CADTH Reimbursement Review
Pembrolizumab (Keytruda)
Sponsor: Merck Canada Inc.
Therapeutic area: Melanoma adjuvant treatment
This multi-part report includes:
Clinical Review
Pharmacoeconomic Review
Stakeholder Input
Clinical Review
Abbreviations
AE
adverse event
CI
confidence interval
CrI
credible interval
DCO
data cut-off
DMFS
distant metastasis–free survival
ECOG
Eastern Cooperative Oncology Group
EORTC QLQ-C30
European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30
HR
hazard ratio
IA
interim analysis
ICI
immune checkpoint inhibitor
ITC
indirect treatment comparison
ITT
intention to treat
LS
least squares
OS
overall survival
PD-1
programmed cell death receptor-1
PD-L1
programmed cell death ligand 1
PET
positron emission tomography
PFS
progression-free survival
QoL
quality of life
RFS
recurrence-free survival
SAE
serious adverse event
SD
standard deviation
VAS
visual analogue scale
WDAE
withdrawal due to adverse event
WLE
wide local excision
Executive Summary
An overview of the submission details for the drug under review is provided in Table 1.
Item | Description |
|---|---|
Drug product | Pembrolizumab (Keytruda), solution for infusion, 100 mg/4 mL vial |
Indication | Indicated for the adjuvant treatment of adult and pediatric (12 years and older) patients with stage IIB or IIC melanoma following complete resection |
Reimbursement request | As per indication |
Health Canada approval status | NOC |
Health Canada review pathway | Priority review |
NOC date | July 5, 2022 |
Sponsor | Merck Canada Inc. |
NOC = Notice of Compliance.
Introduction
Melanoma is a cancer that begins in the melanocyte cells of the skin, also referred to as cutaneous melanoma. Cutaneous melanoma can develop anywhere on the skin, including the eyes, mouth, genitals, and anal area; however, they are most likely to start on the chest, back, and legs. In contrast, noncutaneous melanoma develop from skin cells other than melanocytes, such as basal cells.1 The first signs of melanoma skin cancer are typically a change in the mole colour, size, or shape. Other common signs and symptoms include a mole that is asymmetric, has an uneven or irregular border, is not the same colour throughout, is large in diameter (more than 6 mm), or is evolving.1 The cancerous growth has the potential to grow into and destroy nearby tissue or metastasize to other parts of the body. The Canadian Cancer Society estimated that 9,000 people living in Canada will be diagnosed with melanoma skin cancer in 2022 and 1,200 will die of it. The Public Health Agency of Canada reported that melanoma accounts for approximately 3.8% of new cancer cases and 1.9% of all cancer deaths in men, and 3.3% and 1.2%, respectively, in women.2 Risk factors for melanoma skin cancer include UV radiation; many moles; atypical moles; congenital melanocytic nevi; familial atypical multiple mole melanoma syndrome; other hereditary conditions (xeroderma pigmentosum, Werner syndrome, retinoblastoma); light-coloured skin, eyes, and hair; personal or family history of skin cancer; CDKN2A gene mutation; and a weakened immune system.
A melanoma diagnosis usually begins with a family physician based on reported signs or symptoms and a skin examination. Patients may then be referred to a specialist, such as a dermatologist or surgeon, as needed.1 The presence of cancerous cells and the extent and characteristics of the disease may be identified by skin biopsy, lymph node biopsy, histology, imaging (CT scan, MRI, chest X-ray, PET scan), and/or blood tests.1 Patients with stage IIB and IIC melanoma are defined as having high-risk, node-negative disease. The primary tumour is thick and/or ulcerated (greater than 4 mm thick with or without ulceration or greater than 2 to 4 mm thick with ulceration), but there is no lymph node involvement.3
According to the clinical experts consulted by CADTH, following a diagnostic biopsy, all patients should undergo wide local excision (WLE) of the primary site, which is a curative-intent surgical procedure. Following definitive WLE, the standard of care is to follow patients for surveillance. As per the 2020 Canadian Melanoma Conference recommendations, surveillance should be conducted by an appropriate specialist, including biannual visits and PET/CT scans with brain MRI among the systemic imaging modalities available.4 The Canadian recommendation statement also states that high-risk surveillance should follow a 5-year schedule, beginning with an intensive 2-year period followed by a less-intensive 3-year period because the median time to relapse for stage IIB to III melanoma is less than 2 years after treatment.4
Pembrolizumab is an immune checkpoint inhibitor (ICI) that binds to programmed cell death receptor-1 (PD-1), resulting in the reactivation of tumour-specific cytotoxic T lymphocytes in the tumour microenvironment.5,6 Pembrolizumab is indicated for the adjuvant treatment of adult and pediatric (12 years and older) patients with stage IIB or IIC melanoma following complete resection.5 Pembrolizumab is administered as an IV infusion over 30 minutes.5 For adults, the recommended dosage for adjuvant treatment of melanoma is either 200 mg every 3 weeks or 400 mg every 6 weeks for up to 1 year or until disease recurrence or unacceptable toxicity. For pediatric patients, recommended dosage for adjuvant treatment of melanoma is 2 mg/kg (up to a maximum of 200 mg) every 3 weeks until disease progression or unacceptable toxicity or for a maximum of 12 months.5 The sponsor has requested pembrolizumab be reimbursed as per the indication. The Notice of Compliance was received on July 5, 2022. In December 2021, the FDA approved pembrolizumab for the adjuvant treatment of adult and pediatric (12 years and older) patients with stage IIB, IIC, or III melanoma following complete resection.7 Pembrolizumab was previously reviewed by CADTH for the adjuvant treatment of patients with stage IIIA to stage IIID cutaneous melanoma and received a recommendation for reimbursement with conditions.8
The objective of this report was to perform a systematic review of the beneficial and harmful effects of pembrolizumab (100 mg/4 mL) administered by IV infusion (200 mg every 3 weeks or 400 mg every 6 weeks for adults; 2 mg/kg every 3 weeks for pediatric patients) for the adjuvant treatment of adult and pediatric (12 years and older) patients with stage IIB or IIC melanoma following complete resection.
Stakeholder Perspectives
The information in this section is a summary of input provided by the patient groups who responded to CADTH’s call for patient input and from clinical experts consulted by CADTH for the purpose of this review.
Patient Input
Two patient groups, the Save Your Skin Foundation (SYSF) and Melanoma Canada, submitted patient input for this review. Both groups included patients from across Canada with melanoma, regardless of cancer stage. The SYSF gathered data through online surveys, virtual roundtables, and one-on-one discussions with 25 patients with melanoma (68% female), 18 of whom received the treatment under review. Melanoma Canada received input from 172 patients with melanoma (67% female) and 15 caretakers through an online survey. Twenty patients from the Melanoma Canada submission indicated they had been on treatment with adjuvant pembrolizumab for stage IIB or IIC melanoma following complete resection.
According to the SYSF input, respondents who were diagnosed with stage II melanoma reported having limited access to available treatment options, which increased their initial fear and anxiety. The Melanoma Canada survey respondents indicated that the main day-to-day impacts of their diagnosis included scarring and disfigurement, fear or anxiety, disrupted sleep, as well as pain, fatigue, and depression. Respondents also indicated mobility and lymphedema issues caused by surgery, including lymph node dissection. Their input suggested that there is an unmet need for treatment options to prevent recurrence of disease because there are currently no treatment options available beyond surgery for stage IIB or IIC disease in Canada.
In both submissions, most patients who had experience with the treatment under review reported experiencing at least 1 side effect. In the SYSF submission, the main side effects reported by the survey respondents included fatigue, cognitive impairment, nausea, skin rash, gastrointestinal problems, and weight loss or gain. Most patients found these side effects to be manageable. In the Melanoma Canada submission, the main reported side effects included fatigue or weakness, skin rash, thyroid or pituitary gland issues, and muscle or joint pain. Most respondents indicated they were willing to accept the side effect profile of pembrolizumab if it could potentially mean that they would not have to deal with a recurrence. A common concern among patients was the length of time and the cost of travel to get to a clinical trial site for treatment. In the submissions received, patients expressed a need for future treatments that would be curative, be accessed close to home and delivered in a timely fashion, allow them to work and continue normal day-to-day activities without significant long-term side effects, and be available to them if their disease was to progress or recur.
Clinician Input
Input From Clinical Experts Consulted by CADTH
The following input was provided by 2 clinical specialists with expertise in the diagnosis and management of stage IIB or IIC melanoma who were consulted by CADTH on this review.
The clinical experts described the prognosis of patients with stage IIB or IIC melanoma as similar to that seen in stage III (lymph node–positive) malignant melanoma. The clinical experts stated that the standard of care for patients with resected stage III melanoma involves systemic treatment as adjuvant treatment after surgery. In contrast, the experts noted there are currently no available systemic therapies other than high-dose interferon — which is rarely used — for adjuvant treatment to surgery for patients with resected stage IIB or IIC melanoma. Given the similarities between the prognoses of patients with stage IIB, IIC, and III melanoma diagnoses, the experts indicated that patients and clinicians would likely want access to systemic treatment with similar adjuvant treatment of these patients.
The clinical experts indicated that pembrolizumab would be the first available systemic therapy for adjuvant use in resected stage IIB or IIC melanoma, although clinical trials investigating the efficacy and safety of nivolumab and encorafenib/binimetinib are ongoing. According to the clinical experts, one would expect that pembrolizumab would be used as monotherapy, with a small minority of patients within this category qualifying for consideration of radiation therapy as adjuvant treatment to surgery. The clinical experts felt that approval of pembrolizumab for adjuvant treatment to surgery for patients with resected stage II melanoma would shift the current treatment paradigm. The clinical experts indicated that, for reference, in their experience the incidence of stage II melanoma diagnoses is roughly twice that of stage III, suggesting a significant increase in the number of patients with melanoma eligible for treatment with adjuvant immunotherapy. However, that number may overestimate the effect of introducing pembrolizumab to the patient population with stage II melanoma because presumably a proportion of patients would recur with nodal disease (at which point they may be candidates for treatment with adjuvant systemic therapy).
The clinical experts explained that there are currently no biomarkers in regular clinical use which can guide treatment decision-making in melanoma. The clinical experts felt that patients with stage IIB and IIC melanoma will likely be considered equally for treatment with pembrolizumab as adjuvant treatment to surgery, which is in alignment with the criteria used in the KEYNOTE-716 trial. According to the experts, patient-specific factors, including performance status, the presence or absence of relevant comorbidities, patient age, and patient wishes, will guide decisions about treatment with pembrolizumab for patients with resected stage IIB or IIC melanoma. They also noted that patients with active autoimmune medical comorbidities (i.e., inflammatory bowel disease, rheumatoid arthritis) would not be exempt from treatment, but may be less likely to pursue treatment with adjuvant immunotherapy.
The clinical experts acknowledged that although an improvement in overall survival (OS) is the primary outcome of interest, an improvement in recurrence-free survival (RFS) is still of clinical value. They further described response to treatment, defined by the absence of disease, as a clinically meaningful outcome consistent with outcomes used for other adjuvant indications. According to the clinical experts, most clinicians will restage patients to ensure against disease relapse during adjuvant therapy. They further noted that practices are likely to vary between jurisdictions and it is unlikely that most patients and clinicians will adhere to a schedule as robust as that used in the KEYNOTE-716 trial.
Regarding discontinuation of treatment, the experts indicated that patients should be monitored for treatment-related toxicities during pembrolizumab therapy, and treatment may be discontinued if moderate or severe toxicities occur. The clinical experts referenced the recommendations from the European Society for Medical Oncology9 and the American Society for Clinical Oncology10 as generally accepted algorithms that exist for managing immune-related toxicities. The experts felt that whether adjuvant therapy should be automatically discontinued with disease recurrence is debatable and should be decided on a case-by-case basis. The clinical experts recommended that treatment with pembrolizumab as adjuvant treatment to surgery should be overseen by a qualified medical oncologist, with support from community cancer centres and allied health care providers.
Clinician Group Input
Clinician group input was received from the Ontario Health–Cancer Care Ontario Skin Cancer Drug Advisory Committee, with 5 clinicians contributing to the submission. The clinician group noted that there is currently no treatment for this high-risk patient population and sentinel node–negative patients are currently ineligible for adjuvant treatment, indicating an unmet need. The treatment goals for this patient population would be RFS because it is an important end point for patients and a possible surrogate for OS. The input stated that pembrolizumab would be provided as an adjuvant treatment after appropriate surgical management. The input suggests that treatment should be provided in an outpatient setting, physical exams and CT scans should be used to determine if a patient is responding to treatment, and treatment should be discontinued upon disease recurrence and toxicity.
Drug Program Input
The drug plans were interested in the following:
Should patients be eligible for a downstream PD-1 or programmed cell death ligand 1 (PD-L1) inhibitor if they experience disease recurrence more than 6 months after treatment with an adjuvant PD-1 or PD-L1 inhibitor?
Is a 6-week dosing interval of pembrolizumab appropriate for stage IIB and IIC melanoma?
Should patients with an Eastern Cooperative Oncology Group (ECOG) performance status of 2 or greater be eligible for pembrolizumab for the indication under review?
Should patients with noncutaneous melanoma be considered for treatment with pembrolizumab for the indication under review?
In response to the questions from the drug plans, the clinical experts indicated that the same principle used for other solid tumours could be applied to the treatment setting for patients with stage II melanoma. Although a 21-day schedule does not correspond directly to a 42-day schedule, the experts felt that a 6-week dosing interval for pembrolizumab would be appropriate for most patients. The clinical experts indicated that patients with an ECOG performance status of 2 or greater should be eligible for pembrolizumab, and that the patient selection criteria for noncutaneous stage II melanoma should be similar to what is used for stage III. Additional details are summarized in Table 3.
Clinical Evidence
Pivotal Studies and Protocol-Selected Studies
Description of Studies
The pivotal trial for pembrolizumab (KEYNOTE-716) was the only included study in the CADTH systematic review. KEYNOTE-716 (N = 976) was a randomized, placebo-controlled, parallel-group, crossover and rechallenge, multicentre study of adjuvant pembrolizumab in patients aged 12 years and older with resected stage IIB or IIC cutaneous melanoma. The study consisted of 2 parts: adjuvant treatment in part 1 and crossover and rechallenge after first recurrence in part 2. In part 1, pembrolizumab or placebo was administered every 3 weeks for 17 cycles. The results from part 2 were not available at the time of this review. At the time of this review, data up to the third interim analysis (IA3) was available. The data cut-off (DCO) for interim analyses were December 4, 2020 (IA1); June 21, 2021 (IA2); and January 4, 2022 (IA3).
The primary objective of the KEYNOTE-716 trial was to compare RFS between the treatment groups: pembrolizumab and placebo. Patients included in the trial must have been enrolled within 12 weeks of final surgical resection with complete surgical wound healing and with no evidence of metastatic disease on imaging. The mean age of the included patients was 59.3 years (standard deviation [SD] = 12.9 years); 2 pediatric patients were included (1 randomized to each treatment group). Almost all included patients did not exhibit functional impairment (ECOG performance status of 0 or Karnofsky Performance Status of 100), and the remaining patients (7% in each treatment group) exhibited some functional impairment (ECOG performance status of 1). Most patients had stage IIB melanoma at baseline (64%), and 35% had stage IIC melanoma. In addition to RFS, data were available for the following outcomes as of IA3: distant metastasis–free survival (DMFS), health-related quality of life (HRQoL) measured using the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 (EORTC QLQ-C30), and the 5-level EQ-5D (EQ-5D-5L) visual analogue scale (VAS).
Efficacy Results
OS was identified as the most important outcome for patients with melanoma. At the time of this review, the available evidence did not include an assessment of OS because of data immaturity, and was limited to RFS, an interim analysis of DMFS, and an exploratory analysis of HRQoL. The final OS analysis for the study is not expected to occur until approximately 180 months (15 years) of follow-up. Key efficacy results from the KEYNOTE-716 trial are provided in Table 2.
Table 2: Summary of Key Results From the KEYNOTE-716Trial
Result | Pembrolizumab (N = 487) | Placebo (N = 489) |
|---|---|---|
RFS (ITT population; DCO: June 21, 2021) | ||
Events, n (%) | 72 (14.8) | 115 (23.5) |
Event rate per 100 person-months | 0.9 | 1.4 |
RFSa (months), median (95% CI) | NR (NR to NR) | NR (29.9 to NR) |
RFS ratea at 18 months, % (95% CI) | 85.8 (82.0 to 88.9) | 77.0 (72.6 to 80.7) |
Hazard ratio (95% CI)b | 0.61 (0.45 to 0.82) | |
P valuec | |||||||||||||||||||||||||||| | |
DMFS (ITT population; DCO: January 4, 2022) | ||
Events, n (%) | 63 (12.9) | 95 (19.4) |
Event rate per 100 person-months | 0.6 | 0.9 |
DMFSa (months), median (95% CI) | NR (NR to NR) | NR (NR to NR) |
DMFS ratea at 18 months, % (95% CI) | |||||||||||||||||||||||||||| | |||||||||||||||||||||||||||| |
Hazard ratio (95% CI)b | 0.64 (0.47 to 0.88) | |
P valuec | 0.00292 | |
Change from baseline to week 72 in EORTC QLQ-C30 Global Health Status/QoL Scale (PRO FASd population; DCO: January 4, 2022) | ||
n (%) | |||||||||||||||||||||||||||| | |||||||||||||||||||||||||||| |
Baseline, mean (SD) | |||||||||||||||||||||||||||| | |||||||||||||||||||||||||||| |
Change from baseline, LS mean (95% CI) | |||||||||||||||||||||||||||| | |||||||||||||||||||||||||||| |
Treatment group difference, LS mean (95% CI)e | |||||||||||||||||||||||||||| | |
P valuef | |||||||||||||||||||||||||||| | |
Change from baseline to week 72 in EQ-5D-5L VAS (PRO FASd population; DCO: January 4, 2022) | ||
n (%) | |||||||||||||||||||||||||||| | |||||||||||||||||||||||||||| |
Baseline, mean (SD) | |||||||||||||||||||||||||||| | |||||||||||||||||||||||||||| |
Change from baseline, LS mean (95% CI) | |||||||||||||||||||||||||||| | |||||||||||||||||||||||||||| |
Treatment group difference, LS mean (95% CI)e | |||||||||||||||||||||||||||| | |
P valuef | |||||||||||||||||||||||||||| | |
Harms, n (%) (safety population; DCO: January 4, 2022) | ||
AEs | 462 (95.7) | 445 (91.6) |
SAEs | |||||||||||||||||||||||||||| | |||||||||||||||||||||||||||| |
WDAE (from study treatment) | 83 (17.2) | 22 (4.5) |
Deaths | |||||||||||||||||||||||||||| | |||||||||||||||||||||||||||| |
Notable harms, n (%) (safety population; DCO: January 4, 2022) | ||
Immune-mediated reactions | ||
Colitis | 19 (3.9) | 5 (1.0) |
Pneumonitis | 12 (2.5) | 4 (0.8) |
Severe skin reactions | 15 (3.1) | 3 (0.6) |
SJS | 0 (0.0) | 0 (0.0) |
TEN | 0 (0.0) | 0 (0.0) |
Infusion-related reactions | 3 (0.6) | 7 (1.4) |
Endocrine-related reactions | ||
Hypothyroidism | 83 (17.2) | 18 (3.7) |
Hyperthyroidism | 50 (10.4) | 3 (0.6) |
Adrenal insufficiency | 13 (2.7) | 0 (0.0) |
Type 1 diabetes | 2 (0.4) | 0 (0.0) |
AE = adverse event; CI = confidence interval; DCO = data cut-off; DMFS = distant metastasis–free survival; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; FAS = full analysis set; ITT = intention to treat; LS = least squares; NR = not reached; PRO = patient- reported outcome; RFS = recurrence-free survival; SAE = serious adverse event; SD = standard deviation; SJS = Stevens-Johnson Syndrome; TEN = toxic epidermal necrolysis; VAS = visual analogue scale; WDAE = withdrawal due to adverse event.
aFrom product-limit (Kaplan-Meier) method for censored data.
bBased on Cox regression model with Efron’s method of tie handling with treatment as a covariate stratified by melanoma T category (T3b vs. T4a vs. T4b).
cOne-sided P value based on log-rank test stratified by melanoma T category (T3b vs. T4a vs. T4b).
dThe PRO FAS included 449 patients in the pembrolizumab treatment group and 459 in the placebo treatment group.
eBased on a constrained longitudinal data analysis model with the PRO scores as the response variable with covariates for treatment by time interaction, stratification factor melanoma T category (IIB T3b greater than 2.0 mm to 4.0 mm with ulceration vs. IIB T4a greater than 4.0 mm without ulceration vs. IIC T4b greater than 4.0 mm with ulceration) as covariate.
fThe P value has not been adjusted for multiple testing (i.e., the type I error rate has not been controlled).
Source: Clinical Study Reports.11,12
The final analysis of RFS was based on the DCO of June 21, 2021 (IA2). Recurrence was defined as recurrence of melanoma at any site (local, in-transit, or regional lymph nodes or distant recurrence) or death due to any cause. The median duration of follow-up for all participants (intention-to-treat [ITT] population) was 20.5 months (range, 4.6 to 32.7 months) as of the DCO, with a similar median duration of follow-up across treatment groups. The estimated hazard ratio (HR) suggested a reduction in risk of recurrence at 18 months follow-up based on a HR of 0.61 (95% CI, 0.45 to 0.82; P = |||||||). At that time point, 72 (14.8%) patients randomized to the pembrolizumab group and 115 (23.5%) patients randomized to the placebo group had experienced recurrence of disease. In the pembrolizumab treatment group, 7.8% of events were local, regional, or locoregional recurrence; 6.4% were distant recurrence; and 0.62% were deaths. In the placebo treatment group, 10.2% were local, regional, or locoregional recurrence; 12.3% were distant recurrence; and 1.0% were deaths. The HR for RFS at IA2 was consistent with the results at IA1 (HR = 0.65; 95% CI, 0.46 to 0.92; P = 0.00658) and IA3 (HR = 0.64; 95% CI, 0.50 to 0.84). The 2 sensitivity analyses for RFS accounted for new primary melanomas included in the RFS analysis and different censoring rules; both were consistent with the primary analysis.
The first interim analysis of DMFS was available for this review. Neither patient nor clinician groups highlighted DMFS as an outcome of particular interest compared with RFS and OS. As of IA3, 13% and 19% of patients randomized to pembrolizumab and placebo, respectively, experienced DMFS. The reduction in risk of DMFS at 18 months was in favour of pembrolizumab (HR = 0.64; 95% CI, 0.47 to 0.88; P = 0.00292); however, this was based on a small number of events and immature data.
The analysis of HRQoL outcomes was exploratory but suggested little to no change in HRQoL in the placebo treatment group, and a small numerical reduction in HRQoL in the pembrolizumab treatment group. The results were reported as a change from baseline to week 48 and week 72. At week 72, the least squares (LS) mean of the change from baseline in the EORTC QLQ-C30 global health status/quality of life (QoL) scale was ||||||| (95% CI, ||||||| to |||||||) for patients randomized to pembrolizumab and ||||||| (95% CI, ||||||| to |||||||) for patients randomized to placebo. The LS mean change from baseline to week 72 for the EQ-5D-5L VAS was ||||||| (95% CI, ||||||| to |||||||) for patients randomized to pembrolizumab and ||||||| (95% CI, ||||||| to |||||||) for patients randomized to placebo.
Harms Results
Safety results reported herein were based on the DCO of January 4, 2022. A summary of key safety results is provided in Table 2. A total of ||||||| deaths were reported, ||||||| of which were patients randomized to the placebo group. The frequency of adverse events (AEs) and serious adverse events (SAEs) reported by patients was similar between treatment groups; 95.7% and 91.6% of patients in the pembrolizumab and placebo treatment groups, respectively, reported at least 1 AE. Diarrhea (28% versus 21% for pembrolizumab versus placebo, respectively), pruritus (28% versus 13%), arthralgia (24% versus 17%), rash (19% versus 9%), headache (17% versus 11%), hypothyroidism (17% versus 4%), increased alanine aminotransferase (12% versus 6%), and hyperthyroidism (10% versus 1%) were reported more frequently by patients in the pembrolizumab treatment group than in the placebo group. SAEs were reported by ||||||| of patients in the pembrolizumab treatment group and ||||||| of patients in the placebo treatment group. The most frequently reported SAEs were basal cell carcinoma (||||||| and ||||||| in the pembrolizumab and placebo treatment groups, respectively), squamous cell carcinoma of the skin (||||||| and |||||||), malignant melanoma in situ (||||||| and |||||||, and malignant melanoma (||||||| and |||||||). Neither of the pediatric patients in the study reported an SAE. Numerically, more patients in the pembrolizumab treatment group (17% of patients) discontinued from treatment due to AEs compared with the placebo group (5% of patients); however, discontinuation from treatment did not appear to be the result of any specific AE. The clinical experts consulted by CADTH stated that patients with stage IIB or IIC melanoma following complete resection are overall considered healthy patients. They posed that, as a result, some patients may not be willing to tolerate the AEs associated with pembrolizumab (for which they were involved in a trial; therefore, with unknown benefit) when they felt healthy otherwise.
Notable AEs (i.e., the AEs of special interest for this review), including immune-mediated reactions (colitis and pneumonitis), severe skin reactions (Stevens-Johnson syndrome and toxic epidermal necrolysis), infusion-related reactions, and endocrine-related reactions, were observed in less than 4% of patients in any treatment group, with the exception of hyperthyroidism and hypothyroidism as previously described.
Critical Appraisal
KEYNOTE-716 was a well-designed, randomized, placebo-controlled, parallel-group, multicentre study. Part 1 of the study, which is the focus of this review, was double-blinded. At the time of this review, data from IA3 (DCO of January 4, 2022) was the most recent analysis available. At IA3, the final analysis of RFS and the interim analysis of DMFS were the only primary and key secondary analyses available. OS was identified as the most important outcome for the review of pembrolizumab for stage IIB and IIC melanoma; however, the final OS analysis for the study is not expected to occur until approximately 180 months (15 years) after the first patient was randomized. A study by Suciu et al. provided evidence based on interferon-based therapies to support RFS as a surrogate outcome for a HR of at least 0.77;13 however, a study by Coart et al. concluded that more evidence is needed to confirm the strength of association between RFS and OS for ICI therapies such as pembrolizumab.14 Based on the evidence that is currently available, RFS may be an appropriate surrogate outcome for OS, but this is associated with notable uncertainty given the limited data available for the therapies that are the current standard of care, the small number of events available for analysis, and the relatively short duration of follow-up at this time. Patient-reported HRQoL outcomes (EORTC QLQ-C30 and EQ-5D-5L VAS) were exploratory, subject to potential bias because of missing data, and did not control for multiplicity. As such, conclusions that can be drawn about HRQoL are limited. Subgroup analyses were not prespecified nor powered to show efficacy so should be considered exploratory.
Although the sponsor is requesting reimbursement of pembrolizumab for patients of at least 12 years of age, only 2 pediatric patients (aged 12 to 17 years) were included in the study; therefore, the appropriateness of generalizing the results to pediatric populations is unknown. At the time of this review, the evidence was limited to part 1 of the study, which only included patients who were not previously treated for melanoma beyond complete surgical resection. Additionally, some of the exclusion criteria in the trial — such as patients who had received prior therapy with anti-PD1, anti-PD-L1, or anti-PD-L2 drugs; patients with a known additional malignancy or who had required active antineoplastic therapy or surgery in the past 5 years; and patients with immunodeficiencies — are likely to miss a subset of patients who would be seen in clinical practice (estimated 5% to 10% of patients). The clinical experts indicated that these criteria would not preclude patients from treatment with pembrolizumab in practice, but the safety and efficacy of treatment in these patients is associated with uncertainty. Concomitant medication use described in the trial was considered appropriate and consistent with clinical practice. The evidence is limited to a placebo-controlled trial; however, given the current standard of care is surveillance, this was considered to be a reasonable comparator. At the time of this review, the final analysis was only available for the primary end point: RFS. The clinical experts indicated that approximately one-third of patients who experience recurrence of disease will do so in the first 12 months following resection. Despite having enough events to perform the final analysis of RFS, the small number of events available for analysis may have rendered the effect estimates and corresponding CIs fragile. The duration of follow-up as of IA2 and IA3 is likely too short, causing uncertainty around the generalizability of the estimate for recurrence to what would be expected in clinical practice. In contrast, the clinical experts felt that the duration of follow-up was sufficient to observe AEs of interest.
Indirect Comparisons
A focused literature search for indirect treatment comparisons (ITCs) dealing with melanoma was run in MEDLINE All (1946–) on May 20, 2022. No search limits were applied. No ITCs were identified for this review.
Other Relevant Evidence
A sponsor-submitted ITC was used to support the economic model. This ITC compared the interventions of interest on the outcomes of progression-free survival (PFS) and OS in patients with unresectable stage III or IV melanoma receiving first-line treatment of advanced disease. In the BRAF all-comers/wild-type population, the network meta-analysis (NMA) showed that pembrolizumab may be favourable for PFS relative to ipilimumab monotherapy, dacarbazine, ipilimumab plus dacarbazine, and binimetinib; however, nivolumab plus ipilimumab was favoured relative to pembrolizumab for PFS analysis. For the OS analysis in the BRAF all-comers/wild-type population, the NMA showed that pembrolizumab may be favourable relative to ipilimumab and to dacarbazine. In the population with BRAF mutation–positive melanoma, pembrolizumab may be favourable for PFS relative to ipilimumab monotherapy, dacarbazine, ipilimumab plus dacarbazine, and binimetinib, however, it may be less favourable than nivolumab plus ipilimumab, encorafenib plus binimetinib, vemurafenib plus cobimetinib, atezolizumab plus vemurafenib plus cobimetinib, dabrafenib plus trametinib, and pembrolizumab plus dabrafenib plus trametinib. For the OS analysis in the population with BRAF mutation–positive melanoma, pembrolizumab may be favourable to monotherapy with ipilimumab, dacarbazine, and vemurafenib.
Limitations to this NMA include variation in patient characteristics (BRAF status, PD-L1, M1c metastases, baseline characteristics such as elevated lactate dehydrogenase (LDH), and ECOG status) and trial characteristics (e.g., open label and phase II versus phase III trial), which indicate that the underlying assumption of transitivity is likely to have been violated. Potential heterogeneity was not further investigated, such as with subgroup analyses or meta-regression. Consistency between direct and indirect evidence could not be verified due to the lack of closed loops. All the contributing evidence was indirect, which reduces the certainty of all effects. Additionally, there were limited data available for the NMAs that were conducted for OS and PFS; therefore, fixed-effects models were used for these end points, which is likely to have resulted in estimates that are more precise than in reality. These limitations preclude making conclusions about the comparative effectiveness of pembrolizumab in the setting of advanced melanoma.
Conclusions
One sponsor-submitted, phase III, randomized, placebo-controlled, parallel-group, multicentre study of patients with resected stage IIB or IIC cutaneous melanoma was included in this review. Following complete resection, adjuvant treatment with pembrolizumab as a solution for infusion (2 mg/kg for pediatric patients or 200 mg for adult patients, administered every 3 weeks for 17 weeks) demonstrated a benefit relative to placebo in terms of RFS. This was based on a 39% (95% CI, 18% to 55%) reduction in the hazard of recurrence at 18 months of follow-up. The long-term benefit of adjuvant pembrolizumab treatment of stage IIB and IIC melanoma is currently unknown and, although RFS is a clinically meaningful outcome, the evidence for RFS as a surrogate for OS for ICI regimens is associated with some uncertainty. Overall, the safety profile of pembrolizumab observed in the KEYNOTE-716 trial was considered acceptable, manageable, and consistent with the known safety profile of pembrolizumab. No additional safety signals were identified with adjuvant pembrolizumab monotherapy. Efficacy and safety for pediatric patients is uncertain because only 2 patients aged 12 to 17 years were included in the pivotal trial.
Introduction
Disease Background
Melanoma is a cancer that begins in the melanocyte cells of the skin, also referred to as cutaneous melanoma. Cutaneous melanoma can develop anywhere on the skin, including the eyes, mouth, genitals, and anal area; however, they are most likely to start on the chest, back, and legs. In contrast, noncutaneous melanoma develop from skin cells other than melanocytes, such as basal cells.1 Melanocytes can group together to form moles on the skin, most of which are noncancerous (benign) tumours; however, some changes to melanocytes can lead to melanoma skin cancer.1 The first signs of melanoma are typically a change in the mole colour, size, or shape. Other common signs and symptoms include a mole that is asymmetric, has an uneven or irregular border, is not the same colour throughout, is large in diameter (more than 6 mm), or is evolving.1 The cancerous growth has the potential to grow into and destroy nearby tissue or metastasize to other parts of the body. There are 4 main types of melanoma skin cancer, which include superficial spreading, nodular, lentigo maligna, and acral lentiginous. Superficial spreading melanoma is the most common type, accounting for approximately 70% of all melanoma skin cancers, followed by nodular melanoma, which makes up about 15% to 20% melanoma skin cancers. Lentigo maligna melanoma and acral lentiginous melanoma are less common, affecting 10% to 15% and less than 5% of melanoma skin cancers, respectively.
According to the Canadian Cancer Society, the 5-year observed survival statistics for stage IIB and stage IIC melanoma are 70% and 53%, respectively.1 The Canadian Cancer Society estimated that 9,000 people living in Canada will be diagnosed with melanoma skin cancer in 2022 and 1,200 will die of it. It was reported that melanoma accounts for about 3.8% of new cancer cases and 1.9% of all cancer deaths in men, and 3.3% and 1.2%, respectively, in women.2 The number of new cases of melanoma skin cancer has increased over time, affecting more men than women. The chance of developing melanoma skin cancer increases with age, but it is also found in adolescents and young adults (aged 15 to 29 years). There are a number of risk factors for melanoma (summarized from most to least important): UV radiation; many moles; atypical moles; congenital melanocytic nevi; familial atypical multiple mole melanoma syndrome; other hereditary conditions (xeroderma pigmentosum, Werner syndrome, retinoblastoma); light-coloured skin, eyes, and hair; personal or family history of skin cancer; CDKN2A gene mutation; and a weakened immune system.
A melanoma diagnosis usually begins with a family physician based on reported signs or symptoms and a skin examination. Patients may then be referred to a specialist, such as a dermatologist or surgeon, as needed.1 The clinical experts consulted by CADTH noted that, on occasion, patients may be diagnosed following a referral to dermatology and, more rarely, surgeons may be the first point of contact for patients with primary melanoma. A diagnosis typically involves a review of the patient’s history and risk factors, a skin examination to look for abnormal moles or areas, and a physical examination that may include a check for enlarged lymph nodes. The presence of cancerous cells, extent, and characteristics of the disease may be identified by skin biopsy, lymph node biopsy, histology, imaging (CT scan, MRI, chest X-ray, PET scan), and/or blood tests.1
Patients with stage IIB and IIC melanoma are defined by having high-risk, node-negative disease. The primary tumour is thick and/or ulcerated (greater than 4 mm thick with or without ulceration or greater than 2 mm to 4 mm thick with ulceration), but there is no lymph node involvement.3
Standards of Therapy
According to the clinical experts consulted by CADTH, following a diagnostic biopsy, all patients should undergo WLE of the primary site, which is a curative-intent surgical procedure. Further, the experts indicated that patients with a tumour deeper than 1 mm (or in some cases, deeper than 0.75 mm in the presence of additional high-risk pathological features, such as ulceration) are generally referred for sentinel lymph node biopsy to determine if there is evidence for metastatic melanoma.
Following definitive WLE, patients are generally followed for surveillance. A national expert recommendation statement on high-risk melanoma surveillance was developed at the 2020 Canadian Melanoma Conference.4 Patients with stage IIB to IV were considered high risk. It was recommended that surveillance be conducted by an appropriate specialist, including biannual visits and PET/CT scans with brain MRI among the systemic imaging modalities available.4 The Canadian recommendation statement also stated that high-risk surveillance should follow a 5-year schedule, beginning with an intensive 2-year period followed by a less-intensive 3-year period because the median time to relapse for stage IIB to III melanoma was less than 2 years after treatment.4 Recently updated guidelines published by the National Comprehensive Cancer Network in 2022 include pembrolizumab as an option for patients with stage IIB or IIC following WLE;15 however, the guidelines also indicate that “longer follow-up is needed to evaluate the impact of adjuvant pembrolizumab on OS.” The guidelines further note that clinicians should have a detailed discussion with patients regarding the advantages and disadvantages of treatment with pembrolizumab.15
The clinical experts indicated that surveillance schedules will vary between jurisdictions, but most include a schedule of clinical assessments and diagnostic imaging studies, particularly for patients with resected IIB or IIC disease. Although early detection of disease recurrence has not yet been demonstrated to improve patient survival, given the magnitude of benefit seen with metastatic ICI regimens, most clinicians believe there is an inherent benefit to surveillance. There is historical evidence to support the use of high-dose interferon for patients with resected pT4pN0 disease, but it is rarely prescribed because of the limited evidence for benefit and the fact that the interferon studies were all conducted in the era before ICI therapy.
Drug
Pembrolizumab is commonly known as a drug in the class of ICIs.6 Pembrolizumab is an antibody with high affinity against anti-PD-1. PD-1 is an immune checkpoint receptor that limits the activity of T lymphocytes in peripheral tissues (active T cell immune surveillance). Tumour cells may engage the PD-1 pathway and inhibit active T cell immune surveillance. Pembrolizumab binds to PD-1, thereby preventing it from binding to its ligands (PD-L1 and PD-L2), which results in the reactivation of tumour-specific cytotoxic T lymphocytes in the tumour microenvironment.5
Pembrolizumab is approved by Health Canada for the adjuvant treatment of adult and pediatric (aged 12 years and older) patients with stage IIB or IIC melanoma following complete resection.5 Pembrolizumab is administered as an IV infusion over 30 minutes.5 For adults, the recommended dosage for adjuvant treatment of melanoma is either 200 mg every 3 weeks or 400 mg every 6 weeks for a maximum of 1 year or until disease recurrence or unacceptable toxicity.5 For pediatric patients, recommended dosage for adjuvant treatment of melanoma is 2 mg/kg (up to a maximum of 200 mg) every 3 weeks until disease progression or unacceptable toxicity or for a maximum of 12 months.5
The sponsor has requested that pembrolizumab be reimbursed as per the Health Canada indication. The Notice of Compliance was received on July 5, 2022. In December 2021, the FDA approved pembrolizumab for the adjuvant treatment of adult and pediatric (aged 12 years and older) patients with stage IIB, IIC, or III melanoma following complete resection.7
Pembrolizumab was previously reviewed by CADTH for the adjuvant treatment of patients with stage IIIA to stage IIID cutaneous melanoma and received a recommendation for reimbursement with conditions.8
Stakeholder Perspectives
Patient Group Input
This section was prepared by CADTH staff based on the input provided by patient groups. The full patient group submissions can be found at the end of this report in the Stakeholder Input section.
Two patient groups, SYSF and Melanoma Canada, submitted patient input for this review. Both groups included patients from across Canada with melanoma, regardless of cancer stage. The SYSF gathered data through online surveys, virtual roundtables, and one-on-one discussions with 25 patients with melanoma (68% female, 32% male), 18 of whom received the treatment under review. Melanoma Canada received input from 172 patients with melanoma (67% female) and 15 caretakers through an online survey. Twenty patients from the Melanoma Canada submission indicated they had been treated with adjuvant pembrolizumab for stage IIB or IIC melanoma following complete resection.
According to the SYSF input, respondents who were diagnosed with stage II melanoma reported having limited access to available treatment options which increased their initial fear and anxiety. The Melanoma Canada survey respondents indicated that the main day-to-day impacts of their diagnosis included scarring and disfigurement, fear or anxiety, disrupted sleep as well as pain, fatigue, and depression. Respondents also indicated mobility and lymphedema issues caused by surgery, including lymph node dissection. The input suggested there is an unmet need for treatment options to prevent recurrence of disease because there are currently no treatment options available beyond surgery for stage IIB or IIC disease in Canada.
In both submissions, most patients who had experience with the treatment under review reported experiencing at least 1 side effect. In the SYSF submission, the main side effects reported by the survey respondents included fatigue, cognitive impairment, nausea, skin rash, gastrointestinal problems, and weight loss or gain. Most patients found these side effects to be manageable. In the Melanoma Canada submission, the main reported side effects included fatigue or weakness, skin rash, thyroid or pituitary gland issues, and muscle or joint pain. Most of the respondents indicated they were willing to accept the side effect profile of pembrolizumab if it could potentially mean that they would not have to deal with a recurrence. A common concern among patients was the length of time and the cost of travel to get to a clinical trial site for treatment. In the submissions received, patients expressed a need for future treatments that would be curative, be accessed close to home and delivered in a timely fashion, allow them to work and continue normal day-to-day activities without significant long-term side effects, and be available to them if their disease was to progress or recur.
Clinician Input
Input From Clinical Experts Consulted by CADTH
All CADTH review teams include at least 1 clinical specialist with expertise regarding the diagnosis and management of the condition for which the drug is indicated. Clinical experts are a critical part of the review team and are involved in all phases of the review process (e.g., providing guidance on the development of the review protocol, assisting in the critical appraisal of clinical evidence, interpreting the clinical relevance of the results, and providing guidance on the potential place in therapy). The following input was provided by 2 clinical specialists with expertise in the diagnosis and management of stage IIB or IIC melanoma.
Unmet Needs
The clinical experts described the prognosis of patients with stage IIB and IIC melanoma as similar to that seen in stage III (lymph node–positive) malignant melanoma. For patients with resected stage III melanoma, the use of systemic treatment as adjuvant treatment to surgery has become standard of care, offering an improvement in RFS. The experts stated that apart from high-dose interferon, there are no currently available systemic therapies to be used as adjuvant treatment to surgery for patients with resected stage IIB or IIC melanoma. Given the similarities between the prognoses of patients with stage IIB, IIC, and III melanoma diagnoses, the experts indicated that patients and clinicians would likely want access to systemic treatment for similar adjuvant treatment of these patients.
The experts described how patients endure a significant amount of stress and anxiety following a diagnosis of melanoma, and that the opportunity to pursue adjuvant immunotherapy may reduce a portion of that stress. They noted that this is particularly the case for a treatment that is typically well tolerated with an acceptably low risk of SAEs. The experts indicated that melanoma is an aggressive disease with unpredictable disease recurrence patterns. Furthermore, the experts noted that a proportion of patients with stage IIB or IIC melanoma will have a recurrence that precludes treatment in the metastatic (recurrent) setting. An example is a patient who develops significant intracranial metastatic disease, for which palliative immunotherapy may not be appropriate or possible.
Place in Therapy
The clinical experts indicated that pembrolizumab would be the first available systemic therapy for adjuvant use in resected stage IIB or IIC melanoma, although clinical trials investigating the efficacy and safety of nivolumab and encorafenib-binimetinib are recruiting or in development.
According to the clinical experts, one would expect that pembrolizumab would be used as monotherapy for patients with completely resected stage IIB or IIC melanoma. A small minority of patients within this category may qualify for consideration of radiation therapy as adjuvant treatment to surgery, but the safety profile of pembrolizumab in combination with radiation is such that most clinicians would not prescribe pembrolizumab in these uncommon instances.
If pembrolizumab is approved for use as adjuvant treatment to surgery for patients with resected stage II melanoma, the clinical experts felt there would certainly be a shift in the current treatment paradigm. For reference, the incidence of stage II melanoma diagnoses is roughly twice that of stage III, suggesting a significant increase in the number of patients with melanoma eligible for treatment with adjuvant immunotherapy. However, that number may overestimate the impact of introducing pembrolizumab to the patient population with stage II melanoma because presumably a proportion of patients who would recur with nodal disease (at which point they may be candidates for treatment with adjuvant systemic therapy) would not have recurred with earlier treatment.
Patient Population
The clinical experts explained that there are currently no biomarkers in regular clinical use which would guide treatment decision-making in melanoma. The experts noted that biomarkers such as PD-L1 are used in the treatment of lung cancer; however, reliable predictive biomarkers for melanoma are not routinely used. The experts also noted that presently there are no companion diagnostic testing required to determine eligibility for treatment. The clinical experts felt that patients with stage IIB and IIC melanoma will likely be considered equally for treatment with pembrolizumab as adjuvant treatment to surgery, which is in alignment with the criteria used in the KEYNOTE-716 clinical trial.
According to the experts, patient-specific factors, including performance status, the presence or absence of relevant comorbidities, patient age, and patient wishes, will guide decisions about treatment with pembrolizumab for patients with resected stage IIB or IIC melanoma. The experts felt that most clinicians would be comfortable offering treatment with adjuvant pembrolizumab to patients with an ECOG performance status of 2 or greater. They also noted that patients with active autoimmune medical comorbidities (e.g., inflammatory bowel disease, rheumatoid arthritis), although not absolutely exempt from treatment consideration, may be less likely to pursue treatment with adjuvant immunotherapy.
