
BIRC, blinded independent radiology committee; CI, confidence interval; HR, hazard ratio; ITT, intent to treat; IxRS, interactive voice/web response system; LR, log-rank test.
+indicates value from censored observation
Stratification factors (per IxRS) comprise receipt of prior lenvatinib (yes vs no) and age at informed consent (≤ 65 years vs>65 years).
Source: CSR of Cabozantinib.10
Appendix 4: Description and Appraisal of Outcome Measures
Note that this appendix has not been copy-edited.
Aim
To describe the following outcome measure and review its measurement properties (validity, reliability, responsiveness to change, and MID):
EQ-5D-5L was used to assess health-related quality of life as an additional end point in COSMIC-311 trial.
Findings
Table 22: Summary of Outcome Measures and their Measurement Properties
Outcome measure | Type | Conclusions about measurement properties | MID |
|---|---|---|---|
EQ-5D-5L | A generic, preference-based, HRQoL measure consisting of descriptive questions and a VAS. The descriptive questions cover 5 dimensions, while each dimension is divided into 5 levels of perceived problems. Higher scores indicate worse quality of life in individual scores and better quality of life in population index scores. The VAS records the patient’s self-rated health on a 10 cm scale with anchors from 0 (worst health one can imagine) to 100 (best health one can imagine). | Validity: Strong convergent validity (ρ > 0.5)23 was demonstrated with FACT-G total score (ρ = 0.673) and moderate (ρ = 0.3-0.49)23 to strong convergent validity existed between FACT-G subdomain scores and those of EQ-5D-5L. Construct or known-group validity was demonstrated according to ECOG PS (F stat 5L/3L = 4.11) and cancer stage (F stat 5L/3L = 3.84).24 Reliability: Strong test-retest reliability has been shown in all 5 dimensions (kappa > 0.85) and overall score (ICC = 0.92).24 In patients with papillary thyroid carcinoma, ICC and Spearman correlation (ρ) measured at pre-operation and 6-12 months follow-up were 0.43 and 0.47, respectively, showing moderate reliability.25 Responsiveness: EQ-5D-5L score reflected health status changes observed in patients with papillary thyroid carcinoma during pretreatment (baseline), posttreatment (deterioration), and follow-up (return to baseline) periods, albeit with less sensitivity compared to SF-36.25 | Unknown in patients with thyroid cancer in general. For a subset of patients with papillary thyroid carcinoma, estimate is calculated by distribution-based method26 to be 0.052.25 For VAS, no evidence has been identified for thyroid cancer population. In general population, estimate is 10.0 for VAS based on anchor- and distribution-based methods.27 |
EQ-5D-5L = EuroQoL 5-Dimensions 5-Levels; FACT-G = Functional Assessment of Cancer Therapy – General; HRQoL = health-related quality of life; ICC = intraclass correlation coefficient; MID = minimal important difference; SF-36 = Short Form – 36; VAS = visual analogue scale.
EuroQoL 5-Dimensions 5-Levels Questionnaire
The EQ-5D-5L questionnaire is a generic, preference-based, HRQoL measure consisting of descriptive questions and a VAS.28 EQ-5D-5L has been validated in terms of feasibility, convergent validity, discriminatory power, and ceiling effects in a diverse patient population from 6 countries with chronic conditions.28 Questions were answered based on how the patient felt that day.
The EQ-5D-5L was developed by the EuroQoL Group as an improvement to the EQ-5D 3 level (EQ-5D-3L), to improve sensitivity (measuring small and medium health changes) and reduce ceiling effects.29,30 The instrument is comprised of 5 dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Each dimension is rated on 5 levels: level 1 “no problems,” level 2 “slight problems,” level 3 “moderate problems,” level 4 “severe problems,” and level 5 “extreme problems” or “unable to perform.” Respondents are asked to choose the level that reflects their health state for each of the 5 dimensions. The numerical values assigned to levels 1 to 5 for each dimension reflect rank order categories of function. Data are not used to produce an individual dimension score. A total of 3,125 unique health states are possible, with 55555 representing the worst health state and 11111 representing the best state.
Results from the EQ-5D-5L descriptive system can be converted into a single, country-specific index score using a scoring algorithm taking the local patient and population preferences into account.31 Therefore, the index score is a country-specific value and the lowest EQ-5D index (utility) score varies depending on the scoring algorithm used.28 Even though the range of index scores differs according the scoring algorithm used, in all scoring algorithms of the EQ-5D-5L, a score of 0 represents the health state ‘dead’ and 1.0 reflects ‘perfect health’. Also, negative values are possible to represent health states that a society, not the patient, considers worse than death. Different utility functions are available that reflect the preferences of specific populations, e.g., US, UK. As an example, a Canadian scoring algorithm results in a score of –0.148 for health state 55555 (worst health state).
Another component of the EQ-5D-5L is a visual analogue scale (EQ-VAS), which is 10 cm, continuous scale anchored by 2 verbal descriptors: 0 (worst health imaginable) to 100 (best health imaginable). The respondents are asked to mark an X on the scale that best represents their health on that day.28,31
In summary, the EQ-5D produces 3 types of data for each respondent28,31:
A profile indicating the extent of problems on each of the 5 dimensions represented by a 5-digit descriptor, such as 11121 or 21143.
A population preference-weighted health utility index score based on the descriptive system.
A self-reported assessment of health status based on the EQ-VAS.
Validity
Zeng et al.24 conducted validation study on EQ-5D-5L in a total of 416 patients (and a subset of 90 patients in 2-day follow-up) with 6 commonly diagnosed cancers (lung, breast, liver, colorectal, thyroid, and gastric cancer) in China from December 2016 to July 2017 with Chinese version of questionnaires. They showed a strong correlation (Spearman correlation coefficient, ρ > 0.5),23 i.e., convergent validity, between EQ-5D-5L index and FACT-G total score (ρ = 0.673) in patients with thyroid cancer. In addition, most of subdomains of EQ-5D-5L and FACT-G demonstrated moderate (ρ = 0.3 – 0.49)23 to strong correlations in patients with thyroid cancer as shown below.
Mobility: PWB -0.521b, SFWB 0.309a, EWB 0.102, FWB -0.476b, FACT-G total score -0.188
Self-care: PWB -0.498b, SFWB 0.242, EWB 0.066, FWB -0.447b, FACT-G total score -0.235
Usual activities: PWB -0.619b, SFWB 0.424b, EWB 0.005, FWB -0.488b, FACT-G total score -0.214
Pain/discomfort: PWB -0.448b, SFWB 0.129, EWB -0.17, FWB -0.385b, FACT-G total score -0.367b
Anxiety/depression: PWB -0.045, SFWB -0.057, EWB -0.664b, FWB -0.293a, FACT-G total score -0.560b
Index: PWB 0.816b, SFWB -0.330a, EWB 0.23, FWB 0.890b, FACT-G total score 0.673b
The group also showed that in patients with thyroid cancer, EQ-5D-5L index score decreased as ECOG PS deteriorated and cancer stage increased, i.e., demonstrated known-group validity using parametric F statistic by analysis of variance (ANOVA) and nonparametric area under the receiver operating characteristic curve (AUROC) as shown below. Since results were presented in the ratio formats, i.e., 5L/3L, higher value greater than 1 indicates higher discriminatory power for 5L.
ECOG status 0 – 1 vs. 2 – 3+: F statistic 5L/3L = 4.11, AUROC 5L/3L= 1.32.
Cancer stage I – II vs. III – IV: F statistic 5L/3L = 3.84, AUROC 5L/3L = 1.24.
Reliability
In study by Zeng, et al.,24 48-hour follow-up repeat test in patients with thyroid cancer demonstrated strong test-retest reliability for EQ-5D-5L subdomains, e.g., mobility (kappa statistics = 0.87, 95% CI, = 0.60 to 1.00), self-care (0.89, 95% CI, 0.65 to 1.00), usual activities (0.89, 95% CI, = 0.67 to 1.00), pain/discomfort (0.85, 95% CI, = 0.58 to 1.00), anxiety ot depression (1.00, 95% CI, = 1.00 to 1.00). Similarly, the ICC value was 0.92 (95% CI, 0.98 to 1.00) in thyroid cancer group showing a strong test-retest reliability. In study by Lubitz, et al.,25 ICC agreement and Spearman correlation coefficient (ρ) between preoperative score (n = 117) and 6 to 12 month follow-up score (n = 44) in patients with papillary thyroid carcinoma was 0.43 (95% CI, = 0.15 to 0.64) and 0.47, respectively, demonstrating moderate test-retest reliability.
Responsiveness
Lubitz, et al.25 measured HRQoL changes in patients with papillary thyroid carcinoma at pretreatment (n = 117), posttreatment (n = 95), and follow-up (n = 92) to assess responsiveness of EQ-5D-5L. They hypothesized that all patients would experience a decrease in HRQoL immediately postop, mainly due to physical discomfort, and return to pretreatment health status at follow-up 6 to 12 months after surgery unless patients sustained surgical complications, experienced recurrence, or underwent RAI treatment. They showed that EQ-5D-5L score declined in 53% patients (> MID) from pretreatment to posttreatment period (standardized response mean [SRM] = 0.185), improved in 48% patients (> MID) from posttreatment to follow-up period (SRM = -0.229), and did not change statistically significantly in 41% of patients (> MID) from pretreatment to posttreatment period (SRM = -0.031). For the same periods, proportion of patients that responded (> MID) as measured by SF-36 were 53%, 48%, and 41%, respectively, indicating greater sensitivity than EQ-5D-5L.25
Minimal Important Difference
The MID for EQ-5D-5L, which was calculated based on distribution-based method, i.e., ½ of the standard deviation at pretreatment (0.5x SDT1) state26 in patients with papillary thyroid carcinoma, was shown to be 0.052.25 There is no evidence of MID for VAS in thyroid cancer population. Jin et al. conducted systematic review and estimated VAS to be 10.0 based on anchor- and distribution-methods in general population.27
Other Considerations and Limitations
In Zeng et al. study, EQ-5D-5L utility indices were calculated using the Chinese value sets, which differ from Canadian value sets. Even though EQ-5D-5L demonstrated better measurement properties than 3L in patients with thyroid cancer,24 e.g., smaller ceiling effects (10.1%) for 5L than 3L (17.8%) as well as slightly better test-retest reliability, convergent and known-group validity of 5L compared to those of 3L, other studies showed that SF-36 was more sensitive to HRQoL and treatment effects than EQ-5D-5L in patients with thyroid cancer.25,32 All in all, validation of existing questionnaires in patients with RR DTC32 is still needed because DTC is generally viewed as a curable cancer, whereas RR DTC survival rate is ~10%32 and HRQoL associated with it may differ greatly from treatable DTC.
Pharmacoeconomic Review
Abbreviations
AE
adverse event
BSC
best supportive care
DTC
differentiated thyroid carcinoma
ECOG
Eastern Cooperative Oncology Group
ICER
incremental cost-effectiveness ratio
LY
life-years
NOC
Notice of Compliance
NTRK
neurotrophic tyrosine receptor kinase
OS
overall survival
PD
progressed disease
PFS
progression-free survival
PS
performance score
QALY
quality-adjusted life-year
RAI-R
radioactive iodine-refractory
RDI
relative dose intensity
VEGFR
vascular endothelial growth factor receptor
WTP
willingness to play
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2), and a conclusion.
Item | Description |
|---|---|
Drug product | Cabozantinib (Cabometyx), oral tablets |
Submitted price | Cabozantinib, 20 mg, 40 mg, and 60 mg, oral tablet: $301.29 per tablet |
Indication | For the treatment of adult patients with locally advanced or metastatic differentiated thyroid carcinoma (DTC) that has progressed following prior vascular endothelial growth factor receptor (VEGFR)-targeted therapy and who are radioactive iodine-refractory (RAI-R) or ineligible. |
Health Canada approval status | NOC |
Health Canada review pathway | Priority review |
NOC date | April 27, 2022 |
Reimbursement request | As per indication |
Sponsor | Ipsen Biopharmaceuticals Canada Inc. |
Submission history | Previously reviewed: Yes Indication: Hepatocellular carcinoma Recommendation Date: April 22, 2020 Recommendation: Reimburse with clinical criteria and/or conditions Indication: Renal cell carcinoma Recommendation Date: February 20, 2019 Recommendation: Reimburse with clinical criteria and/or conditions |
DTC = differentiated thyroid carcinoma; NOC = Notice of Compliance; RAI-R = radioactive iodine-refractory; VEGFR = vascular endothelial growth factor receptor.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Partition survival model |
Target population | Adult patients with locally advanced or metastatic differential thyroid carcinoma (DTC) that have progressed following prior vascular endothelial growth factor receptor (VEGFR)-targeted therapies and who are radioactive iodine-refractory (RAI-R) ineligible. |
Treatment | Cabozantinib with BSC; consisting of analgesia, antibiotics for infections, transfusions for anemia, nutritional support, and psychological support with medication or counselling as appropriate. |
Comparator | BSC |
Perspective | Canadian publicly funded health care payer |
Outcomes | QALYs, LYs |
Time horizon | Lifetime (40 years) |
Key data source | COSMIC-311 |
Submitted results | ICER = $206,389 per QALY (incremental costs = $165,563; incremental QALYs = 0.80) |
Key limitations |
|
CADTH reanalysis results |
|
BSC = best supportive care; DTC = differentiated thyroid carcinoma; ICER = incremental cost-effectiveness ratio; LY = life-year; NTRK = neurotrophic tyrosine receptor kinase; OS = overall survival; PFS = progression-free survival; QALY = quality-adjusted life-year; RAI-R = radioactive iodine-refractory; VEGFR = vascular endothelial growth factor receptor.
Conclusions
Evidence from the COSMIC-311 study suggests that cabozantinib prolongs PFS when compared with placebo in patients with progressive RAI-R DTC who have previously failed VEGFR-targeted therapy. However, there is uncertainty related to the OS benefit associated with cabozantinib, primarily given short trial follow-up time (February 8, 2021 data cut-off, median follow-up of 11.9 months). The trial population is generalizable to the Canadian population; however, some uncertainty remains due to the exclusion of patients such as those with brain metastases and Eastern Cooperative Oncology Group (ECOG) performance score of at least 2.
CADTH identified several limitations in the sponsor’s pharmacoeconomic analysis that have notable implications on the cost-effectiveness of cabozantinib. As part of the base-case reanalysis, CADTH addressed the uncertainties associated with long-term treatment efficacy by selecting alternative extrapolation curves to inform OS (for both cabozantinib and BSC) and PFS (cabozantinib only); used the health state utilities values reported by the DECISION trial, and adjusted utility values by age. The CADTH reanalysis resulted in an ICER for cabozantinib plus BSC of $664,742 per QALY (incremental cost: $116,215; incremental quality-adjusted life-years (QALYs): 0.18) versus BSC.
The cost-effectiveness of cabozantinib was sensitive to the assumptions regarding the selected parametric models used to extrapolate OS and the health state utility values. Specifically, the CADTH reanalysis estimated a smaller OS benefit with cabozantinib when compared to the sponsor’s base-case and this translated to a smaller difference in QALYs between cabozantinib plus BSC versus BSC alone (incremental QALYs: 0.80 [sponsor’s base-case] versus 0.18 [CADTH’s reanalysis]). Despite this, 64% of the incremental QALYs in the CADTH reanalysis were accrued in the extrapolated period, in which there are presently no data available to support this benefit. CADTH was able to address the limitation regarding the health state utility values within the CADTH reanalysis. Based on the CADTH reanalysis, a 95% price reduction would be required for cabozantinib, for cabozantinib plus BSC to be considered cost-effective relative to BSC at a $50,000 per QALY threshold, However, as CADTH was unable to fully assess the uncertainty around long-term treatment efficacy due to lack of data and discrepancies in the trial population to those that will be seen in Canadian clinical practice, a higher price reduction may be warranted.
Stakeholder Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, registered clinicians, and drug plans that participated in the CADTH review process.
CADTH received 1 joint patient submission from 2 organizations (i.e., Canadian Cancer Society and Thyroid Cancer Canada). These groups gathered patient input from 2 Canadian patients who identified having differential thyroid carcinoma (DTC) that has progressed following prior treatment who are also radioactive iodine-refractory (RAI-R) or are not eligible for radioactive iodine therapies through a survey. One patient had experience with cabozantinib. Both patients reported that DTC impacted their quality of life, specifically noting that their ability to work, travel, and exercise were moderately effected. Both patients indicated there were financial barriers related to treatment with 1 respondent noting a loss of income due to absence of work while the other noted transportation costs. Both patients had undergone 3 or more lines of previous treatment for their DTC. One patient who had previously tried lenvatinib and is currently taking cabozantinib, said nausea and vomiting were worst while on lenvatinib and diarrhea was worst while taking cabozantinib. Outside of diarrhea, that patient felt that the side effects of cabozantinib were tolerable, and that the medication was easy to use. They also agreed that cabozantinib has been effective at controlling their cancer and that the pill form allowed them to spend less time in the clinic receiving treatment.
Registered clinical input was received from 7 physicians, some of whom are members of the Thyroid Cancer Canada Medical Advisory Panel and some who were investigators of the COSMIC-311 trial. Clinician input noted that the current care pathway for DTC patients who are RAI-R includes first-line lenvatinib. Occasionally, palliative treatment with doxorubicin is tried and BSC is the only remaining option. Clinician input recognized that there are currently no approved or funded options for patients who are RAI-R who progress after vascular endothelial growth factor receptor (VEGFR)-targeted therapies. Cabozantinib is expected to fill an unmet need for patients who progress on prior therapies. Clinicians noted that the inclusion criteria for the COSMIC-311 trial best define the patient population that is best suited for cabozantinib treatment. In addition to the trial inclusion criteria, patients with progressing nonmeasurable disease such as bone metastasis should not be excluded in the real-world clinical setting.
Drug plan input was received for this review. The plans noted that there are no standard comparators funded in Canada at the time of this review for this indication. Plans questioned the eligibility of certain patient subgroups for treatment with cabozantinib including those who experience adverse events (AE) with lenvatinib or sorafenib without progression and patients with ECOG of at least 2.
Several of these concerns were addressed in the sponsor’s model:
The impact of DTC on patient’s quality of life were captured via utility values.
Adverse events (AEs) associated with cabozantinib were included within the analyses.
The sponsor’s model compared cabozantinib to best supportive care (BSC). This reflects its anticipated use given there are no approved or funded options for DTC patients who are RAI-R and have progressed after VEGFR-targeted therapy.
CADTH was unable to address the following concerns raised from stakeholder input:
As the clinical data informing treatment effect of cabozantinib on patients were based on the COSMIC-311 trial, the clinical and cost-effectiveness of cabozantinib in certain patient subpopulations (e.g., DTC patients with known brain metastases, ECOG ≥ 2) remains unknown.
Economic Review
The current review is for cabozantinib (Cabometyx) for patients with locally advanced or metastatic DTC that have progressed following prior VEGFR-targeted therapy and who are RAI-R ineligible.
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted a cost-utility analysis to assess the cost-effectiveness of cabozantinib with BSC as a treatment for patients with DTC that have progressed after prior VEGFR-targeted therapies and who are RAI-R ineligible compared to BSC in Canada. This model population aligned with its Health Canada indication and the reimbursement request.1,2
Cabozantinib is available as 20 mg, 40 mg, and 60 mg oral tablets.1 The recommended dose of cabozantinib is 60 mg orally once daily without food with continued treatment until a patient no longer experience clinical benefit or experiences unacceptable toxicity.1 The submitted price for cabozantinib is $301.2943 per tablet or $8,436 per 28-day cycle.2 The comparator for this analysis was BSC, based on the placebo arm of COSMIC-311.3 It was assumed that patients in both treatment arms would incur the costs of BSC; therefore, BSC acquisition cost was assumed to be $0.
Outcomes of the model included quality-adjusted life-years (QALYs) and life-years (LYs) over a lifetime horizon of 40 years. Discounting (1.5% per annum) was applied for both costs and outcomes and a cycle length of 1 month (30.4375 days) was used with a half-cycle correction applied.2
Model Structure
The sponsor submitted a partitioned survival model consisting of 3 health states: progression free, progressed disease (PD), and death (Figure 1). The proportion of patients who were progression free, experience disease progression, or death at any time was derived from non-mutually exclusive survival curves informed by the COSMIC-311 trial.2 All patients entered the model in the progression-free health state where they were assumed to be stable or responding to therapy.2 Patients can then transition to the death state or to the postprogression state where they remain until they transition to the death state. The proportion of patients in the progression-free state was estimated based on the respective progression-free survival (PFS) curves, where progression was defined as radiographic progression per Response Evaluation Criteria in Solid Tumours 1.1 by blinded independent radiology committee.3 The proportion of patients in the PD state was calculated as the proportion alive (based on the overall survival [OS] curve) minus the proportion of patients alive and progression free (based on the PFS curve).2 It was assumed patients would discontinue treatment at the time of disease progression or death, whichever occurred first. Patients were assumed to receive no subsequent treatment after disease progression.2 Survival curves were further capped in the model using age and gender-specific general population mortality rates.4
Model Inputs
The target population was based on the intention-to-treat population of the phase III COSMIC-311 trial, which enrolled patients with RAI-R DTC (i.e., age = 65.0 years; proportion of females = 54.0%) who had progressed during or after prior VEGFR-targeted therapy (i.e., lenvatinib or sorafenib).2
PFS and OS curves for cabozantinib were generated using unadjusted data from the COSMIC-311 study (February 8, 2021 data cut-off). The placebo arm of COSMIC-311 was used to inform the survival curves of BSC at the same data cut with the PFS curves generated by also using unadjusted data from the COSMIC-311 study. As the COSMIC-311 trial was designed to allow for crossover from placebo at the time of blinded independent radiology committee confirmed progression, rank-preserving structural failure time (RPSFT) adjustment was used to estimate the OS of the placebo arm.2 Extrapolation curves were selected based on clinical plausibility, visual inspection, and statistical fit to the trial’s Kaplan–Meier data. For the sponsor’s base-case analysis, loglogistic and generalized gamma were selected for the PFS curves of cabozantinib and BSC, respectively. The exponential extrapolation curve was used to inform OS for both arms.2 Figure 2 and Figure 3 present the observed and predicted OS and PFS for cabozantinib, respectively. Figure 4 and Figure 5 present the observed and predicted OS (i.e., crossover adjusted placebo) and PFS for BSC, respectively.
The AE rates for both cabozantinib and BSC were informed from the COSMIC-311 trial (August 19, 2020 data cut-off) and were accounted for as a 1-off decrements in utilities and costs in the first cycle of the model.2
Health state utility values in the model were informed by published literature where the PFS and PD states were estimated to have utilities of 0.87 and 0.52, respectively.5 AE-related disutilities values were informed from published literature and adjusted by the mean duration of that AE as reported in the COSMIC-311 trial.6
To inform treatment costs, the number of treatment cycles for cabozantinib was informed from the COSMIC-311 trial with a dose intensity of 100% assumed. The drug acquisition cost of cabozantinib was provided by the sponsor while the cost of BSC was assumed to be $0.2 In addition to treatment acquisition costs, monitoring costs, health care resource use costs, AE management costs, and terminal care costs were included. Treatment monitoring costs and health care resource use costs were sourced from the Ontario Ministry of Health Schedule of Benefits for laboratory and physician services whereas AE management and terminal care costs were informed by published literature.7-10 All costs were expressed as 2021 Canadian dollars.2
Summary of Sponsor’s Economic Evaluation Results
All analyses were run probabilistically (1,000 iterations). Submitted deterministic analysis were aligned with the probabilistic results. The probabilistic findings are presented below.
Base-Case Results
The results of the sponsor’s probabilistic base-case analysis demonstrated that cabozantinib plus BSC was associated with an additional 0.80 QALYs at an additional cost of $165,563. Therefore, the incremental cost-effectiveness ratio (ICER) of cabozantinib plus BSC was $206,389 per QALY gained compared to BSC alone. Based on the deterministic results, the majority (~81%) of the incremental QALYs for cabozantinib were found to be accrued during the extrapolation period (i.e., after the ~1 year of observed COSMIC-311 trial data).
Table 3: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER vs. BSC ($/QALY) |
|---|---|---|---|---|---|
BSC | $37,888 | Ref. | 1.27 | Ref. | Ref. |
Cabozantinib + BSC | $203,451 | $165,563 | 2.07 | 0.80 | $206,389 |
BSC = best supportive care; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; Ref. = reference; vs. = versus.
Note: Results presented were taken from the sponsor’s submitted Excel model.
Source: Sponsor’s pharmacoeconomic submission.2
Sensitivity and Scenario Analysis Results
The sponsor conducted several scenario analyses pertaining to different OS extrapolation selections, time horizon lengths, discounting, health state utilities, treatment duration, and the placebo crossover adjustment for OS. The scenario in which a single exponential model extrapolated the OS data posttrial (i.e., assuming there was no survival benefit for cabozantinib compared to BSC beyond the trial period) had the largest impact on results, with an ICER of $281,727. The remainder of the scenarios had ICERs ranging from $278,891 (health state utility values based on the DECISION trial) to $202,301 (0% discounting).
CADTH Appraisal of the Sponsor’s Economic Evaluation
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the economic analysis:
Uncertainty in cabozantinib treatment efficacy. The efficacy of cabozantinib was informed by the randomized, double-blind, placebo-controlled COSMIC-311 trial. The clinical experts consulted by CADTH noted that, a subset (24.8% of patients in the cabozantinib arm) were previously treated with sorafenib and lenvatinib. The clinical experts noted these patients may be less treatment sensitive; therefore, this may underestimate cabozantinib efficacy compared to Canadian patients who would have only previously failed lenvatinib. These clinical experts further noted that, although the distribution of patient baseline characteristics reflected the current clinical setting, generalizability to certain subgroups of patients may be limited. Specifically, patients with bone metastasis were excluded from COSMIC-311. The clinical experts noted that this exclusion may favour cabozantinib as patients with bone metastasis do not typically respond well to tyrosine kinase inhibitor (TKI) therapies. Although the clinical experts stated that patients in the clinical setting may have higher ECOG performance status (i.e., ≥ 2), they further noted that treating these patients with cabozantinib may not be recommended due to an increased risk of AE.
Furthermore, there was considerable uncertainty in the extrapolated efficacy data for cabozantinib due to the short follow-up duration of COSMIC-311 (a median follow-up of 11.9 months by the second data cut-off [February 8, 2021]). As the median OS was not reached by the second data cut-off, the OS data were considered immature. This limits the interpretability of the long-term survival of RAI-R DTC patients receiving cabozantinib. In the sponsor’s base-case, the exponential curve was used to inform OS of cabozantinib. The selection of this distribution was justified by the sponsor based on the data from the US Surveillance, Epidemiology, and End Results database which suggested that the long-term survival trends for locally advanced or metastatic DTC patients matched a linear model, and in which indicated a fixed rate of survival. However, clinical experts consulted by CADTH stated that this assumption was likely not applicable to patients who have progressed on TKI given their tumour is more biologically aggressive. A linear model would likely overestimate the efficacy of cabozantinib.
Across the parametric survival distributions for PFS, all had similar statistical fit. The sponsor selected the loglogistic distribution for cabozantinib which was associated with the lowest Akaike information criterion (AIC) and Bayesian information criterion (BIC) values. AIC and BIC only reflect statistic fit in the observed trial period and, while data maturity was less of a concern for PFS, the clinical experts noted that this distribution may provide a more optimistic projection of PFS for cabozantinib.
To address the above-mentioned limitations, CADTH selected the gamma curve to inform OS and PFS of cabozantinib to reflect feedback from the clinical experts regarding their expected long-term efficacy of cabozantinib for RAI-R DTC patients in Canada.
Uncertainty in the OS estimates for BSC due to crossover bias. Given the potential crossover bias within the placebo arm of the COSMIC-311 trial, the sponsor used the RPSFT method to adjust for protocol allowed crossover to estimate the OS for BSC within their submitted pharmacoeconomic model. According to the CADTH clinical report, assumptions for this analysis would generally result in a conservative underestimate of the comparative treatment effect for cabozantinib to BSC. Although the results in OS were consistent in the analysis without adjustment when compared to the OS results in the analysis with RPSFT adjustment, uncertainty still remains. Given the lack of real-world survival data on RAI-R DTC patients treated with BSC, it is not possible to verify the validity of the OS predictions. This, in conjunction with other trial limitations stated earlier regarding the trial population, means that the true OS of BSC remains unknown.