Assessing Response to Treatment
The clinical experts indicated that disease-related symptoms are not pertinent to this review because the patient population has been rendered disease-free surgically (except in the sense that a reduction in recurrence rates must equate to a reduction in cancer-related morbidity). The clinical experts acknowledged that although most clinicians and policy-makers want an improvement in OS associated with the use of adjuvant systemic therapy, an improvement in RFS is also of clinical value. They further described response to treatment, defined by the absence of disease, as a clinically meaningful outcome consistent with outcomes used for other adjuvant indications. As with any adjuvant therapy, the experts indicated that the benefit of treatment is theoretical and, in many cases, patients will truly be disease-free and therefore will not benefit from adjuvant systemic therapy. However, the experts also described that there is currently no reliable means by which micrometastatic disease can be absolutely excluded; therefore, all eligible patients should be considered for treatment because the benefit to the population of patients is real.
According to the clinical experts, most clinicians will restage patients to ensure against disease relapse during adjuvant therapy. They further noted that practices are likely to vary between jurisdictions, and it is unlikely that most patients or clinicians will adhere to a schedule as robust as that used in the KEYNOTE-716 trial.
Discontinuing Treatment
Regarding discontinuation of treatment, the clinical experts indicated that patients should be monitored for treatment-related toxicities during pembrolizumab therapy, and treatment may be discontinued if moderate or severe toxicities occur. The clinical experts referenced the recommendations from the European Society for Medical Oncology9 and the American Society for Clinical Oncology10 as generally accepted algorithms that exist for managing immune-related toxicities.
The clinical experts felt that whether adjuvant therapy should be automatically discontinued with disease recurrence is debatable. The experts described that, in many cases, treatment should be discontinued (e.g., in a patient who recurs with extensive, distant metastatic disease); however, in patients who recur locally (e.g., in the draining nodal basin), the treating clinician may elect to continue treatment. Further, the experts noted that this is especially true for patients who recur locally soon after beginning adjuvant immunotherapy because recurrence is thought to reflect a false-negative sentinel lymph node biopsy result rather than primary disease resistance. The experts noted that these cases should be decided on a case-by-case basis.
Prescribing Conditions
The clinical experts recommended that treatment with pembrolizumab as adjuvant treatment after surgery should be overseen by a qualified medical oncologist. The experts indicated that, in most jurisdictions, the use of pembrolizumab in community cancer centres is reasonable, provided access to oncology services is ensured. Allied health care providers (e.g., advanced nurse practitioners, or general practitioner-oncologists) may assume responsibility for individual pre-treatment assessments for patients receiving treatment with a drug such as pembrolizumab but treatment of these patients should still be overseen by a medical oncologist with experience in the setting of cutaneous malignancies.
Clinician Group Input
This section was prepared by CADTH staff based on the input provided by clinician groups. The full original clinician group input received by CADTH has been included in the Stakeholder Input section at the end of this report.
Clinician group input was received from the Ontario Health–Cancer Care Ontario Skin Cancer Drug Advisory Committee, with 5 clinicians contributing to the submission. The clinician group noted that there is currently no treatment for this high-risk patient population and currently sentinel node–negative patients are ineligible for adjuvant treatment, indicating an unmet need. The treatment goals for this patient population would be RFS because it is an important end point for patients and a possible surrogate for OS. The input stated that pembrolizumab would be provided as an adjuvant treatment after appropriate surgical management. The input suggests that treatment should be provided in an outpatient setting, physical exams and CT scans should be used to determine if a patient is responding to treatment, and treatment should be discontinued upon disease recurrence and toxicity.
Drug Program Input
The drug programs provide input on each drug being reviewed through CADTH’s reimbursement review processes by identifying issues that may impact their ability to implement a recommendation. The implementation questions and corresponding responses from the clinical experts consulted by CADTH are summarized in Table 3.
Table 3: Summary of Drug Plan Input and Clinical Expert Response
Drug program implementation questions | Clinical expert response |
|---|---|
Relevant comparators | |
KEYNOTE-716 trial used a placebo comparator. There are no standard funded therapies in Canada for this indication. | For pERC consideration. |
Considerations for initiation of therapy | |
In KEYNOTE-716, patients in the placebo arm who experienced recurrence and patients in the pembrolizumab arm who experienced recurrence greater than 6 months after completing 17 cycles of treatment were eligible to cross over or rechallenge with pembrolizumab for up to 2 years. PAG highlighted that in other solid tumours (e.g., lung, melanoma), patients are eligible for downstream PD-1 or PD-L1 inhibitor provided that disease recurrence (whether locoregional or distant) occurs more than 6 months from the last dose of an adjuvant PD-1 or PD-L1 inhibitor. Can the same principle be applied in this setting? | The clinical experts indicated that the same principle used for other solid tumours could be applied to the treatment setting for patients with stage II melanoma. Overall, the experts felt that stage II melanoma should not be treated any differently from stage III. They noted that the exception is with the use of a PD-1 inhibitor (nivolumab or pembrolizumab) in combination with a CTLA4 inhibitor, such as ipilimumab. Most clinicians would wish to use combination PD-1/CTLA4 inhibition for patients who relapse on (or shortly after completing) treatment with a PD-1 inhibitor. However, that is currently not permitted in most Canadian jurisdictions. |
Considerations for prescribing of therapy | |
Pembrolizumab dosing on KEYNOTE-522 (the phase III trial for triple-negative breast cancer) was 200 mg (2 mg/kg for pediatrics) IV every 21 days × 17 doses. If funded, in line with other indications for pembrolizumab, jurisdictions would implement a weight-based dose of 2 mg/kg (up to a cap of 200 mg) for all patients. Other indications for pembrolizumab use extended dosing intervals of every 6 weeks (4 mg/kg up to a 400 mg cap). Is a dosing interval of every 6 weeks of pembrolizumab appropriate for stage IIB or IIC melanoma? | The clinical experts felt that a dosing interval of every 6-weeks would be appropriate for most patients. They shared that clinicians may wish to initiate treatment on a 21-day schedule, but for the majority of patients, a 42-day schedule will be acceptable (and likely preferred by many patients). However, they also noted that the KEYNOTE-716 clinical trial used a 21-day schedule, and extrapolation of that data to a 42-day schedule is not automatic. |
Generalizability | |
Should patients with ECOG performance status of 2 or greater be eligible for pembrolizumab in this indication? | The clinical experts indicated that patients with an ECOG performance status of 2 or greater should be eligible for pembrolizumab. They stated that it is important to note that within the adjuvant patient population, diminished performance status is not disease-related because patients have been rendered surgically free of disease before treatment. Clinicians and patients will likely be willing to treat patients with stage II performance status with pembrolizumab given the excellent tolerability profile. |
Should patients with noncutaneous melanoma be considered for treatment with pembrolizumab for this indication? Current pembrolizumab indication in stage III adjuvant melanoma allows treatment of mucosal melanoma and excludes ocular or uveal melanoma. | The clinical experts felt it would be reasonable to use the same patient selection criteria for noncutaneous stage II melanoma as that used for stage III.8 |
Care provision issues | |
Pembrolizumab is already prepared and administered at facilities throughout Canada. Health care professionals have extensive experience with it. Preparation and administration time for pembrolizumab are relatively reasonable and would not be expected to create a significant increase to health system resources. | For pERC consideration. |
CTLA4 = cytotoxic T-lymphocyte associated protein 4; ECOG = Eastern Cooperative Oncology Group; PAG = Provincial Advisory Group; pERC = CADTH pan-Canadian Oncology Drug Review Expert Committee; PD-1 = programmed cell death protein 1; PD-L1 = programmed cell death ligand 1.
Clinical Evidence
The clinical evidence included in the review of pembrolizumab is presented in 3 sections. The first section, the Systematic Review, includes pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those studies that were selected according to an a priori protocol. The second section includes indirect evidence selected from the literature that met the selection criteria specified in the review. The third section includes sponsor-submitted long-term extension studies and additional relevant studies that were considered to address important gaps in the evidence included in the systematic review.
Systematic Review (Pivotal and Protocol-Selected Studies)
Objectives
To perform a systematic review of the beneficial and harmful effects of pembrolizumab (100 mg/4 mL) administered by IV infusion (200 mg every 3 weeks or 400 mg every 6 weeks for adults and 2 mg/kg every 3 weeks for pediatric patients) for the adjuvant treatment of adult and pediatric (aged 12 years and older) patients with stage IIB or IIC melanoma following complete resection.
Methods
Studies selected for inclusion in the systematic review will include pivotal studies provided in the sponsor’s submission to CADTH and Health Canada, as well as those meeting the selection criteria presented in Table 4. Outcomes included in the CADTH review protocol reflect outcomes considered to be important to patients, clinicians, and drug plans.
Of note, the systematic review protocol presented was established before the granting of a Notice of Compliance from Health Canada.
Table 4: Inclusion Criteria for the Systematic Review
Criteria | Description |
|---|---|
Population | Adult and pediatric (aged 12 years and older) patients with stage IIB or IIC melanoma following complete resection Subgroups:
|
Intervention | Pembrolizumab (solution for infusion, 100 mg/4 mL vial) administered by IV infusion over 30 minutes, as adjuvant treatment
|
Comparator | Standard of care (surveillance) |
Outcomes | Efficacy outcomes:
Harms outcomes:
|
Study designs | Published and unpublished phase III and IV RCTs |
AE = adverse event; HRQoL = health-related quality of life; RCT = randomized controlled trial; SAE = serious adverse event; SJS = Stevens-Johnson syndrome; TEN = toxic epidermal necrolysis; WDAE = withdrawal due to adverse event.
The literature search for clinical studies was performed by an information specialist using a peer-reviewed search strategy according to the PRESS Peer Review of Electronic Search Strategies checklist.1
Published literature was identified by searching the following bibliographic databases: MEDLINE All (1946–) via Ovid and Embase (1974–) via Ovid. All Ovid searches were run simultaneously as a multi-file search. Duplicates were removed using Ovid deduplication for multi-file searches, followed by manual deduplication in Endnote. The search strategy comprised both controlled vocabulary, such as the National Library of Medicine’s MeSH (Medical Subject Headings), and keywords. The main search concepts were pembrolizumab and melanoma. Clinical trials registries were searched: the US National Institutes of Health’s clinicaltrials.gov, WHO’s International Clinical Trials Registry Platform (ICTRP) search portal, Health Canada’s Clinical Trials Database, and the European Union Clinical Trials Register.
CADTH-developed search filters were applied to limit retrieval to randomized controlled trials or controlled clinical trials. Retrieval was not limited by publication date or by language. Conference abstracts were excluded from the search results. Refer to Appendix 1 for the detailed search strategies.
The initial search was completed on May 19, 2022. Regular alerts updated the search until the meeting of the CADTH pan-Canadian Oncology Drug Review Expert Committee (pERC) on September 14, 2022.
Grey literature (literature that is not commercially published) was identified by searching relevant websites from the Grey Matters: A Practical Tool For Searching Health-Related Grey Literature checklist.2 Included in this search were the websites of regulatory agencies (US FDA and European Medicines Agency). Google was used to search for additional internet-based materials. Refer to Appendix 1 for more information on the grey literature search strategy.
These searches were supplemented by reviewing bibliographies of key papers and through contacts with appropriate experts. In addition, the manufacturer of the drug was contacted for information regarding unpublished studies.
Two CADTH clinical reviewers independently selected studies for inclusion in the review based on titles and abstracts, according to the predetermined protocol. Full-text articles of all citations considered potentially relevant by at least 1 reviewer were acquired. Reviewers independently made the final selection of studies to be included in the review, and differences were resolved through discussion.
Findings From the Literature
A total of 554 studies were identified from the literature for inclusion in the systematic review (Figure 1). The included studies are summarized in Table 5.
Description of the Included Study
The details of included study are summarized in Table 5. One study, KEYNOTE-716, was included in the systematic review for pembrolizumab. KEYNOTE-716 was a randomized, placebo-controlled, parallel-group, crossover and rechallenge, multicentre study of adjuvant pembrolizumab in participants aged 12 years and older with resected stage IIB or IIC cutaneous melanoma. Of the 160 centres involved in the study, 10 were located in Canada. The primary objective of the KEYNOTE-716 trial was to compare RFS between treatment groups: pembrolizumab and placebo. The secondary objectives were to compare DMFS and OS between treatment groups, as well as to assess the safety and tolerability of pembrolizumab compared with placebo based on the proportion of AEs.
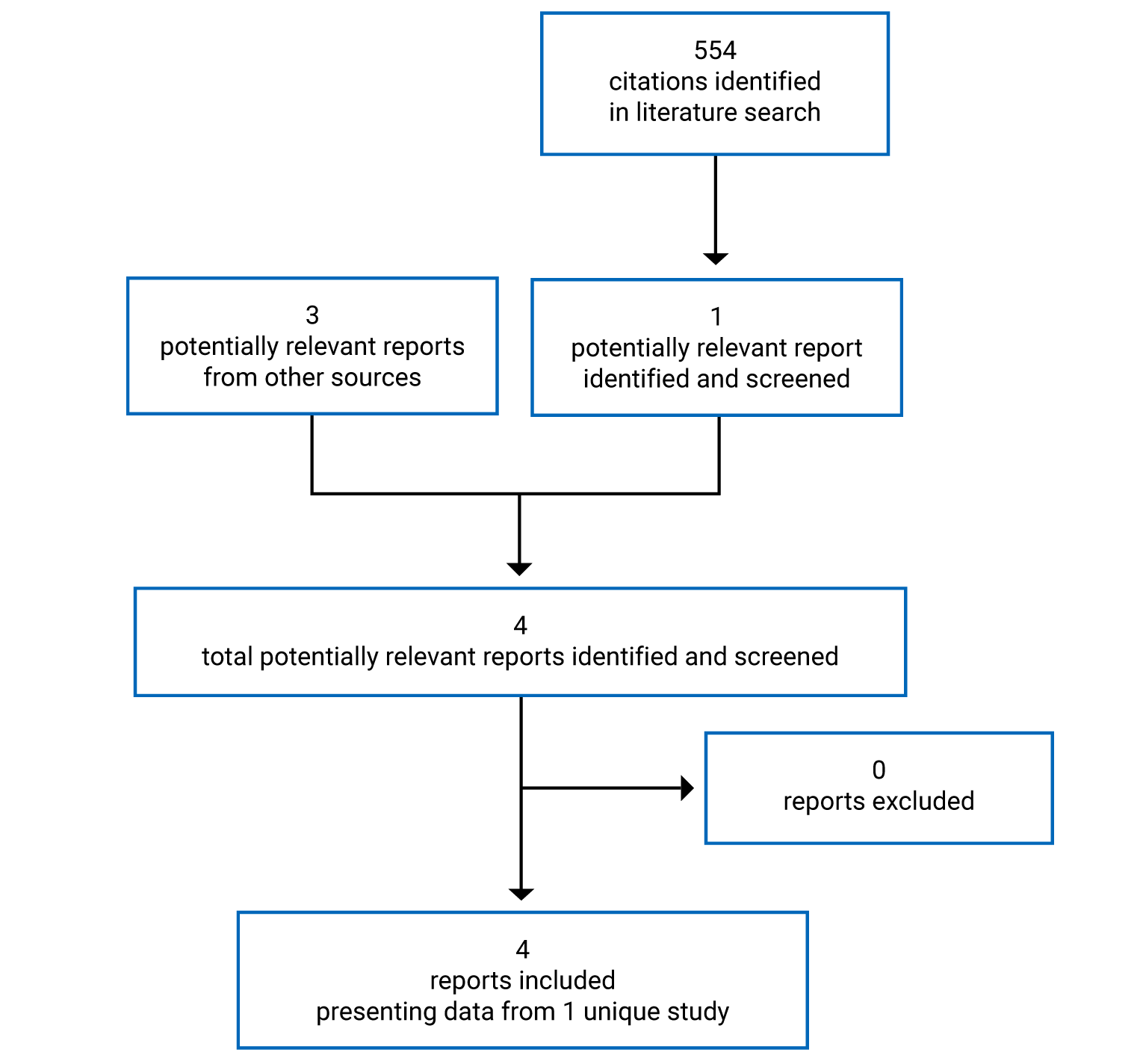
Table 5: Details of Included Studies
Study details | KEYNOTE-716 trial |
|---|---|
Designs and populations | |
Study design | Phase III, randomized, placebo-controlled, parallel-group, crossover and rechallenge, multicentre study |
Locations | 160 centres in 16 countries (US, Canada [10 centres], Brazil, Chile, Belgium, France, Germany, Italy, Spain, Switzerland, UK, Israel, Poland, South Africa, Australia, Japan) |
Patient enrolment dates | September 12, 2018, to December 4, 2020 |
Randomized (N) | 976 |
Inclusion criteria |
|
Exclusion criteria |
|
Drugs | |
Intervention | Pembrolizumab (25 mg/mL) administered by IV infusion via an infusion pump over 30 minutes:
|
Comparator(s) | Placebo (saline solution for infusion via infusion pump):
|
Duration | |
Phase | |
Screening | 28 days |
Part 1, double-blind adjuvant treatment | 17 cycles (each cycle being 3 weeks) |
Part 2, unblinded crossover and rechallenge after first recurrence | 17 (resectable recurrence) or 35 cycles (unresectable recurrence) (each cycle being 3 weeks) Note: Results from part 2 were not available at the time of this review. |
Safety follow-up | 30 days after the last dose is received |
DMFS follow-up | Patients were contacted every 12 weeks until distant metastatic recurrence |
Survival follow-up | Patient with distant metastases that did not enter part 2 were contacted every 12 weeks until death, withdrawal of consent to follow-up, or end of study |
Outcomes | |
Primary end point | RFS (time from randomization to any of the following events: recurrence of melanoma at any site [local, in-transit or regional lymph nodes or distance recurrence] or death due to any cause; does not include new cases of melanoma or second cancer diagnoses) |
Secondary and exploratory end points | Secondary:
Exploratory: HRQoL (EORTC QLQ-C30, EQ-5D-5L VAS) |
Notes | |
Publications | Luke et al. (2022)16 |
AE = adverse event; DB = double-blind; DMFS = distant metastasis–free survival; ECOG = Eastern Cooperative Oncology Group; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; KPS = Karnofsky Performance Status; OS = overall survival; q.3.w. = every 3 weeks; RCT = randomized controlled trial; RFS = recurrence-free survival; VAS = visual analogue scale.
Note: One additional report was included (Luke et al. [2022]).16
Source: Clinical Study Report.11
As described in the overview of the KEYNOTE-716 study design in Figure 2, the study consisted of 2 parts: adjuvant treatment in part 1 and crossover and rechallenge after first recurrence in part 2. During part 1, pembrolizumab or placebo was administered intravenously every 3 weeks (i.e., 1 cycle) for 17 cycles. Patients with confirmed disease recurrence were unmasked and allowed to cross over from placebo to pembrolizumab or to receive repeat treatment with pembrolizumab in part 2 of the study. Of note, the results from part 2 were not available at the time of this review, and part 2 was not aligned with the Health Canada–approved indication. The treatment periods were preceded by a standard 28-day screening period to confirm patient eligibility for the trial. A safety follow-up visit was conducted approximately 30 days after the last dose of study treatment or before the initiation of a new anticancer treatment. Additionally, patients were contacted every 12 weeks as part of the DMFS survival and OS follow-up.
A total of 976 patients were randomized in a 1:1 ratio to receive pembrolizumab or placebo using a centralized interactive response technology system. Randomization was stratified into 3 strata according to T category, which refers to the thickness and ulceration status of the melanoma as per the American Joint Committee on Cancer (AJCC) guidelines 8th edition. The 3 strata were defined as follows: T3b (> 2.0 mm to 4.0 mm with ulceration), T4a (> 4.0 mm without ulceration), or T4b (> 4.0 mm with ulceration). A separate stratum for pediatric patients was also planned, but this ended up including only 2 patients. Part 1 of the study was double-blinded. The patient and the investigator were unaware of treatment assignment, and pembrolizumab and placebo were prepared and dispensed by an unblinded pharmacist or qualified study site personnel. In part 2 of the study, all patients received pembrolizumab as open-label treatment. At the time of this review, data up to the third interim analysis (IA3) were available. The DCO for interim analyses were December 4, 2020 (IA1); June 21, 2021 (IA2); and January 4, 2022 (IA3).
Figure 2: KEYNOTE-716 Study Design
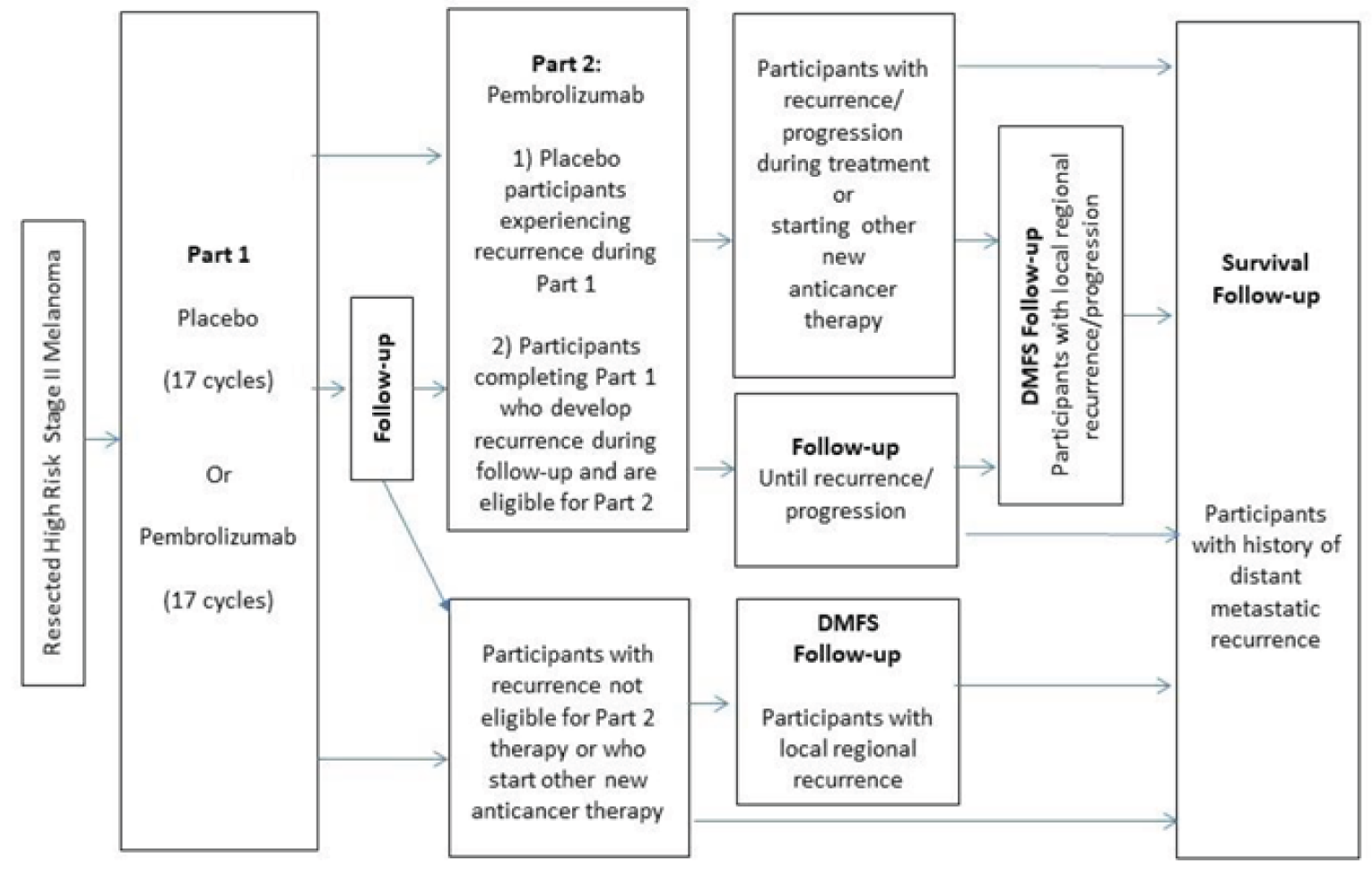
DMFS = distant metastasis–free survival.
Source: Clinical Study Report.17
Populations
Inclusion and Exclusion Criteria
Key inclusion and exclusion criteria for the KEYNOTE-716 trial are described in Table 5. To be eligible for the KEYNOTE-716 trial, patients must have been aged 12 years of age or older with newly diagnosed stage IIB or IIC cutaneous melanoma (tumour [T] category of T3b, T4a, or T4b) with pathologically confirmed negative sentinel lymph node biopsy, and no evidence of regional [N0] or distant metastatic [M0] disease per AJCC 8th edition guidelines. Further, patients must have had completely resected melanoma with negative margins and have not received prior systemic therapy for stage II melanoma. Patients must have been enrolled within 12 weeks of final surgical resection with complete surgical wound healing and no evidence of metastatic disease on imaging, which was determined by the investigator. An ECOG performance status score of 0 or 1, Lansky Performance Status score of at least 50 (for patients aged 16 years or younger), or a Karnofsky Performance Status score of at least 50 (for patients aged between 16 and 18 years) was also required for enrolment.
Patients were excluded from the KEYNOTE-716 trial if they had a diagnosis of immunodeficiency or were receiving chronic systemic steroid therapy or any form of immunosuppressive therapy within 7 days of initiation of treatment. Patients were also excluded if they had a known additional malignancy that was progressing or required active antineoplastic therapy within the past 5 years.
Baseline Characteristics
A summary of the demographic and clinical characteristics of patients at baseline is provided in Table 6. Baseline characteristics were well-balanced across the treatment groups. Of the patients randomized in the KEYNOTE-716 trial, 60% were male and 40% were female; 90% were White, 1% were Black, and 1% were Asian (information for the remainder was missing); and the mean age was 59.3 years (SD = 12.9 years). One pediatric patient (aged between 12 and 17 years) was randomized to each treatment group. The majority of adult patients (93%) had an ECOG score of 0; the remaining had an ECOG score of 1. The 2 pediatric patients had a Karnofsky Performance Status of 100. The T category was T3b for 41% of patients, T4a for 24% of patients, and T4b for 35% of patients. Most patients had stage IIB melanoma at baseline (64%) and 35% had stage IIC melanoma. Less than 1% of patients were at a stage other than IIB or IIC at baseline.
Table 6: Summary of Baseline Characteristics (ITT Population)
Characteristic | Pembrolizumab (N = 487) | Placebo (N = 489) |
|---|---|---|
Sex, n (%) | ||
Male | 300 (61.6) | 289 (59.1) |
Female | 187 (38.4) | 200 (40.9) |
Age (years), mean (SD) | 59.0 (12.6) | 59.6 (13.3) |
Age category (years), n (%) | ||
12 to 17 | 1 (0.2) | 1 (0.2) |
18 to 64 | 302 (62.0) | 294 (60.1) |
65 and older | 184 (37.8) | 194 (39.7) |
Race, n (%) | ||
White | 435 (89.3) | 439 (89.8) |
Black | 4 (0.8) | 4 (0.8) |
Asian | 4 (0.8) | 1 (0.2) |
Other | 2 (0.4) | 0 |
Missing | 42 (8.6) | 45 (9.2) |
Geographic region, n (%) | ||
US | 95 (19.5) | 80 (16.4) |
Non-US | 392 (80.5) | 409 (83.6) |
ECOG PS [adult patients], n (%) | ||
0 | 454 (93.2) | 452 (92.4) |
1 | 32 (6.6) | 35 (7.2) |
2 | 0 | 1 (0.2) |
NA | 1 (0.2) | 1 (0.2) |
KPS status [pediatric patients], n (%) | ||
100 | 1 (0.2) | 1 (0.2) |
N/A | 486 (99.8) | 488 (99.8) |
T category, n (%) | ||
T3a | 2 (0.4) | 0 |
T3b | 200 (41.1) | 201 (41.1) |
T4a | 113 (23.2) | 116 (23.7) |
T4b | 172 (35.3) | 172 (35.2) |
Nodal involvement, n (%) | ||
NX | 2 (0.4) | 1 (0.2) |
N0 | 481 (98.8) | 487 (99.6) |
N1C | 4 (0.8) | 1 (0.2) |
Metastatic staging, n (%) | ||
M0 | 487 (100) | 487 (99.6) |
M1C | 0 (0.0) | 1 (0.2) |
M1D | 0 (0.0) | 1 (0.2) |
Overall cancer stage, n (%) | ||
IIA | 1 (0.2) | 0 (0.0) |
IIB | 309 (63.4) | 316 (64.6) |
IIC | 171 (35.1) | 169 (34.6) |
IIIC | 4 (0.8) | 1 (0.2) |
IV | 0 (0.0) | 2 (0.4) |
Missing | 2 (0.4) | 1 (0.2) |
Stratification, n (%) | ||
Pediatric (age 12 to 17 years) | 1 (0.2) | 1 (0.2) |
IIB T3b > 2.0 mm to 4.0 mm with ulceration | 199 (40.9) | 198 (40.5) |
IIB T4a > 4.0 mm without ulceration | 112 (23.0) | 114 (23.3) |
IIC T4b > 4.0 mm with ulceration | 175 (35.9) | 176 (36.0) |
ECOG = Eastern Cooperative Oncology Group Performance Status; ITT = intention to treat; KPS = Karnofsky Performance Status; NA = not applicable; SD = standard deviation.
Source: Clinical Study Report.11
Interventions
Patients received either pembrolizumab or saline placebo. Both were available as a solution for infusion that was administered intravenously via an infusion pump. Pembrolizumab was provided as a 25 mg/mL vial and the dose used in the study was 2 mg/kg (maximum of 200 mg) for pediatric patients or 200 mg for adult patients administered every 3 weeks (i.e., 1 cycle). Part 1 of the study included 17 cycles of treatment. Part 2 included either 17 or 35 cycles of treatment. All treatments were administered on an outpatient basis.
Discontinuation of Treatment
A patient was discontinued from treatment under the following circumstances:
treatment may have been discontinued if a patient attained complete response following at least 8 cycles (24 weeks) of treatment with at least 2 doses of pembrolizumab beyond the date when complete response was declared
the patient or patient’s legally acceptable representative requests to discontinue study treatment
the patient’s treatment assignment has been purposely unblinded by the investigator, sponsor subsidiary, or through the emergency unblinding call centre during part 1 before recurrence
treatment was interrupted for at least 12 weeks due to a drug-related AE or for non–drug-related or administrative reasons
the patient has a medical condition or personal circumstance that placed the patient at unnecessary risk from continued treatment, as per the opinion of the investigator
the patient has a confirmed positive serum pregnancy test
disease recurrence was confirmed radiographically and/or by examination with subsequent biopsy
any progression or recurrence of any malignancy or any occurrence of another malignancy that requires active treatment (i.e., surgical resection or antineoplastic therapy)
noncompliance with study treatment or procedure requirements
recurrent grade 2 pneumonitis
completion of 17 cycles of therapy during part 1 (note: patients are still eligible for part 2 if they meet the eligibility requirements)
withdrawal of consent to continue in the study by the patient.
Concomitant Therapy
Patients were permitted to use inhaled or topical steroids and systemic steroids at doses 5 mg/m2 per day or less (maximum allowed 10 mg/day) of prednisone or equivalent for pediatric patients (aged ≥ 12 years and < 18 years) and 10 mg/day or less of prednisone or equivalent for adults.
The following is a list of prohibited treatments during the study:
Antineoplastic systemic chemotherapy, immunotherapy, or biological therapy not specified in the protocol. Note: topical 5-fluorouracil use was allowed before enrolment in the study. Treatment of skin cancers other than melanoma with any topical anticancer drugs may be allowed during follow-up after sponsor consultation and approval.
Investigational drugs other than pembrolizumab.
Radiation therapy (with exceptions noted in the eligibility criteria for part 2).
Live vaccines within 30 days before the first dose of study treatment and while participating in the study. Seasonal influenza vaccines for injection are generally killed virus vaccines and were allowed; however, intranasal influenza vaccines are live attenuated vaccines and were not allowed.
Systemic glucocorticoids for any purpose other than to modulate symptoms from an event of clinical interest that is suspected to have an immunologic etiology.
A summary of the most frequently used concomitant medications is provided in Table 7. Overall, ||||||| of patients randomized to the pembrolizumab arm and ||||||| of patients randomized to the placebo arm reported concomitant medication use. Concomitant medication use was reported more frequently (by a difference of at least 10% between treatment groups) by patients randomized to the pembrolizumab arm for the following categories: antidiarrheals, intestinal anti-inflammatory/anti-infective drugs, drugs for acid-related disorders, anti-acne preparations, corticosteroids, dermatological preparations, drugs for obstructive airway diseases, nasal preparations, opthalmologicals, otologicals, corticosteroids for systemic use, and thyroid therapy.
Rescue Therapy and Dose Modification
In general, pembrolizumab was either withheld or permanently discontinued depending on the toxicity grade of immune-related AEs. For example, grade 3 or 4 pneumonitis, AST/ALT elevation or increased bilirubin, nephritis and renal dysfunction, myocarditis, and other immune-related AEs resulted in permanent discontinuation of pembrolizumab. Supportive care to manage AEs with potential immunologic etiology was permitted if deemed necessary by the treating investigator. This may have included oral or IV treatment with corticosteroids as well as additional anti-inflammatory drugs if symptoms did not improve with corticosteroids. Corticosteroids were tapered as the AE improved.
Subsequent Therapies
Subsequent therapies that patients received during part 1 of the KEYNOTE-716 trial following first recurrence is summarized in Table 8. The information presented in the table corresponds to the DCO of January 4, 2022. Subsequent therapies included surgical procedures, radiation, and systemic therapy. Subsequent radiation therapy (|||||||||) and systemic therapy (|||||||||) were more common in the pembrolizumab group versus the placebo group.
Table 7: Concomitant Medication Use (Safety Population, DCO January 4, 2022)
Concomitant medication | Pembrolizumab (N = 483) | Placebo (N = 486) |
|---|---|---|
Patients with 1 or more concomitant medications, n (%) | |||||||||||||| | |||||||||||||| |
Concomitant medication used by at least 10% of patients, n (%) | ||
Antidiarrheals, intestinal anti-inflammatory/anti-infective drugs | |||||||||||||| | |||||||||||||| |
Antiemetics and antinauseants | |||||||||||||| | |||||||||||||| |
Drugs for acid-related disorders | |||||||||||||| | |||||||||||||| |
Drugs for constipation | |||||||||||||| | |||||||||||||| |
Drugs used in diabetes | |||||||||||||| | |||||||||||||| |
Mineral supplements | |||||||||||||| | |||||||||||||| |
Stomatological preparations | |||||||||||||| | |||||||||||||| |
Vitamins | |||||||||||||| | |||||||||||||| |
Antibacterials for systemic use | |||||||||||||| | |||||||||||||| |
Vaccines | |||||||||||||| | |||||||||||||| |
Antithrombotic drugs | |||||||||||||| | |||||||||||||| |
Blood substitutes and perfusion solutions | |||||||||||||| | |||||||||||||| |
Drugs acting on the renin-angiotensin system | |||||||||||||| | |||||||||||||| |
Beta-blocking drugs | |||||||||||||| | |||||||||||||| |
Calcium channel blockers | |||||||||||||| | |||||||||||||| |
Cardiac therapy | |||||||||||||| | |||||||||||||| |
Diuretics | |||||||||||||| | |||||||||||||| |
Lipid modifying drugs | |||||||||||||| | |||||||||||||| |
Vasoprotectives | |||||||||||||| | |||||||||||||| |
Anti-acne preparations | |||||||||||||| | |||||||||||||| |
Antibiotics and chemotherapeutics for dermatologic use | |||||||||||||| | |||||||||||||| |
Antifungals for dermatologic use | |||||||||||||| | |||||||||||||| |
Antipruritics (e.g., antihistamines, anesthetics) | |||||||||||||| | |||||||||||||| |
Corticosteroids, dermatological preparations | |||||||||||||| | |||||||||||||| |
Emollients and protectives | |||||||||||||| | |||||||||||||| |
Other dermatological preparations | |||||||||||||| | |||||||||||||| |
Gynecological anti-infectives and antiseptics | |||||||||||||| | |||||||||||||| |
Other gynecologicals | |||||||||||||| | |||||||||||||| |
Urologicals | |||||||||||||| | |||||||||||||| |
Anti-inflammatory and antirheumatic products | |||||||||||||| | |||||||||||||| |
Topical products for joint and muscular pain | |||||||||||||| | |||||||||||||| |
Analgesics | |||||||||||||| | |||||||||||||| |
Antiepileptics | |||||||||||||| | |||||||||||||| |
Psychoanaleptics | |||||||||||||| | |||||||||||||| |
Psycholeptics | |||||||||||||| | |||||||||||||| |
Antihistamines for systemic use | |||||||||||||| | |||||||||||||| |
Cough and cold preparations | |||||||||||||| | |||||||||||||| |
Drugs for obstructive airway diseases | |||||||||||||| | |||||||||||||| |
Nasal preparations | |||||||||||||| | |||||||||||||| |
Throat preparations | |||||||||||||| | |||||||||||||| |
Opthalmological and ontological preparations | |||||||||||||| | |||||||||||||| |
Opthalmologicals | |||||||||||||| | |||||||||||||| |
Otologicals | |||||||||||||| | |||||||||||||| |
Corticosteroids for systemic use | |||||||||||||| | |||||||||||||| |
Thyroid therapy | |||||||||||||| | |||||||||||||| |
DCO = data cut-off; ITT = intention to treat.
Source: Clinical Study Report.12
Table 8: Subsequent Therapies After First Recurrence (ITT Population, DCO January 4, 2022)
Therapy | Pembrolizumab (N = 487) | Placebo (N = 489) |
|---|---|---|
Patients with RFS events, n | 95 | 139 |
Therapies following first recurrencea | ||
Patients with surgical procedure in part 1 | ||||||||||||||||||| | ||||||||||||||||||| |
Most common proceduresb | ||
Skin excisional biopsy | ||||||||||||||||||| | ||||||||||||||||||| |
Lymph node biopsy | ||||||||||||||||||| | ||||||||||||||||||| |
Skin metastasis resection | ||||||||||||||||||| | ||||||||||||||||||| |
Lymphadenectomy | ||||||||||||||||||| | ||||||||||||||||||| |
Distant metastasis resection | ||||||||||||||||||| | ||||||||||||||||||| |
Patients with radiation in part 1 | ||||||||||||||||||| | ||||||||||||||||||| |
Control of brain metastases | ||||||||||||||||||| | ||||||||||||||||||| |
Control of recurrent disease | ||||||||||||||||||| | ||||||||||||||||||| |
Palliative treatment or symptom control | ||||||||||||||||||| | ||||||||||||||||||| |
Palliative treatment or symptom control of metastatic disease | ||||||||||||||||||| | ||||||||||||||||||| |
Patients with subsequent systemic therapy in part 1 | ||||||||||||||||||| | ||||||||||||||||||| |
Anti-PD-1 therapy | ||||||||||||||||||| | ||||||||||||||||||| |
Anti-CTLA-4 therapy | ||||||||||||||||||| | ||||||||||||||||||| |
Immunotherapy | ||||||||||||||||||| | ||||||||||||||||||| |
Protein kinase inhibitor | ||||||||||||||||||| | ||||||||||||||||||| |
BRAF/MEK-targeted therapy | ||||||||||||||||||| | ||||||||||||||||||| |
Anti-PD-1 and anti-CTLA-4 combination therapy | ||||||||||||||||||| | ||||||||||||||||||| |
Anti-PD-1 and immunotherapy combination therapy | ||||||||||||||||||| | ||||||||||||||||||| |
Anti-PD-1 and anti-CTLA-4 /immunotherapy combination therapy | ||||||||||||||||||| | ||||||||||||||||||| |
Anti-PD-1 and cancer vaccine combination therapy | ||||||||||||||||||| | ||||||||||||||||||| |
Anti-PD-1 and TKI combination therapy | ||||||||||||||||||| | ||||||||||||||||||| |
ITT = intention to treat; RFS = recurrence-free survival.
aPatients with multiple therapies are counted in multiple categories.
bAt least 2 patients in any treatment group.
Source: Clinical Study Report.12
Outcomes
A list of efficacy end points identified in the CADTH review protocol that were assessed in the clinical trials included in this review is provided in Table 9 and end points are further summarized subsequently. A detailed discussion and critical appraisal of the QLQ-C30 and the ED-5D-5L is provided in Appendix 4.
Table 9: Summary of Outcomes of Interest Identified in the CADTH Review Protocol for the KEYNOTE-716 Trial
Outcome measure | Analysis level |
|---|---|
Recurrence-free survival | Primary |
Distant metastasis–free survival | Secondary |
Overall survival | Secondary |
AEs | Secondary |
Discontinuation due to AEs | Secondary |
EORTC QLQ-C30 | Exploratory |
EQ-5D-5L VAS | Exploratory |
AE = adverse event; ECOG = Eastern Cooperative Oncology Group; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30.
Recurrence-Free Survival
In the KEYNOTE-716 trial, RFS was defined as the time from randomization to any of the following events: recurrence of melanoma at any site (local, in-transit, or regional lymph nodes or distant recurrence) or death due to any cause. New incident cases of melanoma and second cancer diagnoses were not counted as events for RFS in the primary analysis. For the primary analysis, the true date of the event was approximated by the date of the first assessment at which the event was objectively documented, after up to 1 missed disease assessment, and before new anticancer therapy was initiated, if any. Participants who experienced a first recurrence immediately after 2 or more consecutive missed disease assessments or after new anticancer therapy was initiated were censored at the last disease assessment before the earlier date of the 2 or more consecutive missed disease assessment or date the new anticancer therapy was initiated. Participants who did not experience a first recurrence event were censored at the last disease assessment before new anticancer therapy was initiated.
The protocol for the KEYNOTE-716 trial indicated a strong preference for tumour imaging to be acquired by CT scan for imaging of the neck, chest, abdomen, and pelvis; contrast-enhanced MRI could be used as an alternative when CT was contraindicated. MRI was strongly preferred for imaging the brain. Tumour imaging was performed every 6 months during the study while on treatment and for the first 3 years off treatment. More frequent imaging was permitted if clinically indicated. Imaging was continued until metastatic disease recurrence was identified, progression in part 2 was identified by the investigator using a modified Response Evaluation Criteria in Solid Tumours for immune based therapeutics (iRECIST) criteria, the patient entered DMFS, or survival follow-up, withdrawal of consent, death, or end of study.
Distant Metastasis–Free Survival
DMFS was defined as the time from randomization to the first diagnosis of a distant metastasis. Distant metastasis refers to cancer that had spread from the original (primary) tumour and beyond local tissues and lymph nodes to distant organs or distant lymph nodes.
Overall Survival
OS was defined as the time from randomization to death due to any cause.
Health-Related Quality of Life
HRQoL was assessed using 2 tools, the EORTC QLQ-C30 version 3 and the EQ-5D-5L VAS. Both HRQoL tools were administered at baseline, during treatment in year 1 (every 4 cycles of treatment), then every 12 weeks during year 2, every 6 months during year 3, at treatment discontinuation, and at the 30-day follow-up visit. The HRQoL tools were administered by trained site personnel and completed electronically by patients. If a patient missed an assessment, the reason for not performing the assessment was reported. Of note, the EORTC QLQ-C30 was restricted to adults in the study because it is not validated in pediatric patients.
The EORTC QLQ-C30 is a cancer-specific HRQoL measure composed of 30 items that include 5 functional dimensions, 3 symptom items, 6 single items, and a global health and QoL scale. The 5 functional dimensions include physical, role, emotional, cognitive, and social. The global health status/QoL scale specifically was reported as a mean change from baseline and included as an exploratory outcome in the KEYNOTE-716 trial. The global health status/QoL scale is informed by 2 items, which are answered using a 7-point Likert-type scale with anchors between 1 (very poor) and 7 (excellent).18 The raw scale score is converted to a standardized score that ranges from 0 to 100, for which a higher score indicates better QoL (i.e., higher scores simply reflect higher levels of response on that scale).18 The KEYNOTE-716 trial defined a clinically meaningful change in the EORTC QLQ-C30 as at least a 10-point change in score from baseline.11,19 Additionally, evidence of validity and reliability of the outcome was identified based on moderate to strong correlations with generic QoL outcomes and an assessment of internal consistency.20,21 Evidence of responsiveness was not identified.
The EQ-5D-5L VAS is a component of the EQ-5D-5L, which is a generic preference-based patient-reported HRQoL outcome. The VAS records the patient’s self-rated health on a 20 cm scale with end points of 0 and 100, with respective anchors of “the worst health you can imagine” and “the best health you can imagine.”22 Evidence of validity and reliability of the EQ-5D-5L was identified, but no data regarding responsiveness was identified. Based on a study that examined various cancers using both anchor and distribution-based methods, the minimal important difference (MID) for the VAS ranged from 7 to 12.23 No estimates for the MID among patients with melanoma were identified. In the KEYNOTE-716 trial, the EQ-5D-5L was used to provided data to develop health utilities for the health economic analyses.
Based on completion and compliance rates, the analysis of change from baseline for the HRQoL outcomes was performed at week 48 and week 72 in IA3.