As part of the CADTH base-case, the gamma curve was used to inform the OS of BSC based on consultation with clinical experts who deemed this to be most clinically plausible.
Health state utility values were not appropriate. In the sponsor’s base-case, health state utility values were informed by Fordham et al., 2015 which was a UK study aimed to estimate health state utilities in individuals with RAI-R DTC.5 In this study, utilities of 0.87 and 0.52 were estimated for the PFS and PD states, respectively.5 However, a recent Canadian Community Health Survey estimates that the average Canadian utility to be 0.863.11 Clinical experts consulted by CADTH noted that it was unlikely that RAI-R DTC patients in the progression-free state would have similar quality of life to the average Canadian given this subset of patients have an advanced, biologically aggressive disease and have been subjected to multiple prior lines of treatment. Therefore, the PFS utility estimate that was selected in the sponsor's base-case overestimated the patient’s quality of life within this state.
By using the Fordham utility estimates, this would further mean that there is a 0.35 utility difference between the progression-free and PD state. This did not align with the COSMIC-311 trial results that found a much smaller difference between these 2 health states (i.e., ||||| for progression-free versus ||||| for PD). However, as noted in the CADTH clinical report, uncertainty remains on how to interpret the health-related quality of life data within the COSMIC-311 trial given the limited follow-up duration.
Finally, the sponsor’s base-case analysis did not include age-adjusted utility values. Given that the model’s starting population had a mean age of 65 (informed by the COSMIC-311 trial) and age is expected to impact an individual’s quality of life as confirmed by the clinical experts consulted by CADTH, this would overestimate the health state utility values seen in the sponsor’s model.
o CADTH addressed these limitations by including the PFS and PD utility values informed by the DECISION trial and by including age-adjusted utilities, using the sponsor-provided option to do so for both. The utility value for PFS in the DECISION trial was more closely aligned to the utility value derived from COSMIC-311 (|||||) while still ensuring a larger incremental difference between the PFS and PD states (i.e., 0.72 for progression-free; 0.64 for PD) compared to the values derived from the COSMIC-311 trial. The DECISION trial utility estimates were considered more in line with the utility values for patients who were progression free and progressed based on consultation by CADTH clinical experts.
No comparative evidence to target-specific treatments for RAI-R DTC. There has been no head-to-head trial or indirect comparison conducted to compare cabozantinib to larotrectinib or selpercatinib in patients with NTRK or rearranged during transfection fusion-positive locally advanced or metastatic DTC that have progressed following prior VEGFR-targeted therapy and who are RAI-R ineligible. As such, the cost-effectiveness of cabozantinib to target-specific treatments remains unknown. Larotrectinib is indicated only in a subset of patients who have NTRK gene fusion while selpercatinib is indicated only in patients with rearranged during transfection fusion-positive solid tumours. Both of these drugs have been reviewed by CADTH12,13 with larotrectinib currently in active negotiation while selpercatinib is under consideration for pCPA negotiations at the time of this review.
CADTH was unable to resolve this issue due to limitations in data availability. Nonetheless, clinical experts consulted by CADTH expected only a small subset of the RAI-R DTC population to be eligible for either treatment options.
Additionally, the following key assumptions were made by the sponsor and have been appraised by CADTH (Refer to Table 4).
CADTH Reanalyses of the Economic Evaluation
Base-Case Results
The CADTH base-case was derived by making changes in the model parameter values, in consultation with clinical experts. These changes, summarized in Table 5, involved the adjustment of survival curve selections for cabozantinib (OS and PFS) and BSC (OS only), the selection of an alternative source to inform health state utilities, and the inclusion of age-adjusted utility values.
Table 4: Key Assumptions of the Submitted Economic Evaluation (Not Noted as Limitations to the Submission)
Sponsor’s key assumption | CADTH comment |
|---|---|
BSC informed by the placebo arm of the COSMIC-311 trial | Reasonable. |
Assumed equal health care resource use between progression-free and progressed health states. | Inappropriate. The clinical expert indicated they would follow-up more closely with progressed patients vs. their progression-free counterpart. However, given that this set of costs had a smaller impact (i.e., its incremental costs contributed less when compared to other costs categories), assumptions regarding health care resource use are unlikely to change the conclusion regarding the cost-effectiveness of cabozantinib. |
Patients remained on treatment until disease progression or death, whichever occurred first. | Uncertain. While this assumption may be true for the majority of patients, patients discontinued treatment for other reasons including AE and clinical deterioration in the COSMIC-311 trial.3 However, the sponsor’s assumption was considered conservative. A scenario analysis was conducted on the CADTH base-case in which treatment discontinuation was informed by the time to treatment discontinuation curve from COSMIC-311. |
Costs and disutilities associated with AEs modelled as a one-off event in the first cycle of the model. | Inappropriate. The sponsor’s base-case modelled costs and disutilities associated with AEs as a one-off event in the first cycle of the model with the AE duration based on COSMIC-311. This was an unreasonable assumption as the clinical experts consulted by CADTH noted that it is not unreasonable for patients to have more than one AE throughout their cabozantinib treatment course, which was further reflected in the COSMIC-311 trial where 22% of patients receiving cabozantinib had 2 dose reductions due to AEs.14 The number of AE were based on the August 2020 data cut-off; these numbers would differ if using the February 2021 data cut-off. This indicates that AEs do not occur only in the first month but rather, AEs can occur at any point while a patient is on treatment. |
AEs associated with BSC informed by the placebo arm of the COSMIC-311 trial. | Inappropriate. The clinical expert consulted by CADTH noted that the AEs associated with the placebo arm in the COSMIC-311 trial were likely related to disease progression. Furthermore, as all patients were assumed to receive BSC regardless of being on cabozantinib or not within the submitted model, the BSC arm of the model should not have additional AEs. However, given the impact of AEs within the economic model applies to only a single cycle, this is unlikely to have a large impact to the overall results. |
No additional administration costs associated with cabozantinib. | Reasonable. Clinical experts consulted by CADTH noted that patients are likely to not require additional physician visits to acquire cabozantinib. |
100% RDI for drug costs. | Reasonable. 100% RDI is a conservative assumption. In real-world clinical practice, the RDI will be uncertain and therefore may reduce the total drug cost of cabozantinib, but this may have a further impact on its effectiveness. |
AE = adverse event; BCS = best supportive care; RDI = relative dose intensity.
Table 5: CADTH Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor’s base-case | ||
1. AE event cost | AE event costs were informed by Meyers 2021; however, costs in the model were not inflated and remain reported in CA$ 2019 | Inflated AE event costs to CA$ 2021 |
2. % Female Input Correction | Probabilistic input was hard coded to use 24% | Updated formula to update value probabilistically |
Changes to derive the CADTH base-case | ||
1.a. Cabozantinib parametric OS distribution | OS: Exponential | OS: Gamma |
1. b. Cabozantinib parametric PFS distribution | PFS: Loglogistic | PFS: Gamma |
2. BSC OS parametric survival distribution | Exponential | Gamma |
3.a. Health State Utilities | PF = 0.87 PD = 0.52 | PF = 0.72 PD = 0.64 |
3.b. Age-adjusted utilities | Age-adjusted utility turned off | Age-adjusted utility turned on |
CADTH base-case | — | 1a + 1b + 2 + 3a + 3b |
AE = adverse event; BSC = best supportive care; CA$ = Canadian dollars; OS = overall survival; PD = progressed; PF = progression free; PFS = progression-free survival.
In the CADTH base-case, cabozantinib plus BSC was associated with estimated total costs and QALYs of $153,974 and 1.46, compared with total costs and QALYs of $37,759 and 1.28 for patients on BSC. Therefore, the ICER for cabozantinib plus BSC compared to BSC was $664,742 per QALY, and the probability of cost-effectiveness at a $50,000 per QALY willingness-to-pay (WTP) threshold was 0%.
The estimated ICER was higher than the sponsor's base-case, driven primarily by changes to the OS distributions and, to some extent, the health state utility values. Specifically, the CADTH reanalysis estimated a smaller OS benefit with cabozantinib when compared to the sponsor’s base-case and this translated to a smaller difference in QALYs between cabozantinib plus BSC versus BSC alone (incremental QALYs: 0.80 [sponsor’s base-case] versus 0.18 [CADTH’s reanalysis]). Despite this, based on the deterministic results, ~64% of the incremental QALYs for cabozantinib plus BSC were found to be accrued during the extrapolated period. This benefit should be interpreted with caution given the lack of OS data to confirm this modelled benefit.
Table 6: Summary of the Stepped Analysis of the CADTH Reanalysis Results
Stepped analysis | Drug | Total costs | Total QALYs | ICER ($/QALY) |
|---|---|---|---|---|
Sponsor’s base-case (probabilistic) | BSC | $37,802 | 1.26 | Ref. |
Cabozantinib + BSC | $203,486 | 2.07 | $206,389 | |
Sponsor’s base-case (corrected; deterministic) | BSC | $37,803 | 1.26 | Ref. |
Cabozantinib + BSC | $203,492 | 2.07 | $205,128 | |
CADTH reanalysis 1a (deterministic) | BSC | $37,803 | 1.26 | Ref. |
Cabozantinib + BSC | $191,562 | 1.61 | $437,732 | |
CADTH reanalysis 1b (deterministic) | BSC | $37,803 | 1.26 | Ref. |
Cabozantinib + BSC | $154,360 | 1.91 | $178,582 | |
CADTH reanalysis 2 (deterministic) | BSC | $37,598 | 1.15 | Ref. |
Cabozantinib + BSC | $203,492 | 2.07 | $180,932 | |
CADTH reanalysis 3a (deterministic) | BSC | $37,803 | 1.43 | Ref. |
Cabozantinib + BSC | $203,492 | 2.02 | $277,028 | |
CADTH reanalysis 3b (deterministic) | BSC | $37,803 | 1.25 | Ref. |
Cabozantinib + BSC | $203,492 | 2.04 | $209,854 | |
CADTH base-case (deterministic) | BSC | $37,598 | 1.28 | Ref. |
Cabozantinib + BSC | $153,864 | 1.46 | $652,952 | |
CADTH base-case (probabilistic) | BSC | $37,759 | 1.28 | Ref. |
Cabozantinib + BSC | $153,974 | 1.46 | $664,742 |
BSC = best supportive care; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; Ref. = reference.
Scenario Analysis Results
A scenario analysis was conducted on the CADTH base-case to investigate the impact of using the time to treatment discontinuation data from COSMIC-311. Results of this scenario analysis are presented in Appendix 4. This analysis resulted in an ICER for cabozantinib of $563,409 per QALY compared to BSC suggesting that, when assuming a shorter treatment duration of cabozantinib, this only had a slight impact on the cost-effectiveness results.
Additionally, CADTH undertook price reduction analyses based on the sponsor’s and CADTH’s base-case. The CADTH base-case suggested a price reduction of 95% would be required to achieve cost-effectiveness of cabozantinib at a WTP threshold of $50,000 per QALY (Table 7).
Table 7: CADTH Price Reduction Analyses
Analysis | ICERs for cabozantinib + BSC vs. BSC ($/QALY) | |
|---|---|---|
Price reduction | Sponsor base-case | CADTH reanalysis |
No price reduction | $206,389 | $664,742 |
10% | $186,113 | $599,798 |
20% | $165,838 | $534,854 |
30% | $145,562 | $469,910 |
40% | $125,287 | $404,966 |
50% | $105,011 | $340,022 |
60% | $84,736 | $275,078 |
70% | $64,460 | $210,134 |
77% | $50,268 | $164,673 |
78% | $48,240 | $158,178 |
80% | $44,185 | $145,190 |
90% | $23,909 | $80,246 |
94% | $15,799 | $54,268 |
95% | $13,772 | $47,774 |
100% | $3,634 | $15,301 |
BSC = best supportive care; ICER = incremental cost-effectiveness ratio; vs. = versus.
Issues for Consideration
Cabozantinib has been previously reviewed by CADTH for hepatocellular carcinoma and renal cell carcinoma, receiving a reimburse with clinical criteria and/or conditions for both submissions.
Entrectinib (Rozlytrek) is currently under review at CADTH for the treatment unresectable locally advanced or metastatic extracranial solid tumours that have a NTRK gene fusion and may represent another NTRK fusion-positive treatment alternative in a subset of DTC patients that have progressed following prior VEGFR-targeted therapy and who are RAI-R ineligible.
Overall Conclusions
Evidence from the COSMIC-311 trial suggests that cabozantinib prolongs PFS when compared with placebo in patients with progressive RAI-R DTC who have previously failed VEGFR-targeted therapy. However, there is uncertainty related to the OS benefit of cabozantinib, largely due to short trial follow-up time (February 8, 2021 data cut-off, median follow-up of 11.9 months). Overall, the trial population assessed is generalizable to the Canadian population; however, uncertainty remains due to the exclusion of patients without characteristics such as brain metastases and ECOG performance scores of 2 and above.
There were several limitations in the sponsor’s pharmacoeconomic identified by CADTH that have notable implication on the cost-effectiveness results of cabozantinib. To address the limitations, CADTH modified the following as part of its base-case: selected alternative extrapolation curves to inform OS (gamma for both cabozantinib and BSC) and PFS (gamma for cabozantinib only), used health state utility values reported by the DECISION trial and included age-adjusted utility values. The CADTH reanalysis resulted in an ICER of $664,742 per QALY (incremental cost: $116,215; incremental QALYs: 0.175) for cabozantinib plus BSC versus BSC. There was a 0% probability that cabozantinib plus BSC would be cost-effective at a $50,000 per QALY threshold.