Harms
Safety events, such as AEs and SAEs, were reported by the patient and documented by the investigator and any associated designees. All AEs that occurred between treatment allocation through 30 days following the end of study treatment were reported.
Statistical Analysis
Primary Outcome
The primary end point of the KEYNOTE-716 trial was RFS. The primary end point was an event-driven outcome with plans to conduct the final analysis after approximately 179 events were observed unless the study was terminated early. The sponsor estimated that the final analysis may occur approximately 48 months after the first participant was randomized, depending on enrolment rate and event accumulation rate.
The nonparametric Kaplan-Meier method was used to estimate the RFS curve in each treatment group. The treatment group difference was assessed by a stratified log-rank test; a stratified Cox proportional hazard model with Efron’s method of tie handling was used to estimate the HR between the treatment arms.
The true date of RFS was approximated based on the first assessment at which the event was objectively documented. Patients who did not experience an event at the time of analysis were censored at the last disease assessment date.
A summary of the censoring rules for the primary end point is provided in Figure 3, as well as the sensitivity analyses performed to evaluate the robustness of the main analysis. Additionally, new primary melanomas were not counted as RFS events for the primary RFS analysis.
Figure 3: Censoring Rules for the Primary End Point (Recurrence-Free Survival)
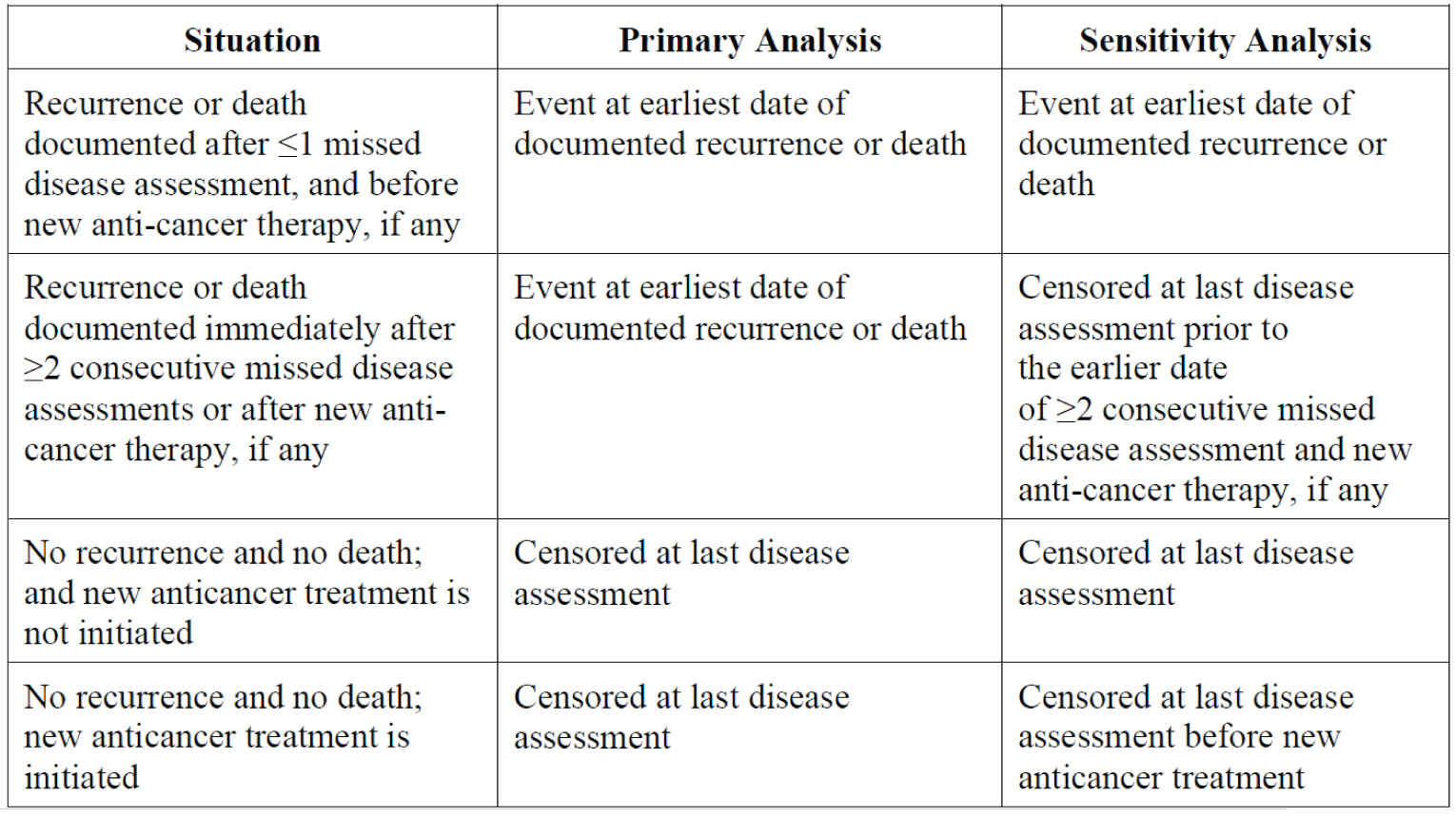
Source: Clinical Study Report.17
Key Secondary Outcomes
The key secondary outcomes of the KEYNOTE-716 trial included DMFS and OS. The key secondary outcomes were estimated using nonparametric “time to metastatic disease” and survival curves for DMFS and OS, respectively, following the same analysis method as for the primary outcome. For DMFS, patients without documented metastatic disease diagnosis were censored at the date of their last disease assessment. For OS, patients without documented death at the time of the analysis were censored at the date of the participant was last known to be alive.
Power Calculation
Based on a target number of 179 events at the final analysis and 1 interim analysis at approximately 71% of the target number of events, the study has approximately 92% power for detecting a HR of 0.6 at 2.5% (1-sided) significance level.
For the key secondary outcome of DMFS, the final analysis was expected to occur at approximately 108 months after the first participant was randomized. It was estimated that approximately 195 DMFS events will have been observed among all participants. The final analysis of OS in this the study was expected to occur at approximately 180 months after the first participant was randomized. It was estimated that approximately 204 OS events will have been observed among all participants.
The above sample size and power calculations were based on the following assumptions:
RFS follows a “cure” model with a long-term RFS of 50% and the 60-month RFS estimated to be 68% for the control group
DMFS follows a cure model with a long-term DMFS of 65% and the 60-month DMFS estimated to be 78% for the control group
OS follows an exponential distribution with the 120-month OS estimated to be 75% for the control group
enrolment period of 16 months
an annual dropout rate of 4.7%
a follow-up period of 32, 92, and 164 months for RFS, DMFS, and OS, respectively, after the last participant is randomized.
Multiplicity
A graphical method (Maurer and Bretz) was used to control the primary and key secondary analyses for multiplicity, as well as the interim analyses. The sponsor reported that, according to this approach, study hypotheses may be tested more than once, and when a particular null hypothesis is rejected, the alpha allocated to that hypothesis can be reallocated to other hypothesis tests. For example, if the primary null hypothesis regarding RFS was rejected, the entire alpha was reallocated to the hypothesis testing for DMFS. Similarly, if the null hypothesis for DMFS was then rejected, the entire alpha would be reallocated to the OS analysis.
Initially, 2.5% alpha (1-sided) was allocated to the primary analysis of RFS. The study was considered successful if RFS demonstrated statistical significance at either an interim analysis or the final analysis while controlled for multiplicity.
A set of boundary properties were set for the interim and final analysis of RFS using a Lan-DeMets O’Brien Fleming approximation spending function. If the RFS events differed from the prespecified boundary properties, the bounds were adjusted. A similar approach was used for the key secondary outcomes of DMFS and OS as well (boundary properties not shown).
Interim Analyses
Five efficacy interim analyses and a final analysis were planned for the KEYNOTE-716 trial, as outlined in Figure 4. At the time of this review, IA3 was the most recent analysis available. The interim and final analysis of the primary end point, RFS, was reported at IA1 and IA2. The interim analysis of DMFS was reported at IA3.
Subgroup Analyses
The primary outcome was analyzed using an unstratified Cox model by the following subgroups of relevance to the CADTH review: T category (T3b versus T4a versus T4b) and age (< 65 years versus ≥ 65 years). The estimate of the between-group treatment effect (with a nominal 95% CI) was reported descriptively. As per the systematic review protocol, the subgroups corresponding to T category and age were summarized for this report.
Secondary Outcomes of the Studies
Patient-reported HRQoL outcomes (EORTC QLQ-C30 and EQ-5D-5L) were considered exploratory; therefore, formal hypothesis testing was not conducted.
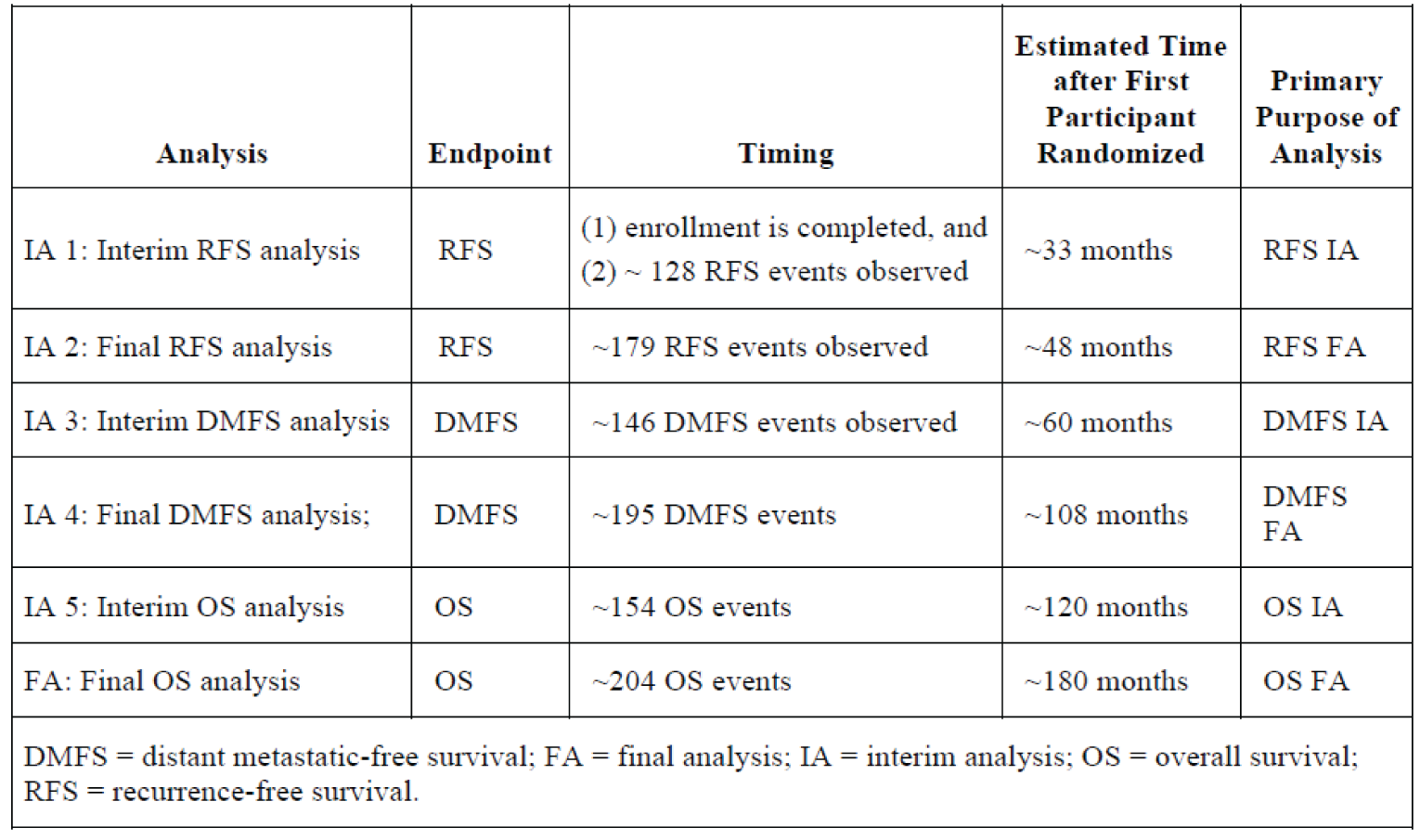
Table 10: Statistical Analysis of Efficacy End Points in the KEYNOTE-716 Trial
End point | Statistical model | Adjustment factors | Sensitivity analyses |
|---|---|---|---|
RFS | Stratified log-rank test Stratified Cox model with Efron’s method of tie handling | Stratification factors:
|
|
DMFS | Same as above | Same as above | None |
OS | Same as above | Same as above | None |
DMFS = distant metastasis–free survival; OS = overall survival; RFS = recurrence-free survival.
Source: Clinical Study Report.11
Analysis Populations
Primary efficacy analyses were conducted using the ITT population. The ITT population included all randomized patients. Patients were analyzed based on the treatment group they were randomized to.
The analysis of safety data was conducted in the “all participants as treated” population, which will be referred to as the safety population herein. The safety population included all randomized patient who received at least 1 dose of study treatment. Patients were analyzed based on the treatment that was received.
Patient-reported outcomes (PROs) were analyzed based on a PRO full analysis set. Patients who had at least 1 PRO assessment available and received at least 1 dose of study treatment were included in the PRO full analysis set.
Results
Patient Disposition
A summary of the patient disposition for the KEYNOTE-716 trial is provided in Table 11. Of the 1,182 patients screened for the KEYNOTE-716 trial, a total of 976 (82.6%) were randomized (487 to pembrolizumab, 489 to placebo).
As of the DCO of January 4, 2022, ||||||| and ||||||| of patients randomized to the pembrolizumab and placebo arms, respectively, had discontinued from the study. The most common reason for discontinuation from the study was death (||||||| and ||||||| for pembrolizumab and placebo, respectively) followed by withdrawal by the patient (||||||| and ||||||| or pembrolizumab and placebo, respectively). The rate of discontinuation from the study was similar at IA2 (DCO June 21, 2021) except fewer patients had died, which was reflected in the overall discontinuation rate (||||||| and ||||||| for pembrolizumab and placebo, respectively).
The proportion of patients who discontinued from treatment was 33.7% of patients randomized to the pembrolizumab arm and 24.3% of patients randomized to the placebo arm. The most common reasons for discontinuation from treatment were AEs (17.6% and 4.7% for pembrolizumab and placebo, respectively), withdrawal by patient (8.3% and 5.6% for pembrolizumab and placebo, respectively), and relapse or recurrence (5.0% and 12.6% for pembrolizumab and placebo, respectively). The rate of discontinuation from treatment was similar at IA2 (DCO June 21, 2021).
Exposure to Study Treatments
A summary of exposure to study drug and placebo during the KEYNOTE-716 trial as of the DCO of January 4, 2022, is provided in Table 12. Patients randomized to the pembrolizumab and placebo arms were on therapy for a mean of ||||||| days (SD = ||||||| days) and ||||||| days (SD = ||||||| days), respectively. Patients randomized to the pembrolizumab arm had received a mean of 14 administrations (SD = 5.2) during this time, and patients randomized to the placebo arm had received a mean of 15 administrations (SD = 4.0).
The duration of follow-up at IA2 and IA3 is summarized in Table 13. At IA2, the median duration of follow-up in months was |||||||||||||||||||||||||||| for pembrolizumab and |||||||||||||||||||||||||||| for placebo. At IA3, the median duration of follow-up in months was |||||||||||||||||||||||||||| for pembrolizumab and ||||||||||||||||||||| for placebo.
Table 11: Patient Disposition in the KEYNOTE-716 Trial (DCO January 4, 2022)
Disposition | Pembrolizumab | Placebo |
|---|---|---|
Screened, N | 1,182 | |
Randomized, N (%) | 976 (82.6) | |
Assigned to treatment, N | 487 | 489 |
Discontinued from study, N (%) | ||||||||||||||||||||| | ||||||||||||||||||||| |
Reason for discontinuation, N (%) | ||
Adverse events | ||||||||||||||||||||| | ||||||||||||||||||||| |
Lost to follow-up | ||||||||||||||||||||| | ||||||||||||||||||||| |
Death | ||||||||||||||||||||| | ||||||||||||||||||||| |
Withdrawal by patient | ||||||||||||||||||||| | ||||||||||||||||||||| |
Discontinued from treatment,a N (%) | 163 (33.7) | 118 (24.3) |
Adverse events | 85 (17.6) | 23 (4.7) |
Lost to follow-up | 0 (0.0) | 1 (0.2) |
Noncompliance with study drug | 0 (0.0) | 1 (0.2) |
Physician decision | 10 (2.1) | 4 (0.8) |
Protocol violation | 4 (0.8) | 1 (0.2) |
Relapse or recurrence | 24 (5.0) | 61 (12.6) |
Withdrawal by patient | 40 (8.3) | 27 (5.6) |
ITT, N | 487 | 489 |
Safety, N | 483 | 486 |
PRO FAS, N | NR | NR |
DCO = data cut-off; FAS = full analysis set; ITT = intention to treat; PP = per protocol; PRO = patient-reported outcome.
aDiscontinuation from treatment includes information from part 1 only.
Source: Clinical Study Report (interim analysis 3).12
Table 12: Exposure (Safety Population, DCO January 4, 2022)
Exposure | Pembrolizumab (N = 483) | Placebo (N = 486) |
|---|---|---|
Number of days on therapya | ||
Mean (SD) | ||||||||||||||||||||| | ||||||||||||||||||||| |
Median (range) | ||||||||||||||||||||| | ||||||||||||||||||||| |
Number of administrations | ||
Mean (SD) | 13.8 (5.2) | 15.1 (4.0) |
Median (range) | ||||||||||||||||||||| | ||||||||||||||||||||| |
Duration of exposure, n (%) | ||
> 0 months | ||||||||||||||||||||| | ||||||||||||||||||||| |
≥ 1 month | ||||||||||||||||||||| | ||||||||||||||||||||| |
≥ 3 months | ||||||||||||||||||||| | ||||||||||||||||||||| |
≥ 6 months | ||||||||||||||||||||| | ||||||||||||||||||||| |
≥ 9 months | ||||||||||||||||||||| | ||||||||||||||||||||| |
≥ 10 months | ||||||||||||||||||||| | ||||||||||||||||||||| |
≥ 12 months | ||||||||||||||||||||| | ||||||||||||||||||||| |
DCO = data cut-off; SD = standard deviation.
aNumber of days on therapy is calculated as last dose date – first dose date + 1.
Source: Clinical Study Report.12
Table 13: Duration of Follow-Up (ITT Population)
Follow-up duration (months)a | Pembrolizumab (N = 487) | Placebo (N = 489) |
|---|---|---|
IA2: DCO June 21, 2021 | ||
Mean (SD) | ||||||||||||||||||||| | ||||||||||||||||||||| |
Median (range) | ||||||||||||||||||||| | ||||||||||||||||||||| |
IA3: DCO January 4, 2022 | ||
Mean (SD) | ||||||||||||||||||||| | ||||||||||||||||||||| |
Median (range) | ||||||||||||||||||||| | ||||||||||||||||||||| |
DCO = database cut-off; IA = interim analysis; ITT = intention to treat; SD = standard deviation.
aFollow-up duration is defined as the time from randomization date to the date of death or the DCO date if the patient was still alive.
Source: Clinical Study Reports.11,12
Efficacy
Only those efficacy outcomes and analyses of subgroups identified in the review protocol are reported below. Refer to Appendix 3 for detailed efficacy data.
Overall Survival
The analysis of OS was not available at the time of this review. The sponsor reported that the final analysis of OS will be conducted when approximately 203 OS events have been observed, which was estimated to occur 15 years after randomization of the first patient.
Disease-Free Survival
Disease-free survival was not reported.
Recurrence-Free Survival
A summary of the results of the final analysis of RFS, the primary outcome for the KEYNOTE-716 trial, based on the DCO of June 21, 2021 (IA2) is provided in Table 14 and Figure 5. The median duration of follow-up for all participants (ITT population) was 20.5 months (range, 4.6 to 32.7 months) as of the DCO, with a similar median duration of follow-up across treatment groups at IA2. At IA2, 72 (14.8%) patients randomized to the pembrolizumab arm and 115 (23.5%) patients randomized to the placebo arm had experienced recurrence of disease. In the pembrolizumab treatment group, 7.8% of events were local, regional, or locoregional recurrence, 6.4% were distant recurrence, and 0.6% were deaths. In the placebo treatment group, 10.2% were local, regional, or locoregional recurrence, 12.3% were distant recurrence, and 1.0% were deaths. At 18 months, the rates of RFS were 85.8% (95% CI, 82.0% to 88.9%) and 77.0% (95% CI, 72.6% to 80.7%) for patients randomized to the pembrolizumab and placebo treatment groups, respectively, which corresponded to a HR of 0.61 (95% CI, 0.45 to 0.82; P = ||||||||||||) or decreased risk of disease recurrence or death in favour of pembrolizumab. The HR for RFS at IA2 was consistent with the results at IA1 (HR = 0.65; 95% CI, 0.46 to 0.92; P = 0.00658) and IA3 (HR = 0.64; 95% CI, 0.50 to 0.84).
Sensitivity analyses for RFS were conducted at IA2. No sensitivity analyses were conducted at IA3. The 2 sensitivity analyses of RFS assessed this outcome accounting for new primary melanomas included in the RFS analysis and using different censoring rules. The results of the sensitivity analyses were consistent with the primary analysis and are presented in Appendix 3.
A descriptive analysis of RFS by subgroup was performed at IA2 and IA3. The results of the subgroup analyses of interest to this review are presented in Table 15. The subgroup analysis of RFS by overall cancer stage resulted in a HR of |||||||||||| (95% CI, ||||||||||||) for patients with stage IIB melanoma and |||||||| (||||||||||||||||||||||||||||||) for patients with stage IIC melanoma for pembrolizumab compared with placebo. For the comparison of pembrolizumab to placebo, the subgroup analysis of RFS by T category resulted in a HR of 0.40 (95% CI, 0.23 to 0.69) for patients with T3b melanoma, 0.49 (95% CI, 0.24 to 1.00) for patients with T4a melanoma, and 0.82 (95% CI, 0.54 to 1.26) for patients with T4b melanoma. For the comparison of pembrolizumab to placebo, the subgroup analysis of RFS by age resulted in a HR of 0.63 (95% CI, 0.41 to 0.97) for patients younger than 65 years and 0.59 (95% CI, 0.4 to 0.89) for patients 65 years and older.
Table 14: Recurrence-Free Survival (ITT Population, DCO June 21, 2021)
RFS | Pembrolizumab (N = 487) | Placebo (N = 489) |
|---|---|---|
Events, n (%) | 72 (14.8) | 115 (23.5) |
Event rate per 100 person-months | 0.9 | 1.4 |
RFSa (months), median (95% CI) | NR (NR to NR) | NR (29.9 to NR) |
RFS ratea at 18 months, % (95% CI) | 85.8 (82.0 to 88.9) | 77.0 (72.6 to 80.7) |
Hazard ratio (95% CI)b | 0.61 (0.45 to 0.82) | |
P valuec | |||||||||||||||||||||||| | |
RFS rate at time point, % (95% CI)a | ||
6 months | 95.6 (||||||||||||) | 93.6 (||||||||||||) |
12 months | 90.8 (||||||||||||) | 83.3 (||||||||||||) |
18 months | 85.8 (||||||||||||) | 77.0 (||||||||||||) |
24 months | 80.5 (||||||||||||) | 71.7 (||||||||||||) |
Type of first event in RFS analysis, n (%) | ||
Local, regional, or locoregional | 38 (7.80) | 50 (10.22) |
Distant (includes distant event diagnosed within 30 days from local, regional, or locoregional event) | 31 (6.37) | 60 (12.27) |
Death | 3 (0.62) | 5 (1.02) |
No event | 415 (85.2) | 374 (76.5) |
CI = confidence interval; DCO = data cut-off; ITT = intention to treat; NR = not reached; RFS = recurrence-free survival.
aFrom product-limit (Kaplan-Meier) method for censored data.
bBased on Cox regression model with Efron’s method of tie handling with treatment as a covariate stratified by melanoma T category (T3b vs. T4a vs. T4b).
cOne-sided P value based on log-rank test stratified by melanoma T category (T3b vs. T4a vs. T4b).
Source: Clinical Study Report.11
Table 15: Recurrence-Free Survival by Subgroup (ITT Population, DCO June 21, 2021)
Subgroup | Events by subgroup, n of N (%) | HR (95% CI) | P valuea | ||
|---|---|---|---|---|---|
Pembrolizumab | Placebo | All patients | |||
Baseline cancer stage (primary censoring rule) | |||||
IIB | |||||||||||| | |||||||||||| | NR | |||||||||||| | NR |
IIC | |||||||||||| | |||||||||||| | NR | |||||||||||| | NR |
T categoryb | |||||
T3b | 18 of 200 (9.0) | 44 of 200 (22.0) | 62 of 400 | 0.40 (0.23 to 0.69) | |||||||||||| |
T4a | 11 of 109 (10.1) | 24 of 116 (20.7) | 35 of 225 | 0.49 (0.24 to 1.00) | |||||||||||| |
T4b | 39 of 171 (22.8) | 45 of 169 (26.6) | 84 of 340 | 0.82 (0.54 to 1.26) | |||||||||||| |
Age | |||||
< 65 | NR | NR | 87 of 598 | 0.63 (0.41 to 0.97) | NR |
≥ 65 | NR | NR | 100 of 378 | 0.59 (0.4 to 0.89) | NR |
CI = confidence interval; DCO = data cut-off; HR = hazard ratio; ITT = intention to treat; NR = not reported; RFS = recurrence-free survival.
aThe P value was not adjusted for multiple testing (i.e., the type I error rate has not been controlled).
bBased on Cox regression model with Efron’s method of tie handling with treatment as a covariate.
Source: Clinical Study Report.11
Figure 5: KM Estimates of Recurrence-Free Survival (Primary Censoring Rule, ITT Population, DCO June 21, 2021)
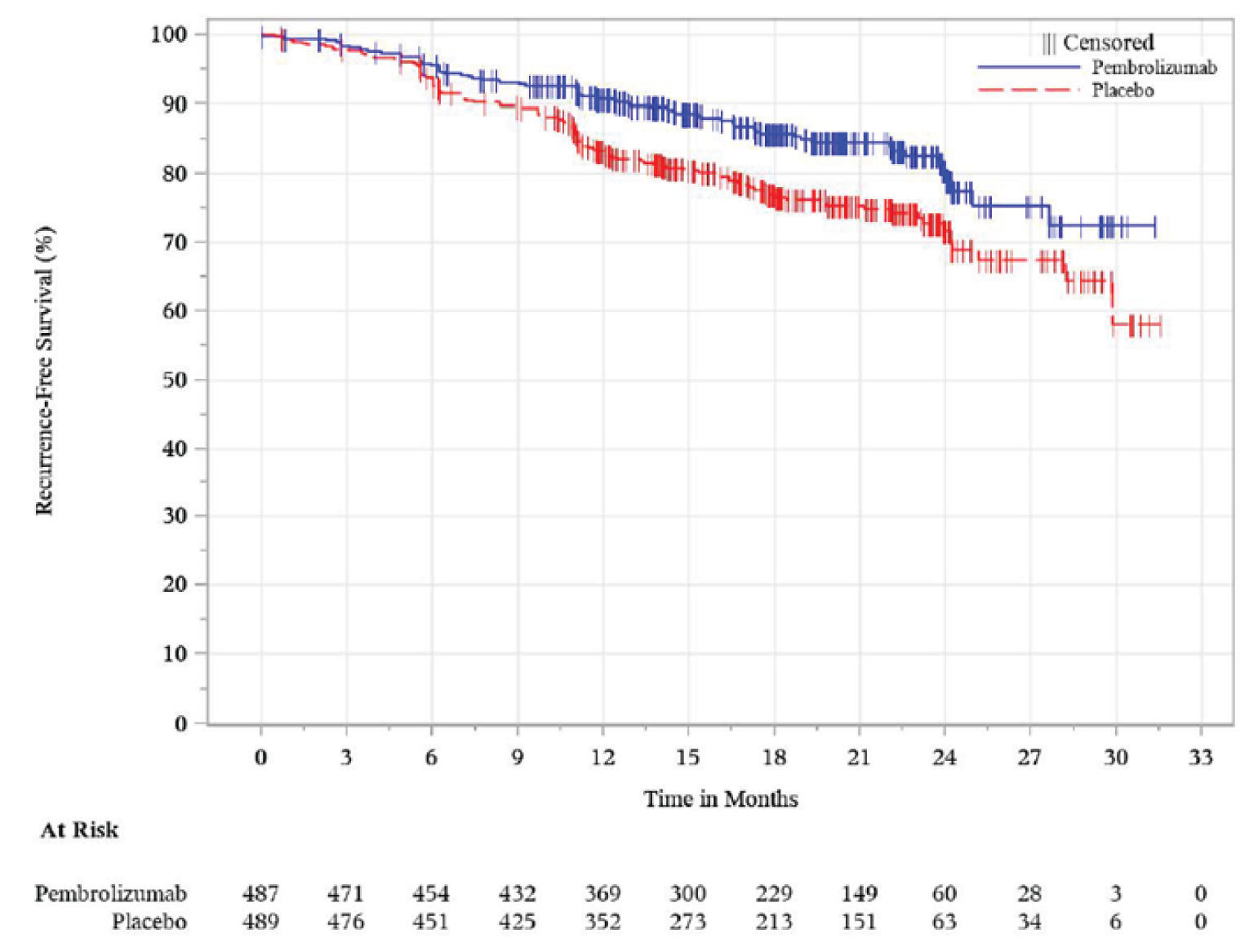
IA2 = interim analysis 2; KM = Kaplan-Meier; RFS = recurrence-free survival
Note: Date cut-off date was June 21, 2021.
Source: Clinical Study Report.11
Distant Metastasis–Free Survival
The results for DMFS based on IA3 are summarized in Table 16 and Figure 6. At the DCO for IA3 (January 4, 2022), the median duration of follow-up was 26.9 months (range, 4.6 to 39.2 months) overall and similar across treatment groups. The median DMFS had not been reached by either treatment group. Distant metastasis was reported for 12.9% of patients randomized to the pembrolizumab group and 19.4% of patients randomized to the placebo group. The DMFS rate at 18 months was 92.7% (95% CI, 89.9% to 94.7%) and 86.5% (95% CI, 83.1% to 89.3%) for the pembrolizumab and placebo treatment groups, respectively. This corresponded to a HR of 0.64 (95% CI, 0.47 to 0.88; P = 0.00292), which represents a decreased risk of experiencing distant metastasis associated with treatment with pembrolizumab.
Table 16: Distant Metastasis–Free Survival (ITT Population, DCO January 4, 2022)
DMFS | Pembrolizumab (N = 487) | Placebo (N = 489) |
|---|---|---|
Events, n (%) | 63 (12.9) | 95 (19.4) |
Event rate per 100 person-months | 0.6 | 0.9 |
DMFSa (months), median (95% CI) | NR (NR to NR) | NR (NR to NR) |
DMFS ratea at 18 months, % (95% CI) | 92.7 |||||||||||| | 86.5 |||||||||||| |
Hazard ratio (95% CI)b | 0.64 (0.47 to 0.88) | |
P valuec | 0.00292 | |
DMFS rate at time point, % (95% CI)a | ||
6 months | |||||||||||| | |||||||||||| |
12 months | 94.7 |||||||||||| | 90.2 |||||||||||| |
18 months | |||||||||||| | |||||||||||| |
24 months | 88.1 (84.4 to 90.9) | 82.2 (78.2 to 85.5) |
30 months | |||||||||||| | |||||||||||| |
36 months | |||||||||||| | |||||||||||| |
CI = confidence interval; DCO = data cut-off; DMFS = distant metastasis–free survival; ITT = intention to treat; NR = not reached.
Note: DMFS is defined as the time from randomization to the first diagnosis of a distant metastasis.
aFrom product-limit (Kaplan-Meier) method for censored data.
bBased on Cox regression model with Efron’s method of tie handling with treatment as a covariate stratified by melanoma T category (T3b vs. T4a vs. T4b).
cOne-sided P value based on log-rank test stratified by melanoma T category (T3b vs. T4a vs. T4b).
Source: Clinical Study Report.12
Health-Related Quality of Life
The results for HRQoL outcomes, the EORTC QLQ-C30 Global Health Status/QoL scale and EQ-5D-5L VAS based on IA3 are provided in Table 17.
The LS mean of the change from baseline to week 48 in the EORTC QLQ-C30 Global Health Status/QoL scale score was |||||||||||||||||||||||| for patients randomized to the pembrolizumab group and |||||||||||||||||||||||||||||||||||| for patients randomized to the placebo group. This corresponded to a LS mean treatment group difference of ||||||||||||||||||||||||||||||||||||. The results for change from baseline to week 48 in EORTC QLQ-C30 at IA3 were similar with the results reported at IA2. The change from baseline to week 72 corresponded to a treatment group difference of ||||||||||||||||||||||||||||||||||||. The results of the Global Health Status/QoL scale score as well as the items of the functional scales at weeks 48 and 72 are presented in Figure 7 and Figure 8, respectively.
The LS mean change from baseline to week 48 for the EQ-5D-5L VAS was |||||||||||||||||||||||||||||||||||| for patients randomized to the pembrolizumab group and |||||||||||||||||||||||||||||||||||| for patients randomized to the placebo group. This corresponded to a LS mean treatment group difference of ||||||||||||||||||||||||||||||||||||||||||||||||. At week 72, the LS mean treatment group difference was ||||||||||||||||||||||||||||||||||||.
Figure 6: KM Estimates of Distant Metastasis–Free Survival (ITT Population, DCO January 4, 2022)
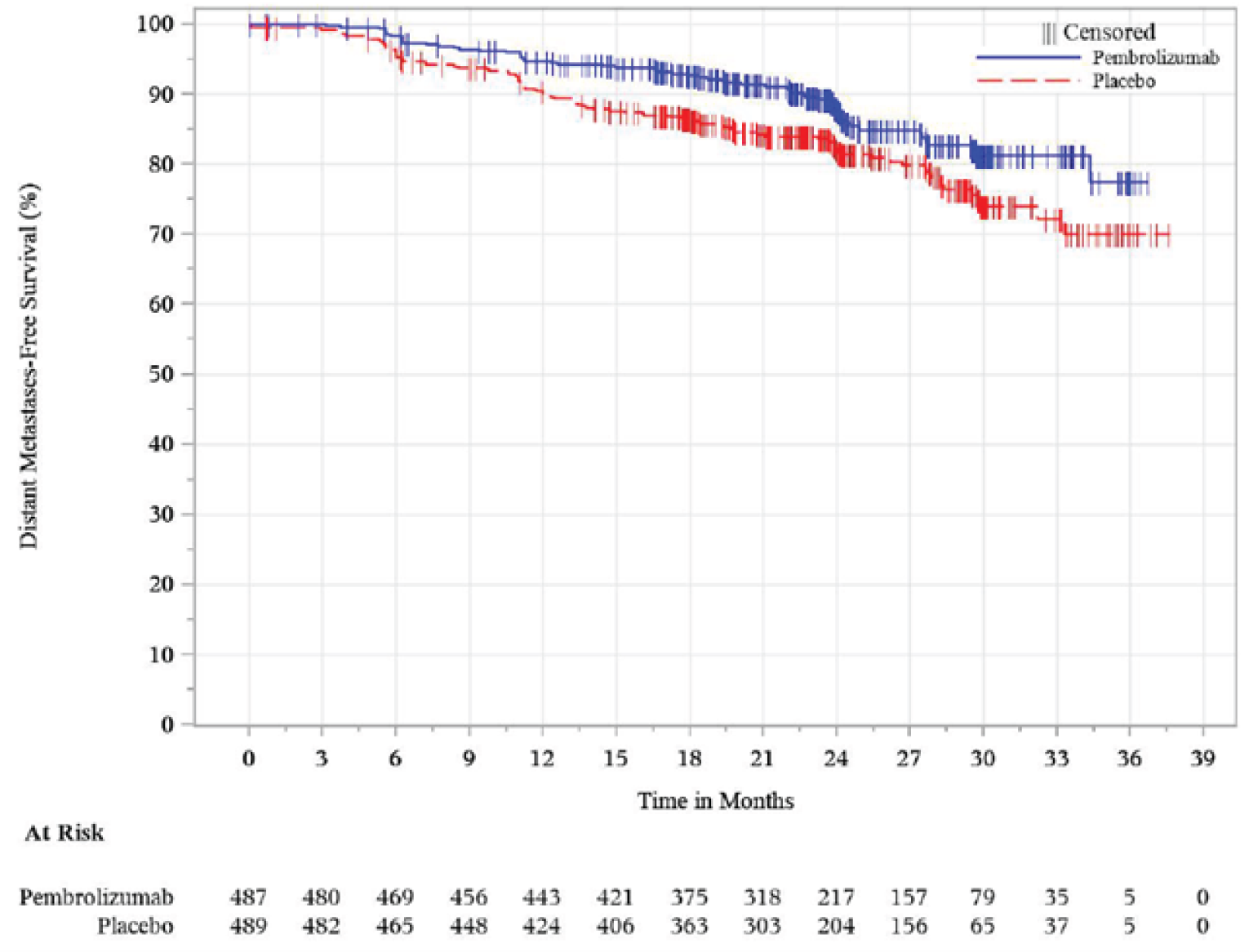
DCO = data cut-off; DMFS = distant metastasis–free survival; ITT = intention to treat; KM = Kaplan-Meier.
Source: Clinical Study Report.12
Table 17: Patient-Reported HRQoL Outcomes (PRO FAS Population, DCO January 4, 2022)
Category | Total N | Baseline, mean (SD) | N at time point, n (%) | Score at time point, mean (SD) | Change from baseline, LS mean (95% CI) | Treatment group difference | |
|---|---|---|---|---|---|---|---|
LS mean (95% CI)a | P valueb | ||||||
Change from baseline in EORTC QLQ-C30, Global Health Status/QoL Scale | |||||||
Week 48 | |||||||
Pembrolizumab | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
Placebo | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | ||
Week 72 | |||||||
Pembrolizumab | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
Placebo | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | ||
Change from baseline in EQ-5D-5L VAS | |||||||
Week 48 | |||||||
Pembrolizumab | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
Placebo | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | ||
Week 72 | |||||||
Pembrolizumab | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| |
Placebo | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | |||||||||||| | ||
CI = confidence interval; DCO = data cut-off; EORTC QLQ-C30 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; FAS = full analysis set; LS = least squares; NR = not reached; SD = standard deviation; VAS = visual analogue scale.
Note: For baseline and week 48, N is the number of patients in each treatment group with non-missing assessments at the specific time point; for change from baseline, N is the number of participants in the analysis population in each treatment group.
aBased on a constrained longitudinal data analysis model with the PRO scores as the response variable with covariates for treatment by time interaction, stratification factor melanoma T category (IIB T3b greater than 2.0 mm to 4.0 mm with ulceration vs. IIB T4a greater than 4.0 mm without ulceration vs. IIC T4b greater than 4.0 mm with ulceration) as covariate.
bThe P value has not been adjusted for multiple testing (i.e., the type I error rate has not been controlled).
Source: Clinical Study Report.12
Figure 7: EORTC QLQ-C30 Functional Scales/Global Health Status/QoL, Change From Baseline to Week 48 (PRO FAS Population, DCO January 4, 2022)

Note: This figure was redacted at the request of the sponsor.
Figure 8: EORTC QLQ-C30 Functional Scales/Global Health Status/QoL, Change From Baseline to Week 72 (PRO FAS Population, DCO January 4, 2022)

Note: This figure was redacted at the request of the sponsor.
Harms
Only those harms identified in the review protocol are reported here. Refer to Table 18 for detailed harms data. The summary of safety events described herein are based on IA3 at which the median duration of follow-up was approximately 27 months.
Adverse Events
At IA3 (DCO January 4, 2022), 95.7% and 91.6% of patients in the pembrolizumab and placebo treatment groups, respectively, reported at least 1 AE. A summary of the most common AEs is available in Table 18. Fatigue, diarrhea, pruritus, arthralgia, rash, headache, and hypothyroidism were reported by at least 17% of patients in the pembrolizumab treatment group. Diarrhea (28% versus 21% for pembrolizumab versus placebo, respectively), pruritus (28% versus 13%), arthralgia (24% versus 17%), rash (19% versus 9%), headache (17% versus 11%), hypothyroidism (17% versus 4%), increased ALT (12% versus 6%), and hyperthyroidism (10% versus 1%) were reported more frequently by patients in the pembrolizumab treatment group than the placebo group.
As described previously, 2 pediatric patients were included in the KEYNOTE-716 trial. The patient randomized to the pembrolizumab arm reported AEs due to an increased lymphocyte count and 1 due to hidradenitis. The patient randomized to the placebo arm did not report any AEs. A summary of harms for older adult populations was also reported and is provided in Table 19. Overall, AEs were more common among patients in the pembrolizumab treatment group than the placebo group.
Serious Adverse Events
SAEs were reported by ||||||| of patients in the pembrolizumab treatment group and ||||||| of patients in the placebo treatment group. The frequency of SAEs was similar between treatment groups in the overall population. The most frequently reported SAEs were basal cell carcinoma (||||||| and ||||||| in the pembrolizumab and placebo treatment groups, respectively), squamous cell carcinoma of the skin (||||||| and |||||||), malignant melanoma in situ (||||||| and |||||||), and malignant melanoma ||||||| and |||||||).
Neither of the pediatric patients in the study reported an SAE. SAEs were reported more frequently among patients who were aged at least 65 years (SAEs for the pembrolizumab and placebo groups were ||||||| and |||||||, respectively) compared with patients who were younger than 65 years (SAEs for the pembrolizumab and placebo arms were ||||||| and |||||||, respectively). An SAE was reported by ||||||| and ||||||| of patients between the ages of 65 and 74 years, and ||||||| and ||||||| of patients between the ages of 75 and 84 years in the pembrolizumab and placebo treatment groups, respectively.
Withdrawals Due to Adverse Events
As of IA3, 17.2% of patients in the pembrolizumab treatment group and 4.5% of patients in the placebo treatment group had discontinued treatment due to AEs (WDAE). Specific reasons for WDAE were varied; the most common reason for WDAE was autoimmune hepatitis (||||||| for the pembrolizumab group and ||||||| for the placebo group) and colitis (||||||| for the pembrolizumab group and ||||||| for the placebo group).
Neither of the pediatric patients in the study withdrew due to an AE. Among older adult patients, the proportion of patients in the pembrolizumab treatment group that withdrew due to an AE increased with age and was similar to the proportion of patients who withdrew due to an AE in the overall population. Similarly, WDAEs among the placebo treatment group was consistent with the overall population.
Mortality
As of the DCO of January 4, 2022, a total of ||||||| patients had died, ||||||| of whom were randomized to the placebo group. Of the ||||||| reported deaths, ||||||| patients (all randomized to the placebo group) were younger than 65 years and ||||||| (||||||| randomized to the pembrolizumab group, ||||||| randomized to the placebo group) were aged 65 years or older.
Notable Harms
A summary of notable harms identified in the CADTH systematic review protocol is described in Table 18. Immune-mediated reactions were more common in the pembrolizumab treatment group than the placebo group. Colitis was reported by 3.9% and 1.0% of patients and pneumonitis was reported by 2.5% and 0.8% of patients in the pembrolizumab and placebo treatment groups, respectively. Severe skin reactions such as Stevens-Johnson syndrome or toxic epidermal necrolysis were not reported by any patients. Infusion-related reactions were reported by 0.6% and 1.4% of patients in the pembrolizumab and placebo treatment groups, respectively. Endocrine-related reactions, such as hypothyroidism and hyperthyroidism, were more commonly reported by patients in the pembrolizumab treatment group than the placebo group, as previously discussed. Adrenal insufficiency was reported by 2.7% and 0 patients, and type 1 diabetes was reported by 0.4% and 0 patients in the pembrolizumab and placebo treatment groups, respectively. Notable harms were not reported by subgroups.
Table 18: Summary of Harms (Safety Population, DCO January 4, 2022)
Harms | Pembrolizumab (N = 483) | Placebo (N = 486) |
|---|---|---|
Patients with ≥ 1 AE | ||
n (%) | 462 (95.7) | 445 (91.6) |
Most common events,a n (%) | ||
Fatigue | 142 (29.4) | 126 (25.9) |
Diarrhea | 136 (28.2) | 100 (20.6) |
Pruritus | 134 (27.7) | 63 (13.0) |
Arthralgia | 115 (23.8) | 84 (17.3) |
Rash | 91 (18.8) | 42 (8.6) |
Headache | 83 (17.2) | 55 (11.3) |
Hypothyroidism | 82 (17.0) | 17 (3.5) |
Nausea | 67 (13.9) | 56 (11.5) |
Cough | 61 (12.6) | 57 (11.7) |
ALT increased | 57 (11.8) | 29 (6.0) |
Asthenia | 55 (11.4) | 52 (10.7) |
Hyperthyroidism | 50 (10.4) | 3 (0.6) |
Myalgia | 50 (10.4) | 28 (5.8) |
Patients with ≥ 1 SAE | ||
n (%) | 103 (21.3) | 94 (19.3) |
Most common events,b n (%) | ||
Basal cell carcinoma | ||||||| | ||||||| |
Squamous cell carcinoma of skin | ||||||| | ||||||| |
Malignant melanoma in situ | ||||||| | ||||||| |
Malignant melanoma | ||||||| | ||||||| |
Patients who stopped treatment due to AEs | ||
n (%) | ||||||| | ||||||| |
Most common events,b n (%) | ||
Autoimmune hepatitis | ||||||| | ||||||| |
Colitis | ||||||| | ||||||| |
Deaths, n (%) | ||
n (%) | ||||||| | ||||||| |
COVID-19 pneumonia | ||||||| | ||||||| |
Pneumonia | ||||||| | ||||||| |
Recurrent cancer | ||||||| | ||||||| |
Completed suicide | ||||||| | ||||||| |
Notable harms, n (%) | ||
Immune-mediated reactions | ||
Colitis | 19 (3.9) | 5 (1.0) |
Pneumonitis | 12 (2.5) | 4 (0.8) |
Severe skin reactions | 15 (3.1) | 3 (0.6) |
SJS | 0 (0.0) | 0 (0.0) |
TEN | 0 (0.0) | 0 (0.0) |
Infusion-related reactions | 3 (0.6) | 7 (1.4) |
Endocrine-related reactions | ||
Hypothyroidism | 83 (17.2) | 18 (3.7) |
Hyperthyroidism | 50 (10.4) | 3 (0.6) |
Adrenal insufficiency | 13 (2.7) | 0 (0.0) |
Type 1 diabetes | 2 (0.4) | 0 (0.0) |
ALT = alanine aminotransferase; AE = adverse event; SAE = serious adverse event; SJS = Stevens-Johnson syndrome; TEN = toxic epidermal necrolysis.
aFrequency ≥ 10.0%.
bFrequency ≥ 1.0%.
Source: Clinical Study Reports.11,12
Table 19: Summary of Harms for Older Adults (Safety Population, DCO January 4, 2022)
Harms | Pembrolizumab (N = 483) | Placebo (N = 486) |
|---|---|---|
Patients with ≥ 1 AE, n (%) | ||
< 65 years | |||||||||||||| | |||||||||||||| |
65 to 74 years | |||||||||||||| | |||||||||||||| |
75 to 84 years | |||||||||||||| | |||||||||||||| |
Patients with ≥ 1 SAE, n (%) | ||
< 65 years | |||||||||||||| | |||||||||||||| |
65 to 74 years | |||||||||||||| | |||||||||||||| |
75 to 84 years | |||||||||||||| | |||||||||||||| |
Patients who stopped treatment due to AEs, n (%) | ||
< 65 years | |||||||||||||| | |||||||||||||| |
65 to 74 years | |||||||||||||| | |||||||||||||| |
75 to 84 years | |||||||||||||| | |||||||||||||| |
Deaths, n (%) | ||
< 65 years | |||||||||||||| | |||||||||||||| |
65 to 74 years | |||||||||||||| | |||||||||||||| |
75 to 84 years | |||||||||||||| | |||||||||||||| |
AE = adverse event; DCO = data cut-off; SAE = serious adverse event.
Source: Clinical Study Reports.12
Critical Appraisal
Internal Validity
The included pivotal study, KEYNOTE-716, was a well-designed, randomized, placebo-controlled, parallel-group, multicentre study. Part 1 of the study, which is the focus of this review, was double-blinded. The study used an appropriate randomization method (i.e., centralized interactive response technology system), and the allocation concealment procedures were clearly described. Treatment groups were well-balanced by baseline demographic and disease characteristics, which indicates that the randomization was successful.
Discontinuations from the study were similar between the treatment groups; discontinuation from treatment was higher in the pembrolizumab treatment group compared with the placebo group (|||||||||||). Notably, discontinuation from treatment due to AEs was more common in the pembrolizumab group (|||||||||||), and discontinuation due to relapse or recurrence was more common in the placebo group (|||||||||||). The imbalance in treatment discontinuation due to AEs may suggest that patients had knowledge of treatment they received (e.g., compromised blinding due to knowledge of common AEs). Although the key outcomes for the trial were objective and unlikely affected by unblinding, this may have impacted reporting of safety outcomes and PROs (EORTC QLQ-C30 and EQ-5D-5L VAS). The magnitude of the bias this may have had on the results is unclear.
Concomitant medications that were permitted in the KEYNOTE-716 trial were considered appropriate. Concomitant medication use was reported more frequently (by a difference of at least 10% between treatment groups) by patients who received pembrolizumab. The clinical experts indicated that many of the AEs that were reported in the study are consistent with the expected safety profile of pembrolizumab as seen in clinical practice. The experts also noted that the AEs associated with treatment are well understood by treating physicians and therefore manageable in clinical practice, which likely explains the concomitant medication usage reported in the trial. However, this may have resulted in an underestimation of AEs associated with pembrolizumab, such as diarrhea and inflammation-related events.
At the time of this review, data from IA3 (DCO January 4, 2022) were the most recent available. Treatment-level results of the efficacy interim analyses were provided by an external unblinded statistician to the external data monitoring committee. At IA3, the final analysis of RFS and the interim analysis of DMFS were the only analyses of the primary and key secondary analyses that were available. Overall survival was identified as the most important outcome for the review of pembrolizumab for stage IIB and IIC melanoma; however, the final OS analysis for the study is not expected to occur until approximately 180 months (15 years) of follow-up. Because a clinical trial of this duration is not feasible, RFS was the primary end point used for the KEYNOTE-716 trial. The power calculation for RFS assumed a long-term RFS of 50%, which was considered appropriate according to the clinical experts consulted by CADTH. Although it was unclear if central adjudication of RFS and DMFS occurred in the trial, these outcomes were assessed by investigators as per Response Evaluation Criteria in Solid Tumours Version 1.1 (RECIST 1.1) criteria, which provide an objective assessment of response to treatment.
Two studies were identified by CADTH that evaluated RFS as a surrogate outcome for OS. The majority of the trials that informed the assessment of RFS as a surrogate outcome for OS evaluated interferon-based treatment regimens. There was evidence to support RFS as a surrogate outcome for a HR of at least 0.77 based on these data,13 which the KEYNOTE-716 trial demonstrated; however, another study that supplemented this analysis with data from a trial comparing ipilimumab (another ICI) with placebo concluded that more evidence is needed to confirm the strength of association between RFS and OS for ICI therapies such as pembrolizumab.14 The clinical experts indicated that although RFS may not translate directly to OS, it is the most appropriate outcome for stage IIB and IIC melanoma because the duration of follow-up to observe the number of events required for a robust analysis of OS is too long given the prognosis of these patients. Based on the evidence that is currently available, RFS may be an appropriate surrogate outcome for OS, but this is associated with notable uncertainty given the limited data available for the therapies that are the current standard of care and the duration of follow-up at this time.
The Kaplan-Meier method was used to estimate the primary and key secondary end points, and Efron’s method of tie handling was used to support the proportional hazards assumption, which was considered appropriate. Censored data were insufficiently reported, which limits the interpretation of the available results for RFS and DMFS. The information size for these analyses was small, consisting of fewer than 200 total events; as such, the effect estimates and corresponding CIs may be considered fragile. The results for DMFS are from an interim analysis, so there is some risk that the magnitude of effect is overestimated. Further follow-up would help to solidify the findings for both RFS and DMFS. Sensitivity analyses of RFS were performed for the final analysis at IA2 and they were supportive of the primary analysis. A graphical method and the Lan-DeMets O’Brien Fleming approximation spending function were used to control the primary (RFS) and key secondary analyses (DMFS and OS) for multiplicity. As described in the FDA guidance for industry, the graphical approach allows hierarchal multiple analysis strategies to be developed and evaluated.24 The patient-reported HRQoL outcomes (EORTC QLQ-C30 and EQ-5D-5L VAS) were assessed as exploratory outcomes. They were based on a subset of the study population that completed the assessments (PRO full analysis set) and were at potential risk of bias because of missing data on these outcomes. Additionally, these outcomes did not control for multiplicity; therefore, the results are at risk of type I error. As such, conclusions that can be drawn about HRQoL are limited.
The primary outcome of RFS was analyzed by subgroups, including overall cancer stage, T category, and age. Randomization was stratified by T category but, as noted by the sponsor, descriptive analyses by baseline T category and overall melanoma cancer stage were not prespecified and the study was not powered to show efficacy in these subgroups. Further, the sponsor noted that the difference in sample size for each of the subgroups limited the interpretation of the data. The exploratory nature of the subgroup analysis is a limitation of this study, particularly given the results of the analysis by T category that is suggestive of a differential treatment effect among subgroups.
External Validity
The KEYNOTE-716 trial included Canadian study centres, but the patient population was predominantly White (89% to 90% of patients). Although the sponsor is requesting reimbursement of pembrolizumab for patients of at least 12 years of age, only 2 pediatric patients (aged 12 to 17 years) were included in the study; therefore, the appropriateness of generalizing the results to pediatric populations is not known. At the time of this review, the evidence was limited to part 1 of the study, which only included patients who were not previously treated for melanoma beyond complete surgical resection. Additionally, some of the exclusion criteria in the trial — such as patients who had received prior therapy with anti-PD1, anti-PD-L1, or anti-PD-L2 drugs, patients with a known additional malignancy or who had required active antineoplastic therapy or surgery in the past 5 years, and patients with immunodeficiencies — are likely to miss a subset of patients who would be seen in clinical practice (estimated 5% to 10% of patients). The clinical experts indicated that these criteria would not preclude patients from treatment with pembrolizumab in the trial, but the safety and efficacy of treatment in these patients is associated with uncertainty. Patients with an ECOG performance status score of 2 or greater were excluded from the pivotal trial. The clinical experts consulted by CADTH indicated that performance status, which is a measure of a patient’s level of functioning, is not particularly relevant in the adjuvant treatment setting because patients are assumed to be surgically rendered free of disease. As such, this exclusion criterion was unlikely to cause a generalizability issue for the study.
The use of pembrolizumab in the KEYNOTE-716 trial was consistent with the product monograph approved by Health Canada.5 Of note, the product monograph recommends adults receive pembrolizumab 200 mg every 3 weeks or 400 mg every 6 weeks, but only the former dosing regimen was evaluated in the trial. The clinical experts consulted by CADTH indicated that dosing every 6 weeks would be appropriate for most patients, but there is some uncertainty about the safety and efficacy of pembrolizumab with this dosing schedule because it was not studied. Concomitant medication use described in the trial was considered appropriate and consistent with clinical practice. The evidence is limited to a placebo-controlled trial; however, given the current standard of care is surveillance, this was considered a reasonable comparator.
The primary outcome in the KEYNOTE-716 trial was RFS. Tumour imaging via CT scan was performed every 6 months while on treatment and 3 years after, which is consistent with Canadian recommendations for surveillance.4 The clinical experts stated that prevention of recurrence of disease is a meaningful outcome. Further, they noted that a reduction in relapse is of value from a clinical perspective because these patients are expected do better in terms of QoL compared with those who take immunotherapy upon relapse but are left with significant toxicities. However, the clinical experts also felt that it is difficult to state whether RFS is an acceptable surrogate for OS without additional data. DMFS was not considered a key outcome by the clinical experts based on clinical relevance. At the time of this review, the final analysis was only available for the primary end point, RFS. The clinical experts indicated that approximately one-third of patients who do experience recurrence of disease will experience it in the first 12 months following resection. Despite having a sufficient number of events to perform the final analysis of RFS, the duration of follow-up as of IA2 and IA3 is likely too short, causing uncertainty about the generalizability of the estimate for recurrence to what would be expected in clinical practice. In contrast, the clinical experts felt that the duration of follow-up was sufficient to observe AEs of interest.
Indirect Evidence
A focused literature search for ITCs dealing with melanoma was run in MEDLINE All (1946–) on May 20, 2022. No search limits were applied.
No ITCs were identified that were relevant to the indication under review (i.e., adjuvant treatment of stage IIB or IIC melanoma following complete resection).
Other Relevant Evidence
This section includes additional relevant studies included in the sponsor’s submission to CADTH that were considered to address important gaps in the evidence included in the systematic review. One ITC of patients with unresectable stage III or IV melanoma, receiving first-line treatment for advanced disease who were either BRAF all comers/wild type or had BRAF-positive melanoma, was submitted by the sponsor to support the evaluation of the economic model.
Methods of Sponsor-Submitted ITC
The sponsor supplied an ITC to relevant comparators based on a systematic review of treatments for patients not previously treated with non-targeted therapy for advanced melanoma to inform the economic model.
Objectives
The objective of the ITC was to assess the comparative efficacy and safety of pembrolizumab for patients not previously treated with non-targeted therapy for advanced melanoma with relevant interventions that are listed in Table 20 to generate economic model inputs.
Study Selection Methods
The systematic review was based on searches of multiple bibliographic databases (from inception until October 15, 2021), reference lists of eligible studies, conference proceedings, HTA agencies, and clinical trial registries. The full search terms are provided in the Appendix 1. No language restrictions were applied. The population of interest did not indicate an age range, although all included studies were among patients aged 18 years and older. It included patients with unresectable stage III or IV melanoma receiving first-line treatment for advanced disease. Eligible studies may have permitted patients with a BRAF V600 mutation to have undergone 1 prior line of therapy targeted at the BRAF or MEK pathways (e.g., BRAF/MEK inhibitor, alone or in combination) in the advanced or metastatic melanoma setting. Patients in the eligible studies may have received prior adjuvant or neoadjuvant systemic therapy for early-stage disease.
Interventions were considered as monotherapy or in combination with another intervention of interest. Other interventions were considered if they were compared in randomized controlled trials to at least 2 interventions (Table 20). Only some of the comparators examined are routinely used in Canada for advanced melanoma (ipilimumab, nivolumab, encorafenib in combination with binimetinib, trametinib in combination with dabrafenib, ipilimumab in combination with nivolumab).
Table 20: Study Selection Criteria and Methods for the Sponsor-Submitted ITC
Criteria | Sponsor-submitted ITC systematic review portion |
|---|---|
Population |
|
Intervention |
|
Comparator | Any interventions administered as monotherapy as well as combination therapies |
Outcome |
|
Study design | RCTs |
Search dates | Database inception to October 15, 2021; 2020 to 2021 for conference proceedings |
Exclusion criteria | Not matching the inclusion criteria |
Databases searched | EMBASE, MEDLINE, Cochrane Central Register of Controlled Trials, Cochrane Database of Systematic reviews, relevant conference abstracts, clinical trials registries |
Selection process | Two reviewers independently screened the retrieved reports at 2 stages (titles and abstracts, and then full articles). Disputes were resolved by discussion or involvement of a third reviewer. |
Data extraction process | Two independent reviewers. Details of the methods used to extract data from the included studies were described. Disputes resolved by discussion or involvement of a third reviewer |
Risk of bias assessment | Cochrane Collaboration’s Risk of Bias tool (version 1). Risk of bias assessment of the selected studies was carried out independently by 2 reviewers, with any disagreements resolved by discussion or involvement of a third reviewer. |
OS = overall survival; PFS = progression-free survival; RCT = randomized controlled trial.
ITC Analysis Methods
The ITC compared interventions of interest for the outcomes of PFS and OS in patients with unresectable stage III or IV melanoma receiving first-line treatment for advanced disease and who were either BRAF all comers/wild type or had BRAF-positive melanoma.
The ITC was an NMA performed with a Bayesian approach using fixed- and random-effects models. If there was insufficient evidence to estimate between-study heterogeneity, fixed-effects models were used. The NMA of reported HRs in terms of PFS and OS assuming proportional hazards between treatments was performed using a generalized linear modelling framework of a regression model with a contrast-based normal likelihood for the log HR (and corresponding standard error) of each trial (or comparison) in the network according to Dias et al.25 Normal noninformative prior distributions for the parameters were estimated with a mean of 0 and a variance of 10,000. Parameters of the models were estimated using Markov Chain Monte Carlo method. A first series of iterations from the Just Another Gibbs Sampler (JAGS)was discarded as “burn-in” and the inferences were based on additional iterations using 2 chains. Sensitivity analysis around the effect of the prior distributions were not described. Deviance information criterion and deviance were reported for each model; however, model convergence was not described.
The results of the NMA for PFS and OS were presented with estimates for treatment effects of each intervention relative to the reference treatment using constant HR models which assumed proportional hazards between treatment. The median and 95% credible intervals (CrIs) were constructed from the 2.5th and 97.5th percentiles of the posterior distributions of relative treatment effects. Homogeneity was assessed by comparing baseline descriptive statistics between the trials for variables considered potential effect modifiers.
Separate analyses were performed for BRAF all comers/wild type and subgroups of those with a BRAF mutation–positive melanoma. A key assumption is that BRAF status is a relative treatment effect modifier for BRAF-targeted therapies: dabrafenib, encorafenib, and vemurafenib. BRAF status was not considered to be an effect modifier for non–BRAF-targeted therapies. Therefore, trials in the population with BRAF mutation receiving non–BRAF-targeted therapies were eligible for inclusion in the BRAF all-comers and BRAF wild-type networks. Across all NMAs, only 1 closed loop was included. Statistical consistency was not presented.
Results of ITC
Summary of Included Studies
A total of 52 publications from 18 unique clinical trials were included in the feasibility assessment, 1 trial was excluded due to a specific patient population (intracranial brain lesions). An enrolment criterion for all but 1 of the trials (RELATIVITY-047) was a restriction to age 18 years or older. The RELATIVITY-047 trial included patients aged 12 years or older; however, no data for patients younger than 18 years were included. Trials included all BRAF wild-type patients (2 trials: CheckMate-066, IMspire170) and all patients with BRAF mutation (7 trials: BRIM-3, coBRIM, COLUMBUS, COMBI-d, COMBI-v, IMspire150, KEYNOTE-022). Other included trials were in a mixed or unknown BRAF status population. A total of up to 17 trials were included in each NMA.
Detailed tables were provided with trial, treatment, patient, and outcome characteristics presented. A risk of bias assessment diagram was reported for the 18 trials considered for the NMA. Overall, 15 studies were rated to be of low risk of bias and 3 were reported to have some concerns for risk of bias due to concerns about the randomization process and selection of the reported result.
NMA results were presented for PFS and OS by BRAF status.
Construction of the Networks
Overall, the NMA included trials with relevant comparators. However, only some regimens are currently used in Canada for the indication of advanced melanoma (trametinib + dabrafenib, cobimetinib + vemurafenib, pembrolizumab monotherapy, ipilimumab monotherapy, nivolumab monotherapy, ipilimumab + nivolumab, and encorafenib + binimetinib).
Trial Characteristics
All 18 trials were head-to-head trials with active comparators. A total of 8 of 18 trials were open label; the remainder were double-masked. Four trials were phase II; the remainder were phase III. All trials were multicentre, and all except 1 were multinational. The number of patients in a study arm ranged from 16 to 368 patients. The earliest year of study initiation was 2006, and the latest study will be completed in 2022. All trials included patients with stage III or IV melanoma (1 trial included patients with brain metastases only and was removed from analysis). All other trials excluded patients with active or untreated brain metastases. Sixteen trials included patients with an ECOG PS of 0 or 1 only; 2 trials included ECOG PS of 0 to 2 (but this consisted of only 1 to 3 patients per trial). Trials were conducted in a BRAF wild-type population (2 trials), patients with BRAF mutation–positive melanoma (7 trials), and unknown or mixed BRAF mutation status (11 trials).
Twelve trials were in the first-line treatment setting, and 3 trials were in the first-line and beyond treatment setting but reported PFS and OS by line of therapy, and 3 trials permitted prior BRAF-inhibitors. On-trial crossover was not permitted in 4 trials and was explicitly allowed in 5 trials (ranged from 9% to 55%); information was not reported for the remaining 9 trials.
Baseline patient characteristics were presented per treatment arm. Mean age at baseline ranged from 52 to 67 years old. The proportion of males across the study treatment arms ranged from 51% to 83%. The proportion of study participants who were White ranged from 85% to 100%, although this information was not recorded for 8 trials. All trials included a majority of patients with an ECOG PS of 0 (58% to 83%) or 1 (15% to 34%); very few patients had an ECOG PS of 2. All patients had stage III (0% to 40%) or stage IV (60% to 100%) melanoma. The proportion of patients with stage M1c (the cancer has spread to any other location that does not involve the central nervous system) ranged from 33% to 70%. The proportion of patients with elevated LDH ranged from 23% to 58%. The proportion of patients who were PD-1– or PD-L1–positive ranged from 21.7% to 80.9% for 9 trials for which it was available. The proportion of patients with a prior treatment with a BRAF or MEK inhibitor ranged from 2% to 7.5% for 3 trials in which this was allowed.
Details of OS and PFS definitions for each of the trials and time of assessment were described in the technical report. A total of 17 trials reported OS (median OS ranged from 9.1 months to 72.1 months and was not evaluable at a median of 31 months for 1 trial). All 18 trials reported PFS (median ranged from 1.6 months to 16.1 months). There were 5 trials with investigator-assessed and independent review committee PFS; in these cases, the independent review committee PFS was used. There were 7 trials in which PFS was investigator-assessed only, and 1 trial in which method of PFS assessment was not described. Duration of follow-up ranged from 12 months to 78 months.
Findings of the NMA
There were 10 trials that reported PFS, and 8 trials reported OS for the BRAF all-comers/wild-type population and were connected in 2 separate networks. Table 21 summarizes the HRs and 95% CrIs for PFS and OS in the BRAF all-comers/wild-type population. Due to sparse networks, fixed-effects models are presented. For PFS analysis in the BRAF all-comers/wild-type population, pembrolizumab may be favourable relative to ipilimumab, dacarbazine, ipilimumab plus dacarbazine, and binimetinib. Nivolumab plus ipilimumab may be favourable relative to pembrolizumab for PFS analysis in the BRAF all-comers/wild-type population. For the OS analysis in the BRAF all-comers/wild-type population, pembrolizumab may be favourable relative to ipilimumab and to dacarbazine.
There were 17 trials that reported PFS and 15 trials that reported OS in the population with BRAF mutation–positive melanoma and were connected in 2 networks. Table 22 summarizes the HRs and 95% CrIs for OS and PFS in the population with BRAF mutation–positive melanoma. Due to sparse networks, fixed-effects models are presented. For PFS analysis in the population with BRAF mutation–positive melanoma, pembrolizumab may be favourable relative to ipilimumab monotherapy, dacarbazine, ipilimumab plus dacarbazine, and binimetinib. Pembrolizumab may be less favourable for PFS than nivolumab plus ipilimumab, encorafenib plus binimetinib, vemurafenib plus cobimetinib, atezolizumab plus vemurafenib plus cobimetinib, dabrafenib plus trametinib, and pembrolizumab plus dabrafenib plus trametinib in the population with BRAF mutation–positive melanoma. For the OS analysis in the population with BRAF mutation–positive melanoma, pembrolizumab may be favourable for OS relative to monotherapy with ipilimumab monotherapy, dacarbazine, and vemurafenib.
Critical Appraisal of Sponsor-Submitted ITC
Table 23 summarizes the critical appraisal of the NMA using the International Society for Pharmacoeconomics and Outcomes (ISPOR) criteria.
Table 21: OS and PFS in BRAF All-Comers and Wild-Type Population for Patients Not Previously Treated With Non-Targeted Therapy for Advanced Melanoma — ITC Resultsa
Pembrolizumab versus | PFS, HR (95% CrI) | OS, HR (95% CrI) |
|---|---|---|
Number of studies, model | |||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||||||||||||| |
Ipilimumab | |||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||||||||||||| |
T-VEC + ipilimumab | |||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||||||||||||| |
Nivolumab + ipilimumab | |||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||||||||||||| |
Nivolumab | |||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||||||||||||| |
Relatlimab + nivolumab | |||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||||||||||||| |
Dacarbazine | |||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||||||||||||| |
Ipilimumab + dacarbazine | |||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||||||||||||| |
Binimetinib | |||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||||||||||||| |
Cobmetinib + atezolizumab | |||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||||||||||||| |
T-VEC + pembrolizumab | |||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||||||||||||| |
CrI = credible interval; HR = hazard ratio; NR = not reported; OS = overall survival; PFS = progression-free survival; RCT = randomized controlled trial; T-VEC = talimogene laherparepvec.
Note: Deviance information criterion (DIC) = 27.62 for PFS model; deviance = 13.65 for PFS model. DIC = 16.77 for OS model; deviance = 8.77 for OS model.
aNMA using proportional hazards model with fixed effects under a Bayesian framework. Results are HRs, with numbers less than 1 favouring pembrolizumab.
Source: Sponsor-submitted ITC.26
Table 22: OS and PFS in Population With BRAF Mutation–Positive Advanced Melanoma and Not Previously Treated With Non-Targeted Therapy — ITC Results
Pembrolizumab versus | PFS, HRa (95% CrI) | OS, HRa (95% CrI) |
|---|---|---|
Number of studies, model | 17 RCTs included, fixed-effects model | 15 RCTs included, fixed-effects model |
Ipilimumab | |||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||||||||||||| |
T-VEC + ipilimumab | |||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||||||||||||| |
Nivolumab + ipilimumab | |||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||||||||||||| |
Nivolumab | |||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||||||||||||| |
Relatlimab + nivolumab | |||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||||||||||||| |
Dacarbazine | |||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||||||||||||| |
Ipilimumab + dacarbazine | |||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||||||||||||| |
Binimetinib | |||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||||||||||||| |
Vemurafenib | |||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||||||||||||| |
Encorafenib + binimetinib | |||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||||||||||||| |
Vemurafenib + cobimetinib | |||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||||||||||||| |
Atezolizumab + vemurafenib + cobimetinib | |||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||||||||||||| |
Dabrafenib + trametinib | |||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||||||||||||| |
Dabrafenib | |||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||||||||||||| |
Pembrolizumab + dabrafenib + Trametinib | |||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||||||||||||| |
Cobmetinib + atezolizumab | |||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||||||||||||| |
T-VEC + pembrolizumab | |||||||||||||||||||||||||||||||||||||||||||| | |||||||||||||||||||||||||||||||||||||||||||| |
CrI = credible interval; HR = hazard ratio; NR = not reported; OS = overall survival; PFS = progression-free survival; RCT = randomized controlled trial; T-VEC = talimogene laherparepvec.
Note: DIC = 33.45 for PFS model; deviance = 16.44 for PFS model. DIC = 32.86 for OS model; deviance = 17.86 for OS model.
aNMA using proportional hazards model with fixed effects under a Bayesian framework. Results are HRs with numbers less than 1 favouring pembrolizumab.
Source: Sponsor-submitted ITC.26
Table 23: ISPOR Questionnaire to Assess the Credibility of an Indirect Treatment Comparison or Network Meta-Analysisa
ISPOR questions | Details and comments |
|---|---|
1. Is the population relevant? | Unclear. The purpose of this NMA was to inform the health economic model. The population for the indication of interest is stage IIB or IIC cutaneous melanoma (based on KEYNOTE 716). The SLR and NMA are based on patients with unresectable stage III or IV melanoma who have not been previously treated with systemic therapy for unresectable or metastatic melanoma. For the purposes of informing the health economics model as to outcomes for patients with advanced melanoma, the patient population is relevant. A comprehensive list of inclusion and exclusion criteria for the studies included in the systematic literature review was included. The inclusion criteria would allow a population that is relevant for the Canadian setting. The comparisons reported in this ITC have generally incorporated relevant treatments for Canadian settings. |
2. Are any critical interventions missing? | No |
3. Are any relevant outcomes missing? | Unclear. Planned analysis was for PFS and OS only. No information was presented in the technical report on other outcomes of interest including response rate (objective response rate, time to objective response, disease control rate, duration of response), HRQoL, disease control rate, disease-related symptoms, productivity (e.g., ability to attend school, work), treatment-free interval, or harms outcomes. |
4. In the context (e.g., settings and circumstances) applicable to your population? | Yes. Trials were multinational and likely applicable to Canada. However, not all comparators included in this NMA are currently used for this indication in Canada. |
5. Did the researchers attempt to identify and include all relevant randomized controlled trials? | Yes. The ITC (NMA) was based on a systematic literature review that identified studies according to a prespecified inclusion criteria. A comprehensive and transparent approach to their systematic review was provided, including the search strategy, and the search was comprehensively conducted over several databases. Study selection and data extraction were appropriate. |
6. Do the trials for the interventions of interest form 1 connected network of randomized controlled trials? | Yes. In total, 52 unique trials were identified for inclusion into the review, and up to 17 trials formed a connected network. |
7. Is it apparent that poor quality studies were included thereby leading to bias? | No. Trials were assessed for risk of bias with the Cochrane risk of bias assessment tool for RCTs. Overall, 3 of 18 trials included in the SLR were deemed to have some concerns. The rest were assessed to be of low risk of bias. However, the risk of bias was not assessed by outcome, as intended by the tool. Therefore, it is unclear whether some elements of potential bias across the outcomes may have been missed. Two trials were only conference abstracts at the time of the NMA; these trials may contribute to uncertainty due to lack of information. |
8. Is it likely that bias was induced by selective reporting of outcomes in the studies? | No. One trial was assessed as having some concerns for risk of bias due to selection of the reported result. |
9. Are there systematic differences in treatment effect modifiers (i.e., baseline patient or study characteristics that impact the treatment effects) across the different treatment comparisons in the network? | Unclear. Inadequate information about baseline patient characteristics as well as variability in baseline patient characteristics that are reported contribute to heterogeneity in the studies included in the ITC. Many individual studies failed to report on factors such as ethnicity, BRAF status, and PD-L1 status. There were differences in the patient populations about prior BRAF inhibitor use and permitted on-trial crossover, which may impact OS. There were differences in follow-up time. There were a large number of trials with unknown or mixed BRAF mutation status (11 trials). The authors assumed that BRAF mutation status did not impact outcomes with other drugs that do not impact the BRAF pathway. The analysis was performed for BRAF all-comers/wild-type and BRAF mutation–positive melanoma separately. |
10. If yes (i.e., there are such systematic differences in treatment effect), were these imbalances in effect modifiers across the different treatment comparisons identified before comparing individual study results? | Potential treatment effect modifiers were explored in the systematic review and NMA feasibility report, which was performed before the NMA. The feasibility assessment to assess heterogeneity in terms of treatment and outcome characteristics, as well as the study and patient characteristics, was performed. Separate analyses were conducted for BRAF all comers/wild type and patients with BRAF mutation–positive melanoma. |
11. Were statistical methods used that preserve within-study randomization? | Yes. There were no naive indirect comparisons. |
12. If both direct and indirect comparisons are available for pairwise contrasts (i.e., closed loops) was agreement in treatment effects (i.e., consistency) evaluated or discussed? | No. There was 1 closed loop; however, it did not include comparisons of interest to this report and was not evaluated or discussed. There were no closed loops of relevance to comparisons with pembrolizumab; therefore, consistency could not be evaluated because all evidence was indirect. |
13. In the presence of consistency between direct and indirect comparisons, were both direct and indirect evidence included in the network meta-analysis? | No. Only indirect evidence was available for the comparisons of interest. |
14. With inconsistency or an imbalance in the distribution of treatment effect modifiers across the different types of comparisons in the network of trials, did the researchers attempt to minimize this bias with the analysis? | Yes, separate analyses were performed for BRAF all-comers/wild-type and patients with a BRAF mutation. No further subgroup analyses were described in the technical report to attempt to investigate other sources of heterogeneity (e.g., population characteristics, different lengths of follow-up for outcomes). |
15. Was a valid rationale provided for the use of random-effects or fixed-effects models? | Yes. Fixed-effects models were used because the sparse network precluded stable estimates of between-study heterogeneity from a random-effects model. Had it been possible, a random-effects model would have been preferred because these models assume that the observed differences among study results are due to a combination of chance and genuine variation in the intervention effects (which is more realistic than the fixed-effects model). In the presence of statistical heterogeneity, random-effects models would result in wider CrIs (more conservative findings). |
16. If a random-effects model was used, were assumptions about heterogeneity explored or discussed? | All analyses were based on fixed-effects models because there was a limited number of included trials per treatment comparison, which precluded estimation of heterogeneity. Using random-effects models to account for heterogeneity was not feasible. This uncertainty is reflected in the 95% CrIs and precludes drawing conclusions from these models. |
17. If there are indications of heterogeneity, were subgroup analyses or meta-regression analyses with prespecified covariates performed? | No. Separate analyses performed for BRAF all-comers/wild-type and patients with BRAF mutation–positive melanoma. No further subgroup nor meta-regression analyses were described in the technical report. |
18. Is a graphical or tabular representation of the evidence network provided with information on the number of RCTs per direct comparison? | Yes |
19. Are the individual study results reported? | Yes |
20. Are results of direct comparisons reported separately from results of the indirect comparisons or network meta-analyses? | No |
21. Are all pairwise contrasts between interventions as obtained with the network meta-analysis reported along with measures of uncertainty? | Yes |
22. Is a ranking of interventions provided given the reported treatment effects and its uncertainty by outcome? | No |
23. Is the impact of important patient characteristics on treatment effects reported? | Separate analyses performed for BRAF all-comers/wild-type and patients with BRAF mutation–positive melanoma. No further subgroup analyses were described in the technical report. |
24. Are the conclusions fair and balanced? | Unclear. No specific conclusions were presented. |
25. Were there any potential conflicts of interest? | Yes; sponsor-submitted ITC |
26. If yes, were steps taken to address these? | No |
CrI = credible interval; ITC = indirect treatment comparison; NMA = network meta-analysis.
aBolded comments are considered a weakness of the ITC.
Source: Adapted from Jansen et al. Indirect Treatment Comparison/Network Meta-Analysis Study Questionnaire to Assess Relevance and Credibility to Inform Health Care Decision Making: An ISPOR-AMCP-NPC Good Practice Task Force Report.27
Other limitations to the NMA are described subsequently.
The degree of heterogeneity between the included studies was difficult to assess because of incomplete reporting of some study characteristics. A description of the trial design (open label versus masked), sample size, duration, and country were reported. There was variability in study design, year study conducted, and sample size. Phase II trials were included, along with phase III. There was variation in the extent to which on-study crossover was allowed, and there were a considerable number of trials for which this information was not reported. Nearly half the trials were open label, which is a limitation. Sensitivity analyses of the effects of these trial design factors on the ITC outcomes were not presented. The direction of bias that the differences in study design would have on the result of the NMA is unclear. Similarly, inadequate information about baseline patient characteristics and variability in baseline patient characteristics reported contribute to the heterogeneity in the studies included in the ITC. Clinical trial eligibility criteria were described for the trials ultimately included in the NMA. However, many individual studies failed to report on such factors such as ethnicity, BRAF status, and PD-L1 status. There was heterogeneity in baseline patient characteristics, including age, elevated LDH, stage III versus IV disease, and presence of stage M1c disease. Although there were differences in the proportion of patients treated with a previous BRAF or MEK inhibitor, the proportion of patients was low (up to 7%) in the 3 studies. The authors assumed that BRAF mutation status is not a strong treatment effect modifier in non–BRAF-targeted therapy; however, this assumption was based on subgroup analyses that were not powered to detect such a difference. There are likely differences in the BRAF mutation status included in the BRAF all-comers/wild-type study patient populations because the BRAF mutation status of the malignancy was unknown for many patients. To account for this, the analysis was performed separately for BRAF all comers/wild type and the population with BRAF mutation–positive melanoma. There was variability in the method of PFS assessment (investigator versus independent review committee). There was heterogeneity in the duration of follow-up and in the results for trial outcomes of OS and PFS, with point estimates ranging widely.
Post-progression treatments may be a limitation of the OS analysis. It is unclear what proportion of patients received crossover therapy because this varied across trials. No sensitivity analysis was performed for trials allowing on-trial crossover. Post-progression treatments may have affected OS across the trials, which would increase uncertainty in the OS results. The direction of potential bias created by post-progression treatments is unclear. Differences in follow-up durations, which varied widely, may also affect PFS and OS outcomes and cause uncertainty in the results.
There may be uncertainty in whether the assumptions related to homogeneity were met. Heterogeneity based on the factors that were reported in combination with the inability to assess those that were not reported contributes to uncertainty in the assumptions about homogeneity. The technical report did not provide sufficient information of assessments of heterogeneity (e.g., graphic representation of baseline characteristics, statistical tests) to fully understand the sources of heterogeneity. In addition, because there were no closed loops, consistency could not be tested. The models assumed constant hazards but did not describe if this assumption was met nor the methods of assessment. Therefore, the potential for heterogeneity to have influenced the comparative efficacy and safety estimates is plausible, and it is not possible to quantify or identify the direction of the bias.
The analytical method used for the ITC was well reported. The authors provided a description of which studies were included in each of the analyses. The analysis of the extracted data followed the framework suggested by the National Institute for Health and Care Excellence (NICE), including using noninformative priors. However, due to sparse networks, all model results were fixed-effects models. Heterogeneity that would have been accounted for by a random-effects model was not accounted for with the fixed-effects model. This uncertainty is reflected in the 95% CrIs and precludes drawing conclusions from these models. In addition, the authors reported that trials that compared pembrolizumab to BRAF-inhibitor trials were mediated by multiple treatment comparisons and are therefore even more uncertain.
Summary
A sponsor-submitted ITC was used to support the economic model. This ITC compared interventions of interest for the outcomes of PFS and OS in patients with unresectable stage III or IV melanoma receiving first-line treatment for advanced disease. In the BRAF all-comers/wild-type population, pembrolizumab may be favourable for PFS relative to ipilimumab monotherapy, dacarbazine, ipilimumab plus dacarbazine, and binimetinib; however, nivolumab plus ipilimumab was favourable relative to pembrolizumab for PFS analysis. For the OS analysis in the BRAF all-comers/wild-type population, pembrolizumab may be favourable relative to ipilimumab and to dacarbazine.
In the population with BRAF mutation–positive melanoma, pembrolizumab may be favourable for PFS relative to ipilimumab monotherapy, dacarbazine, ipilimumab plus dacarbazine, and binimetinib but may be less favourable than nivolumab plus ipilimumab, encorafenib plus binimetinib, vemurafenib plus cobimetinib, atezolizumab plus vemurafenib plus cobimetinib, dabrafenib plus trametinib, and pembrolizumab plus dabrafenib plus trametinib. For the OS analysis in the population with BRAF mutation–positive melanoma, pembrolizumab may be favourable to monotherapy with ipilimumab, dacarbazine, and vemurafenib.
There are several limitations to the NMA describing the effect of pembrolizumab versus comparators on PFS and OS in the setting of advanced melanoma. Limitations to this NMA include variation in patient characteristics (BRAF status, PD-L1, M1c metastases, baseline characteristics such as elevated LDH and ECOG status) and trial characteristics (e.g., open label and phase II versus phase III trial). Additionally, there were limited data available for the NMAs that were conducted for OS and PFS; therefore, fixed-effects models were used for these end points. Data from the current NMA for pembrolizumab in the setting of advanced melanoma may inform transition probabilities in the treatment setting of advanced melanoma, but it would not apply in the setting of stage IIB or IIC melanoma. However, a number of limitations associated with this NMA preclude making conclusions about the comparative effectiveness of pembrolizumab in the setting of advanced melanoma.
Discussion
Summary of Available Evidence
The pivotal trial for pembrolizumab (KEYNOTE-716) was the only study included in the CADTH systematic review. KEYNOTE-716 (N = 976) was a randomized, placebo-controlled, parallel-group, crossover and rechallenge, multicentre study of adjuvant pembrolizumab in participants aged 12 years and older with resected stage IIB or IIC cutaneous melanoma. At the time of this review, data up to the IA3 (database lock: February 20, 2022) were available. The primary objective of the KEYNOTE-716 trial was to compare RFS between treatment groups: pembrolizumab and placebo. Patients included in the trial must have been enrolled within 12 weeks of final surgical resection, with complete surgical wound healing and no evidence of metastatic disease on imaging. The mean age of the included patients was 59.3 years (SD = 12.9), and 2 pediatric patients were included (1 randomized to each treatment group). Almost all included patients did not exhibit functional impairment (ECOG performance status of 0 or Karnofsky Performance Status of 100), and the remaining patients (7% in each treatment group) exhibited some functional impairment (ECOG performance status of 1). Most patients had stage IIB melanoma at baseline (64%), and 35% had stage IIC melanoma. In addition to RFS, data were available for the following outcomes as of IA3: DMFS and HRQoL (measured using the EORTC QLQ-C30, and EQ-5D-5L VAS). Key limitations of the KEYNOTE-716 trial include immaturity of the data, a high rate of discontinuation from treatment, and the lack of control for multiplicity for HRQoL outcomes and subgroup analyses.
One sponsor-submitted NMA of studies that included patients with unresectable stage III or IV melanoma who received first-line treatment for advanced disease was also reviewed as other relevant evidence to inform the economic model. This NMA was affected by multiple limitations, including potential violation of the underlying assumptions of the NMA, which precluded the development of conclusions about the comparative effectiveness of pembrolizumab in the setting of advanced melanoma.
Interpretation of Results
Efficacy
According to the Canadian Cancer Society, the 5-year observed survival statistics for stage IIB and stage IIC melanoma are 70% and 53%, respectively.1 The current standard of care for patients in Canada with stage IIB or IIC melanoma following complete resection is surveillance, although this is considered a high-risk patient population. Input received from patient groups expressed that, as a result, patients feel fear and anxiety about the limited available treatment options and a desire for additional options beyond surgery.
OS was identified as the most important outcome for patients with melanoma. At the time of this review, the available evidence did not include an assessment of OS due to data immaturity and was limited to RFS, an interim analysis of DMFS, and an exploratory analysis of HRQoL. Recurrence was defined as recurrence of melanoma at any site (local, in-transit, or regional lymph nodes or distant recurrence) or death due to any cause. The final analysis of RFS was performed at IA2 and indicated a benefit for patients randomized to pembrolizumab treatment. More specifically, treatment with pembrolizumab corresponded to a 39% reduction in hazard of recurrence (95% CI, 18% to 55%) at 18 months of follow-up. This was based on 15% and 24% of patients randomized to pembrolizumab and placebo, respectively, who had experienced recurrence of disease at that time. A descriptive analysis of RFS was performed at IA3, which was consistent with the results at IA2. As previously described, RFS was used as a surrogate outcome for OS in the KEYNOTE-716 trial. Although this makes sense from a practical perspective given the duration of follow-up required to perform a robust assessment of OS for patients with stage IIB and IIC melanoma, there is some uncertainty in how well RFS translates to OS, particularly with the use of ICI regimens for melanoma in the adjuvant treatment setting. Despite having enough events to perform the final analysis of RFS, the small number of events available for analysis may have rendered the effect estimates and corresponding CIs fragile. Additional trials and long-term follow-up of patients is needed to further define the association between RFS and OS in patients with stage IIB and IIC melanoma. However, patient and clinician groups identified RFS as a meaningful outcome in this context.
Sensitivity analyses for RFS were conducted at IA2. The definition of recurrence used for the primary analysis of RFS did not include new incident cases of melanoma and second cancer diagnoses as events. The sensitivity analyses included new primary melanomas in the definition of RFS and applied different censoring rules, both of which produced RFS results that were consistent with the primary analysis. The effect of second cancer diagnoses on the results of the RFS analysis are unknown.
RFS was also evaluated by subgroups, including baseline cancer stage, T category, and age (younger than 65 years and at least 65 years). The subgroup analyses were descriptive; therefore, it is not possible to draw conclusions for differences across subgroups.
The first interim analysis of DMFS was available for this review. Neither patient nor clinician groups highlighted DMFS as an outcome of interest compared with RFS and OS. As of IA3, 13% and 19% of patients randomized to the pembrolizumab and placebo groups, respectively, experienced DMFS. The reduction in the risk of DMFS at 18 months was approximately 36% (95% CI, 12% to 53% reduction) in favour of pembrolizumab; however, this was based on a small number of events and immature data, so this estimate is associated with uncertainty and there is a risk that the effect is overestimated.
The EORTC QLQ-C30 Global Health Status/QoL scale and EQ-5D-5L VAS were included as patient-reported HRQoL outcomes in the KEYNOTE-716 trial. The former is a cancer-specific outcome, and the latter is a generic, preference-based outcome. The study recorded completion and compliance rates for these outcomes over the course of the study to determine the time point for analyzing the change from baseline. Week 48 was selected for the analysis based on completion rates of 71% and 76% and compliance rates of 83% to 84% and 89% to 90% in the pembrolizumab and placebo treatment groups, respectively. The analysis of HRQoL outcomes were exploratory but suggested little to no change in HRQoL in the placebo treatment group, and a small numerical reduction in HRQoL in the pembrolizumab treatment group. These results should be considered with caution because they were exploratory and did not control for multiplicity.