The analysis showed that costs were largely driven by the drug acquisition cost for cabozantinib with a 95% price reduction required for cabozantinib in order for cabozantinib plus BSC to be considered cost-effective relative to BSC. However, a higher price reduction may be warranted as there remains uncertainty in the clinical effectiveness inputs that could not be addressed in the CADTH reanalysis (i.e., long-term OS benefits). Although the CADTH reanalysis estimated a smaller OS benefit with cabozantinib plus BSC when compared to the sponsor’s base-case, and this translated to a smaller difference in QALYs between cabozantinib plus BSC versus BSC alone (incremental QALYs: 0.80 [sponsor’s base-case] versus 0.18 [CADTH’s reanalysis]), 64% of the incremental QALYs in the CADTH reanalysis were accrued in the extrapolated period. This benefit should be interpreted with caution given the lack of OS data to confirm this modelled benefit.
There remains uncertainty in the treatment effect as generalizability to certain subgroups of patients may be limited. The trial population excluded patients with brain metastasis patients. Lastly, although representing a small subset of RAI-R DTC patients, comparative clinical effectiveness between cabozantinib and larotrectinib (Vitrakvi), and selpercatinib (Retevmo) – which are currently available therapies patients who have NTRK gene fusion or rearranged during transfection (RET)-mutation-positive RAI-R DTC, respectively – remains unknown as there exists no direct or indirect clinical evidence. As such, the cost-effectiveness of cabozantinib plus BSC compared to these 2 treatments is unknown.
References
1.Cabometyx (cabozantinib as cabozantinib (S)-malate): 20 mg, 40 mg, and 60 mg oral tablets [product monograph]. Mississauga (ON): Ipsen Biopharmaceuticals Canada, Inc.; 2022 Apr 27.
2.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Cabometyx (cabozantinib), 20 mg, 40 mg, and 60 mg oral tablets. Mississauga (ON): Ipsen Biopharmaceuticals Canada, Inc.; 2022 May 12.
3.Clinical Study Report: XL184-311. A phase 3, randomized, double-blind, placebo-controlled study of cabozantinib (XL184) in subjects with radioiodine-refractory differentiated thyroid cancer who have progressed after prior VEGFR-targeted therapy [internal sponsor's report]. Alameda (CA): Exelixis, Inc; 2021 Apr 30.
4.Table: 13-10-0114-01. Life expectancy and other elements of the life table, Canada, all provinces except Prince Edward Island. Ottawa (ON): Statistics Canada; 2022: https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310011401. Accessed 2022 May 12.
5.Fordham BA, Kerr C, de Freitas HM, et al. Health state utility valuation in radioactive iodine-refractory differentiated thyroid cancer. Patient Prefer Adherence. 2015;9:1561-1572. PubMed
6.Drug Reimbursement Review sponsor submission: Cabometyx (cabozantinib), 20 mg, 40 mg, and 60 mg oral tablets [internal sponsor's package]. Mississauga (ON): Ipsen Biopharmaceuticals Canada, Inc.; 2022 May 12.
7.Schedule of benefits for laboratory services: effective July 1, 2020. Toronto (ON): Ontario Ministry of Health; 2020: https://www.health.gov.on.ca/en/pro/programs/ohip/sob/lab/lab_mn2020.pdf. Accessed 2022 Aug 22.
8.Schedule of benefits for physician services under the Health Insurance Act: effective October 1, 2021. Toronto (ON): Ontario Ministry of Health; 2022: https://www.health.gov.on.ca/en/pro/programs/ohip/sob/physserv/sob_master.pdf. Accessed 2022 May 12.
9.Meyers BM, Vogel A, Marotta P, et al. The cost-effectiveness of lenvatinib in the treatment of advanced or unresectable hepatocellular carcinoma from a Canadian perspective. Can J Gastroenterol Hepatol. 2021;2021:8811018. PubMed
10.Walker H, Anderson M, Farahati F, et al. Resource use and costs of end-of-Life/palliative care: Ontario adult cancer patients dying during 2002 and 2003. J Palliat Care. 2011;27(2):79-88. PubMed
11.Guertin JR, Feeny D, Tarride JE. Age- and sex-specific Canadian utility norms, based on the 2013-2014 Canadian Community Health Survey. CMAJ. 2018;190(6):E155-E161. PubMed
12.Drug Reimbursement Review: selpercatinib (Retevmo) as monotherapy for the treatment of unresectable advanced or metastatic RET-mutant medullary thyroid cancer in adult and pediatric patients 12 years of age and older with unresectable advanced or metastatic disease - in progress. Ottawa (ON): CADTH; 2022: https://www.cadth.ca/selpercatinib-0. Accessed 2022 Jun 03.
13.Drug Reimbursement Review clinical and pharmacoeconomic reports: larotrectinib (Vitrakvi) for solid tumours with NTRK gene fusion. Can J Health Technol. 2021;1(11). https://www.cadth.ca/sites/default/files/DRR/2021/PC0221-Vitrakvi-combined-report-meta.pdf. Accessed 2022 Jun 03.
14.Clinical Study Report: XL184-311. Addendum 2: a phase 3, randomized, double-blind, placebo-controlled study of cabozantinib (XL184) in subjects with radioiodine-refractory differentiated thyroid cancer who have progressed after prior VEGFR-targeted therapy [internal sponsor's report]. Alameda (CA): Exelixis, Inc; 2021 Aug 19.
15.Retevmo (selpercatinib): 40 mg and 80 mg oral capsules [product monograph]. Toronto (ON): Eli Lilly Canada Inc.; 2022 Apr 19: https://pdf.hres.ca/dpd_pm/00065504.PDF. Accessed 2022 Jun 02.
16.Vitrakvi (larotrectinib as larotrectinib sulfate): 25 mg and 100 mg oral capsules; Vitrakvi (larotrectinib as larotrectinib sulfate): 20 mg/mL oral solution [product monograph]. Mississauga (ON): Bayer Inc.; 2022 Jan 24: https://pdf.hres.ca/dpd_pm/00064510.PDF. Accessed 2022 Jun 03.
17.Budget Impact Analysis [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Cabometyx (cabozantinib), 20 mg, 40 mg, and 60 mg oral tablets. Mississauga (ON): Ipsen Biopharmaceuticals Canada, Inc.; 2022 May 12.
18.Dinh T, Sutherland G. Understanding the gap: a pan-Canadian analysis of prescription drug insurance coverage. Ottawa (ON): The Conference Board of Canada; 2017: https://www.conferenceboard.ca/e-library/abstract.aspx?did=9326. Accessed 2022 May 12.
19.Alignment among public formularies in Canada part 2: oncology medications. Ottawa (ON): Patented Medicine Prices Review Board; 2021: https://www.canada.ca/content/dam/pmprb-cepmb/documents/npduis/analytical-studies/formularies/PMPRB-P2-Formularies-en.pdf. Accessed 2022 Jul 17.
Appendix 1: Cost Comparison Table
Note that this appendix has not been copy-edited.
The comparators presented in the Table 8 have been deemed to be appropriate based on feedback from clinical expert(s). Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in Table 8 and as such, the table may not represent the actual costs to public drug plans.
Table 8: CADTH Cost Comparison Table for Locally Advanced or Metastatic DTC That Have Progressed Following Prior VEGFR-Targeted Therapy and Are Radioactive Iodine-Refractory Ineligible
Treatment | Strength / concentration | Form | Price | Recommended dosagea | Daily cost | 28-day cost |
|---|---|---|---|---|---|---|
Cabozantinib (Cabometyx) | 20 mg 40 mg 60 mg | Tablet | $301.2943b | 60 mg once daily | $301.29 | $8,436.24 |
aRecommended doses are from the respective product monographs, unless otherwise indicated.1
bSponsor submitted price.2
Table 9: CADTH Cost Comparison Table for Locally Advanced or Metastatic NTRK or RET Gene Fusion/Mutation-Positive DTC That Have Progressed Following Prior VEGFR-Targeted Therapy and Are Radioactive Iodine-Refractory Ineligible
Treatment | Strength / concentration | Form | Price | Recommended dosagea | Daily cost | 28-day cost |
|---|---|---|---|---|---|---|
Targeted Kinase Inhibitors | ||||||
Larotrectinib (Vitrakvi) | 25 mg 100 mg 20 mg/mL | Capsule Capsule Oral sol. | $52.3375b $209.3500b $41.8700b | 100 mg twice daily | $418.70 | $11,724 |
Selpercatinib (Retevmo) | 40 mg 80 mg | Capsule | $66.5000c $133.0000c | <50 kg: 120 mg twice daily ≥50 kg: 160 mg twice daily | <50 kg: $399.00 ≥50 kg: $532.00 | <50 kg: $11,172 ≥50 kg: $14,896 |
aRecommended doses are from the respective product monographs, unless otherwise indicated.15,16
bPrice based on the 2021 CADTH submission for Larotrectinib for solid tumours with NTRK gene fusion.13
cPrice based on the 2022 CADTH submission for Selpercatinib as monotherapy for the treatment of RET-mutant medullary thyroid cancer in adult and pediatric patients 12 years of age and older with unresectable advanced or metastatic disease.12
Appendix 2: Submission Quality
Note that this appendix has not been copy-edited.
Description | Yes/No | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing. | Yes | Overall, the trial population assessed is generalizable to the Canadian population; however, uncertainty remains due to the exclusion of patients without characteristics such as brain metastases and ECOG performance scores of 2 and above. |
Model has been adequately programmed and has sufficient face validity. | Yes | No comment. |
Model structure is adequate for decision problem. | Yes | No comment. |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis). | No | CADTH identified several errors relating to how data were incorporated into the model. This included the % female parameter used in probabilistic analysis and the sponsor did not inflate the event costs associated with AEs despite claims that this was done within the sponsor’s submitted report. |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem. | Yes | No comment. |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details). | No | CADTH identified discrepancies in the results reported between the sponsor’s economic report and their submitted model. For example, although both the report and model indicated the probabilistic base-case analysis had an ICER of $206,389, the incremental QALYs and incremental costs were not aligned between the 2 documents ([incremental QALY, model = 0.802 vs report = 0.808]; [incremental costs, model = $165,563 vs report = $165,876]). Additionally, the sponsor did not present discounted LYs despite claiming all modelled outcomes were presented as such. |
AE = adverse event, ECOG = Eastern Cooperative Oncology Group, ICER = incremental cost-effective ratio, LY = life-years, QALY = quality-adjusted life-years.
Appendix 3: Additional Information on the Submitted Economic Evaluation
Note that this appendix has not been copy-edited.