Harms
The safety profile of pembrolizumab has been well established in previous clinical trials, including in the treatment of patients with advanced or stage III melanoma.28 Safety results reported herein were based on the DCO of January 4, 2022. A total of ||||||||| deaths were reported, ||||||||| of which were patients randomized to the placebo group. The frequency of AEs and SAEs reported by patients in the pembrolizumab treatment group appeared similar to that in placebo group in the KEYNOTE-716 trial. AEs such as diarrhea, pruritus, arthralgia, rash, headache, hyperthyroidism, increased ALT, and hyperthyroidism were reported more frequently by patients in the pembrolizumab group than in the placebo group, but this was consistent with clinical expectations according to the clinical experts consulted by CADTH. The experts also indicated that the large difference in incidence of hyperthyroidism and hypothyroidism (9% higher and 13% higher, respectively, in the pembrolizumab groups) was likely due to the objective nature of the AE; however, they also noted that these AEs are usually asymptomatic and easily managed. Numerically, more patients discontinued from treatment due to AEs in the pembrolizumab treatment group (17% of patients) compared with the placebo group (5% of patients); however, discontinuation from treatment did not appear to be the result of any specific AEs. The clinical experts consulted by CADTH stated that patients with stage IIB or IIC melanoma following complete resection are overall healthy patients. They posed that, as a result, some patients may not be willing to tolerate the AEs associated with pembrolizumab (which they were receiving during a trial, therefore the benefits were unclear) when they felt healthy otherwise.
Notable AEs (i.e., the AEs of special interest for this review), including immune-mediated reactions (colitis and pneumonitis), severe skin reactions (Stevens-Johnson syndrome and toxic epidermal necrolysis), infusion-related reactions, and endocrine-related reactions, were observed in less than 4% of patients in any treatment group, with the exception of hyperthyroidism and hypothyroidism as previously described. Overall, the clinical experts indicated that the safety profile of pembrolizumab observed in this study was acceptable, manageable, and consistent with the known safety profile of pembrolizumab. No additional safety signals were identified with adjuvant pembrolizumab monotherapy.
Conclusions
One sponsor-submitted, phase III, randomized, placebo-controlled, parallel-group, multicentre study of patients with resected stage IIB or IIC cutaneous melanoma was included in this review. Following complete resection, adjuvant treatment with pembrolizumab as a solution for infusion (2 mg/kg for pediatric patients or 200 mg for adult patients administered every 3 weeks for 17 weeks) demonstrated a benefit relative to placebo in terms of RFS. This was based on a 39% (95% CI, 18% to 55%) reduction in the hazard of recurrence at 18 months of follow-up. The long-term benefit of adjuvant pembrolizumab treatment of stage IIB and IIC melanoma is currently unknown and, although RFS is a clinically meaningful outcome, the evidence for RFS as a surrogate for OS for ICI regimens is associated with some uncertainty. Overall, the safety profile of pembrolizumab observed in the KEYNOTE-716 trial was considered acceptable, manageable, and consistent with the known safety profile of pembrolizumab. No additional safety signals were identified with adjuvant pembrolizumab monotherapy. Efficacy and safety for pediatric patients is uncertain because only 2 patients aged 12 to 17 years were included in the pivotal trial.
References
1.Canadian Cancer Society. Melanoma. [2022]; https://cancer.ca/en/cancer-information/cancer-types/skin-melanoma. Accessed 2022 Jun 29.
2.Public Health Agency of Canada. Melanoma skin cancer. 2019; https://www.canada.ca/en/public-health/services/chronic-diseases/cancer/melanoma-skin-cancer.html. Accessed 2022 Jun 29.
3.Sosman JA. Adjuvant and neoadjuvant therapy for cutaneous melanoma. . In: Post TW, ed. UpToDate. Waltham (MA): UpToDate; 2022: http://www.uptodate.com. Accessed 2022 May 10.
4.Lee CW, McKinnon JG, Davis N. Canadian melanoma conference recommendations on high-risk melanoma surveillance: a report from the 14th Annual Canadian Melanoma Conference; Banff, Alberta; 20-22 February 2020. Curr Oncol. 2021;28(3):2040-2051. PubMed
5.Keytruda (pembrolizumab): solution for infusion 100 mg/4 mL vial [product monograph]. Kirkland (QC): Merck Canada Inc.; 2022 July 5.
6.Drug Reimbursement Review sponsor submission: Keytruda (pembrolizumab), 100 mg/4 mL vial [internal sponsor's package]. Kirkland (QC): Merck Canada Inc.; 2022 Apr 26.
7.Merck Sharp & Dohme Corp. Highlights of prescribing information: KEYTRUDA® (pembrolizumab) injection, for intravenous use. Silver Spring (MD): U.S. Food and Drug Administration; 2021: https://www.accessdata.fda.gov/drugsatfda_docs/label/2021/125514s112lbl.pdf. Accessed 2022 Jun 29.
8.CADTH pCODR Expert Review Committee (pERC) final recommendation: pembrolizumab (Keytruda). Ottawa (ON): CADTH; 2019 Aug 1: https://www.cadth.ca/sites/default/files/pcodr/Reviews2019/10168PembrolizumabMAT_FnRec_31%20July%202019__Post_01Aug2019_final.pdf. Accessed 2022 Jun 29.
9.Haanen JB, Carbonnel F, Robert C, Larkin J, Jordan K. Management of toxicities from immunotherapy: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2017;28(4): IV119-IV142. PubMed
10.Management of immune-related adverse events in patients treated with immune checkpoint inhibitor therapy: American Society of Clinical Oncology clinical practice guideline (ASCO guidelines) 2018: https://www.asco.org/sites/new-www.asco.org/files/content-files/practice-and-guidelines/2018-management-of-irAEs-summary.pdf. Accessed 2022 Jun 29.
11.Clinical Study Report: P716V02MK3475. Adjuvant therapy with pembrolizumab versus placebo in resected high-risk stage II melanoma: a randomized, double-blind phase 3 study (KEYNOTE 716) [internal sponsor's report]. Kenilworth (NJ): Merck Sharp & Dohme Corp.; 2021 Oct 22.
12.Clinical Study Report: P716V03MK3475. Adjuvant therapy with pembrolizumab versus placebo in resected high-risk stage II melanoma: a randomized, double-blind phase 3 study (KEYNOTE 716) [internal sponsor's report]. Kenilworth (NJ): Merck Sharp & Dohme Corp.; 2022 Jun 6.
13.Suciu S, Eggermont AMM, Lorigan P, et al. Relapse-free survival as a surrogate for overall survival in the evaluation of stage II-III melanoma adjuvant therapy. J Natl Cancer Inst. 2018;110(1):01.
14.Coart E, Suciu S, Squifflet P, et al. Evaluating the potential of relapse-free survival as a surrogate for overall survival in the adjuvant therapy of melanoma with checkpoint inhibitors. Eur J Cancer. 2020;137:171-174. PubMed
15.Melanoma: cutanenous. Version 3.2022. (NCCN clinical practice guidelines in oncology). Plymouth Meeting (PA): National Comprehensive Cancer Network; 2022: https://www.nccn.org. Accessed 2022 Aug 12.
16.Luke JJ, Rutkowski P, Queirolo P, et al. Pembrolizumab versus placebo as adjuvant therapy in completely resected stage IIB or IIC melanoma (KEYNOTE-716): a randomised, double-blind, phase 3 trial. Lancet. 2022;399(10336):1718-1729. PubMed
17.Clinical Study Report: P716V01MK3475. Adjuvant therapy with pembrolizumab versus placebo in resected high-risk stage II melanoma: a randomized, double-blind phase 3 study (KEYNOTE 716) [internal sponsor's report]. Kenilworth (NJ): Merck Sharp & Dohme Corp.; 2021 Apr 5.
18.Fayers PM, Aaronson NK, Bjordal K, et al. The EORTC QLC-C30 scoring manual (3rd Edition). Brussels (BE): European Organisation for Research and Treatment of Cancer (EORTC); 2001: https://www.eortc.org/app/uploads/sites/2/2018/02/SCmanual.pdf. Accessed 2022 Jun 2.
19.Osoba D, Rodrigues G, Myles J, Zee B, Pater J. Interpreting the significance of changes in health-related quality-of-life scores. J Clin Oncol. 1998;16(1):139-144. PubMed
20.Luo N, Fones CS, Lim SE, Xie F, Thumboo J, Li SC. The European Organization for Research and Treatment of Cancer Quality of Life Questionnaire (EORTC QLQ-c30): validation of English version in Singapore. Qual Life Res. 2005;14(4):1181-1186. PubMed
21.Teckle P, Peacock S, McTaggart-Cowan H, et al. The ability of cancer-specific and generic preference-based instruments to discriminate across clinical and self-reported measures of cancer severities. Health Qual Life Outcomes. 2011;9(1):1-10. PubMed
22.van Reenen M, Janssen B. EQ-5D-5L User Guide. Basic information on how to use the EQ-5D-5L instrument. Rotterdam (NL): EuroQol Research Foundation; 2015: https://euroqol.org/publications/user-guides/. Accessed 2022 Jun 02.
23.Pickard AS, Neary MP, Cella D. Estimation of minimally important differences in EQ-5D utility and VAS scores in cancer. Health Qual Life Outcomes. 2007;5:70. PubMed
24.Multiple endpoints in clinical trials guidance for industry: draft guidance. Silver Spring (MD): U.S. Food and Drug Administration; 2017: https://www.fda.gov/files/drugs/published/Multiple-Endpoints-in-Clinical-Trials-Guidance-for-Industry.pdf. Accessed 2022 Jun 29.
25.Dias S, Welton NJ, Sutton AJ, Caldwell DM, Lu G, Ades AE. Evidence synthesis for decision making 4: inconsistency in networks of evidence based on randomized controlled trials. Med Decis Making. 2013;33(5):641-656. PubMed
26.Systematic literature review and network meta-analysis for patients not previously treated with non-targeted therapy for advanced melanoma [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Keytruda (pembrolizumab), 100 mg/4 mL via. Kirkland (QC): Merck Canada Inc.; 2022 Apr 26.
27.Jansen JP, Trikalinos T, Cappelleri JC, et al. Indirect treatment comparison/network meta-analysis study questionnaire to assess relevance and credibility to inform health care decision making: an ISPOR-AMCP-NPC Good Practice Task Force report. Value Health. 2014;17(2):157-173. PubMed
28.Eggermont AMM, Blank CU, Mandala M, et al. Adjuvant pembrolizumab versus placebo in resected stage III melanoma. N Engl J Med. 2018;378(19):1789-1801. PubMed
29.Aaronson NK, Ahmedzai S, Bergman B, et al. The European Organization for Research and Treatment of Cancer QLQ-C30: a quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst. 1993;85(5):365-376. PubMed
30.Cocks K, King M, Velikova G, et al. Evidence-based guidelines for interpreting change scores for the European Organisation for the Research and Treatment of Cancer Quality of Life Questionnaire Core 30. Eur J Cancer. 2012;48(11):1713-1721. PubMed
31.McClure NS, Sayah FA, Xie F, Luo N, Johnson JA. Instrument-defined estimates of the minimally important difference for EQ-5D-5L index scores. Value Health. 2017;20(4):644-650. PubMed
32.Richardson J, Iezzi A, Khan MA, Chen G, Maxwell A. Measuring the sensitivity and construct validity of 6 utility instruments in 7 disease areas. Med Decis Making. 2016;36(2):147-159. PubMed
33.Giesinger JM, Kieffer JM, Fayers PM, et al. Replication and validation of higher order models demonstrated that a summary score for the EORTC QLQ-C30 is robust. J Clin Epidemiol. 2016;69:79-88. PubMed
34.Davda J, Kibet H, Achieng E, Atundo L, Komen T. Assessing the acceptability, reliability, and validity of the EORTC Quality of Life Questionnaire (QLQ-C30) in Kenyan cancer patients: a cross-sectional study. J Patient Rep Outcomes. 2021;5(1):4. PubMed
35.Snyder CF, Blackford AL, Sussman J, et al. Identifying changes in scores on the EORTC-QLQ-C30 representing a change in patients' supportive care needs. Qual Life Res. 2015;24(5):1207-1216. PubMed
36.Herdman M, Gudex C, Lloyd A, et al. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual Life Res. 2011;20(10):1727-1736. PubMed
37.Clinical trial endpoints for the approval of cancer drugs and biologics: guidance for industry. Silver Spring (MD): U.S. Food and Drug Administration; 2018: https://www.fda.gov/media/71195/download. Accessed 2022 Jun 28.
38.Table of surrogate endpoints that were the basis of drug approval or licensure. Silver Spring (MD): U.S. Food and Drug Administration; 2022: https://www.fda.gov/drugs/development-resources/table-surrogate-endpoints-were-basis-drug-approval-or-licensure. Accessed 2022 Jun 24.
39.FDA facts: biomarkers and surrogate endpoints. Silver Spring (MD): U.S. Food and Drug Administration; 2017: https://www.fda.gov/about-fda/innovation-fda/fda-facts-biomarkers-and-surrogate-endpoints. Accessed 2022 June 24.
40.Guideline on the clinical evaluation of anticancer medicinal products. Amsterdam (Netherlands): European Medicines Agency; 2020: https://www.ema.europa.eu/documents/scientific-guideline/draft-guideline-evaluation-anticancer-medicinal-products-man-revision-6_en.pdf. Accessed 2022 Jun 24.
41.Validity of surrogate endpoints in oncology. Version 1.1. (IQWiG reports – commission no. A10-05). Cologne (Germany): Institute for Quality and Efficiency in Health Care (IQWiG); 2011: https://www.iqwig.de/download/a10-05_executive_summary_v1-1_surrogate_endpoints_in_oncology.pdf. Accessed 2022 Jun 24.
42.Gyawali B, Hey SP, Kesselheim AS. Evaluating the evidence behind the surrogate measures included in the FDA's table of surrogate endpoints as supporting approval of cancer drugs. EClinicalMedicine. 2020;21:100332. PubMed
43.Haslam A, Hey SP, Gill J, Prasad V. A systematic review of trial-level meta-analyses measuring the strength of association between surrogate end-points and overall survival in oncology. Eur J Cancer. 2019;106:196-211. PubMed
44.Buyse M, Saad ED, Burzykowski T, Regan MM, Sweeney CS. Surrogacy beyond prognosis: the importance of “trial-level” surrogacy. The Oncologist. 2022;27(4):266-271. PubMed
45.Buyse M, Molenberghs G, Burzykowski T, Renard D, Geys H. The validation of surrogate endpoints in meta-analyses of randomized experiments. Biostatistics. 2000;1(1):49-67. PubMed
46.Eggermont AM, Chiarion-Sileni V, Grob J-J, et al. Prolonged survival in stage III melanoma with ipilimumab adjuvant therapy. N Engl J Med. 2016;375(19):1845-1855. PubMed
Appendix 1: Literature Search Strategy
Note this appendix has not been copy-edited.
Clinical Literature Search
Overview
Interface: Ovid
Databases:
MEDLINE All (1946 to present)
Embase (1974 to present)
Note: Subject headings and search fields have been customized for each database. Duplicates between databases were removed in Ovid.
Date of search: May 19, 2022
Alerts: Bi-weekly search updates until project completion
Search filters applied: Randomized controlled trials; controlled clinical trials.
Limits:
Conference abstracts: excluded
Syntax | Description |
|---|---|
/ | At the end of a phrase, searches the phrase as a subject heading |
MeSH | Medical Subject Heading |
.fs | Floating subheading |
exp | Explode a subject heading |
* | Before a word, indicates that the marked subject heading is a primary topic; or, after a word, a truncation symbol (wildcard) to retrieve plurals or varying endings |
# | Truncation symbol for 1 character |
? | Truncation symbol for 1 or no characters only |
adj# | Requires terms to be adjacent to each other within # number of words (in any order) |
.ti | Title |
.ot | Original title |
.ab | Abstract |
.hw | Heading word; usually includes subject headings and controlled vocabulary |
.kf | Keyword heading word |
.dq | Candidate term word (Embase) |
.pt | Publication type |
.mp | Mapped term |
.rn | Registry number |
.nm | Name of substance word (MEDLINE) |
.yr | Publication year |
.jw | Journal title word (MEDLINE) |
.jx | Journal title word (Embase) |
freq=# | Requires terms to occur # number of times in the specified fields |
medall | Ovid database code: MEDLINE All, 1946 to present, updated daily |
oemezd | Ovid database code; Embase, 1974 to present, updated daily |
cctr | Ovid database code; Cochrane Central Register of Controlled Trials |
Multi-Database Strategy
(Keytruda* or pembrolizumab* or lambrolizumab* or MK 3475 or MK3475 or Merck 3475 or Merck3475 or HSDB 8257 or HSDB8257 or Sch 900475 or Sch900475 or DPT0O3T46P).ti,ab,kf,ot,hw,rn,nm.
exp melanoma/ or exp skin neoplasms/
(melanoma* or melanotic or melanocarcinoma* or melanomalignoma* or naevocarcinoma* or nevocarcinoma* or pigmentary cancer* or dermatoma or ((skin or cutaneous) adj3 (cancer* or neoplas* or tumor* or tumour*))).ti,ab,kf,ot,hw.
2 or 3
1 and 4
5 use medall
*pembrolizumab/
(Keytruda* or pembrolizumab* or lambrolizumab* or MK 3475 or MK3475 or Merck 3475 or Merck3475 or HSDB 8257 or HSDB8257 or Sch 900475 or Sch900475).ti,ab,kf,dq.
7 or 8
exp melanoma/ or exp skin tumor/
(melanoma* or melanotic or melanocarcinoma* or melanomalignoma* or naevocarcinoma* or nevocarcinoma* or pigmentary cancer* or dermatoma or ((skin or cutaneous) adj3 (cancer* or neoplas* or tumor* or tumour*))).ti,ab,kf,dq.
10 or 11
9 and 12
13 use oemezd
(conference abstract or conference review).pt.
14 not 15
6 or 16
(Randomized Controlled Trial or Controlled Clinical Trial or Pragmatic Clinical Trial or Equivalence Trial or Clinical Trial, Phase III).pt.
Randomized Controlled Trial/
exp Randomized Controlled Trials as Topic/
"Randomized Controlled Trial (topic)"/
Controlled Clinical Trial/
exp Controlled Clinical Trials as Topic/
"Controlled Clinical Trial (topic)"/
Randomization/
Random Allocation/
Double-Blind Method/
Double Blind Procedure/
Double-Blind Studies/
Single-Blind Method/
Single Blind Procedure/
Single-Blind Studies/
Placebos/
Placebo/
Control Groups/
Control Group/
(random* or sham or placebo*).ti,ab,hw,kf.
((singl* or doubl*) adj (blind* or dumm* or mask*)).ti,ab,hw,kf.
((tripl* or trebl*) adj (blind* or dumm* or mask*)).ti,ab,hw,kf.
(control* adj3 (study or studies or trial* or group*)).ti,ab,kf.
(Nonrandom* or non random* or non-random* or quasi-random* or quasirandom*).ti,ab,hw,kf.
allocated.ti,ab,hw.
((open label or open-label) adj5 (study or studies or trial*)).ti,ab,hw,kf.
((equivalence or superiority or non-inferiority or noninferiority) adj3 (study or studies or trial*)).ti,ab,hw,kf.
(pragmatic study or pragmatic studies).ti,ab,hw,kf.
((pragmatic or practical) adj3 trial*).ti,ab,hw,kf.
((quasiexperimental or quasi-experimental) adj3 (study or studies or trial*)).ti,ab,hw,kf.
(phase adj3 (III or "3") adj3 (study or studies or trial*)).ti,hw,kf.
or/18-48
17 and 49
remove duplicates from 50
Clinical Trials Registries
ClinicalTrials.gov
Produced by the US National Library of Medicine. Targeted search used to capture registered clinical trials.
[Search terms: (Keytruda OR pembrolizumab) AND melanoma]
WHO ICTRP
International Clinical Trials Registry Platform, produced by the World Health Organization. Targeted search used to capture registered clinical trials.
[Search terms: (Keytruda OR pembrolizumab) AND melanoma]
Health Canada’s Clinical Trials Database
Produced by Health Canada. Targeted search used to capture registered clinical trials.
[Search terms: (Keytruda OR pembrolizumab) AND melanoma]
EU Clinical Trials Register
European Union Clinical Trials Register, produced by the European Union. Targeted search used to capture registered clinical trials.
[Search terms: (Keytruda OR pembrolizumab) AND melanoma]
Grey Literature
Search dates: May 12 to 18, 2022
Keywords: [Search terms: (Keytruda OR pembrolizumab) AND melanoma]
Limits: No limits
Updated: Search updated prior to the completion of stakeholder feedback period
Relevant websites from the following sections of the CADTH grey literature checklist Grey Matters: A Practical Tool for Searching Health-Related Grey Literature were searched:
Health Technology Assessment Agencies
Health Economics
Clinical Practice Guidelines
Drug and Device Regulatory Approvals
Advisories and Warnings
Drug Class Reviews
Clinical Trials Registries
Databases (free)
Health Statistics
Internet Search
Open Access Journals
Appendix 2: Excluded Studies
None of the studies selected for screening from the systematic literature review search were excluded.
Appendix 3: Detailed Outcome Data
Note this appendix has not been copy-edited.
Table 25: Recurrence-Free Survival (ITT Population, DCO January 4, 2022)
RFS | Pembrolizumab (N = 487) | Placebo (N = 489) |
|---|---|---|
Number of events (%) | 95 (19.5) | 139 (28.4) |
Event rate per 100 person-months | 0.9 | 1.4 |
Median RFSa (months) (95% CI) | 37.2 (NR to NR) | NR (NR to NR) |
RFS rate at 18 months in %a (95% CI) | 86.1 (82.6 to 88.9) | 77.8 (73.7 to 81.2) |
Hazard ratio (95% CI)b | 0.64 (0.50 to 0.84) | |
P valuec | Descriptive only | |
RFS rate at time point, % (95% CI)a | ||
6 months | |||||||||||||||||| | |||||||||||||||||| |
12 months | 90.5 |||||||||||||||||| | 83.2 |||||||||||||||||| |
18 months | |||||||||||||||||| | |||||||||||||||||| |
24 months | 81.2 |||||||||||||||||| | 72.8 |||||||||||||||||| |
30 months | |||||||||||||||||| | |||||||||||||||||| |
36 months | |||||||||||||||||| | |||||||||||||||||| |
Type of first event in RFS analysis | ||
Local/regional/locoregional | 46 (9.4) | 56 (11.5) |
Distant (includes distant event diagnosed within 30 days from loco/regional/locoregional event) | 45 (9.2) | 77 (15.8) |
Death | 4 (0.8) | 6 (1.2) |
No event | 392 (80.5) | 350 (71.6) |
CI = confidence interval; DCO = data cut-off; ITT = intention to treat; NR = not reached; RFS = recurrence-free survival.
aFrom product-limit (Kaplan-Meier) method for censored data.
bBased on Cox regression model with Efron’s method of tie handling with treatment as a covariate stratified by melanoma T category (T3b vs. T4a vs. T4b).
cOne-sided P value based on log-rank test stratified by melanoma T category (T3b vs. T4a vs. T4b).
Source: Clinical Study Report.12
Figure 9: KM Estimates of RFS (Primary Censoring Rule; ITT Population)
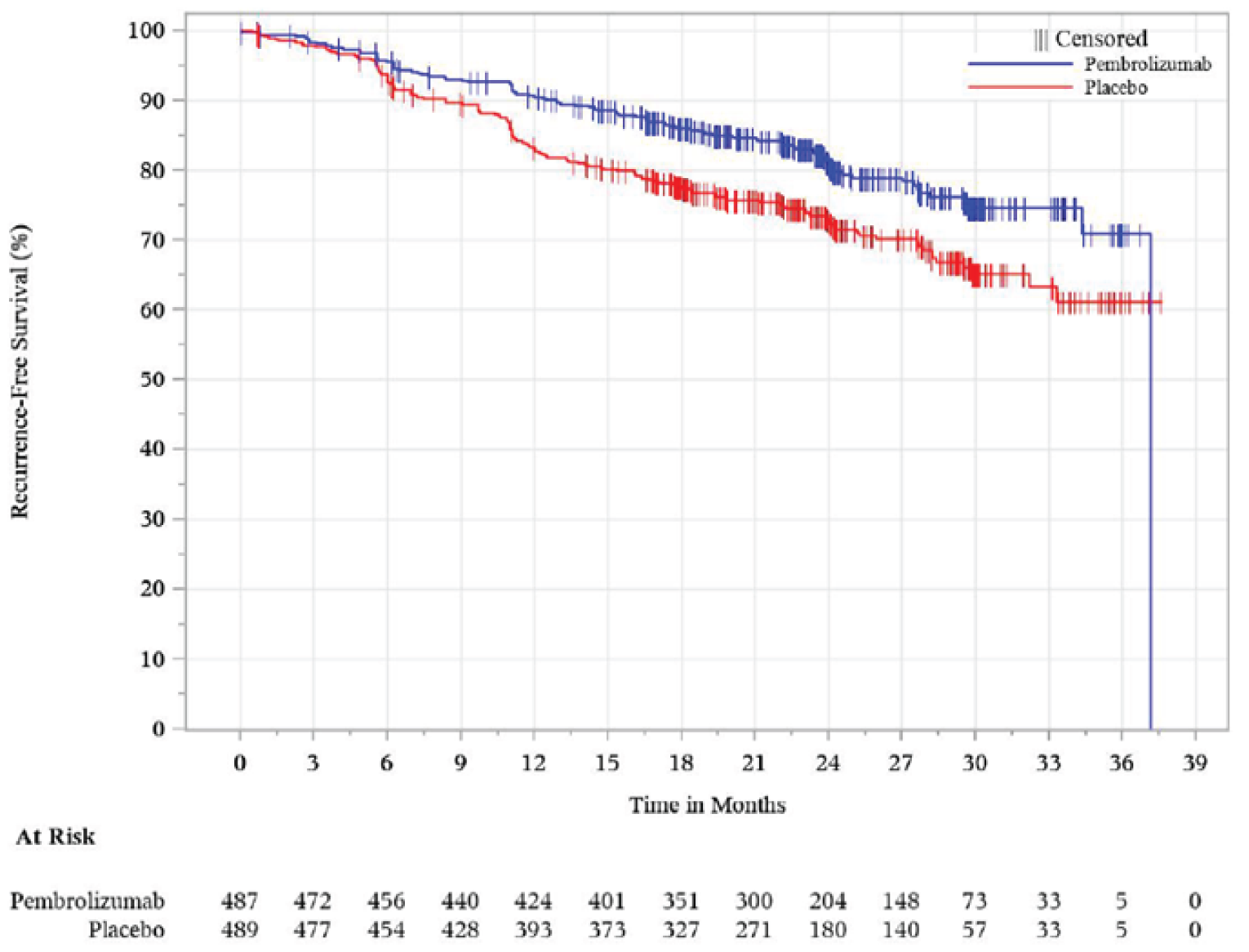
ITT = intention to treat.
Note: Date cut-off date was January 4, 2022.
Source: Clinical Study Report.12
Table 26: Recurrence-Free Survival Sensitivity Analyses (ITT Population, DCO June 21, 2021)
New primary melanomas included as part of the RFS analysis | Pembrolizumab (N = 487) | Placebo (N = 489) |
|---|---|---|
Number of events (%) | 80 (16.4) | 129 (26.4) |
Event rate per 100 person-months | |||||||||||||||||| | |||||||||||||||||| |
Median RFSa (months) (95% CI) | NR (NR to NR) | NR (29.9 to NR) |
RFS rate at 18 months in %a (95% CI) | |||||||||||||||||| | |||||||||||||||||| |
Hazard ratio (95% CI)b | 0.60 (0.45 to 0.79) | |
P valuec,d | |||||||||||||||||| | |
Sensitivity analysis with different censoring rulese | ||
Number of events (%) | |||||||||||||||||| | |||||||||||||||||| |
Event rate per 100 person-months | |||||||||||||||||| | |||||||||||||||||| |
Median RFSa (months) (95% CI) | |||||||||||||||||| | |||||||||||||||||| |
RFS rate at 18 months in %a (95% CI) | |||||||||||||||||| | |||||||||||||||||| |
Hazard ratio (95% CI)b | |||||||||||||||||| | |||||||||||||||||| |
P valuec,d | |||||||||||||||||| | |
CI = confidence interval; DCO = data cut-off; ITT = intention to treat; NR = not reached; RFS = recurrence-free survival.
aFrom product-limit (Kaplan-Meier) method for censored data.
bBased on Cox regression model with Efron’s method of tie handling with treatment as a covariate stratified by melanoma T category (T3b vs. T4a vs. T4b).
cOne-sided P value based on log-rank test stratified by melanoma T category (T3b vs. T4a vs. T4b).
dThe P value has not been adjusted for multiple testing (i.e., the type I error rate has not been controlled).
eSame censoring rules as the primary analysis except that events after 2 consecutive missed disease assessments should be counted as events at the true documented date, and if no events before new anticancer therapy, participants will be censored at last disease assessment.
Source: Clinical Study Report.11
Table 27: Recurrence-Free Survival by Subgroup (ITT Population, DCO January 4, 2022)
IA3 subgroup | # events/N | HR (95% CI) |
|---|---|---|
T categorya | ||
T3b | |||||||||||||||||| | |||||||||||||||||| |
T4a | |||||||||||||||||| | |||||||||||||||||| |
T4b | |||||||||||||||||| | |||||||||||||||||| |
Age | ||
< 65 years | |||||||||||||||||| | |||||||||||||||||| |
≥ 65 years | |||||||||||||||||| | |||||||||||||||||| |
CI = confidence interval; DCO = data cut-off; HR = hazard ratio; ITT = intention to treat.
aBased on actual baseline tumour stage collected on eCRF.
Source: Clinical Study Report.12
Appendix 4: Description and Appraisal of Outcome Measures
Note this appendix has not been copy-edited.
Aim
To describe the following outcome measures and review their measurement properties (validity, reliability, responsiveness to change, and MID):
European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 (EORTC QLQ-C30)
EQ-5D-5L
Findings
The findings about the validity, reliability, responsiveness, and MID of each outcome measure are summarized in Table 28.
Table 28: Summary of Outcome Measures and Their Measurement Properties
Outcome measure | Type | Conclusions about measurement properties | MID |
|---|---|---|---|
EORTC QLQ-C30, version 3.0 | Cancer-specific self-reported measure of HRQoL. A 30-item questionnaire, consisting of 5 functional scales (physical, role, emotional, social, and cognitive), 9 symptom scales (fatigue, nausea/vomiting, pain, dyspnea, insomnia, appetite loss, constipation, diarrhea, and financial difficulties), and a global health status scale. A higher score for functional scales and for GHS scale represents better functioning or HRQoL. A higher score for symptom scales represents worsening of symptoms.29 | In studies examining various cancers: Validity: Moderate to strong correlations with SF-36 scales (r = 0.35 to 0.67) indicating convergent validity.20 GHS scale moderately correlated with EQ-5D-3L index score (r = 0.43) and strongly correlated with EQ VAS (r = 0.73).21 Reliability: Internal consistency assessed using Cronbach alpha; values of ≥ 0.70 for 6 of 9 scales examined.20 Responsiveness: No relevant studies identified. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| Threshold estimates for a small improvement (deterioration) across various cancer sites: GHS: 5 to 8 (–5 to –10) Cognitive: 3 to 7 (–1 to –7) Emotional: 6 to 9 (–3 to –12) Physical: 2 to 7 (–5 to –10) Role: 6 to 12 (–7 to –14) Social: 3 to 8 (–6 to –11) Fatigue: 4 to 9 (–5 to –10) Nausea/vomiting: 3 to 9 (–5 to –11) Pain: 5 to 9 (–3 to –11).30 |
EQ-5D-5L, version 4.0 | Generic preference-based HRQoL scale consisting of a VAS with values between 100 (best imaginable health) and 0 (worst imaginable health) as judged by the patient. A composite index score of 5 dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/ depression. Five response levels for each dimension ranging from experiencing no problems to extreme problems.22 In the Canadian algorithm, index scores ranged from -0.148 to 0.949 for the worst and best health states.31 | In studies examining various cancers: Validity: Moderate to strong correlations with subscales in the SF-36.32 Moderate to poor ability to discriminate between cancer severity by 3 scales: self-reported health status, ECOG PS, cancer stage.21 Reliability: Good internal consistency reliability (alpha > 0.7) for all 5 functioning scales and GHS.21 Responsiveness: No relevant studies identified. | MID for VAS in a study examining various cancers using both anchor and distribution-based methods ranged from 7 to 12.23 For the index score, a Canadian-specific MID of 0.037 for a single-level transition from the baseline health state.31 No estimates for MID among patients with melanoma were identified. |
ECOG PS = Eastern Cooperative Oncology Group Performance Status; EORTC QLQ-C03 = European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; HRQoL = health-related quality of life; GHS = global health scale; MID = minimal important difference; SF-36 = 36-Item Short Form Survey; VAS = visual analogue scale.
EORTC QLQ-C30
The European Organization for Research and Treatment of Cancer (EORTC) Quality of Life Questionnaire Core 30, or EORTC QLQ-C30, is 1 of the most commonly used patient-reported outcome (PRO) measures in oncology clinical trials.33 It is a multi-dimensional, cancer-specific, evaluative measure of HRQoL. It was designed specifically for the purpose of assessing changes in participants’ HRQoL in clinical trials, in response to treatment.33 The core questionnaire of the EORTC QLQ-C30 consists of 30 questions that are scored to create 5 multi-item functional scales (physical, role, emotional, cognitive and social functioning), 3 multi-item symptom scales (fatigue, nausea/vomiting and pain), 6 single-item symptom scales (dyspnea, insomnia, appetite loss, constipation, diarrhea and financial impact), and a 2-item QoL scale. A higher score on the global health status and the functional assessments represents QoL improvement.33
The EORTC QLQ-C30 uses a 1-week recall period in assessing function and symptoms. Most questions have 4 response options (“not at all,” “a little,” “quite a bit,” “very much”), with scores on these items ranging from 1 to 4. The 2 items that inform the global QoL scale are answered using a 7-point Likert-type scale, with anchors between 1 (very poor) and 7 (excellent).18 Raw scores for each scale are computed as the average of the items that contribute to a particular scale. This scaling approach is based upon the assumption that it is appropriate to provide equal weighting to each item that comprises a scale. There is also an assumption that, for each item, the interval between response options is equal (for example, the difference in score between “not at all” and “a little” is the same as “a little” and “quite a bit,” at a value of 1 unit). Each raw scale score is converted to a standardized score that ranges from 0 to 100 using a linear transformation, with a higher score reflecting better function on the function scales, higher symptoms on the symptom scales, and better QoL (i.e., higher scores simply reflect higher levels of response on that scale). Thus, a decline in score on the symptom scale would reflect an improvement, whereas an increase in score on the function and QoL scale would reflect an improvement.18
Psychometric Properties
Validity: There were no studies identified that evaluate the psychometric properties of the EORTC QLQ-C30 specifically for patients with melanoma. One cross-sectional study aimed to validate the EORTC QLQ-C30 in a convenient sample of 57 patients with cancer in Singapore.20 Most patients had breast and colorectal cancer, leukemia, lung cancer, lymphoma, germ cell tumour, and other cancers were also reported. Construct validity was assessed by cross-sectional correlational evidence and discriminative evidence. First, convergent validity was assessed using Spearman’s correlation between QLQ-C30 and Short Form-36 (SF-36) scales, hypothesizing moderate to strong correlation (defined as correlation coefficient of 0.35–0.5, and >0.5, respectively) between scales of these 2 instruments measuring similar dimensions of HRQoL. Results showed moderate to strong correlations between QLQ-C30 and SF-36 scales, ranging from 0.35 to 0.67 across the assessed scales. Next, a known-groups approach was used to compare 6 QLQ-C30 scale scores between patients reporting mild and severe symptoms, as well as by stage of disease and presence of comorbid conditions. Except for emotional functioning, the remaining 5 scales showed better scores in patients with mild symptoms than those with severe symptoms (P<0.05). Patients in early stages of cancer (or with no comorbid conditions) generally had better QLQ-C30 scores than those in advanced disease stages (or with comorbid conditions); however, none of these differences were statistically significant.20
A recent cross-sectional study in Kenya was conducted to evaluate the psychometric properties of the EORTC QLQ-C30, using the English or Kiswahili version in a mix of 100 patients with cancer.34 Most patients had breast cancer, followed by prostate, Kaposi sarcoma, lung, and other cancers. Construct validity was assessed by examining the interscale correlations among the subscales of EORTC QLQ-C30. The interscale correlations were weak to strong, and the absolute magnitude ranged from 0.07 to 0.73.
Teckle et al. conducted a study of patients (N = 184) who had either breast (36%), colorectal (31%), or lung (33%) cancer at the Vancouver Cancer Clinic to investigate if disease severity could be distinguished by cancer-specific and generic preference-based instruments.21 Validity was assessed using Pearson’s correlation coefficient (r) where r between 0 and 0.3 demonstrated weak correlation, between 0.3 and 0.49 was moderate, and greater than 0.5 was considered strong. Teckle et al. found a moderate correlation between the EORTC QLQ-C30 GHS scale and the EQ-5D-3L utility score using the US scoring algorithm (r = 0.43). A strong correlation was found between the EORTC QLQ-C30 GHS scale and the EQ VAS (r = 0.73). Discriminant validity was assessed for cancer severity (self-reported health status, ECOG Performance Status [ECOG PS], and cancer stage).21 An effect size (ES) between 0.2 and 0.5 was considered small, between 0.5 and 0.8 was medium, and greater than 0.8 was large. The EORTC QLQ-C30 was able to discriminate populations based on self-reported health status with a large ES of 1.39, ECOG PS with a medium ES of 0.65, and stage of cancer with a small ES of 0.49. It is worth noting that the comparison with EORTC QLQ-C30 was based solely on the 2 questions in the GHS scale regarding overall health and QoL rather than the questionnaire as a whole.21 This study was a mixed population of 3 types of cancer and the results may not exactly reflect what would be observed in patients with melanoma.
Reliability: The Singaporean cross-sectional study20 described above also assessed internal consistency reliability by calculating Cronbach alpha for all QLQ-C30 scales. Cronbach alpha was ≥ 0.70 for 6 of the 9 QLQ-30 scales including role, emotional, and social functioning, as well as fatigue and nausea and vomiting. Cognitive functioning, physical functioning, and nausea and vomiting did not demonstrate internal consistency reliability based on the 0.70 threshold (Cronbach alpha ranged from 0.19 to 0.68).20
The Kenyan study described above assessed the internal consistency reliability of each scale of the questionnaire using Cronbach alpha-coefficients. With the exception of the cognitive function scale, all of the scales had demonstrated good internal consistency reliability based on a Cronbach alpha ≥ 0.70.34
Responsiveness: Relevant studies evaluating the responsiveness of the instrument were not found.
MID
A clinically meaningful improvement or deterioration in the KEYNOTE-716 trial for the EORTC QLQ-C30 subscales was defined as of a change of 10 points or greater from baseline as defined by Osoba et al. (1998).11,19 This study of patients with breast cancer and small cell lung cancer used an anchor-based approach to estimate the MID in which patients who reported “a little” change (for better or worse) on the subjective significance questionnaire had corresponding changes on a function or symptom scale of the EORTC QLQ-C30 of approximately 5 to 10 points.19 Participants who reported a “moderate” change had corresponding changes in the EORTC QLQ-C30 of about 10 to 20 points and those who reported being “very much” changed had corresponding changes of more than 20 points.19
In the pivotal KEYNOTE-716 trial, changes from baseline in EORTC QLQ-C30 scores for the global health status/QoL and physical functioning subscales were also interpreted according to the minimal important differences (MIDs) derived from a publication by Cocks et al., (2012).11,30 Cocks et al. included a systematic review that examined 118 published studies on various types of cancer such as breast, lung, or head and neck as well as clinician expert input to evaluate meaningful differences and magnitude of change in the EORTC QLQ-C30 scores.30 A meta-analysis was conducted to estimate a weighted average change within each size class for large, medium, small, and trivial changes. Small changes indicated a subtle, clinically relevant change.30 The calculations for symptom subscales were reversed to achieve consistency in improvement or deteriorations over time across all scales. MIDs for improvement and deterioration for small changes in each of the subscales are shown in Table 28.
More recently in 2015, a Canadian study estimated the MIDs of the EORTC QLQ C-30 scales using data from 193 newly diagnosed patients with breast and colorectal cancer.35 The Supportive Care Needs Survey-Short Form-34 (SCNS-SF34) was used as an anchor; mean changes in EORTC QLQ-C30 scales associated with improvement, worsening, and no change in supportive care based on the SCNS-SF34 were then calculated. MIDs were assessed for the following scales: Physical function, role function, emotional function, GHS, pain, and fatigue. For improvement, MIDs associated with a statistically significantly improved supportive care needs ranged from 10 to 32 points. For worsening, MIDs associated with a statistically significantly worsening of supportive care needs ranged from 9 to 21 points. The range for unchanged supportive care needs was from 1-point worsening to 16-point improvement in EORTC QLQ C-30 score.35 Based on this, the authors suggested a 10-point change in EORTC QLQ C-30 score represented changes in supportive care needs, and therefore should be considered for clinical use.35
EQ-5D-5L
The EQ-5D-5L questionnaire is a generic, preference-based, HRQoL measure consisting of descriptive questions and a VAS.22 The descriptive questions comprise of 5 dimensions, mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Each dimension is divided into 5 levels (1, 2, 3, 4, 5) representing “no problems,” “slight problems,” “moderate problems,” “severe problems,” and “extreme problems,” respectively. Respondents are asked to choose 1 level that reflects their own health state for each of the 5 dimensions. A total of 3,125 unique health states are possible, with 55555 representing the worst health state and 11111 representing the best state. The corresponding index ‘utility’ scoring of EQ-5D-5L health states is based on a scoring algorithm that is derived from preference data obtained from interviews using choice-based techniques (e.g., time trade-off) and discrete choice experiment tasks.31,36 The lowest and highest score varies depending on the country-specific scoring algorithm that reflect the preferences of specific populations. The anchors are 0 (dead) and 1 (full health), however negative values are also allowed to represent health states that a population considers worse than death. For example, a Canadian scoring algorithm results in a score of -0.148 for health state 55555 (worst health state) and a score of 0.949 for health state 11111 (best health state). Another component of the EQ-5D-5L is the VAS, which records the participant’s self-rated health on a 20 cm scale with end points 0 and 100, with respective anchors of “the worst health you can imagine” and “the best health you can imagine.”22
Psychometric Properties
Validity and reliability: Richardson et al.32 examined various instruments, including the EQ-5D-5L, in respondents who were healthy and who had a chronic disease (i.e., arthritis, asthma, cancer, depression, diabetes, hearing loss, and heart disease) through an online survey in Australia, Canada, Germany, Norway, the UK, and the US. For discriminant validity, the mean EQ-5D-5L differed between healthy respondents and respondents with a chronic disease (0.88 in healthy, 0.18 in patients with cancer). For construct validity, the EQ-5D-5L was strongly correlated with the physical component of the SF-36 in patients with cancer (r = 0.66) and moderately correlated with the average score of psychosocial content of the mental component of the SF-36, the Capabilities Instrument, and the Subjective Well-Being Instrument of the UK Office of National Statistics (r = 0.50).32
Responsiveness: Relevant studies evaluating the responsiveness of the instrument were not found.
MID: No estimates of the MID were identified for patients with melanoma. Pickard et al. (2007) estimated the MID of the EQ-5D VAS based on cross-sectional data collected from 534 patients with advanced (stage 3 or 4) cancer of the bladder, brain, breast, colon or rectum, head or neck, liver or pancreas, kidney, lung, lymphoma, ovary, or prostate.23 Using both anchor- based and distribution-based methods, estimates of the MID ranged from 8 to 12 based on the ECOG performance status and from 7 to 10 based on the Functional Assessment of Cancer Therapy-General (FACT-G) QoL questionnaire quintiles.23 The MIDs for the index score based on the ECOG performance status and the FACT-G ranged from 0.09 to 0.12 for UK-utility scores and 0.06 to 0.09 for US-utility scores.23
McClure et al. (2017) obtained the MID for the EQ-5D-5L by calculating the average absolute difference between the index score of the baseline health state and the index score of all single-level transitions from the baseline state.31 A single-level transition was defined as a change in a single dimension to the next worse/better level, while holding all other dimensions constant. Such single-level transitions across all 3,125 health states were averaged to arrive at MIDs for various countries, by applying country-specific scoring algorithms. For Canada, transitions between levels 3 and 4 were excluded from the average to form a constant distribution of MID values across the range of baseline scores. This analysis resulted in a Canadian-specific MID of 0.037 for a single-level transition from the baseline health state.31
The following section describes RFS as an outcome measure and summarizes evidence that examines the validity of RFS as surrogate for OS in patients with stage II to IV resected melanoma in the adjuvant setting. Studies discussed in this section were identified through a literature search and by reviewing bibliographies of key papers.
RFS as a Surrogate for OS
In the KEYNOTE-716 trial,11 RFS was the primary outcome used to evaluate the efficacy of pembrolizumab compared to placebo for the adjuvant treatment of adult and pediatric (12 years and older) patients with high-risk stage II melanoma following complete resection in the ITT population. RFS events in the trial were defined as any local, regional (including invasive ipsilateral tumour and invasive locoregional tumour), or distant recurrence as determined by the investigator or death by any cause. During treatment, patients were evaluated for recurrence every 24 weeks in part 1 and every 12 weeks in part 2 of the trial.11
Guideline recommendations: Generally, disease- or recurrence-free survival (herein referred to as RFS) is defined as the time from randomization until disease recurrence or death from any cause.37 In a guidance document assessing end points used in clinical trials for cancer drugs and biologics, the FDA noted the benefits and drawbacks to using RFS as a primary end point.37 Advantages of the RFS outcome include being an objective measure based on quantitative assessment, being evaluable sooner (especially when the survival period is expected to be prolonged), and needing a smaller sample size compared with studies using OS as an end point.37 Using RFS as an end point has disadvantages such as variable definitions across studies, the potential for assessment bias especially in open-label studies, inclusion of non-cancer deaths, and achieving a balanced timing of assessments across treatment groups is essential.37 The FDA guidelines recommend that sponsors clearly define the end point, outline the schedule for assessments, include an estimation of the treatment effect size, and ensure blinding of treatment assignments to help reduce the potential for bias.37 According to the FDA guidance, the Oncology Drug Advisory Committee (ODAC) agreed in December 2003, that RFS prolongation represented clinical benefit if the magnitude of this benefit outweighed the toxicity of the adjuvant treatment.37 According to the FDA, RFS has served as the key outcome for FDA’s Accelerated or Traditional Approvals for adjuvant breast cancer hormonal therapy, adjuvant colon cancer, adjuvant cytotoxic breast cancer, adjuvant therapy for stage III non–small cell lung cancer, melanoma, renal cell cancer, and gastrointestinal stromal tumour.38 The FDA guidance noted that while reasonable likely surrogate end points that have not been validated (i.e., not shown to reliably predict, or correlate with, clinical benefit) may be used under the FDA’s Accelerated Approval program to shorten the time to patient access, sponsors must verify the predicted clinical benefit with post-approval clinical trials.37,39 However, the FDA does not discuss the validity of RFS as surrogate end point for OS in their guidance.37 The European Medicines Agency (EMA) guidance noted that while a benefit in OS is the most convincing outcome, other possible primary end points include PFS, RFS, and PROs.40 The EMA guidance states that while RFS is considered a benefit to a patient regardless of cure, OS data should be reported in the adjuvant setting, as adjuvant therapy may limit treatment options upon disease recurrence.
There are several methods used to assess validity of surrogate outcomes, particularly correlation-based approaches.41 In order to examine the validity of surrogate end points for OS, it has been suggested to evaluate the strength of correlation between OS and the surrogate outcome.42,43 For the purpose of assessing the validity of surrogates for regulatory approval, focus has been placed on trial-level surrogacy, i.e., the correlation of the group-level treatment effect on the surrogate outcome with the treatment effect on OS.43 In contrast, correlations that assess the prognostic validity of a surrogate in individual patients (e.g., correlations of median RFS with median OS), cannot confirm the validity of a surrogate for predicting treatment effects on OS.42 Buyse et al., (2022) similarly suggested that individual-level surrogacy cannot determine how changes in the surrogate will result in changes in OS in a group of patients, therefore the use of trial-level surrogacy is necessary to determine if the effect of treatment on the surrogate can be used to predict the effect of treatment on OS.44
The Institute of Quality and Efficacy in Health Care (IQWiG) suggested that an observed correlation between the surrogate outcome and the clinical end point on its own, cannot adequately demonstrate the validity of a surrogate.41 Instead, comprehensive data are required, preferable a meta-analysis of several randomized trials showing robust results. A requirement for large datasets was also suggested by Buyse et al. (2000), noting that multiple randomized studies are required to obtain precise estimates and to distinguish individual-level from trial-level associations between the end points and effects of interest.45 In the guidance of the IQWiG, it is cautioned that the validity of a surrogate is likely both disease-specific and intervention-specific and that conclusions about the validity of a surrogate cannot be easily applied across different indications or interventions.41 Buyse et al. similarly noted that trial-level surrogacy results in 1 setting may not necessarily apply to a future trial examining a different question. For instance, the effects of a new drug with a novel mechanism of action may have considerably different direct and indirect effects on survival than previous treatments. The IQWiG guidance further suggests that a correlation between the surrogate and a clinical end point could be characterized as strong if the correlation coefficient is at least 0.85, as low if the correlation coefficient is 0.7 or less, and as medium if the correlation coefficient is between 0.85 and 0.7.41
Selected evidence for RFS as a surrogate outcome for OS in resected melanoma: Several trials have used RFS as a surrogate for OS for adjuvant treatment of completely resected melanoma. Suciu et al. (2018) examined the use of RFS as a surrogate for OS among interferon-based regimens for the adjuvant therapy of high-risk resected stage II to III melanoma.13 Authors used a meta-analytic approach and included data from 6,708 patients across 13 randomized controlled trials with a median follow-up time of 6.8 years (range, 4.1 to 17.0 years) which compared interferon to observation or the GM2-KLH/QS-21(GMK) vaccine. RFS was defined as time from randomization to first recurrence (locoregional or distant metastasis) or death due to any cause. Using the Spearman’s correlation coefficient, a strong patient-level association was found between RFS and OS across all trials with rho = 0.90 (95% CI, 0.90 to 0.90) and was similar in the 11 trials without the GMK vaccine with rho = 0.92 (95% CI, 0.84 to 1.00; n = 5,826). The trial-level association between HRs for RFS and OS was high when excluding a small outlier trial with R2 = 0.91 (95% CI, 0.81 to 1.00) and was similar in the trials without the vaccine with R2 = 0.92 (95% CI, 0.84 to 1.00). The authors suggested that RFS appeared to be a valid surrogate end point for OS for randomized studies assessing interferon in this patient population in the adjuvant setting. However, as this review was specific to interferon therapies, these correlations cannot be directly applied to the patient population in the KEYNOTE-716 trial.
A recent study by Coart et al. (2020) examined individual patient data from the European Organisation for Research and Treatment of Cancer (EORTC) 18071 trial46 of ipilimumab versus placebo to determine if RFS was an appropriate surrogate for OS for resected stage II to III melanoma in the adjuvant setting.14 Patients were followed for a median of 5.3 years with 264 patients in the ipilimumab group and 322 in the placebo group. A strong patient-level association was found between RFS and OS using the Spearman’s correlation coefficient with rho = 0.84, (95%: 0.82 to 0.87). The trial (centre) level association between HRs for RFS and OS was determined using the coefficient of determination with R2 = 0.59 (95% CI, 0.08 to 1.00) which is considered low according to the IQWiG guidance criteria, with a wide confidence interval demonstrating considerable uncertainty.14,41 The study also examined associations by adding the HRs from the EORTC 18071 trial to the published HRs of the 12 interferon-based trials in the Suciu et al. publication (excluding a small outlier trial), the results of which revealed an R2 value of 0.77 (95% CI, 0.52 to 1.00). The authors noted that the confidence intervals were too wide to be informative and stated that additional data from adjuvant melanoma trials are required to confirm the strength of association between RFS and OS in this setting of checkpoint inhibitors.14 Furthermore, standard of care has changed since this trial with more effective therapies provided upon recurrence which would have an impact on OS.
Conclusion: Two publications were summarized, which assessed the appropriateness of RFS as a surrogate outcome for OS in for resected stage II to III melanoma in the adjuvant setting. A strength of the Suciu et al. (2018) study was the meta-analytic approach to determine measures of association at both the patient- and trial-level using data across several randomized controlled trials. Coart et al. (2020) later added data from the EORTC 18071 trial to this meta-analysis. However, it has been noted that the validity of a surrogate is likely both disease-specific and intervention-specific as the validity of a surrogate cannot be easily applied across different indications or interventions.41 No study was identified that investigated patient-level and/or trial-level surrogacy of RFS with pembrolizumab in the present target population; therefore, it is unclear if improvements in RFS observed in patients in the pembrolizumab group of the KEYNOTE-716 trial would translate into OS benefits.
Pharmacoeconomic Review
Abbreviations
AE
adverse event
DM
distant metastasis
DMFS
distant metastasis–free survival
ICER
incremental cost-effectiveness ratio
LR
locoregional recurrence
LY
life-year
OS
overall survival
PD-1
programmed cell death receptor-1
PD-L1
programmed cell death ligand 1
QALY
quality-adjusted life-year
RDI
relative dose intensity
RF
recurrence-free
RFS
recurrence-free survival
Executive Summary
The executive summary comprises 2 tables (Table 1 and Table 2) and a conclusion.
Item | Description |
|---|---|
Drug product | Pembrolizumab (Keytruda), 100 mg/4 mL vial of solution for IV infusion |
Submitted price | Pembrolizumab, 100 mg: $4,400.00 |
Indication | Proposed: Adjuvant treatment of adult and pediatric (12 years and older) patients with stage IIB or IIC melanoma following complete resection |
Health Canada approval status | NOC |
Health Canada review pathway | Priority review |
NOC date | July 5, 2022 |
Reimbursement request | As per indication |
Sponsor | Merck |
Submission history | Previously reviewed: Yes Pembrolizumab (Keytruda) has been reviewed for multiple indications at CADTH. The following indications were reviewed in 2020 and 2021: Indication: Esophageal carcinoma, gastroesophageal junction adenocarcinoma
Indication: Classical Hodgkin Lymphoma
Indication: Metastatic or unresectable recurrent head and neck squamous cell carcinoma
Indication: Advanced renal cell carcinoma
|
NOC = Notice of Compliance.
Table 2: Summary of Economic Evaluation
Component | Description |
|---|---|
Type of economic evaluation | Cost-utility analysis Markov model |
Target population | Adult and pediatric (12 years and older) patients with stage IIB or IIC melanoma following complete resection |
Treatment | Pembrolizumab |
Comparator | Observation |
Perspective | Canadian publicly funded health care payer |
Outcome | QALYs, LYs |
Time horizon | Lifetime (50 years) |
Key data source | KEYNOTE-716 trial |
Submitted results | ICER = $31,224 per QALY (incremental costs = $71,034; incremental QALYs = 2.27) |
Key limitations |
|
CADTH reanalysis results |
|
IA2 = Interim analysis 2; ICER = incremental cost-effectiveness ratio; LY = life-year; OS = overall survival; PD-L1 = programmed cell death ligand1; QALY = quality-adjusted life-year; RDI = relative dose intensity; RFS = recurrence-free survival.
Conclusions
Based on an appraisal of the KEYNOTE-716 trial, the CADTH Clinical Review found that, compared with placebo, adjuvant pembrolizumab treatment demonstrated a recurrence-free survival (RFS) benefit in adult and pediatric (12 years and older) patients with stage IIB or IIC cutaneous melanoma after complete surgical resection. This benefit was based on 20.5 months of follow-up; therefore, the long-term benefit of adjuvant pembrolizumab treatment is currently unknown. At the time of this review, only the final analysis of RFS and the interim analysis of distant metastasis–free survival (DMFS) were available for assessment. The CADTH Clinical Review concluded that inferences regarding the efficacy of pembrolizumab on improved overall survival (OS) could not be made due to data immaturity at the time of the planned interim analysis. Further, although RFS is a clinically meaningful outcome, the evidence for RFS as a surrogate for OS for immune checkpoint inhibitor regimens is associated with some uncertainty. Finally, efficacy and safety for pediatric patients were considered uncertain because only 2 patients aged between 12 and 18 years were included in the pivotal trial.
Given the limited OS data from the trial, the cost-effectiveness analysis of adjuvant pembrolizumab relied solely on the assumption that RFS can be translated into OS benefits. Although there was evidence based on interferon-based therapies to support RFS as a surrogate outcome, another study concluded that more evidence is needed to confirm the strength of association between RFS and OS for therapies such as pembrolizumab. Thus, the relationship between RFS and OS is associated with notable uncertainty given the limited data available in terms of the therapies that are the current standard of care and the relatively short duration of follow-up at this time. The RFS benefits modelled by the sponsor were extrapolated to a 50-year time horizon based on data from the KEYNOTE-716 trial, which had a median follow-up of 20.5 months. Furthermore, the sponsor assumed that pembrolizumab’s RFS and OS benefit will increase up to 10 years after pembrolizumab is discontinued. The lack of long-term evidence is particularly of note, given that 99.6% of the estimated incremental life-years (LYs) and 99.0% of the estimated incremental quality-adjusted life-years (QALYs) were generated in the post-trial period for which there is no direct comparative evidence. According to the clinical experts consulted by CADTH for this review, the impact of adjuvant pembrolizumab on long-term RFS or OS, especially once the 1-year treatment period is completed, is unknown for adjuvant treatment of stage IIB and IIC melanoma. This was compounded by the fact that the modelled OS curves submitted by the sponsor lacked face validity compared with the literature; it was also noted that different assumptions about the long-term efficacy have a significant influence on incremental effectiveness and overall cost-effectiveness of pembrolizumab. In addition, the clinical effectiveness of pembrolizumab after multiple lines of prior pembrolizumab treatment is uncertain despite the sponsor’s assumption of identical effectiveness. Evidence also suggested that the effectiveness of pembrolizumab could be potentially reduced when patients were rechallenged with the same drug compared with patients who received pembrolizumab for the first time. Due to all these limitations, CADTH could not derive a base case, and instead explored areas of uncertainty, when possible, and conducted an exploratory reanalysis.
CADTH identified several limitations in the economic analysis submitted by the sponsor, beyond the uncertainty regarding the effect of pembrolizumab on long-term RFS and OS. CADTH conducted an exploratory reanalysis, revising the sponsor’s model by incorporating treatment effect waning, changing market shares of subsequent treatments, and setting the relative dose intensity (RDI) to 100%. Based on the CADTH exploratory reanalysis, adjuvant treatment with pembrolizumab is $107,515 more costly and yields 0.96 more QALYs, resulting in an incremental cost-effectiveness ratio (ICER) of $110,594 per QALY. Given the uncertainty previously mentioned, a price reduction of at least 40.7% would be necessary to achieve an ICER of $50,000 per QALY.
As noted, CADTH was unable to adjust for major limitations, including the substantial uncertainty associated with OS benefit as well as concerns regarding a potential reduction in effectiveness of pembrolizumab in patients who were rechallenged with pembrolizumab at relapse. A scenario analysis reducing the model’s time horizon to 10 years, thus limiting the uncertainty associated with OS benefit, was found to increase the price reduction necessary to achieve an ICER of $50,000 per QALY up to 58.1%. Therefore, longer-term evidence is required to validate OS for patients receiving pembrolizumab as adjuvant therapy for stage IIB or IIC melanoma to reduce the uncertainties identified with this model.
Stakeholder Input Relevant to the Economic Review
This section is a summary of the feedback received from the patient groups, registered clinicians, and drug plans that participated in the CADTH review process.
Patient input was received from Melanoma Canada and Save Your Skin Foundation, both national, nonprofit organizations dedicated to helping patients with skin cancers, including melanoma. Input from these groups was based on online surveys, virtual patient roundtables, and one-on-one conversations, including 196 patients or caregivers from Canada. Patient input highlighted that the diagnosis of melanoma affected their daily activities and quality of life by causing scarring and disfigurement, fear or anxiety, disrupting sleep, as well as causing pain, fatigue, and depression. These factors affected patients’ mobility, increased time off work, and decreased career achievements and overall productivity. Patients also noted that there are currently no funded adjuvant therapy options available in Canada for patients with stage IIB and IIC cutaneous melanoma. Patients were seeking to eliminate the cancer and/or prevent cancer progression. In addition, they were expecting new treatments to have tolerable side effects without long-term quality-of-life effects; minimal impact on finances, including being easily accessible without having to travel long distances; and the possibility of continuation of work or daily activities without significant interruption. Patient input also indicated that some patients would consider their overall health status and the need for frequent travelling to receive the treatment before deciding on adjuvant treatment with pembrolizumab. The inconvenience and the cost to travel to a cancer centre (including gas, parking, and potentially accommodation) were considered key concerns for some patients. A total of 38 patients had experience with pembrolizumab in the adjuvant setting, and most patients reported having minor or mild side effects (e.g., fatigue, nausea, skin rash) that were easily manageable. Of those treated with pembrolizumab, most indicated the side effects were worth the treatment.
Clinician input was received from Ontario Health Skin Cancer Drug Advisory Committee. Clinician feedback highlighted the lack of adjuvant treatment options for stage IIB and IIC cutaneous melanoma and there being an unmet need for adjuvant therapy. Particularly, given that patients with stage IIB and IIC cutaneous melanoma are a higher-risk population for recurrence than those with stage IIIA. Clinician input indicated that treatment goals include improvement in RFS.
CADTH-participating drug plans highlighted several implementation and economic considerations, including whether the patients with noncutaneous melanoma would be considered for treatment with pembrolizumab for this indication. Furthermore, in line with other indications for pembrolizumab, jurisdictions would implement a weight-based dose of 2 mg/kg. Finally, the drug plan considered the possibility of pembrolizumab being used in patients with an Eastern Cooperative Oncology Group (ECOG) performance status of 2 or greater for patients with stage IIB or IIC cutaneous melanoma.
Several of these concerns were addressed in the sponsor’s model:
RFS and OS outcomes were included in the model.
In addition, CADTH addressed some of these concerns as follows:
CADTH included a weight-based dose of 2 mg/kg in a scenario analysis.
CADTH was unable to address the following concerns raised from stakeholder input:
CADTH was unable to evaluate the impact of pembrolizumab being used in patients with an ECOG performance status of 2 or greater.
Economic Review
The current review is for pembrolizumab (Keytruda) for adult and pediatric patients with stage IIB or IIC cutaneous melanoma after complete surgical resection.
Economic Evaluation
Summary of Sponsor’s Economic Evaluation
Overview
The sponsor submitted a cost-utility analysis of pembrolizumab adjuvant therapy in patients with stage IIB or IIC cutaneous melanoma after complete surgical resection compared with observation (i.e., no adjuvant treatment).1 The model population comprised adult and pediatric patients (aged 12 years or older) who have undergone surgical complete resection and have stage IIB or IIC cutaneous melanoma, which aligned with the Health Canada indication.
Pembrolizumab is available as a 100 mg/4 mL solution for infusion in a single-use vial. Pembrolizumab is administered intravenously for 30 minutes. The recommended dosage for pembrolizumab is 200 mg every 3 weeks or 400 mg every 6 weeks until unacceptable toxicity, disease progression, or for up to 12 months (17 doses of 200 mg or 9 doses of 400 mg).
At the submitted price of $4,400 per 4 mL vial, the standard cycle (28 days) cost of pembrolizumab was estimated to be $11,733, assuming 100% RDI. In the base case, the sponsor considered observation (i.e., no adjuvant treatment) as the comparator.
Outcomes of the model included QALYs and LYs over a time horizon of 50 years. The base-case analysis was conducted from the perspective of the Canadian public health care system, with an annual discount rate of 1.5% applied to both costs and outcomes.
Model Structure
The sponsor submitted a Markov model with 4 mutually exclusive health states — recurrence-free (RF), locoregional recurrence (LR), distant metastasis (DM), and death — to track the disease course over time, with a weekly cycle length. The DM state was subdivided in pre- and post-progression distant metastases. A figure of the sponsor’s model structure is available in Appendix 3 (Figure 1). All patients began in the RF health state, where they could remain recurrence-free or transition to the LR or DM states. Patients in the LR state could remain in this health state or transition to the DM state. Patients in the DM state could only transition to death. Patients in any health state could transition to death starting in the first cycle.
The submitted model captured the curative potential of treatment in stage IIB or IIC cutaneous melanoma by reducing the risk of LR and DM from the RF state by 95% after 10 years.
The subsequent therapies in the LR and DM states for patients who received pembrolizumab were defined based on the time when transitions to the LR or DM state occurred. If patients transitioned from RF to LR or from RF to DM before 18 months from treatment initiation with pembrolizumab, these patients would be considered ineligible to receive the following anti–programmed cell death receptor-1 (PD-1) and anti–programmed cell death ligand 1 (PD-L1) therapies, such as pembrolizumab or nivolumab.
A half-cycle correction was not applied to either costs or effectiveness estimates in the base-case analysis.
Model Inputs
The model’s baseline population characteristics and clinical efficacy parameters were characterized by the KEYNOTE-716 trial, a randomized, double-blind, placebo-controlled, multicentre, phase III study designed to evaluate the efficacy of pembrolizumab as an adjuvant therapy following complete surgical resection compared with observation. The sponsor assumed that the patient population in the KEYNOTE-716 trial (baseline characteristics: mean age = 59.3 years; 39.7% female; mean weight = |||| kg; starting age < 18 years = 0.2%; proportion with stage IIB cutaneous melanoma = 64.8%; proportion with IIC stage = 35.2%) reflected the Canadian population.
Transition probabilities were derived using a variety of data sources, including the KEYNOTE-716 trial, real-world retrospective data analysis, a network meta-analysis (NMA) study, Canadian life tables, and other studies in the literature. Data from the KEYNOTE-716 trial was used to model transitions from the RF health state to LR and DM health states. Mortality among those in the RF state was modelled as an exponential distribution based on data from the KEYNOTE-716 trial and assumed to be as high as that of the general Canadian population.
Parametric survival modelling was used to derive health state case-specific hazards of each transition, with survival distributions separately fitted to KEYNOTE-716 trial data for each treatment arm. The base-case parametric functions were selected based on visual inspection of fit, fit based on mean squared error, external validity, and clinical plausibility of long-term projections. A competing-risks approach was taken when modelling transitions from the RF state. In addition, the sponsor’s model considered that when analyzing time to each specific type of RF failure (i.e., LR, DM, or death), the 2 other competing failure types were treated as censored events. Survival distributions were then transformed into transition probabilities.
Adjuvant treatment options following progression to the LR state for patients who received pembrolizumab in the RF state fell into 2 distinct categories: those eligible to receive anti-PD-1 or anti-PD-L1 therapies and those ineligible to receive anti-PD-1 or anti-PD-L1 therapies. While those patients who received no adjuvant therapy in the RF state (i.e., observation) were all eligible to receive anti-PD-1 or anti-PD-L1 therapies. Patients were considered eligible to receive anti-PD-1 or anti-PD-L1 therapies in the LR state if they transitioned from the RF to the LR state 18 months after initiating treatment with pembrolizumab. For both categories, patients were assigned a weighted bucket of treatments, with the weights representing each treatment’s market share (Table 10). Market share estimates were based on the KEYNOTE-054 trial, which assessed adjuvant pembrolizumab for stage III melanoma, and a third-party oncology database (Oncology Continuous Audit of Patients and Prescriptions Syndicated [ONCO-CAPPS]) of patient medical record abstractions, which included 230 adjuvant melanoma cases from Canada. Transition probabilities from the LR to DM states were calculated using trials-based hazard ratios of DMFS for each adjuvant treatment compared with placebo for stage III melanoma. Observation alone was used as reference, and DMFS was informed using data from real-world retrospective database analysis. In addition, mortality among those in the LR state was assumed to be equal to that of the general Canadian population.
The first-line therapy for patients who developed distant metastasis fell into 2 distinct categories: those eligible to receive anti-PD-1 or anti-PD-L1 therapies and those ineligible to receive anti-PD-1 or anti-PD-L1 therapies. Patients were assigned a weighted bucket of treatments, with the weights representing their market shares (Table 11). The market shares were estimated using ONCO-CAPPS data. Patient were considered eligible to receive anti-PD-1 or anti-PD-L1 therapies in the DM state if they transitioned from the RF to the DM state 18 months after initiating treatment with pembrolizumab. Patients who transitioned from the LR to DM state were all considered to be eligible to receive anti-PD-1 or anti-PD-L1 therapies, regardless of the timing of transition. The estimation of OS for each category was calculated as a weighted average of expected OS associated with different first-line treatments. The OS hazard ratios for those first-line treatments for DM were estimated from an NMA, which used pembrolizumab as reference.
In the base-case analysis, initial treatment with adjuvant pembrolizumab in the RF state was assumed to have a persistent treatment effect, without waning in efficacy. The model assumed no ongoing efficacy of the initial adjuvant therapy with pembrolizumab once a patient transitioned to the LR or DM states.
The drug-related grade 3 or higher adverse events (AEs) that occurred with a frequency of more than 5% (all grades) observed in the KEYNOTE-716 trial were incorporated into the model, with an associated cost and disutility. Diarrhea of grade 2 or higher and febrile neutropenia of any grade were also included in the model. Both cost and disutilities for AEs were applied as a one-time decrement in the first model cycle. AEs observed in the post-progression setting were not included in the model.
Health state utility values for the health states RF, LR, and DM pre-progression were derived from the KEYNOTE-716 trial. Health utility for DM post-progression was derived from Beusterien et al.2 because disease progression after DM is not identifiable within the KEYNOTE-716 trial data.
Costs in the model included treatment-acquisition costs for adjuvant pembrolizumab and subsequent therapies, state-specific disease management, AE management, and terminal care costs. The dosing schedule for pembrolizumab adjuvant therapy was derived from ONCO-CAPPS data, which consisted of ||||% of patients receiving 200 mg every 3 weeks and ||||% receiving 400 mg every 6 weeks. Pembrolizumab costs were calculated by multiplying the price per 200 mg per cycle ($8,800 per 200 mg) by the RDI of ||||% (as reflected in the pembrolizumab arm of KEYNOTE-716) to account for any delays or interruptions in administration (e.g., due to AEs). If the patient was younger than 18 years, a weight-based dose (2 mg/kg) was used. The proportion of patients remaining on adjuvant pembrolizumab at each scheduled infusion was based on the observed Kaplan-Meier curve for time to treatment discontinuation in the KEYNOTE-716 trial. The base-case analysis also incorporated the cost of administration of IV pembrolizumab, which was derived from the literature.
Treatment costs for subsequent therapies were sourced from CADTH reports and IQVIA Delta PA.3 Costs of first- and second-line therapy for advanced melanoma (DM state) were included in the model, although transition probabilities from DM to death were assumed to be dependent on the first-line therapy received in the DM state. Drug acquisition and administration costs associated with subsequent therapies (including both first-line and second-line subsequent therapies) were applied as a one-time cost upon entry into the DM state and were calculated in the model as a function of the unit drug cost, defined dosing schedule, and RDI for each drug. Drug wastage was assumed to be 5%.
Disease management costs included routine monitoring of patients in the RF state; these costs were based on a study for ongoing surveillance and active follow-up treatment for cancer recurrence in British Columbia and Ontario. The weekly cost derived from the study was applied in the model. Disease management costs in the LR state included a one-time cost for salvage surgery, obtained from the Ontario Schedule of Benefits; the proportion of patients undergoing each type of salvage surgery was obtained from the KEYNOTE-716 trial. Disease management costs for advanced melanoma (DM state) were obtained from the literature.4
The unit costs of AE management per episode were obtained from several studies in the literature, the Ontario Case Costing Initiative, and the Canadian Institute for Health Information (CIHI) patient cost estimator. Finally, patients who transitioned to death were assumed to incur a one-time cost associated with palliative and terminal care, which was derived from the literature.5
Summary of Sponsor’s Economic Evaluation Results
All analyses were run probabilistically (5,000 iterations for the base case). The deterministic and probabilistic results were similar. The probabilistic findings are presented subsequently.
Base-Case Results
In the sponsor’s base-case analysis, adjuvant treatment with pembrolizumab was associated with an ICER of $31,224 per QALY gained compared with observation. A total of 99.0% of incremental QALYs were gained beyond the median trial period of 20.5 months, indicating nearly all benefit was based on extrapolated data. The probability of pembrolizumab being cost-effective at a willingness-to-pay (WTP) threshold of $50,000 per QALY gained was 64.7%.
The submitted analysis is based on the publicly available prices of all treatments, including subsequent therapies.
Table 3: Summary of the Sponsor’s Economic Evaluation Results
Drug | Total costs ($) | Incremental costs ($) | Total QALYs | Incremental QALYs | ICER vs. observation ($/QALY) |
|---|---|---|---|---|---|
Observation | 265,096 | Reference | 9.56 | Reference | Reference |
Pembrolizumab | 336,130 | 71,034 | 11.83 | 2.27 | 31,224 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year; vs. = versus.
Source: Sponsor’s pharmacoeconomic submission.
Sensitivity and Scenario Analysis Results
The sponsor conducted several sensitivity and scenario analyses. Scenario analysis included a shorter time horizon (30 and 40 years), a societal perspective, no cure rate, alternate assumptions for efficacy and transition probabilities, assuming treatment efficacy waning, and alternate scenarios for subsequent treatment lines (i.e., limit costs to first-line therapy only and do not allow use of immunotherapies in LR or DM states). Of note, the largest driver of the ICER was when the cure assumption was not applied. In this scenario the estimated ICER increased to $53,331 per QALY.
CADTH Appraisal of the Sponsor’s Economic Evaluation
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the economic analysis:
OS benefit is unknown: Neither the median RFS nor the median OS were reached in any of the groups by the data cut-off (June 21, 2021) despite having enough events to perform the final analysis of RFS at interim analysis 2 (IA2). According to the CADTH Clinical Review, OS estimates for the pembrolizumab and placebo arms were expected to be analyzed as part of a fifth interim analysis. Because OS data from the trial were not yet provided, the sponsor submitted a model using RFS estimates as an intermediate outcome to predict the entire 50-year lifetime OS estimates. The RFS data used to populate the model were obtained from extrapolation of the KEYNOTE-716 trial, with a median follow-up time of 20.5 months. In the submitted model, patients treated with pembrolizumab accumulated an additional 2.37 LYs, of which 0.4% were accrued within the trial period (median = 20.5 months) and approximately 60% were accrued between 10 and 30 years after adjuvant treatment. Given the cure assumption used in the model (i.e., patient without a recurrence up to 10 years were considered cured), the submitted model predicts that pembrolizumab would cure 13.8% more patients when compared with observation alone (41.5% and 27.6% of patients were RF at year 10 for pembrolizumab and observation, respectively). Furthermore, because OS data were immature, and only discontinuation due to death from the study was submitted as part of this review (|||% and |||% for pembrolizumab and observation, respectively), there is no direct evidence to suggest pembrolizumab conferred a survival benefit relative to observation or increased the rate of cure.
In addition to the limitations regarding data immaturity, the OS curve provided by the sponsor lacked face validity when compared with melanoma survival estimates for stage IIB and IIC published by the American Joint Committee on Cancer (AJCC) Melanoma Staging Database 7th and 8th editions.6,7 In the KEYNOTE-716 trial, the proportion of patients with stage IIB and IIC melanoma was 64.8% and 35.2%, respectively. Because AJCC’s survival curves only account for melanoma-related events, to validate the OS curve provided by the sponsor, CADTH removed all-cause mortality from the survival estimates. The 5-year survival rate estimated by the sponsor’s model in the observation arm was 79%, which was lower than the AJCC’s 5-year survival rate (between 86% and 90% for stage IIB and 82% for stage IIC melanoma). Because the ACJJ 8th edition only presented 5- and 10-year survival rates, CADTH validated the long-term results against AJCC 7th edition. The 20-year survival rate estimated by the sponsor’s model was 36%, which was similar to the AJCC’s 20-year survival rate for stage IIC melanoma (approximately 36%), but lower than the AJCC’s 20-year survival rate for stage IIB (approximately 45%). Therefore, the OS extrapolation was considered to be unreliable. The lack of face validity of OS curves added to the fact that OS data were exclusively derived from RFS and 99.6% of the incremental LY benefit was accrued after the trial period, resulting in substantial uncertainty about the magnitude of any OS benefit.
The OS benefit is also linked to the choice of subsequent treatment. Patients who develop LR (stage III) or DM (stage IV) within 18 months of starting adjuvant therapy with pembrolizumab will likely be ineligible for treatment with pembrolizumab and other immunotherapies, potentially leading to shorter survival time. Therefore, the choice of treatment in the adjuvant setting is relevant to define further availability of subsequent treatments and needs to be considered in the context of its long-term implication in the stage III and IV prognosis.
CADTH could not address this limitation due to the absence of OS data in a format CADTH could assess and extrapolate, and the lack of face validity of the sponsor’s extrapolated OS curves. As such, the economic analysis is associated with significant uncertainty. Therefore, CADTH was unable to derive a base-case analysis; instead, a CADTH exploratory reanalysis using more appropriate assumptions, when possible, was conducted.
To explore the uncertainty around the OS benefit, CADTH conducted 2 scenario analyses that reduced the time horizon to 2 and 10 years. Given both the unknown short- and long-term OS benefit, CADTH explored the short-term benefit of pembrolizumab when the time horizon was similar to the median follow-up in the KEYNOTE-716 trial (median = 20.5 months). In addition, CADTH explored a second scenario in which the time horizon of the analysis was aligned with the cure assumption (i.e., 10 years).
Waning of treatment effect: The sponsor’s RFS and OS extrapolations assumed RFS and OS benefits of pembrolizumab that are sustained up to 10 years after pembrolizumab is discontinued. According to the clinical experts consulted by CADTH for this review, the effect of adjuvant pembrolizumab on long-term RFS or OS, especially after the 1-year treatment period is complete, is unknown for adjuvant treatment of stage IIB and IIC melanoma. If the clinical benefits of pembrolizumab are not sustained after treatment discontinuation, the pembrolizumab RFS curve would be overestimated because increasing separation of the curves would not be maintained for 10-years post-adjuvant pembrolizumab treatment. Given that adjuvant treatment with pembrolizumab had a maximum duration of 12 months and the median follow-up of the trial was 20.5 months, the long-term extrapolation of persistent RFS benefit of pembrolizumab from the trial data was highly uncertain.
Therefore, assumptions related to continued treatment effects may have a substantial impact on the pharmacoeconomic results. An analysis of the sponsor’s submitted time to event data was performed by CADTH and the results are presented in Figure 2. The line in that figure represents the relative risk of having an event with pembrolizumab versus observation over 3-month periods, based on the raw data from the KEYNOTE-716 clinical trial. Because OS data are not available, CADTH used RFS to analyze the relative risk of having a recurrence. Data shown in the figure were calculated as “1 –RFS at time t + 1 / RFS at time t.” The data suggested a lower relative risk of events up to 15 months. After 15 months, the data showed limited relative effects. This suggests that pembrolizumab prevented disease progression in the first 15 months after treatment initiation, and there was no evidence of a reduction in RFS beyond this period.
Considering the uncertain long-term treatment effect and clinical expert opinion, CADTH incorporated an assumption in its exploratory reanalysis that the treatment effect of pembrolizumab would start to decrease after 2 years and be completed at year 3 because the sponsor’s model was inflexible to changes outside of full-year increments. Of note, the introduction of treatment effect waning does not equate to an assumption of no separation in the RFS curves. The CADTH-revised assumption still leads to long-term separation of the RFS curves of the 2 treatment options beyond trial data, and considers the benefits accrued in the first 3 years after initiation of adjuvant treatment with pembrolizumab.
CADTH conducted a scenario analysis testing an alternative waning effect assumption. It assumed the treatment effect with pembrolizumab would last longer, with waning starting after 3 years and completed at 5 years. This assumption was based on RFS data from the KEYNOTE-054 trial, which assessed the effect of pembrolizumab in patients with stage III melanoma.
Market shares of subsequent treatment in the LR and DM states do not reflect Canadian clinical practice: Within the LR state, market shares for subsequent treatments for the group eligible for anti-PD-1 or anti-PD-L1 therapies and the observation group (Table 10) do not reflect expected use in Canadian clinical practice, according to the clinical experts consulted by CADTH for this review. Furthermore, the market shares within the DM state also did not appear to align with Canadian practice because a high proportion of patients in the group ineligible for anti-PD-1 or anti-PD-L1 therapies were assigned no subsequent therapies (||||%) compared with patients eligible to receive anti-PD-1 or anti-PD-L1 treatments (|||%). According to the clinical experts consulted for this review, patients who were ineligible to receive anti-PD-1 or anti-PD-L1 therapies would have the option to be treated with ipilimumab alone. The market shares provided by the sponsor would underestimate the costs of those ineligible to receive anti-PD-1 or anti-PD-L1 therapies, which would underestimate the costs of those initially treated with adjuvant pembrolizumab.
Effectiveness of pembrolizumab in patients who were rechallenged with pembrolizumab at relapse is uncertain: The evidence used in the model to inform the effectiveness of subsequent therapies after treatment with pembrolizumab was based on clinical trials of patients who were pembrolizumab naive. However, pembrolizumab’s effectiveness when used across multiple lines of therapy is uncertain. A study in patients with stage III melanoma suggested that the effectiveness of pembrolizumab was reduced when patients were rechallenged with the same drug compared with patients who received pembrolizumab for the first time.8 Therefore, the effectiveness of using pembrolizumab in subsequent therapy lines (i.e., stage III and stage IV, both include pembrolizumab as treatment options) after receiving it for earlier treatment of stage IIB or IIC melanoma might be overestimated in the model, which in turn would overestimate pembrolizumab’s clinical benefit.
CADTH could not address this limitation due to uncertainty in pembrolizumab’s effectiveness in patients who were rechallenged with pembrolizumab at relapse.
RDI: The sponsor’s base case incorporated reduced dose intensities for all therapies (i.e., for adjuvant and subsequent therapies). Consistent with previous reviews, given the inability to link reduced dose intensity with outcomes, the CADTH exploratory base case does not incorporate reduced dose intensity. A reduction in RDI can be derived from a delayed dose, a missed dose, or a reduction in dose. When considering wastage, each component can have a different influence on drug costs. Likewise, it is unclear how treatment discontinuation influences RDI.
In the CADTH exploratory reanalysis, RDI calculations were excluded.
Weight-based dosing for pembrolizumab: Pembrolizumab dosing in the KEYNOTE-716 trial was a fixed dose of 200 mg intravenously every 3 weeks or 400 mg every 6 weeks. Input from participating public drug plans indicated that jurisdictions would likely implement a weight-based dose for pembrolizumab of 2 mg/kg (up to a cap of 200 mg) every 3 weeks with the possibility of extended dosing intervals to every 6 weeks (4 mg/kg up to a 400 mg cap). The clinical experts agreed that this approach seemed reasonable given the clear interchangeable use in dosing for other cancer sites. CADTH notes that weight-based dosing will reduce the ICER associated with pembrolizumab and give greater flexibility in dosing. However, CADTH notes that it is not possible to make the direct assumption that the use of weight-based dosing will lead to the same outcomes as the trial’s fixed dose because patients will be exposed to a lower dose, which may impact treatment efficacy.
CADTH conducted a scenario analysis using weight-based dosing based on an average weight of |||| kg for adult patients.
Lack of transparency and flexibility in the model: Several limitations were observed in the submitted model, including the inability to select all-cause AEs without retrieving errors, to adjust vial sharing settings when changing to weight-based dosing, and the probabilistic analysis reporting results that lacked face validity when waning of treatment effect was assumed.
CADTH was unable to address this deficiency and found that results from the submitted economic evaluation could not be fully validated. Due to large discrepancies between the probabilistic and deterministic results when incorporating treatment waning, CADTH’s exploratory base-case results were presented deterministically.
Additionally, the key assumptions presented in Table 4 were made by the sponsor and have been appraised by CADTH.
Table 4: Key Assumptions of the Submitted Economic Evaluation (Not Noted as Limitations to the Submission)
Sponsor’s key assumption | CADTH comment |
|---|---|
Patients were considered to have resectable stage III melanoma upon entry into the LR state. | Acceptable as a simplifying assumption. |
Costs and disutilities related to grade 3+ AEs with an incidence of at least 5% in the KEYNOTE-716 trial and diarrhea of grade 2 or higher and febrile neutropenia of any grade were also included in the model. | Inappropriate. The sponsor selected an arbitrary threshold to capture the impact of treatment-related AEs rather than selecting the most clinically meaningful AEs to include within the model. CADTH’s guidelines recommend that all AEs that have clinical or cost significance be included in the model. As noted in the CADTH Clinical Review, hyperthyroidism and hypothyroidism (all grades) were more common among patients who received pembrolizumab than routine surveillance (hyperthyroidism: 10.4% vs. 0.6%; hypothyroidism: 17.0% vs. 3.5%, respectively). The inclusion of only grade 3+ hyperthyroidism and hypothyroidism in the pharmacoeconomic model may underestimate the cost of treatment associated with these AEs because additional visits to a health care provider and drug treatments may be required. However, the clinical experts consulted by CADTH anticipated that hyperthyroidism and hypothyroidism could be treated with minimal impact on health outcomes. Additionally, the AEs included in the sponsor’s model do not capture the range of AEs deemed to be of special interest based on clinicians’ feedback (i.e., type 1 diabetes mellitus) received by CADTH for this review. Although type 1 diabetes mellitus occurred in approximately 0.4% of patients in the pembrolizumab group, the consequences to both health-related quality of life and costs of treatment are significant and life-long. |
The benefit of pembrolizumab among subgroups in the population is uncertain. | The indication assessed by CADTH, which is aligned with Health Canada indication, included pediatric and adult patients with stage IIB and IIC cutaneous melanoma after complete surgical resection. Of note, the prognosis of stage IIC melanoma (35.2% of the population in the KEYNOTE-716 trial) is significantly worse compared with stage IIB, with a 10-year survival of approximately 40% and 57%, respectively.6 The descriptive analysis of KEYNOTE-716 trial subgroups indicated that patients with stage IIC (which included staging T4b) might not benefit from treatment with pembrolizumab (HR = 0.82; 95%CI, 0.54 to 1.26 for T4b). However, this uncertainty about the effectiveness of pembrolizumab in stage IIC melanoma may resolve as later data cuts become available from the KEYNOTE-716 trial. |
The eligibility to receive treatment with anti-PD-L1 therapies in the DM state (stage IV melanoma), which included pembrolizumab, was modelled as dependent only on the treatment received in the RF state (stage II melanoma). | Inappropriate. The model included 2 subsequent lines of treatment: adjuvant treatment for LR (stage III melanoma), and palliative treatment for DM (stage IV melanoma). Subsequent treatment options for both LR and DM states include anti-PD-1 or anti-PD-L1 options. The eligibility to receive treatment with anti-PD-1 or anti-PD-L1 therapies, which include pembrolizumab, was modelled as dependent only on the treatment received in the RF state (stage II melanoma). However, in clinical practice, the eligibility to receive anti-PD-1 or anti-PD-L1 treatments in the DM state also depends on time of recurrence in the LR state (stage III melanoma). This nuance was not captured in the submitted model and does not reflect current clinical standard of care. In the submitted model, patients who did not receive adjuvant treatment in stage II (i.e., observation arm) were considered eligible to receive anti-PD-1 or anti-PD-L1 therapies in both the LR and DM states, regardless of transition time from LR to DM after being treated with an anti-PD-1 or anti-PD-L1 therapy. |
AE = adverse event; CI = confidence interval; DM = distant metastasis; HR = hazard ratio; LR = locoregional recurrence; PD-1 = programmed cell death receptor-1; PD-L1 = programmed cell death ligand 1; RF = recurrence-free.
CADTH Reanalyses of the Economic Evaluation
Base-Case Results
CADTH was unable to address limitations regarding the uncertainty in the sponsor’s OS estimates and the lack of face validity of the sponsor’s extrapolated OS curves, as well as concerns regarding a potential decrease in effectiveness of anti-PD-1 or anti-PD-L1 therapies used in subsequent treatments in patients who received adjuvant pembrolizumab in stage IIB or IIC melanoma. As such, the changes presented subsequently reflect a CADTH exploratory reanalysis rather than a base-case estimate of the cost-effectiveness for pembrolizumab compared with observation alone. The CADTH exploratory reanalysis was derived by changing model parameter values and assumptions, in consultation with clinical experts.
Table 5 details each change made to derive the CADTH-revised exploratory analysis, which was conducted in a stepwise approach to highlight the effect of each change. The summary of results from the stepped reanalysis are presented in Table 6 and Table 13.
CADTH’s exploratory analysis demonstrates that pembrolizumab was $107,515 more costly than observation alone and yielded 0.96 more QALYs, resulting in an ICER of $110,594 per QALY. The CADTH reanalysis is based on publicly available prices of the comparator and subsequent therapies. In the CADTH exploratory analysis, 98.0% of predicted QALYs were generated through extrapolation beyond the period of the available KEYNOTE-716 trial data (20.5 months).
Scenario Analysis Results
CADTH undertook price reduction analyses based on the CADTH exploratory analysis. These analyses demonstrated that a price reduction of 40.7% would be necessary to achieve cost-effectiveness at a WTP threshold of $50,000 per QALY.
Table 5: CADTH Revisions to the Submitted Economic Evaluation
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
None | — | — |
Changes to derive the CADTH analysis | ||
1. Treatment waning effect | Persistent over time | Treatment waning starts at year 2 and was completed at year 3 |
2. Change in market shares for subsequent treatments | Market shares based on data from ONCO-CAPPS provided by the sponsor | Market shares based on expected current treatments in Canadian practice, with the same market shares in both treatment arms |
3. Change in RDI | Assumed reduced dose intensity with all therapies | Assumed full dose intensity with all therapies |
CADTH exploratory base case | — | 1 + 2 + 3 |
RDI = relative dose intensity.