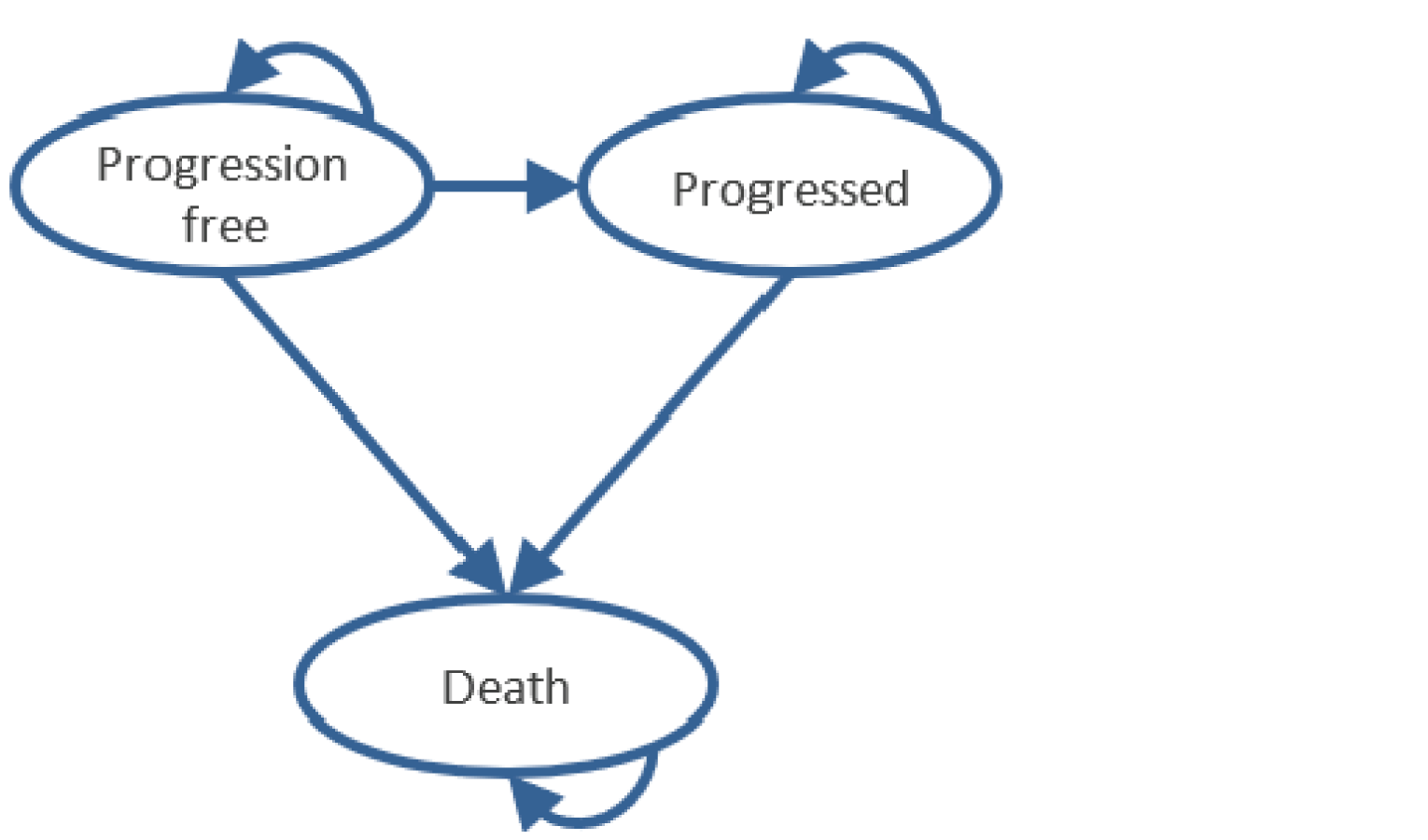
Figure 2: Observed and Extrapolated OS Data for Cabozantinib
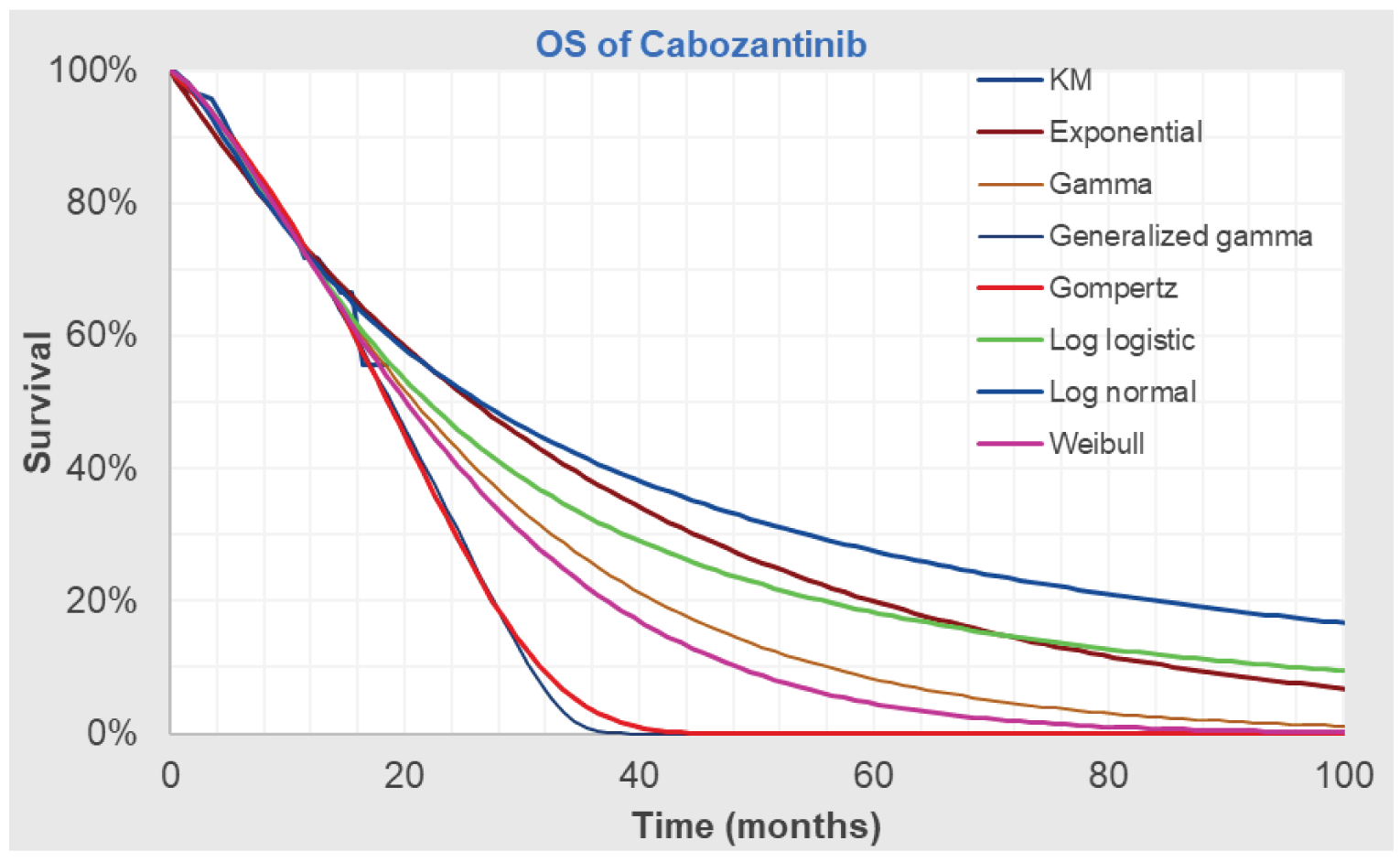
Source: Sponsor’s pharmacoeconomic submission2
Figure 3: Observed and Extrapolated PFS Data for Cabozantinib
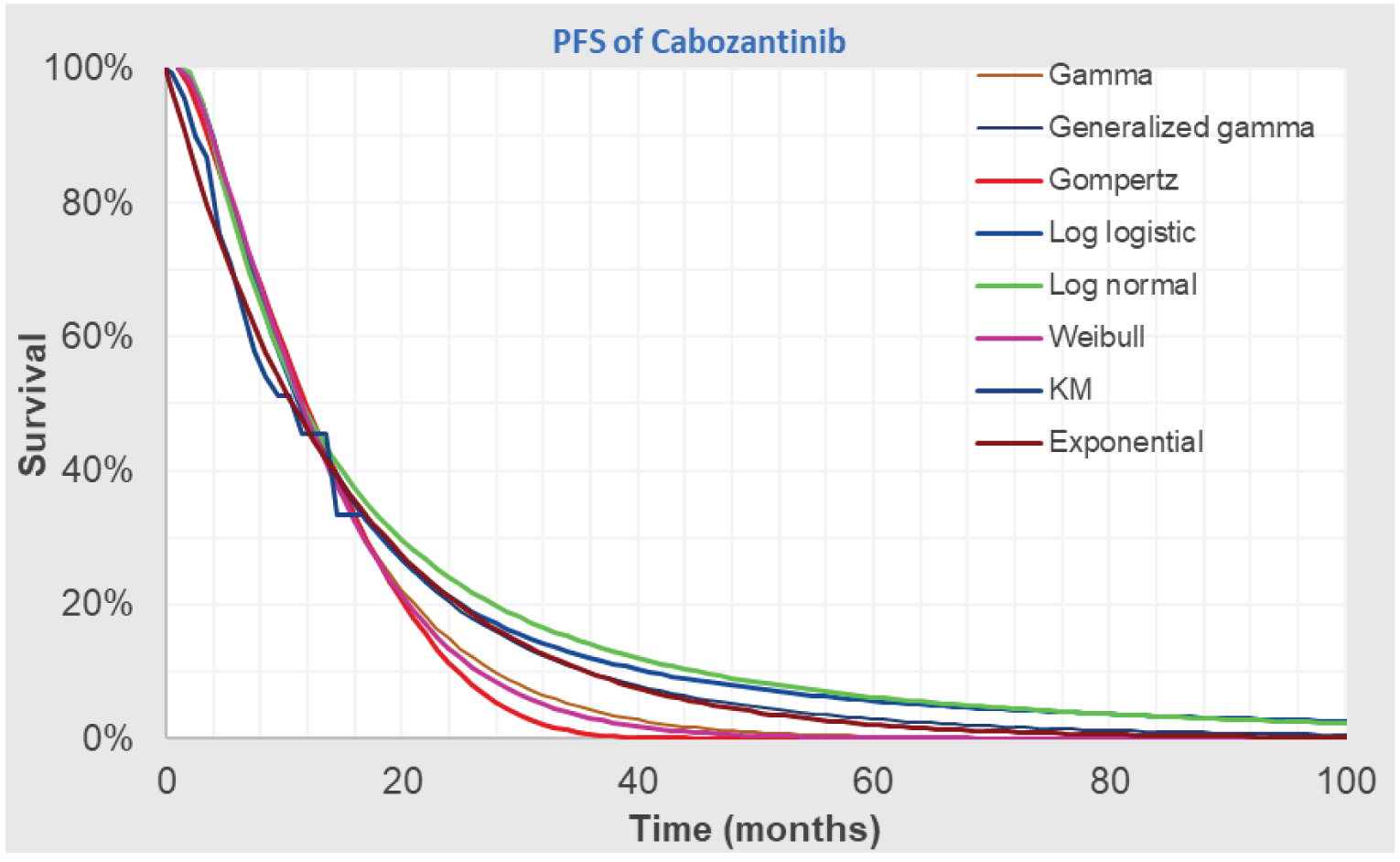
Source: Sponsor’s pharmacoeconomic submission2
Figure 4: Observed and Extrapolated OS Data for BSC (Crossover – RPSFT Adjusted)

Source: Sponsor’s pharmacoeconomic submission2
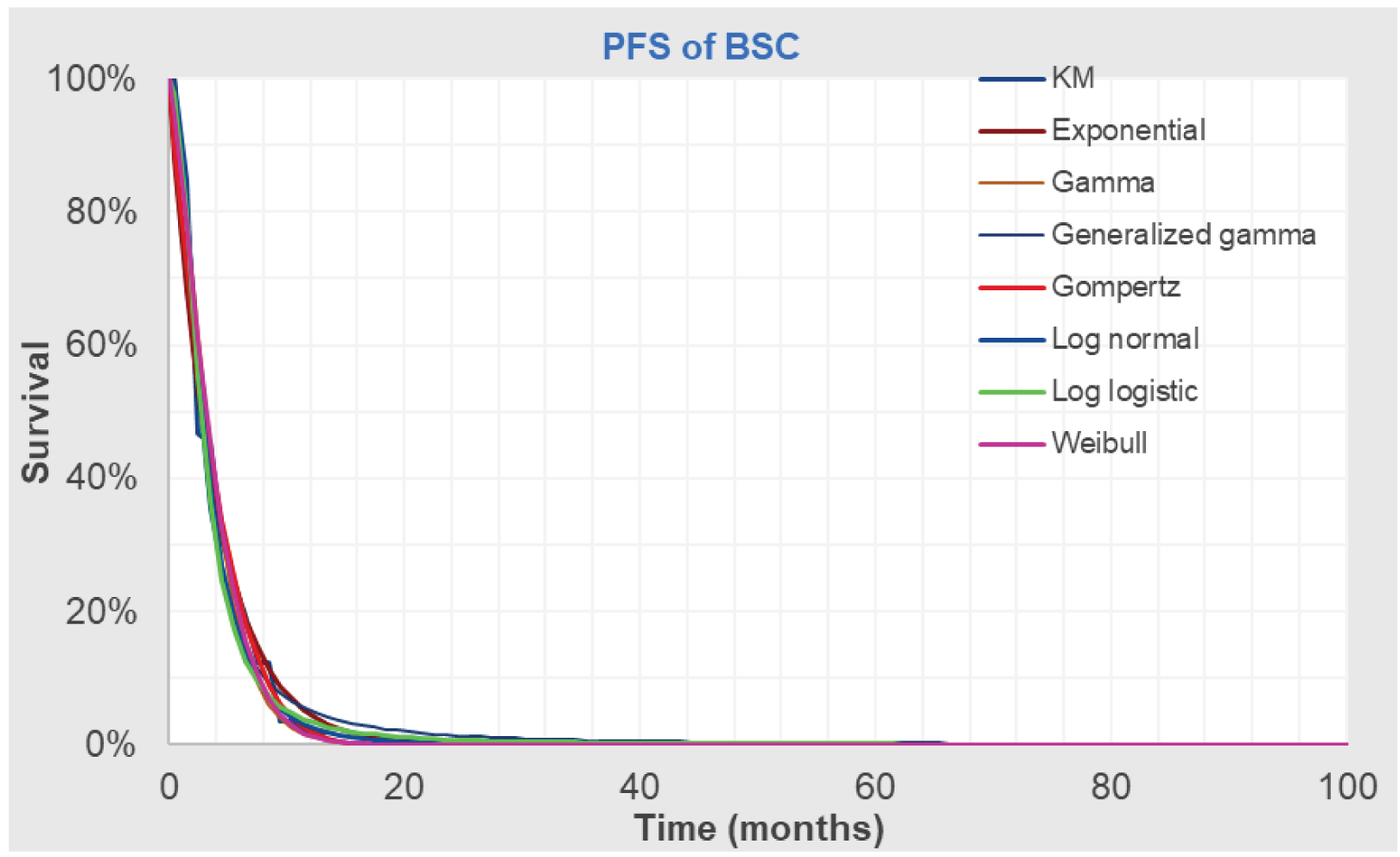
Detailed Results of the Sponsor’s Base-Case
Table 11: Disaggregated Summary of the Sponsor’s Economic Evaluation Results
Parameter | Cabozantinib + BSC | BSC | Incremental |
|---|---|---|---|
Undiscounted LYs | |||
Total | 3.10 | 2.25 | 0.85 |
Progression free | 1.53 | 0.36 | 1.17 |
Progressed | 1.57 | 1.89 | -0.32 |
Discounted QALYs | |||
Total | 2.07 | 1.26 | 0.80 |
Progression free | 1.29 | 0.31 | 0.98 |
Progressed | 0.78 | 0.96 | -0.18 |
Discounted costs ($) | |||
Total | $203,451 | $37,888 | $165,563 |
Total drug acquisition | $163,338 | $0 | $163,338 |
Total drug administration | $0 | $0 | $0 |
Treatment-specific monitoring | $1,278 | $0 | $1,278 |
Disease management – Progression Free | $2,244 | $536 | $1,708 |
Disease management - Progressed | $2,271 | $2,773 | -$502 |
Other Costs (terminal care, AE) | $34,321 | $34,578 | -$257 |
ICER ($/QALY) | $206,389 | ||
AE = adverse event, BSC = best supportive care; ICER = incremental cost-effectiveness ratio; LY= life-year, QALY = quality-adjusted life-year.
Appendix 4: Additional Details on the CADTH Reanalyses and Sensitivity Analyses of the Economic Evaluation
Note that this appendix has not been copy-edited.
Detailed Results of CADTH Base-Case
Table 12: Disaggregated Summary of CADTH’s Economic Evaluation Results
Parameter | Cabozantinib + BSC | BSC | Incremental |
|---|---|---|---|
Undiscounted LYs | |||
Total | 2.22 | 2.03 | 0.19 |
Progression free | 1.05 | 0.36 | 0.69 |
Progressed | 1.17 | 1.67 | -0.50 |
Discounted QALYs | |||
Total | 1.46 | 1.28 | 0.18 |
Progression free | 0.75 | 0.26 | 0.49 |
Progressed | 0.71 | 1.03 | -0.32 |
Discounted costs ($) | |||
Total | $153,974 | $37,759 | $116,215 |
Total drug acquisition | $114,958 | $0 | $114,958 |
Total drug administration | $0 | $0 | $0 |
Treatment-specific monitoring | $890 | $0 | $890 |
Disease management – Progression Free | $1,581 | $537 | $1,044 |
Disease management - Progressed | $1,707 | $2,457 | -$750 |
Other Costs (terminal care, AE) | $34,837 | $34,766 | $71 |
ICER ($/QALY) | $664,742 | ||
AE = adverse event, BSC = best supportive care; ICER = incremental cost-effectiveness ratio; LY= life-year, QALY = quality-adjusted life-year.