Table 6: Summary of the Stepped Analysis of the CADTH Reanalysis Results
Stepped analysis | Drug | Total costs ($) | Total QALYs | ICER ($/QALYs) |
|---|---|---|---|---|
Sponsor’s base case (probabilistic) | Observation | 265,096 | 9.56 | Reference |
Pembrolizumab | 336,130 | 11.83 | 31,224 | |
Sponsor’s base case (deterministic) | Observation | 256,631 | 9.62 | Reference |
Pembrolizumab | 327,336 | 11.76 | 33,036 | |
CADTH reanalysis 1 | Observation | 256,631 | 9.62 | Reference |
Pembrolizumab | 352,271 | 10.52 | 106,322 | |
CADTH reanalysis 2 | Observation | 256,631 | 9.62 | Reference |
Pembrolizumab | 337,457 | 11.82 | 36,860 | |
CADTH reanalysis 3 | Observation | 256,631 | 9.62 | Reference |
Pembrolizumab | 328,781 | 11.76 | 33,711 | |
CADTH exploratory base case (deterministic) | Observation | 256,631 | 9.62 | Reference |
Pembrolizumab | 362,957 | 10.59 | 110,594 |
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
Table 7: CADTH Price Reduction Analyses
Analysis | ICERs for pembrolizumab vs. observation alone | |
|---|---|---|
Price reduction | Sponsor base case | CADTH reanalysis |
No price reduction | 31,224 | 110,594 |
10% | Pembrolizumab dominates | 94,956 |
20% | Pembrolizumab dominates | 80,297 |
30% | Pembrolizumab dominates | 65,638 |
40% | Pembrolizumab dominates | 50,979 |
40.7% | Pembrolizumab dominates | 50,000 |
50% | Pembrolizumab dominates | 36,321 |
60% | Pembrolizumab dominates | 21,662 |
70% | Pembrolizumab dominates | 7,003 |
80% | Pembrolizumab dominates | Pembrolizumab dominates |
90% | Pembrolizumab dominates | Pembrolizumab dominates |
100% | Pembrolizumab dominates | Pembrolizumab dominates |
ICER = incremental cost-effectiveness ratio; vs. = versus.
In addition, CADTH conducted a series of scenario analyses to determine the impact of alternative assumptions on the cost-effectiveness of adjuvant pembrolizumab, which are outlined as follows:
time horizon of 2 years
time horizon of 10 years
treatment effect of pembrolizumab starts to wane at year 3 and completes at year 5
weight-based dosing for pembrolizumab (100% vial sharing).
Results are described in Table 15. CADTH considered 2 scenario analyses to address the substantial uncertainty associated with OS benefits by reducing the time horizon of the analysis to 2 and 10 years. In these scenarios, the ICER increased to $3,561,335 and $275,309 per QALY, respectively. CADTH also considered 1 scenario to address the uncertainty about the duration of marginal treatment effect beyond the trial observational period. In this scenario, the ICER changed to $69,571 per QALY. This finding illustrated the importance of the treatment waning assumption to the estimated cost-effectiveness of pembrolizumab in adjuvant melanoma treatment. CADTH also considered a scenario to address changes in pembrolizumab dose, from fixed dosing to weight-based dosing. In this scenario, vial sharing was assumed to be 100%, resulting in pembrolizumab dominating observation alone. The submitted model did not allow for adjustment of vial sharing when changing to weight-based dosing, so CADTH could not explore other scenario analyses with different assumptions (e.g., 50% and 0% vial sharing).
Issues for Consideration
The requirement for time spent away from work for pembrolizumab infusion (administered every 3 or 6 weeks) was not included in the sponsor’s base case given it does not fit within the health care payer perspective required for submissions to CADTH. In addition to productivity loss, travel costs for patients (and their families) are also relevant for patients who do not live nearby infusion centres. Disparities in funding and treatment access may vary depending on the province or territory, and the requirement for access to a centre where infusions can be performed may have equity of access implications, which were not substantively considered in the economic submission.
It was noted by the clinical experts that the prescription of pembrolizumab might require assessment by an oncologist. Patients living in areas where there are no oncologists to assess patients’ eligibility and prescribe pembrolizumab would incur substantive out-of-pocket costs to travel to specialist appointments.
Overall Conclusions
Based on an appraisal of the KEYNOTE-716 trial, the CADTH Clinical Review found that, compared with placebo, adjuvant pembrolizumab demonstrated RFS benefits in adult patients with stage IIB or IIC cutaneous melanoma. This benefit was based on 20.5 months of follow-up; therefore, the long-term benefit of adjuvant pembrolizumab treatment is currently unknown. At the time of this review, only the final analysis of RFS and the interim analysis of DMFS were available for assessment. The CADTH Clinical Review concluded that inferences regarding whether pembrolizumab increases OS could not be made due to data immaturity at the time of the planned interim analysis. Further, although RFS is a clinically meaningful outcome, the evidence for RFS as a surrogate for OS for immune checkpoint inhibitor regimens is associated with some uncertainty. Finally, the efficacy and safety for pediatric patients were considered uncertain because only 2 patients aged between 12 and 18 years were included in the pivotal trial.
Given the limited OS data from the trial, the cost-effectiveness analysis of adjuvant pembrolizumab relied solely on the assumption that RFS can be translated into OS benefits. Although there was evidence based on interferon-based therapies to support RFS as a surrogate outcome, another study concluded that more evidence is needed to confirm the strength of association between RFS and OS for therapies such as pembrolizumab. Thus, the relationship between RFS and OS is associated with notable uncertainty given the limited data available for the therapies that are the current standard of care and the relatively short duration of follow-up at this time. The RFS benefits modelled by the sponsor were extrapolated to a 50-year time horizon based on data from the KEYNOTE-716 trial, which had a median follow-up time of 20.5 months. Furthermore, the sponsor assumed that pembrolizumab’s RFS and OS benefits would be sustained up to 10 years after pembrolizumab is discontinued. The lack of long-term evidence is particularly of note, given that 99.6% of the estimated incremental LYs and 99.0% of the estimated incremental QALYs were generated in the post-trial period for which there is no direct comparative evidence. According to the clinical experts consulted by CADTH for this review, the impact of adjuvant pembrolizumab treatment on long-term RFS or OS, especially after the 1-year treatment period is completed, is unknown for stage IIB and IIC melanoma. This was compounded by the fact that the modelled OS curves submitted by the sponsor lacked face validity compared with the literature, and it was noted that different assumptions on the long-term efficacy have a significant influence on incremental effectiveness and overall cost-effectiveness of pembrolizumab. In addition, the clinical effectiveness of pembrolizumab after multiple lines of prior pembrolizumab treatment is uncertain despite the sponsor's assumption of identical effectiveness. Evidence suggests that the effectiveness of pembrolizumab could be potentially reduced when patients are rechallenged with the same drug compared with patients who receive pembrolizumab for the first time. Due to all these limitations, CADTH could not derive a base case and instead explored areas of uncertainty, when possible, and conducted an exploratory reanalysis.
CADTH identified several limitations in the economic analysis submitted by the sponsor beyond the uncertainty regarding the effect of pembrolizumab on long-term RFS and OS. These key limitations included uncertainty regarding persistence of treatment effect, market shares of subsequent treatment in LR and DM states do not reflect Canadian clinical practice, and the incorporating of RDI. CADTH conducted an exploratory reanalysis, revising the sponsor’s model by incorporating treatment effect waning, changing market shares of subsequent treatments, and setting RDI to 100%. Based on the CADTH exploratory reanalysis, adjuvant treatment with pembrolizumab is $107,515 more costly and yields 0.96 more QALYs, resulting in an ICER of $110,594 per QALY. Given the uncertainty previously mentioned, a price reduction of at least 40.7% would be necessary to achieve an ICER of $50,000 per QALY.
As noted, CADTH was unable to adjust for major limitations, including the substantial uncertainty associated with OS benefit as well as concerns regarding a potential reduction in effectiveness of pembrolizumab in patients who were rechallenged with pembrolizumab at relapse. A scenario analysis reducing the model’s time horizon to 10 years, thus limiting the uncertainty associated with OS benefit, was found to increase the price reduction necessary to achieve an ICER of $50,000 per QALY up to 58.1%. Therefore, longer-term evidence is required to validate OS for patients receiving pembrolizumab as adjuvant therapy for stage IIB or IIC melanoma to reduce the uncertainties identified with this model.
References
1.Pharmacoeconomic evaluation [internal sponsor's report]. In: Drug Reimbursement Review sponsor submission: Keytruda (pembrolizumab), 100 mg/4 mL vial. Kirkland (QC): Merck Canada Inc.; 2022 Apr 26. In.
2.Beusterien KM, Szabo SM, Kotapati S, et al. Societal preference values for advanced melanoma health states in the United Kingdom and Australia. Br J Cancer. 2009;101(3):387-389. PubMed
3.DeltaPA. In: [Ottawa (ON)]: IQVIA; 2022: https://www.iqvia.com/. Accessed 1800 Jan 1.
4.Gwadry-Sridhar F, Nikan S, Hamou A, et al. Resource utilization and costs of managing patients with advanced melanoma: a Canadian population-based study. Curr Oncol. 2017;24(3):168-175. PubMed
5.Rocchi A, Verma S. Anastrozole is cost-effective vs tamoxifen as initial adjuvant therapy in early breast cancer: Canadian perspectives on the ATAC completed-treatment analysis. Support Care Cancer. 2006;14(9):917-927. PubMed
6.Balch CM, Gershenwald JE, Soong SJ, et al. Final version of 2009 AJCC melanoma staging and classification. J Clin Oncol. 2009;27(36):6199-6206. PubMed
7.Gershenwald JE, Scolyer RA, Hess KR, et al. Melanoma staging: Evidence-based changes in the American Joint Committee on Cancer eighth edition cancer staging manual. CA Cancer J Clin. 2017;67(6):472-492.
8.Eggermont AM, Meshcheryakov A, Atkinson V, et al. Crossover and rechallenge with pembrolizumab in recurrent patients from the EORTC 1325-MG/Keynote-054 phase III trial, pembrolizumab versus placebo after complete resection of high-risk stage III melanoma. Eur J Cancer. 2021;158:156-168. PubMed
Appendix 1: Cost Comparison Table
Note this appendix has not been copy-edited.
The comparators presented in the following table have been deemed to be appropriate based on feedback from clinical expert(s). Comparators may be recommended (appropriate) practice or actual practice. Existing Product Listing Agreements are not reflected in the table and as such, the table may not represent the actual costs to public drug plans.
Table 8: CADTH Cost Comparison Table for Stage IIB and IIC Cutaneous Melanoma
Treatment | Strength/concentration | Form | Price | Recommended dosage | Daily cost | Cost per 28-day cyclea ($) |
|---|---|---|---|---|---|---|
Pembrolizumab (Keytruda) | 100 mg/4mL | 100 mg | 4,400.0000b | 200 mg, every 3 weeks | 419.05 | 11,733 |
400 mg, every 6 weeks |
aCost standardized to 28-day cycles to allow for comparison among regimens of different cycle lengths.
bSponsor’s submitted price.
Appendix 2: Submission Quality
Note this appendix has not been copy-edited.
Description | Yes/No | Comments |
|---|---|---|
Population is relevant, with no critical intervention missing, and no relevant outcome missing | Yes | No comment. |
Model has been adequately programmed and has sufficient face validity | No | See limitations. The model did not allow to change AEs to all-cause, and to adjust vial sharing settings when changing to weight-base dosing. In addition, the survival curves do not meet face validity. |
Model structure is adequate for decision problem | Yes | No comment. |
Data incorporation into the model has been done adequately (e.g., parameters for probabilistic analysis) | Yes | No comment. |
Parameter and structural uncertainty were adequately assessed; analyses were adequate to inform the decision problem | Yes | No comment. |
The submission was well organized and complete; the information was easy to locate (clear and transparent reporting; technical documentation available in enough details) | No | The eligibility criteria for anti-PD-1/PD-L1 therapies were not well described. In addition, unpublished technical documents on market shares lacked crucial information on patient characteristics and database information. |
Appendix 3: Additional Information on the Submitted Economic Evaluation
Note this appendix has not been copy-edited.
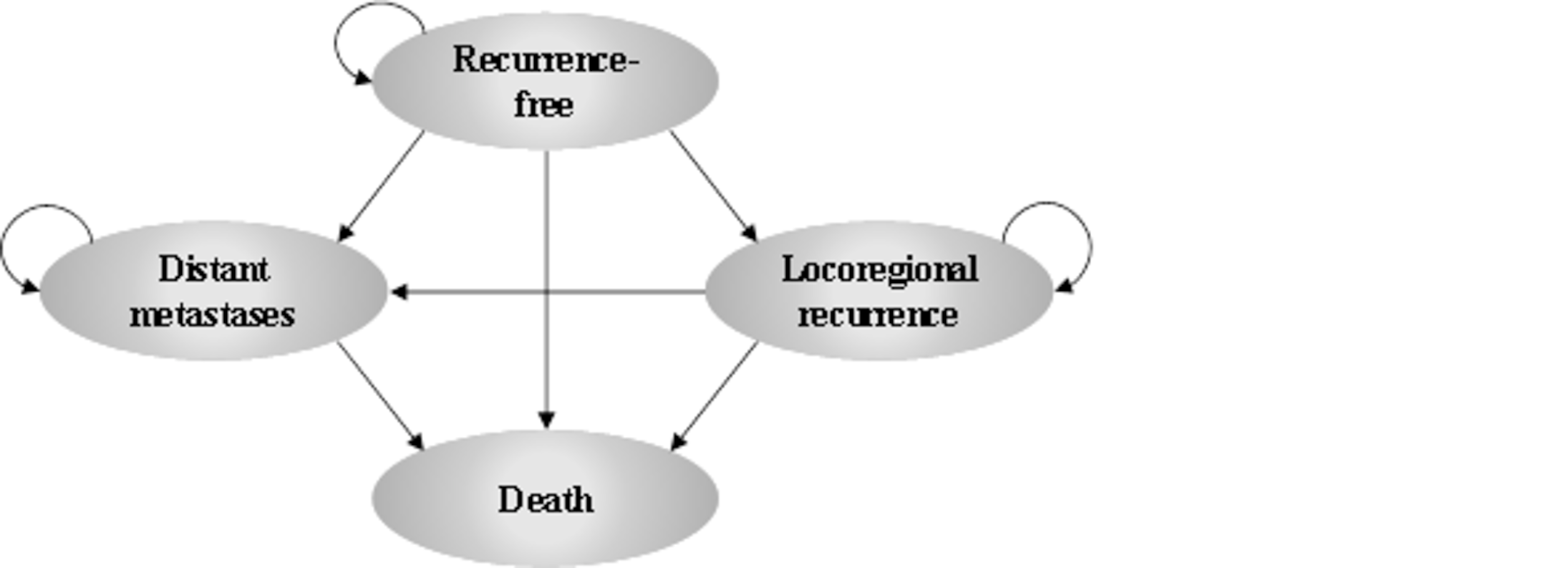
Figure 2: Relative Risk of a Recurrence Event for Pembrolizumab Compared With Observation
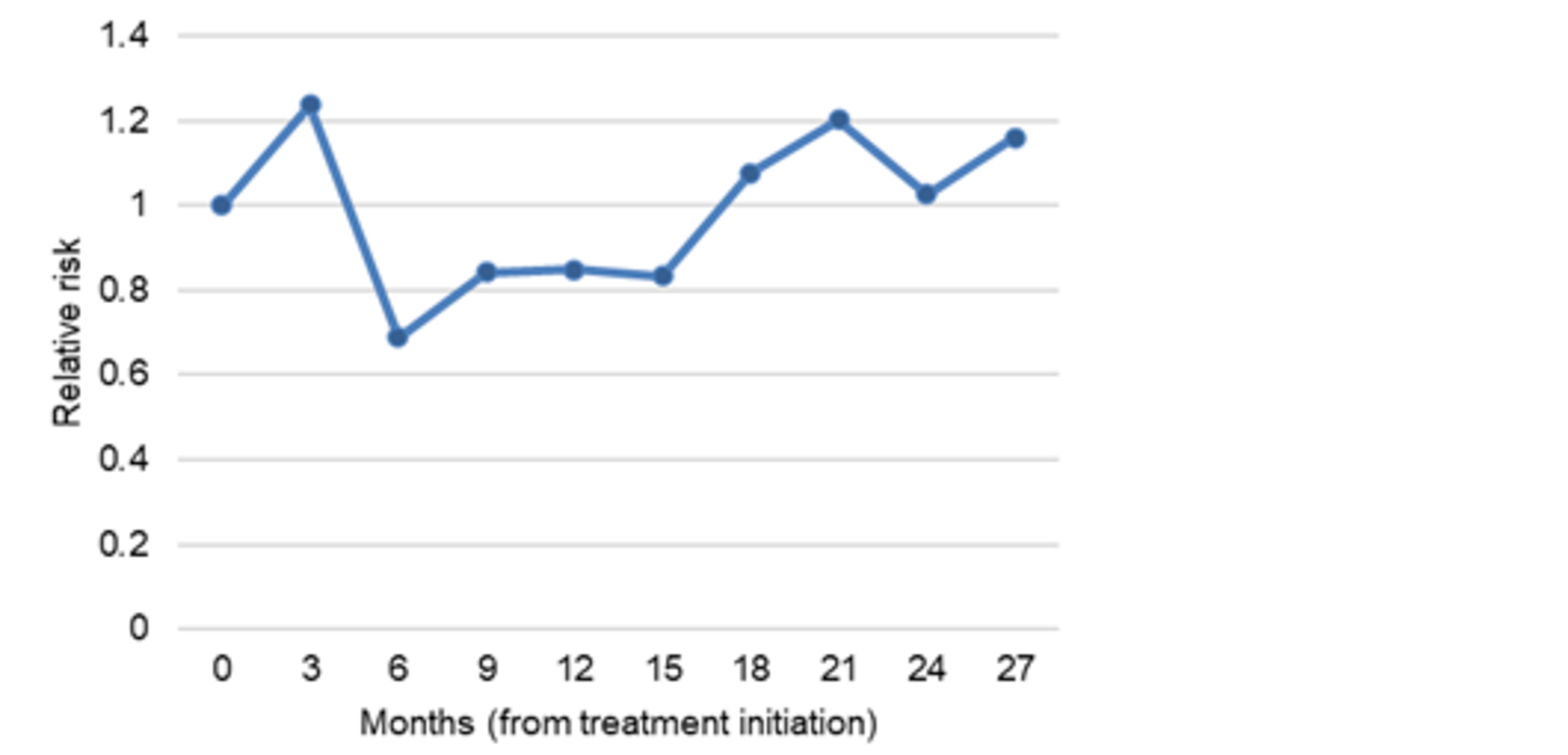
Note: An event was defined as experiencing 1 of the following: locoregional recurrence or distant metastatic recurrence.
Source: CADTH calculation based on the KEYNOTE-716 trial.
Detailed Results of the Sponsor’s Base Case
Table 10: Market Shares of Treatment Options in the LR State
Adjuvant treatments in the LR state | Pembrolizumab | Observation | |
|---|---|---|---|
Anti-PD-1/PD-L1 eligible | Anti-PD-1/PD-L1 ineligible | Anti-PD-1/PD-L1 eligible | |
Pembrolizumab | |||| | || | ||||| |
Nivolumab | ||||| | || | ||||| |
Dabrafenib + Trametinib | ||||| | ||||| | ||||| |
Clinical trials | || | || | || |
Observation | ||||| | ||||| | ||||| |
Source: Adapted from sponsor’s pharmacoeconomic submission.1
Table 11: Market Shares of Treatment Options in the DM State
Adjuvant treatments in the DM state | Pembrolizumab | Observation | |
|---|---|---|---|
Anti-PD-1/PD-L1 eligible | Anti-PD-1/PD-L1 ineligible | Anti-PD-1/PD-L1 eligible | |
Pembrolizumab | ||| | || | ||| |
Ipilimumab | || | || | || |
Nivolumab | ||||| | || | ||||| |
Nivolumab + ipilimumab | ||||| | || | ||||| |
Dabrafenib + Trametinib | ||||| | ||||| | ||||| |
Encorafenib + binimetinib | || | || | || |
Clinical trials | |||| | |||| | |||| |
Observation | |||| | ||||| | |||| |
Source: Adapted from sponsor’s pharmacoeconomic submission.1
Table 12: Disaggregated Summary of Sponsor’s Economic Evaluation Results (Probabilistic)
Parameter | Pembrolizumab | Observation | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 13.52 | 11.15 | 2.37 |
By health state | |||
Recurrence-free | 10.91 | 7.94 | 2.96 |
Locoregional recurrence | 0.85 | 1.05 | –0.16 |
Distant metastasis | 1.76 | 2.19 | –0.43 |
By period | |||
Within trial period (20.5 months) | 1.67 | 1.66 | 0.01 |
After trial period | 11.85 | 9.49 | 2.36 |
Discounted QALYs | |||
Total | 11.83 | 9.56 | 2.27 |
By health state | |||
Recurrence-free | 9.92 | 7.23 | 2.70 |
Locoregional recurrence | 0.75 | 0.89 | –0.14 |
Distant metastasis | 1.16 | 1.44 | –0.28 |
By period | |||
Within trial period (20.5 months) | 1.51 | 1.48 | 0.02 |
After trial period | 10.32 | 8.07 | 2.25 |
Discounted costs ($) | |||
Total | 336,130 | 265,096 | 71,034 |
Adjuvant treatment costs (RF state) | 120,320 | 0 | 120,320 |
Drug acquisition cost | 118,968 | 0 | 118,968 |
Drug administration cost | 1,352 | 0 | 1,352 |
Subsequent treatment costs (LR state) | 15,525 | 25,740 | –10,215 |
Salvage surgery costs | 701 | 786 | –85 |
Drug acquisition cost | 14,749 | 24,728 | –9,979 |
Drug administration cost | 75 | 226 | –151 |
Subsequent treatment costs (DM state) | 128,013 | 166,324 | –38,312 |
Drug acquisition cost | 127,026 | 164,911 | –37,885 |
Drug administration cost | 986 | 1,413 | –427 |
AEs costs | 86 | 4 | 82 |
BRAF testing costs | 328 | 407 | –79 |
Disease management costs | 58,873 | 56,289 | 2,584 |
RF | 37,339 | 29,680 | 7,658 |
LR | 5,269 | 6,327 | –1,058 |
DM | 16,265 | 20,281 | –4,016 |
Terminal care costs | 12,986 | 16,332 | –3,346 |
ICER ($/QALY) | 31,224 | ||
ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year; RF = recurrence-free; LR = locoregional recurrence; DM = distant metastasis; Note: BRAF testing refers to testing for the presence of a BRAF mutation in a tumour.
Appendix 4: Additional Details on the CADTH Reanalyses and Sensitivity Analyses of the Economic Evaluation
Note this appendix has not been copy-edited.
Detailed Results of CADTH Exploratory Analysis
Table 13: Disaggregated Summary of CADTH’s Economic Evaluation Results (Deterministic)
Parameter | Pembrolizumab | Observation | Incremental |
|---|---|---|---|
Discounted LYs | |||
Total | 12.18 | 11.19 | 0.99 |
By health state | |||
Recurrence-free | 9.39 | 8.12 | 1.27 |
Locoregional recurrence | 0.95 | 1.02 | –0.06 |
Distant metastasis | 1.83 | 2.05 | –0.22 |
By period | |||
Within trial period (20.5 months) | 1.67 | 1.66 | 0.01 |
After trial period | 10.51 | 9.53 | 0.98 |
Discounted QALYs | |||
Total | 10.59 | 9.62 | 0.96 |
By health state | |||
Recurrence-free | 8.55 | 7.39 | 1.16 |
Locoregional recurrence | 0.83 | 0.89 | –0.06 |
Distant metastasis | 1.20 | 1.34 | –0.14 |
By period | |||
Within trial period (20.5 months) | 1.50 | 1.48 | 0.02 |
After trial period | 9.08 | 8.14 | 0.94 |
Discounted costs ($) | |||
Total | 362,957 | 256,631 | 106,327 |
Adjuvant treatment costs (RF state) | 121,767 | 0 | 121,767 |
Drug acquisition cost | 120,413 | 0 | 120,413 |
Drug administration cost | 1,354 | 0 | 1,354 |
Subsequent treatment costs (LR state) | 23,650 | 25,514 | –1,863 |
Salvage surgery costs | 757 | 777 | –20 |
Drug acquisition cost | 22,738 | 24,513 | –1,775 |
Drug administration cost | 156 | 224 | –68 |
Subsequent treatment costs (DM state) | 147,739 | 160,153 | –14,000 |
Drug acquisition cost | 146,585 | 158,785 | –13,784 |
Drug administration cost | 1,154 | 1,368 | –216 |
AEs costs | 86 | 4 | 81 |
BRAF testing costs | 364 | 396 | –31 |
Disease management costs | 56,269 | 54,601 | 1,669 |
RF state | 33,105 | 29,113 | 3,992 |
LR state | 5,894 | 6,286 | –391 |
DM state | 17,270 | 19,202 | –1,931 |
Terminal care costs | 14,667 | 15,963 | –1,296 |
ICER ($/QALY) | 110,574 | ||
ICER = incremental cost-effectiveness ratio; LY = life-year; QALY = quality-adjusted life-year; RF = recurrence-free; LR = locoregional recurrence; DM = distant metastasis.
Table 14: Market Shares of Treatment Options in the LR State
Adjuvant treatments in the LR state | Pembrolizumab | Observation | |
|---|---|---|---|
Anti-PD-1/PD-L1 eligible | Anti-PD-1/PD-L1 ineligible | Anti-PD-1/PD-L1 eligible | |
Pembrolizumab | ||||| | 0% | ||||| |
Nivolumab | ||||| | 0% | ||||| |
Dabrafenib + trametinib | ||||| | 43.7% | ||||| |
Clinical trials | || | 0% | || |
Observation | ||||| | 56.3% | ||||| |
Table 15: Market Shares of Treatment Options in the DM State
Adjuvant treatments in the DM state | Pembrolizumab | Observation | |
|---|---|---|---|
Anti-PD-1/PD-L1 eligible | Anti-PD-1/PD-L1 ineligible | Anti-PD-1/PD-L1 eligible | |
Pembrolizumab | ||| | 0% | ||| |
Ipilimumab | || | 51.3% | || |
Nivolumab | ||||| | 0% | ||||| |
Nivolumab + ipilimumab | ||||| | 0% | ||||| |
Dabrafenib + trametinib | ||||| | 43.3% | ||||| |
Encorafenib + binimetinib | || | 0% | || |
Clinical trials | |||| | 0.3% | |||| |
Observation | |||| | 5.1% | |||| |
Scenario Analyses
Stepped analysis | Comparator | Total costs ($) | Total QALYs | ICER ($/QALY) |
|---|---|---|---|---|
CADTH’s exploratory analysis | Observation | 256,631 | 9.62 | Reference |
Pembrolizumab | 362,957 | 10.59 | 110,594 | |
CADTH scenario 1: Time horizon: 2 years | Observation | 72,799 | 1.71 | Reference |
Pembrolizumab | 171,650 | 1.74 | 3,577,067 | |
CADTH scenario 2: Time horizon: 10 years | Observation | 231,198 | 5.97 | Reference |
Pembrolizumab | 339,831 | 6.35 | 283,909 | |
CADTH scenario 3: Treatment effect of pembrolizumab starts to wane at year 3 | Observation | 256,631 | 9.62 | Reference |
Pembrolizumab | 356,358 | 11.06 | 69,571 | |
CADTH scenario 4: Weight-based dosing for pembrolizumab (100% vial sharing) | Observation | 247,579 | 9.62 | Reference |
Pembrolizumab | 239,385 | 10.59 | Dominant |
Appendix 5: Submitted BIA and CADTH Appraisal
Table 17: Summary of Key Take-Aways
Key take-aways of the BIA |
|---|
|
Summary of Sponsor’s BIA
The sponsor submitted a budget impact analysis (BIA) estimating the budget impact of introducing pembrolizumab as adjuvant treatment for adult and pediatric (12 years and older) patients with stage IIB or IIC melanoma following complete resection. The pediatric population accounted for 0.2% of melanoma patients in this BIA, based on KEYNOTE-716 trial data. The BIA base case was undertaken from a publicly funded drug plan perspective, considering drug costs over a 3-year time horizon.
Costs included that of adjuvant therapy and first-line treatments used among patients who progress. Pembrolizumab costs were calculated by incorporating an RDI of ||||| and were based on the duration of pembrolizumab therapy and an increase in RFS, based on data from the KEYNOTE-716 trial.
Costs of first-line subsequent therapies for locoregional and distant recurrence were included in the analysis. The market shares for subsequent treatments were dependent on whether patients received adjuvant pembrolizumab or observation (i.e., no adjuvant therapy), and, whether they recurred within 18 months after starting adjuvant therapy at stage II melanoma.
The subsequent therapies options for patients who received pembrolizumab and developed locoregional or distant recurrences were defined based on the time these recurrences occurred. If patients developed locoregional or distant recurrences before 18 months from treatment initiation with pembrolizumab, patients would be considered ineligible to receive anti-PD-1/PD-L1 therapies (e.g., pembrolizumab, or nivolumab). If patients developed locoregional or distant recurrences after 18 months from treatment initiation with pembrolizumab, patients would be considered eligible to receive the treatment with anti-PD-1/PD-L1 therapies.
The sponsor estimates that pembrolizumab will reach a market share of 80% after 3 years. The sponsor also assumed that 10% of patients would be participating in clinical trials.
The analytic framework, which used an epidemiology-based approach, leveraged data from multiple sources in the literature and assumptions based on clinical expert input to determine the estimated population size (Figure 3). The sponsor compared a reference scenario where pembrolizumab is not reimbursed as adjuvant therapy, with a new drug scenario, where pembrolizumab is funded as adjuvant therapy as per the Health Canada indication. Treatments available in the reference included observation alone, which was assumed to consist of no active treatment, and treatments for recurrence. Key inputs to the BIA are documented in Table 18.
Figure 3: Sponsor’s Estimation of the Size of the Eligible Population
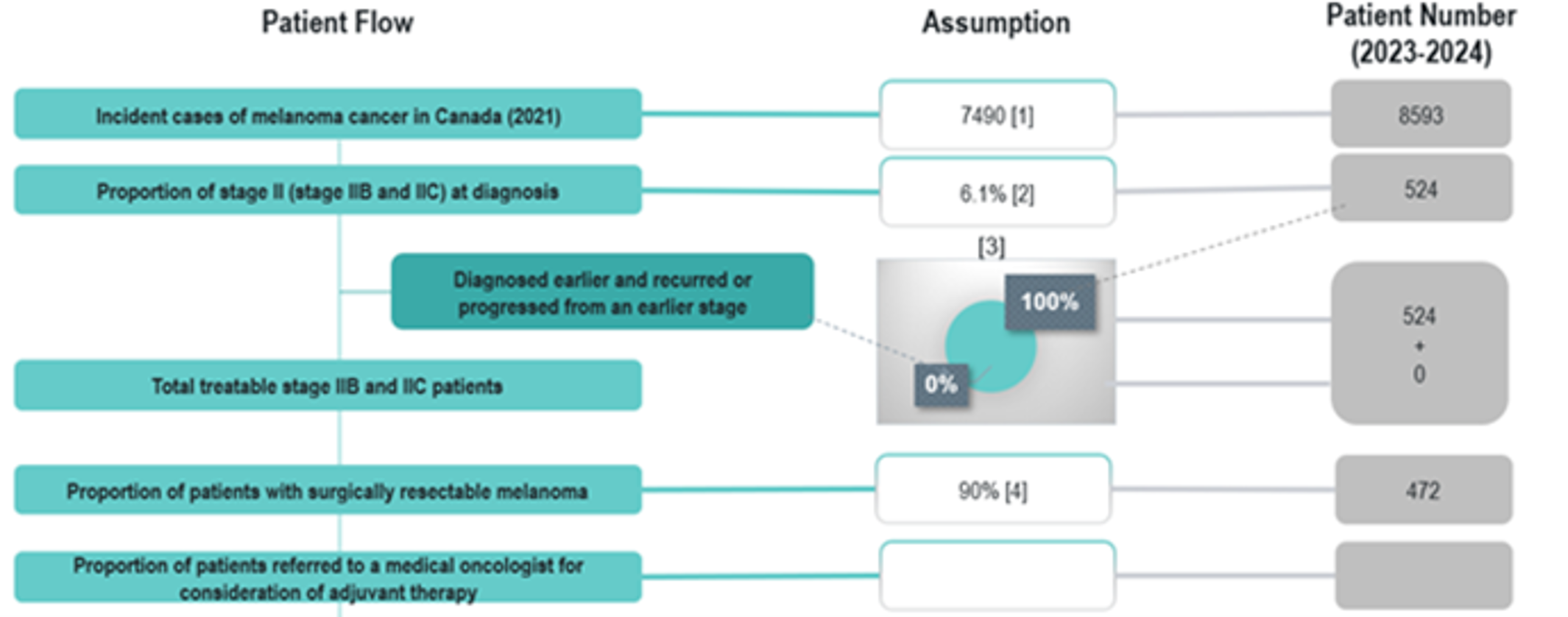
Source: Sponsor’s Budget Impact Submission.
Table 18: Summary of Key Model Parameters
Parameter | Sponsor’s estimate (reported as year 1 / year 2 / year 3 if appropriate) |
|---|---|
Target population | |
Number of patients eligible for drug under review | ||| / ||| / ||| |
Market uptake (3 years) | |
Uptake (reference scenario) | |
Observation | 90% / 90% / 90% |
Clinical trials | 10% / 10% / 10% |
Uptake (new drug scenario) | |
Pembrolizumab | 41.1% / 80% / 80% |
Observation | 48.9% / 10% / 10% |
Clinical trials | 10% / 10% / 10% |
Cost of treatment (per patient) | |
Cost of treatment over 21-days cycle | |
Pembrolizumab | $|||||||| |
Observation | $0 |
Clinical trials | $0 |
Summary of the Sponsor’s BIA Results
The sponsor’s estimated budget impact of funding pembrolizumab for adjuvant treatment of adult and pediatric (12 years and older) patients with stage IIB or IIC melanoma following complete resection from the drug plan perspective was $6,632,024, $26,902,979, $28,840,667 for years 1, 2, and 3, respectively. The 3-year total was $62,375,670.
CADTH Appraisal of the Sponsor’s BIA
CADTH identified several key limitations to the sponsor’s analysis that have notable implications on the results of the BIA:
The sponsor’s assumption regarding patient enrolment in clinical trials as a comparator is uncertain: The sponsor assumed that 10% of patients were enrolled in clinical trials and as they received trial medications, they did not incur treatment/ drug costs. For being in a time limited trial, this decreased the estimated market size and omitted potential treatment costs incurred by patients, thus underestimating the budget impact. Likewise, if pembrolizumab was approved, this may decrease clinical trial use as patients may forego a trial to be placed on a new effective therapy. Further, clinical experts consulted for this review noted that patient enrolment in clinical trials can vary significantly by province.
In the CADTH reanalysis, clinical trials were removed from the market mix; the market share of clinical trials was re-distributed over other comparators.
The sponsor’s assumption regarding the referral rate to a medical oncologist may be underestimated: The sponsor assumed that ||% of patients would be referred to a medical oncologist. According to clinical experts consulted by CADTH for this review, if pembrolizumab is funded, it would be expected that most patients would be referred to a medical oncologist to discuss the option of adjuvant treatment with pembrolizumab.
In the CADTH reanalysis, the referral rate was changed to 90% based on clinical expert opinion.
Market shares of subsequent treatments for patients with locoregional or distant recurrence do not reflect Canadian clinical practice: Differences in market shares for LR subsequent treatments between treatment arms do not reflect Canadian clinical practice. In addition, the market shares within the DM state did not align with Canadian practice as described by clinical experts consulted by CADTH, as a high proportion of patients in the anti-PD-1/PD-L1 ineligible group were assigned no subsequent therapies, instead of treatment with ipilimumab. The market shares provided by the sponsor would underestimate the costs of those ineligible to receive anti-PD-1/PD-L1 therapies, which would underestimate the costs of those initially treated with adjuvant pembrolizumab.
The market shares in the BIA were revised based on input from clinical experts and the drug plans and were consist with the market shares used in CADTH’s base case for the cost-utility analysis.
Use of RDI is inappropriate: The sponsor’s base case incorporates reduced dose intensities for pembrolizumab. Consistent with previous reviews, given the inability to link reduced dose intensity with outcomes, the CADTH base case does not incorporate reduced dose intensity. CADTH notes RDI estimates derived from the trial apply to a fixed based dose and therefore would not be applicable to a weight-based dose.
CADTH used the functionality within the sponsor’s model to exclude reduced dose intensity.
Weight-based dosing for pembrolizumab: Pembrolizumab dosing in KEYNOTE-716 used a fixed dose of 200 mg intravenously every 21 days for adult patients. After consultation, CADTH notes that jurisdictions would likely implement a weight-based dose of 2 mg/kg (up to a cap of 200 mg) every 3 weeks with the possibility of extended dosing intervals every 6 weeks (4 mg/kg up to a 400 mg cap).
In a scenario analysis, CADTH assumed pembrolizumab would be provided using a weight-based dosing based on an average weight of |||| kg for adults and |||| kg for pediatric patients, as per KEYNOTE-716 data.
The budget impact of patients diagnosed in years 1 to 3 are not fully captured: In an attempt to provide a realistic estimate over 3 years, the sponsor assumed those diagnosed with stage IIB/IIC melanoma would gradually enter the BIA over each year. Although CADTH’s base case noted that ||| patients are diagnosed in the final year of the analysis, for some, full adjuvant costs only reflect their first week of treatment (as costs are incurred over a year and some join at the end of the year). Although this approach hopes to represent an accurate estimate of incurred costs over a 3-year period, the analysis omits a substantial proportion of patient costs which are pushed to subsequent years not included in the BIA, thus underestimating the budget impact. Additionally, this approach makes the BIA more complex and difficult to validate.
Given complexities in the sponsor’s modelling approach, CADTH conducted a scenario analysis which estimated the full adjuvant costs for all incident patients diagnosed in years 1 to 3. To calculate this budget impact, CADTH assumed in the new drug scenario: |||, |||, and ||| patients would be diagnosed in years 1 to 3, respectively. In year 1, 41% (||| patients) would receive pembrolizumab, in year 2, 80% (||| patients) would receive pembrolizumab, and in year 3, 80% (||| patients) would receive pembrolizumab. All other patients would remain in observation and not be initially treated with adjuvant pembrolizumab. In the reference scenario, CADTH assumed 100% of patients in all years were under observation.
The total cost of adjuvant therapy, using a fixed dose, was taken from the sponsor’s cost-utility analysis. The total cost was estimated to be $120,413 for those receiving pembrolizumab, and $0 for those receiving observation. For simplicity, CADTH considered that subsequent therapy costs would remain the same as in the CADTH base-case analysis.
CADTH Reanalyses of the BIA
CADTH’s base case revised the proportion of patients on clinical trials, market uptake, RDI, and assumed a weight-base dosing for pembrolizumab.
Table 19: CADTH Revisions to the Submitted Budget Impact Analysis
Stepped analysis | Sponsor’s value or assumption | CADTH value or assumption |
|---|---|---|
Corrections to sponsor’s base case | ||
None | — | — |
Changes to derive the CADTH base case | ||
1. Proportion of patients on clinical trials | 10% | 0% |
2. Referral rate | ||% | 90% |
3. Market shares for subsequent treatment | Market shares based on data from ONCO-CAPPS provided by the sponsor | Market shares based on expected current treatments in Canadian practice, with the same market shares in both treatment arms |
4. Use of RDI | Yes | No |
CADTH base case | 1 + 2 + 3 + 4 | |
RDI = relative dose intensity.
The results of the CADTH stepwise reanalysis are presented in summary format in Table 20 and a more detailed breakdown is presented in Table 21.
Based on CADTH’s base case and using a drug plan perspective, the expected budget impact for funding pembrolizumab as an adjuvant treatment for adult and pediatric (12 years and older) patients with stage IIB or IIC melanoma following complete resection is expected to be in $8,708,492 in year 1, $36,209,278 in year 2, and $41,052,409 in year 3, with a 3-year budget impact of $85,970,178.
Table 20: Summary of the CADTH Reanalyses of the BIA
Stepped analysis | Three-year total |
|---|---|
Submitted base case | $62,375,670 |
CADTH reanalysis 1 | $62,375,670 |
CADTH reanalysis 2 | $80,197,291 |
CADTH reanalysis 3 | $66,010,603 |
CADTH reanalysis 4 | $63,230,761 |
CADTH base case | $85,970,178 |
BIA = budget impact analysis.
Table 21: Detailed Breakdown of the CADTH Reanalyses of the BIA
Stepped analysis | Scenario | Year 0 (current situation) | Year 1 | Year 2 | Year 3 | Three-year total |
|---|---|---|---|---|---|---|
Submitted base case | Observation | $1,085,376 | $7,108,486 | $16,715,852 | $28,467,116 | $52,291,454 |
Pembrolizumab | $1,085,376 | $13,740,510 | $43,618,831 | $57,307,783 | $114,667,124 | |
Budget impact | $0 | $6,632,024 | $26,902,979 | $28,840,667 | $62,375,670 | |
CADTH reanalysis 1 | Observation | $1,085,376 | $7,108,486 | $16,715,852 | $28,467,116 | $52,291,454 |
Pembrolizumab | $1,085,376 | $13,740,510 | $43,618,831 | $57,307,783 | $114,667,124 | |
Budget impact | $0 | $6,632,024 | $26,902,979 | $28,840,667 | $62,375,670 | |
CADTH reanalysis 2 | Observation | $1,395,483 | $9,139,482 | $21,491,810 | $36,600,578 | $67,231,869 |
Pembrolizumab | $1,395,483 | $17,666,370 | $56,081,354 | $73,681,436 | $147,429,160 | |
Budget impact | $0 | $8,526,889 | $34,589,544 | $37,080,858 | $80,197,291 | |
CADTH reanalysis 3 | Observation | $1,031,408 | $6,386,544 | $14,401,537 | $23,862,331 | $44,650,412 |
Pembrolizumab | $1,031,408 | $13,077,546 | $42,213,475 | $55,369,995 | $97,583,470 | |
Budget impact | $0 | $6,691,002 | $27,811,938 | $31,507,664 | $66,010,603 | |
CADTH reanalysis 4 | Observation | $1,085,376 | $7,108,486 | $16,715,852 | $28,467,116 | $52,291,454 |
Pembrolizumab | $1,085,376 | $13,822,780 | $43,969,665 | $57,729,770 | $115,522,215 | |
Budget impact | $0 | $6,714,294 | $27,253,813 | $29,262,654 | $63,230,761 | |
CADTH base case | Observation | $1,326,096 | $8,211,271 | $18,516,262 | $30,680,140 | $57,407,673 |
Pembrolizumab | $1,326,096 | $16,919,763 | $54,725,539 | $71,732,549 | $143,377,851 | |
Budget impact | $0 | $8,708,492 | $36,209,278 | $41,052,409 | $85,970,178 |
BIA = budget impact analysis.
CADTH also conducted additional scenario analyses to address remaining uncertainty, using the CADTH base case. Results are provided in Table 22:
Price reduction of 40.7% in adjuvant pembrolizumab cost.
Weight-based pembrolizumab.
Incident cases of stage IIB/IIC melanoma occurred at the beginning of each year.
Results of CADTH’s scenario analyses demonstrate that both the sponsor’s analysis and CADTH’s base case do not account for a substantial budget impact that will occur in year 4. Of note, it was unclear whether this increase was due entirely to the timing of when individuals were diagnosed, due to the complexity of the sponsor’s model.
Analysis | Scenario | Year 0 (current situation) | Year 1 | Year 2 | Year 3 | Three-year total |
|---|---|---|---|---|---|---|
CADTH’s base case | Observation | $1,326,096 | $8,211,271 | $18,516,262 | $30,680,140 | $57,407,673 |
Pembrolizumab | $1,326,096 | $16,919,763 | $54,725,539 | $71,732,549 | $143,377,851 | |
Budget impact | $0 | $8,708,492 | $36,209,278 | $41,052,409 | $85,970,178 | |
CADTH scenario 1: price reduction of 40.7% | Observation | $1,326,096 | $8,211,271 | $18,516,262 | $30,680,140 | $57,407,673 |
Pembrolizumab | $1,326,096 | $13,332,582 | $39,431,505 | $53,341,287 | $106,105,375 | |
Budget impact | $0 | $5,121,312 | $20,915,244 | $22,661,147 | $48,697,702 | |
CADTH scenario 2: weight-based pembrolizumab dose | Observation | $1,270,887 | $7,835,220 | $17,628,265 | $29,197,059 | $54,660,544 |
Pembrolizumab | $1,270,887 | $15,234,765 | $48,375,325 | $63,971,892 | $127,581,981 | |
Budget impact | $0 | $7,399,544 | $30,747,060 | $34,774,833 | $72,921,437 | |
CADTH scenario 3: incident cases occur at start of each year | Observation | $1,326,096 | $8,211,271 | $18,516,262 | $30,680,140 | $57,407,673 |
Pembrolizumab | $1,326,096 | $29,177,404 | $60,364,482 | $72,156,170 | $161,698,056 | |
Budget impact | $0 | $20,966,133 | $41,848,221 | $41,476,030 | $104,290,383 |
BIA = budget impact analysis.
Stakeholder Input
Patient Input
Melanoma Canada
About Melanoma Canada
Melanoma Canada (formerly Melanoma Network of Canada) was founded in 2009 to provide information resources, support and prevention initiatives for melanoma and skin cancers. We advocate on behalf of patients to ensure timely and effective diagnosis and treatments are available to all patients across Canada. www.melanomanetwork.ca
Information Gathering
Data was gathered for this submission by way of an on-line survey, social media links, and an eblast to our registered network of patients. The survey was made available April 16th to May 19th, 2022.
Demographics: We received a total of 172 individual patient responses and a further 15 caregiver responses. Of the total responses for patients, 115 were female and 57 were male. The survey was open to all patients, regardless of stage. Most respondents were early stage or did not know their staging. We had 1 respondent from outside Canada, 109 of respondents from Ontario, 5 Nova Scotia, 18 BC, 17 Alberta, 9 Quebec, 1 Yukon, 4 Sask, 6 Manitoba and 2 from Newfoundland. It was a very wide representation across the country. 20 patients indicated they had been on treatment with adjuvant pembrolizumab for stage IIB or IIC following complete resection. 42 of the patients had been diagnosed at stage IIB or IIC initially.
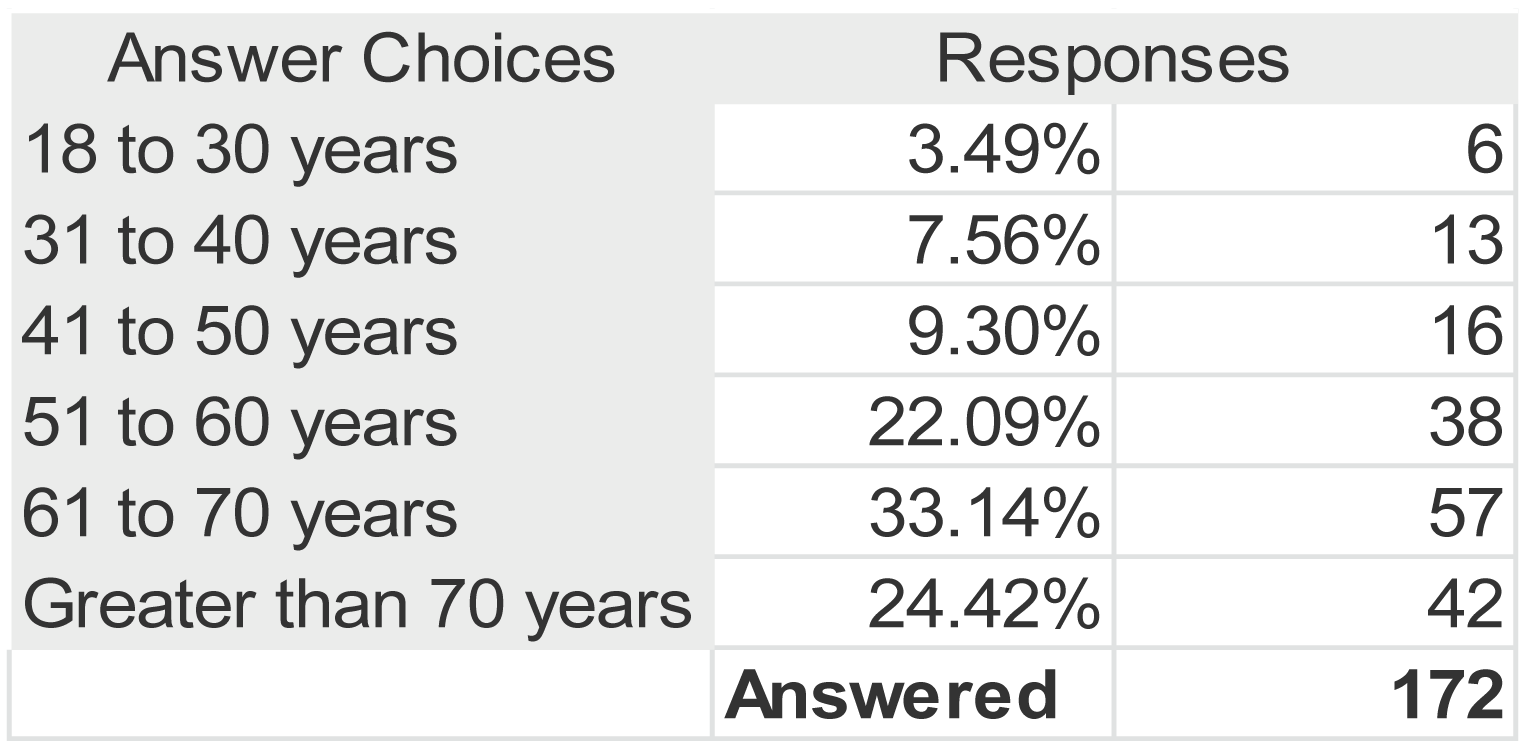
Disease Experience: Patients were asked how their diagnosis of melanoma affects their day-to-day life and quality of life. The most significant impacts reported were 1 – Scarring and Disfigurement; 2. Fear or Anxiety; 3. Disrupted Sleep as well as pain, fatigue, and depression.
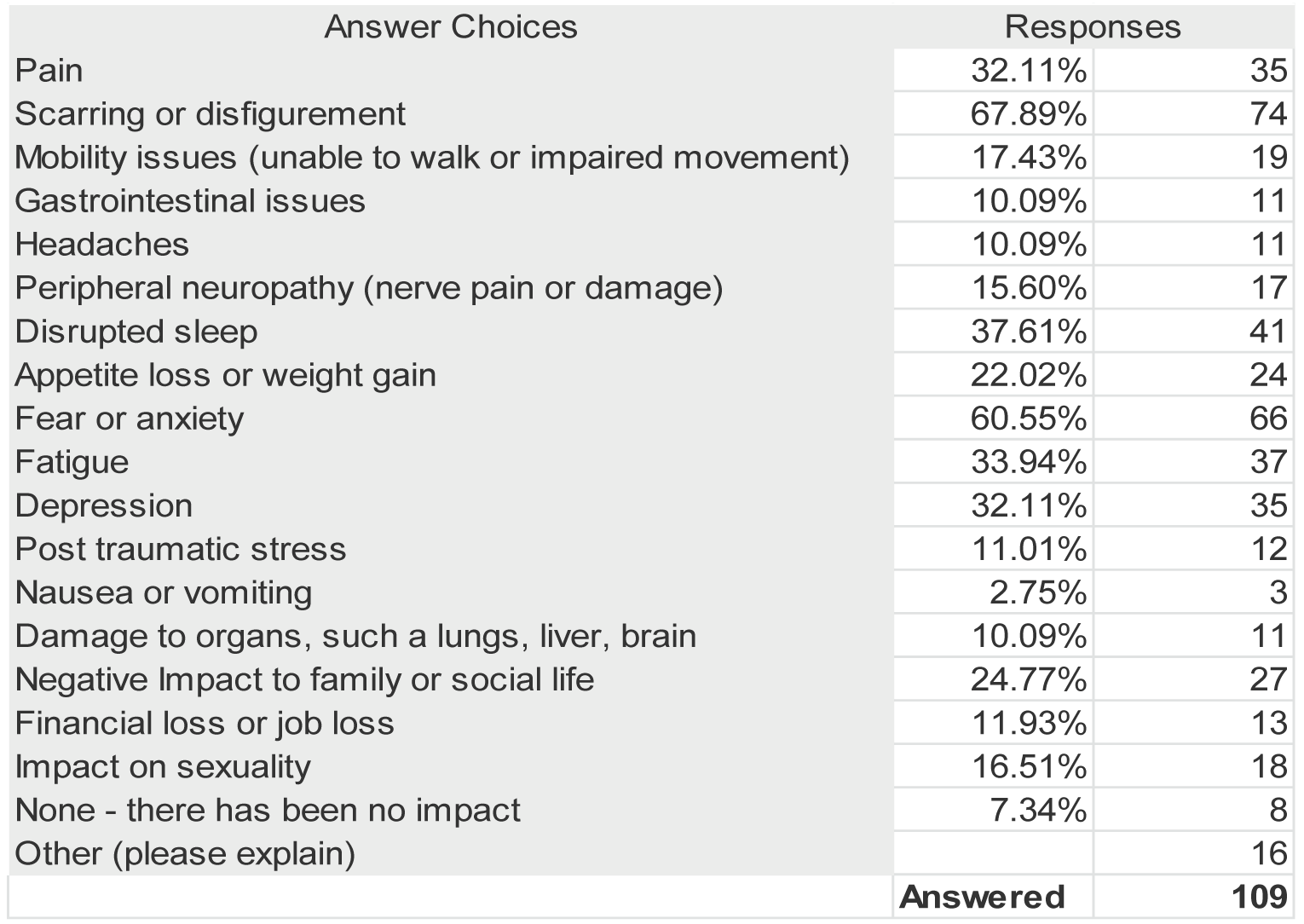
These are just a sample of comments from patients on the impact on their quality of life from the disease include:
Caused permanent damage to my leg and nerves which impacts ability to walk and stand for long periods due to swelling. I have had long term psychological impact – PTSD
Anxiety and emotional impacts for sure. I was warned at the start that this journey would be a roller coaster of emotions, uncertainty, and fear. My medical team was always great but there is the uncertainty of how much time I had left and my determination not to waste the time or my energy on frivolous things or people.
I am anxious about reoccurrence. This anxiety seems to preoccupy many of my thoughts and causes me stress.
I have had to deal with ongoing scarring issues which affect my identity and the mobility of my shoulder. I have to "hide "from the sun and gave up many enjoyable outdoor activities. We moved from our island and now I live mostly indoors.
At the very onset of being diagnosed this event significantly impacted my relationship with my spouse. My view of life changed drastically at the time and my spouse appears to be unable to relate to the anxieties and fear I was feeling as various times. There has been improvements over the past month after having received some good news indicating the cancer has not spread to my lymph nodes.
I tire very easy and due to my steroid of hydrocortisone I have troubles sleeping
I was very concerned about my life expectancy - made it difficult to find joy in life thinking that my life could end within 12 months
Worry about summer weather, going on vacation, always trying to stay out of the sun. Not being able to do things with my children because of sun concerns. Worrying about their getting melanoma in the future.
I find it very hard to walk due to my arterial blockages in both legs , and being limited to carrying no more than 20 lbs , I find it very hard to do groceries , after going through Chemo treatments I am required to go for blood work one a Month for my Cancer D R , I also go for blood work once monthly for My family D R due to My thyroid and diabetic Disease.
As I waited for my specialist appointment from May to Sept. 2021, I had to keep a dressing on the lesion on my calf all last summer, due to ulcerating and how awful it looked. I also didn't swim at all because I got infection and irritated skin around the lesion. It was painful and I had trouble sleeping due to anxiety and discomfort. After both surgeries, I had mobility issues.
I am 11 years from original diagnosis. During the critical treatment time and the following follow up years, fear and anxiety were a real presence. With the progression of time and positive follow ups, that has gradually disappeared. A part of the fear and anxiety is that there were no real post-surgical options for me at that time. It was only watch and wait. I would have truly valued some choices post surgery that improved the odds.
Lymphedema (swelling) of affected arm and hand causes ongoing pain and discomfort
Had to retire
EVERYTHING. Nothing will ever be the same.
The fatigue physically limited me and therefore l couldn't function as normal. Burden fell on my husband. Extremely anxious and that made me uncomfortable and hard on my family.
Time off work, limited physical activities, require more rest.
My nodal melanoma was painful, ulcerated and bleeding from June-Sept. 2021, which made it necessary to keep a dressing on it at all times. I was fearful and had anxiety as I awaited my surgical oncology referral from May 2021.
Surgery was on my upper arm, definitely impacted daily activity including work (typing). Serious anxiety and fears since diagnosis and surgery.
Sleep difficulties. Anxiety. Emotional trauma from scar disfigurement. Social phobia, mild degree.
My husband died of colon cancer in 2000. At the time our sons were 10, 14 and 18 years old. When I was diagnosed with melanoma in 2019, they were concerned that their remaining parent had also diagnosed with cancer.
I have lost some flexibility in the leg that I had two surgeries on. I have scars. I now wear a lymphedema compression stocking, have fittings, and pay for this every 6 months.
Loss of mobility, can no longer ride my bike, swelling and stiffness due to lymphoma, loss of independence.
The fatigue means I've decreased my workdays to 2 per week and have reduced my levels of physical activity. Dealing with depression has reduced my desire to be social and is thus leading to loneliness and isolation.
Nerve pain constantly, deep tissue pain, weakness, hiding disfigured surgical site
Crippling fear and depression, constant thoughts of death and dying of cancer and not being around for my kids, worries for the future, obsession with my skin and all lesions on it.
Having a difficult time with appetite, feelings of nausea, and not able to do much because of these problems. Loss of sleep is also significant.
Having had 2 episodes of melanoma - 25 years apart, I am in constant fear of recurrence. Since my husband had also had melanoma, we fear for our children as well.
Surgery on wrist limits mobility to some extent effecting golf swing; lifting items; gardening and painting. Scarring on forehead from surgery/skin graft effects self image
I do not go outside, therefore no gardening, outside physical activities, picnics, which I used to do prior to the melanomas
Symptoms (from the disease and long-term treatments impacted me in terms of not being able to work fulltime; disease made me modify my daily routine by modifying the time of day I would go outside (fear of the sun), but now am less fearful and use clothing, sunscreen, etc to limit sun exposure
It impacts how I am treated at work. It limits my sports severely. It robs me of sleep (I get 4 hrs max per night). It limits my walking, enjoyment of outings. I have to sit frequently (it was on my ankle). Anxiety improves with each passing year.
I have shortness of breath which has led to mobility issues. I have lymphedema in my arm and neck. I have lost mobility in my arm; can’t lift it and I can’t hold things n my hand. I work from home due to my mobility issues. On medication for nerve damage.
The cancer has impacted my emotional well being. I have post traumatic stress. I have permanent visible scaring. Financial and career impact was huge.
Caregivers also commented on the amount of time it took for appointments and outside care (home care), the enormous financial impact and the unending emotional impact the disease has had on the entire family. A couple mentioned that it has permanently put them on social assistance and food banks as the loss of income was significant.
Experiences With Currently Available Treatments
At this stage of disease (IIB or IIC), there is no treatment available beyond surgery. Yet there is a higher risk of recurrence for this stage than for stage IIIA. As such, there is an obvious unmet need for treatment options to prevent recurrence of disease. There have also been lengthy delays with diagnosis and treatment – beyond the significant delays patients experienced pre-pandemic. A vast majority of patients reported that lasting affects of surgery at this stage and the mental health issues associated with the diagnosis with no treatment beyond surgery (including fear of recurrence and anxiety – knowing the high risk at this stage and no treatment beyond surgery), were the most difficult and lasting impacts on their quality of life. If invasive surgeries could be minimized through use of an effective therapy and the option of adjuvant treatment available, it would go a long way to help patients and their families. Comments from patients included:
Mobility and Lymphedema issues caused by surgery including lymph node dissection (22 patients commented):
Make sure we can still be active and maintain a rigorous exercise program. Also keeping emotions and thoughts in a healthy perspective, which is where psychosocial programs are essential.
Lymphedema – after surgery, affects all of my day-to-day functioning
Depends on the person. I am struggling more with the effects of lymphedema than my prominent graft scar. I have the knowledge I'm at risk of recurrence, but it doesn't cause me problems aside from when I'm already under high stress and it's the times of year significant to my experience (diagnosis, surgery, skin checks etc)
Surgery produced lymphedema, as all nodes were removed from left groin. Leg deformed as a result.
Anxiety and fear caused by the diagnosis and lack of treatment options (mentioned by over 70 patients):
Day to day living without disruption, fear and fatigue would be great, but when I tire it takes about another day or two after to recover
I am anxious about reoccurrence. This anxiety seems to preoccupy many of my thoughts and causes me stress.
Sleep is disrupted all the time. Fear creeps in. Crying comes out of nowhere. I can’t take stress anymore. I wonder sometimes if dying is a better option.
Financial impacts
Traveling to radiation treatments and for appointments takes over an hour from my home. Fuel and parking plus the out of pocket costs to treat Lymphedema
High dose prednisone for 2 years, 100 lbs gained. Four months to put it on, four years to take it off. Poverty. Problems getting ODSP.
Financial - have to spend extra money for dry a lot of dry mouth products and fluoride to make sure my teeth don't rot as a result of surgery on my lymph nodes and my throat.
Financially I lost time at work. I am more vigilant for my health which can be costly with purifiers, naturopathic treatments, and other health care that is not covered. The time commitment is enormous, while also working and having a family life.
Improved Outcomes
The majority of patients indicated they are very willing to accept the side effect profile of pembrolizumab if it would potentially mean that they would not have to deal with a recurrence. Of course, a few more elderly patients suggested they would consider their overall health status and would have to see at the time what their oncologist feels is the best option for them to prevent recurrence of disease, particularly if it meant a lot of travel to receive treatment. Patients would like a therapy that allows them to function as best as possible – ideally able to work and continue normal day to day activities without significant long term side effects. Comments regarding having earlier adjuvant access to treatment included:
Likely if this therapy would have been available to me, it might have meant I didn't have the recurrences and subsequent physical challenges. No interferon, no skin grafts - my life might have been very different.
I would have liked an option to prevent this from spreading. think it would be a game changer.
My stress and anxiety about reoccurrence would be substantially reduced. I would feel that I am doing something to help myself combat the disease.
If I had treatment available, I would hope it would allow me to see my daughter live through to her adult years and be healthy to enjoy my empty nest. She fears having inherited the gene that makes her susceptible to the same melanoma risk as her mother. My mother has melanoma too.
It would give me more hope of survival and improve my emotional well being as I am constantly afraid of the cancer spreading to other areas of my body given the aggressive nature of this disease.
Having a drug that would give me hope to live longer would mean everything to me and my family/friends.
My life is to be here as long as I can and I listen to my Drs as my endocrinologist & oncologist and my family Dr when it comes to taking drugs that will help, and I’m open to advancements in medicine.
Experience With Drug Under Review
20 patients indicated they had been treated with pembrolizumab for stage IIB or C melanoma. All but one indicated the access was through clinical trial. A common issue was the length of time and cost of travel to get to a clinical trial site for treatment. Of those treated, 73% indicated the side effects were worth the treatment and 27% indicated the side effects were not worth the treatment. For those treated, the following is a list of side effects reported:
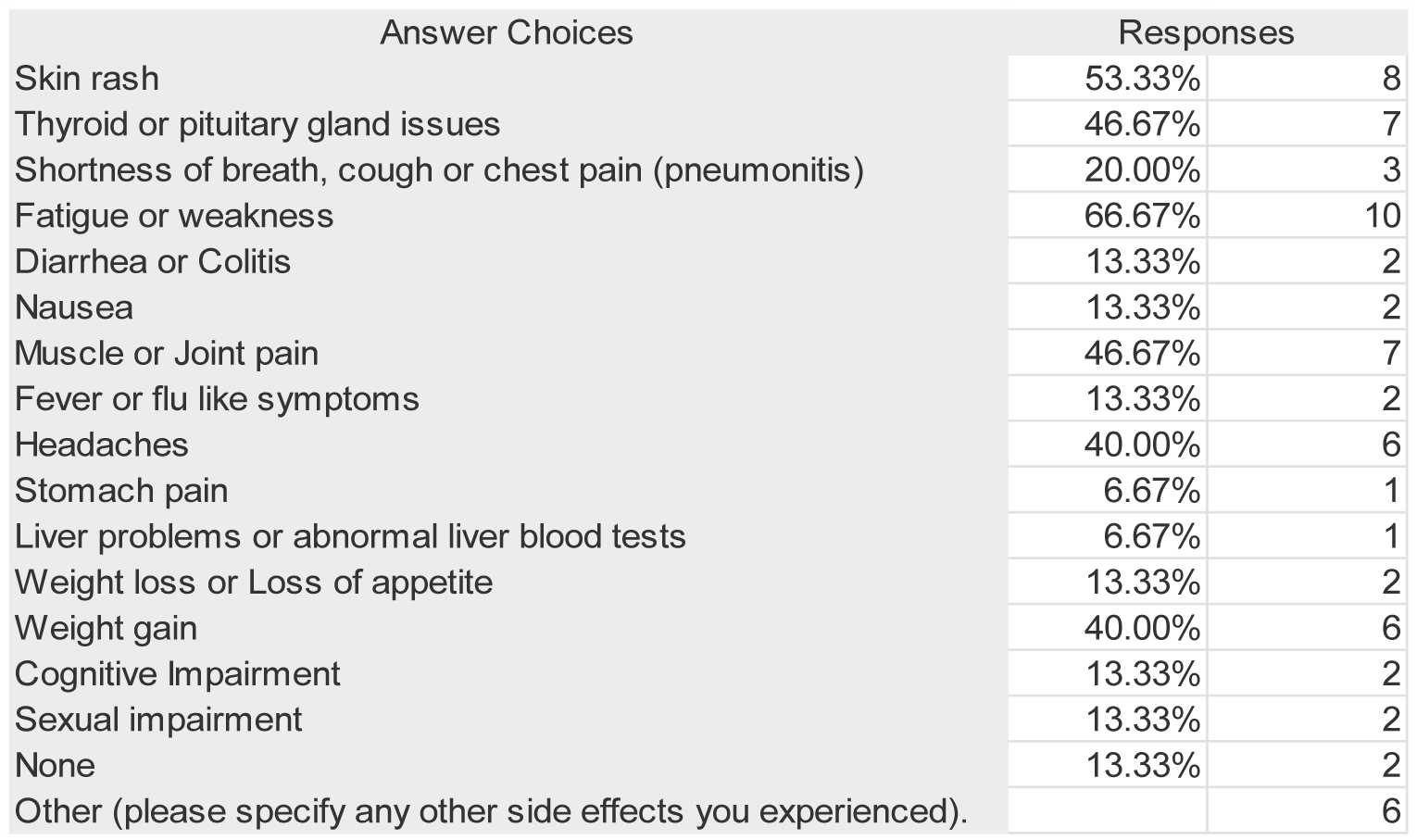
Patients were asked about the outcomes they have experienced with adjuvant treatment. Responses are captured in Figure 4 below:
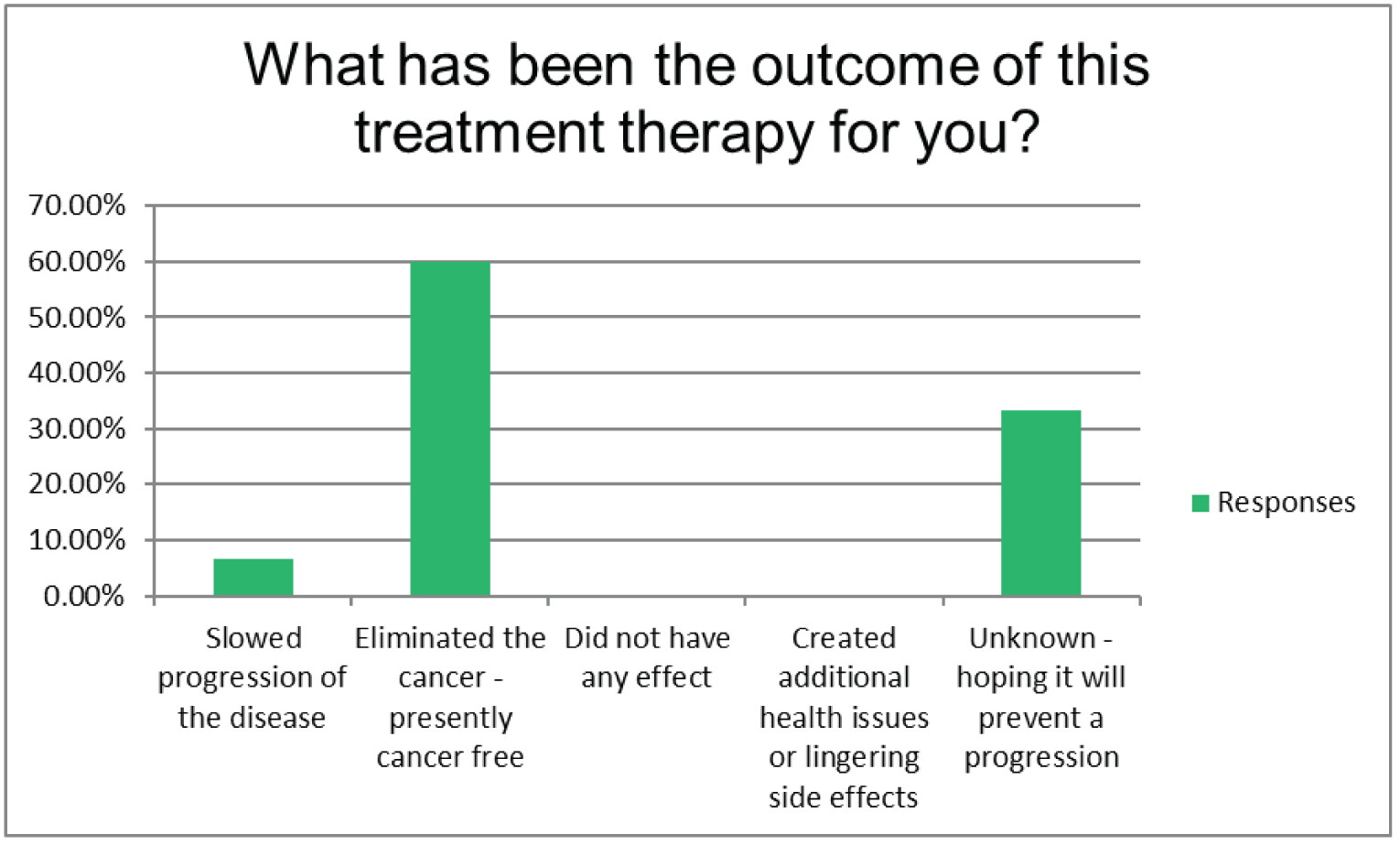
Key values for patients and caregivers for this drug therapy include effectiveness in preventing recurrence of disease; tolerable side effects without long term quality of life impacts; minimal impact on finances including easily accessible without having to travel long distances and the possibility of continuation of work or daily activities without significant interruption.
Companion Diagnostic Test
Not applicable.
Anything Else?
It is so very important to have the option of treatment for this deadly disease at an earlier stage. The research data points to the fact that patients diagnosed at stage IIB or IIC have a very high rate of recurrence and potential metastasis. The financial cost of earlier treatment is far less than the treatment for metastatic disease and as you can see from the patient comments, the emotional, physical and societal impact of melanoma is significant and lasting. This much needed therapy gives not only hope, but a real chance of survival and quality of life for many. It may prevent unnecessary surgical and radiation impacts to quality of life and the burden to patients of ongoing treatment.
Patient Group Conflict of Interest Declaration
Did you receive help from outside your patient group to complete this submission? If yes, please detail the help and who provided it.
No.
Did you receive help from outside your patient group to collect or analyze data used in this submission? If yes, please detail the help and who provided it.
No.
List any companies or organizations that have provided your group with financial payment over the past 2 years AND who may have direct or indirect interest in the drug under review.
Table 1: Financial Disclosures for Melanoma Canada
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Merck Canada | — | — | — | X |
Save Your Skin Foundation
About Save Your Skin Foundation
Save Your Skin Foundation (SYSF) is a national patient-led not-for-profit group dedicated to the fight against non-melanoma skin cancers, melanoma and ocular melanoma through nationwide education, advocacy, and awareness initiatives. SYSF provides a community of oncology patient and caregiver support throughout the entire continuum of care, from prevention and diagnosis to survivorship.
Information Gathering
Information was obtained through online surveys, virtual patient roundtables and one-on-one conversations. Information collected for # 3, 4, and 5 included all melanoma patients, and was gathered over the past 6 months, while section 6 was information from patients treated by drug under review collected over the past 2 weeks.
There were (17) females and (8) males ranging between the ages of 30 – 80+. The breakdown of respondents was (6) between 30- 49, (5) between 50 – 59, (7) 60 – 69 (5) 70-79. And (2) over 80.
(11) respondents were retired, (7) working fulltime, (2) working part-time, (4) not able to work because of health related issues, and
(1) not employed.
There were (9) respondents from BC, (3) from Alberta, (4) from Saskachewan, (2) from Manitoba, (5) from Ontario, (1) from QC, and
(1) from outside of Canada (USA).
Disease Experience
All patient surveyed felt scared, anxious and confused. Most knew nothing about Melanoma, what it meant to have it and what would come next for them. They knew nothing about cancer staging or lymph node dissection. They all noted that they needed and wanted as much information as possible and were reaching out to anyone and everyone for direction.
Once patients got to a cancer centre and/or oncologist some of the anxiety was reduced, but then a sense of doom and fear was exacerbated as they did not qualify for treatment because they were not stage 3 or 4. For the patients diagnosed with stage 2, there was limited access to available treatment in a limited number of centres and provinces. For patients that were not lucky enough to get to special access to treatment, the fear and anxiety of having to “Wait and Watch” was horrific.
“Roller ocaster emotional experience – fear, denial, depression.”
“Mentally exhausting.”
“I still marvel at how well I feel, no pain, no nausea, yet the melanoma marches on.” “I feel lucky it was caught early enough.”fwait
“Stressful on entire family being given a cancer diagnosis.” “Terrifying mentally and physically exhausting and a lot of anxiety.”
Experiences With Currently Available Treatments
There are no treatment options available for stage 2 melanoma.
All patients interviewed over the past 6 months with stage 3 and 4 said that if treatments had of been offered to them at stage 2 or 3 they would not have endured the stress and anxiety of the “wait and watch” approach. All patients interviewed agreed that the most difficult time for them was at diagnosis when they were told they had melanoma but treatments were not available to them. All patients also mentioned that they were surprised when diagnosed with Stage 2 that there were no approved treatment options available to them. (2) patients diagnosed with stage 1 thought that they would be offered treatment and also thought that they would be referred to an oncologist immediately to be monitored in case of disease progression to stage 2.
Improved Outcomes
All patients surveyed would like to be cured, and to have access to treatment close to home and in a timely fashion. If their disease was to progress or reoccur they would hope that there would be other treatment options available to them.
“The new immunotherapy treatments are amazing – I just wish there were more available and more treatment centres accessible to rural areas.”
“Currently the treatment I’m on is very manageable and I can still live lif, work and do everything I could before.”
“Immunotherapies are much more targeted, hence much easier on the patient (usually) than old school treatment of radiation and chemo. I would like to see immunotherapy used more often as a first-line treatment and for other cancers.”
“I would hope that all my treatments would be covered by medical insurance and the decision on which treatment I should received at what time would be determined by me and my oncologist.”
“Patients need access to these life saving treatments – melanoma used to be an instant death sentence, now it is treatable. Had I not had treatment upon diagnosis in the adjuvant stage, I may not have lived to see my daughters graduate hight school – and now college.”
“My experience of being on Keytruda is that life has not changed for me or my family. The side effects are so minimal that no member of my family has been impacted. I have been able to take are of my husband, the house, the pets etc. A couple of hours getting the intravenous and regulars CT scans are a small price to pay if that will extend my life.”
“My quality of life was hardly hindered at all while I was on Keytuda.” “Immunotherapy should be free to all stage patients.”
Experience With Drug Under Review
(3) Patients received treatment through clinical trial, (2) through private payer and (2) through compassionate access. The other (11) were not sure of how they received the treatment. (14) completed the full course of treatment, (2) patients did not and (2) are still on treatment.
(5) Patients received no side effects, while the remainder of patients experienced one or more of the following side effects: Fatigue, cognitive impairment, nausea, skin rash, gasto issues, weight loss or gain.
Only one patient said side effects were not manageable. Others responses were:
“Very manageable.”
“My mom can’t believe how good she feels.”
All patients said that the benefits of treatment far outweighed the side effects. All patients received treatment in a timely manner and treatment costs were covered. The only inconvenience for (4) was having to travel to the cancer center (gas, parking etc).
All patients said that if they were offered a drug therapy on a clinical they would consider it.
“I would want to discuss it and the expectations with my oncologist first, but yes, I would take it.” “FOR SURE!!”
“Assuming that I needed it, now I don’t.”
“I would want to know the positive/negative aspects of the treatment.”
We also asked patients that if they had received a treatment in stage 2 or 3 and their disease was recur at a later stage, what did they feel would be a reasonable next step or option.
“If my melanoma was to recur, I would instantly request additional treatments – I have to fight for my life. If my cancer was to come back, I want to know that I have more treatment options available – and that I would be able to access them.”
“Absolutely if there was a recurrence I would hope that the protocol would be to treat with another option or re-challenge the treatment I had received”
“Yes, I would ask for further treatments. Perhaps combo therapy appropriate to my type of cancer.” “Yes, I would want to continue to receive treatments as long as I can.”
“I would definitely ask for additional treatments. I believe it would be reasonable. I also feel I would ask if any new treatments are available.”
“Yes and I would ask for Keytruda again. I would also be interested in drug studies.”
Companion Diagnostic Test
Not applicable.
Anything Else?
Since 2011 we have seen an onset of treatment options for not only metastatic melanoma patients but stage 3 melanoma patients as well. What we have heard over and over in our surveys and roundtable discussions with patients is that once diagnosed they wish for the process to be seamless, receiving treatment options in a timely fashion and decision for best course of action to be made by themselves along with their medical team. Most early stage melanoma patients were shocked that there were no treatment options for them until their disease progressed. We also heard loud and clear from patients that they were shocked at not only the process of getting treatment but the way in which treatments are approved in Canada and the time delay. Now that we have these innovative treatments in the melanoma space patients are more educated than ever before and they want these treatments within their grasp. And they have wondered why it has taken so long for potential treatment options in an early diagnosis (Stage 1 2 and 3).
What we continue to hear from patients that are on innovative treatments or have had innovative treatments is that the side effects are manageable and far outweigh the risk. As more oncologists are treating in the innovative medicines space it is becoming more common, thereby improving patient outcomes, and potential for long term survivorship. These are comments we hear from patients that have completed treatment in all stages of melanoma:
“Any new drugs and treatments that can help others in this condition are worth investigating.”
“This treatment saved my life, it could not be more important. I have young child, a spouse and parents and friends that would have all been devasted by my passing. I am hoping that Canada speeds up the approval process for new treatments and makes them available to all patients.”
“Life saving, had stage 4 brain and lung and am here 5 years later.”
“There are no words. It game me a chance to see my grandson start school. I am still here enjoying my family and life. In 2013 I was initially told I would not survive beyond 5 years.”
“Very amazing new developments are happening all the time. I would be willing to try any new treatment to have more time with my family.”
“Treatment saved my life! All patients need acces to IO and/or targeted therapy treatments in Canada and not just in a clinical trial.”
Patient Group Conflict of Interest Declaration
To maintain the objectivity and credibility of the CADTH reimbursement review process, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This Patient Group Conflict of Interest Declaration is required for participation. Declarations made do not negate or preclude the use of the patient group input. CADTH may contact your group with further questions, as needed.
Did you receive help from outside your patient group to complete this submission? If yes, please detail the help and who provided it.
No.
Did you receive help from outside your patient group to collect or analyze data used in this submission? If yes, please detail the help and who provided it.
No.
List any companies or organizations that have provided your group with financial payment over the past 2 years AND who may have direct or indirect interest in the drug under review.
Table 2: Financial Disclosures for Save Your Skin Foundation
Company | $0 to 5,000 | $5,001 to 10,000 | $10,001 to 50,000 | In Excess of $50,000 |
|---|---|---|---|---|
Merck | — | — | — | X |
Clinician Group Input
Ontario Health (Cancer Care Ontario) Skin Cancer Drug Advisory Committee
About Ontario Health (Cancer Care Ontario) Skin Cancer Drug Advisory Committee
OH-CCO’s Drug Advisory Committees provide timely evidence-based clinical and health system guidance on drug-related issues in support of CCO’s mandate, including the Provincial Drug Reimbursement Programs (PDRP) and the Systemic Treatment Program.
Information Gathering
This input was jointly discussed at a DAC meeting.
Current Treatments and Treatment Goals
Pembrolizumab prolongs progression-free and overall survival among patients with advanced melanoma and recurrence-free survival in resected stage III disease. Pembrolizumab is not currently available to patients with stage IIB or stage IIC melanoma in the adjuvant setting. There is currently no treatment for this high-risk patient population. Stage IIB and stage IIC are a higher risk population than stage IIIA. Recent trials have shown PFS benefit to 18 months for the stage IIB and stage IIC population.
Treatment goals would be recurrence free survival as it is an important endpoint for patients while being a possible surrogate for overall survival.
Treatment Gaps (Unmet Needs)
Considering the treatment goals, please describe goals (needs) that are not being met by currently available treatments.
There is currently no treatment for this high-risk patient population.
Place in Therapy
How would the drug under review fit into the current treatment paradigm?
Pembrolizumab would be adjuvant treatment after appropriate surgical management. Currently, if these patients are sentinel node negative (even though they are at high risk of recurrence) they do not meet criteria for adjuvant treatment. This treatment is an area of unmet need.
Which patients would be best suited for treatment with the drug under review? Which patients would be least suitable for treatment with the drug under review?
Patients best suited would align with the inclusion criteria of the study. Patients with stage IIB and stage IIC.
Patients least suited would align with the exclusion criteria of the study.
What outcomes are used to determine whether a patient is responding to treatment in clinical practice? How often should treatment response be assessed?
Lack of recurrence by physical exam and CT scans.
What factors should be considered when deciding to discontinue treatment with the drug under review?
Disease recurrence and toxicity.
What settings are appropriate for treatment with [drug under review]? Is a specialist required to diagnose, treat, and monitor patients who might receive [drug under review]?
A medical oncologist would need to diagnose and treat in an outpatient setting.
Additional Information
No other treatment for this very high-risk patient population.
Conflict of Interest Declarations
To maintain the objectivity and credibility of the CADTH drug review programs, all participants in the drug review processes must disclose any real, potential, or perceived conflicts of interest. This conflict of interest declaration is required for participation. Declarations made do not negate or preclude the use of the clinician group input. CADTH may contact your group with further questions, as needed. Please see the Procedures for CADTH Drug Reimbursement Reviews (section 6.3) for further details.
Did you receive help from outside your clinician group to complete this submission? If yes, please detail the help and who provided it.
Ontario Health provided secretariat functions for the DAC.
Did you receive help from outside your clinician group to collect or analyze any information used in this submission? If yes, please detail the help and who provided it.
No.
List any companies or organizations that have provided your group with financial payment over the past two years AND who may have direct or indirect interest in the drug under review. Please note that this is required for each clinician who contributed to the input — please add more tables as needed (copy and paste). It is preferred for all declarations to be included in a single document.
Declaration for Clinician 1
Name: Dr. Frances Wright
Position: Ontario Health Cancer Care Ontario Skin Cancer Drug Advisory Committee Lead
Date: 18/05/2022
Table 3: Conflict of Interest Declaration for Ontario Health (Cancer Care Ontario) Skin Cancer Drug Advisory Committee — Clinician 1
Company | Check appropriate dollar range | |||
|---|---|---|---|---|
$0 to $5,000 | $5,001 to $10,000 | $10,001 to $50,000 | In excess of $50,000 | |
No COI | — | — | — | — |
Declaration for Clinician 2
Name: Dr. Teresa Petrella
Position: Ontario Health Cancer Care Ontario Skin Cancer Drug Advisory Committee Member
Date: 18-05-2022
Table 4: Conflict of Interest Declaration for Ontario Health (Cancer Care Ontario) Skin Cancer Drug Advisory Committee — Clinician 2
Company | Check appropriate dollar range | |||
|---|---|---|---|---|
$0 to $5,000 | $5,001 to $10,000 | $10,001 to $50,000 | In excess of $50,000 | |
No COI | — | — | — | — |
Declaration for Clinician 3
Name: Dr. Marcus Butler
Position: Ontario Health Cancer Care Ontario Skin Cancer Drug Advisory Committee Member
Date: 18-05-2022
Table 5: Conflict of Interest Declaration for Ontario Health (Cancer Care Ontario) Skin Cancer Drug Advisory Committee — Clinician 3
Company | Check appropriate dollar range | |||
|---|---|---|---|---|
$0 to $5,000 | $5,001 to $10,000 | $10,001 to $50,000 | In excess of $50,000 | |
No COI | — | — | — | — |
Declaration for Clinician 4
Name: Dr. Elaine McWhirter
Position: Ontario Health Cancer Care Ontario Skin Cancer Drug Advisory Committee Member
Date: 18-05-2022
Table 6: Conflict of Interest Declaration for Ontario Health (Cancer Care Ontario) Skin Cancer Drug Advisory Committee — Clinician 4
Company | Check appropriate dollar range | |||
|---|---|---|---|---|
$0 to $5,000 | $5,001 to $10,000 | $10,001 to $50,000 | In excess of $50,000 | |
No COI | — | — | — | — |
Declaration for Clinician 5
Name: Dr. Xinni Song
Position: Ontario Health Cancer Care Ontario Skin Cancer Drug Advisory Committee Member
Date: 18-05-2022
Table 7: Conflict of Interest Declaration for Ontario Health (Cancer Care Ontario) Skin Cancer Drug Advisory Committee — Clinician 5
Company | Check appropriate dollar range | |||
|---|---|---|---|---|
$0 to $5,000 | $5,001 to $10,000 | $10,001 to $50,000 | In excess of $50,000 | |
No COI | — | — | — | — |
ISSN: 2563-6596
Disclaimer: The information in this document is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. While patients and others may access this document, the document is made available for informational purposes only and no representations or warranties are made with respect to its fitness for any particular purpose. The information in this document should not be used as a substitute for professional medical advice or as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process. The Canadian Agency for Drugs and Technologies in Health (CADTH) does not endorse any information, drugs, therapies, treatments, products, processes, or services.
While care has been taken to ensure that the information prepared by CADTH in this document is accurate, complete, and up-to-date as at the applicable date the material was first published by CADTH, CADTH does not make any guarantees to that effect. CADTH does not guarantee and is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in any third-party materials used in preparing this document. The views and opinions of third parties published in this document do not necessarily state or reflect those of CADTH.
CADTH is not responsible for any errors, omissions, injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the contents of this document or any of the source materials.
This document may contain links to third-party websites. CADTH does not have control over the content of such sites. Use of third-party sites is governed by the third-party website owners’ own terms and conditions set out for such sites. CADTH does not make any guarantee with respect to any information contained on such third-party sites and CADTH is not responsible for any injury, loss, or damage suffered as a result of using such third-party sites. CADTH has no responsibility for the collection, use, and disclosure of personal information by third-party sites.
Subject to the aforementioned limitations, the views expressed herein are those of CADTH and do not necessarily represent the views of Canada’s federal, provincial, or territorial governments or any third party supplier of information.
This document is prepared and intended for use in the context of the Canadian health care system. The use of this document outside of Canada is done so at the user’s own risk.
This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada.
The copyright and other intellectual property rights in this document are owned by CADTH and its licensors. These rights are protected by the Canadian Copyright Act and other national and international laws and agreements. Users are permitted to make copies of this document for non-commercial purposes only, provided it is not modified when reproduced and appropriate credit is given to CADTH and its licensors.
Redactions: Confidential information in this document may be redacted at the request of the sponsor in accordance with the CADTH Drug Reimbursement Review Confidentiality Guidelines
Stakeholder Input: The views expressed in each submission are those of the submitting organization or individual; not necessarily the views of CADTH or of other organizations. As such, they are independent of CADTH and do not necessarily represent or reflect the view of CADTH. No endorsement by CADTH is intended or should be inferred. By filing with CADTH, the submitting organization or individual agrees to the full disclosure of the information. CADTH does not edit the content of the submissions.
CADTH does use reasonable care to prevent disclosure of personal information in posted material; however, it is ultimately the submitter’s responsibility to ensure no identifying personal information or personal health information is included in the submission. The name of the submitting organization or individual and all conflict of interest information are included in the submission; however, the name of the author, including the name of an individual patient or caregiver submitting the patient input, are not posted.
Accessibility: CADTH is committed to treating people with disabilities in a way that respects their dignity and independence, supports them in accessing material in a timely manner, and provides a robust feedback process to support continuous improvement. All materials prepared by CADTH are available in an accessible format. Where materials provided to CADTH by a submitting organization or individual are not available in an accessible format, CADTH will provide a summary document upon request. More details on CADTH’s accessibility policies can be found here.
About CADTH: CADTH is an independent, not-for-profit organization responsible for providing Canada’s health care decision-makers with objective evidence to help make informed decisions about the optimal use of drugs, medical devices, diagnostics, and procedures in our health care system.
Funding: CADTH receives funding from Canada’s federal, provincial, and territorial governments, with the exception of Quebec.