Scenario Analyses
Table 13: Summary of Scenario Analyses Conducted on CADTH Base-Case
Scenario | Drug | Total Costs | Total QALYs | ICER ($/QALY) |
|---|---|---|---|---|
CADTH base-case | BSC | $37,759 | 1.28 | Ref. |
Cabozantinib + BSC | $153,974 | 1.46 | $664,742 | |
1. TTD informed treatment discontinuation | BSC | $37,549 | 1.25 | Ref. |
Cabozantinib + BSC | $151,849 | 1.45 | $563,409 |
BSC = best supportive care; ICER = incremental cost-effectiveness ratio; OS = overall survival; TTD = time to treatment discontinuation; QALY = quality-adjusted life-year.
Appendix 5: Submitted Budget Impact Analysis and CADTH Appraisal
Note that this appendix has not been copy-edited.
Table 14: Summary of Key Take-Aways
Key Take-aways of the budget impact analysis (BIA) |
|---|
|
Summary of Sponsor’s BIA
The sponsor submitted a BIA to estimate the 3-year budget impact of reimbursing cabozantinib for the treatment of adult patients with locally advanced or metastatic DTC that has progressed following prior VEGFR-targeted therapy and who are RAI-R or ineligible. The analysis was taken from the perspective of the Canadian public drug plan. A 3-year time horizon was used from 2023 to 2025, with 2022 as the base year. Key inputs to the BIA are documented in Table 15.
The sponsor estimated the eligible population using an epidemiological approach. The target population size was estimated using the age-standardized incidence rate of thyroid cancer in the overall population followed by further specifications of population size based on the proportion of patients assumed to have RAI-R DTC, the proportion of patients who have received first-line systemic treatment for their RAI-R, and the proportion of patients who would undergo subsequent treatment after first-line therapy.
The BIA compared 2 scenarios to determine the incremental budget impact of reimbursing cabozantinib. The reference case scenario assumed that 100% of eligible patients would be on BSC.17 The new drug scenario included cabozantinib along with BSC.17 In the sponsor’s base-case, costs related to drug acquisition and markup/dispensing fees were considered.17 BSC was assumed to be equal in both arms and therefore was assigned a treatment cost of $0. Cabozantinib was costed at the recommended dosage of 60 mg once daily.1
Table 15: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as year 1 / year 2 / year 3 if appropriate) |
|---|---|
Target population | |
Incidence of thyroid cancer in adults (18+ years) | 0.0194% |
Proportion of DTC patients | 90.0% |
RAI-R patients | 10.0% |
RAI-R patients treated with first-line systemic treatment | 70.0% |
Average annual percent change | 4.20% |
RAI-R patients who would be treated following first-line treatment | 50% |
Number of patients eligible for drug under review | 118 / 123 / 128 |
Market uptake (3 years) | |
Uptake (reference scenario) BSC alone | 100% / 100% / 100% |
Uptake (new drug scenario) Cabozantinib + BSC BSC alone | 25% / 35% / 45% 75% / 65% / 55% |
Cost of treatment (per patient) | |
Total cost of treatmenta Cabozantinib + BSC BSC Alone | $||||| $0 |
BSC = best standard of care, DTC = differentiated thyroid cancer; RAI-R = radioactive iodine-refractory.
aTotal cost of cabozantinib treatment were calculated assuming a mean dose intensity of 100% and a treatment duration is ||||| months.17
Summary of the Sponsor’s BIA Results
The estimated budget impact of reimbursing cabozantinib for the treatment of adult patients with locally advanced or metastatic DTC that has progressed following prior VEGFR-targeted therapy and who are RAI-R or ineligible in year 1, year 2, year 3 was $2,841,992, $4,145,898, and $5,554,319, respectively. The 3-year total budget impact was $12,542,210.
CADTH Appraisal of the Sponsor’s BIA
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
Cabozantinib market shares were underestimated. The sponsor used clinical expert opinion and internal market research to determine the market share of cabozantinib in the new therapy scenario. Clinical experts consulted by CADTH noted that the market share values for cabozantinib were underestimated. Cabozantinib is expected to capture the market rapidly due to it being the first therapy available for the indicated population. If available, disease specialists are expected to prescribe this drug to most patients except those who have access to alternate investigative therapies or who are reluctant to receive further treatment.
To address this limitation, CADTH set the market share values for cabozantinib to 55%, 65%, and 75% in year 1, 2, and 3 respectively as informed by the clinical experts consulted by CADTH.
Uncertainty in the number of patients eligible for public funding. The sponsor assumed that provinces with cancer agencies (i.e., Alberta, British Columbia, Saskatchewan, Manitoba, and Nova Scotia) and Non-Insured Health Benefits would have 100% coverage rates and that the remaining provinces would have coverage rates between 30% to 50%, as informed by a report from the Conference Board of Canada.18 CADTH noted that given the mean age of patients recruited in the COSMIC-311 trial population was 65 years old and due to the oral formulation of cabozantinib, the public coverage in provinces without cancer agencies may be higher.19
Due to limitations in data availability, CADTH was unable to address this limitation. If a higher proportion of public coverage in provinces without cancer agencies is expected, this would increase the 3-year incremental budget impact of cabozantinib.
CADTH Reanalyses of the BIA
Based on the limitation identified, CADTH’s base-case included a higher proportion of market share for cabozantinib in year 1, 2, and 3.
Table 16: CADTH Revisions to the Submitted BIA
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor’s base-case | ||
1. Cabozantinib Market Share Values for Year 3 | Hard coded market share values for cabozantinib in the new drug scenario | Cell value updated to pull in market share inputs from model input sheet |
Changes to derive the CADTH base-case | ||
1. Cabozantinib Market Share | Year 1: 25% Year 2: 35% Year 3: 45% | Year 1: 55% Year 2: 65% Year 3: 75% |
CADTH base-case | Reanalysis 1 | |
The results of the CADTH stepwise reanalyses are presented in summary format in Table 17 and a more detailed breakdown is presented in Table 18. Based on the CADTH base-case, the estimated incremental budget impact of reimbursing cabozantinib is $6,252,383 in year 1, $7,699,525 in year 2, and $9,257,199 in year 3. The -3-year total budget impact was $23,209,107.
The sponsor estimated that 50% of RAI-R DTC patients would be treated with 2L therapy, based on internal market. However, a clinical expert consulted by CADTH noted that this may be an overestimation as fewer patients would be expected to be able to receive subsequent therapy. Therefore, a scenario analysis was conducted in which the estimated number of RAI-R patients who would be treated following first-line treatment was reduced from 50% to 20%. The budget impact from this analysis was $8,783,122 over 3 years. Thus, the budget impact is highly sensitive to assumptions around the number of eligible patients.
A scenario analysis was conducted in which the price reduction for cabozantinib of 95%, as recommended from the pharmacoeconomic report for RAI-R DTC patients who have progressed following prior VEGFR-targeted therapies, was used. Results of this analysis estimated a 3-year budget impact of $1,239,920.
Table 17: Summary of the CADTH Reanalyses of the BIA
Stepped analysis | Three-year total |
|---|---|
Submitted base-case | $12,542,210 |
CADTH reanalysis 1 and base-case | $23,209,107 |
BIA = budget impact analysis.
Table 18: Detailed Breakdown of the CADTH Reanalyses of the BIA
Stepped analysis | Scenario | Year 0 (current situation) | Year 1 | Year 2 | Year 3 | Three-year total |
|---|---|---|---|---|---|---|
Submitted base-case | BSC | $0 | $0 | $0 | $0 | $0 |
Cabozantinib + BSC | $0 | $2,841,992 | $4,145,898 | $5,554,319 | $12,542,210 | |
Budget impact | $0 | $2,841,992 | $4,145,898 | $5,554,319 | $12,542,210 | |
CADTH base-case | BSC | $0 | $0 | $0 | $0 | $0 |
Cabozantinib + BSC | $0 | $6,252,383 | $7,699,525 | $9,257,199 | $23,209,107 | |
Budget impact | $0 | $6,252,383 | $7,699,525 | $9,257,199 | $23,209,107 | |
CADTH scenario analysis: 95% price reduction (informed by the pharmacoeconomic model) | BSC | $0 | $0 | $0 | $0 | $0 |
Cabozantinib + BSC | $0 | $334,026 | $411,338 | $494,555 | $1,239,920 | |
Budget impact | $0 | $334,026 | $411,338 | $494,555 | $1,239,920 | |
CADTH scenario analysis: proportion of patients who would be treated following first-line treatment (20%) | BSC | $0 | $0 | $0 | $0 | $0 |
Cabozantinib + BSC | $0 | $2,703,209 | $3,328,879 | $4,002,337 | $10,034,424 | |
Budget impact | $0 | $2,703,209 | $3,328,879 | $4,002,337 | $10,034,424 | |
CADTH scenario analysis: exclude markup and dispensing fees | BSC | $0 | $0 | $0 | $0 | $0 |
Cabozantinib + BSC | $0 | $5,915,290 | $7,284,411 | $8,758,103 | $21,957,804 | |
Budget impact | $0 | $5,915,290 | $7,284,411 | $8,758,103 | $21,957,804 |
BSC = best supportive care, BIA = budget impact analysis.
Stakeholder Input
Patient Input
Canadian Cancer Society and Thyroid Cancer Canada
About Canadian Cancer Society and Thyroid Cancer Canada
Website Link for Canadian Cancer Society: https://cancer.ca/en
Our purpose: To unite and inspire all Canadians to take control of cancer.
Our mission: In trusted partnership with donors and volunteers, we improve the lives of all those affected by cancer through world-class research, transformative advocacy and compassionate support.
We set ourselves apart from other cancer charities by taking a comprehensive approach against cancer. We are also the only national charity that supports all Canadians living with all cancers across the country. We shared our survey to endometrial cancer patients and caregivers through our http://CancerConnection.ca forums as well as through patient panels.
Website link for Thyroid Cancer Canada: https://www.thyroidcancercanada.org/
Our Mission: Thyroid Cancer Canada is a national organization of thyroid cancer survivors dedicated to providing emotional support and information to those affected by the disease.
Information Gathering
The Canadian Cancer Society gathered perspectives through survey responses from patients and caregivers. At the Canadian Cancer Society, we reached out to patients through our own thyroid cancer panel and our Cancer Connection forums with a call to action to complete an interview or survey. We also reached out to clinician investigators in the COSMIC-311 trial, the IPSEN Cares program and several Canadian and international thyroid organizations including the Thyroid Foundation of Canada, the American Thyroid Association, the Thyroid Cancer Survivors’ Association, INC, and Thyroid Federation International. Thyroid Cancer Canada also shared these opportunities with their networks through social media. Due to how rare RAI-refractory DTC is, we were unable to secure a patient interview, but were able to secure two patients to complete the survey. Of the 2 survey respondents, one had experience with cabozantinib. Both identified as a patient who currently has differentiated thyroid cancer that has progressed following prior treatments who are also radioactive iodine-resistant or not eligible for radioactive iodine therapies. The data was gathered within the time frame of April 18, 2022 – May 17, 2022.
Due to survey respondents being anonymous, patients will be referred to as Patient 1 and Patient 2 in this report. Patient 2 had tried cabozantinib.
Demographic Information for Survey Respondents
For inclusivity, patients had six options available to identify their gender including man, women, non-binary or third gender, two-spirit, prefer not to say, and prefer to self-describe with an open field. Additionally, patients were provided 16 options to identify their racial or ethnic background.
Patient 1 was a white male from Alberta aged 60 -69 years with an annual household income of $20,000 – $39,999 before tax. Patient 2, who tried cabozantinib, was a white female from Alberta aged 50 – 59 years with an annual household income of $40,000 – $59,999 before tax.
Disease Experience
Patients with RAI-refractory differentiated thyroid cancer who have progressed following prior therapy face aggressive disease, have a poor prognosis and no standard treatment option. This type of thyroid cancer is extremely rare, occurring with an estimated incidence of 4-5 cases per year per million people (Schmidt A, et al 2017). In this survey, patients were asked a series of questions about their disease experience and quality of life.
How much of an impact do symptoms associated with differentiated thyroid cancer have on your day-to-day activities and quality of life?
There were 9 moderate impact selections across the two patients, placing 50% of responses in the moderate impact range. The ability to work, travel and exercise were scored as causing a moderate impact on the day to day and quality of life for both patients. The ability to conduct household chores, fulfill family obligations and maintain mental health also scored in the moderate impact range for Patient 2. Patient 2 also identified three areas in which there was a small impact on their quality of life including the ability to spend time with family and friends, the ability to concentrate and fulfill practical needs (dressing, bathing preparing meals). A detailed breakdown of responses can be viewed in Table 1.
Table 1: Distribution of the Impacts on Day-to-Day Activities and Quality of Life
Task | Not applicable/ No impact | Small impact | Moderate impact | Significant impact | I’m not sure |
|---|---|---|---|---|---|
Ability to work | — | — | Patient 1 and 2 | — | — |
Ability to travel | — | — | Patient 1 and 2 | — | — |
Ability to exercise | — | — | Patient 1 and 2 | — | — |
Ability to conduct household chores | Patient 1 | — | Patient 2 | — | — |
Ability to fulfill family obligations | Patient 1 | — | Patient 2 | — | — |
Ability to spend time with family and friends | Patient 1 | Patient 2 | — | — | — |
Ability to concentrate | — | Patient 2 | — | — | Patient 1 |
Ability to fulfill practical needs (dressing, bathing, preparing meals) | Patient 1 | Patient 2 | — | — | |
Ability to maintain positive mental health | — | — | Patient 2 | — | Patient 1 |
Experiences With Currently Available Treatments
What is the greatest financial barrier related to your treatment(s)?
Respondents had nine potential financial barriers to choose from and selected the one greatest financial barrier they are facing from the list. They also had an open field option if their greatest financial barrier was not present in the list.
Patient 1 indicated that loss of income due to absence from work was his greatest financial barrier. This coincides with their response in Table 1, indicating that his ability to work has been impacted by their cancer. As loss of income from work impacts annual household income, his annual household income would likely be higher than the reported $20,000 – $39,999 if cancer were not a factor.
Patient 2 indicated that transportation (gas, parking fees, public transit etc.) was her greatest financial barrier related to her treatment.
How many lines of treatment have you undergone? Since your diagnosis of differentiated thyroid cancer, which treatments have you tried?
A description of what a line of treatment entails was provided. Both patients indicated they underwent three or more lines of treatment. Patient 1 had tried both surgery and chemotherapy, while Patient 2 had tried radioactive iodine therapy, lenvatinib, cabozantinib, surgery, levothyroxine and external beam radiation. Patients had an opportunity to disclose in an open field if they had tried any additional treatments, however neither of them identified any others. The treatments that each patient had tried to date is depicted below in Table 2.
Table 2: Treatments Tried by Survey Respondents
Treatment | Patient 1 | Patient 2 |
|---|---|---|
Radioactive Iodine therapy | — | Yes |
Lenvatinib (Lenvima) | — | Yes |
Sorafenib (Nexavar) | — | — |
Cabozantinib (Cabometyx) | — | Yes |
Surgery | Yes | Yes |
Thyroid hormone therapy (levothyroxine) | — | Yes |
External beam radiation | — | Yes |
Chemotherapy | Yes | — |
If applicable, please specify which drugs or therapies you are currently using to treat your cancer.
Patient 1 did not disclose any current treatments. Patient 2 indicated that they are currently taking cabozantinib.
How much of an impact do the following cancer treatment side effects have on your daily life?
Table 3 below how impactful prevalent cancer treatment side effects were in general for these two patients. This question was asked to identify which treatment side effects had the most significant negative impacts on patients, and therefore indicate what side effects would be the most ideal to avoid in new treatments or try to avoid in current treatments. For context, refer to Table 2 to review what treatments these patients had tried.
The most significant side effect impacts were different for each patient. Patient 1 indicated fatigue impacted them the most significantly. He also felt small impacts on his life from peripheral neuropathy and concentration and focus.
Patient 2 had a much more diverse and significant range of notable impacts from her treatments. This increase in impactful side effects may correlate, in part, with her more diverse treatment experience as indicated in Table 2. The most significantly impacting treatment side effect for Patient 2 was diarrhea. She also scored fatigue, appetite changes, peripheral neuropathy and pain as having a moderate impact. Patient 2 experienced small impacts from increased liver enzymes, hair loss, nausea and vomiting, weight changes, concentration and focus, changes in libido and sexual function and mouth tongue and throat problems such as sores and pain when swallowing.
There was a total of 14 selections indicating a small to significant side effect impact (35% of responses). Patients had an opportunity to describe any side effects having an impact on their life not included in Table 3, however none were identified.
Table 3: Impact of Treatment Side Effects
Side Effects | Not applicable or no impact | Small impact | Moderate impact | Significant impact | I’m not sure |
|---|---|---|---|---|---|
Increased liver enzymes | — | Patient 2 | — | — | Patient 1 |
Fatigue | — | Patient 2 | Patient 1 | — | |
Hair loss | Patient 1 | Patient 2 | — | — | — |
Easy bruising and bleeding | Patient 1 and Patient 2 | — | — | — | — |
Frequent infections | Patient 1 and Patient 2 | — | — | — | — |
Anemia (low red blood cell counts) | Patient 2 | — | — | — | Patient 1 |
Nausea and vomiting | Patient 1 | Patient 2 | — | — | — |
Appetite changes | Patient 1 | — | Patient 2 | — | — |
Constipation | Patient 1 and Patient 2 | — | — | — | — |
Diarrhea | Patient 1 | — | — | Patient 2 | — |
Peripheral neuropathy (numbness, tingling and pain in the nerves) | — | Patient 1 | Patient 2 | — | — |
Kidney problems | Patient 2 | — | — | Patient 1 | |
Weight changes | Patient 1 | Patient 2 | — | — | — |
Concentration and focus | Patient 1 and 2 | — | — | — | |
Changes in libido and sexual function | Patient 1 | Patient 2 | — | — | — |
Fertility problems | Patient 1 Patient and 2 | — | — | — | — |
Pain | Patient 1 | — | Patient 2 | — | — |
Mouth, tongue and throat problems such as sores and pain when swallowing | Patient 1 | Patient 2 | — | — | — |
Blood pressure changes | Patient 1 and Patient 2 | — | — | — | — |
Hand-Foot Syndrome (redness and swelling of the hands or feet) | Patient 1 and Patient 2 | — | — | — | — |
What improvements would you like to see in new treatments that are not achieved in currently available treatments? For example: effectiveness for relieving certain symptoms or side effects, affordability, ease of use etc.
Patient 2 provided a response to this question and indicated that nausea and vomiting was the worst while taking lenvatanib, while diarrhea was the worst while taking cabozantinib. This coincides with her side effect profile in Table 3, as she scored diarrhea as having a significant impact on her life.
No other treatment improvements were indicated by these two patients in the context of this question, however, more detail was collected from Patient 2 in relation to their experience with cabozantinib as displayed in Section 5 of this report.
Improved Outcomes & Experience with Drug Under Review
Patient 2 indicated she had tried cabozantinib and answered additional questions about her experience. This patient indicated that she accessed cabozantinib though a clinical trial.
What are the side effects that you have experienced with cabozantinib (Cabometyx)? Please rate them on a scale of 1 to 5 (1 is "completely intolerable" and 5 is "very tolerable").
Side effect tolerability was explored to find out if the side effects associated with cabozantinib allowed patients to live an acceptable quality of life. The patient was provided with a list of common and uncommon side effects associated with cabozantinib. She did not experience the following side effects: hair loss, easy bruising and bleeding or anemia, frequent infections, kidney problems, fertility problems or Hand-Foot Syndrome (redness or swelling in the hands or feet). Figure 1 below depicts the tolerability of the side effects the patient experienced. Overall, side effects of cabozantinib were rated as very tolerable with the exception of diarrhea.
When asked if there were any other side effects caused by cabozantinib, the patient indicated she experiences dehydration with no appetite to drink. She did not indicate the tolerability of this side effect.
Patient 2 was asked to rate statements about cabozantinib on a scale of strongly disagree to strongly agree. Overall, she strongly felt the side effects were tolerable, strongly agreed that she would choose to take cabozantinib again considering the side effects, and strongly agreed that this medication was easy to use. She also agreed that cabozantinib has been effective at controlling her cancer and that the pill form allowed her to spend less time in the clinic receiving treatment.
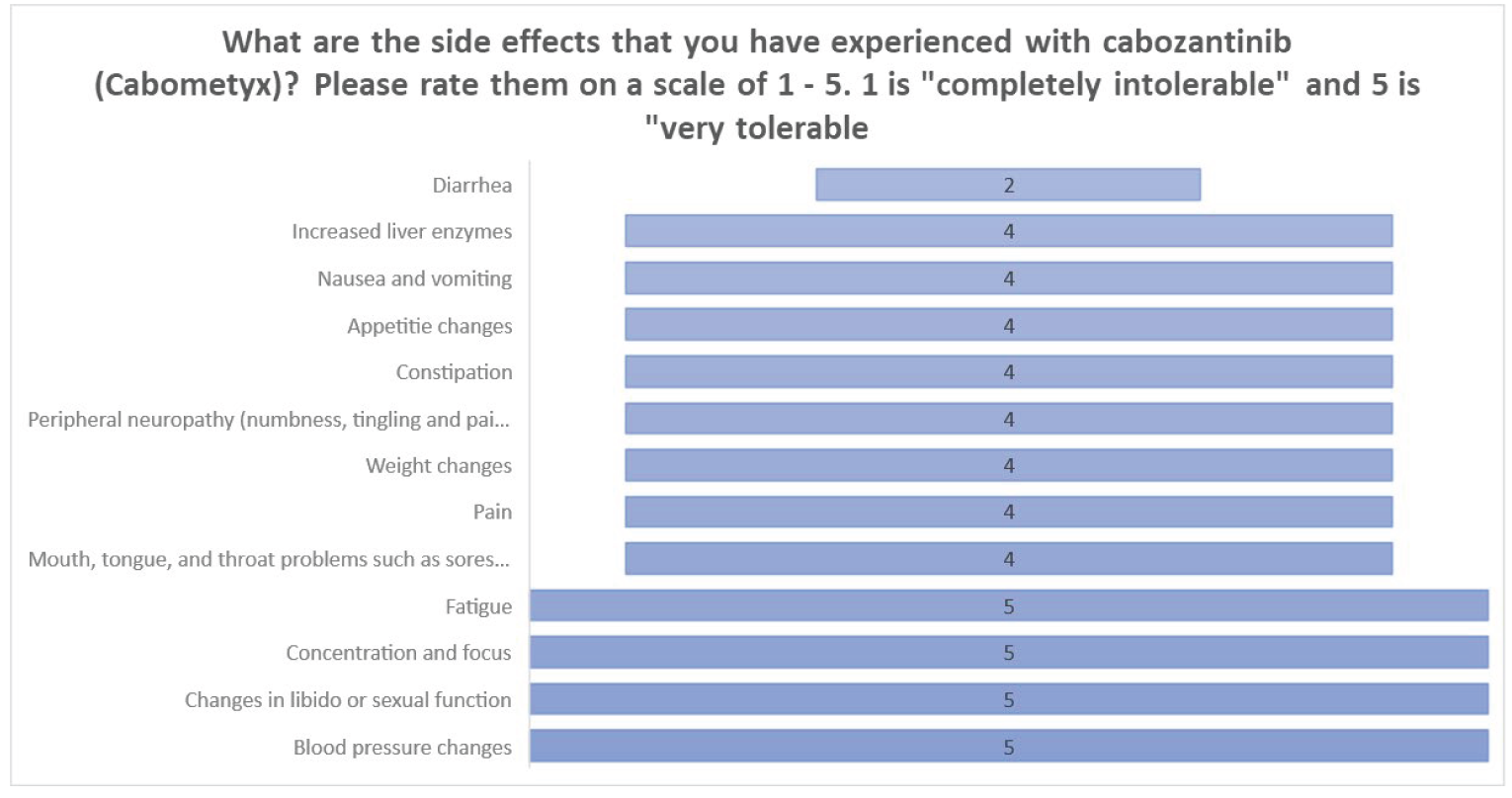
How much do you agree or disagree with the following statements about cabozantinib (Cabometyx)?
Table 4: Patients’ Level of Agreement on Statements Related to Cabozantinib
Statements | Patient response |
|---|---|
Overall the side effects of Cabometyx were tolerable | Strongly agree |
Considering the side effects I experienced so far, I would still choose to take Cabometyx | Strongly agree |
Cabometyx has been effective at controlling my cancer | Agree |
Cabometyx pills allowed me to spend less time in the clinic receiving treatment | Agree |
Cabometyx pills were easy to use | Strongly agree |
Anything Else?
Overall, the sentiments expressed across survey responses include:
Differentiated thyroid cancer caused moderate impacts in the ability to work, travel exercise, conduct household chores, fulfill family obligations and maintain mental health.
The greatest financial burdens for these patients were loss of income from work as well as transportation costs due to cancer treatment.
Fatigue and diarrhea were the most life impacting side effects reported from DTC treatments in general and were deemed significant. In addition, at least one patient indicated moderate impacts related to appetite changes, peripheral neuropathy and pain.
Patient 2 experienced 13 side-effects from cabozantinib, however, she found them all very tolerable with the exception of diarrhea. Patient 2 also strongly agreed that considering the side effects, she would still choose to take cabozantinib.
Patient 2 indicated cabozantinib was effective at controlling her cancer, allowed her to spend less time in the clinic receiving treatment and the pills were east to take.
Considerations for Significant Unmet Need
There are currently no approved/funded treatment options for radioactive iodine-refractory (or ineligible) patients who progress after VEGFR-targeted therapies, creating an urgent medical need for treatments. RAI-refractory DTC is extremely rare, with an estimated incidence of 4-5 cases per year per million people. Considering the rarity of this cancer, the CADTH/pERC recommendations framework that includes Considerations for Significant Unmet Need as described in the Procedures for CADTH Reimbursement Reviews (March 2022), section 9.3.1 should be applied.
In Section 9.3 Rarity of Condition is one of the described considerations for significant unmet need as follows:
is life-threatening, seriously debilitating, or both serious and chronic in nature
affects a relatively small number of patients (incidence of fewer than 5 in 10,000, but typically closer to 1 in 100,000)
In addition, section 9.3 Absence of Alternatives is another one of the described considerations for significant unmet need to be considered. Absence of alternatives is described as follows:
There is an absence of clinically effective drug or non-drug alternative treatments.
Substantial morbidity and mortality exist despite the available drug or non-drug alternative treatments.
In Section 9.3 Clinical Data is one of the described factors that contribute to uncertainty of clinical benefit which is limited to surrogate end points. The COSMIC-311 trial had as its primary endpoints: objective response rate and progression-free survival (Brose MS et al, 2021).
As the treatment and disease under review meets the criteria for application of the deliberative framework that includes Considerations for Significant Unmet Need, this framework should be applied during the evaluation.
References
Angelica Schmidt, Laura Iglesias, Michele Klain,Fabián Pitoia, Martin J. Schlumberger. Radioactive iodine-refractory differentiated thyroid cancer: an uncommon but challenging situation. The Archives of Endocrinology and Metabolism – 2017;61/1
Prof Marcia S Brose, MD, Prof Bruce Robinson, MD, Prof Steven I Sherman, MD, Jolanta Krajewska, MD, Prof Chia- Chi Lin, MD, Fernanda Vaisman, MD et al. Cabozantinib for radioiodine-refractory differentiated thyroid cancer (COSMIC-311): a randomised, double-blind, placebo-controlled, phase 3 trial. The Lancet Oncology – 2021
Conflict of Interest Declaration — Canadian Cancer Society and Thyroid Cancer Canada
To maintain the objectivity and credibility of the CADTH reimbursement review process, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This Patient Group Conflict of Interest Declaration is required for participation. Declarations made do not negate or preclude the use of the patient group input. CADTH may contact your group with further questions, as needed.
Did you receive help from outside your patient group to complete this submission? If yes, please detail the help and who provided it.
Thyroid Cancer Canada shared this survey with their patient networks. Robert Bick provided consultancy.
Did you receive help from outside your patient group to collect or analyze data used in this submission? If yes, please detail the help and who provided it.
The Canadian Cancer Society did not receive help from outside our organization in analysing data or developing this submission.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review.
Table 5: Conflict of Interest Declaration for Canadian Cancer Society and Thyroid Cancer Canada
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
No COI | — | — | — | — |
Ipsen has not provided funds to CCS. Please let us know if you need information related to funding from other pharma companies that provide funds to CCS. To the best of our knowledge there are no existing conflicts of interest.
Clinician Input
The Medical Advisory Panel of Thyroid Cancer Canada and Other Thyroid Cancer-Treating Physicians
About The Medical Advisory Panel of Thyroid Cancer Canada and Other Thyroid Cancer-Treating Physicians
The physicians participating in this input submission are physicians who treat head & neck cancers and endocrine cancers, and who contribute to the knowledge of thyroid cancer and its treatments, including participating in clinical trials, conducting observational research, and involvement in local/provincial and national clinical guideline development and health technology assessment. Some of the participating physicians are members of The Medical Advisory Panel of Thyroid Cancer Canada, and some physicians were investigators in the COSMIC-311 trial: A Study of Cabozantinib Compared With Placebo in Patients With Radioiodine-refractory Differentiated Thyroid Cancer Who Have Progressed After Prior Vascular Endothelial Growth Factor Receptor (VEGFR) -Targeted Therapy.
Information Gathering
Information was gathered through personal experience in treating patients with thyroid cancer, literature review, and virtual discussion among experts. Some of the contributors to this submission were investigators in COSMIC-311 trial.
Current Treatments and Treatment Goals
Differentiated thyroid cancer (DTC) is the most common endocrine malignancy and is increasing in incidence. Curative treatment of DTC requiring surgery, followed in some cases by thyroid stimulating hormone (TSH) suppression and radioactive iodine (RAI) therapy is successful in the majority of patients; however, some patients develop incurable local and/or metastatic disease. The estimated mortality rate associated with incurable disease is 0.5 deaths/100,000 population annually (Faugeras L, Pirson A-S, Donckier J, et al. Refractory thyroid carcinoma: which systemic treatment to use? Ther Adv Med Oncol 2018;10:1758834017752853). Despite the appearance of being differentiated, progressing metastatic DTC is associated with diminishing treatment options with a decreased likelihood of durable response.
While differentiated thyroid cancer (DTC) is the most common endocrine malignancy, radioiodine (RAI)- refractory differentiated thyroid cancer is extremely rare.
In the radioiodine-refractory DTC setting, the first line of therapy is typically a VEGFR-targeted therapy (sorafenib or lenvatinib). Lenvatinib has become the preferred treatment option over sorafenib for 1st line treatment of DTC. Best supportive care is also used in this setting where appropriate. In the practice changing SELECT study comparing lenvatinib 24 mg daily to placebo and noted median PFS was 18.3 months versus 3.6 months (HR, 0.21; P<0.001) and response rate was 64.8% versus 1.5% (P<0.001).
Lenvatinib had a discontinuation rate for toxicity of 14.2%. The post hoc analysis noted an OS benefit in patients with lung metastases > 1 cm regardless of the high cross over rate of 89%. Sorafenib for RAIR DTC in comparison, noted an improvement in PFS compared to placebo (10.8 m vs 5.8 m, HR 0.59, p<0.001) with a discontinuation rate of 18.8% for toxicity. As a result, sorafenib received a negative recommendation from pCODR in 2015 because they were unable to conclude that there was a net clinical benefit with sorafenib compared to placebo in this population. While a statistically significant improvement in PFS was observed, there concerns with the decline in quality of life, the rates of high-grade toxicity, and uncertainty in overall survival benefit of sorafenib versus placebo.
Palliative treatment with doxorubicin (Adriamycin) is occasionally tried where appropriate and best supportive care is the only remaining regular option.
Treatment Gaps (Unmet Needs)
Considering the treatment goals, please describe goals (needs) that are not being met by currently available treatments.
Recognizing that there are currently no approved/funded options for patients who are radioactive iodine- refractory (or ineligible) who progress after VEGFR-targeted therapies, there is an urgent unmet medical need for treatments for these patients.
Place in Therapy
How would the drug under review fit into the current treatment paradigm?
Cabozantinib is expected to fill an urgent unmet need for patients who progress on prior therapy. The progression-free survival benefit demonstrated in the phase III COSMIC-311 trial means cabozantinib is clinically important for patients who otherwise would have run out of options. In the study cabozantinib showed significant improvement in PFS over placebo: median not reached versus 1·9 month; HR 0·22 (96% CI 0·13–0·36; p<0·0001). The discontinuation rate for cabozantinib toxicity was 5%. Median overall survival was not reached in either treatment group (HR 0·54), with overall survival estimates of 85% in the cabozantinib group versus 73% in the placebo group at 6 months. The finding of the COSMIC-311 study was comparable to the PFS benefit observed with lenvatinib in the SELECT study with lower rates of discontinuation due to side effects from treatment. The preliminary OS data is interesting and will be informative with greater maturity. In Canada, no other therapies are funded beyond lenvatinib in first line and cabozantinib demonstrates improvement in disease control with reasonable side effect profile that offer appropriate patients an option for therapy.
Which patients would be best suited for treatment with the drug under review? Which patients would be least suitable for treatment with the drug under review?
We believe the inclusion criteria for the COSMIC-311 trial define the patients best suited for the treatment under review:
Histologically or cytologically confirmed diagnosis of Differentiated Thyroid Cancer (DTC) Radiographic or symptomatic progression of disease on prior VEGFR TKI
Previously treated with or deemed ineligible for treatment with Iodine- 131 for differentiated thyroid cancer (DTC)
Previously treated with at least one of the following vascular endothelial growth factor receptor (VEGFR)-targeting tyrosine kinase inhibitor (TKI) agents for DTC: lenvatinib or sorafenib. Note: Up to two prior VEGFR-targeting TKI agents are allowed Eastern Cooperative Oncology Group (ECOG) performance status (PS) of 0 or 1.
Additionally, we believe that patients with progressing non-measurable disease (such as bone metastases) should not be excluded in a real-world setting.
What outcomes are used to determine whether a patient is responding to treatment in clinical practice? How often should treatment response be assessed?
Clinical assessment, tumour markers and radiological imaging (CT/MRI) is generally done every 3-4 months to assess whether a patient is responding to treatment.
What factors should be considered when deciding to discontinue treatment with the drug under review?
In general, systemic therapy would be stopped when one or more of the following was met:
patient decision to stop
adverse events significant to stop therapy
disease progression
What settings are appropriate for treatment with [drug under review]? Is a specialist required to diagnose, treat, and monitor patients who might receive [drug under review]?
Cabozantinib can be taken at home as prescribed by a medical oncologist. There may be some patients managed by endocrinologists, depending on geographical location.
Additional Information
Radioiodine (RAI)-refractory differentiated thyroid cancer is extremely rare with significant unmet need. As such, we urge CADTH/pERC to apply the recommendations framework that includes Considerations for Significant Unmet Need as described in the Procedures for CADTH Reimbursement Reviews (March 2022), section 9.3.1.
In Section 9.3 Rarity of condition is one of the described considerations for significant unmet need as follows:
is life-threatening, seriously debilitating, or both serious and chronic in nature
affects a relatively small number of patients (incidence of fewer than 5 in 10,000, but typically closer to 1 in 100,000)
Note: RAI-refractory DTC is extremely rare occurring with an estimated incidence of 4-5 cases/year/million people.
In Section 9.3 Absence of alternatives is one of the described considerations for significant unmet need as follows:
There is an absence of clinically effective drug or non-drug alternative treatments.
Substantial morbidity and mortality exist despite the available drug or non-drug alternative treatments.
Note: As stated in 4.1, recognizing that there are currently no approved/funded options for patients who are radioactive iodine-refractory (or ineligible) who progress after VEGFR-targeted therapies, there is an urgent unmet medical need for treatments for these patients. Cabozantinib is expected to fill an urgent unmet need for patients who progress on prior therapy
In Section 9.3 Clinical data is one of the described factors that contribute to uncertainty of clinical benefit that includes:
Limited to surrogate end points
Note: The COSMIC-311 trial had as its primary endpoints: objective response rate and progression-free survival
As the treatment and disease under review clearly meet the criteria for application of the deliberative framework that includes Considerations for Significant Unmet Need we urge CADTH/pERC to apply this framework.
Conflict of Interest Declarations — The Medical Advisory Panel of Thyroid Cancer Canada and Other Thyroid Cancer-Treating Physicians
To maintain the objectivity and credibility of the CADTH drug review programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This conflict of interest declaration is required for participation.
Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please see the Procedures for CADTH Drug Reimbursement Reviews (section 6.3) for further details.
Did you receive help from outside your clinician group to complete this submission? If yes, please detail the help and who provided it.
This submission was completed exclusively by the clinicians listed on page 1. Administrative support (such as aggregating conflict of interest declarations) was provided by the Canadian Cancer Society.
Did you receive help from outside your clinician group to collect or analyze any information used in this submission? If yes, please detail the help and who provided it.
Collection and analysis of information used in this submission was done exclusively by the clinicians listed on page 1, including those clinicians that were investigators in the COSMIC-311 study.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review. Please note that this is required for each clinician who contributed to the input — please add more tables as needed (copy and paste). It is preferred for all declarations to be included in a single document.
Declaration for Clinician 1
Name: Monika Krzyzanowska
Position: Medical Oncologist
Date: 19-05-2022
Table 6: Conflict of Interest Declaration for The Medical Advisory Panel of Thyroid Cancer Canada and Other Thyroid Cancer-Treating Physicians — Clinician 1
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Ipsen | X | — | — | — |
Lilly | X | — | — | — |
Roche | X | — | — | — |
Eisai | X | — | — | — |
Declaration for Clinician 2
Name: Dr. Omar Abdelsalam
Position: Assistant professor
Date: 09-05-2022
Table 7: Conflict of Interest Declaration for The Medical Advisory Panel of Thyroid Cancer Canada and Other Thyroid Cancer-Treating Physicians — Clinician 2
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Roche | X | — | — | — |
Lilly | X | — | — | — |
Ipsen | X | — | — | — |
Eisai | X | — | — | — |
Bayer | X | — | — | — |
Amgen | X | — | — | — |
Declaration for Clinician 3
Name: Cheryl Ho
Position: <Enter currently held position>
Date: 16-05-2020
Table 8: Conflict of Interest Declaration for The Medical Advisory Panel of Thyroid Cancer Canada and Other Thyroid Cancer-Treating Physicians — Clinician 3
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Abbvie | X | — | — | — |
Amgen | — | — | — | — |
AstraZeneca | X | — | — | X |
Bayer | X | — | — | — |
BMS | X | — | — | — |
Eisai | X | — | — | — |
EMD Serono | — | — | X | — |
Janssen | X | — | — | — |
Merck | X | — | — | — |
Novartis | X | — | — | — |
Pfizer | X | — | — | — |
Roche | — | — | — | X |
Takeda | X | — | — | — |
Declaration for Clinician 4
Name: Brandon Meyers
Position: Medical Oncologist, Juravinski Cancer Centre
Date: 16-05-2020
Table 9: Conflict of Interest Declaration for The Medical Advisory Panel of Thyroid Cancer Canada and Other Thyroid Cancer-Treating Physicians — Clinician 4
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Ipsen | — | X | — | — |
Declaration for Clinician 5
Name: Irina Rachinsky
Position: Associate Professor, Staff Nuclear Medicine Physician, Department of Medical Imaging, Division of Nuclear Medicine, Schulich School of Medicine and Dentistry, Western University, London, ON
Date: 13-05-2022
Table 10: Conflict of Interest Declaration for The Medical Advisory Panel of Thyroid Cancer Canada and Other Thyroid Cancer-Treating Physicians — Clinician 5
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
No COI | — | — | — | — |
Declaration for Clinician 6
Name: Sebastien Hotte
Position: Medical Oncologist, Juravinski Cancer Centre
Date: 16-05-2020
Table 11: Conflict of Interest Declaration for The Medical Advisory Panel of Thyroid Cancer Canada and Other Thyroid Cancer-Treating Physicians — Clinician 6
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Ipsen | — | X | — | — |
Eisai | — | X | — | — |
Declaration for Clinician 7
Name: Shereen Ezzat
Position: Professor of Medicine & Oncology, Princess Margaret Cancer Centre
Date: 13-5-2022
Table 12: Conflict of Interest Declaration for The Medical Advisory Panel of Thyroid Cancer Canada and Other Thyroid Cancer-Treating Physicians — Clinician 7
Company | Check Appropriate Dollar Range | |||
|---|---|---|---|---|
$0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 | |
Ipsen-Adboard member | X | — | — | — |
Recordati-Adboard member | X | — | — | — |
Merck | X | — | — | — |
Eisai | X | — | — | — |
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third-party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
Redactions: Confidential information in this document may be redacted at the request of the sponsor in accordance with the CADTH Drug Reimbursement Review Confidentiality Guidelines
Stakeholder Input: The views expressed in each submission are those of the submitting organization or individual; not necessarily the views of CADTH or of other organizations. As such, they are independent of CADTH and do not necessarily represent or reflect the view of CADTH. No endorsement by CADTH is intended or should be inferred. By filing with CADTH, the submitting organization or individual agrees to the full disclosure of the information. CADTH does not edit the content of the submissions.
CADTH does use reasonable care to prevent disclosure of personal information in posted material; however, it is ultimately the submitter’s responsibility to ensure no identifying personal information or personal health information is included in the submission. The name of the submitting organization or individual and all conflict-of-interest information are included in the submission; however, the name of the author, including the name of an individual patient or caregiver submitting the patient input, are not posted.
Accessibility: CADTH is committed to treating people with disabilities in a way that respects their dignity and independence, supports them in accessing material in a timely manner, and provides a robust feedback process to support continuous improvement. All materials prepared by CADTH are available in an accessible format. Where materials provided to CADTH by a submitting organization or individual are not available in an accessible format, CADTH will provide a summary document upon request. More details on CADTH’s accessibility policies can be found here.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.